Geriatric Neuropsychopharmacology: Unmet Needs
13
Cummings and Senanarong PSYCHOGERIATRICS 2001; 1: 14-26. REVIEW Geriatric Neuropsychopharmacology: Unmet Needs Jeffrey L. Cummings*’ and Vorapun Senanarong*2 Received January 9,200 I, accepted February 9, 200 I. ‘‘Department of Neurology and Psychiatry and Biobehavioral Sciences, UCLA School of Medicine ‘ZDivision of Neurology, Department of Medicine, Medicine Siriraj Hospital, Mahidol University Reprint requests to Jeffrey L. Cummings, M.D., Reed Neurological Research Center, UCLA School of Medicine, 710 Westwood Plaza, Los Angeles, CA 90095- 1769, U.S.A. Key words: psychopharmacology, Alzheimer’sdisease, clinical trials, outcomes, translational research Abstract: Substantial progress has been made in developing new pharmacologicalagents for geriatric neurological diseases with behavioral manifestations such as Alzheimer’s disease and Parkinson’s disease as well as new psychotropic agents for psychogeriatric disorders including atypical anti-psychotics, new antidepressants and anti-agitation agents. The growth of the world elderly population demands improved psychogeriatric neuropharmacology. Disease mechanisms are increasingly well understood in geriatric degenerative disorders but remain obscure for idiopathic conditions such as depression, psychosis, and bipolar illness. Classifications of psychiatric disorders underemphasize issues important in psychogeriatrics such as apathy and agitation. Evolving regulatory requirements make it imperativethat clinical trials be performed in geriatric populations if labeling for use in these populationsis sought by pharmaceutical companies. There are unmet needs in almost all phases of drug development including identification of therapeutic targets; optimization of lead compounds; investigation of toxicity and pharmacokinetics;phase I, II and III trials; and post-marketing investigation. Outcomes that are more relevant to clinical practice and more patient-centered are needed in clinical trials. These include assessments of the impact of treatment on quality of life; changes in behavior; functional abilities; delayed pivotal endpoints, such as nursing home placement; and secondary effects on caregivers. Surrogate biological markers of drug effect on disease processes are urgently needed. Resolution of ethical issues including informed consent must be achieved to facilitate advances in drug development. Globalizationof drug discoveries to enable use of therapeutic advances by patientsthroughout the world is necessary. Translational research, changes in public policy to enhance acceptance of new drug development, and harmonization of drug testing and regulatory guidelines will improve globalization of advances in psychogeriatric pharmacotherapy. Identification of these unmet needs in geriatric neuropsychopharmacology suggests an agenda for research activities. GERIATRIC NEUROPSYCHOPHARMACOLOGY: UNMET NEEDS Geriatric neuropsychopharmacology is a burgeoning field. Advances have been made in the development of atypi- cal antipsychoticsfor the treatment of schizophrenia and other psychotic disorders; new types of antidepressants are evolving to control depressive symptoms; a variety of new agents are being investigated to improve treatment of mania and bipolar illness; new therapies have become available for insomnia; several new drugs for the treat- ment of Parkinson’s disease (PD) have emerged in re- cent years; cholinesteraseinhibitors have been developed for the treatment of Alzheimer’s disease (AD); disease- modifying therapies are under investigation for AD and other neurodegenerativediseases; and new therapies for epilepsy, multiple sclerosis and migraine have evolved and are available for elderly patients with persistence of these conditionsfrom earlier ages or who experiencethem as late-onsetdisorders. New psychotropictherapies have, as an underlyingpremise,the assumptionthat major men- tal illnesses are as much disorders of the central nervous system (CNS) as AD or PD and that effective treatment is to be pursued through modification of brain functions. The term “neuropsychopharmacology” encompassesthis unifying assumption. Treatment of psychogeriatric conditions is particularly 14
Transcript of Geriatric Neuropsychopharmacology: Unmet Needs

Cummings and Senanarong PSYCHOGERIATRICS 2001; 1: 14-26.
REVIEW
Geriatric Neuropsychopharmacology: Unmet Needs
Jeffrey L. Cummings*’ and Vorapun Senanarong*2
Received January 9,200 I , accepted February 9, 200 I .
‘‘Department of Neurology and Psychiatry and Biobehavioral Sciences, UCLA School of Medicine ‘ZDivision of Neurology, Department of Medicine, Medicine Siriraj Hospital, Mahidol University
Reprint requests to Jeffrey L. Cummings, M.D., Reed Neurological Research Center, UCLA School of Medicine, 710 Westwood Plaza, Los Angeles, CA 90095- 1769, U.S.A.
K e y words: psychopharmaco logy , Alzheimer’s disease, clinical trials, outcomes, translational research
Abstract: Substantial progress has been made in developing new pharmacological agents for geriatric neurological diseases with behavioral manifestations such as Alzheimer’s disease and Parkinson’s disease as well as new psychotropic agents for psychogeriatric disorders including atypical anti-psychotics, new antidepressants and anti-agitation agents. The growth of the world elderly population demands improved psychogeriatric neuropharmacology. Disease mechanisms are increasingly well understood in geriatric degenerative disorders but remain obscure for idiopathic conditions such as depression, psychosis, and bipolar illness. Classifications of psychiatric disorders underemphasize issues important in psychogeriatrics such as apathy and agitation. Evolving regulatory requirements make it imperative that clinical trials be performed in geriatric populations if labeling for use in these populations is sought by pharmaceutical companies. There are unmet needs in almost all phases of drug development including identification of therapeutic targets; optimization of lead compounds; investigation of toxicity and pharmacokinetics; phase I, II and III trials; and post-marketing investigation. Outcomes that are more relevant to clinical practice and more patient-centered are needed in clinical trials. These include assessments of the impact of treatment on quality of life; changes in behavior; functional abilities; delayed pivotal endpoints, such as nursing home placement; and secondary effects on caregivers. Surrogate biological markers of drug effect on disease processes are urgently needed. Resolution of ethical issues including informed consent must be achieved to facilitate advances in drug development. Globalization of drug discoveries to enable use of therapeutic advances by patients throughout the world is necessary. Translational research, changes in public policy to enhance acceptance of new drug development, and harmonization of drug testing and regulatory guidelines will improve globalization of advances in psychogeriatric pharmacotherapy. Identification of these unmet needs in geriatric neuropsychopharmacology suggests an agenda for research activities.
GERIATRIC NEUROPSYCHOPHARMACOLOGY: UNMET NEEDS Geriatric neuropsychopharmacology is a burgeoning field. Advances have been made in the development of atypi- cal antipsychotics for the treatment of schizophrenia and other psychotic disorders; new types of antidepressants are evolving to control depressive symptoms; a variety of new agents are being investigated to improve treatment of mania and bipolar illness; new therapies have become available for insomnia; several new drugs for the treat- ment of Parkinson’s disease (PD) have emerged in re- cent years; cholinesterase inhibitors have been developed for the treatment of Alzheimer’s disease (AD); disease-
modifying therapies are under investigation for AD and other neurodegenerative diseases; and new therapies for epilepsy, multiple sclerosis and migraine have evolved and are available for elderly patients with persistence of these conditions from earlier ages or who experience them as late-onset disorders. New psychotropic therapies have, as an underlying premise, the assumption that major men- tal illnesses are as much disorders of the central nervous system (CNS) as AD or PD and that effective treatment is to be pursued through modification of brain functions. The term “neuropsychopharmacology” encompasses this unifying assumption.
Treatment of psychogeriatric conditions is particularly
14

urgent because of the growth of the elderly population worldwide. Technologically advanced countries will have a doubling or tripling of their elderly population in the next twenty years, while technologically less advanced coun- tries will have even more marked rises in the number of aged individuals.’) The development of therapies that will prevent, defer the onset, slow the progression, or improve the symptoms of psychogeriatric disorders is imperative.
Despite the progress made in geriatric neuropsychop- harmacology, major unmet needs remain. Disease-modi- fying therapies that have a major impact in terms of pre- venting or deferring disease onset, reducing disease pro- gression, or improving symptoms are lacking for all disor- ders. In the United States (US) there are no agents ap- proved by the Federal Drug Administrators (FDA) for treat- ment of behavioral disorders occurring in patients with neurologic disorders such as AD or PD. Current study designs have major shortcomings and more patient-cen- tered, practitioner-friendly outcomes are needed. Classi- fication of late-onset neuropsychiatric diseases requires modification from nosologies developed for disorders in- volving all age groups such as the 4th edition of the Diag- nostic and Statistical Manual (DSM-IV)2) or the Interna- tional Classification of Diseases 10th edition (ICD-1 O).S
This article reviews some of the areas where there are major unmet needs and provides suggestions for a geri- atric neuropsychopharmacology research agenda. Pre- liminary suggestions for disease classification and differ- ential diagnosis relevant to geriatric neuropsychiatric dis- orders are presented. New policies regarding clinical tri- als and drug development are developed by the US FDA, but relevant to drug development and neuropsychophar- macology worldwide.
CLASSIFICATION OF GERIATRIC NEUROPSYCHIATRIC DISORDERS Current classifications of psychiatric di~orders~.~) have significant omissions relevant to psychogeriatric neurop- sychopharmacology. The behavioral syndrome of aaita- tion, for example, is among the most common symptoms of AD and occurs in other dementing illnesses as well as geriatric depression, psychosis and mania. Despite its fre- quency, it occurs in DSM-IV only in the subcategory of “behavioral disturbance” as an accompanying symptom of dementia of the Alzheimer type. Likewise, apathv is recognized to be a very common geriatric neuropsychiat- ric disorder occurring in AD, frontotemporal dementia
Neuropsy chopharmacology
Table 1. Classification of the major late-occurring psycho- geriatric syndromes (many elderly patients have multiple symptoms simultaneously)
Depression Mania and bipolar illness Delusions Hallucinations Anxiety disorders Obsessive-compulsive disorder Dissociative disorder Apathy Agitation Personality disorders and alterations Sexual disorders Cognitive disorders
Dementia Delirium Domain-specific cognitive disorders
(aphasia, memory impairment, visuospatial disturbances, executive dysfunction)
(FTD), progressive supranuclear palsy (PSP), other neu- rological disorders, depression and s~hizophrenia.4,~) Apa- thy is underrepresented in current classifications and is subsumed under “personality change due to a general medical condition” in DSM-IV.’) The virtual exclusion of these syndromes from the major diagnostic classification systems has adverse consequences for psychogeriatrics. Few studies are devoted to further characterizing these syndromes (compared for example to the number of stud- ies devoted to depression and psychosis), genetic and environmental contributions to the syndromes are not in- vestigated, pharmaceutical companies are not encour- aged to develop treatments, and new therapies and man- agement strategies fail to evolve.
Table 1 provides a preliminary classification of the prin- cipal disorders relevant to psychogeriatrics. This classifi- cation provides a framework for further investigation as well as for drug development. These syndromes may be idiopathic without a specific known etiology at the current time or symptomatic associated with identifiable neuro- logical disorders.
Another problem with current classification systems is their tendency to emphasize isolated neuropsychiatric symptoms. Patients with geriatric neuropsychiatric syn- dromes frequently exhibit multiple neuropsychiatric dis- orders simultaneously.6) Studies with the Neuropsychiat- ric Inventory7) reveal that 90% of AD patients have at least one neuropsychiatric symptom and most exhibit several such symptoms. In a study using the Alzheimer’s Dis-
15

Cummings and Senanarong
ease Assessment Scale Non-Cognitive Portion,8) it was noted that only 30% of patients had one of the three syn- dromes of depression, psychosis or agitation while the other 70% had at least two and 30% had all three condi- t ion~.~) Recognition that most patients with AD and other psychogeriatric disorders have multiple behavioral symp- toms is a key factor in geriatric neuropsychopharmacol-
OgY.
POLICY FOR “INDICATIONS” FOR DRUG THERAPY The US FDA is arguably the most influential regulatory agency for drug development worldwide. Although its poli- cies apply specifically only to pharmaceutical companies and drug development in the US, it often has worldwide influence through communication with regulatory agen- cies in other countries. The large size of the market for new agents makes the US a prime site for new drug de- velopment. The FDA sets exact standards for pharma- ceutical companies to demonstrate drug efficacy and ad- verse events before approval for marketing. These facts enhance the influence exerted by the FDA on global drug development. Thus, FDA policies relevant to psychogeri- atrics and geriatric neuropsychopharmacology influence the unmet needs in this research area.
Granting of an “indication” is the principal goal of a phar- maceutical company applying to the FDA for a new drug application.I0)Granting an indication means that the prod- uct can be labeled and marketed for use in that specific condition. Indications are gained by linking them to the primary outcome measures in randomized clinical trials. For example, an indication for depression is typically ob- tained for an antidepressant by showing a significantly greater reduction in depressive symptoms by the active agent compared to placebo on a rating scale such as the Hamilton Depression Rating Scale.”) In schizophrenia, indications are typically obtained by showing reductions with an antipsychotic agent on the Brief Psychiatric Rat- ing Scale1*) compared to placebo. Formerly, an agent ap- proved for treatment of depression could be marketed as treatment of depression in any disorder exhibiting depres- sive symptoms. It was assumed that drugs efficacious for the treatment of idiopathic depression would also reduce depressive symptoms in conditions such as AD or PD where depression is common. Likewise, an indication for psychosis based on randomized clinical trials of schizo- phrenic patients implied that these same agents could be marketed for treatment of psychosis in other conditions
with psychosis such as PD or AD. Recently, the FDA revised and clarified their policy, link-
ing indications specifically and uniquely to the populations included in randomized controlled trials. To gain an indi- cation for psychosis in AD, the agent must be specifically tested in AD patients with psychosis. Similarly, an indica- tion for treatment of depression in PD must be linked to randomized clinical trials of depressed PD patients. Al- ternatively, an indication for a syndrome such as apathy or agitation can be obtained by showing that an agent is useful for that syndrome across several different popula- tions. For example, an agent could gain an indication for agitation by showing that it reduced symptoms of agita- tion in mania, AD, and mental retardation.
This more restrictive policy has neurobiologic justifica- tion. Patients with AD have neuritic plaques and neurofibril- lary tangles in the cerebral cortex as well as a marked cholinergic deficit’s and these may drastically modify the efficacy or adverse effects associated with agents devel- oped and tested in idiopathic psychiatric disorders. The well known balance between dopamine and acetylcho- line in the brainI4) implies that antipsychotic agents affect- ing dopamine receptors may have differential effects in patients with and without a concomitant cholinergic defi- ciency. Similarly, the serotonergic and noradrenergic defi- cits known to be present in AD and PD may well modify the effects of serotonergic or noradrenergic antidepres- sants developed for treatment of idiopathic depression where such deficits have either not been identified or are less profound and have no pathologic concomitant such as reduction of cells in the raphe nuclei or locus coer- uleus. Patients with geriatric neuropsychiatric disorders may have adverse event profiles that differ from those identified in patients with idiopathic psychiatric conditions. For example, patients with dementia with Lewy bodies (DLB) have markedly exaggerated adverse responses to conventional neur~leptics.’~) Identification of side effect profiles unique to psychogeriatric patients will evolve from clinical trials involving these specific diseases. This new policy will result in the generation of data more specific to psychogeriatric populations and will aid in the appropri- ate management of elderly patients.
The new FDA policy implies that there will be more “off label” prescribing of psychotropic agents for patients with geriatric neuropsychiatric disorders until appropriate clini- cal trials have been performed. There are currently no agents in the US pharmacopoeia that have FDA approval
16

for treatment of behavioral changes in patients with neu- rologic disorders. Off label prescribing has greater liabil- ity risks and requires that patients and caregivers be in- formed that agents are being used in the absence of ap- proved indications for therapy. Such prescribing may also have financial consequences in health care organizations that do not pay for off label use of drugs.
A final issue raised by the new policy is the difficulty of performing randomized clinical trials in populations of pa- tients with relatively rare diseases or unusual neuropsy- chiatric syndromes. FDA approval of drugs will require specific clinical trials of treatment of the condition of inter- est, such as depression in corticobasal degeneration, apathy in PSP, or agitation in Creutzfeldt-Jakob disease. The small size of these populations makes such clinical trials implausible. New policies will be required, such as the development of different standards of evidence for these small populations or the development of new trial strategies or analytic approaches less dependent on large numbers of patients.
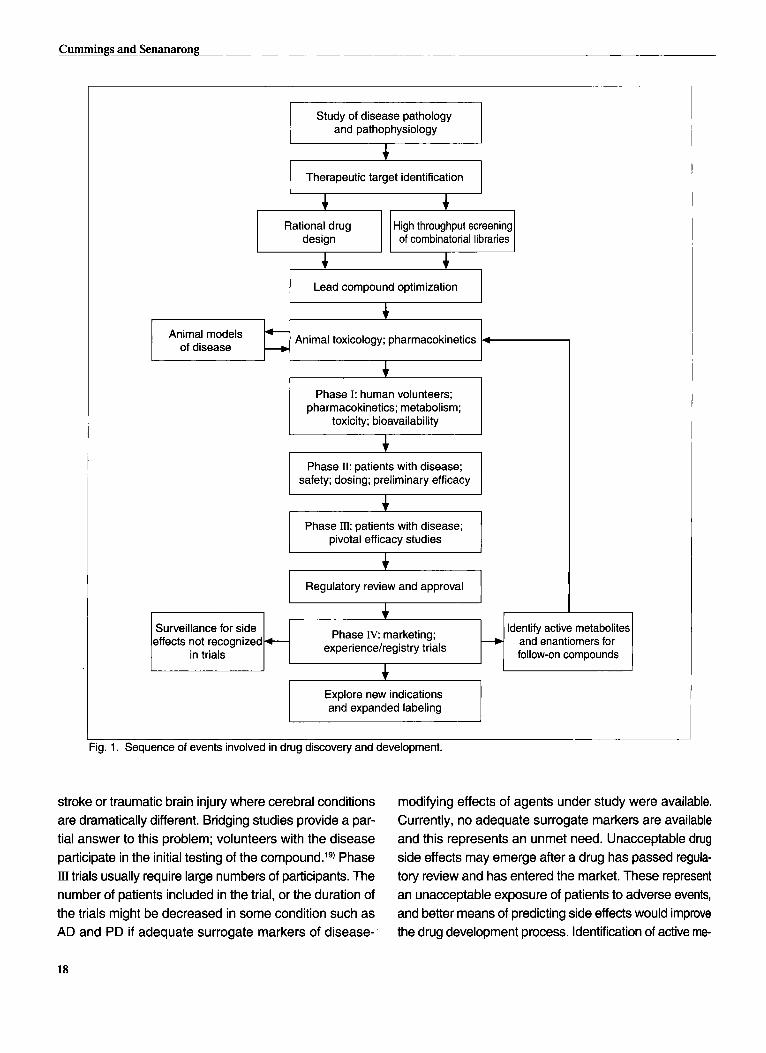
ISSUES IN DRUG DISCOVERY AND DEVELOPMENT Drug discovery and development are complex multi-step processes (Fig. 1). Initial observations on disease pathol- ogy and pathophysiology lead to the search for defined therapeutic targets that may be manipulated through ex- ternally administered interventions. Potential therapeutic compounds are then sought through rational drug design using advanced computer modeling techniques or high throughput screening of combinatorial libraries to identify compounds that have a high likelihood of performing as desired.16) Candidate agents are then further screened and one or more lead compounds are identified. These compounds are then tested for toxicity in animals and pre- liminary pharmacokinetic information is generated. If toxi- cologic observations in animals suggest that the com- pound can be tolerated and has pharmacokinetic proper- ties feasible for use in humans, phase I clinical trials are initiated. These typically involve normal human volunteers. Studies provide information on phamacokinetics, metabo- lism, toxicity, and bioavailability. If these studies suggest that the compound has favorable characteristics, it is rec- ommended for further development and phase II trials are initiated involving patients with the condition of inter- est. Safety, dosing and preliminary efficacy observations emerge from these studies. Compounds that continue to perform favorably in phase II studies are advanced to
Neuropsyc hopharmacology
phase lI studies that are the pivotal efficacy trials submit- ted to regulatory agencies for potential approval of an agent for marketing. After extensive regulatory review, the compound may be approved for treatment of the pa- tient population of the type included in the clinical trial.
Drug development does not stop with approval and marketing of the compound. Surveillance of side effects not recognized in the original clinical trials continues dur- ing this ~eri0d.I~) New indications for the agent and ex- panded labeling also may be sought after a drug is ap- proved for marketing. For example, anticonvulsant com- pounds may be used in bipolar illness or in the treatment of agitation in dementia syndromes. Expanded labeling requires additional clinical trials in the specific population for which labeling is sought. Brand name drugs receive patent protection for a limited period of time (1 7 years from date of issue) during which generic versions of the same compound cannot be marketed.’*) Because of this limited market life-span of any agent imposed by the fi- nite period of patent protection, pharmaceutical compa- nies seek active metabolites of the parent compound or enantiomers that can be developed as follow-on com- pounds. These derivative agents often have improved side effect profiles. They require re-examination in clinical tri- als if regulatory approval is to be obtained.
Unmet needs are present in nearly all phases of the process of drug discovery and development. Understand- ing of the pathology and pathophysiology of nearly every psychogeriatric condition is inadequate. While advances have been made in understanding the pathophysiology of AD, the pathophysiologic bases of depression, late- onset schizophrenia, or geriatric bipolar illness remain obscure. Drug development is based largely on modifica- tion of existing compounds rather than identification of novel targets within the pathophysiological process. Ra- tional drug design and high throughput screening have greatly aided the development of new compounds but both of these techniques are in relatively early phases of development and implementation. Studies of lead com- pound toxicology and establishment of preliminary phar- macokinetic profiles in experimental animals are critical steps in drug development. These experiments, however, have become the focus of substantial social and political controversy and development of surrogate testing sys- tems is an unmet need. Use of normal human volunteers in phase I studies may be of limited relevance for agents that are to be applied in neurodegenerative diseases,
17
Cummings and Senanarong
Surveillance for side effects not recognized
in trials
and pathophysiology
Therapeutic target identification
+ andenantiomers for follow-on compounds
Phase IV: marketing; experiencehegistry trials
+
Rational drug High throughput screening of cornbinatorial libraries
Lead compound optimization
I 1 I I
Animal toxicology; pharmacokinetics Animal models of disease
L
Phase I: human volunteers; pharmacokinetics; metabolism;
toxicity; bioavailability
Phase Il: patients with disease; safety; dosing; preliminary efficacy
Phase m: patients with disease; pivotal efficacy studies
Regulatory review and approval
I ldentifv active metabolites1
Explore new indications and expanded labeling
ig. 1. Sequence of events involved in drug discovety and development.
stroke or traumatic brain injury where cerebral conditions are dramatically different. Bridging studies provide a par- tial answer to this problem; volunteers with the disease participate in the initial testing of the compound.lg) Phase III trials usually require large numbers of participants. The number of patients included in the trial, or the duration of the trials might be decreased in some condition such as AD and PD if adequate surrogate markers of disease-
modifying effects of agents under study were available. Currently, no adequate surrogate markers are available and this represents an unmet need. Unacceptable drug side effects may emerge after a drug has passed regula- tory review and has entered the market. These represent an unacceptable exposure of patients to adverse events, and better means of predicting side effects would improve the drug development process. Identification of active m e
18

tabolites and enantiomers for development of derivative compounds from parent molecules is a common strategy in drug development. These follow-on agents often have fewer side effects but do not expand the spectrum of types of agents available for disease treatment. Enhancement of understanding of disease pathophysiology and identifi- cation of new therapeutic targets would increase the num- ber of novel agents available for disease intervention.
Development of new compounds is driven by three considerations: 1) inadequate efficacy of existing drugs for many patients; 2) existence of groups of patients who are unresponsive to treatment with currently available agents; 3) the presence of adverse events and side ef- fects with currently available compounds. For example, se\ective serotonin reuptake inhibitors are associated with a high frequency of sexual dysfunction and some agents induce weight gain. Atypical antipsychotics are associ- ated with weight gain and sedation and clozapine may induce agranulocytosis. Cholinesterase inhibitors have gastrointestinal side effects when administered at higher doses. Anxiolytic agents may produce sedation, cogni- tive impairment or disinhibition. Neuroleptic antipsychotic agents are associated with extrapyramidal syndromes including parkinsonism and tardive dyskinesia. Selective noradrenergic reuptake inhibitors may produce tachycar- dia or hypertension. Tricyclic antidepressants are associ- ated with anticholinergic side effects including blurred vi- sion, urinary retention, and memory impairment. Time of onset of action is also a critical variable that can be im- proved for many agents. Antidepressants often take sev- eral weeks after appropriate daily doses have been achieved before the antidepressant effect emerges. De- velopment of compounds with better efficacy, fewer side effects, and more rapid onset of action is an unmet need in geriatric neuropsychopharmacology.
CLINICAL TRIALS AND OUTCOME MEASURES Current clinical trials focus on the reduction of rating scale scores by an active agent compared to a placebo or by a new active agent compared to an accepted standard therapy. Antidementia therapies, for example, are required by the FDA to meet the dual outcome criteria of improve- ment on 1) a clinical global scalezo) and 2) a measure of the core neuropsychological symptoms of dementia, typi- cally measured with the Alzheimer's Disease Assessment Scale-Cognitive Portion (ADAS-Cog)?) These outcomes are worthy and reasonable but may not be the most rel-
Neuropsychopharmacology
evant to the patient or caregiver and depend on instru- ments unfamiliar to most practitioners and therefore diffi- cult to translate into routine care of psychogeriatric pa- tients. Changes in behavior, ability to perform activities of daily living, patient quality of life, delay to pivotal points such as nursing home placement, and caregiver quality of life represent alternative measures of the effects of antidementia therapies that have substantial face value for consumers and clinicians. Atypical antipsychotic agents may benefit cognition in individuals with schizophrenia and other psychoses and cognition is a critical outcome in trials of these agents. Likewise, haloperidol appears to produce cognitive decline in patients with AD whereas atypical antipsychotics lack this effect.21) Thus, assess- ment of cognitive effects of psychotropic agents is a criti- cal dimension of clinical trials. Incorporation of such mea- sures into clinical trials is a current unmet need in psychogeriatrics and geriatric neuropsychopharmacology.
In addition to incorporating new outcome measure into antidementia clinical trials, new trial designs may also be warranted and provide important new types of data. For example, a preliminary study with tacrine suggested that this cholinesterase inhibitor may delay nursing home placement.22) Similarly, a randomized clinical trial of vita- min E, selegiline, combined vitamin E plus selegiline, and placebo used death, time to nursing home placement, time to loss of specific activities of daily living, or time to progression to severe dementia as outcome measures.23) Such delay-to-endpoint designs could be employed to provide relevant information on time to decline of specific neuropsychological functions, time to emergence of spe- cific behaviors, (e.g., agitation, psychosis) as well as other milestones in the course of AD or other dementing ill- nesses.
Development of biological markers of therapeutic re- sponses is also urgently needed. Cerebrospinal fluid (CSF) tau and beta-amyloid protein are evolving as bio- logical markers of the underlying neuropathology of ADz4) and could theoretically be used to monitor anti-amyloid or anti-tau therapies. Measures of hippocampus and me- dial temporal structures have been shown to change more rapidly in AD than in normal elderly controls and repre- sent a measure of disease progressi~n.~~) These or other measures might be used to assess disease-modifying effects of agents potentially useful in treating the underly- ing neuropathological processes of AD such as anti-in- flammatory agents, antioxidants, or drugs affecting beta-
19

Cummings and Senanarong
amyloid metabolism. None of these approaches has been used in clinical trials and identification of viable biological markers for use in trials is an unmet need.
Studies using positron emission tomography (PET) or single photon emission computed tomography (SPECT) show regional differences in brain function between psy- chotic and non-psychotic, agitated and non-agitated and depressed versus non-depressed patients with AD.z6 27)
Whether these functional differences can be modified by antipsychotic, antiagitation or antidepressant therapies remains to be investigated. If so, such imaging changes could serve as a surrogate to support clinical trial out- comes in patients with AD and behavioral disturbances. Such supporting studies might allow a reduction in sample size required to demonstrate a drug effect.
Biological markers for idiopathic psychosis and depres- sion in psychogeriatric populations are lacking and their development depends on an improved understanding of the neurobiology of these disorders. Insights into the neu- robiological basis of these conditions might also allow the discovery of disease-modifying therapies; all therapies currently available for these conditions are aimed at relief of symptoms. Investigation of the neurobiological basis and reorientation of pharmacotherapy of these disorders towards disease-modifying interventions is an unmet need in psychogeriatric neuropsychopharmacology.
Clinical trials assess the efficacy of single therapeutic agents. A single cholinesterase inhibitor, antidepressant agent, antipsychotic, or antiagitation agent is compared to placebo in most clinical trial designs. Many patients, however, have multiple symptoms6) and will receive mul- tiple agents simultaneously. Patients with AD may receive a cholinesterase inhibitor, an antioxidant such as vitamin E, and at least one psychotropic compound. Female pa- tients may receive concomitant estrogen replacement therapy. Patients with PD receive multiple dopaminergic compounds plus psychotropic agents. Patients with late- onset schizophrenia may receive an atypical antipsychotic and possibly an antidepressant or sedative-hypnotic. Most psychogeriatric patients will receive treatment for comorbid medical disorder as well as for their neuropsychiatric symp- toms. Studies of combinations of agents in neuropsychi- atric disorders have not been conducted and are urgently needed. On the other hand, there are too many potential combinations for all to be assessed. Development of a means to determine the most rational combinations to be tested is an unmet need in geriatric neuropsychophar-
macology. Agents may have differential therapeutic effects de-
pending on the stage of the disease. Drugs may have different efficacy depending on the stage of the disease- presymptomatic, mild, moderate, or severe. For example, it currently appears that estrogen replacement therapy has benefit in preventing or deferring the onset of AD in postmenopausal womenzR) but these agents are not use- ful therapeutically once patients fulfill all criteria for the presence of
Another critical emerging area in clinical trials involves informed consent and the use of New revi- sions in the Helsinki Accords suggest greatly reducing the use of placebos in the development of new medica- tion. International regulatory agencies have not yet incor- porated these recommendations into new drug applica- tion reviews. The alternative strategy, comparing new agents to active approved compounds, could lead to the approval of ineffective medications because agents per- forming at intermediate levels in clinical trials might pro- duce results similar to an active comparison drug but also similar to a placebo if a placebo was present in the trial. Such a trial would not provide substantial evidence for drug effect but, in the absence of a placebo, could be used as evidence for drug efficacy. Conditioning factors such as the length of the trial, the severity of the condi- tion, the consequence of delaying therapy, the availabil- ity of alternative therapies, and the degree of informed consent of the participant may all contribute in eventual resolution of these issues.
How best to obtain informed consent in cognitively im- paired individuals is controversial. Many patients partici- pating in geriatric neuropsychopharmacology clinical tri- als are mildly or more severely cognitively impaired and may not be able to give fully informed consent for partici- pation. Consent from a caregiver or legally appointed sur- rogate is currently accepted to allow participation in clini- cal trials. This practice, however, raises ethical concerns about protection of the cognitively impaired individual. Such patients must be included in clinical trials for any new drug development to proceed, and policies that opti- mally protect their rights and health require development.
A final group of unresolved issues in clinical trials rel- evant to geriatric neuropsychopharmacology involves fac- tors that condition disease presentation and drug response and are rarely studied or included in clinical trials. For example, premorbid personality may affect disease pre-
20
Research
Research
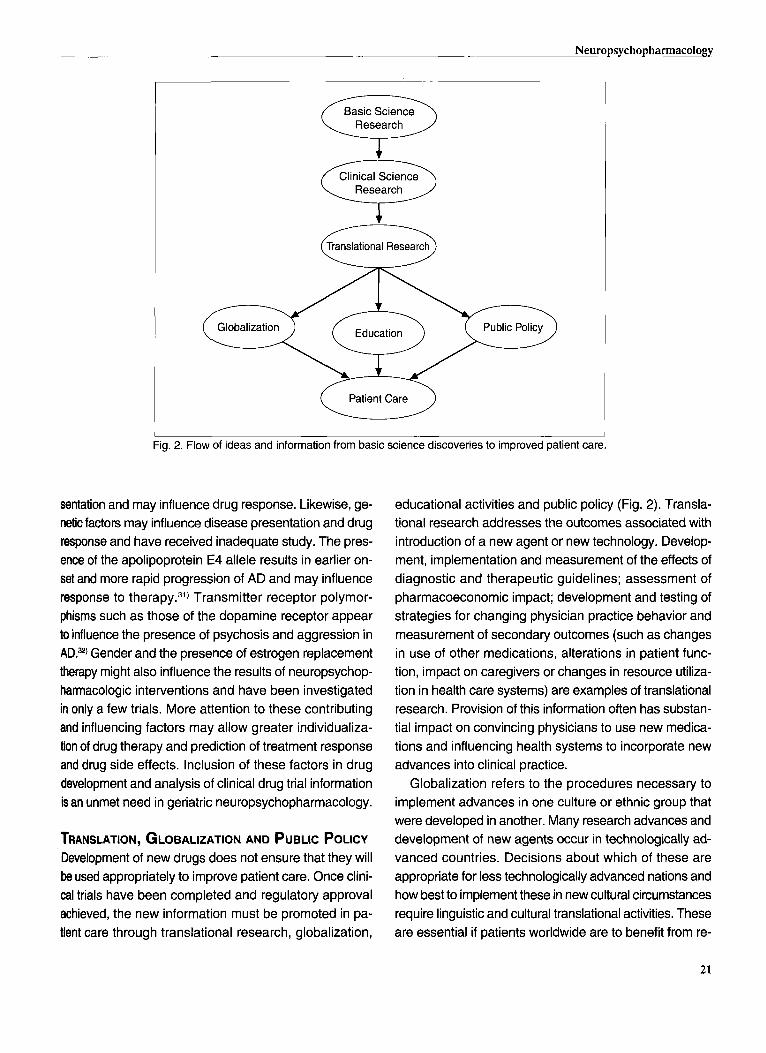
Patient Care u Fig. 2. Flow of ideas and information from basic science discoveries to improved patient care.
sentation and may influence drug response. Likewise, ge- netic factors may influence disease presentation and drug response and have received inadequate study. The pres- ence of the apolipoprotein E4 allele results in earlier on- set and more rapid progression of AD and may influence response to therapy.3i) Transmitter receptor polymor- phisms such as those of the dopamine receptor appear to influence the presence of psychosis and aggression in AD.=) Gender and the presence of estrogen replacement therapy might also influence the results of neuropsychop- harmacologic interventions and have been investigated in only a few trials. More attention to these contributing and influencing factors may allow greater individualiza- tion of drug therapy and prediction of treatment response and drug side effects. Inclusion of these factors in drug development and analysis of clinical drug trial information is an unmet need in geriatric neuropsychopharmacology.
TRANSLATION, GLOBALIZATION AND PUBLIC POLICY Development of new drugs does not ensure that they will be used appropriately to improve patient care. Once clini- cal trials have been completed and regulatory approval achieved, the new information must be promoted in pa- tient care through translational research, globalization,
educational activities and public policy (Fig. 2). Transla- tional research addresses the outcomes associated with introduction of a new agent or new technology. Develop- ment, implementation and measurement of the effects of diagnostic and therapeutic guidelines; assessment of pharmacoeconomic impact; development and testing of strategies for changing physician practice behavior and measurement of secondary outcomes (such as changes in use of other medications, alterations in patient func- tion, impact on caregivers or changes in resource utiliza- tion in health care systems) are examples of translational research. Provision of this information often has substan- tial impact on convincing physicians to use new medica- tions and influencing health systems to incorporate new advances into clinical practice.
Globalization refers to the procedures necessary to implement advances in one culture or ethnic group that were developed in another. Many research advances and development of new agents occur in technologically ad- vanced countries. Decisions about which of these are appropriate for less technologically advanced nations and how best to implement these in new cultural circumstances require linguistic and cultural translational activities. These are essential if patients worldwide are to benefit from re-
21

Cummings and Senanarong
search conducted in research-intensive centers. Public policy can have a major impact on patient care.
When disease screening, disease prevention strategies, health promotion activities or disease treatment are man- dated they are more readily incorporated into clinical prac- tice. Mandating screening for depression and cognitive impairment in aged individuals would improve disease detection, and harmonization of international drug devel- opment and approval guidelines would facilitate interna- tional drug discovery and development efforts. Investiga- tions conducted in one nation might be used to facilitate acceptance of the agent in the other, sparing governmental expenses and facilitating access to new drugs. These are two aspects of public policy that are currently unmet needs in geriatric neuropsychopharmacology.
EFFECTIVENESS RESEARCH Randomized controlled trials determine the efficacy of therapeutic agents in highly selected patient populations receiving therapy in academic clinical settings.m) Typically, patients with unstable medical illnesses or receiving mul- tiple medications are excluded from clinical trials. Most psychogeriatric patients, however, have multiple illnesses, receive several medications and do not obtain their care in specialized settings. Thus, the relevance of efficacy trials to routine clinical practice often is uncertain. To bridge the gap between efficacy studies and routine practice, “effectiveness studies” have emerged. These studies in- clude a broader spectrum of patients, have fewer exclu- sionary criteria, may utilize non-research sites for patient assessment, emphasize outcomes such as employment, hospitalization rates, use of emergency room services, nursing home placement, use of concomitant medications, use of community resources, requirements of caregiver time, and cost-benefit analyses. Such studies also are performed in culturally appropriate settings and employ culturally relevant outcome measures. While efficacy is likely to be determined primarily by neurobiological fac- tors, effectiveness is influenced by many aspects of soci- ety, culture, and healthcare delivery. The performance of more effectiveness trials is an unmet need in geriatric neuropsychopharmacology.
TREATMENT OF BEHAVIORAL ASPECTS OF
ALZHEIMER’S DISEASE AND OTHER DEMENTIAS Alzheimer‘s disease is the most common psychogeriatric disorder and nearly all patients with AD have accompa-
nying neuropsychiatric symptom^.^) Treatment of behav- ioral disorders associated with dementing illnesses has focused almost entirely on off label prescribing of psy- chotropic agents developed for treatment of idiopathic psy- chiatric disorders. These agents often have proved to be efficacious. Atypical antipsychotics including risperidone and olanzapine reduce psychosis and agitation in patients with AD.%.%) Similarly, selective serotonin reuptake inhibi- tors reduce depressive symptoms in patients with AD and depression in small randomized placebo controlled tri- a l ~ . ~ ~ , ~ ~ ) These trials have produced new information re- garding the use of psychotropic agents in patients with AD and also have raised new questions. For example, AD patients residing in nursing homes have large pla- cebo responses when included in randomized controlled trials. In most studies, approximately 30% of patients treated with placebo have at least a 50% reduction in tar- get ~ y m p t o m s . ~ ~ ~ ~ ~ ~ ~ ) Further study of this robust placebo response may provide insights into which patients may respond best to psychosocial interventions and may indi- cate how to structure trials to minimize this confounding effect (e.g., use of placebo lead-in periods, ensuring that patients meet entrance criteria at both screening and baseline assessment, use of wait list controls, etc.).
Agents used to treat the underlying neurobiological changes of dementias such as AD can be anticipated to have behavioral effects. Preventing or deferring the on- set of AD would reduce the number of patients with be- havioral changes. Slowing the progression of AD might defer the emergence of new neuropsychiatric disorders but might prolong the period of occurrence of others (e.g., apathy). Agents that improve cognitive symptoms are likely to affect diverse brain regions and to influence behavioral symptoms. When behavioral data have been collected in randomized controlled trials of antidementia agents, be- havioral changes typically have been observed. In the double-blind controlled trial comparing vitamin E, selegiline, combined therapy and placebo in patients with AD,23) patients on combined therapy exhibited significant reductions in the score of the Behavior Rating Scale for Dementia (BRSD)37) compared to patients in the other arms of the study. Studies of cholinesterase inhibitors revealed that behavioral changes frequently occur in pa- tients experiencing cognitive improvement with these agents and also are present in some patients without demonstrable cognitive changes.%) Similarly, pramipexole has been shown to reduce the emergence of depression
22

Neuropsychopharmacology
in PD patients treated with this dopaminergic agon i~ t .~~) Table 2 provides a conceptual framework for examin-
ing the behavioral changes associated with agents used to treat patients with AD or related dementias. Two gen- eral classes of therapeutic approaches are recognized, mechanism-based and symptom-based. Mechanism- based therapies are further divided into those that are disease-modifying and impact the underlying neurobio- logical disorder and those that are not disease modifying based on transmitter replacement strategies such as cho- linesterase inhibitors. The latter were developed on the basis of disease-related observations but do not change the underlying course of the illness. Symptom-based therapies include psychotropic medications used to re- lieve neuropsychiatric symptoms and whose pathophysi- ological mechanisms remain to be delineated.
GENETIC, NEUROBIOLOGICAL, AND ETIOLOGICAL DETERMINANTS OF GERIATRIC NEUROPSYCHIATRIC SYNDROMES Geriatric neuropsychiatric syndromes are the result of the impact of a disease process on an individual genetic con- stitution with a long history of environmental influences. Genetic and environmental influences must be consid- ered in addition to the neurobiology of the disease itself. A life span developmental approach is as relevant to ge- riatric neuropsychopharmacology as it is to pediatric neu- ropsychopharmacology. Age, gender, educational level and genetic constitution have all been shown to influence the development of AD.‘” Age and gender influence the occurrence of specific types of behavioral disturbances in patients with AD. Older patients are more likely to ex- hibit psychosisg) and women are more likely to experi- ence depression in the course of AD. Past educational experience has been shown to influence the occurrence of cognitive deficits; a finding attributed to the develop- ment of greater cerebral reserve by enhanced educational experience^.'^) Similarly, past emotional experiences might influence the Occurrence of behavioral disturbances in patients with AD and other neuropsychiatric syndromes.
Genetic factors affect the frequency and age of onset of AD. The apolipoprotein E-4 genotype is associated with earlier age of onset and higher frequency of occurrence than the E-2 or E-3 apolipoprotein genotype. Polymor- phisms of both the dopamine receptors and serotonin re- ceptors have been associated with specific neuropsychi- atric disorders in AD.32) Genotype-behavioral phenotype
Table 2. Classification of agents used in geriatric neuropsy- chiatric disorders (behavioral effects may be observed with therapies with any agent of the classification)
Mechanism-based Disease-modifying
Antioxidants Anti-inflammatory agents Amyloid-related agents Tau-related agents Synuclein-related agents
Transmitter replacement therapies Cholinesterase inhibitors Dopaminergic agents
Symptom-based Antidepressants Antipsychotic agents Antiagitation agents Mood stabilizing agents Sedative-hypnotics Anxiolytics Anti-apathetic therapies
studies have been few, and further investigations of ge- netic influences on psychogeriatric syndromes and their response to treatment are an urgent unmet need.
Within diseases, neurobiological differences among patients may influence behavior. Alzheimer’s disease is clinically heterogeneous with patients exhibiting a variety of behavioral changes. In addition, the constellation of neuropsychiatric symptoms among patients with AD changes with evolution of the disease. Recent studies show that at least some of this behavioral heterogeneity is related to the distribution of the underlying neurobio- logical changes. Agitation has been found to be associ- ated with a higher burden of neurofibrillary tangle pathol- ogy in the frontal lobes. Neurofibrillary tangles were not increased in other cortical regions and neuronal loss, Lewy bodies and abundance of neuritic plaques were similar in agitated and non-agitated patients.40) Heterogeneity in the occurrence of agitation thus appears to reflect the under- lying abundance and distribution of neurofibrillary tangle pathology. Neurobiological factors must be considered when developing new therapies for psychogeriatric con- ditions.
Geriatric neuropsychopharmacology must also address a broad range of etiologies of behavioral disorders in the elderly. Table 3 provides a generic approach to consider- ing the diverse array of conditions that may contribute to psychogeriatric disorders. Pharmacologic responses may vary according to the etiology of the underlying disease.
23

Cummings and Senanarong
Table 3. Classification of etiologies of psychogeriatric disorders
Persistent or recurrent in old age Idiopathic With neurologic disorder (epilepsy, multiple sclerosis, Huntington's disease,neoplasms, traumatic brain injury etc.) With medical illness (systemic lupus erythematosus (SLE), etc.) Drug-related (substance abuse disorder, prescribed medications) With adult mental retardation
Idiopathic With neurologic disorder
Late onset
Vascular (vascular dementia, post-stroke syndromes, and white matter ischemic syndromes) Degenerative disorders (Alzheimer's disease, frontotemporal dementia, dementia with Lewy bodies, Parkinson's
Traumatic brain injury Neoplasm Hydrocephalus
disease, Creutzfeldt-Jakob disease, corticobasal degeneration, progressive supranuclear palsy, etc.)
With medical illness Drug-related (substance abuse disorder, prescribed medications)
ANIMAL MODELS Animal models may aid in understanding the pathophysi- ology of psychogeriatric disorders and their treatment. There have been few studies of cognition in existing ani- mal models of neurodegenerative diseases such as transgenic mouse models of AD and essentially no as- sessment of behaviors relevant to the neuropsychiatric aspects of the disorders of interest such as apathy or agi- tation. Animal models of AD could be used to study the effects of the AD-related pathology on vulnerability to the development of behavioral disturbances (e.g., amphet- amine models of psychosis in rodents or stress related models of depression); and animal models of psychoge- riatric conditions with behavioral manifestations could be used to assess the efficacy of psychotropic agents.
On the other hand, most existing animal models are flawed, have limited fidelity to their human disease coun- terpart and cannot at present be used as a decision point as to whether to continue development of a particular com- pound. For example, transgenic models of AD produce amyloid plaques similar to those of the human condition but lack production of neurofibrillary tangles or extensive nerve cell death and therefore fail to model many aspects of the human disease. Development of better animal mod- els of geriatric neuropsychiatric conditions is an unmet need.
CONCLUSION There has been rapid progress in psychogeriatrics and geriatric neuropsychopharmacology. In many cases, these
24
advances have made the unmet needs more apparent. Progress in the development of symptomatic medications makes more obvious the absence of disease-modifying interventions. While mechanism-based and disease-modi fying therapies seem feasible in degenerative disorders, little progress has been made in identifying the underly- ing neurobiological basis and potential interventions in idiopathic neuropsychiatric disorders. Current classifica- tions such as those of DSM-IV and ICD-10 do not em- phasize the occurrence of common psychogeriatric syn- dromes such as agitation and apathy. Changes in FDA requirements for drug approvals will require randomized clinical trials specifically within psychogeriatric populations and point out the current relative absence of such trials. Expansion of clinical trial outcome measures and the implementation of effectiveness trials are urgently needed in geriatric neuropsychopharmacology. Study of the ge netic, developmental and environmental influences on the emergence of behavioral disorders in old age is impera- tive. Finally, improved understanding of the neurobiology of the diverse array of disorders presenting in old age with neuropsychiatric symptoms is a requirement for progress in the development of disease-modifying thera- pies. These unmet needs represent a rich research agenda for geriatric neuropsychopharmacology and prom- ise to provide answers relevant to improved patient care and enhancement of the quality of life of psychogeriatric patients.

ACKNOWLEDGEMENTS This project is supported by a National Institute on Aging Alzheimer‘s Disease Research Center grant (AG 16570), the Alzheimer’s Disease Cooperative Study grant (AG 1 O483), an Alzheimer‘s Disease Research Center of Cali- fornia grant, the Sidell-Kagan Foundation, and the Gen- eral Clinical Research Center grant (RR-00865).
DISCLOSURES Dr. Cummings has provided consultation to Novartis, Pfizer, Esai, Janssen, Lilly and Bristol-Myers Squibb re- garding products potentially relevant to this article.
REFERENCES 1. World Health Organization. World atlas of ageing. Kobe, Ja-
pan. Centre for Health Development, World Health Organiza- tion, 1998.
2. American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-IV. American Psychiatric Association, Washington, DC, 1994.
3. World Health Organization. Clinical descriptions and diagnos- tic guidelines: the ICD X classification of mental disorders. ICD X, Geneva, 1992.
4. Mega M, Cummings JL, Fiorello T, Gombein J. The spectrum of behavioral changes in Alzheimer‘s disease. Neurology 1996; 46: 130-1 35.
5. Marin RS, Fogel BS, Hawkins J, Duffy J, Krupp B. Apathy: a treatable syndrome. J Neuropsychiatry Clin Neurosci 1995; 7: 23-30.
6. Chung JA, Cummings JL. Neurobehavioral and neuropsychi- atric symptoms in Alzheimer‘s disease. Neurologic Clinics 2000; 18: 829-846.
7. Cummings JL, Mega M, Gray K, Rosenberg-Thompson S, Carusi DA, Gornbein J. The neuropsychiatric inventory: com- prehensive assessment of psychopathology in dementia. Neu- rology 1994; 44: 2308-231 4.
8. Rosen WG, Mohs RC, Davis KL. A new rating scale for Alzheimer’s disease. Am J Psychiatry 1984; 141 : 1356-1 364.
9. Levy ML, Cummings JL, Fairbanks LA, Bravi D, Calvani M, Carta A. Longitudinal assessment of symptoms of depression, agitation, and psychosis in 181 patients with Alzheimer’s dis- ease. Am J Psychiatry 1996; 153: 1438-1443.
10. Wooding WM. Planning Pharmaceutical Clinical Trials: Ba- sic Statistical Principles, John Wiley & Sons, New York, 1994.
11. Hamilton M. Development of a rating scale for primary de- pressive illness. Bri J Social Clinical Psychology 1967; 6:
12. Overall JE, Gorham DR. The brief pyschiatric rating scale. Psycho1 Rep 1962; 10: 799-81 2.
13. Cummings JL, Vinters HV, Cole GM, Khachaturian ZS. Alzheimer’s disease: etiologies, pathophysiology, cognitive reserve, and treatment opportunities. Neurology 1998; 51
14. Stahl SM. Essential psychopharmacology. Essential Psy- chopharmacology, 2nd ed., Cambridge University Press,
278-296.
(Suppl): 2-1 7.
Cambridge, England, 2000. 15. McKeith I, Fairbairn A, Perry R, Thompson P, Perry E. Neu-
roleptic sensitivity in patients with senile dementia of Lewy body type. BMJ 1992; 305: 673-678.
16. Rademann J, Jung G. Integrating combinatorial synthesis and bioassays. Science 2000; 287: 1947-1 948.
17. Brewer T, Colditz GA. Postmarketing surveillance and ad- verse drug reactions. JAMA 1999; 281 : 824-829.
18. Friary R. Jobs in the Drug Industry: A Career Guide for Chem- ists, Academic Press, New York, 2000.
19. Sramek JJ, Cutler NR, Kurtz NM, Murphy MF, Carta A. Op- timizing the Development of Antipsychotic Drugs, John Wiley & Sons, New York, 1997.
20. Schneider LS, Olin JT, Lyness SA, Chui HC. Eligibility of Alzheimer’s disease clinic patients for clinical trials. J Am Geriatr SOC 1997; 45: 923-928.
21. De Deyn PP, Rabheru K, Rasmussen A, et al. A random- ized trial of risperidone, placebo, and haloperidol for behav- ioral symptoms of dementia. Neurology 1999; 53: 946-955.
22. Knopman D, Schneider L, Davis K, et al. Long-term tacrine (Cognex) treatment: effects on nursing home placement and mortality. Neurology 1996; 47: 166-1 77.
23. Sano M, Ernest0 C, Thomas RG, et al. For the members of the Alzheimer’s Disease Cooperative Study: a controlled trial of selegiline, alpha-tocopherol, or both as treatment for Alzheimer’s disease. N Engl J Med 1997; 336: 1216-1222.
24. Hulstaert F, Blennow K, lvaniou A, et al. Improved discrimi- nation of AD patients using B-amyloid (1 -42) and tau levels in CSF. Neurology 1999; 52: 1555-1 562.
25. Jack Jr CR, Petersen RC. Structural imaging approaches to Alzheimer’s disease. In Scinto FM, Daffner KR (eds) Early Diagnosis of Alzheimer’s Disease, Humana Press, New Jer- sey; 2000.
26. Sultzer DL, Mahler ME, Mandelkern MA, et al. The relation- ship between psychiatric symptoms and regional cortical me- tabolism in Alzheimer’s disease. J Neuropsychiatry Clin Neurosci 1995; 7: 476-484.
27. Mega MS, Thompson PM, Toga AW, Cummings JL. Brain mapping in dementia. In Mazziotta JC, Toga AW, Frackowiak RSJ (eds) Brain Mapping the Disorders, Academic Press, San Diego, 2000; 21 7-239.
28. Kawas C, Resnick S, Morrison A. A prospective study of estrogen replacement therapy and the risk of developing Alzheimer’s disease: the Baltimore longitudinal study of ag- ing. Neurology 1997; 48: 151 7-1 521.
29. Mulnard RA, Cotman CW, Kawas C, et al. Estrogen replace- ment therapy for treatment of mild to moderate Alzheimer disease: a randomized controlled trial. Alzheimer’s Disease Cooperative Study. JAMA 2000; 283: 1007-1 015.
30. The Ethics and Humanities Subcommittee of the American Academy of Neurology. Ethical issues in clinical research in neurology: advancing knowledge and protecting human re- search subjects. Neurology 1998; 50.
31. Corder EH, Saunders AM, Strittmatter WJ, et al. Gene dose of apolipoprotein E type 4 allele and the risk of Alzheimer’s disease in late onset families. Science 1993; 261 : 921-923.
32. Sweet RA, Limgoankar VL, Kamboh I, Lopez OL, Zhang F, DeKosky ST. Dopamine receptor genetic variation, psycho- sis, and aggression in Alzheimer’s disease. Arch Neurol
25

Cummings and Senanarong -
1998; 55: 1335-1 340. 33. Katz IR, Jeste DV, Mintzer JE, Clyde C, Napolitano J, Brecher
M. Comparison of risperidone and placebo for psychosis and behavioral disturbances associated with dementia: a ran- domized, double-blind trial. Risperidone Study Group. J Clin Psychiatry 1999; 60: 107-1 15.
34. Street J, Clark WS, Gannon KS, et al. Olanzapine treatment of psychotic and behavioral symptoms in patients with Alzheimer’s disease in nursing care facilities. Group tHS. Arch Gen Psychiatry 2000; 57: 968-976.
35. Lyketsos CG, Sheppard J-ME, Steele CD, et al. Random- ized, placebo-controlled, double-blind clinical trial of Sertraline in the treatment of depression complicating Alzheimer’s disease: initial results from the Depression in Alzheimer’s Disease Study. Am J Psychiatry 2000; 157:
36. Taragano FE, Lyketsos CG, Mangone CA, Allegri RF, Comesana-Diaz E. A Double-blind, randomized, fixed-dose
1686-1 689.
trial of fluoxetine vs. amitriptyline in the treatment of major depression complicating Alzheimer’s disease. Psychosomat. ics 1997; 38: 246-252.
37. Tariot PN, Mack JL, Patterson MB, et at., Behavioral Pathol- ogy Committee of the Consortium to Establish a Registry for Alzheimer’s Disease. The behavior rating scale for de- mentia of the consortium to establish a registry for Alzheimer’s disease. Am J Psychiatry 1995; 152: 1349-1 357.
38. Cummings JL. Cholinesterase inhibitors: a new class of psy- chotropic agents. Am J Psychiatry 2000; 157: 4-15.
39. Cummings JL. D-3 receptor agonists: combined action neu- rologic and neuropsychiatric agents. J Neurol Sci 1999; 163:
40. Tekin S, Mega MS, Masterman DL, Chow TW, Vinters HV, Cummings JL. Orbitofrontal and anterior cingulate cortex: neurofibrillary tangle burden is associated with agitation in Alzheimer’s disease. Ann Neurol (in press).
2-3.
26