Community Health Needs Assessment: Emmons County
84
1
-
Upload
academyadmissions -
Category
Documents
-
view
0 -
download
0
Transcript of Community Health Needs Assessment: Emmons County

1

2
Table of Contents Executive Summary .......................................................................................................................... 3
Linton Hospital & Clinics ................................................................................................................... 5
Emmons County Public Health ......................................................................................................... 7
Community Resources ...................................................................................................................... 8
Assessment Process .......................................................................................................................... 9
Demographic Information ................................................................................................................ 14
Health Conditions, Behaviors, and Outcomes .................................................................................. 15
Survey Results .................................................................................................................................. 23
Preventative Care and Public Health Services .................................................................................. 42
Findings of Key Informant Interviews and Focus Group ................................................................... 46
Priority of Health Needs ................................................................................................................... 49
Appendix A – Survey Instruments .................................................................................................... 51
Appendix B – County Health Rankings Model .................................................................................. 68
Appendix C – Emmons County Community Profile .......................................................................... 69
Appendix D – Prioritization of Community’s Health Needs .............................................................. 81
Appendix E—Strategic Plan Notes………………………………….………………………………………………… ………….82

3
Executive Summary To help inform future decisions and strategic planning, Linton Hospital & Clinics in Linton, N.D., along with Emmons County Public Health conducted a community health needs assessment in Emmons County. The Center for Rural Health at the University of North Dakota School of Medicine and Health Sciences facilitated the assessment which included the solicitation of input from area community members and health care professionals as well as analysis of community health-‐related data.
To gather feedback from the community, residents of the health care service area and local health care professionals were given the chance to participate in a survey. Additional information was collected through a Community Group comprised of community members and through key informant interviews with community leaders.
The study took into account input from approximately 131 community members and health care professionals from Emmons County as well as 14 community leaders. This input represented the broad interests of the community served by Linton Hospital & Clinics and Emmons County Public Health. Together with secondary data gathered from a wide range of sources, the information gathered presents a snapshot of health needs and concerns in the community.
Approximately 28% of the population of Emmons County is over age 65. This percentage is double the rate for the rest of North Dakota. In addition, Emmons County has a higher percentage of those individuals over age 65 living alone than either the North Dakota or U.S. averages. Additionally, the median age for Emmons County residents is 50.5, compared to a state median age of 36.9. This likely indicates an increased need for medical services to attend to an aging population. The median household income in Emmons County is significantly lower than for the rest of North Dakota -‐ $31,852 compared to $46,050. The average household size for Emmons County is 2.29 individuals.
The data compiled by County Health Rankings show that with respect to health outcomes, Emmons County was generally faring favorably when compared to the rest of North Dakota, with lower rates of self-‐reported poor physical health days. An examination of health factors, which include health behaviors, clinical care measures, and physical environment, revealed several patterns in the region. Rates of obesity, physical inactivity and access to exercise opportunities were all concerning. Emmons County was performing worse than the state average with respect to ratios of residents to primary care physicians and mental health care providers. Additionally, the number of preventable hospital stays was significantly higher than the state average.
In terms of social and economic factors, several trends stood out for Emmons County. The level of unemployment, the number of children living in poverty and the percentage of those with inadequate social support were all higher than state averages. Relatedly, the percent of those experiencing severe housing problems was also higher.
4
On the positive side, Emmons County placed within the top 10% of counties nationally on the measures of the adult smoking, diabetic screening and violent crime. Emmons County was beating state averages for the number of days residents self-‐reported poor or fair health and poor physical health days. Plus, the County had lower rates of excessive drinking and considerably lower rates of sexually transmitted infections.
Results from the survey revealed that among community members and health care professionals the top five community health concerns were: (1) cost of health insurance, (2) not enough jobs with livable wages, (3) attracting and retaining young families, (4) ability to retain doctors and nurses in the community, and (5) adequacy of health insurance.
The survey also revealed generally good awareness of locally available health care services and that residents choose to receive care locally due to convenience, proximity, familiarity with providers, and because Linton Hospital takes their insurance. Residents travel out of the area for service primarily for access to necessary specialists and because of perceived high quality care.
Input from Community Group members and community leaders provided via a focus group and key informant interviews echoed many of the concerns raised by survey respondents. Thematic concerns emerging from these sessions were (1) meeting mental health needs, (2) increasing activities for youth, (3) inadequate number of jobs with livable wages and affordable housing, (4) attracting and retaining health care staff, and (5) availability of resources to help elderly stay in their homes.
Following careful consideration of the results and findings of this assessment, Community Group members determined that the top health needs or issues in the community are the limited number of primary care physicians, lack of licensed child care capacity and not enough emphasis on wellness and healthy lifestyles.

5
Overview Linton Hospital & Cl inics Opened in 1953, Linton Hospital & Clinics is one of the most important assets in the community and the largest charitable organization in the Linton area. Linton Hospital includes a 14-‐bed, critical access hospital located in Linton. As a hospital and designated level V trauma center, the hospital provides comprehensive care for a wide range of medical and emergency situations. Linton Hospital also has four rural affiliated health clinics which offer health services to residents of Emmons County, N.D. as well as Campbell County, S.D. Linton Hospital provides comprehensive medical care with physician and mid-‐level medical providers and consulting/visiting medical providers. With nearly 100 employees, Linton Hospital is the largest employer in the region. It has 1 part-‐time physician, 3 physician assistants, 5 certified nursing assistants, and 8 nurses for a combined total of 17 health care providers.
A 2009 economic impact study estimated that Linton Hospital had a total economic impact on Emmons County of approximately $3 million.
Linton Hospital & Clinics defines its mission as follows: “To enhance the health, well-‐being, and quality of life of the people we serve.”
Services offered locally by Linton Hospital & Clinics include:
General and Acute Services
• Cardiology (visiting physician) • Clinic • Emergency room • Gynecology (visiting physician) • Hospital (acute care)
• Independent senior housing • Nutrition counseling • Obstetrics (visiting physician) • Orthopedics (visiting physician) • Pharmacy • Podiatry – evaluation and surgery • Swing bed services

6
Surgical Services • Cataracts • Cystoscopy • Biopsy • Hernia repair
• Carpal tunnel release • Hysterectomy • Hemorrhoid repair
Screening/Therapy Services
• Chiropractic services • Chronic disease
management • Holter monitoring • Laboratory services • Lower extremity
circulatory assessment • Massage therapy
• Occupational physicals • Occupational therapy • Pediatric services • Physical therapy • Respiratory care • Sleep studies • Social services
Radiology Services
• CT scan • Digital mammography • Electrocardiograms
• General x-‐ray • MRI (mobile unit) • Ultrasound (mobile unit)
Laboratory
• Hematology • Blood types • Clot times
• Chemistry • Urine testing
Additionally, other services offered locally by other providers include:
• Ambulance • Chiropractic care
• Dental care
_____________________________________________________________________________________________ Community Health Needs Assessment 7
Emmons County Public Health Emmons County Public Health provides public health services that include environmental health, nursing services, the WIC (women, infants and children) program, health screenings and education services. Each of these programs provides a wide variety of services in order to accomplish the mission of public health, which is to assure that North Dakota is a healthy place to live and each person has an equal opportunity to enjoy good health. To accomplish this mission, Emmons County Public Health is committed to the promotion of healthy lifestyles, protection and enhancement of the environment, and provision of quality health care services for the people of North Dakota.
Specific services provided by Emmons County Public Health are:
• Bicycle helmet safety education • Blood pressure checks • Breastfeeding resources—newborn home visits or in office consultation • Car seat program • Child health (well baby checks) • Coordinator for University of Mary Leadership Team • Diabetes screening-‐-‐ at monthly Senior Citizen clinics & in office, anytime. • Emergency Preparedness services • Environmental Health Services (water, sewer, health hazard abatement) • Flu shots • Health Fair activity for KEM Electric Coop • Health Tracks (child health screening) • Home health-‐-‐ In-‐Home Nursing Care • Immunizations-‐-‐ for infants and children through age 18. • Member of Child Protection Team and County Interagency Team • Newborn Home Visits • School health-‐-‐ vision, hearing, scoliosis screenings & health education • Preschool education programs • Assistance with preschool screening • Tobacco Prevention and Control • Tuberculosis testing and management • West Nile program—surveillance and education • WIC (Women, Infants & Children) Program • Worksite Wellness-‐-‐ Coordinator for County Employees & Sheriff’s Dept. • Youth education programs (first aid, bike safety)

8
Community Resources
Linton is located in south central North Dakota, approximately 65 miles southeast of Bismarck, the state’s capital, and 25 miles north of the South Dakota border. Along with the hospital, agricultural operations provide the economic base for Linton and Emmons County. According to the 2010 U.S. Census, Emmons County had a population of 3,550, while the city of Linton had a population of 1,097. Linton has a number of community assets and resources that can be mobilized to address population health improvement. In terms of physical assets and features, the community includes a swimming pool, tennis courts, a golf course, and a baseball/softball diamond. To the north of Linton, Appert Lake National Wildlife Refuge and Long Lake National Refuge offer excellent birding and fishing opportunities. The Missouri River is within a short drive of Linton and offers boating, fishing, swimming and camping. The area’s terrain is suitable for cross country skiing, snowmobiling, and hunting. Pheasant, grouse, turkey, antelope, and deer abound in the area, as well as a variety of raptors, waterfowl, and songbirds. Other community assets include Tae Kwan Do program and a fitness center. The Emmons County school system offers a comprehensive program for students K-‐12. Other health care facilities and services in the area include a pharmacy. The Emmons County Public Health Department is located on the hospital campus.
9
Assessment Process The purpose of conducting a community health needs assessment is to describe the health of local people, identify areas for health improvement, identify use of local health care services, determine factors that contribute to health issues, identify and prioritize community needs, and help health care leaders identify potential action to address the community’s health needs. A health needs assessment benefits the community by:
1) Collecting timely input from the local community, providers, and staff; 2) Providing an analysis of secondary data related to health-‐related behaviors, conditions, risks, and outcomes; 3) Compiling and organizing information to guide decision making, education, and marketing efforts, and to facilitate the development of a strategic plan; 4) Engaging community members about the future of health care; and 5) Allowing the community hospital to meet federal regulatory requirements of the Affordable Care Act, which requires not-‐for-‐profit hospitals to complete a community health needs assessment at least every three years, as well as helping the local public health unit meet accreditation requirements. This assessment examines health needs and concerns in Emmons County. In addition to Linton, located in the county are the communities of Hazelton, Moffit, Strasburg, and Westfield.
Figure 1: Emmons County, North Dakota
The assessment process was highly collaborative. Administrators and other professionals from both Linton Hospital & Clinics and Emmons County Public Health were considerably involved in planning and implementing the process. Along with representatives from the Center for Rural Health, they met regularly by telephone conference and via email. The Community Group (described in more detail below) provided in-‐depth information and informed the assessment in terms of community perceptions, community resources, community needs, and ideas for improving the health of the population and health care services. Representatives from both Linton
10
Hospital & Clinics and Emmons County Public Health were heavily involved in planning the Community Group meetings. The Community Group was comprised of many residents from outside the hospital and health department, including representatives from local government, businesses, and social services.
The survey instrument was developed out of a collaborative effort that took into account input from health organizations around the state. The North Dakota Department of Health’s public health liaison organized a series of meetings that garnered input from the state’s health officer, local public health unit professionals from around North Dakota, representatives of the Center for Rural Health, and representatives from North Dakota State University.
As part of the assessment’s overall collaborative process, the Center for Rural Health spearheaded efforts to collect data for the assessment in a variety of ways:
(1) A survey solicited feedback from area residents, including health care
professionals who work at Linton Hospital & Clinics, Emmons County Public Health, and other health organizations;
(2) Community leaders representing the broad interests of the community took part in one-‐on-‐one key informant interviews;
(3) The Community Group comprised of community leaders and area residents was convened to discuss area health needs and inform the assessment process; and
(4) A wide range of secondary sources of data was examined, providing information on a multitude of measures including demographics; health conditions, indicators, and outcomes; rates of preventive measures; rates of disease; and at-‐risk behavior.
The Center for Rural Health provided substantial support to Linton Hospital & Clinics and Emmons County Public Health in conducting this needs assessment. The Center for Rural Health’s involvement was funded partially through its Medicare Rural Hospital Flexibility (Flex) Program. The Flex Program is federally funded by the Office of Rural Health Policy, part of the Health Resources and Services Administration.
The Center for Rural Health is one of the nation’s most experienced organizations committed to providing leadership in rural health. Its mission is to connect resources and knowledge to strengthen the health of people in rural communities. As the federally designated State Office of Rural Health (SORH) for the state and the home to the North Dakota Medicare Rural Hospital Flexibility (Flex) program, the Center connects the School of Medicine and Health Sciences and the university to rural communities and their health institutions to facilitate developing and maintaining rural health delivery systems. In this capacity the Center works both at a national level and at state and community levels.
Detailed below are the methods undertaken to gather data for this assessment by convening a Community Group, conducting key informant interviews, soliciting feedback about health needs via a survey, and researching secondary data.

11
Community Group A Community Group consisting of 7 community members was convened and first met on May 21, 2014. During this first Community Group meeting, group members were introduced to the needs assessment process, reviewed basic demographic information about Emmons County, and served as a focus group. Focus group topics included community assets and challenges, the general health needs of the community, community concerns, and suggestions for improving the community’s health.
The Community Group met again on July 29, 2014 with 9 community members attending. At this second meeting the Community Group was presented with survey results, findings from key informant interviews and the focus group, and a wide range of secondary data relating to the general health of the population in Emmons County. The group was then tasked with identifying and prioritizing the community’s health needs.
Members of the Community Group represented the broad interests of the community served by Linton Hospital and Emmons County Public Health. They included representatives of the health community, business community, political bodies, law enforcement, education, faith community, and social service agencies. Not all members of the group were present at both meetings.
Interviews One-‐on-‐one interviews with eight key informants were conducted in person in Linton on May 22, 2014. A representative from the Center for Rural Health conducted the interviews. Interviews were held with selected members of the Community Group as well as other key informants who could provide insights into the community’s health needs. Included among the informants were public health professionals with special knowledge in public health acquired through several years of direct experience in the community, including working with medically underserved, low income, and minority populations, as well as with populations with chronic diseases.
Topics covered during the interviews included the general health needs of the community, the general health of the community, community concerns, delivery of health care by local providers, awareness of health services offered locally, barriers to receiving health services, and suggestions for improving collaboration within the community.
Survey A survey was distributed to gather feedback from the community. The survey was not intended to be a scientific or statistically valid sampling of the population. Rather, it was designed to be an additional tool for collecting qualitative data from the community at large – specifically, information related to community-‐perceived health needs.
Two versions of a survey tool were distributed to two different audiences: (1) community members and (2) health care professionals. Copies of both survey instruments are included in Appendix A.
12
Community Member Survey
The community member survey was distributed to various residents of Emmons County. The survey tool was designed to:
• Learn of the good things in the community and the community’s concerns; • Understand perceptions and attitudes about the health of the community, and
hear suggestions for improvement; and • Learn more about how local health services are used by residents.
Specifically, the survey covered the following topics: residents’ perceptions about community assets, levels of collaboration within the community, broad areas of community and health concerns, need for health services, concerns about the delivery of health care in the community, barriers to using local health care, preferences for using local health care versus traveling to other facilities, travel time to a clinic and hospital, use of preventive care, use of public health services, suggestions to improve community health, and basic demographic information.
Approximately 700 community member surveys were available for distribution in Emmons County. The surveys were distributed by Community Group members and were available at Linton Hospital & Clinics, Emmons County Public Health, WIC, the fitness center, banks, a coffee house, the courthouse, the newspaper office, and area business offices. To help ensure anonymity, included with each survey was a postage-‐paid return envelope to the Center for Rural Health. In addition, to help make the survey as widely available as possible, residents also could request a survey by calling Linton Hospital or Emmons County Public Health. The survey period ran from May 21-‐ June 20, 2014. Community members completed 118 surveys.
Area residents also were given the option of completing an online version of the survey, which was publicized in the local newspaper and by Linton Hospital & Clinics and Emmons County Public Health. Eight online surveys were completed. In total, counting both paper and online surveys, 126 community member surveys were completed.
Health Care Professional Survey
Employees of Linton Hospital & Clinics and Emmons County Public Health as well as other local health-‐related organizations were encouraged to complete a version of the survey geared to health care professionals. This health care professional version of the survey was administered online only, and five surveys were completed. The version of the survey for health care professionals covered the same topics as the consumer survey, although it sought less demographic information.
Because a number of health care professionals apparently took the version of the survey intended for community members, the results from both survey versions are being reported in the aggregate only. All results thus reflect the impressions of both community members and health care professionals, although it will not be clear where differences may have existed between the perceptions of community members versus health care professionals. Because only the community member version requested information about employment status, household income, travel times to the hospital
13
and clinic, health status, and health insurance status, results relating to those characteristics should not be compared to the survey totals. They are reported for informational purposes. Counting both versions of the surveys, 131 surveys were completed, equating to a 19% response rate.
Secondary Data Secondary data was collected and analyzed to provide descriptions of: (1) population demographics, (2) general health issues (including any population groups with particular health issues), and (3) contributing causes of community health issues. Data were collected from a variety of sources including the U.S. Census Bureau; the North Dakota Department of Health; the Robert Wood Johnson Foundation’s County Health Rankings (which pulls data from 15 primary data sources); the National Survey of Children’s Health Data Resource Center; the Centers for Disease Control and Prevention; the North Dakota Behavioral Risk Factor Surveillance System; and the National Center for Health Statistics.

14
Demographic Information Table 1 summarizes general demographic and geographic data about Emmons County.
TABLE 1: EMMONS COUNTY INFORMATION AND DEMOGRAPHICS (From 2010 Census/2012 American Community Survey; more recent estimates used where available)
Emmons County North Dakota
Population, 2013 est. 3,486 723,393 Population change, 2010-‐2012 -‐1.8% 7.6% Land area, square miles 1,510 69,001 People per square mile, 2010 2.4 9.7 White persons (not incl. Hispanic/Latino), 2012 est.
98.3% 88.1%
Persons under 18 years, 2012 est. 20.3% 22.1% Persons 65 years or older 27.3% 14.4% Median age 50.5 36.9 Non-‐English spoken at home, 2012 est. 8.9% 5.2% High school graduates, 2012 est. 81.1% 90.5% Bachelor’s degree or higher, 2012 est. 15.0% 27.1% Live below poverty line, 2012 est. 14.7% 12.1%
While the population of North Dakota has grown in recent years, Emmons County has seen a slight decrease in population since 2010, with community members stating it is stabilizing. Demographic information and trends that have implications for the community’s health and the delivery of health care include:
• A rate of people aged 65 and older that is nearly twice the state average indicates an increased need for health care services.
• A rate of residents with at least a bachelor’s degree that is well below the state rate may have health care workforce implications.
• A very low population density, meaning emergency medical services face challenges in responding to emergencies with a population that is dispersed over a large area.

15
Health Condit ions, Behaviors, and Outcomes
As noted above, several sources of secondary data were reviewed to inform this assessment. This data are presented below in three categories: (1) County Health Rankings, (2) the public health community profile, and (3) children’s health.
County Health Rankings
The Robert Wood Johnson Foundation, in collaboration with the University of Wisconsin Population Health Institute, has developed County Health Rankings to illustrate community health needs and provide guidance for actions toward improved health. In this report, Emmons County is compared to North Dakota rates and national benchmarks on various topics ranging from individual health behaviors to the quality of health care.
The data used in the 2014 County Health Rankings are pulled from more than 20 data sources and then are compiled to create county rankings. Counties in each of the 50 states are ranked according to summaries of a variety of health measures. Those having high ranks, such as 1 or 2, are considered to be the “healthiest.” Counties are ranked on both health outcomes and health factors. Below is a breakdown of the variables that influence a county’s rank. A model of the 2014 County Health Rankings – a flow chart of how a county’s rank is determined – may be found in Appendix B. For further information, visit the County Health Rankings website at www.countyhealthrankings.org.
Health Outcomes • Length of life • Quality of life
Health Factors • Health Behavior
o Smoking o Diet and exercise o Alcohol and drug use o Sexual activity
• Clinical Care o Access to care o Quality of care
Health Factors (continued) • Social and Economic Factors
o Education o Employment o Income o Family and social support o Community safety
• Physical Environment o Air and water quality o Housing and transit
Table 2 summarizes the pertinent information gathered by County Health Rankings as it relates to Emmons County. It is important to note that these statistics describe the population of a county, regardless of where county residents choose to receive their medical care. In other words, all of the following statistics are based on the health

16
behaviors and conditions of the county’s residents, not necessarily the patients and clients of Linton Hospital and Emmons County Public Health
For most of the measures included in the rankings, the County Health Rankings’ authors have calculated the “Top U.S. Performers” for 2014. The Top Performer number marks the point at which only 10% of counties in the nation do better, i.e., the 90th percentile or 10th percentile, depending on whether the measure is framed positively (such as high school graduation) or negatively (such as adult smoking).
Emmons County’s ranking also is included in the summary below. For example, Emmons County ranks 29th out of 45 ranked counties in North Dakota on health outcomes and 35th on health factors. The results listed below in red are areas where Emmons County is not measuring up to the state average (and, by extension, on most measures the Top U.S. Performers); the variables listed in blue indicate that the county is faring better than the North Dakota average, but may not be meeting the Top U.S. Performer rate on that measure.
TABLE 2: SELECTED MEASURES FROM COUNTY HEALTH RANKINGS – EMMONS COUNTY
Emmons County
U.S. Top 10%
North Dakota
Ranking: Outcomes 29th (of 45) Premature death 7,473 5,317 6,244 Poor or fair health 11% 10% 12% Poor physical health days (in past 30 days) 2.5 J 2.5 2.7 Poor mental health days (in past 30 days) 2.6 2.4 2.4 % Diabetic 11% -‐ 8%
Ranking: Factors 35th (of 45) Health Behaviors
Adult smoking 12% J 14% 18% Adult obesity 33% 25% 30% Food environment index (10 is best) 7.8 8.7 8.7 Physical inactivity 33% 21% 26% Access to exercise opportunities 37% 85% 62% Excessive drinking 19% 10% 22% Sexually transmitted infections 141 123 358 Teen birth rate N/A 20 28
Clinical Care Uninsured 17% 11% 12% Primary care physicians 1,7731:1 1,051:1 1,320:1 Dentists 3,547:1 1,439:1 1,813:1 Mental health providers N/A 536:1 1,071:1 Preventable hospital stays 78 46 59 Diabetic screening 91% J 90% 86% Mammography screening 69% 71% 68%
Social and Economic Factors

17
Unemployment 5.9% 4.4% 3.1% Children in Poverty 18% 13% 14% Inadequate social support 26% 14% 16% Children in single-‐parent households 21% 20% 26% Violent crime 24 J 64 226
Physical Environment Air pollution – particulate matter 9.7 9.5 10.0 Drinking water violations 0% J 0% 1% Severe housing problems 12% 9% 11%
The data from County Health Rankings show that Emmons County is doing well as compared to the rest of North Dakota on measures of health outcomes, even exceeding the top 10% of counties nationally of some measures of behavioral, social and physical health. Measures that deserve boasting about are:
• Low levels of adult smoking • Low levels of STIs • High levels of diabetic screening • Low crime • Good air and water quality
However, Emmons County is faring worse than other North Dakota Counties on many measures. Emmons County lags the state on premature deaths, poor mental health days and children living in poverty.
Some of the measures are particularly concerning:
• Physical inactivity rate – more than 7 points higher than state rate • Access to exercise opportunities—almost half the state rate • Preventable hospital stays—19 points higher than state rate • Inadequate social & emotional support—10 points higher than state rate
Trends In addition to the reported rates and levels of some of these measures, also concerning are the trends indicating that several measures are rapidly getting worse. For example, as shown in Figure 2, the adult obesity rate has increased considerably since 2008 and at a rate of increase higher than the state and national averages.

18
Figure 2 – Rising rate of adult obesity in Emmons County
Although the rate of sexually transmitted infections is much lower in Emmons County it is important to monitor this measure as it has had a noticeable increase since 2010, as shown in Figure 3.
Figure 3 – Rising rate of sexually transmitted infections in Emmons County
While North Dakota leads the nation with the lowest unemployment rates, Emmons County has higher levels of unemployment, although levels do seem to be lowering in recent years. Results are shown in Figure 4.

19
Figure 4 – Rising rate of unemployment in Emmons County
Similarly, the number of children living in poverty is trending upward, as shown in Figure 5. Figure 5 – Rising rate of children living in poverty in Emmons County
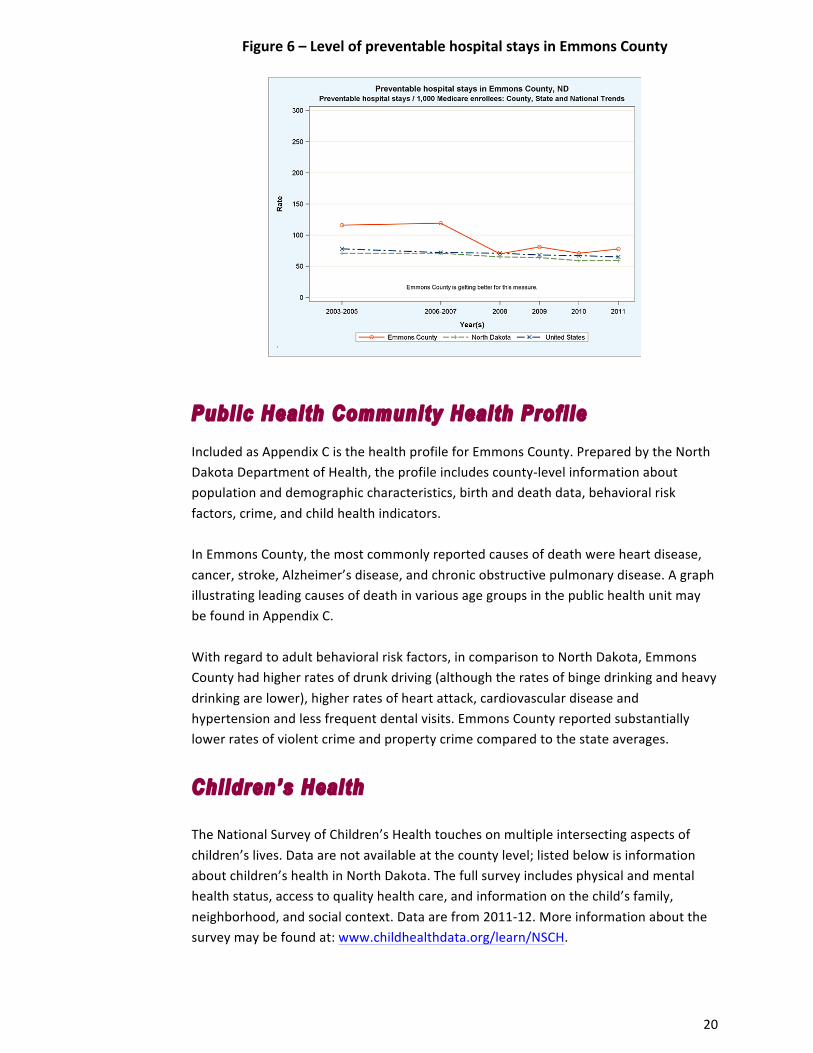
On a positive note, even though Emmons County exceeds the state rate of preventable hospital stays, within the last decade this level has shown some improvement. This factor measures the number of patients being hospitalized for conditions that may be amenable to outpatient care. Thus, it may suggest a tendency to overuse the hospital as a main source of care. This positive trend is illustrated in Figure 6.
20
Figure 6 – Level of preventable hospital stays in Emmons County
Public Health Community Health Profi le Included as Appendix C is the health profile for Emmons County. Prepared by the North Dakota Department of Health, the profile includes county-‐level information about population and demographic characteristics, birth and death data, behavioral risk factors, crime, and child health indicators. In Emmons County, the most commonly reported causes of death were heart disease, cancer, stroke, Alzheimer’s disease, and chronic obstructive pulmonary disease. A graph illustrating leading causes of death in various age groups in the public health unit may be found in Appendix C. With regard to adult behavioral risk factors, in comparison to North Dakota, Emmons County had higher rates of drunk driving (although the rates of binge drinking and heavy drinking are lower), higher rates of heart attack, cardiovascular disease and hypertension and less frequent dental visits. Emmons County reported substantially lower rates of violent crime and property crime compared to the state averages.
Chi ldren’s Health The National Survey of Children’s Health touches on multiple intersecting aspects of children’s lives. Data are not available at the county level; listed below is information about children’s health in North Dakota. The full survey includes physical and mental health status, access to quality health care, and information on the child’s family, neighborhood, and social context. Data are from 2011-‐12. More information about the survey may be found at: www.childhealthdata.org/learn/NSCH.

21
Key measures of the statewide data are summarized below. The rates highlighted in red signify that the state is faring worse on that measure than the national average.
TABLE 4: SELECTED MEASURES REGARDING CHILDREN’S HEALTH
(For children aged 0-‐17 unless noted otherwise) Health Status North Dakota National
Children born premature (3 or more weeks early) 10.8% 11.6% Children 10-‐17 overweight or obese 35.8% 31.3% Children 0-‐5 who were ever breastfed 79.4% 79.2% Children 6-‐17 who missed 11 or more days of school 4.6% 6.2%
Health Care Children currently insured 93.5% 94.5% Children who had preventive medical visit in past year 78.6% 84.4% Children who had preventive dental visit in past year 74.6% 77.2% Young children (10 mos.-‐5 yrs.) receiving standardized screening for developmental or behavioral problems
20.7% 30.8%
Children aged 2-‐17 with problems requiring counseling who received needed mental health care
86.3% 61.0%
Family Life Children whose families eat meals together 4 or more times per week 83.0% 78.4%
Children who live in households where someone smokes 29.8% 24.1% Neighborhood
Children who live in neighborhood with a park, sidewalks, a library, and a community center
58.9% 54.1%
Children living in neighborhoods with poorly kept or rundown housing
12.7% 16.2%
Children living in neighborhood that’s usually or always safe 94.0% 86.6%
The data on children’s health and conditions reveals that while North Dakota is doing better than the national averages on a few measures, it is not measuring up to the national averages with respect to:
• Obese or overweight children • Children with health insurance • Preventive primary care and dentist visits • Developmental/behavioral screening • Children in smoking households
Importantly, more than one in five of the state’s children are not receiving an annual preventive medical visit or a preventive dental visit. Lack of preventive care now affects these children’s future health status.
Table 5 includes selected county-‐level measures regarding children’s health in North Dakota. The data come from North Dakota KIDS COUNT, a national and state-‐by-‐state effort to track the status of children, sponsored by the Annie E. Casey Foundation. KIDS COUNT data focus on main components of children’s well-‐being; more information about KIDS COUNT is available at www.ndkidscount.org. The measures highlighted in

22
red in the table are those on which Emmons County is doing worse than the state average. The year of the most recent data is noted.
The data show that Emmons County is underperforming compared to state averages on many measures. The most marked differences were on the measures of: Uninsured children (with a county rate more than twice the state rate); uninsured children in households below the 200% poverty rate; children enrolled in Health Steps, North Dakota’s Children’s Health Insurance Program (CHIP); and availability of licensed child daycare.
TABLE 5: COUNTY-‐LEVEL MEASURES REGARDING CHILDREN’S HEALTH
Emmons County North Dakota
Uninsured children (% of population age 0-‐18), 2010 14.8% 6.1% Uninsured children below 200% of poverty (% of population), 2010 69.6% 59.6%
Medicaid recipient (% of population age 0-‐20), 2012 19.2% 28.3% Children enrolled in Healthy Steps (% of population age 0-‐18), 2013 9.7% 2.5%
Supplemental Nutrition Assistance Program (SNAP) recipients (% of population age 0-‐18), 2012 14.3% 23.9%
Licensed child care capacity (% of population age 0-‐13), 2013 18.3% 40.2%
High school dropouts (% of grade 9-‐12 enrollment), 2012 0.0% 2.2%

23
Survey Results Survey Demographics To better understand the perspectives being offered by survey respondents, survey-‐takers were asked a few demographic questions. Throughout this report, numbers (N) instead of percentages (%) are reported because percentages can be misleading with smaller numbers. The total number of surveys completed by both community members and health care professionals was 131 (N=131). Survey respondents were not required to answer all survey questions; they were free to skip any questions they wished. With respect to demographics of those who chose to take the survey:
• More than half (N=69) were aged 55 or older, with a quarter (N=30) aged 75 years or older;
• A large majority (N=91) were female; • A quarter (N=29) had some college or technical degrees, a quarter (N=25) had a
high school diploma or GED and another quarter (N=28) had a bachelor’s degree;
• Most (N=59) worked full-‐time, with a substantial number (N=36) also retired; and
• A majority of respondents (N=47) had household incomes between $25,000 to $74,999.
Figure 7 shows these demographic characteristics. It illustrates the wide range of community members’ household income and indicates how this assessment took into account input from parties who represent the broad interests of the community served, including wide age ranges, those in varying work situations, and lower-‐income community members. Of those who provided a household income, 19 community members reported a household income of less than $25,000, with 10 of those indicating a household income of less than $15,000.
Figure 7: Demographics of Survey-‐Takers
4 12
9
21
21
18
30
Age Less than 25 years
25 to 34 years
35 to 44 years
45 to 54 years
55 to 64 years
65 to 74 years
75 years and older

24
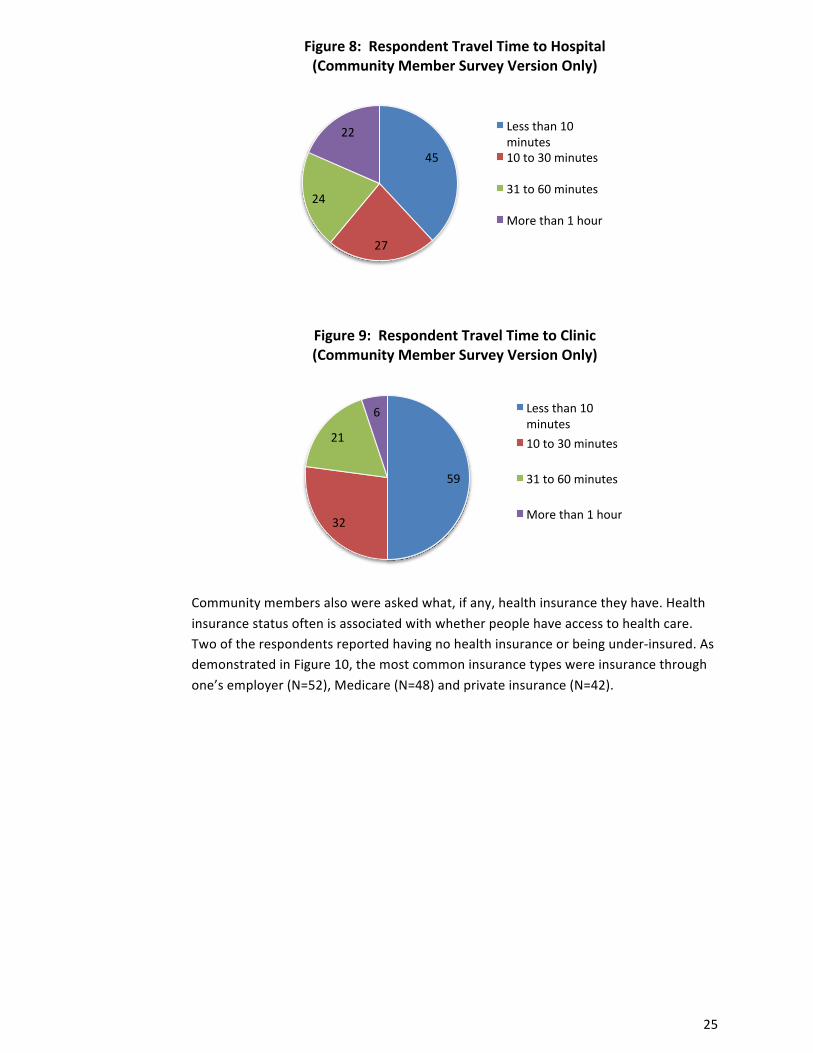
Health Care Access Community members were asked how far they lived from the hospital and clinic they usually go to. A large plurality (N=45) reported living within 10 miles of the hospital they usually go to, while 22 respondents indicated they live more than an hour from the hospital they usually go to. Driving distances, along with lack of transportation options, can have a major effect on access to health care services, especially in winter when weather conditions lead to hazardous driving conditions. With respect to distance to respondents’ clinic of choice, a majority (N=59) said they lived less than 10 minutes from the clinic. Six reported driving more than an hour to the clinic they usually go to. Figures 8 and 9 illustrate these results.
56 12 1 2
2
21
Employment Status (Community Member Version Only)
Full pme
Part pme
Homemaker
Mulpple job holder
Unemployed
Repred
10 9
26
21
15
9
4 13
Household Income (Community Member Version Only)
$0 to $14,999
$15,000 to $24,999
$25,000 to $49,999
$50,000 to $74,999
$75,000 to $99,999
$100,000 to $149,999
$150,000 and over
Prefer not to answer
6
25
29 16
28
8
Educabon Level (Community Member Vesion Only)
Some high school
High school diploma or GED Some college/technical degree Associate's degree
Bachelor's degree
Graduate or professional degree
59
10 7
1
1
36
Employment Status (Community Member Vesion Only)
Full pme
Part pme
Homemaker
Mulpple job holder
Unemployed
Repred
25
Figure 8: Respondent Travel Time to Hospital (Community Member Survey Version Only)
Figure 9: Respondent Travel Time to Clinic (Community Member Survey Version Only)
Community members also were asked what, if any, health insurance they have. Health insurance status often is associated with whether people have access to health care. Two of the respondents reported having no health insurance or being under-‐insured. As demonstrated in Figure 10, the most common insurance types were insurance through one’s employer (N=52), Medicare (N=48) and private insurance (N=42).
45
27
24
22 Less than 10 minutes 10 to 30 minutes
31 to 60 minutes
More than 1 hour
59
32
21
6 Less than 10 minutes 10 to 30 minutes
31 to 60 minutes
More than 1 hour

26
Figure 10: Insurance Status – Community Members
(Community Member Survey Version Only)
Community Assets, Chal lenges, and Collaborat ion
Survey-‐takers were asked what they perceived as the best things about their community in five categories: people, services and resources, quality of life, geographic setting, and activities. In each category, respondents were given a list of choices and asked to pick the top three. Respondents occasionally chose less than three or more than three choices within each category. The results indicate there is consensus (with 80 or more respondents agreeing) that community assets include:
• friendly and helpful people; • a safe place to live; • a good place to raise kids; • health care; • the cleanliness of the area; and • recreational and sporting activities.
Figures 11 to 15 illustrate the results of these questions.
2
3
4
9
42
48
52
0 10 20 30 40 50 60
No insurance/not enough insurance
Other
Medicaid
Veteran's Health Care Benefits
Private insurance
Medicare
Insurance through employer

27
Figure 11: Best Things about the PEOPLE in Your Community
Figure 12: Best Things about the SERVICES AND RESOURCES in Your Community
1
10
10
23
29
30
68
69
104
0 50 100 150
Other
Tolerance, inclusion, open-‐mindedness
Forward-‐thinking ideas (e.g. social values, government)
Government is accessible
Sense that you can make a difference through community engagement
Community is socially and culturally diverse or becoming more diverse
People who live here are involved in the community
Feeling connected to people who live here
People are friendly, helpful, supporpve
8
19
28
32
40
47
64
92
0 50 100
Other
Opportunipes to learn and/or go to college
Restaurants and healthy food
Public services and amenipes
Downtown and shopping
Public transportapon
Quality school systems and programs for youth
Health care

28
Figure 13: Best Things about the QUALITY OF LIFE in Your Community
Figure 14: Best Things about the GEOGRAPHIC SETTING of Your Community
1
7
69
72
104
109
0 50 100 150
Other
Job opportunipes or economic opportunipes
Informal, simple, laidback lifestyle
Healthy place to live
Family-‐friendly; good place to raise kids
Safe place to live, litle/no crime
0
17
29
38
47
48
84
93
0 50 100
Other
Waterfront, rivers, lakes, and/or beaches
Climate and seasons
General proximity to work and acpvipes
General beauty of environment and/or scenery
Natural seung: outdoors and nature
Relapvely small size and scale of community
Cleanliness of area
29
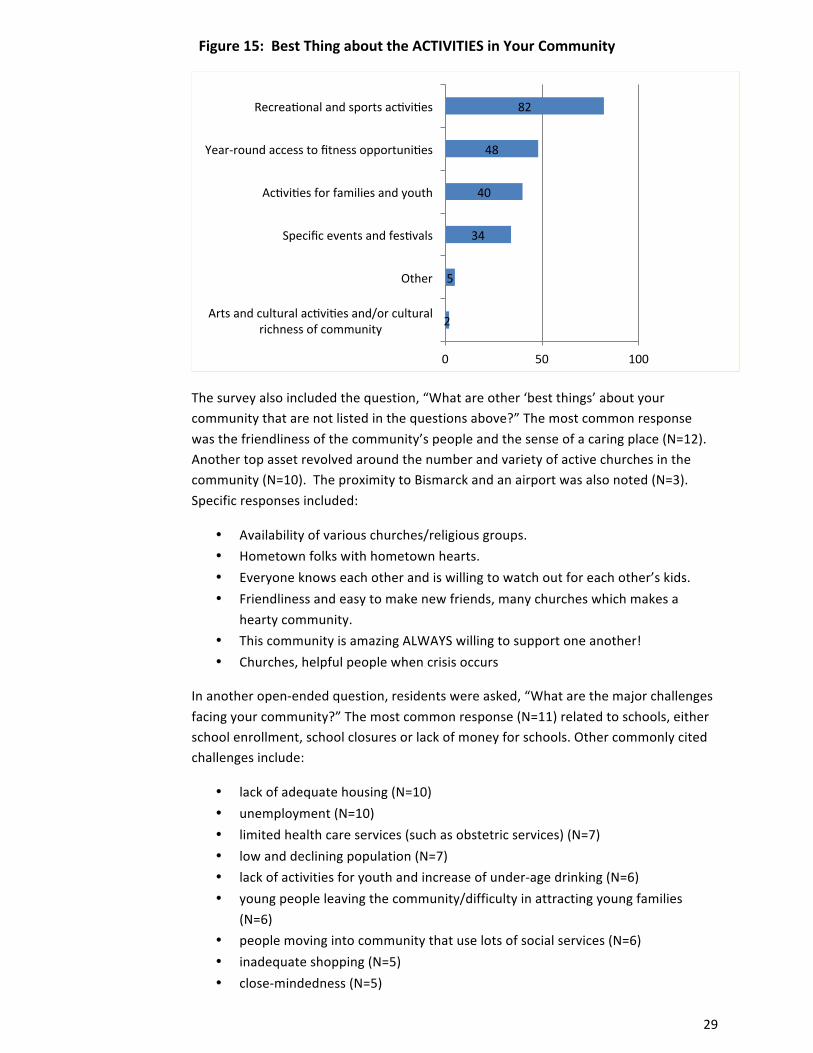
Figure 15: Best Thing about the ACTIVITIES in Your Community
The survey also included the question, “What are other ‘best things’ about your community that are not listed in the questions above?” The most common response was the friendliness of the community’s people and the sense of a caring place (N=12). Another top asset revolved around the number and variety of active churches in the community (N=10). The proximity to Bismarck and an airport was also noted (N=3). Specific responses included:
• Availability of various churches/religious groups. • Hometown folks with hometown hearts. • Everyone knows each other and is willing to watch out for each other’s kids. • Friendliness and easy to make new friends, many churches which makes a
hearty community. • This community is amazing ALWAYS willing to support one another! • Churches, helpful people when crisis occurs
In another open-‐ended question, residents were asked, “What are the major challenges facing your community?” The most common response (N=11) related to schools, either school enrollment, school closures or lack of money for schools. Other commonly cited challenges include:
• lack of adequate housing (N=10) • unemployment (N=10) • limited health care services (such as obstetric services) (N=7) • low and declining population (N=7) • lack of activities for youth and increase of under-‐age drinking (N=6) • young people leaving the community/difficulty in attracting young families
(N=6) • people moving into community that use lots of social services (N=6) • inadequate shopping (N=5) • close-‐mindedness (N=5)
2
5
34
40
48
82
0 50 100
Arts and cultural acpvipes and/or cultural richness of community
Other
Specific events and fespvals
Acpvipes for families and youth
Year-‐round access to fitness opportunipes
Recreaponal and sports acpvipes

30
Specific comments provide some insights into the reasoning behind these issues being singled out as community challenges:
• Closed-‐mindedness and unwilling to change or accept changes. • Lack of people moving here with small families due to school closures. • Money availability to help our smaller school systems to remain open. • All the “outsiders” causing trouble in our community. • We need more “activities”, there used to be a bowling alley and movie theatre,
but no longer. We need to bring those things back, as well as more activities at parks. Also, a dog park would be nice.
• Aging community. Lack of variety of jobs. • That it is too easy to be on welfare, lots of low lifes moving in. • Lack of business, shopping opportunities, clothing, etc. • We are an older community, the young people are leaving to pursue
employment and careers in larger towns. • We are getting people that are not productive members of society. They are just
living off the system.
Those taking the survey generally agreed the various organizations and constituencies in the community collaborated well with one another. Respondents were asked to rate the level of collaboration, or “how well these groups work with others in the community,” on a scale of 1 to 5. The results show that residents perceived emergency services, pharmacies, the hospital and long term care as having the most effective collaboration with other community stakeholders. Groups that were perceived as needing improvement in collaborating included business and industry as well as schools. Figure 16 illustrates community perceptions about collaboration among various organizations and groups. (Indian Health Services and Tribal Health organizations have very limited interactions within Emmons County, which likely accounts for their placement in the ranked list.)

31
Figure 16: Community Collaboration
Survey-‐takers were asked whether they believe health-‐related organizations in the community are working together to improve the overall health of the area population. As shown in Figure 17, by a wide margin residents answered this question in the affirmative.
Figure 17: Coordination to Improve Overall Population Health
1.67
2.00
3.18
3.20
3.45
3.46
3.75
3.75
3.83
3.87
4.00
4.00
4.08
4.23
0.00 2.00 4.00
Indian Health Service
Tribal Health
Schools
Business and industry
Economic development organizapons
Law enforcement
Public Health
Other local providers, such as denpsts, chiropractors
Health and human services agencies
Clinics
Long term care (nursing homes, ass'd living, etc.)
Hospital(s)
Pharmacies
Emergency services, including ambulance and fire
109
14
Yes
No
32
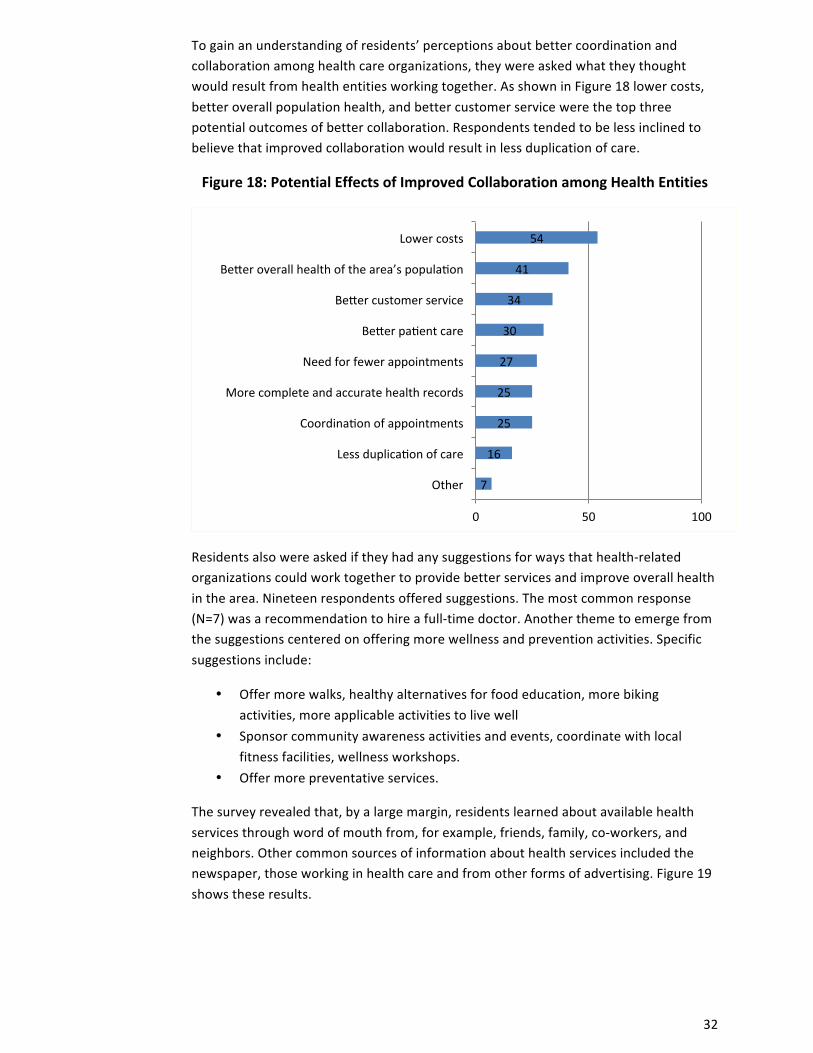
To gain an understanding of residents’ perceptions about better coordination and collaboration among health care organizations, they were asked what they thought would result from health entities working together. As shown in Figure 18 lower costs, better overall population health, and better customer service were the top three potential outcomes of better collaboration. Respondents tended to be less inclined to believe that improved collaboration would result in less duplication of care.
Figure 18: Potential Effects of Improved Collaboration among Health Entities
Residents also were asked if they had any suggestions for ways that health-‐related organizations could work together to provide better services and improve overall health in the area. Nineteen respondents offered suggestions. The most common response (N=7) was a recommendation to hire a full-‐time doctor. Another theme to emerge from the suggestions centered on offering more wellness and prevention activities. Specific suggestions include:
• Offer more walks, healthy alternatives for food education, more biking activities, more applicable activities to live well
• Sponsor community awareness activities and events, coordinate with local fitness facilities, wellness workshops.
• Offer more preventative services.
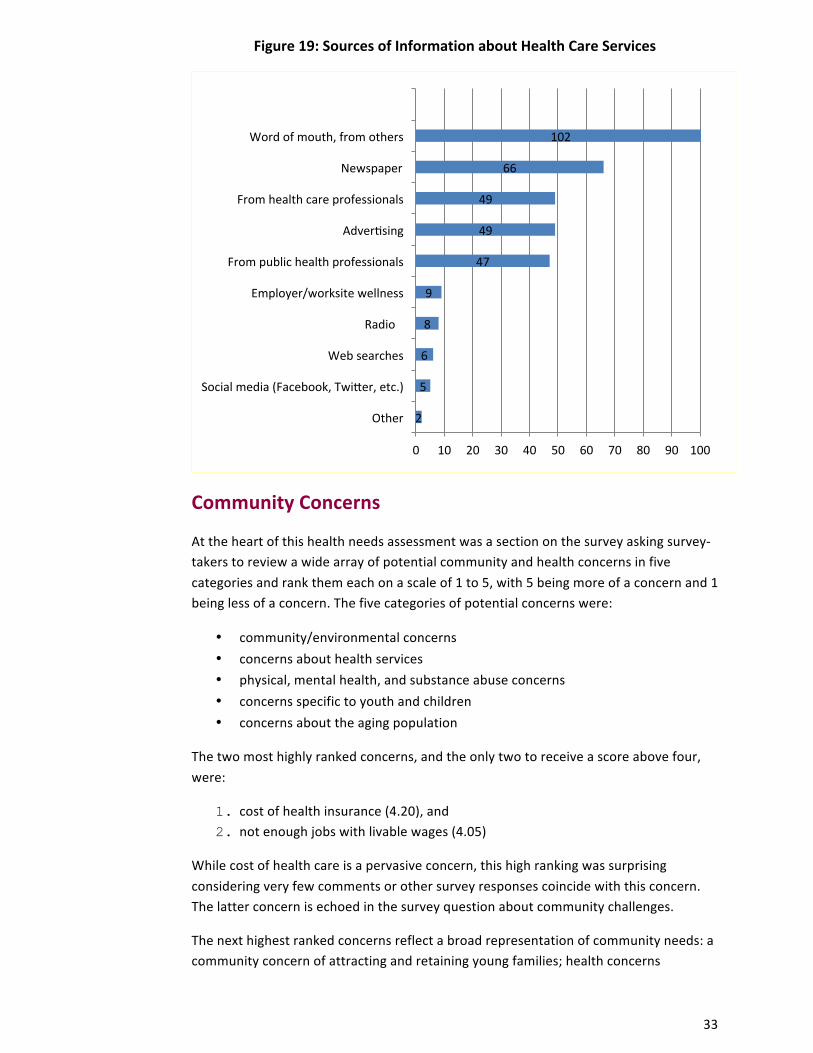
The survey revealed that, by a large margin, residents learned about available health services through word of mouth from, for example, friends, family, co-‐workers, and neighbors. Other common sources of information about health services included the newspaper, those working in health care and from other forms of advertising. Figure 19 shows these results.
7
16
25
25
27
30
34
41
54
0 50 100
Other
Less duplicapon of care
Coordinapon of appointments
More complete and accurate health records
Need for fewer appointments
Beter papent care
Beter customer service
Beter overall health of the area’s populapon
Lower costs
33
Figure 19: Sources of Information about Health Care Services
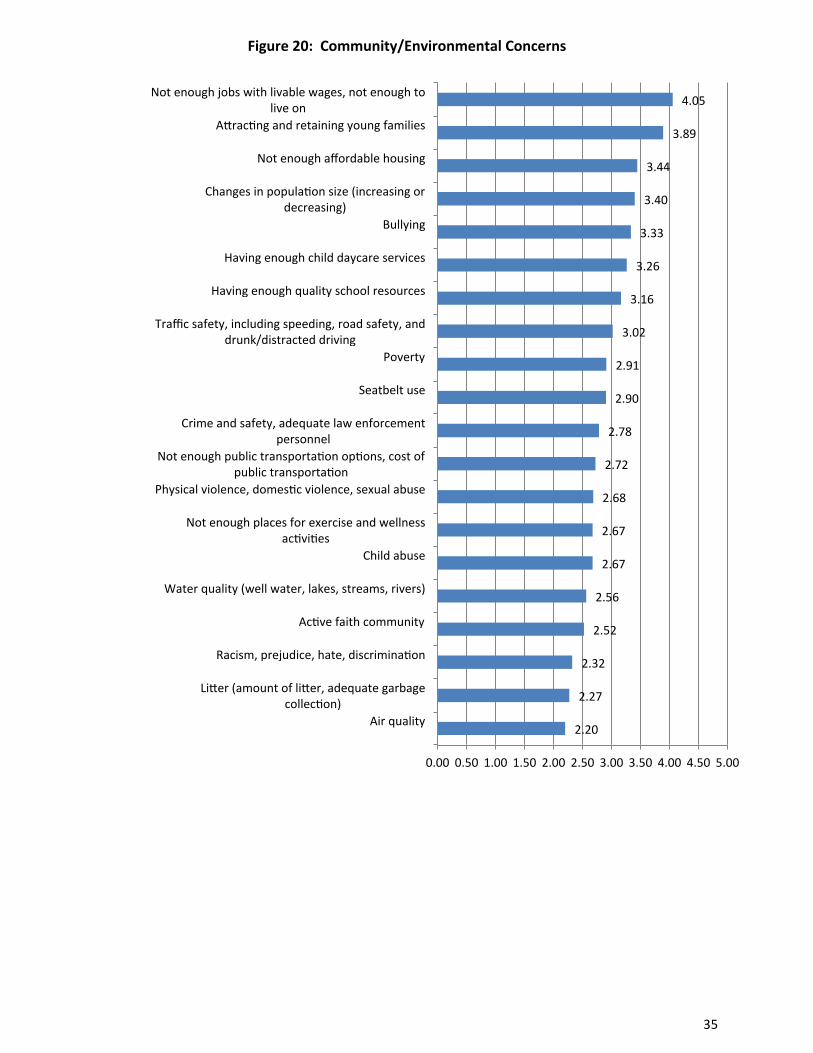
Community Concerns
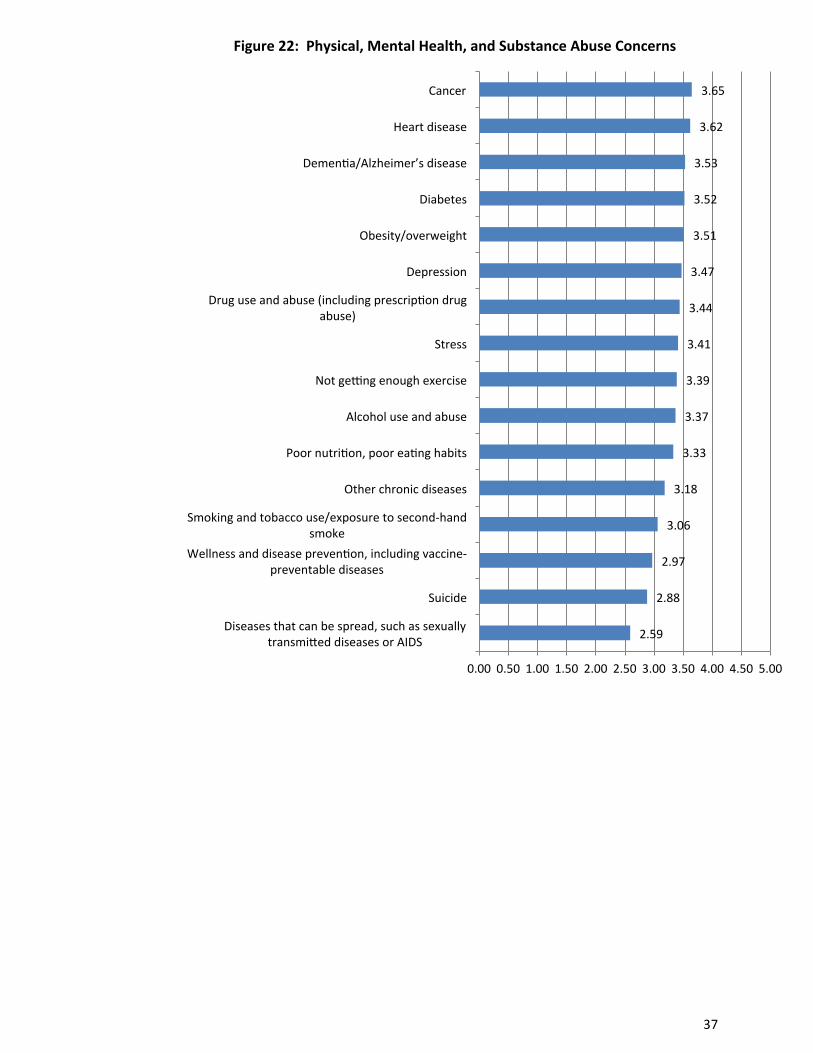
At the heart of this health needs assessment was a section on the survey asking survey-‐takers to review a wide array of potential community and health concerns in five categories and rank them each on a scale of 1 to 5, with 5 being more of a concern and 1 being less of a concern. The five categories of potential concerns were:
• community/environmental concerns • concerns about health services • physical, mental health, and substance abuse concerns • concerns specific to youth and children • concerns about the aging population
The two most highly ranked concerns, and the only two to receive a score above four, were:
1. cost of health insurance (4.20), and 2. not enough jobs with livable wages (4.05)
While cost of health care is a pervasive concern, this high ranking was surprising considering very few comments or other survey responses coincide with this concern. The latter concern is echoed in the survey question about community challenges.
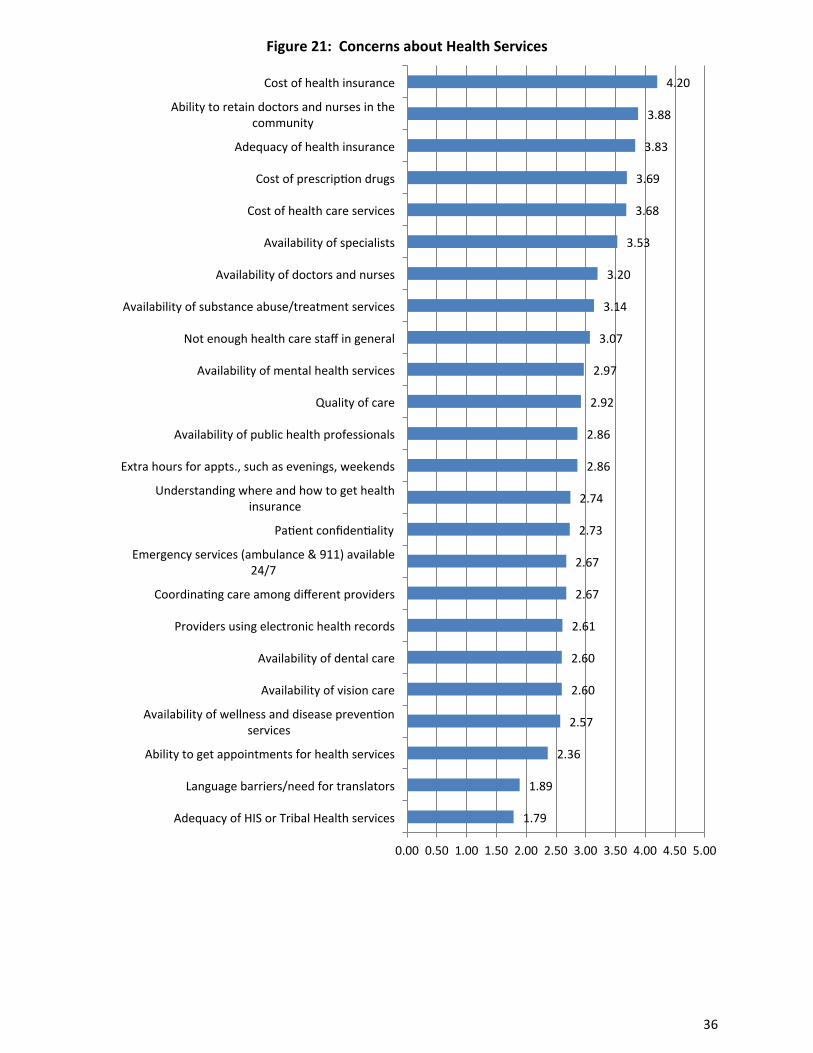
The next highest ranked concerns reflect a broad representation of community needs: a community concern of attracting and retaining young families; health concerns
2
5
6
8
9
47
49
49
66
102
0 10 20 30 40 50 60 70 80 90 100
Other
Social media (Facebook, Twiter, etc.)
Web searches
Radio �
Employer/worksite wellness
From public health professionals
Adverpsing
From health care professionals
Newspaper
Word of mouth, from others
34
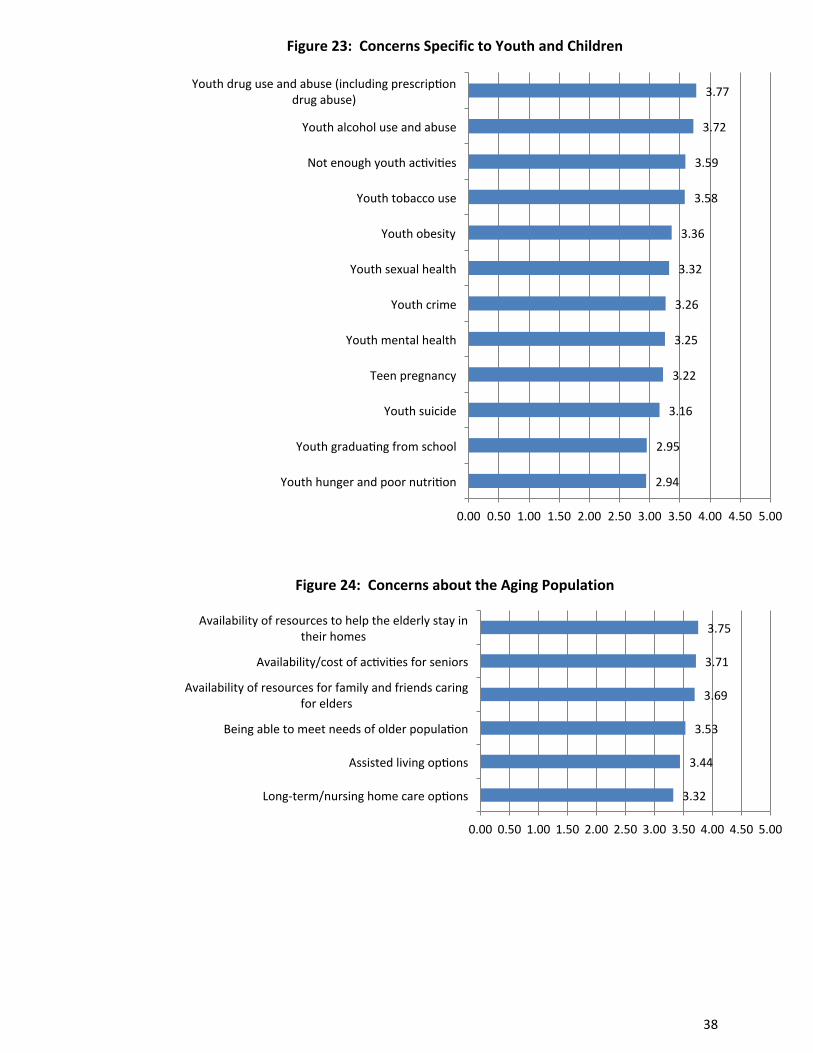
regarding retaining health providers and having adequate health insurance; a concern regarding youth’s drug use and a concern of inadequate resources for the elderly.
3. attracting and retaining young families (3.89) 4. ability to retain doctors and nurses in the community (3.88) 5. adequacy of health insurance (3.83) 6. youth drug use and abuse (3.77) 7. availability of resources to help the elderly stay in their homes (3.75)
Other issues ranked highly (with a mean ranking of at least 3.60 fall into a pattern of concerns for services for the elderly, financial concerns and chronic disease:
• availability/cost of activities for seniors (3.71) • availability of resources for family & friends caring for elders (3.69) • cost of prescription drugs (3.69) • cost of health care services (3.68) • cancer (3.65) • heart disease (3.62)
Figures 20 through 24 illustrate these results.
35
Figure 20: Community/Environmental Concerns
2.20
2.27
2.32
2.52
2.56
2.67
2.67
2.68
2.72
2.78
2.90
2.91
3.02
3.16
3.26
3.33
3.40
3.44
3.89
4.05
0.00 0.50 1.00 1.50 2.00 2.50 3.00 3.50 4.00 4.50 5.00
Air quality
Liter (amount of liter, adequate garbage collecpon)
Racism, prejudice, hate, discriminapon
Acpve faith community
Water quality (well water, lakes, streams, rivers)
Child abuse
Not enough places for exercise and wellness acpvipes
Physical violence, domespc violence, sexual abuse
Not enough public transportapon oppons, cost of public transportapon
Crime and safety, adequate law enforcement personnel
Seatbelt use
Poverty
Traffic safety, including speeding, road safety, and drunk/distracted driving
Having enough quality school resources
Having enough child daycare services
Bullying
Changes in populapon size (increasing or decreasing)
Not enough affordable housing
Atracpng and retaining young families
Not enough jobs with livable wages, not enough to live on
36
Figure 21: Concerns about Health Services
1.79
1.89
2.36
2.57
2.60
2.60
2.61
2.67
2.67
2.73
2.74
2.86
2.86
2.92
2.97
3.07
3.14
3.20
3.53
3.68
3.69
3.83
3.88
4.20
0.00 0.50 1.00 1.50 2.00 2.50 3.00 3.50 4.00 4.50 5.00
Adequacy of HIS or Tribal Health services
Language barriers/need for translators
Ability to get appointments for health services
Availability of wellness and disease prevenpon services
Availability of vision care
Availability of dental care
Providers using electronic health records
Coordinapng care among different providers
Emergency services (ambulance & 911) available 24/7
Papent confidenpality
Understanding where and how to get health insurance
Extra hours for appts., such as evenings, weekends
Availability of public health professionals
Quality of care
Availability of mental health services
Not enough health care staff in general
Availability of substance abuse/treatment services
Availability of doctors and nurses
Availability of specialists
Cost of health care services
Cost of prescrippon drugs
Adequacy of health insurance
Ability to retain doctors and nurses in the community
Cost of health insurance
37
Figure 22: Physical, Mental Health, and Substance Abuse Concerns
2.59
2.88
2.97
3.06
3.18
3.33
3.37
3.39
3.41
3.44
3.47
3.51
3.52
3.53
3.62
3.65
0.00 0.50 1.00 1.50 2.00 2.50 3.00 3.50 4.00 4.50 5.00
Diseases that can be spread, such as sexually transmited diseases or AIDS
Suicide
Wellness and disease prevenpon, including vaccine-‐preventable diseases
Smoking and tobacco use/exposure to second-‐hand smoke
Other chronic diseases
Poor nutripon, poor eapng habits
Alcohol use and abuse
Not geung enough exercise
Stress
Drug use and abuse (including prescrippon drug abuse)
Depression
Obesity/overweight
Diabetes
Demenpa/Alzheimer’s disease
Heart disease
Cancer
38
Figure 23: Concerns Specific to Youth and Children
Figure 24: Concerns about the Aging Population
2.94
2.95
3.16
3.22
3.25
3.26
3.32
3.36
3.58
3.59
3.72
3.77
0.00 0.50 1.00 1.50 2.00 2.50 3.00 3.50 4.00 4.50 5.00
Youth hunger and poor nutripon
Youth graduapng from school
Youth suicide
Teen pregnancy
Youth mental health
Youth crime
Youth sexual health
Youth obesity
Youth tobacco use
Not enough youth acpvipes
Youth alcohol use and abuse
Youth drug use and abuse (including prescrippon drug abuse)
3.32
3.44
3.53
3.69
3.71
3.75
0.00 0.50 1.00 1.50 2.00 2.50 3.00 3.50 4.00 4.50 5.00
Long-‐term/nursing home care oppons
Assisted living oppons
Being able to meet needs of older populapon
Availability of resources for family and friends caring for elders
Availability/cost of acpvipes for seniors
Availability of resources to help the elderly stay in their homes
39
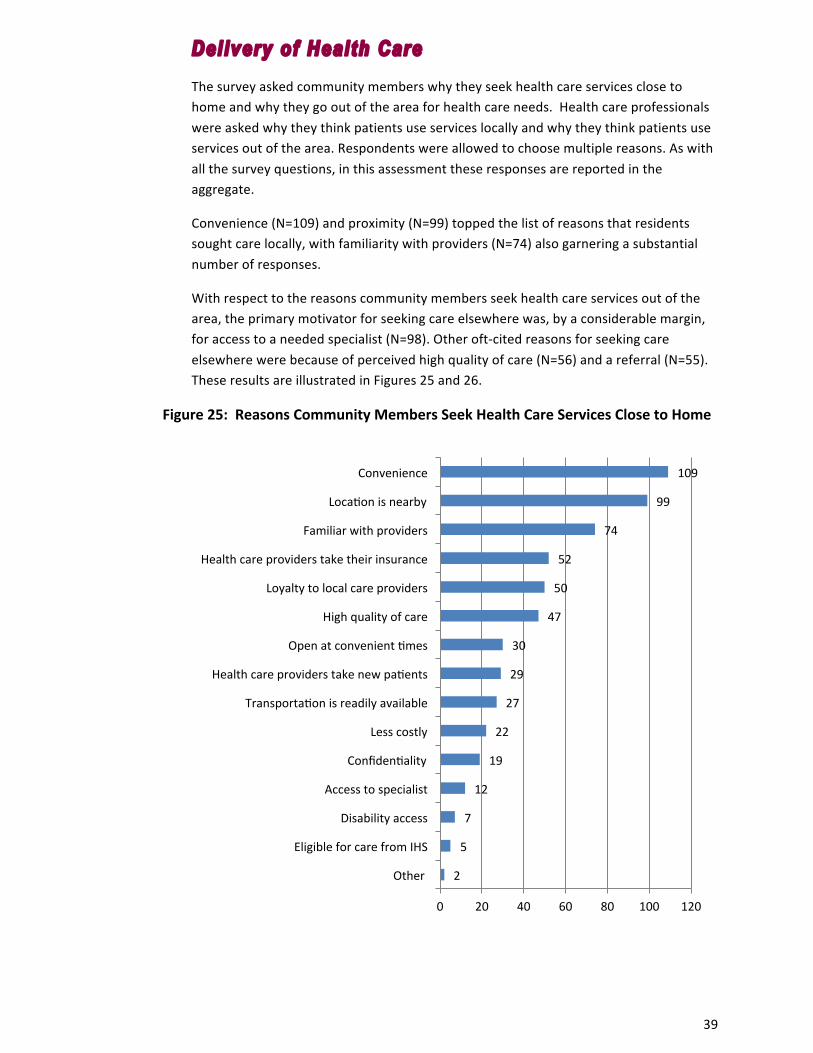
Delivery of Health Care The survey asked community members why they seek health care services close to home and why they go out of the area for health care needs. Health care professionals were asked why they think patients use services locally and why they think patients use services out of the area. Respondents were allowed to choose multiple reasons. As with all the survey questions, in this assessment these responses are reported in the aggregate.
Convenience (N=109) and proximity (N=99) topped the list of reasons that residents sought care locally, with familiarity with providers (N=74) also garnering a substantial number of responses.
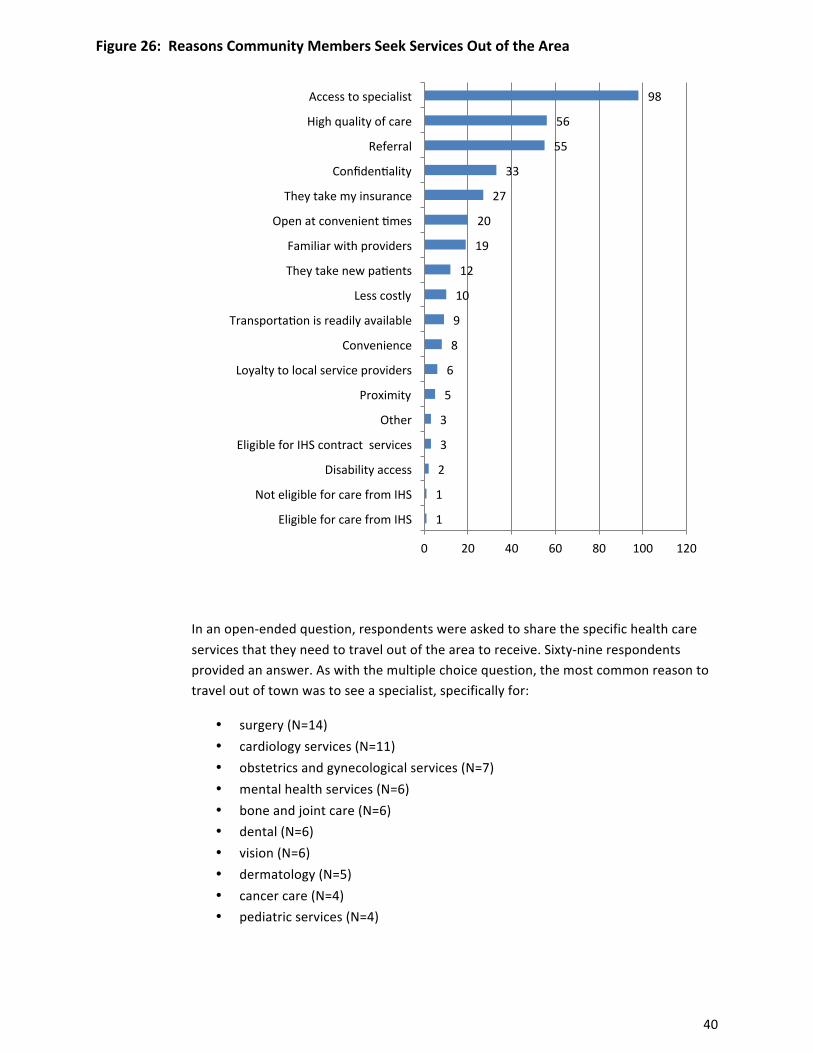
With respect to the reasons community members seek health care services out of the area, the primary motivator for seeking care elsewhere was, by a considerable margin, for access to a needed specialist (N=98). Other oft-‐cited reasons for seeking care elsewhere were because of perceived high quality of care (N=56) and a referral (N=55). These results are illustrated in Figures 25 and 26.
Figure 25: Reasons Community Members Seek Health Care Services Close to Home
2
5
7
12
19
22
27
29
30
47
50
52
74
99
109
0 20 40 60 80 100 120
Other
Eligible for care from IHS
Disability access
Access to specialist
Confidenpality
Less costly
Transportapon is readily available
Health care providers take new papents
Open at convenient pmes
High quality of care
Loyalty to local care providers
Health care providers take their insurance
Familiar with providers
Locapon is nearby
Convenience
40
Figure 26: Reasons Community Members Seek Services Out of the Area
In an open-‐ended question, respondents were asked to share the specific health care services that they need to travel out of the area to receive. Sixty-‐nine respondents provided an answer. As with the multiple choice question, the most common reason to travel out of town was to see a specialist, specifically for:
• surgery (N=14) • cardiology services (N=11) • obstetrics and gynecological services (N=7) • mental health services (N=6) • bone and joint care (N=6) • dental (N=6) • vision (N=6) • dermatology (N=5) • cancer care (N=4) • pediatric services (N=4)
1
1
2
3
3
5
6
8
9
10
12
19
20
27
33
55
56
98
0 20 40 60 80 100 120
Eligible for care from IHS
Not eligible for care from IHS
Disability access
Eligible for IHS contract services
Other
Proximity
Loyalty to local service providers
Convenience
Transportapon is readily available
Less costly
They take new papents
Familiar with providers
Open at convenient pmes
They take my insurance
Confidenpality
Referral
High quality of care
Access to specialist
41
The survey also solicited input about what health care services should be added locally. Twenty-‐six respondents provided suggestions. The most commonly requested service (N=4) was for kidney dialysis. Other commonly requested services were mental health and addiction counseling (N=3) and pediatrics (N=2). The other requests covered the gamut of needs including orthopedics, orthodontics, OB, more senior living, and more surgical services.
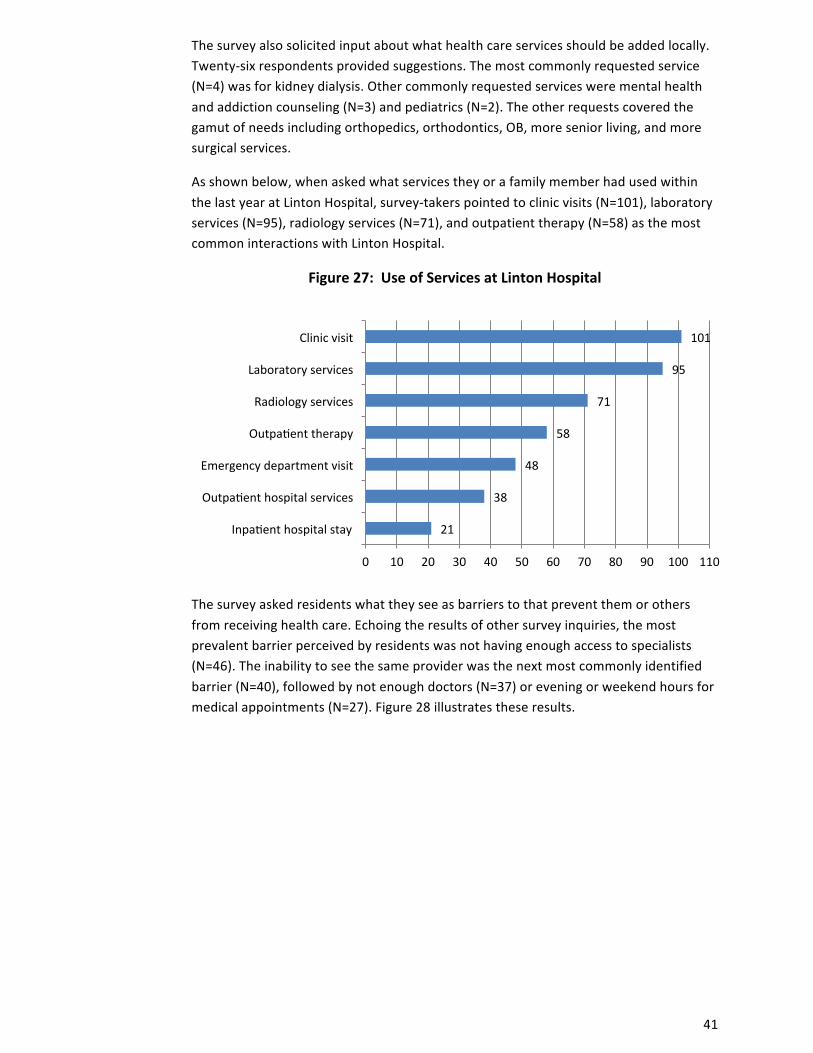
As shown below, when asked what services they or a family member had used within the last year at Linton Hospital, survey-‐takers pointed to clinic visits (N=101), laboratory services (N=95), radiology services (N=71), and outpatient therapy (N=58) as the most common interactions with Linton Hospital.
Figure 27: Use of Services at Linton Hospital
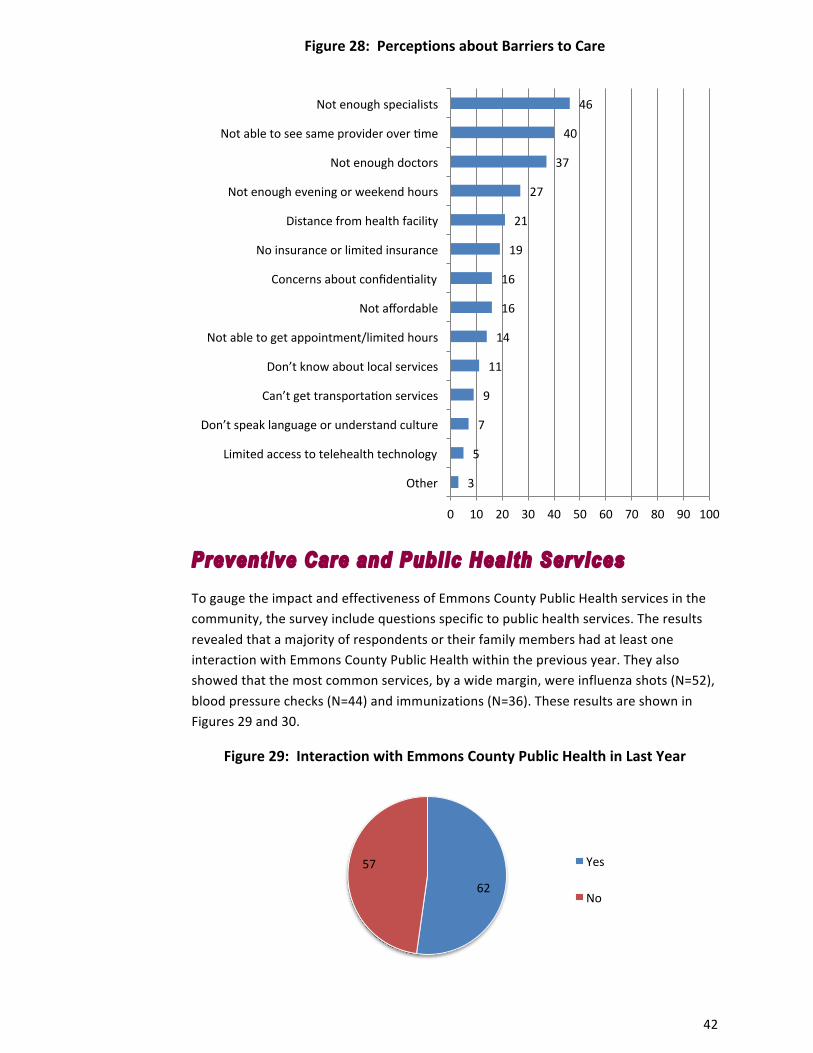
The survey asked residents what they see as barriers to that prevent them or others from receiving health care. Echoing the results of other survey inquiries, the most prevalent barrier perceived by residents was not having enough access to specialists (N=46). The inability to see the same provider was the next most commonly identified barrier (N=40), followed by not enough doctors (N=37) or evening or weekend hours for medical appointments (N=27). Figure 28 illustrates these results.
21
38
48
58
71
95
101
0 10 20 30 40 50 60 70 80 90 100 110
Inpapent hospital stay
Outpapent hospital services
Emergency department visit
Outpapent therapy
Radiology services
Laboratory services
Clinic visit
42
Figure 28: Perceptions about Barriers to Care
Preventive Care and Public Health Services
To gauge the impact and effectiveness of Emmons County Public Health services in the community, the survey include questions specific to public health services. The results revealed that a majority of respondents or their family members had at least one interaction with Emmons County Public Health within the previous year. They also showed that the most common services, by a wide margin, were influenza shots (N=52), blood pressure checks (N=44) and immunizations (N=36). These results are shown in Figures 29 and 30.
Figure 29: Interaction with Emmons County Public Health in Last Year
3
5
7
9
11
14
16
16
19
21
27
37
40
46
0 10 20 30 40 50 60 70 80 90 100
Other
Limited access to telehealth technology
Don’t speak language or understand culture
Can’t get transportapon services
Don’t know about local services
Not able to get appointment/limited hours
Not affordable
Concerns about confidenpality
No insurance or limited insurance
Distance from health facility
Not enough evening or weekend hours
Not enough doctors
Not able to see same provider over pme
Not enough specialists
62
57 Yes
No
43
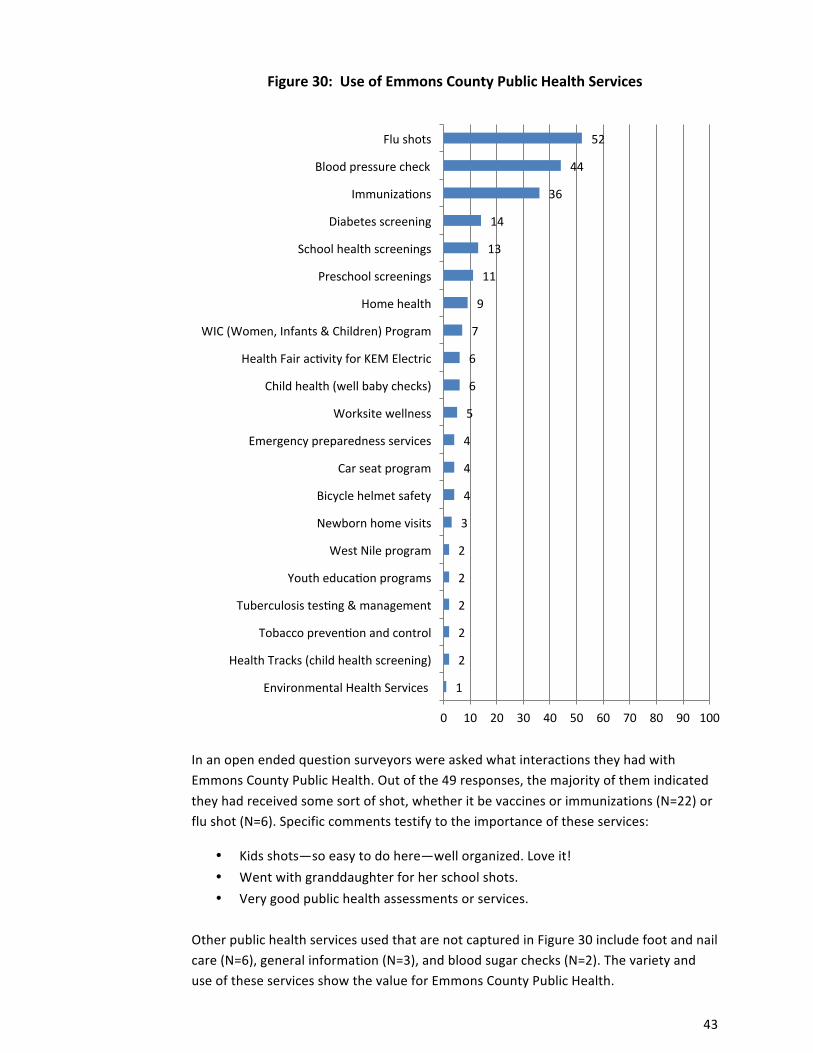
Figure 30: Use of Emmons County Public Health Services
In an open ended question surveyors were asked what interactions they had with Emmons County Public Health. Out of the 49 responses, the majority of them indicated they had received some sort of shot, whether it be vaccines or immunizations (N=22) or flu shot (N=6). Specific comments testify to the importance of these services:
• Kids shots—so easy to do here—well organized. Love it! • Went with granddaughter for her school shots. • Very good public health assessments or services.
Other public health services used that are not captured in Figure 30 include foot and nail care (N=6), general information (N=3), and blood sugar checks (N=2). The variety and use of these services show the value for Emmons County Public Health.
1
2
2
2
2
2
3
4
4
4
5
6
6
7
9
11
13
14
36
44
52
0 10 20 30 40 50 60 70 80 90 100
Environmental Health Services
Health Tracks (child health screening)
Tobacco prevenpon and control
Tuberculosis tespng & management
Youth educapon programs
West Nile program
Newborn home visits
Bicycle helmet safety
Car seat program
Emergency preparedness services
Worksite wellness
Child health (well baby checks)
Health Fair acpvity for KEM Electric
WIC (Women, Infants & Children) Program
Home health
Preschool screenings
School health screenings
Diabetes screening
Immunizapons
Blood pressure check
Flu shots
44
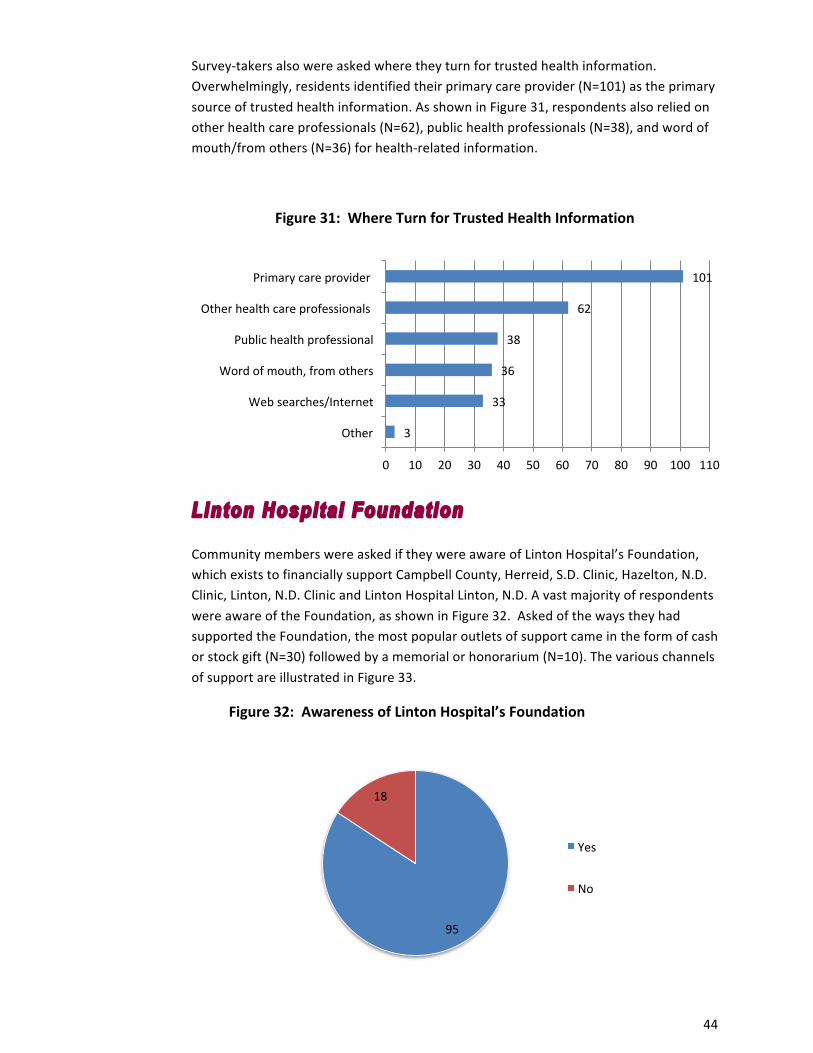
Survey-‐takers also were asked where they turn for trusted health information. Overwhelmingly, residents identified their primary care provider (N=101) as the primary source of trusted health information. As shown in Figure 31, respondents also relied on other health care professionals (N=62), public health professionals (N=38), and word of mouth/from others (N=36) for health-‐related information.
Figure 31: Where Turn for Trusted Health Information
Linton Hospital Foundation
Community members were asked if they were aware of Linton Hospital’s Foundation, which exists to financially support Campbell County, Herreid, S.D. Clinic, Hazelton, N.D. Clinic, Linton, N.D. Clinic and Linton Hospital Linton, N.D. A vast majority of respondents were aware of the Foundation, as shown in Figure 32. Asked of the ways they had supported the Foundation, the most popular outlets of support came in the form of cash or stock gift (N=30) followed by a memorial or honorarium (N=10). The various channels of support are illustrated in Figure 33.
Figure 32: Awareness of Linton Hospital’s Foundation
3
33
36
38
62
101
0 10 20 30 40 50 60 70 80 90 100 110
Other
Web searches/Internet
Word of mouth, from others
Public health professional
Other health care professionals
Primary care provider
95
18
Yes
No

45
Figure 33: Support of Linton Hospital’s Foundation
Other Concerns and Suggestions to Improve Local Health The survey concluded with an open-‐ended question that asked, “Overall, please share concerns and suggestions to improve the delivery of local health care.” Fewer residents responded to this question than to other open-‐ended survey questions, with a total of 15 responses. Respondents shared a wide range of concerns and advice. The only issues that were mentioned by more than one person were: need for permanent, full-‐time doctor that lives in the community (N=7) and need for mental health services (N=2). Other comments expressed gratitude for the availability and quality of health services. Specific comments included:
• Access to counseling, addiction programs, access for eating disorders, alcohol, drugs, gambling, and sex.
• It would be nice to have doctors who stay one time. They don’t want to live here and either do their spouses. More education on mental health would be helpful here. Addictions are prominent but people don’t understand treatment and family counseling.
• There must be good MD’s in charge of each individual’s health care, not Pas who lack education and the needed thought process for good/excellent health care.
• Suggestion for educational information content in small groups and where people gather, especially elderly.
• I am so disgusted with the overall administration of Linton Hospital & Clinic and the injustices that I’ve seen going on. The Hospital Board seems to cater to whims of the Administrator and not to the Community. I have had dealings with
30 1
10
0 4
Cash or stock giz
Endowment gizs
Memorial/honorarium
Planned gizs through wills, trusts or life insurance policies
Other

46
them and you get shut down, no explanations for their actions. I thought this was a Community Hospital.
• I’ve always been pleased with what I needed from them. I’m only a maintenance type person anyway.
• It would be nice to be able to find and maintain a provider. I think we also really need a male doctor for the male population. Our Midlevel staff do an excellent job, and are very thorough.
• They are available almost anytime-‐phone call-‐Quick visit—they go well. Thank you for your interest.
• Thanks for asking!
Findings from Key Informant Interviews and Focus Group
Questions about the health and well-‐being of the community, similar to those posed in the survey, were explored during a focus group session with the Community Group as well as during key informant interviews with community leaders and public health professionals. The themes that emerged from these sources were wide-‐ranging, with some directly associated with health care and others more rooted in broader community matters. Generally, overarching thematic issues that developed during the interviews and focus group can be grouped into five categories (listed in no particular order):
1. Mental health including drug and alcohol use and abuse 2. Not enough activities for children and youth 3. Not enough jobs with livable wages or affordable housing 4. Availability to retain doctors and nurses 5. Availability of resources to help elderly stay in their homes (including hospice)
A more detailed discussion about these issues follows:
1. Mental health including drug & alcohol use & abuse
Mental health was a broad concern that encompassed iterations including use and abuse of alcohol and drugs for all age demographics. There was an overarching concern about the cultural acceptance of alcohol in Emmons County. Some attributed this to the German/Russian heritage. Many community members noted that alcohol was weaved into most events and was socially accepted, even for minors. The youth are perceived to use and abuse alcohol out of boredom. For adults, it was said that there is nothing to do but go to the bars.
Drug use is a pervasive concern, with meth and marijuana more of a concern among high school kids and pain, sleeping pills, depression pills and other prescription drug abuse a concern among the elderly. One commented “mental health is not on the radar

47
but drug abuse is a huge problem.” A need for an addiction counselor was expressed; some community members said they would like to see a substance abuse prevention coordinator added to the list of current hospital offerings, stressing the need for anonymity. Others said they would like to see AA classes and services for depression and bipolar.
Due to the stigma associated with this need and the gossipy nature of small towns, residents recommended the location of this supportive care would need to be outside of the hospital. It was suggested that a counselor from Bismarck could come locally to make it convenient as travel costs deter others from going to Bismarck for care. Keeping a low profile and ensuring confidentiality were stressed.
Others spoke to the unmet mental health needs of those who are in the “sandwich generation” and taking care of both their own children and their parents. It was noted the caretakers try to meet the needs of family members but put their own health on the back burner. Often, they are emotionally exhausted and squeezed in both directions and suffer from depression or anxiety.
2. Not enough activities for youth
The lack of things to do for kids is certainly tied to the first concern of increased use of alcohol and drugs. Many community members noted the absence of kids programming. Apart from the park and pool it was stated that “there was no place for kids.”
A related concern to youth supervision is the lack of daycare. This concern is consistent with the data compiled by KIDS COUNT that shows the licensed child care capacity for children ages 0-‐13 is only at 18.3%.
3. Not enough jobs with l ivable wages or affordable housing
These two concerns were expressed separately but go hand-‐in-‐hand. Residents first expressed the lack of available professional jobs, ones that paid enough for a family to live on. Some phrased it as unemployment. While some pointed out there are job offerings in health care, they said there is nothing for the spouse to do.
Without the availability of jobs it is difficult to attract and retain young families which was another concern often cited. This in turn caused anxiety among some that the community would lose local services like restaurants and health care facilities.
Similarly, the lack of housing was a prioritized concern. It was stated that there are no available lots to buy or build on in Linton. Some noted a high request for rentals but said there “is nothing except low income 1-‐bedroom units.” Some noted more families from the oil patch are moving and though they may be able to find housing, they cannot afford propane to heat their house.
Specific comments included:
• Disconnect in development and demographics—no risk takers to put into building
• No financing

48
4. Availability to retain doctors and nurses
The lack of continuity of care was a frequently expressed concern. The high turnover rate of doctors has resulted in a lack of trust. The lack of trust and confidentiality accounted for a large amount of community members traveling to Bismarck for doctoring. Especially pertinent for an aging population is a reliable and trusted physician. Change does not come easy for this group and the lack of stability creates anxiety. Some noted “You never know who you will see here.” The fact that Linton does not have a full-‐time physician who lives in the community motivates many to travel outside the community for health care.
Additionally, the lack of continuity has caused misunderstandings as patients receive different advice every time they see a different provider. Some acknowledged the difficulty in retaining quality providers by saying “there is a lack of physicians who wish to work in rural America.”
5. Availabil i ty of resources to help elderly stay in their homes
There was an overwhelming concern for the needs of the elderly. Given that Emmons County has a significantly large percentage of persons 65 years and older, almost twice the state rate, there is critical need to attend to their services. Specific requests for services included assisted living apartments, independent senior housing and hospice. Currently, seniors needing hospice are referred to Bismarck and transportation and travel costs are prohibitive.
49
Priority of Health Needs The Community Group held its second meeting on July 29, 2014. Nine members of the group attended the meeting. A representative from the Center for Rural Health presented the group with a summary of this report’s findings, including background and explanation about the secondary data, highlights from the results of the survey (including perceived community health and community concerns, why patients seek care at Linton Hospital, community collaboration, and barriers to care), and findings from the focus group and key informant interviews.
Following the presentation of the assessment findings, and after careful consideration of and discussion about the findings, all members of the group were asked to identify by placing sticker dots on poster boards what they perceived as the top five community health needs. Group members were advised they could consider a number of criteria when prioritizing needs, such as a need’s burden, scope, severity, or urgency, as well as disparities associated with the need and the overall importance the community places on addressing the need. The results were totaled, and the concerns most often cited were:
• Limited number of primary care physicians (6 votes) • Not enough licensed child care capacity (6 votes) • Not enough dentists (3 votes) • Unavailability of resources to help elderly stay in their homes (3 votes) • Elevated rate of severe housing problems (3 votes)
The group then discussed at length the perceptions among community members regarding the lack of primary care physicians and the inability to see the same provider over time. The hospital CEO provided the group with background on the history and financial aspects of recruiting providers to the area. The discussion then migrated to ways to increase community awareness about the challenges of recruiting and retaining providers as well as about better utilization of midlevel providers. The group agreed that many in the community do not fully appreciate the challenges in recruiting providers or the changes taking place in the delivery of health care. While the hospital has been working diligently in bringing more providers to the community, it was suggested that efforts also need to be made to appropriately set community expectations about provider staffing issues. The group then spent time brainstorming ideas on how to raise awareness about this issue.
Following the discussion centered on providers, the group then moved to brainstorming and strategizing for meeting a second identified need. Besides the concern about adequacy of providers, the other concern receiving six votes was the lack of child care capacity. Since another group in the community currently is actively working on this issue, the group decided to address a different issue.
Because the local public health unit is receiving grant money for programming, and because there was some interrelatedness between a number of measures receiving multiple votes (with a total of six votes for rate of obesity, low food environment index, rate of physical inactivity, and access to exercise opportunities), the group decided to

50
cluster these concerns into an additional significant need, labelled “promoting wellness and healthy lifestyles.”
These prioritized needs align well with the survey question asking respondents what suggestions they had for health related organizations to work together to provide better services. As noted earlier in this report, the most common recommendations echo these ranked needs: hire a full time doctor and offer more wellness and prevention activities. When different data sources overlap like this it gives credence to the findings. Moreover, the intersection and consistency of the multiple data outlets strengthen the assessment and bestow a strong foundation to launch the next phase of the assessment, strategic planning and implementation.
Using a logic model, the group then began brainstorming and strategic planning efforts related to meeting this need.
A summary of this prioritization may be found in Appendix D.
Strategic Plan
Using a logic model, the group then began the second portion of the Community Group meeting: a strategic planning session to find ways to address the prioritized significant needs. Because of time constraints, the group did not cover all of planning necessary to create a comprehensive implementation strategy. Instead, they spent their time working on potential ideas to address two of the needs: (1) attracting primary care physicians (and educating the community about these efforts) and (2) promoting wellness and healthy lifestyles.
A steering committee or other group will meet to continue the work that was started by the Community Group and culminate with an implementation strategy that can be executed over the next three years. A preliminary strategic implementation report (to be supplemented as work continues) is included as Appendix E.

51
Appendix A1 – Community Member Survey Instrument
Community Health Survey Linton Hospital and Emmons County Public Health are interested in hearing from you about area health issues and concerns. The focus of this effort is to:
• Learn of the good things in the community and the community’s concerns • Understand perceptions and attitudes about the health of the community, and hear suggestions for
improvement • Learn more about how local health services are used by you and other residents
Please take a few moments to complete the survey. If you prefer, you may take the survey online at http://tinyurl.com/emmonscountysurvey Surveys will be tabulated by the Center for Rural Health at the University of North Dakota School of Medicine and Health Sciences. Your responses are anonymous, and you may skip any question you do not want to answer. Your answers will be combined with other responses and reported only in total. If you have questions about the survey, you may contact Karin Becker at (701) 777-‐4499.
Surveys will be accepted through June 6, 2014. Your opinion matters – thank you in advance!
Community Assets and Collaboration Please tell us about your community by choosing up to three options you most agree with in each category below: Q1. Considering the PEOPLE in your community, the best things are (choose up to THREE):
� Community is socially and culturally diverse or becoming more diverse �
People who live here are involved in the community
� Feeling connected to people who live here �
Sense that you can make a difference through community engagement
� Forward-‐thinking ideas (social values, government) � Tolerance, inclusion, open-‐minded
� Government is accessible � Other (please specify)_________________________
� People are friendly, helpful, supportive
Q2. Considering the SERVICES AND RESOURCES in your community, the best things are (choose up to THREE):
� Downtown and shopping (close by, good variety, availability of goods) � Public services and amenities
� Health care � Public transportation
� Opportunities to learn and/or go to college � Restaurants and healthy food

52
� Quality school systems and programs for youth �
Other (please specify)_________________________
Q3. Considering the QUALITY OF LIFE in your community, the best things are (choose up to THREE):
� Family-‐friendly; good place to raise kids � Job opportunities or economic opportunities
� Healthy place to live � Safe place to live, little/no crime
� Informal, simple, laidback lifestyle � Other (please specify)_________________________
Q4. Considering the ACTIVITIES in your community, the best things are (choose up to THREE):
� Activities for families and youth � Specific events and festivals
� Arts and cultural activities and/or cultural richness of community �
Year-‐round access to fitness opportunities (indoor activities, winter sports, etc.)
� Recreational and sports activities (e.g., outdoor recreation, parks, bike paths, and other activities)
� Other (please specify)_________________________
Q5. Considering the GEOGRAPHIC SETTING in your community, the best things are (choose up to THREE):
� Cleanliness of area (e.g., fresh air, lack of pollution and litter) � Natural setting: outdoors and nature
� Climate and seasons � Relatively small size and scale of community
� General beauty of environment and/or scenery �
Waterfront, rivers, lakes, and/or beaches
� General proximity to work and activities (e.g., short commute, convenient access)
� Other (please specify)_________________________
Q6. What are other “best things” about your community that are not listed in the questions above? _____________________________________________________________________________________ _____________________________________________________________________________________ Q7. What are the major challenges facing your community? _____________________________________________________________________________________ _____________________________________________________________________________________ Q8. For each choice on the next page please rank the level of collaboration, or how well these groups
work with others in the community, on a scale of 1 to 5, with 1 being no collaboration (not working well with others) and 5 being excellent collaboration (working well with others).

53
Community Collaboration No Excellent collaboration collaboration
Don’t Know/Not Applicable
1 2 3 4 5 Business and industry Clinics Economic development organizations Emergency services, including ambulance and fire Health and human services agencies Hospital(s) Indian Health Service Law enforcement Long term care, including nursing homes and assisted living Other local health providers, such as dentists and chiropractors Pharmacies Public Health Schools Tribal Health
Q9. Do you believe that health-‐related organizations in the community are working together to improve
the overall health of the area population? � No � Yes
Q10. Which, if any, of the following do you think would result from better collaboration among health
care providers and health-‐related organizations? (Choose ALL that apply.) ☐ Better customer service ☐Less duplication of care ☐ Better patient care ☐Lower costs ☐ Better overall health of the area’s population ☐More complete and accurate health records ☐ Coordination of appointments ☐ Need for fewer appointments ☐ Other (Please specify)______________________
Q11. What suggestions do you have for health-‐related organizations to work together to provide better services and improve the overall health of the area population?
______________________________________________________________________________ ______________________________________________________________________________ Q12. Where do you find out what health services are available in your area? (Choose ALL that apply.)
� Advertising � From health care professionals � From public health professionals � Social media (Facebook, Twitter, etc.) � Indian Health Service � Tribal health � Newspaper � Web searches � Radio � Employer/worksite wellness � Word of mouth, from others
(friends, neighbors, co-‐workers, etc.) � Other (Please specify)_________________
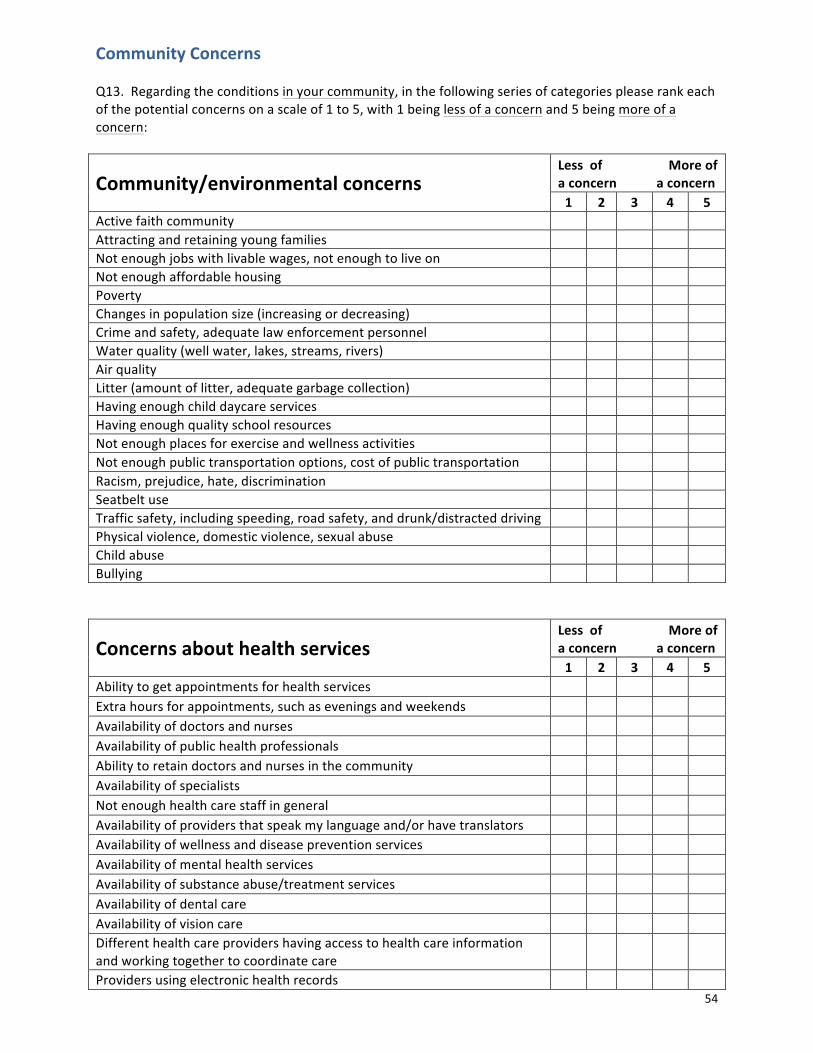
54
Community Concerns Q13. Regarding the conditions in your community, in the following series of categories please rank each of the potential concerns on a scale of 1 to 5, with 1 being less of a concern and 5 being more of a concern:
Community/environmental concerns Less of More of a concern a concern 1 2 3 4 5
Active faith community Attracting and retaining young families Not enough jobs with livable wages, not enough to live on Not enough affordable housing Poverty Changes in population size (increasing or decreasing) Crime and safety, adequate law enforcement personnel Water quality (well water, lakes, streams, rivers) Air quality Litter (amount of litter, adequate garbage collection) Having enough child daycare services Having enough quality school resources Not enough places for exercise and wellness activities Not enough public transportation options, cost of public transportation Racism, prejudice, hate, discrimination Seatbelt use Traffic safety, including speeding, road safety, and drunk/distracted driving Physical violence, domestic violence, sexual abuse Child abuse Bullying
Concerns about health services Less of More of a concern a concern 1 2 3 4 5
Ability to get appointments for health services Extra hours for appointments, such as evenings and weekends Availability of doctors and nurses Availability of public health professionals Ability to retain doctors and nurses in the community Availability of specialists Not enough health care staff in general Availability of providers that speak my language and/or have translators Availability of wellness and disease prevention services Availability of mental health services Availability of substance abuse/treatment services Availability of dental care Availability of vision care Different health care providers having access to health care information and working together to coordinate care
Providers using electronic health records

55
Concerns about health services Less of More of a concern a concern 1 2 3 4 5
Patient confidentiality Quality of care Emergency services (ambulance & 911) available 24/7 Cost of health care services Cost of health insurance Adequacy of health insurance (concerns about out-‐of-‐pocket costs) Adequacy of Indian Health Service or Tribal Health Services Understanding where and how to get health insurance Cost of prescription drugs
Physical, mental health, and substance abuse concerns (Adults)
Less of More of a concern a concern 1 2 3 4 5
Cancer Diabetes Heart disease Other chronic diseases Dementia/Alzheimer’s disease Depression Stress Suicide Alcohol use and abuse Drug use and abuse (including prescription drug abuse) Smoking and tobacco use/exposure to second-‐hand smoke Not getting enough exercise Obesity/overweight Poor nutrition, poor eating habits Diseases that can be spread, such as sexually transmitted diseases or AIDS Wellness and disease prevention, including vaccine-‐preventable diseases
Concerns specific to youth and children Less of More of a concern a concern 1 2 3 4 5
Not enough activities for children and youth Youth obesity Youth hunger and poor nutrition Youth alcohol use and abuse Youth drug use and abuse (including prescription drug abuse) Youth tobacco use Youth mental health Youth suicide Teen pregnancy Youth sexual health Youth crime Youth graduating from school
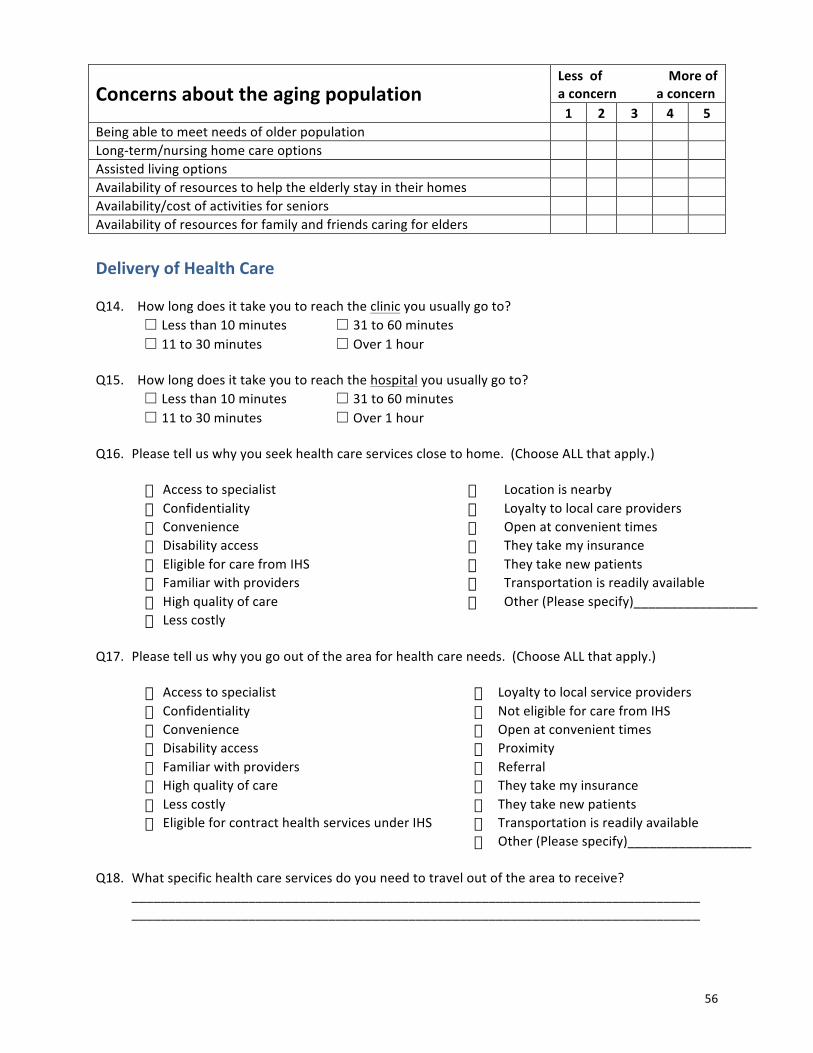
56
Concerns about the aging population Less of More of a concern a concern 1 2 3 4 5
Being able to meet needs of older population Long-‐term/nursing home care options Assisted living options Availability of resources to help the elderly stay in their homes Availability/cost of activities for seniors Availability of resources for family and friends caring for elders Delivery of Health Care Q14. How long does it take you to reach the clinic you usually go to?
☐ Less than 10 minutes ☐ 31 to 60 minutes ☐ 11 to 30 minutes ☐ Over 1 hour
Q15. How long does it take you to reach the hospital you usually go to?
☐ Less than 10 minutes ☐ 31 to 60 minutes ☐ 11 to 30 minutes ☐ Over 1 hour
Q16. Please tell us why you seek health care services close to home. (Choose ALL that apply.)
� Access to specialist � Location is nearby � Confidentiality � Loyalty to local care providers � Convenience � Open at convenient times � Disability access � They take my insurance � Eligible for care from IHS � They take new patients � Familiar with providers � Transportation is readily available � High quality of care � Other (Please specify)_________________ � Less costly �
Q17. Please tell us why you go out of the area for health care needs. (Choose ALL that apply.)
� Access to specialist � Loyalty to local service providers � Confidentiality � Not eligible for care from IHS � Convenience � Open at convenient times � Disability access � Proximity � Familiar with providers � Referral � High quality of care � They take my insurance � Less costly � They take new patients � Eligible for contract health services under IHS � Transportation is readily available � � Other (Please specify)_________________
Q18. What specific health care services do you need to travel out of the area to receive? ______________________________________________________________________________ ______________________________________________________________________________
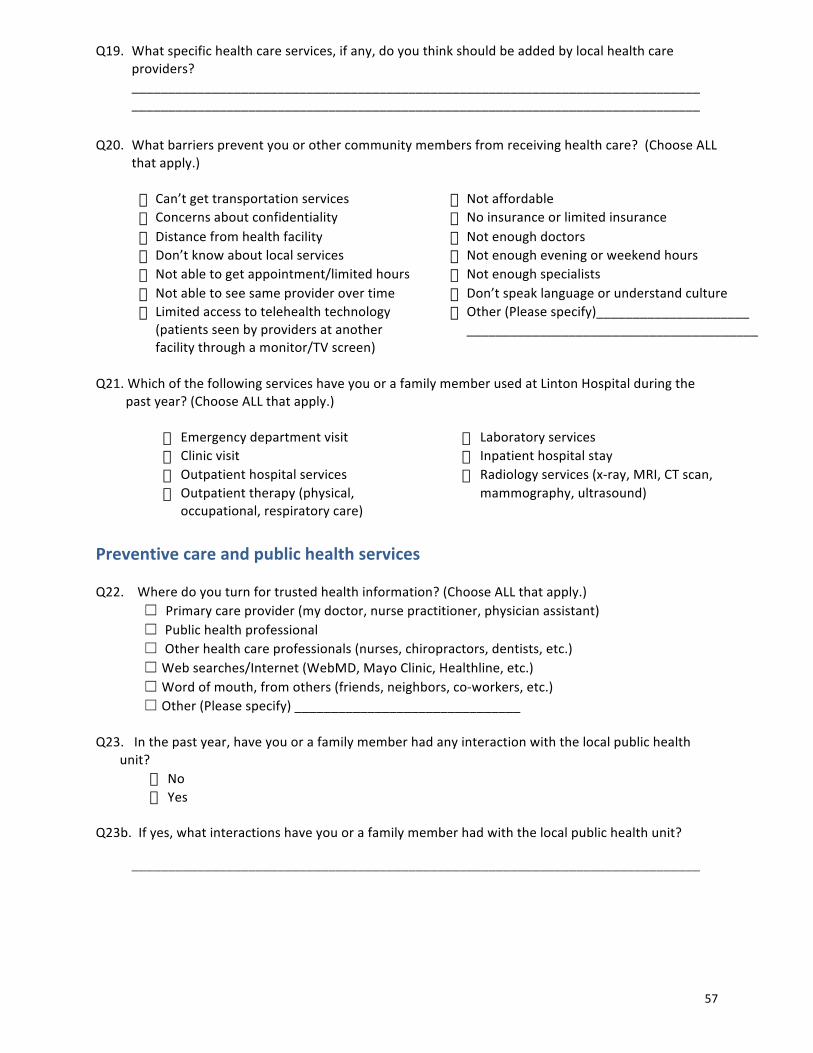
57
Q19. What specific health care services, if any, do you think should be added by local health care providers?
______________________________________________________________________________ ______________________________________________________________________________ Q20. What barriers prevent you or other community members from receiving health care? (Choose ALL
that apply.)
� Can’t get transportation services � Not affordable � Concerns about confidentiality � No insurance or limited insurance � Distance from health facility � Not enough doctors � Don’t know about local services � Not enough evening or weekend hours � Not able to get appointment/limited hours � Not enough specialists � Not able to see same provider over time � Don’t speak language or understand culture � Limited access to telehealth technology
(patients seen by providers at another facility through a monitor/TV screen)
� Other (Please specify)_____________________ ________________________________________
Q21. Which of the following services have you or a family member used at Linton Hospital during the past year? (Choose ALL that apply.)
� Emergency department visit � Laboratory services � Clinic visit � Inpatient hospital stay � Outpatient hospital services � Radiology services (x-‐ray, MRI, CT scan, � Outpatient therapy (physical,
occupational, respiratory care) � mammography, ultrasound)
Preventive care and public health services Q22. Where do you turn for trusted health information? (Choose ALL that apply.) ☐ Primary care provider (my doctor, nurse practitioner, physician assistant) ☐ Public health professional
☐ Other health care professionals (nurses, chiropractors, dentists, etc.) ☐ Web searches/Internet (WebMD, Mayo Clinic, Healthline, etc.) ☐ Word of mouth, from others (friends, neighbors, co-‐workers, etc.) ☐ Other (Please specify) _______________________________
Q23. In the past year, have you or a family member had any interaction with the local public health
unit? � No � Yes
Q23b. If yes, what interactions have you or a family member had with the local public health unit? ______________________________________________________________________________

58
Q24. Which of the following public health services have you or a family member used in the past year? (Choose ALL that apply.)
� Bicycle helmet safety education � Blood pressure checks � Car seat program � Child health (well baby checks) � Diabetes screening � Emergency preparedness services � Environmental health services (water,
sewer, health hazard abatement) � Flu shots � Health Fair activity for KEM Electric
Coop � Health Tracks (child health screening) � Home health
� Immunizations � Newborn home visits � Preschool screenings � School health screenings � Tobacco prevention and control � Tuberculosis testing and management � West Nile program � WIC (Women, Infants & Children)
Program � Worksite wellness � Youth education programs (First Aid,
Bike Safety)
Linton Hospital and Clinics services Q25. Are you aware of Linton Hospital’s Foundation, which exists to financially support Linton Medical Center, Hazelton Clinic and Campbell County Clinic? ☐ Yes ☐ No Q26. Have you supported the Linton Hospital Foundation in any of the following ways? (Choose ALL that apply.)
� Cash or stock gift � Endowment gifts � Memorial/Honorarium � Planned gifts through wills, trusts or life insurance policies � Other: (please specify) ___________________________________________________________________________
Demographic Information Please tell us about yourself. Q27. Health insurance status: (Choose ALL that apply.)
� Insurance through employer � No insurance/not enough insurance � Medicaid � Veteran’s Health Care Benefits � Medicare � Other. Please specify:____________________ � Private insurance
59
Q28: Age:
� Less than 25 years � 25 to 34 years � 35 to 44 years � 45 to 54 years
� 55 to 64 years � 65 to 74 years � 75 years and older
Q29. Highest level of education:
� Some high school � High school diploma or GED � Some college/technical degree
� Associate’s degree � Bachelor’s degree � Graduate or professional degree
Q30. Gender: � Female � Male
Q31. Marital status: � Divorced/separated � Married
� Single/never married � Widowed
Q32. Employment status:
� Full time � Part time � Homemaker
� Multiple job holder � Unemployed � Retired
Q33. Annual household income before taxes:
� Less than $15,000 � $15,000 to $24,999 � $25,000 to $49,999 � $50,000 to $74,999
� $75,000 to $99,999 � $100,000 to $149,999 � $150,000 and over � Prefer not to answer
Q34. Your zip code: ____________
Q35. Overall, please share concerns and suggestions to improve the delivery of local health care.
Thank you for assisting us with this important survey!

60
Appendix A2 – Health Care Professional Survey Instrument
Health Care Professional Health Survey Linton Hospital and Emmons County Public Health are interested in hearing from you about area health issues and concerns. The focus of this effort is to:
• Learn of the good things in the community and the community’s concerns • Understand perceptions and attitudes about the health of the community, and hear suggestions for
improvement • Learn more about how local health services are used by you and other residents
Please take a few moments to complete the survey. If you prefer, you may take the survey online at http://tinyurl.com/emmonscountysurvey Surveys will be tabulated by the Center for Rural Health at the University of North Dakota School of Medicine and Health Sciences. Your responses are anonymous, and you may skip any question you do not want to answer. Your answers will be combined with other responses and reported only in total. If you have questions about the survey, you may contact Karin Becker at (701) 777-‐4499.
Surveys will be accepted through June 30, 2014. Your opinion matters – thank you in advance!
Community Assets and Collaboration Please tell us about your community by choosing up to three options you most agree with in each category below: Q1. Considering the PEOPLE in your community, the best things are (choose up to THREE):
� Community is socially and culturally diverse or becoming more diverse �
People who live here are involved in the community
� Feeling connected to people who live here �
Sense that you can make a difference through community engagement
� Forward-‐thinking ideas (social values, government) � Tolerance, inclusion, open-‐minded
� Government is accessible � Other (please specify)_________________________
� People are friendly, helpful, supportive
Q2. Considering the SERVICES AND RESOURCES in your community, the best things are (choose up to THREE):
� Downtown and shopping (close by, good variety, availability of goods) � Public services and amenities
� Health care � Public transportation
� Opportunities to learn and/or go to college � Restaurants and healthy food
61
� Quality school systems and programs for youth �
Other (please specify)_________________________
Q3. Considering the QUALITY OF LIFE in your community, the best things are (choose up to THREE):
� Family-‐friendly; good place to raise kids � Job opportunities or economic opportunities
� Healthy place to live � Safe place to live, little/no crime
� Informal, simple, laidback lifestyle � Other (please specify)_________________________
Q4. Considering the ACTIVITIES in your community, the best things are (choose up to THREE):
� Activities for families and youth � Specific events and festivals
� Arts and cultural activities and/or cultural richness of community �
Year-‐round access to fitness opportunities (indoor activities, winter sports, etc.)
� Recreational and sports activities (e.g., outdoor recreation, parks, bike paths, and other activities)
� Other (please specify)_________________________
Q5. Considering the GEOGRAPHIC SETTING in your community, the best things are (choose up to THREE):
� Cleanliness of area (e.g., fresh air, lack of pollution and litter) � Natural setting: outdoors and nature
� Climate and seasons � Relatively small size and scale of community
� General beauty of environment and/or scenery �
Waterfront, rivers, lakes, and/or beaches
� General proximity to work and activities (e.g., short commute, convenient access)
� Other (please specify)_________________________
Q6. What are other “best things” about your community that are not listed in the questions above? _____________________________________________________________________________________ _____________________________________________________________________________________ Q7. What are the major challenges facing your community? _____________________________________________________________________________________ _____________________________________________________________________________________ Q8. For each choice on the next page please rank the level of collaboration, or how well these groups
work with others in the community, on a scale of 1 to 5, with 1 being no collaboration (not working well with others) and 5 being excellent collaboration (working well with others).
62
Community Collaboration No Excellent collaboration collaboration
Don’t Know/Not Applicable
1 2 3 4 5 Business and industry Clinics Economic development organizations Emergency services, including ambulance and fire Health and human services agencies Hospital(s) Indian Health Service Law enforcement Long term care, including nursing homes and assisted living Other local health providers, such as dentists and chiropractors Pharmacies Public Health Schools Tribal Health
Q9. Do you believe that health-‐related organizations in the community are working together to improve
the overall health of the area population? � No � Yes
Q10. Which, if any, of the following do you think would result from better collaboration among health
care providers and health-‐related organizations? (Choose ALL that apply.) ☐ Better customer service ☐Less duplication of care ☐ Better patient care ☐Lower costs ☐ Better overall health of the area’s population ☐More complete and accurate health records ☐ Coordination of appointments ☐ Need for fewer appointments ☐ Other (Please specify)______________________
Q11. What suggestions do you have for health-‐related organizations to work together to provide better services and improve the overall health of the area population?
______________________________________________________________________________ ______________________________________________________________________________ Q12. Where do you find out—or where do you think community members find out-‐-‐ what health services are available in your area? (Choose ALL that apply.)
� Advertising � From health care professionals � From public health professionals � Social media (Facebook, Twitter, etc.) � Indian Health Service � Tribal health � Newspaper � Web searches � Radio � Employer/worksite wellness � Word of mouth, from others
(friends, neighbors, co-‐workers, etc.) � Other (Please specify)_________________
63
Community Concerns Q13. Regarding the conditions in your community, in the following series of categories please rank each of the potential concerns on a scale of 1 to 5, with 1 being less of a concern and 5 being more of a concern:
Community/environmental concerns Less of More of a concern a concern 1 2 3 4 5
Active faith community Attracting and retaining young families Not enough jobs with livable wages, not enough to live on Not enough affordable housing Poverty Changes in population size (increasing or decreasing) Crime and safety, adequate law enforcement personnel Water quality (well water, lakes, streams, rivers) Air quality Litter (amount of litter, adequate garbage collection) Having enough child daycare services Having enough quality school resources Not enough places for exercise and wellness activities Not enough public transportation options, cost of public transportation Racism, prejudice, hate, discrimination Seatbelt use Traffic safety, including speeding, road safety, and drunk/distracted driving Physical violence, domestic violence, sexual abuse Child abuse Bullying
Concerns about health services Less of More of a concern a concern 1 2 3 4 5
Ability to get appointments for health services Extra hours for appointments, such as evenings and weekends Availability of doctors and nurses Availability of public health professionals Ability to retain doctors and nurses in the community Availability of specialists Not enough health care staff in general Availability of providers that speak my language and/or have translators Availability of wellness and disease prevention services Availability of mental health services Availability of substance abuse/treatment services Availability of dental care Availability of vision care Different health care providers having access to health care information and working together to coordinate care
Providers using electronic health records
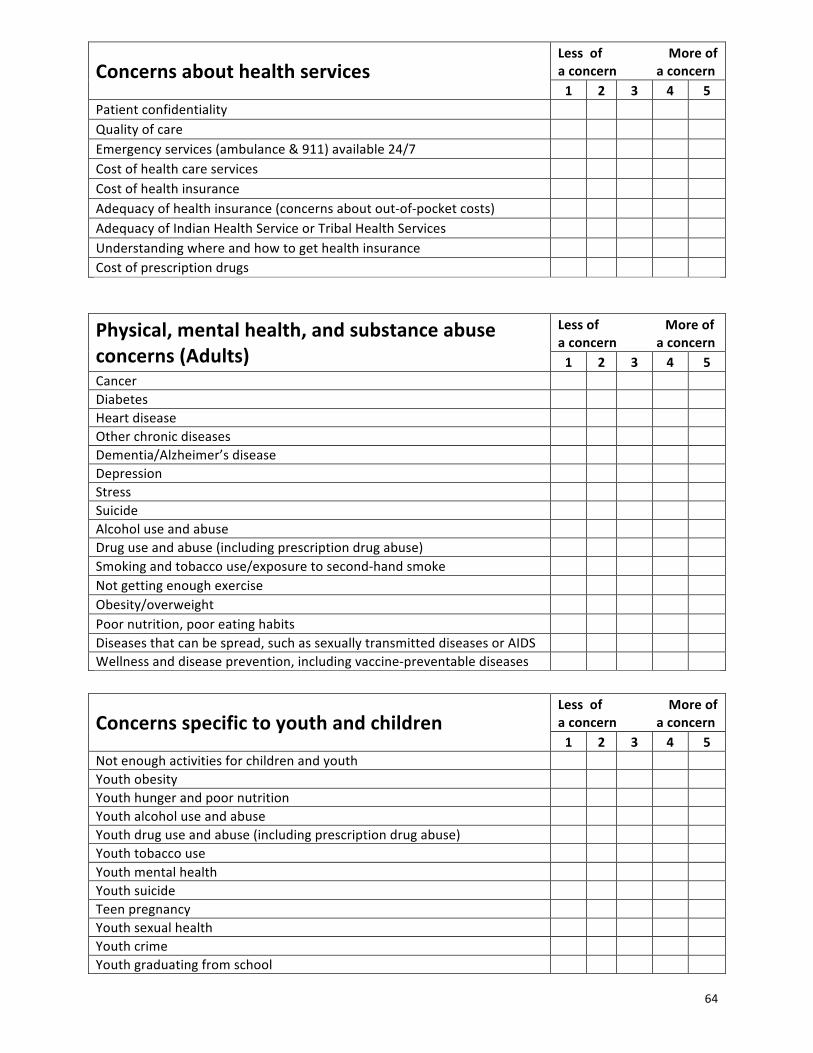
64
Concerns about health services Less of More of a concern a concern 1 2 3 4 5
Patient confidentiality Quality of care Emergency services (ambulance & 911) available 24/7 Cost of health care services Cost of health insurance Adequacy of health insurance (concerns about out-‐of-‐pocket costs) Adequacy of Indian Health Service or Tribal Health Services Understanding where and how to get health insurance Cost of prescription drugs
Physical, mental health, and substance abuse concerns (Adults)
Less of More of a concern a concern 1 2 3 4 5
Cancer Diabetes Heart disease Other chronic diseases Dementia/Alzheimer’s disease Depression Stress Suicide Alcohol use and abuse Drug use and abuse (including prescription drug abuse) Smoking and tobacco use/exposure to second-‐hand smoke Not getting enough exercise Obesity/overweight Poor nutrition, poor eating habits Diseases that can be spread, such as sexually transmitted diseases or AIDS Wellness and disease prevention, including vaccine-‐preventable diseases
Concerns specific to youth and children Less of More of a concern a concern 1 2 3 4 5
Not enough activities for children and youth Youth obesity Youth hunger and poor nutrition Youth alcohol use and abuse Youth drug use and abuse (including prescription drug abuse) Youth tobacco use Youth mental health Youth suicide Teen pregnancy Youth sexual health Youth crime Youth graduating from school

65
Concerns about the aging population Less of More of a concern a concern 1 2 3 4 5
Being able to meet needs of older population Long-‐term/nursing home care options Assisted living options Availability of resources to help the elderly stay in their homes Availability/cost of activities for seniors Availability of resources for family and friends caring for elders Delivery of Health Care Q14. Please tell us why you think community members seek health care services close to home.
(Choose ALL that apply.)
� Access to specialist � Location is nearby � Confidentiality � Loyalty to local care providers � Convenience � Open at convenient times � Disability access � They take my insurance � Eligible for care from IHS � They take new patients � Familiar with providers � Transportation is readily available � High quality of care � Other (Please specify)_________________ � Less costly �
Q15. Please tell us why you think community members go out of the area for health care needs.
(Choose ALL that apply.)
� Access to specialist � Loyalty to local service providers � Confidentiality � Not eligible for care from IHS � Convenience � Open at convenient times � Disability access � Proximity � Familiar with providers � Referral � High quality of care � They take my insurance � Less costly � They take new patients � Eligible for contract health services under IHS � Transportation is readily available � � Other (Please specify)_________________
Q16. What specific health care services do community members need to travel out of the area to
receive? ______________________________________________________________________________ ______________________________________________________________________________
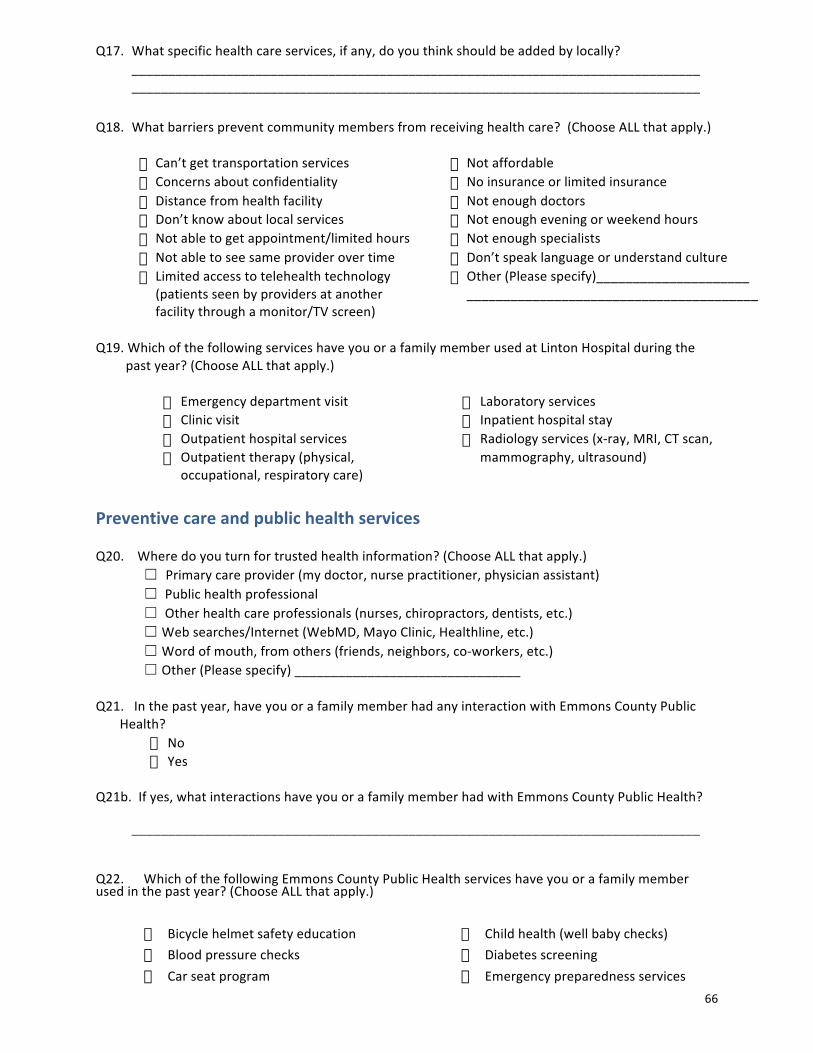
66
Q17. What specific health care services, if any, do you think should be added by locally? ______________________________________________________________________________ ______________________________________________________________________________ Q18. What barriers prevent community members from receiving health care? (Choose ALL that apply.)
� Can’t get transportation services � Not affordable � Concerns about confidentiality � No insurance or limited insurance � Distance from health facility � Not enough doctors � Don’t know about local services � Not enough evening or weekend hours � Not able to get appointment/limited hours � Not enough specialists � Not able to see same provider over time � Don’t speak language or understand culture � Limited access to telehealth technology
(patients seen by providers at another facility through a monitor/TV screen)
� Other (Please specify)_____________________ ________________________________________
Q19. Which of the following services have you or a family member used at Linton Hospital during the past year? (Choose ALL that apply.)
� Emergency department visit � Laboratory services � Clinic visit � Inpatient hospital stay � Outpatient hospital services � Radiology services (x-‐ray, MRI, CT scan, � Outpatient therapy (physical,
occupational, respiratory care) � mammography, ultrasound)
Preventive care and public health services Q20. Where do you turn for trusted health information? (Choose ALL that apply.) ☐ Primary care provider (my doctor, nurse practitioner, physician assistant) ☐ Public health professional
☐ Other health care professionals (nurses, chiropractors, dentists, etc.) ☐ Web searches/Internet (WebMD, Mayo Clinic, Healthline, etc.) ☐ Word of mouth, from others (friends, neighbors, co-‐workers, etc.) ☐ Other (Please specify) _______________________________
Q21. In the past year, have you or a family member had any interaction with Emmons County Public
Health? � No � Yes
Q21b. If yes, what interactions have you or a family member had with Emmons County Public Health? ______________________________________________________________________________ Q22. Which of the following Emmons County Public Health services have you or a family member used in the past year? (Choose ALL that apply.)
� Bicycle helmet safety education � Blood pressure checks � Car seat program
� Child health (well baby checks) � Diabetes screening � Emergency preparedness services
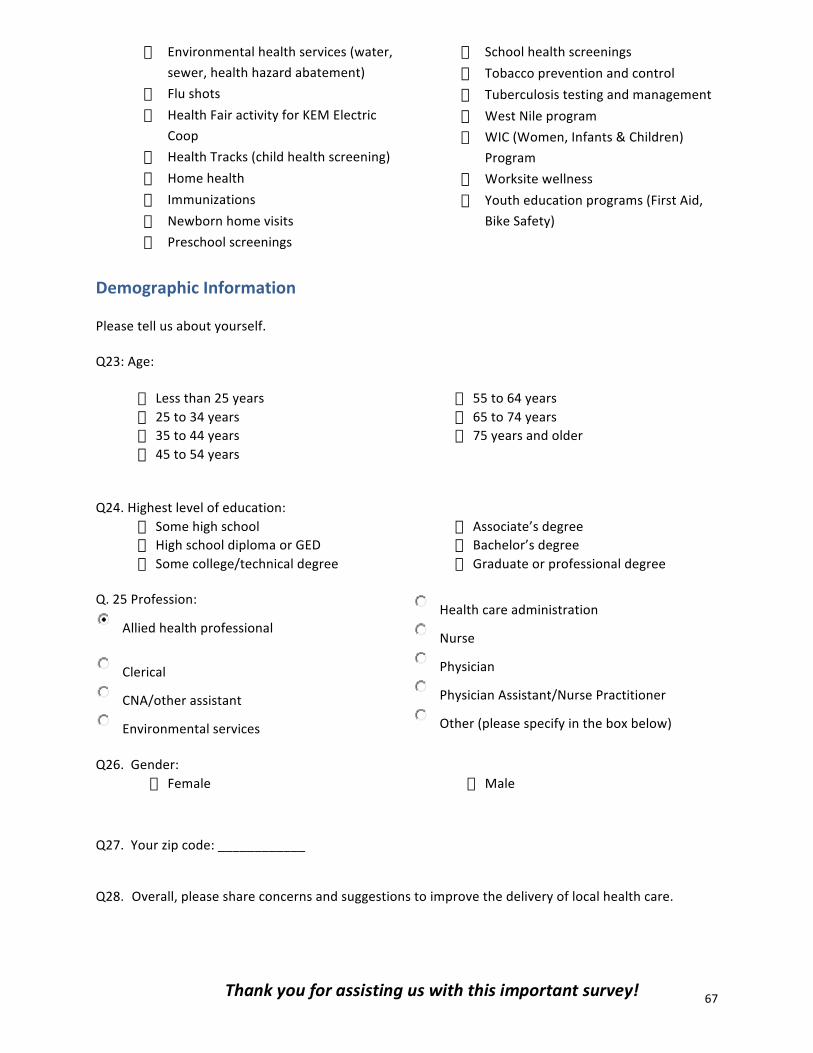
67
� Environmental health services (water, sewer, health hazard abatement)
� Flu shots � Health Fair activity for KEM Electric
Coop � Health Tracks (child health screening) � Home health � Immunizations � Newborn home visits � Preschool screenings
� School health screenings � Tobacco prevention and control � Tuberculosis testing and management � West Nile program � WIC (Women, Infants & Children)
Program � Worksite wellness � Youth education programs (First Aid,
Bike Safety)
Demographic Information Please tell us about yourself. Q23: Age:
� Less than 25 years � 25 to 34 years � 35 to 44 years � 45 to 54 years
� 55 to 64 years � 65 to 74 years � 75 years and older
Q24. Highest level of education:
� Some high school � High school diploma or GED � Some college/technical degree
� Associate’s degree � Bachelor’s degree � Graduate or professional degree
Q. 25 Profession:
Allied health professional
Clerical
CNA/other assistant
Environmental services
Health care administration
Nurse
Physician
Physician Assistant/Nurse Practitioner
Other (please specify in the box below)
Q26. Gender:
� Female � Male
Q27. Your zip code: ____________
Q28. Overall, please share concerns and suggestions to improve the delivery of local health care.
Thank you for assisting us with this important survey!

68
Appendix B – County Health Rankings Model

69
Appendix C – Emmons County Community Health Profile
!""#$% & ' #($ ) * & ' #""($ + ) * & , - . / ) 0 & 1 2 # 3 + / - &!"!#$%&'"()
45-&62#(78("9-2 1-2:-$) 8("9-2 1-2:-$)
!"# $%! &!'&( )*+%,& &-'%(&!"&# *%. &$'&( ),+-%* &$'!(-!"-# &%# *')( &!)+..- &%'&($!"$# -)$ )'!( ,,+#.* &&'%(*!"*# *,- &$'$( )*+.,, &-'%(.!".# .%& &.')( #%+--$ &*'$(%!"%# *)% &$',( %&+#!& #'-(,!",# *!$ &&'*( $#+-&$ .')()!/ $.& #'#( $-+-$% *')(01234 $+..! &!!'!( %,-+.#& &!!'!(!"&, ,.# -&'*( &*#+),& --'$(%./ #,& -,'*( #,+*,, &*'.(
1#7(/.)+#$&9*&45-&62#(7;&<=>=&'-$%(%8#2)0&?.@#).!""#$%&'#($)*
&*+),+-./012*34)5+463.7).8)6*39)0+2.06)4.-+9)80.-)6*+)#5):+79;9)<;0+1;)=>>>?4+79;9?/.@A?))B.96)61CD+9)10+)E+03@+E)+36*+0)80.-)6*+)8;DD)=FGGHA)4+79;9)61I+7)37)JGFG).0)80.-)6*+):.--;736K)!.2;D163.7)5;0@+K)1//0+/016+E).@+0)1)9+@+01D)K+10)2+03.E?))&*+)61CD+)*+1E+0)E+9403C+9)6*+)92+43834)K+109)80.-)>*34*)6*+)E161)39)E+03@+E?))&*+)61CD+)9*.>37/)2+04+76)2.2;D163.7)4*17/+);9+9)4+79;9)E161)80.-)JGGG)1D9.?))&1CD+9)20+9+76)7;-C+0).8)2+09.79)17E)2+04+761/+9)>*34*)37)1D-.96)1DD)4304;-96174+9)0+20+9+76)6*+)416+/.0K)92+43834)2+04+761/+).8)1DD)2+09.79)0+8+0+74+E)CK)6*+)61CD+)=+?/?L)2+04+761/+).8)2+09.79)1/+)FM)17E).DE+0)>*.)10+)-1003+EA?)))%/+)92+43834)2.@+06K)016+9)0+20+9+76)6*+)2+04+761/+).8)+14*)1/+)/0.;2)>*34*)39)37)2.@+06K)=+?/?L)2+04+761/+).8)4*3DE0+7));7E+0)83@+)K+109)37)2.@+06KA?))
F)
J)

70
!""#$% & ' #($ ) * & ' #""($ + ) * & , - . / ) 0 & 1 2 # 3 + / - &!"!#$%&'"()
!"#$%& '%&(%)*+,% !"#$%& '%&(%)*+,%!"##$ %$$&$' ()*"#+% %$$&$'!",+# +-&#' ($#",,+ +$&$'
* $&%' )"+($ %&*'%, $&,' !("#+% #&,'( $&*' ("+$+ %&$'$ $&$' !*$ $&$'( $&*' !"#$+ $&#'*) $&-' %%"-#! %&-'
4.5-6&7898&'-$%(%&
./0123456
70458
!-&*./0+1-*+2##-)3/4-")*5
9:140;<216
4.5-
=>&?@A24@=B24@C45&D?B04@A63E1<63
!"#$%& '%&(%)*+,% !"#$%& '%&(%)*+,%!"(%) %$$&$' (#+"-#- %$$&$'
:$&0#(%-0#/;% !"#!$ +)&(' (!,"()+ +(&*'*"+%( -$&(' #$,"%,- )(&,'(%, %)&$' %!$"#!% %+&-'
:$&<2#(=&>(.2)-2% -) *&,' *#"%)+ !&-'#! %&#' +"()# %&#'!, $&+' %#"#$, *&!'
,#(%-0#/;&1#=(/.)+#$%6&78982##-)3/4-")*5 !-&*./0+1-*+
,#(%-0#/;&?*=-9:140
?@B121/12:@402F6ADG:G/0412:@
?@D@:@H4>20ID<:/B6<:0ABJ
K:@2@B121/12:@402F6ADG:G/0412:@
?@DH4>20ID<:/B6<:0ABJ
@<-&A2#(=B("C-2 1-25-$) B("C-2 1-25-$)
$L+ %)$ ,)&*' ,%!!$ ,-&-'%$L%+ **- ,+&$' ,**)) ,-&,'*$L*+ () !+&(' #$#)% ,(&('!$L!+ %!( ,-&%' !)%,, ,)&(',$L,+ *!! ,+&,' ,%,++ ,+&%'#$L#+ *,! ,!&!' ,)*-! ,+&%'($L(+ *#* #%&+' !$(++ ,+&(')$L)+ %++ ,+&,' *%,#! #,&)'-$M *$* #)&#' *$,)% (!&#'9:140 %")!$ ,-&)' !!*")*) ,+&#'$L%) !), ,+&!' )!$-! ,-&-'(#M #%* #*&)' ##$#$ #(&#'
D-"./-&1#=(/.)+#$&.$;&1-25-$).<-&D-"./-&C*&@<-6&7898&'-$%(%
B#2)0&E.F#).!""#$%&'#($)*
*)
+)
,)
-)
'-$%(%!""#$%&'#($)*
B#2)0&E.F#).
%++$ ,"-!$ (!-"-$$*$$$ ,"!!% L%$&!' (,*"*$$ $&#'*$%$ !"##$ L%-&$' ()*"#+% ,&)'
E-5-$$+./&1#=(/.)+#$&'0.$<-6&9GG8&)#&78886&7888&)#&7898
98&H-.2&'0.$<-&IJK
98&H-.2&'0.$<-&IJK
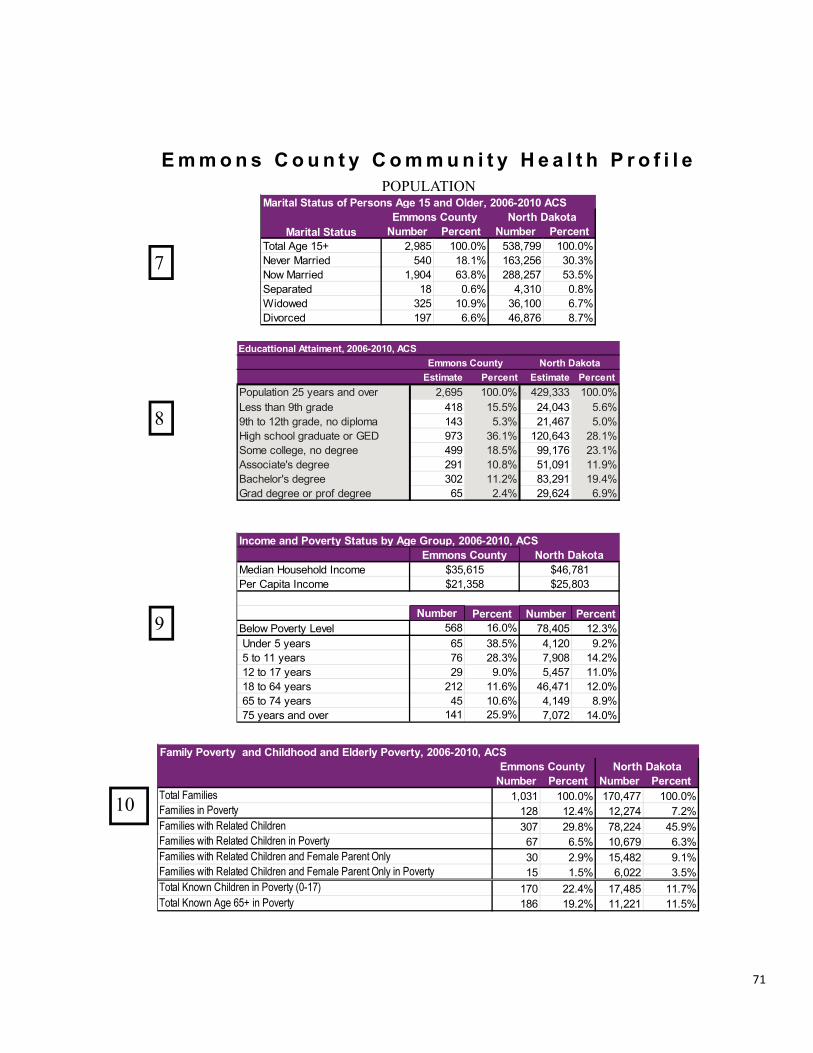
71
!""#$% & ' #($ ) * & ' #""($ + ) * & , - . / ) 0 & 1 2 # 3 + / - &!"!#$%&'"()
4("5-2 1-26-$) 4("5-2 1-26-$)!"# $"%&' (#)*&! $+%,'"! ,#%!' *)$+& -%+'(" +#%,' ()-&# $*%+'+- -%&' !)*!( $$%&'+$+ $$%"' *")*($ $+%&'*! $&%"' *)$*- #%-'$*$ +!%-' ()&(+ $*%&'
.+$),!# .+!)#&,
/01234/!/53647/!/89/$$/53647/$+/89/$(/53647/$#/89/"*/53647/"!/89/(*/53647/(!/53647/612/9:34
;3<9=/>9:3485/?3:3<
7$6#"-&.$8&1#9-2)*&:).)(%&5*&;<-&=2#(>?&@AABC@ADA?&;':!""#$%&'#($)* 4#2)0&E.F#).
@32A61/B9C73D9<2/E1F9G3 .,!)"$! .*")(#$>34/H6IA86/E1F9G3
4("5-2 1-26-$) 4("5-2 1-26-$)$)&,$ $&&%&' $(&)*(( $&&%&'$+# $+%*' $+)+(* (%+',&( +-%#' (#)++* *!%-'"( "%!' $&)"(- "%,',& +%-' $!)*#+ -%$'$! $%!' ")&++ ,%!'$(& ++%*' $()*#! $$%('$#" $-%+' $$)++$ $$%!'
!"#$%$&'($)(*+,&-./
G."+/*&1#9-2)*&&.$8&'0+/80##8&.$8&!/8-2/*&1#9-2)*?&@AABC@ADA?&;':!""#$%&'#($)*& 4#2)0&E.F#).
0+."%(!"#$%$&'
!"#$%$&'(1$.2(3&%".&4(52$%4-&)(")4(!&#"%&(*"-&).(6)%/
!"#$%$&'(1$.2(3&%".&4(52$%4-&)
0+."%(7)+1)(52$%4-&)($)(*+,&-./(89:;<=0+."%(7)+1)(>?&(@AB($)(*+,&-./
!"#$%$&'(1$.2(3&%".&4(52$%4-&)(")4(!&#"%&(*"-&).(6)%/($)(*+,&-./
!"#$%$&'(1$.2(3&%".&4(52$%4-&)($)(*+,&-./
4("5-2 1-26-$) 4("5-2 1-26-$)+)-#! $&&%&' !,#)(-- $&&%&'!*& $#%$' $",)+!" ,&%,'
$)-&* ",%#' +##)+!( !,%!'$# &%"' *),$& &%#',+! $&%-' ,")$&& "%('$-( "%"' *")#(" #%('
H.2+)./&:).)(%&1-2%#$%&;<-&DI&.$8&J/8-2?&@AABC@ADA&;':
H.2+)./&:).)(%4#2)0&E.F#).
J986</KL3/$!M
N3I646832OA29=32PA:94F32
!""#$%&'#($)*
Q3:34/@644A32Q9=/@644A32
!%)+".)- 1-26-$) !%)+".)- 1-26-$)&+)"-! $&&%&' *+-),,, $&&%&'*$# $!%!' +*)&*, !%"'$*, !%,' +$)*"( !%&'-(, ,"%$' $+&)"*, +#%$'*-- $#%!' --)$(" +,%$'+-$ $&%#' !$)&-$ $$%-',&+ $$%+' #,)+-$ $-%*'"! +%*' +-)"+* "%-'
-8D/89/$+8D/L4623)/19/2AI<9G6
!8(6.))+#$./&;)).+"-$)?&@AABC@ADA?&;':!""#$%&'#($)* 4#2)0&E.F#).
>9IC<68A91/+!/53647/612/9:34?377/8D61/-8D/L4623
;6FD3<94R7/23L433
BALD/7FD99</L462C683/94/STPN9G3/F9<<3L3)/19/23L433K779FA683R7/23L433
S462/23L433/94/I49U/23L433
*)
+)
,)
-.)

72
!"#$%&'#$#"(#")(&*$#$&&+,-./'&01*&*20./'&
!""#$% & ' #($ ) * & ' #""($ + ) * & , - . / ) 0 & 1 2 # 3 + / - &
4("5-26.)-&6.)+# 4("5-2&
6.)-&6.)+#
!"# $ ""%"#& !'(#!)* $ "$%$!$ !"()
* * '%''& !+(#* * "%*,# #'("
4("5-2 6.)+# 4("5-2 6.)+#!# $) !"%)*, '#,()#$ !$& !$%!*' '&*($
4("5-2 6.)+# 4("5-2 6.)+#* * #%+!+ ,)(&
7+2)0%8&9::;<&9:=:
-./012345067285401234509:;0<942.0
=7342>24?0<947@77:012345A09:;0<947
4#2)0&>.?#).
@77:0B378:9:C27A09:;0<947
&!("
!""#$%&'#($)*
&*
-2D7012345A09:;0<947B378:9:C27A09:;0<947
EF40.G067;>.CH012345A09:;0<942.EF40.G067;>.CH0B37809:;0<942.
!"#$%&'#$#"(#")(&*$#$&)345(&6734U&9"7#8&$:;&;5$#8&75)37;(&)3%%5)#5;&9<U&'#$#5&36&137#8&*$=3#$&$>>75>$#5;&3?57&$&6"?5&<5$7&@57"3;A&&0%%&9"7#8(&$:;&;5$#8(&75@75(5:#U&)3B:#<&36&75(";5:)5&:3#U&)3B:#<&36&3))B775:)5A&&.85&:B4957&36&5?5:#(&"(&9%3)=5;&"6&65C57$:&("DA&E374B%$(&637&)$%)B%$#":>&7$#5(&$:;&7$#"3(&$75&$(&63%%3C(F&&!"#$%&'($)&G&-5(";5:#&%"?5&9"7#8(&;"?";5;&9<U#$%&75(";5:#&@3@B%$#"3:&D&HIIIA&*#)+,(,-").&G&J"?5&9"7#8(&K&E5#$%&;5$#8(&K&,:;B)5;Ⱦ":$#"3:&36&@75>:$:)<A&*#)+,(,-/&'($)&G&.3#$%&@75>:$:)"5(&;"?";5;&9U#$%&75(";5:#&@3@B%$#"3:&D&HIIIA&0)#$"1"$/&'($)&G&-5(";5:#&%"?5&9"7#8(&;"?";5;&9<&654$%5&@3@B%$#"3:&L$>5&HMNOOP&D&HIIIA&2)),(+)&!"#$%&'($)&G&.55:$>5&9"7#8(&L$>5&QRIP&;"?";5;&9<&654$%57:&@3@B%$#"3:&D&HIIIA&2)),(+)&*#)+,(,-/&'($)&G&.55:$>5&@75>:$:)"5(&L$>5QRIP&;"?";5;&9<&654$%57:&@3@B%$#"3:&D&HIIIA&34$&56&7)815-9&:";)&!"#$%&'($"5&G&-5(";5:#&SST&%"?5&9"7#8(&;"?";5;&9<#$%&75(";5:#&%"?5&9"7#8(&D&HIIIA&34$&56&7)815-9&*#)+,(,-/&'($"5&G&-5(";5:#&SST&@75>:$:)"5(&;"?";5;&9<#$%&@75>:$:)"5(&D&HIIIA&:5<&7)"+%$&'($"5&G&J3C&C5">8#&9"7#8(&L9"7#8&C5">8#&Q&RMII&>7$4(P&;"?";5;&9<#$%&75(";5:#&%"?5&9"7#8(&D&HIIIA&=,6(,$&>)($%&'($"5&G&1B4957&36&":6$:#&;5$#8(&;"?";5;&9<U#$%&75(";5:#&%"?5&9"7#8(&D&HIIIA&?%"18%558&@&A851).-),$&>)($%.&G&*5$#8(&":;"?";B$%(&H&N&HU&<5$7(&36&$>5A&?%"18%558&(,8&A851).-),$&>)($%&'($)&G&1B4957&36&75(";5:#&;5$#8(&L$>5&H&N&HUP&;"?";5;&9<&@3@B%$#"3:&L$>5&H&N&HUP&D&HIIVIIIA&?#48)&>)($%&'($)&G&*5$#8&5?5:#(&;"?";5;&9<&@3@B%$#"3:&D&HIIVIIIA&A+)BA8C4.$)8&>)($%&'($)&G&*5$#8&5?5:#(&C"#8&$>5&(@5)"6")&$;WB(#45:#(&D&HIIVIII&@3@B%$#"3:A&&
4("5-26.)-&6.)+# 4("5-2&
6.)-&6.)+#
* * #$! ,
I, JK #$) ')#$, !,!! #$%+$" $,#
'0+/@&>-.)0%8&9::;<9:=:4#2)0&>.?#).
L:G9:40M7945A09:;0<942.
!""#$%&'#($)*
N52>;09:;0K;.>7AC7:40M7945A09:;0<[email protected]>0M7945A09:;0N3F;70<947
HH&
HR&

73
!"#$%&'#$#"(#")(&*$#$&&+,-./'&01*&*20./'&
!""#$% & ' #($ ) * & ' #""($ + ) * & , - . / ) 0 & 1 2 # 3 + / - &
!"#$%&%'()%**"&+',-%+./-"#(#-0(1-2*+%-3#
456(7849:5:5;+"<"0%
6=>(7=9?@6(78A9
B"CCD/'"'?(78A9
!""#$%&'#($)*4("5-2&6789:&;.)-<
5EA44(785698E5>5(7F=98E>F5(74@98E5@?(7F>9
8E@?6(76598EA4A(7469G-"-&%-&"/-#*(1-H+CI 88(7F59
8A(74F9
?E866(785698@?(76469
4#2)0&=.>#).4("5-2&6789:&;.)-<
=-.)0%&.$8&7?-&789(%)-8&=-.)0&;.)-&5*&'.(%-@&ABBCDABEB
6=E>=A(75=>9J**(B#+'%' 6=5(7?F59
BK,!
L%#C&(!"'%#'%B#-<%C
?(78?9J*3D%".%C'(!"'%#'%
54(785?96@(74?984(7F@9
;&C/M%34&

74
!"#$%&'#$#"(#")(&*$#$&&+,-./'&01*&*20./'&
!""#$% & ' #($ ) * & ' #""($ + ) * & , - . / ) 0 & 1 2 # 3 + / - &
45-
!"#$%&''
()*+&,-&#./01*2
3456N
9&4#"82
!"#$%&
3456&#':
9&4#";:
!"#$%&
9&4#"<
3456
9&4#"
3456&#'<
9&4#"=
1,4>&"&/
1,4>&"&/
6-.7+$5&'.(%-%&8-.)0&9*&45-&:2#(;&3#2&!""#$%&'#($)*<&=>>?@=>A>A =
<8?2:
28?=:
!@,6,A&
!@,6,A&
3456&#
B5,5"&5",$54)0C5D@#E
:8?8:
88?<:
F?:
8?':
'8?7:
78?;:
=8G
B5,5"&5",$54)0C5D@#E
;8?::
B
45-
9&4#";;8
'8?7:
B5,5"&5",$54)0C5D@#E7<
:8?8:
B5,5"&5",$54)0C5D@#E'=:
!@,6,A&H'
9&4#";7
;8?:: 9&4#"H:
6-.7+$5&'.(%-%&8-.)0&9*&45-&:2#(;&3#2&C#2)0&8.D#).<&=>>?@=>A>A = B
F?: 3$5I&5,"4)0(5$-4)E<H
J#&-4"@#,"E::
!C1!0:F
8?':
!@,6,A&'FH
3456F
28?=:
3456&#'FF'
9&4#";:7'
=8G
9&4#"'2H2
()*+&,-&#./01*';H'
3456&#'8<7
3$5I&5,"4)0(5$-4)E<
B5,5"&5",$54)0C5D@#E'2;
B5,5"&5",$54)0C5D@#E'H:
B5,5"&5",$54)0C5D@#E';2
3456&#'HH7
3456&#';87
B5,5"&5",$54)0C5D@#E'<<
88?<:
3456&#==
9&4#"82H
3KJ1;';
<8?2:
3456&#:H;
9&4#"=:;
3KJ1<7<
3456&#'F
78?;:
34&
35&

75
!"#$%&'()!*+,-!$&-+./&0!1%,-.2&344563454&
!""#$% & ' #($ ) * & ' #""($ + ) * & , - . / ) 0 & 1 2 # 3 + / - &
!789:&';<=>?@A=9&-?BC&0=D:@A&7=:=&=A;&7;A?>;7&EA@F&=GGA;G=:;7&7=:=&H:<;&I8FJ;A&@E&K;=AB&BL;D?E?;7&?B&?I&:<;&:=J9;M&D@I:?I8@8B9K&D@99;D:;7&JK&:;9;L<@I;&B8A>;K&EA@F&L;AB@IB&5N&K;=AB&=I7&@97;AO&&!99&7=:=&?B&B;9E6A;L@A:;7&7=:=O&&P8FJ;AB&G?>;I&=A;&L@?I:&;B:?F=:;&L;AD;I:=G;B&E@99@Q;7&JK&RST&D@IE?7;ID;&?I:;A>=9BO&&.:=:?B:?D=9&B?GI?E?D=ID;&D=I&J;&7;:;AF?I;7&JK&D@FL=A?IG&D@IE?7;ID;&?I:;A>=9B&J;:Q;;I&:Q@&G;@GA=L<?D&=A;=BO&%@&J;&B:=:?B:?D=99K&B?GI?E?D=I:2&D@IE?7;ID;&F=K&I@:&@>;A9=LO&&0@A&;U=FL9;&:<;&D@IE?7;ID;&?I:;A>=9B&ROV&HNOV654O3M&=I7&54ON&H54O4655OWM&@>;A9=L&HB;;&L?D:8A;&J;9@QM&B@&:<;&7?EE;A;ID;&J;:Q;;I&:<;&:Q@&I8FJ;AB&?B&I@:&B:=:?B:?D=99K&B?GI?E?D=I:O&&%<=:&F;=IB&:<=:&B8JB:=I:?=9&8ID;A:=?I:K&A;F=?IB&Q<;:<;A&:<;&=LL=A;I:&7?EE;A;ID;&?B&78;&:@&D<=ID;&=9@I;&H78;&:@&B=FL9?IG&>=A?=:?@IM&A=:<;A&:<=I&A;LA;B;I:?IG&=&:A8;&7?EE;A;ID;&?I&:<;&LA;>=9;ID;&@E&:<;&D@I7?:?@I&?I&:<;&:Q@&L@L89=:?@IBO&&%<;&9;BB&:<;K&@>;A9=L2&:<;&F@A;&9?C;9K&?:&?B&:<=:&:<;&&L@?I:&;B:?F=:;B&A;LA;B;I:&:A89K&7?EE;A;I:&LA;>=9;ID;B&?I&:<;&:Q@&L@L89=:?@IBO&&&
45'6,65 !""#$%&'#($)*7
8#2)0&9.:#).7
!"#$%&'("#)"#$*%+,-#.%#/+&01-&(%,-(/%.&2"#$%&.("#)"#$&34&.("#)+&5-(&6%#7&8&.("#)+&5-(&0-6%#9&-#%&-(&6-(%&/"6%+&"#&/1%&,:+/&;<&.:=+>&
?@>A&3?<>8BAA>?9 A?>?&3A<>4BA?>@9
C%:D=&'("#)"#$&*%+,-#.%#/+&01-&(%,-(/%.&1%:D=&.("#)"#$&36-(%&/1:#&A&.("#)+&,%(&.:=&5-(&6%#7&6-(%&/1:#&?&.("#)&,%(&.:=&5-(&0-6%#9&.E("#$&/1%&,:+/&;<&.:=+
;><&3&<>?B&4>F9 4><&3&8>GB&4>;9
'(E#)&'("D"#$&*%+,-#.%#/+&01-&(%,-(/%.&.("D"#$&01%#&/1%=&1:.&/--&6EH1&/-&.("#)&-#%&-(&6-(%&/"6%+&.E("#$&/1%&,:+/&;<&.:=+
I><&3&?><B?8>F9 4>G&3&4>?B&@>A9
4;<,;=<=>
J1(-#"H&K-"#/&L=6,/-6+&
*%+,-#.%#/+&01-&(%,-(/%.&,:"#7&:H1"#$&-5&+/"55&"#&:&M-"#/&.E("#$&/1%&,:+/&;<&.:=+&01"H1&+/:(/%.&6-(%&/1:#&;&6-#/1+&:$-
NO ;4>;&3;8>8B;@>A9
OH/"D"/=&P"6"/:/"-#&'E%&/-&O(/1("/"+
*%+,-#.%#/+&01-&(%,-(/%.&2%"#$&Q"6"/%.&"#&:#=&E+E:Q&:H/"D"/"%+&2%H:E+%&-5&:(/1("/"+&-(&M-"#/&+=6,/-6+>&
?8>I&3&I><BA?>49 ?;><&3?A>8B?;>49
'-H/-(&'":$#-+%.&O(/1("/"+
*%+,-#.%#/+&01-&(%,-(/%.&%D%(&1:D%&2%%#&/-Q.&2=&:&.-H/-(&-(&-/1%(&1%:Q/1&,(-5%++"-#:Q&/1:/&/1%=&1:.&+-6%&5-(6&-(&:(/1("/"+>
;?>8&3AA>GB8<>?9 AG>A&3A@>4BAG>F9
4><,?4&
RD%(&O+/16:*%+,-#.%#/+&01-&(%,-(/%.&%D%(&1:D"#$&2%%#&/-Q.&2=&:&.-H/-(7&#E(+%&-(&-/1%(&1%:Q/1&,(-5%++"-#:Q&/1:/&/1%=&1:.&:+/16:>
?<>;&3&@><B?8>49 ?<>G&3?<>;B??>?9
JE((%#/&O+/16:
*%+,-#.%#/+&01-&(%,-(/%.&%D%(&1:D"#$&2%%#&/-Q.&2=&:&.-H/-(7&#E(+%&-(&-/1%(&1%:Q/1&,(-5%++"-#:Q&/1:/&/1%=&1:.&:+/16:&:#.&01-&+/"QQ&1:D%&:+/16:>
@>;&3&;>;B&F>;9 G>4&3&G>AB&G>F9
@69A&B!=C,<&
SD%(0%"$1/&!E/&N-/&S2%+%
*%+,-#.%#/+&0"/1&:&2-.=&6:++&"#.%T&$(%:/%(&/1:#&-(&%UE:Q&/-&A4&2E/&Q%++&/1:#&;<&3-D%(0%"$1/9 ;8><&3AG>8B8<>@9 ;I>G&3;I><B;F>;9
S2%+%*%+,-#.%#/+&0"/1&:&2-.=&6:++&"#.%T&$(%:/%(&/1:#&-(&%UE:Q&/-&;<&3-2%+%9
AF>F&3A;>8B;@>89 A4>8&3A8>FBA@><9
SD%(0%"$1/&-(&S2%+%
*%+,-#.%#/+&0"/1&:&2-.=&6:++&"#.%T&$(%:/%(&/1:#&-(&%UE:Q&/-&A4&3-D%(0%"$1/&-(&-2%+%9
@;>F&34@>IBG?><9 @8>?&3@;>4B@8>I9
5W&
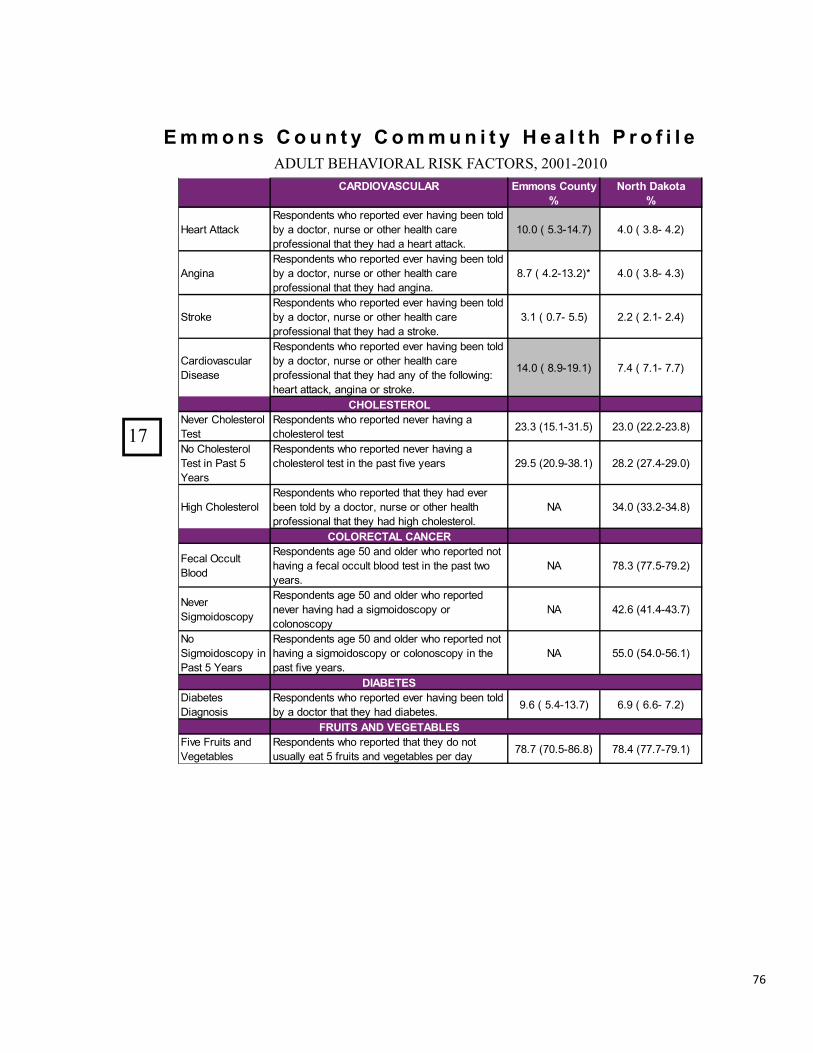
76
!""#$% & ' #($ ) * & ' #""($ + ) * & , - . / ) 0 & 1 2 # 3 + / - &!"#$%&'()!*+,-!$&-+./&0!1%,-.2&344563454&
'4567894:';<45& !""#$%&'#($)*=
>#2)0&6.?#).=
!"#$%&'%%#()*"+,-./".%+&01-&$",-$%"/&"2"$&1#23.4&5"".&%-6/&57&#&/-(%-$8&.9$+"&-$&-%1"$&1"#6%1&(#$"&,$-:"++3-.#6&%1#%&%1"7&1#/&#&1"#$%&#%%#();&
<=;=&>&?;@A<B;CD B;=&>&@;EA&B;FD
'.43.#*"+,-./".%+&01-&$",-$%"/&"2"$&1#23.4&5"".&%-6/&57&#&/-(%-$8&.9$+"&-$&-%1"$&1"#6%1&(#$"&,$-:"++3-.#6&%1#%&%1"7&1#/&#.43.#;
E;C&>&B;FA<@;FDG B;=&>&@;EA&B;@D
H%$-)"*"+,-./".%+&01-&$",-$%"/&"2"$&1#23.4&5"".&%-6/&57&#&/-(%-$8&.9$+"&-$&-%1"$&1"#6%1&(#$"&,$-:"++3-.#6&%1#%&%1"7&1#/&#&+%$-)";
@;<&>&=;CA&?;?D F;F&>&F;<A&F;BD
I#$/3-2#+(96#$&J3+"#+"
*"+,-./".%+&01-&$",-$%"/&"2"$&1#23.4&5"".&%-6/&57&#&/-(%-$8&.9$+"&-$&-%1"$&1"#6%1&(#$"&,$-:"++3-.#6&%1#%&%1"7&1#/&#.7&-:&%1"&:-66-03.4K&1"#$%&#%%#()8&#.43.#&-$&+%$-)";
<B;=&>&E;LA<L;<D C;B&>&C;<A&C;CD
',8<!:@!58<&M"2"$&I1-6"+%"$-6&N"+%
*"+,-./".%+&01-&$",-$%"/&."2"$&1#23.4&#&(1-6"+%"$-6&%"+%& F@;@&><?;<A@<;?D F@;=&>FF;FAF@;ED
M-&I1-6"+%"$-6&N"+%&3.&O#+%&?&P"#$+
*"+,-./".%+&01-&$",-$%"/&."2"$&1#23.4&#&(1-6"+%"$-6&%"+%&3.&%1"&,#+%&:32"&7"#$+ FL;?&>F=;LA@E;<D FE;F&>FC;BAFL;=D
!341&I1-6"+%"$-6*"+,-./".%+&01-&$",-$%"/&%1#%&%1"7&1#/&"2"$&5"".&%-6/&57&#&/-(%-$8&.9$+"&-$&-%1"$&1"#6%1&,$-:"++3-.#6&%1#%&%1"7&1#/&1341&(1-6"+%"$-6;
M' @B;=&>@@;FA@B;ED
'8<85!'@4<&'4>'!5&
Q"(#6&R((96%&S6--/&
*"+,-./".%+"&?=&#./&-6/"$&01-&$",-$%"/&.-%&1#23.4&#&:"(#6&-((96%&56--/&%"+%&3.&%1"&,#+%&%0-&7"#$+;&
M' CE;@&>CC;?ACL;FD
M"2"$&H34T-3/-+(-,7&
*"+,-./".%+"&?=&#./&-6/"$&01-&$",-$%"/&."2"$&1#23.4&1#/&#&+34T-3/-+(-,7&-$&(-6-.-+(-,7&
M' BF;U&>B<;BAB@;CD
M-&H34T-3/-+(-,7&3.&O#+%&?&P"#$+
*"+,-./".%+"&?=&#./&-6/"$&01-&$",-$%"/&.-%&1#23.4&#&+34T-3/-+(-,7&-$&(-6-.-+(-,7&3.&%1"&,#+%&:32"&7"#$+;&
M' ??;=&>?B;=A?U;<D
674A!@!:&J3#5"%"+&J3#4.-+3+
*"+,-./".%+&01-&$",-$%"/&"2"$&1#23.4&5"".&%-6/&57&#&/-(%-$&%1#%&%1"7&1#/&/3#5"%"+;& L;U&>&?;BA<@;CD U;L&>&U;UA&C;FD
B5;7@:&4>6&9!C!@4A<!:&Q32"&Q$93%+&#./&V"4"%#56"+
*"+,-./".%+&01-&$",-$%"/&%1#%&%1"7&/-&.-%&9+9#667&"#%&?&:$93%+&#./&2"4"%#56"+&,"$&/#7 CE;C&>C=;?AEU;ED CE;B&>CC;CACL;<D
57&

77
!""#$% & ' #($ ) * & ' #""($ + ) * & , - . / ) 0 & 1 2 # 3 + / - &!"#$%&'()!*+,-!$&-+./&0!1%,-.2&344563454&
4!5!678&,!789,& !""#$%&'#($)*:
5#2)0&;.<#).:
!"#$%&$%'&&$%()"*+,
-)./&01)0+.%2,&%$)/&$+)1%+,"+%+,)#$%3)0)$"*%,)"*+,%2".%4"#$%&$%/&&$
5675%85579:;;7;< 5;7=%85;7;:5;79<
'&&$%/,>.#?"*%()"*+,%
-)./&01)0+.%2,&%$)/&$+)1%+,)>%,"1%@%&$%A&$)%1">.%#0%+,)%*".+%BC%2,)0%+,)#$%/,>.#?"*%,)"*+,%2".%0&+%3&&1
5C7D%8%=7;:5D7=< 5C7;%8%97@:5C7E<
'&&$%F)0+"*%()"*+,
-)./&01)0+.%2,&%$)/&$+)1%+,)>%,"1%@%&$%A&$)%1">.%#0%+,)%*".+%BC%2,)0%+,)#$%A)0+"*%,)"*+,%2".%0&+%3&&1
67=%8%B79:557;< 97=%8%97;:5C7C<
G?+#H#+>%I#A#+"+#&0%JK)%+&%'&&$%()"*+,
-)./&01)0+.%2,&%$)/&$+)1%+,)>%,"1%@%&$%A&$)%1">.%#0%+,)%*".+%BC%2,)0%/&&$%/,>.#?"*%&$%A)0+"*%,)"*+,%L)/+%+,)A%4$&A%1%+,)#$%K.K"*%"?+#H#+#).7
=7;%8%;7@:%97E< E76%8%E7D:%=7C<
G0>%G?+#H#+>%I#A#+"+#&0
-)./&01)0+.%2,&%$)/&$+)1%M)#03%*#A#+)1%#0%"0>%2">%1K)%+&%/,>.#?"*N%A)0+"*%&$%)A&+#&0"*%/$&M*)A7
567B%85;7B:;;7B< 5=7C%85E7=:5=7E<
,!789,&'76!&7''!==&
()"*+,%O0.K$"0?)-)./&01)0+.%2,&%$)/&$+)1%0&+%,"H#03%"0>%4&$A%&$%,)"*+,%?"$)%?&H)$"3)
5D7;%8%@7E:597@< 557D%8557C:5579<
G??)..%I#A#+)1%M>%P&.+
-)./&01)0+.%2,&%$)/&$+)1%0))1#03%+&%.))%"%1&?+&$%1K$#03%+,)%/".+%5;%A&0+,.%MK+%?&K*1%0&+%1K)%+&%?&.+7%
@7E%8%D7E:5;7D< =7@%8%=7D:%675<
Q&%')$.&0"*%'$&H#1)$
-)./&01)0+.%2,&%$)/&$+)1%+,"+%+,)>%1#1%0&+%,"H)%&0)%/)$.&0%+,)>%?&0.#1)$%+&%M)%+,)#$%/)$.&0"*%1&?+&$%&$%,)"*+,%?"$)%/$&H#1)$7%
5676%85;7D:;B7C<R ;B7E%8;B7C:;D75<
,>1!69!5=?@5&
(#3,%S*&&1%'$)..K$)
-)./&01)0+.%2,&%$)/&$+)1%)H)$%,"H#03%M))0%+&*1%M>%"%1&?+&$N%0K$.)%&$%&+,)$%,)"*+,%/$&4)..#&0"*%+,"+%+,)>%,"1%,#3,%M*&&1%/$)..K$)7%
B=7B%8;67C:DE7=< ;E7C%8;D7D:;E76<
?AAB5?C79?@5&
O04*K)0T"%U"??#0)-)./&01)0+.%"3)%=E%"01%&*1)$%2,&%$)/&$+)1%+,"+%+,)>%1#1%0&+%,"H)%"%4*K%.,&+%#0%+,)%/".+%>)"$
;=75%85E7@:B=7D< ;@7=%8;67=:;97=<
'0)KA&?&??"*%U"??#0)
-)./&01)0+.%"3)%=E%&$%&*1)$%2,&%$)/&$+)1%0)H)$%,"H#03%,"1%"%/0)KA&0#"%.,&+7
QG BC7C%8;@79:B57C<
?5DB6>&
!"**-)./&01)0+.%DE%>)"$.%"01%&*1)$%2,&%$)/&$+)1%+,"+%+,)>%,"1%4"**)0%#0%+,)%/".+%B%A&0+,.
5D7D%8%D75:;D76< 5E7E%85D76:5=7;<
V)"+%S)*+-)./&01)0+.%2,&%$)/&$+)1%0&+%"*2">.%2)"$#03%+,)#$%.)"+M)*+%
E97B%8D97;:=97D< D579%8DC79:D;79<
57&

78
!""#$% & ' #($ ) * & ' #""($ + ) * & , - . / ) 0 & 1 2 # 3 + / - &!"#$%&'()!*+,-!$&-+./&0!1%,-.2&344563454&
4567&,!678,& !""#$%&'#($)*9
:#2)0&;.<#).9
!"#$%&'()*)$ +"*,-#."#$*'/0-'1",-1$".'$0%$'$0"2'0%3"'#-$'0%.'%'."#$%&'3)*)$')#'$0"',%*$'2"%1 4564'78968:4;64< =;6>'7=?6?:8568<
@--$0'A-**+"*,-#."#$*'/0-'1",-1$".'$0"2'0%.'&-*$'B'-1'C-1"',"1C%#"#$'$""$0'.D"'$-'EDC'.)*"%*"'-1'."F%26
=86B'79>6B:896B< 9B65'79>6>:9B6B<
1,=>?'67&6'8?@?8=&+"F-CC"#.'G02*)F%&'HF$)3)$2'
+"*,-#."#$*'/0-'1",-1$".'$0%$'$0"2'.).'#-$'E"$'$0"'1"F-CC"#.".'%C-D#$'-I',02*)F%&'%F$)3)$2 >>6?'74>6?:B>6?< >56>'74;6J:>964<
K-'A")*D1"'G02*)F%&'HF$)3)$2
+"*,-#."#$*'/0-'1",-1$".'$0%$'$0"2',%1$)F),%$".')#'#-'&")*D1"'$)C"',02*)F%&'%F$)3)$2 9868'7'>6B:=965< B6;'7'B6>:'J64<
84A6''4&
LD11"#$'MC-N)#E +"*,-#."#$*'/0-'1",-1$".'$0%$'$0"2'*C-N".'"3"12'.%2'-1'*-C"'.%2* 9B69'7956;:=968< 9;6?'79;68:=564<
B4C!:D>&,!678,&
G%,'MC"%1O-C"#'9?'%#.'-&."1'/0-'1",-1$".'$0%$'$0"2'0%3"'#-$'0%.'%',%,'*C"%1')#'$0"',%*$'$01""'2"%1* 9?64'7'?64:=?68< 9465'79869:9>65<
P%CC-E1%C'HE"'45Q'
O-C"#'45'%#.'-&."1'/0-'1",-1$".'$0%$'$0"2'0%3"'#-$'0%.'%'C%CC-E1%C')#'$0"',%*$'$/-'2"%1*
KH =468'7=868:=>68<
R'H,,1-%F0)#E'*$%$)*$)F%&'*)E#)I)F%#F"M0%.)#E':'M$%$)*$)F%&&2'*)E#)I)F%#$'.)II"1"#F"'I1-C'*$%$"
57&
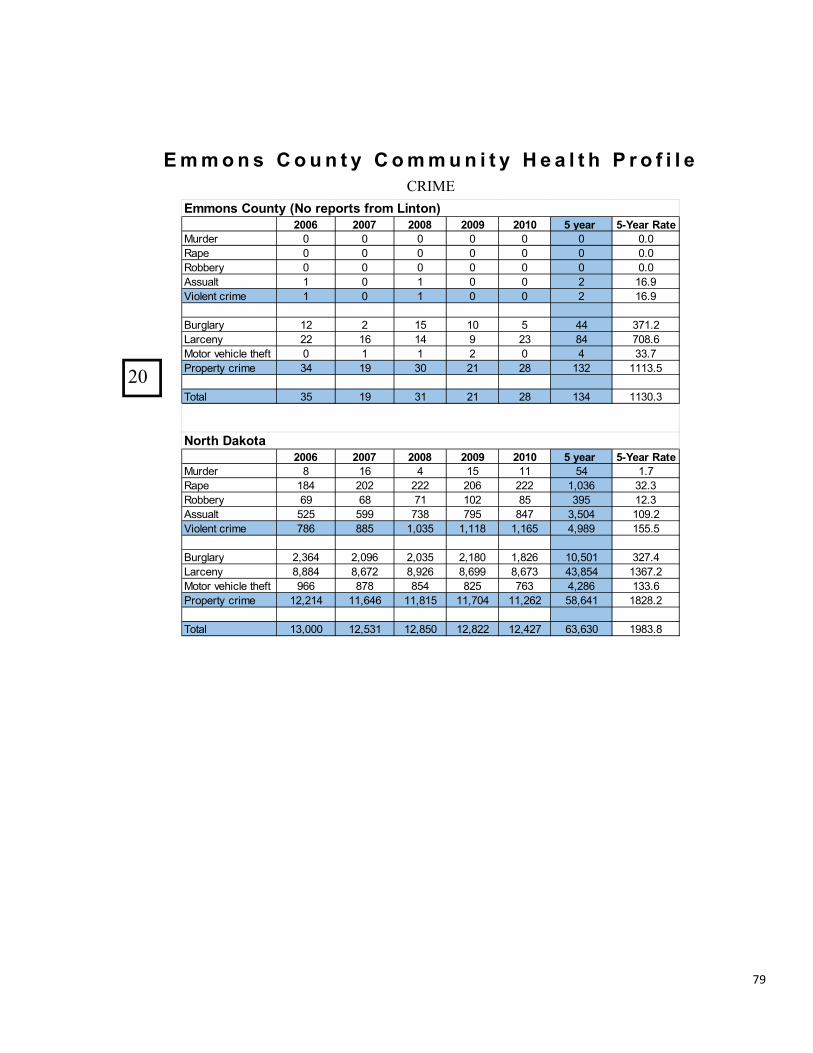
79
!"#$%&!""#$% & ' #($ ) * & ' #""($ + ) * & , - . / ) 0 & 1 2 # 3 + / - &
4556 4557 4558 4559 45:5 ;&*-.2& ;<=-.2&>.)-!"#$%# & & & & & & &'&()*% & & & & & & &'&(+,,%#- & & & & & & &'&.//")01 2 & 2 & & 3 24'567+0%819:#7;% 2 & 2 & & 3 24'5
<"#=0)#- 23 3 2> 2& > ?? @A2'3B)#:%8- 33 24 2? 5 3@ C? A&C'4!+1+#9D%E7:0%91E%F1 & 2 2 3 & ? @@'AG#+*%#1-9:#7;% @? 25 @& 32 3C 2@3 222@'>
H+1)09 @> 25 @2 32 3C 2@? 22@&'@
4556 4557 4558 4559 45:5 ;&*-.2& ;<=-.2&>.)-!"#$%# C 24 ? 2> 22 >? 2'A()*% 2C? 3&3 333 3&4 333 2I&@4 @3'@(+,,%#- 45 4C A2 2&3 C> @5> 23'@.//")01 >3> >55 A@C A5> C?A @I>&? 2&5'367+0%819:#7;% AC4 CC> 2I&@> 2I22C 2I24> ?I5C5 2>>'>
<"#=0)#- 3I@4? 3I&54 3I&@> 3I2C& 2IC34 2&I>&2 @3A'?B)#:%8- CICC? CI4A3 CI534 CI455 CI4A@ ?@IC>? 2@4A'3!+1+#9D%E7:0%91E%F1 544 CAC C>? C3> A4@ ?I3C4 2@@'4G#+*%#1-9:#7;% 23I32? 22I4?4 22IC2> 22IA&? 22I343 >CI4?2 2C3C'3
H+1)09 2@I&&& 23I>@2 23IC>& 23IC33 23I?3A 4@I4@& 25C@'C
!""#$%&'#($)*&?@#&2-A#2)%&32#"&B+$)#$C
@#2)0&D.E#).
'(&

80
!"#$%&"'($)"&#*%#!()+,-&!""#$% & ' #($ ) * & ' #""($ + ) * & , - . / ) 0 & 1 2 # 3 + / - &
'0+/4&5$4+6.)#2%7&&!4(6.)+#$&89:9 !""#$%&'#($)* ;#2)0&<.=#).!"#$%&'()*+',)-)./)0)#()1'2%)3.2&.)45'&6'(.)/7)'$#+#8$')-)./)0)9'2&)/$%,:; 0)4<==: >?@=A)4@B:C(&/$$'%)#()3D'6#2$)C%E62.#/()*+',)-F><)45'&6'(.)/7)D'&,/(,)2+',)-F><: @@)4<>: <-?<A=)4<0:3D''6")/&)G2(+E2+')HID2#&'%)!"#$%&'()#()3D'6#2$)C%E62.#/()45'&6'(.)/7)2$$),D'6#2$)'%E62.#/()6"#$%&'(: >J)400: -?>JK)4>B:L'(.2$$9)12(%#62DD'%)!"#$%&'()#()3D'6#2$)C%E62.#/()45'&6'(.2+')/7)./.2$),D'6#2$)'%E62.#/()6"#$%&'(: <)4<MB: A@-)4BMK:!"#$%&'()N#.")3D'6#7#6)G'2&(#(+)O#,28#$#.9)#()3D'6#2$)C%E62.#/()45'&6'(.2+')/7)./.2$),D'6#2$)'%E62.#/()6"#$%&'(: >@)4-J: 0?<0-)4->:1#+")36"//$)O&/D/E.,)4O&/D/E.,)D'&)<===)D'&,/(,)2+',)<@F>0: <)4=M0: A=<)4>M>:*P'&2+')*!Q)!/ID/,#.')36/&' >=M0 ><MB*P'&2+')CRD'(%#.E&')D'&)3.E%'(.)#()5E8$#6)36"//$ SJ?>J< SJ?K<>)
'0+/4&5$4+6.)#2%7&&!6#$#"+6&,-./)0&89:9 !""#$%&'#($)* ;#2)0&<.=#).Q*TU)V'6#D#'(.,)*+',)=F<J)45'&6'(.)/7)D'&,/(,)2+',)=F<J: -)4=M0: A?K<J)40MA:3T*5)V'6#D#'(.,)*+',)=F<J)45'&6'(.)/7)2$$)6"#$%&'()2+',)=F<J: JB)4<-: -A?BB-)4>0:!"#$%&'()V'6'#P#(+)U&'')2(%)V'%E6'%)5')GE(6"',)45'&6'(.)/7)./.2$),6"//$)'(&/$$I'(. >BK)40B: --?KA=)4--:WH!)5&/+&2I)52&.#6#D2(., <BK >0?--<L'%#62#%)V'6#D#'(.,)*+',)=F>=)45'&6'(.)/7)2$$)D'&,/(,)2+',)=F>=: <-<)4<@: 0J?<<=)4>A:L'%#2()H(6/I')7/&)U2I#$#',)N#.")!"#$%&'()*+',)=F<A); S0J?=J< S@<?=-B)!"#$%&'()*+',)=F<A)G#P#(+)#()CR.&'I')5/P'&.9)45'&6'(.)/7)6"#$%&'()=F<A)7/&)N"/I)D/P'&.9)#,)%'.'&I#('%:; AK)4<=M0: <=?<==)4AM>:;X'2&)>==J)%2.2
'0+/4&5$4+6.)#2%7&&>."+/+-%&.$4&'0+/4&'.2-&89:9 !""#$%&'#($)* ;#2)0&<.=#).!"#$%)!2&')5&/P#%'&,) <> -?<A@!"#$%)!2&')!2D26#.9)4*,)D'&6'(.)/7)2$$)6"#$%&'()=F<-)#()6"#$%)62&': <<B 0<?0AKL/."'&,)N#.")2)!"#$%)*+',)=F<A)#()G28/&)U/&6')45'&6'(.)/7)2$$)I/."'&,)N#.")2)6"#$%)2+',)=F<A:; >B@)4AA: BA?=BJ)4K>:!"#$%&'()*+',)=F<A)G#P#(+)#()2)3#(+$')52&'(.)U2I#$9)45'&6'(.)/7)2$$)6"#$%&'()2+',)=F<A:; <=>)4<-: -=?=BK)4><:!"#$%&'()#()U/,.'&)!2&')45'&6'(.)/7)6"#$%&'()2+',)=F<K: >)4=M-: <?J<>)4<M>:!"#$%&'()*+',)=F<A)N#.")3E,D'6.'%)!"#$%)*8E,')/&)T'+$'6.)4!2,',)D'&)<==)6"#$%&'()=F<A: T* @?-JJ)40M0:!"#$%&'()*+',)=F<A)HID26.)89)O/I',.#6)Y#/$'(6')45'&6'(.)/7)2$$)6"#$%&'()2+',)=F<A: T* 0?<K=)4>MJ:Z#&.",)./)L/."'&,)N#.")H(2%'[E2.')5&'(2.2$)!2&';;) T* -KJ)40M-:;)X'2&)>==J)%2.2
'0+/4&5$4+6.)#2%7&&?(@-$+/-&?(%)+6-&89:9 !""#$%&'#($)* ;#2)0&<.=#).!"#$%&'()*+',)=F<A)V'7'&&'%)./)\EP'(#$')!/E&.)45'&6'(.)/7)2$$)6"#$%&'()2+',)=F<A: -0)4J: B?<-J)4KM<:]77'(,')*+2#(,.)5'&,/()\EP'(#$')!/E&.)V'7'&&2$)45'&6'(.)/7)./.2$)^EP'(#$')6/E&.)&'7'&&2$: <)4>M0: AK0)4KM>:*$6/"/$FV'$2.'%)\EP'(#$')!/E&.)V'7'&&2$)45'&6'(.)/7)2$$)^EP'(#$')6/E&.)&'7'&&2$,: >B)4@<: <?0@0)4<B:
;X'2&)>==K)%2.2./&
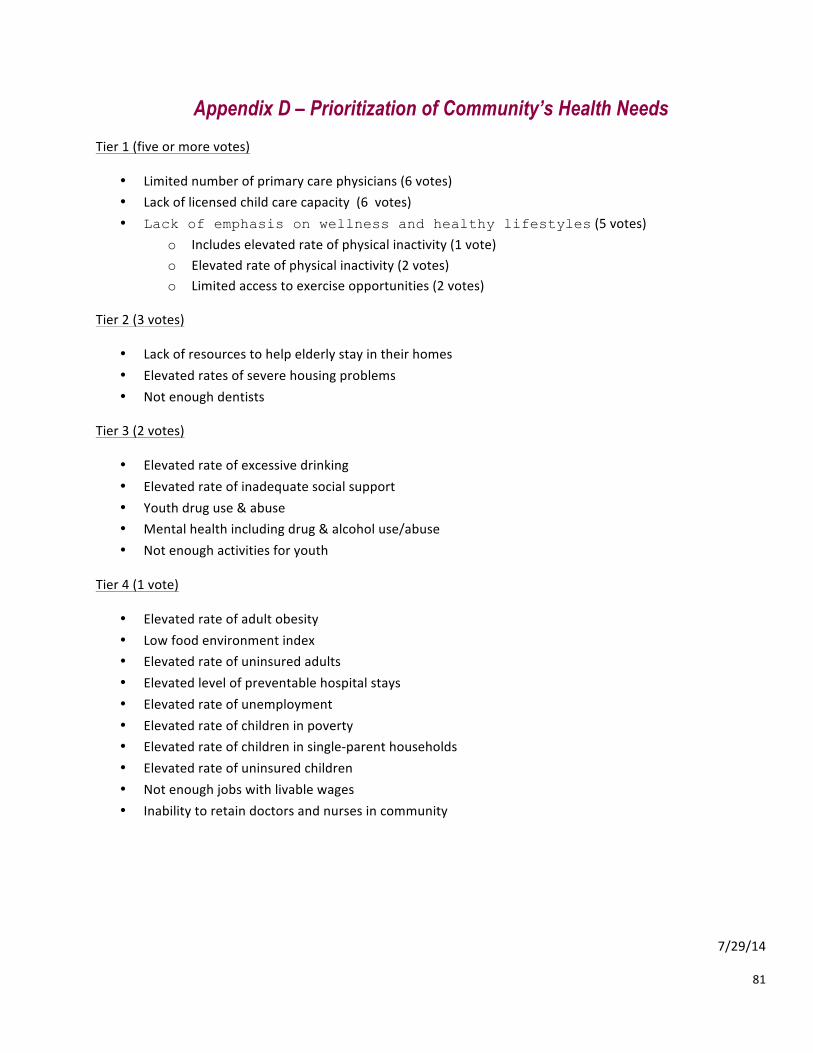
81
Appendix D – Prioritization of Community’s Health Needs Tier 1 (five or more votes)
• Limited number of primary care physicians (6 votes) • Lack of licensed child care capacity (6 votes) • Lack of emphasis on wellness and healthy lifestyles (5 votes)
o Includes elevated rate of physical inactivity (1 vote) o Elevated rate of physical inactivity (2 votes) o Limited access to exercise opportunities (2 votes)
Tier 2 (3 votes)
• Lack of resources to help elderly stay in their homes • Elevated rates of severe housing problems • Not enough dentists
Tier 3 (2 votes)
• Elevated rate of excessive drinking • Elevated rate of inadequate social support • Youth drug use & abuse • Mental health including drug & alcohol use/abuse • Not enough activities for youth
Tier 4 (1 vote)
• Elevated rate of adult obesity • Low food environment index • Elevated rate of uninsured adults • Elevated level of preventable hospital stays • Elevated rate of unemployment • Elevated rate of children in poverty • Elevated rate of children in single-‐parent households • Elevated rate of uninsured children • Not enough jobs with livable wages • Inability to retain doctors and nurses in community
7/29/14
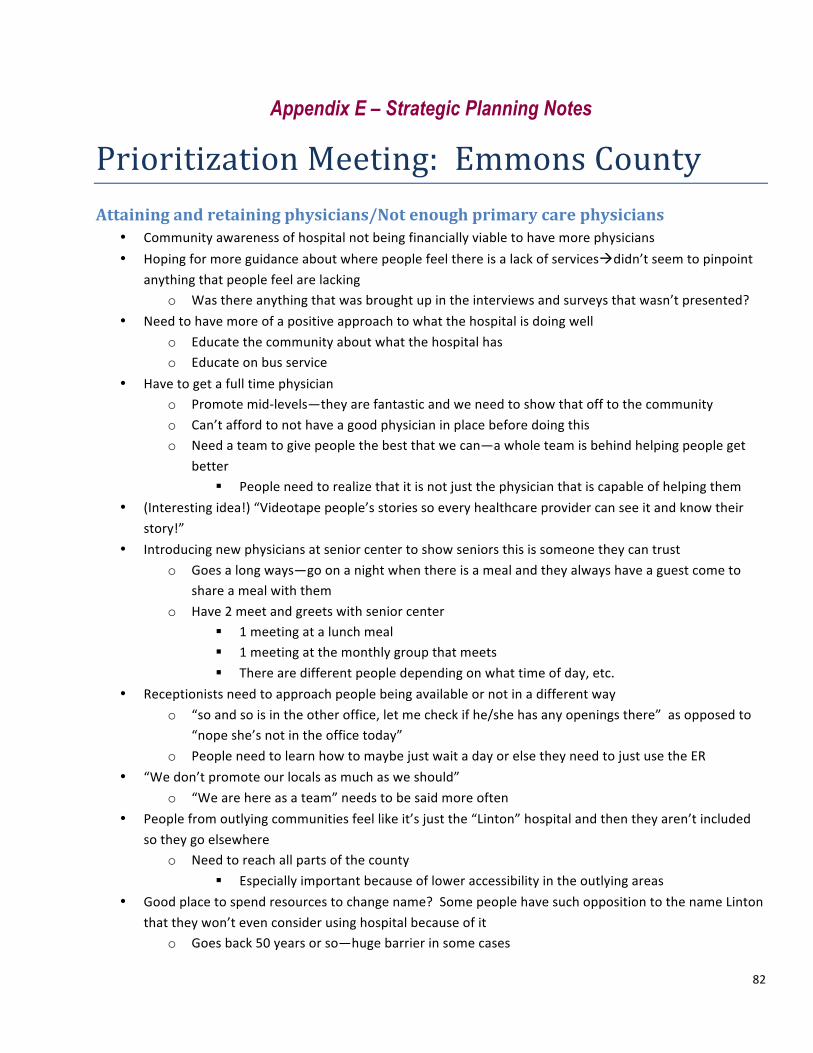
82
Appendix E – Strategic Planning Notes
Prioritization Meeting: Emmons County Attaining and retaining physicians/Not enough primary care physicians
• Community awareness of hospital not being financially viable to have more physicians • Hoping for more guidance about where people feel there is a lack of servicesàdidn’t seem to pinpoint
anything that people feel are lacking o Was there anything that was brought up in the interviews and surveys that wasn’t presented?
• Need to have more of a positive approach to what the hospital is doing well o Educate the community about what the hospital has o Educate on bus service
• Have to get a full time physician o Promote mid-‐levels—they are fantastic and we need to show that off to the community o Can’t afford to not have a good physician in place before doing this o Need a team to give people the best that we can—a whole team is behind helping people get
better § People need to realize that it is not just the physician that is capable of helping them
• (Interesting idea!) “Videotape people’s stories so every healthcare provider can see it and know their story!”
• Introducing new physicians at senior center to show seniors this is someone they can trust o Goes a long ways—go on a night when there is a meal and they always have a guest come to
share a meal with them o Have 2 meet and greets with senior center
§ 1 meeting at a lunch meal § 1 meeting at the monthly group that meets § There are different people depending on what time of day, etc.
• Receptionists need to approach people being available or not in a different way o “so and so is in the other office, let me check if he/she has any openings there” as opposed to
“nope she’s not in the office today” o People need to learn how to maybe just wait a day or else they need to just use the ER
• “We don’t promote our locals as much as we should” o “We are here as a team” needs to be said more often
• People from outlying communities feel like it’s just the “Linton” hospital and then they aren’t included so they go elsewhere
o Need to reach all parts of the county § Especially important because of lower accessibility in the outlying areas
• Good place to spend resources to change name? Some people have such opposition to the name Linton that they won’t even consider using hospital because of it
o Goes back 50 years or so—huge barrier in some cases

83
• Clinics in Hazelton and Herried has helped out considerably • Don’t know how to market the phrase “get over it” • Need a slogan that makes health more of a whole—keep hospital in place for whole county versus just
Linton • Hospital is necessary for nursing home and if that hospital closes so does the nursing home and that
affects a lot of employment • Need to look at all of the resources—hospital works with everyone
o Ex: public health isn’t in competitions with hospital, etc. • If hospital didn’t exist, would we have the ambulance?
o Need resources to keep it running—barrier breaker? • Use people’s stories to spin a positive light to services available in the community
o These impact people’s lives • Key take away points: Educate and raise awareness about services and healthcare workers teamwork,
etc.
Need: Health Lifestyles/Wellness/etc. Encompasses elevated rates of diabetes, elevated rate of adult obesity, low food environment index, elevated rate of physical inactivity, limited access to exercise opportunities
Outcomes: Weight loss o “Less ‘Waist’ in Emmons County” o “Decrease County Obesity” o “Less obesity rates in EC”
• Diabetes o “Reduction noted” o “Active diabetes cases decline”
• Cardiovascular o “High cholesterol decreases in the county” o “Heart attacks and strokes decrease”
• “Emmons County rated among the highest for quality of life” • “Decrease in preventable hospital stays” • “Increase in exercise options for all ages”
Activities • Current resources to utilize:
o Fitness center in Linton o Martial Arts—conditioning challenge program—little kids to seniors o Walking path in Linton
• Easy to develop a walking path in every community and people also like to bike • Need to have a good physical ed program in the schools • Address heart disease, diabetes, obesity on electronic health records and then refer them to hospital • Health fair: do it around free food

84
o Healthy food options o Coincide with community events already in place
*For this last part I missed some areas but between Ken’s notes and mine there should be a complete collection of what people were saying. Everyone was so talkative it was hard to capture every moment!