Mucolitic Ambroxol Versus Hypertonic Saline Nebulizer ...
14
66 TMJ Vol. 02 No. 1 66-79
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of Mucolitic Ambroxol Versus Hypertonic Saline Nebulizer ...

66
TMJ Vol. 02 No. 1 66-79TMJ Vol. 02 No. 1 66-79
Mucolitic Ambroxol Versus Hypertonic Saline NebulizerInduction: For Increasing Sputum Volume And FindingAcid-Fast Bacilli
Sunarto Ang1, Sumardi2, Erna Kristin3*
1Post Graduate Study of Tropical Medicine, Faculty of Medicine, Universitas Gadjah Mada, Yogyakarta.2Division of Pulmonology, Department of Internal Medicine, Faculty of Medicine, Universitas Gadjah Mada/Dr. Sardjito General Hospital, Yogyakarta. 3Department of Pharmacology and Toxicology, Faculty ofMedicine, Universitas Gadjah Mada, Yogyakarta.
Corresponding author: [email protected]
ABSTRACTIntroduction: Tuberculosis, a major killer disease in the community, was caused by Mycobacteriumtuberculosis. According to WHO (2006), pulmonary tuberculosis cases in Indonesia was third ranked inthe world. Prevalence of pulmonary tuberculosis in Eastern Indonesia was higher than in Java and Bali,but the findings of positive smear was lowest. AFB discovery will be decreased because of the poor qualityand quantity of sputum. The useful of mucolitic ambroxol or hypertonic saline nebulizer induction will beto increase quality and quantity of sputum smear.Objectives: The aim of this study was to determine and to compare the effectiveness of ambroxol anduse a hypertonic saline induction on new suspected pulmonary tuberculosis patients to increase sputumvolume and to find AFB.Methods: 76 new suspected pulmonary tuberculosis patients were divided into 2 groups with double-blind and open-label simple random sampling RCT (Randomized Controlled Clinical Trial-Parallel design)study.The sputum induction using ambroxol or 3% hypertonic saline solution.The primary and secondaryoutcome were increasing sputum volume and finding AFB by Ziehl-Neelsen staining to calculate the AFBcount per 100 fields of view. Non parametric statistical analysis and percentage of success.Results: All patients can produce sputum. Only one patient ambroxol group can’t produce it. The qualityand quantity of sputum hypertonic saline induction volume better than ambroxol. AFB finding increaseboth groups, but no significant difference. AFB finding increase 26.47% (9/34) with ambroxol and 27.78%(10/36) with hypertonic saline induction compared than previous negative smear.Conclusions: Significant differences increase sputum volume hypertonic saline induction compared thanambroxol. No significant difference AFB finding improvement hypertonic saline induction compared forambroxol. Finding AFB increase 26.47% with ambroxol and 27.78% with hypertonic saline inductioncompared previous negative smear.
Keywords: Tuberculosis, Ambroxol, Nebulizer induction, Sputum volume, AFB
INTISARIPendahuluan: Penyakit tuberkulosis merupakan pembunuh utama dalam masyarakat, penyakit inidisebabkan oleh Mycobacterium tuberculosis. Menurut WHO (2006) jumlah kasus TB paru di Indonesiaberada di peringkat ketiga di dunia. Prevalensi TB paru di Kawasan Timur Indonesia lebih tinggidibandingkan di Jawa dan Bali, tetapi temuan kasus BTA positif paling rendah. Oleh karena kualitas dan

67
Sunarto Ang., Mucolitic Ambroxol Versus Hypertonic Saline Nebulizer Induction:
For Increasing Sputum Volume And Finding Acid-Fast Bacilli
kuantitas dahak yang kurang baik, sehingga penemuan BTA berkurang. Perlunya upaya penemuan BTAmelalui pemberian ambroxol dan nebulizer salin hipertonis untuk meningkatkan kualitas dan kuantitasdahak.Tujuan: Mengetahui dan membandingkan hasil guna pemberian ambroxol dan nebulizer salin hipertonispada tersangka penderitaTB paru baru untuk meningkatkan volume dahak dan temuan BTA.Metode: 76 orang tersangka TB paru baru yang dibagi dalam 2 kelompok dengan rancangan penelitianRCT (Randomized Controlled Clinical Trial-Parallel design) secara simple random sampling metode doubleblind dan open label. Induksi dahak menggunakan ambroxol dan nebulizer salin hipertonis (NaCl 3%).Pemeriksaan meliputi pengukuran volume dahak dan menghitung angka BTA per 100 lapang pandangdengan pewarnaan Ziehl-Neelsen.Hasil: Adanya peningkatan volume dahak pada kelompok ambroxol (97,37%) dan nebulizer salin hipertonis(100%), volume dahak kelompok nebulizer salin hipertonis lebih baik kualitas dan kuantitas dahakdibandingkan kelompok ambroxol. Adanya peningkatan temuan BTA positif pada kelompok ambroxoldan nebulizer salin hipertonis, tetapi tidak ada perbedaan bermakna kedua kelompok tersebut. TemuanBTA meningkat 26,47% responden kelompok ambroxol dan 27,78% responden kelompok nebulizer salinhipertonis dibandingkan BTA negatif sebelumnya.Simpulan: Ada perbedaan bermakna berupa peningkatan volume dahak kelompok nebulizer salinhipertonis dibandingkan ambroxol. Tidak ada perbedaan bermakna dalam hal peningkatan temuan BTAkelompok nebulizer salin hipertonis dibandingkan ambroxol. Temuan BTA positif meningkat 26,47%responden pada kelompok ambroxol dan 27,78% responden kelompok nebulizer salin hipertonisdibandingkan BTA negatif sebelumnya.
Kata Kunci: Tuberkulosis, Ambroxol, Nebulizer salin hipertonis, Volume dahak, BTA
INDRODUCTIONTuberculosis (TB) is a major killer disease in the
community, caused by Mycobacterium tuberculosis.A third of the world’s population had been infectedand estimated are 8 million new cases and 3 milliondeaths patients per year. One of ten patientsinfected by Mycobacterium tuberculosiswill becomeactive TB1,2,3.
The Pulmonary TB cases in Indonesiacontributed 10% cases in the world1.Based on thesurvey results to indicate the prevalence andincidence rate differences of TB cases in threeregions variation of the estimated incidence ofsmear positive TB cases in Java and Bali 64/100,000;210/100,000 at Eastern Indonesia and 160/100,000in Sumatra. The national prevalence decreased 4%per year and the trend of slower decline in Sumatraand Eastern Indonesia2.
The prevalence of PTB in Indonesia was 253cases per 100,000 population per year and thenumber of new smear positive incidence was 105
cases per 100,000 patients a year, while the deathrate due to TB was still high at 38 cases per 100,000population in a year. TB average second ranked inthe outpatient clinic at the general hospital and thefirst rank in the lung clinic and hospital. In theoutpatient unit of the general hospital, new casesof TB accounted for 19% of all new respiratorycases 2,4. The implementation of tuberculosiseradication program, the tuberculosis diagnosiswas established if found AFB in microscopic smearsputum. To find AFB in sputum examination fortuberculosis was not easy1,5,6,7.
In 2007, the East Kalimantan province has CDR(Case Detection Rate = number of patients findingnew smear positive TB) 29.7% and CNR (CaseNotification Rate) 62.5%. Samarinda has CNR68.7% in 2006 and 55,9% in 2007, its to decreasethe discovery scope new smear positive patients.The national target was 70%8. AFB discovery willbe decreased will the poor quality and quantity ofsputum. To find AFB in sputum smear microscopic

68
TMJ Vol. 02 No. 1 66-79
of suspected tuberculosis was not easy. Theproblem was the quality and quantity of sputum.The ideal sputum for microscopic examination wasmucopurulen about 3-5 ml volume each collection.It takes at least 5,000 AFB per milliliter to be seenmicroscopically. If less of quality and quantity ofsputum, so to find the AFBlessalso7,9,10.
The quality and quantity sputum and sputumphysicochemical the structure affect the resultsmicroscopic examination. Mucopolisaccharidesfibers and mucin acid, it can be difficult to catchmycobacterial cells so make it difficult todetect1,5,11. Microscopic examination of sputumshowed the poor quality sputum smear, so it’s neededucation to health care workers and laboratorypersonnel. The improving sputum collection needcontinuous monitoring12.
Besides sputum physicochemical structure, theacid mucopolisaccharides contains fibers make AFBcapture so difficult to be detected. The sputumcontained mucin can catch mycobacteria cells andprotects them from the decontaminationactivities13. The expectorants can stimulatesecretions from the bronchi and tracheal spending,to increase secretions or to break the acidmucopolisaccharides fibers will be become morewatery sputum and AFB will be spread evenly14. Theuseful of mucokinetic expectorant (ambroxol) wasexpected to improve finding positive smear ratehigher compared than normal procedure.
Ambroxol as an expectorant mucokinetic helpsthe secretion of the bronchi branch and increasekinesis lowering the surface tension by stimulatingan effective spur surfactant transport of mucuswhen coughing14,15. Ambroxol effects can be usedas mucokinetic the respiratory tract16, especiallychronic bronchitis patients17, which to dilute thesputum patients have trouble removing it18.
To find a sputum smear examined using sputuminduction by inhalation hypertonic saline through anebulizer, particularly in patients with dry cough orinadequate sputum volume/ scanty (less than 2milliliters)19-24. Sputum induction was an effectivemethod inhalation to obtain adequate quantity ofsputum. Because of sputum dilution mucus fromsteam hypertonic saline can be separated M.tuberculosis from the trap21.
Hypertonic saline and ambroxol were theexpectorant mucokinetic type, which beneficial toincrease transport of mucus when coughing.Ambroxol to increase coughing because thestimulating effects of surfactant secretion.Hypertonic saline to separate the DNA from theinfected mucus of bacteria, as to reduce the mucusviscosity so it can increase sputum volume smearand findings of previous negative patients15,19,21,22,25.
The aim of this study was to determine and tocompare between ambroxol or hypertonic salinenebulizer induction for increase the sputum volumeand find AFB on suspects pulmonary tuberculosispatients.
MATERIALS AND METHODSThe study design an open-label and double blind
simple random sampling RCTs (randomizedcontrolled Clinical Trial-Parallel design)26,27. Theindependent variables were ambroxol andhypertonic saline nebulizer induction and thedependent variables were sputum volume and AFBfindings. Inclusion criteria were: suspecties newpulmonary tuberculosis patients,who either having adry cough or scanty produce sputum, only producesaliva or quantity sputum less than 2 ml and referralcases that have been examined previously negativesmear, have existence of a written consent (informedconsent)and 18to 55 yearsageold. Exclusion criteria,were:being intreatmentwithanti-tuberculosisdrugs,history of severe respiratory illness, severe illness,hypertension,pregnantorbreastfeeding,allergiesandcontraindications bromhexine or ambroxol andnebulizer induction.
Materials and study tools were ambroxol 30mg tablet and induction instrument uses ultrasonicnebulizer hypertonic saline (NaCl 3% solution).Sputum volume measurements using a measuringcup and sputum smear stained Ziehl-Neelsenmethod.Thedecontaminatenebulizerequipmentwaswashing,decontaminationandsterilization(bysoakingin 2.4% glutaraldehyde for 10-12 hours at 25ºCtemperature).
Ambroxol HCl patients group agree to followthe study (informed consent) will be given the 3tablets ambroxol HCl 30 mg drug to be taken for 1
69
Sunarto Ang., Mucolitic Ambroxol Versus Hypertonic Saline Nebulizer Induction:
For Increasing Sputum Volume And Finding Acid-Fast Bacilli
day every 8 hours and notified via SMS (ShortMessage Service).
Nebulizer induction group will be givenexplanation about hypertonic saline (NaCl 3%solution). A brief description of the procedure wasgiven to the patients. To avoid contamination,patients gargled with normal solution to clear debrisfrom the mouth and oropharynx. All subjects askedto inhale a mist of 3% hypertonic saline solution(sterile) by ultrasonic nebulizer. Inhalation wascontinued until an adequate sputum sample(minimum 3 ml) or maximum period 30 minutes. Thenostrils were closed to prevent nasal inhalation. Theinhalation of hypertonic saline was interruptedevery 5 minutes, so the patient could expectoratesputum. The implementation of induction nebulizerwill be monitoring the patient clinical state andalways O‚ tube and resuscitation equipment.
Ambroxol group performed 3 times sputumcollection, including: Sputum S1 was collected thefirst time visiting. Sputum P was collected themorning of the second day, immediately afterwaking, before breakfast. And sputum S2 wascollected the second day after 6 hours submittedsputum in the morning. The nebulizer inductiongroup 3 times sputum collection also. Sputum S1was collected first visit and prior to the nebulizer.Sputum P was collected conducted by hypertonicsaline nebulizer induction for 5-30 minutes. If thepatient could’t produce the sputum was behospitalized overnight at lung ward, was conductednebulizer 3 times a day. At the following morning(before breakfast) was asked gargle normal saline(NaCl 0.9% solution) to clean detruitus oral cavity.Patients were asked to collect sputum to put in acontainer. The sputum S2 was collected 6 hoursafter sputum induction in the morning.
RESULT1. General description of subjects
129 referral suspected pulmonary TB patients.89 respondents who fulfilled the inclusion criteriaand 40 respondents are excluded because includingexclusion criteria. 76 patients agree and 13 patientsrefused the study. After having history, physical
examination and chest x-ray. The patients will bedivided into 2 groups according computer programthat received ambroxol HCl drug was 38 patientsand received hypertonic saline induction was 38patients. General description of study subjects arepresented in the following table:
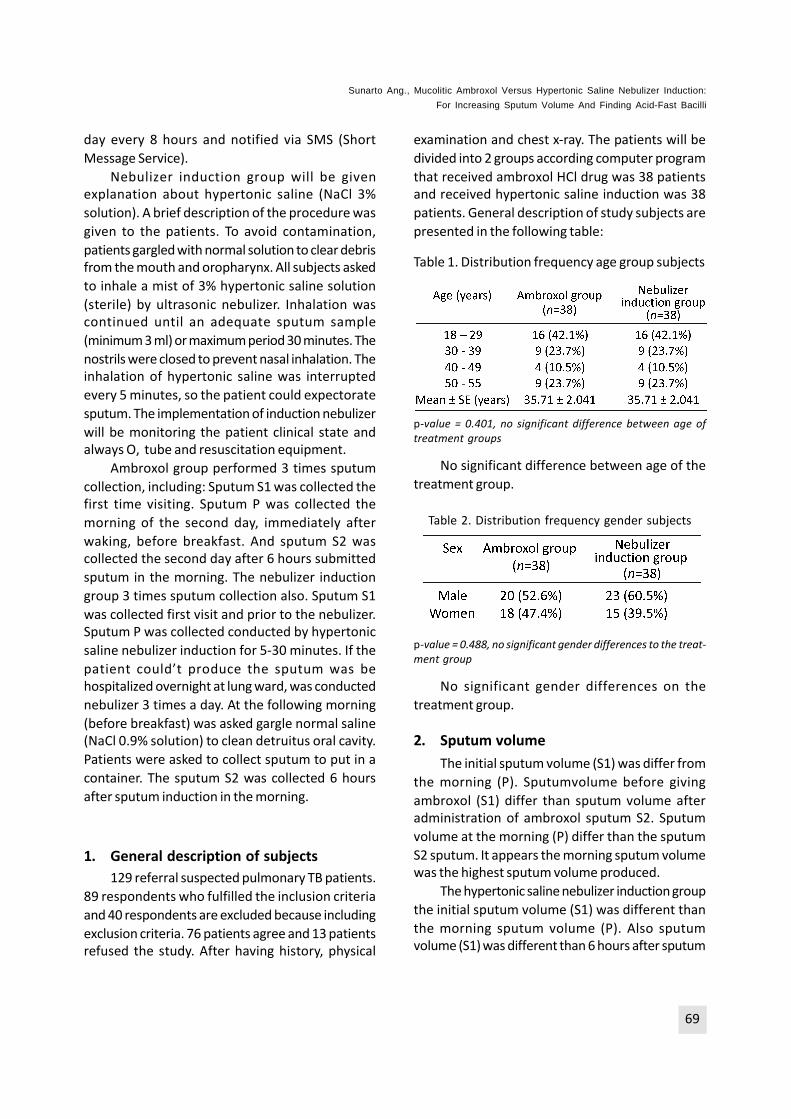
Table 1. Distribution frequency age group subjects
p-value = 0.401, no significant difference between age oftreatment groups
No significant difference between age of thetreatment group.
Table 2. Distribution frequency gender subjects
p-value = 0.488, no significant gender differences to the treat-ment group
No significant gender differences on thetreatment group.
2. Sputum volumeThe initial sputum volume (S1) was differ from
the morning (P). Sputumvolume before givingambroxol (S1) differ than sputum volume afteradministration of ambroxol sputum S2. Sputumvolume at the morning (P) differ than the sputumS2 sputum. It appears the morning sputum volumewas the highest sputum volume produced.
The hypertonic saline nebulizer induction groupthe initial sputum volume (S1) was different thanthe morning sputum volume (P). Also sputumvolume (S1) was different than 6 hours after sputum

70
TMJ Vol. 02 No. 1 66-79
collection time (S2). The morning sputum volume(P) differ than collected after 6 hours post-induction(S2). The highest produce sputum volume at thenebulizer induction time or morning.
A. Comparison of sputum volume betweenambroxol and hypertonic saline nebulizer in-duction group
Table 3. Comparison of sputum volume betweenambroxol and hypertonic saline nebulizerinductiongroups
Description: S1 = the sputum volume at the initial time spu-tum collection (before treatment), P =sputum volume at the time of sputum collection time/ morn-ing; S2 = sputum volume at the time of sputum collection 6hours post-treatment/ morningn = 38 respondents, the data in mean ± 2SE (ml)*Wilcoxon Signed-Ranks Test significantly different betweenambroxol groups if p-value <0.05**Wilcoxon Signed-Ranks Test was significantly differentbetween nebulizer induction groups if p value <0.05***Mann-Whitney U-Test significantly different betweenambroxol and hypertonic saline nebulizer induction groupsif p-value<0,001
Both ambroxol and hypertonic saline nebulizerinduction group were significantly different from toincreasing sputum volume between initial sputumvolume(S1)than morningsputumvolume/time(P)orthe 6 hours post induction sputum volume (S2), so itwas concluded the sputum volume in each groupincreased significantly.
B. The sputum volume test between ambroxoland hypertonic saline nebulizer inductiongroups no pairInitial sputum volume S1 between ambroxol
and hypertonic saline nebulizer induction group. Thecomparison of initial sputum volume (S1) betweenambroxol and hypertonic saline nebulizer induction
group were no significant difference in initialsputum volume group.
Sputum volume P (morning) between mucolyticambroxol and induction hypertonic saline nebulizergroup. Comparison of morning sputum volume (P)between ambroxol and hypertonic saline nebulizerinduction sputum group were significantdifferences. Sputum volume after treatment (P)showed the sputum volume hypertonic salinenebulizer induction more than ambroxol group(Table 3).
Sputum volume S2 between ambroxol andhypertonic saline nebulizer induction group. It wassignificant differences sputum volume (S2) betweenambroxol and hypertonic saline nebulizer inductiongroup, the sputum volume hypertonic salinenebulizer induction group more than the ambroxolgroup (Table 3).
C. Comparison of difference increase sputumvolume between ambroxol and hypertonicsaline nebulizer induction groupsThe excess morning sputum volume (P) with
initial sputum volume (S1) are significantdifferences between each other. Also it significantdifferences between the sputum volume S2 thaninitial sputum volume (S1). Similarly, sputum volumeS2 than morning sputum volume (P). It can beconcluded significant differences between sputumvolume ambroxol than hypertonic saline nebulizerinduction groups, nebulizer induction group washigher than ambroxol group.
Table 4. The difference betweensputum volume ambroxoland nebulizer inductiongroups
The difference p-valueΔ Sputum volume P-S1Δ Sputum volume S2-S1Δ Sputum volume S2-P
0.001*0.001*0.001*
*Mann-Whitney U Test was significantly dif-ferent if p-value <0.05
71
Sunarto Ang., Mucolitic Ambroxol Versus Hypertonic Saline Nebulizer Induction:
For Increasing Sputum Volume And Finding Acid-Fast Bacilli
3. AFB CountSome respondents of study before treatment
were found smear findings each group. At initialsputum (S1) either 4 respondents ambroxol groupfound positive sputum smear and hypertonic salinenebulizer induction group 2 respondents. Finally, theambroxol group had 34 respondents and 36respondents nebulizer induction group.A. Comparative AFB count between
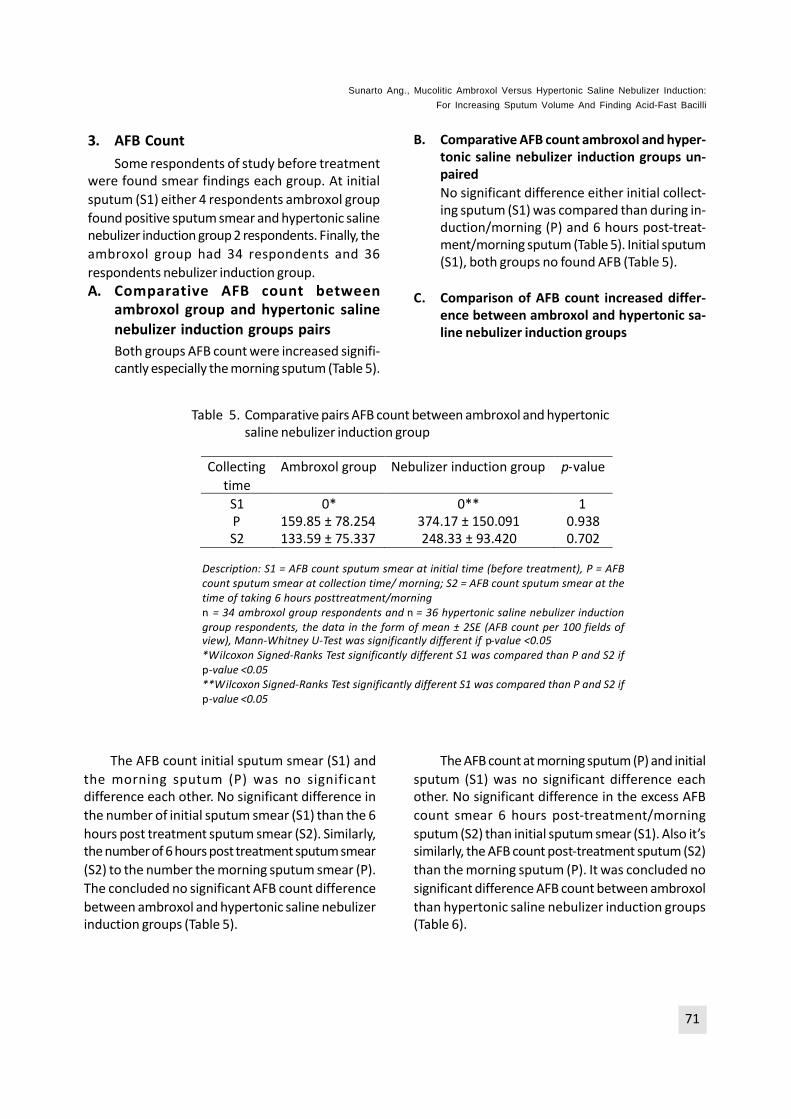
ambroxol group and hypertonic salinenebulizer induction groups pairsBoth groups AFB count were increased signifi-cantly especially the morning sputum (Table 5).
B. Comparative AFB count ambroxol and hyper-tonic saline nebulizer induction groups un-pairedNo significant difference either initial collect-ing sputum (S1) was compared than during in-duction/morning (P) and 6 hours post-treat-ment/morning sputum (Table 5). Initial sputum(S1), both groups no found AFB (Table 5).
C. Comparison of AFB count increased differ-ence between ambroxol and hypertonic sa-line nebulizer induction groups
Table 5. Comparative pairs AFB count between ambroxol and hypertonicsaline nebulizer induction group
Collectingtime
Ambroxol group Nebulizer induction group p-value
S1PS2
0*159.85 ± 78.254133.59 ± 75.337
0**374.17 ± 150.091248.33 ± 93.420
10.9380.702
Description: S1 = AFB count sputum smear at initial time (before treatment), P = AFBcount sputum smear at collection time/ morning; S2 = AFB count sputum smear at thetime of taking 6 hours posttreatment/morningn = 34 ambroxol group respondents and n = 36 hypertonic saline nebulizer inductiongroup respondents, the data in the form of mean ± 2SE (AFB count per 100 fields ofview), Mann-Whitney U-Test was significantly different if p-value <0.05*Wilcoxon Signed-Ranks Test significantly different S1 was compared than P and S2 ifp-value <0.05**Wilcoxon Signed-Ranks Test significantly different S1 was compared than P and S2 ifp-value <0.05
The AFB count initial sputum smear (S1) andthe morning sputum (P) was no significantdifference each other. No significant difference inthe number of initial sputum smear (S1) than the 6hours post treatment sputum smear (S2). Similarly,the number of 6 hours post treatment sputum smear(S2) to the number the morning sputum smear (P).The concluded no significant AFB count differencebetween ambroxol and hypertonic saline nebulizerinduction groups (Table 5).
The AFB count at morning sputum (P) and initialsputum (S1) was no significant difference eachother. No significant difference in the excess AFBcount smear 6 hours post-treatment/morningsputum (S2) than initial sputum smear (S1). Also it’ssimilarly, the AFB count post-treatment sputum (S2)than the morning sputum (P). It was concluded nosignificant difference AFB count between ambroxolthan hypertonic saline nebulizer induction groups(Table 6).

72
TMJ Vol. 02 No. 1 66-79
Table 6. The difference AFB count smear betweenambroxol and nebulizer induction Groups
The difference p-valueΔ AFB count P-S1Δ AFB count S2-S1Δ AFB count S2-P
0.9380.7020.881
*Mann-Whitney U Test was significantly different ifp-value <0.05
4. The percentage of success increased sputumvolumeOnly one person at ambroxol group can’t
exclude the sputum after ambroxol administration,it was increased sputum volume 97.37% (37/38)compared to before ambroxol treatment. Allpatients (100%) at hypertonic saline nebulizerinduction group can increase sputum volumecompared to before treatment.
5. The percentage success rate in AFB onambroxol and hypertonic saline nebulizer in-duction group negative initially sputum (S1).Percentage success rate to find AFB was
different each group. Ambroxol group has 4 positivesmear initial sputum respondents. Thirty fourrespondents whom initial sputum smear (S1) wasnegative. After ambroxol administration were 9respondents found both sputum smear positive inthe morning (P) and the second sputum (S2). It wasincreasing 26.47% (9/34) smear positive findingsambroxol group who previous negative smear.
Two respondents hypertonic saline nebulizerinduction group whom the initial sputum (S1) foundsmear positive. Thirty four respondents initialsputum smear (S1) were negative. After nebulizerinduction treatment were 10 respondents foundboth positivesputum smear in the morning (P) and6 hours after morning sputum (S2). The percentageof success increased to finding positive smear was27.78% (10/36) respondents hypertonic salinenebulizer induction previous negative smear.
DISCUSSION1. Comparison of sputum volumeA. Comparison of sputum volume between
ambroxol and hypertonic saline nebulizer in-duction groups pairThe results of sputum collection in the
ambroxol group was increased sputum volume afteradministration of ambroxol compared before drugadministration. Because to ambroxol was anexpectorants mucokinetic to facilitate or tostimulate the disposal of bronchi and trachealsecretions. The mucolytic physicochemical ofsecretions change, especially lowering the viscosityto be easily expelled by coughing14. Ambroxol hasto process acid mucopolisaccharidespharmacokinetics so the fibers will be break downmucus. It was increasing the production oflysosomes and activates hydrolytic enzymes. It willbe stimulated serous gland cells causes the viscosityof sputum secretions decrease, so it need processtime for metabolism and distribution to the targetorgan15,18,28.
Meanwhile the hypertonic saline nebulizerinduction group to increase sputum volumesignificantly, the results of sputum collection wasincreasing sputum volume induction compared tothe sputum volume before treatment. Thehypertonic saline nebulizer induction to decreaseinvolvement of mucus in the airways. A hydratedmucus in the airways would be more easily movedby mucociliary and cough increased volumesecretion21,23,24,29.Hypertonic saline solution causebronchial irritation and stimulates the secretion ofbronchi. After 10-20 minutes nebulizer will be tomobilize fluid production from lower respiratorytract. Repeated coughing helps to move the productinto the trachea assisted with the expectorant19,30.
Both groups increased sputum volume,especially the morning or sputum induction time ofthe nebulizer. Although it was significant differenceseach other groups, but comparison between groupsinitial sputum volume (S1) between the two groupswas no significant.

73
Sunarto Ang., Mucolitic Ambroxol Versus Hypertonic Saline Nebulizer Induction:
For Increasing Sputum Volume And Finding Acid-Fast Bacilli
Each group shows that significant differencesafter administration of ambroxol and afterinduction to increase the sputum volume product.The high difference significantly in sputum volumewas increased in the morning (P) and sputum S2 eachgroups. The ambroxol group was increasing sputumvolume, but the increased sputum volumehypertonic saline nebulizer induction group morethan it.
The ambroxol group to increase sputum volumeof 97.37% compared to before treatment and thehypertonicsalinenebulizer inductiongrouptoincreaseall suspected pulmonarytuberculosis patients (100%)compared to prior induction treatment.
B. Comparison of sputum volume betweenambroxol and hypertonic saline nebulizer in-duction groups no pairComparison of initial sputum volume (S1)
between ambroxol and hypertonic saline nebulizerinduction groups was no significant difference. Theinitial sputum volume (S1) in both groups did notdiffer significantly. Preliminary data showed samerelatively, because it has been randomized.
Comparison of morning sputum volume (P)between ambroxol and hypertonic saline nebulizerinduction group were significant differences.Sputum volume after treatment showed hypertonicsaline nebulizer induction group more thanambroxol group (Table 3). The hypertonic salinenebulizer induction will be effect faster and moreimmediately19, it was differ the effects ofexpectorant mucolytic drugs must be through thepharmacokinetic mechanism (absorption,distribution, metabolism and excretion) so requiresa time14. Ambroxol has the effect of spur secretionof fluid in conditions of moderate to strongstimulated, to maintain viscosity and sputumvolume in the medium stimulated, becauseambroxol stimulates the secretion of ions Cl¯through Naz / Kz /2Cl ¯ cotransporter at the basalcondition, while the under basal conditionsambroxol will be stop the secretion of Cl¯ andHCO3¯ and does not to affect to the anionssecretion31.
No significant differences between sputumvolume (S2) ambroxol and hypertonic salinenebulizer induction group, which the sputum volumenebulizer induction group more than ambroxolgroup (Table 3).
The useful of hypertonic saline will be moresputum volume production, because it causeirritation to the mucosal bronchial and to stimulatethe secretion of bronchi. The putative mechanismof action to improve mucociliary clearance and orincrease osmolarity fluid of respiratory tract, whereto increase vascular permeability mucosal bronchi,and submucosal glands produce mucus spur. After10-20 minutes nebulizer to mobilizes fluidproduction from lower respiratory tract productsand induction effects of nebulizer will be decrease4 hours later19,32.
According to Rogers25 and Rubin33 thatexpectorant mucokinetics, like: ambroxol andhypertonic saline to work through the sputumtransportation when coughing. The mechanism ofaction alleged by kinesis mucus and coughing canbe removed mucus from lower respiratory tract.â2-adrenoceptor agonist will be stimulate increaseairflow and ciliary beat, Cl¯/water secretion andmucin, increasing the sputum volume and surfactantreduces mucus adhesions to epithelium caused thesputum airway easy to exit.
The inflammatory process due to bacterialinfection occur mucus hypersecretion, ciliadysfunction and changes in the composition ofrespiratory secretions. It contains inflammatorycells, especially neutrophils. The presence ofneutrophils from the release of proinflammatorymediators by epithelial airway damage. It causedthe DNA release and filamentous actin (F-actin) andthe cytoskeleton of DNA and F-actin copolymerize.Mucin degradation in polymers, the release of DNAand actin network. It causes to increase sputumsecretion and to decrease sputum viscosity, soresulting in decreased adhesion to the airwaysurface epithelium. It was caused sputum becomeunsticky to adhesion the respiratory tract surfaceand to cough cause sputum easily out include theAFB contained25,34.

74
TMJ Vol. 02 No. 1 66-79
2. Comparison of AFB findingAmbroxol, as an expectorant to increase
volume and thin sputum, was making it easier forspending sputum from branches of the terminalbronchial. The sputum had contained acidmucopolisaccharides fibers and mucin, couldcomplicate capture mycobacteria cells making itdifficult to detect1,5,11. Mucolytic expectorant willbe describe the bonding acid mucopolisaccharidesfibers so that sputum becomes more dilute andreduced viscosity. To provide sputum release formycobacteria which it trapped by acid mucopoli-saccharides and mucus that are easier to find14,15.After ambroxol treatment led smear easy to find,was reflected significant differences in the AFBnumber of smear before giving ambroxol comparedafter administration of ambroxol primarily onsputum smear rates in the morning or at any rateof sputum smear (S2). Because it possible coincidedwith the melting of the lesions or tubercles next day,especially at the morning2,7,9. Mucolytic has thepharmacokinetic effects, are significant differencesin the increase in sputum volume. It is will be toincrease sputum volume but did not alwayscorrelate with increased AFB count of smear. Thepeak of mucolytic ambroxol levels (Tmax) <1.6hours in plasma despite having a long half-life of10 hours, the effect will be decrease pharmaco-kinetic through oxidative metabolism was triggeredby cytochrome P450 CYP3A4 so mucolytic effectto decline followed a decrease of decompositionof acid mucopolisaccharides also followed by adecrease mucus bronchi biodegradable fibers thatled to the discovery of smear rates declined aswell14,25 .
Ambroxol effects through coughingeffectiveness will spur surfactants secretion. Themechanism of action through the abilitymucokinetic, mucociliary activity, stimulate theproduction of surfactants, anti-inflammatory andantioxidative action alleged role in the ability tostimulate the secretion of bronchi15.
Comparative between the initial sputum smear(S1) is different from the time of the induction rateof sputum smear hypertonic saline nebulizer in themorning (P). The mechanism of mucolytic was to
decrease involvement mucus in the airways. Themechanism of nebulizer induction in osmolaritythrough the saline solution on epithelium airway willbe inhaled and followed by the increase in watercontaining airway mucus. A hydrated mucus in theairways increased volume secretion would be moreeasily moved by mucociliary and cough21,23,24,29,35.Hypertonic saline can also to separate the DNAfrom the infected mucin in the mucus, through areduction in mucus viscosity. Hypertonic solutioncause bronchial irritation and stimulates secretionof bronchi. After 10-20 minutes nebulizer occursthat mobilizes fluid product from lower respiratorytract. Repeated coughing can helps to move theproduct into the trachea, including AFB that trappedin mucopolisaccharides acids that can be helpedwith expectorant, so the discovery of a larger AFBsmear19,30. Nebulizer induction was an effectivemethod as the initiation to discovery of suspectspulmonary tuberculosis who can’t remove sputumor previous negative smear examination results.The chest x-ray on suspected pulmonary tuber-culosis patients who have cavitation and infiltrateswill be to increase 19.9% the findings AFB sputumthrough the hypertonic saline induction36.
The hypertonic saline nebulizer induction groupsmear rates prior to the nebulizer (S1) is differentfrom the AFB count smear after induction (NaCl 3%solution) during or initial morning (P). While AFBcount prior to the nebulizer (S1) was similarcollected after 6 hours AFB sputum collection time/morning S2. Similarly, the AFB count smear duringinduction nebulizer or morning (P) was not differentfrom the AFB count smear was collected after 6hours post-nebulizer induction using hypertonicsaline S2.
This study shows the AFB findings in the initialsputum (S1) was not different than the AFB countsmear after 6 hours nebulizer (S2). Similarly, AFBcount findings at the time of induction nebulizer (P)than AFB count after 6 hours nebulizer (S2). Themajority of respondents had performed inductionnebulizer only one time with a nebulizer inductionwill be to increasing AFB count smear sputum,although there were no significant differences in

75
Sunarto Ang., Mucolitic Ambroxol Versus Hypertonic Saline Nebulizer Induction:
For Increasing Sputum Volume And Finding Acid-Fast Bacilli
the AFB count smear rates after nebulizer 6 hours(S2). After 10-20 minutes fluid production will bemobilizing product of lower respiratory tract.Repeated coughing will be helps moving the productinto the trachea30,37.
It has relationship between to find leukocytesand neutrophils increased with the AFB discoverysmear in pulmonary tuberculosis patients diagnosedafter bronchoscopy are accompanied fever41. TheAFB count smear nebulizer or morning (P) was notdifferent from AFB count smear was collected after6 hours postnebulizer induction use hypertonicsaline (S2). Similarly, the AFB count smear prior tothe nebulizer (S1) was similar collected after 6 hoursAFB count sputum collection time/morning S2.
The mechanism action nebulizer inductionmade solution will become droplets. Smallerdroplets will be deposited into the peripheral lung.Therefore hypertonic saline fluids used fordeposition through a process of osmosis tointerstitial fluid to the lower respiratory tract.Hypertonic saline solution will cause irritation tospur secretion of the bronchi. After 10-20 minutesnebulizer bronchi secretion will be mobilizematerial from lower respiratory tract, including AFB.Repeated coughing will help transfer the materialinto the trachea functions as an expectorant42.Some studies have reported that repeated sputuminduction after initial induction between 8-24 hourswould cause an increase neutrophils count in thesecond sample, so it isn’t recommended sputuminduction with a nebulizer repeated38,39. The 48hours interval time between nebulizer induction willbe to provide a significant number of normal cellsin individuals, so many studyers to advise aminimum time limit for repeat nebulizer inducedsputum isn’t more than 2 days to avoid the effectsof “carry-over” of induction40. Sputum inductionresults to contain a high concentration of liquidphase components such as eosinophil cationicproteins (ECP), mucin glycoprotein and albumin thanin BAL. It was indicates the existence fromrespiratory secretions than space alveolar43.
The sputum smear, which found bacteria, is amucin protein-rich complex medium and a DNA
degradation product. The nebulizer inductionproduce sputum contains many mediatorscompared than bronchoalveolar lavage. Finding AFBsmear rates between the two groups are significantdifferences. The ambroxol group to find smear ratemore survive either the morning sputum (P) andpost-administration drugs, because ambroxol hashalf-life long enough and high volume distribution15.
Comparative sputum volume betweenambroxol and hypertonic saline nebulizer inductiongroups no pair Comparison of initial sputum volume(S1) between ambroxol and hypertonic salinenebulizer induction groups were no significantdifference, because it was randomized.
Comparison of morning sputum volume (P)between ambroxol and hypertonic saline nebulizerinduction groups were significant differences. Thesputum volume hypertonic saline nebulizerinduction group more than the ambroxol group(Table 5).
Because hypertonic saline nebulizer inductioneffect was faster and more immediately19, wasdifferent the effects of expectorant mucolytic drugsthat through the pharmacokinetic mechanism(absorption, distribution, metabolism andexcretion) so requires a certain time14. Surfaceambroxol molecules and its metabolites were notfound in electron-deficient regions, so manycompounds can’t react with glutathione and DNAnucleobase. The existence of electron-rich regionon the surface of the lower respiratory tract andinduction effects will be decline after 4 hours19,32.
The comparison AFB count between ambroxoland hypertonic saline nebulizer induction nebulizergroups
The AFB count sputum smear S1 ambroxol andhypertonic saline nebulizer induction groups. Thestatistical test of AFB count initial sputum/beforetreatment (S1) ambroxol and hypertonic salinenebulizer induction groups are no significantdifference (p-value = 0.639), it were relatively equalsmear both groups because it was randomized. TheAFB finding on sputum smear before treatment (S1)because more careful examination and appropriateprocedures for sputum examination in the hospitalcompared to previous primary care. According to

76
TMJ Vol. 02 No. 1 66-79
Sakundarno12 the quality of sputum was necessaryto find the AFB of smear, so training needed toobtain high quality sputum for laboratoryexamination. If poor quality and quantity ofsputum, to find AFB also lacking. According to ATS9,Siddiqi et al.10 and WHO7, the quality of sputumand microscopic preparations, either increase thesensitivity up to 80% compared than smear culturemethod.
The AFB finding morning sputum (P) smearbetween ambroxol and hypertonic saline nebulizerinduction groups did not differ significantly.Although was a significant increase in sputumvolume at hypertonic saline nebulizer inductioncompared than ambroxol group, but this was notfollowed always increase the AFB findings smear.The mechanism of bronchial mucosal stimulationto irritation can increase sputum volume but notalways increase the AFB count findings, because theAFB need acid mucopolisaccharides decomposition.The previous study (Williams et al45. Brown et al46;Uskul et al47) was showed the induced sputum,gastric washings and bronchoalveolar lavage didnot differ findings smear rates despite increasedsputum volume induction but hypertonic salinenebulizer induction cheaper and more effectivethan other procedures.
The AFB findings post-treatment sputum smear(S2) inbothgroupswasnotsignificant, althoughthereweresignificantdifferencesinsputumvolumebetweeneach groups. It was to increase sputum volumehypertonicsalinenebulizer inductiongroupcomparedthan ambroxol group. It can be explained that thenebulizer induction to increase sputum volume, butwasn’t always followed by increasing AFB findings.Because it has other processes can influence AFBfindings, such as acid mucopolisaccharides bonddecomposition.
The ambroxol and nebulizer induction groupshad significant differences to AFB finding initialsputum compared than the morning sputum/duringsputum induction and 6 hours after morningsputum. Statistical analysis showed that the datawas no significant difference increased BTA findingsboth ambroxol and nebulizer induction groups.Unpaired statistical analysis showed no significantdifference either groups.
3. The percentage of success increased sputumvolumeAmbroxol group was increasing sputum volume
97.37% compared to before giving drugs, while thehypertonic saline nebulizer induction group toincrease entirely (100%) to all suspected pulmonarytuberculosis patients sputum volume increasecompared to before hypertonic saline nebulizerinduction. It was not different to other study.According to Gupta and Garg19 the success of 97%from the quality of less than 2 ml previous sputum.
4. The percentage of success increased AFBcountAmbroxol group has to increase AFB findings
to smear of 26.47% compared to prior treatment,while hypertonic saline nebulizer induction groupwill be increase smear findings of 27.78% comparedto before induction previous negative smear. It wasnot different previous studies at 19-42%, like: 19%(Anderson et al48.); 25% (Parry et al23.; Merrick etal49.); 33.9% (Li et al20.); 34% (Conde et al50.); 42%(Hartung et al51.); 38% (Gupta and Garg19) and 19.9%(Garcia et al36.). Mechanism of action of saline asmucolytic to reduction involving the mucusrespiratory tract. The fluid osmolarity will bedilution during hypertonic saline inhalation. Becausethe hydrated mucus respiratory will be facilitatemovement by mucociliary clearance wasaccompanied by increased sputum volume.Hypertonic saline solution will be separating DNAmucus from the infected mucus smear, causes todecrease viscosity mucus25.
Statisticalanalysisshowedsignificantdifferencesin AFB smear findings in each group like increasedsputum volume, where the nebulizer induced groupmorethanambroxol. ImprovingAFBfinding,especiallythesputumcollectioninthemorning,eitherambroxolor nebulizer induction.
CONCLUSIONThe expectorant ambroxol or saline induction
hypertonic nebulizer will be to increase sputumvolume and AFB count findings on suspectedpulmonary tuberculosis patients. It was significantdifferences between the provision to increase
77
Sunarto Ang., Mucolitic Ambroxol Versus Hypertonic Saline Nebulizer Induction:
For Increasing Sputum Volume And Finding Acid-Fast Bacilli
sputum volume between ambroxol and hypertonicsaline nebulizer induction, where nebulizer inductionmore than ambroxol. No significant difference toincrease AFB findings expectorant betweenambroxol and hypertonic saline nebulizer induction.97.37% ambroxol patients group and all patients(100%) hypertonic saline nebulizer induction groupcan increase quality and quantity sputum compareprevious treatment. 26.47% patients ambroxolgroup were found positive smear and 27.78%patients hypertonic saline nebulizer induction groupcompared than previous negative smear.
SUGGESTIONThe suspects pulmonary tuberculosis patients,
who can’t remove sputum or less than 2 millilitersadvise to take ambroxol first, if failed to proceedhypertonic saline nebulizer induction. The continu-ed study development with a higher standard smearfindings (ie. culture smear).
ACKNOWLEDGEMENTSThe success of this study on supported fund
and study facilities by the East Kalimantan provincialgovernment. We thank Doni Irfandi Alfian, MD., EmilBachtiar Moerad, MD., Mrs. Antasari and Mr.Yatman to assist the implementation of study; SjarifIsmail, MD.,M.Kes, Zulaela, Dipl.Med.Stat,M.Si andDewi Ismimasitoh (CE&BU staff FM GMU), whichprovide inputs in the data study processing, Mrs.Zaimah and all microbiology laboratory staff at A.Wahab Sjahranie General Hospital. The author tothank all who helped and involved in this study.
Ethical approval: The study protocol wasapproved by the ethical review committee of theFaculty of Medicine, Universitas Gadjah Mada,Indonesia.
REFERENCES1. World Health Organization. The Diagnostic
Pipeline, Tuberculosis Diagnosis And DrugSensitivity Testing. StopTB Department. Geneva:World Health Organization, 2006; 4-5.
2. MOH-ROI. Nasional Guideline for TuberculosisTreatment. Jakarta: Ministry of Health Republicof Indonesia, 2007.
3. World Health Organization. The Global BurdenofTB,GlobalTuberculosisControlAShortUpdateTo The 2009 Report. Stop TB Department.Geneva: World Health Organization, 2009;4-6.
4. World Health Organization. Indonesia. GlobalTuberculosis Control, WHO Report. New Delhi:World Health Organization, 2008;113-6.
5. World Health Organization. BacteriologicalResults, Treatment of Tuberculosis Guidelines.Stop TB Department. Geneva: World HealthOrganization, 2010; 25-7.
6. Indonesian Pulmonologist Association.Diagnosis. Tuberculosis Guidelines Diagnosis &Treatment in Indonesia. Jakarta, 2002.
7. World Health Organization. Tuberculosis,Pulmonary–diagnosis. Toman’s TuberculosisCase Detection, Treatment, and Monitoring–Questions and Answers. Geneva: World HealthOrganization, 2004.
8. MOH-ROI. East Kalimantan Province HealthProfile 2008. Available from: URL:http://www.depkes.go.id
9. American Thoracic Society. DiagnosticStandards and Classification of Tuberculosis inAdults and Children. Am J Respir Crit Care Med,2000;161:1376-95
10. Siddiqi K, Lambert M-L, Walley J. Clinicaldiagnosis of smear-negative pulmonarytuberculosis in low-income countries: thecurrent evidence. Lancet, 2003;3:288.
11. Pfyffer GE. Mycobacterium: General Characte-ristics, Laboratory Detection and StainingProcedures. In: Murray PR, Baron EJ, PfallerMA, Tenover FC, Yolken RH, editors. Manual ofClinical Microbiology, Volume 1, 9th ed.Washington: ASM Press, 2007:543 72.
12. Sakundarno M, Nurjazuli N, Jati SP, SariningdyahR, Purwadi S, Alisjahbana B, van der Werf MJ.Insufficient quality of sputum submitted fortuberculosis diagnosis and associated factors,in Klaten district, Indonesia. BMC PulmonaryMedicine, 2009;9(16): 1-11.
13. Nolte FS, Metchcock B. Mycobacterium. In:Murray PR, Baron EJ, Pfaller MA, Tenover FC,Yolken RH, editors. Manual of Clinical

78
TMJ Vol. 02 No. 1 66-79
Microbiology, 6th ed. Washington, D.C.: ASMPress, 1995:400-37.
14. Mutschler E. Arzneimittelwirkungen, 5 volligNeubearbeitete und Erweiterte Auflage.[Translate] Widianto MB, Ranti AS. DinamikaObat Buku Ajar Farmakologi dan Toksikologi.5thed. Bandung: ITB Press, 1999.
15. Malerba M, Ragnoli B. 2008. Ambroxol in The21st Century: Pharmacological and ClinicalUpdate. Expert Opin Drug Metab Toxicol2008;4(8):1119-29.
16. Seligman. Mucolytics. In: Kacmareck, Stoller,editors. Current Respiratory Care. Philadelphia:B.C. Decker, 1988:41-5.
17. Guyatt GH, Townsend M, Kazim F, NewhouseMT. A controlled trial of ambroxol in chronicbronchitis. Chest, 1987;92:618-20.
18. Disse B. Clinical evaluation of new therapiesfor treatment of mucus hypersecretion inrespiratory diseases. Ingelheim: NovartisFound Symp, 2002;248:254-82.
19. Gupta KB, Garg S. Use Of Sputum Induction ForEstablishing Diagnosis In Suspected PulmonaryTuberculosis. Indian J Tuberc, 2005;52:143-6.
20. Li LM, Bai LQ, Yang HL, Xiao CF, Tang RY, ChenYF, Chen SM, Liu SS, Zhang SN, Ou YH, Niu TIM.1999. Sputum induction to improve thediagnostic yield in patients with suspectedpulmonary tuberculosis. Int J Tuberc Lung Dis,1999;3(12):1137–9.
21. Kawada H, Suzuki N, Takeda Y, Takahata M,Suzuki T, Kobayashi N, Kudo K, Kabe J. 1996.The usefulness of induced sputum in thediagnosis of pulmonary tuberculosis. Kekkaku,1996;71(11):603-6.
22. Chang KC, Leung CC, Yew WW, Tam CM.Supervised and induced sputum amongpatients with smear-negative pulmonarytuberculosis. Eur Respir J, 2008;31(5):1085–90.
23. Parry CM, Kamoto O, Hurries AD, Wirima JJ,Nyirenda CM, Nyangulu DS, Hart CA. The useof sputum induction for establishing a diagnosisin patients with suspected pulmonarytuberculosis in Malawi. Tuberc Lung Dis,1995;76:72-6
24. Yue WY, Cohen SS. Sputum Induction by NewerInhalation Methods in Patients with PulmonaryTuberculosis. Chest, 1967;51:614-20.
25. Rogers DF. Mucoactive Agents for AirwayMucus Hypersecretory Diseases. RespiratoryCare, 2007;52(9):1176-97.
26. Harun SR, Putra ST, Wiharta AS, Chair I. Ujiklinis. In: Sastroasmoro S, Ismael S (Ed.): Dasar-Dasar Metodologi Penelitian Klinis. Jakarta:Sagung Seto, 2006; 144-64.
27. Cummings SR, Grady D, Hulley SB. Designing aRandomized Blinded Trial. In: Hulley SB,Cummings SR, Browner WS, Grady DG,Newman TB, editors. Designing Clinical Study,3rd ed. Philadelphia: Lippincott Williams &Wilkins, 2007:147-61.
28. Sharma MK. Role of Mucokinetics inRespiratory Medicine, 2008: Available from:URL:http://www.cdc.gov
29. Economidou F, Samara KD, Antoniou KM,Siafakas NM. Induced Sputum in InterstitialLung Diseases: Novel Insights in the Diagnosis,Evaluation and Study. Respiration,2009;77:351–8.
30. Fireman E. Induced Sputum as a DiagnosticTactic in Pulmonary Diseases.PulmonologyUpdate IMAJ, 2003;5:524-7.
31. Hasegawa I, Niisato N, Iwasaki Y, Marunaka Y.Ambroxol-induced modification of iontransport in human airway Calu-3 epithelia.Biochem Biophys Res Commun, 2006;343:475-82.
32. Sobiecka M, Kus J, Demkow U, Filewska M,Jozwik A, Rohrenschef PR, Wynimko JC.Induced Sputum In Patients With InterstitialLung Disease: A Non- Invasive Surrogate ForCertain Parameters In Bronchoalveolar LavageFluid. J Physiol Pharmacol, 2008;59(6Suppl):645-57.
33. Rubin BK. Mucolytics, Expectorants andMucokinetic Medications. Respiratory Care,2007;52(7):859-64.
34. Rubin BK. The Role of Mucus in Cough Study.Lung, 2009;188(Suppl 1):S69–S72.

79
Sunarto Ang., Mucolitic Ambroxol Versus Hypertonic Saline Nebulizer Induction:
For Increasing Sputum Volume And Finding Acid-Fast Bacilli
35. Rogers DF. Airway Clearance: Physiology,Pharmacology, Techniques, and Practice. The39th Respiratory Care Journal Conference.Cancu´n, 2007 April 21–23.
36. Garcia SB, Perin C, da Silveira MM, Vergani G,Menna-Barreto SS, Dalcin PTR. 2009.Bacteriological analysis of induced sputum forthe diagnosis of pulmonary tuberculosis in theclinical practice of a general tertiary hospital.Am J Respir Crit Care Med, 2009;179:A2600.
37. Gupta KB, Garg S. Sputum induction - A usefultool in diagnosis of respiratory diseases. LungIndia, 2006;23:82-6.
38. Nightingale JA, Rogers DF, Barnes PJ. Effect ofrepeated sputum induction on cell counts innormal volunteers. Thorax, 1998;53:87-90.
39. Holz O, Richter K, Jörres RA, Speckin P, MückeM, Magnussen H. Changes in sputumcomposition between two inductionsperformed on consecutive days. Thorax,1998;53:83-86.
40. Purokivi M, Randell J, Hirvonen M-R, TukiainenH. Reproducibility of measurements of exhaledNO, and cell count and cytokine concentrationsin induced sputum. Eur Respir J, 2000;16:242-6.
41. Um SW, Choi CM, Lee CT, Kim YW, Han SK, ShimYS, Yoo CG. Prospective Analysis of ClinicalCharacteristics and Risk Factors of Post-bronchoscopy Fever. Chest, 2004; 125(3):945-52.
42. Zahrani KA, Jahdali HA, Poirier L, Rene P,Menzies D. Yield of smear, culture andamplification tests from repeated sputuminduction for the diagnosis of pulmonarytuberculosis. Int J Tuberc Lung Dis, 2001;5: 855-60.
43. Alexis NE, Hu SC, Zemen KAT, Bennett WD.2001. Induced sputum derives from the centralairways. Am J Respir Crit Care Med, 2001;164:1964–70.
44. Huq F. Molecular modelling analysis of themetabolism of ambroxol. J. Pharmacol Toxicol,2008;3(2):147-52.
45. Williams TM, Wells AU, Harrison AC, LindstromS, Cameron RJ, Forkin E. Induced sputum andbronchoscopy in the diagnosis of pulmonarytuberculosis. Thorax, 2002; 57:1010-14.
46. Brown M, Varia H, Bassett P, Davidson RN, WallR, Pasvol G. Prospective Study of SputumInduction, Gastric Washing, andBronchoalveolar Lavage for the Diagnosis ofPulmonary Tuberculosis in Patients Who AreUnable to Expectorate. Clin Infect Dis,2007;44:1415–20.
47. Uskul BT, Turker HT, Kant A, Partal M.Comparison of Bronchoscopic Washing andGastric Lavage in the Diagnosis of Smear-Negative Pulmonary Tuberculosis. TheSouthern Medical Association,2009;102(2):154-8.
48. Andersen C, Inhaber N, Menzies D. Comparisonof sputum induction with fiberopticbronchoscopy in the diagnoses of tuberculosis.Am J Respir Crit Care Med, 1995;152:1570-4.
49. Merrick ST, Sepkowitz KA, Walsh J, Damson L,McKinley P, Jacobs JL. Comparison of inducedversus expectorated sputum for diagnosis ofpulmonary tuberculosis by acid-fast smear. AmJ Infect Control, 1997;25:463-6.
50. Conde MB, Soares SLM, Mello FCQ, RezendeVM, Almeida LL, Reingold AL, Daley CL, KritskiAL. Comparison of Sputum Induction withFiberoptic Bronchoscopy in the Diagnosis ofTuberculosis: Experience at an AcquiredImmune Deficiency Syndrome Refence Centerin Rio de Janeiro, Brazil. Am J Respir Crit CareMed, 2000;162:2238–40.
51. Hartung IK, Maulu A, Nash J, Fredlund VG.Suspected pulmonary tuberculosis in ruralSouth Africa – sputum induction as a simplediagnostic tool? S Afr Med J, 2002;92:455-8.