Clinical Pediatric Nephrology - Taylor & Francis eBooks
586
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Clinical Pediatric Nephrology - Taylor & Francis eBooks

K21764.indb 1 02/09/16 6:02 pm
Third Edition
Clinical PediatricTMephrology

CRC Press is an imprint of theTaylor & Francis Group, an informa business
Boca Raton London New York
V i c e C h a i r D e p a r t m e n t o f P e d i a t r i c sN o r t h w e s t e r n U n i v e r s i t yF e i n b e rg S ch o o l o f M e d i c i n ea n d A n n & R o b e r t H . L u r i e C h i l d re n ’s H o s p i t a l o f C h i c a g oC h i c a g o , I L , U S A
D i v i s i o n D i r e c t o r o f P e d i a t r i c N e p h r o l o g yM a rc u s P r o f e s s o r o f P e d i a t r i c sE m o r y U n i v e r s i t y S ch o o l o f M e d i c i n ea n d C h i l d re n ’s H e a l t h c a re o f A t l a n t aA t l a n t a , G A , U S
C h a i r m a n , D e p a r t m e n t o f N e p h r o l o g y P h o e n i x C h i l d re n ’s H o s p i t a lP h o e n i x , A Z , U S A a n d E m e r i t u s P r o f e s s o r o f P e d i a t r i c s G e o rg e Wa s h i n g t o n U n i v e r s i t y S ch o o l o f M e d i c i n eWa s h i n g t o n , D C , U S A
K21764.indb 3 02/09/16 6:02 pm
Third Edition
Clinical PediatricINephrology
CRC PressTaylor & Francis Group
Edited By
Karrwal K. Kher
H. William Schnaper
Larry A. Greenbaum
£9

CRC PressTaylor & Francis Group6000 Broken Sound Parkway NW, Suite 300Boca Raton, FL 33487-2742
© 2017 by Taylor & Francis Group, LLCCRC Press is an imprint of Taylor & Francis Group, an Informa business
No claim to original U.S. Government works
Printed on acid-free paperVersion Date: 20160808
International Standard Book Number-13: 978-1-4822-1462-8 (Pack - Book and Ebook)
This book contains information obtained from authentic and highly regarded sources. While all reasonable efforts have been made to publish reliable data and information, neither the author[s] nor the publisher can accept any legal responsibility or liability for any errors or omissions that may be made. The publishers wish to make clear that any views or opinions expressed in this book by individual editors, authors or contributors are personal to them and do not necessarily reflect the views/opinions of the publishers. The information or guidance contained in this book is intended for use by medical, scientific or health-care professionals and is provided strictly as a supplement to the medical or other professional’s own judgement, their knowledge of the patient’s medical history, relevant manufacturer’s instructions and the appropriate best practice guidelines. Because of the rapid advances in medi-cal science, any information or advice on dosages, procedures or diagnoses should be independently verified. The reader is strongly urged to consult the relevant national drug formulary and the drug companies’ and device or material manufacturers’ printed instructions, and their websites, before administering or utilizing any of the drugs, devices or materials mentioned in this book. This book does not indicate whether a particular treatment is appropriate or suitable for a particular individual. Ultimately it is the sole responsibility of the medical professional to make his or her own professional judgements, so as to advise and treat patients appropriately. The authors and publishers have also attempted to trace the copyright holders of all material reproduced in this publication and apologize to copyright holders if permission to publish in this form has not been obtained. If any copyright material has not been acknowledged please write and let us know so we may rectify in any future reprint.
Except as permitted under U.S. Copyright Law, no part of this book may be reprinted, reproduced, transmitted, or utilized in any form by any electronic, mechanical, or other means, now known or hereafter invented, including photocopying, microfilming, and recording, or in any information storage or retrieval system, without written permission from the publishers.
For permission to photocopy or use material electronically from this work, please access www.copyright.com (http://www.copyright.com/) or contact the Copyright Clearance Center, Inc. (CCC), 222 Rosewood Drive, Danvers, MA 01923, 978-750-8400. CCC is a not-for-profit organization that provides licenses and registration for a variety of users. For organizations that have been granted a photocopy license by the CCC, a separate system of payment has been arranged.
Trademark Notice: Product or corporate names may be trademarks or registered trademarks, and are used only for identification and explanation without intent to infringe.
Visit the Taylor & Francis Web site athttp://www.taylorandfrancis.com
and the CRC Press Web site athttp://www.crcpress.com
K21764.indb 4 02/09/16 6:02 pm

v
Contents
Preface ix
Contributors xi
PART A KIDNEY ANATOMY AND DEVELOPMENT
1 Anatomy and embryology of the urinary tract 3Kurt E. Johnson
2 Molecular basis of developmental renal disease 17Norman D. Rosenblum
PART B DIAGNOSTIC EVALUATION OF KIDNEY DISEASES
3 Urinalysis 31George J. Schwartz
4 Clinical assessment of renal function 45George J. Schwartz
5 Normal and abnormal kidney function in neonates 73Dave T. Selewski and David J. Askenazi
6 Diagnostic imaging of the urinary tract 87Eglal Shalaby-Rana, Bruce Markle, and Dorothy Bulas
7 Radionuclide renal imaging 105Eglal Shalaby-Rana, Mary Andrich, and Massoud Majd
8 Renal biopsy 115Natalie S. Uy, Mihail M. Subtirelu, and Frederick J. Kaskel
9 Hematuria and proteinuria 127Kanwal Kher and Marva Moxey-Mims
PART C DISORDERS OF HOMEOSTASIS
10 Physiology of glomerular filtration 153H. William Schnaper
11 Sodium and volume homeostasis 165Michel Baum
12 Potassium homeostasis 183Caroline Gluck and Lisa M. Satlin
13 Disorders of mineral metabolism 205Farah N. Ali and Craig B. Langman
14 Acid-base homeostasis 235Raymond Quigley
15 Water homeostasis 255Melissa A. Cadnapaphornchai
K21764.indb 5 02/09/16 6:02 pm
vi Contents
PART D GLOMERULAR AND TUBULAR DISEASES
16 Nephrotic syndrome 285Michelle N. Rheault
17 Primary podocytopathies 305Raed Bou Matar, Rudolph P. Valentini, and William E. Smoyer
18 Nephrotic syndrome in the first year of life 353Christer Holmberg and Hannu Jalanko
19 Membranoproliferative glomerulonephritis 367Carla M. Nester and Danniele G. Holanda
20 Membranous nephropathy 385Georges Deschênes
21 Acute glomerulonephritis 401Diego H. Aviles and V. Matti Vehaskari
22 Rapidly progressive glomerulonephritis and vasculitis 419Franca Iorember and V. Matti Vehaskari
23 Immunoglobulin A nephropathy and Henoch-Schönlein purpura nephritis 435M. Colleen Hastings and Robert J. Wyatt
24 Thrombotic microangiopathies 451John D. Mahan and Stephen Cha
25 Tubulointerstitial nephritis 479Rossana Baracco, Gaurav Kapur, and Tej K. Mattoo
PART E KIDNEY IN SYSTEMIC DISEASES
26 Lupus nephritis 499Carla M. Nester, David B. Thomas, and Debbie S. Gipson
27 Kidney disease in sickle cell disease 519Ibrahim F. Shatat and Sherron M. Jackson
28 Kidney disease associated with diabetes mellitus and metabolic syndrome 533Kanwal Kher and Michele Mietus-Snyder
29 Kidney in viral infections 553Jeffrey B. Kopp
PART F KIDNEY FAILURE
30 Acute kidney injury 571Prasad Devarajan and Stuart L. Goldstein
31 Chronic kidney disease 601Kirtida Mistry
32 Anemia in chronic kidney disease 627Meredith Atkinson
33 Chronic kidney disease bone and mineral disorder 639Katherine Wesseling-Perry and Isidro B. Salusky
34 Nutrition in chronic kidney disease 665Sun-Young Ahn and Robert Mak
PART G RENAL REPLACEMENT THERAPIES
35 Continuous renal replacement therapy 679Akash Deep and Timothy E. Bunchman
36 Hemodialysis 703Raj Munshi and Jordan M. Symons
37 Peritoneal dialysis 723Bradley A. Warady
K21764.indb 6 02/09/16 6:02 pm
Contents vii
38 Renal transplantation 743Asha Moudgil and Stanley C. Jordan
PART H HYPERTENSION
39 Hypertension in children and adolescents 777Karen McNiece Redwine
40 Management of hypertension 803Joseph T. Flynn
PART I INHERITED RENAL DISORDERS
41 Tubulopathies 819Detlef Bockenhauer
42 Renal tubular acidosis 839John W. Foreman
43 Cystic kidney disease 863Lisa M. Guay-Woodford
44 Ciliopathies and nephronophthisis 889John Sayer, Shreya Raman, and Shalabh Srivastava
45 Alport syndrome and thin basement membrane nephropathy 899Michelle N. Rheault and Clifford E. Kashtan
46 Renal disease in syndromic disorders 911Patrick Niaudet
PART J UROLOGIC DISORDERS
47 Hydronephrosis and obstructive uropathies 931Ihor V. Yosypiv
48 Vesicoureteral reflux 953Tej K. Mattoo
49 Urinary tract infection 967Brittany Goldberg and Barbara Jantausch
50 Pediatric renal tumors 993Eugene Minevich, Armando J. Lorenzo, W. Robert DeFoor and Martin A. Koyle
51 Urolithiasis in children 1005Uri S. Alon and Tarak Srivastava
52 Voiding disorders 1025Hans G. Pohl
PART K RESEARCH TOOLS
53 Applied clinical biostatistics 1049Shamir Tuchman
Index 1061
K21764.indb 7 02/09/16 6:02 pm

ix
Preface
�is third edition of Clinical Pediatric Nephrology contin-ues to have as its main goal providing a primer of pediat-ric nephrology. Its intended audience includes committed medical students and general trainees, as well as pediatric nephrology fellows and pediatric nephrologists. Our focus remains on the clinical diagnosis and management of pedi-atric renal disorders.
�e book has been thoroughly updated, and each chapter has been rewritten. �e number of chapters has expanded from 37 to 53. In part, this represents a degree of special-ization, with several chapters divided to focus on speci�c disorders as their pathogenesis has been clari�ed. �e organization of the book has also been changed with an additional emphasis on the physiology of kidney diseases. Sections now cover kidney anatomy and development, diagnostic evaluation, disorders of homeostasis, glomeru-lar and tubular diseases, systemic diseases and the kidney, acute and chronic kidney disease, renal replacement thera-pies, hypertension, inherited disorders, urologic disorders, and research tools. We believe that this reorganization and the expansion in the number of chapters better re�ects the status of pediatric nephrology today. Each chapter includes “Key Points” boxes to emphasize issues that the authors and editors believe are important take-aways in the section, a set of review questions for the reader, and where appropri-ate a clinical vignette describing how the information in the chapter could be clinically applied in real life.
An important change has been an evolution in the edi-torship. Dr. Larry Greenbaum has joined the editorial team. He brings immense experience as an academic nephrolo-gist, clinician and a researcher to the editorial team. His role in shaping the content of the third edition is evident in all sections of the book. We also wish to express our sincerest gratitude and thanks to Dr. Sudesh Makker, who guided the editorial work in the �rst two editions of this book.
We wish to thank all the contributors who worked dili-gently with us, under tight time-lines, through several revi-sions of their texts, and who willingly provided elements
for the chapters that are unique to this publication. �e outstanding editorial, production, and marketing teams at Taylor and Francis have provided support that has been essential to our reaching fruition. We are especially grateful to Our sincerest thanks to Henry Spilberg, who has man-aged the publication of the second edition and guided us in the concept design of the third edition of this book at Taylor and Francis. Miranda Bromage, who has taken over the reigns, has been an inspiration to work with. She provided her extraordinary skills in guiding the production of the book. Henry and Miranda were instrumental in advocating for an “all-color” book, which has enhanced its content and visual appeal. We thank both of them from the bottom of our hearts. Amy Blalock and Linda Van Pelt provided their superb expertise in copy editing and composing the galleys. Kyle Meyer, at the Boca Raton o�ce of CRC Press-Taylor and Francis worked patiently with us in the editing of gal-leys of all chapters. Without his help, publication of this book would not have materialized. Figures in this edition were drawn by a very talented pool of artists. �ey are the unsung heroes of this work. We wish to thank each one of them for their contributions.
We owe a major debt of gratitude to two groups. Our students, residents, nephrology fellows and colleagues have provided inspiration and frequently challenged us on com-munication of scienti�c and educational content, as well as the format of this work. Most importantly, our families, who tolerate our busy and o�en distracting schedules have provided consistent support and a sense of perspective as we undertook this task. �ey provide an essential foundation for our lives. It is only with their individual commitments that we have succeeded in completing this task. We owe our heartfelt gratitude and appreciation to each one of them.
Kanwal K. KherLarry A. GreenbaumH. William Schnaper
K21764.indb 9 02/09/16 6:02 pm
xi
Contributors
Sun-Young Ahn, MDMedical director, nephrology inpatient servicesChildren’s National Health System,The George Washington UniversityWashington DC, USA
Farah N. Ali, MD, MSAssistant Professor of PediatricsAnn and Robert H. Lurie Children’s Hospital of ChicagoChicago, Illinois
Uri S. Alon, MDProfessor of PediatricsUniversity of Missouri, Kansas City School of MedicineandSection of Pediatric NephrologyThe Children’s Mercy HospitalKansas City, Missouri
Mary Andrich, MDClinical Associate Professor of Radiology The George Washington University School of MedicineWashington, DC
David Askenszi MD, MSPHAssociate Professor of PediatricsMedical Director - Pediatric and Infant Center for Acute
NephrologyUniversity of Alabama at BirminghamBirmingham Alabama , USA
Meredith Atkinson, MD, MHSAssociate Professor of PediatricsDivision of Pediatric NephrologyJohns Hopkins University School of MedicineBaltimore, Maryland, USA
Diego H. Aviles, MDDivision Chief, Pediatric NephrologyChildren’s Hospital of New OrleansProfessor of Clinical PediatricsLouisiana State University Health Sciences Center
New OrleansNew Orleans, Louisiana
Rossana Baracco, MDAssistant Professor of PediatricsChildren’s Hospital of MichiganWayne State UniversityDetroit, Michigan, USA
Michel Baum, MDSara M. and Charles E. Seay Chair in Pediatric ResearchProfessor of Pediatrics and Internal MedicineDepartment of PediatricsUniversity of Texas Southwestern Medical CenterDallas, Texas
Detlef Bockenhauer, PhDProfessor of Paediatric NephrologyUCL Institute of Child Health and Great Ormond Street
Hospital for ChildrenNHS Foundation TrustLondon, United Kingdom
Raed Bou Matar, MDAssistant Professor of PediatricsCleveland Clinic Lerner College of Medicine of Case
Western Reserve UniversityCenter for Pediatric NephrologyCleveland, Ohio
Dorothy Bulas, MDProfessor of Pediatrics and RadiologyThe George Washington University School of MedicineChildren’s National Health SystemWashington, DC
Timothy E. Bunchman, MDDirector Pediatric NephrologyChildren’s Hospital of RichmondandProfessor of PediatricsVirginia Commonwealth University School of MedicineRichmond, Virginia
Melissa A. Cadnapaphornchai, MDAssociate Professor of Pediatrics and MedicineUniversity of Colorado Anschutz Medical CampusThe Kidney CenterChildren’s Hospital ColoradoAurora, Colorado
K21764.indb 11 02/09/16 6:02 pm
xii Contributors
Stephen Cha, MDClinical Assistant Professor of PediatricsNortheast Ohio Medical UniversityNephrology & Pediatric Hypertension CenterAkron Children’s HospitalAkron , Ohio
Akash Deep MD, FRCPCHHonorary Lecturer, King’s CollegeDirector, Pediatric Intensive Care UnitKing’s College Hospital, London, UK
W. Robert DeFoor, MD, MPHAssociate Professor of SurgeryUniversity of CincinnatiandDirector Clinical ResearchDivision of Pediatric UrologyCincinnati Children’s Hospital Medical CenterCincinnati, Ohio
Georges Deschênes, MD, PhDHead of Pediatric NephrologyAPHP Robert-Debré, Université Sorbonne-Paris-CitéParis, France
Prasad Devarajan, MDLouise M. Williams Endowed ChairProfessor of Pediatrics and Developmental BiologyDirector of Nephrology and HypertensionCincinnati Children’s Hospital Medical CenterUniversity of Cincinnati School of MedicineCincinnati, Ohio
Joseph T. Flynn, MD, MSChief, Division of NephrologySeattle Children’s HospitalProfessor of PediatricsUniversity of Washington School of MedicineSeattle, Washington
John W. Foreman, MDChief, Pediatric NephrologyDepartment of PediatricsDuke University Medical CenterDurham, North Carolina
Debbie S. Gipson, MD, MSProfessor of PediatricsUniversity of Michigan School of MedicineAnn Arbor, Michigan , USA
Caroline Gluck, MDPediatric Nephrology FellowChildren’s Hospital of PhiladelphiaPhiladelphia, Pennsylvania, USA
Brittany Goldberg MD, MSAdjunct Assistant Professor of PediatricsGeorge Washington University School of MedicineDivision of Infectious DiseasesChildren’s National Health SystemWashington, DC
Stuart L. Goldstein, MD, FAAP, FNKFDirector, Center for Acute Care NephrologyDivision of Nephrology and HypertensionThe Heart Institute CincinnatiChildren’s Hospital Medical CenterCincinnati, Ohio, United States of America
Larry Greenbaum, MD, PhD, FAAPMarcus Professor of Pediatric NephrologyChief, Division of NephrologyEmory University School of MedicineandChildren’s Healthcare of AtlantaAtlanta, Georgia USA
Lisa M. Guay-Woodford, MDHudson Professor of PediatricsGeorge Washington UniversityandDirector, Center for Translational ScienceandDirector, Clinical and Translational Institute at
Children’s NationalChildren’s National Health SystemWashington, DC
M. Colleen Hastings, MD, MSAssociate Professor, Pediatrics and MedicineUniversity of Tennessee Health Science CenterandLe Bonheur Children’s HospitalandChildren’s Foundation Research InstituteMemphis, Tennessee
Danniele Gomes Holanda, MDClinical Assistant ProfessorDirector, Electron Microscopy LaboratoryDepartment of PathologyUniversity of Iowa Hospitals and ClinicsIowa City, Iowa, USA
Christer Holmberg, MD, PhDProfessor of pediatricsPediatric Nephrology and TransplantationChildren’s HospitalUniversity of HelsinkiHelsinkiFinland
Franca Iorember, MD, MPHAssociate Professor of PediatricsClinical Division of NephrologyChildren’s Hospital of New OrleansandDepartment of PediatricsLouisiana State University Health Sciences Center
New OrleansNew Orleans, Louisiana
K21764.indb 12 02/09/16 6:02 pm

Contributors xiii
Sherron M. Jackson, MDAssociate Professor, Pediatric
Hematology-OncologyDirector of Pediatric Sickle Cell ClinicMedical University of South CarolinaCharleston, South Carolina USA
Hannu Jalanko, MDProfessor, Head of the Department Pediatric Nephrology and TransplantationChildren’s Hospital, University of HelsinkiHelsinki University Central HospitalHelsinki, Finland
Barbara Jantausch, MDProfessor of PediatricsGeorge Washington University School of MedicineandDivision of Infectious DiseasesChildren’s National Medical CenterWashington, DC
Kurt E. Johnson, PhDProfessor of Anatomy and Regenerative BiologyProfessor of Obstetrics and Gynecology (Research)George Washington University School of Medicine and
Health SciencesWashington, DC
Stanley C. Jordan, MDDirector, NephrologyDirector, HLA and Transplant Immunology LaboratoryComprehensive Transplant CenterMedical Director, Kidney Transplant ProgramCedars-Sinai Medical Center, Los Angeles, California
Gaurav Kapur, MDAssociate Professor, PediatricsDirector, Pediatric DialysisWayne State University School of MedicineChildren’s Hospital of MichiganDetroit, Michigan, USA
Clifford E. Kashtan, MDProfessor of PediatricsChief, Division of Pediatric NephrologyUniversity of Minnesota Amplatz
Children’s HospitalMinneapolis, Minnesota
Frederick J. Kaskel, MD, PhDProfessor and Vice Chair of PediatricsDirector, Life Course Research ProgramBlock Institute for Clinical & Translational
ResearchAlbert Einstein College of MedicineandChildren’s Hospital at MontefioreBronx, NY
Kanwal K. Kher, MDProfessor Emeritus of PediatricsGeorge Washington University School of MedicineWashington, DCand Division Chief, Nephrology and HypertensionPhoenix Children’s HospitalPhoenix, AZ
Jeffrey B. Kopp, MDKidney Disease SectionNational Institute of Diabetes and Digestive and
KidneyBethesda, Maryland
Martin A. Koyle, MDProfessor Department of Surgery University of Toronto Department Head, UrologyThe Hospital for Sick Children Toronto, Canada
Craig B. Langman, MDThe Isaac A Abt MD Professor of Kidney DiseasesFeinberg School of Medicine, Northwestern UniversityHead, Kidney DiseasesThe Ann and Robert H Lurie Children’s Hospital of
ChicagoChicago, Illinois USA
Armando J. Lorenzo, MDAssociate ProfessorDepartment of SurgeryUniversity of Toronto andDepartment of Urology. The Hospital for Sick Children, Toronto, Canada
John D. Mahan, MDProfessor, Department of PediatricsPediatric NephrologyThe Ohio State University College of MedicineandNationwide Children’s HospitalColumbus Ohio
Massoud MajdProfessor of Pediatrics and RadiologyThe George Washington University School of
MedicineandChildren’s National Health SystemWashington, DC
Robert Mak, MD, PhDPediatric NephrologyUniversity of California San DiegoLa Jolla, California
K21764.indb 13 02/09/16 6:02 pm
xiv Contributors
Bruce Markle, MDAssociate Professor of Pediatrics and RadiologyThe George Washington University School of MedicineChildren’s National Health SystemWashington, DC
Tej K. Mattoo, MD, DCH, FRCP (UK)Professor of PediatricsWayne State University School of MedicineChief, Pediatric Nephrology and HypertensionChildren’s Hospital of MichiganDetroit, Michigan
Karen McNiece Redwine, MD, MPHAssociate Professor of PediatricsPediatric NephrologyUniversity of Arkansas for Medical Sciences/Arkansas
Children’s HospitalLittle Rock, Arkansas
Michele Mietus-Snyder, MDAssociate Professor of PediatricsThe George Washington University School of MedicineandChildren’s National Health SystemWashington, DC
Eugene Minevich, MDProfessor of SurgeryDivision of Pediatric UrologyCincinnati Children’s Hospital Medical CenterCincinnati, Ohio
Kirtida Mistry, MBBCh, DCH, MRCPCHAssistant Professor of PediatricsDivision of Pediatric NephrologyThe George Washington University School of MedicineandMedical Director, Dialysis ServicesChildren’s National Medical CenterWashington, DC
Asha Moudgil, MDProfessor of PediatricsGeorge Washington University School of MedicineActing Chief Division of NephrologyandMedical Director, Renal TransplantationChildren’s National Medical CenterWashington, DC
Marva Moxey-Mims, MDKUH Deputy Director for Clinical ResearchDirector, Pediatric Nephrology and Renal Centers
Programs NIH, NIDDK, DKUH Bethesda, Maryland
Raj Munshi, MDSeattle Children’s HospitalSeattle, Washington
Carla M. Nester, MD, MSAAssistant ProfessorDepartments of Internal Medicine and PediatricsDivision of NephrologyUniversity of Iowa Hospital and ClinicsIowa City, Iowa
Patrick Niaudet, MDPediatric NephrologyHôpital Necker-Enfants MaladesUniversité Paris-DescartesParis, France
Hans G. Pohl, MD, FAAPAssociate ProfessorUrology and PediatricsGeorge Washington UniversityandAssociate Chief, Department of UrologyChildren’s National Medical CenterWashington, DC
Raymond Quigley MDDivision of Pediatric NephrologyUniversity of Texas Southwestern Medical CenterDallas, Texas
Shreya Raman, MBBS, MRCP, MSc, FRCPathSpecialist Registrar in HistopathologyRoyal Victoria InfirmaryNewcastle upon Tyne Hospitals NHS Foundation TrustNewcastle upon Tyne, United Kingdom
Michelle N. Rheault, MDAssistant Professor of PediatricsandMedical Director of DialysisDivision of Pediatric NephrologyUniversity of Minnesota Amplatz Children’s HospitalMinneapolis, Minnesota
Norman D. Rosenblum MD, FRCPCPaediatric NephrologistHospital for Sick ChildrenProfessor of Paediatrics, Physiology, and Laboratory
Medicine and PathobiologyCanada Research Chair in Developmental NephrologyUniversity of TorontoPeter Gilgan Centre for Research and LearningHospital for Sick ChildrenToronto, Canada
Isidro B. Salusky, MDDistinguished Professor of PediatricsChief. Division of Pediatric NephrologyDirector, Clinical and Translational Research CenterAssociate Dean for Clinical ResearchDavid Geffen School of Medicine at UCLALos Angeles, California, USA
K21764.indb 14 02/09/16 6:02 pm
Contributors xv
Lisa M. Satlin, MDHerbert H. Lehman Professor and ChairJack and Lucy Clark Department of PediatricsMount Sinai Medical CenterPediatrician-in-ChiefKravis Children’s Hospital at Mount SinaiIcahn School of Medicine at Mount SinaiNew York, New York
John Sayer, MBChB, PhD, FRCPSenior Clinical Lecturer in NephrologyInstitute of Genetic MedicineInternational Centre for LifeNewcastle UniversityNewcastle Upon Tyne, United Kingdom
H. William Schnaper, MDIrene Heinz Given and John Laporte Given Professorship
in Pediatric ResearchVice Chair, Department of PediatricsNorthwestern University Feinberg School of MedicineandAnn & Robert Lurie Children’s Hospital of ChicagoChicago, Illinois
George J. Schwartz, MDProfessor of Pediatrics and MedicineChief, Division of Pediatric NephrologyDepartment of PediatricsUniversity of Rochester School of MedicineRochester, New York
Dave Selewski, MD, MSAssistant ProfessorPediatric NephrologyUniversity of MichiganAnn Arbor, Michigan
Eglal Shalaby-Rana, MDAssistant Professor of Radiology and PediatricsGeorge Washington University School of MedicineandChildren’s National Medical CenterWashington, DC
Ibrahim F. Shatat, MD, MSAssociate Professor of PediatricsDivision of Nephrology and HypertensionMUSC Children’s HospitalCharleston, South Carolina
William E. Smoyer, MDC. Robert Kidder Endowed ChairVice President Clinical and Translational ResearchDirector, Center for Clinical and Translational ResearchThe Research Institute at Nationwide Children’s HospitalProfessor of PediatricsColumbus, Ohio USA
Shalabh Srivastava, MBBS, MRCPSpecialist Registrar in NephrologyInstitute of Genetic MedicineNewcastle UniversityNewcastle upon Tyne, United Kingdom
Tarak Srivastava, MDAssociate Professor of PediatricsUniversity of Missouri, Kansas City School of MedicineandDirector, Nephrology Research LaboratoryChildren’s Mercy HospitalKansas City, Missouri
Mihail M. Subtirelu, MDAdjunct Associate ProfessorUniversity of Missouri, Kansas City Division of Pediatric NephrologyandChildren’s Mercy HospitalKansas City, Missouri
Jordan M. Symons, MDProfessor of PediatricsUniversity of Washington School of MedicineAttending NephrologistSeattle Children’s HospitalSeattle, Washington, USA
David B. Thomas, MDProfessor of PathologyUniversity of Miami Miller School of MedicineUniversity of Miami HospitalMiami, Florida
Shamir Tuchman, MD, MPHAssistant Professor of PediatricsGeorge Washington University School of MedicineandDivision of Pediatric NephrologyChildren’s National Medical CenterWashington, DC
Natalie S. Uy, MDAssistant Professor of PediatricsPediatric NephrologyColumbia University Medical CenterNew York, NY
Rudolph P. Valentini, MDChief Medical OfficerPediatric NephrologyChildren’s Hospital of MichiganClinical Professor of PediatricsWayne State University School of MedicineDetroit, Michigan
K21764.indb 15 02/09/16 6:02 pm
Vesa Matti Vehaskari, MD, PhDProfessor of PediatricsLSU Health Sciences CenterChildren’s Hospital of New OrleansNew Orleans, Louisiana
Bradley A. Warady, MDProfessor of PediatricsUniversity of Missouri, Kansas City School of MedicineandSenior Associate Chairman, Department of PediatricsDirector, Division of Pediatric NephrologyChildren’s Mercy HospitalKansas City, Missouri
Katherine Wesseling-Perry, MDAssociate Professor of PediatricsDivision of Pediatric NephrologyDavid Geffen School of Medicine at UCLAUniversity of California, Los AngelesLos Angeles, California
Robert J. Wyatt, MD, MSProfessor of Pediatrics University of Tennessee Health Science CenterandLe Bonheur Children’s HospitalMemphis, Tennessee
Ihor V. Yosypiv, MDAssociate ProfessorDepartment of PediatricsTulane University Health Sciences CenterNew Orleans, Louisiana
K21764.indb 16 02/09/16 6:02 pm
PART A
Kidney anatomy and development
1 Anatomy and embryology of the urinary tract 3Kurt E. Johnson
2 Molecular basis of developmental renal disease 17Norman D. Rosenblum
K21764.indb 1 02/09/16 6:02 pm
3
1Anatomy and embryology of the urinary tract
KURT E. JOHNSON
Kidneys serve as an important metabolic organ that elimi-nates nitrogenous waste products, maintains �uid and electrolyte balance, and performs important hormonal functions, such as synthesis of 1-25-dihydroxy vitamin D and erythropoietin. Being paired organs, kidneys have also been used in living organ donation for renal replacement therapy in patients with end-stage renal disease (ESRD). Developmental aspects of kidney have received consider-able attention recently and much has now been deciphered about the control of renal and ureteric development. It is also becoming increasingly clear that nephron endowment at birth is an important fetal factor that may determine the development of hypertension and chronic kidney disease (CKD) in adults. �is chapter discusses the clinically rel-evant anatomy and embryogenesis of the kidneys and the urinary tract.
GROSS STRUCTURE AND RELATIONS
In adults, each kidney is reddish-brown, approximately 11 cm long, 5 cm wide, and 3 cm thick, and weighs approxi-mately 130 g. By renal ultrasound measurement, renal length in healthy newborns has been reported to be 4.21 ± 0.45 cm for the right kidney and 4.32 ± 0.46 cm for the le� kidney.1 Kidneys grow with age and achieve adult length by approximately 18 years of age.2,3 Interestingly, renal length is greater in obese children, possibly re�ecting hypertrophy resulting from hyper�ltration.4 Both kidneys are more or less similar in shape, with a convex lateral surface and a deep recess at the hilum of the kidney on the medial sur-face that is called the renal sinus. �e renal artery and vein
and some adipose tissue occupy the renal sinus, along with a funnel-shaped expansion of the ureter known as the renal pelvis. Within the kidney, the renal pelvis is divided into two elongated major calyces and several shorter branches called the minor calyces.
�e two kidneys lie on the posterior abdominal wall along either side of the vertebral column in the retroperito-neal space, but at slightly di�erent levels. �e le� kidney has its superior pole at approximately the level of the middle of T11 vertebral body and its inferior pole at approximately the level of the bottom of L2. In contrast, the right kidney lies slightly lower, with its superior pole at the top of T12 and its inferior pole at the top of L3. �e superior poles of each kidney are in contact with the diaphragm, and their poste-rior surfaces are covered by skeletal muscles (from medial to lateral): psoas major, quadratus lumborum, and transversus abdominis.
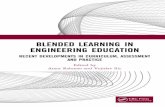
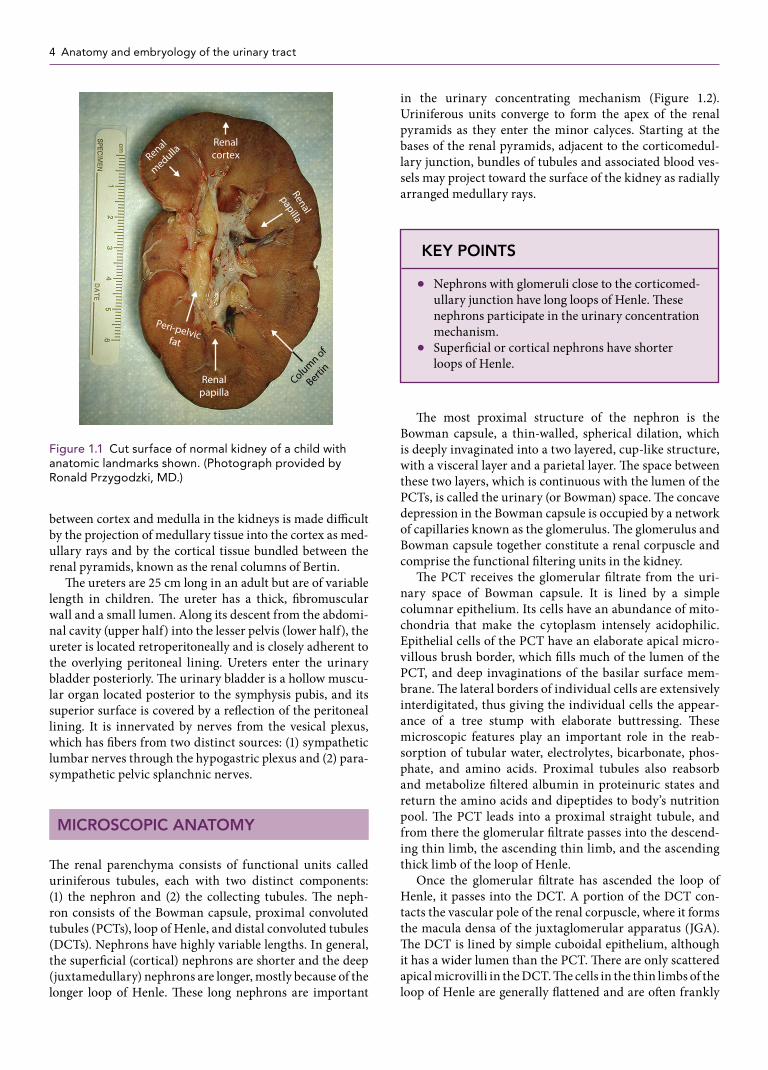
In a longitudinally cut section, the kidney has a darker cortex, whereas the inner medulla is lighter in color. Each kidney has a collection of triangular renal pyramids, or lobes, with a base bordering the cortex and an apex project-ing as renal papillae into the minor calyces (Figure 1.1). Each renal pyramid consists of medullary tissue associated with the corresponding cap of cortical tissue. �e distinction
Gross structure and relations 3Microscopic anatomy 4Renal blood supply 5The renal corpuscle 5
Renal embryology 8References 13Review questions 15Answer key 16
KEY POINT
Newborn kidneys are approximately 4.5 cm long as measured by ultrasound.
K21764.indb 3 02/09/16 6:02 pm
4 Anatomy and embryology of the urinary tract
between cortex and medulla in the kidneys is made di�cult by the projection of medullary tissue into the cortex as med-ullary rays and by the cortical tissue bundled between the renal pyramids, known as the renal columns of Bertin.
�e ureters are 25 cm long in an adult but are of variable length in children. �e ureter has a thick, �bromuscular wall and a small lumen. Along its descent from the abdomi-nal cavity (upper half) into the lesser pelvis (lower half), the ureter is located retroperitoneally and is closely adherent to the overlying peritoneal lining. Ureters enter the urinary bladder posteriorly. �e urinary bladder is a hollow muscu-lar organ located posterior to the symphysis pubis, and its superior surface is covered by a re�ection of the peritoneal lining. It is innervated by nerves from the vesical plexus, which has �bers from two distinct sources: (1) sympathetic lumbar nerves through the hypogastric plexus and (2) para-sympathetic pelvic splanchnic nerves.
MICROSCOPIC ANATOMY
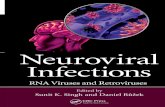
�e renal parenchyma consists of functional units called uriniferous tubules, each with two distinct components: (1) the nephron and (2) the collecting tubules. �e neph-ron consists of the Bowman capsule, proximal convoluted tubules (PCTs), loop of Henle, and distal convoluted tubules (DCTs). Nephrons have highly variable lengths. In general, the super�cial (cortical) nephrons are shorter and the deep (juxtamedullary) nephrons are longer, mostly because of the longer loop of Henle. �ese long nephrons are important
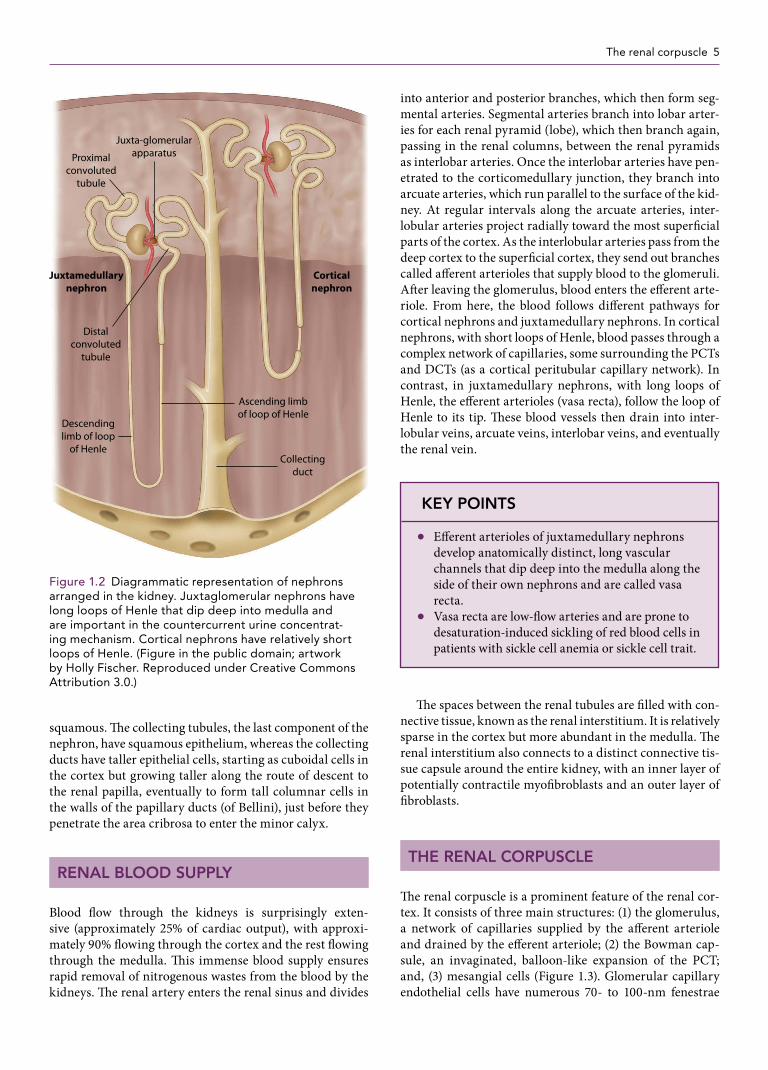
in the urinary concentrating mechanism (Figure 1.2). Uriniferous units converge to form the apex of the renal pyramids as they enter the minor calyces. Starting at the bases of the renal pyramids, adjacent to the corticomedul-lary junction, bundles of tubules and associated blood ves-sels may project toward the surface of the kidney as radially arranged medullary rays.
�e most proximal structure of the nephron is the Bowman capsule, a thin-walled, spherical dilation, which is deeply invaginated into a two layered, cup-like structure, with a visceral layer and a parietal layer. �e space between these two layers, which is continuous with the lumen of the PCTs, is called the urinary (or Bowman) space. �e concave depression in the Bowman capsule is occupied by a network of capillaries known as the glomerulus. �e glomerulus and Bowman capsule together constitute a renal corpuscle and comprise the functional �ltering units in the kidney.
�e PCT receives the glomerular �ltrate from the uri-nary space of Bowman capsule. It is lined by a simple columnar epithelium. Its cells have an abundance of mito-chondria that make the cytoplasm intensely acidophilic. Epithelial cells of the PCT have an elaborate apical micro-villous brush border, which �lls much of the lumen of the PCT, and deep invaginations of the basilar surface mem-brane. �e lateral borders of individual cells are extensively interdigitated, thus giving the individual cells the appear-ance of a tree stump with elaborate buttressing. �ese microscopic features play an important role in the reab-sorption of tubular water, electrolytes, bicarbonate, phos-phate, and amino acids. Proximal tubules also reabsorb and metabolize �ltered albumin in proteinuric states and return the amino acids and dipeptides to body’s nutrition pool. �e PCT leads into a proximal straight tubule, and from there the glomerular �ltrate passes into the descend-ing thin limb, the ascending thin limb, and the ascending thick limb of the loop of Henle.
Once the glomerular �ltrate has ascended the loop of Henle, it passes into the DCT. A portion of the DCT con-tacts the vascular pole of the renal corpuscle, where it forms the macula densa of the juxtaglomerular apparatus (JGA). �e DCT is lined by simple cuboidal epithelium, although it has a wider lumen than the PCT. �ere are only scattered apical microvilli in the DCT. �e cells in the thin limbs of the loop of Henle are generally �attened and are o�en frankly
KEY POINTS
● Nephrons with glomeruli close to the corticomed-ullary junction have long loops of Henle. �ese nephrons participate in the urinary concentration mechanism.
● Super�cial or cortical nephrons have shorter loops of Henle.
Renal
papilla
RenalcortexRenal
medulla
Renalpapilla
Column ofBerti
nPeri-pelvicfat
Figure 1.1 Cut surface of normal kidney of a child with anatomic landmarks shown. (Photograph provided by Ronald Przygodzki, MD.)
K21764.indb 4 02/09/16 6:02 pm
The renal corpuscle 5
squamous. �e collecting tubules, the last component of the nephron, have squamous epithelium, whereas the collecting ducts have taller epithelial cells, starting as cuboidal cells in the cortex but growing taller along the route of descent to the renal papilla, eventually to form tall columnar cells in the walls of the papillary ducts (of Bellini), just before they penetrate the area cribrosa to enter the minor calyx.
RENAL BLOOD SUPPLY
Blood �ow through the kidneys is surprisingly exten-sive (approximately 25% of cardiac output), with approxi-mately 90% �owing through the cortex and the rest �owing through the medulla. �is immense blood supply ensures rapid removal of nitrogenous wastes from the blood by the kidneys. �e renal artery enters the renal sinus and divides
into anterior and posterior branches, which then form seg-mental arteries. Segmental arteries branch into lobar arter-ies for each renal pyramid (lobe), which then branch again, passing in the renal columns, between the renal pyramids as interlobar arteries. Once the interlobar arteries have pen-etrated to the corticomedullary junction, they branch into arcuate arteries, which run parallel to the surface of the kid-ney. At regular intervals along the arcuate arteries, inter-lobular arteries project radially toward the most super�cial parts of the cortex. As the interlobular arteries pass from the deep cortex to the super�cial cortex, they send out branches called a�erent arterioles that supply blood to the glomeruli. A�er leaving the glomerulus, blood enters the e�erent arte-riole. From here, the blood follows di�erent pathways for cortical nephrons and juxtamedullary nephrons. In cortical nephrons, with short loops of Henle, blood passes through a complex network of capillaries, some surrounding the PCTs and DCTs (as a cortical peritubular capillary network). In contrast, in juxtamedullary nephrons, with long loops of Henle, the e�erent arterioles (vasa recta), follow the loop of Henle to its tip. �ese blood vessels then drain into inter-lobular veins, arcuate veins, interlobar veins, and eventually the renal vein.
�e spaces between the renal tubules are �lled with con-nective tissue, known as the renal interstitium. It is relatively sparse in the cortex but more abundant in the medulla. �e renal interstitium also connects to a distinct connective tis-sue capsule around the entire kidney, with an inner layer of potentially contractile myo�broblasts and an outer layer of �broblasts.
THE RENAL CORPUSCLE
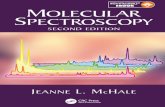
�e renal corpuscle is a prominent feature of the renal cor-tex. It consists of three main structures: (1) the glomerulus, a network of capillaries supplied by the a�erent arteriole and drained by the e�erent arteriole; (2) the Bowman cap-sule, an invaginated, balloon-like expansion of the PCT; and, (3) mesangial cells (Figure 1.3). Glomerular capillary endothelial cells have numerous 70- to 100-nm fenestrae
KEY POINTS
● E�erent arterioles of juxtamedullary nephrons develop anatomically distinct, long vascular channels that dip deep into the medulla along the side of their own nephrons and are called vasa recta.
● Vasa recta are low-�ow arteries and are prone to desaturation-induced sickling of red blood cells in patients with sickle cell anemia or sickle cell trait.
Collectingduct
Descendinglimb of loop
of Henle
Distalconvoluted
tubule
Corticalnephron
Juxtamedullarynephron
Juxta-glomerularapparatus
Ascending limbof loop of Henle
Proximalconvoluted
tubule
Figure 1.2 Diagrammatic representation of nephrons arranged in the kidney. Juxtaglomerular nephrons have long loops of Henle that dip deep into medulla and are important in the countercurrent urine concentrat-ing mechanism. Cortical nephrons have relatively short loops of Henle. (Figure in the public domain; artwork by Holly Fischer. Reproduced under Creative Commons Attribution 3.0.)
K21764.indb 5 02/09/16 6:02 pm

6 Anatomy and embryology of the urinary tract
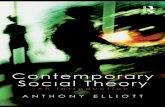
(transcellular pores) without diaphragms, and they rest on a basement membrane (Figure 1.4A). �e glomerular base-ment membrane (GBM) is a multilayered structure with a lamina rara interna (adjacent to capillary endothelium), a lamina densa, and a lamina rara externa (adjacent to the podocytes). �e laminae rarae are rich in polyanions such as heparan sulfate. �ese negatively charged macromolecules presumably repel anions that would otherwise cross from the capillary lumen into the urinary space (and vice versa). In addition, the laminae rarae have an abundance of �bro-nectin, a cell adhesion glycoprotein. Mesangial cells form a
supportive complex between the capillary endothelial cells. �ey can proliferate and produce a basement membrane–like material and appear to have contractile, secretory, and phagocytic activity.
GBM is one of the thickest and most functionally impor-tant basement membranes in the body. �e GBM is a com-plex extracellular matrix that is formed by both capillary endothelial cells and podocytes. It contains type IV colla-gen, laminin, �bronectin, entactin, and proteoglycan com-plex with polyanionic glycosaminoglycans such as heparan sulfate. �e thickness of the GBM varies with age; it is a mean of 373 nm in men and 326 nm in women.5 In children, however, GBM is thinner at birth, rapidly increases in size by the second year of life, and reaches adult proportions by 9 to 11 years of age.6,7 Before 1 year, the thickness of GBM has been reported to be 132 to 208 nm, and it reached 244 to 307 nm by 11 years in one study.6 �inned GBM is usually seen in Alport syndrome, thin basement membrane nephropa-thy (TBMN), and occasionally in immunoglobulin A (IgA) nephropathy.
By electron microscopy, the GBM has a thick, central, electron-dense lamina densa (see Figure 1.4A), with less electron-dense layers adjacent to the capillary endothelial cells (lamina rara interna), and podocytes (lamina rara externa). �e collagen is thought to function as a sca�old for the attachment of other glycoproteins and proteogly-cans that constitute the rest of the GBM. Type IV collagen consists of three intertwined α-chain monomers, each with three distinct domains: the 7S N-terminus, a middle heli-cal collagenous domain, and a C-terminus noncollagenous (NC1) domain.8 �e GBM also allows attachment of epithe-lial cells (through cell surface integrin receptors for extra-cellular matrix molecules such as collagen, laminin, and �bronectin) to itself and one another, and it serves as a part
VC
PC
EMC
Arteriole
DT
MD
MC
Figure 1.3 Light microscopy showing a glomerulus with the juxtaglomerular apparatus. DT, distal tubule; EMC, extraglomerular mesangial cells MC, mesangial cell with mesangial matrix; MD, macula densa; PC, parietal epithe-lial cell; and VC, visceral epithelial cells.
EndC
EpC
(a) (b)
LRELD
LRI
PCPCPC
PC
PCSD
Figure 1.4 (a) Electron micrograph of the basement glomerular capillary. Capillary cross section showing an endothelial cell (EndC), the lamina rara interna (LRT), the lamina rara externa (LRE), the lamina densa (LD), the podocyte foot pro-cesses (PC), the epithelial cell cytoplasm (EpC), and the slit diaphragm (SD). (b) Electron micrograph showing extensive interdigitation of the podocyte foot processes around the basement membrane on the external or urinary side.
K21764.indb 6 02/09/16 6:02 pm
The renal corpuscle / The juxtaglomerular apparatus 7
of the selective �ltration barrier between the lumen of the glomerular capillary (the vascular space) and the lumen of the Bowman capsule (the urinary space).
PODOCYTES
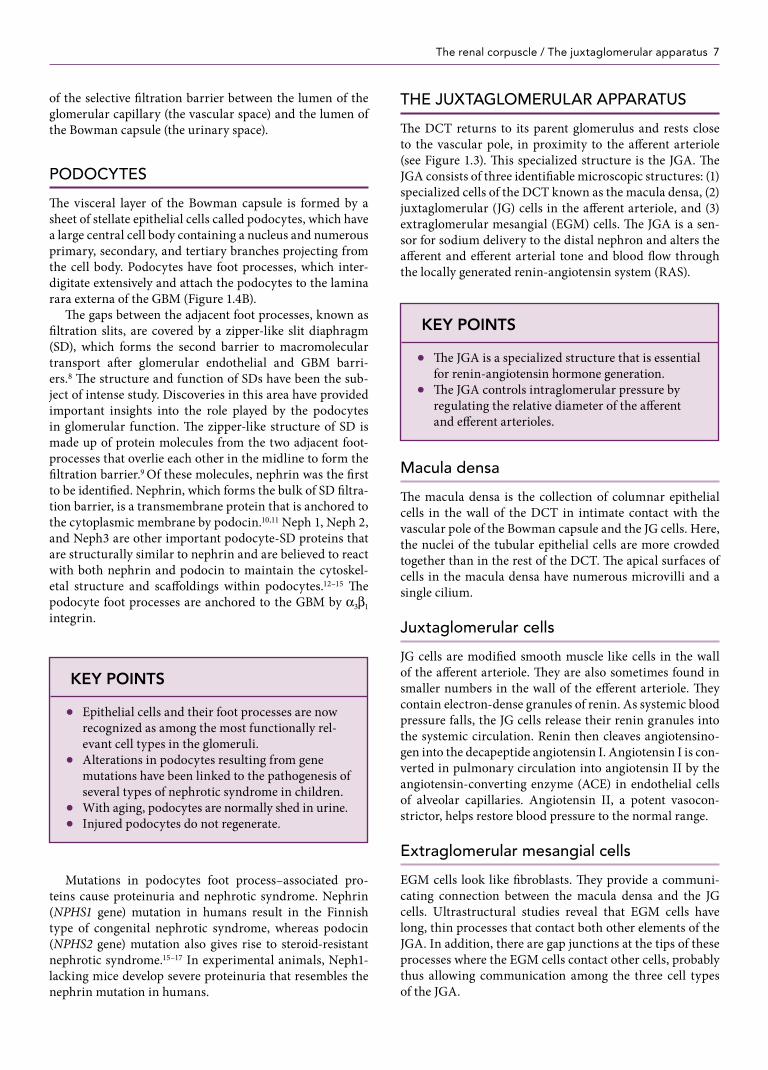
�e visceral layer of the Bowman capsule is formed by a sheet of stellate epithelial cells called podocytes, which have a large central cell body containing a nucleus and numerous primary, secondary, and tertiary branches projecting from the cell body. Podocytes have foot processes, which inter-digitate extensively and attach the podocytes to the lamina rara externa of the GBM (Figure 1.4B).
�e gaps between the adjacent foot processes, known as �ltration slits, are covered by a zipper-like slit diaphragm (SD), which forms the second barrier to macromolecular transport a�er glomerular endothelial and GBM barri-ers.8 �e structure and function of SDs have been the sub-ject of intense study. Discoveries in this area have provided important insights into the role played by the podocytes in glomerular function. �e zipper-like structure of SD is made up of protein molecules from the two adjacent foot-processes that overlie each other in the midline to form the �ltration barrier.9 Of these molecules, nephrin was the �rst to be identi�ed. Nephrin, which forms the bulk of SD �ltra-tion barrier, is a transmembrane protein that is anchored to the cytoplasmic membrane by podocin.10,11 Neph 1, Neph 2, and Neph3 are other important podocyte-SD proteins that are structurally similar to nephrin and are believed to react with both nephrin and podocin to maintain the cytoskel-etal structure and sca�oldings within podocytes.12–15 �e podocyte foot processes are anchored to the GBM by α3β1 integrin.
Mutations in podocytes foot process–associated pro-teins cause proteinuria and nephrotic syndrome. Nephrin (NPHS1 gene) mutation in humans result in the Finnish type of congenital nephrotic syndrome, whereas podocin (NPHS2 gene) mutation also gives rise to steroid-resistant nephrotic syndrome.15–17 In experimental animals, Neph1-lacking mice develop severe proteinuria that resembles the nephrin mutation in humans.
THE JUXTAGLOMERULAR APPARATUS
�e DCT returns to its parent glomerulus and rests close to the vascular pole, in proximity to the a�erent arteriole (see Figure 1.3). �is specialized structure is the JGA. �e JGA consists of three identi�able microscopic structures: (1) specialized cells of the DCT known as the macula densa, (2) juxtaglomerular (JG) cells in the a�erent arteriole, and (3) extraglomerular mesangial (EGM) cells. �e JGA is a sen-sor for sodium delivery to the distal nephron and alters the a�erent and e�erent arterial tone and blood �ow through the locally generated renin-angiotensin system (RAS).
Macula densa
�e macula densa is the collection of columnar epithelial cells in the wall of the DCT in intimate contact with the vascular pole of the Bowman capsule and the JG cells. Here, the nuclei of the tubular epithelial cells are more crowded together than in the rest of the DCT. �e apical surfaces of cells in the macula densa have numerous microvilli and a single cilium.
Juxtaglomerular cells
JG cells are modi�ed smooth muscle like cells in the wall of the a�erent arteriole. �ey are also sometimes found in smaller numbers in the wall of the e�erent arteriole. �ey contain electron-dense granules of renin. As systemic blood pressure falls, the JG cells release their renin granules into the systemic circulation. Renin then cleaves angiotensino-gen into the decapeptide angiotensin I. Angiotensin I is con-verted in pulmonary circulation into angiotensin II by the angiotensin-converting enzyme (ACE) in endothelial cells of alveolar capillaries. Angiotensin II, a potent vasocon-strictor, helps restore blood pressure to the normal range.
Extraglomerular mesangial cells
EGM cells look like �broblasts. �ey provide a communi-cating connection between the macula densa and the JG cells. Ultrastructural studies reveal that EGM cells have long, thin processes that contact both other elements of the JGA. In addition, there are gap junctions at the tips of these processes where the EGM cells contact other cells, probably thus allowing communication among the three cell types of the JGA.
KEY POINTS
● Epithelial cells and their foot processes are now recognized as among the most functionally rel-evant cell types in the glomeruli.
● Alterations in podocytes resulting from gene mutations have been linked to the pathogenesis of several types of nephrotic syndrome in children.
● With aging, podocytes are normally shed in urine. ● Injured podocytes do not regenerate.
KEY POINTS
● �e JGA is a specialized structure that is essential for renin-angiotensin hormone generation.
● �e JGA controls intraglomerular pressure by regulating the relative diameter of the a�erent and e�erent arterioles.
K21764.indb 7 02/09/16 6:02 pm
8 Anatomy and embryology of the urinary tract
RENAL EMBRYOLOGY
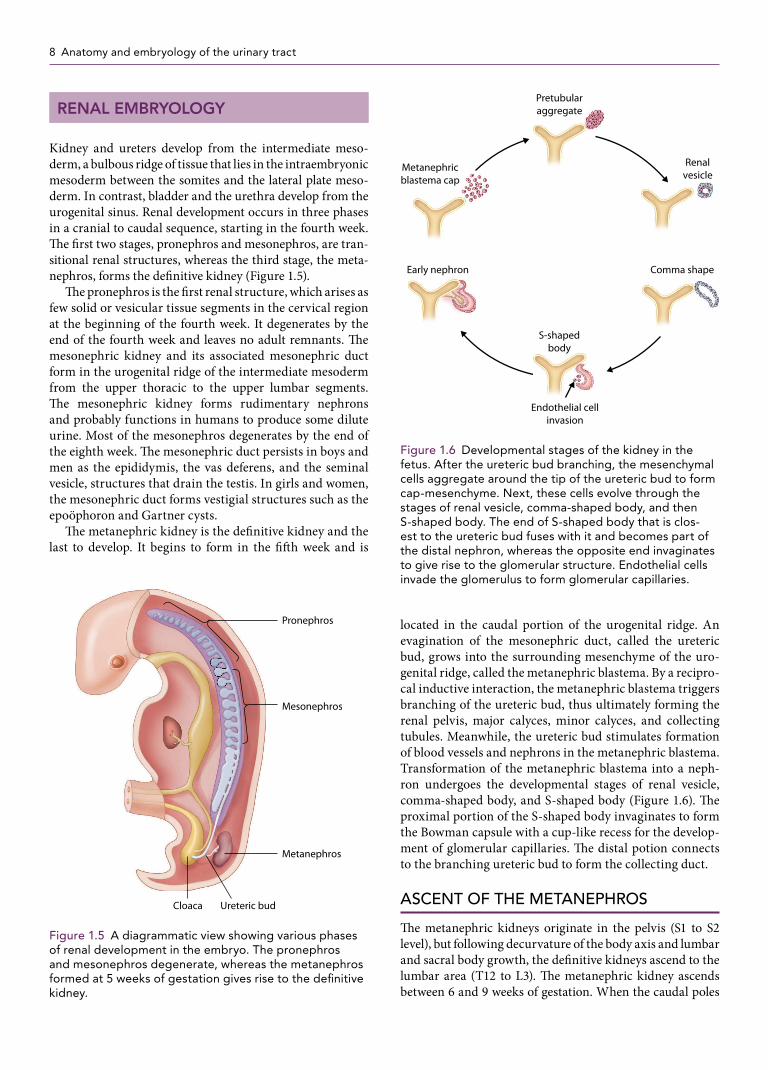
Kidney and ureters develop from the intermediate meso-derm, a bulbous ridge of tissue that lies in the intraembryonic mesoderm between the somites and the lateral plate meso-derm. In contrast, bladder and the urethra develop from the urogenital sinus. Renal development occurs in three phases in a cranial to caudal sequence, starting in the fourth week. �e �rst two stages, pronephros and mesonephros, are tran-sitional renal structures, whereas the third stage, the meta-nephros, forms the de�nitive kidney (Figure 1.5).
�e pronephros is the �rst renal structure, which arises as few solid or vesicular tissue segments in the cervical region at the beginning of the fourth week. It degenerates by the end of the fourth week and leaves no adult remnants. �e mesonephric kidney and its associated mesonephric duct form in the urogenital ridge of the intermediate mesoderm from the upper thoracic to the upper lumbar segments. �e mesonephric kidney forms rudimentary nephrons and probably functions in humans to produce some dilute urine. Most of the mesonephros degenerates by the end of the eighth week. �e mesonephric duct persists in boys and men as the epididymis, the vas deferens, and the seminal vesicle, structures that drain the testis. In girls and women, the mesonephric duct forms vestigial structures such as the epoöphoron and Gartner cysts.
�e metanephric kidney is the de�nitive kidney and the last to develop. It begins to form in the ��h week and is
located in the caudal portion of the urogenital ridge. An evagination of the mesonephric duct, called the ureteric bud, grows into the surrounding mesenchyme of the uro-genital ridge, called the metanephric blastema. By a recipro-cal inductive interaction, the metanephric blastema triggers branching of the ureteric bud, thus ultimately forming the renal pelvis, major calyces, minor calyces, and collecting tubules. Meanwhile, the ureteric bud stimulates formation of blood vessels and nephrons in the metanephric blastema. Transformation of the metanephric blastema into a neph-ron undergoes the developmental stages of renal vesicle, comma-shaped body, and S-shaped body (Figure 1.6). �e proximal portion of the S-shaped body invaginates to form the Bowman capsule with a cup-like recess for the develop-ment of glomerular capillaries. �e distal potion connects to the branching ureteric bud to form the collecting duct.
ASCENT OF THE METANEPHROS
�e metanephric kidneys originate in the pelvis (S1 to S2 level), but following decurvature of the body axis and lumbar and sacral body growth, the de�nitive kidneys ascend to the lumbar area (T12 to L3). �e metanephric kidney ascends between 6 and 9 weeks of gestation. When the caudal poles
Cloaca
Mesonephros
Pronephros
Metanephros
Ureteric bud
Figure 1.5 A diagrammatic view showing various phases of renal development in the embryo. The pronephros and mesonephros degenerate, whereas the metanephros formed at 5 weeks of gestation gives rise to the definitive kidney.
S-shapedbody
Early nephron
Metanephricblastema cap
Pretubularaggregate
Renalvesicle
Comma shape
Endothelial cellinvasion
Figure 1.6 Developmental stages of the kidney in the fetus. After the ureteric bud branching, the mesenchymal cells aggregate around the tip of the ureteric bud to form cap-mesenchyme. Next, these cells evolve through the stages of renal vesicle, comma-shaped body, and then S-shaped body. The end of S-shaped body that is clos-est to the ureteric bud fuses with it and becomes part of the distal nephron, whereas the opposite end invaginates to give rise to the glomerular structure. Endothelial cells invade the glomerulus to form glomerular capillaries.
K21764.indb 8 02/09/16 6:02 pm

Renal embryology / Nephron endowment and future health risks 9
of the metanephroi fuse, the ascent of a horseshoe kidney is halted by the inferior mesenteric artery, a branch from the aorta that supplies hindgut derivatives. Initially, the meta-nephroi are supplied by sacral branches of the aorta, but as they ascend cranially, they take new branches from the dorsal aorta that eventually develop into the renal arteries. �e cau-dal branches usually degenerate, but supernumerary renal arteries sometimes persist, o�en caudal to the main renal artery. During ascent, the fetal kidneys also rotate medially by 90 degrees, so that the renal hilum, with the ureter and renal vessels, faces medially. In arrested ascent, metanephric kidneys may be formed in the pelvis, either unilaterally or bilaterally, resulting in ectopic or pelvic kidneys.
CLOACA AND FORMATION OF THE UROGENITAL SINUS
�e most caudal portion of the early hindgut is the cloaca. �e hindgut precursor and cloaca have a diverticulum, called the allantois, which projects far into the umbili-cal cord. By the ��h week, the proximal part of the cloaca becomes slightly expanded into a precursor of the urinary bladder. During the ��h week and onward, the urorectal septum divides the cloaca into a posterior anal canal and an anterior urogenital sinus. �e urogenital sinus eventually gives rise to major portion of urinary bladder, and the pelvic part that becomes the membranous and prostatic urethra, and phallus. Each ureter enters the urinary bladder more lateral to the midline of the bladder, to form a roughly tri-angular structure called the trigone of the bladder, which is de�ned by the two ureteric inlets superiorly and the urethral outlet inferiorly. �e proximal ends of the ureters become incorporated into the wall of the urinary bladder, so that it is lined transiently by mesodermally derived epithelium in the trigone. Later, the trigone is overgrown by endodermally derived epithelium from the rest of the bladder.
�e distal portion of the allantois eventually degenerates, but the proximal portion persists as a urachal diverticulum that still projects into the umbilical cord. Eventually, the proximal urachal diverticulum forms the median umbili-cal ligament. Rarely, however, persistent urachus can lead to urachal �stula, wherein urine leaks from the bladder into the umbilicus or urachal cysts in the median umbilical ligament.
INTRAUTERINE RENAL FUNCTION
In humans, the pronephros is a rudimentary structure. It does not form functional nephrons and involutes in a short time. �e human mesonephric kidney forms rudimentary renal corpuscles with a Bowman capsule and glomerulus and associated tubules, but there is little substantiation of its function. Mesonephric nephrons have short loops of Henle, a structure suggesting that the small volume of urine produced in the mesonephros is likely to be dilute. By the 16th week of gestation, the mesonephric kidney loses
its functional capacity, and the metanephric kidney devel-ops into a urine-producing structure, with renal corpuscles and well-di�erentiated PCTs with microvillous brush bor-ders at the lumen. However, because the loops of Henle are not fully developed, fetal urine is hypotonic with respect to plasma and is slightly acidic. At term, the human fetus voids approximately 450 mL/day into the amniotic �uid. �e ure-thra is patent in the fetus at approximately 8 weeks.
NEPHRON ENDOWMENT AND FUTURE HEALTH RISKS
Each normal adult kidney has approximately 1 mil-lion nephrons, but this estimate is quite variable. Using mature adult kidneys obtained at autopsy, Nyengaard and Bendtsen18 noted the mean nephron number to be 617,000. A more recent US-Australian, multiethnic autopsy study19 in adults revealed a signi�cant variation in nephron num-ber, ranging from 210,332 to 1,825,380 in each kidney, with a mean of 870,582 ± 31,062.
Nephron number in human fetuses increases through-out gestation, from a mean of 15,000 at 15 weeks to 740,000 in each kidney by 40 weeks.20 �is number appears to pla-teau at approximately 36 weeks.20 Nephrogenesis in full-term fetuses concludes by approximately 34 to 36 weeks of gestation, and new nephrons are not formed a�er birth.20,21 Premature infants, conversely, have fewer nephrons, and nephronogenesis may continue a�er birth for as long as 3 months.22,23 �e clinical impact of low endowed nephron number in premature infants is likely to last a lifetime and is referred to as fetal programming. Indeed, renal length and volume by ultrasonography are known to be signi�cantly lower in young adults who were born prematurely (at less than 32 weeks), a �nding suggesting long term adverse renal consequences and risks in these persons.24 An increased risk for hypertension and CKD associated with prematu-rity, low birth weight, and intrauterine growth retardation was suggested by Brenner et al.,25–27 starting in the 1980s. In an Australian study,28 18-year-old survivors of extreme prematurity (gestational age less than 28 weeks) had higher
KEY POINT
�e urethra is patent by the eighth week of gestation, and urine begins to form a part of amniotic �uid at around that time.
KEY POINT
Poor nephron endowment at birth (fetal program-ming) a�ects blood pressure, development of micro-albuminuria, and can lead to ESRD in adults.
K21764.indb 9 02/09/16 6:02 pm
10 Anatomy and embryology of the urinary tract
ambulatory blood pressure readings, thus lending weight to the hypotheses proposed by Brenner and others. A meta-analysis of studies relating prematurity and blood pressure also demonstrated a higher blood pressure in persons who were born prematurely (range, 28.8 to 34.1 weeks).29
�e link between poor nephron endowment and CKD is plausible, but less well established. Microalbuminuria noted in otherwise healthy nondiabetic adults (46 to 54 years old) has been correlated with low birth weight as a risk factor.30 Increased prevalence of ESRD in adults born with a birth weight of less than 2.5 kg was noted in one study in the United States, and the odds ratio for ESRD was 1.4 (95% con�dence interval [CI], 1.1 to 1.8), as compared with a birth weight of 3 to 3.5 kg.31 Carmody and Charlton32 suggested that apart from low nephron endowment in premature infants, other factors that may enhance the risk for CKD include neona-tal acute kidney injury, use of nephrotoxic antibiotics, poor nutrition, and hypoxia in early life.
CONGENITAL ABNORMALITIES OF THE KIDNEY AND URINARY TRACT
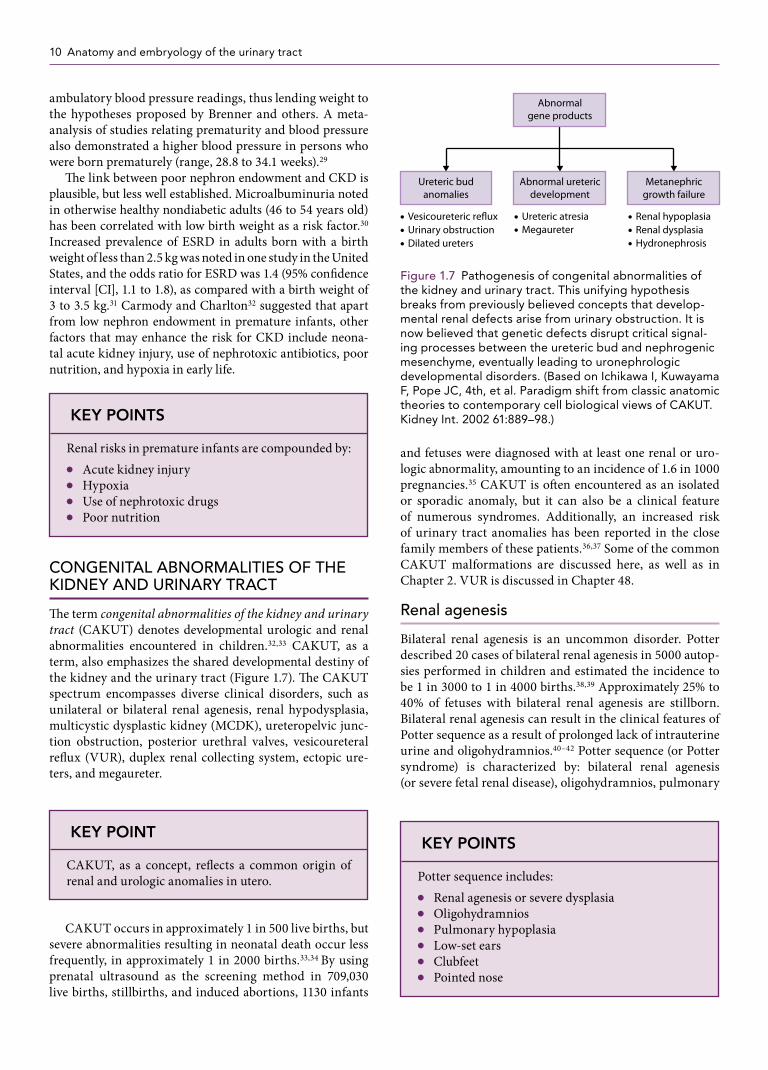
�e term congenital abnormalities of the kidney and urinary tract (CAKUT) denotes developmental urologic and renal abnormalities encountered in children.32,33 CAKUT, as a term, also emphasizes the shared developmental destiny of the kidney and the urinary tract (Figure 1.7). �e CAKUT spectrum encompasses diverse clinical disorders, such as unilateral or bilateral renal agenesis, renal hypodysplasia, multicystic dysplastic kidney (MCDK), ureteropelvic junc-tion obstruction, posterior urethral valves, vesicoureteral re�ux (VUR), duplex renal collecting system, ectopic ure-ters, and megaureter.
CAKUT occurs in approximately 1 in 500 live births, but severe abnormalities resulting in neonatal death occur less frequently, in approximately 1 in 2000 births.33,34 By using prenatal ultrasound as the screening method in 709,030 live births, stillbirths, and induced abortions, 1130 infants
and fetuses were diagnosed with at least one renal or uro-logic abnormality, amounting to an incidence of 1.6 in 1000 pregnancies.35 CAKUT is o�en encountered as an isolated or sporadic anomaly, but it can also be a clinical feature of numerous syndromes. Additionally, an increased risk of urinary tract anomalies has been reported in the close family members of these patients.36,37 Some of the common CAKUT malformations are discussed here, as well as in Chapter 2. VUR is discussed in Chapter 48.
Renal agenesis
Bilateral renal agenesis is an uncommon disorder. Potter described 20 cases of bilateral renal agenesis in 5000 autop-sies performed in children and estimated the incidence to be 1 in 3000 to 1 in 4000 births.38,39 Approximately 25% to 40% of fetuses with bilateral renal agenesis are stillborn. Bilateral renal agenesis can result in the clinical features of Potter sequence as a result of prolonged lack of intrauterine urine and oligohydramnios.40–42 Potter sequence (or Potter syndrome) is characterized by: bilateral renal agenesis (or severe fetal renal disease), oligohydramnios, pulmonary
KEY POINTS
Renal risks in premature infants are compounded by: ● Acute kidney injury ● Hypoxia ● Use of nephrotoxic drugs ● Poor nutrition
KEY POINT
CAKUT, as a concept, re�ects a common origin of renal and urologic anomalies in utero.
KEY POINTS
Potter sequence includes: ● Renal agenesis or severe dysplasia ● Oligohydramnios ● Pulmonary hypoplasia ● Low-set ears ● Clubfeet ● Pointed nose
• Renal hypoplasia• Renal dysplasia• Hydronephrosis
• Vesicoureteric re�ux
Abnormalgene products
• Urinary obstruction• Dilated ureters
• Ureteric atresia• Megaureter
Ureteric budanomalies
Abnormal uretericdevelopment
Metanephricgrowth failure
Figure 1.7 Pathogenesis of congenital abnormalities of the kidney and urinary tract. This unifying hypothesis breaks from previously believed concepts that develop-mental renal defects arise from urinary obstruction. It is now believed that genetic defects disrupt critical signal-ing processes between the ureteric bud and nephrogenic mesenchyme, eventually leading to uronephrologic developmental disorders. (Based on Ichikawa I, Kuwayama F, Pope JC, 4th, et al. Paradigm shift from classic anatomic theories to contemporary cell biological views of CAKUT. Kidney Int. 2002 61:889–98.)
K21764.indb 10 02/09/16 6:02 pm

Renal embryology / Congenital abnormalities of the kidney and urinary tract 11
hypoplasia, clubfeet, micrognathia, a pointed nose, and low-set malformed ears.40 Potter facies refers to the typical facial features seen in Potter sequence. Potter sequence can result from any fetal disorder that leads to prolonged oli-gohydramnios. �ere has been an ongoing speculation that bilateral renal agenesis may be an inherited disorder, pri-marily because of a signi�cantly higher incidence of occult renal defects in close relatives of index cases.43 Recessive mutations in the integrin α8-encoding gene ITGA8 have been described in families with fetal loss secondary to bilat-eral renal agenesis.44 Such �ndings are likely to stimulate investigative pathways to genetic pathogenesis of bilateral renal agenesis.
Accurate information of the incidence of unilateral renal agenesis is di�cult to obtain because many of these cases go undetected as a result of compensatory hypertrophy of the contralateral kidney, as well as normal intrauterine and postnatal renal function. Using renal ultrasound screening in healthy school-age children (6 to 15 years), Sheih et al.45 reported the occurrence of unilateral renal agenesis to be 1 in 290 in the general population of children. European data also suggest the incidence of unilateral renal agenesis to be 1 in 2000 births.46
Unilateral renal agenesis is o�en associated with ipsi-lateral defects in other genital duct derivatives such as the ductus deferens in boys and the uterine tubes and uterus in girls. VUR is common (approximately 25%) in these patients, and extrarenal malformations a�ecting the gastro-intestinal, cardiac, and musculoskeletal systems are seen in approximately 30% of patients.46 An increased incidence of renal anomalies in the children and siblings of patients with unilateral renal agenesis has been noted in some studies.36
Pelvic and horseshoe kidneys
Pelvic kidney and horseshoe kidney are related renal mal-formations that result from failed ascent of the kidneys. In horseshoe kidney, the caudal poles of the metanephric kid-ney are fused. Horseshoe kidney is one of the most common congenital anomalies of the kidney. On the basis of abdomi-nal CT scan data in 15,320 patients, the incidence of horse-shoe kidney was noted to be 1 in 666.47 Approximately half of the patients diagnosed with horseshoe kidney are asymp-tomatic; the remainder present for renal stones and ascend-ing urinary tract infections.48 �e Rovsing sign, consisting of nausea, vomiting, and abdominal pain that is accentu-ated on hyperextension, is seen in a minority of patients with horseshoe kidney.48 Horseshoe kidney can occur as an isolated congenital birth defect but is more frequent in patients with Turner syndrome and trisomy 18 (Edwards syndrome).48,49
Multicystic dysplastic kidneys
MCDKs are developmental, nonfunctional cystic masses caused by abnormalities in metanephric di�erentia-tion. �ese kidneys are characterized by abnormal and
noncommunicating dilated cysts of variable size, with little identi�able renal structure or stroma (Figures 1.8 and 1.9). Renal arterial �ow and excretory functions, as demonstrable by mercaptoacetyltriglycine (MAG3) renal scan, are absent.
MCDK is commonly identi�ed by the presence of a unilateral cystic kidney in the fetus during prenatal ultra-sound evaluation. Cystic kidneys may involute during ges-tation in some cases, and the infant is born with a solitary kidney. Other modes of presentation include an abdominal mass noted by the parents or during a clinical examination within few months of birth. In a study of 97 infants with the diagnosis of MCDK, 85% of the cases were detected by pre-natal ultrasound evaluation, 4% by the presence of a mass postnatally, and 11% by a postnatal ultrasound examination
T
(b)
T
(a)
Figure 1.8 (a) Cut section of a kidney from a neonate shows cystic dysplasia. Renal architecture is poorly defined, numerous cysts are present, and the cortico-medullary differentiation is absent. (b) Microscopic sec-tion of a kidney with renal dysplasia. Arrows shows the presence of cartilage. Tubulointerstitial tissue is poorly organized, and a large dilated renal tubule (T) is shown. (Photomicrograph courtesy of Arthur Cohen, MD.)
Figure 1.9 Renal ultrasound scan showing multiple large cysts in an infant with multicystic dysplastic kidney dis-ease. Nuclear scan demonstrated no blood flow or excre-tory function in this kidney.
K21764.indb 11 02/09/16 6:02 pm

12 Anatomy and embryology of the urinary tract
performed for an unrelated diagnosis.50 MCDK is slightly more common on the le� side in some studies, whereas other investigators have noted a right-sided predominance; these �ndings suggest that both sides can be equally involved.38,39 Contralateral kidneys show abnormalities in approximately 40% of cases that include renal agenesis, renal dysplasia or hypoplasia, VUR, hydroureter or pyelectasis, duplex col-lecting system, and ectopic ureters.39 In a meta-analysis of the abnormalities in the contralateral system, Schreuder et al.51 reported VUR in approximately 20% cases: 15% in the contralateral system, ipsilateral VUR in 3.3%, and bilateral VUR in 2.4% cases. Ureteropelvic junction obstruction was the next most common anomaly in the contralateral renal system, accounting for 4.8% cases in this meta-analysis.
Involution of the cystic mass occurs usually occurs over several years, but the rate of involution is variable. Some patients have complete involution of the MCDK in utero and are thus born with a solitary kidney and unilateral agenesis. Complete involution of the MCDK was noted in 34% at 2 years (165 patients), 47% at 5 years (117 patients), and 59% at 10 years (43 patients) in a study from the United Kingdom.52 �e contralateral normal kidney usually under-goes compensatory hypertrophy.
Hypertension has been well documented in patients with MCDK and is believed to be mediated by the RAS.53 More recent studies, however, point out that the risk of hyperten-sion in MCDK is low. In a review of 29 studies, Narchi et al.54 reported hypertension to be present in only 6 of the 1115 cases, a �nding suggesting the mean probability of devel-oping hypertension in MCDK to be 5.4 in 1000 cases (esti-mated 95% CI, 1.9 to 11.7 per 1000).
A high risk for Wilms tumor and renal cell carcinoma in the MCDK was suggested in older studies. However, the risk of tumors was very low in several more recent, com-prehensive, well-conducted studies.55,56 Surgical resection of the MCDK, which was o�en practiced until the late 1980s for the prevention of hypertension and to protect against development of malignant disease, appears to be di�cult to justify with the evidence-based results.54–57
WAGR syndrome
Wilms tumor, aniridia, genitourinary abnormalities, and mental retardation (WAGR) was �rst reported as a distinct clinical disorder by Miller et al.58 in 1964 (Online Mendelian Inheritance in Man [OMIM] number 194072). It is now well established that the disorder results from deletion in dis-tal band of 11p13 in such a way that WT1 and PAX6 genes, which are adjacent to each other, are a�ected by the dele-tion.59 �e WT1 gene deletion results in renal malforma-tions and risk for Wilms tumor; whereas the PAX6 gene deletion results in aniridia and brain malformations.
�e WT1 gene encodes for Wilms tumor suppressor protein (WT1), a transcription factor containing a DNA binding domain, with four zinc �ngers. WT1 transcrip-tion factor is essential for the development of the neph-ron, as well as the gonads, and is thought to be involved in
mesenchymal-epithelial transition in the renal and germ cell lines.60 With mutations in the WT1 gene, the develop-ment of glomeruli and of the proximal and distal tubules is adversely a�ected, leading to renal malformations. A pro-pensity for Wilms tumor in WAGR and other syndromes with the WT1 gene mutation, such as Denys-Drash syn-drome, results from the presence of undi�erentiated or poorly di�erentiated mesenchymal cells in the kidneys.60,61
�e genital malformations seen in WAGR syndrome include cryptorchidism, ambiguous genitalia, hypospadias, streaked ovaries, and hypoplastic uterus. Renal and urinary tract anomalies encountered in WGAR syndrome include hypoplastic kidneys, unilateral renal agenesis, duplicated ureters,, development of focal segmental glomerulosclerosis, nephrogenic rests, nephroblastomatosis, and renal cysts.62 Aniridia can be partial or complete and results in severe visual impairment. Apart from risk of CKD and ESRD imposed by the development of Wilms tumor, patients with WAGR syndrome are inherently at an increased risk for development of ESRD. �e National Wilms Tumor Study Group reports the incidence of ESRD to be 53% in patients with WAGR syndrome.63,64 Monitoring of kidneys by ultra-sound every 3 months until 6 years of age has been recom-mended in some studies for Wilms tumor surveillance in patients with WAGR syndrome.62
Bladder exstrophy
Bladder exstrophy is an uncommon developmental anom-aly seen in newborn infants. It is caused by a ventral body wall, an anterior bladder wall defect, and eversion of the bladder wall mucosa. �e term exstrophy, which is derived from the Greek word ekstriphein, means “turned inside out.” In the newborn infant, the exposed bladder mucosa is bright red and has a raw appearance. �e exposed mucosa sometimes undergoes metaplasia, forming colonic epithe-lium rather than transitional epithelium. Bladder exstrophy is also associated with other congenital abnormalities of the external genitalia such as bi�d penis, epispadias, and abnor-mal scrotal development
Using the Healthcare Cost and Utilization Project Nationwide Inpatient Sample database, Nelson et al.65 estimated the incidence of bladder exstrophy to be 2.15 in 100,000 live births (or approximately 1 in 40,000 births). �e male-to-female ratio was equal in this study, and the congenital malformation appeared to be more common in whites than in nonwhites. Some genetic analyses have dem-onstrated a higher prevalence of duplication of 22q11.21 in patients with bladder exstrophy.66
Surgical repair of bladder exstrophy has evolved since the 1990s. Both early closure and delayed closure of the defect are acceptable surgical options and are generally dictated by technical preference of the surgical team.67 Postrepair atten-tion to incontinence, recurrent urinary tract infections sec-ondary to associated VUR, and correction of epispadias are common concerns to be addressed during childhood. Many patients require continent urinary diversion procedures,
K21764.indb 12 02/09/16 6:02 pm

Renal embryology / Congenital abnormalities of the kidney and urinary tract 13
as well as bladder augmentation by cystoplasty. However, lower urinary tract symptoms persist in 80% of patients with exstrophy as they grow into adulthood.68 Sexual dysfunction is also a concern in adulthood.69 In addition, adenocarci-nomas occur with higher frequency in the exposed bladder mucosa. Surgical intervention and repair can extend the patient’s life and ensure normal renal function.
Angiotensin-converting enzyme fetopathy
Experimental observations indicate that RAS exerts its in�uence on renal development by promoting the ureteric bud branching process and therefore plays a key role in nephrogenesis.70,71 �e RAS may a�ect ureteric bud branch-ing and nephrogenesis through its in�uence on GDNF, the WT1 gene, and the PAX2 gene. Disruption of the RAS dur-ing nephrogenesis by ACE inhibitors (ACEIs) is well known to cause fetopathy.70,72 ACEI fetopathy risk is low if the drug is consumed in the �rst trimester.72–74 Clinical character-istics of ACEI fetopathy are: oligohydramnios, renal tubu-lar dysgenesis, neonatal anuria, skull defects, intrauterine growth retardation, and patent ductus arteriosus.
REFERENCES
1. Scott JE, Hunter EW, Lee RE, et al. Ultrasound mea-surement of renal size in newborn infants. Arch Dis Child. 1990;65:361–4.
2. Pantoja Zuzuárregui JR1, Mallios R, Murphy J. The effect of obesity on kidney length in a healthy pediatric population. Pediatr Nephrol. 2009;24:2023–7.
3. Alev Kadioglu. Renal measurements, including length, parenchymal thickness, and medullary pyramid thickness, in healthy children: What are the normative ultrasound values? AJR Am J Roentgenol. 2010;194:509–15.
4. Rosenbaum DM, Korngold E, Teele RL. Sonographic assessment of renal length in normal children. AJR Am J Roentgenol. 1984;142:467–9.
5. Steffes MW, Barbosa J, Basgen JM, et al. Quantitative glomerular morphology of the normal human kidney. Lab Invest. 1983;49:82–6.
6. Vogler C, McAdams AJ, Homan SM. Glomerular basement membrane and lamina densa in infants and children: An ultrastructural evaluation. Pediatr Pathol. 1987;7:527–34.
7. Morita M, White RH, Raafat F, et al. Glomerular basement membrane thickness in children: A mor-phometric study. Pediatr Nephrol. 1988;2:190–5.
8. Miner JH. Glomerular basement membrane com-position and the filtration barrier. Pediatr Nephrol. 2011;26:1413–7.
9. Rodewald R, Karnovsky MJ. Porous substructure of the glomerular slit diaphragm in the rat and mouse. J Cell Biol. 1974;60:423–33.
10. Kestilä M1, Lenkkeri U, Männikkö M, et al. Positionally cloned gene for a novel glomerular pro-tein—nephrin—is mutated in congenital nephrotic syndrome. Mol Cell. 1998;1:575–82.
11. Wartiovaara J, Ofverstedt LG, Khoshnoodi J, et al. Nephrin strands contribute to a porous slit dia-phragm scaffold as revealed by electron tomogra-phy. J Clin Invest. 2004;114:1475–83.
12. Sellin L, Huber TB, Gerke P, et al. NEPH1 defines a novel family of podocin interacting proteins. FASEB J. 2003;17:115–7.
13. Liu G, Kaw B, Kurfis J, et al. Neph1 and nephrin inter-action in the slit diaphragm is an important deter-minant of glomerular permeability. J Clin Invest. 2003;112:209–21.
14. Garg P, Verma R, Nihalani D, et al. Neph1 cooperates with nephrin to transduce a signal that induces actin polymerization. Mol Cell Biol. 2007;27:8698–712.
15. Grahammer F, Schell C, Huber TB. The podocyte slit diaphragm: From a thin grey line to a complex signalling hub. Nat Rev Nephrol. 2013;9:587–98.
16. Heeringa SF, Vlangos CN, Chernin G, et al. Thirteen novel NPHS1 mutations in a large cohort of children with congenital nephrotic syndrome. Nephrol Dial Transplant. 2008;23:3527–33.
17. Machuca E, Benoit G, Nevo F, Tête MJ, et al. Genotype-phenotype correlations in non-Finnish congenital nephrotic syndrome. J Am Soc Nephrol. 2010;21:1209–17.
KEY POINTS
● �e RAS plays a crucial role in nephrogenesis. ● Maternal ACEI use a�er the �rst trimester is
associated with fetopathy that includes renal dysgenesis.
SUMMARY
A signi�cant advance in our understanding of the signal pathways involved during development of the kidneys and the urinary tract in fetal life has occurred since the 1990s. What has also become obvious is that the renal development is supported by the development of the rest of the urinary tract, especially the ureteric bud. A disruption in any of these developmental processes can lead to abnor-malities of renal development and CAKUT. Nephron endowment at birth is beginning to be recognized as an important predictor of CKD and hypertension in adults. Attention to prenatal health and prevention of poor nephron endowment may be ways that kidney disease and hypertension can be prevented in adults.
K21764.indb 13 02/09/16 6:02 pm
14 Anatomy and embryology of the urinary tract
18. Nyengaard JR, Bendtsen TF. Glomerular number and size in relation to age, kidney weight, and body surface in normal man. Anat Rec. 1992;232,194–201.
19. Hoy WE, Douglas-Denton RN, Hughson MD, et al. A stereological study of glomerular number and volume: Preliminary findings in a multiracial study of kidneys at autopsy. Kidney Int Suppl. 2003;63, S31–7.
20. Hinchliffe SA, Sargent PH, Howard CV, et al. Human intrauterine renal growth expressed in absolute number of glomeruli assessed by the dissec-tor method and Cavalieri principle. Lab Invest. 1991;64:777–84.
21. Moritz KM, Caruana G, Wintour EM. Development of kidneys and urinary tract. In Rodeck CH, Whittle MF, editors. Fetal Medicine: Basic Science and Clinical Practice, 2nd ed. Philadelphia: Churchill Livingstone; 2009. p. 147.
22. Hinchliffe SA, Lynch MR, Sargent PH, et al. The effect of intrauterine growth retardation on the development of renal nephrons. Br J Obstet Gynaecol. 1992;99:296–301.
23. Mañalich R1, Reyes L, Herrera M, et al. Relationship between weight at birth and the number and size of renal glomeruli in humans: A histomorphometric study. Kidney Int. 2000;58:770–3.
24. Keijzer-Veen MG1, Devos AS, Meradji M, et al. Reduced renal length and volume 20 years after very preterm birth. Pediatr Nephrol. 2010;25:499–507.
25. Brenner BM, Garcia DL, Anderson S. Glomeruli and blood pressure: Less of one, more of the other? Am J Hypertens. 1988;1:335–47.
26. Brenner BM, Mackenzie HS. Nephron mass as a risk factor for progression of renal disease. Kidney Int Suppl. 1997;63 S124–7.
27. Luyckx VA, Bertram JF, Brenner BM, et al. Effect of fetal and child health on kidney development and long-term risk of hypertension and kidney disease. Lancet. 2013 20;382:273–83.
28. Roberts G1, Lee KJ, Cheong JL, et al. Higher ambu-latory blood pressure at 18 years in adolescents born less than 28 weeks’ gestation in the 1990s compared with term controls. J Hypertens. 2014;32:620–6.
29. de Jong F, Monuteaux MC, van Elburg RM, et al. Systematic review and metaanalysis of preterm birth and later systolic blood pressure. Hypertension. 2012;59:226–34.
30. Yudkin JS, Phillips DI, Stanner S. Proteinuria and progressive renal disease: Birth weight and micro-albuminuria. Nephrol Dial Transplant. 1997;12(Suppl 2):10–3.
31. Lackland DT, Bendall HE, Osmond C, et al. Low birth weights contribute to high rates of early-onset chronic renal failure in the Southeastern United States. Arch Intern Med. 2000;160:1472–6.
32. Carmody JB, Charlton JR. Short-term gestation, long-term risk: Prematurity and chronic kidney dis-ease. Pediatrics. 2013;131:1168–79.
33. Ichikawa I, Kuwayama F, Pope JC, 4th, et al. Paradigm shift from classic anatomic theories to con-temporary cell biological views of CAKUT. Kidney Int. 2002;61:889–98.
34. Pope JC 4th, Brock JW, 3rd, Adams MC, et al. How they begin and how they end: Classic and new theories for the development and deterioration of congenital anomalies of the kidney and urinary tract, CAKUT. J Am Soc Nephrol. 1999;10:2018–28.
35. Wiesel A, Queisser-Luft A, Clementi M, et al. Prenatal detection of congenital renal malformations by fetal ultrasonographic examination: An analysis of 709,030 births in 12 European countries. Eur J Med Genet. 2005;48:131–44.
36. McPherson E. Renal anomalies in families of indi-viduals with congenital solitary kidney. Genet Med. 2007;9:298–302.
37. Bulum B, Ozçakar ZB, Ustüner E, et al. High fre-quency of kidney and urinary tract anomalies in asymptomatic first-degree relatives of patients with CAKUT. Pediatr Nephrol. 2013;28:2143–7.
38. Mansoor O, Chandar J, Rodriguez MM, et al. Long-term risk of chronic kidney disease in unilateral multicystic dysplastic kidney. Pediatr Nephrol. 2011;26:597–603.
39. Damen-Elias HA, Stoutenbeek PH, Visser GH, et al. Concomitant anomalies in 100 children with unilat-eral multicystic kidney. Ultrasound Obstet Gynecol. 2005;25:384–8.
40. Potter EL. Bilateral renal agenesis. J Pediatr. 1946;29:68–76.
41. Potter EL. Normal and Abnormal Development of the Kidney. Chicago: Year Book Medical Publishers; 1972. p. 1–305.
42. Wilson RD, Baird PA. Renal agenesis in British Columbia. Am J Med Genet. 1985;21:153–69.
43. Roodhooft AM, Birnholz JC, Holmes LB. Familial nature of congenital absence and severe dysgene-sis of both kidneys. N Engl J Med. 1984;310:1341–5.
44. Humbert C, Silbermann F, Morar B, et al. Integrin alpha 8 recessive mutations are responsible for bilateral renal agenesis in humans. Am J Hum Genet. 2014;94:288–94.
45. Sheih CP, Liu MB, Hung CS, et al. Renal abnormali-ties in schoolchildren. Pediatrics. 1989;84:1086–90.
46. Westland R, Schreuder MF, Ket JC, et al. Unilateral renal agenesis: A systematic review on associated anomalies and renal injury. Nephrol Dial Transplant. 2013;28:1844–55.
47. Weizer AZ, Silverstein AD, Auge BK, et al. Determining the incidence of horseshoe kidney from radiographic data at a single institution. J Urol. 2003;170:1722–6.
48. Glenn JF. Analysis of 51 patients with horseshoe kidney. N Engl J Med. 1959;261:684–7.
49. Bilge I, Kayserili H, Emre S, et al. Frequency of renal malformations in Turner syndrome: Analysis of 82 Turkish children. Pediatr Nephrol. 2000;14:1111–4.
K21764.indb 14 02/09/16 6:02 pm

Review questions / Congenital abnormalities of the kidney and urinary tract 15
50. Kuwertz-Broeking E, Brinkmann OA, Von Lengerke HJ, et al. Unilateral multicystic dysplastic kidney: Experience in children. BJU Int. 2004;93:388–92.
51. Schreuder MF, Westland R, van Wijk JA. Unilateral multicystic dysplastic kidney: A metaanalysis of observational studies on the incidence, associated urinary tract malformations and the contralateral kidney. Nephrol Dial Transplant. 2009;24:1810–8.
52. Aslam M, Watson AR, Trent, and Anglia MCDK Study Group. Unilateral multicystic dysplastic kidney: Long term outcomes. Arch Dis Child. 2006;91:820–3.
53. Snodgrass WT. Hypertension associated with multicystic dysplastic kidney in children. J Urol. 2000;164:472–3.
54. Narchi H. Risk of hypertension with multicystic kidney disease: A systematic review. Arch Dis Child. 2005;90:921–4.
55. Narchi H. Risk of Wilms’ tumour with multicystic kidney disease: A systematic review. Arch Dis Child. 2005;90:147–9.
56. Eickmeyer AB, Casanova NF, He C, et al. The natural history of the multicystic dysplastic kidney: Is limited follow-up warranted? J Pediatr Urol. 2014;10:655–61.
57. Tilemis S, Savanelli A, Baltogiannis D, et al. Is the risk of hypertension an indication for prophylac-tic nephrectomy in patients with unilateral mul-ticystic dysplastic kidney? Scand J Urol Nephrol. 2003;37:429–32.
58. Miller RW, Fraumeni JF Jr, Manning MD. Association of Wilms’ tumor with aniridia, hemihypertophy and other congenital malformations. N Engl J Med. 1964;270:922–7.
59. Francke U, Holmes LB, Atkins L, Riccardi VM. Aniridia-Wilms’ tumor associations: Evidence for specific deletion of 11p13. Cytogenet Cell Genet. 1979;24:185–92.
60. Rauscher FJ. The WT1 Wilms tumor gene product: A developmentally regulated transcription factor in the kidney that functions as a tumor suppressor. FASEB J. 1993;7:896–903.
61. Morrison AA, Viney RL, Saleem MA, et al. New insights into the function of the Wilms tumor sup-pressor gene WT1 in podocytes. Am J Physiol Renal Physiol. 2008;295:F12–7.
62. Fischbach BV, Trout KL, Lewis J, et al. WAGR syndrome: A clinical review of 54 cases. Pediatrics. 2005;116:984–8.
63. Breslow NE, Norris R, Norkool P, et al. Characteristics and outcomes of children with the Wilms’ tumor-aniridia syndrome: A report from the National Wilms’ Tumor Study Group. J Clin Oncol. 2003;24:4579–85.
64. Breslow NE, Collins AJ, Ritchey ML, et al. End stage renal disease in patients with Wilms tumor: Results from the National Wilms Tumor Study Group and the United States Renal Data System. J Urol. 2005;174:1972–5.
65. Nelson CP, Dunn RL, Wei JT. Contemporary epide-miology of bladder exstrophy in the United States. J Urol. 2005;173:1728–31.
66. Draaken M, Baudisch F, Timmermann B, et al. Classic bladder exstrophy: Frequent 22q11.21 duplications and definition of a 414 kb phenocritical region. Birth Defects Res A Clin Mol Teratol. 2014;100:512–7.
67. Dickson AP. The management of bladder exstro-phy: The Manchester experience. J Pediatr Surg. 2014;49:244–50.
68. Taskinen S, Suominen JS. Lower urinary tract symptoms (LUTS) in patients in adulthood with bladder exstrophy and epispadias. BJU Int. 2013;111:1124–9.
69. Gupta AD, Goel SK, Woodhouse CR, et al. Examining long-term outcomes of bladder exstro-phy: A 20-year follow-up. BJU Int. 2014;113:137–41.
70. Yosypiv IV. Renin-angiotensin system in ureteric bud branching morphogenesis: Insights into the mecha-nisms. Pediatr Nephrol. 2011;26:1499–512.
71. Song R, Spera M, Garrett C, et al. Angiotensin II AT2 receptor regulates ureteric bud morphogenesis. Am J Physiol Renal Physiol. 2010;298:F807–17.
72. Pryde PG, Sedman AB, Nugent CE, Barr M. Angiotensin-converting enzyme inhibitor fetopathy. J Am Soc Nephrol. 1993;3:1575–82.
73. Buttar HS. An overview of the influence of ACE inhibitors on fetal-placental circulation and perinatal development. Mol Cell Biochem. 1997;176:61–71.
74. Anonymous. Post marketing surveillance for angio-tensin-converting enzyme inhibitor use during the first trimester of pregnancy: United States, Canada, and Israel, 1987–1995. MMWR Morb Mortal Wkly Rep. 1997;46:240–2.
REVIEW QUESTIONS
1. �e juxtamedullary nephrons have long loops of Henle that participate in:
a. Sodium reabsorption b. Chloride transport c. Urine concentrating mechanism d. None of the above
2. Nephrin constitutes a structural component of: a. Endothelial cytoskeleton b. Podocyte cytoskeleton c. Slit diaphragm d. Bowman capsule
3. Which of the following combinations are transitional embryonic kidneys?
a. Metanephros and mesonephros b. Mesonephros and pronephros c. Pronephros and metanephros d. None of the above
K21764.indb 15 02/09/16 6:02 pm
16 Anatomy and embryology of the urinary tract
4. In a premature infant, nephrogenesis can continue up to 3 months a�er birth:
a. True b. False
5. Characteristic �nding on MAG3 renal scan in a patient with multicystic dysplastic kidney (MCDK) is:
a. Photopenic areas in the a�ected kidney suggesting cysts
b. Arterial �ow from the surrounding tissue c. Adequate blood �ow but no excretory function d. No demonstrable renal blood �ow and no excre-
tory function 6. Vesicoureteral re�ux on the same side or contralateral
side of MCDK occurs in: a. Fewer than 5% cases b. 20% cases c. 50% cases d. Almost always in all patients
7. Wilms tumor, aniridia, genitourinary anomalies, and mental retardation (WAGR) is caused by:
a. Mutation in WT1 gene b. Mutation in PAX6 gene c. Mutation in PAX6 and WT1 d. Mutation in WT1 and GDNF
8. ACEI-induced fetapathy is more common if the drug exposure occurs in:
a. First 2 weeks of pregnancy b. Six to 12 weeks of pregnancy c. Last week of pregnancy d. A�er �rst trimester of pregnancy
9. Horseshoe kidneys are common in: a. Down syndrome b. Turner syndrome c. WAGR syndrome d. Renal coloboma syndrome
10. Low nephron number at birth is associated with: a. Future risk of diabetes mellitus b. Future risk of cardiac disease c. Future risk of hypertension d. No associated risk of disease
ANSWER KEY
1. c 2. c 3. c 4. a 5. d 6. b 7. c 8. d 9. b 10. c
K21764.indb 16 02/09/16 6:02 pm

References
1 Anatomy and embryology of the urinarytract
1. Scott JE, Hunter EW, Lee RE, et al. Ultrasoundmeasurement of renal size in newborn infants. Arch DisChild. 1990;65:361–4. 2. Pantoja Zuzuárregui JR1, MalliosR, Murphy J. The effect of obesity on kidney length in ahealthy pediatric population. Pediatr Nephrol.2009;24:2023–7. 3. Ale v Kadioglu. Renal measurements,including length, parenchymal thickness, and medullarypyramid thickness, in healthy children: What are thenormative ultrasound values? AJR Am J Roentgenol.2010;194:509–15. 4. Rosenbaum DM, Korngold E, Teele RL.Sonographic assessment of renal length in normal children.AJR Am J Roentgenol. 1984;142:467–9. 5. Steffes MW,Barbosa J, Basgen JM, et al. Quantitative glomerularmorphology of the normal human kidney. Lab Invest.1983;49:82–6. 6. Vog ler C, McAdams AJ, Homan SM.Glomerular basement membrane and lamina densa in infantsand children: An ultrastructural evaluation. PediatrPathol. 1987;7:527–34. 7. Morita M, White RH, Raafat F, etal. Glomerular basement membrane thickness in children: Amorphometric study. Pediatr Nephrol. 1988;2:190–5. 8.Miner JH. Glomerular basement membrane composition and thefiltration barrier. Pediatr Nephrol. 2011;26:1413–7. 9.Rodewald R, Karnovsky MJ. Porous substructure of theglomerular slit diaphragm in the rat and mouse. J CellBiol. 1974;60:423–33. 10. Kestilä M1, Lenkkeri U, MännikköM, et al. Positionally cloned gene for a novel glomerularprotein—nephrin—is mutated in congenital nephroticsyndrome. Mol Cell. 1998;1:575–82. 11. Wartiovaara J,Ofverstedt LG, Khoshnoodi J, et al. Nephrin strandscontribute to a porous slit diaphragm scaffold as revealedby electron tomography. J Clin Invest. 2004;114:1475–83.12. Sellin L, Huber TB, Gerke P, et al. NEPH1 defines anovel family of podocin interacting proteins. FASEB J.2003;17:115–7. 13. Liu G, Kaw B, Kurfis J, et al. Neph1and nephrin interaction in the slit diaphragm is animportant determinant of glomerular permeability. J ClinInvest. 2003;112:209–21. 14. Garg P, Verma R, Nihalani D,et al. Neph1 cooperates with nephrin to transduce a signalthat induces actin polymerization. Mol Cell Biol.2007;27:8698–712. 15. Grahammer F, Schell C, Huber TB. Thepodocyte slit diaphragm: From a thin grey line to acomplex signalling hub. Nat Rev Nephrol. 2013;9:587–98.16. Heeringa SF, Vlangos CN, Chernin G, et al. Thirteennovel NPHS1 mutations in a large cohort of children withcongenital nephrotic syndrome. Nephrol Dial Transplant.
2008;23:3527–33. 17. Machuca E, Benoit G, Nevo F, Tête MJ,et al. Genotype-phenotype correlations in non-Finnishcongenital nephrotic syndrome. J Am Soc Nephrol.2010;21:1209–17. KEY POINTS ● �e RAS plays a crucial rolein nephrogenesis. ● Maternal ACEI use a�er the �rsttrimester is associated with fetopathy that includes renaldysgenesis. SUMMARY
A signi�cant advance in our understanding of the
signal pathways involved during development of
the kidneys and the urinary tract in fetal life has
occurred since the 1990s. What has also become
obvious is that the renal development is supported
by the development of the rest of the urinary tract,
especially the ureteric bud. A disruption in any of
these developmental processes can lead to abnor
malities of renal development and CAKUT. Nephron
endowment at birth is beginning to be recognized as
an important predictor of CKD and hypertension in
adults. Attention to prenatal health and prevention of
poor nephron endowment may be ways that kidney
disease and hypertension can be prevented in adults.
18. Nyengaard JR, Bendtsen TF. Glomerular number and sizein relation to age, kidney weight, and body surface innormal man. Anat Rec. 1992;232,194–201.
19. Hoy WE , Douglas-Denton RN, Hughson MD, et al. Astereological study of glomerular number and volume:Preliminary findings in a multiracial study of kidneys atautopsy. Kidney Int Suppl. 2003;63, S31–7.
20. Hinchliffe SA, Sargent PH, Howard CV, et al. Humanintrauterine renal growth expressed in absolute number ofglomeruli assessed by the dissector method and Cavalieriprinciple. Lab Invest. 1991;64:777–84.
21. Moritz KM, Caruana G, Wintour EM. Development ofkidneys and urinary tract. In Rodeck CH, Whittle MF,editors. Fetal Medicine: Basic Science and ClinicalPractice, 2nd ed. Philadelphia: Churchill Livingstone;2009. p. 147.
22. Hinchliffe SA, Lynch MR, Sargent PH, et al. The effectof intrauterine growth retardation on the development ofrenal nephrons. Br J Obstet Gynaecol. 1992;99:296–301.
23. Mañ alich R1, Reyes L, Herrera M, et al. Relationshipbetween weight at birth and the number and size of renalglomeruli in humans: A histomorphometric study. KidneyInt. 2000;58:770–3.
24. Kei jzer-Veen MG1, Devos AS, Meradji M, et al. Reducedrenal length and volume 20 years after very preterm birth.Pediatr Nephrol. 2010;25:499–507.
25. Bre nner BM, Garcia DL, Anderson S. Glomeruli andblood pressure: Less of one, more of the other? Am JHypertens. 1988;1:335–47.
26. Bre nner BM, Mackenzie HS. Nephron mass as a riskfactor for progression of renal disease. Kidney Int Suppl.1997;63 S124–7.
27. Luyckx VA, Bertram JF, Brenner BM, et al. Effect offetal and child health on kidney development and long-termrisk of hypertension and kidney disease. Lancet. 201320;382:273–83.
28. Roberts G1, Lee KJ, Cheong JL, et al. Higher ambulatoryblood pressure at 18 years in adolescents born less than28 weeks’ gestation in the 1990s compared with termcontrols. J Hypertens. 2014;32:620–6.
29. de Jo ng F, Monuteaux MC, van Elburg RM, et al.Systematic review and metaanalysis of preterm birth andlater systolic blood pressure. Hypertension.2012;59:226–34.
30. Yudkin JS, Phillips DI, Stanner S. Proteinuria andprogressive renal disease: Birth weight andmicroalbuminuria. Nephrol Dial Transplant. 1997;12(Suppl2):10–3.
31. Lac kland DT, Bendall HE, Osmond C, et al. Low birthweights contribute to high rates of early-onset chronicrenal failure in the Southeastern United States. Arch
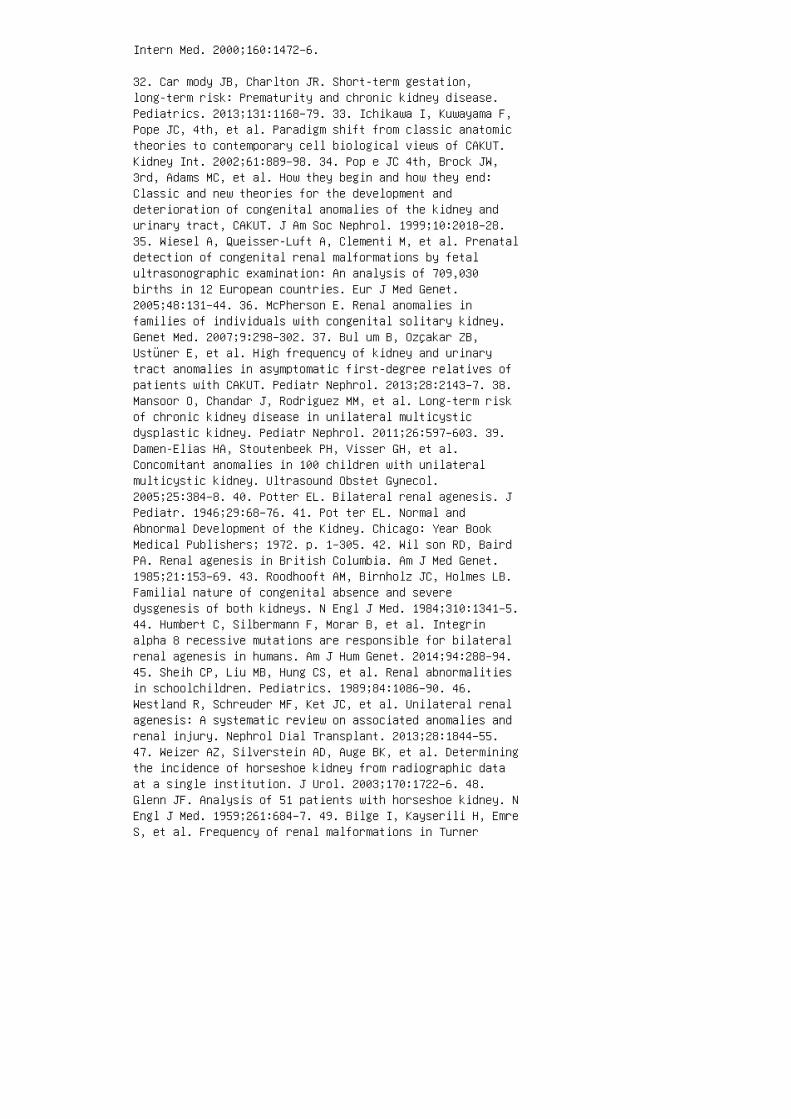
Intern Med. 2000;160:1472–6.
32. Car mody JB, Charlton JR. Short-term gestation,long-term risk: Prematurity and chronic kidney disease.Pediatrics. 2013;131:1168–79. 33. Ichikawa I, Kuwayama F,Pope JC, 4th, et al. Paradigm shift from classic anatomictheories to contemporary cell biological views of CAKUT.Kidney Int. 2002;61:889–98. 34. Pop e JC 4th, Brock JW,3rd, Adams MC, et al. How they begin and how they end:Classic and new theories for the development anddeterioration of congenital anomalies of the kidney andurinary tract, CAKUT. J Am Soc Nephrol. 1999;10:2018–28.35. Wiesel A, Queisser-Luft A, Clementi M, et al. Prenataldetection of congenital renal malformations by fetalultrasonographic examination: An analysis of 709,030births in 12 European countries. Eur J Med Genet.2005;48:131–44. 36. McPherson E. Renal anomalies infamilies of individuals with congenital solitary kidney.Genet Med. 2007;9:298–302. 37. Bul um B, Ozçakar ZB,Ustüner E, et al. High frequency of kidney and urinarytract anomalies in asymptomatic first-degree relatives ofpatients with CAKUT. Pediatr Nephrol. 2013;28:2143–7. 38.Mansoor O, Chandar J, Rodriguez MM, et al. Long-term riskof chronic kidney disease in unilateral multicysticdysplastic kidney. Pediatr Nephrol. 2011;26:597–603. 39.Damen-Elias HA, Stoutenbeek PH, Visser GH, et al.Concomitant anomalies in 100 children with unilateralmulticystic kidney. Ultrasound Obstet Gynecol.2005;25:384–8. 40. Potter EL. Bilateral renal agenesis. JPediatr. 1946;29:68–76. 41. Pot ter EL. Normal andAbnormal Development of the Kidney. Chicago: Year BookMedical Publishers; 1972. p. 1–305. 42. Wil son RD, BairdPA. Renal agenesis in British Columbia. Am J Med Genet.1985;21:153–69. 43. Roodhooft AM, Birnholz JC, Holmes LB.Familial nature of congenital absence and severedysgenesis of both kidneys. N Engl J Med. 1984;310:1341–5.44. Humbert C, Silbermann F, Morar B, et al. Integrinalpha 8 recessive mutations are responsible for bilateralrenal agenesis in humans. Am J Hum Genet. 2014;94:288–94.45. Sheih CP, Liu MB, Hung CS, et al. Renal abnormalitiesin schoolchildren. Pediatrics. 1989;84:1086–90. 46.Westland R, Schreuder MF, Ket JC, et al. Unilateral renalagenesis: A systematic review on associated anomalies andrenal injury. Nephrol Dial Transplant. 2013;28:1844–55.47. Weizer AZ, Silverstein AD, Auge BK, et al. Determiningthe incidence of horseshoe kidney from radiographic dataat a single institution. J Urol. 2003;170:1722–6. 48.Glenn JF. Analysis of 51 patients with horseshoe kidney. NEngl J Med. 1959;261:684–7. 49. Bilge I, Kayserili H, EmreS, et al. Frequency of renal malformations in Turner
syndrome: Analysis of 82 Turkish children. PediatrNephrol. 2000;14:1111–4.
50. Kuwertz-Broeking E, Brinkmann OA, Von Lengerke HJ, etal. Unilateral multicystic dysplastic kidney: Experiencein children. BJU Int. 2004;93:388–92.
51. Sch reuder MF, Westland R, van Wijk JA. Unilateralmulticystic dysplastic kidney: A metaanalysis ofobservational studies on the incidence, associated urinarytract malformations and the contralateral kidney. NephrolDial Transplant. 2009;24:1810–8.
52. Aslam M, Watson AR, Trent, and Anglia MCDK StudyGroup. Unilateral multicystic dysplastic kidney: Long termoutcomes. Arch Dis Child. 2006;91:820–3.
53. Snodgrass WT. Hypertension associated with multicysticdysplastic kidney in children. J Urol. 2000;164:472–3.
54. Narchi H. Risk of hypertension with multicystic kidneydisease: A systematic review. Arch Dis Child.2005;90:921–4.
55. Narchi H. Risk of Wilms’ tumour with multicystickidney disease: A systematic review. Arch Dis Child.2005;90:147–9.
56. Eic kmeyer AB, Casanova NF, He C, et al. The naturalhistory of the multicystic dysplastic kidney: Is limitedfollow-up warranted? J Pediatr Urol. 2014;10:655–61.
57. Til emis S, Savanelli A, Baltogiannis D, et al. Is therisk of hypertension an indication for prophylacticnephrectomy in patients with unilateral multicysticdysplastic kidney? Scand J Urol Nephrol. 2003;37:429–32.
58. Mil ler RW, Fraumeni JF Jr, Manning MD. Association ofWilms’ tumor with aniridia, hemihypertophy and othercongenital malformations. N Engl J Med. 1964;270:922–7.
59. Francke U, Holmes LB, Atkins L, Riccardi VM.Aniridia-Wilms’ tumor associations: Evidence for specificdeletion of 11p13. Cytogenet Cell Genet. 1979;24:185–92.
60. Rauscher FJ. The WT1 Wilms tumor gene product: Adevelopmentally regulated transcription factor in thekidney that functions as a tumor suppressor. FASEB J.1993;7:896–903.
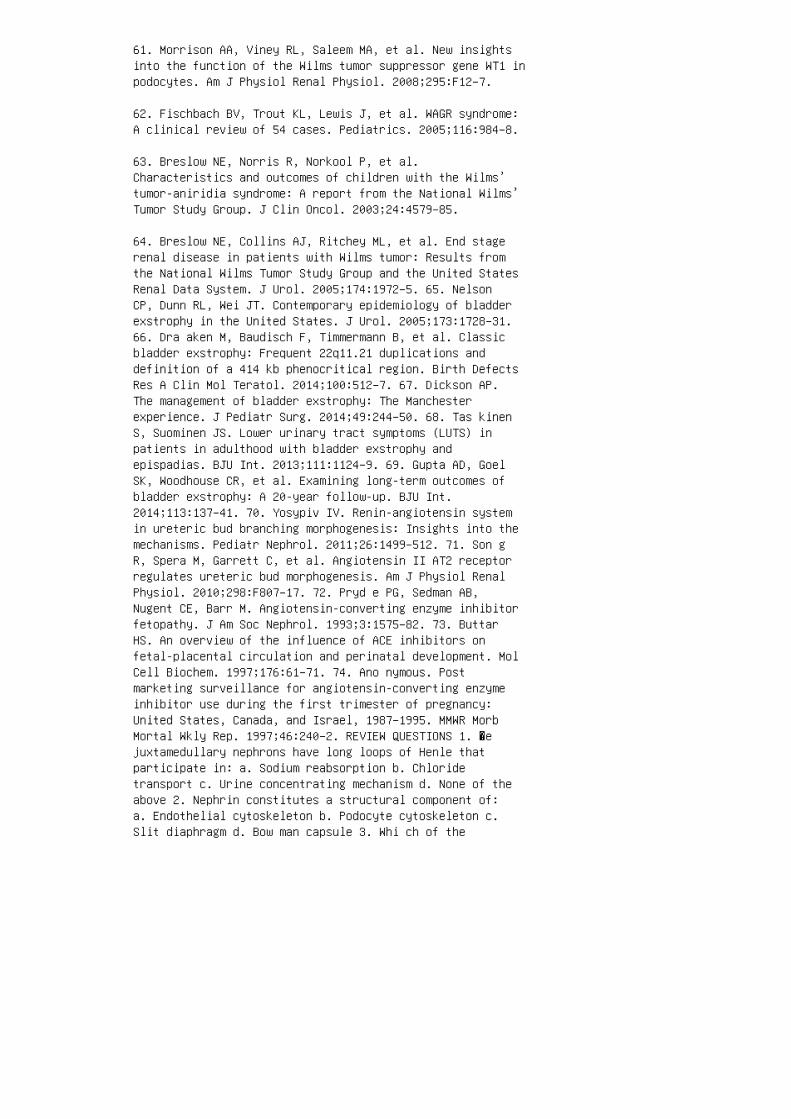
61. Morrison AA, Viney RL, Saleem MA, et al. New insightsinto the function of the Wilms tumor suppressor gene WT1 inpodocytes. Am J Physiol Renal Physiol. 2008;295:F12–7.
62. Fischbach BV, Trout KL, Lewis J, et al. WAGR syndrome:A clinical review of 54 cases. Pediatrics. 2005;116:984–8.
63. Breslow NE, Norris R, Norkool P, et al.Characteristics and outcomes of children with the Wilms’tumor-aniridia syndrome: A report from the National Wilms’Tumor Study Group. J Clin Oncol. 2003;24:4579–85.
64. Breslow NE, Collins AJ, Ritchey ML, et al. End stagerenal disease in patients with Wilms tumor: Results fromthe National Wilms Tumor Study Group and the United StatesRenal Data System. J Urol. 2005;174:1972–5. 65. NelsonCP, Dunn RL, Wei JT. Contemporary epidemiology of bladderexstrophy in the United States. J Urol. 2005;173:1728–31.66. Dra aken M, Baudisch F, Timmermann B, et al. Classicbladder exstrophy: Frequent 22q11.21 duplications anddefinition of a 414 kb phenocritical region. Birth DefectsRes A Clin Mol Teratol. 2014;100:512–7. 67. Dickson AP.The management of bladder exstrophy: The Manchesterexperience. J Pediatr Surg. 2014;49:244–50. 68. Tas kinenS, Suominen JS. Lower urinary tract symptoms (LUTS) inpatients in adulthood with bladder exstrophy andepispadias. BJU Int. 2013;111:1124–9. 69. Gupta AD, GoelSK, Woodhouse CR, et al. Examining long-term outcomes ofbladder exstrophy: A 20-year follow-up. BJU Int.2014;113:137–41. 70. Yosypiv IV. Renin-angiotensin systemin ureteric bud branching morphogenesis: Insights into themechanisms. Pediatr Nephrol. 2011;26:1499–512. 71. Son gR, Spera M, Garrett C, et al. Angiotensin II AT2 receptorregulates ureteric bud morphogenesis. Am J Physiol RenalPhysiol. 2010;298:F807–17. 72. Pryd e PG, Sedman AB,Nugent CE, Barr M. Angiotensin-converting enzyme inhibitorfetopathy. J Am Soc Nephrol. 1993;3:1575–82. 73. ButtarHS. An overview of the influence of ACE inhibitors onfetal-placental circulation and perinatal development. MolCell Biochem. 1997;176:61–71. 74. Ano nymous. Postmarketing surveillance for angiotensin-converting enzymeinhibitor use during the first trimester of pregnancy:United States, Canada, and Israel, 1987–1995. MMWR MorbMortal Wkly Rep. 1997;46:240–2. REVIEW QUESTIONS 1. �ejuxtamedullary nephrons have long loops of Henle thatparticipate in: a. Sodium reabsorption b. Chloridetransport c. Urine concentrating mechanism d. None of theabove 2. Nephrin constitutes a structural component of:a. Endothelial cytoskeleton b. Podocyte cytoskeleton c.Slit diaphragm d. Bow man capsule 3. Whi ch of the

following combinations are transitional embryonic kidneys?a. Met anephros and mesonephros b. Mes onephros andpronephros c. Pro nephros and metanephros d. None of theabove
4. In a premature infant, nephrogenesis can continue up to3 months a�er birth:
a. True
b. False
5. Characteristic �nding on MAG3 renal scan in a patientwith multicystic dysplastic kidney (MCDK) is:
a. Photopenic areas in the a�ected kidney suggesting cysts
b. Arterial �ow from the surrounding tissue
c. Adequate blood �ow but no excretory function
d. No demonstrable renal blood �ow and no excretory function
6. Vesicoureteral re�ux on the same side or contralateralside of MCDK occurs in:
a. Fewer than 5% cases
b. 20% cases
c. 50% cases
d. Almost always in all patients
7. Wilms tumor, aniridia, genitourinary anomalies, andmental retardation (WAGR) is caused by:
a. Mutation in WT1 gene
b. Mutation in PAX6 gene
c. Mutation in PAX6 and WT1
d. Mutation in WT1 and GDNF
8. ACEI-induced fetapathy is more common if the drugexposure occurs in:
a. First 2 weeks of pregnancy

b. Six to 12 weeks of pregnancy
c. Last week of pregnancy
d. A�er �rst trimester of pregnancy 9. Horseshoe kidneysare common in: a. Down syndrome b. Turner syndrome c.WAGR syndrome d. Renal coloboma syndrome 10. Low nephronnumber at birth is associated with: a. Future risk ofdiabetes mellitus b. Future risk of cardiac disease c.Future risk of hypertension d. No associated risk ofdisease ANSWER KEY 1. c 2. c 3. c 4. a 5. d 6. b 7.c 8. d 9. b 10. c
2 Molecular basis of developmental renaldisease
(a)
Figure 2.4 Renal dysplasia. (a) A cut section of dysplastic
kidney with malformed collecting system, lack of well-pat
terned renal parenchyma, and absence of corticomedul
lary differentiation. (b) Microscopic section of the kidney
from the patient demonstrating malformed tubules. Some
tubules are widely dilated (T). Arrows show cartilage
within the renal parenchyma. (Figure courtesy of Arthur
Cohen, MD.)
8. Kume T, Deng K, Hogan BLM. Murine forkhead/ winged helixgenes Foxc1 (Mf1) and Foxc2 (Mfh1) are required for theearly organogenesis of the kidney and urinary tract.Development. 2000;127:1387–95.
9. Miyazaki Y, Oshima K, Fogo A, et al. Bone morphogeneticprotein 4 regulates the budding site and elongation of themouse ureter. J Clin Invest. 2000;105:863–73.
10. Patterson LT, Pembaur M, Potter SS. Hoxa11 and Hoxd11regulate branching morphogenesis of the ureteric bud inthe developing kidney. Development. 2001;128:2153–61.
11. Mendelsohn C, Batourina E, Fung S, et al. Stromalcells mediate retinoid-dependent functions essential forrenal development. Development. 1999;126:1139–48.
12. Batourina E, Gim S, Bello N, et al. Vitamin A controlsepithelial/mesenchymal interactions through Retexpression. Nat Genet. 2001;27:74–8.
13. Qiao J, Uzzo R, Obara-Ishihara T, et al. FGF-7modulates ureteric bud growth and nephron number in thedeveloping kidney. Development. 1999;126:547–54.
14. Ohuchi H, Kimura S, Watamoto M, et al. Involvement offibroblast growth factor (FGF)18-FGF8 signaling inspecification of left-right asymmetry and brain and limbdevelopment of the chick embryo. Mech Dev. 2000;95:55–66.

15. Hu MC , Piscione TD, Rosenblum ND. ElevatedSmad1/beta-catenin molecular complexes and renal medullarycystic dysplasia in ALK3 transgenic mice. Development.2003;130:2753–66.
16. Har twig S, Hu MC, Cella C, et al. Glypican-3 modulatesinhibitory Bmp2-Smad signaling to control renaldevelopment in vivo. Mech Dev. 2005;122:928–38.
17. Karner CM, Chirumamilla R, Aoki S, et al. Wnt9bsignaling regulates planar cell polarity and kidney tubulemorphogenesis. Nat Genet. 2009;41:793–9.
18. Yu J, Carroll TJ, Rajagopal J, et al. A Wnt7bdependentpathway regulates the orientation of epithelial celldivision and establishes the cortico-medullary axis of themammalian kidney. Development. 2009;136:161–71.
19. Yu J, C arroll TJ, McMahon AP. Sonic hedgehogregulates proliferation and differentiation of mesenchymalcells in the mouse metanephric kidney. Development.2002;129:5301–12.
20. Miyazaki Y, Oshima K, Fogo A, et al. Bone morphogeneticprotein 4 regulates the budding site and elongation of themouse ureter. J Clin Invest. 2000;105:863–73.
21. Gre en MC. Mechanism of the pleiotropic effects of theshort-ear mutant gene in the mouse. J Exp Zool.1968;176:129–50.
22. Nis himura H, Yerkes E, Hohenfellner K, et al. Role ofthe angiotensin type 2 receptor gene in congenitalanomalies of the kidney and urinary tract, CAKUT, of miceand men. Mol Cell. 1999;3:1–10. 23. Kreidberg JA, SariolaH, Loring JM, et al. WT-1 is required for early kidneydevelopment. Cell. 1993;74:679–91. 24. Grieshammer U,Cebrian C, Ilagan R, et al. FGF8 is required for cellsurvival at distinct stages of nephrogenesis and forregulation of gene expression in nascent nephrons.Development. 2005;132:3847–57. 25. Dudley AT, Lyons KM,Robertson EJ. A requirement for bone morphogeneticprotein-7 during development of the mammalian kidney andeye. Genes Dev. 1995;9:2795–807. 26. Kob ayashi A,Valerius MT, Mugford JW, et al. Six2 defines and regulatesa multipotent self-renewing nephron progenitor populationthroughout mammalian kidney development. Cell Stem Cell.2008;3:169–81. 27. Brunskill EW, Aronow BJ, Georgas K, etal. Atlas of gene expression in the developing kidney at
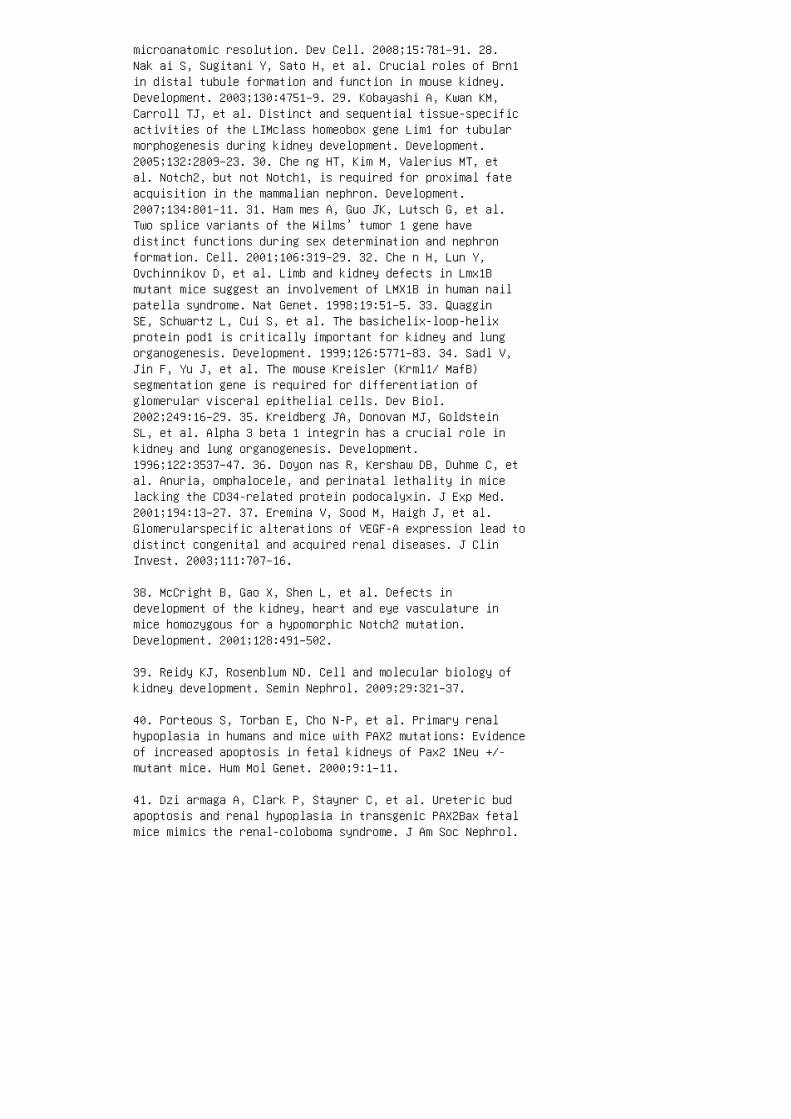
microanatomic resolution. Dev Cell. 2008;15:781–91. 28.Nak ai S, Sugitani Y, Sato H, et al. Crucial roles of Brn1in distal tubule formation and function in mouse kidney.Development. 2003;130:4751–9. 29. Kobayashi A, Kwan KM,Carroll TJ, et al. Distinct and sequential tissue-specificactivities of the LIMclass homeobox gene Lim1 for tubularmorphogenesis during kidney development. Development.2005;132:2809–23. 30. Che ng HT, Kim M, Valerius MT, etal. Notch2, but not Notch1, is required for proximal fateacquisition in the mammalian nephron. Development.2007;134:801–11. 31. Ham mes A, Guo JK, Lutsch G, et al.Two splice variants of the Wilms’ tumor 1 gene havedistinct functions during sex determination and nephronformation. Cell. 2001;106:319–29. 32. Che n H, Lun Y,Ovchinnikov D, et al. Limb and kidney defects in Lmx1Bmutant mice suggest an involvement of LMX1B in human nailpatella syndrome. Nat Genet. 1998;19:51–5. 33. QuagginSE, Schwartz L, Cui S, et al. The basichelix-loop-helixprotein pod1 is critically important for kidney and lungorganogenesis. Development. 1999;126:5771–83. 34. Sadl V,Jin F, Yu J, et al. The mouse Kreisler (Krml1/ MafB)segmentation gene is required for differentiation ofglomerular visceral epithelial cells. Dev Biol.2002;249:16–29. 35. Kreidberg JA, Donovan MJ, GoldsteinSL, et al. Alpha 3 beta 1 integrin has a crucial role inkidney and lung organogenesis. Development.1996;122:3537–47. 36. Doyon nas R, Kershaw DB, Duhme C, etal. Anuria, omphalocele, and perinatal lethality in micelacking the CD34-related protein podocalyxin. J Exp Med.2001;194:13–27. 37. Eremina V, Sood M, Haigh J, et al.Glomerularspecific alterations of VEGF-A expression lead todistinct congenital and acquired renal diseases. J ClinInvest. 2003;111:707–16.
38. McCright B, Gao X, Shen L, et al. Defects indevelopment of the kidney, heart and eye vasculature inmice homozygous for a hypomorphic Notch2 mutation.Development. 2001;128:491–502.
39. Reidy KJ, Rosenblum ND. Cell and molecular biology ofkidney development. Semin Nephrol. 2009;29:321–37.
40. Porteous S, Torban E, Cho N-P, et al. Primary renalhypoplasia in humans and mice with PAX2 mutations: Evidenceof increased apoptosis in fetal kidneys of Pax2 1Neu +/-mutant mice. Hum Mol Genet. 2000;9:1–11.
41. Dzi armaga A, Clark P, Stayner C, et al. Ureteric budapoptosis and renal hypoplasia in transgenic PAX2Bax fetalmice mimics the renal-coloboma syndrome. J Am Soc Nephrol.
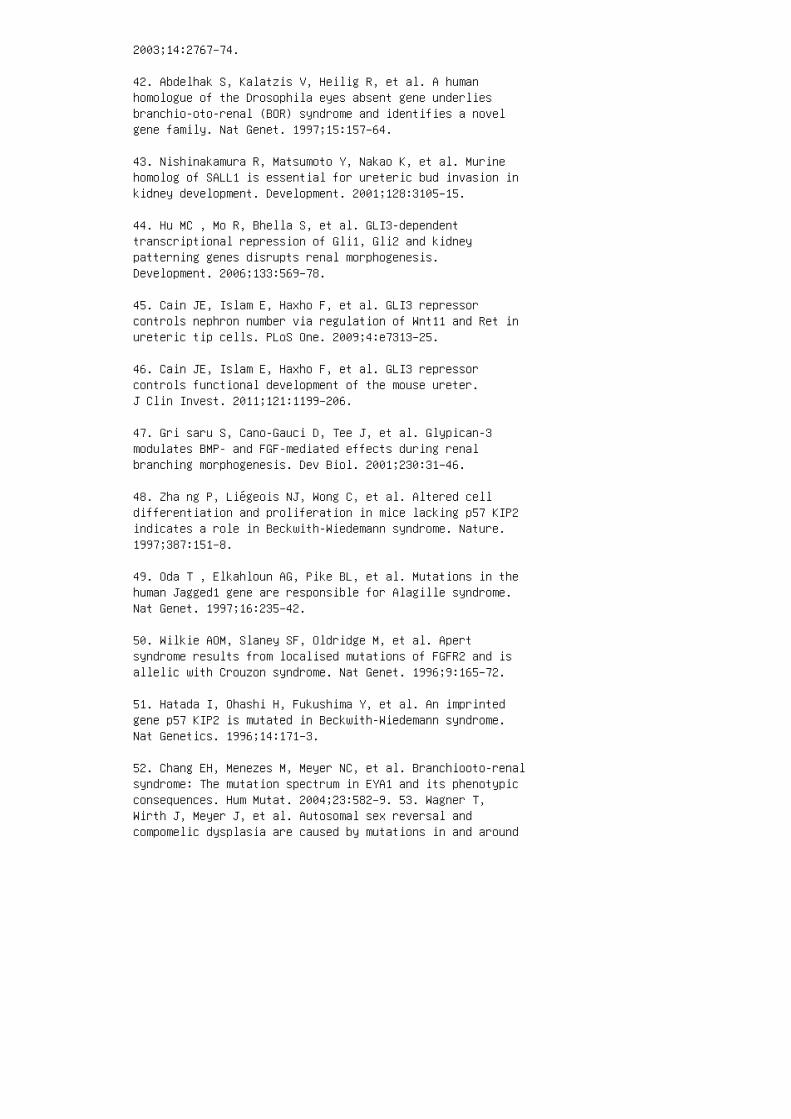
2003;14:2767–74.
42. Abdelhak S, Kalatzis V, Heilig R, et al. A humanhomologue of the Drosophila eyes absent gene underliesbranchio-oto-renal (BOR) syndrome and identifies a novelgene family. Nat Genet. 1997;15:157–64.
43. Nishinakamura R, Matsumoto Y, Nakao K, et al. Murinehomolog of SALL1 is essential for ureteric bud invasion inkidney development. Development. 2001;128:3105–15.
44. Hu MC , Mo R, Bhella S, et al. GLI3-dependenttranscriptional repression of Gli1, Gli2 and kidneypatterning genes disrupts renal morphogenesis.Development. 2006;133:569–78.
45. Cain JE, Islam E, Haxho F, et al. GLI3 repressorcontrols nephron number via regulation of Wnt11 and Ret inureteric tip cells. PLoS One. 2009;4:e7313–25.
46. Cain JE, Islam E, Haxho F, et al. GLI3 repressorcontrols functional development of the mouse ureter.J Clin Invest. 2011;121:1199–206.
47. Gri saru S, Cano-Gauci D, Tee J, et al. Glypican-3modulates BMP- and FGF-mediated effects during renalbranching morphogenesis. Dev Biol. 2001;230:31–46.
48. Zha ng P, Liégeois NJ, Wong C, et al. Altered celldifferentiation and proliferation in mice lacking p57 KIP2indicates a role in Beckwith-Wiedemann syndrome. Nature.1997;387:151–8.
49. Oda T , Elkahloun AG, Pike BL, et al. Mutations in thehuman Jagged1 gene are responsible for Alagille syndrome.Nat Genet. 1997;16:235–42.
50. Wilkie AOM, Slaney SF, Oldridge M, et al. Apertsyndrome results from localised mutations of FGFR2 and isallelic with Crouzon syndrome. Nat Genet. 1996;9:165–72.
51. Hatada I, Ohashi H, Fukushima Y, et al. An imprintedgene p57 KIP2 is mutated in Beckwith-Wiedemann syndrome.Nat Genetics. 1996;14:171–3.
52. Chang EH, Menezes M, Meyer NC, et al. Branchiooto-renalsyndrome: The mutation spectrum in EYA1 and its phenotypicconsequences. Hum Mutat. 2004;23:582–9. 53. Wagner T,Wirth J, Meyer J, et al. Autosomal sex reversal andcompomelic dysplasia are caused by mutations in and around

the SRY-related gene SOX9. Cell. 1994;79:1111–20. 54. McGregor L, Makela V, Darling SM, et al. Fraser syndrome andmouse blebbed phenotype caused by mutations in FRAS1/Fras1encoding a putative extracellular matrix protein. NatGenet. 2003;34:203–8. 55. Van Esch H, Groenen P, NesbitMA, et al. GATA3 haplo-insufficiency causes human HDRsyndrome. Nature. 2000;406:419–22. 56. Franco B, GuioliS, Pragliola A, et al. A gene deleted in Kallmann’ssyndrome shares homology with neural cell adhesion andaxonal path-finding molecules. Nature. 1991;353:529–36.57. Bamshad M, Lin RC, Law DJ, et al. Mutations in humanTBX3 alter limb, apocrine and genital development inulnar-mammary syndrome. Nat Genet. 1997;16:311–5. 58.Barker AR, Thomas R, Dawe HR. Meckel-Gruber syndrome andthe role of primary cilia in kidney, skeleton and centralnervous system development. Organogenesis. 2014;10:96–107.59. Ben zing T, Schermer B. Clinical spectrum andpathogenesis of nephronophthisis. Curr Opin NephrolHypertens. 2012;21:272–8. 60. Sakaki-Yumoto M, KobayashiC, Sato A, et al. The murine homolog of SALL4, a causativegene in Okihiro syndrome, is essential for embryonic stemcell proliferation, and cooperates with Sall1 inanorectal, heart, brain and kidney development.Development. 2006;133:3005–13. 61. Kang S, Graham JM, Jr.,Olney AH, et al. GLI3 frameshift mutations cause autosomaldominant PallisterHall syndrome. Nat Genet. 1997;15:266–8.62. San yanusin P, Schimmenti LA, McNoe LA, et al.Mutation of the PAX2 gene in a family with optic nervecolobomas, renal anomalies and vesicoureteral reflux. NatGenet. 1995;9:358–63. 63. Weber S, Moriniere V, Knuppel T,et al. Prevalence of mutations in renal developmentalgenes in children with renal hypodysplasia: Results of theESCAPE study. J Am Soc Nephrol. 2006;17:2864–70. 64. WeberS, Taylor JC, Winyard P, et al. SIX2 and BMP4 mutationsassociate with anomalous kidney development. J Am SocNephrol. 2008 ;19:891–903. 65. Saisawat P, Tasic V,Vega-Warner V, et al. Identification of two novelCAKUT-causing genes by massively parallel exonresequencing of candidate genes in patients withunilateral renal agenesis. Kidney Int. 2012 ;81:196–200.66. Thomas R, Sanna-Cherchi S, Warady BA, et al. HNF1B andPAX2 mutations are a common cause of renal hypodysplasiain the CKiD cohort. Pediatr Nephrol. 2011;26:897–903. 67.Skinner MA, Safford SD, Reeves JG, et al. Renal aplasia inhumans is associated with RET mutations. Am J Hum Genet.2008 ;82:344–51.
68. Gribouval O, Gonzales M, Neuhaus T, et al. Mutationsin genes in the renin-angiotensin system are associatedwith autosomal recessive renal tubular dysgenesis. Nat
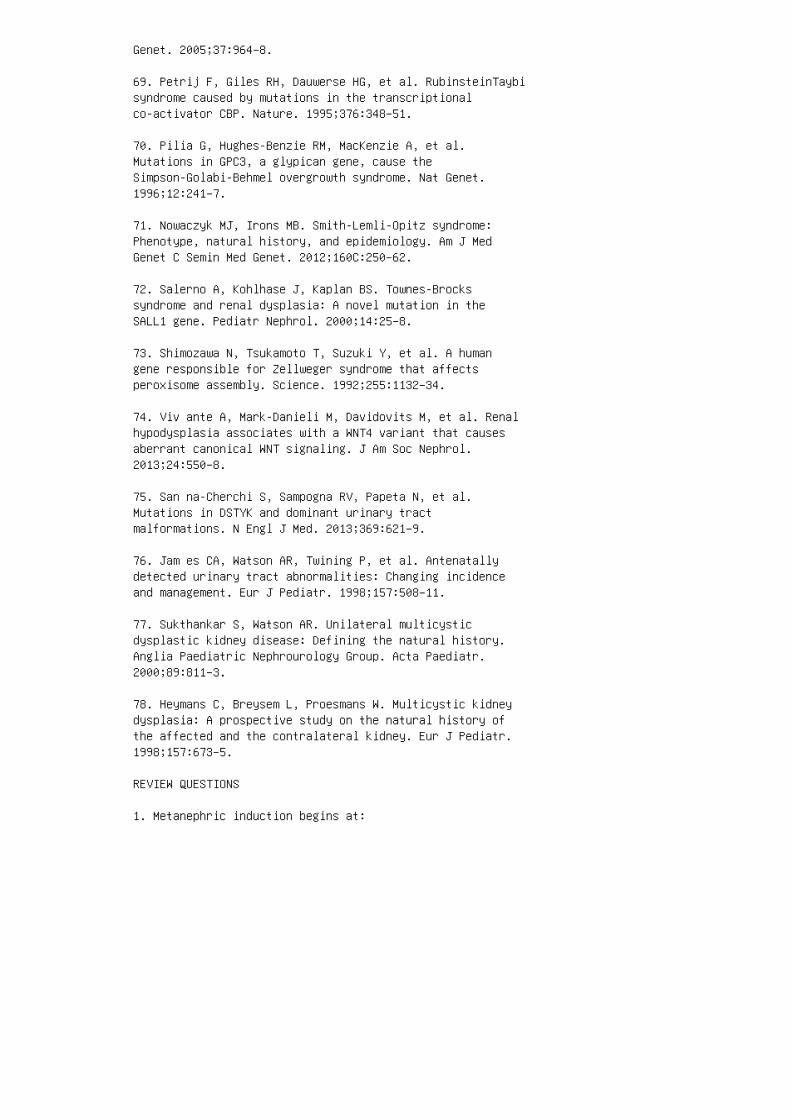
Genet. 2005;37:964–8.
69. Petrij F, Giles RH, Dauwerse HG, et al. RubinsteinTaybisyndrome caused by mutations in the transcriptionalco-activator CBP. Nature. 1995;376:348–51.
70. Pilia G, Hughes-Benzie RM, MacKenzie A, et al.Mutations in GPC3, a glypican gene, cause theSimpson-Golabi-Behmel overgrowth syndrome. Nat Genet.1996;12:241–7.
71. Nowaczyk MJ, Irons MB. Smith-Lemli-Opitz syndrome:Phenotype, natural history, and epidemiology. Am J MedGenet C Semin Med Genet. 2012;160C:250–62.
72. Salerno A, Kohlhase J, Kaplan BS. Townes-Brockssyndrome and renal dysplasia: A novel mutation in theSALL1 gene. Pediatr Nephrol. 2000;14:25–8.
73. Shimozawa N, Tsukamoto T, Suzuki Y, et al. A humangene responsible for Zellweger syndrome that affectsperoxisome assembly. Science. 1992;255:1132–34.
74. Viv ante A, Mark-Danieli M, Davidovits M, et al. Renalhypodysplasia associates with a WNT4 variant that causesaberrant canonical WNT signaling. J Am Soc Nephrol.2013;24:550–8.
75. San na-Cherchi S, Sampogna RV, Papeta N, et al.Mutations in DSTYK and dominant urinary tractmalformations. N Engl J Med. 2013;369:621–9.
76. Jam es CA, Watson AR, Twining P, et al. Antenatallydetected urinary tract abnormalities: Changing incidenceand management. Eur J Pediatr. 1998;157:508–11.
77. Sukthankar S, Watson AR. Unilateral multicysticdysplastic kidney disease: Defining the natural history.Anglia Paediatric Nephrourology Group. Acta Paediatr.2000;89:811–3.
78. Heymans C, Breysem L, Proesmans W. Multicystic kidneydysplasia: A prospective study on the natural history ofthe affected and the contralateral kidney. Eur J Pediatr.1998;157:673–5.
REVIEW QUESTIONS
1. Metanephric induction begins at:

a. Week 7 of gestation
b. Week 10 of gestation
c. Week 5 of gestation
d. Week 20 of gestation
2. Renal dysplasia is characterized by a decreased numberof nephrons, the presence of collecting ducts surroundedby muscular rings, and elements of aberrant development,such as cartilage, or even calci�ed tissue. a. True b.False 3. Branchio-oto-renal (BOR) syndrome results frommutation of: a. PAX2 b. PEX1 c. SOX9 d. EYA1 4. �emost common urinary tract abnormality associated withmulticystic dysplastic kidney (MCDK) is: a. Duplication ofthe collecting system b. Vesicoureteric re�ux c.Posterior urethral valves d. Wilms tumor 5. During renaldevelopment, the WTI gene is important in: a.Glomerulogenesis b. Tubulogenesis c. Formation of therenal pelvis d. Renal ascent 6. BMP4, expressed in themesenchymal cells surrounding the wol�an duct, exerts apositive control in directing the site from which uretericbud would emerge. a. True b. False 7. Patterning of therenal collecting system (renal pelvis and calyces) iscontrolled by: a. Sonic hedgehog (SHH) and BMP gene familyb. Renin, angiotensinogen genes c. JAGGED1 gene d. SIX1and SIX2 genes 8. �e characteristic renal phenotype inAlagille syndrome consists of: a. Renal dysplasia b.Renal aplasia c. Multicystic dysplastic kidney d.Hypoplasia ANSWER KEY 1. c 2. b 3. d 4. b 5. a 6. b7. a 8. a
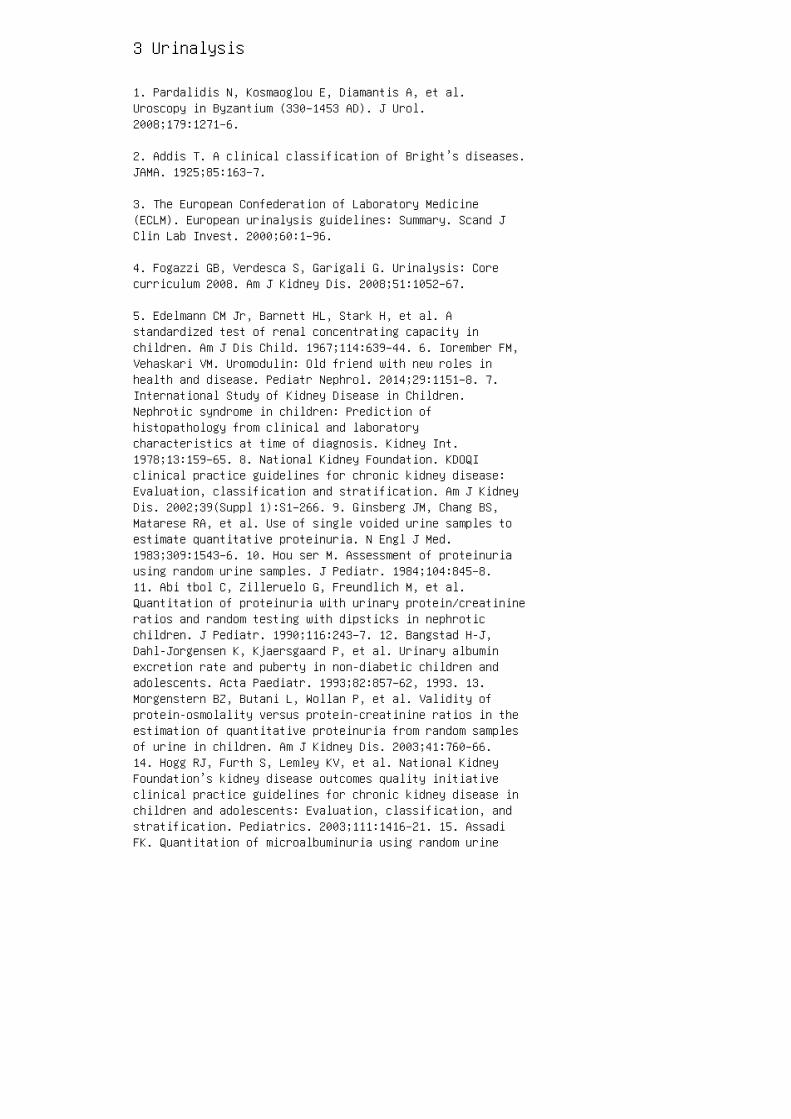
3 Urinalysis
1. Pardalidis N, Kosmaoglou E, Diamantis A, et al.Uroscopy in Byzantium (330–1453 AD). J Urol.2008;179:1271–6.
2. Addis T. A clinical classification of Bright’s diseases.JAMA. 1925;85:163–7.
3. The European Confederation of Laboratory Medicine(ECLM). European urinalysis guidelines: Summary. Scand JClin Lab Invest. 2000;60:1–96.
4. Fogazzi GB, Verdesca S, Garigali G. Urinalysis: Corecurriculum 2008. Am J Kidney Dis. 2008;51:1052–67.
5. Edelmann CM Jr, Barnett HL, Stark H, et al. Astandardized test of renal concentrating capacity inchildren. Am J Dis Child. 1967;114:639–44. 6. Iorember FM,Vehaskari VM. Uromodulin: Old friend with new roles inhealth and disease. Pediatr Nephrol. 2014;29:1151–8. 7.International Study of Kidney Disease in Children.Nephrotic syndrome in children: Prediction ofhistopathology from clinical and laboratorycharacteristics at time of diagnosis. Kidney Int.1978;13:159–65. 8. National Kidney Foundation. KDOQIclinical practice guidelines for chronic kidney disease:Evaluation, classification and stratification. Am J KidneyDis. 2002;39(Suppl 1):S1–266. 9. Ginsberg JM, Chang BS,Matarese RA, et al. Use of single voided urine samples toestimate quantitative proteinuria. N Engl J Med.1983;309:1543–6. 10. Hou ser M. Assessment of proteinuriausing random urine samples. J Pediatr. 1984;104:845–8.11. Abi tbol C, Zilleruelo G, Freundlich M, et al.Quantitation of proteinuria with urinary protein/creatinineratios and random testing with dipsticks in nephroticchildren. J Pediatr. 1990;116:243–7. 12. Bangstad H-J,Dahl-Jorgensen K, Kjaersgaard P, et al. Urinary albuminexcretion rate and puberty in non-diabetic children andadolescents. Acta Paediatr. 1993;82:857–62, 1993. 13.Morgenstern BZ, Butani L, Wollan P, et al. Validity ofprotein-osmolality versus protein-creatinine ratios in theestimation of quantitative proteinuria from random samplesof urine in children. Am J Kidney Dis. 2003;41:760–66.14. Hogg RJ, Furth S, Lemley KV, et al. National KidneyFoundation’s kidney disease outcomes quality initiativeclinical practice guidelines for chronic kidney disease inchildren and adolescents: Evaluation, classification, andstratification. Pediatrics. 2003;111:1416–21. 15. AssadiFK. Quantitation of microalbuminuria using random urine

samples. Pediatr Nephrol. 2002;17:107–10. 16. Santer R,Calado J. Familial renal glucosuria and SGLT2: From amendelian trait to a therapeutic target. Clin J Am SocNephrol. 2010;5:133–41. 17. Nys S, van Merode T, BarteldsAI, et al. Urinary tract infections in general practicepatients: Diagnostic tests versus bacteriological culture.J Antimicrob Chemother. 2006;57:955–8. 18. Williams GJ,Macaskill P, Chan SF, et al. Absolute and relativeaccuracy of rapid urine tests for urinary tract infectionin children: A meta-analysis. Lancet Infect Dis.2010;10:240–50. 19. Rabinovitch A, Sarewitz SJ, WoodcockSM et al. Urinalysis and Collection, Transportation, andPreservation of Urine Specimens. Approved Guideline, 2 ed.Clinical and Laboratory Standards document GP16-A2. Wayne,PA: National Committee for Clinical Laboratory Standards;2001. SUMMARY Urinalysis provides an important insight intorenal physiology and also can provide diagnostic cluesinto many pathologic states. It is o�en the �rstinvestigation in the evaluation of patients with renaldisease. �e technology of urinalysis has been evolvingover the years, especially with the development ofchemical analysis using dipsticks. Screening forproteinuria, hematuria, and UTI in the emergencydepartment and physician o�ces has been particularlyfacilitated by these developments. Microscopic analysis ofthe urine sediment requires knowledge and the experienceof having viewed the sediment in physiologic as well asdisease states. Use of stock images for determining theformed urinary sediment components is evolving but is animperfect technique at this stage.
20. Fairley KF, Birch DF. Hematuria: A simple method foridentifying glomerular bleeding. Kidney Int.1984;21:105–8.
21. Sta pleton FB, Roy SI, Noe HN, et al. Hypercalciuriain children with hematuria. N Engl J Med. 1984;310:1345–8.
22. Andres A, Praga M, Bello I, et al. Hematuria due tohypercalciuria and hyperuricosuria in adult patients.Kidney Int. 1989;36:96–9.
23. Fog azzi GB, Edefonti A, Garigali G, et al. Urineerythrocyte morphology in patients with microscopichaematuria caused by a glomerulopathy. Pediatr Nephrol.2008;23:1093–100.
24. Nolan CR, Kelleher SP. Eosinophiluria. Clin Lab Med.1988;8:555–65.

25. Jen kins RD, Fenn JP, Matsen JM. Review of urinemicroscopy for bacteriuria. JAMA 1986;255:3397–403.
26. Graff L. A Handbook of Routine Urinalysis. St. Louis:JB Lippincott; 1983.
27. Fog azzi GB. Crystalluria: A neglected aspect ofurinary sediment analysis. Nephrol Dial Transplant.1996;11:379–87.
28. Hes s B. Drug-induced urolithiasis. Curr Opin Urol.1998;8:331–4.
29. Sal tel E, Angel JB, Futter NG, et al. Increasedprevalence and analysis of risk factors for indinavirnephrolithiasis. J Urol. 2000;164:1895–7.
30. Cho pra N, Fine PL, Price B, Atlas I. Bilateralhydronephrosis from ciprofloxacin induced crystalluria andstone formation. J Urol. 2000;164:438.
31. Lyon A W, Mansoor A, Trotter MJ. Urinary gems:Acyclovir crystalluria. Arch Pathol Lab Med.2002;126:753–4.
32. Fogazzi GB, Cantù M, Saglimbeni L, et al. Amoxicillin:A rare but possible cause of crystalluria. Nephrol DialTransplant. 2003;18:212–4.
33. Nasr SH, Milliner DS, Wooldridge TD, et al.Triamterene crystalline nephropathy. Am J Kidney Dis.2014;63:148–52.
34. Hufnagle KG, Khan SN, Penn D, et al. Renalcalcifications: A complication of long-term furosemidetherapy in preterm infants. Pediatrics. 1982;70:360–3.
REVIEW QUESTIONS
1. Urine was collected on your 3-year-old febrile patientat home and was stored at room temperature for 18 hours.Urinalysis showed speci�c gravity 1.015, pH 6.5, proteinnegative, blood negative, nitrite positive, and leukocyteesterase negative. Your recommendation is: a. Pat ient hasa UTI, obtain a urine culture and start on antibiotics.b. Patient does not have a UTI, but a culture should beobtained. c. Patient does not have a UTI, and nothing moreneeds to be done. d. Pat ient does not have a UTI, and aurine culture does need to be obtained. Obtain aurinalysis in freshly obtained urine in the clinic. 2.

You need to evaluate urinary sediment in a patient withsuspected glomerulonephritis who has had visible hematuriafor 1 week but is improving, with only faintly pink urine.You are unable to evaluate the urinary sediment for thenext 4 hours. Your laboratory technician labeled the urinesample and froze it at –20° C, with the hope of preservingthe casts and cellular elements for you to evaluate later.When you evaluated the urine sediment later in the daya�er thawing it, you found unclear cell types and noclearly identi�able casts were present. Choose the bestinterpretation of these �ndings. a. Patient does not haveglomerulonephritis. b. Patient’s cellular elements andcasts were likely disrupted by freezing. c. Patient hasglomerulonephritis, but there is no evidence of it in theurinary sediment. d. Patient’s urine sample may have beenlabeled incorrectly. 3. A 3+ positive test for heme ondipstick is diagnostic for the presence of: a. Blood inurine b. Myoglobin in urine c. Hemoglobinuria secondaryto intravascular hemolysis d. All of the above 4. Ameta-analysis of pediatric studies has indicated thaturine nitrite test for UTI: a. Correlates best with arandomly obtained urine. b. Has low speci�city and highsensitivity. c. Has high speci�city and low sensitivity.d. Correlates poorly with UTI. 5. Drug-inducedcrystalluria can result in: a. Acute kidney injury b.Renal stone formation c. Nephrocalcinosis d. All of above6. Which of the following correlates highly with signi�cantbacteria in the urine of a patient with UTI? a. 1bacterium/HPF seen in uncentrifuged urine under 40×magni�cation b. 1 bacterium/oil immersion �eld seen incentrifuged urine stained with Gram stain c. 1bacterium/HPF seen in centrifuged urine stained with Gramstain d. 1 bacterium/oil immersion �eld seen incentrifuged urine stained with Sedi-Stain
7. Urine obtained for urinalysis needs to be collected in aclean container that does not have to be sterile. a. Trueb. False
8. A 10-year-old male patient in septic shock is noted tohave a serum creatinine level of 2.0 mg/dL. Although thepatient has good urine output, the intensive fellow wants anephrology consult. Urinalysis shows speci�c gravity1.010, pH 6.5, blood 3+, protein 2+. Microscopic analysisshows TNTC RBCs, a few granular casts, an occasional muddybrown cast, and many renal tubular epithelial cells. Yourinterpretation of the patient’s urinalysis, given theclinical picture is: a. Patient has prerenal azotemia. b.Patient has acute kidney injury. c. Patient hasglomerulonephritis. d. Patient has acute interstitial
nephritis.
9. Dipstick detection for detection of proteinuria is: a.Speci�c for tubular proteinuria b. Nonspeci�c and detectsall types of urinary proteins c. Able to detectmicroalbuminuria d. Speci�c for albuminuria 10. UTIcaused by Proteus, Pseudomonas, Klebsiella,Staphylococcus, and Mycoplasma that produce theurea-splitting enzyme urease can result in crystalluriaand renal stones. a. True b. False ANSWER KEY 1. d 2. b3. d 4. c 5. d 6. b 7. a 8. b 9. b 10. a
4 Clinical assessment of renal function
1. Kanwar YS, Venkatachalam MA. Ultrastructure ofglomerulus and juxtaglomerular apparatus. In: WindhagerEE, editor. Handbook of Physiology, Section 8: Physiology.New York: Oxford University Press; 1992. p. 3–40.
2. Kanwar YS. Biophysiology of glomerular filtration andproteinuria. Lab Invest. 1984;51:7–21.
3. Rose BD, Post TW. Renal circulation and glomerularfiltration rate. In: Wonsiewicz M, McCullough K, Davis K,editors. Clinical Physiology of Acid-Base and ElectrolyteDisorders. New York: McGraw-Hill; 2001. p. 21–70.
4. Brenner BM, Humes HD. Mechanics of glomerularultrafiltration. N Engl J Med. 1977;297:148–54.
5. Deen WM, Lazzara MJ, Myers BB. Structural determinantsof glomerular permeability. Am J Physiol Renal Physiol.2001;281:F579–96.
6. Brenner BM, Hostetter TH, Humes HD. Molecular basis ofproteinuria of glomerular origin. N Engl J Med.1978;298:826–33.
7. Latta H. An approach to the structure and function ofthe glomerular mesangium. J Am Soc Nephrol. 1992;2:S65–73.
8. Abrahamson DR. Structure and development of theglomerular capillary wall and basement membrane. Am JPhysiol Renal Physiol. 1987;253:F783–94. 9. Schwartz GJ.Does kL/P Cr estimate GFR, or does GFR determine k?Pediatr Nephrol. 1992;6:512–5. 10. Ara nt BS, Jr.,Edelmann CM, Jr., Spitzer A. The congruence of creatinineand inulin clearances in children: Use of the TechniconAutoAnalyzer. J Pediatr. 1972;81:559–61. 11. Dalton RN,Haycock GB. Laboratory investigation. In: Barratt TM,Avner ED, Harmon WE, editors. Pediatric Nephrology, 4thed. Baltimore: Lippincott Williams & Wilkins; 1999. p.343–64. 12. US Re nal Data System, USRDS 2002 Annual DataReport: Atlas of End-Stage Renal Disease in the UnitedStates. Bethesda, MD: National Institutes of Health,National Institute of Diabetes and Digestive and KidneyDiseases; 2002. 13. Col e BR, Giangiacomo J, IngelfingerJR, Robson AM. Measurement of renal function without urinecollection. N Engl J Med. 1972;287:1109–14. 14. SchwartzGJ, Feld LG, Langford DJ. A simple estimate of glomerularfiltration rate in full-term infants during the first yearof life. J Pediatr. 1984;104:849–54. 15. Sch wartz GJ,
Gauthier B. A simple estimate of glomerular filtration ratein adolescent boys. J Pediatr. 1985;106:522–6. 16. Talbot NB. Measurement of obesity by the creatininecoefficient. Am J Dis Child. 2005;55:42–50. 17. GreenblattDJ, Ransil BJ, Harmatz JS, et al. Variability of 24-hoururinary creatinine excretion by normal subjects. J ClinPharmacol. 1976;16:321–8. 18. Ric hardson JA, Philbin PE.The one-hour creatinine clearance rate in healthy men.JAMA. 1971;216:987–90. 19. Hellerstein S, Berenbom M,Alon US, Warady BA. Creatinine clearance followingcimetidine for estimation of glomerular filtration rate.Pediatr Nephrol. 1998;12:49–54. 20. Doolan PD, Alpen EL,Theil GB. A clinical appraisal of the plasma concentrationand endogenous clearance of creatinine. Am J Med.1962;32:65–79. 21. Schwartz GJ, Brion LP, Spitzer A. Theuse of plasma creatinine concentration for estimatingglomerular filtration rate in infants, children, andadolescents. Pediatr Clin North Am. 1987;34:571–90. 22.Schwartz GJ, Haycock GB, Chir B, Spitzer A. Plasmacreatinine and urea concentration in children: Normalvalues for age and sex. J Pediatr. 1976;88:828–30. 23. vanAcker BAC, Koomen GCM, Koopman MG, et al. Creatinineclearance during cimetidine administration for measurementof glomerular filtration rate. Lancet. 1992;340:1326–9.24. Sch utte JE, Longhurst JC, Gaffney FA, et al. Totalplasma creatinine: an accurate measure of total striatedmuscle mass. J Appl Physiol. 1981;51:762–6. 25. Jon es JD,Burnett PC. Implication of creatinine and gut flora in theuremic syndrome: induction of “creatininase” in coloncontents of the rat by dietary creatinine. Clin Chem.1972;18:280–4. SUMMARY Clinical care of children with acuteand chronic kidney diseases requires an assessment of renalfunction from both diagnostic and follow-up perspectives.GFR is long established as the best indicator of overallhuman renal function. Estimation of GFR by clearancemethodology, using exogenously administered and endogenousmarkers, has been the mainstay of evaluations over thepast several decades. An estimation of GFR from endogenousbiomarkers by various mathematical equations has beenattempted since the 1980s, and many of these methods areavailable for clinical use. Because of a lack of steadystate for Cr as well as Cys-C in AKI, application of theGFR equations cannot be advocated. Indeed, to predict earlyrenal injury in AKI, especially when surgical interventionsare necessary or nephrotoxic treatments are planned,several novel markers of renal function are beingevaluated. So far, no gold standard markers have beenestablished, and it is likely that a panel of such markersmay be clinically relevant. For the near future, to obtainan accurate appraisal of renal function, GFR may require
direct measurement by plasma or renal clearancetechniques.
26. Schwartz GJ, Haycock GB, Edelmann CM, Jr., Spitzer A.A simple estimate of glomerular filtration rate inchildren derived from body length and plasma creatinine.Pediatrics. 1976;58:259–63.
27. Drion I, Cobbaert C, Groenier KH, et al. Clinicalevaluation of analytical variations in serum creatininemeasurements: why laboratories should abandon Jaffetechniques. BMC Nephrol. 2012;13:133.
28. Schwartz GJ, Muñoz A, Schneider MF, et al. Newequations to estimate GFR in children with CKD. J Am SocNephrol. 2009;20:629–37.
29. Schwartz GJ, Kwong T, Erway B, et al. Validation ofcreatinine assays utilizing HPLC and IDMS traceablestandards in sera of children. Pediatr Nephrol.2009;24:113–19.
30. Sta ples A, Leblond R, Watkins S, et al. Validation ofthe revised Schwartz estimating equation in a predominantlynon-CKD population. Pediatr Nephrol. 2010;25:2321–6.
31. Counahan R, Chantler C, Ghazali S, et al. Estimationof glomerular filtration rate from plasma creatinineconcentration in children. Arch Dis Child. 1976;51:875–8.
32. Fon g J, Johnston S, Valentino T, et al. Length/serumcreatinine ratio does not predict measured creatinineclearance in critically ill children. Clin Pharmacol Ther.1995;58:192–7.
33. Coc kcroft DW, Gault MH. Prediction of creatinineclearance from serum creatinine. Nephron. 1976;16:31–41.
34. Pie rrat A, Gravier E, Saunders C, et al. PredictingGFR in children and adults: a comparison of theCockcroft-Gault, Schwartz, and modification of diet inrenal disease formulas. Kidney Int. 2003;64:1425–36.
35. Grubb A. Diagnostic value of analysis of cystatin Cand protein HC in biological fluids. Clin Nephrol.1992;38:S20–7.
36. Kaseda R, Iino N, Hosojima M, et al. Megalin-mediatedendocytosis of cystatin C in proximal tubule cells.Biochem Biophys Res Commun. 2007;357:1130–4.

37. Roa ld AB, Aukland K, Tenstad O. Tubular absorption offiltered cystatin-C in the rat kidney. Exp Physiol.2004;89:701–7.
38. Tkaczyk M, Nowicki M, Lukamowicz J. Increased cystatinC concentration in urine of nephrotic children. PediatrNephrol. 2004;19:1278–80.
39. Nejat M, Hill JV, Pickering JW, et al. Albuminuriaincreases cystatin C excretion: implications for urinarybiomarkers. Nephrol Dial Transplant. 2012;27:(Suppl 3)96–103.
40. Mad ero M, Sarnak MJ, Stevens LA. Serum cystatin C asa marker of glomerular filtration rate. Curr Opin NephrolHypertens. 2006;15:610–6.
41. Fis chbach M, Graff V, Terzic J, et al. Impact of ageon reference values for serum concentration of cystatin Cin children. Pediatr Nephrol. 2002;17:104–6. 42. BökenkampA, Domanetzki M, Zinck R, et al. Reference values forcystatin C serum concentrations in children. PediatrNephrol. 1998;12:125–9. 43. Knight EL, Verhave JC,Spiegelman D, et al. Factors influencing serum cystatin Clevels other than renal function and the impact on renalfunction measurement. Kidney Int. 2004;65:1416–21. 44.Fricker M, Wiesli P, Brändle M, et al. Impact of thyroiddysfunction on serum cystatin C. Kidney Int.2003;63:1944–7. 45. Chew-Harris JS, Florkowski CM, GeorgePM, et al. The relative effects of fat versus muscle masson cystatin C and estimates of renal function in healthyyoung men. Ann Clin Biochem. 2013;50:39–46. 46. Xu H, LuY, Teng D, et al. Assessment of glomerular filtration ratein renal transplant patients using serum cystatin C.Transplant Proc. 2006;38:2006–8. 47. Kos J , Štabuc B,Cimerman N, Brunner N. Serum cystatin C, a new marker ofglomerular filtration rate, is increased during malignantprogression. Clin Chem. 1998;44:2556–7. 48. Stevens LA,Schmid CH, Greene T, et al. Factors other than glomerularfiltration rate affect serum cystatin C levels. KidneyInt. 2009;75:652–60. 49. Witzel SH, Butts K, Filler G.Elevated triglycerides may affect cystatin C recovery.Clin Biochem. 2014;47:676–8. 50. Cim erman N, Brguljan PM,Krasovec M, et al. Serum cystatin C, a potent inhibitor ofcysteine proteinases, is elevated in asthmatic patients.Clin Chim Acta. 2000;300:83–95. 51. Ler tnawapan R, BianA, Rho YH, et al. Cystatin C is associated withinflammation but not atherosclerosis in systemic lupuserythematosus. Lupus. 2012;21:279–87. 52. De mirtaş S,

Akan O, Can M, et al. Cystatin C can be affected bynonrenal factors: a preliminary study on leukemia. ClinBiochem. 2006;39:115–8. 53. Deveci K, Gokakin AK, Senel S,et al. Cystatin C in serum as an early marker of renalinvolvement in familial Mediterranean fever patients. EurRev Med Pharmacol Sci. 2013;17:253–60. 54. Wilson ME,Boumaza I, Lacomis D, Bowser R (2010) Cystatin C: acandidate biomarker for amyotrophic lateral sclerosis.PLoS One. 2010;5:e15133. 55. Finney H, Newman DJ, ThakkarH, et al. Reference ranges for plasma cystatin C andcreatinine measurements in premature infants, neonates, andolder children. Arch Dis Child. 2000;82:71–5. 56. Lee JH,Hahn WH, Ahn J, et al. Serum cystatin C during 30postnatal days is dependent on the postconceptional age inneonates. Pediatr Nephrol. 2013;28:1073–8. 57. Filler G,Lepage N. Cystatin C adaptation in the first month oflife. Pediatr Nephrol. 2013;28:991–4. 58. Groesbeck D,Köttgen A, Parekh R, et al. Age, gender, and race effectson cystatin C levels in US adolescents. Clin J Am SocNephrol. 2008;3:1777–85.
59. Bökenkamp A, Domanetzki M, Zinck R, et al. Cystatinserum concentrations underestimate glomerular filtrationrate in renal transplant recipients. Clin Chem.1999;45:1866–8.
60. Hoek FJ, Kemperman FA, Krediet RT. (2003). A comparisonbetween cystatin C, plasma creatinine and the Cockcroftand Gault formula for the estimation of glomerularfiltration rate. Nephrol Dial Transplant. 2003;18:2024–31.
61. Zap pitelli M, Parvex P, Joseph L, et al. Derivationand validation of cystatin C–based prediction equationsfor GFR in children. Am J Kidney Dis. 2006;48:221–30.
62. Schwartz GJ, Schneider MF, Maier PS, et al. Improvedequations estimating GFR in children with chronic kidneydisease using an immunonephelometric determination ofcystatin C. Kidney Int. 2012;82:445–53.63. Bouvet Y,Bouissou F, Coulais Y, et al. GFR is better estimated byconsidering both serum cystatin C and creatinine levels.Pediatr Nephrol. 2006;21:1299–306.
64. Sap irstein LA, Vidt DG, Mandel MJ, et al. Volumes ofdistribution and clearances of intravenously injectedcreatinine in the dog. Am J Physiol. 1955;181:330–6.
65. Bro chner-Mortensen J. A simple method for thedetermination of glomerular filtration rate. Scand J ClinLab Invest. 1972;30:271–4.
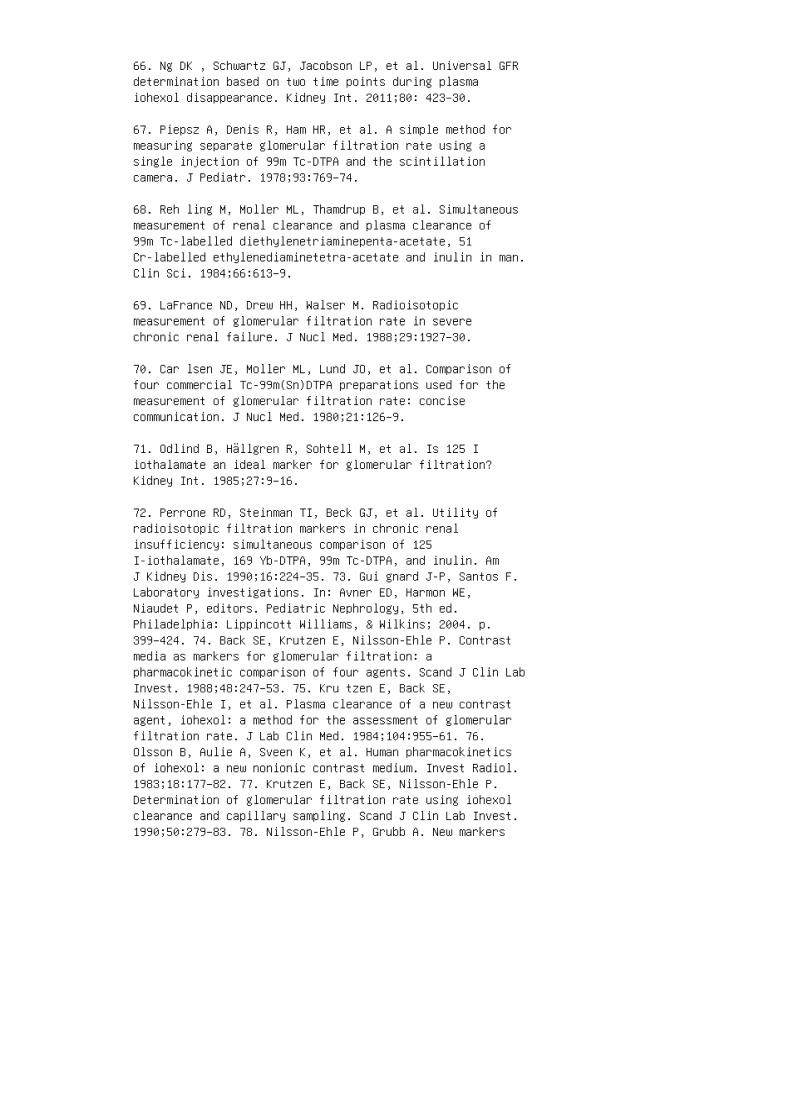
66. Ng DK , Schwartz GJ, Jacobson LP, et al. Universal GFRdetermination based on two time points during plasmaiohexol disappearance. Kidney Int. 2011;80: 423–30.
67. Piepsz A, Denis R, Ham HR, et al. A simple method formeasuring separate glomerular filtration rate using asingle injection of 99m Tc-DTPA and the scintillationcamera. J Pediatr. 1978;93:769–74.
68. Reh ling M, Moller ML, Thamdrup B, et al. Simultaneousmeasurement of renal clearance and plasma clearance of99m Tc-labelled diethylenetriaminepenta-acetate, 51Cr-labelled ethylenediaminetetra-acetate and inulin in man.Clin Sci. 1984;66:613–9.
69. LaFrance ND, Drew HH, Walser M. Radioisotopicmeasurement of glomerular filtration rate in severechronic renal failure. J Nucl Med. 1988;29:1927–30.
70. Car lsen JE, Moller ML, Lund JO, et al. Comparison offour commercial Tc-99m(Sn)DTPA preparations used for themeasurement of glomerular filtration rate: concisecommunication. J Nucl Med. 1980;21:126–9.
71. Odlind B, Hällgren R, Sohtell M, et al. Is 125 Iiothalamate an ideal marker for glomerular filtration?Kidney Int. 1985;27:9–16.
72. Perrone RD, Steinman TI, Beck GJ, et al. Utility ofradioisotopic filtration markers in chronic renalinsufficiency: simultaneous comparison of 125I-iothalamate, 169 Yb-DTPA, 99m Tc-DTPA, and inulin. AmJ Kidney Dis. 1990;16:224–35. 73. Gui gnard J-P, Santos F.Laboratory investigations. In: Avner ED, Harmon WE,Niaudet P, editors. Pediatric Nephrology, 5th ed.Philadelphia: Lippincott Williams, & Wilkins; 2004. p.399–424. 74. Back SE, Krutzen E, Nilsson-Ehle P. Contrastmedia as markers for glomerular filtration: apharmacokinetic comparison of four agents. Scand J Clin LabInvest. 1988;48:247–53. 75. Kru tzen E, Back SE,Nilsson-Ehle I, et al. Plasma clearance of a new contrastagent, iohexol: a method for the assessment of glomerularfiltration rate. J Lab Clin Med. 1984;104:955–61. 76.Olsson B, Aulie A, Sveen K, et al. Human pharmacokineticsof iohexol: a new nonionic contrast medium. Invest Radiol.1983;18:177–82. 77. Krutzen E, Back SE, Nilsson-Ehle P.Determination of glomerular filtration rate using iohexolclearance and capillary sampling. Scand J Clin Lab Invest.1990;50:279–83. 78. Nilsson-Ehle P, Grubb A. New markers
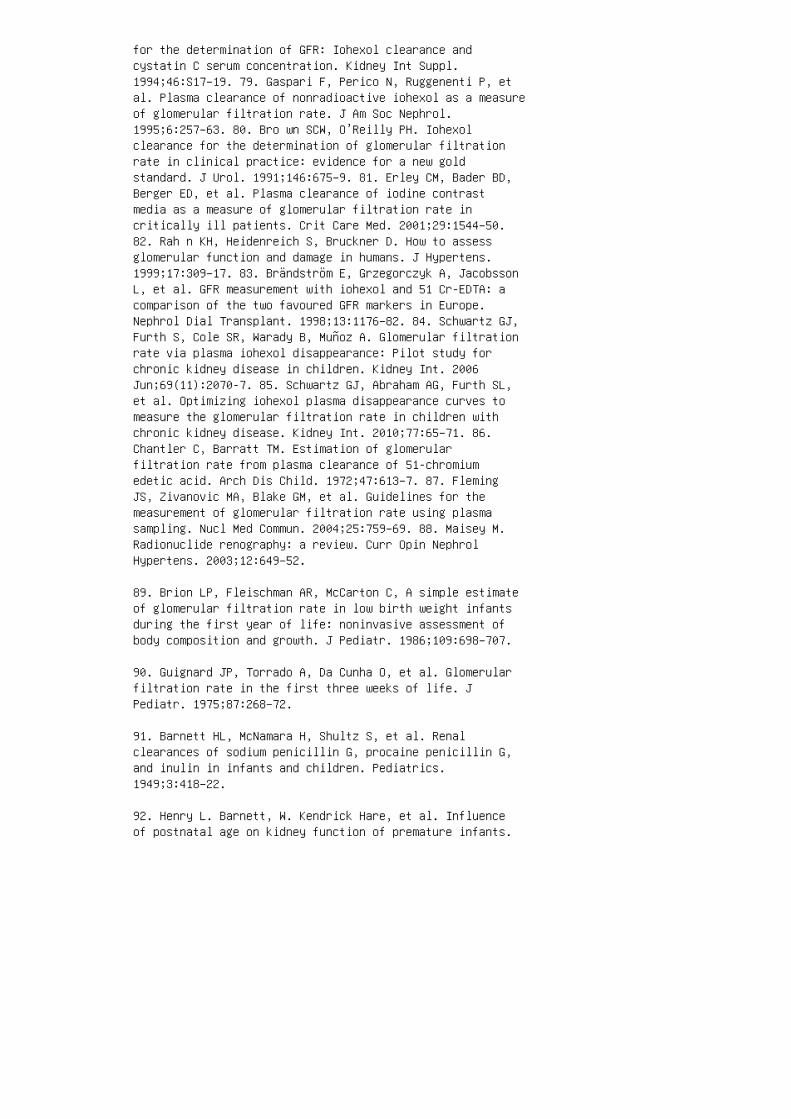
for the determination of GFR: Iohexol clearance andcystatin C serum concentration. Kidney Int Suppl.1994;46:S17–19. 79. Gaspari F, Perico N, Ruggenenti P, etal. Plasma clearance of nonradioactive iohexol as a measureof glomerular filtration rate. J Am Soc Nephrol.1995;6:257–63. 80. Bro wn SCW, O’Reilly PH. Iohexolclearance for the determination of glomerular filtrationrate in clinical practice: evidence for a new goldstandard. J Urol. 1991;146:675–9. 81. Erley CM, Bader BD,Berger ED, et al. Plasma clearance of iodine contrastmedia as a measure of glomerular filtration rate incritically ill patients. Crit Care Med. 2001;29:1544–50.82. Rah n KH, Heidenreich S, Bruckner D. How to assessglomerular function and damage in humans. J Hypertens.1999;17:309–17. 83. Brändström E, Grzegorczyk A, JacobssonL, et al. GFR measurement with iohexol and 51 Cr-EDTA: acomparison of the two favoured GFR markers in Europe.Nephrol Dial Transplant. 1998;13:1176–82. 84. Schwartz GJ,Furth S, Cole SR, Warady B, Muñoz A. Glomerular filtrationrate via plasma iohexol disappearance: Pilot study forchronic kidney disease in children. Kidney Int. 2006Jun;69(11):2070-7. 85. Schwartz GJ, Abraham AG, Furth SL,et al. Optimizing iohexol plasma disappearance curves tomeasure the glomerular filtration rate in children withchronic kidney disease. Kidney Int. 2010;77:65–71. 86.Chantler C, Barratt TM. Estimation of glomerularfiltration rate from plasma clearance of 51-chromiumedetic acid. Arch Dis Child. 1972;47:613–7. 87. FlemingJS, Zivanovic MA, Blake GM, et al. Guidelines for themeasurement of glomerular filtration rate using plasmasampling. Nucl Med Commun. 2004;25:759–69. 88. Maisey M.Radionuclide renography: a review. Curr Opin NephrolHypertens. 2003;12:649–52.
89. Brion LP, Fleischman AR, McCarton C, A simple estimateof glomerular filtration rate in low birth weight infantsduring the first year of life: noninvasive assessment ofbody composition and growth. J Pediatr. 1986;109:698–707.
90. Guignard JP, Torrado A, Da Cunha O, et al. Glomerularfiltration rate in the first three weeks of life. JPediatr. 1975;87:268–72.
91. Barnett HL, McNamara H, Shultz S, et al. Renalclearances of sodium penicillin G, procaine penicillin G,and inulin in infants and children. Pediatrics.1949;3:418–22.
92. Henry L. Barnett, W. Kendrick Hare, et al. Influenceof postnatal age on kidney function of premature infants.

Exp Biol Med (Maywood). 1948;69:55–5.
93. Richmond JB, Kravitz H, Segar W, et al. Renalclearance of endogenous phosphate in infants and children.Exp Biol Med (Maywood). 1951;77:83–7.
94. Broberger U. Determination of glomerular filtrationrate in the newborn: comparison between results obtainedby the single injection technique without collection ofurine and the standard clearance technique. Acta Paediatr.1973;62, 625–8.
95. McCrory WW, Forman CW, McNamara H, et al. Renalexcretion of inorganic phosphate in newborn infants. JClin Invest. 1952;31:357–66.
96. Bro dehl J, Gellissen K, Weber HP. Postnataldevelopment of tubular phosphate reabsorption. ClinNephrol. 1982;17:163–71.
97. Gib b DM, Dalton NR, Barratt MT. Measurement ofglomerular filtration rate in children withinsulin-dependent diabetes mellitus. Clin Chim Acta.1989;82:131–9.
98. Vie ux R, Hascoet JM, Merdariu D, et al. Glomerularfiltration rate reference values in very preterm infants.Pediatrics. 2010;125:e1186–92.
99. Edelmann CM, Jr., Rodriguez-Soriano J, Boichis H, etal. Renal bicarbonate reabsorption and hydrogen ionexcretion in infants. J Clin Invest. 1967;46:1309–17.
100. Oetliker O, Rossi E. The influence of extracellularfluid volume on the renal bicarbonate threshold: a studyof two children with Lowe’s syndrome. Pediatr Res.1969;3:140–8.
101. Sch wartz GJ. Potassium and acid-base. In: Barratt TM,Avner ED, Harmon WE, editors. Pediatric Nephrology, 4thed. Baltimore: Williams & Wilkins; 1999. p. 155–89.
102. Gonzalez SB, Voyer LE, Corti S, et al. Determinationof urinary bicarbonate with the HendersonHasselbalchequation: comparison using two different methods. PediatrNephrol. 2004;19:1371–4.
103. McSherry E. Renal tubular acidosis in childhood.Kidney Int. 1981;20:799–809.
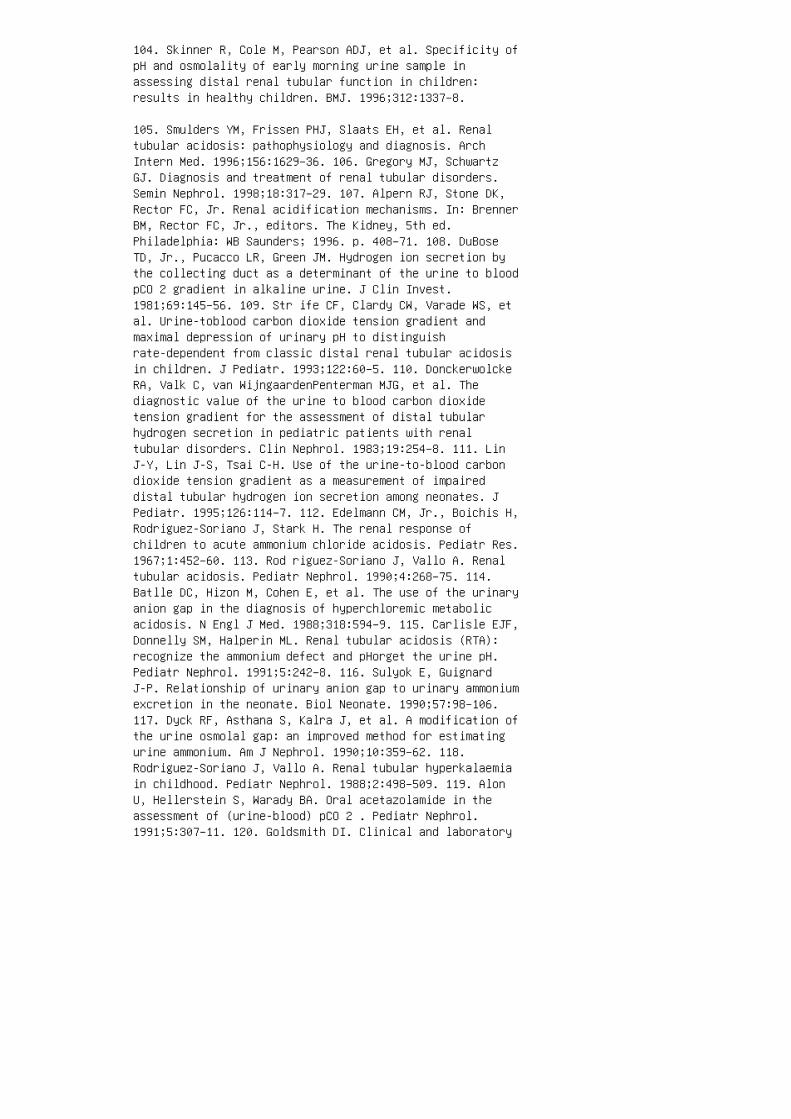
104. Skinner R, Cole M, Pearson ADJ, et al. Specificity ofpH and osmolality of early morning urine sample inassessing distal renal tubular function in children:results in healthy children. BMJ. 1996;312:1337–8.
105. Smulders YM, Frissen PHJ, Slaats EH, et al. Renaltubular acidosis: pathophysiology and diagnosis. ArchIntern Med. 1996;156:1629–36. 106. Gregory MJ, SchwartzGJ. Diagnosis and treatment of renal tubular disorders.Semin Nephrol. 1998;18:317–29. 107. Alpern RJ, Stone DK,Rector FC, Jr. Renal acidification mechanisms. In: BrennerBM, Rector FC, Jr., editors. The Kidney, 5th ed.Philadelphia: WB Saunders; 1996. p. 408–71. 108. DuBoseTD, Jr., Pucacco LR, Green JM. Hydrogen ion secretion bythe collecting duct as a determinant of the urine to bloodpCO 2 gradient in alkaline urine. J Clin Invest.1981;69:145–56. 109. Str ife CF, Clardy CW, Varade WS, etal. Urine-toblood carbon dioxide tension gradient andmaximal depression of urinary pH to distinguishrate-dependent from classic distal renal tubular acidosisin children. J Pediatr. 1993;122:60–5. 110. DonckerwolckeRA, Valk C, van WijngaardenPenterman MJG, et al. Thediagnostic value of the urine to blood carbon dioxidetension gradient for the assessment of distal tubularhydrogen secretion in pediatric patients with renaltubular disorders. Clin Nephrol. 1983;19:254–8. 111. LinJ-Y, Lin J-S, Tsai C-H. Use of the urine-to-blood carbondioxide tension gradient as a measurement of impaireddistal tubular hydrogen ion secretion among neonates. JPediatr. 1995;126:114–7. 112. Edelmann CM, Jr., Boichis H,Rodriguez-Soriano J, Stark H. The renal response ofchildren to acute ammonium chloride acidosis. Pediatr Res.1967;1:452–60. 113. Rod riguez-Soriano J, Vallo A. Renaltubular acidosis. Pediatr Nephrol. 1990;4:268–75. 114.Batlle DC, Hizon M, Cohen E, et al. The use of the urinaryanion gap in the diagnosis of hyperchloremic metabolicacidosis. N Engl J Med. 1988;318:594–9. 115. Carlisle EJF,Donnelly SM, Halperin ML. Renal tubular acidosis (RTA):recognize the ammonium defect and pHorget the urine pH.Pediatr Nephrol. 1991;5:242–8. 116. Sulyok E, GuignardJ-P. Relationship of urinary anion gap to urinary ammoniumexcretion in the neonate. Biol Neonate. 1990;57:98–106.117. Dyck RF, Asthana S, Kalra J, et al. A modification ofthe urine osmolal gap: an improved method for estimatingurine ammonium. Am J Nephrol. 1990;10:359–62. 118.Rodriguez-Soriano J, Vallo A. Renal tubular hyperkalaemiain childhood. Pediatr Nephrol. 1988;2:498–509. 119. AlonU, Hellerstein S, Warady BA. Oral acetazolamide in theassessment of (urine-blood) pCO 2 . Pediatr Nephrol.1991;5:307–11. 120. Goldsmith DI. Clinical and laboratory
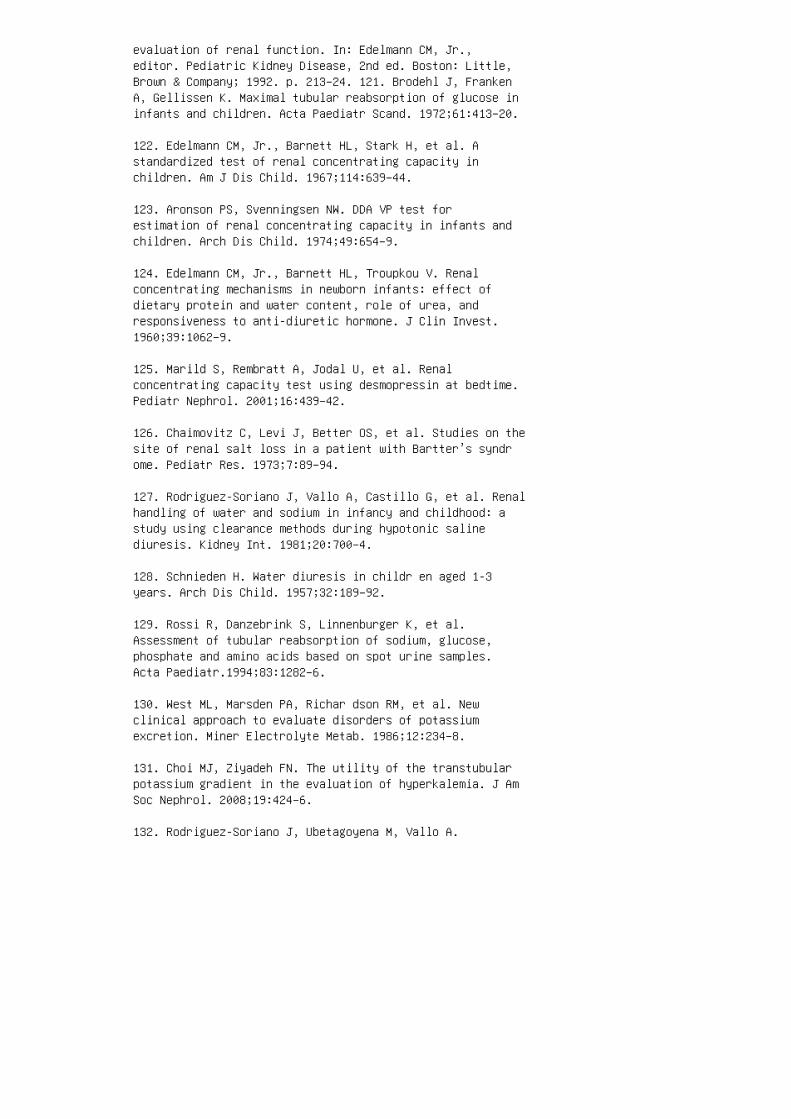
evaluation of renal function. In: Edelmann CM, Jr.,editor. Pediatric Kidney Disease, 2nd ed. Boston: Little,Brown & Company; 1992. p. 213–24. 121. Brodehl J, FrankenA, Gellissen K. Maximal tubular reabsorption of glucose ininfants and children. Acta Paediatr Scand. 1972;61:413–20.
122. Edelmann CM, Jr., Barnett HL, Stark H, et al. Astandardized test of renal concentrating capacity inchildren. Am J Dis Child. 1967;114:639–44.
123. Aronson PS, Svenningsen NW. DDA VP test forestimation of renal concentrating capacity in infants andchildren. Arch Dis Child. 1974;49:654–9.
124. Edelmann CM, Jr., Barnett HL, Troupkou V. Renalconcentrating mechanisms in newborn infants: effect ofdietary protein and water content, role of urea, andresponsiveness to anti-diuretic hormone. J Clin Invest.1960;39:1062–9.
125. Marild S, Rembratt A, Jodal U, et al. Renalconcentrating capacity test using desmopressin at bedtime.Pediatr Nephrol. 2001;16:439–42.
126. Chaimovitz C, Levi J, Better OS, et al. Studies on thesite of renal salt loss in a patient with Bartter’s syndrome. Pediatr Res. 1973;7:89–94.
127. Rodriguez-Soriano J, Vallo A, Castillo G, et al. Renalhandling of water and sodium in infancy and childhood: astudy using clearance methods during hypotonic salinediuresis. Kidney Int. 1981;20:700–4.
128. Schnieden H. Water diuresis in childr en aged 1-3years. Arch Dis Child. 1957;32:189–92.
129. Rossi R, Danzebrink S, Linnenburger K, et al.Assessment of tubular reabsorption of sodium, glucose,phosphate and amino acids based on spot urine samples.Acta Paediatr.1994;83:1282–6.
130. West ML, Marsden PA, Richar dson RM, et al. Newclinical approach to evaluate disorders of potassiumexcretion. Miner Electrolyte Metab. 1986;12:234–8.
131. Choi MJ, Ziyadeh FN. The utility of the transtubularpotassium gradient in the evaluation of hyperkalemia. J AmSoc Nephrol. 2008;19:424–6.
132. Rodriguez-Soriano J, Ubetagoyena M, Vallo A.
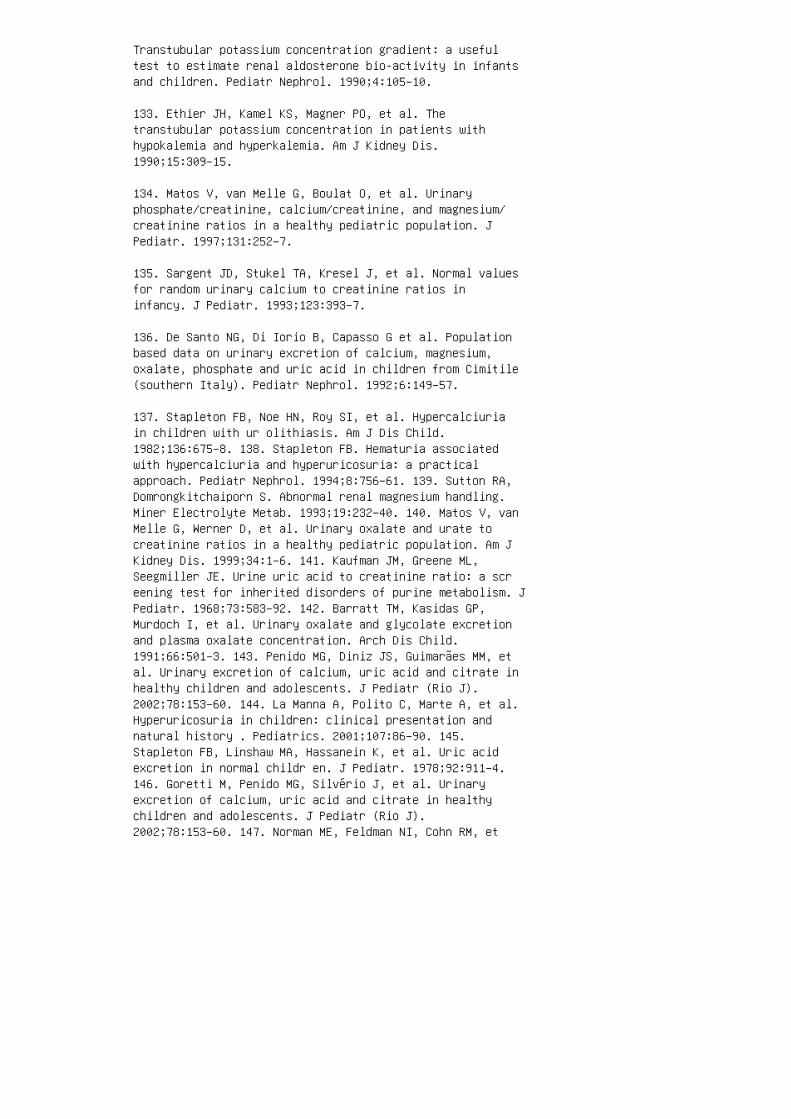
Transtubular potassium concentration gradient: a usefultest to estimate renal aldosterone bio-activity in infantsand children. Pediatr Nephrol. 1990;4:105–10.
133. Ethier JH, Kamel KS, Magner PO, et al. Thetranstubular potassium concentration in patients withhypokalemia and hyperkalemia. Am J Kidney Dis.1990;15:309–15.
134. Matos V, van Melle G, Boulat O, et al. Urinaryphosphate/creatinine, calcium/creatinine, and magnesium/creatinine ratios in a healthy pediatric population. JPediatr. 1997;131:252–7.
135. Sargent JD, Stukel TA, Kresel J, et al. Normal valuesfor random urinary calcium to creatinine ratios ininfancy. J Pediatr. 1993;123:393–7.
136. De Santo NG, Di Iorio B, Capasso G et al. Populationbased data on urinary excretion of calcium, magnesium,oxalate, phosphate and uric acid in children from Cimitile(southern Italy). Pediatr Nephrol. 1992;6:149–57.
137. Stapleton FB, Noe HN, Roy SI, et al. Hypercalciuriain children with ur olithiasis. Am J Dis Child.1982;136:675–8. 138. Stapleton FB. Hematuria associatedwith hypercalciuria and hyperuricosuria: a practicalapproach. Pediatr Nephrol. 1994;8:756–61. 139. Sutton RA,Domrongkitchaiporn S. Abnormal renal magnesium handling.Miner Electrolyte Metab. 1993;19:232–40. 140. Matos V, vanMelle G, Werner D, et al. Urinary oxalate and urate tocreatinine ratios in a healthy pediatric population. Am JKidney Dis. 1999;34:1–6. 141. Kaufman JM, Greene ML,Seegmiller JE. Urine uric acid to creatinine ratio: a screening test for inherited disorders of purine metabolism. JPediatr. 1968;73:583–92. 142. Barratt TM, Kasidas GP,Murdoch I, et al. Urinary oxalate and glycolate excretionand plasma oxalate concentration. Arch Dis Child.1991;66:501–3. 143. Penido MG, Diniz JS, Guimarães MM, etal. Urinary excretion of calcium, uric acid and citrate inhealthy children and adolescents. J Pediatr (Rio J).2002;78:153–60. 144. La Manna A, Polito C, Marte A, et al.Hyperuricosuria in children: clinical presentation andnatural history . Pediatrics. 2001;107:86–90. 145.Stapleton FB, Linshaw MA, Hassanein K, et al. Uric acidexcretion in normal childr en. J Pediatr. 1978;92:911–4.146. Goretti M, Penido MG, Silvério J, et al. Urinaryexcretion of calcium, uric acid and citrate in healthychildren and adolescents. J Pediatr (Rio J).2002;78:153–60. 147. Norman ME, Feldman NI, Cohn RM, et
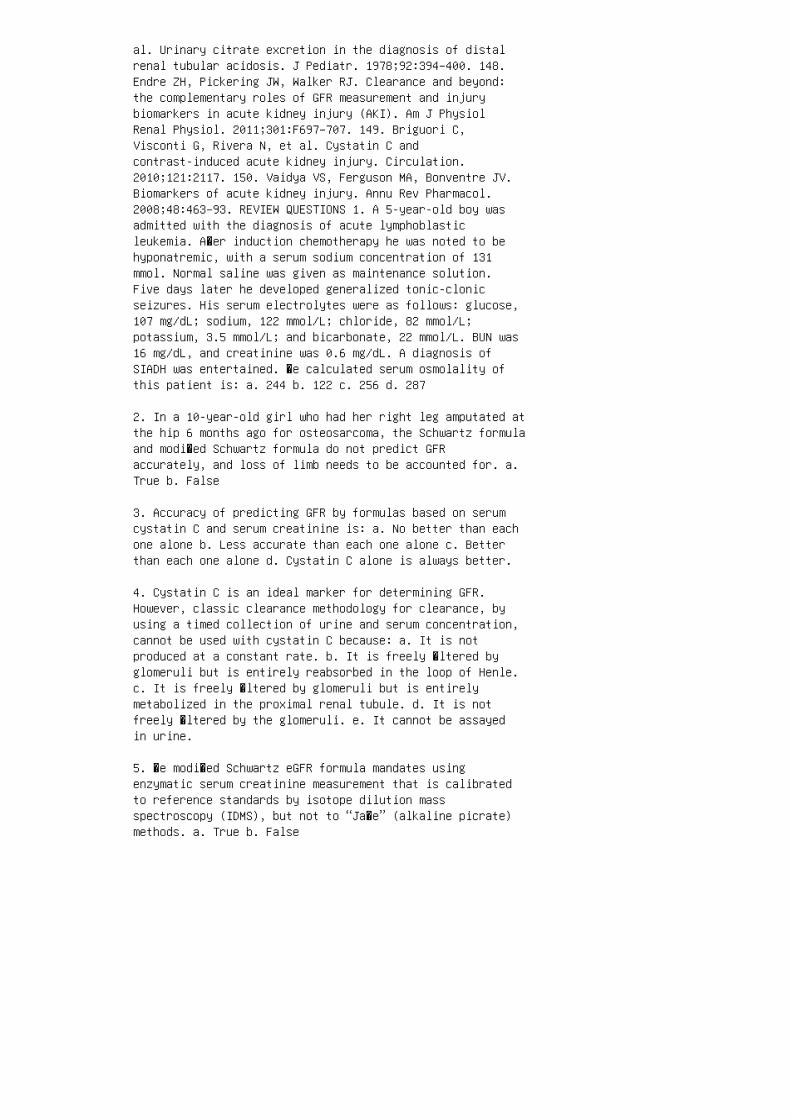
al. Urinary citrate excretion in the diagnosis of distalrenal tubular acidosis. J Pediatr. 1978;92:394–400. 148.Endre ZH, Pickering JW, Walker RJ. Clearance and beyond:the complementary roles of GFR measurement and injurybiomarkers in acute kidney injury (AKI). Am J PhysiolRenal Physiol. 2011;301:F697–707. 149. Briguori C,Visconti G, Rivera N, et al. Cystatin C andcontrast-induced acute kidney injury. Circulation.2010;121:2117. 150. Vaidya VS, Ferguson MA, Bonventre JV.Biomarkers of acute kidney injury. Annu Rev Pharmacol.2008;48:463–93. REVIEW QUESTIONS 1. A 5-year-old boy wasadmitted with the diagnosis of acute lymphoblasticleukemia. A�er induction chemotherapy he was noted to behyponatremic, with a serum sodium concentration of 131mmol. Normal saline was given as maintenance solution.Five days later he developed generalized tonic-clonicseizures. His serum electrolytes were as follows: glucose,107 mg/dL; sodium, 122 mmol/L; chloride, 82 mmol/L;potassium, 3.5 mmol/L; and bicarbonate, 22 mmol/L. BUN was16 mg/dL, and creatinine was 0.6 mg/dL. A diagnosis ofSIADH was entertained. �e calculated serum osmolality ofthis patient is: a. 244 b. 122 c. 256 d. 287
2. In a 10-year-old girl who had her right leg amputated atthe hip 6 months ago for osteosarcoma, the Schwartz formulaand modi�ed Schwartz formula do not predict GFRaccurately, and loss of limb needs to be accounted for. a.True b. False
3. Accuracy of predicting GFR by formulas based on serumcystatin C and serum creatinine is: a. No better than eachone alone b. Less accurate than each one alone c. Betterthan each one alone d. Cystatin C alone is always better.
4. Cystatin C is an ideal marker for determining GFR.However, classic clearance methodology for clearance, byusing a timed collection of urine and serum concentration,cannot be used with cystatin C because: a. It is notproduced at a constant rate. b. It is freely �ltered byglomeruli but is entirely reabsorbed in the loop of Henle.c. It is freely �ltered by glomeruli but is entirelymetabolized in the proximal renal tubule. d. It is notfreely �ltered by the glomeruli. e. It cannot be assayedin urine.
5. �e modi�ed Schwartz eGFR formula mandates usingenzymatic serum creatinine measurement that is calibratedto reference standards by isotope dilution massspectroscopy (IDMS), but not to “Ja�e” (alkaline picrate)methods. a. True b. False

6. Urea splitting organisms, such as Proteus, Pseudomonas,Klebsiella, Staphylococcus, and Mycoplasma hydrolyze ureato ammonium and lead to the following changes: a.Decreased urine pH b. No change in urine pH c. Raisedurine and blood pH d. Raised urine pH only
7. Evaluate this statement: “When C H2O is a positivenumber, it indicates increased free water clearance and adiuretic state.” a. True b. False
8. Novel biomarkers of renal function are useful for: a.Early detection of AKI b. Indicating the onset of AKI a�ercardiovascular surgery or contrast use c. Providinginformation on the potential site of tubular injury in AKId. All of the above
9. A 2½ year old white boy presented with a large rightabdominal mass of 2 weeks’ duration. He also had decreasedappetite. Laboratory studies on presentation were asfollows (in mmol/L): serum sodium, 130; potassium, 3.9;chloride, 92; and bicarbonate, 21. BUN and creatinine were10 mg/dL and 0.4 mg/dL, respectively. �e patient weighed13.7 kg and was 92.5 cm tall. He underwent an open biopsyof the abdominal mass that documented the diagnosis ofrhabdoid tumor of the right kidney. Regional lymph nodesand lungs had metastases. Right nephrectomy was followedby chemotherapy. He also underwent right �ank and wholelung radiation. DTPA nuclear GFR was 48 mL/min/1.73 m 2at 6 months. Serum creatinine was 0.6 mg/dL at 6 months,and the serum cystatin C level was 1.03 mg/L. His heightand weight at 6 months postoperatively (2.5 years of age)were 13.6 kg and 95.7 cm, respectively. Calculated GFR byvarious formulas at 6 months was as follows: 104.5mL/min/1.73 m 2 (original Schwartz), 65 mL/min/1.73 m 2(IDMS-traceable Schwartz GFR formula), and 65.8mL/min/1.73 m 2 (CKiD). �e patient’s estimated GFR isbest re�ected by all, except: a. CKiD formula b. Schwartzoriginal eGFR c. DTPA nuclear GFR d. IDMS-traceablecreatinine based Schwartz GFR 10. In the case given inquestion 9, a poor correlation of DTPA nuclear GFR andserum creatinine–based eGFR is best explained by: a.Patient’s receiving radiation therapy b. Fluid volumeretention c. Chemotherapy causing renal toxicities d.Loss of muscle mass resulting from poor nutrition 11. A30-kg male patient has a 2-day history of gross hematuriaand le� �ank pain. He is treated with intravenous �uids,analgesics, and a blocker agents in the emergencydepartment. He passes a stone in the urine. A 24-h urinestudy shows the following: volume, 1200 mL; citrate, 400

mg/g creatinine; oxalate, 0.05 mg/mg creatinine; and Ca/ Crratio, 0.45. �e stone passed is most likely to be: a. Uricacid b. Calcium phosphate c. Calcium oxalate d. StruviteANSWER KEY 1. c 2. a 3. c 4. c 5. a 6. d 7. a 8. d9. b 10. d 11. c
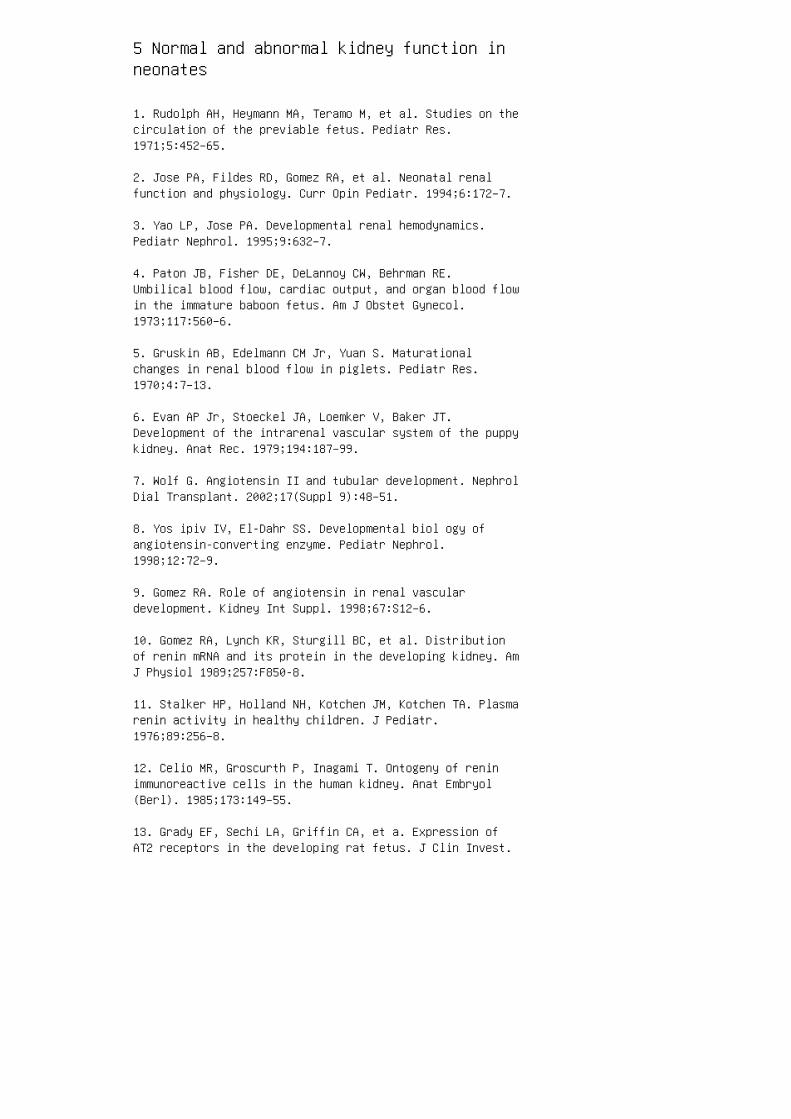
5 Normal and abnormal kidney function inneonates
1. Rudolph AH, Heymann MA, Teramo M, et al. Studies on thecirculation of the previable fetus. Pediatr Res.1971;5:452–65.
2. Jose PA, Fildes RD, Gomez RA, et al. Neonatal renalfunction and physiology. Curr Opin Pediatr. 1994;6:172–7.
3. Yao LP, Jose PA. Developmental renal hemodynamics.Pediatr Nephrol. 1995;9:632–7.
4. Paton JB, Fisher DE, DeLannoy CW, Behrman RE.Umbilical blood flow, cardiac output, and organ blood flowin the immature baboon fetus. Am J Obstet Gynecol.1973;117:560–6.
5. Gruskin AB, Edelmann CM Jr, Yuan S. Maturationalchanges in renal blood flow in piglets. Pediatr Res.1970;4:7–13.
6. Evan AP Jr, Stoeckel JA, Loemker V, Baker JT.Development of the intrarenal vascular system of the puppykidney. Anat Rec. 1979;194:187–99.
7. Wolf G. Angiotensin II and tubular development. NephrolDial Transplant. 2002;17(Suppl 9):48–51.
8. Yos ipiv IV, El-Dahr SS. Developmental biol ogy ofangiotensin-converting enzyme. Pediatr Nephrol.1998;12:72–9.
9. Gomez RA. Role of angiotensin in renal vasculardevelopment. Kidney Int Suppl. 1998;67:S12–6.
10. Gomez RA, Lynch KR, Sturgill BC, et al. Distributionof renin mRNA and its protein in the developing kidney. AmJ Physiol 1989;257:F850-8.
11. Stalker HP, Holland NH, Kotchen JM, Kotchen TA. Plasmarenin activity in healthy children. J Pediatr.1976;89:256–8.
12. Celio MR, Groscurth P, Inagami T. Ontogeny of reninimmunoreactive cells in the human kidney. Anat Embryol(Berl). 1985;173:149–55.
13. Grady EF, Sechi LA, Griffin CA, et a. Expression ofAT2 receptors in the developing rat fetus. J Clin Invest.

1991;88:921–33.
14. Tufro-McReddie A, Harrison JK, Everett AD, Gomez RA.Ontogeny of type 1 angiotensin II receptor gene expressionin the rat. J Clin Invest. 1993;91:530–7.
15. Gleason CA. Prostaglandins and the develop ing kidney.Semin Perinatol 1987;11:12–21. 16. Ext on JH. Calciumsignalling in cells: Molecular mechanisms. Kidney IntSuppl. 1987;23:S68–81. 17. Solhaug MJ, Wallace MR, GrangerJP. Nitric oxide and angiotensin II regulation of renalhemody namics in the developing piglet. Pediatr Res. 1996;39:527–33. 18. Sol haug MJ, Ballevre LD, Guignard JP, etal. Nitric oxide in the developing kidney. PediatrNephrol. 1996;10:529–39. 19. Siragy HM, Jaffa AA,Margolius HS. Bradykinin B2 receptor modulates renalprostaglandin E2 and nitric oxide. Hypertension.1997;29:757–62. 20. El-Dahr SS, Dipp S, Meleg-Smith S, etal. Fetal ontogeny and role of metanephric bradykinin B2receptors. Pediatr Nephrol. 2000;14:288–96. 21. SchanstraJP, Duchene J, Praddaude F, et al. Decreased renal NOexcretion and reduced glomerular tuft area in mice lackingthe bradyki nin B2 receptor. Am J Physiol Heart CircPhysiol. 20 03 ;284:H1904–8. 22. Naicker S, Bhoola KD.Endothelins: Vasoactive modulators of renal function inhealth and disease. Pharmacol Ther. 2001;90:61–88. 23.Pre vot A, Mosig D, Rijtema M, Guignard JP. Renal effectsof adenosine A1-receptor blockade with8-cyclopentyl-1,3-dipropylxanthine in hypoxemic newbornrabbits. Pediatr Res. 2003;54:400–5. 24. Gouyon JB,Guignard JP. Theophylline prevents the hypoxemia-inducedrenal hemodynamic changes in rabbits. Kidney Int.1988;33:1078–83. 25. Huet F, Semama D, Grimaldi M, et al.Effects of theophylline on renal insufficiency in neonateswith respiratory distress syndrome. Intensive Care Med.1995;21:511–4. 26. Jenik AG, Ceriani Cernadas JM,Gorenstein A, et al. A randomized, double-blind,placebocontrolled trial of the effects of prophylactictheophylline on renal function in term neonates withperinatal asphyxia. Pediatrics. 2000;105:E45. 27. Bakr AF.Prophylactic theophylline to prevent renal dysfunction innewborns exposed to perinatal asphyxia: A study in adeveloping country. Pediatr Nephrol. 2005;20:1249–52. 28.Bhat MA, Shah ZA, Makhdoomi MS, Mufti MH. Theophylline forrenal function in term neonates with perinatal asphyxia: Arandomized, placebocontrolled trial. J Pediatr.2006;149:180–4. 29. DiB ona GF, Kopp UC. Neural controlof renal function. Physiol Rev. 1997;77:75–197. 30. JohnsEJ, Kopp UC, DiBona GF. Neural control of renal function.Compr Physiol. 2011;1:731–67. 31. Eliot RJ, Lam R, Leake
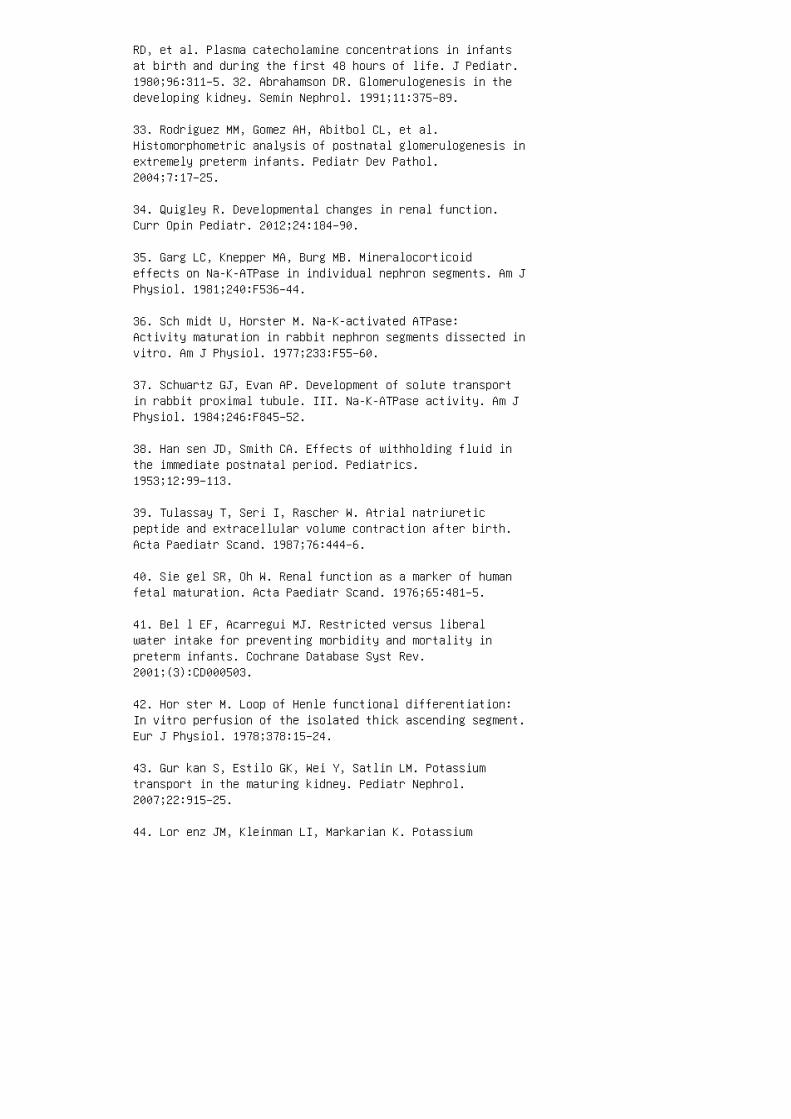
RD, et al. Plasma catecholamine concentrations in infantsat birth and during the first 48 hours of life. J Pediatr.1980;96:311–5. 32. Abrahamson DR. Glomerulogenesis in thedeveloping kidney. Semin Nephrol. 1991;11:375–89.
33. Rodriguez MM, Gomez AH, Abitbol CL, et al.Histomorphometric analysis of postnatal glomerulogenesis inextremely preterm infants. Pediatr Dev Pathol.2004;7:17–25.
34. Quigley R. Developmental changes in renal function.Curr Opin Pediatr. 2012;24:184–90.
35. Garg LC, Knepper MA, Burg MB. Mineralocorticoideffects on Na-K-ATPase in individual nephron segments. Am JPhysiol. 1981;240:F536–44.
36. Sch midt U, Horster M. Na-K-activated ATPase:Activity maturation in rabbit nephron segments dissected invitro. Am J Physiol. 1977;233:F55–60.
37. Schwartz GJ, Evan AP. Development of solute transportin rabbit proximal tubule. III. Na-K-ATPase activity. Am JPhysiol. 1984;246:F845–52.
38. Han sen JD, Smith CA. Effects of withholding fluid inthe immediate postnatal period. Pediatrics.1953;12:99–113.
39. Tulassay T, Seri I, Rascher W. Atrial natriureticpeptide and extracellular volume contraction after birth.Acta Paediatr Scand. 1987;76:444–6.
40. Sie gel SR, Oh W. Renal function as a marker of humanfetal maturation. Acta Paediatr Scand. 1976;65:481–5.
41. Bel l EF, Acarregui MJ. Restricted versus liberalwater intake for preventing morbidity and mortality inpreterm infants. Cochrane Database Syst Rev.2001;(3):CD000503.
42. Hor ster M. Loop of Henle functional differentiation:In vitro perfusion of the isolated thick ascending segment.Eur J Physiol. 1978;378:15–24.
43. Gur kan S, Estilo GK, Wei Y, Satlin LM. Potassiumtransport in the maturing kidney. Pediatr Nephrol.2007;22:915–25.
44. Lor enz JM, Kleinman LI, Markarian K. Potassium
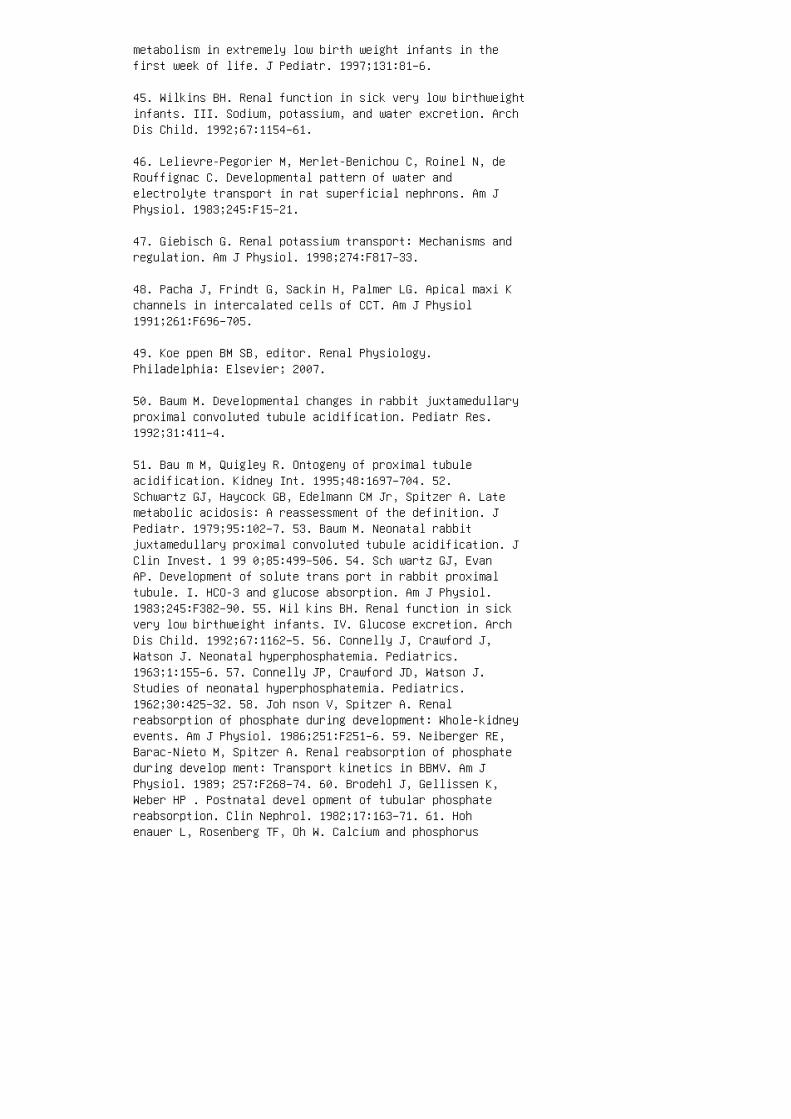
metabolism in extremely low birth weight infants in thefirst week of life. J Pediatr. 1997;131:81–6.
45. Wilkins BH. Renal function in sick very low birthweightinfants. III. Sodium, potassium, and water excretion. ArchDis Child. 1992;67:1154–61.
46. Lelievre-Pegorier M, Merlet-Benichou C, Roinel N, deRouffignac C. Developmental pattern of water andelectrolyte transport in rat superficial nephrons. Am JPhysiol. 1983;245:F15–21.
47. Giebisch G. Renal potassium transport: Mechanisms andregulation. Am J Physiol. 1998;274:F817–33.
48. Pacha J, Frindt G, Sackin H, Palmer LG. Apical maxi Kchannels in intercalated cells of CCT. Am J Physiol1991;261:F696–705.
49. Koe ppen BM SB, editor. Renal Physiology.Philadelphia: Elsevier; 2007.
50. Baum M. Developmental changes in rabbit juxtamedullaryproximal convoluted tubule acidification. Pediatr Res.1992;31:411–4.
51. Bau m M, Quigley R. Ontogeny of proximal tubuleacidification. Kidney Int. 1995;48:1697–704. 52.Schwartz GJ, Haycock GB, Edelmann CM Jr, Spitzer A. Latemetabolic acidosis: A reassessment of the definition. JPediatr. 1979;95:102–7. 53. Baum M. Neonatal rabbitjuxtamedullary proximal convoluted tubule acidification. JClin Invest. 1 99 0;85:499–506. 54. Sch wartz GJ, EvanAP. Development of solute trans port in rabbit proximaltubule. I. HCO-3 and glucose absorption. Am J Physiol.1983;245:F382–90. 55. Wil kins BH. Renal function in sickvery low birthweight infants. IV. Glucose excretion. ArchDis Child. 1992;67:1162–5. 56. Connelly J, Crawford J,Watson J. Neonatal hyperphosphatemia. Pediatrics.1963;1:155–6. 57. Connelly JP, Crawford JD, Watson J.Studies of neonatal hyperphosphatemia. Pediatrics.1962;30:425–32. 58. Joh nson V, Spitzer A. Renalreabsorption of phosphate during development: Whole-kidneyevents. Am J Physiol. 1986;251:F251–6. 59. Neiberger RE,Barac-Nieto M, Spitzer A. Renal reabsorption of phosphateduring develop ment: Transport kinetics in BBMV. Am JPhysiol. 1989; 257:F268–74. 60. Brodehl J, Gellissen K,Weber HP . Postnatal devel opment of tubular phosphatereabsorption. Clin Nephrol. 1982;17:163–71. 61. Hohenauer L, Rosenberg TF, Oh W. Calcium and phosphorus
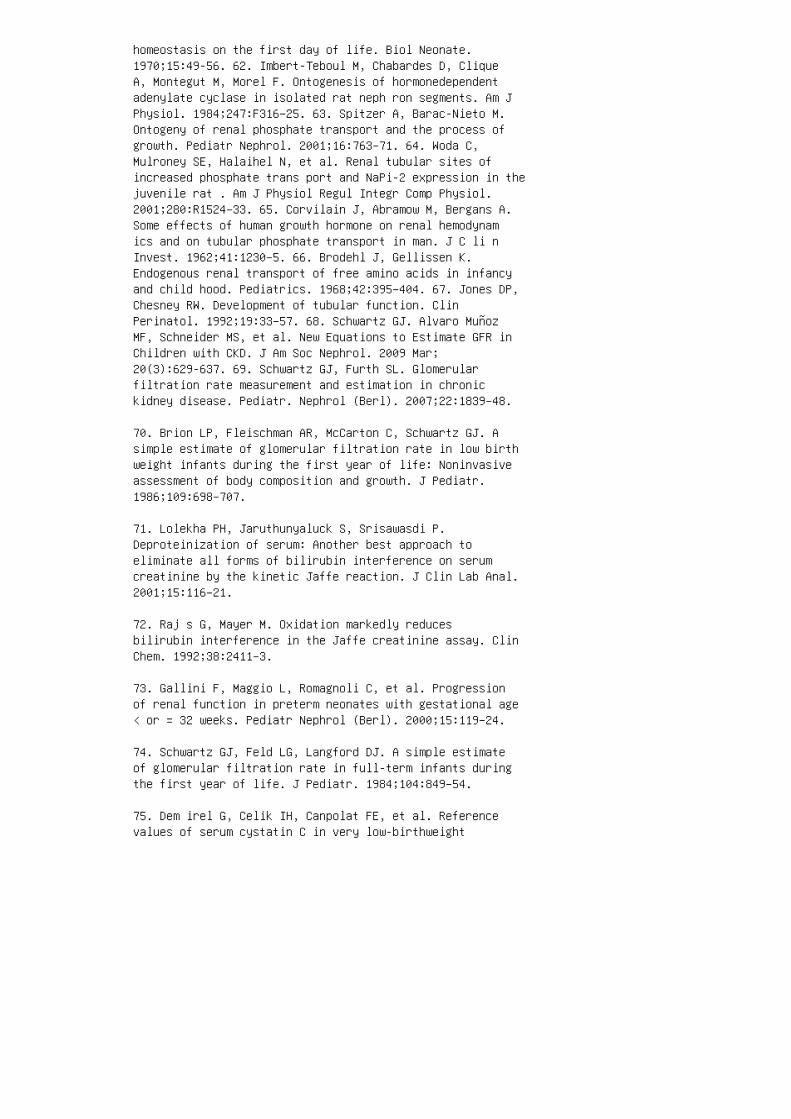
homeostasis on the first day of life. Biol Neonate.1970;15:49-56. 62. Imbert-Teboul M, Chabardes D, CliqueA, Montegut M, Morel F. Ontogenesis of hormonedependentadenylate cyclase in isolated rat neph ron segments. Am JPhysiol. 1984;247:F316–25. 63. Spitzer A, Barac-Nieto M.Ontogeny of renal phosphate transport and the process ofgrowth. Pediatr Nephrol. 2001;16:763–71. 64. Woda C,Mulroney SE, Halaihel N, et al. Renal tubular sites ofincreased phosphate trans port and NaPi-2 expression in thejuvenile rat . Am J Physiol Regul Integr Comp Physiol.2001;280:R1524–33. 65. Corvilain J, Abramow M, Bergans A.Some effects of human growth hormone on renal hemodynamics and on tubular phosphate transport in man. J C li nInvest. 1962;41:1230–5. 66. Brodehl J, Gellissen K.Endogenous renal transport of free amino acids in infancyand child hood. Pediatrics. 1968;42:395–404. 67. Jones DP,Chesney RW. Development of tubular function. ClinPerinatol. 1992;19:33–57. 68. Schwartz GJ. Alvaro MuñozMF, Schneider MS, et al. New Equations to Estimate GFR inChildren with CKD. J Am Soc Nephrol. 2009 Mar;20(3):629-637. 69. Schwartz GJ, Furth SL. Glomerularfiltration rate measurement and estimation in chronickidney disease. Pediatr. Nephrol (Berl). 2007;22:1839–48.
70. Brion LP, Fleischman AR, McCarton C, Schwartz GJ. Asimple estimate of glomerular filtration rate in low birthweight infants during the first year of life: Noninvasiveassessment of body composition and growth. J Pediatr.1986;109:698–707.
71. Lolekha PH, Jaruthunyaluck S, Srisawasdi P.Deproteinization of serum: Another best approach toeliminate all forms of bilirubin interference on serumcreatinine by the kinetic Jaffe reaction. J Clin Lab Anal.2001;15:116–21.
72. Raj s G, Mayer M. Oxidation markedly reducesbilirubin interference in the Jaffe creatinine assay. ClinChem. 1992;38:2411–3.
73. Gallini F, Maggio L, Romagnoli C, et al. Progressionof renal function in preterm neonates with gestational age< or = 32 weeks. Pediatr Nephrol (Berl). 2000;15:119–24.
74. Schwartz GJ, Feld LG, Langford DJ. A simple estimateof glomerular filtration rate in full-term infants duringthe first year of life. J Pediatr. 1984;104:849–54.
75. Dem irel G, Celik IH, Canpolat FE, et al. Referencevalues of serum cystatin C in very low-birthweight
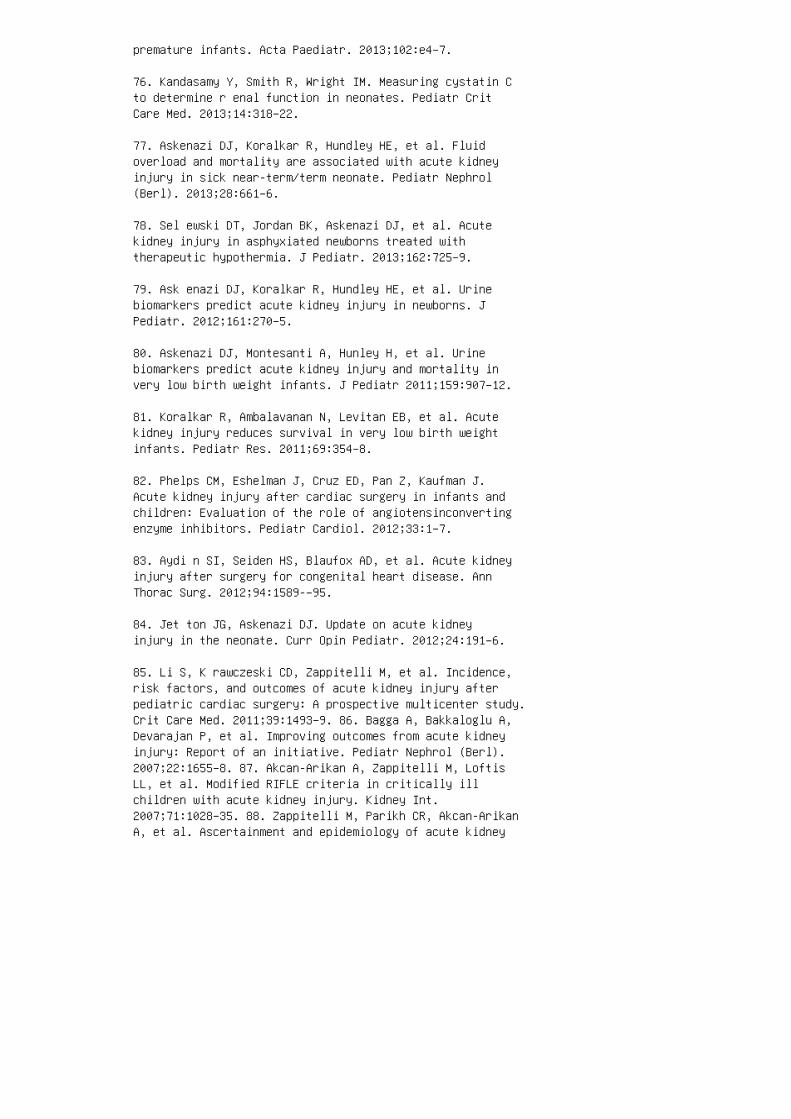
premature infants. Acta Paediatr. 2013;102:e4–7.
76. Kandasamy Y, Smith R, Wright IM. Measuring cystatin Cto determine r enal function in neonates. Pediatr CritCare Med. 2013;14:318–22.
77. Askenazi DJ, Koralkar R, Hundley HE, et al. Fluidoverload and mortality are associated with acute kidneyinjury in sick near-term/term neonate. Pediatr Nephrol(Berl). 2013;28:661–6.
78. Sel ewski DT, Jordan BK, Askenazi DJ, et al. Acutekidney injury in asphyxiated newborns treated withtherapeutic hypothermia. J Pediatr. 2013;162:725–9.
79. Ask enazi DJ, Koralkar R, Hundley HE, et al. Urinebiomarkers predict acute kidney injury in newborns. JPediatr. 2012;161:270–5.
80. Askenazi DJ, Montesanti A, Hunley H, et al. Urinebiomarkers predict acute kidney injury and mortality invery low birth weight infants. J Pediatr 2011;159:907–12.
81. Koralkar R, Ambalavanan N, Levitan EB, et al. Acutekidney injury reduces survival in very low birth weightinfants. Pediatr Res. 2011;69:354–8.
82. Phelps CM, Eshelman J, Cruz ED, Pan Z, Kaufman J.Acute kidney injury after cardiac surgery in infants andchildren: Evaluation of the role of angiotensinconvertingenzyme inhibitors. Pediatr Cardiol. 2012;33:1–7.
83. Aydi n SI, Seiden HS, Blaufox AD, et al. Acute kidneyinjury after surgery for congenital heart disease. AnnThorac Surg. 2012;94:1589-–95.
84. Jet ton JG, Askenazi DJ. Update on acute kidneyinjury in the neonate. Curr Opin Pediatr. 2012;24:191–6.
85. Li S, K rawczeski CD, Zappitelli M, et al. Incidence,risk factors, and outcomes of acute kidney injury afterpediatric cardiac surgery: A prospective multicenter study.Crit Care Med. 2011;39:1493–9. 86. Bagga A, Bakkaloglu A,Devarajan P, et al. Improving outcomes from acute kidneyinjury: Report of an initiative. Pediatr Nephrol (Berl).2007;22:1655–8. 87. Akcan-Arikan A, Zappitelli M, LoftisLL, et al. Modified RIFLE criteria in critically illchildren with acute kidney injury. Kidney Int.2007;71:1028–35. 88. Zappitelli M, Parikh CR, Akcan-ArikanA, et al. Ascertainment and epidemiology of acute kidney
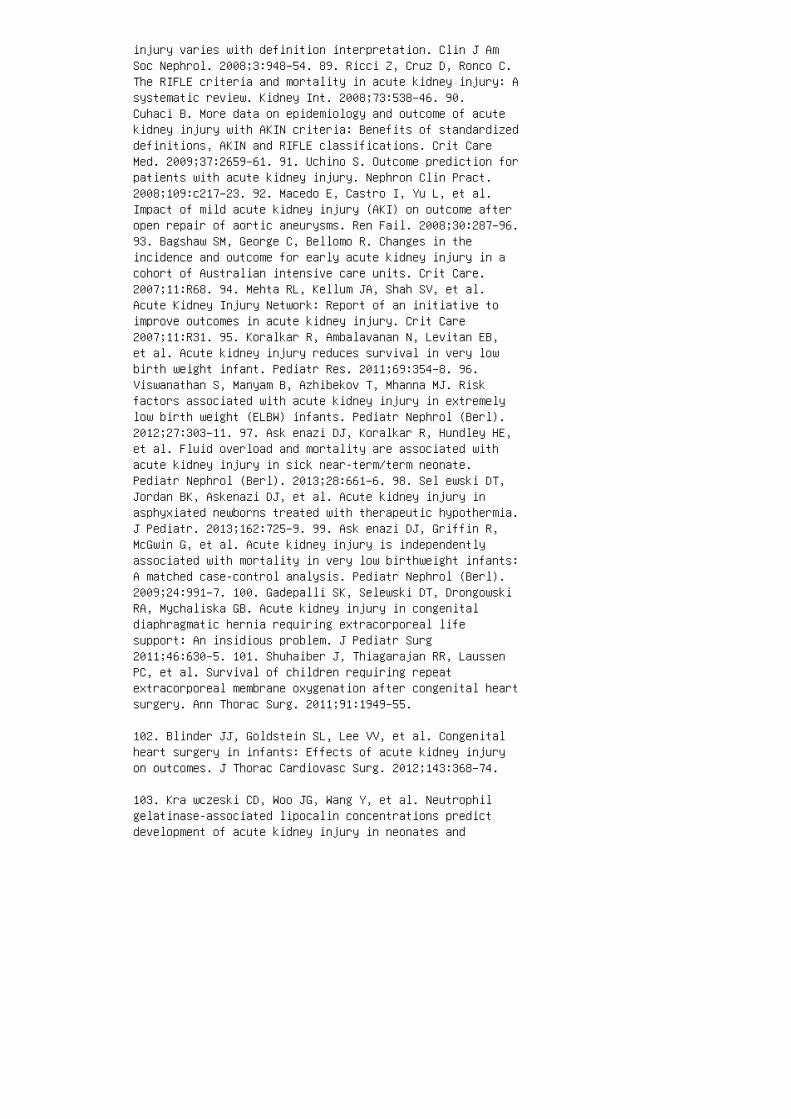
injury varies with definition interpretation. Clin J AmSoc Nephrol. 2008;3:948–54. 89. Ricci Z, Cruz D, Ronco C.The RIFLE criteria and mortality in acute kidney injury: Asystematic review. Kidney Int. 2008;73:538–46. 90.Cuhaci B. More data on epidemiology and outcome of acutekidney injury with AKIN criteria: Benefits of standardizeddefinitions, AKIN and RIFLE classifications. Crit CareMed. 2009;37:2659–61. 91. Uchino S. Outcome prediction forpatients with acute kidney injury. Nephron Clin Pract.2008;109:c217–23. 92. Macedo E, Castro I, Yu L, et al.Impact of mild acute kidney injury (AKI) on outcome afteropen repair of aortic aneurysms. Ren Fail. 2008;30:287–96.93. Bagshaw SM, George C, Bellomo R. Changes in theincidence and outcome for early acute kidney injury in acohort of Australian intensive care units. Crit Care.2007;11:R68. 94. Mehta RL, Kellum JA, Shah SV, et al.Acute Kidney Injury Network: Report of an initiative toimprove outcomes in acute kidney injury. Crit Care2007;11:R31. 95. Koralkar R, Ambalavanan N, Levitan EB,et al. Acute kidney injury reduces survival in very lowbirth weight infant. Pediatr Res. 2011;69:354–8. 96.Viswanathan S, Manyam B, Azhibekov T, Mhanna MJ. Riskfactors associated with acute kidney injury in extremelylow birth weight (ELBW) infants. Pediatr Nephrol (Berl).2012;27:303–11. 97. Ask enazi DJ, Koralkar R, Hundley HE,et al. Fluid overload and mortality are associated withacute kidney injury in sick near-term/term neonate.Pediatr Nephrol (Berl). 2013;28:661–6. 98. Sel ewski DT,Jordan BK, Askenazi DJ, et al. Acute kidney injury inasphyxiated newborns treated with therapeutic hypothermia.J Pediatr. 2013;162:725–9. 99. Ask enazi DJ, Griffin R,McGwin G, et al. Acute kidney injury is independentlyassociated with mortality in very low birthweight infants:A matched case-control analysis. Pediatr Nephrol (Berl).2009;24:991–7. 100. Gadepalli SK, Selewski DT, DrongowskiRA, Mychaliska GB. Acute kidney injury in congenitaldiaphragmatic hernia requiring extracorporeal lifesupport: An insidious problem. J Pediatr Surg2011;46:630–5. 101. Shuhaiber J, Thiagarajan RR, LaussenPC, et al. Survival of children requiring repeatextracorporeal membrane oxygenation after congenital heartsurgery. Ann Thorac Surg. 2011;91:1949–55.
102. Blinder JJ, Goldstein SL, Lee VV, et al. Congenitalheart surgery in infants: Effects of acute kidney injuryon outcomes. J Thorac Cardiovasc Surg. 2012;143:368–74.
103. Kra wczeski CD, Woo JG, Wang Y, et al. Neutrophilgelatinase-associated lipocalin concentrations predictdevelopment of acute kidney injury in neonates and
children after cardiopulmonary bypass. J Pediatr2011;158:1009–15.
104. Alabbas A, Campbell A, Skippen P, et al. Epidemiologyof cardiac surgery-associated acute kidney injury inneonates: A retrospective study. Pediatr Nephrol (Berl).2013;28:1127–34.
105. White SL, Perkovic V, Cass A, et al. Is low birthweight an antecedent of CKD in later life? A systematicreview of observational studies. Am J Kidney Dis.2009;54:248–61.
106. Greenbaum LA, Munoz A, Schneider MF, et al. Theassociation between abnormal birth history and growth inchildren with CKD. Clin J Am Soc Nephrol. 2011;6:14–21.
107. Bas ile DP. The endothelial cell in ischemic acutekidney injury: Implications for acute and chronic function.Kidney Int. 2007;72:151–6.
108. Ask enazi DJ, Feig DI, Graham NM, et al. 3-5 yearlongitudinal follow-up of pediatric patients after acuterenal failure. Kidney Int. 2006;69:184–9.
109. Mammen C, Al Abbas A, Skippen P, et al. Long-termrisk of CKD in children surviving episodes of acute kidneyinjury in the intensive care unit: A prospective cohortstudy. Am J Kidney Dis. 2012;59:523–30.
110. Coc a SG, Singanamala S, Parikh CR. Chronic kidneydisease after acute kidney injury: A systematic review andmeta-analysis. Kidney Int. 2012;81:442–8.
111. Bas ile DP. Rarefaction of peritubular capillariesfollowing ischemic acute renal failure: A potential factorpredisposing to progressive nephropathy. Curr Opin NephrolHypertens. 2004;13:1–7.
112. Guignard JP, Torrado A, Da Cunha O, Gautier E.Glomerular filtration rate in the first three weeks oflife. J Pediatr. 1975;87:268–72.
113. Barnett HL, Hare K, McNamara H, Hare R. Measurementof glomerular filtration rate in premature infants. J ClinInvest. 1948;27:691–9.
114. Vanpee M, Blennow M, Linne T, et al. Renal function invery low birth weight infants: Normal maturity reachedduring early childhood. J Pediatr. 1992;121:784–8.
REVIEW QUESTIONS
1. Which of the following factors is the most important
contributor to the increase in renal blood �ow following
birth?
a. Increased cardiac output
b. Increased renal vascular resistance c. Decreased renalvascular resistance d. Increased circulating plasma volumee. Cha nges in systemic resistance 2. Whi ch of thefollowing statements about the reninangiotensin system isnot true? a. Fetal renin levels are higher than adultlevels. b. Neonatal angiotensin-converting enzyme levelsare higher than adult levels. c. �ere i s a shi� from apredominance of angiotensin receptor type 2 to angiotensinreceptor type 1 following birth. d. Disruptions of theangiotensin type 1 or type 2 receptors are capable ofcausing congenital malformations of the kidney. e. AT-2receptors are coupled to G-proteins. 3. Fetal urine outputbegins at what week during gestation? a. 5th week b. 8thweek c. 12th week d. 20th week e. 36th week 4.Nephrogenesis is completed at: a. 28 we ek s of gestationb. 36 weeks of gestation c. 40 weeks of gestation d. 2weeks following birth e. 2 years of age 5. Which of thefollowing statements about neonatal sodium homeostasis isnot true? a. �ere is an increase in activity of the Na +-H + exchanger in the proximal tubules a�er birth. b. �ereis an initial natriuresis that a�ects term and pretermneonates equally. c. �ere is a shi� toward sodiumconservation at day 4 of life. d. �e loop of Henle has20% of the adult capacity to transport sodium. e. �ereare maturational changes in the distal tubule handling ofsodium a�er birth. 6. When compared to older infants,neonates can be expected to have a lower level of which ofthe following? a. Serum potassium b. Serum phosphorus c.Serum bicarbonate d. Urine glucose e. Urine amino acids7. Which is true of the de�nition of neonatal acute kidneyinjury? a. Oliguria should be the only criterion becauseall neonates with AKI are oliguric. b. An absolute serumcreatinine greater than 1.5 mg/ dL is the best approach.c. �ere are currently no large prospective studies thathave tested di�erent de�nitions against hard clinicaloutcomes. d. Because SCr is stable over the �rst week oflife, looking at an absolute rise in SCr from baselineprovides the best de�nition of neonatal AKI.

e. �e need for dialysis should serve as the de�nition ofAKI.
8. Acute kidney injury has been shown to be associated
with adverse outcomes in which neonatal populations?
a. Infants with very low birth weight
b. Near term/term infants
c. Newborns with perinatal asphyxia treated withtherapeutic hypothermia
d. Newborns undergoing extracorporeal membrane oxygenation
e. Newborns following cardiopulmonary bypass
f. All of the above 9. Compared to the adult kidney,fetal renal blood �ow is typi�ed by which of thefollowing? a. Low renal vascular resistance b. Greaterow to the renal cortex c. Greater �ow to the renal medullad. A larger percentage of the cardiac output ANSWER KEY 1.c 2. e 3. c 4. b 5. b 6. c 7. c 8. f 9. c
6 Diagnostic imaging of the urinary tract
1. Herd D. Anxiety in children undergoing VCUG: Sedationor no sedation? [Review article.] Adv Urol. 2008;498614.
2. Leb owitz RL, Olbing H, Parkkulainen KV, et al.International system of radiographic grading ofvesicoureteric reflux. International Reflux Study inChildren. Pediatr Radiol. 1985;15:105–9.
3. Rosenbaum DM, Korngold E, Teele RL. Sonographicassessment of renal length in normal children. AJR Am JRoentgenol. 1984;142:467–9.
4. Han BK, Babcock DS. Sonographic measurements andappearance of normal kidneys in children. Am J Roentgenol.1985;145:611–16.
5. Moore KI, Persaud TVE. The urogenital system. In: MooreKI, editor. The Developing Human: Clinically OrientedEmbryology, 6th ed. Philadelphia: WB Saunders; 1998. p.303.
6. Thoman DFM. Prenatally detected uropathies:Epidemiological considerations Br J Urol Int.1998;81:8–12.
7. Ngu yen HT, Herndon CD, Cooper C, et al. The Societyfor Fetal Urology consensus statement on the evaluationand management of antenatal hydronephrosis. J Pediatr Urol.2010; 6:212–31.
8. Bas sanese G, Travan L, D’Ottavio G, et al. Prenatalanteroposterior pelvic diameter cutoffs for postnatalreferral for isolated pyelectasis and hydronephrosis: Moreis not always better. J Urol. 2013;190:1858–63.
9. St. A ubin M, Willihnganz-Lawson K, et al. Society forFetal Urology recommendations for postnatal evaluation ofprenatal hydronephrosis: Will fewer voidingcystourethrograms lead to more urinary tract infections? JUrol. 2013;190:1456–61.
10. Laing FC, Burke VD, Wing VW, et al. Postpartumevaluation of fetal hydronephrosis: Optimal timing forfollow up sonography. Radiology. 1984;153:423–4.
11. Eickmeyer AB, Casanova NF, He C, et al. The naturalhistory of the multicystic dysplastic kidney: Is limitedfollow-up warranted? J Pediatr Urol. 2014;10:655–61.
12. Strife JL, Souza AS, Kirks DR, et al. Multicysticdysplastic kidney in children: US follow up. Radiology.1993;186:785–8.
13. England RJ, Haider N, Vujanic GM, et al. Mesoblasticnephroma: A report of the United Kingdom Children’s Cancerand Leukaemia Group (CCLG). Pediatr Blood Cancer.2011;56:744–8
14. Bie ster M, Kolditz D, Kalender WA. Iterativereconstruction methods in X-Ray CT. Phys Med.2012;28:94–108.
15. Mig lioretti DL, Johnson E, Williams A, et al. The useof computed tomography in pediatrics and the associatedradiation exposure and estimated cancer risk. JAMAPediatr. 2013;167:700–7. 16. Boone JM, Hendee WR,Mcnitt-Gray MF, et al. Seltzer SE. Radiation exposure fromCT scans: How to close our knowledge gaps, monitor andsafeguard exposure—Proceedings and recommendations of theRadiation Dose Summit, sponsored by NIBIB, February 24–25,2011. Radiology. 2012;265:544–54. 17. Aspelin P, LaskeyWK, Hermiller JB, et al. Nephrotoxic effects in high riskpatients undergoing angiography. N Engl J Med.2003;348:491–9. 18. Asif A, Epstein M. Prevention ofradiocontrast-induced nephropathy. Am J Kidney Dis.2004;44:12–24. 19. Emch TM, Haller NA. A randomized trialof prophylactic acetylcysteine and theophylline comparedwith placebo for the prevention of renal tubularvacuolization in rats after iohexol administration. ActaRadiol. 2003;10:514–9. 20. Gro bner T. Gadolinium: Aspecific trigger for the development of nephrogenicfibrosing dermopathy and nephrogenic systemic fibrosis?Nephrol Dial Transplant. 2006;21:1104–08. 21. Grobner T,Prischl FC. Gadolinium and nephrogenic systemic fibrosis.Kidney Int. 2007;72:260–4. 22. Mar kova A, Lester J, WangJ, et al. Diagnosis of common dermopathies in dialysispatients: A review and update. Semin Dial. 2012;25:408–18.23. Cow per SE, Robin HS, Steinberg SM, et al.Scleromyxoedema-like cutaneous diseases in renaldialysispatients. Lancet. 2000;356:1000–1. 24. Nar done B,Saddleton E, Laumann AE, et al. Pediatric nephrogenicsystemic fibrosis is rarely reported: A RADAR report.Pediatr Radiol. 2014;4:173–80. 25. Deo A , Fogel M,Cowper SE. Nephrogenic systemic fibrosis: A populationstudy examining the relationship of disease development togadolinium exposure. Clin J Am Soc Nephrol 2007;2:264–7.26. Boyd AS, Zic JA, Abraham JL. Gadolinium deposition innephrogenic fibrosing dermopathy. J Am Acad Dermatol

2007;56:27–30. 27. MacNeil S, Bains S, Johnson C, et al.Gadolinium contrast agent associated stimulation of humanfibroblast collagen production. Invest Radiol. 2011;46:711–7. 28. Vallee JP, Lazeyras F, Khan HG, et al. Absoluterenal blood flow quantification by dynamic MRI andGd-DTPA. Eur Radiol. 2000;10:1245–52. 29. Huang AJ, LeeVS, Rusinek H. Functional renal MR imaging. Magn ResonImaging Clin N Am. 2004;12:469–86. 30. Grenier N,Cornelis F, Le Bras Y, et al. Perfusion imaging in renaldiseases. Diagn Interv Imaging. 2013;94:1313–22. 31. Jones RA, Perez-Brayfield MR, Kirsch AJ, et al. Renal transittime with MR urography in children. Radiology.2004;233:41–50.
32. Zhang H, Prince MR. Renal MR angiography. Magn ResonImaging Clin N Am. 2004;12:487–503.
33. Ley endecker JR, Barnes CE, Zagoria, RJ. MR urography:Techniques and clinical applications. Radiographics.2008;28:23–48.
34. Grattan-Smith JD, Jones RA. MR urography in children.Pediatr Radiol. 2006;36:1119–32.
35. Majd M, Nussbaum Blask AR, et al. Acute pyelonephritis:Comparison of diagnosis with 99mTc-DMSA, SPECT, spiral CT,MR imaging, and power Doppler US in an experimental pigmodel. Radiology. 2001;218:101–8.
36. Lonergan GJ, Pennington DJ, Morrison JC, et al.Childhood pyelonephritis: Comparison of gadolinium-enhancedMR imaging and renal cortical scintigraphy for diagnosis.Radiology. 1998;207:377–84.
37. Goske MJ, Mitchell C, Reslan WA. Imaging of patientswith Wilms’ tumor. Semin Urol Oncol. 1999;17:11–20.
38. Glylys-Morin V, Hoffer FA, Kozakewich, et al. Wilmstumor and nephroblastomatosis: Imaging characteristics atgadolinium-enhanced MR Imaging. Radiology.1999;188:517–21.
39. Hen nigar RA, O’Shea PA, Grattan-Smith JD.Clinicopathologic features of nephrogenic rests andnephroblastomatosis. Adv Anat Pathol 2001;8:276–89.
40. ElMerhi FM, Bae, KT. Cystic renal disease. Magn ResonImaging Clin N Am. 2004;12:449–67.
41. Str and WR, Rushton HG, Markle BM, et al. Autosomal

dominant polycystic kidney disease in infants: Asymmetricdisease mimicking a unilateral renal mass. J Urol.1989;141:1151–3.
42. Bra ncatelli G, Federle MP, Vilgrain V, et al.Fibropolycystic Liver disease: CT and MR imaging findings.Radiographics. 2006;26:659–70.
REVIEW QUESTIONS
1. All of the following are indications for a VCUG except:a. Urinary tract infection b. Hydronephrosis/hydroureterc. To determine kidney function d. Preoperative renaltransplantation
2. Regarding vesicoureteral re�ux, which of the followingis false? a. �ere are �ve grades of re�ux. b. Grade Ire�ux indicates contrast material in the calyces. c. Intrarenal re�ux may be seen with higher grades of re�ux. d.e ur eter is o�en dilated in grades IV and V re�ux. 3.Reg arding the procedure of the VCUG, all statements aretrue, except: a. �e bladder needs to be catheterized. b.Oral sedation with midazolam is available in cases ofextreme anxiety. c. Inf ection is not a complication ofperforming VCUG. d. Parents and child-life specialist mayhelp facilitate the study. 4. Reg arding interpretationof the contrast VCUG, the International Re�ux Studyclassi�es VUR into: a. 4 grades of re�ux b. 5 grades ofre�ux c. Mild, moderate, and severe grades of VUR d. Grade I, Grade II, Grade III 5. Ultrasound is the bestmodality to evaluate for severity of renal obstruction.a. True b. False 6. Echogenic kidneys with loss ofcorticomedullary di�erentiation are speci�c �ndings forglomerulonephritis. a. True b. False 7. At 20 weeks ofgestation, routine ultrasound demonstrates mildpelviectasis (4 to 7 mm) in the fetus. What is thelikelihood of pyelectasis persisting a�er birth in thebaby? a. 20% b. 40% c. 60% d. 80% 8. A good-qualityCT scan of the kidneys should include which of thefollowing? a. Intravenous contrast material administrationb. A three-phase study including delayed excretion imagesc. Multiplanar reconstructions of source images d.Catheter drainage of the bladder e. Hydration and diureticadministration 9. All the following may contribute topotential radiographic contrast material nephrotoxicityexcept: a. Acidosis b. Dehydration c. N-acetyl cysteinetherapy d. Diabetes mellitus e. Prior contrast materialadministration 10. Which of the following is trueregarding nephrogenic systemic �brosis (NSF)? a. It isnot a risk for pediatric-age patients who are not

dehydrated. b. �e serum creatinine is a satisfactoryscreen for administration of gadolinium-based MRI contrastagents (GBCAs). c. A history of dialysis is the onlydetermining factor. d. �ere are a few GBCA agents that areconsidered safe for patients with renal failure (GFR lessthan 30). e. Dissociation of free gadolinium ion from thecontrast agent ligand plays a role.
11. Which imaging modality is best for screening forrecessive polycystic kidney disease? a. x-ray of theabdomen b. Radionuclide renal cortical scan c. CT scan ofabdomen d. Ultrasonography e. Noncontrast MRI ANSWER KEY1. c 2. b 3. c 4. b 5. b 6. b 7. a 8. c 9. c 10. e11. d
7 Radionuclide renal imaging
1. Gelfand MJ, Parisi MT, Treves ST. Pediatric NuclearMedicine Dose Reduction Workgroup. Pediatricradiopharmaceutical administered doses: 2010 NorthAmerican consensus guidelines. J Nucl Med. 2011;52:318–22.
2. Majd M, Rushton HG, Jantausch B, et al. Relationshipamong vesicoureteral reflux, p-fimbriated E. coli andacute pyelonephritis in children with febrile urinarytract infection. J Pediatr. 1991;119:578–85.
3. Rushton HG, Majd M, Chandra R, et al. Evaluation of99m-technetium-dimercaptosuccinic acid renal scans inexperimental acute pyelonephritis in piglets. J Urol.1988;140:1169–74. 4. Par khouse HF, Godley ML, Cooper, Jet al. Renal imaging with 99m Tc-labelled DMSA in thedetection of acute pyelonephritis: An experimental study inthe pig. Nucl Med Commun. 1989;10:63–70. 5. Majd M, BlaskARN, Markle BM, et al. Acute pyelonephritis: Comparison ofdiagnosis with 99m Tc-DMSA SPECT, spiral CT, MR imaging,and power Doppler US in an experimental pig model.Radiology. 2001;218:101–8. 6. Arnold AJ, Brownless SM,Carty HM, et al. Detection of renal scarring by DMSAscanning: An experimental study. J Pediatr Surg.1990;25:391–3. 7. Rushton HG, Majd M, Jantausch B, et al.Renal scarring following reflux and nonrefluxpyelonephritis in children: Evaluation with99mTechnetiumdimercaptosuccinic acid scintigraphy. J Urol.1992;147:1327–32, 8. Patteras JG, Rushton HG, Majd M. Therole of 99mTechnetum dimercapto-succinic acid renal scansin the evaluation of occult ectopic ureters in girls withparadoxical incontinence. J Urol. 199;162:821–5. 9.Gharagozloo AM, Leibowitz RL. Detection of a poorlyfunctioning malpositioned kidney with single ectopicureter in girls with urinary dribbling: Imaging evaluationin 5 patients. Am J Radiol. 1995;164:957–61. 10. Societyof Fetal Urology, Pediatric Nuclear Medicine Council,Society of Nuclear Medicine. The “well-tempered” diureticrenogram: A standard method to examine the asymptomaticneonate with hydronephrosis or hydroureteronephrosis.Report from combined meetings. J Nucl Med.1992;33:2047–51. 11. Ade yoju AAB, Burke D, Atkinson C, etal. The choice of timing for diuresis renography: The F+0method. BJU Int. 2001;88:1–5. 12. Wong DC, Rossleigh MA,Farnsworth RH. Diuretic renography with the addition ofquantitative gravityassisted drainage in infants andchildren. J Nucl Med. 2000;41:1030–6. 13. Ozcan Z,Anderson PJ, Gordon I. Prenatally diagnosed unilateralrenal pelvic dilatation: A dynamic condition on ultrasound
and diuretic renography. J Urol. 2004;172:1456–9. 14.Majd M, Potter BM, Guzzetta PC, et al. Effect of captoprilon the efficacy of renal scintigraphy in the detection ofrenal artery stenosis [Abstract]. J Nucl Med.1983;24:23–8. 15. Lagomarsino E, Orellanna P, Munoz J, etal. Captopril scintigraphy in the study of arterialhypertension in pediatrics. Pediatr Nephrol.2004;19:66–70. 16. Tayl or A. Renovascular hypertension:Nuclear medicine techniques. Q J Nucl Med. 2002;46:268–82.KEY POINTS ● Radionuclide cystography, because of its highsensitivity for VUR and its low radiation burden, isrecommended when serial follow-up studies are required. ●Radionuclide cystography is not adequate for providinginformation on urinary tract anatomy, such as posteriorurethral valve. SUMMARY
Nuclear imaging techniques are a useful adjunct to
other diagnostic imaging modalities in the manage
ment of pediatric nephrology patients. Diuresis renog
raphy provides critical information about conditions
such as obstructive uropathy. Renal cortical scanning
demonstrates the extent of parenchymal involvement in
pyelonephritis and scarring. Radionuclide studies o�er
an opportunity to view the results from a functional
perspective. Together with anatomic imaging, they
assist the pediatric nephrologist in the care of patients
17. Ludwig V, Martin WH, Delbeke D. Calcium channelblockers: A potential cause of false-positive captoprilrenography. Clin Nucl Med. 2003;28:108–12.
18. Sha rfuddin A. Imaging evaluation of kidney transplantrecipients. Semin Nephrol. 2011;31:259–71.
19. Heaf JG, Iversen J. Uses and limitations of renalscintigraphy in renal transplantation monitoring. Eur JNucl Med. 2000;27:871–9.
20. Dubovsky EV, Russell C. Quantitation of renal functionwith glomerular and tubular agents. Semin Nucl Med.1982;12:308–29.

21. Mulligan JS, Blue PW, Hasbargen JA. Methods ofmeasuring GFR with 99mTc-DTPA: An analysis of severalcommon methods. J Nucl Med. 1990;31:1211–9.
22. Coh en ML. Radionuclide clearance techniques. SeminNucl Med. 1974;4:23–8.
23. Piepsz A, Pintelon H, Ham HR. Estimation of normalchromium-51 ethylene diamine tetra-acetic clearance inchildren. Eur J Nucl Med. 1994; 21:12–6.
24. Her d D. Anxiety in children undergoing VCUG: Sedationor no sedation? Adv Urol. 2008:498614.
25. Majd M, Belman AB. Nuclear cystography in infants andchildren. Urol Clin North Am. 1979;6:395–407.
26. Con way JJ, King LR, Belman AB, et al. Detection ofvesicoureteral reflux with radionuclide cystography: Acomparison study with roentgenographic cystography. Am JRoentgenol Radium Ther Nucl Med. 1972;115:720–7.
27. Maj d M. Radionuclide imaging in clinical pediatrics.Pediatr Ann. 1976;15:396–402.
REVIEW QUESTIONS
1. A six-month-old female infant is hospitalized with afebrile urinary tract infection. �e radiopharmaceutical tobe used for assessment for acute pyelonephritis imagingis:
a. 99m Tc-MAG3
b. 99m Tc-pertechnetate
c. 99m Tc-DMSA
d. 99m Tc-DTPA
2. For the patient in question 1, renal cortical imagingdemonstrates multiple areas of photopenia, without loss ofvolume, involving both the upper and lower poles of theright kidney. �e diagnosis is:
a. Renal scarring
b. Multifocal acute pyelonephritis

c. Normal study
3. Clinical indications for DMSA renal corticalscintigraphy include:
a. Urinary tract infection
b. Search for a small ectopic kidney
c. Follow-up in renal trauma
d. All of the above. 4. A 2-month-old male infant wasdiagnosed to have prenatal hydronephrosis in one kidney.Le�-side hydronephrosis was con�rmed by a postnatalultrasound recently. �ere was no evidence of VUR on theVCUG. You should schedule this baby for a: a. DMSA renalscan b. Captopril renal scan c. Radionuclide cystogramd. Diuretic renogram 5. �e in itial imaging on the patientin question 4 demonstrates prompt and symmetric renalfunction with pooling of activity in the dilated le� renalcollecting system and prolonged washout half-time.Drainage on the right side is normal. Renal function isnormal bilaterally. Which of the following would be thebest investigative recommendation? a. MRI of the abdomenb. Repeat diuretic renography in 6 months c. Radionuclidecystogram in 6 months d. DMSA renal scan 6. All of thestatements regarding captopril-enhanced MAG-3 renal scanare true except: a. �e primary use is in the diagnosis ofobstructive uropathy. b. �e primary use is in thediagnosis of renal artery stenosis. c. Calciumchannel–blocking medication should be discontinued for atleast 2 days before the study. d. Either captopril orenalaprilat may be used for ACE blockade. 7. To assessthe function of the transplanted kidney, the best choiceof radionuclide investigation is: a. 99m Tc-DTPA b. 99mTc-pertechnetate c. 99m Tc-DMSA d. 99m Tc-MAG3 8. �emain indication for obtaining a 99m Tc-DTPA renal scanis: a. Evaluate for obstructive uropathy b. Evaluate forvesicoureteral re�ux c. Determine the glomerular �ltrationrate d. �ere are no current indications for obtaining a99m Tc-DTPA renal scan 9. �e following are correctregarding radionuclide cystography except: a. Oralmidazolam may be used for anxiolysis as necessary. b. �eradiotracer used is 99m Tc-pertechnetate. c. It isindicated in the evaluation of vesicoureteral re�ux. d.e bladder does not need to be catheterized. 10. Which oneof the following statements best compares and contraststhe VCUG and the radionuclide cystogram (RNC)? a. �e VCUGhas higher resolution allowing delineation of anatomy andmore accurate grading of re�ux compared to the RNC, which
has higher sensitivity for detecting re�ux and o�ers lessradiation burden.
b. �e RNC has higher resolution allowing delineation ofanatomy and more accurate grading of re�ux compared to theVCUG which has higher sensitivity for detecting re�ux ando�ers less radiation burden.
c. �e RNC and VCUG are very similar to each other, onesimply a radionuclide study and the other a �uoroscopicstudy.
d. None of the above. ANSWER KEY 1. c 2. b 3. d 4. d5. b 6. a 7. d 8. c 9. d 10. a

8 Renal biopsy
1. Pirani CL. Renal biopsy. An historical perspective. In:Silva FG, D’Agati VD, Nadasdy T, editors. Renal BiopsyInterpretation, Churchill Livingstone: New York; 1996:1–19. 2. Iversen P, Brun C. Aspiration biopsy of thekidney. Am J Med. 1951;11:324–30. 3. Korbet SM.Percutaneous renal biopsy. Semin Nephrol. 2002;22:254–67.4. Ric hards NT, Darby S, Howie AJ, et al. Knowledge ofrenal histology alters patient management in over 40% ofcases. Nephrol Dial Transplant. 1994;9:1255–9. 5. Hog gRJ, Portman RJ, Milliner D, et al. Evaluation andmanagement of proteinuria and nephrotic syndrome inchildren: Recommendations from a pediatric nephrology panelestablished at the National Kidney Foundation conferenceon proteinuria, albuminuria, risk, assessment, detection,and elimination (PARADE). Pediatrics. 2000;105:1242–49. 6.Fogo AB. Renal pathology. In: Avner ED, Niaudet P, HarmonWE, editors. Pediatric Nephrology, 5th ed. Philadelphia:Lippincott Williams & Wilkins, 2003; p. 475. 7. Filler G,Young E, Geier P, et al. Is there really an increase innon-minimal change nephrotic syndrome in children? Am JKidney Dis. 2003;42:1107–13. 8. Birk PE, Stannard KM,Konrad HB, et al. Surveillance biopsies are superior tofunctional studies for the diagnosis of acute and chronicrenal allograft pathology in children. Pediatr Transplant.2004;8:29–38. 9. Birnholz JC, Kasinath BS, Corwin HL. Animproved technique for ultrasound guided percutaneousrenal biopsy. Kidney Int. 1985;27:80–2. 10. Wiseman DA,Hawkins R, Numerow LM, Taub KJ. Percutaneous renal biopsyutilizing real time, ultrasonic guidance and asemiautomated biopsy device. Kidney Int. 1990;38:347–9.11. Donovan KL, Thomas DM, Wheeler DC, et al. Experiencewith a new method for percutaneous renal biopsy. NephrolDial Transplant. 1991;6:731–3. 12. Kar k RM, Muehrcke RC.Biopsy of the kidney in the prone position. Lancet1954;1:1047–49. 13. Muehrcke RC, Kark RM, Pirani CL.Technique of percutaneous renal biopsy in the proneposition. J Urol. 1955;74:267–77. 14. Kark RM, MuehrckeRC, Pollak VE, et al. An analysis of 500 percutaneousrenal biopsies. Arch Intern Med. 1958;101:439–351. 15.Komaiko MS, Jordan SC, Querfeld et al. A new percutaneousrenal biopsy device for pediatric patients. PediatrNephrol. 1989;3:191–3. 16. Bur stein DM, Korbet SM,Schwartz MM. The use of the automatic core biopsy systemin percutaneous renal biopsies: A comparative study. Am JKidney Dis. 1993;22:545–52. 17. Feneberg R, Schaefer F,Zieger B, et al. Percutaneous renal biopsy in children: A27-year experience. Nephron. 1998;79:438–46.

SUMMARY
e technical advances in imaging and instruments
have made the percutaneous renal biopsy a safe diag
nostic procedure. Use of real-time ultrasound guid
ance and advanced instruments are the standard of
care in our days. In spite of all the advancements,
there are still a group of well-de�ned contraindica
tions for a percutaneous renal biopsy that the clini
cian must consider carefully. Finally, the success and
safety of the percutaneous renal biopsy in children
require a knowledgeable and experienced pediatric
nephrologist familiar with the technique.
Figure 8.11 Color Doppler evaluation of the kidney dem
onstrating an arteriovenous fistula following a renal biopsy
procedure. The fistula is marked by the area showing the
admixture of blue and red blood flow pattern (arrow).
18. Vidhun J, Masciandro J, Varich L, et al. Safety andrisk stratification of percutaneous biopsies of adultsizedrenal allografts in infant and older pediatric recipients.Transplantation. 2003;76:552–7.
19. Chesney DS, Brouhard BH, Cunningham RJ. Safety andcost effectiveness of pediatric percutaneous renal biopsy.Pediatr Nephrol. 1996;10:493–5.
20. Davis ID, Oehlenschlager W, O’Riordan MA, Avner ED.Pediatric renal biopsy: Should this procedure be performedin an outpatient setting? Pediatr Nephrol. 1998;12:96–100.
21. Simckes AM, Blowey DL, Gyves KM, Alon US. Success andsafety of same-day kidney biopsy in children andadolescents. Pediatr Nephrol. 2000;14:946–52.
22. Hus sain F, Watson AR, Hayes J, Evans J. Standards for

renal biopsies: Comparison of inpatient and day careprocedures. Pediatr Nephrol. 2003;18:53–6.
23. Schow DA, Vinson RK, Morrisseau PM. Percutaneous renalbiopsy of the solitary kidney: A contraindication? J Urol.1992;147:1235–7.
24. Dod ge WF, Daeschner CW Jr, Brennan JC, et al.Percutaneous renal biopsy in children. I. Generalconsiderations. Pediatrics. 1962;30:287–96.
25. Whi te RH. Observations on percutaneous renal biopsyin children. Arch Dis Child. 1963;38:260–6.
26. Karafin L, Kendall AR, Fleisher DS. Urologiccomplications in percutaneous renal biopsy in children. JUrol. 1970;103:332–5.
27. Alt ebarmakian VK, Guthinger WP, Yakub YN, et al.Percutaneous kidney biopsies: Complications and theirmanagement. Urology. 1981;18:118–22.
28. Chan JC, Brewer WH, Still WJ. Renal biopsies underultrasound guidance: 100 consecutive biopsies in children.J Urol. 1983;129:103–7.
29. Sweet M, Brouhard BH, Ramirez-Seijas F, et al.Percutaneous renal biopsy in infants and young children.Clin Nephrol. 1986;26:192–94.
30. Alon U, Pery M. Percutaneous kidney needle biopsy inchildren is less traumatic than in adults. Nephron.1988;50:57–60.
31. al Ra sheed SA, al Mugeiren MM, Abdurrahman MB,Elidrissy AT. The outcome of percutaneous renal biopsy inchildren: An analysis of 120 consecutive cases. PediatrNephrol. 1990;4:600–3.
32. Bohlin AB, Edstrom S, Almgren B. Renal biopsy inchildren: Indications, technique and efficacy in 119consecutive cases. Pediatr Nephrol. 1995;9:201–3.
33. Pel legrini C, Cecconi M, Pieroni G, et al.Percutaneous renal biopsy in children: Use of a fineneedle. Minerva Urol Nefrol. 1996;48:97–101.
34. Ben field MR, Herrin J, Feld L. Safety of kidneybiopsy in pediatric transplantation: A report of theControlled Clinical Trials in Pediatric Transplantation
Trial of Induction Therapy Study Group. Transplantation1999;67: 544–7. 35. Kamitsuji H, Yoshioka K, Ito H.Percutaneous renal biopsy in children: Survey of pediatricnephrologists in Japan. Pediatr Nephrol. 1999;13:693–6.36. Sumboonnanonda A, Srajai K, Vongjirad A, et al.Percutaneous renal biopsy in children. J Med Assoc Thai.2002;85:(Suppl 2)755–61. 37. Proesmans W, Marchal G,Snoeck L, Snoeys R. Ultrasonography for assessment ofbleeding after percutaneous renal biopsy in children. ClinNephrol. 1982;18:257–62. 38. Stegmayr B, Orsten PA. Lysisof obstructive renal pelvic clots with retrogradeinstillation of streptokinase: A case report. Scand J UrolNephrol. 1984;18:347–50. 39. Horowitz MD, Russell E,Abitbol C, et al. Massive hematuria following percutaneousbiopsy of renal allograft: Successful control by selectiveembolization. Arch Surg. 1984;119:1430–3. 40. Fruhwald F,Harmuth P, Kovarik J, et al. Bladder obstruction: A rarecomplication after percutaneous renal biopsy. Eur JRadiol. 1984;4:225–6. 41. Rao K V. Urologicalcomplications associated with a kidney transplant biopsy:Report of 3 cases and review of the literature. J Urol.1986;135:768–70. 42. Sch waighofer B, Fruhwald F, KovarikJ. Sonographically demonstrable changes followingpercutaneous kidney biopsy. Ultraschall Med. 1986;7:44–7.43. Bergman SM, Frentz GD, Wallin JD. Ureteral obstructiondue to blood clot following percutaneous renal biopsy:Resolution with intraureteral streptokinase. J Urol.1990;143:113–5. 44. McDonald MW, Sosnowski JT, Mahin EJ,et al. Automatic spring-loaded biopsy gun with ultrasoniccontrol for renal transplant biopsy. Urology.1993;42:580–2. 45. Mah oney MC, Racadio JM, Merhar GL,First MR. Safety and efficacy of kidney transplant biopsy:TruCut needle vs sonographically guided Biopty gun. AJR AmJ Roentgenol. 1993;160:325–6. 46. Dia z-Buxo JA, DonadioJV Jr. Complications of percutaneous renal biopsy: Ananalysis of 1,000 consecutive biopsies. Clin Nephrol.1975;4:223–7. 47. Bennett AR, Wiener SN. Intrarenalarteriovenous fistula and aneurysm: A complication ofpercutaneous renal biopsy. Am J Roentgenol Radium TherNucl Med. 1965;95:372–82. 48. Eke lund L, Lindholm T.Arteriovenous fistulae following percutaneous renal biopsy.Acta Radiol Diagn (Stockh). 1971;11:38–48. 49. Jor stadS, Borander U, Berg KJ, Wideroe TE. Evaluation ofcomplications due to percutaneous renal biopsy: A clinicaland angiographic study. Am J Kidney Dis. 1984;4:162–5.50. Rollino C, Garofalo G, Roccatello D, et al. ColourcodedDoppler sonography in monitoring native kidney biopsies.Nephrol Dial Transplant. 1994;9:1260–63.
51. Gainza FJ, Minguela I, Lopez-Vidaur I. Evaluation of
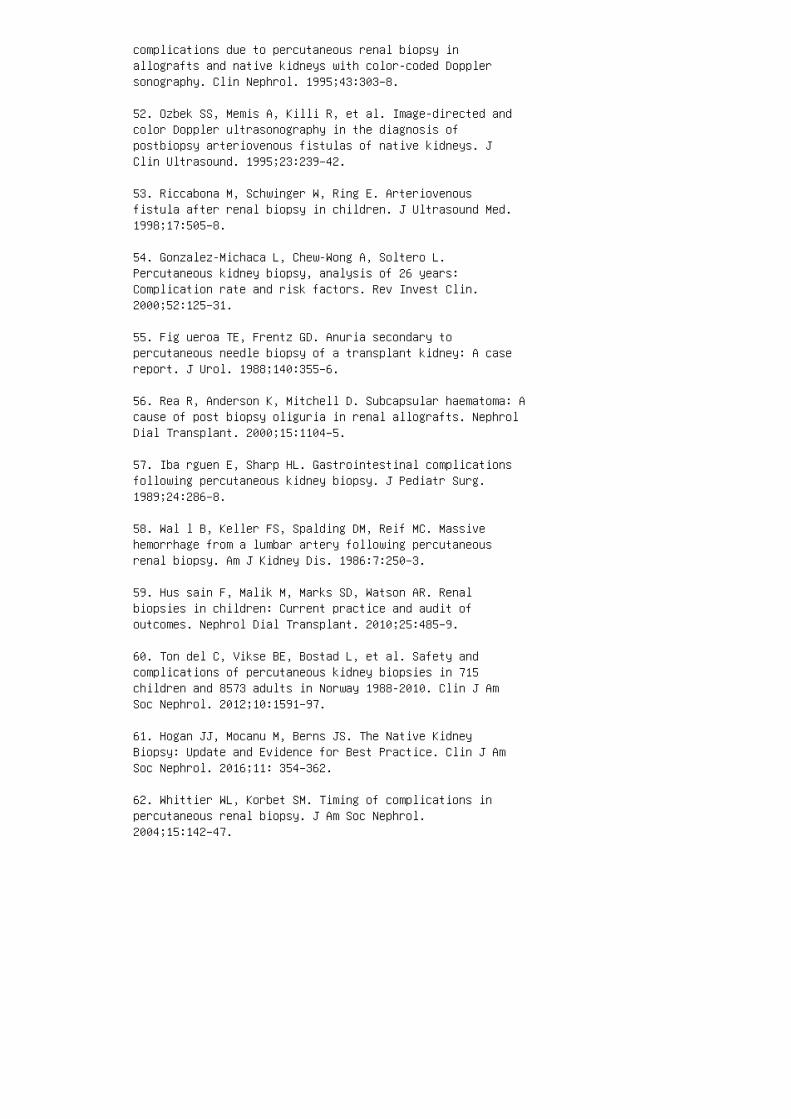
complications due to percutaneous renal biopsy inallografts and native kidneys with color-coded Dopplersonography. Clin Nephrol. 1995;43:303–8.
52. Ozbek SS, Memis A, Killi R, et al. Image-directed andcolor Doppler ultrasonography in the diagnosis ofpostbiopsy arteriovenous fistulas of native kidneys. JClin Ultrasound. 1995;23:239–42.
53. Riccabona M, Schwinger W, Ring E. Arteriovenousfistula after renal biopsy in children. J Ultrasound Med.1998;17:505–8.
54. Gonzalez-Michaca L, Chew-Wong A, Soltero L.Percutaneous kidney biopsy, analysis of 26 years:Complication rate and risk factors. Rev Invest Clin.2000;52:125–31.
55. Fig ueroa TE, Frentz GD. Anuria secondary topercutaneous needle biopsy of a transplant kidney: A casereport. J Urol. 1988;140:355–6.
56. Rea R, Anderson K, Mitchell D. Subcapsular haematoma: Acause of post biopsy oliguria in renal allografts. NephrolDial Transplant. 2000;15:1104–5.
57. Iba rguen E, Sharp HL. Gastrointestinal complicationsfollowing percutaneous kidney biopsy. J Pediatr Surg.1989;24:286–8.
58. Wal l B, Keller FS, Spalding DM, Reif MC. Massivehemorrhage from a lumbar artery following percutaneousrenal biopsy. Am J Kidney Dis. 1986:7:250–3.
59. Hus sain F, Malik M, Marks SD, Watson AR. Renalbiopsies in children: Current practice and audit ofoutcomes. Nephrol Dial Transplant. 2010;25:485–9.
60. Ton del C, Vikse BE, Bostad L, et al. Safety andcomplications of percutaneous kidney biopsies in 715children and 8573 adults in Norway 1988-2010. Clin J AmSoc Nephrol. 2012;10:1591–97.
61. Hogan JJ, Mocanu M, Berns JS. The Native KidneyBiopsy: Update and Evidence for Best Practice. Clin J AmSoc Nephrol. 2016;11: 354–362.
62. Whittier WL, Korbet SM. Timing of complications inpercutaneous renal biopsy. J Am Soc Nephrol.2004;15:142–47.

63. Franke M, Kramarczyk A, Taylan C, et al.Ultrasound-Guided Percutaneous Renal Biopsy in 295Children and Adolescents: Role of Ultrasound and Analysisof Complications. PLoS ONE. 2014: 9(12): e114737.DOI:10.1371/journal.pone.0114737.
REVIEW QUESTIONS
1. Which of the following is not considered an absolute
contraindication for a percutaneous renal biopsy?
a. Uncooperative patient
b. Chronic glomerulonephritis
c. Uncontrolled severe hypertension
d. Acute pyelonephritis
2. Which of the following statements regarding complica
tions of a renal biopsy is false? a. Mic roscopichematuria is the most common complication. b. �eincidence of perinephric hematoma following renal biopsydepends on the modality of evaluation. c. Mos tarteriovenous �stulas require surgical intervention. d.Macroscopic hematuria usually resolves spontaneously within24 to 48 hours. e. Intravenous hydration is su�cient inmost patients to prevent the formation of large clots. 3.e op timal biopsy site for a native kidney is the: a.Upper pole of the right kidney b. Lower pole of the rightkidney c. Upper pole of the le� kidney d. Lower pole ofthe le� kidney 4. Whi ch of the following is not anindication for renal biopsy in children? a. Rapidlyprogressive glomerulonephritis b. Steroid-resistantnephrotic syndrome c. Renal allogra� dysfunction d. Persistent glomerular hematuria e. Steroid responsivenephrotic syndrome 5. Prebiopsy evaluation should include:a. Complete blood count b. Basic metabolic panel c.Ultrasonographic evaluation of the kidneys d. Coagulationpro�le e. All of the above 6. A 10-year-old girlunderwent a percutaneous renal biopsy and was dischargedfrom the outpatient surgical unit a�er 6 hours ofobservation. Next morning the patient complained of le�side abdominal pain, which was noted to be 8 on a 10-pointscale, and was persistent. Her parent gave heracetaminophen 325 mg orally, but there was no resolutionof pain. She is now seen in the emergency room. Patient
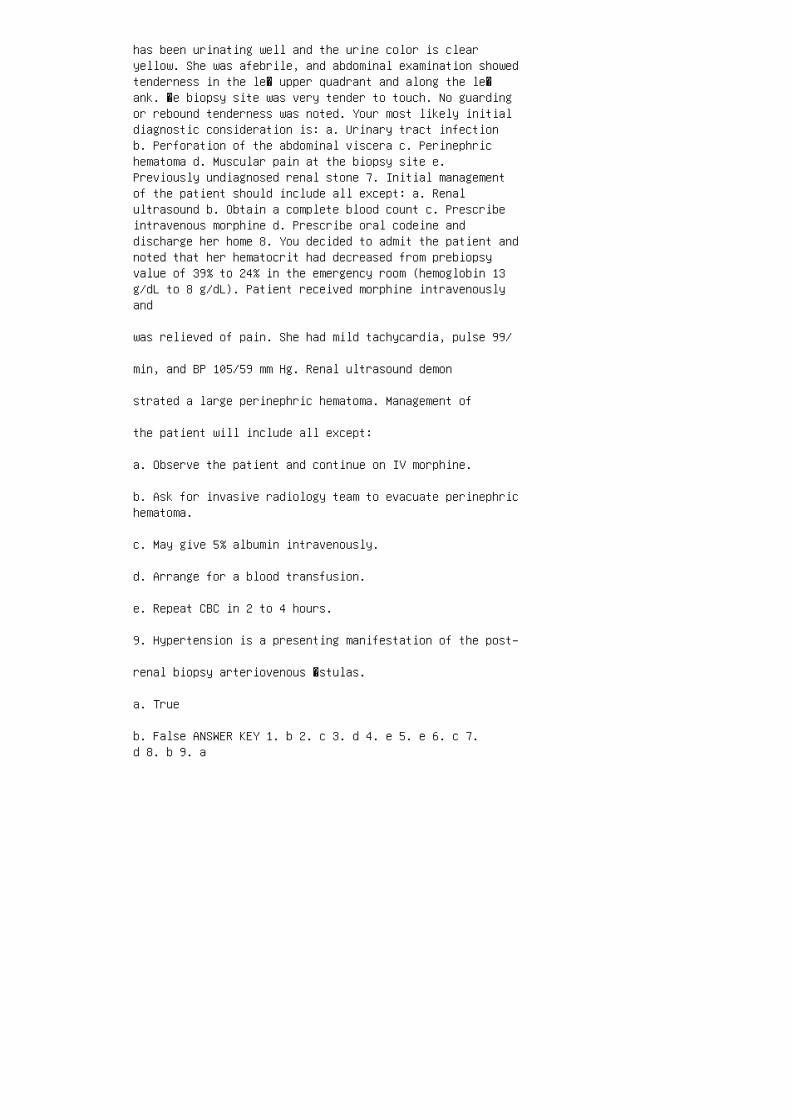
has been urinating well and the urine color is clearyellow. She was afebrile, and abdominal examination showedtenderness in the le� upper quadrant and along the le�ank. �e biopsy site was very tender to touch. No guardingor rebound tenderness was noted. Your most likely initialdiagnostic consideration is: a. Urinary tract infectionb. Perforation of the abdominal viscera c. Perinephrichematoma d. Muscular pain at the biopsy site e.Previously undiagnosed renal stone 7. Initial managementof the patient should include all except: a. Renalultrasound b. Obtain a complete blood count c. Prescribeintravenous morphine d. Prescribe oral codeine anddischarge her home 8. You decided to admit the patient andnoted that her hematocrit had decreased from prebiopsyvalue of 39% to 24% in the emergency room (hemoglobin 13g/dL to 8 g/dL). Patient received morphine intravenouslyand
was relieved of pain. She had mild tachycardia, pulse 99/
min, and BP 105/59 mm Hg. Renal ultrasound demon
strated a large perinephric hematoma. Management of
the patient will include all except:
a. Observe the patient and continue on IV morphine.
b. Ask for invasive radiology team to evacuate perinephrichematoma.
c. May give 5% albumin intravenously.
d. Arrange for a blood transfusion.
e. Repeat CBC in 2 to 4 hours.
9. Hypertension is a presenting manifestation of the post–
renal biopsy arteriovenous �stulas.
a. True
b. False ANSWER KEY 1. b 2. c 3. d 4. e 5. e 6. c 7.d 8. b 9. a
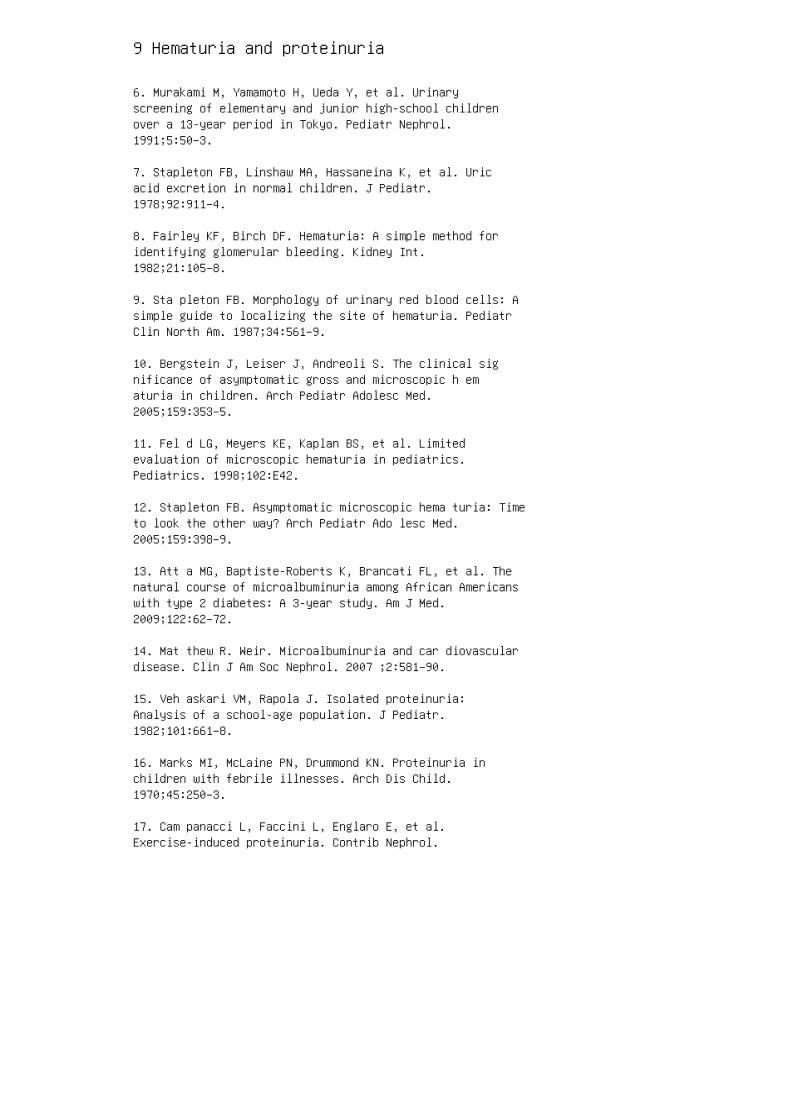
9 Hematuria and proteinuria
6. Murakami M, Yamamoto H, Ueda Y, et al. Urinaryscreening of elementary and junior high-school childrenover a 13-year period in Tokyo. Pediatr Nephrol.1991;5:50–3.
7. Stapleton FB, Linshaw MA, Hassaneina K, et al. Uricacid excretion in normal children. J Pediatr.1978;92:911–4.
8. Fairley KF, Birch DF. Hematuria: A simple method foridentifying glomerular bleeding. Kidney Int.1982;21:105–8.
9. Sta pleton FB. Morphology of urinary red blood cells: Asimple guide to localizing the site of hematuria. PediatrClin North Am. 1987;34:561–9.
10. Bergstein J, Leiser J, Andreoli S. The clinical significance of asymptomatic gross and microscopic h ematuria in children. Arch Pediatr Adolesc Med.2005;159:353–5.
11. Fel d LG, Meyers KE, Kaplan BS, et al. Limitedevaluation of microscopic hematuria in pediatrics.Pediatrics. 1998;102:E42.
12. Stapleton FB. Asymptomatic microscopic hema turia: Timeto look the other way? Arch Pediatr Ado lesc Med.2005;159:398–9.
13. Att a MG, Baptiste-Roberts K, Brancati FL, et al. Thenatural course of microalbuminuria among African Americanswith type 2 diabetes: A 3-year study. Am J Med.2009;122:62–72.
14. Mat thew R. Weir. Microalbuminuria and car diovasculardisease. Clin J Am Soc Nephrol. 2007 ;2:581–90.
15. Veh askari VM, Rapola J. Isolated proteinuria:Analysis of a school-age population. J Pediatr.1982;101:661–8.
16. Marks MI, McLaine PN, Drummond KN. Proteinuria inchildren with febrile illnesses. Arch Dis Child.1970;45:250–3.
17. Cam panacci L, Faccini L, Englaro E, et al.Exercise-induced proteinuria. Contrib Nephrol.
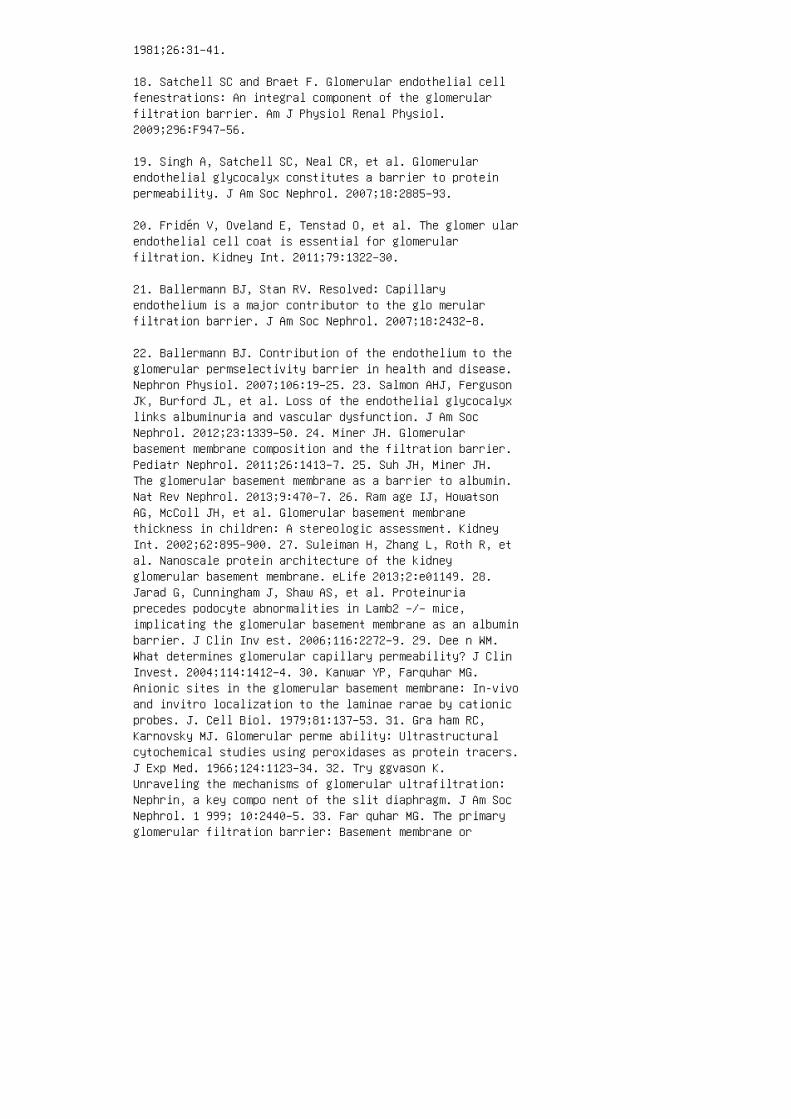
1981;26:31–41.
18. Satchell SC and Braet F. Glomerular endothelial cellfenestrations: An integral component of the glomerularfiltration barrier. Am J Physiol Renal Physiol.2009;296:F947–56.
19. Singh A, Satchell SC, Neal CR, et al. Glomerularendothelial glycocalyx constitutes a barrier to proteinpermeability. J Am Soc Nephrol. 2007;18:2885–93.
20. Fridén V, Oveland E, Tenstad O, et al. The glomer ularendothelial cell coat is essential for glomerularfiltration. Kidney Int. 2011;79:1322–30.
21. Ballermann BJ, Stan RV. Resolved: Capillaryendothelium is a major contributor to the glo merularfiltration barrier. J Am Soc Nephrol. 2007;18:2432–8.
22. Ballermann BJ. Contribution of the endothelium to theglomerular permselectivity barrier in health and disease.Nephron Physiol. 2007;106:19–25. 23. Salmon AHJ, FergusonJK, Burford JL, et al. Loss of the endothelial glycocalyxlinks albuminuria and vascular dysfunction. J Am SocNephrol. 2012;23:1339–50. 24. Miner JH. Glomerularbasement membrane composition and the filtration barrier.Pediatr Nephrol. 2011;26:1413–7. 25. Suh JH, Miner JH.The glomerular basement membrane as a barrier to albumin.Nat Rev Nephrol. 2013;9:470–7. 26. Ram age IJ, HowatsonAG, McColl JH, et al. Glomerular basement membranethickness in children: A stereologic assessment. KidneyInt. 2002;62:895–900. 27. Suleiman H, Zhang L, Roth R, etal. Nanoscale protein architecture of the kidneyglomerular basement membrane. eLife 2013;2:e01149. 28.Jarad G, Cunningham J, Shaw AS, et al. Proteinuriaprecedes podocyte abnormalities in Lamb2 –/– mice,implicating the glomerular basement membrane as an albuminbarrier. J Clin Inv est. 2006;116:2272–9. 29. Dee n WM.What determines glomerular capillary permeability? J ClinInvest. 2004;114:1412–4. 30. Kanwar YP, Farquhar MG.Anionic sites in the glomerular basement membrane: In-vivoand invitro localization to the laminae rarae by cationicprobes. J. Cell Biol. 1979;81:137–53. 31. Gra ham RC,Karnovsky MJ. Glomerular perme ability: Ultrastructuralcytochemical studies using peroxidases as protein tracers.J Exp Med. 1966;124:1123–34. 32. Try ggvason K.Unraveling the mechanisms of glomerular ultrafiltration:Nephrin, a key compo nent of the slit diaphragm. J Am SocNephrol. 1 999; 10:2440–5. 33. Far quhar MG. The primaryglomerular filtration barrier: Basement membrane or

epithelial slits? Kidney Int. 1975;8:197–211. 34.Khoshnoodi J, Tryggvason K. Unraveling the molecularmake-up of the glomerular podocyte slit diaphragm. ExpNephrol. 2001;29:355–9. 35. Chugh SS, Kaw B, Kanwar YS.Molecular struc ture-function relationship in the slitdiaphragm. Semin Nephrol. 2003;6:544–55. 36. Greka A,Mundel P. Cell biology and pathol ogy of podocytes. AnnuRev Physiol. 2012;74:299–323. 37. YujiSato, Wharram BL,Lee SK, et al. Urine podo cyte mRNAs mark progression ofrenal disease. J Am Soc Nephrol. 2009;20:1041–52. 38.Wickman L, Afshinnia F, Wang SQ, et al. Urine podocytemRNAs, proteinuria, and progres sion in human glomerulardiseases. J Am Soc Nephr ol. 2013;24:2081–95. 39. LemleyKV. Protecting podocytes: How good do we need to be?Kidney Int. 2012;81:9–11.
40. Brenner BM, Hostetter TH, Humes HD. Glomerularpermselectivity: Barrier function based on discriminationof molecular size and charge. Am J Physiol.1978;234:F455–60.
41. D’Amico G, Bazzi C. Pathophysiology of proteinuria.Kidney Int. 2003;63, 809–25.
42. Chang RLS, Ueki IF, Troy JL et al. Permselectivity ofthe glomerular capillary wall to macromolecules. II.Experimental studies in rats using neutral dextran.Biophys J. 1975;15:887–906.
43. Dee n WM, Bridges CR, Brenner BM, et al. Heteroporousmodel of glomerular size selectivity: Application tonormal and nephrotic humans. Am J Physiol. 1985;249:F374.
44. Rennke HG, Venkatachalam MA. Glomerular permeability:In vivo tracer studies with polyanionic and polycationicferritins. Kidney Int. 1977;11:44–53.
45. Chang RLS, Deen WM, Robertson CR, et al.Permselectivity of glomerular capillary wall. III.Restricted transport of polyanions. Kidney Int.1975;8:212–8.
46. Ben nett CM, Glassock RJ, Chang RL, et al.Permselectivity of the glomerular capillary wall: Studiesof experimental glomerulonephritis in the rat usingdextran sulfate. J Clin Invest. 1976;57:1287–94.
47. Ren nke, HG, Cotran RS, Venkatachalam MA. Role ofmolecular charge in glomerular permeability: Tracerstudies with cationized ferritins. J Cell Biol.
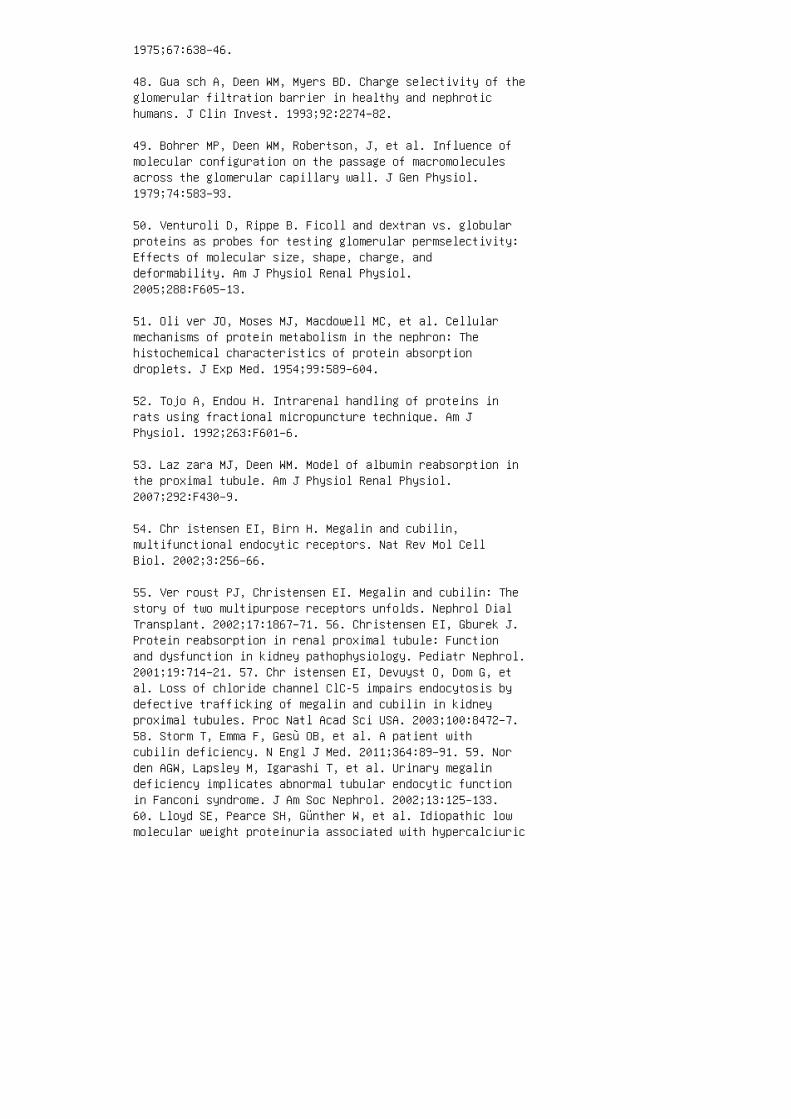
1975;67:638–46.
48. Gua sch A, Deen WM, Myers BD. Charge selectivity of theglomerular filtration barrier in healthy and nephrotichumans. J Clin Invest. 1993;92:2274–82.
49. Bohrer MP, Deen WM, Robertson, J, et al. Influence ofmolecular configuration on the passage of macromoleculesacross the glomerular capillary wall. J Gen Physiol.1979;74:583–93.
50. Venturoli D, Rippe B. Ficoll and dextran vs. globularproteins as probes for testing glomerular permselectivity:Effects of molecular size, shape, charge, anddeformability. Am J Physiol Renal Physiol.2005;288:F605–13.
51. Oli ver JO, Moses MJ, Macdowell MC, et al. Cellularmechanisms of protein metabolism in the nephron: Thehistochemical characteristics of protein absorptiondroplets. J Exp Med. 1954;99:589–604.
52. Tojo A, Endou H. Intrarenal handling of proteins inrats using fractional micropuncture technique. Am JPhysiol. 1992;263:F601–6.
53. Laz zara MJ, Deen WM. Model of albumin reabsorption inthe proximal tubule. Am J Physiol Renal Physiol.2007;292:F430–9.
54. Chr istensen EI, Birn H. Megalin and cubilin,multifunctional endocytic receptors. Nat Rev Mol CellBiol. 2002;3:256–66.
55. Ver roust PJ, Christensen EI. Megalin and cubilin: Thestory of two multipurpose receptors unfolds. Nephrol DialTransplant. 2002;17:1867–71. 56. Christensen EI, Gburek J.Protein reabsorption in renal proximal tubule: Functionand dysfunction in kidney pathophysiology. Pediatr Nephrol.2001;19:714–21. 57. Chr istensen EI, Devuyst O, Dom G, etal. Loss of chloride channel ClC-5 impairs endocytosis bydefective trafficking of megalin and cubilin in kidneyproximal tubules. Proc Natl Acad Sci USA. 2003;100:8472–7.58. Storm T, Emma F, Gesù OB, et al. A patient withcubilin deficiency. N Engl J Med. 2011;364:89–91. 59. Norden AGW, Lapsley M, Igarashi T, et al. Urinary megalindeficiency implicates abnormal tubular endocytic functionin Fanconi syndrome. J Am Soc Nephrol. 2002;13:125–133.60. Lloyd SE, Pearce SH, Günther W, et al. Idiopathic lowmolecular weight proteinuria associated with hypercalciuric
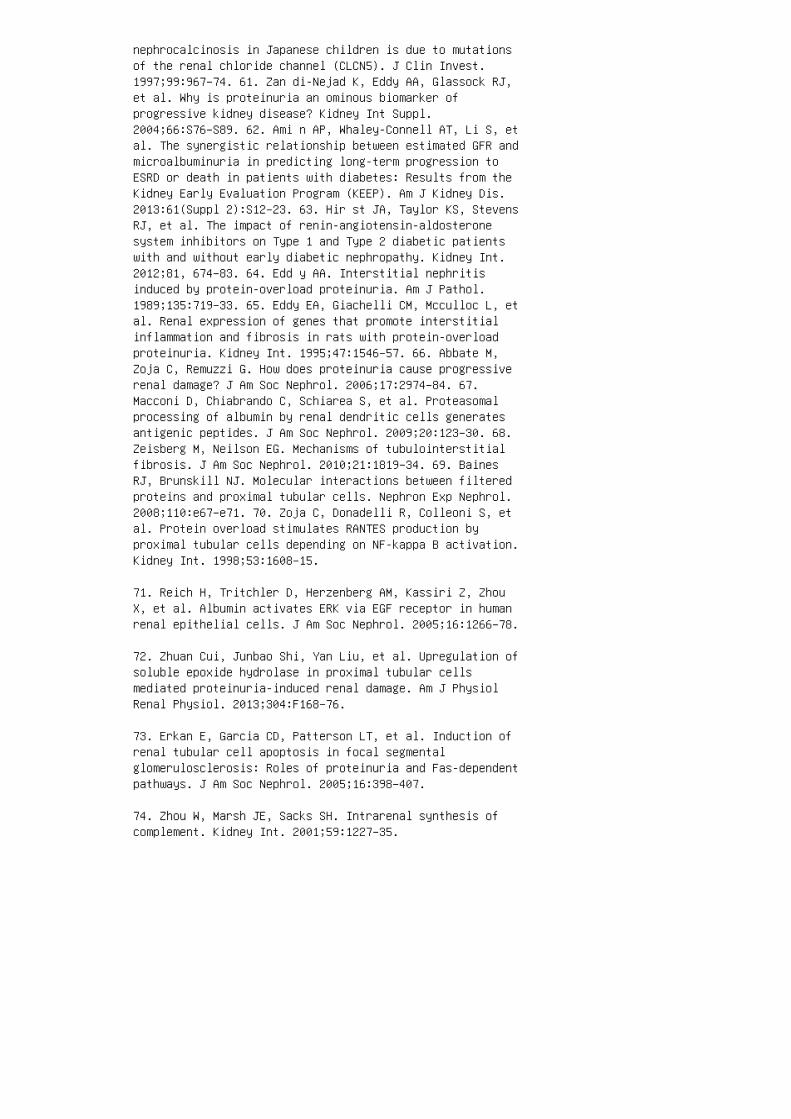
nephrocalcinosis in Japanese children is due to mutationsof the renal chloride channel (CLCN5). J Clin Invest.1997;99:967–74. 61. Zan di-Nejad K, Eddy AA, Glassock RJ,et al. Why is proteinuria an ominous biomarker ofprogressive kidney disease? Kidney Int Suppl.2004;66:S76–S89. 62. Ami n AP, Whaley-Connell AT, Li S, etal. The synergistic relationship between estimated GFR andmicroalbuminuria in predicting long-term progression toESRD or death in patients with diabetes: Results from theKidney Early Evaluation Program (KEEP). Am J Kidney Dis.2013:61(Suppl 2):S12–23. 63. Hir st JA, Taylor KS, StevensRJ, et al. The impact of renin-angiotensin-aldosteronesystem inhibitors on Type 1 and Type 2 diabetic patientswith and without early diabetic nephropathy. Kidney Int.2012;81, 674–83. 64. Edd y AA. Interstitial nephritisinduced by protein-overload proteinuria. Am J Pathol.1989;135:719–33. 65. Eddy EA, Giachelli CM, Mcculloc L, etal. Renal expression of genes that promote interstitialinflammation and fibrosis in rats with protein-overloadproteinuria. Kidney Int. 1995;47:1546–57. 66. Abbate M,Zoja C, Remuzzi G. How does proteinuria cause progressiverenal damage? J Am Soc Nephrol. 2006;17:2974–84. 67.Macconi D, Chiabrando C, Schiarea S, et al. Proteasomalprocessing of albumin by renal dendritic cells generatesantigenic peptides. J Am Soc Nephrol. 2009;20:123–30. 68.Zeisberg M, Neilson EG. Mechanisms of tubulointerstitialfibrosis. J Am Soc Nephrol. 2010;21:1819–34. 69. BainesRJ, Brunskill NJ. Molecular interactions between filteredproteins and proximal tubular cells. Nephron Exp Nephrol.2008;110:e67–e71. 70. Zoja C, Donadelli R, Colleoni S, etal. Protein overload stimulates RANTES production byproximal tubular cells depending on NF-kappa B activation.Kidney Int. 1998;53:1608–15.
71. Reich H, Tritchler D, Herzenberg AM, Kassiri Z, ZhouX, et al. Albumin activates ERK via EGF receptor in humanrenal epithelial cells. J Am Soc Nephrol. 2005;16:1266–78.
72. Zhuan Cui, Junbao Shi, Yan Liu, et al. Upregulation ofsoluble epoxide hydrolase in proximal tubular cellsmediated proteinuria-induced renal damage. Am J PhysiolRenal Physiol. 2013;304:F168–76.
73. Erkan E, Garcia CD, Patterson LT, et al. Induction ofrenal tubular cell apoptosis in focal segmentalglomerulosclerosis: Roles of proteinuria and Fas-dependentpathways. J Am Soc Nephrol. 2005;16:398–407.
74. Zhou W, Marsh JE, Sacks SH. Intrarenal synthesis ofcomplement. Kidney Int. 2001;59:1227–35.
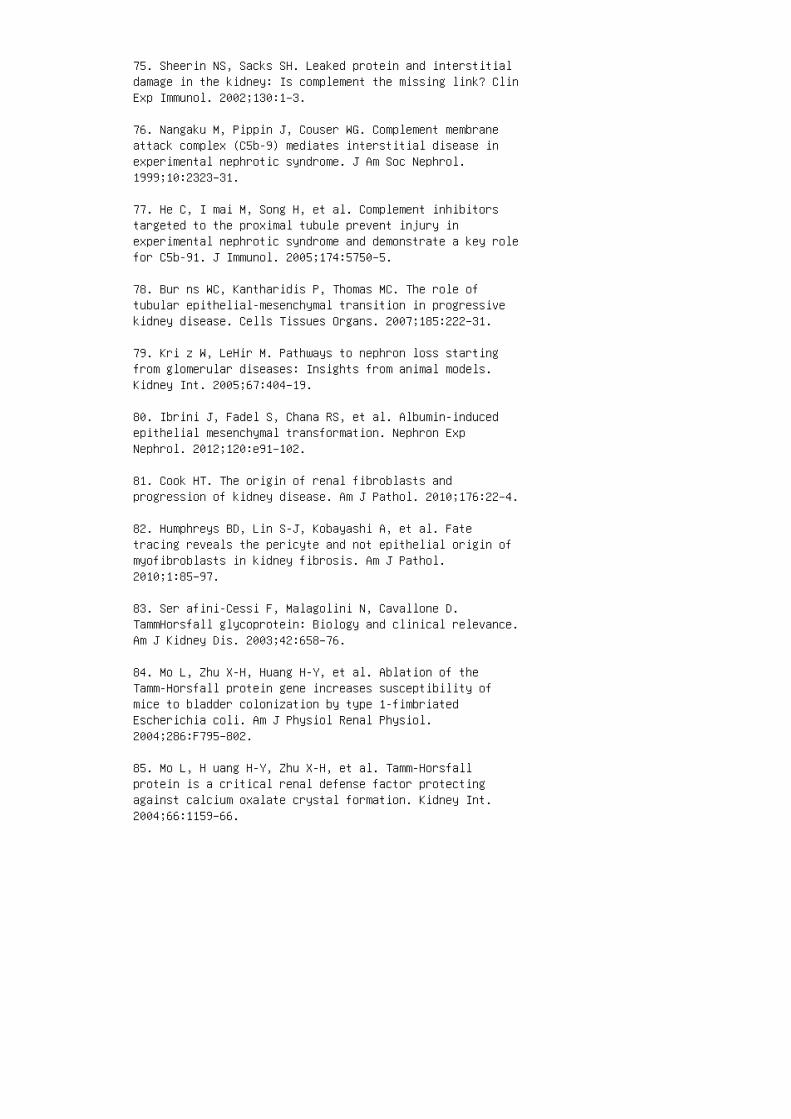
75. Sheerin NS, Sacks SH. Leaked protein and interstitialdamage in the kidney: Is complement the missing link? ClinExp Immunol. 2002;130:1–3.
76. Nangaku M, Pippin J, Couser WG. Complement membraneattack complex (C5b-9) mediates interstitial disease inexperimental nephrotic syndrome. J Am Soc Nephrol.1999;10:2323–31.
77. He C, I mai M, Song H, et al. Complement inhibitorstargeted to the proximal tubule prevent injury inexperimental nephrotic syndrome and demonstrate a key rolefor C5b-91. J Immunol. 2005;174:5750–5.
78. Bur ns WC, Kantharidis P, Thomas MC. The role oftubular epithelial-mesenchymal transition in progressivekidney disease. Cells Tissues Organs. 2007;185:222–31.
79. Kri z W, LeHir M. Pathways to nephron loss startingfrom glomerular diseases: Insights from animal models.Kidney Int. 2005;67:404–19.
80. Ibrini J, Fadel S, Chana RS, et al. Albumin-inducedepithelial mesenchymal transformation. Nephron ExpNephrol. 2012;120:e91–102.
81. Cook HT. The origin of renal fibroblasts andprogression of kidney disease. Am J Pathol. 2010;176:22–4.
82. Humphreys BD, Lin S-J, Kobayashi A, et al. Fatetracing reveals the pericyte and not epithelial origin ofmyofibroblasts in kidney fibrosis. Am J Pathol.2010;1:85–97.
83. Ser afini-Cessi F, Malagolini N, Cavallone D.TammHorsfall glycoprotein: Biology and clinical relevance.Am J Kidney Dis. 2003;42:658–76.
84. Mo L, Zhu X-H, Huang H-Y, et al. Ablation of theTamm-Horsfall protein gene increases susceptibility ofmice to bladder colonization by type 1-fimbriatedEscherichia coli. Am J Physiol Renal Physiol.2004;286:F795–802.
85. Mo L, H uang H-Y, Zhu X-H, et al. Tamm-Horsfallprotein is a critical renal defense factor protectingagainst calcium oxalate crystal formation. Kidney Int.2004;66:1159–66.

86. Bou wman A, Verbeke J, Brand M, et al. Renal medullaryhyperechogenicity in a neonate with oliguria. Clin KidneyJ. 2010;3:176–8. 87. Diabetes and Chronic Kidney DiseaseWork Group. KDOQI clinical practice guidelines andclinical practice recommendations for diabetes and chronickidney disease. Am J Kidney Dis. 2007;49(Suppl 2):S1–180.88. Mahfoud F, Ukena C, Pöss J, et al. Microalbuminuriaindependently correlates to cardiovascular comorbidityburden in patients with hypertension. Clin Res Cardiol.2012;101:761–6. 89. Wit te EC, Heerspink HJL, de Zeeuw,D,et al. First morning voids are more reliable than spoturine samples to assess microalbuminuria. J Am Soc Nephrol.2009;20:436–43. 90. Hogg RJ, Portman RJ, Dawn Milliner D,et al. Evaluation and management of proteinuria andnephrotic syndrome in children: Recommendations from apediatric nephrology panel established at the NationalKidney Foundation Conference on Proteinuria, Albuminuria,Risk, Assessment, Detection, and Elimination (PARADE).Pediatrics. 2000;105:1242–9. 91. Bra ndt JR, Jacobs A,Raissy HH, et al. Orthostatic proteinuria and the spectrumof diurnal variability of urinary protein excretion inhealthy children. Pediatr Nephrol. 2010;25:1131–7. 92.Cho B S, Choi YM, Kang HH, et al.: Diagnosis of nutcrackerphenomenon using renal Doppler ultrasound in orthostaticproteinuria. Nephrol Dial Transplant. 2001;16:1620–5. 93.Lee SJ, You ES, Lee JE, et al. Left renal vein entrapmentsyndrome in two girls with orthostatic proteinuria. PediatrNephrol. 1997;11:218–20. 94. Devarajan P. Mechanisms oforthostatic proteinuria: Lessons from a transplant donor.J Am Soc Nephrol. 1993;4:36–9. 95. Mar ta BM, Mazzoni,ML, Simonetti GD, et al. Renal vein obstruction andorthostatic proteinuria: A review. Nephrol DialTransplant. 2011;26:562–5. 96. Rob inson RR, Glover SN,Phillip PJ, et al. Fixed and reproducible orthostaticproteinuria: Light microscopic studies of the kidney. Am JPathol. 1961;39:405–17. 97. von Bonsdorff M, Tornroth T,Pasternack A. Renal biopsy findings in orthostaticproteinuria. Acta Pathol Microbiol Immunol Scand.1982;90:11–8. 98. Rytand DA, Spreiter S. Prognosis inpostural (orthostatic) proteinuria: Forty to fifty-yearfollow-up of six patients after diagnosis by Thomas Addis.N Engl J Med. 1981;305:618–21. 99. Thompson AL, DurrettRR, Robinson RR. Fixed and reproducible orthostaticproteinuria. VI. Results of a 10-year follow-upevaluation. Ann Intern Med. 1970;73:235–44. 100. Springberg PD, Garrett LE, Jr., Thompson AL, et al. Fixed andreproducible orthostatic proteinuria: Results of a 20-yearfollow-up study. Ann Intern Med. 1982;97:516–9.
101. Committee on Practice and Ambulatory Medicine and

Bright Futures Steering Committee: Recommendations forpreventive pediatric health care. Pediatrics.2007;120:1376.
102. American Academy of Pediatrics. AAP publicationsreaffirmed and retired. Pediatrics. 2011;127:e857.
103. Sekhar DL, Wang L, Hollenbeak CS, et al. Acosteffectiveness analysis of screening urine dipsticks inwell-child care. Pediatrics. 2010;125;660–3.
104. Yap H K, Quek CM, Shen Q, et al. Role of urinaryscreening programs in children in the prevention ofchronic kidney disease. Ann Acad Med Singapore.2005;34:3–7.
105. Murakami M, Hayakawa M, Yanagihara T, et al.Proteinuria screening for children. Kidney Int Suppl.2005;94:S23–7.
106. Boulware LE, Jaar BG, Tarver-Carr ME, et al.Screening for proteinuria in US adults: Acost-effectiveness analysis. JAMA. 2003;290:3101–14.
107. Qaseem A, Hopkins RH, Jr., Sweet DE, et al.Screening, monitoring, and treatment of stage 1 to 3chronic kidney disease: A clinical practice guideline fromthe American College of Physicians. Ann Intern Med.2013;159:835–7.
REVIEW QUESTIONS
1. Mass screening of children for proteinuria andhematuria is a useful strategy for detection of chronickidney disease in children. a. True b. False
2. In a 2-week-old male newborn, parents report that thediaper is occasionally stained red-brown. �ey are concernedthat he has blood in his urine. You reassure the parentswith the suggestion that he probably has uric acidcrystals in the urine and increasing �uid intake would behelpful. Six weeks later, the patients return, with thesymptom that the infant was irritable and that thered-brown staining of the diapers has persisted.Urinalysis of a bagged urine specimen shows no protein orblood. Centrifugation 10 mL of urine shows a large amountof brownish red sediment. Microscopic analysis shows uricacid crystals in the sediment. You would obtain thefollowing investigations: a. Urine for spot uric acid b.Urine for spot uric acid, spot creatinine c.
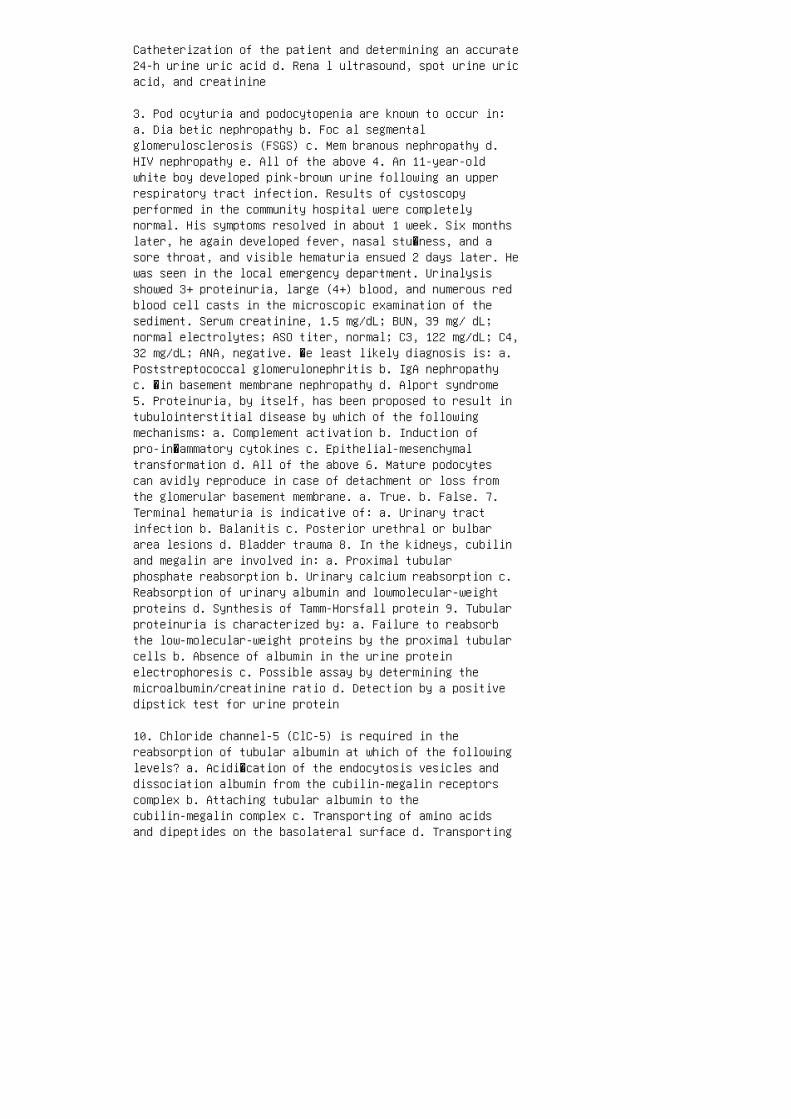
Catheterization of the patient and determining an accurate24-h urine uric acid d. Rena l ultrasound, spot urine uricacid, and creatinine
3. Pod ocyturia and podocytopenia are known to occur in:a. Dia betic nephropathy b. Foc al segmentalglomerulosclerosis (FSGS) c. Mem branous nephropathy d.HIV nephropathy e. All of the above 4. An 11-year-oldwhite boy developed pink-brown urine following an upperrespiratory tract infection. Results of cystoscopyperformed in the community hospital were completelynormal. His symptoms resolved in about 1 week. Six monthslater, he again developed fever, nasal stu�ness, and asore throat, and visible hematuria ensued 2 days later. Hewas seen in the local emergency department. Urinalysisshowed 3+ proteinuria, large (4+) blood, and numerous redblood cell casts in the microscopic examination of thesediment. Serum creatinine, 1.5 mg/dL; BUN, 39 mg/ dL;normal electrolytes; ASO titer, normal; C3, 122 mg/dL; C4,32 mg/dL; ANA, negative. �e least likely diagnosis is: a.Poststreptococcal glomerulonephritis b. IgA nephropathyc. �in basement membrane nephropathy d. Alport syndrome5. Proteinuria, by itself, has been proposed to result intubulointerstitial disease by which of the followingmechanisms: a. Complement activation b. Induction ofpro-in�ammatory cytokines c. Epithelial-mesenchymaltransformation d. All of the above 6. Mature podocytescan avidly reproduce in case of detachment or loss fromthe glomerular basement membrane. a. True. b. False. 7.Terminal hematuria is indicative of: a. Urinary tractinfection b. Balanitis c. Posterior urethral or bulbararea lesions d. Bladder trauma 8. In the kidneys, cubilinand megalin are involved in: a. Proximal tubularphosphate reabsorption b. Urinary calcium reabsorption c.Reabsorption of urinary albumin and lowmolecular-weightproteins d. Synthesis of Tamm-Horsfall protein 9. Tubularproteinuria is characterized by: a. Failure to reabsorbthe low-molecular-weight proteins by the proximal tubularcells b. Absence of albumin in the urine proteinelectrophoresis c. Possible assay by determining themicroalbumin/creatinine ratio d. Detection by a positivedipstick test for urine protein
10. Chloride channel-5 (ClC-5) is required in thereabsorption of tubular albumin at which of the followinglevels? a. Acidi�cation of the endocytosis vesicles anddissociation albumin from the cubilin-megalin receptorscomplex b. Attaching tubular albumin to thecubilin-megalin complex c. Transporting of amino acidsand dipeptides on the basolateral surface d. Transporting

the cubilin-megalin complex to the tubular cell surfaceANSWER KEY 1. b 2. d 3. e 4. a 5. d 6. b 7. c 8. c9. a 10. a

10 Physiology of glomerular filtration
1. Bellomo G. A short history of “glomerulus.” Clin KidneyJ. 2013;6:250–1.
2. Are ndshorst WJ, Gottschalk CW. Glomerularultrafiltration dynamics: Historical perspective. Am JPhysiol. 1985;248:F163–74.
3. Reitsma S, Slaaf DW, Vink H, et al. The endothelialglycocalyx: Composition, functions, and visualization.Pflugers Arch.2007;454:345–59.
4. Bal lermann BJ, Stan RV. Resolved: Capillary endotheliumis a major contributor to the glomerular filtrationbarrier. J Am Soc Nephrol. 2007;18:2432–8.
5. Salmon AH, Ferguson JK, Burford JL, et al. Loss of theendothelial glycocalyx links albuminuria and vasculardysfunction. J Am Soc Nephrol. 2012;23:1339–50.
6. Daniels BS, Hauser EB, Deen WM, Hostetter TH.Glomerular basement membrane: In vitro studies of waterand protein permeability. Am J Physiol. 1992;262:F919–26.
7. St John PL, Abrahamson DR. Glomerular endothelial cellsand podocytes jointly synthesize laminin-1 and -11 chains.Kidney Int. 2001;60:1037–46.
8. Edw ards A, Daniels BS, Deen WM. Hindered transport ofmacromolecules in isolated glomeruli. II. Convection andpressure effects in basement membrane. Biophys J.1997;72:214–22.
9. van d en Heuvel LP, van den Born J, Veerkamp JH, et al.Comparison of heparan sulfate proteoglycans from equineand human glomerular basement membranes. Int J Biochem.1990;22:903–14.
10. Kar asawa R, Nishi S, Suzuki Y, et al. Early increaseof chondroitin sulfate glycosaminoglycan in the glomerularbasement membrane of rats with diabetic glomerulopathy.Nephron. 1997;76:62–71.
11. Kho shnoodi J, Sigmundsson K, Ofverstedt LG, et al.Nephrin promotes cell-cell adhesion through homophilicinteractions. Am J Pathol. 2003;163:2337–46.
12. War tiovaara J, Ofverstedt LG, Khoshnoodi J, et al.Nephrin strands contribute to a porous slit diaphragm

scaffold as revealed by electron tomography. J Clin Invest.2004;114:1475–83.
13. Pat rakka J, Tryggvason K. Molecular make-up of theglomerular filtration barrier. Biochem Biophys Res Commun.2010;396:164–9.
14. Ghitescu L, Desjardins M, Bendayan M.Immunocytochemical study of glomerular permeability toanionic, neutral and cationic albumins. Kidney Int.1992;42:25–32.
15. Ren nke HG, Cotran RS, Venkatachalam MA. Role ofmolecular charge in glomerular permeability: Tracerstudies with cationized ferritins. J Cell Biol.1975;67:638–46.
16. Dee n WM, Troy JL, Robertson CR, Brenner BM. Dynamicsof glomerular ultrafiltration in the rat. IV.Determination of the ultrafiltration coefficient. J ClinInvest. 1973;52:1500–8. 17. Arendshorst WJ, Finn WF,Gottschalk CW. Autoregulation of blood flow in the ratkidney. Am J Physiol. 1975;228:127–33. 18. Kob ori H,Nangaku M, Navar LG, Nishiyama A. The intrarenalrenin-angiotensin system: From physiology to thepathobiology of hypertension and kidney disease. PharmacolRev. 2007;59:251–87. 19. Ichihara A, Imig JD, Navar LG.Cyclooxygenase-2 modulates afferent arteriolar responsesto increases in pressure. Hypertension. 1999;34:843–7.20. Roman RJ. P-450 metabolites of arachidonic acid in thecontrol of cardiovascular function. Physiol Rev.2002;82:131–85. 21. Arendshorst WJ, Navar LG. Renalcirculation and glomerular hemodynamics. In: Coffman TM,Falk RJ, Molitoris BA, et al., editors. Schrier’s Diseasesof the Kidney, 9th ed. Philadelphia: Lippincott Williams &Wilkins; 2013. p. 74–131. 22. Sip os A, Vargas S,Peti-Peterdi J. Direct demonstration of tubular fluid flowsensing by macula densa cells. Am J Physiol Renal Physiol.2010;299:F1087–93. 23. Peti-Peterdi J, Harris RC. Maculadensa sensing and signaling mechanisms of renin release. JAm Soc Nephrol. 2010;21:1093–6. 24. Johns EJ. Role of therenal nerves in modulating renin release during pressurereduction at the feline kidney. Clin Sci (Lond).1985;69:185–95. 25. Bre nner BM, Hostetter TH, Humes HD.Molecular basis of proteinuria of glomerular origin. NEngl J Med. 1978;298:826. 26. Bre nner BM, Hostetter TH,Humes HD. Glomerular permselectivity: Barrier functionbased on discrimination of molecular size and charge. Am JPhysiol. 1978;234:F455. 27. Rodewald R, Karnovsky M.Porous substructure of the glomerular slit diaphragm in
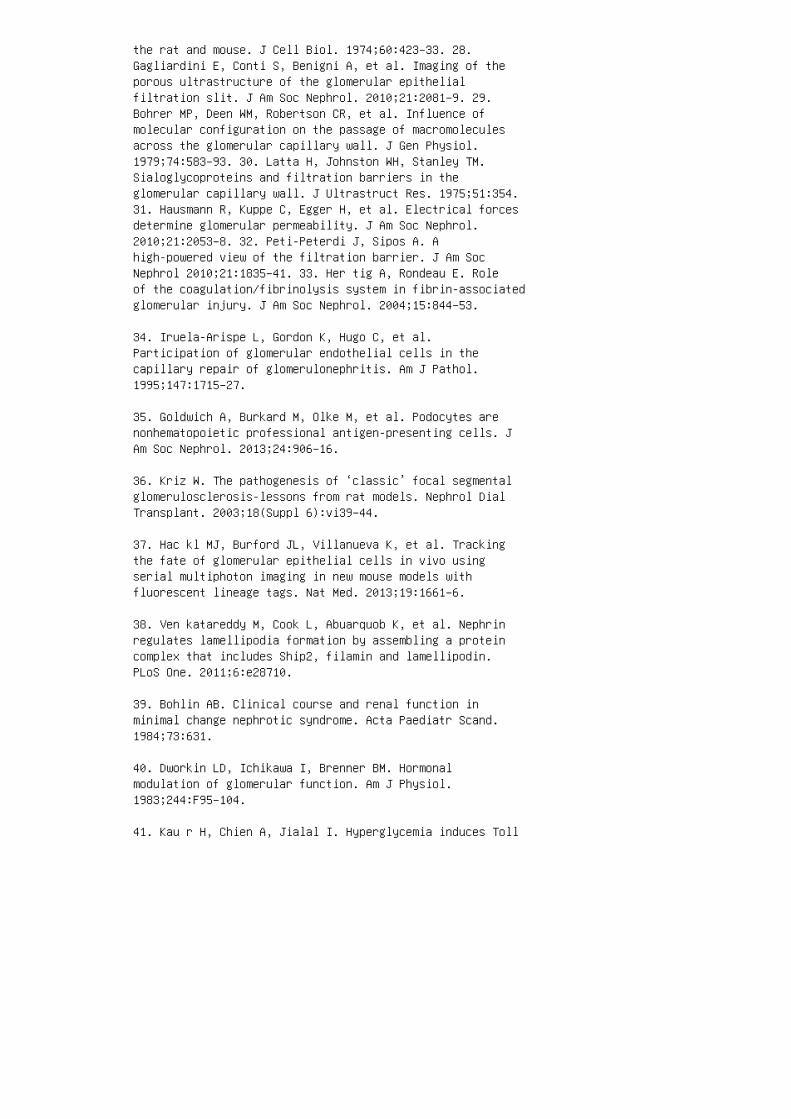
the rat and mouse. J Cell Biol. 1974;60:423–33. 28.Gagliardini E, Conti S, Benigni A, et al. Imaging of theporous ultrastructure of the glomerular epithelialfiltration slit. J Am Soc Nephrol. 2010;21:2081–9. 29.Bohrer MP, Deen WM, Robertson CR, et al. Influence ofmolecular configuration on the passage of macromoleculesacross the glomerular capillary wall. J Gen Physiol.1979;74:583–93. 30. Latta H, Johnston WH, Stanley TM.Sialoglycoproteins and filtration barriers in theglomerular capillary wall. J Ultrastruct Res. 1975;51:354.31. Hausmann R, Kuppe C, Egger H, et al. Electrical forcesdetermine glomerular permeability. J Am Soc Nephrol.2010;21:2053–8. 32. Peti-Peterdi J, Sipos A. Ahigh-powered view of the filtration barrier. J Am SocNephrol 2010;21:1835–41. 33. Her tig A, Rondeau E. Roleof the coagulation/fibrinolysis system in fibrin-associatedglomerular injury. J Am Soc Nephrol. 2004;15:844–53.
34. Iruela-Arispe L, Gordon K, Hugo C, et al.Participation of glomerular endothelial cells in thecapillary repair of glomerulonephritis. Am J Pathol.1995;147:1715–27.
35. Goldwich A, Burkard M, Olke M, et al. Podocytes arenonhematopoietic professional antigen-presenting cells. JAm Soc Nephrol. 2013;24:906–16.
36. Kriz W. The pathogenesis of ‘classic’ focal segmentalglomerulosclerosis-lessons from rat models. Nephrol DialTransplant. 2003;18(Suppl 6):vi39–44.
37. Hac kl MJ, Burford JL, Villanueva K, et al. Trackingthe fate of glomerular epithelial cells in vivo usingserial multiphoton imaging in new mouse models withfluorescent lineage tags. Nat Med. 2013;19:1661–6.
38. Ven katareddy M, Cook L, Abuarquob K, et al. Nephrinregulates lamellipodia formation by assembling a proteincomplex that includes Ship2, filamin and lamellipodin.PLoS One. 2011;6:e28710.
39. Bohlin AB. Clinical course and renal function inminimal change nephrotic syndrome. Acta Paediatr Scand.1984;73:631.
40. Dworkin LD, Ichikawa I, Brenner BM. Hormonalmodulation of glomerular function. Am J Physiol.1983;244:F95–104.
41. Kau r H, Chien A, Jialal I. Hyperglycemia induces Toll

like receptor 4 expression and activity in mouse mesangialcells: Relevance to diabetic nephropathy. Am J PhysiolRenal Physiol. 2012;303:F1145–50.
42. Mer kle M, Ribeiro A, Koppel S, et al. TLR3dependentimmune regulatory functions of human mesangial cells. CellMol Immunol. 2012;9:334–40.
43. Suwanichkul A, Wenderfer SE. Differential expression offunctional Fc-receptors and additional immune complexreceptors on mouse kidney cells. Mol Immunol.2013;56:369–79.
44. Schlondorff D, Banas B. The mesangial cell revisited:No cell is an island. J Am Soc Nephrol. 2009;20:1179–87.
45. Ballermann BJ. Contribution of the endothelium to theglomerular permselectivity barrier in health and disease.Nephron Physiol. 2007;106:19–25.
46. Sis on K, Eremina V, Baelde H, et al. Glomerularstructure and function require paracrine, not autocrine,VEGF-VEGFR-2 signaling. J Am Soc Nephrol.2010;21:1691–701.
47. Lefkowith JB, Schreiner G. Essential fatty aciddeficiency depletes rat glomeruli of resident macrophagesand inhibits angiotensin II–induced eicosanoid synthesis. JClin Invest. 1987;80:947–56. 48. Strutz F, Zeisberg M.Renal fibroblasts and myofibroblasts in chronic kidneydisease. J Am Soc Nephrol. 2006;17:2992–8. 49. Rom agnaniP. Parietal epithelial cells: Their role in health anddisease. Contrib Nephrol. 2011;169:23–36. REVIEW QUESTIONS1. During glomerular �ltration, the passage of largermolecules is restricted by a. �e glycocalyx b. �eglomerular basement membrane c. �e epithelial slitdiaphragm d. All of the above 2. �e podocyte is adi�erentiated cell that provides a static barrier toltration. a. True b. False 3. Inc rease in which of thefollowing does not increase glomerular �ltration? a.E�eren t arteriolar resistance b. Glom erular capillaryhydrostatic pressure c. Glom erular capillary oncoticpressure d. Glo merular capillary blood �ow e. K f 4.Which of the following does not increase macromolecularclearance by the glomerulus? a. Fever b. Shock c.Flexible molecules d. Hypertrophy 5. Fenestration of theglomerular endothelium is maintained in part by productionof a. VEGF b. TGF-β c. COX-2 d. Endothelin e.Glycosaminoglycans ANSWER KEY 1. d 2. b 3. c 4. b 5. a
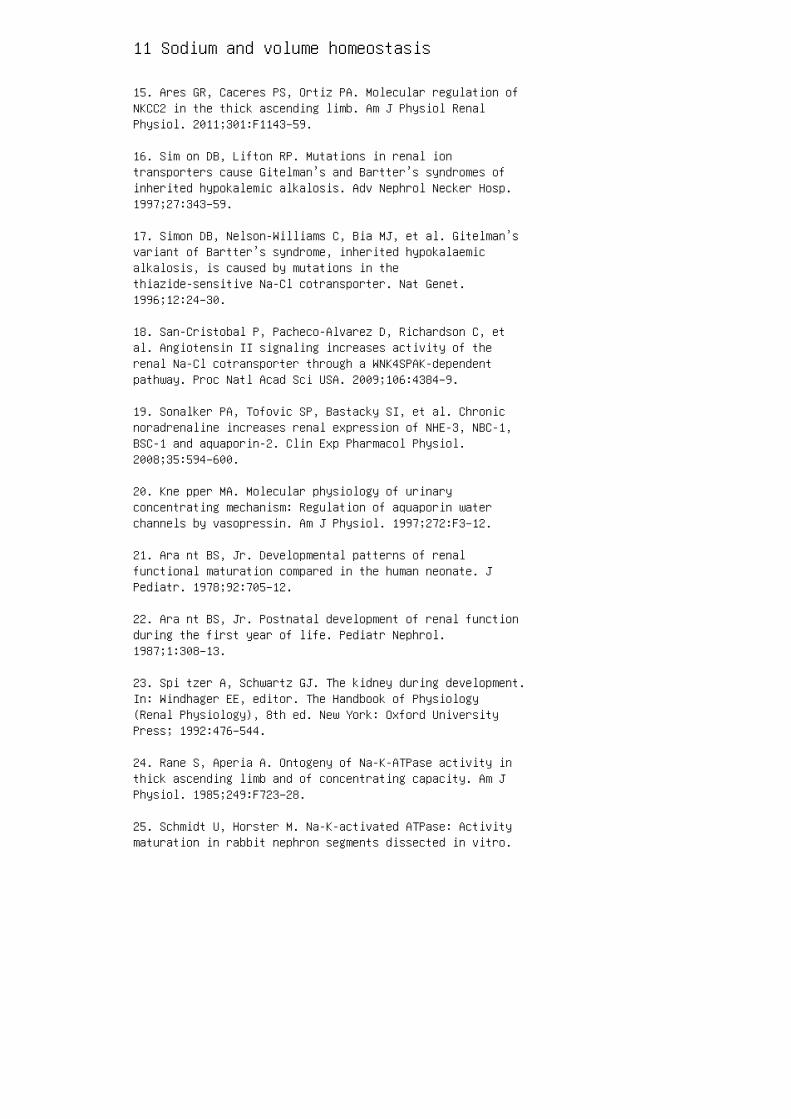
11 Sodium and volume homeostasis
15. Ares GR, Caceres PS, Ortiz PA. Molecular regulation ofNKCC2 in the thick ascending limb. Am J Physiol RenalPhysiol. 2011;301:F1143–59.
16. Sim on DB, Lifton RP. Mutations in renal iontransporters cause Gitelman’s and Bartter’s syndromes ofinherited hypokalemic alkalosis. Adv Nephrol Necker Hosp.1997;27:343–59.
17. Simon DB, Nelson-Williams C, Bia MJ, et al. Gitelman’svariant of Bartter’s syndrome, inherited hypokalaemicalkalosis, is caused by mutations in thethiazide-sensitive Na-Cl cotransporter. Nat Genet.1996;12:24–30.
18. San-Cristobal P, Pacheco-Alvarez D, Richardson C, etal. Angiotensin II signaling increases activity of therenal Na-Cl cotransporter through a WNK4SPAK-dependentpathway. Proc Natl Acad Sci USA. 2009;106:4384–9.
19. Sonalker PA, Tofovic SP, Bastacky SI, et al. Chronicnoradrenaline increases renal expression of NHE-3, NBC-1,BSC-1 and aquaporin-2. Clin Exp Pharmacol Physiol.2008;35:594–600.
20. Kne pper MA. Molecular physiology of urinaryconcentrating mechanism: Regulation of aquaporin waterchannels by vasopressin. Am J Physiol. 1997;272:F3–12.
21. Ara nt BS, Jr. Developmental patterns of renalfunctional maturation compared in the human neonate. JPediatr. 1978;92:705–12.
22. Ara nt BS, Jr. Postnatal development of renal functionduring the first year of life. Pediatr Nephrol.1987;1:308–13.
23. Spi tzer A, Schwartz GJ. The kidney during development.In: Windhager EE, editor. The Handbook of Physiology(Renal Physiology), 8th ed. New York: Oxford UniversityPress; 1992:476–544.
24. Rane S, Aperia A. Ontogeny of Na-K-ATPase activity inthick ascending limb and of concentrating capacity. Am JPhysiol. 1985;249:F723–28.
25. Schmidt U, Horster M. Na-K-activated ATPase: Activitymaturation in rabbit nephron segments dissected in vitro.
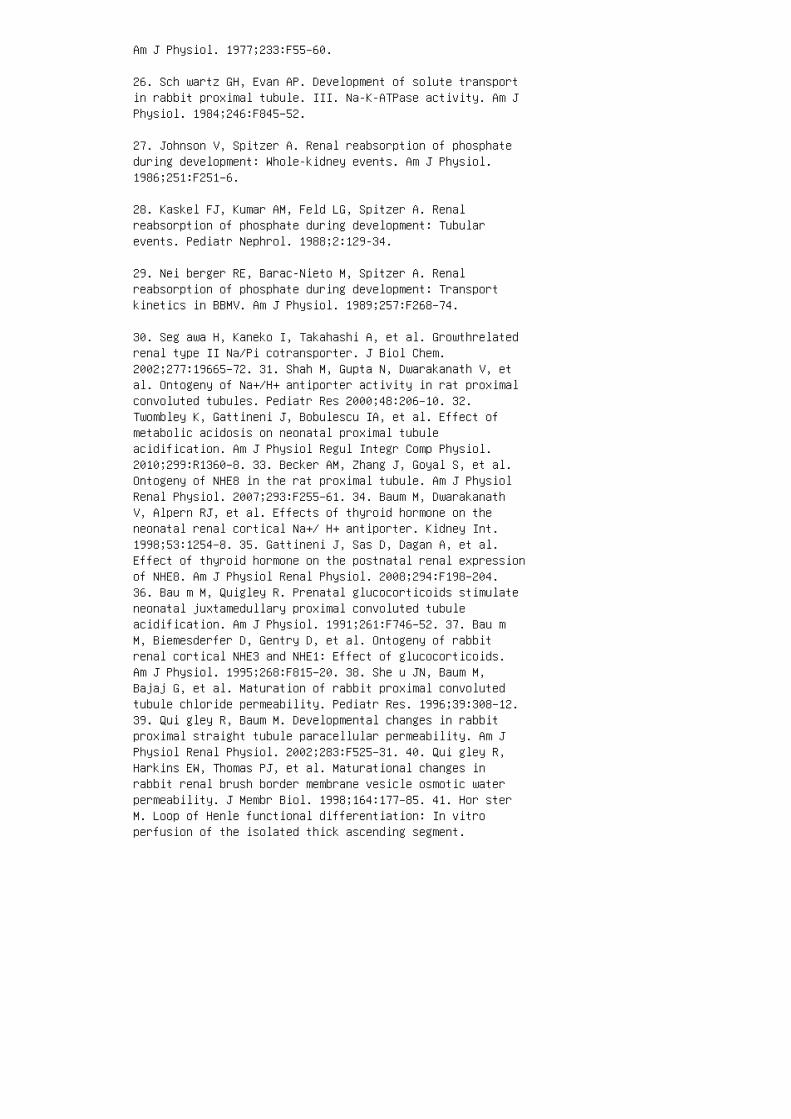
Am J Physiol. 1977;233:F55–60.
26. Sch wartz GH, Evan AP. Development of solute transportin rabbit proximal tubule. III. Na-K-ATPase activity. Am JPhysiol. 1984;246:F845–52.
27. Johnson V, Spitzer A. Renal reabsorption of phosphateduring development: Whole-kidney events. Am J Physiol.1986;251:F251–6.
28. Kaskel FJ, Kumar AM, Feld LG, Spitzer A. Renalreabsorption of phosphate during development: Tubularevents. Pediatr Nephrol. 1988;2:129-34.
29. Nei berger RE, Barac-Nieto M, Spitzer A. Renalreabsorption of phosphate during development: Transportkinetics in BBMV. Am J Physiol. 1989;257:F268–74.
30. Seg awa H, Kaneko I, Takahashi A, et al. Growthrelatedrenal type II Na/Pi cotransporter. J Biol Chem.2002;277:19665–72. 31. Shah M, Gupta N, Dwarakanath V, etal. Ontogeny of Na+/H+ antiporter activity in rat proximalconvoluted tubules. Pediatr Res 2000;48:206–10. 32.Twombley K, Gattineni J, Bobulescu IA, et al. Effect ofmetabolic acidosis on neonatal proximal tubuleacidification. Am J Physiol Regul Integr Comp Physiol.2010;299:R1360–8. 33. Becker AM, Zhang J, Goyal S, et al.Ontogeny of NHE8 in the rat proximal tubule. Am J PhysiolRenal Physiol. 2007;293:F255–61. 34. Baum M, DwarakanathV, Alpern RJ, et al. Effects of thyroid hormone on theneonatal renal cortical Na+/ H+ antiporter. Kidney Int.1998;53:1254–8. 35. Gattineni J, Sas D, Dagan A, et al.Effect of thyroid hormone on the postnatal renal expressionof NHE8. Am J Physiol Renal Physiol. 2008;294:F198–204.36. Bau m M, Quigley R. Prenatal glucocorticoids stimulateneonatal juxtamedullary proximal convoluted tubuleacidification. Am J Physiol. 1991;261:F746–52. 37. Bau mM, Biemesderfer D, Gentry D, et al. Ontogeny of rabbitrenal cortical NHE3 and NHE1: Effect of glucocorticoids.Am J Physiol. 1995;268:F815–20. 38. She u JN, Baum M,Bajaj G, et al. Maturation of rabbit proximal convolutedtubule chloride permeability. Pediatr Res. 1996;39:308–12.39. Qui gley R, Baum M. Developmental changes in rabbitproximal straight tubule paracellular permeability. Am JPhysiol Renal Physiol. 2002;283:F525–31. 40. Qui gley R,Harkins EW, Thomas PJ, et al. Maturational changes inrabbit renal brush border membrane vesicle osmotic waterpermeability. J Membr Biol. 1998;164:177–85. 41. Hor sterM. Loop of Henle functional differentiation: In vitroperfusion of the isolated thick ascending segment.

Pflugers Arch. 1978;378:15–24. 42. Sat lin LM, Palmer LG.Apical K+ conductance in maturing rabbit principal cell.Am J Physiol. 1997;272:F397–404. 43. Satlin LM, PalmerLG. Apical Na+ conductance in maturing rabbit principalcell. Am J Physiol. 1996;270:F391–97. 44. Satlin LM.Postnatal maturation of potassium transport in rabbitcortical collecting duct. Am J Physiol. 1994;266:F57–65.45. Woda CB, Miyawaki N, Ramalakshmi S, et al. Ontogeny offlow-stimulated potassium secretion in rabbit corticalcollecting duct: Functional and molecular aspects. Am JPhysiol Renal Physiol. 2003;285:F629–39. 46. GoldsmithDI, Drukker A, Blaufox MD, et al. Hemodynamic andexcretory response of the neonatal canine kidney to acutevolume expansion. Am J Physiol. 1979;237:F392–7. 47.Aperia A, Elinder G. Distal tubular sodium reabsorption inthe developing rat kidney. Am J Physiol. 1981;240:F487–91.
48. Chevalier RL, Thornhill BA, Belmonte DC, et al.Endogenous angiotensin II inhibits natriuresis after acutevolume expansion in the neonatal rat. Am J Physiol.1996;270:R393–7.
49. Paintal AS. Vagal sensory receptors and their reflexeffects. Physiol Rev. 1973;53:159–227.
50. Henry JP, Gauer OH, Reeves JL. Evidence of the atriallocation of receptors influencing urine flow. Circ Res.1956;4:85–90.
51. de Bo ld AJ, Borenstein HB, Veress AT, et al. A rapidand potent natriuretic response to intravenous injectionof atrial myocardial extract in rats. Life Sci.1981;28:89–94.
52. Nagaya N, Nishikimi T, Goto Y, et al. Plasma brainnatriuretic peptide is a biochemical marker for theprediction of progressive ventricular remodeling afteracute myocardial infarction. Am Heart J. 1998;135:21–8.
53. Cogan MG. Angiotensin II: A powerful controller ofsodium transport in the early proximal tubule.Hypertension. 1990;15:451–8.
54. Qua n A, Baum M. Regulation of proximal tubuletransport by angiotensin II. Semin Nephrol.1997;17:423–30.
55. Bel lo-Reuss E. Effect of catecholamines on fluidreabsorption by the isolated proximal convoluted tubule.Am J Physiol. 1980;238:F347–52.
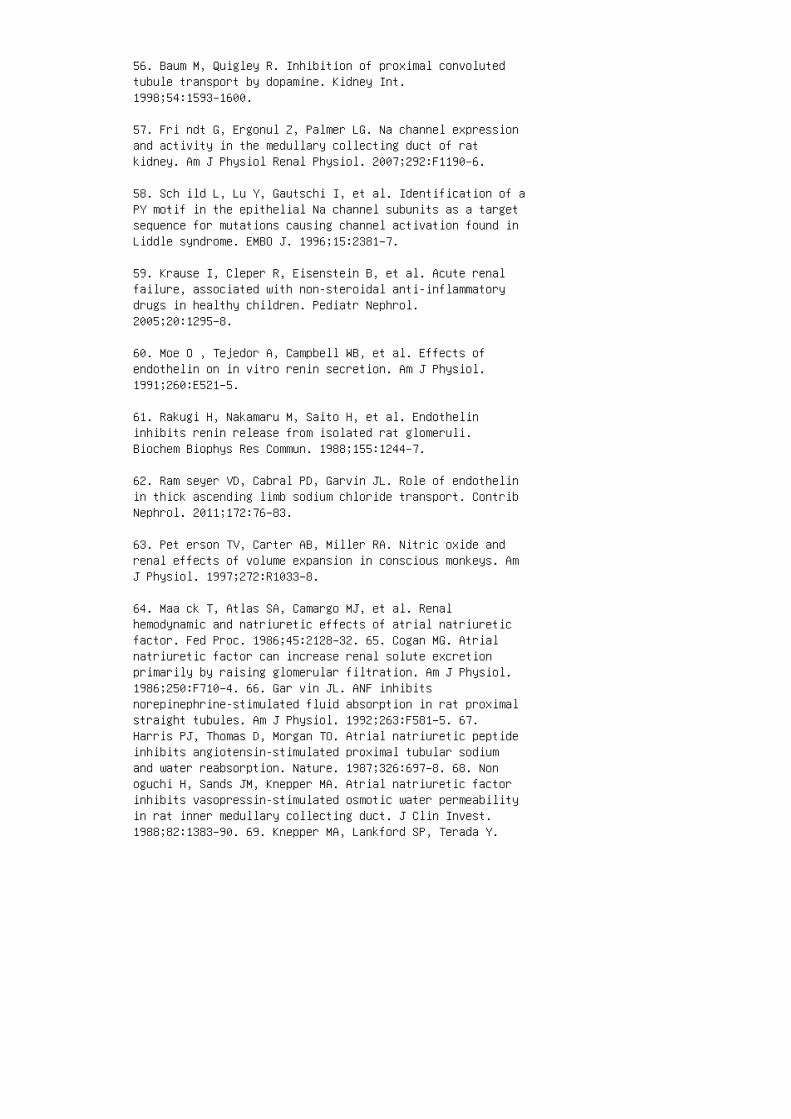
56. Baum M, Quigley R. Inhibition of proximal convolutedtubule transport by dopamine. Kidney Int.1998;54:1593–1600.
57. Fri ndt G, Ergonul Z, Palmer LG. Na channel expressionand activity in the medullary collecting duct of ratkidney. Am J Physiol Renal Physiol. 2007;292:F1190–6.
58. Sch ild L, Lu Y, Gautschi I, et al. Identification of aPY motif in the epithelial Na channel subunits as a targetsequence for mutations causing channel activation found inLiddle syndrome. EMBO J. 1996;15:2381–7.
59. Krause I, Cleper R, Eisenstein B, et al. Acute renalfailure, associated with non-steroidal anti-inflammatorydrugs in healthy children. Pediatr Nephrol.2005;20:1295–8.
60. Moe O , Tejedor A, Campbell WB, et al. Effects ofendothelin on in vitro renin secretion. Am J Physiol.1991;260:E521–5.
61. Rakugi H, Nakamaru M, Saito H, et al. Endothelininhibits renin release from isolated rat glomeruli.Biochem Biophys Res Commun. 1988;155:1244–7.
62. Ram seyer VD, Cabral PD, Garvin JL. Role of endothelinin thick ascending limb sodium chloride transport. ContribNephrol. 2011;172:76–83.
63. Pet erson TV, Carter AB, Miller RA. Nitric oxide andrenal effects of volume expansion in conscious monkeys. AmJ Physiol. 1997;272:R1033–8.
64. Maa ck T, Atlas SA, Camargo MJ, et al. Renalhemodynamic and natriuretic effects of atrial natriureticfactor. Fed Proc. 1986;45:2128–32. 65. Cogan MG. Atrialnatriuretic factor can increase renal solute excretionprimarily by raising glomerular filtration. Am J Physiol.1986;250:F710–4. 66. Gar vin JL. ANF inhibitsnorepinephrine-stimulated fluid absorption in rat proximalstraight tubules. Am J Physiol. 1992;263:F581–5. 67.Harris PJ, Thomas D, Morgan TO. Atrial natriuretic peptideinhibits angiotensin-stimulated proximal tubular sodiumand water reabsorption. Nature. 1987;326:697–8. 68. Nonoguchi H, Sands JM, Knepper MA. Atrial natriuretic factorinhibits vasopressin-stimulated osmotic water permeabilityin rat inner medullary collecting duct. J Clin Invest.1988;82:1383–90. 69. Knepper MA, Lankford SP, Terada Y.
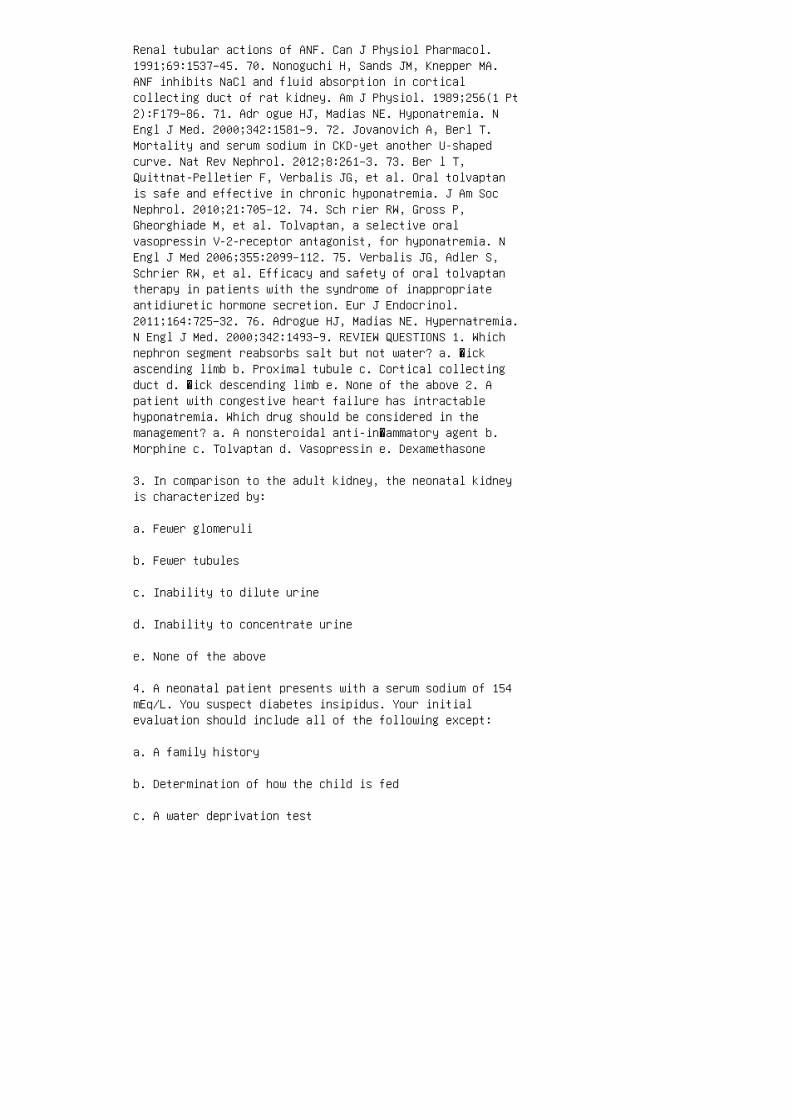
Renal tubular actions of ANF. Can J Physiol Pharmacol.1991;69:1537–45. 70. Nonoguchi H, Sands JM, Knepper MA.ANF inhibits NaCl and fluid absorption in corticalcollecting duct of rat kidney. Am J Physiol. 1989;256(1 Pt2):F179–86. 71. Adr ogue HJ, Madias NE. Hyponatremia. NEngl J Med. 2000;342:1581–9. 72. Jovanovich A, Berl T.Mortality and serum sodium in CKD-yet another U-shapedcurve. Nat Rev Nephrol. 2012;8:261–3. 73. Ber l T,Quittnat-Pelletier F, Verbalis JG, et al. Oral tolvaptanis safe and effective in chronic hyponatremia. J Am SocNephrol. 2010;21:705–12. 74. Sch rier RW, Gross P,Gheorghiade M, et al. Tolvaptan, a selective oralvasopressin V-2-receptor antagonist, for hyponatremia. NEngl J Med 2006;355:2099–112. 75. Verbalis JG, Adler S,Schrier RW, et al. Efficacy and safety of oral tolvaptantherapy in patients with the syndrome of inappropriateantidiuretic hormone secretion. Eur J Endocrinol.2011;164:725–32. 76. Adrogue HJ, Madias NE. Hypernatremia.N Engl J Med. 2000;342:1493–9. REVIEW QUESTIONS 1. Whichnephron segment reabsorbs salt but not water? a. �ickascending limb b. Proximal tubule c. Cortical collectingduct d. �ick descending limb e. None of the above 2. Apatient with congestive heart failure has intractablehyponatremia. Which drug should be considered in themanagement? a. A nonsteroidal anti-in�ammatory agent b.Morphine c. Tolvaptan d. Vasopressin e. Dexamethasone
3. In comparison to the adult kidney, the neonatal kidneyis characterized by:
a. Fewer glomeruli
b. Fewer tubules
c. Inability to dilute urine
d. Inability to concentrate urine
e. None of the above
4. A neonatal patient presents with a serum sodium of 154mEq/L. You suspect diabetes insipidus. Your initialevaluation should include all of the following except:
a. A family history
b. Determination of how the child is fed
c. A water deprivation test

d. A urine osmolality
e. An assessment of volume status of the child 5. Whichstatement about the collecting tubule is incorrect? a. Itis responsive to aldosterone. b. It is responsive tovasopressin. c. It reabsorbs 1% to 3% of the �lteredsodium. d. It has a lumen positive potential di�erence.e. It has an apical epithelial sodium channel. ANSWER KEY1. a 2. c 3. e 4. c 5. d

12 Potassium homeostasis
1. Delgado MM, Rohatgi R, Khan S, et al. Sodium andpotassium clearances by the maturing kidney:Clinical-molecular correlates. Pediatr Nephrol.2003;18:759–67. 2. Sulyok E, Nemeth M, Tenyi I, et al.Relationship between maturity, electrolyte balance and thefunction of the renin-angiotensin-aldosterone system innewborn infants. Biol Neonate. 1979;35:60–5. 3. Fly nnMA, Woodruff C, Clark J, Chase G. Total body potassium innormal children. Pediatr Res. 1972;6:239–45. 4. ButteNF, Hopkinson JM, Wong WW, et al. Body composition duringthe first 2 years of life: An updated reference. PediatrRes. 2000;47:578–85. 5. Dickerson JW, Widdowson EM.Chemical changes in skeletal muscle during development.Biochem J. 1960;74:247–57. 6. Rodriguez-Soriano J, ValloA, Castillo G, Oliveros R. Renal handling of water andsodium in infancy and childhood: A study using clearancemethods during hypotonic saline diuresis. Kidney Int.1981;20:700–4. 7. Lorenz JM, Kleinman LI, Markarian K.Potassium metabolism in extremely low birth weight infantsin the first week of life. J Pediatr. 1997;131:81–6. 8.Hol brook JT, Patterson KY, Bodner JE, et al. Sodium andpotassium intake and balance in adults consumingself-selected diets. Am J Clin Nutr. 1984;40:786–93. 9.Bia MJ, DeFronzo RA. Extrarenal potassium homeostasis. Am JPhysiol. 1981;240:F257–68. 10. Tudvad F, McNamarh NH,Barnett HL. Renal response of premature infants toadministration of bicarbonate and potassium. Pediatrics.1954;13:4–16. 11. Gie bisch G. Renal potassium transport:Mechanisms and regulation. Am J Physiol. 1998;274:F817–33.12. Lelievre-Pegorier M, Merlet-Benichou C, Roinel N, deRouffignac C. Developmental pattern of water andelectrolyte transport in rat superficial nephrons. Am JPhysiol. 1983;245:F15–21. 13. Solomon S. Absolute ratesof sodium and potassium reabsorption by proximal tubule ofimmature rats. Biol Neonate. 1974;25:340–51. 14. Zink H,Horster M. Maturation of diluting capacity in loop ofHenle of rat superficial nephrons. Am J Physiol.1977;233:F519–24. 15. Schmidt U, Horster M.Na-K-activated ATPase: Activity maturation in rabbitnephron segments dissected in vitro. Am J Physiol.1977;233:F55–60. 16. Ho K, Nichols CG, Lederer WJ, et al.Cloning and expression of an inwardly rectifyingATP-regulated potassium channel. Nature. 1993;362:31–8.17. Zhou H, Tate SS, Palmer LG. Primary structure andfunctional properties of an epithelial K channel. Am JPhysiol. 1994;266:C809–24. 18. Konrad M, Köckerling A,Ziegler A, et al. Mutations in the gene encoding theinwardly-rectifying renal potassium channel, ROMK, cause

the antenatal variant of Bartter syndrome: Evidence forgenetic heterogeneity. International Collaborative StudyGroup for Bartter-like Syndromes. Hum Mol Genet.1997;6:17–26.
19. Satlin LM. Postnatal maturation of potassium transportin rabbit cortical collecting duct. Am J Physiol.1994;266:F57–65.
20. Gur kan S, Estilo GK, Wei Y, Satlin LM. Potassiumtransport in the maturing kidney. Pediatr Nephrol.2007;22:915–25.
21. Woda CB, Bragin A, Kleyman TR, Satlin LM.Flowdependent K+ secretion in the cortical collecting ductis mediated by a maxi-K channel. Am J Physiol RenalPhysiol. 2001;280:F786–93.
22. Liu W , Xu S, Woda C, Kim P, et al. Effect of flowand stretch on the [Ca2+]i response of principal andintercalated cells in cortical collecting duct. Am JPhysiol Renal Physiol. 2003;285:F998–1012.
23. Bailey MA, Cantone A, Yan Q, et al. Maxi-K channelscontribute to urinary potassium excretion in theROMK-deficient mouse model of type II Bartter’s syndromeand in adaptation to a high-K diet. Kidney Int.2006;70:51–9.
24. Pacha J, Frindt G, Sackin H, et al. Apical maxi Kchannels in intercalated cells of CCT. Am J Physiol.1991;261:F696–705.
25. Constantinescu AR, Lane JC, Mak J, et al.Na+-K+ATPase-mediated basolateral rubidium uptake in thematuring rabbit cortical collecting duct. Am J PhysiolRenal Physiol. 2000;279:F1161–8.
26. Satlin LM, Evan AP, Gattone VH, 3rd, Schwartz GJ.Postnatal maturation of the rabbit cortical collectingduct. Pediatr Nephrol. 1988;2:135–45.
27. Ben chimol C, Zavilowitz B, Satlin LM. Developmentalexpression of ROMK mRNA in rabbit cortical collectingduct. Pediatr Res. 2000;47:46–52.
28. Zolotnitskaya A, Satlin LM. Developmental expressionof ROMK in rat kidney. Am J Physiol. 1999;276:F825–36.
29. Satlin LM, Palmer LG. Apical K+ conductance in
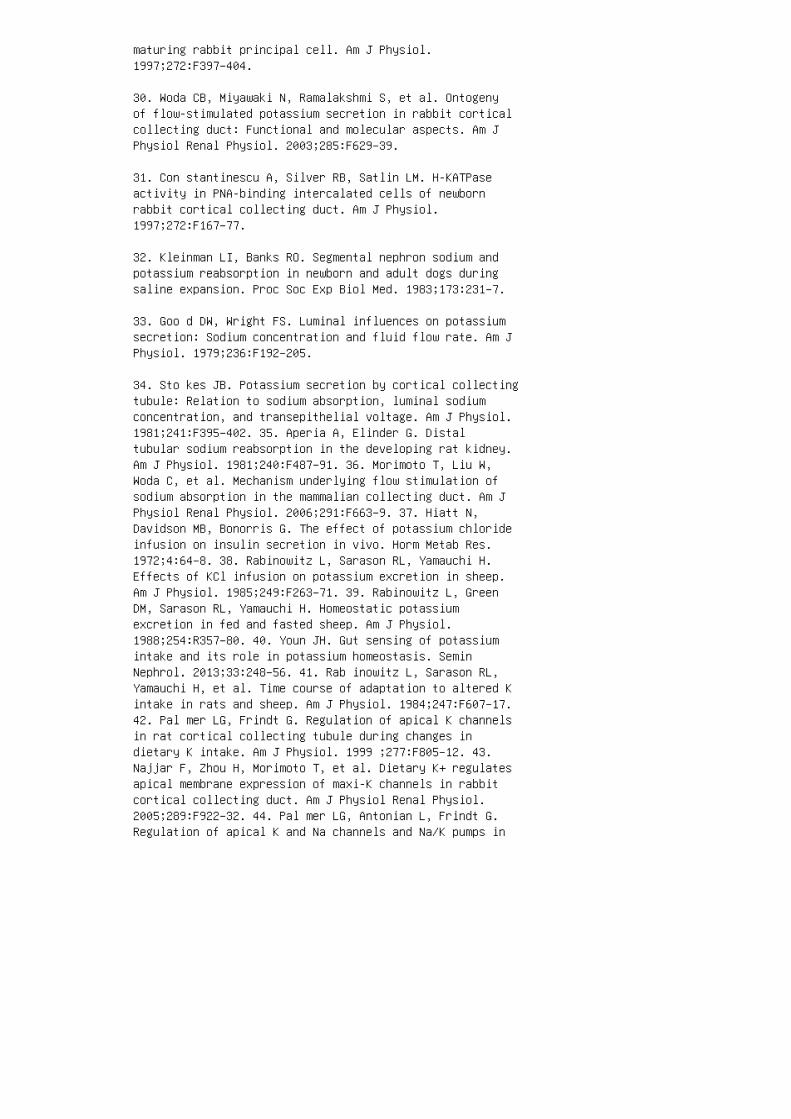
maturing rabbit principal cell. Am J Physiol.1997;272:F397–404.
30. Woda CB, Miyawaki N, Ramalakshmi S, et al. Ontogenyof flow-stimulated potassium secretion in rabbit corticalcollecting duct: Functional and molecular aspects. Am JPhysiol Renal Physiol. 2003;285:F629–39.
31. Con stantinescu A, Silver RB, Satlin LM. H-KATPaseactivity in PNA-binding intercalated cells of newbornrabbit cortical collecting duct. Am J Physiol.1997;272:F167–77.
32. Kleinman LI, Banks RO. Segmental nephron sodium andpotassium reabsorption in newborn and adult dogs duringsaline expansion. Proc Soc Exp Biol Med. 1983;173:231–7.
33. Goo d DW, Wright FS. Luminal influences on potassiumsecretion: Sodium concentration and fluid flow rate. Am JPhysiol. 1979;236:F192–205.
34. Sto kes JB. Potassium secretion by cortical collectingtubule: Relation to sodium absorption, luminal sodiumconcentration, and transepithelial voltage. Am J Physiol.1981;241:F395–402. 35. Aperia A, Elinder G. Distaltubular sodium reabsorption in the developing rat kidney.Am J Physiol. 1981;240:F487–91. 36. Morimoto T, Liu W,Woda C, et al. Mechanism underlying flow stimulation ofsodium absorption in the mammalian collecting duct. Am JPhysiol Renal Physiol. 2006;291:F663–9. 37. Hiatt N,Davidson MB, Bonorris G. The effect of potassium chlorideinfusion on insulin secretion in vivo. Horm Metab Res.1972;4:64–8. 38. Rabinowitz L, Sarason RL, Yamauchi H.Effects of KCl infusion on potassium excretion in sheep.Am J Physiol. 1985;249:F263–71. 39. Rabinowitz L, GreenDM, Sarason RL, Yamauchi H. Homeostatic potassiumexcretion in fed and fasted sheep. Am J Physiol.1988;254:R357–80. 40. Youn JH. Gut sensing of potassiumintake and its role in potassium homeostasis. SeminNephrol. 2013;33:248–56. 41. Rab inowitz L, Sarason RL,Yamauchi H, et al. Time course of adaptation to altered Kintake in rats and sheep. Am J Physiol. 1984;247:F607–17.42. Pal mer LG, Frindt G. Regulation of apical K channelsin rat cortical collecting tubule during changes indietary K intake. Am J Physiol. 1999 ;277:F805–12. 43.Najjar F, Zhou H, Morimoto T, et al. Dietary K+ regulatesapical membrane expression of maxi-K channels in rabbitcortical collecting duct. Am J Physiol Renal Physiol.2005;289:F922–32. 44. Pal mer LG, Antonian L, Frindt G.Regulation of apical K and Na channels and Na/K pumps in
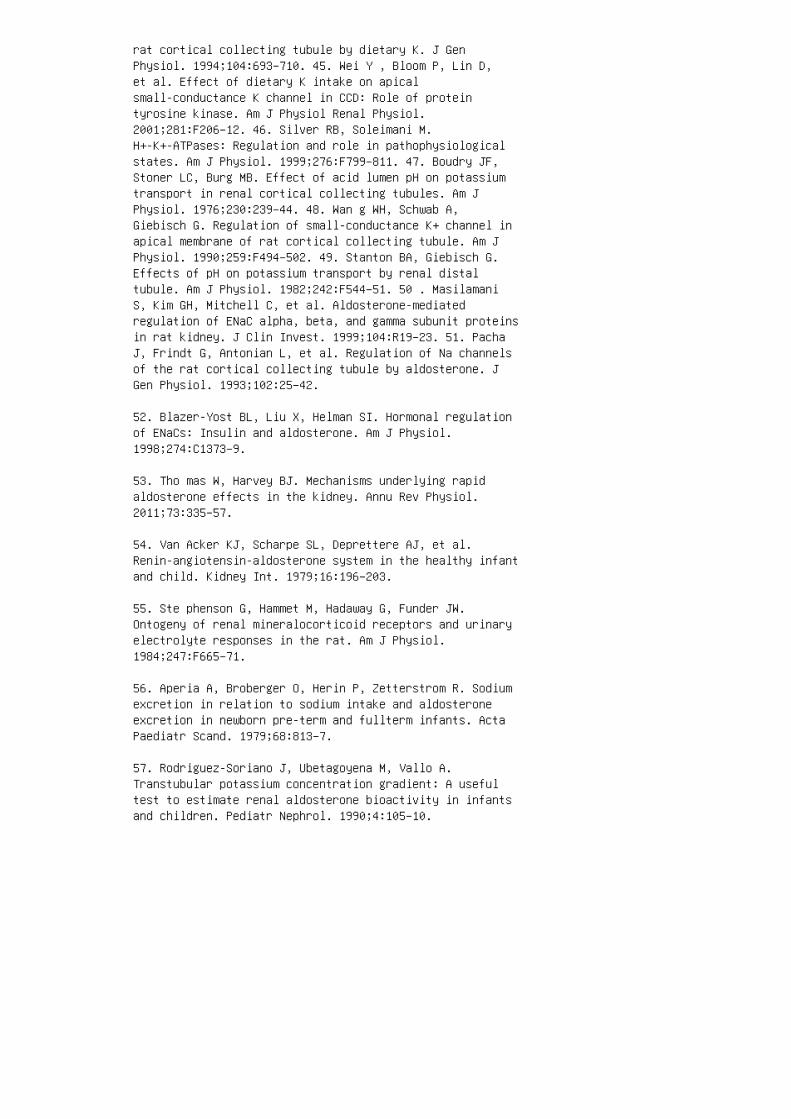
rat cortical collecting tubule by dietary K. J GenPhysiol. 1994;104:693–710. 45. Wei Y , Bloom P, Lin D,et al. Effect of dietary K intake on apicalsmall-conductance K channel in CCD: Role of proteintyrosine kinase. Am J Physiol Renal Physiol.2001;281:F206–12. 46. Silver RB, Soleimani M.H+-K+-ATPases: Regulation and role in pathophysiologicalstates. Am J Physiol. 1999;276:F799–811. 47. Boudry JF,Stoner LC, Burg MB. Effect of acid lumen pH on potassiumtransport in renal cortical collecting tubules. Am JPhysiol. 1976;230:239–44. 48. Wan g WH, Schwab A,Giebisch G. Regulation of small-conductance K+ channel inapical membrane of rat cortical collecting tubule. Am JPhysiol. 1990;259:F494–502. 49. Stanton BA, Giebisch G.Effects of pH on potassium transport by renal distaltubule. Am J Physiol. 1982;242:F544–51. 50 . MasilamaniS, Kim GH, Mitchell C, et al. Aldosterone-mediatedregulation of ENaC alpha, beta, and gamma subunit proteinsin rat kidney. J Clin Invest. 1999;104:R19–23. 51. PachaJ, Frindt G, Antonian L, et al. Regulation of Na channelsof the rat cortical collecting tubule by aldosterone. JGen Physiol. 1993;102:25–42.
52. Blazer-Yost BL, Liu X, Helman SI. Hormonal regulationof ENaCs: Insulin and aldosterone. Am J Physiol.1998;274:C1373–9.
53. Tho mas W, Harvey BJ. Mechanisms underlying rapidaldosterone effects in the kidney. Annu Rev Physiol.2011;73:335–57.
54. Van Acker KJ, Scharpe SL, Deprettere AJ, et al.Renin-angiotensin-aldosterone system in the healthy infantand child. Kidney Int. 1979;16:196–203.
55. Ste phenson G, Hammet M, Hadaway G, Funder JW.Ontogeny of renal mineralocorticoid receptors and urinaryelectrolyte responses in the rat. Am J Physiol.1984;247:F665–71.
56. Aperia A, Broberger O, Herin P, Zetterstrom R. Sodiumexcretion in relation to sodium intake and aldosteroneexcretion in newborn pre-term and fullterm infants. ActaPaediatr Scand. 1979;68:813–7.
57. Rodriguez-Soriano J, Ubetagoyena M, Vallo A.Transtubular potassium concentration gradient: A usefultest to estimate renal aldosterone bioactivity in infantsand children. Pediatr Nephrol. 1990;4:105–10.
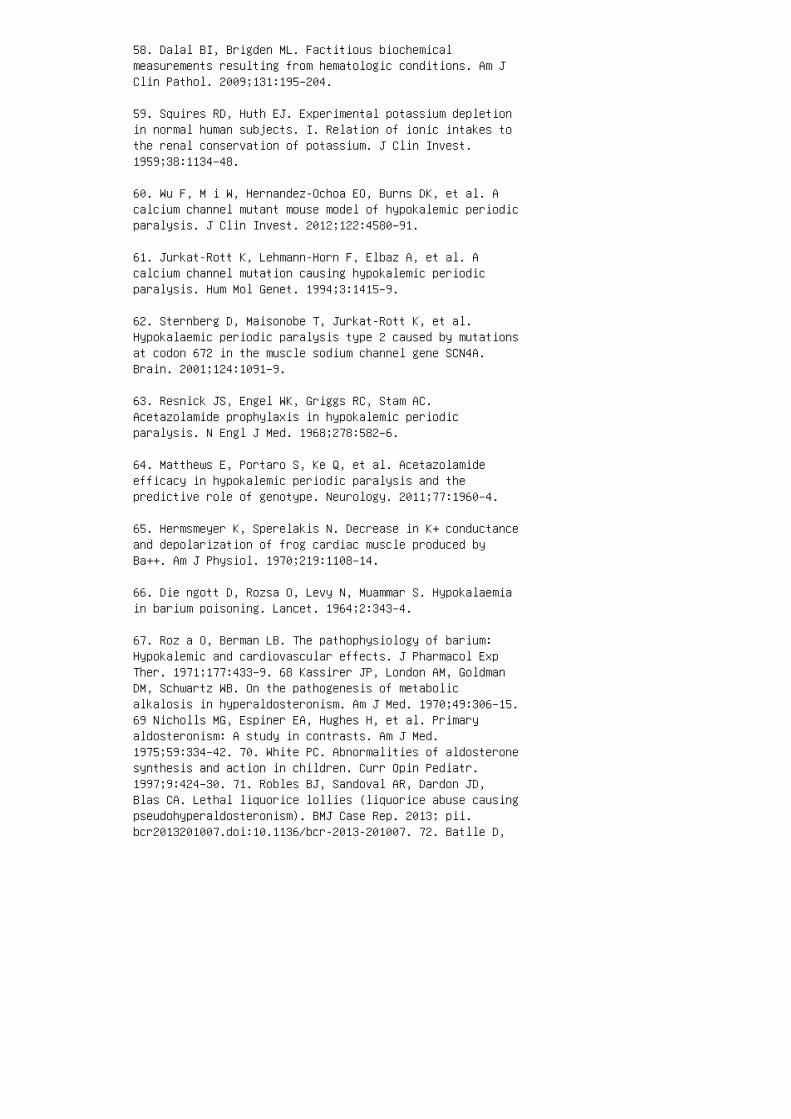
58. Dalal BI, Brigden ML. Factitious biochemicalmeasurements resulting from hematologic conditions. Am JClin Pathol. 2009;131:195–204.
59. Squires RD, Huth EJ. Experimental potassium depletionin normal human subjects. I. Relation of ionic intakes tothe renal conservation of potassium. J Clin Invest.1959;38:1134–48.
60. Wu F, M i W, Hernandez-Ochoa EO, Burns DK, et al. Acalcium channel mutant mouse model of hypokalemic periodicparalysis. J Clin Invest. 2012;122:4580–91.
61. Jurkat-Rott K, Lehmann-Horn F, Elbaz A, et al. Acalcium channel mutation causing hypokalemic periodicparalysis. Hum Mol Genet. 1994;3:1415–9.
62. Sternberg D, Maisonobe T, Jurkat-Rott K, et al.Hypokalaemic periodic paralysis type 2 caused by mutationsat codon 672 in the muscle sodium channel gene SCN4A.Brain. 2001;124:1091–9.
63. Resnick JS, Engel WK, Griggs RC, Stam AC.Acetazolamide prophylaxis in hypokalemic periodicparalysis. N Engl J Med. 1968;278:582–6.
64. Matthews E, Portaro S, Ke Q, et al. Acetazolamideefficacy in hypokalemic periodic paralysis and thepredictive role of genotype. Neurology. 2011;77:1960–4.
65. Hermsmeyer K, Sperelakis N. Decrease in K+ conductanceand depolarization of frog cardiac muscle produced byBa++. Am J Physiol. 1970;219:1108–14.
66. Die ngott D, Rozsa O, Levy N, Muammar S. Hypokalaemiain barium poisoning. Lancet. 1964;2:343–4.
67. Roz a O, Berman LB. The pathophysiology of barium:Hypokalemic and cardiovascular effects. J Pharmacol ExpTher. 1971;177:433–9. 68 Kassirer JP, London AM, GoldmanDM, Schwartz WB. On the pathogenesis of metabolicalkalosis in hyperaldosteronism. Am J Med. 1970;49:306–15.69 Nicholls MG, Espiner EA, Hughes H, et al. Primaryaldosteronism: A study in contrasts. Am J Med.1975;59:334–42. 70. White PC. Abnormalities of aldosteronesynthesis and action in children. Curr Opin Pediatr.1997;9:424–30. 71. Robles BJ, Sandoval AR, Dardon JD,Blas CA. Lethal liquorice lollies (liquorice abuse causingpseudohyperaldosteronism). BMJ Case Rep. 2013; pii.bcr2013201007.doi:10.1136/bcr-2013-201007. 72. Batlle D,

Haque SK. Genetic causes and mechanisms of distal renaltubular acidosis. Nephrol Dial Transplant.2012;27:3691–704. 73. Alper SL. Familial renal tubularacidosis. J Nephrol. 2010;23(Suppl 16):S57–76. 74. HaqueSK, Ariceta G, Batlle D. Proximal renal tubular acidosis:A not so rare disorder of multiple etiologies. NephrolDial Transplant. 2012;27:4273–87. 75. McS herry E. Renaltubular acidosis in childhood. Kidney Int.1981;20:799–809. 76. Fre mont OT, Chan JC. UnderstandingBartter syndrome and Gitelman syndrome. W J Pediatr.2012;8:25–30. 77. Sey berth HW, Schlingmann KP. Bartter-and Gitelman-like syndromes: Salt-losing tubulopathieswith loop or DCT defects. Pediatr Nephrol.2011;26:1789–802. 78. Warnock DG. Liddle syndrome: Anautosomal dominant form of human hypertension. Kidney Int.1998;53:18–24. 79. Han sson JH, Nelson-Williams C, SuzukiH, et al. Hypertension caused by a truncated epithelialsodium channel gamma subunit: Genetic heterogeneity ofLiddle syndrome. Nat Genet. 1995;11:76–82. 80. Shi mketsRA, Warnock DG, Bositis CM, et al. Liddle’s syndrome:Heritable human hypertension caused by mutations in thebeta subunit of the epithelial sodium channel. Cell.1994;79:407–14. 81. Jeunemaitre X, Bassilana F, Persu A,et al. Genotype-phenotype analysis of a newly discoveredfamily with Liddle’s syndrome. J Hypertens.1997;15:1091–100. 82. Manitius A, Levitin H, Beck D,Epstein FH. On the mechanism of impairment of renalconcentrating ability in potassium deficiency. J ClinInvest. 1960;39:684–92. 83. Sch wartz WB, Relman AS.Effects of electrolyte disorders on renal structure andfunction. N Engl J Med. 1967;276:452–8. 84. Ber l T,Linas SL, Aisenbrey GA, et al. On the mechanism of polyuriain potassium depletion: The role of polydipsia. J ClinInvest. 1977;60:620–5.
85. Conn JW. Hypertension, the potassium ion and impairedcarbohydrate tolerance. N Engl J Med. 1965;273:1135–43.
86. Wel t LG, Hollander W, Jr, Blythe WB. The consequencesof potassium depletion. J Chronic Dis. 1960;11:213-54.
87. Wilde WS. Potassium. In: Comar C.L. and Bronner F,eds. Mineral Metabolism: An Advanced Treatise. Volume UUB.New York: Academic Press; 1962. pp. 73–107.
88. Bro nson WR, DeVita VT, Carbone PP, et al.Pseudohyperkalemia due to release of potassium from whiteblood cells during clotting. N Engl J Med.1966;274:369–75.
89. Hartmann RC, Auditore JV, Jackson DP. Studies onthrombocytosis. I. Hyperkalemia due to release ofpotassium from platelets during coagulation. J ClinInvest. 1958;37:699–707.
90. Seimiya M, Yoshida T, Sawabe Y, et al. Reducing theincidence of pseudohyperkalemia by avoiding making a fistduring phlebotomy: A quality improvement report. Am JKidney Dis. 2010;56:686–92.
91. DeFronzo RA, Bia M, Smith D. Clinical disorders ofhyperkalemia. Annu Rev Med. 1982;33:521–54.
92. Aro nson PS, Giebisch G. Effects of pH on potassium:New explanations for old observations. J Am Soc Nephrol.2011;22:1981–9.
93. Her tz P, Richardson JA. Arginine-induced hyperkalemiain renal failure patients. Arch Intern Med.1972;130:778–80.
94. Coo perman LH. Succinylcholine-induced hyperkalemia inneuromuscular disease. JAMA. 1970;213:1867–71.
95. Wal ton JD, Farman JV. Suxamethonium hyperkalaemia inuraemic neuropathy. Anaesthesia. 1973;28:666–8.
96. Gronert GA, Theye RA. Pathophysiology of hyperkalemiainduced by succinylcholine. Anesthesiology. 1975;43:89–99.
97. Reza MJ, Kovick RB, Shine KI, Pearce ML. Massiveintravenous digoxin overdosage. N Engl J Med.1974;291:777–8.
98. Cha rles G, Zheng C, Lehmann-Horn F, et al.Characterization of hyperkalemic periodic paralysis: Asurvey of genetically diagnosed individuals. J Neurol2013;260:2606–13.
99. Jurkat-Rott K, Lehmann-Horn F. Hyperkalemic periodicparalysis type 1. In: Pagon RA, Adam MP, Bird TD, et al.,editors. GeneReviews. Seattle, 19932014.http://www.ncbi.nlm.nih.gov/books/NBK1496/. AccessedDecember 27, 2014.
100. Bri on LP, Schwartz GJ, Campbell D, et al. Earlyhyperkalaemia in very low birthweight infants in theabsence of oliguria. Arch Dis Child. 1989;64:270–2.
101. Mil denberger E, Versmold HT. Pathogenesis and

therapy of non-oliguric hyperkalaemia of the prematureinfant. Eur J Pediatr. 2002;161:415–22. 102. Stefano JL,Norman ME, Morales MC, et al. Decreased erythrocyteNa+,K+-ATPase activity associated with cellular potassiumloss in extremely low birth weight infants withnonoliguric hyperkalemia. J Pediatr. 1993;122:276–84.103. Sato K, Kondo T, Iwao H, et al. Internal potassiumshift in premature infants: Cause of nonoligurichyperkalemia. J Pediatr. 1995;126:109–13. 104. Oma r SA,DeCristofaro JD, Agarwal BI, et al. Effect of prenatalsteroids on potassium balance in extremely low birthweight neonates. Pediatrics. 2000;106:561–7. 105. LordonRE, Burton JR. Post-traumatic renal failure in militarypersonnel in Southeast Asia: Experience at Clark USAFhospital, Republic of the Philippines. Am J Med.1972;53:137–47. 106. Strauss MB. Acute renal insufficiencydue to lower-nephron nephrosis. N Engl J Med.1948;239:693–700. 107. Speiser PW, White PC. Congenitaladrenal hyperplasia. N Engl J Med. 2003;349:776–88. 108.Whi te PC. Aldosterone synthase deficiency and relateddisorders. Mol Cell Endocrinol. 2004;217:81–7. 109. Cheek DB, Perry JW. A salt wasting syndrome in infancy. ArchDis Child. 1958;33:252–6. 110. Fur geson SB, Linas S.Mechanisms of type I and type II pseudohypoaldosteronism.J Am Soc Nephrol. 2010;21:1842–5. 111. Gur an T,Degirmenci S, Bulut IK, et al. Critical points in themanagement of pseudohypoaldosteronism type 1. J Clin ResPediatr Endocrinol. 2011;3:98–100. 112. Xie J , Craig L,Cobb MH, et al. Role of with-no-lysine [K] kinases in thepathogenesis of Gordon’s syndrome. Pediatr Nephrol.2006;21:1231–6. 113. Bon ny O, Rossier BC. Disturbances ofNa/K balance: Pseudohypoaldosteronism revisited. J Am SocNephrol. 2002;13:2399–414. 114. Har ris RC, Breyer MD.Update on cyclooxygenase-2 inhibitors. CJASN.2006;1:236–45. 115. Flores D, Liu Y, Liu W, et al.Flow-induced prostaglandin E2 release regulates Na and Ktransport in the collecting duct. Am J Physiol RenalPhysiol. 2012;303:F632–8. 116. Schlanger LE, Kleyman TR,Ling BN. K+-sparing diuretic actions of trimethoprim:Inhibition of Na+ channels in A6 distal nephron cells.Kidney Int. 1994;45:1070–6. 117. Kle yman TR, Roberts C,Ling BN. A mechanism for pentamidine-induced hyperkalemia:Inhibition of distal nephron sodium transport. Ann InternMed. 1995;122:103–6. 118. Fried LF, Emanuele N, Zhang JH,et al. Combined angiotensin inhibition for the treatmentof diabetic nephropathy. N Engl J Med. 2013;369:1892–903.
119. Hoorn EJ, Walsh SB, McCormick JA, et al. Thecalcineurin inhibitor tacrolimus activates the renal sodiumchloride cotransporter to cause hypertension. Nat Med.
2011;17:1304–9.
120. Ethier JH, Kamel KS, Magner PO, et al. Thetranstubular potassium concentration in patients withhypokalemia and hyperkalemia. Am J Kidney Dis.1990;15:309–15.
121. Choi MJ, Ziyadeh FN. The utility of the transtubularpotassium gradient in the evaluation of hyperkalemia. J AmSoc Nephrol. 2008;19:424–6.
122. Hegenbarth MA; American Academy of PediatricsCommittee on Drugs. Preparing for pediatric emergencies:Drugs to consider. Pediatrics. 2008;121:433–43.
123. Leh nhardt A, Kemper MJ. Pathogenesis, diagnosis andmanagement of hyperkalemia. Pediatr Nephrol.2011;26:377–84.
124. Blumberg A, Weidmann P, Shaw S, et al. Effect ofvarious therapeutic approaches on plasma potassium andmajor regulating factors in terminal renal failure. Am JMed. 1988;85:507–12.
125. McClure RJ, Prasad VK, Brocklebank JT. Treatment ofhyperkalaemia using intravenous and nebulised salbutamol.Arch Dis Child. 1994;70:126–8.
126. Kam el KS, Wei C. Controversial issues in thetreatment of hyperkalaemia. Nephrol Dial Transplant2003;18:2215–8.
127. Mor gan AG, Burkinshaw L, Robinson PJ, Rosen SM.Potassium balance and acid-base changes in patientsundergoing regular haemodialysis therapy. Brit Med J. 197028;1:779–83.
128. Yaseen H, Khalaf M, Dana A, et al. Salbutamol versuscation-exchange resin (Kayexalate) for the treatment ofnonoliguric hyperkalemia in preterm infants. J Perinatol.2008;25:193–7.
129. Ohlsson A, Hosking M. Complications following oraladministration of exchange resins in extremelylowbirth-weight infants. Eur J Pediatr. 1987;146:571–4.
130. Rashid A, Hamilton SR. Necrosis of thegastrointestinal tract in uremic patients as a result ofsodium polystyrene sulfonate (Kayexalate) in sorbitol: Anunderrecognized condition. Am J Sur Pathol. 1997;21:60–9.

131. Emmett M, Hootkins RE, Fine KD, et al. Effect ofthree laxatives and a cation exchange resin on fecalsodium and potassium excretion. Gastroenterology.1995;108:752–60.
REVIEW QUESTIONS
1. A 16-year-old girl is noted to have a plasma K + concen
tration of 7.0 mEq/L with peaked T waves on ECG. �e
first step of management should be:
a. Administration of IV insulin with glucose
b. Administration of IV sodium bicarbonate c. Administration of nebulized albuterol d. Administration of IVcalcium gluconate e. Administration of IV furosemide 2.Severe hypokalemia may be associated with: a. Hyp otensionb. Rena l concentrating defect c. Skeletal muscle weaknessd. ST depression and appearance of U wave on ECG e. All ofthe above 3. K + is freely �ltered in the glomerulus. �emajority of �ltered K + is reabsorbed in the ________,and the net urinary K + secretion, and thus excretion,occurs in the ____________. a. TALH; distal nephron(distal convoluted tubule and collecting duct) b.Proximal tubule; distal nephron (distal convoluted tubuleand collecting duct) c. Distal nephron (distal convolutedtubule and collecting duct); TALH d. Proximal tubule; TALHe. Distal nephron (distal convoluted tubule and collectingduct); proximal tubule 4. A 10-year-old patient withhistory of acute lymphoblastic anemia is noted to be inseptic shock and disseminated intravascular coagulation.She is paralyzed with succinylcholine for intubation andplaced on pressors for hypotension. Her sedation ismaintained with propofol, and the patient requires multipleunits of pRBCs for severe anemia. Arterial blood gas (ABG)reveals that she is acidotic, with an elevated lactate.Her ABG also reveals a K + of 7.5 mEq/L. �e team sends o�a sample to verify the K + result. You are concerned thatthe value is real because: a. Succinylcholine can promoteK + release from muscle cells. b. �e patient may havesustained acute kidney injury secondary to herhypotension. c. �e patient received a large K + load viaboth intravascular hemolysis and pRBC transfusion. d. Allof the above. 5. An 8-year-old boy with obstructiveuropathy is noted to have chronic hypokalemia and non-gapmetabolic acidosis. Despite his acidosis, his urine pHremains 6.0. His urine is negative for glucose and
protein. Given his underlying uropathy, the patient mostlikely has: a. Type 1 RTA involving the inability of theproximal tubule to reabsorb HCO 3 – b. Type 1 RTAinvolving the inability of the distal nephron to secrete H+ c. Type 2 RTA involving the inability of the proximaltubule to reabsorb HCO 3 – d. Type 2 RTA involving theinability of the distal nephron to secrete H + 6. A2-week-old girl is brought to the emergency department forvomiting and lethargy. She is noted to have thready pulsesand poor capillary re�ll. She has not yet regained birthweight. Samples for CBC, chemistry,
VBG, blood culture, urine culture, and CSF culture are
sent to the laboratory, and the patient is started on IV
antibiotics. Results are signi�cant for acidosis, severe
hyponatremia and hyperkalemia. Based on the patient’s
presumed diagnosis, you expect urine electrolytes to
show:
a. FeNa <1%, TTKG > 8
b. FeNa <1%, TTKG > 8
c. FeNa <1%, TTKG < 4
d. FeNa >10%, TTKG < 4
e. FeNa >10%, TTKG > 8
FeNa = fractional excretion of sodium; TTKG = transtubularpotassium gradient.
7. Patients with nephrotic syndrome are predisposed to
developing hypokalemia because of:
a. Treatment with loop diuretics
b. Impaired reabsorption of �ltered K +
c. Secondary hyperaldosteronism
d. Increased K + �ltration by the glomerulus
e. Choices a and c

8. Bartter syndrome is characterized by the following
derangements:
a. Hypernatremia, hypochloremia, hyperkalemia,hyperprostaglandinemia, metabolic alkalosis
b. Hyponatremia, hyperchloremia, hypokalemia,hypoprostaglandinemia metabolic acidosis c. Hyponatremia,hypochloremia, hypokalemia, hyperprostaglandinemia,metabolic alkalosis d. Hypernatremia, hyperchloremia,hyperkalemia, hyperprostaglandinemia, metabolic acidosisANSWER KEY 1. d 2. e 3. b 4. d 5. b 6. d 7. e 8. c
13 Disorders of mineral metabolism
Figure 13.13 A suggested algorithm for evaluation ofhyperphosphatemia in children.
2. Friedman PA, Gesek FA. Cellular calcium transport inrenal epithelia: Measurement, mechanisms, and regulation.Physiol Rev. 1995;75:429–71.
3. Hoenderop JG, Willems PH, Bindels RJ. Toward acomprehensive molecular model of active cal ciumreabsorption. Am J Physiol Renal Physiol.2000;278:F352–60.
4. Rei lly RF, Ellison DH. Mammalian distal tubule,physiology, pathophysiology, and molecular anatomy.Physiol Rev. 2000;80:277–313.
5. Brown EM, MacLeod RJ. Extracellular calcium sensing andextracellular calcium signaling. Physiol Rev.2001;81:239–97.
6. Houillier P, Paillard M. Calcium-sensing recep tor andrenal cation handling. Nephrol Dial Transplant.2003;18:2467–70.
7. Bru nette MG, Chan M, Ferriere C, Roberts KD. Site of1,25-dihydroxyvitamin D 3 synthesis in the kidney.Nature. 1978;276:287–9.
8. Kawashima H, Torikai S, Kurokawa K. Localization of25-hydroxyvitamin D 3 1a-hydroxylase and 24-hydroxylasealong the rat nephron. Proc Natl Acad Sci U S A.1981;78:1199–203.
10. Bro wn AJ, Dusso A, Slatopolsky E. Vitamin D. Am JPhysiol. 1999;277:F157–75.
11. Scarpace PJ, Neuman WF, Raisz LG. Metabolism ofradioiodinated salmon calcitonin in rats. Endocrinology.1977;100:1260–67.
12. Buc lin T, Cosma Rochat M, Burckhardt P, et al.Bioavailability and biological efficacy of a new oralformulation of salmon calcito nin in healthy volunteers. JBone Miner Res. 2 00 2;17:1478–85.
13. Zal ups RK, Knox FG. Calcitonin decreases the renaltubular capacity for phosphate reabsorp tion. Am J Physiol.1983;245:F345–8.

14. Shinki T, Ueno Y, DeLuca HF, Suda T. Calcitonin is amajor regulator for the expression of renal25-hydroxyvitamin D 3 -1a-hydroxylase gene innormocalcemic rats. Proc Natl Acad Sci U S A.1999;96:8253–8.
15. Davis TME, Singh B, Choo KE, et al. Dynamic assessmentof the electrocardiographic QT interval during citrateinfusion in healthy volun teers. Br Heart J. 1995;73:523–6.
16. Lehmann G, Deisenhofer I, Ndrepepa G, et al. ECGchanges in a 25-year-old woman with hypocalcemia due tohypoparathyroidism: Hypocalcemia mimicking acutemyocardial infarction. Chest. 2000;118:260–2.
17. Bashour T, Basha HS, Cheng TO. Hypocalcemiccardiomyopathy. Chest. 1980;78:663. 18. Lang RM, FellnerSK, Neumann A, et al. Left ventricular contractilityvaries directly with blood ionized calcium. Ann InternMed. 1988;108:524–9. 19. Salle BL, Delvin E, Glorieux F,David L. Human neonatal hypocalcemia. Biol Neonate.1990;58(Suppl 1):22–31. 20. Driscoll DA, Budarf ML,Emanuel BS. A genetic etiology for DiGeorge syndrome:Consistent deletions and microdeletions of 22q11. Am J HumGenet. 1992;50:924–33. 21. Thakker RV. Genetics ofendocrine and metabolic disorders: Parathyroid. Rev EndocrMetab Disord. 2004;5:37–51. 22. Nesbit MA, Bowl MR,Harding B, et al. Characterization of GATA3 mutations inthe hypoparathyroidism, deafness, and renal dysplasia (HDR)syndrome. J Biol Chem. 2004;279:22624–34. 23. Baron J,Winer KK, Yanovski JA, et al. Mutations in the Ca( 2+)-sensing receptor gene cause autosomal dominant andsporadic hypoparathyroidism. Hum Mol Genet. 1996;5:601–6.24. Marguet C, Mallet E, Basuyau JP, et al. Clinical andbiological heterogeneity in pseudohypoparathyroidismsyndrome: Results of a multicenter study. Horm Res.1997;48:120–30. 25. Elli FM, Bordogna P, de Sanctis L,Giachero F, Verrua E, Segni M, Mazzanti L, Boldrin V,Toromanovic A, Spada A, Mantovani G. Screening of PRKAR1Aand PDE4D in a Large Italian Series of Patients ClinicallyDiagnosed with Albright Hereditary Osteodystrophy and/ orPseudohypoparathyroidism. J Bone Miner Res. 2016 Jan 13.doi: 10.1002/jbmr.2785. 26. Ana st CS, Mohs JM, Kaplan SL,Burns TW. Evidence for parathyroid failure in magnesiumdeficiency. Science. 1972;177:606–8. 27. Rude RK, OldhamSB, Singer FR. Functional hypo parathyroidism andparathyroid hormone endorga n resistance in human magnesiumdeficiency. Clin Endocrinol (Oxf). 1976;5:209-24. 28.Dusso AS, Brown AJ, Slatopolsky E. Vitamin D. Am J Physiol
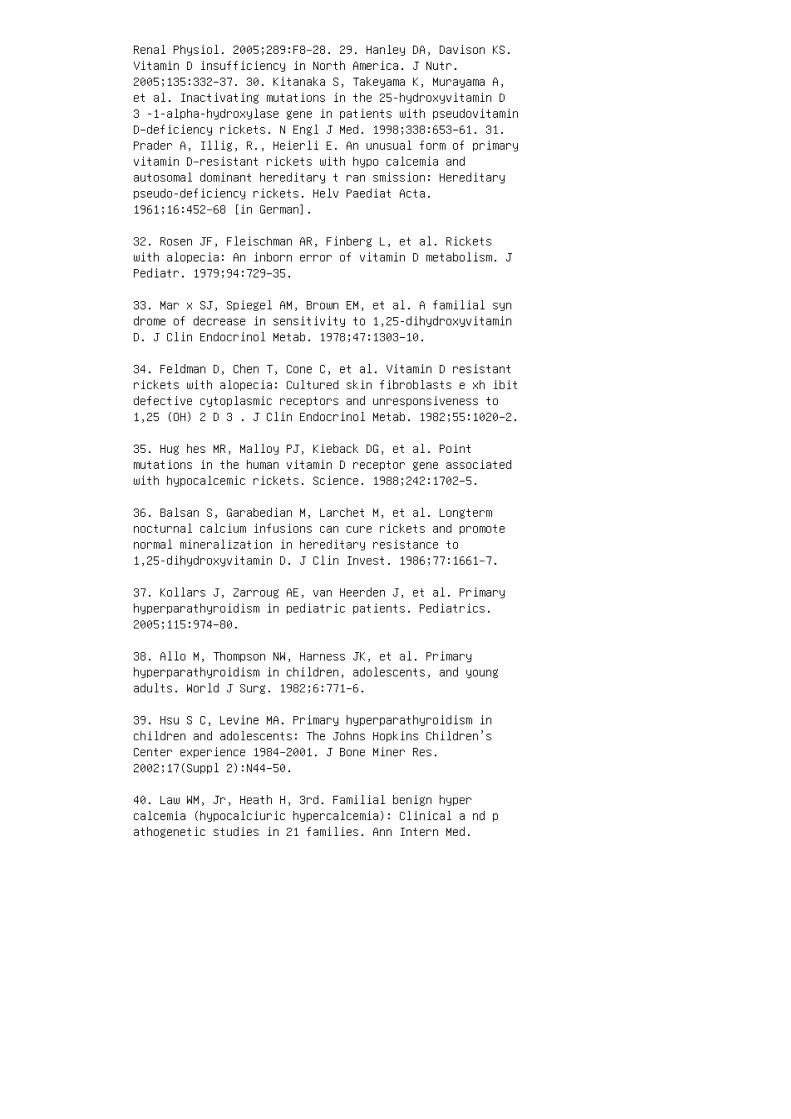
Renal Physiol. 2005;289:F8–28. 29. Hanley DA, Davison KS.Vitamin D insufficiency in North America. J Nutr.2005;135:332–37. 30. Kitanaka S, Takeyama K, Murayama A,et al. Inactivating mutations in the 25-hydroxyvitamin D3 -1-alpha-hydroxylase gene in patients with pseudovitaminD–deficiency rickets. N Engl J Med. 1998;338:653–61. 31.Prader A, Illig, R., Heierli E. An unusual form of primaryvitamin D–resistant rickets with hypo calcemia andautosomal dominant hereditary t ran smission: Hereditarypseudo-deficiency rickets. Helv Paediat Acta.1961;16:452–68 [in German].
32. Rosen JF, Fleischman AR, Finberg L, et al. Ricketswith alopecia: An inborn error of vitamin D metabolism. JPediatr. 1979;94:729–35.
33. Mar x SJ, Spiegel AM, Brown EM, et al. A familial syndrome of decrease in sensitivity to 1,25-dihydroxyvitaminD. J Clin Endocrinol Metab. 1978;47:1303–10.
34. Feldman D, Chen T, Cone C, et al. Vitamin D resistantrickets with alopecia: Cultured skin fibroblasts e xh ibitdefective cytoplasmic receptors and unresponsiveness to1,25 (OH) 2 D 3 . J Clin Endocrinol Metab. 1982;55:1020–2.
35. Hug hes MR, Malloy PJ, Kieback DG, et al. Pointmutations in the human vitamin D receptor gene associatedwith hypocalcemic rickets. Science. 1988;242:1702–5.
36. Balsan S, Garabedian M, Larchet M, et al. Longtermnocturnal calcium infusions can cure rickets and promotenormal mineralization in hereditary resistance to1,25-dihydroxyvitamin D. J Clin Invest. 1986;77:1661–7.
37. Kollars J, Zarroug AE, van Heerden J, et al. Primaryhyperparathyroidism in pediatric patients. Pediatrics.2005;115:974–80.
38. Allo M, Thompson NW, Harness JK, et al. Primaryhyperparathyroidism in children, adolescents, and youngadults. World J Surg. 1982;6:771–6.
39. Hsu S C, Levine MA. Primary hyperparathyroidism inchildren and adolescents: The Johns Hopkins Children’sCenter experience 1984–2001. J Bone Miner Res.2002;17(Suppl 2):N44–50.
40. Law WM, Jr, Heath H, 3rd. Familial benign hypercalcemia (hypocalciuric hypercalcemia): Clinical a nd pathogenetic studies in 21 families. Ann Intern Med.
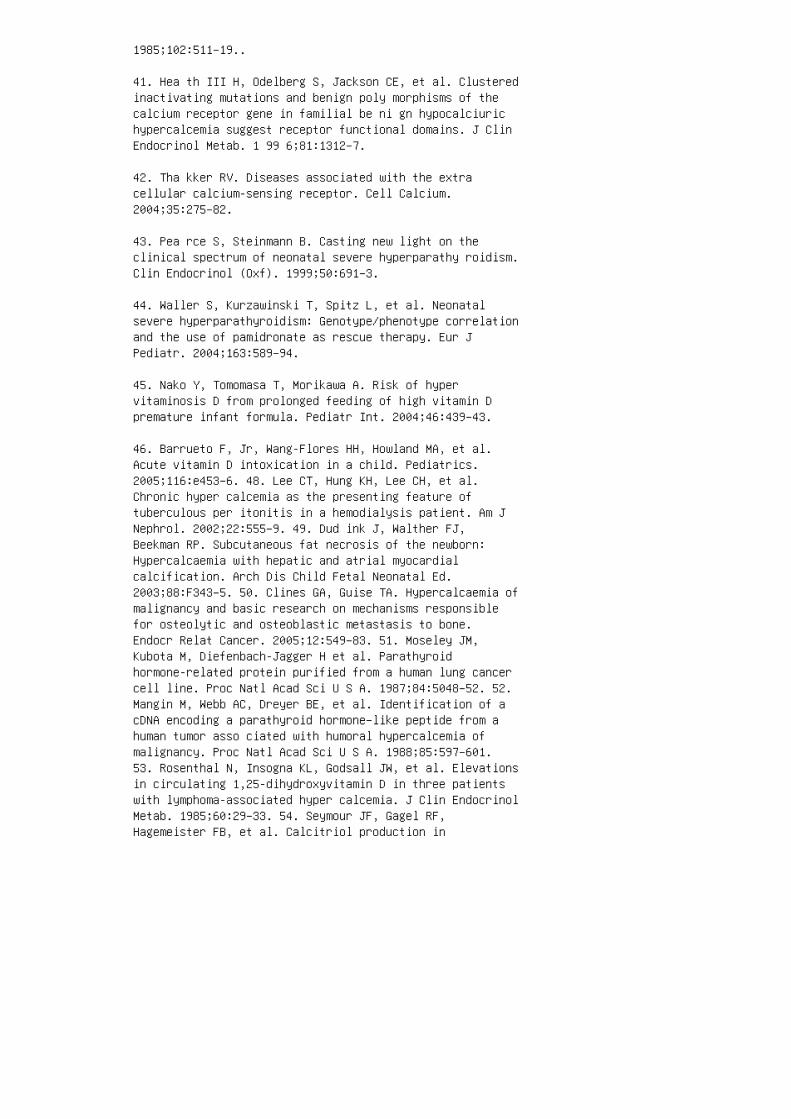
1985;102:511–19..
41. Hea th III H, Odelberg S, Jackson CE, et al. Clusteredinactivating mutations and benign poly morphisms of thecalcium receptor gene in familial be ni gn hypocalciurichypercalcemia suggest receptor functional domains. J ClinEndocrinol Metab. 1 99 6;81:1312–7.
42. Tha kker RV. Diseases associated with the extracellular calcium-sensing receptor. Cell Calcium.2004;35:275–82.
43. Pea rce S, Steinmann B. Casting new light on theclinical spectrum of neonatal severe hyperparathy roidism.Clin Endocrinol (Oxf). 1999;50:691–3.
44. Waller S, Kurzawinski T, Spitz L, et al. Neonatalsevere hyperparathyroidism: Genotype/phenotype correlationand the use of pamidronate as rescue therapy. Eur JPediatr. 2004;163:589–94.
45. Nako Y, Tomomasa T, Morikawa A. Risk of hypervitaminosis D from prolonged feeding of high vitamin Dpremature infant formula. Pediatr Int. 2004;46:439–43.
46. Barrueto F, Jr, Wang-Flores HH, Howland MA, et al.Acute vitamin D intoxication in a child. Pediatrics.2005;116:e453–6. 48. Lee CT, Hung KH, Lee CH, et al.Chronic hyper calcemia as the presenting feature oftuberculous per itonitis in a hemodialysis patient. Am JNephrol. 2002;22:555–9. 49. Dud ink J, Walther FJ,Beekman RP. Subcutaneous fat necrosis of the newborn:Hypercalcaemia with hepatic and atrial myocardialcalcification. Arch Dis Child Fetal Neonatal Ed.2003;88:F343–5. 50. Clines GA, Guise TA. Hypercalcaemia ofmalignancy and basic research on mechanisms responsiblefor osteolytic and osteoblastic metastasis to bone.Endocr Relat Cancer. 2005;12:549–83. 51. Moseley JM,Kubota M, Diefenbach-Jagger H et al. Parathyroidhormone-related protein purified from a human lung cancercell line. Proc Natl Acad Sci U S A. 1987;84:5048–52. 52.Mangin M, Webb AC, Dreyer BE, et al. Identification of acDNA encoding a parathyroid hormone–like peptide from ahuman tumor asso ciated with humoral hypercalcemia ofmalignancy. Proc Natl Acad Sci U S A. 1988;85:597–601.53. Rosenthal N, Insogna KL, Godsall JW, et al. Elevationsin circulating 1,25-dihydroxyvitamin D in three patientswith lymphoma-associated hyper calcemia. J Clin EndocrinolMetab. 1985;60:29–33. 54. Seymour JF, Gagel RF,Hagemeister FB, et al. Calcitriol production in

hypercalcemic and normocalcemic patients with non-Hodgkinlym phoma. Ann Intern Med. 1994;121:633–40. 55. Zhang J,Kumar A, Roux K, et al. Elastin region deletions inWilliams syndrome. Genet Test. 1999;3:357–9. 56. AmentaS, Sofocleous C, Kolialexi A, et al. Clinicalmanifestations and molecular investiga tion of 50 patientswith Williams syndrome in the Greek population. PediatrRes. 2005;57:789–95. 57. Ame rican Academy of Pediatrics.Committee on Genetics 2001 health care supervision forchildren with Williams syndrome. Pediatrics.2001;107:1192–204. 58. Sch lingmann KP, Kaufmann M, WeberS, et al. Mutations in CYP24A1 and idiopathic infantilehypercalcemia. N Engl J Med. 2011;365:410–21. 59. DinourD, Davidovits M, Aviner S, et al. Maternal and infantilehypercalcemia caused by vitaminD-hydroxylase mutations andvitamin D intake. Pediatr Nephrol. 2015;30:145–52. 60.Cal vi LM, Schipani E. The PTH/PTHrP receptor in Jansen’smetaphyseal chondrodysplasia. J Endocrinol Invest.2000;23:545-54. 61. Bastepe M, Raas-Rothschild A, SilverJ, et al. A form of Jansen’s metaphyseal chondro dysplasiawith limited metabolic and skeletal abnormalities iscaused by a novel activating parathyroid hormone(PTH)/PTH-related pep tide receptor mutation. J ClinEndocrinol Metab. 200 4;89:3595–600.
62. Dai LJ, Ritchie G, Kerstan D, et al. Magnesiumtransport in the renal distal convoluted tubule. PhysiolRev. 2001;81:51–84.
63. Kon rad M, Schlingmann KP, Gudermann T. Insights intothe molecular nature of magne sium homeostasis. Am JPhysiol Renal Physiol. 2 00 4;286:F599–605.
64. Fli nk EB. Magnesium deficiency: Etiology and clinicalspectrum. Acta Med Scand Suppl. 1981;647:125–37.
65. Gitelman HJ, Graham JB, Welt LG. A new famil ialdisorder characterized by hyopokalemia and hypomagnesemia. Trans Assoc Am Physicians. 1966;79:221–35.
66. Shaer A J. Inherited primary renal tubular hypoka lemicalkalosis: A review of Gitelman and Bartter syn dromes. AmJ Med Sci. 2001;322:316–32.
67. Sabath E, Meade P, Berkman J, et al. Pathophysiologyof functional mutations of the thiazide-sensitive Na-Clcotransporter in Gitelman disease. Am J Physiol RenalPhysiol. 2004;287:F195–203.
68. Lin SH, Cheng NL, Hsu YJ, Halperin ML. Intrafamilial

phenotype variability in patients with Gitelman syndromehaving the same mutations in their thiazide-sensitivesodium/chloride cotrans porter. Am J Kidney Dis.2004;43:304–12.
69. Ea HK, Blanchard A, Dougados M, Roux C.Chondrocalcinosis secondary to hypomagnesemia inGitelman’s syndrome. J Rheumatol. 2005;32:1840–2.
70. Bartter FC, Pronove P, Gill JR, Jr, et al. Hyperplasiaof the juxtaglomerular complex with hyperaldoste ronism andhypokalemic alkalosis: A new syndrome. Am J Med.1962;33:811–28.
71. Jeck N, Konrad M, Peters M, et al. Mutations in thechloride channel gene, CLCNKB, leading to a mixedBartter–Gitelman phenotype. Pediatr Res. 2000;48:754–8.
72. Skyberg D, Stromme JH, Nesbakken R, et al. Neonatalhypomagnesemia with selective malab sorption of magnesium:A clinical entity. Scand J Cli n Lab Invest.1968;21:355–63.
73. Sch lingmann KP, Weber S, Peters M, et al.Hypomagnesemia with secondary hypocalcemia is caused bymutations in TRPM6, a new member of the TRPM gene family.Nat Genet. 2002;31:166–70.
74. Geve n WB, Monnens LA, Willems HL, et al. Renalmagnesium wasting in two families with autosomal dominantinheritance. Kidney Int. 1987;31:1140–44.
74. Meij IC, Koenderink JB, van Bokhoven H, et al.Dominant isolated renal magnesium loss is caused bymisrouting of the Na(+), K(+)−ATPase gammasubunit. NatGenet. 2000;26:265–66.
75. Balon TW, Jasman A, Scott S, et al. Genetic heterogeneity in familial renal magnesium wasting. J Cli nEndocrinol Metab. 2002;87:612–7. 76. Geven WB, Monnens LA,Willems JL, et al. Isolated autosomal recessive renalmagnesium loss in two sisters. Clin Genet.1987;32:398–402. 77. Michelis MF, Drash AL, Linarelli LG,et al. Decreased bicarbonate threshold and renal magnesiumwasting in a sibship with distal renal tubular acidosis.(Evaluation of the pathophysiological role of para thyroidhormone). Metabolism. 1972;21:905–20. 78. Benigno V,Canonica CS, Bettinelli A, et al.Hypomagnesaemia-hypercalciurianephrocalcinosis: A report ofnine cases and a review. Nephrol Dial Transplant.
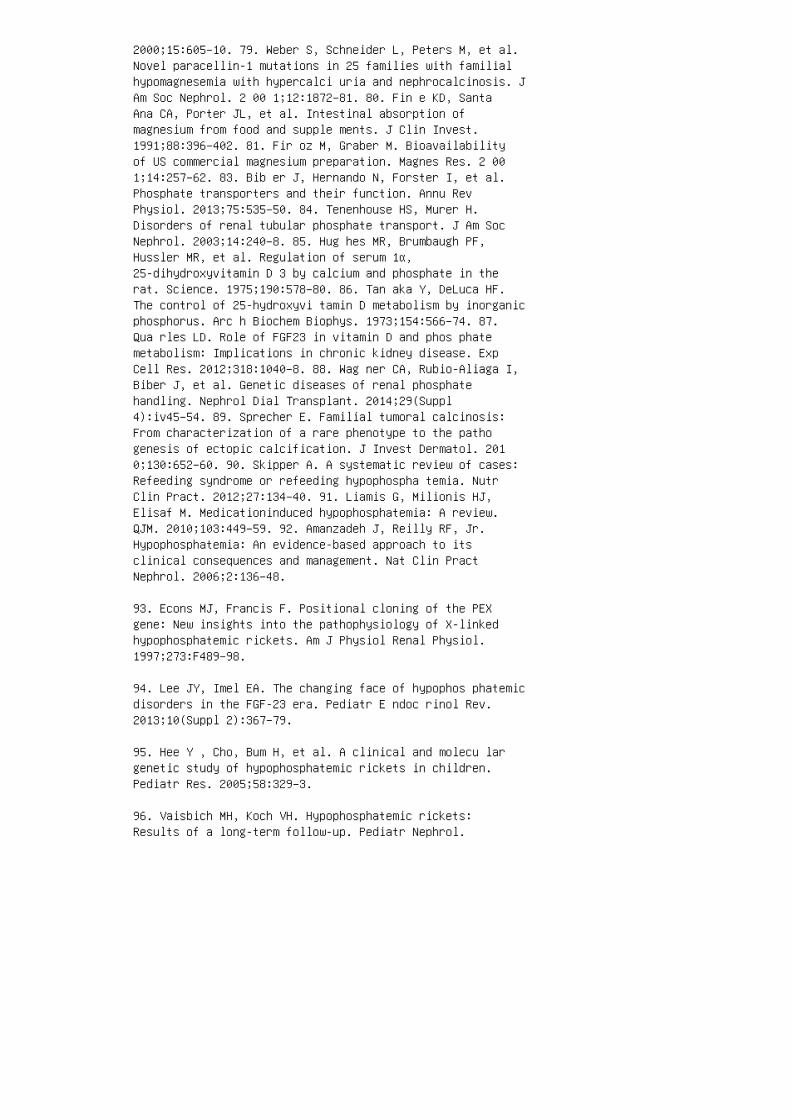
2000;15:605–10. 79. Weber S, Schneider L, Peters M, et al.Novel paracellin-1 mutations in 25 families with familialhypomagnesemia with hypercalci uria and nephrocalcinosis. JAm Soc Nephrol. 2 00 1;12:1872–81. 80. Fin e KD, SantaAna CA, Porter JL, et al. Intestinal absorption ofmagnesium from food and supple ments. J Clin Invest.1991;88:396–402. 81. Fir oz M, Graber M. Bioavailabilityof US commercial magnesium preparation. Magnes Res. 2 001;14:257–62. 83. Bib er J, Hernando N, Forster I, et al.Phosphate transporters and their function. Annu RevPhysiol. 2013;75:535–50. 84. Tenenhouse HS, Murer H.Disorders of renal tubular phosphate transport. J Am SocNephrol. 2003;14:240–8. 85. Hug hes MR, Brumbaugh PF,Hussler MR, et al. Regulation of serum 1α,25-dihydroxyvitamin D 3 by calcium and phosphate in therat. Science. 1975;190:578–80. 86. Tan aka Y, DeLuca HF.The control of 25-hydroxyvi tamin D metabolism by inorganicphosphorus. Arc h Biochem Biophys. 1973;154:566–74. 87.Qua rles LD. Role of FGF23 in vitamin D and phos phatemetabolism: Implications in chronic kidney disease. ExpCell Res. 2012;318:1040–8. 88. Wag ner CA, Rubio-Aliaga I,Biber J, et al. Genetic diseases of renal phosphatehandling. Nephrol Dial Transplant. 2014;29(Suppl4):iv45–54. 89. Sprecher E. Familial tumoral calcinosis:From characterization of a rare phenotype to the pathogenesis of ectopic calcification. J Invest Dermatol. 2010;130:652–60. 90. Skipper A. A systematic review of cases:Refeeding syndrome or refeeding hypophospha temia. NutrClin Pract. 2012;27:134–40. 91. Liamis G, Milionis HJ,Elisaf M. Medicationinduced hypophosphatemia: A review.QJM. 2010;103:449–59. 92. Amanzadeh J, Reilly RF, Jr.Hypophosphatemia: An evidence-based approach to itsclinical consequences and management. Nat Clin PractNephrol. 2006;2:136–48.
93. Econs MJ, Francis F. Positional cloning of the PEXgene: New insights into the pathophysiology of X-linkedhypophosphatemic rickets. Am J Physiol Renal Physiol.1997;273:F489–98.
94. Lee JY, Imel EA. The changing face of hypophos phatemicdisorders in the FGF-23 era. Pediatr E ndoc rinol Rev.2013;10(Suppl 2):367–79.
95. Hee Y , Cho, Bum H, et al. A clinical and molecu largenetic study of hypophosphatemic rickets in children.Pediatr Res. 2005;58:329–3.
96. Vaisbich MH, Koch VH. Hypophosphatemic rickets:Results of a long-term follow-up. Pediatr Nephrol.
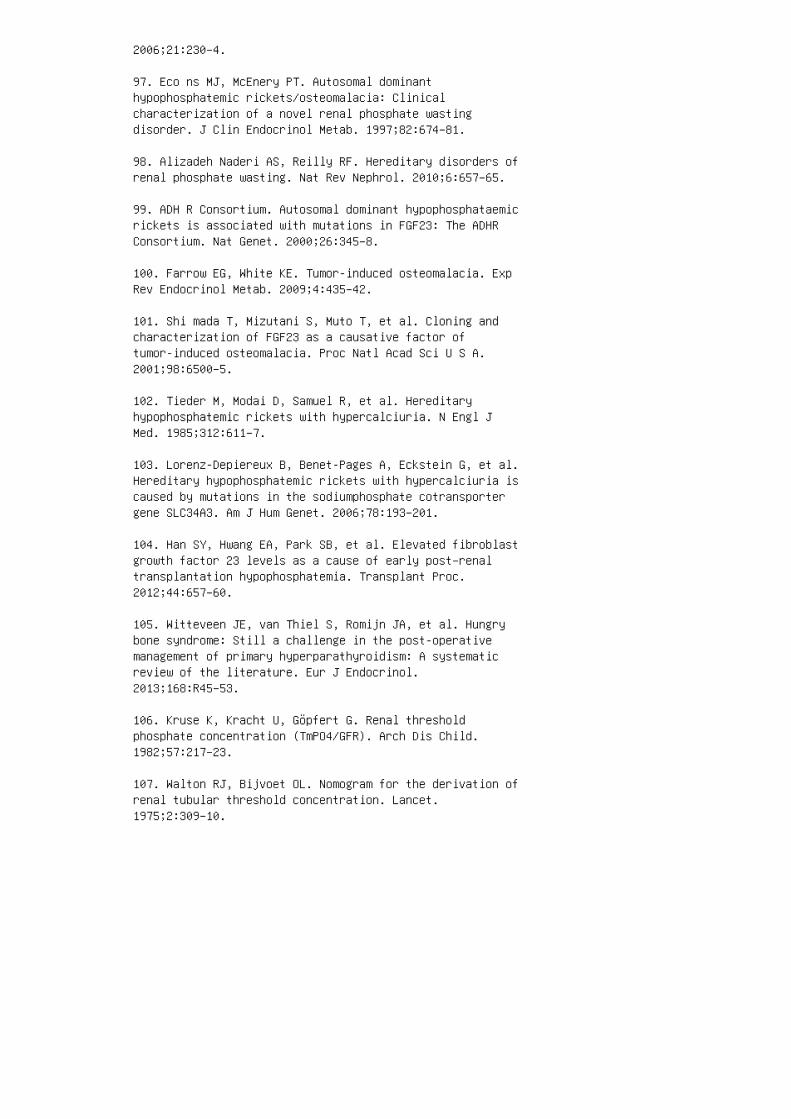
2006;21:230–4.
97. Eco ns MJ, McEnery PT. Autosomal dominanthypophosphatemic rickets/osteomalacia: Clinicalcharacterization of a novel renal phosphate wastingdisorder. J Clin Endocrinol Metab. 1997;82:674–81.
98. Alizadeh Naderi AS, Reilly RF. Hereditary disorders ofrenal phosphate wasting. Nat Rev Nephrol. 2010;6:657–65.
99. ADH R Consortium. Autosomal dominant hypophosphataemicrickets is associated with mutations in FGF23: The ADHRConsortium. Nat Genet. 2000;26:345–8.
100. Farrow EG, White KE. Tumor-induced osteomalacia. ExpRev Endocrinol Metab. 2009;4:435–42.
101. Shi mada T, Mizutani S, Muto T, et al. Cloning andcharacterization of FGF23 as a causative factor oftumor-induced osteomalacia. Proc Natl Acad Sci U S A.2001;98:6500–5.
102. Tieder M, Modai D, Samuel R, et al. Hereditaryhypophosphatemic rickets with hypercalciuria. N Engl JMed. 1985;312:611–7.
103. Lorenz-Depiereux B, Benet-Pages A, Eckstein G, et al.Hereditary hypophosphatemic rickets with hypercalciuria iscaused by mutations in the sodiumphosphate cotransportergene SLC34A3. Am J Hum Genet. 2006;78:193–201.
104. Han SY, Hwang EA, Park SB, et al. Elevated fibroblastgrowth factor 23 levels as a cause of early post–renaltransplantation hypophosphatemia. Transplant Proc.2012;44:657–60.
105. Witteveen JE, van Thiel S, Romijn JA, et al. Hungrybone syndrome: Still a challenge in the post-operativemanagement of primary hyperparathyroidism: A systematicreview of the literature. Eur J Endocrinol.2013;168:R45–53.
106. Kruse K, Kracht U, Göpfert G. Renal thresholdphosphate concentration (TmPO4/GFR). Arch Dis Child.1982;57:217–23.
107. Walton RJ, Bijvoet OL. Nomogram for the derivation ofrenal tubular threshold concentration. Lancet.1975;2:309–10.
108. Barth JH, Jones RG, Payne RB. Calculation of renaltubular reabsorption of phosphate: The algorithm performsbetter than the nomogram. Ann Clin Biochem. 2000;37:79–81.109. Payne RB. Renal tubular reabsorption of phosphate(TmP/GFR): Indications and interpretation. Ann ClinBiochem. 1998;35:201–6. 110. Felsenfeld AJ, Levine BS.Approach to treatment of hypophosphatemia. Am J Kidney Dis.2012;60:655–61. 111. Scanni R, vonRotz M, Jehle S, et al.The human response to acute enteral and parenteralphosphate loads. J Am Soc Nephrol. 2014;25:2730–9. 112.Domico MB, Huynh V, Anand SK, et al. Severehyperphosphatemia and hypocalcemic tetany after orallaxative administration in a 3-month-old infant.Pediatrics. 2006;118:e1580–3. 113. Wilson FP, Berns JS.Tumor lysis syndrome: New challenges and recent advances.Adv Chronic Kidney Dis. 2014;21:18–26. 114. Hebert LA,Lemann J, Jr, Petersen JR, et al. Studies of the mechanismby which phosphate infusion lowers serum calciumconcentration. J Clin Invest. 1966;45:1886–94. 115.Agarwal B, Walecka A, Shaw S, et al. Is parenteralphosphate replacement in the intensive care unit safe?Ther Apher Dial. 2014;18:31–6. 116. Llach F, FelsenfeldAJ, Haussler MR. The pathophysiology of altered calciummetabolism in rhabdomyolysis-induced acute r en alfailure: Interactions of parathyroid hormone,25-hydroxycholecalciferol, and1,25-dihydroxycholecalciferol. N Engl J Med.1981;305:117–23. 117 Finer G, Price HE, Shore RM, WhiteKE, Langman CB. Hyperphosphatemic familial tumoralcalcinosis: Response to acetazolamide and postulatedmechanisms. Am J Med Genet A. 2014 Jun;164A(6):1545-9.doi: 10.1002/ ajmg.a.36476 118. Oliveira RB, Cancela AL,Graciolli FG, et al. Early control of PTH and FGF23 innormophosphatemic CKD patients: A new target in CKD-MBDtherapy? Clin J Am Soc Nephrol. 2010;5:286–91. 119. ArayaK, Fukumoto S, Backenroth R, et al. Fibroblast growthfactor (FGF)23 gene as a cause of tumoral calcinosis. JClin Endocrinol Metab. 2005;90:5523–7. 120. Shah A,Miller CJ, Nast CC, et al. Severe vascular calcificationand tumoral calcinosis in a family with hyperphosphatemia:A fibroblast growth factor 23 mutation identified by exomesequencing. Nephrol Dial Transplant. 2014;29:2235–43.121. Favia G, Lacaita MG, Limongelli L, et al.Hyperphosphatemic familial tumoral calcinosis:Odontostomatologic management a nd p athological features.Am J Case Rep. 2014;15:569–75.
REVIEW QUESTIONS
1. All of the following hormones have a net e�ect of reduc
ing serum phosphorus values except:
a. Parathyroid hormone
b. Calcitonin
c. Calcitriol
d. FGF-23
2. Which of the following conditions leads to
hypocalcemia?
a. Pseudohypoparathyroidism
b. Jansen syndrome
c. Vitamin A intoxication
d. �yrotoxicosis
3. When conducting an evaluation of hypocalcemia,
which of the following blood levels WILL NOT be
a�ected by recent administration of intravenous cal
cium therapy?
a. Parathyroid hormone
b. 25(OH) vitamin D
c. Ionized calcium
d. 1,25(OH) 2 vitamin D
4. Hypophosphatemia in Fanconi syndrome leads to
which of the following hormonal changes?
a. Elevated blood FGF-23 levels
b. Elevated blood cortisol levels
c. Lowered blood levels of calcitriol
d. No distinct pattern in calciotropic hormones

e. Elevated blood levels of calcitonin
5. Which of the following segments of the kidney handle
the majority of magnesium homeostasis
A. Proximal tubule
B. �ick ascending limb
C. �in ascending limb
D. Distal convoluted tubule
E. Collecting ducts
a. D and E
b. B and D
c. A and C
d. A and B
e. All of the above
6. Which of the following is not associated with
hypophosphatemia?
a. Tumoral calcinosis
b. Refeeding syndrome
c. XLH
d. Calcitonin therapy
7. Ionized calcium is the biologically active component of
total body calcium and comprises: a. 50% of the total bodycalcium b. 1% of the serum calcium c. 1% of the totalbody calcium d. 50% of the serum calcium 8. �e vastmajority of phosphorus handling occurs in this part of thenephron: a. Proximal tubule b. Loop of Henle c. Distaltubule d. Collecting duct 9. Which of the following isnot associated with hypomagnesemia? a. Chronic diarrheab. Addison disease c. Gitelman syndrome d. Loop diuretics10. When calculating the fractional excretion of magnesium,

the plasma magnesium must be multiplied by 0.7 because:a. �e majority of magnesium is albumin bound. b. �emajority of magnesium is not ultra�ltrable. c. �at is theultra�ltrable percentage of magnesium d. �at is thepercentage of magnesium that is reabsorbed distally. ANSWERKEY 1. c 2. a 3. b 4. d 5. d 6. d 7. d 8. a 9. b10. c
14 Acid-base homeostasis
As discussed previously, the acid-base homeostasis
is determined by respiratory function and metabolic
function. �e challenge has always been to determine
how much of a disturbance is due to the respiratory
or the metabolic components. �e fundamentals of
acid-base physiology were developed during the early
to mid-20th century. Much of this information is
reviewed by Davenport. 2 Henderson had expressed theionization reaction
for a general acid using the principle of mass action
that had been developed in the late 19th century.
Hasselbalch then converted the Henderson equation
into the familiar logarithmic form that is well known
as the Henderson–Hasselbalch equation. As tech
niques improved for the measurement of the com
ponents of the blood gases (i.e. pH and pCO 2 ) e�orts
to determine the two components, respiratory versus
metabolic, began to develop. �e �rst was the stan
dard base. �is was measured by taking the sample of
blood and allowing it to equilibrate with gas to yield
a pCO 2 of 40 mm Hg. �us, a sample with a low stan
dard bicarbonate would indicate a metabolic acidosis. �econcept of base excess was then developed. It is
de�ned as the amount of acid or base needed to titrate the
bicarbonate concentration to 24 mEq/L while keeping the

pCO 2 at 40 mm Hg. �e advantage to this approach was
that it would also take into account the other bu�ers pres
ent in the blood sample, including hemoglobin. During
this time, the approach taken by investigators in Boston
was directed at estimating the predicted values of the
blood gas determinants to understand the patient’s acid
base disturbance, while the approach in Copenhagen was
based on the measured base excess. �is resulted in the
“Great Trans-Atlantic Acid-Base Debate.” 69 Currently,
most physicians use the base excess approach. Morerecently, Stewart reintroduced the concept of
the “strong ion di�erence.” 70 �is is a more physico
chemical approach to the understanding of acid-base
physiology. �e merits of this approach continue to
be debated. 71–74 Even the more practical tools that are
used in the assessment of the patient with acid-base
disorders have evolved. �e acid-base nomogram (see
Figure 14.5) used to be complicated and di�cult to
use, but mobile platform adoption and computing
so�ware are making its clinical applications easier. 75 �ecauses of increased anion gap acidosis have
shi�ed over time. �e occurrence of paraldehyde
overdose is rare, but the �nding of 5-oxoproline over
dose has been reported several times. �us, the mne
monic for increased anion gap acidosis, MUDPILES,
becomes less relevant. A new mnemonic for the 21st

century designated GOLD MARK (see Table 14.2)
has been proposed by Mehta and colleagues. 76
9. Quigley R. Proximal renal tubular acidosis. J Nephrol.2006;19(Suppl 9):S41–5.
10. Fry A C, Karet FE. Inherited renal acidoses.Physiology (Bethesda). 2007;22:202–11.
11. Nakhoul NL, Hamm LL. Vacuolar H(+)-ATPase in thekidney. J Nephrol. 2002;15(Suppl 5):S22–31.
12. Good DW. The thick ascending limb as a site of renalbicarbonate reabsorption. Semin Nephrol. 1993;13:225–35.
13. Lee S , Lee HJ, Yang HS, et al. Sodium-bicarbonatecotransporter NBCn1 in the kidney medullary thickascending limb cell line is upregulated under acidicconditions and enhances ammonium transport. Exp Physiol.2010;95:926–37.
14. Lee Hamm L, Hering-Smith KS, Nakhoul NL. Acid-baseand potassium homeostasis. Semin Nephrol. 2013;33:257–64.
15. Weiner ID, Verlander JW. Renal ammonia metabolism andtransport. Compr Physiol. 2013;3:201–20.
16. DuBose TD, Jr, Good DW, Hamm LL, Wall SM. Ammoniumtransport in the kidney: New physiological concepts andtheir clinical implications. J Am Soc Nephrol.1991;1:1193–203.
17. Tan nen RL. Ammonia metabolism. Am J Physiol.1978;235:F265–77.
18. Pit ts RF. Renal production and excretion of ammonia.Am J Med. 1964;36:720–42.
19. Wei ner ID, Hamm LL. Molecular mechanisms of renalammonia transport. Annu Rev Physiol. 2007;69:317-40.
20. Sel din DW, Teng HC, Rector FC, Jr. Ammonia excretionand renal glutaminase activity during administration ofstrong acid and buffer acid. Proc Soc Exp Biol Med.1957;94:366–8.
21. Halperin ML, Vinay P, Gougoux A, et al. Regulation ofthe maximum rate of renal ammoniagenesis in the acidoticdog. Am J Physiol. 1985;248:F607–15.

22. Curthoys NP, Moe OW. Proximal tubule function andresponse to acidosis. Clin J Am Soc Nephrol.2014;9:1627–38.
23. Curthoys NP, Watford M. Regulation of glutaminaseactivity and glutamine metabolism. Annu Rev Nutr.1995;15:133–59.
24. Quigley R. Developmental changes in renal func tion.Curr Opin Pediatr. 2012;24:184–90.
25. Quigley R, Baum M. Neonatal acid base balance anddisturbances. Semin Perinatol. 2004;28:97–102.
26. Carmody JB, Norwood VF. A clinical approach topaediatric acid-base disorders. Postgrad Med J.2012;88:143–51.
27. Har rison RA. Acid-base balance. Respir Care Clin NAm. 1995;1:7–21.
28. Whittier WL, Rutecki GW. Primer on clinical acidbaseproblem solving. Dis Mon. 2004;50:122–62.
29. Kuma r V, Karon BS. Comparison of measured andcalculated bicarbonate values. Clin Chem. 2008;54:1586–7.30. Kraut JA, Madias NE. Metabolic acidosis:Pathophysiology, diagnosis and management. Nat RevNephrol. 2010;6:274–85. 31. Emmett M, Narins RG. Clinicaluse of the anion gap. Medicine (Baltimore). 1977;56:38–54.32. Kra ut JA, Madias NE. Serum anion gap: Its uses andlimitations in clinical medicine. Clin J Am Soc Nephrol.2007;2:162–74. 33. Kellum JA. Closing the gap onunmeasured anions. Crit Care. 2003;7:219–20. 34. MehtaAN, Emmett JB, Emmett M. GOLD MARK: An anion gap mnemonicfor the 21st century. Lancet. 2008;372:892. 35. SadjadiSA, Manalo R, Jaipaul N, et al. Ion-selective electrodeand anion gap range: What should the anion gap be? Int JNephrol Renovasc Dis. 2013;6:101–5. 36. Oh MS , CarrollHJ. The anion gap. N Engl J Med. 1977;297:814–7. 37. Emmett M. Anion gap, anion gap corrected for albumin, andbase deficit fail to accurately diagnose clinicallysignificant hyperlactatemia in critically ill patients. JIntensive Care Med. 2008;23:350. 38. Pau lson WD. Effectof acute pH change on serum anion gap. J Am Soc Nephrol.1996;7:357–63. 39. Halperin ML, Bear RA, Hannaford MC,Goldstein MB. Selected aspects of the pathophysiology ofmetabolic acidosis in diabetes mellitus. Diabetes1981;30:781–7. 40. Ham meke M, Bear R, Lee R, et al.
Hyperchloremic metabolic acidosis in diabetes mellitus: Acase report and discussion of pathophysiologic mechanisms.Diabetes. 1978;27:16–20. 41. Fal l PJ, Szerlip HM. Lacticacidosis: From sour milk to septic shock. J Intensive CareMed. 2005;20:255–71. 42. Rob ergs RA, Ghiasvand F,Parker D. Biochemistry of exercise-induced metabolicacidosis. Am J Physiol Regul Integr Comp Physiol.2004;287:R502–16. 43. Gladden LB. Lactate metabolism: Anew paradigm for the third millennium. J Physiol.2004;558:5–30. 44. Gladden LB. A lactatic perspective onmetabolism. Med Sci Sports Exerc. 2008;40:477–85. 45.Gun nerson KJ, Saul M, He S, Kellum JA. Lactate versusnon-lactate metabolic acidosis: A retrospective outcomeevaluation of critically ill patients. Crit Care.2006;10:R22. 46. Bakker J, Nijsten MW, Jansen TC. Clinicaluse of lactate monitoring in critically ill patients. AnnIntensive Care. 2013;3:12. 47. Seashore MR. The organicacidemias: An overview. In: Pagon RA, Adam MP, ArdingerHH, et al., editors. GeneReviews. Seattle: University ofWashington Press; 1993. 48. Ting SM, Ching I, Nair H, etal. Early and late presentations of ethylene glycolpoisoning. Am J Kidney Dis. 2009;53:1091–7.
49. Velez LI, Shepherd G, Lee YC, Keyes DC. Ethyleneglycol ingestion treated only with fomepizole. J MedToxicol. 2007;3:125–8.
50. Kra ut JA, Kurtz I. Toxic alcohol ingestions: Clinicalfeatures, diagnosis, and management. Clin J Am SocNephrol. 2008;3:208–25.
51. Fenves AZ, Kirkpatrick HM, 3rd, Patel VV, et al.Increased anion gap metabolic acidosis as a result of5-oxoproline (pyroglutamic acid): A role foracetaminophen. Clin J Am Soc Nephrol. 2006;1:441–7.
52. Verma R, Polsani KR, Wilt J, Loehrke ME.5-Oxoprolinuria as a cause of high anion gap metabolicacidosis. Br J Clin Pharmacol. 2012;73:489–91.
53. Moe O W, Fuster D. Clinical acid-base pathophysiology:Disorders of plasma anion gap. Best Pract Res ClinEndocrinol Metab. 2003;17:559–74.
54. Batlle DC, Hizon M, Cohen E, et al. The use of theurinary anion gap in the diagnosis of hyperchloremicmetabolic acidosis. N Engl J Med. 1988;318:594–9.
55. Kamel KS, Ethier JH, Richardson RM, et al. Urineelectrolytes and osmolality: When and how to use them. Am

J Nephrol. 1990;10:89–102.
56. Oh MS , Phelps KR, Lieberman RL, Carroll HJ.Determination of urinary ammonia by osmometry. Anal Chem.1979;51:2247–8.
57. Wre nn K. The delta (delta) gap: An approach to mixedacid-base disorders. Ann Emerg Med. 1990;19:1310–3.
58. Ras tegar A. Use of the DeltaAG/DeltaHCO3– ratio inthe diagnosis of mixed acid-base disorders. J Am SocNephrol. 2007;18:2429–31.
59. Seldin DW, Rector FC, Jr. Symposium on acid-basehomeostasis: The generation and maintenance of metabolicalkalosis. Kidney Int. 1972;1:306–21.
60. Tutay GJ, Capraro G, Spirko B, et al. Electrolyteprofile of pediatric patients with hypertrophic pyloricstenosis. Pediatr Emerg Care. 2013;29:465–8.
61. Kennedy JD, Dinwiddie R, Daman-Willems C, et al.Pseudo-Bartter’s syndrome in cystic fibrosis. Arch DisChild. 1990;65:786–7.
62. Bates CM, Baum M, Quigley R. Cystic fibrosis presentingwith hypokalemia and metabolic alkalosis in a previouslyhealthy adolescent. J Am Soc Nephrol. 1997;8:352–5.
63. Kere J, Lohi H, Hoglund P. Genetic disorders ofmembrane transport III: Congenital chloride diarrhea. Am JPhysiol. 1999;276:G7–13.
64. Can non PJ, Heinemann HO, Albert MS, et al.“Contraction” alkalosis after diuresis of edematouspatients with ethacrynic acid. Ann Intern Med 62: 979–990,1965
65. Luk e RG, Galla JH. It is chloride depletion alkalosis,not contraction alkalosis. J Am Soc Nephrol.2012;23:204–7. 66. Shaer AJ. Inherited primary renaltubular hypokalemic alkalosis: A review of Gitelman andBartter syndromes. Am J Med Sci 2001;322:316–32. 67. Javaheri S, Kazemi H. Metabolic alkalosis and hypoventilationin humans. Am Rev Respir Dis. 1987;136:1011–6. 68.Javaheri S, Shore NS, Rose B, Kazemi H. Compensatoryhypoventilation in metabolic alkalosis. Chest.1982;81:296–301. 69. Seve ringhaus JW. Siggaard-Andersenand the “Great Trans-Atlantic Acid-Base Debate.” Scand JClin Lab Invest Suppl. 1993;214:99–104. 70. Morgan TJ. The
Stewart approach: One clinician’s perspective. ClinBiochem Rev. 2009;30:41–54. 71. Kurtz I, Kraut J,Ornekian V, Nguyen MK. Acidbase analysis: A critique of theStewart and bicarbonate-centered approaches. Am J PhysiolRenal Physiol. 2008;294:F1009–31. 72. Kellum JA.Clinical review: Reunification of acidbase physiology. CritCare. 2005;9:500–7. 73. Sig gaard-Andersen O,Fogh-Andersen N. Base excess or buffer base (strong iondifference) as measure of a non-respiratory acid-basedisturbance. Acta Anaesthesiol Scand Suppl.1995;107:123–8. 74. Seve ringhaus JW. Blood gascalculator. J Appl Physiol. 1966;21:1108-16. 75. Pronicka E, Piekutowska-Abramczuk DH, Popowska E, et al.Compulsory hyperventilation and hypocapnia of patientswith Leigh syndrome associated with SURF1 gene mutationsas a cause of low serum bicarbonates. J Inherit Metab Dis.2001;24:707–14. 76. Meh ta AN, Emmett JB, Emmett M. GOLDMARK: An anion gap mnemonic for the 21st century. Lancet.2008; 372:892. REVIEW QUESTIONS 1. A 3-year-old boypresents with a 3-week history of progressive eyeswelling. He also has some swelling in his legs, and hismom reports his abdomen to be more distended. Onexamination, his blood pressure is 110/50 mm Hg and heartrate is 85 beats/min. He is afebrile. He has 2+periorbital edema and 2+ pitting edema of his legs. Hiscardiac and lung examinations were normal. His urinalysisshowed 4+ protein and is negative for blood. His serumchemistries are creatinine, 0.3 mg/dL; sodium, 132 mEq/L;potassium, 4.5 mEq/L; chloride 107 mEq/L; and bicarbonate,25 mEq/L. �is yields an anion gap of zero. Which of thefollowing is the most likely cause of the low anion gap?a. �e laboratory made an error. b. �e serum calcium mustbe elevated.
c. His gamma-globulin fraction must be elevated.
d. His serum albumin is very low.
e. He has bromide intoxication.
2. A 1-year-old infant was admitted with a 3-day history ofdiarrhea. �e laboratory analysis on the day of admissionrevealed sodium, 135 mEq/L; chloride, 115 mEq/L; andbicarbonate 15 mEq/L. A�er 2 days, the diarrhea hasstopped and the patient has been volume expanded with 0.9%saline, the electrolytes were measured again and found tobe sodium 138 mEq/L; chloride, 115 mEq/L; and bicarbonateof 17 mEq/L. �e urinary electrolytes were found to besodium of 35 mEq/L; potassium 75 mEq/L; and chloride of105 mEq/L. �e urine pH was 7.0. �e most likely explanation
for these �ndings is:
a. �e patient has distal RTA.
b. �e patient has cystinosis.
c. �e 0.9% saline has caused dilutional alkalosis.
d. �e ability to increase ammoniagenesis is impairedbecause of the patient’s age.
3. A 15-year-old male patient has reportedly attemptedsuicide by drinking antifreeze containing ethylene glycol.His electrolytes were found to be sodium, 142 mEq/L;chloride, 111 mEq/L; and bicarbonate, 21 mEq/L. Otherlaboratory �ndings were glucose, 72 mg/dL, BUN, 28 mg/dL;and serum osmolality, 345 mOsm/kg water. �e best evidencethat he actually drank the ethylene glycol is:
a. �e history of drinking antifreeze
b. �e elevated anion gap
c. �e high osmolar gap
d. No evidence for ethylene glycol ingestion
4. A 14-year-old female presents with a 3-week history ofpolyuria and polydipsia. �e family also reports that shehas lost 6 lb during this period. On examination, her bloodpressure is 110/59 mm Hg, heart rate is 140 beats/min, andrespiratory rate is 26 breaths/min. Serum chemistriesdemonstrated sodium, 132 mEq/L; potassium, 5.8 mEq/L;chloride, 98 mEq/L; and bicarbonate, 8 mEq/L (anion gap,26). Her serum glucose was 820 mg/dL. Her urinalysisreveals no protein or blood, but had 4+ glucose. Her aniongap is most likely elevated because of:
a. Decreased serum albumin
b. Increased serum acetoacetate
c. Increased serum acetone
d. Increased serum calcium
e. Increased serum lactate
5. �e primary source of acid in our diet is:
a. Fatty acids
b. Citric acid
c. Phosphate
d. Ascorbic acid
e. Sulfur-containing amino acids
6. A 10-kg patient generates 10 mEq of H + /day that needto be excreted in her urine. If the patient’s urine had nobu�ers and he made 1 L of urine, what would be the �nal pHof the urine? a. 1 b. 2 c. 5 d. 6 e. Cannot calculatewith the given information 7. A 6-week-old male infant hashad nonbilious emesis for the past 2 days and appearsvolume depleted. �e electrolyte values were sodium, 132mEq/L; potassium, 2.8 mEq/L; chloride, 88 mEq/L; andbicarbonate 36 mEq/L. �e most likely source for the lossof his potassium is: a. Emesis b. Stool c. Urine d. Hehas not lost any potassium, but it has shi�ed into theintracellular compartment e. Sweat 8. A 2-year-old,ex–29-week preterm infant with bronchopulmonary dysplasiais being seen for diarrhea. He has lost 0.6 kg in the past2 days and now weighs 9.5 kg. His blood pressure is 98/45mm Hg, and his heart rate is 112 bpm. His respiratory rateis 32 breaths/ min, and his lungs have coarse bronchithroughout. His skin turgor is decreased, with positivetenting. Laboratory studies revealed sodium, 136 mEq/L;potassium, 3.6 mEq/L; chloride, 90 mEq/L; and bicarbonate,24 mEq/L. An arterial blood gas sample showed the pH to be7.22 and pCO 2 to be 60 mm Hg. Serum creatinine is 0.5mg/dL. �e most likely explanation for these �ndings is: a.e laboratory made an error in the ABG result. b. �epatient has acute respiratory acidosis that isuncompensated. c. �e patient has chronic respiratoryacidosis with acute metabolic acidosis. d. �e patientmust have had some vomiting. 9. A 3-year-old infant isbeing evaluated for stridor and hyperventilation. Duringthe workup, serum electrolyte examination results revealedsodium, 138 mEq/L; potassium, 4.3 mEq/L; chloride, 108mEq/L; and bicarbonate, 15 mEq/L. To assess the concernregarding the low bicarbonate, the most appropriate nextstep would be: a. Perform a cortisone stimulation test.b. Obtain arterial blood gas sample to assess pH and pCO 2. c. Collect urine for anion gap. d. Perform bicarbonateloading to determine transport maximum for bicarbonate.10. A 13-year-old female presents for the evaluation ofhypertension. Her blood pressure is 165/112 mm Hg. Herfamily history is positive for many individuals with

hypertension, including her mother and two uncles. Herphysical examination is otherwise normal. Laboratoryvalues showed sodium, 145 mEq/L; potassium, 2.8 mEq/L;chloride, 99 mEq/L; and bicarbonate 36 mEq/L. An arterialblood gas has a pH of 7.5 and pCO 2 50 mm Hg. Her urinaryelectrolytes were sodium, 78 mEq/L; potassium 56 mEq/L;and chloride, 148 mEq/L. �ese laboratory values wouldindicate:
a. She is wasting chloride and should be given extrachloride.
b. She most likely has renal tubular acidosis.
c. She needs to be examined for chronic lung disease.
d. She has chloride-unresponsive alkalosis. ANSWER KEY 1.d 2. d 3. c 4. b 5. e 6. b 7. c 8. c 9. b 10. d
15 Water homeostasis
1. Darwin C. On the Origin of Species by Means of NaturalSelection. London: John Murray; 1859.
2. Smith HW. From Fish to Philosopher. Boston: Little,Brown and Company; 1953.
3. Bernard C. Leçons sur lex phénomènes de la vie communsaux animaux et auz végétaux. Paris: JB Baillerre et Fils;1885.
4. Kuhn W, Ryffel K. Herstellung konzentrierter Losungenaus verdunnten durch blosse Membranwirking: einModellversuch zur der Niere. Z Physiol Chem.1942;276:145–80.
5. Kok ko JP, Rector FCJ. Countercurrent multiplicationsystem without active transport in inner medulla. KidneyInt. 1972;2:214–23.
6. Sands JM, Kokko JP. Countercurrent system. Kidney Int1990;38:695–9.
7. Ste phenson JL. Concentration of urine in a centralcore model of the renal counterflow system. Kidney Int.1972;2:85–94.
8. Molony DA, Reeves WB, Andreoli TE. Na + :K + :2Clcotransport and the thick ascending limb. Kidney Int.1989;36:418–26. 9. Dunn FL, Brennan TJ, Nelson AE,Robertson GL. The role of blood osmolality and volume inregulating vasopressin secretion in the rat. J ClinInvest. 1973;52:3212–9. 10. Robertson GL, Berl T.Pathophysiology of water metabolism. In: Brenner BM,editor. The Kidney. 6th ed. Philadelphia: WB Saunders;2000. p. 866–924. 11. Morgenthaler NG, Struck J, AlonsoC, Bergmann A. Assay for the measurement of copeptin, astable peptide derived from the precursor of vasopressin.Clin Chem. 2006;52:112–9. 12. Robertson GL. Abnormalitiesof thirst regulation. Kidney Int. 1984;25:460–9. 13.Schrier RW. Pathogenesis of sodium and water retention inhigh-output and low-output cardiac failure, nephroticsyndrome, cirrhosis, and preg nancy (1). N Engl J Med.1988;319:1065–72. 14. Schrier RW. Pathogenesis of sodiumand water retention in high-output and low-output cardiacfailure, nephrotic syndrome, cirrhosis, and preg nancy (2).N Engl J Med. 1988;319:1127–34. 15. Saito T, Ishikawa SE,Sasaki S, et al. Alteration in water channel AQP-2 byremoval of AVP stimulation in collecting duct cells of
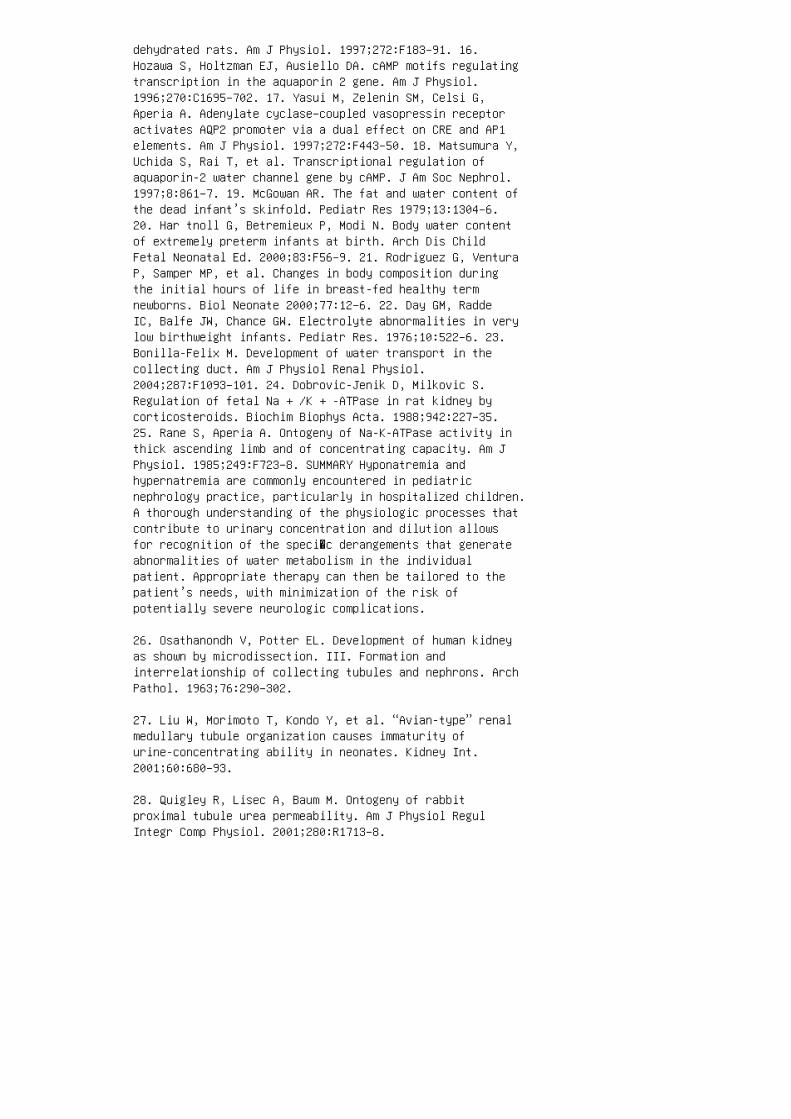
dehydrated rats. Am J Physiol. 1997;272:F183–91. 16.Hozawa S, Holtzman EJ, Ausiello DA. cAMP motifs regulatingtranscription in the aquaporin 2 gene. Am J Physiol.1996;270:C1695–702. 17. Yasui M, Zelenin SM, Celsi G,Aperia A. Adenylate cyclase–coupled vasopressin receptoractivates AQP2 promoter via a dual effect on CRE and AP1elements. Am J Physiol. 1997;272:F443–50. 18. Matsumura Y,Uchida S, Rai T, et al. Transcriptional regulation ofaquaporin-2 water channel gene by cAMP. J Am Soc Nephrol.1997;8:861–7. 19. McGowan AR. The fat and water content ofthe dead infant’s skinfold. Pediatr Res 1979;13:1304–6.20. Har tnoll G, Betremieux P, Modi N. Body water contentof extremely preterm infants at birth. Arch Dis ChildFetal Neonatal Ed. 2000;83:F56–9. 21. Rodriguez G, VenturaP, Samper MP, et al. Changes in body composition duringthe initial hours of life in breast-fed healthy termnewborns. Biol Neonate 2000;77:12–6. 22. Day GM, RaddeIC, Balfe JW, Chance GW. Electrolyte abnormalities in verylow birthweight infants. Pediatr Res. 1976;10:522–6. 23.Bonilla-Felix M. Development of water transport in thecollecting duct. Am J Physiol Renal Physiol.2004;287:F1093–101. 24. Dobrovic-Jenik D, Milkovic S.Regulation of fetal Na + /K + -ATPase in rat kidney bycorticosteroids. Biochim Biophys Acta. 1988;942:227–35.25. Rane S, Aperia A. Ontogeny of Na-K-ATPase activity inthick ascending limb and of concentrating capacity. Am JPhysiol. 1985;249:F723–8. SUMMARY Hyponatremia andhypernatremia are commonly encountered in pediatricnephrology practice, particularly in hospitalized children.A thorough understanding of the physiologic processes thatcontribute to urinary concentration and dilution allowsfor recognition of the speci�c derangements that generateabnormalities of water metabolism in the individualpatient. Appropriate therapy can then be tailored to thepatient’s needs, with minimization of the risk ofpotentially severe neurologic complications.
26. Osathanondh V, Potter EL. Development of human kidneyas shown by microdissection. III. Formation andinterrelationship of collecting tubules and nephrons. ArchPathol. 1963;76:290–302.
27. Liu W, Morimoto T, Kondo Y, et al. “Avian-type” renalmedullary tubule organization causes immaturity ofurine-concentrating ability in neonates. Kidney Int.2001;60:680–93.
28. Quigley R, Lisec A, Baum M. Ontogeny of rabbitproximal tubule urea permeability. Am J Physiol RegulIntegr Comp Physiol. 2001;280:R1713–8.

29. Forrest JN, Jr, Stanier MW. Kidney composition andrenal concentration ability in young rabbits. J Physiol.1966;187:1–4.
30. Edelmann CM, Barnett HL, Troupkou V. Renalconcentrating mechanisms in newborn infants: Effect ofdietary protein and water content, role of urea, andresponsiveness to antidiuretic hormone. J Clin Invest.1960;39:1062–9.
31. Edelmann CM, Jr, Barnett HL, Stark H. Effect of ureaon concentration of urinary nonurea solute in prematureinfants. J Appl Physiol. 1966;21:1021–5.
32. Imran S, Eva G, Christopher S, Flynn E, Henner D. Isspecific gravity a good estimate of urine osmolality? JClin Lab Anal. 2010;24:426–30.
33. Lee ch S, Penney MD. Correlation of specific gravityand osmolality of urine in neonates and adults. Arch DisChild. 1987;62:671–3.
34. Lord RC. Osmosis, osmometry, and osmoregulation.Postgrad Med. J 1999;75:67–73.
35. Aw TC, K iechle FL. Pseudohyponatremia. Am J EmergMed. 1985;3:236–9.
36. Katz MA. Hyperglycemia-induced hyponatremia:Calculation of expected serum sodium depression. N Engl JMed. 1973;289:843–4.
37. Hillier TA, Abbott RD, Barrett EJ. Hyponatremia:Evaluating the correction factor for hyperglycemia. Am JMed. 1999;106:399–403.
38. Moritz ML, Ayus JC. The changing pattern ofhypernatremia in hospitalized children. Pediatrics.1999;104:435–9.
39. Mor itz ML, Ayus JC. Prevention of hospital-acquiredhyponatremia: A case for using isotonic saline.Pediatrics. 2003;111:227–30.
40. Moritz ML, Ayus JC. Preventing neurologicalcomplications from dysnatremias in children. PediatrNephrol. 2005;20:1687–700.
41. Armon K, Riordan A, Playfor S, et al. Hyponatraemia

and hypokalaemia during intravenous fluid administration.Arch Dis Child. 2008;93:285–7.
42. Has egawa H, Okubo S, Ikezumi Y, et al. Hyponatremiadue to an excess of arginine vasopressin is common inchildren with febrile disease. Pediatr Nephrol.2009;24:507–11.
43. Mor itz ML, Ayus JC. Disorders of water metabolism inchildren: Hyponatremia and hypernatremia. Pediatr Rev.2002;23:371–80. 44. Ayus JC, Achinger SG, Arieff A. Braincell volume regulation in hyponatremia: Role of sex, age,vasopressin, and hypoxia. Am J Physiol Renal Physiol. 2 008;295:F619–24. 45. Sza talowicz VL, Miller PD, Lacher JW,et al. Comparative effect of diuretics on renal waterexcretion in hyponatraemic oedematous disor ders. Clin Sci(Lond). 1982;62:235–8. 46. Kim GH, Lee JW, Oh YK, et al.Antidiuretic effect of hydrochlorothiazide inlithium-induced nephro genic diabetes insipidus isassociated with upregulation of aquaporin-2, Na-Clco-transporter, and epi thelial sodium channel. J Am SocNephrol. 2004;15:2836–43. 47. Hsi eh S, White PC.Presentation of primary adre nal insufficiency inchildhood. J Clin Endocrinol Met ab. 2011;96:E925–8. 48.Bet tinelli A, Longoni L, Tammaro F, et al. Renalsalt-wasting syndrome in children with intracranialdisorders. Pediatr Nephrol. 2012;27:733–9. 49. Moritz ML.Syndrome of inappropriate antidiure sis and cerebral saltwasting syndrome: Are they dif ferent and does it matter?Pediatr Nephrol. 2012;27:689–93. 50. Har desty DA,Kilbaugh TJ, Storm PB. Cerebral salt wasting syndrome inpost-operative pedi atric brain tumor patients. NeurocritCare. 2 01 2;17:382–7. 51. von BP , Ankermann T, EggertP, et al. Diagnosis and management of cerebral saltwasting (CSW) in children: The role of atrial natriureticpeptide (ANP) and brain natriuretic peptide (BNP). ChildsNerv Syst. 2006;22:1275–81. 52. Costa KN, Nakamura HM,Cruz LR, et al. Hyponatremia and brain injury: Absence ofalterations of serum brain natriuretic peptide andvasopressin. Arq Neuropsiquiatr. 2009;67:1037–44. 53.Bitew S, Imbriano L, Miyawaki Net al. More on renal saltwasting without cerebral disease: Response to salineinfusion. Clin J Am Soc Nephrol. 2009;4:309–15. 54.Maesaka JK, Imbriano LJ, Ali NM, Ilamathi E. Is itcerebral or renal salt wasting? Kidney Int. 2009;76:934–8.55. Maesaka JK, Miyawaki N, Palaia T, et al. Renal saltwasting without cerebral disease: Diagnostic value ofurate determinations in hyponatremia. Kidney Int.2007;71:822–6. 56. Maesaka JK, Gupta S, Fishbane S.Cerebral salt-wasting syndrome: Does it exist? Nephron.

1999;82:100–9. 57. Bartter FC, Schwartz WB. The syndromeof inappropriate secretion of antidiuretic hormone. Am JMed. 1967;42:790–806. 58. Fenske W, Stork S, BlechschmidtA, et al. Copeptin in the differential diagnosis ofhyponatremia. J Clin Endocrinol Metab. 2009;94:123–9.
59. Carpentier E, Greenbaum LA, Rochdi D, et al.Identification and characterization of an activating F229Vsubstitution in the V2 vasopressin recep tor in an infantwith NSIAD. J Am Soc Nephrol. 2012;23:1635–40.
60. Che ung CC, Cadnapaphornchai MA, Ranadive SA, et al.Persistent elevation of urine aquaporin-2 during waterloading in a child with nephrogenic syndrome ofinappropriate antidiuresis (NSIAD) caused by a R137Lmutation in the V2 vasopressin receptor. Int J PediatrEndocrinol. 2012;2012:3.
61. Rosenthal SM, Feldman BJ, Vargas GA, Gitelman SE.Nephrogenic syndrome of inappropriate antidiuresis(NSIAD): A paradigm for activating mutations causingendocrine dysfunction. Pediatr Endocrinol Rev.2006;4(Suppl 1):66–70.
62. Tenenbaum J, Ayoub MA, Perkovska S, et al. Theconstitutively active V2 receptor mutants confer ring NSIADare weakly sensitive to agonist and antagonist regulation.PLoS One. 2009;4:e8383.
63. Bockenhauer D, Penney MD, Hampton D, et al. A familywith hyponatremia and the nephrogenic syndrome ofinappropriate antidiuresis. Am J Kidney Dis.2012;59:566–8.
64. Decaux G, Vandergheynst F, Bouko Y, et al. Nephrogenicsyndrome of inappropriate antidi uresis in adults: Highphenotypic variability in m en a nd women from a largepedigree. J Am Soc Nephrol. 2007;18:606–2.
65. Wan g W, Li C, Summer SN, et al. Molecular analy sis ofimpaired urinary diluting capacity in glucocorticoiddeficiency. Am J Physiol Renal Physiol. 2 006;290:F1135–42.
66. Che n YC, Cadnapaphornchai MA, Yang J, et al.Nonosmotic release of vasopressin and renal aquaporins inimpaired urinary dilution in hypothyroidism. Am J PhysiolRenal Physiol. 2005;289:F672–8.
67. Hanna FW, Scanlon MF. Hyponatraemia, hypothy roidism,
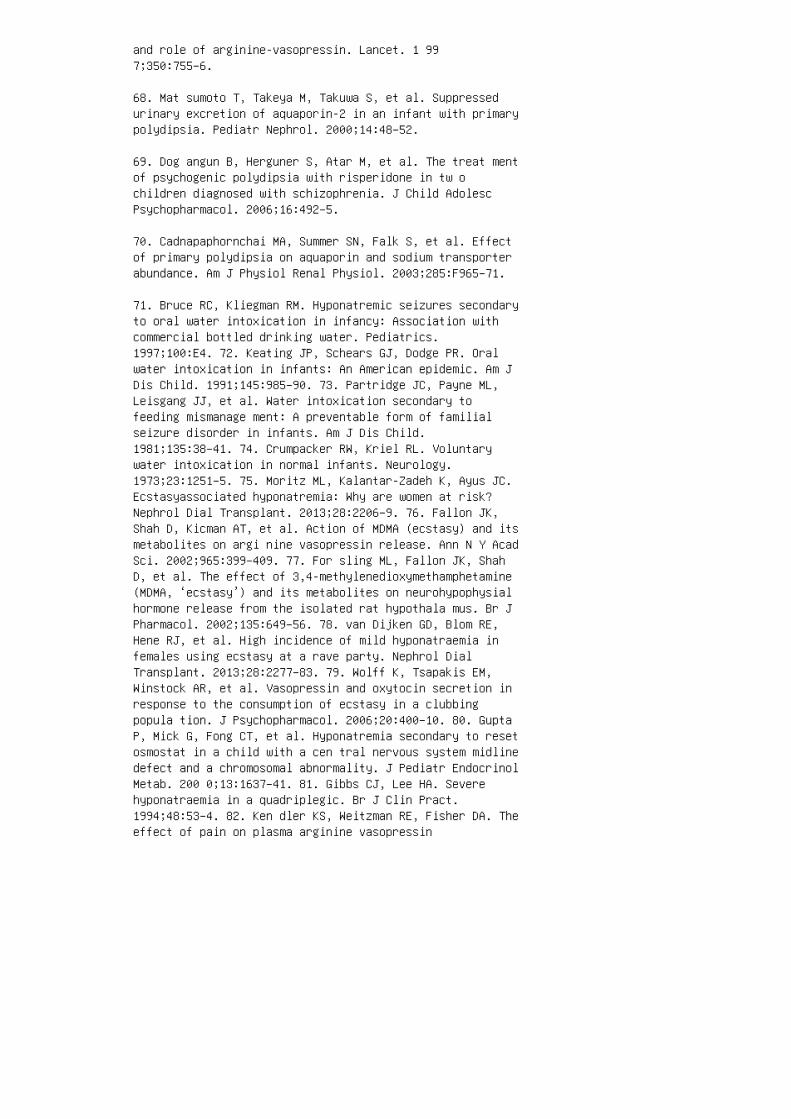
and role of arginine-vasopressin. Lancet. 1 997;350:755–6.
68. Mat sumoto T, Takeya M, Takuwa S, et al. Suppressedurinary excretion of aquaporin-2 in an infant with primarypolydipsia. Pediatr Nephrol. 2000;14:48–52.
69. Dog angun B, Herguner S, Atar M, et al. The treat mentof psychogenic polydipsia with risperidone in tw ochildren diagnosed with schizophrenia. J Child AdolescPsychopharmacol. 2006;16:492–5.
70. Cadnapaphornchai MA, Summer SN, Falk S, et al. Effectof primary polydipsia on aquaporin and sodium transporterabundance. Am J Physiol Renal Physiol. 2003;285:F965–71.
71. Bruce RC, Kliegman RM. Hyponatremic seizures secondaryto oral water intoxication in infancy: Association withcommercial bottled drinking water. Pediatrics.1997;100:E4. 72. Keating JP, Schears GJ, Dodge PR. Oralwater intoxication in infants: An American epidemic. Am JDis Child. 1991;145:985–90. 73. Partridge JC, Payne ML,Leisgang JJ, et al. Water intoxication secondary tofeeding mismanage ment: A preventable form of familialseizure disorder in infants. Am J Dis Child.1981;135:38–41. 74. Crumpacker RW, Kriel RL. Voluntarywater intoxication in normal infants. Neurology.1973;23:1251–5. 75. Moritz ML, Kalantar-Zadeh K, Ayus JC.Ecstasyassociated hyponatremia: Why are women at risk?Nephrol Dial Transplant. 2013;28:2206–9. 76. Fallon JK,Shah D, Kicman AT, et al. Action of MDMA (ecstasy) and itsmetabolites on argi nine vasopressin release. Ann N Y AcadSci. 2002;965:399–409. 77. For sling ML, Fallon JK, ShahD, et al. The effect of 3,4-methylenedioxymethamphetamine(MDMA, ‘ecstasy’) and its metabolites on neurohypophysialhormone release from the isolated rat hypothala mus. Br JPharmacol. 2002;135:649–56. 78. van Dijken GD, Blom RE,Hene RJ, et al. High incidence of mild hyponatraemia infemales using ecstasy at a rave party. Nephrol DialTransplant. 2013;28:2277–83. 79. Wolff K, Tsapakis EM,Winstock AR, et al. Vasopressin and oxytocin secretion inresponse to the consumption of ecstasy in a clubbingpopula tion. J Psychopharmacol. 2006;20:400–10. 80. GuptaP, Mick G, Fong CT, et al. Hyponatremia secondary to resetosmostat in a child with a cen tral nervous system midlinedefect and a chromosomal abnormality. J Pediatr EndocrinolMetab. 200 0;13:1637–41. 81. Gibbs CJ, Lee HA. Severehyponatraemia in a quadriplegic. Br J Clin Pract.1994;48:53–4. 82. Ken dler KS, Weitzman RE, Fisher DA. Theeffect of pain on plasma arginine vasopressin
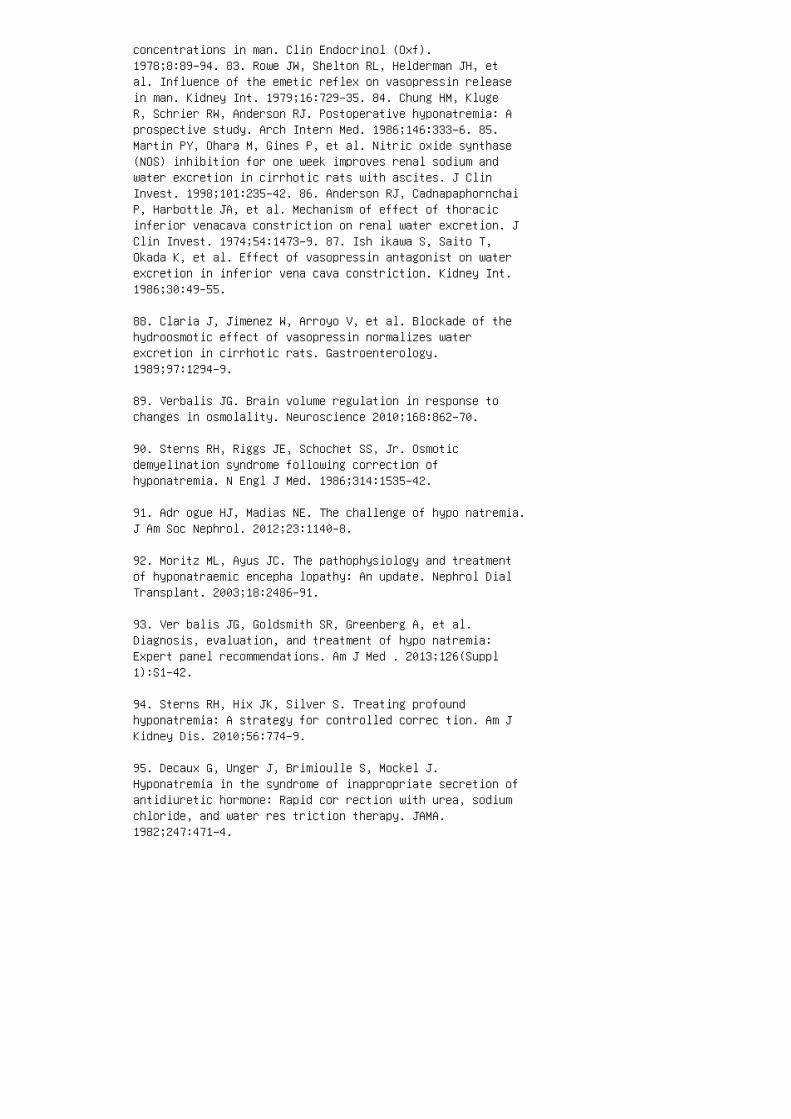
concentrations in man. Clin Endocrinol (Oxf).1978;8:89–94. 83. Rowe JW, Shelton RL, Helderman JH, etal. Influence of the emetic reflex on vasopressin releasein man. Kidney Int. 1979;16:729–35. 84. Chung HM, KlugeR, Schrier RW, Anderson RJ. Postoperative hyponatremia: Aprospective study. Arch Intern Med. 1986;146:333–6. 85.Martin PY, Ohara M, Gines P, et al. Nitric oxide synthase(NOS) inhibition for one week improves renal sodium andwater excretion in cirrhotic rats with ascites. J ClinInvest. 1998;101:235–42. 86. Anderson RJ, CadnapaphornchaiP, Harbottle JA, et al. Mechanism of effect of thoracicinferior venacava constriction on renal water excretion. JClin Invest. 1974;54:1473–9. 87. Ish ikawa S, Saito T,Okada K, et al. Effect of vasopressin antagonist on waterexcretion in inferior vena cava constriction. Kidney Int.1986;30:49–55.
88. Claria J, Jimenez W, Arroyo V, et al. Blockade of thehydroosmotic effect of vasopressin normalizes waterexcretion in cirrhotic rats. Gastroenterology.1989;97:1294–9.
89. Verbalis JG. Brain volume regulation in response tochanges in osmolality. Neuroscience 2010;168:862–70.
90. Sterns RH, Riggs JE, Schochet SS, Jr. Osmoticdemyelination syndrome following correction ofhyponatremia. N Engl J Med. 1986;314:1535–42.
91. Adr ogue HJ, Madias NE. The challenge of hypo natremia.J Am Soc Nephrol. 2012;23:1140–8.
92. Moritz ML, Ayus JC. The pathophysiology and treatmentof hyponatraemic encepha lopathy: An update. Nephrol DialTransplant. 2003;18:2486–91.
93. Ver balis JG, Goldsmith SR, Greenberg A, et al.Diagnosis, evaluation, and treatment of hypo natremia:Expert panel recommendations. Am J Med . 2013;126(Suppl1):S1–42.
94. Sterns RH, Hix JK, Silver S. Treating profoundhyponatremia: A strategy for controlled correc tion. Am JKidney Dis. 2010;56:774–9.
95. Decaux G, Unger J, Brimioulle S, Mockel J.Hyponatremia in the syndrome of inappropriate secretion ofantidiuretic hormone: Rapid cor rection with urea, sodiumchloride, and water res triction therapy. JAMA.1982;247:471–4.
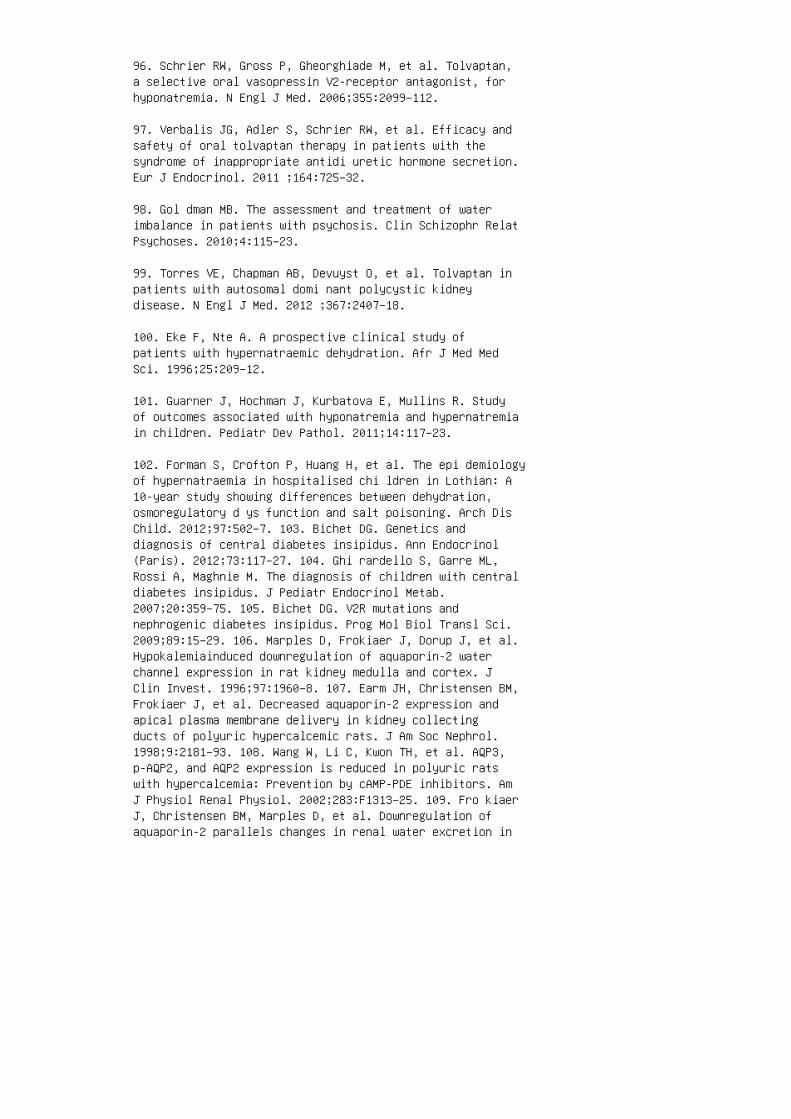
96. Schrier RW, Gross P, Gheorghiade M, et al. Tolvaptan,a selective oral vasopressin V2-receptor antagonist, forhyponatremia. N Engl J Med. 2006;355:2099–112.
97. Verbalis JG, Adler S, Schrier RW, et al. Efficacy andsafety of oral tolvaptan therapy in patients with thesyndrome of inappropriate antidi uretic hormone secretion.Eur J Endocrinol. 2011 ;164:725–32.
98. Gol dman MB. The assessment and treatment of waterimbalance in patients with psychosis. Clin Schizophr RelatPsychoses. 2010;4:115–23.
99. Torres VE, Chapman AB, Devuyst O, et al. Tolvaptan inpatients with autosomal domi nant polycystic kidneydisease. N Engl J Med. 2012 ;367:2407–18.
100. Eke F, Nte A. A prospective clinical study ofpatients with hypernatraemic dehydration. Afr J Med MedSci. 1996;25:209–12.
101. Guarner J, Hochman J, Kurbatova E, Mullins R. Studyof outcomes associated with hyponatremia and hypernatremiain children. Pediatr Dev Pathol. 2011;14:117–23.
102. Forman S, Crofton P, Huang H, et al. The epi demiologyof hypernatraemia in hospitalised chi ldren in Lothian: A10-year study showing differences between dehydration,osmoregulatory d ys function and salt poisoning. Arch DisChild. 2012;97:502–7. 103. Bichet DG. Genetics anddiagnosis of central diabetes insipidus. Ann Endocrinol(Paris). 2012;73:117–27. 104. Ghi rardello S, Garre ML,Rossi A, Maghnie M. The diagnosis of children with centraldiabetes insipidus. J Pediatr Endocrinol Metab.2007;20:359–75. 105. Bichet DG. V2R mutations andnephrogenic diabetes insipidus. Prog Mol Biol Transl Sci.2009;89:15–29. 106. Marples D, Frokiaer J, Dorup J, et al.Hypokalemiainduced downregulation of aquaporin-2 waterchannel expression in rat kidney medulla and cortex. JClin Invest. 1996;97:1960–8. 107. Earm JH, Christensen BM,Frokiaer J, et al. Decreased aquaporin-2 expression andapical plasma membrane delivery in kidney collectingducts of polyuric hypercalcemic rats. J Am Soc Nephrol.1998;9:2181–93. 108. Wang W, Li C, Kwon TH, et al. AQP3,p-AQP2, and AQP2 expression is reduced in polyuric ratswith hypercalcemia: Prevention by cAMP-PDE inhibitors. AmJ Physiol Renal Physiol. 2002;283:F1313–25. 109. Fro kiaerJ, Christensen BM, Marples D, et al. Downregulation ofaquaporin-2 parallels changes in renal water excretion in

unilateral ureteral obstruction. Am J Physiol.1997;273:F213–23. 110. Shi Y , Li C, Thomsen K, et al.Neonatal ureteral obstruction alters expression of renalsodium transporters and aquaporin water channels. KidneyInt. 2004;66:203–15. 111. Mar ples D, Christensen S,Christensen EI, et al. Lithium-induced downregulation ofaquaporin-2 water channel expression in rat kidneymedulla. J Clin Invest. 1995;95:1838–45. 112. Bockenhauer D, Bichet DG. Inherited secondary nephrogenicdiabetes insipidus: Concentrating on humans. Am J PhysiolRenal Physiol. 2013;304:F1037–42. 113. Bockenhauer D,van’t HW, Dattani M, et al. Secondary nephrogenic diabetesinsipidus as a complication of inherited renal diseases.Nephron Physiol. 2010;116:23–9. 114. Lin nanvuo-LaitinenM, Pirttiaho H, Simila S, Lautala P. [Familial nephrogenicdiabetes insipidus and mental retardation]. Duodecim.1985;101:778–82. 115. Schofer O, Beetz R, Bohl J, et al.Mental retardation syndrome with renal concentrationdeficiency and intracerebral calcification. Eur J Pediatr.1990;149:470–4. 116. Bro oks BS, el GT, Allison JD,Hoffman WH. Frequency and variation of the posteriorpituitary bright signal on MR images. AJNR Am JNeuroradiol. 1989;10:943–8. 117. Mootha SL, Barkovich AJ,Grumbach MM, et al. Idiopathic hypothalamic diabetesinsipidus, pituitary stalk thickening, and the occultintracranial g er minoma in children and adolescents. JClin Endocrinol Metab. 1997;82:1362–7.
118. Cesar KR, Magaldi AJ. Thiazide induces waterabsorption in the inner medullary collecting duct ofnormal and Brattleboro rats. Am J Physiol.1999;277:F756–60.
119. Pedersen RS, Bentzen H, Bech JN, Pedersen EB. Effectof an acute oral ibuprofen intake on urinary aquaporin-2excretion in healthy humans. Scand J Clin Lab Invest.2001;61:631–40.
120. Bernier V, Lagace M, Lonergan M, et al. Functionalrescue of the constitutively internalized V2 vasopressinreceptor mutant R137H by the phar macological chaperoneaction of SR49059. Mol E nd ocrinol. 2004;18:2074–84.
121. Mor ello JP, Salahpour A, Laperriere A, et al.Pharmacological chaperones rescue cell-sur face expressionand function of misfolded V2 vas opressin receptormutants. J Clin Invest. 2000;105:887–95.
122. Chr istensen BM, Marples D, Kim YH, et al. Changes incellular composition of kidney collect ing duct cells in
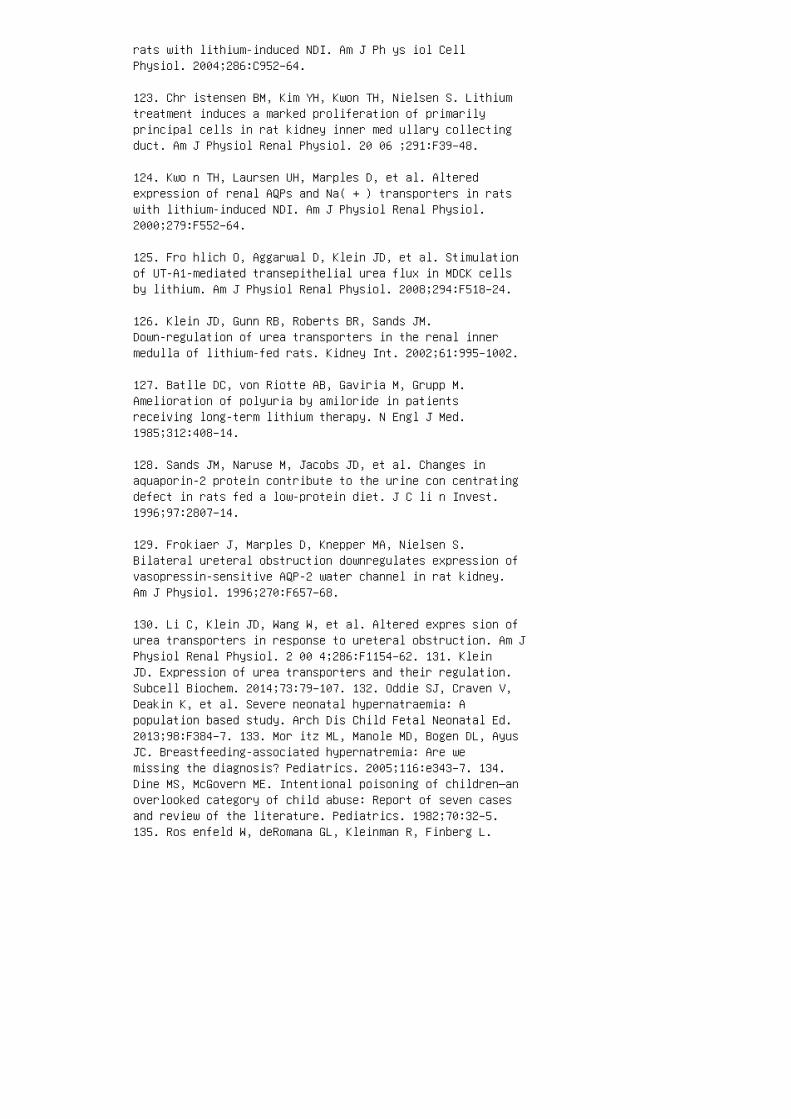
rats with lithium-induced NDI. Am J Ph ys iol CellPhysiol. 2004;286:C952–64.
123. Chr istensen BM, Kim YH, Kwon TH, Nielsen S. Lithiumtreatment induces a marked proliferation of primarilyprincipal cells in rat kidney inner med ullary collectingduct. Am J Physiol Renal Physiol. 20 06 ;291:F39–48.
124. Kwo n TH, Laursen UH, Marples D, et al. Alteredexpression of renal AQPs and Na( + ) transporters in ratswith lithium-induced NDI. Am J Physiol Renal Physiol.2000;279:F552–64.
125. Fro hlich O, Aggarwal D, Klein JD, et al. Stimulationof UT-A1-mediated transepithelial urea flux in MDCK cellsby lithium. Am J Physiol Renal Physiol. 2008;294:F518–24.
126. Klein JD, Gunn RB, Roberts BR, Sands JM.Down-regulation of urea transporters in the renal innermedulla of lithium-fed rats. Kidney Int. 2002;61:995–1002.
127. Batlle DC, von Riotte AB, Gaviria M, Grupp M.Amelioration of polyuria by amiloride in patientsreceiving long-term lithium therapy. N Engl J Med.1985;312:408–14.
128. Sands JM, Naruse M, Jacobs JD, et al. Changes inaquaporin-2 protein contribute to the urine con centratingdefect in rats fed a low-protein diet. J C li n Invest.1996;97:2807–14.
129. Frokiaer J, Marples D, Knepper MA, Nielsen S.Bilateral ureteral obstruction downregulates expression ofvasopressin-sensitive AQP-2 water channel in rat kidney.Am J Physiol. 1996;270:F657–68.
130. Li C, Klein JD, Wang W, et al. Altered expres sion ofurea transporters in response to ureteral obstruction. Am JPhysiol Renal Physiol. 2 00 4;286:F1154–62. 131. KleinJD. Expression of urea transporters and their regulation.Subcell Biochem. 2014;73:79–107. 132. Oddie SJ, Craven V,Deakin K, et al. Severe neonatal hypernatraemia: Apopulation based study. Arch Dis Child Fetal Neonatal Ed.2013;98:F384–7. 133. Mor itz ML, Manole MD, Bogen DL, AyusJC. Breastfeeding-associated hypernatremia: Are wemissing the diagnosis? Pediatrics. 2005;116:e343–7. 134.Dine MS, McGovern ME. Intentional poisoning of children—anoverlooked category of child abuse: Report of seven casesand review of the literature. Pediatrics. 1982;70:32–5.135. Ros enfeld W, deRomana GL, Kleinman R, Finberg L.

Improving the clinical management of hypernatremicdehydration: Observations from a study of 67 infants withthis disorder. Clin Pediatr (Phila). 1977;16:411–7. REVIEWQUESTIONS 1. A 3-month-old male infant presents withseizures. He is euvolemic on examination. Initiallaboratory studies include serum sodium of 118 mEq/L withserum osmolality 240 mOsm/kg H 2 O and urine osmolality85 mOsm/kg H 2 O. Further investigation should be directedtoward: a. Family history of diabetes insipidus b. Homepreparation of infant formula c. Central nervous systeminfection as a cause of SIADH d. History of sustainedfever with increased insensible losses 2. A teenage malepatient presents with altered mental status and is foundto have a cerebrospinal �uid specimen positive for herpessimplex virus by polymerase chain reaction. He is mildlyvolume depleted and hypernatremic on admission. What isthe most likely cause of his hypernatremia? a. Table saltingestion b. Poor �uid intake related to altered mentalstatus c. Nephrogenic diabetes insipidus d. Surreptitiousdiuretic use 3. A�er a few days the patient described inquestion 2 returns to his usual diet. He then developshyponatremia with serum sodium of 125 mEq/L, SOsm 258mOsm/kg H 2 O, and UOsm 300 mOsm/kg H 2 O. He isclinically euvolemic. He most likely has: a. Primarypolydipsia related to increased thirst from hypothalamicdysfunction b. Pseudohyponatremia c. Central diabetesinsipidus d. SIADH
4. A 4-week old male infant is admitted with hypovolemia,failure to thrive, and chronic irritability. He ishypernatremic (serum sodium of 159 mEq/L) with UOsm 50mOsm/kg H 2 O. �e most likely cause of his hypernatremiais: a. Child abuse with chronic �uid deprivation b.Chronic diarrhea c. Nephrogenic diabetes insipidus d.Chronic vomiting
5. A 6-month-old male infant with known congenitalX-linked nephrogenic diabetes insipidus has been vomitingeverything he eats or drinks for the past 36 hours. Onpresentation, his weight is decreased 1 kg from baseline.His is afebrile with heart rate 165 bpm and capillaryre�ll 4 seconds. Which of the following parenteral �uidtherapies is most appropriate at this time? a. Fluidbolus with normal saline b. Fluid bolus with D5W c. D50.5 NS at maintenance rate d. D5 0.2 NS at maintenancerate
6. A 16-year-old female patient presents to the adolescentmedicine clinic with fatigue and recent-onset headache. Sheis mildly volume depleted with weight stable from 1 month

ago at 37 kg. Laboratory tests reveal serum sodium of 122mEq/L, SOsm 250 mOsm/kg H 2 O, urine chloride 47 mEq/L,and UNa 55 mEq/L. �e most likely cause of her hyponatremiais: a. Surreptitious diuretic use b. Chronic laxativeabuse c. Bulimia with chronic vomiting d. Primarypolydipsia as a means to reduce hunger
7. A 3-year-old girl undergoes a water deprivation test forpolyuria and polydipsia. Over the course of a 6-hour test,serum sodium increases from 139 to 142 mEq/L, and UOsmchanges from 250 mOsm/kg H 2 O to 850 mOsm/kg H 2 O. �emost likely cause of the polyuria is: a. Primarypolydipsia b. Nephrogenic diabetes insipidus c. Partialnephrogenic diabetes insipidus d. Central diabetesinsipidus 8. A 3-year-old boy undergoes a waterdeprivation test for polyuria and polydipsia. Over thecourse of a 6-hour test, serum sodium increases from 142to 148 mEq/L, whereas UOsm remains lower than 100 mOsm/kgH 2 O. dDAVP is administered and UOsm increases to 850mOsm/kg H 2 O. �e most likely cause of the polyuria is: a.Primary polydipsia b. Nephrogenic diabetes insipidus c.Partial nephrogenic diabetes insipidus d. Central diabetesinsipidus 9. A 12-month-old boy presents with hyponatremicseizures. He is euvolemic. �e following treatment shouldbe provided now: a. Hypertonic saline b. Fluidrestriction c. Conivaptan d. Normal saline bolus 10. A12-month-old boy presents with hypernatremic dehydrationwith associated seizures. Serum sodium is 162 mEq/L.Following �uid resuscitation, his �uid management planshould include: a. Administer normal saline because thishas a lower concentration than the current serum sodium.b. Provide maintenance parenteral �uid support. c.Calculate and correct the free water de�cit whileproviding additional support for maintenance and ongoinglosses. d. Administer D5 0.2 NS at maintenance. ANSWER KEY1. b 2. b 3. d 4. c 5. a 6. a 7. a 8. d 9. a 10.c
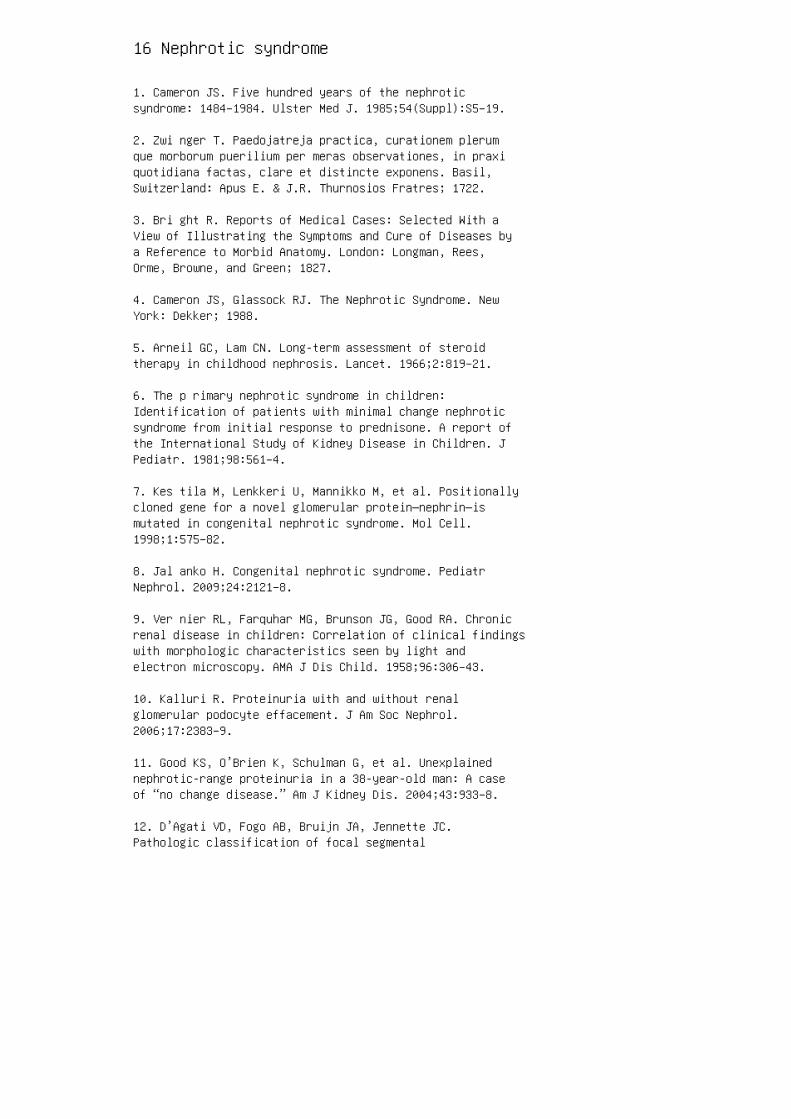
16 Nephrotic syndrome
1. Cameron JS. Five hundred years of the nephroticsyndrome: 1484–1984. Ulster Med J. 1985;54(Suppl):S5–19.
2. Zwi nger T. Paedojatreja practica, curationem plerumque morborum puerilium per meras observationes, in praxiquotidiana factas, clare et distincte exponens. Basil,Switzerland: Apus E. & J.R. Thurnosios Fratres; 1722.
3. Bri ght R. Reports of Medical Cases: Selected With aView of Illustrating the Symptoms and Cure of Diseases bya Reference to Morbid Anatomy. London: Longman, Rees,Orme, Browne, and Green; 1827.
4. Cameron JS, Glassock RJ. The Nephrotic Syndrome. NewYork: Dekker; 1988.
5. Arneil GC, Lam CN. Long-term assessment of steroidtherapy in childhood nephrosis. Lancet. 1966;2:819–21.
6. The p rimary nephrotic syndrome in children:Identification of patients with minimal change nephroticsyndrome from initial response to prednisone. A report ofthe International Study of Kidney Disease in Children. JPediatr. 1981;98:561–4.
7. Kes tila M, Lenkkeri U, Mannikko M, et al. Positionallycloned gene for a novel glomerular protein—nephrin—ismutated in congenital nephrotic syndrome. Mol Cell.1998;1:575–82.
8. Jal anko H. Congenital nephrotic syndrome. PediatrNephrol. 2009;24:2121–8.
9. Ver nier RL, Farquhar MG, Brunson JG, Good RA. Chronicrenal disease in children: Correlation of clinical findingswith morphologic characteristics seen by light andelectron microscopy. AMA J Dis Child. 1958;96:306–43.
10. Kalluri R. Proteinuria with and without renalglomerular podocyte effacement. J Am Soc Nephrol.2006;17:2383–9.
11. Good KS, O’Brien K, Schulman G, et al. Unexplainednephrotic-range proteinuria in a 38-year-old man: A caseof “no change disease.” Am J Kidney Dis. 2004;43:933–8.
12. D’Agati VD, Fogo AB, Bruijn JA, Jennette JC.Pathologic classification of focal segmental
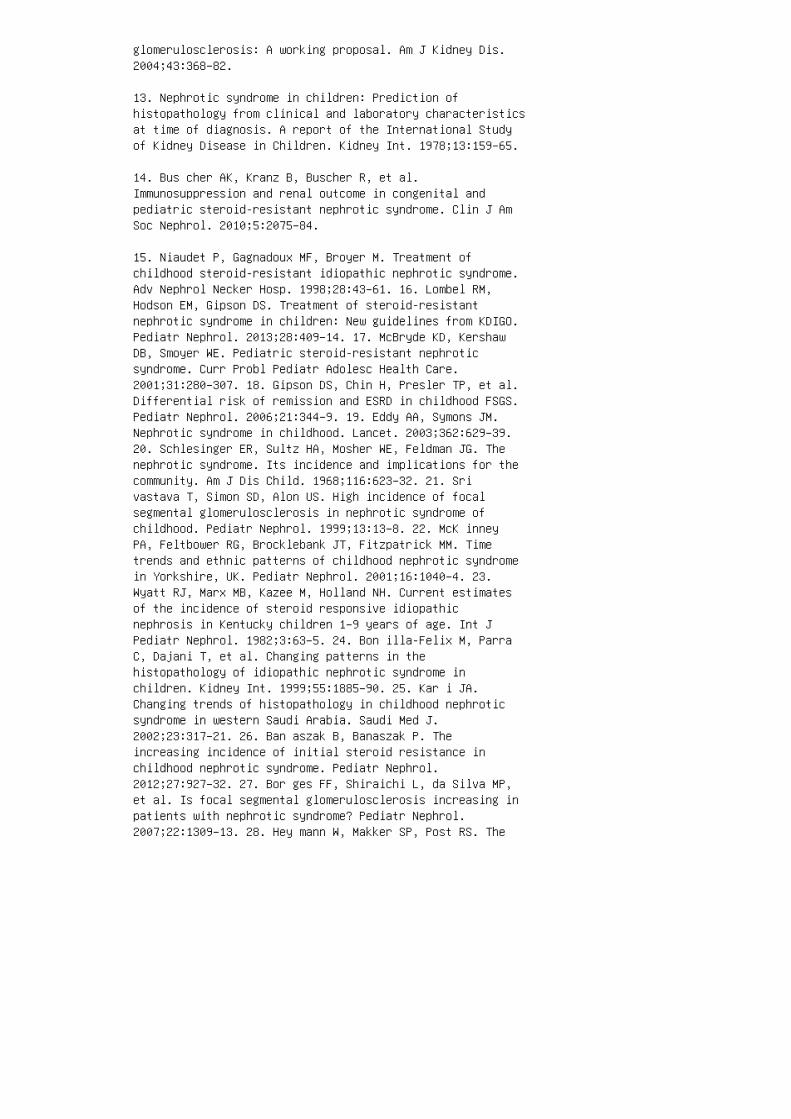
glomerulosclerosis: A working proposal. Am J Kidney Dis.2004;43:368–82.
13. Nephrotic syndrome in children: Prediction ofhistopathology from clinical and laboratory characteristicsat time of diagnosis. A report of the International Studyof Kidney Disease in Children. Kidney Int. 1978;13:159–65.
14. Bus cher AK, Kranz B, Buscher R, et al.Immunosuppression and renal outcome in congenital andpediatric steroid-resistant nephrotic syndrome. Clin J AmSoc Nephrol. 2010;5:2075–84.
15. Niaudet P, Gagnadoux MF, Broyer M. Treatment ofchildhood steroid-resistant idiopathic nephrotic syndrome.Adv Nephrol Necker Hosp. 1998;28:43–61. 16. Lombel RM,Hodson EM, Gipson DS. Treatment of steroid-resistantnephrotic syndrome in children: New guidelines from KDIGO.Pediatr Nephrol. 2013;28:409–14. 17. McBryde KD, KershawDB, Smoyer WE. Pediatric steroid-resistant nephroticsyndrome. Curr Probl Pediatr Adolesc Health Care.2001;31:280–307. 18. Gipson DS, Chin H, Presler TP, et al.Differential risk of remission and ESRD in childhood FSGS.Pediatr Nephrol. 2006;21:344–9. 19. Eddy AA, Symons JM.Nephrotic syndrome in childhood. Lancet. 2003;362:629–39.20. Schlesinger ER, Sultz HA, Mosher WE, Feldman JG. Thenephrotic syndrome. Its incidence and implications for thecommunity. Am J Dis Child. 1968;116:623–32. 21. Srivastava T, Simon SD, Alon US. High incidence of focalsegmental glomerulosclerosis in nephrotic syndrome ofchildhood. Pediatr Nephrol. 1999;13:13–8. 22. McK inneyPA, Feltbower RG, Brocklebank JT, Fitzpatrick MM. Timetrends and ethnic patterns of childhood nephrotic syndromein Yorkshire, UK. Pediatr Nephrol. 2001;16:1040–4. 23.Wyatt RJ, Marx MB, Kazee M, Holland NH. Current estimatesof the incidence of steroid responsive idiopathicnephrosis in Kentucky children 1–9 years of age. Int JPediatr Nephrol. 1982;3:63–5. 24. Bon illa-Felix M, ParraC, Dajani T, et al. Changing patterns in thehistopathology of idiopathic nephrotic syndrome inchildren. Kidney Int. 1999;55:1885–90. 25. Kar i JA.Changing trends of histopathology in childhood nephroticsyndrome in western Saudi Arabia. Saudi Med J.2002;23:317–21. 26. Ban aszak B, Banaszak P. Theincreasing incidence of initial steroid resistance inchildhood nephrotic syndrome. Pediatr Nephrol.2012;27:927–32. 27. Bor ges FF, Shiraichi L, da Silva MP,et al. Is focal segmental glomerulosclerosis increasing inpatients with nephrotic syndrome? Pediatr Nephrol.2007;22:1309–13. 28. Hey mann W, Makker SP, Post RS. The
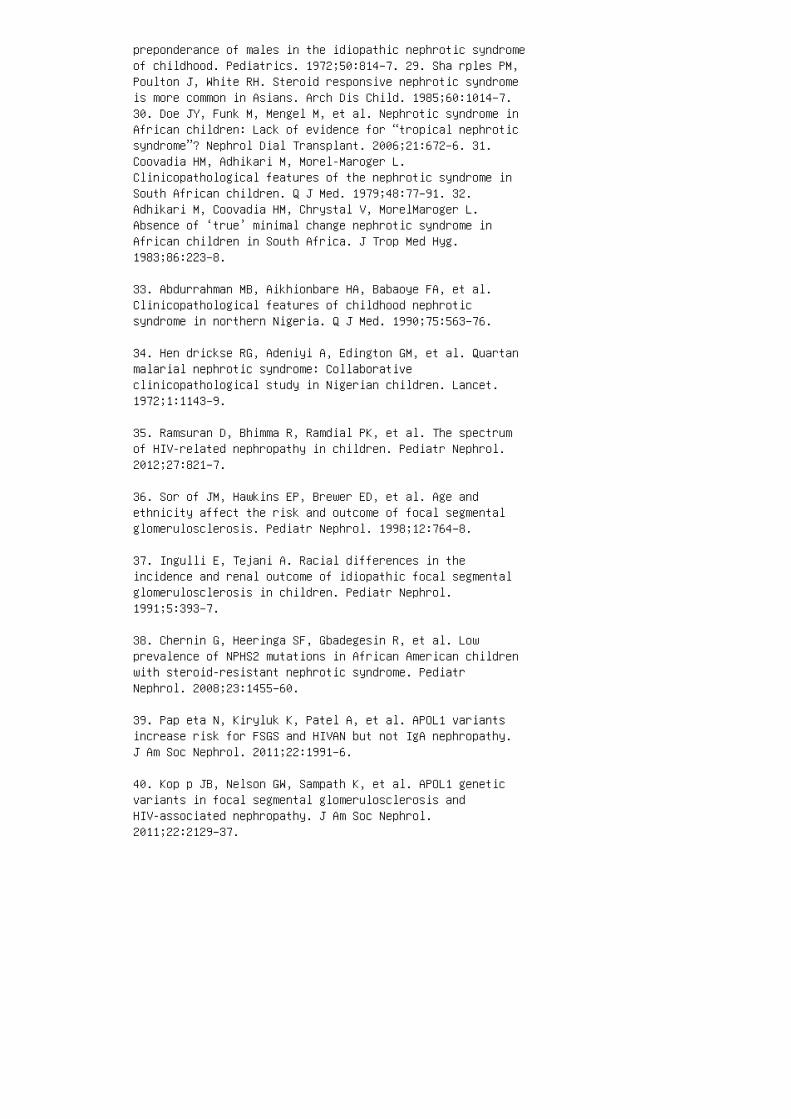
preponderance of males in the idiopathic nephrotic syndromeof childhood. Pediatrics. 1972;50:814–7. 29. Sha rples PM,Poulton J, White RH. Steroid responsive nephrotic syndromeis more common in Asians. Arch Dis Child. 1985;60:1014–7.30. Doe JY, Funk M, Mengel M, et al. Nephrotic syndrome inAfrican children: Lack of evidence for “tropical nephroticsyndrome”? Nephrol Dial Transplant. 2006;21:672–6. 31.Coovadia HM, Adhikari M, Morel-Maroger L.Clinicopathological features of the nephrotic syndrome inSouth African children. Q J Med. 1979;48:77–91. 32.Adhikari M, Coovadia HM, Chrystal V, MorelMaroger L.Absence of ‘true’ minimal change nephrotic syndrome inAfrican children in South Africa. J Trop Med Hyg.1983;86:223–8.
33. Abdurrahman MB, Aikhionbare HA, Babaoye FA, et al.Clinicopathological features of childhood nephroticsyndrome in northern Nigeria. Q J Med. 1990;75:563–76.
34. Hen drickse RG, Adeniyi A, Edington GM, et al. Quartanmalarial nephrotic syndrome: Collaborativeclinicopathological study in Nigerian children. Lancet.1972;1:1143–9.
35. Ramsuran D, Bhimma R, Ramdial PK, et al. The spectrumof HIV-related nephropathy in children. Pediatr Nephrol.2012;27:821–7.
36. Sor of JM, Hawkins EP, Brewer ED, et al. Age andethnicity affect the risk and outcome of focal segmentalglomerulosclerosis. Pediatr Nephrol. 1998;12:764–8.
37. Ingulli E, Tejani A. Racial differences in theincidence and renal outcome of idiopathic focal segmentalglomerulosclerosis in children. Pediatr Nephrol.1991;5:393–7.
38. Chernin G, Heeringa SF, Gbadegesin R, et al. Lowprevalence of NPHS2 mutations in African American childrenwith steroid-resistant nephrotic syndrome. PediatrNephrol. 2008;23:1455–60.
39. Pap eta N, Kiryluk K, Patel A, et al. APOL1 variantsincrease risk for FSGS and HIVAN but not IgA nephropathy.J Am Soc Nephrol. 2011;22:1991–6.
40. Kop p JB, Nelson GW, Sampath K, et al. APOL1 geneticvariants in focal segmental glomerulosclerosis andHIV-associated nephropathy. J Am Soc Nephrol.2011;22:2129–37.

41. Mad havan SM, O’Toole JF, Konieczkowski M, et al.APOL1 localization in normal kidney and nondiabetic kidneydisease. J Am Soc Nephrol. 2011;22:2119–28.
42. Reeves-Daniel AM, DePalma JA, Bleyer AJ, et al. TheAPOL1 gene and allograft survival after kidneytransplantation. Am J Transplant. 2011;11:1025–30.
43. Epstein A. Concerning the causation of edema inchronic parenchymatous nephritis. Am J Med Sci.1917;154:638.
44. Siddall EC, Radhakrishnan J. The pathophysiology ofedema formation in the nephrotic syndrome. Kidney Int.2012;82:635–42.
45. Sta rling EH. On the Fluids of the Body. Chicago: W.T. Keener & Co.; 1909.
46. Meltzer JI, Keim HJ, Laragh JH, et al. Nephroticsyndrome: Vasoconstriction and hypervolemic typesindicated by renin-sodium profiling. Ann Intern Med.1979;91:688–96.
47. Vande Walle JG, Donckerwolcke RA, Koomans HA.Pathophysiology of edema formation in children withnephrotic syndrome not due to minimal change disease. J AmSoc Nephrol. 1999;10:323–31.
48. Man ning RD, Jr. Effects of hypoproteinemia on renalhemodynamics, arterial pressure, and fluid volume. Am JPhysiol. 1987;252:F91–8.
49. Ras cher W, Tulassay T. Hormonal regulation of watermetabolism in children with nephrotic syndrome. Kidney IntSuppl. 1987;21:S83–9. 50. Usberti M, Federico S,Meccariello S, et al. Role of plasma vasopressin in theimpairment of water excretion in nephrotic syndrome.Kidney Int. 1984;25:422–9. 51. Gee rs AB, Koomans HA,Boer P, Dorhout Mees EJ. Plasma and blood volumes inpatients with the nephrotic syndrome. Nephron.1984;38:170–3. 52. Vande Walle J, Donckerwolcke R, Boer P,et al. Blood volume, colloid osmotic pressure and F-cellratio in children with the nephrotic syndrome. Kidney Int.1996;49:1471–7. 53. Koo mans HA, Geers AB, Dorhout MeesEJ, Kortlandt W. Lowered tissue-fluid oncotic pressureprotects the blood volume in the nephrotic syndrome.Nephron. 1986;42:317–22. 54. Fauchald P, Noddeland H,Norseth J. Interstitial fluid volume, plasma volume and

colloid osmotic pressure in patients with nephroticsyndrome. Scand J Clin Lab Invest. 1984;44:661–7. 55. Russi E, Weigand K. Analbuminemia. Klin Wochenschr.1983;61:541–5. 56. Toye J M, Lemire EG, Baerg KL.Perinatal and childhood morbidity and mortality incongenital analbuminemia. Paediatr Child Health.2012;17:e20–3. 57. Shapiro MD, Hasbargen J, Hensen J,Schrier RW. Role of aldosterone in the sodium retention ofpatients with nephrotic syndrome. Am J Nephrol.1990;10:44–8. 58. Brown EA, Markandu ND, Sagnella GA, etal. Evidence that some mechanism other than the reninsystem causes sodium retention in nephrotic syndrome.Lancet. 1982;2:1237–40. 59. Bro wn EA, Markandu ND,Sagnella GA, et al. Lack of effect of captopril on thesodium retention of the nephrotic syndrome. Nephron.1984;37:43–8. 60. Ichikawa I, Rennke HG, Hoyer JR, et al.Role for intrarenal mechanisms in the impaired saltexcretion of experimental nephrotic syndrome. J ClinInvest. 1983;71:91–103. 61. Kim SW, Wang W, Nielsen J, etal. Increased expression and apical targeting of renal ENaCsubunits in puromycin aminonucleoside-induced nephroticsyndrome in rats. Am J Physiol Renal Physiol.2004;286:F922–35. 62. Kim SW, de Seigneux S, Sassen MC, etal. Increased apical targeting of renal ENaC subunits anddecreased expression of 11betaHSD2 in HgCl2inducednephrotic syndrome in rats. Am J Physiol Renal Physiol.2006;290:F674–87. 63. Des chenes G, Doucet A. Collectingduct (Na + /K + )ATPase activity is correlated with urinarysodium excretion in rat nephrotic syndromes. J Am SocNephrol. 2000;11:604–15. 64. Deschenes G, Gonin S, ZoltyE, et al. Increased synthesis and AVP unresponsiveness ofNa,K-ATPase in collecting duct from nephrotic rats. J AmSoc Nephrol. 2001;12:2241–52.
65. Carattino MD, Hughey RP, Kleyman TR. Proteolyticprocessing of the epithelial sodium channel gamma subunithas a dominant role in channel activation. J Biol Chem.2008;283:25290–5.
66. Svenningsen P, Bistrup C, Friis UG, et al. Plasmin innephrotic urine activates the epithelial sodium channel. JAm Soc Nephrol. 2009;20:299–310.
67. Andersen RF, Buhl KB, Jensen BL, et al. Remission ofnephrotic syndrome diminishes urinary plasmin content andabolishes activation of ENaC. Pediatr Nephrol.2013;28:1227–34.
68. Deschenes G, Wittner M, Stefano A, et al. Collectingduct is a site of sodium retention in PAN nephrosis: A

rationale for amiloride therapy. J Am Soc Nephrol.2001;12:598–601.
69. Sch rier RW, Fassett RG. A critique of the overfillhypothesis of sodium and water retention in the nephroticsyndrome. Kidney Int. 1998;53:1111–7.
70. Bockenhauer D. Over- or underfill: Not all nephroticstates are created equal. Pediatr Nephrol. 2013;28:1153–6.
71. Van de Walle JG, Donckerwolcke RA. Pathogenesis ofedema formation in the nephrotic syndrome. PediatrNephrol. 2001;16:283–93.
72. Kap ur G, Valentini RP, Imam AA, Mattoo TK. Treatmentof severe edema in children with nephrotic syndrome withdiuretics alone: A prospective study. Clin J Am SocNephrol. 2009;4:907–13.
73. Stur gill BC, Shearlock KT. Membranous glomerulopathyand nephrotic syndrome after captopril therapy. JAMA.1983;250:2343–5.
74. Rad ford MG, Jr, Holley KE, Grande JP, et al.Reversible membranous nephropathy associated with the useof nonsteroidal anti-inflammatory drugs. JAMA.1996;276:466–9.
75. Habib GS, Saliba W, Nashashibi M, Armali Z.Penicillamine and nephrotic syndrome. Eur J Intern Med.2006;17:343–8.
76. Gipson DS, Massengill SF, Yao L, et al. Management ofchildhood onset nephrotic syndrome. Pediatrics.2009;124:747–57.
77. Las kin BL, Goebel J, Starke JR, et al.Costeffectiveness of latent tuberculosis screening beforesteroid therapy for idiopathic nephrotic syndrome inchildren. Am J Kidney Dis. 2013;61:22–32.
78. Pickering L, editor. Red Book: 2012 Report of theCommittee on Infections Diseases, 29th ed. Elk GroveVillage, IL: American Academy of Pediatrics Committee onInfectious Diseases; 2012.
79. Ker lin BA, Haworth K, Smoyer WE. Venousthromboembolism in pediatric nephrotic syndrome. PediatrNephrol. 2014;29:989–97.
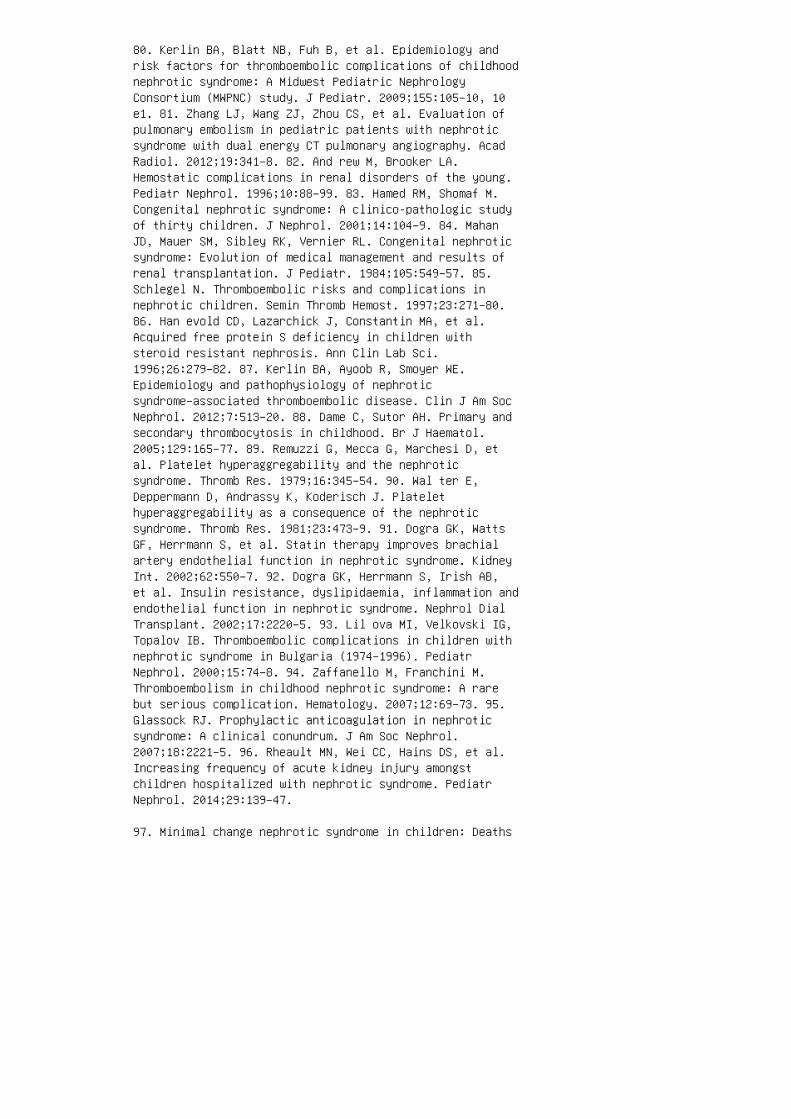
80. Kerlin BA, Blatt NB, Fuh B, et al. Epidemiology andrisk factors for thromboembolic complications of childhoodnephrotic syndrome: A Midwest Pediatric NephrologyConsortium (MWPNC) study. J Pediatr. 2009;155:105–10, 10e1. 81. Zhang LJ, Wang ZJ, Zhou CS, et al. Evaluation ofpulmonary embolism in pediatric patients with nephroticsyndrome with dual energy CT pulmonary angiography. AcadRadiol. 2012;19:341–8. 82. And rew M, Brooker LA.Hemostatic complications in renal disorders of the young.Pediatr Nephrol. 1996;10:88–99. 83. Hamed RM, Shomaf M.Congenital nephrotic syndrome: A clinico-pathologic studyof thirty children. J Nephrol. 2001;14:104–9. 84. MahanJD, Mauer SM, Sibley RK, Vernier RL. Congenital nephroticsyndrome: Evolution of medical management and results ofrenal transplantation. J Pediatr. 1984;105:549–57. 85.Schlegel N. Thromboembolic risks and complications innephrotic children. Semin Thromb Hemost. 1997;23:271–80.86. Han evold CD, Lazarchick J, Constantin MA, et al.Acquired free protein S deficiency in children withsteroid resistant nephrosis. Ann Clin Lab Sci.1996;26:279–82. 87. Kerlin BA, Ayoob R, Smoyer WE.Epidemiology and pathophysiology of nephroticsyndrome–associated thromboembolic disease. Clin J Am SocNephrol. 2012;7:513–20. 88. Dame C, Sutor AH. Primary andsecondary thrombocytosis in childhood. Br J Haematol.2005;129:165–77. 89. Remuzzi G, Mecca G, Marchesi D, etal. Platelet hyperaggregability and the nephroticsyndrome. Thromb Res. 1979;16:345–54. 90. Wal ter E,Deppermann D, Andrassy K, Koderisch J. Platelethyperaggregability as a consequence of the nephroticsyndrome. Thromb Res. 1981;23:473–9. 91. Dogra GK, WattsGF, Herrmann S, et al. Statin therapy improves brachialartery endothelial function in nephrotic syndrome. KidneyInt. 2002;62:550–7. 92. Dogra GK, Herrmann S, Irish AB,et al. Insulin resistance, dyslipidaemia, inflammation andendothelial function in nephrotic syndrome. Nephrol DialTransplant. 2002;17:2220–5. 93. Lil ova MI, Velkovski IG,Topalov IB. Thromboembolic complications in children withnephrotic syndrome in Bulgaria (1974–1996). PediatrNephrol. 2000;15:74–8. 94. Zaffanello M, Franchini M.Thromboembolism in childhood nephrotic syndrome: A rarebut serious complication. Hematology. 2007;12:69–73. 95.Glassock RJ. Prophylactic anticoagulation in nephroticsyndrome: A clinical conundrum. J Am Soc Nephrol.2007;18:2221–5. 96. Rheault MN, Wei CC, Hains DS, et al.Increasing frequency of acute kidney injury amongstchildren hospitalized with nephrotic syndrome. PediatrNephrol. 2014;29:139–47.
97. Minimal change nephrotic syndrome in children: Deaths

during the first 5 to 15 years’ observation. Report of theInternational Study of Kidney Disease in Children.Pediatrics. 1984;73:497–501.
98. Hingorani SR, Weiss NS, Watkins SL. Predictors ofperitonitis in children with nephrotic syndrome. PediatrNephrol. 2002;17:678–82.
99. Matsell DG, Wyatt RJ. The role of I and B inperitonitis associated with the nephrotic syndrome ofchildhood. Pediatr Res. 1993;34:84–8.
100. McL ean RH, Forsgren A, Bjorksten B, et al. Decreasedserum factor B concentration associated with decreasedopsonization of Escherichia coli in the idiopathicnephrotic syndrome. Pediatr Res. 1977;11:910–6.
101. Anderson DC, York TL, Rose G, Smith CW. Assessment ofserum factor B, serum opsonins, granulocyte chemotaxis,and infection in nephrotic syndrome of children. J InfectDis. 1979;140:1–11.
102. Ballow M, Kennedy TL, 3rd, Gaudio KM, et al. Serumhemolytic factor D values in children withsteroidresponsive idiopathic nephrotic syndrome. J Pediatr.1982;100:192–6.
103. Krensky AM, Ingelfinger JR, Grupe WE. Peritonitis inchildhood nephrotic syndrome: 1970–1980. Am J Dis Child.1982;136:732–6.
104. Gia ngiacomo J, Cleary TG, Cole BR, et al. Serumimmunoglobulins in the nephrotic syndrome: A possible causeof minimal-change nephrotic syndrome. N Engl J Med.1975;293:8–12.
105. Fod or P, Saitua MT, Rodriguez E, et al. T-celldysfunction in minimal-change nephrotic syndrome ofchildhood. Am J Dis Child. 1982;136:713–7.
106. Haddy RI, Perry K, Chacko CE, et al. Comparison ofincidence of invasive Streptococcus pneumoniae diseaseamong children before and after introduction of conjugatedpneumococcal vaccine. Pediatr Infect Dis J. 2005;24:320–3.
107. Wei CC, Yu IW, Lin HW, Tsai AC. Occurrence ofinfection among children with nephrotic syndrome duringhospitalizations. Nephrology (Carlton). 2012;17:681–8.
108. Unc u N, Bulbul M, Yildiz N, et al. Primary

peritonitis in children with nephrotic syndrome: Resultsof a 5-year multicenter study. Eur J Pediatr.2012;169:73–6.
109. Tain YL, Lin G, Cher TW. Microbiological spectrum ofsepticemia and peritonitis in nephrotic children. PediatrNephrol. 1999;13:835–7.
110. McIntyre P, Craig JC. Prevention of serious bacterialinfection in children with nephrotic syndrome. J PaediatrChild Health. 1998;34:314–7.
111. Mil ner LS, Berkowitz FE, Ngwenya E, et al. Penicillinresistant pneumococcal peritonitis in nephrotic syndrome.Arch Dis Child. 1987;62:964–5.
112. Ily as M, Roy S, 3rd, Abbasi S, et al. Seriousinfections due to penicillin-resistant Streptococcuspneumoniae in two children with nephrotic syndrome.Pediatr Nephrol. 1996;10:639–41. 113. Wu HM, Tang JL, CaoL, et al. Interventions for preventing infection innephrotic syndrome. Cochrane Database Syst Rev.2012;4:CD003964. 114. Chen T, Lv Y, Lin F, Zhu J. Acutekidney injury in adult idiopathic nephrotic syndrome. RenFail. 2011;33:144–9. 115. Cho udhry S, Bagga A, Hari P, etal. Efficacy and safety of tacrolimus versus cyclosporinein children with steroid-resistant nephrotic syndrome: Arandomized controlled trial. Am J Kidney Dis.2009;53:760–9. 116. Olowu WA, Adenowo OA, Elusiyan JB.Reversible renal failure in hypertensive idiopathicnephrotics treated with captopril. Saudi J Kidney DisTranspl. 2006;17:216–21. 117. Milliner DS, MorgensternBZ. Angiotensin converting enzyme inhibitors for reductionof proteinuria in children with steroid-resistantnephrotic syndrome. Pediatr Nephrol. 1991;5:587–90. 118.Low enstein J, Schacht RG, Baldwin DS. Renal failure inminimal change nephrotic syndrome. Am J Med.1981;70:227–33. 119. Koomans HA. Pathophysiology of edemaand acute renal failure in idiopathic nephrotic syndrome.Adv Nephrol Necker Hosp. 2000;30:41–55. 120. Vande WalleJ, Mauel R, Raes A, et al. ARF in children with minimalchange nephrotic syndrome may be related to functionalchanges of the glomerular basal membrane. Am J Kidney Dis.2004;43:399–404. 121. Hol mberg C, Antikainen M, RonnholmK, et al. Management of congenital nephrotic syndrome ofthe Finnish type. Pediatr Nephrol. 1995;9:87–93. 122. Dagan A, Cleper R, Krause I, et al. Hypothyroidism inchildren with steroid-resistant nephrotic syndrome.Nephrol Dial Transplant. 2012;27:2171–5. 123. FreundlichM, Bourgoignie JJ, Zilleruelo G, et al. Calcium and
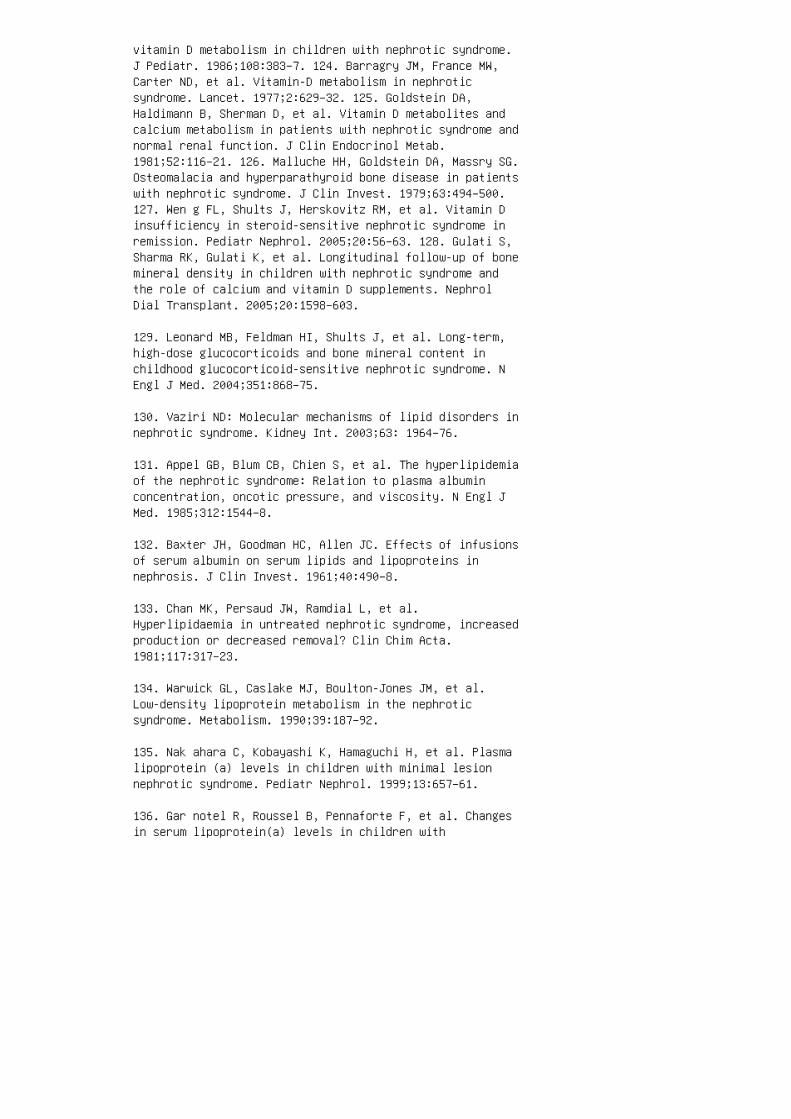
vitamin D metabolism in children with nephrotic syndrome.J Pediatr. 1986;108:383–7. 124. Barragry JM, France MW,Carter ND, et al. Vitamin-D metabolism in nephroticsyndrome. Lancet. 1977;2:629–32. 125. Goldstein DA,Haldimann B, Sherman D, et al. Vitamin D metabolites andcalcium metabolism in patients with nephrotic syndrome andnormal renal function. J Clin Endocrinol Metab.1981;52:116–21. 126. Malluche HH, Goldstein DA, Massry SG.Osteomalacia and hyperparathyroid bone disease in patientswith nephrotic syndrome. J Clin Invest. 1979;63:494–500.127. Wen g FL, Shults J, Herskovitz RM, et al. Vitamin Dinsufficiency in steroid-sensitive nephrotic syndrome inremission. Pediatr Nephrol. 2005;20:56–63. 128. Gulati S,Sharma RK, Gulati K, et al. Longitudinal follow-up of bonemineral density in children with nephrotic syndrome andthe role of calcium and vitamin D supplements. NephrolDial Transplant. 2005;20:1598–603.
129. Leonard MB, Feldman HI, Shults J, et al. Long-term,high-dose glucocorticoids and bone mineral content inchildhood glucocorticoid-sensitive nephrotic syndrome. NEngl J Med. 2004;351:868–75.
130. Vaziri ND: Molecular mechanisms of lipid disorders innephrotic syndrome. Kidney Int. 2003;63: 1964–76.
131. Appel GB, Blum CB, Chien S, et al. The hyperlipidemiaof the nephrotic syndrome: Relation to plasma albuminconcentration, oncotic pressure, and viscosity. N Engl JMed. 1985;312:1544–8.
132. Baxter JH, Goodman HC, Allen JC. Effects of infusionsof serum albumin on serum lipids and lipoproteins innephrosis. J Clin Invest. 1961;40:490–8.
133. Chan MK, Persaud JW, Ramdial L, et al.Hyperlipidaemia in untreated nephrotic syndrome, increasedproduction or decreased removal? Clin Chim Acta.1981;117:317–23.
134. Warwick GL, Caslake MJ, Boulton-Jones JM, et al.Low-density lipoprotein metabolism in the nephroticsyndrome. Metabolism. 1990;39:187–92.
135. Nak ahara C, Kobayashi K, Hamaguchi H, et al. Plasmalipoprotein (a) levels in children with minimal lesionnephrotic syndrome. Pediatr Nephrol. 1999;13:657–61.
136. Gar notel R, Roussel B, Pennaforte F, et al. Changesin serum lipoprotein(a) levels in children with
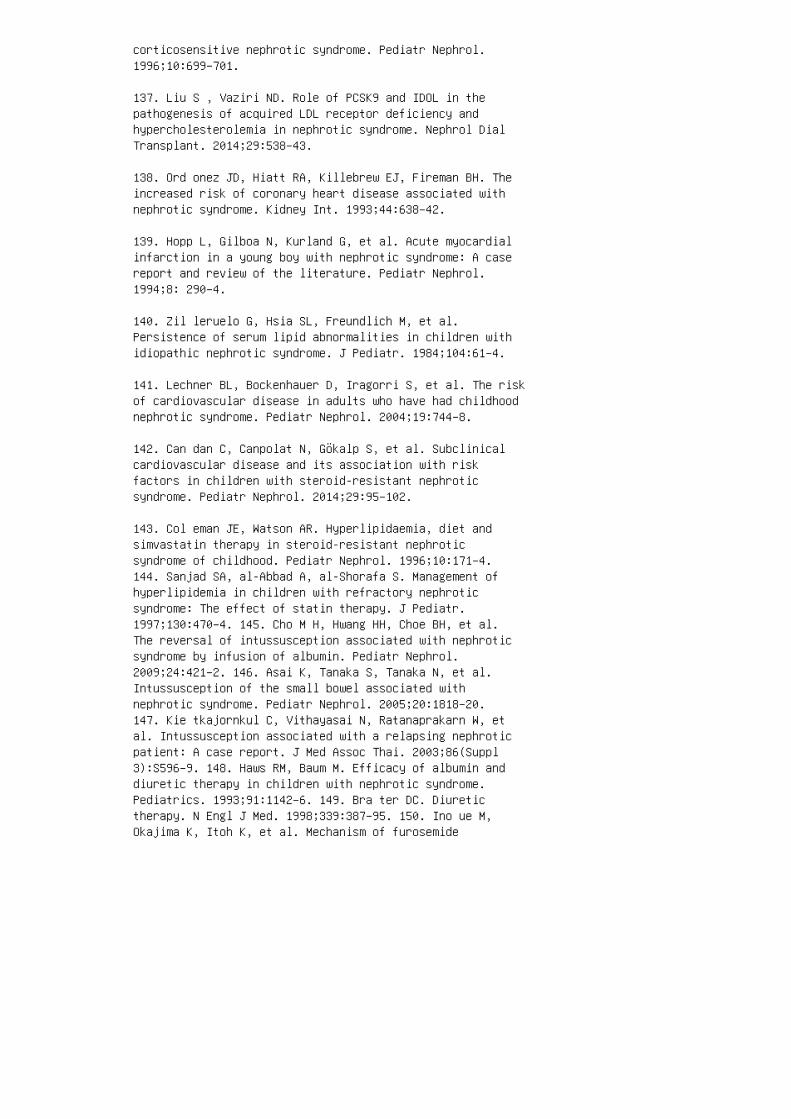
corticosensitive nephrotic syndrome. Pediatr Nephrol.1996;10:699–701.
137. Liu S , Vaziri ND. Role of PCSK9 and IDOL in thepathogenesis of acquired LDL receptor deficiency andhypercholesterolemia in nephrotic syndrome. Nephrol DialTransplant. 2014;29:538–43.
138. Ord onez JD, Hiatt RA, Killebrew EJ, Fireman BH. Theincreased risk of coronary heart disease associated withnephrotic syndrome. Kidney Int. 1993;44:638–42.
139. Hopp L, Gilboa N, Kurland G, et al. Acute myocardialinfarction in a young boy with nephrotic syndrome: A casereport and review of the literature. Pediatr Nephrol.1994;8: 290–4.
140. Zil leruelo G, Hsia SL, Freundlich M, et al.Persistence of serum lipid abnormalities in children withidiopathic nephrotic syndrome. J Pediatr. 1984;104:61–4.
141. Lechner BL, Bockenhauer D, Iragorri S, et al. The riskof cardiovascular disease in adults who have had childhoodnephrotic syndrome. Pediatr Nephrol. 2004;19:744–8.
142. Can dan C, Canpolat N, Gökalp S, et al. Subclinicalcardiovascular disease and its association with riskfactors in children with steroid-resistant nephroticsyndrome. Pediatr Nephrol. 2014;29:95–102.
143. Col eman JE, Watson AR. Hyperlipidaemia, diet andsimvastatin therapy in steroid-resistant nephroticsyndrome of childhood. Pediatr Nephrol. 1996;10:171–4.144. Sanjad SA, al-Abbad A, al-Shorafa S. Management ofhyperlipidemia in children with refractory nephroticsyndrome: The effect of statin therapy. J Pediatr.1997;130:470–4. 145. Cho M H, Hwang HH, Choe BH, et al.The reversal of intussusception associated with nephroticsyndrome by infusion of albumin. Pediatr Nephrol.2009;24:421–2. 146. Asai K, Tanaka S, Tanaka N, et al.Intussusception of the small bowel associated withnephrotic syndrome. Pediatr Nephrol. 2005;20:1818–20.147. Kie tkajornkul C, Vithayasai N, Ratanaprakarn W, etal. Intussusception associated with a relapsing nephroticpatient: A case report. J Med Assoc Thai. 2003;86(Suppl3):S596–9. 148. Haws RM, Baum M. Efficacy of albumin anddiuretic therapy in children with nephrotic syndrome.Pediatrics. 1993;91:1142–6. 149. Bra ter DC. Diuretictherapy. N Engl J Med. 1998;339:387–95. 150. Ino ue M,Okajima K, Itoh K, et al. Mechanism of furosemide
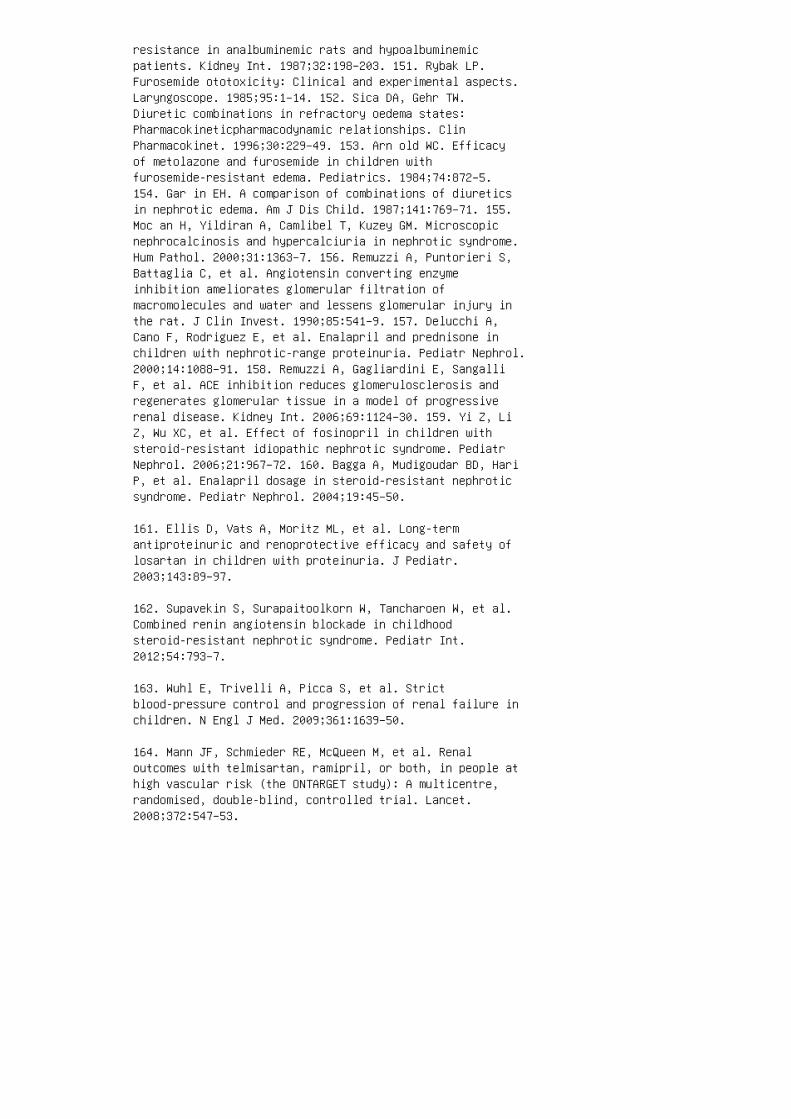
resistance in analbuminemic rats and hypoalbuminemicpatients. Kidney Int. 1987;32:198–203. 151. Rybak LP.Furosemide ototoxicity: Clinical and experimental aspects.Laryngoscope. 1985;95:1–14. 152. Sica DA, Gehr TW.Diuretic combinations in refractory oedema states:Pharmacokineticpharmacodynamic relationships. ClinPharmacokinet. 1996;30:229–49. 153. Arn old WC. Efficacyof metolazone and furosemide in children withfurosemide-resistant edema. Pediatrics. 1984;74:872–5.154. Gar in EH. A comparison of combinations of diureticsin nephrotic edema. Am J Dis Child. 1987;141:769–71. 155.Moc an H, Yildiran A, Camlibel T, Kuzey GM. Microscopicnephrocalcinosis and hypercalciuria in nephrotic syndrome.Hum Pathol. 2000;31:1363–7. 156. Remuzzi A, Puntorieri S,Battaglia C, et al. Angiotensin converting enzymeinhibition ameliorates glomerular filtration ofmacromolecules and water and lessens glomerular injury inthe rat. J Clin Invest. 1990;85:541–9. 157. Delucchi A,Cano F, Rodriguez E, et al. Enalapril and prednisone inchildren with nephrotic-range proteinuria. Pediatr Nephrol.2000;14:1088–91. 158. Remuzzi A, Gagliardini E, SangalliF, et al. ACE inhibition reduces glomerulosclerosis andregenerates glomerular tissue in a model of progressiverenal disease. Kidney Int. 2006;69:1124–30. 159. Yi Z, LiZ, Wu XC, et al. Effect of fosinopril in children withsteroid-resistant idiopathic nephrotic syndrome. PediatrNephrol. 2006;21:967–72. 160. Bagga A, Mudigoudar BD, HariP, et al. Enalapril dosage in steroid-resistant nephroticsyndrome. Pediatr Nephrol. 2004;19:45–50.
161. Ellis D, Vats A, Moritz ML, et al. Long-termantiproteinuric and renoprotective efficacy and safety oflosartan in children with proteinuria. J Pediatr.2003;143:89–97.
162. Supavekin S, Surapaitoolkorn W, Tancharoen W, et al.Combined renin angiotensin blockade in childhoodsteroid-resistant nephrotic syndrome. Pediatr Int.2012;54:793–7.
163. Wuhl E, Trivelli A, Picca S, et al. Strictblood-pressure control and progression of renal failure inchildren. N Engl J Med. 2009;361:1639–50.
164. Mann JF, Schmieder RE, McQueen M, et al. Renaloutcomes with telmisartan, ramipril, or both, in people athigh vascular risk (the ONTARGET study): A multicentre,randomised, double-blind, controlled trial. Lancet.2008;372:547–53.
165. Hanevold CD. Acute renal failure during lisinopril andlosartan therapy for proteinuria. Pharmacotherapy.2006;26:1348–51.
166. Cooper WO, Hernandez-Diaz S, Arbogast PG, et al.Major congenital malformations after firsttrimesterexposure to ACE inhibitors. N Engl J Med.2006;354:2443–51.
167. Kust er S, Mehls O, Seidel C, Ritz E. Blood pressurein minimal change and other types of nephrotic syndrome.Am J Nephrol. 1990;10(Suppl 1):76–80.
168. Kon tchou LM, Liccioli G, Pela I. Blood pressure inchildren with minimal change nephrotic syndrome duringoedema and after steroid therapy: The influence of familialessential hypertension. Kidney Blood Press Res.2009;32:258–62.
169. Ishikura K, Ikeda M, Hamasaki Y, et al. Nephroticstate as a risk factor for developing posterior reversibleencephalopathy syndrome in paediatric patients withnephrotic syndrome. Nephrol Dial Transplant.2008;23:2531–6.
170. The fourth report on the diagnosis, evaluation, andtreatment of high blood pressure in children andadolescents. Pediatrics. 2004;114:555–76.
171. Wiegering V, Schick J, Beer M, et al. Varicella-zostervirus infections in immunocompromised patients: A singlecentre 6-years analysis. BMC Pediatr. 2011;11:31.
172. Mufson MA, Stanek RJ. Epidemiology of invasiveStreptococcus pneumoniae infections and vaccineimplications among children in a West Virginia community,1978–2003. Pediatr Infect Dis J 2004;23:779–81.
173. McC arthy HJ, Bierzynska A, Wherlock M, et al.Simultaneous sequencing of 24 genes associated withsteroid-resistant nephrotic syndrome. Clin J Am SocNephrol. 2013;8:637–48.
174. Rei ser J, Gupta V, Kistler AD. Toward the developmentof podocyte-specific drugs. Kidney Int. 2010;77:662–8.REVIEW QUESTIONS 1. �e most likely �nding on kidneyhistopathologic examination for a 2-year-old child withsteroid-sensitive nephrotic syndrome is: a. Minimal changenephrotic syndrome b. Focal segmental glomerulosclerosisc. Membranous nephropathy d. Membranoproliferative

glomerulonephritis e. Mesangial proliferativeglomerulonephritis 2. Sequence variants in the followinggene account for a large fraction of observed FSGS risk inAfrican Americans: a. NPHS2 b. WT1 c. MYH9 d. APOL1e. COQ6 3. Which of the following is not a component ofthe “under�ll hypothesis” of edema formation in nephroticsyndrome? a. Decreased plasma oncotic pressure withleakage of �uid into the interstitial space b.Hypovolemia with renal hypoperfusion c. Activation of therenin-angiotensin-aldosterone system d. Vasopressinrelease e. Increased sodium reabsorption through ENaC 4.Children with an initial presentation of nephroticsyndrome should have all of the following performed,except: a. Complement C3 level b. Genetic testing forNPHS2 mutations c. Serum albumin d. PPD e. Cholesterollevel 5. �e following factors cause increased risk forthrombosis in nephrotic syndrome, except: a. Increasedproduction of protein S by the liver b. Loss of ATIII inthe urine c. Platelet hyperaggregability d. Diminishedbrinolytic activity e. Hyperlipidemia 6. Complications offurosemide therapy for treatment of edema in nephroticsyndrome can include all of the following except: a.Hypokalemia b. Acute kidney injury c. Nephrocalcinosisd. Metabolic acidosis e. �rombosis 7. Live vaccines(varicella, MMR) can be given to which population ofchildren with nephrotic syndrome? a. Children receivingcyclophosphamide b. Children receiving 2 mg/kg/day ofprednisone
c. Children who have been o� high-dose steroids for 1 month
d. Children who have been o� high-dose steroids for 1 week
e. Children receiving 2 mg/kg/day of prednisone andexposed to varicella
8. Complications of 25% albumin infusions in nephroticpatients can include all of the following, except:
a. Pseudotumor cerebri
b. Respiratory distress
c. Congestive heart failure
d. Acute hypertension
e. Pulmonary edema
9. Which of the following is most suggestive of a cause of

nephrotic syndrome other than MCNS?
a. Age 2 years
b. No hematuria
c. Anasarca
d. Stage II hypertension
e. Normal complement 3
10. A�er receiving intravenous furosemide, a 2-year-oldgirl with SSNS develops gross hematuria and hypertension.What study should be performed �rst to evaluate for thecause of the hematuria?
a. Urine calcium-to-creatinine ratio
b. Urine protein-to-creatinine ratio c. Lasix renogram d.Renal ultrasound with Doppler e. Voiding cystourethrogramANSWER KEY 1. a 2. d 3. e 4. b 5. a 6. d 7. c 8. a9. d 10. d
17 Primary podocytopathies
SUMMARY
Nephrotic syndrome is one of the most commonly
encountered kidney diseases in children. Advances in
genetic testing and molecular diagnostics have allowed
for better classi�cation of the disease. Moreover, ani
mal and human research studies have contributed
to an improved understanding of the underlying
pathophysiology. However, many questions remain
unanswered in terms of the pathogenesis behind the
primary glomerular injury, as well as the mechanisms
of edema and dyslipidemia. Furthermore, the path
ways by which the most commonly used medications,
such as corticosteroids, exert their e�ect have not been
fully elucidated. Despite the monumental improve
ments in the mortality and morbidity of children with
this disease, many children with refractory SRNS,
particularly those with underlying genetic mutations,
may not fully respond to the currently available thera
peutic options. Unfortunately, such children continue
to face signi�cant challenges in regard to their quality
of life, and they remain at increased risk for treatment
related toxicities as well as infectious, thrombotic, and
cardiovascular complications. Additional research is
needed to promote a deeper understanding of the

underlying pathogenesis and to provide a wider spec
trum of safe and e�ective treatments.
9. Reiser J, Polu KR, Moller CC, et al. TRPC6 is aglomerular slit diaphragm–associated channel required fornormal renal function. Nat Genet. 2005;37:739–44.
10. Winn MP, Conlon PJ, Lynn KL, et al. A muta tion in theTRPC6 cation channel causes familial f oc al segmentalglomerulosclerosis. Science. 2005;308:1801–4.
11. Sch warz K, Simons M, Reiser J, et al. Podocin, araft-associated component of the glomerular slitdiaphragm, interacts with CD2AP and nephrin. J ClinInvest. 2001;108:1621–9.
12. Sorensson J, Ohlson M, Lindstrom K, Haraldsson B.Glomerular charge selectivity for horseradish peroxidaseand albumin at low and normal ionic strengths. ActaPhysiol Scand. 1998;163:83–91.
13. Ciarimboli G, Schurek HJ, Zeh M, et al. Role ofalbumin and glomerular capillary wall charge dis tributionon glomerular permselectivity: Studies on th eperfused-fixed rat kidney model. Pflugers Arch.1999;438:883–91.
14. Russo LM, Sandoval RM, McKee M, et al. The normalkidney filters nephrotic levels of albumin retrieved byproximal tubule cells: Retrieval is disrupted in nephroticstates. Kidney Int. 2007;71:504–13.
15. Kitano Y, Yoshikawa N, Nakamura H. Glomerular anionicsites in minimal change nephrotic syndrome and focalsegmental glomerulosclerosis. Clin Nephrol.1993;40:199–204.
16. Carrie BJ, Salyer WR, Myers BD. Minimal changenephropathy: An electrochemical disorder of the glomerularmembrane. Am J Med. 1981;70:262–8.
17. van den Born J, van den Heuvel LP, Bakker MA, et al. Amonoclonal antibody against GBM heparan sulfate induces anacute selective proteinuria in rats. Kidney Int.1992;41:115–23.
18. Taylor GM, Neuhaus TJ, Shah V, et al. Charge and sizeselectivity of proteinuria in children with idiopathicnephrotic syndrome. Pediatr Nephrol. 1997;11:404–10.
19. Levin M, Smith C, Walters MD, Gascoine P, Barratt TM.Steroid-responsive nephrotic syndrome: A generaliseddisorder of membrane negative charge. Lancet.1985;2:239–42.
20. Clark A, Barrat T. Steroid-responsive nephroticsyndrome. In: Barrat T, Avner E, Harmon W, editors.Pediatric Nephrology. Baltimore: Lippincott Williams &Wilkins; 1998. p. 731.
21. Nash M, Edelman C, Bernstein J. The nephrotic syndrome.In: Edelman C, editor. Pediatric Kidney Disease. Boston:Little, Brown and Company; 1992. p. 1247.
22. Sri vastava T, Simon SD, Alon US. High incidence offocal segmental glomerulosclerosis in nephrotic syndrome ofchildhood. Pediatr Nephrol. 1999;13:13–8.
23. Hogg RJ, Portman RJ, Milliner D, et al. Evaluation andmanagement of proteinuria and nephrotic syndrome inchildren: Recommendations from a pediatric nephrologypanel established at the National Kidney Foundationconference on proteinuria, albuminuria, risk, assessment,detection, and elimination (PARADE). Pediatrics.2000;105:1242–9. 24. McEnery PT, Strife CF. Nephroticsyndrome in childhood:. management and treatment inpatients with minimal change disease, mesangialproliferation, or focal glomerulosclerosis. Pediatr ClinNorth Am. 1982;29:875–94. 25. Ano nymous. Nephroticsyndrome in children: Prediction of histopathology fromclinical and laboratory characteristics at time ofdiagnosis. A report of the International Study of KidneyDisease in Children. Kidney Int. 1978;13:159–65. 26.Sharples PM, Poulton J, White RH. Steroid responsivenephrotic syndrome is more common in Asians. Arch DisChild. 1985;60:1014–7. 27. Bhimma R, Coovadia HM, AdhikariM. Nephrotic syndrome in South African children: Changingperspectives over 20 years. Pediatr Nephrol.1997;11:429–34. 28. Kopp JB, Smith MW, Nelson GW, et al.MYH9 is a major-effect risk gene for focal segmentalglomerulosclerosis. Nat Genet. 2008;40:1175–84. 29.Bonilla-Felix M, Parra C, Dajani T, et al. Changingpatterns in the histopathology of idiopathic nephroticsyndrome in children. Kidney Int. 1999;55:1885–90. 30.McCurdy FA, Butera PJ, Wilson R. The familial occurrenceof focal segmental glomerular sclero sis. Am J Kidney Dis.1987;10:467–9. 31. Naruse T, Hirokawa N, Maekawa T, et al.Familial nephrotic syndrome with focal glomerular sclerosis. Am J Med Sci. 1980;280:109–13. 32. White RH. The

familial nephrotic syndrome. I. A European survey. ClinNephrol. 1973;1:215–9. 33. Cha ndra M, Mouradian J, HoyerJR, Lewy JE. Familial nephrotic syndrome and focalsegmental glomerulosclerosis. J Pediatr. 1981;98:556–60.34. Mon crieff MW, White RH, Glasgow EF, et al. Thefamilial nephrotic syndrome. II. A clinicopathologi calstudy. Clin Nephrol. 1973;1:220–9. 35. Roy S, 3rd, PitcockJA. Idiopathic nephrosis in identical twins. Am J DisChild. 1971;121:428–30. 36. Shalhoub RJ. Pathogenesis oflipoid nephro sis: A disorder of T-cell function. Lancet.1974 ;2:556–60. 37. Yang T, Nast CC, Vo A, Jordan SC.Rapid remis sion of steroid and mycophenolate mofetil(MMF)–resistant minimal change nephrotic syndrome afterrituximab therapy. Nephrol Dial Transplant.2008;23:377–80. 38. Aggarwal N, Batwara R, McCarthy ET, etal. Serum permeability activity in steroid-resistant minimal change nephrotic syndrome is abolished by treatment ofHodgkin disease. Am J Kidney Dis. 2007;50:826–9.
39. Ali AA, Wilson E, Moorhead JF, et al. Minimalchangeglomerular nephritis: Normal kidneys in an abnormalenvironment? Transplantation. 1994;58:849–52.
40. Abdel-Hafez M, Shimada M, Lee PY, et al. Idiopathicnephrotic syndrome and atopy: Is there a common link? Am JKidney Dis. 2009;54:945–53.
41. Audard V, Larousserie F, Grimbert P, et al. Minimalchange nephrotic syndrome and classical Hodgkin’slymphoma: Report of 21 cases and review of the literature.Kidney Int. 2006;69:2251–60.
42. Sasdelli M, Cagnoli L, Candi P, et al. Cell mediatedimmunity in idiopathic glomerulonephritis. Clin ExpImmunol. 1981;46:27–34.
43. Yan K , Nakahara K, Awa S, et al. The increase ofmemory T cell subsets in children with idiopathicnephrotic syndrome. Nephron. 1998;79:274–8.
44. Fodor P, Saitua MT, Rodriguez E, et al. T-cell dysfunction in minimal-change nephrotic syndrome of childhood. Am J Dis Child. 1982;136:713–7.
45. Sellier-Leclerc AL, Duval A, Riveron S, et al. Ahumanized mouse model of idiopathic nephrotic syndromesuggests a pathogenic role for imma ture cells. J Am SocNephrol. 2007;18:2732–9.
46. Tasic V. Nephrotic syndrome in a child after a bee

sting. Pediatr Nephrol. 2000;15:245–7.
47. Swa nson GP, Leveque JA. Nephrotic syndrome associatedwith ant bite. Tex Med. 1990;86:39–41.
48. Cuoghi D, Venturi P, Cheli E. Bee sting and relapse ofnephrotic syndrome. Child Nephrol Urol. 1988;9:82–3.
49. Lag rue G, Laurent J, Rostoker G. Food allergy andidiopathic nephrotic syndrome. Kidney Int Suppl.1989;27:S147–51.
50. Sah ali D, Pawlak A, Valanciute A, et al. A novelapproach to investigation of the pathogenesis of activeminimal-change nephrotic syndrome using subtracted cDNAlibrary screening. J Am Soc Nephrol. 2002;13:1238–47.
51. Ishimoto T, Shimada M, Araya CE, et al. Minimal changedisease: A CD80 podocytopathy? Semin Nephrol.2011;31:320–5.
52. Okuyama S, Komatsuda A, Wakui H, et al. Up-regulationof TRAIL mRNA expression in peripheral blood mononuclearcells from patients with minimal-change nephroticsyndrome. Nephrol Dial Transplant. 2005;20:539–44.
53. Gonzalez E, Neuhaus T, Kemper MJ, Girardin E.Proteomic analysis of mononuclear cells of patients withminimal-change nephrotic syndrome of childhood. NephrolDial Transplant. 2009;24:149–55.
54. Gar in EH. A comparison of combinations of diureticsin nephrotic edema. Am J Dis Child. 1987;141:769–71.
55. van den Berg JG, Weening JJ. Role of the immune systemin the pathogenesis of idiopathic nephrotic syndrome. ClinSci (Lond). 2004;107:125–36. 56. Cheung W, Wei CL, SeahCC, et al. Atopy, serum IgE, and interleukin-13 insteroid-responsive nephrotic syndrome. Pediatr Nephrol.2004;19:627–32. 57. Lai KW, Wei CL, Tan LK, et al.Overexpression of interleukin-13 inducesminimal-change–like nephropathy in rats. J Am Soc Nephrol.2007;18:1476–85. 58. Yok oyama H, Kida H, Abe T, et al.Impaired immunoglobulin G production in minimal changenephrotic syndrome in adults. Clin Exp Immunol.1987;70:110–5. 59. McAdams AJ, Valentini RP, Welch TR. Thenonspecificity of focal segmental glomerulosclerosis: Thedefining characteristics of primary focalglomerulosclerosis, mesangial proliferation, and minimalchange. Medicine (Baltimore). 1997;76:42–52. 60. Ell is D,
Kapur S, Antonovych TT, et al. Focal glomerulosclerosis inchildren: Correlation of histology with prognosis. JPediatr. 1978;93:762–8. 61. Hara M, Yanagihara T, TakadaT, et al. Urinary excretion of podocytes reflects diseaseactivity in children with glomerulonephritis. Am JNephrol. 1998;18:35–41. 62. Har a M, Yanagihara T, KiharaI. Urinary podocytes in primary focal segmentalglomerulosclerosis. Nephron. 2001;89:342–7. 63. Dantal J,Bigot E, Bogers W, et al. Effect of plasma proteinadsorption on protein excretion in kidneytransplantrecipients with recurrent nephrotic syndrome. N Engl J Med.1994;330:7–14. 64. Crave di P, Kopp JB, Remuzzi G. Recentprogress in the pathophysiology and treatment of FSGSrecurrence. Am J Transplant. 2013;13:266–74. 65.Avila-Casado M del C, Perez-Torres I, Auron A, et al.Proteinuria in rats induced by serum from patients withcollapsing glomerulopathy. Kidney Int. 2004;66:133–43.66. Kem per MJ, Wolf G, Muller-Wiefel DE. Transmission ofglomerular permeability factor from a mother to her child.N Engl J Med. 2001;344:386–7. 67. Wei C, Trachtman H, LiJ, et al. Circulating suPAR in two cohorts of primaryFSGS. J Am Soc Nephrol. 2012;23:2051–9. 68. Wei C, ElHindi S, Li J, et al. Circulating urokinase receptor as acause of focal segmental glomerulosclerosis. Nat Med.2011;17:952–60. 69. Huang J, Liu G, Zhang YM, et al.Plasma soluble urokinase receptor levels are increased butdo not distinguish primary from secondary focal segmentalglomerulosclerosis. Kidney Int. 2013;84:366–72. 70. MaasRJ, Deegens JK, Wetzels JF. Serum suPAR in patients withFSGS: Trash or treasure? Pediatr Nephrol. 2013;28:1041–8.71. Boc k ME, Price HE, Gallon L, Langman CB. Serumsoluble urokinase-type plasminogen activator receptorlevels and idiopathic FSGS in children: A single-centerreport. Clin J Am Soc Nephrol. 2013;8:1304–11.
72. Franco Palacios CR, Lieske JC, Wadei HM, et al. Urinebut not serum soluble urokinase receptor (suPAR) mayidentify cases of recurrent FSGS in kidney transplantcandidates. Transplantation. 2013;96:394–9.
73. Brown EJ, Schlondorff JS, Becker DJ, et al. Mutationsin the formin gene INF2 cause focal segmentalglomerulosclerosis. Nat Genet. 2010;42:72–6.
74. Mel e C, Iatropoulos P, Donadelli R, et al. MYO1Emutations and childhood familial focal segmentalglomerulosclerosis. N Engl J Med. 2011;365:295–306.
75. He N, Zahirieh A, Mei Y, et al. Recessive NPHS2(podocin) mutations are rare in adult-onset idiopathic
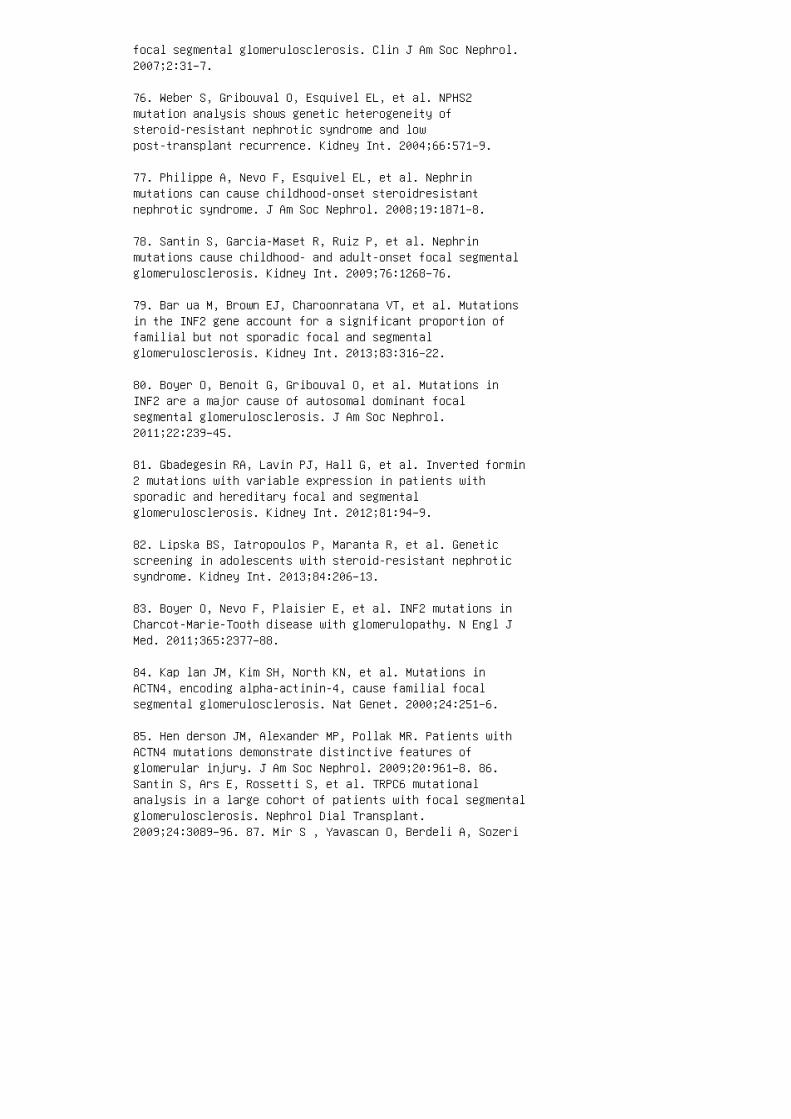
focal segmental glomerulosclerosis. Clin J Am Soc Nephrol.2007;2:31–7.
76. Weber S, Gribouval O, Esquivel EL, et al. NPHS2mutation analysis shows genetic heterogeneity ofsteroid-resistant nephrotic syndrome and lowpost-transplant recurrence. Kidney Int. 2004;66:571–9.
77. Philippe A, Nevo F, Esquivel EL, et al. Nephrinmutations can cause childhood-onset steroidresistantnephrotic syndrome. J Am Soc Nephrol. 2008;19:1871–8.
78. Santin S, Garcia-Maset R, Ruiz P, et al. Nephrinmutations cause childhood- and adult-onset focal segmentalglomerulosclerosis. Kidney Int. 2009;76:1268–76.
79. Bar ua M, Brown EJ, Charoonratana VT, et al. Mutationsin the INF2 gene account for a significant proportion offamilial but not sporadic focal and segmentalglomerulosclerosis. Kidney Int. 2013;83:316–22.
80. Boyer O, Benoit G, Gribouval O, et al. Mutations inINF2 are a major cause of autosomal dominant focalsegmental glomerulosclerosis. J Am Soc Nephrol.2011;22:239–45.
81. Gbadegesin RA, Lavin PJ, Hall G, et al. Inverted formin2 mutations with variable expression in patients withsporadic and hereditary focal and segmentalglomerulosclerosis. Kidney Int. 2012;81:94–9.
82. Lipska BS, Iatropoulos P, Maranta R, et al. Geneticscreening in adolescents with steroid-resistant nephroticsyndrome. Kidney Int. 2013;84:206–13.
83. Boyer O, Nevo F, Plaisier E, et al. INF2 mutations inCharcot-Marie-Tooth disease with glomerulopathy. N Engl JMed. 2011;365:2377–88.
84. Kap lan JM, Kim SH, North KN, et al. Mutations inACTN4, encoding alpha-actinin-4, cause familial focalsegmental glomerulosclerosis. Nat Genet. 2000;24:251–6.
85. Hen derson JM, Alexander MP, Pollak MR. Patients withACTN4 mutations demonstrate distinctive features ofglomerular injury. J Am Soc Nephrol. 2009;20:961–8. 86.Santin S, Ars E, Rossetti S, et al. TRPC6 mutationalanalysis in a large cohort of patients with focal segmentalglomerulosclerosis. Nephrol Dial Transplant.2009;24:3089–96. 87. Mir S , Yavascan O, Berdeli A, Sozeri
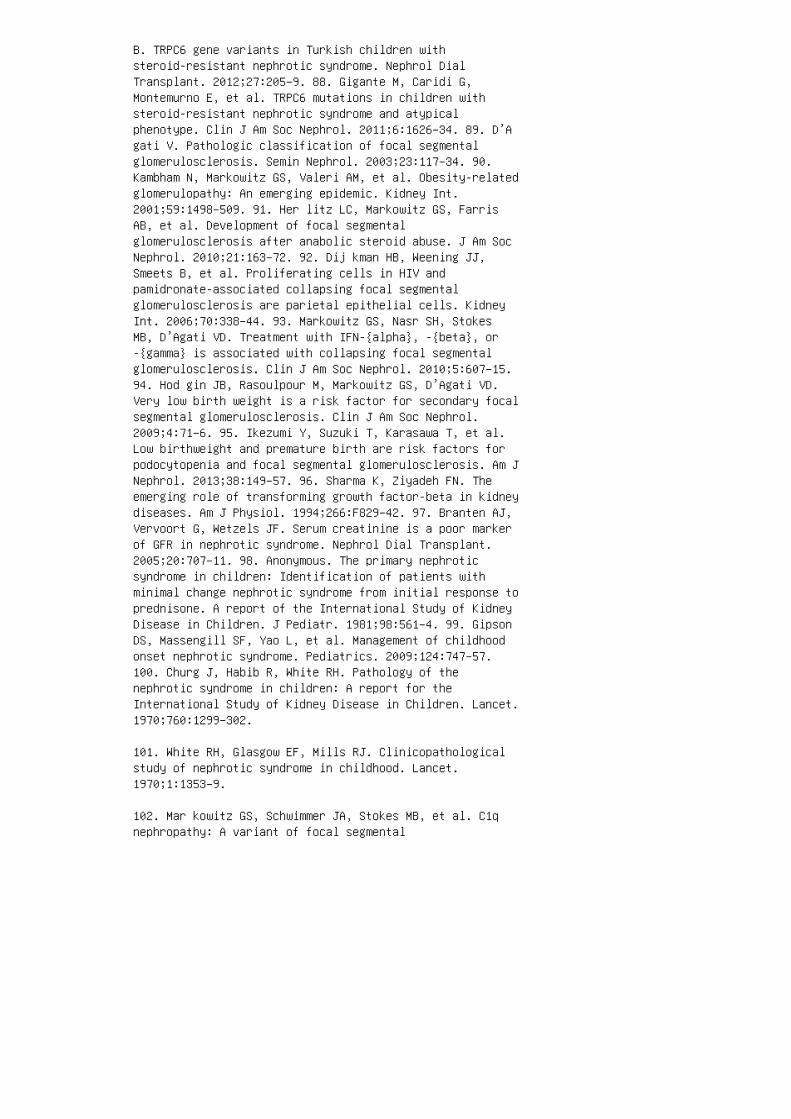
B. TRPC6 gene variants in Turkish children withsteroid-resistant nephrotic syndrome. Nephrol DialTransplant. 2012;27:205–9. 88. Gigante M, Caridi G,Montemurno E, et al. TRPC6 mutations in children withsteroid-resistant nephrotic syndrome and atypicalphenotype. Clin J Am Soc Nephrol. 2011;6:1626–34. 89. D’Agati V. Pathologic classification of focal segmentalglomerulosclerosis. Semin Nephrol. 2003;23:117–34. 90.Kambham N, Markowitz GS, Valeri AM, et al. Obesity-relatedglomerulopathy: An emerging epidemic. Kidney Int.2001;59:1498–509. 91. Her litz LC, Markowitz GS, FarrisAB, et al. Development of focal segmentalglomerulosclerosis after anabolic steroid abuse. J Am SocNephrol. 2010;21:163–72. 92. Dij kman HB, Weening JJ,Smeets B, et al. Proliferating cells in HIV andpamidronate-associated collapsing focal segmentalglomerulosclerosis are parietal epithelial cells. KidneyInt. 2006;70:338–44. 93. Markowitz GS, Nasr SH, StokesMB, D’Agati VD. Treatment with IFN-{alpha}, -{beta}, or-{gamma} is associated with collapsing focal segmentalglomerulosclerosis. Clin J Am Soc Nephrol. 2010;5:607–15.94. Hod gin JB, Rasoulpour M, Markowitz GS, D’Agati VD.Very low birth weight is a risk factor for secondary focalsegmental glomerulosclerosis. Clin J Am Soc Nephrol.2009;4:71–6. 95. Ikezumi Y, Suzuki T, Karasawa T, et al.Low birthweight and premature birth are risk factors forpodocytopenia and focal segmental glomerulosclerosis. Am JNephrol. 2013;38:149–57. 96. Sharma K, Ziyadeh FN. Theemerging role of transforming growth factor-beta in kidneydiseases. Am J Physiol. 1994;266:F829–42. 97. Branten AJ,Vervoort G, Wetzels JF. Serum creatinine is a poor markerof GFR in nephrotic syndrome. Nephrol Dial Transplant.2005;20:707–11. 98. Anonymous. The primary nephroticsyndrome in children: Identification of patients withminimal change nephrotic syndrome from initial response toprednisone. A report of the International Study of KidneyDisease in Children. J Pediatr. 1981;98:561–4. 99. GipsonDS, Massengill SF, Yao L, et al. Management of childhoodonset nephrotic syndrome. Pediatrics. 2009;124:747–57.100. Churg J, Habib R, White RH. Pathology of thenephrotic syndrome in children: A report for theInternational Study of Kidney Disease in Children. Lancet.1970;760:1299–302.
101. White RH, Glasgow EF, Mills RJ. Clinicopathologicalstudy of nephrotic syndrome in childhood. Lancet.1970;1:1353–9.
102. Mar kowitz GS, Schwimmer JA, Stokes MB, et al. C1qnephropathy: A variant of focal segmental

glomerulosclerosis. Kidney Int. 2003;64:1232–40.
103. Border WA. Distinguishing minimal-change disease frommesangial disorders. Kidney Int. 1988;34:419–34.
104. Myllymaki J, Saha H, Mustonen J, et al. IgMnephropathy: Clinical picture and long-term prognosis. Am JKidney Dis. 2003;41:343–50.
105. Waldherr R, Gubler MC, Levy M, et al. The significanceof pure diffuse mesangial proliferation in idiopathicnephrotic syndrome. Clin Nephrol. 1978;10:171–9.
106. Ano nymous. Childhood nephrotic syndrome associatedwith diffuse mesangial hypercellularity: A report of theSouthwest Pediatric Nephrology Study Group. Kidney Int.1983;24:87–94.
107. Swartz SJ, Eldin KW, Hicks MJ, Feig DI. Minimalchange disease with IgM+ immunofluorescence: A subtype ofnephrotic syndrome. Pediatr Nephrol. 2009;24:1187–92.
108. Viz jak A, Ferluga D, Rozic M, et al. Pathology,clinical presentations, and outcomes of C1q nephropathy. JAm Soc Nephrol. 2008;19:2237–44.
109. Kersnik Levart T, Kenda RB, Avgustin Cavic M, et al.C1Q nephropathy in children. Pediatr Nephrol.2005;20:1756–61.
110. His ano S, Fukuma Y, Segawa Y, et al.Clinicopathologic correlation and outcome of C1qnephropathy. Clin J Am Soc Nephrol. 2008;3:1637–43.
111. Fogo A, Glick AD, Horn SL, Horn RG. Is focalsegmental glomerulosclerosis really focal? Distribution oflesions in adults and children. Kidney Int.1995;47:1690–6.
112. Morel-Maroger L, Leathem A, Richet G. Glomerularabnormalities in nonsystemic diseases: Relationshipbetween findings by light micros copy andimmunofluorescence in 433 renal biopsy s pe cimens. Am JMed. 1972;53:170–84.
113. Fog o A, Hawkins EP, Berry PL, et al. Glomerularhypertrophy in minimal change disease predicts subsequentprogression to focal glomerular scle rosis. Kidney Int.1990;38:115–23.
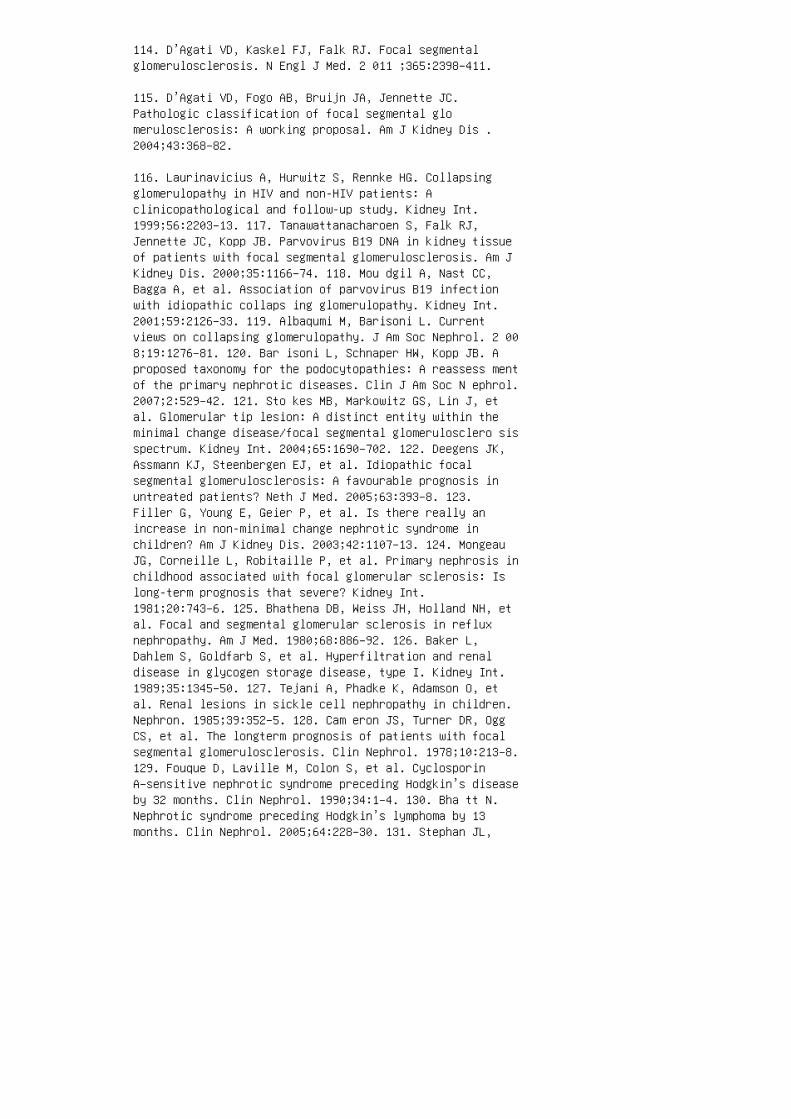
114. D’Agati VD, Kaskel FJ, Falk RJ. Focal segmentalglomerulosclerosis. N Engl J Med. 2 011 ;365:2398–411.
115. D’Agati VD, Fogo AB, Bruijn JA, Jennette JC.Pathologic classification of focal segmental glomerulosclerosis: A working proposal. Am J Kidney Dis .2004;43:368–82.
116. Laurinavicius A, Hurwitz S, Rennke HG. Collapsingglomerulopathy in HIV and non-HIV patients: Aclinicopathological and follow-up study. Kidney Int.1999;56:2203–13. 117. Tanawattanacharoen S, Falk RJ,Jennette JC, Kopp JB. Parvovirus B19 DNA in kidney tissueof patients with focal segmental glomerulosclerosis. Am JKidney Dis. 2000;35:1166–74. 118. Mou dgil A, Nast CC,Bagga A, et al. Association of parvovirus B19 infectionwith idiopathic collaps ing glomerulopathy. Kidney Int.2001;59:2126–33. 119. Albaqumi M, Barisoni L. Currentviews on collapsing glomerulopathy. J Am Soc Nephrol. 2 008;19:1276–81. 120. Bar isoni L, Schnaper HW, Kopp JB. Aproposed taxonomy for the podocytopathies: A reassess mentof the primary nephrotic diseases. Clin J Am Soc N ephrol.2007;2:529–42. 121. Sto kes MB, Markowitz GS, Lin J, etal. Glomerular tip lesion: A distinct entity within theminimal change disease/focal segmental glomerulosclero sisspectrum. Kidney Int. 2004;65:1690–702. 122. Deegens JK,Assmann KJ, Steenbergen EJ, et al. Idiopathic focalsegmental glomerulosclerosis: A favourable prognosis inuntreated patients? Neth J Med. 2005;63:393–8. 123.Filler G, Young E, Geier P, et al. Is there really anincrease in non-minimal change nephrotic syndrome inchildren? Am J Kidney Dis. 2003;42:1107–13. 124. MongeauJG, Corneille L, Robitaille P, et al. Primary nephrosis inchildhood associated with focal glomerular sclerosis: Islong-term prognosis that severe? Kidney Int.1981;20:743–6. 125. Bhathena DB, Weiss JH, Holland NH, etal. Focal and segmental glomerular sclerosis in refluxnephropathy. Am J Med. 1980;68:886–92. 126. Baker L,Dahlem S, Goldfarb S, et al. Hyperfiltration and renaldisease in glycogen storage disease, type I. Kidney Int.1989;35:1345–50. 127. Tejani A, Phadke K, Adamson O, etal. Renal lesions in sickle cell nephropathy in children.Nephron. 1985;39:352–5. 128. Cam eron JS, Turner DR, OggCS, et al. The longterm prognosis of patients with focalsegmental glomerulosclerosis. Clin Nephrol. 1978;10:213–8.129. Fouque D, Laville M, Colon S, et al. CyclosporinA–sensitive nephrotic syndrome preceding Hodgkin’s diseaseby 32 months. Clin Nephrol. 1990;34:1–4. 130. Bha tt N.Nephrotic syndrome preceding Hodgkin’s lymphoma by 13months. Clin Nephrol. 2005;64:228–30. 131. Stephan JL,
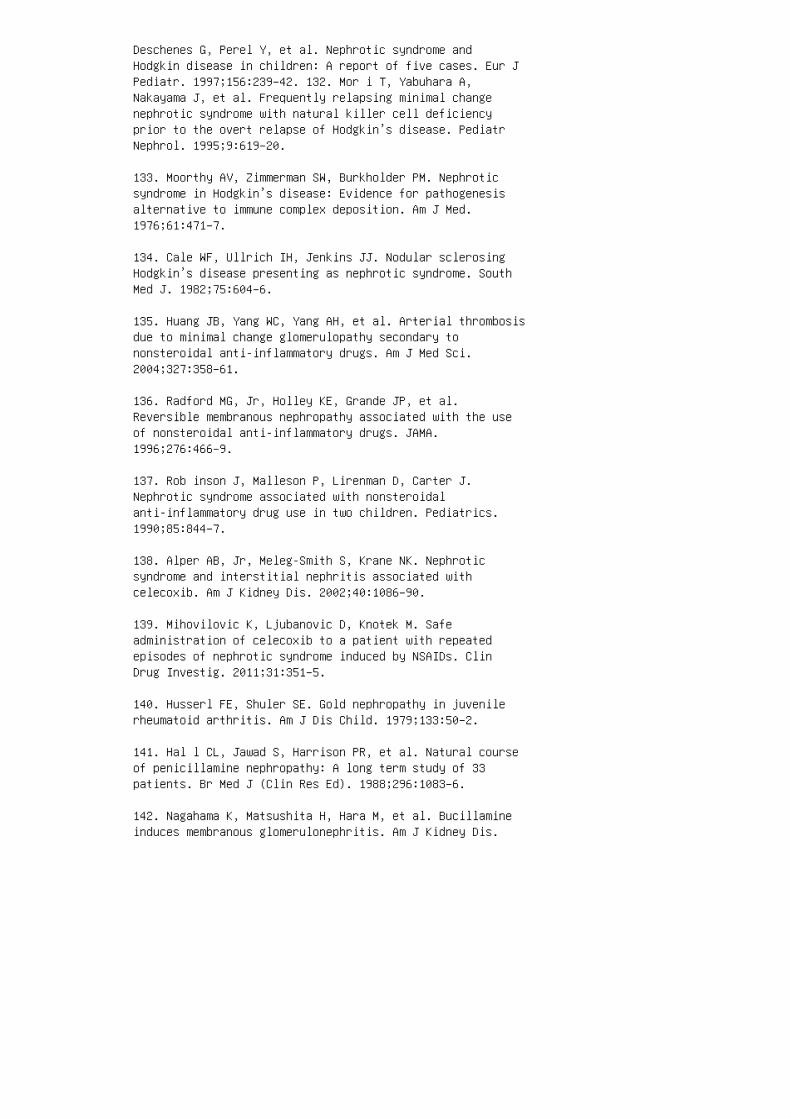
Deschenes G, Perel Y, et al. Nephrotic syndrome andHodgkin disease in children: A report of five cases. Eur JPediatr. 1997;156:239–42. 132. Mor i T, Yabuhara A,Nakayama J, et al. Frequently relapsing minimal changenephrotic syndrome with natural killer cell deficiencyprior to the overt relapse of Hodgkin’s disease. PediatrNephrol. 1995;9:619–20.
133. Moorthy AV, Zimmerman SW, Burkholder PM. Nephroticsyndrome in Hodgkin’s disease: Evidence for pathogenesisalternative to immune complex deposition. Am J Med.1976;61:471–7.
134. Cale WF, Ullrich IH, Jenkins JJ. Nodular sclerosingHodgkin’s disease presenting as nephrotic syndrome. SouthMed J. 1982;75:604–6.
135. Huang JB, Yang WC, Yang AH, et al. Arterial thrombosisdue to minimal change glomerulopathy secondary tononsteroidal anti-inflammatory drugs. Am J Med Sci.2004;327:358–61.
136. Radford MG, Jr, Holley KE, Grande JP, et al.Reversible membranous nephropathy associated with the useof nonsteroidal anti-inflammatory drugs. JAMA.1996;276:466–9.
137. Rob inson J, Malleson P, Lirenman D, Carter J.Nephrotic syndrome associated with nonsteroidalanti-inflammatory drug use in two children. Pediatrics.1990;85:844–7.
138. Alper AB, Jr, Meleg-Smith S, Krane NK. Nephroticsyndrome and interstitial nephritis associated withcelecoxib. Am J Kidney Dis. 2002;40:1086–90.
139. Mihovilovic K, Ljubanovic D, Knotek M. Safeadministration of celecoxib to a patient with repeatedepisodes of nephrotic syndrome induced by NSAIDs. ClinDrug Investig. 2011;31:351–5.
140. Husserl FE, Shuler SE. Gold nephropathy in juvenilerheumatoid arthritis. Am J Dis Child. 1979;133:50–2.
141. Hal l CL, Jawad S, Harrison PR, et al. Natural courseof penicillamine nephropathy: A long term study of 33patients. Br Med J (Clin Res Ed). 1988;296:1083–6.
142. Nagahama K, Matsushita H, Hara M, et al. Bucillamineinduces membranous glomerulonephritis. Am J Kidney Dis.
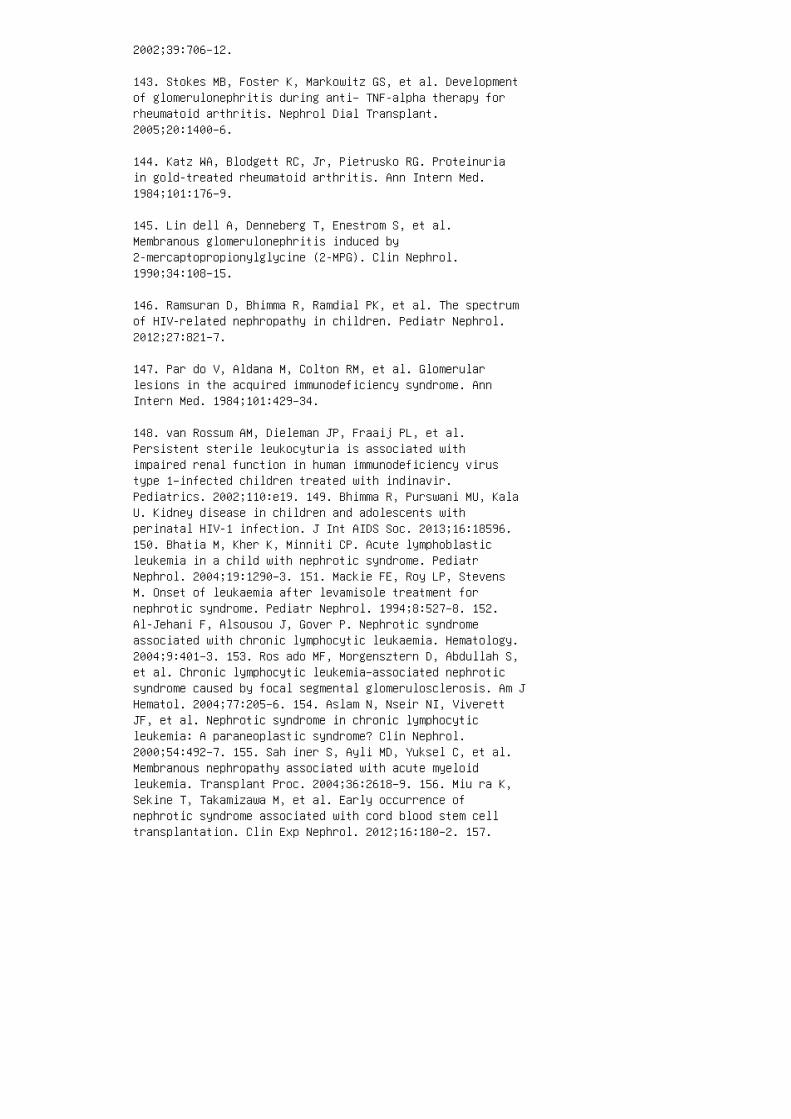
2002;39:706–12.
143. Stokes MB, Foster K, Markowitz GS, et al. Developmentof glomerulonephritis during anti– TNF-alpha therapy forrheumatoid arthritis. Nephrol Dial Transplant.2005;20:1400–6.
144. Katz WA, Blodgett RC, Jr, Pietrusko RG. Proteinuriain gold-treated rheumatoid arthritis. Ann Intern Med.1984;101:176–9.
145. Lin dell A, Denneberg T, Enestrom S, et al.Membranous glomerulonephritis induced by2-mercaptopropionylglycine (2-MPG). Clin Nephrol.1990;34:108–15.
146. Ramsuran D, Bhimma R, Ramdial PK, et al. The spectrumof HIV-related nephropathy in children. Pediatr Nephrol.2012;27:821–7.
147. Par do V, Aldana M, Colton RM, et al. Glomerularlesions in the acquired immunodeficiency syndrome. AnnIntern Med. 1984;101:429–34.
148. van Rossum AM, Dieleman JP, Fraaij PL, et al.Persistent sterile leukocyturia is associated withimpaired renal function in human immunodeficiency virustype 1–infected children treated with indinavir.Pediatrics. 2002;110:e19. 149. Bhimma R, Purswani MU, KalaU. Kidney disease in children and adolescents withperinatal HIV-1 infection. J Int AIDS Soc. 2013;16:18596.150. Bhatia M, Kher K, Minniti CP. Acute lymphoblasticleukemia in a child with nephrotic syndrome. PediatrNephrol. 2004;19:1290–3. 151. Mackie FE, Roy LP, StevensM. Onset of leukaemia after levamisole treatment fornephrotic syndrome. Pediatr Nephrol. 1994;8:527–8. 152.Al-Jehani F, Alsousou J, Gover P. Nephrotic syndromeassociated with chronic lymphocytic leukaemia. Hematology.2004;9:401–3. 153. Ros ado MF, Morgensztern D, Abdullah S,et al. Chronic lymphocytic leukemia–associated nephroticsyndrome caused by focal segmental glomerulosclerosis. Am JHematol. 2004;77:205–6. 154. Aslam N, Nseir NI, ViverettJF, et al. Nephrotic syndrome in chronic lymphocyticleukemia: A paraneoplastic syndrome? Clin Nephrol.2000;54:492–7. 155. Sah iner S, Ayli MD, Yuksel C, et al.Membranous nephropathy associated with acute myeloidleukemia. Transplant Proc. 2004;36:2618–9. 156. Miu ra K,Sekine T, Takamizawa M, et al. Early occurrence ofnephrotic syndrome associated with cord blood stem celltransplantation. Clin Exp Nephrol. 2012;16:180–2. 157.
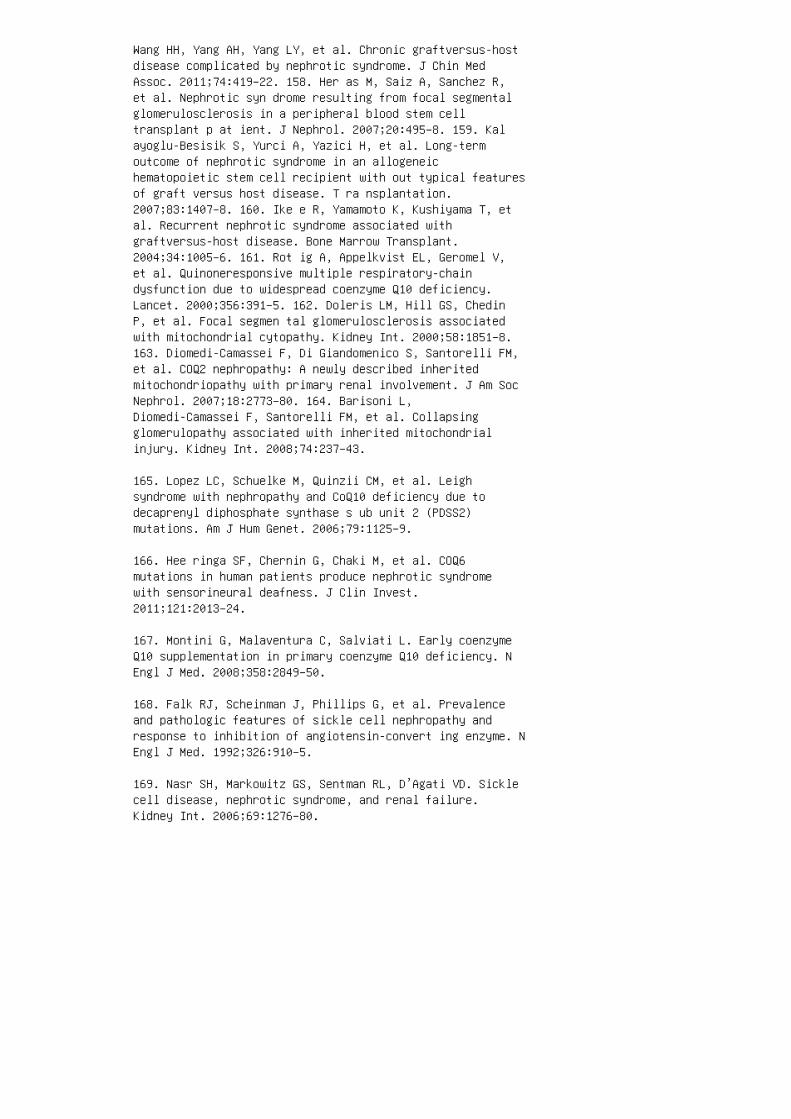
Wang HH, Yang AH, Yang LY, et al. Chronic graftversus-hostdisease complicated by nephrotic syndrome. J Chin MedAssoc. 2011;74:419–22. 158. Her as M, Saiz A, Sanchez R,et al. Nephrotic syn drome resulting from focal segmentalglomerulosclerosis in a peripheral blood stem celltransplant p at ient. J Nephrol. 2007;20:495–8. 159. Kalayoglu-Besisik S, Yurci A, Yazici H, et al. Long-termoutcome of nephrotic syndrome in an allogeneichematopoietic stem cell recipient with out typical featuresof graft versus host disease. T ra nsplantation.2007;83:1407–8. 160. Ike e R, Yamamoto K, Kushiyama T, etal. Recurrent nephrotic syndrome associated withgraftversus-host disease. Bone Marrow Transplant.2004;34:1005–6. 161. Rot ig A, Appelkvist EL, Geromel V,et al. Quinoneresponsive multiple respiratory-chaindysfunction due to widespread coenzyme Q10 deficiency.Lancet. 2000;356:391–5. 162. Doleris LM, Hill GS, ChedinP, et al. Focal segmen tal glomerulosclerosis associatedwith mitochondrial cytopathy. Kidney Int. 2000;58:1851–8.163. Diomedi-Camassei F, Di Giandomenico S, Santorelli FM,et al. COQ2 nephropathy: A newly described inheritedmitochondriopathy with primary renal involvement. J Am SocNephrol. 2007;18:2773–80. 164. Barisoni L,Diomedi-Camassei F, Santorelli FM, et al. Collapsingglomerulopathy associated with inherited mitochondrialinjury. Kidney Int. 2008;74:237–43.
165. Lopez LC, Schuelke M, Quinzii CM, et al. Leighsyndrome with nephropathy and CoQ10 deficiency due todecaprenyl diphosphate synthase s ub unit 2 (PDSS2)mutations. Am J Hum Genet. 2006;79:1125–9.
166. Hee ringa SF, Chernin G, Chaki M, et al. COQ6mutations in human patients produce nephrotic syndromewith sensorineural deafness. J Clin Invest.2011;121:2013–24.
167. Montini G, Malaventura C, Salviati L. Early coenzymeQ10 supplementation in primary coenzyme Q10 deficiency. NEngl J Med. 2008;358:2849–50.
168. Falk RJ, Scheinman J, Phillips G, et al. Prevalenceand pathologic features of sickle cell nephropathy andresponse to inhibition of angiotensin-convert ing enzyme. NEngl J Med. 1992;326:910–5.
169. Nasr SH, Markowitz GS, Sentman RL, D’Agati VD. Sicklecell disease, nephrotic syndrome, and renal failure.Kidney Int. 2006;69:1276–80.
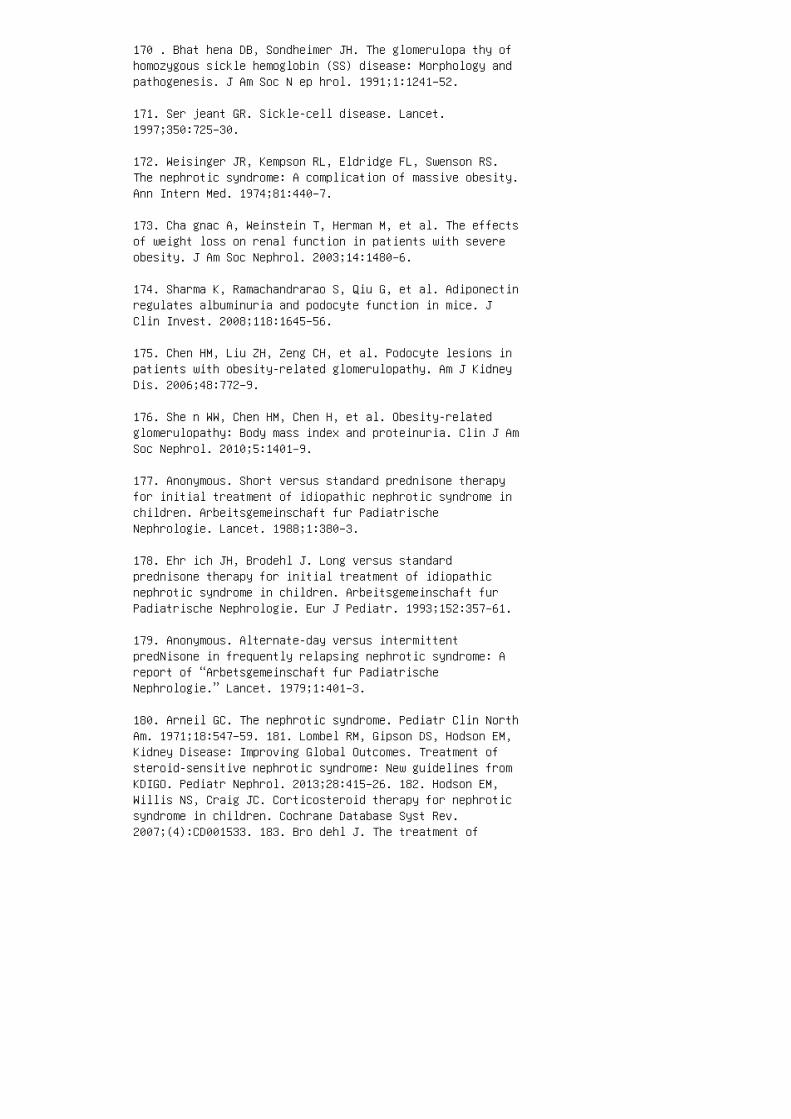
170 . Bhat hena DB, Sondheimer JH. The glomerulopa thy ofhomozygous sickle hemoglobin (SS) disease: Morphology andpathogenesis. J Am Soc N ep hrol. 1991;1:1241–52.
171. Ser jeant GR. Sickle-cell disease. Lancet.1997;350:725–30.
172. Weisinger JR, Kempson RL, Eldridge FL, Swenson RS.The nephrotic syndrome: A complication of massive obesity.Ann Intern Med. 1974;81:440–7.
173. Cha gnac A, Weinstein T, Herman M, et al. The effectsof weight loss on renal function in patients with severeobesity. J Am Soc Nephrol. 2003;14:1480–6.
174. Sharma K, Ramachandrarao S, Qiu G, et al. Adiponectinregulates albuminuria and podocyte function in mice. JClin Invest. 2008;118:1645–56.
175. Chen HM, Liu ZH, Zeng CH, et al. Podocyte lesions inpatients with obesity-related glomerulopathy. Am J KidneyDis. 2006;48:772–9.
176. She n WW, Chen HM, Chen H, et al. Obesity-relatedglomerulopathy: Body mass index and proteinuria. Clin J AmSoc Nephrol. 2010;5:1401–9.
177. Anonymous. Short versus standard prednisone therapyfor initial treatment of idiopathic nephrotic syndrome inchildren. Arbeitsgemeinschaft fur PadiatrischeNephrologie. Lancet. 1988;1:380–3.
178. Ehr ich JH, Brodehl J. Long versus standardprednisone therapy for initial treatment of idiopathicnephrotic syndrome in children. Arbeitsgemeinschaft furPadiatrische Nephrologie. Eur J Pediatr. 1993;152:357–61.
179. Anonymous. Alternate-day versus intermittentpredNisone in frequently relapsing nephrotic syndrome: Areport of “Arbetsgemeinschaft fur PadiatrischeNephrologie.” Lancet. 1979;1:401–3.
180. Arneil GC. The nephrotic syndrome. Pediatr Clin NorthAm. 1971;18:547–59. 181. Lombel RM, Gipson DS, Hodson EM,Kidney Disease: Improving Global Outcomes. Treatment ofsteroid-sensitive nephrotic syndrome: New guidelines fromKDIGO. Pediatr Nephrol. 2013;28:415–26. 182. Hodson EM,Willis NS, Craig JC. Corticosteroid therapy for nephroticsyndrome in children. Cochrane Database Syst Rev.2007;(4):CD001533. 183. Bro dehl J. The treatment of

minimal change nephrotic syndrome: Lessons learned frommulticentre co-operative studies. Eur J Pediatr.1991;150:380–7. 184. Hodson EM, Knight JF, Willis NS,Craig JC. Corticosteroid therapy in nephrotic syndrome: Ameta-analysis of randomised controlled trials. Arch DisChild. 2000;83:45–51. 185. Bagga A, Hari P, Srivastava RN.Prolonged versus standard prednisolone therapy for initialepisode of nephrotic syndrome. Pediatr Nephrol.1999;13:824–7. 186. Feber J, Al-Matrafi J, Farhadi E, etal. Prednisone dosing per body weight or body surface areain children with nephrotic syndrome: Is it equivalent?Pediatr Nephrol. 2009;24:1027–31. 187. Saadeh SA, BaraccoR, Jain A, et al. Weight or body surface area dosing ofsteroids in nephrotic syndrome: Is there an outcomedifference? Pediatr Nephrol. 2011;26:2167–71. 188. HoyerPF, Brodeh J. Initial treatment of idiopathic nephroticsyndrome in children: Prednisone versus prednisone pluscyclosporine A. A pro spective, randomized trial. J Am SocNephrol. 200 6;17:1151–7. 189. Viv arelli M, MoscaritoloE, Tsalkidis A, et al. Time for initial response tosteroids is a major prognostic factor in idiopathicnephrotic syndrome. J Pediatr. 2010;156:965–71. 190. Wingen AM, Muller-Wiefel DE, Scharer K. Spontaneousremissions in frequently relapsing and steroid dependentidiopathic nephrotic syn drome. Clin Nephrol.1985;23:35–40. 191. Tarshish P, Tobin JN, Bernstein J,Edelmann CM, Jr. Prognostic significance of the earlycourse of minimal change nephrotic syndrome: Report of theInternational Study of Kidney Disease in Children. J AmSoc Nephrol. 1997;8:769–76. 192. Mat too TK, Mahmoud MA.Increased maintenance corticosteroids during upperrespiratory infection decrease the risk of relapse innephrotic syndrome. Nephron. 2000;85:343–5. 193. ElzoukiAY, Jaiswal OP. Long-term, small dose prednisone therapyin frequently relapsing nephrotic syndrome of childhood:Effect on remis sion, statural growth, obesity, andinfection rate. Cli n Pediatr (Phila). 1988;27:387–92.194. Srivastava RN, Vasudev AS, Bagga A, Sunderam KR.Long-term, low-dose prednisolone therapy in frequentlyrelapsing nephrotic syndrome. Pediatr Nephrol.1992;6:247–50.
195. Allen DB. Growth suppression by glucocorticoidtherapy. Endocrinol Metab Clin North Am. 1996 ;25:699–717.
196. All en DB, Julius JR, Breen TJ, Attie KM. Treatmentof glucocorticoid-induced growth suppression with growthhormone: National Cooperative Growth Study. J ClinEndocrinol Metab. 1998;83:2824–9.

197. Donatti TL, Koch VH, Fujimura MD, Okay Y. Growth insteroid-responsive nephrotic syndrome: A study of 85pediatric patients. Pediatr Nephrol. 2003;18:789–95.
198. Emma F, Sesto A, Rizzoni G. Long-term linear growthof children with severe steroid-respon sive nephroticsyndrome. Pediatr Nephrol. 2003 ;18:783–8.
199. Ree s L, Greene SA, Adlard P, et al. Growth andendocrine function in steroid sensitive nephroticsyndrome. Arch Dis Child. 1988;63:484–90.
200. Leroy V, Baudouin V, Alberti C, et al. Growth in boyswith idiopathic nephrotic syndrome on longterm cyclosporinand steroid treatment. Pediatr Nephrol. 2009;24:2393–400.
201. Simmonds J, Grundy N, Trompeter R, Tullus K.Long-term steroid treatment and growth: A study insteroid-dependent nephrotic syndrome. Arch Dis Child.2010;95:146–9.
202. Padilla R, Brem AS. Linear growth of children withnephrotic syndrome: Effect of alkylating agents.Pediatrics. 1989;84:495–9.
203. Pol ito C, Oporto MR, Totino SF, et al. Normal growthof nephrotic children during long-term alternate-dayprednisone therapy. Acta Paediatr Scand. 1986;75:245–50.
204. Jones JP, Jr. Fat embolism and osteonecrosis. OrthopClin North Am. 1985;16:595–633.
205. Sol omon L. Idiopathic necrosis of the femoral head:Pathogenesis and treatment. Can J Surg. 1981;24:573–8.
206. Nishimura T, Matsumoto T, Nishino M, Tomita K.Histopathologic study of veins in steroid treated rabbits.Clin Orthop Relat Res. 1997;334:37–42.
207. Malizos KN, Karantanas AH, Varitimidis SE, et al.Osteonecrosis of the femoral head: Etiology, imag ing andtreatment. Eur J Radiol. 2007;63:16–28.
208. Limaye SR, Pillai S, Tina LU. Relationship of steroiddose to degree of posterior subcapsular cata racts innephrotic syndrome. Ann Ophthalmol. 1988;20:225–7.
209. Hayasaka Y, Hayasaka S, Matsukura H. Ocular findingsin Japanese children with nephrotic syn drome receivingprolonged corticosteroid therapy. Oph thalmologica.
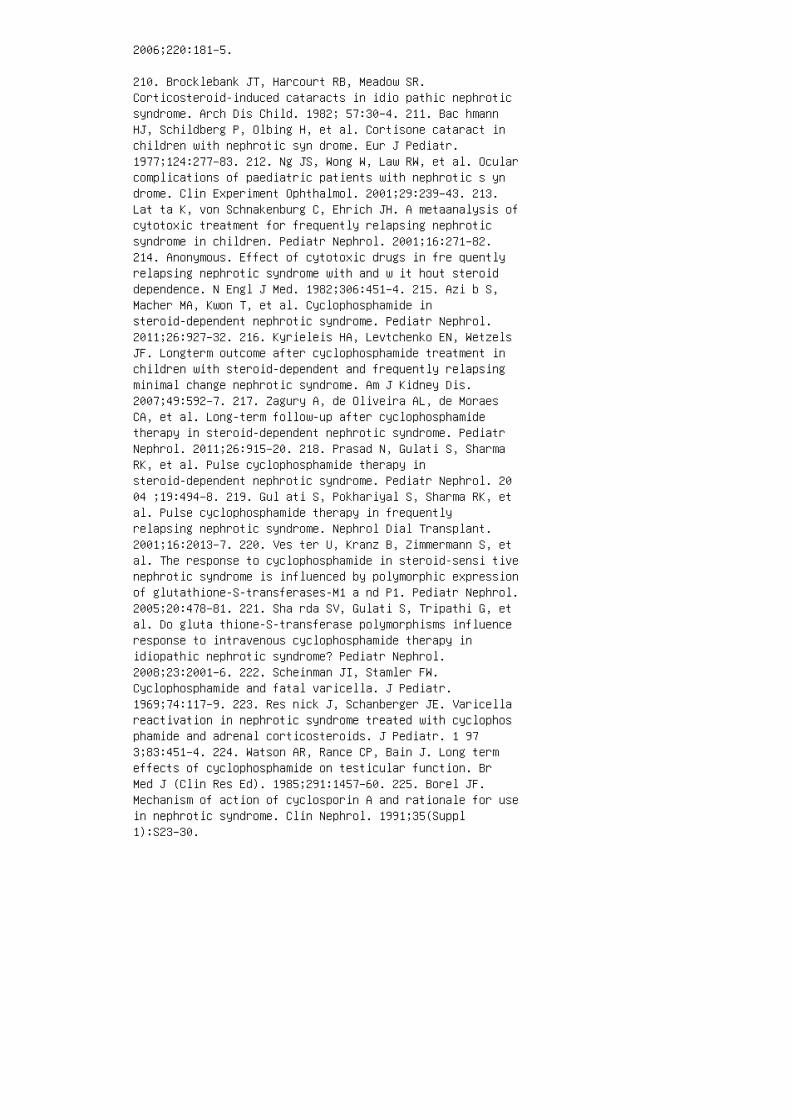
2006;220:181–5.
210. Brocklebank JT, Harcourt RB, Meadow SR.Corticosteroid-induced cataracts in idio pathic nephroticsyndrome. Arch Dis Child. 1982; 57:30–4. 211. Bac hmannHJ, Schildberg P, Olbing H, et al. Cortisone cataract inchildren with nephrotic syn drome. Eur J Pediatr.1977;124:277–83. 212. Ng JS, Wong W, Law RW, et al. Ocularcomplications of paediatric patients with nephrotic s yndrome. Clin Experiment Ophthalmol. 2001;29:239–43. 213.Lat ta K, von Schnakenburg C, Ehrich JH. A metaanalysis ofcytotoxic treatment for frequently relapsing nephroticsyndrome in children. Pediatr Nephrol. 2001;16:271–82.214. Anonymous. Effect of cytotoxic drugs in fre quentlyrelapsing nephrotic syndrome with and w it hout steroiddependence. N Engl J Med. 1982;306:451–4. 215. Azi b S,Macher MA, Kwon T, et al. Cyclophosphamide insteroid-dependent nephrotic syndrome. Pediatr Nephrol.2011;26:927–32. 216. Kyrieleis HA, Levtchenko EN, WetzelsJF. Longterm outcome after cyclophosphamide treatment inchildren with steroid-dependent and frequently relapsingminimal change nephrotic syndrome. Am J Kidney Dis.2007;49:592–7. 217. Zagury A, de Oliveira AL, de MoraesCA, et al. Long-term follow-up after cyclophosphamidetherapy in steroid-dependent nephrotic syndrome. PediatrNephrol. 2011;26:915–20. 218. Prasad N, Gulati S, SharmaRK, et al. Pulse cyclophosphamide therapy insteroid-dependent nephrotic syndrome. Pediatr Nephrol. 2004 ;19:494–8. 219. Gul ati S, Pokhariyal S, Sharma RK, etal. Pulse cyclophosphamide therapy in frequentlyrelapsing nephrotic syndrome. Nephrol Dial Transplant.2001;16:2013–7. 220. Ves ter U, Kranz B, Zimmermann S, etal. The response to cyclophosphamide in steroid-sensi tivenephrotic syndrome is influenced by polymorphic expressionof glutathione-S-transferases-M1 a nd P1. Pediatr Nephrol.2005;20:478–81. 221. Sha rda SV, Gulati S, Tripathi G, etal. Do gluta thione-S-transferase polymorphisms influenceresponse to intravenous cyclophosphamide therapy inidiopathic nephrotic syndrome? Pediatr Nephrol.2008;23:2001–6. 222. Scheinman JI, Stamler FW.Cyclophosphamide and fatal varicella. J Pediatr.1969;74:117–9. 223. Res nick J, Schanberger JE. Varicellareactivation in nephrotic syndrome treated with cyclophosphamide and adrenal corticosteroids. J Pediatr. 1 973;83:451–4. 224. Watson AR, Rance CP, Bain J. Long termeffects of cyclophosphamide on testicular function. BrMed J (Clin Res Ed). 1985;291:1457–60. 225. Borel JF.Mechanism of action of cyclosporin A and rationale for usein nephrotic syndrome. Clin Nephrol. 1991;35(Suppl1):S23–30.

226. Faul C, Donnelly M, Merscher-Gomez S, et al. Theactin cytoskeleton of kidney podocytes is a direct targetof the antiproteinuric effect of cyclosporine A. Nat Med.2008;14:931–8.
227. Niaudet P, Habib R. Cyclosporine in the treat ment ofidiopathic nephrosis. J Am Soc N ep hrol. 1994;5:1049–56.
228. Nia udet P, Broyer M, Habib R. Treatment of idiopathic nephrotic syndrome with cyclosporin A in children.Clin Nephrol. 1991;35(Suppl 1):S31-6.
229. Kan o K, Kyo K, Yamada Y, et al. Comparison betweenpre- and posttreatment clinical and renal biopsies inchildren receiving low dose ciclospo rine-A for 2 years forsteroid-dependent nephrotic s yn drome. Clin Nephrol.1999;52:19–24.
230. Hab ib R, Niaudet P. Comparison between pre- andposttreatment renal biopsies in children receivingciclosporine for idiopathic nephrosis. Clin Nephrol.1994;42:141–6.
231. Mahmoud I, Basuni F, Sabry A, et al. Singlecentreexperience with cyclosporin in 106 children withidiopathic focal segmental glo merulosclerosis. NephrolDial Transplant. 200 5;20:735–42.
232. Niaudet P. Comparison of cyclosporin and chlorambucilin the treatment of steroid-dependent idiopathic nephroticsyndrome: A multicentre randomized controlled trial. TheFrench Society of Paediatric Nephrology. Pediatr Nephrol.1992;6:1–3.
233. Ponticelli C, Edefonti A, Ghio L, et al. Cyclosporinversus cyclophosphamide for patients with steroiddependentand frequently relapsing idiopathic nephrotic syndrome: Amulticentre randomized controlled trial. Nephrol DialTransplant. 1993;8:1326–32.
234. Ishikura K, Yoshikawa N, Nakazato H, et al. Twoyearfollow-up of a prospective clinical trial of cyclosporinefor frequently relapsing nephrotic syndrome in children.Clin J Am Soc Nephrol. 2012;7:1576–83.
235. Iij ima K, Hamahira K, Tanaka R, et al. Risk factorsfor cyclosporine-induced tubulointerstitial lesions inchildren with minimal change nephrotic syndrome. KidneyInt. 2002;61:1801–5.
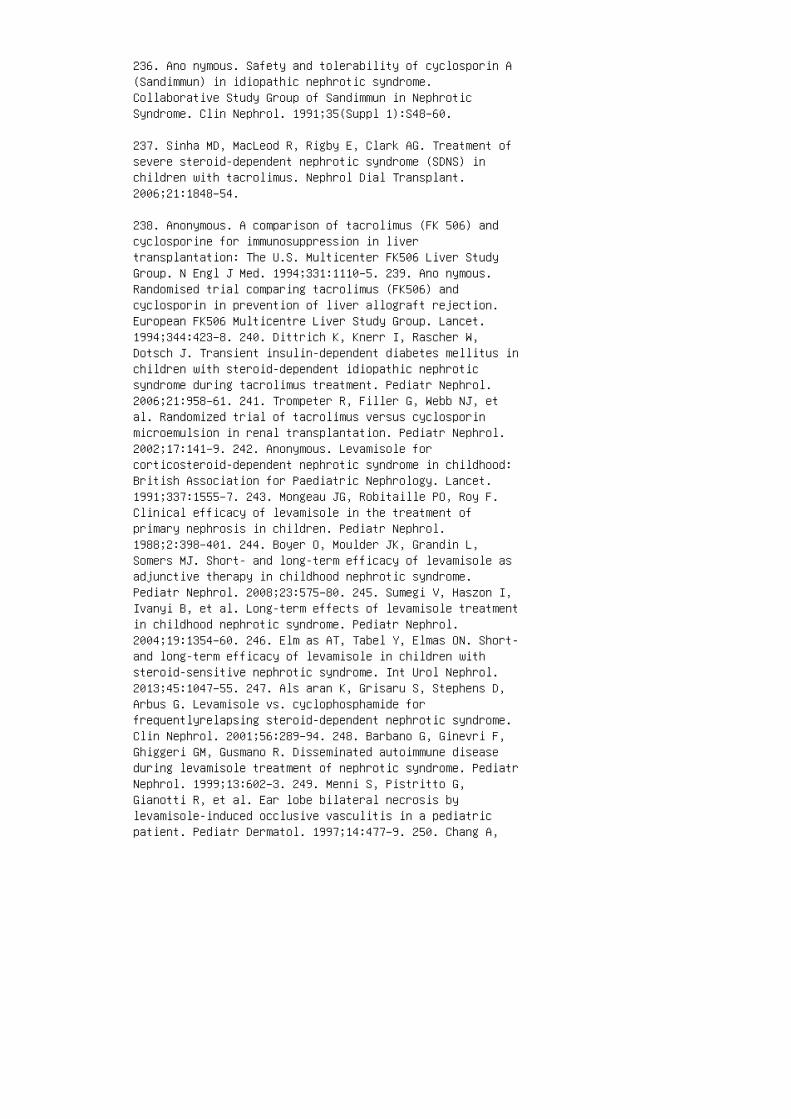
236. Ano nymous. Safety and tolerability of cyclosporin A(Sandimmun) in idiopathic nephrotic syndrome.Collaborative Study Group of Sandimmun in NephroticSyndrome. Clin Nephrol. 1991;35(Suppl 1):S48–60.
237. Sinha MD, MacLeod R, Rigby E, Clark AG. Treatment ofsevere steroid-dependent nephrotic syndrome (SDNS) inchildren with tacrolimus. Nephrol Dial Transplant.2006;21:1848–54.
238. Anonymous. A comparison of tacrolimus (FK 506) andcyclosporine for immunosuppression in livertransplantation: The U.S. Multicenter FK506 Liver StudyGroup. N Engl J Med. 1994;331:1110–5. 239. Ano nymous.Randomised trial comparing tacrolimus (FK506) andcyclosporin in prevention of liver allograft rejection.European FK506 Multicentre Liver Study Group. Lancet.1994;344:423–8. 240. Dittrich K, Knerr I, Rascher W,Dotsch J. Transient insulin-dependent diabetes mellitus inchildren with steroid-dependent idiopathic nephroticsyndrome during tacrolimus treatment. Pediatr Nephrol.2006;21:958–61. 241. Trompeter R, Filler G, Webb NJ, etal. Randomized trial of tacrolimus versus cyclosporinmicroemulsion in renal transplantation. Pediatr Nephrol.2002;17:141–9. 242. Anonymous. Levamisole forcorticosteroid-dependent nephrotic syndrome in childhood:British Association for Paediatric Nephrology. Lancet.1991;337:1555–7. 243. Mongeau JG, Robitaille PO, Roy F.Clinical efficacy of levamisole in the treatment ofprimary nephrosis in children. Pediatr Nephrol.1988;2:398–401. 244. Boyer O, Moulder JK, Grandin L,Somers MJ. Short- and long-term efficacy of levamisole asadjunctive therapy in childhood nephrotic syndrome.Pediatr Nephrol. 2008;23:575–80. 245. Sumegi V, Haszon I,Ivanyi B, et al. Long-term effects of levamisole treatmentin childhood nephrotic syndrome. Pediatr Nephrol.2004;19:1354–60. 246. Elm as AT, Tabel Y, Elmas ON. Short-and long-term efficacy of levamisole in children withsteroid-sensitive nephrotic syndrome. Int Urol Nephrol.2013;45:1047–55. 247. Als aran K, Grisaru S, Stephens D,Arbus G. Levamisole vs. cyclophosphamide forfrequentlyrelapsing steroid-dependent nephrotic syndrome.Clin Nephrol. 2001;56:289–94. 248. Barbano G, Ginevri F,Ghiggeri GM, Gusmano R. Disseminated autoimmune diseaseduring levamisole treatment of nephrotic syndrome. PediatrNephrol. 1999;13:602–3. 249. Menni S, Pistritto G,Gianotti R, et al. Ear lobe bilateral necrosis bylevamisole-induced occlusive vasculitis in a pediatricpatient. Pediatr Dermatol. 1997;14:477–9. 250. Chang A,
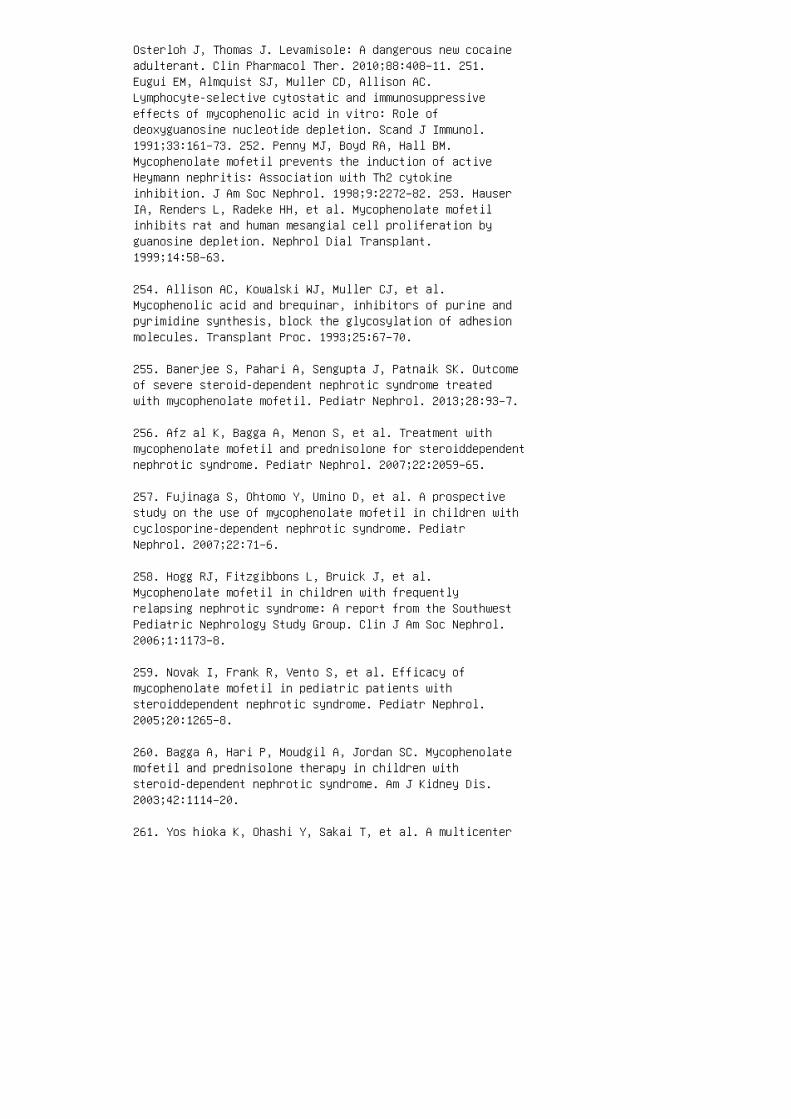
Osterloh J, Thomas J. Levamisole: A dangerous new cocaineadulterant. Clin Pharmacol Ther. 2010;88:408–11. 251.Eugui EM, Almquist SJ, Muller CD, Allison AC.Lymphocyte-selective cytostatic and immunosuppressiveeffects of mycophenolic acid in vitro: Role ofdeoxyguanosine nucleotide depletion. Scand J Immunol.1991;33:161–73. 252. Penny MJ, Boyd RA, Hall BM.Mycophenolate mofetil prevents the induction of activeHeymann nephritis: Association with Th2 cytokineinhibition. J Am Soc Nephrol. 1998;9:2272–82. 253. HauserIA, Renders L, Radeke HH, et al. Mycophenolate mofetilinhibits rat and human mesangial cell proliferation byguanosine depletion. Nephrol Dial Transplant.1999;14:58–63.
254. Allison AC, Kowalski WJ, Muller CJ, et al.Mycophenolic acid and brequinar, inhibitors of purine andpyrimidine synthesis, block the glycosylation of adhesionmolecules. Transplant Proc. 1993;25:67–70.
255. Banerjee S, Pahari A, Sengupta J, Patnaik SK. Outcomeof severe steroid-dependent nephrotic syndrome treatedwith mycophenolate mofetil. Pediatr Nephrol. 2013;28:93–7.
256. Afz al K, Bagga A, Menon S, et al. Treatment withmycophenolate mofetil and prednisolone for steroiddependentnephrotic syndrome. Pediatr Nephrol. 2007;22:2059–65.
257. Fujinaga S, Ohtomo Y, Umino D, et al. A prospectivestudy on the use of mycophenolate mofetil in children withcyclosporine-dependent nephrotic syndrome. PediatrNephrol. 2007;22:71–6.
258. Hogg RJ, Fitzgibbons L, Bruick J, et al.Mycophenolate mofetil in children with frequentlyrelapsing nephrotic syndrome: A report from the SouthwestPediatric Nephrology Study Group. Clin J Am Soc Nephrol.2006;1:1173–8.
259. Novak I, Frank R, Vento S, et al. Efficacy ofmycophenolate mofetil in pediatric patients withsteroiddependent nephrotic syndrome. Pediatr Nephrol.2005;20:1265–8.
260. Bagga A, Hari P, Moudgil A, Jordan SC. Mycophenolatemofetil and prednisolone therapy in children withsteroid-dependent nephrotic syndrome. Am J Kidney Dis.2003;42:1114–20.
261. Yos hioka K, Ohashi Y, Sakai T, et al. A multicenter
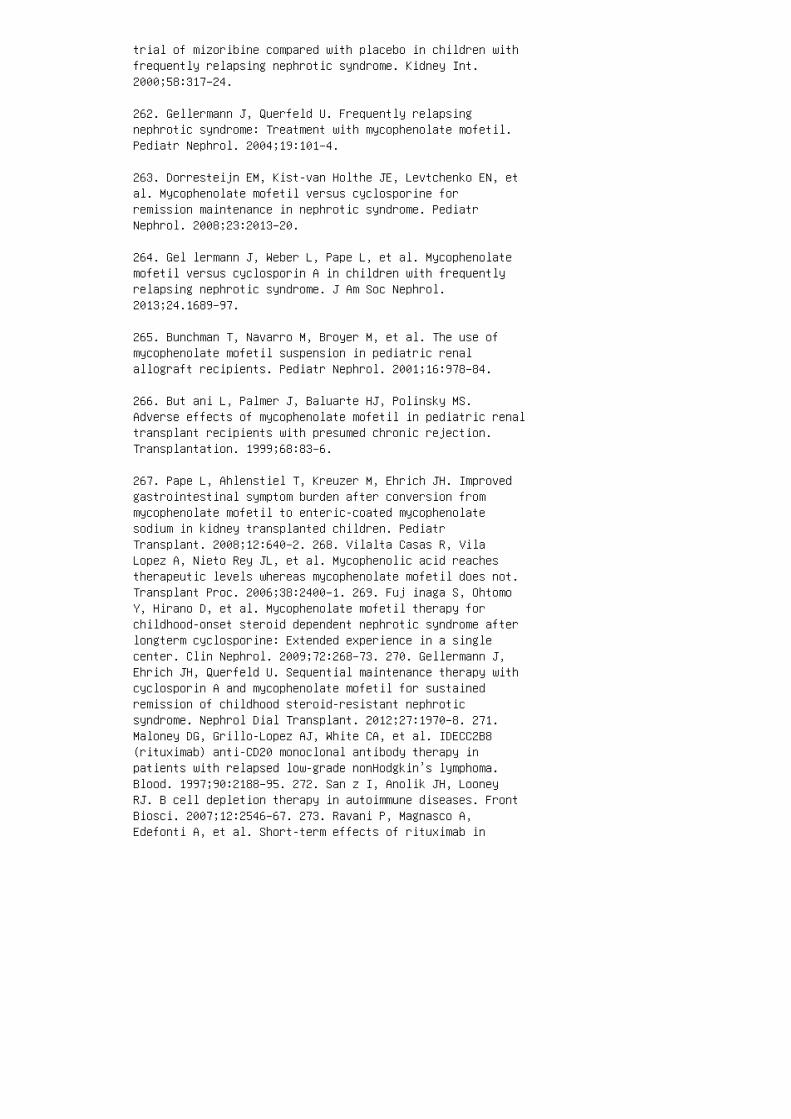
trial of mizoribine compared with placebo in children withfrequently relapsing nephrotic syndrome. Kidney Int.2000;58:317–24.
262. Gellermann J, Querfeld U. Frequently relapsingnephrotic syndrome: Treatment with mycophenolate mofetil.Pediatr Nephrol. 2004;19:101–4.
263. Dorresteijn EM, Kist-van Holthe JE, Levtchenko EN, etal. Mycophenolate mofetil versus cyclosporine forremission maintenance in nephrotic syndrome. PediatrNephrol. 2008;23:2013–20.
264. Gel lermann J, Weber L, Pape L, et al. Mycophenolatemofetil versus cyclosporin A in children with frequentlyrelapsing nephrotic syndrome. J Am Soc Nephrol.2013;24.1689–97.
265. Bunchman T, Navarro M, Broyer M, et al. The use ofmycophenolate mofetil suspension in pediatric renalallograft recipients. Pediatr Nephrol. 2001;16:978–84.
266. But ani L, Palmer J, Baluarte HJ, Polinsky MS.Adverse effects of mycophenolate mofetil in pediatric renaltransplant recipients with presumed chronic rejection.Transplantation. 1999;68:83–6.
267. Pape L, Ahlenstiel T, Kreuzer M, Ehrich JH. Improvedgastrointestinal symptom burden after conversion frommycophenolate mofetil to enteric-coated mycophenolatesodium in kidney transplanted children. PediatrTransplant. 2008;12:640–2. 268. Vilalta Casas R, VilaLopez A, Nieto Rey JL, et al. Mycophenolic acid reachestherapeutic levels whereas mycophenolate mofetil does not.Transplant Proc. 2006;38:2400–1. 269. Fuj inaga S, OhtomoY, Hirano D, et al. Mycophenolate mofetil therapy forchildhood-onset steroid dependent nephrotic syndrome afterlongterm cyclosporine: Extended experience in a singlecenter. Clin Nephrol. 2009;72:268–73. 270. Gellermann J,Ehrich JH, Querfeld U. Sequential maintenance therapy withcyclosporin A and mycophenolate mofetil for sustainedremission of childhood steroid-resistant nephroticsyndrome. Nephrol Dial Transplant. 2012;27:1970–8. 271.Maloney DG, Grillo-Lopez AJ, White CA, et al. IDECC2B8(rituximab) anti-CD20 monoclonal antibody therapy inpatients with relapsed low-grade nonHodgkin’s lymphoma.Blood. 1997;90:2188–95. 272. San z I, Anolik JH, LooneyRJ. B cell depletion therapy in autoimmune diseases. FrontBiosci. 2007;12:2546–67. 273. Ravani P, Magnasco A,Edefonti A, et al. Short-term effects of rituximab in
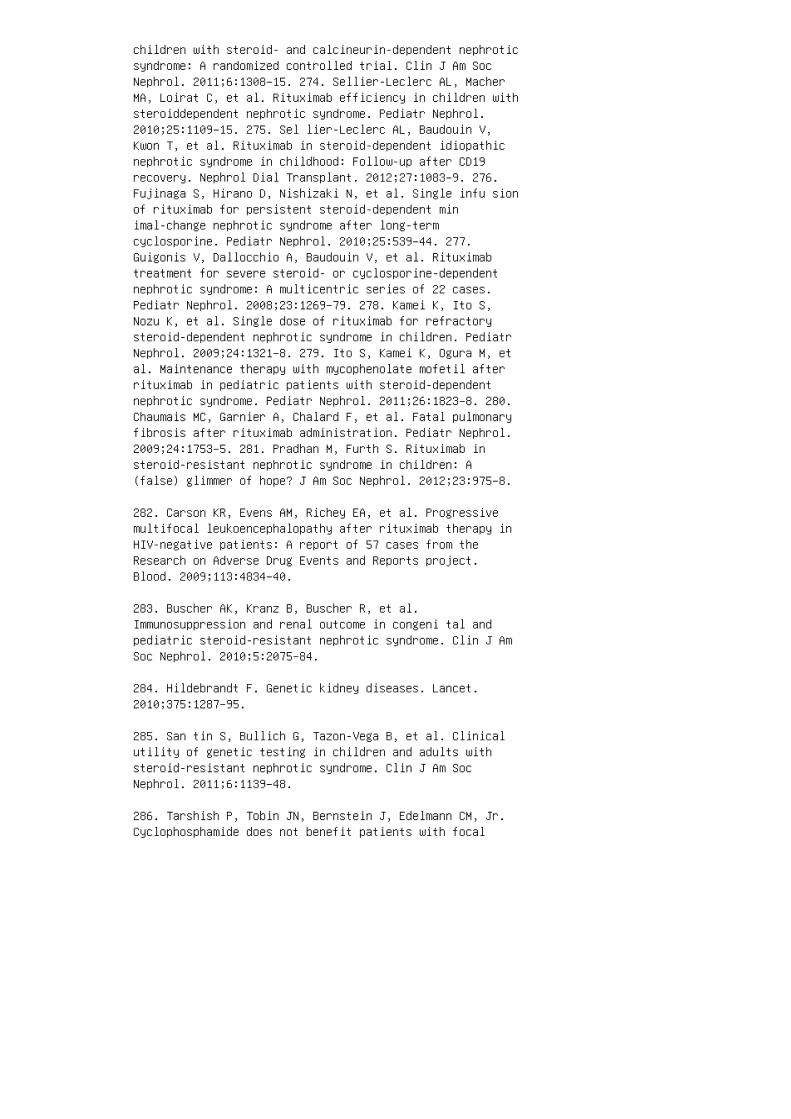
children with steroid- and calcineurin-dependent nephroticsyndrome: A randomized controlled trial. Clin J Am SocNephrol. 2011;6:1308–15. 274. Sellier-Leclerc AL, MacherMA, Loirat C, et al. Rituximab efficiency in children withsteroiddependent nephrotic syndrome. Pediatr Nephrol.2010;25:1109–15. 275. Sel lier-Leclerc AL, Baudouin V,Kwon T, et al. Rituximab in steroid-dependent idiopathicnephrotic syndrome in childhood: Follow-up after CD19recovery. Nephrol Dial Transplant. 2012;27:1083–9. 276.Fujinaga S, Hirano D, Nishizaki N, et al. Single infu sionof rituximab for persistent steroid-dependent minimal-change nephrotic syndrome after long-termcyclosporine. Pediatr Nephrol. 2010;25:539–44. 277.Guigonis V, Dallocchio A, Baudouin V, et al. Rituximabtreatment for severe steroid- or cyclosporine-dependentnephrotic syndrome: A multicentric series of 22 cases.Pediatr Nephrol. 2008;23:1269–79. 278. Kamei K, Ito S,Nozu K, et al. Single dose of rituximab for refractorysteroid-dependent nephrotic syndrome in children. PediatrNephrol. 2009;24:1321–8. 279. Ito S, Kamei K, Ogura M, etal. Maintenance therapy with mycophenolate mofetil afterrituximab in pediatric patients with steroid-dependentnephrotic syndrome. Pediatr Nephrol. 2011;26:1823–8. 280.Chaumais MC, Garnier A, Chalard F, et al. Fatal pulmonaryfibrosis after rituximab administration. Pediatr Nephrol.2009;24:1753–5. 281. Pradhan M, Furth S. Rituximab insteroid-resistant nephrotic syndrome in children: A(false) glimmer of hope? J Am Soc Nephrol. 2012;23:975–8.
282. Carson KR, Evens AM, Richey EA, et al. Progressivemultifocal leukoencephalopathy after rituximab therapy inHIV-negative patients: A report of 57 cases from theResearch on Adverse Drug Events and Reports project.Blood. 2009;113:4834–40.
283. Buscher AK, Kranz B, Buscher R, et al.Immunosuppression and renal outcome in congeni tal andpediatric steroid-resistant nephrotic syndrome. Clin J AmSoc Nephrol. 2010;5:2075–84.
284. Hildebrandt F. Genetic kidney diseases. Lancet.2010;375:1287–95.
285. San tin S, Bullich G, Tazon-Vega B, et al. Clinicalutility of genetic testing in children and adults withsteroid-resistant nephrotic syndrome. Clin J Am SocNephrol. 2011;6:1139–48.
286. Tarshish P, Tobin JN, Bernstein J, Edelmann CM, Jr.Cyclophosphamide does not benefit patients with focal

segmental glomerulosclerosis: A report of theInternational Study of Kidney Disease in Children. PediatrNephrol. 1996;10:590–3.
287. Straatmann C, Ayoob R, Gbadegesin R, et al. Treatmentoutcome of late steroid-resistant nephrotic syndrome: Astudy by the Midwest Pediatric Nephrology Consortium.Pediatr Nephrol. 2013;28:1235–41.
288. Abrantes MM, Cardoso LS, Lima EM, et al. Predictivefactors of chronic kidney disease in primary focalsegmental glomerulosclerosis. Pediatr Nephrol.2006;21:1003–12.
289. Gip son DS, Chin H, Presler TP, et al. Differentialrisk of remission and ESRD in childhood FSGS. PediatrNephrol. 2006;21:344–9.
290. Troyanov S, Wall CA, Miller JA, et al. Focal andsegmental glomerulosclerosis: Definition and relevance ofa partial remission. J Am Soc Nephrol. 2005;16:1061–8.
291. Rhe ault MN, Wei CC, Hains DS, et al. Increasingfrequency of acute kidney injury amongst childrenhospitalized with nephrotic syndrome. Pediatr Nephrol.2014;29:139–47.
292. Haws RM, Baum M. Efficacy of albumin and diuretictherapy in children with nephrotic syndrome. Pediatrics.1993;91:1142–6.
293. Bagga A, Mudigoudar BD, Hari P, Vasudev V. Enalaprildosage in steroid-resistant nephrotic syndrome. PediatrNephrol. 2004;19:45–50.
294. Ellis D, Vats A, Moritz ML, et al. Long-termantiproteinuric and renoprotective efficacy and safety oflosartan in children with proteinuria. J Pediatr.2003;143:89–97.
295. Montane B, Abitbol C, Chandar J, et al. Novel therapyof focal glomerulosclerosis with mycophenolate andangiotensin blockade. Pediatr Nephrol. 2003;18:772–7.
296. Ame rican Academy of Pediatrics. Immunocompromisedchildren. In: Pickering LK, Baker CJ, Kimberlin DW,editors. Red Book: Report of the Committee on InfectiousDiseases, 29th ed. Elk Grove Village, IL: American Academyof Pediatrics; 2012. p. 74–90. 297. Close GC, Houston IB.Fatal haemorrhagic chickenpox in a child on long-term
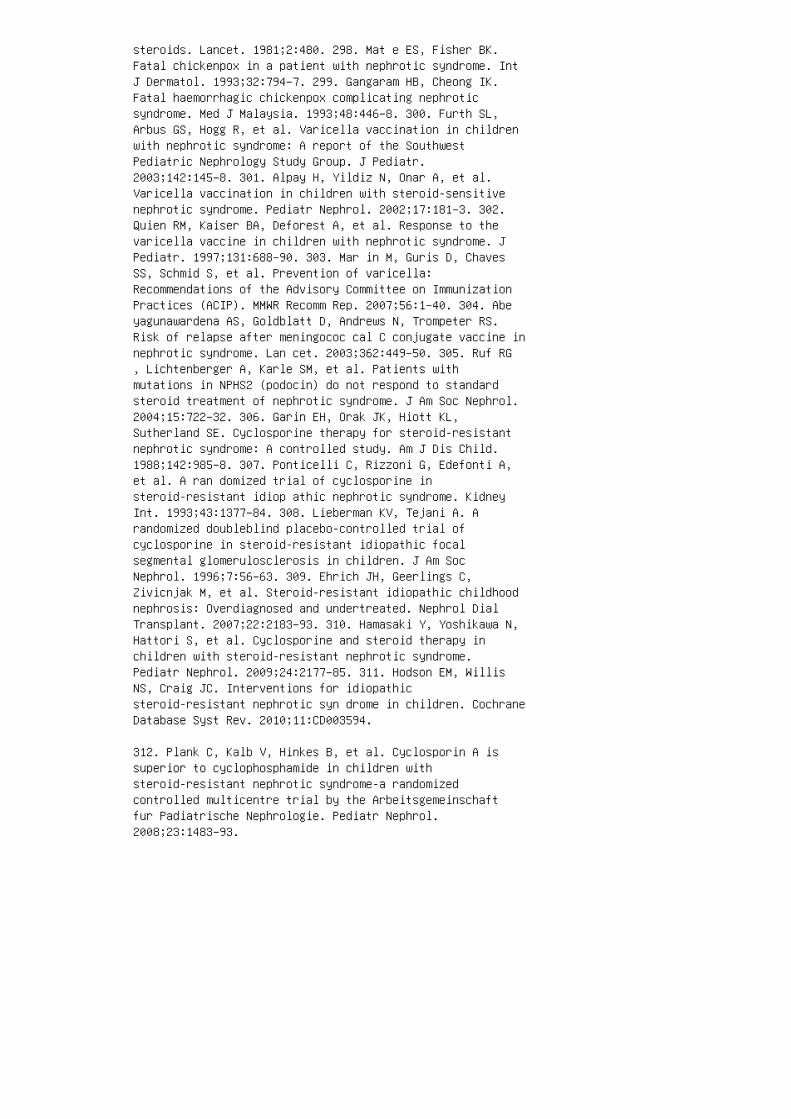
steroids. Lancet. 1981;2:480. 298. Mat e ES, Fisher BK.Fatal chickenpox in a patient with nephrotic syndrome. IntJ Dermatol. 1993;32:794–7. 299. Gangaram HB, Cheong IK.Fatal haemorrhagic chickenpox complicating nephroticsyndrome. Med J Malaysia. 1993;48:446–8. 300. Furth SL,Arbus GS, Hogg R, et al. Varicella vaccination in childrenwith nephrotic syndrome: A report of the SouthwestPediatric Nephrology Study Group. J Pediatr.2003;142:145–8. 301. Alpay H, Yildiz N, Onar A, et al.Varicella vaccination in children with steroid-sensitivenephrotic syndrome. Pediatr Nephrol. 2002;17:181–3. 302.Quien RM, Kaiser BA, Deforest A, et al. Response to thevaricella vaccine in children with nephrotic syndrome. JPediatr. 1997;131:688–90. 303. Mar in M, Guris D, ChavesSS, Schmid S, et al. Prevention of varicella:Recommendations of the Advisory Committee on ImmunizationPractices (ACIP). MMWR Recomm Rep. 2007;56:1–40. 304. Abeyagunawardena AS, Goldblatt D, Andrews N, Trompeter RS.Risk of relapse after meningococ cal C conjugate vaccine innephrotic syndrome. Lan cet. 2003;362:449–50. 305. Ruf RG, Lichtenberger A, Karle SM, et al. Patients withmutations in NPHS2 (podocin) do not respond to standardsteroid treatment of nephrotic syndrome. J Am Soc Nephrol.2004;15:722–32. 306. Garin EH, Orak JK, Hiott KL,Sutherland SE. Cyclosporine therapy for steroid-resistantnephrotic syndrome: A controlled study. Am J Dis Child.1988;142:985–8. 307. Ponticelli C, Rizzoni G, Edefonti A,et al. A ran domized trial of cyclosporine insteroid-resistant idiop athic nephrotic syndrome. KidneyInt. 1993;43:1377–84. 308. Lieberman KV, Tejani A. Arandomized doubleblind placebo-controlled trial ofcyclosporine in steroid-resistant idiopathic focalsegmental glomerulosclerosis in children. J Am SocNephrol. 1996;7:56–63. 309. Ehrich JH, Geerlings C,Zivicnjak M, et al. Steroid-resistant idiopathic childhoodnephrosis: Overdiagnosed and undertreated. Nephrol DialTransplant. 2007;22:2183–93. 310. Hamasaki Y, Yoshikawa N,Hattori S, et al. Cyclosporine and steroid therapy inchildren with steroid-resistant nephrotic syndrome.Pediatr Nephrol. 2009;24:2177–85. 311. Hodson EM, WillisNS, Craig JC. Interventions for idiopathicsteroid-resistant nephrotic syn drome in children. CochraneDatabase Syst Rev. 2010;11:CD003594.
312. Plank C, Kalb V, Hinkes B, et al. Cyclosporin A issuperior to cyclophosphamide in children withsteroid-resistant nephrotic syndrome-a randomizedcontrolled multicentre trial by the Arbeitsgemeinschaftfur Padiatrische Nephrologie. Pediatr Nephrol.2008;23:1483–93.
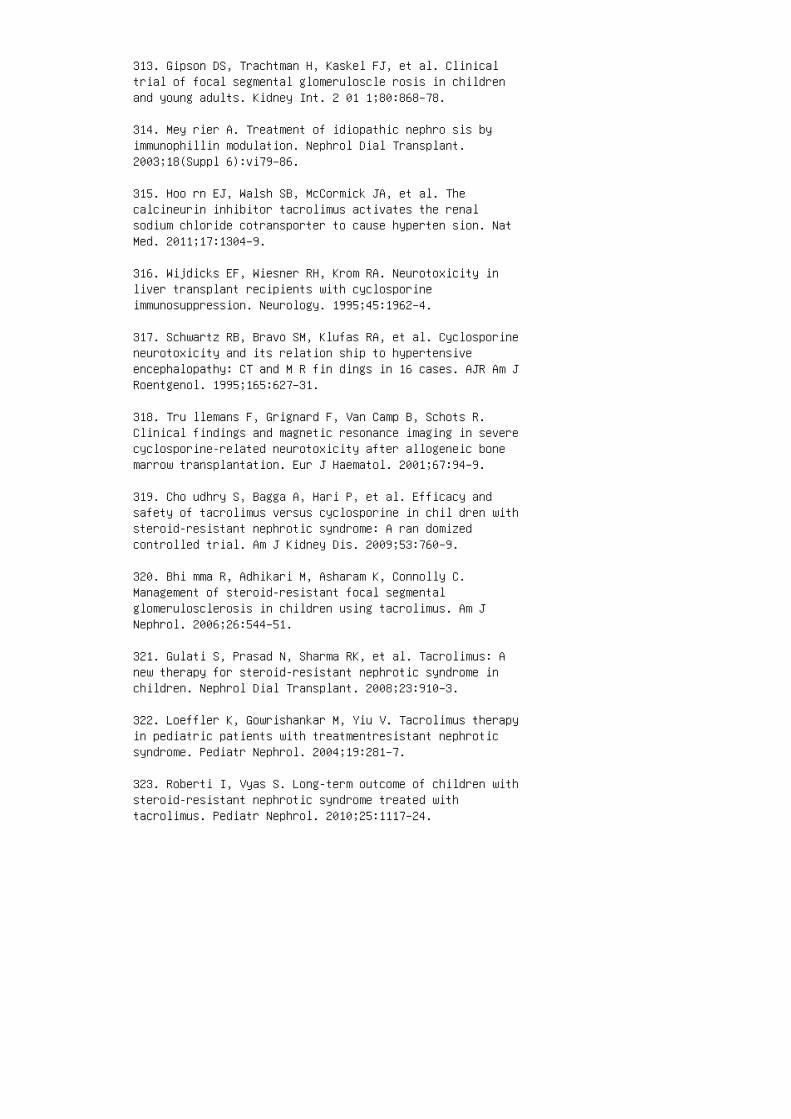
313. Gipson DS, Trachtman H, Kaskel FJ, et al. Clinicaltrial of focal segmental glomeruloscle rosis in childrenand young adults. Kidney Int. 2 01 1;80:868–78.
314. Mey rier A. Treatment of idiopathic nephro sis byimmunophillin modulation. Nephrol Dial Transplant.2003;18(Suppl 6):vi79–86.
315. Hoo rn EJ, Walsh SB, McCormick JA, et al. Thecalcineurin inhibitor tacrolimus activates the renalsodium chloride cotransporter to cause hyperten sion. NatMed. 2011;17:1304–9.
316. Wijdicks EF, Wiesner RH, Krom RA. Neurotoxicity inliver transplant recipients with cyclosporineimmunosuppression. Neurology. 1995;45:1962–4.
317. Schwartz RB, Bravo SM, Klufas RA, et al. Cyclosporineneurotoxicity and its relation ship to hypertensiveencephalopathy: CT and M R fin dings in 16 cases. AJR Am JRoentgenol. 1995;165:627–31.
318. Tru llemans F, Grignard F, Van Camp B, Schots R.Clinical findings and magnetic resonance imaging in severecyclosporine-related neurotoxicity after allogeneic bonemarrow transplantation. Eur J Haematol. 2001;67:94–9.
319. Cho udhry S, Bagga A, Hari P, et al. Efficacy andsafety of tacrolimus versus cyclosporine in chil dren withsteroid-resistant nephrotic syndrome: A ran domizedcontrolled trial. Am J Kidney Dis. 2009;53:760–9.
320. Bhi mma R, Adhikari M, Asharam K, Connolly C.Management of steroid-resistant focal segmentalglomerulosclerosis in children using tacrolimus. Am JNephrol. 2006;26:544–51.
321. Gulati S, Prasad N, Sharma RK, et al. Tacrolimus: Anew therapy for steroid-resistant nephrotic syndrome inchildren. Nephrol Dial Transplant. 2008;23:910–3.
322. Loeffler K, Gowrishankar M, Yiu V. Tacrolimus therapyin pediatric patients with treatmentresistant nephroticsyndrome. Pediatr Nephrol. 2004;19:281–7.
323. Roberti I, Vyas S. Long-term outcome of children withsteroid-resistant nephrotic syndrome treated withtacrolimus. Pediatr Nephrol. 2010;25:1117–24.

324. Wang W, Xia Y, Mao J, et al. Treatment of tacro limusor cyclosporine A in children with idiopathic nephroticsyndrome. Pediatr Nephrol. 2 01 2;27:2073–9.
325. Butani L, Ramsamooj R. Experience with tacroli mus inchildren with steroid-resistant nephrotic syn drome.Pediatr Nephrol. 2009;24:1517–23. 326. de Me llo VR,Rodrigues MT, Mastrocinque TH, et al. Mycophenolatemofetil in children withsteroid/cyclophosphamide-resistant nephrotic syndrome.Pediatr Nephrol. 2010;25:453–60. 327. Li Z, Duan C, He J,et al. Mycophenolate mofetil therapy for children withsteroid-resistant nephrotic syndrome. Pediatr Nephrol.2010;25:883–8. 328. Cat tran DC, Wang MM, Appel G, et al.Mycophenolate mofetil in the treatment of focal segmentalglomerulosclerosis. Clin Nephrol. 2004;62:405–11. 329.Segarra Medrano A, Vila Presas J, Pou Clave L, et al.Efficacy and safety of combined cyclosporin A andmycophenolate mofetil therapy in patients withcyclosporin-resistant focal segmental glo merulosclerosis.Nefrologia. 2011;31:286–91. 330. Kemper MJ, Altrogge H,Ganschow R, MullerWiefel DE. Serum levels ofimmunoglobulins and IgG subclasses in steroid sensitivenephrotic syndrome. Pediatr Nephrol. 2002;17:413–7. 331.Val lerskog T, Gunnarsson I, Widhe M, et al. Treatmentwith rituximab affects both the cellular and the humoralarm of the immune system in patients with SLE. ClinImmunol. 2007;122:62–74. 332. Bru neau S, Dantal J. Newinsights into the patho physiology of idiopathic nephroticsyndrome. Clin Imm unol. 2009;133:13–21. 333. For noni A,Sageshima J, Wei C, et al. Rituximab targets podocytes inrecurrent focal segmental glomerulosclerosis. Sci TranslMed. 2011;3:85ra46. 334. Chan AC. Rituximab’s newtherapeutic target: The podocyte actin cytoskeleton. SciTransl Med. 2011;3:85ps21. 335. Ala chkar N, Wei C, ArendLJ, et al. Podocyte effacement closely links to suPARlevels at time of posttransplantation focal segmentalglomerulo sclerosis occurrence and improves with therapy.T ra nsplantation. 2013;96:649–56. 336. Van csa A, SzaboZ, Szamosi S, et al. Long-term effects of rituximab on Bcell counts and autoan tibody production in rheumatoidarthritis: Use of hig h-sensitivity flow cytometry formore sensitive assessment of B cell depletion. J Rheumatol.2 013 ;40:565–71. 337. Fernandez-Fresnedo G, Segarra A,Gonzalez E, et al. Rituximab treatment of adult patientswith steroid-resistant focal segmental glomerulosclerosis. Clin J Am Soc Nephrol. 2009;4:1317–23. 338. PetersHP, van de Kar NC, Wetzels JF. Rituximab in minimal changenephropathy and focal segmental glomerulosclerosis: Reportof four cases and review of the literature. Neth J Med.
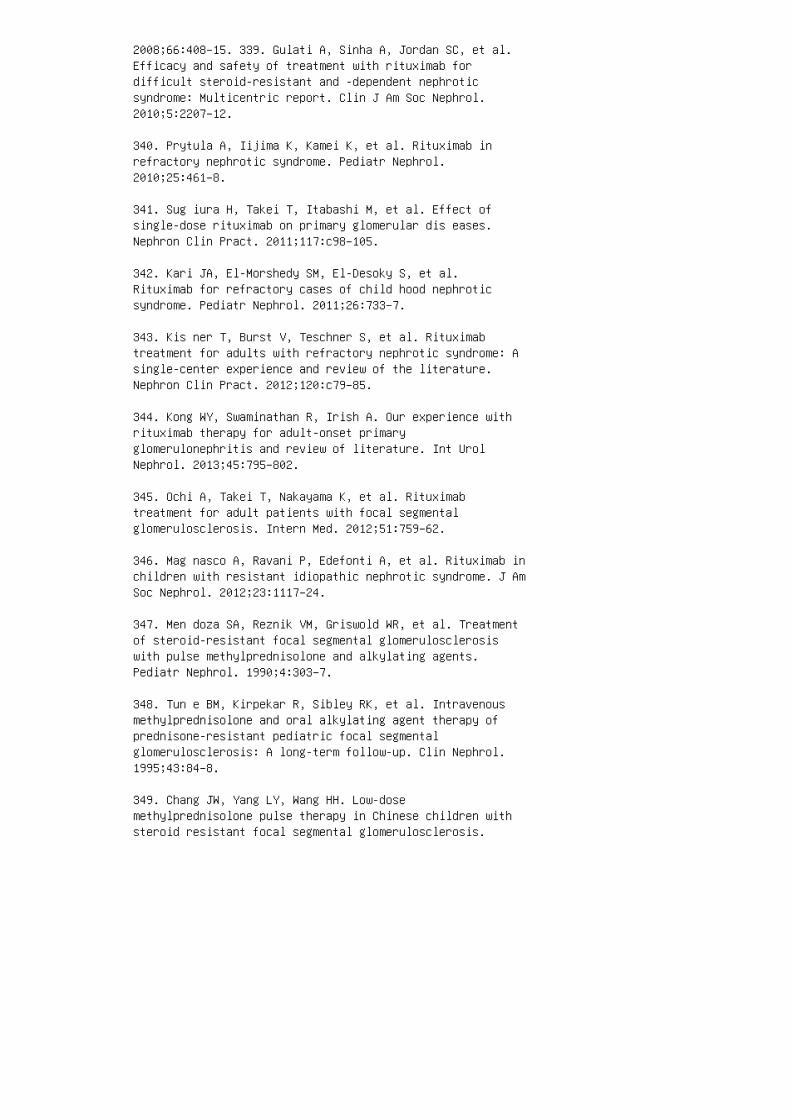
2008;66:408–15. 339. Gulati A, Sinha A, Jordan SC, et al.Efficacy and safety of treatment with rituximab fordifficult steroid-resistant and -dependent nephroticsyndrome: Multicentric report. Clin J Am Soc Nephrol.2010;5:2207–12.
340. Prytula A, Iijima K, Kamei K, et al. Rituximab inrefractory nephrotic syndrome. Pediatr Nephrol.2010;25:461–8.
341. Sug iura H, Takei T, Itabashi M, et al. Effect ofsingle-dose rituximab on primary glomerular dis eases.Nephron Clin Pract. 2011;117:c98–105.
342. Kari JA, El-Morshedy SM, El-Desoky S, et al.Rituximab for refractory cases of child hood nephroticsyndrome. Pediatr Nephrol. 2011;26:733–7.
343. Kis ner T, Burst V, Teschner S, et al. Rituximabtreatment for adults with refractory nephrotic syndrome: Asingle-center experience and review of the literature.Nephron Clin Pract. 2012;120:c79–85.
344. Kong WY, Swaminathan R, Irish A. Our experience withrituximab therapy for adult-onset primaryglomerulonephritis and review of literature. Int UrolNephrol. 2013;45:795–802.
345. Ochi A, Takei T, Nakayama K, et al. Rituximabtreatment for adult patients with focal segmentalglomerulosclerosis. Intern Med. 2012;51:759–62.
346. Mag nasco A, Ravani P, Edefonti A, et al. Rituximab inchildren with resistant idiopathic nephrotic syndrome. J AmSoc Nephrol. 2012;23:1117–24.
347. Men doza SA, Reznik VM, Griswold WR, et al. Treatmentof steroid-resistant focal segmental glomerulosclerosiswith pulse methylprednisolone and alkylating agents.Pediatr Nephrol. 1990;4:303–7.
348. Tun e BM, Kirpekar R, Sibley RK, et al. Intravenousmethylprednisolone and oral alkylating agent therapy ofprednisone-resistant pediatric focal segmentalglomerulosclerosis: A long-term follow-up. Clin Nephrol.1995;43:84–8.
349. Chang JW, Yang LY, Wang HH. Low-dosemethylprednisolone pulse therapy in Chinese children withsteroid resistant focal segmental glomerulosclerosis.
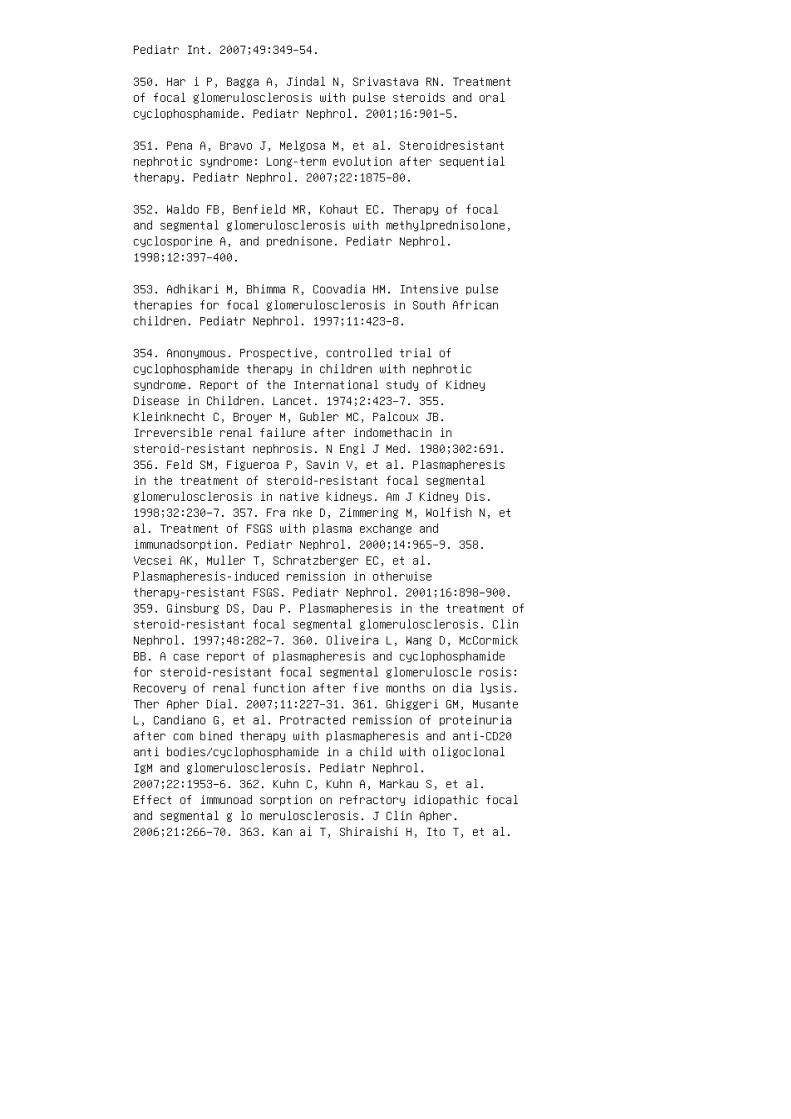
Pediatr Int. 2007;49:349–54.
350. Har i P, Bagga A, Jindal N, Srivastava RN. Treatmentof focal glomerulosclerosis with pulse steroids and oralcyclophosphamide. Pediatr Nephrol. 2001;16:901–5.
351. Pena A, Bravo J, Melgosa M, et al. Steroidresistantnephrotic syndrome: Long-term evolution after sequentialtherapy. Pediatr Nephrol. 2007;22:1875–80.
352. Waldo FB, Benfield MR, Kohaut EC. Therapy of focaland segmental glomerulosclerosis with methylprednisolone,cyclosporine A, and prednisone. Pediatr Nephrol.1998;12:397–400.
353. Adhikari M, Bhimma R, Coovadia HM. Intensive pulsetherapies for focal glomerulosclerosis in South Africanchildren. Pediatr Nephrol. 1997;11:423–8.
354. Anonymous. Prospective, controlled trial ofcyclophosphamide therapy in children with nephroticsyndrome. Report of the International study of KidneyDisease in Children. Lancet. 1974;2:423–7. 355.Kleinknecht C, Broyer M, Gubler MC, Palcoux JB.Irreversible renal failure after indomethacin insteroid-resistant nephrosis. N Engl J Med. 1980;302:691.356. Feld SM, Figueroa P, Savin V, et al. Plasmapheresisin the treatment of steroid-resistant focal segmentalglomerulosclerosis in native kidneys. Am J Kidney Dis.1998;32:230–7. 357. Fra nke D, Zimmering M, Wolfish N, etal. Treatment of FSGS with plasma exchange andimmunadsorption. Pediatr Nephrol. 2000;14:965–9. 358.Vecsei AK, Muller T, Schratzberger EC, et al.Plasmapheresis-induced remission in otherwisetherapy-resistant FSGS. Pediatr Nephrol. 2001;16:898–900.359. Ginsburg DS, Dau P. Plasmapheresis in the treatment ofsteroid-resistant focal segmental glomerulosclerosis. ClinNephrol. 1997;48:282–7. 360. Oliveira L, Wang D, McCormickBB. A case report of plasmapheresis and cyclophosphamidefor steroid-resistant focal segmental glomeruloscle rosis:Recovery of renal function after five months on dia lysis.Ther Apher Dial. 2007;11:227–31. 361. Ghiggeri GM, MusanteL, Candiano G, et al. Protracted remission of proteinuriaafter com bined therapy with plasmapheresis and anti-CD20anti bodies/cyclophosphamide in a child with oligoclonalIgM and glomerulosclerosis. Pediatr Nephrol.2007;22:1953–6. 362. Kuhn C, Kuhn A, Markau S, et al.Effect of immunoad sorption on refractory idiopathic focaland segmental g lo merulosclerosis. J Clin Apher.2006;21:266–70. 363. Kan ai T, Shiraishi H, Ito T, et al.
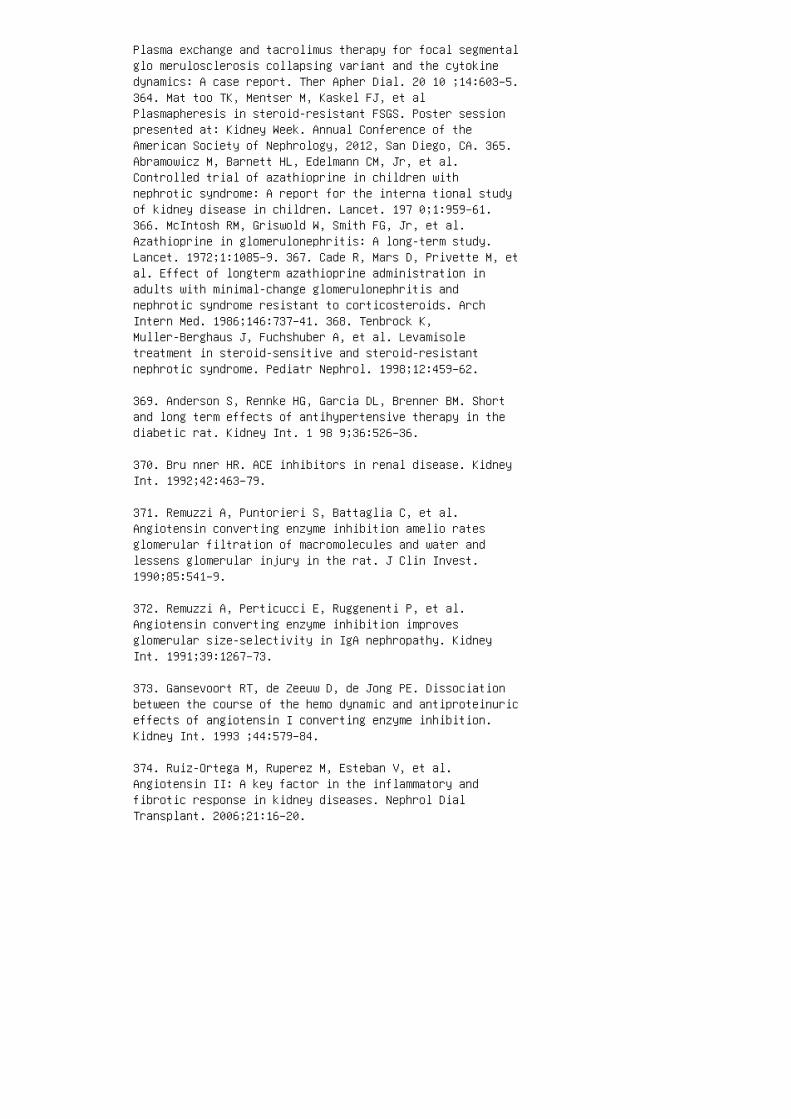
Plasma exchange and tacrolimus therapy for focal segmentalglo merulosclerosis collapsing variant and the cytokinedynamics: A case report. Ther Apher Dial. 20 10 ;14:603–5.364. Mat too TK, Mentser M, Kaskel FJ, et alPlasmapheresis in steroid-resistant FSGS. Poster sessionpresented at: Kidney Week. Annual Conference of theAmerican Society of Nephrology, 2012, San Diego, CA. 365.Abramowicz M, Barnett HL, Edelmann CM, Jr, et al.Controlled trial of azathioprine in children withnephrotic syndrome: A report for the interna tional studyof kidney disease in children. Lancet. 197 0;1:959–61.366. McIntosh RM, Griswold W, Smith FG, Jr, et al.Azathioprine in glomerulonephritis: A long-term study.Lancet. 1972;1:1085–9. 367. Cade R, Mars D, Privette M, etal. Effect of longterm azathioprine administration inadults with minimal-change glomerulonephritis andnephrotic syndrome resistant to corticosteroids. ArchIntern Med. 1986;146:737–41. 368. Tenbrock K,Muller-Berghaus J, Fuchshuber A, et al. Levamisoletreatment in steroid-sensitive and steroid-resistantnephrotic syndrome. Pediatr Nephrol. 1998;12:459–62.
369. Anderson S, Rennke HG, Garcia DL, Brenner BM. Shortand long term effects of antihypertensive therapy in thediabetic rat. Kidney Int. 1 98 9;36:526–36.
370. Bru nner HR. ACE inhibitors in renal disease. KidneyInt. 1992;42:463–79.
371. Remuzzi A, Puntorieri S, Battaglia C, et al.Angiotensin converting enzyme inhibition amelio ratesglomerular filtration of macromolecules and water andlessens glomerular injury in the rat. J Clin Invest.1990;85:541–9.
372. Remuzzi A, Perticucci E, Ruggenenti P, et al.Angiotensin converting enzyme inhibition improvesglomerular size-selectivity in IgA nephropathy. KidneyInt. 1991;39:1267–73.
373. Gansevoort RT, de Zeeuw D, de Jong PE. Dissociationbetween the course of the hemo dynamic and antiproteinuriceffects of angiotensin I converting enzyme inhibition.Kidney Int. 1993 ;44:579–84.
374. Ruiz-Ortega M, Ruperez M, Esteban V, et al.Angiotensin II: A key factor in the inflammatory andfibrotic response in kidney diseases. Nephrol DialTransplant. 2006;21:16–20.
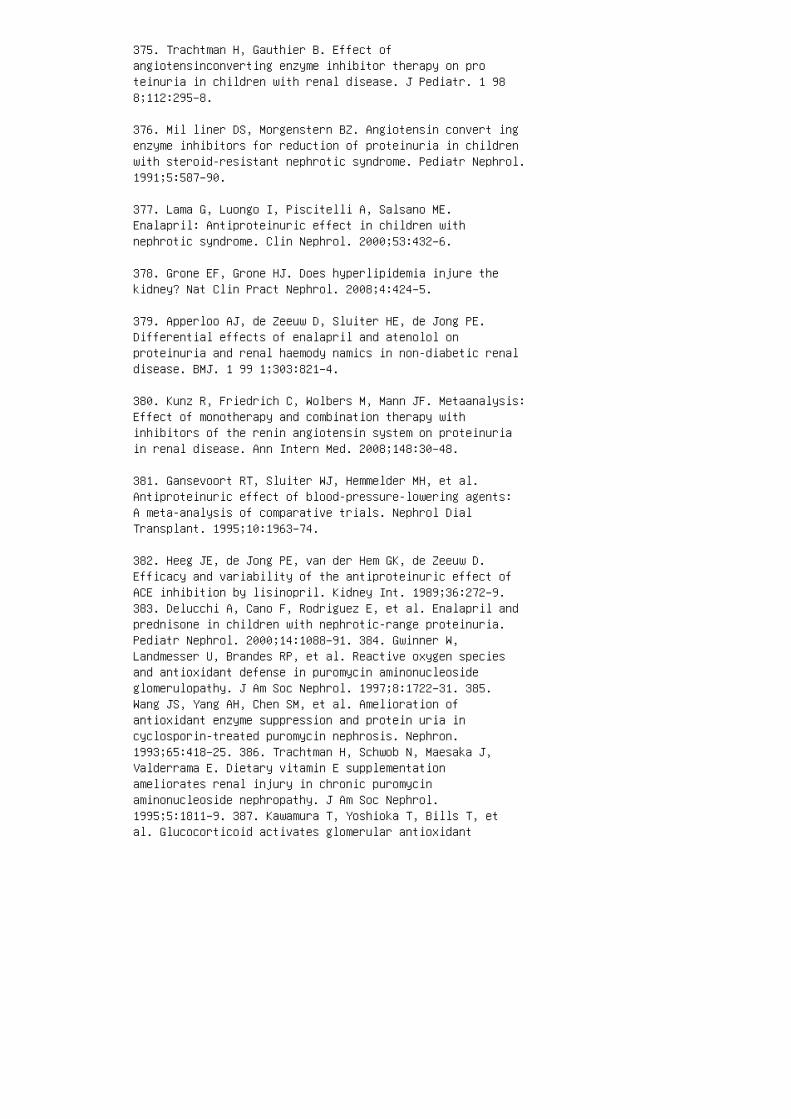
375. Trachtman H, Gauthier B. Effect ofangiotensinconverting enzyme inhibitor therapy on proteinuria in children with renal disease. J Pediatr. 1 988;112:295–8.
376. Mil liner DS, Morgenstern BZ. Angiotensin convert ingenzyme inhibitors for reduction of proteinuria in childrenwith steroid-resistant nephrotic syndrome. Pediatr Nephrol.1991;5:587–90.
377. Lama G, Luongo I, Piscitelli A, Salsano ME.Enalapril: Antiproteinuric effect in children withnephrotic syndrome. Clin Nephrol. 2000;53:432–6.
378. Grone EF, Grone HJ. Does hyperlipidemia injure thekidney? Nat Clin Pract Nephrol. 2008;4:424–5.
379. Apperloo AJ, de Zeeuw D, Sluiter HE, de Jong PE.Differential effects of enalapril and atenolol onproteinuria and renal haemody namics in non-diabetic renaldisease. BMJ. 1 99 1;303:821–4.
380. Kunz R, Friedrich C, Wolbers M, Mann JF. Metaanalysis:Effect of monotherapy and combination therapy withinhibitors of the renin angiotensin system on proteinuriain renal disease. Ann Intern Med. 2008;148:30–48.
381. Gansevoort RT, Sluiter WJ, Hemmelder MH, et al.Antiproteinuric effect of blood-pressure-lowering agents:A meta-analysis of comparative trials. Nephrol DialTransplant. 1995;10:1963–74.
382. Heeg JE, de Jong PE, van der Hem GK, de Zeeuw D.Efficacy and variability of the antiproteinuric effect ofACE inhibition by lisinopril. Kidney Int. 1989;36:272–9.383. Delucchi A, Cano F, Rodriguez E, et al. Enalapril andprednisone in children with nephrotic-range proteinuria.Pediatr Nephrol. 2000;14:1088–91. 384. Gwinner W,Landmesser U, Brandes RP, et al. Reactive oxygen speciesand antioxidant defense in puromycin aminonucleosideglomerulopathy. J Am Soc Nephrol. 1997;8:1722–31. 385.Wang JS, Yang AH, Chen SM, et al. Amelioration ofantioxidant enzyme suppression and protein uria incyclosporin-treated puromycin nephrosis. Nephron.1993;65:418–25. 386. Trachtman H, Schwob N, Maesaka J,Valderrama E. Dietary vitamin E supplementationameliorates renal injury in chronic puromycinaminonucleoside nephropathy. J Am Soc Nephrol.1995;5:1811–9. 387. Kawamura T, Yoshioka T, Bills T, etal. Glucocorticoid activates glomerular antioxidant
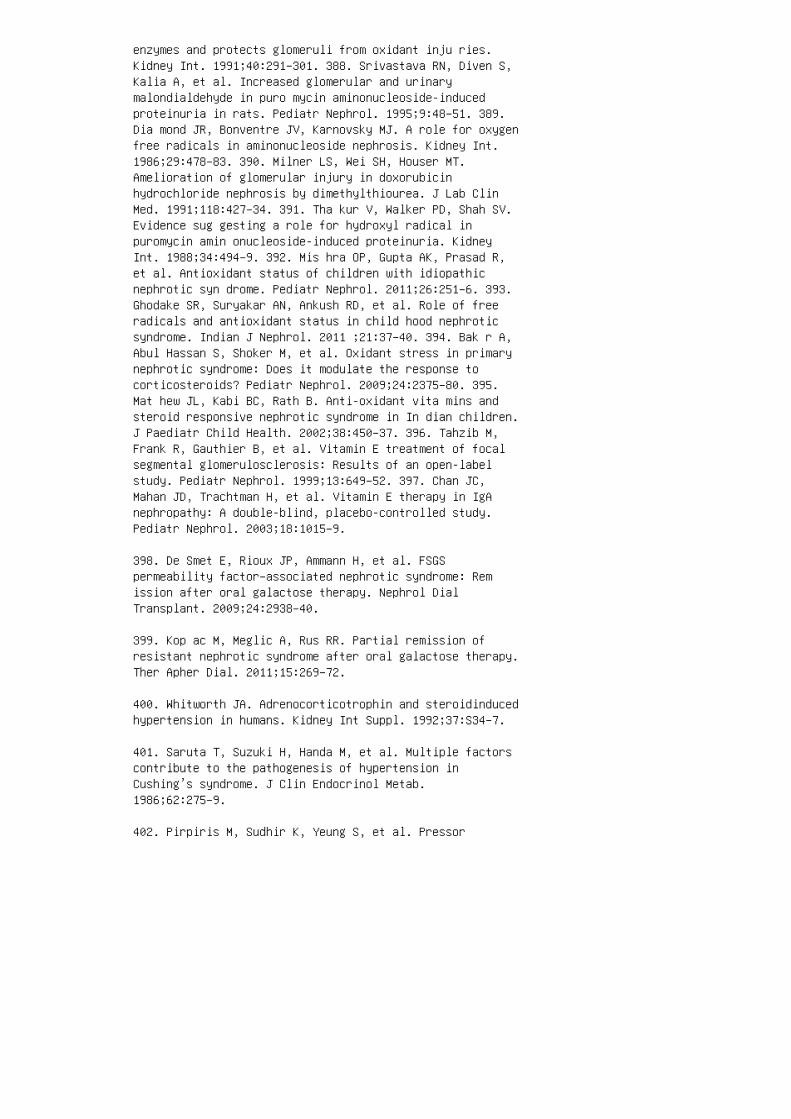
enzymes and protects glomeruli from oxidant inju ries.Kidney Int. 1991;40:291–301. 388. Srivastava RN, Diven S,Kalia A, et al. Increased glomerular and urinarymalondialdehyde in puro mycin aminonucleoside-inducedproteinuria in rats. Pediatr Nephrol. 1995;9:48–51. 389.Dia mond JR, Bonventre JV, Karnovsky MJ. A role for oxygenfree radicals in aminonucleoside nephrosis. Kidney Int.1986;29:478–83. 390. Milner LS, Wei SH, Houser MT.Amelioration of glomerular injury in doxorubicinhydrochloride nephrosis by dimethylthiourea. J Lab ClinMed. 1991;118:427–34. 391. Tha kur V, Walker PD, Shah SV.Evidence sug gesting a role for hydroxyl radical inpuromycin amin onucleoside-induced proteinuria. KidneyInt. 1988;34:494–9. 392. Mis hra OP, Gupta AK, Prasad R,et al. Antioxidant status of children with idiopathicnephrotic syn drome. Pediatr Nephrol. 2011;26:251–6. 393.Ghodake SR, Suryakar AN, Ankush RD, et al. Role of freeradicals and antioxidant status in child hood nephroticsyndrome. Indian J Nephrol. 2011 ;21:37–40. 394. Bak r A,Abul Hassan S, Shoker M, et al. Oxidant stress in primarynephrotic syndrome: Does it modulate the response tocorticosteroids? Pediatr Nephrol. 2009;24:2375–80. 395.Mat hew JL, Kabi BC, Rath B. Anti-oxidant vita mins andsteroid responsive nephrotic syndrome in In dian children.J Paediatr Child Health. 2002;38:450–37. 396. Tahzib M,Frank R, Gauthier B, et al. Vitamin E treatment of focalsegmental glomerulosclerosis: Results of an open-labelstudy. Pediatr Nephrol. 1999;13:649–52. 397. Chan JC,Mahan JD, Trachtman H, et al. Vitamin E therapy in IgAnephropathy: A double-blind, placebo-controlled study.Pediatr Nephrol. 2003;18:1015–9.
398. De Smet E, Rioux JP, Ammann H, et al. FSGSpermeability factor–associated nephrotic syndrome: Remission after oral galactose therapy. Nephrol DialTransplant. 2009;24:2938–40.
399. Kop ac M, Meglic A, Rus RR. Partial remission ofresistant nephrotic syndrome after oral galactose therapy.Ther Apher Dial. 2011;15:269–72.
400. Whitworth JA. Adrenocorticotrophin and steroidinducedhypertension in humans. Kidney Int Suppl. 1992;37:S34–7.
401. Saruta T, Suzuki H, Handa M, et al. Multiple factorscontribute to the pathogenesis of hypertension inCushing’s syndrome. J Clin Endocrinol Metab.1986;62:275–9.
402. Pirpiris M, Sudhir K, Yeung S, et al. Pressor
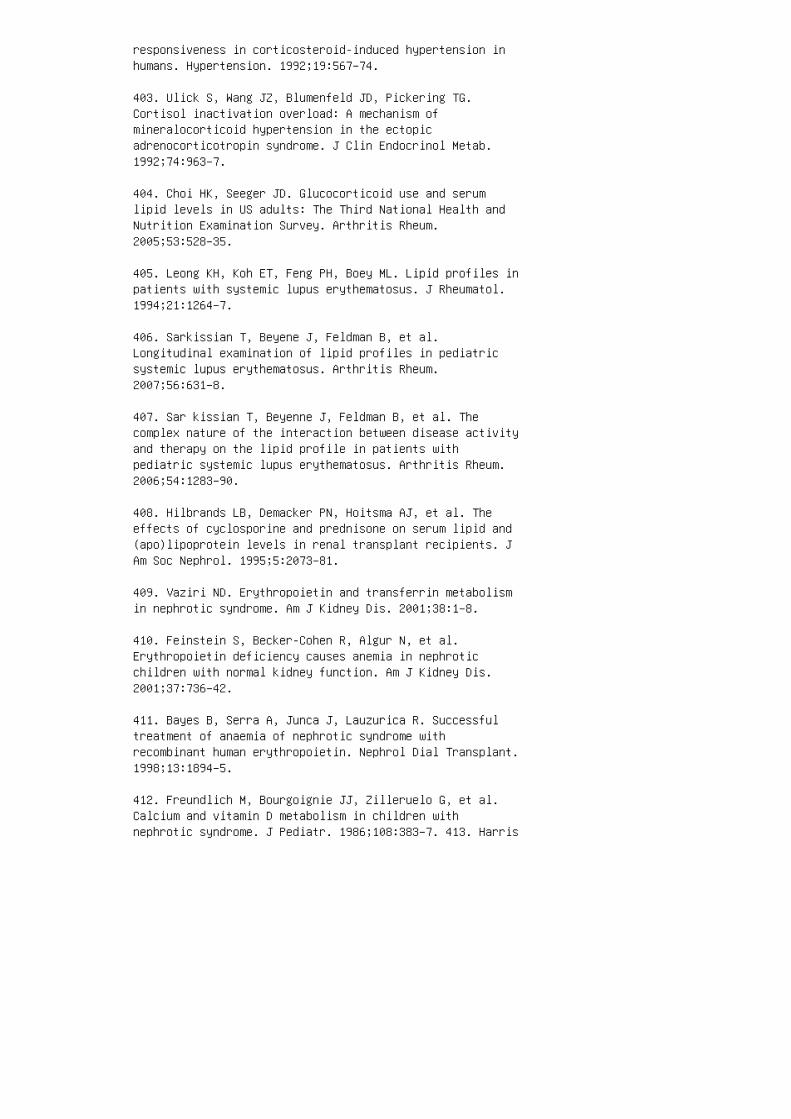
responsiveness in corticosteroid-induced hypertension inhumans. Hypertension. 1992;19:567–74.
403. Ulick S, Wang JZ, Blumenfeld JD, Pickering TG.Cortisol inactivation overload: A mechanism ofmineralocorticoid hypertension in the ectopicadrenocorticotropin syndrome. J Clin Endocrinol Metab.1992;74:963–7.
404. Choi HK, Seeger JD. Glucocorticoid use and serumlipid levels in US adults: The Third National Health andNutrition Examination Survey. Arthritis Rheum.2005;53:528–35.
405. Leong KH, Koh ET, Feng PH, Boey ML. Lipid profiles inpatients with systemic lupus erythematosus. J Rheumatol.1994;21:1264–7.
406. Sarkissian T, Beyene J, Feldman B, et al.Longitudinal examination of lipid profiles in pediatricsystemic lupus erythematosus. Arthritis Rheum.2007;56:631–8.
407. Sar kissian T, Beyenne J, Feldman B, et al. Thecomplex nature of the interaction between disease activityand therapy on the lipid profile in patients withpediatric systemic lupus erythematosus. Arthritis Rheum.2006;54:1283–90.
408. Hilbrands LB, Demacker PN, Hoitsma AJ, et al. Theeffects of cyclosporine and prednisone on serum lipid and(apo)lipoprotein levels in renal transplant recipients. JAm Soc Nephrol. 1995;5:2073–81.
409. Vaziri ND. Erythropoietin and transferrin metabolismin nephrotic syndrome. Am J Kidney Dis. 2001;38:1–8.
410. Feinstein S, Becker-Cohen R, Algur N, et al.Erythropoietin deficiency causes anemia in nephroticchildren with normal kidney function. Am J Kidney Dis.2001;37:736–42.
411. Bayes B, Serra A, Junca J, Lauzurica R. Successfultreatment of anaemia of nephrotic syndrome withrecombinant human erythropoietin. Nephrol Dial Transplant.1998;13:1894–5.
412. Freundlich M, Bourgoignie JJ, Zilleruelo G, et al.Calcium and vitamin D metabolism in children withnephrotic syndrome. J Pediatr. 1986;108:383–7. 413. Harris
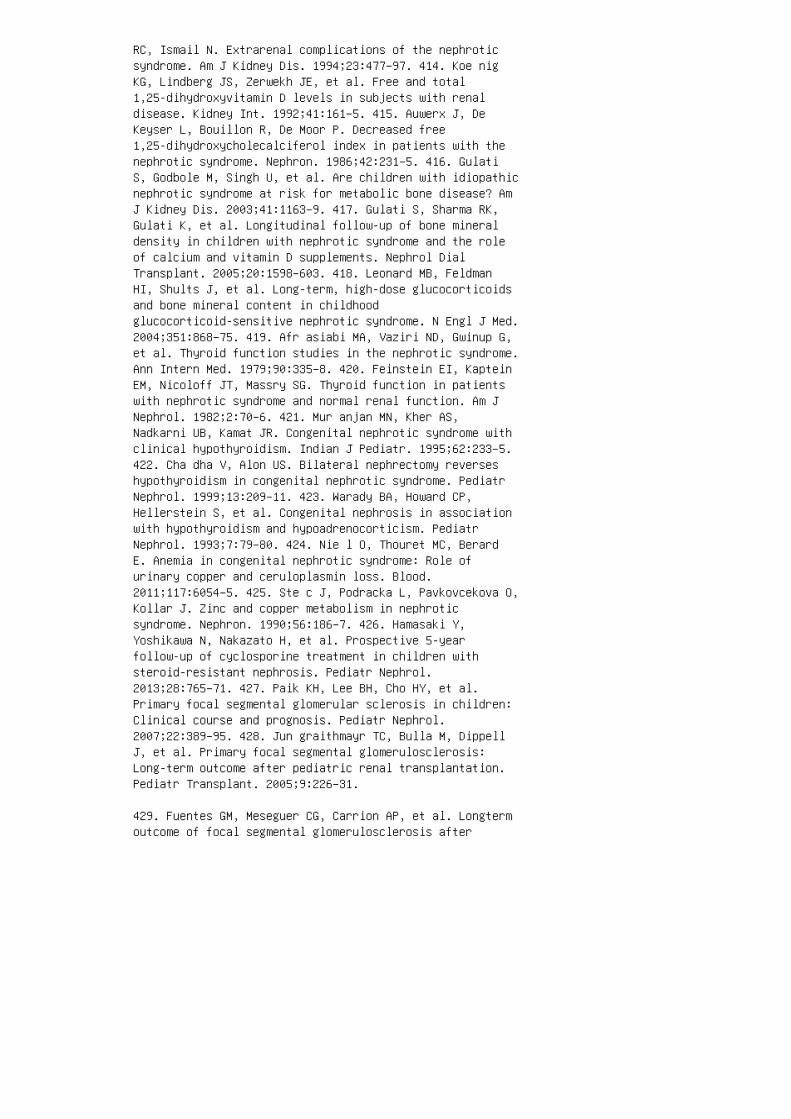
RC, Ismail N. Extrarenal complications of the nephroticsyndrome. Am J Kidney Dis. 1994;23:477–97. 414. Koe nigKG, Lindberg JS, Zerwekh JE, et al. Free and total1,25-dihydroxyvitamin D levels in subjects with renaldisease. Kidney Int. 1992;41:161–5. 415. Auwerx J, DeKeyser L, Bouillon R, De Moor P. Decreased free1,25-dihydroxycholecalciferol index in patients with thenephrotic syndrome. Nephron. 1986;42:231–5. 416. GulatiS, Godbole M, Singh U, et al. Are children with idiopathicnephrotic syndrome at risk for metabolic bone disease? AmJ Kidney Dis. 2003;41:1163–9. 417. Gulati S, Sharma RK,Gulati K, et al. Longitudinal follow-up of bone mineraldensity in children with nephrotic syndrome and the roleof calcium and vitamin D supplements. Nephrol DialTransplant. 2005;20:1598–603. 418. Leonard MB, FeldmanHI, Shults J, et al. Long-term, high-dose glucocorticoidsand bone mineral content in childhoodglucocorticoid-sensitive nephrotic syndrome. N Engl J Med.2004;351:868–75. 419. Afr asiabi MA, Vaziri ND, Gwinup G,et al. Thyroid function studies in the nephrotic syndrome.Ann Intern Med. 1979;90:335–8. 420. Feinstein EI, KapteinEM, Nicoloff JT, Massry SG. Thyroid function in patientswith nephrotic syndrome and normal renal function. Am JNephrol. 1982;2:70–6. 421. Mur anjan MN, Kher AS,Nadkarni UB, Kamat JR. Congenital nephrotic syndrome withclinical hypothyroidism. Indian J Pediatr. 1995;62:233–5.422. Cha dha V, Alon US. Bilateral nephrectomy reverseshypothyroidism in congenital nephrotic syndrome. PediatrNephrol. 1999;13:209–11. 423. Warady BA, Howard CP,Hellerstein S, et al. Congenital nephrosis in associationwith hypothyroidism and hypoadrenocorticism. PediatrNephrol. 1993;7:79–80. 424. Nie l O, Thouret MC, BerardE. Anemia in congenital nephrotic syndrome: Role ofurinary copper and ceruloplasmin loss. Blood.2011;117:6054–5. 425. Ste c J, Podracka L, Pavkovcekova O,Kollar J. Zinc and copper metabolism in nephroticsyndrome. Nephron. 1990;56:186–7. 426. Hamasaki Y,Yoshikawa N, Nakazato H, et al. Prospective 5-yearfollow-up of cyclosporine treatment in children withsteroid-resistant nephrosis. Pediatr Nephrol.2013;28:765–71. 427. Paik KH, Lee BH, Cho HY, et al.Primary focal segmental glomerular sclerosis in children:Clinical course and prognosis. Pediatr Nephrol.2007;22:389–95. 428. Jun graithmayr TC, Bulla M, DippellJ, et al. Primary focal segmental glomerulosclerosis:Long-term outcome after pediatric renal transplantation.Pediatr Transplant. 2005;9:226–31.
429. Fuentes GM, Meseguer CG, Carrion AP, et al. Longtermoutcome of focal segmental glomerulosclerosis after
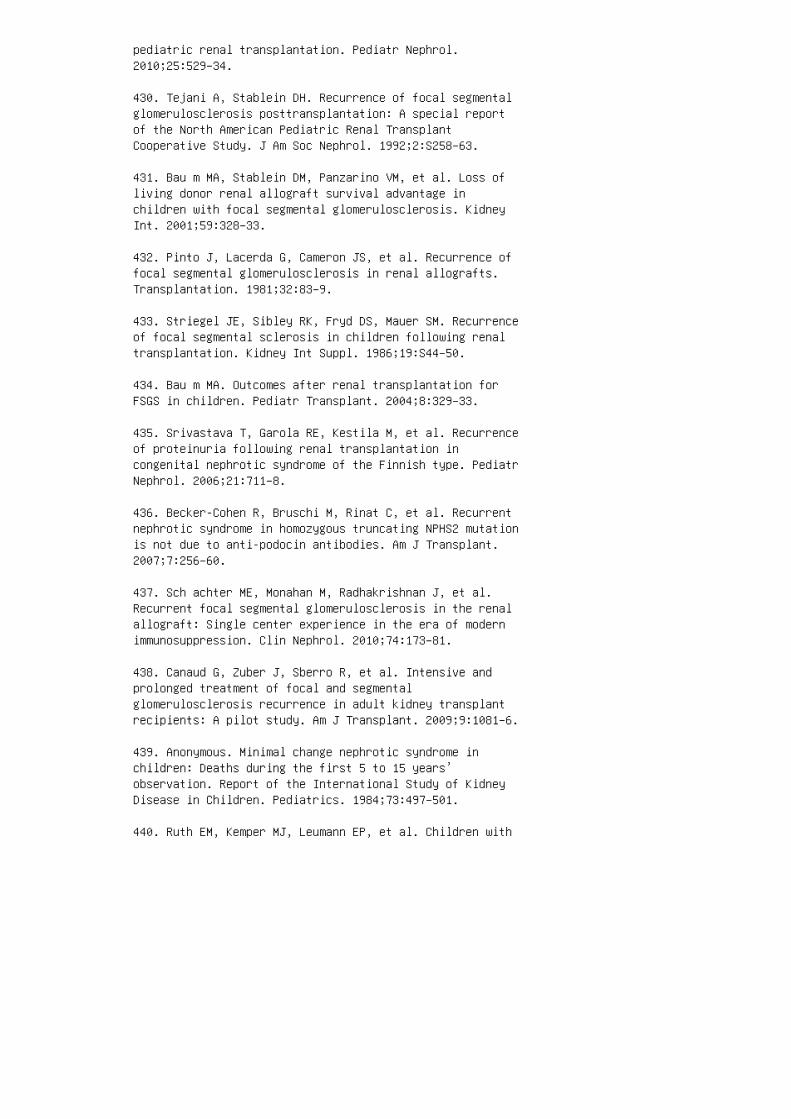
pediatric renal transplantation. Pediatr Nephrol.2010;25:529–34.
430. Tejani A, Stablein DH. Recurrence of focal segmentalglomerulosclerosis posttransplantation: A special reportof the North American Pediatric Renal TransplantCooperative Study. J Am Soc Nephrol. 1992;2:S258–63.
431. Bau m MA, Stablein DM, Panzarino VM, et al. Loss ofliving donor renal allograft survival advantage inchildren with focal segmental glomerulosclerosis. KidneyInt. 2001;59:328–33.
432. Pinto J, Lacerda G, Cameron JS, et al. Recurrence offocal segmental glomerulosclerosis in renal allografts.Transplantation. 1981;32:83–9.
433. Striegel JE, Sibley RK, Fryd DS, Mauer SM. Recurrenceof focal segmental sclerosis in children following renaltransplantation. Kidney Int Suppl. 1986;19:S44–50.
434. Bau m MA. Outcomes after renal transplantation forFSGS in children. Pediatr Transplant. 2004;8:329–33.
435. Srivastava T, Garola RE, Kestila M, et al. Recurrenceof proteinuria following renal transplantation incongenital nephrotic syndrome of the Finnish type. PediatrNephrol. 2006;21:711–8.
436. Becker-Cohen R, Bruschi M, Rinat C, et al. Recurrentnephrotic syndrome in homozygous truncating NPHS2 mutationis not due to anti-podocin antibodies. Am J Transplant.2007;7:256–60.
437. Sch achter ME, Monahan M, Radhakrishnan J, et al.Recurrent focal segmental glomerulosclerosis in the renalallograft: Single center experience in the era of modernimmunosuppression. Clin Nephrol. 2010;74:173–81.
438. Canaud G, Zuber J, Sberro R, et al. Intensive andprolonged treatment of focal and segmentalglomerulosclerosis recurrence in adult kidney transplantrecipients: A pilot study. Am J Transplant. 2009;9:1081–6.
439. Anonymous. Minimal change nephrotic syndrome inchildren: Deaths during the first 5 to 15 years’observation. Report of the International Study of KidneyDisease in Children. Pediatrics. 1984;73:497–501.
440. Ruth EM, Kemper MJ, Leumann EP, et al. Children with
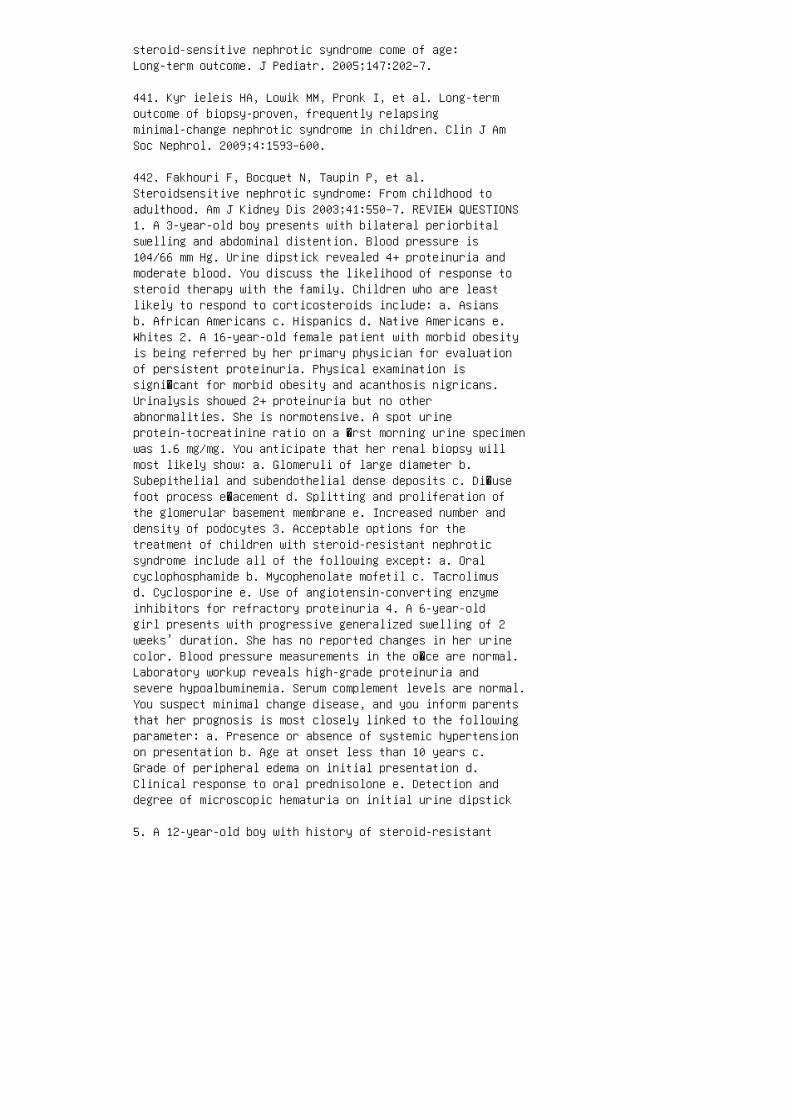
steroid-sensitive nephrotic syndrome come of age:Long-term outcome. J Pediatr. 2005;147:202–7.
441. Kyr ieleis HA, Lowik MM, Pronk I, et al. Long-termoutcome of biopsy-proven, frequently relapsingminimal-change nephrotic syndrome in children. Clin J AmSoc Nephrol. 2009;4:1593–600.
442. Fakhouri F, Bocquet N, Taupin P, et al.Steroidsensitive nephrotic syndrome: From childhood toadulthood. Am J Kidney Dis 2003;41:550–7. REVIEW QUESTIONS1. A 3-year-old boy presents with bilateral periorbitalswelling and abdominal distention. Blood pressure is104/66 mm Hg. Urine dipstick revealed 4+ proteinuria andmoderate blood. You discuss the likelihood of response tosteroid therapy with the family. Children who are leastlikely to respond to corticosteroids include: a. Asiansb. African Americans c. Hispanics d. Native Americans e.Whites 2. A 16-year-old female patient with morbid obesityis being referred by her primary physician for evaluationof persistent proteinuria. Physical examination issigni�cant for morbid obesity and acanthosis nigricans.Urinalysis showed 2+ proteinuria but no otherabnormalities. She is normotensive. A spot urineprotein-tocreatinine ratio on a �rst morning urine specimenwas 1.6 mg/mg. You anticipate that her renal biopsy willmost likely show: a. Glomeruli of large diameter b.Subepithelial and subendothelial dense deposits c. Di�usefoot process e�acement d. Splitting and proliferation ofthe glomerular basement membrane e. Increased number anddensity of podocytes 3. Acceptable options for thetreatment of children with steroid-resistant nephroticsyndrome include all of the following except: a. Oralcyclophosphamide b. Mycophenolate mofetil c. Tacrolimusd. Cyclosporine e. Use of angiotensin-converting enzymeinhibitors for refractory proteinuria 4. A 6-year-oldgirl presents with progressive generalized swelling of 2weeks’ duration. She has no reported changes in her urinecolor. Blood pressure measurements in the o�ce are normal.Laboratory workup reveals high-grade proteinuria andsevere hypoalbuminemia. Serum complement levels are normal.You suspect minimal change disease, and you inform parentsthat her prognosis is most closely linked to the followingparameter: a. Presence or absence of systemic hypertensionon presentation b. Age at onset less than 10 years c.Grade of peripheral edema on initial presentation d.Clinical response to oral prednisolone e. Detection anddegree of microscopic hematuria on initial urine dipstick
5. A 12-year-old boy with history of steroid-resistant
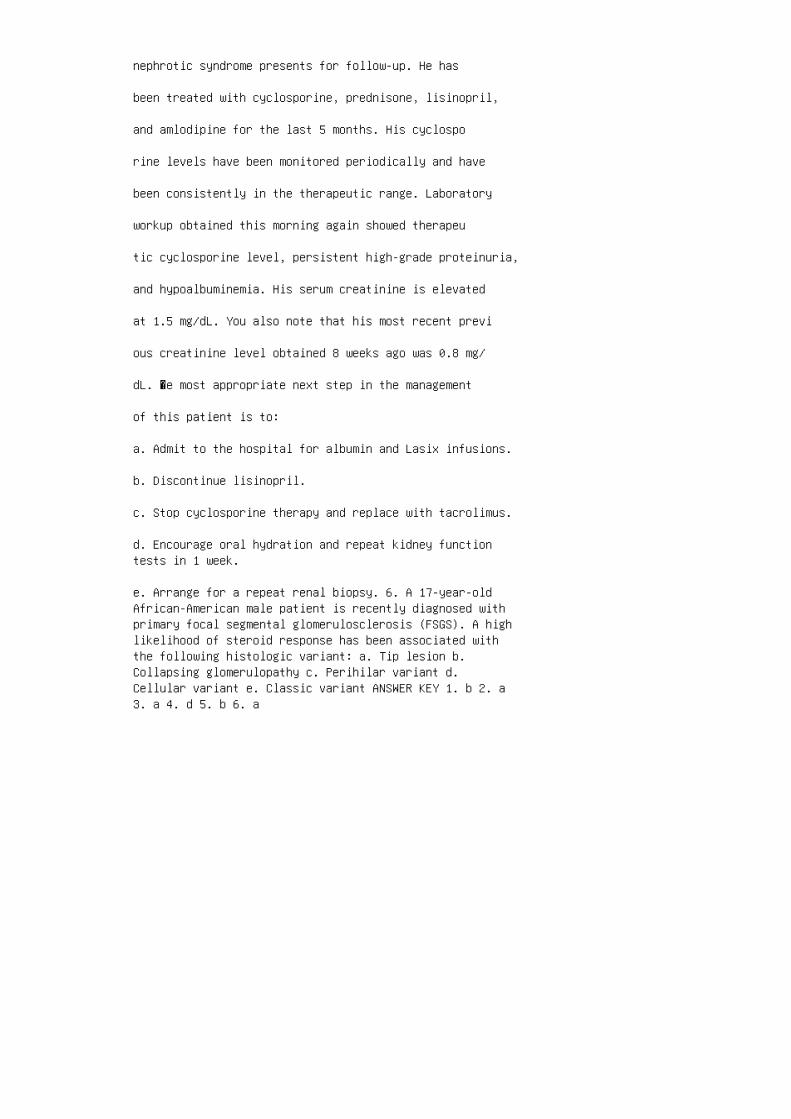
nephrotic syndrome presents for follow-up. He has
been treated with cyclosporine, prednisone, lisinopril,
and amlodipine for the last 5 months. His cyclospo
rine levels have been monitored periodically and have
been consistently in the therapeutic range. Laboratory
workup obtained this morning again showed therapeu
tic cyclosporine level, persistent high-grade proteinuria,
and hypoalbuminemia. His serum creatinine is elevated
at 1.5 mg/dL. You also note that his most recent previ
ous creatinine level obtained 8 weeks ago was 0.8 mg/
dL. �e most appropriate next step in the management
of this patient is to:
a. Admit to the hospital for albumin and Lasix infusions.
b. Discontinue lisinopril.
c. Stop cyclosporine therapy and replace with tacrolimus.
d. Encourage oral hydration and repeat kidney functiontests in 1 week.
e. Arrange for a repeat renal biopsy. 6. A 17-year-oldAfrican-American male patient is recently diagnosed withprimary focal segmental glomerulosclerosis (FSGS). A highlikelihood of steroid response has been associated withthe following histologic variant: a. Tip lesion b.Collapsing glomerulopathy c. Perihilar variant d.Cellular variant e. Classic variant ANSWER KEY 1. b 2. a3. a 4. d 5. b 6. a

18 Nephrotic syndrome in the first yearof life
KEY POINT
Transplanting an a dult kidney into an infant requires
excessive �uids (2500 mL/m 2 /day) to provide ade
quate perfusion of the gra�. SUMMARY NS in the �rst year oflife is a rare, usually severe disease that in most casescan be treated only with RTx a�er nephrectomy of thediseased native kidneys. However, the long-term outcomefor these children critically depends on early diagnosisand early institution of supportive treatment withsubsequent PD and RTx.
12. Patrakka J, Kestilä M, Wartiovaara J, et al. Congenitalnephrotic syndrome (NPHS1): Features resulting fromdifferent mutations in Finnish patients. Kidney Int.2000;58:972–80.
13. Philippe A, Nevo F, Esquivel EL, et al. Nephrinmutations can cause childhood-onset steroid resistantnephrotic syndrome. J Am Soc Nephrol. 2008;19:1871–8.
14. Bolk S, Puffenberg EG, Hudson J, et al. Elevatedfrequency and allelic heterogeneity of congenitalnephrotic syndrome, Finnish type, in the old orderMennonites. Am J Hum Genet. 1999;65:1785–90.
15. Koziell A, Grech V, Hussain S, et al.Genotype/phenotype correlations of NPHS1 and NPHS2mutations in nephrotic syndrome advocate a functionalinterrelationship in glomerular filtration. Hum Mol Genet.2002;11:379–88.
16. Seppälä M, Rapola J, Huttunen NP, et al. Congenitalnephrotic syndrome: Prenatal diagnosis and geneticcounselling by estimation of amniotic-fluid and maternalserum alpha-fetoprotein. Lancet. 1976;2:123–5.
17. Patrakka J, Martin P, Salonen R, et al. Proteinuriaand prenatal diagnosis of congenital nephrosis in fetalcarriers of nephrin gene mutations. Lancet.2002;359:1575–7.
18. Laakkonen H, Lönnqvist T, Uusimaa J, et al. Musculardystonia and athetosis in six patients with congenitalnephrotic syndrome of the Finnish type (NPHS1). Pediatri

Nephrol. 2006;21:182–9.
19. Jal anko H, Holmberg C. Congenital nephrotic syndrome.In: Avner E, Harmon WE, Niaudet P, Yoshikawa N, editors.Pediatric Nephrology. New York: Springer, 2009. pp.601–19.
20. Roselli S, Moutkine I, Gribouval O, et al. Plasmamembrane targeting of podocin through the classicalexocytic pathway: Effect of NPHS2 mutations. Traffic.2004;5:37–44.
21. Weber S, Gribouval O, Esquivel EL, et al. NPHS2mutation analysis shows genetic heterogeneity ofsteroid-resistant nephrotic syndrome and low posttransplantrecurrence. Kidney Int. 2004;66:571–9.
22. Hin kes B, Vlangos C, Heeringa S, et al. Specificpodocin mutations correlate with age of onset insteroidresistant nephrotic syndrome. J Am Soc Nephrol.2008;19:365–71.
23. Machua E, Benoit G, Nevo F, et al. Genotypephenotypecorrelations in non-Finnish congenital nephrotic syndrome.J Am Soc Nephrol. 2010;21:1209–17.
24. Ruf RG , Lichtenberger A, Karle SM, et al. Patientswith mutations in NPHS2 (podocin) do not respond tostandard steroid treatment of nephrotic syndrome. J Am SocNephrol. 2004;15:722–32.
25. Fri schberg Y, Feinstein S, Rinat C, et al. The heartof children with steroid-resistant nephrotic syndrome: Isit all podocin? J Am Soc Nephrol. 2006;17:227–31. 26. CallKM, Glaser T, Ito CY, et al. Isolation and characterizationof a zinc finger polypeptide gene at the human chromosome11 Wilms’ tumor locus. Cell. 1990;60:509–20. 27. Nia udetP, Gubler MC. WT1 and glomerular disease. Pediatr Nephrol.2006;21:1653–60. 28. Denys P, Malvaux P, Van Den Berghe H,et al. Association of an anatomo-pathological syndrome ofmale pseudohermaphroditism, Wilms’ tumor, parenchymatousnephropathy and XX/XY mosaicism. Arch Fr Pediatr.1967;24:729–39. 29. Dra sh A, Sherman F, Hartmann WH, etal. A syndrome of pseudohermaphroditism, Wilms’ tumor,hypertension, and degenerative renal disease. J Pediatr.1970;76:585–93. 30. Barbaux S, Niaudet P, Gubler MC, etal. Donor splicesite mutations in WT1 are responsible forFrasier syndrome. Nat Genet. 1997;17:467–70. 31. Kla mtB, Koziell A, Poulat F, et al. Frasier syndrome is causedby defective alternative splicing of WT1 leading to an
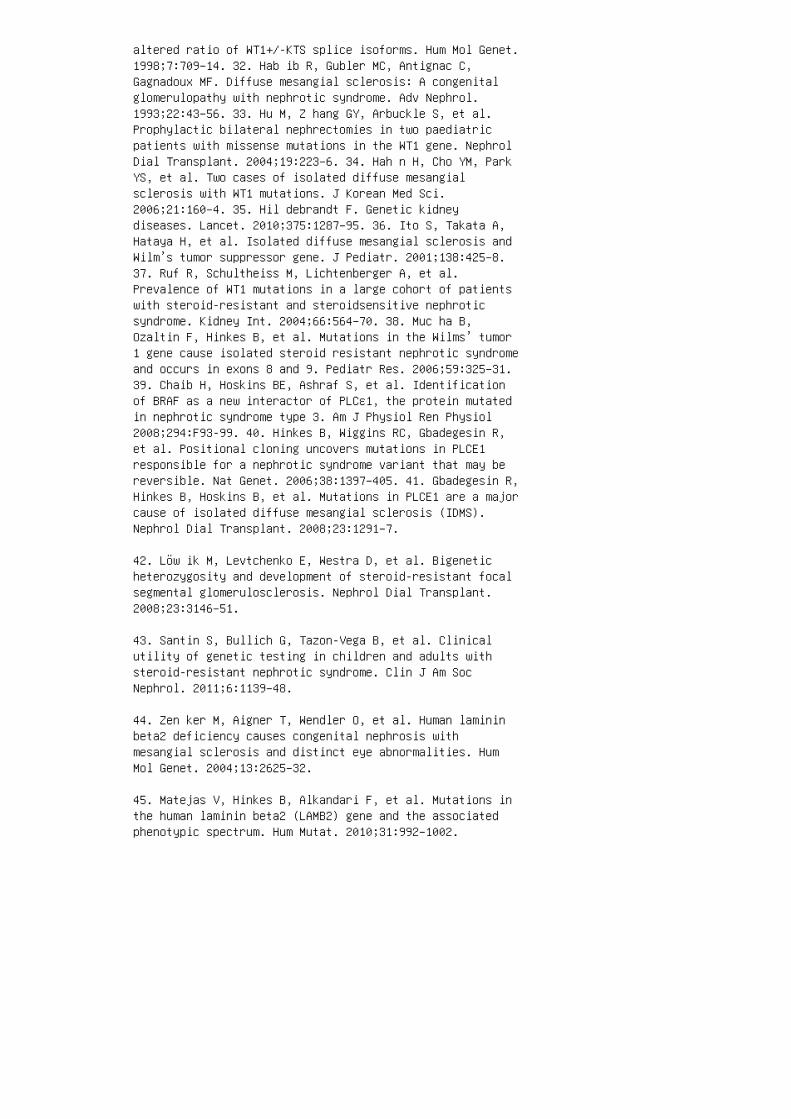
altered ratio of WT1+/-KTS splice isoforms. Hum Mol Genet.1998;7:709–14. 32. Hab ib R, Gubler MC, Antignac C,Gagnadoux MF. Diffuse mesangial sclerosis: A congenitalglomerulopathy with nephrotic syndrome. Adv Nephrol.1993;22:43–56. 33. Hu M, Z hang GY, Arbuckle S, et al.Prophylactic bilateral nephrectomies in two paediatricpatients with missense mutations in the WT1 gene. NephrolDial Transplant. 2004;19:223–6. 34. Hah n H, Cho YM, ParkYS, et al. Two cases of isolated diffuse mesangialsclerosis with WT1 mutations. J Korean Med Sci.2006;21:160–4. 35. Hil debrandt F. Genetic kidneydiseases. Lancet. 2010;375:1287–95. 36. Ito S, Takata A,Hataya H, et al. Isolated diffuse mesangial sclerosis andWilm’s tumor suppressor gene. J Pediatr. 2001;138:425–8.37. Ruf R, Schultheiss M, Lichtenberger A, et al.Prevalence of WT1 mutations in a large cohort of patientswith steroid-resistant and steroidsensitive nephroticsyndrome. Kidney Int. 2004;66:564–70. 38. Muc ha B,Ozaltin F, Hinkes B, et al. Mutations in the Wilms’ tumor1 gene cause isolated steroid resistant nephrotic syndromeand occurs in exons 8 and 9. Pediatr Res. 2006;59:325–31.39. Chaib H, Hoskins BE, Ashraf S, et al. Identificationof BRAF as a new interactor of PLCε1, the protein mutatedin nephrotic syndrome type 3. Am J Physiol Ren Physiol2008;294:F93-99. 40. Hinkes B, Wiggins RC, Gbadegesin R,et al. Positional cloning uncovers mutations in PLCE1responsible for a nephrotic syndrome variant that may bereversible. Nat Genet. 2006;38:1397–405. 41. Gbadegesin R,Hinkes B, Hoskins B, et al. Mutations in PLCE1 are a majorcause of isolated diffuse mesangial sclerosis (IDMS).Nephrol Dial Transplant. 2008;23:1291–7.
42. Löw ik M, Levtchenko E, Westra D, et al. Bigeneticheterozygosity and development of steroid-resistant focalsegmental glomerulosclerosis. Nephrol Dial Transplant.2008;23:3146–51.
43. Santin S, Bullich G, Tazon-Vega B, et al. Clinicalutility of genetic testing in children and adults withsteroid-resistant nephrotic syndrome. Clin J Am SocNephrol. 2011;6:1139–48.
44. Zen ker M, Aigner T, Wendler O, et al. Human lamininbeta2 deficiency causes congenital nephrosis withmesangial sclerosis and distinct eye abnormalities. HumMol Genet. 2004;13:2625–32.
45. Matejas V, Hinkes B, Alkandari F, et al. Mutations inthe human laminin beta2 (LAMB2) gene and the associatedphenotypic spectrum. Hum Mutat. 2010;31:992–1002.
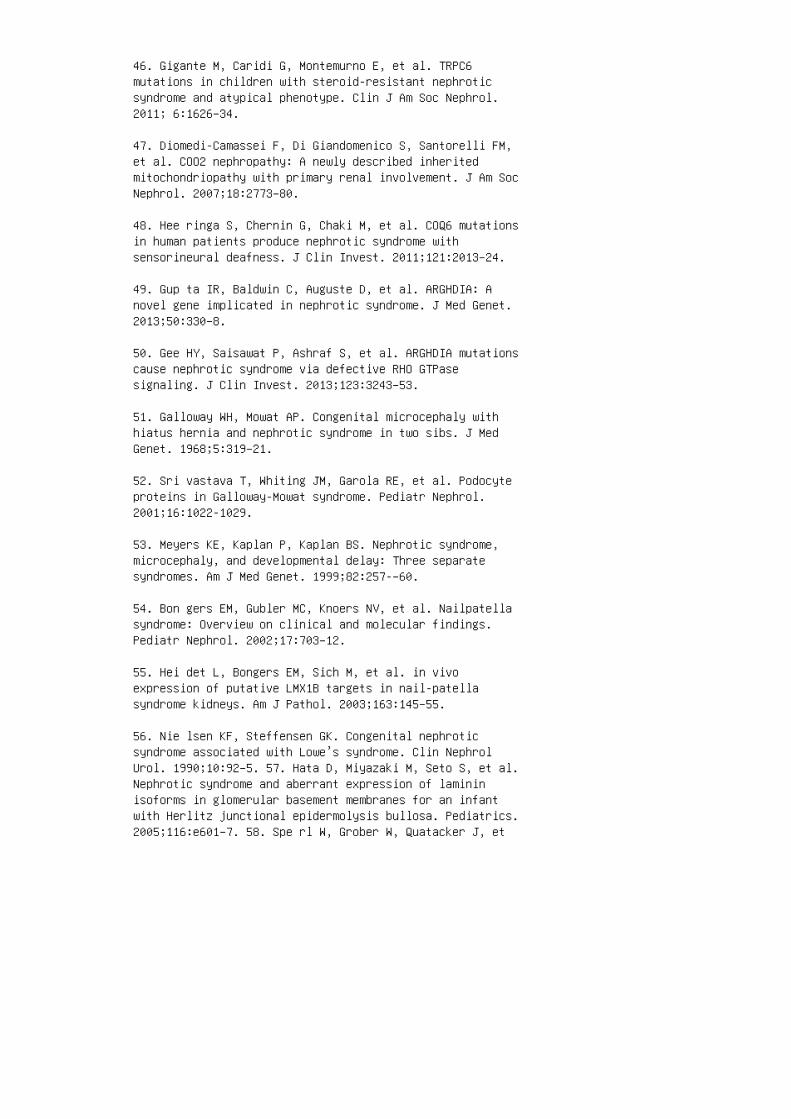
46. Gigante M, Caridi G, Montemurno E, et al. TRPC6mutations in children with steroid-resistant nephroticsyndrome and atypical phenotype. Clin J Am Soc Nephrol.2011; 6:1626–34.
47. Diomedi-Camassei F, Di Giandomenico S, Santorelli FM,et al. COO2 nephropathy: A newly described inheritedmitochondriopathy with primary renal involvement. J Am SocNephrol. 2007;18:2773–80.
48. Hee ringa S, Chernin G, Chaki M, et al. COQ6 mutationsin human patients produce nephrotic syndrome withsensorineural deafness. J Clin Invest. 2011;121:2013–24.
49. Gup ta IR, Baldwin C, Auguste D, et al. ARGHDIA: Anovel gene implicated in nephrotic syndrome. J Med Genet.2013;50:330–8.
50. Gee HY, Saisawat P, Ashraf S, et al. ARGHDIA mutationscause nephrotic syndrome via defective RHO GTPasesignaling. J Clin Invest. 2013;123:3243–53.
51. Galloway WH, Mowat AP. Congenital microcephaly withhiatus hernia and nephrotic syndrome in two sibs. J MedGenet. 1968;5:319–21.
52. Sri vastava T, Whiting JM, Garola RE, et al. Podocyteproteins in Galloway-Mowat syndrome. Pediatr Nephrol.2001;16:1022-1029.
53. Meyers KE, Kaplan P, Kaplan BS. Nephrotic syndrome,microcephaly, and developmental delay: Three separatesyndromes. Am J Med Genet. 1999;82:257-–60.
54. Bon gers EM, Gubler MC, Knoers NV, et al. Nailpatellasyndrome: Overview on clinical and molecular findings.Pediatr Nephrol. 2002;17:703–12.
55. Hei det L, Bongers EM, Sich M, et al. in vivoexpression of putative LMX1B targets in nail-patellasyndrome kidneys. Am J Pathol. 2003;163:145–55.
56. Nie lsen KF, Steffensen GK. Congenital nephroticsyndrome associated with Lowe’s syndrome. Clin NephrolUrol. 1990;10:92–5. 57. Hata D, Miyazaki M, Seto S, et al.Nephrotic syndrome and aberrant expression of lamininisoforms in glomerular basement membranes for an infantwith Herlitz junctional epidermolysis bullosa. Pediatrics.2005;116:e601–7. 58. Spe rl W, Grober W, Quatacker J, et
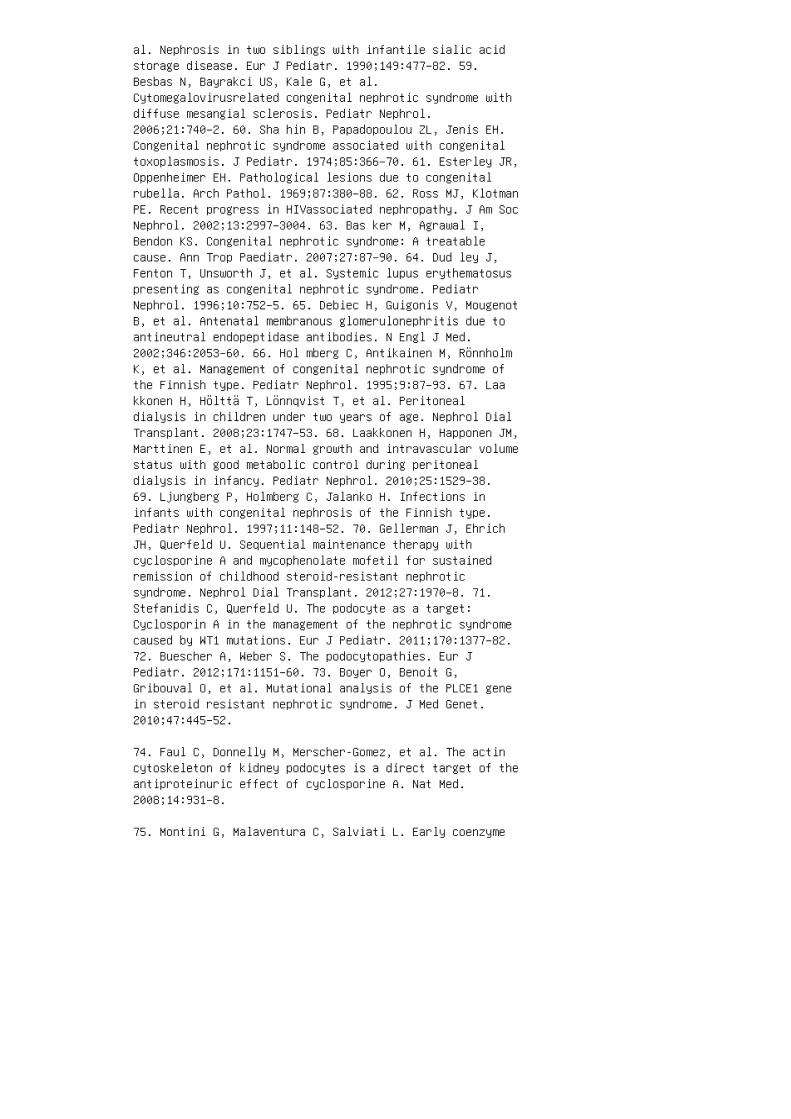
al. Nephrosis in two siblings with infantile sialic acidstorage disease. Eur J Pediatr. 1990;149:477–82. 59.Besbas N, Bayrakci US, Kale G, et al.Cytomegalovirusrelated congenital nephrotic syndrome withdiffuse mesangial sclerosis. Pediatr Nephrol.2006;21:740–2. 60. Sha hin B, Papadopoulou ZL, Jenis EH.Congenital nephrotic syndrome associated with congenitaltoxoplasmosis. J Pediatr. 1974;85:366–70. 61. Esterley JR,Oppenheimer EH. Pathological lesions due to congenitalrubella. Arch Pathol. 1969;87:380–88. 62. Ross MJ, KlotmanPE. Recent progress in HIVassociated nephropathy. J Am SocNephrol. 2002;13:2997–3004. 63. Bas ker M, Agrawal I,Bendon KS. Congenital nephrotic syndrome: A treatablecause. Ann Trop Paediatr. 2007;27:87–90. 64. Dud ley J,Fenton T, Unsworth J, et al. Systemic lupus erythematosuspresenting as congenital nephrotic syndrome. PediatrNephrol. 1996;10:752–5. 65. Debiec H, Guigonis V, MougenotB, et al. Antenatal membranous glomerulonephritis due toantineutral endopeptidase antibodies. N Engl J Med.2002;346:2053–60. 66. Hol mberg C, Antikainen M, RönnholmK, et al. Management of congenital nephrotic syndrome ofthe Finnish type. Pediatr Nephrol. 1995;9:87–93. 67. Laakkonen H, Hölttä T, Lönnqvist T, et al. Peritonealdialysis in children under two years of age. Nephrol DialTransplant. 2008;23:1747–53. 68. Laakkonen H, Happonen JM,Marttinen E, et al. Normal growth and intravascular volumestatus with good metabolic control during peritonealdialysis in infancy. Pediatr Nephrol. 2010;25:1529–38.69. Ljungberg P, Holmberg C, Jalanko H. Infections ininfants with congenital nephrosis of the Finnish type.Pediatr Nephrol. 1997;11:148–52. 70. Gellerman J, EhrichJH, Querfeld U. Sequential maintenance therapy withcyclosporine A and mycophenolate mofetil for sustainedremission of childhood steroid-resistant nephroticsyndrome. Nephrol Dial Transplant. 2012;27:1970–8. 71.Stefanidis C, Querfeld U. The podocyte as a target:Cyclosporin A in the management of the nephrotic syndromecaused by WT1 mutations. Eur J Pediatr. 2011;170:1377–82.72. Buescher A, Weber S. The podocytopathies. Eur JPediatr. 2012;171:1151–60. 73. Boyer O, Benoit G,Gribouval O, et al. Mutational analysis of the PLCE1 genein steroid resistant nephrotic syndrome. J Med Genet.2010;47:445–52.
74. Faul C, Donnelly M, Merscher-Gomez, et al. The actincytoskeleton of kidney podocytes is a direct target of theantiproteinuric effect of cyclosporine A. Nat Med.2008;14:931–8.
75. Montini G, Malaventura C, Salviati L. Early coenzyme
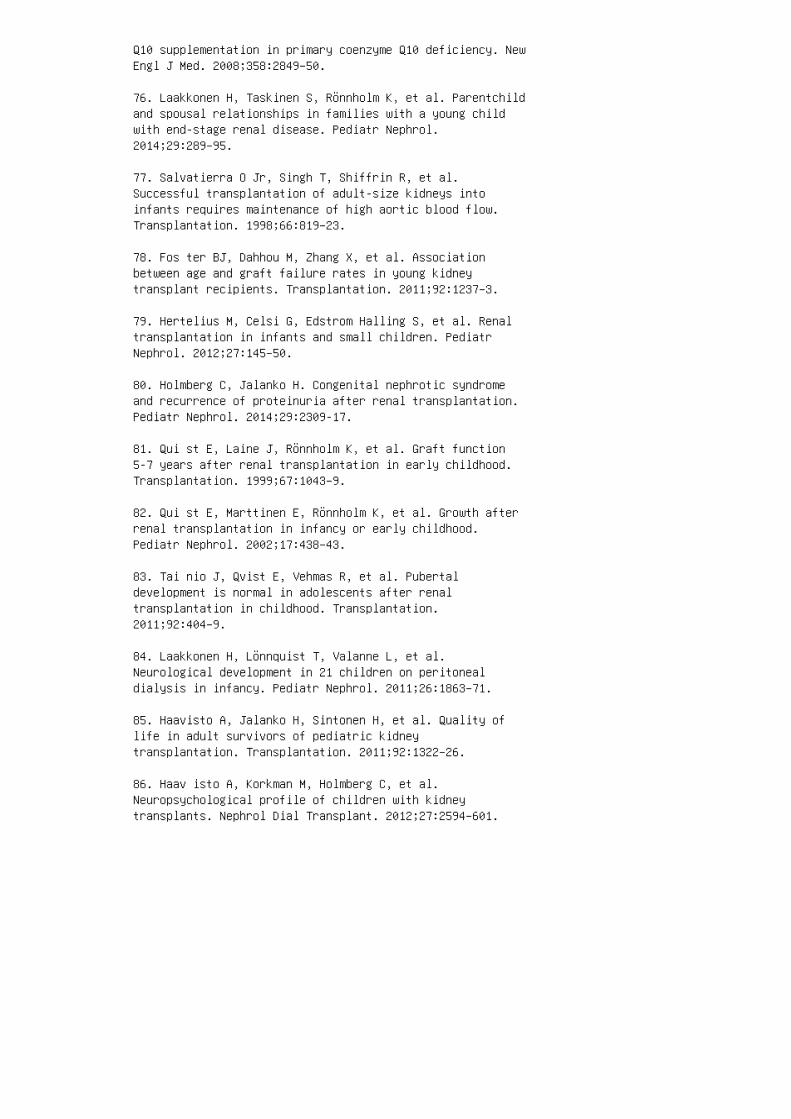
Q10 supplementation in primary coenzyme Q10 deficiency. NewEngl J Med. 2008;358:2849–50.
76. Laakkonen H, Taskinen S, Rönnholm K, et al. Parentchildand spousal relationships in families with a young childwith end-stage renal disease. Pediatr Nephrol.2014;29:289–95.
77. Salvatierra O Jr, Singh T, Shiffrin R, et al.Successful transplantation of adult-size kidneys intoinfants requires maintenance of high aortic blood flow.Transplantation. 1998;66:819–23.
78. Fos ter BJ, Dahhou M, Zhang X, et al. Associationbetween age and graft failure rates in young kidneytransplant recipients. Transplantation. 2011;92:1237–3.
79. Hertelius M, Celsi G, Edstrom Halling S, et al. Renaltransplantation in infants and small children. PediatrNephrol. 2012;27:145–50.
80. Holmberg C, Jalanko H. Congenital nephrotic syndromeand recurrence of proteinuria after renal transplantation.Pediatr Nephrol. 2014;29:2309-17.
81. Qui st E, Laine J, Rönnholm K, et al. Graft function5-7 years after renal transplantation in early childhood.Transplantation. 1999;67:1043–9.
82. Qui st E, Marttinen E, Rönnholm K, et al. Growth afterrenal transplantation in infancy or early childhood.Pediatr Nephrol. 2002;17:438–43.
83. Tai nio J, Qvist E, Vehmas R, et al. Pubertaldevelopment is normal in adolescents after renaltransplantation in childhood. Transplantation.2011;92:404–9.
84. Laakkonen H, Lönnquist T, Valanne L, et al.Neurological development in 21 children on peritonealdialysis in infancy. Pediatr Nephrol. 2011;26:1863–71.
85. Haavisto A, Jalanko H, Sintonen H, et al. Quality oflife in adult survivors of pediatric kidneytransplantation. Transplantation. 2011;92:1322–26.
86. Haav isto A, Korkman M, Holmberg C, et al.Neuropsychological profile of children with kidneytransplants. Nephrol Dial Transplant. 2012;27:2594–601.

87. Johnson RJ, Warady BA. Long-term neurocognitiveoutcomes of patients with end-stage renal disease duringinfancy. Pediatr Nephrol. 2013;28:1283–91.
88. van S trahlen KJ, Borzych-Duzalka D, Hataya H, et al.Survival and clinical outcomes of children starting renalreplacement therapy in the neonatal period. Kidney Int.2014;86:168–74. REVIEW QUESTIONS 1. Congenital nephroticsyndrome is best defined as: a. Nephrotic syndrome duringthe �rst year of life b. Nephrotic syndrome during therst 6 years of life c. Nephrotic syndrome during the �rst3 months of life d. End-stage renal disease andproteinuria in infancy e. Proteinuria and hematuria withuremia at birth 2. �e most common causes of congenitalnephrotic syndrome are: a. WT1 mutations b. WT1 and PLCε1mutations c. Neonatal infections d. Galloway-Mowatsyndrome e. NPHS1 and NPHS2 mutations 3. Which of thefollowing is most important in regulating glomerularprotein �ltration? a. �e capillary endothelium b.Mesangial cell function c. �e basement membrane d. �eslit diaphragm e. �e podocyte cell bodies 4. Congenitalnephrotic syndrome secondary to NPHS1 mutation: a. Ismost commonly seen in Turkish children b. Is caused by amutation in the podocin gene c. Usually manifests a�er therst 3 months of life d. Is caused by a nephrin genemutation e. Reacts to cyclosporin A medication 5.Congenital nephrotic syndrome secondary to NPHS2 mutation:a. Presents during the �rst month of life b. Ischaracterized by severe NS and ocular malformations c. Iscaused by a mutation in the podocin gene d. Shows DMS inrenal biopsy e. Reacts to ACE inhibitors and indomethacin6. �e most typical symptoms of congenital nephroticsyndrome is (are): a. Severe nephrosis during the �rst 3months of life b. Malformations and end-stage renalfailure c. Hematuria, high fever, and a typical rash d.Proteinuria and gastrointestinal malformations e. Edema,high creatinine level, and high blood pressure during therst months of life 7. Congenital nephrotic syndrome ismost effectively treated by: a. Dialysis and early renaltransplantation b. ACE inhibitors and indomethacin withcyclosporin A c. �e patients recover spontaneously d.Penicillin e. High-dose immunosuppression
8. Which of the following best represents the long-term
outcome of congenital nephrotic syndrome?
a. Remains poor, with death during the �rst years of life
b. Has improved, because most patients respond to the
medication
c. Is poor regardless of intervention, because the diseasemostly reappears in the gra
d. Is good with early support, dialysis, and renaltransplantation
e. Is poor because gra� survival is still only 50% at 5years ANSWER KEY 1. c 2. e 3. d 4. d 5. c 6. a 7. a8. d
19 Membranoproliferativeglomerulonephritis
1. Habib R, Gubler MC, Loirat C, et al. Dense depositdisease: A variant of membranoproliferativeglomerulonephritis. Kidney Int. 1975;7:204–15.
2. Wal ker PD, Ferrario F, Joh K, et al. Dense depositdisease is not a membranoproliferative glomerulonephritis.Mod Pathol. 2007;20:605–16.
3. Sibley RK, Kim Y. Dense intramembranous depositdisease: New pathologic features. Kidney Int.1984;25:660–70.
4. Raz zaque MS, Yamaguchi K, Taguchi T. An unusual caseof dense deposit disease with nodular sclerotic lesions ofthe glomeruli. Clin Nephrol. 1999;51:326–8.
5. Joh K, Aizawa S, Matsuyama N, et al. Morphologicvariations of dense deposit disease: Light and electronmicroscopic, immunohistochemical and clinical findings in10 patients. Acta Pathol Jpn. 1993;43:552–65.
6. The S outhwest Pediatric Nephrology Study Group. Densedeposit disease in children: Prognostic value of clinicaland pathologic indicators. Am J Kidney Dis. 1985;6:161–9.
7. Davi s AE, Schneeberger EE, Grupe WE, et al.Membranoproliferative glomerulonephritis (MPGN type I) anddense deposit disease (DDD) in children. Clin Nephrol.1978;9:184–93.
8. Bel giojoso GB, Tarantino A, Bazzi C, et al.Immunofluorescence patterns in chronicmembranoproliferative glomerulonephritis (MPGN). ClinNephrol. 1976;6:303–10.
9. Bur kholder PM, Bradford WD. Proliferativeglomerulonephritis in children: A correlation of variedclinical and pathologic patterns utilizing light,immunofluorescence, and electron microscopy. Am J Pathol.1969;56:423–67.
10. Jen is EH, Sandler P, Hill GS, et al.Glomerulonephritis with basement membrane dense deposits.Arch Pathol. 1974;97:84–91.
11. Kim Y , Vernier RL, Fish AJ, et al. Immunofluorescencestudies of dense deposit disease: The presence of railroad
tracks and mesangial rings. Lab Invest. 1979;40:474–80.
12. Wes t CD, Witte DP, McAdams AJ. Composition ofnephritic factor-generated glomerular deposits inmembranoproliferative glomerulonephritis type 2. Am JKidney Dis. 2001;37:1120–30.
13. Pickering MC, D’Agati VD, Nester CM, et al. C3glomerulopathy: Consensus report. Kidney Int.2013;84:1079–89.
14. Ser vais A, Noel LH, Roumenina LT, et al. Acquired andgenetic complement abnormalities play a critical role indense deposit disease and other C3 glomerulopathies. KidneyInt. 2012;82:454–64.
15. Gal e DP, de Jorge EG, Cook HT, et al. Identificationof a mutation in complement factor H-related protein 5 inpatients of Cypriot origin with glomerulonephritis. Lancet2010;376:794–801. 16. Athanasiou Y, Voskarides K, Gale DP,et al. Familial C3 glomerulopathy associated with CFHR5mutations: Clinical characteristics of 91 patients in 16pedigrees. Clin J Am Soc Nephrol. 2011;6:1436–46. 17.Martinez-Barricarte R, Heurich M, Valdes-Canedo F, et al.Human C3 mutation reveals a mechanism of dense depositdisease pathogenesis and provides insights into complementactivation and regulation. J Clin Invest.2010;120:3702–12. 18. Mal ik TH, Lavin PJ, Goicoechea deJorge E, et al. A hybrid CFHR3-1 gene causes familial C3glomerulopathy. J Am Soc Nephrol. 2012;23:1155–60. 19.Tortajada A, Yebenes H, Abarrategui-Garrido C, et al. C3glomerulopathy-associated CFHR1 mutation alters FHRoligomerization and complement regulation. J Clin Invest.2013;123:2434–46. 20. Med jeral-Thomas N, Malik TH, PatelMP, et al. A novel CFHR5 fusion protein causes C3glomerulopathy in a family without Cypriot ancestry. KidneyInt. 2014;85:933–7. 21. Lic ht C, Heinen S, Jozsi M, etal. Deletion of Lys224 in regulatory domain 4 of factor Hreveals a novel pathomechanism for dense deposit disease(MPGN II). Kidney Int. 2006;70:42–50. 22. Ser vais A,Fremeaux-Bacchi V, Lequintrec M, et al. Primaryglomerulonephritis with isolated C3 deposits: A new entitywhich shares common genetic risk factors with haemolyticuraemic syndrome. J Med Genet. 2007;44:193–9. 23. Set hiS, Nester CM, Smith RJ. Membranoproliferativeglomerulonephritis and C3 glomerulopathy: Resolving theconfusion. Kidney Int. 2012;81:434–41. 24. Set hi S,Fervenza FC, Zhang Y, et al. C3 glomerulonephritis:Clinicopathological findings, complement abnormalities,glomerular proteomic profile, treatment, and follow-up.

Kidney Int. 2012;82:465–73. 25. Servais A, Noel LH,Fremeaux-Bacchi V, et al. C3 glomerulopathy. ContribNephrol. 2013;181:185–93. 26. Pic kering M, Cook HT.Complement and glomerular disease: New insights. Curr OpinNephrol Hypertens. 2011;20:271–7. 27. Gol ay V, TrivediM, Abraham A, et al. The spectrum of glomerular diseases ina single center: A clinicopathological correlation. IndianJ Nephrol. 2013;23:168–75. 28. Naw az Z, Mushtaq F, MousaD, et al. Pattern of glomerular disease in the Saudipopulation: A singlecenter, five-year retrospective study.Saudi J Kidney Dis Transpl. 2013;24:1265–70. 29. KawamuraT, Usui J, Kaseda K, et al. Primary membranoproliferativeglomerulonephritis on the decline: Decreased rate from the1970s to the 2000s in Japan. Clin Exp Nephrol.2013;17:248–54. 30. Swaminathan S, Leung N, Lager DJ, etal. Changing incidence of glomerular disease in OlmstedCounty, Minnesota: A 30-year renal biopsy study. Clin J AmSoc Nephrol. 2006;1:483–7.
31. Bra den GL, Mulhern JG, O’Shea MH, et al. Changingincidence of glomerular diseases in adults. Am J KidneyDis. 2000;35:878–83.
32. Maisonneuve P, Agodoa L, Gellert R, et al.Distribution of primary renal diseases leading toend-stage renal failure in the United States, Europe, andAustralia/New Zealand: Results from an internationalcomparative study. Am J Kidney Dis. 2000;35:157–65.
33. Hanko JB, Mullan RN, O’Rourke DM, et al. The changingpattern of adult primary glomerular disease. Nephrol DialTransplant. 2009;24:3050–4.
34. Briganti EM, Dowling J, Finlay M, et al. The incidenceof biopsy-proven glomerulonephritis in Australia. NephrolDial Transplant. 2001;16:1364–7.
35. Study Group of the Spanish Society of Nephrology.Decreasing incidence of membranoproliferativeglomerulonephritis in Spanish c hi ldren. Pediatr Nephrol.1990;4:266–7.
36. Iitaka K, Saka T, Yagisawa K, et al. Decreasinghypocomplementemia and membranoprolifera tiveglomerulonephritis in Japan. Pediatr Nephrol 2000;14:794–6.
37. Wes t CD. Idiopathic membranoproliferativeglomerulonephritis in childhood. Pediatr Nephrol.1992;6:96–103.
38. Daha MR, Fearon DT, Austen KF. C3 nephritic factor(C3NeF): Stabilization of fluid phase and cell-boundalternative pathway convertase. J Immunol. 1976;116:1–7.
39. Sco tt DM, Amos N, Sissons JG, et al. The immunogloblin nature of nephritic factor (NeF). Clin Exp Immunol. 1978;32:12–24.
40. Tho mpson RA. C3 inactivating factor in the serum of apatient with chronic hypocomplementaemic proliferativeglomerulo-nephritis. Immunology. 1972;22:147–58.
41. Spi tzer RE, Vallota EH, Forristal J, et al. Serum C3lytic system in patients with glomerulonephritis. Science.1969;164:436–7.
42. Cameron JS, Turner DR, Heaton J, et al. Idiopathicmesangiocapillary glomerulonephritis: Comparison of typesI and II in children and adults and longterm prognosis. AmJ Med. 1983;74:175–92.
43. Swa inson CP, Robson JS, Thomson D, MacDonald MK.Mesangiocapillary glomeru lonephritis: A long-term study of40 cases. J Pathol. 1983;141:449–68.
44. Schwertz R, Rother U, Anders D, et al. Complementanalysis in children with idiopathic membranoproliferativeglomerulonephritis: A long-term follow-up. Pediatr AllergyImmunol. 2001;12:166–72.
45. Pickering MC, Cook HT. Translational mini-reviewseries on complement factor H: Renal diseases associatedwith complement factor H—Novel insights from humans andanimals. Clin Exp Immunol. 2008;151:210–30. 46. Wong EK,Anderson HE, Herbert AP, et al. Characterization of afactor H mutation that per turbs the alternative pathway ofcomplement in a f am ily with membranoproliferative GN. JAm Soc Nephrol. 2014;25:2425–33. 47. Xia o X, PickeringMC, Smith RJ. C3 glomerulopa thy: The genetic and clinicalfindings in dense depos it disease and C3glomerulonephritis. Semin Thromb Hemost. 2014;40:465–71.48. Ser vais A, Noel LH, Dragon-Durey MA, et al.Heterogeneous pattern of renal disease associ ated withhomozygous factor H deficiency. Hum P at hol.2011;42:1305–11. 49. Vaziri-Sani F, Holmberg L, SjoholmAG, et al. Phenotypic expression of factor H mutations inpatients with atypical hemolytic uremic syndrome. KidneyInt. 2006;69:981–8. 50. Bom back AS, Smith RJ, Barile GR,et al. Eculizumab for dense deposit disease and C3

glomerulonephritis. Clin J Am Soc Nephrol. 2012;7:748–56.51. Alp er CA, Abramson N, Johnston RB, Jr, et al.Increased susceptibility to infection associated withabnormalities of complement-mediated functions and of thethird component of complement (C3). N Engl J Med.1970;282:350–4. 52. Neary J, Dorman A, Campbell E, et al.Familial membranoproliferative glomerulonephritis typeIII. Am J Kidney Dis. 2002;40:E1. 53. Don adio JV, Jr,Slack TK, Holley KE, et al. DM. Idiopathicmembranoproliferative (mesangiocapillary)glomerulonephritis: A clinicopathologic study. Mayo ClinProc. 1979;54:141–50. 54. Bohle A, Gartner HV, FischbachH, et al. The morphological and clinical features ofmembranoproliferative glomerulonephritis in adults.Virchows Arch A Pathol Anat Histol. 1974;363:213–24. 55.Lu DF , Moon M, Lanning LD, et al. Clinical features andoutcomes of 98 children and adults with dense depositdisease. Pediatr Nephrol. 2012;27:773–81. 56. Park SJ,Kim YJ, Ha TS, et al. Dense deposit disease in Koreanchildren: A multicenter clinicopathologic study. J KoreanMed Sci. 2012;27:1215–21. 57. Duv all-Young J, MacDonaldMK, McKechnie NM. Fundus changes in (type II)mesangiocapillary glomerulonephritis simulating drusen: Ahistopathological report. Br J Ophthalmol. 1989;73:297–302.58. Appel GB, Cook HT, Hageman G, et al.Membranoproliferative glomerulonephritis type II (densedeposit disease): An update. J Am Soc Nephrol.2005;16:1392–403. 59. Sethi S, Fervenza FC.Membranoproliferative glomerulonephritis: A new look at anold entity. N Engl J Med. 2012;366:1119–31.
60. McEnery PT. Membranoproliferative glomerulonephritis:The Cincinnati experience—Cumulative renal survival from1957 to 1989. J Pediatr. 1990;116:S109–14.
61. Ford DM, Briscoe DM, Shanley PF, et al. Childhoodmembranoproliferative glomerulonephritis type I: Limitedsteroid therapy. Kidney Int. 1992;41:1606–12.
62. Tarshish P, Bernstein J, Tobin JN, et al. Treatment ofmesangiocapillary glomerulonephritis with alternatedayprednisone: A report of the International Study of KidneyDisease in Children. Pediatr Nephrol. 1992;6:123–30.
63. Nasr SH, Valeri AM, Appel GB, et al. Dense depositdisease: Clinicopathologic study of 32 pediatric and adultpatients. Clin J Am Soc Nephrol. 2009;4:22–32.
64. De S, Al-Nabhani D, Thorner P, et al. Remission ofresistant MPGN type I with mycophenolate mofetil and

steroids. Pediatr Nephrol. 2009;24:597–600.
65. Sin gh A, Tejani C, Tejani A. One-center experiencewith cyclosporine in refractory nephrotic syndrome inchildren. Pediatr Nephrol. 1999;13:26–32.
66. Erb ay B, Karatan O, Duman N, et al. The effect ofcyclosporine in idiopathic nephrotic syndrome resistant toimmunosuppressive therapy. Transplant Proc.1988;20:289–92.
67. Bag heri N, Nemati E, Rahbar K, et al. Cyclosporine inthe treatment of membranoproliferative glomerulonephritis.Arch Iran Med. 2008;11:26–9.
68. Jan sen JH, Hogasen K, Harboe M, Hovig T. In situcomplement activation in porcine membranoproliferativeglomerulonephritis type II. Kidney Int. 1998;53:331–49.
69. Pickering MC, Cook HT, Warren J, et al. UncontrolledC3 activation causes membranoproliferativeglomerulonephritis in mice deficient in complement factorH. Nat Genet. 2002;31:424–8.
70. McGinley E, Watkins R, McLay A, et al. Plasma exchangein the treatment of mesangiocapillary glomerulonephritis.Nephron. 1985;40:385–90.
71. Obe rkircher OR, Enama M, West JC, et al. Regressionof recurrent membranoproliferative glomerulonephritis typeII in a transplanted kidney after plasmapheresis therapy.Transplant Proc. 1988;20:418–23.
72. Guiard E, Karras A, Plaisier E, et al. Patterns ofnoncryoglobulinemic glomerulonephritis with monoclonal Igdeposits: Correlation with IgG subclass and response torituximab. Clin J Am Soc Nephrol. 2011;6:1609–16.
73. Kat tah AG, Fervenza FC, Roccatello D. Rituximabbasednovel strategies for the treatment of immunemediatedglomerular diseases. Autoimmun Rev. 2013;12:854–9. 74.Radhakrishnan S, Lunn A, Kirschfink M, et al. Eculizumaband refractory membranoproliferative glomerulonephritis. NEngl J Med. 2012;366:1165–6. 75. Vivarelli M, Pasini A,Emma F. Eculizumab for the treatment of dense-depositdisease. N Engl J Med. 2012;366:1163–5. 76. Dai na E,Noris M, Remuzzi G. Eculizumab in a patient withdense-deposit disease. N Engl J Med. 2012;366:1161-3. 77.Marks SD, Rees L. Spontaneous clinical improvement in densedeposit disease. Pediatr Nephrol. 2000;14:322–4. 78.

Ikeda M, Honda M, Hasegawa O. Another example ofspontaneous improvement in a case of dense depositdisease. Pediatr Nephrol. 2001;16:609–10. 79. West CD,McAdams AJ, Witte DP. Acute non-proliferative glomerulitis:A cause of renal failure unique to children. PediatrNephrol. 2000;14:786–93. 80. di Belgiojoso B, Tarantino A,Colasanti G, et al. The prognostic value of some clinicaland histological parameters in membranoproliferativeglomerulonephritis (MPGN): Report of 112 cases. Nephron.1977;19:250–8. 81. Som ers M, Kertesz S, Rosen S, et al.Non-nephrotic children with membranoproliferativeglomerulonephritis: Are steroids indicated? PediatrNephrol. 1995;9:140–4. 82. Little MA, Dupont P, CampbellE, et al. Severity of primary MPGN, rather than MPGN type,determines renal survival and post-transplantationrecurrence risk. Kidney Int. 2006;69:504–11. 83. ÇaltikYilmaz A, Aydog Ö, Ayküz SG, et al. The relation betweentreatment and prognosis of childhood membranoproliferativeglomerulonephritis. Ren Fail. 2014;36:1221–5. 84. Nas rSH, Valeri AM, Appel GB, et al. Dense deposit disease:Clinicopathologic study of 32 pediatric and adult patients.Clin J Am Soc Nephrol. 2009;4:22–32. 85. Bra un MC,Stablein DM, Hamiwka LA, et al. Recurrence ofmembranoproliferative glomerulonephritis type II in renalallografts: The North American Pediatric Renal TransplantCooperative Study experience. J Am Soc Nephrol.2005;16:2225–33. 86. Kotanko P, Pusey CD, Levy JB.Recurrent glomerulonephritis following renaltransplantation. Transplantation. 1997;63:1045–52. 87.Mathew TH. Recurrence of disease following renaltransplantation. Am J Kidney Dis. 1988;12:85–96. 88. Cameron JS. Recurrent disease in renal allografts. KidneyInt. (Suppl) 1993;43:S91–4. 89. Cam eron JS. Recurrentrenal disease after renal transplantation. Curr OpinNephrol Hypertens. 1994;3:602–7.
90. Ramos EL, Tisher CC. Recurrent diseases in the kidneytransplant. Am J Kidney Dis. 1994;24:142–54.
91. Har iharan S, Adams MB, Brennan DC, et al. Recurrentand de novo glomerular disease after renaltransplantation: A report from Renal Allograft DiseaseRegistry (RADR). Transplant 1999;68:635–41.
92. Lorenz EC, Sethi S, Leung N, et al. Recurrentmembranoproliferative glomerulonephritis after kidneytransplantation. Kidney Int. 2010;77:721–8.
REVIEW QUESTIONS
1. What is the major distinguishing pathologic feature ofthe MPGN kidney biopsy?
a. Immunoglobulin deposition on immuno�uorescence
b. Mes angial interposition into the glomerular basementmembrane
c. Mes angial cell proliferation
d. Pod ocyte e�acement
2. Why w as the name MPGN II changed to dense depositdisease?
a. Only 25 % of patients actually had MPGN.
b. MPG N II is the only MPGN with intramembranous deposits.
c. Dens e deposits were the sole disease-de�ningcharacteristic.
3. Whi ch is the classic laboratory �nding in MPGNpatients?
a. Low platelet count
b. Hyp ocomplementemia
c. Gen etic abnormality
d. Pos itive bacterial cultures
4. Which of the following is not a known cause of secondaryMPGN?
a. Systemic lupus erythematosus
b. Viral infection
c. Licorice intoxication
d. Immunoglobulin de�ciency
5. Name the required immune deposit location for densedeposit disease.
a. Subendothelial deposits
b. Intramembranous deposits
c. Subepithelial deposits
d. Mesangial deposits.
6. What is the ratio of MPGN presentation in childrencompared to that in adults?
a. ¼:1
b. ½:1
c. ¾:1
d. 1:1 7. �e most likely pathologic cause of dense depositdisease is: a. A genetic mutation b. An autoantibody c.A protein inhibitor d. An exposure 8. What is the riskfor end-stage renal disease for a patient with MPGN? a.25% b. 50% c. 75% d. 100% 9. Of the MPGN diseases,which is the most likely to result in end-stage renaldisease? a. DDD b. MPGN I c. MPGN III d. C3GN 10. Whatis the risk for recurrence a�er transplant for MPGN? a.25% b. 50% c. 75% d. 100% 11. Which treatment for MPGNis supported by a randomized controlled trial? a. Steroidtherapy b. None c. Mycophenolate mofetil d. Rituximab12. What is the presentation biomarker that is associatedwith the greatest likelihood of advancing to end-stagerenal disease? a. Proteinuria greater than 2 g b. Degreeof interstitial �brosis on presentation biopsy c. Degreeof creatinine elevation at time of kidney biopsy d.Unknown ANSWER KEY 1. b 2. a 3. b 4. c 5. b 6. a 7.b 8. b 9. a 10. b 11. a 12. d
20 Membranous nephropathy
1. Wasserstein AG. Membranous glomerulonephritis. J Am SocNephrol. 1997;8:664–74.
2. Glassock RJ. Attending rounds: An older patient withnephrotic syndrome. Clin J Am Soc Nephrol. 2012;7:665–70.
3. Hla dunewich MA, Troyanov S, Calafati J, et al. Thenatural history of the non-nephrotic membranous nephropathypatient. Clin J Am Soc Nephrol. 2009;4:1417–22.
4. Lee BH, Cho HY, Kang HG, et al. Idiopathic membranousnephropathy in children. Pediatr Nephrol. 2006;21:1707–15.
5. Chen A, Frank R, Vento S, et al. Idiopathic membranousnephropathy in pediatric patients: Presentation, responseto therapy, and long-term outcome. BMC Nephrol. 2007;8:11.
6. Menon S, Valentini RP. Membranous nephropathy inchildren: Clinical presentation and therapeutic approach.Pediatr Nephrol. 2010;25:1419–28.
7. International Study of Kidney Disease in Children.Nephrotic syndrome in children: Prediction ofhistopathology from clinical and laboratory characteristicsat time of diagnosis: A report of the International Studyof Kidney Disease in Children. Kidney Int. 1978;13:159–65.
8. Takekoshi Y, Tanaka M, Shida N, et al. Strongassociation between membranous nephropathy and hepatitis-Bsurface antigenaemia in Japanese children. Lancet.1978;18;2:1065–8.
9. Hsu HC, Wu CY, Lin CY, et al. Membranous nephropathy in52 hepatitis B surface antigen (HBsAg) carrier children inTaiwan. Kidney Int. 1989;36:1103–7. 10. Mox ey-Mims MM,Stapleton FB, Feld LG. Applying decision analysis tomanagement of adolescent idiopathic nephrotic syndrome.Pediatr Nephrol. 1994;8:660–4. 11. 2013 U.S. Renal DataSystem annual data, report. Pediatric ESRD. Available at:http://www.usrds. org/2013/pdf/v2_ch8_13.pdf. Accessed onJanuary 2, 2015. 12. Hendrickse RG, Adeniyi A, EdingtonGM, et al. Quartan malarial nephrotic syndrome:Collaborative clinicopathological study in Nigerian schoolchildren. Lancet. 1972;1:1143–9. 13. Liao MT, Chang MH,Lin FG, et al. Universal hepatitis B vaccination reduceschildhood hepatitis B virusassociated membranousnephropathy. Pediatrics. 2011;128:e600–4. 14. Olowu WA,Adelusola KA, Adefehinti O, et al. Quartan

malaria-associated childhood nephrotic syndrome: Now a rareclinical entity in malaria endemic Nigeria. Nephrol DialTransplant. 2010;25:794–801. 15. Doi T, Mayumi M, KanatsuK, et al. Distribution of IgG subclasses in membranousnephropathy. Clin Exp Immunol. 1984;58:57–62. 16. NoëlLH, Aucouturier P, Monteiro RC, et al. Glomerular andserum immunoglobulin G subclasses in membranousnephropathy and anti-glomerular basement membranenephritis. Clin Immunol Immunopathol. 1988;46:186–94. 17.Troyanov S, Roasio L, Pandes M, et al. Renal pathology inidiopathic membranous nephropathy: A new perspective.Kidney Int. 2006;69:1641–8. 18. Rodriguez EF, Nasr SH,Larsen CP, et al. Membranous nephropathy with crescents: Aseries of 19 cases. Am J Kidney Dis. 2014;64:66–73. 19.Churg J, Sobin LH. Renal disease: Classification and atlasof glomerular diseases. Tokyo: Igaku-shoin, 1982, p. 52.20. Tsukahara H, Takahashi Y, Yoshimoto M, et al. Clinicalcourse and outcome of idiopathic membranous nephropathy inJapanese children. Pediatr Nephrol. 1993;7:387–91. 21.Ardalan M. Triggers, bullets and targets, puzzle ofmembranous nephropathy. Nephrourol Mon. 2012;4:599–602.22. Ronco P, Debiec H, Imai H. Circulating antipodocyteantibodies in membranous nephropathy: Pathophysiologic andclinical relevance. Am J Kidney Dis. 2013;62:16–9 23.Debiec H, Lefeu F, Kemper MJ, et al. Early-childhoodmembranous nephropathy due to cationic bovine serumalbumin. N Engl J Med. 2011;364:2101–10. 24. Wong SN, ChanWK, Hui J, et al. Membranous lupus nephritis in Chinesechildren: A case series and review of the literature.Pediatr Nephrol. 2009;24:1989–96.
25. Aline-Fardin A, Rifle G, Martin L, et al. Recurrent andde novo membranous glomerulopathy after kidneytransplantation. Transplant Proc 2009; 41: 669–671.
26. Wan g HH, Yang AH, Yang LY, et al. Chronicgraftversus-host disease complicated by nephrotic syndrome.J Chin Med Assoc. 2011;74:419-22.
27. Palcoux JB, Gaulme J, Demeocq F, et al.Extramembranous glomerulonephritis during congenitalsyphilis. Arch Fr Pediatr. 1979;36:691–5.
28. Deb iec H, Guigonis V, Mougenot B, et al. Antenatalmembranous glomerulonephritis due to antineutralendopeptidase antibodies. N Engl J Med. 2002;346:2053–60.
29. Purswani MU, Chernoff MC, Mitchell CD, et al. Chronickidney disease associated with perinatal HIV infection inchildren and adolescents. Pediatr Nephrol. 2012;27:981–9.
30. Araya CE, Gonzalez-Peralta RP, Skoda-Smith S, et al.Systemic Epstein-Barr virus infection associated withmembranous nephropathy in children. Clin Nephrol.2006;65:160–4.
31. Stur gill BC, Shearlock KT. Membranous glomerulopathyand nephrotic syndrome after captopril therapy. JAMA.1983;250:234–5.
32. Naw az FA, Larsen CP, Troxell ML. Membranousnephropathy and nonsteroidal anti-inflammatory agents. AmJ Kidney Dis. 2013;62:1012–7.
33. Hal l CL. The natural course of gold and penicillaminenephropathy: A long-term study of 54 patients. Adv Exp MedBiol. 1989;252:247–56.
34. Kaw asaki Y, Suzuki J, Sike T, et al.Bucillamineinduced nephropathy in a child with juvenilerheumatoid arthritis and Kartagener’s syndrome. PediatrInt. 2000;42:316–8.
35. Theodoni G, Printza N, Karyda S, et al.D-penicillamine induced membranous glomerulonephritis in achild with Wilson’s disease. Hippokratia. 2012;16:94.
36. Heymann W, Hackel DB, Harwod S. et al. Production ofthe nephrotic syndrome in rats by Freund’s adjuvants andrat kidney suspensions. Proc Soc Exp Biol Med.1959;10:60–4.
37. Cou ser WG, Steinmuller DR, Stilmant MM, et al.Experimental glomerulonephritis in the isolated perfusedrat kidney. J Clin Invest. 1978; 62:1275–87.
38. Farquhar MG, Saito A, Kerjaschki D, et al. The Heymannnephritis antigenic complex: Megalin (gp330) and RAP. J AmSoc Nephrol. 1995;6:35–47.
39. Bec k LH Jr, Bonegio RG, Lambeau G, et al. M-typephospholipase A2 receptor as target antigen in idiopathicmembranous nephropathy. N Engl J Med. 2009;361:11–21.
40. Tomas NM, Beck LH Jr, Meyer-Schwesinger C, et al.Thrombospondin type-1 domain-containing 7A in idiopathicmembranous nephropathy. N Engl J Med. 2014;371:2277–8741. Border WA, Ward HJ, Kamil ES, et al. Induction ofmembranous nephropathy in rabbits by administration of anexogenous cationic antigen. J Clin Invest. 1982;69:451–61.
42. Fujigaki Y, Nagase M, Honda N. Intraglomerularbasement membrane translocation of immune complex (IC) inthe development of passive in situ IC nephritis of rats.Am J Pathol. 1993;142:831–842. 43. Tak ekoshi Y, Tanaka M,Miyakawa Y, et al. Free “small” and IgG associated “large”hepatitis B e antigen in the serum and glomerularcapillary walls of two patients with membranousglomerulonephritis. N Engl J Med. 1979;300:814–9. 44. BeckLH Jr, Salant DJ. Membranous nephropathy: From models toman. J Clin Invest. 2014;124:2307–14. 45. Cyb ulsky AV,Quigg RJ, Salant DJ. Experimental membranous nephropathyredux. Am J Physiol Renal Physiol. 2005;289:F660–71. 46.Nangaku M, Shankland SJ, William G. Couser WG. Cellularresponse to injury in membranous nephropathy. J Am SocNephrol. 2005;16:1195–204. 47. Kon S P, Coupes B, ShortCD, et al. Urinary C5b-9 excretion and clinical course inidiopathic human membranous nephropathy. Kidney Int.1995;48:1953–8. 48. Pap agianni AA, Alexopoulos E,Leontsini M, et al. C5b-9 and adhesion molecules in humanidiopathic membranous nephropathy. Nephrol DialTransplant. 2002;17:57–63. 49. Ano nymous. Collaborativestudy of the adult idiopathic nephritic syndrome: Acontrolled study of short-term prednisone treatment inadults with membranous nephropathy. N Engl J Med.1979;301:1301–6. 50. Cam eron JS, Healy MJ, Adu D. TheMedical Research Council Trial of short-term high-dosealternate day prednisone in idiopathic membranousnephropathy with nephritic syndrome in adults. Q J Med.1990;274:133–56. 51. Cat tran DC, Delmore T, Roscoe J, etal. A randomized controlled trial of prednisone in patientswith idiopathic membranous nephropathy. N Engl J Med.1989;320:210–5. 52. International Society of Nephrology.Kidney disease: Improving global outcomes (KDIGO) clinicalpractice guideline for glomerulonephritis. Idiopathicmembranous nephropathy. Kidney Int Suppl. 2012;2:186–97.53. Ponticelli C, Zucchelli P, Passerini P, et al. Arandomized trial of methylprednisolone and chlorambucil inidiopathic membranous nephropathy. N Engl J Med.1989;320:8–13. 54. How man A, Chapman TL, Langdon MM, etal. Immunosuppression for progressive membranousnephropathy: A UK randomised controlled trial. Lancet.2013;381:744–51.
55. Cattran DC, Greenwood C, Ritchie S, et al. Acontrolled trial of cyclosporine in patients withprogressive membranous nephropathy. CanadianGlomerulonephritis Study Group. Kidney Int.1995;47:1130–5.
56. Alexopoulos E, Papagianni A, Tsamelashvili M, et al.
Induction and long-term treatment with cyclosporine inmembranous nephropathy with the nephrotic syndrome.Nephrol Dial Transplant. 2006;21:3127–32.
57. Amb alavanan S, Fauvel JP, Sibley RK, et al. Mechanismof the antiproteinuric effect of cyclosporine in membranousnephropathy. J Am Soc Nephrol. 1996;7:290–8.
58. Schönenberger E, Ehrich JH, Haller H, et al. Thepodocyte as a direct target of immunosuppressive agents.Nephrol Dial Transplant. 2011;26:18–24.
59. Faul C, Donnelly M, Merscher-Gomez S, et al. The actincytoskeleton of kidney podocytes is a direct target of theantiproteinuric effect of cyclosporine A. Nat Med.2008;14:931–8.
60. Pra ga M, Barrio V, Juárez GF, et al. Tacrolimusmonotherapy in membranous nephropathy: A randomizedcontrolled trial. Kidney Int. 2007;71:924–30.
61. Xu J, Z hang W, Xu Y, et al. Tacrolimus combined withcorticosteroids in idiopathic membranous nephropathy: Arandomized, prospective, controlled trial. ContribNephrol. 2013;181:152–62.
62. Che n M, Li H, Li XY, Lu FM, et al. Tacrolimus combinedwith corticosteroids in treatment of nephrotic idiopathicmembranous nephropathy: A multicenter randomized controlledtrial. Am J Med Sci. 2010;339:233–8.
63. Che n Y, Schieppati A, Chen X, et al.Immunosuppressive treatment for idiopathic membranousnephropathy in adults with nephrotic syndrome. CochraneDatabase Syst Rev. 2014;(10):004293.
64. Miller G, Zimmerman R 3rd, Radhakrishnan J, et al. Useof mycophenolate mofetil in resistant membranousnephropathy. Am J Kidney Dis. 2000;36:250–6.
65. Branten AJ, du Buf-Vereijken PW, Vervloet M, et al.Mycophenolate mofetil in idiopathic membranousnephropathy: A clinical trial with comparison to ahistoric control group treated with cyclophosphamide. Am JKidney Dis. 2007;50:248–56.
66. Dussol B, Morange S, Burtey S, et al. Mycophenolatemofetil monotherapy in membra nous nephropathy: A 1-yearrandomized controlled trial. Am J Kidney Dis.2008;52:699–705.

67. Annonymus. Package insert of Rituxan. Available at:http://www.gene.com/download/pdf/rituxan_ prescribing.pdf.Accessed January 5, 2015. 68. Fer venza FC, Cosio FG,Erickson SB, et al. Rituximab treatment of idiopathicmembranous nephropathy. Kidney Int. 2008;73:117–25. 69.Beck LH Jr, Fervenza FC, Beck DM, et al. Rituximab-induceddepletion of anti-PLA2R autoantibodies predicts responsein mem branous nephropathy. J Am Soc Nephrol.2011;22:1543–50. 70. Rug genenti P, Cravedi P, Chianca A,et al. Rituximab in idiopathic membranous nephropa thy. JAm Soc Nephrol. 2012; 23:1416–25. 71. Approval package forH.P. Acthar Gel. Available athttp://www.accessdata.fda.gov/drugsatfda_ docs/nda/2010/022432Orig1s000Approv.pdf. Accessed August 8,2015. 72. Ponticelli C, Passerini P, Salvadori M, et al. Arandomized pilot trial comparing methylpred nisolone plus acytotoxic agent versus synthetic adreno corticotropichormone in idiopathic membranous nephropathy. Am J KidneyDis. 2006;47:233-40. 73. Rau en T, Michaelis A, Floege J,et al. Case series of idiopathic membranous nephropathywith longterm beneficial effects of ACTH peptide 1-24. ClinNephrol. 2009 ;71:637-42. 74. Hla dunewich MA, Cattran D,Beck LH, et al. A pilot study to determine the dose andeffectiveness of adrenocorticotrophic hormone (H.P.Acthar® Gel) in nephrotic syndrome due to idiopathic membranous nephropathy. Nephrol Dial Transplant. 2014;29:1570-7. 75. van d en Brand JA, van Dijk PR, HofstraJM, Wetzels JF. Long-term outcomes in idiopathicmembranous nephropathy using a restric tive treatmentstrategy. J Am Soc Nephrol. 20 14 ;25:150–8. 76. Wuh l E,Trivelli A, Picca S, et al. Strict bloodpressure controland progression of renal failure in children. N Engl JMed. 2009;361:1639–50. 77. Daniels SR, Greer FR; Committeeon Nutrition. Lipid screening and cardiovascular health inchild hood. Pediatrics. 2008;122:198–208. 78. Noel LH,Zanetti M, Droz D, Barbanel C: Longterm prognosis ofidiopathic membranous glo merulonephritis: Study of 116untreated patients. Am J Med. 1079;66:82–90. 79. ZhangLJ, Zhang Z, Li SJ, et al. Pulmonary embolism and renalvein thrombosis in patients with nephrotic syndrome:Prospective evaluation of prevalence and risk factors withCT. Radiology. 2014;273:897–906. 80. Hsu HF, Huang SY.Carotid artery thrombosis in a child with membranousnephropathy associated with factor V Leiden mutation.Pediatr Int. 2012;54:573–4.
81. Mahmoodi BK, ten Kate MK, Waanders F, et al. Highabsolute risks and predictors of venous and arterialthromboembolic events in patients with nephrotic syndrome:

Results from a large retrospective cohort study.Circulation. 2008;117:224–30.
82. Kerlin BA, Blatt NB, Fuh B, et al. Epidemiology andrisk factors for thromboembolic complications of childhoodnephrotic syndrome: A Midwest Pediatric NephrologyConsortium (MWPNC) study. J Pediatr. 2009;155:105–110.
83. Ker lin BA, Ayoob R, Smoyer WE. Epidemiology andpathophysiology of nephrotic syndrome-associatedthromboembolic disease. Clin J Am Soc Nephrol.2012;7:513–20.
84. Donadio JV Jr, Torres VE, Velosa JA, et al. Idiopathicmembranous nephropathy: The natural history of untreatedpatients. Kidney Int. 1988;33:708–15.
85. Schieppati A, Mosconi L, Perna A, et al. Prognosis ofuntreated patients with idiopathic membranous nephropathy.N Engl J Med. 1993;229:85–89, 1993.
86. Pol anco N, Gutiérrez E, Covarsí A, et al. Spontaneousremission of nephrotic syndrome in idiopathic membranousnephropathy. J Am Soc Nephrol. 2010;21:697–704.
87. Hei det L, Gagnadoux ME, Beziau A, et al. Recurrenceof de novo membranous glomerulonephritis on renal grafts.Clin Nephrol 1994;41:31
REVIEW QUESTIONS
1. Membranous nephropathy is:
a. �e leading cause of nephrotic syndrome in adults
b. �e leading cause of nephrotic syndrome in children c.Idiopathic in most cases, whatever the patient age d.Mainly associated with lupus nephropathy 2. �e diagnosisof membranous nephropathy relies on: a. Nephrotic-rangeproteinuria b. �e age at onset of nephrotic syndrome c.Renal biopsy �ndings of thickened glomerular capillarywall, immunopathology, and electron microscopy showingsubepithelial deposits d. Low circulating C3 and C4 in theplasma 3. �e treatment of idiopathic membranousnephropathy includes all except: a. Prednisone +calcineurin antagonists b. Prednisone + alkylating agentsc. Immunosuppression and ACE inhibitors d.Immunosuppression and ARBs e. Complement blockade byeculizumab 4. Circulating anti-PLA2R antibodies are seenin patients with: a. Membranous nephropathy associated
with systemic lupus erythematosus b. Membranousnephropathy associated with drugs and toxins c. Primaryor idiopathic membranous nephropathy d. Membranousnephropathy associated with hepatitis B 5.Corticosteroids, as a monotherapy, can producelong-lasting remission in patients with membranousnephropathy. a. True b. False ANSWER KEY 1. a 2. c 3.e 4. c 5. b
21 Acute glomerulonephritis
12. Rodríguez-Iturbe B, Rubio L, García R. Attack rate ofpoststreptococcal nephritis in families: A prospectivestudy. Lancet. 1981;1:401–3.
13. Tas ic V, Polenakovic M. Occurrence of subclinicalpost-streptococcal glomerulonephritis in family contacts. JPaediatr Child Health. 2003;39:177–9.
14. Sagel I, Treser G, Ty A, et al. Occurrence and natureof glomerular lesions after group A streptococcalinfections in children. Ann Intern Med. 1973;79:492–9.
15. Lew y JE, Salinas-Madrigal L, Herdson PB, et al.Clinico-pathologic correlations in acute poststreptococcalglomerulonephritis: A correlation between renal functions,morphologic damage and clinical course of 46 children withacute poststreptococcal glomerulonephritis. Medicine(Baltimore) 1971;50:453–501.
16. Modai D, Pik A, Behar M, et al. Biopsy proven evolutionof post streptococcal glomerulonephritis to rapidlyprogressive glomerulonephritis of a post infectious type.Clin Nephrol. 1985;23:198–202.
17. Bat son BN, Baliga R. Post-streptococcal hypertensiveencephalopathy with normal urinalysis. Pediatr Nephrol.2003;18:73.
18. Zak i SA, Shanbag P. Unusual presentation ofpoststreptococcal glomerulonephritis as posteriorreversible encephalopathy syndrome. J Pediatr Neurosci.2014;9:42–4.
19. Rova ng RD, Zawada ET Jr, Santella RN, et al. Cerebralvasculitis associated with acute poststreptococcalglomerulonephritis. Am J Nephrol. 1997;17:89–92.
20. Nasr SH, Radhakrishnan J, D’Agati VD. Bacterialinfection-related glomerulonephritis in adults. KidneyInt. 2013;83:792–803.
21. Jennings RB, Earle DP. Post-streptococcalglomerulonephritis: Histopathologic and clinical studies ofthe acute, subsiding acute and early chronic latentphase’s. J Clin Invest. 1961;40:1525–95.
22. Wong W, Morris MC, Zwi J. Outcome of severe acutepost-streptococcal glomerulonephritis in New Zealand
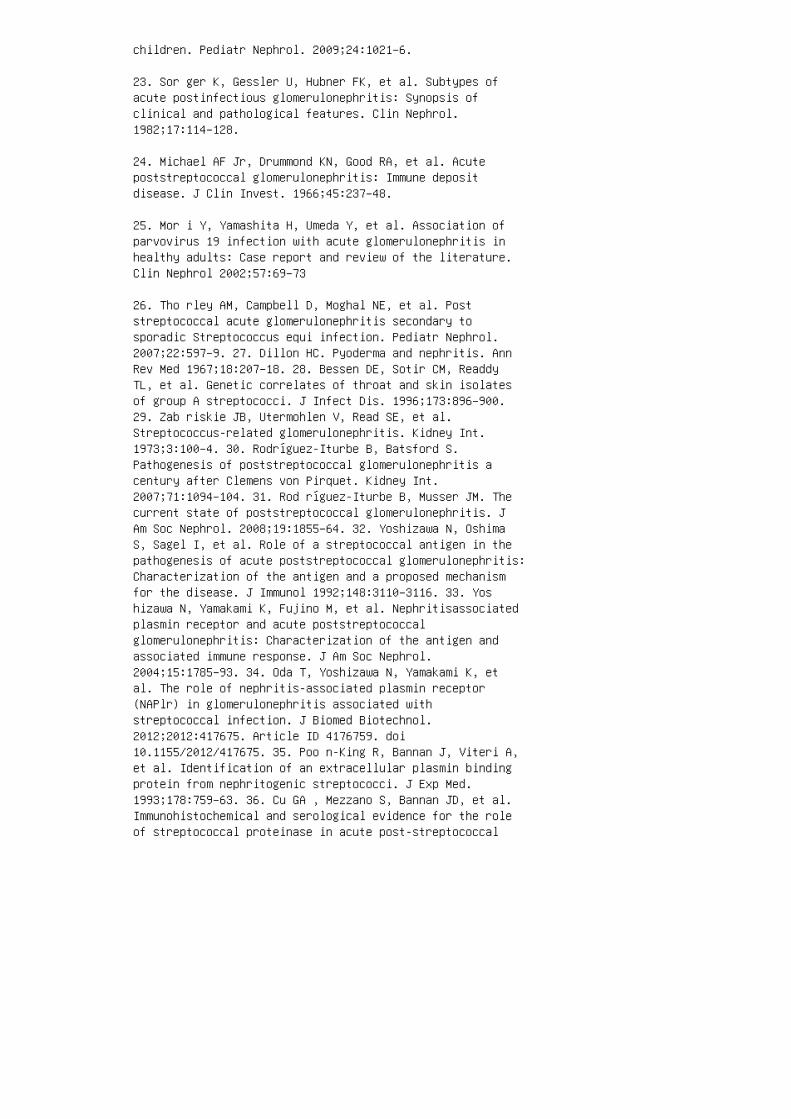
children. Pediatr Nephrol. 2009;24:1021–6.
23. Sor ger K, Gessler U, Hubner FK, et al. Subtypes ofacute postinfectious glomerulonephritis: Synopsis ofclinical and pathological features. Clin Nephrol.1982;17:114–128.
24. Michael AF Jr, Drummond KN, Good RA, et al. Acutepoststreptococcal glomerulonephritis: Immune depositdisease. J Clin Invest. 1966;45:237–48.
25. Mor i Y, Yamashita H, Umeda Y, et al. Association ofparvovirus 19 infection with acute glomerulonephritis inhealthy adults: Case report and review of the literature.Clin Nephrol 2002;57:69–73
26. Tho rley AM, Campbell D, Moghal NE, et al. Poststreptococcal acute glomerulonephritis secondary tosporadic Streptococcus equi infection. Pediatr Nephrol.2007;22:597–9. 27. Dillon HC. Pyoderma and nephritis. AnnRev Med 1967;18:207–18. 28. Bessen DE, Sotir CM, ReaddyTL, et al. Genetic correlates of throat and skin isolatesof group A streptococci. J Infect Dis. 1996;173:896–900.29. Zab riskie JB, Utermohlen V, Read SE, et al.Streptococcus-related glomerulonephritis. Kidney Int.1973;3:100–4. 30. Rodríguez-Iturbe B, Batsford S.Pathogenesis of poststreptococcal glomerulonephritis acentury after Clemens von Pirquet. Kidney Int.2007;71:1094–104. 31. Rod ríguez-Iturbe B, Musser JM. Thecurrent state of poststreptococcal glomerulonephritis. JAm Soc Nephrol. 2008;19:1855–64. 32. Yoshizawa N, OshimaS, Sagel I, et al. Role of a streptococcal antigen in thepathogenesis of acute poststreptococcal glomerulonephritis:Characterization of the antigen and a proposed mechanismfor the disease. J Immunol 1992;148:3110–3116. 33. Yoshizawa N, Yamakami K, Fujino M, et al. Nephritisassociatedplasmin receptor and acute poststreptococcalglomerulonephritis: Characterization of the antigen andassociated immune response. J Am Soc Nephrol.2004;15:1785–93. 34. Oda T, Yoshizawa N, Yamakami K, etal. The role of nephritis-associated plasmin receptor(NAPlr) in glomerulonephritis associated withstreptococcal infection. J Biomed Biotechnol.2012;2012:417675. Article ID 4176759. doi10.1155/2012/417675. 35. Poo n-King R, Bannan J, Viteri A,et al. Identification of an extracellular plasmin bindingprotein from nephritogenic streptococci. J Exp Med.1993;178:759–63. 36. Cu GA , Mezzano S, Bannan JD, et al.Immunohistochemical and serological evidence for the roleof streptococcal proteinase in acute post-streptococcal
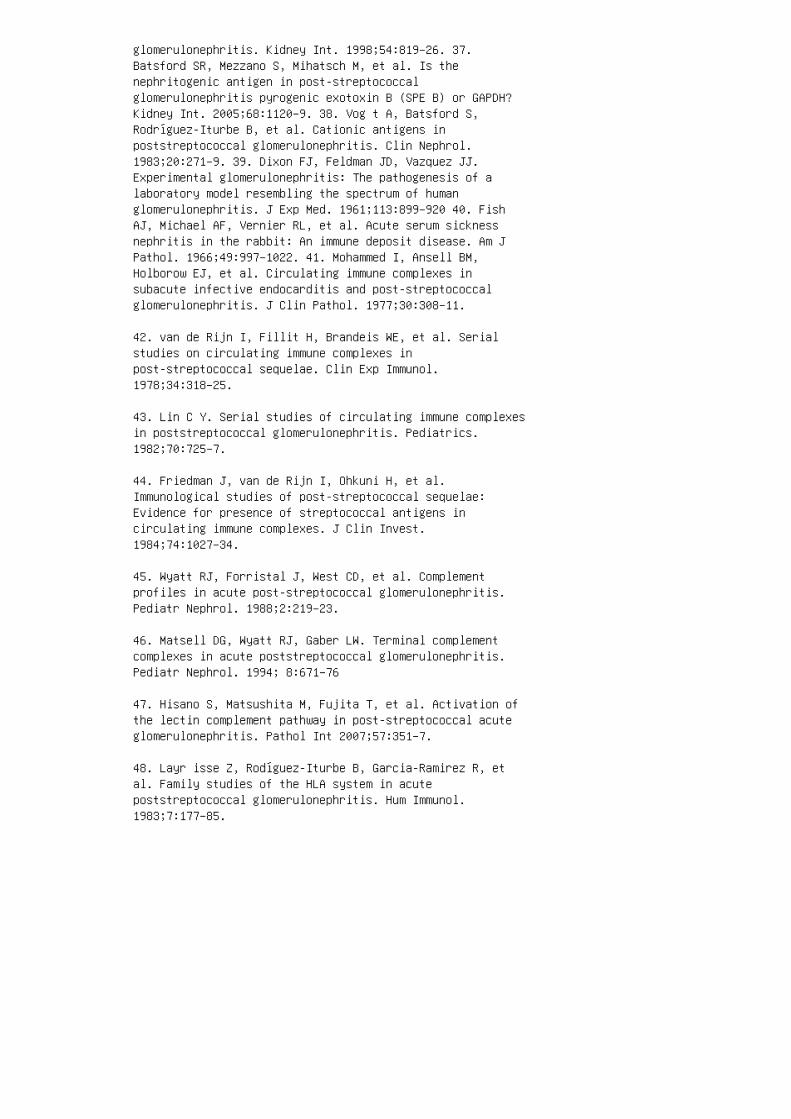
glomerulonephritis. Kidney Int. 1998;54:819–26. 37.Batsford SR, Mezzano S, Mihatsch M, et al. Is thenephritogenic antigen in post-streptococcalglomerulonephritis pyrogenic exotoxin B (SPE B) or GAPDH?Kidney Int. 2005;68:1120–9. 38. Vog t A, Batsford S,Rodríguez-Iturbe B, et al. Cationic antigens inpoststreptococcal glomerulonephritis. Clin Nephrol.1983;20:271–9. 39. Dixon FJ, Feldman JD, Vazquez JJ.Experimental glomerulonephritis: The pathogenesis of alaboratory model resembling the spectrum of humanglomerulonephritis. J Exp Med. 1961;113:899–920 40. FishAJ, Michael AF, Vernier RL, et al. Acute serum sicknessnephritis in the rabbit: An immune deposit disease. Am JPathol. 1966;49:997–1022. 41. Mohammed I, Ansell BM,Holborow EJ, et al. Circulating immune complexes insubacute infective endocarditis and post-streptococcalglomerulonephritis. J Clin Pathol. 1977;30:308–11.
42. van de Rijn I, Fillit H, Brandeis WE, et al. Serialstudies on circulating immune complexes inpost-streptococcal sequelae. Clin Exp Immunol.1978;34:318–25.
43. Lin C Y. Serial studies of circulating immune complexesin poststreptococcal glomerulonephritis. Pediatrics.1982;70:725–7.
44. Friedman J, van de Rijn I, Ohkuni H, et al.Immunological studies of post-streptococcal sequelae:Evidence for presence of streptococcal antigens incirculating immune complexes. J Clin Invest.1984;74:1027–34.
45. Wyatt RJ, Forristal J, West CD, et al. Complementprofiles in acute post-streptococcal glomerulonephritis.Pediatr Nephrol. 1988;2:219–23.
46. Matsell DG, Wyatt RJ, Gaber LW. Terminal complementcomplexes in acute poststreptococcal glomerulonephritis.Pediatr Nephrol. 1994; 8:671–76
47. Hisano S, Matsushita M, Fujita T, et al. Activation ofthe lectin complement pathway in post-streptococcal acuteglomerulonephritis. Pathol Int 2007;57:351–7.
48. Layr isse Z, Rodíguez-Iturbe B, Garcia-Ramirez R, etal. Family studies of the HLA system in acutepoststreptococcal glomerulonephritis. Hum Immunol.1983;7:177–85.

49. Bak r A, Mahmoud LA, Al-Chenawi F, Salah A. HLADRB1alleles in Egyptian children with poststreptococcal acuteglomerulonephritis. Pediatr Nephrol. 2007;22:376–9.
50. Dur sun H, Noyan A, Matyar S, et al. Endothelial nitricoxide synthase gene intron 4 a/b VNTR polymorphism inchildren with APSGN. Pediatr Nephrol. 2006; 21:1661–5.
51. Lem e CE, Ribeiro CA Jr, Silva HB. Renal tubularsodium reabsorption during the recovery from the oliguricphase of acute nephritis. Biomedicine. 1975;23:92–6.
52. Mota-Hernandez F, Feiman R, Gordillo-Paniagua G.Predictive value of fractional excretion of filteredsodium for hypertension in acute post-streptococcalglomerulonephritis. J Pediatr. 1984;104:560–3.
53. Ozd emir S, Saatçi U, Beşbaş N, et al. Plasma atrialnatriuretic peptide and endothelin levels in acutepoststreptococcal glomerulonephritis. Pediatr Nephrol.1992;6:519–22.
54. Powell HR, Rotenberg E, Williams AL, Credie MC. Plasmarenin activity in acute post-streptococcalglomerulo-nephritis and the haemolytic-uraemic syndrome.Arch Dis Child. 1974;49:802–7.
55. Mae kawa S, Fukuda K, Yamauchi T, et al. Follow-upstudy of pharyngeal carriers of beta-hemolyticstreptococci among s3chool children in Sapporo City duringa period of 2 years and 5 months. J Clin Microbiol.1981;13:101–22.
56. Str ömberg A, Schwan A, Cars O. Throat carrier ratesof beta-hemolytic streptococci among healthy adults andchildren. Scand J Infect Dis. 1988;20:411–7. 57. Parks T,Smeesters PR, Curtis N, et al. ASO titer or not? When touse streptococcal serology: A guide for clinicians. Eur JClin Microbiol Infect Dis. 2015;34:945–9. 58. Dod ge WF,Spargo BH, Travis LB, et al. Poststreptococcalglomerulonephritis: A prospective study in children. N EnglJ Med. 1972; 286: 273–8. 59. Meekin GE, Martin DR, DawsonKP. Probable association of M type 57 streptococcal skininfection with acute glomerulonephritis in the Taurangaarea. N Z Med J. 1980;91:456–60. 60. Wes t CD, NorthwayJD, Davis NC. Serum levels of beta-1C globulin, acomplement component, in the nephritidies, lipoidnephrosis and other conditions. J Clin Invest. 1964;43:1507-17. 61. Cameron JS, Vick RM, Ogg SC, et al. PlasmaC3 and C4 concentrations in management of
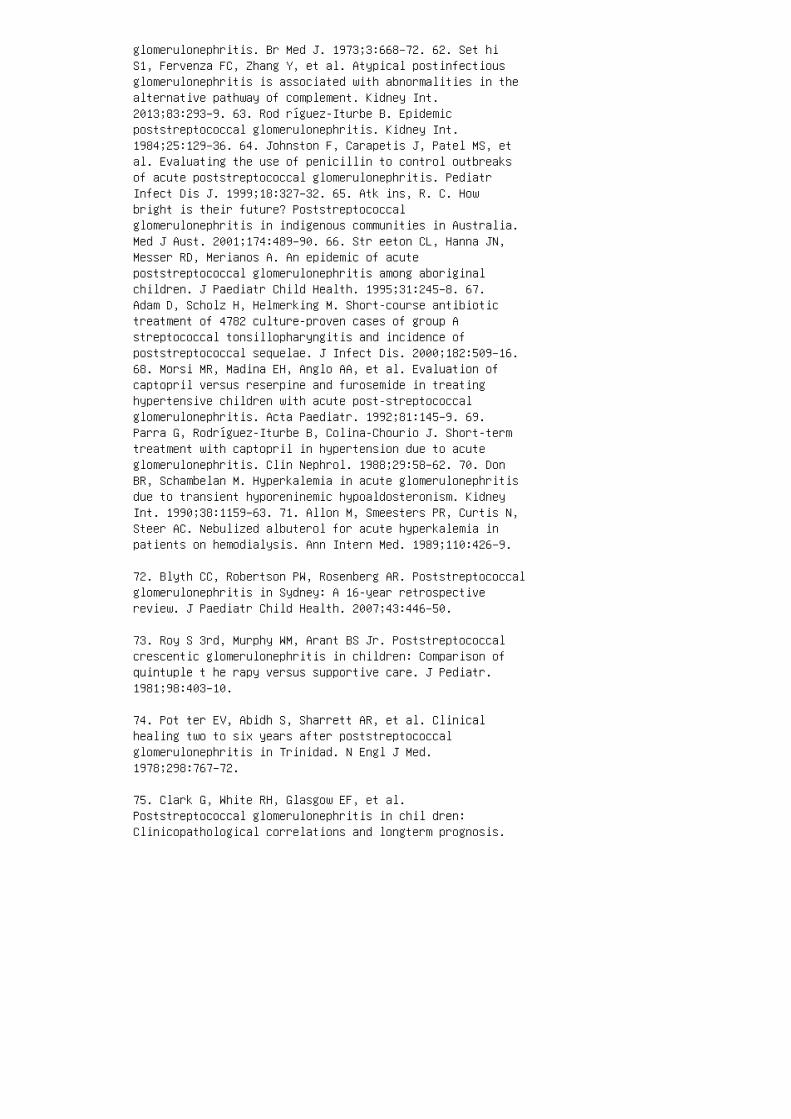
glomerulonephritis. Br Med J. 1973;3:668–72. 62. Set hiS1, Fervenza FC, Zhang Y, et al. Atypical postinfectiousglomerulonephritis is associated with abnormalities in thealternative pathway of complement. Kidney Int.2013;83:293–9. 63. Rod ríguez-Iturbe B. Epidemicpoststreptococcal glomerulonephritis. Kidney Int.1984;25:129–36. 64. Johnston F, Carapetis J, Patel MS, etal. Evaluating the use of penicillin to control outbreaksof acute poststreptococcal glomerulonephritis. PediatrInfect Dis J. 1999;18:327–32. 65. Atk ins, R. C. Howbright is their future? Poststreptococcalglomerulonephritis in indigenous communities in Australia.Med J Aust. 2001;174:489–90. 66. Str eeton CL, Hanna JN,Messer RD, Merianos A. An epidemic of acutepoststreptococcal glomerulonephritis among aboriginalchildren. J Paediatr Child Health. 1995;31:245–8. 67.Adam D, Scholz H, Helmerking M. Short-course antibiotictreatment of 4782 culture-proven cases of group Astreptococcal tonsillopharyngitis and incidence ofpoststreptococcal sequelae. J Infect Dis. 2000;182:509–16.68. Morsi MR, Madina EH, Anglo AA, et al. Evaluation ofcaptopril versus reserpine and furosemide in treatinghypertensive children with acute post-streptococcalglomerulonephritis. Acta Paediatr. 1992;81:145–9. 69.Parra G, Rodríguez-Iturbe B, Colina-Chourio J. Short-termtreatment with captopril in hypertension due to acuteglomerulonephritis. Clin Nephrol. 1988;29:58–62. 70. DonBR, Schambelan M. Hyperkalemia in acute glomerulonephritisdue to transient hyporeninemic hypoaldosteronism. KidneyInt. 1990;38:1159–63. 71. Allon M, Smeesters PR, Curtis N,Steer AC. Nebulized albuterol for acute hyperkalemia inpatients on hemodialysis. Ann Intern Med. 1989;110:426–9.
72. Blyth CC, Robertson PW, Rosenberg AR. Poststreptococcalglomerulonephritis in Sydney: A 16-year retrospectivereview. J Paediatr Child Health. 2007;43:446–50.
73. Roy S 3rd, Murphy WM, Arant BS Jr. Poststreptococcalcrescentic glomerulonephritis in children: Comparison ofquintuple t he rapy versus supportive care. J Pediatr.1981;98:403–10.
74. Pot ter EV, Abidh S, Sharrett AR, et al. Clinicalhealing two to six years after poststreptococcalglomerulonephritis in Trinidad. N Engl J Med.1978;298:767–72.
75. Clark G, White RH, Glasgow EF, et al.Poststreptococcal glomerulonephritis in chil dren:Clinicopathological correlations and longterm prognosis.
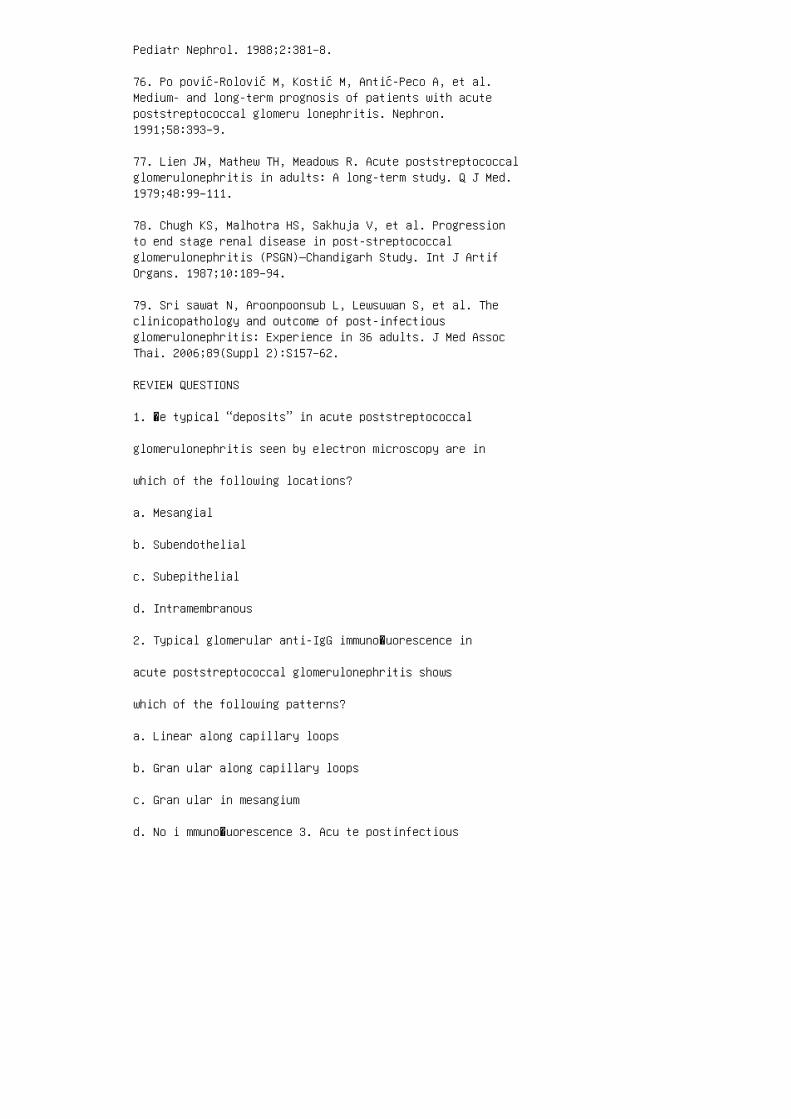
Pediatr Nephrol. 1988;2:381–8.
76. Po pović-Rolović M, Kostić M, Antić-Peco A, et al.Medium- and long-term prognosis of patients with acutepoststreptococcal glomeru lonephritis. Nephron.1991;58:393–9.
77. Lien JW, Mathew TH, Meadows R. Acute poststreptococcalglomerulonephritis in adults: A long-term study. Q J Med.1979;48:99–111.
78. Chugh KS, Malhotra HS, Sakhuja V, et al. Progressionto end stage renal disease in post-streptococcalglomerulonephritis (PSGN)—Chandigarh Study. Int J ArtifOrgans. 1987;10:189–94.
79. Sri sawat N, Aroonpoonsub L, Lewsuwan S, et al. Theclinicopathology and outcome of post-infectiousglomerulonephritis: Experience in 36 adults. J Med AssocThai. 2006;89(Suppl 2):S157–62.
REVIEW QUESTIONS
1. �e typical “deposits” in acute poststreptococcal
glomerulonephritis seen by electron microscopy are in
which of the following locations?
a. Mesangial
b. Subendothelial
c. Subepithelial
d. Intramembranous
2. Typical glomerular anti-IgG immuno�uorescence in
acute poststreptococcal glomerulonephritis shows
which of the following patterns?
a. Linear along capillary loops
b. Gran ular along capillary loops
c. Gran ular in mesangium
d. No i mmuno�uorescence 3. Acu te postinfectious

glomerulonephritis most commonly follows infection bywhich of the following organisms? a. Group A β-hemolyticstreptococcus b. Group B β-hemolytic streptococcus c.Group C β-hemolytic streptococcus d. Gro up Cstreptococcus 4. Which of the following is true regardingscabies-associated acute postinfectiousglomerulonephritis? a. �e latent period is longer than intonsillitisassociated disease. b. It is usually not causedby group A β-hemolytic streptococcus. c. Complement C3 istypically not decreased. d. An antigen from Sarcoptesscabiei is present in the glomeruli. 5. Which of thefollowing statements is true regarding the epidemiology ofacute poststreptococcal glomerulonephritis? a. It is morecommon in a�uent societies. b. During epidemics,subclinical disease is more common than symptomaticdisease. c. Epidemics are usually caused by non–group Astreptococci. d. Antibiotic prophylaxis is not e�ective.6. A 9-year-old boy presents with symptomless grosshematuria. He has had a sore throat for 2 days. His basicmetabolic panel is normal. Which of the following is themost helpful diagnostic test? a. Complement C3 level b.Complement C4 level c. �roat culture d. ASO titer 7. A6-year-old girl has painless gross hematuria and pu�yeyes. She denies any recent illness. Her BP is 139/76;BUN, 34 mg/dL; creatinine, 1.3 mg/dL; serum albumin, 2.9g/dL; and complement, C3 23 mg/dL. Urine is positive forblood and protein. Which of the following is the mostappropriate treatment? a. Amoxicillin b. Intravenoussteroids c. Chlorothiazide or furosemide d. Observationonly 8. A 9-year-old boy presents with pu�y eyes andheadache. He remembers having a recent sore throat. His BPis 150/90 mm Hg, and he has mild periorbital and pretibialedema. Blood urea nitrogen (BUN) is 30 mg/dL; creatinine,1.3 mg/ dL; and complement C3, 20 mg/dL. Intravenousnicardipine and furosemide are started to control hishypertension. �e next day his metabolic panel showssodium, 132 mmol/L; potassium, 4.8 mmol/L; chloride, 100mmol/L; carbon dioxide, 20
mmol/L; BUN, 60 mg/dL; and creatinine, 3.2 mg/
dL. Which of the following is the most appropriate
next step?
a. Hemodialysis
b. Continuous venovenous hemo�ltration
c. Renal biopsy

d. Intravenous steroid treatment
9. Hypertension in acute postinfectious glomerulonephri
tis is mainly due to which of the following?
a. Activated sympathomimetic nervous system
b. Decreased glomerular �ltration rate
c. Elevated plasma renin level secondary to nephritis
d. Increased �uid volume expansion resulting fromincreased tubular sodium absorption ANSWER KEY 1. c 2. b3. a 4. a 5. b 6. a 7. c 8. c 9. d

22 Rapidly progressive glomerulonephritisand vasculitis
1. Markowitz GS, Radhakrishnan J, D’Agati VD. Anoverlapping etiology of rapidly progressiveglomerulonephritis. Am J Kidney Dis. 2004;43: 388–93.
2. Kambham N. Crescentic glomerulonephritis: An update onpauci-immune and anti-GBM disease. Adv Anat Pathol.2012;19:111–24.
3. Jennette JC. Rapidly progressive crescenticglomerulonephritis. Kidney Int. 2003;63:1164–77.
4. Flossmann O, Berden A, de Groot K, et al. Longtermpatient survival in ANCA-associated vasculitis. Ann RheumDis. 2011;70:488–94.
5. Li Z, G ou S, Chen M, et al. Predictors for outcomes inpatients with severe ANCA-associated glomerulonephritis whowere dialysis-dependent at presentation: A study of 89cases in a single Chinese center. Semin Arthritis Rheum.2013;42:515–21.
6. de Lindvan Wijngaarden RA, Hauer HA, Wolterbeek R, etal. Clinical and histologic determinants of renal outcomein ANCA-associated vasculitis: A prospective analysis of100 patients with severe renal involvement. J Am SocNephrol. 2006;17:2264–74.
7. Ozen S, Ruperto N, Dillon MJ, et al. EULAR/PReSendorsed consensus criteria for the classification ofchildhood vasculitides. Am Rheum Dis. 2006;65:936–41.
8. Ruperto N, Ozen S, Pistorio A, et al. EULAR/ PRINTO/PREScriteria for Henoch-Schonlein purpura, childhoodpolyarteritis nodosa, childhood Wegener granulomatosis andchildhood Takayasu arteritis: Ankara 2008. Part I. Overallmethodology and clinical characterization. Ann Rheum Dis.2010;69:790–7. 9. Oe Y, Nakaya I, Yahata M, et al. Classicpolyarteritis nodosa presenting with rapidly progressiverenal insufficiency. Clin Nephrol. 2010;74:315–8. 10.Bakkaloglu SA, Ekim M, Tumer N, et al. Severe renalimpairment in the case of classic polyarteritis nodosa.Pediatr Nephrol. 2001;16:148–50. 11. Sinha A, Puri K, HariP, et al. Etiology and outcome of crescenticglomerulonephritis. Indian Pediatr. 2013;50:283–8. 12.Gardner-Medwin JM, Dolezalova P, Cummins C, et al.Incidence of Henoch-Schonlein purpura, Kawasaki disease,and rare vasculitides in children of different ethnic
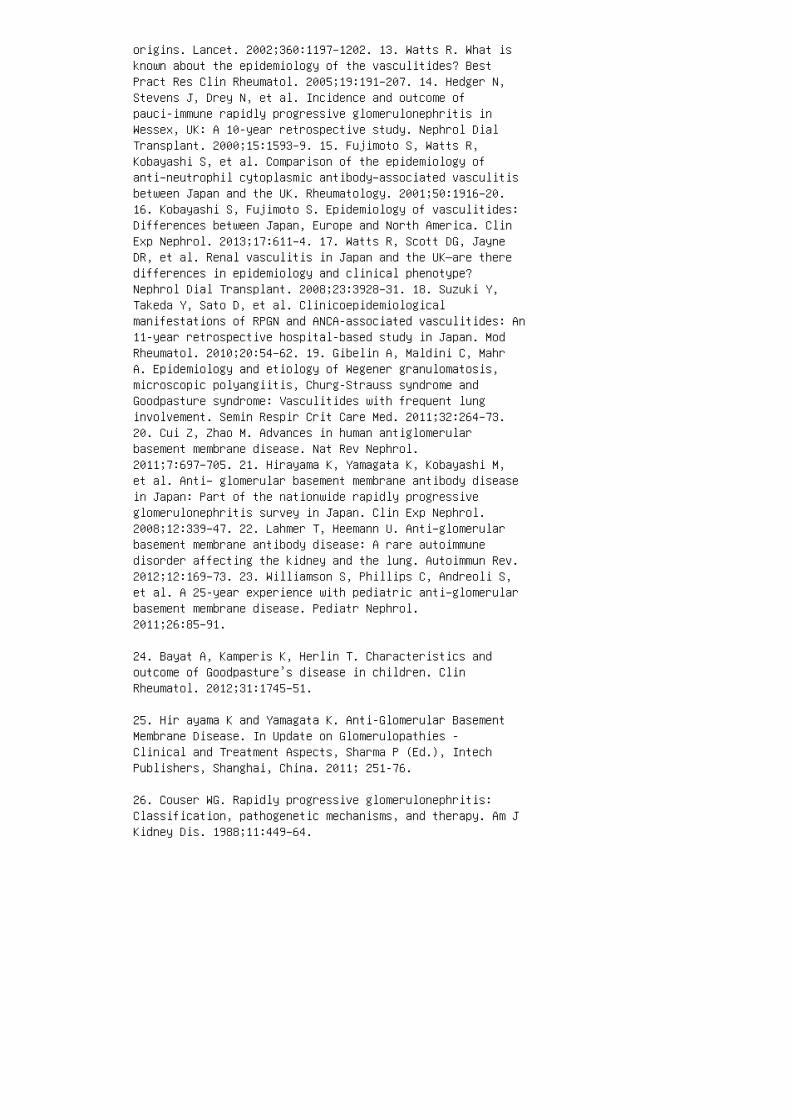
origins. Lancet. 2002;360:1197–1202. 13. Watts R. What isknown about the epidemiology of the vasculitides? BestPract Res Clin Rheumatol. 2005;19:191–207. 14. Hedger N,Stevens J, Drey N, et al. Incidence and outcome ofpauci-immune rapidly progressive glomerulonephritis inWessex, UK: A 10-year retrospective study. Nephrol DialTransplant. 2000;15:1593–9. 15. Fujimoto S, Watts R,Kobayashi S, et al. Comparison of the epidemiology ofanti–neutrophil cytoplasmic antibody–associated vasculitisbetween Japan and the UK. Rheumatology. 2001;50:1916–20.16. Kobayashi S, Fujimoto S. Epidemiology of vasculitides:Differences between Japan, Europe and North America. ClinExp Nephrol. 2013;17:611–4. 17. Watts R, Scott DG, JayneDR, et al. Renal vasculitis in Japan and the UK—are theredifferences in epidemiology and clinical phenotype?Nephrol Dial Transplant. 2008;23:3928–31. 18. Suzuki Y,Takeda Y, Sato D, et al. Clinicoepidemiologicalmanifestations of RPGN and ANCA-associated vasculitides: An11-year retrospective hospital-based study in Japan. ModRheumatol. 2010;20:54–62. 19. Gibelin A, Maldini C, MahrA. Epidemiology and etiology of Wegener granulomatosis,microscopic polyangiitis, Churg-Strauss syndrome andGoodpasture syndrome: Vasculitides with frequent lunginvolvement. Semin Respir Crit Care Med. 2011;32:264–73.20. Cui Z, Zhao M. Advances in human antiglomerularbasement membrane disease. Nat Rev Nephrol.2011;7:697–705. 21. Hirayama K, Yamagata K, Kobayashi M,et al. Anti– glomerular basement membrane antibody diseasein Japan: Part of the nationwide rapidly progressiveglomerulonephritis survey in Japan. Clin Exp Nephrol.2008;12:339–47. 22. Lahmer T, Heemann U. Anti–glomerularbasement membrane antibody disease: A rare autoimmunedisorder affecting the kidney and the lung. Autoimmun Rev.2012;12:169–73. 23. Williamson S, Phillips C, Andreoli S,et al. A 25-year experience with pediatric anti–glomerularbasement membrane disease. Pediatr Nephrol.2011;26:85–91.
24. Bayat A, Kamperis K, Herlin T. Characteristics andoutcome of Goodpasture’s disease in children. ClinRheumatol. 2012;31:1745–51.
25. Hir ayama K and Yamagata K. Anti-Glomerular BasementMembrane Disease. In Update on Glomerulopathies -Clinical and Treatment Aspects, Sharma P (Ed.), IntechPublishers, Shanghai, China. 2011; 251-76.
26. Couser WG. Rapidly progressive glomerulonephritis:Classification, pathogenetic mechanisms, and therapy. Am JKidney Dis. 1988;11:449–64.
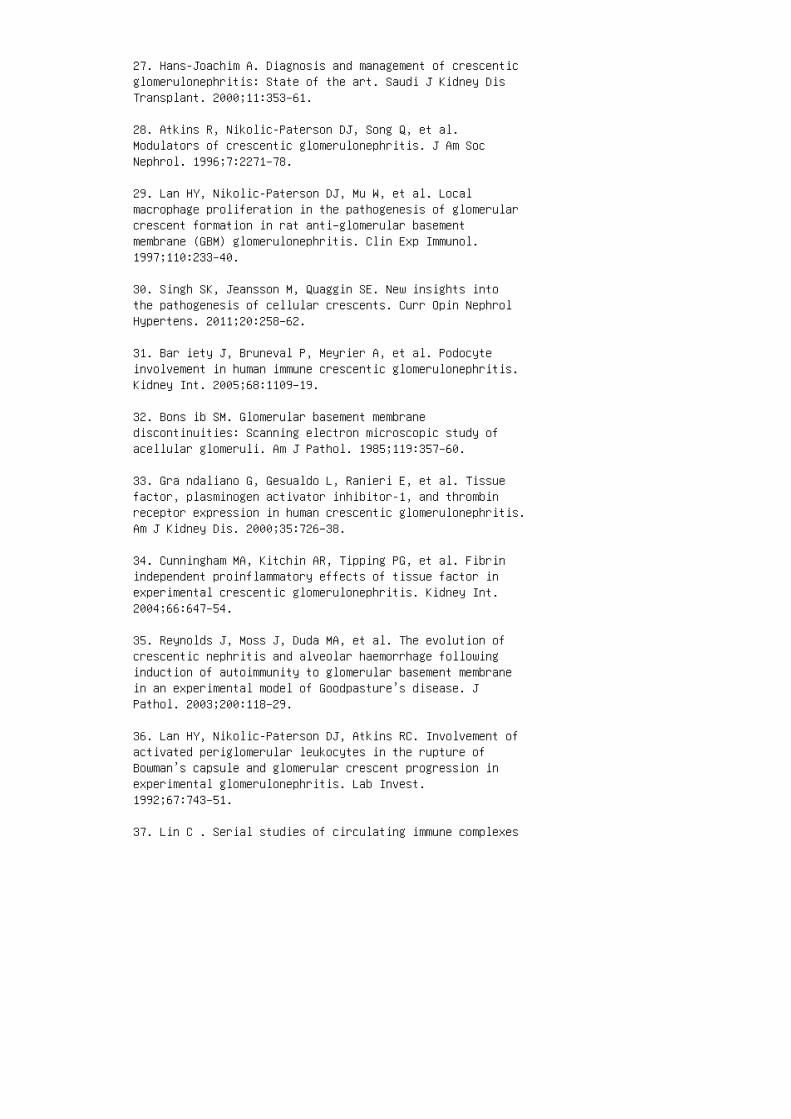
27. Hans-Joachim A. Diagnosis and management of crescenticglomerulonephritis: State of the art. Saudi J Kidney DisTransplant. 2000;11:353–61.
28. Atkins R, Nikolic-Paterson DJ, Song Q, et al.Modulators of crescentic glomerulonephritis. J Am SocNephrol. 1996;7:2271–78.
29. Lan HY, Nikolic-Paterson DJ, Mu W, et al. Localmacrophage proliferation in the pathogenesis of glomerularcrescent formation in rat anti–glomerular basementmembrane (GBM) glomerulonephritis. Clin Exp Immunol.1997;110:233–40.
30. Singh SK, Jeansson M, Quaggin SE. New insights intothe pathogenesis of cellular crescents. Curr Opin NephrolHypertens. 2011;20:258–62.
31. Bar iety J, Bruneval P, Meyrier A, et al. Podocyteinvolvement in human immune crescentic glomerulonephritis.Kidney Int. 2005;68:1109–19.
32. Bons ib SM. Glomerular basement membranediscontinuities: Scanning electron microscopic study ofacellular glomeruli. Am J Pathol. 1985;119:357–60.
33. Gra ndaliano G, Gesualdo L, Ranieri E, et al. Tissuefactor, plasminogen activator inhibitor-1, and thrombinreceptor expression in human crescentic glomerulonephritis.Am J Kidney Dis. 2000;35:726–38.
34. Cunningham MA, Kitchin AR, Tipping PG, et al. Fibrinindependent proinflammatory effects of tissue factor inexperimental crescentic glomerulonephritis. Kidney Int.2004;66:647–54.
35. Reynolds J, Moss J, Duda MA, et al. The evolution ofcrescentic nephritis and alveolar haemorrhage followinginduction of autoimmunity to glomerular basement membranein an experimental model of Goodpasture’s disease. JPathol. 2003;200:118–29.
36. Lan HY, Nikolic-Paterson DJ, Atkins RC. Involvement ofactivated periglomerular leukocytes in the rupture ofBowman’s capsule and glomerular crescent progression inexperimental glomerulonephritis. Lab Invest.1992;67:743–51.
37. Lin C . Serial studies of circulating immune complexes
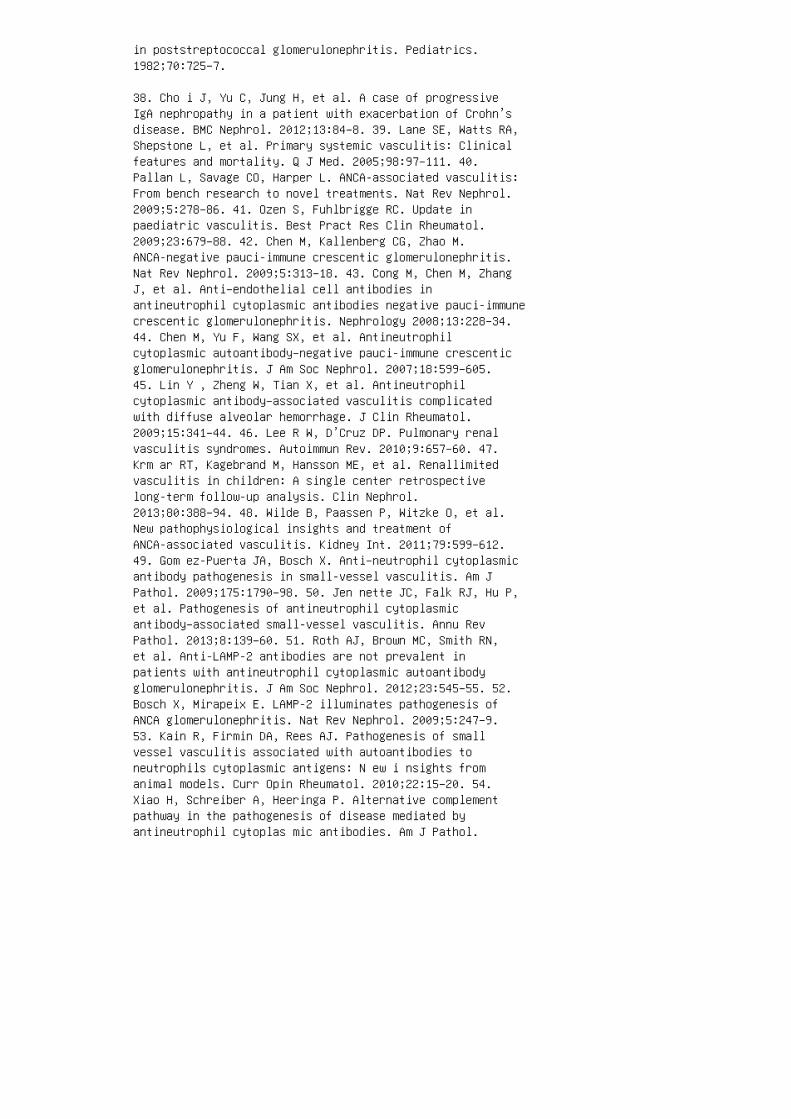
in poststreptococcal glomerulonephritis. Pediatrics.1982;70:725–7.
38. Cho i J, Yu C, Jung H, et al. A case of progressiveIgA nephropathy in a patient with exacerbation of Crohn’sdisease. BMC Nephrol. 2012;13:84–8. 39. Lane SE, Watts RA,Shepstone L, et al. Primary systemic vasculitis: Clinicalfeatures and mortality. Q J Med. 2005;98:97–111. 40.Pallan L, Savage CO, Harper L. ANCA-associated vasculitis:From bench research to novel treatments. Nat Rev Nephrol.2009;5:278–86. 41. Ozen S, Fuhlbrigge RC. Update inpaediatric vasculitis. Best Pract Res Clin Rheumatol.2009;23:679–88. 42. Chen M, Kallenberg CG, Zhao M.ANCA-negative pauci-immune crescentic glomerulonephritis.Nat Rev Nephrol. 2009;5:313–18. 43. Cong M, Chen M, ZhangJ, et al. Anti–endothelial cell antibodies inantineutrophil cytoplasmic antibodies negative pauci-immunecrescentic glomerulonephritis. Nephrology 2008;13:228–34.44. Chen M, Yu F, Wang SX, et al. Antineutrophilcytoplasmic autoantibody–negative pauci-immune crescenticglomerulonephritis. J Am Soc Nephrol. 2007;18:599–605.45. Lin Y , Zheng W, Tian X, et al. Antineutrophilcytoplasmic antibody–associated vasculitis complicatedwith diffuse alveolar hemorrhage. J Clin Rheumatol.2009;15:341–44. 46. Lee R W, D’Cruz DP. Pulmonary renalvasculitis syndromes. Autoimmun Rev. 2010;9:657–60. 47.Krm ar RT, Kagebrand M, Hansson ME, et al. Renallimitedvasculitis in children: A single center retrospectivelong-term follow-up analysis. Clin Nephrol.2013;80:388–94. 48. Wilde B, Paassen P, Witzke O, et al.New pathophysiological insights and treatment ofANCA-associated vasculitis. Kidney Int. 2011;79:599–612.49. Gom ez-Puerta JA, Bosch X. Anti–neutrophil cytoplasmicantibody pathogenesis in small-vessel vasculitis. Am JPathol. 2009;175:1790–98. 50. Jen nette JC, Falk RJ, Hu P,et al. Pathogenesis of antineutrophil cytoplasmicantibody–associated small-vessel vasculitis. Annu RevPathol. 2013;8:139–60. 51. Roth AJ, Brown MC, Smith RN,et al. Anti-LAMP-2 antibodies are not prevalent inpatients with antineutrophil cytoplasmic autoantibodyglomerulonephritis. J Am Soc Nephrol. 2012;23:545–55. 52.Bosch X, Mirapeix E. LAMP-2 illuminates pathogenesis ofANCA glomerulonephritis. Nat Rev Nephrol. 2009;5:247–9.53. Kain R, Firmin DA, Rees AJ. Pathogenesis of smallvessel vasculitis associated with autoantibodies toneutrophils cytoplasmic antigens: N ew i nsights fromanimal models. Curr Opin Rheumatol. 2010;22:15–20. 54.Xiao H, Schreiber A, Heeringa P. Alternative complementpathway in the pathogenesis of disease mediated byantineutrophil cytoplas mic antibodies. Am J Pathol.
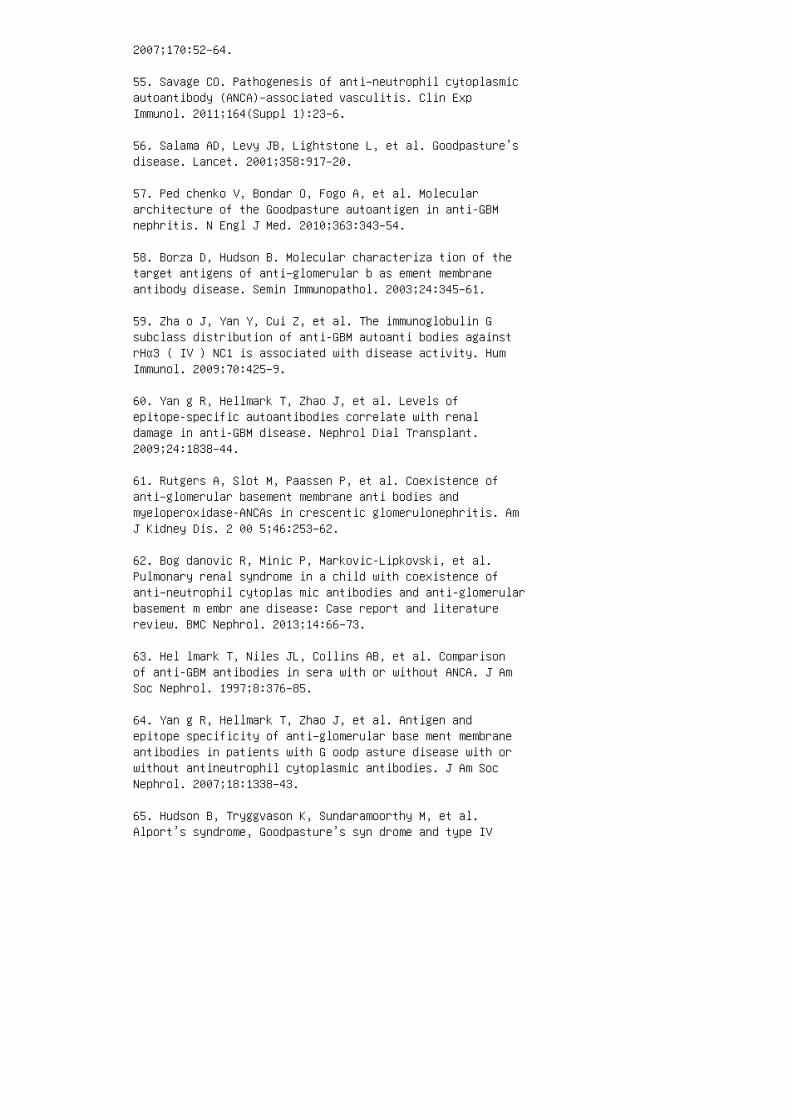
2007;170:52–64.
55. Savage CO. Pathogenesis of anti–neutrophil cytoplasmicautoantibody (ANCA)–associated vasculitis. Clin ExpImmunol. 2011;164(Suppl 1):23–6.
56. Salama AD, Levy JB, Lightstone L, et al. Goodpasture’sdisease. Lancet. 2001;358:917–20.
57. Ped chenko V, Bondar O, Fogo A, et al. Moleculararchitecture of the Goodpasture autoantigen in anti-GBMnephritis. N Engl J Med. 2010;363:343–54.
58. Borza D, Hudson B. Molecular characteriza tion of thetarget antigens of anti–glomerular b as ement membraneantibody disease. Semin Immunopathol. 2003;24:345–61.
59. Zha o J, Yan Y, Cui Z, et al. The immunoglobulin Gsubclass distribution of anti-GBM autoanti bodies againstrHα3 ( IV ) NC1 is associated with disease activity. HumImmunol. 2009;70:425–9.
60. Yan g R, Hellmark T, Zhao J, et al. Levels ofepitope-specific autoantibodies correlate with renaldamage in anti-GBM disease. Nephrol Dial Transplant.2009;24:1838–44.
61. Rutgers A, Slot M, Paassen P, et al. Coexistence ofanti–glomerular basement membrane anti bodies andmyeloperoxidase-ANCAs in crescentic glomerulonephritis. AmJ Kidney Dis. 2 00 5;46:253–62.
62. Bog danovic R, Minic P, Markovic-Lipkovski, et al.Pulmonary renal syndrome in a child with coexistence ofanti–neutrophil cytoplas mic antibodies and anti-glomerularbasement m embr ane disease: Case report and literaturereview. BMC Nephrol. 2013;14:66–73.
63. Hel lmark T, Niles JL, Collins AB, et al. Comparisonof anti-GBM antibodies in sera with or without ANCA. J AmSoc Nephrol. 1997;8:376–85.
64. Yan g R, Hellmark T, Zhao J, et al. Antigen andepitope specificity of anti–glomerular base ment membraneantibodies in patients with G oodp asture disease with orwithout antineutrophil cytoplasmic antibodies. J Am SocNephrol. 2007;18:1338–43.
65. Hudson B, Tryggvason K, Sundaramoorthy M, et al.Alport’s syndrome, Goodpasture’s syn drome and type IV
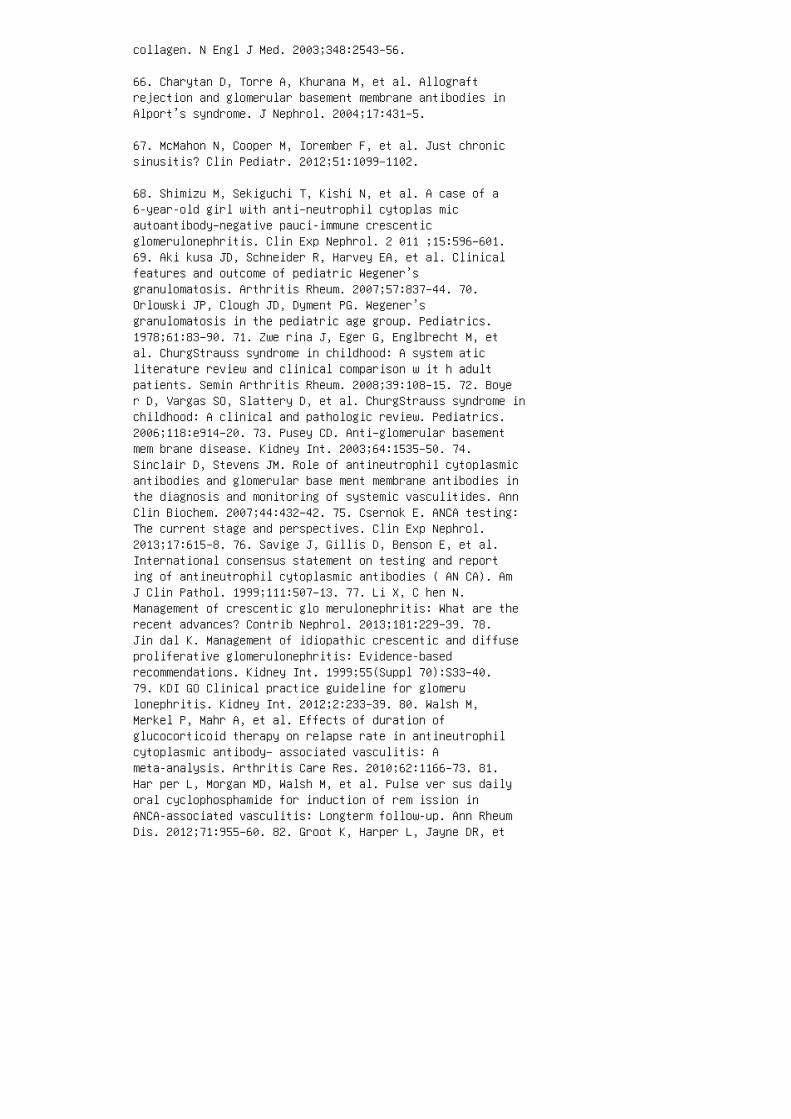
collagen. N Engl J Med. 2003;348:2543–56.
66. Charytan D, Torre A, Khurana M, et al. Allograftrejection and glomerular basement membrane antibodies inAlport’s syndrome. J Nephrol. 2004;17:431–5.
67. McMahon N, Cooper M, Iorember F, et al. Just chronicsinusitis? Clin Pediatr. 2012;51:1099–1102.
68. Shimizu M, Sekiguchi T, Kishi N, et al. A case of a6-year-old girl with anti–neutrophil cytoplas micautoantibody–negative pauci-immune crescenticglomerulonephritis. Clin Exp Nephrol. 2 011 ;15:596–601.69. Aki kusa JD, Schneider R, Harvey EA, et al. Clinicalfeatures and outcome of pediatric Wegener’sgranulomatosis. Arthritis Rheum. 2007;57:837–44. 70.Orlowski JP, Clough JD, Dyment PG. Wegener’sgranulomatosis in the pediatric age group. Pediatrics.1978;61:83–90. 71. Zwe rina J, Eger G, Englbrecht M, etal. ChurgStrauss syndrome in childhood: A system aticliterature review and clinical comparison w it h adultpatients. Semin Arthritis Rheum. 2008;39:108–15. 72. Boyer D, Vargas SO, Slattery D, et al. ChurgStrauss syndrome inchildhood: A clinical and pathologic review. Pediatrics.2006;118:e914–20. 73. Pusey CD. Anti–glomerular basementmem brane disease. Kidney Int. 2003;64:1535–50. 74.Sinclair D, Stevens JM. Role of antineutrophil cytoplasmicantibodies and glomerular base ment membrane antibodies inthe diagnosis and monitoring of systemic vasculitides. AnnClin Biochem. 2007;44:432–42. 75. Csernok E. ANCA testing:The current stage and perspectives. Clin Exp Nephrol.2013;17:615–8. 76. Savige J, Gillis D, Benson E, et al.International consensus statement on testing and reporting of antineutrophil cytoplasmic antibodies ( AN CA). AmJ Clin Pathol. 1999;111:507–13. 77. Li X, C hen N.Management of crescentic glo merulonephritis: What are therecent advances? Contrib Nephrol. 2013;181:229–39. 78.Jin dal K. Management of idiopathic crescentic and diffuseproliferative glomerulonephritis: Evidence-basedrecommendations. Kidney Int. 1999;55(Suppl 70):S33–40.79. KDI GO Clinical practice guideline for glomerulonephritis. Kidney Int. 2012;2:233–39. 80. Walsh M,Merkel P, Mahr A, et al. Effects of duration ofglucocorticoid therapy on relapse rate in antineutrophilcytoplasmic antibody– associated vasculitis: Ameta-analysis. Arthritis Care Res. 2010;62:1166–73. 81.Har per L, Morgan MD, Walsh M, et al. Pulse ver sus dailyoral cyclophosphamide for induction of rem ission inANCA-associated vasculitis: Longterm follow-up. Ann RheumDis. 2012;71:955–60. 82. Groot K, Harper L, Jayne DR, et

al. Pulse versus daily oral cyclophosphamide for inductionof remission in antineutrophil cytoplasmic antibody–associated vasculitis. Ann Intern Med.2009;150:670–80. 83. Lind van Wijngaarden RA, Hauer HA,Wolterbreek R, et al. Chances of recovery fordialysis-dependent ANCA–associated glomerulonephritis. JAm Soc Nephrol. 2007;18:2189–97.
84. Jayne DR, Gaskin G, Rasmussen N, et al. Randomizedtrial of plasma exchange or highdosage methylprednisoloneas adjunctive therapy for severe renal vasculitis. J AmSoc Nephrol. 2007;18:2180–88.
85. Walters GD, Willis NS, Craig JC. Interventions forrenal vasculitis in adults: A systematic review. BMCNephrol. 2010;11:12–34.
86. Gregersen JW, Kristensen T, Krag SR, et al. Earlyplasma exchange improves outcome in PR3-ANCA–positiverenal vasculitis. Clin Exp Rheumatol. 2012;30(Suppl70):S39–47.
87. Levy JB, Turner AN, Rees AJ, et al. Long-term outcomeof anti–glomerular basement mem brane antibody diseasetreated with plasma e xc hange and immunosuppression. AnnIntern Med. 2001;134:1033–42.
88. Lin d van Wijngaarden RA, Hauer HA, Wolterbreek R, etal. Clinical and histologic determinants of renal outcomein ANCAassociated vasculitis: A prospective analysis of100 patients with severe renal involvement. J Am SocNephrol. 2006;17:2264–74.
89. Klemmer PJ, Chalermskulrat W, Reif MS, et al.Plasmapheresis therapy for diffuse alveolar hemorrhage inpatients with small-vessel vascu litis. Am J Kidney Dis.2003;42:1149–53.
90. Cui Z, Zhao J, Jia X, et al. Anti–glomerular basementmembrane disease: Outcomes of different therapeuticregimens in a large single-center Chinese cohort study.Medicine (Baltimore). 2011;90:303–11.
91. Wal sh M, Catapano F, Szpirt W, et al. Plasma exchangefor renal vasculitis and idiopathic rapidly progressiveglomerulone phritis: A meta-analysis. Am J Kidney Dis. 2011;57:566–74.
92. Muk htyar C, Guillevin L, Cid MC, et al. EULARrecommendations for the management of pri mary small and
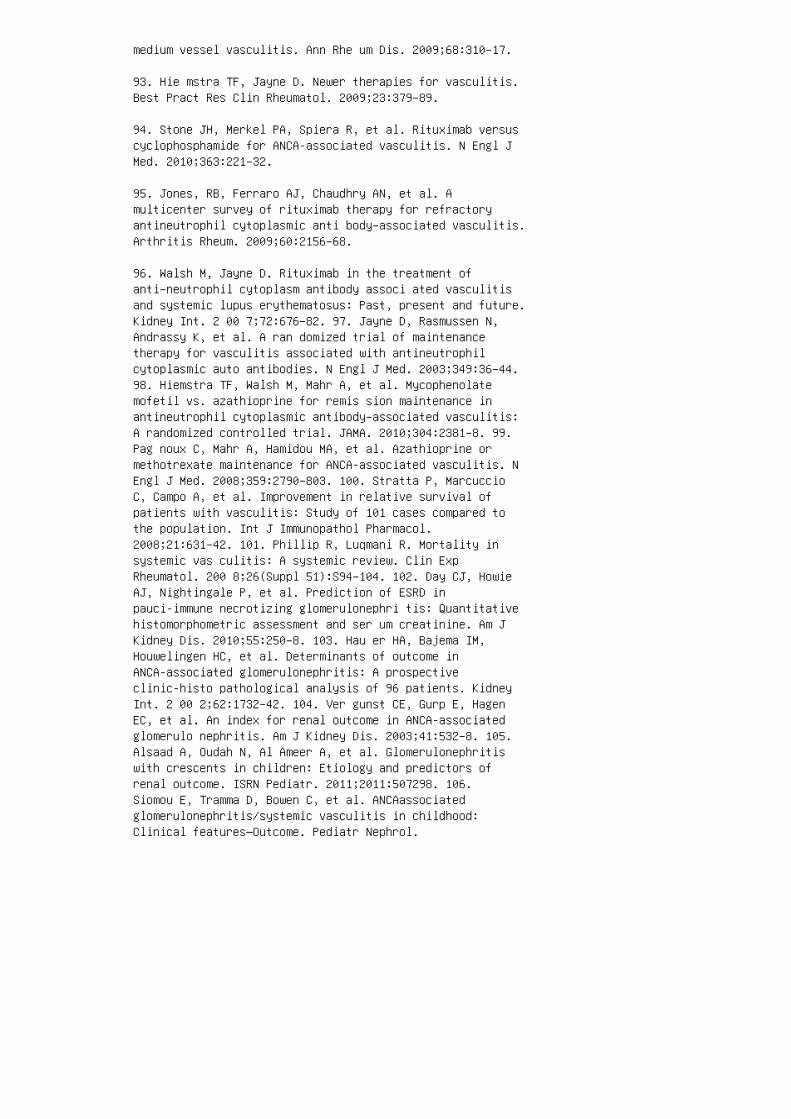
medium vessel vasculitis. Ann Rhe um Dis. 2009;68:310–17.
93. Hie mstra TF, Jayne D. Newer therapies for vasculitis.Best Pract Res Clin Rheumatol. 2009;23:379–89.
94. Stone JH, Merkel PA, Spiera R, et al. Rituximab versuscyclophosphamide for ANCA-associated vasculitis. N Engl JMed. 2010;363:221–32.
95. Jones, RB, Ferraro AJ, Chaudhry AN, et al. Amulticenter survey of rituximab therapy for refractoryantineutrophil cytoplasmic anti body–associated vasculitis.Arthritis Rheum. 2009;60:2156–68.
96. Walsh M, Jayne D. Rituximab in the treatment ofanti–neutrophil cytoplasm antibody associ ated vasculitisand systemic lupus erythematosus: Past, present and future.Kidney Int. 2 00 7;72:676–82. 97. Jayne D, Rasmussen N,Andrassy K, et al. A ran domized trial of maintenancetherapy for vasculitis associated with antineutrophilcytoplasmic auto antibodies. N Engl J Med. 2003;349:36–44.98. Hiemstra TF, Walsh M, Mahr A, et al. Mycophenolatemofetil vs. azathioprine for remis sion maintenance inantineutrophil cytoplasmic antibody–associated vasculitis:A randomized controlled trial. JAMA. 2010;304:2381–8. 99.Pag noux C, Mahr A, Hamidou MA, et al. Azathioprine ormethotrexate maintenance for ANCA-associated vasculitis. NEngl J Med. 2008;359:2790–803. 100. Stratta P, MarcuccioC, Campo A, et al. Improvement in relative survival ofpatients with vasculitis: Study of 101 cases compared tothe population. Int J Immunopathol Pharmacol.2008;21:631–42. 101. Phillip R, Luqmani R. Mortality insystemic vas culitis: A systemic review. Clin ExpRheumatol. 200 8;26(Suppl 51):S94–104. 102. Day CJ, HowieAJ, Nightingale P, et al. Prediction of ESRD inpauci-immune necrotizing glomerulonephri tis: Quantitativehistomorphometric assessment and ser um creatinine. Am JKidney Dis. 2010;55:250–8. 103. Hau er HA, Bajema IM,Houwelingen HC, et al. Determinants of outcome inANCA-associated glomerulonephritis: A prospectiveclinic-histo pathological analysis of 96 patients. KidneyInt. 2 00 2;62:1732–42. 104. Ver gunst CE, Gurp E, HagenEC, et al. An index for renal outcome in ANCA-associatedglomerulo nephritis. Am J Kidney Dis. 2003;41:532–8. 105.Alsaad A, Oudah N, Al Ameer A, et al. Glomerulonephritiswith crescents in children: Etiology and predictors ofrenal outcome. ISRN Pediatr. 2011;2011:507298. 106.Siomou E, Tramma D, Bowen C, et al. ANCAassociatedglomerulonephritis/systemic vasculitis in childhood:Clinical features—Outcome. Pediatr Nephrol.
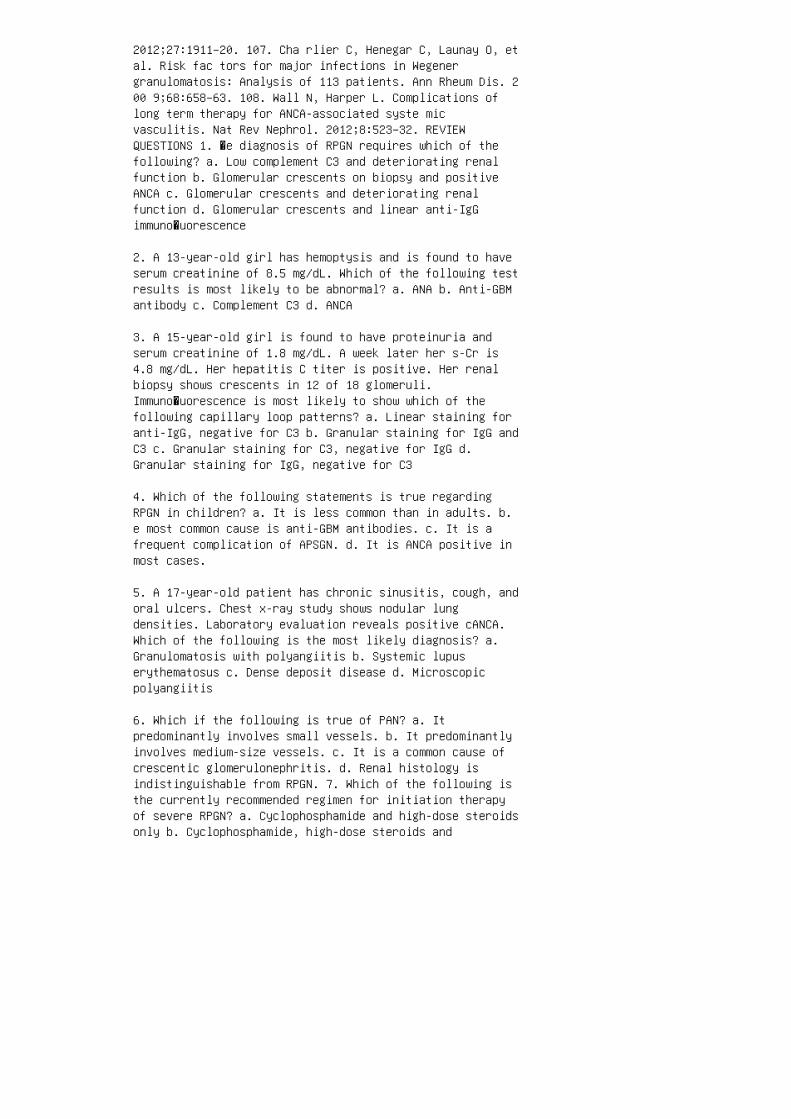
2012;27:1911–20. 107. Cha rlier C, Henegar C, Launay O, etal. Risk fac tors for major infections in Wegenergranulomatosis: Analysis of 113 patients. Ann Rheum Dis. 200 9;68:658–63. 108. Wall N, Harper L. Complications oflong term therapy for ANCA-associated syste micvasculitis. Nat Rev Nephrol. 2012;8:523–32. REVIEWQUESTIONS 1. �e diagnosis of RPGN requires which of thefollowing? a. Low complement C3 and deteriorating renalfunction b. Glomerular crescents on biopsy and positiveANCA c. Glomerular crescents and deteriorating renalfunction d. Glomerular crescents and linear anti-IgGimmuno�uorescence
2. A 13-year-old girl has hemoptysis and is found to haveserum creatinine of 8.5 mg/dL. Which of the following testresults is most likely to be abnormal? a. ANA b. Anti-GBMantibody c. Complement C3 d. ANCA
3. A 15-year-old girl is found to have proteinuria andserum creatinine of 1.8 mg/dL. A week later her s-Cr is4.8 mg/dL. Her hepatitis C titer is positive. Her renalbiopsy shows crescents in 12 of 18 glomeruli.Immuno�uorescence is most likely to show which of thefollowing capillary loop patterns? a. Linear staining foranti-IgG, negative for C3 b. Granular staining for IgG andC3 c. Granular staining for C3, negative for IgG d.Granular staining for IgG, negative for C3
4. Which of the following statements is true regardingRPGN in children? a. It is less common than in adults. b.e most common cause is anti-GBM antibodies. c. It is afrequent complication of APSGN. d. It is ANCA positive inmost cases.
5. A 17-year-old patient has chronic sinusitis, cough, andoral ulcers. Chest x-ray study shows nodular lungdensities. Laboratory evaluation reveals positive cANCA.Which of the following is the most likely diagnosis? a.Granulomatosis with polyangiitis b. Systemic lupuserythematosus c. Dense deposit disease d. Microscopicpolyangiitis
6. Which if the following is true of PAN? a. Itpredominantly involves small vessels. b. It predominantlyinvolves medium-size vessels. c. It is a common cause ofcrescentic glomerulonephritis. d. Renal histology isindistinguishable from RPGN. 7. Which of the following isthe currently recommended regimen for initiation therapyof severe RPGN? a. Cyclophosphamide and high-dose steroidsonly b. Cyclophosphamide, high-dose steroids and
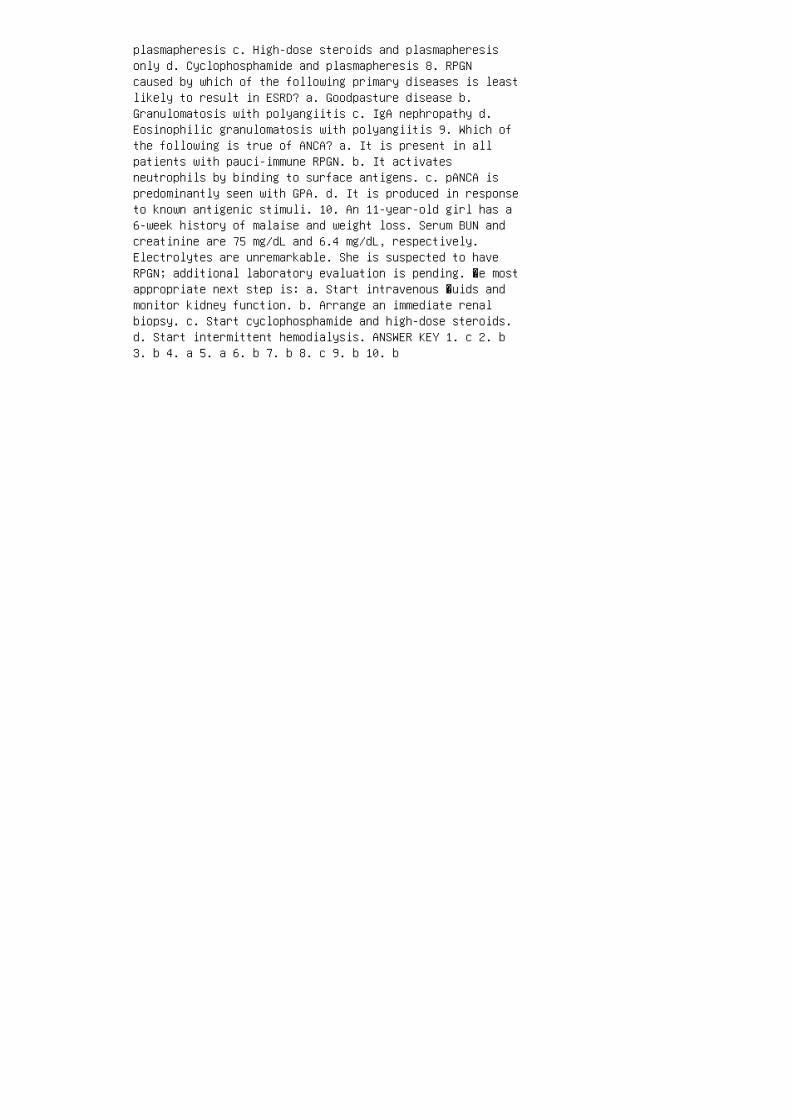
plasmapheresis c. High-dose steroids and plasmapheresisonly d. Cyclophosphamide and plasmapheresis 8. RPGNcaused by which of the following primary diseases is leastlikely to result in ESRD? a. Goodpasture disease b.Granulomatosis with polyangiitis c. IgA nephropathy d.Eosinophilic granulomatosis with polyangiitis 9. Which ofthe following is true of ANCA? a. It is present in allpatients with pauci-immune RPGN. b. It activatesneutrophils by binding to surface antigens. c. pANCA ispredominantly seen with GPA. d. It is produced in responseto known antigenic stimuli. 10. An 11-year-old girl has a6-week history of malaise and weight loss. Serum BUN andcreatinine are 75 mg/dL and 6.4 mg/dL, respectively.Electrolytes are unremarkable. She is suspected to haveRPGN; additional laboratory evaluation is pending. �e mostappropriate next step is: a. Start intravenous �uids andmonitor kidney function. b. Arrange an immediate renalbiopsy. c. Start cyclophosphamide and high-dose steroids.d. Start intermittent hemodialysis. ANSWER KEY 1. c 2. b3. b 4. a 5. a 6. b 7. b 8. c 9. b 10. b
23 Immunoglobulin A nephropathy andHenoch-Schönlein purpura nephritis
3. Wyatt RJ, Julian BA. IgA nephropathy. N Engl J Med.2013;368:2402–14.
4. Ber ger J. IgA glomerular deposits in renal disease.Transplant Proc. 1969;1:939–44.
5. Waldo FB. Is Henoch-Schönlein purpura the systemic formof IgA nephropathy? Am J Kidney Dis. 1988;12:373–7.
6. Meadow SR, Scott DG. Berger disease: HenochSchönleinsyndrome without the rash. J Pediatr. 1985;106:27–32.
7. Hug hes FJ, Wolfish NM, McLaine PN. HenochSchönleinsyndrome and IgA nephropathy: A case report suggesting acommon pathogenesis. Pediatr Nephrol. 1988;2:389–92.
8. Watanabe T, Takada T, Kihara I, Oda Y. Three cases ofHenoch-Schönlein purpura preceded by IgA nephropathy.Pediatr Nephrol. 1995;9:674.
9. Cho BS, Kim SD, Choi YM, Kang HH. School urinalysisscreening in Korea: Prevalence of chronic renal disease.Pediatr Nephrol. 2001;16:1126–8.
10. Uts unomiya Y, Kado T, Koda T, et al. Features of IgAnephropathy in preschool children. Clin Nephrol.2000;54:443–8.
11. Yos hikawa N, Tanaka R, Iijima K. Pathophysiology andtreatment of IgA nephropathy in children. Pediatr Nephrol.2001;16:446–57.
12. Coppo R, Gianoglio B, Porcellini MG, Maringhini S.Frequency of renal diseases and clinical indications forrenal biopsy in children (report of the Italian NationalRegistry of Renal Biopsies in Children). Group of RenalImmunopathology of the Italian Society of PediatricNephrology and Group of Renal Immunopathology of theItalian Society of Nephrology. Nephrol Dial Transplant.1998;13:293–7.
13. Wyatt RJ, Julian BA, Baehler RW, et al. Epidemiologyof IgA nephropathy in central and eastern Kentucky for theperiod 1975 through 1994. Central Kentucky Region of theSoutheastern United States IgA Nephropathy DATABANKProject. J Am Soc Nephrol. 1998;9:853–8.
14. Cop po R, Camilla R, Alfarano A, et al. Upregulationof the immunoproteasome in peripheral blood mononuclearcells of patients with IgA nephropathy. Kidney Int.2009;75:536–41.
15. Utsunomiya Y, Koda T, Kado T, et al. Incidence ofpediatric IgA nephropathy. Pediatr Nephrol. 2003;18:511–5.
16. Kir yluk K, Li Y, Sanna-Cherchi S, et al. Geographicdifferences in genetic susceptibility to IgA nephropathy:GWAS replication study and geospatial risk analysis. PLoSGenet. 2012;8:e1002765.
17. Jennette JC, Wall SD, Wilkman AS. Low incidence of IgAnephropathy in blacks. Kidney Int. 1985;28:944–50.
18. See dat YK, Nathoo BC, Parag KB, et al. IgAnephropathy in blacks and Indians of Natal. Nephron.1988;50:137–41. 19. Sehic AM, Gaber LW, Roy S, et al.Increased recognition of IgA nephropathy inAfrican-American children. Pediatr Nephrol. 1997;11:435–7.20. Lau KK, Gaber LW, Delos Santos NM, et al. PediatricIgA nephropathy: Clinical features at presentation andoutcome for African-Americans and Caucasians. ClinNephrol. 2004;62:167–72. 21. Lévy M, Gonzalez-Burchard G,Broyer M, et al. Berger’s disease in children: Naturalhistory and outcome. Medicine (Baltimore). 1985;64:157–80.22. Wyatt RJ, Kritchevsky SB, Woodford SY, et al. IgAnephropathy: Long-term prognosis for pediatric patients. JPediatr. 1995;127:913–9. 23. Levy M, Broyer M, Arsan A,Levy-Bentolila D, et al. Anaphylactoid purpura nephritisin childhood: Natural history and immunopathology. AdvNephrol Necker Hosp. 1976;6:183–228. 24. Cop po R,Mazzucco G, Cagnoli L, et al. Long-term prognosis ofHenoch-Schönlein nephritis in adults and children. ItalianGroup of Renal Immunopathology Collaborative Study onHenoch-Schönlein purpura. Nephrol Dial Transplant.1997;12:2277–83. 25. Sch arer K, Krmar R, Querfeld U,Ruder H, et al. Clinical outcome of Schönlein-Henochpurpura nephritis in children. Pediatr Nephrol.1999;13:816–23. 26. Ronkainen J, Nuutinen M, Koskimies O.The adult kidney 24 years after childhood Henoch-Schönleinpurpura: A retrospective cohort study. Lancet.2002;360:666–70. 27. Yos hikawa N, Ito H, Yoshiya K,Nakahara C, et al. Henoch-Schöenlein nephritis and IgAnephropathy in children: A comparison of clinical course.Clin Nephrol. 1987;27:233–7. 28. Davi n JC.Henoch-Schönlein purpura nephritis: Pathophysiology,treatment, and future strategy. Clin J Am Soc Nephrol.2011;6:679–89. 29. Eva ns DJ, Williams DG, Peters DK, et

al. Glomerular deposition of properdin in Henoch-Schönleinsyndrome and idiopathic focal nephritis. Br Med J.1973;3:326–8. 30. Wyatt RJ, Julian BA, Bhathena DB, et al.IgA nephropathy: Presentation, clinical course, andprognosis in children and adults. Am J Kidney Dis.1984;4:192–200. 31. Conley ME, Cooper MD, Michael AF.Selective deposition of immunoglobulin A1 inimmunoglobulin A nephropathy, anaphylactoid purpuranephritis, and systemic lupus erythematosus. J ClinInvest. 1980;66:1432–6. 32. Rob erts IS, Cook HT,Troyanov S, et al. The Oxford classification of IgAnephropathy: Pathology definitions, correlations, andreproducibility. Kidney Int. 2009;76:546–56. 33. CattranDC, Coppo R, Cook HT, et al. The Oxford classification ofIgA nephropathy: Rationale, clinicopathologicalcorrelations, and classification. Kidney Int.2009;76:534–45.
34. Hogg RJ, Silva FG, Wyatt RJ, et al. Prognosticindicators in children with IgA nephropathy: Report of theSouthwest Pediatric Nephrology Study Group. PediatrNephrol. 1994;8:15–20.
35. Andreoli SP, Yum MN, Bergstein JM. IgA nephropathy inchildren: Significance of glomerular basement membranedeposition of IgA. Am J Nephrol. 1986;6:28–33.
36. Yoshikawa N, Ito H, Nakamura H. Prognostic indicatorsin childhood IgA nephropathy. Nephron. 1992;60:60–7.
37. Barratt J, Feehally J. IgA nephropathy. J Am SocNephrol. 2005;16:2088–97.
38. Haas M. IgA nephropathy and HenochSchöenlein purpuranephritis. In: Jennette JC, Olsen JL, Schwartz MM, FG S,editors. Heptinstall’s Pathology of the Kidney. vol I. 6thed. Philadelphia: Lippincott, Williams and Wilkins; 2007.pp. 423–86.
39. Ikezumi Y, Suzuki T, Imai N, et al. Histologicaldifferences in new-onset IgA nephropathy between childrenand adults. Nephrol Dial Transplant. 2006;21:3466–74.
40. Cop po R, Troyanov S, Camilla R, et al. The Oxford IgAnephropathy clinicopathological classification is validfor children as well as adults. Kidney Int. 2010;77:921–7.
41. Suz uki H, Kiryluk K, Novak J, et al. Thepathophysiology of IgA nephropathy. J Am Soc Nephrol.2011;22:1795–803.

42. Lau K K, Suzuki H, Novak J, Wyatt RJ. Pathogenesis ofHenoch-Schönlein purpura nephritis. Pediatr Nephrol.2010;25:19–26.
43. Bar ratt J, Feehally J, Smith AC. Pathogenesis of IgAnephropathy. Semin Nephrol. 2004;24:197–217.
44. Mestecky J, Tomana M, Crowley-Nowick PA, et al.Defective galactosylation and clearance of IgA1 moleculesas a possible etiopathogenic factor in IgA nephropathy.Contrib Nephrol. 1993;104:172–82.
45. Tomana M, Matousovic K, Julian BA, et al.Galactose-deficient IgA1 in sera of IgA nephropathypatients is present in complexes with IgG. Kidney Int.1997;52:509–16.
46. Allen AC, Willis FR, Beattie TJ, et al. Abnormal IgAglycosylation in Henoch-Schönlein purpura restricted topatients with clinical nephritis. Nephrol Dial Transplant.1998;13:930–4.
47. Ber thoux F, Suzuki H, Thibaudin L, et al.Autoantibodies targeting galactose-deficient IgA1associate with progression of IgA nephropathy. J Am SocNephrol. 2012;23:1579–87.
48. Tomana M, Novak J, Julian BA, et al. Circulatingimmune complexes in IgA nephropathy consist of IgA1 withgalactose-deficient hinge region and antiglycanantibodies. J Clin Invest. 1999;104:73–81. 49. Novak J,Julian BA, Tomana M, et al. Progress in molecular andgenetic studies of IgA nephropathy. J Clin Immunol.2001;21:310–27. 50. Novak J, Vu HL, Novak L, et al.Interactions of human mesangial cells with IgA andIgA-containing immune complexes. Kidney Int.2002;62:465–75. 51. Novak J, Tomana M, Matousovic K, etal. IgA1containing immune complexes in IgA nephropathydifferentially affect proliferation of mesangial cells.Kidney Int. 2005;67:504–13. 52. Novak J, Julian BA,Mestecky J, et al. Glycosylation of IgA1 and pathogenesisof IgA nephropathy. Semin Immunopathol. 2012;34:365–82.53. Amore A, Conti G, Cirina P, et al. Aberrantlyglycosylated IgA molecules downregulate the synthesis andsecretion of vascular endothelial growth factor in humanmesangial cells. Am J Kidney Dis. 2000;36:1242–52. 54.Lai K N. Pathogenesis of IgA nephropathy. Nat Rev Nephrol.2012;8:275–83. 55. Jul ian BA, Quiggins PA, Thompson JS,et al. Familial IgA nephropathy: Evidence of an inherited
mechanism of disease. N Engl J Med. 1985;312:202–8. 56.Wya tt RJ, Rivas ML, Julian BA, et al. Regionalization inhereditary IgA nephropathy. Am J Hum Genet. 1987;41:36–50.57. Lavi gne KA, Woodford SY, Barker CV, et al. FamilialIgA nephropathy in southeastern Kentucky. Clin Nephrol.2010;73:115–21. 58. Sco lari F, Amoroso A, Savoldi S, etal. Familial clustering of IgA nephropathy: Furtherevidence in an Italian population. Am J Kidney Dis.1999;33:857–65. 59. Lev y M. Familial cases of Berger’sdisease and anaphylactoid purpura: More frequent thanpreviously thought. Am J Med. 1989;87:246–8. 60. GharaviAG, Yan Y, Scolari F, et al. IgA nephropathy, the mostcommon cause of glomerulonephritis, is linked to 6q22-23.Nat Genet. 2000;26:354–7. 61. Gharavi AG, Moldoveanu Z,Wyatt RJ, et al. Aberrant IgA1 glycosylation is inheritedin familial and sporadic IgA nephropathy. J Am SocNephrol. 2008;19:1008–14. 62. Kiryluk K, Moldoveanu Z,Sanders JT, et al. Aberrant glycosylation of IgA1 isinherited in both pediatric IgA nephropathy andHenoch-Schönlein purpura nephritis. Kidney Int.2011;80:79–87. 63. Hastings MC, Moldoveanu Z, Julian BA,et al. Galactose-deficient IgA1 in African Americans withIgA nephropathy: Serum levels and heritability. Clin J AmSoc Nephrol. 2010;5:2069–74. 64. Moldoveanu Z, Wyatt RJ,Lee JY, et al. Patients with IgA nephropathy haveincreased serum galactosedeficient IgA1 levels. Kidney Int.2007;71:1148–54. 65. Lin X, Ding J, Zhu L, Shi S, et al.Aberrant galactosylation of IgA1 is involved in the geneticsusceptibility of Chinese patients with IgA nephropathy.Nephrol Dial Transplant. 2009;24:3372–5.
66. Wellcome Trust Case Control Consortium. Genome-wideassociation study of 14,000 cases of seven common diseasesand 3,000 shared controls. Nature. 2007;447:661–78.
67. Kher KK, Makker SP, Moorthy B. IgA nephropathy(Berger’s disease): A clinicopathologic study in children.Int J Pediatr Nephrol. 1983;4:11–8.
68. Coppo R. Pediatric IgA nephropathy: Clinical andtherapeutic perspectives. Semin Nephrol. 2008;28:18–26.
69. San tos NM, Ault BH, Gharavi AG, et al.Angiotensinconverting enzyme genotype and outcome inpediatric IgA nephropathy. Pediatr Nephrol.2002;17:496–502.
70. Kitajima T, Murakami M, Sakai O. Clinicopathologicalfeatures in the Japanese patients with IgA nephropathy. JpnJ Med. 1983;22:219–22.
71. Southwest Pediatric Nephrology Study Group.Association of IgA nephropathy with steroidresponsivenephrotic syndrome. Am J Kidney Dis. 1985;5:157–64.
72. Wya tt RJ, Hogg RJ. Evidence-based assessment oftreatment options for children with IgA nephropathies.Pediatr Nephrol. 2001;16:156–67.
73. Hur ley RM, Drummond KN. Anaphylactoid purpuranephritis: Clinicopathological correlations. J Pediatr.1972;81:904–11.
74. Calvino MC, Llorca J, Garcia-Porrua C, et al.HenochSchönlein purpura in children from northwesternSpain: A 20-year epidemiologic and clinical study.Medicine (Baltimore). 2001;80:279–90.
75. Amo li MM, Thomson W, Hajeer AH, et al. Interleukin 1receptor antagonist gene polymorphism is associated withsevere renal involvement and renal sequelae inHenoch-Schönlein purpura. J Rheumatol. 2002;29:1404–7.
76. Stewart M, Savage JM, Bell B, et al. Long-term renalprognosis of Henoch-Schönlein purpura in an unselectedchildhood population. Eur J Pediatr. 1988;147:113–5.
77. Saulsbury FT. Henoch-Schönlein purpura in children:Report of 100 patients and review of the literature.Medicine (Baltimore). 1999;78:395–409.
78. Has tings MC, Moldoveanu Z, Suzuki H, et al.Biomarkers in IgA nephropathy: Relationship topathogenetic hits. Expert Opin Med Diagn. 2013;7:615–27.
79. Mills JA, Michel BA, Bloch DA, et al. The AmericanCollege of Rheumatology 1990 criteria for theclassification of Henoch-Schönlein purpura. ArthritisRheum. 1990;33:1114–21.
80. Eva ns DJ, Williams DG, Peters DK, et al. Glomerulardeposition of properdin in HenochSchönlein syndrome andidiopathic focal nephritis. Br Med J. 1973;3:326–8.
81. Lev y M, Gonzalez-Burchard G, Broyer M, et al.Berger’s disease in children: Natural history and outcome.Medicine (Baltimore). 1985;64:157–80. 82. Wyatt RJ, JulianBA, Rivas ML. Role for specific complement phenotypes anddeficiencies in the clinical expression of IgAnephropathy. Am J Med Sci. 1991;301:115–23. 83. Gar
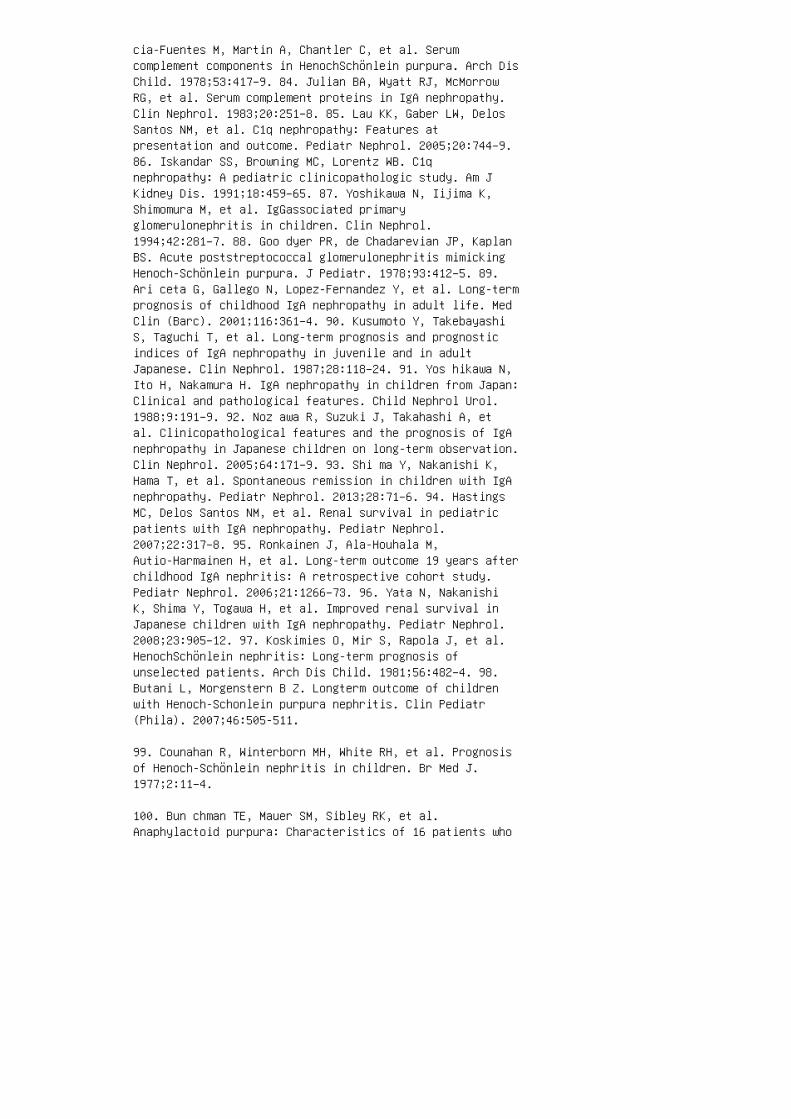
cia-Fuentes M, Martin A, Chantler C, et al. Serumcomplement components in HenochSchönlein purpura. Arch DisChild. 1978;53:417–9. 84. Julian BA, Wyatt RJ, McMorrowRG, et al. Serum complement proteins in IgA nephropathy.Clin Nephrol. 1983;20:251–8. 85. Lau KK, Gaber LW, DelosSantos NM, et al. C1q nephropathy: Features atpresentation and outcome. Pediatr Nephrol. 2005;20:744–9.86. Iskandar SS, Browning MC, Lorentz WB. C1qnephropathy: A pediatric clinicopathologic study. Am JKidney Dis. 1991;18:459–65. 87. Yoshikawa N, Iijima K,Shimomura M, et al. IgGassociated primaryglomerulonephritis in children. Clin Nephrol.1994;42:281–7. 88. Goo dyer PR, de Chadarevian JP, KaplanBS. Acute poststreptococcal glomerulonephritis mimickingHenoch-Schönlein purpura. J Pediatr. 1978;93:412–5. 89.Ari ceta G, Gallego N, Lopez-Fernandez Y, et al. Long-termprognosis of childhood IgA nephropathy in adult life. MedClin (Barc). 2001;116:361–4. 90. Kusumoto Y, TakebayashiS, Taguchi T, et al. Long-term prognosis and prognosticindices of IgA nephropathy in juvenile and in adultJapanese. Clin Nephrol. 1987;28:118–24. 91. Yos hikawa N,Ito H, Nakamura H. IgA nephropathy in children from Japan:Clinical and pathological features. Child Nephrol Urol.1988;9:191–9. 92. Noz awa R, Suzuki J, Takahashi A, etal. Clinicopathological features and the prognosis of IgAnephropathy in Japanese children on long-term observation.Clin Nephrol. 2005;64:171–9. 93. Shi ma Y, Nakanishi K,Hama T, et al. Spontaneous remission in children with IgAnephropathy. Pediatr Nephrol. 2013;28:71–6. 94. HastingsMC, Delos Santos NM, et al. Renal survival in pediatricpatients with IgA nephropathy. Pediatr Nephrol.2007;22:317–8. 95. Ronkainen J, Ala-Houhala M,Autio-Harmainen H, et al. Long-term outcome 19 years afterchildhood IgA nephritis: A retrospective cohort study.Pediatr Nephrol. 2006;21:1266–73. 96. Yata N, NakanishiK, Shima Y, Togawa H, et al. Improved renal survival inJapanese children with IgA nephropathy. Pediatr Nephrol.2008;23:905–12. 97. Koskimies O, Mir S, Rapola J, et al.HenochSchönlein nephritis: Long-term prognosis ofunselected patients. Arch Dis Child. 1981;56:482–4. 98.Butani L, Morgenstern B Z. Longterm outcome of childrenwith Henoch-Schonlein purpura nephritis. Clin Pediatr(Phila). 2007;46:505-511.
99. Counahan R, Winterborn MH, White RH, et al. Prognosisof Henoch-Schönlein nephritis in children. Br Med J.1977;2:11–4.
100. Bun chman TE, Mauer SM, Sibley RK, et al.Anaphylactoid purpura: Characteristics of 16 patients who
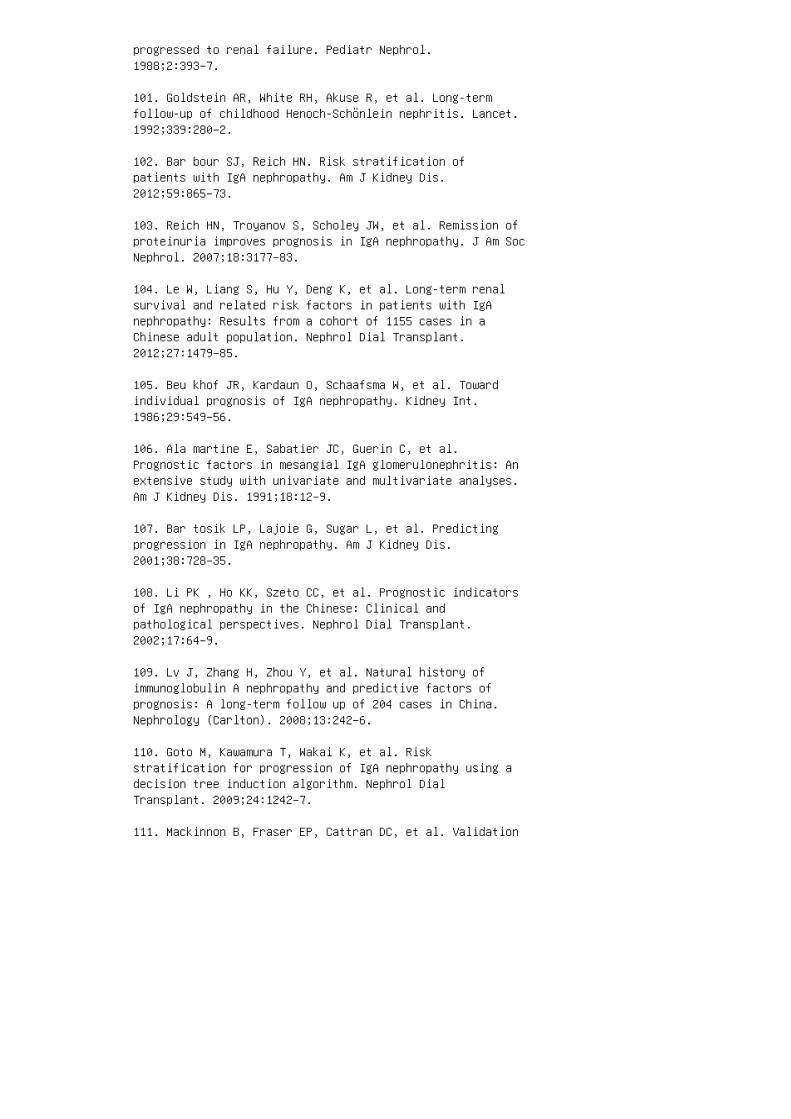
progressed to renal failure. Pediatr Nephrol.1988;2:393–7.
101. Goldstein AR, White RH, Akuse R, et al. Long-termfollow-up of childhood Henoch-Schönlein nephritis. Lancet.1992;339:280–2.
102. Bar bour SJ, Reich HN. Risk stratification ofpatients with IgA nephropathy. Am J Kidney Dis.2012;59:865–73.
103. Reich HN, Troyanov S, Scholey JW, et al. Remission ofproteinuria improves prognosis in IgA nephropathy. J Am SocNephrol. 2007;18:3177–83.
104. Le W, Liang S, Hu Y, Deng K, et al. Long-term renalsurvival and related risk factors in patients with IgAnephropathy: Results from a cohort of 1155 cases in aChinese adult population. Nephrol Dial Transplant.2012;27:1479–85.
105. Beu khof JR, Kardaun O, Schaafsma W, et al. Towardindividual prognosis of IgA nephropathy. Kidney Int.1986;29:549–56.
106. Ala martine E, Sabatier JC, Guerin C, et al.Prognostic factors in mesangial IgA glomerulonephritis: Anextensive study with univariate and multivariate analyses.Am J Kidney Dis. 1991;18:12–9.
107. Bar tosik LP, Lajoie G, Sugar L, et al. Predictingprogression in IgA nephropathy. Am J Kidney Dis.2001;38:728–35.
108. Li PK , Ho KK, Szeto CC, et al. Prognostic indicatorsof IgA nephropathy in the Chinese: Clinical andpathological perspectives. Nephrol Dial Transplant.2002;17:64–9.
109. Lv J, Zhang H, Zhou Y, et al. Natural history ofimmunoglobulin A nephropathy and predictive factors ofprognosis: A long-term follow up of 204 cases in China.Nephrology (Carlton). 2008;13:242–6.
110. Goto M, Kawamura T, Wakai K, et al. Riskstratification for progression of IgA nephropathy using adecision tree induction algorithm. Nephrol DialTransplant. 2009;24:1242–7.
111. Mackinnon B, Fraser EP, Cattran DC, et al. Validation

of the Toronto formula to predict progression in IgAnephropathy. Nephron Clin Pract. 2008;109:c148–53.
112. Berthoux F, Mohey H, Laurent B, et al. Predicting therisk for dialysis or death in IgA nephropathy. J Am SocNephrol. 2011;22:752–61.
113. Fri mat L, Briançon S, Hestin D, et al. IgAnephropathy: Prognostic classification of end-stage renalfailure. L’Association des Néphrologues de l’Est. NephrolDial Transplant. 1997;12:2569–75.
114. Rad ford MG, Donadio JV, Bergstralh EJ, et al.Predicting renal outcome in IgA nephropathy. J Am SocNephrol. 1997;8:199–207. 115. Manno C, Strippoli GF,D’Altri C, et al. A novel simpler histologicalclassification for renal survival in IgA nephropathy: Aretrospective study. Am J Kidney Dis. 2007;49:763–75.116. D’A mico G, Minetti L, Ponticelli C, et al. Prognosticindicators in idiopathic IgA mesangial nephropathy. Q JMed. 1986;59:363–78. 117. Edström Halling S, Söderberg MP,Berg UB. Predictors of outcome in paediatric IgAnephropathy with regard to clinical and histopathologicalvariables (Oxford classification). Nephrol Dial Transplant.2012;27:715-22. 118. Shi ma Y, Nakanishi K, Hama T, et al.Validity of the Oxford classification of IgA nephropathyin children. Pediatr Nephrol. 2012;27:783–92. 119.Niaudet P, Murcia I, Beaufils H, Broyer M, et al. PrimaryIgA nephropathies in children: Prognosis and treatment.Adv Nephrol Necker Hosp. 1993;22:121–40. 120. Nia udet P,Habib R. Methylprednisolone pulse therapy in the treatmentof severe forms of SchönleinHenoch purpura nephritis.Pediatr Nephrol. 1998;12:238–43. 121. One r A, TinaztepeK, Erdogan O. The effect of triple therapy on rapidlyprogressive type of Henoch-Schönlein nephritis. PediatrNephrol. 1995;9:6–10. 122. Bergstein J, Leiser J,Andreoli SP. Response of crescentic Henoch-Schöenleinpurpura nephritis to corticosteroid and azathioprinetherapy. Clin Nephrol. 1998;49:9–14. 123. Kid ney DiseaseIGO Clinical practice guidelines for glomerulonephritis.Immunoglobulin A nephropathy. Kidney Int Suppl.2012;S209–17. 124. Cop po R, Peruzzi L, Amore A, et al.IgACE: A placebo-controlled, randomized trial ofangiotensin-converting enzyme inhibitors in children andyoung people with IgA nephropathy and moderateproteinuria. J Am Soc Nephrol. 2007;18:1880–8. 125.Bhattacharjee R, Filler G. Additive antiproteinuric effectof ACE inhibitor and losartan in IgA nephropathy. PediatrNephrol. 2002;17:302–4. 126. Hog g RJ, Wyatt RJ,Scientific Planning Committee of the North American IgA

Nephropathy Study. A randomized controlled trial ofmycophenolate mofetil in patients with IgA nephropathyISRCTN62574616. BMC Nephrol. 2004;5:3. 127. Hogg RJ, LeeJ, Nardelli N, Julian BA, et al. Clinical trial toevaluate omega-3 fatty acids and alternate day prednisonein patients with IgA nephropathy: Report from theSouthwest Pediatric Nephrology Study Group. Clin J Am SocNephrol. 2006;1:467–74. 128. Coppo R. Is a legacy effectpossible in IgA nephropathy? Nephrol Dial Transplant.2013;28:1657–62.
REVIEW QUESTIONS
1. Which of the following histopathologic features is notincluded as a part of the Oxford classi�cation? a.Mesangial hypercellularity b. Endocapillaryhypercellularity c. Segmental glomerulosclerosis d.Tubular atrophy/interstitial �brosis e. Crescent formation
2. �e increased incidence of IgA nephropathy in Asiancountries such as Japan may be due to all of the following,except: a. True racial or ethnic di�erences in incidenceb. Increased detection through school screening programsc. An aggressive approach by pediatric nephrologists inthese countries for performing renal biopsies in childrenwith isolated microscopic hematuria or low levels ofproteinuria d. Increased serum levels of immunoglobulin Ain these populations
3. On renal biopsy, IgA nephropathy is characterized bywhich of the following: a. Dominant or codominantdeposition of immunoglobulin A, mainly in the glomerularmesangium b. Subepithelial humps c. Patchy foot processe�acement d. Prominent subendothelial deposits e.Apple-green birefringence under polarized light
4. A multi-hit hypothesis may explain the pathogenesis ofIgA nephropathy. �e �rst hit is thought to be due to: a.e presence in the serum of galactose-de�cient (orunderglycosylated) IgA1 in which in some carbohydrate sidechains (O-glycans) of the hinge region terminate inN-acetylgalactosamine (GalNAc) or sialylated GalNac ratherthan galactose b. �e generation of antiglycan antibodiesrecognizing this terminal GalNac c. �e formation ofnephritogenic circulating immune complexes containinggalactose-de�cient IgA1 and antiglycan antibody d.Secretion of extracellular matrix components, induction ofnitric oxide synthase, and the release various mediatorsof renal injury such as angiotensin II, proin�ammatory andpro�brotic cytokines, and growth factors

5. Which of the following statements is false? a. Serumgalactose-de�cient IgA1 level is elevated in approximately75% patients with IgA nephropathy; this is a heritabletrait. b. �e majority of �rst-degree relatives withelevated serum galactose-de�cient IgA1 levels do notdevelop clinical manifestations of IgA nephropathy of HSPnephritis. c. A locus at 6q22-23 named IgAN1 is associatedwith the production of galactose-de�cient immunoglobulinA. d. Susceptibility loci for IgA nephropathy have beenfound on chromosome 6p21 in the major histocompatibilitycomplex and on chromosome 1q32 in the complement factor H(CFH) gene cluster. 6. In the United States, thepercentage of children who have gross hematuria at thetime of presentation with IgA nephropathy isapproximately: a. 10% b. 25% c. 50% d. 75% e. 90% 7.e peak incidence of Henoch-Schönlein purpura is betweenages: a. 1 to 3 years b. 2 to 4 years c. 4 to 6 yearsd. 6 to 8 ye ars e. 10 to 1 2 years 8. �e percentage ofchildren with IgA nephropathy who present with overtnephrotic syndrome is: a. Less than 10% b. 10% to 25% c.25% to 5 0% d. 50% to 75% e. Grea ter than 75% 9. �e diagnosis of IgA nephropathy is dependent on: a. Serumgalactose-de�cient IgA1 and antiglycan antibody levels b.Serum immunoglobulin A levels c. Low C 3 levels d. Genetic testing for IgAN1 e. Examination of cortical renaltissue obtained via kidney biopsy 10. A normal urinalysismay eventually be seen in what percentage of pediatricpatients diagnosed with IgA nephropathy? a. 10% b. 20%c. 33% d. 70% e. 90% 11 . All o f the followingfeatures may predict loss of renal function in childrenand adults with IgA nephropathy, except: a. Serialmeasurements of urinary protein excretion averaged over 6month intervals a�er renal biopsy b. Sev ere histologicfeatures on kidney biopsy c. Hyp ertension d. Rena lfunction at time of presentation e. Pers istent hematuria
12. �e mainstay of treatment for persistent proteinuria inthe setting of IgA nephropathy is: a. High-doseintravenous corticosteroids b. Low-dose oralcorticosteroids c. Angiotensin-converting enzymeinhibitors or angiotensin receptor blockers d.Tonsillectomy e. Cyclophosphamide
ANSWER KEY
1. e
2. d 3. a 4. a 5. c 6. d 7. b 8. a 9. e 10. c 11.e 12. c

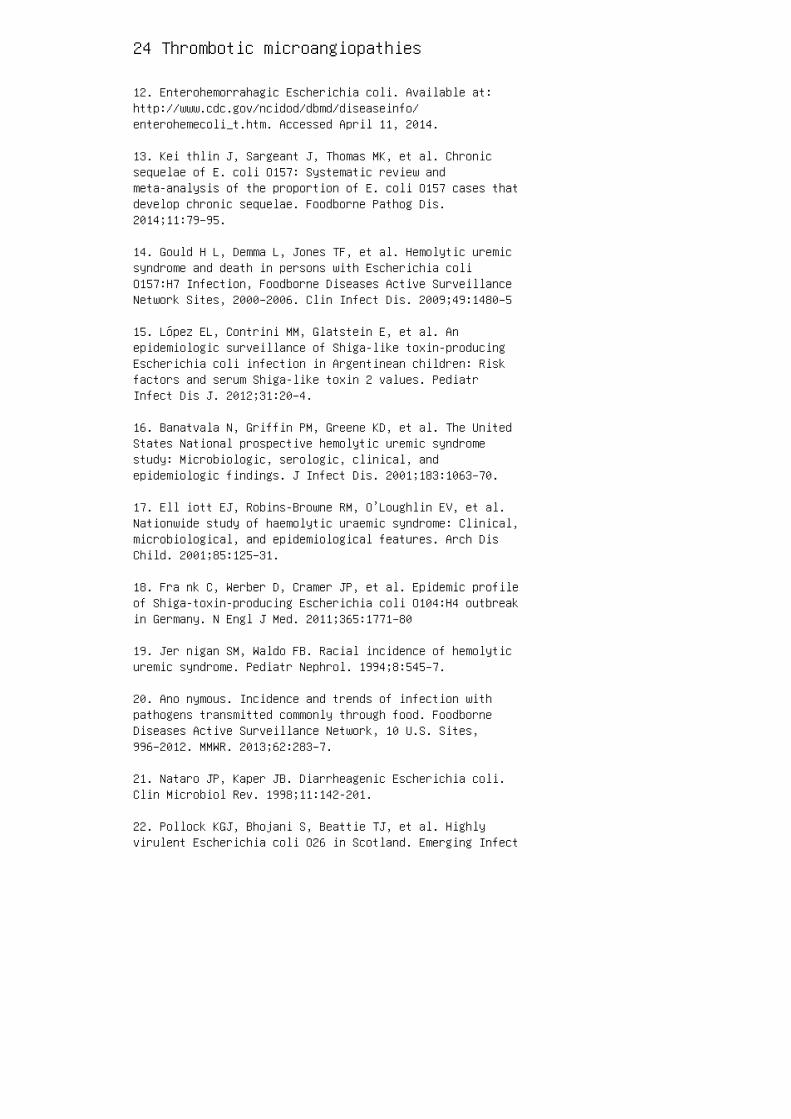
24 Thrombotic microangiopathies
12. Enterohemorrahagic Escherichia coli. Available at:http://www.cdc.gov/ncidod/dbmd/diseaseinfo/enterohemecoli_t.htm. Accessed April 11, 2014.
13. Kei thlin J, Sargeant J, Thomas MK, et al. Chronicsequelae of E. coli O157: Systematic review andmeta-analysis of the proportion of E. coli O157 cases thatdevelop chronic sequelae. Foodborne Pathog Dis.2014;11:79–95.
14. Gould H L, Demma L, Jones TF, et al. Hemolytic uremicsyndrome and death in persons with Escherichia coliO157:H7 Infection, Foodborne Diseases Active SurveillanceNetwork Sites, 2000–2006. Clin Infect Dis. 2009;49:1480–5
15. López EL, Contrini MM, Glatstein E, et al. Anepidemiologic surveillance of Shiga-like toxin-producingEscherichia coli infection in Argentinean children: Riskfactors and serum Shiga-like toxin 2 values. PediatrInfect Dis J. 2012;31:20–4.
16. Banatvala N, Griffin PM, Greene KD, et al. The UnitedStates National prospective hemolytic uremic syndromestudy: Microbiologic, serologic, clinical, andepidemiologic findings. J Infect Dis. 2001;183:1063–70.
17. Ell iott EJ, Robins-Browne RM, O’Loughlin EV, et al.Nationwide study of haemolytic uraemic syndrome: Clinical,microbiological, and epidemiological features. Arch DisChild. 2001;85:125–31.
18. Fra nk C, Werber D, Cramer JP, et al. Epidemic profileof Shiga-toxin-producing Escherichia coli O104:H4 outbreakin Germany. N Engl J Med. 2011;365:1771–80
19. Jer nigan SM, Waldo FB. Racial incidence of hemolyticuremic syndrome. Pediatr Nephrol. 1994;8:545–7.
20. Ano nymous. Incidence and trends of infection withpathogens transmitted commonly through food. FoodborneDiseases Active Surveillance Network, 10 U.S. Sites,996–2012. MMWR. 2013;62:283–7.
21. Nataro JP, Kaper JB. Diarrheagenic Escherichia coli.Clin Microbiol Rev. 1998;11:142-201.
22. Pollock KGJ, Bhojani S, Beattie TJ, et al. Highlyvirulent Escherichia coli O26 in Scotland. Emerging Infect
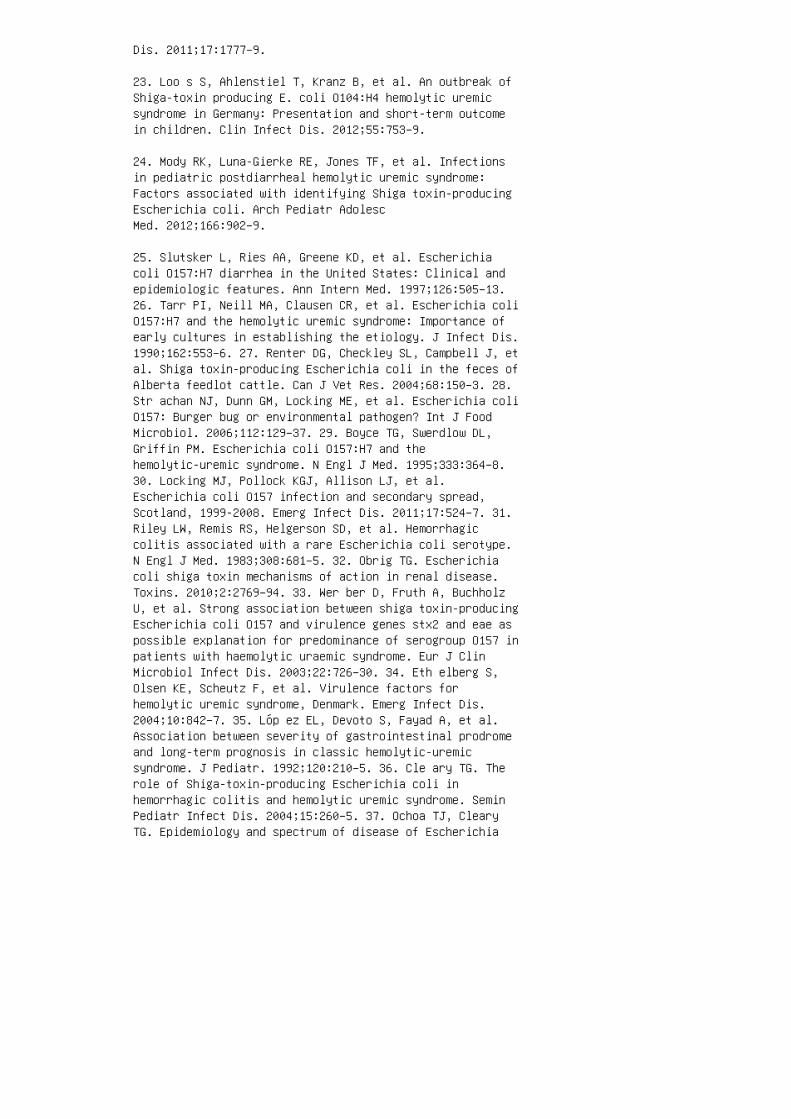
Dis. 2011;17:1777–9.
23. Loo s S, Ahlenstiel T, Kranz B, et al. An outbreak ofShiga-toxin producing E. coli O104:H4 hemolytic uremicsyndrome in Germany: Presentation and short-term outcomein children. Clin Infect Dis. 2012;55:753–9.
24. Mody RK, Luna-Gierke RE, Jones TF, et al. Infectionsin pediatric postdiarrheal hemolytic uremic syndrome:Factors associated with identifying Shiga toxin-producingEscherichia coli. Arch Pediatr AdolescMed. 2012;166:902–9.
25. Slutsker L, Ries AA, Greene KD, et al. Escherichiacoli O157:H7 diarrhea in the United States: Clinical andepidemiologic features. Ann Intern Med. 1997;126:505–13.26. Tarr PI, Neill MA, Clausen CR, et al. Escherichia coliO157:H7 and the hemolytic uremic syndrome: Importance ofearly cultures in establishing the etiology. J Infect Dis.1990;162:553–6. 27. Renter DG, Checkley SL, Campbell J, etal. Shiga toxin-producing Escherichia coli in the feces ofAlberta feedlot cattle. Can J Vet Res. 2004;68:150–3. 28.Str achan NJ, Dunn GM, Locking ME, et al. Escherichia coliO157: Burger bug or environmental pathogen? Int J FoodMicrobiol. 2006;112:129–37. 29. Boyce TG, Swerdlow DL,Griffin PM. Escherichia coli O157:H7 and thehemolytic-uremic syndrome. N Engl J Med. 1995;333:364–8.30. Locking MJ, Pollock KGJ, Allison LJ, et al.Escherichia coli O157 infection and secondary spread,Scotland, 1999‐2008. Emerg Infect Dis. 2011;17:524–7. 31.Riley LW, Remis RS, Helgerson SD, et al. Hemorrhagiccolitis associated with a rare Escherichia coli serotype.N Engl J Med. 1983;308:681–5. 32. Obrig TG. Escherichiacoli shiga toxin mechanisms of action in renal disease.Toxins. 2010;2:2769–94. 33. Wer ber D, Fruth A, BuchholzU, et al. Strong association between shiga toxin-producingEscherichia coli O157 and virulence genes stx2 and eae aspossible explanation for predominance of serogroup O157 inpatients with haemolytic uraemic syndrome. Eur J ClinMicrobiol Infect Dis. 2003;22:726–30. 34. Eth elberg S,Olsen KE, Scheutz F, et al. Virulence factors forhemolytic uremic syndrome, Denmark. Emerg Infect Dis.2004;10:842–7. 35. Lóp ez EL, Devoto S, Fayad A, et al.Association between severity of gastrointestinal prodromeand long-term prognosis in classic hemolytic-uremicsyndrome. J Pediatr. 1992;120:210–5. 36. Cle ary TG. Therole of Shiga-toxin-producing Escherichia coli inhemorrhagic colitis and hemolytic uremic syndrome. SeminPediatr Infect Dis. 2004;15:260–5. 37. Ochoa TJ, ClearyTG. Epidemiology and spectrum of disease of Escherichia
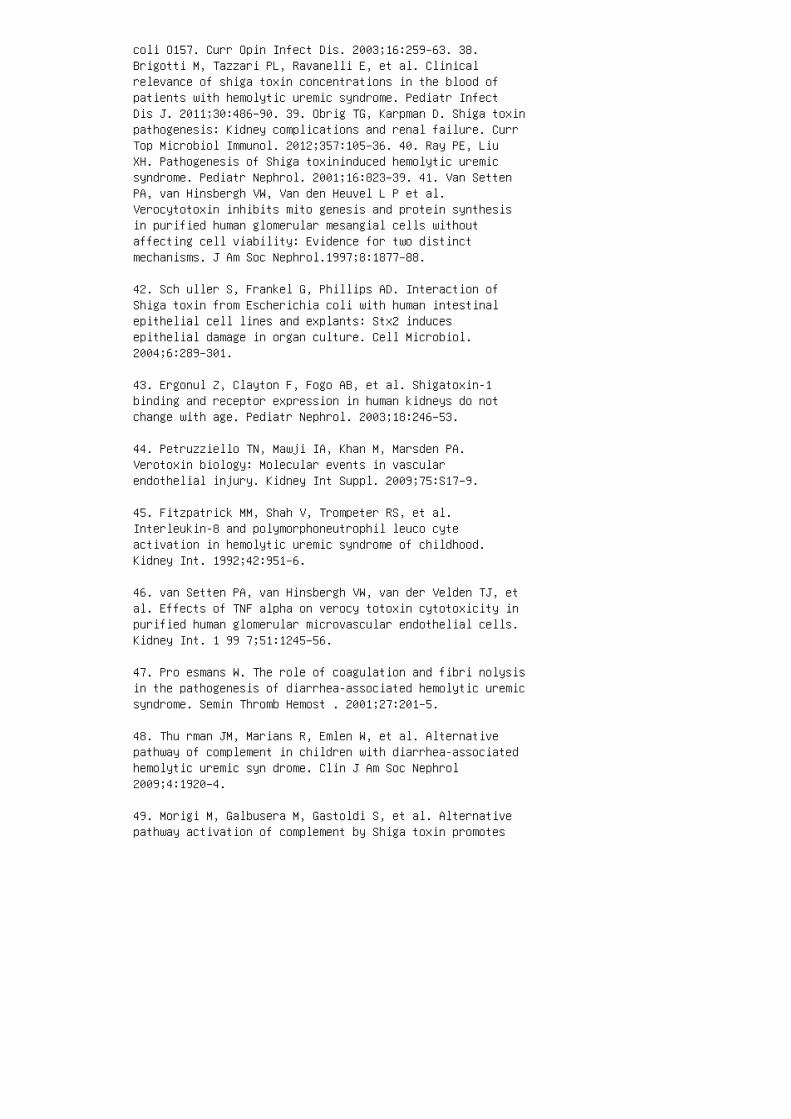
coli O157. Curr Opin Infect Dis. 2003;16:259–63. 38.Brigotti M, Tazzari PL, Ravanelli E, et al. Clinicalrelevance of shiga toxin concentrations in the blood ofpatients with hemolytic uremic syndrome. Pediatr InfectDis J. 2011;30:486–90. 39. Obrig TG, Karpman D. Shiga toxinpathogenesis: Kidney complications and renal failure. CurrTop Microbiol Immunol. 2012;357:105–36. 40. Ray PE, LiuXH. Pathogenesis of Shiga toxininduced hemolytic uremicsyndrome. Pediatr Nephrol. 2001;16:823–39. 41. Van SettenPA, van Hinsbergh VW, Van den Heuvel L P et al.Verocytotoxin inhibits mito genesis and protein synthesisin purified human glomerular mesangial cells withoutaffecting cell viability: Evidence for two distinctmechanisms. J Am Soc Nephrol.1997;8:1877–88.
42. Sch uller S, Frankel G, Phillips AD. Interaction ofShiga toxin from Escherichia coli with human intestinalepithelial cell lines and explants: Stx2 inducesepithelial damage in organ culture. Cell Microbiol.2004;6:289–301.
43. Ergonul Z, Clayton F, Fogo AB, et al. Shigatoxin-1binding and receptor expression in human kidneys do notchange with age. Pediatr Nephrol. 2003;18:246–53.
44. Petruzziello TN, Mawji IA, Khan M, Marsden PA.Verotoxin biology: Molecular events in vascularendothelial injury. Kidney Int Suppl. 2009;75:S17–9.
45. Fitzpatrick MM, Shah V, Trompeter RS, et al.Interleukin-8 and polymorphoneutrophil leuco cyteactivation in hemolytic uremic syndrome of childhood.Kidney Int. 1992;42:951–6.
46. van Setten PA, van Hinsbergh VW, van der Velden TJ, etal. Effects of TNF alpha on verocy totoxin cytotoxicity inpurified human glomerular microvascular endothelial cells.Kidney Int. 1 99 7;51:1245–56.
47. Pro esmans W. The role of coagulation and fibri nolysisin the pathogenesis of diarrhea-associated hemolytic uremicsyndrome. Semin Thromb Hemost . 2001;27:201–5.
48. Thu rman JM, Marians R, Emlen W, et al. Alternativepathway of complement in children with diarrhea-associatedhemolytic uremic syn drome. Clin J Am Soc Nephrol2009;4:1920–4.
49. Morigi M, Galbusera M, Gastoldi S, et al. Alternativepathway activation of complement by Shiga toxin promotes
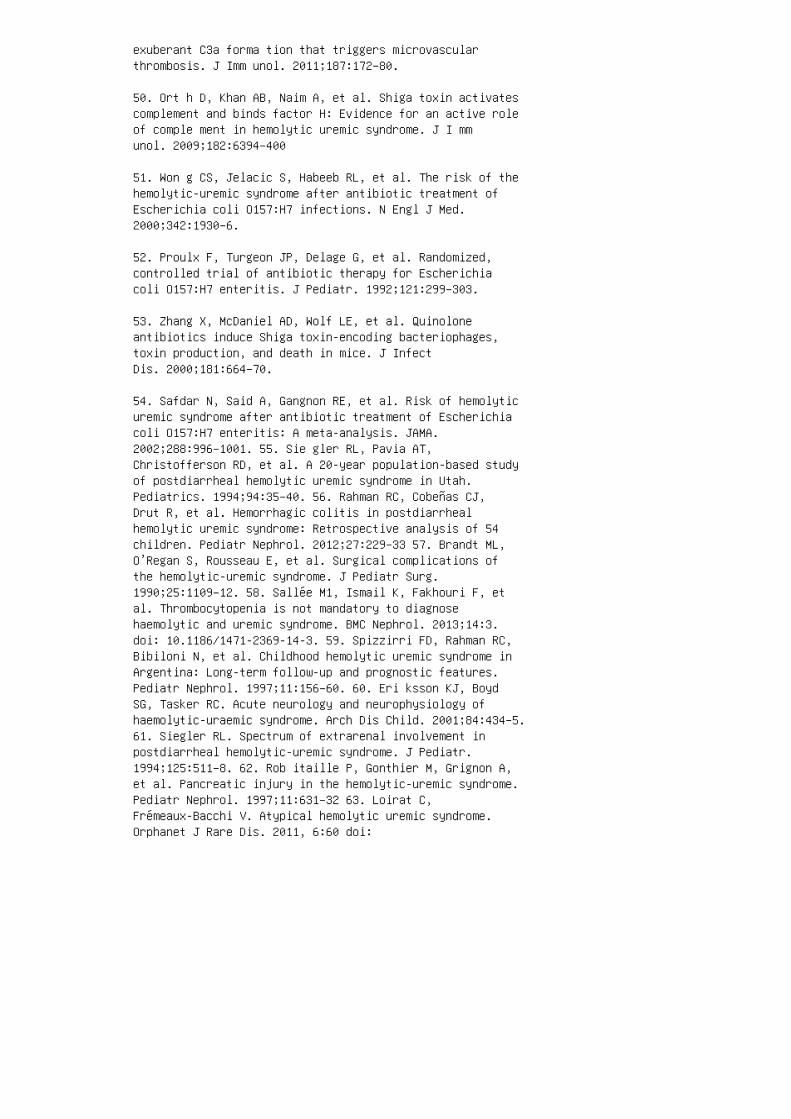
exuberant C3a forma tion that triggers microvascularthrombosis. J Imm unol. 2011;187:172–80.
50. Ort h D, Khan AB, Naim A, et al. Shiga toxin activatescomplement and binds factor H: Evidence for an active roleof comple ment in hemolytic uremic syndrome. J I mmunol. 2009;182:6394–400
51. Won g CS, Jelacic S, Habeeb RL, et al. The risk of thehemolytic-uremic syndrome after antibiotic treatment ofEscherichia coli O157:H7 infections. N Engl J Med.2000;342:1930–6.
52. Proulx F, Turgeon JP, Delage G, et al. Randomized,controlled trial of antibiotic therapy for Escherichiacoli O157:H7 enteritis. J Pediatr. 1992;121:299–303.
53. Zhang X, McDaniel AD, Wolf LE, et al. Quinoloneantibiotics induce Shiga toxin-encoding bacteriophages,toxin production, and death in mice. J InfectDis. 2000;181:664–70.
54. Safdar N, Said A, Gangnon RE, et al. Risk of hemolyticuremic syndrome after antibiotic treatment of Escherichiacoli O157:H7 enteritis: A meta-analysis. JAMA.2002;288:996–1001. 55. Sie gler RL, Pavia AT,Christofferson RD, et al. A 20-year population-based studyof postdiarrheal hemolytic uremic syndrome in Utah.Pediatrics. 1994;94:35–40. 56. Rahman RC, Cobeñas CJ,Drut R, et al. Hemorrhagic colitis in postdiarrhealhemolytic uremic syndrome: Retrospective analysis of 54children. Pediatr Nephrol. 2012;27:229–33 57. Brandt ML,O’Regan S, Rousseau E, et al. Surgical complications ofthe hemolytic-uremic syndrome. J Pediatr Surg.1990;25:1109–12. 58. Sallée M1, Ismail K, Fakhouri F, etal. Thrombocytopenia is not mandatory to diagnosehaemolytic and uremic syndrome. BMC Nephrol. 2013;14:3.doi: 10.1186/1471-2369-14-3. 59. Spizzirri FD, Rahman RC,Bibiloni N, et al. Childhood hemolytic uremic syndrome inArgentina: Long-term follow-up and prognostic features.Pediatr Nephrol. 1997;11:156–60. 60. Eri ksson KJ, BoydSG, Tasker RC. Acute neurology and neurophysiology ofhaemolytic-uraemic syndrome. Arch Dis Child. 2001;84:434–5.61. Siegler RL. Spectrum of extrarenal involvement inpostdiarrheal hemolytic-uremic syndrome. J Pediatr.1994;125:511–8. 62. Rob itaille P, Gonthier M, Grignon A,et al. Pancreatic injury in the hemolytic-uremic syndrome.Pediatr Nephrol. 1997;11:631–32 63. Loirat C,Frémeaux-Bacchi V. Atypical hemolytic uremic syndrome.Orphanet J Rare Dis. 2011, 6:60 doi:

10.1186/1750-1172-6-60. 64. Constantinescu AR, Bitzan M,Weiss LS, et al. Non-enteropathic hemolytic uremicsyndrome: Causes and short-term course. Am J KidneyDis. 2004;43:976–82. 65. Noris M, Caprioli J, Bresin E, etal. Relative role of genetic complement abnormali ties insporadic and familial aHUS and their imp act on clinicalphenotype. Clin J Am Soc Nephrol. 2010;5:1844–59. 66.Frémeaux-Bacchi V, Fakhouri F, Garnier A, et al. Geneticsand outcome of atypical hemolytic uremic syndrome: Anationwide French series comparing children and adults.Clin J Am Soc Nephrol. 2013;8:554–62. 67. Maga TK,Nishimura CJ, Weaver AE, et al. Mutations in alternativepathway complement proteins in American patients with a typical hemolytic uremic syndrome. Hum Mut.2010;31:E1445–60. 68. Landau D, Shalev H, Levy-Finer G, etal. Familial hemolytic uremic syndrome associated withcomplement factor H deficiency. J Pediatr.2001:138:412–17.
69. Warwicker P, Donne RL, Goodship JA, et al. Familialrelapsing haemolytic uraemic syndrome and complementfactor H deficiency. Nephrol Dial Transplant.1999;14:1229–33.
70. Richards A, Kemp EJ, Liszewski MK, et al. Mutations inhuman complement regulator, membrane cofactor protein(CD46), predis pose to development of familial hemolyticure mic syndrome. Proc Natl Acad Sci U S A.2003;100:12966–71.
71. Nor is M, Brioschi S, Caprioli J, et al. Familialhaemolytic uraemic syndrome and an MCP mutation. Lancet.2003;362:1542–7.
72. Bresin E, Rurali E, Caprioli J, et al.; EuropeanWorking Party on Complement Genetics in Renal Diseases.Combined complement gene mutations in atypical hemolyticuremic syn drome influence clinical phenotype. J Am SocNephr ol. 2013;24:475–86.
73. Kava nagh D, Richards A, Frémeaux-Bacchi V, et al.Screening for complement sys tem abnormalities in patientswith atypical hem olytic uremic syndrome. Clin J Am SocNephrol. 2007;2:591–6.
74. Lem aire M, Frémeaux-Bacchi V, Schaefer F, et al.Recessive mutations in DGKE cause atypi calhemolytic-uremic syndrome. Nat Genet. 2 01 3;45:53–6.
75. Jan eway CA Jr, Travers P, Walport M, et al.
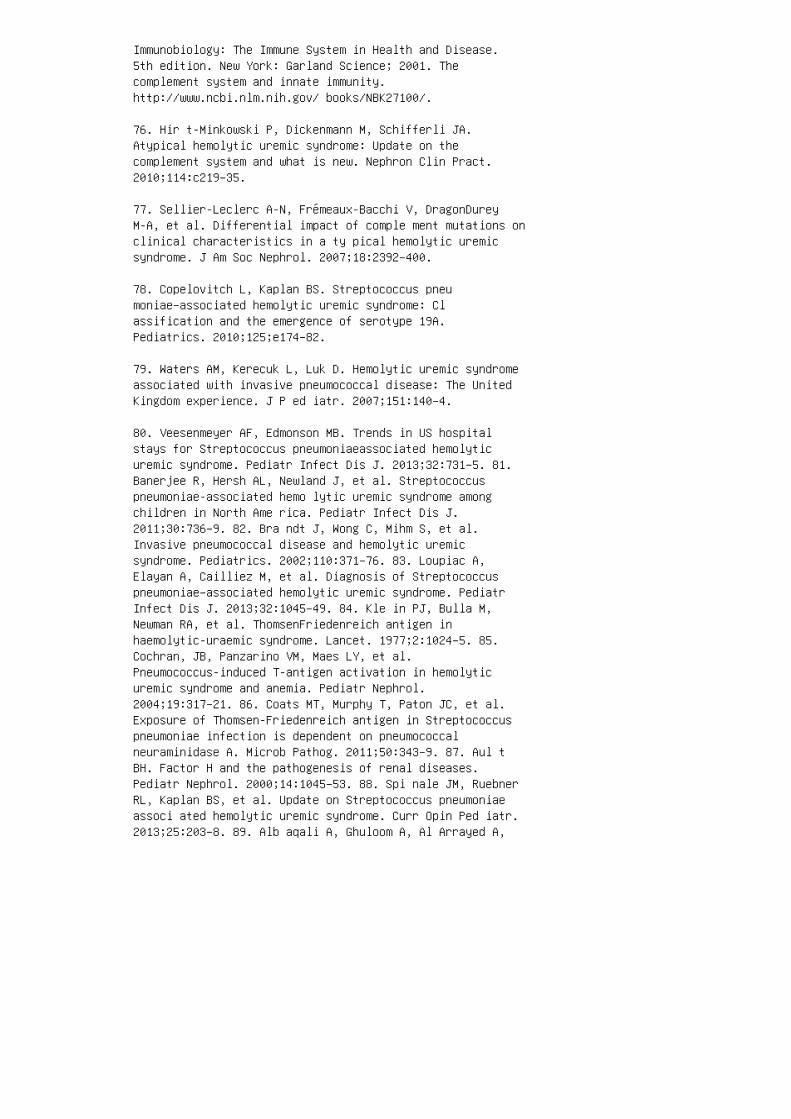
Immunobiology: The Immune System in Health and Disease.5th edition. New York: Garland Science; 2001. Thecomplement system and innate immunity.http://www.ncbi.nlm.nih.gov/ books/NBK27100/.
76. Hir t-Minkowski P, Dickenmann M, Schifferli JA.Atypical hemolytic uremic syndrome: Update on thecomplement system and what is new. Nephron Clin Pract.2010;114:c219–35.
77. Sellier-Leclerc A-N, Frémeaux-Bacchi V, DragonDureyM-A, et al. Differential impact of comple ment mutations onclinical characteristics in a ty pical hemolytic uremicsyndrome. J Am Soc Nephrol. 2007;18:2392–400.
78. Copelovitch L, Kaplan BS. Streptococcus pneumoniae–associated hemolytic uremic syndrome: Classification and the emergence of serotype 19A.Pediatrics. 2010;125;e174–82.
79. Waters AM, Kerecuk L, Luk D. Hemolytic uremic syndromeassociated with invasive pneumococcal disease: The UnitedKingdom experience. J P ed iatr. 2007;151:140–4.
80. Veesenmeyer AF, Edmonson MB. Trends in US hospitalstays for Streptococcus pneumoniaeassociated hemolyticuremic syndrome. Pediatr Infect Dis J. 2013;32:731–5. 81.Banerjee R, Hersh AL, Newland J, et al. Streptococcuspneumoniae-associated hemo lytic uremic syndrome amongchildren in North Ame rica. Pediatr Infect Dis J.2011;30:736–9. 82. Bra ndt J, Wong C, Mihm S, et al.Invasive pneumococcal disease and hemolytic uremicsyndrome. Pediatrics. 2002;110:371–76. 83. Loupiac A,Elayan A, Cailliez M, et al. Diagnosis of Streptococcuspneumoniae–associated hemolytic uremic syndrome. PediatrInfect Dis J. 2013;32:1045–49. 84. Kle in PJ, Bulla M,Newman RA, et al. ThomsenFriedenreich antigen inhaemolytic-uraemic syndrome. Lancet. 1977;2:1024–5. 85.Cochran, JB, Panzarino VM, Maes LY, et al.Pneumococcus-induced T-antigen activation in hemolyticuremic syndrome and anemia. Pediatr Nephrol.2004;19:317–21. 86. Coats MT, Murphy T, Paton JC, et al.Exposure of Thomsen-Friedenreich antigen in Streptococcuspneumoniae infection is dependent on pneumococcalneuraminidase A. Microb Pathog. 2011;50:343–9. 87. Aul tBH. Factor H and the pathogenesis of renal diseases.Pediatr Nephrol. 2000;14:1045–53. 88. Spi nale JM, RuebnerRL, Kaplan BS, et al. Update on Streptococcus pneumoniaeassoci ated hemolytic uremic syndrome. Curr Opin Ped iatr.2013;25:203–8. 89. Alb aqali A, Ghuloom A, Al Arrayed A,
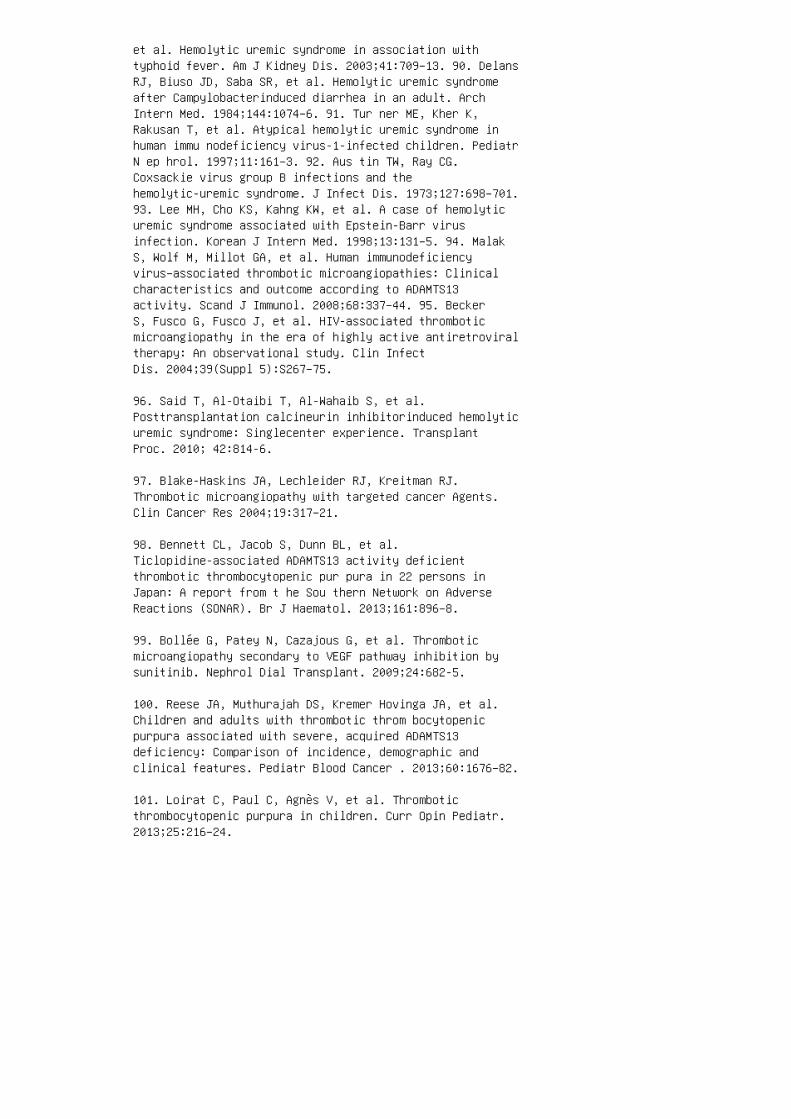
et al. Hemolytic uremic syndrome in association withtyphoid fever. Am J Kidney Dis. 2003;41:709–13. 90. DelansRJ, Biuso JD, Saba SR, et al. Hemolytic uremic syndromeafter Campylobacterinduced diarrhea in an adult. ArchIntern Med. 1984;144:1074–6. 91. Tur ner ME, Kher K,Rakusan T, et al. Atypical hemolytic uremic syndrome inhuman immu nodeficiency virus-1-infected children. PediatrN ep hrol. 1997;11:161–3. 92. Aus tin TW, Ray CG.Coxsackie virus group B infections and thehemolytic-uremic syndrome. J Infect Dis. 1973;127:698–701.93. Lee MH, Cho KS, Kahng KW, et al. A case of hemolyticuremic syndrome associated with Epstein-Barr virusinfection. Korean J Intern Med. 1998;13:131–5. 94. MalakS, Wolf M, Millot GA, et al. Human immunodeficiencyvirus–associated thrombotic microangiopathies: Clinicalcharacteristics and outcome according to ADAMTS13activity. Scand J Immunol. 2008;68:337–44. 95. BeckerS, Fusco G, Fusco J, et al. HIV-associated thromboticmicroangiopathy in the era of highly active antiretroviraltherapy: An observational study. Clin InfectDis. 2004;39(Suppl 5):S267–75.
96. Said T, Al-Otaibi T, Al-Wahaib S, et al.Posttransplantation calcineurin inhibitorinduced hemolyticuremic syndrome: Singlecenter experience. TransplantProc. 2010; 42:814-6.
97. Blake-Haskins JA, Lechleider RJ, Kreitman RJ.Thrombotic microangiopathy with targeted cancer Agents.Clin Cancer Res 2004;19:317–21.
98. Bennett CL, Jacob S, Dunn BL, et al.Ticlopidine-associated ADAMTS13 activity deficientthrombotic thrombocytopenic pur pura in 22 persons inJapan: A report from t he Sou thern Network on AdverseReactions (SONAR). Br J Haematol. 2013;161:896–8.
99. Bollée G, Patey N, Cazajous G, et al. Thromboticmicroangiopathy secondary to VEGF pathway inhibition bysunitinib. Nephrol Dial Transplant. 2009;24:682-5.
100. Reese JA, Muthurajah DS, Kremer Hovinga JA, et al.Children and adults with thrombotic throm bocytopenicpurpura associated with severe, acquired ADAMTS13deficiency: Comparison of incidence, demographic andclinical features. Pediatr Blood Cancer . 2013;60:1676–82.
101. Loirat C, Paul C, Agnès V, et al. Thromboticthrombocytopenic purpura in children. Curr Opin Pediatr.2013;25:216–24.
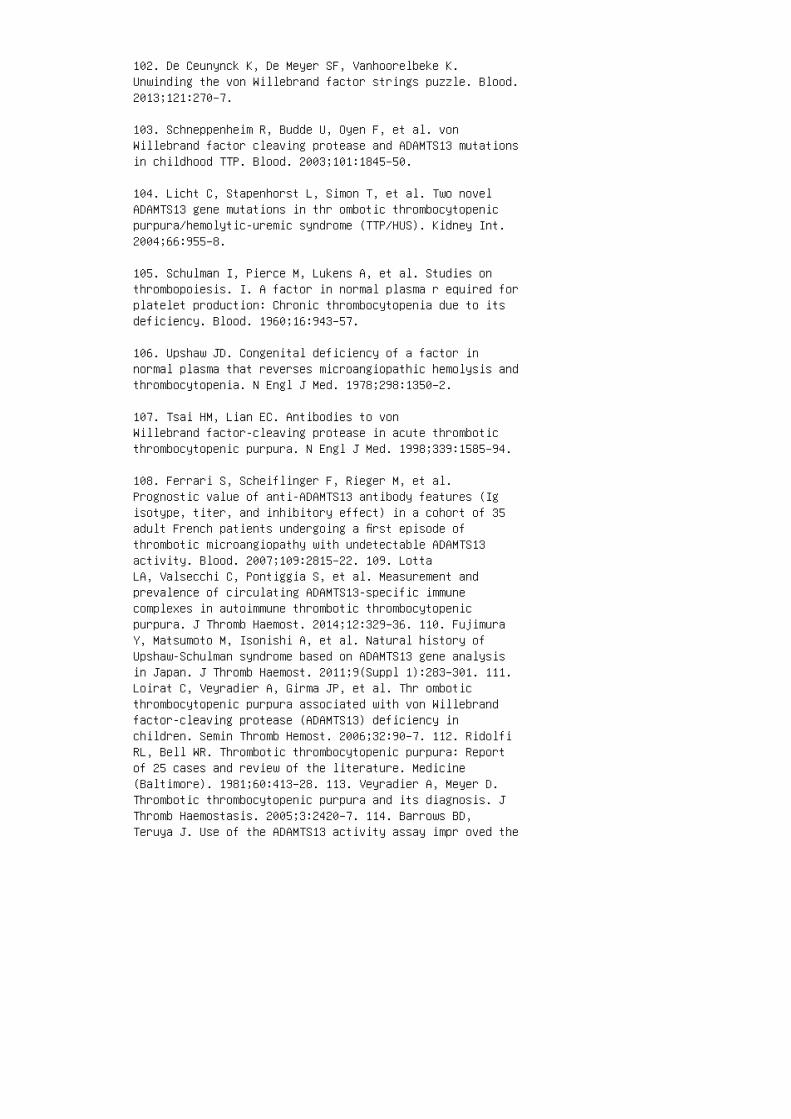
102. De Ceunynck K, De Meyer SF, Vanhoorelbeke K.Unwinding the von Willebrand factor strings puzzle. Blood.2013;121:270–7.
103. Schneppenheim R, Budde U, Oyen F, et al. vonWillebrand factor cleaving protease and ADAMTS13 mutationsin childhood TTP. Blood. 2003;101:1845–50.
104. Licht C, Stapenhorst L, Simon T, et al. Two novelADAMTS13 gene mutations in thr ombotic thrombocytopenicpurpura/hemolytic-uremic syndrome (TTP/HUS). Kidney Int.2004;66:955–8.
105. Schulman I, Pierce M, Lukens A, et al. Studies onthrombopoiesis. I. A factor in normal plasma r equired forplatelet production: Chronic thrombocytopenia due to itsdeficiency. Blood. 1960;16:943–57.
106. Upshaw JD. Congenital deficiency of a factor innormal plasma that reverses microangiopathic hemolysis andthrombocytopenia. N Engl J Med. 1978;298:1350–2.
107. Tsai HM, Lian EC. Antibodies to vonWillebrand factor-cleaving protease in acute thromboticthrombocytopenic purpura. N Engl J Med. 1998;339:1585–94.
108. Ferrari S, Scheiflinger F, Rieger M, et al.Prognostic value of anti-ADAMTS13 antibody features (Igisotype, titer, and inhibitory effect) in a cohort of 35adult French patients undergoing a first episode ofthrombotic microangiopathy with undetectable ADAMTS13activity. Blood. 2007;109:2815–22. 109. LottaLA, Valsecchi C, Pontiggia S, et al. Measurement andprevalence of circulating ADAMTS13-specific immunecomplexes in autoimmune thrombotic thrombocytopenicpurpura. J Thromb Haemost. 2014;12:329–36. 110. FujimuraY, Matsumoto M, Isonishi A, et al. Natural history ofUpshaw-Schulman syndrome based on ADAMTS13 gene analysisin Japan. J Thromb Haemost. 2011;9(Suppl 1):283–301. 111.Loirat C, Veyradier A, Girma JP, et al. Thr omboticthrombocytopenic purpura associated with von Willebrandfactor-cleaving protease (ADAMTS13) deficiency inchildren. Semin Thromb Hemost. 2006;32:90–7. 112. RidolfiRL, Bell WR. Thrombotic thrombocytopenic purpura: Reportof 25 cases and review of the literature. Medicine(Baltimore). 1981;60:413–28. 113. Veyradier A, Meyer D.Thrombotic thrombocytopenic purpura and its diagnosis. JThromb Haemostasis. 2005;3:2420–7. 114. Barrows BD,Teruya J. Use of the ADAMTS13 activity assay impr oved the

accuracy and efficiency of the diagnosis and treatment ofsuspected acquired thrombotic thrombocytopenic purpura.Arch Pathol Lab Med. 2014;138:546–9. 115. Ruggenenti P,Noris M, Remuzzi G. Thrombotic microangiopathy, hemolyticuremic syndrome, and thrombotic thrombocytopenic purpura.Kidney Int. 2001;60:831–46. 116. Zoja C, Morigi M,Remuzzi G. The role of the endothelium in hemolytic uremicsyndrome. J Nephrol. 2001;4:S58–82. 117. Taylor CM, ChuaC, Howie AJ, et al. Clinicopathological findings indiarrhoea-negative haemolytic uraemic syndrome. PediatrNephrol. 2004;19:419–25. 118. Inward CD, Howie AJ,Fitzpatrick MM, et al.: Renal histopathology in fatalcases of diarrhoeaassociated haemolytic uraemic syndrome.British Association for Paediatric Nephrology. PediatrNephrol. 1997;11:556–9. 119. Koster FT, BoonpucknavigV, Sujaho S, et al. Renal histopathology in thehemolytic-ure mic syndrome following shigellosis. ClinNephr ol. 1984;21:126–33. 120. Halevy D, Radhakrishnan J,Markowitz G, et al. Thrombotic microangiopathies. CritCare Clin. 2002;18:309–20. 121. Buteau C, Proulx F,Chaibou M, et al. Leukocytosis in children withEscherichia coli O157:H7 enteritis developing the hemolytic-uremic syndrome. Pediatr Infect Dis J. 2000;9:642–7.
122. Gould LH, Bopp C, Strockbine N, et al.Recommendations for diagnosis of shiga toxin– producingEscherichia coli Infections by clinical laboratories.MMWR. 2009;58:12–4.
123. Klein EJ, Stapp JR, Clausen CR, et al. Shigatoxin-producing Escherichia coli in children withdiarrhea: Prospective point-of-care study. JPediatr. 2002;141:172–7.
124. Cohen MB. Shiga toxin–producing E. coli: Two testsare better than one. J Pediatr 2002;141:155–6.
125. Tazzari PL, Ricci F, Carnicelli D, et al.: Flow cytometry detection of Shiga toxins in the blood from childrenwith hemolytic uremic syndrome. Cytometry B Clin Cytom.2004;61:40–4.
126. Ariceta G, Besbas N, Johnson S, et al. Guideline forthe investigation and initial therapy of diarrheanegativehemolytic uremic syndrome. Pediatr Nephrol. 2009;24:687–96.
127. Peyvandi F, Palla R, Lotta LA, et al. ADAMTS-13assays in thrombotic thrombocytopenic purpura. J ThrombHaemost. 2010;8:631–40.
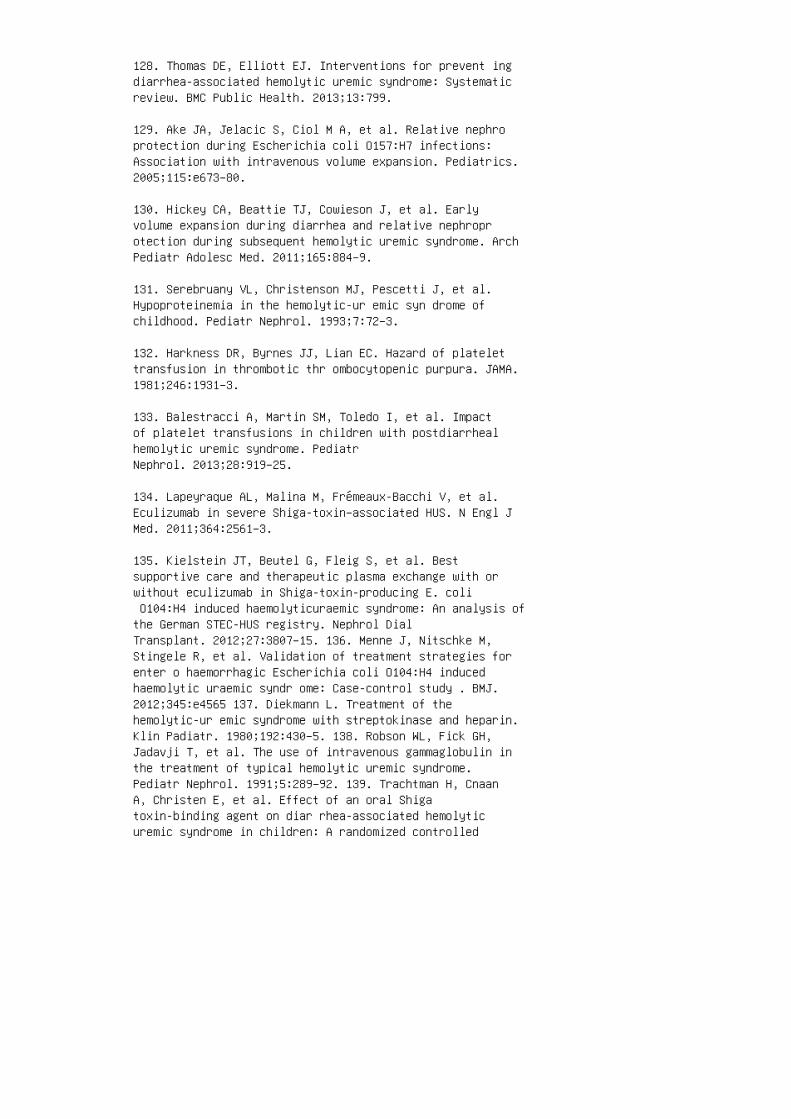
128. Thomas DE, Elliott EJ. Interventions for prevent ingdiarrhea-associated hemolytic uremic syndrome: Systematicreview. BMC Public Health. 2013;13:799.
129. Ake JA, Jelacic S, Ciol M A, et al. Relative nephroprotection during Escherichia coli O157:H7 infections:Association with intravenous volume expansion. Pediatrics.2005;115:e673–80.
130. Hickey CA, Beattie TJ, Cowieson J, et al. Earlyvolume expansion during diarrhea and relative nephroprotection during subsequent hemolytic uremic syndrome. ArchPediatr Adolesc Med. 2011;165:884–9.
131. Serebruany VL, Christenson MJ, Pescetti J, et al.Hypoproteinemia in the hemolytic-ur emic syn drome ofchildhood. Pediatr Nephrol. 1993;7:72–3.
132. Harkness DR, Byrnes JJ, Lian EC. Hazard of platelettransfusion in thrombotic thr ombocytopenic purpura. JAMA.1981;246:1931–3.
133. Balestracci A, Martin SM, Toledo I, et al. Impactof platelet transfusions in children with postdiarrhealhemolytic uremic syndrome. PediatrNephrol. 2013;28:919–25.
134. Lapeyraque AL, Malina M, Frémeaux-Bacchi V, et al.Eculizumab in severe Shiga-toxin–associated HUS. N Engl JMed. 2011;364:2561–3.
135. Kielstein JT, Beutel G, Fleig S, et al. Bestsupportive care and therapeutic plasma exchange with orwithout eculizumab in Shiga-toxin-producing E. coli O104:H4 induced haemolyticuraemic syndrome: An analysis ofthe German STEC-HUS registry. Nephrol DialTransplant. 2012;27:3807–15. 136. Menne J, Nitschke M,Stingele R, et al. Validation of treatment strategies forenter o haemorrhagic Escherichia coli O104:H4 inducedhaemolytic uraemic syndr ome: Case-control study . BMJ.2012;345:e4565 137. Diekmann L. Treatment of thehemolytic-ur emic syndrome with streptokinase and heparin.Klin Padiatr. 1980;192:430–5. 138. Robson WL, Fick GH,Jadavji T, et al. The use of intravenous gammaglobulin inthe treatment of typical hemolytic uremic syndrome.Pediatr Nephrol. 1991;5:289–92. 139. Trachtman H, CnaanA, Christen E, et al. Effect of an oral Shigatoxin-binding agent on diar rhea-associated hemolyticuremic syndrome in children: A randomized controlled

trial. JAMA. 2003;290:1337–44. 140. Perez N, Spizzirri F,Rahman R, et al. Ster oids in the hemolytic uremicsyndrome. Pediatr Nephrol. 1998;12:101–4. 141. Reill, A.Prevention and control of enterohaem orrhagic Escherichiacoli (EHEC) infections: Memorandum from a WHO meeting.World Health Or ganization consultation on prevention andcontrol of enterohaemorrhagic Escherichia coli (EHEC)infections. Bull World Health Organ. 1998;76:245–55. 142.Legendre CM, Licht C, Muus P, et al. T erminal complementinhibitor eculizumab in atypical hemolytic uremicsyndrome. N Engl J Med. 2013;368:2169–81. 143. KavanaghD, Goodship TH, Richards A. Atypical hemolytic uremicsyndrome. Semin Nephrol. 2013;33:508–30. 144. U.S. Foodand Drug Administration. Highlights of PrescribingInformation: Soliris [online], 2011. Available at:http://www .accessdata.fda.gov/drugsatfda_docs/label/2011/125166s172lbl.pdf. AccessedApril 14, 2014. 145. Carr R, Cataland SR. Relapse of aHUSafter discontinuation of therapy with eculizumab in apatient with aHUS and factor H mutation. AnnHematol. 2013;92:845–6. 146. Bresin E, Daina E, Noris M,et al. Outcome of renal transplantation in patients withnon-Shiga toxin-associated hemolytic uremic syndrome:Prognostic significance of genetic background. Clin J AmSoc Nephrol. 2006;1:88–99. 147. Saland JM, RuggenentiP, Remuzzi G; Consensus Study Group. Liver-kidneytransplantation to cure atypical hemolytic uremicsyndrome. J Am Soc Nephrol. 2009;20:940–9. 148. Saland J.Liver-kidney transplantation to cure atypi cal HUS: Stillan option post-eculizumab? Pediatr Nephrol. 2014;29:329–32.
149. Nester C, Stewart Z, Myers D, et al. Pre-emptiveeculizumab and plasmapheresis for renal transplant inatypical hemolytic uremic syndrome. Clin J Am Soc Nephrol.2011;6:1488–94.
150. George JN. Thrombotic thrombocytopenic pur pura. NEngl J Med. 2006;354:1927–35.
151. von Baeyer H. Plasmapheresis in thromboticmicroangiopathy-associated syndromes: Review of outcomedata derived from clinical trials and open studies. TherApher. 2002;6:320–8
152. Rock GA, Shumak KH, Buskard NA, et al. Comparison ofplasma exchange with plasma infusion in the treatment ofthrombotic thrombocytopenic purpura. N Engl J Med.1991;325:393–7.
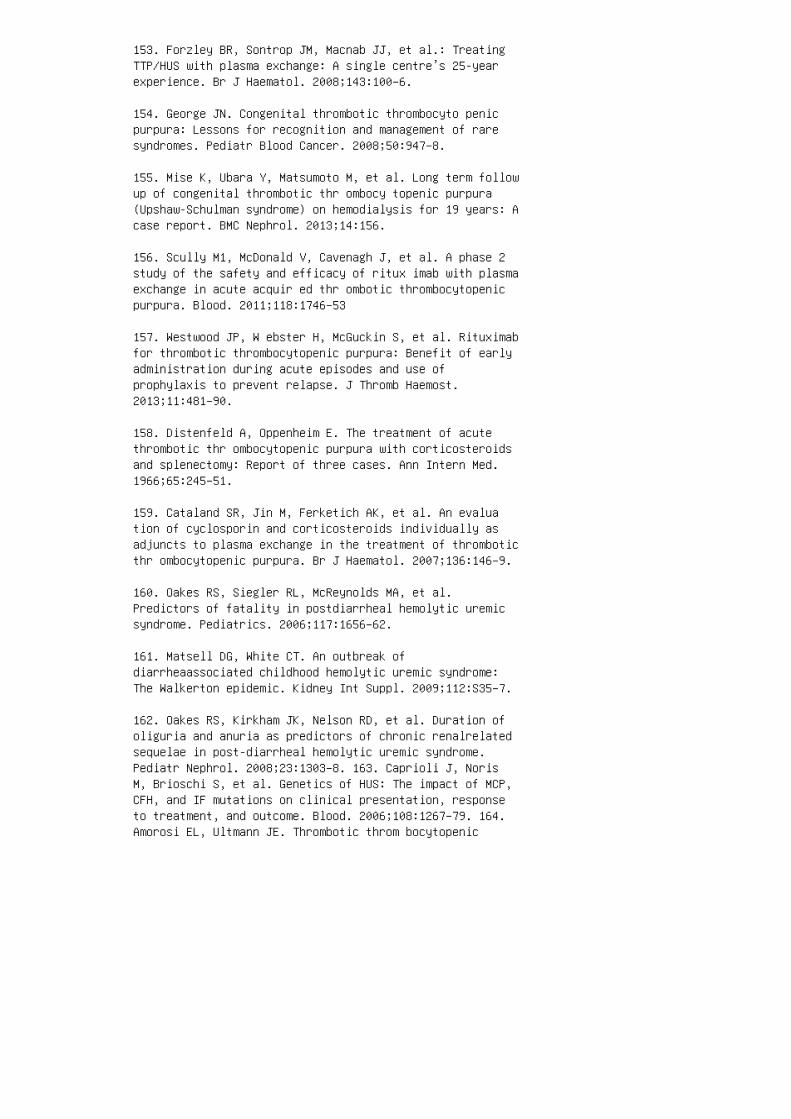
153. Forzley BR, Sontrop JM, Macnab JJ, et al.: TreatingTTP/HUS with plasma exchange: A single centre’s 25-yearexperience. Br J Haematol. 2008;143:100–6.
154. George JN. Congenital thrombotic thrombocyto penicpurpura: Lessons for recognition and management of raresyndromes. Pediatr Blood Cancer. 2008;50:947–8.
155. Mise K, Ubara Y, Matsumoto M, et al. Long term followup of congenital thrombotic thr ombocy topenic purpura(Upshaw-Schulman syndrome) on hemodialysis for 19 years: Acase report. BMC Nephrol. 2013;14:156.
156. Scully M1, McDonald V, Cavenagh J, et al. A phase 2study of the safety and efficacy of ritux imab with plasmaexchange in acute acquir ed thr ombotic thrombocytopenicpurpura. Blood. 2011;118:1746–53
157. Westwood JP, W ebster H, McGuckin S, et al. Rituximabfor thrombotic thrombocytopenic purpura: Benefit of earlyadministration during acute episodes and use ofprophylaxis to prevent relapse. J Thromb Haemost.2013;11:481–90.
158. Distenfeld A, Oppenheim E. The treatment of acutethrombotic thr ombocytopenic purpura with corticosteroidsand splenectomy: Report of three cases. Ann Intern Med.1966;65:245–51.
159. Cataland SR, Jin M, Ferketich AK, et al. An evaluation of cyclosporin and corticosteroids individually asadjuncts to plasma exchange in the treatment of thromboticthr ombocytopenic purpura. Br J Haematol. 2007;136:146–9.
160. Oakes RS, Siegler RL, McReynolds MA, et al.Predictors of fatality in postdiarrheal hemolytic uremicsyndrome. Pediatrics. 2006;117:1656–62.
161. Matsell DG, White CT. An outbreak ofdiarrheaassociated childhood hemolytic uremic syndrome:The Walkerton epidemic. Kidney Int Suppl. 2009;112:S35–7.
162. Oakes RS, Kirkham JK, Nelson RD, et al. Duration ofoliguria and anuria as predictors of chronic renalrelatedsequelae in post-diarrheal hemolytic uremic syndrome.Pediatr Nephrol. 2008;23:1303–8. 163. Caprioli J, NorisM, Brioschi S, et al. Genetics of HUS: The impact of MCP,CFH, and IF mutations on clinical presentation, responseto treatment, and outcome. Blood. 2006;108:1267–79. 164.Amorosi EL, Ultmann JE. Thrombotic throm bocytopenic
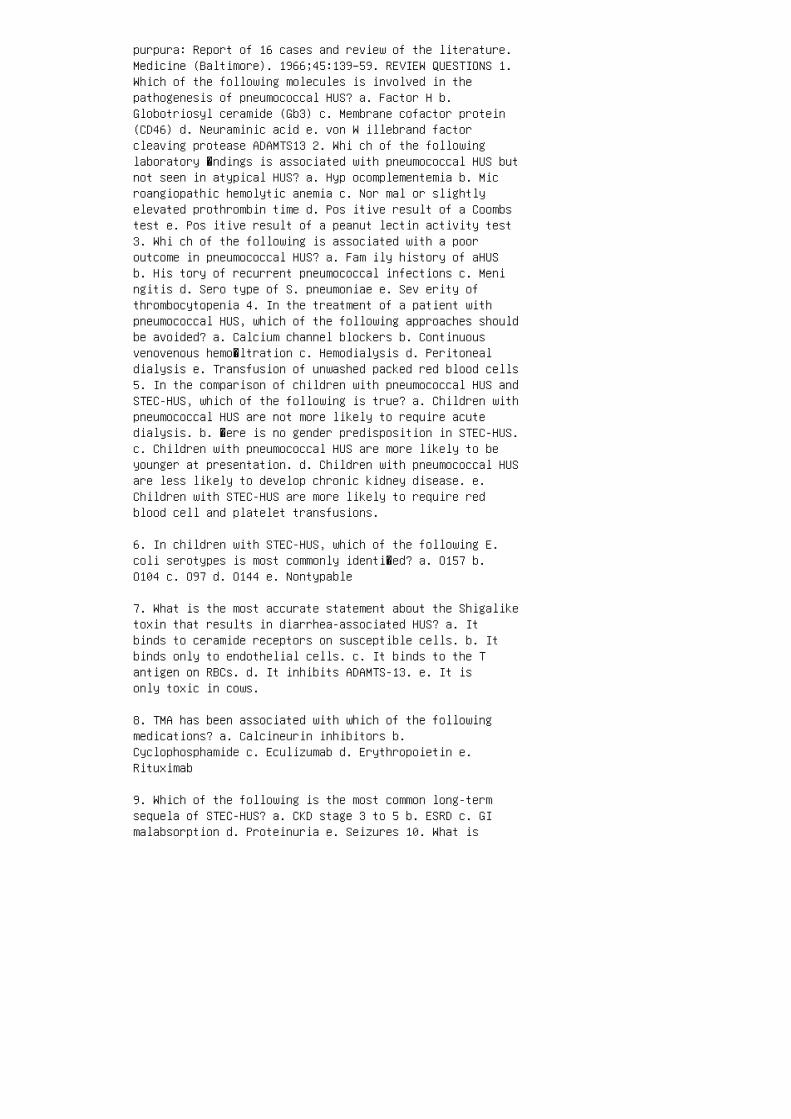
purpura: Report of 16 cases and review of the literature.Medicine (Baltimore). 1966;45:139–59. REVIEW QUESTIONS 1.Which of the following molecules is involved in thepathogenesis of pneumococcal HUS? a. Factor H b.Globotriosyl ceramide (Gb3) c. Membrane cofactor protein(CD46) d. Neuraminic acid e. von W illebrand factorcleaving protease ADAMTS13 2. Whi ch of the followinglaboratory �ndings is associated with pneumococcal HUS butnot seen in atypical HUS? a. Hyp ocomplementemia b. Microangiopathic hemolytic anemia c. Nor mal or slightlyelevated prothrombin time d. Pos itive result of a Coombstest e. Pos itive result of a peanut lectin activity test3. Whi ch of the following is associated with a pooroutcome in pneumococcal HUS? a. Fam ily history of aHUSb. His tory of recurrent pneumococcal infections c. Meningitis d. Sero type of S. pneumoniae e. Sev erity ofthrombocytopenia 4. In the treatment of a patient withpneumococcal HUS, which of the following approaches shouldbe avoided? a. Calcium channel blockers b. Continuousvenovenous hemo�ltration c. Hemodialysis d. Peritonealdialysis e. Transfusion of unwashed packed red blood cells5. In the comparison of children with pneumococcal HUS andSTEC-HUS, which of the following is true? a. Children withpneumococcal HUS are not more likely to require acutedialysis. b. �ere is no gender predisposition in STEC-HUS.c. Children with pneumococcal HUS are more likely to beyounger at presentation. d. Children with pneumococcal HUSare less likely to develop chronic kidney disease. e.Children with STEC-HUS are more likely to require redblood cell and platelet transfusions.
6. In children with STEC-HUS, which of the following E.coli serotypes is most commonly identi�ed? a. O157 b.O104 c. O97 d. O144 e. Nontypable
7. What is the most accurate statement about the Shigaliketoxin that results in diarrhea-associated HUS? a. Itbinds to ceramide receptors on susceptible cells. b. Itbinds only to endothelial cells. c. It binds to the Tantigen on RBCs. d. It inhibits ADAMTS-13. e. It isonly toxic in cows.
8. TMA has been associated with which of the followingmedications? a. Calcineurin inhibitors b.Cyclophosphamide c. Eculizumab d. Erythropoietin e.Rituximab
9. Which of the following is the most common long-termsequela of STEC-HUS? a. CKD stage 3 to 5 b. ESRD c. GImalabsorption d. Proteinuria e. Seizures 10. What is

the most commonly de�ned genetic abnormality in individualswith aHUS? a. C3 b. Factor H c. Factor I d. Factor 2e. �rombomodulin ANSWER KEY 1. d 2. d 3. c 4. e 5. c6. a 7. a 8. a 9. d 10. b

25 Tubulointerstitial nephritis
6. Cavallo T. Tubulointerstitial nephritis. In: JenetteJC, Olson JL, Schwartz MM, Silva FG, editors.Heptinstall’s Pathology of the Kidney, 5th ed.Philadelphia: Lippincott-Raven; 1998.
7. Wilson DM, Turner DR, Cameron JS, et al. Value of renalbiopsy in acute intrinsic renal failure. Br Med J.1976;2:459–61.
8. Linton AL, Clark WF, Driedger AA, et al. Acuteinterstitial nephritis due to drugs: Review of theliterature with a report of nine cases. Ann Intern Med.1980;93:735–41.
9. Far rington K, Levison DA, Greenwood RN, et al. Renalbiopsy in patients with unexplained renal impairment andnormal kidney size. Q J Med. 1989;70:221–33.
10. Ekonayan G. Tubulointerstitial nephropathies. In:Massry SG, Glasscock RJ, editors. Textbook of Nephrology,3rd ed. Baltimore: Williams & Wilkins; 1995.
11. Greising J, Trachtman H, Gauthier B, Valderrama E.Acute interstitial nephritis in adolescents and youngadults. Child Nephrol Urol. 1990;10:189–95.
12. Jon es CL, Eddy AA. Tubulointerstitial nephritis.Pediatr Nephrol. 1992;6:572–86.
13. Pettersson E, von Bonsdorff M, Tornroth T, Lindholm H.Nephritis among young Finnish men. Clin Nephrol.1984;22:217–22.
14. Mur ray T, Goldberg M. Chronic interstitial nephritis:Etiologic factors. Ann Intern Med. 1975;82:453–9.
15. Ros tand SG, Kirk KA, Rutsky EA, et al. Racialdifferences in the incidence of treatment for end stagerenal disease. N Engl J Med. 1982;306:1276–9.
16. Tej ani A, Butt K, Glassberg K, et al. Predictors ofeventual end stage renal disease in children withposterior urethral valves. J Urol. 1986;136:857–60.
17. Smi th GH, Canning DA, Schulman SL, et al. Thelong-term outcome of posterior urethral valves treatedwith primary valve ablation and observation. J Urol.1996;155:1730–4.

18. Hostetter TH, Nath KA, Hostetter MK. Infectionrelatedchronic interstitial nephropathy. Semin Nephrol.1988;8:11–6.
19. Alon US. Tubulointerstitial nephritis. In: Avner ED,Harmon WE, Niaudet P, editors. Pediatric Nephrology, 5thed. Philadelphia: Lippincott Williams & Wilkins; 2004.
20. North American Pediatric Renal Transplant CooperativeStudy (NAPRTCS). 2004 annual report. Boston: NAPRTCS;2004:8-4, 13-4.
21. Alpers CE. The kidney. In: Kumar V, Abbas AK, Faust N,editors. Robbins and Cotran Pathologic Basis of Disease,7th ed. Philadelphia: WB Saunders; 2004. p. 1483.
22. Kel ly CJ, Neilson EG. Tubulointerstitial disease. In:Brenner BM, editor. Brenner & Rector’s The Kidney, 7th ed.Philadelphia: WB Saunders; 2004. p. 1483.
23. Ber gstein J, Litman N. Interstitial nephritis withanti-tubular-basement-membrane antibody. N Engl J Med.1975;292:875–8. 24. Baker RJ, Pusey CD. The changingprofile of acute tubulointerstitial nephritis. NephrolDial Transplant. 2004;19:8–11. 25. Toto RD. Acutetubulointerstitial nephritis. Am J Med Sci.1990;299:392–410. 26. Haw kins EP, Berry PL, Silva FG.Acute tubulointerstitial nephritis in children: Clinical,morphologic, and lectin studies. A report of the SouthwestPediatric Nephrology Study Group. Am J Kidney Dis.1989;14:466–71. 27. Koskimies O, Holmberg C. Interstitialnephritis of acute onset. Arch Dis Child. 1985;60:752–5.28. Ell is D, Fried WA, Yunis EJ, Blau EB. Acuteinterstitial nephritis in children: A report of 13 casesand review of the literature. Pediatrics. 1981;67:862–72.29. Kobayashi Y, Honda M, Yoshikawa N, Ito H. Acutetubulointerstitial nephritis in 21 Japanese children. ClinNephrol. 2000;54:191–7. 30. Mey ers C. Acute interstitialnephritis. In: Greenberg A, editor. Primer on KidneyDiseases, 3rd ed. San Diego: Academic Press; 2001. 31.Inaba H, Jones DP, Gaber LW, et al. BK virusinducedtubulointerstitial nephritis in a child with acutelymphoblastic leukemia. J Pediatr. 2007;151:215–7. 32.Brentjens JR, Matsuo S, Fukatsu A, et al. Immunologicstudies in two patients with antitubular basement membranenephritis. Am J Med. 1989;86:603–8. 33. Clayman MD,Michaud L, Brentjens J, et al. Isolation of the targetantigen of human anti-tubular basement membraneantibody-associated interstitial nephritis. J Clin Invest.
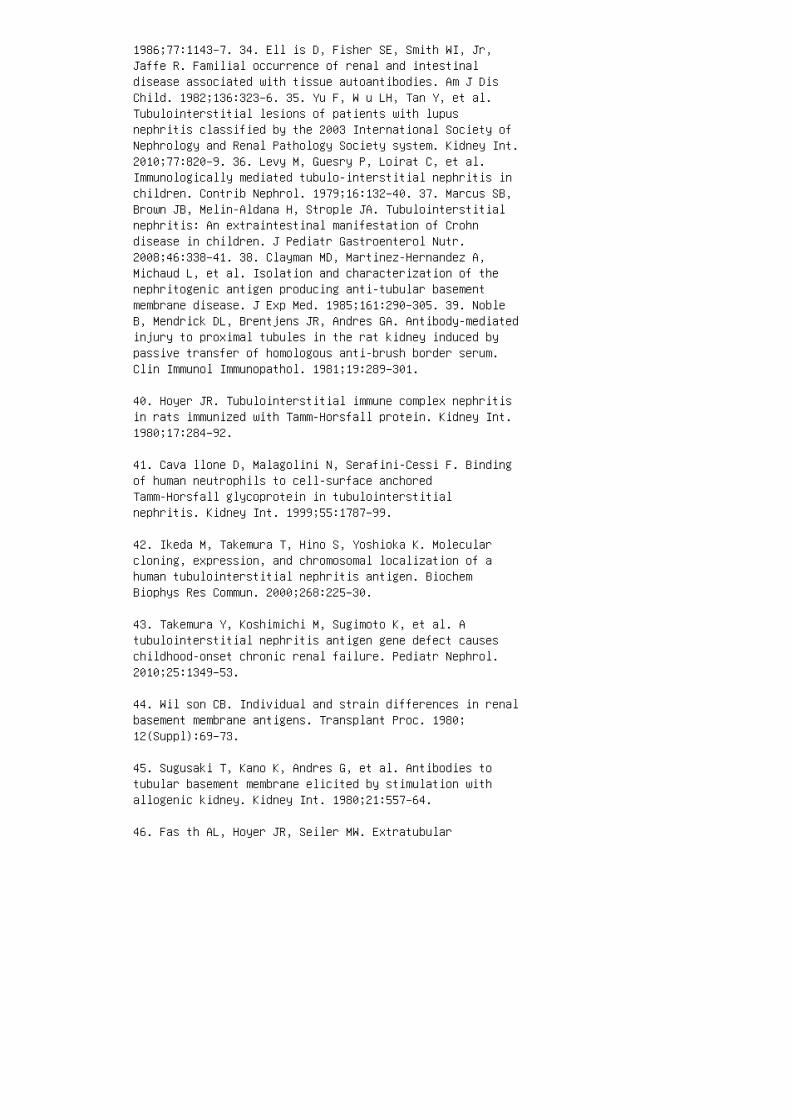
1986;77:1143–7. 34. Ell is D, Fisher SE, Smith WI, Jr,Jaffe R. Familial occurrence of renal and intestinaldisease associated with tissue autoantibodies. Am J DisChild. 1982;136:323–6. 35. Yu F, W u LH, Tan Y, et al.Tubulointerstitial lesions of patients with lupusnephritis classified by the 2003 International Society ofNephrology and Renal Pathology Society system. Kidney Int.2010;77:820–9. 36. Levy M, Guesry P, Loirat C, et al.Immunologically mediated tubulo-interstitial nephritis inchildren. Contrib Nephrol. 1979;16:132–40. 37. Marcus SB,Brown JB, Melin-Aldana H, Strople JA. Tubulointerstitialnephritis: An extraintestinal manifestation of Crohndisease in children. J Pediatr Gastroenterol Nutr.2008;46:338–41. 38. Clayman MD, Martinez-Hernandez A,Michaud L, et al. Isolation and characterization of thenephritogenic antigen producing anti-tubular basementmembrane disease. J Exp Med. 1985;161:290–305. 39. NobleB, Mendrick DL, Brentjens JR, Andres GA. Antibody-mediatedinjury to proximal tubules in the rat kidney induced bypassive transfer of homologous anti-brush border serum.Clin Immunol Immunopathol. 1981;19:289–301.
40. Hoyer JR. Tubulointerstitial immune complex nephritisin rats immunized with Tamm-Horsfall protein. Kidney Int.1980;17:284–92.
41. Cava llone D, Malagolini N, Serafini-Cessi F. Bindingof human neutrophils to cell-surface anchoredTamm-Horsfall glycoprotein in tubulointerstitialnephritis. Kidney Int. 1999;55:1787–99.
42. Ikeda M, Takemura T, Hino S, Yoshioka K. Molecularcloning, expression, and chromosomal localization of ahuman tubulointerstitial nephritis antigen. BiochemBiophys Res Commun. 2000;268:225–30.
43. Takemura Y, Koshimichi M, Sugimoto K, et al. Atubulointerstitial nephritis antigen gene defect causeschildhood-onset chronic renal failure. Pediatr Nephrol.2010;25:1349–53.
44. Wil son CB. Individual and strain differences in renalbasement membrane antigens. Transplant Proc. 1980;12(Suppl):69–73.
45. Sugusaki T, Kano K, Andres G, et al. Antibodies totubular basement membrane elicited by stimulation withallogenic kidney. Kidney Int. 1980;21:557–64.
46. Fas th AL, Hoyer JR, Seiler MW. Extratubular
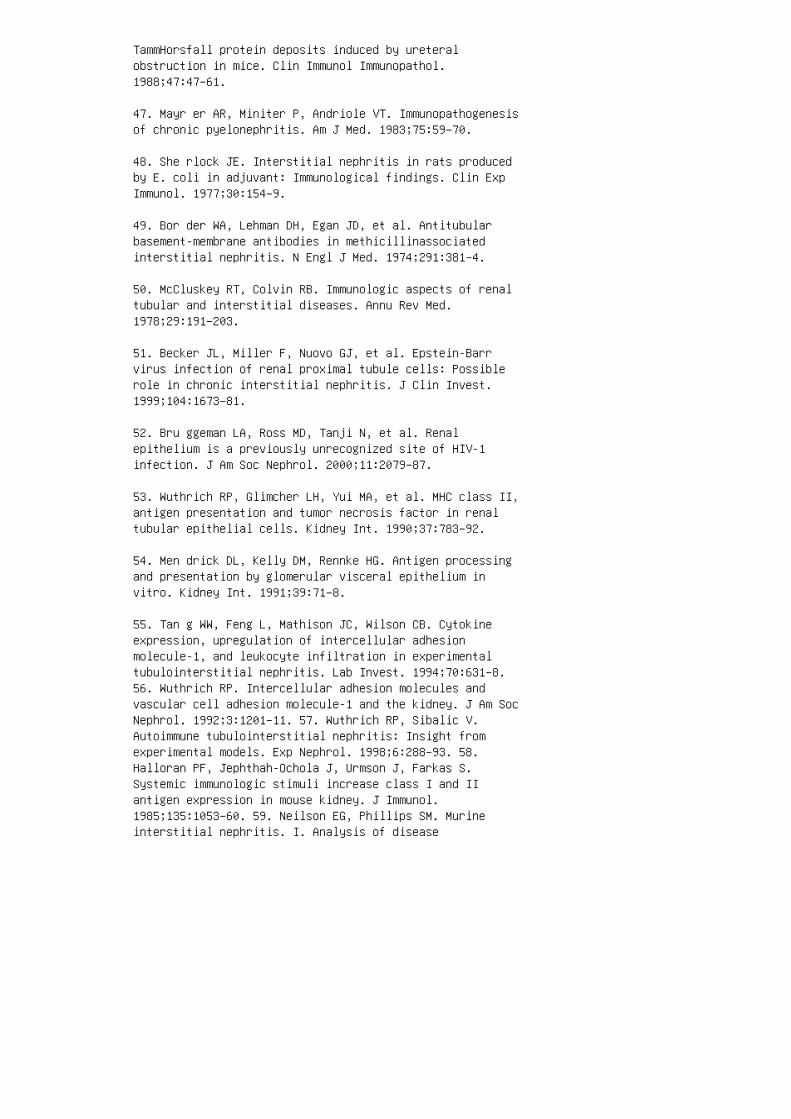
TammHorsfall protein deposits induced by ureteralobstruction in mice. Clin Immunol Immunopathol.1988;47:47–61.
47. Mayr er AR, Miniter P, Andriole VT. Immunopathogenesisof chronic pyelonephritis. Am J Med. 1983;75:59–70.
48. She rlock JE. Interstitial nephritis in rats producedby E. coli in adjuvant: Immunological findings. Clin ExpImmunol. 1977;30:154–9.
49. Bor der WA, Lehman DH, Egan JD, et al. Antitubularbasement-membrane antibodies in methicillinassociatedinterstitial nephritis. N Engl J Med. 1974;291:381–4.
50. McCluskey RT, Colvin RB. Immunologic aspects of renaltubular and interstitial diseases. Annu Rev Med.1978;29:191–203.
51. Becker JL, Miller F, Nuovo GJ, et al. Epstein-Barrvirus infection of renal proximal tubule cells: Possiblerole in chronic interstitial nephritis. J Clin Invest.1999;104:1673–81.
52. Bru ggeman LA, Ross MD, Tanji N, et al. Renalepithelium is a previously unrecognized site of HIV-1infection. J Am Soc Nephrol. 2000;11:2079–87.
53. Wuthrich RP, Glimcher LH, Yui MA, et al. MHC class II,antigen presentation and tumor necrosis factor in renaltubular epithelial cells. Kidney Int. 1990;37:783–92.
54. Men drick DL, Kelly DM, Rennke HG. Antigen processingand presentation by glomerular visceral epithelium invitro. Kidney Int. 1991;39:71–8.
55. Tan g WW, Feng L, Mathison JC, Wilson CB. Cytokineexpression, upregulation of intercellular adhesionmolecule-1, and leukocyte infiltration in experimentaltubulointerstitial nephritis. Lab Invest. 1994;70:631–8.56. Wuthrich RP. Intercellular adhesion molecules andvascular cell adhesion molecule-1 and the kidney. J Am SocNephrol. 1992;3:1201–11. 57. Wuthrich RP, Sibalic V.Autoimmune tubulointerstitial nephritis: Insight fromexperimental models. Exp Nephrol. 1998;6:288–93. 58.Halloran PF, Jephthah-Ochola J, Urmson J, Farkas S.Systemic immunologic stimuli increase class I and IIantigen expression in mouse kidney. J Immunol.1985;135:1053–60. 59. Neilson EG, Phillips SM. Murineinterstitial nephritis. I. Analysis of disease
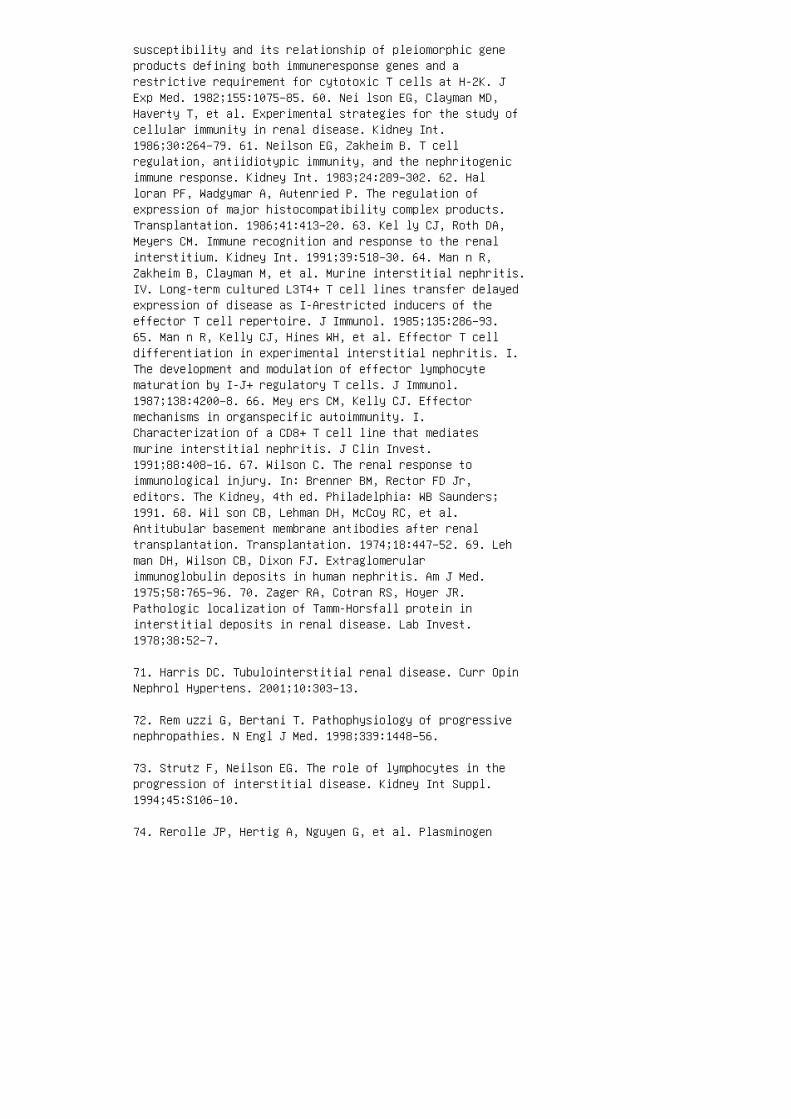
susceptibility and its relationship of pleiomorphic geneproducts defining both immuneresponse genes and arestrictive requirement for cytotoxic T cells at H-2K. JExp Med. 1982;155:1075–85. 60. Nei lson EG, Clayman MD,Haverty T, et al. Experimental strategies for the study ofcellular immunity in renal disease. Kidney Int.1986;30:264–79. 61. Neilson EG, Zakheim B. T cellregulation, antiidiotypic immunity, and the nephritogenicimmune response. Kidney Int. 1983;24:289–302. 62. Halloran PF, Wadgymar A, Autenried P. The regulation ofexpression of major histocompatibility complex products.Transplantation. 1986;41:413–20. 63. Kel ly CJ, Roth DA,Meyers CM. Immune recognition and response to the renalinterstitium. Kidney Int. 1991;39:518–30. 64. Man n R,Zakheim B, Clayman M, et al. Murine interstitial nephritis.IV. Long-term cultured L3T4+ T cell lines transfer delayedexpression of disease as I-Arestricted inducers of theeffector T cell repertoire. J Immunol. 1985;135:286–93.65. Man n R, Kelly CJ, Hines WH, et al. Effector T celldifferentiation in experimental interstitial nephritis. I.The development and modulation of effector lymphocytematuration by I-J+ regulatory T cells. J Immunol.1987;138:4200–8. 66. Mey ers CM, Kelly CJ. Effectormechanisms in organspecific autoimmunity. I.Characterization of a CD8+ T cell line that mediatesmurine interstitial nephritis. J Clin Invest.1991;88:408–16. 67. Wilson C. The renal response toimmunological injury. In: Brenner BM, Rector FD Jr,editors. The Kidney, 4th ed. Philadelphia: WB Saunders;1991. 68. Wil son CB, Lehman DH, McCoy RC, et al.Antitubular basement membrane antibodies after renaltransplantation. Transplantation. 1974;18:447–52. 69. Lehman DH, Wilson CB, Dixon FJ. Extraglomerularimmunoglobulin deposits in human nephritis. Am J Med.1975;58:765–96. 70. Zager RA, Cotran RS, Hoyer JR.Pathologic localization of Tamm-Horsfall protein ininterstitial deposits in renal disease. Lab Invest.1978;38:52–7.
71. Harris DC. Tubulointerstitial renal disease. Curr OpinNephrol Hypertens. 2001;10:303–13.
72. Rem uzzi G, Bertani T. Pathophysiology of progressivenephropathies. N Engl J Med. 1998;339:1448–56.
73. Strutz F, Neilson EG. The role of lymphocytes in theprogression of interstitial disease. Kidney Int Suppl.1994;45:S106–10.
74. Rerolle JP, Hertig A, Nguyen G, et al. Plasminogen
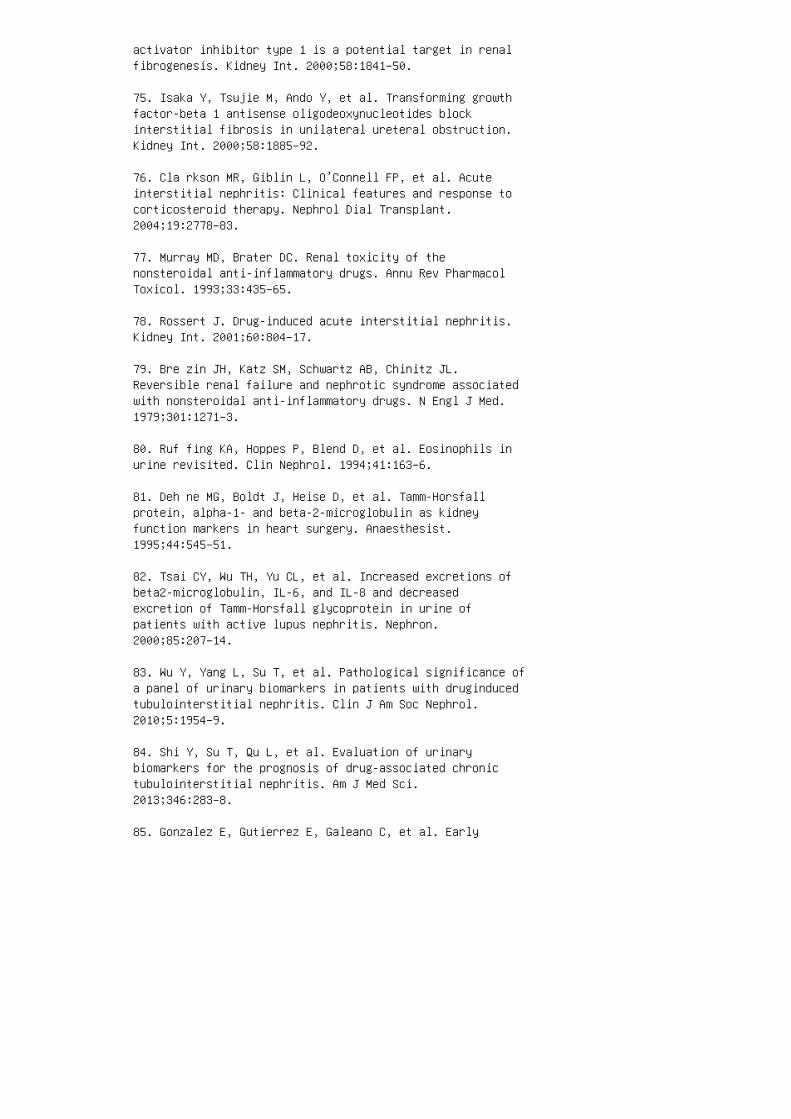
activator inhibitor type 1 is a potential target in renalfibrogenesis. Kidney Int. 2000;58:1841–50.
75. Isaka Y, Tsujie M, Ando Y, et al. Transforming growthfactor-beta 1 antisense oligodeoxynucleotides blockinterstitial fibrosis in unilateral ureteral obstruction.Kidney Int. 2000;58:1885–92.
76. Cla rkson MR, Giblin L, O’Connell FP, et al. Acuteinterstitial nephritis: Clinical features and response tocorticosteroid therapy. Nephrol Dial Transplant.2004;19:2778–83.
77. Murray MD, Brater DC. Renal toxicity of thenonsteroidal anti-inflammatory drugs. Annu Rev PharmacolToxicol. 1993;33:435–65.
78. Rossert J. Drug-induced acute interstitial nephritis.Kidney Int. 2001;60:804–17.
79. Bre zin JH, Katz SM, Schwartz AB, Chinitz JL.Reversible renal failure and nephrotic syndrome associatedwith nonsteroidal anti-inflammatory drugs. N Engl J Med.1979;301:1271–3.
80. Ruf fing KA, Hoppes P, Blend D, et al. Eosinophils inurine revisited. Clin Nephrol. 1994;41:163–6.
81. Deh ne MG, Boldt J, Heise D, et al. Tamm-Horsfallprotein, alpha-1- and beta-2-microglobulin as kidneyfunction markers in heart surgery. Anaesthesist.1995;44:545–51.
82. Tsai CY, Wu TH, Yu CL, et al. Increased excretions ofbeta2-microglobulin, IL-6, and IL-8 and decreasedexcretion of Tamm-Horsfall glycoprotein in urine ofpatients with active lupus nephritis. Nephron.2000;85:207–14.
83. Wu Y, Yang L, Su T, et al. Pathological significance ofa panel of urinary biomarkers in patients with druginducedtubulointerstitial nephritis. Clin J Am Soc Nephrol.2010;5:1954–9.
84. Shi Y, Su T, Qu L, et al. Evaluation of urinarybiomarkers for the prognosis of drug-associated chronictubulointerstitial nephritis. Am J Med Sci.2013;346:283–8.
85. Gonzalez E, Gutierrez E, Galeano C, et al. Early
steroid treatment improves the recovery of renal functionin patients with drug-induced acute interstitialnephritis. Kidney Int. 2008;73:940–6.
86. Raz a MN, Hadid, Keen CE, et al. Acutetubulointerstitial nephritis, treatment with steroid andimpact on renal outcomes. Nephrology. 2012;17:748–53. 87.Jahnukainen T, Ala-Houhala M, Karikoski R, et al. Clinicaloutcome and occurrence of uveitis in children withidiopathic tubulointerstitial nephritis. Pediatr Nephrol.2011;26:291–9. 88. Jahnukainen T, Saarela V, Arikoski P,et al. Prednisone in the treatment of tubulointerstitialnephritis in children. Pediatr Nephrol. 2013;28:1253–60.89. Pre ddie DC, Markowitz GS, Radhakrishnan J, et al.Mycophenolate mofetil for the treatment of interstitialnephritis. Clin J Am Soc Nephrol. 2006;1:718–22. 90.Moudgil A, Przygodzki RM, Kher KK. Successfulsteroid-sparing treatment of renal limited sarcoidosis withmycophenolate mofetil. Pediatr Nephrol. 2006;21:281–5.91. Leeaphorn N, Stokes MB, Ungprasert P, et al.Idiopathic granulomatous interstitial nephritis responsiveto mycophenolate mofetil therapy. Am J Kidney Dis.2014;63:696–9. 92. Laberke HG, Bohle A. Acute interstitialnephritis: Correlations between clinical and morphologicalfindings. Clin Nephrol. 1980;14:263–73. 93. Iva nyi B,Hamilton-Dutoit SJ, Hansen HE, Olsen S. Acutetubulointerstitial nephritis: Phenotype of infiltratingcells and prognostic impact of tubulitis. Virchows Arc.1996;428:5–12. 94. Bha umik SK, Kher V, Arora P, et al.Evaluation of clinical and histological prognostic markersin drug-induced acute interstitial nephritis. Ren Fail.1996;18:97–104. 95. Kid a H, Abe T, Tomosugi N, et al.Prediction of the long-term outcome in acute interstitialnephritis. Clin Nephrol. 1984;22:55–60. 96. Mye rs BD,Ross J, Newton L, et al. Cyclosporineassociated chronicnephropathy. N Engl J Med. 1984;311:699–705. 97. Dob rinR, Vernier R, Fish A. Acute eosinophilic interstitialnephritis and renal failure with bone marrow– lymph nodegranulomas and anterior uveitis. Am J Med. 1975;59:325–33.98. Man deville JT, Levinson RD, Holland GN. Thetubulointerstitial nephritis and uveitis syndrome. SurvOphthalmol 2001;46:195–208. 99. Dusek J, Urbanova I,Stejskal J, et al. Tubulointerstitial nephritis anduveitis syndrome in a mother and her son. Pediatr Nephrol.2008;23:2091–3. 100. Saa rela V, Nuutinen M, Ala-Houala Met al. Tubulointerstitial nephritis and uveitis syndromein children: A prospective multicenter study.Ophthalmology. 2013;120:1476–81. 101. Lev inson RD, ParkMS, Rikkers SM, et al. Strong associations among specificHLA-DQ and HLA-DR alleles and the tubulointerstitial
nephritis and uveitis syndrome. Invest Ophthalmol Vis Sci.2003;44:653–7.
REVIEW QUESTIONS
1. Which of the following is true regarding drug-inducedATIN? a. ATIN secondary to NSAIDs can present asnephrotic syndrome. b. �e triad of fever, rash, andarthralgia is present in the majority of patients withdrug-induced ATIN. c. Eosinophiluria is pathognomonic forATIN. d. Renal injury always develops soon a�er startingthe o�ending drug. e. Drug-induced ATIN is dose-dependent.
2. �e typical features on light microscopy of a kidneybiopsy in a patient with ATIN are: a. Tubular atrophy andinterstitial �brosis with minimal interstitial in�ammatorycell in�ltration b. Di�use endocapillary proliferationwith crescents and necrosis c. Di�use thickening of theglomerular basement membrane d. Di�use mesangialproliferation e. Interstitial mononuclear cell in�ltrationwith variable degrees of tubular necrosis and regeneration
3. A 15-year-old boy with a history of obstructiveuropathy who received a kidney transplant 8 years ago hasan elevated creatinine level. Renal biopsy showsinterstitial stripe �brosis and tubular atrophy. �esendings are characteristic of: a. Interstitial nephritissecondary to BK virus b. Acute cellular rejection c.Calcineurin inhibitor chronic interstitial damage d.Interstitial nephritis secondary to NSAIDs use e. Chronictransplant nephropathy
4. A 5-year-old girl presents with fever, fatigue, andabdominal pain and is admitted to the hospital because ofAKI with a creatinine value of 1.3. According to historyobtained, she had been taking amoxicillin for 4 days forstrep throat. Her physical examination is normal; herurinalysis reveals a speci�c gravity of 1.009, negativendings for blood and protein, 10 to 20 white blood cells,and no casts. You suspect ATIN secondary to amoxicillin.Which of the following is the next best step in hermanagement? a. Schedule her for a renal biopsy. b.Discontinue amoxicillin and follow creatinine trend. c.Administer pulse corticosteroids followed by oralprednisone. d. Check eosinophils in the urine, ifnegative, continue workup looking for other causes of AKI.e. Change amoxicillin to a cephalosporin. 5. Which of thefollowing urinary biomarkers has been associated with theacute changes seen in ATIN? a.N-acetyl-β-D-glucosaminidase (NAG) b. Kidney injury

molecule-1 (KIM-1) c. Neutrophil gelatinase-associatedlipocalin (NGAL) d. Monocyte chemotactic peptide-1 (MCP-1)e. β 2 -Microglobulin 6. A 10-year-old boy presents withnonoliguric AKI. He has a renal biopsy performed thatshows severe interstitial in�ammation with predominantmononuclear cell in�ltrate and no granulomas;immuno�uorescence is negative. �ere is no history ofmedication use or evidence of any viral or bacterialinfection. �e patient receives corticosteroids and hisrenal function returns to normal. Regarding furtherevaluation and follow-up, which of the following is themost accurate statement? a. He will need follow-up with anephrologist for at least 1 year. b. He can follow upwith his primary care physician for yearly checkups onlyand does not need specialty care. c. He needs anophthalmology evaluation now and every 3 months for thenext year in addition to follow-up with a nephrologist.d. He needs follow-up with a rheumatologist because of thepossibility of underlying autoimmune disease. 7. A12-year-old girl, previously healthy, presents with nauseaand vomiting. She has been taking ibuprofen for a kneeinjury for the last 7 days. She has mild pitting edema onboth lower extremities. Her laboratory results revealsigni�cant proteinuria with a ratio of urine protein tocreatinine of 5.9, elevated serum creatinine of 3.5 mg/dL,normal electrolytes, and a low serum albumin of 2.0 g/dL.You suspect ATIN secondary to NSAIDs and stop themedication. Over the next 2 days her creatinine continuesto rise and you decide to perform a renal biopsy. Which ofthe following would be the most appropriate step in hermanagement while you wait for the results of her biopsy?a. Administer albumin followed by furosemide b. Administerintravenous �uids c. Check complements and serologicndings and test for viral and bacterial infections d.Start intravenous methylprednisolone 10 mg/kg e. Startmycophenolate mofetil 8. Which of the following conditioncan cause secondary tubulointerstitial nephritis? a.Membranous nephropathy b. In�ammatory bowel disease c.Systemic lupus erythematosus d. IgA nephropathy e. All ofthe above
9. Regarding CTIN, which of the following statements istrue? a. In children, the most common cause of CTIN islupus nephritis. b. NSAIDs are the most common causes ofdrugrelated CTIN in children. c. CTIN progresses rapidlyto end-stage renal disease. d. Polyuria, polydipsia, andnocturnal enuresis may be the only manifesting symptoms inchildren with CTIN. e. Corticosteroids are e�ective inthe treatment of CTIN.

10. Regarding prognosis of ATIN in children, which of thefollowing statements is true? a. �e recovery of renalfunction depends on the severity of disease atpresentation. b. Prognosis is independent from thepresence of tubular atrophy. c. Prognosis is worse inpatients with underlying renal disease and when there isprolonged oliguria (more than 3 weeks). d. Most childrenwith ATIN progress slowly to CTIN. e. All of the above.ANSWER KEY 1. a 2. e 3. c 4. b 5. a 6. c 7. d 8. e9. d 10. c
26 Lupus nephritis
Figure 26.9 Renal biopsy findings in the patient. The
glomerulus on the right has endocapillary hypercellularity
in the 5 to 10 o’clock position. In contrast, othercapillary
loops are open, with luminal red blood cells present.
4. Benseler SM, Silverman ED. Systemic lupus erythematosus.Rheum Dis Clin North Am. 2007;33:471– 98, vi.
5. Mok C C, Mak A, Chu WP, et al. Long-term survival ofsouthern Chinese patients with systemic lupuserythematosus: A prospective study of all age-groups.Medicine (Baltimore). 2005;84:218–24.
6. Lilleby V, Flato B, Forre O. Disease duration,hypertension and medication requirements are associatedwith organ damage in childhood-onset systemic lupuserythematosus. Clin Exp Rheumatol. 2005;23:261–9.
7. Gutierrez-Suarez R, Ruperto N, Gastaldi R, et al. Aproposal for a pediatric version of the Systemic LupusInternational Collaborating Clinics/American College ofRheumatology Damage Index based on the analysis of 1,015patients with juvenile-onset systemic lupus erythematosus.Arthritis Rheum. 2006;54:2989–96.
8. Ramirez Gomez LA, Uribe Uribe O, Osio Uribe O, et al.Childhood systemic lupus erythematosus in Latin America:The GLADEL experience in 230 children. Lupus.2008;17:596–604.
9. Tuc ker LB, Uribe AG, Fernandez M, et al. Adolescentonset of lupus results in more aggressive disease andworse outcomes: Results of a nested matched case-controlstudy within LUMINA, a multiethnic US cohort (LUMINALVII). Lupus. 2008;17:314–22.
10. Hir aki LT, Benseler SM, Tyrrell PN, et al. Ethnicdifferences in pediatric systemic lupus erythematosus. JRheumatol. 2009;36:2539–46.
11. Hersh AO, Trupin L, Yazdany J, et al. Childhoodonsetdisease as a predictor of mortality in an adult cohort ofpatients with systemic lupus erythematosus. Arthritis CareRes (Hoboken). 2010;62:1152–9.
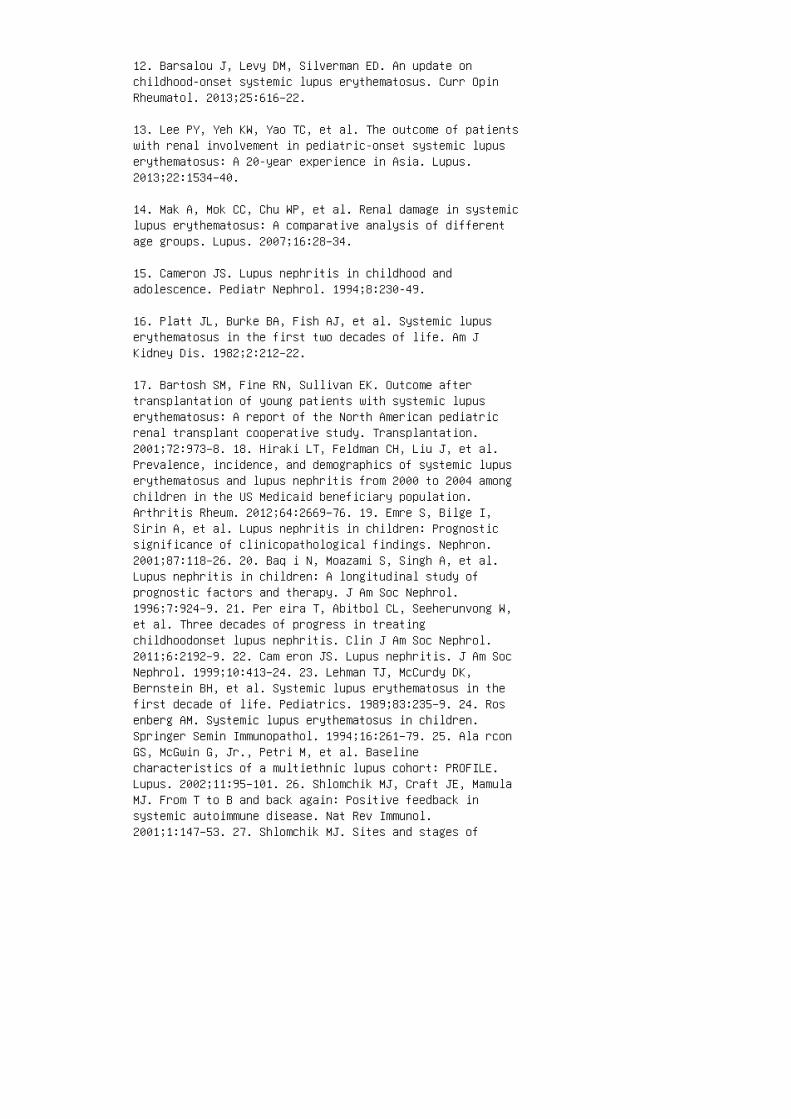
12. Barsalou J, Levy DM, Silverman ED. An update onchildhood-onset systemic lupus erythematosus. Curr OpinRheumatol. 2013;25:616–22.
13. Lee PY, Yeh KW, Yao TC, et al. The outcome of patientswith renal involvement in pediatric-onset systemic lupuserythematosus: A 20-year experience in Asia. Lupus.2013;22:1534–40.
14. Mak A, Mok CC, Chu WP, et al. Renal damage in systemiclupus erythematosus: A comparative analysis of differentage groups. Lupus. 2007;16:28–34.
15. Cameron JS. Lupus nephritis in childhood andadolescence. Pediatr Nephrol. 1994;8:230-49.
16. Platt JL, Burke BA, Fish AJ, et al. Systemic lupuserythematosus in the first two decades of life. Am JKidney Dis. 1982;2:212–22.
17. Bartosh SM, Fine RN, Sullivan EK. Outcome aftertransplantation of young patients with systemic lupuserythematosus: A report of the North American pediatricrenal transplant cooperative study. Transplantation.2001;72:973–8. 18. Hiraki LT, Feldman CH, Liu J, et al.Prevalence, incidence, and demographics of systemic lupuserythematosus and lupus nephritis from 2000 to 2004 amongchildren in the US Medicaid beneficiary population.Arthritis Rheum. 2012;64:2669–76. 19. Emre S, Bilge I,Sirin A, et al. Lupus nephritis in children: Prognosticsignificance of clinicopathological findings. Nephron.2001;87:118–26. 20. Baq i N, Moazami S, Singh A, et al.Lupus nephritis in children: A longitudinal study ofprognostic factors and therapy. J Am Soc Nephrol.1996;7:924–9. 21. Per eira T, Abitbol CL, Seeherunvong W,et al. Three decades of progress in treatingchildhoodonset lupus nephritis. Clin J Am Soc Nephrol.2011;6:2192–9. 22. Cam eron JS. Lupus nephritis. J Am SocNephrol. 1999;10:413–24. 23. Lehman TJ, McCurdy DK,Bernstein BH, et al. Systemic lupus erythematosus in thefirst decade of life. Pediatrics. 1989;83:235–9. 24. Rosenberg AM. Systemic lupus erythematosus in children.Springer Semin Immunopathol. 1994;16:261–79. 25. Ala rconGS, McGwin G, Jr., Petri M, et al. Baselinecharacteristics of a multiethnic lupus cohort: PROFILE.Lupus. 2002;11:95–101. 26. Shlomchik MJ, Craft JE, MamulaMJ. From T to B and back again: Positive feedback insystemic autoimmune disease. Nat Rev Immunol.2001;1:147–53. 27. Shlomchik MJ. Sites and stages of
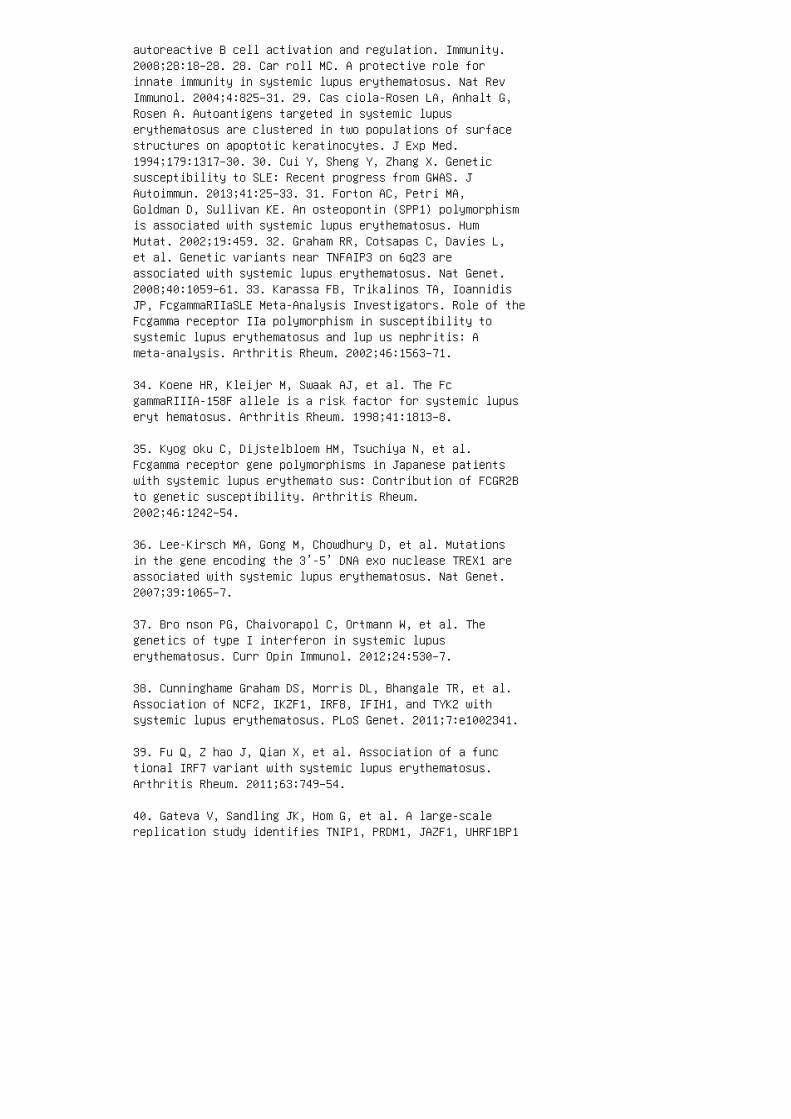
autoreactive B cell activation and regulation. Immunity.2008;28:18–28. 28. Car roll MC. A protective role forinnate immunity in systemic lupus erythematosus. Nat RevImmunol. 2004;4:825–31. 29. Cas ciola-Rosen LA, Anhalt G,Rosen A. Autoantigens targeted in systemic lupuserythematosus are clustered in two populations of surfacestructures on apoptotic keratinocytes. J Exp Med.1994;179:1317–30. 30. Cui Y, Sheng Y, Zhang X. Geneticsusceptibility to SLE: Recent progress from GWAS. JAutoimmun. 2013;41:25–33. 31. Forton AC, Petri MA,Goldman D, Sullivan KE. An osteopontin (SPP1) polymorphismis associated with systemic lupus erythematosus. HumMutat. 2002;19:459. 32. Graham RR, Cotsapas C, Davies L,et al. Genetic variants near TNFAIP3 on 6q23 areassociated with systemic lupus erythematosus. Nat Genet.2008;40:1059–61. 33. Karassa FB, Trikalinos TA, IoannidisJP, FcgammaRIIaSLE Meta-Analysis Investigators. Role of theFcgamma receptor IIa polymorphism in susceptibility tosystemic lupus erythematosus and lup us nephritis: Ameta-analysis. Arthritis Rheum. 2002;46:1563–71.
34. Koene HR, Kleijer M, Swaak AJ, et al. The FcgammaRIIIA-158F allele is a risk factor for systemic lupuseryt hematosus. Arthritis Rheum. 1998;41:1813–8.
35. Kyog oku C, Dijstelbloem HM, Tsuchiya N, et al.Fcgamma receptor gene polymorphisms in Japanese patientswith systemic lupus erythemato sus: Contribution of FCGR2Bto genetic susceptibility. Arthritis Rheum.2002;46:1242–54.
36. Lee-Kirsch MA, Gong M, Chowdhury D, et al. Mutationsin the gene encoding the 3’-5’ DNA exo nuclease TREX1 areassociated with systemic lupus erythematosus. Nat Genet.2007;39:1065–7.
37. Bro nson PG, Chaivorapol C, Ortmann W, et al. Thegenetics of type I interferon in systemic lupuserythematosus. Curr Opin Immunol. 2012;24:530–7.
38. Cunninghame Graham DS, Morris DL, Bhangale TR, et al.Association of NCF2, IKZF1, IRF8, IFIH1, and TYK2 withsystemic lupus erythematosus. PLoS Genet. 2011;7:e1002341.
39. Fu Q, Z hao J, Qian X, et al. Association of a functional IRF7 variant with systemic lupus erythematosus.Arthritis Rheum. 2011;63:749–54.
40. Gateva V, Sandling JK, Hom G, et al. A large-scalereplication study identifies TNIP1, PRDM1, JAZF1, UHRF1BP1
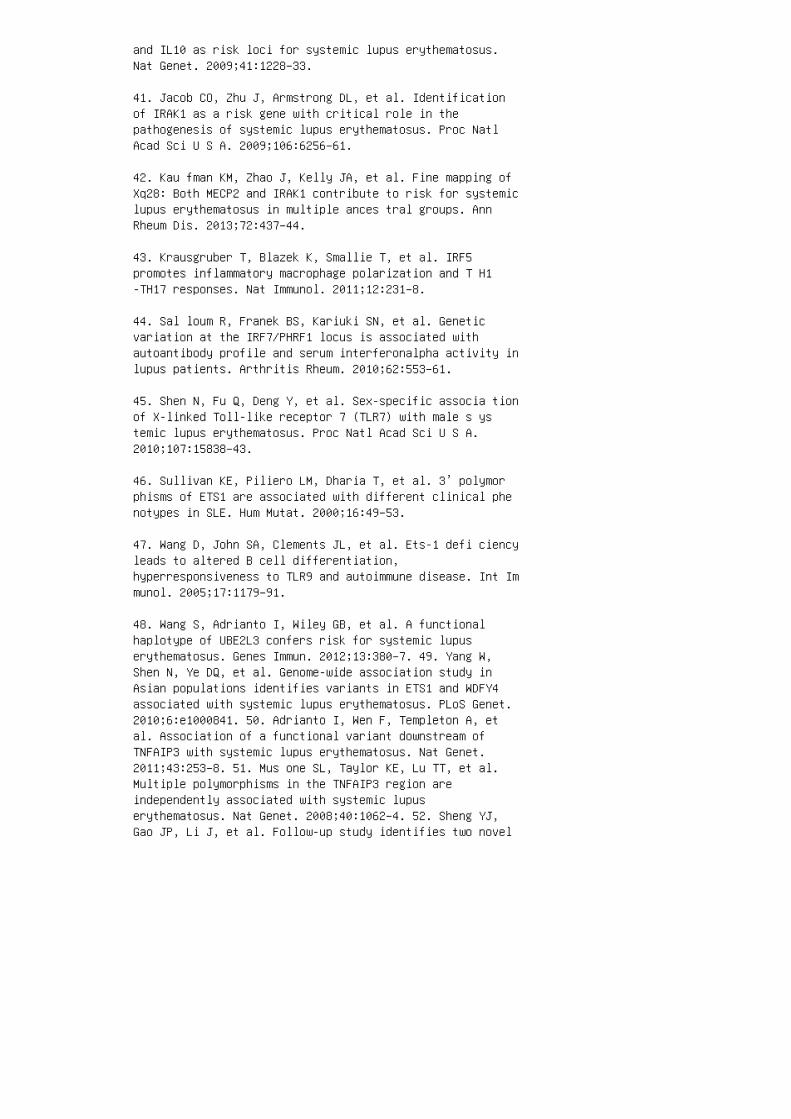
and IL10 as risk loci for systemic lupus erythematosus.Nat Genet. 2009;41:1228–33.
41. Jacob CO, Zhu J, Armstrong DL, et al. Identificationof IRAK1 as a risk gene with critical role in thepathogenesis of systemic lupus erythematosus. Proc NatlAcad Sci U S A. 2009;106:6256–61.
42. Kau fman KM, Zhao J, Kelly JA, et al. Fine mapping ofXq28: Both MECP2 and IRAK1 contribute to risk for systemiclupus erythematosus in multiple ances tral groups. AnnRheum Dis. 2013;72:437–44.
43. Krausgruber T, Blazek K, Smallie T, et al. IRF5promotes inflammatory macrophage polarization and T H1-TH17 responses. Nat Immunol. 2011;12:231–8.
44. Sal loum R, Franek BS, Kariuki SN, et al. Geneticvariation at the IRF7/PHRF1 locus is associated withautoantibody profile and serum interferonalpha activity inlupus patients. Arthritis Rheum. 2010;62:553–61.
45. Shen N, Fu Q, Deng Y, et al. Sex-specific associa tionof X-linked Toll-like receptor 7 (TLR7) with male s ystemic lupus erythematosus. Proc Natl Acad Sci U S A.2010;107:15838–43.
46. Sullivan KE, Piliero LM, Dharia T, et al. 3’ polymorphisms of ETS1 are associated with different clinical phenotypes in SLE. Hum Mutat. 2000;16:49–53.
47. Wang D, John SA, Clements JL, et al. Ets-1 defi ciencyleads to altered B cell differentiation,hyperresponsiveness to TLR9 and autoimmune disease. Int Immunol. 2005;17:1179–91.
48. Wang S, Adrianto I, Wiley GB, et al. A functionalhaplotype of UBE2L3 confers risk for systemic lupuserythematosus. Genes Immun. 2012;13:380–7. 49. Yang W,Shen N, Ye DQ, et al. Genome-wide association study inAsian populations identifies variants in ETS1 and WDFY4associated with systemic lupus erythematosus. PLoS Genet.2010;6:e1000841. 50. Adrianto I, Wen F, Templeton A, etal. Association of a functional variant downstream ofTNFAIP3 with systemic lupus erythematosus. Nat Genet.2011;43:253–8. 51. Mus one SL, Taylor KE, Lu TT, et al.Multiple polymorphisms in the TNFAIP3 region areindependently associated with systemic lupuserythematosus. Nat Genet. 2008;40:1062–4. 52. Sheng YJ,Gao JP, Li J, et al. Follow-up study identifies two novel
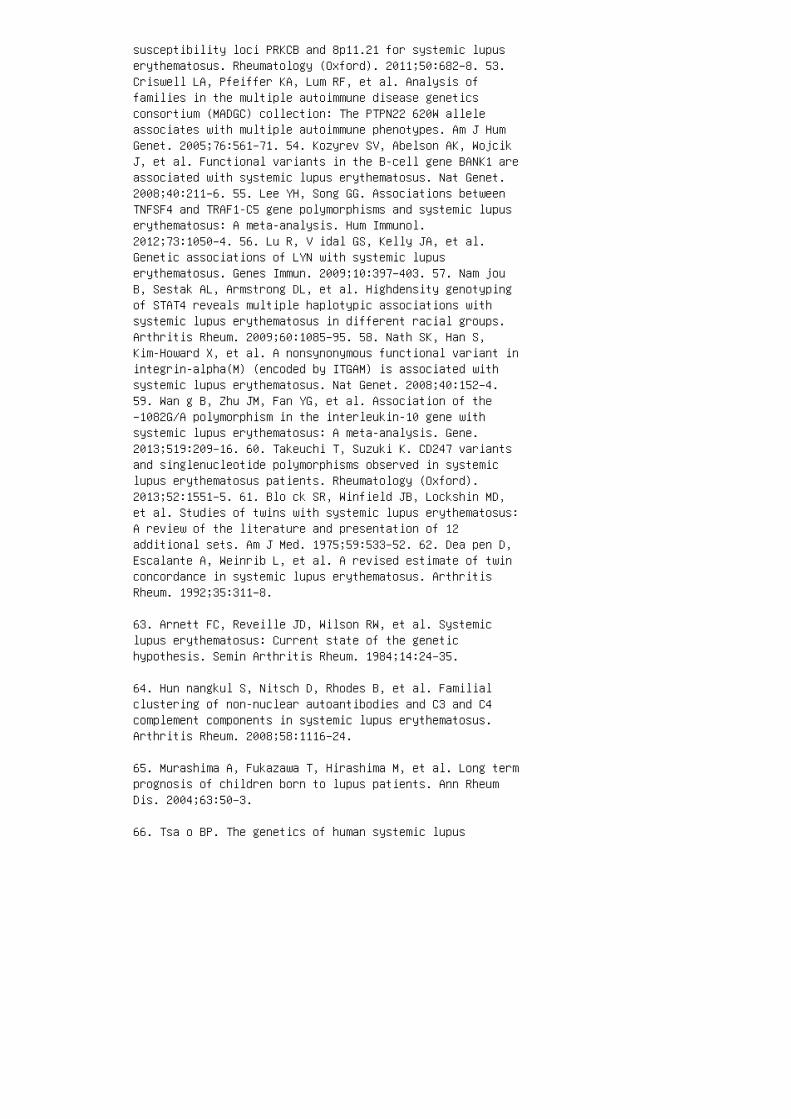
susceptibility loci PRKCB and 8p11.21 for systemic lupuserythematosus. Rheumatology (Oxford). 2011;50:682–8. 53.Criswell LA, Pfeiffer KA, Lum RF, et al. Analysis offamilies in the multiple autoimmune disease geneticsconsortium (MADGC) collection: The PTPN22 620W alleleassociates with multiple autoimmune phenotypes. Am J HumGenet. 2005;76:561–71. 54. Kozyrev SV, Abelson AK, WojcikJ, et al. Functional variants in the B-cell gene BANK1 areassociated with systemic lupus erythematosus. Nat Genet.2008;40:211–6. 55. Lee YH, Song GG. Associations betweenTNFSF4 and TRAF1-C5 gene polymorphisms and systemic lupuserythematosus: A meta-analysis. Hum Immunol.2012;73:1050–4. 56. Lu R, V idal GS, Kelly JA, et al.Genetic associations of LYN with systemic lupuserythematosus. Genes Immun. 2009;10:397–403. 57. Nam jouB, Sestak AL, Armstrong DL, et al. Highdensity genotypingof STAT4 reveals multiple haplotypic associations withsystemic lupus erythematosus in different racial groups.Arthritis Rheum. 2009;60:1085–95. 58. Nath SK, Han S,Kim-Howard X, et al. A nonsynonymous functional variant inintegrin-alpha(M) (encoded by ITGAM) is associated withsystemic lupus erythematosus. Nat Genet. 2008;40:152–4.59. Wan g B, Zhu JM, Fan YG, et al. Association of the−1082G/A polymorphism in the interleukin-10 gene withsystemic lupus erythematosus: A meta-analysis. Gene.2013;519:209–16. 60. Takeuchi T, Suzuki K. CD247 variantsand singlenucleotide polymorphisms observed in systemiclupus erythematosus patients. Rheumatology (Oxford).2013;52:1551–5. 61. Blo ck SR, Winfield JB, Lockshin MD,et al. Studies of twins with systemic lupus erythematosus:A review of the literature and presentation of 12additional sets. Am J Med. 1975;59:533–52. 62. Dea pen D,Escalante A, Weinrib L, et al. A revised estimate of twinconcordance in systemic lupus erythematosus. ArthritisRheum. 1992;35:311–8.
63. Arnett FC, Reveille JD, Wilson RW, et al. Systemiclupus erythematosus: Current state of the genetichypothesis. Semin Arthritis Rheum. 1984;14:24–35.
64. Hun nangkul S, Nitsch D, Rhodes B, et al. Familialclustering of non-nuclear autoantibodies and C3 and C4complement components in systemic lupus erythematosus.Arthritis Rheum. 2008;58:1116–24.
65. Murashima A, Fukazawa T, Hirashima M, et al. Long termprognosis of children born to lupus patients. Ann RheumDis. 2004;63:50–3.
66. Tsa o BP. The genetics of human systemic lupus

erythematosus. Trends Immunol. 2003;24:595–602.
67. Weening JJ, D’Agati VD, Schwartz MM, et al. Theclassification of glomerulonephritis in systemic lupuserythematosus revisited. J Am Soc Nephrol. 2004;15:241–50.
68. Wee ning JJ, D’Agati VD, Schwartz MM, et al. Theclassification of glomerulonephritis in sys temic lupuserythematosus revisited. Kidney Int. 2 00 4;65:521–30.
69. Tucker LB, Menon S, Schaller JG, Isenberg DA. Adult-and childhood-onset systemic lupus erythematosus: Acomparison of onset, clinical features, serology, andoutcome. Br J Rheumatol. 1995;34:866–72.
70. Mei slin AG, Rothfield N. Systemic lupus erythe matosusin childhood: Analysis of 42 cases, with c om parativedata on 200 adult cases followed concurrently. Pediatrics.1968;42:37–49.
71. Hoc hberg MC. Updating the American College ofRheumatology revised criteria for the classification ofsystemic lupus erythematosus. Arthritis Rheum.1997;40:1725.
72. Carreno L, Lopez-Longo FJ, Monteagudo I, et al. Immunological and clinical differences between juvenile andadult onset of systemic lupus erythe matosus. Lupus.1999;8:287–92.
73. Rood MJ, ten Cate R, van Suijlekom-Smit LW, et al.Childhood-onset systemic lupus erythematosus: Clinicalpresentation and prognosis in 31 patients. Scand JRheumatol. 1999;28:222–6.
74. Tan EM, Feltkamp TE, Smolen JS, et al. Range ofantinuclear antibodies in “healthy” individuals. ArthritisRheum. 1997;40:1601–11.
75. Shiel WC, Jr., Jason M. The diagnostic associations ofpatients with antinuclear antibodies referred to acommunity rheumatologist. J Rheumatol. 1989;16:782–5.
76. Massengill SF, Hedrick C, Ayoub EM, et al.Antiphospholipid antibodies in pediatric lupus nephritis.Am J Kidney Dis. 1997;29:355–61.
77. Mol ta C, Meyer O, Dosquet C, et al. Childhood-onsetsystemic lupus erythematosus: Antiphospholipid antibodiesin 37 patients and their first-degree relatives.
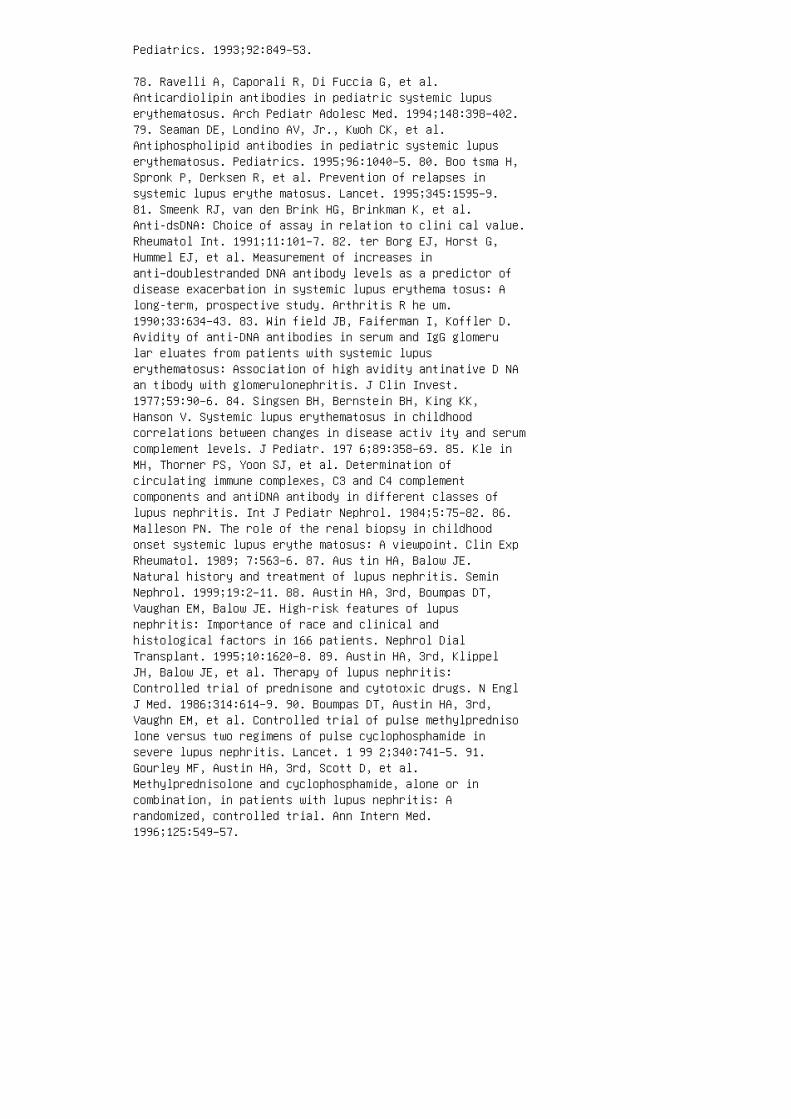
Pediatrics. 1993;92:849–53.
78. Ravelli A, Caporali R, Di Fuccia G, et al.Anticardiolipin antibodies in pediatric systemic lupuserythematosus. Arch Pediatr Adolesc Med. 1994;148:398–402.79. Seaman DE, Londino AV, Jr., Kwoh CK, et al.Antiphospholipid antibodies in pediatric systemic lupuserythematosus. Pediatrics. 1995;96:1040–5. 80. Boo tsma H,Spronk P, Derksen R, et al. Prevention of relapses insystemic lupus erythe matosus. Lancet. 1995;345:1595–9.81. Smeenk RJ, van den Brink HG, Brinkman K, et al.Anti-dsDNA: Choice of assay in relation to clini cal value.Rheumatol Int. 1991;11:101–7. 82. ter Borg EJ, Horst G,Hummel EJ, et al. Measurement of increases inanti–doublestranded DNA antibody levels as a predictor ofdisease exacerbation in systemic lupus erythema tosus: Along-term, prospective study. Arthritis R he um.1990;33:634–43. 83. Win field JB, Faiferman I, Koffler D.Avidity of anti-DNA antibodies in serum and IgG glomerular eluates from patients with systemic lupuserythematosus: Association of high avidity antinative D NAan tibody with glomerulonephritis. J Clin Invest.1977;59:90–6. 84. Singsen BH, Bernstein BH, King KK,Hanson V. Systemic lupus erythematosus in childhoodcorrelations between changes in disease activ ity and serumcomplement levels. J Pediatr. 197 6;89:358–69. 85. Kle inMH, Thorner PS, Yoon SJ, et al. Determination ofcirculating immune complexes, C3 and C4 complementcomponents and antiDNA antibody in different classes oflupus nephritis. Int J Pediatr Nephrol. 1984;5:75–82. 86.Malleson PN. The role of the renal biopsy in childhoodonset systemic lupus erythe matosus: A viewpoint. Clin ExpRheumatol. 1989; 7:563–6. 87. Aus tin HA, Balow JE.Natural history and treatment of lupus nephritis. SeminNephrol. 1999;19:2–11. 88. Austin HA, 3rd, Boumpas DT,Vaughan EM, Balow JE. High-risk features of lupusnephritis: Importance of race and clinical andhistological factors in 166 patients. Nephrol DialTransplant. 1995;10:1620–8. 89. Austin HA, 3rd, KlippelJH, Balow JE, et al. Therapy of lupus nephritis:Controlled trial of prednisone and cytotoxic drugs. N EnglJ Med. 1986;314:614–9. 90. Boumpas DT, Austin HA, 3rd,Vaughn EM, et al. Controlled trial of pulse methylprednisolone versus two regimens of pulse cyclophosphamide insevere lupus nephritis. Lancet. 1 99 2;340:741–5. 91.Gourley MF, Austin HA, 3rd, Scott D, et al.Methylprednisolone and cyclophosphamide, alone or incombination, in patients with lupus nephritis: Arandomized, controlled trial. Ann Intern Med.1996;125:549–57.
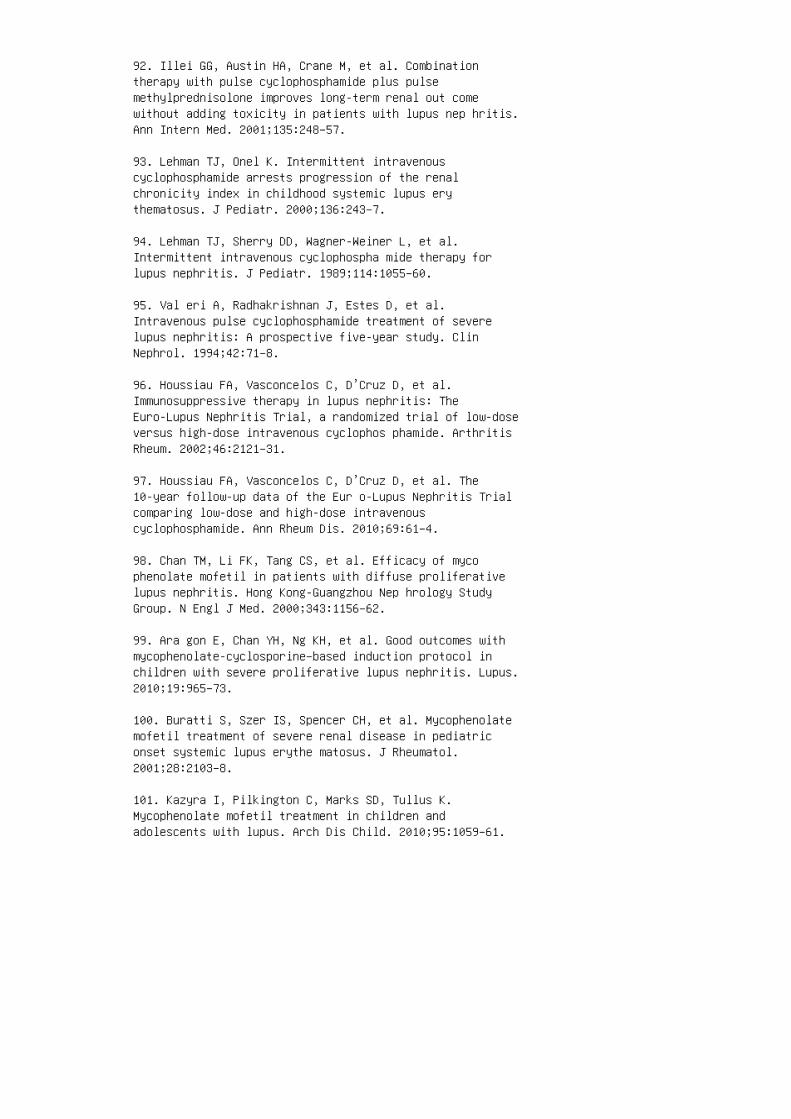
92. Illei GG, Austin HA, Crane M, et al. Combinationtherapy with pulse cyclophosphamide plus pulsemethylprednisolone improves long-term renal out comewithout adding toxicity in patients with lupus nep hritis.Ann Intern Med. 2001;135:248–57.
93. Lehman TJ, Onel K. Intermittent intravenouscyclophosphamide arrests progression of the renalchronicity index in childhood systemic lupus erythematosus. J Pediatr. 2000;136:243–7.
94. Lehman TJ, Sherry DD, Wagner-Weiner L, et al.Intermittent intravenous cyclophospha mide therapy forlupus nephritis. J Pediatr. 1989;114:1055–60.
95. Val eri A, Radhakrishnan J, Estes D, et al.Intravenous pulse cyclophosphamide treatment of severelupus nephritis: A prospective five-year study. ClinNephrol. 1994;42:71–8.
96. Houssiau FA, Vasconcelos C, D’Cruz D, et al.Immunosuppressive therapy in lupus nephritis: TheEuro-Lupus Nephritis Trial, a randomized trial of low-doseversus high-dose intravenous cyclophos phamide. ArthritisRheum. 2002;46:2121–31.
97. Houssiau FA, Vasconcelos C, D’Cruz D, et al. The10-year follow-up data of the Eur o-Lupus Nephritis Trialcomparing low-dose and high-dose intravenouscyclophosphamide. Ann Rheum Dis. 2010;69:61–4.
98. Chan TM, Li FK, Tang CS, et al. Efficacy of mycophenolate mofetil in patients with diffuse proliferativelupus nephritis. Hong Kong-Guangzhou Nep hrology StudyGroup. N Engl J Med. 2000;343:1156–62.
99. Ara gon E, Chan YH, Ng KH, et al. Good outcomes withmycophenolate-cyclosporine–based induction protocol inchildren with severe proliferative lupus nephritis. Lupus.2010;19:965–73.
100. Buratti S, Szer IS, Spencer CH, et al. Mycophenolatemofetil treatment of severe renal disease in pediatriconset systemic lupus erythe matosus. J Rheumatol.2001;28:2103–8.
101. Kazyra I, Pilkington C, Marks SD, Tullus K.Mycophenolate mofetil treatment in children andadolescents with lupus. Arch Dis Child. 2010;95:1059–61.
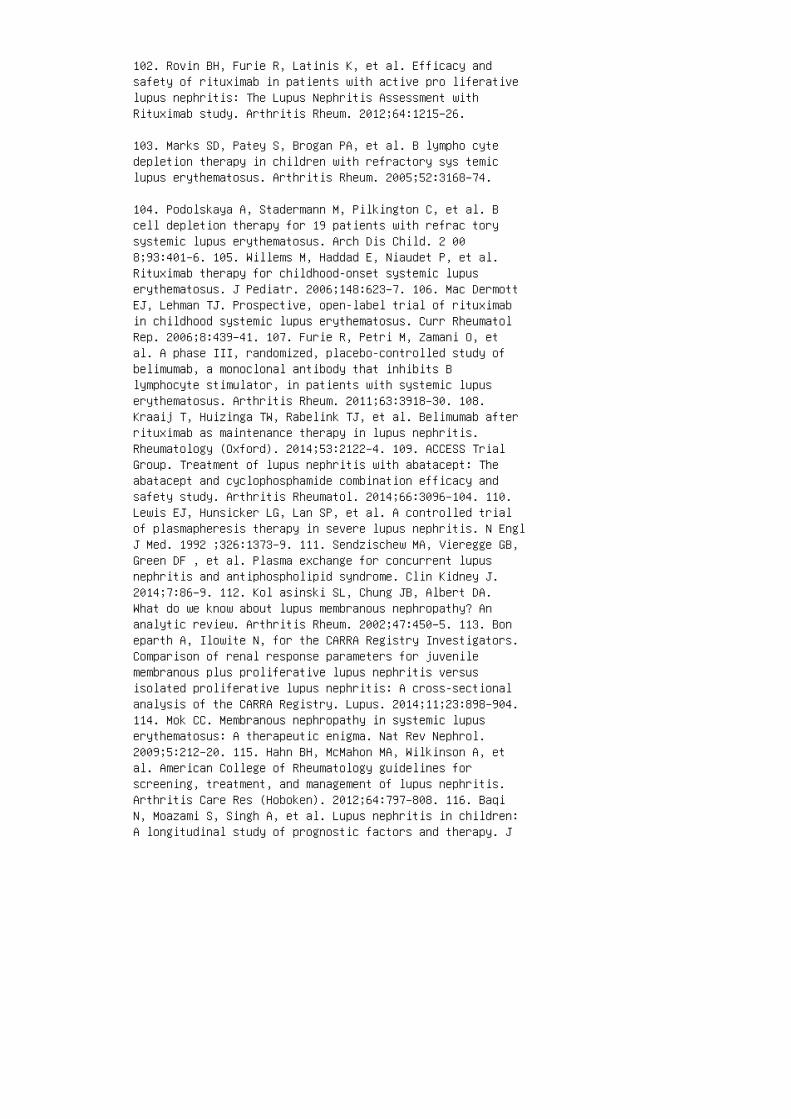
102. Rovin BH, Furie R, Latinis K, et al. Efficacy andsafety of rituximab in patients with active pro liferativelupus nephritis: The Lupus Nephritis Assessment withRituximab study. Arthritis Rheum. 2012;64:1215–26.
103. Marks SD, Patey S, Brogan PA, et al. B lympho cytedepletion therapy in children with refractory sys temiclupus erythematosus. Arthritis Rheum. 2005;52:3168–74.
104. Podolskaya A, Stadermann M, Pilkington C, et al. Bcell depletion therapy for 19 patients with refrac torysystemic lupus erythematosus. Arch Dis Child. 2 008;93:401–6. 105. Willems M, Haddad E, Niaudet P, et al.Rituximab therapy for childhood-onset systemic lupuserythematosus. J Pediatr. 2006;148:623–7. 106. Mac DermottEJ, Lehman TJ. Prospective, open-label trial of rituximabin childhood systemic lupus erythematosus. Curr RheumatolRep. 2006;8:439–41. 107. Furie R, Petri M, Zamani O, etal. A phase III, randomized, placebo-controlled study ofbelimumab, a monoclonal antibody that inhibits Blymphocyte stimulator, in patients with systemic lupuserythematosus. Arthritis Rheum. 2011;63:3918–30. 108.Kraaij T, Huizinga TW, Rabelink TJ, et al. Belimumab afterrituximab as maintenance therapy in lupus nephritis.Rheumatology (Oxford). 2014;53:2122–4. 109. ACCESS TrialGroup. Treatment of lupus nephritis with abatacept: Theabatacept and cyclophosphamide combination efficacy andsafety study. Arthritis Rheumatol. 2014;66:3096–104. 110.Lewis EJ, Hunsicker LG, Lan SP, et al. A controlled trialof plasmapheresis therapy in severe lupus nephritis. N EnglJ Med. 1992 ;326:1373–9. 111. Sendzischew MA, Vieregge GB,Green DF , et al. Plasma exchange for concurrent lupusnephritis and antiphospholipid syndrome. Clin Kidney J.2014;7:86–9. 112. Kol asinski SL, Chung JB, Albert DA.What do we know about lupus membranous nephropathy? Ananalytic review. Arthritis Rheum. 2002;47:450–5. 113. Boneparth A, Ilowite N, for the CARRA Registry Investigators.Comparison of renal response parameters for juvenilemembranous plus proliferative lupus nephritis versusisolated proliferative lupus nephritis: A cross-sectionalanalysis of the CARRA Registry. Lupus. 2014;11;23:898–904.114. Mok CC. Membranous nephropathy in systemic lupuserythematosus: A therapeutic enigma. Nat Rev Nephrol.2009;5:212–20. 115. Hahn BH, McMahon MA, Wilkinson A, etal. American College of Rheumatology guidelines forscreening, treatment, and management of lupus nephritis.Arthritis Care Res (Hoboken). 2012;64:797–808. 116. BaqiN, Moazami S, Singh A, et al. Lupus nephritis in children:A longitudinal study of prognostic factors and therapy. J
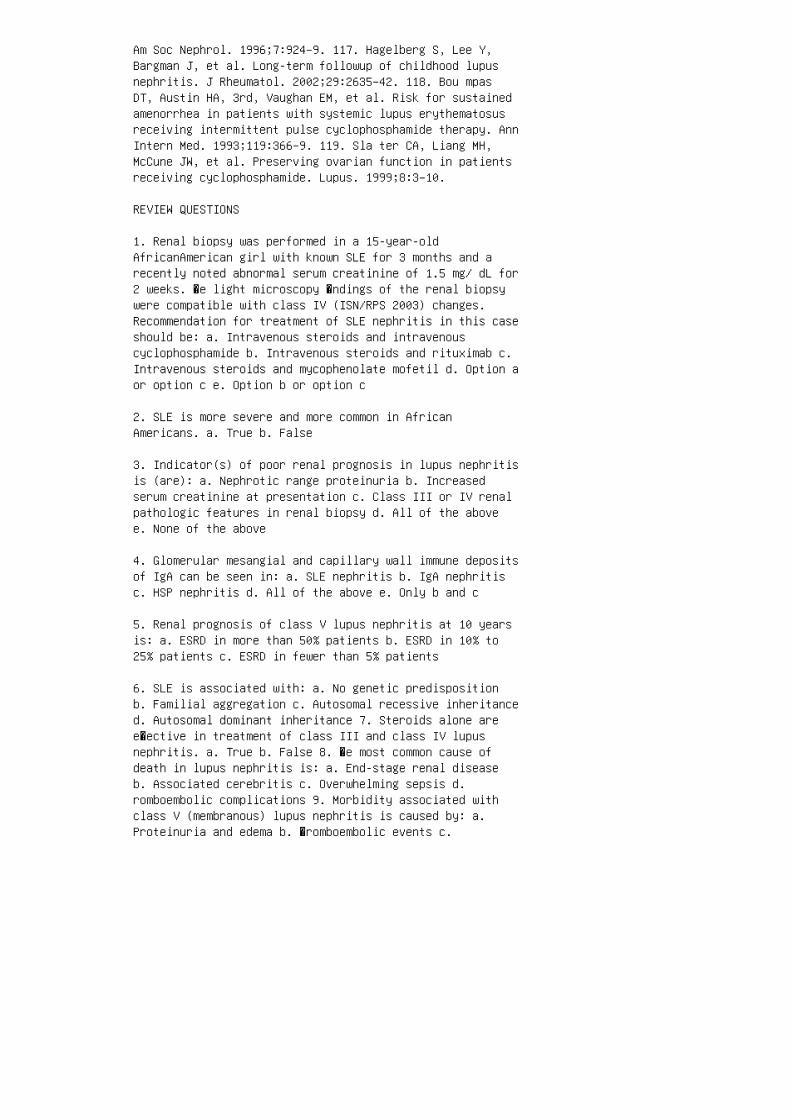
Am Soc Nephrol. 1996;7:924–9. 117. Hagelberg S, Lee Y,Bargman J, et al. Long-term followup of childhood lupusnephritis. J Rheumatol. 2002;29:2635–42. 118. Bou mpasDT, Austin HA, 3rd, Vaughan EM, et al. Risk for sustainedamenorrhea in patients with systemic lupus erythematosusreceiving intermittent pulse cyclophosphamide therapy. AnnIntern Med. 1993;119:366–9. 119. Sla ter CA, Liang MH,McCune JW, et al. Preserving ovarian function in patientsreceiving cyclophosphamide. Lupus. 1999;8:3–10.
REVIEW QUESTIONS
1. Renal biopsy was performed in a 15-year-oldAfricanAmerican girl with known SLE for 3 months and arecently noted abnormal serum creatinine of 1.5 mg/ dL for2 weeks. �e light microscopy �ndings of the renal biopsywere compatible with class IV (ISN/RPS 2003) changes.Recommendation for treatment of SLE nephritis in this caseshould be: a. Intravenous steroids and intravenouscyclophosphamide b. Intravenous steroids and rituximab c.Intravenous steroids and mycophenolate mofetil d. Option aor option c e. Option b or option c
2. SLE is more severe and more common in AfricanAmericans. a. True b. False
3. Indicator(s) of poor renal prognosis in lupus nephritisis (are): a. Nephrotic range proteinuria b. Increasedserum creatinine at presentation c. Class III or IV renalpathologic features in renal biopsy d. All of the abovee. None of the above
4. Glomerular mesangial and capillary wall immune depositsof IgA can be seen in: a. SLE nephritis b. IgA nephritisc. HSP nephritis d. All of the above e. Only b and c
5. Renal prognosis of class V lupus nephritis at 10 yearsis: a. ESRD in more than 50% patients b. ESRD in 10% to25% patients c. ESRD in fewer than 5% patients
6. SLE is associated with: a. No genetic predispositionb. Familial aggregation c. Autosomal recessive inheritanced. Autosomal dominant inheritance 7. Steroids alone aree�ective in treatment of class III and class IV lupusnephritis. a. True b. False 8. �e most common cause ofdeath in lupus nephritis is: a. End-stage renal diseaseb. Associated cerebritis c. Overwhelming sepsis d.romboembolic complications 9. Morbidity associated withclass V (membranous) lupus nephritis is caused by: a.Proteinuria and edema b. �romboembolic events c.

Infective events d. All of the above 10. Patients withclass V (membranous) lupus nephritis should receiveinduction therapy with pulse IV steroids and IV Cytoxanprotocol. a. True b. False 11. In treatment ofproliferative lupus nephritis (class III and IV),mycophenolate mofetil (MMF) induction therapy is: a. Lesse�ective than NIH regimen of IV Cytoxan b. More e�ectivethan NIH regimen of IV Cytoxan c. At least as e�ective asNIH regimen of IV Cytoxan d. �ere are no convincingcomparative data available. ANSWER KEY 1. d 2 a 3. d4. d 5. b 6. b 7. b 8. c 9. d 10. b 11. c

27 Kidney disease in sickle cell disease
1. Lonsdorfer A, Comoe L, Yapo AE, et al. Proteinuria insickle cell trait and disease: An electrophoreticanalysis. Clin Chim Acta. 1989;181:239–47.
2. Stallworth JR, Tripathi A, Jerrell JM. Prevalence,treatment, and outcomes of renal conditions in pediatricsickle cell disease. South Med J. 2011;104:752–6.
3. Pham PT, Pham PC, Wilkinson AH, et al. Renalabnormalities in sickle cell disease. Kidney Int.2000;57:1–8.
4. Sklar AH, Campbell H, Caruana RJ, et al. A populationstudy of renal function in sickle cell anemia. Int J ArtifOrgans. 1990;13:231–6.
5. Wigfall DR, Ware RE, Burchinal MR, et al. Prevalenceand clinical correlates of glomerulopathy in children withsickle cell disease. J Pediatr. 2000;136:749–53.
6. McPherson Yee M, Jabbar SF, et al. Chronic kidneydisease and albuminuria in children with sickle celldisease. Clin J Am Soc Nephrol. 2011;6:2628–33. 7. McKieKT, Hanevold CD, Hernandez C, et al. Prevalence,prevention, and treatment of microalbuminuria andproteinuria in children with sickle cell disease.J.Pediatr Hematol Oncol. 2007;29:140–4. 8. Alvarez O,Lopez-Mitnik G, Zilleruelo G. Short-term follow-up ofpatients with sickle cell disease and albuminuria. PediatrBlood Cancer. 2008;50:1236–9. 9. Becton LJ, Kalpatthi RV,Rackoff E, et al. Prevalence and clinical correlates ofmicroalbuminuria in children with sickle cell disease.Pediatr Nephrol. 2010;25:1505–11. 10. Aygun B, MortierNA, Smeltzer MP, et al. Glomerular hyperfiltration andalbuminuria in children with sickle cell anemia. PediatrNephrol. 2011;26:1285–90. 11. Dha rnidharka VR, Dabbagh S,Atiyeh B, et al. Prevalence of microalbuminuria inchildren with sickle cell disease. Pediatr Nephrol.1998;12:475–8. 12. Powars DR, Elliott-Mills DD, Chan L, etal. Chronic renal failure in sickle cell disease: Riskfactors, clinical course, and mortality. Ann Intern Med.1991;115:614–20. 13. Thompson J, Reid M, Hambleton I, etal. Albuminuria and renal function in homozygous sicklecell disease: Observations from a cohort study. ArchIntern Med. 2007;167:701–8. 14. Guasch A, Navarrete J,Nass K, et al. Glomerular involvement in adults withsickle cell hemoglobinopathies: Prevalence and clinicalcorrelates of progressive renal failure. J Am Soc Nephrol.

2006;17:2228–35. 15. Platt OS, Brambilla DJ, Rosse WF, etal. Mortality in sickle cell disease: Life expectancy andrisk factors for early death. N Engl J Med. 19949;330:1639–44. 16. Lebensburger J, Johnson SM, AskenaziDJ, et al. Protective role of hemoglobin and fetalhemoglobin in early kidney disease for children withsickle cell anemia. Am J Hematol. 2011;86:430–2. 17.Powars DR, Meiselman HJ, Fisher TC, et al. Beta-S genecluster haplotypes modulate hematologic and hemorheologicexpression in sickle cell anemia: Use in predictingclinical severity. Am J Pediatr Hematol Oncol.1994;16:55–61. 18. Guasch A, Zayas CF, Eckman JR, et al.Evidence that microdeletions in the alpha globin geneprotect against the development of sickle cellglomerulopathy in humans. J Am Soc Nephrol. 1999;10:1014–9.19. Allon M. Renal abnormalities in sickle cell disease.Arch Intern Med. 1990;150:501–4. 20. Sabatini S.Pathophysiologic mechanisms of abnormal collecting ductfunction. Semin Nephrol. 1989;9:179–202. 21. Statius vanEps LW, Schouten H, La Porte-Wijsman LW, et al. Theinfluence of red blood cell transfusions on thehyposthenuria and renal hemodynamics of sickle cellanemia. Clin Chim Acta. 1967;17:449–61. 22. Davies SC,Hewitt PE. Sickle cell disease. Br J Hosp Med.1984;31:440–4.
SUMMARY
SCD is a multiorgan disorder that can a�ect the
kidney and lead to CKD and ESRD. Renal injury or
SCN starts early in childhood. E�orts to prevent sick
ling, examine potential renoprotective agents, and
develop biomarkers to identify early kidney injury
and patients at risk of disease progression are among
the most important avenues in understanding and
preventing the renal consequences of SCD.
Kidney transplantation o�ers better survival option
for patients with ESRD. With advances in the trans
plant �eld, bone marrow coupled with kidney trans
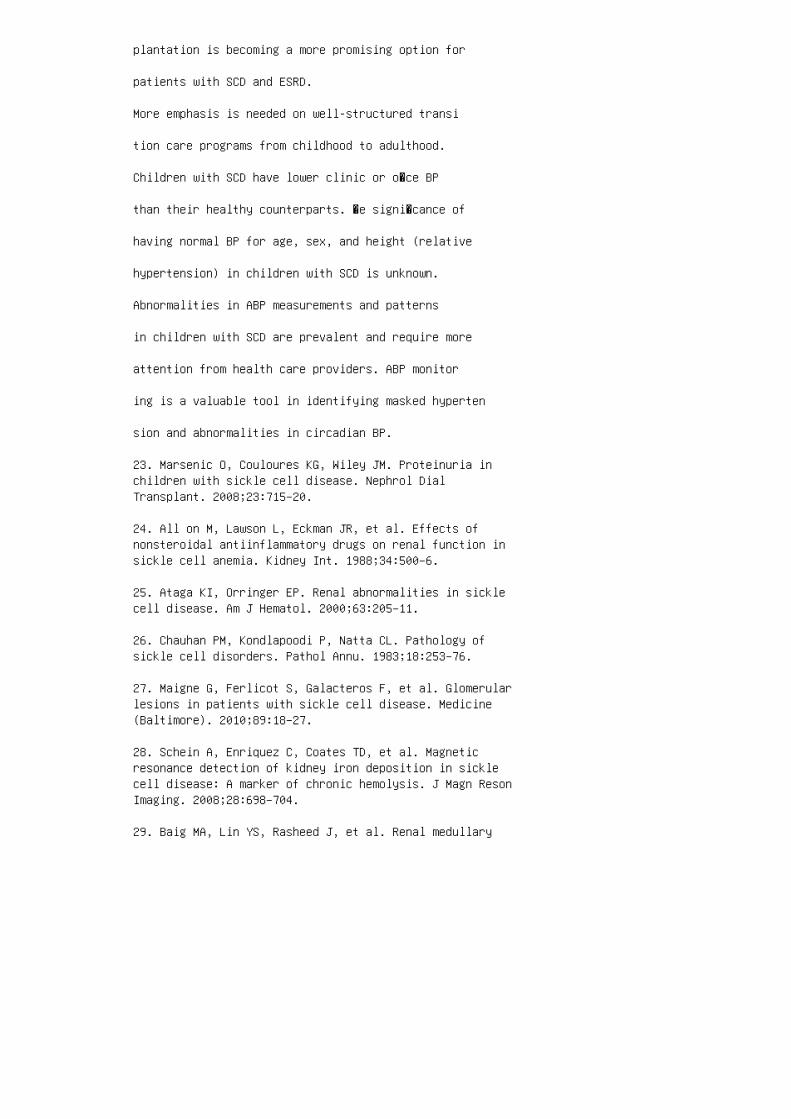
plantation is becoming a more promising option for
patients with SCD and ESRD.
More emphasis is needed on well-structured transi
tion care programs from childhood to adulthood.
Children with SCD have lower clinic or o�ce BP
than their healthy counterparts. �e signi�cance of
having normal BP for age, sex, and height (relative
hypertension) in children with SCD is unknown.
Abnormalities in ABP measurements and patterns
in children with SCD are prevalent and require more
attention from health care providers. ABP monitor
ing is a valuable tool in identifying masked hyperten
sion and abnormalities in circadian BP.
23. Marsenic O, Couloures KG, Wiley JM. Proteinuria inchildren with sickle cell disease. Nephrol DialTransplant. 2008;23:715–20.
24. All on M, Lawson L, Eckman JR, et al. Effects ofnonsteroidal antiinflammatory drugs on renal function insickle cell anemia. Kidney Int. 1988;34:500–6.
25. Ataga KI, Orringer EP. Renal abnormalities in sicklecell disease. Am J Hematol. 2000;63:205–11.
26. Chauhan PM, Kondlapoodi P, Natta CL. Pathology ofsickle cell disorders. Pathol Annu. 1983;18:253–76.
27. Maigne G, Ferlicot S, Galacteros F, et al. Glomerularlesions in patients with sickle cell disease. Medicine(Baltimore). 2010;89:18–27.
28. Schein A, Enriquez C, Coates TD, et al. Magneticresonance detection of kidney iron deposition in sicklecell disease: A marker of chronic hemolysis. J Magn ResonImaging. 2008;28:698–704.
29. Baig MA, Lin YS, Rasheed J, et al. Renal medullary

carcinoma. J Natl Med Assoc. 2006;98:1171–4.
30. Swa rtz MA, Karth J, Schneider DT, et al. Renalmedullary carcinoma: Clinical, pathologic,immunohistochemical, and genetic analysis with pathogeneticimplications. Urology. 2002;60:1083–9.
31. Wal sh A, Kelly DR, Vaid YN, et al. Complete responseto carboplatin, gemcitabine, and paclitaxel in a patientwith advanced metastatic renal medullary carcinoma.Pediatr Blood Cancer. 2010;55:1217–20.
32. Kir yluk K, Jadoon A, Gupta M, et al. Sickle cell traitand gross hematuria. Kidney Int. 2007;71:706–10.
33. Fal k RJ, Scheinman J, Phillips G, et al. Prevalenceand pathologic features of sickle cell nephropathy andresponse to inhibition of angiotensin-converting enzyme. NEngl J Med. 1992;326:910–5.
34. Bhathena DB, Sondheimer JH. The glomerulopathy ofhomozygous sickle hemoglobin (SS) disease: Morphology andpathogenesis. J Am Soc Nephrol. 1991;1:1241–52.
35. Hatch FE, Crowe LR, Miles DE, et al. Altered vascularreactivity in sickle hemoglobinopathy: A possibleprotective factor from hypertension. Am J Hypertens.1989;2:2–8.
36. Wood KC, Hsu LL, Gladwin MT. Sickle cell diseasevasculopathy: A state of nitric oxide resistance. FreeRadic Biol Med. 2008;44:1506–28.
37. Shatat IF, Jakson SM, Blue AE, et al. Maskedhypertension is prevalent in children with sickle celldisease: A Midwest Pediatric Nephrology Consortium study.Pediatr Nephrol. 2013;28:115–20.
38. DeB aun MR, Armstrong FD, McKinstry RC, et al. Silentcerebral infarcts: A review on a prevalent and progressivecause of neurologic injury in sickle cell anemia. Blood.2012;119:4587–96.
39. Ale em A. Renal abnormalities in patients with sicklecell disease: A single center report from Saudi Arabia.Saudi J Kidney Dis Transpl. 2008;19:194–9. 40. Osegbe DN.Haematuria and sickle cell disease: A report of 12 casesand review of the literature. Trop Geogr Med.1990;42:22–7. 41. Pegelow CH, Colangelo L, Steinberg M, etal. Natural history of blood pressure in sickle cell
disease: Risks for stroke and death associated withrelative hypertension in sickle cell anemia. Am J Med.1997;102:171–7. 42. Guasch A, Cua M, You W, et al. Sicklecell anemia causes a distinct pattern of glomerulardysfunction. Kidney Int. 1997;51:826–33. 43. Joh nson CS,Giorgio AJ. Arterial blood pressure in adults with sicklecell disease. Arch Intern Med. 1981;141:891–3. 44.Dimashkieh H, Choe J, Mutema G. Renal medullary carcinoma:A report of 2 cases and review of the literature. ArchPathol Lab Med. 2003;127:e135–8. 45. Bak ir AA, HathiwalaSC, Ainis H, et al. Prognosis of the nephrotic syndrome insickle glomerulopathy: A retrospective study. Am JNephrol. 1987;7:110–5. 46. Fou can L, Bourhis V, Bangou J,et al. A randomized trial of captopril formicroalbuminuria in normotensive adults with sickle cellanemia. Am J Med. 1998;104:339–42. 47. Bodas P, Huang A,O’Riordan MA, et al.The prevalence of hypertension andabnormal kidney function in children with sickle celldisease: A cross sectional review. BMC Nephrol.2013;14:237. 48. Derebail VK, Nachman PH, Key NS, et al.High prevalence of sickle cell trait in African Americanswith ESRD. J Am Soc Nephrol. 2010;21:413–7. 49. Nai k RP,Derebail VK, Grams ME, et al. Association of sickle celltrait with chronic kidney disease and albuminuria inAfrican Americans. JAMA. 2014;312:2115–25. 50. Abb ott KC,Hypolite IO, Agodoa LY. Sickle cell nephropathy atend-stage renal disease in the United States: Patientcharacteristics and survival. Clin Nephrol. 2002;58:9–15.51. Hassell KL, Eckman JR, Lane PA. Acute multiorganfailure syndrome: A potentially catastrophic complicationof severe sickle cell pain episodes. Am J Med.1994;96:155–62. 52. Sklar AH, Perez JC, Harp RJ, et al.Acute renal failure in sickle cell anemia. Int J ArtifOrgans. 1990;13:347–51. 53. Audard V, Homs S, Habibi A, etal. Acute kidney injury in sickle patients with painfulcrisis or acute chest syndrome and its relation topulmonary hypertension. Nephrol Dial Transplant.2010;25:2524–9. 54. Sim ckes AM, Chen SS, Osorio AV, etal. Ketorolacinduced irreversible renal failure in sicklecell disease: A case report. Pediatr Nephrol.1999;13:63–7. 55. Koppes GM, Daly JJ, Coltman CA, Jr., etal. Exertion-induced rhabdomyolysis with acute renalfailure and disseminated intravascular coagulation insickle cell trait. Am J Med. 1977;63:313–7.
56. Keitel HG, Thompson D, Itano HA. Hyposthenuria insickle cell anemia: A reversible renal defect. J ClinInvest. 1956;35:998–1007.
57. Mil ler ST, Wang WC, Iyer R, et al. Urine concen
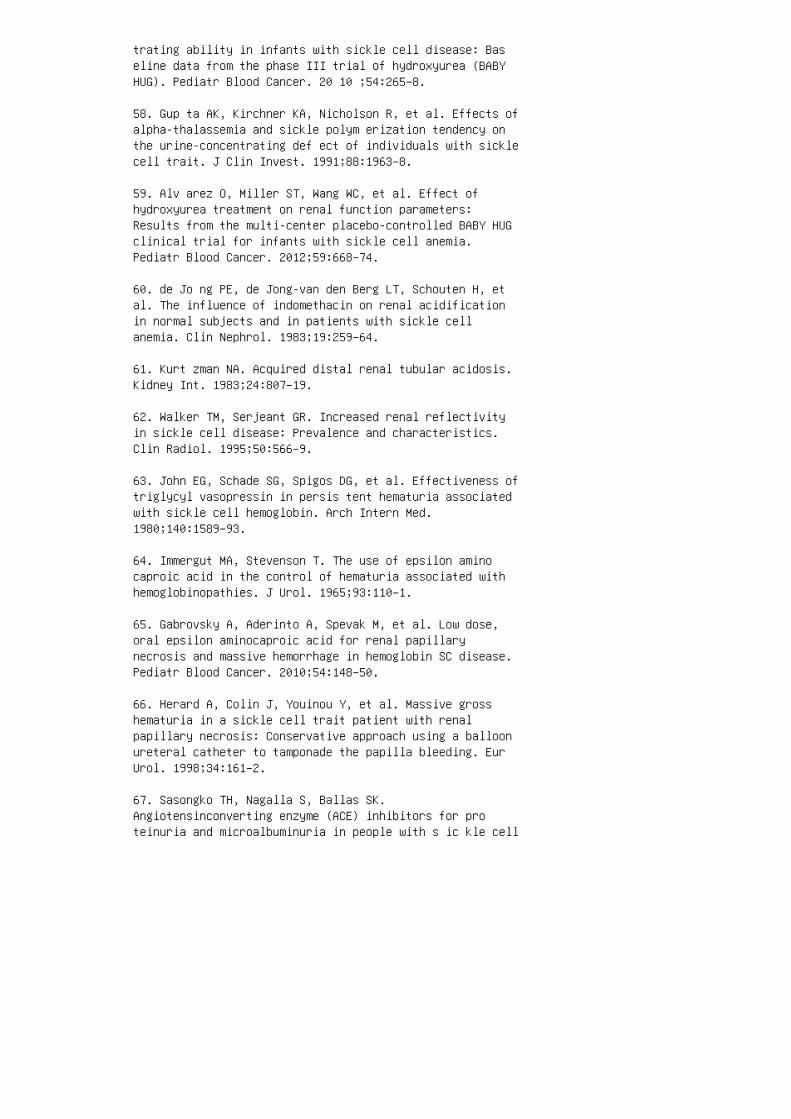
trating ability in infants with sickle cell disease: Baseline data from the phase III trial of hydroxyurea (BABYHUG). Pediatr Blood Cancer. 20 10 ;54:265–8.
58. Gup ta AK, Kirchner KA, Nicholson R, et al. Effects ofalpha-thalassemia and sickle polym erization tendency onthe urine-concentrating def ect of individuals with sicklecell trait. J Clin Invest. 1991;88:1963–8.
59. Alv arez O, Miller ST, Wang WC, et al. Effect ofhydroxyurea treatment on renal function parameters:Results from the multi-center placebo-controlled BABY HUGclinical trial for infants with sickle cell anemia.Pediatr Blood Cancer. 2012;59:668–74.
60. de Jo ng PE, de Jong-van den Berg LT, Schouten H, etal. The influence of indomethacin on renal acidificationin normal subjects and in patients with sickle cellanemia. Clin Nephrol. 1983;19:259–64.
61. Kurt zman NA. Acquired distal renal tubular acidosis.Kidney Int. 1983;24:807–19.
62. Walker TM, Serjeant GR. Increased renal reflectivityin sickle cell disease: Prevalence and characteristics.Clin Radiol. 1995;50:566–9.
63. John EG, Schade SG, Spigos DG, et al. Effectiveness oftriglycyl vasopressin in persis tent hematuria associatedwith sickle cell hemoglobin. Arch Intern Med.1980;140:1589–93.
64. Immergut MA, Stevenson T. The use of epsilon aminocaproic acid in the control of hematuria associated withhemoglobinopathies. J Urol. 1965;93:110–1.
65. Gabrovsky A, Aderinto A, Spevak M, et al. Low dose,oral epsilon aminocaproic acid for renal papillarynecrosis and massive hemorrhage in hemoglobin SC disease.Pediatr Blood Cancer. 2010;54:148–50.
66. Herard A, Colin J, Youinou Y, et al. Massive grosshematuria in a sickle cell trait patient with renalpapillary necrosis: Conservative approach using a balloonureteral catheter to tamponade the papilla bleeding. EurUrol. 1998;34:161–2.
67. Sasongko TH, Nagalla S, Ballas SK.Angiotensinconverting enzyme (ACE) inhibitors for proteinuria and microalbuminuria in people with s ic kle cell
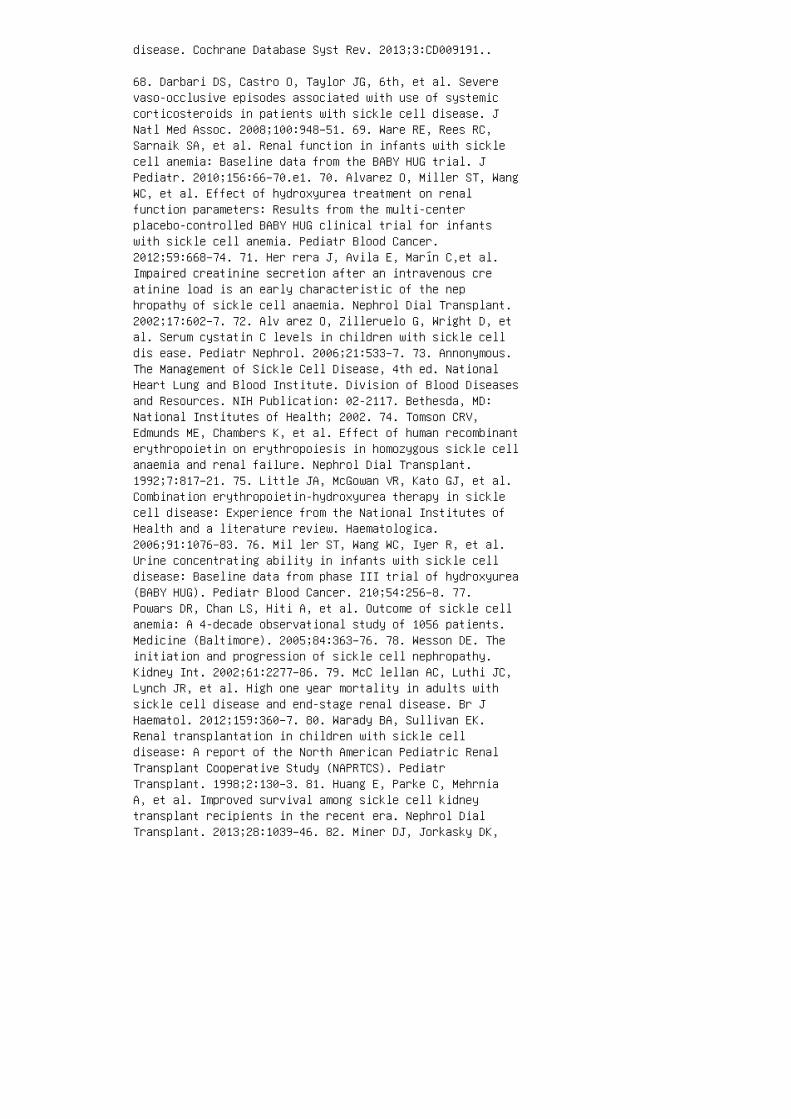
disease. Cochrane Database Syst Rev. 2013;3:CD009191..
68. Darbari DS, Castro O, Taylor JG, 6th, et al. Severevaso-occlusive episodes associated with use of systemiccorticosteroids in patients with sickle cell disease. JNatl Med Assoc. 2008;100:948–51. 69. Ware RE, Rees RC,Sarnaik SA, et al. Renal function in infants with sicklecell anemia: Baseline data from the BABY HUG trial. JPediatr. 2010;156:66–70.e1. 70. Alvarez O, Miller ST, WangWC, et al. Effect of hydroxyurea treatment on renalfunction parameters: Results from the multi-centerplacebo-controlled BABY HUG clinical trial for infantswith sickle cell anemia. Pediatr Blood Cancer.2012;59:668–74. 71. Her rera J, Avila E, Marín C,et al.Impaired creatinine secretion after an intravenous creatinine load is an early characteristic of the nephropathy of sickle cell anaemia. Nephrol Dial Transplant.2002;17:602–7. 72. Alv arez O, Zilleruelo G, Wright D, etal. Serum cystatin C levels in children with sickle celldis ease. Pediatr Nephrol. 2006;21:533–7. 73. Annonymous.The Management of Sickle Cell Disease, 4th ed. NationalHeart Lung and Blood Institute. Division of Blood Diseasesand Resources. NIH Publication: 02-2117. Bethesda, MD:National Institutes of Health; 2002. 74. Tomson CRV,Edmunds ME, Chambers K, et al. Effect of human recombinanterythropoietin on erythropoiesis in homozygous sickle cellanaemia and renal failure. Nephrol Dial Transplant.1992;7:817–21. 75. Little JA, McGowan VR, Kato GJ, et al.Combination erythropoietin-hydroxyurea therapy in sicklecell disease: Experience from the National Institutes ofHealth and a literature review. Haematologica.2006;91:1076–83. 76. Mil ler ST, Wang WC, Iyer R, et al.Urine concentrating ability in infants with sickle celldisease: Baseline data from phase III trial of hydroxyurea(BABY HUG). Pediatr Blood Cancer. 210;54:256–8. 77.Powars DR, Chan LS, Hiti A, et al. Outcome of sickle cellanemia: A 4-decade observational study of 1056 patients.Medicine (Baltimore). 2005;84:363–76. 78. Wesson DE. Theinitiation and progression of sickle cell nephropathy.Kidney Int. 2002;61:2277–86. 79. McC lellan AC, Luthi JC,Lynch JR, et al. High one year mortality in adults withsickle cell disease and end-stage renal disease. Br JHaematol. 2012;159:360–7. 80. Warady BA, Sullivan EK.Renal transplantation in children with sickle celldisease: A report of the North American Pediatric RenalTransplant Cooperative Study (NAPRTCS). PediatrTransplant. 1998;2:130–3. 81. Huang E, Parke C, MehrniaA, et al. Improved survival among sickle cell kidneytransplant recipients in the recent era. Nephrol DialTransplant. 2013;28:1039–46. 82. Miner DJ, Jorkasky DK,
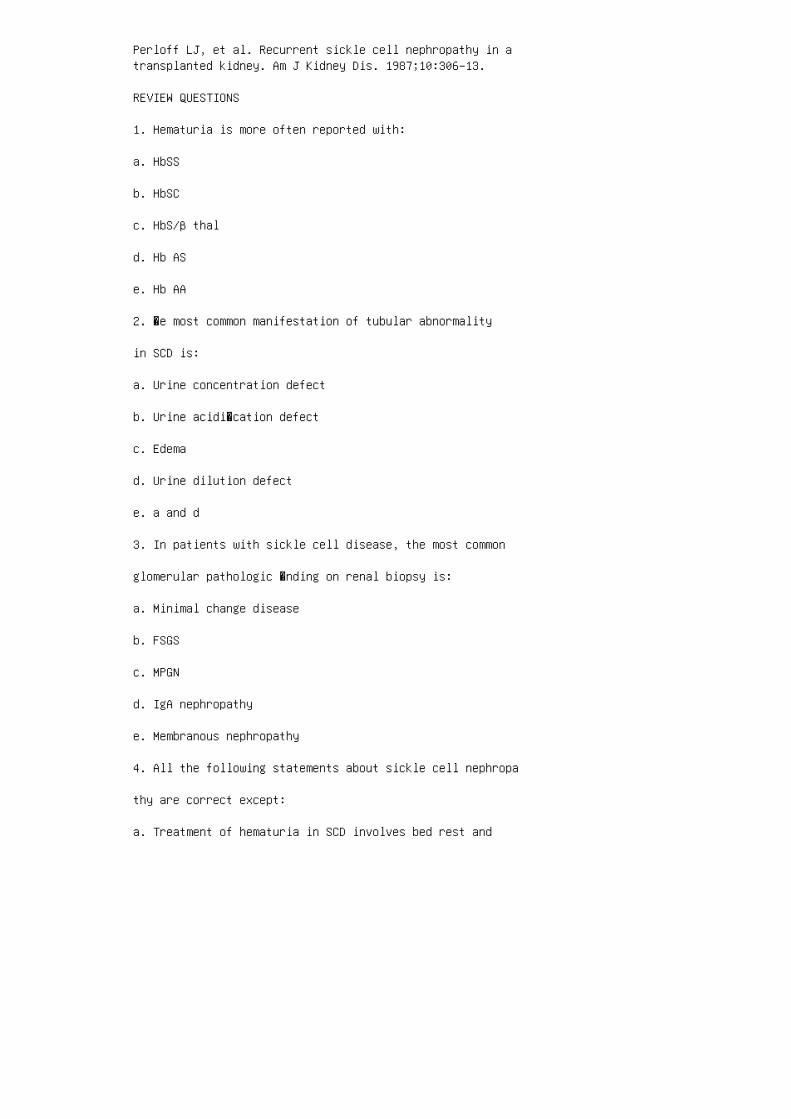
Perloff LJ, et al. Recurrent sickle cell nephropathy in atransplanted kidney. Am J Kidney Dis. 1987;10:306–13.
REVIEW QUESTIONS
1. Hematuria is more often reported with:
a. HbSS
b. HbSC
c. HbS/β thal
d. Hb AS
e. Hb AA
2. �e most common manifestation of tubular abnormality
in SCD is:
a. Urine concentration defect
b. Urine acidi�cation defect
c. Edema
d. Urine dilution defect
e. a and d
3. In patients with sickle cell disease, the most common
glomerular pathologic �nding on renal biopsy is:
a. Minimal change disease
b. FSGS
c. MPGN
d. IgA nephropathy
e. Membranous nephropathy
4. All the following statements about sickle cell nephropa
thy are correct except:
a. Treatment of hematuria in SCD involves bed rest and

maintenance of a high urinary �ow.
b. Patients with sickle cell disease are at a lower risk ofdeveloping hyperkalemia when treated with ACEIs and βblockers.
c. �e reported prevalence of microalbuminuria andproteinuria in patients with sickle cell disease rangesfrom 16% to 40%.
d. Renal medullary carcinoma is present almost exclusivelyin young black patients with sickle cell trait.
e. Children with sickle cell disease have lower clinic BPmeasurements than their age-, sex-, heightmatchedcounterparts.
5. All of the following statements regarding tubular
function in patients with sickle cell disease are correct
except:
a. Sodium reabsorption is increased.
b. Phosphate reabsorption is increased. c. Potassiumreabsorption is increased. d. Urate secretion isincreased. e. Creatinine secretion is increased. 6. �eearliest manifestation of kidney injury in childhood is:a. Acidosis b. Enuresis c. Hyposthenuria d. Hypertensione. Proteinuria 7. Mechanisms of renal injury include allof the following except: a. Immune complex deposits inthe basement membrane b. Hypoxia in the vasa recta c.Polymerization of sickle hemoglobin d. Hyper�ltration inthe glomerulus e. Medullary �brosis 8. All of thefollowing factors are strong predictors of chronic kidneydisease except: a. Proteinuria b. Hematuria c. CARhaplotype d. Nephrotoxic medications e. Nephroticsyndrome 9. All of the following are known correlates ofmicroalbuminuria and proteinuria except: a. Degree ofhemolysis b. Increasing age c. Elevated blood pressured. Pulmonary hypertension e. Higher hemoglobin levelsANSWER KEY 1. d 2. a 3. b 4. b 5. c 6. c 7. a 8. d9. e

28 Kidney disease associated withdiabetes mellitus and metabolic syndrome
1. Pinhas-Hamiel O, Zeitler P. The global spread of type 2diabetes mellitus in children and adolescents. J Pediatr.2005;146:693–700.
2. Pettit DJ, Talton J, Dabelea D, et al.; SEARCH forDiabetes in Youth Study Group. Prevalence of diabetesmellitus in U.S. youth in 2009. The SEARCH for Diabetes inYouth Study. Diabetes Care. 2014;37:402–8.
3. Fagot-Campagna A, Pettitt DJ, Engelgau M, et al. Type 2diabetes among North American children and adolescents: Anepidemiologic health perspective. J Pediatr.2000;136:664–72.
4. United States Renal Data System. US Renal Data System2012 Annual Data Report: Atlas of EndStage Renal Disease inthe United States. Bethesda, MD: National Institutes ofHealth, National Institute of Diabetes and Digestive andKidney Diseases. Available at: http://www.usrds.org.Accessed September 9, 2013. 5. Raile K, Galler A, HoferS, et al. Diabetic nephropathy in 27,805 children,adolescents, and adults with type 1 diabetes: Effect ofdiabetes duration, A1C, hypertension, dyslipidemia,diabetes onset, and sex. Diabetes Care. 2007;30:2523–28.6. Dahlquist G, Stattin E-L, Rudberg S. Urinary albuminexcretion rate and glomerular filtration rate in theprediction of diabetic nephropathy: A long‐term follow‐upstudy of childhood onset type‐1 diabetic patients. NephrolDial Transplant. 2001;16:1382–86. 7. Salgado PP, Silva IN,Vieira EC, et al. Risk factors for early onset of diabeticnephropathy in pediatric type 1 diabetes. J PediatrEndocrinol Metab. 2010;23:1311–20. 8. Finne P, ReunanenA, Stenman S, et al. Incidence of end-stage renal diseasein patients with type 1 diabetes. JAMA. 2005;294:1782–7.9. Maa hs DM, Snively BM, Bell RA, et al. Higherprevalence of elevated albumin excretion in youth withtype 2 than type 1 diabetes. The SEARCH for Diabetes inYouth Study. Diabetes Care. 2007;30:2593–8. 10. EppensM, Craig ME, Cusumano J, et al. Prevalence of diabetescomplications in adolescents with type 2 compared withtype 1 diabetes. Diabetes Care. 2006;29:1300–6. 11.Vallon V, Komers R. Pathophysiology of the diabetickidney. Compr Physiol. 2011;1:1175–232. 12. Noh H, KingGL. The role of protein kinase C activation in diabeticnephropathy. Kidney Int. 2007;106(Suppl):S49–53. 13.Kanwar YS, Sun L, Xie P, et al. A glimpse of variouspathogenetic mechanisms of diabetic nephropathy. Annu Rev
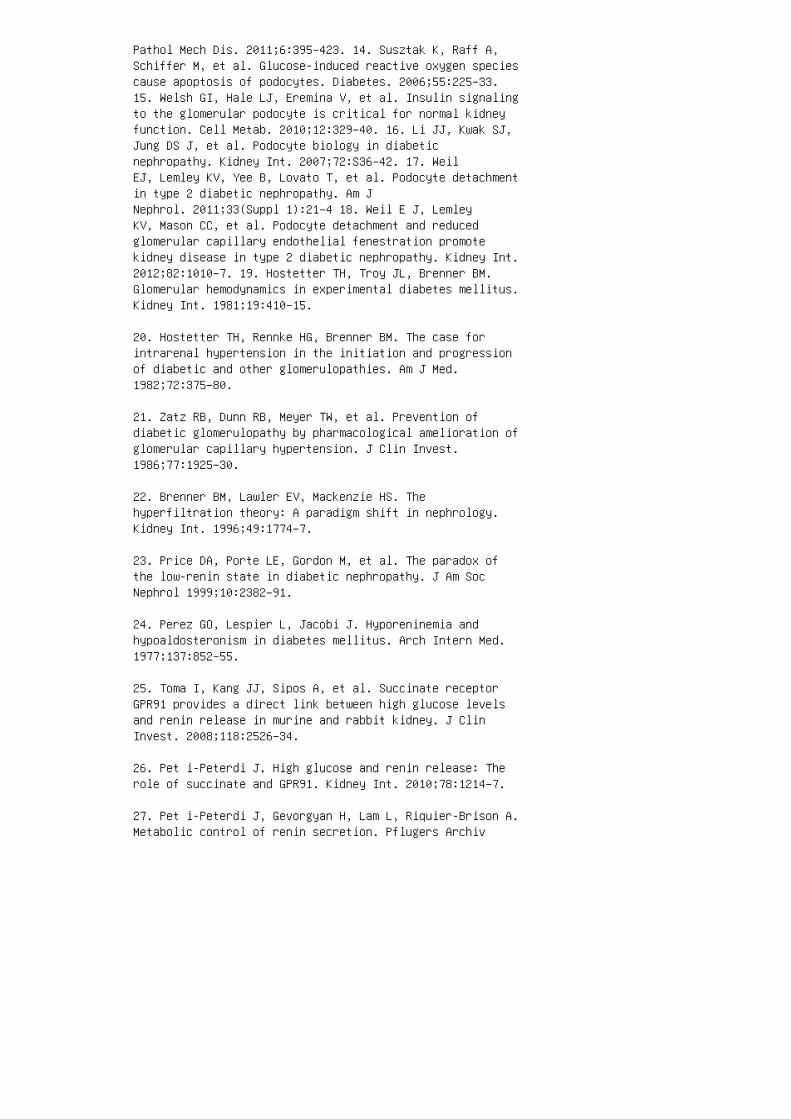
Pathol Mech Dis. 2011;6:395–423. 14. Susztak K, Raff A,Schiffer M, et al. Glucose-induced reactive oxygen speciescause apoptosis of podocytes. Diabetes. 2006;55:225–33.15. Welsh GI, Hale LJ, Eremina V, et al. Insulin signalingto the glomerular podocyte is critical for normal kidneyfunction. Cell Metab. 2010;12:329–40. 16. Li JJ, Kwak SJ,Jung DS J, et al. Podocyte biology in diabeticnephropathy. Kidney Int. 2007;72:S36–42. 17. WeilEJ, Lemley KV, Yee B, Lovato T, et al. Podocyte detachmentin type 2 diabetic nephropathy. Am JNephrol. 2011;33(Suppl 1):21–4 18. Weil E J, LemleyKV, Mason CC, et al. Podocyte detachment and reducedglomerular capillary endothelial fenestration promotekidney disease in type 2 diabetic nephropathy. Kidney Int.2012;82:1010–7. 19. Hostetter TH, Troy JL, Brenner BM.Glomerular hemodynamics in experimental diabetes mellitus.Kidney Int. 1981;19:410–15.
20. Hostetter TH, Rennke HG, Brenner BM. The case forintrarenal hypertension in the initiation and progressionof diabetic and other glomerulopathies. Am J Med.1982;72:375–80.
21. Zatz RB, Dunn RB, Meyer TW, et al. Prevention ofdiabetic glomerulopathy by pharmacological amelioration ofglomerular capillary hypertension. J Clin Invest.1986;77:1925–30.
22. Brenner BM, Lawler EV, Mackenzie HS. Thehyperfiltration theory: A paradigm shift in nephrology.Kidney Int. 1996;49:1774–7.
23. Price DA, Porte LE, Gordon M, et al. The paradox ofthe low-renin state in diabetic nephropathy. J Am SocNephrol 1999;10:2382–91.
24. Perez GO, Lespier L, Jacobi J. Hyporeninemia andhypoaldosteronism in diabetes mellitus. Arch Intern Med.1977;137:852–55.
25. Toma I, Kang JJ, Sipos A, et al. Succinate receptorGPR91 provides a direct link between high glucose levelsand renin release in murine and rabbit kidney. J ClinInvest. 2008;118:2526–34.
26. Pet i-Peterdi J. High glucose and renin release: Therole of succinate and GPR91. Kidney Int. 2010;78:1214–7.
27. Pet i-Peterdi J, Gevorgyan H, Lam L, Riquier-Brison A.Metabolic control of renin secretion. Pflugers Archiv
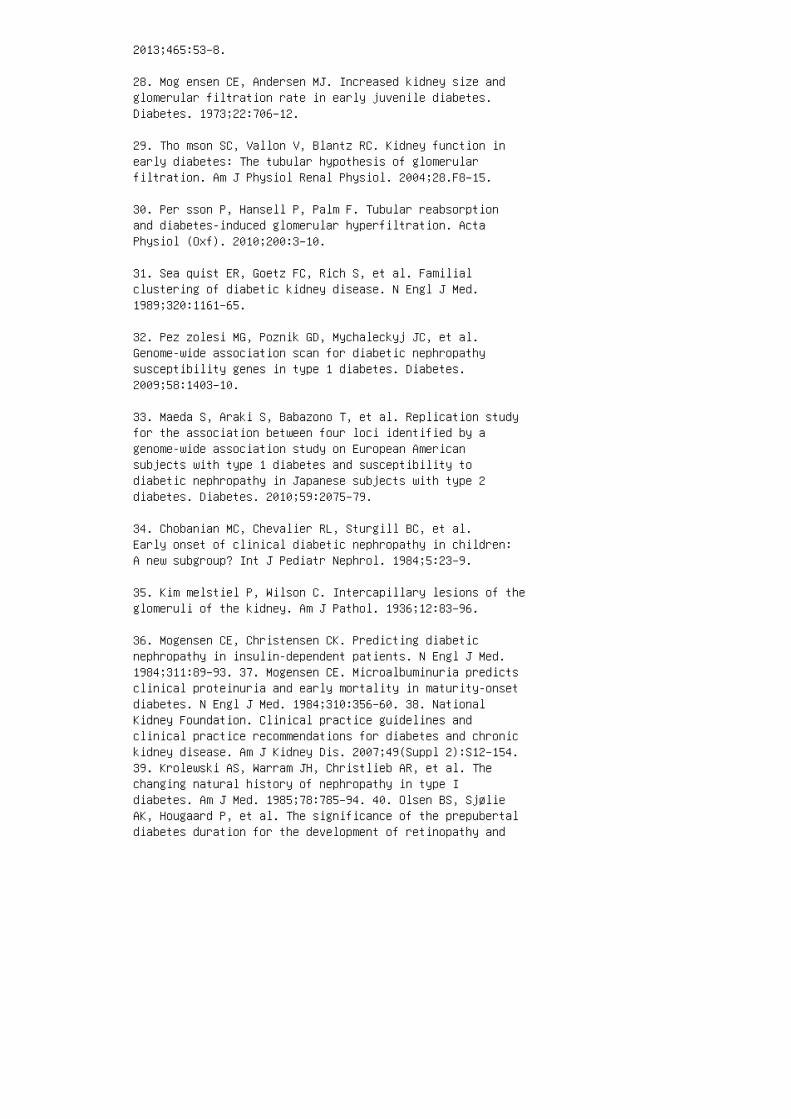
2013;465:53–8.
28. Mog ensen CE, Andersen MJ. Increased kidney size andglomerular filtration rate in early juvenile diabetes.Diabetes. 1973;22:706–12.
29. Tho mson SC, Vallon V, Blantz RC. Kidney function inearly diabetes: The tubular hypothesis of glomerularfiltration. Am J Physiol Renal Physiol. 2004;28.F8–15.
30. Per sson P, Hansell P, Palm F. Tubular reabsorptionand diabetes-induced glomerular hyperfiltration. ActaPhysiol (Oxf). 2010;200:3–10.
31. Sea quist ER, Goetz FC, Rich S, et al. Familialclustering of diabetic kidney disease. N Engl J Med.1989;320:1161–65.
32. Pez zolesi MG, Poznik GD, Mychaleckyj JC, et al.Genome-wide association scan for diabetic nephropathysusceptibility genes in type 1 diabetes. Diabetes.2009;58:1403–10.
33. Maeda S, Araki S, Babazono T, et al. Replication studyfor the association between four loci identified by agenome-wide association study on European Americansubjects with type 1 diabetes and susceptibility todiabetic nephropathy in Japanese subjects with type 2diabetes. Diabetes. 2010;59:2075–79.
34. Chobanian MC, Chevalier RL, Sturgill BC, et al.Early onset of clinical diabetic nephropathy in children:A new subgroup? Int J Pediatr Nephrol. 1984;5:23–9.
35. Kim melstiel P, Wilson C. Intercapillary lesions of theglomeruli of the kidney. Am J Pathol. 1936;12:83–96.
36. Mogensen CE, Christensen CK. Predicting diabeticnephropathy in insulin-dependent patients. N Engl J Med.1984;311:89–93. 37. Mogensen CE. Microalbuminuria predictsclinical proteinuria and early mortality in maturity-onsetdiabetes. N Engl J Med. 1984;310:356–60. 38. NationalKidney Foundation. Clinical practice guidelines andclinical practice recommendations for diabetes and chronickidney disease. Am J Kidney Dis. 2007;49(Suppl 2):S12–154.39. Krolewski AS, Warram JH, Christlieb AR, et al. Thechanging natural history of nephropathy in type Idiabetes. Am J Med. 1985;78:785–94. 40. Olsen BS, SjølieAK, Hougaard P, et al. The significance of the prepubertaldiabetes duration for the development of retinopathy and
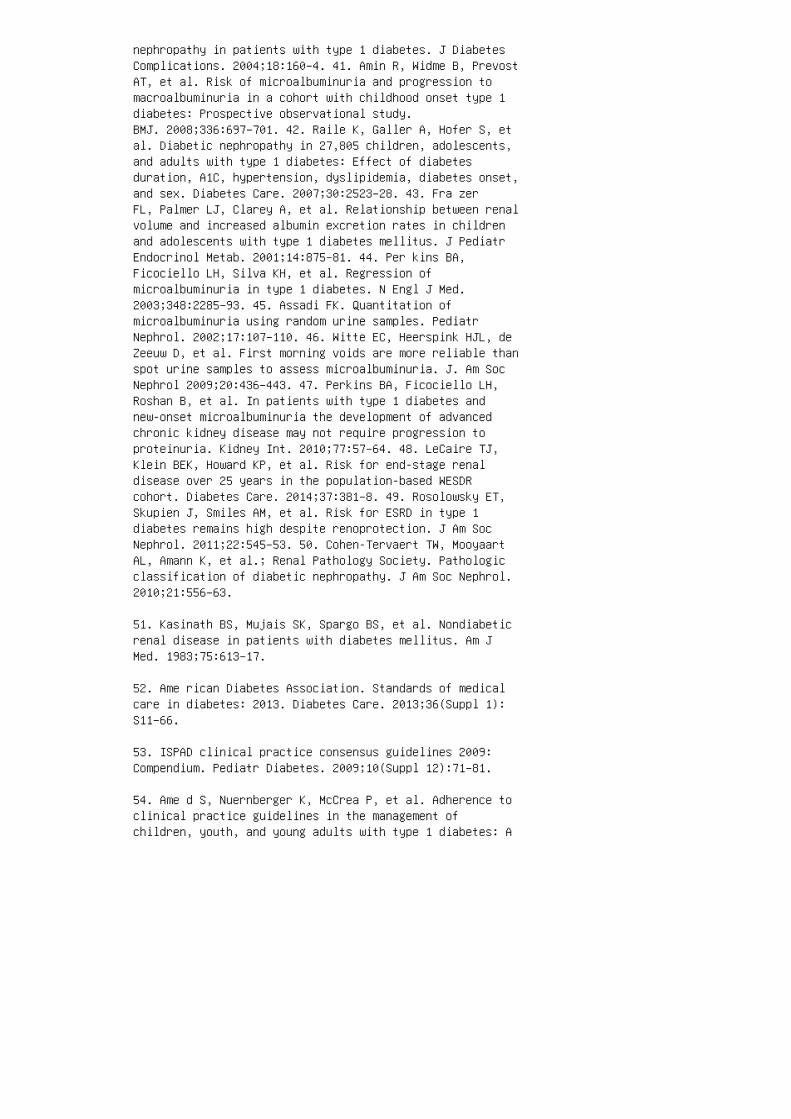
nephropathy in patients with type 1 diabetes. J DiabetesComplications. 2004;18:160–4. 41. Amin R, Widme B, PrevostAT, et al. Risk of microalbuminuria and progression tomacroalbuminuria in a cohort with childhood onset type 1diabetes: Prospective observational study.BMJ. 2008;336:697–701. 42. Raile K, Galler A, Hofer S, etal. Diabetic nephropathy in 27,805 children, adolescents,and adults with type 1 diabetes: Effect of diabetesduration, A1C, hypertension, dyslipidemia, diabetes onset,and sex. Diabetes Care. 2007;30:2523–28. 43. Fra zerFL, Palmer LJ, Clarey A, et al. Relationship between renalvolume and increased albumin excretion rates in childrenand adolescents with type 1 diabetes mellitus. J PediatrEndocrinol Metab. 2001;14:875–81. 44. Per kins BA,Ficociello LH, Silva KH, et al. Regression ofmicroalbuminuria in type 1 diabetes. N Engl J Med.2003;348:2285–93. 45. Assadi FK. Quantitation ofmicroalbuminuria using random urine samples. PediatrNephrol. 2002;17:107–110. 46. Witte EC, Heerspink HJL, deZeeuw D, et al. First morning voids are more reliable thanspot urine samples to assess microalbuminuria. J. Am SocNephrol 2009;20:436–443. 47. Perkins BA, Ficociello LH,Roshan B, et al. In patients with type 1 diabetes andnew-onset microalbuminuria the development of advancedchronic kidney disease may not require progression toproteinuria. Kidney Int. 2010;77:57–64. 48. LeCaire TJ,Klein BEK, Howard KP, et al. Risk for end-stage renaldisease over 25 years in the population-based WESDRcohort. Diabetes Care. 2014;37:381–8. 49. Rosolowsky ET,Skupien J, Smiles AM, et al. Risk for ESRD in type 1diabetes remains high despite renoprotection. J Am SocNephrol. 2011;22:545–53. 50. Cohen-Tervaert TW, MooyaartAL, Amann K, et al.; Renal Pathology Society. Pathologicclassification of diabetic nephropathy. J Am Soc Nephrol.2010;21:556–63.
51. Kasinath BS, Mujais SK, Spargo BS, et al. Nondiabeticrenal disease in patients with diabetes mellitus. Am JMed. 1983;75:613–17.
52. Ame rican Diabetes Association. Standards of medicalcare in diabetes: 2013. Diabetes Care. 2013;36(Suppl 1):S11–66.
53. ISPAD clinical practice consensus guidelines 2009:Compendium. Pediatr Diabetes. 2009;10(Suppl 12):71–81.
54. Ame d S, Nuernberger K, McCrea P, et al. Adherence toclinical practice guidelines in the management ofchildren, youth, and young adults with type 1 diabetes: A
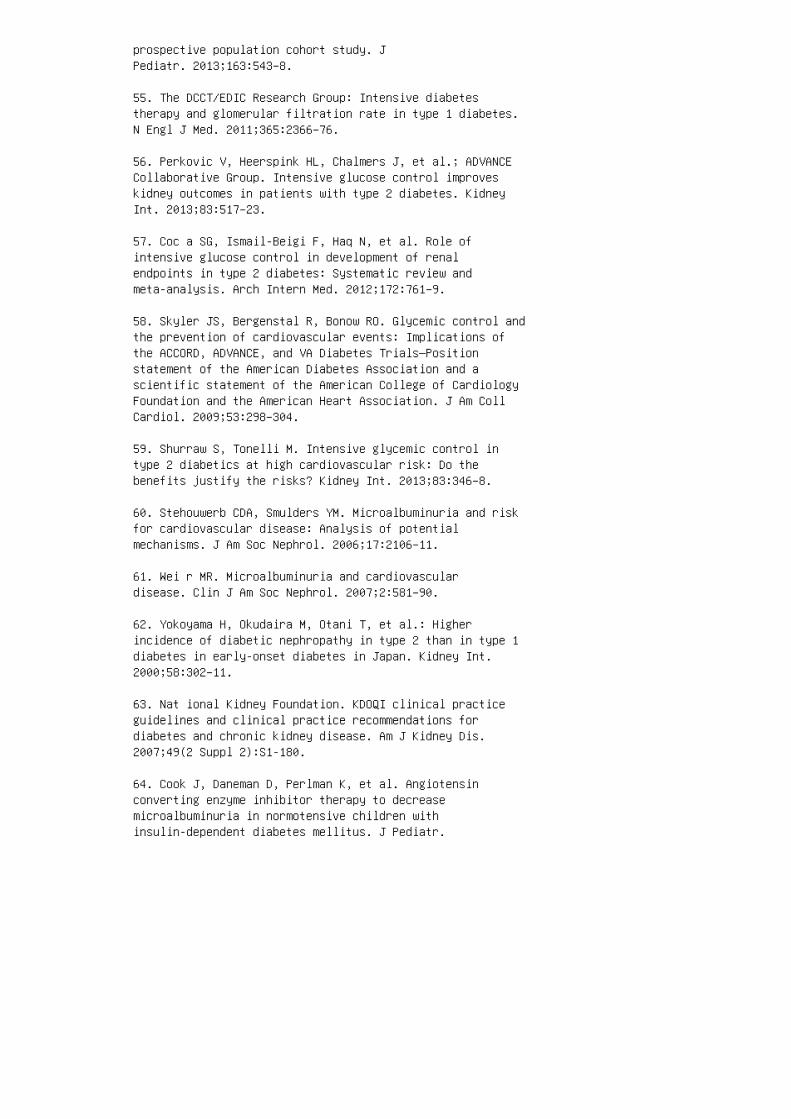
prospective population cohort study. JPediatr. 2013;163:543–8.
55. The DCCT/EDIC Research Group: Intensive diabetestherapy and glomerular filtration rate in type 1 diabetes.N Engl J Med. 2011;365:2366–76.
56. Perkovic V, Heerspink HL, Chalmers J, et al.; ADVANCECollaborative Group. Intensive glucose control improveskidney outcomes in patients with type 2 diabetes. KidneyInt. 2013;83:517–23.
57. Coc a SG, Ismail-Beigi F, Haq N, et al. Role ofintensive glucose control in development of renalendpoints in type 2 diabetes: Systematic review andmeta-analysis. Arch Intern Med. 2012;172:761–9.
58. Skyler JS, Bergenstal R, Bonow RO. Glycemic control andthe prevention of cardiovascular events: Implications ofthe ACCORD, ADVANCE, and VA Diabetes Trials—Positionstatement of the American Diabetes Association and ascientific statement of the American College of CardiologyFoundation and the American Heart Association. J Am CollCardiol. 2009;53:298–304.
59. Shurraw S, Tonelli M. Intensive glycemic control intype 2 diabetics at high cardiovascular risk: Do thebenefits justify the risks? Kidney Int. 2013;83:346–8.
60. Stehouwerb CDA, Smulders YM. Microalbuminuria and riskfor cardiovascular disease: Analysis of potentialmechanisms. J Am Soc Nephrol. 2006;17:2106–11.
61. Wei r MR. Microalbuminuria and cardiovasculardisease. Clin J Am Soc Nephrol. 2007;2:581–90.
62. Yokoyama H, Okudaira M, Otani T, et al.: Higherincidence of diabetic nephropathy in type 2 than in type 1diabetes in early-onset diabetes in Japan. Kidney Int.2000;58:302–11.
63. Nat ional Kidney Foundation. KDOQI clinical practiceguidelines and clinical practice recommendations fordiabetes and chronic kidney disease. Am J Kidney Dis.2007;49(2 Suppl 2):S1-180.
64. Cook J, Daneman D, Perlman K, et al. Angiotensinconverting enzyme inhibitor therapy to decreasemicroalbuminuria in normotensive children withinsulin-dependent diabetes mellitus. J Pediatr.
1990;117:39–45. 65. EUCLID Study Group. Randomisedplacebocontrolled trial of lisinopril in normotensivepatients with insulin dependent diabetes andnormoalbuminuria or microalbuminuria. Lancet.1997;349:1787–92. 66. ACE I nhibitors in DiabeticNephropathy Trialist Group. Should all patients with type1 diabetes mellitus and microalbuminuria receiveangiotensin-converting enzyme inhibitors? A metaanalysis ofindividual patient data. Ann Intern Med. 2001;134:370–9.67. Par ving H-H, Hommel E, Jensen BR, et al. Longtermbeneficial effect of ACE inhibition on diabeticnephropathy in normotensive type 1 diabetic patients.Kidney Int. 2001;60:228–34. 68. Brenner BM, Cooper ME, deZeeuw D, et al. Effects of losartan on renal andcardiovascular outcomes in patients with type 2 diabetesand nephropathy. N Engl J Med. 2001;345:861–9. 69. Bilous R, Chaturvedi N, Sjolie AK, et al. Effect ofcandesartan on microalbuminuria and albumin excretion ratein diabetes: Three randomized trials. Ann Intern Med.2009;151:11–20. 70. Mau er M, Zinman B, Gardiner R, et al.Renal and retinal effects of enalapril and losartan intype 1 diabetes. N Engl J Med. Jul 2 2009;361:40-51 71.Hir st JA, Taylor KS, Stevens RJ, et al. The impact ofrenin–angiotensin–aldosterone system inhibitors on type 1and type 2 diabetic patients with and without earlydiabetic nephropathy. Kidney Int. 2012;81:674–83. 72. National Kidney Foundation. KDOQI clinical practiceguidelines for diabetes and CKD: 2012 Update. Am J KidneyDis. 2012;60:850–86. 73. Jen nings DL, Kalus JS, ColemanCI, et al. Combination therapy with an ACE inhibitor andan angiotensin receptor blocker for diabetic nephropathy:A meta-analysis. Diabet Med. 2007;24:486–93. 74. JuarezGF, Luño J, Barrio V, et al. Effect of dual blockade ofthe renin-angiotensin system on the progression of type 2diabetic nephropathy: A randomized trial. Am J Kidney Dis.2013;61:211–8. 75. Mann JF, Schmieder RE, McQueen M, etal. Renal outcomes with telmisartan, ramipril, or both, inpeople at high vascular risk (the ONTARGET study): Amulticentre, randomised, double-blind, controlledtrial. Lancet. 2009;372:547–53. 76. Fried LF, Emanuele N,Zhang JH, et al. Combined angiotensin inhibition for thetreatment of diabetic nephropathy. N Engl J Med.2013;369:1892–903. 77. Parving H-H, Persson F, Lewis JB,et al.; AVOID Study Investigators. Aliskiren combined withlosartan in type 2 diabetes and nephropathy. N Engl J Med.2008;358:2433–46. 78. Parving H-H, Brenner BM, McMurrayJJV, et al. Cardiorenal end points in a trial of aliskirenfor type 2 diabetes. N Engl J Med. 2012;367:2204–13.
79. U.S. Food and Drug Administration. FDA drug safety
communication: New warning and contraindication for bloodpressure medicines containing aliskiren (Tekturna):4-20-2012. http://www.fda.gov/drugs/drugsafety/ucm300889.htm. Accessed on November 10, 2013.
80. Krolewski AS, Kosinski EJ, Warram JH, et al. Magnitudeand determinants of coronary artery disease injuvenile-onset, insulin-dependent diabetes mellitus. Am JCardiol. 1987;59:750–5.
81. Pre is SR, Hwang SJ, Coady S, et al. Trends in allcauseand cardiovascular disease mortality among women and menwith and without diabetes mellitus in the Framingham HeartStudy, 1950 to 2005. Circulation. 2009;119:1728–35.
82. Rod riguez BL, Fujimoto WY, Mayer-Davis EJ, et al.Prevalence of cardiovascular disease risk factors in U.S.children and adolescents with diabetes: The SEARCH fordiabetes in youth study. Diabetes Care. 2006;29:1891–6.
83. Chr istlieb AR, Warram JH, Krolewski AS, et al.Hypertension: The major risk factor in juvenileonsetinsulin-dependent diabetics. Diabetes. 1981;30(Suppl2):90–6.
84. Ame rican Diabetes Association. Standards of medicalcare in diabetes: 2013. Diabetes Care. 2013;36(Suppl1):S11–66.
85. The A CCORD Study Group: Effects of intensiveblood-pressure control in type 2 diabetes mellitus. N EnglJ Med. 2010;362:1575–85.
86. Arg uedas JA, Leiva V, Wright JM. Blood pressuretargets for hypertension in people with diabetes mellitus.Cochrane Database Syst Rev. 2013;(10)008277.
87. Nos adini R, Tonolo G. Cardiovascular and renalprotection in type 2 diabetes mellitus: The role ofcalcium channel blockers. J Am Soc Nephrol. 2002;13(Suppl3):S216–23.
88. Xu G, Chen J, Jing G, et al. Preventing β-cell loss anddiabetes with calcium channel blockers. Diabetes.2012;61:848–56.
89. Guy J, Ogden L, Wadwa RP, et al.: Lipid and lipoproteinprofiles in youth with and without type 1 diabetes: TheSEARCH for Diabetes in Youth Case-Control Study. DiabetesCare. 2009;32:416–20.

90. Vergès B. Lipid disorders in type 1 diabetes. DiabetesMetab. 35: 353–60, 2009.
91. Kershnar AK, Daniels SR, Imperatore G, et al. Lipidabnormalities are prevalent in youth with type 1 and type2 diabetes: The SEARCH for Diabetes in Youth Study. JPediatr. 2006;149:314–9.
92. Reh C M, Mittelman SD, Wee C-P, et al. A longitudinalassessment of lipids in youth with type 1 diabetes. PediatrDiabetes. 2011:12:365–71.
93. Won g HK, Ong KL, Cheung CL, Utilization of glucose,blood pressure, and lipid lowering medications amongpeople with type II diabetes in the United States,1999-2010. Ann Epidemiol. 2014;24:516–21. 94. Reaven GM.Banting lecture 1988: Role of insulin resistance in humandisease. Diabetes. 1988;37:1595–607. 95. Reaven GM. Roleof insulin resistance in human disease (syndrome X): Anexpanded definition. Annu Rev Med. 1993;44:121-31. 96.Anonymous. Third report of the National CholesterolEducation Program Expert Panel on Detection, Evaluation,and Treatment of High Blood Cholesterol in Adults (AdultTreatment Panel III). NIH Publication No. 02-5215,September 2002. Bethesda, MD: National Institutes ofHealth; 2002. 97. Alb erti KG, Zimmet PZ. Definition,diagnosis and classification of diabetes mellitus and itscomplications. I. Diagnosis and classification of diabetesmellitus provisional report of a WHO consultation. DiabetMed. 1998;15:539–53. 98. Wor ld Health Organization.Report of a WHO consultation: Definition of metabolicsyndrome in definition, diagnosis, and classification ofdiabetes mellitus and its complications. I. Diagnosis andclassification of diabetes mellitus. Geneva: World HealthOrganization, Department of Noncommunicable DiseaseSurveillance; 1999. 99. Steinberger J, Daniels SR, EckelRH, et al. Progress and challenges in metabolic syndromein children and adolescents. Circulation. 2009;119:628–47.100. Fox CS, Massaro JM, Hoffmann U, et al. Abdominalvisceral and subcutaneous adipose tissue compartments.association with metabolic risk factors in the FraminghamHeart Study. Circulation. 2007;116:39–48. 101. Kuba V M,Leone C, Damiani D. Is waist-to-height ratio a usefulindicator of cardio-metabolic risk in 6-10-year-oldchildren? BMC Pediatr. 2013,13:91. 102. Alberti KG, EckelRH, Grundy SM, et al. Harmonizing the metabolic syndrome:A joint interim statement of the International DiabetesFederation Task Force on Epidemiology and Prevention;National Heart, Lung, and Blood Institute; American Heart

Association; World Heart Federation; InternationalAtherosclerosis Society; and International Association forthe Study of Obesity. Circulation. 2009;120:1640–5. 103.Cook S, Weitzman M, Auinger P, et al. Prevalence of ametabolic syndrome phenotype in adolescents: Findings fromthe third National Health and Nutrition ExaminationSurvey, 1988-1994. Arch Pediatr Adolesc Med.2003;157:821–7. 104. Wei ss R, Dziura J, Burgert TS, etal. Obesity and the metabolic syndrome in children andadolescents. N Engl J Med. 2004;350:2362–74. 105.Bosy-Westphal A, Onur S, Geisler C, et al. Common familialinfluences on clustering of metabolic syndrome traits withcentral obesity and insulin resistance: The Kiel obesityprevention study. Int J Obes (Lond). 2007;31:784–90.
106. Cameron AJ, Shaw JE, Zimmet PZ. The metabolicsyndrome: Prevalence in worldwide populations. EndocrinolMetab Clin North Am. 2004;33:351–75.
107. van D ongen J, Willemsen G, Chen WM, et al.Heritability of metabolic syndrome traits in a largepopulation-based sample. J Lipid Res. 2013;54:2914–23.
108. Povel CM, Boer JM, Reiling E, Feskens EJ. Geneticvariants and the metabolic syndrome: A systematic review.Obes Rev. 2011;12:952–67.
109. Mon da KL, North KE, Hunt SC, et al. The genetics ofobesity and the metabolic syndrome. Endocr Metab ImmuneDisord Drug Targets. 2010;10:86–108.
110. Sjögren M, Lyssenko V, Jonsson A, et al. The searchfor putative unifying genetic factors for components of themetabolic syndrome. Diabetologia. 2008;51:2242–51.
111. Parker VE, Semple RK. Genetics in endocrinology:Genetic forms of severe insulin resistance: Whatendocrinologists should know. Eur J Endocrinol.20131;169:R71–80.
112. Ever ard A, Cani PD. Diabetes, obesity and gutmicrobiota. Best Pract Res Clin Gastroenterol.2013;27:73–83.
113. Wis se BE. The inflammatory syndrome: The role ofadipose tissue cytokines in metabolic disorders linked toobesity. J Am Soc Nephrol. 2004;15:2792–800.
114. Stu mvoll M, Goldstein BJ, van Haeften TW. Type 2diabetes: Principles of pathogenesis and therapy. Lancet.

2005;365:1333–46.
115. Mie tus-Snyder M, Krauss RM. Lipid metabolism inchildren and adolescents: Impact on vascular biology. JClin Lipidol. 2008;2:127–37.
116. Riccardi G. Dietary treatment of the metabolicsyndrome: The optimal diet. Br J Nutr. 2000;83(Suppl1):S143–8.
117. Huth PJ, Fulgoni VL 3rd, Keast DR, et al. Major foodsources of calories, added sugars, and saturated fat andtheir contribution to essential nutrient intakes in theU.S. diet: Data from the National Health and NutritionExamination Survey (2003-2006). Nutr J. 2013;12:116. doi10.1186/1475-2891-12-116.
118. Huffman MD, Capewell S, Ning H, et al. Cardiovascularhealth behavior and health factor changes (1988-2008) andprojections to 2020: Results from the National Health andNutrition Examination Surveys. Circulation.2012;125:2595–602.
119. Bre mer AA, Mietus-Snyder M, Lustig RH. Toward aunifying hypothesis of metabolic syndrome. Pediatrics.2012;129:557–70.
120. Bays HE. Is “sick fat” a cardiovascular disease?Stateof-the-art paper. J Am Coll Cardiol. 2011;57:2461–73.
121. Kam bham N, Markowitz G, Valeri A, et al.Obesityrelated glomerulopathy: An emerging epidemic.Kidney Int. 59:1498–509, 200. 122. Cohen AH. Massiveobesity and the kidney: A morphologic and statisticalstudy. Am J Pathol. 1975;81:117–30. 123. Hsu CY,McCulloch CE, Iribarren C, et al.: Body mass index andrisk for end-stage renal disease. Ann Intern Med.2006;144:21–8. 124. Serra A, Romero R, Lopez D, et al.Renal injury in the extremely obese patients with normalrenal function. Kidney Int. 2008;73:947–55. 125. AdelmanRD, Restaino IG, Alon US, Blowey DL. Proteinuria and focalsegmental glomerulosclerosis in severely obeseadolescents. J Pediatr. 2001;138:481–5. 126. She n WW,Chen HM, Chen H, et al. Obesity-related glomerulopathy:Body mass index and proteinuria. Clin J Am Soc Nephrol.2010;5:1401–9. 127. Goumenos DS, Kawar B, El Nahas M, etal. Early histological changes in the kidney of peoplewith morbid obesity. Nephrol Dial Transplant.2009;24:3732–8. 128. Hayde n MR, Sowers JR.Childhood-adolescent obesity in the cardiorenal syndrome:

Lessons from animal models. Cardiorenal Med. 2011;1:75–86.129. Che n HM, Li SJ, Chen HP, et al. Obesity-relatedglomerulopathy in China: A case series of 90 patients. AmJ Kidney Dis. 2008;52:58–65. 130. Danilewicz M,Wagrowska-Danielwicz M. Morphometric andimmunohistochemical insight into focal segmentalglomerulosclerosis in obese and non-obese patients.Nefrologia 2009;29:35–41. 131. Dar ouich S, Goucha R,Jaafoura MH, et al. Clinicopathological characteristics ofobesity-associated focal segmental glomerulosclerosis.Ultrastruct Pathol. 2011;35:176–2. 132. Orc hard TJ,Temprosa M, Goldberg R, et al. The effect of metformin andintensive lifestyle intervention on the metabolic syndrome:The Diabetes Prevention Program randomized trial. AnnIntern Med. 2005;142:611–9. 133. Knowler WC,Barrett-Connor E, Fowler SE, et al. Reduction in theincidence of type 2 diabetes with lifestyle interventionor metformin. N Engl J Med. 2002;346:393–403. 134. JensenDE, Nguo K, Baxter KA, et al. Fasting gut hormone levelschange with modest weight loss in obese adolescents.Pediatr Obes. 2015, doi: 10.1111/ijpo.275. 135. RojasLBA, Gomes MB. Metformin: An old but still the besttreatment for type 2 diabetes. Diabetol Metab Syndr.2013;5:6. 136. God arzi MO, Brier-Ash M. Metforminrevisited: Re-evaluation of its properties and role in thepharmacopoeia of modern antidiabetic agents. Diabetes ObesMetab. 2005;6:654–65. 137. Mogul HR, Freeman R, Nguyen K,et al. Carbohydrate modified diet & insulin sensitizersreduce body weight & modulate metabolic syndrome measuresin EMPOWIR (enhance the metabolic profile of women withinsulin resistance): A randomized trial of normoglycemicwomen with midlife weight gain. PLoS One. 2014;9:e108264.doi 10.1371/journal.pone.0108264.
138. Sharma AM. Is there a rationale for angiotensinblockade in the management of obesity hypertension?Hypertension. 2004;44:12–9.
139. Sattar N, Preiss D, Murray HM, et al. Statins and riskof incident diabetes: A collaborative meta-analysis ofrandomized statin trials. Lancet. 2010; 375:735–42.
140. Eil and LS, Luttrell PK. Use of statins fordyslipidemia in the pediatric population. J PediatrPharmacol Ther. 2010;15:160–72.
141. Expert Panel on Integrated Guidelines forCardiovascular Health and Risk Reduction in Children andAdolescents. Summary report. Pediatrics. 2011;128(Suppl5):S213–56.

142. Ejerblad E, Fored CM, Lindblad P, et al. Obesity andrisk for chronic renal failure. J Am Soc Nephrol.2006;17:1695–702.
REVIEW QUESTIONS
1. In the pediatric age group (up to 19 years), diabetesmellitus accounts for ESRD in: a. 10% to 15% b. 20% to50% c. >1% d. >10%
2. Advanced glycation products result from nonenzymaticreaction of glucose with proteins, lipids, and nucleicacids. a. True b. False
3. Podocyes lack insulin receptors. a. True b. False
4. Renin-angiotensin induces glomerular injury in diabeticnephropathy by: a. Systemic hypertension b. Glomerularhypertension c. Increasing podocyte apoptosis d.Increasing tubular sodium concentration and inducingtubuloglomerular feedback
5. The classic pathologic lesion in diabetic nephropathyis: a. Kimmelstiel-Wilson lesion b. Large glomeruli(glomerulomegaly) c. Focal segmental glomerulosclerosisd. Wire loop lesion
6. The la tent phase of diabetic nephropathy in diabetesmellitus type 1 lasts: a. <5 yea rs b. 5 to 10 y ears c.10 to 1 5 years d. 30 to 4 0 years 7. Microalbuminuria ina diabetic 17-year-old girl is best tested in a: a.Random sample obtained in any time b. Random sampleobtained late in the afternoon c. First morning urinesample d. Random sample obtained after ambulating for 4hours 8. Microalbuminuria in a patient with diabetesmellitus type 1 indicates: a. Early diabetic nephropathyb. No clinical significance c. Onset of ESRD d.Development of Kimmelstiel-Wilson lesion 9. A 25-year-oldman with onset of diabetes mellitus at 3 years of age hadbeen lost to follow-up in nephrology for 3 years. He hadsporadic visits with his internist and endocrinologist.Upon his return to the nephrology clinic, his estimatedGFR was 100 mL/min/1.73 m 2 , and he now haswell-documented microalbuminuria and his hemoglobin A1cwas 11.5%. His previous known GFR, obtained 3 years ago,was 135 mL/min/1.73 m 2 . Which of the following bestreflects diabetic nephropathy in this patient? a. Hisdisease has not progressed, because he has a normal GFR.b. He is now cured of diabetic nephropathy, because he
does not have hyperfiltration c. Microalbuminuria inpresence of normal GFR has no clinical significance. d.His renal disease has progressed, because he now hasalbuminuria and his GFR has should be considered to havedeclined from a state of hyperfiltration to “normal.” 10.Which of the following statements best characterizes theuse of angiotensin-converting enzyme inhibitors indiabetic nephropathy? a. ACEIs are ideally started at thetime of the diagnosis of diabetes mellitus to preventdevelopment of microalbuminuria. b. Evidence to suggestthat ACEIs prevent development of microalbuminuria islacking. c. ACEIs improve diabetes control. d. ACEIsprevent progression of microalbuminuria. 11. The centralfindings of metabolic syndrome are: a. Insulin resistanceand hyperglycemia b. Hypertension c. Obesity withincreased waist circumference d. Dyslipidemia e.Microabluminuria f. All of the above g. Only a, b, and e12. Obesity and metabolic syndrome are characterized bymolecular markers of systemic inflammation. a. True. b.False.
13. Renal pathologic findings in obesity and metabolicsyndrome characteristically demonstrate: a.Glomerulomegaly (large glomeruli) b. FSGS with lesspronounced morphologic changes c. Basement membranethickening d. Lesser degree of foot-process fusion e. Allof the above f. Only a, b, and d
ANSWER KEY
1. d
2. a 3. b 4. b 5. a 6. c 7. c 8. a 9. d 10. d 11.f 12. a 13. e
29 Kidney in viral infections
4. Strauss J, Abitbol C, Zilleruelo G, et al. Renal diseasein children with the acquired immunodeficiency syndrome. NEngl J Med. 1989;321:625–30.
5. Con nor E, Gupta S, Joshi V, et al. Acquiredimmunodeficiency syndrome-associated renal disease inchildren. J Pediatr. 1988;113:39–44.
6. Kopp JB. Renal dysfunction in HIV-1-infected patients.Curr Infect Dis Rep. 2002;4:449–60.
7. Ross MJ, Klotman PE. Recent progress in HIVassociatednephropathy. J Am Soc Nephrol. 2002;13:2997–3004.
8. Herman ES, Klotman PE. HIV-associated nephropathy:Epidemiology, pathogenesis, and treatment. Semin Nephrol.2003;23:200–8.
9. Kimmel PL, Barisoni L, Kopp JB. Pathogenesis andtreatment of HIV-associated renal diseases: Lessons fromclinical and animal studies, molecular pathologiccorrelations, and genetic investigations. Ann Intern Med.2003;139:214–26.
10. Weiner NJ, Goodman JW, Kimmel PL. The HIVassociatedrenal diseases: Current insight into pathogenesis andtreatment. Kidney Int. 2003;63:1618–31.
11. Winston JA, Bruggeman LA, Ross MD, et al. Nephropathyand establishment of a renal reservoir of HIV type 1during primary infection. N Engl J Med. 2001;344:1979–84.
12. Abbott KC, Hypolite I, Welch PG, et al. Humanimmunodeficiency virus/acquired immunodeficiencysyndrome-associated nephropathy at end-stage renal diseasein the United States: Patient characteristics and survivalin the pre highly active antiretroviral therapy era. JNephrol. 2001;14:377–83.
13. Freedman BI, Soucie JM, Stone SM, et al. Familialclustering of end-stage renal disease in blacks withHIV-associated nephropathy. Am J Kidney Dis.1999;34:254–8.
14. Kopp JB, Winkler C. HIV-associated nephropathy inAfrican Americans. Kidney Int Suppl. 2003;63(Suppl83):S43–9.
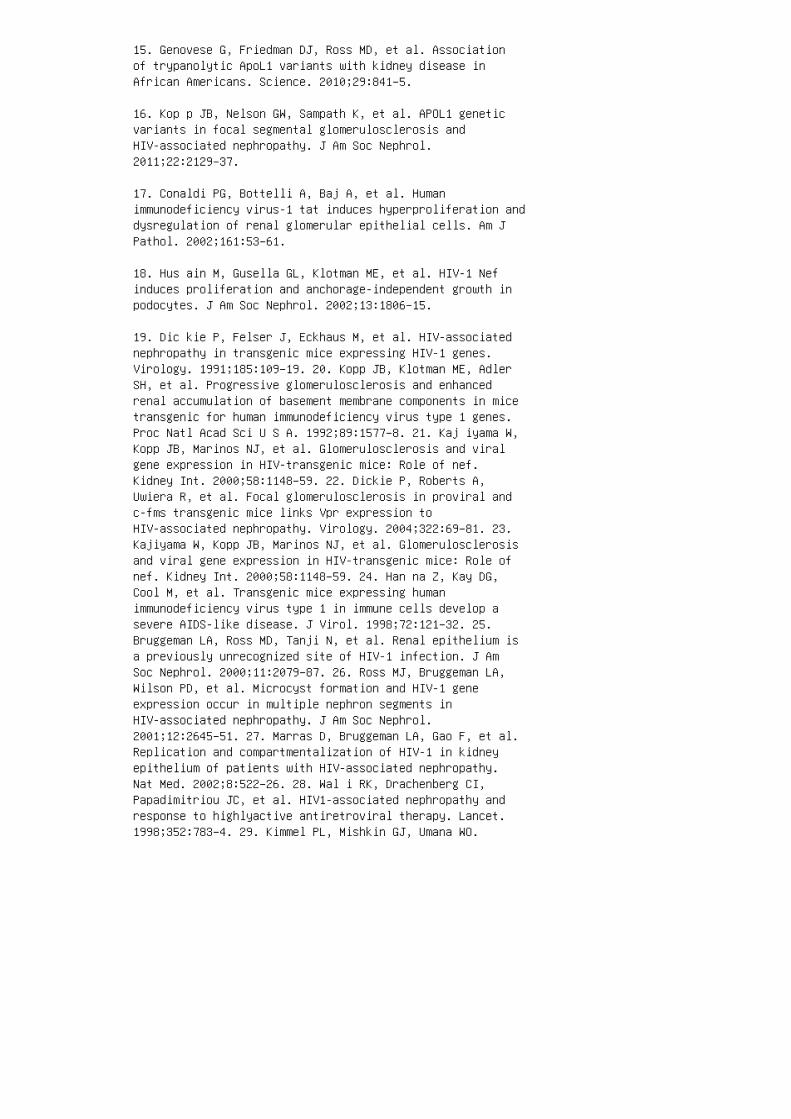
15. Genovese G, Friedman DJ, Ross MD, et al. Associationof trypanolytic ApoL1 variants with kidney disease inAfrican Americans. Science. 2010;29:841–5.
16. Kop p JB, Nelson GW, Sampath K, et al. APOL1 geneticvariants in focal segmental glomerulosclerosis andHIV-associated nephropathy. J Am Soc Nephrol.2011;22:2129–37.
17. Conaldi PG, Bottelli A, Baj A, et al. Humanimmunodeficiency virus-1 tat induces hyperproliferation anddysregulation of renal glomerular epithelial cells. Am JPathol. 2002;161:53–61.
18. Hus ain M, Gusella GL, Klotman ME, et al. HIV-1 Nefinduces proliferation and anchorage-independent growth inpodocytes. J Am Soc Nephrol. 2002;13:1806–15.
19. Dic kie P, Felser J, Eckhaus M, et al. HIV-associatednephropathy in transgenic mice expressing HIV-1 genes.Virology. 1991;185:109–19. 20. Kopp JB, Klotman ME, AdlerSH, et al. Progressive glomerulosclerosis and enhancedrenal accumulation of basement membrane components in micetransgenic for human immunodeficiency virus type 1 genes.Proc Natl Acad Sci U S A. 1992;89:1577–8. 21. Kaj iyama W,Kopp JB, Marinos NJ, et al. Glomerulosclerosis and viralgene expression in HIV-transgenic mice: Role of nef.Kidney Int. 2000;58:1148–59. 22. Dickie P, Roberts A,Uwiera R, et al. Focal glomerulosclerosis in proviral andc-fms transgenic mice links Vpr expression toHIV-associated nephropathy. Virology. 2004;322:69–81. 23.Kajiyama W, Kopp JB, Marinos NJ, et al. Glomerulosclerosisand viral gene expression in HIV-transgenic mice: Role ofnef. Kidney Int. 2000;58:1148–59. 24. Han na Z, Kay DG,Cool M, et al. Transgenic mice expressing humanimmunodeficiency virus type 1 in immune cells develop asevere AIDS-like disease. J Virol. 1998;72:121–32. 25.Bruggeman LA, Ross MD, Tanji N, et al. Renal epithelium isa previously unrecognized site of HIV-1 infection. J AmSoc Nephrol. 2000;11:2079–87. 26. Ross MJ, Bruggeman LA,Wilson PD, et al. Microcyst formation and HIV-1 geneexpression occur in multiple nephron segments inHIV-associated nephropathy. J Am Soc Nephrol.2001;12:2645–51. 27. Marras D, Bruggeman LA, Gao F, et al.Replication and compartmentalization of HIV-1 in kidneyepithelium of patients with HIV-associated nephropathy.Nat Med. 2002;8:522–26. 28. Wal i RK, Drachenberg CI,Papadimitriou JC, et al. HIV1-associated nephropathy andresponse to highlyactive antiretroviral therapy. Lancet.1998;352:783–4. 29. Kimmel PL, Mishkin GJ, Umana WO.

Captopril and renal survival in patients with humanimmunodeficiency virus nephropathy. Am J Kidney Dis.1996;28:202–08. 30. Burns GC, Paul SK, Toth IR, et al.Effect of angiotensin-converting enzyme inhibition inHIV-associated nephropathy. J Am Soc Nephrol.1997;8:1140–6. 31. Smith MC, Austen JL, Carey JT, et al.Prednisone improves renal function and proteinuria inhuman immunodeficiency virus-associated nephropathy. Am JMed. 1996;101:41–8. 32. Eustace JA, Nuermberger E, Choi M,et al. Cohort study of the treatment of severeHIV-associated nephropathy with corticosteroids. KidneyInt. 2000;58:1253–60. 33. Navarrete JE, Pastan S. Effectof highly active antiretroviral treatment and prednisonein biopsyproven HIV-associated nephropathy (abstract). J AmSoc Nephrol. 2000;11:93A. 34. Ingulli E, Tejani A, FikrigS, et al. Nephrotic syndrome associated with acquiredimmunodeficiency syndrome in children. J Pediatr.1991;119:710–16.
35. Nelson PJ, Gelman IH, Klotman PE. Suppression of HIV-1expression by inhibitors of cyclin-dependent kinasespromotes differentiation of infected podocytes. J Am SocNephrol. 2001;12:2827–31.
36. Gherardi D, D’Agati V, Chu TH, et al. Reversal ofcollapsing glomerulopathy in mice with the cyclindependentkinase inhibitor CYC202. J Am Soc Nephrol.2004;15:1212–22.
37. Ratnam KK, Feng X, Chuang PY, et al. Role of theretinoic acid receptor-α in HIV-associated nephropathy.Kidney Int. 2011;79:624–34.
38. Sharma M, Magenheimer LK, Home T, et al. Inhibition ofNotch pathway attenuates the progression of humanimmunodeficiency virus-associated nephropathy. Am J PhysiolRenal Physiol. 2013;304:F1127–36.
39. Kimmel PL, Phillips TM, Ferreira-Centeno A, et al.Brief report: Idiotypic IgA nephropathy in patients withhuman immunodeficiency virus infection. N Engl J Med.1992;327:702–6.
40. Mat tana J, Siegal FP, Schwarzwald E, et al.AIDSassociated membranous nephropathy with advanced renalfailure: Response to prednisone. Am J Kidney Dis.1997;30:116–9.
41. Ala rcon-Zurita A, Salas A, Anton E, et al. Membranousglomerulonephritis with nephrotic syndrome in a HIV
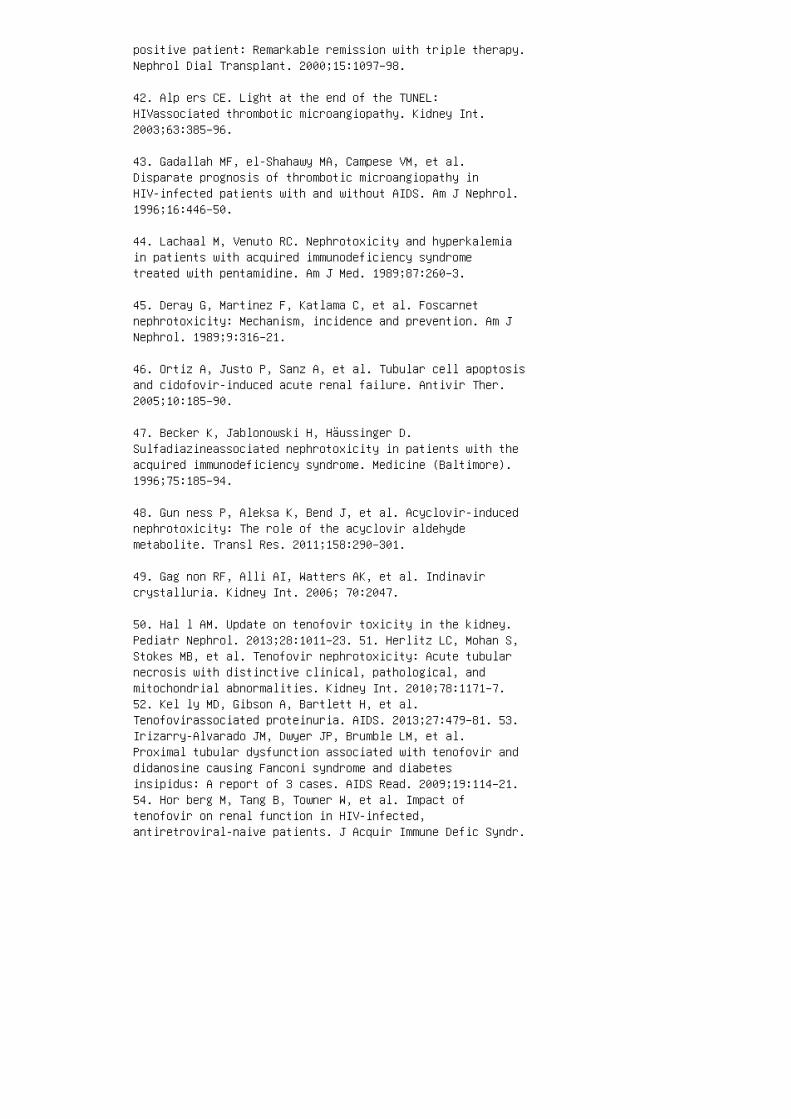
positive patient: Remarkable remission with triple therapy.Nephrol Dial Transplant. 2000;15:1097–98.
42. Alp ers CE. Light at the end of the TUNEL:HIVassociated thrombotic microangiopathy. Kidney Int.2003;63:385–96.
43. Gadallah MF, el-Shahawy MA, Campese VM, et al.Disparate prognosis of thrombotic microangiopathy inHIV-infected patients with and without AIDS. Am J Nephrol.1996;16:446–50.
44. Lachaal M, Venuto RC. Nephrotoxicity and hyperkalemiain patients with acquired immunodeficiency syndrometreated with pentamidine. Am J Med. 1989;87:260–3.
45. Deray G, Martinez F, Katlama C, et al. Foscarnetnephrotoxicity: Mechanism, incidence and prevention. Am JNephrol. 1989;9:316–21.
46. Ortiz A, Justo P, Sanz A, et al. Tubular cell apoptosisand cidofovir-induced acute renal failure. Antivir Ther.2005;10:185–90.
47. Becker K, Jablonowski H, Häussinger D.Sulfadiazineassociated nephrotoxicity in patients with theacquired immunodeficiency syndrome. Medicine (Baltimore).1996;75:185–94.
48. Gun ness P, Aleksa K, Bend J, et al. Acyclovir-inducednephrotoxicity: The role of the acyclovir aldehydemetabolite. Transl Res. 2011;158:290–301.
49. Gag non RF, Alli AI, Watters AK, et al. Indinavircrystalluria. Kidney Int. 2006; 70:2047.
50. Hal l AM. Update on tenofovir toxicity in the kidney.Pediatr Nephrol. 2013;28:1011–23. 51. Herlitz LC, Mohan S,Stokes MB, et al. Tenofovir nephrotoxicity: Acute tubularnecrosis with distinctive clinical, pathological, andmitochondrial abnormalities. Kidney Int. 2010;78:1171–7.52. Kel ly MD, Gibson A, Bartlett H, et al.Tenofovirassociated proteinuria. AIDS. 2013;27:479–81. 53.Irizarry-Alvarado JM, Dwyer JP, Brumble LM, et al.Proximal tubular dysfunction associated with tenofovir anddidanosine causing Fanconi syndrome and diabetesinsipidus: A report of 3 cases. AIDS Read. 2009;19:114–21.54. Hor berg M, Tang B, Towner W, et al. Impact oftenofovir on renal function in HIV-infected,antiretroviral-naive patients. J Acquir Immune Defic Syndr.

2010;53:62–9. 55. Young J, Schäfer J, Fux CA, Furrer H, etal.; The Swiss HIV Cohort Study. Renal function inpatients with HIV starting therapy with tenofovir andeither efavirenz, lopinavir or atazanavir. J Acquir ImmuneDefic Synd. 2012;26:567–75. 56. Weve r K, van Agtmael MA,Carr A. Incomplete reversibility of tenofovir-related renaltoxicity in HIV-infected men. J Acquir Immune Defic Syndr.2010;55:78–81. 57. Mar tin JL, Brown CE, Matthews-Davis N,et al. Effects of antiviral nucleoside analogs on humanDNA polymerases and mitochondrial DNA synthesis.Antimicrob Agents Chemother. 1994;38:2743–9. 58.Perazella MA. Tenofovir-induced kidney disease: Anacquired renal tubular mitochondriopathy. Kidney Int.2010;78:1060–3. 59. Mal lipattu SK, Salem F, Wyatt CM. Thechanging epidemiology of HIV-related chronic kidneydisease in the era of antiretroviral therapy. Kidney Int.2014;86:259–65. 60. Paula AA, Falcão MC, Pacheco AG.Metabolic syndrome in HIV-infected individuals: Underlyingmechanisms and epidemiological aspects. AIDS Res Ther.2013;10:32–9. 61. Maynard JE. Hepatitis B: Globalimportance and need for control. Vaccine.1990;8(Suppl):S18–20. 62. Bhimma R, Coovadia HM. HepatitisB virus-associated nephropathy. Am J Nephrol.2004;24:198–211. 63. Gil bert RD, Wiggelinkhuizen J. Theclinical course of hepatitis B virus-associatednephropathy. Pediatr Nephrol. 1994;8:11–14. 64. Hirose H,Udo K, Kojima M, et al. Deposition of hepatitis Be antigenin membranous glomerulonephritis: Identification byF(ab¢)2 fragments of monoclonal antibody. Kidney Int.1984;26:338–41. 65. Takekoshi Y, Tochimaru H, Nagata Y, etal. Immunopathogenetic mechanisms of hepatitis Bvirus-related glomerulopathy. Kidney Int Suppl.1991;35:S3–39. 66. Lai KN, Lai FM, Lo S, et al. IgAnephropathy associated with hepatitis B virus antigenemia.Nephron. 1987;47:141–3.
67. Bhimma R, Coovadia HM, Adhikari M. Hepatitis Bvirus-associated nephropathy in black South Africanchildren. Pediatr Nephrol. 1998;12:479–84.
68. Lee H S, Choi Y, Yu SH, et al. A renal biopsy study ofhepatitis B virus-associated nephropathy in Korea. KidneyInt. 1988;34:537–43.
69. Pagnoux C, Seror R, Henegar C, et al. Clinical featuresand outcomes in 348 patients with polyarteritis nodosa: Asystematic retrospective study of patients diagnosedbetween 1963 and 2005 and entered into the FrenchVasculitis Study Group Database. Arthritis Rheum.2010;62:616–26.

70. Ruiz-Moreno M, Rua MJ, Molina J, et al. Prospective,randomized controlled trial of interferon-alpha inchildren with chronic hepatitis B. Hepatology.1991;13:1035–9.
71. Barbera C, Bortolotti F, Crivellaro C, et al.Recombinant interferon-alpha 2a hastens the rate of HBeAgclearance in children with chronic hepatitis B.Hepatology. 1994;20:287–90.
72. Sok al EM, Conjeevaram HS, Roberts EA, et al.Interferon alfa therapy for chronic hepatitis B inchildren: A multinational randomized controlled trial.Gastroenterology. 1998;114:988–95.
73. Lai C L, Lok AS, Lin HJ, et al. Placebo-controlledtrial of recombinant alpha 2-interferon in ChineseHBsAg-carrier children. Lancet.1987;2:877–80.
74. Lai C L, Lin HJ, Lau JN, et al. Effect of recombinantalpha 2 interferon with or without prednisone in ChineseHBsAg carrier children. Q J Med. 1991;78:155–63.
75. Jon as MM, Mizerski J, Badia IB, et al. Clinical trialof lamivudine in children with chronic hepatitis B. N EnglJ Med. 2002;346:1706–13.
76. Marcellin P, Chang TT, Lim SG, et al. Adefovirdipivoxil for the treatment of hepatitis B eantigen-positive chronic hepatitis B. N Engl J Med.2003;348:808–16.
77. Lai FM, Tam JS, Li PK, et al. Replication of hepatitisB virus with corticosteroid therapy in hepatitis B virusrelated membranous nephropathy. Virchows Arch A PatholAnat Histopathol. 1989;414:279–84.
78. Gui llevin L, Lhote F. Treatment of polyarteritisnodosa and microscopic polyangiitis. Arthritis Rheum.1988;41:2100–5.
79. Alter MJ, Kruszon-Moran D, Nainan OV, et al. Theprevalence of hepatitis C virus infection in the UnitedStates, 1988 through 1994. N Engl J Med. 1999;341:556–62.
80. Jon as MM. Children with hepatitis C. Hepatology.2002;36(5 Suppl 1):S173–8.
81. Yeu ng LT, King SM, Roberts EA. Mother-to-infant
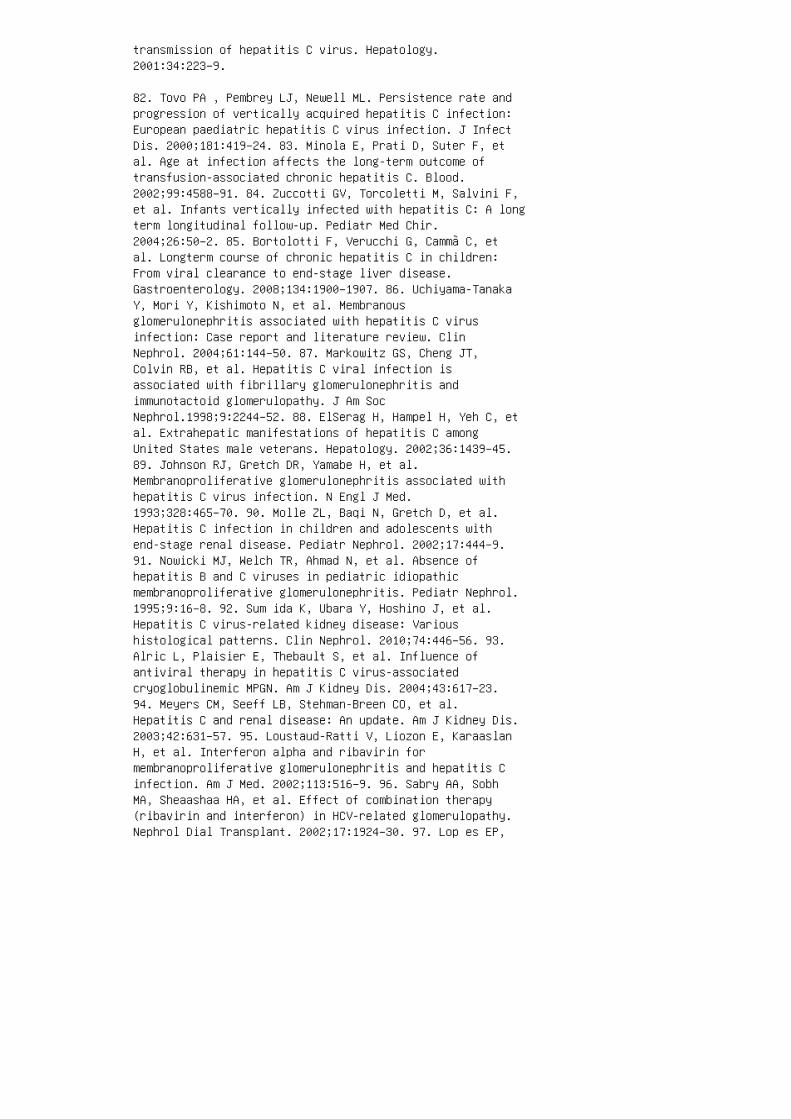
transmission of hepatitis C virus. Hepatology.2001:34:223–9.
82. Tovo PA , Pembrey LJ, Newell ML. Persistence rate andprogression of vertically acquired hepatitis C infection:European paediatric hepatitis C virus infection. J InfectDis. 2000;181:419–24. 83. Minola E, Prati D, Suter F, etal. Age at infection affects the long-term outcome oftransfusion-associated chronic hepatitis C. Blood.2002;99:4588–91. 84. Zuccotti GV, Torcoletti M, Salvini F,et al. Infants vertically infected with hepatitis C: A longterm longitudinal follow-up. Pediatr Med Chir.2004;26:50–2. 85. Bortolotti F, Verucchi G, Cammà C, etal. Longterm course of chronic hepatitis C in children:From viral clearance to end-stage liver disease.Gastroenterology. 2008;134:1900–1907. 86. Uchiyama-TanakaY, Mori Y, Kishimoto N, et al. Membranousglomerulonephritis associated with hepatitis C virusinfection: Case report and literature review. ClinNephrol. 2004;61:144–50. 87. Markowitz GS, Cheng JT,Colvin RB, et al. Hepatitis C viral infection isassociated with fibrillary glomerulonephritis andimmunotactoid glomerulopathy. J Am SocNephrol.1998;9:2244–52. 88. ElSerag H, Hampel H, Yeh C, etal. Extrahepatic manifestations of hepatitis C amongUnited States male veterans. Hepatology. 2002;36:1439–45.89. Johnson RJ, Gretch DR, Yamabe H, et al.Membranoproliferative glomerulonephritis associated withhepatitis C virus infection. N Engl J Med.1993;328:465–70. 90. Molle ZL, Baqi N, Gretch D, et al.Hepatitis C infection in children and adolescents withend-stage renal disease. Pediatr Nephrol. 2002;17:444–9.91. Nowicki MJ, Welch TR, Ahmad N, et al. Absence ofhepatitis B and C viruses in pediatric idiopathicmembranoproliferative glomerulonephritis. Pediatr Nephrol.1995;9:16–8. 92. Sum ida K, Ubara Y, Hoshino J, et al.Hepatitis C virus-related kidney disease: Varioushistological patterns. Clin Nephrol. 2010;74:446–56. 93.Alric L, Plaisier E, Thebault S, et al. Influence ofantiviral therapy in hepatitis C virus-associatedcryoglobulinemic MPGN. Am J Kidney Dis. 2004;43:617–23.94. Meyers CM, Seeff LB, Stehman-Breen CO, et al.Hepatitis C and renal disease: An update. Am J Kidney Dis.2003;42:631–57. 95. Loustaud-Ratti V, Liozon E, KaraaslanH, et al. Interferon alpha and ribavirin formembranoproliferative glomerulonephritis and hepatitis Cinfection. Am J Med. 2002;113:516–9. 96. Sabry AA, SobhMA, Sheaashaa HA, et al. Effect of combination therapy(ribavirin and interferon) in HCV-related glomerulopathy.Nephrol Dial Transplant. 2002;17:1924–30. 97. Lop es EP,
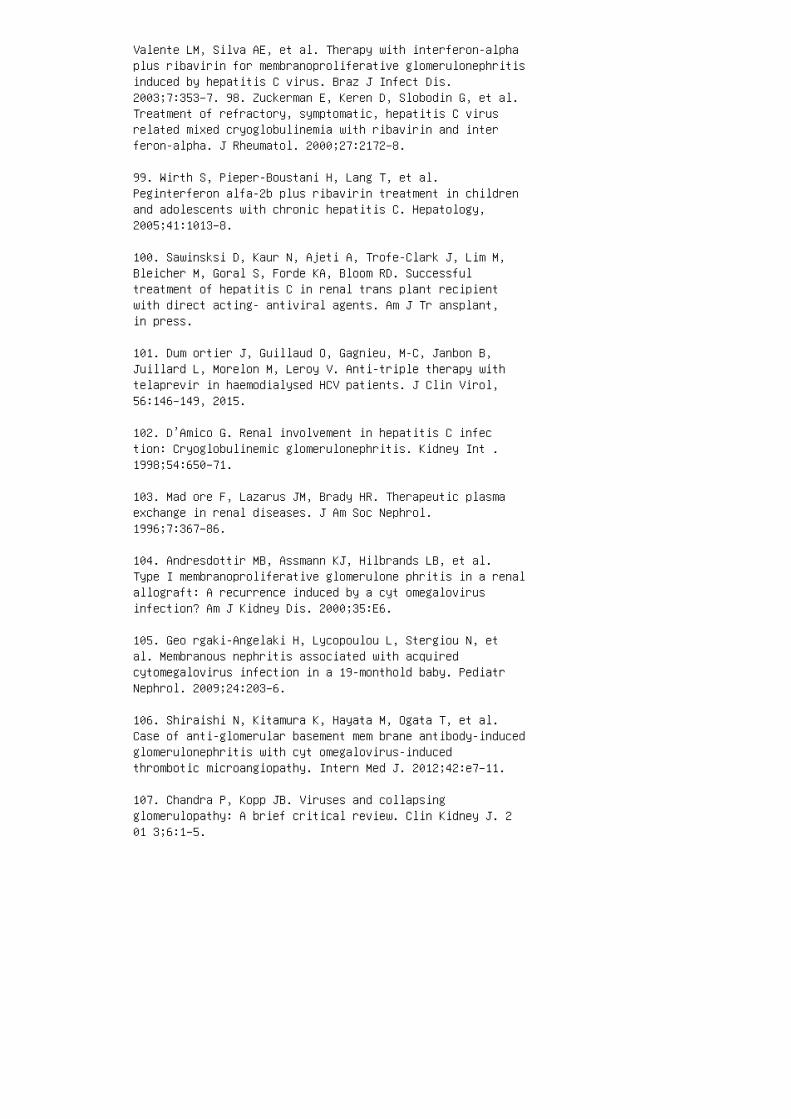
Valente LM, Silva AE, et al. Therapy with interferon-alphaplus ribavirin for membranoproliferative glomerulonephritisinduced by hepatitis C virus. Braz J Infect Dis.2003;7:353–7. 98. Zuckerman E, Keren D, Slobodin G, et al.Treatment of refractory, symptomatic, hepatitis C virusrelated mixed cryoglobulinemia with ribavirin and interferon-alpha. J Rheumatol. 2000;27:2172–8.
99. Wirth S, Pieper-Boustani H, Lang T, et al.Peginterferon alfa-2b plus ribavirin treatment in childrenand adolescents with chronic hepatitis C. Hepatology,2005;41:1013–8.
100. Sawinsksi D, Kaur N, Ajeti A, Trofe-Clark J, Lim M,Bleicher M, Goral S, Forde KA, Bloom RD. Successfultreatment of hepatitis C in renal trans plant recipientwith direct acting- antiviral agents. Am J Tr ansplant,in press.
101. Dum ortier J, Guillaud O, Gagnieu, M-C, Janbon B,Juillard L, Morelon M, Leroy V. Anti-triple therapy withtelaprevir in haemodialysed HCV patients. J Clin Virol,56:146–149, 2015.
102. D’Amico G. Renal involvement in hepatitis C infection: Cryoglobulinemic glomerulonephritis. Kidney Int .1998;54:650–71.
103. Mad ore F, Lazarus JM, Brady HR. Therapeutic plasmaexchange in renal diseases. J Am Soc Nephrol.1996;7:367–86.
104. Andresdottir MB, Assmann KJ, Hilbrands LB, et al.Type I membranoproliferative glomerulone phritis in a renalallograft: A recurrence induced by a cyt omegalovirusinfection? Am J Kidney Dis. 2000;35:E6.
105. Geo rgaki-Angelaki H, Lycopoulou L, Stergiou N, etal. Membranous nephritis associated with acquiredcytomegalovirus infection in a 19-monthold baby. PediatrNephrol. 2009;24:203–6.
106. Shiraishi N, Kitamura K, Hayata M, Ogata T, et al.Case of anti-glomerular basement mem brane antibody-inducedglomerulonephritis with cyt omegalovirus-inducedthrombotic microangiopathy. Intern Med J. 2012;42:e7–11.
107. Chandra P, Kopp JB. Viruses and collapsingglomerulopathy: A brief critical review. Clin Kidney J. 201 3;6:1–5.
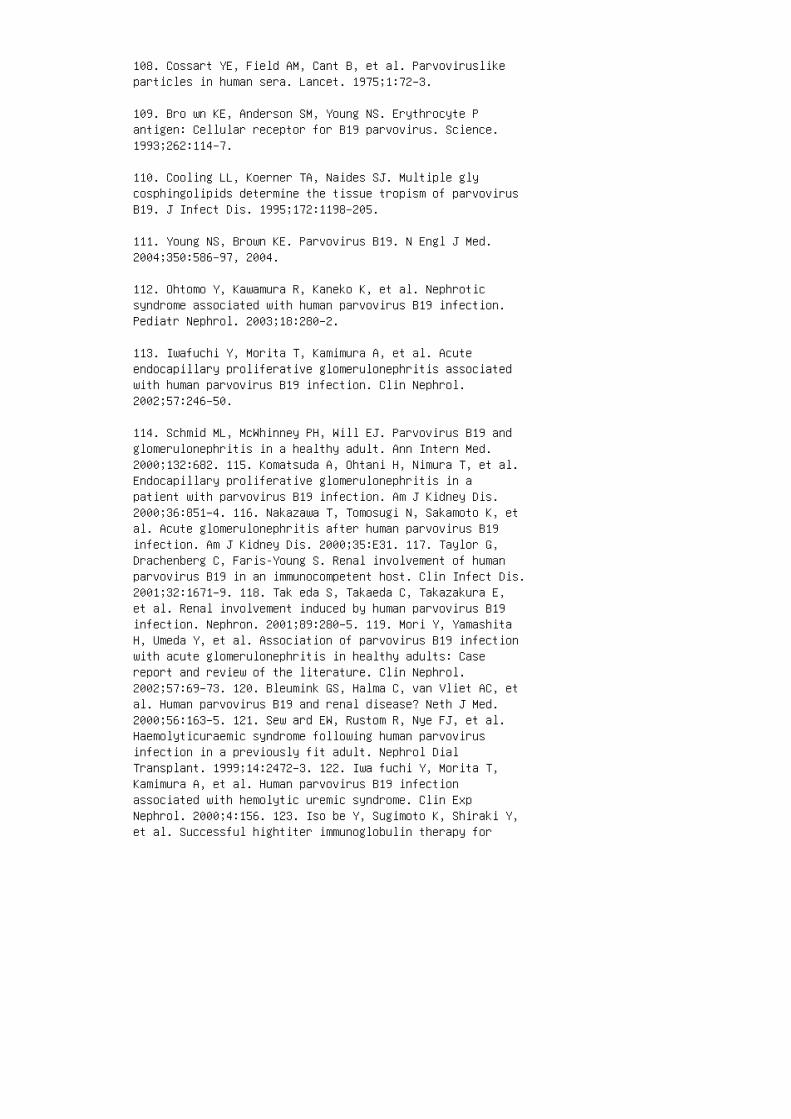
108. Cossart YE, Field AM, Cant B, et al. Parvoviruslikeparticles in human sera. Lancet. 1975;1:72–3.
109. Bro wn KE, Anderson SM, Young NS. Erythrocyte Pantigen: Cellular receptor for B19 parvovirus. Science.1993;262:114–7.
110. Cooling LL, Koerner TA, Naides SJ. Multiple glycosphingolipids determine the tissue tropism of parvovirusB19. J Infect Dis. 1995;172:1198–205.
111. Young NS, Brown KE. Parvovirus B19. N Engl J Med.2004;350:586–97, 2004.
112. Ohtomo Y, Kawamura R, Kaneko K, et al. Nephroticsyndrome associated with human parvovirus B19 infection.Pediatr Nephrol. 2003;18:280–2.
113. Iwafuchi Y, Morita T, Kamimura A, et al. Acuteendocapillary proliferative glomerulonephritis associatedwith human parvovirus B19 infection. Clin Nephrol.2002;57:246–50.
114. Schmid ML, McWhinney PH, Will EJ. Parvovirus B19 andglomerulonephritis in a healthy adult. Ann Intern Med.2000;132:682. 115. Komatsuda A, Ohtani H, Nimura T, et al.Endocapillary proliferative glomerulonephritis in apatient with parvovirus B19 infection. Am J Kidney Dis.2000;36:851–4. 116. Nakazawa T, Tomosugi N, Sakamoto K, etal. Acute glomerulonephritis after human parvovirus B19infection. Am J Kidney Dis. 2000;35:E31. 117. Taylor G,Drachenberg C, Faris-Young S. Renal involvement of humanparvovirus B19 in an immunocompetent host. Clin Infect Dis.2001;32:1671–9. 118. Tak eda S, Takaeda C, Takazakura E,et al. Renal involvement induced by human parvovirus B19infection. Nephron. 2001;89:280–5. 119. Mori Y, YamashitaH, Umeda Y, et al. Association of parvovirus B19 infectionwith acute glomerulonephritis in healthy adults: Casereport and review of the literature. Clin Nephrol.2002;57:69–73. 120. Bleumink GS, Halma C, van Vliet AC, etal. Human parvovirus B19 and renal disease? Neth J Med.2000;56:163–5. 121. Sew ard EW, Rustom R, Nye FJ, et al.Haemolyticuraemic syndrome following human parvovirusinfection in a previously fit adult. Nephrol DialTransplant. 1999;14:2472–3. 122. Iwa fuchi Y, Morita T,Kamimura A, et al. Human parvovirus B19 infectionassociated with hemolytic uremic syndrome. Clin ExpNephrol. 2000;4:156. 123. Iso be Y, Sugimoto K, Shiraki Y,et al. Successful hightiter immunoglobulin therapy for
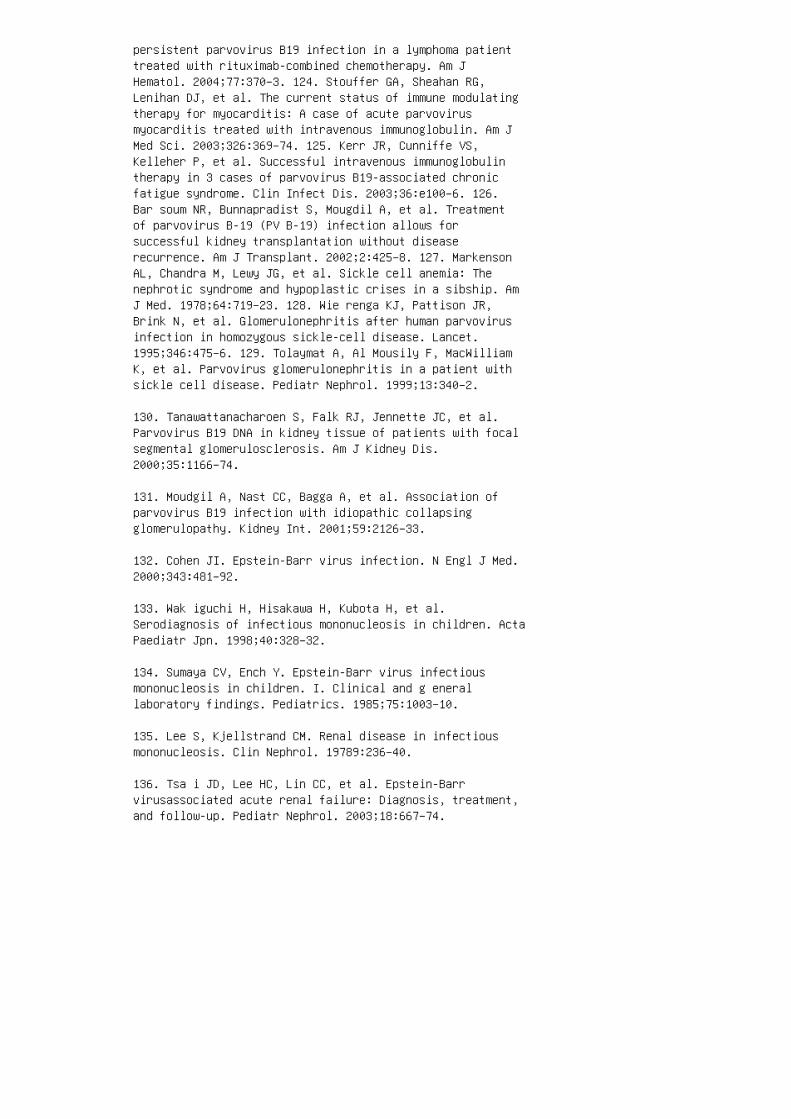
persistent parvovirus B19 infection in a lymphoma patienttreated with rituximab-combined chemotherapy. Am JHematol. 2004;77:370–3. 124. Stouffer GA, Sheahan RG,Lenihan DJ, et al. The current status of immune modulatingtherapy for myocarditis: A case of acute parvovirusmyocarditis treated with intravenous immunoglobulin. Am JMed Sci. 2003;326:369–74. 125. Kerr JR, Cunniffe VS,Kelleher P, et al. Successful intravenous immunoglobulintherapy in 3 cases of parvovirus B19-associated chronicfatigue syndrome. Clin Infect Dis. 2003;36:e100–6. 126.Bar soum NR, Bunnapradist S, Mougdil A, et al. Treatmentof parvovirus B-19 (PV B-19) infection allows forsuccessful kidney transplantation without diseaserecurrence. Am J Transplant. 2002;2:425–8. 127. MarkensonAL, Chandra M, Lewy JG, et al. Sickle cell anemia: Thenephrotic syndrome and hypoplastic crises in a sibship. AmJ Med. 1978;64:719–23. 128. Wie renga KJ, Pattison JR,Brink N, et al. Glomerulonephritis after human parvovirusinfection in homozygous sickle-cell disease. Lancet.1995;346:475–6. 129. Tolaymat A, Al Mousily F, MacWilliamK, et al. Parvovirus glomerulonephritis in a patient withsickle cell disease. Pediatr Nephrol. 1999;13:340–2.
130. Tanawattanacharoen S, Falk RJ, Jennette JC, et al.Parvovirus B19 DNA in kidney tissue of patients with focalsegmental glomerulosclerosis. Am J Kidney Dis.2000;35:1166–74.
131. Moudgil A, Nast CC, Bagga A, et al. Association ofparvovirus B19 infection with idiopathic collapsingglomerulopathy. Kidney Int. 2001;59:2126–33.
132. Cohen JI. Epstein-Barr virus infection. N Engl J Med.2000;343:481–92.
133. Wak iguchi H, Hisakawa H, Kubota H, et al.Serodiagnosis of infectious mononucleosis in children. ActaPaediatr Jpn. 1998;40:328–32.
134. Sumaya CV, Ench Y. Epstein-Barr virus infectiousmononucleosis in children. I. Clinical and g enerallaboratory findings. Pediatrics. 1985;75:1003–10.
135. Lee S, Kjellstrand CM. Renal disease in infectiousmononucleosis. Clin Nephrol. 19789:236–40.
136. Tsa i JD, Lee HC, Lin CC, et al. Epstein-Barrvirusassociated acute renal failure: Diagnosis, treatment,and follow-up. Pediatr Nephrol. 2003;18:667–74.
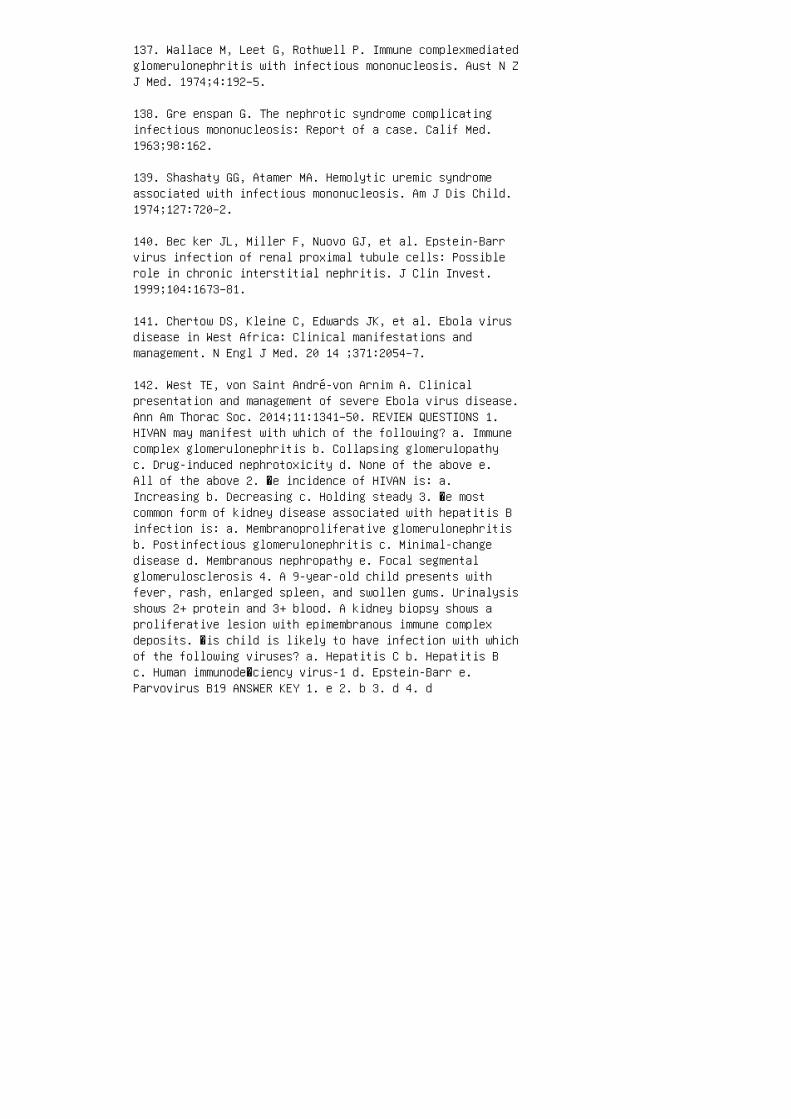
137. Wallace M, Leet G, Rothwell P. Immune complexmediatedglomerulonephritis with infectious mononucleosis. Aust N ZJ Med. 1974;4:192–5.
138. Gre enspan G. The nephrotic syndrome complicatinginfectious mononucleosis: Report of a case. Calif Med.1963;98:162.
139. Shashaty GG, Atamer MA. Hemolytic uremic syndromeassociated with infectious mononucleosis. Am J Dis Child.1974;127:720–2.
140. Bec ker JL, Miller F, Nuovo GJ, et al. Epstein-Barrvirus infection of renal proximal tubule cells: Possiblerole in chronic interstitial nephritis. J Clin Invest.1999;104:1673–81.
141. Chertow DS, Kleine C, Edwards JK, et al. Ebola virusdisease in West Africa: Clinical manifestations andmanagement. N Engl J Med. 20 14 ;371:2054–7.
142. West TE, von Saint André-von Arnim A. Clinicalpresentation and management of severe Ebola virus disease.Ann Am Thorac Soc. 2014;11:1341–50. REVIEW QUESTIONS 1.HIVAN may manifest with which of the following? a. Immunecomplex glomerulonephritis b. Collapsing glomerulopathyc. Drug-induced nephrotoxicity d. None of the above e.All of the above 2. �e incidence of HIVAN is: a.Increasing b. Decreasing c. Holding steady 3. �e mostcommon form of kidney disease associated with hepatitis Binfection is: a. Membranoproliferative glomerulonephritisb. Postinfectious glomerulonephritis c. Minimal-changedisease d. Membranous nephropathy e. Focal segmentalglomerulosclerosis 4. A 9-year-old child presents withfever, rash, enlarged spleen, and swollen gums. Urinalysisshows 2+ protein and 3+ blood. A kidney biopsy shows aproliferative lesion with epimembranous immune complexdeposits. �is child is likely to have infection with whichof the following viruses? a. Hepatitis C b. Hepatitis Bc. Human immunode�ciency virus-1 d. Epstein-Barr e.Parvovirus B19 ANSWER KEY 1. e 2. b 3. d 4. d

30 Acute kidney injury
1. Hui-Stickle S, Brewer ED, Goldstein SL. Pediatric ARFepidemiology at a tertiary care center from 1999 to 2001.Am J Kidney Dis. 2005;45:96–101.
2. Devarajan P. Update on mechanisms of ischemic acutekidney injury. J Am Soc Nephrol. 2006;17:1503–20.
3. Goldstein SL. Advances in pediatric renal replacementtherapy for acute kidney injury. Semin Dialy.2011;24:187–91.
4. Uchino S, Kellum JA, Bellomo R, et al. Acute renalfailure in critically ill patients: A multinational,multicenter study. JAMA. 2005;294:813–8. 5. Askenazi DJ,Ambalavanan N, Goldstein SL. Acute kidney injury incritically ill newborns: What do we know? What do we needto learn? Pediatr Nephrol. 2009;24:265–74. 6. Sin gbartlK, Kellum JA. AKI in the ICU: Definition, epidemiology,risk stratification, and outcomes. Kidney Int.2012;81:819–25. 7. Kellum JA, Angus DC. Patients are dyingof acute renal failure. Crit Care Med. 2002;30:2156–7. 8.Bellomo R, Ronco C, Kellum JA, et al. Acute renalfailure—Definition, outcome measures, animal models, fluidtherapy and information technology needs: The SecondInternational Consensus Conference of the Acute DialysisQuality Initiative (ADQI) Group. Crit Care.2004;8:R204–12. 9. Akcan-Arikan A, Zappitelli M, LoftisLL, et al. Modified RIFLE criteria in critically illchildren with acute kidney injury. Kidney Int.2007;71:1028–35. 10. Srisawat N, Hoste EE, Kellum JA.Modern classification of acute kidney injury. Blood Purif.2010;29:300–7. 11. Slater MB, Anand V, Uleryk EM,Parshuram CS. A systematic review of RIFLE criteria inchildren, and its application and association withmeasures of mortality and morbidity. Kidney Int.2012;81:791–8. 12. Meh ta RL, Kellum JA, Shah SV, et al.Acute Kidney Injury Network: Report of an initiative toimprove outcomes in acute kidney injury. Crit Care.2007;11. 13. Chertow GM, Burdick E, Honour M, et al. Acutekidney injury, mortality, length of stay, and costs inhospitalized patients. J Am Soc Nephrol. 2005;16:3365–70.14. Price JF, Mott AR, Dickerson HA, et al. Worseningrenal function in children hospitalized with decompensatedheart failure: Evidence for a pediatric cardiorenalsyndrome? Pediatr Crit Care Med. 2008;9:279–84. 15.Kidney Disease: Improving Global Outcomes (KDIGO) AcuteKidney Injury Work Group—KDIGO clinical practice guidelinefor acute kidney injury. Kidney Int Suppl. 2012;2:1–138.
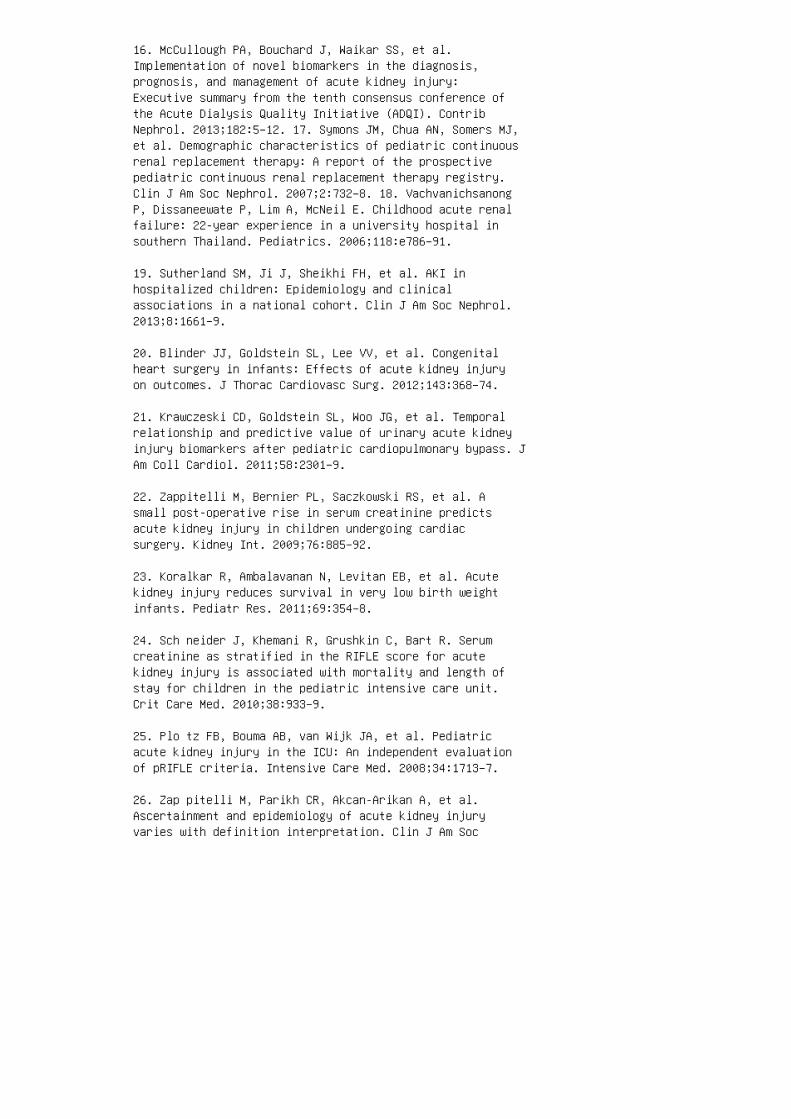
16. McCullough PA, Bouchard J, Waikar SS, et al.Implementation of novel biomarkers in the diagnosis,prognosis, and management of acute kidney injury:Executive summary from the tenth consensus conference ofthe Acute Dialysis Quality Initiative (ADQI). ContribNephrol. 2013;182:5–12. 17. Symons JM, Chua AN, Somers MJ,et al. Demographic characteristics of pediatric continuousrenal replacement therapy: A report of the prospectivepediatric continuous renal replacement therapy registry.Clin J Am Soc Nephrol. 2007;2:732–8. 18. VachvanichsanongP, Dissaneewate P, Lim A, McNeil E. Childhood acute renalfailure: 22-year experience in a university hospital insouthern Thailand. Pediatrics. 2006;118:e786–91.
19. Sutherland SM, Ji J, Sheikhi FH, et al. AKI inhospitalized children: Epidemiology and clinicalassociations in a national cohort. Clin J Am Soc Nephrol.2013;8:1661–9.
20. Blinder JJ, Goldstein SL, Lee VV, et al. Congenitalheart surgery in infants: Effects of acute kidney injuryon outcomes. J Thorac Cardiovasc Surg. 2012;143:368–74.
21. Krawczeski CD, Goldstein SL, Woo JG, et al. Temporalrelationship and predictive value of urinary acute kidneyinjury biomarkers after pediatric cardiopulmonary bypass. JAm Coll Cardiol. 2011;58:2301–9.
22. Zappitelli M, Bernier PL, Saczkowski RS, et al. Asmall post-operative rise in serum creatinine predictsacute kidney injury in children undergoing cardiacsurgery. Kidney Int. 2009;76:885–92.
23. Koralkar R, Ambalavanan N, Levitan EB, et al. Acutekidney injury reduces survival in very low birth weightinfants. Pediatr Res. 2011;69:354–8.
24. Sch neider J, Khemani R, Grushkin C, Bart R. Serumcreatinine as stratified in the RIFLE score for acutekidney injury is associated with mortality and length ofstay for children in the pediatric intensive care unit.Crit Care Med. 2010;38:933–9.
25. Plo tz FB, Bouma AB, van Wijk JA, et al. Pediatricacute kidney injury in the ICU: An independent evaluationof pRIFLE criteria. Intensive Care Med. 2008;34:1713–7.
26. Zap pitelli M, Parikh CR, Akcan-Arikan A, et al.Ascertainment and epidemiology of acute kidney injuryvaries with definition interpretation. Clin J Am Soc
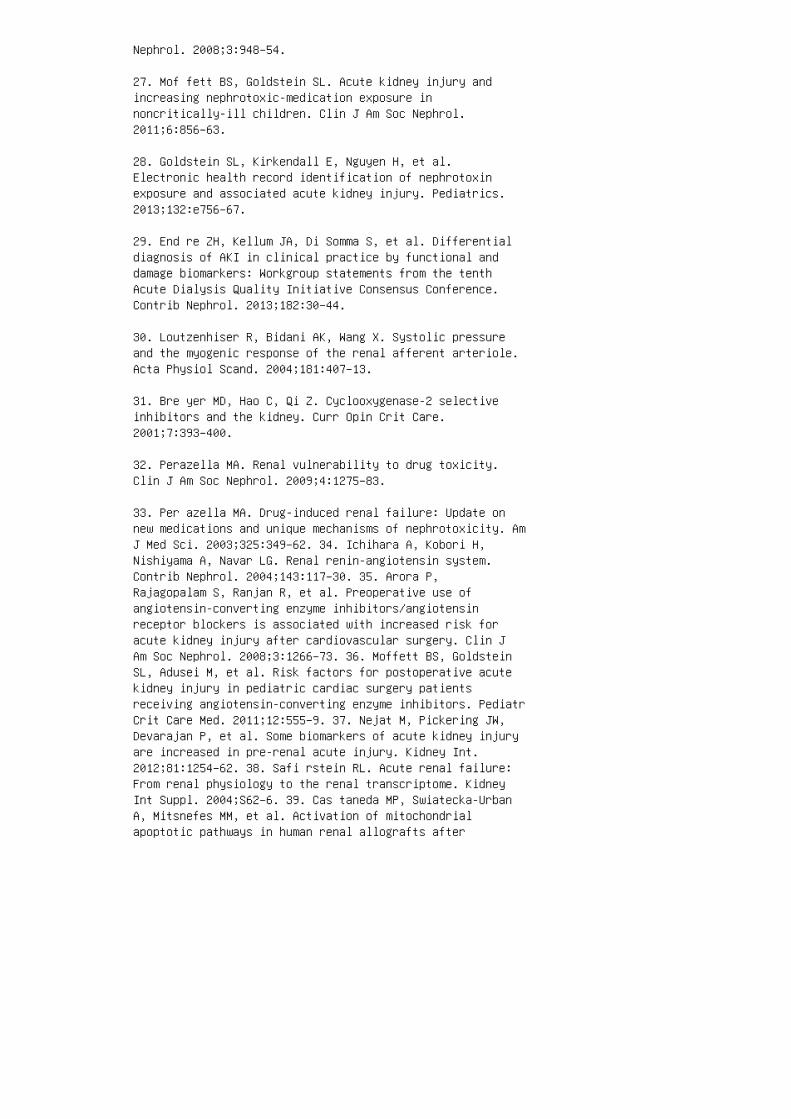
Nephrol. 2008;3:948–54.
27. Mof fett BS, Goldstein SL. Acute kidney injury andincreasing nephrotoxic-medication exposure innoncritically-ill children. Clin J Am Soc Nephrol.2011;6:856–63.
28. Goldstein SL, Kirkendall E, Nguyen H, et al.Electronic health record identification of nephrotoxinexposure and associated acute kidney injury. Pediatrics.2013;132:e756–67.
29. End re ZH, Kellum JA, Di Somma S, et al. Differentialdiagnosis of AKI in clinical practice by functional anddamage biomarkers: Workgroup statements from the tenthAcute Dialysis Quality Initiative Consensus Conference.Contrib Nephrol. 2013;182:30–44.
30. Loutzenhiser R, Bidani AK, Wang X. Systolic pressureand the myogenic response of the renal afferent arteriole.Acta Physiol Scand. 2004;181:407–13.
31. Bre yer MD, Hao C, Qi Z. Cyclooxygenase-2 selectiveinhibitors and the kidney. Curr Opin Crit Care.2001;7:393–400.
32. Perazella MA. Renal vulnerability to drug toxicity.Clin J Am Soc Nephrol. 2009;4:1275–83.
33. Per azella MA. Drug-induced renal failure: Update onnew medications and unique mechanisms of nephrotoxicity. AmJ Med Sci. 2003;325:349–62. 34. Ichihara A, Kobori H,Nishiyama A, Navar LG. Renal renin-angiotensin system.Contrib Nephrol. 2004;143:117–30. 35. Arora P,Rajagopalam S, Ranjan R, et al. Preoperative use ofangiotensin-converting enzyme inhibitors/angiotensinreceptor blockers is associated with increased risk foracute kidney injury after cardiovascular surgery. Clin JAm Soc Nephrol. 2008;3:1266–73. 36. Moffett BS, GoldsteinSL, Adusei M, et al. Risk factors for postoperative acutekidney injury in pediatric cardiac surgery patientsreceiving angiotensin-converting enzyme inhibitors. PediatrCrit Care Med. 2011;12:555–9. 37. Nejat M, Pickering JW,Devarajan P, et al. Some biomarkers of acute kidney injuryare increased in pre-renal acute injury. Kidney Int.2012;81:1254–62. 38. Safi rstein RL. Acute renal failure:From renal physiology to the renal transcriptome. KidneyInt Suppl. 2004;S62–6. 39. Cas taneda MP, Swiatecka-UrbanA, Mitsnefes MM, et al. Activation of mitochondrialapoptotic pathways in human renal allografts after
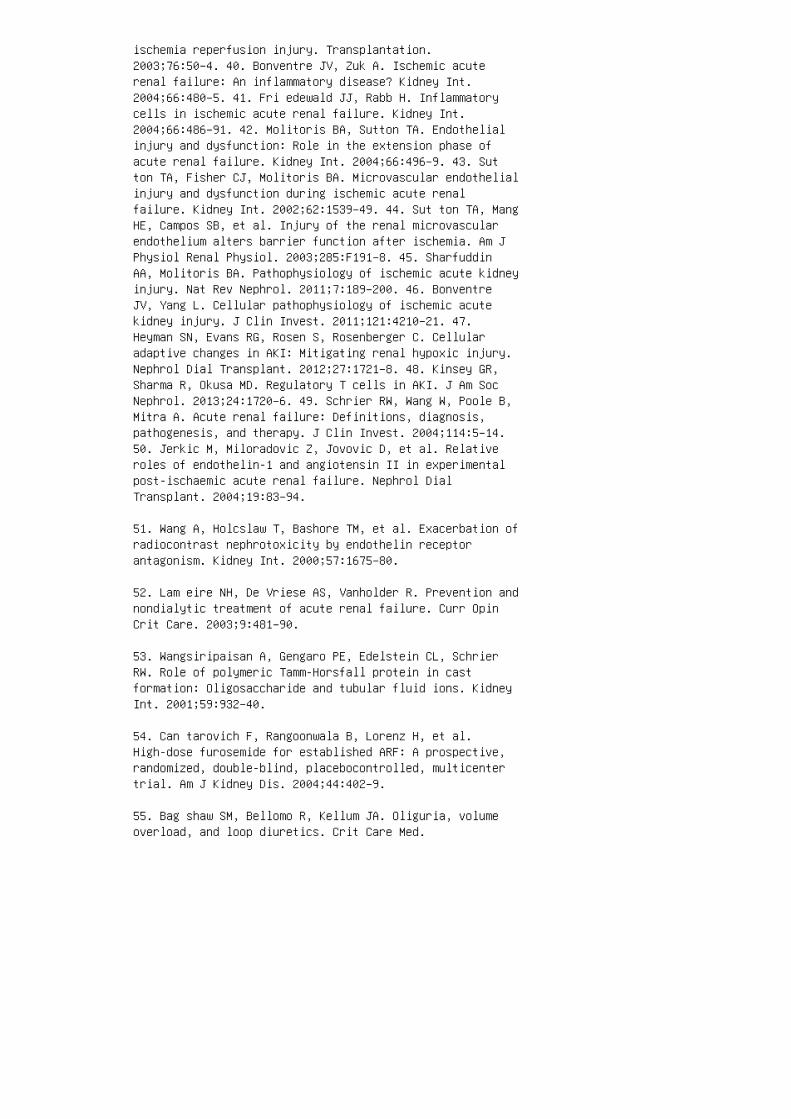
ischemia reperfusion injury. Transplantation.2003;76:50–4. 40. Bonventre JV, Zuk A. Ischemic acuterenal failure: An inflammatory disease? Kidney Int.2004;66:480–5. 41. Fri edewald JJ, Rabb H. Inflammatorycells in ischemic acute renal failure. Kidney Int.2004;66:486–91. 42. Molitoris BA, Sutton TA. Endothelialinjury and dysfunction: Role in the extension phase ofacute renal failure. Kidney Int. 2004;66:496–9. 43. Sutton TA, Fisher CJ, Molitoris BA. Microvascular endothelialinjury and dysfunction during ischemic acute renalfailure. Kidney Int. 2002;62:1539–49. 44. Sut ton TA, MangHE, Campos SB, et al. Injury of the renal microvascularendothelium alters barrier function after ischemia. Am JPhysiol Renal Physiol. 2003;285:F191–8. 45. SharfuddinAA, Molitoris BA. Pathophysiology of ischemic acute kidneyinjury. Nat Rev Nephrol. 2011;7:189–200. 46. BonventreJV, Yang L. Cellular pathophysiology of ischemic acutekidney injury. J Clin Invest. 2011;121:4210–21. 47.Heyman SN, Evans RG, Rosen S, Rosenberger C. Cellularadaptive changes in AKI: Mitigating renal hypoxic injury.Nephrol Dial Transplant. 2012;27:1721–8. 48. Kinsey GR,Sharma R, Okusa MD. Regulatory T cells in AKI. J Am SocNephrol. 2013;24:1720–6. 49. Schrier RW, Wang W, Poole B,Mitra A. Acute renal failure: Definitions, diagnosis,pathogenesis, and therapy. J Clin Invest. 2004;114:5–14.50. Jerkic M, Miloradovic Z, Jovovic D, et al. Relativeroles of endothelin-1 and angiotensin II in experimentalpost-ischaemic acute renal failure. Nephrol DialTransplant. 2004;19:83–94.
51. Wang A, Holcslaw T, Bashore TM, et al. Exacerbation ofradiocontrast nephrotoxicity by endothelin receptorantagonism. Kidney Int. 2000;57:1675–80.
52. Lam eire NH, De Vriese AS, Vanholder R. Prevention andnondialytic treatment of acute renal failure. Curr OpinCrit Care. 2003;9:481–90.
53. Wangsiripaisan A, Gengaro PE, Edelstein CL, SchrierRW. Role of polymeric Tamm-Horsfall protein in castformation: Oligosaccharide and tubular fluid ions. KidneyInt. 2001;59:932–40.
54. Can tarovich F, Rangoonwala B, Lorenz H, et al.High-dose furosemide for established ARF: A prospective,randomized, double-blind, placebocontrolled, multicentertrial. Am J Kidney Dis. 2004;44:402–9.
55. Bag shaw SM, Bellomo R, Kellum JA. Oliguria, volumeoverload, and loop diuretics. Crit Care Med.
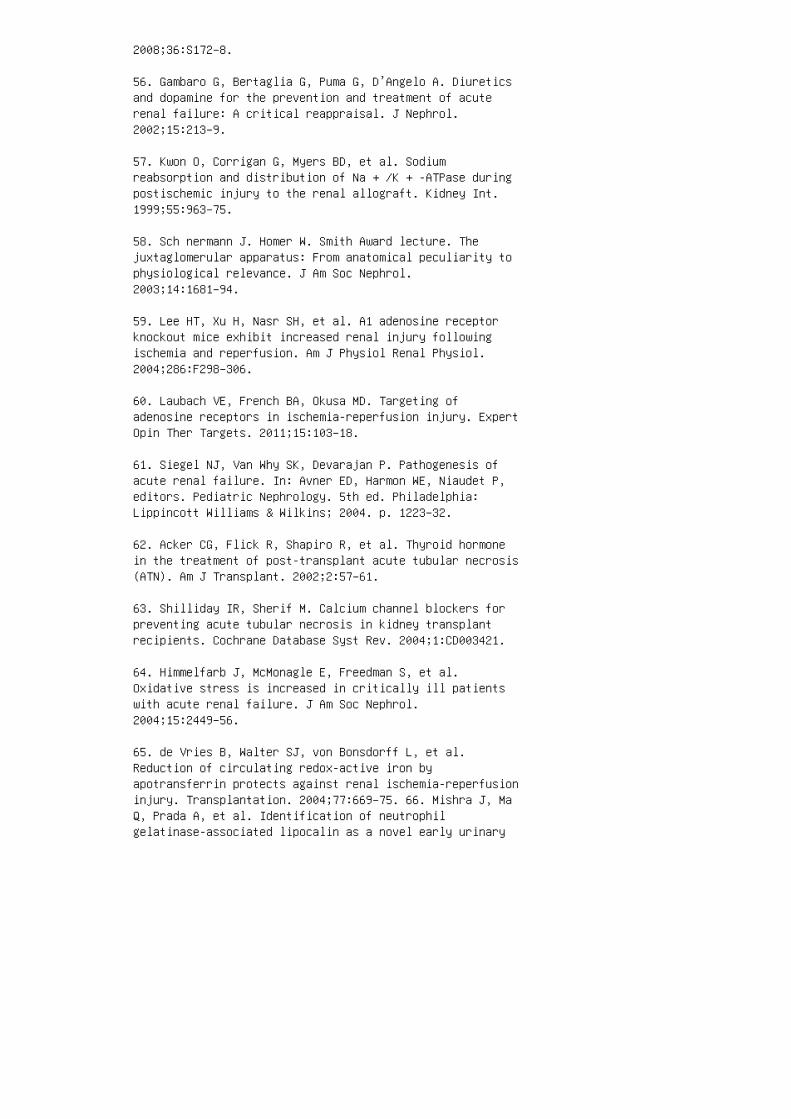
2008;36:S172–8.
56. Gambaro G, Bertaglia G, Puma G, D’Angelo A. Diureticsand dopamine for the prevention and treatment of acuterenal failure: A critical reappraisal. J Nephrol.2002;15:213–9.
57. Kwon O, Corrigan G, Myers BD, et al. Sodiumreabsorption and distribution of Na + /K + -ATPase duringpostischemic injury to the renal allograft. Kidney Int.1999;55:963–75.
58. Sch nermann J. Homer W. Smith Award lecture. Thejuxtaglomerular apparatus: From anatomical peculiarity tophysiological relevance. J Am Soc Nephrol.2003;14:1681–94.
59. Lee HT, Xu H, Nasr SH, et al. A1 adenosine receptorknockout mice exhibit increased renal injury followingischemia and reperfusion. Am J Physiol Renal Physiol.2004;286:F298–306.
60. Laubach VE, French BA, Okusa MD. Targeting ofadenosine receptors in ischemia-reperfusion injury. ExpertOpin Ther Targets. 2011;15:103–18.
61. Siegel NJ, Van Why SK, Devarajan P. Pathogenesis ofacute renal failure. In: Avner ED, Harmon WE, Niaudet P,editors. Pediatric Nephrology. 5th ed. Philadelphia:Lippincott Williams & Wilkins; 2004. p. 1223–32.
62. Acker CG, Flick R, Shapiro R, et al. Thyroid hormonein the treatment of post-transplant acute tubular necrosis(ATN). Am J Transplant. 2002;2:57–61.
63. Shilliday IR, Sherif M. Calcium channel blockers forpreventing acute tubular necrosis in kidney transplantrecipients. Cochrane Database Syst Rev. 2004;1:CD003421.
64. Himmelfarb J, McMonagle E, Freedman S, et al.Oxidative stress is increased in critically ill patientswith acute renal failure. J Am Soc Nephrol.2004;15:2449–56.
65. de Vries B, Walter SJ, von Bonsdorff L, et al.Reduction of circulating redox-active iron byapotransferrin protects against renal ischemia-reperfusioninjury. Transplantation. 2004;77:669–75. 66. Mishra J, MaQ, Prada A, et al. Identification of neutrophilgelatinase-associated lipocalin as a novel early urinary

biomarker for ischemic renal injury. J Am Soc Nephrol.2003;14:2534–43. 67. Mis hra J, Mori K, Ma Q, et al.Amelioration of ischemic acute renal injury by neutrophilgelatinase–associated lipocalin. J Am Soc Nephrol.2004;15:3073–82. 68. Mol itoris BA. Actin cytoskeleton inischemic acute renal failure. Kidney Int. 2004;66:871–83.69. Woroniecki R, Ferdinand JR, Morrow JS, Devarajan P.Dissociation of spectrin-ankyrin complex as a basis forloss of Na-K-ATPase polarity after ischemia. Am J PhysiolRenal Physiol. 2003;284:F358–64. 70. Horton MA.Arg-gly-Asp (RGD) peptides and peptidomimetics astherapeutics: Relevance for renal diseases. Exp Nephrol.1999;7:178–84. 71. Kaushal GP, Basnakian AG, Shah SV.Apoptotic pathways in ischemic acute renal failure. KidneyInt. 2004;66:500–6. 72. Sup avekin S, Zhang W,Kucherlapati R, et al. Differential gene expressionfollowing early renal ischemia/reperfusion. Kidney Int.2003;63:1714–24. 73. Kelly KJ, Plotkin Z, Vulgamott SL,Dagher PC. P53 mediates the apoptotic response to GTPdepletion after renal ischemia-reperfusion: Protectiverole of a p53 inhibitor. J Am Soc Nephrol. 2003;14:128–38.74. Del R io M, Imam A, DeLeon M, et al. The death domainof kidney ankyrin interacts with Fas and promotesFas-mediated cell death in renal epithelia. J Am SocNephrol. 2004;15:41–51. 75. Burns AT, Davies DR, McLarenAJ, et al. Apoptosis in ischemia/reperfusion injury ofhuman renal allografts. Transplantation. 1998;66:872–6.76. Obe rbauer R, Rohrmoser M, Regele H, et al. Apoptosisof tubular epithelial cells in donor kidney biopsiespredicts early renal allograft function. J Am Soc Nephrol.1999;10:2006–13. 77. Sch warz C, Hauser P, Steininger R,et al. Failure of BCL-2 up-regulation in proximal tubularepithelial cells of donor kidney biopsy specimens isassociated with apoptosis and delayed graft function. LabInvest. 2002;82:941–8. 78. Hoffmann SC, Kampen RL, Amur S,et al. Molecular and immunohistochemical characterizationof the onset and resolution of human renal allograftischemia-reperfusion injury. Transplantation.2002;74:916–23. 79. Hauser P, Schwarz C, Mitterbauer C, etal. Genomewide gene-expression patterns of donor kidneybiopsies distinguish primary allograft function. LabInvest. 2004;84:353–61. 80. Devarajan P, Mishra J,Supavekin S, et al. Gene expression in early ischemicrenal injury: Clues towards pathogenesis, biomarkerdiscovery, and novel therapeutics. Mol Genet Metab.2003;80:365–76.
81. Devarajan P. Apoptosis and necrosis. In: Ronco C,Bellomo R, Kellum JA, eds. Critical Care Nephrology, 2nded. Philadelphia: Saunders Elsevier; 2009.

82. Mol itoris BA, Dagher PC, Sandoval RM, et al. siRNAtargeted to p53 attenuates ischemic and cisplatininducedacute kidney injury. J Am Soc Nephrol. 2009;20:1754–64.
83. Bonventre JV. Dedifferentiation and proliferation ofsurviving epithelial cells in acute renal failure. J AmSoc Nephrol. 2003;14(Suppl 1):S55–61.
84. Ham merman MR. Recapitulation of phylogeny by ontogenyin nephrology. Kidney Int. 2000;57:742–55.
85. Rookmaaker MB, Verhaar MC, van Zonneveld AJ, RabelinkTJ. Progenitor cells in the kidney: Biology andtherapeutic perspectives. Kidney Int. 2004;66:518–22.
86. Morigi M, Imberti B, Zoja C, et al. Mesenchymal stemcells are renotropic, helping to repair the kidney andimprove function in acute renal failure. J Am Soc Nephrol.2004;15:1794–804.
87. Sal mela K, Wramner L, Ekberg H, et al. A randomizedmulticenter trial of the anti–ICAM-1 monoclonal antibody(enlimomab) for the prevention of acute rejection anddelayed onset of graft function in cadaveric renaltransplantation: A report of the European Anti–ICAM-1Renal Transplant Study Group. Transplantation.1999;67:729–36.
88. Sim mons EM, Himmelfarb J, Sezer MT, et al. Plasmacytokine levels predict mortality in patients with acuterenal failure. Kidney Int. 2004;65:1357–65.
89. Doi K , Hu X, Yuen PS, et al. AP214, an analogue ofalpha-melanocyte–stimulating hormone, amelioratessepsis-induced acute kidney injury and mortality. KidneyInt. 2008;73:1266–74.
90. Peng Q, Li K, Smyth LA, et al. C3a and C5a promoterenal ischemia-reperfusion injury. J Am Soc Nephrol.2012;23:1474–85.
91. Lewis AG, Kohl G, Ma Q, et al. Pharmacologicaltargeting of C5a receptors during organ preservationimproves kidney graft survival. Clin Exp Immunol.2008;153:117–26.
92. Zar jou A, Agarwal A. Sepsis and acute kidney injury.J Am Soc Nephrol. 2011;22:999–1006.

93. Wan L, Bagshaw SM, Langenberg C, et al.Pathophysiology of septic acute kidney injury: What do wereally know? Crit Care Med. 2008;36:S198–203.
94. Fahimi D, Mohajeri S, Hajizadeh N, et al. Comparisonbetween fractional excretions of urea and sodium inchildren with acute kidney injury. Pediatr Nephrol.2009;24:2409–12.
95. Sch wartz GJ, Munoz A, Schneider MF, et al. Newequations to estimate GFR in children with CKD. J Am SocNephrol. 2009;20:629–37.
96. Fol and JA, Fortenberry JD, Warshaw BL, et al. Fluidoverload before continuous hemofiltration and survival incritically ill children: A retrospective analysis. CritCare Med. 2004;32:1771–6. 97. Goldstein SL, Somers MJ,Baum MA, et al. Pediatric patients with multi-organdysfunction syndrome receiving continuous renalreplacement therapy. Kidney Int. 2005;67:653–8. 98. Sutherland SM, Zappitelli M, Alexander SR, et al. Fluidoverload and mortality in children receiving continuousrenal replacement therapy: The Prospective PediatricContinuous Renal Replacement Therapy Registry. Am J KidneyDis. 2010;55:316–25. 99. Devarajan P. Biomarkers for theearly detection of acute kidney injury. Curr Opin Pediatr.2011;23:194–200. 100. Devarajan P. Neutrophilgelatinase–associated lipocalin: A promising biomarker forhuman acute kidney injury. Biomark Med. 2010;4:265–80.101. Mishra J, Dent C, Tarabishi R, et al. Neutrophilgelatinase–associated lipocalin (NGAL) as a biomarker foracute renal injury after cardiac surgery. Lancet.2005;365:1231–8. 102. Kra wczeski CD, Woo JG, Wang Y, etal. Neutrophil gelatinase–associated lipocalinconcentrations predict development of acute kidney injuryin neonates and children after cardiopulmonary bypass. JPediatr. 2011;158:1009–15e1. 103. Parikh CR, Devarajan P,Zappitelli M, et al. Postoperative biomarkers predictacute kidney injury and poor outcomes after pediatriccardiac surgery. J Am Soc Nephrol. 2011;22:1737–47. 104.Haa se M, Devarajan P, Haase-Fielitz A, et al. The outcomeof neutrophil gelatinase–associated lipocalinpositivesubclinical acute kidney injury: A multicenter pooledanalysis of prospective studies. J Am Coll Cardiol.2011;57:1752–61. 105. Bri enza N, Giglio MT, Marucci M,Fiore T. Does perioperative hemodynamic optimizationprotect renal function in surgical patients? Ameta-analytic study. Crit Care Med. 2009;37:2079–90. 106.Filler G. Acute renal failure in children: Aetiology andmanagement. Paediatr Drugs. 2001;3:783–92. 107. Michael M,
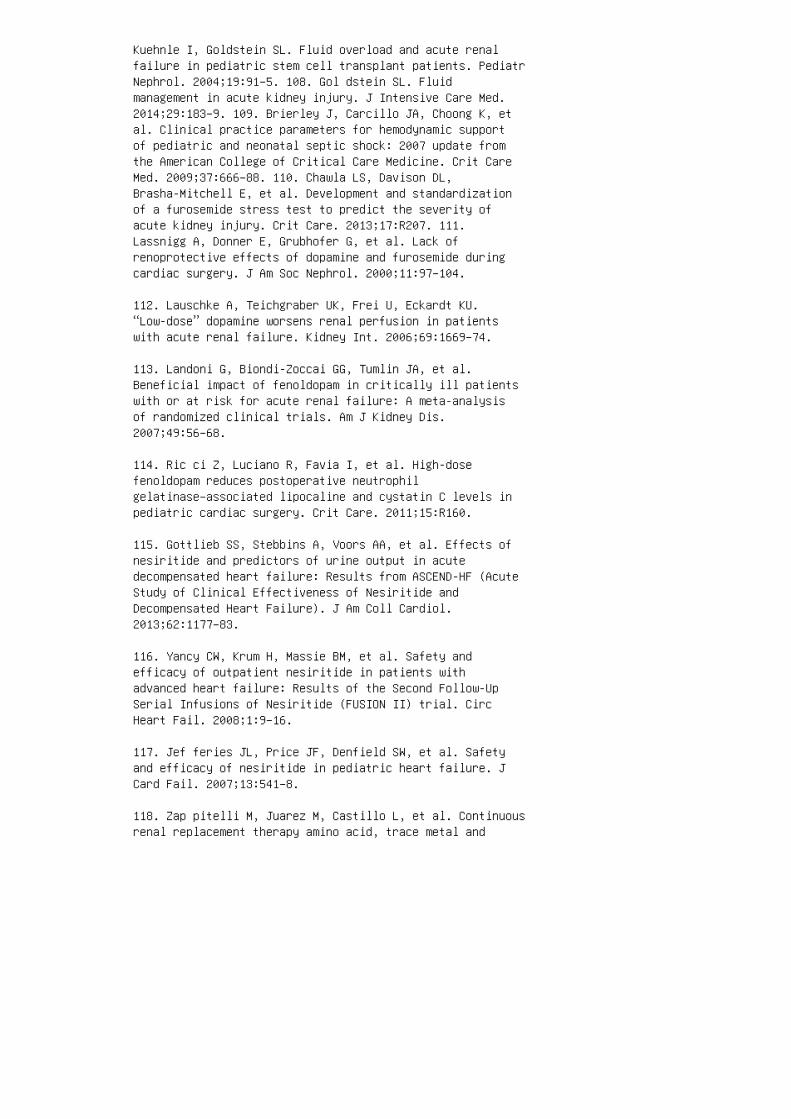
Kuehnle I, Goldstein SL. Fluid overload and acute renalfailure in pediatric stem cell transplant patients. PediatrNephrol. 2004;19:91–5. 108. Gol dstein SL. Fluidmanagement in acute kidney injury. J Intensive Care Med.2014;29:183–9. 109. Brierley J, Carcillo JA, Choong K, etal. Clinical practice parameters for hemodynamic supportof pediatric and neonatal septic shock: 2007 update fromthe American College of Critical Care Medicine. Crit CareMed. 2009;37:666–88. 110. Chawla LS, Davison DL,Brasha-Mitchell E, et al. Development and standardizationof a furosemide stress test to predict the severity ofacute kidney injury. Crit Care. 2013;17:R207. 111.Lassnigg A, Donner E, Grubhofer G, et al. Lack ofrenoprotective effects of dopamine and furosemide duringcardiac surgery. J Am Soc Nephrol. 2000;11:97–104.
112. Lauschke A, Teichgraber UK, Frei U, Eckardt KU.“Low-dose” dopamine worsens renal perfusion in patientswith acute renal failure. Kidney Int. 2006;69:1669–74.
113. Landoni G, Biondi-Zoccai GG, Tumlin JA, et al.Beneficial impact of fenoldopam in critically ill patientswith or at risk for acute renal failure: A meta-analysisof randomized clinical trials. Am J Kidney Dis.2007;49:56–68.
114. Ric ci Z, Luciano R, Favia I, et al. High-dosefenoldopam reduces postoperative neutrophilgelatinase–associated lipocaline and cystatin C levels inpediatric cardiac surgery. Crit Care. 2011;15:R160.
115. Gottlieb SS, Stebbins A, Voors AA, et al. Effects ofnesiritide and predictors of urine output in acutedecompensated heart failure: Results from ASCEND-HF (AcuteStudy of Clinical Effectiveness of Nesiritide andDecompensated Heart Failure). J Am Coll Cardiol.2013;62:1177–83.
116. Yancy CW, Krum H, Massie BM, et al. Safety andefficacy of outpatient nesiritide in patients withadvanced heart failure: Results of the Second Follow-UpSerial Infusions of Nesiritide (FUSION II) trial. CircHeart Fail. 2008;1:9–16.
117. Jef feries JL, Price JF, Denfield SW, et al. Safetyand efficacy of nesiritide in pediatric heart failure. JCard Fail. 2007;13:541–8.
118. Zap pitelli M, Juarez M, Castillo L, et al. Continuousrenal replacement therapy amino acid, trace metal and
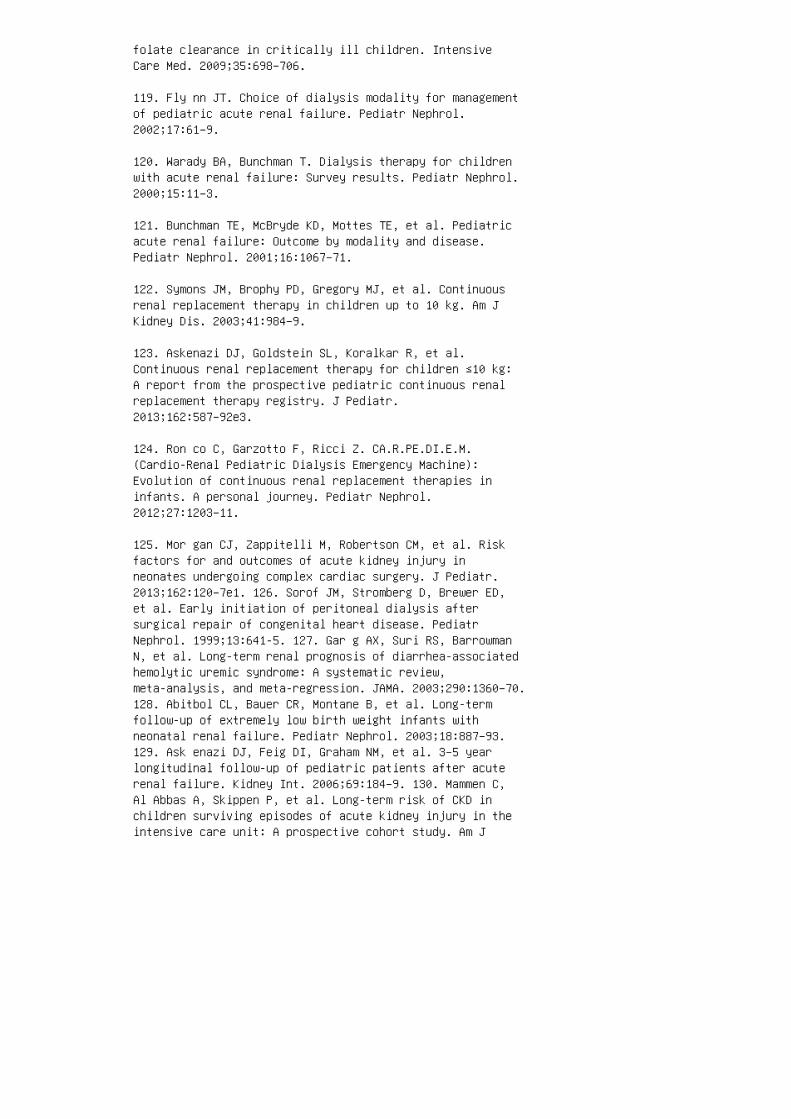
folate clearance in critically ill children. IntensiveCare Med. 2009;35:698–706.
119. Fly nn JT. Choice of dialysis modality for managementof pediatric acute renal failure. Pediatr Nephrol.2002;17:61–9.
120. Warady BA, Bunchman T. Dialysis therapy for childrenwith acute renal failure: Survey results. Pediatr Nephrol.2000;15:11–3.
121. Bunchman TE, McBryde KD, Mottes TE, et al. Pediatricacute renal failure: Outcome by modality and disease.Pediatr Nephrol. 2001;16:1067–71.
122. Symons JM, Brophy PD, Gregory MJ, et al. Continuousrenal replacement therapy in children up to 10 kg. Am JKidney Dis. 2003;41:984–9.
123. Askenazi DJ, Goldstein SL, Koralkar R, et al.Continuous renal replacement therapy for children ≤10 kg:A report from the prospective pediatric continuous renalreplacement therapy registry. J Pediatr.2013;162:587–92e3.
124. Ron co C, Garzotto F, Ricci Z. CA.R.PE.DI.E.M.(Cardio-Renal Pediatric Dialysis Emergency Machine):Evolution of continuous renal replacement therapies ininfants. A personal journey. Pediatr Nephrol.2012;27:1203–11.
125. Mor gan CJ, Zappitelli M, Robertson CM, et al. Riskfactors for and outcomes of acute kidney injury inneonates undergoing complex cardiac surgery. J Pediatr.2013;162:120–7e1. 126. Sorof JM, Stromberg D, Brewer ED,et al. Early initiation of peritoneal dialysis aftersurgical repair of congenital heart disease. PediatrNephrol. 1999;13:641-5. 127. Gar g AX, Suri RS, BarrowmanN, et al. Long-term renal prognosis of diarrhea-associatedhemolytic uremic syndrome: A systematic review,meta-analysis, and meta-regression. JAMA. 2003;290:1360–70.128. Abitbol CL, Bauer CR, Montane B, et al. Long-termfollow-up of extremely low birth weight infants withneonatal renal failure. Pediatr Nephrol. 2003;18:887–93.129. Ask enazi DJ, Feig DI, Graham NM, et al. 3–5 yearlongitudinal follow-up of pediatric patients after acuterenal failure. Kidney Int. 2006;69:184–9. 130. Mammen C,Al Abbas A, Skippen P, et al. Long-term risk of CKD inchildren surviving episodes of acute kidney injury in theintensive care unit: A prospective cohort study. Am J

Kidney Dis. 2012;59:523–30. REVIEW QUESTIONS 1. You havejust initiated peritoneal dialysis for a 5-yearold boy withacute kidney injury (AKI) resulting from hemolytic-uremicsyndrome following infection with Shiga toxin–producing E.coli. �e family is inquiring about the chances of renalfunction recovery. Of the following, the most appropriatestatement regarding the natural history of AKI is: a.Complete renal recovery is the rule. b. Kidneytransplantation is the only hope for renal recovery. c.Progression to chronic kidney disease occurs in 25% ofchildren with dialysis requiring HUS. d. Renal recovery isaided by the use of diuretics. e. Renal recovery isunusual in children with dialysisrequiring AKI. 2. A4-week-old infant with cyanotic heart disease, renaldysplasia, and a baseline serum creatinine of 1.2 mg/dLundergoes a diagnostic cardiac catheterization withcontrast. Five days later, in preparation for cardiacsurgery, the anesthesiologist checks a renal panel andnotes that the serum creatinine is now 2.2 mg/dL. �e urineoutput is normal, and the urinalysis shows a trace amountof protein. Of the following options, the most likelyexplanation for the increase in serum creatinine is: a.Contrast nephropathy b. Laboratory error c. Prerenalazotemia d. Worsening cardiac function e. Wor seningchronic kidney disease 3. A 3-d ay-old infant was born at36 weeks of gestation by emergency cesarean section forfetal distress and placental abruption. Apgar scores were2 and 3 at 1 and 5 minutes, respectively. He was placed onmechanical ventilation and given intravenous hydration. Healso received a single dose of ampicillin and gentamicin,
which was not continued because the result of admis
sion blood culture was negative. Today, the serum cre
atinine is 2.5 mg/dL. Of the following, the most likely
cause of the acute kidney injury is:
a. Nephrotoxicity
b. Perinatal asphyxia
c. Prematurity
d. Respiratory distress syndrome
e. Sepsis
4. You have initiated therapy with enalapril for essential
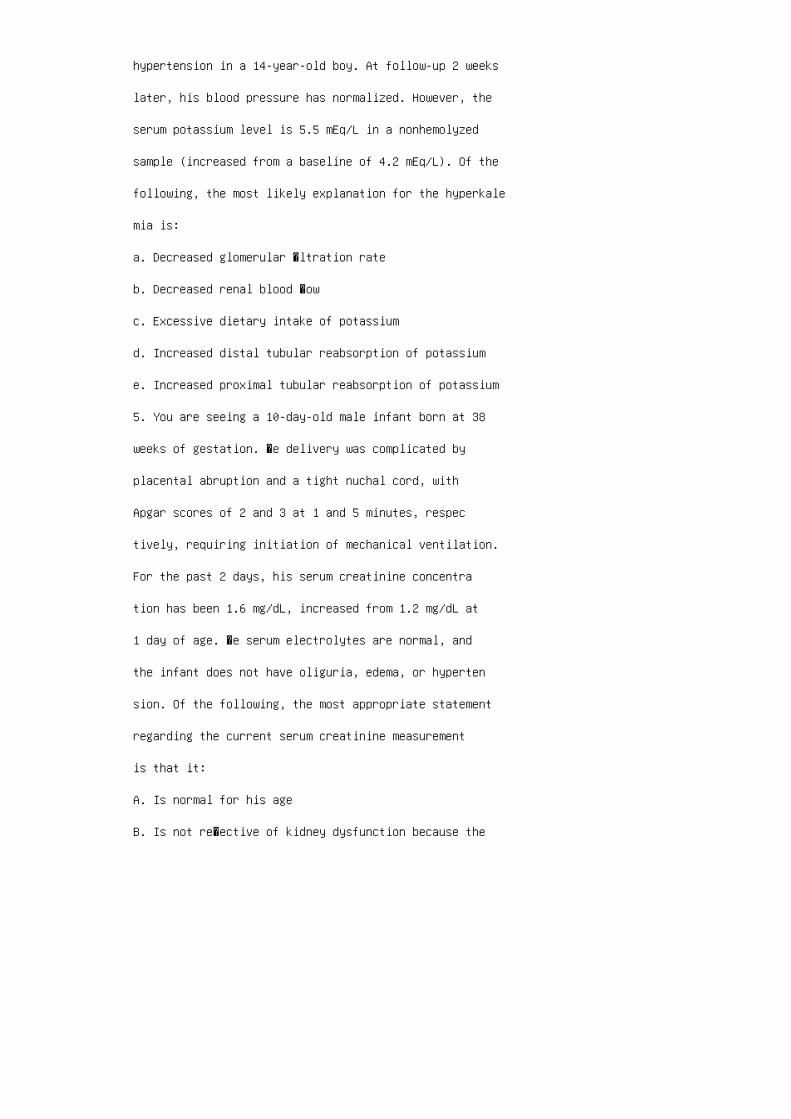
hypertension in a 14-year-old boy. At follow-up 2 weeks
later, his blood pressure has normalized. However, the
serum potassium level is 5.5 mEq/L in a nonhemolyzed
sample (increased from a baseline of 4.2 mEq/L). Of the
following, the most likely explanation for the hyperkale
mia is:
a. Decreased glomerular �ltration rate
b. Decreased renal blood �ow
c. Excessive dietary intake of potassium
d. Increased distal tubular reabsorption of potassium
e. Increased proximal tubular reabsorption of potassium
5. You are seeing a 10-day-old male infant born at 38
weeks of gestation. �e delivery was complicated by
placental abruption and a tight nuchal cord, with
Apgar scores of 2 and 3 at 1 and 5 minutes, respec
tively, requiring initiation of mechanical ventilation.
For the past 2 days, his serum creatinine concentra
tion has been 1.6 mg/dL, increased from 1.2 mg/dL at
1 day of age. �e serum electrolytes are normal, and
the infant does not have oliguria, edema, or hyperten
sion. Of the following, the most appropriate statement
regarding the current serum creatinine measurement
is that it:
A. Is normal for his age
B. Is not re�ective of kidney dysfunction because the
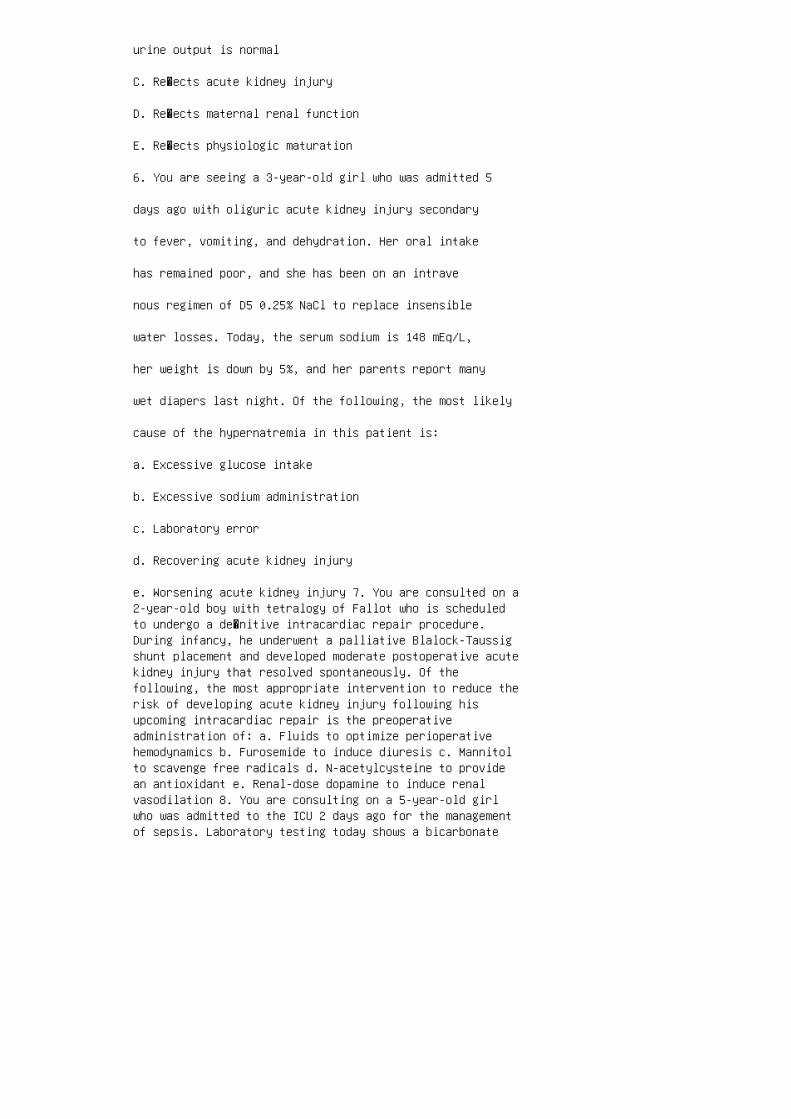
urine output is normal
C. Re�ects acute kidney injury
D. Re�ects maternal renal function
E. Re�ects physiologic maturation
6. You are seeing a 3-year-old girl who was admitted 5
days ago with oliguric acute kidney injury secondary
to fever, vomiting, and dehydration. Her oral intake
has remained poor, and she has been on an intrave
nous regimen of D5 0.25% NaCl to replace insensible
water losses. Today, the serum sodium is 148 mEq/L,
her weight is down by 5%, and her parents report many
wet diapers last night. Of the following, the most likely
cause of the hypernatremia in this patient is:
a. Excessive glucose intake
b. Excessive sodium administration
c. Laboratory error
d. Recovering acute kidney injury
e. Worsening acute kidney injury 7. You are consulted on a2-year-old boy with tetralogy of Fallot who is scheduledto undergo a de�nitive intracardiac repair procedure.During infancy, he underwent a palliative Blalock-Taussigshunt placement and developed moderate postoperative acutekidney injury that resolved spontaneously. Of thefollowing, the most appropriate intervention to reduce therisk of developing acute kidney injury following hisupcoming intracardiac repair is the preoperativeadministration of: a. Fluids to optimize perioperativehemodynamics b. Furosemide to induce diuresis c. Mannitolto scavenge free radicals d. N-acetylcysteine to providean antioxidant e. Renal-dose dopamine to induce renalvasodilation 8. You are consulting on a 5-year-old girlwho was admitted to the ICU 2 days ago for the managementof sepsis. Laboratory testing today shows a bicarbonate

level of 14 mmol/L, BUN 50 mg/dL, and serum creatinine 2.0mg/ dL. �e ICU team is contemplating bicarbonate therapyfor the metabolic acidosis. Of the following, the mostlikely consequence of bicarbonate therapy in this situationis: a. Hyperchloremia b. Hyperkalemia c.Hyperphosphatemia d. Hypocalcemia e. Hyponatremia 9. Youare seeing a 6-yearold boy who was admitted to thecritical care unit 3 days ago with septic shock. He hasrequired multiple boluses of crystalloids and colloids forhypotension and multiple blood products for disseminatedintravascular coagulation. His urine output has beendecreasing for the past 24 h, and he has been anuric forthe past 12 h. He has developed generalized edema, and hisweight is now 26 kg (up from an admission weight of 20kg). He has received two doses of intravenous furosemide(3 mg/kg) during the past 12 h, with no diuretic response.Of the following, the most appropriate next step in hismanagement is: a. Continue furosemide every 6 h. b.Initiate mannitol diuresis. c. Start fenoldopam. d.Initiate a trial of IV normal saline bolus. e. Prepare forrenal replacement therapy. 10. You are seeing a 5-year-oldboy who initially presented to the emergency departmentabout 24 h ago with a 3-day history of fever, vomiting,poor oral intake, and 1 day of no urine output. Initialassessment in the emergency department found tachycardia,hypotension, lethargy, and di�use abdominal tenderness. Hewas given �uid resuscitation, started on intravenousvancomycin (10 mg/kg/dose every 6 h) and gentamicin (2.5mg/kg/ dose every 8 h), and admitted for close observation.He continues to have anuria. �e serum creatinineconcentration today is 1.6 mg/dL (increased from 0.8 mg/dLat
initial presentation). Of the following, the most appro
priate next step in the management of this patient’s
intravenous antibiotic regimen is:
a. Adjust the antibiotics for a glomerular �ltration rate(GFR) of 75 mL/min.
b. Adjust the antibiotics for a GFR of 50 mL/min.
c. Adjust the antibiotics for a GFR of 10 mL/min.
d. Continue the current regimen of antibiotics.
e. Stop all antibiotics. ANSWER KEY 1. c 2. a 3. b 4. a5. c 6. d 7. a 8. d 9. e 10. c


31 Chronic kidney disease
1. U.S. Renal Data System. USRDS 2013 Annual Data Report:Atlas of Chronic Kidney Disease and End-Stage RenalDisease in the United States. Bethesda, MD: NationalInstitutes of Health, National Institute of Diabetes andDigestive and Kidney Diseases; 2013.
2. Kidney Disease Outcomes Quality Initiative. Clinicalpractice guidelines for chronic kidney dis ease:Evaluation, classification, and stratification. A m J Kidney Dis. 2002;39:S1–266.
3. Kid ney Disease: Improving Global Outcomes CKD WorkGroup. KDIGO 2012 clinical practice guide line for theevaluation and management of chronic kid ney disease.Kidney Int Suppl. 2013;3:1–150.
4. Leve y AS, Eckardt KU, Tsukamoto Y, et al. Definitionand classification of chronic kidney dis ease: A positionstatement from Kidney Disease: Imp roving Global Outcomes(KDIGO). Kidney Int. 2005;67:2089–100.
5. Sch wartz GJ, Brion LP, Spitzer A. The use of plasmacreatinine concentration for estimat ing glomerularfiltration rate in infants, children, and adolescents.Pediatr Clin North Am. 1 987 ;34:571–90.
6. Sch wartz GJ, Furth SL. Glomerular filtration ratemeasurement and estimation in chronic kidney disease.Pediatr Nephrol. 2007;22:1839–48.
7. Counahan R, Chantler C, Ghazali S, et al. Estimation ofglomerular filtration rate from plasma creatinineconcentration in children. Arch Dis Child. 1976;51:875–8.
8. App le F, Bandt C, Prosch A, et al. Creatinineclearance: Enzymatic vs Jaffe determinations of creatininein plasma and urine. Clin Chem. 1986;32:388–90.
9. Levey AS, Stevens LA, Schmid CH, et al. A new equationto estimate glomerular filtration rate. Ann Intern Med.2009;150:604–12.
10. Coresh J, Selvin E, Stevens LA, et al. Prevalence ofchronic kidney disease in the United States. JAMA.2007;298:2038–47.
11. Ard issino G, Dacco V, Testa S, et al. Epidemiology ofchronic renal failure in children: Data from the ItalKid

project. Pediatrics. 2003;111:e382–7.
12. Warady BA, Chadha V. Chronic kidney disease inchildren: The global perspective. Pediatr Nephrol.2007;22:1999–2009.
13. Esbjorner E, Berg U, Hansson S. Epidemiology ofchronic renal failure in children: A report from Sweden1986-1994. Swedish Pediatric Nephrology Association.Pediatr Nephrol. 1997;11:438–42.
14. Deleau J, Andre JL, Briancon S, Musse JP. Chronicrenal failure in children: An epidemiological survey inLorraine (France) 1975-1990. Pediatr Nephrol.1994;8:472–6. 15. Ishikura K, Uemura O, Ito S, et al.Pre-dialysis chronic kidney disease in children: Resultsof a nationwide survey in Japan. Nephrol Dial Transplant.2013;28:2345–55. 16. U.S . Renal Data System. USRDS 2005Annual Data Report: Atlas of End-Stage Renal Disease inthe United States, Bethesda, MD: National Institutes ofHealth, National Institute of Diabetes and Digestive andKidney Diseases; 2005. 17. North American Pediatric RenalTrials and Collaborative Studies. 2008 Annual Report:Renal Transplantation, Dialysis, Chronic RenalInsufficiency. 2008. Available athttps://web.emmes.com/study/ped/annlrept/Annual%20Report%20-2008.pdf. AccessedDecember 25, 2015. 18. Harambat J, van Stralen KJ, Kim JJ,Tizard EJ. Epidemiology of chronic kidney disease inchildren. Pediatr Nephrol. 2012;27:363–73. 19. Orr NI,McDonald SP, McTaggart S, et al. Frequency, etiology andtreatment of childhood end-stage kidney disease inAustralia and New Zealand. Pediatr Nephrol.2009;24:1719–26. 20. Lew is MA, Shaw J, Sinha MD, et al.Demography of the UK paediatric renal replacement therapypopulation in 2008. Nephron Clin Pract. 2008;115(Suppl1):c278–88. 21. Eur opean Renal Association and EuropeanDialysis and Transplant Association. Registry 2011.Available at http://www.espn-reg.org/files/ESPN%20ERAEDTA%20AR2011.pdf. Accessed March 16, 2015. 22. Hattori S, Yosioka K, Honda M, Ito H. The 1998 report of theJapanese National Registry data on pediatric end-stagerenal disease patients. Pediatr Nephrol. 2002:17:456–61.23. Nor th American Pediatric Renal Trials andCollaborative Studies. 2011 annual report: Dialysis. 2011.24. Hostetter TH, Olson JL, Rennke HG, et al.Hyperfiltration in remnant nephrons: A potentially adverseresponse to renal ablation. Am J Physiol. 1981;241:F85–93.25. Hostetter TH, Troy JL, Brenner BM. Glomerularhemodynamics in experimental diabetes mellitus. Kidney
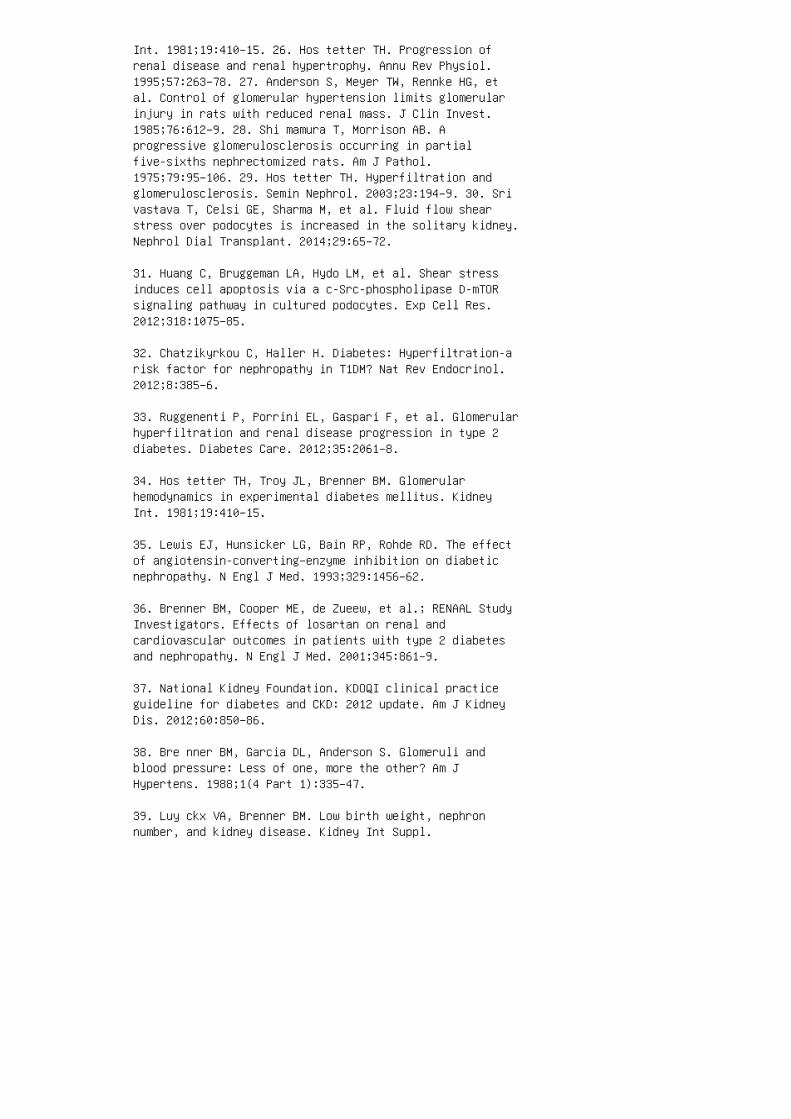
Int. 1981;19:410–15. 26. Hos tetter TH. Progression ofrenal disease and renal hypertrophy. Annu Rev Physiol.1995;57:263–78. 27. Anderson S, Meyer TW, Rennke HG, etal. Control of glomerular hypertension limits glomerularinjury in rats with reduced renal mass. J Clin Invest.1985;76:612–9. 28. Shi mamura T, Morrison AB. Aprogressive glomerulosclerosis occurring in partialfive-sixths nephrectomized rats. Am J Pathol.1975;79:95–106. 29. Hos tetter TH. Hyperfiltration andglomerulosclerosis. Semin Nephrol. 2003;23:194–9. 30. Srivastava T, Celsi GE, Sharma M, et al. Fluid flow shearstress over podocytes is increased in the solitary kidney.Nephrol Dial Transplant. 2014;29:65–72.
31. Huang C, Bruggeman LA, Hydo LM, et al. Shear stressinduces cell apoptosis via a c-Src-phospholipase D-mTORsignaling pathway in cultured podocytes. Exp Cell Res.2012;318:1075–85.
32. Chatzikyrkou C, Haller H. Diabetes: Hyperfiltration-arisk factor for nephropathy in T1DM? Nat Rev Endocrinol.2012;8:385–6.
33. Ruggenenti P, Porrini EL, Gaspari F, et al. Glomerularhyperfiltration and renal disease progression in type 2diabetes. Diabetes Care. 2012;35:2061–8.
34. Hos tetter TH, Troy JL, Brenner BM. Glomerularhemodynamics in experimental diabetes mellitus. KidneyInt. 1981;19:410–15.
35. Lewis EJ, Hunsicker LG, Bain RP, Rohde RD. The effectof angiotensin-converting–enzyme inhibition on diabeticnephropathy. N Engl J Med. 1993;329:1456–62.
36. Brenner BM, Cooper ME, de Zueew, et al.; RENAAL StudyInvestigators. Effects of losartan on renal andcardiovascular outcomes in patients with type 2 diabetesand nephropathy. N Engl J Med. 2001;345:861–9.
37. National Kidney Foundation. KDOQI clinical practiceguideline for diabetes and CKD: 2012 update. Am J KidneyDis. 2012;60:850–86.
38. Bre nner BM, Garcia DL, Anderson S. Glomeruli andblood pressure: Less of one, more the other? Am JHypertens. 1988;1(4 Part 1):335–47.
39. Luy ckx VA, Brenner BM. Low birth weight, nephronnumber, and kidney disease. Kidney Int Suppl.
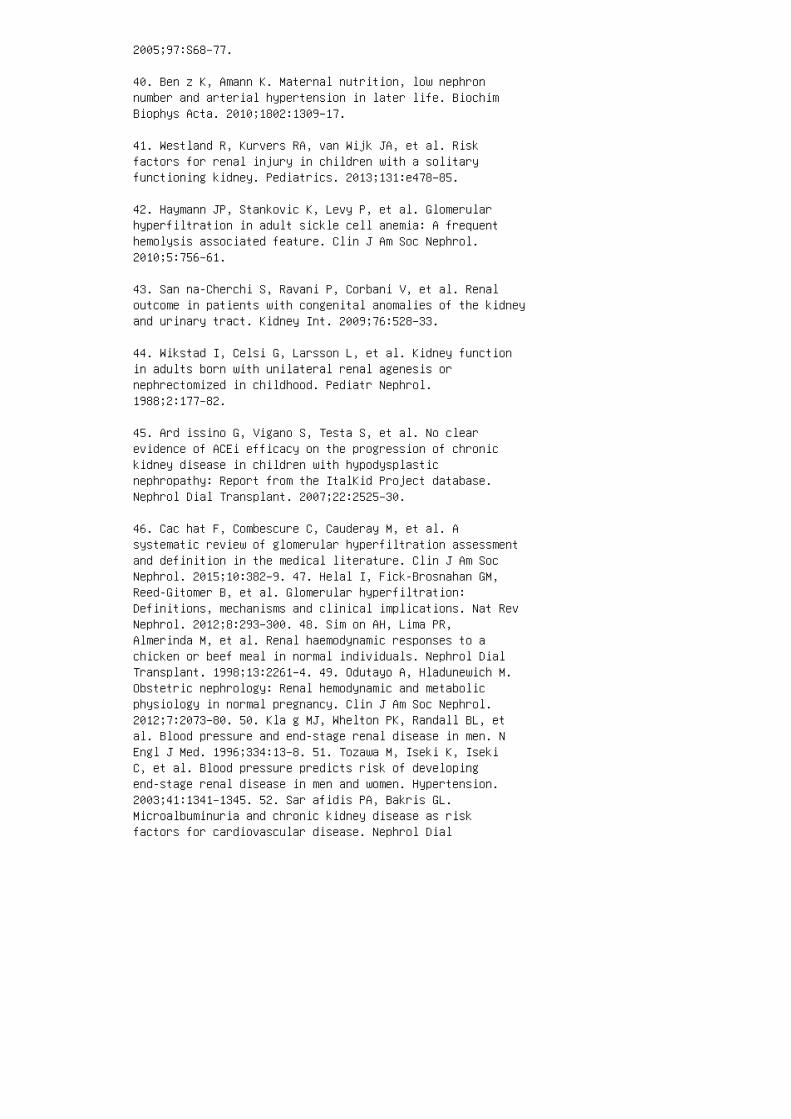
2005;97:S68–77.
40. Ben z K, Amann K. Maternal nutrition, low nephronnumber and arterial hypertension in later life. BiochimBiophys Acta. 2010;1802:1309–17.
41. Westland R, Kurvers RA, van Wijk JA, et al. Riskfactors for renal injury in children with a solitaryfunctioning kidney. Pediatrics. 2013;131:e478–85.
42. Haymann JP, Stankovic K, Levy P, et al. Glomerularhyperfiltration in adult sickle cell anemia: A frequenthemolysis associated feature. Clin J Am Soc Nephrol.2010;5:756–61.
43. San na-Cherchi S, Ravani P, Corbani V, et al. Renaloutcome in patients with congenital anomalies of the kidneyand urinary tract. Kidney Int. 2009;76:528–33.
44. Wikstad I, Celsi G, Larsson L, et al. Kidney functionin adults born with unilateral renal agenesis ornephrectomized in childhood. Pediatr Nephrol.1988;2:177–82.
45. Ard issino G, Vigano S, Testa S, et al. No clearevidence of ACEi efficacy on the progression of chronickidney disease in children with hypodysplasticnephropathy: Report from the ItalKid Project database.Nephrol Dial Transplant. 2007;22:2525–30.
46. Cac hat F, Combescure C, Cauderay M, et al. Asystematic review of glomerular hyperfiltration assessmentand definition in the medical literature. Clin J Am SocNephrol. 2015;10:382–9. 47. Helal I, Fick-Brosnahan GM,Reed-Gitomer B, et al. Glomerular hyperfiltration:Definitions, mechanisms and clinical implications. Nat RevNephrol. 2012;8:293–300. 48. Sim on AH, Lima PR,Almerinda M, et al. Renal haemodynamic responses to achicken or beef meal in normal individuals. Nephrol DialTransplant. 1998;13:2261–4. 49. Odutayo A, Hladunewich M.Obstetric nephrology: Renal hemodynamic and metabolicphysiology in normal pregnancy. Clin J Am Soc Nephrol.2012;7:2073–80. 50. Kla g MJ, Whelton PK, Randall BL, etal. Blood pressure and end-stage renal disease in men. NEngl J Med. 1996;334:13–8. 51. Tozawa M, Iseki K, IsekiC, et al. Blood pressure predicts risk of developingend-stage renal disease in men and women. Hypertension.2003;41:1341–1345. 52. Sar afidis PA, Bakris GL.Microalbuminuria and chronic kidney disease as riskfactors for cardiovascular disease. Nephrol Dial
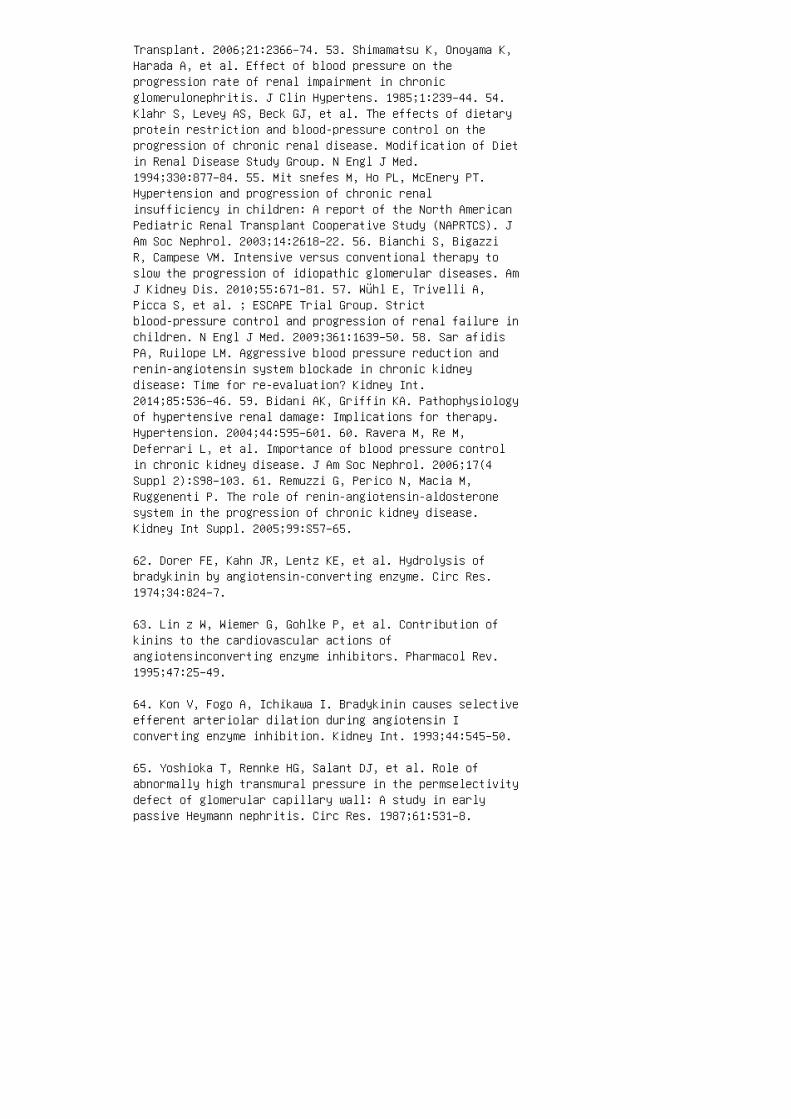
Transplant. 2006;21:2366–74. 53. Shimamatsu K, Onoyama K,Harada A, et al. Effect of blood pressure on theprogression rate of renal impairment in chronicglomerulonephritis. J Clin Hypertens. 1985;1:239–44. 54.Klahr S, Levey AS, Beck GJ, et al. The effects of dietaryprotein restriction and blood-pressure control on theprogression of chronic renal disease. Modification of Dietin Renal Disease Study Group. N Engl J Med.1994;330:877–84. 55. Mit snefes M, Ho PL, McEnery PT.Hypertension and progression of chronic renalinsufficiency in children: A report of the North AmericanPediatric Renal Transplant Cooperative Study (NAPRTCS). JAm Soc Nephrol. 2003;14:2618–22. 56. Bianchi S, BigazziR, Campese VM. Intensive versus conventional therapy toslow the progression of idiopathic glomerular diseases. AmJ Kidney Dis. 2010;55:671–81. 57. Wühl E, Trivelli A,Picca S, et al. ; ESCAPE Trial Group. Strictblood-pressure control and progression of renal failure inchildren. N Engl J Med. 2009;361:1639–50. 58. Sar afidisPA, Ruilope LM. Aggressive blood pressure reduction andrenin-angiotensin system blockade in chronic kidneydisease: Time for re-evaluation? Kidney Int.2014;85:536–46. 59. Bidani AK, Griffin KA. Pathophysiologyof hypertensive renal damage: Implications for therapy.Hypertension. 2004;44:595–601. 60. Ravera M, Re M,Deferrari L, et al. Importance of blood pressure controlin chronic kidney disease. J Am Soc Nephrol. 2006;17(4Suppl 2):S98–103. 61. Remuzzi G, Perico N, Macia M,Ruggenenti P. The role of renin-angiotensin-aldosteronesystem in the progression of chronic kidney disease.Kidney Int Suppl. 2005;99:S57–65.
62. Dorer FE, Kahn JR, Lentz KE, et al. Hydrolysis ofbradykinin by angiotensin-converting enzyme. Circ Res.1974;34:824–7.
63. Lin z W, Wiemer G, Gohlke P, et al. Contribution ofkinins to the cardiovascular actions ofangiotensinconverting enzyme inhibitors. Pharmacol Rev.1995;47:25–49.
64. Kon V, Fogo A, Ichikawa I. Bradykinin causes selectiveefferent arteriolar dilation during angiotensin Iconverting enzyme inhibition. Kidney Int. 1993;44:545–50.
65. Yoshioka T, Rennke HG, Salant DJ, et al. Role ofabnormally high transmural pressure in the permselectivitydefect of glomerular capillary wall: A study in earlypassive Heymann nephritis. Circ Res. 1987;61:531–8.
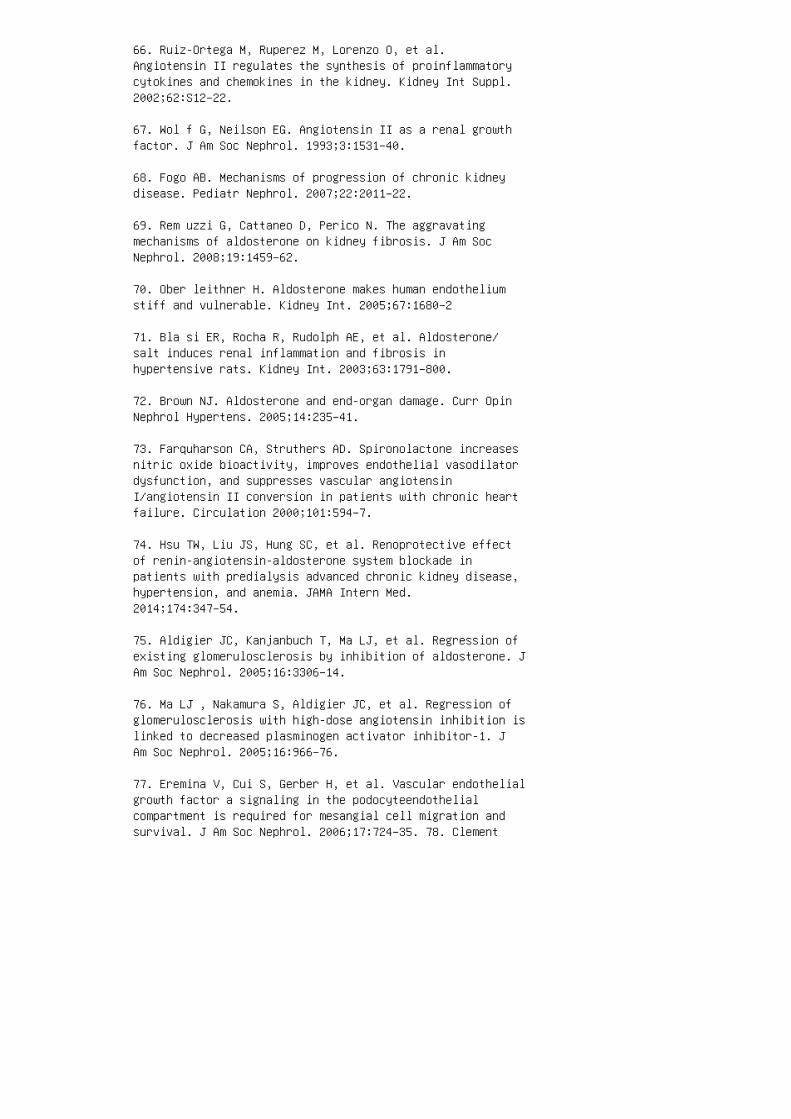
66. Ruiz-Ortega M, Ruperez M, Lorenzo O, et al.Angiotensin II regulates the synthesis of proinflammatorycytokines and chemokines in the kidney. Kidney Int Suppl.2002;62:S12–22.
67. Wol f G, Neilson EG. Angiotensin II as a renal growthfactor. J Am Soc Nephrol. 1993;3:1531–40.
68. Fogo AB. Mechanisms of progression of chronic kidneydisease. Pediatr Nephrol. 2007;22:2011–22.
69. Rem uzzi G, Cattaneo D, Perico N. The aggravatingmechanisms of aldosterone on kidney fibrosis. J Am SocNephrol. 2008;19:1459–62.
70. Ober leithner H. Aldosterone makes human endotheliumstiff and vulnerable. Kidney Int. 2005;67:1680–2
71. Bla si ER, Rocha R, Rudolph AE, et al. Aldosterone/salt induces renal inflammation and fibrosis inhypertensive rats. Kidney Int. 2003;63:1791–800.
72. Brown NJ. Aldosterone and end-organ damage. Curr OpinNephrol Hypertens. 2005;14:235–41.
73. Farquharson CA, Struthers AD. Spironolactone increasesnitric oxide bioactivity, improves endothelial vasodilatordysfunction, and suppresses vascular angiotensinI/angiotensin II conversion in patients with chronic heartfailure. Circulation 2000;101:594–7.
74. Hsu TW, Liu JS, Hung SC, et al. Renoprotective effectof renin-angiotensin-aldosterone system blockade inpatients with predialysis advanced chronic kidney disease,hypertension, and anemia. JAMA Intern Med.2014;174:347–54.
75. Aldigier JC, Kanjanbuch T, Ma LJ, et al. Regression ofexisting glomerulosclerosis by inhibition of aldosterone. JAm Soc Nephrol. 2005;16:3306–14.
76. Ma LJ , Nakamura S, Aldigier JC, et al. Regression ofglomerulosclerosis with high-dose angiotensin inhibition islinked to decreased plasminogen activator inhibitor-1. JAm Soc Nephrol. 2005;16:966–76.
77. Eremina V, Cui S, Gerber H, et al. Vascular endothelialgrowth factor a signaling in the podocyteendothelialcompartment is required for mesangial cell migration andsurvival. J Am Soc Nephrol. 2006;17:724–35. 78. Clement

LC, Avila-Casado C, Macé C, et al. Podocyte-secretedangiopoietin-like-4 mediates proteinuria inglucocorticoid-sensitive nephrotic syndrome. Nat Med.2011;17:117–22. 79. Wha rram BL, Goyal M, Wiggins JE, etal. Podocyte depletion causes glomerulosclerosis:Diphtheria toxin-induced podocyte depletion in ratsexpressing human diphtheria toxin receptor transgene. J AmSoc Nephrol. 2005;16:2941–52. 80. Fukuda A, Chowdhury MA,Venkatareddy MP, et al. Growth-dependent podocyte failurecauses glomerulosclerosis. J Am Soc Nephrol.2012;23:1351–63. 81. Gerritsen ME, Bloor CM. Endothelialcell gene expression in response to injury. FASEB J.1993;7:523–32. 82. Liu Y. Renal fibrosis: New insightsinto the pathogenesis and therapeutics. Kidney Int.2006;69:213–7. 83. Fat hallah-Shaykh SA, Flynn JT, PierceCB, et al. Progression of Pediatric CKD of nonglomerularorigin in the CKiD cohort. Clin J Am Soc Nephrol.2015;10:571–7. 84. Sanc hez-Niño MD, Fernandez-FernandezB, PerezGomez MV, et al. Albumin-induced apoptosis oftubular cells is modulated by BASP1. Cell Death Dis.2015;6:e1644. 85. She erin NS, Sacks SH. Leaked proteinand interstitial damage in the kidney: Is complement themissing link? Clin Exp Immunol. 2002;130:1–3. 86. Boo rP, Konieczny A, Villa L, et al. Complement C5 mediatesexperimental tubulointerstitial fibrosis. J Am SocNephrol. 2007;18:1508–15. 87. Gor riz JL,Martinez-Castelao A. Proteinuria: Detection and role innative renal disease progression. Transplant Rev (Orlando).2012;26:3–13. 88. de Goeij MC, Liem M, de Jager DJ, et al.Proteinuria as a risk marker for the progression ofchronic kidney disease in patients on predialysis care andthe role of angiotensin-converting enzymeinhibitor/angiotensin II receptor blocker treatment.Nephron Clin Pract. 2012;121:c73–82. 89. Ruan XZ,Varghese Z, Moorhead JF. An update on the lipidnephrotoxicity hypothesis. Nat Rev Nephrol. 2009;5:713–21.90. Chawla V, Greene T, Beck GJ, et al. Hyperlipidemia andlong-term outcomes in nondiabetic chronic kidney disease.Clin J Am Soc Nephrol. 2010;5:1582–7. 91. Kasiske BL,O’Donnell MP, Schmitz PG, Kim Y, Keane WF. Renal injury ofdiet-induced hypercholesterolemia in rats. Kidney Int.1990;37:880–91. 92. Chen SC, Hung CC, Kuo MC, et al.Association of dyslipidemia with renal outcomes in chronickidney disease. PLoS One. 2013;8:e55643. 93. Cases A,Coll E. Dyslipidemia and the progression of renal diseasein chronic renal failure patients. Kidney Int Suppl.2005;99:S87–93.
94. Abrass CK. Cellular lipid metabolism and the role oflipids in progressive renal disease. Am J Nephrol.
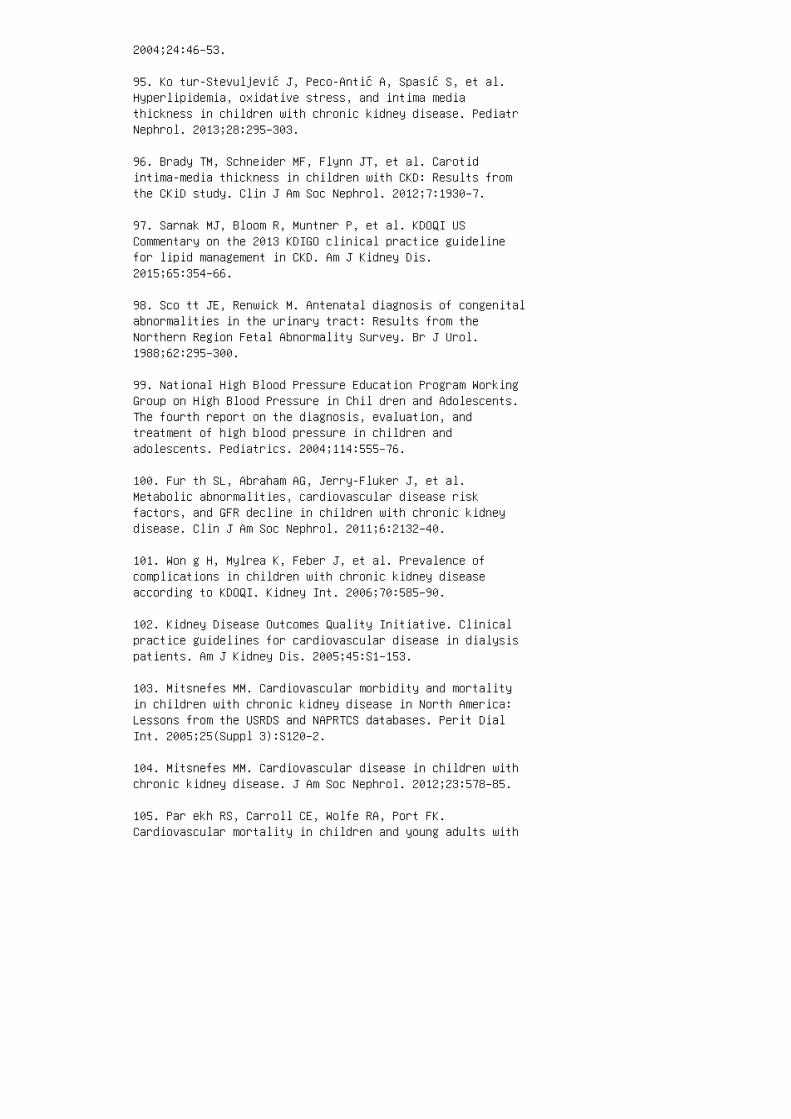
2004;24:46–53.
95. Ko tur-Stevuljević J, Peco-Antić A, Spasić S, et al.Hyperlipidemia, oxidative stress, and intima mediathickness in children with chronic kidney disease. PediatrNephrol. 2013;28:295–303.
96. Brady TM, Schneider MF, Flynn JT, et al. Carotidintima-media thickness in children with CKD: Results fromthe CKiD study. Clin J Am Soc Nephrol. 2012;7:1930–7.
97. Sarnak MJ, Bloom R, Muntner P, et al. KDOQI USCommentary on the 2013 KDIGO clinical practice guidelinefor lipid management in CKD. Am J Kidney Dis.2015;65:354–66.
98. Sco tt JE, Renwick M. Antenatal diagnosis of congenitalabnormalities in the urinary tract: Results from theNorthern Region Fetal Abnormality Survey. Br J Urol.1988;62:295–300.
99. National High Blood Pressure Education Program WorkingGroup on High Blood Pressure in Chil dren and Adolescents.The fourth report on the diagnosis, evaluation, andtreatment of high blood pressure in children andadolescents. Pediatrics. 2004;114:555–76.
100. Fur th SL, Abraham AG, Jerry-Fluker J, et al.Metabolic abnormalities, cardiovascular disease riskfactors, and GFR decline in children with chronic kidneydisease. Clin J Am Soc Nephrol. 2011;6:2132–40.
101. Won g H, Mylrea K, Feber J, et al. Prevalence ofcomplications in children with chronic kidney diseaseaccording to KDOQI. Kidney Int. 2006;70:585–90.
102. Kidney Disease Outcomes Quality Initiative. Clinicalpractice guidelines for cardiovascular disease in dialysispatients. Am J Kidney Dis. 2005;45:S1–153.
103. Mitsnefes MM. Cardiovascular morbidity and mortalityin children with chronic kidney disease in North America:Lessons from the USRDS and NAPRTCS databases. Perit DialInt. 2005;25(Suppl 3):S120–2.
104. Mitsnefes MM. Cardiovascular disease in children withchronic kidney disease. J Am Soc Nephrol. 2012;23:578–85.
105. Par ekh RS, Carroll CE, Wolfe RA, Port FK.Cardiovascular mortality in children and young adults with

end-stage kidney disease. J Pediatr. 2002;141:191–7.
106. Chavers BM, Li S, Collins AJ, Herzog CA.Cardiovascular disease in pediatric chronic dialysispatients. Kidney Int. 2002;62:648–53.
107. Mit snefes MM, Daniels SR, Schwartz SM, et al. Severeleft ventricular hypertrophy in pediatric dialysis:Prevalence and predictors. Pediatr Nephrol.2000;14:898–902.
108. Mat teucci MC, Wuhl E, Picca S, et al. Leftventricular geometry in children with mild to moderatechronic renal insufficiency. J Am Soc Nephrol.2006;17:218–26. 109. Mitsnefes MM, Daniels SR, SchwartzSM, et al. Changes in left ventricular mass in childrenand adolescents during chronic dialysis. Pediatr Nephrol.2001;16:318–23. 110. Goo dman WG, Goldin J, Kuizon BD, etal. Coronaryartery calcification in young adults withend-stage renal disease who are undergoing dialysis. NEngl J Med. 2000;342:1478–83. 111. Civilibal M, CaliskanS, Adaletli I, et al. Coronary artery calcifications inchildren with end-stage renal disease. Pediatr Nephrol.2006;21:1426–33. 112. Kid ney Disease Outcomes QualityInitiative. Clinical practice guidelines and clinicalpractice recommendations for anemia in chronic kidneydisease. Am J Kidney Dis. 2006;47:S11–145. 113. Levin NW.Quality of life and hematocrit level. Am J Kidney Dis.1992;20:16–20. 114. Wol cott DL, Marsh JT, La Rue A, etal. Recombinant human erythropoietin treatment may improvequality of life and cognitive function in chronichemodialysis patients. Am J Kidney Dis. 1989;14:478–85.115. Moreno F, Sanz-Guajardo D, Lopez-Gomez JM, et al.Increasing the hematocrit has a beneficial effect onquality of life and is safe in selected hemodialysispatients. J Am Soc Nephrol. 2000;11:335–42. 116. FadrowskiJJ, Pierce CB, Cole SR, et al. Hemoglobin decline inchildren with chronic kidney disease: Baseline resultsfrom the chronic kidney disease in children prospectivecohort study. Clin J Am Soc Nephrol. 2008;3:457–62. 117.Ast or BC, Muntner P, Levin A, et al. Association ofkidney function with anemia: The Third National Health andNutrition Examination Survey (19881994). Arch Intern Med.2002;162:1401–8. 118. Don nelly S. Why is erythropoietinmade in the kidney? The kidney functions as a critmeter.Am J Kidney Dis. 2001;38:415–25. 119. Ganz T. Hepcidin, akey regulator of iron metabolism and mediator of anemia ofinflammation. Blood 2003;102:783–8. 120. Coyne DW.Hepcidin: Clinical utility as a diagnostic tool andtherapeutic target. Kidney Int. 2011;80:240–4. 121.
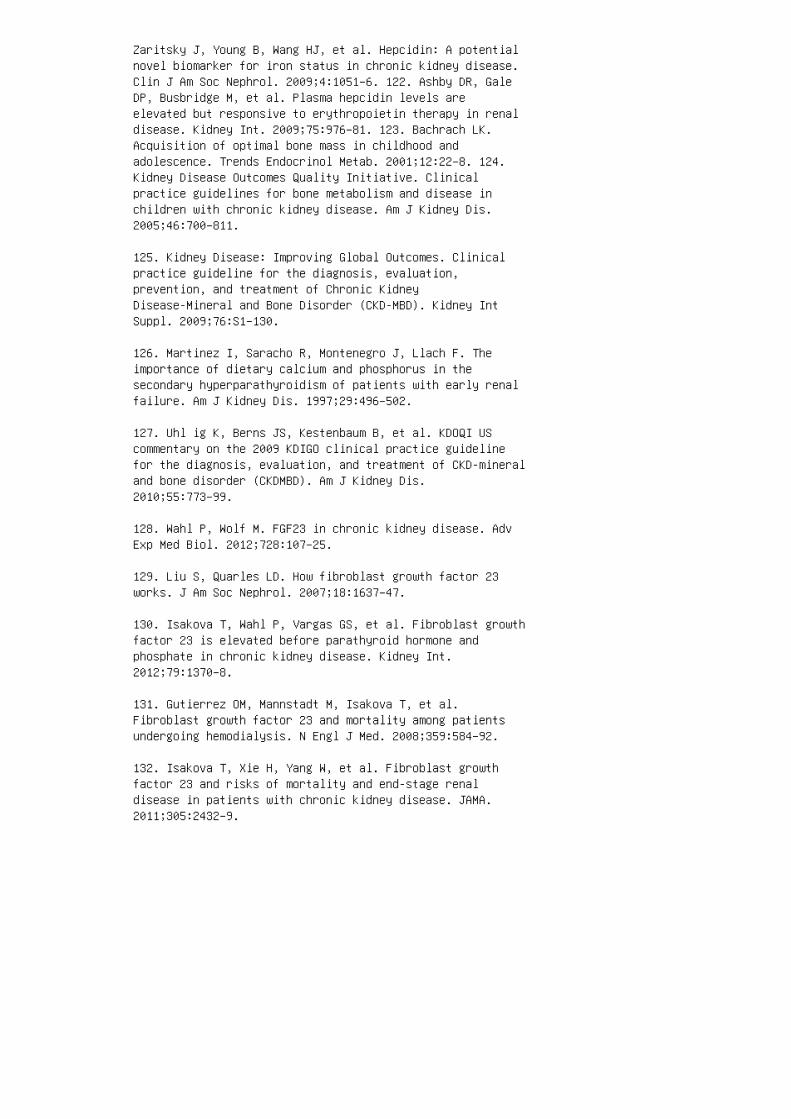
Zaritsky J, Young B, Wang HJ, et al. Hepcidin: A potentialnovel biomarker for iron status in chronic kidney disease.Clin J Am Soc Nephrol. 2009;4:1051–6. 122. Ashby DR, GaleDP, Busbridge M, et al. Plasma hepcidin levels areelevated but responsive to erythropoietin therapy in renaldisease. Kidney Int. 2009;75:976–81. 123. Bachrach LK.Acquisition of optimal bone mass in childhood andadolescence. Trends Endocrinol Metab. 2001;12:22–8. 124.Kidney Disease Outcomes Quality Initiative. Clinicalpractice guidelines for bone metabolism and disease inchildren with chronic kidney disease. Am J Kidney Dis.2005;46:700–811.
125. Kidney Disease: Improving Global Outcomes. Clinicalpractice guideline for the diagnosis, evaluation,prevention, and treatment of Chronic KidneyDisease-Mineral and Bone Disorder (CKD-MBD). Kidney IntSuppl. 2009;76:S1–130.
126. Martinez I, Saracho R, Montenegro J, Llach F. Theimportance of dietary calcium and phosphorus in thesecondary hyperparathyroidism of patients with early renalfailure. Am J Kidney Dis. 1997;29:496–502.
127. Uhl ig K, Berns JS, Kestenbaum B, et al. KDOQI UScommentary on the 2009 KDIGO clinical practice guidelinefor the diagnosis, evaluation, and treatment of CKD-mineraland bone disorder (CKDMBD). Am J Kidney Dis.2010;55:773–99.
128. Wahl P, Wolf M. FGF23 in chronic kidney disease. AdvExp Med Biol. 2012;728:107–25.
129. Liu S, Quarles LD. How fibroblast growth factor 23works. J Am Soc Nephrol. 2007;18:1637–47.
130. Isakova T, Wahl P, Vargas GS, et al. Fibroblast growthfactor 23 is elevated before parathyroid hormone andphosphate in chronic kidney disease. Kidney Int.2012;79:1370–8.
131. Gutierrez OM, Mannstadt M, Isakova T, et al.Fibroblast growth factor 23 and mortality among patientsundergoing hemodialysis. N Engl J Med. 2008;359:584–92.
132. Isakova T, Xie H, Yang W, et al. Fibroblast growthfactor 23 and risks of mortality and end-stage renaldisease in patients with chronic kidney disease. JAMA.2011;305:2432–9.

133. Fau l C, Amaral AP, Oskouei B, et al. FGF23 inducesleft ventricular hypertrophy. J Clin Invest.2011;121:4393–408.
134. Mal luche HH, Mawad HW, Monier-Faugere MC. Renalosteodystrophy in the first decade of the new millennium:Analysis of 630 bone biopsies in black and white patients.J Bone Miner Res. 2011;26:1368–76.
135. Wong CS, Gipson DS, Gillen DL, et al. Anthropometricmeasures and risk of death in children with end-stage renaldisease. Am J Kidney Dis. 2000;36:811–9.
136. Fur th SL, Hwang W, Yang C, et al. Growth failure,risk of hospitalization and death for children withend-stage renal disease. Pediatr Nephrol. 2002;17:450–5.
137. Rosenkranz J, Reichwald-Klugger E, Oh J, et al.Psychosocial rehabilitation and satisfaction with life inadults with childhood-onset of end-stage renal disease.Pediatr Nephrol. 2005;20:1288–94.
138. AlUzri A, Matheson M, Gipson DS, et al. The impact ofshort stature on health-related quality of life inchildren with chronic kidney disease. J Pediatr.2013;163:736–41.
139. Kid ney Disease Outcomes Quality Initiative. Clinicalpractice guideline for nutrition in children with CKD:2008 update—Executive summary. Am J Kidney Dis.2009;53:S11–104. 140. Karlberg J. A biologically-orientedmathematical model (ICP) for human growth. Acta PaediatrScand Suppl. 1989;350:70–94. 141. Clark PA, Rogol AD.Growth hormones and sex steroid interactions at puberty.Endocrinol Metab Clin North Am. 1996;25:665–81. 142.Ravelli AM, Ledermann SE, Bisset WM, et al. Foregut motorfunction in chronic renal failure. Arch Dis Child.1992;67:1343–7. 143. Mak RH, Cheung W, Cone RD, Marks DL.Leptin and inflammation-associated cachexia in chronickidney disease. Kidney Int. 2006;69:794–7. 144. Uta ka S,Avesani CM, Draibe SA, et al. Inflammation is associatedwith increased energy expenditure in patients with chronickidney disease. Am J Clin Nutr. 2005;82:801–5. 145.Parekh RS, Flynn JT, Smoyer WE, et al. Improved growth inyoung children with severe chronic renal insufficiency whouse specified nutritional therapy. J Am Soc Nephrol.2001;12:2418–26. 146. Roe lfsema V, Clark RG. The growthhormone and insulin-like growth factor axis: Itsmanipulation for the benefit of growth disorders in renalfailure. J Am Soc Nephrol. 2001;12:1297–306. 147. Yakar

S, Rosen CJ, Beamer WG, et al. Circulating levels of IGF-1directly regulate bone growth and density. J Clin Invest.2002;110:771–81. 148. Haffner D, Schaefer F, Girard J, etal. Metabolic clearance of recombinant human growthhormone in health and chronic renal failure. J ClinInvest. 1994;93:1163–71. 149. Sch aefer F, Chen Y, TsaoT, et al. Impaired JAKSTAT signal transduction contributesto growth hormone resistance in chronic uremia. J ClinInvest. 2001;108:467–75. 150. Sun DF, Zheng Z, Tummala P,et al. Chronic uremia attenuates growth hormone-inducedsignal transduction in skeletal muscle. J Am Soc Nephrol.2004;15:2630–6. 151. Rabkin R, Sun DF, Chen Y, et al.Growth hormone resistance in uremia, a role for impairedJAK/STAT signaling. Pediatr Nephrol. 2005;20:313–8. 152.Kaysen GA. The microinflammatory state in uremia: Causesand potential consequences. J Am Soc Nephrol.2001;12:1549–57. 153. Juul A, Flyvbjerg A, Frystyk J, etal. Serum concentrations of free and total insulin-likegrowth factor-I, IGF binding proteins -1 and -3 andIGFBP-3 protease activity in boys with normal orprecocious puberty. Clin Endocrinol (Oxf). 1996;44:515–23.154. Tonshoff B, Blum WF, Wingen AM, Mehls O. Seruminsulin-like growth factors (IGFs) and IGF bindingproteins 1, 2, and 3 in children with chronic renalfailure: Relationship to height and glomerular filtrationrate. The European Study Group for Nutritional Treatmentof Chronic Renal Failure in Childhood. J Clin EndocrinolMetab. 1995;80:2684–91.
155. Wren AM, Seal LJ, Cohen MA, et al. Ghrelin enhancesappetite and increases food intake in humans. J ClinEndocrinol Metab. 2001;86:5992.
156. Koj ima M, Hosoda H, Date Y, et al. Ghrelin is agrowth-hormone-releasing acylated peptide from stomach.Nature. 1999;402:656–60.
157. Bock GH, Conners CK, Ruley J, et al. Disturbances ofbrain maturation and neurodevelopment during chronic renalfailure in infancy. J Pediatr. 1989;114:231–8.
158. Gre enbaum LA, Warady BA, Furth SL. Current advancesin chronic kidney disease in children: Growth,cardiovascular, and neurocognitive risk factors. SeminNephrol. 2009;29:425–34.
159. Schnaper HW, Cole BR, Hodges FJ, Robson AM. Cerebralcortical atrophy in pediatric patients with end-stagerenal disease. Am J Kidney Dis. 1983;2:645–50.
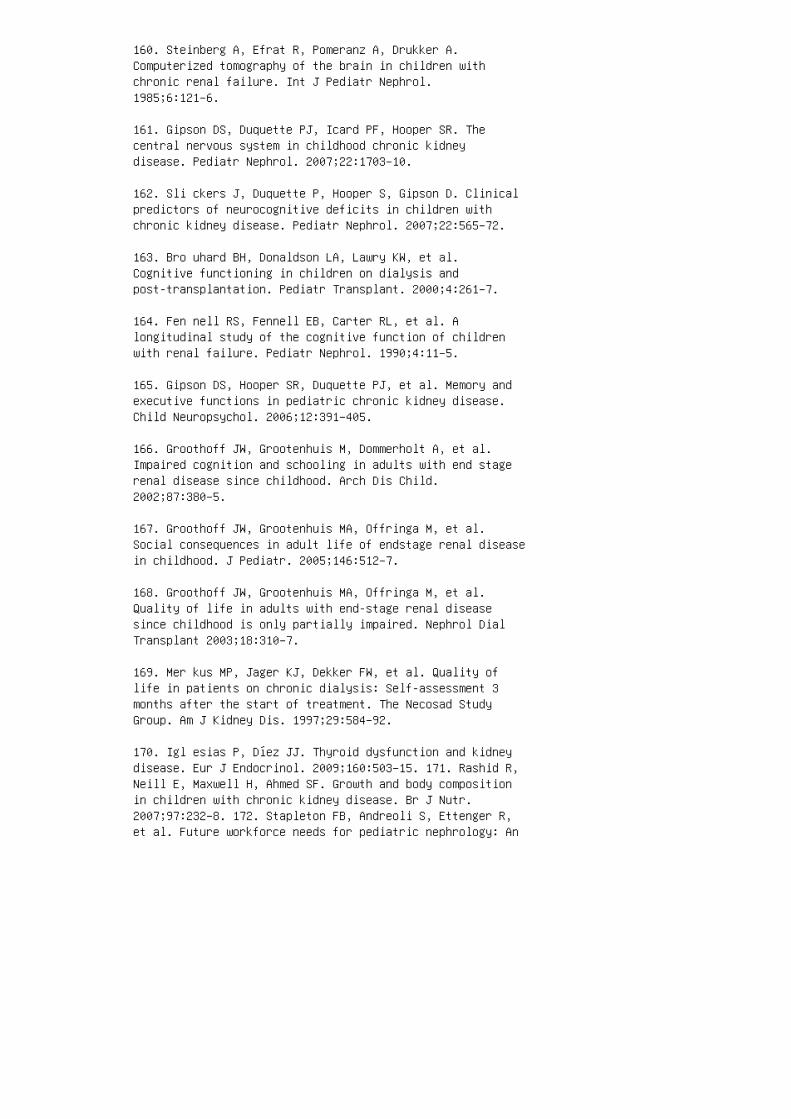
160. Steinberg A, Efrat R, Pomeranz A, Drukker A.Computerized tomography of the brain in children withchronic renal failure. Int J Pediatr Nephrol.1985;6:121–6.
161. Gipson DS, Duquette PJ, Icard PF, Hooper SR. Thecentral nervous system in childhood chronic kidneydisease. Pediatr Nephrol. 2007;22:1703–10.
162. Sli ckers J, Duquette P, Hooper S, Gipson D. Clinicalpredictors of neurocognitive deficits in children withchronic kidney disease. Pediatr Nephrol. 2007;22:565–72.
163. Bro uhard BH, Donaldson LA, Lawry KW, et al.Cognitive functioning in children on dialysis andpost-transplantation. Pediatr Transplant. 2000;4:261–7.
164. Fen nell RS, Fennell EB, Carter RL, et al. Alongitudinal study of the cognitive function of childrenwith renal failure. Pediatr Nephrol. 1990;4:11–5.
165. Gipson DS, Hooper SR, Duquette PJ, et al. Memory andexecutive functions in pediatric chronic kidney disease.Child Neuropsychol. 2006;12:391–405.
166. Groothoff JW, Grootenhuis M, Dommerholt A, et al.Impaired cognition and schooling in adults with end stagerenal disease since childhood. Arch Dis Child.2002;87:380–5.
167. Groothoff JW, Grootenhuis MA, Offringa M, et al.Social consequences in adult life of endstage renal diseasein childhood. J Pediatr. 2005;146:512–7.
168. Groothoff JW, Grootenhuis MA, Offringa M, et al.Quality of life in adults with end-stage renal diseasesince childhood is only partially impaired. Nephrol DialTransplant 2003;18:310–7.
169. Mer kus MP, Jager KJ, Dekker FW, et al. Quality oflife in patients on chronic dialysis: Self-assessment 3months after the start of treatment. The Necosad StudyGroup. Am J Kidney Dis. 1997;29:584–92.
170. Igl esias P, Díez JJ. Thyroid dysfunction and kidneydisease. Eur J Endocrinol. 2009;160:503–15. 171. Rashid R,Neill E, Maxwell H, Ahmed SF. Growth and body compositionin children with chronic kidney disease. Br J Nutr.2007;97:232–8. 172. Stapleton FB, Andreoli S, Ettenger R,et al. Future workforce needs for pediatric nephrology: An

analysis of the nephrology workforce and trainingrequirements by the Workforce Committee of the AmericanSociety of Pediatric Nephrology. J Am Soc Nephrol.1997;8:S5–8. 173. Khan SS, Xue JL, Kazmi WH, et al. Doespredialysis nephrology care influence patient survivalafter initiation of dialysis? Kidney Int. 2005;67:1038–46.174. The G ISEN Group (Gruppo Italiano di StudiEpidemiologici in Nefrologia). Randomised placebocontrolledtrial of effect of ramipril on decline in glomerularfiltration rate and risk of terminal renal failure inproteinuric, non-diabetic nephropathy. Lancet.1997;349:1857–63. 175. Jac obsen P, Andersen S, Rossing K,Jensen BR, Parving H-H. Dual blockade of therenin-angiotensin system versus maximal recommended doseof ACE inhibition in diabetic nephropathy. Kidney Int.2003;63:1874–80. 176. Bia nchi S, Bigazzi R, Campese VM.Long-term effects of spironolactone on proteinuria andkidney function in patients with chronic kidney disease.Kidney Int. 2006;70:2116–23. 177. Flynn JT, Mitsnefes M,Pierce C, et al. Blood pressure in children with chronickidney disease: A report from the Chronic Kidney Diseasein Children study. Hypertension. 2008;52:631–7. 178. Mitsnefes M, Flynn J, Cohn S, et al. Masked hypertensionassociates with left ventricular hypertrophy in childrenwith CKD. J Am Soc Nephrol. 2010;21:137–44. 179. Kid neyDisease Outcomes Quality Initiative. Clinical practiceguidelines on hypertension and antihypertensive agents inchronic kidney disease. Am J Kidney Dis. 2004;43:S1–290.180. Mitch WE. Dietary protein restriction in chronic renalfailure: Nutritional efficacy, compliance, and progressionof renal insufficiency. J Am Soc Nephrol. 1991;2:823–31.181. Bernhard J, Beaufrere B, Laville M, Fouque D.Adaptive response to a low-protein diet in predialysischronic renal failure patients. J Am Soc Nephrol.2001;12:1249–54. 182. Fukui M, Nakamura T, Ebihara I, etal. Low-protein diet attenuates increased gene expressionof platelet-derived growth factor and transforming growthfactor-beta in experimental glomerular sclerosis. J LabClin Med. 1993;121:224–34. 183. Chaturvedi S, Jones C.Protein restriction for children with chronic renalfailure. Cochrane Database Syst Rev. 2007;(4)006863. 184.Madero M, Sarnak MJ, Wang X, et al. Uric acid andlong-term outcomes in CKD. Am J Kidney Dis.2009;53:796–803.
185. Goicoechea M, de Vinuesa SG, Verdalles U, et al.Effect of allopurinol in chronic kidney diseaseprogression and cardiovascular risk. Clin J Am SocNephrol. 2010;5:1388–93.
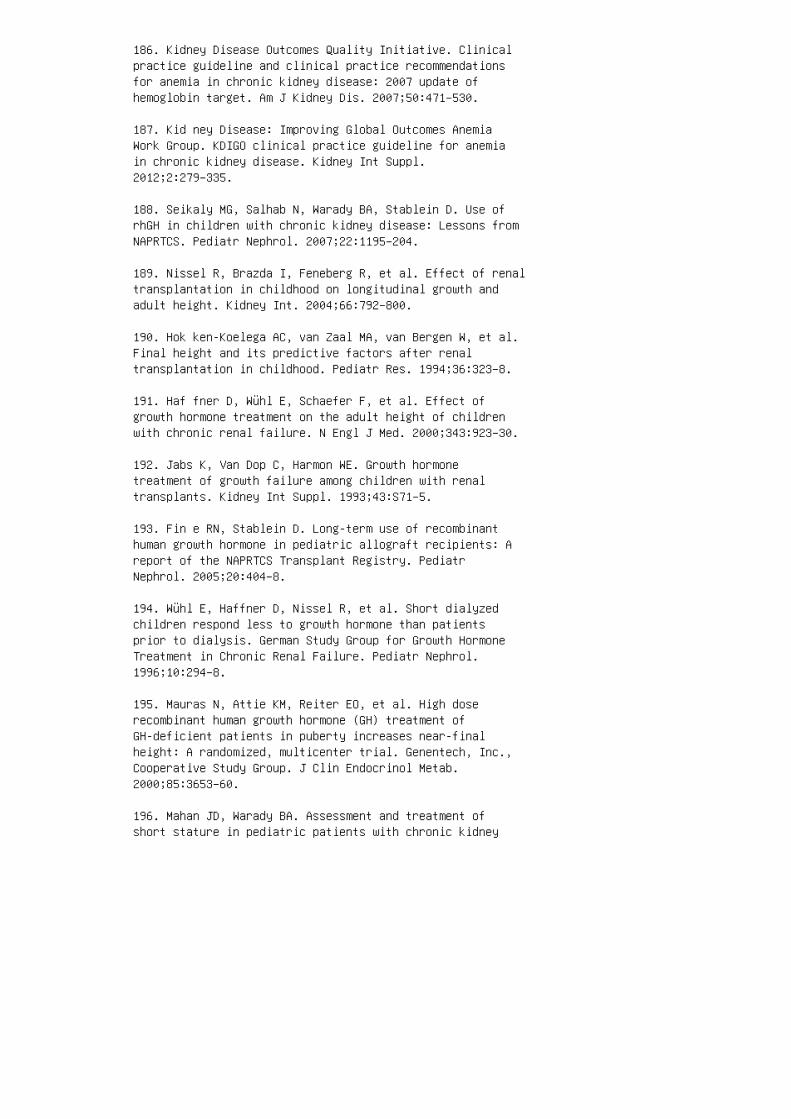
186. Kidney Disease Outcomes Quality Initiative. Clinicalpractice guideline and clinical practice recommendationsfor anemia in chronic kidney disease: 2007 update ofhemoglobin target. Am J Kidney Dis. 2007;50:471–530.
187. Kid ney Disease: Improving Global Outcomes AnemiaWork Group. KDIGO clinical practice guideline for anemiain chronic kidney disease. Kidney Int Suppl.2012;2:279–335.
188. Seikaly MG, Salhab N, Warady BA, Stablein D. Use ofrhGH in children with chronic kidney disease: Lessons fromNAPRTCS. Pediatr Nephrol. 2007;22:1195–204.
189. Nissel R, Brazda I, Feneberg R, et al. Effect of renaltransplantation in childhood on longitudinal growth andadult height. Kidney Int. 2004;66:792–800.
190. Hok ken-Koelega AC, van Zaal MA, van Bergen W, et al.Final height and its predictive factors after renaltransplantation in childhood. Pediatr Res. 1994;36:323–8.
191. Haf fner D, Wühl E, Schaefer F, et al. Effect ofgrowth hormone treatment on the adult height of childrenwith chronic renal failure. N Engl J Med. 2000;343:923–30.
192. Jabs K, Van Dop C, Harmon WE. Growth hormonetreatment of growth failure among children with renaltransplants. Kidney Int Suppl. 1993;43:S71–5.
193. Fin e RN, Stablein D. Long-term use of recombinanthuman growth hormone in pediatric allograft recipients: Areport of the NAPRTCS Transplant Registry. PediatrNephrol. 2005;20:404–8.
194. Wühl E, Haffner D, Nissel R, et al. Short dialyzedchildren respond less to growth hormone than patientsprior to dialysis. German Study Group for Growth HormoneTreatment in Chronic Renal Failure. Pediatr Nephrol.1996;10:294–8.
195. Mauras N, Attie KM, Reiter EO, et al. High doserecombinant human growth hormone (GH) treatment ofGH-deficient patients in puberty increases near-finalheight: A randomized, multicenter trial. Genentech, Inc.,Cooperative Study Group. J Clin Endocrinol Metab.2000;85:3653–60.
196. Mahan JD, Warady BA. Assessment and treatment ofshort stature in pediatric patients with chronic kidney

disease: A consensus statement. Pediatr Nephrol.2006;21:917–30.
197. Kas iske BL, Snyder JJ, Matas AJ, et al. Preemptivekidney transplantation: The advantage and the advantaged.J Am Soc Nephrol. 2002;13:1358–64.
198. Vat s AN, Donaldson L, Fine RN, Chavers BM.Pretransplant dialysis status and outcome of renaltransplantation in North American children: A NAPRTCSStudy. North American Pediatric Renal TransplantCooperative Study. Transplantation. 2000;69:1414–9. 199.Mitch WE, Walser M, Buffington GA, et al. A simple methodof estimating progression of chronic renal failure.Lancet. 1976;2:1326–8. 200. Ham ilton BE, Hoyert DL,Martin JA, et al. Annual summary of vital statistics:2010-2011. Pediatrics. 2013;131:548–58. 201. McDonald SP,Craig JC. Long-term survival of children with end-stagerenal disease. N Engl J Med. 2004;350:2654–62. REVIEWQUESTIONS 1. �e most common cause of CKD in children is:a. Focal segmental glomerulosclerosis b. Polycystic kidneydisease c. Congenital anomalies of the kidneys and urinarytract (CAKUT) d. Imm une-mediated glomerulonephritis e.Hemo lytic-uremic syndrome 2. �e in cidence of ESRD inchildren: a. Dec reases with increasing age b. Rema insthe same throughout childhood and adolescence c. Is highest in children younger than 4 years d. Inc reases withadvancing age 3. In th e United States, FSGS is thepredominant cause of CKD in: a. Afr ican Americans b.His panics c. Whit es d. Nati ve Americans e. Asi anAmericans 4. Mor tality of children with ESRD is highestin which age group? a. 0 to 4 years b. 5 to 14 years c.15 to 19 years 5. Angiotensin II plays a role inprogression of CKD by: a. Causing predominant a�erent overe�erent arteriolar vasoconstriction b. Decreasingsingle-nephron GFR c. Increasing proin�ammatory cytokines,chemokines, and cell adhesion molecules d. Stimulatingaldosterone, which itself is injurious to the kidney e.a, b, and d f. c and d 6. What is the most commoncomplication of CKD in children? a. Anemia b.Hypertension c. Fluid and electrolyte abnormalities d.Growth failure e. Mineral and bone disorder
7. �e prevalence of LVH in pediatric dialysis patients is:a. 10% b. 20% c. 30% d. Up to 50% e. Up to 75%
8. In children the fastest rate of growth occurs: a.During infancy b. Age 1 to 4 years c. Age 4 to 10 yearsd. During puberty

9. All of the following contribute to growth impairment inchildren with CKD, except: a. Malnutrition b. Anemia c.GH de�ciency d. Altered post–receptor signaling of JAK2and STAT proteins e. Reduced bioavailability of IGF-1
10. All of the following central and neurocognitive de�citsoccur in children with CKD except: a. Cerebral atrophy b.Speech and language delay c. Lower educational attainmentd. Lower IQ scores e. Macrocephaly and hydrocephalus 11.In children with CKD, all but one of the followingtherapeutic interventions slow progression. a.ACE-inhibitors or angiotensin receptor blockers b. Bloodpressure control c. Minimizing proteinuria d.Cholesterol-lowering therapy ANSWER KEY 1. c 2. d 3. a4. a 5. f 6. b 7. e 8. a 9. c 10. e 11. d

32 Anemia in chronic kidney disease
Adjustment of ESA dosing should be controlled to
minimize large �uctuations in Hb level. KEY POINTS ●Hyporesponsiveness to ESA therapy is common. ● �e risksand bene�ts of escalation of ESA dose versus red bloodcell transfusion must be balanced for individual patients.SUMMARY Anemia is prevalent and is associated with adverseoutcomes in children with CKD. Although various factorscontribute to anemia risk, EPO insu�ciency and ironde�ciency are the major underlying etiologic factors, andthey are the mechanisms most commonly targeted by currenttherapies. Ongoing therapeutic challenges includehepcidin-mediated iron-restricted erythropoiesis andconcerns about the safety and e�cacy of escalating ESAdoses for refractory anemia. Most recommendations regardingESA use and dosing are based on data from adult trials;there have been no interventional studies examining thee�ects of ESA administration on clinical outcomes inchildren. Nevertheless, ESAs continue to be importantcomponents of CKD care in children; use of ESAs shouldbalance the risks and bene�ts.
5. Hollowell JG, van Assendelft OW, Gunter EW, et al.Hematological and iron-related analytes— Reference data forpersons aged 1 year and over: United States, 1988–94. Datafrom the Third National Health Examination Survey. VitalHealth Stat 11. 2005;(247):1–156.
6. Jackson RT. Separate hemoglobin standards for blacksand whites: A critical review of the case for separate andunequal hemoglobin standards. Med Hypotheses.1990;32:181–9.
7. Atkinson MA, Pierce CB, Zack RM, et al. Hemoglobindifferences by race in children with CKD. Am J Kidney Dis.2010;55:1009–17.
8. Filler G, Mylrea K, Feber J, et al. How to define anemiain children with chronic kidney disease? Pediatr Nephrol.2007;22:702–7.
9. Greenbaum LA. Anemia in children with chronic kidneydisease. Adv Chronic Kidney Dis. 2005;12:385–96.
10. Atkinson MA, Martz K, Warady BA, et al. Risk foranemia in pediatric chronic kidney disease patients: Areport of NAPRTCS. Pediatr Nephrol. 2010;25:1699–706.
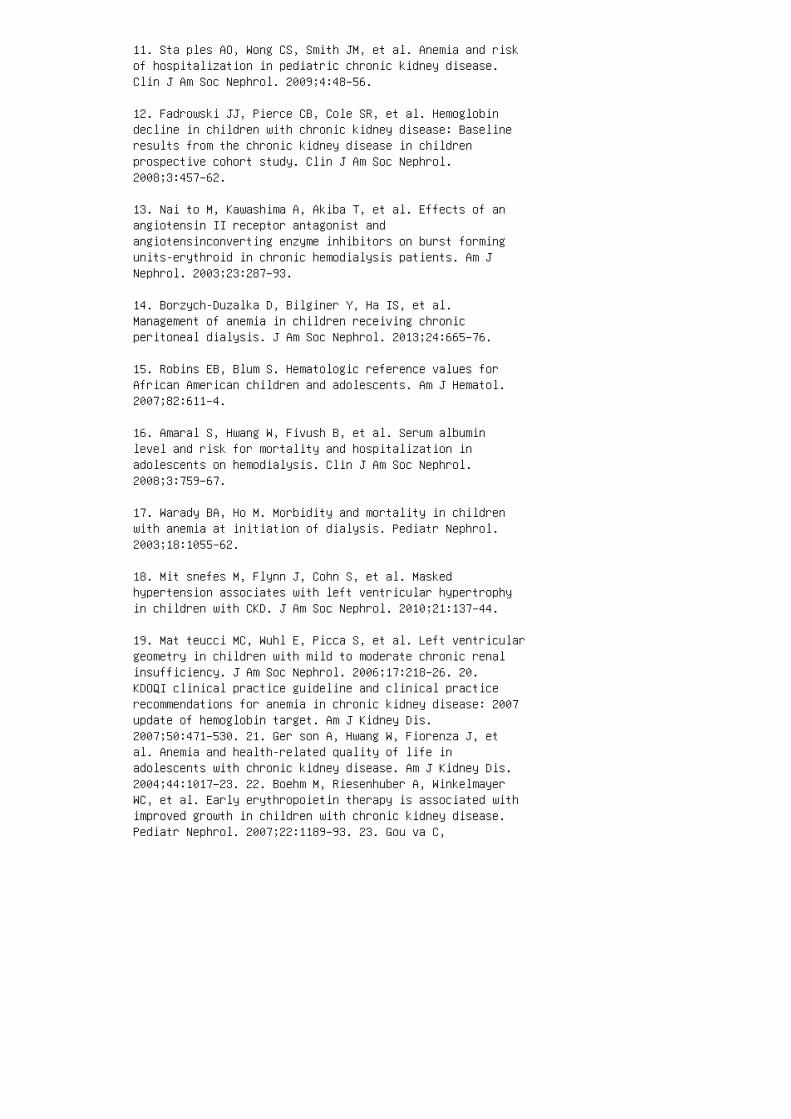
11. Sta ples AO, Wong CS, Smith JM, et al. Anemia and riskof hospitalization in pediatric chronic kidney disease.Clin J Am Soc Nephrol. 2009;4:48–56.
12. Fadrowski JJ, Pierce CB, Cole SR, et al. Hemoglobindecline in children with chronic kidney disease: Baselineresults from the chronic kidney disease in childrenprospective cohort study. Clin J Am Soc Nephrol.2008;3:457–62.
13. Nai to M, Kawashima A, Akiba T, et al. Effects of anangiotensin II receptor antagonist andangiotensinconverting enzyme inhibitors on burst formingunits-erythroid in chronic hemodialysis patients. Am JNephrol. 2003;23:287–93.
14. Borzych-Duzalka D, Bilginer Y, Ha IS, et al.Management of anemia in children receiving chronicperitoneal dialysis. J Am Soc Nephrol. 2013;24:665–76.
15. Robins EB, Blum S. Hematologic reference values forAfrican American children and adolescents. Am J Hematol.2007;82:611–4.
16. Amaral S, Hwang W, Fivush B, et al. Serum albuminlevel and risk for mortality and hospitalization inadolescents on hemodialysis. Clin J Am Soc Nephrol.2008;3:759–67.
17. Warady BA, Ho M. Morbidity and mortality in childrenwith anemia at initiation of dialysis. Pediatr Nephrol.2003;18:1055–62.
18. Mit snefes M, Flynn J, Cohn S, et al. Maskedhypertension associates with left ventricular hypertrophyin children with CKD. J Am Soc Nephrol. 2010;21:137–44.
19. Mat teucci MC, Wuhl E, Picca S, et al. Left ventriculargeometry in children with mild to moderate chronic renalinsufficiency. J Am Soc Nephrol. 2006;17:218–26. 20.KDOQI clinical practice guideline and clinical practicerecommendations for anemia in chronic kidney disease: 2007update of hemoglobin target. Am J Kidney Dis.2007;50:471–530. 21. Ger son A, Hwang W, Fiorenza J, etal. Anemia and health-related quality of life inadolescents with chronic kidney disease. Am J Kidney Dis.2004;44:1017–23. 22. Boehm M, Riesenhuber A, WinkelmayerWC, et al. Early erythropoietin therapy is associated withimproved growth in children with chronic kidney disease.Pediatr Nephrol. 2007;22:1189–93. 23. Gou va C,
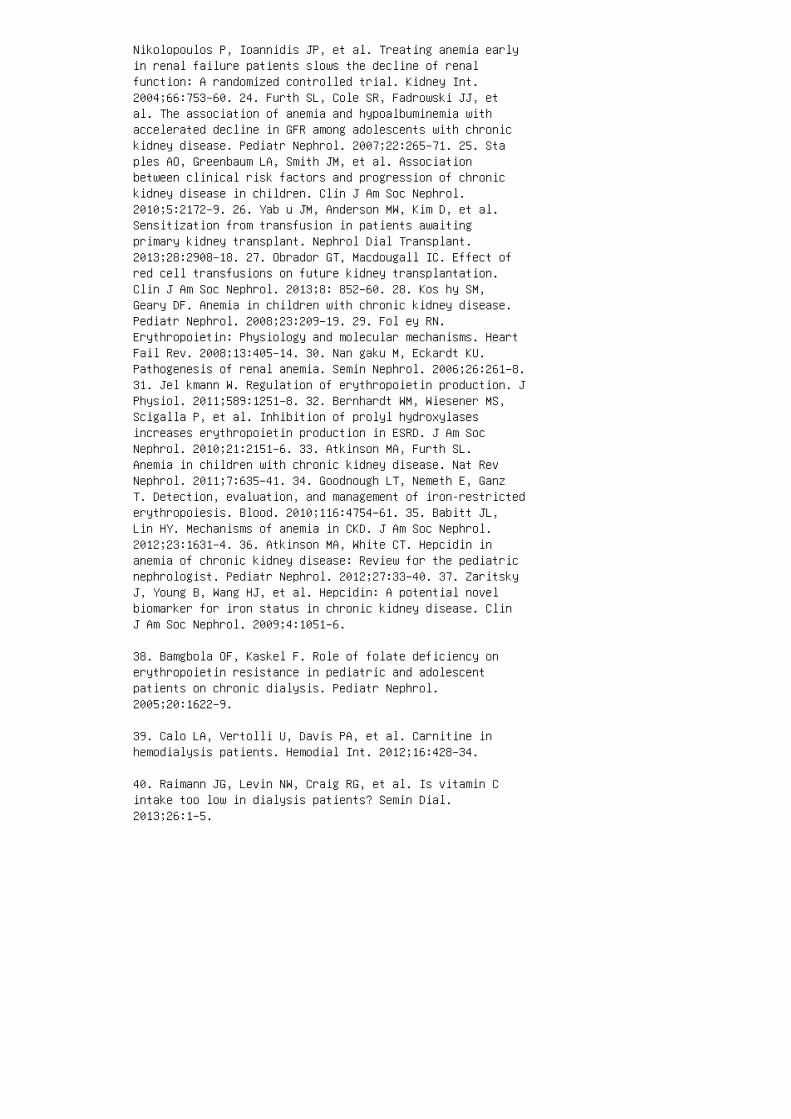
Nikolopoulos P, Ioannidis JP, et al. Treating anemia earlyin renal failure patients slows the decline of renalfunction: A randomized controlled trial. Kidney Int.2004;66:753–60. 24. Furth SL, Cole SR, Fadrowski JJ, etal. The association of anemia and hypoalbuminemia withaccelerated decline in GFR among adolescents with chronickidney disease. Pediatr Nephrol. 2007;22:265–71. 25. Staples AO, Greenbaum LA, Smith JM, et al. Associationbetween clinical risk factors and progression of chronickidney disease in children. Clin J Am Soc Nephrol.2010;5:2172–9. 26. Yab u JM, Anderson MW, Kim D, et al.Sensitization from transfusion in patients awaitingprimary kidney transplant. Nephrol Dial Transplant.2013;28:2908–18. 27. Obrador GT, Macdougall IC. Effect ofred cell transfusions on future kidney transplantation.Clin J Am Soc Nephrol. 2013;8: 852–60. 28. Kos hy SM,Geary DF. Anemia in children with chronic kidney disease.Pediatr Nephrol. 2008;23:209–19. 29. Fol ey RN.Erythropoietin: Physiology and molecular mechanisms. HeartFail Rev. 2008;13:405–14. 30. Nan gaku M, Eckardt KU.Pathogenesis of renal anemia. Semin Nephrol. 2006;26:261–8.31. Jel kmann W. Regulation of erythropoietin production. JPhysiol. 2011;589:1251–8. 32. Bernhardt WM, Wiesener MS,Scigalla P, et al. Inhibition of prolyl hydroxylasesincreases erythropoietin production in ESRD. J Am SocNephrol. 2010;21:2151–6. 33. Atkinson MA, Furth SL.Anemia in children with chronic kidney disease. Nat RevNephrol. 2011;7:635–41. 34. Goodnough LT, Nemeth E, GanzT. Detection, evaluation, and management of iron-restrictederythropoiesis. Blood. 2010;116:4754–61. 35. Babitt JL,Lin HY. Mechanisms of anemia in CKD. J Am Soc Nephrol.2012;23:1631–4. 36. Atkinson MA, White CT. Hepcidin inanemia of chronic kidney disease: Review for the pediatricnephrologist. Pediatr Nephrol. 2012;27:33–40. 37. ZaritskyJ, Young B, Wang HJ, et al. Hepcidin: A potential novelbiomarker for iron status in chronic kidney disease. ClinJ Am Soc Nephrol. 2009;4:1051–6.
38. Bamgbola OF, Kaskel F. Role of folate deficiency onerythropoietin resistance in pediatric and adolescentpatients on chronic dialysis. Pediatr Nephrol.2005;20:1622–9.
39. Calo LA, Vertolli U, Davis PA, et al. Carnitine inhemodialysis patients. Hemodial Int. 2012;16:428–34.
40. Raimann JG, Levin NW, Craig RG, et al. Is vitamin Cintake too low in dialysis patients? Semin Dial.2013;26:1–5.
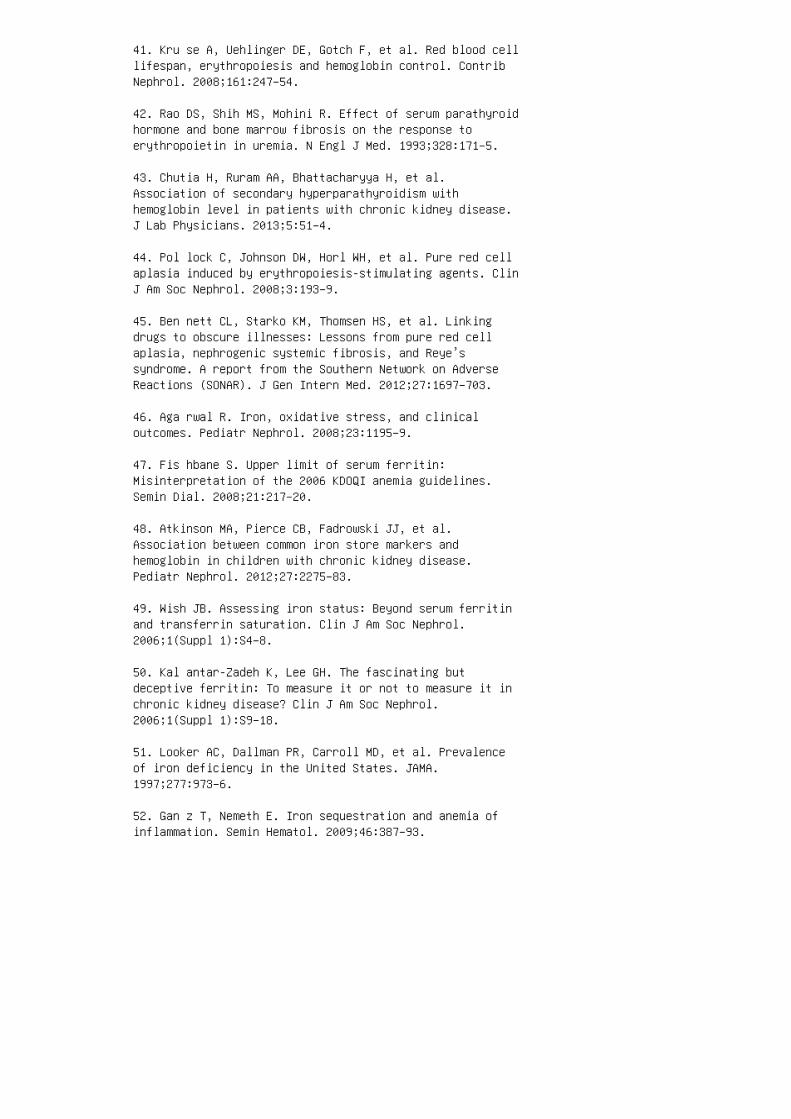
41. Kru se A, Uehlinger DE, Gotch F, et al. Red blood celllifespan, erythropoiesis and hemoglobin control. ContribNephrol. 2008;161:247–54.
42. Rao DS, Shih MS, Mohini R. Effect of serum parathyroidhormone and bone marrow fibrosis on the response toerythropoietin in uremia. N Engl J Med. 1993;328:171–5.
43. Chutia H, Ruram AA, Bhattacharyya H, et al.Association of secondary hyperparathyroidism withhemoglobin level in patients with chronic kidney disease.J Lab Physicians. 2013;5:51–4.
44. Pol lock C, Johnson DW, Horl WH, et al. Pure red cellaplasia induced by erythropoiesis-stimulating agents. ClinJ Am Soc Nephrol. 2008;3:193–9.
45. Ben nett CL, Starko KM, Thomsen HS, et al. Linkingdrugs to obscure illnesses: Lessons from pure red cellaplasia, nephrogenic systemic fibrosis, and Reye’ssyndrome. A report from the Southern Network on AdverseReactions (SONAR). J Gen Intern Med. 2012;27:1697–703.
46. Aga rwal R. Iron, oxidative stress, and clinicaloutcomes. Pediatr Nephrol. 2008;23:1195–9.
47. Fis hbane S. Upper limit of serum ferritin:Misinterpretation of the 2006 KDOQI anemia guidelines.Semin Dial. 2008;21:217–20.
48. Atkinson MA, Pierce CB, Fadrowski JJ, et al.Association between common iron store markers andhemoglobin in children with chronic kidney disease.Pediatr Nephrol. 2012;27:2275–83.
49. Wish JB. Assessing iron status: Beyond serum ferritinand transferrin saturation. Clin J Am Soc Nephrol.2006;1(Suppl 1):S4–8.
50. Kal antar-Zadeh K, Lee GH. The fascinating butdeceptive ferritin: To measure it or not to measure it inchronic kidney disease? Clin J Am Soc Nephrol.2006;1(Suppl 1):S9–18.
51. Looker AC, Dallman PR, Carroll MD, et al. Prevalenceof iron deficiency in the United States. JAMA.1997;277:973–6.
52. Gan z T, Nemeth E. Iron sequestration and anemia ofinflammation. Semin Hematol. 2009;46:387–93.

53. Kal antar-Zadeh K, McAllister CJ, Lehn RS, et al. Alow serum iron level is a predictor of poor outcome inhemodialysis patients. Am J Kidney Dis. 2004;43:671–84.
54. Mor gan HE, Gautam M, Geary DF. Maintenanceintravenous iron therapy in pediatric hemodialysispatients. Pediatr Nephrol. 2001;16:779–83. 55. Warady BA,Kausz A, Lerner G, et al. Iron therapy in the pediatrichemodialysis population. Pediatr Nephrol. 2004;19:655–61.56. Morgan HE, Holt RC, Jones CA, et al. Intravenous irontreatment in paediatric chronic kidney disease patientsnot on erythropoietin. Pediatr Nephrol. 2007;22:1963–5.57. Shander A, Sazama K. Clinical consequences of ironoverload from chronic red blood cell transfusions, itsdiagnosis, and its management by chelation therapy.Transfusion. 2010;50:1144–55. 58. Bes arab A, Bolton WK,Browne JK, et al. The effects of normal as compared withlow hematocrit values in patients with cardiac disease whoare receiving hemodialysis and epoetin. N Engl J Med.1998;339:584–90. 59. Singh AK, Szczech L, Tang KL, et al.Correction of anemia with epoetin alfa in chronic kidneydisease. N Engl J Med. 2006;355:2085–98. 60. Pfe ffer MA,Burdmann EA, Chen CY, et al. A trial of darbepoetin alfain type 2 diabetes and chronic kidney disease. N Engl JMed. 2009;361:2019–32. 61. Bad ve SV, Hawley CM, JohnsonDW. Is the problem with the vehicle or the destination?Does high-dose ESA or high haemoglobin contribute to pooroutcomes in CKD? Nephrology (Carlton). 2011;16:144–53. 62.Goo dkin DA, Fuller DS, Robinson BM, et al. Naturallyoccurring higher hemoglobin concentration does notincrease mortality among hemodialysis patients. J Am SocNephrol. 2011;22:358–65. 63. Ung er EF, Thompson AM, BlankMJ, et al. Erythropoiesis-stimulating agents: Time for areevaluation. N Engl J Med. 2010;362:189–92. 64. Kli gerAS, Foley RN, Goldfarb DS, et al. KDOQI US commentary onthe 2012 KDIGO clinical practice guideline for anemia inCKD. Am J Kidney Dis. 2013;62:849–59. 65. Lestz RM,Fivush BA, Atkinson MA. Association of highererythropoiesis stimulating agent dose and mortality inchildren on dialysis. Pediatr Nephrol. 2014;29: 2021–8.66. Covic A, Cannata-Andia J, Cancarini G, et al.Biosimilars and biopharmaceuticals: What the nephrologistsneed to know—A position paper by the ERAEDTA council.Nephrol Dial Transplant. 2008;23:3731–7. 67. Horl WH.Differentiating factors between erythropoiesis-stimulatingagents: An update to selection for anaemia of chronickidney disease. Drugs. 2013;73:117–30. 68. KDO QIclinical practice guidelines and clinical practicerecommendations for anemia in chronic kidney disease. Am J
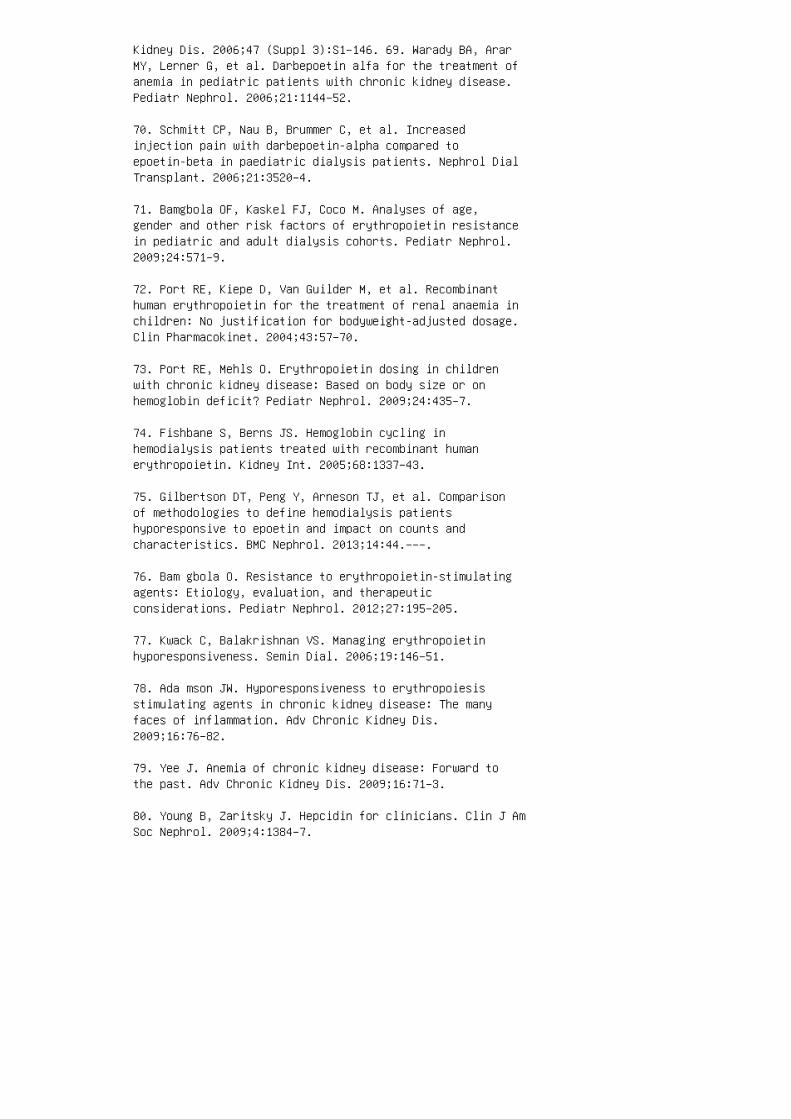
Kidney Dis. 2006;47 (Suppl 3):S1–146. 69. Warady BA, ArarMY, Lerner G, et al. Darbepoetin alfa for the treatment ofanemia in pediatric patients with chronic kidney disease.Pediatr Nephrol. 2006;21:1144–52.
70. Schmitt CP, Nau B, Brummer C, et al. Increasedinjection pain with darbepoetin-alpha compared toepoetin-beta in paediatric dialysis patients. Nephrol DialTransplant. 2006;21:3520–4.
71. Bamgbola OF, Kaskel FJ, Coco M. Analyses of age,gender and other risk factors of erythropoietin resistancein pediatric and adult dialysis cohorts. Pediatr Nephrol.2009;24:571–9.
72. Port RE, Kiepe D, Van Guilder M, et al. Recombinanthuman erythropoietin for the treatment of renal anaemia inchildren: No justification for bodyweight-adjusted dosage.Clin Pharmacokinet. 2004;43:57–70.
73. Port RE, Mehls O. Erythropoietin dosing in childrenwith chronic kidney disease: Based on body size or onhemoglobin deficit? Pediatr Nephrol. 2009;24:435–7.
74. Fishbane S, Berns JS. Hemoglobin cycling inhemodialysis patients treated with recombinant humanerythropoietin. Kidney Int. 2005;68:1337–43.
75. Gilbertson DT, Peng Y, Arneson TJ, et al. Comparisonof methodologies to define hemodialysis patientshyporesponsive to epoetin and impact on counts andcharacteristics. BMC Nephrol. 2013;14:44.–––.
76. Bam gbola O. Resistance to erythropoietin-stimulatingagents: Etiology, evaluation, and therapeuticconsiderations. Pediatr Nephrol. 2012;27:195–205.
77. Kwack C, Balakrishnan VS. Managing erythropoietinhyporesponsiveness. Semin Dial. 2006;19:146–51.
78. Ada mson JW. Hyporesponsiveness to erythropoiesisstimulating agents in chronic kidney disease: The manyfaces of inflammation. Adv Chronic Kidney Dis.2009;16:76–82.
79. Yee J. Anemia of chronic kidney disease: Forward tothe past. Adv Chronic Kidney Dis. 2009;16:71–3.
80. Young B, Zaritsky J. Hepcidin for clinicians. Clin J AmSoc Nephrol. 2009;4:1384–7.

81. Atkinson MA, White CT. Hepcidin in anemia of chronickidney disease: Review for the pediatric nephrologist.Pediatr Nephrol. 2012;27:33–40.
REVIEW QUESTIONS
1. �e initial laboratory evaluation for anemia in a childwith CKD should include which of the following?
a. Complete blood count
b. Reticulocyte count
c. Ferritin
d. Transferrin saturation
e. All of the above
2. Which of the following is not associated with the anemiaof CKD in children?
a. Increased risk for hospitalization
b. Increased fracture risk
c. Decreased quality of life
d. Increased risk for mortality
e. Increased risk for le� ventricular hypertrophy 3. �eprimary site of endogenous erythropoietin production inchildren is: a. Hepa tocytes b. Renal tubular epithelialcells c. Erythroid progenitor cells in bone marrow d.Peritubular �broblasts in the renal cortex e.Juxtaglomerular apparatus 4. Whi ch is the primaryphysiologic stimulus for increased EPO gene expression?a. Hypoxia b. Anemia c. Increased distal tubular sodiumreabsorption d. Urem ia e. Decrease in blood pressure 5.Iron-restricted erythropoiesis can include: a. Absoluteiron de�ciency b. Depletion of accessible iron stores byESAstimulated bone marrow c. In�ammation-associatedimpairment in iron tra�cking d. a and b only e. a, b,and c 6. Children receiving ESA therapy should receiveiron supplementation as indicated to maintain: a.Ferritin greater than 50 ng/mL and transferrin saturationgreater than 20% b. Ferritin greater than 100 ng/mL andtransferrin saturation greater than 10% c. Ferritingreater than 100 ng/mL and transferrin saturation greater

than 20% d. Ferritin greater than 500 ng/mL andtransferrin saturation greater than 30% e. Ferritingreater than 100 ng/mL and transferrin saturation greaterthan 30% 7. All of the following are possible indicationsfor IV iron administration except: a. Poor enteral ironabsorption b. Poor adherence to oral iron supplementationregimen c. Long-term hemodialysis status d. Activesystemic infection e. ESA hyporesponsiveness 8.Short-acting recombinant human erythropoietin formulationshave longer half-lives and are more e�ective whenadministered: a. Subcutaneously b. Intravenously c.Enterally d. Peritoneally e. With hemodialysis 9.Potential advantages of darbepoetin alfa compared withshort-acting recombinant human erythropoietin include: a.Longer interval between doses b. Improved adherence c.Decreased pain with administration d. a and b only e. a,b, and c
10. �e goal rate of hemoglobin increase a�er initiation ofan ESA is:
a. 1 to 2 g/dL per week
b. 1 to 2 g/dL per month
c. 1 to 2 g/dL over 3 months
d. Increase to goal hemoglobin of 11 g/dL over 1 month
e. Increase to goal hemoglobin of 12 g/dL over 3 monthsANSWER KEY 1. e 2. b 3. d 4. a 5. e 6. c 7. d 8. a9. d 10. b
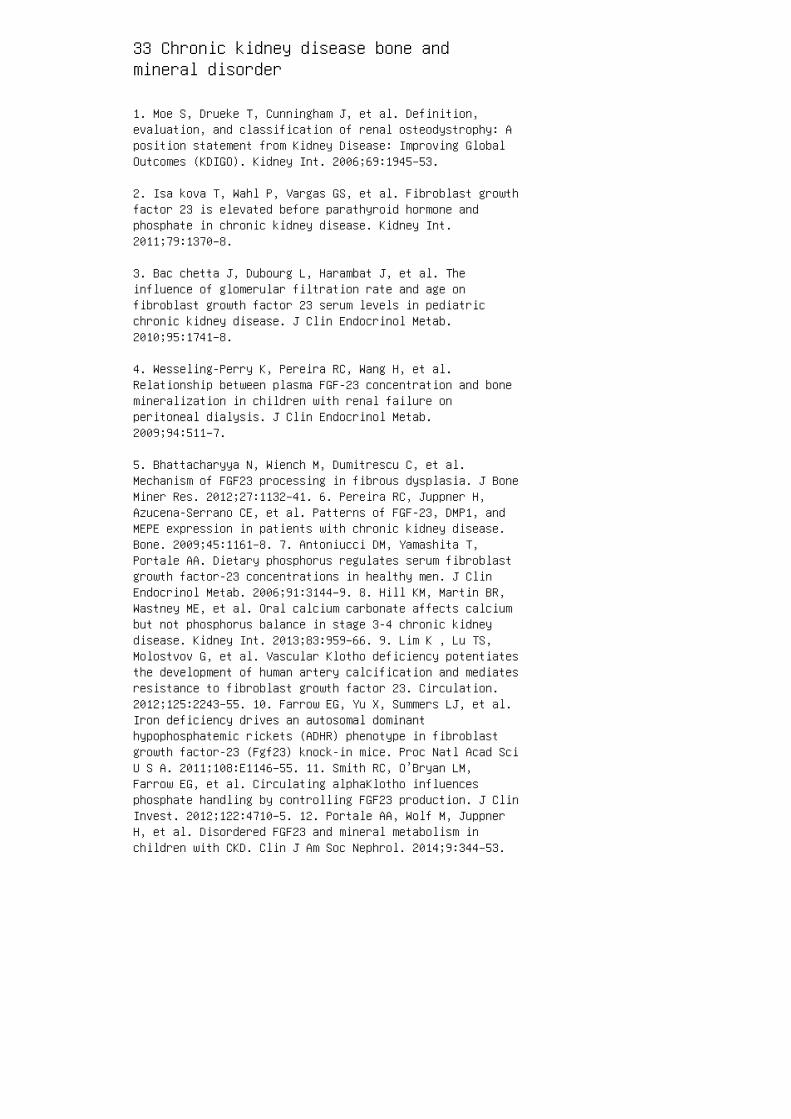
33 Chronic kidney disease bone andmineral disorder
1. Moe S, Drueke T, Cunningham J, et al. Definition,evaluation, and classification of renal osteodystrophy: Aposition statement from Kidney Disease: Improving GlobalOutcomes (KDIGO). Kidney Int. 2006;69:1945–53.
2. Isa kova T, Wahl P, Vargas GS, et al. Fibroblast growthfactor 23 is elevated before parathyroid hormone andphosphate in chronic kidney disease. Kidney Int.2011;79:1370–8.
3. Bac chetta J, Dubourg L, Harambat J, et al. Theinfluence of glomerular filtration rate and age onfibroblast growth factor 23 serum levels in pediatricchronic kidney disease. J Clin Endocrinol Metab.2010;95:1741–8.
4. Wesseling-Perry K, Pereira RC, Wang H, et al.Relationship between plasma FGF-23 concentration and bonemineralization in children with renal failure onperitoneal dialysis. J Clin Endocrinol Metab.2009;94:511–7.
5. Bhattacharyya N, Wiench M, Dumitrescu C, et al.Mechanism of FGF23 processing in fibrous dysplasia. J BoneMiner Res. 2012;27:1132–41. 6. Pereira RC, Juppner H,Azucena-Serrano CE, et al. Patterns of FGF-23, DMP1, andMEPE expression in patients with chronic kidney disease.Bone. 2009;45:1161–8. 7. Antoniucci DM, Yamashita T,Portale AA. Dietary phosphorus regulates serum fibroblastgrowth factor-23 concentrations in healthy men. J ClinEndocrinol Metab. 2006;91:3144–9. 8. Hill KM, Martin BR,Wastney ME, et al. Oral calcium carbonate affects calciumbut not phosphorus balance in stage 3-4 chronic kidneydisease. Kidney Int. 2013;83:959–66. 9. Lim K , Lu TS,Molostvov G, et al. Vascular Klotho deficiency potentiatesthe development of human artery calcification and mediatesresistance to fibroblast growth factor 23. Circulation.2012;125:2243–55. 10. Farrow EG, Yu X, Summers LJ, et al.Iron deficiency drives an autosomal dominanthypophosphatemic rickets (ADHR) phenotype in fibroblastgrowth factor-23 (Fgf23) knock-in mice. Proc Natl Acad SciU S A. 2011;108:E1146–55. 11. Smith RC, O’Bryan LM,Farrow EG, et al. Circulating alphaKlotho influencesphosphate handling by controlling FGF23 production. J ClinInvest. 2012;122:4710–5. 12. Portale AA, Wolf M, JuppnerH, et al. Disordered FGF23 and mineral metabolism inchildren with CKD. Clin J Am Soc Nephrol. 2014;9:344–53.
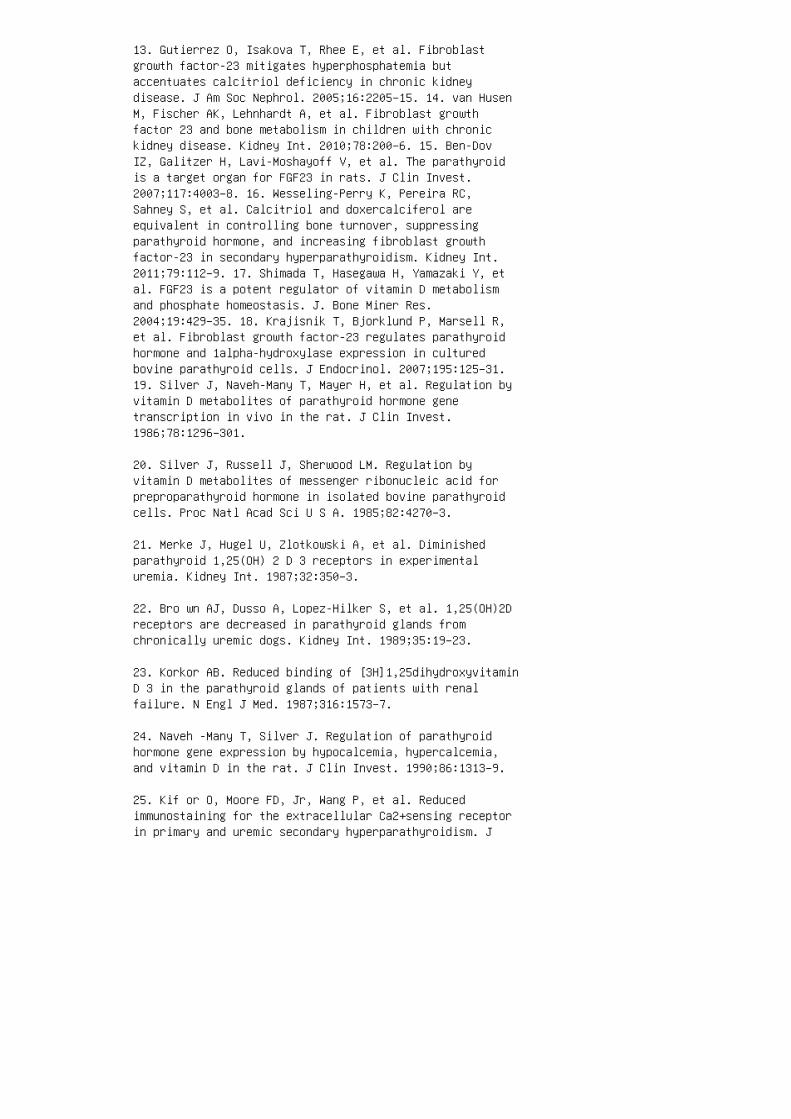
13. Gutierrez O, Isakova T, Rhee E, et al. Fibroblastgrowth factor-23 mitigates hyperphosphatemia butaccentuates calcitriol deficiency in chronic kidneydisease. J Am Soc Nephrol. 2005;16:2205–15. 14. van HusenM, Fischer AK, Lehnhardt A, et al. Fibroblast growthfactor 23 and bone metabolism in children with chronickidney disease. Kidney Int. 2010;78:200–6. 15. Ben-DovIZ, Galitzer H, Lavi-Moshayoff V, et al. The parathyroidis a target organ for FGF23 in rats. J Clin Invest.2007;117:4003–8. 16. Wesseling-Perry K, Pereira RC,Sahney S, et al. Calcitriol and doxercalciferol areequivalent in controlling bone turnover, suppressingparathyroid hormone, and increasing fibroblast growthfactor-23 in secondary hyperparathyroidism. Kidney Int.2011;79:112–9. 17. Shimada T, Hasegawa H, Yamazaki Y, etal. FGF23 is a potent regulator of vitamin D metabolismand phosphate homeostasis. J. Bone Miner Res.2004;19:429–35. 18. Krajisnik T, Bjorklund P, Marsell R,et al. Fibroblast growth factor-23 regulates parathyroidhormone and 1alpha-hydroxylase expression in culturedbovine parathyroid cells. J Endocrinol. 2007;195:125–31.19. Silver J, Naveh-Many T, Mayer H, et al. Regulation byvitamin D metabolites of parathyroid hormone genetranscription in vivo in the rat. J Clin Invest.1986;78:1296–301.
20. Silver J, Russell J, Sherwood LM. Regulation byvitamin D metabolites of messenger ribonucleic acid forpreproparathyroid hormone in isolated bovine parathyroidcells. Proc Natl Acad Sci U S A. 1985;82:4270–3.
21. Merke J, Hugel U, Zlotkowski A, et al. Diminishedparathyroid 1,25(OH) 2 D 3 receptors in experimentaluremia. Kidney Int. 1987;32:350–3.
22. Bro wn AJ, Dusso A, Lopez-Hilker S, et al. 1,25(OH)2Dreceptors are decreased in parathyroid glands fromchronically uremic dogs. Kidney Int. 1989;35:19–23.
23. Korkor AB. Reduced binding of [3H]1,25dihydroxyvitaminD 3 in the parathyroid glands of patients with renalfailure. N Engl J Med. 1987;316:1573–7.
24. Naveh -Many T, Silver J. Regulation of parathyroidhormone gene expression by hypocalcemia, hypercalcemia,and vitamin D in the rat. J Clin Invest. 1990;86:1313–9.
25. Kif or O, Moore FD, Jr, Wang P, et al. Reducedimmunostaining for the extracellular Ca2+sensing receptorin primary and uremic secondary hyperparathyroidism. J
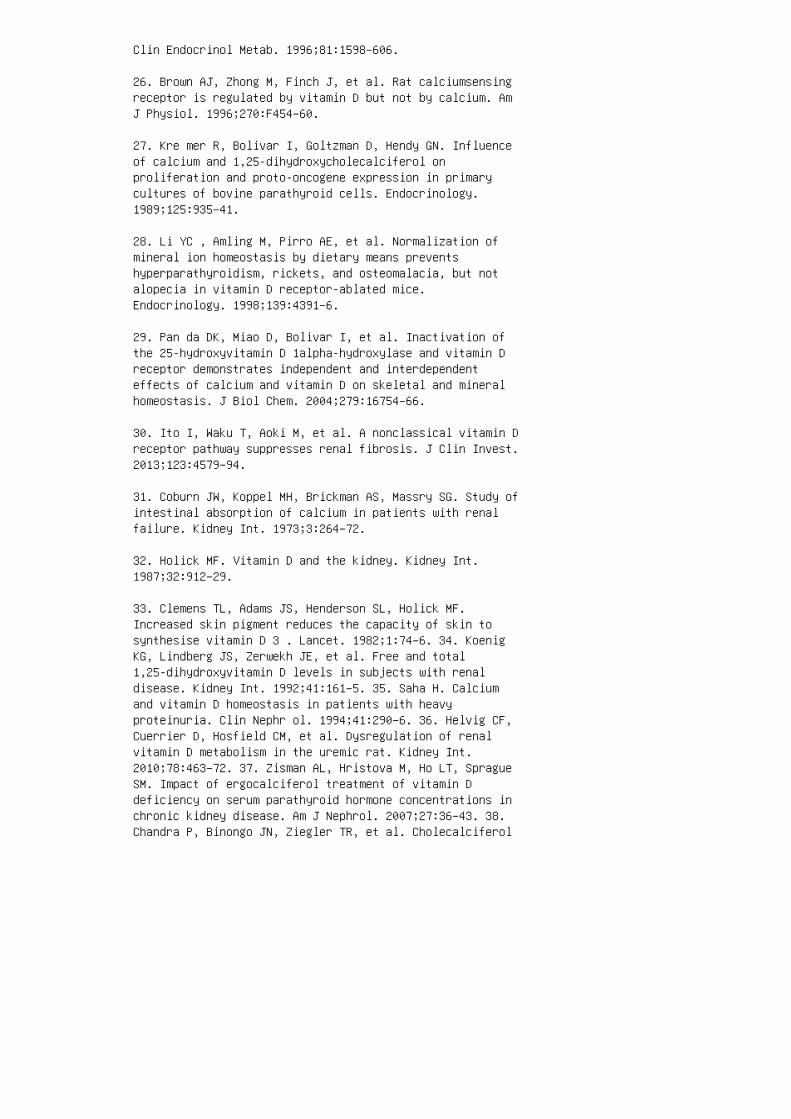
Clin Endocrinol Metab. 1996;81:1598–606.
26. Brown AJ, Zhong M, Finch J, et al. Rat calciumsensingreceptor is regulated by vitamin D but not by calcium. AmJ Physiol. 1996;270:F454–60.
27. Kre mer R, Bolivar I, Goltzman D, Hendy GN. Influenceof calcium and 1,25-dihydroxycholecalciferol onproliferation and proto-oncogene expression in primarycultures of bovine parathyroid cells. Endocrinology.1989;125:935–41.
28. Li YC , Amling M, Pirro AE, et al. Normalization ofmineral ion homeostasis by dietary means preventshyperparathyroidism, rickets, and osteomalacia, but notalopecia in vitamin D receptor-ablated mice.Endocrinology. 1998;139:4391–6.
29. Pan da DK, Miao D, Bolivar I, et al. Inactivation ofthe 25-hydroxyvitamin D 1alpha-hydroxylase and vitamin Dreceptor demonstrates independent and interdependenteffects of calcium and vitamin D on skeletal and mineralhomeostasis. J Biol Chem. 2004;279:16754–66.
30. Ito I, Waku T, Aoki M, et al. A nonclassical vitamin Dreceptor pathway suppresses renal fibrosis. J Clin Invest.2013;123:4579–94.
31. Coburn JW, Koppel MH, Brickman AS, Massry SG. Study ofintestinal absorption of calcium in patients with renalfailure. Kidney Int. 1973;3:264–72.
32. Holick MF. Vitamin D and the kidney. Kidney Int.1987;32:912–29.
33. Clemens TL, Adams JS, Henderson SL, Holick MF.Increased skin pigment reduces the capacity of skin tosynthesise vitamin D 3 . Lancet. 1982;1:74–6. 34. KoenigKG, Lindberg JS, Zerwekh JE, et al. Free and total1,25-dihydroxyvitamin D levels in subjects with renaldisease. Kidney Int. 1992;41:161–5. 35. Saha H. Calciumand vitamin D homeostasis in patients with heavyproteinuria. Clin Nephr ol. 1994;41:290–6. 36. Helvig CF,Cuerrier D, Hosfield CM, et al. Dysregulation of renalvitamin D metabolism in the uremic rat. Kidney Int.2010;78:463–72. 37. Zisman AL, Hristova M, Ho LT, SpragueSM. Impact of ergocalciferol treatment of vitamin Ddeficiency on serum parathyroid hormone concentrations inchronic kidney disease. Am J Nephrol. 2007;27:36–43. 38.Chandra P, Binongo JN, Ziegler TR, et al. Cholecalciferol
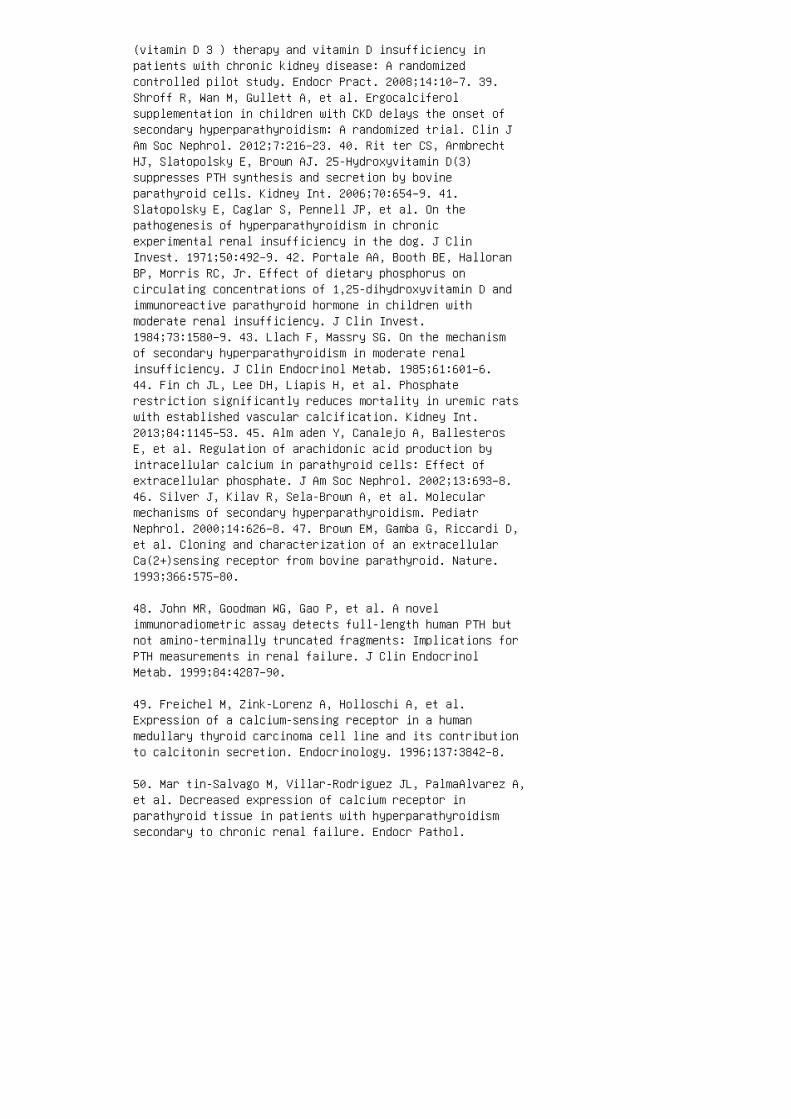
(vitamin D 3 ) therapy and vitamin D insufficiency inpatients with chronic kidney disease: A randomizedcontrolled pilot study. Endocr Pract. 2008;14:10–7. 39.Shroff R, Wan M, Gullett A, et al. Ergocalciferolsupplementation in children with CKD delays the onset ofsecondary hyperparathyroidism: A randomized trial. Clin JAm Soc Nephrol. 2012;7:216–23. 40. Rit ter CS, ArmbrechtHJ, Slatopolsky E, Brown AJ. 25-Hydroxyvitamin D(3)suppresses PTH synthesis and secretion by bovineparathyroid cells. Kidney Int. 2006;70:654–9. 41.Slatopolsky E, Caglar S, Pennell JP, et al. On thepathogenesis of hyperparathyroidism in chronicexperimental renal insufficiency in the dog. J ClinInvest. 1971;50:492–9. 42. Portale AA, Booth BE, HalloranBP, Morris RC, Jr. Effect of dietary phosphorus oncirculating concentrations of 1,25-dihydroxyvitamin D andimmunoreactive parathyroid hormone in children withmoderate renal insufficiency. J Clin Invest.1984;73:1580–9. 43. Llach F, Massry SG. On the mechanismof secondary hyperparathyroidism in moderate renalinsufficiency. J Clin Endocrinol Metab. 1985;61:601–6.44. Fin ch JL, Lee DH, Liapis H, et al. Phosphaterestriction significantly reduces mortality in uremic ratswith established vascular calcification. Kidney Int.2013;84:1145–53. 45. Alm aden Y, Canalejo A, BallesterosE, et al. Regulation of arachidonic acid production byintracellular calcium in parathyroid cells: Effect ofextracellular phosphate. J Am Soc Nephrol. 2002;13:693–8.46. Silver J, Kilav R, Sela-Brown A, et al. Molecularmechanisms of secondary hyperparathyroidism. PediatrNephrol. 2000;14:626–8. 47. Brown EM, Gamba G, Riccardi D,et al. Cloning and characterization of an extracellularCa(2+)sensing receptor from bovine parathyroid. Nature.1993;366:575–80.
48. John MR, Goodman WG, Gao P, et al. A novelimmunoradiometric assay detects full-length human PTH butnot amino-terminally truncated fragments: Implications forPTH measurements in renal failure. J Clin EndocrinolMetab. 1999;84:4287–90.
49. Freichel M, Zink-Lorenz A, Holloschi A, et al.Expression of a calcium-sensing receptor in a humanmedullary thyroid carcinoma cell line and its contributionto calcitonin secretion. Endocrinology. 1996;137:3842–8.
50. Mar tin-Salvago M, Villar-Rodriguez JL, PalmaAlvarez A,et al. Decreased expression of calcium receptor inparathyroid tissue in patients with hyperparathyroidismsecondary to chronic renal failure. Endocr Pathol.

2003;14:61–70.
51. Can aff L, Hendy GN. Human calcium-sensing receptorgene: Vitamin D response elements in promoters P1 and P2confer transcriptional responsiveness to1,25-dihydroxyvitamin D. J Biol Chem. 2002;277:30337–50.
52. Li YC , Pirro AE, Amling M, et al. Targeted ablation ofthe vitamin D receptor: An animal model of vitaminD-dependent rickets type II with alopecia. Proc Natl AcadSci U S A. 1997;94:9831–5.
53. Bro wn AJ, Zhong M, Ritter C, et al. Loss of calciumresponsiveness in cultured bovine parathyroid cells isassociated with decreased calcium receptor expression.Biochem Biophys Res Commun. 1995;212:861–7.
54. Wad a M, Furuya Y, Sakiyama J, et al. The calcimimeticcompound NPS R-568 suppresses parathyroid cellproliferation in rats with renal insufficiency: Control ofparathyroid cell growth via a calcium receptor. J ClinInvest. 1997;100:2977–83.
55. Massry SG, Stein R, Garty J, et al. Skeletalresistance to the calcemic action of parathyroid hormone inuremia: Role of 1,25 (OH)2 D3. Kidney Int. 1976;9:467–74.
56. Wesseling-Perry K, Harkins GC, Wang HJ, et al. Thecalcemic response to continuous parathyroid hormone(PTH)(1-34) infusion in end-stage kidney disease variesaccording to bone turnover: A potential role for PTH(7-84).J Clin Endocrinol Metab. 2010;95:2772–80.
57. D’Amour P, Brossard JH, Rousseau L, et al. Structureof non-(1-84) PTH fragments secreted by parathyroid glandsin primary and secondary hyperparathyroidism. Kidney Int.2005;68:998–1007.
58. Div ieti P, John MR, Juppner H, et al. Human PTH(7-84)inhibits bone resorption in vitro via actions independentof 59
59. Lan gub MC, Monier-Faugere MC, Wang G, et al.Administration of PTH-(7-84) antagonizes the effects ofPTH-(1-84) on bone in rats with moderate renal failure.Endocrinology. 2003;144:1135–8. 60. Nguyen-Yamamoto L,Rousseau L, Brossard JH, et al. Syntheticcarboxyl-terminal fragments of parathyroid hormone (PTH)decrease ionized calcium concentration in rats by acting ona receptor different from the PTH/PTH-related peptide
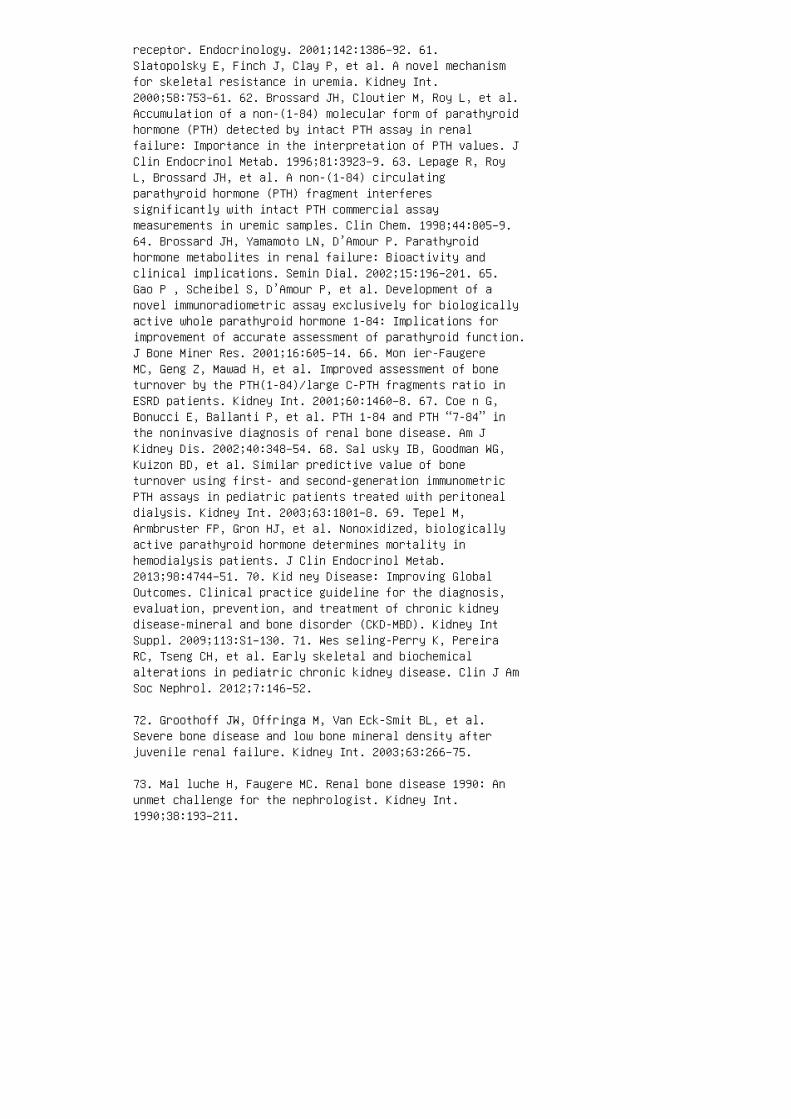
receptor. Endocrinology. 2001;142:1386–92. 61.Slatopolsky E, Finch J, Clay P, et al. A novel mechanismfor skeletal resistance in uremia. Kidney Int.2000;58:753–61. 62. Brossard JH, Cloutier M, Roy L, et al.Accumulation of a non-(1-84) molecular form of parathyroidhormone (PTH) detected by intact PTH assay in renalfailure: Importance in the interpretation of PTH values. JClin Endocrinol Metab. 1996;81:3923–9. 63. Lepage R, RoyL, Brossard JH, et al. A non-(1-84) circulatingparathyroid hormone (PTH) fragment interferessignificantly with intact PTH commercial assaymeasurements in uremic samples. Clin Chem. 1998;44:805–9.64. Brossard JH, Yamamoto LN, D’Amour P. Parathyroidhormone metabolites in renal failure: Bioactivity andclinical implications. Semin Dial. 2002;15:196–201. 65.Gao P , Scheibel S, D’Amour P, et al. Development of anovel immunoradiometric assay exclusively for biologicallyactive whole parathyroid hormone 1-84: Implications forimprovement of accurate assessment of parathyroid function.J Bone Miner Res. 2001;16:605–14. 66. Mon ier-FaugereMC, Geng Z, Mawad H, et al. Improved assessment of boneturnover by the PTH(1-84)/large C-PTH fragments ratio inESRD patients. Kidney Int. 2001;60:1460–8. 67. Coe n G,Bonucci E, Ballanti P, et al. PTH 1-84 and PTH “7-84” inthe noninvasive diagnosis of renal bone disease. Am JKidney Dis. 2002;40:348–54. 68. Sal usky IB, Goodman WG,Kuizon BD, et al. Similar predictive value of boneturnover using first- and second-generation immunometricPTH assays in pediatric patients treated with peritonealdialysis. Kidney Int. 2003;63:1801–8. 69. Tepel M,Armbruster FP, Gron HJ, et al. Nonoxidized, biologicallyactive parathyroid hormone determines mortality inhemodialysis patients. J Clin Endocrinol Metab.2013;98:4744–51. 70. Kid ney Disease: Improving GlobalOutcomes. Clinical practice guideline for the diagnosis,evaluation, prevention, and treatment of chronic kidneydisease-mineral and bone disorder (CKD-MBD). Kidney IntSuppl. 2009;113:S1–130. 71. Wes seling-Perry K, PereiraRC, Tseng CH, et al. Early skeletal and biochemicalalterations in pediatric chronic kidney disease. Clin J AmSoc Nephrol. 2012;7:146–52.
72. Groothoff JW, Offringa M, Van Eck-Smit BL, et al.Severe bone disease and low bone mineral density afterjuvenile renal failure. Kidney Int. 2003;63:266–75.
73. Mal luche H, Faugere MC. Renal bone disease 1990: Anunmet challenge for the nephrologist. Kidney Int.1990;38:193–211.
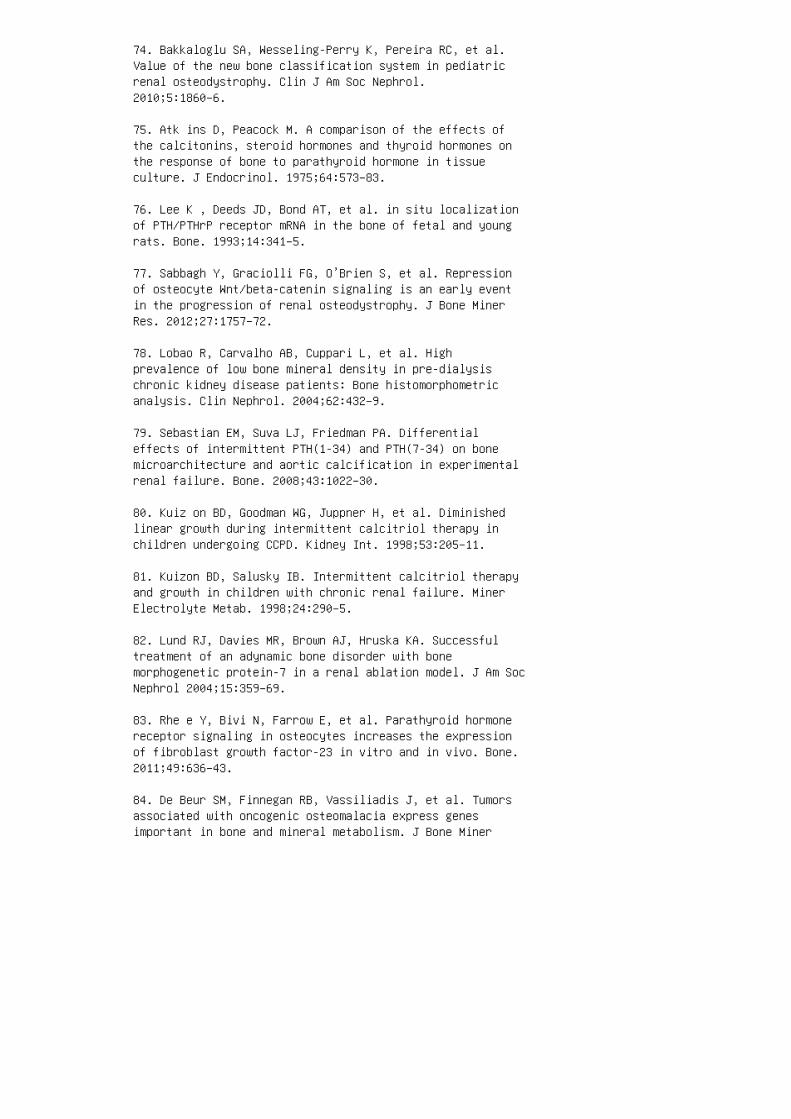
74. Bakkaloglu SA, Wesseling-Perry K, Pereira RC, et al.Value of the new bone classification system in pediatricrenal osteodystrophy. Clin J Am Soc Nephrol.2010;5:1860–6.
75. Atk ins D, Peacock M. A comparison of the effects ofthe calcitonins, steroid hormones and thyroid hormones onthe response of bone to parathyroid hormone in tissueculture. J Endocrinol. 1975;64:573–83.
76. Lee K , Deeds JD, Bond AT, et al. in situ localizationof PTH/PTHrP receptor mRNA in the bone of fetal and youngrats. Bone. 1993;14:341–5.
77. Sabbagh Y, Graciolli FG, O’Brien S, et al. Repressionof osteocyte Wnt/beta-catenin signaling is an early eventin the progression of renal osteodystrophy. J Bone MinerRes. 2012;27:1757–72.
78. Lobao R, Carvalho AB, Cuppari L, et al. Highprevalence of low bone mineral density in pre-dialysischronic kidney disease patients: Bone histomorphometricanalysis. Clin Nephrol. 2004;62:432–9.
79. Sebastian EM, Suva LJ, Friedman PA. Differentialeffects of intermittent PTH(1-34) and PTH(7-34) on bonemicroarchitecture and aortic calcification in experimentalrenal failure. Bone. 2008;43:1022–30.
80. Kuiz on BD, Goodman WG, Juppner H, et al. Diminishedlinear growth during intermittent calcitriol therapy inchildren undergoing CCPD. Kidney Int. 1998;53:205–11.
81. Kuizon BD, Salusky IB. Intermittent calcitriol therapyand growth in children with chronic renal failure. MinerElectrolyte Metab. 1998;24:290–5.
82. Lund RJ, Davies MR, Brown AJ, Hruska KA. Successfultreatment of an adynamic bone disorder with bonemorphogenetic protein-7 in a renal ablation model. J Am SocNephrol 2004;15:359–69.
83. Rhe e Y, Bivi N, Farrow E, et al. Parathyroid hormonereceptor signaling in osteocytes increases the expressionof fibroblast growth factor-23 in vitro and in vivo. Bone.2011;49:636–43.
84. De Beur SM, Finnegan RB, Vassiliadis J, et al. Tumorsassociated with oncogenic osteomalacia express genesimportant in bone and mineral metabolism. J Bone Miner
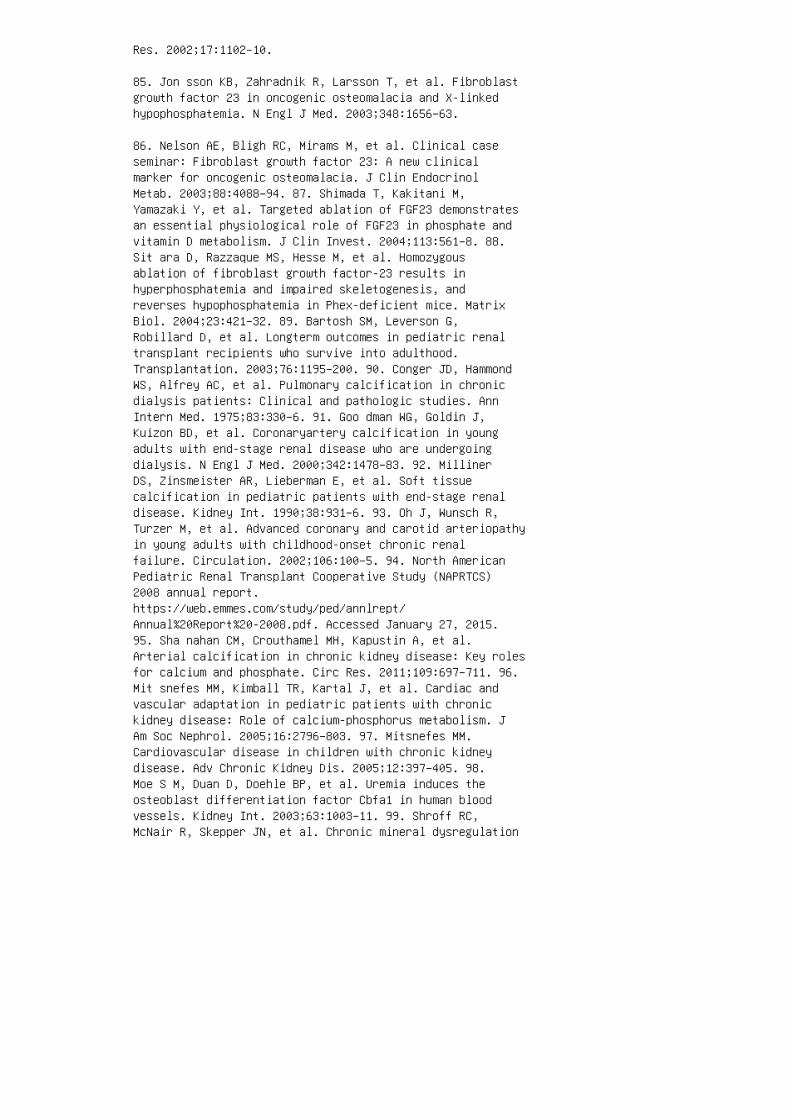
Res. 2002;17:1102–10.
85. Jon sson KB, Zahradnik R, Larsson T, et al. Fibroblastgrowth factor 23 in oncogenic osteomalacia and X-linkedhypophosphatemia. N Engl J Med. 2003;348:1656–63.
86. Nelson AE, Bligh RC, Mirams M, et al. Clinical caseseminar: Fibroblast growth factor 23: A new clinicalmarker for oncogenic osteomalacia. J Clin EndocrinolMetab. 2003;88:4088–94. 87. Shimada T, Kakitani M,Yamazaki Y, et al. Targeted ablation of FGF23 demonstratesan essential physiological role of FGF23 in phosphate andvitamin D metabolism. J Clin Invest. 2004;113:561–8. 88.Sit ara D, Razzaque MS, Hesse M, et al. Homozygousablation of fibroblast growth factor-23 results inhyperphosphatemia and impaired skeletogenesis, andreverses hypophosphatemia in Phex-deficient mice. MatrixBiol. 2004;23:421–32. 89. Bartosh SM, Leverson G,Robillard D, et al. Longterm outcomes in pediatric renaltransplant recipients who survive into adulthood.Transplantation. 2003;76:1195–200. 90. Conger JD, HammondWS, Alfrey AC, et al. Pulmonary calcification in chronicdialysis patients: Clinical and pathologic studies. AnnIntern Med. 1975;83:330–6. 91. Goo dman WG, Goldin J,Kuizon BD, et al. Coronaryartery calcification in youngadults with end-stage renal disease who are undergoingdialysis. N Engl J Med. 2000;342:1478–83. 92. MillinerDS, Zinsmeister AR, Lieberman E, et al. Soft tissuecalcification in pediatric patients with end-stage renaldisease. Kidney Int. 1990;38:931–6. 93. Oh J, Wunsch R,Turzer M, et al. Advanced coronary and carotid arteriopathyin young adults with childhood-onset chronic renalfailure. Circulation. 2002;106:100–5. 94. North AmericanPediatric Renal Transplant Cooperative Study (NAPRTCS)2008 annual report.https://web.emmes.com/study/ped/annlrept/Annual%20Report%20-2008.pdf. Accessed January 27, 2015.95. Sha nahan CM, Crouthamel MH, Kapustin A, et al.Arterial calcification in chronic kidney disease: Key rolesfor calcium and phosphate. Circ Res. 2011;109:697–711. 96.Mit snefes MM, Kimball TR, Kartal J, et al. Cardiac andvascular adaptation in pediatric patients with chronickidney disease: Role of calcium-phosphorus metabolism. JAm Soc Nephrol. 2005;16:2796–803. 97. Mitsnefes MM.Cardiovascular disease in children with chronic kidneydisease. Adv Chronic Kidney Dis. 2005;12:397–405. 98.Moe S M, Duan D, Doehle BP, et al. Uremia induces theosteoblast differentiation factor Cbfa1 in human bloodvessels. Kidney Int. 2003;63:1003–11. 99. Shroff RC,McNair R, Skepper JN, et al. Chronic mineral dysregulation

promotes vascular smooth muscle cell adaptation andextracellular matrix calcification. J Am Soc Nephrol.2010;21:103–12. 100. Jono S, McKee MD, Murry CE, et al.Phosphate regulation of vascular smooth muscle cellcalcification. Circ Res. 2000;87:E10–17. 101. Ahmed S,O’Neill KD, Hood AF, et al. Calciphylaxis is associatedwith hyperphosphatemia and increased osteopontinexpression by vascular smooth muscle cells. Am J KidneyDis. 2001;37:1267–76.
102. Bostrom K. Insights into the mechanism of vascularcalcification. Am J Cardiol. 2001;88:20E–2E.
103. Moe S M, O’Neill KD, Duan D, et al. Medial arterycalcification in ESRD patients is associated withdeposition of bone matrix proteins. Kidney Int.2002;61:638–47.
104. Chen NX, O’Neill KD, Duan D, et al. Phosphorus anduremic serum up-regulate osteopontin expression in vascularsmooth muscle cells. Kidney Int. 2002;62:1724–31.
105. Sch afer C, Heiss A, Schwarz A, et al. The serumprotein alpha 2-Heremans-Schmid glycoprotein/fetuin-A is asystemically acting inhibitor of ectopic calcification. JClin Invest. 2003;112:357–66.
106. Schinke T, Amendt C, Trindl A, et al. The serumprotein alpha2-HS glycoprotein/fetuin inhibits apatiteformation in vitro and in mineralizing calvaria cells: Apossible role in mineralization and calcium homeostasis. JBiol Chem. 1996;271:20789–96.
107. Sweatt A, Sane DC, Hutson SM, et al. Matrix Glaprotein (MGP) and bone morphogenetic protein-2 in aorticcalcified lesions of aging rats. J Thromb Haemost.2003;1:178–85.
108. Koh N , Fujimori T, Nishiguchi S, et al. Severelyreduced production of Klotho in human chronic renalfailure kidney. Biochem Biophys Res Commun.2001;280:1015–20.
109. Rus so D, Battaglia Y, Buonanno E. Phosphorus andcoronary calcification in predialysis patients. KidneyInt. 2010;78:818.
110. Rus so D, Palmiero G, De Blasio AP, et al. Coronaryartery calcification in patients with CRF not undergoingdialysis. Am J Kidney Dis. 2004;44:1024–30.

111. Gut ierrez OM, Mannstadt M, Isakova T, et al.Fibroblast growth factor 23 and mortality among patientsundergoing hemodialysis. N Engl J Med. 2008;359:584–92.
112. Jean G, Bresson E, Terrat JC, et al. Peripheralvascular calcification in long-haemodialysis patients:Associated factors and survival consequences. Nephrol DialTransplant. 2009;24:948–55.
113. Sci alla JJ, Lau WL, Reilly MP, et al. Fibroblastgrowth factor 23 is not associated with and does notinduce arterial calcification. Kidney Int.2013;83:1159–68.
114. Faul C, Amaral AP, Oskouei B, et al. FGF23 inducesleft ventricular hypertrophy. J Clin Invest.2011;121:4393–408.
115. Buizert PJ, van Schoor NM, Simsek S, et al. PTH: Anew target in arteriosclerosis? J Clin Endocrinol Metab.2013;98:1583–90.
116. Ton elli M, Keech A, Shepherd J, et al. Effect ofpravastatin in people with diabetes and chronic kidneydisease. J Am Soc Nephrol. 2005;16:3748–54.
117. Hol daas H, Fellstrom B, Cole E, et al. Long-termcardiac outcomes in renal transplant recipients receivingfluvastatin: The ALERT extension study. Am J Transplant.2005;5:2929–36. 118. Wanner C, Krane V, Marz W, et al.Atorvastatin in patients with type 2 diabetes mellitusundergoing hemodialysis. N Engl J Med. 2005;353:238-–48.119. Block GA, Spiegel DM, Ehrlich J, et al. Effects ofsevelamer and calcium on coronary artery calcification inpatients new to hemodialysis. Kidney Int. 2005;68:1815–24.120. Block GA, Raggi P, Bellasi A, et al. Mortality effectof coronary calcification and phosphate binder choice inincident hemodialysis patients. Kidney Int.2007;71:438–41. 121. Jam al SA, Vandermeer B, Raggi P, etal. Effect of calcium-based versus non-calcium-basedphosphate binders on mortality in patients with chronickidney disease: An updated systematic review andmetaanalysis. Lancet. 2013;382:1268–77. 122. Oliveira RB,Cancela AL, Graciolli FG, et al. Early control of PTH andFGF23 in normophosphatemic CKD patients: A new target inCKD-MBD therapy? Clin J Am Soc Nephrol. 2010;5:286–91.123. Gon zalez-Parra E, Gonzalez-Casaus ML, Galan A, etal. Lanthanum carbonate reduces FGF23 in chronic kidneydisease stage 3 patients. Nephrol Dial Transplant.
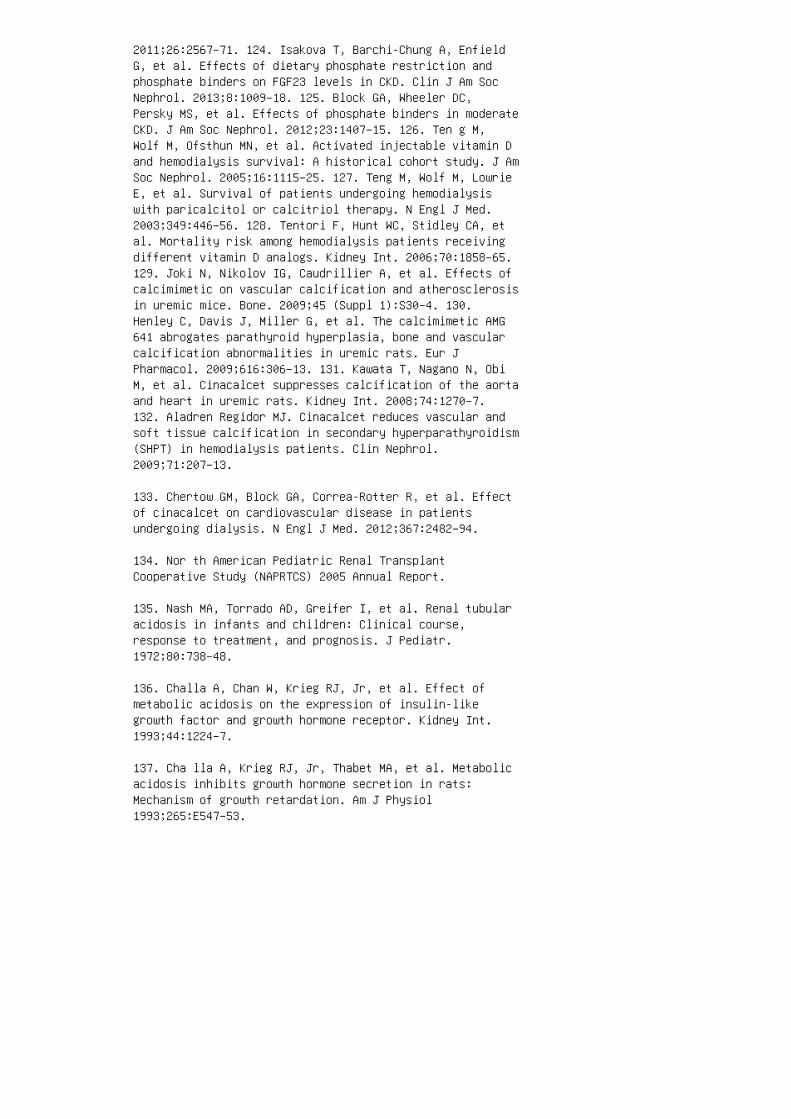
2011;26:2567–71. 124. Isakova T, Barchi-Chung A, EnfieldG, et al. Effects of dietary phosphate restriction andphosphate binders on FGF23 levels in CKD. Clin J Am SocNephrol. 2013;8:1009–18. 125. Block GA, Wheeler DC,Persky MS, et al. Effects of phosphate binders in moderateCKD. J Am Soc Nephrol. 2012;23:1407–15. 126. Ten g M,Wolf M, Ofsthun MN, et al. Activated injectable vitamin Dand hemodialysis survival: A historical cohort study. J AmSoc Nephrol. 2005;16:1115–25. 127. Teng M, Wolf M, LowrieE, et al. Survival of patients undergoing hemodialysiswith paricalcitol or calcitriol therapy. N Engl J Med.2003;349:446–56. 128. Tentori F, Hunt WC, Stidley CA, etal. Mortality risk among hemodialysis patients receivingdifferent vitamin D analogs. Kidney Int. 2006;70:1858–65.129. Joki N, Nikolov IG, Caudrillier A, et al. Effects ofcalcimimetic on vascular calcification and atherosclerosisin uremic mice. Bone. 2009;45 (Suppl 1):S30–4. 130.Henley C, Davis J, Miller G, et al. The calcimimetic AMG641 abrogates parathyroid hyperplasia, bone and vascularcalcification abnormalities in uremic rats. Eur JPharmacol. 2009;616:306–13. 131. Kawata T, Nagano N, ObiM, et al. Cinacalcet suppresses calcification of the aortaand heart in uremic rats. Kidney Int. 2008;74:1270–7.132. Aladren Regidor MJ. Cinacalcet reduces vascular andsoft tissue calcification in secondary hyperparathyroidism(SHPT) in hemodialysis patients. Clin Nephrol.2009;71:207–13.
133. Chertow GM, Block GA, Correa-Rotter R, et al. Effectof cinacalcet on cardiovascular disease in patientsundergoing dialysis. N Engl J Med. 2012;367:2482–94.
134. Nor th American Pediatric Renal TransplantCooperative Study (NAPRTCS) 2005 Annual Report.
135. Nash MA, Torrado AD, Greifer I, et al. Renal tubularacidosis in infants and children: Clinical course,response to treatment, and prognosis. J Pediatr.1972;80:738–48.
136. Challa A, Chan W, Krieg RJ, Jr, et al. Effect ofmetabolic acidosis on the expression of insulin-likegrowth factor and growth hormone receptor. Kidney Int.1993;44:1224–7.
137. Cha lla A, Krieg RJ, Jr, Thabet MA, et al. Metabolicacidosis inhibits growth hormone secretion in rats:Mechanism of growth retardation. Am J Physiol1993;265:E547–53.
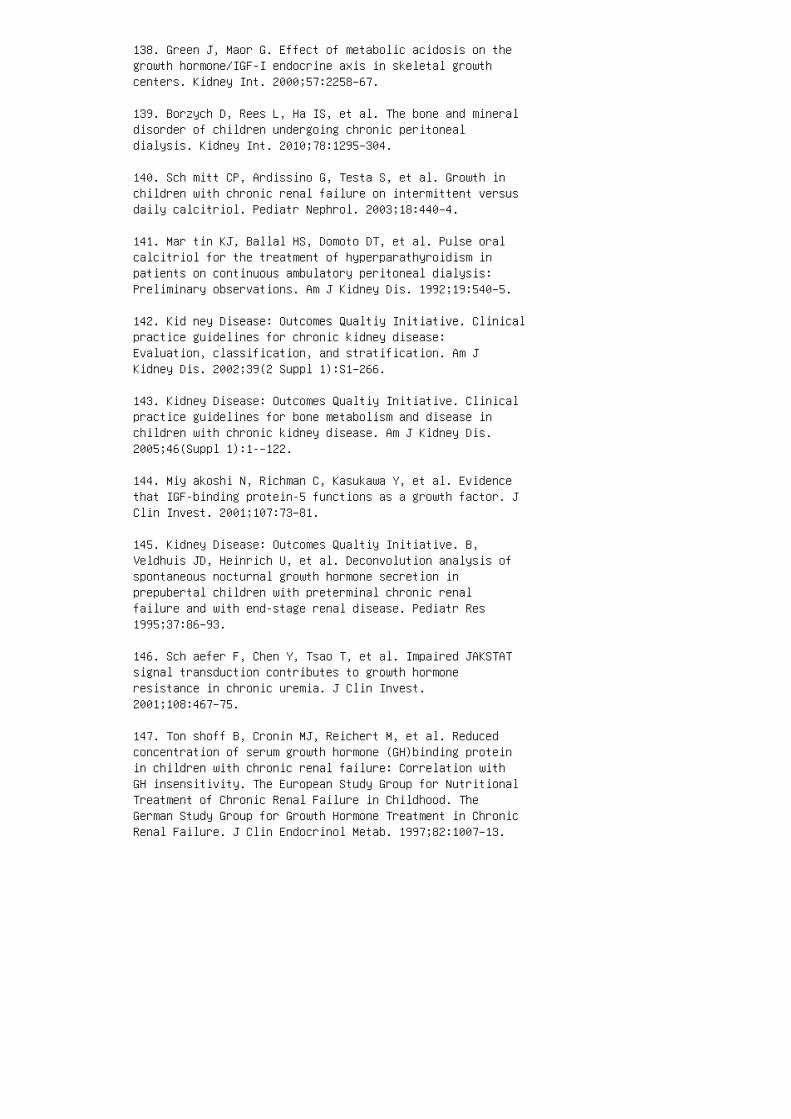
138. Green J, Maor G. Effect of metabolic acidosis on thegrowth hormone/IGF-I endocrine axis in skeletal growthcenters. Kidney Int. 2000;57:2258–67.
139. Borzych D, Rees L, Ha IS, et al. The bone and mineraldisorder of children undergoing chronic peritonealdialysis. Kidney Int. 2010;78:1295–304.
140. Sch mitt CP, Ardissino G, Testa S, et al. Growth inchildren with chronic renal failure on intermittent versusdaily calcitriol. Pediatr Nephrol. 2003;18:440–4.
141. Mar tin KJ, Ballal HS, Domoto DT, et al. Pulse oralcalcitriol for the treatment of hyperparathyroidism inpatients on continuous ambulatory peritoneal dialysis:Preliminary observations. Am J Kidney Dis. 1992;19:540–5.
142. Kid ney Disease: Outcomes Qualtiy Initiative. Clinicalpractice guidelines for chronic kidney disease:Evaluation, classification, and stratification. Am JKidney Dis. 2002;39(2 Suppl 1):S1–266.
143. Kidney Disease: Outcomes Qualtiy Initiative. Clinicalpractice guidelines for bone metabolism and disease inchildren with chronic kidney disease. Am J Kidney Dis.2005;46(Suppl 1):1-–122.
144. Miy akoshi N, Richman C, Kasukawa Y, et al. Evidencethat IGF-binding protein-5 functions as a growth factor. JClin Invest. 2001;107:73–81.
145. Kidney Disease: Outcomes Qualtiy Initiative. B,Veldhuis JD, Heinrich U, et al. Deconvolution analysis ofspontaneous nocturnal growth hormone secretion inprepubertal children with preterminal chronic renalfailure and with end-stage renal disease. Pediatr Res1995;37:86–93.
146. Sch aefer F, Chen Y, Tsao T, et al. Impaired JAKSTATsignal transduction contributes to growth hormoneresistance in chronic uremia. J Clin Invest.2001;108:467–75.
147. Ton shoff B, Cronin MJ, Reichert M, et al. Reducedconcentration of serum growth hormone (GH)binding proteinin children with chronic renal failure: Correlation withGH insensitivity. The European Study Group for NutritionalTreatment of Chronic Renal Failure in Childhood. TheGerman Study Group for Growth Hormone Treatment in ChronicRenal Failure. J Clin Endocrinol Metab. 1997;82:1007–13.

148. Bac chetta J, Wesseling-Perry K, Kuizon B, et al. Theskeletal consequences of growth hormone therapy indialyzed children: A randomized trial. Clin J Am SocNephrol. 2013;8:824–32. 149. Foley RN, Parfrey PS, SarnakMJ. Clinical epidemiology of cardiovascular disease inchronic renal disease. Am J Kidney Dis. 1998;32:S112–S9.150. Sha nahan CM. Mechanisms of vascular calcification inrenal disease. Clin Nephrol. 2005;63:146–57. 151. Ducy P,Zhang R, Geoffroy V, et al. Osf2/Cbfa1: A transcriptionalactivator of osteoblast differentiation. Cell.1997;89:747–54. 152. Raz zaque MS, Sitara D, Taguchi T, etal. Premature aging-like phenotype in fibroblast growthfactor 23 null mice is a vitamin D-mediated process. FASEBJ. 2006;20:720–2. 153. Gutierrez OM, Januzzi JL, IsakovaT, et al. Fibroblast growth factor 23 and left ventricularhypertrophy in chronic kidney disease. Circulation.2009;119:2545–52. 154. Gipstein RM, Coburn JW, Adams DA,et al. Calciphylaxis in man: A syndrome of tissue necrosisand vascular calcification in 11 patients with chronicrenal failure. Arch Intern Med. 1976;136:1273–80. 155. Bleyer AJ, Choi M, Igwemezie B, et al. A case control studyof proximal calciphylaxis. Am J Kidney D. 1998;32:376–83.156. Maw ad HW, Sawaya BP, Sarin R, et al. Calcific uremicarteriolopathy in association with low turnover uremic bonedisease. Clin Nephrol. 1999;52:160–6. 157. Goldsmith DJ.Calciphylaxis, thrombotic diathesis and defects incoagulation regulation. Nephrol Dial Transplant.1997;12:1082–3. 158. Mohammed IA, Sekar V, Bubtana AJ, etal. Proximal calciphylaxis treated with calcimimetic‘cinacalcet’. Nephrol Dial Transplant. 2008;23:387–9.159. Rogers NM, Teubner DJ, Coates PT. Calcific uremicarteriolopathy: Advances in pathogenesis and treatment.Semin Dial. 2007;20:150–7. 160. Hernandez JD, Wesseling K,Pereira R, et al. Technical approach to iliac crestbiopsy. Clin J Am Soc Nephrol. 2008;3(Suppl 3):S164–9.161. Mucsi I, Hercz G, Uldall R, et al. Control of serumphosphate without any phosphate binders in patientstreated with nocturnal hemodialysis. Kidney Int.1998;53:1399–404. 162. Fischbach M, Terzic J, Menouer S,et al. Intensified and daily hemodialysis in childrenmight improve statural growth. Pediatr Nephrol.2006;21:1746–52. 163. Goodman WG. Aluminum and renalosteodystrophy. In: Bushinsky DA, editor. RenalOsteodystrophy. Philadelphia: Lippincott-Raven; 1998. p.317.
164. Salusky IB, Foley J, Nelson P, et al. Aluminumaccumulation during treatment with aluminum hydroxide anddialysis in children and young adults with chronic renaldisease. N Engl J Med. 1991;324:527–31.

165. Coburn JW, Mischel MG, Goodman WG, et al. Calciumcitrate markedly enhances aluminum absorption fromaluminum hydroxide. Am J Kidney Dis. 1991;17:708–11.
166. Andreoli SP, Dunson JW, Bergstein JM. Calciumcarbonate is an effective phosphorus binder in childrenwith chronic renal failure. Am J Kidney Dis.1987;9:206-–10.
167. Salusky IB, Goodman WG. Adynamic renal osteodystrophy:Is there a problem? J Am Soc Nephrol. 2001;12:1978–85.
168. Nat ional Kidney Foundation. KDOQI clinical practiceguideline for nutrition in children with CKD: 2008 update.Executive summary. Am J Kidney Dis. 2009;53:S11–104.
169. Wallot M, Bonzel KE, Winter A, et al. Calcium acetateversus calcium carbonate as oral phosphate binder inpediatric and adolescent hemodialysis patients. PediatrNephrol. 1996;10:625–30.
170. Cus hner HM, Copley JB, Lindberg JS, et al. Calciumcitrate, a nonaluminum-containing phosphatebinding agentfor treatment of CRF. Kidney Int. 1988;33:95–9.
171. Bir ck R, Zimmermann E, Wassmer S, et al. Calciumketoglutarate versus calcium acetate for treatment ofhyperphosphataemia in patients on maintenancehaemodialysis: A cross-over study. Nephrol DialTransplant. 1999;14:1475–9.
172. Chertow GM, Burke SK, Dillon MA, et al. Longtermeffects of sevelamer hydrochloride on the calcium xphosphate product and lipid profile of haemodialysispatients. Nephrol Dial Transplant. 1999;14:2907–14.
173. Delmez J, Block G, Robertson J, et al. A randomized,double-blind, crossover design study of sevelamerhydrochloride and sevelamer carbonate in patients onhemodialysis. Clin Nephrol. 2007;68:386–91.
174. O’D onovan R, Baldwin D, Hammer M, et al.Substitution of aluminium salts by magnesium salts incontrol of dialysis hyperphosphataemia. Lancet.1986;1:880–2.
175. Hergesell O, Ritz E. Stabilized polynuclear ironhydroxide is an efficient oral phosphate binder in uraemicpatients. Nephrol Dial Transplant. 1999;14:863–7.
176. D’H aese PC, Spasovski GB, Sikole A, et al. Amulticenter study on the effects of lanthanum carbonate(Fosrenol) and calcium carbonate on renal bone disease indialysis patients. Kidney Int Suppl. 2003;85:S73–8.
177. Sla topolsky E, Liapis H, Finch J. Progressiveaccumulation of lanthanum in the liver of normal and uremicrats. Kidney Int. 2005;68:2809–13. 178. Ross C A, TaylorCL, Yaktine AL, Del Valle HB. Dietary Reference Intakesfor Calcium and Vitamin D. Washington, DC: NationalAcademies Press; 2011. 179. Salusky IB, Goodman WG, SahneyS, et al. Sevelamer controls parathyroid hormone-inducedbone disease as efficiently as calcium carbonate withoutincreasing serum calcium levels during therapy with activevitamin D sterols. J Am Soc Nephrol. 2005;16:2501–8. 180.Salusky IB, Kuizon BD, Belin TR, et al. Intermittentcalcitriol therapy in secondary hyperparathyroidism: Acomparison between oral and intraperitonealadministration. Kidney Int. 1998;54:907–14. 181. Nat ionalKidney Foundation. K/DOQI clinical practice guidelines forbone metabolism and disease in chronic kidney disease. Am JKidney Dis. 2003;42:S1–201. 182. Fukagawa M, Okazaki R,Takano K, et al. Regression of parathyroid hyperplasia bycalcitriol-pulse therapy in patients on long-termdialysis. N Engl J Med. 1990;323:421–2. 183. Pie ridesAM, Ellis HA, Simpson W, et al Variable response tolong-term 1alpha-hydroxycholecalciferol in haemodialysisosteodystrophy. Lancet. 1976;1:1092–5. 184. Dobrez DG,Mathes A, Amdahl M, et al. Paricalcitoltreated patientsexperience improved hospitalization outcomes compared withcalcitriol-treated patients in real-world clinicalsettings. Nephrol Dial Transplant. 2004;19:117–81. 185.Sjo den G, Smith C, Lindgren U, DeLuca HF. 1alpha-Hydroxyvitamin D 2 is less toxic than 1alphahydroxyvitamin D 3 in the rat. Proc Soc Exp Biol Med.1985;178:432–6. 186. And ress DL, Norris KC, Coburn JW, etal. Intravenous calcitriol in the treatment of refractoryosteitis fibrosa of chronic renal failure. N Engl J Med.1989;321:274–9. 187. Tha dhani R, Appelbaum E, PritchettY, et al. Vitamin D therapy and cardiac structure andfunction in patients with chronic kidney disease: ThePRIMO randomized controlled trial. JAMA. 2012;307:674–84.188. Schwarz U, Amann K, Orth SR, et al. Effect of 1,25(OH)2 vitamin D 3 on glomerulosclerosis in subtotallynephrectomized rats. Kidney Int. 1998;53:1696–705. 189.Agarwal R, Acharya M, Tian J, et al. Antiproteinuriceffect of oral paricalcitol in chronic kidney disease.Kidney Int. 2005;68:2823–8. 190. Nakane M, Ma J, Ruan X,et al. Mechanistic analysis of VDR-mediated renin

suppression. Nephron Physiol. 2007;107:35–44. 191. WadaM, Nagano N. Control of parathyroid cell growth bycalcimimetics. Nephrol Dial Transplant. 2003;18(Suppl3):iii13-7. 192. Arnold A, Brown MF, Urena P, et al.Monoclonality of parathyroid tumors in chronic renalfailure and in primary parathyroid hyperplasia. J ClinInvest. 1995;95:2047–53.
193. Quarles LD, Yohay DA, Carroll BA, et al. Prospectivetrial of pulse oral versus intravenous calcitriol treatmentof hyperparathyroidism in ESRD. Kidney Int.1994;45:1710–21.
194. Froment DP, Molitoris BA, Buddington B, et al. Siteand mechanism of enhanced gastrointestinal absorption ofaluminum by citrate. Kidney Int. 1989;36:978-84.
195. Jorna FH, Tobe TJ, Huisman RM, et al. Earlyidentification of risk factors for refractory secondaryhyperparathyroidism in patients with long-term renalreplacement therapy. Nephrol Dial Transplant.2004;19:1168–73.
196. Andress DL, Ott SM, Maloney NA, Sherrard DJ. Effectof parathyroidectomy on bone aluminum accumulation inchronic renal failure. N Engl J Med. 1985;312:468–73.
197. de Barros Gueiros JE, Chammas MC, Gerhard R, et al.Percutaneous ethanol (PEIT) and calcitriol (PCIT)injection therapy are ineffective in treating severesecondary hyperparathyroidism. Nephrol Dial Transplant.2004;19:657–63.
198. Diethelm AG, Edwards RP, Whelchel JD. The naturalhistory and surgical treatment of hypercalcemia before andafter renal transplantation. Surg Gynecol Obstet.1982;154:481–90.
199. D’Alessandro AM, Melzer JS, Pirsch JD, et al. Tertiaryhyperparathyroidism after renal transplantation: Operativeindications. Surgery. 1989;106:1049–55.
200. Ber gua C, Torregrosa JV, Fuster D, et al. Effect ofcinacalcet on hypercalcemia and bone mineral density inrenal transplanted patients with secondaryhyperparathyroidism. Transplantation. 2008;86:413–7.
201. Borchhardt K, Sulzbacher I, Benesch T, et al.Lowturnover bone disease in hypercalcemichyperparathyroidism after kidney transplantation. Am J
Transplant. 2007;7:2515–21.
202. Bhan I, Shah A, Holmes J, et al. Post-transplanthypophosphatemia: Tertiary ‘hyper-phosphatoninism’? KidneyInt. 2006;70:1486–94.
203. Even epoel P, Naesens M, Claes K, et al. Tertiary‘hyperphosphatoninism’ accentuates hypophosphatemia andsuppresses calcitriol levels in renal transplantrecipients. Am J Transplant. 2007;7:1193–200.
204. Bonomini V, Feletti C, Di FA, Buscaroli A. Boneremodelling after renal transplantation (RT). Adv Exp MedBiol. 1984;178:207–16.
205. Nie lsen HE, Melsen F, Christensen MS. Asepticnecrosis of bone following renal transplantation: Clinicaland biochemical aspects and bone morphometry. Acta MedScand. 1977;202:2–32.
206. Grotz WH, Mundinger FA, Gugel B, et al. Bone mineraldensity after kidney transplantation: A cross-sectionalstudy in 190 graft recipients up to 20 years aftertransplantation. Transplantation. 1995;59:982–6. 207.Julian BA, Laskow DA, Dubovsky J, et al. Rapid loss ofvertebral mineral density after renal transplantation. NEngl J Med. 1991;325:544–50. 208. Slatopolsky E, Martin K.Glucocorticoids and renal transplant osteonecrosis. AdvExp Med Biol. 1984;171:353–9. 209. Parfrey PS, Farge D,Parfrey NA, et al. The decreased incidence of asepticnecrosis in renal transplant recipients: A case controlstudy. Transplantation. 1986;41:182–7. 210. Isono SS,Woolson ST, Schurman DJ. Total joint arthroplasty forsteroid-induced osteonecrosis in cardiac transplantpatients. Clin Orthop Relat Res. 1987:201–8. 211. EnrightH, Haake R, Weisdorf D. Avascular necrosis of bone: Acommon serious complication of allogeneic bone marrowtransplantation. Am J Med. 1990;89:733–8. 212. Velasquez-Forero F, Mondragon A, Herrero B, Pena JC. Adynamicbone lesion in renal transplant recipients with normalrenal function. Nephrol Dial Transplant. 1996;11(Suppl3):58–64. 213. San chez CP, Salusky IB, Kuizon BD, et al.Bone disease in children and adolescents undergoingsuccessful renal transplantation. Kidney Int.1998;53:1358–64. 214. Lin dberg JS, Culleton B, Wong G, etal. Cinacalcet HCl, an oral calcimimetic agent for thetreatment of secondary hyperparathyroidism in hemodialysisand peritoneal dialysis: A randomized, doubleblind,multicenter study. J Am Soc Nephrol. 2005;16:800–7. 215.All en DB, Goldberg BD. Stimulation of collagen synthesis
and linear growth by growth hormone inglucocorticoid-treated children. Pediatrics.1992;89:416–21. 216. Roo t AW, Bongiovanni AM, EberleinWR. Studies of the secretion and metabolic effects ofhuman growth hormone in children withglucocorticoid-induced growth retardation. J Pediatr.1969;75:826–32. 217. Wehrenberg WB, Bergman PJ, Stagg L,et al. Glucocorticoid inhibition of growth in rats:Partial reversal with somatostatin antibodies.Endocrinology. 1990;127:2705–8. 218. Aubia J, Serrano S,Marinoso L, et al. Osteodystrophy of diabetics in chronicdialysis: A histomorphometric study. Calcif Tissue Int.1988;42:297–301. 219. Movs owitz C, Epstein S, Fallon M,et al. Cyclosporin-A in vivo produces severe osteopeniain the rat: Effect of dose and duration of administration.Endocrinology. 1988;123:2571–7. 220. Bryer HP, Isserow JA,Armstrong EC, et al. Azathioprine alone is bone sparingand does not alter cyclosporin A-induced osteopenia in therat. J Bone Miner Res. 1995;10:132–8.
221. Hokken-Koelega AC, van Zaal MA, van BW, et al. Finalheight and its predictive factors after renaltransplantation in childhood. Pediatr Res. 1994;36:323–8.
222. Fin e RN, Yadin O, Nelson PA, et al. Recombinanthuman growth hormone treatment of children following renaltransplantation. Pediatr Nephrol. 1991;5:147–51.
223. Mitsnefes MM, Kimball TR, Border WL, et al. Abnormalcardiac function in children after renal transplantation.Am J Kidney Dis. 2004;43:721–6.
224. Ish itani MB, Milliner DS, Kim DY, et al. Earlysubclinical coronary artery calcification in young adultswho were pediatric kidney transplant recipients. Am JTransplant. 2005;5:1689–93.
225. Wolf M, Molnar MZ, Amaral AP, et al. Elevatedfibroblast growth factor 23 is a risk factor for kidneytransplant loss and mortality. J Am Soc Nephrol.2011;22:956–66.
226. Wesseling-Perry K, Tsai EW, Ettenger RB, et al.Mineral abnormalities and long-term graft function inpediatric renal transplant recipients: A role for FGF-23?Nephrol Dial Transplant. 2011;26:3779–84.
REVIEW QUESTIONS
A 12-year-old boy has come to a pediatrician’s o�ce for a

school physical. He wakes up several times at night to uri
nate. On examination, he is found to be a pale boy with a
height and a weight that are both below the 3rd percentile.He
has Tanner 1 pubertal development and normal blood pres
sure. Serum electrolytes are sodium, 136 mmol/L; potassium,
3.8 mmol/L; chloride, 108 mmol/; total carbon dioxide, 18
mmol/L; blood urea nitrogen, 40 mg/dL; creatinine, 1.8 mg/
dL (stage 3 CKD); phosphorus, 4 mg/dL; calcium, 9.9 mg/dL;
parathyroid hormone, 170 pg/mL, and hematocrit, 28%.
1. An appropriate serum PTH level for this child with this
degree of renal insu�ciency is:
a. 10 to 65 pg/mL
b. 65 to 110 pg/mL
c. 200 to 300 pg/mL
d. >400 pg/mL
2. Growth hormone therapy should be initiated:
a. Immediately, to maximize �nal height potential
b. A�er correction of acidosis, anemia, and secondaryhyperparathyroidism c. A�er the initiation of dialysis d.A�er successful renal transplantation e. Growth hormonetherapy is contraindicated in this child 3. An 8-year-oldgirl presents with re�ux nephropathy and growth failureand has the following serum biochemical determinations:Serum creatinine, 2.5 mg/dL (CKD stage 4); calcium, 8.9mg/dL; phosphorus, 6 mg/dL; and PTH, 140 pg/mL. �e �rststep in serum phosphorus management is: a. Initiation ofa non–calcium-containing phosphate binder b. Nutritionalassessment and phosphate restriction c. Vitamin D steroltherapy d. Growth hormone therapy 4. A 14-year-old boywith obstructive uropathy and stage 3 CKD has been treatedwith growth hormone therapy for the past 2 years. His

growth velocity has been decreasing over the past 6 months.An indication to stop therapy would be: a. Serum PTH of150 pg/mL b. Height at percentile corresponding to themean parental height c. Tanner 2 pubertal development d.Increasing alkaline phosphatase activity 5. A 10-year-oldboy receiving maintenance hemodialysis is treated withcalcium carbonate and thrice weekly calcitriol to controlhis renal osteodystrophy. His serum PTH level is 700pg/mL; phosphorus, 5 mg/dL; and calcium, 11.5 mg/dL. Toameliorate his hypercalcemia, the next step in his therapyshould include: a. Dietary calcium restriction b. Bonebiopsy c. Switching to a non–calcium-containing phosphatebinder d. Increasing the calcitriol therapy ANSWER KEY 1.a 2. b 3. b 4. b 5. c
34 Nutrition in chronic kidney disease
1. Kidney Disease Outcomes Quality Initiative, NationalKidney Foundation. Clinical practice guidelines fornutrition in chronic renal failure. Am J Kidney Dis.2000;35:S1–140.
2. Furth SL, Stablein D, Fine RN, et al. Adverse clinicaloutcomes associated with short stature at dialysisinitiation: A report of the North American Pediatric RenalTransplant Cooperative Study. Pediatrics. 2002;109:909–13.3. Wong CS, Gipson DS, Gillen DL, et al. Anthropometricmeasures and risk of death in children with end-stagerenal disease. Am J Kidney Dis. 2000;36:811–9. 4. Fos terBJ, McCauley L, Mak RH. Nutrition in infants and veryyoung children with chronic kidney disease. PediatrNephrol. 2012;27:1427–39. 5. Kar lberg J, Schaefer F,Hennicke M, et al. Early age-dependent growth impairmentin chronic renal failure. European Study Group forNutritional Treatment of Chronic Renal Failure inChildhood. Pediatr Nephrol. 1996;10:283–7. 6. KidneyDisease Outcomes Quality Initiative, Clinical PracticeGuideline for Nutrition in Children with CKD: 2008 update.Executive summary. Am J Kidney Dis. 2009;53:S11–104. 7.Zivicnjak M, Franke D, Filler G, et al. Growth impairmentshows an age-dependent pattern in boys with chronic kidneydisease. Pediatr Nephrol. 2007;22:420–9. 8. Schaefer F,Wuhl E, Feneberg R, et al. Assessment of body compositionin children with chronic renal failure. Pediatr Nephrol.2000;14:673–8. 9. Rees L, Shaw V. Nutrition in childrenwith CRF and on dialysis. Pediatr Nephrol.2007;22:1689–702. 10. Van D yck M, Proesmans W. Headcircumference in chronic renal failure from birth. ClinNephrol. 2001;56:S13–6. 11. Warady BA, Belden B, KohautE. Neurodevelopmental outcome of children initiatingperitoneal dialysis in early infancy. Pediatr Nephrol.1999;13:759–65. 12. Borah MF, Schoenfeld PY, Gotch FA, etal. Nitrogen balance during intermittent dialysis therapyof uremia. Kidney Int. 1978;14:491–500. 13.Juarez-Congelosi M, Orellana P, Goldstein SL. Normalizedprotein catabolic rate versus serum albumin as a nutritionstatus marker in pediatric patients receiving hemodialysis.J Ren Nutr. 2007;17:269–74. 14. Kopple JD, Jones MR,Keshaviah PR, et al. A proposed glossary for dialysiskinetics. Am J Kidney Dis. 1995;26:963–81. 15. EdefontiA, Picca M, Damiani B, et al. Models to assess nitrogenlosses in pediatric patients on chronic peritonealdialysis. Pediatr Nephrol. 2000;15:25–30. 16. Leavey SF,Strawderman RL, Jones CA, et al. Simple nutritionalindicators as independent predictors of mortality in

hemodialysis patients. Am J Kidney Dis. 1998;31:997–1006.17. Stenvinkel P, Barany P, Chung SH, et al. A comparativeanalysis of nutritional parameters as predictors of outcomein male and female ESRD patients. Nephrol Dial Transplant.2002;17:1266–74. 18. Wong CS, Hingorani S, Gillen DL, etal. Hypoalbuminemia and risk of death in pediatricpatients with end-stage renal disease. Kidney Int.2002;61:630–7.
SUMMARY
e association between mortality and extremes of
BMI in children with CKD heightens the impor
tance of careful nutritional management in this
patient population. Close assessment, monitoring,
and management of nutritional status in CKD may
have a critical impact on growth and neurodevelop
ment, especially in younger children. 4 �erefore, the
active involvement of a registered dietitian, health
care professionals, and caregivers is essential for pro
viding proper nutritional care to children with CKD.
Moreover, further clinical trials are needed to estab
lish evidence-based guidelines for nutritional assess
ment and management in pediatric CKD.
Table 34.4 Recommended target ranges for serum
parathyroid hormone
Chr onic kidney
disease stage Serum PTH level (pg/mL) 2 35–70 3 35–70 470–110 5 200–300
Source: National Kidney Foundation: K/DOQI clinicalpractice guidelines for bone metabolism and disease inchildren with chronic kidney disease. Am J Kidney Dis2005; 46: S1-121. Reprinted with permission

Abbreviation: PTH, parathyroid hormone.
19. Quan A, Baum M. Protein losses in children oncontinuous cycle peritoneal dialysis. Pediatr Nephrol.1996;10:728–31.
20. Ras hid R, Neill E, Smith W, et al. Body compositionand nutritional intake in children with chronic kidneydisease. Pediatr Nephrol. 2006;21:1730–8.
21. Tsampalieros A, Kalkwarf HJ, Wetzsteon RJ, et al.Changes in bone structure and the muscle-bone unit inchildren with chronic kidney disease. Kidney Int.2013;83:495–502.
22. Mak R H, Cheung WW, Zhan JY, et al. Cachexia andprotein-energy wasting in children with chronic kidneydisease. Pediatr Nephrol. 2012;27:173–81.
23. Gunta SS, Mak RH. Ghrelin and leptin pathophysiology inchronic kidney disease. Pediatr Nephrol. 2013;28:611–6.
24. Gunta SS, Thadhani RI, Mak RH. The effect of vitamin Dstatus on risk factors for cardiovascular disease. Nat RevNephrol. 2013;9:337–47.
25. Ledermann SE, Shaw V, Trompeter RS. Longterm enteralnutrition in infants and young children with chronic renalfailure. Pediatr Nephrol. 1999;13:870–5.
26. Mar ques de Aquino T, Avesani CM, Brasileiro RS, deAbreu Carvalhaes JT. Resting energy expenditure ofchildren and adolescents undergoing hemodialysis. J RenNutr. 2008;18:312–9.
27. Pol lock C, Voss D, Hodson E, Crompton C. The CARIguidelines: Nutrition and growth in kidney disease.Nephrology (Carlton) 2005;10(Suppl 5):S177–230.
28. Ede fonti A, Picca M, Damiani B, et al. Dietaryprescription based on estimated nitrogen balance duringperitoneal dialysis. Pediatr Nephrol. 1999;13:253–8.
29. Salusky IB, Fine RN, Nelson P, et al. Nutritionalstatus of children undergoing continuous ambulatoryperitoneal dialysis. Am J Clin Nutr. 1983;38:599–611.
30. Coleman JE, Watson AR, Rance CH, Moore E. Gastrostomybuttons for nutritional support on chronic dialysis.

Nephrol Dial Transplant. 1998;13:2041–6.
31. Ree d EE, Roy LP, Gaskin KJ, Knight JF. Nutritionalintervention and growth in children with chronic renalfailure. J Ren Nutr. 1998;8:122–6.
32. Van Dyck M, Bilem N, Proesmans W. Conservativetreatment for chronic renal failure from birth: A 3-yearfollow-up study. Pediatr Nephrol. 1999;13:865–9.
33. Bon thuis M, van Stralen KJ, Verrina E, et al.Underweight, overweight and obesity in paediatric dialysisand renal transplant patients. Nephrol Dial Transplant.2013;28(Suppl 4):iv195–iv204.
34. Sec ker D, Mak R. Nutritional challenges in pediatricchronic kidney disease. In: Geary DF, Schaefer F, editors.Comprehensive Pediatric Nephrology, 1st ed. Philadelphia:Mosby; 2008. pp. 743–59. 35. Dello Strologo L, PrincipatoF, Sinibaldi D, et al. Feeding dysfunction in infants withsevere chronic renal failure after long-term nasogastrictube feeding. Pediatr Nephrol. 1997;11:84–6. 36. Col emanJE, Watson AR. Growth posttransplantation in childrenpreviously treated with chronic dialysis and gastrostomyfeeding. Adv Perit Dial. 1998;14:269–73. 37. Pugh P,Watson AR. Transition from gastrostomy to oral feedingfollowing renal transplantation. Adv Perit Dial.2006;22:153–7. 38. Gol dstein SL, Baronette S, GambrellTV, et al. nPCR assessment and IDPN treatment ofmalnutrition in pediatric hemodialysis patients. PediatrNephrol. 2002;17:531–4. 39. Krause I, Shamir R,Davidovits M, et al. Intradialytic parenteral nutrition inmalnourished children treated with hemodialysis. J RenNutr. 2002;12:55–9. 40. Ore llana P, Juarez-Congelosi M,Goldstein SL. Intradialytic parenteral nutrition treatmentand biochemical marker assessment for malnutrition inadolescent maintenance hemodialysis patients. J Ren Nutr.2005;15:312–7. 41. Kop ple JD, Levey AS, Greene T, et al.Effect of dietary protein restriction on nutritionalstatus in the Modification of Diet in Renal Disease Study.Kidney Int. 1997;52:778–91. 42. Menon V, Kopple JD, WangX, et al. Effect of a very low-protein diet on outcomes:Long-term follow-up of the Modification of Diet in RenalDisease (MDRD) Study. Am J Kidney Dis. 2009;53:208–17.43. Cha turvedi S, Jones C. Protein restriction forchildren with chronic renal failure. Cochrane DatabaseSyst Rev. 2007:(17)006863. 44. Win gen AM, Fabian-Bach C,Schaefer F, Mehls O. Randomised multicentre study of alow-protein diet on the progression of chronic renalfailure in children. European Study Group of Nutritional

Treatment of Chronic Renal Failure in Childhood. Lancet.1997;349:1117–23. 45. Boaz M, Smetana S. Regressionequation predicts dietary phosphorus intake from estimateof dietary protein intake. J Am Diet Assoc.1996;96:1268–70. 46. Uri barri J. Phosphorus homeostasisin normal health and in chronic kidney disease patientswith special emphasis on dietary phosphorus intake. SeminDial. 2007;20:295–301. 47. Van Horn L. Fiber, lipids, andcoronary heart disease: A statement for healthcareprofessionals from the Nutrition Committee, American HeartAssociation. Circulation. 1997;95:2701–4. 48. Keane WF,Tomassini JE, Neff DR. Lipid abnormalities in patients withchronic kidney disease. Contrib Nephrol. 2011;171:135–42.49. Saland JM, Pierce CB, Mitsnefes MM, et al.Dyslipidemia in children with chronic kidney disease.Kidney Int. 2010;78:1154–63.
50. Querfeld U, Salusky IB, Nelson P, et al.Hyperlipidemia in pediatric patients undergoing peritonealdialysis. Pediatr Nephrol 1988;2:447–52.
51. Kavey R E, Allada V, Daniels SR, et al. Cardiovascularrisk reduction in high-risk pediatric patients: Ascientific statement from the American Heart AssociationExpert Panel on Population and Prevention Science; theCouncils on Cardiovascular Disease in the Young,Epidemiology and Prevention, Nutrition, Physical Activityand Metabolism, High Blood Pressure Research,Cardiovascular Nursing, and the Kidney in Heart Disease;and the Interdisciplinary Working Group on Quality of Careand Outcomes Research: Endorsed by the American Academy ofPediatrics. Circulation. 2006;114:2710–38.
52. Sch aefer B, Wuhl E. Progression in chronic kidneydisease and prevention strategies [educational paper]. EurJ Pediatr. 2012;171:1579–88.
53. Kidney Disease Outcomes Quality Initiative. Clinicalpractice guidelines for cardiovascular disease in dialysispatients. Am J Kidney Dis. 2005;45:S1–153.
54. American Academy of Pediatrics. National CholesterolEducation Program: Report of the Expert Panel on BloodCholesterol Levels in Children and Adolescents.Pediatrics. 1992;89:525–84.
55. Gidding SS, Dennison BA, Birch LL, et al. Dietaryrecommendations for children and adolescents: A guide forpractitioners. Consensus statement from the American HeartAssociation. Circulation. 2005;112:2061–75.
56. Nii nikoski H, Lapinleimu H, Viikari J, et al. Growthuntil 3 years of age in a prospective, randomized trial ofa diet with reduced saturated fat and cholesterol.Pediatrics. 1997;99:687–94.
57. Cabo J, Alonso R, Mata P. Omega-3 fatty acids andblood pressure. Br J Nutr. 2012;107(Suppl 2): S195–200.
58. Rangel-Huerta OD, Aguilera CM, Mesa MD, Gil A. Omega-3long-chain polyunsaturated fatty acids supplementation oninflammatory biomarkers: A systematic review of randomisedclinical trials. Br J Nutr. 2012;107(Suppl 2):S159–70.
59. Vedtofte MS, Jakobsen MU, Lauritzen L, Heitmann BL.The role of essential fatty acids in the control ofcoronary heart disease. Curr Opin Clin Nutr Metab Care.2012;15:592–6.
60. Calder PC, Yaqoob P. Marine omega-3 fatty acids andcoronary heart disease. Curr Opin Cardiol. 2012;27:412–9.
61. Gor en A, Stankiewicz H, Goldstein R, Drukker A. Fishoil treatment of hyperlipidemia in children andadolescents receiving renal replacement therapy.Pediatrics. 1991;88:265–8.
62. Per eira AM, Hamani N, Nogueira PC, Carvalhaes JT.Oral vitamin intake in children receiving long-termdialysis. J Ren Nutr. 2000;10:24–9. 63. Dibas BI, WaradyBA. Vitamin D status of children receiving chronicdialysis. Pediatr Nephrol. 2012;27:1967–73. 64. Kri leyM, Warady BA. Vitamin status of pediatric patientsreceiving long-term peritoneal dialysis. Am J Clin Nutr.1991;53:1476–9. 65. Warady BA, Kriley M, Alon U,Hellerstein S. Vitamin status of infants receivinglong-term peritoneal dialysis. Pediatr Nephrol.1994;8:354–6. 66. Goo dman WG, Coburn JW. The use of1,25-dihydroxyvitamin D3 in early renal failure. Annu RevMed. 1992;43:227–37. 67. Kidney Disease Outcomes QualityInitiative, National Kidney Foundation. Clinical practiceguidelines for bone metabolism and disease in childrenwith chronic kidney disease. Am J Kidney Dis.2005;46:S1–121. 68. Wang M, Hercz G, Sherrard DJ, et al.Relationship between intact 1-84 parathyroid hormone andbone histomorphometric parameters in dialysis patientswithout aluminum toxicity. Am J Kidney Dis.1995;26:836–44. 69. Rees L. What parathyroid hormonelevels should we aim for in children with stage 5 chronickidney disease: What is the evidence? Pediatr Nephrol.
2008;23:179–84. REVIEW QUESTIONS 1. Which one of thefollowing statements is true? a. No association has beenfound between low body mass index and increased risk formortality in children. b. Growth failure in infants withCKD is mainly due to malnutrition. c. Rates of lineargrowth and neurodevelopment are highest during the seconddecade of life. d. �e nutritional status of children withCKD should be evaluated with the same frequency as insameaged healthy children. 2. Which one of the followingparameters is not included in the typical nutritionalassessment for a child with CKD? a. Headcircumference-for-age percentile for children younger than3 years of age b. Height-for-age percentile c.Weight-for-age percentile d. Triceps skinfold thickness3. Whi ch one of the following statements most accuratelydescribes the factors contributing to cachexia in CKD? a.Ghr elin is an orexigenic hormone that may play a role inthe pathogenesis of cachexia in CKD. b. �e fo urcirculating gene products of ghrelin include acyl ghrelin,des-acyl-ghrelin, obestatin, and melatonin.
c. Leptin is an anorexigenic hormone secreted fromleukocytes.
d. Vitamin supplementation has been shown to have littlee�ect on cachexia in experimental CKD.
4. Which one of the following statements is false?
a. �e energy requirements of children with CKD are higherthan those of healthy children.
b. �e caloric intake for children with CKD should bedetermined from national recommendations of the estimatedenergy requirements based on chronologic age and gender.
c. Children on chronic dialysis who receive nutritionalsupport through gastrostomy tube feedings show improvementin weight and height SDS.
d. �e energy intake from dialysate glucose is approximately8 to 12 kcal/kg/day.
5. For children older than 3 years of age, which of thefollowing distributions of calories from carbohydrates,fat, and protein is recommended?
a. Carbohydrates 25% to 35%, fat 45% to 65%, protein 10%to 30%

b. Carbohydrates 10% to 30%, fat 45% to 65%, protein 25%to 35%
c. Carbohydrates 25% to 35%, fat 10% to 30%, protein 45%to 65%
d. Carbohydrates 45% to 65%, fat 25% to 35%, protein 10%to 30%
6. Which of the following macronutrients is lost throughthe peritoneal dialysate ultra�ltrate?
a. Protein
b. Carbohydrates
c. Lipids
d. None of the above
7. Which of the following statements is true?
a. Dyslipidemia is rare in patients with CKD.
b. Children on PD have low prevalence rates (30% to 40%)of hypertriglyceridemia. c. Dyslipidemia potentiallyaccelerates the progression of CKD. d. Restricting dietaryfat to 30% of the total caloric intake has adverse e�ectson growth. 8. Which one of the following vitaminsupplements is recommended in children on dialysis? a.Vitamin A b. Vitamin E c. Vitamin B d. Vitamin K 9.Which one of the following vitamins inhibits PTH secretionand at large doses causes adynamic bone disease? a.Vitamin A b. Vitamin E c. Vitamin C d. Vitamin D 10.Which of the following medications inhibits PTH secretionby increasing the sensitivity of calcium-sensing receptorsto extracellular calcium? a. Calcitriol b. Paricalcitolc. Cinacalcet hydrochloride d. Doxercalciferol ANSWER KEY1. b 2. d 3. a 4. a 5. d 6. a 7. c 8. c 9. d 10. c

35 Continuous renal replacement therapy
1. Haq NU, Nolph KD. Past, present, and future ofquantified peritoneal dialysis. Semin Dial. 2001;14:263-7.
2. Van S tone JC. Dialysis equipment and dialysate, past,present and the future. Semin Nephrol. 1997;17:214-7.
3. Merrill JP. The use of the artificial kidney in thetreatment of uremia. J Urban Health. 1998;75:911-18.
4. Kramer P, Schrader J, Bohnsack W, et al. Continuousarteriovenous haemofiltration: A new kidney replacementtherapy. Proc Eur Dial Transplant Assoc. 1981;18:743–9.
5. Maxvold NJ, Bunchman TE. Renal failure and replacementtherapy. Crit Care Clin. 2003;19:563-75.
6. Kramer P, Wigger W, Rieger J, et al. Arteriovenoushaemofiltration: A new and simple method for treatment ofover-hydrated patients resistant to diuretics. KlinWochenschr .1977;55:1121-2.
7. Bellomo R, Ronco C. An introduction to continuous renalreplacement therapy. In: Bellomo R, Baldwin I, Ronco C,Golper T, editors. Atlas of Hemofiltration. Philadelphia:Saunders; 2001. p. 1–9.
8. Forni LG, Hilton PJ. Continuous hemofiltration in thetreatment of acute renal failure. N Engl J Med.1997;336:1303-9.
9. Lebedo I. Principles and practice of hemofiltration andhemodiafiltration. Artif Organs. 1998;22:20-5.
10. Par akininkas D, Greenberg LA. Comparison of soluteclearance in three modes of continuous renal replacementtherapy. Pediatr Crit Care Med. 2004;5:269-74. 11.Jenkins R, Harrison H, Chen B, et al. Accuracy ofintravenous infusion pumps in continuous renal replacementtherapies. ASAIO J. 1992;38:808-10. 12. Flores FX, BrophyPD, Symons JM, et al. CRRT after stem celltransplantation: A report from the Prospective PediatricCRRT Registry Group. Pediatr Nephrol. 2008;23:625–63. 13.Hackbarth R, Bunchman TW, Chua AN, et al. The effect ofvascular access location and size on circuit survival inpediatric continuous renal replacement therapy: A reportfrom the PPCRRT registry. Int J Artif Organs.2007;12:1116–21. 14. Davenport A, Aulton K, Payne PB, etal. Hyperlactatemia and increasing metabolic acidosis due

to the use of lactate based fluid during haemofiltration.Intensive Care Med. 1989;15:546-7. 15. Davenport A, WillEJ, Davison AM. The effect of lactate-buffered solutionson the acid-base status of patients with renal failure.Nephrol Dial Transplant. 1989;4:800-4. 16. Davenport A,Aulton K, Payne RB, et al. Hyperlactatemia and increasingmetabolic acidosis in hepatorenal failure treated byhemofiltration. Ren Fail. 1990;12:99-101. 17. DavenportA, Will EJ, Davison AM. Hyperlactataemia and metabolicacidosis during haemofiltration using lactate-bufferedfluids. Nephron. 1991;59:461-5. 18. Thomas AN, Guy JM,Kishen R, et al. Comparison of lactate and bicarbonatebuffered haemofiltation fluids: Use in critically illpatients. Nephrol Dial Transplant. 1997;12:1212-7. 19.Zim merman D, Cotman P, Ting R, et al. Continuousveno-venous haemodialysis with a novel bicarbonatedialysis solution: Prospective cross-over comparison with alactate buffered solution. Nephrol Dial Transplant.1999;14:2387-91. 20. Maxvold NJ, Flynn JT, Smoyer WE, etal. Prospective, crossover comparison of bicarbonate vslactate-based dialysate for pediatric CVVHD. Blood Purif.1999;17:27 (abstract). 21. Barenbrock M, Hausberg M,Matzkies F, et al. Effects of bicarbonate- andlactate-buffered replacement fluids on cardiovascularoutcome in CVVH patients. Kidney Int. 2000;58:1751-7. 22.McLean AG, Davenport A, Cox D, et al. Effects oflactate-buffered and lactate-free dialysate in CAVHDpatients with and without liver dysfunction. Kidney Int.2000;58:1765-72. 23. Bunchman TE, Maxvold NJ, Barnett J,et al. Pediatric hemofiltration: Normocarb® dialysatesolution with citrate anticoagulation. Pediatr Nephrol.2002;17:150-4. 24. Bunchman TE, Maxvold NJ, Brophy PD.Pediatric convective hemofiltration (CVVH): Normocarbreplacement fluid and citrate anticoagulation. Am J KidneyDis. 2003;42:1248-52.
SUMMARY
CRRT has evolved since the 1980s as an e�cient
and safe treatment for AKI in both adult and pedi
atric patients. Newer dialysate and replacement �uid
solutions are available, and now one can safely use
bicarbonate as the bu�er to minimize cardiovascular
instability, as well as to minimize the possibility of con
founding the serum lactic acid levels. Anticoagulation
for maintenance of the CRRT circuit is critical to pro
viding adequate �uid and electrolyte therapy in the
pediatric patient with AKI, and citrate anticoagulation
appears to have multiple bene�ts over heparin anti
coagulation. Prostacyclin is an emerging anticoagu
lant with great promise. Vascular access is critical for
proper functioning of a CRRT circuit, and ideally it
should use the largest catheter possible. Finally, CRRT
may be a useful therapy in other clinical conditions,
such as hyperosmolality, intoxications, hematopoietic
cell transplantation, tumor lysis syndrome prevention,
extracorporeal hepatic support, and plasmapheresis.
25. Karvellas CJ, Farhat MR, Sajjad I, et al. A comparisonof early versus late initiation of renal replacementtherapy in critically ill patients with acute kidneyinjury: A systematic review and meta-analysis. Crit Care.2011;15:R72. doi:10.1186/cc10061
26. Bouman CS, Oudemans-Van Straaten HM, Tijssen JG, etal. Effects of early high-volume continuous venovenoushemofiltration on survival and recovery of renal functionin intensive care patients with acute renal failure: Aprospective, randomized trial. Crit Care Med.2002;30:2205–11.
27. Bai M, Zhou M, He L, et al. Citrate versus heparinanticoagulation for continuous renal replacement therapy:An updated meta-analysis of RCTs. Intensive Care Med.2015;41:2098-110.
28. O’S hea SI, Oftel TL, Kovalik EC. Alternative methodsof anticoagulation for dialysis-dependent patients withheparin-induced thrombocytopenia. Semin Dial.2003;16:61-7.
29. Mehta RL, McDonald BR, Aguilar MM, et al. Regional

citrate anticoagulation for continuous arteriovenoushemodialysis in critically ill patients. Kidney Int.1990;38:976-81.
30. Cha dha V, Garg U, Warady BA, et al. Citrate clearancein children receiving continuous venovenous renalreplacement therapy. Pediatr Nephrol. 2002;17:819-24.
31. Mei er-Kriesche HU, Gitomer J, Finkel K, et al.Increased total to ionized calcium ratio during continuousvenovenous hemodialysis with regional citrateanticoagulation. Crit Care Med. 2001;29:748-52.
32. Monchi M, Berghams D, Ledoux D, et al. Citrate vs.heparin for anticoagulation in continuous venovenoushemofiltration: A prospective randomized study. IntensiveCare Med. 2004;30:260-5.
33. Brophy PD, Somers MJG, Baum MA, et al. Multicentreevaluation of anticoagulation in patients receivingcontinuous renal replacement therapy (CRRT). Nephrol DialTransplant. 2005;20:1416–21.
34. Gainza FJ, Quintanilla N, Pijoan JI, et al. Role ofprostacyclin (epoprostenol) as anticoagulant in continuousrenal replacement therapies: Efficacy, safety and costanalysis. J Nephrol. 2006;19:648–55.
35. Arcangeli A, Rocca B, Salvatori G, et al. Heparinversus prostacyclin in continuous hemodiafiltration foracute renal failure: Effects on platelet function in thesystemic circulation and across the filter. Thromb Res.2010;126:24–31.
36. Bal ik M, Waldauf P, Plasil P, et al. Prostacyclinversus citrate in continuous hemodiafiltration: Anobservational study in patients with high risk of bleeding.Blood Purif. 2005;23:325–29.
37. Ven kataraman R, Kellum JA, Palevsky P. Dosing patternsfor continuous renal replacement therapy at a largeacademic medical center in the United States. J Crit Care2002;17:246-250. 38. Ronco C. Fluid balance in CRRT: Acall to attention! Int J Artif Organs. 2005;28:763-4. 39.Soysal DD, Karaböcüoğlu M, Citak A, et al. Metabolicdisturbances following the use of inadequate solutions forhemofiltration in acute renal failure. Pediatr Nephrol.2007;22: 715-9. 40. Fiaccadori E, Lombardi M, Leonardi, etal. Prevalence and clinical outcomes associated withpreexisting malnutrition in acute renal failure: A

prospective cohort study. J Am Soc Nephrol.1999;10:581-93. 41. Macias WL, Alaka KJ, Murphy MH, et al.Impact of the nutritional regimen on protein catabolismand nitrogen balance in patients with acute renal failure.JPEN J Parenter Enteral Nutr. 1996;20:56-62. 42. KoppleJD. The nutrition management of the patient with acuterenal failure. J Parenter Enteral Nutr. 1996;20:3-12. 43.Chi ma CS, Meyer L, Hummell AC, et al. Protein catabolicrate in patients with acute renal failure on continuousarteriovenous hemofiltration and total parenteralnutrition. J Am Soc Nephrol. 1993;3:1516-21. 44. Davi esSP, Reaveley DA, Brown EA, et al. Amino acid clearance anddaily losses in patients with acute renal failure treatedby continuous arteriovenous hemodialysis. Crit Care Med.1991;19:1510-5. 45. Max vold NJ, Smoyer WE, Custer JR, etal. Amino acid loss and nitrogen balance in critically illchildren with acute renal failure: A prospectivecomparison between classic hemofiltration andhemofiltration with dialysis. Crit Care Med.2000;28:1161-5. 46. Ber ger MM, Shenkin A, Revelly JP, etal. Copper, selenium, zinc, and thiamine balances duringcontinuous venovenous hemodiafiltration in critically illpatients. Am J Clin Nutr. 2004;80:410-6. 47. Brophy PD,Mottes TA, Kudelka TL, et al. AN-69 membrane reactions arepH-dependent and preventable. Am J Kidney Dis.2001;38:173-8. 48. Parshuram CS, Cox PN. Neonatalhyperkalemichypocalcemic cardiac arrest associated withinitiation of blood-primed continuous venovenoushemofiltration. Pediatr Crit Care Med. 2002;3:67-9. 49.Pasko DA, Mottes TA, Mueller BA. Pre dialysis of bloodprime in continuous hemodialysis normalizes pH andelectrolytes. Pediatr Nephrol. 2003;18:1177 -83. 50.Hackbarth RM, Eding D, Smith CG, et al. Zero-balanceultrafiltration (Z-BUF) in blood-primed CRRT circuitsachieves electrolyte and acid-base homeostasis prior topatient connection. Pediatr Nephrol. 2005;20:1328-33. 51.Symons JM, Brophy PD, Gregory MJ, et al. Continuous renalreplacement therapy in children up to 10 kg. Am J KidneyDis. 2003;41:984-9. 52. Smoyer WE, Maxvold NJ, RemenappRT, et al. Pediatric renal replacement therapy. In:Fuhrman BP, Zimmerman JJ, editors. Pediatric CriticalCare, 2nd ed. St. Louis: Mosby–Year Book; 1998. p. 767.
53. Sell LL, Cullen ML, Whittlesey GC, et al. Experiencewith renal failure during extracorporeal membraneoxygenation: Treatment with continuous hemofiltration. JPediatr Surg. 1987;22:600-2.
54. Meyer RJ, Brophy PD, Bunchman TE, et al. Survival andrenal function in pediatric patients following
extracorporeal life support with hemofiltration. PediatrCrit Care Med. 2001;2:238-42.
55. Braun MC, Welch TR. Continuous venovenoushemodiafiltration in the treatment of acute hyperammonemia.Am J Nephrol. 1998;18:531-3.
56. Sperl W, Geiger R, Maurer H, et al. Continuousarteriovenous haemofiltration in hyperammonemia of newbornbabies. Lancet. 1990;336:1192-3.
57. Sperl W, Geiger R, Maurer H, et al. Continuousarteriovenous haemofiltration in a neonate withhyperammonaemic coma due to citrullinaemia. J InheritMetab Dis. 1992;15:158-9.
58. Thompson GN, Butt WW, Shann FA, et al. Continuousvenovenous hemofiltration in the management of acutedecompensation in inborn errors of metabolism. J Pediatr.1991;118:879-84.
59. Jouvet P, Poggi F, Rabier D, et al. Continuousvenovenous haemodiafiltration in the acute phase ofneonatal maple syrup urine disease. J Inherit Metab Dis.1997;20:463-72.
60. Falk MC, Knight JF, Roy LP, et al. Continuousvenovenous haemofiltration in the acute treatment of inbornerrors of metabolism. Pediatr Nephrol. 1994;8:330-3.
61. Won g KY, Wong SN, Lam SY, et al. Ammonia clearance byperitoneal dialysis and continuous arteriovenoushemodiafiltration. Pediatr Nephrol. 1998;12:589 -91.
62. Picca S, Dionisi-Vici C, Abeni D, et al. Extracorporealdialysis in neonatal hyperammonemia: Modalities andprognostic indicators. Pediatr Nephrol. 2001;16:862-7.
63. Deodato F, Boenzi S, Rizzo C, et al. Inborn errors ofmetabolism: An update on epidemiology and onneonatal-onset hyperammonemia. Acta Paediatr Suppl.2004;93:18-21.
64. Beal AL, Cerra FB. Multiple organ failure syndrome inthe 1990s. JAMA. 1994;271:226-33.
65. Pro ulx F, Fayon M, Farrell CA, et al. Epidemiology ofsepsis and multiple organ dysfunction syndrome inchildren. Chest. 1996;109:1033-7.
66. Goldstein SL, Somers MJ, Baum MA, et al. Pediatricpatients with multi-organ dysfunction syndrome receivingcontinuous renal replacement therapy. Kidney Int.2005;67:653–8.
67. Rus s KB, Stevens TM, Singal AK. Acute Kidney Injuryin Patients with Cirrhosis. J Clin Transl Hepatol.2015;3:195-204.
68. du Ch eyron D, Bouchet B, Parienti JJ, et al. Theattributable mortality of acute renal failure in criticallyill patients with liver cirrhosis. Intensive Care Med.2005;31:1693-9. 69. Bernal W, Hall C, Karvellas CJ, et al.Arterial ammonia and clinical risk factors forencephalopathy and intracranial hypertension in acuteliver failure. Hepatology. 2007;46:1844–52. 70. AgarwalB, Shaw S, Shankar Hari M, et al. Continuous renalreplacement therapy (CRRT) in patients with liver disease:Is circuit life different? J Hepatol. 2009;51:504–9. 71.Sac cente SL, Kohaut EC, Berkow RL. Prevention of tumorlysis syndrome using continuous veno-venoushemofiltration. Pediatr Nephrol. 1995;9:569–73. 72 WilsonFP, Berns JS. Tumor lysis syndrome: New challenges andrecent advances. Adv Chronic Kidney Dis. 2014;21 :18-26.73. Hingorani SR, Guthrie K, Batchelder A, et al. Acuterenal failure after myeloablative hematopoietic celltransplant: Incidence and risk factors. Kidney Int.2005;67:272-7. 74. DiCarlo JV, Alexander SR, Agarwal R, etal. Continuous veno-venous hemofiltration may improvesurvival from acute respiratory distress syndrome afterbone marrow transplantation or chemotherapy. J PediatrHematol Oncol. 2003;25:801-5. 75. McB ryde KD, BunchmanTE, Kudelka TL, et al. Hyperosmolar solutions incontinuous renal replacement therapy for hyperosmolar acuterenal failure: A preliminary report. Pediatr Crit Care Med.2005;6:220-5. 76. Borkan SC. Extracorporeal therapies foracute intoxications. Crit Care Clin. 2002;18:393-40. 77.Mokhlesi B. Leikin JB, Murray P, et al. Adult toxicology incritical care. Part I. General approach to the intoxicatedpatient. Chest. 2003;123:577-92. 78. Mok hlesi B. LeikinJB, Murray P, et al. Adult toxicology in critical care.Part II. Specific poisonings. Chest. 2003;123:897-922.79. Goe bel J, Ananth M, Lewy JE. Hemodiafiltration forvancomycin overdose in a neonate with end-stage renalfailure. Pediatr Nephrol. 1999;13:423-5. 80. Mey er RJ,Flynn JT, Brophy PD, et al. Hemodialysis followed bycontinuous hemofiltration for treatment of lithiumintoxication in children. Am J Kidney Dis. 2001;37:1044-7.81. Christiansson LK, Kaspersson KE, Kulling PE, et al.Treatment of severe ethylene glycol intoxication with
continuous arteriovenous hemofiltration dialysis. JToxicol Clin Toxicol. 1995;33:267-70. 82. Domoto DT, BrownWW, Bruggensmith P. Removal of toxic levels ofN-acetylprocainamide with continuous arteriovenoushemofiltration or continuous arteriovenoushemodiafiltration. Ann Intern Med. 1987;106:550-2. 83.Oka da S, Teramoto S, Matsuoka R. Recovery fromtheophylline toxicity by continuous hemodialysis withfiltration. Ann Intern Med. 2000;133:922.
84. Vilay AM, Mueller BA, Haines H, et al. Treatment ofmethotrexate intoxication with various modalities ofcontinuous extracorporeal therapy and glucarpidase.Pharmacotherapy. 2010;30:111.
85. Jalan R, Sen S. Extracorporeal albumin dialysis forintoxication from protein-bound agents. Crit Care Med.2004. 32:1436-7.
86. Askenazi DJ, Goldstein SL, Chang IF, et al. Managementof a severe carbamazepine overdose using albumin-enhancedcontinuous venovenous hemodialysis. Pediatrics.2004;113:406-9.
87. Churchwell MD, Pasko DA, Smoyer W, et al. Enhancedclearance of highly protein-bound drugs byalbumin-supplemented dialysate during modeled continuoushemodialysis. Nephrol Dial Transplant. 2009;24:231–38.
88. Bunchman TE. Plasmapheresis and renal replacementtherapy in children. Curr Opin Pediatr. 2002;14:310-4.
89. Yorgin PD, Eklund DK, Al-Uzri A, et al. Concurrentcentrifugation plasmapheresis and continuous venovenoushemodiafiltration. Pediatr Nephrol. 2000;14:18-21.
90. Pon ikvar R, Kandus A, Urbančič A, et al. Continuousrenal replacement therapy and plasma exchange in newbornsand infants. Artif Organs. 2002;26:163-8.
91. Lex mond WS, Van Dael CM, Scheenstra R, et al.Experience with molecular adsorbent recirculating systemtreatment in 20 children listed for highurgency livertransplantation. Liver Transpl. 2015; 21:369-80.
92. Vaid A, Chweich H, Balk EM, et al. Molecular adsorbentrecirculating system as artificial support therapy forliver failure: A meta-analysis. ASAIO J. 2012;58:51–9.
93. Kortgen A, Rauchfuss F, Götz M, et al. Albumin dialysis
in liver failure: Comparison of molecular adsorbentrecirculating system and single pass albumin dialysis-aretrospective analysis. Ther Apher Dial. 2009;13:419–25.
94. Sau er IM, Goetz M, Steffen I, et al. In vitrocomparison of the molecular adsorbent recirculation system(MARS) and single-pass albumin dialysis (SPAD).Hepatology. 2004;39:1408–14.
95. Ringe H, Varnholt V, Zimmering M, et al. Continuousveno-venous single-pass albumin hemodiafiltration inchildren with acute liver failure. Pediatr Crit Care Med.2011;12:257–64.
96. Kre ymann B, Seige M, Schweigart U, et al. Albumindialysis: Effective removal of copper in a patient withfulminant Wilson disease and successful bridging to livertransplantation. A new possibility for the elimination ofprotein-bound toxins. J Hepatol. 1999;31:1080-5. 97.Collins KL, Roberts EA, Adeli K, et al. Single passalbumin dialysis (SPAD) in fulminant wilsonian liverfailure: A case report. Pediatr Nephrol. 2008;23:1013–16.98. Chawla LS, Georgescu F, Abell B, S et al. Modificationof continuous venovenous hemodiafiltration with single-passalbumin dialysate allows for removal of serum bilirubin.Am J Kidney Dis. 2005;45:e51–6. 99. Smoy er WE, McAdamsC, Kaplan BS, et al. Determinants of survival in pediatriccontinuous hemofiltration. J Am Soc Nephrol.1995;6:1401-9. 100. Goldstein SL, Currier H, Graf JM, etal. Outcomes in children receiving continuous venovenoushemofiltration. Pediatrics. 2001;107:1309-12. 101. Sym onsJM, Chua AN, Somers MJG, et al. Demographiccharacteristics of pediatric continuous renal replacementtherapy: A report of the Prospective Pediatric ContinuousRenal Replacement Therapy Registry. Clin J Am Soc Nephrol.2007;2:732–8. 102. Ask enazi DJ, Goldstein SL, Koralkar R,et al. Continuous renal replacement therapy for children≤10 kg: A report from the Prospective Pediatric ContinuousRenal Replacement Therapy Registry. J Pediatr.2013;162:587–92. 103. López-Herce J, Santiago MJ, SolanaMJ, et al. Clinical course of children requiring prolongedcontinuous renal replacement therapy. Pediatr Nephrol.2010;25:523–28. 104. Ped ersen O, Jepsen SB, and Toft P.Continuous renal replacement therapy for critically illinfants and children. Dan Med J. 2012;59:A4385. REVIEWQUESTIONS CASE 1 A 6-year-old, 20-kg child with leukemiaduring induction develops Gram-negative septic shock withmultiorgan system failure. �e child is intubated on 70% FIO2 and a PEEP of 10 cm. �e child is oliguric and is 18%uid overloaded. �e child’s laboratory tests include the

following: sodium, 140 mmol/L; potassium, 6.9 mmol/L;chloride, 105 mmol/L; bicarbonate, 14 mmol/L; BUN, 100mg/dL; and lactate, 4.5 mmol/L. A recent ABG showed: pH,7.23; pAO 2 of 90; and pCO 2 of 43. �e child isreceiving norepinephrine for maintaining hemodynamicstability. Current blood pressure is 90/60 mm Hg. �e childis to be placed on CRRT. 1. Optimal size and site ofplacement of the vascular access is: a. 11-Fr dual-lumencatheter in subclavian vein. b. 8- or 9-Fr dual-lumencatheter in right internal jugular vein
c. 8- or 9-Fr dual-lumen catheter in femoral vein
d. 11-Fr dual-lumen catheter in femoral vein
2. Use of AN 69 membrane based hemo�lter in this patient
may be associated with the risk of:
a. Hemo�lter clotting more frequently
b. Poor clearance, if used in convective mode
c. Anaphylaxis
d. AN69 membrane has less clinical risk than polysulfonemembrane
3. If AN69 membrane hemo�lter is used in CRRT, blood
prime should be avoided in this patient due to presence
of metabolic acidosis and enhanced risk of anaphylaxis.
a. True
b. False
4. To allow optimal functioning of CRRT, the ideal arterial
and venous pressures (as noted on the CRRT monitors)
should be:
a. Greater than 50 mm and less than 400 mm
b. Greater than −50 mm and less than −400 mm
c. Greater than −150 mm and less than 200 mm
d. Greater than −150 mm and less than −200 mm
5. In this septic patient, the best modality of CRRT is:
a. Di�usive method (CVVHD)
b. Convective method (CVVH)
c. Slow continuous ultra�ltration (SCUF)
d. Both convestive and di�usive methods (CVVHDF)
6. Small molecular solutes are removed equally well by
convection and di�usion.
a. True
b. False
7. To optimize solute clearance, the optimal total volume of
dialysate and replacement �uid (if using CVVHDF) is:
a. 2000 mL/h/1.73 m 2
b. 35 mL/kg/h
c. Either a or b
d. Neither a nor b
8. Target net �uid ultra�ltration rate to be ordered should
be:
a. 10 mL/h
b. 1 to 2 mL/kg/h
c. 10 mL/kg/h
d. 25 mL/kg/h
CASE 2
A 14-year-old female patient is admitted with new-onset
AKI, oliguria, hyperkalemia, IDDM, dehydration. Her
laboratory tests show: serum sodium, 175 mmol/L (uncor
rected); glucose, 1300 mg/dL; and BUN, 90 mg/dL.
1. What is this patient’s calculated serum osmolality
(mOsm/L)?
a. 280
b. 380
c. 480
d. 542 2. Osmolality (mOsm/L) of the peritoneal dialysate(PD), 1.5% dextrose, low-calcium solution is: a. 280 b.300 c. 320 d. 344 3. Osmolality (mOsm/L) of hemodialysisdialysate is: a. 280 b. 300 c. 320 d. 340 4.Osmolality (mOsm/L) of dialysate used in CRRT is: a. 280b. 300 c. 320 d. 340 CASE 3 A 16-year-old male patient isadmitted to the intensive care unit with multimedicationoverdose. He has AKI and oliguria. He is unresponsive andbut is hemodynamically stable. No seizures have beennoted. If started on CRRT, 1. �e most important factor(s)in determining drug clearance is(are): a. Protein bindingb. Molecular weight c. Volume of distribution d. All ofthe above 2. �e preferred form of renal replacementtherapy (RRT) in this case is: a. PD b. CRRT convectivec. CRRT di�usive d. CRRT convective and di�usive e. HDstandard f. HD sigh �ux CASE 4 A 3-day-old male newborninfant is admitted to the intensive care unit withsomnolence, refusal to feed for 2 days, and twitching ofthe face today. �e child weighs 2.9 kg (240 mLintravascular blood volume). Serum electrolytes show:sodium, 140 mmol/L; potassium, 5 mmol/L;, CO 2, 14mmol/L; and arterial blood pH, 7.02. Ammonia level was1500 μmol/L. 1. �e best type of renal replacement therapy(RRT) that will lower ammonia most rapidly is: a. PD b.CRRT c. Hemodialysis, standard d. Hemodialysis, high �ux
ANSWER KEY
CASE 1
1. b
2. c
3. a
4. c
5. b
6. a
7. c
8. b CASE 2 1. c 2. d 3. a 4. a CASE 3 1. d 2. f CASE4 1. c

36 Hemodialysis
Figure 36.7 Incident and point prevalent patients withend-stage renal disease, 0 to 19 years old, by treatmentmodality
in the United States. HD, hemodialysis; Inc, incidence; PD,peritoneal dialysis; Prev, prevalence; Tx, transplantation.(From
US Renal Data System. USRDS 2013 Annual Data Report: Atlasof Chronic Kidney Disease and End-Stage Renal Disease in
the United States. Bethesda, MD: National Institutes ofHealth, National Institute of Diabetes and Digestive andKidney
Diseases; 2013.)
7. Fine RN, DePalma JR, Lieberman E, Donnel GN, Gordon A,Maxwell MH. Extended hemodialysis in children with chronicrenal failure. J Pediatr. 1968;73:706–13.
8. Kjellstrand CM, Shideman, JR, Santiago, EA, et al.Technical advances in hemodialysis of very small pediatricpatients. Proc Clin Dial Transplant Forum. 1971;1:124–32.
9. Brescia M, Cimino JE, Appel K, Hurwich BJ. Chronichemodialysis using venipuncture and a surgically createdarteriovenous fistula. N Engl J Med. 1966;275:1089–92.
10. Mahan JD, Mayer M, Nevins TE. The Hickman catheter: Anew hemodialysis access device for infants and children.Kidney Int. 1983;24:694–97.
11. War d RA. New AAMI standards for dialysis fluids.Nephrol News Issues. 2011;25:33–6.
12. Aljama P, Bird PA, Ward MK, et al. Hemodialysisinducedleucopenia and activation of complement: Effects ofdifferent membranes. Proc Eur Dial Transplant Assoc.1978;15:144–53.
13. Car uana RJ, Hamilton RW, Pearson FC. Dialyzerhypersensitivity syndrome: Possible role of allergy toethylene oxide. Report of 4 cases and review of theliterature. Am J Nephrol. 1985;5:271–4.
14. Kia li M, Djurdev O, Farah M, et al. Use ofelectronbeam sterilized hemodialysis membranes and the
risk of thrombocytopenia. JAMA. 2011;306:1679–87.
15. Bon omini V, Feletti C, Stefoni S, Vangelista A. Earlydialysis and renal transplantation. Nephron.1986;44:267–71.
16. Bon omini V, Vangelista A, Stefoni S. Early dialysisin renal substitutive programs. Kidney Int Suppl.1978;8:S112–6.
17. Tattersall J, Greenwood R, Farrington K. Urea kineticsand when to commence dialysis. Am J Nephrol.1995;15:283–9.
18. Cooper BA, Branley P, Bulfone L, et al. A randomized,controlled trial of early versus late initiation ofdialysis. N Engl J Med. 2010;363:609–19.
19. Silva MB, Jr, Hobson RW, 2nd, Pappas PJ, et al. Astrategy for increasing use of autogenous hemodialysisaccess procedures: Impact of preoperative noninvasiveevaluation. J Vasc Surg. 1998;27:302–7.
20. Davenport A. Alternatives to standard unfractionatedheparin for pediatric hemodialysis treatments. PediatrNephrol. 2012;27:1869–97.
21. Thijssen S, Kruse A, Raimann J, et al. A mathematicalmodel of regional citrate anticoagulation in hemodialysis.Blood Purif. 2005;29:197–203.
22. Han evold C, Lu S, Yonekawa K. Utility of citratedialysate in management of acute kidney injury inchildren. Hemodial Int. 2011;14(Suppl 1):S2–6.
23. Hoe nich NA, Woffindin C, Matthews JN, et al. Clinicalcomparison of high-flux cellulose acetate and syntheticmembranes. Nephrol Dial Transplant. 1994;9:60–6. 24. JainSR, Smith L, Brewer ED, Goldstein SL. Noninvasiveintravascular monitoring in the pediatric hemodialysispopulation. Pediatr Nephrol. 2001;16:15–8. 25. Michael M,Brewer ED, Goldstein SL. Blood volume monitoring to achievetarget weight in pediatric hemodialysis patients. PediatrNephrol. 2004;19:432–37. 26. Gotch FA Sargent JA. Amechanistic analysis of the National Cooperative DialysisStudy (NCDS). Kidney Int. 1985;28:526–34. 27. Owen WF,Jr, Lew NL, Liu Y, et al. The urea reduction ratio andserum albumin concentrations as predictors of mortality inpatients undergoing hemodialysis. N Engl J Med.1993;329:1001–6. 28. Rocco MV. Revisions to KDOQI

guidelines released at the NKF 2006 spring clinicalmeetings. Nephrol News Issues. 2006;20:40, 42. 29. Daugirdas JT. Simplified equations for monitoring kt/V, PCRn,eKt/V and ePCRn. Adv Ren Replace Ther. 1995;2:295–304.30. Got ch FA. The current place of urea kinetic modelingwith respect to different dialysis modalities. NephrolDial Transplant. 1998;13:10–14. 31. Ley poltd JK, JaberBL, Zimmerman DL. Predicting treatment dose for noveltherapies using urea standard kt/V. Semin Dial.2004;17:142–5. 32. Sur i RS, Garg AX, Chertow GM, et al.Frequent Hemodialysis Network (FHN) randomized trials:Study design. Kidney Int. 2007;71:349–59. 33. Lin dsay RM,Nesrallah G, Suri R, et al. Is more frequent hemodialysisbeneficial and what is the evidence? Curr Opin NephrolHypertens. 2004;13:631–5. 34. Rai mann JG, Thijssen S,Ramos R, Levin NW. More frequent hemodialysis: What do weknow? Where do we stand? Contrib Nephrol. 2011;171:10–6.35. Tom A, McCauley L, Bell L, et al. Growth duringmaintenance hemodialysis: Impact of enhanced nutrition andclearance. J Pediatr. 1999;134:464–71. 36. I. NKF-K/DOQIclinical practice guidelines for hemodialysis adequacy:Update 2000. Am J Kidney Dis. 2001;37(Suppl 1):S7–64. 37.Sarkar SR, Kaitwatcharachai C, Levin NW. Complicationsduring hemodialysis. In: Nissenson AR, Fine RN, editors.Clinical Dialysis. 4th ed. New York: McGraw-Hill; 2005. p.237. 38. Mandal AK, Abernathy T, Nelluri SN, Stitzel V. Isquinine effective and safe in leg cramps? J ClinPharmacol. 1995;35:588–93. 39. Daugirdas JT, Ing TS.First-use reactions during hemodialysis: A definition ofsubtypes. Kidney Int Suppl. 1988;24:S37–43. 40. SchulmanG, Hakim R, Arias R, et al. Bradykinin generation bydialysis membranes: Possible role in anaphylactic reaction.J Am Soc Nephrol. 1993;3:1563–9. 41. Muth CM, Shank ES.Gas embolism. N Engl J Med. 2000;342:476–82.
42. Warady BA, Bunchman T. Dialysis therapy for childrenwith acute renal failure: Survey results. Pediatr Nephrol.2000;15:11–13.
43. Mey er RJ, Flynn JT, Brophy PD, et al. Hemodialysisfollowed by continuous hemofiltration for treatment oflithium intoxication in children. Am J Kidney Dis.2001;37:1044–7.
44. US Renal Data System. USRDS 2013 Annual Data Report:Atlas of Chronic Kidney Disease and EndStage Renal Diseasein the United States. Bethesda, MD: National Institutes ofHealth, National Institute of Diabetes and Digestive andKidney Diseases; 2013.

REVIEW QUESTIONS
1. A 16-year-old boy with a history of end-stage renaldisease from focal segmental glomerulosclerosis has afailing renal allogra� and will need to return to dialysiswithin the next 6 months. He and his family choosehemodialysis as their preferred modality. He is highlysensitized, and although he will be listed for renaltransplant again, you anticipate that his waiting timewill be at least 1 to 2 years. Of the following, the mostappropriate recommendation for hemodialysis vascularaccess is: a. Art eriovenous �stula b. Art eriovenousgra� c. Femo ral venous catheter d. Int ernal jugularvenous catheter e. Sub clavian venous catheter
2. You a re determining the appropriate hemodialysisprescription for a new patient in your hemodialysis unit.When choosing a dialyzer, you obtain the manufacturer’sspeci�cations regarding the K uf . Of the following, themost accurate statement about K uf is that it de�nes: a.e maximum theoretical limit for ultra�ltration at in�nitetransmembrane pressure b. �e maximum theoretical limit forurea clearance at in�nite blood and dialysate �ow rate c.e minimum required transmembrane pressure necessary toprevent back-�ltration d. �e volume of blood cleared ofurea in 1 min at a given blood �ow rate e. �e volume ofuid that will cross the membrane in 1 h at a giventransmembrane pressure
3. A 12-year-old patient presenting to the emergencydepartment with several weeks of fatigue, malaise, andweight loss is found to have renal failure with BUN 110mg/dL and Cr 11.7 mg/dL. Renal ultrasound demonstratessmall, echogenic kidneys bilaterally. You believe that thepatient likely has had undiagnosed renal dysplasia and nowhas end-stage renal disease. �e patient is tired and thinbut alert without signs of volume overload. You makearrangements to initiate hemodialysis. Of the following,the most appropriate consideration in the initialhemodialysis prescriptions would be: a. Ensure vascularaccess that can provide blood �ow of at least 300 mL/min.b. Avo id heparin anticoagulation for the �rst week. c.Preferentially choose a polysulfone dialyzer membrane. d.Target urea clearance of no more than 30%. e. Use adialyzer with a high KoA. 4. During the dialysis process,several factors are responsible for molecular transport.Of the following, the most accurate statement regardingthe physical principles of molecular transport that areactive in hemodialysis is: a. Adsorption favors movementof smaller molecules over larger molecules. b. Convection

favors movement of smaller molecules over largermolecules. c. Di�usion favors movement of smallermolecules over larger molecules. d. Ultra�ltration favorsmovement of smaller molecules over larger molecules. e.Under most circumstances in hemodialysis, small and largemolecules transport equally. 5. �e hemodialysis apparatusis complex and has multiple components designed to providesafe and e�ective therapy to the patient. Of thefollowing, the option that best describes the two maincomponents of the dialysis apparatus is: a. �e bloodcircuit and the dialysate circuit b. �e hemodialyzer andthe vascular access c. �e arterial segment and the venoussegment d. �e proportioning system and the ultra�ltrationcontroller e. �e “A” concentrate and the “B” concentrate6. An 11-year-old girl is admitted to the intensive careunit with meningococcemia and renal failure as a secondarye�ect of her multiorgan dysfunction syndrome. Herpotassium level has risen to 7.2 mEq/L, with changes onher electrocardiogram suggesting evidence for cardiace�ects. You are preparing to perform emergency hemodialysisto correct the hyperkalemia. Of the following, the mostappropriate option for vascular access would be: a.Arteriovenous �stula b. Arteriovenous gra� c. Bilateralsingle-lumen cephalic vein catheters d. Femoraldouble-lumen venous catheter e. Subclavian double-lumenvenous catheter 7. A 19-year-old male patient has beenreceiving hemodialysis for acute kidney injury for 8 weeksbecause of complications following liver transplantation.He has tolerated his sessions well, but he remainsintubated in the intensive care unit. Over the last week,his platelet count has dropped, and the intensive careunit team is concerned that he may have heparin-inducedthrombocytopenia. �ey ask whether there are options toperform his hemodialysis sessions but limit his heparinexposure. Of the following, the method most likely toensure e�ective hemodialysis sessions and also address theconcern for heparin-induced thrombocytopenia would be to:a. Change unfractionated heparin to low-molecularweightheparin. b. Eliminate heparin and use citrate-containingdialysate. c. Give a heparin bolus at the start ofhemodialysis but avoid use of continuous infusion. d.Perform hemodialysis without anticoagulation. e. Use halfthe previous dose of unfractionated heparin.
8. A 10-month-old boy with end-stage renal disease fromposterior urethral valves who is maintained on peritonealdialysis develops fungal peritonitis and must make atemporary transition to hemodialysis. He weighs 7.7 kg andis polyuric. Of the following, the most accurate statementabout plans for hemodialysis is that: a. Extended session
length is likely required to achieve ultra�ltration goals.b. Heparin cannot be used as the anticoagulant. c. Highmetabolic needs will obligate use of a dialyzer with ahigh KoA. d. Outcome data indicate that the single-poolKt/V target for this age group is 1.6. e. �e patient willlikely need blood prime of the hemodialysis circuit.
9. You are preparing the prescription for a 10-year-oldgirl with end-stage renal disease from renal dysplasia whowill initiate hemodialysis. �e patient has a newright-sided 10-French internal jugular catheter that youanticipate will deliver a blood �ow rate of 150 mL/ min.You have chosen a hemodialyzer with K D for urea of 120mL/min at that blood �ow rate. �e patient weighs 35 kg;she does not appear volume overloaded. You would like totarget a urea clearance of approximately 30% for this �rstsession. Of the following, the dialysis time that willmost likely give a urea clearance closest to the target of30% is: a. 30 min b. 60 min c. 90 min d. 120 min e.180 min 10. You are reviewing the dialysis adequacystudies for your unit and notice that a patient has Kt/Vthis month of 1.1. �e patient has been doing well onhemodialysis, growing, thriving and participating inschool. Results of blood testing have been stable.Previous values for Kt/V over the last 6 months have been1.4 to 1.6. His current prescription is as follows:Dialyzer: KoA 1100 mL/min Vascular access: 12-Frenchright-sided internal jugular catheter Blood �ow rate: 250mL/min Session length: 3 h Schedule: Tuesday, �ursday,Saturday Of the following, the most appropriate next stepto address the low Kt/V for this patient would be to: a.Adjust the dialysis schedule to Monday, Tuesday, �ursday,and Saturday. b. Change to a larger dialyzer with KoA 1400mL/ min. c. Increase dialysis time to 4 h/session. d.Refer the patient for urgent placement of an arteriovenousstula. e. Review session characteristics and repeat Kt/Vmeasurement. ANSWER KEY 1. a 2. e 3. d 4. c 5. a 6. d7. b 8. e 9. b 10. e
37 Peritoneal dialysis
1. Blackfan K, Maxcy K. The intraperitoneal injection ofsaline solution. Am J Dis Child. 1918;15:19.
2. Bloxsom A, Powell N. The treatment of acute temporarydysfunction of the kidneys by peritoneal irrigation.Pediatrics. 1948;1:52–7.
3. Swan H, Gordon HH. Peritoneal lavage in the treatmentof anuria in children. Pediatrics. 1949;4:586–95.
4. Odel H, Ferris D, Power M. Peritoneal lavage as aneffective means of extra-renal excretion. Am J Med.1950;9:63–77.
5. Max well MH, Rockney RE, Kleeman CR, et al. Peritonealdialysis. 1. Technique and applications. JAMA.1959;170:917–24.
6. Segar WE, Gibson RK, Rhamy R. Peritoneal dialysis ininfants and small children. Pediatrics 1961;27:603–13.
7. Etteldorf JN, Dobbins WT, Sweeney MJ, et al.Intermittent peritoneal dialysis in the management of acuterenal failure in children. J Pediatr. 1962;60:327–39.
8. Feldman W, Baliah T, Drummond KN. Intermittentperitoneal dialysis in the management of chronic renalfailure in children. Am J Dis Child. 1968;116:30–6.
9. Palmer RA, Quinton WE, Gray JE. Prolonged peritonealdialysis for chronic renal failure. Lancet. 1964;1:700–2.
10. Palmer RA, Newell JE, Gray EJ, et al. Treatment ofchronic renal failure by prolonged peritoneal dialysis. NEngl J Med. 1966;274:248–54.
11. Tenckhoff H, Schechter H. A bacteriologically safeperitoneal access device. Trans Am Soc Artif InternOrgans. 1968;14:181–7.
12. Boen ST, Mion CM, Curtis FK, et al. Periodic peritonealdialysis using the repeated puncture technique and anautomatic cycling machine. Trans Am Soc Artif InternOrgans. 1964;10:409–14.
13. Tenckhoff H, Meston B, Shilipetar G. A simplifiedautomatic peritoneal dialysis system. Trans Am Soc ArtifIntern Organs. 1972;18:436–40.
14. Popovich R, Moncrief J, Decherd J, et al. Thedefinition of a novel portable/wearable equilibriumdialysis technique (Abstract). Trans Am Soc Artif InternOrgans. 1976;5:64.
15. Oreopoulos DG, Katirtzoglou A, Arbus G, et al.Dialysis and transplantation in young children. Br Med J.1979;1:1628–9. 16. Balfe JW, Irwin M. Continuousambulatory peritoneal dialysis in children. In: Legrain M,editor. Continuous Ambulatory Peritoneal Dialysis.Amsterdam: Excerpta Medica; 1980. p. 131–-6. 17. SchaeferF, Warady BA. Peritoneal dialysis in children withend-stage renal disease. Nat Rev Nephrol. 2011;7:659–68.18. Warady BA, Hebert D, Sullivan EK, et al. Renaltransplantation, chronic dialysis, and chronic renalinsufficiency in children and adolescents: The 1995 AnnualReport of the North American Pediatric Renal TransplantCooperative Study. Pediatr Nephrol. 1997;11:49–64. 19.Honda M, Iitaka K, Kawaguchi H, et al. The JapaneseNational Registry data on pediatric CAPD patients: Aten-year experience. A report of the Study Group ofPediatric PD Conference. Perit Dial Int. 1996;16:269–75.20. Ale xander S, Warady B. The demographics of dialysisin children. In: Warady B, Schaefer F, Fine R, AlexanderS, editors. Pediatric Dialysis. Dordrecht: Kluwer; 2004.p. 35. 21. North American Pediatric Renal Trials andCollaborative Studies (NAPRTCS) Annual Dialysis Report.Rockville, MD: Emmes Corporation; 2011. 22. Fur th SL,Powe NR, Hwang W, et al. Does greater pediatric experienceinfluence treatment choices in chronic disease management?Dialysis modality choice for children with end-stage renaldisease. Arch Pediatr Adolesc Med. 1997;151:545–50. 23.US Re nal Data System (USRDS) 2013 Annual Data Report:Atlas of Chronic Kidney Disease and EndStage Renal Diseasein the United States. Bethesda, MD: National Institutes ofHealth, National Institute of Diabetes and Digestive andKidney Diseases; 2013. 24. van der Heijden BJ, van DijkPC, Verrier-Jones K, et al. Renal replacement therapy inchildren: Data from 12 registries in Europe. PediatrNephrol. 2004;19:213–21. 25. Watson AR, Hayes WN, VondrakK, et al. Factors influencing choice of renal replacementtherapy in European paediatric nephrology units. PediatrNephrol. 2013;28:2361–8. 26. Rip pe B, Stelin G.Simulations of peritoneal solute transport during CAPD:Application of two-pore formalism. Kidney Int.1989;35:1234–44. 27. Schaefer F, Haraldsson B, Haas S, etal. Estimation of peritoneal mass transport by three-poremodel in children. Kidney Int. 1998;54:1372–9. 28.Fischbach M, Haraldsson B. Dynamic changes of the total
pore area available for peritoneal exchange in children. JAm Soc Nephrol. 2001;12:1524–9. 29. Flessner MF. Theperitoneal dialysis system: Importance of each component.Perit Dial Int. 1997;17(Suppl 2):S91–7. 30. Flessner MF.Peritoneal ultrafiltration: Physiology and failure.Contrib Nephrol. 2009;163:7-14.
31. Popovich R, Moncrief J, Okutan M, et al. A model ofthe peritoneal dialysis system. Proceedings of the 25thAnnual Conference on Engineering in Medicine andBiolology. 1972. p. 172.
32. Morgenstern B. Structure and function of the pediatricperitoneal membrane. In: Richard F, Alexander S, Warady B,editors. CAPD/CCPD in Children. Norwell, MA: Kluwer;1998:73–85.
33. Krediet R. The physiology of peritoneal solute, water,and lymphatic transport. In: Khanna R, Krediet R, editors.Nolph and Gokal’s Textbook of Peritoneal Dialysis, 3rd ed.New York: Springer; 2009. p. 137–72.
34. Haraldsson B. Assessing the peritoneal dialysiscapacities of individual patients. Kidney Int.1995;47:1187–98.
35. Mor genstern BZ, Baluarte HJ. Peritoneal dialysiskinetics in children. In: Fine RN, editor. ChronicAmbulatory Peritoneal Dialysis (CAPD) and Chronic CyclingPeritoneal Dialysis in Children. Boston: Martinus Nijhoff;1987. p. 47–61.
36. Pop ovich R, Pyle W, Rosenthal D, et al. Kinetics ofperitoneal dialysis in children. In: Moncrief J, PopovichR, editors. CAPD Update. New York: Masson; 1981. p. 227.
37. Gea ry D, Harvey E, Balfe J. Mass transfer areacoefficients in children. Perit Dial Int. 1994;14:30–3.
38. Warady BA, Alexander SR, Hossli S, et al. Peritonealmembrane transport function in children receiving long-termdialysis. J Am Soc Nephrol. 1996;7:2385–91.
39. Bou ts AH, Davin JC, Groothoff JW, et al.Standardperitoneal permeability analysis in children. J Am SocNephrol. 2000;11:943–50.
40. Gru skin AB, Rosenblum H, Baluarte HJ, et al.Transperitoneal solute movement in children. Kidney IntSuppl. 1983;15:S95–100.
41. Pyle W. Mass transfer in peritoneal dialysis. PhDthesis, University of Texas at Austin. Ann Arbor, MI:University Microfilms International; 1987.
42. de Boer AW, Schroder CH, van Vliet R, et al. Clinicalexperience with icodextrin in children: Ultrafiltrationprofiles and metabolism. Pediatr Nephrol. 2000;15:21–4.
43. Schroder CH. New peritoneal dialysis fluids: Practicaluse for children. Pediatr Nephrol. 2003;18:1085–8.
44. Finkelstein F, Healy H, Abu-Alfa A, et al. Superiorityof icodextrin compared with 4.25% dextrose for peritonealultrafiltration. J Am Soc Nephrol. 2005;16:546–54.
45. Dar t A, Feber J, Wong H, Filler G. Icodextrinre-absorption varies with age in children on automatedperitoneal dialysis. Pediatr Nephrol. 2005;20:683–5.
46. Mactier RA, Khanna R, Moore H, et al. Kinetics ofperitoneal dialysis in children: Role of lymphatics.Kidney Int. 1988;34:82–8.
47. Rip pe B. Is lymphatic absorption important forultrafiltration? Perit Dial Int. 1995;15:203–4. 48.Schroder CH, Reddingius RE, van Dreumel JA, et al.Transcapillary ultrafiltration and lymphatic absorptionduring childhood continuous ambulatory peritoneal dialysis.Nephrol Dial Transplant. 1991;6:571–3. 49. Twa rdowski Z,Nolph K, Khanna R, et al. Peritoneal equilibration test.Perit Dial Bull. 1987;7:378. 50. KDOQI clinical practiceguidelines and clinical practice recommendations for 2006updates: Hemodialysis adequacy, peritoneal dialysisadequacy and vascular access. Am J Kidney Dis. 2006;28:S1.51. Kohaut EC, Waldo FB, Benfield MR. The effect ofchanges in dialysate volume on glucose and ureaequilibration. Perit Dial Int. 1994;14:236–9. 52. SlimanGA, Klee KM, Gall-Holden B, et al. Peritonealequilibration test curves and adequacy of dialysis inchildren on automated peritoneal dialysis. Am J KidneyDis. 1994;24:813–8. 53. Sch aefer F, Langenbeck D, HeckertKH, et al. Evaluation of peritoneal solute transfer by theperitoneal equilibration test in children. Adv Perit Dial.1992;8:410–5. 54. Warady BA, Jennings J. The short PET inpediatrics. Perit Dial Int. 2007;27:441–5. 55. Can o F,Sanchez L, Rebori A, et al. The short peritonealequilibration test in pediatric peritoneal dialysis.Pediatr Nephrol. 2010;25:2159–64. 56. Gea ry D, Warady B.The peritoneal equilibration test in children. In: Fine R,
Alexander S, Warady B, editors. Chronic AmbulatoryPeritoneal Dialysis (CAPD) and Chronic Cycling PeritonealDialysis (CCPD) in Children, 2nd ed. Boston: Kluwer Group;1998. 57. Roc co MV, Jordan JR, Burkart JM. Changes inperitoneal transport during the first month of peritonealdialysis. Perit Dial Int. 1995;15:12–7. 58. Borzych-Duzalka D, Bilginer Y, Ha IS, et al. Management ofanemia in children receiving chronic peritoneal dialysis.J Am Soc Nephrol. 2013;24:665–76. 59. Dolan NM,Borzych-Duzalka D, Suarez A, et al. Ventriculoperitonealshunts in children on peritoneal dialysis: A survey of theInternational Pediatric Peritoneal Dialysis Network.Pediatr Nephrol. 2013;28:315–9. 60. Warady B, Alexander S,Schaefer F. Peritoneal dialysis in children. In: Khanna R,Krediet R, editors. Nolph and Gokal’s Textbook ofPeritoneal Dialysis. New York: Springer; 2009. p. 803–59.61. Zaritsky J, Warady BA. Peritoneal dialysis in infantsand young children. Semin Nephrol. 2011;31:213–24. 62.Zur owska AM, Fischbach M, Watson AR, et al. Clinicalpractice recommendations for the care of infants withstage 5 chronic kidney disease (CKD5). Pediatr Nephrol.2013;28:1739–48. 63. Hölttä T, Holmberg C, Rönnholm K.Peritoneal dialysis during infancy. In: Warady B, SchaeferF, Alexander S, editors. Pediatric Dialysis, 2nd ed. NewYork: Springer; 2012. p. 219–29.
64. Vidal E, Edefonti A, Murer L, et al. Peritonealdialysis in infants: The experience of the ItalianRegistry of Paediatric Chronic Dialysis. Nephrol DialTransplant. 2012;27:388–95.
65. Lantos JD, Warady BA. The evolving ethics of infantdialysis. Pediatr Nephrol. 2013;28:1943–7.
66. Watson AR. Stress and burden of care in families withchildren commencing renal replacement therapy. Adv PeritDial. 1997;13:300–4.
67. Jon es L, Aldridge M. Organization and management of apediatric dialysis program. In: Warady B, Schaefer F,Alexander S, editors. Pediatric Dialysis, 2nd ed. NewYork: Springer; 2012. p. 53–72.
68. Watson AR. Psychosocial support for children andfamilies requiring renal replacement therapy. PediatrNephrol. 2014; 29:1169–74.
69. Warady B, Andrews W. Peritoneal dialysis access. In:Geary D, Schaefer F, editors. Comprehensive PediatricNephrology. Philadelphia: Mosby Elsevier; 2008. p. 823–34.
70. Rin aldi S, Sera F, Verrina E, et al. Chronicperitoneal dialysis catheters in children: A fifteen-yearexperience of the Italian Registry of Pediatric ChronicPeritoneal Dialysis. Perit Dial Int. 2004;24:481–6.
71. Fur th SL, Donaldson LA, Sullivan EK, et al. Peritonealdialysis catheter infections and peritonitis in children: Areport of the North American Pediatric Renal TransplantCooperative Study. Pediatr Nephrol. 2000;15:179–82.
72. Whi te CT, Gowrishankar M, Feber J, et al. Clinicalpractice guidelines for pediatric peritoneal dialysis.Pediatr Nephrol. 2006;21:1059–66.
73. Lo WK, Lui SL, Li FK, et al. A prospective randomizedstudy on three different peritoneal dialysis catheters.Perit Dial Int. 2003;23(Suppl 2):S127–31.
74. Lindley RM, Williams AR, Fraser N, et al. Synchronouslaparoscopic-assisted percutaneous endoscopic gastrostomyand peritoneal dialysis catheter placement is a validalternative to open surgery. J Pediatr Urol.2012;8:527–30.
75. Cribbs RK, Greenbaum LA, Heiss KF. Risk factors forearly peritoneal dialysis catheter failure in children. JPediatr Surg. 2010;45:585–9.
76. Daschner M, Gfrorer S, Zachariou Z, et al.Laparoscopic Tenckhoff catheter implantation in children.Perit Dial Int. 2002;22:22–6.
77. Piraino B, Bernardini J, Brown E, et al. ISPD positionstatement on reducing the risks of peritonealdialysis-related infections. Perit Dial Int.2011;31:614–30.
78. War ady BA, Bakkaloglu S, Newland J, et al. Consensusguidelines for the prevention and treatment ofcatheter-related infections and peritonitis in pediatricpatients receiving peritoneal dialysis: 2012 update. PeritDial Int. 2012;32(Suppl 2):S32–86. 79. Chadha V, JonesLL, Ramirez ZD, et al. Chest wall peritoneal dialysiscatheter placement in infants with a colostomy. Adv PeritDial. 2000;16:318–20. 80. Warchol S, Ziolkowska H,Roszkowska-Blaim M. Exit-site infection in children onperitoneal dialysis: Comparison of two types of peritonealcatheters. Perit Dial Int. 2003;23:169–73. 81. Rah im KA,Seidel K, McDonald RA. Risk factors for catheter-related

complications in pediatric peritoneal dialysis. PediatrNephrol. 2004;19:1021–8. 82. Twardowski ZJ, Prowant BF.Current approach to exit-site infections in patients onperitoneal dialysis. Nephrol Dial Transplant.1997;12:1284–95. 83. Bender FH, Bernardini J, Piraino B.Prevention of infectious complications in peritonealdialysis: Best demonstrated practices. Kidney Int Suppl.2006:S44–54. 84. Schaefer F, Feneberg R, Aksu N, et al.Worldwide variation of dialysis-associated peritonitis inchildren. Kidney Int. 2007;72:1374–9. 85. Chu a AN,Goldstein SL, Bell D, et al. Topical mupirocin/sodiumhypochlorite reduces peritonitis and exit-site infectionrates in children. Clin J Am Soc Nephrol. 2009;4:1939–43.86. War ady BA, Sullivan EK, Alexander SR. Lessons fromthe peritoneal dialysis patient database: A report of theNorth American Pediatric Renal Transplant CooperativeStudy. Kidney Int Suppl. 1996;53:S68–71. 87. Tra naeus A.Peritonitis in pediatric continuous peritoneal dialysis.In: Fine RN AS, Warady BA, editors. CAPD/CCPD in Children.Norwell, MA: Kluwer; 1998. p. 301–47. 88. War ady BA,Feneberg R, Verrina E, et al. Peritonitis in children whoreceive long-term peritoneal dialysis: A prospectiveevaluation of therapeutic guidelines. J Am Soc Nephrol.2007;18:2172–9. 89. War ady BA, Ellis EN, Fivush BA, etal. “Flush before fill” in children receiving automatedperitoneal dialysis. Perit Dial Int. 2003;23:493–8. 90.Strippoli GF, Tong A, Johnson D, et al. Catheterrelatedinterventions to prevent peritonitis in peritonealdialysis: A systematic review of randomized, controlledtrials. J Am Soc Nephrol. 2004;15:2735–46. 91. BakkalogluSA. Prevention of peritonitis in children: Emergingconcepts. Perit Dial Int. 2009;29(Suppl 2):S186–9. 92.Holloway M, Mujais S, Kandert M, et al. Pediatricperitoneal dialysis training: Characteristics and impacton peritonitis rates. Perit Dial Int. 2001;21:401–4. 93.War ady BA, Bashir M, Donaldson LA. Fungal peritonitis inchildren receiving peritoneal dialysis: A report of theNAPRTCS. Kidney Int. 2000;58:384–9. 94. Wong SF, Leung MP,Chan MY. Pharmacokinetics of fluconazole in childrenrequiring peritoneal dialysis. Clin Ther. 1997;19:1039–47.
95. Reuman PD, Neiberger R, Kondor DA. Intraperitoneal andintravenous fluconazole pharmokinetics in a pediatricpatient with end stage renal disease. Pediatr Infect DisJ. 1992;11:132–3.
96. Blowey DL, Garg UC, Kearns GL, et al. Peritonealpenetration of amphotericin B lipid complex andfluconazole in a pediatric patient with fungal peritonitis.Adv Perit Dial. 1998;14:247–50.
97. Honda M, Warady BA. Long-term peritoneal dialysis andencapsulating peritoneal sclerosis in children. PediatrNephrol. 2010;25:75–81.
98. Vidal E, Edefonti A, Puteo F, et al. Encapsulatingperitoneal sclerosis in paediatric peritoneal dialysispatients: The experience of the Italian Registry ofPediatric Chronic Dialysis. Nephrol Dial Transplant.2013;28:1603–9.
99. da Silva N, Rocha S, Rocha L, et al.Posttransplantation encapsulating peritoneal sclerosis ina pediatric patient. Pediatr Nephrol. 2012;27:1583–8.
100. Korte MR, Habib SM, Lingsma H, et al.Posttransplantation encapsulating peritoneal sclerosiscontributes significantly to mortality after kidneytransplantation. Am J Transplant. 2011;11:599–605.
101. Sch mitt CP. Peritoneal dialysis solutions. In: WaradyB, Schaefer F, Alexander SR, editors. Pediatric Dialysis,2nd ed. New York: Springer; 2012. p. 205-18.
102. Verrina E, Cappelli V, Perfumo F. Selection ofmodalities, prescription, and technical issues in childrenon peritoneal dialysis. Pediatr Nephrol. 2009;24:1453–64.
103. Cha dha V, Schaefer F, Warady B. Peritonitis andexitsite infections. In: Warady B, Schaefer F, AlexanderS, editors. Pediatric Dialysis, 2nd ed. New York:Springer; 2012. p. 231–56.
104. Pir aino B. Staphylococcus aureus infections indialysis patients: Focus on prevention. ASAIO J.2000;46:S13–7.
105. Uttley L, Vardhan A, Mahajan S, et al. Decrease ininfections with the introduction of mupirocin cream at theperitoneal dialysis catheter exit site. J Nephrol.2004;17:242–5.
106. Bernardini J, Bender F, Florio T, et al. Randomized,double-blind trial of antibiotic exit site cream forprevention of exit site infection in peritoneal dialysispatients. J Am Soc Nephrol. 2005;16:539–45.
107. Schaefer F, Klaus G, Muller-Wiefel DE, et al.Intermittent versus continuous intraperitonealglycopeptide/ceftazidime treatment in children with

peritoneal dialysis-associated peritonitis: The MidEuropeanPediatric Peritoneal Dialysis Study Group (MEPPS). J AmSoc Nephrol. 1999;10:136–45.
108. von Li lien T, Salusky IB, Yap HK, et al. A frequentcomplication in children treated with continuousperitoneal dialysis. Am J Kidney Dis. 1987;10:356–60.
109. Ara nda RA, Romao Junior JE, Kakehashi E, et al.Intraperitoneal pressure and hernias in children onperitoneal dialysis. Pediatr Nephrol. 2000;14:22–4. 110.Bakkaloglu A. Non-infectious compolications of peritonealdialysis in children. In: Warady BA, Schaefer F, AlexanderS, editors. Pediatric Dialysis, 2nd ed. New York:Springer; 2012. p. 257–71. 111. Levin NW, Zasuwa G.Relationship between dialyser type and signs and symptoms.Nephrol Dial Transplant. 1993;8(Suppl 2):30–9. 112. Rockel A, Klinke B, Hertel J, et al. Allergy to dialysismaterials. Nephrol Dial Transplant. 1989;4:646–52. 113.Purello D’Ambrosio F, Savica V, Gangemi S, et al. Ethyleneoxide allergy in dialysis patients. Nephrol DialTransplant. 1997;12:1461–3. 114. Hothi D, Harvey E. Commoncomplications of haemodialysis. In: Warady B, Schaefer F,Alexander S, editors. Pediatric Dialysis, 2nd ed. NewYork: Springer; 2012:345–74. 115. Boeschoten EW, KredietRT, Roos CM, et al. Leakage of dialysate across thediaphragm: An important complication of continuousambulatory peritoneal dialysis. Neth J Med. 1986;29:242–6.116. Cop po R, Amore A, Cirina P, et al. Bradykinin andnitric oxide generation by dialysis membranes can beblunted by alkaline rinsing solutions. Kidney Int.2000;58:881–8. 117. Hak im RM, Schafer AI.Hemodialysis-associated platelet activation andthrombocytopenia. Am J Med. 1985;78:575–80. 118. SilverSM, DeSimone JA, Jr, Smith DA, et al. Dialysisdisequilibrium syndrome (DDS) in the rat: Role of the“reverse urea effect.” Kidney Int. 1992;42:161–6. 119.Fischbach M, Warady BA. Peritoneal dialysis prescription inchildren: Bedside principles for optimal practice. PediatrNephrol. 2009;24:1633–42; quiz 40, 42. 120. War ady BA,Watkins SL, Fivush BA, et al. Validation of PD Adequest2.0 for pediatric dialysis patients. Pediatr Nephrol.2001;16:205–11. 121. Ver rina E, Amici G, Perfumo F, etal. The use of the PD Adequest mathematical model inpediatric patients on chronic peritoneal dialysis. PeritDial Int. 1998;18:322–8. 122. Morgenstern BZ, Wuhl E, NairKS, et al. Anthropometric prediction of total body waterin children who are on pediatric peritoneal dialysis. JAm Soc Nephrol. 2006;17:285–93. 123. Verrina E, Perri K.Technical aspects and prescription of peritoneal dialysis

in children. In: Warady BA Schaefer F, Alexander S,editors. Pediatric Dialysis, 2nd ed. New York: Springer;2012. p. 169–203. 124. Bakkaloglu SA, Borzych D, Soo Ha I,et al. Cardiac geometry in children receiving chronicperitoneal dialysis: Findings from the InternationalPediatric Peritoneal Dialysis Network (IPPN) registry.Clin J Am Soc Nephrol. 2011;6:1926–33. 125. Gerson A,Hwang W, Fiorenza J, et al. Anemia and health-relatedquality of life in adolescents with chronic kidneydisease. Am J Kidney Dis. 2004;44:1017–23.
126. Goldstein SL, Graham N, Burwinkle T, et al.Healthrelated quality of life in pediatric patients withESRD. Pediatr Nephrol. 2006;21:846–50.
127. Mit snefes MM, Laskin BL, Dahhou M, et al. Mortalityrisk among children initially treated with dialysis forend-stage kidney disease, 1990-2010. JAMA.2013;309:1921–9.
REVIEW QUESTIONS
1. �e greatest percentage of prevalent pediatric patientsreceives which of the following renal replacementmodalities? a. Peritoneal dialysis b. Hemodialysis c.Kidney transplant
2. Which of the following peritoneal membrane porescomprise 90% to total pore area? a. Aquaporins b. Sma llpores c. Lar ge pores
3. Con vective mass transfer is responsible for only asmall portion of large solute removal. a. Tru e b. Fals e
4. �e PE T test should be performed with which one of thefollowing solutions for all older children and adolescentsundergoing PD? a. Icodex trin b. �e re gular clinical �llvolume for that patient c. 110 0 mL/m 2 of a mixture of2.5% and 4.25% PD solution d. 1100 mL/m 2 of 2.5% PDsolution
5. Which one of the following is not an absolutecontraindication to long-term PD? a. Gastroschisis b.Ventriculoperitoneal shunt c. Omphalocele d. Obliteratedperitoneal cavity
6. Which of the following measures has not led to adecreased rate of peritonitis in children and adults?(Choose one) a. Topical application of antibiotic atcatheter exit site b. Flush before �ll technique c.

Disconnect systems d. Use of Tenckho� catheter with curledintraperitoneal portion 7. Which of the following is nottrue about hernias that develop in pediatric patientsundergoing PD? (Choose one) a. �e incidence is directlyproportional to the patient’s age. b. More than 75%require surgical repair. c. Raised IPP is a risk factorfor hernia development. d. Surgical repair should befollowed by no/low-volume dialysis. 8. �e achievement ofPD adequacy should take all but which one of the followingfactors into consideration? a. Peritoneal membrane solutetransport capacity b. Frequency of peritonitis c.Patient’s body surface area d. Residual renal function 9.e term “V” in Kt/V is equivalent to which one of thefollowing? a. Volume of the peritoneal dialysis solutionb. Total blood volume c. Total body water d. Volume ofultra�ltrate 10. An important cause of mortality inpediatric patients undergoing PD includes which one of thefollowing? a. Cardiovascular disease b. Inadequate Kt/Vc. Poor catheter function d. Loss of residual kidneyfunction ANSWER KEY 1. c 2. b 3. b 4. d 5. b 6. d 7.a 8. b 9. c 10. a
38 Renal transplantation
1. North American Pediatric Renal Trials and CollaborativeStudy. 2010 Annual transplant report. 2010 Available athttps://web.emmes. com/study/ped/annlrept/2010_Report.pdf.
2. Moudgil A. Primer on renal transplantation. Indian JPediatr. 2012;79:1076–83.
3. Kasiske BL, Cangro CB, Hariharan S, et al. Theevaluation of renal transplantation candidates: Clinicalpractice guidelines. Am J Transplant 2001;1(Suppl 2):3–95.
4. Lubrano R, Perez B, Elli M. Methylmalonic acidemia andkidney transplantation. Pediatr Nephrol. 2013;28:2067–8.
5. McGuire PJ, Lim-Melia E, Diaz GA, et al. Combinedliver-kidney transplant for the man agement ofmethylmalonic aciduria: A case rep ort and review of theliterature. Mol Genet Metab. 2008;93:22–9.
6. Rumsby G, Cochat P. Primary hyperoxaluria. N Engl JMed. 2013;369:2163.
7. El Sayegh S, Keller MJ, Huprikar S, Murphy B. Solidorgan transplantation in HIV-infected recipients. PediatrTransplant. 2004;8:214–21.
8. Morales JM, Aguado JM. Hepatitis C and renaltransplantation. Curr Opin Organ Transplant.2012;17:609–15. 9. 42 CFR 482.90. Condition ofparticipation: Patient and living donor selection.Available at http://www.ecfr.gov/cgi-bin/text-idx?SID=63359829bd75a679b008b46384d49373&node=42:5.0.1.1.1&rgn =div5#42:5.0.1.1.1.5.6.11. Accessed August 31, 2015. 10.Goldberg A, Amaral S, Moudgil A. Developing a frameworkfor evaluating kidney transplantation candidacy inchildren with multiple co-morbidities. Pediatr Nephrol.2015;30:5–13. 11. Ria nthavorn P, Ettenger RB. Medicationnonadherence in the adolescent renal transplant recipient:A clinician’s viewpoint. Pediatr Transplant.2005;9:398–407. 12. Kasiske BL, Ramos EL, Gaston RS, etal. The evaluation of renal transplant candidates:Clinical practice guidelines. JASN. 1995;6:1–34. 13.Matas AJ, Smith JM, Skeans MA, et al. OPTN/SRTR 2011annual data report: Kidney. Am J Transplant 2013;13(Suppl1):11–46. 14. Wood KJ, Goto R. Mechanisms of rejection:Current perspectives. Transplantation. 2012;93:1–10. 15.Uni ted Network for Organ Sharing. Available at

http://www.unos.org/. 16. Org an Allocation. 2013.Available at http://www.unos.org/donation/index.php?topic=organ_allocation. 17. KDPI Calculator. 2013.Available at http://optn.transplant.hrsa.gov/resources/allocationcalculators.Accessed August 31, 2015. 18. Org an Procurement andTransplantation Network. Available athttp://optn.transplant.hrsa. gov/. Accessed August 31,2015. 19. Gebel HM, Liwski RS, Bray RA. Technicalaspects of HLA antibody testing. Curr Opin OrganTransplant. 2013;18:455–62. 20. Becker LE, Susal C,Morath C. Kidney transplantation across HLA and ABOantibody barriers. Curr Opin Organ Transplant.2013;18:445–54. 21. Takahashi K, Saito K.ABO-incompatible kidney transplantation. Transplant Rev(Orlando). 2013;27:1–8. 22. Duq uesnoy RJ, Claas FH. 14thInternational HLA and Immunogenetics Workshop: Report onthe structural basis of HLA compatibility. Tissue Antigens.2007;69(Suppl 1):180–4. 23. Ling M, Marfo K, Masiakos P,et al. Pretransplant anti-HLA-Cw and anti-HLA-DPantibodies in sensitized patients. Human Immunol.2012;73:879–83. 24. Gin evri F, Nocera A, Comoli P, etal. Posttransplant de novo donor-specific HLA antibodiesidentify pediatric kidney recipients at risk for lateantibody-mediated rejection. Am J Transplant.2012;12:3355–62. 25. Cecka JM. Calculated PRA (CPRA): Thenew measure of sensitization for transplant candidates. AmJ T ransplant 2010;10:26–9.
26. Halloran PF. Immunosuppressive drugs for kidneytransplantation. N Engl J Med. 2004;351:2715–29.
27. Mou dgil A, Puliyanda D. Induction therapy in pediatricrenal transplant recipients: An overview. Paediatr Drugs.2007;9:323–41.
28. Jordan SC, Toyoda M, Kahwaji J, Vo AA. Clinicalaspects of intravenous immunoglobulin use in solid organtransplant recipients. Am J Transplant. 2011;11:196–202.
29. Zub er J, Le Quintrec M, Krid S, et al. Eculizumab foratypical hemolytic uremic syndrome recurrence in renaltransplantation. Am J Transplant. 2012;12:3337–54.
30. Matasic R, Dietz AB, Vuk-Pavlovic S. Dexamethasoneinhibits dendritic cell maturation by redirectingdifferentiation of a subset of cells. J Leukocy Biol.1999;66:909–14.
31. Vincenti F. Are calcineurin inhibitors-free regimens

ready for prime time? Kidney Int. 2012;82:1054–60.
32. Kin near G, Jones ND, Wood KJ. Costimulation blockade:Current perspectives and implications for therapy.Transplantation. 2013;95:527–35.
33. Phas e II Pharmacokinetics, efficacy, and safety ofbelatacept in pediatric renal transplant recipients: 2013.Available at http://clinicaltrials.gov/ct2/show/NCT01791491. Accessed September 4, 2015.
34. Abu ali MM, Arnon R, Posada R. An update onimmunizations before and after transplantation in thepediatric solid organ transplant recipient. PediatrTransplant. 2011;15:770–7.
35. Kas iske BL, Bia MJ. The evaluation and selection ofliving kidney donors. Am J Kidney Dis. 1995;26:387–98.
36. Piros L, Langer RM. Laparoscopic donor nephrectomytechniques. Curr Opin Organ Transplant. 2012;17:401–5.
37. Shapiro M, Sarwal MM. Pediatric kidney transplantation.Pediatr Clin North Am. 2010;57:393–400.
38. Sarwal MM, Ettenger RB, Dharnidharka V, et al.Complete steroid avoidance is effective and safe inchildren with renal transplants: A multicenter randomizedtrial with three-year follow-up. Am J Transplant.2012;12:2719–29.
39. The American Society of Transplantation infectiousdiseases guidelines, ed 3. Am J Transplant. 2013;13:1–371.
40. Kidney paired donation pilot program. Available athttp://optn.transplant.hrsa.gov/. Accessed September 4,2015.
41. Kid ney Disease Improving Global Outcomes. Clinicalpractice guideline for the care of kidney transplantrecipients. Am J Transplant. 2009;9(Suppl 3):S1–155
42. Har tono C, Muthukumar T, Suthanthiran M. Noninvasivediagnosis of acute rejection of renal allografts. CurrOpin Organ Transplant. 2010;15:35–41. 43. Halloran PF,Pereira AB, Chang J, et al. Potential impact of microarraydiagnosis of T cell-mediated rejection in kidneytransplants: The INTERCOM study. Am J Transplant.2013;13:2352–63. 44. Sie dlecki A, Irish W, Brennan DC.Delayed graft function in the kidney transplant. Am J
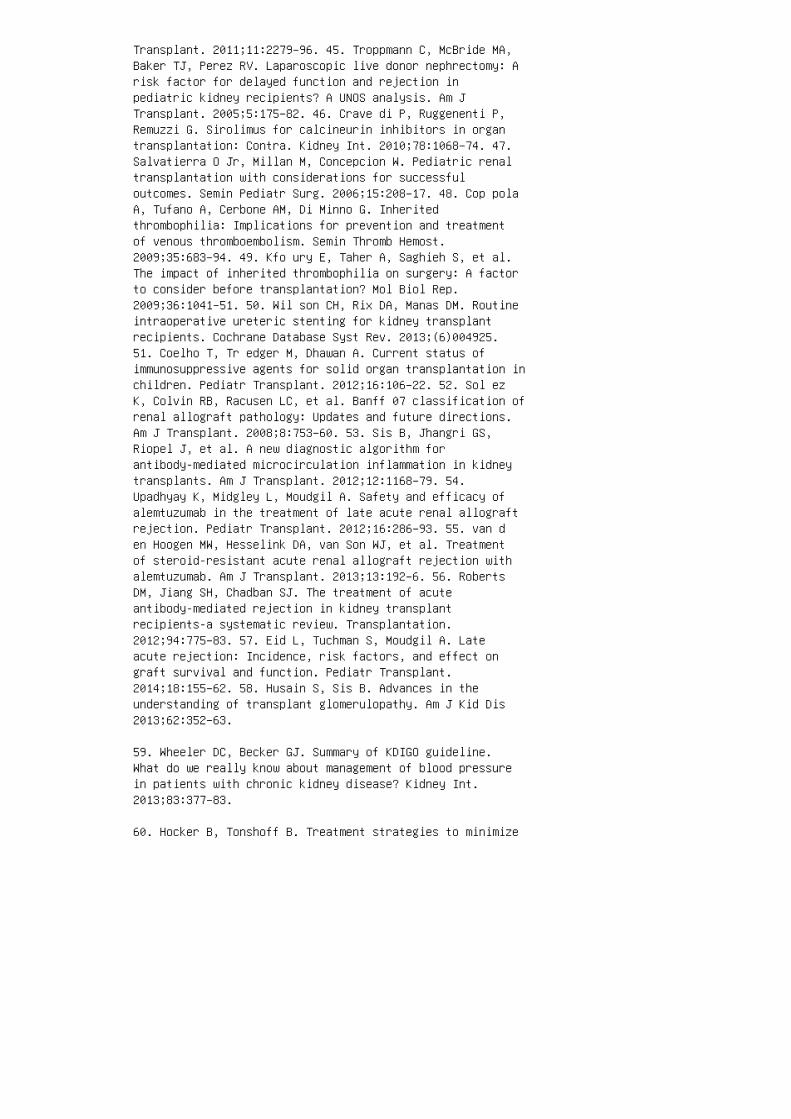
Transplant. 2011;11:2279–96. 45. Troppmann C, McBride MA,Baker TJ, Perez RV. Laparoscopic live donor nephrectomy: Arisk factor for delayed function and rejection inpediatric kidney recipients? A UNOS analysis. Am JTransplant. 2005;5:175–82. 46. Crave di P, Ruggenenti P,Remuzzi G. Sirolimus for calcineurin inhibitors in organtransplantation: Contra. Kidney Int. 2010;78:1068–74. 47.Salvatierra O Jr, Millan M, Concepcion W. Pediatric renaltransplantation with considerations for successfuloutcomes. Semin Pediatr Surg. 2006;15:208–17. 48. Cop polaA, Tufano A, Cerbone AM, Di Minno G. Inheritedthrombophilia: Implications for prevention and treatmentof venous thromboembolism. Semin Thromb Hemost.2009;35:683–94. 49. Kfo ury E, Taher A, Saghieh S, et al.The impact of inherited thrombophilia on surgery: A factorto consider before transplantation? Mol Biol Rep.2009;36:1041–51. 50. Wil son CH, Rix DA, Manas DM. Routineintraoperative ureteric stenting for kidney transplantrecipients. Cochrane Database Syst Rev. 2013;(6)004925.51. Coelho T, Tr edger M, Dhawan A. Current status ofimmunosuppressive agents for solid organ transplantation inchildren. Pediatr Transplant. 2012;16:106–22. 52. Sol ezK, Colvin RB, Racusen LC, et al. Banff 07 classification ofrenal allograft pathology: Updates and future directions.Am J Transplant. 2008;8:753–60. 53. Sis B, Jhangri GS,Riopel J, et al. A new diagnostic algorithm forantibody-mediated microcirculation inflammation in kidneytransplants. Am J Transplant. 2012;12:1168–79. 54.Upadhyay K, Midgley L, Moudgil A. Safety and efficacy ofalemtuzumab in the treatment of late acute renal allograftrejection. Pediatr Transplant. 2012;16:286–93. 55. van den Hoogen MW, Hesselink DA, van Son WJ, et al. Treatmentof steroid-resistant acute renal allograft rejection withalemtuzumab. Am J Transplant. 2013;13:192–6. 56. RobertsDM, Jiang SH, Chadban SJ. The treatment of acuteantibody-mediated rejection in kidney transplantrecipients-a systematic review. Transplantation.2012;94:775–83. 57. Eid L, Tuchman S, Moudgil A. Lateacute rejection: Incidence, risk factors, and effect ongraft survival and function. Pediatr Transplant.2014;18:155–62. 58. Husain S, Sis B. Advances in theunderstanding of transplant glomerulopathy. Am J Kid Dis2013;62:352–63.
59. Wheeler DC, Becker GJ. Summary of KDIGO guideline.What do we really know about management of blood pressurein patients with chronic kidney disease? Kidney Int.2013;83:377–83.
60. Hocker B, Tonshoff B. Treatment strategies to minimize

or prevent chronic allograft dysfunction in pediatricrenal transplant recipients: An overview. Paediatr Drugs.2009;11:381–96.
61. Touma J, Costanzo A, Boura B, et al. Endovascularmanagement of transplant renal artery stenosis. J VascSurg. 2014;59:1058–65
62. Marinella MA. Hematologic abnormalities followingrenal transplantation. Int Urol Neph. 2010;42:151–64.
63. Kahwaji J, Barker E, Pepkowitz S, et al. Acutehemolysis after high-dose intravenous immunoglobulintherapy in highly HLA sensitized patients. CJASN.2009;4:1993–7.
64. Wu Y, Cheng W, Yang XD, et al. Growth hormone improvesgrowth in pediatric renal transplant recipients: Asystemic review and meta-analysis of randomized controlledtrials. Pediatr Nephrol. 2013;28:129–33.
65. Fine RN, Stablein D, Cohen AH, et al. Recombinanthuman growth hormone post-renal transplantation inchildren: A randomized controlled study of the NAPRTCS.Kidney Int. 2002;62:688–96.
66. Ponticelli C, Glassock RJ. Posttransplant recurrence ofprimary glomerulonephritis. CJASN. 2010;5:2363–72.
67. Vin ai M, Waber P, Seikaly MG. Recurrence of focalsegmental glomerulosclerosis in renal allograft: Anin-depth review. Pediatr Transplant. 2010;14:314–25.
68. Sgambat K, Banks M, Moudgil A. Effect of galactose onglomerular permeability and proteinuria insteroid-resistant nephrotic syndrome. Pediatr Nephrol.2013;28:2131–5.
69. Yu CC, Fornoni A, Weins A, et al. Abatacept inB7-1-positive proteinuric kidney disease. N Engl J Med.2013;369:2416-–23.
70. Caires RA, Marques ID, Repizo LP, et al. De novothrombotic microangiopathy after kidney transplantation:Clinical features, treatment, and long-term patient andgraft survival. Transplantation Proc. 2012;44:2388–90.
71. Ponticelli C, Glassock RJ. De novo membranousnephropathy (MN) in kidney allografts: A peculiar form ofalloimmune disease? Transpl Int. 2012;25:1205–10.
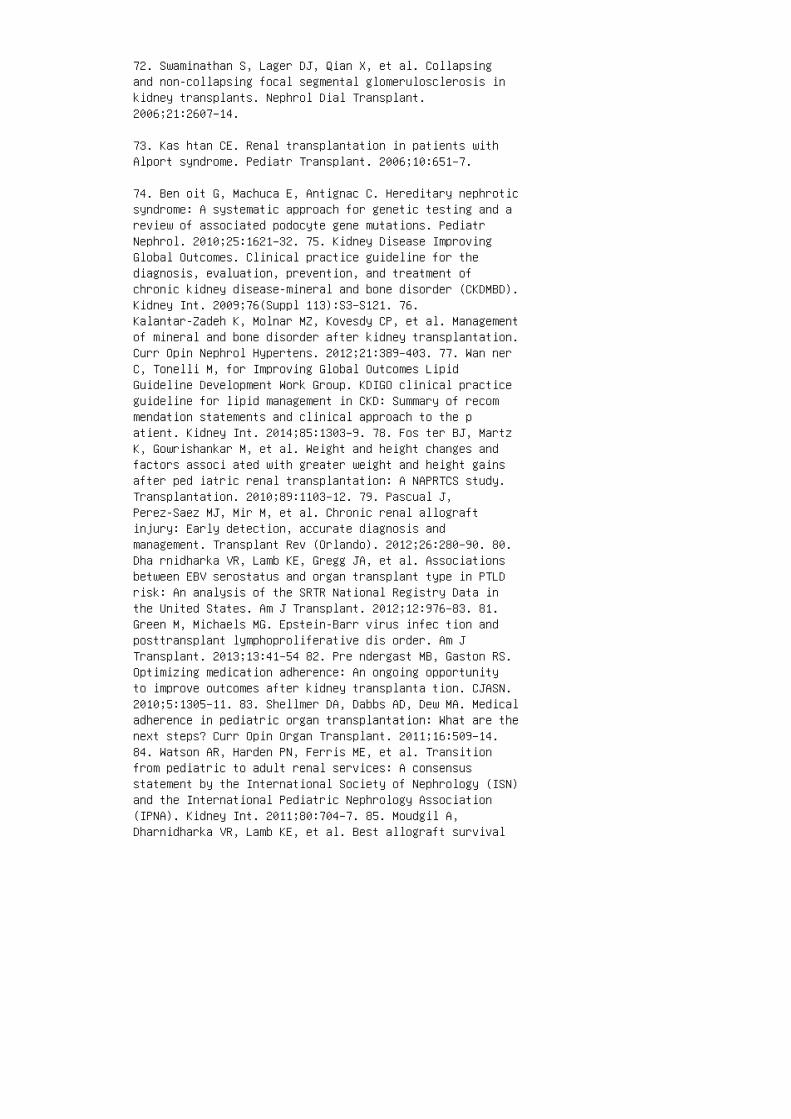
72. Swaminathan S, Lager DJ, Qian X, et al. Collapsingand non-collapsing focal segmental glomerulosclerosis inkidney transplants. Nephrol Dial Transplant.2006;21:2607–14.
73. Kas htan CE. Renal transplantation in patients withAlport syndrome. Pediatr Transplant. 2006;10:651–7.
74. Ben oit G, Machuca E, Antignac C. Hereditary nephroticsyndrome: A systematic approach for genetic testing and areview of associated podocyte gene mutations. PediatrNephrol. 2010;25:1621–32. 75. Kidney Disease ImprovingGlobal Outcomes. Clinical practice guideline for thediagnosis, evaluation, prevention, and treatment ofchronic kidney disease-mineral and bone disorder (CKDMBD).Kidney Int. 2009;76(Suppl 113):S3–S121. 76.Kalantar-Zadeh K, Molnar MZ, Kovesdy CP, et al. Managementof mineral and bone disorder after kidney transplantation.Curr Opin Nephrol Hypertens. 2012;21:389–403. 77. Wan nerC, Tonelli M, for Improving Global Outcomes LipidGuideline Development Work Group. KDIGO clinical practiceguideline for lipid management in CKD: Summary of recommendation statements and clinical approach to the patient. Kidney Int. 2014;85:1303–9. 78. Fos ter BJ, MartzK, Gowrishankar M, et al. Weight and height changes andfactors associ ated with greater weight and height gainsafter ped iatric renal transplantation: A NAPRTCS study.Transplantation. 2010;89:1103–12. 79. Pascual J,Perez-Saez MJ, Mir M, et al. Chronic renal allograftinjury: Early detection, accurate diagnosis andmanagement. Transplant Rev (Orlando). 2012;26:280–90. 80.Dha rnidharka VR, Lamb KE, Gregg JA, et al. Associationsbetween EBV serostatus and organ transplant type in PTLDrisk: An analysis of the SRTR National Registry Data inthe United States. Am J Transplant. 2012;12:976–83. 81.Green M, Michaels MG. Epstein-Barr virus infec tion andposttransplant lymphoproliferative dis order. Am JTransplant. 2013;13:41–54 82. Pre ndergast MB, Gaston RS.Optimizing medication adherence: An ongoing opportunityto improve outcomes after kidney transplanta tion. CJASN.2010;5:1305–11. 83. Shellmer DA, Dabbs AD, Dew MA. Medicaladherence in pediatric organ transplantation: What are thenext steps? Curr Opin Organ Transplant. 2011;16:509–14.84. Watson AR, Harden PN, Ferris ME, et al. Transitionfrom pediatric to adult renal services: A consensusstatement by the International Society of Nephrology (ISN)and the International Pediatric Nephrology Association(IPNA). Kidney Int. 2011;80:704–7. 85. Moudgil A,Dharnidharka VR, Lamb KE, et al. Best allograft survival

from share-35 kidney donors occurs in middle-aged adultsand young children: An analysis of OPTN data.Transplantation. 2013;95:319–25. 86. Mengel M, Sis B, HaasM, et al. Banff 2011 Meeting report: New concepts inantibodymediated rejection. Am J Transplant.2012;12:563–70. 87. Sol ez K, Racusen LC. The Banffclassification revisited. Kidney Int. 2013;83:201–6.
REVIEW QUESTIONS
1. A 5-year-old previously healthy child developed acutekidney injury as a result of septic shock. He receivedcontinuous renal replacement therapy for 1 month and thentransitioned to peritoneal dialysis as his kidneys failedto recover. He received a number of blood transfusionsduring his stay in the ICU. His parents ask about theoption of kidney transplant. He has otherwise completelyrecovered and weighs 15 kg. He is CMV IgG positive and EBVIgG negative. �e most important challenge posed for kidneytransplant in this child is:
a. Size of 15 kg
b. Potential for sensitization because of number of bloodtransfusions
c. EBV negative status
d. CMV positive status
2. A 10-year-old with ESRD secondary to FSGS underwentliving kidney transplant from a family friend. �e kidneyworked immediately with good urine output and decrease increatinine. At 36 hours later, he developed severeoliguria and creatinine started to increase. �e next stepin workup of gra� dysfunction includes which of thefollowing?
a. Uri nalysis and urine for ratio of protein to creatinine
b. Rena l ultrasound with Doppler
c. MAG -3 renal scan
d. VCUG
3. A 15year-old girl under went kidney transplant 4 yearsago for ESRD secondary to renal dysplasia with stable serumcreatinine level of 0.6 mg/ dL. For the past year, she o�enmissed clinic appointments, and her tacrolimus trough
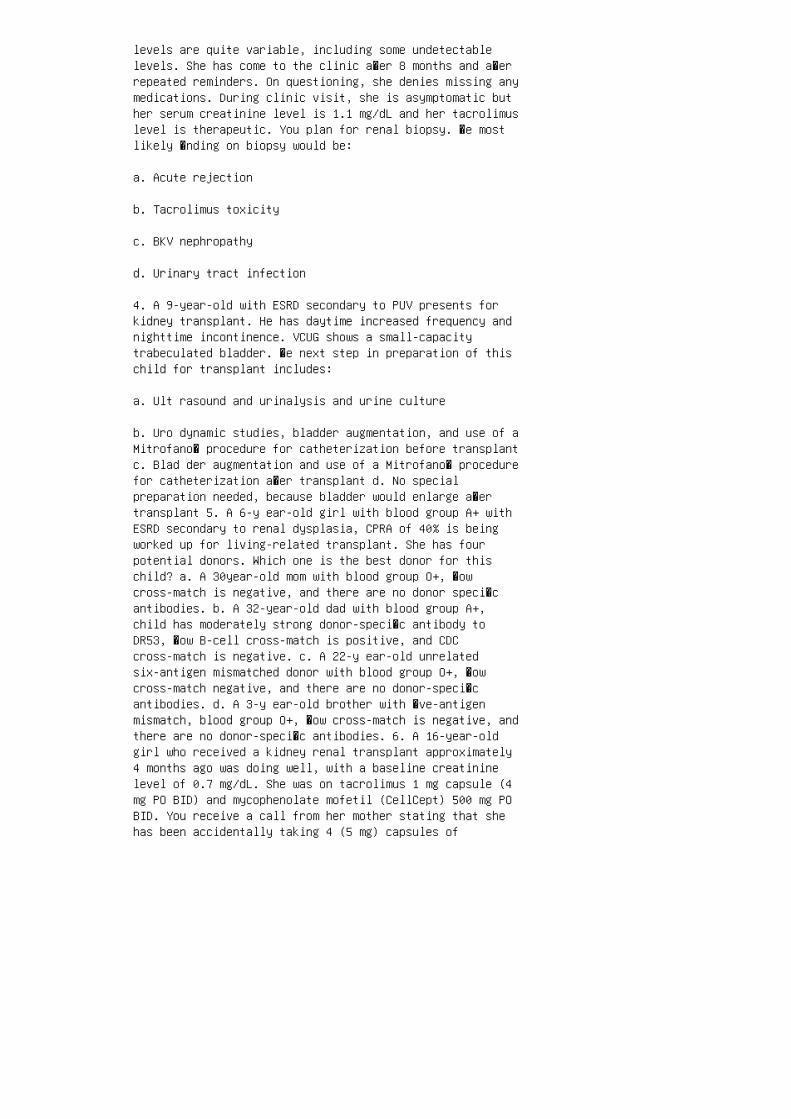
levels are quite variable, including some undetectablelevels. She has come to the clinic a�er 8 months and a�errepeated reminders. On questioning, she denies missing anymedications. During clinic visit, she is asymptomatic buther serum creatinine level is 1.1 mg/dL and her tacrolimuslevel is therapeutic. You plan for renal biopsy. �e mostlikely �nding on biopsy would be:
a. Acute rejection
b. Tacrolimus toxicity
c. BKV nephropathy
d. Urinary tract infection
4. A 9-year-old with ESRD secondary to PUV presents forkidney transplant. He has daytime increased frequency andnighttime incontinence. VCUG shows a small-capacitytrabeculated bladder. �e next step in preparation of thischild for transplant includes:
a. Ult rasound and urinalysis and urine culture
b. Uro dynamic studies, bladder augmentation, and use of aMitrofano� procedure for catheterization before transplantc. Blad der augmentation and use of a Mitrofano� procedurefor catheterization a�er transplant d. No specialpreparation needed, because bladder would enlarge a�ertransplant 5. A 6-y ear-old girl with blood group A+ withESRD secondary to renal dysplasia, CPRA of 40% is beingworked up for living-related transplant. She has fourpotential donors. Which one is the best donor for thischild? a. A 30year-old mom with blood group O+, �owcross-match is negative, and there are no donor speci�cantibodies. b. A 32-year-old dad with blood group A+,child has moderately strong donor-speci�c antibody toDR53, �ow B-cell cross-match is positive, and CDCcross-match is negative. c. A 22-y ear-old unrelatedsix-antigen mismatched donor with blood group O+, �owcross-match negative, and there are no donor-speci�cantibodies. d. A 3-y ear-old brother with �ve-antigenmismatch, blood group O+, �ow cross-match is negative, andthere are no donor-speci�c antibodies. 6. A 16-year-oldgirl who received a kidney renal transplant approximately4 months ago was doing well, with a baseline creatininelevel of 0.7 mg/dL. She was on tacrolimus 1 mg capsule (4mg PO BID) and mycophenolate mofetil (CellCept) 500 mg POBID. You receive a call from her mother stating that shehas been accidentally taking 4 (5 mg) capsules of

tacrolimus for the past 2 days. When seen in the emergencyroom, you expect to see: a. Hypertension, tremors, andheadache b. Increase in creatinine, high serum potassium,low CO 2 and magnesium, and high tacrolimus level inblood c. A and B d. Stable creatinine, normal serum K andCO 2 , and high magnesium and tacrolimus level 7. A12-year-old kidney transplant recipient presents to theclinic with unexplained weight loss and intermittent vagueabdominal pain for the past 2 to 3 months. He had ESRDsecondary to nephronophthisis and received a kidneytransplant 8 years ago from a deceased donor. He has beenstable until recently and has not had any acuterejections. He has no fever and denies any other symptoms.His physical examination is normal, except for weightloss of 6 kg. His BP is normal and his creatinine is atits baseline of 0.6 mg/dL and urinalysis is normal. Youwould like to start the workup of his weight loss, and thetests that would be most useful are: a. CMV and BKV viralloads b. Interferon-γ release assay for tuberculosis c.LDH, uric acid, EBV viral load
d. CT scan of abdomen, chest, and pelvis
e. Hemoglobin A 1c
8. A 9-year-old child transplanted with his father’skidney 9 days ago is seen for post-transplant followup inthe clinic. You notice that he has a swelling near theallogra� and in the suprapubic area, which is mildlytender to touch. He had ESRD secondary to renal dysplasia,his Foley catheter was removed on postoperative day 5, andhe was discharged home on postoperative day 6 with a serumcreatinine of 0.7 mg/dL. His serum creatinine today is 1.3mg/dL. Renal ultrasound with Doppler shows good perfusionand normal renal transplant morphology and resistiveindex. An anechoic �uid collection is present next to histransplant and in the pelvis, which was not present 4 daysago. Which tests would help in determining the cause ofacute renal dysfunction in this child?
a. Renal biopsy
b. Pharmacokinetics of tacrolimus
c. MAG-3 renal scan and VCUG
d. Needle aspiration of �uid and measurement of creatininein this �uid
e. c and d
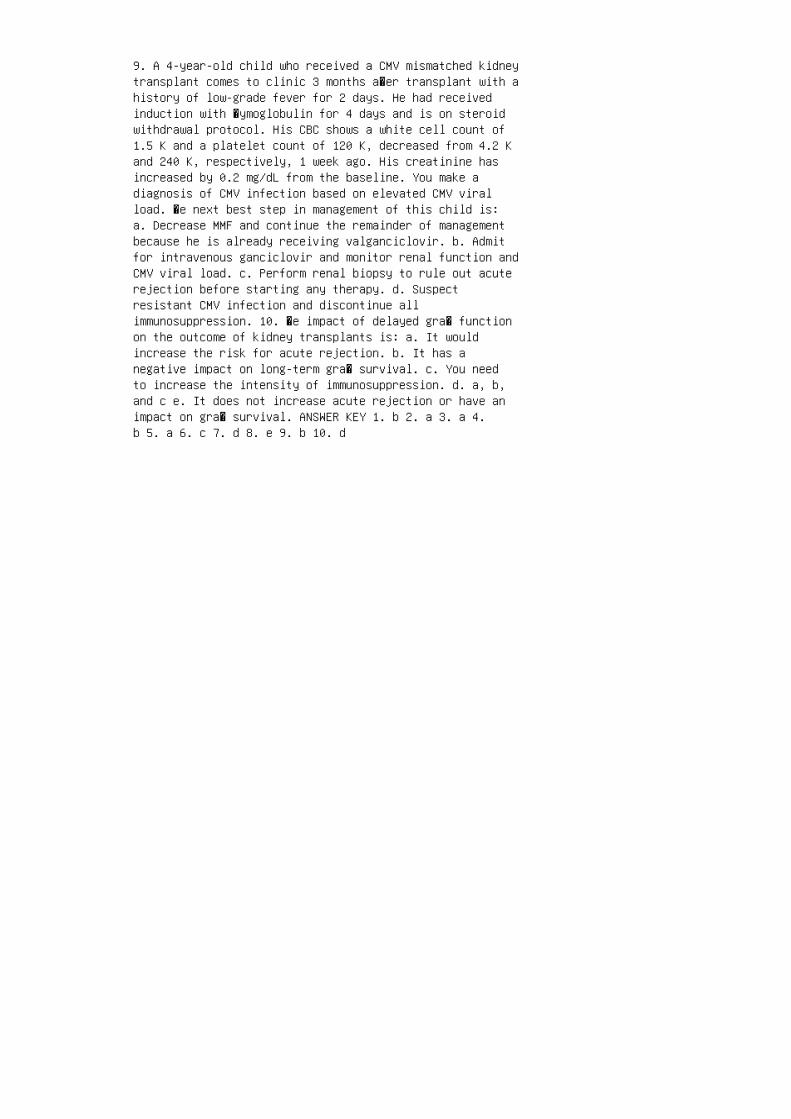
9. A 4-year-old child who received a CMV mismatched kidneytransplant comes to clinic 3 months a�er transplant with ahistory of low-grade fever for 2 days. He had receivedinduction with �ymoglobulin for 4 days and is on steroidwithdrawal protocol. His CBC shows a white cell count of1.5 K and a platelet count of 120 K, decreased from 4.2 Kand 240 K, respectively, 1 week ago. His creatinine hasincreased by 0.2 mg/dL from the baseline. You make adiagnosis of CMV infection based on elevated CMV viralload. �e next best step in management of this child is:a. Decrease MMF and continue the remainder of managementbecause he is already receiving valganciclovir. b. Admitfor intravenous ganciclovir and monitor renal function andCMV viral load. c. Perform renal biopsy to rule out acuterejection before starting any therapy. d. Suspectresistant CMV infection and discontinue allimmunosuppression. 10. �e impact of delayed gra� functionon the outcome of kidney transplants is: a. It wouldincrease the risk for acute rejection. b. It has anegative impact on long-term gra� survival. c. You needto increase the intensity of immunosuppression. d. a, b,and c e. It does not increase acute rejection or have animpact on gra� survival. ANSWER KEY 1. b 2. a 3. a 4.b 5. a 6. c 7. d 8. e 9. b 10. d
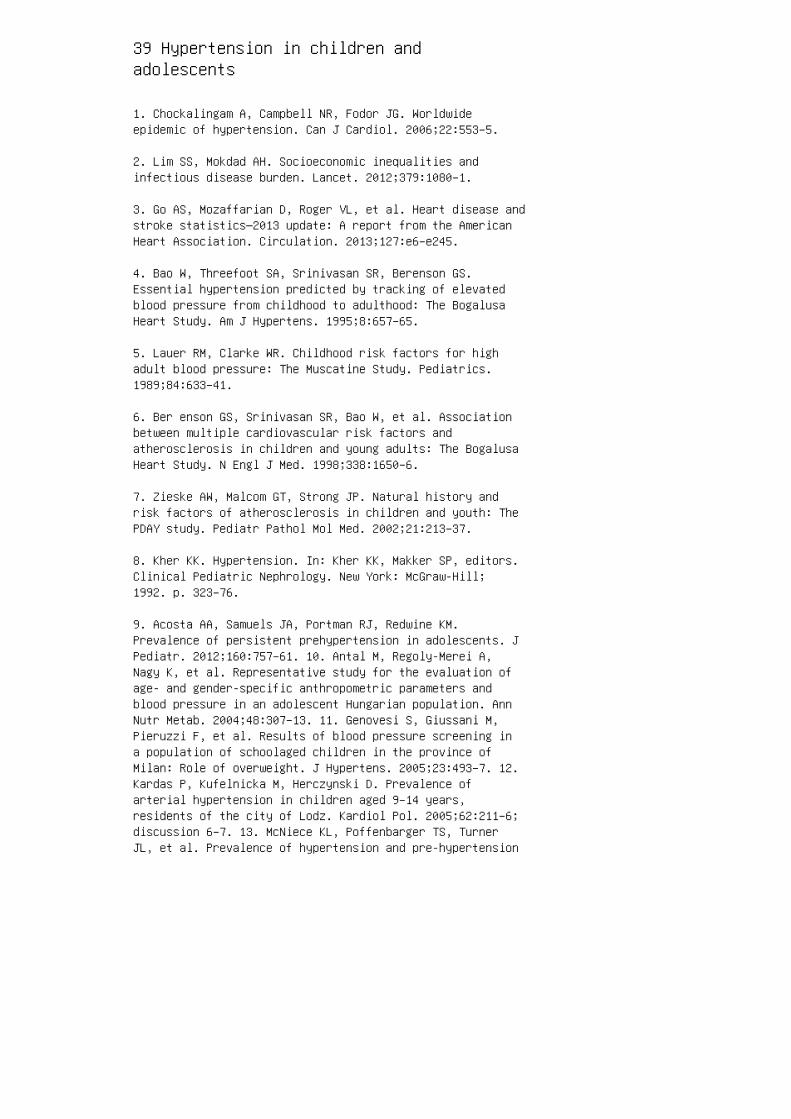
39 Hypertension in children andadolescents
1. Chockalingam A, Campbell NR, Fodor JG. Worldwideepidemic of hypertension. Can J Cardiol. 2006;22:553–5.
2. Lim SS, Mokdad AH. Socioeconomic inequalities andinfectious disease burden. Lancet. 2012;379:1080–1.
3. Go AS, Mozaffarian D, Roger VL, et al. Heart disease andstroke statistics—2013 update: A report from the AmericanHeart Association. Circulation. 2013;127:e6–e245.
4. Bao W, Threefoot SA, Srinivasan SR, Berenson GS.Essential hypertension predicted by tracking of elevatedblood pressure from childhood to adulthood: The BogalusaHeart Study. Am J Hypertens. 1995;8:657–65.
5. Lauer RM, Clarke WR. Childhood risk factors for highadult blood pressure: The Muscatine Study. Pediatrics.1989;84:633–41.
6. Ber enson GS, Srinivasan SR, Bao W, et al. Associationbetween multiple cardiovascular risk factors andatherosclerosis in children and young adults: The BogalusaHeart Study. N Engl J Med. 1998;338:1650–6.
7. Zieske AW, Malcom GT, Strong JP. Natural history andrisk factors of atherosclerosis in children and youth: ThePDAY study. Pediatr Pathol Mol Med. 2002;21:213–37.
8. Kher KK. Hypertension. In: Kher KK, Makker SP, editors.Clinical Pediatric Nephrology. New York: McGraw-Hill;1992. p. 323–76.
9. Acosta AA, Samuels JA, Portman RJ, Redwine KM.Prevalence of persistent prehypertension in adolescents. JPediatr. 2012;160:757–61. 10. Antal M, Regoly-Merei A,Nagy K, et al. Representative study for the evaluation ofage- and gender-specific anthropometric parameters andblood pressure in an adolescent Hungarian population. AnnNutr Metab. 2004;48:307–13. 11. Genovesi S, Giussani M,Pieruzzi F, et al. Results of blood pressure screening ina population of schoolaged children in the province ofMilan: Role of overweight. J Hypertens. 2005;23:493–7. 12.Kardas P, Kufelnicka M, Herczynski D. Prevalence ofarterial hypertension in children aged 9–14 years,residents of the city of Lodz. Kardiol Pol. 2005;62:211–6;discussion 6–7. 13. McNiece KL, Poffenbarger TS, TurnerJL, et al. Prevalence of hypertension and pre-hypertension
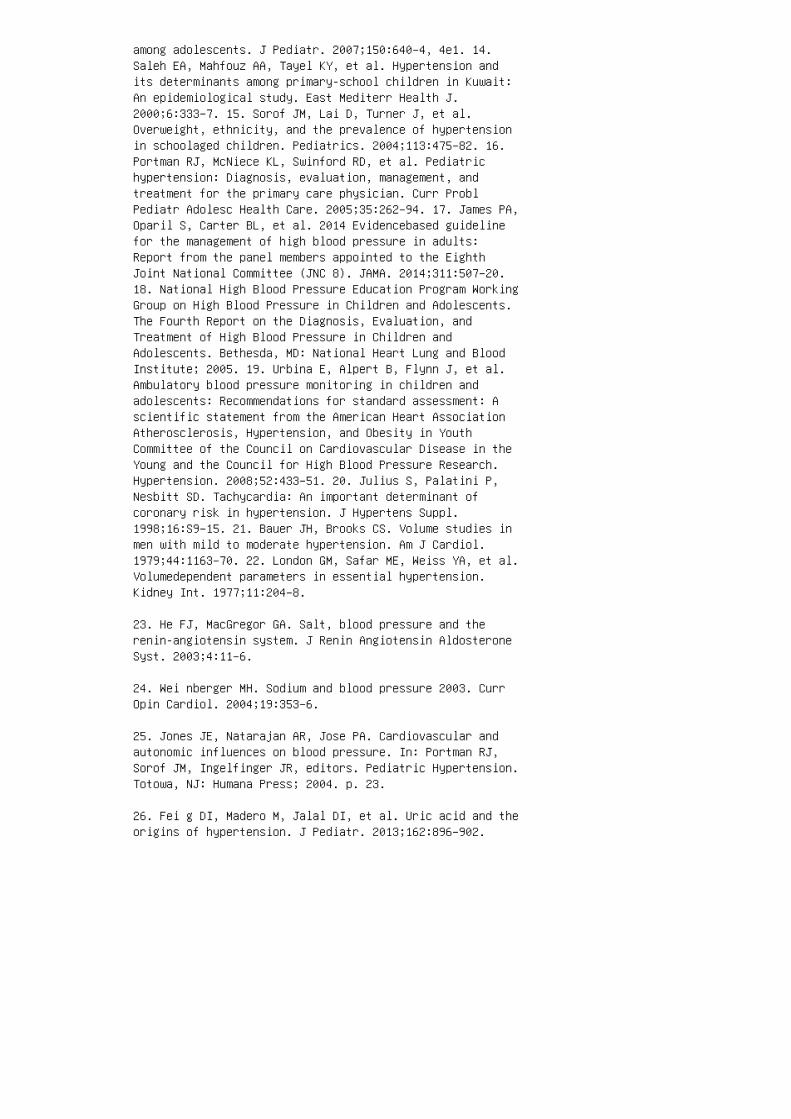
among adolescents. J Pediatr. 2007;150:640–4, 4e1. 14.Saleh EA, Mahfouz AA, Tayel KY, et al. Hypertension andits determinants among primary-school children in Kuwait:An epidemiological study. East Mediterr Health J.2000;6:333–7. 15. Sorof JM, Lai D, Turner J, et al.Overweight, ethnicity, and the prevalence of hypertensionin schoolaged children. Pediatrics. 2004;113:475–82. 16.Portman RJ, McNiece KL, Swinford RD, et al. Pediatrichypertension: Diagnosis, evaluation, management, andtreatment for the primary care physician. Curr ProblPediatr Adolesc Health Care. 2005;35:262–94. 17. James PA,Oparil S, Carter BL, et al. 2014 Evidencebased guidelinefor the management of high blood pressure in adults:Report from the panel members appointed to the EighthJoint National Committee (JNC 8). JAMA. 2014;311:507–20.18. National High Blood Pressure Education Program WorkingGroup on High Blood Pressure in Children and Adolescents.The Fourth Report on the Diagnosis, Evaluation, andTreatment of High Blood Pressure in Children andAdolescents. Bethesda, MD: National Heart Lung and BloodInstitute; 2005. 19. Urbina E, Alpert B, Flynn J, et al.Ambulatory blood pressure monitoring in children andadolescents: Recommendations for standard assessment: Ascientific statement from the American Heart AssociationAtherosclerosis, Hypertension, and Obesity in YouthCommittee of the Council on Cardiovascular Disease in theYoung and the Council for High Blood Pressure Research.Hypertension. 2008;52:433–51. 20. Julius S, Palatini P,Nesbitt SD. Tachycardia: An important determinant ofcoronary risk in hypertension. J Hypertens Suppl.1998;16:S9–15. 21. Bauer JH, Brooks CS. Volume studies inmen with mild to moderate hypertension. Am J Cardiol.1979;44:1163–70. 22. London GM, Safar ME, Weiss YA, et al.Volumedependent parameters in essential hypertension.Kidney Int. 1977;11:204–8.
23. He FJ, MacGregor GA. Salt, blood pressure and therenin-angiotensin system. J Renin Angiotensin AldosteroneSyst. 2003;4:11–6.
24. Wei nberger MH. Sodium and blood pressure 2003. CurrOpin Cardiol. 2004;19:353–6.
25. Jones JE, Natarajan AR, Jose PA. Cardiovascular andautonomic influences on blood pressure. In: Portman RJ,Sorof JM, Ingelfinger JR, editors. Pediatric Hypertension.Totowa, NJ: Humana Press; 2004. p. 23.
26. Fei g DI, Madero M, Jalal DI, et al. Uric acid and theorigins of hypertension. J Pediatr. 2013;162:896–902.

27. Gruskin AB. The adolescent with essential hypertension.Am J Kidney Dis. 1985;6:86–90.
28. Johnson RJ, Segal MS, Srinivas T, et al. Essentialhypertension, progressive renal disease, and uric acid: Apathogenetic link? J Am Soc Nephrol. 2005;16:1909–19.
29. Brunner H, Cockcroft JR, Deanfield J, et al.Endothelial function and dysfunction. Part II. Associationwith cardiovascular risk factors and diseases: A statementby the Working Group on Endothelins and EndothelialFactors of the European Society of Hypertension. JHypertens. 2005;23:233–46.
30. Mou rad A, Carney S, Gillies A, et al. Arm positionand blood pressure: A risk factor for hypertension? J HumHypertens. 2003;17:389–95.
31. Net ea RT, Lenders JW, Smits P, Thien T. Both body andarm position significantly influence blood pressuremeasurement. J Hum Hypertens. 2003;17:459–62.
32. Gil lman MW, Cook NR. Blood pressure measurement inchildhood epidemiological studies. Circulation.1995;92:1049–57.
33. Jon es DW, Appel LJ, Sheps SG, et al. Measuring bloodpressure accurately: New and persistent challenges. JAMA.2003;289:1027–30.
34. Bailey RH, Knaus VL, Bauer JH. Aneroidsphygmomanometers: An assessment of accuracy at auniversity hospital and clinics. Arch Intern Med.1991;151:1409–12.
35. Canzanello VJ, Jensen PL, Schwartz GL. Are aneroidsphygmomanometers accurate in hospital and clinicsettings? Arch Intern Med. 2001;161:729–31.
36. Ramsey M, 3rd. Blood pressure monitoring: Automatedoscillometric devices. J Clin Monit. 1991;7:56–67.
37. Barker ME, Shiell AW, Law CM. Evaluation of theDinamap 8100 and Omron M1 blood pressure monitors for usein children. Paediatr Perinat Epidemiol. 2000;14:179–86.
38. Par k MK, Menard SW, Yuan C. Comparison of bloodpressure in children from three ethnic groups. Am JCardiol. 2001;87:1305–8.

39. Dea l JE, Barratt TM, Dillon MJ. Management ofhypertensive emergencies. Arch Dis Child. 1992;67:1089–92.40. Daniels SR, Loggie JM, McEnery PT, Towbin RB. Clinicalspectrum of intrinsic renovascular hypertension inchildren. Pediatrics. 1987;80:698–704. 41. Watson AR,Balfe JW, Hardy BE. Renovascular hypertension inchildhood: A changing perspective in management. JPediatr. 1985;106:366–72. 42. Harms MM, Rotteveel JJ, KarNC, Gabreels FJ. Recurrent alternating facial paralysisand malignant hypertension. Neuropediatrics.2000;31:318–20. 43. Browning AC, Mengher LS, Gregson RM,Amoaku WM. Visual outcome of malignant hypertension inyoung people. Arch Dis Child. 2001;85:401–3. 44.Strandgaard S, Olesen J, Skinhoj E, Lassen NA.Autoregulation of brain circulation in severe arterialhypertension. Br Med J. 1973;1:507–10. 45. Sch wartz RB,Mulkern RV, Gudbjartsson H, Jolesz F. Diffusion-weightedMR imaging in hypertensive encephalopathy: Clues topathogenesis. AJNR Am J Neuroradiol. 1998;19:859–62. 46.Tuor UI. Acute hypertension and sympathetic stimulation:Local heterogeneous changes in cerebral blood flow. Am JPhysiol. 1992;263:H511–8. 47. Uha ri M, Saukkonen AL,Koskimies O. Central nervous system involvement in severearterial hypertension of childhood. Eur J Pediatr.1979;132:141–6. 48. Tro mpeter RS, Smith RL, Hoare RD, etal. Neurological complications of arterial hypertension.Arch Dis Child. 1982;57:913–7. 49. Adelman RD, Coppo R,Dillon MJ. The emergency management of severehypertension. Pediatr Nephrol. 2000;14:422–7. 50. HulseJA, Taylor DS, Dillon MJ. Blindness and paraplegia insevere childhood hypertension. Lancet. 1979;2:553–6. 51.Isl es CG. Hypertensive emergencies: Malignanthypertension and hypertensive encephalopathy. In: SwalesJD, editor. Textbook of Hypertension. Oxford: BlackwellScientific; 1994. p. 1233. 52. Ledingham JG, RajagopalanB. Cerebral complications in the treatment of acceleratedhypertension. Q J Med. 1979;48:25–41. 53. Taylor D,Ramsay J, Day S, Dillon M. Infarction of the optic nervehead in children with accelerated hypertension. Br JOphthalmol. 1981;65:153–60. 54. Flynn JT, Mitsnefes M,Pierce C, et al. Blood pressure in children with chronickidney disease: A report from the Chronic Kidney Diseasein Children study. Hypertension. 2008;52:631–7. 55.Tullus K. Secondary forms of hypertension. In: Flynn JT,Ingelfinger JR, Portman RJ, editors. PediatricHypertension, 2nd ed. New York: Humana Press; 2011. 56.Mar tinez-Maldonado M. Hypertension in end-stage renaldisease. Kidney Int Suppl. 1998;68:S67–72. 57. Deal JE,Snell MF, Barratt TM, Dillon MJ. Renovascular disease in

childhood. J Pediatr. 1992;121:378–84.
58. Loirat C, Pillion G, Blum C. Hypertension in children:Present data and problems. Adv Nephrol. 1982;11:65.
59. Fos sali E, Signorini E, Intermite RC, et al.Renovascular disease and hypertension in children withneurofibromatosis. Pediatr Nephrol. 2000;14:806–10.
60. Greene JF, Jr, Fitzwater JE, Burgess J. Arteriallesions associated with neurofibromatosis. Am J ClinPathol. 1974;62:481–7.
61. Halpern M, Currarino G. Vascular lesions causinghypertension in neurofibromatosis. N Engl J Med.1965;273:248.
62. Leumann EP. Blood pressure and hypertension inchildhood and adolescence. Ergeb Inn Med Kinderheilkd.1979;43:109–83.
63. Mena E, Bookstein JJ, Holt JF, Fry WJ.Neurofibromatosis and renovascular hypertension inchildren. Am J Roentgenol Radium Ther Nucl Med.1973;118:39–45.
64. Loughridge LW. Renal abnormalities in the Marfansyndrome. Q J Med. 1959;28:531–44.
65. Wig gelinkhuizen J, Cremin BJ. Takayasu arteritis andrenovascular hypertension in childhood. Pediatrics.1978;62:209–17.
66. Pro esmans W, Van Damme B, Marchal G, et al.Klippel-Trenaunay syndrome with systemic hypertension andchronic renal failure. Ann Pediatr (Paris). 1982;29:671[in French].
67. Lon de S. Causes of hypertension in the young. PediatrClin North Am. 1978;25:55–65.
68. O’N eill JA, Jr, Berkowitz H, Fellows KJ, Harmon CM.Midaortic syndrome and hypertension in childhood. JPediatr Surg. 1995;30:164–71; discussion 71–2.
69. Sumboonnanonda A, Robinson BL, Gedroyc WM, et al.Middle aortic syndrome: Clinical and radiological findings.Arch Dis Child. 1992;67:501–5.
70. Wiltse HE, Goldbloom RB, Antia AU, et al. Infantile
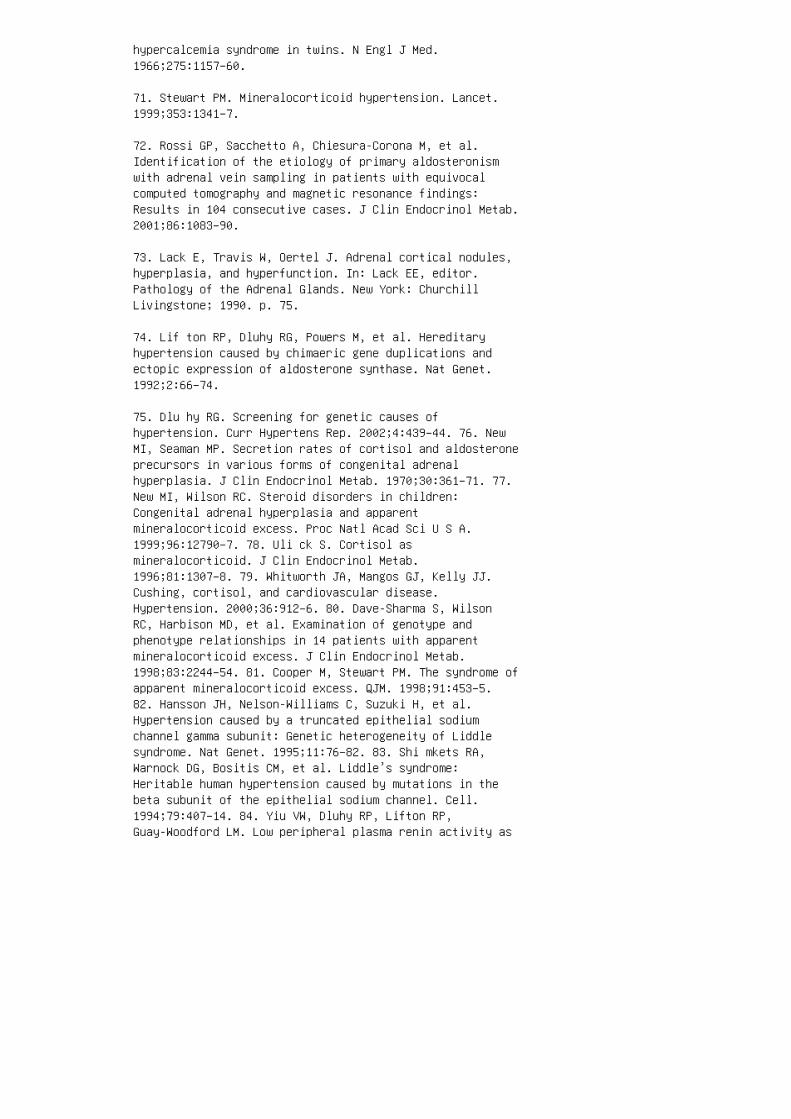
hypercalcemia syndrome in twins. N Engl J Med.1966;275:1157–60.
71. Stewart PM. Mineralocorticoid hypertension. Lancet.1999;353:1341–7.
72. Rossi GP, Sacchetto A, Chiesura-Corona M, et al.Identification of the etiology of primary aldosteronismwith adrenal vein sampling in patients with equivocalcomputed tomography and magnetic resonance findings:Results in 104 consecutive cases. J Clin Endocrinol Metab.2001;86:1083–90.
73. Lack E, Travis W, Oertel J. Adrenal cortical nodules,hyperplasia, and hyperfunction. In: Lack EE, editor.Pathology of the Adrenal Glands. New York: ChurchillLivingstone; 1990. p. 75.
74. Lif ton RP, Dluhy RG, Powers M, et al. Hereditaryhypertension caused by chimaeric gene duplications andectopic expression of aldosterone synthase. Nat Genet.1992;2:66–74.
75. Dlu hy RG. Screening for genetic causes ofhypertension. Curr Hypertens Rep. 2002;4:439–44. 76. NewMI, Seaman MP. Secretion rates of cortisol and aldosteroneprecursors in various forms of congenital adrenalhyperplasia. J Clin Endocrinol Metab. 1970;30:361–71. 77.New MI, Wilson RC. Steroid disorders in children:Congenital adrenal hyperplasia and apparentmineralocorticoid excess. Proc Natl Acad Sci U S A.1999;96:12790–7. 78. Uli ck S. Cortisol asmineralocorticoid. J Clin Endocrinol Metab.1996;81:1307–8. 79. Whitworth JA, Mangos GJ, Kelly JJ.Cushing, cortisol, and cardiovascular disease.Hypertension. 2000;36:912–6. 80. Dave-Sharma S, WilsonRC, Harbison MD, et al. Examination of genotype andphenotype relationships in 14 patients with apparentmineralocorticoid excess. J Clin Endocrinol Metab.1998;83:2244–54. 81. Cooper M, Stewart PM. The syndrome ofapparent mineralocorticoid excess. QJM. 1998;91:453–5.82. Hansson JH, Nelson-Williams C, Suzuki H, et al.Hypertension caused by a truncated epithelial sodiumchannel gamma subunit: Genetic heterogeneity of Liddlesyndrome. Nat Genet. 1995;11:76–82. 83. Shi mkets RA,Warnock DG, Bositis CM, et al. Liddle’s syndrome:Heritable human hypertension caused by mutations in thebeta subunit of the epithelial sodium channel. Cell.1994;79:407–14. 84. Yiu VW, Dluhy RP, Lifton RP,Guay-Woodford LM. Low peripheral plasma renin activity as
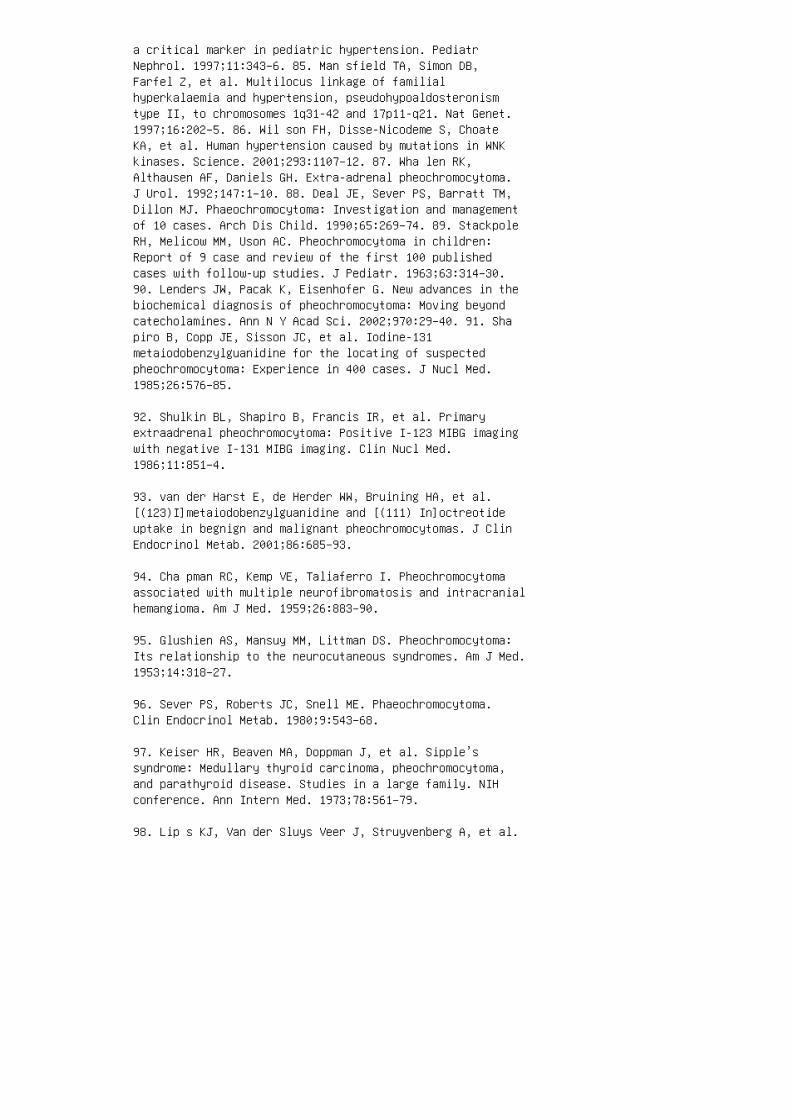
a critical marker in pediatric hypertension. PediatrNephrol. 1997;11:343–6. 85. Man sfield TA, Simon DB,Farfel Z, et al. Multilocus linkage of familialhyperkalaemia and hypertension, pseudohypoaldosteronismtype II, to chromosomes 1q31-42 and 17p11-q21. Nat Genet.1997;16:202–5. 86. Wil son FH, Disse-Nicodeme S, ChoateKA, et al. Human hypertension caused by mutations in WNKkinases. Science. 2001;293:1107–12. 87. Wha len RK,Althausen AF, Daniels GH. Extra-adrenal pheochromocytoma.J Urol. 1992;147:1–10. 88. Deal JE, Sever PS, Barratt TM,Dillon MJ. Phaeochromocytoma: Investigation and managementof 10 cases. Arch Dis Child. 1990;65:269–74. 89. StackpoleRH, Melicow MM, Uson AC. Pheochromocytoma in children:Report of 9 case and review of the first 100 publishedcases with follow-up studies. J Pediatr. 1963;63:314–30.90. Lenders JW, Pacak K, Eisenhofer G. New advances in thebiochemical diagnosis of pheochromocytoma: Moving beyondcatecholamines. Ann N Y Acad Sci. 2002;970:29–40. 91. Shapiro B, Copp JE, Sisson JC, et al. Iodine-131metaiodobenzylguanidine for the locating of suspectedpheochromocytoma: Experience in 400 cases. J Nucl Med.1985;26:576–85.
92. Shulkin BL, Shapiro B, Francis IR, et al. Primaryextraadrenal pheochromocytoma: Positive I-123 MIBG imagingwith negative I-131 MIBG imaging. Clin Nucl Med.1986;11:851–4.
93. van der Harst E, de Herder WW, Bruining HA, et al.[(123)I]metaiodobenzylguanidine and [(111) In]octreotideuptake in begnign and malignant pheochromocytomas. J ClinEndocrinol Metab. 2001;86:685–93.
94. Cha pman RC, Kemp VE, Taliaferro I. Pheochromocytomaassociated with multiple neurofibromatosis and intracranialhemangioma. Am J Med. 1959;26:883–90.
95. Glushien AS, Mansuy MM, Littman DS. Pheochromocytoma:Its relationship to the neurocutaneous syndromes. Am J Med.1953;14:318–27.
96. Sever PS, Roberts JC, Snell ME. Phaeochromocytoma.Clin Endocrinol Metab. 1980;9:543–68.
97. Keiser HR, Beaven MA, Doppman J, et al. Sipple’ssyndrome: Medullary thyroid carcinoma, pheochromocytoma,and parathyroid disease. Studies in a large family. NIHconference. Ann Intern Med. 1973;78:561–79.
98. Lip s KJ, Van der Sluys Veer J, Struyvenberg A, et al.

Bilateral occurrence of pheochromocytoma in patients withthe multiple endocrine neoplasia syndrome type 2A(Sipple’s syndrome). Am J Med. 1981;70:1051–60.
99. Pry s-Roberts C. Phaeochromocytoma: Recent progress inits management. Br J Anaesth. 2000;85:44-57.
100. Ulc haker JC, Goldfarb DA, Bravo EL, Novick AC.Successful outcomes in pheochromocytoma surgery in themodern era. J Urol. 1999;161:764–7.
101. Sorof J, Daniels S. Obesity hypertension in children:A problem of epidemic proportions. Hypertension.2002;40:441–7.
102. Sacks FM, Svetkey LP, Vollmer WM, et al. Effects onblood pressure of reduced dietary sodium and the DietaryApproaches to Stop Hypertension (DASH) diet: DASH-SodiumCollaborative Research Group. N Engl J Med. 2001;344:3–10.
103. Vol lmer WM, Sacks FM, Ard J, et al. Effects of dietand sodium intake on blood pressure: Subgroup analysis ofthe DASH-sodium trial. Ann Intern Med. 2001;135:1019–28.
104. Whelton SP, Chin A, Xin X, He J. Effect of aerobicexercise on blood pressure: A meta-analysis of randomized,controlled trials. Ann Intern Med. 2002;136:493–503.
105. Sim ons-Morton DG, Hunsberger SA, Van Horn L, et al.Nutrient intake and blood pressure in the DietaryIntervention Study in Children. Hypertension.1997;29:930–6.
106. Sim ons-Morton DG, Obarzanek E. Diet and bloodpressure in children and adolescents. Pediatr Nephrol.1997;11:244–9. 107. Cornoni-Huntley J, LaCroix AZ, HavlikRJ. Race and sex differentials in the impact ofhypertension in the United States: The National Health andNutrition Examination Survey I Epidemiologic Follow-upStudy. Arch Intern Med. 1989;149:780–8. 108. Eis ner GM.Hypertension: Racial differences. Am J Kidney Dis.1990;16:35–40. 109. Treiber FA, Musante L, Strong WB, LevyM. Racial differences in young children’s blood pressure:Responses to dynamic exercise. Am J Dis Child.1989;143:720–3. 110. Southard DR, Coates TJ, Kolodner K,et al. Relationship between mood and blood pressure inthe natural environment: An adolescent population. HealthPsychol. 1986;5:469–80. 111. Blowey DL, Duda PJ, Stokes P,Hall M. Incidence and treatment of hypertension in theneonatal intensive care unit. J Am Soc Hypertens.
2011;5:478–83. 112. Sel iem WA, Falk MC, Shadbolt B, KentAL. Antenatal and postnatal risk factors for neonatalhypertension and infant follow-up. Pediatr Nephrol.2007;22:2081–7. 113. Singh HP, Hurley RM, Myers TF.Neonatal hypertension: Incidence and risk factors. Am JHypertens. 1992;5:51–5. 114. Abman SH, Warady BA, Lum GM,Koops BL. Systemic hypertension in infants withbronchopulmonary dysplasia. J Pediatr. 1984;104:928–31.115. Becker JA, Short BL, Martin GR. Cardiovascularcomplications adversely affect survival duringextracorporeal membrane oxygenation. Crit Care Med.1998;26:1582–6. 116. Boe dy RF, Goldberg AK, Howell CG,Jr, et al. Incidence of hypertension in infants onextracorporeal membrane oxygenation. J Pediatr Surg.1990;25:258–61. 117. Fri edman AL, Hustead VA.Hypertension in babies following discharge from a neonatalintensive care unit: A 3-year follow-up. Pediatr Nephrol.1987;1:30–4. 118. Plouin PF, Chatellier G, Rougeot MA, etal P. Plasma renin activity in phaeochromocytoma: Effectsof beta-blockade and converting enzyme inhibition. JHypertens. 1988;6:579–85. 119. Kupferman JC, AronsonFriedman L, Cox C, et al. BP control and left ventricularhypertrophy regression in children with CKD. J Am SocNephrol. 2014;25:167–74. 120. Litwin M, Niemirska A,Sladowska-Kozlowska J, et al. Regression of target organdamage in children and adolescents with primaryhypertension. Pediatr Nephrol. 2010;25:2489–99. 121.Matteucci MC, Chinali M, Rinelli G, et al. Change incardiac geometry and function in CKD children during strictBP control: A randomized study. Clin J Am Soc Nephrol.2013;8:203–10. 122. Binkert CA, Debatin JF, Schneider E,et al. Can MR measurement of renal artery flow and renalvolume predict the outcome of percutaneous transluminalrenal angioplasty? Cardiovasc Intervent Radiol.2001;24:233–9.
123. Debatin JF, Spritzer CE, Grist TM, et al. Imaging ofthe renal arteries: Value of MR angiography. AJR Am JRoentgenol. 1991;157:981–90.
124. Mar cos HB, Choyke PL. Magnetic resonance angiographyof the kidney. Semin Nephrol. 2000;20:450–5.
125. Shahdadpuri J, Frank R, Gauthier BG, et al. Yield ofrenal arteriography in the evaluation of pediatrichypertension. Pediatr Nephrol. 2000;14:816–9.
126. Cho banian AV, Bakris GL, Black HR, et al. Seventhreport of the Joint National Committee on Prevention,Detection, Evaluation, and Treatment of High Blood
Pressure. Hypertension. 2003;42:1206–52.
127. World Health Organization, editor. The World HealthReport 2002: Reducing Risks, Promoting Healthy Life.Geneva: World Health Organization; 2002.
128. US Renal Data System (USRDS) 2013 Annual Data Report:Atlas of Chronic Kidney Disease and EndStage Renal Diseasein the United States. Bethesda, MD: National Institutes ofHealth, National Institute of Diabetes and Digestive andKidney Diseases; 2013.
129. Bel sha CW, Wells TG, McNiece KL, et al. Influence ofdiurnal blood pressure variations on target organabnormalities in adolescents with mild essentialhypertension. Am J Hypertens. 1998;11:410–7.
130. Bra dy TM, Fivush B, Flynn JT, Parekh R. Ability ofblood pressure to predict left ventricular hypertrophy inchildren with primary hypertension. J Pediatr.2008;152:73–8, 8 e1.
131. Hanevold C, Waller J, Daniels S, et al. The effects ofobesity, gender, and ethnic group on left ventricularhypertrophy and geometry in hypertensive children: Acollaborative study of the International PediatricHypertension Association. Pediatrics. 2004;113:328–33.
132. McNiece KL, Gupta-Malhotra M, Samuels J, et al. Leftventricular hypertrophy in hypertensive adolescents:Analysis of risk by 2004 National High Blood PressureEducation Program Working Group staging criteria.Hypertension. 2007;50:392–5.
133. Sor of JM, Alexandrov AV, Cardwell G, Portman RJ.Carotid artery intimal-medial thickness and leftventricular hypertrophy in children with elevated bloodpressure. Pediatrics. 2003;111:61–6.
134. Khoury PR, Mitsnefes M, Daniels SR, Kimball TR.Age-specific reference intervals for indexed leftventricular mass in children. J Am Soc Echocardiogr.2009;22:709–14.
135. Lev y D, Garrison RJ, Savage DD, et al. Prognosticimplications of echocardiographically determined leftventricular mass in the Framingham Heart Study. N Engl JMed. 1990;322:1561–6.
136. Mes serli FH, Sundgaard-Riise K, Reisin ED, et al.

Dimorphic cardiac adaptation to obesity and arterialhypertension. Ann Intern Med. 1983;99:757–61. 137. SniderAR, Gidding SS, Rocchini AP, et al. Doppler evaluation ofleft ventricular diastolic filling in children withsystemic hypertension. Am J Cardiol. 1985;56:921–6. 138.Ino u T, Lamberth WC, Jr, Koyanagi S, et al. Relativeimportance of hypertension after coronary occlusion inchronic hypertensive dogs with LVH. Am J Physiol.1987;253:H1148–58. 139. Zehender M, Meinertz T, HohnloserS, et al. Prevalence of circadian variations andspontaneous variability of cardiac disorders and ECGchanges suggestive of myocardial ischemia in systemicarterial hypertension. Circulation. 1992;85:1808–15. 140.Agu NC, McNiece Redwine K, Bell C, et al. Detection ofearly diastolic alterations by tissue Doppler imaging inuntreated childhood-onset essential hypertension. J Am SocHypertens. 2014;8:303–11. 141. Dan iels SR, Witt SA,Glascock B, et al. Left atrial size in children withhypertension: The influence of obesity, blood pressure,and left ventricular mass. J Pediatr. 2002;141:186–90.142. Hei ss G, Sharrett AR, Barnes R, et al. Carotidatherosclerosis measured by B-mode ultrasound inpopulations: Associations with cardiovascular risk factorsin the ARIC study. Am J Epidemiol. 1991;134:250–6. 143.Lande MB, Carson NL, Roy J, Meagher CC. Effects ofchildhood primary hypertension on carotid intima mediathickness: A matched controlled study. Hypertension.2006;48:40–4. 144. Urb ina EM, Khoury PR, McCoy C, et al.Cardiac and vascular consequences of pre-hypertension inyouth. J Clin Hypertens (Greenwich). 2011;13:332–42. 145.Ska lina ME, Annable WL, Kliegman RM, Fanaroff AA.Hypertensive retinopathy in the newborn infant. J Pediatr.1983;103:781–6. 146. Williams KM, Shah AN, Morrison D,Sinha MD. Hypertensive retinopathy in severelyhypertensive children: Demographic, clinical, andophthalmoscopic findings from a 30-year British cohort. JPediatr Ophthalmol Strabismus. 2013;50:222–8. 147. GargJP, Bakris GL. Microalbuminuria: Marker of vasculardysfunction, risk factor for cardiovascular disease. VascMed. 2002;7:35–43. 148. Gerstein HC, Mann JF, Yi Q, et al.Albuminuria and risk of cardiovascular events, death, andheart failure in diabetic and nondiabetic individuals.JAMA. 2001;286:421–6. 149. Jen sen JS, Feldt-Rasmussen B,Strandgaard S, et al. Arterial hypertension,microalbuminuria, and risk of ischemic heart disease.Hypertension. 2000;35:898–903. 150. Radhakishun NN, vanVliet M, von Rosenstiel IA, et al. Limited value ofroutine microalbuminuria assessment in multi-ethnic obesechildren. Pediatr Nephrol. 2013;28:1145–9.
REVIEW QUESTIONS
1. According to current guidelines, the initial evaluationof all children with con�rmed hypertension should includeall of the following except:
a. Renal ultrasound
b. Electrocardiogram
c. Urinalysis
d. Complete history and physical
e. Echocardiogram
2. All of the following low-renin hypertensive disordersare associated with hypokalemia except:
a. Liddle syndrome
b. Adrenal hyperplasia
c. Apparent mineralocorticoid excess
d. Glucocorticoid-remediable aldosteronism
e. Gordon syndrome
3. Renin secretion is increased by all of the followingexcept:
a. Decreased intravascular volume
b. Activation of the sympathetic nervous system
c. Increased aldosterone secretion
d. Hypotension
e. Renal artery stenosis
4. Oscillometric blood pressure monitors directly measure:
a. Pulse pressure
b. Systolic blood pressure
c. Diastolic blood pressure
d. Mean arterial pressure
e. Diurnal blood pressure variation
5. A previously healthy 14-year-old male patient is seenfor a routine school physical examination. His bloodpressure at this visit is 132/70 (95th percentile: 130/83).He is asymptomatic, and the rest of his physicalexamination is normal. �e next step in his evaluation andmanagement should be:
a. Urinalysis
b. Renal ultrasound.
c. Repeat blood pressure in 1 to 2 weeks.
d. Reassurance that his blood pressure is normal
e. Initiation of antihypertensive medication
6. All of the following are associated with a higher riskfor hypertension in the neonatal period except:
a. Umbilical artery catheterization
b. Large for gestational age
c. Bronchopulmonary dysplasia
d. Patent ductus arteriosus
e. Maternal drug use 7. CT imaging of a child withhypertensive encephalopathy will most commonly show changesin the: a. Parieto-occipital white matter b. Hypothalamusc. Pituitary gland d. Prefrontal cortex e. Optic nerve8. All of the following may raise the blood pressure of achild with chronic hypertension who is being treated foran acute asthma exacerbation and allergy symptoms except:a. Prednisone b. Albuterol c. Phenylephrine d. Ibuprofene. Cetirizine 9. Normal blood pressure levels in childrenare based on the child’s: a. Age b. Gender c. Body massindex d. Height e. a, b, and d 10. Children whose BP isgreater than the 90th percentile (or greater than 120/80mm Hg) but less than the 95th percentile should beclassi�ed as prehypertensive. However, these childrenshould be treated as if they were hypertensive if theyhave any of the following conditions except: a. Le�ventricular hypertrophy b. Diabetes mellitus c. Renaldysplasia d. Short stature e. Retinopathy ANSWER KEY 1.

b 2. e 3. c 4. d 5. c 6. b 7. a 8. e 9. e 10. d

40 Management of hypertension
KEY POINT
In patients with renovascular hypertension, anti
hypertensive medications are used frequently—in
the initial management until anatomic correction is
achieved and long term when there is residual hyper
tension or vascular lesions that cannot be corrected.SUMMARY �e management of pediatric hypertension begins bystaging the hypertension based on standard tables,evaluating the patient for the presence of symptoms ortarget organ damage, and determining if there is anunderlying medical condition that warrants more aggressivetreatment. Most patients are initially treated withnonpharmacologic intervention initially, although severe,symptomatic hypertension may warrant intravenousmedications in an intensive care unit. �ere are increasingdata on the safety and e�cacy of antihypertensivemedications in children, but few comparative or long-termdata are available to guide use of a speci�c agent.However, in some instances a speci�c agent is indicated.
3. Chobanian AV, Bakris GL, Black HR, et al. The SeventhReport of the Joint National Committee on Prevention,Detection, Evaluation, and Treatment of High BloodPressure. The JNC 7 report. JAMA 2003;289:2560–72.
4. National High Blood Pressure Education Program WorkingGroup on High Blood Pressure in Children and Adolescents.The fourth report on the diagnosis, evaluation, andtreatment of high blood pressure in children andadolescents. Pediatrics. 2004;114:555–576.
5. Expert Panel on Integrated Guidelines forCardiovascular Health and Risk Reduction in Children andAdolescents; National Heart, Lung, and Blood Institute.Expert panel on integrated guidelines for cardiovascularhealth and risk reduction in children and adolescents:Summary report. Pediatrics. 2011;128(Suppl 5):S213–56.
6. Lauer RM, Clarke WR. Childhood risk factors for highadult blood pressure: The Muscatine study. Pediatrics1989;84:633–641.
7. Luepker RV, Jacobs DR, Prineas RJ, Sinaiko AR. Secular
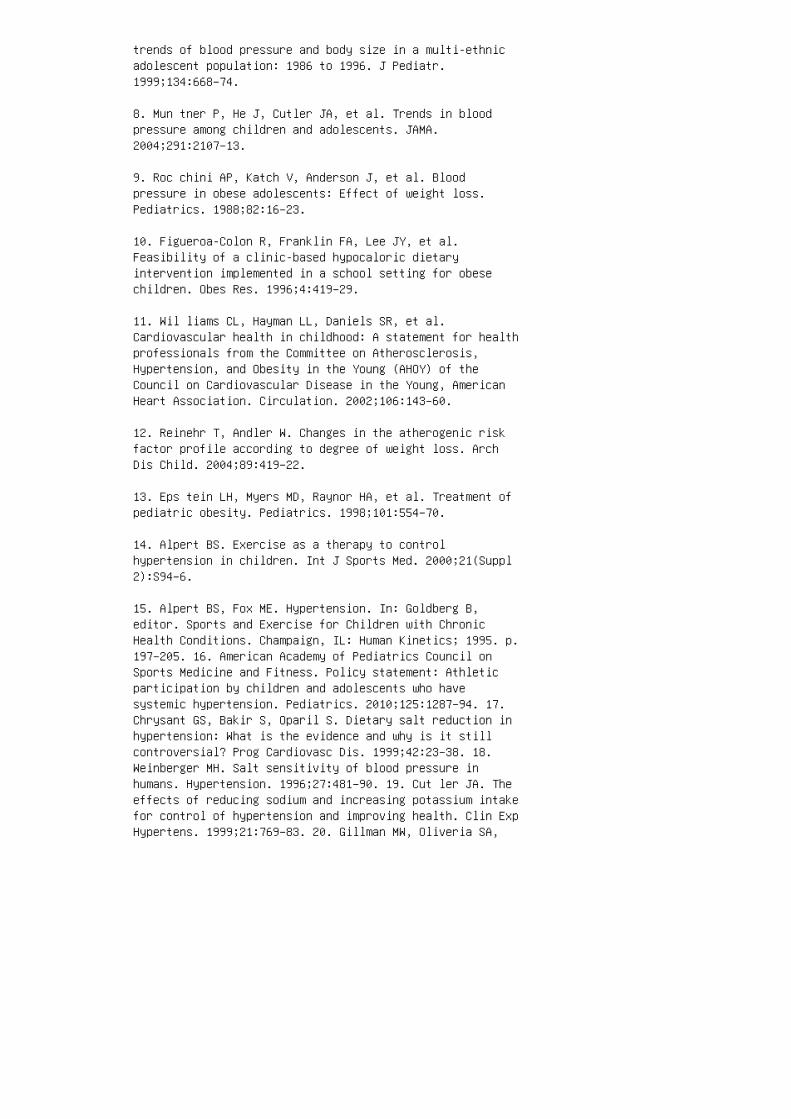
trends of blood pressure and body size in a multi-ethnicadolescent population: 1986 to 1996. J Pediatr.1999;134:668–74.
8. Mun tner P, He J, Cutler JA, et al. Trends in bloodpressure among children and adolescents. JAMA.2004;291:2107–13.
9. Roc chini AP, Katch V, Anderson J, et al. Bloodpressure in obese adolescents: Effect of weight loss.Pediatrics. 1988;82:16–23.
10. Figueroa-Colon R, Franklin FA, Lee JY, et al.Feasibility of a clinic-based hypocaloric dietaryintervention implemented in a school setting for obesechildren. Obes Res. 1996;4:419–29.
11. Wil liams CL, Hayman LL, Daniels SR, et al.Cardiovascular health in childhood: A statement for healthprofessionals from the Committee on Atherosclerosis,Hypertension, and Obesity in the Young (AHOY) of theCouncil on Cardiovascular Disease in the Young, AmericanHeart Association. Circulation. 2002;106:143–60.
12. Reinehr T, Andler W. Changes in the atherogenic riskfactor profile according to degree of weight loss. ArchDis Child. 2004;89:419–22.
13. Eps tein LH, Myers MD, Raynor HA, et al. Treatment ofpediatric obesity. Pediatrics. 1998;101:554–70.
14. Alpert BS. Exercise as a therapy to controlhypertension in children. Int J Sports Med. 2000;21(Suppl2):S94–6.
15. Alpert BS, Fox ME. Hypertension. In: Goldberg B,editor. Sports and Exercise for Children with ChronicHealth Conditions. Champaign, IL: Human Kinetics; 1995. p.197–205. 16. American Academy of Pediatrics Council onSports Medicine and Fitness. Policy statement: Athleticparticipation by children and adolescents who havesystemic hypertension. Pediatrics. 2010;125:1287–94. 17.Chrysant GS, Bakir S, Oparil S. Dietary salt reduction inhypertension: What is the evidence and why is it stillcontroversial? Prog Cardiovasc Dis. 1999;42:23–38. 18.Weinberger MH. Salt sensitivity of blood pressure inhumans. Hypertension. 1996;27:481–90. 19. Cut ler JA. Theeffects of reducing sodium and increasing potassium intakefor control of hypertension and improving health. Clin ExpHypertens. 1999;21:769–83. 20. Gillman MW, Oliveria SA,
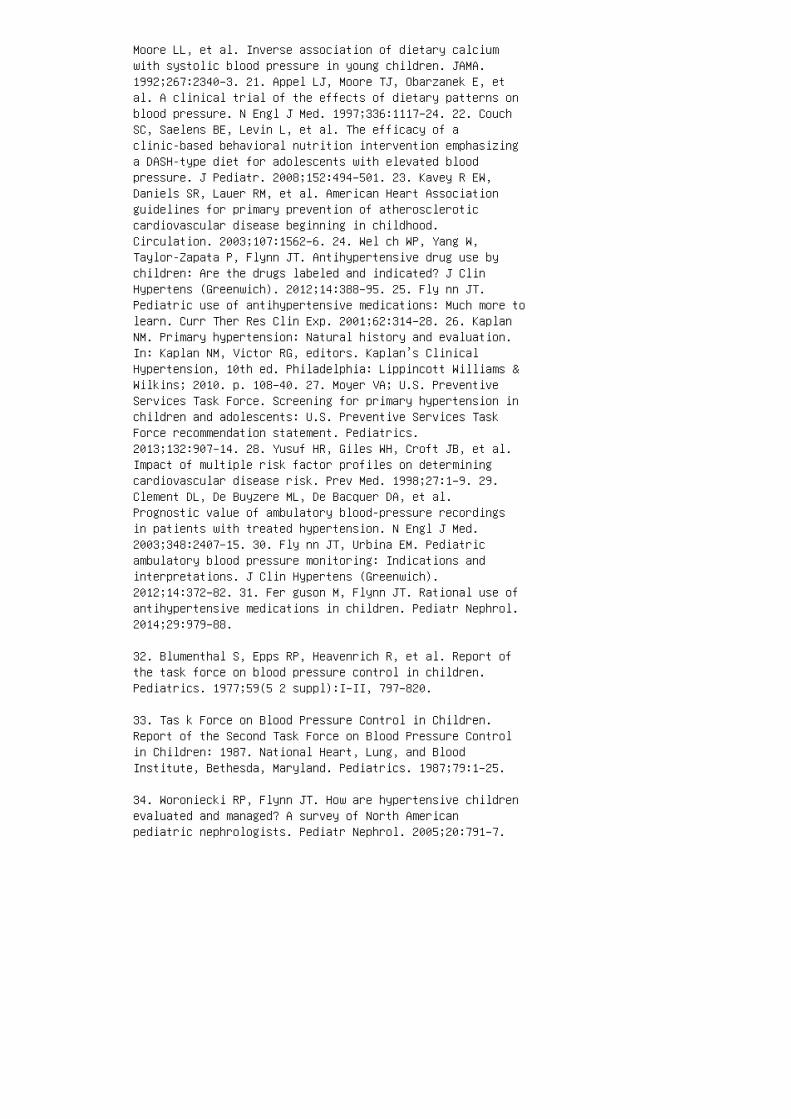
Moore LL, et al. Inverse association of dietary calciumwith systolic blood pressure in young children. JAMA.1992;267:2340–3. 21. Appel LJ, Moore TJ, Obarzanek E, etal. A clinical trial of the effects of dietary patterns onblood pressure. N Engl J Med. 1997;336:1117–24. 22. CouchSC, Saelens BE, Levin L, et al. The efficacy of aclinic-based behavioral nutrition intervention emphasizinga DASH-type diet for adolescents with elevated bloodpressure. J Pediatr. 2008;152:494–501. 23. Kavey R EW,Daniels SR, Lauer RM, et al. American Heart Associationguidelines for primary prevention of atheroscleroticcardiovascular disease beginning in childhood.Circulation. 2003;107:1562–6. 24. Wel ch WP, Yang W,Taylor-Zapata P, Flynn JT. Antihypertensive drug use bychildren: Are the drugs labeled and indicated? J ClinHypertens (Greenwich). 2012;14:388–95. 25. Fly nn JT.Pediatric use of antihypertensive medications: Much more tolearn. Curr Ther Res Clin Exp. 2001;62:314–28. 26. KaplanNM. Primary hypertension: Natural history and evaluation.In: Kaplan NM, Victor RG, editors. Kaplan’s ClinicalHypertension, 10th ed. Philadelphia: Lippincott Williams &Wilkins; 2010. p. 108–40. 27. Moyer VA; U.S. PreventiveServices Task Force. Screening for primary hypertension inchildren and adolescents: U.S. Preventive Services TaskForce recommendation statement. Pediatrics.2013;132:907–14. 28. Yusuf HR, Giles WH, Croft JB, et al.Impact of multiple risk factor profiles on determiningcardiovascular disease risk. Prev Med. 1998;27:1–9. 29.Clement DL, De Buyzere ML, De Bacquer DA, et al.Prognostic value of ambulatory blood-pressure recordingsin patients with treated hypertension. N Engl J Med.2003;348:2407–15. 30. Fly nn JT, Urbina EM. Pediatricambulatory blood pressure monitoring: Indications andinterpretations. J Clin Hypertens (Greenwich).2012;14:372–82. 31. Fer guson M, Flynn JT. Rational use ofantihypertensive medications in children. Pediatr Nephrol.2014;29:979–88.
32. Blumenthal S, Epps RP, Heavenrich R, et al. Report ofthe task force on blood pressure control in children.Pediatrics. 1977;59(5 2 suppl):I–II, 797–820.
33. Tas k Force on Blood Pressure Control in Children.Report of the Second Task Force on Blood Pressure Controlin Children: 1987. National Heart, Lung, and BloodInstitute, Bethesda, Maryland. Pediatrics. 1987;79:1–25.
34. Woroniecki RP, Flynn JT. How are hypertensive childrenevaluated and managed? A survey of North Americanpediatric nephrologists. Pediatr Nephrol. 2005;20:791–7.
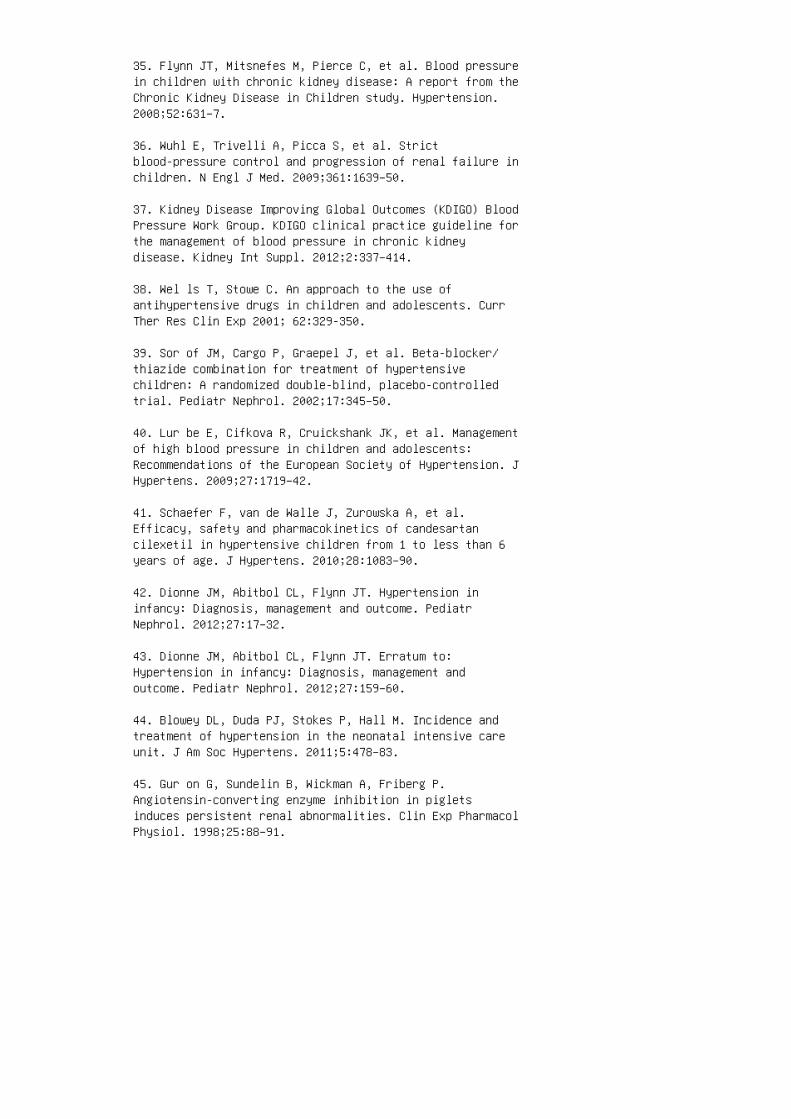
35. Flynn JT, Mitsnefes M, Pierce C, et al. Blood pressurein children with chronic kidney disease: A report from theChronic Kidney Disease in Children study. Hypertension.2008;52:631–7.
36. Wuhl E, Trivelli A, Picca S, et al. Strictblood-pressure control and progression of renal failure inchildren. N Engl J Med. 2009;361:1639–50.
37. Kidney Disease Improving Global Outcomes (KDIGO) BloodPressure Work Group. KDIGO clinical practice guideline forthe management of blood pressure in chronic kidneydisease. Kidney Int Suppl. 2012;2:337–414.
38. Wel ls T, Stowe C. An approach to the use ofantihypertensive drugs in children and adolescents. CurrTher Res Clin Exp 2001; 62:329-350.
39. Sor of JM, Cargo P, Graepel J, et al. Beta-blocker/thiazide combination for treatment of hypertensivechildren: A randomized double-blind, placebo-controlledtrial. Pediatr Nephrol. 2002;17:345–50.
40. Lur be E, Cifkova R, Cruickshank JK, et al. Managementof high blood pressure in children and adolescents:Recommendations of the European Society of Hypertension. JHypertens. 2009;27:1719–42.
41. Schaefer F, van de Walle J, Zurowska A, et al.Efficacy, safety and pharmacokinetics of candesartancilexetil in hypertensive children from 1 to less than 6years of age. J Hypertens. 2010;28:1083–90.
42. Dionne JM, Abitbol CL, Flynn JT. Hypertension ininfancy: Diagnosis, management and outcome. PediatrNephrol. 2012;27:17–32.
43. Dionne JM, Abitbol CL, Flynn JT. Erratum to:Hypertension in infancy: Diagnosis, management andoutcome. Pediatr Nephrol. 2012;27:159–60.
44. Blowey DL, Duda PJ, Stokes P, Hall M. Incidence andtreatment of hypertension in the neonatal intensive careunit. J Am Soc Hypertens. 2011;5:478–83.
45. Gur on G, Sundelin B, Wickman A, Friberg P.Angiotensin-converting enzyme inhibition in pigletsinduces persistent renal abnormalities. Clin Exp PharmacolPhysiol. 1998;25:88–91.
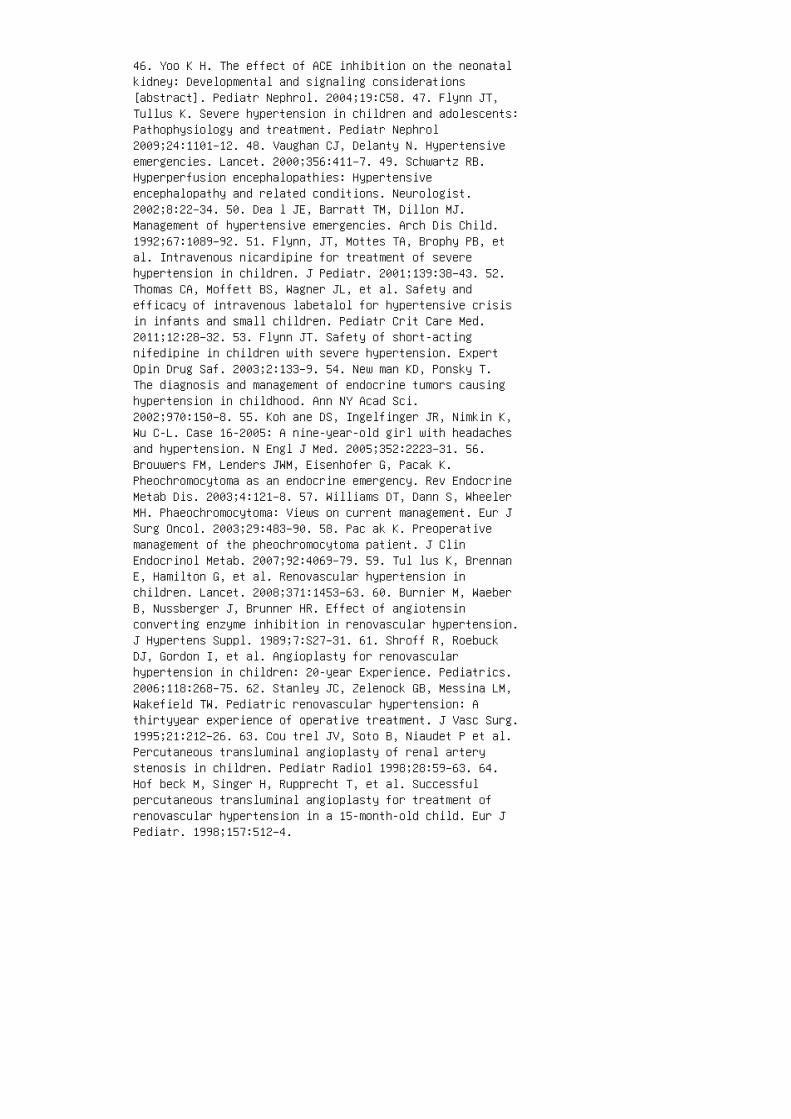
46. Yoo K H. The effect of ACE inhibition on the neonatalkidney: Developmental and signaling considerations[abstract]. Pediatr Nephrol. 2004;19:C58. 47. Flynn JT,Tullus K. Severe hypertension in children and adolescents:Pathophysiology and treatment. Pediatr Nephrol2009;24:1101–12. 48. Vaughan CJ, Delanty N. Hypertensiveemergencies. Lancet. 2000;356:411–7. 49. Schwartz RB.Hyperperfusion encephalopathies: Hypertensiveencephalopathy and related conditions. Neurologist.2002;8:22–34. 50. Dea l JE, Barratt TM, Dillon MJ.Management of hypertensive emergencies. Arch Dis Child.1992;67:1089–92. 51. Flynn, JT, Mottes TA, Brophy PB, etal. Intravenous nicardipine for treatment of severehypertension in children. J Pediatr. 2001;139:38–43. 52.Thomas CA, Moffett BS, Wagner JL, et al. Safety andefficacy of intravenous labetalol for hypertensive crisisin infants and small children. Pediatr Crit Care Med.2011;12:28–32. 53. Flynn JT. Safety of short-actingnifedipine in children with severe hypertension. ExpertOpin Drug Saf. 2003;2:133–9. 54. New man KD, Ponsky T.The diagnosis and management of endocrine tumors causinghypertension in childhood. Ann NY Acad Sci.2002;970:150–8. 55. Koh ane DS, Ingelfinger JR, Nimkin K,Wu C-L. Case 16-2005: A nine-year-old girl with headachesand hypertension. N Engl J Med. 2005;352:2223–31. 56.Brouwers FM, Lenders JWM, Eisenhofer G, Pacak K.Pheochromocytoma as an endocrine emergency. Rev EndocrineMetab Dis. 2003;4:121–8. 57. Williams DT, Dann S, WheelerMH. Phaeochromocytoma: Views on current management. Eur JSurg Oncol. 2003;29:483–90. 58. Pac ak K. Preoperativemanagement of the pheochromocytoma patient. J ClinEndocrinol Metab. 2007;92:4069–79. 59. Tul lus K, BrennanE, Hamilton G, et al. Renovascular hypertension inchildren. Lancet. 2008;371:1453–63. 60. Burnier M, WaeberB, Nussberger J, Brunner HR. Effect of angiotensinconverting enzyme inhibition in renovascular hypertension.J Hypertens Suppl. 1989;7:S27–31. 61. Shroff R, RoebuckDJ, Gordon I, et al. Angioplasty for renovascularhypertension in children: 20-year Experience. Pediatrics.2006;118:268–75. 62. Stanley JC, Zelenock GB, Messina LM,Wakefield TW. Pediatric renovascular hypertension: Athirtyyear experience of operative treatment. J Vasc Surg.1995;21:212–26. 63. Cou trel JV, Soto B, Niaudet P et al.Percutaneous transluminal angioplasty of renal arterystenosis in children. Pediatr Radiol 1998;28:59–63. 64.Hof beck M, Singer H, Rupprecht T, et al. Successfulpercutaneous transluminal angioplasty for treatment ofrenovascular hypertension in a 15-month-old child. Eur JPediatr. 1998;157:512–4.

REVIEW QUESTIONS
1. A 16-year-old obese boy with hypertension and type 2diabetes has been referred to you for evaluation. His o�ceblood pressure is 145/82 mm Hg. He has LVH on anechocardiogram and a mildly elevated urinarymicroalbumin-to-creatinine ratio. �e referring physicianprescribed hydrochlorothiazide 50 mg daily. Yourrecommendation should be:
a. Order ambulatory blood pressure monitoring to assesshis blood pressure control.
b. Add metoprolol 100 mg daily to further reduce his bloodpressure.
c. Start regular aerobic exercise and a low-sodium diet.
d. Stop the hydrochlorothiazide and start lisinopril 10 mgdaily.
2. An 8-year-old girl has been found to have con�rmed o�cehypertension. Her weight and BMI are both at the 97thpercentile for age, and her height is at the 40thpercentile. Which of the following changes should be madeto her daily routine?
a. Restriction of caloric intake to 1500 calories/day
b. Supplementation with potassium chloride
c. 30 minutes of brisk walking around the block with hermother a�er school
d. Scheduling for an assessment of obesity in a pediatricendocrinology clinic
3. A 12 year-old girl treated with quinapril for primaryhypertension needs the following issues addressed at herquarterly follow-up appointments:
a. Use of contraception
b. CBC monitoring
c. Edema assessment
d. a and b

e. a, b, and c
4. When deciding whether to start an antihypertensivemedication, the following is the most importantconsideration:
a. �e age of the child
b. �e presence of obesity
c. �e presence of le� ventricular hypertrophy
d. �e success of lifestyle modi�cation
5. A 12-year-old girl with pheochromocytoma has beenreferred to you by the oncology service for assistancewith blood pressure management until surgery, which isscheduled to take place in 2.5 weeks. Which of thefollowing strategies should be employed to control her BP?
a. Sodium restriction and bedrest
b. Start treatment with oral labetalol
c. Start treatment with oral propranolol
d. Sodium restriction and start phenoxybenzamine
e. Start treatment with doxazosin 6. An 8-year-old boypresents to the emergency department a�er having twotonic-clonic seizures. Blood pressures obtained byambulance personnel were 150 to 168/95 to 118 mm Hg.Ativan has been given and seizures have stopped. Which ofthe following measures would not be appropriate? a.Reduction of blood pressure with sublingual nifedipine to110/70 mm Hg b. Insertion of an arterial monitoring linec. Obtain a comprehensive medical history d. Ordernicardipine from the pharmacy 7. A 12-year-old boy isreferred from the urology department with new-onset bloodpressure elevation in the setting of known re�uxnephropathy. In the clinic, his blood pressuremeasurements ful�ll criteria for stage 2 hypertension.Initial evaluations are notable for an estimated GFR of 65mL/min/1.73 m 2 and 3+ proteinuria by dipstick. Which ofthe following drug classes would be considered mostappropriate in this setting? a. Nondihydropyridinecalcium channel blockers b. Loop diuretics c. Angiotensinreceptor antagonists d. Direct-acting vasodilators e.β-Adrenergic blockers 8. Which of the following medicationclasses should be avoided as primary therapy in the
hypertensive female athlete? a. Angiotensin-convertingenzyme inhibitors b. Diuretics c. β-blockers d. Calciumchannel blockers e. a and b 9. Recommendations forstaging hypertension in children and adolescents provideguidance for clinicians in evaluating and managingpatients with elevated blood pressure. �e new stagingsystem recommends immediate institution ofantihypertensive medications for patients with bloodpressure in which of the following stages? a. Stage 2hypertension b. Normal blood pressure c. Stage 1hypertension d. Pre-hypertension e. a and c 10. Youreceive a phone call from a neonatologist in a neighboringcommunity. She has been caring for a now 6-week-old,former 28 weeks of gestation premature infant. She isconcerned about some high blood pressure readings andwants your recommendations regarding treatment. Whatadditional information do you need to make the bestrecommendation? a. �e infant’s current weight and lengthb. �e infant’s medication list c. Details about how theinfant’s blood pressure is being measured
d. a and b
d. b and c
11. An otherwise healthy 16-year-old boy presents witho�ce blood pressure readings of 160/100 mm Hg in bothupper extremities. He is not obese, but there is a strongfamily history of cardiovascular disease. He initiallydenies any symptoms, but at the end of the visit, hismother tells you that he occasionally complains of his legsaching during soccer, and that he sometimes has abdominalpain a�er eating. What medication should you prescribewhile you are waiting for test results to come back?
a. Lisinopril
b. Felodipine
c. Valsartan
d. Metoprolol ANSWERS 1. d 2. c 3. d 4. c 5. e 6. a7. c 8. e 9. a 10. e 11. b
41 Tubulopathies
11. Schneider JA, Bradley K, Seegmiller JE. Increasedcystine in leukocytes from individuals homozygous andheterozygous for cystinosis. Science. 1967;157:1321–2.
12. Wilmer MJ, Emma F, Levtchenko EN. The pathogenesis ofcystinosis: Mechanisms beyond cystine accumulation. Am JPhysiol Renal Physiol. 2010;299:F905–16.
13. Norden AG, Scheinman SJ, Deschodt-Lanckman MM, et al.Tubular proteinuria defined by a study of Dent’s (CLCN5mutation) and other tubular diseases. Kidney Int.2000;57:240–9.
14. Bockenhauer D, van’t Hoff W, Dattani M, et al.Secondary nephrogenic diabetes insipidus as a complicationof inherited renal diseases. Nephron Physiol.2010;116:p23–9.
15. Gahl WA, Kuehl EM, Iwata F, et al. Corneal crystals innephropathic cystinosis: Natural history and treatment withcysteamine eyedrops. Mol Genet Metab. 2000;71:100–20.
16. Ani kster Y, Shotelersuk V, Gahl WA. CTNS mutations inpatients with cystinosis. Hum Mutat. 1999;14:454–8.
17. Tho ene JG, Oshima RG, Crawhall JC, et al. Cystinosis:Intracellular cystine depletion by aminothiols in vitro andin vivo. J Clin Invest. 1976;58:180–9.
18. Nesterova G, Gahl WA. Cystinosis: The evolution of atreatable disease. Pediatr Nephrol. 2013;28:51–9.
19. Bes ouw MT, Bowker R, Dutertre JP, et al. Cysteaminetoxicity in patients with cystinosis. J Pediatr.2011;159:1004–11.
20. Loi M . Lowe syndrome. Orphanet J Rare Dis. 2006;1:16.
21. Lowe CU, Terrey M, Mac LE. Organic-aciduria, decreasedrenal ammonia production, hydrophthalmos, and mentalretardation: A clinical entity. AMA Am J Dis Child.1952;83:164–84.
22. Attree O, Olivos IM, Okabe I, et al. The Lowe’soculocerebrorenal syndrome gene encodes a protein highlyhomologous to inositol polyphosphate5-phosphatase. Nature.1992;358:239–42.
23. Zhang X, Jefferson AB, Auethavekiat V, Majerus PW. Theprotein deficient in Lowe syndrome is aphosphatidylinositol-4,5-bisphosphate 5-phosphatase. ProcNatl Acad Sci U S A. 1995;92:4853–6.
24. Toker A. The synthesis and cellular roles ofphosphatidylinositol 4,5-bisphosphate. Curr Opin Cell Biol.1998;10:254–61.
25. Pirruccello M, De Camilli P. Inositol 5-phosphatases:Insights from the Lowe syndrome protein OCRL. TrendsBiochem Sci. 2012;37:134–43.
26. Erd mann KS, Mao Y, McCrea HJ, et al. A role of theLowe syndrome protein OCRL in early steps of the endocyticpathway. Dev. Cell. 2007;13:377–90.
27. Mao Y , Balkin DM, Zoncu R, et al. A PH domain withinOCRL bridges clathrin-mediated membrane trafficking tophosphoinositide metabolism. EMBO J. 2009;28:1831–42. 28.Swan LE, Tomasini L, Pirruccello M, et al. Two closelyrelated endocytic proteins that share a commonOCRL-binding motif with APPL1. Proc Natl Acad Sci U S A.2010;107:3511–6. 29. Noa kes CJ, Lee G, Lowe M. The PHdomain proteins IPIP27A and B link OCRL1 to receptorrecycling in the endocytic pathway. Mol Biol Cell.2011;22:606–23. 30. Pasternack SM, Bockenhauer D, Refke M,et al. A premature termination mutation in a patient withLowe syndrome without congenital cataracts: Dropping the“O” in OCRL. Klin Padiatr. 2013;225:29–33. 31. Hichri H,Rendu J, Monnier N, et al. From Lowe syndrome to Dentdisease: Correlations between mutations of the OCRL1 geneand clinical and biochemical phenotypes. Hum Mutat.2011;32:379–88. 32. Kle ta R. Fanconi or not Fanconi? Lowesyndrome revisited. Clin J Am Soc Nephrol. 2008;3:1244–5.33. Bockenhauer D, Bokenkamp A, van’t Hoff W, et al. Renalphenotype in Lowe syndrome: A selective proximal tubulardysfunction. Clin J Am Soc Nephrol. 2008;3:1430–6. 34.Recker F, Reutter H, Ludwig M. Lowe syndrome/ Dent-2disease: A comprehensive review of known and novelaspects. J Pediatr Genet. 2013; 2 (2):53-68. DOI:10.3233/PGE-13049. 35. Las ne D, Baujat G, Mirault T, etal. Bleeding disorders in Lowe syndrome patients: Evidencefor a link between OCRL mutations and primary haemostasisdisorders. Br J Haematol. 2010;150:685–8. 36. Nyk jaer A,Dragun D, Walther D, et al. An endocytic pathway essentialfor renal uptake and activation of the steroid 25-(OH)vitamin D 3 . Cell. 1999;96:507–15. 37. Arr on K, OliverC, Moss J, et al. The prevalence and phenomenology ofself-injurious and aggressive behaviour in genetic

syndromes. J Intellect Disabil Res. 2011;55:109–20. 38.Gob ernado JM, Lousa M, Gimeno A, Gonsalvez M.Mitochondrial defects in Lowe’s oculocerebrorenalsyndrome. Arch Neurol. 1984;41:208–9. 39. Madhivanan K,Mukherjee D, Aguilar RC. Lowe syndrome: Between primarycilia assembly and Rac1mediated membrane remodeling. CommunIntegr Biol. 2012;5:641–4. 40. Gah l WA, Bernardini I,Dalakas M, et al. Oral carnitine therapy in children withcystinosis and renal Fanconi syndrome. J Clin Invest.1988;81:549–60. 41. Wrong OM, Norden AG, Feest TG. Dent’sdisease; a familial proximal renal tubular syndrome withlowmolecular-weight proteinuria, hypercalciuria,nephrocalcinosis, metabolic bone disease, progressiverenal failure and a marked male predominance. QJM.1994;87:473–93.
42. Lloyd SE, Pearce SH, Fisher SE, et al. A commonmolecular basis for three inherited kidney stone diseases.Nature. 1996;379:445–9.
43. Piw on N, Gunther W, Schwake M, thet al. ClC-5 Cl −-channel disruption impairs endocytosis in a mouse modelfor Dent’s disease. Nature. 2000;408:369–73.
44. Iga rashi T, Hayakawa H, Shiraga H, et al.Hypercalciuria and nephrocalcinosis in patients withidiopathic low-molecular-weight proteinuria in Japan: Isthe disease identical to Dent’s disease in United Kingdom?Nephron. 1995;69:242–7.
45. Reinhart SC, Norden AG, Lapsley M, et al.Characterization of carrier females and affected maleswith X-linked recessive nephrolithiasis. J Am Soc Nephrol.1995;5:1451–61.
46. Nijenhuis T, Vallon V, van der Kemp AW, et al.Enhanced passive Ca 2+ reabsorption and reduced Mg 2+channel abundance explains thiazide-induced hypocalciuriaand hypomagnesemia. J Clin Invest. 2005;115:1651–8.
47. Raja KA, Schurman S, D’Mello RG, et al. Responsivenessof hypercalciuria to thiazide in Dent’s disease. J Am SocNephrol. 2002;13:2938–44.
48. Ludwig M, Utsch B, Balluch B, et al. Hypercalciuria inpatients with CLCN5 mutations. Pediatr Nephrol.2006;21:1241–50.
49. Hoopes RR, Jr, Shrimpton AE, Knohl SJ, et al. Dentdisease with mutations in OCRL1. Am J Hum Genet.
2005;76:260–7.
50. Dent CE, Friedman M. Hypercalcuric rickets associatedwith renal tubular damage. Arch Dis Child. 1964;39:240–9.
51. Shr impton AE, Hoopes RR, Jr, Knohl SJ, et al. OCRL1mutations in Dent 2 patients suggest a mechanism forphenotypic variability. Nephron Physiol. 2009;112:27–36.
52. Bokenkamp A, Bockenhauer D, Cheong HI, et al. Dent-2disease: A mild variant of Lowe syndrome. J Pediatr.2009;155:94–9.
53. Curhan GC, Willett WC, Rimm EB, Stampfer MJ. Aprospective study of dietary calcium and other nutrientsand the risk of symptomatic kidney stones. N Engl J Med.1993;328:833–8.
54. Lemann J, Jr, Pleuss JA, Worcester EM, et al. Urinaryoxalate excretion increases with body size and decreaseswith increasing dietary calcium intake among healthyadults. Kidney Int. 1996;49:200–8.
55. Col ussi G, De Ferrari ME, Brunati C, Civati G.Medical prevention and treatment of urinary stones. JNephrol. 2000;13 Suppl 3:S65–70.
56. Scheinman SJ. X-linked hypercalciuric nephrolithiasis:Clinical syndromes and chloride channel mutations. KidneyInt. 1998;53:3–17.
57. Gill JR, Jr. The role of chloride transport in thethick ascending limb in the pathogenesis of Bartter’ssyndrome. Klin Wochenschr. 1982;60:1212–4. 58. Rudin A.Bartter’s syndrome: A review of 28 patients followed for10 years. Acta Med Scand. 1988;224:165–71. 59. Ji W, FooJN, O’Roak BJ, et al. Rare independent mutations in renalsalt handling genes contribute to blood pressure variation.Nat Genet. 2008;40:592–9. 60. Simon DB, Karet FE, HamdanJM, et al. Bartter’s syndrome, hypokalaemic alkalosis withhypercalciuria, is caused by mutations in the Na-K-2Clcotransporter NKCC2. Nat Genet. 1996;13:183–8. 61. SimonDB, Karet FE, Rodriguez-Soriano J, et al. Geneticheterogeneity of Bartter’s syndrome revealed by mutationsin the K + channel, ROMK. Nat Genet. 1996;14:152–6. 62.Sim on DB, Bindra RS, Mansfield TA, et al. Mutations inthe chloride channel gene, CLCNKB, cause Bartter’ssyndrome type III. Nat Genet. 1997;17:171–8. 63. EstevezR, Boettger T, Stein V, et al. Barttin is a Cl − channelbeta-subunit crucial for renal Cl − reabsorption and inner
ear K + secretion. Nature. 2001;414:558–61. 64. Brochard K, Boyer O, Blanchard A, et al. Phenotypegenotypecorrelation in antenatal and neonatal variants of Barttersyndrome. Nephrol Dial Transplant. 2009;24:1455–64. 65.Jec k N, Konrad M, Peters M, et al. Mutations in thechloride channel gene, CLCNKB, leading to a mixedBartter-Gitelman phenotype. Pediatr Res. 2000;48:754–8.66. Konrad M, Vollmer M, Lemmink HH, et al. Mutations inthe chloride channel gene CLCNKB as a cause of classicBartter syndrome. J Am Soc Nephrol. 2000;11:1449–59. 67.Peters M, Jeck N, Reinalter S, et al. Clinical presentationof genetically defined patients with hypokalemicsalt-losing tubulopathies. Am J Med. 2002;112:183–90. 68.Pressler CA, Heinzinger J, Jeck N, et al. Late-onsetmanifestation of antenatal Bartter syndrome as a result ofresidual function of the mutated renal Na + -K + -2Cl −co-transporter. J Am Soc Nephrol. 2006;17:2136–42. 69.Noz u K, Fu XJ, Kaito H, et al. A novel mutation in KCNJ1in a Bartter syndrome case diagnosed aspseudohypoaldosteronism. Pediatr Nephrol. 2007;22:1219–23.70. Boc kenhauer D, Cruwys M, Kleta R, et al. AntenatalBartter’s syndrome: Why is this not a lethal condition?QJM. 2008;101:927–42. 71. Bockenhauer D, Bichet DG.Inherited secondary nephrogenic diabetes insipidus:Concentrating on humans. Am J Physiol Renal Physiol.2013;304:F1037–42. 72. Bet tinelli A, Ciarmatori S,Cesareo L, et al. Phenotypic variability in Barttersyndrome type I. Pediatr Nephrol. 2000;14:940–5.
73. Bartter FC, Pronove P, Gill JR, Jr, Maccardle RC.Hyperplasia of the juxtaglomerular complex withhyperaldosteronism and hypokalemic alkalosis: A newsyndrome. Am J Med. 1962;33:811–28.
74. Brum S, Rueff J, Santos JR, Calado J. Unusualadultonset manifestation of an attenuated Bartter’ssyndrome type IV renal phenotype caused by a mutation inBSND. Nephrol Dial Transplant. 2007;22:288–9.
75. Schlingmann KP, Konrad M, Jeck N, et al. Salt wastingand deafness resulting from mutations in two chloridechannels. N Engl J Med. 2004;350:1314–9.
76. Watanabe S, Fukumoto S, Chang H, et al. Associationbetween activating mutations of calcium-sensing receptorand Bartter’s syndrome. Lancet. 2002;360:692–4.
77. Heb ert SC. Bartter syndrome. Curr Opin NephrolHypertens. 2003;12:527–32.

78. Goto Y, Itami N, Kajii N, et al. Renal tubularinvolvement mimicking Bartter syndrome in a patient withKearns-Sayre syndrome. J Pediatr. 1990;116:904–10.
79. Nia udet P, Rotig A. Renal involvement in mitochondrialcytopathies. Pediatr Nephrol. 1996;10:368–73.
80. Emm a F, Pizzini C, Tessa A, et al. “Bartter-like”phenotype in Kearns-Sayre syndrome. Pediatr Nephrol.2006;21:355–60.
81. Koshida R, Sakazume S, Maruyama H, et al. A case ofpseudo-Bartter’s syndrome due to intestinal malrotation.Acta Paediatrica Jpn. 1994;36:107–11.
82. Mat hot M, Maton P, Henrion E, et al. Pseudo-Barttersyndrome in a pregnant mother and her fetus. PediatrNephrol. 2006;21:1037–40.
83. Vanhaesebrouck S, Van Laere D, Fryns JP, Theyskens C.Pseudo-Bartter syndrome due to Hirschsprung disease in aneonate with an extra ring chromosome 8. Am J Med Genet A.2007;143A:2469–72.
84. Horvatovich K, Orkenyi M, Biro E, et al. PseudoBarttersyndrome in a case of cystic fibrosis caused by C1529G andG3978A compound heterozygosity. Orv Hetil. 2008;149:325–8[in Hungarian].
85. Choi M, Scholl UI, Ji W, et al. Genetic diagnosis bywhole exome capture and massively parallel DNA sequencing.Proc Natl Acad Sci U S A. 2009;106:19096–101.
86. Kleta R, Bockenhauer D. Bartter syndromes and othersalt-losing tubulopathies. Nephron Physiol.2006;104:73–80.
87. Seyberth HW. An improved terminology and classificationof Bartter-like syndromes. Nat Clin Pract Nephrol.2008;4:560–7.
88. Kle ta R, Basoglu C, Kuwertz-Broking E. New treatmentoptions for Bartter’s syndrome. N Engl J Med.2000;343:661–2.
89. Rei nalter SC, Jeck N, Brochhausen C, et al. Role ofcyclooxygenase-2 in hyperprostaglandin E syndrome/antenatalBartter syndrome. Kidney Int. 2002;62:253–60. 90. DogneJM, Hanson J, Supuran C, Pratico D. Coxibs andcardiovascular side-effects: From light to shadow. Curr
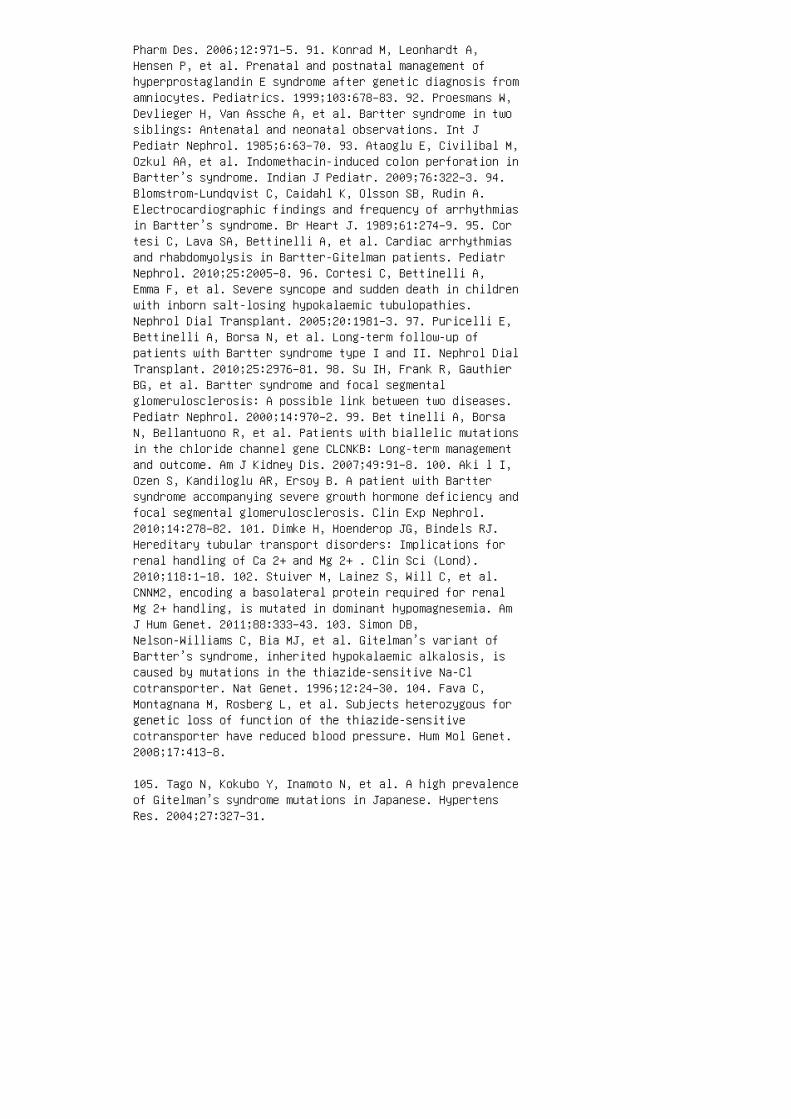
Pharm Des. 2006;12:971–5. 91. Konrad M, Leonhardt A,Hensen P, et al. Prenatal and postnatal management ofhyperprostaglandin E syndrome after genetic diagnosis fromamniocytes. Pediatrics. 1999;103:678–83. 92. Proesmans W,Devlieger H, Van Assche A, et al. Bartter syndrome in twosiblings: Antenatal and neonatal observations. Int JPediatr Nephrol. 1985;6:63–70. 93. Ataoglu E, Civilibal M,Ozkul AA, et al. Indomethacin-induced colon perforation inBartter’s syndrome. Indian J Pediatr. 2009;76:322–3. 94.Blomstrom-Lundqvist C, Caidahl K, Olsson SB, Rudin A.Electrocardiographic findings and frequency of arrhythmiasin Bartter’s syndrome. Br Heart J. 1989;61:274–9. 95. Cortesi C, Lava SA, Bettinelli A, et al. Cardiac arrhythmiasand rhabdomyolysis in Bartter-Gitelman patients. PediatrNephrol. 2010;25:2005–8. 96. Cortesi C, Bettinelli A,Emma F, et al. Severe syncope and sudden death in childrenwith inborn salt-losing hypokalaemic tubulopathies.Nephrol Dial Transplant. 2005;20:1981–3. 97. Puricelli E,Bettinelli A, Borsa N, et al. Long-term follow-up ofpatients with Bartter syndrome type I and II. Nephrol DialTransplant. 2010;25:2976–81. 98. Su IH, Frank R, GauthierBG, et al. Bartter syndrome and focal segmentalglomerulosclerosis: A possible link between two diseases.Pediatr Nephrol. 2000;14:970–2. 99. Bet tinelli A, BorsaN, Bellantuono R, et al. Patients with biallelic mutationsin the chloride channel gene CLCNKB: Long-term managementand outcome. Am J Kidney Dis. 2007;49:91–8. 100. Aki l I,Ozen S, Kandiloglu AR, Ersoy B. A patient with Barttersyndrome accompanying severe growth hormone deficiency andfocal segmental glomerulosclerosis. Clin Exp Nephrol.2010;14:278–82. 101. Dimke H, Hoenderop JG, Bindels RJ.Hereditary tubular transport disorders: Implications forrenal handling of Ca 2+ and Mg 2+ . Clin Sci (Lond).2010;118:1–18. 102. Stuiver M, Lainez S, Will C, et al.CNNM2, encoding a basolateral protein required for renalMg 2+ handling, is mutated in dominant hypomagnesemia. AmJ Hum Genet. 2011;88:333–43. 103. Simon DB,Nelson-Williams C, Bia MJ, et al. Gitelman’s variant ofBartter’s syndrome, inherited hypokalaemic alkalosis, iscaused by mutations in the thiazide-sensitive Na-Clcotransporter. Nat Genet. 1996;12:24–30. 104. Fava C,Montagnana M, Rosberg L, et al. Subjects heterozygous forgenetic loss of function of the thiazide-sensitivecotransporter have reduced blood pressure. Hum Mol Genet.2008;17:413–8.
105. Tago N, Kokubo Y, Inamoto N, et al. A high prevalenceof Gitelman’s syndrome mutations in Japanese. HypertensRes. 2004;27:327–31.
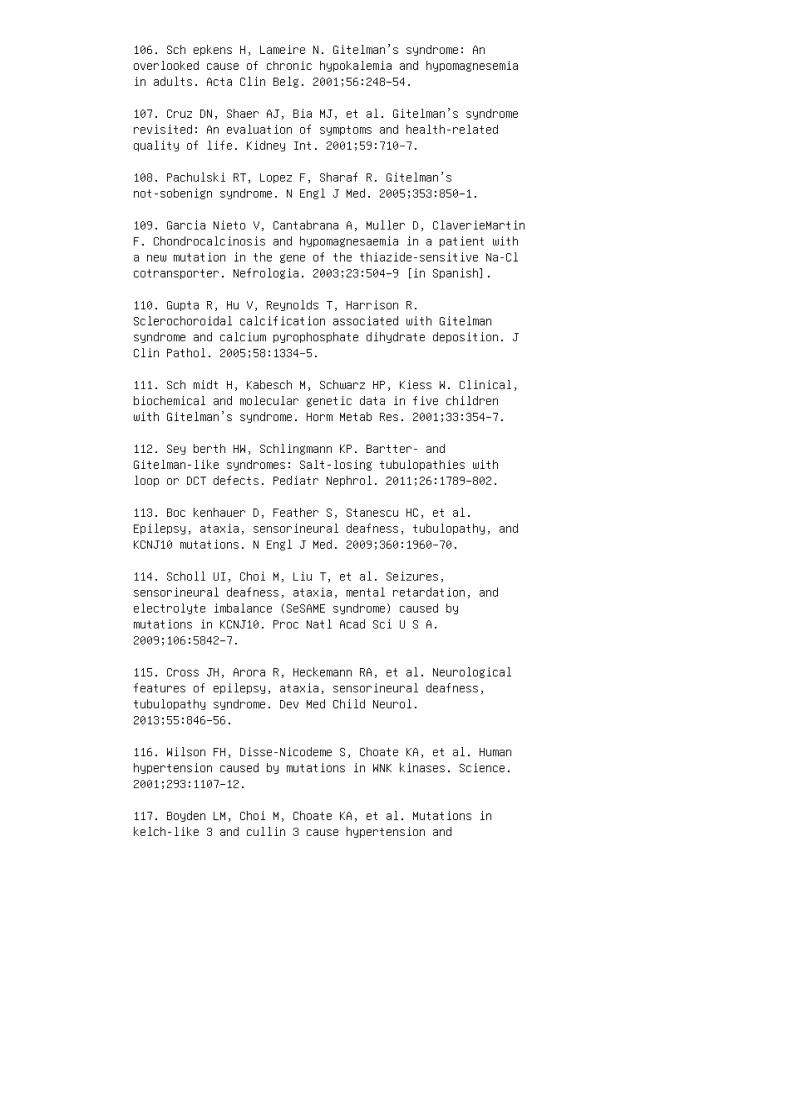
106. Sch epkens H, Lameire N. Gitelman’s syndrome: Anoverlooked cause of chronic hypokalemia and hypomagnesemiain adults. Acta Clin Belg. 2001;56:248–54.
107. Cruz DN, Shaer AJ, Bia MJ, et al. Gitelman’s syndromerevisited: An evaluation of symptoms and health-relatedquality of life. Kidney Int. 2001;59:710–7.
108. Pachulski RT, Lopez F, Sharaf R. Gitelman’snot-sobenign syndrome. N Engl J Med. 2005;353:850–1.
109. Garcia Nieto V, Cantabrana A, Muller D, ClaverieMartinF. Chondrocalcinosis and hypomagnesaemia in a patient witha new mutation in the gene of the thiazide-sensitive Na-Clcotransporter. Nefrologia. 2003;23:504–9 [in Spanish].
110. Gupta R, Hu V, Reynolds T, Harrison R.Sclerochoroidal calcification associated with Gitelmansyndrome and calcium pyrophosphate dihydrate deposition. JClin Pathol. 2005;58:1334–5.
111. Sch midt H, Kabesch M, Schwarz HP, Kiess W. Clinical,biochemical and molecular genetic data in five childrenwith Gitelman’s syndrome. Horm Metab Res. 2001;33:354–7.
112. Sey berth HW, Schlingmann KP. Bartter- andGitelman-like syndromes: Salt-losing tubulopathies withloop or DCT defects. Pediatr Nephrol. 2011;26:1789–802.
113. Boc kenhauer D, Feather S, Stanescu HC, et al.Epilepsy, ataxia, sensorineural deafness, tubulopathy, andKCNJ10 mutations. N Engl J Med. 2009;360:1960–70.
114. Scholl UI, Choi M, Liu T, et al. Seizures,sensorineural deafness, ataxia, mental retardation, andelectrolyte imbalance (SeSAME syndrome) caused bymutations in KCNJ10. Proc Natl Acad Sci U S A.2009;106:5842–7.
115. Cross JH, Arora R, Heckemann RA, et al. Neurologicalfeatures of epilepsy, ataxia, sensorineural deafness,tubulopathy syndrome. Dev Med Child Neurol.2013;55:846–56.
116. Wilson FH, Disse-Nicodeme S, Choate KA, et al. Humanhypertension caused by mutations in WNK kinases. Science.2001;293:1107–12.
117. Boyden LM, Choi M, Choate KA, et al. Mutations inkelch-like 3 and cullin 3 cause hypertension and

electrolyte abnormalities. Nature. 2012;482:98–102.
118. Ros er M, Eibl N, Eisenhaber B, et al. Gitelmansyndrome. Hypertension. 2009;53:893–7.
119. Chang SS, Grunder S, Hanukoglu A, et al. Mutations insubunits of the epithelial sodium channel cause saltwasting with hyperkalaemic acidosis,pseudohypoaldosteronism type 1. Nat Genet. 1996;12:248–53.120. Geller DS, Rodriguez-Soriano J, Vallo Boado A, et al.Mutations in the mineralocorticoid receptor gene causeautosomal dominant pseudohypoaldosteronism type I. NatGenet. 1998;19:279–81. 121. Riepe FG. Clinical andmolecular features of type 1 pseudohypoaldosteronism. HormRes. 2009;72:1–9. 122. Narchi H, Santos M, Kulaylat N.Polyhydramnios as a sign of fetal pseudohypoaldosteronism.Int J Gynaecol Obstet. 2000;69:53–4. 123. Won g GP,Levine D. Congenital pseudohypoaldosteronism presenting inutero with acute polyhydramnios. J Matern Fetal Med.1998;7:76–8. 124. Kerem E, Bistritzer T, Hanukoglu A, etal. Pulmonary epithelial sodium-channel dysfunction andexcess airway liquid in pseudohypoaldosteronism. N Engl JMed. 1999;341:156–62. 125. Martin JM, Calduch L,Monteagudo C, et al. Clinicopathological analysis of thecutaneous lesions of a patient with type Ipseudohypoaldosteronism. J Eur Acad Dermatol Venereol.2005;19:377–9. 126. Gur an T, Degirmenci S, Bulut IK, etal. Critical points in the management ofpseudohypoaldosteronism type 1. J Clin Res PediatrEndocrinol. 2011;3:98–100. 127. Gel ler DS, Farhi A,Pinkerton N, et al. Activating mineralocorticoid receptormutation in hypertension exacerbated by pregnancy. Science.2000;289:119–23. 128. Han sson JH, Schild L, Lu Y, et al.A de novo missense mutation of the beta subunit of theepithelial sodium channel causes hypertension and Liddlesyndrome, identifying a proline-rich segment critical forregulation of channel activity. Proc Natl Acad Sci U S A.1995;92:11495–9. 129. Lifton RP, Dluhy RG, Powers M, etal. Hereditary hypertension caused by chimaeric geneduplications and ectopic expression of aldosteronesynthase. Nat Genet. 1992;2:66–74. 130. Stewart PM,Krozowski ZS, Gupta A, et al. Hypertension in the syndromeof apparent mineralocorticoid excess due to mutation of the11 betahydroxysteroid dehydrogenase type 2 gene. Lancet.1996;347:88–91. 131. Pal ermo M, Quinkler M, Stewart PM.Apparent mineralocorticoid excess syndrome: An overview.Arq Bras Endocrinol Metabol. 2004;48:687–96. 132. LiftonRP. Genetic dissection of human blood pressure variation:Common pathways from rare phenotypes. Harvey Lect.2004;100:71–101. REVIEW QUESTIONS 1. Hyperkalemia can be
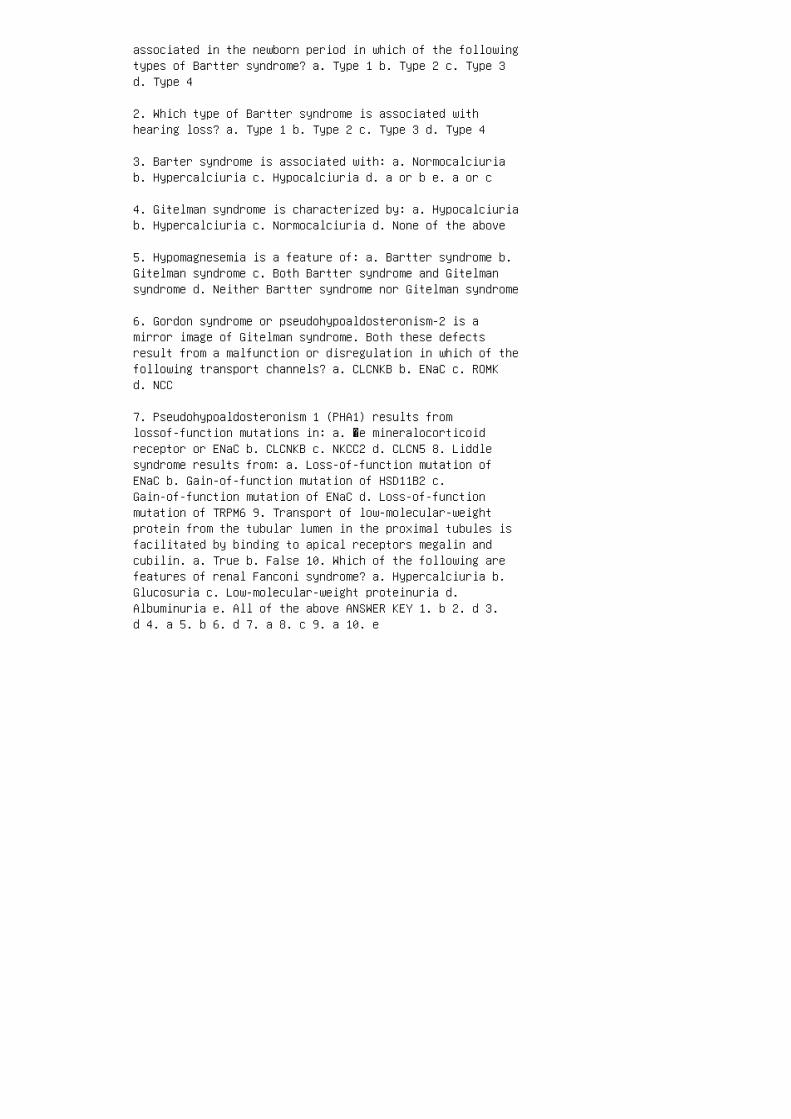
associated in the newborn period in which of the followingtypes of Bartter syndrome? a. Type 1 b. Type 2 c. Type 3d. Type 4
2. Which type of Bartter syndrome is associated withhearing loss? a. Type 1 b. Type 2 c. Type 3 d. Type 4
3. Barter syndrome is associated with: a. Normocalciuriab. Hypercalciuria c. Hypocalciuria d. a or b e. a or c
4. Gitelman syndrome is characterized by: a. Hypocalciuriab. Hypercalciuria c. Normocalciuria d. None of the above
5. Hypomagnesemia is a feature of: a. Bartter syndrome b.Gitelman syndrome c. Both Bartter syndrome and Gitelmansyndrome d. Neither Bartter syndrome nor Gitelman syndrome
6. Gordon syndrome or pseudohypoaldosteronism-2 is amirror image of Gitelman syndrome. Both these defectsresult from a malfunction or disregulation in which of thefollowing transport channels? a. CLCNKB b. ENaC c. ROMKd. NCC
7. Pseudohypoaldosteronism 1 (PHA1) results fromlossof-function mutations in: a. �e mineralocorticoidreceptor or ENaC b. CLCNKB c. NKCC2 d. CLCN5 8. Liddlesyndrome results from: a. Loss-of-function mutation ofENaC b. Gain-of-function mutation of HSD11B2 c.Gain-of-function mutation of ENaC d. Loss-of-functionmutation of TRPM6 9. Transport of low-molecular-weightprotein from the tubular lumen in the proximal tubules isfacilitated by binding to apical receptors megalin andcubilin. a. True b. False 10. Which of the following arefeatures of renal Fanconi syndrome? a. Hypercalciuria b.Glucosuria c. Low-molecular-weight proteinuria d.Albuminuria e. All of the above ANSWER KEY 1. b 2. d 3.d 4. a 5. b 6. d 7. a 8. c 9. a 10. e
42 Renal tubular acidosis
4. Dubose TD, Jr. Reclamation of filtered bicarbonate.Kidney Int. 1990;38:584–9.
5. Wan g T, Hropot M, Aronson PS, Giebisch G. Role of NHEisoforms in mediating bicarbonate reabsorption along thenephron. Am J Physiol Renal Physiol. 2001;281:F1117–22.
6. Boron WF. Acid-base transport by the renal proximaltubule. J Am Soc Nephrol. 2006;17:2368–82.
7. Rilly RF, Ellison DH. Mammalian distal tubule:Physiology, pathophysiology, and molecular anatomy. PhysiolRev. 2000;80:277–313.
8. Eladari D, Chambrey R, Peti-Peterdi J. A new look atelectrolyte transport in the distal tubule. Annu RevPhysiol. 2012;74:325–49.
9. Kleyman TR, Satlin LM, Hallows KR. Opening lines ofcommunication in the distal nephron. J Clin Invest.2013;123:4139–41.
10. Gueutin V, Vallet M, Jayat M, et al. Renalβ-intercalated cells maintain body fluid and electrolytebalance. J Clin Invest. 2013;123:4219–31.
11. Thomas W, Harvey BJ. Mechanisms underlying rapidaldosterone effects in the kidney. Annu Rev Physiol.2011;73:335–57.
12. Wei ner ID, Verlander JW. Renal ammonia metabo lism andtransport. Compr Physiol. 2013;3:201–20.
13. Weiner ID, Verlander JW. Role of NH 3 and NH4+transporters in renal acid-base transport. Am J PhysiolRenal Physiol. 2011;300:F11–23.
14. Rod iguez Soriano J, Vallo A, Castillo G, Olveros R.Natural history of primary distal renal tubu lar acidosistreated since infancy. J Pediatr. 1 98 2;101:669–76.
15. Cau ana RJ, Buckalew VM, Jr. The syndrome of distal(type 1) renal tubular acidosis: Clinical and laboratoryfindings in 58 cases. Medicine. 1988;67:84–99.
16. Cal das A, Broyer M, Dechaux M, Kleinknecht C. Primarydistal tubule acidosis in childhood: Clinical study andlong-term follow up of 28 patients. J Pediatr.

1992;121:233–41.
17. Karet FE, Finberg KE, Nelson RD, et al. Mutations inthe gene encoding B1 subunit of the H + -ATPase causerenal tubular acidosis with sensorineural deafness. NatGenet. 1999;21:8–90.
18. Karet FE, Finberg KE, Nayir A, et al. Localization ofa gene for autosomal recessive distal renal tubularacidosis with normal hearing (rdRTA2) to 7q33-34. Am HumGenet. 1999;65:1656–65.
19. Bruce LJ, Cope, Jones GK, et al. Familial distal renaltubular acidosis is associated with muta tions in the redcell anion exchanger (Band 3), AE1 g ene. J Clin Invest.1997;100:1693–707.
20. Jarolim P, Shayakul C, Prabakaran D, et al. Autosomaldistal renal tubular acidosis is associ ated in threefamilies with heterozygosity for the R589 H mutation inthe AE1 (Band 3) Cl /HCO 3 exchanger. J Biol Chem.1998;273:6380–8. 21. Kar et FE, Gainza FJ, Gyory AZ, etal. Mutations in the chloride-bicarbonate exchanger geneAE1 cause autosomal dominant but not reces sive distalrenal tubular acidosis. Proc Natl A ca d Sci U S A.1997;95:6337–42. 22. Tanph aichitr VS, Sumboonnanonda A,Ideguchi H, et al. Novel AE1 mutations in recessivedistal renal tubular acidosis: Loss of function is rescuedby glycophorin A. J Clin Invest. 1998;2173–9. 23.Vasuvattakul S, Yenchitsomanus PT, Vachuanichsanong P, etal. Autosomal reces sive distal renal tubular acidosisassociated with Southeast Asian ovalocytosis. Kidney Int.1999;56:1674–82. 24. Levine AS, Michael AF, Jr.Ehlers-Danlos syndrome with renal tubular acidosis andmedullary spo nge kidneys. J Pediatr. 1967;71:107–13. 25.Bae hner RI, Gilchrist GS, Anderson FJ. Hereditaryelliptocytosis and primary renal tubular acidosis in asingle family. Am J Dis Child. 1968;115:414–9. 26. PhamPT, Pham PC, Wilkinson AH, et al. Renal abnormalities insickle cell disease. Kidney Int. 2000;57:1–8. 27.Buckalew VM, Jr, Pyrvis ML, Schulman MG, et al. Hereditaryrenal tubular acidosis: Report of a 64 member kindred withvariable clinical expression including idiopathichypercalciuria. Medicine. 1974;53:229–54. 28. Ham ed JA,Czerwinski AW, Coates B, et al. Familial absorptivehypercalciuria and renal tubular acidosis. Am J Med.1979;67:385–91. 29. Restano I, Kaplan BS, Stanley C, BakerL. Nephrolithiasis, hypocitraturia, and a dis tal renaltubular acidification defect in typ e 1 glycogen storagedisease. J Pediatr. 1993;122:392–6. 30. Falik-Borenstein

ZC, Jordan SC, Saudubray J-M, et al. Renal tubularacidosis in carnitine palmi toyltransferase type Ideficiency. N Engl J Med 1 99 2;327:24–7. 31. Fab ris A1,Anglani F, Lupo A, et al. Medullary sponge kidney: Stateof the art. Nephrol Dial Transplant. 2013;28:1111–9. 32.Brenner RJ, Spring DB, Sebastian A, et al. Incidence ofradiographically evident bone disease, nephrocalcinosis,and nephrolithiasis in various types of renal tubularacidosis. N Engl J Med. 1982;307:217–21. 33. Mutalen C,Montoreano R, Labarrere C. Early skeletal effects ofalkali therapy upon the osteomalacia of renal tubularacidosis. J Clin Endocrinol Metab. 1976;42:875–81. 34.Nor man ME, Feldman NI, Cohn RM, et al. Urinary citrate inthe diagnosis of renal tubular acidosis. J Pediatr.1978;92:394–400.
35. Morris RC Jr, Frudenberg HH. Impaired renalacidification in patients with hypergammaglobulinemia.Medicine. 1967;46:57–69.
36. Caruana RJ, Barish CF, Buckalew VM, Jr. Completedistal renal tubular acidosis in sys temic lupus: Clinicaland laboratory findings. Am J of Kid Dis. 1985;6:59–63.
37. Tal al N. Sjögren syndrome, lymphoprolifera tion andrenal tubular acidosis. Ann Intern Med. 1971;74:633–4.
38. Coh en EP, Bastani B, Cohen MR, et al. Absence of H +-ATPase in cortical collecting tubules of a patient withSjögren’s syndrome and distal renal tubular acidosis. J AmSoc Nephrol. 1 99 2;3:264–72.
39. Bat lle DC, von Riotte A, Schlueter W. Urinary sodiumin the evaluation of hyperchlo remic metabolic acidosis. NEngl J Med. 198 7;316:140–4.
40. Izraeli s, Rachmel A, Frishberg Y, et al. Transientrenal acidification defect during acute infantilediarrhea: The role of urinary sodium. J Pediatr.1990;117:711–6.
41. Strife CF, Clardy CW, Varade WS, et al. Urine to bloodcarbon dioxide tension gradient and maximal depression ofurine pH to distinguish ratedependent from classic distalrenal tubule acidosis in children. J Pediatr.1993;122:60–5.
42. Bat lle DC, Grupp M, Gaviria M, Kurtzman NA. Distalrenal tubular acidosis with intact capacity to lower urinepH. Am J Med. 1982;72:751–6.
43. McCurdy DK, Frederick M, Elkington JR. Renal tubuleacidosis due to amphotericin B. N Engl J Med.1968;278:124–31.
44. Bat lle D, Gaviria M, Grupp M, et al. Distal nephronfunction in patients receiving chronic lithium therapy.Kidney Int. 1982;21:477–85.
45. Yong JM, Sanderson KV. Photosensitive dermatitis andrenal tubular acidosis after ingestion of calciumcyclamate. Lancet. 1969;2:1273–5.
46. Ste ele TW, Gyory AZ, Edwards KD. Renal function inanalgesic nephropathy. Br Med J. 1969;2:213–6.
47. Navarro JF, Quereda C, Quereda C, et al. Nephrogenicdiabetes insipidus and renal tubular acidosis secondary tofoscarnet therapy. Am J of Kidney Dis. 1996;27:431–4.
48. Gyory AZ, Stewart JH, George CRP, et al. Renal tubularacidosis, acidosis due to hyperkalemia, hypercalcemia,disordered citrate metabolism, and other tubulardysfunction following human renal transplantation. Q JMed. 1969;38:231.
49. Better OS, Chasnowitz C, Naveh Y, et al. Syndrome ofincomplete renal tubular acidosis after cadaveric renaltransplantation. Ann Intern Med. 1969;71:39–46.
50. Jordan J, Cohen EP, Roza A, et al. An immunochemicalstudy of H + -ATPase in kidney transplant rejection. J LabClin Med. 1996;127:310–4. 51. Ber lyne GM. Distal tubularfunction in chronic hydronephrosis. Q J Med.1961;30:339–55. 52. Hut cheon RA, Kaplan BS, Drummond KN.Distal renal tubular acidosis in children with chronichydronephrosis. J Pediatr. 1976;89:372–6. 53. Guizar JM,Kornhauser C, Malacaro M, et al. Renal tubular acidosis inchildren with vesicoureteral reflux. J Urol.1996;156:193–5. 54. Vai nder M, Kelly J. Rebal tubulardysfunction secondary to jejunoileal bypass. JAMA.1976;235:1257–8. 55. Drutz DJ, Gutman RA. Renal tubularacidosis in leprosy. Ann Intern Med. 1971;75:475–6. 56.Cochran M, Peacock M, Smith DA, Nordin BEC. Renal tubularacidosis of pyelonephritis with renal stone disease. BrMed J. 1968;2:721–9. 57. McS herry E, Morris RC, Jr.Attainment and maintenance of normal stature with alkalitherapy in infants and children with classic renal tubularacidosis. J Clin Invest. 1978;61:509–27. 58. Rod riguezSoriano J, Boichis H, Stark H, Edelmann CM, Jr. Proximal
renal tubular acidosis: A defect in bicarbonatereabsorption with normal urinary acidification. PediatrRes. 1967;1:81–98. 59. Foreman JW. Roth KS. Human renalFanconi syn drome: Then and now. Nephron.1989; 51:301–6.60. Brenes LG, Brenes JN, Hernandez MM. Familial proximalrenal tubular acidosis. Am J Med. 1977;63:244–52. 61.Winsnes A, Monn E, Stokke O, Feyling T. Congenital,persistent proximal type of renal tubule acidosis in twobrothers. Acta Paediatr Scand 1979;60;861–8. 62. IgarashiT, Ishii T, Watanabe K, et al. Persistent isolatedproximal renal tubular acidosis: A sys temic disease with adistinct clinical entity. Pediatr Nep hrol. 1994;8:70–1.63. Iga rashi T, Inatomi J, Sekine T, et al. Mutations inSLC4A4 cause permanent isolated proximal tubu lar acidosiswith ocular abnormalities. Nat Genet. 199 9;23:264–266.64. Kle ta R, Bernardini I, Ueda M, et al. Long-termfollow-up of well-treated nephropathic cystinosispatients. J Pediatr. 2004;145:555-60. 65. McSherry E,Sebastian A, Morris RC Jr. Renal tubular acidosis ininfants: The several kinds, including bicarbonate-wasting,classic renal tubu lar acidosis. J Clin Invest. 197251:499-514. 66. Sly WS, Whyte MP, Sundaram V, et al.Carbonic anhydrase II deficiency in 12 families with theautosomal recessive syndrome of osteopetrosis with renaltubular acidosis and cerebral calcifica tion. N Engl J Med.1985;313:139–5. 67. Karet FE. Mechanisms in hyperkalemicrenal tubular acidosis. J Am Soc Nephrol 2009;20:251–4.68. Oetliker O, Zurbrugg RP. Renal regulation of fluid,electrolytes and acid-base homeostasis in the salt los ingform of congenital adrenal hyperplasia (SL-CAH). ECFvolume a compensating factor in aldosterone deficiency.Clin Endocrinol Metab. 1978;46:543–51
69. New M I. Inborn errors of steroidogenesis. Mol CellEndocrinol. 2003;211:75–83.
70. Stratakis CA, Bossis I. Genetics of the adrenal gland.Rev Endocr Metab Dis. 2004;5:53–68
71. Geller DS, Rodriguez Soriano J, Vallo Boado A, et al.Mutations in the mineralocorticoid receptor gene causeautosomal pseudohypoaldosteronism type 1. Nat Genet.1998;19:279–81.
72. Chang SS, Grunder S Hanukoglu A, et al. Mutations inthe subunits of the epithelial sodium channel cause saltwasting with hyperkalemia acidosis, pseudohypoaldosteronism type 1. Nat Genet. 1996;l12:248–53.
73. Grunder S, Firsou D, Chang SS, et al. A mutation
causing pseudohypoaldosteronism type 1 identi fies aconserved glycine that is involved in the gating of theepithelial sodium channel. EMBO J. 1997;16:899–907.
74. Bar ker PM, Nguyen MS, Gatzy JT, at al. Role of gammaENaC subunit in lung liquid clearance and electrolytebalance in newborn mice: Insights into perinataladaptation and pseudohypoaldosteron ism. J Clin Invest.1998;102:1634–40.
75. Achard JM, Disse-Nicoderm S, Fiquet-Kempf B, et al.Phenotypic and genetic heterogeneity of famil ialhyperkalemic hypertension (Gordon syndrome). Cli n ExpPharmacol Physiol. 2001;28:1048–52.
76. Wil son FH, Disse-Nicoderm S, Choate KA, et al. Humanhypertension caused by mutations in WNK kinases. Science2001;293:1107–11.
77. Boyden LM, Choi M, Choate KM, et al. Mutations inKelch-like 3 and Cullin 3 cause hypertension andelectrolytes abnormalities. Nature 2012;482:98–102.
78. Daven port MW, Zipser RD. Association of hypoten sionwith hyperreninemic hypoaldosteronism in the criticallypatient. Ach Intern Med. 1983;143:735–75.
79. DeFr onzo RA. Hyperkalemia and hyporeninemichypoaldosteronism. Kidney Int. 1980;17:118–34.
80. Assadi FK, Ziai M. Impaired renal acidification ininfants with fetal alcohol syndrome. Pediatr Res.1985;19:850–3.
81. Alon U, Kodroff MB, Broecker B, et al. Renal tubu laracidosis in neonatal unilateral kidney diseases. J P ediatr. 1984;104:855–60.
82. Batlle DC, Arruda JAL, Kurtzman NA. Hyperkalemicdistal renal tubular acidosis associated with obstruc tiveuropathy. N Engl J Med. 1981;304:373–80.
83. Henrich WL. Nephrotoxicity of nonsteroidalantiinflammatory agents. Am J Kidney Dis. 1983;2:478–84.
84. O’Kelly R, Magee F, McKenna TJ. Routine heparintherapy inhibits adrenal aldosterone production. J ClinEndocrinol Metab. 1983;56:108–12.
85. Hulter HN, Bonner EL, Jr, Glynn RD, Sebastian A. Renal
and acid-base effects of chronic spi ronolactoneadministration. Am J Physiol. 1 89 1;240:F381–7. 86. Ponce SP, Jennings AE, Madias NE, et al. Druginducedhyperkalemia. Medicine (Baltimore). 1985;64:357–70. 87.Valazquez H, Perazella MN, Wright FS, et al. Renalmechanisms of trimethoprim induced hyperkale mia. AnnIntern Med. 1993;119:296–302. 88. Kleyman TR, Roberts C,Ling BN. A mechanism for pentamidine-induced hyperkalemia:Inhibition of distal sodium nephron sodium transport. AnnIntern Med. 1995;122:103–6. 89. Kamel DS, Ethier JH,Quaggin S, et al. Studies to determine the basis of thehyperkalemia in recipients of a renal transplant who aretreated with cyclosporine. J Am Soc Nephrol.1991;2:1279–84. 90. Sands JM, McMahan SJ, Tumlin JA.Evidence that the inhibition of Na + /K + -ATPase activityby FK506 involves a calcineurin. Kidney Int.1994;46:647–52. 91. Wes t ML, Marsden PA, Richardson MA,et al. New clinical approach to evaluate disorders ofpotassium excretion. Miner Electrolyte Metab.1986;12:234–38. 92. Kraut JA, Madias N. Serum anion gap:Its uses and limitations in clinical medicine. Clin J AmSoc Nephrol. 2007;2:162–74. 93. Car lisle EJF, DonnellySM, Halperin ML. Renal tubular acidosis (RTA): Recognizethe ammonium defect and pHorget the urine pH. PediatrNephrol. 1991;5:242–48. 94. Schloeder FX, Stinebaugh BJ.Defect of urinary acidification during fasting. Metabolism.1966;15:17–25. 95. Mad ison LL, Seldin DW. Ammoniumexcretion and renal enzymatic adaptation in humansubjects, as disclosed by administration of precursoramino acids. J Clin Invest. 1958;37:1615–27. 96. KrautJA, Madias NE. Differential diagnosis of nongap metabolicacidosis: Value of a systematic approach. Clin J Am SocNephrol. 2012;7:671-9. 97. Halperin ML, Goldstein MB, HaigA, et al. Studies on the pathogenesis of type I (distal)renal tubular acidosis as revealed by the urinary pCO 2 . JClin Invest. 1974;53:669–677. 98. Alo n U, Hellerstein S,Warady BA. Oral acetazolamide in the assessment of(urine-blood) pCO 2 . Pediatr Nephrol. 1991;5:307–11. 99.Edelmann CM, Jr, Biochis H, Rodriguez Soriano J, Stark H.The renal response of children to acute ammonium chloriseacidosis. Pediatr Res. 1967;1:452–60. 100. Edelmann CM,Jr, Rodriguez Soriano J, Biochis H, et al. Renalbicarbonate and hydrogen ion excretion in normal infants.J Clin Invest. 1967;46:1309–17. 101. Oster JR, Hotchkiss,Carbon M, et al. A short duration renal acidification testusing calcium chloride. Nephron. 1975;14:281–92. 102.Loney LC, Norling LL, Robson A. The use of argininehydrochloride infusion to assess urinary acidification. JPediatr. 1982;100:95–8.

103. Lash JP, Arruda JAL. Laboratory evaluation of renaltubular acidosis. Clin Lab Med. 1993;13:117–29.
104. Ras togi SP, Crawford C, Wheeler R, et al. Effect offurosemide in urinary acidification in distal renaltubular acidosis. J Lab Clin Med. 1984;271–82.
REVIEW QUESTIONS
1. �e normal acid production of children is:
a. <1 mEq/kg/day
b. 1 to 3 mEq/kg/day
c. 4 to 6 mEq/kg/day
d. >6 mEq/kg/day
2. �e most important way of excreting acid duringincreased acid production is:
a. Increased ammonium excretion
b. Increased phosphate excretion
c. Increased urea excretion
d. Decreased bicarbonate excretion
3. Pro ximal tubule bicarbonate reabsorption occursbecause of which of the following?
a. Amm onia generation from glutamine
b. Hyd rogen ion excretion by the K + /H + ATPase
c. AE1 in the basolateral membrane
d. Carbonic anhydrase on the brush border membrane
4. For adequate distal tubule acid excretion, there mustbe adequate:
a. Sodium reabsorption
b. Potassium absorption
c. Ammonium absorption
d. Sodium excretion
5. Ammoniagenesis occurs in the:
a. �ick ascending limb
b. Cortical collecting tubule
c. Medullary collecting tubule
d. Proximal tubule
6. Fanconi syndrome involves RTA type:
a. Type I
b. Type II
c. Type III
d. Type IV
7 In RTA, the urine anion gap is:
a. Positive
b. Negative
c. Neutral
8. Type 1 is associated with a mutation in the gene codingfor:
a. NBC1
b. 2Cl /Na/K
c. AE1
d. CA
9. An ab normal β 1 subunit of H + -ATPase is associatedwith:
a. Skeletal dysplasia
b. Early onset deafness c. Cardiac defect d. Mentalretardation 10. �e main abnormality of RTA type 4 is: a.Hyperkalemia causing decreased ammoniagenesis b.Hypokalemia causing decreased ammoniagenesis c.
Hyperkalemia causing increased ammoniagenesis d.Hypokalemia causing increased ammoniagenesis 11.Nephrocalcinosis is associated with: a. Type I RTA b.Type II RTA c. Type IV RTA d. None of above 12. �eanticonvulsant medication, topiramate, is associated with:a. Type I RTA b. Type II RTA c. Type III RTA d. Type IVRTA 13. �e type of RTA requiring the largest dose ofsupplemental alkali to correct the acidosis is: a. Type Ib. Type II c. Type IV 14. �e major urinary bu�er oftitratable acid is: a. Citrate b. Phosphate c. Urate d.Creatinine 15. A simple way of testing the distalnephron’s ability to acidify the urine is to administerorally: a. Phosphate b. Citrate c. Furosemide d.Hydrochlorothiazide ANSWER KEY 1. b 2. a 3. d 4. a 5.d 6. b 7. a 8. c 9. b 10. a 11. a 12. b 13. b 14.b 15. c
43 Cystic kidney disease
1. Wilson PD. Polycystic kidney disease. N Engl J Med.2004;350:151–64.
2. Arts HH, Knoers NV. Current insights into renalciliopathies: What can genetics teach us? Pediatr Nephrol.2013;28:863–74.
3. Guay-Woodford LM, Desmond RA. Autosomal recessivepolycystic kidney disease: The clinical experience in NorthAmerica. Pediatrics. 2003;111:1072–80.
4. Ber gmann C, Senderek J, Windelen E, et al. Clinicalconsequences of PKHD1 mutations in 164 patients withautosomal-recessive polycystic kidney disease (ARPKD).Kidney Int. 2005;67:829–48.
5. Bergmann C, Kupper F, Dornia C, et al. Algorithm forefficient PKHD1 mutation screening in autosomal recessivepolycystic kidney disease (ARPKD). Hum Mutat.2005;25:225–31.
6. Adeva M, El-Youssef M, Rossetti S, et al. Clinical andmolecular characterization defines a broadened spectrum ofautosomal recessive polycystic kidney disease (ARPKD).Medicine (Baltimore). 2006;85:1–21. 7. Gunay-Aygun M,Font-Montgomery E, Lukose L, et al. Correlation of kidneyfunction, volume and imaging findings, and PKHD1 mutationsin 73 patients with autosomal recessive polycystic kidneydisease. Clin J Am Soc Nephrol. 2010;5:972–84. 8. Kas htanCE, Primack WA, Kainer G, et al. Recurrent bacteremia withenteric pathogens in recessive polycystic kidney disease.Pediatr Nephrol. 1999;13:678–82. 9. Davis ID, Ho M,Hupertz V, et al. Survival of childhood polycystic kidneydisease following renal transplantation: The impact ofadvanced hepatobiliary disease. Pediatr Transplant.2003;7:364–9. 10. Chalhoub V, Abi-Rafeh L, Hachem K, etal. Intracranial aneurysm and recessive polycystic kidneydisease: The third reported case. JAMA Neurol.2013;70:114–6. 11. Onu chic LF, Furu L, Nagasawa Y, et al.PKHD1, the polycystic kidney and hepatic disease 1 gene,encodes a novel large protein containing multipleimmunoglobulin-like plexin-transcription-factor domainsand parallel beta-helix 1 repeats. Am J Hum Genet.2002;70:1305–17. 12. Mutation Database Autosomal RecessivePolycystic Kidney Disease (ARPKD/PKHD1). 2013. Availableat http://www.humgen.rwth-aachen.de. Accessed October 1,2015. 13. Ros setti S, Harris PC. Genotype-phenotypecorrelations in autosomal dominant and autosomal recessive

polycystic kidney disease. J Am Soc Nephrol.2007;18:1374–80. 14. Menezes LF, Cai Y, Nagasawa Y, et al.Polyductin, the PKHD1 gene product, comprises isoformsexpressed in plasma membrane, primary cilium, andcytoplasm. Kidney Int. 2004;66:1345–55. 15. Kerkar N,Norton K, Suchy FJ. The hepatic fibrocystic diseases. ClinLiver Dis. 2006;10:55–71, v–vi. 16. Yod er BK. Role ofprimary cilia in the pathogenesis of polycystic kidneydisease. J Am Soc Nephrol. 2007;18:1381–8. 17. Hildebrandt F, Benzing T, Katsanis N. Ciliopathies. N Engl JMed. 2011;364:1533–43. 18. Guay-Woodford L. Other cysticdiseases. In: Feehally J, Johnson R, editors.Comprehensive Clinical Nephrology, 4th ed. London: Mosby;2010. p. 543–59. 19. Capisonda R, Phan V, Traubuci J, etal. Autosomal recessive polycystic kidney disease:Outcomes from a single-center experience. Pediatr Nephrol.2003;18:119–26. 20. Srinath A, Shneider BL. Congenitalhepatic fibrosis and autosomal recessive polycystic kidneydisease. J Pediatr Gastroenterol Nutr. 2012;54:580–7. 21.Gunay-Aygun M, Font-Montgomery E, Lukose L, et al.Characteristics of congenital hepatic fibrosis in a largecohort of patients with autosomal recessive polycystickidney disease. Gastroenterology. 2013;144:112–21 e2.SUMMARY Cystic renal diseases are diverse disorders, manyof which are genetically transmitted. �ese disorders arealso diverse in their age of presentation, clinicalmanifestations, and progression to ESRD. With the growinguse of fetal ultrasound evaluation, these disorders areincreasingly diagnosed prenatally. Although ARPKD is themost common genetically inherited cystic disorder inchildren, ADPKD can also be clinically signi�cant duringchildhood. Several syndromes are associated with renalcysts and must be considered in the evaluation of childrenfound to have cysts on ultrasound evaluation. Cysticdiseases are now classi�ed as ciliopathies because ciliarydysfunction in renal eipthelia is a major contributor todisease pathogenesis in most of these conditions. Treatmentmodalities for most renal cystic diseases are limited atthe present time, and these disorders o�en progress toESRD. Future development of drugs that reduce cyst size,attenuate interstitial �brosis, and prevent progressivedecline in renal function could reduce the evolution ofESRD in these patients.
22. Rossetti S, Consugar MB, Chapman AB, et al.Comprehensive molecular diagnostics in autosomal dominantpolycystic kidney disease. J Am Soc Nephrol.2007;18:2143–60.
23. Gigarel N, Frydman N, Burlet P, et al. Preimplantation

genetic diagnosis for autosomal recessive polycystickidney disease. Reprod Biomed Online. 2008;16:152–8.
24. Zvereff V, Yao S, Ramsey J, et al. Identification ofPKHD1 multiexon deletions using multiplexligation-dependent probe amplification and quantitativepolymerase chain reaction. Genet Test Mol Biomarkers.2010;14:505–10.
25. Guay-Woodford LM, Knoers NV. Genetic testing:Considerations for pediatric nephrologists. Semin Nephrol.2009;29:338–48.
26. Beaunoyer M, Snehal M, Li L, et al. Optimizingoutcomes for neonatal ARPKD. Pediatr Transplant.2007;11:267–71.
27. Van De Voorde RG, Mitsnefes MM. Hypertension and CKD.Adv Chronic Kidney Dis. 2011;18:355–61.
28. Tel ega G, Cronin D, Avner ED. New approaches to theautosomal recessive polycystic kidney disease patient withdual kidney-liver complications. Pediatr Transplant.2013;17:328–35.
29. Gun ay-Aygun M, Turkbey BI, Bryant J, et al.Hepatorenal findings in obligate heterozygotes forautosomal recessive polycystic kidney disease. Mol GenetMetab. 2011;104:677–81.
30. Cha pal M, Debout A, Dufay A, et al. Kidney and livertransplantation in patients with autosomal recessivepolycystic kidney disease: A multicentric study. NephrolDial Transplant. 2012;27:2083–8.
31. Tor res VE, Harris PC, Pirson Y. Autosomal dominantpolycystic kidney disease. Lancet. 2007;369:1287–301.
32. Rizk D, Chapman A. Treatment of autosomal dominantpolycystic kidney disease (ADPKD): The new horizon forchildren with ADPKD. Pediatr Nephrol. 2008;23:1029–36.
33. Boyer O, Gagnadoux MF, Guest G, et al. Prognosis ofautosomal dominant polycystic kidney disease diagnosed inutero or at birth. Pediatr Nephrol. 2007;22:380–8.
34. Harris PC. 2008 Homer W. Smith Award: Insights intothe pathogenesis of polycystic kidney disease from genediscovery. J Am Soc Nephrol. 2009;20:1188–98.

35. Gar cia-Gonzalez MA, Jones JG, Allen SK, et al.Evaluating the clinical utility of a molecular genetictest for polycystic kidney disease. Mol Genet Metab.2007;92:160–7.
36. Qian F, Watnick TJ, Onuchic LF, et al. The molecularbasis of focal cyst formation in human autosomal dominantpolycystic kidney disease type I. Cell. 1996;87:979–87.37. Torres VE, Harris PC. Polycystic kidney disease in2011: Connecting the dots toward a polycystic kidneydisease therapy. Nat Rev Nephrol. 2012;8:66–8. 38. NauliSM, Alenghat FJ, Luo Y, et al. Polycystins 1 and 2 mediatemechanosensation in the primary cilium of kidney cells.Nat Genet. 2003;33:129–37. 39. Reed B, Nobakht E, DadgarS, et al. Renal ultrasonographic evaluation in children atrisk of autosomal dominant polycystic kidney disease. Am JKidney Dis.2010;56:50–6. 40. Mekahli D, Woolf AS,Bockenhauer D. Similar renal outcomes in children withADPKD diagnosed by screening or presenting with symptoms.Pediatr Nephrol. 2010;25:2275–82. 41. Harris PC, RossettiS. Molecular diagnostics of ADPKD coming of age. Clin J AmSoc Nephrol. 2008;3:1–2. 42. Bergmann C, Bruchle NO,Frank V, et al. K. Perinatal deaths in a family withautosomal dominant polycystic kidney disease and a PKD2mutation. N Engl J Med. 2008;359:318–9. 43. Vuj ic M,Heyer CM, Ars E, et al. Incompletely penetrant PKD1 allelesmimic the renal manifestations of ARPKD. J Am Soc Nephrol.2010;21:1097–102. 44. Har ris PC. The TSC2/PKD1 contiguousgene syndrome. Contrib Nephrol. 1997;122:76–82. 45. Sujansky E, Kreutzer SB, Johnson AM, et al. Attitudes ofat-risk and affected individuals regarding presymptomatictesting for autosomal dominant polycystic kidney disease.Am J Med Genet. 1990;35:510–5. 46. Cadnapaphornchai MA,McFann K, Strain JD, et al. Prospective change in renalvolume and function in children with ADPKD. Clin J Am SocNephrol. 2009;4:820–9. 47. Nat ional High Blood PressureEducation Working Group on High Blood Pressure in Childrenand Adolescents. The fourth report on the diagnosis,evaluation, and treatment of high blood pressure inchildren and adolescents. Pediatrics.2004;114(Suppl):555–76. 48. Helal I, Reed B, McFann K, etal. Glomerular hyperfiltration and renal progression inchildren with autosomal dominant polycystic kidney disease.Clin J Am Soc Nephrol. 2011;6:2439–43. 49. Wong H, VivianL, Weiler G, Filler G. Patients with autosomal dominantpolycystic kidney disease hyperfiltrate early in theirdisease. Am J Kidney Dis. 2004;43:624–8. 50. Baj wa ZH,Sial KA, Malik AB, et al. Pain patterns in patients withpolycystic kidney disease. Kidney Int. 2004;66:1561–9.51. Hog an MC, Norby SM. Evaluation and management of pain
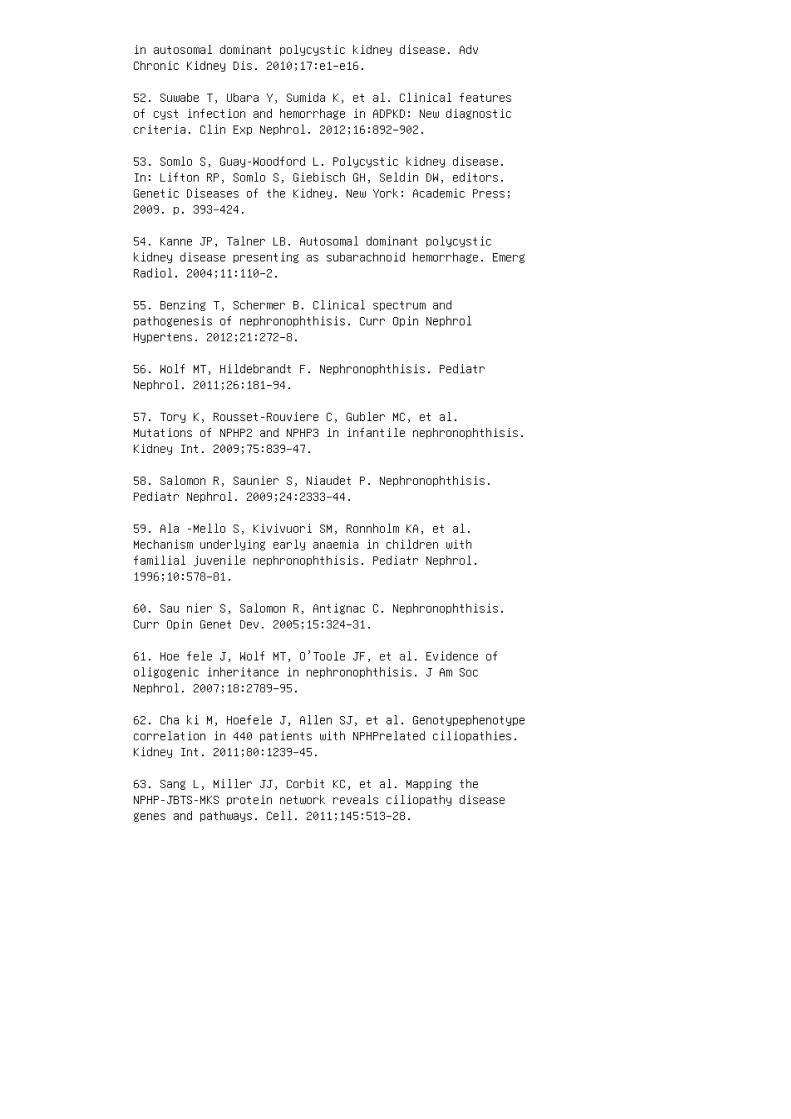
in autosomal dominant polycystic kidney disease. AdvChronic Kidney Dis. 2010;17:e1–e16.
52. Suwabe T, Ubara Y, Sumida K, et al. Clinical featuresof cyst infection and hemorrhage in ADPKD: New diagnosticcriteria. Clin Exp Nephrol. 2012;16:892–902.
53. Somlo S, Guay-Woodford L. Polycystic kidney disease.In: Lifton RP, Somlo S, Giebisch GH, Seldin DW, editors.Genetic Diseases of the Kidney. New York: Academic Press;2009. p. 393–424.
54. Kanne JP, Talner LB. Autosomal dominant polycystickidney disease presenting as subarachnoid hemorrhage. EmergRadiol. 2004;11:110–2.
55. Benzing T, Schermer B. Clinical spectrum andpathogenesis of nephronophthisis. Curr Opin NephrolHypertens. 2012;21:272–8.
56. Wolf MT, Hildebrandt F. Nephronophthisis. PediatrNephrol. 2011;26:181–94.
57. Tory K, Rousset-Rouviere C, Gubler MC, et al.Mutations of NPHP2 and NPHP3 in infantile nephronophthisis.Kidney Int. 2009;75:839–47.
58. Salomon R, Saunier S, Niaudet P. Nephronophthisis.Pediatr Nephrol. 2009;24:2333–44.
59. Ala -Mello S, Kivivuori SM, Ronnholm KA, et al.Mechanism underlying early anaemia in children withfamilial juvenile nephronophthisis. Pediatr Nephrol.1996;10:578–81.
60. Sau nier S, Salomon R, Antignac C. Nephronophthisis.Curr Opin Genet Dev. 2005;15:324–31.
61. Hoe fele J, Wolf MT, O’Toole JF, et al. Evidence ofoligogenic inheritance in nephronophthisis. J Am SocNephrol. 2007;18:2789–95.
62. Cha ki M, Hoefele J, Allen SJ, et al. Genotypephenotypecorrelation in 440 patients with NPHPrelated ciliopathies.Kidney Int. 2011;80:1239–45.
63. Sang L, Miller JJ, Corbit KC, et al. Mapping theNPHP-JBTS-MKS protein network reveals ciliopathy diseasegenes and pathways. Cell. 2011;145:513–28.
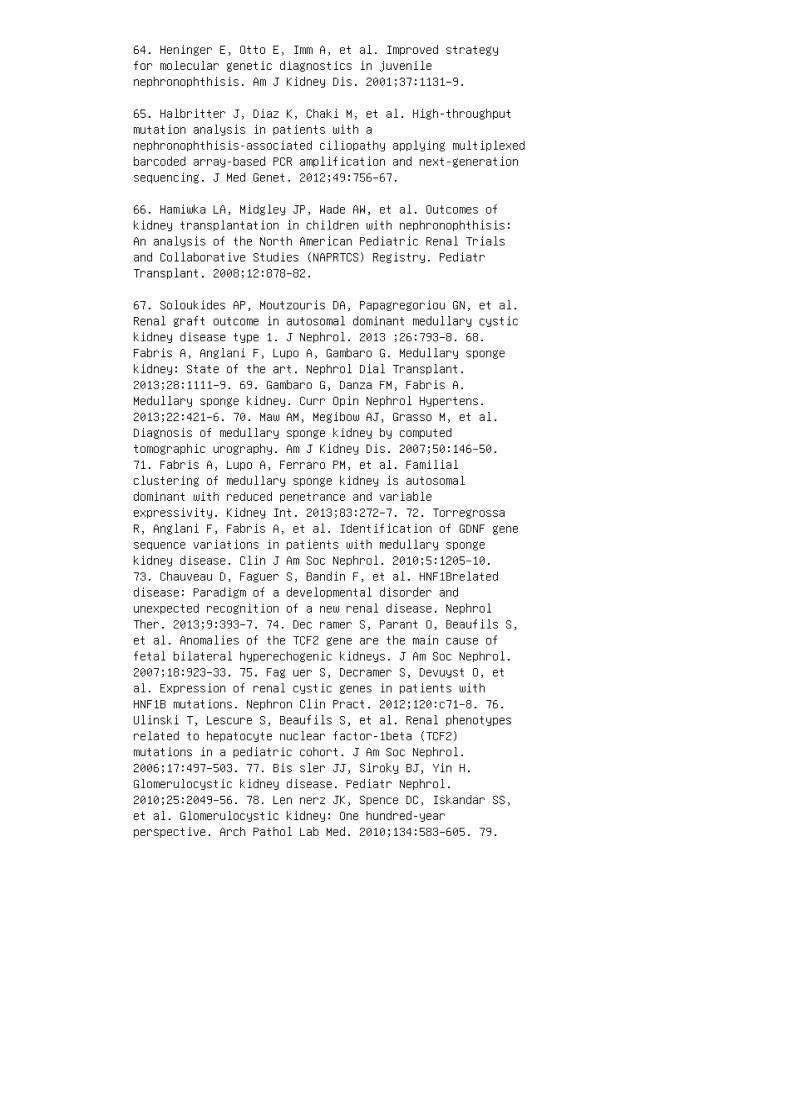
64. Heninger E, Otto E, Imm A, et al. Improved strategyfor molecular genetic diagnostics in juvenilenephronophthisis. Am J Kidney Dis. 2001;37:1131–9.
65. Halbritter J, Diaz K, Chaki M, et al. High-throughputmutation analysis in patients with anephronophthisis-associated ciliopathy applying multiplexedbarcoded array-based PCR amplification and next-generationsequencing. J Med Genet. 2012;49:756–67.
66. Hamiwka LA, Midgley JP, Wade AW, et al. Outcomes ofkidney transplantation in children with nephronophthisis:An analysis of the North American Pediatric Renal Trialsand Collaborative Studies (NAPRTCS) Registry. PediatrTransplant. 2008;12:878–82.
67. Soloukides AP, Moutzouris DA, Papagregoriou GN, et al.Renal graft outcome in autosomal dominant medullary cystickidney disease type 1. J Nephrol. 2013 ;26:793–8. 68.Fabris A, Anglani F, Lupo A, Gambaro G. Medullary spongekidney: State of the art. Nephrol Dial Transplant.2013;28:1111–9. 69. Gambaro G, Danza FM, Fabris A.Medullary sponge kidney. Curr Opin Nephrol Hypertens.2013;22:421–6. 70. Maw AM, Megibow AJ, Grasso M, et al.Diagnosis of medullary sponge kidney by computedtomographic urography. Am J Kidney Dis. 2007;50:146–50.71. Fabris A, Lupo A, Ferraro PM, et al. Familialclustering of medullary sponge kidney is autosomaldominant with reduced penetrance and variableexpressivity. Kidney Int. 2013;83:272–7. 72. TorregrossaR, Anglani F, Fabris A, et al. Identification of GDNF genesequence variations in patients with medullary spongekidney disease. Clin J Am Soc Nephrol. 2010;5:1205–10.73. Chauveau D, Faguer S, Bandin F, et al. HNF1Brelateddisease: Paradigm of a developmental disorder andunexpected recognition of a new renal disease. NephrolTher. 2013;9:393–7. 74. Dec ramer S, Parant O, Beaufils S,et al. Anomalies of the TCF2 gene are the main cause offetal bilateral hyperechogenic kidneys. J Am Soc Nephrol.2007;18:923–33. 75. Fag uer S, Decramer S, Devuyst O, etal. Expression of renal cystic genes in patients withHNF1B mutations. Nephron Clin Pract. 2012;120:c71–8. 76.Ulinski T, Lescure S, Beaufils S, et al. Renal phenotypesrelated to hepatocyte nuclear factor-1beta (TCF2)mutations in a pediatric cohort. J Am Soc Nephrol.2006;17:497–503. 77. Bis sler JJ, Siroky BJ, Yin H.Glomerulocystic kidney disease. Pediatr Nephrol.2010;25:2049–56. 78. Len nerz JK, Spence DC, Iskandar SS,et al. Glomerulocystic kidney: One hundred-yearperspective. Arch Pathol Lab Med. 2010;134:583–605. 79.

Bin gham C, Hattersley AT. Renal cysts and diabetessyndrome resulting from mutations in hepatocyte nuclearfactor-1beta. Nephrol Dial Transplant. 2004;19:2703–8.80. Oliva MR, Hsing J, Rybicki FJ, et al. Glomerulocystickidney disease: MRI findings. Abdom Imaging.2003;28:889–92. 81. Eknoyan G. A clinical view of simpleand complex renal cysts. J Am Soc Nephrol. 2009;20:1874–6.82. Nas cimento AB, Mitchell DG, Zhang XM, et al. Rapid MRimaging detection of renal cysts: Age-based standards.Radiology. 2001;221:628–32. 83. Hon g S, Lim JH, Jeong IG,et al. What association exists between hypertension andsimple renal cyst in a screened population? J HumHypertens. 2013 ;27:539–44. 84. Israel GM, Bosniak MA. Anupdate of the Bosniak renal cyst classification system.Urology. 2005;66:484–8.
85. Warren KS, McFarlane J. The Bosniak classification ofrenal cystic masses. BJU Int. 2005;95:939–42.
86. Aki nci D, Gumus B, Ozkan OS, et al. Single-sessionpercutaneous ethanol sclerotherapy in simple renal cystsin children: Long-term follow-up. Pediatr Radiol.2005;35:155–8.
87. Skolarikos A, Laguna MP, de la Rosette JJ.Conservative and radiological management of simple renalcysts: A comprehensive review. BJU Int. 2012;110:170–8.
88. Sil ver IM, Boag AH, Soboleski DA. Best cases from theAFIP: Multilocular cystic renal tumor: Cystic nephroma.Radiographics. 2008;28:1221–5.
89. Freire M, Remer EM. Clinical and radiologic features ofcystic renal masses. AJR Am J Roentgenol.2009;192:1367–72.
90. Moch H. Cystic renal tumors: New entities and novelconcepts. Adv Anat Pathol. 2010;17:209–14.
91. Boybeyi O, Karnak I, Orhan D, et al. Cystic nephromaand localized renal cystic disease in children: Diagnosticclues and management. J Pediatr Surg. 2008;43:1985–9.
92. Sun Y, Zhou J, Stayner C, et al. Magnetic resonanceimaging assessment of a murine model of recessivepolycystic kidney disease. Comp Med. 2002;52:433–8.
93. Chapman AB, Guay-Woodford LM, Grantham JJ, et al.Renal structure in early autosomal-dominant polycystickidney disease (ADPKD): The Consortium for Radiologic
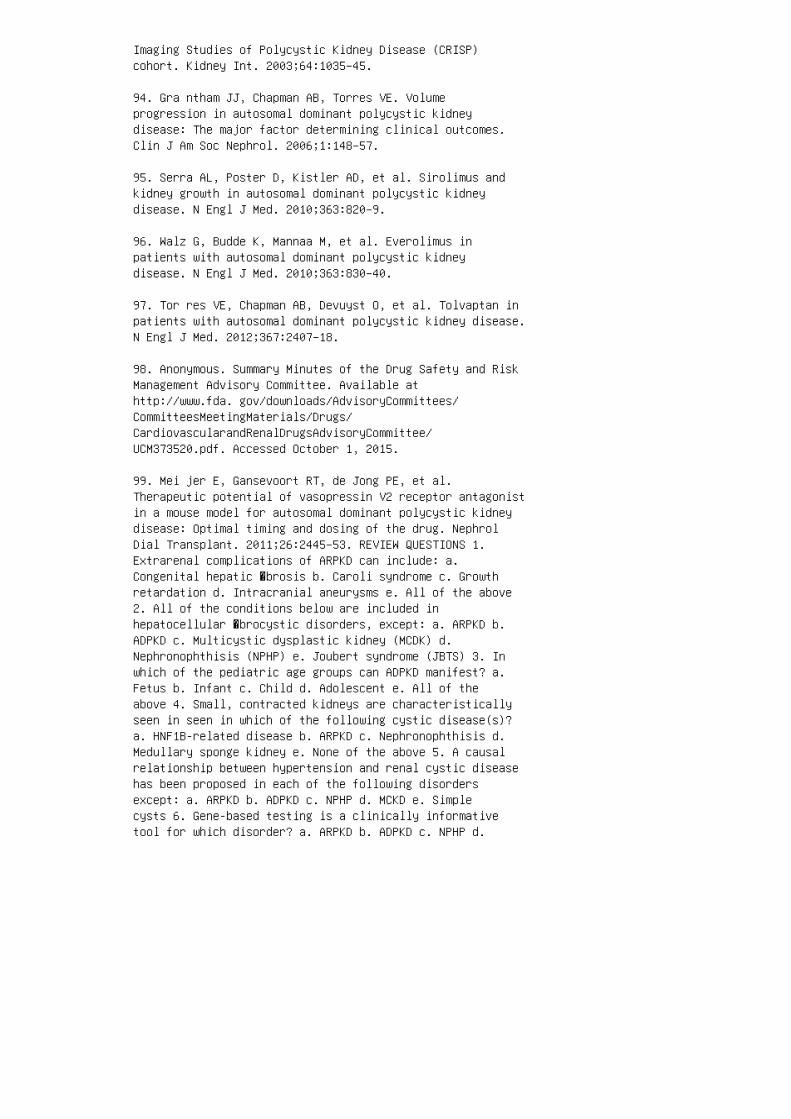
Imaging Studies of Polycystic Kidney Disease (CRISP)cohort. Kidney Int. 2003;64:1035–45.
94. Gra ntham JJ, Chapman AB, Torres VE. Volumeprogression in autosomal dominant polycystic kidneydisease: The major factor determining clinical outcomes.Clin J Am Soc Nephrol. 2006;1:148–57.
95. Serra AL, Poster D, Kistler AD, et al. Sirolimus andkidney growth in autosomal dominant polycystic kidneydisease. N Engl J Med. 2010;363:820–9.
96. Walz G, Budde K, Mannaa M, et al. Everolimus inpatients with autosomal dominant polycystic kidneydisease. N Engl J Med. 2010;363:830–40.
97. Tor res VE, Chapman AB, Devuyst O, et al. Tolvaptan inpatients with autosomal dominant polycystic kidney disease.N Engl J Med. 2012;367:2407–18.
98. Anonymous. Summary Minutes of the Drug Safety and RiskManagement Advisory Committee. Available athttp://www.fda. gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/CardiovascularandRenalDrugsAdvisoryCommittee/UCM373520.pdf. Accessed October 1, 2015.
99. Mei jer E, Gansevoort RT, de Jong PE, et al.Therapeutic potential of vasopressin V2 receptor antagonistin a mouse model for autosomal dominant polycystic kidneydisease: Optimal timing and dosing of the drug. NephrolDial Transplant. 2011;26:2445–53. REVIEW QUESTIONS 1.Extrarenal complications of ARPKD can include: a.Congenital hepatic �brosis b. Caroli syndrome c. Growthretardation d. Intracranial aneurysms e. All of the above2. All of the conditions below are included inhepatocellular �brocystic disorders, except: a. ARPKD b.ADPKD c. Multicystic dysplastic kidney (MCDK) d.Nephronophthisis (NPHP) e. Joubert syndrome (JBTS) 3. Inwhich of the pediatric age groups can ADPKD manifest? a.Fetus b. Infant c. Child d. Adolescent e. All of theabove 4. Small, contracted kidneys are characteristicallyseen in seen in which of the following cystic disease(s)?a. HNF1B-related disease b. ARPKD c. Nephronophthisis d.Medullary sponge kidney e. None of the above 5. A causalrelationship between hypertension and renal cystic diseasehas been proposed in each of the following disordersexcept: a. ARPKD b. ADPKD c. NPHP d. MCKD e. Simplecysts 6. Gene-based testing is a clinically informativetool for which disorder? a. ARPKD b. ADPKD c. NPHP d.
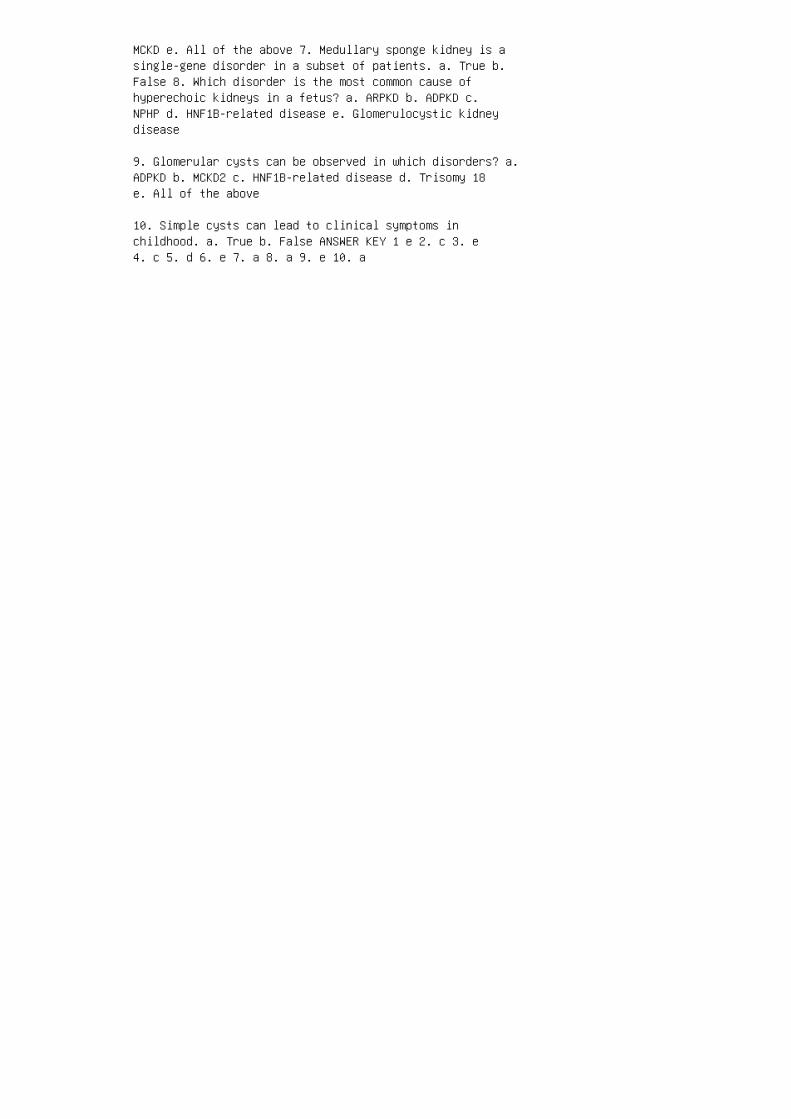
MCKD e. All of the above 7. Medullary sponge kidney is asingle-gene disorder in a subset of patients. a. True b.False 8. Which disorder is the most common cause ofhyperechoic kidneys in a fetus? a. ARPKD b. ADPKD c.NPHP d. HNF1B-related disease e. Glomerulocystic kidneydisease
9. Glomerular cysts can be observed in which disorders? a.ADPKD b. MCKD2 c. HNF1B-related disease d. Trisomy 18e. All of the above
10. Simple cysts can lead to clinical symptoms inchildhood. a. True b. False ANSWER KEY 1 e 2. c 3. e4. c 5. d 6. e 7. a 8. a 9. e 10. a
44 Ciliopathies and nephronophthisis
17. Basten SG, Giles RH. Functional aspects of primarycilia in signaling, cell cycle and tumorigenesis. Cilia.2013;2:6.
18. Sim ms RJ, Hynes AM, Eley L, Sayer JA.Nephronophthisis: A genetically diverse ciliopathy. Int JNephrol. 2011;2011:527137.
19. Leitch CC, Zaghloul NA, Davis EE, et al. Hypomorphicmutations in syndromic encephalocele genes are associatedwith Bardet-Biedl syndrome. Nat Genet. 2008;40:443–8.
20. Kri shnan R, Eley L, Sayer JA. Urinary concentrationdefects and mechanisms underlying nephronophthisis. KidneyBlood Press Res. 2008;31:152–62.
21. Hildebrandt F, Zhou W. Nephronophthisis-associatedciliopathies. J Am Soc Nephrol. 2007;18:1855–71.
22. Hil debrandt F, Otto E, Rensing C, et al. A novel geneencoding an SH3 domain protein is mutated innephronophthisis type 1. Nat Genet. 1997;17:149–53.
23. Potter DE, Holliday MA, Piel CF, et al. Treatment ofend-stage renal disease in children: A 15-year experience.Kidney Int. 1980;18:103–9.
24. Wal dherr R, Lennert T, Weber HP, et al. Thenephronophthisis complex: A clinicopathologic study inchildren. Virchows Arch A Pathol Anat Histol.1982;394:235–54.
25. Ala -Mello S, Koskimies O, Rapola J, Kaariainen H.Nephronophthisis in Finland: Epidemiology and comparisonof genetically classified subgroups. Eur J Hum Genet.1999;7:205–11.
26. Sal omon R, Saunier S, Niaudet P. Nephronophthisis.Pediatr Nephrol. 2009;24:2333–44.
27. Hal britter J, Porath JD, Diaz KA, et al.Identification of 99 novel mutations in a worldwide cohortof 1,056 patients with a nephronophthisis-relatedciliopathy. Hum Genet. 2013;132:865–84.
28. Otto EA, Schermer B, Obara T, et al. Mutations in INVSencoding inversin cause nephronophthisis type 2, linkingrenal cystic disease to the function of primary cilia and
left-right axis determination. Nat Genet. 2003;34:413–20.
29. Olbrich H, Fliegauf M, Hoefele J, et al. Mutations ina novel gene, NPHP3, cause adolescent nephronophthisis,tapeto-retinal degeneration and hepatic fibrosis. NatGenet. 2003;34:455–9.
30. Antignac C, Arduy CH, Beckmann JS, et al. A gene forfamilial juvenile nephronophthisis (recessive medullarycystic kidney disease) maps to chromosome 2p. Nat Genet.1993;3:342–5.
31. Ele y L, Moochhala SH, Simms R, et al. Nephrocystin-1interacts directly with Ack1 and is expressed in humancollecting duct. Biochem Biophys Res Commun.2008;371:877–82.
32. Georges B, Cosyns JP, Dahan K, et al. Late-onset renalfailure in Senior-Loken syndrome. Am J Kidney Dis.2000;36:1271–5. 33. Apostolou T, Nikolopoulou N,Theodoridis M, et al. Late onset of renal disease innephronophthisis with features of Joubert syndrome type B.Nephrol Dial Transplant. 2 001;16:2412–5. 34. Hoe fele J,Nayir A, Chaki M, et al. Pseudodominant inheritance ofnephronophthi sis caused by a homozygous NPHP1 deletion.Ped iatr Nephrol. 2011;26:967–71. 35. Nag C , Ghosh M, DasK, Ghosh T. Joubert syn dro me: The molar tooth sign of themid-brain. Ann Med Health Sci Res. 2013;3:291–4. 36.Simms RJ, Eley L, Sayer JA. Nephronophthisis. Eur J HumGenet. 2008;17:406–16. 37. Chaki M, Airik R, Ghosh AK, etal. Exome capture reveals ZNF423 and CEP164 muta tions,linking renal ciliopathies to DNA damage responsesignaling. Cell. 2012;150:533–48. 38. Gee H Y, Otto EA,Hurd TW, et al. Whole-exome resequencing distinguishescystic kidney dis eases from phenocopies in renalciliopathies. Kid ney Int. 2014;85:880–7. 39. Saye r JA,Simms RJ. The challenges and sur prises of a definitivemolecular genetic diagnosis. Kidney Int. 2014;85:748–9.40. Mihatsch MJ, Gudat F, Zollinger HU, et al. Systemickaryomegaly associated with chronic interstitialnephritis: A new disease entity? Clin Nephrol.1979;12:54–62. REVIEW QUESTIONS 1. Clinical features of aciliopathy may include: a. Renal cysts b. Retinal diseasec. Cerebral malformations d. All of above e. None ofabove 2. Nephronopthisis may be associated with which ofthe following syndromes? a. Joubert syndrome b. Long QTsyndrome c. Medullary cystic kidney disease d.Senior-Loken syndrome e. a and d f. b and c 3. �e mostcommon genetic cause of nephronophthisis is: a. NPHP1 b.NPH P4 c. SDC CAG8 d. NPHP 5
4. A molecular genetic diagnosis can be made in whatpercentage of cases of NPHP?
a. 25%
b. 40%
c. 60%
d. 10%
5. �e histologic features of nephronophthisis may include:
a. Glomerular basement membrane thinning
b. Interstitial �brosis
c. Karyomegaly d. Cortical microcysts e. b and d f. aand c ANSWER KEY 1. d 2. e 3. a 4. c 5. e

45 Alport syndrome and thin basementmembrane nephropathy
1. Alport AC. Hereditary familial congenital haemorrhagicnephritis. Br Med J. 1927;1:504–6.
2. Barker DF, Hostikka SL, Zhou J, et al. Identificationof mutations in the COL4A5 collagen gene in Alportsyndrome. Science. 1990;248:1224–7.
3. Moc hizuki T, Lemmink HH, Mariyama M, et al.Identification of mutations in the alpha 3(IV) and alpha4(IV) collagen genes in autosomal recessive Alportsyndrome. Nat Genet. 1994;8:77–81.
4. Rogers PW, Kurtzman NA, Bunn SM, Jr., White MG.Familial benign essential hematuria. Arch Intern Med.1973;131:257–62.
5. van Paassen P, van Breda Vriesman PJ, et al. Signs andsymptoms of thin basement membrane nephropathy: Aprospective regional study on primary glomerulardisease—The Limburg Renal Registry. Kidney Int.2004;66:909–13.
6. Lem mink HH, Nillesen WN, Mochizuki T, et al. Benignfamilial hematuria due to mutation of the type IV collagenalpha4 gene. J Clin Invest. 1996;98:1114–8.
7. Levy M, Feingold J. Estimating prevalence insingle-gene kidney diseases progressing to renal failure.Kidney Int. 2000;58:925–43.
8. Haas M. Thin glomerular basement membrane nephropathy:Incidence in 3471 consecutive renal biopsies examined byelectron microscopy. Arch Pathol Lab Med.2006;130:699–706. 9. Trachtman H, Weiss RA, Bennett B,Greifer I. Isolated hematuria in children: Indications fora renal biopsy. Kidney Int. 1984;25:94–9. 10. SchroderCH, Bontemps CM, Assmann KJ, et al. Renal biopsy andfamily studies in 65 children with isolated hematuria.Acta Paediatr Scand. 1990;79:630–6. 11. Piq ueras AI,White RH, Raafat F, Moghal N, Milford DV. Renal biopsydiagnosis in children presenting with haematuria. PediatrNephrol. 1998;12:386–91. 12. U.S. Renal Data System. USRDS2013 Annual Data Report: Atlas of Chronic Kidney Diseaseand EndStage Renal Disease in the United States. Bethesda,MD: USRDS; 2013. 13. Abrahamson DR. Origin of theglomerular basement membrane visualized after in vivolabeling of laminin in newborn rat kidneys. J Cell Biol.
1985;100:1988–2000. 14. Abrahamson DR, Hudson BG,Stroganova L, et al. Cellular origins of type IV collagennetworks in developing glomeruli. J Am Soc Nephrol.2009;20:1471–9. 15. Miner JH. The glomerular basementmembrane. Exp Cell Res. 2012;318:973–8. 16. Poschl E,Pollner R, Kuhn K. The genes for the alpha 1(IV) and alpha2(IV) chains of human basement membrane collagen type IVare arranged head-tohead and separated by a bidirectionalpromoter of unique structure. EMBO J. 1988;7:2687–95. 17.Segal Y, Zhuang L, Rondeau E, et al. Regulation of thepaired type IV collagen genes COL4A5 and COL4A6: Role ofthe proximal promoter region. J Biol Chem.2001;276:11791–7. 18. Khoshnoodi J, Cartailler JP, AlvaresK, et al. Molecular recognition in the assembly ofcollagens: Terminal noncollagenous domains are keyrecognition modules in the formation of triple helicalprotomers. J Biol Chem. 2006;281:38117–21. 19. Hudson BG.The molecular basis of Goodpasture and Alport syndromes:Beacons for the discovery of the collagen IV family. J AmSoc Nephrol. 2004;15:2514–27. 20. Kalluri R, Gattone VH,2nd, Hudson BG. Identification and localization of type IVcollagen chains in the inner ear cochlea. Connect TissueRes. 1998;37:143–50. 21. Hud son BG, Reeders ST,Tryggvason K. Type IV collagen: Structure, geneorganization, and role in human diseases: Molecular basisof Goodpasture and Alport syndromes and diffuseleiomyomatosis. J Biol Chem. 1993;268:26033–6. 22. MinerJH, Sanes JR. Collagen IV alpha 3, alpha 4, and alpha 5chains in rodent basal laminae: Sequence, distribution,association with laminins, and developmental switches. JCell Biol. 1994;127:879–91.
23. Gunwar S, Ballester F, Noelken ME, et al. Glomerularbasement membrane: Identification of a noveldisulfide-cross-linked network of alpha3, alpha4, andalpha5 chains of type IV collagen and its implications forthe pathogenesis of Alport syndrome. J Biol Chem.1998;273:8767–75.
24. Zeisberg M, Khurana M, Rao VH, et al. Stage-specificaction of matrix metalloproteinases influences progressivehereditary kidney disease. PLoS Med. 2006;3:e100.
25. Pes cucci C, Mari F, Longo I, et al. AutosomaldominantAlport syndrome: Natural history of a disease due toCOL4A3 or COL4A4 gene. Kidney Int. 2004;65:1598–603.
26. Fallerini C, Dosa L, Tita R, et al. Unbiased nextgeneration sequencing analysis confirms the existence ofautosomal dominant Alport syndrome in a relevant fraction
of cases. Clin Genet. 2014;86:252–7.
27. Crockett DK, Pont-Kingdon G, Gedge F, et al. TheAlport syndrome COL4A5 variant database. Hum Mutat.2010;31:e1652–7.
28. Rana K, Wang YY, Buzza M, et al. The genetics of thinbasement membrane nephropathy. Semin Nephrol.2005;25:163–70.
29. Jef ferson JA, Lemmink HH, Hughes AE, et al.Autosomal dominant Alport syndrome linked to the type IVcollage alpha 3 and alpha 4 genes (COL4A3 and COL4A4).Nephrol Dial Transplant. 1997;12:1595–9.
30. Ran a K, Wang YY, Powell H, et al. Persistent familialhematuria in children and the locus for thin basementmembrane nephropathy. Pediatr Nephrol. 2005;20:1729–37.
31. Jais JP, Knebelmann B, Giatras I, et al. X-linkedAlport syndrome: Natural history in 195 families andgenotype-phenotype correlations in males. J Am SocNephrol. 2000;11:649–57.
32. Jais JP, Knebelmann B, Giatras I, et al. X-linkedAlport syndrome: Natural history and genotypephenotypecorrelations in girls and women belonging to 195 families:A European Community Alport Syndrome Concerted Actionstudy. J Am Soc Nephrol. 2003;14:2603–10.
33. Kashtan CE, Ding J, Gregory M, et al. Clinical practicerecommendations for the treatment of Alport syndrome: Astatement of the Alport Syndrome Research Collaborative.Pediatr Nephrol. 2013;28:5–11.
34. Rhe ault MN, Kren SM, Hartich LA, et al.X-inactivation modifies disease severity in femalecarriers of murine X-linked Alport syndrome. Nephrol DialTransplant. 2010;25:764–9.
35. Zehnder AF, Adams JC, Santi PA, et al. Distributionof type IV collagen in the cochlea in Alport syndrome.Arch Otolaryngol Head Neck Surg. 2005;131:1007–13. 36.Harvey SJ, Mount R, Sado Y, et al. The inner ear of dogswith X-linked nephritis provides clues to the pathogenesisof hearing loss in X-linked Alport syndrome. Am J Pathol2001;159:1097–104. 37. Storey H, Savige J, Sivakumar V,et al. COL4A3/ COL4A4 mutations and features in individualswith autosomal recessive Alport syndrome. J Am SocNephrol. 2013;24:1945–54. 38. Col ville DJ, Savige J.
Alport syndrome: A review of the ocular manifestations.Ophthalmic Genet. 1997;18:161–73. 39. Nielsen CE.Lenticonus anterior and Alport’s syndrome. Acta Ophthalmol(Copenh). 1978;56:518–30. 40. Perrin D, Jungers P,Grunfeld JP, et al. Perimacular changes in Alport’ssyndrome. Clin Nephrol. 1980;13:163–7. 41. TeekhasaeneeC, Nimmanit S, Wutthiphan S, et al. Posterior polymorphousdystrophy and Alport syndrome. Ophthalmology.1991;98:1207–15. 42. Bur ke JP, Clearkin LG, Talbot JF.Recurrent corneal epithelial erosions in Alport’s syndrome.Acta Ophthalmol (Copenh). 1991;69:555–7. 43. Kashtan CE,Kleppel MM, Gubler MC. Immunohistologic findings in Alportsyndrome. Contrib Nephrol. 1996;117:142–53. 44. Gub lerMC, Knebelmann B, Beziau A, et al. Autosomal recessiveAlport syndrome: Immunohistochemical study of type IVcollagen chain distribution. Kidney Int. 1995;47:1142–7.45. Tryggvason K, Patrakka J. Thin basement membranenephropathy. J Am Soc Nephrol. 2006;17:813–22. 46. Savi geJ, Rana K, Tonna S, et al. Thin basement membranenephropathy. Kidney Int. 2003;64:1169–78. 47. Gre goryMC. The clinical features of thin basement membranenephropathy. Semin Nephrol. 2005;25:140–5. 48. Vogler C,McAdams AJ, Homan SM. Glomerular basement membrane andlamina densa in infants and children: An ultrastructuralevaluation. Pediatr Pathol. 1987;7:527–34. 49. Cosio FG,Falkenhain ME, Sedmak DD. Association of thin glomerularbasement membrane with other glomerulopathies. Kidney Int.1994;46:471–4. 50. Savige J, Gregory M, Gross O, et al.Expert guidelines for the management of Alport syndrome andthin basement membrane nephropathy. J Am Soc Nephrol.2013;24:364–75. 51. Her tz JM, Thomassen M, Storey H,Flinter F. Clinical utility gene card for: Alportsyndrome. Eur J Hum Genet. 2012;20. 52. Web b NJ,Shahinfar S, Wells TG, et al. Losartan and enalapril arecomparable in reducing proteinuria in children with Alportsyndrome. Pediatr Nephrol. 2013;28:737–43.
53. Gross O, Licht C, Anders HJ, et al. Earlyangiotensin-converting enzyme inhibition in Alportsyndrome delays renal failure and improves lifeexpectancy. Kidney Int. 2012;81:494–501.
54. Gross O, Beirowski B, Koepke ML, et al. Preemptiveramipril therapy delays renal failure and reduces renalfibrosis in COL4A3-knockout mice with Alport syndrome.Kidney Int. 2003;63:438–46.
55. Gross O, Friede T, Hilgers R, et al. Safety andefficacy of the ACE-inhibitor ramipril in Alport syndrome:The double-blind, randomized, placebocontrolled,
multicenter phase III EARLY PRO-TECT Alport Trial inPediatric Patients. ISRN Pediatr 2012;436046.
56. Temme J, Kramer A, Jager KJ, et al. Outcomes of malepatients with Alport syndrome undergoing renal replacementtherapy. Clin J Am Soc Nephrol. 2012;7:1969–76.
57. Gross O, Weber M, Fries JW, Muller GA. Living donorkidney transplantation from relatives with mild urinaryabnormalities in Alport syndrome: Long-term risk, benefitand outcome. Nephrol Dial Transplant. 2009;24:1626–30.
58. Bro wne G, Brown PA, Tomson CR, et al.Retransplantation in Alport post-transplant antiGBMdisease. Kidney Int. 2004;65:675–81.
59. Kashtan CE. Renal transplantation in patients withAlport syndrome. Pediatr Transplant. 2006;10:651–7.
REVIEW QUESTIONS
1. In a patient with persistent microscopic hematuria,which of the following �ndings is suggestive of a diagnosisof Alport syndrome rather than thin basement membranenephropathy?
a. Male gender
b. Family history of hematuria
c. Failed newborn hearing screen
d. Anterior lenticonus
e. Elevated cholesterol
2. X-linked Alport syndrome is caused by mutations inwhich gene?
a. COL4A3
b. COL4A4
c. COL4A5
d. MYH9
e. PAX2
3. Het erozygous females with COL4A5 mutations are at risk

for:
a. Micr oscopic hematuria
b. Pro teinuria
c. End -stage renal disease d. Deafness e. All of theabove 4. ACEIs are NOT indicated for treatment of whichpatient? a. Male with XLAS and proteinuria b. Male withXLAS and microalbuminuria with family history of ESRD atage 20 c. Male with XLAS and microalbuminuria with familyhistory of ESRD at age 50 d. Female with XLAS andproteinuria e. Female with ARAS and proteinuria 5. �istype of mutation in COL4A5 is associated with a milderAlport phenotype: a. Missense mutation b. Large deletionc. Splice site mutation d. Nonsense mutation e. Largerearrangement 6. �e following ophthalmologic �ndings arefrequently observed in patients with Alport syndrome,except: a. Anterior lenticonus b. Myopia c. Cornealerosion d. Maculopathy e. Posterior polymorphousdystrophy 7. α5(IV) may be absent from the GBM and presentin the Bowman capsule in which disorder? a. Males withXLAS b. Females with XLAS c. TBMN d. ARAS e. ARAS andADAS 8. TBMN can be caused by mutations in: a. COL4A3 b.COL4A4 c. COL4A5 d. Both a and b e. Both a and c ANSWERS1. d 2. c 3. e 4. c 5. a 6. b 7. e 8. d
46 Renal disease in syndromic disorders
1. Lin F, Patel V, Igarashi P. Renal dysgenesis. In:Lifton RP, Somlo S, Giebish GH, Seldin DW, editors.Genetic Diseases of the Kidney. New York: Academic Press;2009. p. 463–93. 2. Limwongse C. Syndromes andmalformations of the urinary tract. In: Avner E, Harman,WE, Niaudet, P, Yoshikawa, N, editors. PediatricNephrology, 6th ed. New York: Springer; 2010. p. 121–56.3. Spi tzer AA, editor. Inheritance of Kidney and UrinaryTract Diseases. Boston: Kluwer Academic Publishers; 1989.4. Turnpenny PD, Ellard S. Alagille syndrome:Pathogenesis, diagnosis and management. Eur J Hum Genet.2012;20:251–7. 5. Ber ard E, Sarles J, Triolo V, et al.Renovascular hypertension and vascular anomalies inAlagille syndrome. Pediatr Nephrol. 1998;12:121–4. 6.Salem JE, Bruguiere E, Iserin L, et al. Hypertension andaortorenal disease in Alagille syndrome. J Hypertens.2012;30:1300–6. 7. Hab ib R, Dommergues JP, Gubler MC, etal. Glomerular mesangiolipidosis in Alagille syndrome(arteriohepatic dysplasia). Pediatr Nephrol.1987;1:455–64. 8. Green JS, Parfrey PS, Harnett JD, et al.The cardinal manifestations of Bardet-Biedl syndrome, aform of Laurence-Moon-Biedl syndrome. N Engl J Med.1989;321:1002–9. 9. Bea les PL, Elcioglu N, Woolf AS, etal. New criteria for improved diagnosis of Bardet-Biedlsyndrome: Results of a population survey. J Med Genet.1999;36:437–46. 10. Putoux A, Attie-Bitach T, MartinovicJ, Gubler MC. Phenotypic variability of Bardet-Biedlsyndrome: Focusing on the kidney. Pediatr Nephrol.2012;27:7–15. 11. Imhoff O, Marion V, Stoetzel C, et al.Bardet-Biedl syndrome: A study of the renal andcardiovascular phenotypes in a French cohort. Clin J Am SocNephrol. 2011;6:22-9. 12. Dippell J, Varlam DE. Earlysonographic aspects of kidney morphology in Bardet-Biedlsyndrome. Pediatr Nephrol. 1998;12:559–63. 13. Janssen S,Ramaswami G, Davis EE, et al. Mutation analysis inBardet-Biedl syndrome by DNA pooling and massivelyparallel resequencing in 105 individuals. Hum Genet.2011;129:79–90. 14. Zaghloul NA, Katsanis N. Mechanisticinsights into Bardet-Biedl syndrome, a model ciliopathy. JClin Invest. 2009;119:428–37. 15. Schurman SJ, ScheinmanSJ. Inherited cerebrorenal syndromes. Nat Rev Nephrol.2009;5:529–38. 16. Pettenati MJ, Haines JL, Higgins RR, etal. Wiedemann-Beckwith syndrome: Presentation of clinicaland cytogenetic data on 22 new cases and review of theliterature. Hum Genet. 1986;74:143–54. 17. Weksberg R,Shuman C, Beckwith JB. BeckwithWiedemann syndrome. Eur JHum Genet. 2010;18:8–14. 18. Choufani S, Shuman C,Weksberg R. Molecular findings in Beckwith-Wiedemann

syndrome. Am J Med. Genet. C Semin Med Genet.2013;163C:131–40. SUMMARY Genetic and syndromic disorderscan be associated renal malformations, the presence ofrenal cysts, hypercalciuria, nephrocalcinosis, andproteinuria. Progressive loss of renal function, chronickidney disease, and ESRD can also result from some ofthese disorders. Recognition of syndromes that areassociated with renal disease requires the input of agenetics team in addition to the nephrologist. Complexsurgical management in disorders such as VATER or VACTERLassociation requires the involvement of urologic and othersurgical expertise. Genetic diagnosis of many syndromicdisorders is possible now, and the array of availablediagnostic tests for clinical use is ever increasing. �ischapter provides an overview of the common syndromes andgenetic diseases associated with renal manifestations. �ereader is referred to the broader literature on thesubject for a deeper understanding, if needed.
19. Melnick M, Bixler D, Silk K, et al. Autosomal dominantbranchiootorenal dysplasia. Birth Defects Orig Artic Ser.1975;11:121–8.
20. Che n A, Francis M, Ni L, et al. Phenotypicmanifestations of branchio-oto-renal syndrome. Am J MedGenet. 1995;58:365–70.
21. Fraser FC, Ling D, Clogg D, Nogrady B. Genetic aspectsof the BOR syndrome: Branchial fistulas, ear pits, hearingloss, and renal anomalies. Am J Med Genet. 1978;2:241–52.
22. Rod riguez Soriano J. Branchio-oto-renal syndrome. JNephrol. 2003;16:603–5.
23. Orten DJ, Fischer SM, Sorensen JL, et al.Branchiooto-renal syndrome (BOR): Novel mutations in theEYA1 gene, and a review of the mutational genetics of BOR.Hum Mutat. 2008;29:537–44.
24. Abdelhak S, Kalatzis V, Heilig R, et al. A humanhomologue of the Drosophila eyes absent gene underliesbranchio-oto-renal (BOR) syndrome and identifies a novelgene family. Nat Genet. 1997;15:157–64.
25. Xu PX , Adams J, Peters H, et al. Eya1-deficient micelack ears and kidneys and show abnormal apoptosis of organprimordia. Nat Genet. 1999;23:113–7.
26. Hos kins BE, Cramer CH, Silvius D, et al.Transcription factor SIX5 is mutated in patients with
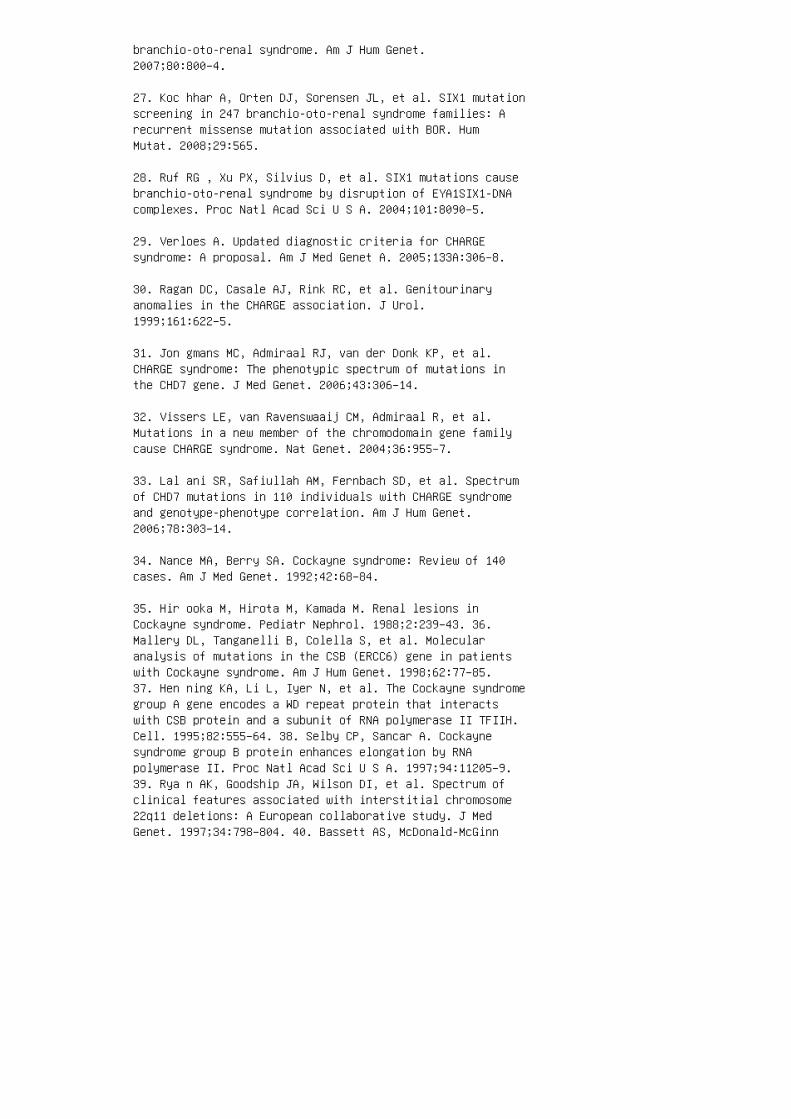
branchio-oto-renal syndrome. Am J Hum Genet.2007;80:800–4.
27. Koc hhar A, Orten DJ, Sorensen JL, et al. SIX1 mutationscreening in 247 branchio-oto-renal syndrome families: Arecurrent missense mutation associated with BOR. HumMutat. 2008;29:565.
28. Ruf RG , Xu PX, Silvius D, et al. SIX1 mutations causebranchio-oto-renal syndrome by disruption of EYA1SIX1-DNAcomplexes. Proc Natl Acad Sci U S A. 2004;101:8090–5.
29. Verloes A. Updated diagnostic criteria for CHARGEsyndrome: A proposal. Am J Med Genet A. 2005;133A:306–8.
30. Ragan DC, Casale AJ, Rink RC, et al. Genitourinaryanomalies in the CHARGE association. J Urol.1999;161:622–5.
31. Jon gmans MC, Admiraal RJ, van der Donk KP, et al.CHARGE syndrome: The phenotypic spectrum of mutations inthe CHD7 gene. J Med Genet. 2006;43:306–14.
32. Vissers LE, van Ravenswaaij CM, Admiraal R, et al.Mutations in a new member of the chromodomain gene familycause CHARGE syndrome. Nat Genet. 2004;36:955–7.
33. Lal ani SR, Safiullah AM, Fernbach SD, et al. Spectrumof CHD7 mutations in 110 individuals with CHARGE syndromeand genotype-phenotype correlation. Am J Hum Genet.2006;78:303–14.
34. Nance MA, Berry SA. Cockayne syndrome: Review of 140cases. Am J Med Genet. 1992;42:68–84.
35. Hir ooka M, Hirota M, Kamada M. Renal lesions inCockayne syndrome. Pediatr Nephrol. 1988;2:239–43. 36.Mallery DL, Tanganelli B, Colella S, et al. Molecularanalysis of mutations in the CSB (ERCC6) gene in patientswith Cockayne syndrome. Am J Hum Genet. 1998;62:77–85.37. Hen ning KA, Li L, Iyer N, et al. The Cockayne syndromegroup A gene encodes a WD repeat protein that interactswith CSB protein and a subunit of RNA polymerase II TFIIH.Cell. 1995;82:555–64. 38. Selby CP, Sancar A. Cockaynesyndrome group B protein enhances elongation by RNApolymerase II. Proc Natl Acad Sci U S A. 1997;94:11205–9.39. Rya n AK, Goodship JA, Wilson DI, et al. Spectrum ofclinical features associated with interstitial chromosome22q11 deletions: A European collaborative study. J MedGenet. 1997;34:798–804. 40. Bassett AS, McDonald-McGinn
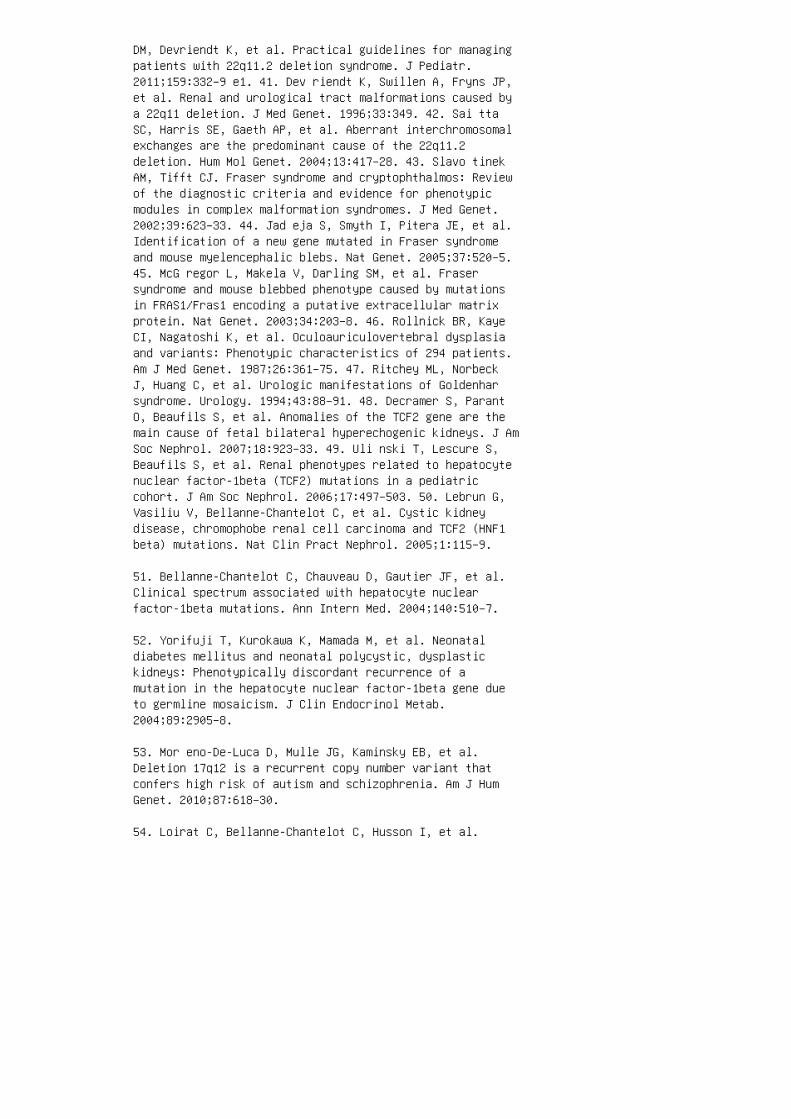
DM, Devriendt K, et al. Practical guidelines for managingpatients with 22q11.2 deletion syndrome. J Pediatr.2011;159:332–9 e1. 41. Dev riendt K, Swillen A, Fryns JP,et al. Renal and urological tract malformations caused bya 22q11 deletion. J Med Genet. 1996;33:349. 42. Sai ttaSC, Harris SE, Gaeth AP, et al. Aberrant interchromosomalexchanges are the predominant cause of the 22q11.2deletion. Hum Mol Genet. 2004;13:417–28. 43. Slavo tinekAM, Tifft CJ. Fraser syndrome and cryptophthalmos: Reviewof the diagnostic criteria and evidence for phenotypicmodules in complex malformation syndromes. J Med Genet.2002;39:623–33. 44. Jad eja S, Smyth I, Pitera JE, et al.Identification of a new gene mutated in Fraser syndromeand mouse myelencephalic blebs. Nat Genet. 2005;37:520–5.45. McG regor L, Makela V, Darling SM, et al. Frasersyndrome and mouse blebbed phenotype caused by mutationsin FRAS1/Fras1 encoding a putative extracellular matrixprotein. Nat Genet. 2003;34:203–8. 46. Rollnick BR, KayeCI, Nagatoshi K, et al. Oculoauriculovertebral dysplasiaand variants: Phenotypic characteristics of 294 patients.Am J Med Genet. 1987;26:361–75. 47. Ritchey ML, NorbeckJ, Huang C, et al. Urologic manifestations of Goldenharsyndrome. Urology. 1994;43:88–91. 48. Decramer S, ParantO, Beaufils S, et al. Anomalies of the TCF2 gene are themain cause of fetal bilateral hyperechogenic kidneys. J AmSoc Nephrol. 2007;18:923–33. 49. Uli nski T, Lescure S,Beaufils S, et al. Renal phenotypes related to hepatocytenuclear factor-1beta (TCF2) mutations in a pediatriccohort. J Am Soc Nephrol. 2006;17:497–503. 50. Lebrun G,Vasiliu V, Bellanne-Chantelot C, et al. Cystic kidneydisease, chromophobe renal cell carcinoma and TCF2 (HNF1beta) mutations. Nat Clin Pract Nephrol. 2005;1:115–9.
51. Bellanne-Chantelot C, Chauveau D, Gautier JF, et al.Clinical spectrum associated with hepatocyte nuclearfactor-1beta mutations. Ann Intern Med. 2004;140:510–7.
52. Yorifuji T, Kurokawa K, Mamada M, et al. Neonataldiabetes mellitus and neonatal polycystic, dysplastickidneys: Phenotypically discordant recurrence of amutation in the hepatocyte nuclear factor-1beta gene dueto germline mosaicism. J Clin Endocrinol Metab.2004;89:2905–8.
53. Mor eno-De-Luca D, Mulle JG, Kaminsky EB, et al.Deletion 17q12 is a recurrent copy number variant thatconfers high risk of autism and schizophrenia. Am J HumGenet. 2010;87:618–30.
54. Loirat C, Bellanne-Chantelot C, Husson I, et al.

Autism in three patients with cystic or hyperechogenickidneys and chromosome 17q12 deletion. Nephrol. DialTransplant. 2010;25:3430–3.
55. Heidet L, Decramer S, Pawtowski A, et al. Spectrum ofHNF1B mutations in a large cohort of patients who harborrenal diseases. Clin J Am Soc Nephrol. 2010;5:1079–90.
56. Karstensen HG, Tommerup N. Isolated and syndromic formsof congenital anosmia. Clin Genet. 2012;81:210–5.
57. Har delin JP, Dode C. The complex genetics of Kallmannsyndrome: KAL1, FGFR1, FGF8, PROKR2, PROK2, et al. SexDev. 2008;2:181–93.
58. Dod e C, Teixeira L, Levilliers J, et al. Kallmannsyndrome: Mutations in the genes encoding prokineticin-2and prokineticin receptor-2. PLoS Genet. 2006;2:e175.
59. Hardelin JP, Julliard AK, Moniot B, et al. Anosmin-1 isa regionally restricted component of basement membranes andinterstitial matrices during organogenesis: Implicationsfor the developmental anomalies of X chromosome-linkedKallmann syndrome. Dev Dyn. 1999;215:26–44.
60. Kirk JM, Grant DB, Besser GM, et al. Unilateral renalaplasia in X-linked Kallmann’s syndrome. Clin Genet.1994;46:260–2.
61. Mor cel K, Camborieux L, Guerrier D.MayerRokitansky-Kuster-Hauser (MRKH) syndrome. Orphanet JRare Dis. 2007;2:13.
62. Devriendt K, Moerman P, Van Schoubroeck D, et al.Chromosome 22q11 deletion presenting as the Pottersequence. J Med Genet. 1997;34:423–5.
63. Alexiev BA, Lin X, Sun CC, Brenner DS. MeckelGrubersyndrome: Pathologic manifestations, minimal diagnosticcriteria, and differential diagnosis. Arch Pathol Lab Med.2006;130:1236–8.
64. Bla nkenberg TA, Ruebner BH, Ellis WG, et al.Pathology of renal and hepatic anomalies in Meckelsyndrome. Am J Med Genet Suppl. 1987;3:395–410.
65. Art s HH, Knoers NV. Current insights into renalciliopathies: What can genetics teach us? Pediatr Nephrol.2013;28:863–74. 66. Di Donato S. Multisystemmanifestations of mitochondrial disorders. J Neurol.

2009;256:693–710. 67. DiMauro S, Schon EA. Mitochondrialrespiratorychain diseases. N Engl J Med. 2003;348:2656–68.68. And erson S, Bankier AT, Barrell BG, et al. Sequenceand organization of the human mitochondrial genome.Nature. 1981;290:457–65. 69. Niaudet P, Rotig A. Renalinvolvement in mitochondrial cytopathies. Pediatr Nephrol.1996;10:368–73. 70. Au KM, Lau SC, Mak YF, et al.Mitochondrial DNA deletion in a girl with Fanconi’ssyndrome. Pediatr Nephrol. 2007;22:136–40. 71. Maj anderA, Suomalainen A, Vettenranta K, et al. Congenitalhypoplastic anemia, diabetes, and severe renal tubulardysfunction associated with a mitochondrial DNA deletion.Pediatr Res. 1991;30:327–30. 72. Niaudet P, Heidet L,Munnich A, et al. Deletion of the mitochondrial DNA in acase of de Toni-DebreFanconi syndrome and Pearson syndrome.Pediatr Nephrol. 1994;8:164–8. 73. de Lo nlay P, ValnotI, Barrientos A, et al. A mutant mitochondrial respiratorychain assembly protein causes complex III deficiency inpatients with tubulopathy, encephalopathy and liverfailure. Nat Genet. 2001;29:57–60. 74. Barakat AY,D’Albora JB, Martin MM, Jose PA. Familial nephrosis, nervedeafness, and hypoparathyroidism. J Pediatr. 1977;91:61–4.75. Goldenberg A, Ngoc LH, Thouret MC, et al. Respiratorychain deficiency presenting as congenital nephroticsyndrome. Pediatr Nephrol. 2005;20:465–9. 76. Mon tini G,Malaventura C, Salviati L. Early coenzyme Q10supplementation in primary coenzyme Q10 deficiency. N EnglJ Med. 2008;358:2849–50. 77. Rot ig A, Appelkvist EL,Geromel V, et al. Quinoneresponsive multiplerespiratory-chain dysfunction due to widespread coenzymeQ10 deficiency. Lancet. 2000;356:391–5. 78. Emma F,Bertini E, Salviati L, Montini G. Renal involvement inmitochondrial cytopathies. Pediatr Nephrol.2012;27:539–50. 79. Rotig A, Goutieres F, Niaudet P, etal. Deletion of mitochondrial DNA in patient with chronictubulointerstitial nephritis. J Pediatr. 1995;126:597–601.80. Tzen CY, Tsai JD, Wu TY, et al. Tubulointerstitialnephritis associated with a novel mitochondrial pointmutation. Kidney Int. 2001;59:846–54. 81. Rustin P,Chretien D, Bourgeron T, et al. Biochemical and molecularinvestigations in respiratory chain deficiencies. ClinChim Acta. 1994;228:35–51. 82. Rotig A, Munnich A. Geneticfeatures of mitochondrial respiratory chain disorders. J AmSoc Nephrol. 2003;14:2995–3007. 83. Goto Y, Nonaka I,Horai S. A mutation in the tRNA(Leu)(UUR) gene associatedwith the MELAS subgroup of mitochondrialencephalomyopathies. Nature. 1990;348:651–3.
84. Sweeney E, Fryer A, Mountford R, et al. Nail patellasyndrome: A review of the phenotype aided by developmental
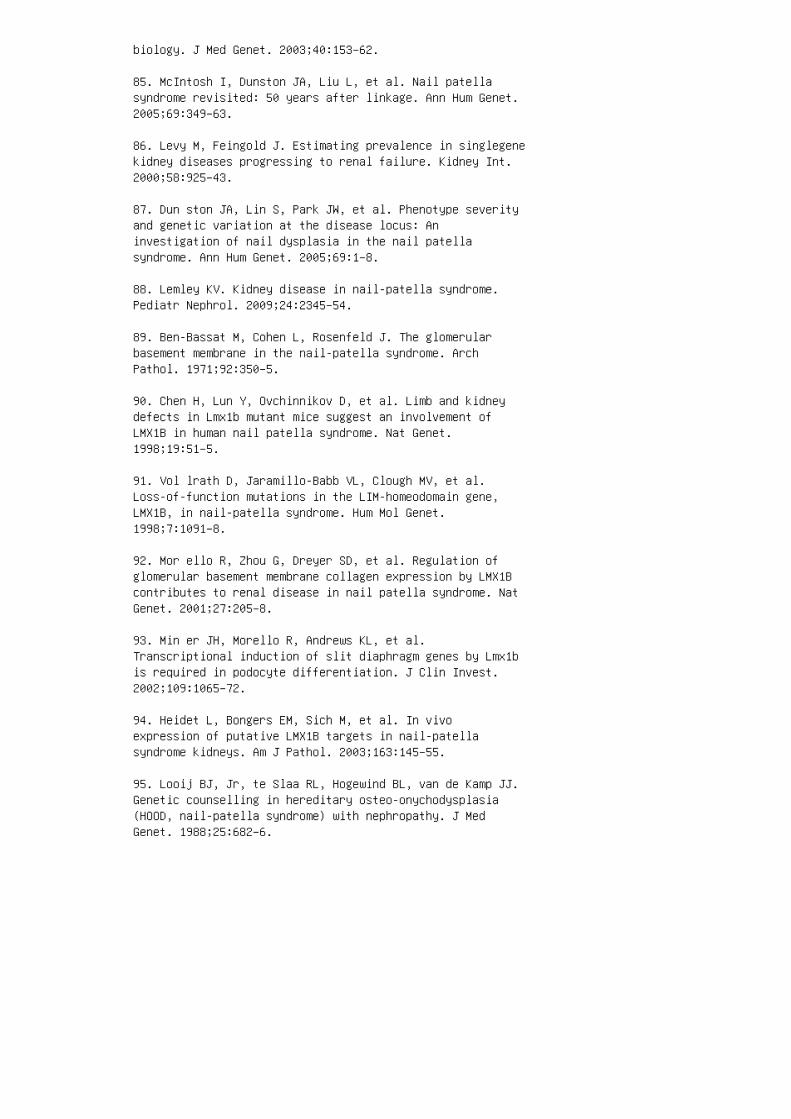
biology. J Med Genet. 2003;40:153–62.
85. McIntosh I, Dunston JA, Liu L, et al. Nail patellasyndrome revisited: 50 years after linkage. Ann Hum Genet.2005;69:349–63.
86. Levy M, Feingold J. Estimating prevalence in singlegenekidney diseases progressing to renal failure. Kidney Int.2000;58:925–43.
87. Dun ston JA, Lin S, Park JW, et al. Phenotype severityand genetic variation at the disease locus: Aninvestigation of nail dysplasia in the nail patellasyndrome. Ann Hum Genet. 2005;69:1–8.
88. Lemley KV. Kidney disease in nail-patella syndrome.Pediatr Nephrol. 2009;24:2345–54.
89. Ben-Bassat M, Cohen L, Rosenfeld J. The glomerularbasement membrane in the nail-patella syndrome. ArchPathol. 1971;92:350–5.
90. Chen H, Lun Y, Ovchinnikov D, et al. Limb and kidneydefects in Lmx1b mutant mice suggest an involvement ofLMX1B in human nail patella syndrome. Nat Genet.1998;19:51–5.
91. Vol lrath D, Jaramillo-Babb VL, Clough MV, et al.Loss-of-function mutations in the LIM-homeodomain gene,LMX1B, in nail-patella syndrome. Hum Mol Genet.1998;7:1091–8.
92. Mor ello R, Zhou G, Dreyer SD, et al. Regulation ofglomerular basement membrane collagen expression by LMX1Bcontributes to renal disease in nail patella syndrome. NatGenet. 2001;27:205–8.
93. Min er JH, Morello R, Andrews KL, et al.Transcriptional induction of slit diaphragm genes by Lmx1bis required in podocyte differentiation. J Clin Invest.2002;109:1065–72.
94. Heidet L, Bongers EM, Sich M, et al. In vivoexpression of putative LMX1B targets in nail-patellasyndrome kidneys. Am J Pathol. 2003;163:145–55.
95. Looij BJ, Jr, te Slaa RL, Hogewind BL, van de Kamp JJ.Genetic counselling in hereditary osteo-onychodysplasia(HOOD, nail-patella syndrome) with nephropathy. J MedGenet. 1988;25:682–6.
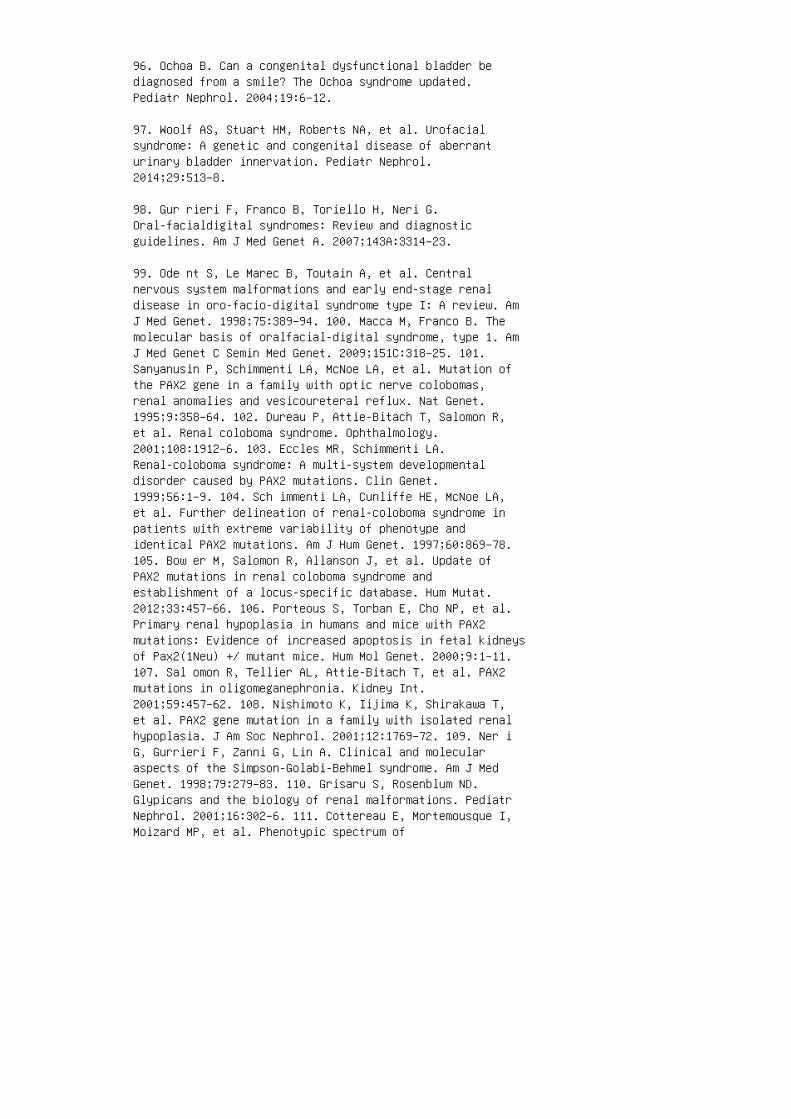
96. Ochoa B. Can a congenital dysfunctional bladder bediagnosed from a smile? The Ochoa syndrome updated.Pediatr Nephrol. 2004;19:6–12.
97. Woolf AS, Stuart HM, Roberts NA, et al. Urofacialsyndrome: A genetic and congenital disease of aberranturinary bladder innervation. Pediatr Nephrol.2014;29:513–8.
98. Gur rieri F, Franco B, Toriello H, Neri G.Oral-facialdigital syndromes: Review and diagnosticguidelines. Am J Med Genet A. 2007;143A:3314–23.
99. Ode nt S, Le Marec B, Toutain A, et al. Centralnervous system malformations and early end-stage renaldisease in oro-facio-digital syndrome type I: A review. AmJ Med Genet. 1998;75:389–94. 100. Macca M, Franco B. Themolecular basis of oralfacial-digital syndrome, type 1. AmJ Med Genet C Semin Med Genet. 2009;151C:318–25. 101.Sanyanusin P, Schimmenti LA, McNoe LA, et al. Mutation ofthe PAX2 gene in a family with optic nerve colobomas,renal anomalies and vesicoureteral reflux. Nat Genet.1995;9:358–64. 102. Dureau P, Attie-Bitach T, Salomon R,et al. Renal coloboma syndrome. Ophthalmology.2001;108:1912–6. 103. Eccles MR, Schimmenti LA.Renal-coloboma syndrome: A multi-system developmentaldisorder caused by PAX2 mutations. Clin Genet.1999;56:1–9. 104. Sch immenti LA, Cunliffe HE, McNoe LA,et al. Further delineation of renal-coloboma syndrome inpatients with extreme variability of phenotype andidentical PAX2 mutations. Am J Hum Genet. 1997;60:869–78.105. Bow er M, Salomon R, Allanson J, et al. Update ofPAX2 mutations in renal coloboma syndrome andestablishment of a locus-specific database. Hum Mutat.2012;33:457–66. 106. Porteous S, Torban E, Cho NP, et al.Primary renal hypoplasia in humans and mice with PAX2mutations: Evidence of increased apoptosis in fetal kidneysof Pax2(1Neu) +/ mutant mice. Hum Mol Genet. 2000;9:1–11.107. Sal omon R, Tellier AL, Attie-Bitach T, et al. PAX2mutations in oligomeganephronia. Kidney Int.2001;59:457–62. 108. Nishimoto K, Iijima K, Shirakawa T,et al. PAX2 gene mutation in a family with isolated renalhypoplasia. J Am Soc Nephrol. 2001;12:1769–72. 109. Ner iG, Gurrieri F, Zanni G, Lin A. Clinical and molecularaspects of the Simpson-Golabi-Behmel syndrome. Am J MedGenet. 1998;79:279–83. 110. Grisaru S, Rosenblum ND.Glypicans and the biology of renal malformations. PediatrNephrol. 2001;16:302–6. 111. Cottereau E, Mortemousque I,Moizard MP, et al. Phenotypic spectrum of

Simpson-Golabi-Behmel syndrome in a series of 42 caseswith a mutation in GPC3 and review of the literature. Am JMed Genet C Semin Med Genet. 2013;163C:92–105. 112.Powell CM, Michaelis RC. Townes-Brocks syndrome. J MedGenet. 1999;36:89–93. 113. Koh lhase J, Wischermann A,Reichenbach H, et al. Mutations in the SALL1 putativetranscription factor gene cause Townes-Brocks syndrome.Nat Genet. 1998;18:81–3. 114. Miller EM, Hopkin R, Bao L,Ware SM. Implications for genotype-phenotype predictionsin TownesBrocks syndrome: Case report of a novel SALL1deletion and review of the literature. Am J Med Genet A.2012;158A:533–40. 115. Nishinakamura R, Takasato M.Essential roles of Sall1 in kidney development. KidneyInt. 2005;68:1948–50.
116. Borozdin W, Steinmann K, Albrecht B, et al. Detectionof heterozygous SALL1 deletions by quantitative real timePCR proves the contribution of a SALL1 dosage effect inthe pathogenesis of TownesBrocks syndrome. Hum Mutat.2006;27:211–2.
117. Quan L, Smith DW. The VATER association. Vertebraldefects, anal atresia, T-E fistula with esophagealatresia, radial and renal dysplasia: A spectrum ofassociated defects. J Pediatr. 1973;82:104–7.
118. Sol omon BD. VACTERL/VATER Association. Orphanet JRare Dis. 2011;6:56.
119. Ahn SY, Mendoza S, Kaplan G, et al. Chronic kidneydisease in the VACTERL association: Clinical course andoutcome. Pediatr Nephrol. 2009;24:1047–53.
REVIEW QUESTIONS
1. Children a�ected with one of the following syndromesare at higher risk of developing Wilms tumor.
a. Bran chio-oto-renal syndrome
b. Ren al-coloboma syndrome
c. Tow nes-Brocks syndrome
d. Bec kwith-Wiedemann syndrome
e. Coc kayne syndrome
2. Whi ch of the following anomalies is not observed inpatients with HNF1B-mutation?
a. Ch olestasis
b. Hypo magnesemia
c. Mul ticystic kidney disease
d. Ver tebral malformations
e. Dia betes mellitus
3. Chi ldren a�ected with one of the following syndromesmay develop proteinuria and a nephrotic syndrome.
a. CHA RGE syndrome
b. Nai l-patella syndrome
c. Ochoa syndrome
d. Fraser syndrome
e. Simpson-Golabi-Behmel syndrome 4. Concerningmitochondrial disorders, which of the following assertionsis not applicable? a. �ey are secondary to defects ofoxidative phosdphorylation. b. Mitochondrial DNA isinherited from the father. c. �e most frequent renalmanifestation is proximal tubulopathy. d. Patients maypresent with hyperlactatemia. e. Patients may develop anephrotic syndrome. 5. All of the following are seen inpatients with Alagille syndrome, except: a. Chroniccholestasis b. Pulmonary artery stenosis c. Posteriorembryotoxon d. Hearing loss e. Vascular abnormalities 6.Which of the following does not apply to nail-patellasyndrome? a. It is an autosomal dominant disease. b.Iliac horns are a pathognomonic radiologic feature of thedisease. c. Urinary tract malformations are frequentlyobserved in nail-patella syndrome. d. Nail-patellasyndrome is caused by mutations of the LMX1B gene. e.End-stage renal disease develops in 10% to 15% of cases.ANSWER KEY 1. d 2. d 3. b 4. b 5. d 6. c

47 Hydronephrosis and obstructiveuropathies
1. Chevalier RL, Peters CA. Congenital urinary tractobstruction: Proceedings of the State-Of-The-Art StrategicPlanning Workshop—National Institutes of Health, Bethesda,MD, 11–12 March 2002. Pediatr Nephrol. 2003;18:576–606.
2. Collins A J, Foley R N, Herzog C, et al. US renal datasystem 2012 annual data report. Am J Kidney Dis.2013;61:A7, e1–476.
3. Song R, Yosypiv IV. Genetics of congenital anomalies ofthe kidney and urinary tract. Pediatr Nephrol.2011;26:353–64.
4. Leb owitz RL. Neonatal hydronephrosis: 146 cases.Radiol Clin North Am. 1977;15:49–54.
5. Flashner SC. Ureteroplevic junction. In: Kelalis PP,King LR, Belman AB, editors. Clinical Pediatric Urology.Philadelphia: Saunders; 1992. pp 693–705.
6. Woodward M, Frank D. Postnatal management of antenatalhydronephrosis. BJU Int. 2002;89:149–56.
7. Brown T, Mandell J, Lebowitz RL. Neonatal hydronephrosisin the era of sonography. Am J Radiol 1992; 148:959–964.
8. Sanna-Cherchi S, Ravani P, Corbani V, et al. Renaloutcome in patients with congenital anomalies of the kidneyand urinary tract. Kidney Int. 2009;76:528–33.
9. Kim KM, Bogaert GA, Nguyen HT, et al. Hemodynamicchanges after complete unilateral ureteral obstruction inthe young lamb. J Urol. 1997;158:1090–3.
10. Moody TE, Vaughan ED, Gillenwater JY. Relationshipbetween renal blood flow and ureteral pressure during 18hours of total unilateral ureteral occlusion:Iimplications for changing sites of increased renalresistance. Invest Urol. 1975;13,246–51.
11. Cha abane W, Praddaude F, Buleon M, et al. Renalfunctional decline and glomerulotubular injury arearrested but not restored by release of unilateralureteral obstruction (UUO). Am J Physiol Renal Physiol.304:F432–F439, 2013.
12. Yosypiv IV. Renin-angiotensin system in ureteric bud

branching morphogenesis: Insights into the mechanisms.Pediatr Nephrol. 2011;26:1499–512.
13. Gribouval O, Gonzales M, Neuhaus T, et al. Mutationsin genes in the renin-angiotensin system are associatedwith autosomal recessive renal tubular dysgenesis. NatGenet 2005;37:964–8. 14. Hiraoka M, Taniguchi T, Nakai Het al. No evidence for AT2R gene derangement in humanurinary tract anomalies. Kidney Int 2001; 59:1244. 15.Yokoyama H, Wada T, Kobayashi K, et al. A disintegrin andmetalloproteinase with thrombospondin motifs (ADAMTS)-1null mutant mice develop renal lesions mimickingobstructive nephropathy. Nephrol Dial Transplant.2002;17:39–41. 16. Gamp AC, Tanaka Y, Lüllmann-RauchR, etal. LIMP-2/LGP85 deficiency causes ureteric pelvicjunction obstruction, deafness and peripheral neuropathy inmice. Hum Mol Genet 2003;12:631–46. 17. Chang CP, McDillBW, Neilson JR, et al. Calcineurin is required inurinarytract mesenchyme for the development of the pyeloureteralperistaltic machinery. J Clin Invest 2004;113:1051–8. 18.Singh S, Robinson M, Nahi F, et al. Identification of aunique transgenic mouse line that develops mega bladder,obstructive uropathy, and renal dysfunction. J Am SocNephrol 2007; 18:461–71. 19. Cain JE, Islam E, Haxho F, etal. GLI3 repressor controls functional development of themouse ureter. J Clin Invest. 2011;121:1199–2006. 20.Tripathi P, Wang Y, Casey AM, et al. Absence of canonicalSMAD signaling in ureteral and bladder mesenchyme causesureteropelvic junction obstruction. J Am Soc Nephrol.2012;23:618–28. 21. Wei ss RM, Guo S, Shan A, et al. Brg1determines urothelial cell fate during ureter development.J Am Soc Nephrol. 2013;24:618–26. 22. Chevalier RL.Perinatal obstructive nephropathy. Semin Nephrol.2004cx;28:124–129. 23. Peters CA. Animal models of fetalrenal disease. Prenat Diagn. 2001;21:917–22. 24. MatsellDG, Mok A, Tarantal AF. Altered primate glomerulardevelopment due to in utero urinary tract obstruction.Kidney Int. 2002;61:1263–9. 25. Chevalier RL.Pathophysiology of obstructive nephropathy in the newborn.Semin Nephrol. 1998;18:585–9. 26. Chevalier RL, ThornhillBA, Wolstenholme JT, et al. Unilateral ureteralobstruction in early development alters renal growth:Dependence on the duration of obstruction. J Urol.1999;161:309–14. 27. Thornhill BA, Burt LA, Chen C et al.Variable chronic partial ureteral obstruction in theneonatal rat: A new model of ureteropelvic junctionobstruction. Kidney Int. 2005;67:42–7. 28. Chung KH,Chevalier RL. Arrested development of the neonatal kidneyfollowing chronic ureteral obstruction. J Urol.1996;155:1139–1144. 29. Chevalier RL, Peach MJ.
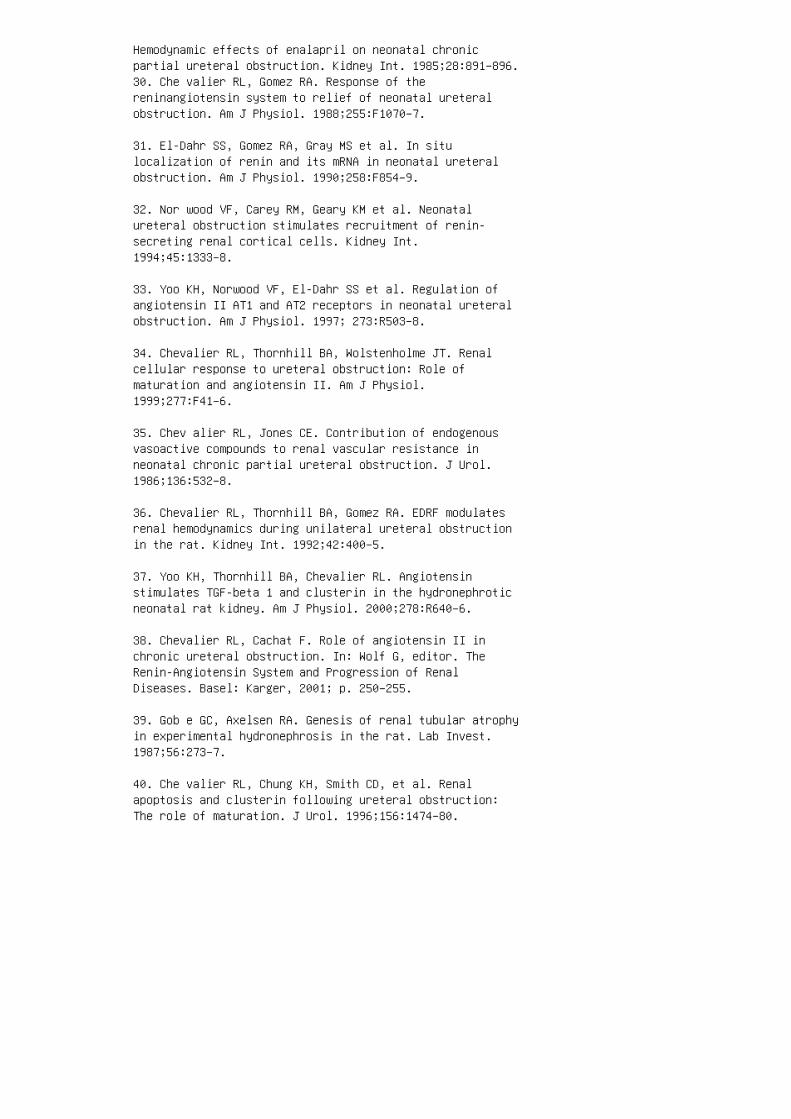
Hemodynamic effects of enalapril on neonatal chronicpartial ureteral obstruction. Kidney Int. 1985;28:891–896.30. Che valier RL, Gomez RA. Response of thereninangiotensin system to relief of neonatal ureteralobstruction. Am J Physiol. 1988;255:F1070–7.
31. El-Dahr SS, Gomez RA, Gray MS et al. In situlocalization of renin and its mRNA in neonatal ureteralobstruction. Am J Physiol. 1990;258:F854–9.
32. Nor wood VF, Carey RM, Geary KM et al. Neonatalureteral obstruction stimulates recruitment of renin-secreting renal cortical cells. Kidney Int.1994;45:1333–8.
33. Yoo KH, Norwood VF, El-Dahr SS et al. Regulation ofangiotensin II AT1 and AT2 receptors in neonatal ureteralobstruction. Am J Physiol. 1997; 273:R503–8.
34. Chevalier RL, Thornhill BA, Wolstenholme JT. Renalcellular response to ureteral obstruction: Role ofmaturation and angiotensin II. Am J Physiol.1999;277:F41–6.
35. Chev alier RL, Jones CE. Contribution of endogenousvasoactive compounds to renal vascular resistance inneonatal chronic partial ureteral obstruction. J Urol.1986;136:532–8.
36. Chevalier RL, Thornhill BA, Gomez RA. EDRF modulatesrenal hemodynamics during unilateral ureteral obstructionin the rat. Kidney Int. 1992;42:400–5.
37. Yoo KH, Thornhill BA, Chevalier RL. Angiotensinstimulates TGF-beta 1 and clusterin in the hydronephroticneonatal rat kidney. Am J Physiol. 2000;278:R640–6.
38. Chevalier RL, Cachat F. Role of angiotensin II inchronic ureteral obstruction. In: Wolf G, editor. TheRenin-Angiotensin System and Progression of RenalDiseases. Basel: Karger, 2001; p. 250–255.
39. Gob e GC, Axelsen RA. Genesis of renal tubular atrophyin experimental hydronephrosis in the rat. Lab Invest.1987;56:273–7.
40. Che valier RL, Chung KH, Smith CD, et al. Renalapoptosis and clusterin following ureteral obstruction:The role of maturation. J Urol. 1996;156:1474–80.
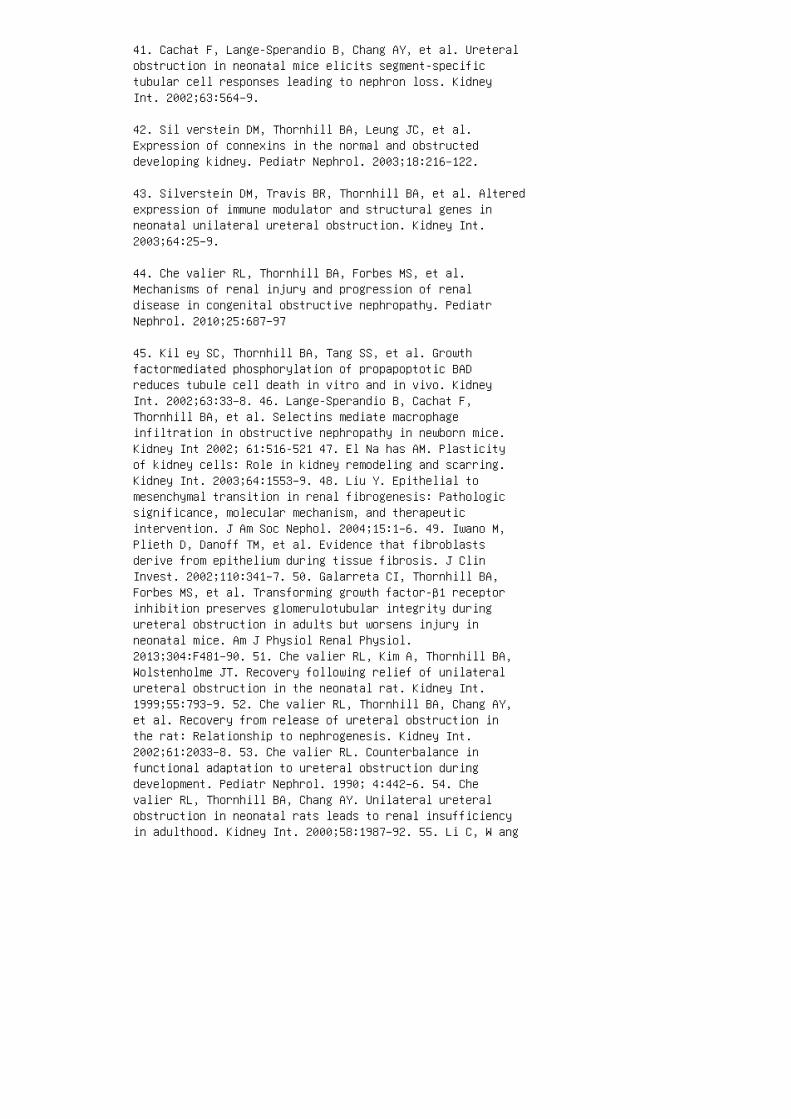
41. Cachat F, Lange-Sperandio B, Chang AY, et al. Ureteralobstruction in neonatal mice elicits segment-specifictubular cell responses leading to nephron loss. KidneyInt. 2002;63:564–9.
42. Sil verstein DM, Thornhill BA, Leung JC, et al.Expression of connexins in the normal and obstructeddeveloping kidney. Pediatr Nephrol. 2003;18:216–122.
43. Silverstein DM, Travis BR, Thornhill BA, et al. Alteredexpression of immune modulator and structural genes inneonatal unilateral ureteral obstruction. Kidney Int.2003;64:25–9.
44. Che valier RL, Thornhill BA, Forbes MS, et al.Mechanisms of renal injury and progression of renaldisease in congenital obstructive nephropathy. PediatrNephrol. 2010;25:687–97
45. Kil ey SC, Thornhill BA, Tang SS, et al. Growthfactormediated phosphorylation of propapoptotic BADreduces tubule cell death in vitro and in vivo. KidneyInt. 2002;63:33–8. 46. Lange-Sperandio B, Cachat F,Thornhill BA, et al. Selectins mediate macrophageinfiltration in obstructive nephropathy in newborn mice.Kidney Int 2002; 61:516-521 47. El Na has AM. Plasticityof kidney cells: Role in kidney remodeling and scarring.Kidney Int. 2003;64:1553–9. 48. Liu Y. Epithelial tomesenchymal transition in renal fibrogenesis: Pathologicsignificance, molecular mechanism, and therapeuticintervention. J Am Soc Nephol. 2004;15:1–6. 49. Iwano M,Plieth D, Danoff TM, et al. Evidence that fibroblastsderive from epithelium during tissue fibrosis. J ClinInvest. 2002;110:341–7. 50. Galarreta CI, Thornhill BA,Forbes MS, et al. Transforming growth factor-β1 receptorinhibition preserves glomerulotubular integrity duringureteral obstruction in adults but worsens injury inneonatal mice. Am J Physiol Renal Physiol.2013;304:F481–90. 51. Che valier RL, Kim A, Thornhill BA,Wolstenholme JT. Recovery following relief of unilateralureteral obstruction in the neonatal rat. Kidney Int.1999;55:793–9. 52. Che valier RL, Thornhill BA, Chang AY,et al. Recovery from release of ureteral obstruction inthe rat: Relationship to nephrogenesis. Kidney Int.2002;61:2033–8. 53. Che valier RL. Counterbalance infunctional adaptation to ureteral obstruction duringdevelopment. Pediatr Nephrol. 1990; 4:442–6. 54. Chevalier RL, Thornhill BA, Chang AY. Unilateral ureteralobstruction in neonatal rats leads to renal insufficiencyin adulthood. Kidney Int. 2000;58:1987–92. 55. Li C, W ang
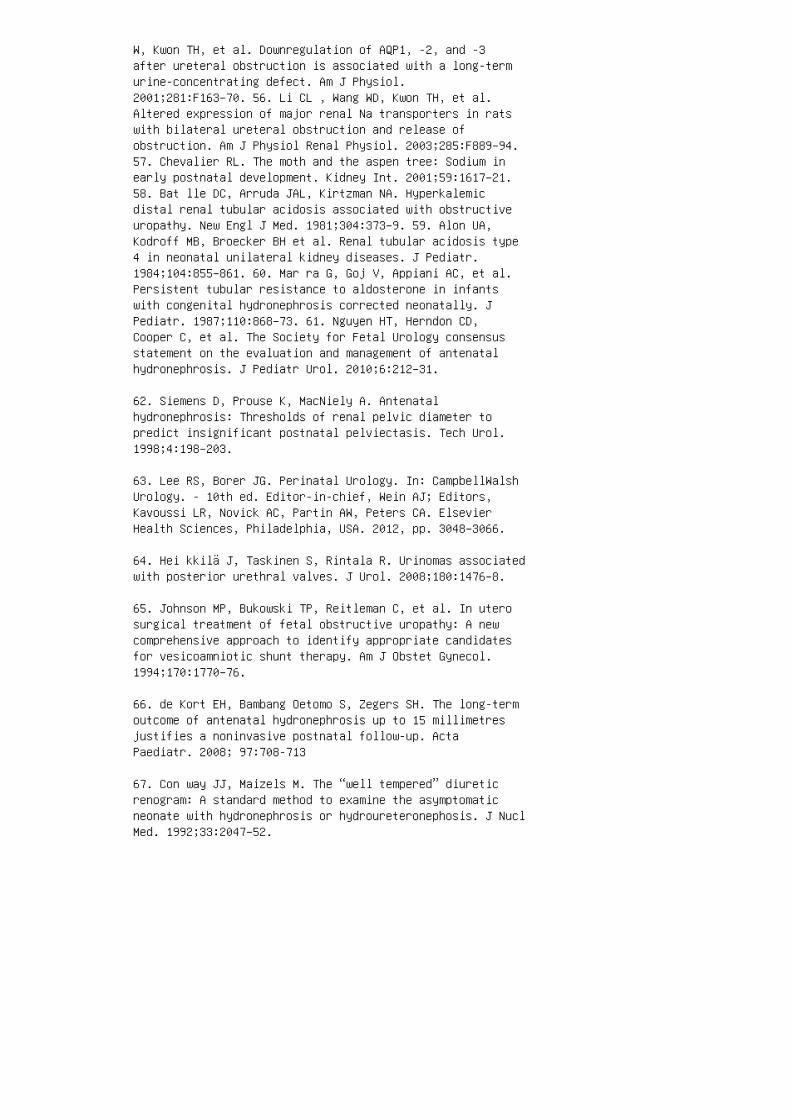
W, Kwon TH, et al. Downregulation of AQP1, -2, and -3after ureteral obstruction is associated with a long-termurine-concentrating defect. Am J Physiol.2001;281:F163–70. 56. Li CL , Wang WD, Kwon TH, et al.Altered expression of major renal Na transporters in ratswith bilateral ureteral obstruction and release ofobstruction. Am J Physiol Renal Physiol. 2003;285:F889–94.57. Chevalier RL. The moth and the aspen tree: Sodium inearly postnatal development. Kidney Int. 2001;59:1617–21.58. Bat lle DC, Arruda JAL, Kirtzman NA. Hyperkalemicdistal renal tubular acidosis associated with obstructiveuropathy. New Engl J Med. 1981;304:373–9. 59. Alon UA,Kodroff MB, Broecker BH et al. Renal tubular acidosis type4 in neonatal unilateral kidney diseases. J Pediatr.1984;104:855–861. 60. Mar ra G, Goj V, Appiani AC, et al.Persistent tubular resistance to aldosterone in infantswith congenital hydronephrosis corrected neonatally. JPediatr. 1987;110:868–73. 61. Nguyen HT, Herndon CD,Cooper C, et al. The Society for Fetal Urology consensusstatement on the evaluation and management of antenatalhydronephrosis. J Pediatr Urol. 2010;6:212–31.
62. Siemens D, Prouse K, MacNiely A. Antenatalhydronephrosis: Thresholds of renal pelvic diameter topredict insignificant postnatal pelviectasis. Tech Urol.1998;4:198–203.
63. Lee RS, Borer JG. Perinatal Urology. In: CampbellWalshUrology. - 10th ed. Editor-in-chief, Wein AJ; Editors,Kavoussi LR, Novick AC, Partin AW, Peters CA. ElsevierHealth Sciences, Philadelphia, USA. 2012, pp. 3048–3066.
64. Hei kkilä J, Taskinen S, Rintala R. Urinomas associatedwith posterior urethral valves. J Urol. 2008;180:1476–8.
65. Johnson MP, Bukowski TP, Reitleman C, et al. In uterosurgical treatment of fetal obstructive uropathy: A newcomprehensive approach to identify appropriate candidatesfor vesicoamniotic shunt therapy. Am J Obstet Gynecol.1994;170:1770–76.
66. de Kort EH, Bambang Oetomo S, Zegers SH. The long-termoutcome of antenatal hydronephrosis up to 15 millimetresjustifies a noninvasive postnatal follow-up. ActaPaediatr. 2008; 97:708-713
67. Con way JJ, Maizels M. The “well tempered” diureticrenogram: A standard method to examine the asymptomaticneonate with hydronephrosis or hydroureteronephosis. J NuclMed. 1992;33:2047–52.
68. Ric cabona M. Obstructive diseases of the urinarytract in children: Lessons from the last 15 years. PediatrRadiol. 2010;40:947–55.
69. Mor ris R, Malin G, Khan K, et al. Systematic reviewof the effectiveness of antenatal intervention for thetreatment of congenital lower urinary tract obstruction.BJOG 2010;117:382–90.
70. Mor ris RK, Malin GL, Quinlan-Jones E, et al.Percutaneous vesicoamniotic shunting versus conservativemanagement for fetal lower urinary tractobstruction(PLUTO): A randomized trial. Lancet. 2013;382:1496–506.
71. Biard JM, Johnson MP, Carr MC, et al. Long-termoutcomes in children treated by prenatal vesicoamnioticshunting for lower urinary tract obstruction. ObstetGynecol. 2005;106:503–8.
72. Timberlake MD, Herndon CDA. Mild to moderate postnatalhydronephrosis: Grading systems and management. Nat RevUrol. 2013;10:649–5.
73. Koff SA, Campbell K. Nonoperative management ofunilateral neonatal hydronephrosis. J Urol.1992;148:525–30.
74. King LR, Coughlin PWF, Bloch EC, et al. The case forimmediate pyeloplasty in the neonate with ureteropelvicjunction obstruction. J Urol 1984;132:725–9.
75. Che rtin B, Fridmans A, Knizhnik M, et al. Does earlydetection of ureteropelvic junction obstruction improvesurgical outcome in terms of renal function? J Urol1999;162:1037–42.
76. Ulm an I, Jayanthi VR, Koff SA. The long-termfollow-up of newborns with severe unilateral hydronephrosisinitially treated nonoperatively. J Urol. 2000;164:1101–7.77. Palmer LS, Maizels M, Cartwright PC, et al. Surgeryversus observation for managing obstructive grade 3 to 4unilateral hydronephrosis: A report from the society forfetal urology. J Urol. 1998;159:222–7. 78. DiSa ndro MJ,Kogan BA. Ureteropelvic junction obstruction. Urol Clin NoAm. 1998; 25:187–92. 79. Eskild-Jensen A, Jorgensen TM,Olsen LH, et al. Renal function may not be restored whenusing decreasing differential function as the criterion forsurgery in unilateral hydronephrosis. BJU Int.2003;92:779–84. 80. Onen A, Jayanthi VR, Koff SA.
Long-term follow up of prenatally detected severebilateral newborn hydronephrosis initially managednonoperatively. J Urol. 2002;168:1118–22. 81. Peters CA.Editorial: The long-term follow up of prenatally detectedsevere bilateral newborn hydronephrosis initially managednonoperatively. J Urol. 2002;168:1121–26. 82. Ter zi F,Assael BM, Claris AA, et al. Increased sodium requirementfollowing early postnatal surgical correction of congenitaluropathies in infants. Pediatr Nephrol. 1990;4:581–6. 83.Zha ng PL, Peters CA, Rosen S. Ureteropelvic junctionobstruction: Morphological and clinical studies. PediatrNephrol. 2000;14:820–6. 84. Kumar S, Walia S, Ikpeme O, etal. Postnatal outcome of prenatally diagnosed severe fetalrenal pelvic dilatation. Prenat Diagn. 2012;32:519–22.85. Stock JA, Krous HF, Heffernan J, et al. Correlation ofrenal biopsy and radionuclide renal scan differentialfunction in patients with unilateral ureteropelvicjunction obstruction. J Urol. 1995;154:716–21. 86. Capolicchio G, Leonard MP, Wong C, et al. Prenatal diagnosisof hydronephrosis: Impact on renal function and itsrecovery after pyeloplasty. J Urol. 1999;162:1029–34. 87.Bou baker A, Prior JO, Meyrat B, et al. Unilateral ureteropelvic junction obstruction in children: Longterm follow upafter unilateral pyeloplasty. J Urol. 2003;170:575–9. 88.Roth KS, Carter WH, Jr, Chan JCM. Obstructive nephropathyin children: Long-term progression after relief ofposterior urethral valve. Pediatrics 2001; 107:1004-1009.89. Heikkilä J, Holmberg C, Kyllönen L, et al. Long-termrisk of end stage renal disease in patients with posteriorurethral valves. J Urol. 2011;186:2392–6. 90. Kibar Y,Ashley RA, Roth CC, et al. Timing of posterior urethralvalve diagnosis and its impact on clinical outcome. JPediatr Urol. 2011;7:538–42. 91. Kousidis G, Thomas DF,Morgan H, et al. The longterm outcome of prenatallydetected posterior urethral valves: A 10 to 23-yearfollow-up study. BJU Int. 2008;102:1020–4. 92. DeFoor W,Clark C, Jackson E, et al. Risk factors for end stagerenal disease in children with posterior urethral valves.J Urol. 2008;180:1705–8.
93. Koff SA, Peller PA, Young DC, et al. The assessment ofobstruction in the newborn with unilateral hydronephrosisby measuring the size of the opposite kidney. J Urol.1994;152:596–601.
94. Garcia-Pena BM, Keller MS, Schwartz DS et al. Theultrasonographic differentiation of obstructive versusnonobstructive hydronephrosis in children: A multivariatescoring system. J Urol. 1997;158:560–6.

95. Brandell RA, Brock JW, III, Hamilton BD, et al.Unilateral hydronephrosis in infants: Are measurements ofcontralateral-renal length useful? J Urol. 1996;156:188–94.
96. Koff SA. Letter. Unilateral hydronephrosis in infants:Are measurements of contralateral renal length useful? JUrol. 1997;157:962–3.
97. Wanner C, Luscher TF, Schollmeyer P, Vetter W.Unilateral hydronephrosis and hypertension: Cause orcoincidence? Nephron. 1987;45:236–9.
98. Hohenfellner K, Wingen A-M, Nauroth O, et al. Impactof ACE I/D gene polymorphism on congenital renalmalformations. Pediatr Nephrol. 2001;16:356–61.
99. Heb ert LA, Wilmer WA, Falkenhain ME et al.Renoprotection: One or many therapies? Kidney Int.2001;59:1211–6.
100. Gur on G, Friberg P. An intact renin-angiotensinsystem is a prerequisite for normal renal development. JHypertens. 2000;18:123–8.
101. Gur on G, Marcussen N, Nilsson A, et al. Postnataltime frame for renal vulnerability to enalapril in rats. JAm Soc Nephol. 2000;10:155–9.
102. O’D ea RF, Mirkin BL, Alward CT, et al. Treatment ofneonatal hypertension with captopril. J Pediatr.1988;113:403–8.
103. Che valier RL, Thornhill BA, Belmonte DC, et al.Endogenous angiotensin II inhibits natriuresis followingacute volume expansion in the neonatal rat. Am J Physiol.1996;270:R393 –7.
104. Elder JS, Stansbrey R, Dahms BB, et al. Renalhistological changes secondary to ureteropelvic junctionobstruction. J Urol. 1995;154:719–24.
105. Chevalier RL. Biomarkers of congenital obstructivenephropathy: Past, present and future. J Urol.2004;172:852–6.
106. Yang SP, Woolf AS, Quinn F, et al. Deregulation ofrenal transforming growth factor-beta 1 after experimentalshort-term ureteric obstruction in fetal sheep. Am JPathol. 2001;159:109–113.
107. Furness PD, III, Maizels M, Han SW, et al. Elevatedbladder urine concentration of transforming growthfactor-b1 correlates with upper urinary tract obstructionin children. J Urol. 1999;162:1033–38.
108. Trn ka P, Ivanova L, Hiatt MJ, et al. Urinarybiomarkers in obstructive nephropathy. Clin J Am SocNephrol. 2012;7:1567–75. 109. Grandaliano G, Gesualdo L,Bartoli F, et al. MCP-1 and EGF renal expression and urineexcretion in human congenital obstructive nephropathy.Kidney Int. 2000;58:182–8. 110. Li Z, Zhao Z, Liu X, etal. Prediction of the outcome of antenatal hydronephrosis:Significance of urinary EGF. Pediatr Nephrol.2012;27:2251–9. 111. Wasilewska A, Taranta-Janusz K, DębekW, et al. KIM-1 and NGAL: New markers of obstructivenephropathy. Pediatr Nephrol. 2011;26:579–86. REVIEWQUESTIONS 1. �e most common cause of antenatal obstructiveuropathy is: a. Posterior urethral valves b.Vesicoureteric re�ux c. Ureterovesicular junctionobstruction d. Uret eropelvic junction obstruction 2. Routine antenatal ultrasound detects most cases of antenatalhydronephrosis. a. Fals e b. Tru e 3. In pr enatallydetected hydronephrosis, no evidence of urinary tractobstruction is seen in: a. 10% b. 90% c. 50% d. 30% 4.A pren atal ultrasound in a male fetus demonstratebilateral hydronephrosis and a thickened bladder wall. Adiagnosis of posterior urethral valves is beingentertained. �e most important clinical concern in theneonatal period in this patient will be: a. Reducednephron mass b. Urinary tract infection c. Pulmonaryhypoplasia d. Diaphragmatic hernia 5. Risk for CKD andESRD risk in patients with posterior urethral valves isdetermined by: a. Severity of hydronephrosis b. Severityof renal dysplasia c. Frequency of urinary tractinfections d. Amniotic �uid sodium concentration 6. Amale baby at the age of 37 weeks of gestation is born viacesarean section delivery and requires mechanicalventilation a�er resuscitation. His mother had poorprenatal follow-up, and there is no record of her havinghad any prenatal ultrasound evaluations. �e patientdeveloped right-sided pneumothorax on day 2. He did noturinate for 12 hours, urinary bladder catheterization wasdone, and an indwelling catheter was le� in place. Renalultrasound showed bilateral hydronephrosis, bilateralhydroureters and a distended urinary bladder withthickened wall. �e most important next investigative stepin this patient should be:
a. Monitor renal ultrasound for worsening of hydronephrosis
b. Monitor serum creatinine for renal function
c. A DMSA renal scan
d. A nuclear cystogram
e. A contrast vesicocystourethrogram
7. Following are the features of lower urinary tractobstruction in neonates, except:
a. Hematuria following birth
b. Bilateral antenatal hydronephrosis
c. Hypospadias
d. Fetal or neonatal urinary ascites
8. Urinary incontinence is a clinical manifestation oflower urinary tract obstruction:
a. True
b. False
9. Of prenatally detected cases ofpyelectasis/hydronephrosis, 50% to 70% are due to:
a. Ureteropelvic junction obstruction
b. Vesicoureteric re�ux
c. Transient or physiologic neonatal changes
d. Potter syndrome
10. Which of the following disorders can mimichydronephrosis in an antenatal sonogram?
a. Multicystic dysplastic kidney
b. Megaureter
c. Large renal cysts
d. All of the above
11. A 6-year-boy complains of right-side abdominal painevery time he goes out with his parents for dinner or when
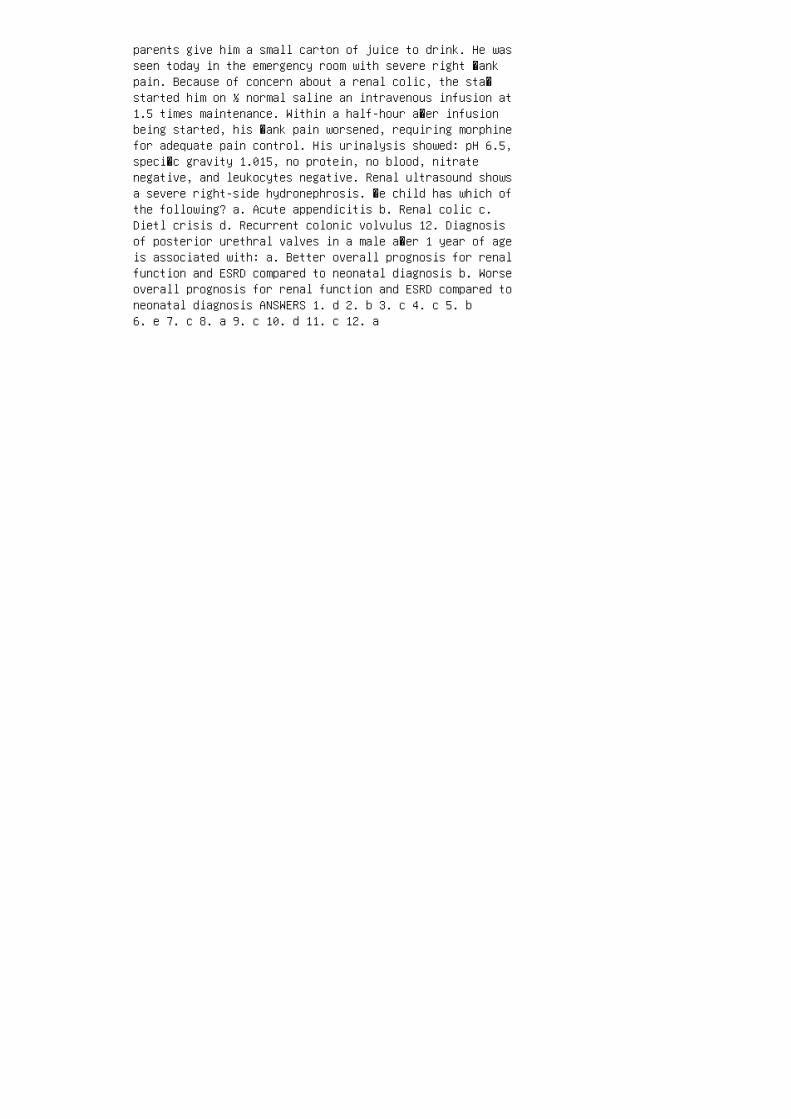
parents give him a small carton of juice to drink. He wasseen today in the emergency room with severe right �ankpain. Because of concern about a renal colic, the sta�started him on ½ normal saline an intravenous infusion at1.5 times maintenance. Within a half-hour a�er infusionbeing started, his �ank pain worsened, requiring morphinefor adequate pain control. His urinalysis showed: pH 6.5,speci�c gravity 1.015, no protein, no blood, nitratenegative, and leukocytes negative. Renal ultrasound showsa severe right-side hydronephrosis. �e child has which ofthe following? a. Acute appendicitis b. Renal colic c.Dietl crisis d. Recurrent colonic volvulus 12. Diagnosisof posterior urethral valves in a male a�er 1 year of ageis associated with: a. Better overall prognosis for renalfunction and ESRD compared to neonatal diagnosis b. Worseoverall prognosis for renal function and ESRD compared toneonatal diagnosis ANSWERS 1. d 2. b 3. c 4. c 5. b6. e 7. c 8. a 9. c 10. d 11. c 12. a

48 Vesicoureteral reflux
(a)
(b)
Figure 48.8 The Cohen procedure is the most widely
used technique for surgical correction of vesicoureteral
reflux. (a) The ureters (the procedure is often bilateral)
are mobilized intravesically. (b) Two separate submuco
sal tunnels are created so that each ureter opens on the
opposite side from its hiatus. (Reproduced with permis
sion from: Capozza N, Caione P. Vesicoureteral reflux:
surgical and endoscopic treatment. Pediatr Nephrol.
2007;22:1261–5.)
12. Snodgrass W. The impact of treated dysfunctionalvoiding on the nonsurgical management of vesicoureteralreflux. J Urol. 1998;160:1823–5.
13. Dra chman R, Valevici M, Vardy PA. Excretory urographyand cystourethrography in the evaluation of children withurinary tract infection. Clin Pediatr (Phila).1984;23:265–7.
14. Askari A, Belman AB. Vesicoureteral reflux in blackgirls. J Urol. 1982;127:747–8.
15. Kuni n CM. A ten-year study of bacteriuria inschoolgirls: Final report of bacteriologic, urologic, andepidemiologic findings. J Infect Dis. 1970;122:382–93.
16. Skoog SJ, Belman AB. Primary vesicoureteral reflux inthe black child. Pediatrics. 1991;87:538–43.
17. Cha nd DH, Rhoades T, Poe SA, et al. Incidence andseverity of vesicoureteral reflux in children related toage, gender, race and diagnosis. J Urol. 2003;170:1548–50.
18. Zerin JM, Ritchey ML, Chang AC. Incidentalvesicoureteral reflux in neonates with antenatally detectedhydronephrosis and other renal abnormalities. Radiology.
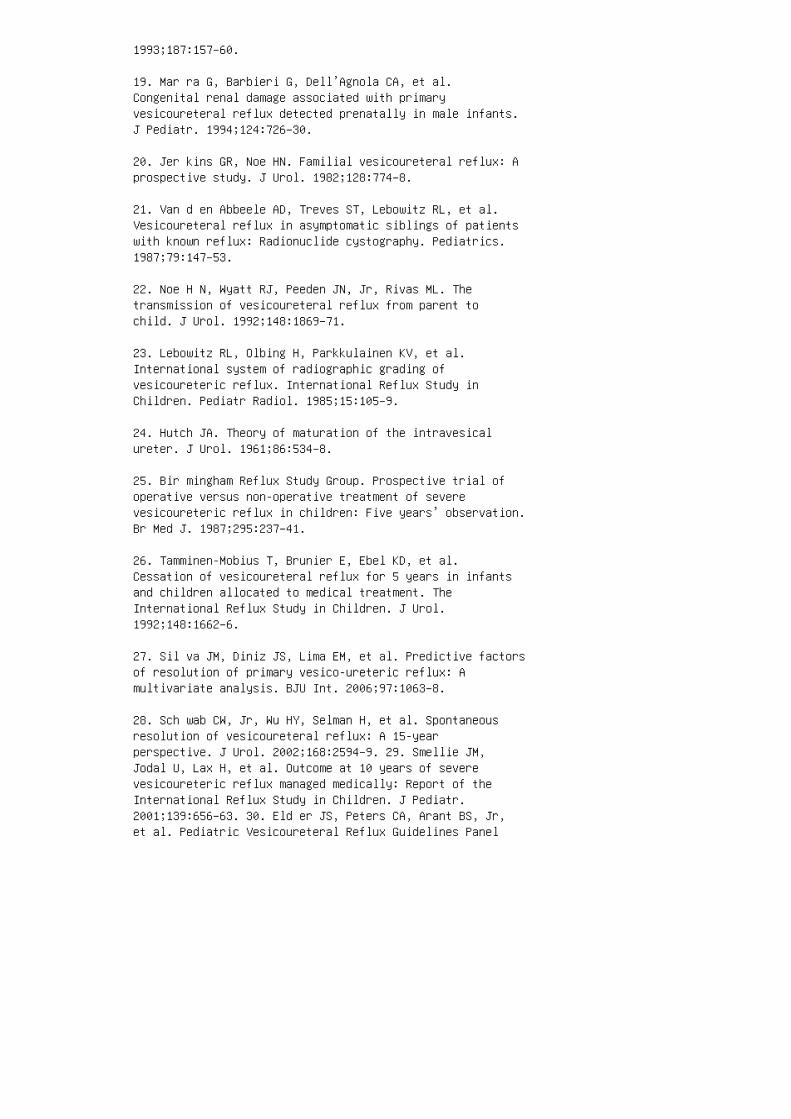
1993;187:157–60.
19. Mar ra G, Barbieri G, Dell’Agnola CA, et al.Congenital renal damage associated with primaryvesicoureteral reflux detected prenatally in male infants.J Pediatr. 1994;124:726–30.
20. Jer kins GR, Noe HN. Familial vesicoureteral reflux: Aprospective study. J Urol. 1982;128:774–8.
21. Van d en Abbeele AD, Treves ST, Lebowitz RL, et al.Vesicoureteral reflux in asymptomatic siblings of patientswith known reflux: Radionuclide cystography. Pediatrics.1987;79:147–53.
22. Noe H N, Wyatt RJ, Peeden JN, Jr, Rivas ML. Thetransmission of vesicoureteral reflux from parent tochild. J Urol. 1992;148:1869–71.
23. Lebowitz RL, Olbing H, Parkkulainen KV, et al.International system of radiographic grading ofvesicoureteric reflux. International Reflux Study inChildren. Pediatr Radiol. 1985;15:105–9.
24. Hutch JA. Theory of maturation of the intravesicalureter. J Urol. 1961;86:534–8.
25. Bir mingham Reflux Study Group. Prospective trial ofoperative versus non-operative treatment of severevesicoureteric reflux in children: Five years’ observation.Br Med J. 1987;295:237–41.
26. Tamminen-Mobius T, Brunier E, Ebel KD, et al.Cessation of vesicoureteral reflux for 5 years in infantsand children allocated to medical treatment. TheInternational Reflux Study in Children. J Urol.1992;148:1662–6.
27. Sil va JM, Diniz JS, Lima EM, et al. Predictive factorsof resolution of primary vesico-ureteric reflux: Amultivariate analysis. BJU Int. 2006;97:1063–8.
28. Sch wab CW, Jr, Wu HY, Selman H, et al. Spontaneousresolution of vesicoureteral reflux: A 15-yearperspective. J Urol. 2002;168:2594–9. 29. Smellie JM,Jodal U, Lax H, et al. Outcome at 10 years of severevesicoureteric reflux managed medically: Report of theInternational Reflux Study in Children. J Pediatr.2001;139:656–63. 30. Eld er JS, Peters CA, Arant BS, Jr,et al. Pediatric Vesicoureteral Reflux Guidelines Panel

summary report on the management of primary vesicoureteralreflux in children. J Urol. 1997;157:1846–51. 31. UpadhyayJ, McLorie GA, Bolduc S, et al. Natural history of neonatalreflux associated with prenatal hydronephrosis: Long-termresults of a prospective study. J Urol. 2003;169:1837–41;discussion 41; author reply 41. 32. Con nolly LP, TrevesST, Zurakowski D, Bauer SB. Natural history ofvesicoureteral reflux in siblings. J Urol.1996;156:1805–7. 33. Shaikh N, Ewing AL, Bhatnagar S,Hoberman A. Risk of renal scarring in children with afirst urinary tract infection: A systematic review.Pediatrics. 2010;126:1084–91. 34. Peters CA, Skoog SJ,Arant BS, et al. Summary of the AUA guideline onmanagement of primary vesicoureteral reflux in children. JUrol. 2010;184:1134–44. 35. Chen JJ, Pugach J, West D, etal. Infant vesicoureteral reflux: A comparison betweenpatients pr es enting with a prenatal diagnosis and thosepresenting with a urinary tract infection. Urology.2003;61:442–6; discussion 6–7. 36. Shaikh N, Hoberman A,Wise B, et al. Dysfunctional elimination syndrome: Is itrelated to urinary tract infection or vesicoureteralreflux diagnosed early in life? Pediatrics.2003;112:1134–7. 37. Nor gaard JP, van Gool JD, Hjalmas K,et al. Standardization and definitions in lower urinarytract dysfunction in children. International Children’sContinence Society. Br J Urol. 1998;81(Suppl 3):1–16. 38.Koff SA, Wagner TT, Jayanthi VR. The relationship amongdysfunctional elimination syndromes, pri maryvesicoureteral reflux and urinary tract infections inchildren. J Urol. 1998;160:1019–22. 39. Seruca H.Vesicoureteral reflux and voiding dysfunction: Aprospective study. J Urol. 1989;142:494–8; di sc ussion501. 40. Kof f SA. Relationship between dysfunctional voiding and reflux. J Urol. 1992;148:1703–5. 41. van Gool JD,Hjalmas K, Tamminen-Mobius T, Olbing H. Historical cluesto the complex of dys functional voiding, urinary tractinfection and vesicoureteral reflux. The InternationalReflux Study in Chi ldren. J Urol. 1992;148:1699–702. 42.Rushton HG. Wetting and functional voiding disor ders. UrolClin North Am. 1995;22:75–93. 43. O’Regan S, Yazbeck S,Schick E. Constipation, bladder instability, urinary tractinfection syndrome. Clin N ep hrol. 1985;23:152–4. 44.Neumann PZ, DeDomenico IJ, Nogrady MB. Constipation andurinary tract infection. Pediatrics. 1973;52:241–5.
45. Chase JW, Homsy Y, Siggaard C, et al. Functionalconstipation in children. J Urol. 2004;171:2641–3.
46. Win berg J, Andersen HJ, Bergstrom T, et al.Epidemiology of symptomatic urinary tract infection in
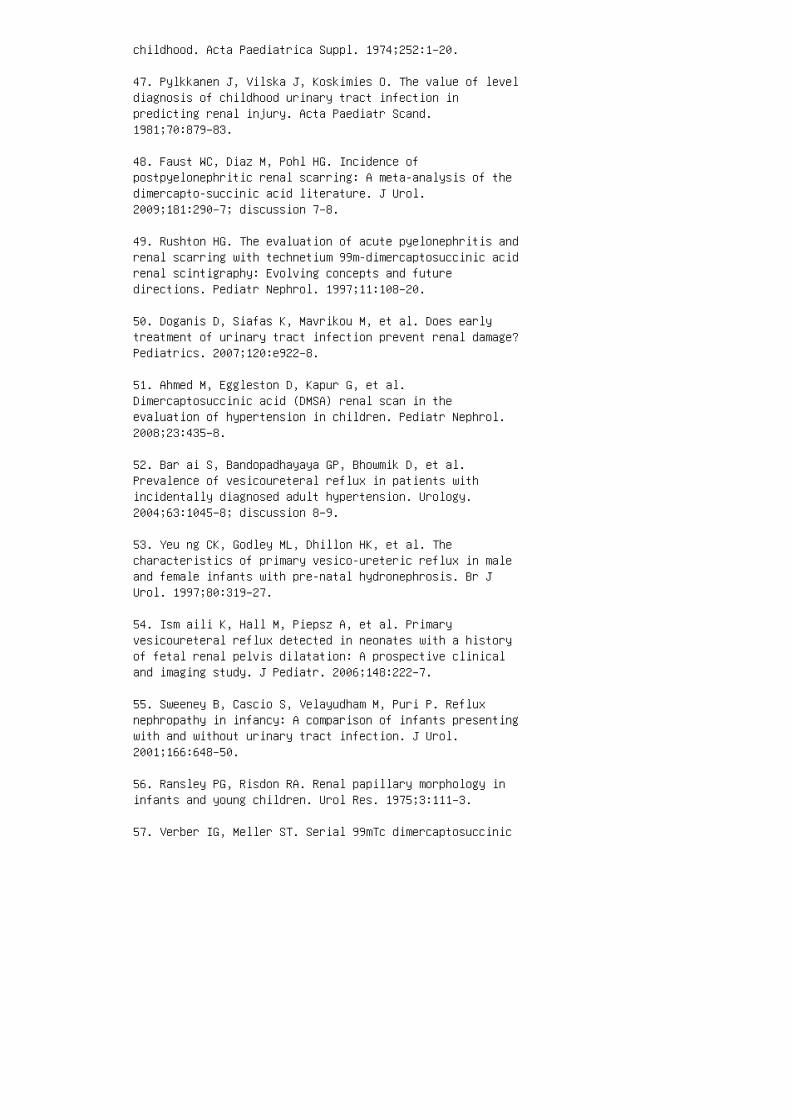
childhood. Acta Paediatrica Suppl. 1974;252:1–20.
47. Pylkkanen J, Vilska J, Koskimies O. The value of leveldiagnosis of childhood urinary tract infection inpredicting renal injury. Acta Paediatr Scand.1981;70:879–83.
48. Faust WC, Diaz M, Pohl HG. Incidence ofpostpyelonephritic renal scarring: A meta-analysis of thedimercapto-succinic acid literature. J Urol.2009;181:290–7; discussion 7–8.
49. Rushton HG. The evaluation of acute pyelonephritis andrenal scarring with technetium 99m-dimercaptosuccinic acidrenal scintigraphy: Evolving concepts and futuredirections. Pediatr Nephrol. 1997;11:108–20.
50. Doganis D, Siafas K, Mavrikou M, et al. Does earlytreatment of urinary tract infection prevent renal damage?Pediatrics. 2007;120:e922–8.
51. Ahmed M, Eggleston D, Kapur G, et al.Dimercaptosuccinic acid (DMSA) renal scan in theevaluation of hypertension in children. Pediatr Nephrol.2008;23:435–8.
52. Bar ai S, Bandopadhayaya GP, Bhowmik D, et al.Prevalence of vesicoureteral reflux in patients withincidentally diagnosed adult hypertension. Urology.2004;63:1045–8; discussion 8–9.
53. Yeu ng CK, Godley ML, Dhillon HK, et al. Thecharacteristics of primary vesico-ureteric reflux in maleand female infants with pre-natal hydronephrosis. Br JUrol. 1997;80:319–27.
54. Ism aili K, Hall M, Piepsz A, et al. Primaryvesicoureteral reflux detected in neonates with a historyof fetal renal pelvis dilatation: A prospective clinicaland imaging study. J Pediatr. 2006;148:222–7.
55. Sweeney B, Cascio S, Velayudham M, Puri P. Refluxnephropathy in infancy: A comparison of infants presentingwith and without urinary tract infection. J Urol.2001;166:648–50.
56. Ransley PG, Risdon RA. Renal papillary morphology ininfants and young children. Urol Res. 1975;3:111–3.
57. Verber IG, Meller ST. Serial 99mTc dimercaptosuccinic
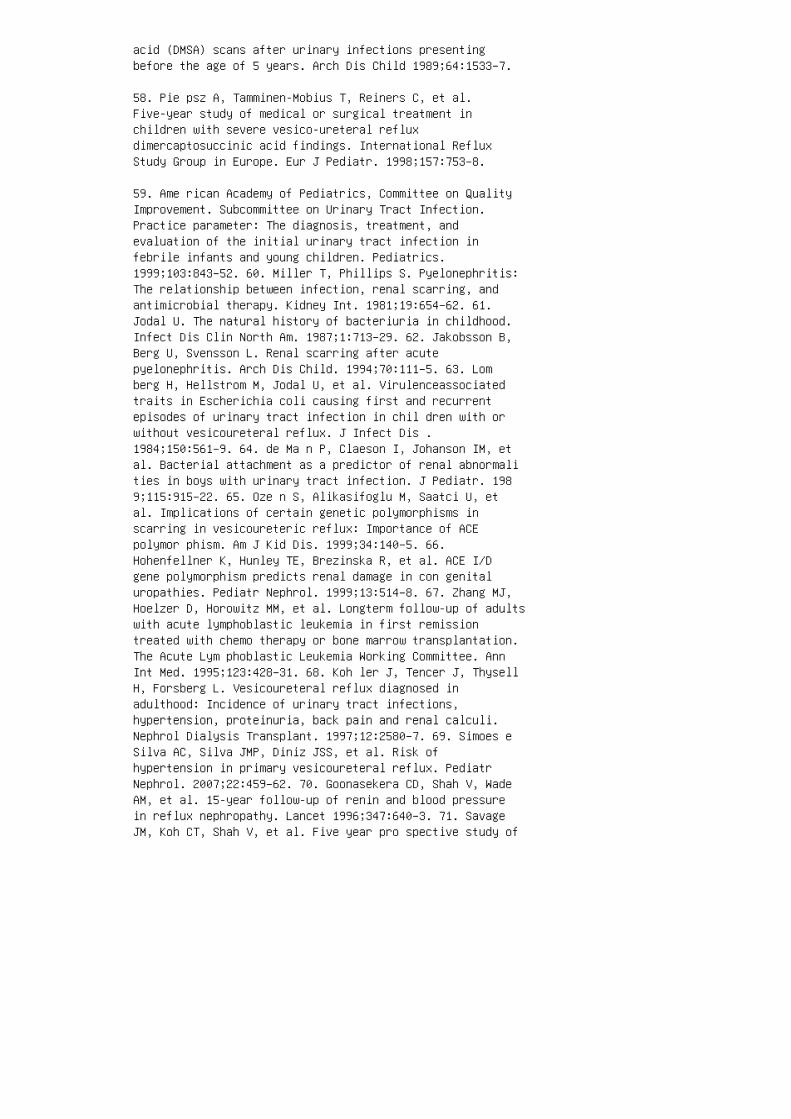
acid (DMSA) scans after urinary infections presentingbefore the age of 5 years. Arch Dis Child 1989;64:1533–7.
58. Pie psz A, Tamminen-Mobius T, Reiners C, et al.Five-year study of medical or surgical treatment inchildren with severe vesico-ureteral refluxdimercaptosuccinic acid findings. International RefluxStudy Group in Europe. Eur J Pediatr. 1998;157:753–8.
59. Ame rican Academy of Pediatrics, Committee on QualityImprovement. Subcommittee on Urinary Tract Infection.Practice parameter: The diagnosis, treatment, andevaluation of the initial urinary tract infection infebrile infants and young children. Pediatrics.1999;103:843–52. 60. Miller T, Phillips S. Pyelonephritis:The relationship between infection, renal scarring, andantimicrobial therapy. Kidney Int. 1981;19:654–62. 61.Jodal U. The natural history of bacteriuria in childhood.Infect Dis Clin North Am. 1987;1:713–29. 62. Jakobsson B,Berg U, Svensson L. Renal scarring after acutepyelonephritis. Arch Dis Child. 1994;70:111–5. 63. Lomberg H, Hellstrom M, Jodal U, et al. Virulenceassociatedtraits in Escherichia coli causing first and recurrentepisodes of urinary tract infection in chil dren with orwithout vesicoureteral reflux. J Infect Dis .1984;150:561–9. 64. de Ma n P, Claeson I, Johanson IM, etal. Bacterial attachment as a predictor of renal abnormalities in boys with urinary tract infection. J Pediatr. 1989;115:915–22. 65. Oze n S, Alikasifoglu M, Saatci U, etal. Implications of certain genetic polymorphisms inscarring in vesicoureteric reflux: Importance of ACEpolymor phism. Am J Kid Dis. 1999;34:140–5. 66.Hohenfellner K, Hunley TE, Brezinska R, et al. ACE I/Dgene polymorphism predicts renal damage in con genitaluropathies. Pediatr Nephrol. 1999;13:514–8. 67. Zhang MJ,Hoelzer D, Horowitz MM, et al. Longterm follow-up of adultswith acute lymphoblastic leukemia in first remissiontreated with chemo therapy or bone marrow transplantation.The Acute Lym phoblastic Leukemia Working Committee. AnnInt Med. 1995;123:428–31. 68. Koh ler J, Tencer J, ThysellH, Forsberg L. Vesicoureteral reflux diagnosed inadulthood: Incidence of urinary tract infections,hypertension, proteinuria, back pain and renal calculi.Nephrol Dialysis Transplant. 1997;12:2580–7. 69. Simoes eSilva AC, Silva JMP, Diniz JSS, et al. Risk ofhypertension in primary vesicoureteral reflux. PediatrNephrol. 2007;22:459–62. 70. Goonasekera CD, Shah V, WadeAM, et al. 15-year follow-up of renin and blood pressurein reflux nephropathy. Lancet 1996;347:640–3. 71. SavageJM, Koh CT, Shah V, et al. Five year pro spective study of

plasma renin activity and blood pressure in patients withlongstanding reflux nephropathy. Arch Dis Child.1987;62:678–82. 72. Wolfish NM, Delbrouck NF, Shanon A, etal. Prevalence of hypertension in children with primaryvesicoureteral reflux. J Pediatr. 1993;123:559–63. 73.Wennerstrom M, Hansson S, Hedner T, et al. Ambulatoryblood pressure 16-26 years after the first urinary tractinfection in childhood. J Hypertens. 2000;18:485–91. 74.Zhang Y, Bailey RR. A long term follow up of adults withreflux nephropathy. N Z Med J. 1995;108:142–4.
75. Karlen J, Linne T, Wikstad I, Aperia A. Incidence ofmicroalbuminuria in children with pyelonephritic scarring.Pediatr Nephrol (Berlin) 1996;10:705–8.
76. Craig JC, Irwig LM, Knight JF, Roy LP. Does treatmentof vesicoureteric reflux in childhood prevent end-stagerenal disease attributable to reflux nephropathy?Pediatrics 2 000;105:1236–41.
77. Kin caid-Smith P. Glomerular lesions in atrophicpyelonephritis and reflux nephropathy. Kidney Int Suppl.1975;4:S81–3.
78. North American Pediatric Renal Transplant CooperativeStudies. 2008 Annual Report, Boston, NAPRTCS; 2008.
79. Furth SL, Abraham GA, Jerry-Fluker J, et al. Metabolicabnormalities, CVD risk factors and GFR decline inchildren with CKD. Clin J Am Soc Nephrol. 2011;6:2132–40.
80. Bailey RR, Lynn KL, Smith AH. Long-term followup ofinfants with gross vesicoureteral reflux. J Urol.1992;148:1709–11.
81. Lah des-Vasama T, Niskanen K, Ronnholm K. Outcome ofkidneys in patients treated for vesicoureteral reflux(VUR) during childhood. Nephrol Dial Transplant.2006;21:2491–7.
82. el-Khatib M, Packham DK, Becker GJ, KincaidSmith P.Pregnancy-related complications in women with refluxnephropathy. Clin Nephrol. 1994;41:50–5.
83. Jun gers P, Houillier P, Chauveau D, et al. Pregnancyin women with reflux nephropathy. Kidney Int.1996;50:593–9.
84. Hollowell JG. Outcome of pregnancy in women with ahistory of vesico-ureteric reflux. BJU Int.

2008;102:780–4.
85. Gru neberg RN, Leakey A, Bendall MJ, Smellie JM. Bowelflora in urinary tract infection: Effect of chemotherapywith special refer ence to cotrimoxazole. Kidney Int Suppl.1 975 ;4:S122–9.
86. Sme llie JM, Tamminen-Mobius T, Olbing H, et al.Five-year study of medical or surgical treat ment inchildren with severe reflux: Radiological rena l findings.The International Reflux Study in Children. PediatrNephrol. 1992;6:223–30.
87. Jodal U, Smellie JM, Lax H, Hoyer PF. Ten-year resultsof randomized treatment of children with severevesicoureteral reflux: Final report of the InternationalReflux Study in Children. Pediatr Nephrol. 2006;21:785–92.
88. Brandstrom P, Esbjorner E, Herthelius M, et al. TheSwedish reflux trial in children. III. Urinary tractinfection pattern. J Urol. 2010;184:286–91.
89. Brandstrom P, Neveus T, Sixt R, et al. The Swedishreflux trial in children. IV. Renal dam age. J Urol.2010;184:292–7. 90. Shakil A, Reed L, Wilder L, Strand WR.Clinical inquiries: Do antibiotics prevent recurrent UTIin children with anatomic abnormalities? J Fam Pract.2004;53:498–500. 91. Cooper CS, Chung BI, Kirsch AJ, etal. The outcome of stopping prophylactic antibiotics inold er children with vesicoureteral reflux. J Urol.2000;163:269–72; discussion 72–3. 92. Tam minen-Mobius T,Brunier E, Ebel KD, et al. Cessation of vesicoureteralreflux for 5 years in infants and children allocated tomedical treatment. The International Reflux Study inChildren. J Urol. 1992;148:1662–6. 93. Allen UD, MacDonaldN, Fuite L, et al. Risk factors for resistance to“first-line” anti microbials among urinary tract isolatesof Esc herichia coli in children. Can Med Assoc J.1999;160:1436–40. 94. Kar pman E, Kurzrock EA. Adversereactions of nitrofurantoin, trimethoprim and sulfamethoxazole in children. J Urol. 2004;172:448–53. 95. Uhari M,Nuutinen M, Turtinen J. Adverse reactions in childrenduring long-term anti microbial therapy. Pediatr Infect DisJ. 199 6;15:404–8. 96. Bol lgren I. Antibacterialprophylaxis in chil dren with urinary tract infection. ActaPaediatr Suppl. 1999;88:48–52. 97. Wil liams G, Lee A,Craig J. Antibiotics for the prevention of urinary tractinfection in children: A systematic review of randomizedcontrolled trials. J Pediatr. 2001;138:868–74. 98. Wheeler D, Vimalachandra D, Hodson EM, et al. Antibiotics and

surgery for vesicoureteric reflux: A meta-analysis ofrandomised con trolled trials. Arch Dis Child.2003;88:688–94. 99. Gordon I, Barkovics M, Pindoria S, etal. Primary vesicoureteric reflux as a predic tor of renaldamage in children hospitalized wit h urinary tractinfection: A systematic review and meta-analysis. J Am SocNephrol. 2003;14:739–44. 100. Williams GJ, Wei L, Lee A,Craig JC. Long-term antibiotics for preventing recurrenturinary tract infection in children. Cochrane DatabaseSyst Rev. 2006;(3):001534. 101. Garin EH, Olavarria F,Garcia Nieto V, et al. Clinical significance of primaryvesicoureteral reflux and urinary antibiotic prophylaxisafter acute pyelonephritis: A multicenter, randomized,controlled study. Pediatrics. 2006;117:626–32. 102.Roussey-Kesler G, Gadjos V, Idres N, et al. Antibiotic prophylaxis for the prevention of recurrent urinary tractinfection in children with low grade vesicoureteralreflux: Results from a prospective randomized study. JUrol. 2008;179:674–9.
103. Pennesi M, Travan L, Peratoner L, et al. Is antibioticprophylaxis in children with vesicoureteral refluxeffective in pr eventing pyelonephritis and renal scars? Arandomized, controlled trial. Pediatrics.2008;121:e1489–94.
104. Montini G, Rigon L, Zucchetta P, et al. Prophylaxisafter first febrile urinary tract infection in children? Amulticenter, randomized, controlled, noninferiority trial.Pediatrics. 2008;122:1064–71.
105. Craig JC, Simpson JM, Williams GJ, et al. Antibioticprophylaxis and recurrent urinary tract infection inchildren. N Engl J Med. 2009;361:1748–59.
106. Subcommittee on Urinary Tract Infection, SteeringCommittee on Quality Improvement and Management. Urinarytract infection: Clinical practice guideline for thediagnosis and management of the initial UTI in febrileinfants and children 2 to 24 months. Pediatrics.2011;128:595–610.
107. Randomized Intervention for Children withVesicoureteral Reflux Trial Investigators. Antimicrobialprophylaxis for children with vesicoureteral reflux. N EnglJ Med. 2014;370:2367–76.
108. Diamond DA, Mattoo TK. Endoscopic treatment ofprimary vesicoureteral reflux. N Engl J Med.2012;366:1218–26.
109. Elder JS, Diaz M, Caldamone AA, et al. Endoscopictherapy for vesicoureteral reflux: A meta-analysis. I.Reflux resolution and urinary tract infection. J Urol.2006;175:716–22.
110. Vandersteen DR, Routh JC, Kirsch AJ, et al.Postoperative ur eteral obstruction after subureteralinjection of dextranomer/hyaluronic acid copolymer. JUrol. 2006;176:1593–5.
111. Nelson CP, Chow JS. Dextranomer/hyaluronic acidcopolymer (Deflux) implants mimicking distal ur eteralcalculi on CT. Pediatr Radiol. 2008;38:104–6.
112. Lendvay TS, Sorensen M, Cowan CA, et al. The evolutionof vesicoureteral reflux management in the era ofdextranomer/hyaluronic acid copolymer: A Pediatric HealthInformation System database study. J Urol.2006;176:1864–7.
113. Kutikov A, Guzzo TJ, Canter DJ, Casale P. Initialexperience with laparoscopic transvesical ureteralreimplantation at the Children’s Hospital of Philadelphia.J Urol. 2006;176:2222–5; discussion 5–6.
114. Lakshmanan Y, Fung LC. Laparoscopic extravesicular ureteral reimplantation for vesicoureteral reflux: Recenttechnical advances. J Endourol. 2000;14:589– 93; discussion593–4.
115. Kaplan WE, Firlit CF. Management of reflux in themyelodysplastic child. J Urol. 1983;129:1195–7.
116. Kennelly MJ, Bloom DA, Ritchey ML, Panzl AC. Outcomeanalysis of bilateral Cohen cross-trigonalureteroneocystostomy. Urology. 1995;46:393–5.
117. Bisignani G, Decter RM. Voiding cystourethr ographyafter uncomplicated ureteral reimplantation in children:Is it necessary? J Urol. 1997;158:1229–31. 118. Hoenig DM,Diamond DA, Rabinowitz R, Caldamone AA. Contralateralreflux after unilateral ureteral reimplantation. J Urol.1996;156:196–7. 119. Sung J, Skoog S. Surgical managementof vesicoureteral reflux in children Pediatr Nephrol.2012;27:551–61 120. O’Regan S, Yazbeck S, Hamberger B,Schick E. Constipation a commonly unrecognized cause ofenuresis. Am J Dis Child. 1986;140:260–1. 121. Herndon CD,Decambre M, McKenna PH. Interactive computer games fortreatment of pelvic floor dysfunction. J Urol.
2001;166:1893–8. 122. Upadhyay J, Bolduc S, Bagli DJ, etal. Use of the dysfunctional voiding symptom score topredict resolution of vesicoureteral reflux in childrenwith voiding dysfunction. J Urol. 2003;169:1842–6;discussion 6; author reply 6. 123. Schulman SL, Quinn CK,Plachter N, Kodman-Jones C. Comprehensive management ofdysfunctional voiding. Pediatrics. 1999;103:E31. 124.Praga M, Hernandez E, Montoyo C, et al. Long-termbeneficial effects of angiotensin-converting enzymeinhibition in patients with nephrotic proteinuria. Am JKidney Dis. 1992;20:240–8. 125. Ohtomo Y, Nagaoka R,Kaneko K, et al. Angiotensin converting enzyme genepolymorphism in primary vesicoureteral reflux. PediatrNephrol. 2001;16:648–52. 126. Risdon RA. The smallscarred kidney in childhood. Pediatr Nephrol.1993;7:361–4. REVIEW QUESTIONS 1. Which of the followingis associated with a higher incidence of primaryvesicoureteral re�ux diagnosed a�er urinary tractinfection? a. Older age b. Male gender c. AfricanAmerican race d. Family history of vesicoureteral re�ux inparent or sibling 2. Which of the following is a riskfactor for renal scarring a�er a UTI? a. African Americanrace b. High grade vesicoureteral re�ux c. Absence ofvesicoureteral re�ux d. Diarrhea e. Pyuria 3. Hypertension is most directly associated with which of thefollowing? a. His tory of urinary tract infections b. Vesicoureteral re�ux c. Use o f De�ux d. Rena l scarring
4. Which of the following is a risk factor for unsuccessfulendoscopic repair of vesicoureteral re�ux?
a. Neurogenic bladder
b. Congenital re�ux
c. History of UTI
d. Caucasian race
e. Grade I or II re�ux
5. �e success rate of open surgical repair ofvesicoureteral re�ux is approximately:
a. 65%
b. 75%
c. 85%

d. 90%
e. 98% 6. Which of the following is the preferred agentfor treating hypertension in a patient with re�uxnephropathy? a. Calcium channel blocker b. Beta blockerc. ACE inhibitor d. �iazide diuretic ANSWER KEY 1. d 2.b 3. d 4. a 5. e 6. c

49 Urinary tract infection
SUMMARY
Infections of the urinary tract are a common child
hood disorder that can lead to signi�cant morbid
ity and hospitalizations. Our understanding of the
structural and molecular predispositions to UTI
makes it possible to develop a uni�ed diagnostic and
therapeutic approach that can be practiced in ter
tiary care centers and in the community. Such a uni
ed management approach may result in a lowered
long-term risk for renal damage. Recent data suggest
that the renal scarring resulting from UTI may be
determined by host in�ammatory response, pres
ence of urinary tract abnormalities, and the bacte
rial virulence. UTI and chronic pyelonephritis is, by
itself, an uncommon cause of CKD and ESRD.
5. Winberg J, Anderson HJ, Bergstrom T, et al.Epidemiology of symptomatic urinary tract infection inchildhood. Acta Paediatr Scand. 1974;252:1–20.
6. Hellstrom A, Hanson E, Hansson S, et al. Associationbetween urinary symptoms at 7 years old and previousurinary tract infection. Arch Dis Child. 1991;66:232–4.
7. Marild S, Jodal U. Incidence rate of first-time symptomatic urinary tract infection in children under 6 y ears of age. Acta Paediatr. 1998;87:549–52.
8. Ber gstrom T, Larson H, Loncoln K, et al. Studies ofurinary tract infections in infancy and childhood. XII.Eighty consecutive patients with neonatal infections. JPediatr. 1972;80:858–66.
9. Drew JH, Acton CM. Radiological findings in new born
infants with urinary tract infection. Arch Dis Chi ld.1976;51:628–30.
10. Wet tergren B, Jodal U, Jonasson G. Epidemiology ofbacteriuria during the first year of life. Acta PaeditrScand. 1985;74:925–33.
11. To T, Agha M, Dick PT, et al. Cohort study on circumcision of newborn boys and subsequent risk of urinary-tract infection. Lancet. 1998;352:1813-6.
12. Gin sburg CM, McCracken Jr, GH. Urinary tractinfections in young infants. Pediatrics. 1982;69:409–12.
13. Schnadower D, Kuppermann N, Macias CG, et al.;American Academy of Pediatrics Pediatric EmergencyMedicine Collaborative Research Committee. Febrile infantswith urinary tract infections at very low risk for adverseevents and bacteremia. Pediatrics. 2010;126:1074–83.
14. Newman TB, Bernzweig JA, Takayama JI, et al. Urinetesting and urinary tract infection in febrile infantsseen in office settings. Arch Pediatr Adolesc Med.2002;156:44–54.
15. Hob erman A, Wald ER. Treatment of urinary tractinfection. Pediatr Infect Dis J. 1999;18:1020–1.
16. Majd M, Rushton HG, Jantausch B, et al. Relationshipamong vesicoureteral reflux, P-fimbriated Escherichia coliand acute pyelone phritis in children with febrile urinarytract infection. J Pediatr. 1991;19:578–85.
17. Zorc JJ, Levine DA, Platt SL, et al. Clinical anddemographic factors associated with urinary tractinfection in young febrile infants. Pediatrics.2005;116:644–8.
18. Didier C, Streicher MP, Chognot D, et al. Lateonsetneonatal infections: Incidences and patho gens in the eraof antenatal antibiotics. Eur J Ped iatr. 2012;171:681–7.
19. Abrahamsson K, Hansson S, Jodal U. Staphylococcussaprophyticus urinary tract infec tions in children. Eur JPediatr. 1993;152:69–71.
20. Dougherty FE, Gottlieb RP, Gross GW. Neonatal renalabscess caused by Staphylococcus aureus. Pediatr InfectDis J. 1991;10:463–6. 21. Wippermann CF, Schofer O, BeetzR. Renal abscess in childhood: Diagnostic and therapeutic
progress. Pediatr Infect Dis J. 1991;10:446–50. 22. Bus hK. Extended-spectrum beta-lactamases in North America,1987-2006. Clin Microbiol Infect. 2008;14:134–43. 23.Bertrand X, Dowzicky MJ. Antimicrobial suscep tibilityamong Gram-negative isolates collected fro m intensivecare units in North America, Europe, the Asia-Pacific Rim,Latin America, the Middle East, and Africa between 2004and 2009 as part of the Tigecycline Evaluation andSurveillance Trial. Clin Ther. 2012;34:124–37. 24. MolandES, Hanson ND, Black JA, et al. Prevalence of newerbeta-lactamases in Gramnegative clinical isolates collectedin the United States from 2001 to 2002.J Clin Microbiol.2006;44:3318–24. 25. Chandramohan L, Revell PA. Prevalenceand molecular characterization ofextended-spectrumβ-lactamase-producing Enterobacteriaceaein a pediatric patient population. Antimicrob AgentsChemother. 2012;56:4765–70. 26. Plos K, Carter T, Hull S,et al. Frequency and orga nization of pap homologous DNA inrelation to c li nical origin of uropathogenic Escherichiacoli. J Infect Dis. 1990;161:518–24. 27. Kor honen TK,Vaisanen V, Kallio P, et al. The role of pili in theadhesion of Escherichia coli to human urinary tractepithelial cells. Scand J Infect Dis. 1982;33:26–31. 28.Spurbeck RR, Stapleton AE, Johnson JR, et al. Fimbrialprofiles predict virulence of uropatho genic Escherichiacoli strains: Contribution of y gi and yad fimbriae.Infect Immun. 2011;79:4753–63. 29. Sch illing JD, MulveyMA, Huttgren SJ. Structure and function of Escherichiacoli type I pilli: New insight into the pathogenesis ofurinary tract infections. J Infect Dis. 2001;183:S36–40.30. Kallenius G, Mollby R, Svenson SB. Occurrence ofP-fimbriated Escherichia coli in urinary tract infec tions.Lancet. 1981;2:1369–72. 31. Nowicki B, Svanborg-Eden C,Hull R. Molecular analysis and epidemiology of the Drhemag glutinin of uropathogenic Escherichia coli. InfectImmun. 1989;57:446–51 32. Rama G, Chhina DK, Chhina RS, etal. Urinary tract infections-microbial virulencedeterminants and reactive oxygen species. Comp ImmunolMicrobiol Infect Dis. 2005;28:339–49. 33. Azpiroz MF, PoeyME, Laviña M. Microcins and urovirulence in Escherichiacoli. Microb Pathog. 2009;47:274–80. 34. Kunin C.Detection, Prevention and Management of Urinary TractInfections, ed 4. Philadelphia: Lea & Febiger; 1987. p.130.
35. Orskov I, Orskov F, Birch-Andersen A, et al. O, K, Hand fimbrial antigens in Escherichia coli serotypesassociated with pyelonephritis and cystitis. Scand JInfect Dis. 1982;33:18–25.
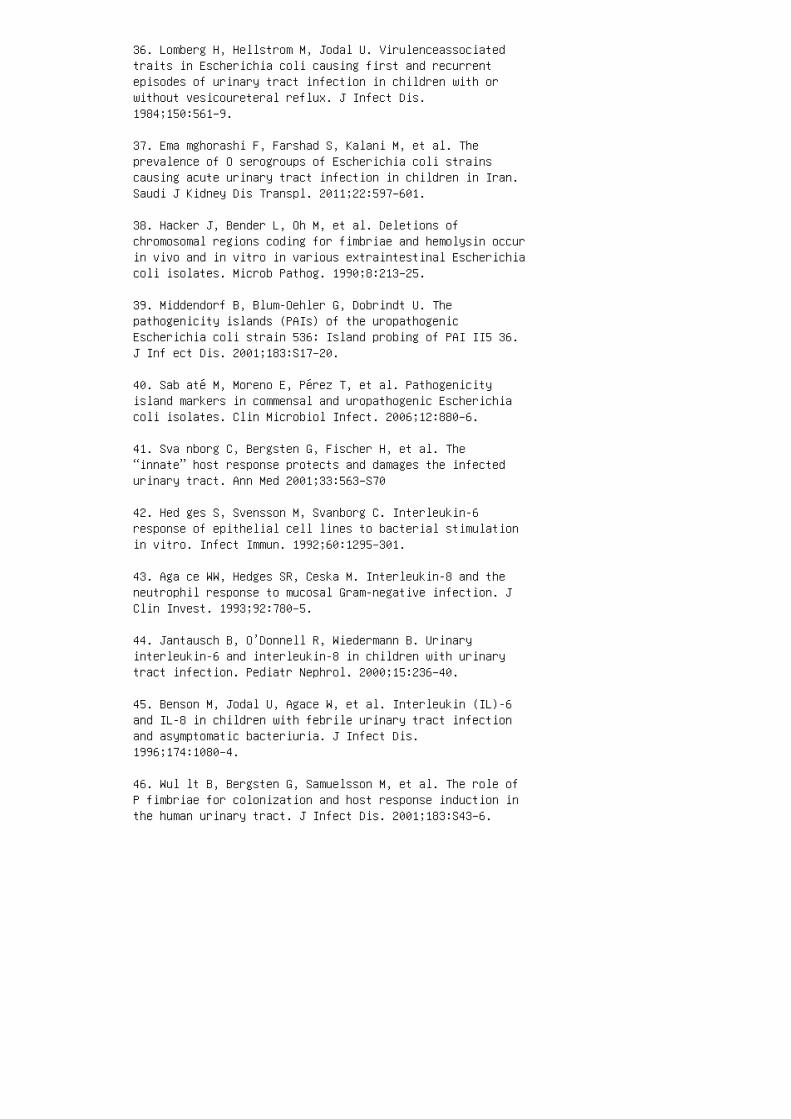
36. Lomberg H, Hellstrom M, Jodal U. Virulenceassociatedtraits in Escherichia coli causing first and recurrentepisodes of urinary tract infection in children with orwithout vesicoureteral reflux. J Infect Dis.1984;150:561–9.
37. Ema mghorashi F, Farshad S, Kalani M, et al. Theprevalence of O serogroups of Escherichia coli strainscausing acute urinary tract infection in children in Iran.Saudi J Kidney Dis Transpl. 2011;22:597–601.
38. Hacker J, Bender L, Oh M, et al. Deletions ofchromosomal regions coding for fimbriae and hemolysin occurin vivo and in vitro in various extraintestinal Escherichiacoli isolates. Microb Pathog. 1990;8:213–25.
39. Middendorf B, Blum-Oehler G, Dobrindt U. Thepathogenicity islands (PAIs) of the uropathogenicEscherichia coli strain 536: Island probing of PAI II5 36.J Inf ect Dis. 2001;183:S17–20.
40. Sab até M, Moreno E, Pérez T, et al. Pathogenicityisland markers in commensal and uropathogenic Escherichiacoli isolates. Clin Microbiol Infect. 2006;12:880–6.
41. Sva nborg C, Bergsten G, Fischer H, et al. The“innate” host response protects and damages the infectedurinary tract. Ann Med 2001;33:563–S70
42. Hed ges S, Svensson M, Svanborg C. Interleukin-6response of epithelial cell lines to bacterial stimulationin vitro. Infect Immun. 1992;60:1295–301.
43. Aga ce WW, Hedges SR, Ceska M. Interleukin-8 and theneutrophil response to mucosal Gram-negative infection. JClin Invest. 1993;92:780–5.
44. Jantausch B, O’Donnell R, Wiedermann B. Urinaryinterleukin-6 and interleukin-8 in children with urinarytract infection. Pediatr Nephrol. 2000;15:236–40.
45. Benson M, Jodal U, Agace W, et al. Interleukin (IL)-6and IL-8 in children with febrile urinary tract infectionand asymptomatic bacteriuria. J Infect Dis.1996;174:1080–4.
46. Wul lt B, Bergsten G, Samuelsson M, et al. The role ofP fimbriae for colonization and host response induction inthe human urinary tract. J Infect Dis. 2001;183:S43–6.

47. Bitsori M, Karatzi M, Dimitriou H, et al. Urine IL-8concentrations in infectious and non-infectious urinarytract conditions. Pediatr Nephrol. 2011;26:2003–7.
48. She u JN, Chen SM, Meng MH, et al. The role of serumand urine interleukin-8 on acute pyelonephritis andsubsequent renal scarring in children. Pediatr Infect DisJ. 2009;28:885–90.
49. Due ll BL, Carey AJ, Tan CK, et al. Innatetranscriptional networks activated in bladder in responseto uropathogenic Escherichia coli drive diverse biologicalpathways and rapid synthesis of IL-10 for defense againstbacterial urinary tract infection. J Immunol.2012;188:781–92. 50. Frendeus B, Wachtler C, Hedlund M, etal. Escherichia coli P fimbriae utilize the Toll-likereceptor 4 pathway for cell activation. Mol Microbiol.2001;40:37–51. 51. Luster AD. Chemokines: Chemotactic cytokines that mediate inflammation. N Engl J Med. 1 998;338:436–45. 52. Sva nborg C, Frendeus B, Godaly G, etal. Tolllike receptor signaling and chemokine receptorexpression influence the severity of urinary tractinfection. J Infect Dis. 2001;183:S61–5. 53. Olszyna DP,Opal SM, Prins JM, et al. Chemotactic activity of CXCchemokines inter leukin-8, growth-related oncogene-alpha,and e pi thelial cell-derived neutrophil-activatingprotein-78 in urine of patients with urosepsis. J InfectDis. 2000;182:1731–7. 54. Ott o G, Burdick M, Strieter R,et al. Chemokine response to febrile urinary tractinfection. Kidney Int. 2005;68:62–70. 55. Fre ndeus B,Godaly G, Hang L, et al.: Interleukin-8 receptordeficiency confers sus ceptibility to acute experimentalpyelonephritis and m ay have a human counterpart. J ExpMed. 2000;192:881–90. 56. Lun dstedt AC, Leijonhufvud I,Ragnarsdottir B, et al. Inherited susceptibility to acutepyelone phritis: A family study of urinary tract infection.J I nf ect Dis. 2007;195:1227–34. 57. Haw n TR, ScholesD, Wang H, et al. Genetic variation of the human urinarytract innate immune response and asymptomatic bacteriuriain women. PLoS One. 2009;4:e8300 58. Kar oly E, Fekete A,Banki NF, et al. Heat shock protein 72 (HSPA1B) genepolymorphism and Toll-like receptor (TLR) 4 mutation areassociated with increased risk of urinary tract infectionin children. Pediatr Res. 2007;61:371–4. 59. Yin X, HouT, Liu Y, et al. Association of Toll-like receptor 4 genepolymorphism and expression with urinary tract infectiontypes in adults. PLoS One. 2010;5:e14223 60. Tramma D,Hatzistylianou M, Gerasimou G, et al. Interleukin-6 andinterleukin-8 levels in the urine of children with renalscarring. Pediatr Nephrol. 2012;27:1525–30 61. Haraoka,
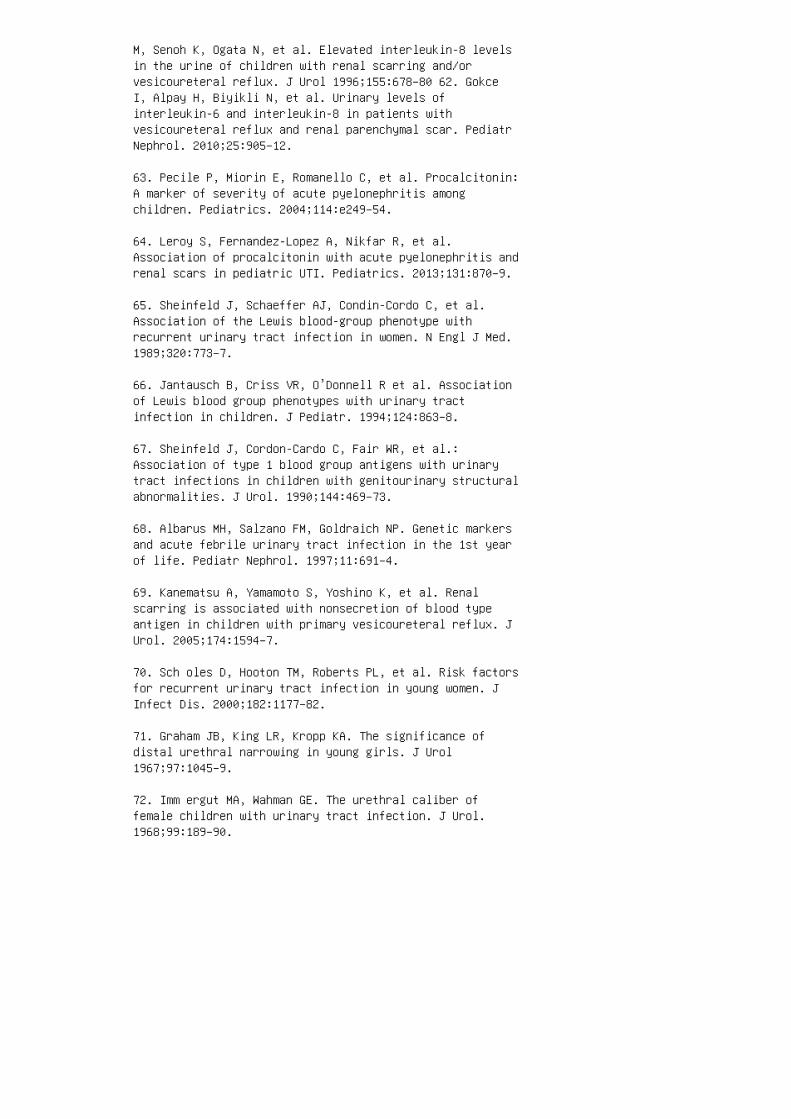
M, Senoh K, Ogata N, et al. Elevated interleukin-8 levelsin the urine of children with renal scarring and/orvesicoureteral reflux. J Urol 1996;155:678–80 62. GokceI, Alpay H, Biyikli N, et al. Urinary levels ofinterleukin-6 and interleukin-8 in patients withvesicoureteral reflux and renal parenchymal scar. PediatrNephrol. 2010;25:905–12.
63. Pecile P, Miorin E, Romanello C, et al. Procalcitonin:A marker of severity of acute pyelonephritis amongchildren. Pediatrics. 2004;114:e249–54.
64. Leroy S, Fernandez-Lopez A, Nikfar R, et al.Association of procalcitonin with acute pyelonephritis andrenal scars in pediatric UTI. Pediatrics. 2013;131:870–9.
65. Sheinfeld J, Schaeffer AJ, Condin-Cordo C, et al.Association of the Lewis blood-group phenotype withrecurrent urinary tract infection in women. N Engl J Med.1989;320:773–7.
66. Jantausch B, Criss VR, O’Donnell R et al. Associationof Lewis blood group phenotypes with urinary tractinfection in children. J Pediatr. 1994;124:863–8.
67. Sheinfeld J, Cordon-Cardo C, Fair WR, et al.:Association of type 1 blood group antigens with urinarytract infections in children with genitourinary structuralabnormalities. J Urol. 1990;144:469–73.
68. Albarus MH, Salzano FM, Goldraich NP. Genetic markersand acute febrile urinary tract infection in the 1st yearof life. Pediatr Nephrol. 1997;11:691–4.
69. Kanematsu A, Yamamoto S, Yoshino K, et al. Renalscarring is associated with nonsecretion of blood typeantigen in children with primary vesicoureteral reflux. JUrol. 2005;174:1594–7.
70. Sch oles D, Hooton TM, Roberts PL, et al. Risk factorsfor recurrent urinary tract infection in young women. JInfect Dis. 2000;182:1177–82.
71. Graham JB, King LR, Kropp KA. The significance ofdistal urethral narrowing in young girls. J Urol1967;97:1045–9.
72. Imm ergut MA, Wahman GE. The urethral caliber offemale children with urinary tract infection. J Urol.1968;99:189–90.
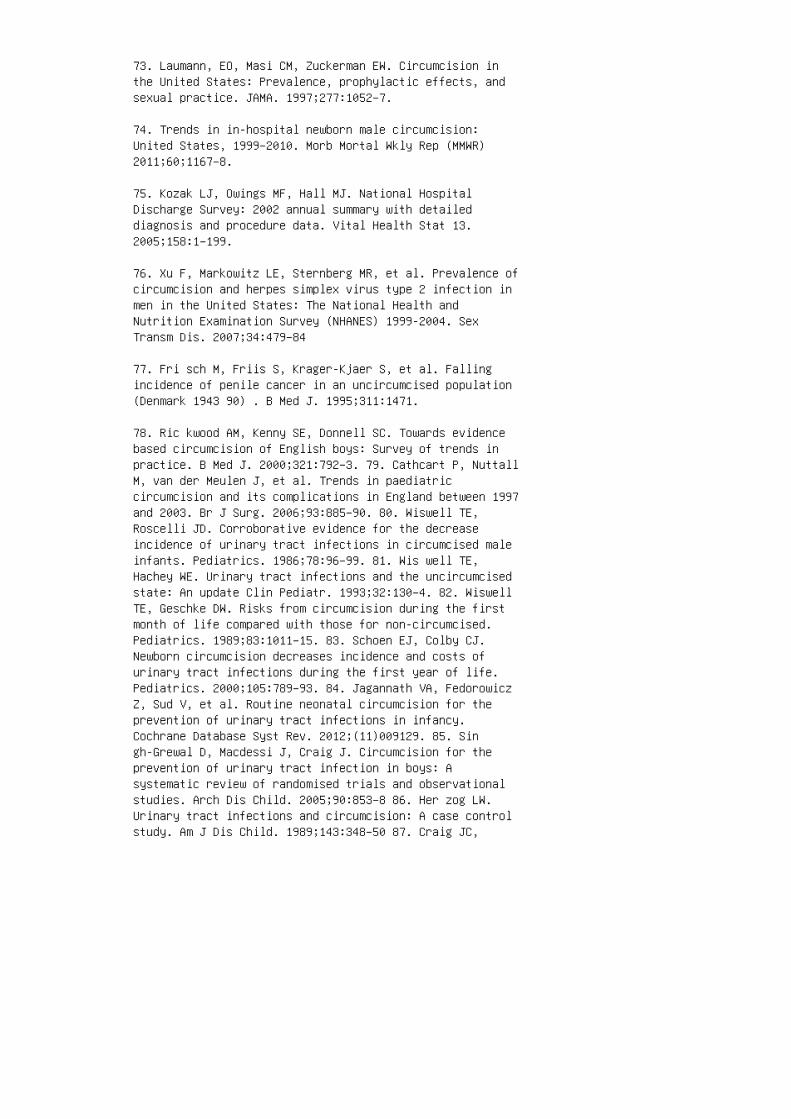
73. Laumann, EO, Masi CM, Zuckerman EW. Circumcision inthe United States: Prevalence, prophylactic effects, andsexual practice. JAMA. 1997;277:1052–7.
74. Trends in in-hospital newborn male circumcision:United States, 1999–2010. Morb Mortal Wkly Rep (MMWR)2011;60;1167–8.
75. Kozak LJ, Owings MF, Hall MJ. National HospitalDischarge Survey: 2002 annual summary with detaileddiagnosis and procedure data. Vital Health Stat 13.2005;158:1–199.
76. Xu F, Markowitz LE, Sternberg MR, et al. Prevalence ofcircumcision and herpes simplex virus type 2 infection inmen in the United States: The National Health andNutrition Examination Survey (NHANES) 1999-2004. SexTransm Dis. 2007;34:479–84
77. Fri sch M, Friis S, Krager-Kjaer S, et al. Fallingincidence of penile cancer in an uncircumcised population(Denmark 1943 90) . B Med J. 1995;311:1471.
78. Ric kwood AM, Kenny SE, Donnell SC. Towards evidencebased circumcision of English boys: Survey of trends inpractice. B Med J. 2000;321:792–3. 79. Cathcart P, NuttallM, van der Meulen J, et al. Trends in paediatriccircumcision and its complications in England between 1997and 2003. Br J Surg. 2006;93:885–90. 80. Wiswell TE,Roscelli JD. Corroborative evidence for the decreaseincidence of urinary tract infections in circumcised maleinfants. Pediatrics. 1986;78:96–99. 81. Wis well TE,Hachey WE. Urinary tract infections and the uncircumcisedstate: An update Clin Pediatr. 1993;32:130–4. 82. WiswellTE, Geschke DW. Risks from circumcision during the firstmonth of life compared with those for non-circumcised.Pediatrics. 1989;83:1011–15. 83. Schoen EJ, Colby CJ.Newborn circumcision decreases incidence and costs ofurinary tract infections during the first year of life.Pediatrics. 2000;105:789–93. 84. Jagannath VA, FedorowiczZ, Sud V, et al. Routine neonatal circumcision for theprevention of urinary tract infections in infancy.Cochrane Database Syst Rev. 2012;(11)009129. 85. Singh-Grewal D, Macdessi J, Craig J. Circumcision for theprevention of urinary tract infection in boys: Asystematic review of randomised trials and observationalstudies. Arch Dis Child. 2005;90:853–8 86. Her zog LW.Urinary tract infections and circumcision: A case controlstudy. Am J Dis Child. 1989;143:348–50 87. Craig JC,

Knight JF, Sureshkumar P, et al. Effect of circumcision onincidence of urinary tract infection in preschool boys. JPediatr. 1996;128:23–7. 88. Nayir A. Circumcision for theprevention of significant bacteriuria in boys. PediatrNephrol. 200 1;16:1129–34 89. Wis well TE, Miller GM,Gelston, HM, Jr, et al.: Effect of circumcision status onperiurethral bac terial flora during the first year oflife. J. Pediatr. 198 8;113:442–6 90. Wis well TE: JohnK. Lattimer Lecture. Prepuce pres ence portends prevalenceof potentially perilous periurethral pathogens. J Urol.1992;148:739–42. 91. Law ay MA, Wani ML, Patnaik R, et al.Does circumci sion alter the periurethral uropathogenicbacterial flora. Afr J Paediatr Surg. 2012;9:109–12 92.Price LB, Liu CM, Johnson KE, et al. The effects ofcircumcision on the penis microbiome. PLoS ONE2010;5:e8422 93. Fussell EN, Kaack MB, Cherry R, et al.Adherence of bacteria to human foreskin. J Urol.1988;140:997–1001 94. Bonacorsi S, Lefevre S, Clermont O.Escherichia coli strains causing urinary tract infectionin uncircum cised infants resemble urosepsis-like adultstrains. J Uro l. 2005;173:195–7. 95. American Academy ofPediatrics Task Force on Circumcision. Male circumcision.Pediatrics. 2012;130:e756–85
96. Loening-Baucke V. Urinary incontinence and urinarytract infection and their resolution with treatment ofchronic constipation of child hood. Pediatrics.1997;100:228–32.
97. McKenna PH, Herndon CDA. Voiding dysfunction associatedwith incontinence, vesicoureteral reflux and recurrenturinary tract i nfections. Curr Opin Urol.2000;10:599–606.
98. Kof f SA, Wagner TT, Jayanthi VR. The rela tionshipamong dysfunctional elimination syndromes, primaryvesicoureteral reflux and urinary tract infections inchildren. J Urol. 1998;160:1019–22.
99. Elder JS, Diaz M. Vesicoureteral reflux: The role ofbladder and bowel dysfunction. Nat Rev Urol.2013;10:640–8.
100. Honkinen O, Lehtonen O-P, Ruuskanen O, et al. Cohortstudy of bacterial species causing urinary tract infectionand urinary tract abnormalities in children. B Med J.1999;318:770–1.
101. Hobermann A, Wald ER. Urinary tract infec tions infebrile children. Pediatr Infect Dis. 199 7;16:11–7.
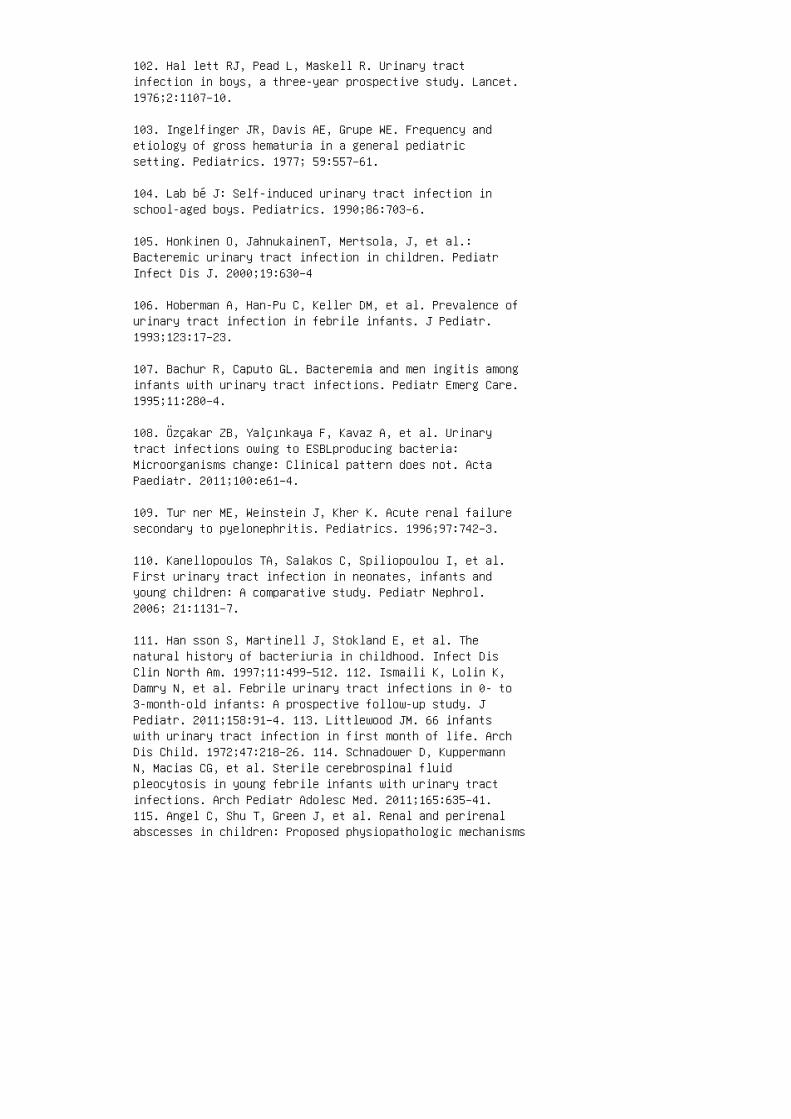
102. Hal lett RJ, Pead L, Maskell R. Urinary tractinfection in boys, a three-year prospective study. Lancet.1976;2:1107–10.
103. Ingelfinger JR, Davis AE, Grupe WE. Frequency andetiology of gross hematuria in a general pediatricsetting. Pediatrics. 1977; 59:557–61.
104. Lab bé J: Self-induced urinary tract infection inschool-aged boys. Pediatrics. 1990;86:703–6.
105. Honkinen O, JahnukainenT, Mertsola, J, et al.:Bacteremic urinary tract infection in children. PediatrInfect Dis J. 2000;19:630–4
106. Hoberman A, Han-Pu C, Keller DM, et al. Prevalence ofurinary tract infection in febrile infants. J Pediatr.1993;123:17–23.
107. Bachur R, Caputo GL. Bacteremia and men ingitis amonginfants with urinary tract infections. Pediatr Emerg Care.1995;11:280–4.
108. Özçakar ZB, Yalçınkaya F, Kavaz A, et al. Urinarytract infections owing to ESBLproducing bacteria:Microorganisms change: Clinical pattern does not. ActaPaediatr. 2011;100:e61–4.
109. Tur ner ME, Weinstein J, Kher K. Acute renal failuresecondary to pyelonephritis. Pediatrics. 1996;97:742–3.
110. Kanellopoulos TA, Salakos C, Spiliopoulou I, et al.First urinary tract infection in neonates, infants andyoung children: A comparative study. Pediatr Nephrol.2006; 21:1131–7.
111. Han sson S, Martinell J, Stokland E, et al. Thenatural history of bacteriuria in childhood. Infect DisClin North Am. 1997;11:499–512. 112. Ismaili K, Lolin K,Damry N, et al. Febrile urinary tract infections in 0- to3-month-old infants: A prospective follow-up study. JPediatr. 2011;158:91–4. 113. Littlewood JM. 66 infantswith urinary tract infection in first month of life. ArchDis Child. 1972;47:218–26. 114. Schnadower D, KuppermannN, Macias CG, et al. Sterile cerebrospinal fluidpleocytosis in young febrile infants with urinary tractinfections. Arch Pediatr Adolesc Med. 2011;165:635–41.115. Angel C, Shu T, Green J, et al. Renal and perirenalabscesses in children: Proposed physiopathologic mechanisms

and treatment algorithm. Pediatr Surg Int. 2003;19:35–9.116. Wippermann CF, Schofer O, Beetz R, et al. Renalabscess in childhood: Diagnostic and therapeutic progress.Pediatr Infect Dis J. 1991;10:446–50. 117. Dem bry LM,Andriole VT. Renal and peri renal abscesses. Infect DisClin North Am. 1997 ;11:663–80. 118. Wang, YT, Lin KY,Chen MJ, et al. Renal abscess in children: A clinicalretrospective study, Acta Paediatr. 2003;44:197–201. 119.Angel T, Shu J, Green E, et al. Renal and perirenalabscesses in children: Proposed physiopathologic mechanismsand treatment algorithm. Pediatr Surg Int. 2003;19:35–9.120. Shu T, Green JM, Orihuela E. Renal and peri renalabscesses in patients with otherwise anat omically normalurinary tracts. J Urol. 2004;172:148–50. 121. Coe lho RF,Schneider-Monteiro ED, Mesquita JL, et al. Renal andperinephric abscesses: Analysis of 65 consecutive cases.World J Surg. 2007;31:431–6. 122. Delanghe J, SpeeckaertM. Preanalytical require ments of urinalysis. Biochem Med(Zagreb). 2 014 ;24:89–104. 123. Dow ns SM. Technicalreport: Urinary tract infections in febrile infants andyoung children. Pediatrics. 1999;103:e54. 124. Rawal K,Senguttuvan P, Morris M, et al. Significance of crystalclear urine. Lancet. 1990;335:1228. 125. Bulloch B,BausherJC, Pomerantz WJ, et al.: Can urine clarity excludethe diagnosis of urinary tract infection? Pediatrics2000;106.e60. 126. Struthers S, Scanlon J, Parker K, etal.: Parental reporting of smelly urine and urinary tractinfec tion. Arch Dis Child. 2003;88:250–2. 127. GorelicMD, Shaw KN. Screening tests for urinary tract infection inchildren: A meta-analysis. P ed iatrics. 1999;104:e54.128. Kunin CN, DeGroot JE, Uehling D, et al.: Detection ofurinary tract infection in 3-5 year old girls by mothersusing a nitrite strip indicator. Pediatrics.1976;57:829–35.
129. Al-Ori F, McGillivray D, Tange S, et al. Urine culturefrom bag specimens in young children: Are the r isks toohigh? J Pediatr. 2000;137:221–6.
130. Hob erman A, Wald ER, Reynolds EA, et al. Pyuria andbacteriuria in urine specimens obtained by catheter fromyoung children with fever. J Pediatr. 1994;124:513–9.
131. Giorgi LJ, Bratslavsky G, Kogan BA. Febrile uri narytract infections in infants: Renal ultrasound rem ainsnecessary. J Urol. 2005;173:568–70
132. Hob erman A, Charron M, Hickey RW, et al. Imagingstudies after a first febrile urinary tract infection inyoung children. N Engl J Med. 2003;348:195–202.

133. Alon US, Ganapathy S. Should renal ultrasonogra phy bedone routinely in children with first urinary tra ctinfection? Clin Pediatr. 1999;38:21–5.
134. Zam ir W, Sakran Y, Horowitz, A et al. Urinary tractinfection: Is there a need for routine renal ultrasonography? Arch Dis Child. 2004;89:466–8.
135. Mas sanyi EZ, Preece J, Gupta A, et al. Utility ofscreening ultrasound after first febrile UTI amongpatients with clinically significant vesicoureteralreflux. Urology. 2013;82:905–9.
136. Mori R, Lakhanpaul M, Verrier-Jones K. Diagnosis andmanagement of urinary tract infection in children: Summaryof NICE guidance. BMJ. 2007;335:395–7.
137. Deader R, Tiboni SG, Malone PS, et al. Will theimplementation of the 2007 National Institute for Healthand Clinical Excellence (NICE) guidelines on childhoodurinary tract infection (UTI) in the UK miss significanturinary tract pathology? BJU Int. 2012;110:454–8.
138. Han nula A, Venhola M, Renko M, et al. Vesicouretericreflux in children with suspected and proven urinary tractinfection. Pediatr Nephrol. 2010;25:1463–9.
139. Berry CS, Vander Brink BA, Koff SA, et al. Is VCUGstill indicated following the first episode of urinarytract infection in boys? Urology. 2012;80:1351–5.
140. Lee JH, Kim MK, Park SE. Is a routine voidingcystourethrogram necessary in children after the firstfebrile urinary tract infection? Acta Paediatr.2012;101:e105–9.
141. Pennesi M, L’Erario I, Travan L, et al., ManagingChildren under 36 months of age with febrile urinary tractinfection: A new approach. Pediatr Nephrol. 2012;4:611–5.
142. Spe ncer JD, Bates CM, Mahan JD, et al. The accuracyand health risks of a voiding cystoure throgram after afebrile urinary tract infection. J P ed iatr Urol.2012;8:72–6.
143. Craig JC, Knight JF, Sureshkumar P, et al.Vesicoureteral reflux and timing of micturatingcystourethrography after urinary tract infection. Arch DisChild. 1997;76:275–7. 144. Mahant S, To T, Friedman J.
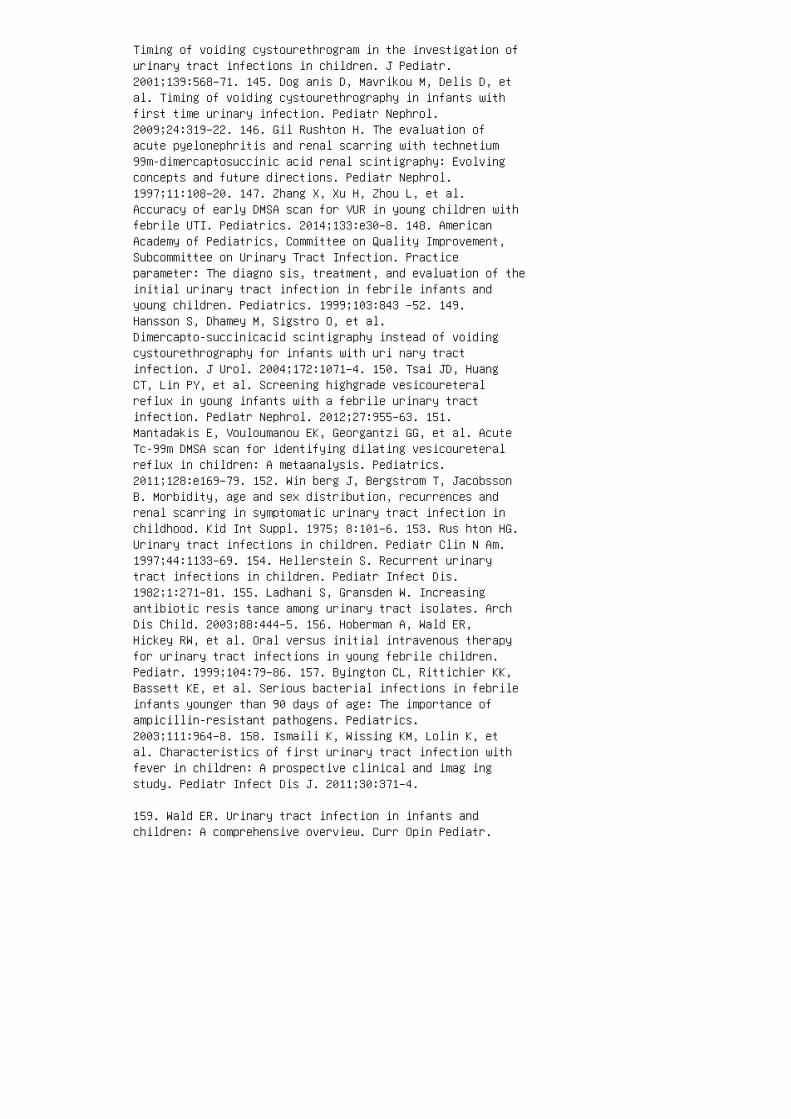
Timing of voiding cystourethrogram in the investigation ofurinary tract infections in children. J Pediatr.2001;139:568–71. 145. Dog anis D, Mavrikou M, Delis D, etal. Timing of voiding cystourethrography in infants withfirst time urinary infection. Pediatr Nephrol.2009;24:319–22. 146. Gil Rushton H. The evaluation ofacute pyelonephritis and renal scarring with technetium99m-dimercaptosuccinic acid renal scintigraphy: Evolvingconcepts and future directions. Pediatr Nephrol.1997;11:108–20. 147. Zhang X, Xu H, Zhou L, et al.Accuracy of early DMSA scan for VUR in young children withfebrile UTI. Pediatrics. 2014;133:e30–8. 148. AmericanAcademy of Pediatrics, Committee on Quality Improvement,Subcommittee on Urinary Tract Infection. Practiceparameter: The diagno sis, treatment, and evaluation of theinitial urinary tract infection in febrile infants andyoung children. Pediatrics. 1999;103:843 –52. 149.Hansson S, Dhamey M, Sigstro O, et al.Dimercapto-succinicacid scintigraphy instead of voidingcystourethrography for infants with uri nary tractinfection. J Urol. 2004;172:1071–4. 150. Tsai JD, HuangCT, Lin PY, et al. Screening highgrade vesicoureteralreflux in young infants with a febrile urinary tractinfection. Pediatr Nephrol. 2012;27:955–63. 151.Mantadakis E, Vouloumanou EK, Georgantzi GG, et al. AcuteTc-99m DMSA scan for identifying dilating vesicoureteralreflux in children: A metaanalysis. Pediatrics.2011;128:e169–79. 152. Win berg J, Bergstrom T, JacobssonB. Morbidity, age and sex distribution, recurrences andrenal scarring in symptomatic urinary tract infection inchildhood. Kid Int Suppl. 1975; 8:101–6. 153. Rus hton HG.Urinary tract infections in children. Pediatr Clin N Am.1997;44:1133–69. 154. Hellerstein S. Recurrent urinarytract infections in children. Pediatr Infect Dis.1982;1:271–81. 155. Ladhani S, Gransden W. Increasingantibiotic resis tance among urinary tract isolates. ArchDis Child. 2003;88:444–5. 156. Hoberman A, Wald ER,Hickey RW, et al. Oral versus initial intravenous therapyfor urinary tract infections in young febrile children.Pediatr. 1999;104:79–86. 157. Byington CL, Rittichier KK,Bassett KE, et al. Serious bacterial infections in febrileinfants younger than 90 days of age: The importance ofampicillin-resistant pathogens. Pediatrics.2003;111:964–8. 158. Ismaili K, Wissing KM, Lolin K, etal. Characteristics of first urinary tract infection withfever in children: A prospective clinical and imag ingstudy. Pediatr Infect Dis J. 2011;30:371–4.
159. Wald ER. Urinary tract infection in infants andchildren: A comprehensive overview. Curr Opin Pediatr.
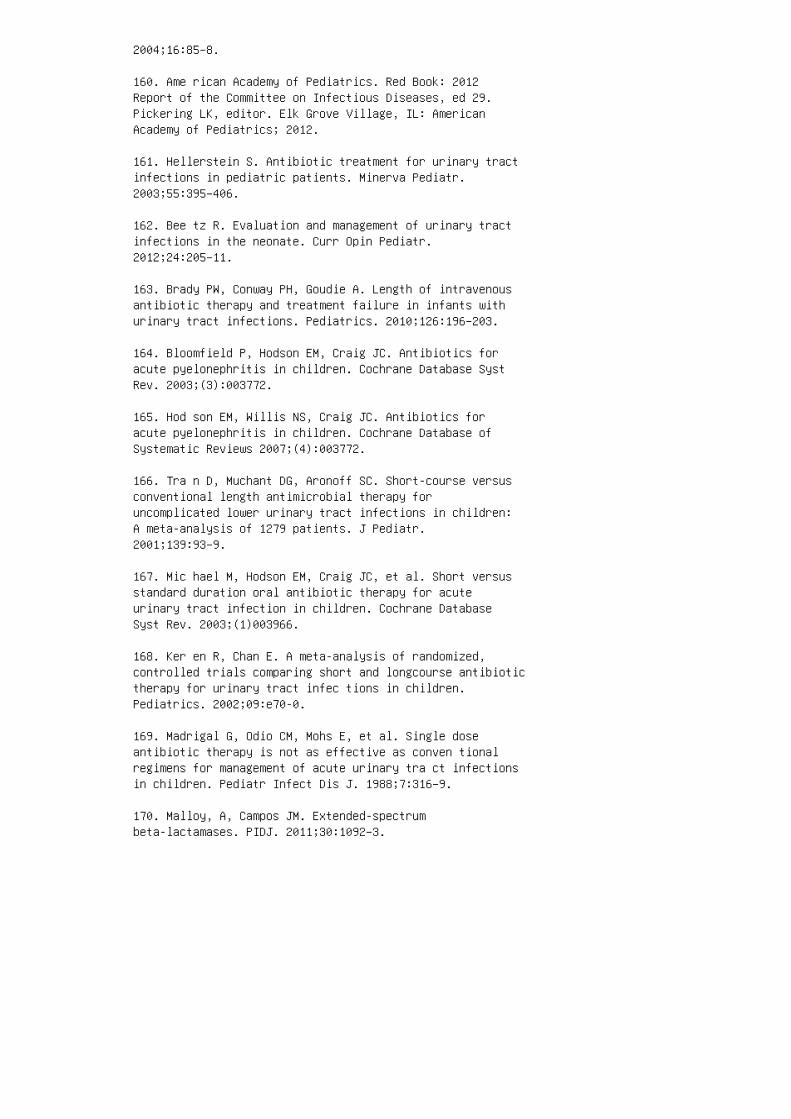
2004;16:85–8.
160. Ame rican Academy of Pediatrics. Red Book: 2012Report of the Committee on Infectious Diseases, ed 29.Pickering LK, editor. Elk Grove Village, IL: AmericanAcademy of Pediatrics; 2012.
161. Hellerstein S. Antibiotic treatment for urinary tractinfections in pediatric patients. Minerva Pediatr.2003;55:395–406.
162. Bee tz R. Evaluation and management of urinary tractinfections in the neonate. Curr Opin Pediatr.2012;24:205–11.
163. Brady PW, Conway PH, Goudie A. Length of intravenousantibiotic therapy and treatment failure in infants withurinary tract infections. Pediatrics. 2010;126:196–203.
164. Bloomfield P, Hodson EM, Craig JC. Antibiotics foracute pyelonephritis in children. Cochrane Database SystRev. 2003;(3):003772.
165. Hod son EM, Willis NS, Craig JC. Antibiotics foracute pyelonephritis in children. Cochrane Database ofSystematic Reviews 2007;(4):003772.
166. Tra n D, Muchant DG, Aronoff SC. Short-course versusconventional length antimicrobial therapy foruncomplicated lower urinary tract infections in children:A meta-analysis of 1279 patients. J Pediatr.2001;139:93–9.
167. Mic hael M, Hodson EM, Craig JC, et al. Short versusstandard duration oral antibiotic therapy for acuteurinary tract infection in children. Cochrane DatabaseSyst Rev. 2003;(1)003966.
168. Ker en R, Chan E. A meta-analysis of randomized,controlled trials comparing short and longcourse antibiotictherapy for urinary tract infec tions in children.Pediatrics. 2002;09:e70-0.
169. Madrigal G, Odio CM, Mohs E, et al. Single doseantibiotic therapy is not as effective as conven tionalregimens for management of acute urinary tra ct infectionsin children. Pediatr Infect Dis J. 1988;7:316–9.
170. Malloy, A, Campos JM. Extended-spectrumbeta-lactamases. PIDJ. 2011;30:1092–3.
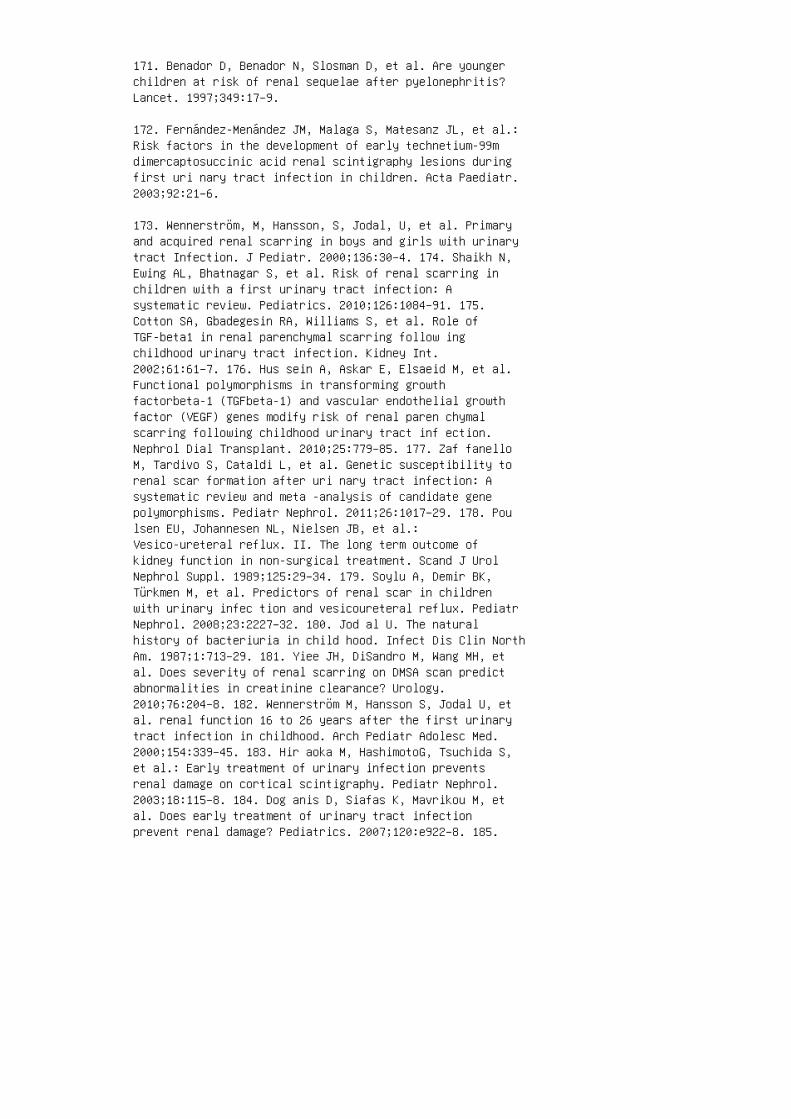
171. Benador D, Benador N, Slosman D, et al. Are youngerchildren at risk of renal sequelae after pyelonephritis?Lancet. 1997;349:17–9.
172. Fernández-Menández JM, Malaga S, Matesanz JL, et al.:Risk factors in the development of early technetium-99mdimercaptosuccinic acid renal scintigraphy lesions duringfirst uri nary tract infection in children. Acta Paediatr.2003;92:21–6.
173. Wennerström, M, Hansson, S, Jodal, U, et al. Primaryand acquired renal scarring in boys and girls with urinarytract Infection. J Pediatr. 2000;136:30–4. 174. Shaikh N,Ewing AL, Bhatnagar S, et al. Risk of renal scarring inchildren with a first urinary tract infection: Asystematic review. Pediatrics. 2010;126:1084–91. 175.Cotton SA, Gbadegesin RA, Williams S, et al. Role ofTGF-beta1 in renal parenchymal scarring follow ingchildhood urinary tract infection. Kidney Int.2002;61:61–7. 176. Hus sein A, Askar E, Elsaeid M, et al.Functional polymorphisms in transforming growthfactorbeta-1 (TGFbeta-1) and vascular endothelial growthfactor (VEGF) genes modify risk of renal paren chymalscarring following childhood urinary tract inf ection.Nephrol Dial Transplant. 2010;25:779–85. 177. Zaf fanelloM, Tardivo S, Cataldi L, et al. Genetic susceptibility torenal scar formation after uri nary tract infection: Asystematic review and meta -analysis of candidate genepolymorphisms. Pediatr Nephrol. 2011;26:1017–29. 178. Poulsen EU, Johannesen NL, Nielsen JB, et al.:Vesico-ureteral reflux. II. The long term outcome ofkidney function in non-surgical treatment. Scand J UrolNephrol Suppl. 1989;125:29–34. 179. Soylu A, Demir BK,Türkmen M, et al. Predictors of renal scar in childrenwith urinary infec tion and vesicoureteral reflux. PediatrNephrol. 2008;23:2227–32. 180. Jod al U. The naturalhistory of bacteriuria in child hood. Infect Dis Clin NorthAm. 1987;1:713–29. 181. Yiee JH, DiSandro M, Wang MH, etal. Does severity of renal scarring on DMSA scan predictabnormalities in creatinine clearance? Urology.2010;76:204–8. 182. Wennerström M, Hansson S, Jodal U, etal. renal function 16 to 26 years after the first urinarytract infection in childhood. Arch Pediatr Adolesc Med.2000;154:339–45. 183. Hir aoka M, HashimotoG, Tsuchida S,et al.: Early treatment of urinary infection preventsrenal damage on cortical scintigraphy. Pediatr Nephrol.2003;18:115–8. 184. Dog anis D, Siafas K, Mavrikou M, etal. Does early treatment of urinary tract infectionprevent renal damage? Pediatrics. 2007;120:e922–8. 185.
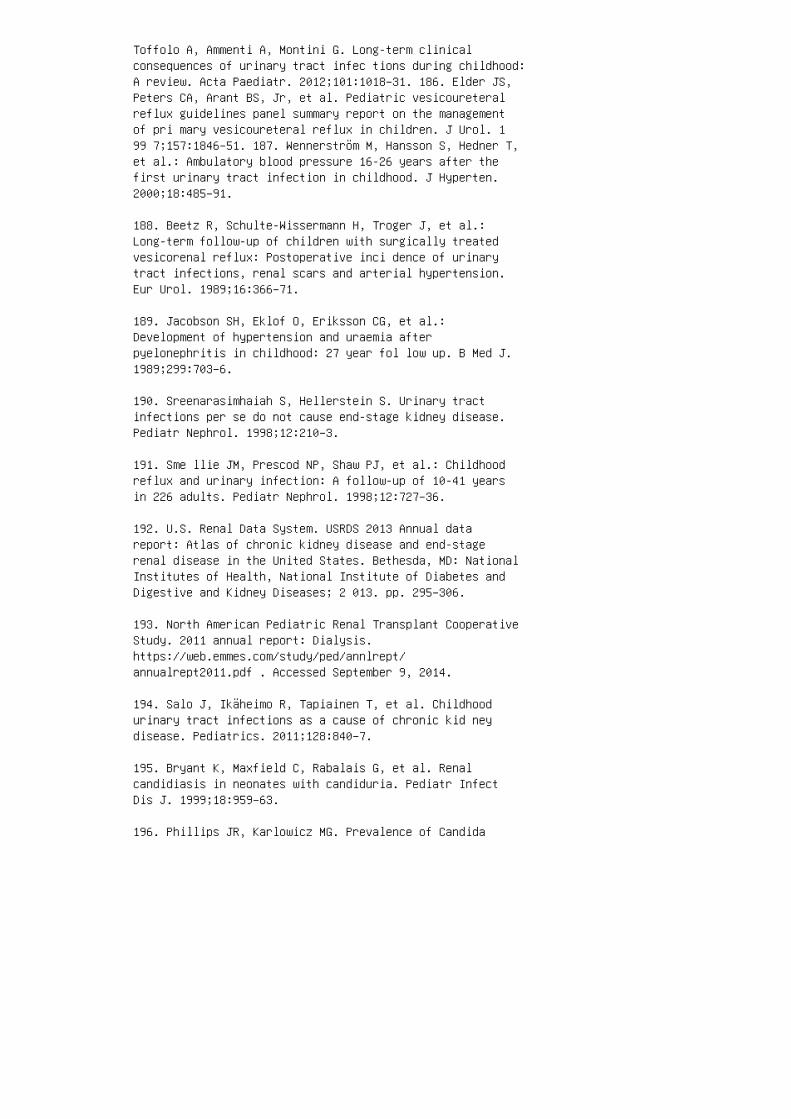
Toffolo A, Ammenti A, Montini G. Long-term clinicalconsequences of urinary tract infec tions during childhood:A review. Acta Paediatr. 2012;101:1018–31. 186. Elder JS,Peters CA, Arant BS, Jr, et al. Pediatric vesicoureteralreflux guidelines panel summary report on the managementof pri mary vesicoureteral reflux in children. J Urol. 199 7;157:1846–51. 187. Wennerström M, Hansson S, Hedner T,et al.: Ambulatory blood pressure 16-26 years after thefirst urinary tract infection in childhood. J Hyperten.2000;18:485–91.
188. Beetz R, Schulte-Wissermann H, Troger J, et al.:Long-term follow-up of children with surgically treatedvesicorenal reflux: Postoperative inci dence of urinarytract infections, renal scars and arterial hypertension.Eur Urol. 1989;16:366–71.
189. Jacobson SH, Eklof O, Eriksson CG, et al.:Development of hypertension and uraemia afterpyelonephritis in childhood: 27 year fol low up. B Med J.1989;299:703–6.
190. Sreenarasimhaiah S, Hellerstein S. Urinary tractinfections per se do not cause end-stage kidney disease.Pediatr Nephrol. 1998;12:210–3.
191. Sme llie JM, Prescod NP, Shaw PJ, et al.: Childhoodreflux and urinary infection: A follow-up of 10-41 yearsin 226 adults. Pediatr Nephrol. 1998;12:727–36.
192. U.S. Renal Data System. USRDS 2013 Annual datareport: Atlas of chronic kidney disease and end-stagerenal disease in the United States. Bethesda, MD: NationalInstitutes of Health, National Institute of Diabetes andDigestive and Kidney Diseases; 2 013. pp. 295–306.
193. North American Pediatric Renal Transplant CooperativeStudy. 2011 annual report: Dialysis.https://web.emmes.com/study/ped/annlrept/annualrept2011.pdf . Accessed September 9, 2014.
194. Salo J, Ikäheimo R, Tapiainen T, et al. Childhoodurinary tract infections as a cause of chronic kid neydisease. Pediatrics. 2011;128:840–7.
195. Bryant K, Maxfield C, Rabalais G, et al. Renalcandidiasis in neonates with candiduria. Pediatr InfectDis J. 1999;18:959–63.
196. Phillips JR, Karlowicz MG. Prevalence of Candida
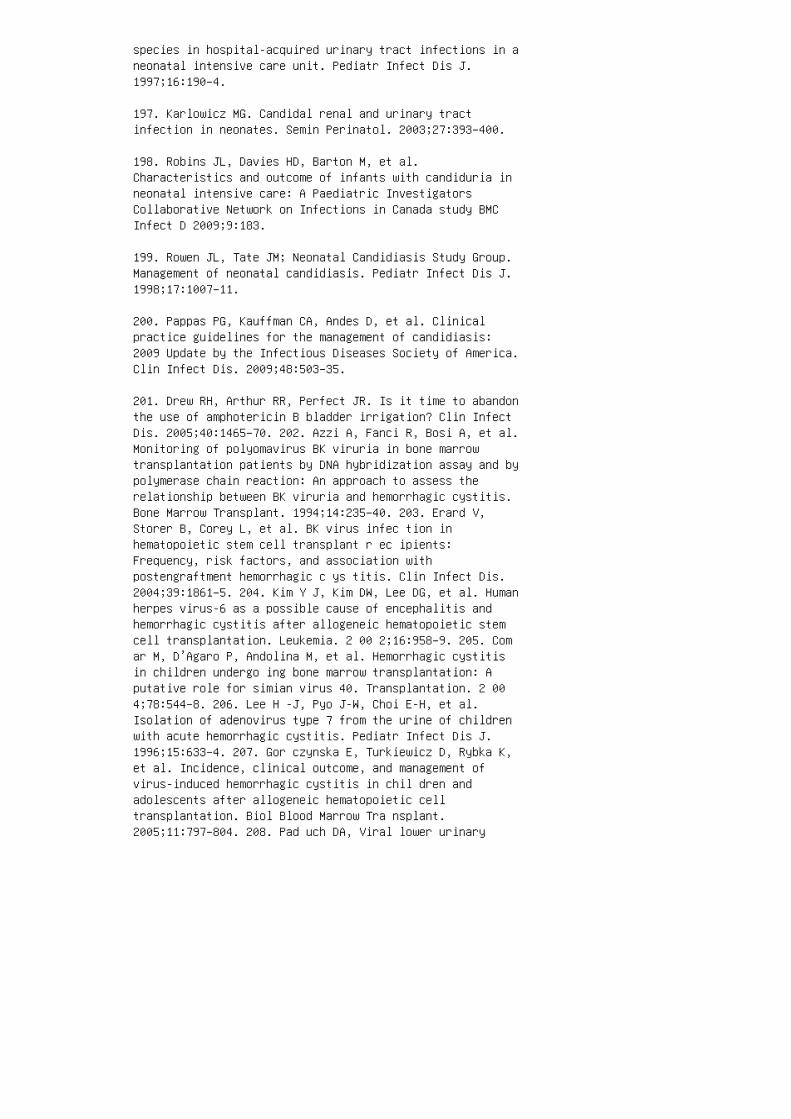
species in hospital-acquired urinary tract infections in aneonatal intensive care unit. Pediatr Infect Dis J.1997;16:190–4.
197. Karlowicz MG. Candidal renal and urinary tractinfection in neonates. Semin Perinatol. 2003;27:393–400.
198. Robins JL, Davies HD, Barton M, et al.Characteristics and outcome of infants with candiduria inneonatal intensive care: A Paediatric InvestigatorsCollaborative Network on Infections in Canada study BMCInfect D 2009;9:183.
199. Rowen JL, Tate JM; Neonatal Candidiasis Study Group.Management of neonatal candidiasis. Pediatr Infect Dis J.1998;17:1007–11.
200. Pappas PG, Kauffman CA, Andes D, et al. Clinicalpractice guidelines for the management of candidiasis:2009 Update by the Infectious Diseases Society of America.Clin Infect Dis. 2009;48:503–35.
201. Drew RH, Arthur RR, Perfect JR. Is it time to abandonthe use of amphotericin B bladder irrigation? Clin InfectDis. 2005;40:1465–70. 202. Azzi A, Fanci R, Bosi A, et al.Monitoring of polyomavirus BK viruria in bone marrowtransplantation patients by DNA hybridization assay and bypolymerase chain reaction: An approach to assess therelationship between BK viruria and hemorrhagic cystitis.Bone Marrow Transplant. 1994;14:235–40. 203. Erard V,Storer B, Corey L, et al. BK virus infec tion inhematopoietic stem cell transplant r ec ipients:Frequency, risk factors, and association withpostengraftment hemorrhagic c ys titis. Clin Infect Dis.2004;39:1861–5. 204. Kim Y J, Kim DW, Lee DG, et al. Humanherpes virus-6 as a possible cause of encephalitis andhemorrhagic cystitis after allogeneic hematopoietic stemcell transplantation. Leukemia. 2 00 2;16:958–9. 205. Comar M, D’Agaro P, Andolina M, et al. Hemorrhagic cystitisin children undergo ing bone marrow transplantation: Aputative role for simian virus 40. Transplantation. 2 004;78:544–8. 206. Lee H -J, Pyo J-W, Choi E-H, et al.Isolation of adenovirus type 7 from the urine of childrenwith acute hemorrhagic cystitis. Pediatr Infect Dis J.1996;15:633–4. 207. Gor czynska E, Turkiewicz D, Rybka K,et al. Incidence, clinical outcome, and management ofvirus-induced hemorrhagic cystitis in chil dren andadolescents after allogeneic hematopoietic celltransplantation. Biol Blood Marrow Tra nsplant.2005;11:797–804. 208. Pad uch DA, Viral lower urinary
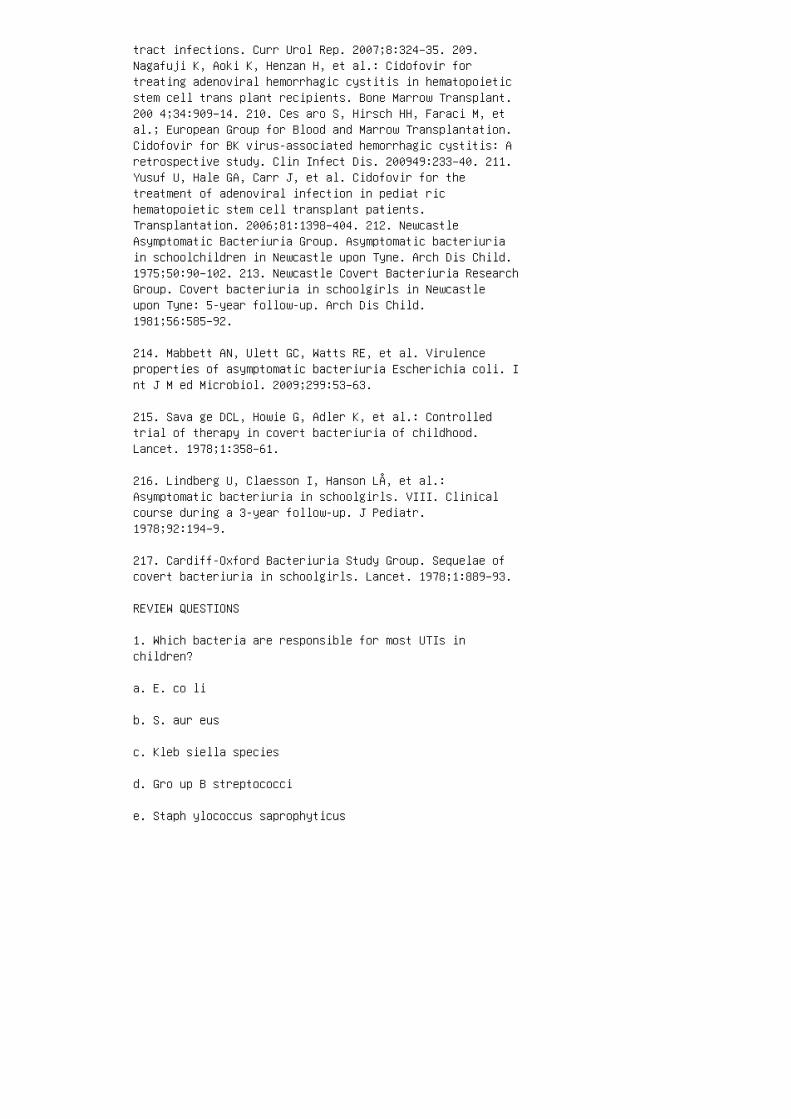
tract infections. Curr Urol Rep. 2007;8:324–35. 209.Nagafuji K, Aoki K, Henzan H, et al.: Cidofovir fortreating adenoviral hemorrhagic cystitis in hematopoieticstem cell trans plant recipients. Bone Marrow Transplant.200 4;34:909–14. 210. Ces aro S, Hirsch HH, Faraci M, etal.; European Group for Blood and Marrow Transplantation.Cidofovir for BK virus-associated hemorrhagic cystitis: Aretrospective study. Clin Infect Dis. 200949:233–40. 211.Yusuf U, Hale GA, Carr J, et al. Cidofovir for thetreatment of adenoviral infection in pediat richematopoietic stem cell transplant patients.Transplantation. 2006;81:1398–404. 212. NewcastleAsymptomatic Bacteriuria Group. Asymptomatic bacteriuriain schoolchildren in Newcastle upon Tyne. Arch Dis Child.1975;50:90–102. 213. Newcastle Covert Bacteriuria ResearchGroup. Covert bacteriuria in schoolgirls in Newcastleupon Tyne: 5-year follow-up. Arch Dis Child.1981;56:585–92.
214. Mabbett AN, Ulett GC, Watts RE, et al. Virulenceproperties of asymptomatic bacteriuria Escherichia coli. Int J M ed Microbiol. 2009;299:53–63.
215. Sava ge DCL, Howie G, Adler K, et al.: Controlledtrial of therapy in covert bacteriuria of childhood.Lancet. 1978;1:358–61.
216. Lindberg U, Claesson I, Hanson LÅ, et al.:Asymptomatic bacteriuria in schoolgirls. VIII. Clinicalcourse during a 3-year follow-up. J Pediatr.1978;92:194–9.
217. Cardiff-Oxford Bacteriuria Study Group. Sequelae ofcovert bacteriuria in schoolgirls. Lancet. 1978;1:889–93.
REVIEW QUESTIONS
1. Which bacteria are responsible for most UTIs inchildren?
a. E. co li
b. S. aur eus
c. Kleb siella species
d. Gro up B streptococci
e. Staph ylococcus saprophyticus

2. �e 20 12 AAP Task Force on Circumcision states that allmale infants should undergo circumcision.
a. Tru e
b. Fals e
3. Whi ch symptoms or laboratory test results di�erentiatecystitis from acute pyelonephritis?
a. Abd ominal pain
b. Exc essive crying
c. Hem aturia
d. Feve r
e. Dysu ria
4. According to the 2011 AAP UTI Practice Guideline, whatis the minimum colony count diagnostic of urinary tractinfection?
a. 100,000 CFU/mL
b. 50,000 CFU/mL
c. 20,000 CFU/mL
d. 10,000 CFU/mL
5. All children under 2 years of age should have a renalultrasound a�er diagnosis of UTI.
a. True
b. False
6. A 6-year-old girl with a history of spina bi�darequiring routine urinary catheterization has a history ofmultiple episodes of UTI. She has been on multiple coursesof antibiotics and was recently admitted a�er failingoutpatient therapy on ce�xime. You are suspicious she mayhave developed an ESBL infection. What is the best choiceof empiric therapy for this child? a. Ce�riaxone b.Ce�azidime c. Meropenem d. Ampicillin-sulbactam 7. Amale infant is born at 25 weeks’ gestation and developscandiduria at two weeks of age while in the neonatalintensive care unit. Which antimicrobial agent should be

empirically started? a. Fluconazole b. Micafungin c.Itraconazole d. Amphotericin 8. Which of the followingviruses may cause cystitis in an immunocompromisedpatient? a. Adenovirus b. BK virus c. HHV-6 d. CMV e.All of the above 9. Which of the following therapies isindicated in a 16-year-old girl with Proteus mirabilisbacteriuria found during a routine health screen? a.Ce�xime b. Trimethoprim-sulfamethoxazole c. Cipro�oxacind. Amoxicillin e. No therapy. 10. E. coli associated withasymptomatic bacteriuria have fewer virulence factors thanpathogenic E. coli. a. True b. False ANSWER KEY 1. a 2.b 3. d 4. b 5. a 6. c 7. d 8. e 9. e 10. b
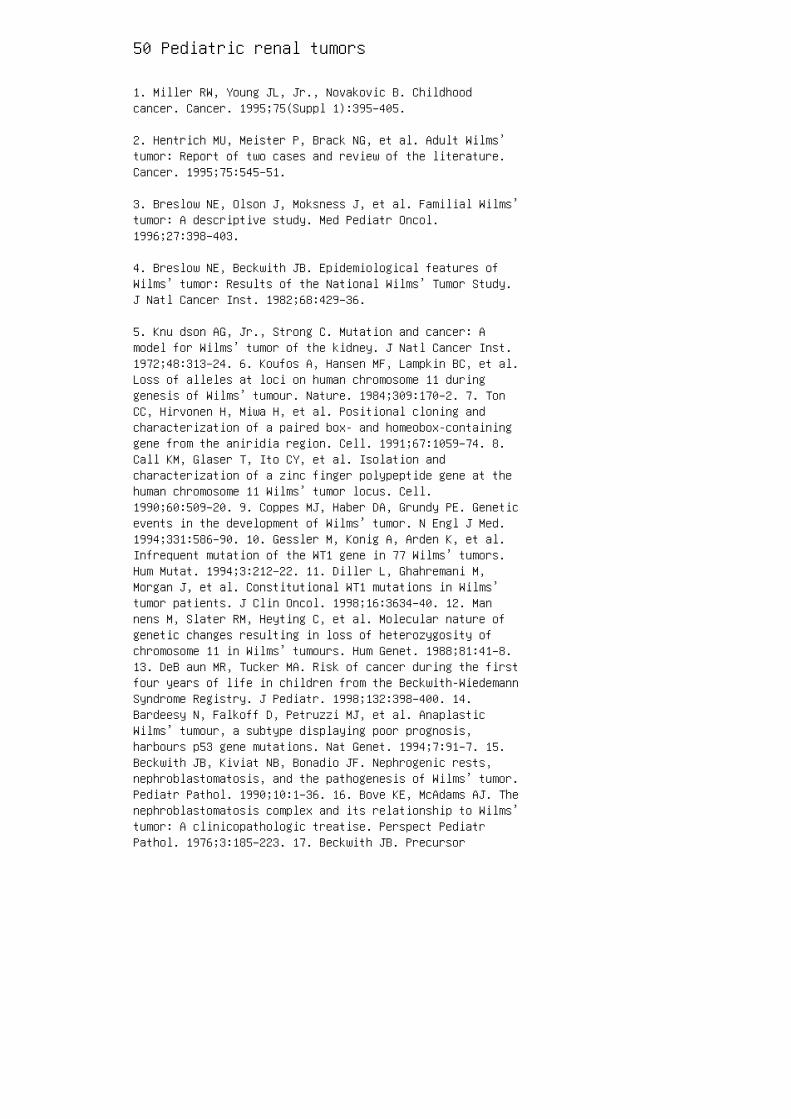
50 Pediatric renal tumors
1. Miller RW, Young JL, Jr., Novakovic B. Childhoodcancer. Cancer. 1995;75(Suppl 1):395–405.
2. Hentrich MU, Meister P, Brack NG, et al. Adult Wilms’tumor: Report of two cases and review of the literature.Cancer. 1995;75:545–51.
3. Breslow NE, Olson J, Moksness J, et al. Familial Wilms’tumor: A descriptive study. Med Pediatr Oncol.1996;27:398–403.
4. Breslow NE, Beckwith JB. Epidemiological features ofWilms’ tumor: Results of the National Wilms’ Tumor Study.J Natl Cancer Inst. 1982;68:429–36.
5. Knu dson AG, Jr., Strong C. Mutation and cancer: Amodel for Wilms’ tumor of the kidney. J Natl Cancer Inst.1972;48:313–24. 6. Koufos A, Hansen MF, Lampkin BC, et al.Loss of alleles at loci on human chromosome 11 duringgenesis of Wilms’ tumour. Nature. 1984;309:170–2. 7. TonCC, Hirvonen H, Miwa H, et al. Positional cloning andcharacterization of a paired box- and homeobox-containinggene from the aniridia region. Cell. 1991;67:1059–74. 8.Call KM, Glaser T, Ito CY, et al. Isolation andcharacterization of a zinc finger polypeptide gene at thehuman chromosome 11 Wilms’ tumor locus. Cell.1990;60:509–20. 9. Coppes MJ, Haber DA, Grundy PE. Geneticevents in the development of Wilms’ tumor. N Engl J Med.1994;331:586–90. 10. Gessler M, Konig A, Arden K, et al.Infrequent mutation of the WT1 gene in 77 Wilms’ tumors.Hum Mutat. 1994;3:212–22. 11. Diller L, Ghahremani M,Morgan J, et al. Constitutional WT1 mutations in Wilms’tumor patients. J Clin Oncol. 1998;16:3634–40. 12. Mannens M, Slater RM, Heyting C, et al. Molecular nature ofgenetic changes resulting in loss of heterozygosity ofchromosome 11 in Wilms’ tumours. Hum Genet. 1988;81:41–8.13. DeB aun MR, Tucker MA. Risk of cancer during the firstfour years of life in children from the Beckwith-WiedemannSyndrome Registry. J Pediatr. 1998;132:398–400. 14.Bardeesy N, Falkoff D, Petruzzi MJ, et al. AnaplasticWilms’ tumour, a subtype displaying poor prognosis,harbours p53 gene mutations. Nat Genet. 1994;7:91–7. 15.Beckwith JB, Kiviat NB, Bonadio JF. Nephrogenic rests,nephroblastomatosis, and the pathogenesis of Wilms’ tumor.Pediatr Pathol. 1990;10:1–36. 16. Bove KE, McAdams AJ. Thenephroblastomatosis complex and its relationship to Wilms’tumor: A clinicopathologic treatise. Perspect PediatrPathol. 1976;3:185–223. 17. Beckwith JB. Precursor

lesions of Wilms tumor: Clinical and biologicalimplications. Med Pediatr Oncol. 1993;21:158–68. 18.Ganguly A, Gribble J, Tune B, et al. Renin-secretingWilms’ tumor with severe hypertension: Report of a caseand brief review of renin-secreting tumors. Ann InternMed. 1973;79:835–7. 19. Suresh I, Suresh S, Arumugam R, etal. Antenatal diagnosis of Wilms tumor. J Ultrasound Med.1997;16:69–72. 20. Romão RL, Pippi SJL, Shuman C, et al.Nephron sparing surgery for unilateral Wilms tumor inchildren with predisposing syndromes: Single centerexperience over 10 years. J Urol. 2012;188(Suppl4):1493–8. 21. Gunther P, Schenk JP, Wunsch R, et al.Abdominal tumours in children: 3-D visualisation andsurgical planning. Eur J Pediatr Surg. 2004;14:316–21.
SUMMARY
Renal tumors in children are rare. Advances in man
agement have been the result of cooperative stud
ies enrolling patients from di�erent centers. �is
strategy is bound to be the basis for future improve
ments in diagnosis and therapy. �e introduction of
nephron-sparing procedures and minimally invasive
surgery is expected to change current surgical man
agement. Long-term complications from surgery,
chemotherapy, and radiation need to be addressed as
survivors grow into adulthood.
22. Wootton-Gorges SL, Albano EA, et al. Chest radiographyversus chest CT in the evaluation for pulmonary metastasesin patients with Wilms’ tumor: A retrospective review.Pediatr Radiol. 2000;30:533–7; discussion 537–9.
23. D’Angio GJ. Pre- or post-operative treatment for Wilmstumor? Who, what, when, where, how, why— And which. MedPediatr Oncol. 2003;41:545–9.
24. D’Angio GJ. Pre- or postoperative therapy for Wilms’tumor? J Clin Oncol. 2008;26:4055–7.
25. Pow is M, Messahel B, Hobson R, et al. Surgical
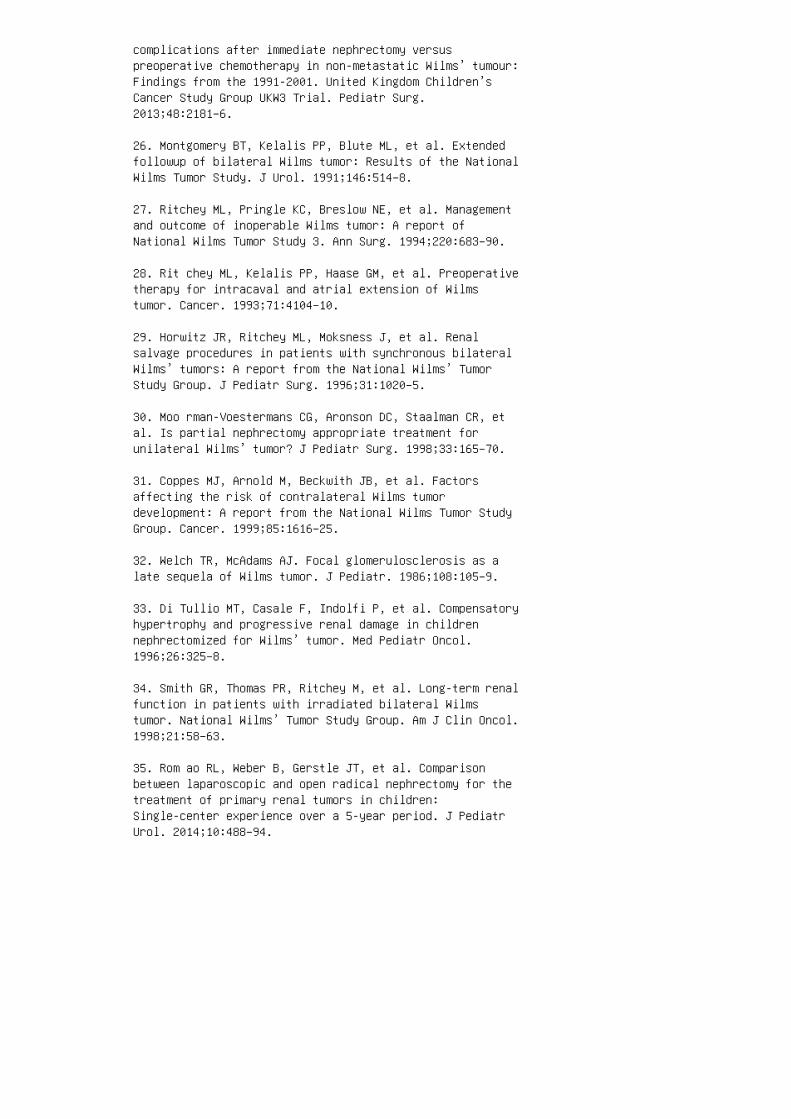
complications after immediate nephrectomy versuspreoperative chemotherapy in non-metastatic Wilms’ tumour:Findings from the 1991-2001. United Kingdom Children’sCancer Study Group UKW3 Trial. Pediatr Surg.2013;48:2181–6.
26. Montgomery BT, Kelalis PP, Blute ML, et al. Extendedfollowup of bilateral Wilms tumor: Results of the NationalWilms Tumor Study. J Urol. 1991;146:514–8.
27. Ritchey ML, Pringle KC, Breslow NE, et al. Managementand outcome of inoperable Wilms tumor: A report ofNational Wilms Tumor Study 3. Ann Surg. 1994;220:683–90.
28. Rit chey ML, Kelalis PP, Haase GM, et al. Preoperativetherapy for intracaval and atrial extension of Wilmstumor. Cancer. 1993;71:4104–10.
29. Horwitz JR, Ritchey ML, Moksness J, et al. Renalsalvage procedures in patients with synchronous bilateralWilms’ tumors: A report from the National Wilms’ TumorStudy Group. J Pediatr Surg. 1996;31:1020–5.
30. Moo rman-Voestermans CG, Aronson DC, Staalman CR, etal. Is partial nephrectomy appropriate treatment forunilateral Wilms’ tumor? J Pediatr Surg. 1998;33:165–70.
31. Coppes MJ, Arnold M, Beckwith JB, et al. Factorsaffecting the risk of contralateral Wilms tumordevelopment: A report from the National Wilms Tumor StudyGroup. Cancer. 1999;85:1616–25.
32. Welch TR, McAdams AJ. Focal glomerulosclerosis as alate sequela of Wilms tumor. J Pediatr. 1986;108:105–9.
33. Di Tullio MT, Casale F, Indolfi P, et al. Compensatoryhypertrophy and progressive renal damage in childrennephrectomized for Wilms’ tumor. Med Pediatr Oncol.1996;26:325–8.
34. Smith GR, Thomas PR, Ritchey M, et al. Long-term renalfunction in patients with irradiated bilateral Wilmstumor. National Wilms’ Tumor Study Group. Am J Clin Oncol.1998;21:58–63.
35. Rom ao RL, Weber B, Gerstle JT, et al. Comparisonbetween laparoscopic and open radical nephrectomy for thetreatment of primary renal tumors in children:Single-center experience over a 5-year period. J PediatrUrol. 2014;10:488–94.
36. Koo A S, Koyle MA, Hurwitz RS, et al. The necessity ofcontralateral surgical exploration in Wilms tumor withmodern noninvasive imaging technique: A reassessment. JUrol. 1990;144:416–7; discussion 422. 37. Martin LW, ReyesPM, Jr. An evaluation of 10 years’ experience withretroperitoneal lymph node dissection for Wilms’ tumor. JPediatr Surg. 1969;4:683–7. 38. Ritchey ML, Shamberger RC,Haase G, et al. Surgical complications after primarynephrectomy for Wilms’ tumor: Report from the NationalWilms’ Tumor Study Group. J Am Coll Surg. 2001;192:63–8.39. Ritchey ML, Kelalis PP, Breslow N, et al. Surgicalcomplications after nephrectomy for Wilms’ tumor. SurgGynecol Obstet. 1992;175:507–14. 40. Neville HL, RitcheyML. Wilms’ tumor: Overview of National Wilms’ Tumor StudyGroup results. Urol Clin North Am. 2000;27:435–42. 41.Green DM, Breslow NE, Evans I, et al. Relationship betweendose schedule and charges for treatment on National Wilms’Tumor Study-4: A report from the National Wilms’ TumorStudy Group. J Natl Cancer Inst Monogr. 1995;21–5. 42.Rit chey ML, Green DM, Thomas PR, et al. Renal failure inWilms’ tumor patients: A report from the National Wilms’Tumor Study Group. Med Pediatr Oncol. 1996;26:75–80. 43.Blu te ML, Kelalis PP, Offord KP, et al. GJ, BilateralWilms tumor. J Urol. 1987;138:968–73. 44. Green DM, ThomasPR, Shochat S. The treatment of Wilms tumor: Results ofthe National Wilms Tumor Studies. Hematol Oncol Clin NorthAm. 1995;9:1267–74. 45. Grundy P, Breslow N, Green DM, etal. Prognostic factors for children with recurrent Wilms’tumor: Results from the Second and Third National Wilms’Tumor Study. J Clin Oncol. 1989;7:638–47. 46. Dom e JS,Liu T, Krasin M, et al. Improved survival for patientswith recurrent Wilms tumor: The experience at St. JudeChildren’s Research Hospital. J Pediatr Hematol Oncol.2002;24:192–8. 47. Abu -Ghosh AM, Krailo MD, Goldman SC,et al. Ifosfamide, carboplatin and etoposide in childrenwith poor-risk relapsed Wilms’ tumor: A Children’s CancerGroup report. Ann Oncol. 2002;13:460–9. 48. Pein F, MichonJ, Valteau-Couanet D, et al. High-dose melphalan,etoposide, and carboplatin followed by autologousstem-cell rescue in pediatric high-risk recurrent Wilms’tumor: A French Society of Pediatric Oncology study. JClin Oncol. 1998;16:3295–301. 49. Green DM, Grigoriev YA,Nan B, et al. Congestive heart failure after treatment forWilms’ tumor: A report from the National Wilms’ TumorStudy group. J Clin Oncol. 2001;19:1926–34. 50. Gre enDM, Peabody EM, Nan B, et al. Pregnancy outcome aftertreatment for Wilms tumor: A report from the NationalWilms Tumor Study Group. J Clin Oncol. 2002;20:2506–13.51. Kinsella TJ, Trivette G, Rowland J, et al. Long-term
follow-up of testicular function following radiationtherapy for early-stage Hodgkin’s disease. J Clin Oncol1989;7:718–24.
52. Stillman RJ, Schinfeld JS, Schiff I, et al. Ovarianfailure in long-term survivors of childhood malignancy. AmJ Obstet Gynecol. 1981;139:62–6.
53. Bre slow NE, Takashima JR, Whitton JA, et al. Secondmalignant neoplasms following treatment for Wilm’s tumor:A report from the National Wilms’ Tumor Study Group. JClin Oncol. 1995;13:1851–9.
54. Schmidt D, Beckwith JB. Histopathology of childhoodrenal tumors. Hematol Oncol Clin North Am.1995;9:1179–200.
55. D’A ngio GJ, Breslow N, Beckwith JB, et al. Treatmentof Wilms’ tumor: Results of the Third National Wilms’Tumor Study. Cancer. 1989;64:349–60.
56. Argani P, Perlman EJ, Breslow NE, et al. Clear cellsarcoma of the kidney: A review of 351 cases from theNational Wilms Tumor Study Group Pathology Center. Am JSurg Pathol. 2000;24:4–18.
57. Tomlinson GE, Breslow NE, Dome J, et al. Rhabdoidtumor of the kidney in the National Wilms’ Tumor Study:Age at diagnosis as a prognostic factor. J Clin Oncol.2005;23:7641–5.
58. Wee ks DA, Beckwith JB, Mierau GW, et al. Rhabdoidtumor of kidney: A report of 111 cases from the NationalWilms’ Tumor Study Pathology Center. Am J Surg Pathol.1989;13:439–58.
59. Mal ik R. Rhabdoid tumor of the kidney. Med PediatrOncol. 1988;16:203–5.
60. Eck schlager T, Kodet R. Renal cell carcinoma inchildren: A single institution’s experience. Med PediatrOncol. 1994;23:36–9.
61. Ren shaw AA, Granter SR, Fletcher JA, et al. Renal cellcarcinomas in children and young adults: Increasedincidence of papillary architecture and unique subtypes. AmJ Surg Pathol. 1999;23:795–802.
62. Carcao MD, Taylor GP, Greenberg ML, et al. Renal-cellcarcinoma in children: A different disorder from its adult

counterpart? Med Pediatr Oncol. 1998;31:153–8.
63. Aronson DC, Medary I, Finlay JL, et al. Renal cellcarcinoma in childhood and adolescence: A retrospectivesurvey for prognostic factors in 22 cases. J Pediatr Surg.1996;31:183–6.
64. Ind olfi P, Spreafico F, Collini P, et al. Metastaticrenal cell carcinoma in children and adolescents: A30-year unsuccessful story. J Pediatr Hematol Oncol;2012;34:e277–81.
65. Howell CG, Othersen HB, Kiviat NE, et al. Therapy andoutcome in 51 children with mesoblastic nephroma: A reportof the National Wilms’ Tumor Study. J Pediatr Surg.1982;17:826–31.
66. She n SC, Yunis EJ. A study of the cellularity andultrastructure of congenital mesoblastic nephroma. Cancer.1980;45:306–14.
67. Vujanic GM, Delemarre JF, Moeslichan S, et al.Mesoblastic nephroma metastatic to the lungs and heart:Another face of this peculiar lesion—Case report andreview of the literature. Pediatr Pathol. 1993;13:143–53.68. Cook HT, Taylor GM, Malone P, et al. Renin inmesoblastic nephroma: An immunohistochemical study. HumPathol. 1988;19:1347–51. 69. O’H agan AR, Ellsworth R,Secic M, et al. Renal manifestations of tuberous sclerosiscomplex. Clin Pediatr (Phila). 1996;35:483–9. 70.Fittschen A, Wendlik I, Oeztuerk S, et al. Prevalence ofsporadic renal angiomyolipoma: A retrospective analysis of61,389 in- and out-patients. Abdom Imaging.2014;39:1009–13. 71. Dic kinson M, Ruckle H, Beaghler M,et al. Renal angiomyolipoma: Optimal treatment based onsize and symptoms. Clin Nephrol. 1998;49:281–6. REVIEWQUESTIONS CASE 1 A 2-day-old boy is found to have a hard,palpable abdominal mass on routine newborn examination. �epregnancy and delivery were unremarkable. �ere is norelevant family history. Both parents and an older7-year-old sibling are healthy. No other abnormalities areencountered on physical examination. �e baby appears well.He underwent an abdominal ultrasound and, subsequently, aCT scan of the abdomen, shown. 1. Based on thepresentation and �ndings on imaging studies, the �ndingson the le� kidney are most likely to represent: a. Wilmstumor b. Congenital mesoblastic nephroma c. Clear cellsarcoma d. Renal cell carcinoma e. Multilocular cysticnephroma
2. �e best next step in management is:
a. Percutaneous biopsy
b. Open biopsy
c. Chemotherapy (Wilms tumor protocol) and repeat imagingin 6 weeks
d. Partial nephrectomy
e. Radical nephrectomy
CASE 2
A 3-year-old boy presents with rapid increase in abdomi
nal girth. He has been healthy and has no signi�cant medi
cal or surgical history. His family history is unremarkable.
Physical examination demonstrated a normal blood pres
sure for age, no dismorphic features, and a palpable abdom
inal mass. CT evaluation is shown below.
3. Based on these �ndings, all of the following are indi
cated except:
a. Chest CT scan
b. Doppler ultrasound of the renal vein and vena cava
c. Port placement for chemotherapy
d. Bilateral nephrectomies
e. Screen for predisposition syndromes
4. Which of the following are associated with a predisposi
tion to Wilms tumor?
a. Macroglossia
b. Aniridia
c. Hemihypertrophy

d. Cryptorchidism
e. All of the above
5. Which of the following surgical principles regarding
the management of renal masses consistent with Wilms
tumor is true: a. Ipsilateral adrenalectomy is alwaysindicated. b. Removal almost always includes radicalresection of adjacent structures, such as spleen, tail ofpancreas, bowel segment, and liver segment. c. Earlyintraoperative tumor rupture demands aborting the procedureand proceeding with chemotherapy and radiation. d.Ipsilateral lymph node sampling always should be done. e.Nephron-sparing surgical procedures should not be o�ered.CASE 3 A 14-year-old patient with tuberous sclerosis hasthe following �ndings on a routine CAT scan imaging study.6. Which one of the following is an accepted step inmanagement for the lesion highlighted with an arrow? a.Serial imaging with ultrasound b. Reimage every 3 monthswith CT scan c. Open biopsy d. Radical nephrectomy e.Partial nephrectomy and lymph node dissection ANSWER KEY1. b 2. e 3. d 4. e 5. d 6. a
51 Urolithiasis in children
3. Hamm LL, Alpern RJ. Regulation of acid-base balance,citrate, and urine pH. In: Coe FL, Favus MS, Pak CYC, etal., editors. Kidney Stones: Medical and SurgicalManagement. Philadelphia: LippincottRaven; 1996. p 289–302.
4. Robertson WG, Peacock M. The pattern of urinary stonedisease in Leeds and in the United Kingdom in relation toanimal protein intake during the period 1960-1980. UrolInt. 1982;37:394–9.
5. Bet ter OS, Shabtai M, Kedar S, et al. Increasedincidence of nephrolithiasis in lifeguards in Israel. AdvExp Med Biol. 1980;128:467–72.
6. Lattimer JK, Hubbard M. Pediatric urologic admissions. JUrol. 1951:66:289–93.
7. Bass HN, Emanuel B. Nephrolithiasis in childhood. JUrol. 1966;95:749–53.
8. Troup CW, Lawnicki CC, Bourne RB, Hodgson NB. Renalcalculus in children. J Urol. 1972;107:306–7.
9. Malek RS, Kelalis PP. Pediatric nephrolithiasis. J Urol.1975;113:545–51.
10. Sta pleton FB, McKay CP, Noe HN. Urolithiasis inchildren: The role of hypercalciuria. Pediatr Ann.1987;16:980–1, 984–92.
11. Mil liner DS, Murphy ME. Urolithiasis in pediatricpatients. Mayo Clin Proc. 1993;68:241–8.
12. Osorio AV, Alon US. The relationship between urinarycalcium, sodium, and potassium excretion and the role ofpotassium in treating idiopathic hypercalciuria.Pediatrics. 1997;100:675–81.
13. Pen ido MG, Srivastava T, Alon US. Pediatric primaryurolithiasis: 12-year experience at a MidwesternChildren’s Hospital. J Urol. 2013;189:1493–7.
14. Rou th JC, Graham DA, Nelson CP. Epidemiologicaltrends in pediatric urolithiasis at United Statesfreestanding pediatric hospitals. J Urol. 2010;184:1100–4.
15. Sas DJ, Hulsey TC, Shatat IF, Orak JK. Increasingincidence of kidney stones in children evaluated in the
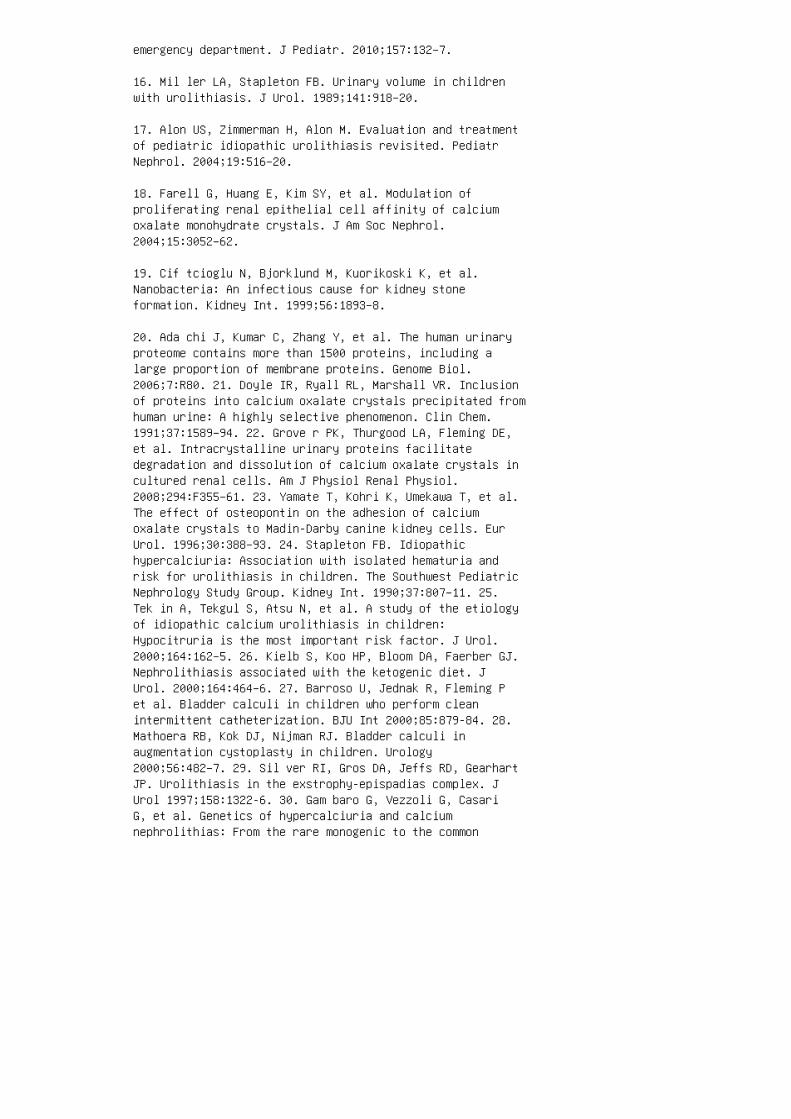
emergency department. J Pediatr. 2010;157:132–7.
16. Mil ler LA, Stapleton FB. Urinary volume in childrenwith urolithiasis. J Urol. 1989;141:918–20.
17. Alon US, Zimmerman H, Alon M. Evaluation and treatmentof pediatric idiopathic urolithiasis revisited. PediatrNephrol. 2004;19:516–20.
18. Farell G, Huang E, Kim SY, et al. Modulation ofproliferating renal epithelial cell affinity of calciumoxalate monohydrate crystals. J Am Soc Nephrol.2004;15:3052–62.
19. Cif tcioglu N, Bjorklund M, Kuorikoski K, et al.Nanobacteria: An infectious cause for kidney stoneformation. Kidney Int. 1999;56:1893–8.
20. Ada chi J, Kumar C, Zhang Y, et al. The human urinaryproteome contains more than 1500 proteins, including alarge proportion of membrane proteins. Genome Biol.2006;7:R80. 21. Doyle IR, Ryall RL, Marshall VR. Inclusionof proteins into calcium oxalate crystals precipitated fromhuman urine: A highly selective phenomenon. Clin Chem.1991;37:1589–94. 22. Grove r PK, Thurgood LA, Fleming DE,et al. Intracrystalline urinary proteins facilitatedegradation and dissolution of calcium oxalate crystals incultured renal cells. Am J Physiol Renal Physiol.2008;294:F355–61. 23. Yamate T, Kohri K, Umekawa T, et al.The effect of osteopontin on the adhesion of calciumoxalate crystals to Madin-Darby canine kidney cells. EurUrol. 1996;30:388–93. 24. Stapleton FB. Idiopathichypercalciuria: Association with isolated hematuria andrisk for urolithiasis in children. The Southwest PediatricNephrology Study Group. Kidney Int. 1990;37:807–11. 25.Tek in A, Tekgul S, Atsu N, et al. A study of the etiologyof idiopathic calcium urolithiasis in children:Hypocitruria is the most important risk factor. J Urol.2000;164:162–5. 26. Kielb S, Koo HP, Bloom DA, Faerber GJ.Nephrolithiasis associated with the ketogenic diet. JUrol. 2000;164:464–6. 27. Barroso U, Jednak R, Fleming Pet al. Bladder calculi in children who perform cleanintermittent catheterization. BJU Int 2000;85:879-84. 28.Mathoera RB, Kok DJ, Nijman RJ. Bladder calculi inaugmentation cystoplasty in children. Urology2000;56:482–7. 29. Sil ver RI, Gros DA, Jeffs RD, GearhartJP. Urolithiasis in the exstrophy-epispadias complex. JUrol 1997;158:1322-6. 30. Gam baro G, Vezzoli G, CasariG, et al. Genetics of hypercalciuria and calciumnephrolithias: From the rare monogenic to the common
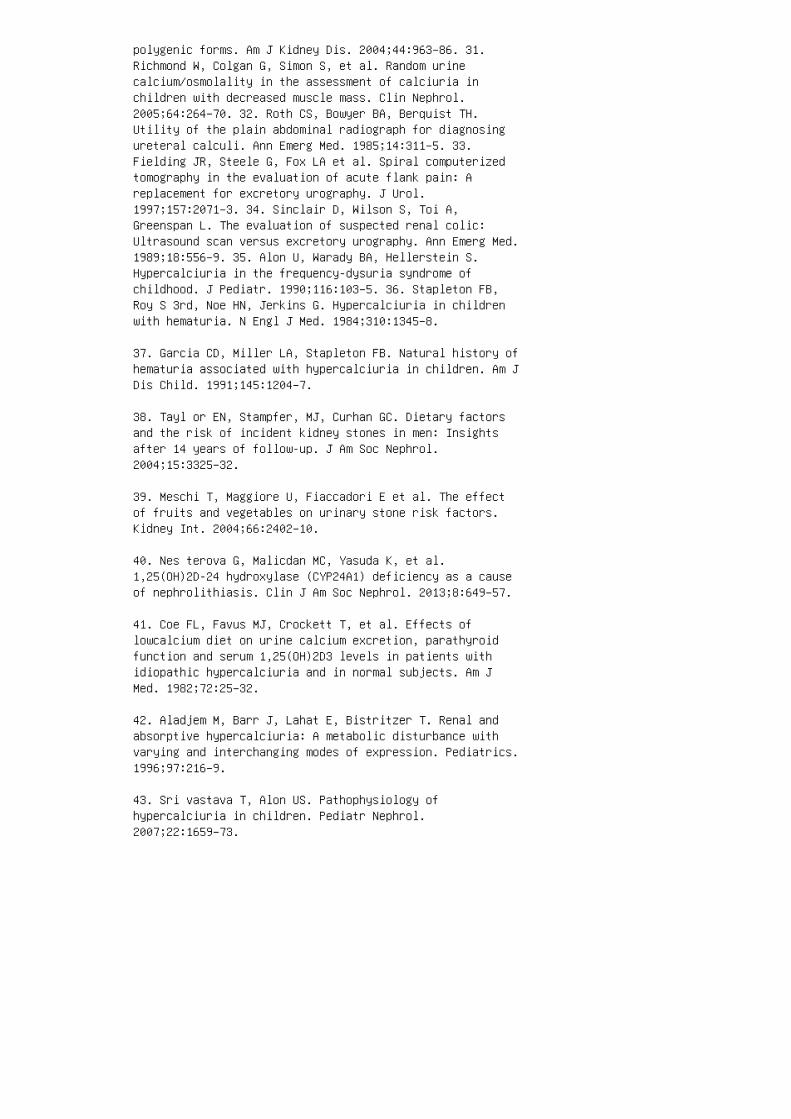
polygenic forms. Am J Kidney Dis. 2004;44:963–86. 31.Richmond W, Colgan G, Simon S, et al. Random urinecalcium/osmolality in the assessment of calciuria inchildren with decreased muscle mass. Clin Nephrol.2005;64:264–70. 32. Roth CS, Bowyer BA, Berquist TH.Utility of the plain abdominal radiograph for diagnosingureteral calculi. Ann Emerg Med. 1985;14:311–5. 33.Fielding JR, Steele G, Fox LA et al. Spiral computerizedtomography in the evaluation of acute flank pain: Areplacement for excretory urography. J Urol.1997;157:2071–3. 34. Sinclair D, Wilson S, Toi A,Greenspan L. The evaluation of suspected renal colic:Ultrasound scan versus excretory urography. Ann Emerg Med.1989;18:556–9. 35. Alon U, Warady BA, Hellerstein S.Hypercalciuria in the frequency-dysuria syndrome ofchildhood. J Pediatr. 1990;116:103–5. 36. Stapleton FB,Roy S 3rd, Noe HN, Jerkins G. Hypercalciuria in childrenwith hematuria. N Engl J Med. 1984;310:1345–8.
37. Garcia CD, Miller LA, Stapleton FB. Natural history ofhematuria associated with hypercalciuria in children. Am JDis Child. 1991;145:1204–7.
38. Tayl or EN, Stampfer, MJ, Curhan GC. Dietary factorsand the risk of incident kidney stones in men: Insightsafter 14 years of follow-up. J Am Soc Nephrol.2004;15:3325–32.
39. Meschi T, Maggiore U, Fiaccadori E et al. The effectof fruits and vegetables on urinary stone risk factors.Kidney Int. 2004;66:2402–10.
40. Nes terova G, Malicdan MC, Yasuda K, et al.1,25(OH)2D-24 hydroxylase (CYP24A1) deficiency as a causeof nephrolithiasis. Clin J Am Soc Nephrol. 2013;8:649–57.
41. Coe FL, Favus MJ, Crockett T, et al. Effects oflowcalcium diet on urine calcium excretion, parathyroidfunction and serum 1,25(OH)2D3 levels in patients withidiopathic hypercalciuria and in normal subjects. Am JMed. 1982;72:25–32.
42. Aladjem M, Barr J, Lahat E, Bistritzer T. Renal andabsorptive hypercalciuria: A metabolic disturbance withvarying and interchanging modes of expression. Pediatrics.1996;97:216–9.
43. Sri vastava T, Alon US. Pathophysiology ofhypercalciuria in children. Pediatr Nephrol.2007;22:1659–73.
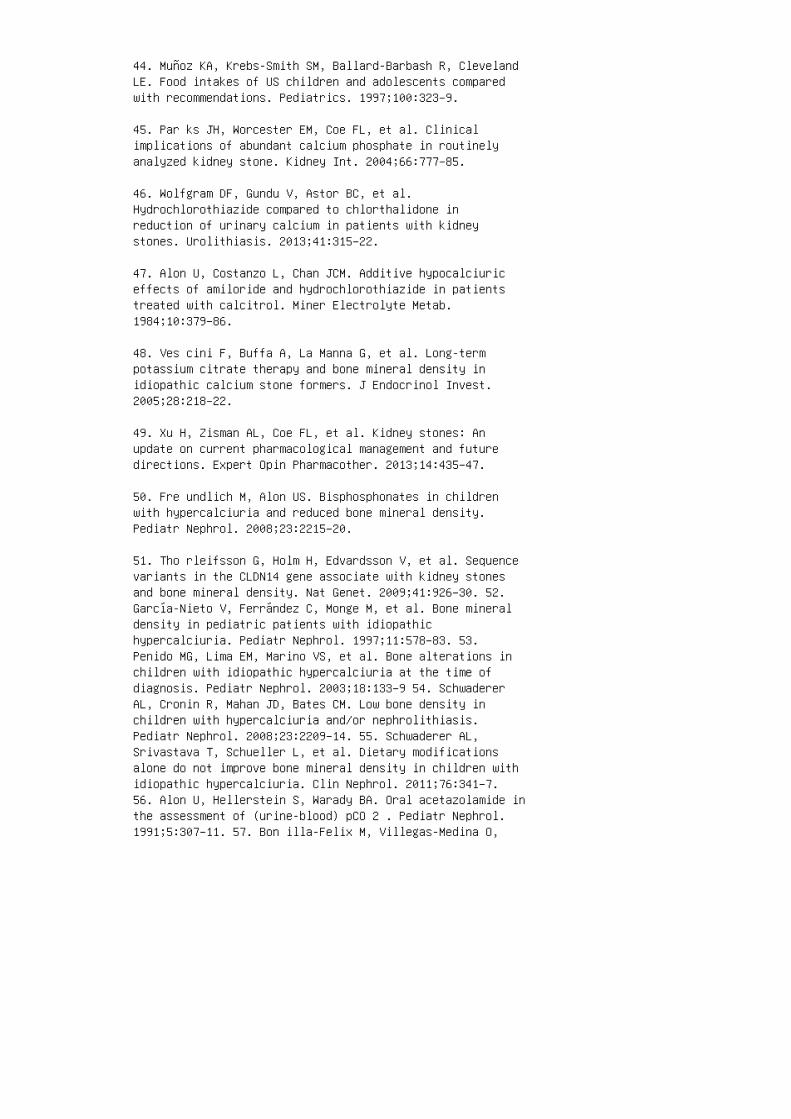
44. Muñoz KA, Krebs-Smith SM, Ballard-Barbash R, ClevelandLE. Food intakes of US children and adolescents comparedwith recommendations. Pediatrics. 1997;100:323–9.
45. Par ks JH, Worcester EM, Coe FL, et al. Clinicalimplications of abundant calcium phosphate in routinelyanalyzed kidney stone. Kidney Int. 2004;66:777–85.
46. Wolfgram DF, Gundu V, Astor BC, et al.Hydrochlorothiazide compared to chlorthalidone inreduction of urinary calcium in patients with kidneystones. Urolithiasis. 2013;41:315–22.
47. Alon U, Costanzo L, Chan JCM. Additive hypocalciuriceffects of amiloride and hydrochlorothiazide in patientstreated with calcitrol. Miner Electrolyte Metab.1984;10:379–86.
48. Ves cini F, Buffa A, La Manna G, et al. Long-termpotassium citrate therapy and bone mineral density inidiopathic calcium stone formers. J Endocrinol Invest.2005;28:218–22.
49. Xu H, Zisman AL, Coe FL, et al. Kidney stones: Anupdate on current pharmacological management and futuredirections. Expert Opin Pharmacother. 2013;14:435–47.
50. Fre undlich M, Alon US. Bisphosphonates in childrenwith hypercalciuria and reduced bone mineral density.Pediatr Nephrol. 2008;23:2215–20.
51. Tho rleifsson G, Holm H, Edvardsson V, et al. Sequencevariants in the CLDN14 gene associate with kidney stonesand bone mineral density. Nat Genet. 2009;41:926–30. 52.García-Nieto V, Ferrández C, Monge M, et al. Bone mineraldensity in pediatric patients with idiopathichypercalciuria. Pediatr Nephrol. 1997;11:578–83. 53.Penido MG, Lima EM, Marino VS, et al. Bone alterations inchildren with idiopathic hypercalciuria at the time ofdiagnosis. Pediatr Nephrol. 2003;18:133–9 54. SchwadererAL, Cronin R, Mahan JD, Bates CM. Low bone density inchildren with hypercalciuria and/or nephrolithiasis.Pediatr Nephrol. 2008;23:2209–14. 55. Schwaderer AL,Srivastava T, Schueller L, et al. Dietary modificationsalone do not improve bone mineral density in children withidiopathic hypercalciuria. Clin Nephrol. 2011;76:341–7.56. Alon U, Hellerstein S, Warady BA. Oral acetazolamide inthe assessment of (urine-blood) pCO 2 . Pediatr Nephrol.1991;5:307–11. 57. Bon illa-Felix M, Villegas-Medina O,

Vehaskari VM. Renal acidification in children withidiopathic hypercalciuria. J Pediatr. 1994;124:529–34. 58.Srivastava T, Winston MJ, Auron A, et al. Urinecalcium/citrate ratio in children with hypercalciuricstones. Pediatr Res. 2009;66:85–90. 59. Arr abal-Polo MA,Arrabal-Martin M, Arias-Santiago S, et al. Importance ofcitrate and the calcium: Citrate ratio in patients withcalcium renal lithiasis and severe lithogenesis. BJU Int.2013;111:622–7. 60. MacDougall L, Taheri S, Crofton P.Biochemical risk factors for stone formation in a Scottishpaediatric hospital population. Ann Clin Biochem.2010;47:125–30. 61. Baia Lda C, Baxmann AC, Moreira SR, etal. Noncitrus alkaline fruit: A dietary alternative forthe treatment of hypocitraturic stone formers. J Endourol.2012;26:1221–6. 62. Pen niston KL, Steele TH, Nakada SY.Lemonade therapy increases urinary citrate and urinevolumes in patients with recurrent calcium oxalate stoneformation. Urology. 2007;70:856–60. 63. Sidhu H, Hoppe B,Hesse A, et al. Absence of Oxalobacter formigenes incystic fibrosis patients: A risk factor for hyperoxaluria.Lancet. 1998;352:1026–9. 64. Monico CG, Olson JB,Milliner DS. Determinants of pyridoxine responsiveness inprimary hyperoxaluria type I. Pediatr Res. 2004:55:576A65. Van Woerden CS, Groothoff JW, Wijburg FA, et al.Clinical implications of mutations analysis in primaryhyperoxaluria type 1. Kidney Int. 2004;66:746–52. 66.Stapleton FB, Nash DA. A screening test forhyperuricosuria. J Pediatr. 1983102:88–90. 67. Matos V,Van Melle G, Werner D, et al. Urinary oxalate and urate tocreatinine ratios in a healthy pediatric population. Am JKidney Dis. 1999;34:e6. 68. Cameron JS, Moro F, SimmondsHA. Gout, uric acid and purine metabolism in paediatricnephrology. Pediatr Nephrol. 1993;7:105–18.
69. Maalouf NM, Sakhaee K, Parks JH, et al. Association ofurinary pH with body weight in nephrolithiasis. KidneyInt. 2004;65:1422–5.
70. Del lo-Strologo L, Pras E, Pontesilli C, et al.Comparison between SLC3A1 and SLC7A9 cystinuria patientsand carriers: A need for a new classification. J Am SocNephrol. 2002;13:2547–53.
71. Font-Llitjós M, Jiménez-Vidal M, Bisceglia L, et al.New insights into cystinuria: 40 new mutations,genotype-phenotype correlation, and digenic inheritancecausing partial phenotype. J Med Genet. 2005;42:58–68.
72. Sakhaee K, Poindexter JR, Pak CY. The spectrum ofmetabolic abnormalities in patients with cystine
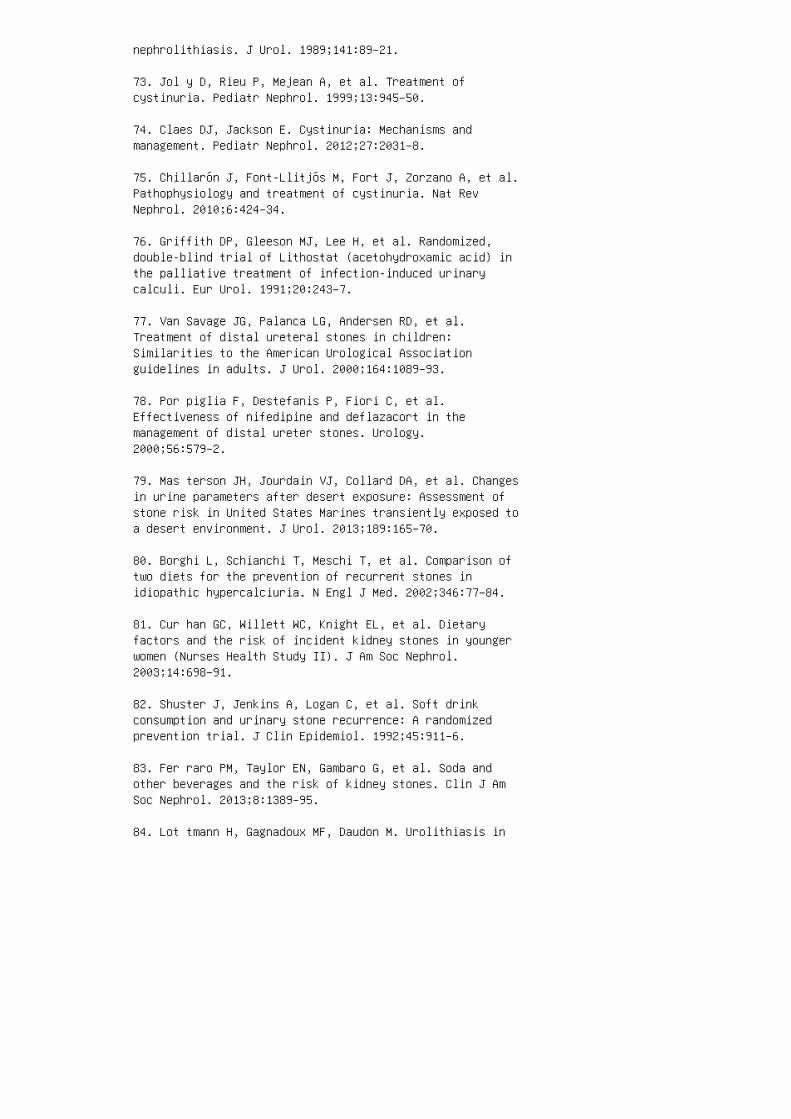
nephrolithiasis. J Urol. 1989;141:89–21.
73. Jol y D, Rieu P, Mejean A, et al. Treatment ofcystinuria. Pediatr Nephrol. 1999;13:945–50.
74. Claes DJ, Jackson E. Cystinuria: Mechanisms andmanagement. Pediatr Nephrol. 2012;27:2031–8.
75. Chillarón J, Font-Llitjós M, Fort J, Zorzano A, et al.Pathophysiology and treatment of cystinuria. Nat RevNephrol. 2010;6:424–34.
76. Griffith DP, Gleeson MJ, Lee H, et al. Randomized,double-blind trial of Lithostat (acetohydroxamic acid) inthe palliative treatment of infection-induced urinarycalculi. Eur Urol. 1991;20:243–7.
77. Van Savage JG, Palanca LG, Andersen RD, et al.Treatment of distal ureteral stones in children:Similarities to the American Urological Associationguidelines in adults. J Urol. 2000;164:1089–93.
78. Por piglia F, Destefanis P, Fiori C, et al.Effectiveness of nifedipine and deflazacort in themanagement of distal ureter stones. Urology.2000;56:579–2.
79. Mas terson JH, Jourdain VJ, Collard DA, et al. Changesin urine parameters after desert exposure: Assessment ofstone risk in United States Marines transiently exposed toa desert environment. J Urol. 2013;189:165–70.
80. Borghi L, Schianchi T, Meschi T, et al. Comparison oftwo diets for the prevention of recurrent stones inidiopathic hypercalciuria. N Engl J Med. 2002;346:77–84.
81. Cur han GC, Willett WC, Knight EL, et al. Dietaryfactors and the risk of incident kidney stones in youngerwomen (Nurses Health Study II). J Am Soc Nephrol.2003;14:698–91.
82. Shuster J, Jenkins A, Logan C, et al. Soft drinkconsumption and urinary stone recurrence: A randomizedprevention trial. J Clin Epidemiol. 1992;45:911–6.
83. Fer raro PM, Taylor EN, Gambaro G, et al. Soda andother beverages and the risk of kidney stones. Clin J AmSoc Nephrol. 2013;8:1389–95.
84. Lot tmann H, Gagnadoux MF, Daudon M. Urolithiasis in

children. In: Gearhart JP, Rink RC, Mouriquano PDE,editors. Pediatric Urology. Philadelphia: WB Saunders;2001. p 828–59. 85. Esen T, Krautschick A, Alken P.Treatment update on pediatric urolithiasis. World J Urol.1997;15:195-202. 86. Goe l MC, Baserge NS, Babu RV, et al.Pediatric kidney: Functional outcome after extracorporealshock wave lithotripsy. J Urol. 1996;155:2044–6. 87.Lottmann HB, Archambaud F, Hellal B, et al.99mTechnetium-dimercapto-succinic acid renal scan in theevaluation of potential long-term renal parenchymal damageassociated with extracorporeal shock wave lithotripsy inchildren. J Urol. 1998;159:521–4. 88. Sal erno A, NappoSG, Matarazzo E, et al. Treatment of pediatric renalstones in a Western country: A changing pattern. J PediatrSurg. 2013;48:835–9. 89. El-Zoghby ZM, Lieske JC, FoleyRN, et al. Urolithiasis and the risk of ESRD. Clin J AmSoc Nephrol. 2012;7:1409–15. 90. Alexander RT, HemmelgarnBR, Wiebe N, et al. Kidney stones and kidney functionloss: A cohort study. BMJ. 2012;345:e5287. 91. Noe HN.Hypercalciuria and pediatric stone recurrences with andwithout structural abnormalities. J Urol. 2000;164:1094–6.92. Soygur T, Akbay A, Kupeli S. Effect of potassiumcitrate therapy on stone recurrence and residual fragmentsafter shockwave lithotripsy in lower caliceal calciumoxalate urolithiasis: A randomized controlled trial. JEndourol. 2002;16:149–52. REVIEW QUESTIONS 1. �e greatestrisk factor for pediatric stone formation is: a.Hypercalciuria b. Low urine �ow c. Hypocitraturia d.Hyperoxaluria 2. A child with body weight of 50 kg has a24-hour urine volume of 700 mL. �e additional daily �uidintake recommended for this child will be: a. 300 mL b.400 mL c. 500 mL d. 600 mL 3. In a teenager withidiopathic hypercalciuria, dietary intervention willinclude: a. Sodium intake of 2000 to 2300 and potassiumintake of 3000 to 3500 mg/day b. Sodium intake of 1500 to1800 and potassium intake of 3000 to 3500 mg/day c. Sodium intake of 1500 to 1800 and potassium intake of 2000 to2500 mg/day d. Sod ium intake of 2000 to 2300 andpotassium intake of 2000 to 2500 mg/day 4. �e ri sk inadministrating potassium citrate is: a. Upse t stomachb. Dev elopment of hypercholesterolemia
c. Severe diarrhea
d. Rendering the urine too alkaline
5. When employing thiazide diuretics:
a. Sodium intake should be liberalized
b. K-citrate should not be used concomitantly
c. �e addition of amiloride is bene�cial
d. Osteopenia may worsen
6. Numerical goals in managing children withhypercalciuria-to-hypocitraturia include:
a. Urine calcium/citrate ratio < 0.20 and Na/K ratio < 2.5
b. Urine calcium/citrate ratio < 0.33 and Na/K ratio < 2.5
c. Urine calcium/citrate ratio < 0.20 and Na/K ratio < 3.5
d. Urine calcium/citrate ratio < 0.33 and Na/K ratio < 3.5
7. Gastrointestinal issues causing hypocitraturia areusually associated with:
a. Severe constipation
b. Fat malabsorption
c. Gastroesophageal re�ux
d. Chronic diarrhea
8. Mild absorptive hyperoxaluria is best treated by:
a. Dietary oxalate restriction
b. Administration of Oxalobacter formigenes
c. Dietary calcium supplementation
d. Avoidance of food high in fat 9. High incidence of uricacid stones in obese population is due to: a. Diet richin purines b. Diet rich in salt c. Decreased ammoniaproduction d. Insu�cient �uid intake 10. To protectagainst stone formation in children on ketogenic diets, itis advisable to give: a. Potassium citrate b. �iazidediuretics c. Allopurinol d. Magnesium oxide ANSWER KEY1. b 2. c 3. a 4. d 5. c 6. b 7. d 8. c 9. c 10. a

52 Voiding disorders
20. Hellstrom AL, Hanson E, Hansson S, et al. Micturitionhabits and incontinence in 7-yearold Swedish schoolentrants. Eur J Pediatr. 1990;149:434–7.
21. Bakwin H. Enuresis in children. J Pediatr.1961;58:806–19.
22. Hagstroem S, Kamperis K, Rittig S, et al.Monosymptomatic nocturnal enuresis is associated withabnormal nocturnal bladder emptying. J Urol.2004;171:2562–6; discussion 6.
23. Geo rge CP, Messerli FH, Genest J, et al. Diurnalvariation of plasma vasopressin in man. J Clin EndocrinolMetab. 1975;41:332–8.
24. Rittig S, Knudsen UB, Nørgaard JP, Pedersen EB,Djurhuus JC. Abnormal diurnal rhythm of plasmavasopressin and urinary output in patients with enuresis.Am J Physiol. 1989 Apr;256(4 Pt 2):F664-71.
25. Frokiaer J, Nielsen S. Do aquaporins have a role innocturnal enuresis? Scand J Urol Nephrol Suppl.1997;183:31–2.
26. Nor gaard JP, Hansen JH, Nielsen JB, et al. Nocturnalstudies in enuretics: A polygraphic study of sleep-EEG andbladder activity. Scand J Urol Nephrol Suppl.1989;125:73–8.
27. Kof f SA. Why is desmopressin sometimes ineffec tive atcuring bedwetting? Scand J Urol Nephrol S up pl.1995;173:103–8.
28. Boyd MM . The depth of sleep in enuretic schoolchildrenand in non-enuretic controls. J Psychosom Res.1960;4:274–81.
29. Kales A, Kales JD. Sleep disorders: Recent findings inthe diagnosis and treatment of disturbed sleep. N Engl JMed. 1974;290:487–99.
30. Wol fish N. Sleep arousal function in enuretic males.Scand J Urol Nephrol Suppl. 1999;202:24–6.
31. Wolfish NM. Sleep/arousal and enuresis sub types. JUrol. 2001;166:2444–7.

32. Houts AC. Behavioural treatment for enuresis. Scand JUrol Nephrol Suppl. 1995;173:83–6; discussion 7.
33. Monda JM, Husmann DA. Primary nocturnal enuresis: Acomparison among observation, imip ramine, desmopressinacetate and bed-wetting a la rm systems. J Urol.1995;154:745–8.
34. Ellerker AG. The extravesical ectopic ureter. Br JSurg. 1958;45:344–53.
35. Bukowski TP, Lewis AG, Reeves D, et al. Epididymitisin older boys: Dysfunctional voiding as an etiology. JUrol. 1995;154:762–5.
36. Umeyama T, Kawamura T, Hasegawa A, Ogawa O. Ectopicureter presenting with epididy mitis in childhood: Reportof 5 cases. J Urol. 1985;134:131–3.
37. Pattaras JG, Rushton HG, Majd M. The role of99mtechnetium dimercapto-succinic acid renal scans in theevaluation of occult ectopic ureters in girls withparadoxical incontinence. J Urol. 1999;162:821–5. 38.Brave rman RM, Lebowitz RL. Occult ectopic ureter in girlswith urinary incontinence: Diagnosis by using CT. AJR Am JRoentgenol. 1991;156:365–6. 39. Bozorgi F, Connolly LP,Bauer SB, et al. Hypoplastic dysplastic kidney with avaginal ectopic ureter identified by technetium-99m-DMSAscintigraphy. J Nucl Med. 1998;39:113–5. 40. Ruarte AC,Podesta ML, Medel R. Detrusor aftercontractions in childrenwith normal urinary tracts. BJU Int. 2002;90:286–93. 41.Koff SA, Solomon MH, Lane GA, Lieding KG. Urodynamicstudies in anesthetized children. J Urol. 1980;123:61-–3.42. Nash DF. The development of micturition control withspecial reference to enuresis. Ann R Coll Surg Engl.1949;5:318–44, illust. 43. Lapides J, Diokno AC.Persistence of the infant bladder as a cause for urinaryinfection in girls. Trans Am Assoc Genitourin Surg.1969;61:51–6. 44. Bauer SB, Retik AB, Colodny AH, et al.The unstable bladder in childhood. Urol Clin North Am.1980;7:321–36. 45. Vincent SA. Postural control of urinaryincontinence: The curtsy sign. Lancet. 1966;2:631–2. 46.Upa dhyay J, Bolduc S, Bagli DJ, et al. Use of thedysfunctional voiding symptom score to predict resolutionof vesicoureteral reflux in children with voidingdysfunction. J Urol. 2003;169:1842–6; discussion 6; authorreply 6. 47. Cha ndra M, Saharia R, Hill V, Shi Q.Prevalence of diurnal voiding symptoms and difficultarousal from sleep in children with nocturnal enuresis. JUrol. 2004;172:311–6. 48. Koff SA, Lapides J, Piazza DH.

Association of urinary tract infection and reflux withuninhibited bladder contractions and voluntary sphinctericobstruction. J Urol. 1979;122:373–6. 49. Curran MJ,Kaefer M, Peters C, et al. The overactive bladder inchildhood: Long-term results with conservative management.J Urol. 2000;163:574–7. 50. Parekh DJ, Pope JCt, Adams MC,Brock JW, 3rd. The use of radiography, urodynamic studiesand cystoscopy in the evaluation of voiding dysfunction. JUrol. 2001;165:215–8. 51. Homsy YL. Dysfunctional voidingsyndromes and vesicoureteral reflux. Pediatr Nephrol.1994;8:116–21. 52. Homsy YL, Nsouli I, Hamburger B, etal. Effects of oxybutynin on vesicoureteral reflux inchildren. J Urol. 1985;134:1168–71. 53. Koff SA, MurtaghD. The uninhibited bladder in children: Effect oftreatment on vesicoureteral reflux resolution. ContribNephrol. 1984;39:211–20. 54. Scholtmeijer RJ, van MastrigtR. The effect of oxyphenonium bromide and oxybutyninhydrochloride on detrusor contractility and reflux inchildren with vesicoureteral reflux and detrusorinstability. J Urol. 1991;146:660–2.
55. Seruca H. Vesicoureteral reflux and voidingdysfunction: A prospective study. J Urol. 1989;142:494–8;discussion 501.
56. Kof f SA, Wagner TT, Jayanthi VR. The relationshipamong dysfunctional elimination syndromes, primaryvesicoureteral reflux and urinary tract infections inchildren. J Urol. 1998;160:1019–22.
57. O’Regan S, Yazbeck S, Schick E. Constipation, bladderinstability, urinary tract infection syndrome. ClinNephrol. 1985;23:152–4.
58. Yaz beck S, Schick E, O’Regan S. Relevance ofconstipation to enuresis, urinary tract infection andreflux: A review. Eur Urol. 1987;13:318–21.
59. Hinman F, Jr. Nonneurogenic neurogenic bladder (theHinman syndrome): 15 years later. J Urol. 1986;136:769–77.
60. Van Gool J, Tanagho EA. External sphincter activityand recurrent urinary tract infection in girls. Urology.1977;10:348–53.
61. Snodgrass W. Relationship of voiding dysfunction tourinary tract infection and vesicoureteral reflux inchildren. Urology. 1991;38:341–4.
62. Mayo ME, Burns MW. Urodynamic studies in children who
wet. Br J Urol. 1990;65:641–5.
63. Oli ver JL, Campigotto MJ, Coplen DE, et al.Psychosocial comorbidities and obesity are associated withlower urinary tract symptoms in children with voidingdysfunction. J Urol. 2013;190:1511–5.
64. Wen ske S, Combs AJ, Van Batavia JP, Glassberg KI. Canstaccato and interrupted/fractionated uroflow patternsalone correctly identify the underlying lower urinarytract condition? J Urol. 2012;187:2188–93.
65. Wen ske S, Van Batavia JP, Combs AJ, Glassberg KI.Analysis of uroflow patterns in children with dysfunctionalvoiding. J Pediatr Urol. 2014;10:240–4.
66. Wein AJ. Emerging role of botulinum toxin in thetreatment of neurogenic and non-neurogenic voidingdysfunction. J Urol. 2003;170:1044.
67. Smith CP, Somogyi GT, Chancellor MB. Emerging role ofbotulinum toxin in the treatment of neurogenic andnon-neurogenic voiding dysfunction. Curr Urol Rep.2002;3:382–7.
68. Young HH. Strictures of the prostatico-membranousurethra: Newer methods in the management of difficultlesions. Ann Surg. 1936;104:267–78.
69. Robertson WB, Hayes JA. Congenital diaphragmaticobstruction of the male posterior urethra. Br J Urol.1969;41:592–8.
70. Ros enfeld B, Greenfield SP, Springate JE, Feld LG.Type III posterior urethral valves: Presentation andmanagement. J Pediatr Surg. 1994;29:81–5.
71. Greenfield SP. Posterior urethral valves: Newconcepts. J Urol. 1997;157:996–7.
72. Par khouse HF, Barratt TM, Dillon MJ, et al. Longtermoutcome of boys with posterior urethral valves. Br J Urol.1988;62:59–62. 73. Holmdahl G. Bladder dysfunction in boyswith posterior urethral valves. Scand J Urol Nephrol Suppl.1997;188:1–36. 74. Bauer SB, Labib KB, Dieppa RA, RetikAB. Urodynamic evaluation of boy with myelodysplasia andincontinence. Urology. 1977;10:354–62. 75. Bauer SB,Hallett M, Khoshbin S, et al. Predictive value ofurodynamic evaluation in newborns with myelodysplasia.JAMA. 1984;252:650–2. 76. Lais A, Kasabian NG, Dyro FM,
et al. The neurosurgical implications of continuousneurourological surveillance of children withmyelodysplasia. J Urol. 1993;150:1879–83. 77. Sidi AA,Dykstra DD, Gonzalez R. The value of urodynamic testing inthe management of neonates with myelodysplasia: Aprospective study. J Urol. 1986;135:90–3. 78. Jus t M,Schwarz M, Ludwig B, et al. Cerebral and spinalMR-findings in patients with postrepair myelomeningocele.Pediatr Radiol. 1990;20:262–6. 79. Ede lstein RA, BauerSB, Kelly MD, et al. The longterm urological response ofneonates with myelodysplasia treated proactively withintermittent catheterization and anticholinergic therapy.J Urol. 1995;154:1500–4. 80. Geraniotis E, Koff SA,Enrile B. The prophylactic use of clean intermittentcatheterization in the treatment of infants and youngchildren with myelomeningocele and neurogenic bladderdysfunction. J Urol. 1988;139:85–6. 81. Kas abian NG,Bauer SB, Dyro FM, et al. The prophylactic value of cleanintermittent catheterization and anticholinergicmedication in newborns and infants with myelodysplasia atrisk of developing urinary tract deterioration. Am J DisChild. 1992;146:840–3. 82. Duc kett JW, Jr. Cutaneousvesicostomy in childhood: The Blocksom technique. Urol ClinNorth Am. 1974;1:485–95. 83. Mandell J, Bauer SB, ColodnyAH, Retik AB. Cutaneous vesicostomy in infancy. J Urol.1981;126:92–3. 84. Kuban KC, Leviton A. Cerebral palsy. NEngl J Med. 1994;330:188–95. 85. Mur phy KP, Molnar GE,Lankasky K. Medical and functional status of adults withcerebral palsy. Dev Med Child Neurol. 1995;37:1075–84.86. Decter RM, Bauer SB, Khoshbin S, et al. Urodynamicassessment of children with cerebral palsy. J Urol.1987;138:1110–2. 87. Bro dak PP, Scherz HC, Packer MG,Kaplan GW. Is urinary tract screening necessary forpatients with cerebral palsy? J Urol. 1994;152:1586–7.88. Robson WL, Jackson HP, Blackhurst D, Leung AK.Enuresis in children with attention-deficit hyperactivitydisorder. South Med J. 1997;90:503–5. 89. Diamond IR,Tannock R, Schachar RJ. Response to methylphenidate inchildren with ADHD and comorbid anxiety. J Am Acad ChildAdolesc Psychiatry 1999;38:402–9.
90. Alo n US, Berenbom A. Idiopathic hypercalciuria ofchildhood: 4- to 11-year outcome. Pediatr Nephrol.2000;14:1011–5.
91. Heiliczer JD, Canonigo BB, Bishof NA, Moore ES.Noncalculi urinary tract disorders secondary to idiopathichypercalciuria in children. Pediatr Clin North Am.1987;34:711–8.

92. Par ekh DJ, Pope JI, Adams MC, Brock JW, 3rd. The roleof hypercalciuria in a subgroup of dysfunctional voidingsyndromes of childhood. J Urol. 2000;164:1008–10.
93. Vachvanichsanong P, Malagon M, Moore ES. Urinaryincontinence due to idiopathic hypercalciuria in children.J Urol. 1994;152:1226–8.
94. Stapleton FB. What is the appropriate evaluation andtherapy for children with hypercalciuria and hematuria?Semin Nephrol. 1998;18:359–60.
95. Bomalaski MD, Anema JG, Coplen DE, et al. Delayedpresentation of posterior urethral valves: A not so benigncondition. J Urol. 1999;162:2130–2.
96. Ritchey ML, Sinha A, DiPietro MA, et al. Significanceof spina bifida occulta in children with diurnal enuresis.J Urol. 1994;152:815–8.
97. Pip pi Salle JL, Capolicchio G, Houle AM, et al.Magnetic resonance imaging in children with voidingdysfunction: Is it indicated? J Urol. 1998;160:1080–3.
98. Kae fer M, Zurakowski D, Bauer SB, et al. Estimatingnormal bladder capacity in children. J Urol. 1997;158:2261-4.
99. Gue rrero RA, Cavender CP. Constipation: Physical andpsychological sequelae. Pediatr Ann. 1999;28:312–6.
100. Blethyn AJ, Verrier Jones K, Newcombe R, et al.Radiological assessment of constipation. Arch Dis Child.1995;73:532–3.
101. Dohil R, Roberts E, Jones KV, Jenkins HR.Constipation and reversible urinary tract abnormalities.Arch Dis Child. 1994;70:56–7.
102. Bolann BJ, Sandberg S, Digranes A. Implications ofprobability analysis for interpreting results of leukocyteesterase and nitrite test strips. Clin Chem.1989;35:1663–8.
103. Pezzlo M. Detection of urinary tract infections byrapid methods. Clin Microbiol Rev. 1988;1:268–80.
104. Parrott TS. Urologic implications of imperforateanus. Urology. 1977;10:407–13.

105. Gre enfield SP, Fera M. Urodynamic evaluation of thepatient with an imperforate anus: A prospective study. JUrol. 1991;146:539–41.
106. Mathews R, Jeffs RD, Reiner WG, et al. Cloacalexstrophy: Improving the quality of life—The Johns Hopkinsexperience. J Urol. 1998;160:2452–6.
107. Khoury AE, Hendrick EB, McLorie GA, et al. Occultspinal dysraphism: Clinical and urodynamic outcome afterdivision of the filum terminale. J Urol. 1990;144:426–8;discussion 8–9, 43–4. 108. Sutow WW, Pryde AW. Incidenceof spina bifida occulta in relation to age. AMA J DisChild. 1956;91:211–7. 109. Wen JG, Tong EC. Cystometry ininfants and children with no apparent voiding symptoms. BrJ Urol. 1998;81:468–73. 110. Chin-Peuckert L, Salle JL. Amodified biofeed back program for children withdetrusor-sphincter dyssynergia: 5-year experience. J Urol.200 1;166:1470–5. 111. Com bs AJ, Glassberg AD, Gerdes D,Horowitz M. Biofeedback therapy for children with dysfunctional voiding. Urology. 1998;52:312–5. 112. De PaepeH, Hoebeke P, Renson C, et al. Pelvicfloor therapy in girlswith recurrent urinary tract infections and dysfunctionalvoiding. Br J Urol. 1998;81(Suppl 3):109–13. 113. DePaepe H, Renson C, Van Laecke E, et al. Pelvic-floortherapy and toilet training in young children withdysfunctional voiding and obstipa tion. BJU Int.2000;85:889–93. 114. De Paepe H, Renson C, Hoebeke P, etal. The role of pelvic-floor therapy in the treatment oflower urinary tract dysfunctions in children. Scand J UrolNephrol. 2002;36:260–7. 115. Duel BP. Biofeedback therapyand dysfunc tional voiding in children. Curr Urol Rep.2003 ;4:142–5. 116. Gla zier DB, Ankem MK, Ferlise V, etal. Utility of biofeedback for the daytime syndrome ofurinary frequency and urgency of childhood. Urology.2001;57:791–3; discussion 3–4. 117. Her ndon CD, DecambreM, McKenna PH. Interactive computer games for treat mentof pelvic floor dysfunction. J Urol. 2 00 1;166:1893–8.118. Hoe beke P, Vande Walle J, Theunis M, et al.Outpatient pelvic-floor therapy in girls with day timeincontinence and dysfunctional voiding. Uro logy.1996;48:923–7. 119. Kjo lseth D, Knudsen LM, Madsen B, etal. Urodynamic biofeedback training for children withbladder-sphincter dyscoordination during voiding.Neurourol Urodyn. 1993;12:211–21. 120. McK enna PH,Herndon CD, Connery S, Ferrer FA. Pelvic floor muscleretraining for pediatric voiding dysfunction usinginteractive computer games. J Urol. 1999;162:1056–62;discussion 62–3. 121. Wennergren H, Oberg B. Pelvic floorexercises for children: A method of treating dysfunctional

voiding. Br J Urol. 1995;76:9–15. 122. Sugar EC, FirlitCF. Urodynamic biofeedback: A new therapeutic approach forchildhood incon tinence/infection (vesical voluntarysphincter dys synergia). J Urol. 1982;128:1253–8.
123. Austin PF, Homsy YL, Masel JL, et al. AlphaAdrenergicblockade in children with neuropathic and nonneuropathicvoiding dysfunction. J Urol 1999;162:1064–7.
124. Cain MP, Wu SD, Austin PF, et al. Alpha blockertherapy for children with dysfunc tional voiding andurinary retention. J Urol. 2003;170:1514–5; discussion6–7.
125. Yan g SS, Wang CC, Chen YT. Effectiveness ofalpha1-adrenergic blockers in boys with low urinary flowrate and urinary incontinence. J Formos Med Assoc.2003;102:551–5.
126. Blackwell B, Currah, J. The psychopharma cology ofnocturnal enuresis. In: Kolvin IM, Mack eith RC, MeadowSR, editors. Bladder Control and Enuresis. Philadelphia:JB Lippincott; 1973.
127. Kaneko K, Fujinaga S, Ohtomo Y, et al. Combinedpharmacotherapy for nocturnal enuresis. Pediatr Nephrol.2001;16:662–4.
128. Kla uber GT. Clinical efficacy and safety ofdesmopressin in the treatment of nocturnal enuresis. JPediatr. 1989;114:719–22.
129. Wil le S. Comparison of desmopressin and enuresisalarm for nocturnal enuresis. Arch Dis Child.1986;61:30–3.
130. Hjalmas K, Hanson E, Hellstrom AL, et al. Long-termtreatment with desmopressin in children with primarymonosymptomatic noc turnal enuresis: An open multicentrestudy. Swe dish Enuresis Trial (SWEET) Group. Br J Urol.1998;82:704–9.
131. Ell er DA, Austin PF, Tanguay S, Homsy YL. Daytimefunctional bladder capacity as a pre dictor of response todesmopressin in monosymptomatic nocturnal enuresis. EurUrol. 1 99 8;33(Suppl 3):25–9.
132. Rus hton HG, Belman AB, Zaontz MR, et al. Theinfluence of small functional blad der capacity and otherpredictors on the res ponse to desmopressin in the
management of monosymptomatic nocturnal enuresis. J Urol.1996;156:651–5.
133. Watanabe H, Kawauchi A, Kitamori T, Azuma Y.Treatment system for nocturnal enuresis according to anoriginal classification system. Eur Urol. 1994;25:43–50.
134. Yeung CK, Sreedhar B, Leung VT, Metreweli C.Ultrasound bladder measurements in patients with primarynocturnal enuresis: A urodynamic and treatment outcomecorrelation. J Urol. 2004;171:2589–94.
135. Smith EM, Elder JS. Double antimicrobial prophylaxisin girls with breakthrough UTI. Urology. 1994 ;43:708-–12.136. Pohl HG, Bauer SB, Borer JG, et al. The outcome ofvoiding dysfunction managed with clean intermittentcatheterization in neurologically and anatomically normalchildren. BJU Int. 2002;89:923–7. 137. Tanagho EA, MillerER, Lyon RP, Fisher R. Spastic striated external sphincterand urinary tract infection in girls. Br J Urol.1971;43:69–82. 138. Steinhardt GF, Naseer S, Cruz OA.Botulinum toxin: Novel treatment for dramatic urethraldilatation associated with dysfunctional voiding. J Urol.1997;158:190–1. REVIEW QUESTIONS 1. A 2-year-old girl isexpected to begin toilet training in which of thefollowing sequences: a. Daytime bowel, daytime bladder,nocturnal bladder, nocturnal bowel b. Noc turnal bowel,daytime bowel, daytime bladder, nocturnal bladder c. Daytime bladder, nocturnal bladder, nocturnal bowel, daytimebowel d. Nocturnal bladder, nocturnal bowel, daytimebowel, daytime bladder 2. A 6-year-old boy is referredshortly a�er the beginning of second grade with new-onseturinary frequency occurring every 15 minutes. He does nothave nocturnal enuresis and has not had daytime wetting. Hehas never had a urinary tract infection and was completelyasymptomatic before the school year began. His physicalexamination is normal. Your treatment recommendationsinclude: a. Reassurance b. Renal bladder sonography withprevoid and postvoid views of the bladder to investigatewhether he is retaining urine c. An MRI of the sacralspine d. Anticholinergic medication 3. A 7-year-old obesegirl presents with daytime incontinence lasting over ayear. She has been evaluated with multiple urine culturesand only mixed bacterial growth found. She denies urgencyto void, voids approximately �ve times daily, and neverwets the bed. Her mother states that her underpants aresporadically wet, with wetting occurring shortly a�er thegirl voids. Her physical examination is normal. Yourtreatment recommendations include: a. Renal bladdersonography with prevoid and postvoid views of the bladder

to investigate whether she is retaining urine b. An MR Iof the sacral spine c. Ant icholinergic medication d. Reassurance and encouragement to void with her legs widelyspaced
4. An 8-year-old girl presents with incontinence occurringwhen she laughs hard. Her physical examination,urinalysis, and remainder of her history are normal. Youdiagnose giggle incontinence and o�er a prescription for:a. Amitriptyline b. Oxybutynin c. Vasopressin d.Methylphenidate
5. A 9-year-old boy presents with nighttime wetting. Hehas never been completely dry at night and wets the bedapproximately three nights of the week. His father had thesame problem until the age of 13 years. A review of theboy’s voiding patterns shows that he is dry during theday, denies urgency, and has normal bowel movements. He isinterested in becoming dry soon because he is planning tojoin the Boy Scouts. Your treatment recommendationsinclude: a. Nothing, because he will grow out of it around13 years of age, just like his father b. Oxybutynin and abowel program c. Vasopressin d. Amitriptyline
6. A 9-year-old boy presents with nighttime wetting. Hehas never been completely dry at night and wets the bedapproximately three nights out of the week. His fathersu�ered from the same problem until the age of 13 years. Areview of the boy’s voiding patterns shows that heoccasionally has episodes of mild incontinence during theday preceded by the need to void and has bowel movementsevery several days. He is interested in becoming dry soonbecause he is planning to join the Boy Scouts. Yourtreatment recommendations include: a. Nothing as he willgrow out of it around 13 years of age, just like hisfather. b. Oxybutynin and a bowel program c. Vasopressind. Amitriptyline
7. A 6-year-old girl has never been completely dry.Despite that she has no symptoms other than persistentlydamp underpants, her pediatrician has evaluated her forsuspected UTIs. Each urine culture has demonstrated eitherno growth or fewer than 10,000 CFU/mL of mixed growth. Shewas toilet trained at 23 months of age. She voids �vetimes during the day, with normal sensation to void beforeand no evidence of urgency. Her panties are always wet,day and night. She does not wake up to urinate in themiddle of the night. Your initial recommendation includes:a. Timed voiding to make certain that she is not inover�ow incontinence b. A renal-bladder sonogram c. A KUB
examination d. Renal scan e. A VCUG 8. A 6-year-old girlpresents with a history of �ve culture-proved urinarytract infections. She has never had fever with them.Instead, the cultures are obtained because of her chronicurinary incontinence. She wets most every day, generallybeginning around midday and into the a�ernoons. Herincontinence is never preceded by a sense of urgency. Shewill generally stay dry throughout the night, wakes around7 am, but doesn’t void until around lunchtime. She mightvoid once more before bedtime. Which condition is shelikely to have? a. Paradoxical incontinence b. Sensoryde�cient bladder c. Detrusor overactivity d. Primarynocturnal enuresis 9. A 4-year-old girl presents with ahistory of three culture-proved febrile urinary tractinfections. Her only medications include MiraLAX forchronic constipation, though she takes it rarely andcomplains of abdominal pain. She is frequently wet duringthe day, and her incontinence is preceded by urgency. Yourinitial recommendations include: a. Timed voiding andbetter adherence to her bowel program b. Oxybutynin and abowel program c. Trimethoprim-sulfamethoxazole nightly d.Renal bladder sonogram with prevoid and postvoid views anda contrast voiding cystourethrogram, andtrimethoprim-sulfamethoxazole, nightly 10. A 5-year-oldgirl is diagnosed with dysfunctional voiding syndrome a�eran evaluation for wetting, constipation, and recurrentfebrile UTIs. A VCUG was negative. Your treatmentrecommendation includes: a. Timed voiding b. Timedvoiding, bladder program c. Timed voiding, bladderprogram, anticholinergics d. Timed voiding, bladderprogram, antibiotic prophylaxis 11. Identify theincorrect statement regarding voiding abnormalities. a.Hinman syndrome, which is a discoordination between thedetrusor contraction and sphincter relaxation, isinitially managed by injecting Botox (botulinum toxin)into the sphincter. b. Bladder dysfunction from posteriorurethral valve is not static. Whereas detrusoroveractivity predominates in childhood, myogenic failure isseen in adolescence. c. Most infants with neurogenicbladder have complete paralysis of detrusor function. d.Children with cerebral palsy are incontinent only as aresult of their physical limitation, because they cannotreach the toilet in time.
ANSWER KEY
1. b
2. a

3. d
4. d 5. c 6. b 7. d 8. b 9. d 10. d 11. b
53 Applied clinical biostatistics
Figure 53.3 Receiver operating characteristic plot com
paring tests (a) and (b). AUC, area under the curve; Test
x, theoretically perfect discriminatory test; Test c, test
without discriminatory ability. model. All covariates weremeasured only once at the entry into the study. Gender wascoded as 1 for male and 2 for female. U p/c is the urineprotein-to-creatinine ratio on a �rst morning specimen.
Covariate β-Coef�cient P Value 95% Con�dence interval
Age (yr) 6.625 0.024 0.762, 14.012
Gender –6.761 0.003 –8.682, –4.839
Systolic BP 2.322 0.041 0.157, 4.487
Diastolic BP 5.208 0.109 –1.638, 12.054
U p/c 8.312 0.0001 7.926, 8.698
Constant(α ) 3.224 0.000 1.471, 4.977
Answer:
is regression analysis reveals that age, gender, systolic
blood pressure, and a �rst morning urine protein-to-cre
atinine ratio are all signi�cant determinants of the change
(e.g., decline) in eGFR. Based on a nonsigni�cant P value,
diastolic blood pressure was not found to be a determinant
of change in eGFR in the multivariate models despite being
signi�cant in univariate analyses. �ere may be two poten
tial reasons for this. �e �rst is that diastolic blood pres
sure is intimately related to systolic blood pressure.Because
they o�en run together (e.g., co-linear), placing both inthe

model may make one insigni�cant when adjusted for the
other. �e additional possibility is that there was not suf
cient power in the study to detect a signi�cant e�ect of
diastolic blood pressure on eGFR. Although not provided,
if there were insu�cient numbers of patients in the study
to perform a regression with �ve covariates, the diastolic
blood pressure may have been a�ected by this. In looking
at the remaining determinants, age, systolic blood pressure,
and the �rst morning urine protein-to-creatinine ratio,
all had positive and statistically signi�cant β-coe�cients
in the regression. �ese data suggest that there is a direct
relationship with these variables and eGFR in that older
children with higher systolic blood pressures and higher
urine protein-to-creatinine ratios had a higher absolute
change in the eGFR over the year of the study. Conversely,
gender had a negative association with eGFR, implying that
females have a lesser change in eGFR (e.g., protectivee�ect).
Furthermore, looking at the P values and con�dence inter
vals associated with the regression show that the strength
of the association is strongest between the �rst morning
urine protein-to-creatinine ratio and the eGFR. �is can be
inferred because of the narrow con�dence interval and very
low associated P values.
2. Given the results of the multivariate regression inQuestion 1, write the regression equation associated with
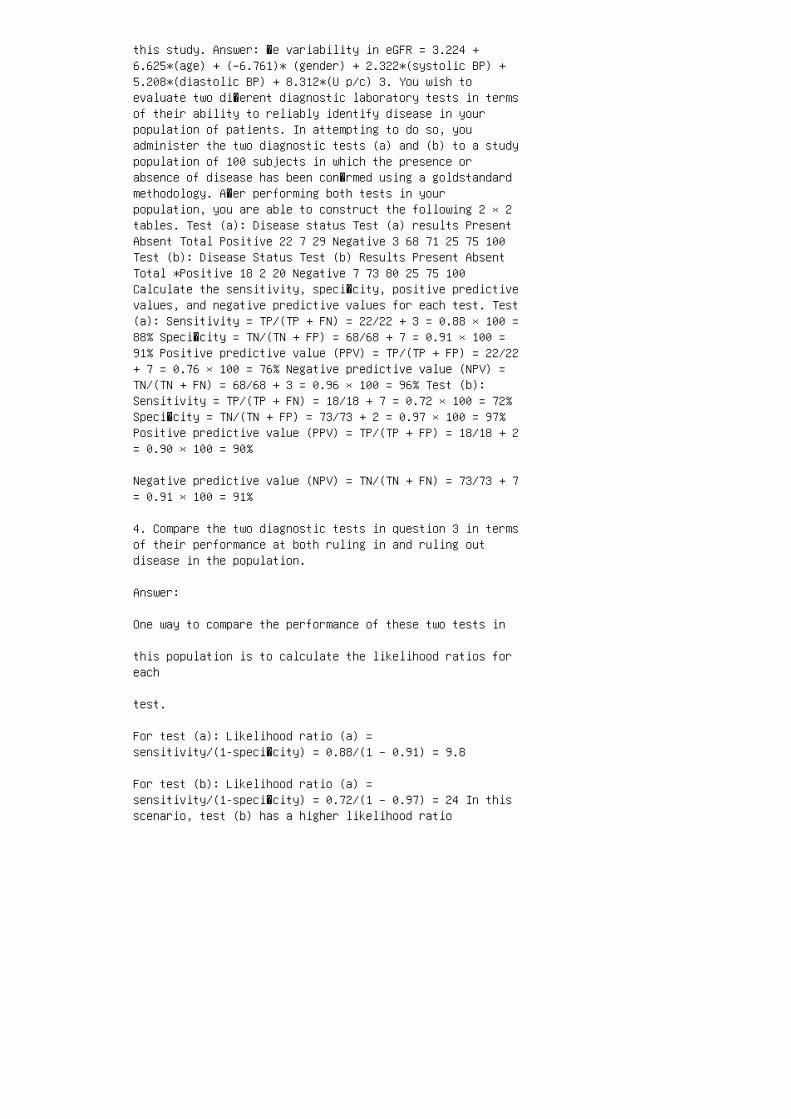
this study. Answer: �e variability in eGFR = 3.224 +6.625*(age) + (–6.761)* (gender) + 2.322*(systolic BP) +5.208*(diastolic BP) + 8.312*(U p/c) 3. You wish toevaluate two di�erent diagnostic laboratory tests in termsof their ability to reliably identify disease in yourpopulation of patients. In attempting to do so, youadminister the two diagnostic tests (a) and (b) to a studypopulation of 100 subjects in which the presence orabsence of disease has been con�rmed using a goldstandardmethodology. A�er performing both tests in yourpopulation, you are able to construct the following 2 × 2tables. Test (a): Disease status Test (a) results PresentAbsent Total Positive 22 7 29 Negative 3 68 71 25 75 100Test (b): Disease Status Test (b) Results Present AbsentTotal *Positive 18 2 20 Negative 7 73 80 25 75 100Calculate the sensitivity, speci�city, positive predictivevalues, and negative predictive values for each test. Test(a): Sensitivity = TP/(TP + FN) = 22/22 + 3 = 0.88 × 100 =88% Speci�city = TN/(TN + FP) = 68/68 + 7 = 0.91 × 100 =91% Positive predictive value (PPV) = TP/(TP + FP) = 22/22+ 7 = 0.76 × 100 = 76% Negative predictive value (NPV) =TN/(TN + FN) = 68/68 + 3 = 0.96 × 100 = 96% Test (b):Sensitivity = TP/(TP + FN) = 18/18 + 7 = 0.72 × 100 = 72%Speci�city = TN/(TN + FP) = 73/73 + 2 = 0.97 × 100 = 97%Positive predictive value (PPV) = TP/(TP + FP) = 18/18 + 2= 0.90 × 100 = 90%
Negative predictive value (NPV) = TN/(TN + FN) = 73/73 + 7= 0.91 × 100 = 91%
4. Compare the two diagnostic tests in question 3 in termsof their performance at both ruling in and ruling outdisease in the population.
Answer:
One way to compare the performance of these two tests in
this population is to calculate the likelihood ratios foreach
test.
For test (a): Likelihood ratio (a) =sensitivity/(1-speci�city) = 0.88/(1 – 0.91) = 9.8
For test (b): Likelihood ratio (a) =sensitivity/(1-speci�city) = 0.72/(1 – 0.97) = 24 In thisscenario, test (b) has a higher likelihood ratio

mostly because of its high speci�city. However, the choiceof
which test is most favorable in this example hinges primar
ily on the characteristics of the disease under study.Should
the disease in this example be serious and potentially fatal
if undetected and/or curable on detection, test (a) may be
preferable because of its higher sensitivity. �is is due tothe
lower rate of false-negative results associated with test(a).
A false-negative result in this scenario would have serious
consequences for the health of this population because of
disease severity. However, in a situation in which a disease
is relatively mild and not associated with signi�cant mor
bidity and mortality and/or further testing associated with
a positive test result is both expensive and associated with
its own risks, then test (b) may be preferable. �is isbecause
of its lower rate of false-positive test results (e.g.,higher
speci�city). 5. You have conducted a case-control studyexamining whether maternal exposure to drug x duringpregnancy is associated with the development ofhypertension in children younger than 10 years of age. Inperforming this study, you retrospectively collect data ona group of children diagnosed with hypertension with age-and gender-matched controls sampled from the same generalpopulation. You retrospectively collect exposure data fromthe mothers of these children to drug x during pregnancy.From your data, you are able to construct the following 2 ×2 table: Hypertension status Exposure history HypertensiveNormotensive Total Exposed 20 25 45 Unexposed 5 50 55 25 75100 Calculate the odds of developing hypertension withexposure relative to not being exposed. How does this

metric relate to the calculation of a relative risk?Answer: �is question is asking for a calculation of theodds ratio from this case-control study. �e odds ratio(OR) is calculated from the number of those with diseasedivided by those without disease for each exposure group.In this question this becomes: OR = ad/b c = 20 × 50/5 ×25 = 1000/125 = 8. In the situation in which a case-controlstudy is examining a relatively rare disease, the oddsratio can be a good approximation of the relative risk.However, in this scenario in which hypertension ishypothetically present in 25% of the population, therelative risk for disease associated with exposure x isdi�cult to estimate.