comparative study of extra amniotic saline
105
“COMPARATIVE STUDY OF EXTRA AMNIOTIC SALINE INFUSION THROUGH INTRACERVICAL BALLOON CATHETER AND FOLEYS BULB INDUCTION FOR INDUCTION OF LABOUR” Dissertation submitted to THE TAMILNADU Dr. M.G.R MEDICAL UNIVERSITY CHENNAI – 600032 with partial fulfillment of the regulations for the award of the degree of M.S OBSTETRICS AND GYNAECOLOGY (BRANCH – II ) UNIVERSITY REGISTRATION NO. 221816302 COIMBATORE MEDICAL COLLEGE, COIMBATORE MAY 2020
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of comparative study of extra amniotic saline

“COMPARATIVE STUDY OF EXTRA AMNIOTIC SALINE
INFUSION THROUGH INTRACERVICAL BALLOON
CATHETER AND FOLEYS BULB INDUCTION FOR
INDUCTION OF LABOUR”
Dissertation submitted to
THE TAMILNADU Dr. M.G.R MEDICAL UNIVERSITY
CHENNAI – 600032
with partial fulfillment of the regulations for the award of the degree of
M.S OBSTETRICS AND GYNAECOLOGY (BRANCH – II )
UNIVERSITY REGISTRATION NO. 221816302
COIMBATORE MEDICAL COLLEGE,
COIMBATORE
MAY 2020

CERTIFICATE
This is to certify that this dissertation on “COMPARATIVE
STUDY OF EXTRA AMNIOTIC SALINE INFUSION THROUGH
INTRACERVICAL BALLOON CATHETER AND FOLEYS BULB
INDUCTION FOR INDUCTION OF LABOUR” is a bonafide
research work done by Dr.GEETHA RAJAGOPALAN , under my
guidance and supervision during the academic year 2018-19. This has
been submitted in partial fulfillment for the award of M.S Degree in
OBSTETRICS AND GYNAECOLOGY (Branch II) by THE
TAMILNADU DR. M.G.R MEDICAL UNIVERSITY, CHENNAI –
600032.
Date: Guide
Prof. Dr.K. Murugalakshmi, M.D., D.G.O.,
Department of Obstetrics & Gynaecology
Coimbatore Medical College Hospital.
Date: Prof. Dr. R.Manonmani M.D., D.G.O.,
HOD,
Department of Obstetrics & Gynaecology
Coimbatore Medical College Hospital.
Date: Prof. Dr. B. Asokan M.S., M.ch.,
The Dean,
Coimbatore Medical College Hospital.

CERTIFICATE
This is to certify that this dissertation work titled
“COMPARATIVE STUDY OF EXTRA AMNIOTIC SALINE
INFUSION THROUGH INTRACERVICAL BALLOON
CATHETER AND FOLEYS BULB INDUCTION FOR
INDUCTION OF LABOUR” of the candidate Dr. GEETHA
RAJAGOPALAN with registration number 221816302 for the award of
M.S Degree in OBSTETRICS AND GYNAECOLOGY (Branch II) . I
personally verified the urkund.com website for the purpose of plagiarism
check I found that the uploaded thesis file contains from introduction to
conclusion pages and result shows Nine percentage (9%) of plagiarism in
the dissertation.
Guide and Supervisor sign with seal



DECLARATION
I solemnly declare that this dissertation entitled
“COMPARATIVE STUDY OF EXTRA AMNIOTIC SALINE
INFUSION THROUGH INTRACERVICAL BALLOON
CATHETER AND FOLEYS BULB INDUCTION FOR
INDUCTION OF LABOUR” was done by me at Coimbatore Medical
College Hospital, Coimbatore during the period of September 2018
to September 2019 under the guidance and supervision of
Prof.Dr.K.MURUGALAKSHMI MD DGO., This dissertation is
submitted to THE TAMILNADU DR. M.G.R MEDICAL
UNIVERSITY , towards partial fulfillment of the regulation for the
award of M.S DEGREE IN OBSTETRICS AND GYNAECOLOGY
(BRANCH II) .
PLACE :
DATE :
DR.GEETHA RAJAGOPALAN

ACKNOWLEDGEMENT
It gives me great pleasure in preparing this dissertation and I take
this opportunity to thank everyone who has made this possible.
It is most appropriate that I begin by expressing my gratitude to my
parents for their blessings.
My profound thanks to the Dean. Prof. Dr. B. ASOKAN M.S.,
M.ch., Coimbatore Medical College Hospital for permitting me to make
use of the clinical materials of our hospital.
My sincere thanks to Prof. Dr. R. MANONMANI M.D., D.G.O.,
Professor and Head of the Department, Department of Obstetrics &
Gynaecology, Coimbatore Medical College Hospital, Coimbatore, for her
profound enthusiasm and keen supervision of this work.
It gives me immense pleasure to express my deep sense of
gratitude and heartfelt thanks to Prof. Dr. K. MURUGALAKSHMI,
M.D., D.G.O., Professor, Department of Obstetrics & Gynaecology,
Coimbatore Medical College Hospital, Coimbatore, for her invaluable
guidance, constant encouragement, immense patience and great care
towards this dissertation.
I wish to express my heartfelt gratitude to Prof.Dr.N. GEETHA,
M.D., Professor, Department of Obstetrics & Gynaecology, Coimbatore
Medical College Hospital, Coimbatore, whose knowledge and experience
have guided and inculcated in me a sense of confidence.

My heartfelt thanks to Associate Professors Dr.Thilagavathy,
M.D(O.G)., Dr.Mohanasundari,M.D(O.G).,D.Ch., for their support
and encouragement in this study.
I am extremely thankful to all our Assistant Professors of
Department of Obstetrics and Gynaecology for their guidance and help
during this study.
I am ever grateful to my husband and family for being a constant
source of support and encouragement.
I extend my thanks to my entire Postgraduate colleagues for their
help and support.
I wish to thank, Statistician, for his suggestions and for providing a
scientific meaning to this study.
I would like to thank all my patients without whose cooperation,
this dissertation would never have seen the light of the day.
Dr. GEETHA RAJAGOPALAN

CONTENTS
S.NO CONTENTS PAGE NO
1. INTRODUCTION 1
2. AIMS AND OBJECTIVES 5
3. REVIEW OF LITERATURE 8
4. MATERIALS AND METHODS 31
5. STATISTICAL ANALYSIS AND RESULTS 38
6. DISCUSSION 71
7. SUMMARY 76
8. CONCLUSION 77
9. BIBLIOGRAPHY
10. ANNEXURES
PROFORMA
CONSENT FORM
MASTER CHART

1
INTRODUCTION
Labour starts spontaneously at term or near term in majority of
women. Induction of labour has become mandatory in modern day
obstetrics, because of medical or obstetric complications of pregnancy.
Definition of induction of labour
Stimulation of regular uterine contractions in a viable pregnancy
before the spontaneous onset of labour with or without rupture of
membranes after 28 wkw of gestation using mechanical or pharmacological
methods in order to generate progressive cervical dilatation and subsequent
delivery after fetus has attained maturity.
History of labour induction deals back to Hippocrates original
description of mammary stimulating and mechanical dilatation of cervical
canal.
Induction of labour is as old as Soraners of Greece, who was the first
person to induce labour in 100 A.D. Starting from the olden days of Soraners
to the modern days of obstetrics, induction of labour has gone through
different methods and modifications over the period of time by different
people.
2
Steamens started inducing labour electively for the convenience of
obstetricians or the expectant mother. Moshion was the first to describe
manual dilatation of cervix for induction of labour.
Induction of labour is accepted as an option in the management of
high risk pregnancies in which the continuation of pregnancy is likely to
adversely affect the maternal condition or the perinatal outcome.
Success of labour induction depends on the patient selection. Patient
to be induced must be term or nearing term with adequatepelvis, favorable
cervix & with a viable fetus.
“Mechanical induction of labour is defined as “Stimulation of
uterine contractions by means of non-pharmacological agents administered
intracervically to the patients with the aim of starting labour”
Mechanical methods for induction promote cervical ripening and
promote onset of labour by stretching of cervix.They are amongst the oldest
methods used to initiate labour.
Safety aspect of induction methods becomes most important, although
this could be at the expenses of effectiveness. Mechanical methods have
advantages over pharmacological methods as they are widely available, low
in cost with fewer side effects such as less uterine hyperstimulation.

3
Failed induction is termed when the uterus to fail to contract after
recommended attempts of stimulation, or the uterus contracts abnormally, or
cervix does not dilate, or the fetus is in jeopardy.
Although induction of labour is aimed at achieving vaginal delivery,
there is always an increased risk of caesarean section. Hence individual
variation is more important each patient needs to be viewed in the context of
her past obstetrical history and complications in the present pregnancy
cervical status before deciding on the mode of induction.

4
Risks of induction of labour
1. OPERATIVE DELIVERY: In both primi and muti IOL increases risk of
caesarean section. About 3 fold increase in primi compared to those
labouring spontaneously.
In muti it is doubled from 3.4% to 8.5%
2. UTERINE HYPERCONTRACTILITY: any agent used in IOL can
over stimulate the uterus which leads to prolonged or tonic uterine
contractions, fetal compromise and abnormal FHR patterns
3. UTERINE RUPTURE: rare but occurs in patients with uterine scar like
caesarean section or uterine perforation
4. FAILED INDUCTION: rates of failed induction is about 3%
5. IATROGENIC PREMATURITY
6. PAIN
No method of induction is free from complications, aim of this study
is to find the effective method with least complications. The study was
undertaken with the objective of observing difference in the responses of two
different mechanical methods of induction of labour. The Study was
conducted in Coimbatore Medical College, Coimbatore.

5
AIM AND OBJECTIVES
AIM :
The study is carried out to assess the effectiveness of Extra amniotic
saline infusion through intracervical balloon catheter and Foleys bulb
induction for induction of labour.
OBJECTIVES OF THE STUDY
• To study the effect of cervical ripening
• To study the oxytocin augmentation need
• To see the effect on the labour outcome
• To study the response difference in primi and multi
• To assess the maternal and fetal outcome
Study Centre
The study was undertaken in the Department of Obstetrics and
Gynaecology, Coimbatore Medical College, Coimbatore.
Study design
Prospective randomized control study conducted between September
2018-2019.

6
Sample size
100 antenatal mothers admitted in the hospital were included in this
study.
Inclusion criteria
1. Singleton pregnancy
2. Cephalic presentation
3. Absence of infection
4. Bishop score <5
5. Intact fetal membrane
Exclusion criteria
1. Low lying placenta
2. Malpresentation
3. Maternal infection
4. Rupture of membranes
5. Maternal comorbid illnesses like Gestational diabetes, Heart disease,
Chronic kidney disease

7
Induction indications
1. Post EDD pregnancies
2. oligohydroamnios
3. Intra uterine growth restriction
4. Gestational hypertension
5. Severe preeclampsia
CONCLUSION
EASI group showed more effective cervical ripening as compared to the
Foleys bulb induction group. Mean induction to active labour interval was
shorter in EASI as compared to Foleys bulb. Mean induction to delivery
interval was shorter in EASI group as compared to Foleys bulb induction.
Oxytocin augmentation necessity was more in Foleys bulb group. In both the
groups fetal outcome and maternal outcome were similar. EASI was found to
be more effective than Foleys bulb for cervical ripening and induction of
labour.

8
REVIEW OF LITERATURE
• Induction of labour is unavoidable in modern obstetrics because of the
maternal obstetrical and medical complications.
• The outcome of successful induction depends on the perfect balance
between the hazards of meddling and risks of avoidable complications
by non – intervention.
• Methods of induction of labour are listed here, some of which are
sexual intercourse, breaststimulation, purgatives, enemas,
acupuncture, stripping of membranes, amniotomy etc...
• Stripping of membrane was tried in 1810 by HAMILTON in England.
This was used mainly for cervical ripening and labour induction.
Risks include infection, premature rupture of membranes and bleeding from
placental contact.
• THOMAS DENMON first reported AMNIOTOMY –artificial rupture
of membranes in 1956 in London. It was effective only when the
cervix is favourable

9
• In 1820- BRUNNING HAUSEN introduced spongy tests to dilate the
cervix and thereby induce labour.
• In 1843 SCHREIBER stimulated labour electrically. In 1846
KIWISCH used hot vaginal douche. In the same year COHEN used
the extraamniotic fluid administration for labour induction.
• In 1865 WILSON used laminaria tents. Assumed probably function
through the disturbance of chorio amniotic decidual interphase and
thereby bringing lysosomal destruction and prostaglandin synthesis.
• In 1935 VANEULER, introduced the term prostaglandins. In
1971KARIM & SHARMA first induced labour with use of oral PGE2.
Since then a large number of reports have appeared in literature,
evaluating the efficacy of oral PGE2 for induction of labour.
• Oral PGE2 induces normal uterine contraction and soften the cervix
,and hence decreasing the resistance of the cervix to dilation.
• Cervical dilatation with a balloon catheter was introduced to BARNES
by WOODMAN in 1863. Since then several modifications of this
method are reported. One method is the infusion of extra amniotic
normal saline and is referred as EASI.

10
• In 1989 SCHREYER etal., found that extra amniotic saline infusion
resulted in greater increase in cervical dilatation
• SHERMAN in 1996 summarized the results of 13 trials with balloon
catheters and concluded that with or without saline infusion the
method cause rapid improvement in Bishop score and shortened
labours.
• VENGALIL and colleagues in 1998 proved that extra amniotic saline
infusion resulted in greater increase in Bishop score compared.
• HELMIN & MOLLER In 1998 reported catheter infusion to be
efficacious for cervical ripening than prostaglandin E2 gel.
• GOLDMAN & WIGTON in 1999 demonstrated a significantly higher
Bishop score with extra amniotic catheter infusion compared with
intracervical dinoprostone.
• GUINN & colleagues in 2000 compared induction of labour with
intracervical dinoprostone, laminaria plus intravenous oxytocin and
extraamniotic saline infusion. It was proved that induction to delivery
interval was less with extra amniotic saline infusion than laminaria or
dinoprostone gel.

11
• BUCCELLATO and associates in 2000 proved that there was greater
increase in Bishop score with extra amniotic saline infusion when
compared with 50ug of misoprostol.
• GUINN DAVIES , JK JONES, SULLIVAN L, WOLF D in 2004
conducted randomized control study for labour induction and
compared foley catheter with concurrent oxytocin and foley catheter
with extraamniotic saline infusion and proved that saline infusion was
effective.
• SHARAMI, MILANI in 2005 conducted randomized control trial
compared cervical ripening with PGE2 gel & extra amniotic
salineinfusion and demonstrated that extra amniotic saline infusion
was effective.
• KARJANE NW, BROCK EC in 2006 done a prospective study for
induction of labour using foley balloon with and without amniotic
saline infusion and showed with saline infusion induction is more
effective.
• SAIMA QAMAR, ADELLAR in 2012 conducted a comparative study
of PGE2 gel, PGE2 pessary and extra amniotic saline infusion with

12
oxytocin for induction of labour and found saline infusion have greater
increase in Bishop score compared to PGE2 gel and pessary.
Induction of labour
Induction implies stimulation of contractions before the spontaneous
onset of labour ,with or without ruptured membranes.
Indications include membrane rupture without labour, gestational
hypertension, nonreassuring fetal status, post term pregnancy, diabetes.
Contraindications include macrosomia, multifetal gestation, severe
hydrocephalus, malpresentation, uterine incision type, contracted or distorted
pelvic anatomy, abnormal placentation, active genital herpes etc.
Risks –Maternal complication rates that are increased in association with
labour induction ---caesarean delivery, chorioamnionitis and uterine atony.
Caesarean delivery: This is especially increased in nulliparous
undergoing induction.
Rate of caesarean delivery following elective induction was increased in
women without antepartum complications and with a Bishops score of 7 or
greater when compared with spontaneous labour.

13
Chorioamnionitis: Women whose labour is induced have an increased
incidence of chorioamnionitis compared with spontaneous labour.
Uterine atony: Postpartum atony and hemorrhage are more common in
women undergoing induction.
Regimens for labour induction
Pharmacological techniques:
Prostaglandin E2
Prostaglandin E1
Mechanical techniques:
• Foleys catheter
• Extra amniotic saline infusion (EASI)
• Hygroscopic cervical dilators
• Membrane stripping
APPLIED PHYSIOLOGY
• Uterine cervix contain extra cellular material proteins, Collagen (type
I &III), elastin, glycosaminoglycan, especially dermatin sulfate,

14
hyaluronic acid, heparin sulphate, water. Only 10- 15% cervical tissue
is composed of smooth muscle.
• It is well recognized that the cervix loses its firmness in late pregnancy
and becomes soft and compliant. During labour it further loses its
elasticity , viscosity and plasticity.
• Hyaluronic acid contributes to accumulation of water within the
substance of cervix, which destabilizes the collagen fibrils,
contributing to cervical ripening.
• Glycosaminoglycans increase and dermatin sulphate decrease at
labour. Proteolytic enzymes in cervix degrade cross linked collagen.
• Collagenase is an enzyme that breaks down collagen. Leucocyte
elastase is another enzyme that breaks elastin, proteoglycans.
• Apart from enzymatic change, cervical remodeling takes place with
advancing gestation. Abnormal remodeling of collagen may contribute
to dysfunctional labour.
• Based on current evidence, both prostaglandins and relaxin hormones
playa key role in process of cervical ripening. Cervical ripening occur
with increase in formation of gap junctions and increase in myometrial
contractility.

15
PHYSIOLOGY OF CERVICAL RIPENING

16
CERVICAL RIPENING

17

18
Human uterine cervix is a complex heterogeneous organ that
undergoes intensive changes throughout gestation and parturition.
The external os is connected to the internal os by a slender passage
called endocervical canal.
Cervical mucosa is lined with tall columnar epithelium and contains
many large glands which are lined by columnar epithelium which ends

19
abruptly at the level of external os, giving way to stratified squamous
epithelium that covers the portiovaginalis and extends to the vagina proper.
Cervix is composed of an extra cellular matrix consisting
predominantly of collagen with elastin and proteoglycans and celluar
portion consisting of smooth muscle and fibroblasts, epithelium and blood
vessels. Abnormal remodeling of collagen contribute to dysfunctional
labour.
Extensive remodeling of cervix occurs from early gestation to
postpartum period. Water content of cervix increases from 80% in non-
active state to 86% in late pregnancy, the remodeling process involves
properly timed biochemical cascades, interaction between the cellular
matrix and cervical stromal inflammatory cells such as neutrophils and
macrophages.
Cervical undergoes destructive procedure process through which the
cervix dilates to facilitate delivery.
Extracellular matrix (ECM)
Collagen is the predominant content of the ECM. Cervical collagen
consists of type II (70%) and type III (30%).

20
These proteins are rigid and arranged as a triple helix, the collagen can
be crossed-lined into fibrils, fibers and bundles. Elastin is another important
component of Extra Cellular Matrix (E.C.M) of cervix. Elastin fibers are
organized in parallel to and between collagen fibers.
Cellular component
Smooth muscle cells (20%) and fibroblasts (60%) make up the cellular
component of uterine cervix. Smooth muscle cells are embedded in an ECM
composed mainly of collagen fibers.

21
Role of hormones in cervical ripening
Hormonal manipulation may also have a role in cervical ripening.
Human cervical connective tissue contains both estrogen and progesterone
receptors.
As term approaches, there is a down regulation of both estrogen and
progesterone receptor, which may be caused by increased turnover of the
receptor proteins.
Estrogen and its precursors stimulate collagenase production in the
pregnant human cervix and progesterone maintain high level of enzyme that
degrade hyaluronic acid, thereby keeping its level in the cervix low until
term when progesterone and progesterone receptor level decrease.
Relaxin, an ovarian hormone released during gestation (H 1 is
expressed by ovary and H2 by both deciduas and trophoblast), it softens the
cervix.
The IL’s (interleukins) have also been suggested to play an important
role in the process because they are chemotactic for neutrophils. IL-8
involved in neutrophils mediated cervical ripening. IL-6 is known to
stimulate the production of PGE2 by amnion and deciduas.Recent studies

22
have indicated that IL-6 and TNF levels in amniotic fluid are elevated in the
active phase of both preterm and term labour.
Onset of labour
Uterine stretch and parturition
Fetal growth significantly increases in myometrial tensile stress and
amniotic fluid pressure.
With uterine activation, stretch is required for inductionspecific
contraction-associated proteins (CAPs).
Stretch increases expression of the gap junction protein-connexin 43,
as well as oxytocin receptors.
Clinical report for a role of stretch comes from the observation that
multifetal pregnancies and hydramnios are at a much greater risk for preterm
labour than singletons.

23
CERVICAL RIPENING
Methods of cervical ripening
1. NON MEDICAL:
• Sexual intercourse
• Herbal remedies
• Castor oil
• Hot baths
• Breast stimulation
• Acupuncture
• Sweeping of membranes
2. MECHANICAL:
• Foleys catheter
• Extraamniotic saline infusion
• Laminaria tent

24
3. PHARMACOLOGICAL:
• Oxytocin
• PGS
• Relaxin ,
• Estrogen
4. SURGICAL
ARM
Non- medical methods
• Sexual intercourse was said to induce labor as the human semen is a
source of natural PGS
• Nipple stimulation does not have any effect in IOL
• Herbal remedies, castor oil, enema, accupuncture had notbeen
adequately proved.
• Sweeping of membranes or stripping is an age old method of IOL .

25
• Simple technique were a finger is inserted through the cervix and
swept around the lower uterine segment above the internal os in a
circular motion.
• It works by the release of PGS .
• It often stimulates uterine contractions and ripens the cevix.
Mechanism of action of EXTRA AMNIOTIC SALINE INFUSION
• Mechanical action of Foley’s catheter is similar to stripping and
causes the release of prostaglandins, cytokines in the decidual cells.
• The lytic enzymes like Phospholipase A, which acts on phospholipids
to form Arachidonic acid, which in turn converted to Prostoglandins.
• Saline infusion cause mechanical stretching of isthmial region thereby
production of PGE & F
Success of induction depends on
• Period of gestation – uterus is more sensitive near term or post term.
• Gravida – induction is more successful in parous women.
• Sensitivity of uterus

26
• Pre induction scoring – patients with Bishop score >6 respond well to
induction than those with unfavorable Bishop score <5
Pre induction scoring
In this study, Bishop scoring system and partogram is used. It is a
time– honored fact that Bishop score is a sensitive indicator that predicts
successful induction of labour.
Bishop Score 0 1 2 3
Dilatation 0 1-2 3-4 5-6
Effacement 0-30 4-60 60-70 80+
Station -3 -2 -1/0 +1/+2
Consistency Firm Medium Soft
Os Position Posterior Mid Position Anterior

27
MODIFIED BISHOPS SCORE
Factor / Score 0 1 2 3
Dilatation (cm) <1 1-2 2-4 >4
Cervical length (cm) >4 2-4 1-2 <1
Station (cm) -3 -2 -1/0 +1/+2
Consistency Firm Moderate Soft -
Position Posterior Mid; Anterior - -

28

29
Partogram
It is graphic representation of progress of labour together with information
about fetal and maternal condition against time.
The components of partogram are
1. Cervical dilatation in cm
2. Descent of the presenting part
3. Frequency & duration of uterine contractions
4. Fetal heart rate
5. Rupture of membranes and color of amniotic fluid
6. Maternal pulse rate
7. Blood pressure
8. Urine output
9. Drugs used

30
• An alert line is drawn at the rate of expected progress that is
1cm/hr. An action line is drawn parallel to alert line but 4 hours
apart. If labour is abnormal , then cervicograph deviates towards
rjght or crosses the action line when definite action is required.
• Partogram is universally accepted method to assess the progress of
labour.

31
METHODOLOGY
The subjects of the study were selected from the patients who came to
the labour ward in Coimbatore medical college & Hospital from September
2018-september 2019 as a time bound study.
The study was done in 100 women after counselling about the
methods of induction.50 women were assigned to induction by extra
amniotic saline infusion and 50 assigned to Foleys bulb induction.
Both the groups were randomly selected and reactivated.
A prospective study of all cases of pregnant women who got admitted
to labour ward requiring induction of labour were randomly assigned to
EASI/Foleys bulb induction between September 2018-September 2019.
Patients were selected as per the inclusion criteria and the exclusion
criteria.
After obtaining informed consent from the patients, a detailed history,
complete physical examination, Bishops score assessment, routine
investigations were done for all the patients .
Group A—Extra amniotic saline infusion with Foleys catheter
(20-22).

32
Group B---Foleys bulb induction with Foleys catheter .
Patients with Bishop score 0-5 and meeting inclusion and exclusion
criteria were included .50 patients in each group were studied. The groups
were compared with respect to maternal age, parity, gestational age, reason
for induction, initial Bishops scores, side effects, intrapartum complications,
delivery mode ,induction delivery interval, apgar scores.
The statistical methods used were students t-test, chi square test.

33
PROCEDURE
After informed consent was obtained, women were assigned to receive
EASI or Foleys bulb induction.
Group A—Extra amniotic saline infusion group
• All women were done a speculum examination in lithotomy position
.Vulva, vagina and cervix cleaned with betadine solution.
• Prophylactic antibiotics given.20-22F Foleys was inserted into the
cervical canal beyond the internal os under strict aseptic precautions
and under direct visualisation and the balloons were inflated with 30
ml normal saline water.
• Outlet of Foleys catheter was connected to a normal saline bottle
through a drip set and 150 ml of normal saline was injected into the
extra amniotic space and catheter was blocked and taped to the medial
aspect of thigh.
• By monitoring pulse rate, uterine contractions and fetal heart rate
every 1/2hourly and BP 4th hourly and was watched for bleeding
PV/draining PV.

34
• Cervix was assessed for Bishop score after 6hrs, 12hrs,18 hrs or when
the catheter was expelled whichever occurred first.
• Oxytocin induction/augmentation was done as per the labour induction
protocol.
Group B—Foleys bulb induction
• All women were done a speculum examination lithotomy position.
Vulva, vagina and cervix cleaned with betadine solution.
• Prophylactic antibiotics given.20-22F Foleys was inserted into the
cervical canal beyond the internal os under strict aseptic precautions
and under direct visualisation and the balloons were inflated with 80
ml normal saline water and the catheter was placed in traction by
taping it to the medial aspect of thigh.
• Maternal pulse rate, uterine contractions, fetal heart rate was
monitered every 1/2hourly and BP 4th hourly and was watched for
bleeding PV.

35
• Cervix was assessed for Bishop score after 6hrs, 12hrs ,18 hrs or when
the catheter was expelled whichever occurred first.
• Further oxytocin induction/augmentation was done as per the labour
induction protocol by syntocin infusion of 5U in 500 ml normal saline
starting with 30 minutes interval.

36
Extra Amniotic Saline Induction

37
Foley Bulb Induction

38
STATISTICAL ANALYSIS
In both the groups, the patients selected belonged to similar age group,
parity and weeks of gestation and Bishops score. The mean Bishops score
was significantly increased in 6,12 hours in primi gravid as compared to
Foleys bulb induction.
In patients with extra amniotic saline infusion, majority went in for
active labour 6-12 hours, whereas in Foleys bulb induction ,majority went in
for active labour in 2-24 hours. Induction delivery interval was significantly
reduced in primigravida in cases of EASI as compared to Foleys bulb
induction.
Usage of oxytocin augmentation was increased in Foleys group of
patients with Foleys bulb induction.
Vaginal delivery was found to be more in EASI group 53.1% as
compared to 46.9% in Foleys bulb group.
There was no significant difference in the neonatal outcome in both
the groups.

39
RESULTS
Table 1: Distribution of study participants
Groups Frequency Percent (%)
EXTRA AMNIOTIC
SALINE INFUSION
50 50.0
FOLEYS BULB
INDUCTION
50 50.0
Total 100 100.0
50%50%
Distribution of study participants
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB INDUCTION

40
Table 2: Mean age of the study group
Groups N Mean SD
EXTRA AMNIOTIC
SALINE INFUSION
50 25.06 3.930
FOLEYS BULB
INDUCTION
50 25.98 5.220
24.6
24.8
25
25.2
25.4
25.6
25.8
26
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB INDUCTION
25.06
25.98
Mean age

41
Table 3: Age distribution among study groups
Age in groups
EXTRA AMNIOTIC
SALINE INFUSION
FOLEYS BULB
INDUCTION
P value
No % No %
<20 years 6 46.2% 7 53.8%
.627
21-25 years 23 53.5% 20 46.5%
26-30 years 17 53.1% 15 46.9%
>31 years 4 33.3% 8 66.7%
0
5
10
15
20
25
<20 21-25 26-30 >31
6
23
17
4
7
20
15
8
Age distribution
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB INDUCTION

42
Table 4: Gravida distribution among study groups
Gravida
EXTRA AMNIOTIC
SALINE INFUSION
FOLEYS BULB
INDUCTION
P value
No % No %
G1 22 56.4% 17 43.6%
.458
G2 18 52.9% 16 47.1%
G3 8 36.4% 14 63.6%
G4 2 40.0% 3 60.0%
0
5
10
15
20
25
G1 G2 G3 G4
22
18
8
2
1716
14
3
Gravida distribution
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB INDUCTION

43
Table 5: Gestational age distribution among study groups
Gestational age
EXTRA AMNIOTIC
SALINE INFUSION
FOLEYS BULB
INDUCTION
P value
No % No %
<36 weeks 50 50% 50 50%
.889 37-40 weeks 38 51.4% 36 48.6%
>41 weeks 9 45.9% 11 55.0%
0
5
10
15
20
25
30
35
40
45
50
<36 37-40 41
50
38
9
50
36
11
Gestational age
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB INDUCTION
44
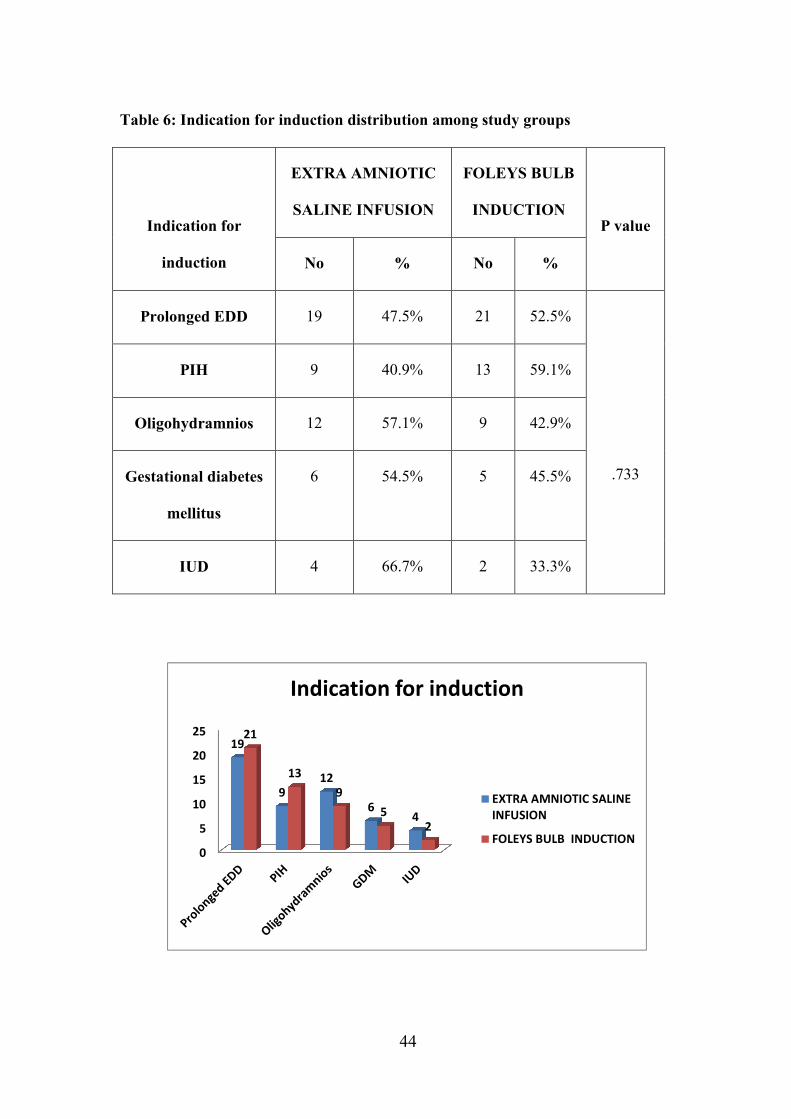
Table 6: Indication for induction distribution among study groups
Indication for
induction
EXTRA AMNIOTIC
SALINE INFUSION
FOLEYS BULB
INDUCTION
P value
No % No %
Prolonged EDD 19 47.5% 21 52.5%
.733
PIH 9 40.9% 13 59.1%
Oligohydramnios 12 57.1% 9 42.9%
Gestational diabetes
mellitus
6 54.5% 5 45.5%
IUD 4 66.7% 2 33.3%
0
5
10
15
20
2519
9
12
64
21
13
9
5
2
Indication for induction
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB INDUCTION

45
Table 7: Bishop score at 0 hour among study groups
0 hour
EXTRA AMNIOTIC
SALINE INFUSION
FOLEYS BULB
INDUCTION
P value
No % No %
1 1 50.0% 1 50.0%
.979 2 29 49.2% 30 50.8%
3 20 51.3% 19 48.7%
0
5
10
15
20
25
30
0 1 2
1
29
20
1
30
19
Bishop score at 0 hour
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB INDUCTION

46
Table 8: Bishop score at 6 hours among study groups
6 hours
EXTRA AMNIOTIC
SALINE INFUSION
FOLEYS BULB
INDUCTION
P value
No % No %
<5 16 61.5% 10 38.5%
.161 6-10 34 45.9% 40 54.1%
0
5
10
15
20
25
30
35
40
<5 6-10
16
34
10
40
Bishop score at 6 hours
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB INDUCTION

47
Table 9: Bishop score at 12 hours among study groups
12 hours
EXTRA AMNIOTIC
SALINE INFUSION
FOLEYS BULB
INDUCTION
P value
No % No %
<5 6 100.0% 0 0.0%
.001* 6-10 36 42.4% 49 57.6%
>11 8 88.9% 1 11.1%
0
5
10
15
20
25
30
35
40
45
50
<5 6-10 >11
6
36
8
0
49
1
Bishop score at 12 hours
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB INDUCTION

48
Table 10: Bishop score at 18 hours among study groups
18 hours
EXTRA AMNIOTIC
SALINE INFUSION
FOLEYS BULB
INDUCTION
P value
No % No %
<5 0 0.0% 1 100.0%
.043* 6-10 5 83.3% 1 16.7%
>11 1 16.7% 5 83.3%
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
<5 6-10 >11
0
5
11 1
5
Bishop score at 18 hours
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB INDUCTION

49
Table 11 : Mean Bishop score at 0of parity among the study group
EXTRA AMNIOTIC SALINE
INFUSION FOLEYS BULB INDUCTION
P
value
Mean Bishop
score at 0
PRIMI
N=22
MULTI
N=28
PRIMI
N=17
MULTI
N=33
Mean SD Mean SD Mean SD Mean SD
2.09 .426 2.61 .497 1.94 .243 2.58 .502 .000*
EXTRA AMNIOTICFOLEYS BULB
SALINE INFUSIONINDUCTION
0
0.5
1
1.5
2
2.5
3
Primi Multi Primi Multi
2.09
2.61
1.94
2.58
Mean Bishop score at 0

50
Table12 : Mean Bishop score at 6of parity among the study group
EXTRA AMNIOTIC SALINE
INFUSION FOLEYS BULB INDUCTION
P
value
Mean Bishop
score at 6
PRIMI
N=22
MULTI
N=28
PRIMI
N=17
MULTI
N=33
Mean SD Mean SD Mean SD Mean SD
7.05 1.21 5.46 .793 5.82 1.01 6.36 .653 .000*
EXTRA AMNIOTICFOLEYS BULB
SALINE INFUSIONINDUCTION
0
1
2
3
4
5
6
7
8
Primi Multi Primi Multi
7.05
5.465.82
6.36
Mean Bishop score at 6

51
Table 13 : Mean Bishop score at 12of parity among the study group
EXTRA AMNIOTIC SALINE
INFUSION FOLEYS BULB INDUCTION
P
value
Mean Bishop
score at 12
PRIMI
N=22
MULTI
N=28
PRIMI
N=17
MULTI
N=33
Mean SD Mean SD Mean SD Mean SD
9.64 1.52 6.43 1.47 8.47 .624 9.15 .795 .000*
EXTRA AMNIOTICFOLEYS BULB
SALINE INFUSIONINDUCTION
0
1
2
3
4
5
6
7
8
9
10
Primi Multi Primi Multi
9.64
6.43
8.479.15
Mean Bishop score at 12

52
Table 14 : Incidence of LSCS
Mode of
delivery
EXTRA AMNIOTIC
SALINE INFUSION
FOLEYS BULB
INDUCTION
No % No %
LSCS 13 46.4% 15 53.6%
12
12.5
13
13.5
14
14.5
15
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB INDUCTION
13
15
LSCS

53
Table 15 : Incidence of LSCS
LSCS
EXTRA AMNIOTIC SALINE
INFUSION
N=13
FOLEYS BULB
INDUCTION
P
value PRIMI MULTI PRIMI MULTI
No % No % No % No %
LSCS 7 53.8% 6 46.2% 6 40.0% 9 60.0% .837
EXTRA AMNIOTICFOLEYS BULB
SALINE INFUSIONINDUCTION
0
1
2
3
4
5
6
7
8
9
Primi Multi Primi Multi
7
6 6
9
LSCS

54
Table 16: Mode of induction among study groups
Mode of
induction
EXTRA AMNIOTIC
SALINE INFUSION
FOLEYS BULB
INDUCTION
P value
No % No %
0 50 100.0% 0 0.0%
.000* 1 0 0.0% 5 100.0%
0
5
10
15
20
25
30
35
40
45
50
1 2
50
00
5
Mode of induction
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB INDUCTION

55
Table 17: Oxytocin infusion among study groups
Oxytocin
Infusion
EXTRA AMNIOTIC
SALINE INFUSION
FOLEYS BULB
INDUCTION P value
No % No %
0 24 54.5% 20 45.5%
0.420
1 26 46.4% 30 53.6%
0
5
10
15
20
25
30
0 1
24
20
26
30
Oxytocin infusion
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB INDUCTION

56
Table 18: Oxytocin infusion among parity in study groups
Oxytocin
infusion
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB
INDUCTION
P
value PRIMI MULTI PRIMI MULTI
No % No % No % No %
0 19 79.2% 5 20.8% 5 75.0% 15 75.0%
.000* 1 3 11.5% 23 88.5% 12 40.0% 18 60.0%
0
5
10
15
20
25
Primi Multi Primi Multi
19
5 5
15
3
23
12
18
Oxytocin infusion among parity

57
Table19: Mean Induction labour intervalof the study group
Groups N Mean SD P VALUE
EXTRA AMNIOTIC
SALINE INFUSION
50 9.80 2.753
.949
FOLEYS BULB
INDUCTION
50 9.83 1.834
9.785
9.79
9.795
9.8
9.805
9.81
9.815
9.82
9.825
9.83
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB INDUCTION
9.8
9.83
Mean Induction labour interval

58
Table 20: Induction Labour Interval among study groups
Induction
Labour Interval
EXTRA AMNIOTIC
SALINE INFUSION
FOLEYS BULB
INDUCTION
P value
No % No %
<6 5 83.3% 1 16.7%
.007* 7-12 32 41.6% 45 58.4%
>13 10 66.7% 5 33.3%
0
5
10
15
20
25
30
35
40
45
<6 7-12 >13
5
32
10
1
45
5
Induction Labour Interval
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB INDUCTION

59
Table 21: Induction Labour Interval among parity in study groups
Induction
Labour
Interval
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB
INDUCTION
P
value PRIMI MULTI PRIMI MULTI
No % No % No % No %
<6 6 100.0% 0 0.0% 0 0.0% 0 0.0%
.000* 7-12 16 47.1% 18 52.9% 12 26.7% 33 73.3%
>13 0 0.07% 10 100.0% 5 100.0% 0 66.0%
EXTRA AMNIOTIC FOLEYS BULB
SALINE INFUSION INDUCTION
- < 6 - 7-12 - >13
0
5
10
15
20
25
30
35
Primi Multi Primi Multi
6
0 0 0
1618
12
33
0
10
5
0
Induction Labour Interval among
parity

60
Table 22: Mean Induction labour intervalof parity among the study group
EXTRA AMNIOTIC SALINE
INFUSION FOLEYS BULB INDUCTION
P
value
Induction
labour
interval
PRIMI
N=22
MULTI
N=28
PRIMI
N=17
MULTI
N=33
Mean SD Mean SD Mean SD Mean SD
7.68 1.60 28 11.4 11.94 1.24 8.74 .885 .000*
0
5
10
15
20
25
30
Primi Multi Primi Multi
7.68
28
11.94
8.74
Mean Induction labour interval

61
Table 23: Mean Induction delivery intervalof the study group
Groups N Mean SD P VALUE
EXTRA AMNIOTIC
SALINE INFUSION
50 15.96 2.962
.000*
FOLEYS BULB
INDUCTION
50 17.86 2.138
15
15.5
16
16.5
17
17.5
18
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB INDUCTION
15.96
17.86
Mean Induction delivery interval

62
Table 24: Mean Induction delivery intervalof parity among the study group
EXTRA AMNIOTIC SALINE
INFUSION FOLEYS BULB INDUCTION
P
value
Induction
delivery
interval
PRIMI
N=22
MULTI
N=28
PRIMI
N=17
MULTI
N=33
Mean SD Mean SD Mean SD Mean SD
14.00 2.30 17.50 2.48 20.24 1.25 16.64 1.29 .000*
EXTRA AMNIOTIC FOLEYS BULB
SALINE INFUSION INDUCTION
0
5
10
15
20
25
Primi Multi Primi Multi
14
17.5
20.24
16.64
Mean Induction delivery interval of
parity

63
Table 25: Mean Induction delivery intervalof gravida among study groups
Induction
delivery
interval
EXTRA AMNIOTIC SALINE
INFUSION FOLEYS BULB INDUCTION
PRIMI MULTI PRIMI MULTI
No % No % No % No %
6-12 6 85.7% 1 14.3% 1 50.0% 1 50.0%
13-24 16 37.2% 27 62.8% 17 34.0% 33 66.0%
EXTRA AMNIOTIC FOLEYS BULB
SALINE INFUSION INDUCTION
- < 6-12 - 13-24
0
5
10
15
20
25
30
35
Primi Multi Primi Mult
6
1 1 1
16
27
17
33
Mean Induction delivery interval of
gravida

64
Table 26: Mode of delivery among study groups
Mode of delivery
EXTRA AMNIOTIC
SALINE INFUSION
FOLEYS BULB
INDUCTION
P value
No % No %
Labour natural 26 53.1% 23 46.9%
.940 LSCS 13 46.4% 15 53.6%
Forceps 5 50.0% 5 50.0%
Vacuum 6 46.2% 7 53.8%
0
5
10
15
20
25
30
Labour
natural
LSCS Forceps Vacuum
26
13
56
23
15
57
Mode of delivery
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB INDUCTION
65
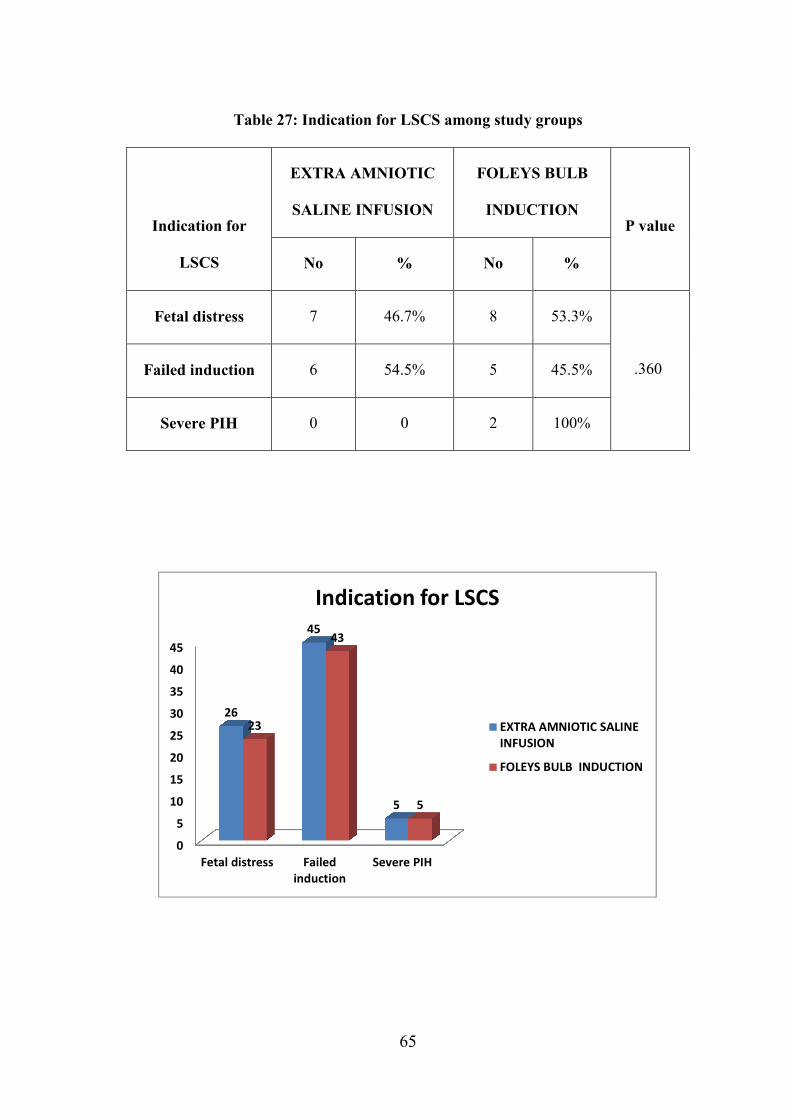
Table 27: Indication for LSCS among study groups
Indication for
LSCS
EXTRA AMNIOTIC
SALINE INFUSION
FOLEYS BULB
INDUCTION
P value
No % No %
Fetal distress 7 46.7% 8 53.3%
.360 Failed induction 6 54.5% 5 45.5%
Severe PIH 0 0 2 100%
0
5
10
15
20
25
30
35
40
45
Fetal distress Failed
induction
Severe PIH
26
45
5
23
43
5
Indication for LSCS
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB INDUCTION

66
Table 28:Neonatal outcome among study groups
Neonatal outcome
EXTRA AMNIOTIC
SALINE INFUSION
FOLEYS BULB
INDUCTION
P value
No % No %
NICU admission 6 50.0% 6 50.0%
1.000 Good outcome 44 50.0% 44 50.0%
0
5
10
15
20
25
30
35
40
45
NICU admission Good outcome
6
44
6
44
Neonatal outcome
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB INDUCTION

67
Table 29: Intrapartum maternal distress among study groups
Intrapartum
maternal distress
EXTRA AMNIOTIC
SALINE INFUSION
FOLEYS BULB
INDUCTION
P value
No % No %
No 46 50.0% 46 50.0%
1.000 Yes 4 50.0% 4 50.0%
0
5
10
15
20
25
30
35
40
45
50
NO YES
46
4
46
4
Intrapartum maternal distress
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB INDUCTION

68
Table 30: PPH among study groups
PPH
EXTRA AMNIOTIC
SALINE INFUSION
FOLEYS BULB
INDUCTION
P value
No % No %
No 46 50.0% 46 50.0%
1.000 Yes 4 50.0% 4 50.0%
0
5
10
15
20
25
30
35
40
45
50
NO YES
46
4
46
4
PPH
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB INDUCTION

69
Table 31:Intrapartum Pyrexia among study groups
Intrapartum
Pyrexia
EXTRA AMNIOTIC
SALINE INFUSION
FOLEYS BULB
INDUCTION
P value
No % No %
No 48 51.1% 46 48.9%
.400 Yes 2 33.3% 4 66.7%
0
5
10
15
20
25
30
35
40
45
50
NO YES
48
2
46
4
Intrapartum Pyrexia
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB INDUCTION

70
Table 32: Postpartum sepsis among study groups
Postpartum
sepsis
EXTRA AMNIOTIC
SALINE INFUSION
FOLEYS BULB
INDUCTION
P value
No % No %
No 48 50.0% 48 50.0%
1.000 Yes 2 50.0% 2 50.0%
0
5
10
15
20
25
30
35
40
45
50
NO YES
48
2
48
2
Postpartum sepsis
EXTRA AMNIOTIC SALINE
INFUSION
FOLEYS BULB INDUCTION

71
DISCUSSION
The study was conducted in Institute of Obstetrics and Gynaecology,
Coimbatore to compare the efficacy of Extra amniotic saline infusion and
Foleys bulb for induction of labour. The study was done in 100 patients.50
patients were induced with extra amniotic saline and 50 patients were
induced with Foleys bulb induction. Both the groups has patients of similar
age, parity and gestational age.
Change in Bishops score
In my study, both the groups had patient who were induced with
almost similar Bishops score initially.
Mean Bishops score at 0 hours was 2.09 in primi with EASI and 1.94
with Foleys bulb induction. Mean Bishops score at 6 hours was 7.05 in primi
with EASI and 5.82 with Foleys bulb induction. Mean Bishops score at 12
hours was 9.64 in primi with EASI and 8.47 with Foleys bulb induction.
Mean Bishops score at 0 hours was 2.61 in multigravida with EASI
and 2.58 with Foleys bulb induction. Mean Bishops score at 6 hours was
5.46 in multigravida with EASI and 6.36 with Foleys bulb induction. Mean
Bishops score at 12 hours was 6.43 in multigravida with EASI and 9.15 with
Foleys bulb induction.

72
Mean Bishops score improved in higher rate in EASI in primi as
compared to Foleys bulb induction. The difference is statistically significant
(P<0.01)
Induction to Active labour interval
In my study, majority of patients induced with EASI established
active labour within 9.8 hours ,whereas in Foleys bulb induction ,active
labour was established in 9.83 hours. Mean induction active labour interval
in primi with EASI was 7.68 hours and in Foleys bulb induction was 11.94
hours . Mean induction active labour interval in multi with EASI was 28 and
in Foleys bulb induction was 8.74 hours . The difference between the two
groups is statistically significant(P<0.01).EASI was found to be more
effective in causing cervical ripening than Foleys bulb induction in primi.
OXYTOCIN AUGMENTATION
In my study ,oxytocin usage in EASI was 46.4% and Oxytocin usage
in Foleys induction group was about 53.6% for augmentation of labour. The
difference is statistically significant(P<0.01).

73
Induction to Delivery interval
In my study, majority of patients induced with EASI delivered within
14 hours in primi and 17.5 hours in multi where as in Foleys bulb induction
,delivered within 20.24 hours in primi and 16.64 in Multigravida .Mean
induction delivery interval in induced with EASI was 15.96 hours and with
Foleys bulb induction was 17.86 hours .The difference between the two
groups is ststistically significant(P<0.01)
Mode of delivery
In my patients induced with EASI 53.1% of patients delivered
vaginally, whereas in patients with Foleys bulb induction 46.9% had vaginal
delivery. LSCS rate was only 46.4%in EASI as compared to about 53.6% in
patients with Foleys bulb induction.
Indication of caesarean delivery
In my study, incidence of caesarean delivery was significantly lower
in 46.4% in EASI as compared to 53.6% Foleys bulb induction . Incidence of
failed induction in EASI 54.5% and Foleys bulb induction is 45.5%.
Incidence of fetal distress was 46.7 % in EASI whereas it was 56.3% in
patients with Foleys bulb induction.

74
Bucecellate et al (2000)also reported that failure to progress and non
reassuring fetal heart rate were the common cause for caesarean delivery.
GUNN et al (2004) reported that fetal distress was the most common cause
for LSCS. Sharami et al (2005)reported that cervical dystonia was the most
common cause for LSCS.
Fetal Outcome
In my study fetal outcome and admission in NICU was similar in both
the groups. The most common cause for NICU admission was birth asphyxia
and meconium aspiration. GUNN et al reported no significant maternal and
neonatal morbidities.
Maternal outcome
In my study puerperal pyrexia was comparable in both the groups.
There was no difficulty in intra cervical Foleys catheter insertion.
JANET et al reported technical difficulty in one patient due to cervix
partition. SCREYER et al reported mild bleeding after Foleys bulb insertion.
SHERMAN et al reported rupture of membranes at the time of
insertion. Majority of the patients who were induced belonged to the age
group 20-25 years. Study conducted by JANEI et al (1999),

75
SHARAMI(2005)showed that the majority of patients belonged to 20-30
years of age.
Majority of patients were Primigravida –56.4%.The study conducted
by JANEI et al (1999)and GUNN et al (2004)also had maximum number of
primigravidas.
Majority of the patients were induced between 40=41 weeks of
gestation. EASI—19,Foleys --- 21.The study of KARJANE et al
(2006)showed that post delivery was the most common cause for induction.

76
SUMMARY
Improvement in Bishops score was more in EASI than the Foleys bulu
induction. Mean induction to active labour interval (ILI) was shorter in EASI
than Foleys bulb induction .Mean induction to delivery interval was shorter
in EASI than Foleys bulb induction.
Mean induction to active labour interval and mean induction to
delivery interval were shorter in multi of both the groups as compared to
primi of both the groups . Regarding age parity, gestational age and the
indication for induction there was no significant difference in both the
groups.
53.1% of patients in EASI infusion had labour naturale when
compared to 46.9% Foleys bulb induction. LSCS incidence for failed
induction in EASI was 46.4% as compared to 53.6% in Foleys bulb
induction.

77
CONCLUSION
Cervical ripening was more effective in the EASI group in primi as
compared to Foleys bulb induction. Mean induction to active labour interval
was shorter in the EASI when compared to Foleys bulb induction. Mean
induction to delivery interval was shorter in the EASI when compared to
Foleys bulb induction.
Oxytocin usage was lower in EASI group than Foleys bulb induction.
Response to primi are better than multi in both the groups. Fetal and
maternal outcome were similar in both the groups.
EASI was found to be more effective, cheeper and readily available
method for cervical ripening and induction of labour. Incidence of LSCS in
EASI was 46.4% as compared to Foleys induction which was 53.6%.
Neonatal admissions were similar in both the groups.
BIBLIOGRAPHY
1. Allot HA, Palmer CR: Sweeping the membranes; A valid
procedure instimulating the onset of labour? Br J ObstetGynecol
100:898, 1993
2. American college of Obstetricians and Gynecologists. Induction
and augmentation of Labour. ACOG technical bulletin no.217,
Washington DCAmericancollege of obstetricians and
Gynecologists, 1995
3. Bakos O, Back strom T: Induction of labour: A prospective
randomized study into amniotomy and oxytocin as induction
methods. ActaObstetGynecolScand 66: 537, 1987
4. Bernstein P: Prostaglandin E2 gel for cervical ripening and labour
induction: Amulticentered placebo controlled trial.Can med assoc
J 145:1249, 1991
5. Bishop EH Pelvic scoring for elective induction ObstetGynecol
1964; 24:266-8
6. Bishop EH. Pelvic scoring for elective induction. ObstetGynecol
24:266, 1964.

7. Blumenthal PD, RamanauskasR.Randomized trial of dilapan and
Laminaria as cervical ripening agents before induction of labor.
ObstetGynecol 1990;75:365-8
8. Buccellato CA, Stika CS, Frederiksen MC. A randomised trial of
misoprostolversus extra amniotic saline infusion with oxytocin
for induction of labour AMJ ObstetGynecol 2000 May; 182(5):
1039-44
9. Buser D, Mora G, Arias F: A randomised comparison between
misoprostol andDinoprostone for cervical ripening and labour
induction in patients withunfavourable cervices. ObstetGynecol
89: 581, 1997
10. Calder AA Review of prostaglandin use in labour induction Br J
ObstetGynecol 1997; 104(Suppl 15): 2-7
11. Chammas MF, Nguyen TM, Vasavada RA, Nuwayhid BS, Castro
LC.Sequential use of Prepidil and Extra amniotic saline infusion
for the inductionof labour in nulliparous women with very low
Bishop score. J MaternFetalMed 2001 Jun; 10(3): 193-6
12. Chuck F, HuffakerBJ.Labor induction with Intravaginal
Misoprostol versusIntracervical Prostaglandin E2 gel (prepidil)
:randomised comparison. Am JObstetGynecol 1995; 173:1137-42

13. Debra A.Guinn, MD, Alice R.Goepfert MD, Michelle Christine,
MD JohnOwen, MD and John C.Hauth, MD. ObstetGynecol
2000; 96:106-12
14. Ekman G, Forman A, Marsal K, Ulmesten U: Intravaginal versus
intracervical application of Prostaglandin E2 in viscous gel for
cervical priming andinduction of labour at term in patients with
an unfavorable cervical state. Am JObstetGynecol 147: 657, 1983
15. Embrey MP, Mollison BG The unfavorable cervix and induction
of labor usinga cervical balloon J ObstetGynecol Br Commonw
1967; 74:44-8
16. Fait G, Grisaru D, Shenhav M, Kupfermine MJ, Lessing JB,
Peyser MR, JaffaA Balloon catheter with extra amniotic saline
instillation: a method ofinduction in Pregnancies at 41 or more
Gestational weeks. Aust N Z J ObstetGynecol 1997May; 37(2):
174-6
17. Fletcher HM, Mitchell S, Simeon D, Frederick T, Brown D.
IntravaginalMisoprostol as a cervical ripening agent. Br J
ObstetGynaecol 1993; 100:641-4
18. Ghezzi F, Massimo F, Raio L, Di Naro E, Balasteri D, Bolis P.
Extra amniotic Foley catheter and Prostaglandin E2 gel for

cervical ripening at term gestation.Eur J ObstetGynecol
ReprodBiol 2001 Aug;97(2): 183-7.
19. Gilson GJ, Russell DJ, Izquierdo LA, Quails CR, Curet LB. A
prospectiverandomized evaluation of a hygroscopic cervical
dilator, Dilipan, in thepreinduction ripening of patients
undergoing induction of labor. Am J ObstetGynecol 1996;
175:145-9
20. Goldman JB, Wigton TR, A randomised comparison of extra
amniotic salinesaline infusion and Dinoprostone gel for cervical
ripening ObstetGynecol1999 Feb; 93(2): 271-4
21. Guinn DA, Goepfert AR, Christine M, Owen J, Huth JC, Extra
amnioticSaline, Laminaria, or Prostaglandin E2 gel For Labour
induction withUnfavourable cervix: a randomised controlled trial.
ObstetGynecol 2000 Jul;96(1): 106-12
22. Hale RW, Pion RJ: Laminaria: An under utilized clinical adjunct.
ClinObstetGynecol 15:829, 1972.
23. HemlinJ ,MoIler B: Extra amniotic saline infusion is promising in
preparingthe cervix, for induction of labour. ActaObstetGynecol
Scan 77: 45, 1998

24. Hofmeyer GJ, Gulmezoglu AM, Alferevic Z: Misoprostol for
induction oflabour: A systematic review. Br J ObstetGynecol
106: 798,1999
25. Keirse MJ. Prostaglandins in pre-induction cervical ripening:
Prostaglandins inmetanalysis of worldwide clinical experience. J
Reprod Med 1993; 38:89-100.
26. Krammer J, O'Brien WF, Mechanical methods of cervical
ripening ClinObstetGynecol 1995; 38:280-92.
27. Laube DW, Induction of labor. ClinObstetGynecol 1997;40:485-
95
28. Laube DW, Induction of labour. ClinObstetGynecol 1997;
40:485-95
29. Lin A, Kupferminc M, Dooley SL, A randomised trial of extra
amniotic salineinfusion versus laminaria for cervical ripening
ObstetGynecol 1995 Oct; 86(4Pt 1): 545-9
30. Lyndrup J, Nickelson C, Guldbaek E, Weber T. Induction of
labor byprostaglandin E2: intracervical gel or vaginal pessaries?
Eur J ObstetGynecolReprod.biol 1991; 42:101-9

31. Macer CA, Macer CL, Chan LS. Elective induction versus
spontaneous labor: A retrospective study of complications and
outcome. Am J ObstetGynecol1991; 166:1690-7
32. Mahomed K, Jayaguru AS Extra amniotic Saline infusion for
induction of labour in antepartum fetaldeath:a cost effective
method worthy of use Br J ObstetGynaecol 1997 Sep; 104(9):
1058-61
33. ManabeY,ManabeR.Nelaton. Catheter versus laminaria for a safe
and gradualcervical dilatation. Contraception 1981; 24:53-60
34. Ma wire CJ, hipato T, Rusakaniko S. Extra amniotic saline
infusion versusextra amniotic Prostaglandin F2 for cervical
ripening and induction of labourInt J Gynaecolobstet 1999 Jan;
64(1): 35-41
35. O' driscollCarrol and coughlan. Selective induction of labour.
BMJ4 : 727-29
36. Perry KG, Larmon JE, May WL, Robinette LG, Martin RW.
Cervical ripening:a randomised comparison between Intravaginal
misoprostol and anIntracervical balloon catheter combined with
IntravaginalDinoprostone. Am JObstetGynecol 1998; 178:1333-
40

37. Rouben D, Arias F, A randomised trial of Extra amniotic saline
infusion plusintracervical Foley catheter balloon versus
Prostaglandin E2 vaginal gel forripening the cervix and inducing
labor in patients with unfavourable cervicesObstetGynecol 1993
Aug; 82(2): 290-4
38. Sanchez Ramos L, Kaunitz AM, Del valleGO,DeIke I, Schroeder
P, Briones D.
39. Labor induction with the prostaglandin El versus oxytocin; a
randomised trial.ObstetGynecol 1993; 81:332-6
40. Sawai SK, Williams MC, O'Brien W, et al. Sequential outpatient
application of intravaginal PGE2 gel in the management of Post
date pregnancies. ObstetGynecol 1991; 78:19-22
41. Sciscione AC, McCullough H, Manley JS ,Shlossman PA,
Colmorgen GHC:A prospective randomised comparison of Foley
catheter insertion versus intra cervical Prostaglandin E2 gel for
pre induction cervical ripening. Am J ObstetGynecol 180:55,
1999
42. Sherman DJ, Frenkel E, Pansky M, Caspi E, Bukovsky I, Langer
R Balloon cervical ripening with Extra-amniotic Saline infusion

or PGE2: a double -blind, randomised controlled study
ObstetGynecol 2001 Mar; 97(3): 375-80
43. Sherman DJ, FrenkelEJovbin J, Arieli S, Caspi E, Bukovsky I
Ripening of the unfavorable cervix with extraamniotic catheter
balloon: Clinical experienceand review ObstetGynecolSurv 1996;
51:627-7
44. Srisomboon J, Tongsong T, Tosiri V. Preinduction cervical
ripening with intra vaginal Prostaglandin El: a randomised
controlled trial. J obstetGynecol Res1996; 22:119-24
45. Trofatter, Cervical ripening. Clin. Obstet Gynecoll992: 35:476-86
46. Trootwijk AL, Vanveen JBC, Doesburg WH. Pre-induction intra-
cervicalapplication of a highly viscous Prostaglandin E2 gel in
pregnant women withan unripe cervix. Eur J
obstetGynecolReprodbiol 1992; 43:105-11
47. Vengalil SR, Guinn DA, Olabi NF, Burd LI, Owen. A
randomised trial of misoprostol and Extra amniotic saline
infusion for Cervical ripening and laborinduction J
ObstetGynecol 1998 May; 91(5 Pt 1): 774-9

48. Wing D, Jones M, Rahall A, Goodwin M, Paul R. A comparison
of Misoprostol and Prostaglandin E2 gel for Pre induction
Cervical ripening andLabour induction. Am J ObstetGynecol
1995; 173:1137-42
49. Wing DA, Ortiz -Omphroy G, and Paul RH. A comparison of
intermittent vaginal administration of misoprostol with
continuous dinoprostone forcervical ripening and labor induction.
Am J ObstetGynecol 1995; 172:1811-6
50. Woodman WB. Induction of labor at the eight month, and
delivery of a living child i n less than four hours by Dr.Barne's
method Lancet 1863; 1:10-11
51. Zanini A, Guidini A, Norchi S, Beretta E, Cortinovis I, Bottino S,
Preinductioncervical ripening with PGE2 gel: Intracervical versus
intravaginalroute. ObstetGynecol 1990; 76: 681-3

PROFORMA
NAME:
AGE:
IP NO:
ADDRESS:
DATE OF EXAMINATION:
OBSTERTIC SCORE:
HISTORY OF PRESENTING ILLNESS:
MENSTRUAL HISTORY:
MARITAL HISTORY:
OBSTETRICS HISTORY:
PAST HISTORY:
FAMILY HISTORY:

GENERAL EXAMINATION:
HEIGHT: WEIGHT:
RESPIRATORY RATE:
PULSE RATE: BLOOD PRESSURE:
TEMPERATURE:
PALLOR: PEDAL EDEMA:
ICTERUS:
BREAST: THYROID:
SYSTEMIC EXAMINATION
CVS: RESPIRATORY SYSTEM:
PER ABDOMEN:
PER VAGINAL EXAMINATION:
PROVISIONAL DIAGNOSIS:
USG FINDINGS

CONSENT FORM
I Mr/Mrs hereby volunteer to participate in the study
"“COMPARATIVE STUDY OF EXTRA AMNIOTIC SALINE
INFUSION THROUGH INTRACERVICAL BALLOON
CATHETER AND FOLEYS BULB INDUCTION FOR
INDUCTION OF LABOUR”. I was explained about the nature of the
study by the doctor, knowing which I fully give my consent to participate
in this study. I also give consent to take clinical photographs for the
purpose of the study.
Date :
Place :
Signature of the Patient

xg;g[jy; gotk;
bgah; :
taJ/ ghypdk; :
Kfthp :
muR nfhit kUj;Jtf; fy;Y}hp kUj;Jtkidapy; kfsph; kw;Wk; kfg;ngW kUj;Jtg; gphptpy; gl;lnkw;gog;g[ gapYk; khztp kU.fPjh,uh$nfhghyd; mth;fs; nkw;bfhs;Sk; “COMPARATIVE STUDY OF EXTRA AMNIOTIC SALINE INFUSION THROUGH INTRACERVICAL BALLOON CATHETER AND FOLEYS BULB INDUCTION FOR INDUCTION OF LABOUR” Fwpj;j Ma;tpy; bra;Kiw kw;Wk; midj;J tpgu';fisa[k; nfl;Lf; bfhz;L vdJ re;njf';fis bjspt[g;gLj;jpf; bfhz;nld; vd;gij bjhptpj;Jf; bfhs;fpnwd;.
vdJ ,e;jMa;tpy; fye;Jbfhs;s KG rk;kkj;JlDk;/ Ra rpe;jida[lDk; rk;kjpf;fpnwd;.
,e;jMa;tpy; vd;Dilatpgu';fs; ghJfhf;fg;gLtJld; ,jd; Kot[fs; Ma;tpjHpy; btspaplg;gLtjpy; Ml;nrgid ,y;iy vd;gij bjhptpj;Jf; bfhs;fpnwd;. ve;j neuj;jpYk; ,e;j Ma;tpypUe;J ehd; tpypfpf; bfhs;s vdf;F chpik cz;L vd;gija[k; mwpntd;.
,lk; : ifbahg;gk;
ehs; :
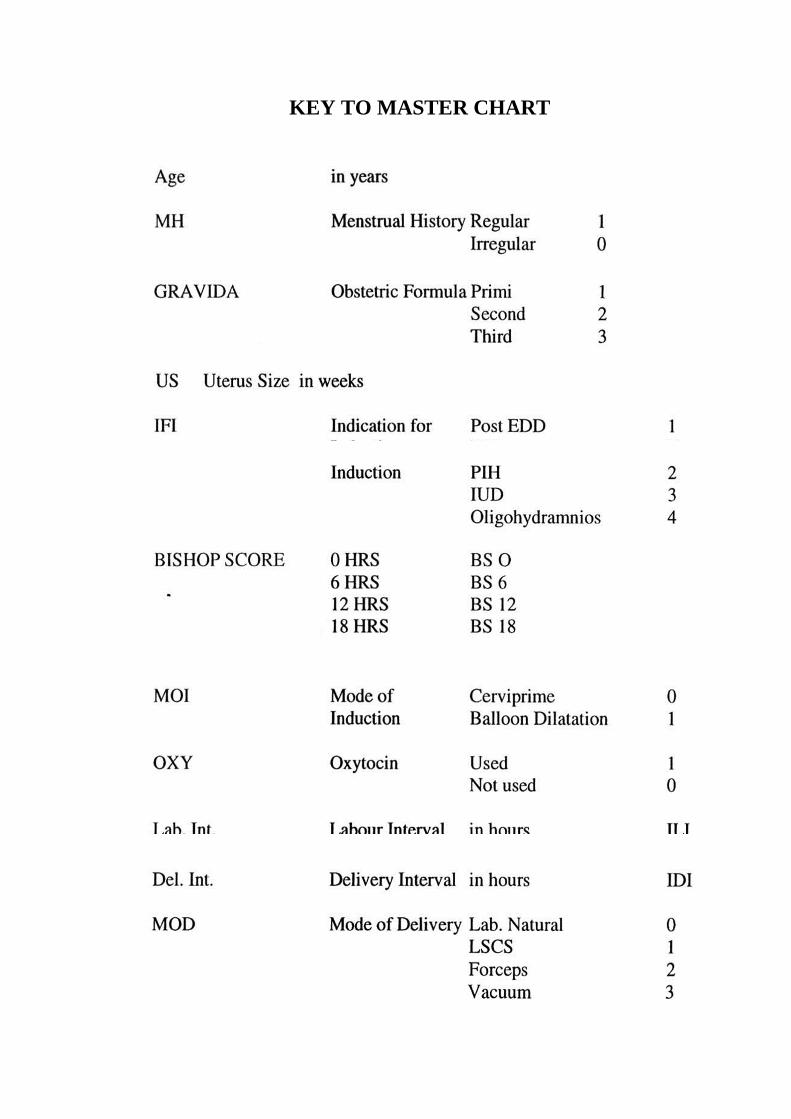
KEY TO MASTER CHART


S.N
o
Nam
e
IP.N
o
Age
Gra
vida
US
IFI
BS
0
BS
6
BS
12
BS
18
MO
I
Oxy ILI
IDI
MO
D
Ind-
CS
NO
Int.
MD
Int.
PPH
Int.
Pyr
Post
Sep
1 Chitra 67582 21 1 38 2 2 6 10 - 0 0 9 12 0 - Good 0 0 0 02 Menaka 89765 19 1 41 1 3 5 11 - 0 0 8 11 1 0 Good 0 0 0 03 Anushya 85623 24 2 41 1 2 6 6 8 0 1 7 13 1 1 Adm 0 0 0 04 Sathya 86237 22 1 39 2 3 7 11 - 0 0 6 10 0 0 Good 0 0 0 05 Priya 89385 26 2 37 3 2 7 7 - 0 1 9 15 1 0 Good 0 1 0 06 Krithiga 68251 22 1 38 5 2 8 10 - 0 1 8 13 0 0 Adm 0 0 0 07 Geetha 73279 20 1 39 2 3 9 8 - 0 0 9 14 0 0 Good 0 0 0 08 Meena 56821 23 2 37 3 2 6 6 - 0 1 9 18 1 1 Good 0 0 0 09 Anjali 61521 27 3 38 2 3 5 5 - 0 1 13 20 0 0 Good 0 0 1 0
10 Madhu 63991 25 3 38 3 3 6 6 - 0 1 11 20 2 0 Good 0 0 0 011 Keerthana 57892 30 1 40 1 2 8 8 - 0 0 8 15 0 0 Adm 0 0 0 012 Mylathal 63589 33 4 36 5 3 5 5 - 0 1 13 18 0 0 Good 0 0 0 013 Rammayi 58960 37 2 41 1 2 6 6 - 0 1 14 16 3 0 Good 0 0 0 014 Devi 67432 20 1 38 4 2 5 8 - 0 0 9 13 1 0 Good 1 0 0 015 Fathima 63740 24 3 37 2 3 6 6 - 0 1 12 18 0 0 Good 0 0 0 016 Jaya 70452 26 2 38 3 2 5 5 - 0 1 14 20 3 0 Good 0 0 0 017 Gowri 68466 28 1 41 1 2 8 10 - 0 0 7 10 0 0 Good 0 0 0 018 Bhagyalakshmi 62538 21 1 39 3 2 9 9 - 0 0 8 14 0 0 Good 1 0 0 019 Chandrakala 67753 23 1 36 5 2 8 8 - 0 1 6.5 16 1 0 Adm 0 0 0 020 Dhanalakshmi 63997 26 2 40 1 3 6 7 - 0 1 10 14 2 0 Good 0 0 0 121 Seetha 64308 25 2 38 4 2 6 7 - 0 1 9 18 0 0 Good 0 0 0 022 Kavitha 64270 21 3 41 1 3 7 7 - 0 1 11 16 0 0 Good 0 0 0 023 Poornima 56848 28 1 38 2 2 8 10 - 0 0 6 12 0 0 Good 0 0 0 024 Divya 62960 22 4 38 3 3 6 6 - 0 1 12 18 2 0 Good 0 0 0 025 Lakshmi 57265 26 2 37 3 2 6 6 - 0 1 13 18 0 0 Good 0 0 1 0
MASTER CHART

26 Preethi 43226 23 1 41 1 1 7 11 - 0 0 6 14 1 0 Adm 0 0 0 027 Shanthi 41063 20 3 38 4 3 5 6 - 0 1 12 20 3 0 Good 0 0 0 028 Jeeva 32475 32 2 37 3 3 5 6 - 0 1 10 19 0 0 Good 0 0 0 029 Gomathi 35162 23 1 40 1 2 7 10 - 0 0 6.5 15 2 0 Good 1 0 0 030 Saranaya 62831 29 3 38 4 3 4 5 - 0 1 15 20 0 0 Good 0 0 0 031 Muniyammal 64522 25 2 37 2 2 5 6 - 0 1 11 18 1 1 Good 0 0 0 032 Kaleeshwari 93286 29 1 41 1 2 8 10 - 0 0 6 15 0 0 Good 0 0 0 033 Sowmya 94360 21 2 36 3 3 6 7 - 0 1 14 14 0 0 Good 0 0 0 034 Sivashakthi 86253 30 2 40 1 2 6 8 - 0 0 9 16 1 1 Good 0 0 0 035 Nandhini 32351 19 1 40 1 2 6 9 - 0 0 10 16 0 0 Good 0 1 0 036 Radha 45298 27 2 38 3 3 5 5 - 0 1 14 18 0 0 Good 0 0 0 037 Sunitha 42063 24 1 39 2 2 6 8 - 0 0 8 15 0 0 Good 0 0 0 038 Ameena 57061 28 3 41 1 3 5 5 - 0 1 15 20 1 0 Good 0 0 0 039 Sandhiya 95896 23 2 38 4 2 6 8 - 0 0 10 19 0 0 Good 0 0 0 040 Thavamani 90157 25 1 40 1 2 8 11 - 0 0 7 14 3 0 Good 0 0 0 041 Sudha 89753 31 2 38 2 3 5 12 - 0 0 8 10 0 0 Good 0 1 0 042 Nilofer 75625 20 1 37 3 2 6 6 - 0 1 11 16 3 0 Good 0 0 0 043 Anitha 73204 22 1 40 1 2 8 11 - 0 0 7 19 1 1 Good 0 0 0 044 Jasmine 87529 24 3 38 5 3 5 6 - 0 1 12 18 0 0 Good 1 0 0 145 Nithya 35941 28 1 39 1 2 6 12 - 0 0 6 14 2 0 Good 0 0 0 046 Sindhu 74250 29 2 41 1 3 5 9 - 0 0 8 19 3 0 Good 0 0 0 047 Punitha 86635 28 2 39 3 2 4 6 - 0 1 12 20 0 0 Good 0 0 0 048 Pavithra 25739 25 1 40 1 2 6 9 - 0 0 11 18 1 0 Adm 0 0 0 049 Bhavya 30263 27 2 38 4 3 4 6 - 0 0 14 17 0 0 Good 0 1 0 050 Elamathy 63257 22 1 40 1 2 6 12 - 0 0 6 12 1 0 Good 0 0 0 0

S.N
o
Nam
e
IP.N
o
Age
Gra
vida
US
IFI
BS 0
BS 6
BS 1
2
BS 1
8
MO
I
Oxy ILI
IDI
MO
D
Ind-
CS
NO
Int.
MD
Int.
PPH
Int.
Pyr
Post
Sep
1 Rani 42561 20 1 40 1 2 5 8 0 1 1 14 18 0 good 0 0 0 0
2 Swetha 32620 26 1 36 2 2 6 9 12 1 0 12 20 0 good 0 0 0 0
3 Saranya 41575 28 2 40 1 2 6 8 1 1 8 15 1 0 good 0 0 0 0
4 Akila 56738 22 3 38 3 2 7 9 1 1 9 16 0 good 0 1 0 0
5 Bhuvana 54022 36 4 38 4 3 6 9 1 1 7 15 0 good 0 0 0 0
6 Thilaka 23842 29 3 41 1 3 6 8 1 0 9 17 1 0 good 0 0 1 0
7 Varalakshmi 38035 32 2 39 2 3 7 10 1 1 9 18 0 1 good 1 0 0 0
8 Yalini 20846 21 1 41 1 2 5 9 1 1 13 22 1 adm 0 0 0 0
9 Bhavana 34283 38 2 39 3 2 7 8 1 0 10 18 0 good 0 0 0 0
10 Seetha 36848 27 3 37 2 3 6 9 1 0 10 15 0 1 good 0 0 0 0
11 Gokila 54627 24 1 40 1 2 5 8 1 1 12 21 1 adm 0 0 0 0
12 Amala 38646 39 4 39 4 3 6 9 1 0 9 16 2 good 0 0 0 0
13 Punitha 49560 23 2 41 1 2 7 8 1 1 8 18 0 0 good 0 0 0 0
14 Ranjitha 49428 30 3 38 2 3 6 9 1 0 9 15 1 adm 0 1 0 0
15 Sathya 58736 34 1 41 1 2 5 8 12 1 1 13 22 0 good 0 0 0 0
16 Preetha 48269 26 2 39 3 3 6 9 1 1 10 18 3 good 0 0 0 1
17 Priya 43097 20 3 40 1 2 6 10 1 0 9 16 0 good 0 0 0 0
18 Aruna 89675 27 2 38 2 2 7 10 1 1 10 18 0 good 0 0 1 0
19 Anitha 86758 22 1 41 1 1 6 9 1 1 12 20 0 1 good 0 0 0 0
20 Priyanka 68344 28 1 39 3 2 5 8 1 1 11 21 1 good 0 0 0 0
21 Chandra 67489 21 2 36 5 3 7 10 1 1 10 18 2 adm 0 0 0 0
22 Kaviya 64038 23 1 40 1 2 6 8 1 0 12 20 3 0 good 1 0 0 0
23 Hema 59879 36 3 38 2 3 6 8 12 1 1 9 15 1 good 0 0 0 0
24 Sheela 56841 19 1 41 1 2 6 8 1 0 10 19 0 good 0 0 0 0
25 Vasantha 39756 24 2 39 4 2 5 9 1 0 9 18 0 good 0 0 0 0
ER CHART MASTER

26 Kavitha 49274 29 2 41 1 3 6 10 1 1 8 16 0 1 adm 0 0 0 0
27 Renuka 37156 22 1 39 3 2 5 8 1 1 12 20 1 good 0 0 0 0
28 Pavithra 59689 25 1 40 1 2 5 9 1 0 13 19 3 good 0 0 0 0
29 Ilakiya 39256 32 3 38 2 2 6 8 1 0 10 18 2 good 0 0 0 0
30 Fathima 78372 34 4 39 3 3 7 9 1 1 9 16 1 2 good 0 0 0 0
31 Anjali 79458 19 1 40 1 2 6 8 1 0 14 20 0 good 1 0 0 0
32 Sangeetha 46582 25 3 39 2 3 7 9 1 1 10 18 0 good 0 1 0 0
33 Sunitha 49283 22 2 41 1 2 6 8 12 1 0 9 19 1 0 good 0 0 0 0
34 Surya 65826 27 3 38 3 2 8 9 1 1 8 16 3 good 0 0 1 0
35 Arpitha 89647 20 2 41 1 2 6 9 1 1 8 18 1 0 good 0 0 0 0
36 Aruna 85731 25 1 39 2 2 8 10 1 1 11 19 2 good 0 0 0 0
37 Jayasudha 96528 28 3 38 4 3 7 10 1 0 7.5 16 0 good 0 0 0 0
38 Ramayee 93842 21 1 40 1 2 6 9 1 1 12 22 1 1 good 0 0 0 0
39 Vanitha 65639 30 2 37 2 2 7 10 1 1 8 16 3 good 1 0 0 1
40 Krithika 53741 24 3 39 3 3 6 11 1 0 9 15 0 good 0 0 0 0
41 Deivasudha 56748 29 1 41 1 2 7 9 1 1 10 19 1 0 adm 0 0 0 0
42 Janani 93743 20 2 38 3 3 7 10 1 1 8 16 0 good 0 0 0 0
43 Padma 82058 23 3 39 4 3 6 9 1 0 8 15 0 good 0 1 0 0
44 Gowri 72583 30 1 36 5 2 8 8 11 1 1 10 20 0 good 0 0 0 0
45 Srilakshmi 82746 23 2 40 1 2 6 9 1 0 9 17 1 2 good 0 0 1 0
46 vidhya 95842 22 3 38 2 3 7 9 1 1 8 15 2 good 0 0 0 0
47 Chitra 97537 29 2 39 2 2 5 10 1 1 7 18 3 good 0 0 0 0
48 Saranya 89359 19 2 41 1 3 6 9 1 0 8 18 1 0 good 0 0 0 0
49 Nithiya 42673 25 3 38 2 3 6 10 1 0 9 16 3 good 0 0 0 0
50 Selvi 84254 21 1 40 1 2 5 8 10 1 1 12 22 0 good 0 0 0 0