Volume 6 - Depression - Taylor & Francis eBooks
240
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Volume 6 - Depression - Taylor & Francis eBooks


The Scienceof Mental Health
Volume 6
Depression

Series Content
Volume 1BIPOLAR DISORDER
Volume 2AUTISM
Volume 3SCHIZOPHRENIA
Volume 4ATTENTION-DEFICIT HYPERACTIVITY DISORDERS
Volume 5ADDICTION
Volume 6DEPRESSION
Volume 7PERSONALITY AND PERSONALITY DISORDER
Volume 8COMPULSIVE DISORDER AND TOURETTE'SSYNDROME
Volume 9STRESS AND THE BRAIN
Volume 10FEAR AND ANXIETY

The Scienceof Mental Health
Volume 6
Depression
Edited with introductions by
Steven HymanNational Institute ofMental Health
ROUTLEDGENew York/London

Published in 2001 by
Routledge711 Third AvenueNew York, NY 10017
Published in Great Britain byRoutledge2 Park Square, Milton ParkAbingdon, Oxon OX14 4RN
Routledge is an Imprint of Taylor & Francis Books, Inc.Copyright e 2001 by Routledge
All rights reserved. No part of this book may be reprinted or reproduced or utilized in any form or byany electronic, mechanical, or other means, now known or hereafter invented, including anyphotocopying and recording, or in any information storage or retrieval system, without permission inwriting from the publishers.
Library of Congress Cataloging-in-Publication Data
The science ofmental health / edited with introductions by Steven Hyman.p. cm.
Includes bibliographical references.ISBN 0-8153-3743-4 (set)1. Mental health. 1. Hyman, Steven E.
RA790 .S435 2002616.89--dc21
2001048491
POD ISBN:Set ISBN:Vol 1:Vol 2:Vol 3:Vol 4:Vol 5:Vol 6:Vol 7:Vol 8:Vol 9:Vol 10:
978041553252597808153374309780815337447978081533745497808153374619780815337478978081533748597808153374929780815337508978081533751597808153375229780815337539

Contents
IX Introduction
Epidemiology1 The Prevalence and Distribution of Major Depression in a National
Community Sample: The National Comorbidity SurveyD. G. Blazer, R. C Kessler, K. A. McGonagle, and M. S. Swartz
9 Comparing Age at the Outset of Major Depression and Other PsychiatricDisorders by Birth Cohorts in Five U.S. Community Populations
K. C Burke, j. D. Burke, D. S. Rae,and D. A. Regier17 Socioeconomic Burden of Subsyndromal Depressive Symptoms and
Major Depression in a Sample of the General PopulationL. L. judd, M. P. Paulus, K. B. Wells, and M. H Rapoport
24 Boundaries of Major Depression: An Evaluation of DSM-IV CriteriaK. S. Kendlerand C O. Gardner
31 Prevalence of and Risk Factors for Lifetime Suicide Attempts in theNational Cornorbidity Survey
R. C Kessler, G. Borges, and E. E. Walters41 A 40-Year Perspective on the Prevalence of Depression
j. M. Murphy, N. M. Laird, R. R. Monson, A. M. Sobol,and A. H Leighton
Natural History49 Depressive Symptomatology and Incident Cognitive Decline in an Elderly
Community SampleS. S. Bassuk, L. F. Berkman, and D. Wypij
58 Lost Human Capital from Early-Onset Chronic DepressionE.R. Berndt, L. M. Koran, S. N. Finkelstein, A. L. Gelenberg, etat.
67 The Effects of Stressful Life Events on DepressionR. C Kessler
92 Natural Course of Adolescent Major Depressive Disorder in aCommunity Sample: Predictors of Recurrence in Young Adults
P. M. Lewinsohn, P.Rohde,J R. Seeley, D. N. Klein, andI A. Gotlib100 Recurrence after Recovery from Major Depressive Disorder during 15
Years of Observational Follow-upT. 1.Mueller, A. C Leon, M. B. Keller, et at.
107 Association between Depression and Mortality in Older AdultsR. Schulz, S. R. Beach, D. G. Iues, L. M. Martire, A. A. Ariyo,and WJ Kop
v

VI Contents
Depression and Medical Disorders115 MRI Defined Vascular Depression
K. R. Krishnan, j. C. Hays, and D. G. Blazer120 The Relationship of Depression to CardiovascularDisease:Epidemiology,
Biology, and TreatmentD. L. Musselman, D. L. Evans, and C. B. Nemeroff
Genes and Environment133 Symptoms of Anxiety and Symptoms of Depression: Same Genes,
Different Environments?K. S. Kendler, A . C Heath, N G. Martin, and L. l. Eaves
141 Stressful LifeEvents, Genetic Liability, and Onset of an Episode of MajorDepression in Women
K. S. Kendler, R . C. Kessler, E. E. Walters, et at.151 The Genetics of Major Depressive Disorder
G. S. Malhi, j . Moore, and P. McGuffin156 Genetic Epidemiology of Major Depression: Review and Meta-analysis
P. F. Sullivan, M. C. Neale, and K. S. Kendler168 Childhood Sexual Abuse as a Risk Factor for Depression in Women:
Psychosocial and Neurobiological CorrelatesE. L. Weiss,! G. Longhurst, and C.Mazure
Evolution182 Is Depression an Adaptation?
R . M. Nesse
Neurobiology and Behavior190 Subgenual Prefrontal Cortex Abnormalities in Mood Disorders
W C. Dreuets.]. L. Price.]. R . Simpson, R . D. Todd, T. Reich,M. Vannier, and M. E. Raichle
195 A Molecular and Cellular Theory of DepressionR . S. Duman, G. R .. Heninger, and E.! Nestler
205 The Impact of Early Adverse Experiences on Brain SystemsInvolved inthe Pathophysiology of Anxiety and Affective Disorders
C. Heim and C. B. Nemeroff219 The Corticosteroid Receptor Hypothesis of Depression
F. Holsboer .245 Reciprocal Limbic-Cortical Function and Negative Mood: Converging
PET Findings in Depression and Normal SadnessH S. Mayberg, M. Liotti, S. K Brannan, S. McGinnis, R. K.Mahurin,P. A. [erabek.]. A. Silva,! L. Tekell, C. C.Martin,! L. Lancaster,and P. T. Fox
254 Depression Duration but Not Age PredictsHippocampal Volume LossinMedically Healthy Women with Recurrent Major Depression
y. 1. Sheline, M. Sanghavi, M. A. Mintun, and M. H Gado

Contents Vll
Treatment Outcomes265 Natural History and Preventative Treatment of Recurrent Mood
DisordersE. Frank and M. E. Thase
282 A Comparison of Nefazodone, the Cognitive Behavioral-AnalysisSystemof Psychotherapy, and Their Combination for the Treatment of ChronicDepression
M. B. Keller,]P. McCullough, D. N Klein, B. Arnow,D.L. Dunner,A. J. Gelenberg, J. c. Markowitz, C. B. Nemeroff, J. M. Russell,M. E. Thase, M. H Trivedi, and J. Zajecka
291 Functioning and Utility for Current Health of Patients with Depression orChronic Medical Conditions in Managed, Primary Care Practices
K. B. Wells and C. D. Sherbourne
299 Acknowledgments

This page intentionally left blank

Introduction
In common usage, the term "depression" can refer to the state of being sad orblue, but it also signifies a serious clinical syndrome that affectsapproximately 10percent of people at some point in their lives. This clinical syndrome may occur asa primary illness or as a complication of ("secondary to") another mental disordersuch as schizophrenia, a medical condition such as hypothyroidism, or the effectsof a drug. Based on studies of clinical courses and outcomes, treatment responses,and familial patterns of depression, primary depressive illness is dichotomized intounipolar (depressions only) and bipolar. In bipolar disorder, or manic-depressiveillness, depressions are interspersed with manias- periods of elevated mood, highenergy, and lack of sleep. Bipolar disorder is described in a separate volume.
"Major depression" is the term used in the DiagnosticandStatisticalManual
a/MentalDisorders, 4th edition (DSM-IV),1of the American Psychiatric Association
to describe primary unipolar depressive illnessof significant severity and duration.Characteristic symptoms include a disturbance of mood, general sadness (oftenaccompanied by irritability), loss of interest in one's usual pursuits, and inability toexperience pleasure (anhedonia). Major depression is also characterized by bodilysymptoms, including sleep disturbance, generally insomnia (but occasionallyexcessive sleeping), change in appetite (usually loss of appetite but occasionallyovereating), decreased energy, and, when the depression is severe, a slowing ofthought, speech, and movement (psychomotor retardation) . Cognitively, patientsoften complain of difficulty concentrating, ruminations on negativethoughts, guilt,a loss of hope, and suicidal thoughts. In a small percentage of severe cases,peoplemay develop psychotic symptoms (most commonly delusions- fixed, culturallyinappropriate falsebeliefsthat are congruent with their depressedmood). Grief andbereavement may have many symptoms similar to those of depression. Griefshould not be medicalized, but major losses may also trigger major depression. It isa difficult matter of judgment to determine when grieving has slipped intodepression, but the diagnosis must be based on the duration, trajectory, andseverity of the symptoms.
The course of major depression is often episodic, but recurrences are therule , especially when the illness begins early in life. Between episodes of majordepression many individuals- even with treatment- do not recover fully and mayexperience chronic low-level symptoms of depression. In perhaps 20 percent ofpeople with major depression, severe symptoms become chronic and relativelyunremitting. The term "dysthymia" is applied by the DSM-IV to chronicdepression in which symptoms are not severe enough to quality for the diagnosisofa major depressive episode . We have learned, however, that despite diminished
ix

x Introduction
severity of symptoms, dysthymia can lead to substantial impairments, perhapsrelated to the chronicity of the symptoms that may wear people down.
The most serious complication of both major depression (unipolar) andbipolar depression is suicide. It has been estimated that 10 to 15 percent of peoplewith recurrent depression commit suicide, and the most common reason forsuicide is depression. Other disorders commonly associated with suicide areschizophrenia and alcoholism. Suicide is currently the eighth leadingcauseof deathin the United States and the third leading cause of death among young peoplebetween the ages of 15 and 24.
In all its forms depression causes serious impairments in life roles. Basedon a systematic review of data, the World Health Organization ranked majordepression as the leading cause of disability in the developed world and the fifthleading cause of disease burden worldwide (defined as years of healthy life lost to
premature mortality or disability).2As in all of the volumes in this series, articles are included that cover a
diverse range of issues needed to understand depression. The studies included hereare derived from the scientific literature, but several books provide poignant
personal accounts of the experience of depression that supplement this list.3
Theorganization of this volume includes the subjects of epidemiology, genetics, thenatural history of depression (for example , the course of depressive illness over alifetime), examples of the relationship of depression to general medical disorders,an evolutionary view of depression, the neurobiology and behavioral science ofdepression, and, finally, the treatment of depression.
The epidemiological studies included here reveal that depression is anextremely common illness (Blazer et al., 1994)that creates a substantial economicburden. The negative socioeconomic impact of depression extends even to its lesssevere forms (Judd et al., 1996). An article in the section on natural historycomplements the epidemiological findings, demonstrating a potent negative impactof depression on educational attainment (Berndt et al., 2000). An entry on theepidemiology of suicide attempts is also included (Kessleret al., 1999).This articlediscusses the important role of epidemiology beyond tallying the incidence (newoccurrences) and prevalence (total number of cases during a defined period) of acondition and goes into the identification of possible risk factors contributing toillness or mortality, in this case suicide attempts.
The major current controversy in the epidemiology of depression is thequestion of whether the age of onset of major depression is getting progressivelyyounger in Western countries and whether the rates of depression are increasing.This unsettled question (Murphy et al., 2000) has important implications. Basedonthe known natural history of depression, if onsets are indeed getting earlier in life,there would be a greater number of recurrences and, likely, increased levels ofdisability. Such findings would also suggest important public health efforts to findthe reasons for such a change comb ined with increased attention to casefinding inchildren. The central question is whether the findings of Klerman and Weissmanand several later investigators reflect real trends or result from artifacts of recentversus distant recall, decreasing stigma associatedwith talking about depression in

Introduction Xl
younger generations, and an increased awareness of depress ion in the generalpopulation.
Another active area of research represented in this collection isthe impactof stress on depression (Kessler, 1997). Fixing the relationship of stress todepression is difficult because different individuals perceive and respond to stressin different ways . Moreover, there is an important chicken-and-eggquestion thatremains unsettled. Do negative life events independently create a risk of depression,or do individuals at risk for depression or who are already depressed have a greaterliability- as a result of their symptoms- of putting themselves in harm's way?
The negative impact of depression on functioning is illustrated by itseffects on cognitive functioning with aging (Bassuk et al., 1998) and on overallmortality (Schulz et al., 2000). Until recently the interaction among depression,medical illness, and mortality was conceptualized in a rather simplistic manner. Itwas thought that a medical illnesssuch asa stroke, a heart attack, or diabetes was aserious life stressor (which of course it is) and thus caused depression. Depressionwould then have a negative impact on overall recovery by diminishing themotivation of the affected person to adhere to medical treatments and engage inself-care and rehabilitation. The situation, however, appears to be far morecomplex. First, there is good evidence that certain strokes (primarily in thedominant hemisphere) can directly trigger depression independently of the degreeof disability. More recently , data have been brought forward to suggestdepressionthat appears later in life may result from cerebrovascular disease (Krishnan et al.,1997).If this hypothesis is corroborated, prevention strategiesfor depression mightcome to include diet, exercise, and cardiovascular medicat ions.
Even more unexpected, research has shown that the negative impact ofdepression on the outcome of cardiovascular disease extends far beyond issuesofself-care and motivation. Musselman et al. (1998) review some of the data thatestablish biological effects of depression that can influence the outcome ofcardiovascular disease. There is increasing evidence that depression may be themost potent modifiable risk factor for mortality in individualswho have had a heartattack or who suffer from congestive heart failure .
The origins of depression ate to be found neither in genes alone nor inlife events alone but in an interaction among multiple genes,developmental events,and stressful environmental triggers. These complex issuesare addressed in articlesby Kendler et al. (1987, 1995). One of the major emerging developmental riskfactors for depression in women is a history of childhood sexual abuse rweisset al.,1999). No one would doubt that early abuse is a profound stressor, but furtherresearch on the mechanisms by which it leads to later illness isvery much in need ifwe are to develop better preventive interventions for abused children. A history ofchildhood abuse, including sexual abuse, is also a potential risk factor for othermental disorders, for example, borderline personality disorder. Thus we must alsolearn the mediators by which this more general risk factor leads down one path oranother, and we must learn about the resilience of those who do not develop asubsequent disorder.
Genes exert a less powerful effect in major depression than they do inautism, schizophrenia, or bipolar disorder; yet genesstill playa significant role in

xii Introduction
the risk of depression, at about the same level that they do in risk of type II (adultonset) diabetes. As with all mental illnesses, however, the genetic risks of majordepression are not straightforward. The evidence from family studies and fromcurrent attempts at gene discovery (for example, by linkage analysis) indicates thatrisk of depression is the result of the impact of multiple genes that interact witheach other and with nongenetic factors. Pinning down the genetic variations thatconfer risk of depression is made more difficult by the almost certain likelihoodthat depression is heterogeneous, with multiple and different genetic andenvironmental pathways of risk. Overall, there may be no one gene or no one typeof environmental event that is both necessary and sufficient to cause depression.This complexity is reviewed in Malhi et al. (2000). The high frequency ofdepression in the population suggests that the genetic variations that produce riskare also very common in the population. This raises the question of whether thosegenes have some adaptive value; one view of this evolutionary question isaddressed by Nesse (2000).
Emotions such as fear or happiness represent transient responses tospecific stimuli; mood represents the predominant long-term emotional state.It hasbeen far easier to study emotion (short-term and stimulus-induced) than mood,partly because there are convincing animal models for some emotions, such asfear,and partly because certain emotions can be reliably induced in human researchvolunteers (see volumes on Fear, Anxiety, and the Brain) . In contrast, althoughthere is strong indirect evidence that animals have moods, such states have provenvery difficult to measure or study. There are animal models that the pharmaceuticalindustry has used to identify drugs that may act as antidepressants, but these drugdiscovery paradigms are not satisfactory models of the state of depression. Despitethese challenges, there has been steady progress during the last decade in theinvestigation of the neural substrates of depression. For example, studies usingnoninvasive neuroimaging technologies such as positron emission tomography(pET) to study brain activity and studies using postmortem brain tissue have begunto identify brain structures that might be involved in depression (Drevets et al.,1997; Mayberg et al., 1999) and suicide.
Another important clue as to what goes wrong in the brain in depressionis the long-standing observation that approximately half the people with seriousmajor depression have excessive secretion of cortisol, the major stress hormone.Cortisol is the end product of activation of a stress-response system called thehypothalamic-pituitary-adrenal (HPA) axis.Heim and Nemeroff (1999) addresstherole of stress, including the role of early stress, in risk of depression . This biologicaland behavioral investigation complements the more epidemiologically orientedstudies reviewed by Kessler (1997). Holsboer (2000) has argued that the HPA axismay playa central role in the pathogenesis of depression. His views yield severalhypotheses that must be tested in the coming years. One hypothesized effect oflong-term disruption of the HPA axis by depression includes atrophy of thehippocampus, a brain structure that plays a central role in explicit (conscious)memory. (See volume on Stress and the Brain.) While much more needs to bedone, including longitudinal studies correlating hippocampal volumes with stress,depression, and cortisol measurements, as well as with cognitive function, initial

Introduction Xlll
work suggests that depression may indeed produce hippocampal atrophy (Shelineet al., 1999).
Treatment of depression involves certain well-tested psychotherapies,medications, or their combination. Treatment issues are addressedby a review fromFrank and Thase (1999) and by Keller et al. (2000), who have developed acombination treatment for chronic depression. The benefits of treatment forfunctioning are addressed by Wells and Sherbourne (1999).The overall value oftreatment must be kept front and center because, unfortunately, many individualswith serious depression still do not receive an appropriate diagnosis and, even ifthey do, may not get adequate treatment.
References1. American Psychiatric Association. Diagnostic and Statistical Manual0/MentalDisorders, 4th ed. Washington, D.C.: American Psychiatric Press, 1994.2. C.J. L. Murray and A. D. Lopez. 1heGlobal Burden o/Disease. Cambridge, Mass.:Harvard University Press, 1996.3. William Styron. Darkness Visible: A Memoiro/Madness. New York: Vintage, 1992;Andrew Solomon. TbeNoondayDemon. New York: Scribner, 2001.

This page intentionally left blank

Regular Articles
The Prevalence and Distributionof Major Depression in a National Community Sample:
The National Comorbidity Survey
Dan G. Blazer, M.D., Ph.D., Ronald C. Kessler, Ph.D.,Katherine A. McGonagle, Ph.D., and Marvin S. Swartz, M.D.
~ Maior depression is a frequent and disabling psychiatri c disorder in the UnitedStates. Th is report exam ines the prevalence and risk factor profile ofboth pure and comorbidmajor depression according to data from the Nat ional Com orbidity Survey . Mu1l!Jd;. To estimat e the prevalence ofpsychiatric como rbidity in the United States, a national sample of 8,098persons 15-54 years of age from the 48 conterminous states was surveyed with a modifiedversion of the Comp osite Int ernational Diagnostic Interview. 8.a.JdLl; From the survey datathe prevalence of current (30-day) malor depression was estimated to be 4.9%, with a relat ivelyhigher prevalence in females, young adults, and persons with less than a college education.The prevalence estimate for lifetim e major depression was 17.1%, with a similar dem ographicdistribution. Both 30 -day and lifetime prevalence estimates were higher than estimates fromthe earlier Epidemio logic Catchment Area study . When pure major depression was comparedwith majo r depression co-occurring with other psychiatric disorders, the risk factor profilesexh ibited clear differences. Conclusions' These findings suggest a greater burden of maio«depression in community -dwelling persons than has been estimated from previous communitysam ples. The risk factor profile showed significant differen ces betwe en persons with pure andcombined major depression.
(Am) Psychiatry 1994; 151:979-986)
D epression is co nsidered a major public hea lthprobl em (1-3). Commu nity-based epidemiologic
st udies of DSM -II1·d ef ined ma jor depression haveyielded varyi ng prevalence estimate s, pr imarily becauseof vary ing methods of case ascertainment (4-6). By farthe most amb itious effort to estimate the prevalence of
Received March 22, 1993i revision received Oct . 21, 1993; accepred Nev. 18, 1993. From Duke UniveniryMedicalCenter andEbeSurvey Research Center, University of Michigan, AnnArbor. Addressreprintrequests to Dr. Blazer, Duke University Medical Center, Box300S, Durham, NC 27710.
The NationalComorbiditySurveyis supported bygrantMH..-46376from the U.S. Alcohol, Drug Abuse, and Mental Health Administration, with supplementa l suppo rt from the W.T. Grant Foundation.Preparation of this report was also supportedby Research ScientistDevelopment Award MH-00507 from NIMH to Dr. Blazer.
Am] Psychiatry 151:7, ]uIy 1994
major depre ssion was the Epidemiologic Cat chmentArea (ECA) study in five U.S. communities (7). Theprevalence estimates of major depression from the ECAstudy were criticized for at least twO reasons. First, atrue nat ional estimate could not be abstra cted becausethe investigators sampled only five communities. Second, the prevalence estimates of major depression weremuch lower than those from previous studies, The 1month prevalence estimate for the United States, basedon dat a on depress ion accord ing to the DSM-I1Icriteriafrom the five sites of the ECA study , wa s 1.6% for menand 2.9 % for women. In contrast, in a retrospectiveanaly sis of the Sterling County study (8), the rate wasestimated to be 5 .3 %, and in the New Haven, Conn.,study (4), which used the Research Diagn ostic Criteria,the rates were 3.2 % for men and 5.2 % for wom en. Es-
979
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission .
1

PREVALENCE OF MAJOR DEPRESSION
TABLE 1. Democrlphk: Cho<oc:tlfl. t ic. o! the Subjects In the Nation.1Cornorbldlt)'Survey and In the U.S. Popu~ ion
NationalComorbid ity U.S.
Survey Populatio nCha racteristic IN=8.09811 %)' (%)b
Age (years)15-24 24.7 25.525-34 30 .1 30.835-44 27 .1 25.945-54 18.1 17.8
SexMale 49 .5 49.1Female 50 .5 50 .9
RacelethniciryWhit e 75 .3 75.0Blade 11.5 11.9Hispan ic 9.7 8.6Ot her 3.5 4.5
Educarlon fyears)0-11 22 .3 22.512 37.4 36 .813- 15 21. 7 21.216 or mere 18.6 19.5
Ma rital statusMa rried 62.9 59 .8Separated/widowed/ divorced 10 .6 10.1Nevermarried 27 .1 30 .1
RegionNortheast 20 .2 20.0Midwest 23.8 24 .6South 36 .4 33 .7Wes, 19.6 21. 7
UrbaniciryLarge metropo litan area 67.8 71.2Sma ll metr opol ita n area 7.5 8.1Rura l area 24 .7 20.7
· Weighted to the population.bFro m the Nat ional Health Interview Survey, U.S. Department ofHealth an d Human Services, National Cente r for Health Statistic s,1989.
t imates of lifetime prevalence from the ECA study werealso lower than those foun d in previous studies (9).
T he genera l methodology applied in the ECA studyhas been transpaned to studies th rough out the world.For exa mple, studies using case-finding meth ods similar to that of the ECA study (the National Institut e ofMental Health Diagnostic Inte rview Schedule) andstudies that apply DSM·IIJ and DSM· ll! ·R criteria havebeen conducted in a number of other countries) including Canada (10), Puerto Rico (11), Italy (12), New Zealand (13), and Taiwan (14).
The National Comorbidity Survey represents the firstepidemiologic data from a national sample of cornmunity residents from which estimates of preva lence distr ibution and risk factors for selected DSM·I1I-R psychiatric disorders in the United States can be derived. Inthis artic le, preva lence estima tes for bot h curre nt (30day) and lifetime major depr ession are presented. Also,a risk factor profile is presented for both "p ure" majordepressi on and major depression occurring with othe rpsychiatric disorders, a presen tation nor emphasized inmost community-based epidemiologic studies of majo rdepression . The case ascertainment methods of the Na-
980
tionaI Comorbidity Survey were similar but not identical to those used in the ECA study . The different approach to case ascertainment for lifetime major depression in the N at ional Comorbidity Survey was expectedto lead to higher national estimates than those from theECA study, and the estimates presented here confirmthis assumption.
MElliOD
The National ComcrbiditySurvey isa nationwidestudyof the U.s.population, ages 1.5-54 yun. th.1 was designed to estimate theprevale nce, risk faeton , lind consequences of p,yc hiatric morbidityand como rb idiry, It is based on a strati fied, multistage arca probabil ity sample of the noninstiturionaliud civilian popula tion in the 48con terminous states, wirna supplementa l sample of srudents living incampus gro up ho using. The survey was adm inistered by the field suffof the Survey Research Cente r at the Univen ity of Michigan betweenSept. 1-4, 1990, and Feb. 6, 1992 . The 158 Na tional Como rbiditySurvey interviewers were experi enced interviewers who completed arigor ous program of training to administer the Composite Internationa l Diagn ost ic Inrerview reliabl y.
Several special design features of the Na tion al Como rbid ity Surveyarc note worthy . A eonresponse survey was carried out in which asample of persons who did not respo nd mitially to the survey wereoffered a substantial financial incentive to complete a shan fo rm ofthe d iagnostic interview. Significantly higher preva lence of both lifetime and curr ent psychiatric diso rders was found among these initia lnon respondents than among respo ndents in the main survey. Thisresult is consistent with previous resea rch showing that persons withhistories of psychiatric disord er are under repre sented in crcss-nat iona l surveys as well as in relm erview surveys of the general popula tion (1.5, 16). The survey data were .....eighted to compensate for thisnonresponse. The data were also weighted to adjust for var iation inprobabilities of selection across and wit hin households and wereposrseradfied by means of an interactive procedure to appr cxunatethe nat iona l popula tion distr ibution of the cro ss-classif icar ionof age,KX, racclcthn iciry, marital status , educat ion, living arrangements, region, and urbani city as defined by the 1989 U.S. Nati on al Hea lthInterview Survey (17) . A mo re detailed discussion of the Na tionalComorbidity Survey sampling, designing, and weighting proceduresis presented in the overv iew of the surve y by Kessler er at. (1g).
The overa ll response rate for the survey was 82.4% . The distribution of demographic character istics in the samp le of 8,098 respon dents and in the U.S. population in the same age gro ups, acco rding tothe National Health Interview Survey, is presented in ta ble 1.
The contro l variables prese nted in Ihis analy sis arc primarily demograp hic variab les. Age represents the range of the overa ll sample , 15.54 yean. Two questions were asked to determ ine racclethnicity. Thefirst asked abo ut Hispanic backgrou nd and the second abo ut the selfperceptio n of racclethnicity (white, black , o r other). Responden tswho repo n ed a Hispanic background in respo nse to the firSt questionwere coded as such regardless of the ir answer to the secon d question .Level of education was deter mined by asking the respo nden t the number of yean of fonnal schoo ling she or he had com pleted. A hierarchyof coding rules was used to dete rmine employment status: all respo ndents who reponed tha t they were students wet(' coded as studentregardl ess of ether reponed categor ies; nonstu dent respo nden ts whoreponed being employed were coded as wo rking regardlCS$of otherrepone d categories; and nonstudent, une mployed respo ndents whorepo n ed being homemaken were cod ed as home maker regar dless ofother reponed categories. Income represen ts total family income before taxes during the year befor e the interview, includ ing salaries,wages, Social Security , welfare , and any o ther income.
Religious affiliations were grouped into Protestant, Catholi c, and"oth er " categories . Th e Catholic categ ory included Roman Catholic,Cat ho lic, Orthodox , Eastern Orthodox, and GreckJRuss ian Orthodox . "Other" included Christian Science, Jehovah 's WitnetSCs, Lat.rer-Day Saints, Q uaker , and Unita rian, as well u Jewish, M uslim, andEastern religions such as Buddhist and Hin du. For detenni ning ur-
Am] Psychiatry 151:7.]u/y 1994
~ epr odu c ed with pe rmiss ion of the co pyright owner . Furthe r re production prohibited without permission.
2

Bl.AZER. KESSl.ER,MCGONAGLE,ET AI..
TABLE 2. PrevalenceorCurrent(30-0,)') andLifetime MajorDepressiye Episode, by fbcelEthnicfty, Sex,and Ap, Fromthe NationalComor·bidity Surtey IN=8 ,09 81
Males Females Totol
RacelEthnicity ~ lifetime 30-Day Lifetime ~ Lifetime----and Age 'Yo' SE 'Yo' SE 'Yo' SE 'Yo' SE 'Yo ' SE %a SE
AU15-24 years 4.3 1.1 11.0 1.8 8.2 1.3 20.8 1.9 6.1 0.9 15.7 1.325-3 4 years 4.0 0.9 13.1 1.3 4.3 0.8 19.4 1.3 4.2 0.6 16.5 0.9JS-44 years 4.2 1.0 14.7 1.6 6.4 1.1 23.8 1.9 5.3 0.8 19.2 1.445- 54 years 2.3 0.8 11.8 1.9 5.0 1.0 21.8 2.3 3.6 0.7 16.7 1.5Total 3.8 0.5 12.7 0.9 5.9 0.6 21.3 0.9 4.9 0.4 17.1 0.7
White15-2 4 years 4.1 1.2 11.6 2.1 8.6 1.6 23.1 2.3 6.2 1.0 16.9 U25-3 4 years 4.3 1.0 14.0 1,4 3.5 0.5 19.6 U 3.9 0.6 17.0 1.135-4 4 years 4.7 1.2 15.2 2.0 5.7 1.1 24.2 2.4 5.2 0.9 19.5 1.845-54 years 2.6 1.0 12.7 2.0 4.8 1.1 23.1 2.9 3.7 0.8 17.9 1.6Total 4.0 0.5 13.5 1.0 5.4 0.6 22.3 1.0 4.7 0,4 17.9 0.8
Black15- 24 years U' 1.1 4.7 2.2 4.5 2.0 9.2 2.7 3.1 1.2 7.1 1.825-3 4 years 1.0' 0.9 9.0 4.1 5.6' 3.6 18.6 4,4 3.8' 2.3 14.5 3.335-44 yean 2.1' 1.1 5.9 1.8 9.7 3.1 21.1 4.5 6.4 1.9 14.9 3.345- 54 years 0.0 0.0 10.2 6.2 1.0b 0.7 9.0 3.9 0.5' 0.3 9.6 4.1Toul 1.2 0.5 7.2 1.9 5.7 1.7 15.s 2.2 3.8 1.0 11.9 1.6
Hispanic8.5'J5-2 4 years 5.1 10.8 5.1 12.7 4,4 22.6 5.7 10.5 3.4 16.5 3.6
25-3 4 years 3.7 1.6 10.0 3.2 7.5 3.2 19.8 4.2 5.7 1.8 15.1 2.235-4 4 years 3.0b 1.8 17.6 6.7 11.2' 6.1 30.2 9.0 7.3 3.5 24.2 6.045-54 years 3.1' 2.3 9.3 5.0 19.6' 11.4 30.2 11.7 8,4' 5.5 16.0 6.6Total 5.3 1.9 11.7 2.4 11.1 2.4 23.9 3.6 8.1 1.6 17.7 1.9
-Weighted to the population.bl ow precision, no p reval ence reported.
ban icity, persons were categorized as living in a large metropolitanarea iftheywerepartof the core of a standardmetropolitan statisticalareaof 250,000 personsor moreoron the fringe of such a metropolitan area. Small metropolitan area included individuals who wert inthe core or on the fringe of areas of fewer than 250,000 persons.Rural area included individuals who lived in ncnmerropohtan counties having fewer than 20,000 persons.
The one variable with a substantial amount of missing data wasincome. Acomplex, regression-based scheme was developed to assignesu mared values of income for cases in which data were missing.Missingdata for other variables were few but wereestimated as wellwhen necessary.
DSM-IJI ·R diagnoses were based on a modified version of theComposite International Diagnostic Interview (19). This structuredinterview was developed in a collaborative project of the WorldHealth Organization and the Alcohol, Drug Abuse, and MentalHealth Administration (20)to fosterepidemiologicandcross-cu ltura lcomparativeresearch by producing diagn oses according to both thedefinitions and criteria of DSM·Hl-R and the diagnostic criteria forresearch of ICD-IO. Diagnoses were generatedby che Composite International Diagnostic Interview computerprogram. "Pure major depressiveepisode," derived from the interview, is major depressionwithout current generalized anxi ery disorder, panicdisorder, phobia,substance abuse or dependence. manic episode, or non affecnve p s y ~chcsis. "Comorbid major depressiveepisode" is major depressionthat is diagnosed concurrent with any of the diagnoses just me ntioned. Dysthymia was not included as a comorbid diagnosis, since"double depression" is a unique condition char will be explored inseparateanalyses.
The approach to case ascertainmen t in the National ComorbiditySurvey, as compared to the useof the Diagnostic Interview Schedule(DIS) in the ECA study (21). is critical to interpretingthe results teported in thisarticle. First, there arc three stem questions in the Composite Imernational Diagnostic Interview, compared to one questionin ehe DIS,to elicit a positive responsethat can beusedin determininglifetime rates of major depression. These three questionswere placed
Am] Psychiatry lSl :7, ]u/y 1994
early in the interview,embedded ina seriesof questionsabout lifetimesymptoms so as co facilitate recall of previous depressive episodes,Fifty-sixpercentof the total sample reported at least one "ycs" tothese stem questions. In contrast, approximately 32% of the ECAstudy respondents gave a positive response to the stem question (22).In addition, the probability of identifying a case among individualswho gave a positiveanswer to a stem question was higherinthe NationalComorbidirySurvey thanin the ECAstudy, In the survey. 30%of persons giving a positive answer to a stem question received a diagnosis of major depression, comparedto approximately 20% in theECAstudy. Althoughthe ECA study used DSM-II1 ratherthanDSM·IIl-R criteria, the criteria for major depression in these two versionsof DSM arc virtually identical. Therefore. use of the revised editionof DSM·II1 in the National Comorbidiry Survey should have had noeffect on diffcrencrs in prevalence estimates.
Data analyzed in this article were obtained from a stratified, muitatage sample and were subsequently weighted to adjust for differential probabilities of selection andnonresponsc. As a resultof th is complex sample design and weighting, estimatesof standard error basedon the usual assumption of equal-probabilitysimple random sampling would be biased. Since more complex methods of analysis wererequiredto obtainappropriatestandarderro rs, estimatesof standarderrorsof proportions were obtainedbytheTaylorSeries linearizationmethod (23)_Adjusted ratesweredeveloped by usingmultiplelogisticregression, com roll ing for the demographic factorsthat were significant in the crude analyses.
RESULTS
A total of 394 of the 8,098 subjects (weighted numbers) included in the sample were diagnosed as havinga curr en t (30·day) episode of major depression, aprevalence of 4.9%. One hundred seventy-two respondents experienced a pure episode of major depression,
981
Reproduced with permission of Ihe copyright owner . Further reproduction prohibited without permission.
3
PREVALENCE OF MAJOR DEPRESSION
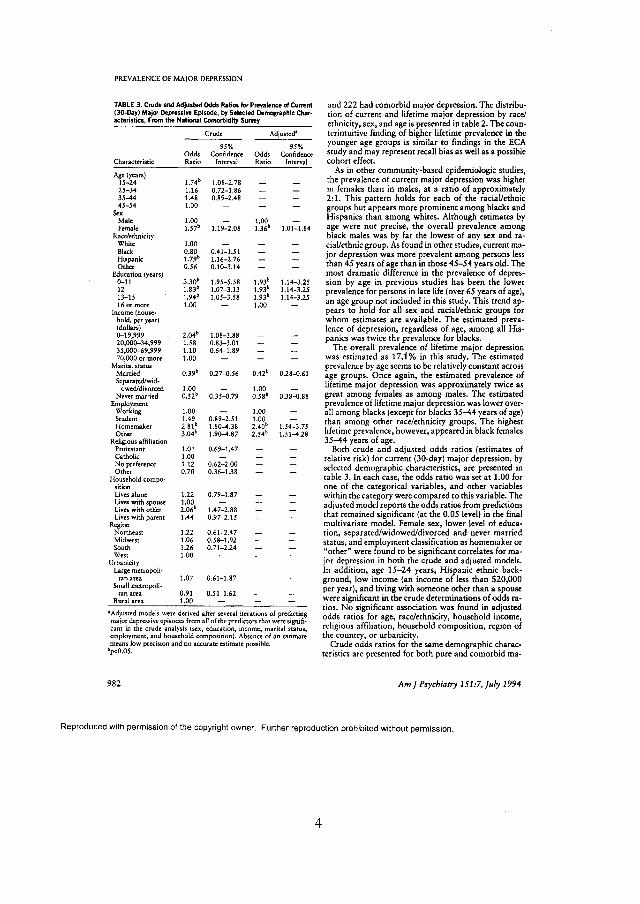
TABLE 3. CrudeandAdjusted OddsRltiOi forPrevalence of Current(30·00y) MajorDepressi.. Episode, by Selected Demographic Char.acteristlcs. From theNational Comorbidtty Survey
Crude Adjusted'
95% 95%Odds Confidence Odds Confidence
Characteristic Ratio Interval Ratio Interval
Age (years)1.74'15-24 1.08- 2.78
25-34 1.16 0.72-1.8635-44 1.48 0.89-2.4845-54 1.00
SexMale 1.00 - 1.00Female 1.57' 1.19-2.08 1.36' 1.01-1.84
Racezeehn iciryWhite 1.00Black 0.80 0.41- 1.51Hispanic 1.79' 1.16-2.76Other 0.56 0.10-3 .14
Education (years)3.30' 1.93'0-11 1.95-5 .58 1.14-3.25
12 1.83' 1.07-3.13 1.93' 1.14-3.2513-15 1.94' 1.05-3.58 1.93' 1.14-3.25160r more 1.00 - 1.00
Income [house-hold, per year)(dollars)
2.04'0- 19,999 1.08-3.8820,000-34,999 1.58 0.83-3.0135,000-69,999 1.10 0.64-1.8970,000 or more 1.00
Marital statusMarried 0.39' 0.27-0 .56 0.42' 0.28-0. 61Separated/wid-
owed/divorced 1.00 - 1.00Nevermarried 0.52' 0.35-0.79 0.58' 0.38-0.88
EmploymentWorking 1.00 - 1.00Student 1.49 0.89-2 .51 1.00Homemaker 2.81' 1.80-4.38 2.40' 1.54-3.75Other 3.04' 1.90-4.87 2.54' 1.51-4.28
ReligiousaffiliationProeestanr 1.01 0.69-1.47Catholic 1.00 -No preference 1.12 0.62- 2.00Other 0.70 0.36-1.38
Household compo-sitionLivesalone 1.22 0.79- 1.87Liveswith spouse 1.00 -Liveswith other 2.06' 1.47-2.88Lives withparent 1.44 0.97-2.15
RegionNortheast 1.22 0.61- 2.47Midwest 1.06 0.58- 1.92Soum 1.26 0.71-2.24West 1.00
UrbanlciryLargemetropoli-
tan area 1.07 0.61-1.87Smallmetr opo ll-
tan area 0.91 0.51-1.62Ruralarea 1.00
'Adjusted models were derived after several iterations of predictingmajordepressiveepisodes from allof the predictors that weresignifi-cant in the crude analysis (sex, education. income, marital status,employment, and household composition). Absence of an estimatemeans low precision and no accurate estimatepossible. .
' p<O.05.
982
and 222 had comorbid major depression. T he distr ibution of current and lifetime major depress ion by racelethniciry , sex, and age is presented in table 2. The counterintuitive finding of higher lifetime prevalence in theyounger age groups is similar 10 findings in the ECAstud y and may represent recall bias as well as a possiblecohort effect.
As in other community-based epidemiologic studies ,the prevalence of current major depre ssion was higherin females than in males , at a ratio of approximately2:1. Th is pattern holds for each of the raci al/ethnicgroups but app ears more prominent among blacks andHispanics than among whites . Although estimates byage were not precise, the overall prevalence amongblack males was by far the lowest of any sex and racial/ethnic group. As found in other studies , current major depressio n was more prevalent among persons lessthan 45 years of age than in those 45-54 years old. Themost dramatic difference in the prevalence of depression by age in pre vious studies has been the lowerprevalence for persons in late life (over 65 years of age),an age group not included in this study . This trend appears to hold for all sex and racial/ethnic gro ups forwhom estimates are available. The estimated prevalence of depre ssion, regardless of age, among all Hispanics was twice the preval ence for blacks.
The overall prevalence of lifetime major depressionwas estimated as 17.1 % in th is study. The estimat edpreval ence by age seems 10 be relat ively constant acrossage groups. Once again, the estimated prevalence oflifetime major depression was approx imately twice asgreat among females as among males. The estimatedprevalence of lifetime major depression was lower overall among blacks (except for blacks 35-44 years of age)than amon g other race/erhniclry groups. The highestlifetime prevalence, however, appeared in black females35-44 years of age.
Both crude and ad justed odds ratios (estimate s ofrelative risk) for current (30-day) major depression, byselected demographic characterist ics, are presented intable 3. In each case, the odds ratio was ser at 1.00 forone of the ca tegorical var iables, and other variableswithin the category were compared to this var iable. Thead justed model reports the odds ratios from pred ictionsthat rema ined significant (at the 0.05 level) in the finalmultivariate model . Female sex, lower level of education, separated/widowed/d ivorced and never marriedstatus, and emplo yment classification as homemaker or"other" were found to be significant correlates for major depre ssion in both the crude and adjusted models.In addition , age 15-24 years, Hispanic ethn ic background, low income (an income of less than $20 ,000per year), and living with someone other than a spousewere significant in the crude determinations of odds ratics . No significant associat ion was found in adjustedodds ratios for age, race/ethniciry, household income,religious affiliat ion, hous ehold composition , region ofthe country, or urbaniciry.
Crude odds ratios for the same demographic characteristics are presented for both pure and comorbid rna-
Am] Psychiatry 151:7, ]uly 1994
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.
4

BLAZER, KESSLER, MCGONAGLE,ETAL.
TABU 4. Crude Odds Ratios for Prevalence of Current (3o-D.ay) Pureand Comorbid MajorDepressive Episode. by Selected DemographicCharac1eristics. Fromthe National Comorbklity Survet
Pure ComorbidDepressive Episode Depressive Episode Comorbid Versus Pure
95% 95% 95%Odds Confidence Odds Confidence Odds Confidence
Characteristic Ratio Interval Ratio Interval Ratiob Interval
Age (years)15-24 1.03 0.46-2.26 3.00' 1.43-6.30 2.86 0.85-9 .6025-3 4 0.85 0.47-1.56 1.71 0.72-4 .05 1.98 0.66-5 .9435-44 0.76 0.35-1.66 2.80' 1.21-6.45 3.57' 1.06- 12.0145-54 1.00 - 1.00 - 1.00
SexMale 1.00 - 1.00 - 1.00Female l. S6( 1.09-2.22 1.56' 1.03-2 .35 1.00 0.58-1 .70
Rece/erhniciryWhite 1.00 - 1.00 - 1.00Black 0.36" 0.21-0.63 1.22 0.56-2 .65 3.32' 1.51-7.31Hispanic 1.19 0.68-2.08 2.31' 1.29-4 .15 1.90 0.85-4 .25Other 0.25' 0.07-0.88 0.86 0.10-7.66 3.40 0.19-6.26
Education(years)0-1 1 1.69 0.75- 3.77 6.82c 2.71-17.19 3.93c 1.10-14 .0212 1.12 0.56-2.22 3.45" 1.50-7.95 3.04' 1.12-8.2013-15 1.13 0.56-2 .26 3.79c 1.51-9 .53 3.30' 1.18- 9.1716 or more 1.00 - 1.00 - 1.00
Income (household, per year) (dollars)0-19 ,999 1.60 0.62-4.17 2.48 0.80-7.68 1.53 0.33-6 .9920,000-34,999 1.30 0.49-3.45 1.87 0.58-6 .03 1.43 0.29-7 .0635,000-69,999 0.82 0.35-1.92 1.43 0.53-3.85 1.73 0.44-6 .8270,000 or more 1.00 - 1.00 - 1.00
MaritalstatusMarried O.42c 0.22-0.79 0.39' 0.23-0.65 0.94 0.40-2.2 1Separated/widowed/divorced 1.00 - 1.00 - 1.00 -Never married o.sr- 0.28-0 .93 a.56' 0.31-1.00 1.11 0.47-2.59
FmpJoymentWorking 1.00 - 1.00 - 1.00Student 1.17 0.57-2 .42 1.75 0.88-3.4 5 1.48 0.58- 3.74Homemaker 2.S3' 1.26-6.35 2.61c 1.55-4 .39 0.92 0.35-2 .40Other 1.76 0.93-3 .33 4.03' 2.09-7.77 2.19 0.87-5.47
ReligiousaffiliationProtestant 1.06 0.64-1 .77 0.96 0.55-1.69 0.91 0.43-1.93Catholic 1.00 - 1.00 - 1.00 -No preference 1.50 0.57- 3.99 0.84 0.43-1.64 0.57 0.18-1.85Other 0.63 0.26-1.52 0.76 0.28-2 .08 1.20 0.32-4 .56
Householdcompositionlives alone 1.48 0.55-4 .02 1.00 0.63-1.58 0.68 0.20-2.32Liveswithspouse 1.00 - 1.00 - 1.00 -Liveswithother 1.83c 1.07-3 .12 2.16' 1.27-3 .69 1.17 0.52-2.66Liveswith parent 1.26 0.71-2.23 1.57 0.91-2 .73 1.24 0.57-2 .70
RegionNortheast 0.81 0.46-1.44 1.60 0.47-5.39 1.93 0.53-7 .04Midwest 0.93 0.55-1.56 1.18 0.40-3 .48 1.27 0.40-4.03South 1.25 0.83-1 .89 1.25 0.43-3.63 1.00 0.34-2.95We" 1.00 - 1.00 - 1.00
UrbaniciryLargemetropolitan area 1.05 0.52-2 .11 1.08 0.57-2 .02 1.02 0.50-2 .09Small metropolitan area 0.86 0.40-1.87 0.95 0.51-1.77 1.10 0.52-2.34Rural area 1.00 - 1.00 - 1.00
aAIlodds ratiosare adjusted estimates.bOddsratioof the odds ratios forcomorbid and puremajordepressiveepisode.cp<O.OS .
jar depression in table 4. The last column repr esents the lence estimates for both pure and comorbid depressionratio of the odds rat ios for como rbid versus pure major were higher for females than for males, for the otherdepress ion by these same categories and shows whether facto rs the estimates were less likely to coincide. Blacksthis ratio of ratios is significant. The pattern of crude were less likely to be depressed ingenera l, but during aodds ratios for pure versus comorbid major depression single episode they were more likely to have a como rb idexhibits subs tantial varia bility . Although the preva- disord er. Hispanics had higher crud e rates of como rbid
Am] Psychiatry151:7,]u/y 1994 983
Reproduced with permission of the copyrigh t owner. Further reproduction prohibited without permission .
5
PREVALENCEOF MAJOR DEPRESSION
depression than ot her racial/ ethn ic gro ups, and amo ngth emselves they demon str ated a trend toward higherrates of comorbid than pure depression . A lower levelo f edu cat ion was a risk factor for co mo rbid depression ,and at the level of less than 16 yea rs, the odds rat io forcom orbid depr ession was signi ficantl y higher than forpure depre ssion . H omemaker status was signi ficantlyrelated to both pure and co morbid depre ssion, al th ou gh neith er ty pe of depre ssion predom inat ed amongho memakers . Living w ith another person wa s a significant correlate of comorbid as well as pure depression,but thi s associatio n disappear ed in the ad justed ana lyses, where factors such as marital status co nfo unded theassociation, since the prevalence of depression was highamo ng wo men living with children but not for wo menliving with th eir spo uses . Th e 15- 24 and 35-44 agegroups were mo re likely than older indivi dua ls to havecom orb id depression; in the 35-44 age gro up, cornorbid depr ession pred om inated.
DISCUSSION
Prevalence estimates for current and lifetime majordepre ssion in th e Na tion al Co morbidity Survey wer ehigher than those in the ECA st udy bu t similar to thosefound with the Sched ule for Affective Disor de rs andSchizoph renia/Research D iagnostic Criteria ap proa chto case finding in a comm unity survey of New Haven,Co nn. (4 , 6 ): 4 .9 % versus 4.3 % for current prevalenceand 17 .1% versus 20 .0% for lifet ime prevalence in theN ati onal Co mo rbidity Survey versus the New Havenstudy.
To place in context these prevalence estimatesof major depr ession fro m a larg e nat ion al sample (which usedcase-ide nti ficatio n procedures that are somewhat butnot dramaticall y different from those used in previouslarge surveys wit hin the Un ited States), three topic ssho uld be addressed . First, the higher pr evalence esti mate s of curren t and lifetim e majo r depression in theNatio na l Co mo rbidity Survey, compared to the ECAstud y, should be exp lored. Second, th e risk facto r pro file fro m th e N at ion al Com orbidity Survey overallsho uld be com pared w ith the exist ing literature on major depression rega rding risk fact ors. T hird, the d ifference in the risk facto r pr ofiles of pure ma jor depressionan d como rb id major depre ssion sho uld be address ed.
A number of factor s may hav e co ntributed to thehigher pr evalence o f maj or depr ession in the Nat ionalCo mo rbi dity Surv ey as com pa red to the ECA study .O ne possibili ty is tha t the approach to probi ng fo r anepisode of major depressio n led to a higher proportiono f true lifetime cas es being reported in the survey. Thisco uld have occurred becaus e each respond ent was giventhree chances to respond to a stem question for majordepr ession (ques tio ns asking abo ut episodes of feeling"sad, blue, or depressed," feel ing "down in the dump sand gloo my, " and " losing int erest in th ings you usuall yenjoy ") rather than the one que stion in the DIS. A seco nd possibility is that th is more detailed pr ob ing caused
984
overrepo rti ng and false positives. In an effort to investigate thi s possi bility, a br ief Composite Intern at ionalD iagn ostic Interview/major depressive episode validation was perform ed in rhe Nation al Co mo rbidi ty Sur vey. T hirty person s from the survey-20 wh o reporteda lifet ime h istory of major depression accord ing tothe structured inte rview and 10 wh o gave a positive an swer to a stem question for ma jor depr ession but failedto meet th e DSM-I11-R criteria - were reinterviewed,These va lidat ing interv iews were performed by clin icians, blind to the Co mposite International DiagnosticIn terview diagnosis, who used th e Structured Clin icalInterview for DSM -m-R (SCID) (24 ). Fourteen (70 %)of the 20 subj ects who had lifetime ma jor depressionaccording to th e Co mposit e International Dia gn osticInterview wer e classified as hav ing lifetime ma jor depre ssion acco rding to the SCID , while eight (80 %) ofth e 10 cla ssified as not hav ing lifetime ma jor depre ssionby the interview wer e clas sified the same wa y by theSCID. These va lida tio n resul ts ar e simil a r to th os efound for major depression accord ing to the DIS in theECA study, in wh ich findings from a structured qu estionnaire were compared w ith tho se from a standardized diagnostic interv iew . Differences in prevalencebetw een the ECA study and th e N at ion al ComorbiditySurvey therefo re may result from th e use of a differe ntva lidation instr ument, the scm, in th e Nation al Comorbidity Survey. In additio n, the resul ts of the ECAvalida tio n srudies varied widel y (25 , 26) .
There ma y be ad d iti o nal reas ons fo r th e greaterpreval ence o f major depression in the N ati on al Cornerbidi ty Survey. Fir st , indiv id ua ls in the sa m ple wereyo unger, an d therefo re the overall rat es wo uld be expecte d to be higher , given th at th e lowest rat es for major depress ion were am ong the o ver~65 age gro up in theECA sam ple (l ). Seco nd , secul a r tre nds could also account for these differences, as the Nation al Co mo rbidity Surv ey was con ducte d approxi mately 10 years afterthe ECA study (3). T his explanation , ho we ver, is mored ifficu lt to defend , since the inte rva l of 10 years isvery short for o bservi ng bistorical tre nds. Theref ore,th e best ex planation is a meth od olog ical one, namel y,that the Co mposite International Diagnostic Interviewis a mor e sensitive instrument than the DIS in community population studies . A tbird possible reason for thediscrep ancy between the prevalen ce estima tes of thetwo st udies is tha t a nat ional sam ple may yield a higherpr evalence than adjusted rates from local surv eys, whichwere used in the ECA study.
Another issue to be addr essed is the o vera ll ris k fact orp rofil e o f major depre ssion in th is study compared toother studies of ma jor depress ion . The co nsensus frommost co mmun ity -based ep idemiologic stud ies is that 1)younger person s a re at greater risk for ma jor depressionthan older per son s; 2) blacks are som ewhat less at riskthan whites; 3 ) wom en are at greater risk for majordepression than men; 4 ) person s of a lower socioeconom ic status are at greater risk than those w ho aremor e well -off econ om ically ; 5) pers on s who are separat ed or div orced have higher rates of maj or depression
Am ] Psychiatry 1S1:7,]uly 1994
Re pro du ced with permission of the co pyrigh t owner. Fu rthe r reproduction prohibited witho ut permission .
6

than persons who are married or have never married;and 6) persons in urban areas are at greater risk thanpersons in rural areas (3, 4, 6,27-30). The risk factorprofile for J-month prevalence could vary from the profile for 6-month or I -year prevalence. However, it isprobable that comorbidiry would be even greater forthe latter . Therefore, the I-month estimate of comerbidity is a lower -boundary estimate of the percentage ofpersons with comorbid depress ion.
In general , the risk factor profile from the NationalCom orbidity Survey does not var y from the profilefound in other epidemi ologic studies. There are, however, two excepti ons. First, the lower prevalence of major depre ssion in rural ar eas compared to urban areasthat was reported from the ECA study (27) was notreplicated in this study . The reason for this differencemay be that in the ECA study, urba n-rural differenceswere comp ared in areas where the urban and ruralcounties are conterminou s, as opposed to comparisonsfrom a nationwide sample. Urban versus rural factorsvary considerably by region of the country. Unless urban-rural comparisons are made in the same geographic area, urban-rural differences may be obscuredby other geographic and demographic factors such asregion of the country. Second, the finding of a muchhigher prevalence of major depression among homemakers than among persons in other categories of employment has not been reponed in most major surveysbut accord s with the work of Brown and Harris in England . These investigators, in a much smaller study (3J ),found an exceptionally high pr evalence of depressionam ong homem akers with small children as comparedto other women .
The final topic to be discussed relates specifically tothe purpose of the N ati onal Com orbidity Survey,namely, to determine the comorbidity of psychiatricdisord ers and consider var iations in the risk factor profiles for pure versus comorbid expre ssions of those disorders. Therefore, the National Comorbidity Surveybreak s new ground in cons idering risk factor profiles ofpure versus comorbid major depression. The findingsare striking. Many risk factor s that have been associated with major depression, i.e., younger age, lowerlevel of education, and lower income, were associatedwith major depressi on only among persons with comorbid, as opposed to pure, major depr ession. In contrast, one pot ential risk for major depression , nonbJackracelethnicity, was found for pure but not comorbid depression. Could it be that comorbid major depression isa more environmentally dr iven disorder (even thoughthe symptoms of major depr ession in thi s circumstanceare similar to tho se of pure major depress ion) ?Stressorsin the environment that lead to the symptoms of majordepression may also lead to symptoms of anxiety andother psychiatric disorders, such as substance and alcoho l ab use, suggest ing a maj or etiologic role forpsychosocial adversity in many of the more prevalentdisorders. In contrast, individuals with pure major depression may be expressing a disorder less affected bypsychosocial stress or perhaps a unique profile of psy-
AmJ Psychiatry 15J:7.July /994
BLAZER.KESSLER. MCGONAGLE,ET AL.
chosocial correlates. The higher prevalence of depr ession in females and am ong homemakers is apparent forboth pure and comorbid depression.
ACKNOWLEDGMENTS
The National Comorbidiry Survey (Ronald G. Kessler. PrincipalInvestigator) is a collaborative epidemiologic investigation of theprevalence, causes, and consequences of psychiatr ic morbidity andcomorbidi ty in the United States. Co llaborating Na tional Comorbid·icy Survey sites and invest igators are: The Addiction Research Foun dation (Robin Room) ; Dulce University Med ical Center (Dan Blazer.Marvin Swarul;J oMs Hopkins University Uarms Anthony, WilliamEaton, Philipleaf); the Max Planck Institute of Ps)'chiarry (Hans -Ulrich Winchen); the Medical College of Virginia (Kennelh Kendler);the University of Michigan (lloyd j ohns ton, Ronald Knslcr ); NIMH(Darrell Kirsch. Dam: 1Regier); New York Uni vc~i ty (Patrick Shrout);State University of New York at Stony Brook (Evelyn Brometh Universiry of Tcreme (R.JayTurner); and Washingt on University Schoolof Medicine (Linda Cottier).
REfERENCES
1. RegierDA , BoydJH, BurkeJD Jr, Rae DS, MyersJK, Kramer M,Robins LN, George LK, Kam o M, Locke BZ: One -month prevalence of mental disorders in the United States: based on five Epidemiologic Catchmenr Area sites. Arch Gen Psychiatry 1988; 45:977-986
2. Wells KB, Stewart A, Hays RD, Burna m MA, Rogen W, Dan ielsM, Berry S, Greenfield S. Ware J: The-funct ioning and well-beingof depressed pat ients: results from the Medical Outcomes Srudy.JAMA 1989,262,914-919
3. Cross-National Co llaborative Group: Th e changing rare of major depression: cress -national comparisons. JAMA 1992; 268:3098-3105
4. Weissman MM , Myers JK: Affective disorde rs in a US urbancommun iry: the use of Research Diagnostic Criteria in an epidemiologic survey. Arch Gen Psych iatry 1978; 35:1304-1311
5. Blazer 0 , WiUiams CD: Epidemiology of dysphoria and dep ression in an elderly population. Am) Psychiatry 1980; 137 : 439 ~
6. Myers JK, Weissman MM , TIschler GL, Holur CE Ill, leaf Pl,Orvaschel H, Anthony Je, Boyd JH , Burke JO Jr, Kramer M,Srolnman R: Six-month prevalence of psychiatric disorder s inthree communities: 1980 to 1982. Arch Gc:n Psychiatry 1984;41,959-967
7. Re-gierDA, MycrsJK , Kramer M, Robins LN, Blazer DG, HoughRL.,Eaton WW, Locke BZ: The NIMH Epidemiologic Catchment Area program: historical context. major objectives, andstudy population characteristics. Arch Gen Psychiatry 1984; 41:934-941
8. Murph y jM, Sobol AM, Neff RK, Olivier DC, Leighton AH,Stability of prevalence: depression and anxiety diso rders. ArchOen Psychiatry 1984; 41:99()-997
9. Robins LN, Helser JE, Weissman MM , Orvaschel H, GruenbergE., Burke JD Jr, Regier DA: Lifetime prevalence of specific psy·chiatric disorders in thr ee sites . Arch Cen Psychiatry 1984; 41:949-958
10. Orn H, Newman se, Bland RC: Design and field methods of theEdmonton Survey of P,ychiauK:Disorders . Acta Psychiatr Scand(Suppl) 1988; 38;17- 23
11. Canino GJ. Bird HR, Shrout PE: The prevalence of specific psy·chiatric disorders in Puerto Rico. Arch Gcn Psychiatry 198 7; .... :727- 735
12. Faravelli C, Degl'Ien ocent i BG, Aiaui L, Incerpi G, Pallanti S:Epidem iolog y o f mood d isorders: a co mmunity survey inFl or ~ nce.J Affect Disord 1990; 20:135- 141
13. W,II.jE, Bu.hn,lIjA. Homblow AR,joycePRoOakley-BrowneMA: Christchurch Psychiatric Epidemiology Srudy, part I: methodology and lifetime prevalence for specific psychiatr ic dlsorders . Aust NZ J Psychiarry 1989; 23:315-326
985
Reproduced with permissi on of the copyright owner. Further reproduction proh ibited without permission.
7

PREVALENCE OF MAJOR DEPRESSION
14. Hwu HG. Yeb EK, Chang LY: Prevalence of psych iatr ic disorders in T aiwan defined by the Ch inese Diagnostic InterviewSchedule. Acta Psychiatr Scand 1989; 79: 136-147
15. Allgulander C: Psychoacti ve dru g use in a genera l populationsample, Sweden: corr elate s with perceived health, psychiatric diagnoses, and mortality in an automated record-linkage study.Amj Public Health 1989; 79,1006-1010
16. Eaton WW, Anthony j C, Tepper S, Dryman A: Psychop athologyand attriti on in the Epidemiologic Catchment Area Study. Am JEpidemiol 1992; I3 H 05 1- 1059
17. US Departm ent of He alth and Human Services: National HealthInterview Surve y, 1989 (computer file). Hyatt sville, Md, National Center for Health Statisti cs. 1992
18. Kessler Re,McGonagle KA, Zhao S, Nelson CB, Hughes M,Eshleman 5, Winchen H, Kendl er KS: Lifetime and 12·monthpreva lence of DSM-III-R psychiatric disorders in the UnitedStates: results from the Na tional Co morbldiry Survey. Arch GenPsychiatry 1994; 51 :8-19
19. World Health Organization : Com posite Interna tional Diagnos tic Interview (CIDI, Version 1.0 ). Geneva , WHO, 1990
20 . RobinsLN, WUl8J, Wincl>en 00, Holur J£, The Composite laternational Diagno stic Interv iew: an epidemiologic instrument suitable for use in conjunctio n with d ifferent diagn ostic systems andin different cultures. Arch Gen Psychiatry 1988 ;45:1069-1077
21. Rob ins LN. Helzer JE.Croughan J. Ratcliff KS: The Na tionalInstitute of Mental Health Diagnostic Interview Schedule: its history , charac teristics, and validi ry. Arch Gen Psychiatry 1981 ; 38 :381-389
22 . Weissman MM, Bruce ML, Leaf P], Flor io LP, Holzer C: Affecw
rive disord ers. in Psychiatric Disorders In America. Edited byRegier DA, Robin s LN. New York, Free Press, 1991
986
23. Woodruff RS, Cau sey BD: Computerized method for appr oximating the variance of a comp licated estimate. 1Am StatisticalAssoc 1976; 71 ,315 -321
24 . Spitzer RL, WilliamsJBW, Gibboo M, Fin, MB,The StructuredClinica l Interview for DSM·llI-R (SCID), I: history, rat ionale,and descrip tion. Arch Gen Psychiatry 1992 ; 49:624--629
25 . Helzer JE, Robins LN, McEvo y L], Spitznage l EL,Stolnman RK,Farmer A, Brock ington IF: A compa rison of clinical and Diagnosric Interview Schedule diagnoses: physician reexam inatio n oflay-interv iewed cases in the general population. Arch Gee Psychiatry 1985 ; 42 ,657-666
26 . Anthonyle ,Folstein M, Romanoski AJ, Von Korff MR, NestadtC R, Chahal R, Merchant A, Brown CHI Shapiro S, Kramer M,Gruenberg EM : Comparison of the lay Diagnostic Interv iewSchedule and a srandardized psychiatric diagn osis: exper ience ineastern Baltimore . Arcb Gen Psychiatry 1985 ; 42 :667-675
27. Blazer D. George LK. Lend erman R. Pennybacker M, MelvilleML, Woodbury M, Man ton KG, Jordan K, Locke B: Psychiatr icdisorders: a ruraVurban comparison . Arch Gen Psychiatry 1985;42 ,651-656
28. Somervdl PO, Leaf PJ, Weissman MM, Blazer DG, Bruce ML:The prevalence of ma jor depress ion in black and white adults infive United Srates cornmunines. AmJ Epidemiol 1989 ; 130:725735
29 . Tennant C: Femal e vu lnerability to depression. Psychol Med1985; 15,133-737
30. Jorm AF: Sex and age differences in depress ion : a quantitativesynthes is of published research. Aust NZ 1Psychiatry 1987; 21:46-53
31. Brown CW, Harris T : Social Or igins of Depressi on : A Study ofPsychiat ric Diso rder in Women. New York. Free Press, 1978
Am J Psychiatry 151:7, July 1994
Reproduced with permission of the copyrighl owner. Further reproduction prohibited without permission .
8

Article
Comparing Age at Onset of Major Depressionand Other Psychiatric Disorders by Birth Cohorts
in Five US Community PopulationsKimberly Christi e Burke, MS; Jack D. Burke, I t. MD, MPH; Donald S. Rae, MS; Darrel A. Regier, MD, MPH
• Using data collected in the National Institute of MentalHealth (Rockville, Md) Epidemiologic Catchment Area Program, we examined the proposed hypothesis that there hasbeen a shift in major depression to younger ages at onset,or increased prevalence in younger age periods, for recentbirth cohorts. life-table survival methods were used to examine the hazard rates for major dep ression as well as forother specific mental disorders. The findings are consistentwith a gradual shift to increased rates for major depressionbetween the ages of 15 and 19 yea rs for Epidem iologicCatchment Area respondents born more recently. The findings also suggest a similar shift for drug abuse/dependence;similar but less pronounced changes were found for alcoholabuse/dependence and obsessive-compulsive disorder.However, in thi s study, bipolar disorder, panic disorder, andphob ias did not exhibit a cons istent increase in onset atyounger ages . Further research is requ ired to determine ifthe shifts in major depression, drug abuse/dependence, andpossibly alcohol abuse/dependence are linked . It is irnportantto note that these shifts to adolescent onset are occurring when nearly half the 31 million Americans withouthealth insurance are aged 24 years or younger.
(Arch Cen Psychiatry. 1991 ;48:789-795)
A recent life-table an alysis of the age at onset of mentaldi sorders am ong respondents from th e Nationa l In
sti tu te of Men tal Health (NIMH, Rockville , Md) Epidemiologic Catchment Area (ECA) Program'" suggested theimportance of on set in adolescence and early adulthoodfor several specific mental d isorders, including major depression.tThis find ing is consistent with the suggestion byK1erman et al..11and othe rs":" that members of recent generations are displaying higher rates and/or younger agesat onset for major depression compared with members ofolder generations.
K1erman and Weissm an ll recently reviewed evid ence sug-
AccepledT6Tpublication September 20, 1990.From the Office of the Institute Director (M s Burke) , Division of
'-:,":l : ,.,, ~ ~ _ , .r c. ~ _ :. ~, ~, ':'. ~ ~ ~ .., ~,.. t. I l""\ ~ 'l . ~ I.: ~ \ ~ ... ~ n :,,: ')i,... ... 'if C': .., ! r.~ 1
Health , Rockville . ,v'0 . ,V\SBurxe ISnow wr tn sco« anc ~"'m l ;:e ~ ; , (; l <': ,
Temple, Tex.Reprint requests to Scott and White Clinic, 2401 5 31st 51, Alexander
Bldg, Temple, TX 76508 (Ms Burke).
.ArchGen Psychiatry-Vol 4B, September 1991
gesting an increase in the rate of major depression amongpeople born since World War II. In 1976, K1erman' hypothesized that western societies were entering an "Age of Melancholy" and reported that clinical depression was increasing in adolescence and young adulthood. Later, results froma longi tudinal study conducted between 1947 and 1972 inLundby, Sweden , demonstrated that the probability of suffering a mild or moderate case of depression increased during that 25-year period for both sexes ." More recent studiesexamining relatives of patients ha ve also reported evidencein support of increased rates of major depression,' earlieronset of major depression in successive birth cohorts ," and astatistically significant difference between the hazard ratesfor major depression developing for patients born before1940 and patients born after 1940." Simillrly, a-study examinin g ho spital reco rds in Zurich, Switzerland, reported thatth e number of admissions for major depression increasedsubstantially from 1920 to 1982," Most recently, Wickramara tne et al" examined birthcohort trends am onga subsampleof N IMH ECA respondents. For the 10640 white ECA respondents, the y reported increased rates of major depressive episode for both men and women born after 1935, withevidence of a peri od effect on respondents of all ages after1960.
Three studies have also examined data relative to bipolar disorders . Angst's" study of Zurich admission recordsalso showe d increases for bipolar d isorder since 1920, andtw o reports exami ning relatives in famil y studies havesuggested increases for bipolar I disorder" or a categorycombining bipolar and sch izoaffective disorders ."
Although findings from these recent investigations suggest a temporal change in recent generations, with ma jordepression and possibly bipolar disorder having earlier agesat onset and/or higher rate s than had been true in oldergenerations, the studies ha ve to varying degrees been subject to two limitations. First, these studies generally have notexamined other nonaffective disorders to investigatew hether the shift to earlier ages at onset is a generalphenomenon displayed in all disorders or perhaps a meth,-delo"': crtifac!. '3 ~ C0 ,.. . d , these stud ies typ ically have notused large, represent at ive general population samples. ;.
To address these problems, this analysis exammes selected Diagnostic Interview Schedule (DIS)-DSM-lII psychi atric d isorders, in addition to major depression, in the
Age at Onset-Burke et al 789
9

' •.:L: . ,-,MH ECA sa mple of community and in sti tutionalre sidents in terms of two qu es tions , (1) Fo r m ajor d epression, has there b een a sh ift to you nger ages at onset inmore recent birth co horts? (2) Has any suc h sh ift for majo r d epression been m at ch ed by similar shifts for otherdi sorder s , incl u d ing drug or a lcohol ab use/depend ence,th e anxie ty di sorders , o r bi p olar disorder? In this analysis , self-reported onset ex p erie nce for th e firs t 30 yea rs oflife will be co m p a re d fo r all NIMH EC A re spondentsgrouped in to fo u r birth cohorts ove r the p ast century.
SUBJECTS AND METHODSNIMH ECA Program
Th e da ta used to ana lyze the hypothesized shift in the age atonset and/or the increase in rates for major depression w ere collecte d as part of the NIMH ECA Program . The NIMH ECA Program was a combined hou sehold and insti tu tional survey ofmental disord ers conducted in five sites throu ghout the UnitedState s, and it has been described in detail elsewhere.""" Thisanalysis is based on data from 20 745 hou sehold and institutionalres po nde nts who were aged 18 yea rs and olde r at time of entryint o the study . Data were exclude d for an addi tional 116 resp ondents for whom year of birth was missing.
Diagnoses of specific ment al d isorders were mad e using theDIS." Designed for use by no nclinicians in epidemiologic studies, thi s instrument uses self-reported informati on about symptoms to make diagnoses of specific mental disorders based onDSM-lI/ criteria." If a positive diagnosis can be made based onth e symptoms rep orted, an inquiry is made to determine th e ageat first occurre nce of the symp toms. Although it is possible thatthis first occurrence may not have been seve re eno ugh to passth e threshold for a DSM-1lldiagn osis, tha t initial episo de is generally used as the o ~ for da ting onset of the disorder in theNIMH ECA da ta se t and appears to be most relevan t for datingonset in general.7,II .n
The NIMH ECA Progra m invo lved complex multi stage sampling procedures" : therefore, the respondents have beenweig hted to reflect th eir probab ility of selection and then havebeen weighted to th e 1980 US Census on the basis of age , sex,and racelethnicity as described previously,16,21
life-Table Survival Methods
Life-ta ble survival methods, similar to those used in a recentexamination of the age at onset of mental disorders in the N IMHECA.' were used to compare the age at onset of selected mentaldisorders by birth cohorts. Surviv al meth ods were used toexamine average yea rly hazard rates for specific 5-year agein tervals. A hazard rate gives th e probability that a disorder willdevelop during a time interval in a respondent who en ters thatin terval and who is free of a disord er at the begin ning of tha t intervaJ.7·22.2J In this analvsis, the time interval was defined as arange of 5 years during which age at onset could occur, for example, 15 to 19 yea rs or 20 to 24 year s .
Using th e Statisti cal Package for the Social Sciences (SPSS)Survival progra m." hazard rates to age 30 years were examinedacross four birth cohorts . The birth cohorts examin ed were thoseborn before 1917 (unweighted n = 6566), betwe en 1917 and 1936(n = 4432), betwee n 1937 and 1952 (n = 4981), and between 1953and 1966 (n = 4766). Using an observa tion pe riod from birth to30 years of age allowe d the comparison of each birth coho rt forequivalent periods of risk; 30 years was the oldest age possiblefor a respond ent born in the youngest birth coho rt (1953 to 1966)at th e time of int ervi ew . The younges t birth cohort is th e onl y onewhose members may have bee n less than 30 years of age, but lifetables have the advantage of adjusting for the fact that subjectshave different ages, or, in analogy to treahne nt outcome studies, that they have bee n followed up for differen t pe riods ."
For each disord er, the hazard rates of the four birth cohortswere compared using the Lee-Desu" statistic, which follo ws a X]distribution with g - 1 df, where g is the number of groups un-
790 Arch Cen Psychiatry-Vol 48, Septemb er 1991
der comparison. This approach tests whether the distribution sof ons et in the first 30 years of life for the fou r birth cohorts we redrawn from the same population or we re sign ificantly differen t.It compares th e pr obabilities in the coh orts in all age int ervals simultaneou sly" and is similar to othe r anal yses of the coho rt eff eet . 1 5 .2 ~ However, there is no method (eg, based on proportionalhazards models) to test specifically for shifts in the peak age atonse t wh ile ap plying the complex weig hts of the ECA data."Rather than using unw eight ed data, which would be inapp ropriate for th e total ECA sample, we have relied on a graphic approach to identify appa rent shifts in peak age at ons et ." However, these apparent shifts cannot be tested for statisticalsignificance by th is approa ch."
The SPSS softwa re program appropriately weighted the databased on the samp ling procedures to produce estimates of hazard rates . However, the program cannot accurately de termineth e varia nce associated with comp lex sampling design s like thatused in the NIMH ECA Progra m. Therefore, two adjus tme ntswere necessary before tests of significa nce could be performedto determine if the onse t experie nce differed by birth cohorts.'Firs t, to assure that the sampling weig hts did not inflate the statistica l power of comp arison s, the weighted ' sam ple was ad justed to the same size as the total actua l sample; to accomplishthis , the sampling weig ht used for th e five sites was mul tipliedby the number of resp ond ent s in the NIMH ECA sample andth en divid ed by the 1980 US Census po pu lation . Second , the x'test statistics were divided by the es tima ted sample design effectbefore calculation of Pvalues. This conservative adjustm ent wasdon e based on repeated estimates of th e design effect for pr evalences in these condi tions that ranged from 1.5 to 2.0' ·",; thesedes ign effect estima tes were produ ced by th e programSESUDAAN" deve loped for analyzing such complex surveys.These adjustments are equivalent to reducing the samp le size bythe design effect. "
RESULTS
Hazard rates were plotted and compared for sta tistically significant differences. The four cohorts examined will be referred to ascohort 1 (respondents born betwe en 1953 and 1966), cohort 2 (respon den ts born betwee n 1937 and 1952), cohort 3 (respondentsborn between 1917 and 1936), and cohort 4 (respo nde nts born hefore 1917). These cohorts were similar to those used by Weissma net al" in the initial analysis of NIMH ECA da ta from New Have n(Conn ) respo ndents. Since the five NIMH ECA sites en tered thefield at different times in the early 19805, the end point for cohort1 is shown as 1966, which is the latest year of birth of any NIMHECA respond ent and applies to the Los Angeles (Calif) site.
Mood Disorders
Unipolar Ma jor Depressive Episode. - For th e first 30 years oflife in each cohort, Fig 1 plots the hazard rates for develop mentof Unipolar major depressive episode (with no lifetime history ofman ic episodes) . For those NIMH ECA respondents bornbe tween 1953 an d 1966, the hazard rates for unipolar major depression developing peak duri ng two age intervals : 15101 9 and25 to 29 years of age . In the age int erval 15 to 19 yea rs , there alsoappears to be an increase in the magnitude of th e hazard rate forrespondents in cohort 1 compared with those respondents incoh ort 2, and similarly for cohort 2 compared with cohort 3. Thistrend is made ap pa rent by examining the ratio of the hazard ratefor ages 15 to 19 yea rs to the hazard rate for ages 25 to 29 years:cohort 1, 0.005510.0064=0.86; cohort 2, 0.0032/0.0062 =0.52; andcohort 3, 0.0005/0.0019 = 0.26. The ratio for coh ort 4 goes againstthi s trend, but it is based on much smaller hazard rates (0.0003/0.0002 = 1.50).
The haza rd rates for major de pressio n deve lopi ng for respondent s born in cohort 1 and for those responden ts born in coh ort2 are sign ificantly different (x' = 14.2, df = I , P = .00( 2). The hazard rates for major dep ression developing for res pondents incohort 2 compa red with cohort 3 are also signi ficantly d ifferent(x'=85 .3, df = l. P<.OOOI).
ABeat Onset-Burke et al
10

19 37·1 952
1953 · 1966
1917 ·1936
I " ! I ! - - ! " , 1 Before 1917t'\ A "n ' n'A 1c:'n., .... .,.'2S_29
0.0020
0.00 15
%'" 0.0010'EeI
0.0005
0 .0000
Age at Onset. y
195) ·1 96619]7· 1952
':.J· 29
7.,9'.
0.0070
0.0065
0.0060
0.0055
0 .0050
11.1 0.004 5
~ 0.0040
~ 0.0035
~ 0 .0030
0.0025
0 .0020
0.0015
0.00 10
~~:~ IO ~ : ; - :~ ; : ; ~ :,::: - . ::, :~ : ?B e' O" '9"Age at O nset. y
These cu.....es rep resent dat a from all respo ndents in all li...e sites of theNIMH Epidemiologic Catchment Area Program, weighll!d for sampling designand ad jus.led by age , sex . and ra c ~ e l h n i c il y to the 1980 US Ce nsus.
Major dep ressive episode with no history of a manic ep isode .
O nset expe rience is from birth 10 age 30, wilh average yearly haurd tales foreac h S'y t'OJ r lime tnte rv..l calc ulated by life-table survival method s.
These CUI'\le'S reptes.en l data from all respo ndents in all f ve Sites 01 theNIMH Epidem io logic Catchm@nt Area Program. weigh ted for sampling dnignan d adj usted by age . sex . and racPiethni city to the 1980 U5 Census.
On set ex per ience is from birt h to age 30. w ith ave rage yearly haza rd r a f ~ foreach 5-year lime interva l ca lculated by life- table survival met hods .
f ig l. - Hazard rate by year o f birth for unipolar majo r depression(with no history of a manic episode), by Oiasnostic Interview5chedul....DSM·III crite ria. for cohorts born befo re 1917 (dashedfine), from 1917to 1936 (broke n line). from 1937 to 1952(solid line).and from 1953 to 1966(lightly shaded lin e). NIM H indica tes Natio nalInstitu te of Mental Health .
Bipolar Disorder.-For those respondents with a diagnosis ofmania, there is no apparen t shift to an earlier age at onse t for themanic episode for those born most recentl y (Fig 2). The haza rdrates for respondents born in cohort 1 compared with the haz ard rates for those born in cohort 2 are not significantly different(X' =1.4, dl= I , P= .240). However, for those respo ndents bornin cohort 2 compared with those born in cohort 3, the hazardrates are significantly different (X'=24.0, dl= I. P<.oool) .
In Fig 3. addi tional information on bipolar disorder is presented . For those ECA responde nts with a lifetime diagnosis ofmania, the age at onset information presented is the youngest ageat which either a major depr essive or manic episod e occurred,using the age for whichever episode came first. As with mani cepisode alone (Fig ~ ) , there does no t ap pear to have been a changein age at onset for respondents born in cohort 1 compared withthose born in cohort 2 (X'=0.18, dl= I, P= .6705). The hazardrates for respondent s born in cohort 2 compared with those bornin cohort 3 are significantly different (X'= 27.2, df = I , P<.0001).
Anxiety DisordersPanic Disorde r.-For ECA respond ents, the re has been no
apparent shift in the age at onse t for panic disorder (Fig 4), Thepeak hazard occurs in the age interval 25 to 29 years for birth cohorts I , 2, and 3. The re is no Significant difference between thehazard rates for respondents born after 1953 compared with thehazard rates for resp ond ent s born in cohort 2 (X'= 0.5, dl= l.P= ,5). However, the rates for birth cohort 2 are significantlydifferent from the rates for respon dents born in coho rt 3(X'=20.2. dl= I. P<.oool) .
Obsessive-Compulsive Disorder.- For obsessive-eompulsivediso rde r, there appears to have been a shift to a younger age atonse t for the most recent birth cohor t (cohort I). Figure 5, a plotof the hazard rates by birth coho rts, shows that the peak hazardrate for cohort I occurs during the age interval 20 to 24 years.while the peak hazard s for cohort s 2 and 3 both occur in the age
Arch Gen Psychiatry-Vol 48, September 1991
Fig 2.-Hazard rate by year of bi rth for mania by same crite ria andfor same cohorts as in Fig 1. NIMH ind icates National Institu te ofMental Health .
interval 25 to 29 years . The haza rd rates for respondents born incohort 1 compared with the rates for respondent s born in cohort2 are signi ficantly different (X'=9.5, dl= I , P= .(02). The hazardrates for respondents born in cohort 2 and respo ndents born incohort 3 (X'=16.3, dl= I . P<.oool) are also ~ gnifi c an tl y different.
Phob ias.- Figur e 6 de monstrates that the hazard rate for development of phobia s is highest for cohort I in the age inte rval10 to 14 year s. while the peak hazard for cohorts 2. 3, and 4 occurs in the interval 5 to 9 years . The difference between cohortI and cohort 2 just reaches statistical significance (X'= 4.3, df= I ,P= .04). A significant difference in developin g phobias for thoserespondents born in cohort 2 and those resp ond ent s born in cohort 3 is found (X'= 21.1, df= I. P<.oool ).
Drug and Alcohol Use Disorders
Drug Abu seIDependence,-In addition to the much higherrates in the youngest coho rt, wh ich may be observed by the needto break the vertical axis of the grap h. there also appears to bea shift to a younger age at onset for respondents born in cohortI compared with cohort 2 for dru g abuse /depend ence (Fig7). Thepeak hazard occurs between the ages of 15 and 19 years for cohort I and between the ages of 20 and 24 years for coho rt 2; thedifference between the hazard rates for respond ent s born in cohort I and for respond ent s born in cohort 2 is signi ficant(X'= 179.4. df = I. P<.OOOI ). There is also a significant differencebetween the hazard rates for resf.0ndents born in coho rt 2 andrespondents born in cohort 3 (X = 159.1, dl= I, P< .OOOI).
Alcohol Abu se/Dependence, -Like drug abuse/dependence,the hazard rates for alcohol abuse/de pendence are highest forthose NIMH ECA resp onden ts born between 1953 and 1966 (Fig8). The difference betwee n the hazard rates for cohort Icompa red with cohort 2 (X' = 58.0, dl= I . P<.oool) is sign ifican t.A Significant difference is also foun d between the hazard ratesfor respondents born in coho rt 2 and rates for respo nde nts bornin coho rl3 (X'= 62.3, dl = I , P<.oool). As with major depression ,a trend toward increasi ng impo rtance of the 15- to 19-year ageinterval is also seen in Fig 8 across the four coho rts.
Age at Onset -Burke et al 791
11

0.0020
0 .0015
1953-1960
!!~ 0.0010]:i!
0.0005
I , Before 19170.0000 ~. . " 10-14 15-19 20-24 25.29
Earliest Age at Onset. y
0.0020
0.0015
~" 0.0010
~:i!
0.0005
0.0000
19 37-1952
1953-19&&
These curves represent data from all respo ndents in all five ii l ~ of theNIMH Epidemiologic Catchm ent Are.. Program. we ighted for ~ mp l i ng dei ignand ad justed b)' age , sell, and race/e lhnic ilY10 the 1980 US Cen sus.
Mania wilh or without ma jor d ep ressive episode; onset Is for mania unlessmajor dep ressive ep isode occur red earher.
Onse t experie nce is from birth 10 age 3D. w ith average yearly halol rd rale s toreach S·ve.,time interva l caleul,lIed by hte-table survival methods.
Age 31 O nset, y
These curv es represent d..ua from " II respondenls in all five sites of theNIMH Epidemio log ic (alchmen l Are. Progra m, we ighted for sampl ing design"nd ad jusled by age . sell, and race/ethnicilY10 the 1980 US (ensus.
O nset e xce-eoce is from birth 10 018<' 30. with average year ly ha za rd rail'S forea ch 5.yea, lime inte rval calc ulated by life· lable survival method s.
Fig 3.-Hazard rate by year of birth for mania (with or with ou t a major depressive episode. onse t is for mania unless major dep ressiveepisod e occurred earlier) by same criteria and for same coho rts asin Fig 1. NIMH tndtcstes National Institute of Mental Healt h.
Fig S.-Hazard rate by year of birth for obsessive-compulsive disorder by same criteria and for same coh orts as in Fig 1, NIM H indica tesNational Instit ute of Mental Health.
Fig 4.- Hazard rate by year of birth for panic disorder by same criteria and for same cohorts as in Fig 1. NIMH indicates Natio nal in sti tut e of Mental Health.
Fig 6.-Hazard rate by year of birth for phobias (agoraphobia, simp le phobia, or social ph obia) by same criteria and for same coh ortsas in Fig 1. NIMH ind icates Natio nal Insti tute of Mental Health .
0.0025
Ag e a l O nset, y
Age et O n set , Y
19 37· 19 52
19 5] · 19&6
~ 91 7 . , 9 3 &
0.0070
0.0065
0.0060
0.0055
0.0050
0.0045
0.0035
0.0030
0.0025
0.0020
0.0015
0.0010
0.0005ooooo ' , , ,8efo,e 191 7
. 0-4 5-9 10· 14 15-19 20-24 25.29
~ 0.0040
"~:i!
The se curve s represent do1 li1from a ll respondents in all Iive s ile~ o f IheNIMH Epide miolog ic Cal("hmenl Area Progr am , weiRhted for samplinR desi $:nao d ad jusled by age , sell. and race!e lhn icity 10 the 1960 US Censu s.
19 17-.1936
10-14 15·19 20-24 25-29
Before 19 17
0.0015
!!~
"0.0010
~:i!
0.0005
0.0020
These curve s repr f'sf'nl data from all rf'Spo ndf'nls in all five s itt's of theNIMH Epidf'miologic Catch ment Area Prog ram, weigh ted for sampling de signand "djuSll'Clby age , sell, and race/e lhnici lY10 the 1980 US Ce nsus.
Onset el,pe rience is from binh 10 "Ilf' 3D, w ith ave rage yearl y hau rd ra tes foreach S .~ar lime inlerva l cakulo1 led by li(e·l. ble survival mel hods .
-"Roro1phob io1 , simp le ph obia . o r soci ,,1pho hia .
O n~1 expe rien ce is from binh 10 .tIce 30 , w ith average yead v h.tlu td rates foreac h S·yea, lime interval celc uta ted by Iife·labl e surv ival melhod s.
792 Arch Gen Psychiatry- Vo l 48 , Sept embe r 1991 Age at Onset-Burk e e t al
12
9 ] · 19&9 17 .1936
9 17 .1936
5-9 10· 14 15-19 20-24 25.29
5-9 10· 14 15-19 20-24 25.29
953 19&&
953 19&&
953 19&&
953 19&&
~.
0-4 5-9 10.0005

.....-29
0.
025
0 .0200
0 .0150
0 .0100
0.0100
• 0.0090
~ 0.0080
~ 0.0070
~ 0.0060
0.0050
0.0040
0.00 30
0.0020
0 .00 10" ,
0.0000 0•4 • n . n .. .. , n ' n" ,.
19]7 · 1952
1917· 19] 6~ a e i or e 1 9 1 7
5·9 10·14 15· 19 20·24 25·29
0.D25}0.0200
0.0150
0.0100....0 .0100
~ 0.0090
~ 0.0080
~ 0.0070
r. 0.0060
0 .0050
0.0040
0 .0030
0.0020
0.00 10
0.0000 0.4
Age at Onset, yAge at O nset, Y
These curves represent data from aUresp ondent s in all five sites of theNIM H Epidemiologic C. tchmenl Area Program, weighted for sampling designand ad justed by age, sex, and race!elhnicity to the 1980 US Census .
O nset e..ceue nce is from birth 10 age 3D. with average' yearly haz ard rates foreach 5·yeolf lime interval calculated by nre-u bte survival methods.
These curves represent dala Irom all respond ents in aU five sites of theNIMH Epidem iolog ic Catchmenl Area Prog ram, we ighled for u, mp ling de-signand adjusted by age, sex. and r a c ~ e l hn i ci ty 10 the 1980 US Census.
O nset experience is from birth to age 30, with average yea rly haz ard r a l ~ forea ch 5-year lime interva l calc ulated by Iife·t.lb le surviva l methods.
Fig 7.- Hazard rate by year of birth for drug abuse/dependence bysame criteria and for same cohorts as in Fig 1. NIM H indicates Nstional Institu te of Mental Health.
Fig 8.-Hazard rate by year of birth for alcohol abuse/depende nceby same crit eria and for same cohorts as in Fig 1. NIMH indicatesNatio nal Institute of Mental Health .
COMMENTFor unipolar major depression, there appea rs to have
been a gradua l increase in the hazard rate for the interv al15 to 19 years of age across the three cohorts born since1917. These findings are consistent with Klennan'shypo thesisv" and the findin gs of other studies " '\' thatmembers of recent birth cohorts have a higher risk of having a major depressive episode . One interesting but unexplained finding is the apparent importance of the 15-to19-year age interval for theoldes tcohort, born before 1917.Gersh on et al" reported a similar, unexplainable increasein hazard rates fur relatives born from 1910 to 1919 in anearlier family study, compared with other decade s ofbirthbefore 1940. That study, and the current findings from theECA, depend on retrospective recall from respondents fordocumenting lifetime history and age at onset, but the similarity may suggest the need to examine possible commonalities between that cohort and the more recent ones thatappear to experience higher onset rates in adolescence.
For bipolar disorder, these results are not able tocorroborate sugges tions of a cohort effect shown insome earlier stud ies.P " Wheth er this difference iscaused by differences in sampling, as those studiesused either relatives of proband s or admission rates toa psychiatric hospital, or by differences in diagnosticass essment is not clear. It is also possible that a smalleffect that could be detected in a sample of high-riskfamily members could not be demonstrated in a general population stud y for a relatively uncommon disorder such as bipolar disorder .
For drug abuse/dependence, there has been a shift to ayounger age at onse t for the most recent cohort as well as
Arrh Cen Psvchlatrv-cvol 48, Septembe r 1991
an increase in the magnitud e of the hazard rate for thoserespondents born between 1953 and 191>6. For alcoholabuse/depe ndence, there has not been a shift in the peakage at onset, since the age period 15 to 19 years was alsoof predominant importance for cohort 2, but ther e hasbeen a progressive increase in the magnitude and predominance of the hazard rate in the 15-to 19-year age interval.
EarlierStudiesThese findings are interesting for several reasons . They
corroborate earlier analyses of a subsample of ECArespondents and findings from other, more targeted ,samples for major depr ession. It is noteworthy that theearlier result s can be shown in a large general populationsamp le that includ es both sexes, multiple racial and ethnic groups, and five different community sites . They alsodemonstrate that some disorders, particularly drugabuse /dependence, exhibit the same changes. The demonstration of widely different patterns of onset across thetwo most recent birth cohorts for the specific disordersexamined her ein suggests that the shifts observed formajor depression and drug abuse/dependence are not theresult of a simple methodologic artifact.
The evidence of increasing onset from 15 to 19 years ofage for major depression, drug abuse/dependence, andpossibly alcoholabuse /dependence raises important ques tions about the possible association of these conditions.Prior analyses of a subset of ECA respondents in the 18to 3D-year age range have shown that an earlier major depressive or anxie ty disorder approximately doubles therisk of subsequent drug abuse/dependence for both menand women (but not alcohol abuse/dependence)." Find-
Age at Onset -Burke et al 793
13
19]7 · 1952
19]7 · 195219]7 · 1952
19]7 · 195219]7 · 1952
19]7 · 1952
19]7 · 1952

ings from the Yale University (New Haven) FamilyStudyhave also shown that major depression occurring beforethe age of 30 years is linked with panic and drug use dis0 r C f:'!"5 ~ KJE':;;!z r, and '-\ lei~~-; ";;:.n ll }- , .~~ . '(' cE : . (' :.·{"~'?':: ~: ' ,.' ;
ronmental factor s that n°,a)' co.irriuu re ~( . ~ ~ "l'; :. aF? '" ;\; ~ ·'~ ~ ; l. ~ :\
to earlier onset for depression and higher rates in youngercohorts, such as changing family structure and increasingurbanization. In this analysis of ECA data , the youngestcohort also appears to have increased onset ofdrug abuse /dependence in adolescence. While it has been known thatfirst use of drugs typically occurs in this age period, it is notclear whether the earlier occurrence of major depressionsomehow contributes to an earlier onset of clinicaldisorders of drug abuse /dependence in adolescents who mayhave only experimented with drug use in earlier cohorts .If so, the shift to an earlier age at onset formajor depressioncould be one of the factors leading to increased drug abuse /dependence in the same period of late adolescence .
For obsessive-compulsive disorder, the peak hazardhas shifted to a somewhat younger age at onset for themost recently born cohort (respondents born between1953and 1966). The onset has shifted from 25 to 29 yearsof age to 20 to 24 years of age . This demonstration of anapparent shift in onset of an anxiety disorder, if it is foundin other stud ies, may raise the possibility of studyingwhether onset of the disorder is also possibly linked to theshifts in depression and drug abuse/dependence, or atleast whether it results from similar factors.
By restrictinganalysis to the first30yearsof lifeforeach cohort, this approach does not permit identification ofperiod effectslikethose showa by Lavoriet aI" for the 19705 and Wickramaratneet aIu for the 1960s and 19705. A periodeffectwouldoperateuniformlyon respondents without regard to their ageat a particular.time in history. The analysis is restrictedhereintolifebeforetheageof30years toallow meaningfultestsof significance ofany clifferences observedbetweencohorts. Forthatreason, there is no adequate basis forexaminingthe effectsofparticularcalendaryears to determine if allrespondents showincreasedrates (periodeffect)or only thoseborn morerecently(cohorteffect).
For all disorders examined, a significant difference wasfound in onset between cohorts 3 and 2. This finding is consistent with earlier reports of the cohort effect for major depression for persons born after 1940. However, the uniformfinding foralldisorders may represent either a profound effectora methodologic limitation resulting from retrospectivereporting. Further efforts to understand the basis of this apparently uniform effect would be of great importance, especially if methodologic limitations can be ruled out.
limitationsFindings from epidemi ologic studies must be inter
preted cautiously, especially when they are early and information is available from only a few other similar studies. In addition to this general caution, there are two possible limitations in this specific analysis that deservefurther consideration.
First, test-retest reliability of age-at-onset questionsfrom the DIS suggests that agreement is adequate for alldisorders examined herein, with the possible exception ofphobias, where agreement with independent clinical examiners was weaker." However, the test-retest agreement has not been good enough to justify use of narrow,3-year age intervals, so this analysis has used 5-year
794 Arch Gen Psychiatry- Vol 48, September 1991
intervals; onset patterns cannot be determined as precisely as desired in this retrospective analysis. For thatreason, the apparent shift for obsessive-compulsive dis~ "df' ~- ( ~ "" m 2~ to ] 0 . ,n ?;~ to 2r to 'JL v r: c. r~ ) an d for dru r-...-- _ :.:. """r _. , ' ,"~ \ - . - . - " ~ -- . ' " ..- .. ~ ~ .::. : ~ )
may be less robust than the larger shifts for majordepression (from 25 to 29 years to 15 to 19 years) .
Second , poor recall or poor reporting by older respondents of either symptom or onset data , or earlier mortality of those respondents with psychiatric disorders in theolder cohorts, are also of concern in this retrospectiveanalysis of cross-sectional data .' ·" Recent evidence fromone study that examined the reliability of recall forself-reported age at onset for specific mental disordersdemonstrated a tendency for older respondents to increase their reported age at onset for major depression bya few years across interviews"; another more recent studyfound the opposite, that older subjects tend to lowerrather than raise their estimated age at onset." If oldersubjects do increase their reported age at onset, our finding of a uniform significant difference in the risk of devel oping disorders for respondents in cohort 2 (born between 1937 and 1952) and for respondents in cohort 3(born from 1917 to 1936)forall disorders may be explainedby this tendency. This finding may also support the cautious recommendation by Lavori et aP' not to rely on ageat-ons et report s for subjects older than 50 years . In theNIMH ECA study, there are no data that allow evaluationof recall problems in older subjects or the differentialmortality problems in aging cohorts . However, the consistent demonstration of differences between cohorts 2and 3 may indicate methodologic problems rather than acohort effect applying to every disorder examined herein .While the shift around World War II was found in earlierstudies for major depression, its considerably strongshowing for every disorder may raise skepticism aboutthe validity of such retrospective reporting for the oldestrespondents (eg, > 50 years).
CONCLUSIONWith the apparent shift to earlier ages at onset, and with
the general demonstration that childhood and adolescence are important periods for development of mentaldisorders, both research and policy issues arise . Ideally,research on the age at onset of psychiatric disordersshould be conducted prospectively to improve accuracy ofthe onset data and to distinguish cohort and period effectsmore directly . However, prospective studies to examinethe proposed shift for recent birth cohorts have not beenreported. As a result , increased study of the onset of disorders in adolescence and early adulthood appears to beof great importance, especially to examine palterns of cooccurrence of depressive and drug use disorders. Asnoted by Klerman and Weissman ,11 research that is crosscultural would be especially important in examining howdifferent genetic and environmental factors interact toproduce these changes in age at onset. 39
In terms of policy implications, it should be noted thatof the estimated 31 million Americans with no health insurance coverage in 1987, almost half (46%)were 24yearsold or younger." As a result, the general problem of ensuring adequate access to mental health services in thiscountry is even more serious for the age group most likelyto experience onset of these disorders.
Age at Onset-Burke et al
14

The ECA is a series of five epidemiologic research studie sperformed by independent research teams in collaboration with staffof the NIMH.
NIMH Principal Collaborators. - Darrel A. Regier, MD, MPH, BenZ. Locke, M5PH , and Jack D. Burke, [r. MD, MPH .
NIM H Project Offi cer. - Carl A . Taube, PhD (1978-1985), and isnow William Huber.
Principal Investigators and Coin vestigators.c-j erorne K, Myers,PhD, Myrna M. Weissman, PhD, and Gary L. Tischler, MD, YaleUnivers ity (grant VOl MH-34224); Morton Kramer, DSc, ErnestGruenberg, MO, and Sam Shapiro, MS, The John s Hopkins University, Baltimore, Md (grant UOI MH·33870); LeeN , Robins, PhD, andJohn Helzer, MD, Washin gton University, St Louis , Mo (grant U01MH·33883); Linda George, PhD, and Dan Blazer, MD. Duke University, Durham, NC (grant UOI MH 35386);and Marvin Karno, MD ,Richard L. Hough, PhD, Javier l. Escobar, MD . M. Audrey Burnam,PhD, and Dianne Timbers, PhD, UCLA (grant UOI MH-35865).
Helpful comm ents on earlier drafts of the manuscript by SusanAhmed. PhD, are gratefully acknow ledged.
References
1. Regier DA, Myers JK, Kramer M . Rob ins LN, Blazer DG ,Hough RL, Eaton WW , Locke . BZ. The NIMH Epid emiologicCatchment Area program . Arch Cen Psychiatry. 1984;41:934-941 .
2. Eaton WW , Ho lzer CE, Von Korff M , Anthony JC, HelzerJE, Ceorge L, Burn am A, Boyd JH, Kessler LG, Locke BZ. Thedesign of the Epidem iologic Catchment Area surv eys. Arch CenPsychiatry. 1984;41 :942-948.
3. Rob ins LN, Helzer IE, W eissman MM, O rvasche l H, C ruenberg E, Burke JD, Regier DA . Lifet ime prevalence o f speci ficpsychiatric d isorders in three sites. Arch Cen Psychiatry.1984;41 :949-958.
4. Myers JK, Wei ssman MM, Tischler GL, Holzer CE, Leaf PJ.Orva schel H, Anthony JC, Boyd JH, Burke JD, Kramer M ,5tol tzm an R. Six-mo nth prevalen ce o f psych iatri c d isorders inthree commu niti es. Arch Gen Psychiatry. 1984;41 :959-%7.
5. Shapiro 5, Skinner EA, Kessler LC, Von Korff M , GermanP5, Tischler GL, Leaf PJ. Benham L, Cottier L, Regier DA . Uti li zation of health and menta l health servi ces. Arch Cen Psychi·atry. 1984;41 :971-982.
6. Boyd JH, Burke ID , Gruenberg E, Holze r CE, Rae D5 ,George LK, Karno M , 5toltzman R, McEvoy L, Nestadt C . Exclu sion criteria o f DSM-I/I . Arch Cen Psychiatry . 1984;41 :983-9B9.
7. Burke KC, Burk e JD, Regier DA, Rae D5. Age at o nset o fselected ment al disorders in five communi ty populations. ArchCen Psychiatry. 1990;47:511-51B.
8. Klerm an GL. Age and clinical depression : today 's yo uth inthe twenty-f irst century. I Cerontol. 1976;31:318-323.
9. Klerman GL, Lavori PW, Rice J. Reich T, Endicott J. An dreasen NC , Keller MB , Hirs chfeld RMA. Birth-cohort trends inrates of major depressive disorder among relatives of pat ientswith affecti ve disor der . Arch Cen Psychiatry. 1985;42:689-693.
10. Klerman CL. The current age of youthf ul melancholia. BrI Psychiatry. 1988;152:4-14.
11. Klerman GL, Weissman MM. Increas ing rates of depression ./AMA. 1989;261 :2229·2235.
12. Wickramaratne PJ.Weissman MM, Leaf PI, Ho lford TR.Age , per iod, and cohort effects on the risk of major depression .I Clin Epidemio/. 1989;42:333-343.
13. Hagn ell 0 , Lanke J, Rorsman B, O jesjo L. Are w e entering an age of melancholy ? de pres sive illness in a prospectiveepi demiologic al stud y over 25 years: the Lundby stud y, Sweden . Psychol Med. 1982;12:279-282.
14. Lavori PW, Klerman GL. Keller MB , Reich T, Rice J. Endi cott I . Age-period-cohort analysis o f secula r tr end s in on set o fmajor depression. I Psychiatr Res. 1987;21 :23-35.
15. Gersh on ES, Hamovit JH. Guroff /I. Nurnberger JI. Birthcohort changes in manic and depre ssive disorde rs in relativesof bipolar and schizoaffeeti ve patients. Arch Cen Psychiatry.1987;44 ;314-319.
16. Angs t J. Swit ch from depression to mania . Psychopathology.1985;18:140-154.
Arch Gen Psychiatry-Vol 48. September 1991
15
17. Price RA. Kidd KK, Paul DL, Ger shon ES, Prusoff BA,W eissman MM , Goldin LR. Mu ltiple thresho ld models for theaff ecti ve disorders . I Psychiatr Res. 1985;19:533-546.
18. Regier DA. Boyd JH, Burke )0, Rae D5, M yers JK, KramerM , Rob in s LN, George LK, Karno M , Locke BZ. One-month pr evalen ce of mental d isorders in the U .S.: based on five epidemio logic catchment sites. Arch Gen Psychiatry. 1988;45 :977-986.
19. Robins LN, Helz er IE. Croughan), Ratcliff KS. NIMH DIS :its hi story, characterislics , and valid ity. Arch Cen Psychiatry.1981;38; 381-389.
20. Amer ican Psychiatric Association , Committee on No ~
menclature and Stati stics . Diagnostic and Statist ical Manual ofMental Disord ers, Third Edition . Washington, DC : AmericanPsychiat ri c Association; 1980;215.
21. Eaton WW , Kessler LG, eds . Epidemiologic Fie ld Methodsin Psychiatry . Orlando, Fla: Academic Press Inc ; 1985.
22. Gr oss A, Clark V. Survival Distribution: Reliability Applications With Biomedical Science. New Yor k, NY : Jo hn Wiley &Sons In c ; 1975.
23. Kalbfleisch JD, Prentice RL. The Statistical Anal ysis ofFailure Time Data. New Yor k, NY: [o hn Wi ley & Sons Inc ; 1980.
24. SPSSUser's Guide. 2nd ed . New York . NY: McGraw-H iliInt ern ati on al Book Co ; 1986:875-887.
25. Flei ss JL, Dunner DL, Stallone F, Fieve RR. The life table.Arch Cen Psychiatry. 1976;33:107-112.
26. Lee ET, Desu MM. A comput er program for comparing Ksamples w ith right censored data. Comput Methods ProgramsBiomed. 1972;2:315-321.
27. Robertson CO , Gehan EA. A computer SUb-program fo rcalcu lati ng the generalized Wilcoxon test. Comput MethodsPrograms Biomed. 1972;2 :315-321.
28. Weis sman MM , Leaf PJ.Holzer CE, M yer s )K, Tischler GL.The epidem iol ogy o f dep ression : an update on sex difference sin rate s. I Affective Disord. 1984;7:179-188.
29. Wickr amar atne PJ.Prusoff BA, Me rikangas KR, W eissmanMM . The use o f survival time models w ith nonproportionalhazard functio ns to investigate age of onset in family studies.I Chron ic Dis. 1986;39:389-397.
30. Kessler LG. Folsom R, Royall R, Fors,1he A, McEvoy L,Holzer CEoRae D5, Wo odbury M . Parameter and var iance estima tion. In : Eaton WW , Kessler LG, eds. Epidemiologic FieldMeth ods in Psychiatry. O rlando, Fla: Academic Press Inc ;1985:327-349.
31. Shah BV. SESUDAAN : Standard Errors Program for Com pu t ing of Standardized Rates from Sample Survey Data. Research Triangle Park , NC: Research Triangle In stitute; 1981.
32. Kish L. Survey Sampling. New York, NY : John Wiley &Sons Inc ; 1%5 :575-577.
33. Ch ri stie KA. Burke ID , RegierDA. RaeDS, Boyd JH, LockeBZ. Ep idemio logic evidence for early onset of mental disordersand hi ghe r risk of drug abuse in young adu lts . Am I Psychiatry.1988;145:971-975.
34. Price RA. Kidd KK, W eissman MM . Early on set (under age30 years) and panic disord er as markers fo r etiologic hom ogeneity in major depression. Arch Gen Psychiatry , 1987;44 :434440.
35. W itt ehen HU , Burke )0 , Semlar G, Pfister H, VonCranach M , Zaudig M . Recall and dating of psychiatric symp toms . Arch Gen Psychiatry . 1989;46 :437-443.
36. Hasin D, Link B. Age and recognition of depression. Psycho l Med. 1988; 18:683-688.
37. Prusoff BA, Merikangas KR, Weissman MM. Lifetim epr evalence and age of onset of psychiatric d isorders : recall 4years later . I Psychiatr Res. 1988;22:107-117.
38. Farrer LA. Flor io LP, Bruce ML , Leaf PJ, Weissman MM .Reliabil ity of self-reported age at onset of major depression. IPsychiatr Res. 1989;23:35-47.
39. Sartorius N, Nielsen lA, Stromgren E. Changes in fre quency o f mental d isorder over t ime . Acta Psychiatr Scand.1989;79:suppI348.
40. Moyer ME. A revised look at the number of un insuredAm ericans . Health Affairs. 1989(.ummer);8 :102-110.
Age at Onset-Burke et al i9.:i

This page intentionally left blank
15

Socioeconomic Burden of Subsyndromal Depressive Symptomsand Major Depression in a Sample of the General Population
Lewis 1. Judd , M.D., Martin P. Paulus, M.D.,Kenneth B. Wells, M.D., M.P.H., and Mark H. Rapaport, M.D.
~ The autho rs' goal was to eualuate the associat ion between impairment in daily(unction and suhsyndrornal depressive symptoms as well as major depr ession to determine theeconom ic and societal significance of these condition s. ~ Using l Z-month prevalencedata gathered lry the Na tiona l institute of Men tal Health (NIM H) Epidem iologic CatchmentArea Program (ECA), based on responses to the N IMH Diagnostic Interview Schedule, theau thors divided the 2,.393 subjects from the Los Angeles ECA site into three groups: subjectswith subsyndromal depre ssive symptoms (N ;270), major depression (N ; 102), and no depr essive disorder or symptoms (,\1; 2,02 1). The groups w ere compared Otl 10 domains offunc tionaloutcome and well-being. Baulsu Significantl)'more subjects with depressive symptoms thansubjects who had no disorder repo rted high levels ofho usehold strain, socia l irri tab ility , andfinancial strain as ioell as limitat ions in physical or job functioni ng. restricted activity days ,bed days , and poor health statu s. Significatlll y more subjects with major depre ssion thansub jects with no diso rder reported major finan cial losses, bed days, high levels of financialstrain, limitat ions in physic al or job functioning, and poor health statu s. Except for lowerself-ratings of health status , no significant differ ettces were [ound between subjects with sub syn dromal symptoms and those with major depression. Conclusjons 'Significantly more peop lewith sub syndrom al depress iue symptoms or major depression repor ted impairment in eight of10 [unctional domains than did subjects wi th 110 disorder. 'The high I-year prevalence ofsubsyndromal depres sive symp toms , combined with the associa ted functional impairment .emphasizes the clinical and public health im portance and need for additional investiga tionsinto these symptoms.
(Am ] Psychiatr y 1996; 153:14 11- 1417)
I nterest in subthreshold depressio n has increasedsince rhc repo rt oi Wells et a ]. ( I ) that sub th reshold
depressive symptoms in medica l and psychia tr ic ou tpatienrs were assoc iated with significant levels of psychosocial dysfunctio n. Epidemiologic studies have con firmed that, co mpared with no depressive symptoms,subthreshold depressions, variously defined, are associa ted wit h more d isabi lirv and wo rk da vs lost (1-3 ),grea ter use oi serv ices for menta l health prob lems (3) .
Received July 12. 1~9 5 ; revision s received Jan. 11 and April 16.1996; accepted June 3. 1996. From rhe Dep artmen t of Psychiatry,University ofCahtorn ia. San Oit'go; the P"ychiiuryService, 5:l11 DiegoVA Medical Center: the Depnrrmeruof Jls}'chiarr)'end BiobchovioralS..-icnces, Uruvcrsu y of California. Los A Il~ d l' s; and the Ran d Cc rp c ration, S .lI}( :1 Mon ica, Caht. Add ress reprint req uests to Dr. Judd.UCSD Departmen t of I'sychiarrr. ':1 500 Gilman Dr., t.a Julia, CA92093·0603 .
Sup po rted h)' N II\H ~ C hui..-nl Resea rch Cen ter grnu t :.,.IIt -'wYloiand the Rohrer Fund.
The autho rs thank Bernade ne Benjamin of rbc RandCorporationfor her assisrancc in co nd ucting rhe statisdl.:al analysis,
AmI Psychiat ry JS3 :1l. November 19%
poor self-ra tings of emotional heal th (1.3. 4), and morelifetime suicid e attempts (5 ).
To clar ify the clinica l sign ificance of sub threshol d depressive symptoms , we defined a more restrictive condirion , subsyndro ma l depressive symptoms, as at leasttwo or more current depressive symp toms , present formost or all of the time, lasting for at least 2 weeks, inindividua ls w ho did not meet criteria for major depression or dysthymia. Usiog this defin ition. we found tha t11.8% of 9,160 comm unity residents in the NationalInst itu te o f Me nta l Health (N IM H ) Epid em iologicCatchment Area Program (ECA) met criteria fo r sub syndroma l depressive symptoms during a l-y ear period(6). T wo-third s of th e sub jects with subsy nd rom al depressive symptoms were women; the most comm on depressive symptoms were insomnia, fatigue, and recurrent tho ughts of death. Significa nt ly more su bjects withsubsyndrornal depressive symptoms than ot her subjectsreponed lifetime disabili ty benefits, raising the questiono f whether subsyndromal depressive symp toms are associated with sufficient disruptio n in the dom ains of
1411
Reproduced with permission of the co pyrighl owner. Further reproduction proh ibited wilho ut permi s s ion .
17

SOCIOECONO.\UC BURD EN OF DEPRESSION
everyday func tio n to have demon strable public hea lth,societal, and economic impact.
To address this quest ion, we ana lyzed the database(ro m the Los Angeles site o f the ECA, where the inves tigators syste ma tica lly probed do ma ins o f da ily function no t o btained a t o the r ECA sites. Results of respon de nts with su bsyn drorna l depressive symptoms werecompared w ith th ose of respondents who had no dep ressive diso rde r o r symptoms. Because the severe impa irment associated with major depression has been establis hed unequ ivoca lly (1--4, 7), subjects with majordepress ion were included for reference compa rison ofdisability. T wo a priori hypot heses were tes ted : 1) Significantly more su bjects with su bsyn d rorna l de pressivesymptoms tha n sub jects with no depressive d isorder orsymptoms will report func tio nal impai rment. 2) Significantly mor e subjects with major depression than sub jeers with su bsynd romal de pr essive symptoms or no depressive d iso rde r or symptoms wi ll report function alim pai rment. Mil ita tin g agai nst hypoth esis 2 are emp irica l reports th at su bjects wit h su bsyn dromal depr essivesym pto ms, even thou gh sign ificantly less impai red, a rere latively co mpa ra ble in impairment to subjects withmajor de press ion (1--4).
lvtETHOD
The sampling methodolo gy. human loubjeci consent procedures.stud )' design. survey method s, and demographic characreristics of th erCA sam ple have been repo ned elsewhere (H- IO). ECA DSM-1I1 Ji agnoses ......ere develop ed from responses 10 the ~ IMH Diagnostic ln rcrvicw Sched ule (DIS). previously descr ibed in the lireranrre (1 1. 12).A Spa nish-langua ge version o f the DIS was also used at the Los Angclcs site o f the ECA (13, 14).
At three ECAsites, including Los Angeles, dora we re co llected fureac h ind ividua l me ntal symptom pruned by the [)IS and the timef" lI11eS when symptoms occurred u.c.•1 month. f, months, 1 year, orlifetime). T he DIS speci fics a sta ndardized threshold to dete rmine if asymptom is chnic ally sign ificant " For example, de pressive symptomsmust ha ve been present for at least 2 weeks and substa nt ial enoughthat the respondent had either talked ro a hcnlrh pro fessio nal or hadta ken med icenons because of it or felt the symp rom had inter fer edsubst antia lly wirh his or her everyday activities. Depressive symptomsident ified b~' the DIS are clinica lly subsrannal in severity and duratio n. exten ding well beyond no rmal moo d vicissitudes. Th e DIS req uires that depressive or othe r mental symp toms shou ld no t he associa red ......uh current medical illnesses and shou ld not be side effects ofdr ug or alcohol cons umption or problems: symptoms associated wirhthese conditions are excl uded .
The Los Angeles ECA interviews included questions probing 10domains of function al outcomes and well-being, Details of the content and merhodologv of th ese measures ha ve been report ed elsewhere (lS -IH) hut wi ll he summar ized here ,
Domains of Daily Function
I. High or low soda l irtitabilit)' in previous 6 mon ths, Respo nden ts were asked how often over the last 6 months they had felt ups et,irr itated, or angry in six types o f socia l relationsh ips: with friends .wit h spouse, wit h other adu lts in the household, with family membersand relat ives not living with the respondent, w irh boss or supe rviso rat work. ,1mJ ..... irh co-wor kers. Response caregcnes we re not at ell,less than o nce a mon th. once a month, ,I few times a mo nth. and oncea week or more. Responses were averaged for filch respondent acrossall ap plicable categories and then, due to high skewness . were di-
141 2
chotornized into 1) being irri tab le less than once a month o r 1) beingirritable mo re than o nce a month.
2. Higb or low household strain. T his domain of function isbased O il the employmen t slrain sca le of Pearli n and Lieberman( 19) hUI app lied to ho useh old responsibilit ies by Go lding (20), Re spondents we re asked to a nswe r )'es or no to fuu r items: " I havemore home (and fa mily) d ut ies than I a m able to do:' " I spend toomany hours ta king care o f Illy horne (<IOU fa mily}," " I do mo rewo rk around the hous e than I should have woo," and "Househo ldand fam ily res po nsibilities keep me fro m do ing th ings I wo uld rc ally like to do." Dic hot omous sco ring recommended by Golding(201 was used. in which responses we re scored as high when an~ ' ofthe four items was endorsed.
3. High or lou' sod ill contacts in prerim u month, Num ber of conraces (visits ur telep hone calls] dur ing th e last month with friends.family membe rs. or ot her adu lts (but no t incl udi ng any persons livingin household ) were sum med. Skewed respo nse dist ributio n requireddic hotomized scoring: a ra ring of high was given to reports of 13 ormore co ntac ts in the la st month, and a raring of low W3S given torep orts of fewer than 13 in the last mo nth.
4. Ma;or [inancial loss in pr ~ l'io"s 6 months, Th is do main wasscore d present if one or mor e o f th e following five items occ urredd ur ing the last 6 mon ths: jo b loss, someone impo rta nt to the respon dent was out of wor k fo r 1 month or mo re, loss of home or anythingelse impo rtant , or the financial situation of someone the respo ndentdepen ded o u Kot much worse.
J. High or low financial strain. In this funct ion al domain , develope d hy Pea rlin a nd Lieberman (19) and Go lding (201. res pondentswe re as ked to answer yes o r no to five negat ive or positive items,The nega tive items wer e " It is difficult fo r me to affo rd the kind ofmedical care I shou ld have ," "It is difficult for me to pay all themon rhlv hills," ant i ..It is diffic ult to afford needed fur niture (If
hOllse h~ ld applia nces," The posi tive item s were " I have enoughmo ney to pay for the kin d of fo od I sho u ld havc '' and "I hav eenough mo ney to pay for the k ind of clothes ) sho uld ha ve," Asde scribed by Gold ing (20). lo w financial s train was present if anypositive item was endorsed and high financia l strai n was prcse nt ifany negat ive item was endo rsed.
6. Talked to somcollc about most personal problems. fears. andhopes ill pret·ious 6 months. Respondents were ask ed to answer yesor no to the question, "I n the last 6 mo nth s. is there someone youhave tal ked to abo ut you r most persona l problems, hopes. o r fears}'
7. Any day with restricted aail'it)' due to ph)'sical illness in preI.';O/IS 2 wet.'ks. Res pondents were aske d, "During the last 2 weeks,how many days d id ph ysical illn C' ss or you r physica l conditionmake )'ou cur down on things you woul d like to do . such as gellinga round or having visitors?" Scor es ......ere d ichotom ized ;110 presen to r absent .
8. An)' dily in bed due 10 physical illness in previous 2 weeks. Responden ts Were aske d , "During the last 2 weeks. how manydays d id)'OU stay in bed all o r most of th e day because o f feeling physical painor illness?" Scoring was d ichotomized as present o r ab sent .
9. Any chronic limitation in physical or ;ob function ing due 10ph)'si'lJl illness. Responden ts were asked to answer yes or no toseven items . similar to the H ispa nic Health and Nu tri tion Exa mina tion Sur vey (17, 18) : " Does yo ur physi ca l health or physical con d it io n ma ke it d ifficult for you to ca rry o ut you r daily act ivuies!""Does your physica l hea lth or physica l co nditi on keep you fromtaking th e kind of job you would like?" "Does your ph ysical hea ltho r phvsicc l co ndition lim it the wo rk )'OU C;In do on your job?"" Does your physical hea lth o r physical co ndition make it difficu ltfo r you to get ar o un d (outside th e hom e. in th is place)?" "Doesyou r physical hea lth o r physica l con di tio n prev ent you from gettingthe kind of job rou wo uld like ?" "A rc yo u able to dr ess you rselfco mpletely. or do yo u nee d help ?" and " Do you ha ve an y pro blemsgoing to the ba throom. Hkc not being able 10 get th ere in rime, o rneeding help to ~ er th ere ?" Due to skewing of responses, scoringwas dichoto mized as pres ent if o ne o r more items were endo rsed orabsent if no items were endo rsed.
10. General health status. Respon dents were asked one item fromth e Ran d Hea lth Insu rance Expe riment : " Wo uld )'OU sa)' rha r yourhea lth is exc ellent , good, fair ) o r poor ?" Th is item was score d 3S
l eexcellcnr, 2=gnod, -'=fair , or -te poor .
Am ] Psychiatry 153:1 1, November 1996
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission .
18

.JUDO, PAULUS, WELI.S.ET AL.
TABLE 1. Demographic Characte rist ics of 2 .393 Subjects in the Los Angeles Site of the NIMH Epidemiologic Catch ment Area Survey Dividedby Depression Status Into Three Mutually Exclusive Groups
Sobiccrs \Virh No Subjec ts WithDep ressive Disord er or Subsyndronu l Depressive Subiecrs \,(-'ith Major
Ch ar,ld t'rist i..: SrlllplO lilS (N;:,2 .02 1) Sym ptoms IN =270 1 De pr..'ssinn (N =101 ,
.'i '% N ";" N %Gende r
:\Ob I", 1.01 4 50.2 % 35.6 35 343fema le 1.00 7 4' :U ~ 174 fl4.4 67 65.i
Ma rital sta tusMarr ied wilh children 575 28.5 52 19.3 14 I FM arr ied wirhour children 467 2.1.1 51 18.9 12 11.8Singll' with children 242 12.0 4.1 15.9 24 2.1.5Single without ..children 71 8 3.1.1 122 4 5.2 .'>2 5 1.0
ErhmcitvNilti \ ' ~ Hisp an ic 4j J 21.4 78 IN.9 27 26.5lmmigrnnr Hispanic 643 J U I 48 17.8 15 14.7No n-Hispamc wh itt' 94S 46 .S 144 53..3 60 58.8
.lkdfl SO Mel1lf SO M£,.111 SIl
A ~(' i ~' e : :m) 4UJ 17.06 ,;7.29 14)~S .16. IS 11.00Education itot a l yt'ar ".1 11..14 4.511 12 . 14 3.M3 I l ..U 3. 114
Effect oi DepressionSr;l( U~ ( ~ t A ~ O V A)
TABLE 2 . EHect of Depression Status' on 10 Domains of Funct ionand Well-Being in 2.393 Subj ect s in the los Angeles Sit e of theNIMI-I Epide mio logic Catchment Area Survey
"N o depr essive disorder or symp tom s tN =2,02 11. subsyndroma l d epressive symp rnms IN =2 70 1,o r ma jor deprt'ssio ll (N =102 ).
I'Tht, s.:nrt's o f ,suh jeo:rs ' .... ith suh,,}"ndrnm41ll1epres ..iw symptoms andsu h jt'l'ls with ma jo r Jeprc s~ i on ",,"'rt' s i~n i (k>1 nt ly higher (ind i.:alinFgreilte r imp:'lirmem ) rhilll rhe Sl'ores o f su bjt'crs with no dep r t 's~ivl '
J isordl'r or sym plt>ll1S (p<O,lJ5. T ukt'y's Srudt'lII izl'd Ralll-\t"fl'st !.
Description of Samp le
Demographic charactcnsr i...s of rbc Los Angeles ECA site s:lInp ll'hove been de scribe d in grea ter detai l elsewhe re ( B , 16 ). Using the11 -01omh DISdata , we dividedthe 2.393 subiccrs into three mllfu"lhexclus ive suhgnlup s: rhosc with sub wnd roma l sympto runnc dcprcs ..io n. defined or rhc presence o f <H leas t rwo or more depressive symp rom s ill respondent s 1I0t IlIt'c ring .:rite ri;l fo r majo r de pression or dyst hYl11i ~l ~ those \vith major depression J ~ defineJ h ~' DS!\·I-III;and thosewith 110 de press ive disorde r or symptoms,
Duriug c lZvmonth period , 270 subjccrs mer crlreria for subsvndro ma l de p ressive svmpro ms. 102 met DS!\.I-Ill .:ritt'ria for major de rrl.'....ion . and 2.01 1 were assigned to rhe su bgr oup subjects with nodepressivedisorder or symptoms . The demographic cha racrcnsr ics ofrhe three groups are given in table I. Th e groups wir h sobsvndromu lde p ressive sym pt o ms and majo r depression had approximately arwo -ro-o ne prepcnderu ncc of wome n to men. ;1I1d the ~ w u p with TlO
dep ressive d isor de r or sym pto ms had a balan ced sex distr ibutio n,Co mpa red with the group with no depressive disord er or svmpr o ms,rhc gro up with subsvndromat dc pressive symp tom s had fewer marr ied people and th t' group with ma jor depression even fewe r. The~roll PS with su bsvndrom al dcpre..sin' sympto ms and ma jo r depression we re. on the ave rag e, yo unge r an d bet ter educa ted . T hen' was >1s li~ h cl~ ' hi!tl1l'r prevalence of non -I i ispa llil' whi rl'Sand na tive Hispanks and fewe r imm igr'lIU Hi sp anic .. in the groups wit h subsynd rom alJ q lr t' ~ s i vc .~ Y ll1 p r ( ) m s illld OIa jo r dl'p h.·"..io n than in tht, gflh lp with nodt'prl''isin- d iso rd l'r or symplUlns.
Sldtistic:al Methods.
Doma in of Function
High socia l irririlh tlity"H igh hou sehold struin!'High socia l con tactsT alk ed ro ..o rncon c about mo st person al
problems.fears. and hopes in lasr6 monrbs''Ma jor finaucmlloss in last 6 mo nths"High financ ial strain!'Am' dav with rcsmc red actrvitv due 10
ph )' s i ~ ' a l i ll ll t's~ in pr evious fw(,,'eksh
Any dav in bed due to physical illness inprevious 2 weeks"
Any chronic lunit ari on in physicel or jo b
c~~~ ,~:i [l ~ l;~r. hi ~ ~~ :::sf,hysic;II iI/nessr,
f tuf=2.2255;
l L ll <O.Ot/H !10,72 <0,000 1
1.5 2 n.s.
1.1.67 <11.000127.46 <0.000 121.95 <0 ,000 1
28 ..19 <0,000 1
1~ . 9 5 <0.1)00 1
3 1.93 <0.00012 1.16 <0,000 1
Dm' to Ihc eo mp le.xsam plillAd e~ign ilnJ th l' nHlltiplt.· ..: o mp:l r iS()Il~inwllH'd. Iwo d i ~l in o: t sra risriO::l1 aprw ,KIlt's \wrt' Ilsed ro de rerm ineth t· dtt'o.:ts of depr c'ision o n IUll...·t io nal sriltus , First, il mu lt iple an alys is01\-,;lri;lIKe f1\ IA NO V.-\ j (~AS) was ":<l rr ied o ur rholt induJed all \'ar i;lbks d , ;lr,l..:t.... rizins, flln..:tiotlil! sra lus i1<; dcpl'ntlC'llt JnC'ilS\lreS and deprt'ss inn SrJ tu,> li.e.. no dc pre!>sivc diso rder or <;ympro ms . ,>uhs)'ndro1ll;11 d (,, 'p re s~i\'e ~ r lll p tt ) m :), or Ill;l jm dt' pr e ~~klO) as rhl' indltpendt'nrmt';lStltt' to dt'lt'nnil\C' wht'tht'r dep rl'ssio l\ s riltu~ hilll ,I sigllifi':illlr d fed Oil IUllel ioll;l1StiltUS, Th is illl alvsis ind udeJ nne 'WilV A~OVAs;m..! Tuhy's Sllldc nli:led Ran ~ .... Pll~t hoc l·omr.lriso ns I;, dl,tenn illethe di......·t of depress ion sta w s o n rht' indi viJ u'll \';niahlt's d l;H,l...·re r i7.ing iun...-rion ill SUitt'>, Sl'l'ond, il Oltlltinom iilll llHlst io:r t ' ~r t' s ~ i o n an alysis 'lltl pred ior rhl' multiSliltt' s;ll tl pli l1~ d l ' s i ~n W;lS llsed to obra inprt'di l:rion\ fo r r h ~ pre ...a lcn.:e oi d i~ t ll rb .lIKt' S in fUlleri llllid ~r a lUs due
Am J Psychiatry 153:11, Nov em ber 1996
to th...dfe..:r of dt'pr cssion sriHUS(2 I . 22 J. TI l(' STAT A st:lt i ~ , i ''';1 1 pad agl\ whi .:h ena bles rht' ilJ juStme nt of srandard er ror ..:ak ulal ions orme.l l1S of Tll)'lor l i n e ~ 1t i 7. d r i ol1 , wa~ used fo r Ihis teKfession ;m ;lIysis.fo r t':l..:h de pC'nd em v:lri;lble, ;1 sc p;lrd re Huher fc~ rt:'ssi on ;lni) l y~is
was c.lku l:lICd (22). Ca nd idJre va ri.lh les illd lldl·d educa lion. age.11\;lr iml Sta tu s. l·th llil..'iry. gl' lldc r. o.: urren t eh rn nk llledka ll..'ond it io n.eOlllorh iJ nwnt.11di soru e:r . .:omorbiJ ak ohol ust' d iso rder 112-mont h,tnd liferinlc) • ..:omo rh id drug use: d i,sllrd l' r ( 12-month ;Ind liferime).<Iudrhl' rh rt'(,,· d iagnosril' groups (110 depressive di'''ordl' r or symptoms,suh'iYlIdromal J c p re s ~i v ..., ~~ ' m pw ms, and major dep ression ), T he 1:0
mo rb id men ta l d iso rde r variilble ind l1Jed rnanio:episo de. J~ 's rh)' m ia(life t imt' Hnly), hipololr di so rder (lifetime o nly). a r~ 'pio: a J hipntH distlr ·d l'r (lift"rime on ly I. l:i1nnjhis ahuse o r J l'pend enc e, so.:hilUp hrenia ,
1413
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.
19

SOClorCONOMIC BURDEN OF IJr PRESS IO~
TABLE 3. Adjusted Percentages- of Subjects in the l os Angeles Site of the NIMH Epidemiologic Catchment AreaSurvey, Divided by DepressionStatus, Who Reported Impairment in Social, Financial, and Physical or Role Funct ion
Sll h il '(f ~
WiThNoDepressiveDisord er orSytllprolllsiN: 2.01 11
Subiccrs\,(!jrh
SubsvndromnlI ) ~ ' rr t' s s i n 'Svmp eoms(N",270)
Subjects\'\!it h
MajorDepressionIN: 1(2 )
C"I t'gory of Funct ion ~ , ; , sr SE ' ~ ; , Sf. Significant Difference
Social functionHigh SIKi:-l! con tact [~ I . ~ !iO
contacts pe r month IT;tlhd ro someone " hou r 64
your most persona lproblems , fears, andhOPl'S in last ,; months
Financia l st atu stv!'lint financial 10:-<; in 14
last 6 mo nths
High financial strain 53
I'hysical or role limi rarionsAm' chronic limitatio ns
i ~ physical or jo b [unctioning due to physicalillness
Am rest ricted ac rivin t ild:1Y due to pny"il:a( ill-ness in I,lsr 2 wee ks
Any bed day due to physical illness in previous 1wCI,..k~
4 1
69
17
6 1
1"
18
11
.17
7J
25
69
24
16
11
N OIH'
NOlle
Between subjects with maie r depression :.Illdthose with no depressi ve d isor der o r symptomsIt: 3.1. 01:22 89. p:O.002j h
Between subjects wirh subsynd roma l depressivesvm pro ms an"! those with no dep ressive disorder or symptoms ((=2.1 , df=2253 . p=O,oW'and between subjects with ma jor dep ressionand th o se with no depressive d isorder I,It
symptoms ((=1.3. df=1153. r =O.01 jl'
I\l't\\,('\'11 sub jects with subsvn drom al depressivesymptoms an d tho se with no dep ressive dis,order or svmproms (t=4.3, dt= lJ05. r <O.OOOIII>an d betw een subiecrs with major depr essiona nd these with no dep ressive disorder orsymprorns it=6 .1. df=230$. p<OJ)0011
Betwe en subjects with sub syndrornal depressivesymp tom s and those with no depressive dis,order or symprnOls lr=3.7. df=ll96. p<O.OOO I )
between suhiec rs wirh subwndromal depressivesymptoms and those wir h nu depressive dis.order or symptoms (1=2.9. df=2JO O, p<0.004 )1and between subj ects with ma jo r de pressionand those w ith 110 depressive disorder orsymptoms U=2,J . df=1300. p=O,(l.W'
- Pcrccnrages a re adjusted for educunon. age. marital srnrus, erhnicn v, gender, current chronic mcdicalcondinons, comor bid mental disorder s.co r norbid alcohol IISCdisorder I J Lrnonth and hferimer, and ...omorbid drug u'>e disorder tl Lrnonrh ,lOJ lifetim e t.
hCon firllleJ h,\' Tukcv's Srudennzcd Rilll1.\\' tt'st (p<0.05). 111 a ll cases. rbc scores o f subjects with suh svndrom nl depressivesymptoms and subjectswith major depression were lughcr iinJ i..'JtinJ:, greater irnpairmenr ! rhan those oj subjects with no depressive disorder or sympto ms,
schizophrcnifcrm disorder, obsessive-compulsive disorder, phobias,so matization d isor der, panic disorder. ilnrisllcial personolitv disorderIliferime onlv), and anorexia nervus" (l.ferime onlvt.
Bused on the calcu la ted logisnc regre ssion mo d ~l . predicted prevalena ' s for the following depen dent variable s were obtained: socia l irritability {hig h versus lo w), household strain (high vcrstlS low ), socialconmcrs (high l ~ IJ l versus low Is1211. rnlking 10 SOO\\'O O(,' abour per'sonal problems. financiatlcss, financia l strai n, restr icted activity daysd ue rn physkal illness. IX'd da y~ due ro physi...<l l i1 111e ~s, chronk limilillinns in physic<l \ or joh illll c t i () o i n ~ , ;lIld ~cncTil l he,llth ~ rilH1 s (ex.:ellent. gooJ . ia ir, ponrl, -\'hrt'e diifcrCl1f statistica l ani \ ly~\' s wt'rt: llsed10 Jd d rt"ss tht' t w o h)·purht=ses.
Tht' hn",othese" advillKt'd here were r\'sred h)' llsi n~ thc two sr.u islic:l1'lpproil..:he" alrea dy dt'scrihed h"r:, Sredfka lly. rh ~ ' hyp ot he~isrhilt d\'prcssioll status sil{nijicanr ly ilffech dOOl:lins oj il1lKtion wastt'sled h ~ ' a M..\NOVA followed hy posr hOI: comp ar il>ulls usingT uk('y'.. Srndt'nr il.('d RanJ.:e resT s fur alpha <0,05. t>.1ur('O\"cr. sp('cijicpredicrions oj prev~kn ct' ra tC'soj distllfbancl's ill dom;;tins of functiun wcre obta in('d fu r ehe grou ps \\-,Ih no d('pressive di~order ors ~ 'm rtom ... suhsynJroma l dep rcssi\ 'e s~ ·mprolll s. :.Iud milint dt'p ression. Thl,' aH 't;l~e predictions .Uldthl,' s;and;\fd crro rs were suhj \'\'rt'd10 it I :o.C()fE' ..-omp:trison, Only rhuso:o.:cmp;lrisons \\'hi\'h \\'eT(,' fou nd
1414
ro he significant hy using Tukcv's test .1lId rhe r score differences ohrained from rhe regression ana lysis are report ed as significant in thisillV\"srigall(IIl,
RESUl.TS
The MA NOVA for effects of depre ssion status on do main s of funct ion revei.lled tha t signi ficant effects werepresent for nine of the! 0 do ma ins of everyday function(tab le 2).
Table 3 includes results of regression analys es forseven of the 10 functional domains. Sub jects with majo rdep ress ion differed signif icantly from those with no depressive disorder or sym pto ms on two fina ncial sta tusJoma ins and from the gro up wit h subsyndroma l depress ive sympto ms on one financial status domain. Sig·nifica ntly more of the subjects wirh suhsyndromal 'depress ive symptoms than of those \\' irh no de press ive
Am .l Psychiatry 153:11. November 1996
Reproduced with permission of th e copyright owner. Further reprodu ction prohibited without permi ssion .
20

JUDD. PAUl.l ;S. WEll'>, F.TAL.
FIGURE 1. Adjust ed Percen tages of Subjects With No De pre ssiveDisorde r or Symp toms, SUbsyndl oma l Dep ress ive Symptoms, or Major Depression Repo rting High l evels of Household Strain or Soc ialIrritabil ity'
HIGH SOCiAlIRRlTABIUTYc
HIGH HOUSEHOLDSTRAIN
b
o NO DISORDER OR DEPRESSIVE SYMPTOMS (N'2.021)
o SUBSYNDROMAL DEPRESSIVE SYMPTOMS (N. 270j
o MAJOR DEPRESSION (N.l02j
)
)
I
o 70Z>= 6a:Ii' 5wa:~ 40
w 30
M 20
~ 10If
- I' crccrnagcs M e adjusted tur cd ucnnon ••rgc, mar ital St .HU~ , ~ " rl \l l i..: i l~"gender, current ch rou ic l.·l)illOrhid medi..:nrcond u iou , co morbid ment;11diso rder. cnmc rbid a lcohol usc disorder Il f -month and Iitet jnll' )and com c rbid t lr lljot use disor der ( 12' mo m h nnd hfetimej.
"Signific llu diffe ren ce between rh ~ ' ~rn u p wirh sub synd rom ...1dcpr cssit·C' symptoms and rbe orher two I:trn u p~ It: ] , I, df=2270. pd ),nOll(,i gl1ilil';ln l ac..:ordlOK to Tu kev's Stude urizcd Rang e resr, p<0 ,0 5i,
'Significant diffe rence be tween tht' gruup with subs ynd rorn al deprc csi\"t' svmproms and the oth er I W U group s H: .1.3. df.2174. I'<U,lllli Itsig ni tican r ;l ..:..:orl lin~ tn Tuh'(l< Stuurlui / cll R31lJl"t"Il.'fo l , r <tl U5),
ment a l di so rd ers, a nd curre nt c hro nic med ica l co nd itio ns, An add iriona l co nrro l in redu cing the infl uence ofco mo rbid co ndit ions wa s pro vided by th e D IS itself,w hich requires tha t w hen a depressive sym pto m is reco rde d it nor be asso ciated with a medica l illnes s o r hea side effec t (ro m a lcohol o r dr ug use o r d isor der s ,Th ese da ta su ppo rt an d extend findi ngs from six p revio us stud ies rep o rt ing sig ni fica nt associa tions betw eensubthreshold depressive sym ptoms and greate r impairrnenr in everyday func tion (1- 6), T here is now strongevidence th a t subsv ndro ma l depressive symptoms a reassocia ted with substantial d isa bili ty in many spheresof human activ ity. placing no ta ble burdens on indiv id uills an d the so cie ty.
Co mpa red with respon dent s wh o ha d no dep ressivedisorder or symptoms, ind ivid ua ls w ith major depression repo rted imp a irment in five of 10 fu nct ion a l doma ins. Significa ntly mo re su bjects w ith ma jor dcp ression repo n ed ma jor finan cia l loss in th e last 6 mo nths(1 5%), more suffered from high fina ncia l stra in (69 'Xd,mo re rep on ed phys ica l o r jo b limita tion s d ue to illness(24 % ). mor e rep orted bed da ys (1 1fyO), an d their se lfra tings o f hea lt h were poo rest. These da ta streng the nth e confl uence of scientific evidence tha t ma jor dep rcss ion is associa ted unquestio nably wi th severe per vasivedisability in man)' aspects of da ily func tioning, w hichhas a pa lpab le imp act Oil society a nd th e eco no my (1,2,4 , 7, 23). Fo r exa mple, 24 % of the subjects wi th majo r depr ession reported limi mtion s in physica l o r joh
The full Los Angele s ECA sample included ap p rox ima rely equa l num bers o f Hi sp an ic a nd nun -Hispanicwhites, which d iffer s fro m rhe genera l U.S, populnrinn( 15. 16 ). O ur co nclu sio ns here. ther efo re. sho uld betested in mo re rep rese nta tive sa mples: however . the reported find ings a pply fo r bot h Hi spanic a nd non -H ispanic groups , and ethnic ity was co nt ro lled fo r in thea na lysis.
Signi fica ntly mor e subjects wi th suhsynd rom al de prcss ive symptoms th an su bjec ts with no dep ressi ve disor de r o r symptoms repo rted di sa hility on seve n o f 10doma ins of funct ion: high social irritab ility (61% ), highhouseh old st ra in (45 CXd , hig h fina ncial str ai n (63 % ),restricted activity days due to physica l illn ess ( I ~r : ~ ),bed days due to physica l illness (1 1%) , chronic limira lio n in phys ica l o r job fun cti on ing (18 ' ; {,) ~ a nd sel f-ra ting o f hea lth as poo r.
Althoug h one pr ima ry st udy goa l wa s to eva luat e assoctanons betwee n " pure" suhsyndro ma! d epress ionund ma jnr depression and Iun ct iuna l irupai rmcnt, so meidentified impainne nr co uld he assoc iated w ith otherconditio ns. The log ist ic regr ession a nalysis was designed to co nt ro l for the: co mo rbid effects o f lifet imeand Current (12-monr hl a lco ho l and d ru ~ use d iso rd ers ,
d isorder o r sym pto ms repo rted impa irment in thr eeph ysica l or ro le limita tio n d oma ins; significa ntly mo reof th e subjec ts wit h major depression than of th ose wi thno depress ive d iso rder o r sy mpto ms repo rted disab ilityin two of th ese dom a ins, There were no si~n i f ica fl( d ifferences betwe en th e sub jects with ma jor dep ressionand th ose wi th sub syn dro rna l depressive sympto ms inthese domains o f function,
Figure 1 cornpar es the res ults of the reg ressi o n analyses on rhe do ma ins of househo ld stra in and SOd .11irr ita bility . Co mpa red with the subjects who bad no depressive diso rd er or sym ptoms. signi ficantly mo re o fthe sub jects wi th subsyndro mal depressive symptomsrepo rted high levels o f hou seho ld srra in and socia l irr itab ility. No signi fica nt d iffe rences we re fou nd betweenthe sub jects wi th maj o r depressio n an d those wit h nodepr essive d iso rd er o r th ose wi th subsyndrornul depressive sympto ms,
Estimates ol general beattb status , On t he 4-pointhea lth sca le ( Iepuor to 4~ e xc e llent ) , the su b jects wit hsuhsynd rornal dep ressive symptoms gave th em selves asign ifica ntly poo re r mean hea lth rat ing (llle,m =2.9 1.S£~ O .O.i) th an d id the subjects wi th no depr essive diso rder o r sympto ms (rneane L'l J, S E ~ O. 0 21 (t ~4 . 5 , df=2289, p<O.OO1). Resp onden ts w ith major depr essio na lso gave rhernsclves a significa nt ly poorer mea n hea lthraring ( l11e ",1~2 . 6 7, SF.~0 .0 9 ) th an did those wi th nodepress ive diso rde r o r sym ptoms (t=5 .03 , df ~22 89 , p<0 .0001), Th e respondents with major dep ress ion ga veth emsel ves .1 significaurly poo rer mean hea lth ra tingthan d id the sub jects wit h subsyu d rorn a l de p ressivesympto ms (td .6, d f ~2305 , p ~ O . 0 5 ) .
DISCUSSION
Am JPs,'cbiatry 15.1:11, No,' ember 19% 141 5
Re pro duc e d with pe rmis sion of the copyrig ht own e r. Further re produ ction pro hibited witho ut pe rmission .
21

SOCIOECONOMI C BURDEN OF DEPRESSION
functioning, and this is consistent with annual C0 5t cstirnates for mood di sorders, which found that the twolargest cosr categori es were increased absenteeism andreduced worker producti vity (23).
No large consistent differences in impairment in thedomains o f function emerged between the subj ect s withsubsyndromal depressive sym ptoms and those with 111.)
ior depression . apa rt from their self-ratings of theirhealth stJ[US, which could have occurred bv chancealone. This does not support one of our a priori hypotheses-e-rhar more subject s with ma jor depre ssionthan those with subsyndrom al depressive sym pto mswill report impairment . However, every other study using different out com e measures than tho se reportedhere, such as absenteeism , lise of health services, use ofpublic ass istance, and suicide att empts, have found sigruficanrly more adv erse outcom e associated with majordepression than subsyndrornal depressive sympto ms(1-6). \Vic d id find that higher ab solute percentages ofsub jects with major depr ession than of subjects withsubsyndrorna l depressi ve sym pto ms reponed impairment in five of 10 functional domains, but the differences were not sufficient ly rob ust to survi ve formal testing. further, the functio~al measurements used in thisSTUd)' were primarily dichotomou s; it is apparent thatthere a re d ifference s betw een subsynd ro ma l depr essivesympto ms an d major depression that we did not ha vethe power to detect. It should he not ed that our findingsar e also consistent with thos e of previous investigations(1-4), which fo und th a t the impairments in subjectswith subsyndroma l depress ive sym pto ms a nd thosew ith major depression a re qualit ativel y comparableand more simila r to each other than thev are to anyimp airm ent found in subjects w itho ut suhs yndromaldepr essive symptoms or maj or depression.
It is not fully clear what suhsyndromal sym pto maticdep ression repr esent s clinically, bur we do know fromthe studies of Broadhead er al. (2) and Howarth ct a l.(5) that subthreshol d depres sive sym pto ms ar e associated with gr eater risk for future major depr essive epi sodes. In a large sample of medic al and psychiatric outpatients (24), we found th at the demographic a ndclinical characteristics of subjects with subsyndro rnaldepressive svrnprorns signific..mrl y more closely reser nhied thos e of subjects with major depre ssion than thoseo f nondepressl'J medical outpati ent s. Fo r exa mple, wefound that 41 IX, of outpatients with su hsyndrom"ll dc ~pre ssive sym pto ms had famil y histories of depr ession , ...ra re ne<.Hl y as high as thar for subiects wirh major de press ion (59%). We ha ve proposed that suns yndromaldepressive symptoms represl'nt. respectivel y, either pro·dromal manifestations o r residual (kpressive symptoms from impending O( incompletel y resolv ed majordepr ession or dysthymia (25 ). Suhsyndromal depressivesympfo ms may also he a low-gmde chronic co nd irion,placing patients at higher risk fo r future major d e·pre ssive episodes (25). Thi s has ltd us to conclude thatsuhsynd ro mal depressive symptoms arc a clinicallymc.mingful, subthres ho ld vari•.1Ilt of uni polm m ~,jor depres sion .
1416
The fact that a ppro xima tely o ne in 10 people in thiscommunity sample met crit eria for subsynd ro mal depress ive sympto ms dur ing I yea r, when com hined withthe associ ated functional impairment reported by usand others (1-6 ), suppo rts the conclusion that subsyndrornal depressive sympto ms arc J clinic al condirion ofpublic health significance. Pro spective, controlled studies of subsynd romal depr essive symptoms in unipola rmajor depression are needed. especial ly treatment investigations, becau se no data a re available indic atingthar su bsynd ro mal depressive sym pto ms respond torreatmenr or if the y should he treated at a ll. lr is pos siblethat effecti ve t reatment of subs yndromal depressiv esymptoms may not only reduce the associated functiona I disability identified but also prevent more severel y disabling futur e episodes of major depr ession o rdysthymia.
HHTHE NCES
I. We lls KB. Ste wa rt A. H ,l ~ "S RD . I~llfllilm ~( ;\ . RtJ ~t't ~ \\:0' . Dauicb~I . Jkrry S. ( ;rcelltidd ..... War l·.l : The tUtKfjollin t: <lllliwC'II·ht- ingof depressed r, l t kl1 t~: result.. from the :\ll·die.ll O utcomes Stl1Jy..1:\:\1:\ 1~ H~: 1n2:914-".>19
1. Bn),IJh(',ld \VI:. nLlll'r 1)( ;. (;t:or,.:,t:LJ(.'1\ 1'LK: Depression. dis' I h i l i r ~· llay\ and davs los t fron t w ur k in n prospec tive cpid vuuoltl~i..: sur vev. .IA.\IA 1l::l9\h 164 :1514-252 H
.). lohnsou J. \Vl·issm.lll M:\l, Klcnuun {; I.: Ser vice urilizuti on .llld'SO,:i,l l morbidirv ,1s"ol,," i.H(.'J w ith depressive svmproms in till'(,·Oll1munity. .IAMA 11J92. 26 7:14 7 ~ -r4~ 3
4. Spitler RL. Kroenke Kcl.m zer ~ 1. I I " hn SR. \X : ill i 'lll\ s.l n.l k( ; r tl ~FV III. Rrod y DeDavie s 1\1 : Hcnlrh-rclared quahrv of litl ' ill pnmar v 1."Hl' paticn rs wi rh uu-nrn l dis o rders: rcsul r-, hOlll t herRI~IE · 1\1D IOUO ..tud v. JA~lA 191;)5: 174:1511-1 51 7
5. Howa rth E. johnson]. Klenn au (it" \'(.'CiSSIll.lll :\1: Depressivesympto llls as rela tive a nd orrributablc risk f,"':tm" tor tir,,(·on..ermu iur depr ession . Arch (;(.'1\ Psych i:my I'j9 2: 4 Y :~ 17-:-l2.l
6 . j udd 1.1.. Rapaport !o.l.I\Hllus ~ I , Brown.!: Suhsynd ro m:d Symp toruaric· Dt'prt', ,,ion. .J<:Iil\ PS~l" h ia tr~\ " 11.)")4: 55l April ..uppll
7. M int z] . ~ Iillt:l " T H . ,\ ruda ~1.1, H wan g SS: Trennuent 01' ..lcp rcssion ,lIHI f U l\" ·t i n lu ll. " ,, p. K i r~ " (0 work . Ard l (;(.' 1\ PSYl·hi.ltry IlJ92:49:i61 - i6 l\
x. R (. ' ~i(. ·r DA. :-'lYl·rs.lK. Kramer M. Robin-, l.!'o:.RI.1Zl'r D( ; ,I-ICl\l~h
R!.. Eaton W\'f . Locke HZ: TIll.' :" 1 ~ I H f pidl'miolu!-\il- Catchmcnt Afl·..l I' ro ~r i\ll\ : historical con text, ll\;1jur obi ecrivcs. andsrud v population characwrbticv. Arc h (j(. '11l'syd li;\lry 1l.Jl'l4. 41 :9.'4-941
s. E:HOIl WW, Holzer CE III. Von Korff ~L :\ nrhuny .le. Helzer.IE.G l'O r ~l' I .. HUfll<lIU A. HoyJ .Iii , KI.·..., lcr 1.(;. 1.(1.;\,(. HZ: The dl'sigll u f til(: E riJ c lll ioll, ~i l ' ClI,,'hnll'nl Ar(.·:l ~1l f\ ' l ' Y~ : th e l'o nt ru l;llld 1lll' :\SlIrl'melll of (,·rrm . Al·d l ( it'll P S \"l 'hi~ltr\ " IIjS-1:41 :1:142-~ 4H . .
10. bWIl \y!.I(C' ssler L.k Jsl : Epi J ~ 'm iulo~ ; l ' Field ~lerhoJ, in Psydl i;ltry: Th l' NrMH Epil.klllitllu~ i..: C u d mll' nt Ar(';l I'rol-l,r:lln .Or land o, H'l. A(.",HII.·m il· I'ress. llJ l<"'
I I. Rollin s IS. Hdzcr.lE. Cmtlcr l.. (; oIJ ill14 [ : ;\i;HiOIl'lll n,>li n1t(.·ot' f\.! (.·!H.111 kalth Di'\14llU'li..: hm'f\'ie \\' S....h(.·Julc. \'t"r...ion 111. re\' i~ (. 'J . St Loui...., W; l~hin ~ton lln in·r ...it \". O';" pilrlll 1l'llt of I' S ~dl i ,lt ( ~ ·. IlJl'llJ
12. Roh ins I.N . I kl7.cr.lF. C ruUj.:!lilll.l. R.Hdiff KS: '11ll' ;"':<ltion"lIn"otiWt(.· of "hom,l l He.llrh D j ;l~ll l)s t k IIlft"n "il'w S ~ 'h l'dllk ; i r~ h i. ·ron ·. ..:h:Hilcrerifiti(.-s, and \";lliJ it\". Ard l (;(..1\ P, n "hi;Hf\ ' Il::l ~ I ; .~~ :
. u .:i -.~ l'l lJ ...
1.1 . K,HllO ~I. KUtn.Hll 1\IA, E s ~oh:lr 1.lioUl:h RL E.no ll W\X': DC'\'t'IOr ml'llt 01the Sr ;lIIi sh·klll~U .J it' \·t"f!<il'lI\ I,f thl' N;\f; lmil[ Ill..ti tUl(.'of ~l('llt 'll Hl'ahh I) ;i\~n() ..ti.: Inren·i(.·\\· S .: h (. · d ~ ll (.·. Ardl {;(.'11Pw chi;ltn' IlJ~3: 40: II M.l- I I 8M
14. lh ;rna m ~I A, K,lrllO1\1. HI 1U~h RI.• FS,,'I)h ,l r .II. Fllrfirrh l' AB: ' n l l"
Am.l Psychiatry 153:11, N(",ember 19%
Reptoduced with permission of the copyright owner . Further reproduction ptohibited without permission .
22

Sp.tn ish Di J, ~ n l) s t i ~ · hHC' f\ 'it,W Scbed ule: rdiJ bility and ~ ' C1111p ;lt i ·
von w ill, dlll i( ;ll J i a ~lI o s c !o. , .Arc h C CIl Psp:hi.lIr J 19M3: 40; I IS'I1196
I.t \·(-'dl ... Kn . (; o l t! in~ ./."- 1. Bur na m .\ 1..\: I' ... p,:hi,urk disorder .H1 dlimimno ns in ph ~ ' ~i ~ " 1 1 tlillnio l\ing i ll .l ...Illlplt, ot the Los Angclc-,gene ral (l\ lpu hu jOrl . , \ 111 JP..y ~ - h i J ( ry 1938; 145 :7 12-7 17
16, W ~II ~ KB. G ll l ~lill !-\ VI'!. Bum.nu ~, t t\ : Psvch iatnc diso rder in ;I
....ample of rhe geller;1!jlupuhltio/l \....uh an d withou r ~ ' hru nit ' mcdi(<II wndirinns. Am J P... ~ ·, hialr Y 19H8: )45:Y7fi- 9JolI
17, D.HJ Collecnon Furnl ~ uf th e His panic HANES; Adu lt Samrh:Person Questionnai re Form PHSh20 f') . W ;l< .h ill ~tn/l . DC. USDep... mn en t 01Health :lII J H uma n Services. 19H1
IH. \'('ildn COS: Health Characrcnsricsof Perso ns With Chr o nic Acrivirv l.irnu anon : f)al ,l Fro lll rhe N at;u n;l l l lc.l lth Sun!;'\' . S c r i ~' "
10 , ~ ll m ~ r 112: Departmen t ( II Healt h, [t! ~I ';lt io o ;1nJ \X1t'll;lfl 'Publicanon HHA 77· 15.\9 . R o ..:k\ ' ill ~ · , Md, N...rion a l Ce nte r fmHealth Srans rics. 1976
19, I 'earliu Ll.Lie be rrnan :\-1:\ : SU.:iilJ sour ces nt crnouon al di :'itrt '~ sRcs Co nunumtv Meut Hcchh 19i 'l : 1:2 17- 14:::
2U, (; nlt ling .1"'1: n i\·il'iull (It hll u~ d l\l l d lahor, \t r;l ill ,111(1 dep r l"~ s i H'
Am J Psychiatry 153: II , 1'010""",1,,, 1996
JUD I). PAUI.US. Wfl LS, ET ..I L.
symptnrm . H n tl n ~ Mexican A Il\ (' r i ' ; ln ~ end non- Hisp .nuc w hi r c ~ ,
Psvchcl \X1onWIl Q 1l::l'lU; 14:10 .1-1 I i2 1. Schl och rcr l\-ID: AIl31J's is o f inco mplete ruuhi variure Ja r.l USi ll ~
linear mud d ... wi th ..trth :(Ur t" ~ t cova rian ce murr iccv. Sr;le Med19H8: i :317- .U 4
.." l lubcr PJ: T he:hl'!l.1\'iw o f ma ximumlikelih ood csnmn rcs undernonsmuda rd cond inon s, ill Fihh l krkd l'~ ' ~~' l1lposi u l11 , 1 9f i . ~ .
berkeley, UniH'n.ity of CJ lllurni.\ Press. 196 7, pp 22 1- 13313. C rn'n he rg.1'1::. Sng lin t., Finkelst ein S. Berudr E: The econ om ic
burd en of depn- , sio n in 1'J90 . J Clinl'sychiarrv 19 9.1: .' 4:4tH41H
24. Sherbuumc CI>. \'\-'t'1I1o KB. 1iJp RD. RU~l"T :'i \'(.', Burnam :\ IA..ludd 1,1,: Subrbresbol d depression nud depressive disord er : chnical t · h M a ~· tt: r i s ( i", IIf ~ l ' n er31I1l eJ I ' J, 1 and menrul ht';lhh ,p .:d ,lIryourpancnr s. Am J r S J ~ ·h ial r y 1994; 15 1: 1777- 17N4
2.' . Ju dd L: C lini'J. 1 " l.1 r 'l ~ 'r e r i ..tics 01 su l n ~ 'n d r t )I1l , 1 1 ~ Y ll1 p t tl m J. t i ~ 'dcp re....ion, in C r i r i,a l l" ~ll l' '' in th e Tre.mu eur tlf M l~ ,t:t i vc Disor der s. vol 9 , Edit ed hy L lll ~ ~'r SZ . )\nll lc/ Ill N. R ,h :. l ~ ll i G.M cndl e....-icz J, Basvl, ~ w i l/ , l · r t l n d . Karge r l ln r~ 'rn ' lli tlll 'l l AI,.';IJ ·('m y tn r Biutlll't1il,.·;11and I>n lR Rcscar chl , 1'1'14 , I'll fl7- 74
141 7
Reproduced with permiss ion of the copy right owner. Further reproduction prohibit ed without permi ssion.
23

Boundaries of Major Depression:An Evaluation of DSM-IV Criteria
Kenneth S. Kend ler, M.D ., and Charles O. Gard ner, Jr. , Ph.D .
~ Little is k ninon about the boundaries between rnaior depr ession and mil der subsvndrn ma! depressive states . \Vith respect 10 dep ressive symptoms , does V SM · IV "fuTz 'e "a lu re' at its ;oin ts"? Method: III perso nally inte rnieu/ed [emalc twill s fro m d pop ulatio n-basedregistr», the authors exami ned wh ether ,1 ran}<e of vaiues uhmJ< th ree dim ension s of the depressiv« syndrome "SSeSS( ,tI ill the last )'('ilr (number of symptoms listed ill DSM· III·R underdiag nost ic criteri on A (or rnainr depre ssive episod e. It.,peIo{s£'llt' rit)' or impairm ent requi tedtv score s)'m/J(om s as present, and duration of episo de) predicted [uture depress;" ,' t'fJisol/esin the ind ex twill and risk of maior depression ill the co-tunn. Bssulu: A ll increasing numbero{criteriw zA sym ptoms predicted, in a monotnn ic [asbion, a greater risk (or [ut ure depressiveepisodes in tin' index ttuin as wdl as a greJ t"r risk [or ma tor depression in th e co -twin. ,'\'0sucb co nsistent relutions hip was seen unth duration CJ;episode. Fe" nn -erity, u single numutuni c[unction I" edid ed risk in the cv -twin. while ind ex twins unth seL'erc' impairment had " substanthlll" high a risk (o r future episodes than did those with less H'l 'el'(' impairment, Four or[eu -crcriterion A symptnm«, syndromes comp osed ofsymptoms im'oll/ing no or minimal impairment, 1.1Itd cpis.idesl}f less than 14 days' duration all signific,mt ly predictedboth future depressiveelJisode s ill the index twill and risk of mdior depression in the to-twin. Co nclusio ns ' Theauth urs linmd little cmpirica! suppor t (o r the DSM - IV requireme nts fo r 2 w eeks ' duration,fif'" s)'m ptoms, or dinic,l/1)' signifi cant impairment. i\'1ost [unctions a/JI}c',lred continuous.These results suggl!st that maior depression- as articulated hy VS A1·!V-may he a diagn ostica nu -entiun im posed WI" conti nuum uldepressivl! sym ptoms of l'"rying sl'l!erity (HId duration .
(Am J Psychiat ry 199H; 155: 172-1 77 }
T he: depressive syndrome is o ne o r" the o ldes t in psychia t ry, ha ving been clearl y descr ibed hy the phy
sicians o f antiquity ( 11. Man y issu es have long heen dehal ed in rhe nosology o f depression, includi ng therelationship between " mela ncholic" and "neurotic/react ive" depression (2-6 ), (he va lue o f the primary-seconda ry distiucrion t" , HIand "familia!" subtypes (7. 9) .a nd the dia gnost ic inter face betw een depression an dsc hizo ph renia (10- 12) , However, less at tention ha sbeen paid to th e bou nd arie s of the de press ive syndro meitself. Perhaps thi s is becau se the key di agno stic qucs-
Received jan. II. 1'1'17; rt'\'iloiclll received Auj.t.'\ , 1'1'17; accep tedA u ~ , I I. 1'1'17. FWl1llhL' VirKin i;J II\'irilUtL' fur 1l1oyL"hi<l t rk and B chavior,ll ( ;L'nL'l il:) uml IhL' Dcpa nm ent of P ) ~y h ...rry and rhcDcparr mcmIH H uman (it·llt'Ut..lo , ;\h·d i.,:.d C \l I Ic ~L ' HI Vi r~l1li J ti t V l r~ Il H , \ ( :0111 IIIUlHH',lhh lIn iH'r"iry. Richmoud . Add rc..) rcp riut requcvrs Iu Dr.Kcndler. I',ll , Bel;'; IJ ~OI1(,. Ri..hmoud. VA 2,l.!I1X-tH26: h· ndlt r<.ah ~ ~ .\' lo: U . C JU (l'ol1hlil,.
SUf'f' tlf h:J hy ~ 1 !\ I H wanr", ~tH ·4 11 xl H , M II ·4'1491 . MH-Ol 1 77.JlIJ r>. IH ·54 1,\11. T h ~ ' V lr~il1l , ll\\il1 Kq,:...rry . t · "' t .\hh ~ h ~ 'J J llI.llll;.t \Il
t'llnl·J hr \X' . ~ ; llKL'. ~ l.n . , Ph.n., ,llld 1.. CUft") . Ph.D.• i ~ ", u rp "r1 t' ~1hy gra nt HI>·lh 74h tro m rhl' r--:J tiullal ln",rilutt' uf ChdJ HC:lhh Jl1JHuman Dl·..·d llr Il1Cl1t ,tnd ~f;\lH NS· \ I ) f!4 trolll tht' N.Hillllal !lh£i ·Hilt' tli N~ · ll rtl l lljll.i~ · 'l l ,llld C U ll ll ll\ lIl l ". lt i \ " ~ I ) j'ordl.'I S ;JnJ Stroke
172
tion in patients wi th depr ess ive sympto ms in clin icalset tin gs. where mo st depr ession resear ch has been car ried ou t, is usua lly, "Wh at is the hc.:st d iag no sis?" How ever , in epidem iol ogic studies , wh ere th e ran ge of syrnp toms is broader a nd mild ca ses are common, the mor erelevant que stion in ind ivid ua ls wi th dep ressive symp toms is ofte n, "I s thi s a C.1St' o f maj o r depression ?"
Wl' eval uat ed two mut ua lly ex clusive hyp othesesa bout the synd rome o f ma jo r depression- as arri cu lated in DSM·IV,
1. is major depression a discre te syn d ro me with" po ints o f rarity" at its bounda ries! That is, is there adi scon ti nuity in et iol ogic processes so chat maj or de-pression differs qua lirativ ely a nd nor [ust qu a nti tativelyfrom subsvnd rom a l conditio ns?
2. Is m ~i or depression a diagn ostic conve ntion irnposed UI1 a cont inuum o f depressive sym pto ms of varyin~ severity a nd dunHion ?
We eva lua ted three ke~ ' features o f Ihe s)'nd ro me ofmajor ut.·pre ssio n: I ) numher o f sym pto ms listed und ernirerion A io r maj o r depress ive ep iso de IDSM-IV reoqu ires tha I al lea st iiVl' be pfl'sen t}, 2 ) b 'el o f severil)'o r impa irtnt..'nt req uired for ra ting indivi duJ ) s)'mpw ms
Am/l's)'chidlr)' I.H :2, Fehru,,, )' 1YY8
Reproduced with permission of the copyright owner, Further reproduc tion prohibited without permission,
24

KI't' NETH S. KI'Nll l.fH ANIl CH ARI.ES O . ( ;AllI>Nf:R. JR.
Number ot Symptoms. Level 01Impairment and Duration
Hypomests 1
Hypothesis 2
e~ c
~ ~~8CI £
~~
<;~c
~~~ 6~ uoo.f
~ .~. 00Ii
FIGURE 1. Two Hypoth esized Relationships Between Levels of Diag.nost ic Crite ria for Major Depression and Validating Variabl es"
MET HOD
Sdmp!t·
as p rese n t (DSrvl· fV req ui res either significant d ist ressor significant irnpai nucnr in tuno ioni ng fur the entiresyndrome }, and J) d ur a tion (DSM · IV requires a minimum tlf 2 wee ks) , Ou r strategy W ;l S to evaminc, ill .11\
epidem iologic sa m ple of (l' 111.1I" twi ns, individuals withdepr essive sym ptoms wh o rep orted vary ing num bers (Ifsymptoms, dur ation, and levels of severity o r impairmenr, both above an d below the DS\ l · IV di"gno sticthr eshold , III these individuals, we ex ami ned how varving levels of these feat ures predicted nor only future episod es of major de pr ession bur also risk for ma jor depression in the co -twi n-two o f the va lidati ng uitl'r i.\most wid ely used for ps ych iat r ic d iso rden, ( 131.
As sho wn in figure I, and previously a rticula ted hyKendell and Brockingto n (12). hypoth", is I predicts J
disconrinu iry in the relationship among sym pto ms , du ration. and imp ai rment and th e validat ing criteria. Forexample, th is hypothesis predicts J much larger difference in the risk of major de press iou in co- rwin v hcrwe euind ivid ua ls having tour versus fin' of the criterion Asympto ms th an her ween those having three versus fo ursympto ms or five ver sus six . Bycunrrast, hypoth l'sis .1pre di ct s th at rhc rela t ion sh ip am on g s~ m p t( ll1 1'\ . d ura rion, a nd im pair rncn r wil l be rd atively ,,111011(h and ( on tinuous with no appa rent " hrea ks" .1(the po ints a rt iculated in DS\ ·l · IV.
Tb v ( :;lUt:;l",i;lll t"' Ill;llt- \ ;llIl,,"W \ twill.. "!Udlnl lll rlu.. n-purr M I.'
rM( of ;1 IOll1lolluJ ill;ll "lUJy H i ~ ~ · l l\,'l i.: and ,,·Il\·lfl)llIIWIlf.ll ri..k t.rc.ten s io r ..·ClllI I1lO Il I' syf.:h l,ltf i,: J i\llfd,,·r... T Ill' rwm -• .1\<: l·rt ,lillnIIr Cl Ill,h i' pllplIl.lfioll ·Il;l\rd V tr ~ill i J l win R I.'J . :.i\ lr ~ ' , wen-,·hgihk hi pM
ncip arv in l1,is " IU J ~ ' it hurh lll\·llIh,,·r .. HI ,hl' p.ur had ph·v i H u s l ~r"'spll ndeJ Itt .l m.nlcd yunriunn.lir\·, I I I which rlu- lnJl\ iJu.lI rc SPW1Sl' rare WJs. 64·l{,. ln (lUI' ti"r sene.. tit p\·r..0 11 ;11 in terviews , wvsucceeded in interviewin g 1J1 ·};. (S =2. 1h.l l til t he dir.:. ihlt' iudividuJb.. Nirll'ry pt'rl:t'lllllt thl.'iunrview.. were b ,,·t··IO· I.l( \";th t· rvsr '\'t' f,'com pleted h~ ' telephone. ~ : rill t'll ml\ lrmt'J cunwnr W; IS ob tainedbefore J II f a,, · t' ·to -f J ~ · t' interviews . illlJ ~'wr " CII1JI il\WIlt was nht ailll'dlor JIl tdephnn(' i lH ~ ' n it ' ''''' '' . Tht" n1\'illl .l~ t' li t tllt' 1" , lrti~' l p.lli llgtwin !» was .lll, l Y\'ars l ~l> = i'. 6 I. Z n !.llsity Wi'" dt'h..rmim·J h lilld l ~ h ~using sra ndard qut'ui ons 1141. phu tu}:.r,lrh ... ,Ind. w h"'11 1l~ ·": t '\" ;I r y .D:"A t('sting ( I. ~ J .
Sint:r thr o r i ~l na l int('fI,'lt'w, we h;l\'t' ,,:ulllpk cl.'d tWI)aJJHiunJI M:rirs (If tdl:'phonr int\"·fI,,il:'ws. wkt..:h 'oUf.:I.:c,·\,.·Jed in i n t l n ' i l' w i n ~ 1.110 I(1J1.5"'/ul and 1, ~ 9 H 187,7'1." 01 t h~ ' nr i~ i n J lly illh.'fI,it'Wl·J suh ic..:ts.r(,spc'l.: ti\'dy. The mean nUlnhcr uf month.. hc.' lwl·r ll rh,,' fir..t .Illd thirdinter\'it ws wa'li, "1..\ I S D=~ . ll .
Fur thl'st"ana lpC'!Io ' W I' \Ist·d t\\ 11 'olIhSJ lllr 1t·s: I I inJ i...idu 'l ls whuf.: omr1t' tt'd 01 11 thrrr rrr !loUnilJ i nr t' n ' i ~ ' w s IN=I.X12i, in whunl WI.'anrmptcd w prt'J ilo:( rbl.. lur major J t·prn ..ion ,It tht' tiln,,· nf t'ithc:rIht' st'lo: und IIr th ird inrervi,'w il!lo ;1 IUIlt:tiOIl o r rht· ..:hilt.l,,·[eri..t....... lJfd cpn ' s ~i \ 'e s ~ 'n J romt's It'pu rled at Ih\· fjr..c lIllcn ·iew. 3lHIl lmcm ·bers lit pair s ui knuwn l~ w , ..i r ~ · wh"f\' both lIwmher",Wl'H' inrer\·it'..... t'J oil l('ast oo..:c' l)\It'r the fir..t. Sl''''UlId, 311..! third int t'n ·i,,·......IN .2 .0.lH).
Mell$ures
Info rnu tion ..... o)!Io ~ ' II I1 t' c.:rt · J lrom J IJ f ~ ' sp ond t'lH s J t l·..,,·h ui thl'Ihre(' i 1H t' n 'i t' w ~ lin th~ ' o..: ..: ur ren,,·\' III 20 indi \'idll id SY l1lpttllll\ J Ufi n~ tht' )'car hdor t' int l.'r\·it'w. h HlrtC('1l o t' rh,'w \ ~ ' l1l flt O Ill\ wt' r ~ '
Number 01 Symploms. Levelat Impairment and Duralion
.1\X-'u h h Y Pl)t ht'~ i .. 1, ;1 sba rp discounnuirj i!lo IIh",,·r\'!,.'J III the " .l li J ; llI n ~
vari.tblc Iri..s" IIf recurrence ol maimdepression or n sk ut mujnr J~ '
I""·....ion ill <l ...o- twim " So i1 ililKtioll o f the level IIi the J i,lKnosti,,'\'rit"ri;1(ent· num ber III ..ymptllllls lisred tor I.: rirt'riu ll A in the nS .'.1·11 1·1{;.IiJKIlO:>i:> of major J ~ ' p r e :> li i H ' ejusod c. Ihe k'vrl II I impninnenrn'411 in:J for r ;lIi ll~ ,1 SylllJ"1II1l1 as present. and tbv durarion (Ii epi..oJ\ ·~ ) . SUf.:h.1 di""·C1ll1inuit.\· Il l.l ~ ' indi,,'at";1 " true" Ji .\ ~ ll l) s t i l.: bound Jry ill Hallin '. Ky co ntrast. ....-itb h ~ 'P Cll h l ' s i ll 2, con tinuity is observedb ~ · t w l · l ·lI the validating \'ilri.lhlt' and Ihl: Ji agllu..tk ..:riteria, Su.:h apJrt t'rn uf r"'\ ults would . " ~ U t · thJ t, with n:sflt',,'1 10 fht' valida w rst'xJll\ illed, thl.'J iJgn usti,,' <:riteri.l rdl (,l:t a wntllluum o r sevc:ritf andnot ,I Ji"""t'tt' synd rum,,·. Thi\ 'igurr is ilJ apled frllm Kendell andBrod . \Ilgtun ( 11 1,
J i s <l jo: .!t r q ~ J ( ,, 'd \·t'rsions of the nillt' s ~'n1Jl rom s Jistt'J unde r ~ r i t r r i Cl nA lor lI1 ajor J cprc\si\',· r r l",mtt' in D!'lM·llI·R (p. 221). Si", of Iht'nint' symptoms wcre t'J..:h n .'pre ~em rd by ;J singlt' itt'm. Two s)'mp'IUIlIS werc= u is J~r t' K.lI" 'J illlu t.....o items 1'.Il.:h; .:ri lerion A4 ....'as di·\' ilk d into "cr.l ran: insllmn i;J .lnu h)·per)()tnni3 j't' ms, whi l(' ..: ritr riull A.' W ~l S di\,jJ l.'c.l inru "ep<lt:.l tt' itc,'m!lo iUSC:SSill)t ps y~ h ()mo torJj.:. it<lr inn dod rt'tJ rdat iu ll, Crih.'rillll Al ......15d I S:.l g ~ n · ~i It I: J into fou ritem ,,: J el:rt'ilscd 3pret ile . in" re.1s('d otppedt c. dt', 'rras('d weight.Jn d inl.:n·ils,,·d ...... ei1loh t ,
S ~ ' lI1 r t I) I11S Wl'rt' rt'c.ju ireJ ICJ h;I\·l.' a dUrJl iUllut 01 1It'Jst 5 dilys. For~,\ ·t'r y "'ympwlll report ed prl'Sl'llI h ~ ' Ihe suhjel:[. th\· intef\'i('wer inquir c:u ;lSW th,,' po ,, ~ i h il i t y tha t it Wil " due to r hysit:al illness or mrdi·..:ati"n . Ii in ,h e intervit'wt'r 's juJ gm,,·nt th is was thc,' ..:asc, whit:h IX",,'urn'U 17.4% of tht' rimt' .1 ~ " OS S ,Ill 'lo)'rnptoms. then Iht' symptom was~ " lIl ~ id ~ ' r cd llUl prt lol:" llt.
Fur t' ol ,,'h symptom r t'p ort~ 'd :IS prC'SCllt, we ;l1"u inquirrd abo ulth.... !in"r ic)' uf rhe sympwlll and/o r s)'mptom-n:la l"d impairmcnt.
tim J PsychioJlry I.H :2 . Feb",.,,)' 1'1'18 173
25

I\OlI N\)ARIf:~ Of: ~ IA I () R flf:PRf: ~ SI() :>:
TABLE 1. Num ber of Criterio n A Symptoms for DSM·lIl ·R Major Depressive Episode as a Boundary of Major Depression in a Studyof Female Twins
Number otCrite rion A ~ Y I1l P h JII 1~
x or ~ )
Ri..k of ;\,:hl jur Depression at Ri..k of I. dt" (j lll~· .\I;l imS~ nll1d or Third lruervicw
." L1 tll ht' f of Indt ,\Dcprcsvion in Co -T wiu 01...1
~l S ;1 Function of X um ber o f Function 'Ii ~ u lll l lt"r ofNumbvr of I l1 d ~ ' 1( Criterio n ,ASymptoms in "l' ,·\';ns R t'port i ll~ C riter ion :\ Sy m r tlJ l1lS inTwin e f l.t ·Pl l rtlll ~ Episod car Hrsr lnrcrvic v S p e ~..ifi..: N umb er ot First Fpi "Olk ' elf InJl.'<O: Twi n
~ r ~ · \ ,: i ii ..: Numbe r Ilt' ~ ymp fOrn :io at First,~Y l1l r t \ l l1 h at Fir,r Od ds p tou v- Second , o r'! hirJ Ri," P (UIl\··
lnn-rvu-w' Rat io " railed ! lnrcrvicw'' Ratio z r.llk·d l
1> 4 I.NN 3.9 4 O.tJ2 14~ 1..17 fl.W 0 .00 7(,J 1.M IO,nS IJ.{lOO '5 1 5 . ~ 1.4 ~ ~ I . IJ Y O.tlll i5 S _ ~ ,4 S 17.16 1.1.000 1 124 1.47 ,"i.IHI IJ.00146 1.i7 12.0U U.l}()01 11~ I. N.' ~ 1 .! W iI.OO!)l4 1 6.S0 l l3R IlOOlll 99 1.~4 1 1.X.'\ (I.1I1l0 1n 1.l.26 44.4 5 U.OtH)1 72 2..'.' ~ 'f •.'\g 0 .000 1
- N um bc r Itt ind e x (Will!> wh o JiJ Ill)( ha ve a uu nim al dep ressive !>ynJ n >1111." in the prl."\iotl') ~ t'" : lJ at t' i l '~ l illh:r\ ir \\ \\";1'. 1,3 I ~ .I·NlIIllhl,.' r of index (wins who JiJ no r havea rninimal dcprcsvivcsvndrum e in previou s Yt·;lJ .H li r ~ r . ~ C ....II11J • •1f third inrcr vi..· ~ \ W .I" 1.-4 47.
Thi .. W.l .\ ,ISS"' \SL'J in wvern l W :l\~ . Usuall v. Wi..' asked how much the"1'\·,:i1il..· S ~ ' l1l rHn l ll ( q ~ .• r"t.' t.' li n~ ~ d Jerr ~ · s~; o ll . lin ·JIl l'", ~/f.1tig,lll·) inr ~ · rf ~· r ~ ' d wirh rhc ..ubj vct ' .. daily lill,.' . Th e respon se options were"hotrdly ut . , I 1. ~ ~ S O l\ W . M "u lo t. " und "vomplere!v. " For weightuain.nul lo\ !> . we avkcd rIll.' num ber 01 f"oLlllJ .. losr or gained. rc')IW..:riH'ly. lur insomni u and h Yr ~ · r ~ (Jml1 i " . we asked rill' number ofhtlur ~ nt lost sleep or hour .. spen t ill exrru ~ In' r . respectively. Foriuc rcawd or Jt·(r l'oI SI,.·J ; \ r rt· t i t~ , ,md for p"y...hom orur agi r..mon, inn-rvicwvrv , " ftl,.· f J1r ohill~ . ta red th e "rl1lJ'l ttlln a-, ..everc. mo dcm re,o r mild . ' '(' l' rn lul,.·I,.·J r ,, " i l\~s 01 " ~ ' \'l 'r i r y or illlJ'l" irml'])( r"or ":;\I,.·h'.VOlJ'lWlll inttl th rl·t.' ..: , \t c~ urics -ll1 ilc.J . 1l1Odt:"nlll·• •\IId sl....c:rt: . t or~ ~ ' IIl J'l fll InS \\rhl,.·fl· Wt.'illl,.lllircJ ,llllllll illlJ'l"iTllh'llt . \W ":01l\'I,.· rtl·J til\'r ,lIil1 ~ " ,lS full ow !>: lII ilJ = h ;lrJI ~ ' .H .111. lHuJ n:l tt"="llln l,.· .. 'llhi "1,."\, ·rr :;.11m IIr ( Il m J'l l l · l d ~ . For \\c i ~ h( ~ ; li ll :lnd w"i ~hl luss. W \' dl"lillt:J mild. lIIuJ erJIl', .1oJ sn ...·r l,.· iPi ,Ul t"r i" ,J ,'. rd.Ht·d w " l~ h l.... h .tn ~t ·.,t < In Ih, IO- I-I lh. JnJ ~ 1 5 1 h , n,"sll"·I,.·riw) r . Fur i lhUlnni' l;1 nJ h ~ ·pt ::r sull1 ni a . Wl' dd'in"d llulJ. nlOJt'r.He. ;, nd !>t·\·..· f(· ;lSan t"pi!>uJ t.'·rd.lh·d ..: h . \lI~ I,. · in ..In·p 01<1 htlurs ...l - 4 hllurs. anJ ~ .'5 huur').rl,.'"pl·t:tivdy . Fur () \ ~ I ·IJl - J{ l'ri(c.' ri.\ (hiH \\Wl' r l,. ·rr l · ~e: 1He,1 h~ ' mu Tt,'dl;IU un c i(ClU. WI,.' IUU\.; the HU b( s,'n'rl' ..y m p w lll· r d a ( ~· d illljl;lir1l1l:nt n·ptlTtt·tl.
Altt' r inl,.luirilll-: ,lho Ul thl' il\J i\'iJ Il'll \ ~ · m pllJl11~. thl' iIHl·n·ie:Wt.'r; l ~k t: J rhl,.' rwin whi,:h il ,111\ of rht' t'mlllr!>l'J ,,\'mr rnlT1 ' ..:o·tk:.... llrn ·dill t1U ·la ~1 ~" " lr. Fur rlH' pu r p n ,) l' ~ nl rhis 'HlldY.'Wl·Jciinc:J a minimaldl'rr l'sslvt" ~~ ' n d ro n l\' ,h l,.·on..i\ (inJ.:, of .l( Ic,1\[ th rt.'l' l"1l- (J....,· u rri n ~ de>r,,' s~i\ !!oymplOnlS. reJ..\,\rJI..·s!!o ul lt"\'el01'l 'n'l"i t ~ · or impolirmelH- Ol1l'(II whi h haJ to hI,.' J l · prt ' ~ ",J mood or I m ~ 01 i1HL'rt's r / p k '~ ls ll r e: - ;\ l1 d
I,l"ting ;l[ le,1M 5" dilyS.Tu ,,·xaminl,.· (ht' impa.:t (JI (ht' numhl'r of s}' lnpWllls reported. WI,.'
rl·quirl,.·J .1 min imum dllr;Hiun of illlI\'s') Ilf 1 \\ t'eb and, in <1(cOI'dwith DSt-. I·III·R. Jid litH r r: l,.lll i r ~ · illlYk\"d til " .\ t.'ri (~ · or impai rll1entr'ur ,lll ind i\' iJll ,11 ~ y m rt l)m TO hI,.' t:llullteJ as pr,,·wnt . Tn eX,llninl'lhl" imp:h:t li t 1L'n.·1or' ~ c \'l,.' r i t y ur imp iliml l·]} t. Wl' reqlli rl,.·d " min i·mu m du r.ltinn (If 1 Wl·l·ks .lnJ ill 1':<1 S1 fiw 1'1lJmseJ ..-ri(l·rinn A!>Ylllr rtlllls. \\::c tht'n J t.'lllll"J rhrt'l' hl...r;lr.... h i..: ;l ll ~ · . lr ~ :ln i le d ~fflUr S _Suhjl''':IS whu hiltl fin ::nr murt.' 01IIH' ..:rilcrion A .;y m p (Um .. :a1 rhl'~ \ ·\ ·\ · r t.' In d Wt.'ft· d . 1'. ~ijil,. 'J ;\~ Sl:\·crl,.' , Th OSt' who h:ltl iin::nr mure:.... rilt.'riu n A :' ~ ' lIl p t u lll') <11 1"(" moJ ..·r;l(\· It,::ycl hlU wen: no( d :a..sifi...Jin lh\· St' \'("U' ~ W Il P wcrt dassili\·tI ;h lUudcr;lh::, Thu sl' whu nll'r li..t'tlr nll)rc t:ritl'riil unit-Jt the-milJ It''''d l,tnd (hu.. JiJ nO( ml.'ct l"ritt'ri;(IlIr eith t'r (he m uJ l " ~;H l ' or ..n l'fl' ~ r tlur) Wr:rt' d assilit"d;h mild. Ton ;lmint' rlH' impi1l"l III Ju r.Hitltl.. \u' r l '~uir t'J .\ minimu lll uf five~ ' r i t rr i o ll A symptllflh hut no '\I,.\:llmpi' l1}1Il1-: 1~ " 'l ' l of st'\'l' riry Dr illl'1""inm'Ill JnJ h'ld no rn"lllirtl lll,.·IH I t l( J r tl" tl rt~ ' J Jurat ion longerth'1I1 .' diln•.
In .1J diiioll to i n~uirill~ ,lhllUI tbt.' h i !>tor ~ ' ut Jcprl"~si\"L ' ~r lT1 I l( O l mill th...· I"st yl,.· ,H. ,n horh tht· li r ~t ~ lI1 J third imcrv it'ws Wt" inquired, \ ~(l llt rht· iir"t"r illll,.· h l o;rur ~ ()f 1lI .1jor dcpr \·s..i'll1. ll si n~ a se:crjoni1J Jr tt'd from tht' Srn l":UlTl,.·J Clink 'll llUt.',,· iew ttl( DS?vl-III-R (16).\'('\, d .lSo;i til'd il twill ;l" h Jv ill~ ,I l i l~ 'tll1l ~ ' hi~ tor} 01 m;ljor lk prl.'ssiollit ,h i' rt:portl'J 01lt.'or lllOTe l'p isoJ t'" l\l l,. ·~ · tirlg, DS\!·lIl ·H nitt"ria dllr·in~ ;ll1r IITlt' ul rht"rhn '(' illle(\,il,.'w:-, .
174
Statistical Mt,tlJOd$
Our <lll.tlyse:!> t.';": ~l lll i ll t' d two pot enr iu] va lulato r-, of the n u "lJln~il,. ·
boundaries of major dcprvs..illl1 , Th e firsr llf th c ~\ ' \V.1\ risk ( I t recurren ce01 DS:-d·IIl· J{·J d ined lI1;ljor J tpr t'!>..ion at the secon d and third interviews .1$ predicted ~y chnra...'teristics of the dcprcs-ovcsynJronl\' ." .sessed ut the first iurervicw. These analyses were ....onducrcd hy \\\ inJ..\ll) ~i s ri .... regression, 11rH:r;1(iclfl;lli/t'J h ~ ' PR(X: I . ( ) ( ; I ~ r! ( : in Sr\ S 11'71.Subgroups of twins with .\ J ...pressive synd rome l\ ' . ~ .. those with three .lour. lin', or more ..:ritl·ritlll A "rmplmn'il wrre I,.·wnpilred with twill!>who denicd J minim.tl d l:p r~ !o si \ '\" s~ 1It.lmm l,.· .H dw fir..r ill(t",·it.'w.
'1hI.''it'wnJ \·:1liJ .lt ur l'\ alllint.'ow:\s rhl,.· hJ/;lrJ r.He:of lift' rimt' Il l.!'
illr J t·prt:s, itm. J di m'd h ~ ' DSM· III·H . ill Iht.'( O ·IWlll ;h.1 IUll..: tillll ul(t"alures of thl' first minimal d <r r t' ~ !'iin' synJ ru ml' ' ·'I",,·ricl\I,.·,,·J in rill'tin ,l, ..e: (" n n~ 1. ur (hirJ iml·n ·icw. Thi'i Wih p,:rfurl11<J h,. u..in~ th...C tl~
rmpurtin n.tl H.tl'.1fd lUl'lhlkl. .l~ 1I 1 ~rilti un ;l li j/' n l ill rh" rIiHf': ( i pm ·l"cuur..· III ~ t\ S ( 171.[',,,'h l-\wup W .h l·llln l".Iu·t l wirh rwin') whll J I,.·lIinlt'n 'r '-'i:perie:n.... lll~ t"ot'n J minor J l'prc!o')in ' ..ynJ rulllt' ;l( .111 ...\o;l·....·lIll ·1U ~ . If a (w ill w ; , ~ nor illlt·t \·i("\\,t.'J ill ;111 ,hre:l,.· imn ' i"'w!I .111 " rl,.··purred no likrim l"hi!iwry lit" Ill.ljor dq lr t', !> iull. t1l\' 1l lit,!" ' l J..\ ~ · ,II 1.1';1inre"'It:w \\" .1 ~ t r ~ ' ,ll~ ' J a ~ ht'r ; l ~ t' .
For bot h rhl' IOg.lsti\' ;H10 Cll;': <I n ;l l ~ · 'ses . \\.... rer llrt (Iw t c: ~ r t.' ~ ~ i u l1.... lldfil,.·i~·nr. on whkh t\,st.. for l i l1 t" :l r i t ~ · art' apprupri;Jldy IllJJ I,.·, .mdl"hi-squa n ' wit h dl:d . O nt'-mikJ p \',1Iue') :\(1,.' rCl'llrn'J hr l,.·;lUSl' \\"1,.'
haJ ,1 .... It:ar a priori Ji r e ~ti ()ll .l1 hypo lht.'sis. For thl,.· I() ~ i s l i .... ;J1ll1 e ll\
re~re~ 'iion Jllillyses. Wt.' ;,I!>II pn· sl·IH. he":,HISt' (If tl1t'ir t:J.;l.'IIf intl·rp rl,.'·mtioll . (he odds ratin .lIlt! ri..k riUin. rrsr t." .... t i \· c1 ~.
T o orre~t lur the 1,.·lIrrl,.·latl·t! llbser\,;1tiol1s in f} 1I,.'1ll!l\'rS of :l twinp'lir l· nllllliplil::J (he \';lfliITKe ul lhe:: par amt.'tl'f 1,.·,Slil ll,lt...• initiallyoht .,illl·Uhy tht.'follllwillj.; cql lJl io n: tI l +f 1 ~+ y l/L\+ ~ J, wheTt· , t""'l.l,I :II'ith l,.· inrr ,l.... l"s\ I,.·orr e-klrioll ill t\"'ln p<1 irs for (hl' J \'p"nJe::lil \ ari.lhl\'. ,\.e q u a l~ till' tHll11 hc:r Il l' ":UlHrlt't..· rwill p"ir !>, 'IllJ ." n lllOlb rh\· llumllt.'ruf ullpaired individm\ls in the:: , \ n " l ~ s i$ . This (nrlllub \\,a.. , d ~l.' h r.l i .(<lily J eri \'eJ frum thl' lor mu la lor dUHnt'll !>;m11,lin)( :l" J"·....: rillt.·Jl'oy "ish ( IS). Chi-s\lu.u ,,· ,md r ..alut'!O " we Tl·I,."I!..:UL! (t:"J h;tseJ 1111rhl!>nt'w :mo hUl!-I,.· r " ~lilll :W : 01Ihe ~; u n r l j n ~ \·;1fian( I,.·.
" h' wi..ht.'ll fU Il.'SI ~ (: lt i S ( it'; l ll } · wherh\' r rh~' rc:l.:IIIUlh hir !> I" 'r\\'\"\'n(Iur prt.'tli..:tor;wd v;.li•.b tut \ ar i;tl"k!oWl'rt.'l'nnrlnUtlUS(hYJ1u(hc..i ~ 1in figure I )or l.:ont a ill\,t! ,I di....:ulIlinuil r { h ~ ·p t ll hc s i .. I in fl ~ u r,, ' JI. Tudu !'ill . we l"lImrHl'd tht' r'il-mC,I'iUtt'd in lu}t likc-hhnoJ unih__ )f "s~'ril '~ uf loj.:istk: and Cu, rc:p t·!>')illn llloJ d !o, il1dlld lO ~ only suhi!;'I,. "wirh 'l minilll,11 J t"pre"!oo i\'Csyndro l'1t.'. \X:t' Ilr!>1 iiI ,1 " ~ 'o \ ';lt i ,lI"" ~ olllr "lIloJ el, wht"rl,.' rh\' soil' prnJi l,.·tor \''In:11, lt''Wi'" ~e ~ lT III hirth . Nt:xl. w,'t'xa lllilll,.·J Ihe Illlpro \'\'IlH'llr in til uht:lim·J when .1 ,ill ~k lint':\r Inn..·•tion \\' ;l \> aJJeJ . Thi s Ill\l~ ·ll tll\ , .\S ,kp;..:r,,·d in f i~ll r \ ' I lhyporhc:\ i\ 11.a!>!>lIm c ~ ;l .... n ml nuo ll~ lilW.lT rd .Hion!<hip hl'tWt"t"1l thl,.· rfl·dil..·lllr .1llL1v:lliJ,11or fm ' ;I ~urc s ;lntl l.';ln ht" sr ~ ' I:i1 l rd hy ~ 1 s i n~ dt.' r; \f:\n1cte- r. ~i ·n;1II>', \\'1,.' fin t"..!., f<111~l ' or' mo rt.' ,,:olllplcx mnJds ~tln t.\illil\~ r ~ \ 'l1 IIrmo rl' p:Harn~ 'tl' rs , whil,.'h int roJ lll:l·J di " nmtill Uiti~ '~ into thl,.' rd .uitl n·ship l·itht.'rin rhl,.· form III ,1 , c~on d lillt".lr11I lll'ticJI1 ol".1dUlllmy \';lTi;lbkspcl' if yin~ th;1tall indi\ 'idu;11 \ ' ;H\ '~~ Clr y nf (hc r r\ ' Ji~ ' (I) r \ ;lTi"bl,' h.h J
Am ,/ 1'5)'<" ;l1l r)' 15.\:2. Fe/mlar)' 19\18
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.
26

K E ~ N ET H S. KIS DIER AN D ( :H.~ R L ES O. ( ; . ~R PN E R . IR.
TABLE 2. SeverityofCriterion ASymptoms tor DSM-III-R Major Depressive Episode as a Boundaryof MajorDepression in a Studyof Female Twins
SI,'\'t' rtf \' or ImpairmentIll'Cw t rinn ,\ S Y lll ~'lt ll m :o.
.\I ilJ
.\ loJ "'fa!..,Sever e
N um ber o t Ind..-,'l wins R t'r Clrl ill ~
~ I J i or Deprvssiou\'('jrb S ~ 'm p w m ~ ofSpecific St' \t' r i l ~ tIT
lmp airmenr ar FirstInter view'
1710 140
Risk o f ~ I J i or D"'pr t'\s ioll atSecond or Thin) lnrervi..-w
J ) ,1 Fnncnon of Scvcr irv o fS ~ ' m p t lJ m ~ in lpisode ~ H
First lnrerview
Odd, r too c"R,H!u X' (ailed l
3.1)7 I ,'i.07 Il.Ol)OI.\.42 1~ .9.'i O.(X)()1
I1. M 47.99 II.UOO I
')2176%
Ri..k p U IIH' -
Rat io X' l ~lI k JI
1.';1\ 4.U1 11.1131.:"9 .W.- .'i n .nOIlI1.22 '" - r 1I,IIOl l!
-X umber who did nut meet DSt-.I ·IJl·R criteria fur l11 :ljur depressionin previous yvar ct fj r ~ t iurcrview wav l,<l4 4 ,n:-":\Imlx' r who J ld 11111 rnccr DS.\I-II1-R ( rih 'r ;'l fur m"ior depression in previous yC';lr ;H first. second. or third in ter vie w w.,,, I. (, ~ ~ .
umq ur- ' ,11m'. Thr lits or rh""t, mudd s were com pared hy - .! );: {I ' l ~Iikt..'lilumd J. \\ hich .lrrw:-.:il1UIt'S a clu-squa rc Ulslrih uliu ll,
RESUI.TS
Number ofCriterion A Symptoms
Comp ared with su bjects who denied a minima l depressive synd rome du ring rhe previous year at rhe firstinterview , the futur e risk fo r an episode of OSM-III-Rmajo r depression was significantl y higher for individ uals with a dep ressive episode that included only threeo r tou r crit erion A syrn proms (rablc 1), In genera l, thegre ater the numb er of cr irer io n A sym pto m s p resen t ,rhe gre;.l u: r rhe risk fo r a futu re episode of ma jor depression. No suhsta nrial d isco ntinu ity wa s apparentbetween four and five criterion A symptoms as hypothesized by 05"1-IV. Howe ver, the risk for futur e depressive episodes was substan tially greate r in subjects withseven o r mor e than for those with six or fewer criterionA sympto ms.
In model ing the rela tionship between the numbe r ofcriterion A symptoms in subjects with a minimal deprcssivc synd rome and the risk for futur e depressiveepisodes, we found tha t, compared with a covuria teson ly mode l• •1 marked impro...ernent in fit was obtainedby a sim ple mo del wit h a sin g le linc a r .fu ncnonIX'= 20 .6 1. di =1, p<O.OOO1). No other significant improvements in fit could he found , the closest being theaddition of a second linear func tion, which increasedthe slope of rhc regression line between six and sevencri terion A sympto ms (X' =1.60, df= I. n.s.),
COIl1 p<Hed wit h sub jects who denied a minimal depressive synd rome dur ing the previous year at the first- ,second - I and third interview, the risk for lifet ime majo rdepression in the co-tw ins was significantly greater fortho se twin s who reponed a depressive syndro me withonly th ree o r fo ur cr iterion A symptoms (ta ble 1). Ingenera l, the risk of maj or depression in the co-twin increased with an increas ing numb er of criterion A syruproms. J'\o discolltinuitv \vas seen hetween four ..md fivesympto ms. as h)'pothe'sized by OSM·IV. or hetween six..lOd seven s ~ ' m p t o l1ls . as seen \.... ith the pred iction of riskfor future depressi....e episodes.
Am] PS)'chi,lIry 1J.\ :2 , fe l",,,,ry 19911
27
In modeling th is relationship, co mpared with ..l covariates-only model• •1 huge impro vement in fit was ohrained by a simple model with a single linear functionIX1=Ll.94, df=l, p=O.0002 ). No signi ficant improvements in fit could he found hv the introduction of all"d iscontinuities in the relations hip between number (;fcr iterion A sympto ms and risk for major depres sion inthe co-twin.
Seve rity or Im pairment
Co mpared wirh subjects who did not endorse nSM1I1· R criteria fo r major depression in rhe previous year.those who met cr ireria for major depression only whe nsympto ms were defined as having mild sev erity o r im pairment still had a significantly greater risk for ma jordepression in futur e years (rah le 21. The magnitude ofthe increase d futur e risk was ncruallv less for rhove whomet criteria when individual symptoms were requir edto have ..rr least moderate severity or irnpa ir rnenr (ruhle2 ) and su bsta nt ia lly g reater for those wh o met enterinwhen sympto ms had to have severe irnpair rnenr or severity to be count ed present trahle 2).
In model ing th is relat ionship, compared with a cova ria rcs-on ly model , a significant improvement in titwas obtained by a simple model wit h a single Iinearfunction (X' =4.97, df= I, p=O.03 ). T he addi tion oL, second, steeper linear function between moderate and severe produ ce-d a furth er significa nr improvement in fit(X1=5.16, dfel , p=O.02 ). No ot her sil:nifi'''1111 improvements in fit cou ld he found .
The level o f severity or impairment requ ired for depressive sympto ms predic ted an increasing risk for major depression in the co- rwin in whar app eared to he- ;,l
mon otonic cont inuo us fashion (table 2), Fo r subjectswho met cri teria for major depre ssion o nly when symprom s were defined as having mild seve-rity or impairment . their co-twins had a sign ifican tly h i~h er risk formajo r depression than co-twins of subjects who d id normeet DSM·IIl-R criter ia (ta ble 2 ). These relative risksincreased to 1.79 and 2.22 , respective ly. when, to becoun ted present, symptoms had to have mod erate orSt'Vl' rc..· levels of severity or impairment .
In ('xa mining a sta tistica l mod el o f rhi!<o n: larinnship.we found th;\(, (o mp<\ red with a covi.u iatt'..-only model.
175
Risk o f ~ I J i or D"'pr t'\s ioll atSecond or Thin) lnrervi..-w
J ) ,1 Fnncnon of Scvcr irv o fS ~ ' m p t lJ m ~ in lpisode ~ H
First lnrerview
N um ber o t Ind..-,'l wins R t'r Clrl ill ~
~ I J i or Deprvssiou\'('jrb S ~ 'm p w m ~ ofSpecific St' \t' r i l ~ tIT
lmp airmenr ar FirstInter view'
First lnrerview

K(1l 1~j)A K IES Of ~ IA JO K DfP RES S IO~
TABLE3. Duration of DSM·III-R MajorDepressive Episodeas a Boundaryof MajorDepression in a Study of Female Twins
Risk of J.ifctimc ~t .l iorNumber of Index
Risk uf l.iferime .\:la jo rDep ression in Co- Tw in o1Sa Dep ression in Co -Twin 3!> a
Xumber of' Index Function of Durat ion of Twins Reponing Funct ion 01 Dura tion of"l winv H t'l lllrrill~ fp i\oot' at FirM Inter view Specific Duration of First Episode of Index Twin
~pt' l. :di c Dur ation j)1 Episode ,H first,Fri~\lJt' ar flr'l Odds r (o ne- Second. or Third Kisk r tone-
Dur.niou of Fri ...odt· ( d ;l~ ~l huerview' Ra tio X' tailed ) Imcr" it'w" Ratio X.! railed !
:; - 1" "" .U O ,7.92 u.ooo: 144 LS I 10. M } o.ooo«l-t -29 56 4.42 26.65 0.0 00 1 154 L iS 14 .7 9 OJ'OOI.l O- ,) 4 44 4." 3 22.4 1 0.11001 88 1.,,8 IIAO o.ooos(,( )-y() 38 " .19 28.89 0,000 1 84 2. h4 4\."1} 0.000 1~ <j l 40 5.93 28.29 0.0 00 1 10" 1.65 1.1.97 (1.000 1
.1;-":Ulll ba or ' 1l 1 ~l l ' d ~ who did not meer DSJ\I -JIl·R criteria for major dep ression tcxclud ing dura tion) in previous year at first inter view wasI. ' S4.
1 ' ~ ll l1l l w r ol ..ubi ccrs who did not meet DS!\t·III·R cr iteri a for r naior dep ress ion (exclud ing J ura tion ) in previo us yea r at first . second, or th in'!interview was I .S"i7.
a sign ifica nt im pro vement in fit was o btai ned by a sirnpic' mode l with 0 sing le linea r function (X2=5.77, df=l ,p=O,0 2). No other significant imp ro vem ent s in fit co uldbe found.
Duration
Compa red with th ose twins w ho rep oned no ma jordepressive epis od e in the last year , twi ns with a n ep isodelast ing 5 to IJ day s ha d a signi fica ntly higher risk for afurure ep isode of DSM -lII-R major de pression (ta ble 3).T he odds rat io for future episodes was slightly low er forthos e wi th dep ressive episo des last ing 14-29 o r 30 - 59days (ta ble 3). A mod estl y greate r risk for futu re ep isodeswas ass ociated with d urations of gr ea ter tha n 60 days .
Co mp ared w ith a covariares-on ly model , no significam improveme nt in fit was fo und with the add itio n ofa sing le linea r functi on (X2=0 ,22 , df =1, n.s.), indicatingno star ist ically sign ifica nt rela tio ns hip bet ween duration an d future risk for ma jor de pressio n. No significa nt improvements in fit for th is mo de l co uld he fo und.
Du ration o f the reported depre ssive episode in the indextw in was an inconsis tent index of th e risk for ma jo r depression in the co-rw in. For episodes sho rter than 90 da ys,the risk in th e co -twin increased mod estly wi th incr easingduration hut decreased aga in with epi sodes of 91 or moreJ ~ lYS in length . Co -twins of subj ects with a dep ressive ep isod e of less than 14 da ys durati o n had a highl y sign ifican tly increased risk for maj o r depressio n (tabl e 3),
In mode ling thi s relat ion sh ip, we found that , com paredwi th a covariares-on ly mode l, no significant impr ovementin fit was ob ta ined by a model wi th a single linea r function (X2=2,44, d f=l , p=O.12 ). Th e on ly significan t impro vem ent to thi s wa s fo und with a mod el in which thetwins wi th depressive ep isod es lastin g for 60-90 days di ffered from all o ther ca tegories (X2=8 ,05, df=l , p=0 .00 5 ).
DISCUSSION
Our goa l was to eva lua te two co nt ras t ing hypothesesa bo ut the na ture of the bounda ries of th e ma jor de pressive syndrome , illust rated in figure 1. Do DSM -IV cri-
176
reria for maj or depressio n "ca rve na ture at its jo ints"or is major depression a manmad e co ncept imposed o na diagn ost ic continuum? \'(Ie tested three fundamentalfeatures o f th e de pres sive syn d ro me aga inst two keyvali da t ing crite ria lon g used in psychi at ric research: oc currence of fut ur e de press ive episodes a nd risk of majordepress ion in a co -tw in . \'(Ie fa iled to find ev iden ce fora d isco ntin u ity a t th e bo un da ries proposed by DSM-IV.Syndromes that met fewer th an five criter io n A symp toms, lasted fo r less than 2 wee ks, or were formed ofsymptoms that we re qu ite m ild o r produced no imp a irme nt had considerable predi ct ive an d fam ilial val idi ty.That is, th ese s ubsynd romes cons istent ly pr ed icted, a th igh levels o f significa nce, the risk fo r subsequent DSM·III-R-defined episodes o f ma jo r de pression and the riskfo r ma jor depression in a co -twi n. We found sta t ist icalevide nce for o nly a sing le d iscontinuity in the predict iono f future depressive episodes (between th ose meet ingsym pto m definition s req uir ing m ild o r mo de ra te vers ussevere impairment), bur thi s discontinu ity was no r inline wi th DSM-IV cri te ria , nor was it repli cated in th epr edi ct ion of risk o f illn ess in the co -twin .
Noso logic Implications
W e hav e shown that, tak en one at a tim e, three ma jor"ga te keeping" DSM-IV cr iteri a for maj o r dep ressionsym pto m number , im pai rme nt , an d du ration-s-do no tappea r to carve nature at its joints (121. \'(Ie d id notpe rfo rm a formal taxonomic ana lysis. T her efor e, ou rresu lts do not directly add ress the q ues ti on o f whethera discrete dep res sive synd rome ex ists in nature, as ha sbeen suggested by a number of sta tistica l me thods suchas duster an alysis (19 , 20 ), gra de of membership analysis (2 1,22) , and lat ent class analys is (20, 23-25 ), Ho weve r, o ur res u lts do sugges t th at if a d iscrete depressivesyndrome exis ts in nature, th e cur ren r DSM-1 V crit eri ath at we eva lua ted do not perform well in det ecting it.
O ur results suggest ing a continuity of risk betweensub syn d ro rna l a nd syndroma l maj or depression a re notwithout p receden t. Sub synd rorn al depressive sy mpto ms ha ve been ass ociated wi th subs tantia l soc ia l morbidity (26- 28) , a much greater risk for first- on set ma jo r
AmI Psychiatry 155:2, February 1998
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission ,
28

depression (29), ;1l1J Cl greater risk for mood disordersill first-degree relatives (301. In " recent analysis of theNotional Comorbidity Survey, Kessler er al. (3 1) examined three definition s of depression : minor (meetingtwo, three, or four criterion A symptoms), major (meeting five or six crite rion A sympto ms), and severe ma jortmeering seven or mo re cr iterion A symptoms). Th eyfou nd, across the th ree categories, mon oton ic increasesfor average number of episodes, average length of longest episodes, impairment, comorbidiry, and parentalhistory of psychiatr ic disorders.
Although the use of operarionalized diagnostic criteria has resulted in substantial improvement in the reli.thility of psychiatric diagnoses, demonstrating their " ;.1
lidity has been more problematic. These results suggestthat our current DS:\,l · IV diagnostic convent ions formajor depression. derived largely from the WashingtonUniversity criteria 132) and Research Diagnostic Criteria 1,33), rnav he arbirrarv and nor reflective of a natu raldisconrin uiry in depressive symptoms as experienced inthe general popul ation .
Limitations
Th e sam ple stud ied was en rirely female. Resultsmight differ in male subjects. The history of depressivesymptoms was assessed, at different points in the inter view, for the last year and for lifetime. Given problemsin the recall of depressive episodes (34. 351. it is possiblethat errors of memory might have produced a hlurringof a true diagnostic boundary.
R E H RENrF .~
I. !.h:k \cm S\\;'; .\ ld '1l1l:ho l1'1 Jl1d 1>t' l" rl' SSiUll : Fro m Ilipp0l,:r:Hil..'Tim,,·.. to ~ l mlt" rn Timn. !\,I,'\\' !i an'n . C Ull ll . )' ,11(' ll ni\'\'rSlt\ 'r'r\.·.....19HIl .
1. J',,'nd l·lI R[ ; Tht" ..:b ~ ..iii"';Hiun o f J I, 'l"r C $ ~ I (l l1'i : .1 r('" ic,\'- C)t .;o n1 1, 'lIl r tl r ; l r ~ ' I..'Hllf1 I' io n . HI'J P ' ~ Io · h i ;. m y 197b: 129: IS- 2H
.\. F:lrllwr A. ~k Gu ;t i n P: Th ,,' d ; h ~ i f i .: ;ltill ll of t h", dl'prl'ssio ll'i:..·. lnl l·t1lp. lr.l ry ';Clll tus ilm n: "j , iICtl. Hr .l P ~ ~ ' \' :hi ;lI r y 1 9 H ~ : 15::;:4 . \ ~ -44 . \
..I. \X!j llllk ur c:: T lw \'l d j d i r ~ ' o f lI t"lIrOl i,,··n·;l l·rin· tkprl,'\sion: tH ·\ \
doll ;l .ll1d H:o'!'!'T;!i ..:l!. Ar..: h { ;,,' 11 P s ~ · ..: h i .ll r y 19S5: 41: I I 16- 1112' . 7. i l11l11l,·r Ol '111 .\ 1. Sr it/,t"r RL: :-'1t"! 'llh.:huJia : fWIll D S~ I -Ill TO
I) S.\\ · III· R . .\ 1\1 I P S \ ' ~ ' h i illT\ ' 1 9 ~ 1J : 14 li:211-2S6. Ru,h .\ 1. \ \ \ 'i s ' ~ : ll h l ' ~ ~ l ' r .IE; ~ Id 'lIli;h" Ii.,: s~ nlpto m fl." .lturl's .11ld
J) S ~ I · I\' . ..\ 111 .1 Jl s, · ~ · h i .ur \ 'I 'J ~4 : 1:; 1 : 4~ 9 - 49X":" . AIl Jn ' ; \S ~ '1l ~ c. \~ " i ll Cl k ;l r (;: Sl'...( llt J .H ~· \k prn!lio n : f'lm i!i.ll,
dmi\·;ll. ;lIal H ' '' \ '' l r ~ ' h rl·rspf,.·..rin·lo. Alii J I·..~ " ,: h l .;u r r 19 79.; 136:(,1- (,(,
N..\ ki, I.:'11H ~ . lt o !lf,.'lHh.t ] RH, K ll s ~ ·nt h . l l Tt. K'1..h~ :Ir i ; ln f\1.Kh:lni~ I l( . l' u I..lll ri'll1 VR: Dil t'\·n.:lIt i.u iull of p r i n1 'lr~ · .1ti ei;rin' ilhll''isfrnm situ.u illll.l l. <' r m r lUl11 iui ~ · • •1nd ') ~ ...unJllr~ · J epr\·!lsiu!l!l. :\ r.:h( ir n r sn:h i,l[f\ ' 1\}71.J: .l h :fl.H -64 .\
\). \X'illlll.:;.r G: U;l ir o l.lr Jf,.' pn ·, ..iull: i<, il di \·j, ih ll' inw :HlIo nOlllllllS'1 Ibf~ lw,,? -' rdl (i~ ' l1 P..y \ h i; Hr ~ · I ":l 7lJ; 36 :47-n
Il l. () lkn ·n..h,lW 1)1' : 'l' lw ~ Lt s ..i'-i\:'ll lll11 01 rh\' lwKti0l1.11 pSydlO WS.I\r ,I P..\\ :hi.Hr \ 1'17'; : 111:5 J '7- .\.11)
I I. l' o p ~ ' .H i J r . · l. i p il1lo l i .l ~ .Ir: Di .1J.:,ll m i.. ill s.:hiz o ph n' n iil ;IIlJlll;l1li...· J f,.' r rn "in· i l l ll ~ ..S: .1 r ~ ·.h ~f,. ·SS Ill ~' llt uf Ih ~ ' s p n · i f i .: i r ~ nf~,, ~ · hi/ o r h r ~ n i ..·" "~' l11 p to tllS in lh ~ ' l i ~ l' lI of .:u rreIH rt' ';(''l r..:h . Ar..:h( i~ ' 11 I'sw hi'ltr \' I '''is : ~5 : S 11 - ~ l1 S
I! . 1.:\" I J~· l i It t". . 1\ ~ 1 1 \ ·l.:i ll ~rtlll IF: " Iw idc lirli ic 1rilll1o j J i sl ' ;l ~ e ~ · n ri( i c ...l lld th ~ ' rd .Hillll ship h l'l \\' ~ 'n1 ...:h il.lIphn' n il.· ;lnd afi l ' ~ l j H' I'sydw·..~ .... Ur .l I''' y\·hiiIlrY I'lXll : 1.l 7" :.t ! 4- .n l
Am.l Ps)'chi,lIr)' 1.' .1:2, /-"dm 'ar)' 1998
HN" ETH S. KEM lLm ANI>CHAHLESP . C;.'R D:-JEI\. 11\.
13. Ro bin s L ( iUll' SR: Est.\hl i!oh m f,.·1Htl i dic gno ..nc ' ''I li d it ~ · in p..y.ch iat ric illn ess: i t ~ 'l lll' li".u in n In schixop hren i.i. Am] P ~ ~ ' l ' hli 1tr ~1'170; 12lo:':'S.l-'JS7
(4. Eaves LJ, E ~ ' lo t' ll " ' l H]. ~ l. m il1 l\'(j • .Ia rJ m<,' R. Heath .-\L Feingold L. Y lH ll l~ PA. Kendlcr l( ~ : (i r m·s. Culturv and r \ ' r s u ll . \ li r ~ · :;\ 11 Empirical ,\ pproih:h. LClIIdull , (h im ..!Ullj n 'r !1.i l ~ P r ~ · s !o . I '1s t.,
I.S. Spcnccjli, Co rcv 1.0\ , Nnncc W'E, ,\ liH.lzif;1 \ 11.. Kcndlcr KS.Schicken RM: Xlolccular ' lO" l y s i ~ 01(\\,;n z n : n ~ i r ~' m.illA V:'\:TRON A probe s (.lhsrr.I.... I!. Amj H uru Cc uc r 19 :-1 X; 4 .\: ..\ 159
I lo. Sp it:£t'r RI.• \X' ilk m ls .lB\\' . Gibbon ~ I : Struct ured Cluucnllnn-r.view tor nS:\ I· Il I·R (Sel f)) . :"l'W Yor k. :"\f,.'\\' Yo rk St.trv P ~ ' \ ' l ll 'amc In-airurc, RillT1Wrri(s Research, I ':IS'7" .
17. S,\5!ST AT (J,\t'r's Guide . ver sion 6. 4 th vd, \'Il l, I. 1. Ca n '. ~ <:.S,.\S lnsnt urc, 1\)9(\ .
18. "ish L: St.Hi'iri..:,11 D~ · s i ~ t l tor Resea rch. :'\:\'\\' York. .Juhn \\ ·il\·,&: So ns, 1984
19. I'avkcl E ~ : C1assir'i\'';llinll or depre....~ · J p;u i\' nls : , I .:I lI , r~ ·r .!tlO1 lr lo i,derived ~rnup i n~ . l\r.l r..y..-hi.ury 1"01 7"1; I l g : .! - ~ - l x S
20. ( ;rm 'C \X :~1. And rea..en N <:. YUUIlJ.l, ~ I . FI1\!L...m], Keller .\ lItHi r!l....bfcld RMI\ • •h ·it;h T: 1..ol.mon JI1\1 ..:h.lr.h ·[l·ri / .u iu l1 CIt anuclea r de p ressive wud rmuc r <' ~ · I. · hlll ~I f,.'l l 1\)";" ; 1 7 :4 7 1 - 4 ~ 4
21 . Blazer D. Swar tz ,\ 1. \'('Ufklhllr\ ' ~1 . .\!allllill 1\(; . Huuh c, D. ( it'o rl:l'I.K: Dep ressive wmproms ' Hl ~ 1 \ 1~· l' r \· ....ivc J i" J.l, lIl1Sl:S in .1 ~ '11 11 1111 ~ 1 'n it ~ · pop ulunon . usv of ,I !H'W l' rn..v du rc tor '11l.1Iylo i, nt' I h ~ .: h i . lt ·r ic classificurion . Arch (;1.'11 I'..v..·hi.lt n I':'XS; 4 ' : IOi N- II)H4
22. \'(. 'clO d hu r ~ ·M A . \ t1nwn l( ; :·( ;r .1J\,'ot 11ll'm "" rsh il' '1l1.11 y..i'\ o fdep ression-relat ed r ..y~ h i., r r i\ · di ..orders. SIJ..: il ,II'v,k i11 .\ k lh. ,d ..and Res 19H9 ; I H : 1l 6 -l n , ~
2 3 . Yo u ng .\l A. Sche rmer \V.\. Klc rnum Gl.. Atulrcnvcn :--.:c.Hir schfeld R ~ I A: Th e c l1 J o~ cnl)u s , t1h · typ\· o t dq ' n ·'i..iu ll: asrudvof irs internal w nslnh:t validitv. Br ,J l'sn ·hi.m \' I ~~ti: 14 ~ :.25 7":'267 " .
24 . Fa ron \'(,,\Y/ . Drvman A. Sorenson A. ~ k C ur dl c lll1 .-\: l.>S.\1· IIImajor dep ressive di,orJt'r in tin' co mm uni rv: 01Lrrcur d .\.;,s .\ 11.111. .sis o f da ra from the :'\1\ lff F.piJ t·rnio l0J:k · c. lI d 1 m ~ · 1lt An·.\ pro ·g,r:ll11ml.'. Br J P,,-y..:hi.Hry 19 M'1; 1.'5 :4l'l- .i4
2 5 . Kend ler KS. E: l\'e ~ LJ. \\'"lt t'rs F.E. N"'"k' .\ Ic' 1re.n h AC I\e ~~I \ 'rRC: Th e idenriiil';u iun ., ,,d \·:tlid.lt iu n I)t di st illd J c:prt'ss i\'t' ~ ~ ' Il
d ro m ~s in '1 r n r ul.lt illll ·h:l..eJ !l'lfllr1e oi le lll.llt· IWilh . Ar.:h (i " nPsn-h i.Ht \· 19'16: 5.1:\9 1- .\9 ')
26. } ') hn ~ . m j. \·(.'e i....m .Ul ~ I\ l . )\I ~ ' rnlil n Gl.: S~ · t\ i,'( ul ilit .lI i,m ;llIJ\O\,'iil l mu rh id iry 'l..~ c K i .\t ed wi lh d~ ' pr~ ' s ~ ' H ' '~ ' l1l I H O lll lo ill tht'
l. orlll n u n i r ~ ' . J A :\ I. -\ 199.!: 1 6 " : 1 4 7 ~ -14 t U
17. .Judd Lt ., !'.w lll' \I I" \'('d ls KB. K;lp.lrorr ,\ 111: SUI.' iuC'I.'o l1mlli ..:h u r d~ ' n o f suhsy ndrn ma J d t'l'r c !l ~ i \'\,.' sy ll1p rUl\l'i :\lld 11I,l jo r lil.'·press ion in 'l sa m ple of rh\' ~ t · ll~ r ' ll po r u l;u inn . Am .l P \ y \ ' h i . Ht ~19% : I.H :14 11-14 17
l X. OIt'Stlll ~ t. Brn .ldh~ "ld WE, \'(\' iss m.lIl ~ l ~t. l. \ · ll ll " CohHhf,.·r I..• icwl"n C. « Mho l R: S u h r h r ~s h () l d p \ ~ ·\ ·h i .Hr i ~ · ..~ mp u 1m.;,ill .1pr i.nury ~ ' ;I r\ ' J.:,rtlUp I' r . \ ~ · r i .: c . Ar~h (i t'll r !l~ · t,.: h i.lrr r I " W~ : .U :XSO- Nl'ln
19 . H orwat h E, ,Jo h nso n I. t..:lc: rm an ( ;1., \X"CiSSllli\1l ~ I j\l : D~ ' r n ' ~ s i \'l '
'ym plollh as r t'la liw ,1I1d 'Itt r ih uI'l hlt' r i'\l.:f,l( t' lr\ fu r t i r<, t · l ll ,.. ~ ' r1Il'1jnr ,k r rcssio l1. Ard1 (it' ll I'syd, i;ltr r 19\)2: 4'1:X 17-Xl .l
.In. I h ' lll i ~l R.-\. Sadomid; ;\ f) .I "lm R\\!. 7. i ~ :\ 1'. h ' t ' I ~ l l : ~ l:I inrd \ ·p r~ 's ..itlll. m ino r d"l ' (\ 's!lio u . •IIlJ dou hk' d ~ 'l' n ' " i tJ ll : ;HI,' I h \ ' ~\Ii..rinl·[ d ini":.ll l·m irk s? Am J ~ It 'd (; e l1et Ne ufl lr sy.:hi.lCr ( ; ~ ' l l\ '(
19% ; (,7:34 7- .153.\ 1. I\ c s s l ~'r RC, Z hi1U S. m,I;.',·r DC . ~ \\" ;Hrt ~l : 1'(\-\ " I,·n.:t' . 1.·lIrr\·
LHes. i1m l ~ C) ll r Sl ' of rninur d ~ · r r f,. · ~ ..illLl ;\ 111.1Ill;.l jcor \ If,.·rn ·ssiu ll in [hf,.·~ . H i () I1'1 1 COllul rhid i[\ ' Su rw \'.1 .\ tt'c..:r Di, .u d 1'I 'J7: 4 . ' : 1~ - , \(1
. ~ 2 . F ~ i~hu c r J r . Rn hin.. ~ : . f iU/_t''s K, 'X'uo d ru ff R.\ J r. \\ ' illcokur (; ..\ tUll o2 R: D i ;l ~ nn'\ [ io,; .:r irt·ri,l fur ll"e in r..~ d 1 i ;l rr i .: ro,;,\\,:lt dl .:\ r....h (it' n P s~ ' ~ ·h i ;ttr ~ · I l,I:"1; l (, : 5 '7" - ( , .~
.l.l . S ri t 7. ~ ·r nl .• f.lldi \',I (t J. Rl,h in.. E: Rl·, C';Jrdl I )l" !-lltl)\ rk ( :r ih·ri.1I RDO fur .1 Sd \·.... tcd (jruup o f h UKCio ll,l l I h'in rJ\'rs , 2nd ".J,~ l'\\' Yo rk. Nl'\\' Ym k S r; u~' P'\\·..:h iMrio,; Inst ilUh', B i Clll 1 ~ ·rr i f,. " Ih '·" ~· ' H..:h . l~i 5 .
3 4. Bronnl 'r [.I, Ounn t o . (c mlld l ~I ~I . D ~ '\\' ~I ;\ . ~ : hu lh \ 'r l-\ He:1.11 11g-tt>rm rdi .1hility li t Jial-\l1os illA l i t' f,. ·[i lll ~ · major J ~ 'p r c '\ ~ i tll1 ina \ - n ll lln u l1 i r ~ ' ...111\1'1\·. Ardl (;\'n I' s ~ ·.: h i . lfr ~ - II.J Xti; 4 , ~ :4 \ ,'-H tl
.H. KrllJ lt'r KS. !\' l·.l ll' !\IC, Is: l·s..J ~ · r nCo"-k:u h :\ C . L1 \'(,' ~ 1..1 : T lwlifet ime hi '\ w r ~ ' u f 1ll.l jm J l' pn '....tOll ill wClm ~' n : rdlilhili ty o i J i;lg nos i!lalld Ill' r ;r,l h ility. ;\ r.:h (; ~ ' 11 r " Y ~ ' h i i H r y 19 '13 ; ' 1l :~(,3-S '7 n
177
29

References
Introduction
Disorders, 4th ed. Washington, D.C.: American PsychiatricPress, 1994.
2. C. J. L. Murray and A. D. Lopez. 1heGlobal Burdeno/Disease. Cambridge, Mass.:
Harvard University Press, 1996.
3. William Styron. Darkness Visible: A Memoiro/Madness. NewYork: Vintage, 1992;
Andrew Solomon. TbeNoondayDemon. New York: Scribner, 2001.

This page intentionally left blank
R eproduced with permissi on of the copyright owner.Further reproduction proh ibited without permission. 14.Hwu HG. Yeb EK, Chang LY: Prevalence of psych iatr icdisorders in T aiwan defined by the Ch inese DiagnosticInterview Schedule. Acta Psychiatr Scand 1989; 79: 13 6-14715. Allgulander C: Psychoacti ve dru g use in a genera lpopulation sample, Sweden: corr elate s with perceivedhealth, psychiatric diagnoses, and mortality in anautomated record-linkage study. Amj Public Health 1989;79,1006-1010 16. Eaton WW, Anthony j C, Tepper S, Dryman A:Psychop athology and attriti on in the EpidemiologicCatchment Area Study. Am J Epidemiol 1992; I3 H 05 1105917. US Departm ent of He alth and Human Services: NationalHealth Interview Surve y, 1989 (computer file). Hyattsville, Md, National Center for Health Statisti cs. 199218. Kessler Re,McGonagle KA, Zhao S, Nelson CB, Hughes M,Eshleman 5, Winchen H, Kendl er KS: Lifetime and 12 ·monthpreva lence of DSM-III-R psychiatric disorders in theUnited States: results from the Na tional Co morbldirySurvey. Arch Gen Psychiatry 1994; 51 :8-19 19. World HealthOrganization : Com posite Interna tional Diagnos ticInterview (CIDI, Version 1.0 ). Geneva , WHO, 1990 20 .RobinsLN, WUl8J, Wincl>en 00, Holur J£, The Compositelaternational Diagno stic Interv iew: an epidemiologicinstrument suitable for use in conjunctio n with d ifferentdiagn ostic systems and in different cultures. Arch GenPsychiatry 1988 ;45:1069-1077 21. Rob ins LN. HelzerJE.Croughan J. Ratcliff KS: The Na tional Institute ofMental Health Diagnostic Interview Schedule: its history ,charac teristics, and validi ry. Arch Gen Psychiatry 1981 ;38 : 381 -389 22 . Weissman MM, Bruce ML, Leaf P], Flor ioLP, Holzer C: Affec w rive disord ers. in PsychiatricDisorders In America. Edited by Regier DA, Robin s LN. NewYork, Free Press, 1991 986 23. Woodruff RS, Cau sey BD:Computerized method for appr oximating the variance of acomp licated estimate. 1Am Statistical Assoc 1976; 71 ,315-321 24 . Spitzer RL, WilliamsJBW, Gibboo M, Fin, MB,TheStructured Clinica l Interview for DSM·llI-R (SCID), I:history, rat ionale, and descrip tion. Arch Gen Psychiatry1992 ; 49:624--629 25 . Helzer JE, Robins LN, McEvo y L],Spitznage l EL,Stolnman RK, Farmer A, Brock ington IF: Acompa rison of clinical and Diagnosric Interview Schedulediagnoses: physician reexam inatio n of lay-interv iewedcases in the general population. Arch Gee Psychiatry 1985 ;42 ,657-666 26 . Anthonyle ,Folstein M, Romanoski AJ, VonKorff MR, Nestadt C R, Chahal R, Merchant A, Brown CHIShapiro S, Kramer M, Gruenberg EM : Comparison of the layDiagnostic Interv iew Schedule and a srandardized

psychiatric diagn osis: exper ience in eastern Baltimore .Arcb Gen Psychiatry 1985 ; 42 :667-675 27. Blazer D. GeorgeLK. Lend erman R. Pennybacker M, Melville ML, Woodbury M,Man ton KG, Jordan K, Locke B: Psychiatr ic disorders: aruraVurban comparison . Arch Gen Psychiatry 1985; 42,651-656 28. Somervdl PO, Leaf PJ, Weissman MM, Blazer DG,Bruce ML: The prevalence of ma jor depress ion in black andwhite adults in five United Srates cornmunines. AmJEpidemiol 1989 ; 130:725735 29 . Tennant C: Femal e vulnerability to depression. Psychol Med 1985; 15,133-737 30.Jorm AF: Sex and age differences in depress ion : aquantitative synthes is of published research. Aust NZ1Psychiatry 1987; 21: 46-53 31. Brown CW, Harris T : SocialOr igins of Depressi on : A Study of Psychiat ric Diso rderin Women. New York. Free Press, 1978 Am J Psychiatry 151:7,July 1994
Reproduced with permission of the copyrighl owner. Furtherreproduction prohibited without permission . 8 ComparingAge at Onset of Major Depression and Other PsychiatricDisorders by Birth Cohorts in Five US Community PopulationsKimberly Christi e Burke, MS; Jack D. Burke, I t. MD, MPH;Donald S. Rae, MS; Darrel A. Regier, MD, MPH
• Using data collected in the National Institute of Mental
Health (Rockville, Md) Epidemiologic Catchment Area Pro
gram, we examined the proposed hypothesis that there has
been a shift in major depression to younger ages at onset,
or increased prevalence in younger age periods, for recent
birth cohorts. life-table survival methods were used to ex
amine the hazard rates for major dep ression as well as for
other specific mental disorders. The findings are consistent
with a gradual shift to increased rates for major depression
between the ages of 15 and 19 yea rs for Epidem iologic
Catchment Area respondents born more recently. The find
ings also suggest a similar shift for drug abuse/dependence;
similar but less pronounced changes were found for alcohol

abuse /dependence and obsessive-compulsive disorder.
However, in thi s study, bipolar disorder, panic disorder,and
phob ias did not exhibit a cons istent increase in onset at
younger ages . Further research is requ ired to determine if
the shifts in major depression, drug abuse/dependence, and
possibly alcohol abuse/dependence are linked . It is irnpor
tantto note that these shifts to adolescent onset are occur
ring when nearly half the 31 million Americans without
health insurance are aged 24 years or younger. (Arch CenPsychiatry. 1991 ;48:789-795)
A recent life-table an alysis of the age at onset of mentaldi sorders am ong respondents from th e Nationa l In
sti tu te of Men tal H ealth (NIMH, Rockville , Md) Epidemi
ologic Catchment Area (ECA) Program'" suggested the
importance of on set in adolescence and early adulthood
for several specific mental d isorders, including major de
pression.tThis find ing is consistent with the suggestion by
K1erman et al.. 11 and othe rs":" that members of recent gen
erations are displaying higher rates and/or younger ages
at onset for major depression compared with members of
older generations. K1erman and Weissm an ll recentlyreviewed evid ence sugAccepl edT6Tpublication September 20,1990. From the Office of the Institute Director (M s Burke), Division of
'-:,":l : ,.,, ~ ~ _ , .r c. ~ _ :. ~, ~, ':'. ~ ~ ~ ..,~,.. t. I l""\ ~ 'l . ~ I.: ~ \ ~ ... ~ n :,,: ')i,... ...'if C': .., ! r.~ 1
Health , Rockville . ,v'0 . ,V\SBurxe ISnow wr tn sco« anc~"'m l ;:e ~ ; , (; l <': ,

Temple, Tex.
Reprint requests to Scott and White Clinic, 2401 5 31st 51, Alexander
Bldg, Temple, TX 76508 (Ms Burke).
.ArchGen Psychiatry-Vol 4B, September 1991 gesting anincrease in the rate of major depression among people bornsince World War II. In 1976, K1erman' hypothesized thatwestern societies were entering an "Age of Melancholy" andreported that clinical depression was increasing inadolescence and young adulthood. Later, results from alongi tu dinal study conducted between 1947 and 1972 inLundby, Sweden , demonstrated that the probability of suffering a mild or moderate case of depression increasedduring that 25-year period for both sexes ." More recentstudies examining relatives of patients ha ve also reportedevidence in support of increased rates of majordepression,' earlieronset of major depression in successivebirth cohorts ," and a statistically significant differencebetween the hazard rates for major depression developingfor patients born before 1940 and patients born after1940." Simillrl y , a-study examinin g ho spital reco rdsin Zurich, Switzerland, reported that th e number ofadmissions for major depression increased substantiallyfrom 1920 to 1982," Most recently, Wickramara tne et al" examined birthcohort trends am onga subsample of N IMH ECArespondents. For the 10640 white ECA respondents, the yreported increased rates of major depressive episode forboth men and women born after 1935, with evidence of a period effect on respondents of all ages after 1960. Threestudies have also examined data relative to bipolardisorders . Angst's" study of Zurich admission records alsoshowe d increases for bipolar d isorder since 1920, and two reports exami ning relatives in famil y studies havesuggested increases for bipolar I disorder" or a categorycombining bipolar and sch izoaffective disorders ."Although findings from these recent investigations suggesta temporal change in recent generations, with ma jordepression and possibly bipolar disorder having earlierages at onset and/or higher rate s than had been true inolder generations, the studies ha ve to varying degreesbeen subject to two limitations. First, these studiesgenerally have not examined other nonaffective disorders toinvestigate w hether the shift to earlier ages at onset isa general phenomenon displayed in all disorders or perhapsa meth,-delo"': crtifac!. '3 ~ C0 ,.. . d , these stud iestyp ically have not used large, represent at ive general

population samples. ;. To address these problems, thisanalysis exammes selected Diagnostic Interview Schedule(DIS)-DSM-lII psychi atric d isorders, in addition to majordepression, in the Age at Onset-Burke et al 789 ' •.:L: andin re sidents in terms of two qu es tions , (1) Fo r m ajord epression, has there b een a sh ift to you nger ages atonset in more recent birth co horts? (2) Has any suc h shift for majo r d epression been m at ch ed by similarshifts for other di sorder s , incl u d ing drug or alcohol ab use/depend ence, th e anxie ty di sorders , o rbi p olar disorder? In this analysis , s elf-reported onsetex p erie nce for th e firs t 30 yea rs of life will be com p a re d fo r all NIMH EC A re spondents grouped in to fou r birth cohorts ove r the p ast century. SUBJECTS ANDMETHODS NIMH ECA Program Th e da ta used to ana lyze thehypothesized shift in the age at onset and/or the increasein rates for major depression w ere collecte d as part ofthe NIMH ECA Program . The NIMH ECA Program was a comb inedhou sehold and insti tu tional survey of m ental disord ersconducted in five sites throu ghout the United State s, andit has been described in detail elsewhere.""" This analysisis based on data from 20 745 hou sehold and institutionalres po nde nts who were aged 18 yea rs and olde r at timeof entry int o the study . Data were exclude d for an additional 116 resp ond ents for whom year of birth wasmissing. Di agnoses of specific ment al d isorders were made using the DIS." Designed for use by no nclinicians inepidemiologic studies, thi s instrument uses self-reportedinformati on about symptoms to make diagnoses of specificmental disorders based on DSM-lI/ criteria." If a positivediagnosis can be made based on th e sy mptoms rep orted, aninquiry is made to determine th e age at first occurre nceof the symp toms. Although it is possible that this firstoccurrence may not have been seve re eno ugh to pass th ethreshold for a DSM-1lldiagn osis, tha t initial episo deis generally used as the o ~ for da ting onset of thedisorder in the NIMH ECA da ta se t and appears to be mostrelevan t for dating onset in general. 7 ,II .n The NIMHECA Progra m invo lved complex multi stage samplingprocedures" : therefore, the respondents have been weighted to reflect th eir probab ility of selection and thenhave been weighted to th e 1980 US C ensus on the basis ofage , sex, and racelethnicity as described previously,16,21life-Table Survival Methods Life-ta ble survival methods,similar to those used in a recent examination of the age atonset of mental disorders in the N IMH ECA.' were used tocompare the age at onset of selected mental disorders bybirth cohorts. Surviv al meth ods were used to examineaverage yea rly hazard rates for specific 5-year age intervals. A hazard rate gives th e probability that a dis

order will develop during a time interval in a respondentwho en ters that in terval and who is free of a disord erat the begin ning of tha t intervaJ.7·22.2J In thisanalvsis, the time interval was defined as a range of 5years during which age at onset could occur, for example,15 to 19 yea rs or 20 to 24 year s . Using th e Statistical Package for the Social Sciences (SPSS) Survival program." hazard rates to age 30 years were examined across fourbirth cohorts . The birth cohorts examin ed were those bornbefore 1917 (unweighted n = 6566), betwe en 1917 and 1936(n = 4432), betwee n 1937 and 1952 (n = 4981), and b etween1953 and 1966 (n = 4766). Using an observa tion pe riodfrom birth to 30 years of age allowe d the comparison ofeach birth coho rt for equivalent periods of risk; 30 yearswas the oldest age possible for a respond ent born in theyoungest birth coho rt (1953 to 1966) at th e time of intervi ew . The younges t birth cohort is th e onl y onewhose members may have bee n less than 30 years of age, butlife tables have the advantage of adjusting for the factthat subjects have different ages, or, in analogy totreahne nt outcome studies, that they have bee n followedup for differen t pe riods ." For each disord er, thehazard rates of the four birth cohorts were compared usingthe Lee-Desu" statistic, which follo ws a X] distributionwith g 1 df, where g is the number of groups un790 Arch CenPsyc hiatry-Vol 48, Septemb er 1991 whether of ons et inthe first 30 years of life for the fou r birth cohorts were drawn from the same population or we re sign ificantlydifferen t. It compares th e pr obabilities in the coh ortsin all age int ervals simultaneou sly" and is similar toothe r anal yses of the coho rt eff eet . 1 5 .2 ~ However,there is no method (eg, based on proportional hazardsmodels) to test specifically for shifts in the peak age atonse t wh ile ap plying the complex weig hts of the ECAdata." Rather than using unw eight ed data, which would beinapp ropriate for th e total ECA sample, we have relied ona graphic approach to identify appa rent shifts in peak ageat ons et ." However, these apparent shifts cannot betested for statistical significance by th is approa ch."The SPSS softwa re program appropriately weighted the databased on the samp ling procedures to pr oduce estimates ofhazard rates . However, the program cannot accurately determine th e varia nce associated with comp lex samplingdesign s like that used in the NIMH ECA Progra m.Therefore, two adjus tme nts were necessary before tests ofsignifica nce c ould be performed to determine if the onset experie nce differed by birth cohorts.' Firs t, to assurethat the sampling weig hts did not inflate the statistica lpower of comp arison s, the weighted ' sam ple was ad justed to the same size as the total actua l sample; to

accomplish this , the sampling weig ht used for th e fivesites was mul tiplied by the number of resp ond ent s inthe NIMH ECA sample and th en divid ed by the 1980 USCensus po pu lation . Second , the x' test statistics weredivided by the es tima ted sample design effect beforecalculation of Pvalues. This conservative adjustm ent wasdon e based on repeated estimates of th e design effect forpr evalences in these condi tions that ranged from 1.5 to2.0' ·",; these des ign effect estima tes were produ ced byth e program SESUDAAN" deve loped for analyzing suchcomplex surveys. These adjus tments are equivalent toreducing the samp le size by the design effect. " RESULTSHazard rates were plotted and compared for sta tisticallysignificant differences. The four cohorts examined will bereferred to as cohort 1 (resp ondents born betwe en 1953and 1966), cohort 2 (respon den ts born betwee n 1937 and1952), cohort 3 (respondents born between 1917 and 1936),and cohort 4 (respo nde nts born hefore 1917). Thesecohorts were similar to those used by Weissma n et al" inthe initial analysis of NIMH ECA da ta from New Have n(Conn ) respo ndents. Since the five NIMH ECA sites entered the field at different times in the early 19805, theend point for cohort 1 is shown as 1966, which is thelatest year of birth of any NIMH ECA respond ent andapplies to the Los Angeles (Calif) site. Mood Disorders Unipolar Ma jor Depressive Episode. For th e first 30 yearsof life in each cohort, Fig 1 plots the hazard rates fordevelop ment of Unipolar major depressive episode (with nolifetime history of man ic episodes) . For those NIMH ECAres pondents born be tween 1953 an d 1966, the hazard ratesfor unipolar major depression developing peak duri ng twoage intervals : 15101 9 and 25 to 29 years of age . In theage int erval 15 to 19 yea rs , there also appears to be anincrease in the magnitude of th e hazard rate for respondents in cohort 1 compared with those respondents in cohort 2, and similarly for cohort 2 compared with cohort 3.This trend is made ap pa rent by examining the ratio of theh azard rate for ages 15 to 19 yea rs to the hazard ratefor ages 25 to 29 years: cohort 1, 0.005510.0064 =0.86;cohort 2, 0.0032/0.0062 =0.52; and cohort 3, 0.0005/0.0019= 0.26. The ratio for coh ort 4 goes against thi s tr end,but it is based on much smaller hazard rates (0.0003/0.0002 = 1.50). The haza rd rates for major de pressio ndeve lopi ng for re spondent s born in cohort 1 and forthose res ponden ts born in coh ort 2 are sign ificantlydifferent (x' = 14.2, df = I , P = .00( 2). The hazardrates for major dep ression developing for res pondents incohort 2 compa red with cohort 3 are also signi ficantly differ ent (x'=85 .3, df = l. P<.OOOI). ABeat Onset-Burke etal 19 37·1 952 1953 · 1966 1917 ·1936 I " ! I ! ! " , 1

Before 1917 t'\ A "n ' n'A 1c:'n., .... .,.'2S_29 0.00200.00 15 % '" 0.0010 'E e I 0.0005 0 .0000 Age at Onset. y195) ·1 966 1 9]7· 1952 ':.J· 29 7.,9'. 0.0070 0.00650.0060 0.0055 0 .0050 11.1 0.004 5 ~ 0.0040 ~ 0.0035 ~ 0.0030 0.0025 0 .0020 0.0015 0.00 10 ~~:~ IO ~ : ; :~ ; : ;~ :,::: . ::, :~ : ?B e' O" '9" Age at O nset. y Thesecu.....es rep resent dat a from all respo ndents in allli...e sites of the NIMH Epidemiologic Catchment AreaProgram, weighll!d for sampling design and ad jus.led byage , sex . and ra c ~ e l h n i c il y to the 1980 US Census. Major dep ressive episode with no history of a manicep isode . O nset expe rience is from birth 10 age 30, wilhaverage yearly h aurd tales for eac h S'y t' OJ r lime tnterv..l calc ulated by life-table survival method s. TheseCUI'\l e'S reptes.en l data from all respo ndents in all fve Sites 01 the NIMH Epidem io logic Catchm@nt AreaProgram. weigh ted for sampling dnign an d adj usted by age. sex . and racPiethni city to the 1980 U5 Census. On setex per ience is from birt h to age 30. w ith ave rageyearly haza rd r a f ~ for each 5-year lime interva l calculated by lifetable survival met hods . f ig l. Hazardrate by year o f birth for unipolar majo r depression (withno history of a manic episode), by Oiasnostic Interview5chedul....DSM·III crite ria. for cohorts born befo re 1917(dashed fine), from 1917to 1936 (broke n line). from 1937to 1952(solid line). and from 1953 to 1966(lightly shadedlin e). NIM H indica tes Natio nal Institu te of MentalHealth . Bipolar Disorder.-For those respondents with adiagnosis of mania, there is no apparen t shift to anearlier age at onse t for the manic episode for those bornmost recentl y (Fig 2). The haza rd rates for respondentsborn in cohort 1 compared with the haz ard rates for thoseborn in cohort 2 are not significantly different (X' =1.4,dl= I , P= .240). However, for those respo ndents born incohort 2 compared with those born in cohort 3, the hazardrates are significantly different (X'=24.0, dl= I. P<.oool). In Fig 3. addi tional information on bipolar disorder ispresented . For those ECA responde nts with a lifetimediagnosis of mania, the age at onset information presentedis the youngest age at which either a major depr essive ormanic episod e occurred, using the age for whicheverepisode came first. As with mani c episode alone (Fig ~ ) ,there does no t ap pear to have been a change in age atonset for respondents born in cohort 1 compared with thoseborn in cohort 2 (X'=0.18, dl= I, P= .6705). The hazardrates for resp ondent s born in cohort 2 compared withthose born in cohort 3 are significantly different (X'=27.2, df = I , P<.0001). Anxiety Disorders Panic Disorder.-For ECA respond ents, the re has been no

apparent shift in the age at onse t for panic disorder (Fig4), The
peak hazard occurs in the age interval 25 to 29 years forbirth co
horts I , 2, and 3. The re is no Significant differencebetween the
hazard rates for respondents born after 1953 compared withthe
hazard rates for resp ond ent s born in cohort 2 (X'= 0.5,dl= l.
P= ,5). However, the rates for birth cohort 2 aresignificantly
different from the rates for respon dents born in coho rt 3
(X'=20.2. dl= I. P<.oool) . Obsessive-CompulsiveDisorder.For obsessive-eompulsive
diso rde r, there appears to have been a shift to a youngerage at
onse t for the most recent birth cohor t (cohort I). Figure5, a plot
of the hazard rates by birth coho rts, shows that the peakhazard
rate for cohort I occurs during the age interval 20 to 24years.
while the peak hazard s for cohort s 2 and 3 both occur inthe age
Arch Gen Psychiatry-Vol 48, September 1991 Fig 2.-Hazardrate by year of bi rth for mania by same crite ria and forsame cohorts as in Fig 1. NIMH ind icates National Institute of Mental Health . interval 25 to 29 years . The haza rdrates for respondents born in cohort 1 compared with therates for respondent s born in cohort 2 are signi ficantlydifferent (X'=9.5, dl= I , P= .(02). The hazard rates forresp ondents born in cohort 2 and respo ndents born incohort 3 (X'=16.3, dl= I . P<.oool) are also ~ gnifi c antl y different. Phob ias.Figur e 6 de monstrates that thehazard rate for develo pment of phobia s is highest forcohort I in the age inte rval 10 to 14 year s. while the

peak hazard for cohorts 2. 3, and 4 occurs in the interval5 to 9 years . The difference between co hort I and cohort2 just reaches statistical significance (X'= 4.3, df= I , P= .04). A significant difference in developin g phobias forthose respondents born in cohort 2 and those resp ond ent sborn in cohort 3 is found (X'= 21.1, df= I. P<.oool ). Drugand Alcohol Use Disorders Drug Abu seIDependence,-Inaddition to the much higher rates in the youngest coho rt,wh ich may be observed by the need to break the verticalaxis of the grap h. there also appears to be a shift to ayounger age at onset for respondents born in cohort Icompared with cohort 2 for dru g abuse /depend ence (Fig7).The peak ha zard occurs between the ages of 15 and 19 yearsfor cohort I and between the ages of 20 and 24 years forcoho rt 2; the difference between the hazard rates forrespond ent s born in cohort I and for respond ent s bornin cohort 2 is signi ficant (X'= 179.4. df = I. P<.OOOI ).There is also a significant difference between the hazardrates for resf.0ndents born in coho rt 2 and respond entsborn in cohort 3 (X = 159.1, dl= I, P< .OOOI). Alcohol Abuse/Dependence, -Like drug abuse/dependence, the hazardrates for alcohol abuse/de pendence are highest for thoseNIMH ECA resp onden ts born between 1953 and 1966 (Fig 8).The difference betwee n the hazard rates for cohort I compared with cohort 2 (X' = 58.0, dl= I . P<.oool) is significan t. A Significant difference is also foun d betweenthe hazard rates for respondents born in coho rt 2 andrates for respo nde nts born in coho rl3 (X'= 62.3, dl = I, P<.oool). As with major depression , a trend towardincreasi ng impo rtance of the 15to 19-year age interval isalso seen in Fig 8 across the four coho rts. Age at Onset-Burke et al 791 0.0020 0 .0015 1953-1960 !! ~ 0.0010 ] :i!0.0005 I , Before 1917 0.0000 ~. . " 10-14 15-19 20-2425.29 Earliest Age at Onset. y 0.0020 0.0015 ~ " 0.0010 ~:i! 0.0005 0.0000 19 37-1952 1953-19&& These curvesrepresent data from all respo ndents in all five ii l ~ ofthe NIMH Epidemiologic Catchm ent Are.. Program. we ightedfor ~ mp l i ng dei ign and ad justed b)' age , sell, andrace/e lhnic ilY10 the 1980 US Cen sus. Mania wilh orwithout ma jor d ep ressive episode; onset Is for maniaunless major dep ressive ep isode occur red earher. Onse texperie nce is from birth 10 age 3D. w ith average yearlyhalol rd rale s tor each S·ve.,time interva l caleul,lIedby hte-table survival methods. Age 31 O nset, y These curves represent d..ua from " II respondenls in all five sitesof the NIMH Epidemio log ic (alchmen l Are. Progra m, weighted for sampl ing design "nd ad jusled by age . sell,and race/ethnicilY10 the 1980 US (ensus. O nset e xce-eoceis from birth 10 018<' 30. with average year ly ha za rdrail'S for ea ch 5.yea, lime inte rval calc ulated by life·

lable survival method s. Fig 3.-Hazard rate by year ofbirth for mania (with or with ou t a major depressiveepisode. onse t is for mania unless major dep ressiveepisod e occurred earlier) by same criteria and for samecoho rts as in Fig 1. NIMH tndtcstes National Institute ofMental Healt h. Fig S.-Hazard rate by year of birth forobsessive-compulsive disorder by same criteria a nd forsame coh orts as in Fig 1, NIM H indica tes National Institute of Mental Health. Fig 4.Hazard rate by year of birthfor panic disorder by same criteria and for same cohorts asin Fig 1. NIMH indicates Natio nal in sti tut e of MentalHealth. Fig 6.-Hazard rate by year of birth for phobias(agoraphobia, simp le phobia, or social ph obia) by samecriteria and for same coh orts as in Fig 1. NIMH ind icatesNatio nal Insti tute of Mental Health . 0.0025 Ag e a l Onset, y Age et O n set , Y 19 37· 19 52 19 5] · 19&6 ~ 91 7. , 9 3 & 0.0070 0.0065 0.0060 0.0055 0.0050 0.0045 0.00350.0030 0.0025 0.0020 0.0015 0.0010 0.0005 ooooo ' , ,,8efo,e 191 7 . 0-4 5-9 10· 14 15-19 20-24 25.29 ~ 0.0040 "~ :i! The se curve s represent do1 li1from a ll respondentsin all Iive s ile~ o f Ihe NIMH Epide miolog ic Cal("hmenlArea Progr am , weiRhted for samplinR desi $:n ao d adjusled by age , sell. and race!e lhn icity 10 the 1960 USCensu s. 19 17-.1936 10-14 15·19 20-24 25-29 Before 19 170.0015 !! ~ " 0.0010 ~ :i! 0.0005 0.0020 These curve s reprf'sf'nl data from all rf'Spo ndf'nls in all five s itt's ofthe NIMH Epidf'miologic Catch ment Area Prog ram, weigh tedfor sampling de sign and "djuSll'Clby age , sell, andrace/e lhnici lY10 the 1980 US Ce nsus. Onset el,pe rienceis from binh 10 "Ilf' 3D, w ith ave rage yearl y hau rd rates for each S .~ar lime inlerva l cakulo1 led by li(e·l.ble survival mel hods . -"Roro1phob i o1 , simp le ph obia. o r soci ,,1pho hia . O n~1 expe rien ce is from binh 10.tIce 30 , w ith average yead v h.tlu td rates for eac hS·yea, lime interval celc uta ted by Iife·labl e surv ivalmelhod s. 792 Arch Gen PsychiatryVo l 48 , Sept embe r 1991Age at Onset-Burk e e t al 9 ] · 19& 17 .1936 9 17 .19365-9 10· 14 15-19 20-24 25.29 5-9 10· 14 15-19 20-24 25.29953 19&& 953 19&& 953 19&& 953 19&& ~. 0-4 5-9 10 .0005....-29 0. 025 0 .0200 0 .0150 0 .0100 0.0100 • 0.0090 ~0.0080 ~ 0.0070 ~ 0.0060 0.0050 0.0040 0.00 30 0.0020 0 .0010 " , 0.0000 0 • 4 • n . n .. .. , n ' n" ,. 19]7 · 19521917· 19] 6 ~ a e i or e 1 9 1 7 5·9 10·14 15· 19 20·2425·29 0.D25} 0.0200 0.0150 0.0100 .... 0 .0100 ~ 0.0090 ~0.0080 ~ 0.0070 r. 0.0060 0 .0050 0.0040 0 .0030 0.00200.00 10 0.0000 0.4 Age at Onset, y Age at O nset, Y Thesecurves represent data from aUresp ondent s in all fivesites of the NIM H Epidemiologic C. tchmenl Area Program,weighted for sampling design and ad justed by age, sex, andrace!elhnicity to the 1980 US Census . O nset e..ceue nce

is from birth 10 age 3D. with average' yearly haz ard ratesfor each 5·yeolf lime interval calculated by nre-u btesurvival methods. These curves represent dala Irom allrespond ents in aU five sites of the NIMH Epidem iolog icCatchmenl Area Prog ram, we ighled for u, mp ling de-signand adjusted by age, sex. and r a c ~ e l hn i ci ty 10 the1980 US Census. O nset experience is from birth to age 30,with average yea rly haz ard r a l ~ for ea ch 5-year limeinterva l calc ulated by Iife·t.lb le surviva l methods.Fig 7.Hazard rate by year of birth for drugabuse/dependence by same criteria and for same cohorts asin Fig 1. NIM H indicates Nstional Institu te of MentalHealth. Fig 8.-Hazard rate by year of birth for alcoholabuse/depende nce by same crit eria and for same cohorts asin Fig 1. NIMH indicates Natio nal Institute of MentalHealth . COMMENT For unipolar major depression, there appears to have been a gradua l increase in the hazard rate forthe interv al 15 to 19 years of age across the threecohorts born since 1917. These findings are consistent withKlennan's hypo thesisv" and the findin gs of other studies" '\' that members of recent birth cohorts have a higherrisk of having a major depressive episode . One interestingbut unexplained finding is the apparent importance of the15-to 19-year age interval for theoldes tcohort, bornbefore 1917. Gersh on et al" reported a similar,unexplainable increase in hazard rates fur relatives bornfrom 1910 to 1919 in an earlier family study, compared withother decade s ofbirth before 1940. That study, and thecurrent findings from the ECA, depend on retrospectiverecall from respondents for documenting lifetime historyand age at onset, but the similarity may suggest the needto examine possible common
alities between that cohort and the more recent ones thatappear to experience higher onset rates in adolescence. Forbipolar disorder, these results are not able to
corroborate sugges tions of a cohort effect shown in
some earlier stud ies.P " Wheth er this difference is
caused by differences in sampling, as those studies
used either relatives of proband s or admission rates to
a psychiatric hospital, or by differences in diagnostic
ass essment is not clear. It is also possible that a small
effect that could be detected in a sample of high-risk

family members could not be demonstrated in a gen
eral population stud y for a relatively uncommon disor
der such as bipolar disorder . For drug abuse/dependence,there has been a shift to a
younger age at onse t for the most recent cohort as well as
I Clin Epidemio/. 1989;42:333-343. 13. Hagn ell 0 , LankeJ, Rorsman B, O jesjo L. Are w e entering an age ofmelancholy ? de pres sive illness in a prospective epidemiologic al stud y over 25 years: the Lundby stud y, Swe
den . Psychol Med. 1982;12:279-282. 14. Lavori PW, KlermanGL. Keller MB , Reich T, Rice J. Endi
cott I . Age-period-cohort analysis o f secula r tr end sin on set o f
major depression. I Psychiatr Res. 1987;21 :23-35. 15.Gersh on ES, Hamovit JH. Guroff /I. Nurnberger JI. Birth
cohort changes in manic and depre ssive disorde rs inrelatives
of bipolar and schizoaffeeti ve patients. Arch CenPsychiatry.
1987;44 ;314-319. 16. Angs t J. Swit ch from depression tomania . Psychopathol
ogy .1985;18:140-154.
Arch Gen Psychiatry-Vol 48. September 1991 shon ld aff ective dis orders . I Psychiatr Res. 1985;19:533-546. 18.Regier DA. Boyd JH, Burke )0, Rae D5, M yers JK, Kramer M ,Rob in s LN, G eorge LK, Karno M , Locke BZ. One-month prevalen ce of mental d isorders in the U .S.: based on fiveepidemio logic catchment sites. Arch Gen Psychiatry.1988;45 :977-986. 19. Robins LN, Helz er IE. Croughan),Ratcliff KS. NIMH DIS : its hi st ory, characterislics ,and valid ity. Arch Cen Psychiatry. 1981;38; 381-389. 20.Amer ican Psychiatric Association , Committee on No ~menclature and Stati stics . Diagnostic and Statist icalManual of Mental Disord ers, Third Edition . Washington, DC: American Psychiat ri c Association; 1980;215. 21. EatonWW , Kessler LG, eds . Epidemiologic Fie ld Methods inPsychiatry . Orlando, Fla: Academic Press Inc ; 1985. 22.

Gr oss A, Clark V. Survival Distribution: ReliabilityApplications With Biomedical Science. New Yor k, NY : Jo hnWiley & Sons In c ; 1975. 23. Kalbfleisch JD, Prentice RL.The Statistical Anal ysis of Failure Time Data. New Yor k,NY: [o hn Wi ley & Sons Inc ; 1980. 24. SPSSUser's Guide.2nd ed . New York . NY: McGraw-H ili Int ern ati on al BookCo ; 1986:875-887. 25. Flei ss JL, Dunner DL, Stallone F,Fieve RR. The life table. Arch Cen Psychiatry.1976;33:107-112. 26. Lee ET, Desu MM. A comput er programfor comparing K samples w ith right censored data. ComputMethods Programs Bi omed. 1972;2:315-321. 27. Robertson CO, Gehan EA. A computer SUb-program fo r calcu lati ng thegeneralized Wilcoxon test. Comput Methods Programs Bi omed.1972;2 :315-321. 28. Weis sman MM , Leaf PJ.Holzer CE, Myer s )K, Tischler GL. The epidem iol ogy o f dep ression :an update on sex difference s in rate s. I AffectiveDisord. 1984;7:179-188. 29. Wickr amar atne PJ.Prusoff BA,Me rikangas KR, W eissman MM . The use o f survival timemodels w ith nonproportional hazard functio ns toinvestigate age of onset in family studies. I Chron ic Dis.1986;39:389-397. 30. Kessler LG. Folsom R, Royall R,Fors,1he A, McEvoy L, Holzer CEoRae D5, Wo odbury M .Parameter and var iance estima t ion. In : Eaton WW ,Kessler LG, eds. Epidemiologic Field Meth ods inPsychiatry. O rlando, Fla: Academic Press Inc ;1985:327-349. 31. Shah BV. SESUDAAN : Standard ErrorsProgram for Com pu t ing of Standardized Rates from SampleSurvey Data. Research Triangle Park , NC: Research TriangleIn stitute; 1981. 32. Kish L. Survey Sampling. New York, NY: John Wiley & Sons Inc ; 1%5 :575-577. 33. Ch ri stie KA.Burke ID , Reg ierDA. RaeDS, Boyd JH, Locke BZ. Ep idemiologic ev idence for early onset of mental disorders and highe r risk of drug abuse in young adu lts . Am IPsychiatry. 1988;145:971-975. 34. Price RA. Kidd KK, Weissman MM . Early on set (under age 30 years) and panicdisord er as markers fo r etiologic hom ogeneity in majordepression. Arch Gen Psychiatry , 1987;44 :434440. 35. Witt ehen HU , Burke )0 , Semlar G, Pfister H, Von Cranach M, Zaudig M . Recall and dating of psychiatric symp toms .Arch Gen Psychiatry . 1989;46 :437-443. 36. Hasin D, LinkB. Age and recognition of depression. Psycho l Med. 1988;18:683-688. 37. Prus off BA, Merikangas KR, Weissman MM.Lifetim e pr eva lence and age of onset of psychiatric disorders : recall 4 years later . I Psychiatr Res.1988;22:107-117. 38. Farrer LA. Flor io LP, Bruce ML , LeafPJ, Weissman MM . Reliabil ity of self-reported age atonset of major depression. I Psychiatr Res. 1989;23:35-47.39. Sartorius N, Nielsen lA, Stromgren E. Changes in frequency o f mental d isorder over t ime . Acta PsychiatrScand. 1989;79:suppI348. 40. Moyer ME. A revised look at

the number of un insured Am ericans . Health Affairs.1989(.ummer);8 :102-110. Age at Onset-Burke et al i9.:iThis page intentionally left blank

Lost
Reproduced with permission of the copyright owner. Furtherreproduction prohibited without permission. 24. Keller MB.cet en berg Aj, Hirschfeld RMA. Rush Aj . r hase ME,KocsisJH, M arkowitz JC, Fawcett JA,Koran lM , Klein ON,zcs seu JM. Kornste in SG, McCu lloug h JP. Davis SM. Harrison WM: The treat me nt of ch ro nic dep ression. part 2: adouble-blin d , ran domized tria l 01 sertr atin e and imip ramine . j Clin pw chiatry 1998 ; 59:598-607 25 . Spitzer Rl , Williams JBW. Gibbon M, First MB: The Structu redClinica l Interview for DSM·III ·R (SO D). I: hi story,rationa le, and description. Arch Gen Psychia tr y 1992;49:624 -629 26 . Miller IW, Keitner GI, Scha tzberg AF.Klein ON. rhase ME. Rush AJ, Markow itz JC. Scb tager D.xomst eln $G, Davi s SM, Harrison WM. Keller MB: Th etreatment 01 chronic depression , part 3: psychoso cialfunc.t ioning befo re and afte r t reatment wit h sertraline or im i pramine. j Clin Psychia lr y 1998 ; 59:608-617 27. rertov AR, Ware JEJr, Greenfie ld S. NelsonEC,Perrin E, ZubkoH M: Medica l Outcomes Stud y: an application of methods for evaluating the resul ts 01 medica lcare. JAMA 1989 ; 262 :907 913 28 Ware JE Ir . Sherbo u rneCD: The MOS 36-ltem Short .Form Health Survey (SF-36). I:conc ept uat Irernework and item selection. Med Care 1992 ;30:473-483 29. US Bureau of the Census: Current PopulationSurvey: Curr ent Population Reports , Series P·20 and P·GO.washington 0(; US Government Printi ng Office , March 199730. Bernd t f;R: Analyzing determ inants of wages and measuring wage d iscrimination: dummy vari ables in regressionmodels, in The Practi ce of Econometrics: (la ssie andContemporary. Ed· i ted by Berndt ER. Reading. Malos,Addison -we sley, 1991 . pp 150 -223 31, Kocsis JH. f rances AJ,VossC, Mason Bj, Mann JJ, Sweeney J; tm ipram ine andsocial -v ocational adju stmen t in ch ronic dep ressian .Am J P!>ychiatry 1988 ; 145:997999 32. Komstein $G , SChatzberg AF, these ME, Yonkers KA, M<· Cul lough JP,xeun erGI. Gclenbe rg Aj , Ryan CE, Hess Al . Harri son WM, Davi sSM, Kell er MB : Gende r d ifferences in ch ron ic ma jo rand double dep ression . JAttect Disord (in press) Am JPsychiatry 157:6 , June 20 00 BERNDT , KORAN , FINKelSTEIN,ET Al. 33. Pave M, Alpert [E, eorus )S. Nierenberg AA, PavaJA. Rosenbaum JF: Pattern s 01personality d isordercomorbidi ty in earl yonset versus tare -onset majordepression . Am J Psychiatry 1996; 153:1308-1312 34. KashKl . Klein ON: The relat ionship between age at onset andcomorbidit v in psychiat ric disorders . j Nerv Ment Dis1996 ; 184:703 -707 35. Rohde p. tewrnsobn PM. Seeley JR:Comorbidity of unipolar depression . II: c urnorbiditv with oth er mental disorders in adoles cents and adu lts. J

Abno rm P!>ychoI1991 ; 100:2 14-222 36. Klein ON,SChatzberg AF, McCu llough JP, Keller MB, Dowling f ,Goodman 0, Howland RH, Mar kowitz lC. Smith C, Miceli RJ,Harrison WM: The earl y versus late disti nction indysthymic di sorder: com pa rison on demographic and clinica l variab les, family history, and treatmen t responsein ou tpa tients with sup erimposed ma jor depressive episodes. J Attect Diso rd 1999 ; 52:187196 37. Keller MS,Shapir o RW, t avori PW, Wolfe N: Recovery in majordepressive disorder. Ar<h Gen Psvctnatrv 1982 ; 39:905-91038. Keller MO, Lavcri ew, Endicott J, Coryell W, KlermanGl: "Dou ble dep ression " : tw o-yea r tonow-up . Am JPsychiatry 1983 ; 140 :689-694 39. Kelle r MS. Klerman GL,Lavon PW, Coryell WA. Endicott J. Taylo r J: t ong-term outcome of epi sodes of major depression . JAMA 1984 ; 252:788 -792 40. Keller MB, t avo rl PW, Rice JB, Coryell W.Hirschf eld RMA: The persis tent risk of cbronkttv inrecurre nt episodes of non bipolar ma jo r depressivedisorder : a prospecti ve tcnow-up. Am J Psvchtetrv 1986 ;143:24 -28 41. Emslie GJ, Rush AJ, Weinb erg \VA, kowa tcbRA, Hughe s CW, carmo dy T, Ri ntelman J: A do uble-bli nd,random ized . placebo controll ed tria l o f f1uoxetine inchildren and adolescents with dep ression. Arch GenPsychiatry 1997 ; 54:1031-1037 42. Ettner Sl , Frank RG.Kessler R(; The impact of psychiat ric d.sorders on labormarket outcomes. lnd l abo r aetat Rev 1997 ; 51: 64-81 947
Reproduced with permission of the copyright owner. Furtherreproduction prohibited without permission.

This page intentionally left blank
Reproduced with permission of the copyright owner. Furtherreproduction prohibited without permission. 99 RegularArticles Recurrence After Recovery From Major DepressiveDisorder During 15 Years of Observational Follow-Up TimothyI. Mueller, M.D., Andrew C. Leon, Ph.D., Martin B. Keller,M.D., David A. Solomon, M.D., Jean Endicott, Ph.D., WilliamCoryell, M.D., Meredith Warshaw, M.S.S., M.A., and Jack D.Maser, Ph.D. Objective: The recurrence of an affectivedisorder in people who initially recove r from majordepressive disorder was characterized by using the uniquelongitudinal prospective follow-up data from the NationalInstitute of Mental Health Collaborative Program on thePsychobio logy of Depress ion-Clinical Studies . Method: Upto 15 years of prospec tive follow-up data on the course ofmajor depressive disorder were available for 380 subjectswho recovered from an index episode of major depressivedisorder and for 105 subjects who subsequentl y remainedwell for at least 5 years after recovery. Baselinedemograph ic and clinical characteristics were examined aspredictors of recurrence of an affective disorder. Theauthors also examined naturalistically appliedantidepressant therapy. Results : A cumulative proportionof 85% (Kaplan-Meier estimate) of the 380 recoveredsubjects expertenced a recurrence, as did 58% (Kaplan-Meier estimate) of those who remained well for at least 5years . Female sex. a longer depressive episode beforeintake. more prior episodes. and never marry ing weresignificant predictors of a recurrence . None of these orany other characteristic persisted as a predictor ofrecurrence in subjects who recovered and were subsequentlywell for at least 5 years. Subjects reported receiving lowlevels of antidepressant treatment during the indexepisode, which further decreased in amount and extentduring the well interval. Conclusions: Few baselinedemographic or clinical characte ristics predict who willor will not experience a recurrence of an affectivedisorder after recovery from an index episode of majordepress ive disorder. even in person s with lengthy wellintervals. Naturalistically applied levels ofantidepressant treatment are well belo w those showneffective in maintenance pharmacotherapy studies. (Am JPsychiatry 1999; 156:1000-1006) "Single episode s areextrenu..·ly rare if the per iod of O b SlT ' "a rion issigni ficantly extended ." -Angst cr al. ( II Presented inpart at the 149th annual meeting of the AmericanPsychiatric Association , New York, May 4-9,1996. Rece ivedJune 12,1 998; revision received Oct. 21.1998, acceptedNOli. 17, 1998. From the NIMH Collaborative Program on me

Psychobiology 01 Depress ion-Clinical Studies; and theDepartm ent of Psychiatry and Human Behavior. BrownUniversity School of Medicine. Address reprint requests toOr. Mueller, Department of Psychiatry and Human Behavior,Brown University School of Medicin e. cia Butler HospitaL345 Blackstone Blvd " Providence. RI 02906;Timothy_.Mueller @brown.edu (e-mai l) This manuscript hasbeen reviewed by the Publication Committee of theCollaborative Depression Study and has its endorsement .The authors thank Rita Misek lor manuscript preparation.1000 For the maj orit y of people with ma jor de pressivedis orde r, recurren ce a it er reco vcr v is th e rule .Alth ou gh resol utio n of th e signs and 'symptoms o fdepr essio n is t he: maj o r goal o f tr ..-arrnenr, themai nreJ1;,lIKc: of that st ate o f well -being is o m: ofthe current ch allenge s for the mental he alth field .Both natural istic 'IOU treatment stud ies o f majordepression ha ve high li ghted the high ra re of recurrence a fter recover y (2-6) . A g rCJtl' r n urn ber of pr ior e pisodes o f maj o r de p ression is the strongestbaseline predictor o f the dura tion of the well interva l;th e great er th e number of prior ep isodes , the mor t'rapid the recurrence (4-6) . Oth er factor s rhar predi cta mo re ra pid recurrence a re secondary su htvp e o fdepression (6 ) and the persistence of su bsyndro rna lsymp to ms (L l.. Judd et a l., 1998 unpublish t'd pap er). T hL' literatu re is inco ns istent regar di ng t hedfe(t of age 0 \1 recurrence r isk . Lo wer age has bee nAm J Psychiat ry 156:7, July 1999
Reproduced with permission of the copyright owner. Furtherreproduct ion prohibited without permission. Fo positivelyassociated with greater risk in some studies of clinicalsamples (4, 7) and a nonclinica! samp le (8) and negatively associated with great er risk in other clinicalsamples (6), The Na tional Institute of Mental HealthCollaborative Program on the Psychob iology ofDepressionClinica l Studies is a pro spective natur alisticstudy of a cohort of people who sought treatment ior anaffective diso rder at one of five universirv medicalcenters between 1978 and 198 J. This coh~rt has beenfollowed since intake with att ent ion to course and outcome of their mental disorders. We have reported (9) on the10year course of the index episode of ma jor depressi vedisord er, focusing on the subjects who remain ed ill for 5years of pro spective follow-up. Over the 10 years of follow-up, 401 (93 % by Kapl an -Meier estimate) out of 431subjects event ually recovered. In the 35 subj ects whowere continuously ill for'; years, 13 (38 % by Kaplan-Meier estimate) su bsequently reco vered in the next 5

years. The current report complements the descr iption of10 years of observation of the first cycle of majordepressive disord er by describing the well interval following recover y from the intak e episode , on the basis of15 years of follo w-updata, which have recentl y become available. In addit ion to the sub jects who recovered at somepoint in the 15 years, we focus on the subgro up o fsubjects who rec o ver ed from th e inde x episode ofdepres sion and subsequently remained well for at least 5years. We cho se 5 years to par alle l the time frame usedin the pr ior work (9). In this report we specifica llyaddress the following quest ions: 1) What pro por tion ofsubjects with major depre ssive disord er develop an otherepi sod e of a ffective disord er ? 2) Do subject age,number of prior episodes, and presence of secondary majordepression persist as significant baseline predictors ofrecurrence? 3) What clinical o r de mographic feat ures distinguish the group of subjects who recovered an d thenstayed well for at least 5 yea rs after recovery? 4) Dosubje cts co nti nue to exper ience recurrence s after 5years of recovery? and 5) What was the level ofantidepressant treatment in the groups who stayed well fo rat least 5 years after recovery? METHOD Between the year s1978 and J9fll . 955 pati ent s who sou ght psy· ch ia Hklrl'atm ent fo r il moo d d isurde r alone of five U.S. medicJI centers (in Bosro n. C h i\: a ~o. Iowa Citro Kew York. and St. Loui s) .....ere emered int o ;) prosp e~ t i ve, natu ra listi..: f ( )lIo Y>~up s tu d ~ '. Th is re portcoxtends to 1.5 YC;lni of fo llo w· up pre .... iou sanal)'ses on t he 431 SUbjCl'ts with onl y ma jor de pr tsslve J isnrdl' r;'lt intake w ho h'ld no pr io r hist or r of milni .). hYPo nlit ni a. ~ chil.O a ff ec tiv e disorder. ('hu mic int ermittent depr essive diso rder, ormino r de pression of at lettst 2 ~' ea rs ' dur ati on iltintah-. After ..:umplete dc:S(:riptio n o f the stud y tothe subje..:ts, writte n in formed co ns('nt W,IS o btained . We ha l'e di.. ti n ~ uis h c: d two nested grn ups. Th<:first co nsists o f the 380 sub;e..:ts who reco wredfrom the index (·r isod e.n some time w hile st ill in ;l~t i\' e follo w -up during tht, 15 year s of ob serviltiona l follow -up . From th em co mt' the s el,,'ondgroup uf 105, a suh set who re..:uverl",d frum the indexepisod..:ilnd subseq uently rem.lined well for at lc;1st Sre;)r ... Am J Psychialry 156:7, July 1999 Assessments Th edeta ils o f [he assessment procedures are describ edelsewhere 16 .9). Briefly,;111 sub jects were assessed atint ake with the Sched ule for Affccn ve Disor der s andSchizophrenia (SADS) (101.and this informat ion was usedwith medical records to make dia gnos es according to theResear ch Dia gn osti c Crit er ia (ROC) ( I J ), T he

subiecrs were inrervie .....ed ever y fomonths for thefirst 5 years and every year thereafter by means of theLongitudinal lnrcrval Follo w-Up Evaluation (12). Thisfollo w-up instr ument mea sure.. the levelo f psycbopatholog )' for each ROC m' lim af fecti ve disorder Oil ae-poin r scale called the " psychiatric sta tus rat ing"(9), A scor e of I denot es no sym pto ms of t he disorders, and :1 score of (, denotes fulfillm ent of the fulldiagnos t ic ' riteria with psychosi s or severeimpairment. For these 431 subjects with major depr ession,recove ry was cons ider ed to begin with the firsr Ilf Hconsecut ive weeks of no or minimal sympto ms {psychiatricstatus ratill~ o f I or 2). Unti l recovery oc curr ed , asubjec t remained in an episo de of m aier dep ressive disorder, with ps vchiamc status rat ings of 1-6. Thecontinuous string o f psychiat ric sta tus rati ngs for major depre s..ive di so rder lasting up to ?SO weeks was thesource o f date fo r the analys es uf the course ofillness. Predictorsof Course We examine d demogr aphic.\lIJ cliuical char a..rer istics determined at int ake aspredict ors of the subseq uent cour se of major depr essivediso rder, In addition, we used t he cvt rac red score onthe Hamilton Dep ression Rating $..: ,,1,,' ( ItH and thesco re on the Glo bal ASSl'SSrneu t Scale (GAS) fro m J.n:l collec ted at the , ~ · ye .u poin t to reflecr the "cur rent" st.HUS for the subg rou p of subject s who remained well tor at least $ ~' C;H S . Treatment Ant idepressant rrcarm eur was co ded weekl y by using a 5-point composite an ridcprcs sunt scale, which quumifics a llantide pressant somaror hera py, includin g EeT an d pharmacot hera py (91. A score of a means that lUI auridcprcssa nt so matic rrc.nm enr W ;lS provi ded for tha tweek. A score of J repr esents ;l daily dose o f 1-99 mg ofimipramin c or its eq uivale nt, A sco re of 1 represent sa dail y Jose of 100-1 99 mg o f imipramine or equivalent,J repres en ts 200299 rng of imipram ine cquivaleur• •tnd 4repr esents .;00 mg or mo re o f imipramine equivalcur. The study p rotocol did not influence the treat mentprovided hy the patient 's physician. Statistical MethodsThe ou tcome of interest ill rhcse ; I n :l I ~ ' SC i wasrec urrence of an atfcc tive disorder. The data werecensored either by loss HI follow-up or end of theassessment per iod . Surviva l nnnlysis W ;\ S used to analyze time unti l recurrence during the follow-up. TheKapla n-Meie r prod uct limit was used 10 estimat e thecumulative pro babil ity of recurrence ( UJ. Analyse s werecond ucrcd fur the entire group o f 3HO subjects with major depr essive disord er at buscliuc who experienced nrecover)' and to r the I05 subj ects who subsequen tlyremained well for 20 1 least 5 r ear s ufter reco very from

the index ep isode a nd for whu m <ldd it iOlu l follo......-ur d.na Wer,,' :w ail., hle. for predi....tor.\Oalrses ,lnd to a..:count for h :n~th uf ful\u w-lIp. dini\:;11 a llu delllogr Jph ic \";Ici"bles W"' fl 't'ntl'red into;) Cu x regressiun to e\·.lIUah' the strenv,rh o f thei r i I SS o d a [ i t) n~ with ret:urrence<I fter oth er variahlcs in the m(ldei Wt're \:ontr olledfor. A two -tailed 201 · rh:t o( 0,05 WM. l'onsidered st atisr kall ~ ' si ~n i ( i can t . For anal yses uf treatment. the t test and fi sher's eX;Kt ""st wer t used . To;)c o.:ount for lHultiple univ;u i' ltC.' rests. a two·taill'll a lph;1of 0.0 I w ;) S used to derermim' b:e1 o fstat istic ,ll si ~n i fi";1 11ce , RESULTS Th e result sare or g'\lIized to reflect the two groups Ihat are theiocus of Ihis study: the comp lete coh or t who recoveredwithin 15 rears (N=3S0) and the subset 1001
Reproduced with permission of the copyright owner, Furtherre production proh ibited without pe rmission. Wald l. 2.__ .?5% CI ~ ;1 1..._ P Adjusted Odds Ratio Recurrence (N;279 ) Mean SO No Recurrence (N;101j Mean SO TABLE 1.Relation of Clinical and Demographic Features to RecurrenceOver 15 Years tor 380 Subjects Who Recovered From an IndexEpisode at Major Depressive Oisord_e_, ---:-;-r-r-r-r-rCharacteris tic Age at intake (years) Durati on 01depressiveepisode before intake (weeks ) (Odds rat io calculated pe ryear) Hamilton depression score before i n t a k e ~ GASScore before inlake a 39 .6 50 19.4 42 3 14.2 37 .7 85 687.3 20.3 108 40.4 14.7 108 7.1 11.0 1.00 1.11 1.01 1.00 0.99-1.01 1.05-1.1 8 0.99-1 .03 099-101 0.18 12.59 0 .80 0.00 0.6 7 0 .0004 0.37 0.97 N % N % Female gender 52 Numberof episodes of majo r depr essive diso rder before intake oq 1 U 2 10 ~3 17 Primary major depressive disorder atm take60 Psychotic subtype al intake 7 Mar ital status at intakeMarried 58 Divorced. separate d. or widowed 24 hi ... .." ,........ ,,,,,.-1 19 VWlng 10 Ul l s slng O~Ii1, 1'\1=95and N=271. respectively, 51 48 26 10 17 59 7 57 24 19 17893 64 40 82 164 29 133 56 90 64 33 23 14 29 59 10 48 20 321.43 1.18 080 117 1.00 1.01 1.55 1.10-1 .86 1.06-1.31 062-1.03 077-1 .79 7.20 9.51 2.91 0 .53 0 .00 7 .83 0,00 7 0.002 0 .09 0.47 096 0.005 Week Aller Recovery 0 2 -1 0.0 I, o 52 10.:1 156 208 260 312 364 ,0 6 468 520 572 624 676728 780 FIGURE 1. Time 10 Recurrence or Affective Disorderfor 380 SUbjects Who Recovered From an Index Episode 01Majo r Depressive Disorder predict or of recurrence. Womenwert' 43'}:. mort likely ro exp erience a rec urrence .Those who had ne ver mar ried weft' 55% more likelv toexperience a recurrence th an tho se in th e other two caregones o( marital status. Longer du rati on o f depressi vee p iso de before intake W;lS asso c ia ted w ith a higher

risk . such [hat 1:00(h a dd ition a I yea r \\' a~ asso ciured with .111 I I 'Yo, grearer likel ihood of recurrence. Simil arl y, ea ch addit ional ep isode o f majordepressi on before inta ke was associated with an I H(Y.,incre ase in the risk o f recu rrence. f igu re I presentsrhe survival curve for th e 3:;0 sub[ect s. Subjects beganth ei r \\'l.'11 inrervuls at different calendar dale s andthus hove different lengths of follow-up. from 2X wee ks 1015 full yea rs In o weeks to tal). The rncdiau rime torecur ren ce (It'ngth of rhe well interval) wa s IJ 2 weeks, and rhc cumulati ve pruporrion (Ka p la nMeie r) ofrecurrvnce ut 15 ycars W i:1S 85(Y" . The mean rim e torecu rrence in the roral gr o up o f s ubjec ts ( in cl u din g cen sored s u b jec ts ] was 14 5 weeks (51)= 160 1.Some' ot the 27Y s ll h j e'l ,,: r~ with major depressive:di so rd er .H intake who had .1 rl'(UTrI:IKe receivcda diffcreur di agnosis Jurill ~ the recu rrence: n ine: (3%, de veloped sc h izoa ffect ive d isorder (d ep res sed,mani c, or mi xedl ; 17 ( 6 · ~ ';.) develop ed mania. and36 ( 13 '~ { ,) de velo ped hyp omania . For 7 8 1~t, tN=217 ), ho wever, the rec urr enc e wa s majur de:prl:~~ i\'1: di sorde r. To a ssess rhe level o f u urural isr icsomatic anr id eprcssanr treatment, WI: determined rheproportion of weeks d u r ing the l " r i~ () t ltof illness that a ny suc h rreurmenr was rece ived, the me anscores o n rhe cornposir e a nr ide pressaur sca le du ringtho se week s o f rre armcnr, a nd rh e p roporri on of sub icc rs who recei vcd no ; H lt i dl.' p rt' '''~ ' 1 11ttrv a tmcnt . Dur ing th eir in ~: ~\ ~ 0.6 s i 0 4 £ of rhis group w ho ~ lI hSl'L .Jl h : ll rly rcm .iincd well for at k a't,; yea " i:\= 10'; ). Complete Cohort Of rhe ,HW"'llhjl ·,.:r~ ill rhi ... ~rlld y group, 279 WI:H:followed until a recurrence. (,(, rcru aincd well a nd werefo llowed unt il oo ios l to foll ow-u p, " a nd ,, 5 re mained we ll and were follo wed to rhl' 15-Yl·.lr point. Inrhl' sur vi vnl an ;ll y st '~ rh .rr fo lio \\", thl·... l· 1" ... 1 two groups a rc d 'l ssifit..'d ;1... ccn ...orcd . Table I vum m.mzes the demographic an d clinica lfl·;1tul'l·... to r rhc g ro u p who recov e red and did 110t han' ,1 recurrence Ii' :: 101) and for thosl' who recovered an d l·\'l,.·llfu;llly did exp erience a rec u rrence (;\ ::2 l)1; it al ... tl prl·.... l ·nt ~ the re sultsof a Cox rq~rl · ", .... ion llludd th .u l,·x .ll ll illl·d 1,';l l."1 l v.uiable ,lS 'l 1002 Ali i ,J /-':;yl:hI8( ry ' 0,61 .July 1999
Reproduced with permission of the copyright owner. Furtherreproduction prohibited without permission, 062-1 .03 077-1.79 TABLE 2. Relation of Clinical and Demographic Features10 Recurrence Over 15 Years for 105 SUbjects Who Rema ined

Well tor at Least 5 Years After Recovery From an IndexEpisode of Major Depressive Disorder No Adiusted RecurrenceRecurrence Odds Wald X' Characteristi c (N=53) (N=52) Ratio95% CI (dl=1) -------_._----._Mean SO Mean SO Age at intake(years) 39.5 12.8 38.5 15.8 1.01 0.981.03 0.40 0.52Duration of depressive episo de before intake (weeks)(Oddsratio calculated per year) 56 103 42 50 0.97 0.73-1.29 0.05 0.82 Hamilton depression score before intake d18.1 7.0 20.8 7.7 1.00 0.951.05 0 .Q1 0.92 GAS score beforeintake 43.1 11.7 37.8 13.3 0.99 0.96-1 .01 0.87 0.35Hamilton depression score at 5 vee rs" 4.1 3.8 4.8 3.9 1.080.97-1.19 1.96 0.16 GAS score at 5 years 77.0 9.7 72.7 11.80.99 0.961.03 0.11 0.74 N % N % Female gender 26 49 32 621.16 0.62-2. 16 0.22 0.64 Number 01episodesof majordepressivedisorder before intake 1.15 0.88-1.50 1.05 0.31 024 45 18 35 1 13 25 11 21 2 6 11 10 19 ~3 10 19 13 25Primary major depressive disorder at intake 33 62 33 630.69 0.37-130 1.33 025 Marital status at intake Married 3260 28 54 1.00 Divorced, separated, or widowed 13 25 7 131.04 0.42-2 .60 0.01 0.93 Never married 8 15 17 33 1.920.92-4 .02 3.04 0.08 aOwing to missing data, N=51 and N=52. respectively. b Owing to missing data. N=42 and N=49,respectively. dex episode of ma jor depress ive diso rder,the gro up w ith a rec urrence (N =279) an d the gro up with out a recurre nce (N : 1( 1) rece ived ant idepre ssanr tr eat ment fo r s imilar perc ent ages of the weeksduring fol lo w-up lmean =68 (~~lt S D = 3 6 ~ , . versusmean=i Ouj" , 50 =40 %, respe ct ivel y) (t:0 .40, d f:.ln,p:0.6 9) . These groups a lso receive d simi la r levels ofa nu de pressan r treat ment , as represent ed by the scoreon t he compos ite ant idep ressan t sca h(mea n= 1.70 , SO= I .Os , versu s mean: 1,64, 51): I .Os ) It: 0 .4 5, df=378, p: 0 ,66) . In a dd ition, 1 1% 01 the group wit h arec urrence 130 of 279) vers us 16 % of the gro up with norecurrence (16 o f \Oll receiv ed no antide pressa nt t reatment du ring the index ep isod e of major depressi ve diso rd er (;(":1.8 1, d f: l , p=O.l S). Subjects WhoRemained Well tor at Least 5 Years In th is subsarnple oflOS subjec ts, 52 were followed until a recur ren ce, IXremained we ll and we re fo llowed unt il "l o st tofollowup," and 35 rema ined well a nd we re fo llowed to the IS -year poi nt. In t he survival analyses tha t follow,these last two gro ups are classified as cens ore d. Tabl e2 pre sent s the d emographic an d clinica l info rmationfor the J05 subje cts w ho ex perienced a well in te rva lof 5 years or lo nger and we re fo llo wed fo r lip to 10ad ditional yea rs (15 years total ). .\-tan)" of thesesubje cts remai ne d wel l; however, 52 158 % Kap lan -Meier estima te] exp er ie nc ed a recurrence o f an affectivedisorde r du ring the subseq uen t prospec t ive fo llo wup

period . T he subjec ts w ho d id not expe rience <1recurrence we re foll o wed for a mean of 676 weeks ISD:I65), wher eas th ose who did experie nce a recu rrencewere Foll o wed for i22 week s (51)= Am J Psychiatry 156:7,July 1999 FIGURE 2. Time to Recurrence of Affective Disorder for 105 Subjects Who Rema ined Well for at Least 5 YearsAfter Recovery From an Index Episode of Major Depress iveDisorder 1.0 I 0' ~ 0.e ~ &O' £ o.a 00 o 52 104 156 208 260312364 416 468 520 572 624 676 728780 Week After R-eov.ry 116 ). SCOfl'S on th e GAS and H amilto n dep ression sca leat 5 yea rs ind icat ed a relat ively high level of functio ning and few dep ressive sym ptoms. The varia bles intable 2 were ente re d into a Cox reg ress io n mo de l.None of thes e cl inica l or demograph ic va r ia blespredicted rime to recurrence, Figure 2 illustrates the surviva l cu rve for this subgroup of subjects. T he mediantime to recurre nce w as 39 4 wee ks, or 134 weeks beyo ndthe requ isite 260 week s of reco very. Most o f th ose who ex perienced a recu rrence of an a ffective disorder afrerS vear s of well ness (N :.52) developed on ly ma jordepressive disor der IN : 47, 90%) , However, five (10% )develo ped h ypom ani a ; nom.. de velopedschizo..affective disorder or man ia. Th e part...' f11 ofrecu rren ce of major affec tive disor1003
Reproduced with permission of the copyr ight owne r.Further reproduction proh ibited without permission. TABLE3. Relation of Recu rrence Over 15 Years to AntidepressantTreatment Rece ived During the Wellintervar for 105SUbjects Who Remained Well tor at Least 5 Years AfterRecovery From an Index Episode of Major Depre ssiveDisorder Period and Measure No Recurrence tN.53) Recurrence(N. 52) N % Mean SO N % Mean SO Analysis dl 30 58 37 71Year 1 of well interval Subjects who received noantidepressanttrealment Percentage of weeksinwhichantidepressant treatment was received Scoreoncompositeantidepressant scaleforsubjects receiving antidepressanttreatmeot" Year 2 of welt interval Subjects who received noanndepressant treatment Percentage of weeksinwhichantidepressant treatment was receivedScoreoncompositeantidepressant scalelor subjectsreceivingantidepressant treatme nt? Years3-5 of wellinterval Subjects who received no antidepressant treatmentPercentage of weeksinwhich antidepressant treatmentwasreceived Score onco mposite antidepressantscale forsubjectsreceiving antidepressant treatmenj '' 17 66 35 91 32 70 3237 66 22 60 40 1.54 199 1.49 0.99 0.95 109 2 1 40 80 1 8666 1.37 62 1.34 26 0.91 38 1.10 41 0.95 1.68 -1 .39 2.471.89 0.54 0.43 O.42 a 65 0.10 65 0.17 O.43 a 38 0.02 380.07 0.31' 34 0.59 34 0.67 aFisher's exact test. b A score

of 1 represents 199 mg/day 0' imipramineor equivalent; 4represents~ 3 00 mg/day of imipramineor equivalent. de r inthis subgro up is simila r to th e " vera II pattern in thelarger g ro up of 279 subjects described ea rlie r who recovered from t he index e piso de an d subsequently had arecurrence, Recurrence of ma jor depressive disorder is thepredom inant pattern. The anti depressant tr eat ment fo rth e g roup of subjec ts who sta yed well fo r a t lea st 5years was examined . For the index e pisode of major depression we determined the proport ion of weeks in whichan)' antidepressant treatmen t wa s received, the meanlevel of ant ide pre ssa nt treatment in tho se week s, andthe proporti on of subjects who received no anti depressant treatment. In addition, fo r all of these subj ects we determined th e same dat a a t yea rs I, 2 , and 3-5of t he we ll int erval to gai n a view of nat u ra listicall y applied "maintenance antidep ressa nt treatment ,"and fo r the subjec ts with a recurrence we determined theanridepressanr treatment during the 4 week s just beforerecurrence , Those remaining well received antidepre ssantt rea tment fo r a mea n o f 63 % (SI) =44%) of the ind exepisode o f major depress ive disorder, compared to 65(YQ(5D=40%) for those w ho experienced a rec ur renc e, andthose who did and did no t rem ai n well had treatmentlevels correspon ding to mea n score s o n the composite antide pressa nt sca le of 1.4 8 (5D =1.151 and 1.5 9 (5D=1.15). Neithe r o f th ese small d iffe renc es was sta tistically sign ifica nt. In ad d it ion, du ring the indexep isode, 21 % of the we ll group (1 1 of 53 ) and 19% ofthe group who experienced a recu rrence ( 10 o f 52) received no antidepressan t tr eatment (X 2 =O.04. dfe 1,p=0.85 ). After r ecovery fro m the in dex epi so de , thes ubjects cont in ue d to receive antid epressan t somatictherapy. Table 3 su mma rizes the an tidepressant treatmentreceived du ring the first 5 yea rs o f the well interva l.Using a co nse rvatively set a lp ha of 0.0 I for sta tistica l significance, we fo un d no d ifferences be tweenth ose who di d and did no t ha ve a recurr ence in theproport ion o f 1004 wee ks in wh ich any antidepressan ttreatment was received, the mean sco re o n the compositeantidepressant scale for those who did receive treatment,or the proportion w ho rece ived no ne. Fo r the grou p whoexperienced a recurrence (N =52). we exami ned the level ofant idepressant t reat ment during the month JUSt beforerecurrence. The mean scores on the composite anridepressantsca le for th is rime period were d istributed CISfollows:scorceO (no t reat ment }, N =40 (77% ); score ~ l, N= 12(2YXI' score 2:2 , N=8 (15( ~~ ); sco re ~3, N :::: l (2%);sco re 2'4. N =O. DISCUSSION It may be that recurrenceafter recovery from major dep ressive disorder is not inevi

ta b le. T hese resu lts ex tend o ur kno wledge throu ghca re ful prospective ob ser va tion. lr appears rhar somepeople w ith major depression do not develop ano therepisode with observatio nal perio ds of up to 15 years. Wha t basel ine cha racrerist ics dis ti nguish th ese people from those who do ha ve recurrences ? In the entire group o f 3HO subjects w ho recovered, a grea te r like lihoodnf recurrence o f an af fective d iso rder was asso cia tedwi th being fem ale, having mo re prior ep isodes, nevermarrying, and havi ng a longer du ration of de press ionbefo re intake. Age and primary versus seco nd a ry depressive episode did not distinguish the [ \\,0 groups inthis long-term study, a finding contr a ry to rhc find ingso f reports fro m the co llabora ti ve d epress ion studyba sed o n br iefer follo w-up pe riods (6 ). No ne of theo th er cli n ical or dem ogr aphic characte risticsassesse d at base line di stingu ished the two groups.Recent wor k by o ur group (unpublished 1998 pa pe r) , which broade ns th e str ic tly synd ro ma l view of majo r depressi ve diso rd er 10 include s u bsynd ro rna l Am JPsychiatry 156:7. July 1999 Reproduced with permiss ion ofthe copyright owne r. Further reproduction prohibitedwithout permiss ion . dl dl sy mp toms, illus t rates tha trill" pers iste nce of subsyndr om al symptoms in subjectsw ho wou ld class ically he ca tego rized as reco ver edpred icts ;1 th reefold sho rte r t ime to rec u r renee than rha t seen in su b jects w ho achi eve a full y asymptoma ri ...· s ta rt' (68 versus 23 t wee ks}. Infc1I..,t , th is prospeci ivcly obse rved cl ini calcharacteristic a ppea rs ro be a stronge r pre dic to r o frccurren ce th an th e aforemen t ion ed basel ine measures . T he pres ence o f psyc ho tic tea rures was not asignificant pred ictor in th is sample . Cory ell and collea gu es (14 ) demonstra ted that the pr esence o f psychotic fcaturcs in sub jects w ith ol.'preSSIOJ1 in the coll abo rat ive dep ress io n st udy p red ict ed grea te rpsychoso cial irnpa irrnent , lon ger illness episo des. and shorter times to first a nd seco nd recurr ences. We didno t find this to he t he case in th is g ro up. Th eimportant d isn ncrion is th at the current gro up was more rest r ict ive a nd d id J1 0{ include a ny sub jec t swit h schizo. if fcc rive disorde r. w here as th e gr o upin th e stu d y by Co rye ll cr a l. did . A mean ingfulrnin oriry o f sub jects developed mania a s themanifestati on o f thei r recurrent a ffective d isorder,Th e rat e o f 6 .1% fo r the larger gro up ("I=.l~O) is compa rable to th e 5,2 1 Y, ) in the coll ab o rat ivedepressio n st udy ( 15), wh ich was ba sed on 10 years offollow-up dat a . As reviewed in the rep o rt Oil tha tstudy. p revious inve stigators usin g w idel y differing

me thods and pati ent pop ulation s re po rt a rate o fswitching fro m un ipol a r to bipo lar depression thatr"lnges from O'Yo to J7. 5 'Yo, wi th a medi an of 9, 7 ~ kTh e lo ngi tud inal des ign of th is st udy lends st rength to o ur findi ng , w hich ind ica tes a slight increase fro m 10 years o f fo llow -up to the c urrentl y re port ed 15 years. The gender d iffe rence in d iag no:-.edmajo r dep ressive d isorder is we ll kno wn , Mosr but nota ll studies revea l a 2: t (fema le to ma le) rat io inprevalence and an ea rlier o nset of d epression and morerecurrence for women [ha n fo r men ( 16). Th e g rea te rrisk of recu rr ence fo r women is no t uni versall y reported ; in fact, in stud ies using retros pec t ively collecte d da ta an d so ph istic a ted meth ods of a nal ysis, no gender effe ct wa s a ppare nt ( 17, 1~ ) . Earli crreports irom the co llabo rative depression stu d )' o n pro bauds and Iamil v mem bers (6. 8), incl udi ng work on only s ubjects wit h a first ep isod e of major depressivedi sorder (1 9 ), reveal ed no gender d ifterenc e in t imeto re currenc e. However, another analvsis o f d at a fro mth e coll a bor a t i n :" de pression st udy, based o nlon ger fo llowup n mcs, sho wed a ge nde r di fIerencc among a group wi th het ero gen eou s nu mb ers of episodes(20) , Th ar ana lys is indicates th at a lon ger follow-up is need ed to de mon srr ure a gender ef fect o nrecurrence, Thi s effect disa ppea rs when th e gr o up isrvsrric ted to subjec ts w ith,) y(".trs of r~l :OVt' r y,suggesting (h at thi s su hg ro up · ·heh.l ves" like th efirst-episo de g ro up in rega rd to th e e ffe('t of gende r on rl'(urren(c. The sec.:o nd su h ject g ruup in o urst udy rep resents a uniq ue co llcl,:riun o f peo plc. Too ur kllo wl l'dge , rh is is the first rep ort o f a group o f people with nMjor depressive dis o rder w ho recov c..'red from an ep isode o f illne ss, subse q ut'm lyrem a ine d well for 5 )'t'ar ~. ~11l J we re pro srectiVl'ly fo llowed for lip to 10 'H.ld irio na l years, OurAm J Psychiatry 156:7. July 1999 . ea rlier wo rk (~)demonst rated th at a lthough 67'X. (Kapl an-M eier es timate ] rec o ver fr o m major dep ressive d i sorderwithin the first vea r, wi th a med ian tim e to recoveryof 16 weeks (Ka plan-Meier) , a sma ll hut meaningfulfr..action o f people co nt inue to reco ver for up to th eI(J-ycar follow-up po int. The persistently we ll su b[ects(N = I05) reported here recovered fair ly promptly a fte rinta ke (medi an rim e to rC( OH'r y= 13.27 weeks), a nd80°1.. were well a t I year o f foll o w-up. Even w ith thelen gt hy we ll interval, 5 8% (Ka plan-M eier esti ma rc)su bsequently ex peri ence d a recurrence. N one o f the baseline de mo gr a ph ic ..md cl inical charucrcri st icsth at pr edicted recu rr ence in {he la rger gro up

persisted as sig nif ica nt in this well g ro up. Ouranalysis o f the a nti de p ressa n t rrea rrn en rreceived by the ent ire grou p of 380 subject s w ho recover ed pro vid es so me insi g h ts in to natural ist ically ap pli ed t rea tme nt s as prospecti vely observed o ver15 yea rs. T he sub ject s wh o d id and di d not have arec urren ee received simil ar amou nts of a nti de pressant tre a tmc nr during the index episod e, a nd theyreceived t rea tm en t for sim ila r proportions o f th eindex e p iso de, Inso far as t reatmen t is a re flect ion o f clinical charac teristics of the d epression , th eco mpar ability o f th e tr eat men t received lend sfurther support ro the cl inical sirnilariry o f th e index ep isodes of de pressi o n fo r th e two gr o ups . T hesm alk-r group o f 105 su b jects whn ex perienced at least5 yea rs of recov ery pro vide a no ther view of nar u ralisrica lly a pplied rrcatmenrs. As th e well inte rva l progressed , the proport ion of week s rh ar any a nrideprcs sant rn.-a unen t was received and the mean level o f{ha t t rea tmen t d id no t di ffer to a srarisricallysignifi(ant degree herween the ~ r oup w ho d id not experience a recurrence .lJHJ th e g rou p who did , In addition, th e p ropo rt ion o f s ub jects rece iving no anti de p ressa n t treanu cnt increased fro m a rou nd 35(Yoto 650/0 over th e 5 years, • F urthe rmore, o f the subjects who eventually ex pericnc ed a re cur rence , 77~j jwer e recei vin g no a nri depressanr rre.ir rncnt duringrh e month just befor e th e rec urrence . In th e rem aini ng 23 lX, who d id re ceive tr eatmen t, th e modallevel of tre atment was bet wee n a nt idep ressant scalesco res o f 2 a nd 3, or between 100 and 199 mg of imipra mine eq uival ents per da y. It appear s th at wh eth er illor \\I~ II, [h is cohort uf af fecrivc ly ill suhjecrsrecei ved r oughly eq uiva lent and rather lo w levels ofsomar ic a nt idcpressa n r the rap y during the leng thywe ll int er val , an d the ruaj or it y of subjects received no a nr ide p rcssan r therap y just before recur renee . Whe the r or no t the recu r rence rat e would he reduced if th l.' le vel of an t idep ressa n t t re at ment\\'er e gre. trc r .... ,ltltlOt IX' det l'rm ined bytht.'st, da ta . O ur dat a o n llOnSOJl'l i.lt ic t hera pies . s u('h as psy( hother a py or f'lmi ly th erap y. are no t sys tem at ic or ( ompreh en sive t.'no ugh for usto com ml'tlf on th eir appl icat io n in th is gro up ,Being fcm al e, hnving a lon ge r ep isod e o f illne sshefo re sel.'ki ng rrC;\[Il1t:nt , never heing ma rried, and having m or e pri o r episodes ar e ('ha ra .... tc risti cs that m ay 1005
Reproduced with perm iss ion of the copyright owner,

Further reproduclion prohibited wilhout permission, 105sugges t to th e treating clin ician th at <1 pati ent will have a rec ur renee after rec ov er ing from maj o rdepressive di sorder. fro m th e dat il we a rc rep oningit was d iscourag ing to find so linkin fo rma t io n withwhich to pr edict wh ich subjects ,In..' s t ill at ri skfur recurrence even after half a decad e of recovery,Unfortunately, in thi s stu dy group we found th at peoplecontinu e ( 0 expericnce recu rrences even a fter longperiods of wel lness. The paucity of predictors and th e pers isten t po ss ib ility of recurrence s ho u ld ~lIiJ eclinicians a nd patients to he ever vig ilan t for .,recurrence of depression and the pernic ious suhsyndromalsymptoms of depressi on (our 1998 unpubl ished paper) . This someW h M d iscouragin g ad mo n iti o n is temper ed byour rep ort (9) rh.u some people (all reco ver after evenextremely long a nd seem ingly interminable epi sodes ofmajor deprt.' ssivl' dis order a nd hy other s' find ings(2) that suggest that effec t ive application of long-terman ridepressanr ph arrnaccuhernpy may maintain a sta te o fwell being . AC KNOWLEDG MENT S The ~ 1 l\.' I H Co ll..rhora rivc l'rogram 0 11 the Psychob iology of Depression-c-Clinicnl Studi es was condu cted wit h the p.. \Tricipanon of th e following inn 'stig..rtor s: M.B. Keller,M.D. (chairperson. Provide nce, R.I. ): 'X'. Cory ell, M.D.(co-chairpe rson , 10\v.1 Ci ty): J .D . Ma ser. Ph.D .i\'V;1$ h i n ~ to n , D. C. ); T.1. Mueller, ~'I.0 . ,M.T. Shea, Ph.D. (Providence, R.I. );./ . Haley (lowa Ciry):]. Endico tt , Ph.D.. A.C. Leon, Ph.O.,./ . Loth• .vI.S.W.INl'w York); und] . Rice.. Ph.D.•T. Reich, M.D. (Sf. Louis). Orbcr contributor s includ e H.S. Akiskal , 1\:I.D" N.e.And reasen, M.D .. Ph .D ., 1'.j . C luvro u, ~I.D ., j ,Croughan, M.D., R.M .A. Hir schfeld , M.D., M.M . Katz,Ph.D.. P.W. l.nvor i, Ph .D ., R.t.. Spitzer, M.D. , andM.A. Young. Ph.D. Deceased : G .l.. Klerrnun, ,M.D., E.Rohius, 1\'1.0.• R.W. Sh..rpiro, f\:l.D.• and G.\X!illokur, M .D. REFERENCE S 1. Angst J. Baastrup P, GrofP, Hippius H, Poldinge r W, wets P: The course of monopolarcep ressron and bipolar psychoses. Psychiatr NeuralNeurochir 1973: 76:489-500 2. Frank E, Kupfer OJ. Peral JM, Carn es C. Janet! DB. Mallinger AG. Tha se ME. McEach ranAS, Grochocinsk i VJ: Thre e-year out comes lor maintenancetherapies in recu rrent depre ssion . Arch Ge n Psychiatry1990: 47 :1093-1099 3. Hoy-Byrne P, Post AM, Uhde TW. PcrcuT. Davis 0 : The longitudinal course of recurrent affectiveillness: life cha rt data 1006 from research patients atthe NIM H. Acta Psychia tr Scand Supp l 1985: 71 :3-34 4.Gonza les LA , Lewinsohn PM, Clarke GN : Longi tudinalfollow up of unipolar depressives : an investiga tion ofpredic tors of relapse . J Consult Clin Psychol1985:

53:461-469 5. Maj M, Veltro F.Pirozz i A. Lobrace S, Magliano L: Patt ern of recurrence of illness atler recoveryfrom an episode of major depression : a pros pective study.Am J Psychiatry 1992; 149: 795--800 6. Keller MB, Lever tPW, Lewis CE, Klerman GL: Predict ors of relapse in majordepressive disorde r. JAMA 1983; 250 :32993304 7, Giles DE,Jarrett RS, Biggs MM. Guzick OS. Rush AJ: Clinicalpredictors of recurren ce in depression. Am J Psychia try1989; 146:764767 8. Corye ll W, Endicott J, Keller MB:Predictors of relapse into maj or depressive disorder in anonchnical population. Am J Psychia try 1991 :148:1353-1358 9. Muelle r TI. Keller MS, Leon AC. Solom onDA, Shea MT, Coryell W, Endicott J: Recovery after fiveyears of unremitted major depressive disorder. Arch Ge nPsychiatry 1996 ; 53: 794-799 10. Endicott J. Spitze r RL:A diagnostic interview: the Schedule for Affective Disorders and Schizophrenia. Arch Gan Psychiatry 1978: 35 :837-84411. Spitze r RL, Endicott J, Robins E: Research DiagnosticCrite ria: rationa le and reliability. Arch Gen Psychiatry1978; 35: 773-782 12. Keller MS, Levert PW, Friedman B,Nielsen E, Endicott J, McDonald-Scott P, Andreasen NC: TheLongitudinal Interv al Follow -Up Evalu ation: acomprehensive method lo r ass ess ing outcome in prospective longitudinal studies. Arch Gen Psyc hiatry 1987 :44:540-548 13. Kaplan EL, Me ier P: Nonparametriceslimation from incomplete observations. J Am Stat Assoc1958; 53 :457-481 14. Coryell W, Leon A, WinokurG.EndicaUJ, Keller M, Akiskal H, Solomon 0 : Imparlance ofpsyc holic features to long-term cour se in majo rdepressive disorder. Am J Psychiatry 1996; 153:483-489 15.Coryell W, Endicott J, Maser JD, Keller MB, Leon AC,Akiskal HS: Long -te rm stability of polarity distinct ionsin the affective disorders. Am J Psychiatry 1995 :152:385--390 16. Pajer K: New strategies in the treatmentof depression in women . J Clin Psychia try 1995 : 56(Febsupp l):30-37 17. Kessler ac, McGonagle KA, Swartz M,Blazer OG, Nelson CS: Sex and depression in the Natio nalComorbidity Survey, I: lifetime prevale nce. ch ronicityand recurrence. J Affect Oisord 1993 : 29:85--96 18.Kessing LV: Recurrence in affective disorder, II: effec tof age and gender. Br J Psychiatry 1998; 172:29-34 19.Simpson H8 . Nee JC , Endicotl J : Firs t-episode majordepres sion: few sex differences in cou rse . Arc h GenPsychiatry 1997 : 54:633-839 20. Winokur G, Corye ll W,Keller M, Endicott J , Akiska l H: A prospective fellow-upof patient s with bipo lar and primary unipolar affectivedisorder. Arc h Gen Psychiatry 1993; 50:457-465 Am JPsychiatry 156:7, July 1999
Reproduced with permission of the copy right owner .

Further reproduction prohibited without permission.Association Between Depression and Mortality in OlderAdults The Cardiovascular Health Study Richard Schulz, PhD;Scott R. Beach, PhD; Diane G. Ives, MPH; Lynn M. Martire,PhD; Abraham A. Ariyo, MD, MPH; Willem). Kop, PhDBackground. Stud ies of th e associatio n betweendepressive sympto ms and mort ality in elde rly populationshave yielded cont radictory findi ngs. To address thesediscrepancies , we test this associa tion using the mostextensive array of sociode mo graphic and ph ysical hea lthcont rol variables ever studied . to our kn owledge, in alarge pop ula tion-based sample of elde rly ind ivid uals.Oblectlve: To examine th e relati on between base line depressive sympto ms and 6-year all -cau se mo rtali ty inolde r pe rson s, systematica lly cont ro lling forsociodemographic fa ctors , clini cal di sease, subclinical disease, and health risk facto rs . Methods: A totalof 5201 men and wome n aged 65 years and olde r f rom 4 UScom munities participated in the study . Depressive symptoms and 4 categories of covariates were assesse d atbaseline . The pri mary outco me measure was 6-yearmortalit y. Results: Of th e 5 20 1 parti cip ants , 98 4(1 8 .9%) died with in 6 years. High baselin e depressiv esymptoms were assoc iated wi th a higher mo rta lity rate(23 .9%) than low baselin e depression sco res (17.7%)(unadjus ted relativ e risk IRRJ, 1.4 1; 95 % confidenceinterval IClJ, 1.22-1.63). Depression was also an independen t pr edi ctor of mortality when co nt ro lling forsociode mogra phic factor s (RR, 1.43; 95% Cl, 1.23-1.66) ,pr evalent clini cal disease (RR, 1.25 ; 95% CI, 1.07 -1.45), subclinical dis ease indicators (RR, 1.35 ; 95% Cl ,1.15-1.58) , or biological or behavioral risk factor s (RR,1.42 ; 95% Cl, 1.22 -1.65 ) . Wh en the bes t predictorsfrom all 4 classes of var iab les wer e included as covariates , high depressiv e sympto ms remained an independent pr ed ictor o f mort alit y (RR, 1.24 ; 95% CI ,1.06-1.46) . Conclusions: High levels o f depr essivesymptoms are an independent risk fact or for mort a lit yin com m unityresidi ng olde r ad ults . Mo tivati ona ldep icti on may be a key underlying mechanism for the depression -mortality effect, Arch Intern Med.2000;160:1761-1768 From the Department oj Psychiatry (DrsSchulz and Martire), the University Cenler for Social andUrban Research (Drs Schulz, Bead" and Martire), and theDepartment of Epidemiology, Graduate School of PublicHealth (Ms Ives) . University of Pillsburgh, Pillsburgh,Pa; the Deparlmerd of Cardiology. University oj California,Davis Medical Center. Sacramento (Dr Ariyo); and theDepartment of Medical and Clinical Psychology, UnifonnedServices Universityof the Health Sciences, and the Division

oj Cardiology, Georgetown University Medical Center,Wasl,ingtoll, DC (Dr Kop). T li E t.I NK between depression and mortality in older pers ons co ntin ues to be a h otl y debat ed issue ,J.2 with some investiga tors"!' demonstra ting that depressio n is an ind ependent risk factorfor mortality and othe rs"'" failing to find this association . Although resea rch ers may argue about the rea son sfo r these inconsistent findings (measu res o f d epressionused , sam ple used , th e length of the observa tion period for ascertaining mortality, and cho ice of covariates), individuals in both camps wou ld agre e tha t a fair test of the depression-morta li ty hypothesis req uires th atkn own demographi c and physica l hea lth sta tus predictors of mortality be con trolled. More over,the be tterand mor e extensive the health controls used in a study,the more con clus ive would be a finding linking depressionto mortality. The Card io vasc ular Healt h Stu dy (CHS), ala rge popula tion-bas ed stud y of olde r person s ,affords a unique oppo rtunity to test the asso ciatio nbetw een depre ssion and mort ality becau se of the ex tensi ve arra y o f soc io de mog ra p hic, obj ec ti ve clin ica l di sease, subcl in ica l di sease , and healthrisk fact or variab les available as cova riates . Th eassocia tion between mor e th an 70 pr ed ictor varia blesFor editorial comment see page 1731 and 5-year mortalit yfor this sa m p le was rec ently rep orted by Fri ed andcolleagu es ." Whil e Fri ed and co lleagues us ed anexplora to ry approach, relying on st epwise Cox prop o rtional ha zard s regression procedures to det ermine the bestpredictors o f mort ality , we use a mor e the oretica l,hyp othesis-based approach in thi s art icle. W e extendthe work of Fr ied and colleagu es by testing speci fic multi varia te models link ing depr ession to 6-yea r mortality in this sample. Five distinct mod(REPRIN TED) ARCHINTERN MED/ VOL 160, JUNE 26. 2000 WWW.ARCHI NTERNMED .COM<01000 American Medical Associali on. All right s reserved.107 in Older Adults

PARTICIPANTS AND METHODS
Symptoms of Anxiety and
Symptoms of Depression
Same Genes, Different Environments?
~enne t h S. Kendler, MD; Andrew C. Heath, DPhil; NicholasG. Martin , PhD; LindonJ. Eaves, DSc • While tradlUonalmultivariate ataUsllcal methods cen de
scribe patle rna 01 psychiatric symptoma, they cannotprovide
Insight Into why certa in aymptoma tend to co-occur In a
populallon. Howaver, thla can ba achieved ualng recantly
developed methods 01 muillvariata genellc analyala . Examin
Ing sell-report symptoms In a clinically unselected twin sam
ple (3798 pairs), traditional lactor analysis Indicates that
symptoms 01 depression and anxiety tend to lorm separate
symptom clustera. Muillvariate ganellc analys is shows that
genes act la rgely In a nonspecilic way to Inlluence theoverall
level 01 psychiatric symptoma. Noevldance could be lound lor
genes that specilically a"act symptoms 01 depression without
,Iso st rongly Influencing symptoms 01 anxiety. By contrast,
the environment seems to have speclllc effects, te, certain
leatures 01 the environment strongly Inlluence symptoms 01
snxlety while having Iltlle Impact on symptoms 01depreaslon.
These results, which are rapIleated across sexas, suggeatthat
theseparable anxiety and depression symptom clusters In the

general popu lallon are largely the result 01 env ironmental
factors. (Arch Gen Psychlalry 1987:44:451-457)
I ndividual psychiatric sympto ms are not independe ntlydis tributed in th e populati on. Rath er, sy mptoms tendto
clust er to form recognizable psychiatric sy ndromes. Al
though initially the pr ovince of th e diagno st ician ,the task of
recogni zing and describ ing clinical syndrome s has been
supplemented , for several decades, by multi variate stat is
tical methods.'.2 These methods can ident ify syndromes by
showing that certain symptoms often occur togeth er in
individuals in a population; howev er, th ey prov ide noins ight
into why th ese sym pto ms tend to co vary. In thi sarticle, we apply newly developed methods of
multivariate g enetic analysis' th at can move beyond tradi
tional factor analys is to clarify why cer tain symptomstend
toclu ster. We app ly th ese methods to self-report symptoms
ofanxi ety and depression from a large clinically unselected
twin sample.' Our goal is to und erstand why certain individ
uals disp lay depr essive sympto ms, while for oth ers th e
symptoms of anxiety are more pronounced.t " We wish to testtwo major hypothese s. The first is th at
ce rtain gen es specifically influence the liability todepres
sive sympto ms and other genes specifically influ ence the

liability to sym ptoms of anxiety. The second hypothesi sis Accepted for pub licat ion Aug 29, 1986. From theDepartment s of Psychiatr y (Dr KendJer) and Human Genetics
/Drs Kendler, Heath, Martin , and Eaves), Medical Collegeof Virginia,
Virginia Commonwealth University. Richmond. Dr Mart in isnow with
Queensland Insti tute for Medical Resear ch, Herston ,Queensland , Aus
tralia. Reprint requests to Department of Psychiatry,Medical College of Vir
ginia, Virginia Commonwealth Universit y, PO Box 710,Richmond, VA
23298(Dr Kendler).
Arch Surg-Vol122, May1987 that certain environmentalfactors ar e specifically depressogenic and oth ers arespecifically anx iogenic . METHODS Sampla This study isbased on completed postal questionnaires, mailed during theperiod from 1980to 1982, receivedfrom 1978 same-sex female,and 918 same-sex male, and 902 opposite-sex volunteer twinpairs older than the age of 18 years from the AustralianNational Health and Medical Research Council (NHMRC) TwinRegister, Canberra . As described elsewhere,' zygosity wasdetermined by questionnaire items shown to be at least95%accurate . The questionna ire contained a seven-itemanxiety and a seven-item depression subscale from theDelusione-Symptom s-States Inventory (DSSI), developed andvalidated by Bedford et aJ." Respondents were asked toindicate whether they had experienced symptoms "recently":1, not at all; 2, a little ; 3, a lot; and 4, unbearably.The prevalence ofsymptoms ofanxiety anddepression asassessed by this scale was similar in the twin sample andin genera l population samples from Austr alia.' Frequen cyofcontact among members of a twin pair was shown to beunrelated to concordance for symptoms. To simplify theanalyses, the 902 opposite-sex twin pairs were excludedfrom the multivariate genetic analyses. Because fewindividuals checked the most extreme response <unbearably), response categories 3 and 4 were collapsed into asingle category for the purposes of these analyses.Furthermore, because of the low response rate , the lastitem of the depressi on scale (depressed, thoughts ofsuicide) was eliminated from the multivariate analysis.

Since the fun text of these items has been presentedpreviously,' in this report, we will use the abbreviateditem versions. Data Analysis : An Ovarvlew Because of thestatist ical complexity of some of the material in thisarticle, in this section, a relatively nontechnicaloverview of the methods of data analysis is presented. Moretechnical aspects are outlined in the "Data Analysis:Methods" section. Finally, the first paragraph of the"Comment" section contains a nontechnical summary of theimportant results . There are thr ee major steps to thedata analysis presented in this art icle. First , atraditional factor analysis of the twin responses to theDSSI items is presented . Second, the fit of various modelsto these responses is examined using multivariate geneticanalysis. Third, after the det ermination of the mostappropriate multivariate genetic model, the results of thatmodelare presented in detail. Factor analysis attempts toaccount for the observed correlations between a relativelylarge number of symptoms in terms of the effects ofa smallnumber oflatent dimensions or factors. Factor analysis utilizes as "raw" data only the cross-correlations ofsymptoms within individuals. Thus, factor analysis ispurely a descriptive technique that can succinctlysummarize patterns of symptomcovariation. For example, ifthe DSSIitems are providing only a gross measure of overall"psychiatric distress," we would expect a single-factorsolution. If the items are able to discriminate between twodimensions of symptomatology (eg, symptoms of anxiety vsdepression), at least two factors would be needed toexplain the observed pattern of symptoms correlations. Thenext step in the data analysis is multivariate geneticAnxiety and Oepression-Kendlar et al 451 133 Common-PathwayModel Anx 1 Anx 2 Dep 1 Dep 2 Independent-Pathway Model Dep1 Anx 2 Anx 1 Relationship, as dep icted by schematic pathdiagrams, among hypothe sized genetic lactors (G, and G,),hypothes ized environmental factors (E, or E, and E,), twohypothesized symptoms of anxiety (Anx 1 and Anx 2), and twohypothesized symptoms of depression (Dep 1 and Dep 2).Strong relationships among variables are reprasented byblack arrows and weak relationsh ips by gray arrows . Incommon-pathway model, genetic and environmental factorsaffect symptoms by both acting on same latent variable .That Is, one genetic (G,land one environmental (E,) lactorspecifically Influence latent variable anxiety (Anx),whilesecond genetic (G,) and second environmental (E,) faclorspecifically influence latent variable depression (Dep).Individual symptoms are in turn influenced by latentvariables . In this model, genes and environment , by theirInfluence on latent variables, are equally specific (ornonspecific) In their Influence on symptoms of anxiety and

depress ion. In Independent-pathway model, genes andenvironment directiy and separately Influence individualsymptoms. One 01many possible configurations Is depictedhere with this model In which two genetic lactors (G, andG,) and one environmental lactor (E,) directiy Influencethe lour symptoms . G, is relatively specific for symptoms01anxiety and G, for symploms 01depression, but E, Isnonspecific and Influences approximately equally symptomsof both anxiety and depression. Thus , in this specificconfiguration , genes and not environment are responsiblefor tendency of symptoms of anxiety to correlate morehighly with other symptoms of anxiety than with symptoms ofdepression, and vice versa. In another possibleconfiguration of Independent-pathway model, and one moreconsistent with results of this articla, environmentalfactors would be relatively specific In their Impact onsymptoms of anxiety and symptoms of depression while agenetic factor would nonspeclfically Influence both sets ofsymptoms . analysis. This techniquecanbe understood as ageneralization of factoranalysis that permits theestimationofseparategenetic and environmentalfactors. Byusinginfonnation fromthe correlations between monozygotic(MZ) and dizygotic (DZ) twin pairs for the same symptom andcross-correlations between and within twins for differentsymptoms, multivariate genetic analysis permits theseparation of the genetic from the environmental impact onsymptom covarietlcn . We wish to test two models in ourmultivariate genetic analysis that represent different waysin which genes and environment might affect multiplesymptoms (Figure~ The lIrst, or "commonpathway." modelassumes that genes andenvironmentboth contribute to one ormore intermediate lstent varisbl es (eg, liability to"anxiety" and liabiUty to "depression," denoted .. "Anx"and "Dep" in the upper section of the Figure), which are inturn responsible for the observed pattern of symptomcovariation . In other words, this modelassumes that genesandenvironmentact on symptom covariati on by sflnal commonpathway. Under the second, or "independent-pathway,' model,genes and environment msy have different effects on thepattern of symptom covariation . Fbr example ( .. picturedin the bottom section of the Figure), there could be twosets of genes-one of which was relstively selective forsymptoms of anxiety and the other for symptoms of depression-but environmental intluences thst pre dispose equallyto both sets of symptoms . It can be shown algebraicallythat the common-psthway model can be subsumed .. s submodelof the independent-psthway model, so that the lit oflhe twomodels can be tested statistically (by means of slikelihood ratio t test), U The lInai step in the "Result..section is to present in detail the lIndings of the most

appropriate multivariste genetic model. This presentationpermits s detailed comparison of results between theconventional and multivariate genetic factor analyses andan examinstlon of the consistency of the findings aerosssexes. . Dete Anelye'e: Methode Methods of data summary andanalysis designed for continuous variables areInapproprlste fordiscontlnuoUBvariables , such as our Itemscores , which have only three-point seales. The approachthst we hsve used ..sumes the existence, for each Item, ofa normslly cIIetributed liability that determin.. theprobabiUty of response to thst item . The observeddistribution is related to the latent distribution byabrupt "threshold" superimposed on the latent distribution. With multicategory data .. those used in th isar-ticle, it is possible to te st statistically thevalidity of these assump tions. As describ ed previously,'the fit of th is "threshold" model to the observed data wasgood. The lIrot step in our dsta analysis was a traditionalfactor analysis of the twin responses. The sample wassubdivided by seX and th en into lIrst and second membersfrom each twin pair. A factor snslysis was performedseparstely for each of the four resulting subsamples.Foetor loadings were estimated by the unweighted le..t-equarea method ." In each analysis, the number offactors extracted w .. determined by the number ofeigenvalues greater than unity. We estimated uncorrelated("orthogonal") factors for comparsbility with themultivariate genetic analysis . To select for study one "fthe jnl\nite number of statistically equivalent solutions("fsctor rotations"), we used the simplest techniq~' offixing to 0 the Ioadings of one depression Item ("lostinterest III everything") on the second and third factors,and of an anxiety item ("pain or tension in head") on thethird fsetor. U This method of rotationensuredcomparabilityof factorrotationsbetween sexes, between first andsecondtwins, andbetween the traditional andmultivariategenetic factoranalyses. These items were chosenby performing varimax rotations u on the results from thefour subsamples and then selecting the items for which themean-squared rsctor loadlnga were highest on the observeddepression snd anxiety faetora, In lItting three factors,th is traditional fsctor anslysis required the estimationof 36 common fsctor loadings for 13 items on the firstlatent factor, 12on the second , and 11on the third. Item-specific fsctor loadlngs, which explain the varisnce notaccounted for by the common factors loadings, were obtainedby subtracting from unity the variance accounted for by thecommon fsctor Icadinge . By convention , theseitem-specillc loadings are not tabulated. Althoughsolutions that permit correlated ("oblique") factors""

sometimes preferred for deocriptlVll purposes, our chiefintereS~ was in causal analysis for whlch uncorrelatedfacton are IIlUC simpler to Interpret. This ia particularlytrue with respeet to the action of different genes thst, inthe absence of gametic-phSs' disequllibrium, should beuncorrelated In the population. . Theoretlcally, the bestdata summaries for multivariate analysIS 452 Arch GenPsychiatry-Vol «, May 1987 Anxiety and Depresslon-Kendleret al Anx 2 Dep 1 Dep 2 Tabla I .-Factor Loadings(x 100) ofSymptoms 01 Anxlaty and Depression on PhenotypicFactortl InFemelas end Malas' Femlll.. Molos '1Wln 1 '1Wln 2 'lWln 1'1Wln 2 ItBm I II m I II III I II III I II III Anxietysubscale 1. Wo<rled aboul .""'rythlng 62 37 16 63 26 22 5537 20 55 33 29 2. Breath less or heart poundIng 37 34 0 4242 -8 43 44 1 35 55 0 3. Worked up, can', sit stl1l 57 44 361 34 11 SO SO 23 57 37 19 4. Feelings of panic 66 40 8 7227 0 71 29 1 63 42 7 5. Pain or tension in head 41 44 lit41 44 lit 49 4S lit 36 59 lit 6. WorryIngkepi me awake 5831 39 60 25 51 54 25 58 55 27 56 7. Anxious. can 't make upmy mind 78 32 -7 79 21 -2 73 16 14 74 34 6 Depressionsubscakl 1. Miserable ditflculty with sleep 68 31 74 72 2463 68 27 52 68 29 57 2. Dep... esed without knowingwhy 7023 -3 71 18 -2 72 19 -2 72 22 1 3. Gone 10bed not caring 841 7 55 7 2 63 -3 -4 83 11 4 4. Low in spirits . just sat 806 I 80 10 2 76 5 -5 78 7 2 5. Futureseems hopeless 83 3 855 -6 9 63 -18 7 84 10 4 6. Lost interest in everything 89lit lit 92 lit lit 86 lit lit 91 lit at ·Orthogonal factors . tParameter fixed to o.
of our discontinuous data would be l3-way contingencytables,
,ross-e1assifyi ng th e scores of individuals on each ofthe 13items,
for factor analysis, or 26-way tables , cross -classifyingresponses of
first and second twins on each of the 13 items, formultivariate
genetic analysis. In practice, fitt ing models to suchcontingency
tables , which would require the rep eated numeri calintegr ation of
the mult ivariate normal distribution, would be infeasiblewith

current computer resources. Instead, we have obtain edmaximum
likelihood e stimates of the "polychoric corr elat ion?"between
every pair of variables, separately for each twin group(male and
female first and second twins for factor analysis; male andfemale
MZ and DZ pairs for the multivariate gene tic analysis ).We then
fitted models to 13x 13 or 26 x 26 mat rices of pclychoriccorrela
tions. The factor analyses were performed separately on each
13 x 13 matrix, but the multivariate geneti c analysieinvolved
simulta neous analys is of two matrices, one for MZ pairsand the
other for DZ pairs ofa given sex. Models were fitted byunweighted
least squares, in the case of the factor analysis , but byweighted
least squares, using estimates of the reciprocal of thesampling
variance of each polychoric correlation as noniterativeweights, J,8.1ll
for the multivariate geneti c analysts . The latterapproach gives
us an approximate 'I goodness-of-fit test of the absolutefit
of the model with the number of degrees oHreedom equal tothe
number of uniqu e cor relations (650 if we are analyzingtwo 26x 26

correl ation matrices) minus the number of estimatedparameters.
We can also compute an approx imate likelihood ratio 'I (or"'I
difference") te st of the relative fit of each modelcompared with
more complete models . For the full model , only a goodness-of-fit
test is available. For subsidiary models, the likelihoodratio 'I
provides a more powerful test . Thus , it is possible thatby a
goodness-of-fit test a model msy provide an acceptable fitto the
data , yet be re jected in favor of a different model by slikelihood
ratio test. In our multivariate genetic analys is using theindependent
pathway model , we estimated simultaneously item loadingson the
common genetic factors, the common (nonfamilial)environmental
factors , and Ite m-speciflc genetic factors. Loadings onthe common
genetic fae tors contribute both to the withinindividualand to th e
between-twin cross-correlations between items . Loadings onthe
common (nonfamilial) environmental factors contribute to the
within-individual but not to the between-twin itemcroes-correla
tions, Loadings of the item-specific genetic factorscontribute to

the correlation between twins for a specific item, but notthe CfOSS
correlations between items . Finally, item-specificenvironmental
factors , which expla in the residual variance, areobtained by
Arch Gen Psychialry-Vol44, May 1987 subtraction. Bothcommon and item-specific loadings are expected to be thesame for both members of a twin pair. An independentpathway model that allow. for three common genetic, three commonenvironmental, and item-specific genetic factors requiresthe estimation of 85 parameters: 36 (13 +12+11)commongenetic factor ite m loadings , 36 common environmentalfactor loadings, and 13 ite m-specific genetic factorloadings. Using the common-pathway model, we estimated asbefore common genetic, item-specific genetic , anditem-specific environ .. mental loadings. However, underthis model, the item loadings of each common environmen talfactor are expected to be a constant multiple of theloadings on the corresponding common genetic factor.Therefore, it was necessary to estimate only a singlescalar multiplier for each common genetic foetor from whichloadings on the corresponding common environmental factorcould be derived. In the three-factor common-pathway model,it was therefore necessary to estimate only 62 parameters:36 common genetic loadings, three scalar mult ipliers, and13 item-specific genetic loadings . The previous univariateanalys is' indicated that the overall effect of commonenvironmental or genetic dominance on symptoms of anxietyand depression in this sample wassmall or undetectable. Ifa variable accounts for a small proportion of variance inan item, sta tistical princ iples dictate that it cannotmake a major contribution to the covariat ion ofthat ite mwith othe r items . Therefore, our multi variate analyse sconsidered only additive gene tic and non.. familial (orrandom) environmental effects , both of which were shown,in our univariate analysis , to have a large impact onsymptom s of anxiety and depression.' For an estimate ofthe simil arity of factor loadings obtained on diff erentsamples (eg, twin 1 vs twin 2 or males vs females), thecongruency coefficient (T t ) was used." RESULTS FeelorAnalysl. Using the eigenvalue criterion, three orthogonalfactors were e xtracted in each case for the first andsecond members of the male and female twin pairs . Theresults of this traditional, or phenotyp ic, factoranalyaia are seen in Table 1. Fac:torloadings (which, in anorthogonal solution, are equivalent to the correlation of

an ite m with the underlying latent factor) are given forthe rotated solution. The first phenotypic factor, whichaccounted for between 46.8% and 60.5% of the totalvariation, was similar aeroas groups. The congruencycoefficients were above .99 for all six possibleeompariAnxialy and Dapression-Kendler at al 453 Table2.-Factor Loadings [ x 100) of Symptoms of AnxietyandDepression on GeneticandEnvironmental Fadors in FemaleandMaleTwins· Genetic Factor. Envlronmental Factors Item I IIIII Spec ilic I II III Specific Females Anxiely subscale 1.WOrriedabout everything 51 2 10 33 40 32 21 56 2.Breathlessor heart pounding 31 39 9 25 29 25 -1 73 3.Woric;ed up. can't sit still 50 11 2 35 36 37 8 59 4.Feelings of panic 59 14 1 20 41 26 -3 60 5. Painor tensionin head 33 34 Of 34 28 34 Of 68 6. Worrying kept me awake40 13 29 29 43 25 39 50 7. Anxious, can't make up my mind68 2 10 0 45 25 6 51 Depressionsubscale 1. Miserable ,difficulty with sleep 46 10 45 0 51 28 50 0; 2. Depressedwithout knowingwhy 53 2 13 21 47 21 -16 61 3. Gone to bednot caring 51 18 13 43 71 -2 1 17 4. Low in spirits , justsat 60 1 17 32 53 9 11 46 5. Futureseems hopell!SS 53 2 134 69 11 14 32 6. Lost interestin everything 63 Of Of 17 68Ot Of 37 Males Anxiety subsea's 1. Worriedabouteverything33 8 46 0 40 35 3 63 2. 8feathless or heart pounding 42 447 0 14 28 -2 73 3. Worked up,can't sit still 38 22 19 36 3145 13 58 4. Feelingsof panic 74 1 15 0 17 31 -5 55 5.Painor tension in head 32 34 or 37 24 44 Of 63 6. Worryingkept me 8'Nake 44 6 23 29 29 25 72 0; 7. Anxious.can'tmakeup my mind 60 13 18 6 45 25 1 57 Depressionsubscale 1.Miserable , difficulty with sleep 44 4 29 9 46 32 37 50 2.DepressedwithoutknowingWhy 57 -7 5 23 39 35 8 58 3.Gone10bed notcaring 57 -4 12 5 56 -3 4 59 4. LowIn spirits.just sat 85 1 -16 0 48 10 4 55 5. Futureseems hopeless 51-1 7 32 68 -2 2 41 6. Lost interestIn everything 62 Of Of 064 Of Of 45 Orthogonallactors. weighted least-squaresolution . tParameter fixed to O. :f:Paramelervalueconstrained to be positive. sons across the four groups .The highest factor loadings in all gr oups were found onfour core depression items: "gone to bed not caring," "lowin spirits. just sat ," "future seems hopeless," and "lostinterest in everything." However, the factor was not highlyspecific for depression as all items loaded positively (ie,> +0.30) on th is factor . This factor was tJ!rmed"depression-dist ress" to signify that depression itemsconsistently loaded highest on thi s factor, but it wasalso, in part, a general psychiatric distress factor. Thesecond phenotypic factor, which accounted for between 6.5%and 10.9% of the total variation, was also Quite similar inthe four groups. Five of the six possible congruencycoefficients were above .96 and the sixth (between male

twin I and male twin 2) was .93. The four highest loadingsin all groups were from among five anxiety items: "worri edabout everything," "breathless or heart pounding," "workedup, can't sit st ill,' "feelings of panic ," and "pain ortens ion in head." Unlike the first factor , the secondfactor was relatively specific. The loadings of all anxiety items except "anxious, can't make up my mind" were inexcess of .26, while the loadings for the four coredepression ite ms never exceeded .11. This factor wastermed "general anxiety." A third factor, which accountedfor between 6.6% and 6.9% of the total variation, had inall four groups by far the highest loading on the twoinsomnia items : "worrying kept me awake" and "miserable,difficulty with aleep." Five of the six poss iblecongruency coefficient! were above ,90 and the sixth(between female twin I and 454 Arch Gen Psych iatry-Vol 44,May 1987 male twin 1) was .87. This factor was tenned"insomnia." A useful way to quantify the contribution ofthe first two phenotypic factor s to the original anxietyand depression subscales is to compare the proportion oftotal varia nce accounted for in the two subscales by thefirst two factors. Across all four group s, the mean (:tSD) proportion of variance in the anxiety and dep re~ sionsub scales accounted for by the "depression-distress"factor was, respectively, 33.8%,=2.8% and 63.4%,=1.9%. Inother words , the "depresslon-d istress" factor accountedfor one third of the total var iance of the anxietyeubscale, but for nearly two thirds of the total variancefor the depression subscale. The mean proportion ofvariance in the anxiety and depress ion subseales accountedfor by the "general anx iety " factor was, respectively,14.1%:t 3.W and 2.4%:: 0.4%. The "general anxiety" factoraccounted for over five times as much variance in theanxiety as in the depression subscale. Multlvarlata GanotlcAnalyala: Modol Fitting We considered two majormultivariste models: the common' pathway andindependent-pathwsy models (Figure). By a X' good· ness-of-flt test, the fit of a "full" independent-pathway modelwith three genetic and three environmental tactors wasexcellent for both female' (X'=470.8: 4(=666: P =.98) andmales (x'=556.8: 4(=666: P= .69). For females , all subsidiary models with fewer than three genetic and threeenvironmental factors could be Anxiety andDepression-Kendler at al ",jected by likelihood ratio X'tests . For males, sll subsidiary models could also be rejected except that whichcontained sll three environmentalfactors and only the first two genetic factors IX' =16.3;<if= 11; P = .13). . The twoand one-factor common-pathwaymodels could be r <'i ,-cted at high levels of statist icalsignificance (P < .OOOOI) for both males and females .

However, the three-factor common-pathwav model produced areasonable fit in both females (X' = 550.0; d ( ~ 598; P =.92) and males (x' =638.4; df= 598; P = ,12). However,compared with the full independent-pat hway model, thethreeractor common-pathway modelcouldbe rejected bylikelihoodratio tl-,ts at high levels of signifiesnee forboth females (X' = 79.3; d( =33;P< .OOOI) and males (x'=81.6; df=33; P <.OOOI). . Finally, we fitted the fullindependent-pathway model to both :;l'xes simultaneously.The likelihood rat io test of heterogeneit y was veryhighly significant (X' = 222.9;df=85; P < .OOOI),indicating that although this model was appropriate foreach sex, the factor loadings differed significantlybetween females and males . Reaults 01 Best·FI"lng ModelGene t ic and environmental factor loadings are given underthe full independent-pathway model separately for femalesand for males (Table 2). Although a slightly simplermodelalso provided an adequate fit in males (ie , twogenetic and three env ironme ntal (al'tors) , th e fullmodel was somewhat superior in fit and had the advantage ofsimplifying the comparison of the results acros s sexes .In comparing these results with .the phenotypic factorloadings shown in Table I, it should be remember ed that wear e now fi tting a total of six (three genetic and threeenvironmental) factors rather than three phenotypicfactors, so that the individual factor loadings will, inalmost all cases, be lowerinTable 2 than inTable J. Acomparison of the se tables should focus on the patternrather than the absolute value of the factor loadings. Thefirst genetic factor, which accounted for 26.7% of thetotal phenotypic var iance in females and 27.8% in males,was very similar in both sexe s (r, =.986). The four items'lith highest load ing in both sexes were two anxietyitems, "feelings of panic" and "anxious , can 't make up mymind," and two depr ession items , "low in spirits , justsat" and "lost interest in everything." Like the firstphenotypic "depression-distress" factor, all items tendedto load highly and positively on this factor. Unlike thefirst phenotypic factor, the average loading for anxietyitems was almost as high as that found for depressionitems. Because of the appare nt lack of specificity of thisfacto r, it was termed the "genetic distress" factor. Thesecond genetic factor accounted for 2.8% of the totalvariance in females and 3.0% in males and was reasonablysimila r across sexes (r(= .837). In both sexes , only twoitems had subs tantial loadings on thi s f actor:"breathless or heart pounding" and "pain or tension in head." This factor differed from the second phenotyp ic"general anxiety" factor in having low loading s for othe ranxiety item s, es pecially "worr ied about everyt hing"

and "feelings of pan ic." Therefore, this factor was termedthe "genetic somatic anxiety" fact or, The third geneticfactor, which accounted for 2.9% of the total variat ion infema les and 3.8% in males, was only modestly stable acrosssexes (r, = .510). In females, substantial loading s wereseen only for the two insomnia items. In males, the highestloading was seen on the first anxiety ite m "wor ried abouteve rything," followed by the two insomnia item s. Thisfactor was broadly similar to th e thir d phen otypic factor and, hence, was ter med the "genetic insomnia" factor. The second and third genetic factors, alth ough statistica lly significant because of the large size of thesample , account for a small proportion of total variancein liability to sympto ms in the twin population . The genetic specific loadings , which refle ct the geneticinfluences unique to each symptom, were , a ll the average,relativel y modest , accounting for only 7.8% of the totalvari at ion in liabilit y to symptoms in female s and 4.0%in males. These results sugg est that the majority of genetic variance in these sympto ms is accounted for by thethre e e xtracted factors. The first environmental factor,which accounted for 24.5% of the total phen otypic variance in females and 18.8% in males was similar acrosssexes (r e =.984). In both sexes, the four highest loadings
were on the core depression items : "gone to bed notcaring," "Jaw in
spirit s, just sat," "future seemed hopeless ," and "lostinte rest in everyt hing." This factor was relativelysimiJar to the first phe
notypic "depression-distress" factor, but the specificityfor depres
ArchGen Psychiatry-Vol 44, May1987 sive symptoms'Y.'8.8somewhat greater. Therefore, th is factor was termedthe "env ironmental depression" factor. , The secondenvironmental factor, which accounted for 5.8% of thephenotypic variance in femalesand8.1%in males, wasalsoverysimilar in the two eexes(T,=.986), In both sexes, the threehighest loadings were on the core anxiety aymptoms "worriedabout ever ything," "worked up, can't sit still ," and"pain or tension in head ," This factor was quite similarto the second phenotypic "general anxiety" factor inloading more equally on all the anxiety items and hence wastermed the "environmental general anx iety" factor. The third environmental factor, which accounted for 4.0%of thetota l variance in females and 5.3% in males, was alsoreasonably similar in males and females (T e = .836). In

both sexes , this factor had substantial loadings on onlythe two insomnia items. This fa ctor was broad ly similarto both the "insomnia" and "gene tic insomnia" factors andwas termed the "environmental insomnia" factor . For almostaU the items, item-specific environmental loadings thatrepre sen t environm ental effects (including measurementerror) influen cing one item but no others, accounted (or asubstantial proportion of the total variation . For allitems , specific environmental variation accounted for26.0% of the total phenotyp ic variation in female s and30.0% in males . A useful way to contra st the contributionof the firat genetic and environmental factors to theanxiety and depr ession subscales is to compare theproportion of variance accounted for in these subscales bythe two factors. The "genetic -d istress" factorcontributed more to the total variat ion in the depress ionthan to the anxiety subscale in both females (29.8% vs24.1%) and malea (31.8% va 23.3%), but the differences werequite small. This is in contrast to the "environmentaldepression" factor , which contributed more than 21> timesthe total variance to the depression than to the anxiet ysubscale in females (36.3% vs 14 .4%~ In males, this ratiowas over 3:1(30.0% vs 9.3%). These result s support theconclusion that the first genetic factor is nonspecific ,while the first environment al factor is relativelyspecific (or symptoms of depression. COMMENT This articlerepresents, to our knowledge , the first a pplica t ion ofmultivariate gen etic methods to individual psych iatricsymptoms. We analyzed responses of 3978 twin pa irs to theanxiety and depress ion subscales of the DSSJ. Our majorgoal was to clari fy the role of genes vs the environmentin the etiology of separable anxiety and depression symptomclusters in the general population. Three major results arenoteworthy. F irst, a traditional factor an alysis consistently identi fied two important factors termed "depression-dis t ress" and "general anx iety." Second, infitting multivariate genetic models, the commonpathwaymodel could be clearly rejected in favor of the inde pe ndent -pa thway model. Third, fitting the fullindependent-pathway model produced three factors ofparticular interest, termed :"genetic distress ,""environmental depres sion, Jl and "environmental anxiety." We could find little evid ence that genes influencedspecifically either sy mptoms of de pression or symptoms ofanxiety. However, ce r t ain envi ronme nt s appe are d tobe speci fica lly depressogenic a nd others a nxiogenic,Phenotypic Factor Analysis In thi s large volunteer twinsample, the traditional eige nva lue cri terion readily identi fied three phenotypic factors that were st able acrossfour groups (ie, twin I and 2 in fem ales and males). After

rotation, the first of these phenotypic fact ors, termed"de pr ession-dist ress ," accounted for about half of thetotal variation. As the name implies , this factor loadedsubstantially on alm ost all items, but loadings wereconsistently highest on the depression items. The secondphenotypic factor, wh ich accounted for between 6% and 11%of the total variance, was termed a "general anxiety"factor. Loadings for this factor were both relativelyspecific for the anxiety subscale, and were similar Anxielyand Depression-Kendler el al 455 for almost all the anxietyitems. The third or "insomnia" factor had highest loadingson the two insomnia items with only quite modest loadingson all other items. Controversy over the discriminationbetween symptoms of anxiety and depression has a longhistory. ',U," Twomajor viewpoints, which have been termedthe "distinct-syndrome" and "unitary-syndrome" positions,'have been articulated. The distinct-syndrome position viewsdepression and anxiety as qualitatively distinct, albeitwith some overlap of symptomatology. The unitary-syndromeviewpoint, by contrast, argues that these two states are ona single continuum, and that any differences between themare basically quantitative and not qualitative. As recentlyreviewed, U,. empirical studies using a variety ofmultivariate techniques have tended to support thedistinct-syndrome position, although these results are notunequivocal. In addition , follow-up studies have stronglysupported the discrimination between anxiety states anddepression . ",28 Previous multivariate studies oftherelationship between anxiety and depression have, with rareexception," been performed on samples obtained in atreatment setting, Such an approach introduces an importantpossible bias. Individuals with symptoms of both disordersare more likely to present for treatment than those withsymptoms from only one disorder. This bias can create aspurious covariation of symptoms . By contrast, no suchbias can be operating in the general population samplestudied in this article. The Australian NHMRC Twin Registryrepresents a large, volunteer twin population, in whichreported levels of anxiety and depression do not differfrom those observed in the general Australian population .'Results from this sample provide some support for the"distinct-syndrome" position in that two phenotypic factorsthat could be identified as depression and anxiety wereextracted from each of the four subject groups . However,these symptom dimensions were not completely independent,as anxiety items consistently loaded positively on thefirst "depression-distress factor." By contrast, mostdepression items had very low loadings on the second"general anxiety" factor. Contrary to expectation,consistent evidence was found for a third "insomnia"

factor. We are unaware of any similar results that suggestan insomnia factor can be discriminated from anxiety anddepression in the general population . These insomniaitems, along with other questionnaire data about sleepduration and quality, are the focus of another report inpreparation. Multlv.rl.t. Genatlc Modal FI"lng Threeaspects of model fitting were examined: (1) thebest-fitting model, (2) the required number of genetic andenvironmental factors, and (3) the consistency of resultsacross sexes. We considered two different models of howgenetic and environmental factors might influence symptomcovariation. The first, or common-pathway model, assumedthat both genes and environment act on symptoms byinfluencing the same latent variables . The second, orindependent-pathway model, permitted genes and environmentto influence symptom covariation in different ways. Thecommon-pathway model could be clearly rejected in favor ofthe independent-pathway model. These findings indicate thatin this sample genes and environment are influencing thepattern of covariation of individual symptoms of anxietyand depression in qualitatively different ways. Thepreviously reported univariate analysis of these symptomsincluded an examination of the genetic and environmentalcorrelation of liability between sexes.' These analysesrequ ired the consideration of opposite-sex DZtwin pairs,the inclusion of which in the present multi458 Arch G.nPsychiatry-Vol44, May 1987 In the multivariate geneticanalyses, our consideration of sex differences was limitedto showing that, although the same model produced the bestfit in both sexes, the individual factor loadings differedsignificantly between the sexes . These results requiredthe separate analysis of results in females and males,which had the advantage of permitting an assessment of thesimilarity of results across sexes. Results 01Best-FittingMultivariate Genetic Model The results of thebest-fitting multivariate model gave a strikingconfirmation ofthe previous finding that genes andenvironment were influencing symptom covariation in aqualitatively different fashion. Ofthe three geneticfactors, the first two were relatively stable across sexes,while the third was only modestly so. The first"genetic-distress" factor was so named because factorloadings were high on all items with relatively littledifference found between depression and anxiety items .Compared with the first phenotypic factor, the firstgenetic factor was substantially less specific fordepression. This "genetic-distress" factor, which accountedfor around 27% of the total phenotypic variance and overtwo thirds of the total genetic variance in both sexes,indicated that genes were largely acting nonspecifically to

influence the predisposition to symptoms of psychiatricdistress. The second and third genetic factors were quiteminor, each accounting for less than 4% of the totalphenotypic variance . The second, or "genetic somaticanxiety" factor, loaded highly on only two anxiety items,both of which reflected the somatic symptoms of anxiety.This factor differed from the phenotypic "general anxiety"factor in the low loadings found for several key symptomsreflecting cognitive aspects ofanxiety. Although genes seemto "code" specifically for symptoms of anxiety to a modestdegree, they apparently influence only the somatic symptomsof anxiety. The third, or "genetic insomnia" factor, wasbroadly similar to the third phenotypic factor in loadingmost prominently on the two insomnia items. Genetic factorsthat influence complaints of insomnia are, at least inpart, separable from those that influence general levels ofdistress or symptoms of physical anxiety. Of the threeenvironmental factors, the first two were stable and thethird relatively stable across sexes. The first or"environmental depression" factor loaded consistentlyhighest on four core depression items. This factor was morespecific for depression than the first phenotypic"depression-distress" factor, as reflected by the fact thatthe "environmental depression" factor accounted for over2'" times the total variance in the depression subscalethan in the anxiety subscale . The second, or"environmental general anxiety" factor, was quite similarto the phenotypic "general anxiety " factor. Loadings wereconsistently highest on both physical and cognitivesymptoms ofanxiety , while loadings were low on the coredepression symptoms . The third, or "environ' mentalinsomnia" factor, like the two other insomnia factors, hadhighest loadings on the two insomnia items. Theenvironmental factors that influence insomnia also appearto be in part separable from those that cause anxiety anddepression. This is not surprising in that nighttime noisemight be expected to produce precisely this effect.Limitation. One potential limitation of this report isnoteworthy. The symptoms studied were obtained byselfreport from the general population. As noted above,this has distinct advan· tages for the kind of multivariateanalyses performed. The AnXiety and Depresslon-Kendler el81
use of the
aS50ciat ed with help-seeking behavior. However, it does
mean that the re sults obtained here on sympt oms ofanxiety

and d epression cannot necessarily be extrapolated to
clinical syndromes. For example, if there were genes spe
cifiC for panic disorder, individuals with such genes couldbe
rare enough in our sample to prevent detection of a separa
ble "panic" gen etic factor. SIgnlllc8nce The re sults of this study sugges t that the tendency in the
genera l populatio n for symptoms ofanxiety to co-occur with
ather symptoms of anxiety and symptoms of depress ion to
co-occur with oth er symptoms of depression is largely the
re5ult of environmental factor s. Contrary to our expecta
tion. genetic influences on these symptoms were largely
non5pecific. That is , while genes may "set" the vulnerability
ofan indiv idual to symptoms of psychiatric dist ress, theydo
not see m to code specifically for symptoms ofdepression or
anxiety. These finding s are consis tent with a previous
analysis of th e t otal anxiety and depre ssion scale scores
performed with the Au stralian NHMRC Twin Registry
data analyzed her e." In that report, high genetic correla
tions w ere found between transformed total scores on the
anxiety and d epression subscales, indicating that the same
genes were l argely respo nsible for genetic variat ion inthe
two subscales. The one notable exception to the apparentnonspecificity
of gene act ion on symptoms of anxiety and depression was

the consisten t emerge nce of a minor "genetic somatic
anxiety" f actor. These results sugges t that genes may be
responsible for the frequentl y observe d partial indepen
ment of psyc hopathology. Br J Psy chiatry1971;119:647·656. 2. PaykeJ ES: Have multivariate statistics contributed to classification?
Br J P,ychia ''1I 1981;139:357·362. 3. Martin NG, E avel W:The genetical analysis oCcovariance structure .
Heredit y 1977;38:79-96. -I. Kend ler KS, Hea t h A. Martin NG, Eave s LJ: Symploms ofanxiety and
depress ion In a volunte er t win populatio n: The etiologic role of geneti c and
enviro nment al (acton . A rch Gen P'IIchial't'Y1986;43:213-221. 5. Fahy TJ, Brandon S, Gars ideRF : Clinical syndromes in a sample of
depres sed patient s: A gener al practice material. Proc RSoc Med 1969;62:
331·335 . 6. Derog atl s LR, Klerman GL, Lipma n RS:Anxiety states and depre s
she neurosis : Issues in nosologic discrimination. J NtrVMent Dis 1972;155:
392-'03. i . Derogatis LR , Lipman RS, Covi L, Rickels K:Facto rial Invar ianc e of
symptom dime nsions in anxious and depressive neuroses .Arc h Gen Psychi
" ' y 1972;27:659-665. Eo . Men delsJ, Weinste in N,Cohrane C: The relationship between depres
sion and anxie ty. Arch Gfln P,ychiatry 1972;27:649-653. ~. Roth M, Gurney C, Ganide RF, Ker r TA: St udies in theclassi ficatio n
ofatfect ive diso rde rs: The relationship bet .....eenanxiety states and depres
sive' illnes ses-e-L Br J P't/cltiatry 1972;121:147-161.

10. Gurney C, Roth M, Gar side RF, Kerr TA, Schapira K:Studies in the
classiflcati cn of affective diso rders : The relationshipbetwe en anxiety states
and depre ssive Illnesses-c-H . Br J P.ychiatry1972;121:162-166. 11. Pr usote B, Klerman GL: Differentiating depressed from anxious
outpatients . Arch Gen P, vchiat ry 1974;30:302-308. 12.Roth M, Mountj oy CQ: The dist inction between anxiety states and
depress ive disord ers , in Paykel ES (ed): Handbook ofAffective Disorders.
};e w York , Guilford Pre ss, 1982, pp 70-92. 13. MullaneyJA: The relat ionsh ip bet ween anxiety and depres sion: A
revle ..... of some prin cipal compone nt analyt ic studies. J Aff ect Di, 1984;7:
139·148.
14. Bedford A, Foulds GA, Sheffield BF : A new pers onaldisturbance
" , I, (OOSIfSAD). S rJ Soc Cli o P6yc hia ''1I1976;15:387-394.
15. Jc res kog KG, Sob rom 0 , Lis ret VI: Analy.iI of Linear S tro ctttral
Rtlatio ndip, bV the MeOwd of Ma%imu m Likeli kood.Chicago, Interna
tional Educa t ional Services , 1983.
16. Hannan HH: Factor Anafy.u, ed 3. Chicago, Univers ityor Chicago
Press, 1976.
Arch Gan Psychiatry-Vol 44, May 1987 17. Olsson U: Maximumlikelihood esti mation of the polychoric cor re lationcoefficient . P. ychomdrika 1979;44:443-460. 18. Heat h AC,Berg K: Effects of soclal policy on t he heritability ofeducation achieveme nt , in Berg K (ed): Medical Genetic':Paat, Pre,tm , Futur e. New York, Alan R Liss Inc , 1985.

19. H eath AC, Berg K, Eaves LJ , 801uII MH, 8un det J,Nance WE, Corey LA, Magnu s P: No decline in ass ortativemat ing for edu cati on level. Behav Genet 1985;15:349-369.20. Heath AC, Berg K, Ea ves W, 801&&1 MH, Corey LA, SundetJ, Magnu s P, Nan ce WE : Educa tion policy and theheritability of educational a ttainment. Nature 1985;314:734·736. 21. Derogatis LR, SerioJ C, Cleary PA: An empirical comparison of three indices of fact orial similari ty.P, ychol Rep 1972;30:791-804. 22. Mapoth er E: Discussionon manic-depressive pllychosis. Br M.d J 1926;2:872-S79 .23. KerrTA, Roth M, Schapira K, Gurney C: The allsessmentand prediction of outcome in affective disorders . BTJ P.ychialry 1972;121 :167·174, 24. Murph y JM , Neff RK, SobolAM, Rice J X, Olivier DC: Computer diagnos is of depression and anxiety: The St irling Country Study. P't/chalMed 1985;15:99-112. 25. Jardine R, Mart in NG, Henders onAS: Genet ic covar iat ion between neu ro ticism and thesymptoms of anxiet y and depression. Genet Epidemiol1984;1:89-107. 26. Scballi ng D, Cron holm B, Asbe rg M,Eepmerk S: Rati ngs or psychi c and somatic anxietyindicants: l nter ra ter reliab ility and re lat ions topersonality vari ables . Acta P.vchia1r Scand1973;49:363-368. 27. Par ker G: Reporte d paren talcharacteris ti cs in re latio n to tra it d epression andanxiet y levels in I non-clinical grou p. Att, CNZ JP.ychiatry 1979;13:260-264 . 28, Parker G: Pare ntal characteri stic s in relation todepreesive diecrd er a. SrJP,ychia''1I1979;134:138-147. 29. Parker G: Pare nta l repreaentations of pati ents with an xiet y neurosis. A ctaP'1/chiatr Scand 1981;63:33-36. 30. Barrett JE: The relationship of life event s to the onaet of neurotic dis orders,in Barrett JE (ed): Streu and M.ntal Dilorder. New York ,Raven Pre as, 1979, pp 87·109. 31. F inlay.Jo nes R , BrownGW: Types of stressful live events and th e o nset of anxiety and depreest ve disorden . P'1/chol Med 1981;U:803..s15.32. To rgersen 8 : Developm ental difreren tia Uon ofanxiety and atr'ecti ve neuroeee. Acta P'1/chiatr Scand1985;71:304·310. Anxiety and Depresslon-Kendler et at 457

This page intentionally left blank
Reproduced with permission of the copyright owner. Furtherreproduct ion prohibited wilhout permission. STRESSFUL LIFEEVENTS AND DEPRESSION enviro nment on liab ility topsychiatr ic illness. Am J Psychiatry 1986; 1 4H79-289 13 .Rothma n KJ: Mo der n Epidemiology. Bosto n, Little, Brown, 1986 14. Kendler KS, Neale Me,Kessler Re,Heath AC, EavesLJ: A longitudin al twi n stud y of t -reat preva lence ofmajor depression in women . Arch Ceo Psychiatr y 199 3; 50:843-8 52 1S. Kendler KS, Kessler Re, NealeMe, Heath AC,Eaves LJ: The pred iction of major de pression in women :towa rd an integrated etiologic model. Am J Psychiatr y1993; 150:1139-1148 16. Paykel ES: Co ntributio n of lifeevents to causation of psychiatric illness. Psychol Med1978 ; 8:245 -253 17. Coste llo CG: Social facto rs associated with depr ession: a rerrospective community stud y.Psychol Med 1982; 12 :329-339 18. Sut tees PC , Miller PM ,Ingham JG, Kreitma n NB, Rennie 0 , Sashidharan SP: Lifeevents and the onset of affective disorder : a longitudinal general po pulation study .] Afff'ct Disord 1986; 10:37-50 19. Bebbi ngtc n PE. Stutt E, Tenna nt C, Hurry J:Misfortu ne and resilience: a commun ity n udy of women.Psychol Med 1984 ; 14: 347-3 63 20 . Bebbingto n PE, Tennan t C, Hu rry j : Adversiry and the natu re of psychiatric disorder in the com mu nity. J Affect Diso rd 1981 ; 3: 345-366 21. Finlay-jones R, Brown GW: Types of stressfu llife (Vents and the onset of anxiety and depr essivedisorder s. Psychol Med 198 1; 11,803 -815 22. Gilbert P:Depr ession : The Evoluti on of Powerlessness. New York ,Guilford Press, 1992 23 . Brown GW, Harr is TO : Depression, in life Events and Illness. Edited by Brown GW.Harris TO . New York, Guilford Press, 198 9 24. Bohma n M.Sigvard sson S, Cloninger CR: Matern al inheritance of alcoho l abus e: cross-fos tering analysis of adopted women.Arch Gen Psychiat ry 1981; 38,9 65-96 9 25 . Cloninger C R,B ohman M, Slgvardsson S: Inheritance of alcoho l ab use:cross -fostering analysis of ad opt ed men. Arch GenPsychi.tTy 1981; 38,86 1868 26 . Cado ret RJ, Trough ronE., O'Gonnan N : Genetic and environ menta l factors inalcohol ab use:and antisoci al perso nali ry. ] StudAlcohol 1987; 48<1-8 842 27. Cadoret R] , Ca in CA, CroweRR: Evidence for gene-envircm ent interaction in thedevelopment of ado lescent antisocial behavio r. BehavG<nCl I983; 1),30131 0 28 . 'T ienari P: Interac tionbetween genet ic vulnerab ility and family environment: theFinnish Adopt ive Family Study of Schizophre nia. ActaPsychiatr Scand 1991j 84:46 ()-465 29 . Ever itt BS, SmithAMR : Inte ractions in co ntingency tab les: a briefdiscussion of alternat ive definitions. Psychol Med 1979;

9: 581-583 30. Kish L, Frankel MR: Inferences from complexsamples. J Royal Statistica l Society Series B 1974 ; 36 :1-37 31. Neale Me, Cardo n LR: Method olo gy for GeneticStud ies of Tw ins and Fam ilies. Dordrecbt , The Netherland s, Kluwer Academ ic,1 992 32 . Sham PC, Walters EE,Neale Me. Heath AC. M aclean CJ, Kendler KS: Logisticregression ana lysis of twin dara: estimat ion ofparameters of the muh i faaor ialliability-th resho ld model. Behav Genet 1994; 24:22 9238 33. Allison PO: EventHistory Analysis. Beverl y Hills, Ca lif, Sage. 1984 34.Kendle r KS. Neale MC, Kessler RC. Heat h AC. Eaves Lj : Atwin stud y of recent life events and difficuhies. Arch CenPsychiatry 1993 ; 50, 589-596 35 . Allison PO: Discrete-rime me thods for the analysis of event histories, inSociological Meth od ology. Edited by Leinhardt S. SanFrancisco, j essey-Bass, 1982 36 . Laird N, O livier 0 :Covariance a nalysis of censored survival dat a usinglog-linear ana lysis techniques. JAm Statist ical Assoc1981; 76 ,231-240 37. Falconer OS: Introduction to Quantitative Generics, 3rd ed. New York , John Wiley &. Sons,1989 38 . Defries jC, Fulker OW: Mul tip le regression analysis of twin data . Behav Genet 1985; 15:46 7-474 39.Falconer OS: The inher itance of liability co cen aindiseases. estimated from the incidence amo ng relat ives.Ann Hum Gene t 1965; 29 ,51-76 40. SASISTAT User's Guide,version 6, 4th ed, vols I , 2. Cary , NC, SAS Institu te,1990 41 . Co x DR: Th e Analysis of Binar y Data . London.Methuen , 1970 42 . Fleiss j : Sta tistical Meth ods (orRat es and Pro portions, 2nd ed. New York, Joh n Wiley &.Sons, 1981 Am J Psychiat ry 152:6, June 1995
Reproduced with permission of the copyright owner. Furtherreproduction prohibited without permission. The Genetics ofMajor Depressive Disorder Gin S. Malhi, MB, MRCPsych,Janette Moore, MB, MRCPsych, and Peter McGuffin, MB, PhD,FRCP, FRCPsych • Address SGDP Research Centre. Institute ofPsychiatry, DeCrespigny Park, Denmark Hill, LondonSE5 8AF.UK, E-mail: [email protected] Current PsychiatryReports 2000, 2:165-169 Current Science Inc. ISSN 1523-3812Copyright © 2000byCurrent Science Inc.
Introduction
Compared with the general population , the relativ es of
depressed pro band s have at least a thre e-fold increase in
their risk of developing major depress ive disorder (MOD)[I J. In a recent study using narrow ICD-IO (International

Classification of Diseases ofthe World Health Organization ,
edn 10) criteria, depression was nine times as frequent inthe
siblings of depressed pro band s compared with siblings of
healthy controls [2-J. Some family studies have also shown
that the prevalence of MOD is greater among the relatives of
those who experience their first depressive episode before
the age of 20 [3]. and childhood onset was recently reported
as being associated with an increased familial risk [4J. How
ever, the relationship between age of onset and family load
ing for depression is by no means clear. For example, in one
study veryearlyonset (before puberty) was associated with a
high rate of antisocial behavior amon g relatives, ratherthan "pure" depression [5]. and a twin study ofdepressivesymptoms in childho od found that they werefamilial, but in children below age 11 ; th is resultedfrom shared environm ent rather than shared genes [6J. TwinStudies Broadly speaking, twin studies of MOD in adult ssuggest that genes and specific environmental factors areimporta nt , and that shared env ironmental factors, although important in less severe subtypes of depression, areperhaps of less significance in thi s pat ient group [7J,It is of interest to note that the heritability of unipolar depression appears to be higher than was once thought,with estimates in the region of 40% to 70%. Recent largetwin registry studies have explored the influence ofgenetic factors on major depression in male twins [8,9-J,In both studies, the best fitt ing biometri c twin modelfor major depression again contained only genetic andnonshared environmental factors, Lyons et ai, [gJ in afurther analysis stratified the diagnosis of majordepression according to severity and found that thisparticular model held only for severe or psychot icdepression. Dysthymia, as well as mild and moderatedepression, were best explained by a n ongenet ic modelcontai ning only c ommon family enviro nment and nonsha redenv ironment. This is further evide nce that perhaps moresevere forms of depression differ in their etiology frommild er disorders. Kendler et al, [8-] used an ap proach

based on bivariate path analysis to further explore thegenetic correl ation in th e liability to major depressio nin men and women , and found it to be +0.57 , Theyconcluded th at although major depression is equallyheritable in men and women and most genetic risk factorsinfluence liability to major depression similarly in bothsexes, genes may exist that act differently on the risk forthe disorder between the two sexes, Multivariate approacheshave also been applied to the investigation of the geneticor igins of comorb idity in disorder s such as panicdisorder, phobia, bulimia, and alcoholism, as well as majordepression and generali zed anxiety disorder (GAD) (10J.Two sets of shared genetic factors have been suggested bythis analysis, The first contributes to major depressionand GAD, and the second to 166 phobia, panic disorder, andbulimia. Genetic effects for alcoholism appear to bespecific in nature , It is not clear, however, whetherthese findings can be extrapolated to clinical samples,given the somewhat more liberal interpretation of thediagnostic criteria that suggest the lifetime prev alenceof major depression and GAD as 31% and 24%, respectively.There is also evidence that the covartation of anxiety anddepressive symptoms in childhood (maternally rated) may beexplained by a common set of genes [6J. However, this studyalso suggested a role for nonshared environmental factorsin the comorbidity of these symptoms and the influence ofspecific genetic effects for depressive symptomatology.Gene-Environment Interplay Although older terminologysuggested that some forms of depression were reactive andothers endogenous, there is little genetic evidence tosupport such a separation. A recent twinfamily analysisshowed that it is unlikely that there are two broadsubtypes of depression, one mainly genetic and the othermainly nongenetic [11] , Rather, it seems probable thatdepression generally results from a combination of geneticliability and environmental adversity. However, therelationship between these factors is complicated. One ofthe first studies to explore gene-environment interplayfound an increased rate not only of depression amongrelatives of depressiveprobands [12], but also anincreasein reported life events . The authors suggestedthat part of the association between lifeeventsanddepression may be due to this familial aggregation.Suchfindingssuggestthe possibllitythat familial factors may beinfluencing the liability to major depression indirectly,by predisposing an individual to a more aversiveenvironment [13 ..J. Severalstudies have supported thesurprising proposition that life events may be partlygenetically influenced [13--,14J. Kendler [13] categorizedlife events, according to their likely range of impact,

into personal events, which focused primarily on theproband, and network events where the impact extended toother individuals in the proband's social circle. Fornetwork events twin resemblance appeared to result purelyfrom common environmental effects , whereas for personalevents twin resemblance appeared to be due to geneticinfluence only. In a third category, interpersonaldifficulties, both genetic and common environmental factorsappeared to operate. The distinct familial origins ofdifferent categories of events are underlined by a recentsib pair study (2-J.Thisstudy showed positivecorrelationsbetweensiblings for eventsclassifiedas independent (thatis, not likely to result from the subject's deliberateactions) , but this wasalmost entirelyexplained by sharedeventssuch as death or illnessof a parent. Nevertheless, itremains that some life events (or how they are reported)are influenced by genetic factors, and there is evidencethat the genetic factors operating in depression and in thepredisposition to life events are positivelycorrelated,thereby implying an association via a common set of genes[I5,16,17-J. To what degree, therefore, is the relationshipbetweenstressful life events and depression due to a causalrelationship, with life events contributing directlyto theonset of major depression? Kendler et al. [18]exploredthisquestion in their population-based sample of female twinsand found strong evidence that th eobservedassociationwas,at least in part, causal. MolecularGenetics Having demonstrated a genetic contribution toanxiety and depressive disorders, the next stage of theinvestigation draws on molecular genetic methods in anattempt to locate and identify the genes involved .Depression does not follow mendelian segregation patterns,thereby indicating a complex mode of inheritance. It islikely that the genetic influences on these disorders aremultigenic in nature, acting in concert with environmentalfactors. Segregation analyses have been unable to confirmspecific modes of inheritance. Given that the genomecontains 3 billion base pairs and over 100,000 genes, thetask of locating a susceptibility gene for a particulardisease is formidable. Linkage analysis, by detecting theco-inheritance of chromosomal regions and disorder withinfamilies, offers a possibility of achieving this. LinkageStudies Linkagestudies of affectivedisorder have primarilyfocused on the bipolar phenotype and there have been fewrecent linkage studies of major depression. Older studies,predating the availability of DNA markers, made use ofclassical genetic markers such as blood group antigens andprotein polymorphisms with inconclusive results. Morerecently analyses using DNA polymorphisms have concentratedon excluding linkage to chromosomal regions known to

contain possible candidate genes, such as those involved inneuroendocrine or neurotransmitter systems [19,20], orthose implicated in bipolar disorder [21]. These haveemployed parametric linkage methods . Such conventional lodscore linkage analysis requires precise knowledge of thedisease mode of transmission and assumes a gene of majoreffect is operating [22J. As stated previously, the mode ofinheritance is unknown for depressive disorders, andparametric linkage analysis requires reasonably accuratespecification of parameters such as gene frequency andpenetrance. Mls-speciflcation of the parameters of such amodel introduces the possibility of error. An alternativelinkage strategy requiring no information about the mod eof inheritance, and useful in disease involvtng several(oligogenic) or many genes (polygenic), is the affected sibpair method. This non parametric linkage method isassociated with some loss of statistical power, Althoughsuch analysis has been used in linkage studies ofdepression [23J only a small number of pedigrees wereinvolved, whereas very large samples sizes (many hundredsof families) are likely to be required to detect genes ofsmall effect [24J. GenomeMalhi wide screen s of severa lhundred roughly evenly spaced DNA mark ers are commencingin a number of cent ers. These should be successful ifthere are relatively common genes that contribute at leasta moderate relative risk of around 2 or more, but ifdepression turns out to be highly polygenic oth er methodswill be required [24J. Association Studies This methodallows the detection of much smaller effects (relativerisks of less than 2) but is limited by the fact thatallelic association result s eit her from very tightlinkage between a marker and a disease susceptibility locus(resulting in linkage disequilibrium) or from the markerlocus itself conferring susceptibility. This means thatuntil recently it has not been feasible to consider a wholegenome scan for association (although methods are nowemerging to accomplish this [241. Therefore, researchhasfocused on candidate genes. Candidate genes for majordepression and anxiety disorders have primarily beensuggestedbythe molecular mechanisms implicated in theaction of therapeuticdrugs and the putativepathophysiologyfor these disorders. Of particular interestare
genes associated with neurotransmitter systems. Manyof the
association studi es associated with these phenotypes have
focused on the serotonergicsystem and in particular the sero

tonin transporter gene located on chromosome 17 (17q11.117q 12) . Many antidepressant and anxiolytic drugs suchas
tricyclic antidepressants and the newer serotonin selective
reuptake inhibitors influence the transporter facilitated
uptake of serotonin . Several polymorphlsms of the serotonin
transporter (SER7) gene have been described. A 44 bpinsertion /de letion polymorphism in the tran
scriptional control region of the gene has been described
by Heils etal. [25). The short version of this promoter poly
morphism was shown to be associated with decreased tran
scr iptional effict ency result ing in reduced serotonin
transporter expression. Since an original report of associa
tion between this genetic variant and personality traitsthat
are likely to be relevant to vulnerability to depression[26),
various studies have explored this further . Katsuragi eta1.
[27) replicated the finding in a Japanese sample but several
other studies have failed to do so [2830J. Ohara et al. [31)
described a tendency for the sho rter variant of this po ly
morphism to be more frequent in patients diagnosed with
an anxiety disorder using DSM-lV (Diagnostic and Statisti
cal Manual of Menta l Disorders , edn 4) criteria. Associa
tions of this polymorphism with affective disorders have
also been described [32). Similar associatio ns have been
shown for both unipolar and bipolar subtypes separately

[33), altho ugh this too has not been replicated [34] . Afurther variabl e number tandem repea t po lymor
phism, in the second intron of the sero tonin transporter
gene, has also been described [35). Several variants ofthis
polymorphism were found to be associated with affectivedisorder [36,37J. In particular an association of the nin ecopy variant with unipolar dep ression has been reported[38,39J.However, this has not been replicated in independent studies [40). Gelernter et a1. [41J investiga ted therange of allele frequency variation for both the promoterand second intron polymorphisms of the seroton intransporter gene in seven different populations and foundsignificant globa l variation . Linkage diseq uilibr iumvaried among the pop ulations suggesting a large potentialfor pop ulation stratification in association studiesemploying population controls : as the majo rity of studiesexploring depressive and anxiety rela ted phenotypes havedone. Taken as a whole, therefore , the various associationfindings suggest that polymorphic variation at this generesults in some pheno typic effect but it is unclear atpresent what phenotypic construct best captures this [30).Othe r candidate gene association studies in depression andanxiety have investigated the dopamine receptor genes [42),the tryosine hydroxylase gene [43), genes related to thegamma -aminobutyric acid system (44), and the catechol-o-methyltransferase gene [45,46). Candidate geneapproaches are limited In that they are on ly as good asthe current understanding of the disease pathophysiology[47). However, the possibility of a genome-wide search forassociation, similar to that for linkage studies, isincreasingly feasibl e with the development of highthroughput genotyping techniques such as DNA pooling [48J.In order to scan systematically for allelic association,however, a much denser map of polymorphic markers wo uld berequi red and biallelic single nucleotide polymorphisms arelikely to provide this in the near future [24). ConclusionsThe genetics of unipolar depression is a neglected area incomparison with bipolar disorder or schi zophren ia despitebeing a much mo re common disorder. This may be because therole of psychosocial adversity has seemed so obviouslyimportant and depress ion appears as an unde rstandab lereaction to st ress . However famili al agg r egation is aconsistent finding and recent twin s tudies sugges t tha theritabi lity is substantial. Studies trying to incorporateenviro nme ntal measures within a genetic des ign have onlyreally taken place in the past 10 to 15 years an d suggesta complicated pi cture where measures of stress are

actually confounded by familial or genetic effects. Thefutu re is likely to see an increasing emphasis on tryingto elucidate gene-environment inte rplay. Molecular geneticstudies of unipolar disorder have scarcely begun and haveso far been ma inly restricted to ca ndidate genes but isli kely t ha t more systematic approaches using linkage andlinkage d isequilibrium mapping will identify suscepti bility loci with in th e foreseeab le future.

mmended
Papers of particular interest . published recently, havebee n
h igh light ed as : O f importan ce O f major Importan ce
1. McGuffinP, Katz R: Nature . nurture and affectivedisorder. In The BioJogy of Depression. Edited by Deakin)WE Londo n: Gaskell: 1986:2651.
2.· Farmer A. Harr is T, Redm an K. et aJ.:The Card iffDepress ion Study: a sib pair study of life events andfamHiality in major depr ession . Br) Psychlauy 2000,176:150-1 55.
The most recent attempt to study the famlliallty of bothdepression
and social adversitywith In a clinically ascertainedsample. Depressive
disorder as defined by ICD 10washighly famllial.Independent life
events were also familial but this largely resulted fromboth members
of sib pairssharing the same events.
3. Weissman MM. Warner V, Wlckramaratne P. Prusoff BA: Earlyonset major depression in parents and their children.JAffect Dlsord 1988 , 15:269277.
4. Kovacs M, Devlin B, Pollock M, et aI.: Acon trolle dfamily history study of childhoo d-onset depressivedisorder. Arch Cen Psychiatry 1997. 54:13-623.
5. Harrington RC, Rutter M. Weissman M, et al.: Psychiatricdisorders in the relatives of depressed probands I:comparison of prepubertal, adolescent and early adult onsetcases. JAffect Dlsord 1997. 42:922.
6. Thapar A. McGuffin P: Anxiety an d depr essive sym ptomsin child hood a genetic study of comorbidity. ) ChildPsychol Psychiatry 1997 , 38:651-656.
7. McGuffin P. Katz R. Watkins S, Rutherford ): A ho spital-based twin register of the heritability ofDSM-IVunipolar depression. ArchCen Psychiatry 1996.

53:129136.
8. ' Kendler KS,Prescott CA: A population based twin studyof lifetime majo r depression in men and women . Arch GenPsychiatry1999. 56:3944.
The first large scale population-based twin study toexamine the
extent to which the same genes influence depression in thetwo sexes.
In both men and women depression showed substantial andsignifi
cant he rUabUHy. but therewasevidence of both common genetic
effects and genetic effects that differbetween the sexes.
9.· Lyon s Mj, Elsen SA,Goldberg ). et al.:A registrybasedtwin study of depr ession in men . Arch Cen Psychiatry 1998, 55 : 468-4 72.
A large scale study confirming that major depression in menis sub
stantially heritable but that certain affectivedisordersubtypes such
as dythysmia may be largely envlronrnental ln origin.
10. Kend ler KS, Walters EE. Neale MC, er aJ. :The structure of the genetic and environmental risk factors for sixmajor psychiatric disorders in WOmen. Phobia. generalisedanxiety disorder. panicdisorder. bulimia. major depressionand alco ho lism . Arch Cen Psychlalry 1995. 52:374383.
11. Andrew M, McGuffin P. Katz R: Genetic and non -geneticsubtypes of ma jor depr essive disord er. Br) Psychialry1998. 173:523526.
12. McGuffin P, Katz R.Bebbington P: The Cam berwellCollaborative Study III.Depressio n and adversityin therelatives of dep ressed probands. Br) Psychiatry, 1988.152:775-782.
13.·· Kan dler K: Major depression and the environment: apsychiatric gene tic perspective . Phannacopsychlatry1998,31:59.

A masterlyaccount of the ways in which genes andenvironment are
likely to co-act and interact to cause depression.
14. Plom ln R, Lichtenseln P, Pedersen NL, el al.: Geneticinfluence on life events during the last half of the lifespa n . Psychol Ageing 1990,5:25-30.
15. Kendler KS, Karkowskl·Shuma n L: Stressful life eventsand genetic liability to major depression: genetic controlof exposure to the envlronment7 Psychol Med 199 7,27:539-547. 16 .' Silberg ), Pickles A, Rutter M, etal.:The Influence of genetic factors and life stress ondepression among adolescent girls. Arch CenPsychiatry1999,56:225232. This paper. like the paper by Thapar el aI. 117·J. Is an import ant attempt to study depression and lifeevents in the context of a twin study. 17.· Thap ar A. Harold G, McGuffin P: Life events and depr essive symptoms inchildhood · shared genes or shared adversity? A researchnote. ) ChildPsychoJPsychiatry 199B. 39:115311 58. Thefocus here is on depressive symptoms ratherthan disorder.There is evidence that lire events. at least when reportedby questionnaire, are in partInfluenced by the same genesthat are associated with reporti ng depressive symptoms. lB. Kend ler KS, Karkowskl LM, Prescott CA: Causa l relationsh ip between stressful life events and the o nset of majordepressio n. Am ) Psychiatry 1999,1 56:837841. 19.Netswanger K. Zubenko CS. C Ues DE. er aJ.: Linkage a ndassociation analysis of chromoso mal regions containinggenes related to neuroendocrine or serotonin function infamilies with early-onse t. recurrent major depression.AmJMoo Genet 1998.81 :443439. 20. Wang Z. Crowe RR, TannaVL. Winokur C: Alpha 2 adre nergic receptor subtypes indepression: a candidate gene study. ) Affect Dlsord 1992.25:191-1 96. 21. Bak tuniene ]. Yuan QP. Engstrom C, etaI.: Linkage anaIysis of candidate loci in families withrecurrent major depression . Mol Psychiatry1998, 3:162-168. 22. McGuffin P, Owen M): Molecular Genetic Studies ofSchizo ph ren ia. CoJd Spring HarborSymposia onQuanlitalive BloJogy 1996, 61:815822. 23. Wilson AF. ElstonRC, Malle tt DB. et al.:The curren t status of geneticlinkage studies of alcoholism and unipolar dep ression .Psychlatr Cenet 1991. 2:107124 . 24. McGuffin P. Martin N:Behavio ur an d Genes. Br Moo) 1999, 319:3740. 25. Hells A,Teufel A, Petri S. er al.: AUeUc var iation of hu manserotonin transporter gene expression . JNeurochem 1996.66:26212624. 26 . Lesch KP, Bengel D, Hells A, et aI.:Assoclanon of anx ietyrelated traitswith a polymorphism inthe serotonin transporter gene regulat ory region . Science

1996 , 274:1527-1 531. 27. Katsuragt S, Kun ugl H. Sano A.et al.:Assoc iation between sero tonin transporter genepolymorphism and anxiety-related trait s.BioiPsychiatry1999, 45:368370. 28. BaUD, Hlll L. Freeman B,er al.:The serotonin transport er gene and peer-ratedneuroticism. Neuroreport 1997. 8: 1301-1 304. 29. EbstetnRP, Gritsenko I. Nemanov L. ef al.: No assoc ialion betweenthe serotonin transporter gene regulatory regionpolymorphism and the Tridimensional PersonalityQuestionnaire (TPQ) temperament of harm avoidance. MolPsychiatry 1997. 2:224226. 30. Gelemter ), Kranzler H.Coccaro EF, et aJ.: Serot onin tran sporterprotein genepolymorphism and personality measures in AfricanAmericanand European American subjects. Am ) Psychiatry 1998,155:1332-1 338. 31. Ohara K, Nagai M. Suzuki Y. et aI.:Association be tween anxiety disorders and a functionalpolymorphism in the serotonin transporter gene.PsychiatryRes1998,81 :277279. 32 . Collier DA. Stob er G.LiT, et al.:A novel fun ction al po lymorphism within thepromot er of the serotonin transporter gene: possible rolein the susceptibility to affective diso rder. MolPsychiatry 1996. 1:453460. 33 . Furlong RA. Ho L, Walsh C,et al.: Analysis and meta-an alysis of two serotonintransporter gene polymorphisms in bipolar and unipolaraffective disord ers. Am ) Med Cenet 1998, 81:5863. 34. Ohara K, Nagai M, Tsuka moto T, et aI.: Functio nal polymorphism in the sero tonin transporter promoter at theSLC6A4 locu s and mood disorders. Bioi Psychialry 1998 ,44:550554. Malhi
35. Lesch KP. Balling U. Gross ], ef aI.: Organi sation ofthe human serotonin transporter gene .] Neural Transmission1994, 95:157-162 .
36. Collier DA. Arranz Ml. Sham P, ef aJ.: The serotonintransporter is a potential susceptibility factor forbipolar affective disorder. Neurorepof( 1996, 7:167 5-1679.
37. Rees M, Norton N. jones 1,eraI.: Association studies ofbipolar disorder at the human serotonin transportergene(hSERT; 5HIT). Molecular Psychlally 1997. 2:398-402.
38. BattersbyS, Ogtlvje AD,Smith CAD,ef aI.: Structure of avariablenumber tandem repeat of the serotonin transportergene and association with affective disorder. PsychiarrGenet 1996,6:177-181.
39. Ogtlvte AD. Battersby S. Bubb Vj, er aI.: Polymorphismin serotonin transportergene associated with susceptibilityto major depression. Lancer 1996, 347 :731 ~733 .

40. Kunugi H. Hattori M, Kato T, er al.:Serotonintransporter gene polymorphisms: ethnic difference andpossible association with bipolar affective disorder.MolPsychiatry 1991, 2:457-462.
41.· Gelemter j, Cubells jF,Kldd jR, er al.:Populationstudies of polymorphisms of the serotonin transporterprotein gene. Am] Moo Genef 1999,88:61-66 .
An attempt to explicatethe population geneticsof theserotonin
transportergene. a candidategene that has provokedmuchinterest
and controversy in association studies of depression. 42.Serretti A. Macciardi F. Cusin C. er al.:Dopamine receptorD4 gene is associated with delusional symptomatology inmood disorders. Psychiatry Res 1998. 80:129136. 43.Serrettl A, Macciardi F, Verga M, et al.:Tyrosinehydroxylase gene associated with depressive symptomatologyin mood disorder. Am] Moo Gener 1998.81 :127-1 30. 44. OrucL. Verheyen GR, Furac 1, er aI.:Positive associationbetween the GABRA5 gene and unipolar recurrentmajor depression . Neuropsychobio/ogy 1997. 36:62-64 . 45. Ohara K,Nagai M, Suzuki Y, er al.:No association between anxietydisorders and catechol-o-methyltransferase polymorphism.Psyrhiatry Res1998, 80:145-148. 46. Kunugi H,ValladaHP,Hoda F. er aI.: No evidence for an association ofaffective disorders with high or low activity allele ofcatechol-o-methyltransferase gene. BioI Psychlarry1997,42:282-285. 47. Craddock N, Owen Ml: Modern moleculargenet ic approaches to psychiatric disease. Br Med8u111996,52:434-4 52. 48. Daniels J.Holman s P. Williams N, ef aJ.:A simple method for analyzing microsatellite allele imagepatternsgeneratedfrom DNA pools and its application toallelic association studies. Am] Hum Gener 1998,62:1189-1197 .

Reviews
1. Well s JE, Bushnell JA, Horn blow AR. Joyce PR,Oakley-Browne MA: Chnstc burc h psych iat r ic ep idemiology study, part I: m ethodology and lif eti me prevalence fo r specific psychiat ric dlsc rders. Aust NZ jPsychia try 1989; 23:315326
2. Weissman MM, Bruce ML, leaf PJ, Florio lp, Holzer C III: Affective disorders, in Psychiatr ic Disor ders inAmerica : The Epidem io log ic Catch ment Area Study.Edited by Robins l N, Regier DA. New Yo rk. Free Press,1991 . pp 53 -80
3. Kend ler K, Neale MC. Kessler Re, Heath AC. Eaves L]: Apop ulation-based tw in study of major de pression in women: the impact of va ryin g definit ion s of illness. ArchGen Psychiatry 1992; 49:257-266
4. Kessler RC. McGon agle KA, Zhao S, Nelson ce, Hughes M,Eshleman S,Wittchen H-U. Kendl er KS: li feti m e and12-month prev alen ce of DSM-III-R psych iatric di sord ersin the Uni ted States : results fro m the Natio nal Comorbiditv Survey. Arch Gen Psvchiat rv 1994 ; 51:819
5. Greenberg PE. Stiglin LE, Finke lstein SN. Bernd t ER:The ceonomic burden of depression in 1990. J Clin Psychiatry 1993; 54:405-4 18
6. Piccin ell i M. Wilkinson G: Out com e of depr ession inpsyc hiatric setti ngs. Br J Psychia try 1994 ; 164 :297-304
7. Wells KB. Stewart A, Hays RD.Bu rnam MA, Rogers W.Daniels M, Berry S. Greenfie ld S. Ware J: The fun ctioning and well -being of depressed pat ien ts: result s fromth e Medi cal Outco me s Study. lAMA1989 ; 262: 9 14-919
8. Broadh ead WE. Blazer DG, George lK, Tse CK: Depression.disabi lity days, and days lost from wo rk in a prospective epidernlolo gic s urvey. JAMA 1990 ; 264:2524-2528
9 . Jud d Ll., Pau lus MP, Wells KB, Rapaport MH:Socioeconomic burden of subsvndro mat depressive sym ptomsand major depression in a samp le of the general po pu lation . Am J Psvchiatr y 1996: 153:1411-141 7
10. Ustun TB, Re hm J, Chatterj i S. Saxena S, Trott er R,Room R, Bickenbac b J (WHO/NIH Join t Pro ject CAR StudyGroup ): Multi . p ie informant ranki ng o f th e di sab li

ng effects of d iffe rent healt h condi t ions in 14 countri es. l ancet 1999; 354 :111115
11. Harr is EC, Barraclo ugh BB: Excess morta lity ofmental disor der. Sr J Psychiat ry 1998; 173:1153
12. Murray (Jl . Lopez AD: Evidenc e-based health poli cy:lesso ns from th e Glo bal Burden of Disease Study .Science 1996: 274 : 740-743
13. Pincus HA. Tanlelian 'n.. Marcus Sc. Olfson M, Zari nDA, Thom pso n J, Magno Zito J: Prescrib ing trends inpsychotropic medic ation s: pri mary care. psych iat ry.and oth er m edi cal we«antes. JAMA 1998; 279 :526-531
14. McGuffi n P, Katz R: The gene tics of depressio n and mani c-depr essive disorde r. a J Psych iatr y 1989 :155:294304
15. Tsuang MT, Far ao ne SV: The Genet ics of MoodDisorders. Balt imo re, John s H opkins University Press,1990
1560 16. Merikangas KR. Kupf er OJ: Mood disord ers: genetic aspects, in Comprehensive Textb ook of Psy chiat ry,6th ed. '0'011. Edited by Kapl an HI. Sadoc k BJ. Baltimore . Wi ll iam s & Wilk ins, 1995 . p p 1102-1116 17.Plom ln R, DeFries JC.McClearn GE, Rutter M: BehavioralGenet ics. New York. WH Freeman , 1997 18. Glass GV.McGawB. Smith ML: Me ta-Analvsts in Social Research. Beverl yHills , Cali f. Sage Publica t ions, 1981 19. Sm ith Ml,Glass GV, Miller TI: The Bene fits of Psychotherapy. Baltim ore, John s Hop kins University Press. 198 0 20 . ThackerSB: Meta-anal ysis: a qu antita tive appro ach to researchin tegrati on . JAMA 1988; 2 59 : 168 ~1 689 21. PetittiDB: Meta-Analysi s, Decisio n Analy sis, and rosr-euecttveness Analysis. New York, Oxfo rd Un iversityPress, 1994 22. Ken dler KS. Pedersen Nl , Neale MC. Math ~A: A pilot Swedish twin stu dy 01 aff ect ive illnessincluding hospit al and population -ascertai ned subsamptes: res ults of model fitting. Beha v Genet 1995; 25 :217-232 23. Angst J, Frey R, Lohmever B. Zerbin-ROdin E:Bipolar mani c-depr essive psychosis: res ults of a genetic investi ga ti o n. Hum Genet 1980 ; 55 :237-2 54 24.Gersho n ES. Mark A. Cohen N, Beliz on N, Baron M, KnobeKE: Tran smitted fact or s in the mo rbi d risk of affective di sord ers: a cont rolled study. J Psychiatr Res1975 ; 12 :~8 329 9 25. McGuffin P, Katz R, Bebbi ngto n P:Hazard . heredit y, and depression : a f amily study. JPsvchiatr Res 1987; 4:365-375 26. Perri s C: A study of

bipolar (manicdepr essive) and un ipol ar recu rrentdepressiv e psych oses. Act a Psychi a1r Scand Suppl 1966;194:1-188 27. Scharfe t ter C: Subdivid ing th e fu ncti onal psychoses: a famil y hereditar y approach . Psycho! Med1981 : 11:637640 28. Smerald i E, Negri F. Mefica AM: Agene tic study of affect ive disorder s. Acta Psychiat rScan d 1977; 56:382 -398 29 . Sta ncer HC. Persad E,Wagener OK, joma T: Evid ence fo r hom ogene ity of m ajordep ression and b ipo lar affect ive di s order. JPsvchiatr Res 1987; 21:3753 30. Winok ur G, Cador et R.Oorzab J, Baker M: Dep ressive di sease: a genet ic stu dy.Arch Gen Psy chiatry 1971; 24 :135-144 31. Allen MG. CohenS, Polli n W, Greenspan SI: Affect ive illn ess in veterantwins: a di agnostic review. Am J Psychiatry 1974 ; 131:1234-1239 32. Bertelsen A. Harv ald B. Hau ge M: A Dan ishtw in stud y of mani c-depressive di s orders. Br JPsychiat ry 1977 : 130:330351 33. Slater E, Shie lds J:Psycho tic and Neuroti c Illn esses in Twins. l ondon , HerMajesty 's Statlo nerv Off ice, 195 3 34. Torgersen S:Genet ic teeter s in m oderately severe and m ild affective disorders. Arch Gen Psychiat ry 1986 ; 43: 222-226 35.Schlesselma n JJ : Case-Control Studi es: Design , Conduct,Anal ysis. New York, Oxfo rd universit y Press. 1982 36.SAS/STAT So ftware : Changes and Enhancements ThroughRelease 6.11. Cary, NC, SASIns titute. 1996 37. Neale MC,Cardon lR: Meth odol ogy for the Study of Twin s and Families. Dordre cht, the Nether lan ds, Kluwer. 1992 38 .Fakoner OS; The inheritan ce of l iabili ty to certa in diseases, estim at ed from th e incidence among relati ves.Ann Hum Genet (London) 1965; 29:51-76 39. Neale Me. Boke rS. Xie G, Maes H: Mx: Statistica l Mode ling. R ichmond .Medical College of Virginia, Department of Psychiatry, 199940. Ham agarni F: A rev iew of the Mx computer program forstructural equat io n model ing. Struc tu ral Equati onModelin g 1997: 4:157-1 75 41 . Nea le Me , Mill er MB: Theuse of likel iho od -based conf iden ce intervals ingenetic m odels. Behav Gene1 1997; 27:113-1 20 42. WeissmanMM , M erikangas KR, John K. wickramar atn e P,Pru sott BA,Kidd KK: Fam ily-gene ti c stud ies of psych iatric di sorAm ) Psych iat ry 157;10, October 2000 der s: devel opin gtechnologies. Arch Gen Psychia try 198 6; 43 : 1104-1116
43 . Khou ry MJ. Beaty TH. Cohen BH: Fundam ent als ofGenet ic Epide miology. New York. Oxford University Press.199 3
44. Gersho n ES. Ham ovit J. Guroft JJ. DIb ble E. Leckm anJF. Sceerv W. Targurn SO. Nurnberger JI Jr. Goldin lR. Bunney WE: Ir: A family study of sctuzoa ttec rive . bipolarI. bipolar II. un ipolar. and n ormal control p ro band s.

Arch Gen Psychi at ry 1982 ; 39: 1157-11 67
45. Maier W. licht ermann O. Minges j, Hallmayer J, Heun R.Benkert O. Le vinson OF: Continuity and discontinuit y ofaff ecti ve di so rders and sch izo phre nia: results of acon trolle d famil y study. Arch Gen Psychiatry 1993; 50:871--883
46 . Tsuang MT. Winokur G. Crowe RR: Morbidity risks of schizophrenia and affe ct ive disord ers amo ng first-degreerelati ves of patients with schizop hrenia . m an ia. depression . and surgi cal c ondition s. erJ Psychi at ry 1980;137 :497 -504
47. Weissman MM . Gershon ES.Kidd KK, Prusoff SA. l eckmanJF. D ibble E. Hamovit J. Thompson WD, Pauls DL. Guro ffJj: Psvchi
atr ic disord ers in th e relativ es of proband s w ithaffective di sor
ders : the Yale Universit y-NIMH Colla borative Study. ArchGen Psychi at ry 1984 : 41 :13-21
48 . Weissma n MM . Wickram aratne P. Adams PS. lish JO.Horwath
E. Charne y D. Wood s SW. Leem an E. Frosch E: Therelationship
b etween panic d isord er and major depression : a newfamily
study. Arch Gen Psychiatry 19 93 ; 50 :767-780
49 . Kendler KS: Is seeking treatm ent for depression predicted by a
hist ory 01 de pre ssion in relatives? implicati on s forfamily stud
ies of atf ect ive di sorder. Psvchot Med 1995; 25 :807 81 4
50. Sullivan PF. we lls jE. Joyce PRoBush nell JA. Muld erRT. o akle v
Browne MA: Fam il y hi stor y of depre ssio n in clini cand commu
nity sam ples. J Affect Disord 1996 ; 40:159-1 68

51. Tsuang MT. Fleming lA. Kendler KS. Gruenb er g AS:Selecti on of
cont rols fo r family studies : b iases and im pli cations. Arch Gen
Psvchia trv 198 8 ; 4 5:1006-1 008
52 . Schw artz S, link BG: Th e "w ell control" arte factin case/co ntro l
stud ies of specific psychiatri c di sorders. Psychol Med1989; 19:
737 -74l
53. Kendler KS: The su per-no rm al contro l group inpsychiat r ic ge
neti cs: possible artifactual evidence for coaggregation.Psvchi
atr Genet 1990; 1:45-53
54 . Kendler KS: Tw in stu d ies of psychiatric illn ess:cur rent status
and future dir ect ion s. Arch Gen Psychiatry 199 3:50:90591 5
55. vo n Kno rrin g A·l. Cloninger CR. Bohman M. Sigvardsson S: An
ad option studv of dep ressive disord ers and substanceabus e.
Arch Gen Psych iatry 198 3; 40 :943 -950
56. Cadoret Rj, O'Gorman TW. Heyw ood E. Trought on E:Geneti c
and en vironmental factors in major depre ssion . JAffectDisord
1985; 9 ;155-164
57. Wende r PH. Ketv SS. Rosenthal O. SChulsinger F,Ortmann J.

Lund e I : Psych iatr ic disorders in the biological and adoptive
f amilies of adopted indiv id ua ls with affe ctive disorders. Arch
Gen Psvchia tr v 198 6 ; 43 :923-929
58. Regier OA, Goldberg 10. Taub e CA: The de facto USmental
health servic es system : a public health perspecti ve.Arch Gen
Psychiatry 1978 ; 35 :68 5-693
59. Regier DA. Narrow WE, Rae OS. Mand erscheid RW. lockeBZ,
G oodwin FK: Th e de facto US m ent al and addicti ve disorders
service system : Epid em iol ogic Cat chment Area prospective 1
year pre valence rates of d isorde rs and serv ices. ArchGen Psy
chiatry 1993 ; 50 :85-94
60. Bieru t L], Heath AC. Bucholz KK. Din widdie SH. Madden PAF.
Statham OJ. Dunne MP. Mart in NG: Major depressive di sorder
in a com m uni ty -based tw in sam ple: are th eredifferent genetic
and envi ro n mental contributions for m en and women? Arch
Gen Psychiatr y 1999: 56 :557-563
Am JPsychiatry 15 7:10 . October 2000 61 . Kendl er KS.Prescott CA:A populati on-ba sed twin study of lif etime majo r depression in m en and women. Arch Gen Psychia try1999; 56 ;39-14; co rre ct io n. 2000; 57 :94-95 62. l yons Mj . Eisen SA. Gold berg J, Tru e W. Lin N. Meyer JM.Toom ey R. Faraone SV. Merten J. Tsuang MT: A registry-based twin stu dy of depr ession in males. Arch GenPsychiat ry 1998; 5 5:468-47l 63. McGuffin p. Katz R,

Watkins S, Rutherford J: A hospital-based t win register ofth e heritability of OSM-1V unipolar depression. Arch GenPsy chiatry 199 6; 53:129 -136 64 . Kendler KS. Gardner CO.Prescott CA: Corrections to two prior published art icles(lett er). Arch Gen Psychiatry 2000; 57:94-95 65 . AndrewsG. Stewart G. Allen R. Henderson AS: The genet ics of six neurotic disorders: a twin stud y. J Affe ct Oisord 1990; 19: zs-zs 66. Neale MC, Eaves lJ, Kendler KS: The power ofthe classical twin study to resolve varia t io n inthreshold traits. Beha v Genet 1994 ; l4 :lJ9-l58 67.Weissman MM . Bland R. Joyce PRo Newman S. Wells JE, Wittchen H-U: Sex differences in rat es of depression :cross-national perspectiv es. J Affe ct Disord 1993: 29:77-84 68 . Kessler Re . McGonagle KA. Swartz M. BlazerOG.Nelson CB: sex and depression in th e NationalComorbidity Survey. I: lifetime pr eval ence, chronicityand recu rrence . J Aff ect Disord 1993; 19 :85-96 69 .Gater R. Tansella M. Korten A. Tiemens BG. Mavreas VG.Otata wura MO : Sex difference s in the prevalence anddetection of depressive and anxiety disorders in generalhealth care settings . Arch Gen Psychiatry 19 98 ;55:405--4 13 70. Faraon e SV. Lyons MJ. Tsuang MT: Sex differences in affect ive disorder: genet ic tr an smission. Genet Epid em iol 1987; 4 :331343 71 . Merika ngas KR.Weissm an MM . Pauls DL: Genet ic factors in the sex ratioo f maj or depression . Psychol Med 1985; 15 :63-69 72 .Reich T. Van Eerdewegh P, Rice J. Mullaney J. Endicott 1.Kler man Gl : The familial tr an smission of pri mary majordepr essive di s order. J Psychiatr Res 198 7; 21 :613-62473. Kendler KS, Neale MC. Kessler RC. Heath AC. Eaves u.Parental tr eat ment and the eq ua l en v iro nm entassumpt ion in twin studies of psychiatric illness. Psvchol Med 1994 ; 24 :579-590 74. Kendler KS.Gardener co: Twinstudies of adult psychiatric and substance d ependencedisorders: are they biased by differences in the environment al experiences of monoand dizygotic t wins inchildhood and adolescence? Psycho! Med 1998; l 8 : 6l5-63375 . Bryan E: Twins and Higher Multiple Births: A Guide toTheir Nature and Nurture . london, Edward Arnold. 1992 76.Kendler KS. Pedersen NL. Farahmand BY. Persson p·G: Th e treated incidence of psych otic and affect ive illness intwins com pared to population expect atio n. Psvchc l Med1996; 26 : 1135-1144 77. Kendler KS, Martin NG, Heath AC.Eaves LJ: Self-report psychiat ric s ymptoms in twins andtheir non -twin relatives: are tw ins differe nt ? Am J MedGen et Neuropsych iatr Genet 19 95; 60 : 58 8-591 78 .Reich T. Clon inger CR. Guze SB: Th e multifactorial modelof disease transmission, I: descr iption of the model andits use in psychiatry. Br J Psychiatry 19 75 ; 127 :1-10 79. Cadoret RJ. Woolson R. Winokur G: The relationship of age

of on set in un ip olar affective illness to risk of alcoholism and depression in parents . J Psychiatr Res 1977; 13:137-142 80. Gershon ES. Weissman MM. Guroff JJ. Prusc ttSA. leckman JF: validatio n of criteria for majordepression through controlled family study. J Affect Disord19 86; 11:125--131 81 . Kendler KS. Neal e MC. Kessler RC.Heath AC. Eaves lJ: The cunical characte rist ics of majordepression as indices of the familial risk to illness . BrJ Psychiatry 1994; 165:66-72 1561
82. K endler KS, Gardne r CO, Prescott CA: Clin icalcharacteristics of ma jo r de pressio n tha t predi ct riskof dep ression in relat ives. Arch Gen Psych iatry 1999;56:322 327; cor rect ion, 2000; 57: 94-95
83. Led ma n JF.Weissman MM, Prusoff BA. Caruso KA. Menkangas KR, Paul s Dt, Kidd Kt<: Subty pes of depression .Arch Gen Psvchla trv 19 84 ; 41 :833-838
84 . l eckma n JF, Caruso KA, Prusott SA. Weissman MM.Merikangas KR. Pauls m : Appetite disturba nce andexcessive guilt in ma jor depres sio n. Arch Gen Psychiatry 1984; 41 :839-844
85. Mendlewicz J. Baron M: Morbidity risks in subty pes ofunipola r depre ssive illness: differen ces between earlyand lat e on set for ms. Br J Psychia try 1981; 139:463-466
86 . Weissman MM. Merik angas KR, Wick rama rat ne P, KiddKK, Prusoft SA, te ck man JF, Pauls OL: Unde rsta ndi ngthe clinical het· erogen eitv of m aj or depre ssion usingfamil y da ta . Arch Gen Psychi at ry 198 6; 43 :43<H 34
81. Berkson J: Limitat ion s of the appl icat ion offourfold t able anal ysis to hospital data. Biom etricsBull 194 6; 2:47-53
88 . Cohen P, Cohen J: The clini cian 's ill usio n. ArchGen Psychiat ry 1984; 41 :11 78-1182
89 . Klerman Gl , Weissman MM: Increasing rate s of depression . JAMA1989; 261 :2229-2235
90 . NIMH Genetics Work grou p : Genet ics and Ment alDisorde rs. Beth esda. Md , Nati onal Institute of MentalHealth, 1998
91 . Kendl er KS, Eaves lj, Walter s EE, Neale Me, Heat hAC, Kessler RC:The identi fi cation and validat ion of

distin ct depressive syndromes in a po pulat ionbased sample of fem ale tw in s. Arch Gen Psychiatry 1996; 53:391-399
92. Benk elfat c . Ellenb ogen MA, Dean P, Palmour RM,Young SN: Mood -lowerin g effe ct of t ryptoph an depl etion . Arch Gen Psychia try 1994; 51:687 69 1
93. Giles DE, Kup fer DJ, Rush AJ,Roffwarg HP: Contro lledcomparison of ete ctrophvsiol ogical sleep in fam ilie s ofpro band s w ith unipolar depressio n. Am J Psych iat ry1998 ; 155:192-199
94. Kendler KS: Overv iew : a current perspect ive on tw instudies of schi z ophren ia. Am J Psychia try 198 3 ; 140:14 13 1425
95. Land er ES, Scho rk NJ: Genet ic dissect io n of complex tr aits. scie nce 1994; 265:20 37-2048
1562 96 . Hill AB: The environm ent and disease: association or causat io n. Proc R Soc Med 1965; 58 :29 5300 97 .Rothman KJ: Modern Epidem iol ogy. Boston , Little, Brown,19 86 98 . Brom et EJ, Dunn l O, Co nne ll MM, Dew MA,Schul berg HC: l on g-term reliability of diagn osing lifeti me major dep ression in a communit y sample. Arch GenPsychiatry 1986; 43:43 5440 99 . Kendl er KS, Neale MC,Kessler RC, Heath AC, Eaves u: The l ifet im e history of majo r depr ession in wom en : reliabili ty of dtagnosis andherita bili ty. Arch Gen Psychiatry 1993; 50 :86 3-870 100.Keller MB. Klein ON, Hir schfeld RMA, Kocsis JH, McCullough JP, Mill er I, First MB. Hol zer CP 111 , Keltner GI,Mari n DB. Shea T: Results of the DSM·IV mo od d isord ersfi eld tr ial. Am J Psychiat ry 1995; 152:843-849 101 .Buli k eM, Sullivan PF, Kendl er KS: Her itabil ity andreliabili ty of binge -eating and bul imia nervosa. BioiPsych iat ry 1998; 44 : 1210-1218 102 . Foley OL, Neale MC,Kendler KS: Reliab ili ty of a li fet ime history of maj ord epression: im pli cat io ns for h eritabili ty andco-rnerbid ity. Psvcbot Med 1998 ; 28 :857-870 10 3. Kendler KS, Kessler Re, Walte rs EE, Maclean CJ. Neale MC, HeathAC, Eaves LJ: Stressful life eve nts, gene tic liabi lity,and onset of an epi sode o f ma jo r dep ress ion in women. Am J Psych iat ry 1995; 152 :833-842 104 . Rutte r M,Plomin R: Opportunities for psychiat ry from genetic findings . Br J P, ychiat ry 1997; 17 1:209-21 9 105. AndreasenNC, Rice J, Endicott J, Reich T, Coryell W: The fam ilyhistory approach to dia gnosis: how useful is it? Arch GenPsychia t ry 1986 ; 43 :421-429 10 6. Cha pman 1F, MannuzzaS, Klein OF, Fyer AJ: Effects of infor mant mental disord

er on psychiatric fam ily history data. Am J Psychiatry1994; 151 :574-579 107. Orvaschel H, Tho mps on WOoBelangerA, PrusoH SA. Kidd KK: Com pa rison of th e fam il y hist ory method to direct int erv iew : fac tors affect ing th edi agn osis o f depression . J Affec t Disord 1982; 4:49-59 108 . Tho m pson WD, Orvaschel H, Prusott BA, Kidd KK:An evalua tion of the family history for ascertain ingpsych iatr ic di so rders. Arch Gen Psych iat ry 1982 : 39:53-58 Am J Psychiatry 157:10, October 200 0

This page intentionally left blank
Reproduced with permission of the copyright owner . Furtherreproduction prohibited without permission. This pageintentionally left blank Is Depression an Adaptation?RandolphM. Nesse, MD M any functions have been suggestedfor low mood or depression, including communicating a needfor help, signaling yielding in a hierarchy conflict ,fostering disengagement from commitments to unrea chablegoals, and regulating patterns of investment. A morecomprehensive evolutionary explanation may emerge fromattempts to identify how the characteristics of low moodincrease an organism's ability to cope with the adaptivechallenges charact eristic of unpropitious situations inwhich effort to pursue a major goal will likely result indanger, loss, bodily damage, or wasted effort. In suchsituations, pessimism and lack of motivation may give afitness advantage by inhibiting certain actions, especiallyfutile or dangerous challenges to dominant figures ,actions in the absence of a crucial resource or a viableplan , efforts that would damage the body ,and actions thatwould disrupt a currently unsatisfactory majorlifeenterprise when it might recover or the alternative islikely to be even worse. These hypotheses are consistentwith considerable evidence and suggest specific tests .Arch Cen Psychiatry. 2000;57:14-20 Pain or suJJering ojanyhind, iJlong continued, causesdepressionand lessensthepower oj action;yet it is well adapted to make acreatureguard itself againstany great or sudden evil . TheLifeand Letters of CharlesDarwin, Charles Darwin, 1887 Somemanifestations of disease arise directly from a defect inthe body's machinery while others are defenses ordysregulations of defenses.l-' Manifestations of diseasethat arise directly from defects, such as jaundice orseizures , have no utility. However, defenses such as painor diarrhea are adaptations shaped by natural selec tion.Dysregulated or extreme defenses cause many diseases, suchas chronic pain or dehydration from diar rhea .Distinguishing manifestations of disease that arise fromthese 3 causes is important. Correcting a defect is almostalways useful , but blocking a defense can be harmful. Forinstance, drug treatment of Shigella-induced diarrhea oftencauses complications.' Searching for the cause of a defectstarts with the defect itself, but the From theDepartmentof Psychiatry. University oj Michigan, AnnArbor. cause of adefense, such as cough, is sought in the abnormality thatarouses it, not in its mediating mechanisms. Is depressionan adaptation , an adaptation gone awry, or a pathologicalstate unrelated to any function? Opinions range fromdismissal of the possibility that depression or low mood

could be useful to the conviction that even severedepression is an adaptation with a specific function.'These opinions have important practical consequences .Patients who believe that depression is normal may refusedrug treatment for fear of "covering up the real problem,"while those who believe depression is purely a product ofbrain pathology may be reluctant to examine how theirrelationships may contribute to their symptoms . Clinicianswho believe depression is an adaptation may spend yearstrying to help a patient understand its significance ,while other clinicians actively discourage such inquiry.The physiological changes associated with depression areassumed to be defects by many research ers, while otherssee them as merely reflecting the activity of moodregulation mechanisms. Despite huge advances in our abilityto treat depression and growing recARCH GEN PSYCHIATRY/VOl57, JAN 2000 WWW .ARCHGENPSYCHIATRY.COM CC2000 AmericanMedical Association. AU rights reserved . Adaptation?ognition that it is often a medical disease resulting frommultiple pathways,' fundamental disagreements continueabout its adaptive significanc e. Terminology isinconsistent in this area. Those who see depression asintrinsi cally pathological tend to reserve the wordforsevere states that are mostly unrelated to ordinary moodvariation, while those who see it as a defense use the sameword to cover a wide range of normal and abnormal states.In this article , depression will refer to severe states ofnegative affect that are often but not necessarily pathological , and low mood will refer to states in thecommon range of normal experience . Low mood and depressionhave been difficult to distinguish from each other and fromrelated states such as sadness, grief, demoralization,guilt , and boredom. This difficulty may reflect the nature of the organism. Natur al select ion may have graduallyand part ially differ entiated a generic state of inhibition into subtypes specialized to cope with particularkinds of situations. Sadness, depression, guilt , and griefmay be partially differenti ated members of a "fuzzyset,,6.7 whose commo nali ties are explained partially byphylogeny and partially by the benefits certain responsesoffer in any unpropitious situatio n. Many people believethat low mood is normal and probably useful in certainsituations, but when excessive, prol onged , or expressedin the wrong situation , it becomes patho logicaldepression . This plausible starting posi tion gives riseto several qu e stions: In what situations is low mooduseful? How does it give a selective advantage? At whatlevel of severity does low mood become pathologicaldepression? Is some depre ssion unrelated to low mood? Firmanswers to these questions will not be possible until we

better und erstand the evolutionary origins and functionsof low mood . These questions about why the capacity formood exists at all are separat e and distinct fromproximate questions about the psychological and bra inmechanisms that cause low mood , and from the question ofwhy people differ in their vulnerability to low mood ordepression . The match between the eye's complex form andits function demonstrates that it is an adaptation , whileseizures are obviously a defect. Do th e glob al characteristics of low mood or depr ession give clues totheir adaptive significance? Depression is painful andinterfe res with norm al function, so it seems obviouslymaladaptive . However , other useful capacities, such aspain , nausea, and fatigue, are also aversive anddisruptive. In fact, their very aversiveness is likely aproduct of natural selection, prob ably because theypromote escape and avoidance of situations that decreasefitness. From this perspective , the intrinsic aversivenessof most low mood and depression suggests that they may berelated to a defense. The epidemiology of mood disordersoffers other clues . If depression were rare, like schizophrenia, and had symptoms unrel ated to the e xperiencesof most people, this would suggest it was a disease unrelated to any defense. In fact, major depr essive disorderaffects about 10% of the US populati on in a year"Depressive syndromes that do not meet diagnostic criteriaare even more common."!" Furthermore, there is no point ofrarity in the distribution that can differentiatepathologic from nonpathologic depression ," and subjectsmove frequently between syndromal and subthresholddepression over time ."· " Also, the incidence of depression is highest at the ages where reproductive value peaks, a patt ern characteristic of few diseases. Defenses areregulated by cues associated with situations in which theyare useful; defects are not. " ·17 The regularity of therelationship between loss and negative affect and theproportionality of low mood to the magnitude of a 10ss's.19imply that mood is regulated . However, the relationship ofdepression to events is less consistent. While about 80% offirst episodes in women are pr eceded by a severe lifeevent, 'S .2. only about one sixth of previously well womendevelop a depre ssion after a severe lifeevent. 21 Forthird and subsequent episodes of endogenous depression ,onset is unrelated to life pressive episodes are notdefenses. The global evidence undermines the idea that lowmood and depression are defects unrelated to a defense butis insufficient to sup port any firm conclusion about theiradaptive signlficance .just as for most other traits, anyconclusion about the ir utilit y requires consideration ofspecific hypotheses about how they could have offered a

selective advantage. POSSIBLE FUNCTIONS OF LOW MOOD ANDDEPRESSION Signaling benefits of several kinds have beenattributed to low mood or depr ession ." An infant 'scrying motivates its mother to help , an essentialmechanism shaped by kin selection . H .23 While cryingmakes a strong link to adult dep ression , it is less clearthat states of passive Withdrawal benefit Infants." Lewis"suggested that depression in adults is a plea for help.This view remains prevalent , but the evidence is mixed.The capacity to arouse pity in others may be helpful , butthere are few data to support this . However , reactions topatients with chronic depression are mainly negative ."Depression has also been interpreted as a communicationdesigned to manipulate others into providing resources.P"Following Lewis" and Meyer," and citing studies of infants,Klerman concluded: "depression isclearly adaptive,especially for infant primates, including man, "3Z(pIl 5lbut , "My current view is that the adult depressive episoderepresentsanattemptat adaptationthat has failed,""t "",presumablybecause help was not forthcoming. Engel andSchmale" ·" used the phrase conservation-wilhdrawal torefer to the presumed utility of the "despair " phase ofthe behavior pattern of a lost infant monkey. Depression inadults after a loss has been interpr eted as analogous tothis pattern of infant behavior, and many authors,"including Beck," emphasize a role for depr ession inconserving resources. However , unlike hibernation,depression is rarelya state of calm conservation, does notaffect all individuals in a group synchronously, and, withthe possible ARCH GEN PSYCH lATRY/V OL 57, JAN 2000WWW.ARCHGENPSYCHIATRYCOM C>2000American Medical Association. All rights reserved. exception of seasonal depression ,"is not usually correc ted by the mere passage of time.While conserving ene rgy du ring bad tim es is sensible,depress ion seems poorly designed for th is purpose . Bowlby" emphasized the value of attach men t and of aversivefeelings when an attachment is threatened or lost. He andhis followers have generally treated grief and depressionin adul ts as an epiphenomenon of auachmen t." However, itremains to be determined wh ether grief is merely a designconstraint or an adaptation in its own right .'? Price andothers." :" have suggested the ut ility of depression as ayield ing signa l in hie rarchy conflicts. Basing the irthe ory on animal models , they recogniz ed that many oftheir patient s with depr ession we re unwilling to yieldto a more powerful adversary. If they did finally yiel d ,th is signa led to th e dom inant figure that the personwas no longer a threat, ended the conflict , and resolvedthe dep ression ." This theory suggests a possible role forhigh as well as low moo d in negoua ung hierar chies" and

is supported by clinica l evidence of episodes of dep ression precipitated by social compe tition and resolved byreconciliatlon .P:" Har tung" hassugges ted a varia tion inwhic h se lfdeception abou t one's abilities C'deceivingdown ") lulls superiors into th inking one is no thr eat.Clinicians have long noted that depression is commo n inpeople who are pursu ing unreachable goals." :" "Failure toyie ld" may be an example, in the status competitiondomain, of this more genera l situation. When currentlifeplans are not working, the distr ess and lack ofmotivation that characterize depression may mo tivate planning an d reassessme nt" or escape, even by suicide."Hamburg summarized possible functions of depression ,saying, [when] the subject estimates the probability ofeffective action is low . . . the depressive responses canbe viewed as adaptive. . . . Feelingsofsadnessanddiscourageme nt may be a useful stimulus toconsiderwaysofchanging [the] situation . . . . Moreover ,[the] state of sadness may elicit heigh tened interes t andsym pathetic co nsideration on the part of Significantotherpeople.5Hp240) The lated view but emp hasizes thefrequency and costs of incorrect percep tions of lack ofcontro l instead of the benefi ts of a passive s tra tegy."·" Tiger" offers an exp licitly evolutio nary view ofopumism. The role of depression in disengaging mo tivationfrom an unreachab le goal was specified more explicitly inthe incentive-disengagement theory of Klinger. 56 . 57 If acommitm ent to pursue a goal enco unters an obstacle,efforts increase and become aggress ive. If the obs tacleca nno t be overco me , low moo d hel ps to di s engage theco mmitment and end the cycle . If the ind ividual canno tdisengage, low mood escalates. Klinger concludes,"depression is ordinarily, therefore , a normal, adaptivepart ofdisengaging oneself from an incentive . " 56' p2l )Many othe r researchers also see a close relationshipbetween depression and difficulty in disengaging from majorcommuments.Y" This pos ition has been elaborated in theframework of contro l theory,which suggests that low moodmotivates consideration of alternative strategieswhen thedistance from the goal is being reduced more slowly thananticipated.""" Several related theories have led toevidence that low mood is aroused by a mismatch be{weenachieve ments and expec ts tions" ··'-6'Closely related iswork on the informati on functions of mood.... Low mood shifts cogn ition to the more syste mat i c" and perhaps themore realistic· 7 ." Many studies support the relationshipof goal pursuit to low mood," but few have addressedclinical depression. My previous auernpts to explain moo dhave emphas ized the benefits of regul ating investm ent strateg ies as a function of changes in ant icipated levels

of payoffs. 70 . 72 In a pro pitio us situatio n , organisms gain by upregulating effort and risk takin g. In anunp rop itious silUation, downr egulation of effort andrisk takin g is adaptive. Mood thus regulates theallocation of effort and res ources-toward enterprises,strategies, and times likely to give a high payoff and awayfrom unp rofitable enterp rises and times when efforts willlikely be wasted or dange rous. As Wend er and Klein putit, based and mood in general-seems to us to have evo lutionary utility . . If one is subject to a series of defeats,it pays to adopt a conse rvative game plan of sitting backand waiting and leuing others take the risks . Such waitingwould be fostered by a pess imistic outloo k. Similarly ifone is raking in the chips of life , it pays to ado pt anexpansive risk taking approach, and thus maximiz e accessto scarce resources.P'r'?" IN WHAT SITUATIONS IS LOW MOODUSEFUL? Most aue mp ts to explain low mood have beenformulated in ter ms of specific funct ions, especiallycommun icat ion, motivati on, and regulat ion of effort.However , a single emot ional s tate may serve severaldifferent functio ns, and dif f erent emotio ns have functio ns in common. Emotions differ from one anothe r no tbecause they have different functions, but because theywere sha ped to cope with di fferent situations.64.70.74.7. After all, the global func tion of an emo tionor affect is to create a specia l state in an organism thatall ows it to co pe effectively with the adaptivechallenges characteristic of so me si tuation that hasrecurr ed an d influ enced fitness ove r th e course of many gene rations. Thus , the crucia l ques tion abo ut lowmood is not its function but in what situation s itsvarious characteristics offers fitn ess advantages. Thecharacteristics oflow mood and the situations tha t arouseit offer clu es to wh en and how it has been useful.Decreased motivation and activity wou ld obviously beuseful mainly in si tua tions in which action would befutil e or dangero us . Organisms carefully regula te whenand where they exert effort; foraging theory offers robu stpredictions for one such kind of effort . 79.80As the foodin a patch is depleted, organisms give up on that patch atclose to the op timal time, namel y, when the rate ofreturn in the current patch declines below the average rateof return over all patch es. If the overall rate of returnfrom all patches drops below the cos t, for aging stops.When the snow is deep and the temperature is low, foragingmay cost a deer more ene rgy per hour than it ARCHGENPSYCHIATRY/ VOL 57. JAN 2000 WWW.ARCHGENPSYCH1ATRY.COM©2000 American Medical Association. An rights reserved. canits is starv ing , is to stand still and wa il. 3':> Humanbehavior is far more complex and is organized around the

pursuit of personal goals. In recent years, psychologistshave inc reasingly viewe d emot ions as arisin g from anindividual'sappraisal ofhow an event will influe nce goalattainment. ,, · 81 .•zAn enormous body of literature nowdesc ribes the role ofaffect in regulating goalpursuit"'·oo.s,.., bu t little of th is wo rk has made itsway into psychiatry and even less is grounded in evolutionary biology. Specific emotions have been matched to part icular situa tio ns,' and contro l theorists have documented how e mo tions are in fluenced by success or failurein the pursu it ofgoa ls." Situations that regu larly arisein the pu r suit of goals aro use spec ial sta tes ("m indsets") to deal w ith them effecuvely ." Failing to reach agoal is an especia lly potent elicito r of negativeaffect,'6.59 Th ere is consi de rable agreemen t that lowmood helps to disengage individua ls from unprod uctiveefforts. ARE THE CORE ASPECTS OF DEPRESSION EVER USEFUL? Itis easy to see how lack of mo tivation for one act ivitycould free effort for som eth ing more productive, bu t depression is characterized by a more pervasive pessimism, low
self-esteem, and reduced initiative. These character isticspose the core conu ndrum ofdepress ion. They are the exactopposite of the op timism, ene rgy, and a willingness tomake
changes that would help a person get
ou t of a bad situa tion. However, there are situatio ns inwhich active
efforts just make things worse. One,
well descr ibed by Price," is when
challenging a dominant figure starts
fights that canno t be won. In this
situa tion , it is far better to inhibit
str iving and signa l sub mission and
a wish for reconciliation ." Anoth er
situation is the failure of a major life
enterprise. The purs uit ofla rge goals
requires const ruc ting expensive so

cial ente rprises that are difficult to
rep lace-marriages, friendships, ca
reers , reputatio n, status , and grou p
memberships. Majo r se tbac ks in these ses. In suchsituations, it is often useful to inhibit any tendency toshift quickly to a different endeavo r. The startup costsfor a new enter prise are huge, there is often no certaintythat another enterpr ise can be found at all, and theattractiveness of alterna tives may be illusory . Hastilygiving up on an unsa tisfying marriage or job often takes aperson out of the frying pan and into the fire. In thissitua tion, pessimism, lack of energy, low self-esteem,lack of initiative, and fearfulness can prevent calamityeven while they perpetuate misery. Th ere are also man yother kinds of unpropitious si tuations, suc h as lacking aviable life plan or so me crucia l resource or being sostresse d that striv ing would cause bodily damage . Ju stas anxiety inhib its dangerous actions, depression inhibitsfutile efforts. This see ms to contra dic t the idea thatdepressio n facilitates disengage ment from unr eachableincentives . Which is it? Does depression foster giving upand moving on when efforts to reach a goal are no tworking, or does it motivate persisting despite litt lelikelihood of success? Th is apparent contradiction arisesfrom trying to frame the explana tion in terms of onefunction . When depression is instead seen as a stateshaped to cope with unp ropitious situat ions, it is clearhow it could be useful, both to decrease investmen t in thecurrent unsatisfying life enterprise and also to preven tth e prema tu re p urs u it of alternatives. Failure todisengage can cause depression,and depression can make itharder to disengage. This may explain why the low-moodsystem is so prone to gelling stuck in positive feedbackloops· · '" Mood dysregulation may now be so prevalentbecause we are bereft of kin , beliefs, and rituals thatroutinely extrac ted our ances tors from suc h cycles."Also, the costs of low mood may be small compa red withthose of inappropriate high mood , so in certain situations the "smoke detector prin ciple" biases the systemtoward low mood .' Usua lly, th e dil emm a is resolved bychanging or accepting the current situatio n or by movingon. When it is not , serious pa thology ticle has so farbeen presented in the cold quasiecono mic terms ofbehavioral eco logy. However, for mos t people theresources at issue are relationships that are mediated no tby calcu lated reciprocity, bu t by power ful emot iona l

commitme nts . To break such commit ments and turn energieselsewhere is far different from just moving to a differentforaging patch . At least as important as th e ris ks andcos ts o f mak ing a change is the thr eat to the person'sident ity, r eputation , and sense of a secure place in asocial ne twork and the cosmos. As a result , most peopledo not treat others as objects , to be explo ited optimallyan d then replaced when convenient. Instead,despite the difficultie s, they persist in their relationsh ips, forbetter and for worse. Ambivalent relationships can causevas t su ffering.Q3 TESTS The several theses presentedherein requi re different kind s of assessment .?' :" Thefirst , that it is important to determ ine if depression isa defense, a dysregulated defense, or a defect, extends awell-recognized dist inction from the res t of medicine topsychia try. The second, that evolutionary hypotheses aboutlow mood and depression are beu er formulated in terms ofthe situa tions that shaped them instead ofjust theirfunctions either will or will not prove itself useful. Thethird, that generic low mood and related negative affecthave been shaped to dea l with unpropitious situations,predicts that the effect of a life event on mood willdepend primaril y on how it changes the antici pa tedpayoff of fu ture efforts. Many data exist to test thisproposal, and in itial forays have been made. For instance, dep ression is precipi ta ted not so much by life eventsthat involve loss, but by those that a re humilia tin g o rent rap ping.'o .'6 Life events research has moved steadilyfrom lists of events to examination of the individualcontext of the even t." A furthe r step in this dir ectionis to assess an individual's major life goals and abilityto achieve them . This requires the ideographic study ofwhy an individual is commilled to certain goals ARCH GENPSYCHtATRY/ VOL 57. JAN 2000 WWW.ARCHGENP$YCHIATRYCOM ©2000American Medical Associ ation. All rights reserved . andthat individu al's values , relatio nships, enterprises,strategies , obstacles. anticipated success or failure ,stra tegic con flicts and trade-offs, and decisions abo utwhat to do nex t in life· ' A related thes is, that naturalselectio n has pa rt ially differ entiat ed severalnegative affects to deal with di fferent kinds of unpropitious situatio ns , predicts subs tant ial overlap for thecha rac teristics of low mood , depression , anx iety, guilt, and grief. Likewise, the brain mec hanisms that mediatethem sho uld be tightly intert wined parts of thebehavioral inhibiti on system ." Dru gs th at relievedepress ion sho uld (and do) also relieve anx iety.Substant ial com orbidity of depression and an xiety disorders" is ex pec ted, not only because relate d brainmechanisms give sha red diatheses, but also because

situations that involve persistence in fut ile efforts alsoinvo lve risk and loss . Much work rem ains to consider howsubtypes of negat ive af[ec ts may match certain situations, suc h as seasona l low mood in cold , dark sea sonsand grief after a loss. Th e simp les t un tes tedprediction is th at depr essi on sho u ld be com mon inpeople who are una ble to disengage from unreachable goals.Gradua te s tudents who are failing and faculty who are unlikely to make tenure are obv ious candida tes for study,but ot her situa tions ar e far more common: unrequit edlov e , inability to get work, pursuing an elusive largelife goa l, or tryin g to lose weight, stop using drugs,sat isfy a fetish , be morally exemplary, get famou s, orpl ease a crit ica l pa ren t. Ability to rep ress suchwishes should prevent depression. Negative thi nking andlack of mo tiva tion shou ld be espec ia lly co mmon insitua tio ns charac terized by temptation to cha llenge adomi nant fi gure, failure of a major life en terp rise, orlack of a viable life plan. Th ey sho uld be less com mo nafier discrete losses, even large ones. Low self-estee m should be an especially promine nt part of those depressions that arise from inabil ity to yield in a sta tus competition . Furthermore, if negative thin king functionspartly to keep people from prematurely leaving badsituations, then ant idepressant treatment sho uld increaseleave. It wo uld be interesting to see if drug treatment ofspouses who are abuse d and have depression ma kes th emmore likel y to leave or to tolerate a bad si tuat ion. The bene fits of cog nitive thera py sho uld be mediated notju st by corre ctin g negative distortions, but more specifically by in cr easin g the pe rso n's ex pectations ofthe effectiveness of futur e action s. Thi s pe rspectivealso suggests an imal and ne ura l mode ls . If th e bra inmec ha nisms tha t regula te foraging are related to thosethat mediate depr ession , then a ntidepres sants shou ldcha nge the duration of foraging time in a depleted patchand the willingness to exe rt effort even when the net rateof r eturn is negative. They might also cha nge preferences for working hard for a large intermitten t reward vseas ily ge lting sma ll, frequent rewards. If low mood isan active coordina ted state, the n the bra in mechanismsthat mediate it can be blocked at different points, so antidep ressants sho uld be effective via multiple mechanisms . This perspective predicts that d epressi on sho uld b e frequ en t in peo ple who are anx io us, dutybound,amb itious , or lacking alternatives beca use such individuals are especially likely to get themse lves into situations in which they are unable to give up a major goal."People wh o lack th e resour ces or power to accomp lish their goals may be especially vulnera ble. "'0Subjective

wellbei ng sh ould be (and is) low er in those pursuinglarge lon ger -t erm projects,lOUO' especially conflic tingones.'?' It is interesting, in this context , to note thatsome of the gene tic p re d is pos itio n to d epress ionis med iated by different ial exposure to severe li feevenLS. IO'i,l0 5 Fina lly , this pers pec tive pre dictsthat soc ial factor s s hould influence ra tes of depressio n . Depres sion s hou ld be more common in cult ureswith rigid hierarchies and in th ose in whic h life ente rprises tend to be hu ge, vulnerable, an d irreplaceable.Media exposure sho uld increase depression , not j us t byfosterin g nega tive soc ial compa riso ns , but also bymotivating the pursu it of u nreachable goa ls. Relevanthere are cross-c ultural data tha t find subing to becieties with grea ter income equa lity"" and da ta show ingincr easing rates of dep ression in developed socteues .':" CONC LUSIONS Is depression an adaptat ion? At present ,we do no t have th e evide nce needed to say for su re.However , it seems likely tha t low mood and relatednegative affects were shaped to help organisms cope wi thunpropitiou s situa tio ns. Some negat ive and passiveaspec ts of depression may be useful becau se they inhibitdangero us or was te ful ac tions in situations char acterized by co mm itted pu rsu it of an unreach abl e goa l, temptati ons to cha llenge author ity , insu fficient intern al reserves to allow action witho ut damage, or lack ofa viable life stra tegy. Howeve r, it is esse ntia l toemphasi ze that many depress ions are clearly diseasestates: so me caused by dysregulation s of nega tive affectand othe rs by brain defec ts unrelated to low mood . Th efact th at low mood , and pe rha ps some dep ressi on , maybe usefu l sho uld not d istr act a ttention from recognition that dep ression is one of h u m anity's mos t serious me dia l probl ems. lOB A deep er understan ding of theadaptive sign ificance of low moo d and depression willimprove our ability to prevent and relieve bot h mood disorde rs and low moods that are normal, but un necessary .Acceptedfor publicationSeptember28, 1999 Preparation ofthis article was made possible by a grant f rom the KaplanFoundation, Englewood, Nj, and by support f rom theDepartment of Psychiatry and the InstitUl efor Social Research, University of Michigan, Ann Arbor. I thank LindaBrake!,MD, Deborah Carr, PhD, He/ena Cronin, PhD, AllanGibba rd, PhD, Paul Gilbert, PhD, Ursula Goodenough,PhD,john Greden, MD, Annette Hollander, PhD, Gordon Kane,PhD, Lois Kane, Mat thew Keller, BA, Kevin Kerber, MD,Timothy Kete/a ar, PhD, Raymond Kloss, MD, Richard Lempert,PhD, Dav id Lyons, MD, ja cquelyn Murphy , PhD, MargaretNesse , MS, ARCH GEN PSYCHIATRY/VOL 57 . JAN 200 0WWW.ARCHGENPSYCHIATRY.COM ©2000 American Medical Associ

ation. All righ ts reserved. Price, PhD, Peter RailLOn,PhD, Barbara Smuts, PhD, Charles Webster, PhD,BrantWenegral, MD, andElizabeth Young, MDJor comments on theideas preserlted and on early draJts oj this article.Corresponding author: RaMo/ph M. Nesse, MD, InstitutelorSocial Research. University of Michigan, Room 5057, 426ThompsonSI. AnnArbor, MI48106·1248 (e-mail:nesse@umich,edu). IllI1Ill1TilNII~ ••~ t , WilliamsGW,Nesse RM. Thedawnof Darwinian medicine. aRev8 iol.1991;66:1-22. 2. NesseRM, Williams GC. Why WeGet Sick: TheNewSCience 01DarwmianMedicine. New York, NY: VintageBooks:1994. 3. DuPont HL. Hornick RB. Adverse ell eet of10motutherapy in shigellosis. JAMA. 1973;226: 1525·1526. 4.McGuireMi, TroisiA, Raleigh MM. Depression inevolutionarycontext. In: Baron-CohenS, ed. TheMaladaptedMmd. Hillsdale. NJ: lawrence AErfbaumAssociates:1997:255-282, 5. Aklskal HS, McKinney WTJr.Depressiveeisorders: towardaunifiedhypothesis.Science.1973; 162:20·29. 6. Shaver P, Schwartz J, Kirson 0,O'Connor C. Emotionknowledge: turtnerexplorationofapro'totypeapproach. J Pers SocPsychol. 1987;52: 1061-1066. 7.Watson 0, Clark LAoANects separable andinseparable:onthehierarchicalarr angement 01the negativeattects. J Pers Soc Pwcnat. 1992;62: 469-505. 8. KesslerAC,McGonagleKA.SwartzM, Blazer OG. Nelson CB. Sexanddepression in theNational ComorbidftySurvey.f:utenmeprevalence,cnronrcny andrecurrence. J ANectDisord. 1993;29: 65-96. 9. OnsonM, Broadhead WE,WeissmanMM,le on AC, Farber l , Hoven C, KatholR.Subthreshold psychiatric symptoms in a primarycare grouppractice. ArchGen Psychiatry. 1996;53:880666 10. Juddu.Akiskal HS, Paulus MP. The role and clinical significance01subsyndromal depressivesymptoms (SSO) inunipolar majordepressive disorder. J Affecl ouom.1997;45:5-17. 11.Kendler KS, Gardner COJr. Boundaries of rnaror depression:an evaluation 01DSM-IVcriteria. Am J Psychiatry.1998;155:172-177. 12. Whybrow PC, Akiskal HS, McKinney WT.Mood Disorders: Toward aNewPSychobiology, New York, NY:Plenum PublishingCorp; 1984 13. Aklskal HS, Juddl l .GillinJC, lemmi H. SUbthreshOlddepressions:clinicalandpo'yscmnographic validation 01dysthymic, residual and ma sked lorms. J Aflect D/sord.1997;45:53-63. 14. AngstJ, Merikangas KR, Presig M.SubthreshOldsyndromes01depressionandanxietyin thecommunity. J CfinPsychiatry, 1997;58:6-10. 15. Janzen OH.Evolutionary physiology 01 personal detense.In: TownsendCR,Calow P, ecs. Physioloaical Ecology: An EvolutionaryApproach to Resource Use. Cambridge, Mass: BlackwellPublishers: 1981:145-164. 16. Vander A, Sherman JH, LucianoOS. Human Physiology: The Mechanisms of Body Function. 5th

ed. NewYork, NY; McGraw-Hill Book Co: 1965. 17. fordUniversity Press; 1990. 18. BrownGW. Harris T. SocialOrigins 01Depression. NewYork, NY: TheFreePress; 1978. 19.MonroeSM, SimonsAD. Diathe sis-stress theories inthecontextof lifestress research: impficationslorthedepressivedisorders.Psychol Bull. 1991:110 406-42520. Brown GW. HarrisTO, Hepworth C. l oss, humiliation andentrapmentamongwomen developingdepression:a patientandnon-patientcomparison. Psychol Med. 1995;25:7-21. 21.MonroeSM, SimonsAD,Thase ME.Onset01depressionandtimetotreatment entry: roles olli lestress.J Consult Clin Psycho/.1991;59:566-573. 22. Frank E,AM erson B, ReynoldsCFIll, Ritenour A, KupferOJ. lifeeventsandtheresearchdiagnosticcriteriae ndogenoussubtype:aconlirmation01thedistinctionusingtheBedfordCollegemethods. Arch Gen Psychiatry. 1994;51:519524. 23. Johnson-laird PN, Oatley K. The language 01 emotions: ananalysis01asemantic field. Cogn Emouon. 1989;3:81·123. 24. BarrAG.Theeanycryingparadox:amodest proposal. HumNature.1990;1:355-389. 25. l ummaa V,Vuorisalo T, BarrRG,Lehtonen L. Whycry?adaptivesignificanceof intensivecryinginhumaninfants.EvolutionHumBehav.1998: 19:193·202. 26.RosenblumLA PlimptonEH. Theinfant'setten to copewithseparation. In: l ewis M, Rosenblum LA,eds. TheUncommonChild. NewYork, NY: PlenumPublishingCorp; 1981 :225·257.27. lewis AJ. Melancholia: aclinical survey01depressivestates. J Mental Sci. 1934;80:1-43 28. CoyneJC,Kessler RC, Tal M, Turnbull J. living with a depressedperson. J Consult ClinPsychol. 1967:55:347-352. 29.HagenEH.Thefunctions01postpartumdepression. Evo/ution HumBetuv. In press. 30. WatsonPW,And rews PW.Anevolutionarytheory
depressed and 1.11 eight weeks later while manic. Althoughthese preliminary observations in mania require replicationin a larger
sample. they suggest that subgenual prefrontal cortexmetabolism is
mood-state dependent. Decreased blood flow and metabolismin the subgenual pre
frontal cortex in depression could reflect a regionalreduction in
either synaptic activity" or tissue volume (because of thelow spatial
resolution of PET) reductions in tissue associated with

atrophy or
hypoplasia reduce the magnitude of local blood flow andmetabolic
measures from PET images, a phenomenon known as the partialvolume averaging effect)", The grey matter volume of thecorrespondi ng cortex was therefore measured in MRl imagesacquired in mood-disordered and control subjects (Figs 2.3). MRI scans were not available for the subjects in groupsA and B, so to improv e the sensitivity for detectingintergroup differences (regional brain volume measures havegreater variability than PET measures), the sample sizeswere increased by adding MRJ data from subjects no tinvolved in the PET comparisons. The expanded bipolar groupincluded the unrnedicated, bipolar depressives from group Ctogether with two medicated-depressed, four manic and eightremirted (six medicated) subjects with bipolar disorder'(total n =21; age = 35 :!: 8.2; 13 female; 20 right-handed;all had a parent or sibling with bipolar disorder). Theexpand ed unipolar group combined the FPDD group with sevenadditional unipolar depressives who met criteria forrecurrent , major depressive disorder' , but not for FPDD12 (total n = 17j mean age = 35 :!:9.4; 10 female. 16right-handed). Additional controls were combined with thosefrom group C (total n =21; age =34 :!: 8.2; 11 female; 19right-handed). The left subgenual prefrontal cortex greymatter volum e was reduced by 39% in the bipolar subjectsand 48% in the unipolar depressives relative to the controls (F =9.8; P < 0.0002, after covarying for age, genderand whole brain volume: Fig. 3») and did not significantlydiffer between the unipolar and bipolar groups. (Notably,post hoc tests showed that the volumet ric differencesidentified in the expanded group of bipolar subjects werealso significant when the cont rols were compared either tothe seven bipolar subjects from group C (P < 0.05) or tothe 14 bipolar subjects not included in group C (P <0.005).) No significant differences in mean volume werefound between the bipolar and contro l groups in otherportions of the anteri or cingulate gyrus, including theright subgenual prefrontal cortex (219 :!: 95 and 209 :!:66 mm ', respectively) or the dorsal anterior cingulatecortex (left: 418:!: 184 and 389:!: 211mm' , respectively"= 0.47; right : 456 :!: 134 and 406 :!: 134mm' ,respectively. ,= 1.2). Post hoc analysis indicated that thevolumetric difference in the subgenual prefrontal cortex ispresent irrespective of mood state in bipolar disorder(mean values for the symptomatic (manic or depressed) andremirted subsamples were 131:!: 72 and 146:!: 99 mm',respectively). The anatomical abnormality also persisted du

ring antidepressantdrug treatm ent in 15 of the unipolardepressives who were reimaged following a mean treatmentperiod of 3.2 :!: 3.5 months (the mean volume was 126:!: 66mm' pretreatment and 123 :!:61 mm' post-treatrnnent). Thus, the reduction in the left subgenual prefrontal cortexgrey matter volume in mood disorders. localized bysynergistic use of PET and MRJ image data. could reflecteither an abnormallty of brain development related to thetendency to develop mood episodes or a degenerative changeresulting from recurrent illness. In monkeys and otherexperimental animals. the subgenual prefrontal cortex hasextensive connections with structures implicated inemotional behaviour and autono mic/neuroendocrine responsesto stressors, including the amygdala) the lateral hypotha
NA11JRE IVOL386124 APRJL 1991 8211 'FPOO····· letters tonature 300 1,00 l ~ 100 Carlltol _21 Bipolar _ 21 Unipolar_17 Figure 2 COronal (y . 31mm) and saginal ~ "'" 3mmjsections showing negat ive voxer r values w here metabolismis decreas ed in depressives relative to COntro ls. Thisimage. generated post hoc to provide optimal localizationof the su bge nua! PFC abnormal ity, compares all unmedicated dep ressives scanned w ith the 9538 (bipola r depressives from group C plus unipolar depressives wi th FPDDjwith the group C controls . The stereotaxic cenrre-ot-massof th is differ· ence (x ... 2.y a: 32,z . 2) laywilhin oneFWHM (17mm tor PET VI) from the pea k SF difference ingroup A (Fig . 1) and from Ihe ce ntre-of-mess of the SFdiffer ence computed pos t nee lor Ihe entire PET VI imageset (g roups A plus Bj: )( >: l ,y _ 25.z _ 6.All tnreecooromate sets localizeto the agranula r region of theenrertor cingu late gyru s ventral to the CC (Fig . I). Thespa tia l resolution of PET precludes c lear lateralityorsuecnons. Anterior , or lett. is to the lett. lamus, thenucleus accumbens, and the brainstem sero tone rgic, no radrenergi c and dopami nergic nuclei (the function of theseneurotransmi tte r systems appears to be blunte d duringdep ressive ep isode s and to be augmented by anti depressan t dru g treatments)l.U-7. H umans with lesion s thatinclude the subgen ual prefr on tal co rtex demons trat eabno rmal a utonomic respon ses to emo tional exper iences,inabi lity to experience emo tion related to concepts thato rd inarily evoke emotion, and imp aired comprehension ofthe advers e conseque nces of pernicious socialbehaviours'" , Based partly upon these observa tions,Damasio et al. B • IO prop osed that the ability to discernthe outcome of social beha viour in term s of punishment and reward depend s upon visceral feedback med iated thr oughin teractions between the ventro media l prefrontal co rtexand autono mic centres. If so, d isordered in terac tio ns

between the subgen uai prefron tal cortex and interconnected structures may be related to the pathological guilto r anxi ety characterizing depression, or the rapid shifts between inapp ropriate eup ho ria and anger seen inmania u . Th e neura l networ k formed by the se structures may contain a disease proce ss that is not confinedto the subgenuai prefront al cortex, as reduced leftamygdala volu me" and third ventri cle enla rgement" (thesubgenual prefrontal cortex shares substantial, predo minantly ipsilate ral connections with the amygdala and themedial thalamic nuclei surro unding the third ventric le')have also been repo rted in bipolar d isorder . Post-mortem histop ath ological assessments with in th iscircu itry may elucidate the neurobiology of familialmooddisorders. 0 Me thod s Subject s . Characteristics ofsubgroups appear in Table I , The bipolardepre ssed (BP-D)subje cts met criteria for bipolar d isorder, dep ressedphas e', and had a parent o r sibling with probab leordefinite bip olar d isorde r. Hamilt on
I Depre ssion Rating Scale (H DRS) scores (21 items)" werein th e mod erately-to severely-d epressed range (mean =24.2 =: 3.5 (20-29) for gro up s A and B, and 23,4 :: 6.5(l6-3 5) for gro up C). Subjects had not received psychotro pic or 826 Figure 3 MRI-based vo lumes 01 the leftsubgenual prefrontal co rtex (PFC) grey matte r differedbetween the dipolar disordered. unipo lar dep resse d andco ntrol groups (ANOVA,F =9.8;P < 0.0002,co-vary ing lorgender. age andwh ole brai n VOlume) . POSI hoc test s(Tukey-Krame r) showed sign ihc8nt volu metric decreases intne bipolar and uni polar groups relative to the co ntrolgroup. Who le-bra in MRI volume and skull x-raymeasures(produ ct of anterior-poster ior distance betwe en the inner tables at the skull at the estimated bico mmissuralseqmen r" and perpendicular dista nce from the midpoi nt ofthe biccmmissure! segmen t to the vertex") were slightlysmaller in the unipo lar group compared with the bipo larand control groups , and did not diNer between the bipolarand control gro ups . The len subqenuat PFC /whole brainvolume ratio was also redu ced in the bipolar and unipolargro ups, being 1.8 x 10 · ' ::;0.74 x 10 ·', 1.1 x 10-'::0.64 x 10·', and 1.1x 10 · ' :: 0.51 x 10·' in the control. bipolar . and ur nporer groups. rescecuvev IF =:8.4; P < 0.001). o the r drugs likdy to alter bloo d flow(OF) o r glucose metabolism for > 4 weeks. Exclusioncriteria inclu ded substance abu se within on e year and major medical disorders. Co ntrols met the same exclusionsand den ied having had majo r psychiatric disorder s. GroupA con trol s con sisted o f 24 subjects involved in our previous ' study of unipolar depression" , who also denied a

famil y history o f psychia tr ic diso rders. This large,carefully screened co ntrol gro up was used to genera tethe co mpos ite nonnative image for the r-image com putation. Gro up B co ntrols were matched withbipo lar subjects ingroup B (40% female in each) and group C co ntro ls withthe bipolar subjects in gro up C (50 and 57% fema le,respectively) fo r age, hand edn ess and gend er. Im ageacquisltl o n. PETsca ns were acqui red as subjects restedwith eyes closed . For grou ps A and B. ima ges wereobtained usin g PEn VI and 6080 mCi of Hz'sQ (ref. 25).Tissue rad ioactivi ty was measured , which over th e range tested accurately reflects di fferences in regiona l BF16 • For group C, images were acquir ed with a Siemens 9538tom ogra ph (resolution was 5 m m FWHM , septa insert ed ).Glucose metabo lism was measured using 5IOmCi o f j"F}2.tluorodeoxyglucose , adapt ion s o f the Sokoloff method,"and art erial blood sampling. A linear no nnalization wasapp lied by d ivid ing regional-by-global metabolic rat efor glucose (MRglu; mean global values did notsignificantly differ acro ss the contro l,bipolardepressed, and unipolar-dep ressed (FPDD ) groups.being 6.0 :: 0.95,6 .2 :: 1.2 and 5.7:: 1. 1 mg per 100 mgper min , respective ly). The metabolic images were notfiltered (that is, FWHM was 5 rnrn ). Region al OF was alsomeasured" and th e reconstructed BF im ages were filteredto a '-dim ensional resolu tio n of 14 m m FWHM, Technicalproblems precluded acq uisition o f the metabolic image forone bipo lar depressive and the BF image for anothe r.Image a na lysis . To guide regional analyses. PET scan sfrom group A were used to com pute a compos ite statistical im age high lighti ng differences between bipolardepressives and co ntrols. After remapping primary im agesinto a common, stereotaxic arr ayl.1', an imag e of unpaired r-values was com pu ted , with eachvoxelrepresenting the d ifference in mean OFbetwe en depressives and controls divide d by th e local varia nce" .The t ima ge was searched for t values above a thres hold1tl th at wou ld correspond to P < 0.05 in a single test ,ROI NATURE IVOL 386124APRIL1997 were defined to encompassthe voxel containing the peak I tl value and adjacentvoxels with similar r values. The size of each ROI wasoptimized by computing regional rfo r progressively largerROI. and the ROI for which the regional rwas maximized wasselected. Eleven ROI were defined, located in the followingregio ns (per cent difference in mean norm alized flow indepressives relative to co ntrols app ears in parentheses): subgenual prefrontal cortex (PFC) ( 7.7% ), righ t(R) insula ( 7.5%), R and left (1) temporopa rietal cort ex( 7.4 and 6.7%, respectively), R and l lentifo rm nucleus (6.3 and 5.7%, respectively), rostral thalamus (6.1%), pos

terio r cing ulate ( 5.6%), L hippocampus ( 5.2% ), lfrontal po le (4.4%) and R precuneat e (4.5%). Thehypothesis that SF differed between dep ressives andcontrols in each ROI was tested bycomp aring the mean BFofthe depressed and contro l samples I fro m gro up B inone-tailed r-tests. corr ected for mult iple compa risons
" (Bonferroni), with degrees of freedom corre cted forunequa l variance (Sanerthwaite). Thu s, the RO I used toobt ain the BF measures for both gro ups A and B were identical in size and location, having been generated from ther-image from group A, and stereotaxically placed in eachsubject's PET I imagt'll·lI..l'lThe only mean BF differencebetween the de pressives and cont rols from groupBachieving significance after corrections from II tests wasfound in the subgenual PFC. Because of the higher spatialresolution of the 9538 image s, regional measures in gro upC were obtained using the smaller ROI sho wn in Fig. 1.
Thus. they were not guided by informa tion regardi nginherent d ifferences
between the dep ressives and contro ls from grou ps B or C.Neuromorphometrle mea s ure s . MR images acqu ired using aSiemens
VISION 1.5Tscanner and a 3D MPRAGE sequ ence (TI , 300 ms:TR, 9.7; TE. 4;
flip angle, 12 0 ; matrix , 256 X 256 X 128, I X 1 X 25 mmvoxels) were resliced
to I mm' voxels with coronal sections orie nte d perpendicul ar to the bicom
mis suralline using ANALYZE. The grey matter was manu allytraced for the first
full gyrus beneath the corpus callosum in all coro nalslices between the
anterio rmost po int of the callosum and the anterio rmostplane where the
in ternal capsule no longer divided the striatum.Segmentation was perfo rmed
by one investigato r (W.C.D.) blinded to diagnos is.Virtually ident ical mean

in tergroup differences were obtained by a second rate r (l.R-S.) blinded to the
measur es of the first. Variance compo nents estimates {intraclass correl ation
coefficients) showed that 1.0% of the total variability wasdu e to Interrater
di fferences and 99% to inter-subject differences.
R ru iv rd I 2~ p tr mbtr l996 ;ic c epl rdItl Frbru i ryl9'.l ' .
I. lMl"0Jtic oNJ Sultisriu l MOII...u of Mn ",J DisDrdm(DSM· /tt -R) IAmrnCln Pl:rchialric A»ocia · lion .Wuhinflon , DC, 1987}. Good win. f . K.&I Jami son . K,R.M""i ,.dq> trSsiw JU" w IO rl"ord Univtrlity PTn3, NrwYork. 1990). D, rvru. w. C.&I Todd. R. D. in ....dLfltP1yth... try lrd . Guu.s. B.) 991" 2 IMo, by. SI l.ou i, .1997). M Ulion a. I. c.. Phrl p, . M. E.• Plurnmrr . D. &:KIlh.I. D. .E.Qua nli lauon in pos it ron rm i",ion computed lomography: S. PhYliul · anal omical rlfrcu.} .CompO" . ,wut. To,""1". 5. 7,.. -14' ( 11181).
5. Ci rmicharl, S. T. &r Pria. 1L Um bic;·co nnrction, ofthr orbi t.al and mrdia1 prr ftont.al co n u in macaq uemon krys . }. Comp. N~ .., l 36) . 6 105-6041 fI9ll o5 ).
6. Nea" ry. E. J..Terreberry, R. R.. Hutl ry. K.M.. Ruil.K. G, &:fryntak. R. J. in N"" .obiologyof CutfUl<l rr Un(:(II,", Limbic 1'aaI<lmLf,J (rdl VOSt. B. A &I Gibnrl, M.l206-213 (Bitk,hluxt. Boslo n. 199').
7. Srwd<. S. Il , Drulc h. A..Y.,RoTh. R. H. &Bunn ry, B.o5. Topos ~phic o rsaniutio n of thr dt"r rtnl pr ojrrtion,of Thr mtd ial prtfronlaJ cc rtex in the TlII:In an terograde tract' lnc1nl! ' Ndy lUin8 PIrOJn lw vvlf'l rU kuco.ogglulini n. l: CA...p. NrLf'ol. 190, 2 1' _242 (1989).
8. DamiLIio, A R.. Tranr l, D. 8rDi miLIio. H. Indi vidualsWith sociopalhic brh arior Clustd by fton w dami8t fail 10respond iu tomi t:ica.U y to social slimuli. atJutv. B."i "Ru . 41. 81_94 ( 1990 ).
9. B«han. A.. Tra.nd. D.. Damuio. H.&:Damuio. A. R. Fa ilur ~t om po n d au l o n omi uIJ y t o an tici p a t tdfutul't ou tcomn folJowin8 dimi ,r to thr prdront.alco n t.l. u,.,br.Cort. .. 21~ -22S ( 1996).

10. D.miLIio. A. R.[)rJ(.Ilru't EfTOr:Emorioll,Rt4UIlI,""d"ot HLfm"" B." i... (G, ourtlPutnlJTl.Nrw York, 1994; Piudor MacMi1I&n. lo ndo n. 1995).
II . Dr rvru, w.e."1ll.A functional anatomM:.al studyofunipolar drp rusion . , . N ~",Jri 11. 36283641 ( 19112).
IZ. Winoku r. G. Tbr drvdopmml and validity of familial ,ubtypn in pn ma ty unipolar drp ru,ion. P/wanrwacopsyc/ri.uryU, 142I46f I9U ).
13. Butn, L R.dill. Ct rtbral mtubolic ntes for &lucosr inmood <fuordr n . Arch.Grn. Psyclowu. -41, "'1-""7 (II1U) .
14. But rr. L R. " Ill. Rtduction of prr fron W (onu.s1ucoSt mt Ubolism (ommon to thr (t rypors of dtpreuion.Arm Gc-n. Psych;"t 46, 20250 (1\189).
I ~ . BuchaNum. M. S. n aLFrontal conu and ba.wJ ganpiamrubolK TlIln ~ by pos itron nnWion l omop phrwithll"IZ~UCOStinafJ«tiw illn-., .A fl ra.DiJ.IO .U 1-1 5 2(1986 ) .
16. Cobm. R. M. nlll. Evidt:DCrfor comm on aJlrntionl incrrr bral g1uCO$rm~ bolism in mljot affr'CUvt &sordrn andKhiz ophrmq. N....ro p ~tmiWJ lI1fy 1. 241-2S4 (11119).
11. Oolan. R. J.n ..J.. Donollt r nJ ptt front.al (on udY'function in thr major PlychOK$: symptom or diwut sptcifIcityf). N~. oJ. N ~ 'O MJ. P1yt/r;" ,. ~ 1290-129.. (199 )).
18. DrrvtU, W. e. &-BontTo n. K.in ;.d LfIlPsyc/r"' try( td. Gu.u:,S . B.) 53-82 (Mosby.SI Louil. 19116).
19. Dr rwu. W. C. &: R.a i chJ ~ . M. E. Rtci proaJ ,uppreuion of rtJi o ruJ Ctrrilral bIocxIflow dUM, rmot:ionaJvtnlU hiR,hrr cognit:ivr p' OCftW'S: impli u tion l for int (~ eti on ' ~ern ( motio n and copt ition. CApit. £"'01.(in tht p~ ) .
20. Drrvru, W. e., Spittnal!rl . EoL. MacLrod. AIe.&IWch1r, M. .E.DiKriminltory u p.ability of PET mr iLIut~mr nu of ,r-gional blood flow in familial purr drp rruivrdist iLIr. Abur. Soc. Nnl. o.n. I ll, 15% (l99ZI.
NATUREIVOL 386124 APRIL 199 7 leners to 21. Yo ung.1l C .Biw. l. T., Z i ~ ~ r . V. E. &I Mqrr. D. A A n tinl sulr

for mani a: rr lil bility. valid ity and srn,iuYlty.Bn'.'.Pryt:/rwu. lJ ) ,429-005{l978 ). 2~ . n taocee,R.J.• Ka8ry.ml , G. H. & Won 8·Rilry, M.T. Thr rrhlionshi pbetweenCNS mr laboli, m and <y!oarchi ftctu u : • ,rvi rw of '·C ·cko rrBlucosr JNdin with COfrda tion 10 cylochro mrori dllW' hiltodl ~mistry . CAmp. Mrd . lmlll· GNp/r, U ,8192 ( 1989 ). B . Purlson. G. D. " ol Mtd ial i nd superio r t~ mpo n.l gyraJ volumrs and u ~b r aJ asymmrt ty inKhlJ:oph ~ nii vrnu, bipola r d isordrt . 8iol 1'I)I'C ;'~t. oil , 1_1 4 ( 1997). Z4. Hamilton . M. A ~ti n8 saltfor drpr rNion . ,. N ~ rol N ~ro 'Lf'l. P1yt/ritu. D ,S6-62 11%01. 205. Raiehlr, M. E... Muti n. W. R. W..Hrncovll ch. P.. Mintun, M. A. 8r Marlr.ham, I. Brain bloodflo w mr iLIu ,td with inln .,. nou, :110. II . Implr.-nution and validat ion . l. NwcLMd 24, 71lO-i98( 1IIUj. 26, 1'01. P, T. &I Mlntu n. M. A. Noninv,uiv r funcuonalbn.in m. pp in 8 by ch in lf( dillribU lion .in&1 y m 01 I·.vrra!ed PETl m'8 n of Ht O h u ue aetlvtly. l. NueL Mtd.)O, 141_ 1411 ( 11189). 2•. Phrlp .. M. E. t1 oiL TomOlfraphic mr llurrmmu of loal cerebral glucose IT>tllbolic me Inhumam With 11'· 18J2.tlu oro .l .dro.lY-o-g1ucosr:va/idalto n of mtl hod . A"". Nr", ,,l ,, 311J88 119791.28, TaI.irach, J. & To u mo ~. P. in Co-PUr"" . Strr rorAric Atltu of flor H"moln 8 ,oi" 1122 I Thr im~ . Slu" 8"n. 1988). 29. Fo", P. T.. Prrlm ultrt . I. S. 8r lUich! r.M. E. A IIrr rol.l ctic mr rhod of ~" it omiul locaIiuuo nfo r pennon rm issio n tomo8raphy. 1. u mpLft. ....uut.Tom.",. 9. 141-I S) (J98 5). JO. Cannichwl.S. T. &-1'riu .1. L Archi ltQ on i<su bdivision of thr orb iw andmtdlaJp,tfn,"W con u in Utt macaqu r monkry. , . Comp.Nfil.oL J.46.366402 (I994) . AckPowltdrrmn"lt.l. This workWaJI Up poMtd by tht US NIH and thr Charln A Dana Foundation , Wt Lhanl T. Vidn'1'Iand I. HaJkJ. for advict o ninliit analysa. W. Powt'u fo r guid .tnet on meubol:i(imlpna . E. Spi LZ n' !-r l and T. Pil8l'am for usiSlancrwilh Sla tistic.aJan aJY'il , and L Ga,dnr r fo, trdmiul assistanct CotT tspondtnCt and rtqu t!lu for mltrnallshoul d be adciraard10 W.C.D. 827 This page intentionallyleft blank A Molecular and Cellular Theory of DepressionRonaldS. Duman, PhD; George R. Heninger, MD; Eric].Nestler, MD, PhD R ecent studies have begun to characterizethe actions of stress and antidepressant treatmen ts beyondthe neurotransmitter and receptor level. This work hasdemonstrated that long-term antidepressant treatmentsresult in the sustained activation of the cyclic adenosine3' ,5' -monophosphate system in specific brain regions,including the increased function and expression of thetranscription factor cyclic adenosine monophosphateresponse element-binding protein. The activated cyclicadenosine 3' ,5'-monophosphate system leads to the

regulation of specific target genes, including theincreased expression of brain-derived neu rotrophic factorin certain populations of neurons in the hippoc ampus andcerebral cortex . The importance of these changes ishighlighted by the discovery that stress can decrease theexpression of brain-derived neurotrophic factor and lead toatrophy of these same populations of stressvulnerablehippocampal neurons. The possibility that the decreasedsize and impaired function of these neurons may be involvedin depression is supported by recent clinical imagingstudies, which demonstrate a decreased volume of certainbrain structures. These findings constitute the frameworkfor an updated molecular and cellular hypothesis ofdepression, which posits that stressinduced vulnerabilityand the therapeutic action of antidepressant treatmentsoccur via intracellular mechanisms that decrease orincrease , respectively, neurotrophic factors necessary forthe survival and function of particular neurons. Thishypothesis also explains how stress and other types ofneuronal insult can lead to depression in vulnerableindividuals and it outlines novel targets for the rationaldesign of fundamentally new therapeutic agents . Arch GenPsychiatry. 1997;54:597-606 Depression is thought to be aheterogenous illness that can result from the dysfunctionof several neurotransmitter or For editorial comment seepage 607 metabolic systems. Basicand clinical studies haveprovided evidence that the serotonin and norepinephrine(NE) neurotransmitter systems are involved in the treatmentof depression. These studies have led to a series ofhypotheses concerning the mechanism of the action of anti.~; . .iS well as th e ?<It:-;.-,Fromthe Ll1boratory ofMolecularPsychiatry, Departmentsof Psychiatry andPhannacol(lg)', Yale UniversitySchoolof Medicine.Connecticut Mental H~ alrJI Center, New Haven. ARCH GENPSYCHIATRYN OL 54 , JULY 1997 physiologyof depression, thathave focused on alterations in levels of these monoaminesor their receptors . Although these models have guidedresearch efforts in the field for 3 decades, they have notgenerated a compelling model of antidepressant action orthe pathophysiology of depression. For example, studies todate have failed to identify a common action ofantidepressant treatments at the level of monoamines ortheir receptors. This is not surprising given thatdifferent types of antidepressant treatments exert widelydifThis article is also available onoti'i.i:l Web site:ama-assn.orglpsych.· ," , Depression systems. II is alsopossible that there is more than a single mechan ism bywhich antidepressant treatments exert their therapeuticactions. An updat ed hyp othesis tha t bu ilds on pr eviouswor k suggests that thc long-term , therapeuti c action of

antidep ressant treatm ents is mediated by postrecepto rintracellul ar targets . Advances in molecular and cellularbiology have elucidated the in tracellul ar machinery throu gh w hich monoamines ull imately act to cont rol thefunctioning of neurons. These advances have made itpossible to begin the process of delin eating the specificsignal transdu ction path ways that med ia te the sho rt term effec ts o f diff er ent types of ant idep ressanttreatm en ts and that underlie the adapta tions in neuronal f unction respo nsible for the long-term effects ofthese treatments. We present a brief review of the basicand clinical work about the role of serotonin and NEsystems in the treatment ofdepression.We also discuss, ingreater J etail , recent advances that demonstrate a rolefor intr acell ul ar s igna l tr ans d u ct ion pathwaysand die regulation ofspecific target genes in antidepressant tre a tm ent s. Spec ifica lly , we describerecent findings that demonstrate that the transcriptionfactor cyclic adenosine 3' ,5 '-monophosphate (cAMP)response element -binding pr otein (CREB) is one intracellular target of long-term ant idepressant treatmen tand that brain-de rived neurotrophi c factor (BDNF) is onetarget gene of CREB. These studies supp ort an emerginghypothesis of the mechanisms by which stress and oth erenvironmenta l in sults may damage specific populations ofneurons and. thereby, cont ribute to the p athophysiologyof depre ssion in vu lne rable indivi dua ls. Thi sprovides a framework for futur e studies needed to testthis potentially unifying hypoth esis for ant idepressantaction and the pathophysiology of at least certain formsofdepression . MONOAMINES AND DEPRESSION Early studiesindic ated that agents that deplete monoamines,such as reasmall perc cntage of indi viduals. This led to the theo rythat reduced availability of mon oam ine neurotransmitters.part icularly NE and s(rotonin , could play a role in theforrnat i on of depress ion ." ) Th is hypothesis wassupported by the discovery that pr ototypicalantidepressant treatm ents, the tricyclics and monoamineoxidase inhibitors, cause a short-term increase in synapticlevels of mon oam ines. However, despite extensive research, it remains unclear whether long-term ant idepressanttreatments result in the increased or decreased function ofthe man y mon oamin e pathways located throughout thebrain. The role of mon oamines in depression has be enfurther examined with the use of sero t onin and NEdepletion par adigms in norm al and drug-remittedindividuals with depression . '· 6 The results of thesestudies demo nstrate that although the depl etion of serotonin or NE does not lead to depr essive symptom s in normal individuals , pa tients who experi enced remission on

either seroto nin or NE selec tive reuptake inh ibitors arevulnerable to relapse on depl eti on of the correspondi ngmo noami ne. This indicates that se roto n in and NE aresomehow in volved in the maintena nce o f an an t ide pressan t response , but canno t alone explain eith er themech an ism of act ion of ant idepress ant treatments or the pathoph ysiology of depression. This conclusio n is alsosupported by the time required for the therapeut ic actionof antidepressant treatm en ts (several weeks) , eventhough levels of monoamines are increased rapidly by thesetreatm ent s. Togeth er, the results suggest that additional facto rs co ntribu te to an udepres. sant responsesand the onset of depression . MONOAMINE RECEPT ORS ANDDEPRESSION A conse que nce of antidepr essant treatment andelevated levels of serot onin or NE is th e ac tivat ion ofmono amine recep tors . One possibilit y is that persistent activation of these recept ors would lead toadaptations in th e receptors that would ARCH GENPSVCHIATRYN Ol 5i . JULY 1997 to thc peutic actionofantidcprcssant treatm ents. " Indeed . ca rly stud iesdemonstrated that lonc-rr: ",,: ' . dep ressan t l rca lm t;l\ S U0W Oregulate the density of receptor sites for serot onin and NE . Th e best characterized example is tha tthe lon g-t erm, but n ot sh ort-t erm , administrationofmany lypes ofantidepressant treatmen ts decreases levelsof l3-adrenergic recept or ( I3AR) ligand -bind ing sitesin limb ic bra in regions. such as the cerebral cortex andthe hipp oc ampus.P:'! The ability of I3ARs to stimu latethe formation of cAMP is similarly decreased in theseregions by long-term antidepressant treatm en ts. Serotonin jrecept orbind in g sites wer e also found to bedown-regulated by many antidepressant treatments ." Theseand other receptor studies led to various receptorsensitivity hypothes esfor example, that the action of antidepressant treatm en ts is dependent on the down -regulation of I3AR or se ro ro n l n, recep tors an d tha tenhanced sens itivity of these receptors may lead todepression .I" However, there are many problemswith thesehypotheses. First. not all ant idepressant treatm en tseffectively regulate the levels of I3AR orserotoninj-receptor si tes' This could mean that the actionof different antidepressant treatments is mediated bydifferent receptors or that other sites are more relevan t.Second, the time course for down-regulation of I3 AR an dse ro to n in, recep torbinding sites is more rapid thanthe therap eutic on se t of th ese tre atments. ' .Il.14Third. levels of sero tonin, receptors are increased, notdecreased. by long-term electroshoc k seizure treatment,one of the most effective therapies for depression . ' .14Fourth , the reduction of I3AR function by the adm inist

ration of selective I3ARrecept or an tagonists is not aneffective treatment for depre ssion and actuall y producesdepression in some individuals. 1>.16 In fact, theactivation or facilitation of I3AR function by theadministration of thyroid hormone or a speci fic receptoragonist can have antidepressant efficacy in some patien ts.17 Aserotontn ., receptor sensitivity hypothesis has alsobeen put forth by Blier and de Monugny." This hyFigure 1.Amodel demonstrating antidepressant regulation ofthe~-adrenergic receptor (J3AR)-<:oupled cyclicadenosine 3',S'-monophosphate(cAMP) system. Whenthereis no treatment.basalevels ot norepinephrine (Nf) stimulate the~AR~oupledcAMP system. snon-tetmadministrationofcertain typesofantidepressantselevates levelsofNE. increasinglevelsatpARstimulated cAMPformation. Long-termadministration ofmany types ofantidepressantscausesdown-regulationoftlltJ number of f3 AR-bindingsitesavailable tostimulate cAMP production. Thisinturnleadstoa decrease intilemaximal levelofJ3ARstimulated cAMP formation. However, withsynapticlevelsofNEstillelevatedasa resultofcontinuedanlidepressant treatment, tilelevel ofcAMP formedremainselevated relative tothe no-treatment condition.Thispossibilityrequires furthertestingtodetermineiflevelsof(jARstimulated cAMPformationareindeed elevated. However, thismodel providesamechanism toexplainhow long-terman tidepressanttreatmentsactivatethecAMPpathwayeven though levelsof(jARaredecreased. INTRACELLULAR MESSENGE RS, NEU ROTRO PHICFACTORS, AND DEPRESSION Adva nces in molecula r andcellular biology have paved the way for studies to de termi ne how antidepressant treatments ult imately regulatethe function of target neurons in the bra in. There aremany comp rehensive reviews on intracellu lar signa ltransd uction path ways,""" and this inf ormation will notbe discussed in deta il herein except as it pertains toantidepressant treatm ents. In general, these pa thways canbe divided into 2 broad categories. The first catcades thatmedia te the actions of monoamine receptors. Such intracellular factors represent potentia l comm on targets formany different types of antidepressant treatm ents becausethey could be regulated by the activation of either theserotonin or NE receptor syst ems . This could include theactivat ion of serotoni n and NE recept or subtypes thatare not themselves regu lated by antidepressant trea tments. It will be impo rtant in future studies to determin e which serotonin and NE rec epto r sub types medi a te thereleva n t th e r a p eu t i c a c t ions of an t idep ressan t tr eatm en ts , al though identifica tion of the critical int racellular targets will likely facilitate this

process. Treatment (Allfative to No Tfeafmenf) egoryincludes those pathways that are controlled by receptor-cou pled second messengers (eg, cAMP, inositoltriphosphate, Ca H , and nitric oxide) and are usuallyregulated by classicneurotr ansmi tters, such as themonoamine s, amino acids, and neuropep tides (Figure 2 ).The second category includes those pathways that arecontrolled by receptors tha t conta in, or in.teract with ,protein tyros ine kinases and are usually regu lated byneurotr ophic factors and cytoki nes ; ac tiva tion ofthese receptors leads to the regu lation of otherintracellula r cascades, suc h as the mitogen-activated protein kinase pathway (Figure 2). As the pro tein kinasesand phos pharases, phosp hoproteins, transcrip tion factors , and target genes that make up these pathways areincreasingly identified and characterized , it is becomingpossible to examine how adaptatio ns of these complexpathways are involved in the long-term ac tions o f antidep ressa nt treatments and other psychotrop ic dru gs.The ability to study these adaptations is a criticaladvance because these path ways control all aspects ofneuronal function and ultimately underlie the ability ofthe brain to adapt and respond to pharmacological and enviro nme nta l inputs. The fun ctional consequences of suchmolecular adaptations can be determ ined at the cellularlevel by analysis of the electro physiological and morphoAcufeAntidepressant Treatment No Treatment depressanttreatments increase the function of postsynapticserotonin.; receptors in the hipp ocamp us. Dependi ng onthe type of antidepressant treatment, they propose thatthis could occur by eithe r the increasedsensitivityofpostsynapticserotonln ., receptors or thedesensitization ofserotonin aut orecep tors , One problemwith this hypothesis is that directacting seroton in .,receptor agonists are not clearly effective antidepress ant tr ea tme nts , a lt ho ugh the sero toni nj; agoniststested (buspirone hydrochloride and gepirone) are thoughtto be partial agonists at postsynapt ic serotorun.,receptors and may not adequately test the hypoth esis.Anoth er possibility is that increased serotonin.,neurotransmission is necessary, bu t insufficient, forantid epressant efficacy and that the ac tiva tion o fadditiona l factors is required, Several other monoaminereceptor subtypes are repo rted to be regulated by antidepressant treat men ts· ·, However, as with the I3AR,seroronin. , and serotonin., Tecep· tors, regulation ofthese other monoamine rec eptors alon e cann ot acco untfor the mecha nism of action of antidepressant treatments .Rather, alterati on s in the levels of these recep tors orin their functional sensitivity probably represent adap

tations to increased levels of mono
amine s. In fact, it can be argued that
t he obs erved recept o r down
regulatlons are indicative of contin
ued receptor activation secondary to
co ntin ue d eleva tio ns in mon o
amine levels after long-term antide
pressant treatments. Indeed, levels
of these receptors are decreased, and
not completely elimina ted, by long
term antidepressant treatments, rais
ing the possibility that there cou ld
be sufficient levels of receptor re
maining to respo nd to the elevated
l eve ls of s e r o to ni n and NE
(Figure 1 ) . If this is the case, the
fun ct ion al ou tp ut of the mon o
a mine recep tor s wo u ld be in
creased, not decr eased , by long
term treatm ent s , a possib ility that
was en tertai ned in an ea rly re
view." This wouldsuggest that long
term antidepressant treatme nts re
sult in the sustained activation of the
intracellular signal transdu ction casARCH GENPSVCHIATRVNOL H , JULY 1997 Stress Stress igure igure igure

igure igure i r i r igure igure igure Figure3, Amodeltorthemolecularmechanism ofactionat tonq-termantidepressanttreatments. Antidepressantscauseashort-termincreaseinlevels atserotoninandnoreprinephrine (Nf) by inhibiting thereuptakeor breakdown ofthesemonoamines.Long-termantidepressantadministrationdecreases thetunctionandexpression ofcertainserotoninandNEreceptors(eg,r,-adrenergicreceptor {PAR} and sero tonin!), butthe cyclicadenosine 3', S'-monophosphate (cAMP) signaltransductionpathway is in creasedbylong-termantidepressanttreatments, includingincreasedlevelsat adenylyl cyclase andcAMP·dependentproteinkinase(PKA), as weJl as thetranslocation of PKA tothecef! nucleus. Moreover, recentstudiesdem onstrate thatexpressionandfunctionotthetranscription factorcAMP responseelement-bind ing
. l ular mo del s of learn in g an d memory.''' '' Morphological changes includ e atrophy or the sprout ing ofneurons in response to damaging or growth-promoting stim ulLlO32 These types of responses can be viewedasprototypical ways in which the brain adapts 10 repeatedperturbations. Our hypothesis is that similar types ofmolecular and cellu lar adaptations occur in response toantidepressant treatments and are involved in the pathophysiology of depression. These types of adaptations arecomplicated and, in many cases, are difficult to identify ,bu t recog niti on of the ir po tential imp ortance hasstimulated studies that have investiga ted the role of intracellular pat hways and their cellular adaptations in antidepressant action and in depression . Characterization ofsuch adaptat ions is at a relat ively early stage , but hasalready led to no table conceptua l advances in the field.ANTIDEPRESSANT TREATMENTS ACTI VATE THE cAMP SIGNALTRANSDUCTION PATHWAY There are many pote nti alintracellular pathways that could mediate the action of antidepressant treatments. One suc h path way that isregulated by the serotonin and NE systems is the cAMPsignal transdu ction cascade (Figure 3 ). Receptoractivation leads 10 the form ation ofcAMPby coupling toadenylyl cyclase via the stimulatory G pro tein subt ype,Gs. Certain forms of adenylyl cyclase can be activatedindepen dent of Gs in respon se to elevated cellula r Ca"levels." The effects of cAMP are then mediated by theactivation of cAMP-de pende nt pro tein kinase, which , inturn , leads 10 the regu lation of cellu lar fun ction bythe phosph orylation of spe cific proteins. One of these isth e tran scription facto r CREB, whic h mediates many of

the actions of the cA MP sy s te m on ge ne ex pr es sion."·" In addition to its regulaARCH GEN P5VCHIATRYIVO L 5",JULY 1997 Vehicle CREB mANA FluoxetineHydrochloride ControlStress Vehicle Fluoxenne CREBFigure 5. Stressdecreasesandantidepressant treatments increasetheexpressionof brain-derived neurotrophic factorin thehippocampus. The influenceofacuterestraintstress(90minutes)orlong-termttuoxetinehydrochloride administration (21days) on levelsofbrain-derived neurotrophic factor messenger RNA weredetermined by insituhybridization analysis. The CA3 andCA1pyramidal and dentategyrus granulecell layersofthehippocampus areindicated. Pretreatment with fluoxetineorother antidepressantsalsoblocksthedown-regulationofbrain-derivedneurotrophic factorinresponse to stress" C Fluoxeline C ECS HydrOChloride =ssCREBC ECS C ECS C ECS Antibody "'CREM CREe Figule 4.Long-term antidepressant treatments increase tevetsofcyclicadenosine 3', 5' -monopnosptute (cAMP)response element-bindingprotein (CREB) messenger RNA (mRNA)andbindingin the hippoCJmpus. The findingthatlong-termantidepressanttreatmentsincreasethe expressionandfunction of CREBinthehippocampusisillustrated. The influence of long-term(21 days) fluoxetine hydrochlorideadministrationonlevelsofCREB messenger RNA wasdetermined byinsituhybridizationanalysis. LevelsofCREB messenger RNA wereincreasedinthemsior subuetas ofthe hippocampus,includingCA3andCA 1pyramidal anddentategyrusgranule celllayers.LevelsofCREB bindingwere also increasedby long-termfJuoxetinetreatment, as well aselectroshock seizures (ECS)(10days). For this assay. homogenates ofthe hippocampusareincubatedwith a radiolabeled, synthetic fragment ofDNAthat contains a consensus cAMPresponseelement. Binding ofCREB shiffsthemigrationof theradiolabeled DNA throughthogel. The identity of CREB is co nfirmed inseveral ways.First, the CREB binding is reduced bycompetition withunlabeledD NA containingthecAMP response element,butnotwith DNA containing amutated cAMP response elementsequence (notshown). Secona, supershin (55)studies(tiottom) demonstrate that a specificantibody toCRfB.butnotCREM (cAMP response etemem modulatory protein), snetsthecAMP response element-binding band. For ssanalysis, thehomogenate ispreincubated with antibodyoetoretheradiolabeled DNA is added. If the specificantibodybinds totheprotein-DNA complex, it either disrupts thecomplex or supershiftsthemigrationofthe complex through thegel. 44 tion by pho sphorylation, recent stud ies havedemonstrated that expression of the total amount ofCREB isanother mechanism by which the fun cti on of CREB can beregu lated . J5.J7 The cAMP system is a potential c ommon

target for serotonin and NE because there are receptorsubtypes for both monoamines that s timulate the formationof this second messenger (Figure 3). In addition to theI3AR, there are 3 serotonin receptor subtypes thatstimulate the cAMPsystem (serotonin,.e., ), and one of these (serotonin) is reported to be regulated by long-termantid epres sant treatments." Moreover, CREB may representa common intracellular target for antidepre ssant treatments because other serotonin or NE recep tors (eg,serotonin ZA.c and " tadrenergic receptors) could alsoactivate CREB via the stimulation of Ca? -dependeru protein kinases (Figure 4)." '" Several studies havedemonstrated that the postreceptor components of the cAMPsystem are regulated by long-term antidepressant treatments(Figure 3) . Levelsof guanine nucleotid e-stimulatedadenylyl cyclas e and cAMP-dependent prot ein kinase enzymeactivity are reported to be increased by longtermantidepressant treatrnents .P" In addition , we have foundthat the levels of CREB messenger RNA and protein in thehippocampus are incr eased by longterm antidepressant treatments, including serotonin and NE selective r euptakeinhibitors (Figure 4 and Figure 5)." The time course forthe indu ct ion of CREB is consistent with that for thetherapeutic ac tions of antidepressant treatments (ie ,10-21 davs of treatment) . To furth er test 'the hypothesis that CREB is involved in antidepressant actions , itwill be important to determine whether the time course forthe reversal of these effects is consistent with the offsetof therapeutic actions. Increased expression of CREB couldbe mediated by the up-regulation of cAMP functi ondiscussed previ ously because CREB expression can beinduced in cultured cells by the activation of thecAMPcascad e." These findings contrast to those of a recentstudy of CREBfunction in pcn cells,an adrenal chromafincell line." However , in the l atter study, th e short-termincubalion ofPCn cells with antid epressant treatmentsinhibited depolarization-indu ced activation of CREB, aneffect owing to the blockad e of Ca?" channels. To ourknowledge , such inhibition of CREBhas not beendemonstrated in vivo . Increased function and expression ofCREBprovides direct support for the proposal that the cAMPSignal transduction system is increased in the hippocampusby long-term antidepressan t tr eatments . Induction of theintracellular components of the cAMP cascad e may alsoexpla in the requirement for long-term antidepressanttreatments, even though levels of cAMP may be elevated byshort-term an tidepressant treatments (Figure 1 and Figure3) . Our results also indicate the types of specific geneelements likely to be regulated by long-term antidepressanttreatments; that is, those with functional cAMP response

elements, However, not all genes with a cAMP responseelement CREB mANA would be expected to bc activated byantid epressant treatments. First, up-regulation of thecAMP system and CREB is not obse rved in all brain regions(there is evidence for down -regulation of the cAMP systemin the locus coeruleus" ). Second, regulation of geneexpression is dependent on the ac tivity and int eractionof several different promo ter elements and transcript ionfactor s. Thus , acti vati on o f the cAMP system and CREBmay lead to the regulation of a specific set of genes inthe hippocampus that are invo lved in the action of antidepr essan t treatmen ts. One goa l of curren t studiesis to identi fy these genes and to determine theirrelevance to the clinical responses to anti depressanttreatm ent s. Recent s tudies have ident ified BDNF and itsrecepto r, trkB, as 2 potential target genes of interest.ANTIDEPRESSANT TREATMENTS REGULATE NEUROTROPHINSBrain-derived n e~ ro tr o phi c factor is a member of thenerve growt h factor family, which also includ es theprototype nerve growth factor as well as neu ro tro p hi n-3 and neu rotrop hin-4. These growth factors are invol vedin the differenti ation and grow th of many types ofneurons in the developing brain as well as the mai ntenance and surv ival of neurons in the m ature brain.,o.nil For example, the survival and growth of serotoninneurons in the adult brain is increased by BDNF and, to alesser degree, by neur otrophin-B, but not by the nervegrowth facto r." Also, neur otr o phins can rap idlyinfluence the function of n euron s, as de mo nstra ted bythe finding tha t sho rt-term exposure of hippocampalslices to BDNF inc reases th e strength ofcertain synapticconnections. 28 . 29 These types of findin gs, along withan incr easing app reciation of the neurotrophic actio nsof the monoa mines ,":" highlight the lar ge ove rlap between th e rol es played by neurotroph ins and monoami nes inthe regulation of brai n function. The actions ofneurotrophins are mediated by bindin g to specificreceptors, referred 10 as trkBrecept ors, which lead to theactivation of protein tyrosine kinase activity located onthc int racellular domain of the receptors. Recent stud ieshave provided sup pon for the notion that neurotrophins andneuro nal plasticity and survival may be involved in thetreatment of depression. First, BDNF is repon ed to haveant idepre ssant effects in 2 behavio ral models of depressio n, th e forced swim and learn ed helples snessparadigms" Second, lon g-term , bu t not short term , antidep ressa nt adm inistration , including seroto nin and NEsele cti ve « u p take in h ibit or s, a mon o amineoxidase inhibi tor, an atypical ant idepressant, as well aselectros hock seizures, increases the express ion of BDNF

and trkBin the hipp ocampus (Figure 3 and Figure 5) .41."Third , BDNF is repone d to enhance the growth of serotonin and NE neu rons, as well as to pr otect these neuronsfrom neurotoxic damage.'· '" While these findings support arole for BDNF in the actions of an tidepressant treatments, studies of add itional antidepressa nt and non an tidepress ant age nts are required to further test this hypothesis. In addition , the role of other neu r otro phic factor s (eg, nerv e grow th factor , neurotrophin-3, and neurotrophin -4) should be examined . The poss ibility tha tincrease d expression ofBDNF results from the activatio nof CREBis suppone d by severa l lines of evidence . First,the lime course for the up-regulation of CREBis simila rtothat of BDNF. Second , th e regulation of CREB and BDNF isobserved in the same populations of neuro ns in thehippocampus (Figur e 4 and Figure 5) . Third , s tu dies inprimary neu ron al cultur es have dem onstrated that the stimu la t io n o f cAMPo r Ca" activated pro tein kinasesincreases th e ex p ression of BDNF."·" Finally, thereduction of CREBlevels in the hippocampu s by theadministration of anti sense oligonucleotides to CREBmessenger RNA decreases basal levels of BDNF an d blocksthe induction of BDNF by anti depressa n t treatme nts."Additional in vitro and in vivo studies are needed todemonstrate a dir ect link between CREB and the expressionofBDNF. ARCH GEN PSYCHIATRYNOL 54, JULY 1997 A ROLE FORNEUROTROPHINS IN DEPRESSION There is also evidenc e of aneurotrophi c element in the pathophysiology of cenain forms of depre ssion. First , immobiliza tion s tress causes adramatic reduction in BDNF expression in the hippocam pusof rats (Figure 5).56 Th e relevance of this findingrequires further examination , For example, do other typesof stress (eg, psychosocial) , which can precipitate orexacerbate depression , also decrease the exp ression ofBDNF? Second, chronic stress of several types (ie, restraint or psychosocial) o r gl ucoco rt ico id tr eat men tsare reported to cause atrophy, or even death, of vulnerableneurons in the hipp ocampu s in rats and n onhumanprimates."·· J The CA3 pyramidal neurons seem to be mostvuln erable to stress, although other populations ofneurons seem 10 be sensitive to stress, glucoco rt lcoids ,cytoki nes , and other types of neuron al in sult , such ash yp o xiaischemia or hypoglycemia." Third, the ability ofthe hipp ocampu s to inhibit the hypothalamic-pituitaryadrenal axis is reduced in certain patients withdepression, cons istent with a deficit of hipp ocampal function in these individua ls." Fou nh, there is a smalldecrease in hippocampa l volume as det ermined by magneticresonance imaging in patient s with depression or posttrauma tic st ress disord er. ...ee In addition, a recent

review of the literatur e provides evidence to sugges tthat there may be a decr ease in the size of certain brainstru ctures in depressio n." Down-regulation of BDNF maycont ribute to th e atrophy of neurons in the hipp ocampusin response to s tress. However , not all episodes ofdepression are associated with stress, and the modelpresented may be limited to certain subtyp es of depression . Postm ort em studies to dem onstrate atrophy or neuronal death dire ctly in the hip poc ampus of patients withdepression are required to further test this hypoth esis.These studies form the basis of a molecular and cellularmodel ofdepression and antidepressant actio n (Figure 6 ) .Depre ssion , part icularly stress-associated cases, mayreFigure 6. Amolecularandcellularmodel fortheactionofantidepressant treatments andthe pathophysiology01sttess-tetstea disorders. This model 01thehippoCJmpusshows themajorcelltypes inthe hippocampus andhowstressandantidepressant treatments may influence CA3 pyramidalcells. The 3 major sublields ot tnehippocampus (CA3 andCA1pyramidalcells anddentate gyrus granule cells)areconnected bythemossy fiber andSchaffer collateralpathways. Recent studies demonstrate that chronic stressdecreases the expression ofbrain-derivedneurotrophic factor(BDNF) inthe hippocampus. This couldcontributetotheatrophyordeath ofneurons in theCA3 pyramidalijeillayerotm« hippocampus. Long-term elevationofglucocorticoid levels isalso known todecrease thesurvival of th ese neurons. Other types ofneuronal insultsuch ashypoxia-ischemia, hypoglycemia, neurotoxins, andviralinfections could also cause atrophy ordamage ofneuronsandCOUld. thereby, make anindividual vulnerabletosubsequent insults. These types ofinteractionscouldunderlie the observations of de creased function andvolumeofhippocampus inpatients with affective disorders andcouldexplain the selective vulnerability ofcertainindividualstobecome depressed. Long-term antidepressanttreatments increase the expression ofBDNF. aswell astrkB,andprevent the down-regulation ofBDNF elicited by stress.This could increase thegrowth orsurvival ofneurons. orhelprepair orprotect neurons from totmerdamage. Increasedexpression olBDNFandtrkBseems 10 bemedialed bythesustainedelevation ofthe serotonin andnorepinephrine (Nf)systemsandthecyclic adenosine monophosphate cascade. Normalizationofglucocorticoid levels bylong-term antidepressanttreatments could also contribute to the recovery ofCA3neurons. specific genes that may predispose certainindividuals to depression and render others relativelyresistant. Studies of the cAMP pathway, CREB, and BDNF,discussed previously, demonstrate the enormous number ofgenes that could be involved. Indeed , these studies

highlight the naivete of candidate gene strategies toidentify depression vulnerability genes, which remainfocused on monoamine metabolic enzymes, receptors , andreuptake proteins. These studies indicate the need for moreopen-ended investigations of the genetic factors involvedin depression. However, it could be immediately informativeto examine how SchaHerCollateral Hippocampus A HYPOTHESISFOR GENETIC AND ENVIRONMENTAL VULNERABILITIES ..GIUCOCriCOidS ... Sero,onirand NE ... BON' B~N'.GIUCOC~rtiCOidS pal neurons could be involved in theaffective, neuroendocrine , cognitive,and vegetativeabnormalities observed in depression. However, theseabnormalities are also likely to be influenced by severalother limbic brain structures and it is possible thatstress alters the structure and function of neurons inthese brain regions as well. It is widely believed thatdepression results from a combination of genetic andenvironmental factors . Yet, virtually nothing is knownabout the nerable pyramidal neurons in the CA3 region ofthe hippocampus. This could be a consequence, at least inpart, of the decreased levels of BDNF available to theseneurons. Elevated levels of glucocorticoids are also knownto playa notable role in stress-induced damage of CA3neurons "·63 Antidepressant treatments could reverse thisatrophy by increasing BDNF expression and function. Infact, we have found that long-term antidepressantpretreatment blocks the down-regulation of BDNF in responseto stress" Normalization of glucocorticoid levels byantidepressant treatments in some individuals could be anadditional mechanism for the prevention of further neuronaldamage ." Further studies are required to determine whetherantidepressant treatments have direct neuroprotectiveeffects or neurotrophic actions on hippocampal neurons assuggested by early studies .71.n Recent studies areencouraging. We have found that long-term electroshocktreatment causes sprouting of granule neurons in thehippocampus. " Unlike the sprouting observed in response tokindling or excitotoxin treatment, there was no obviouscell dam age after long-term electroshock treatment. Inaddition, electroshockinduced sprouting was markedlyattenuated in mutant knockout mice that express reducedlevels ofBDNF. These results indicate that electroshockinduces sprouting of certain hippocampal neurons and thatthe response is mediated by the increased expression ofBDNFin these neurons. The observation that antidepressanttreatments can lead to the reinstatement of hippocampalcontrol of the hypothalamic-pituitaryadrenal axis in somepatients further supports the possibtlity that the functionof these neurons, indeed, can be improved." One challengein depression research is the difficulty of identifying

specific anatomical substrates involved in the disorder.The hippocampus is involved in the control of emotion,learning and memory, and the regulation of thehypothalamicpituitary-adrenal axis, as well as othervegetative processes. Changes in the structure or functionof hippocamGIUCOCriCOidS GIUCOCriCOidS GIUCOCriCOidSGIUCOCriCOidS GIUC CriCOidS GIUCOCriCOidS HippocampusHippocampus Hippocampus Hippocampus Hippocampus HippocampusHippocampus Hippocampus Hippocampus Hippocampus HippocampusHippocampus GIUCOCriCOidS GIUCOCriCOidS GIUCOCrSchaHerCollatera Hippocampus Hippocampus GIUCOCr GIUCOCrSero GIUCOCriCOidS Hippocampus Hippocampus GIUCOCr tors maypredispose cer tain individuals to mood disorders based onour hypothesi s. One possibility is that many individual swho become depr essed may have had a prior exposure tostress that causes a small amount of neuronal damagc,butnot enough to precipitat e a behavioral change . Ifadditional damag e occurs, either as a result of normalaging or further stressful stimuli, these effects may thenbe manifested in the symptoms ofa mood disorder. Thesetypes of events could explain the decreased volume of specific brain structures in depression. This model couldalso explain how other types of neuronal insult predisposean individual to mood disorders. Insults such ashypoxia-ischemia, hypoglycemia, neurotoxins, or viralinfections could cause direct neuronal damage or renderneurons more vulnerable to psychosocial stress (Figure 6) .Such changes could lead to depression at later times or ,if severe enough, could immediately precipitate adepressive episode. For example,a high iJ\cidence ofdepression is well docum ented in patients who have had astroke.' '"'' The possible involvement of myriad environmental factors implicates many additional sets of genes that could conceivably alter an individual's inherentresponses to stress and establish a diath esis for depression . The possible role of a subtle neur odegenerati vec ontribution to th e pathophysi ol ogy of depressi on should be dir ectl y exa mined by analysis ofpostmortemtissue, as discussed previously. RATIONAL DESIGN OF NOVELTHERAPEUTIC AGENTS New information indicating a role forthe cAMPpathwa y and CREBin the a ctions of antidepressanttreatments suggests novel approach es to developfaster-acting and mor e effectiveagents. The developmentand testing ofsuch agents will also help to further testour hypothesi s. First , receptor agonist s could betargeted at the specific serotonin or NE receptors that stimula te cAMPor Ca" -activated prote in kinases andmediate the ant idepres sant induelion of BDNF. Thesereceptor sites must 13AR and the serotonin.j, receptorsites are likely candidates. Second, identifi cation of

other neurotrans mill er recep to rs th at s ti mulatecAMPor Ca?"-acnvated protein kinases in the hippo campuscould be additional targets. Third, agents that dir ectlystimulate cAMPor Ca' ·activated kinases, or that directlyactiva te CREB, could be developed. F ourth , th e inhibition of cAMP breakdown would enhance the function ofCREBand increase BDNF expression . Fifth , agents thatactivate the BDNF-trkB signaling pathwa y may be of someuse. The first 2 possibilities have the potential forregulating the function of CREBand the expre ssion of BDNFspecifically in the hippo campu s, depending on the distribution of the recept ors targeted , but may not bemuch more effective than available treatments. Conversely,the last 3 possibilities may be less specific becau se theywould be expec ted to influence man y brain regions as wellas periph eral tissues that express these intracellu lartargets, but may be more effective. There has beenlegitimate concern regarding the specifrciryand safety ofsuch agents. However, it is impossible to pred ict theeffects of such agents unti l prototypi cal compounds areavailable for evalu ation . Moreover, some agents, such aslith ium and nons teroidal anti inflamma tory agents (whichaffect arachidon ic acid metabolism ), are enorm ousl yeffective for their respective indications despite theirgeneralized actions. The possibilit y that the inhib itionof cAMP breakd own increases BDNF expression has beenexamined . Long-t erm administration of inhibitors ofphosphodiesterases, the enzymes that metabolize cAMP,increases the expression of CREBand BDNF in the hippocampus of rats. .... Mor eover, coadministration of a phosph odi esterase inhibitor with a tricyclic antidepressantresults in a more rapid induction of CREBand BDNF ." Thesefindings provid e additional support for the hypothesisthat the cAMP system regula tes the expression of BDNFandsuggest that the inhibition of cAMPmetabolism may provide amechanism fora more rapid treatm ent of depression. The AkCH GEN PSYCHtATRYNOL 54. JULY t997 metabolism may have antidepressant effects was raised several years ago" and wassupported by preliminary clinical studi es with rolipram, apotent phosphodiesteras e inhibitor ." The lack of furtherprogress on the therapeu tic potential of phosphodiesteraseinhibitors raises questions abou t the efficacy of the seagents in the treatm ent of depression. However, given therecent observations, it may be time to reevaluate the therapeutic pot ential of phosphodiesterase inhibitors. Onepotential application tha t has not been investigated isthe use of pho sphodiesteras e inhibitors as augmentingagents with oth er antidepressant treatments that block thereuptake or metabolism of mon oamines. This appro ach couldallow the cAMP system to be augmented in specific brain

regions that contain the appropriate serotonin and NEreceptors. COMMENT Although th e regulation of CREB andBDNF may be important in the actio ns of ant ide p ressanttreatments, it would be preliminary and naive to suggestthat these are the so le tar g ets of the se tr eatm ents.Th er e are m any ge nes th at a re kn own to be regula tedby the cAMP system and certain antidepressanttreatments.70.79. 86 In addition , th e cAMP cascade isjust one of many int racellular pathwa ys that could beregulated by serotonin and NE and could be important to theaction of antidepressant treatmenrs. One example is theregulation of the phosphatidylinositol system and proteinkinase C by lnhium.":" The findings discussed hereinindicate that antidepressant action is not mediated by thesimple upor down-regulation ofmonoamines and theirreceptors. Elucidation of the role of the cAMP system andBDNF in the r esponse to ant idepressant treatments provides fundamentally new leads in understandingantidepressant action and the pathophysiology of depression . Although the studies discu ssed provide aframework for a unifying hypothesis, it requires furthertesting of its several components. However, the modelincorpora tes th e im portant role of th e mon oam ines inthese ph enom ena and begins to elab ora te the many m ol ecular a nd c e ll u la r m ec han is ms in flu e nce d byth e mo no arnines that are more proximal to the co mp lexadapt at i ons in brain function tha t underlie d epressionand its trea tm ent. AcceptedforpublicationJune 18, 1996,Thi s study was supported by grants MH4548 1, MH53 199, and2 PO 1MH25642from theNational1nstitute of Mental Health,National InstiM es of Health, Belhesda, Md;aVeteransAdministration NalionalCenter Grant,VeteransAffairs Medical Center, West Haven, Conn; andtheAbraham RibicoffR esearch Faci lit ies of theConnecticut Mental Health Center, State of ConnecticutDepartment of Mental Health and Addiction Services, NewHaven. Corresponding author:Ronald S. Duman, PhD, Con necticut Mental Heallh Cm ter, 34 Park St, New Haven, CT 06508.lIll1I1Illil[lj!l:~ 1. Schildkaut JJ. The catecholaminehypothesis of attectlve disorders: a review of supportingevidence. Am J Psychiatry. 1965;122:509· 522. 2. Bunney WE.Davis J. Ncrepinepnnne in depressive reactions: a review.Arcn GenP SyChiatry. 1965:t3:483-494. 3. Coppen A. Thebiochemistry 01affectivedisorders. 8r J Psychiatry.1967:113:1237·1264. 4. Shopsin 8, GershonS,GoldsteinM. Friedman E, Wilk S. Use 01synthesis inhibitors in defining aroleforbiogenicaminesduringimipraminetreatment in depressedpatients. Psycnopharmacol Cammun. 1975:1:239·249. 5.Delgado Pl , Price l H, Miller Hl , Salomon RM, AghajanianG.HeninerGR, CharneyD. Serotonin andtheneurobio lOQY

ofdepression.ArchGenPsyChiatry. 1994:51:865-874. 6. MillerHl . DelgadoPL. Salomon RM, Berman R. KrystalJH. HeningerGR.CharneyOS.Clinicaland biochemicaleffects ofcatecholaminedepletionon antidepressant· induced remissionof depression. Arch Gen Psychiatry. 1996;53:117-128. 7.Sulser F. VetulaniJ. MobleyP. Modeof action ofantidepressant drugs. BiochemPharmacal.1978; 27:257·261. 8.CharneyOS. MenkesDB,HeningerGR. Receptor sensitivity andthemechanism of action of antidepressant treatment:implications lor the euerogyand therapy 01depression. ArChGen Psychiatry. 1981;38:1160-1180. 9. Heninger GR. Charneyas. Mechanisms of actionofantidepre ssant treatments:implicationslor the etiology and treatment 01depressivedisorders. In:Meltzer HY.ed. Psychopharmacology: The ThirdGeneration 01 Progress. New York, NY: RavenPress:1987:535-544. 10, sant treatments reduces reactivity01noradrenergiccAMP·generating system in limbic forebrain.Nature. 1975:257:495-496. 11. BanerjeeSP. Kung LS, RiggiSJ. Chanda SK. Develo pment of ~ -adrenergi c receptorsubsensitivity byantidepressants.Nature. 1977;268:455-456.12. Peroutka st.SnyderSH. tong-term antidepressanttreatment decreases spiroperidol-Iabeledserotoninreceptorbinding. Science. 1980:210:8890. 13. Riva MA. Dreese LRe-evaluation of the regulationof a-adrenemicreceptorbindingby desipramine treatment.Mol Pturmscot.1989:36:211218. 14. ButlerMO, MorinobuS, Duman RS.Chronicelectroconvulsive seizures increase theexpressionofserotonin2receptor m RNA in ratIrontal cortex.JNeurachem.1993:61:1270·1276. 15.PaykelES,FlemingerA.WatsonJP.Psychiatricsideeffectsofantihyperte nsive drugsotherthanreserpine. JClinPsychopharmacol. 1982;2;14-39. 16. AvornJ. Everitt DE.Weiss S. Increased a n t i d e ~ pressant use inpatientsprescribed l3-blockers. JAMA. 1986:255:357-360. 17.GoodwinFK, PrangeN . PostRM, MuscenolaG, Upton MA.Potentiation of antidepressant effect bytriiodothyronineintricyclic ronrespcnoers.Am J Psychiatry. 1982;139:34-38.18. Blier P, de Montigny C. Current advances andtrendsinthetreatmentofdep ression. TrendsPharmacal SCi.1994:15:220·226. 19. StoneEA. Problemswiththecurrenthypotheses01antidepressantagents:speculationsleading toanewhypothesis. Behav Brain Sci. 1983:6:535577. 20.Berridge MJ.lnositol lriphosohateandcalciumsignaling.Nature. 1993:361:315-325. 21. Blenis J. Signal transductionvia the MAP klnases: proceed atyour ownRSK. ProeNatlAcadSciUSA. 1993;90:5889·5892. 22. HudsonCJ. Young LT.LiPP.WarshJJ. CNSsignal transductioninthepathophysiologyandpharmacotherapy 01affective disordersand schizophrenia. Synapse. 1993;13;278-293. 23, Darnell

JE. Kerr 1M. Stark GR. Jak-STAT pathwaysandtranscriptionalactivation in responseto t FNsandotherextracellularsignaling proteins.Science.1994:264:1415·1421. 24. Nestler EJ, Duman RS. G proteinsand cyclic nucl eotides in the nervous system. In; SiegelG. Aoranoff B.AlbersRW.Molinoff P.ecs.Basic Neurochemistry. 5thed. NewYork.NY; RavenPress; 1994:429-448.25. Duman RS. Nestler EJ.$ignal transductionpathways lorcalecholaminereceptors. In; MeltzerH, ed.Psychopharmacology: The Fourth Generation of Progress.NewYork. NY: RavenPress; 1995:303·320. 26. Madison DV.Malenka RC. Nicoll RA. Mechanisms underlyinglong-termpotentiation ot synaptic transmission. Ann RevNeurosci. 1991;14: 379·397. 27. Bliss TVP. CoUingridge G. Asynaptic model 0' memory: long-termpotentiationinthehippocampus. Nature. 1993:361:31,39. 28.KangH,SChumanEM.Long-lastingneurctrcphlninducedenhancement01synaptictransmission in theadult hippocampus.Science.1995:267:16SS1662. 29. levine ES. DreyfusCF, arack18. Plummer MR. Brain-derived neurotrophic lactor rapidlyenhancestransmission inhippocampal neuronsvia postsynaptictyrosinekinasereceptors. ProcNail Acad SCt USA.1995;92:6074'8077. ARCl I GEN PSYCHIATRYN O L 54. JULY1997 Neurotrophic tactors: from molecule to man.TrendsNecrose: 1994;17:182-190. 31. Lindvall 0, KokaiaZ.BengzonJ. ElmerE, Kokaia M. Neurotrophinsandbrain insults.Trends Neurosci. 1994;17:490·496. 32. IhcenenH.Neurotrophins andneuronal plasticl!y. Science.1995;270:593·598. 33. Meyer TE. Habener JF. Cyclicadenosine 3'.5'monophosphate response element-bindinqprotein(CREB) andrelatedtranscnpt ion-activatinqdeoxyribonucleicacid-bindingproteins. EndocrRev.1993:14:269·290. 34. GhoSh A.GreenbergME.Calciumsionaiinginneurons:molecular mechanismsandcellularconsequences. Science. 1995:268:239-247. 35. WalkerWHoFucci L, Habener JF. Expression ofthegeneencodingtr.lOScriptionfactor cyclicadenosine3',S'·monophosphate(cAMP)responseelement-bindingprotein(CREB): regulationby ' 01· li c ll ~ -stimulati nghormone-inducedcAMP signaifino inprimary ratSertori cells.Endocrinology. 1995; 136:3534-3545. 36. WidnellKL,RussellOS. NestlerEJ. Regulationof expresnon of cAMPresponseelement·binding proteinin thelocuscoeruleusinvivoand ina locuscoe ruleus-likecelllineinvitro.ProcNatlAcad SCi US A.1994:91:10947·10951. 37,Widnell Kl . Sell OW, Lanesa,RussellDS,VaidyaVA,MiserendinoMJD. Rubin CR. DumanRS,NestlerEJ.Regulationof CREBexpression: invivoevidencefor a functionalrole in morphineaction in thenucleus accumbens. J PharmicolExpTher. 1996:276:306-315. 38. Sleight IU,CaroloC. Petit

N,ZwingelsteinC. BoursonA.ldentification of5-hydroxytryptamine, receptor bindingsitesin rat hypothalamus:sensitivity to chronic antide pressant treatments. MOlPharmacal. 1995;47:99·103. 39. MenkesDB. Hasenick MM.Wheeler MA, BitenskyMW. Guanosine triphosphate activationof brain adenylate cyClase: enhancementby longtermantidepressant treatment. Science. 1983; 129:65·67. 40.Ozawa H. Basenick MM. Chronicelectroconvulsive treatmentaugments coupling 01the GTPbinding protein Gs tothecatalytic moietyof adenylylcyclaseina manner similartothatseenwith chronican tidepressant drugs.J Neurochem.1991; 56:330-338. 41. Colin SF. ChangHC. Mollner S.PfeufferT. Reed RR. Duman AS.NestlerEJ.Chroniclithiumregulates theexpression0'adenylatecyclaseand Giproteinalphainrat cerebralcortex.Proc NatlACdd Sci USA. 1991:88:10634,10637. 42. NestlerEJ,Terwilliger RZ. DumanRS.Chronicantidepressantadministration alters thesubcellulardistributionof cyclic AMP-dependentproteinkinasein rat frontal cortex. J Neurochem. 1989;53:1644-1647. 43. PerezJ. TIneliiO. Brunella N,Racagni G.cAMPdependent phosphorylation01solubleand crude microtubuletracnons of ratcerebral cortex after prolongeddesmethylimipraminetreatment. Eur J Pharmacal.1989:172:305·316. 44. NibuyaM, Nestler EJ. Duman RS.Chronicantidepressant administration increases theexpressionalcAMPresponseelement-binding protein (CREB)inrathippocampus. J Neurosci. 1996;16: 2365-2372. 45. SchwaningerM, ScheelC. BlumeR, Rosslg L, KnepelW. Inhibition byantidepressant drugs 0' cyclic AMP response element-bindingproteinl cyclicAMPresponseelement-directedgenetranscription, Mol P harmacol.1995;47:1112-1118. __46. RZ, Nestler EJ, Duman RS. Coordinateregulationof firingrate, tyrosinehydroxylase, andthecyclic AMP system in rat locus coeruleus: effects01chronicstress anc: no r epi ne ~~ I : ; :1 f Ci ~pietingagents. J Neutccnem. 1992;58:.11 94-502. 47. La DC.Neurotrophic factors andsynaptic plasticity. Neuron.1995;15:979-981 . 48. Mamounas LA. Blue ME, SiuciakJA,AltarCA. BDNF promotes thesurvivalandsproutmgofserotonergic axons intherat brain.JNeurosci.1995;15:7929·7939. 49. Duman RS, Vaidya VA. Nibuya M, MorinobuS, Rydele k-Filzgerardl. Stress.antidepressant treatments,and neurotrophic factors: molecularand cellular mechanisms.Neuroscientist.1995;1:351360. 50. Azmitia EC, RubensteinVJ,StrataciJA, AiosJC. Whitaker-Azmilia PM.5-HT,.agonistanddexamethasone reversalofpara-chloruamphetamineinducedlossof MAP-2 andsynaptophysinimmun oreactivityinadultratbrain.BrainRes.1995; 677:181-192. 51.

The Impact of Early Adverse Experiences on Brain
Systems Involved in the Pathophysiology of Anxiety
and Affective Disorders
Christine Heim and Charles B. Nemeroff
The relative contribu tion of genetic and environmental
fa ctors to the developm ent of the major psych iatric disor
ders has long been debated . Recently. considerable atten
tion has been given to the observatio ns that adverse
experiences early in life predispose individuals to the
development of affective and anxiety disorders in adult
hood. Corticotropin-releasing factor (CRF) is the central
coordinator of the endocrinologic. autonomic, immuno
logic, and behavioral stress responses. When centrally
admin istered, CRF produces many physiologic and behav
ioral changes reminiscent ofboth acute stress and depres
sion. Moreover, CRF has also been implica ted in the
pathogenesis of a variety of anxiety disorders , mainly
through CRF neurocircuits connecting the amygdala and
the locus ceruleus. Clinical studies have provided convinc
ing evidence for central CRF hypersecretion in depres
sion, and, to a lesser extent , in some anxiety disorders .
Evidence mainly from preclinical studies sugges ts that
stress early in l ife results in persistent centra l CRF
hyperacti vity and increased stress reactivity in adulthood.
Thus, genetic dispos ition coupled with early stress in

critical phases ofdevelopment may result in a pheno type
that is neurobiologicall y vulnerable to stress and may
lower an individual 's threshold for deve loping depression
and anxiety upon further stress exposure . This pathophys
iologic model may provide novel approaches to the pre
vention and treatment ofpsychopathology associated with
stress early in life. Bioi Psychiatry 1999;46:15091522
© 1999 Society of Biologica l Psychiatry
Key Words: Anxiety, depression, deve lopment, stress,
corticotropin-releasing factor Are neuroses exogenous orendogenous illnesses? Are they the inevitable result of aparticular constitution or the product of certaindetrimental (traumatic) experiences in life? (Freud 1895)
From the Department of Psychiatry and Behavioral Sciences.Emory University School of Medicine. Atlanta. Georg ia.
Address reprint requests to Charles B. Nemeroff. Departmentof Psychiatry and Behavioral Sciences. Emory UniversitySchool of Medicine, 1639 Pierce Drive, WMRB. Suite 4000.Atlanta. GA 30322.
Received April 6. 1999; revised August 3, 1999; acceptedAugust 10. 1999.
C' 1999 Society of Biological Psychiatry Introduction F romthe past to present times, the relative eontribution ofdisposition and experience to the pathogenesis of mentaldisorders has been explored in numerous studies. Evidencefrom these studies suggests a strong genetic contributionto the development of the ma jor psychiatric disorders. Inaddit ion, a preeminent role of stressful life events hasbeen documented for several disorders, especially mood andanxiety disorders, but schizophrenia as well. A number ofstudies have shown that the onset of depression is oftenpreceded by stress ful life events, and there is evidencethat concomitant chronic stress enhances the effects ofmajor life events on depression (Kessler 1997). Likewise,stressful life events along with recent minor difficultieshave been identified as predictors of an episode of

depression in a monozygotic female twin study (Kendlcr andMagee 1993). Moreover, genetically vulnerable individualsare more likely to develop major dcpression in response tostress than individuals without genetic loading (Kendler etal 1995). The strong impact of untoward life events inchildhood on the development of mood and anxiety disordersin adulthood has been well documented in recent years . Onestudy compris ing almost 2000 women revealed that womenwith a history of childhood sexual or physical abuseexhibited more symptoms of depression and anxiety and hadmore frequently attempted suicide than women without ahistory of childhood abuse (McCauley ct al 1997). Anotherrecent study reported that women who had been abused inchildhood were four times more likely to develop majordepressio n in adulthood than women who had not been abused(Mullen et al 1996). The magnitude of childhood abuse iscorrelated to the severity of depression in adulthood.Moreover, child abuse is associa ted with the early onsetof depression and a greater likelihood for chronicdepression (Young et al 1997; Zlotnick et al 1995).Childhood abuse also has been shown to predispose for thedevelopment of severa l anxiety disorders in adulthood,including panic disorder and generalized anxiety disorder0006·) 223/99/520.00 PII 50006·3223(99)00224·3
1510 1999;46;1509 -1522 Heim
Figure I. Major CRF-slained cell groups (dots) and tibersystems in the rat brain. cc, corpus callosum ; HIP,hippocampus; SEPT, septal
region; AC, anterior commissure ; BST, bed nucleus of thestria terminalis; SI, substantia innominata; CeA. centralnucleus of the
amygdala; MPO, medial preoptic area ; PVH, paraventricularnucleus of the hypothalamus; ME, median eminence; PP.posterior
pituitary; LHA, lateral hypothalamic area; rnfb, medialforebrain bundle ; MID THAL, midline thalamic nuclei ; st,stria terminal is;
POR, perioculomotor nucleus ; CG, central gray; DR, dorsalraphe; MR, median raphe, LOT, laterodorsal tegmentalnucleus; LC. locus
ceruleus; PB, parabrachial nucleus; MVN , medial vestibularnucleus; DVC, dorsal vagal complex; As. A" noradrenergiccell groups.

(Reproduced with permission from Swanson et al 1983.)
(Portegijs et al 1996; Stein et al 1996). Moreover, post
traumatic stress disorder (PTSD), an anxiety disorder
consisting of symptoms of intrusion, avoidance , and in
creased arousal related to the experience of a traumatic
event, has also been related to childhood adversities;
PTSD may be a direct consequence of the experience of
childhood abuse. Childhood abuse, however, appears to
increase an individual's risk to develop PTSD in response
to extreme stressors in adulthood (Bremner et al 1993;
Browne and Finkelhor 1986; Zaidi and Foy 1993). In additionto childhood physical and sexual abuse,
parental loss and other childhood adversities have also
been related to the development of depression and anxiety
disorders, including PTSD, in adulthood (Kendler et al
1993; Kessler and Magee 1993; McCranie et al 1992).
Several studies have shown that depression and anxiety
disorders are often comorbid in individuals with a history
of childhood adversities , whereas there is littlespecificity
regarding the consequences of different kinds of experi
ences (Mullen et al 1996; Saunders et al 1992). Based onthese observations, we assume that genetic
predisposition coupled with early adverse experiences in
critical phases of development induce a persistent vulner
ability to the effects of stress later in life and, thus,

increase vulnerability of an individual to develop mood
and anxiety disorders. This stress vulnerability was posited
to be mediated by persistent changes in stress-responsiveneurobiological systems involved in both mood and anxietydisorders. Corticotropin-Releasing Factor It is likely thatpersistent changes in central nervous system (CNS)corticotropin-releasing factor (CRF) systems mediate theassociation between stressful experiences and thedevelopment of mood and anxiety disorders. The 4I-aminoacid sequence of CRF was isolated and characterized by Valeet al (1981). Subsequent immunohistochemical andradioimmunoassay mapping suggested a heterogeneousdistribution of CRF neurons throughout the CNS (see Owensand Nemeroff 1991 for review; Figure I). Cell bodies thatcontain CRF are found in high densities in the medialparvocellular region of the hypothalamic paraventrieularnucleus (PVN). These neurons project mainly to the medianeminence, where CRF is released from nerve terminals intothe portal vascular system connecting the hypothalamus andthe pituitary gland (Antoni et al 1983). The parvoeellularCRF neurons of the hypothalamic PVN, thus, form the centralconstituent of the neuroendocrine stress-response system.Outside the hypothalamus , an abundant presence ofCRFcontaining neurons is found in cortical regions. TheseCRF neurons may be involved in the mediation of behavioralstress responses as well as the cognitive appraisal of
Early 1999;46;1509 -1 522
stressful situations. A high density of CRF neurons is also
found in the central nucleus of the amygdala (CeA), a
limbic brain region involved in the process ing of emo
tions. The presence of CRF in the CeA suggests a role for
CRF in the modulation of affective stress responses.
Amygdaloid CRF neurons project directly to the parvo
cellular division of the PVN and to brain stem regions.
There are also indirect projections to these regions passing
to (and through) the bed nucleus of the stria terminalis
(BNST). These projections likely mediate endocrine and

autonomic nervous system function (Gray et al 1989).
Finally, CRF immunoreactivity has been measured in
brain stem nuclei, which comprise the source of the major
noradrenergic and serotonergic projections to the fore
brain. These include the locus ceruleus, the parabrachial
nucleus, and the raphe nuclei. These findings plausibly
infer a role of CRF in modulating monoaminergic neuro
transmitter systems, long believed to be involved in the
pathophysiology of mood and anxiety disorders. An equallywidespread distr ibution of CRF messenger
ribonucleic acid (mRNA) in those brain regions that also
contain CRF has been descr ibed (Beyer et al 1988). Two
subtypes of CRF receptors have further been identified,
both G-protei n-linked receptors (Chalmers et al 1996).
The CRF 1 receptors are found in high density in the
anterior pituitary gland, but arc also found in a variety of
subcortical and cortical brain regions. The CRF 2 receptors
are expresse d mostly in peripheral tissues, e.g., heart,
testes, and in some brain areas , including the septum,
hypothalamus, and the dorsal raphe nuclei. Only recently,
urocortin has been identified, which shows partial se
quence homology with CRF and binds to both CRF
receptors. It has been posited to be the endogenous ligand
for the CRF 2 -receptor subtype. The functiona lsignificance
and relevance of urocortin for neuropsychiatric disorders

is currently unknown (Arborelius et al 1999). Thus, CRF
appears to function not only as a releasing factor, but also
as a neurotransmitter that functions as primary CNS
mediator of the endocrine, autonomic, immune, and be
havioral responses to stress .
CRF and the Stress Responses
Endocrinologically, the stress response is largely charac
terized by activation of the hypothalamicpituitary-adre
nal (HPA) axis. Stress-activated neurotransmitter systems
are believed to stimulate both the synthesis and secretion
of CRF into the hypothalam ohypophysial portal circula
tion. The CRF binds to receptors of the adenohypophysial
cort icotrophs and thereby stimulates the production and
release of the pro-opiomelanocortin (POMC) derivatives
derivatives, adrenocorticotropi n (ACTH) and l3-endor
phin. In tum , ACTH, stimulates the synthesis and secretionof glucocorticoid s from the adrenal cortex. The metabolicand immune-modulating effects of glucocorticoids (cortisolin primates and cort icosterone in most rodents) maintainhomeostatic balance during stress. Circulatingglucocorticoids control the activity of the HPA axis bynegative-feedback inhibition (Dallman et al 1987). Thereare two types of adrenal steroid receptors, themineralocorticoid (MR) and the glucocorticoid receptors(GR). High-affinity MR arc located in the hippocampus andare believed to be involved in the circadian regulation ofthe HPA axis. Low-affinity GR, in contrast, are widelydistributed throughout the CNS and in the pituitary and arethought to regulate HPA axis reactivity to stress inconcert with MR (DeKloet ct al 1991). During the feedbackprocess, glucocorticoids bind to the cytoplasmic receptor,which then undergoes a conforma tional change (activation)and translocates to the nucleus of the cell to alter levelsof gene expression. The ability of these receptors to

dampen HPA-axis responses to stress is critical to theadaptation of an organism. Interestingly, there is apositive feed-forward cascade between glucocorticoids andextrahypothalamic CRF, in which stressinduced increases inglucocorticoid secretion may further enhance CRF neuronalactivity in circuits involved in behaviora l responses tostress . As noted previously, an extensive literature hasprovided evidence that CRF mediates autonomic, immune, andbehaviora l stress responses beyond its role as ahypothalamic hypophysiotropic hormone (see Figure 2).Direct CNS administration of CRF to laboratory animalsresults in many physiologic and behavioral changes thatclose ly parallel signs of stress (Dunn and Berridge 1990).These changes include activation of the autonomic nervoussystem and subsequent elevations of peripheralcatecholamines, increases in heart rate and mean arterialpressure, and changes in gastrointestinal activ ity.Behavioral effec ts of central CRF administration includedeereased reproductive behavior, decrease d food intake andfeeding behavior, disruption of slow-wave sleep, increasedgroomi ng behavior, and increased locomotor activity in afamiliar environment. In nonhuman primates, CRF applicationresults in a behav ioral despair syndrome, characterized byinactivity, frequen t vocalizations, reclining, andhuddling (Kalin 1990). Many of these CRF-induced changesare reminiscent of the symptoms of depression, includingloss of libido and appetite, sleep disturbances, changes inmotor activity, and loss of interest. Centrallyadministered CRF also produces many behavioral changes thatare indicative of anxiety. These include suppression' ofexploratory behavior in a novel environment, potentiationof acoustic startle responses, facilitation of fearconditioning, and enhancement of shock-induced freezing andfighting behavior (Dunn and Berridge 1990;
1512 1999,46:1509 -1 522 Figure 2. Effec ts of centralcorticotropin-releasing factor (CRF). Triangles, increase:inverted triangles. decrease; diamonds, bidirectionalchanges: ACTH, adrenocorticotropin: GI, gastrointestinal;FR, firing rate; SW, slow wave.
Koob et al 1994; Owens and Nemeroff 199 1). The behavioral
effects of CRF can be blocked by central administration of
CRF-receptor antagonists or a CRF antisense oligo-de
oxynucleotide (Dunn and Berridge 1990; Skutella et al 1994).
Findings of an attenuating effect of CRF receptor

antagonists
on stress-induced behavior and findings of increased or
decreased anxiety in transgenic mice overexpressing CRF or
lacking CRF I receptors, respectively, substantiate a rolefor
endogenous CRF in the mediation of anxiety (Arborelius et a1
1999). There is increasing evidence that the CRF neuronal
system connecting the amygdala with the noradrenergic
neurons of the locus cerulcus is involved in the mediation
of the anxiogenic effects of the peptide. The amygdala has
long been implicated in the regulation of emotions (Le
Doux 1994). Stress increases CRF conce ntrations in the
amygdala (Pich et al 1993). Microinj ection of CRF di
rcctly into the amyg dala suppresses cxploratory behavior
in an open-field test and facilitates fear conditioning
(Liang and Lee J988). Corticotrop in-releasing factor
receptor antagonists locally administered into the amyg
dala attenuate shock-induced freezing behavior. Further
more, lesions of the amygdala completely abolish CRF
induced potentiation of startle respo nses as well asconditioned emotional responses, suggesting a role for CRFin the encoding of emotional memories (Hitchcock and Davis1996; LeDoux 1994). Orig inating from the amygdala, CRFneurons project to the locus ceruleus and synapse ontonoradrenergic neurons (van Bockstaele et al 1996). Thelocus ceruleus has also been implicated in the mediation ofanxiety (Schulkin et al 1994). Acute and chronic stressincrease CRF concentrations in the locus eeruleus (Chappellet al 1986). Microinjection of CRF directly into the locusceruleus increases neuronal firing rates and the release ofexc itatory amino acids (Singewa ld et al 1996; Valentinoet al 1983). The presence of CRF in the locus ceruleu s

appears to increase tyrosine hydroxylase activity, therate-limiting step in norepinephrine synthesis (Melia andDuman 199\ ). Along with these modulatory effec ts of CRFon the locus ceruleus, CRF may be involved in theregulation of arousal and vigilance. Microinjections of CRFinto the locus ceruleus and into the neighboringparabrachial nucleus also induce anxiety-like behavior,includin g decreased exploratory behavior in a novelenvironment and increased confl ict behavior (Butler et al1990; Weiss et al 1994). The CRF-induced increases indefensive withd rawal behavior can be reversed by infusionof CRF-r eceptor antagonists BIOL PSYCHIATRY
BIOL PSYCHIATRY 1512
BIOL PSYCHIATRY
Early Life Stress, Anxiety, and Depression 1999;46:1S09 l l22
Table I. Comparison of Neurobiological Correlates of Major
Depression and Anxiety Disorders ACTlI, adrenocorticotropichormone; e RF. corticotropin-releasing (actor;
DEX, dexamethasone; GAD. generalized anxiety disorder; GR,glucocorticoid
receptor; OeD . obsessive-compulsive disorder; PBMC.peripheral blood mononu
clear cells: PD. panic disorder. PTSD, posttraumatic stressdisorder; SP, social
phobia.
into the locus ceruleus (Smagin et al 1996). Benzodiaz
epines have been shown to attenuate several of the
anxiogcnic effects of CRF, and this anxiolytic effect may,
in part, depend on a reduction of CRF concentrations in
the locus ceruleus (Owens et al 1989). Thus, extrahypo
thalamic CRF pathways projecting from the amygdala to
the locus ceruleus may serve as the major neurotr ansmitter

system mediating various anxiety states. By these path
ways, enhanced CRF activity may explain many symp
toms of anxiety disorders, including PTSD, such as im
printed emotional memories, symptoms of avoidance, and
increased vigilance, along with enhanced startle reactivity.
A comparable dysregulation of CNS CRF systems may be
the biological basis for the high symptom overlap and
frequent comorbidit y between depression and anxiety
disorders.
Clinical Findings in Depression
Increased HPA-axis activity in major depression is one of
the most robust findings in the history of biological
psychiatry (see Table I) . Board et al ( 1957) reported
increased adrenocort ical activity in depressed patients,and
this finding has now been replicated in numerous studies
(Holsboer 199 I). Aftcr the intake of a standard dose of
dexamethasone, a synthetic glucocorticoid that suppresses
pituitaryadrenal activity through negative-feedback inhi
bition in healthy subjects, the majority of depressed
patients exhibit nonsuppression of ACTH, l3-endorphin,
and cortisol (Carroll et al 198I). Nonsuppression in the
dexamethasone suppression test (DST) is more prevalent
among patients with severe forms of depression, such as
depression with psychotic features. Consistent withimpaired feedback inhibition, decreasedglucocorticoid-receptor binding and function has been

measured in peripheral mononuclear cells of depressedpatients (see Pariante et al 1995). All of these featuresare state rather than trait dependent and reverse withclinical remission. When administered exogenous CRFintravenously, which stimulates pituitary ACTH release,depressed patients exhibit a reduced ACTH response whencompared with normal control subjects (Gold et al 1984;Holsboer et al 1985). Cortisol responses to CRF indepressed patients are normal, and this suggests anincreased adrenocortical reactivity to endogenouslysecreted ACTH. Indeed, increased cortisol responses indepressed patients after exogenously administered ACTH I _24 , a biologically active fraction of ACTH, has beenreported (Amsterdam et a1 1983). Potential mechanismsunderlying thc blunted ACTH response to CRF in depressedpatients include down-regul ation of pituitary CRFreceptors in response to chronic hypersecretion ofhypothalamic CRF andlor increased feedback inhibition ofthe corticotrophs to the basal hypercortisolemia. Similarto other HPA-axis alterations in depression, the bluntedACTH response to CRF is state dependent and normalizes uponclinical recovery (Amsterdam et al 1988). When pretreatedwith dexamethasone and subsequently administered CRFintravenously, depressed patients exhibit "escape" fromdexameth asone suppression that cannot be observed inhealthy subjects (von Bardeleben and Holsboer 1989). Thisfinding strongly suggests that increased hypothalamic CRFrelease mediates the development of DST nonsuppressionobserved in depressed patients. The combined DST/CRFstimulation test appears to be a highly sensitivediagnostic test for depression, which also detects traitvulnerability, because of its relative persistence afterrecovery and its documented alterations in asymptomaticfirst-degree relatives of depressed patients (Heuser et al1994). In direct support of the hypothesis of CNS CRFhypersecretion in depression is the well-documentedincrease in CRF concentrations in lumbar cerebrospinalfluid (CSF) of depressed patients compared with healthycontrol subjects and patients with other psychiatricdisorders in a series of studies (Banki et al 1987, 1992a;Nemeroff et al 1984; Widerlov et al 1988). Increased CRFconcentrations were also observed in cisternal CSF ofsuicide victims, most of whom presumably suffered fromdepression (Arato et al 1989). Other studies failed to findelevated CRF levels in CSF of patients with majordepression (Kling et al 1991), although these findingsappear to be explained by the inclusion of patients withatypical depression. Indeed, a recent study has providedevidence for decreased rather than increased CSF CRFconcentrations in eucortisolemic depressed patients with at

least one atypical symptom (Geracioti et al 1997). t PTSD tt! PO, ! PTSD t PO Anxiety disorders ! PTSD PO, ! PTSD !GAD, ! OCD,PD, t PTSD,SP PD,PTSD -PO, t PTSD, t OCD Majordepression
Basal cortisol levels
Cortisol suppression by dexamethasone
GR bindin g in PBMC
ACT H response to CRF challenge
Cortisol response to CRF challenge
ACT H response to DEXlCRF challenge
Cerebrospinal fluid CRF levels
Hippocampal volume 1514 1999:46:I509 -1 522 Heim BecauseCSF measures likely reflect overall peptide
release from several brain areas, it is difficult to infer
conclusions on increases in CRF neuronal activity in
specific regions, such as the hypothalamus or the cortex.
Postmortem studies can, however , provide such informa
tion. Thus, increased CRF concentrations, as well as
increased CRF mRNA expression, has been observed in
hypothalamic tissue obtained from depressed patients
compared with control subjects (Raadsheer et al 1994,1995). Moreover, decreased CRF-receptor binding in the
frontal cortex of suicide victims, likely due to chronic CRF
hypersecretion, has been reported (Nemeroff et al 1988)
and confirmed in a second study (Owens and Nemeroff,
unpublished observations). Consistent with findings fromanimal studies (Brady et
al 1992), severa l classes of antidepressant drugs have been

shown to reduce central CRF activity in humans. Antide
pressant treatment and symptom remission appear to be
associated with normalization of central CRF activity.
Twenty-four hours after a regimen of electroconvulsive
therapy, depressed patients exhibited a decrease in CSF
CRF levels (Nemero ff et al 1992). Short-term treatment
with desipramine reduces CSF CRF concentrations in
normal volunteers (Veith et al 1993). Chronic treatment of
depressed patients with fluoxetine results in a decrease in
CSF CRF concentrations that is associa ted with clinical
recovery (De Bellis et al 1993). Patients who remain
depression-free during a 6-month antidepressant treatment
period exhibit reduced CSF CRF concentrations, whereas
patients with persistently elevated CSF CRF concentra
tions did not exhibit remission (Banki et al 1992b). Thus,
central CRF hyperactivity is a state, rather than a trait
marker of depression. Reducti on of CNS CRF activity
appears to be one final cornmon pathway of antidepressant
action. Consistent with the neuroend ocrine findings are the
radiologically demonstrable increases in pituitary and
adrenal gland volumes in depressed patients that have
been reported (Krishnan et a1 1991; Ne meroffet al 1993).
Research from laboratory animal studies provides evi
dence that chronic ACTH stimulation of the adrenal gland
results in increased adrenal gland volumes (Orth et al

1992). In a recent study, chronic intracerebroventricular
infusion of CRF induced adrenal gland hyperplasia (Bu
walda et al 1997). Sustained hypercortisolemia in depres
sion may contribute to the developm ent of hippocampal
atrophy due to the direct neurotoxic effec ts of corticos te
roids. Although we failed to find atrophy of the hippocam
pus in depressed patients in an early study (Axelson et al
1993), a higher-resolution magneti c resonance imaging
study detected significant reductions in hippocampal vol
ume in women with a history of recurrent depression
(Sheline et al 1996). Moreover, there was a correlationbetween the total duration of depressive episodes and theextent of atrophy. Because of the seminal role of thehippocampus in inhibiting paraventricular nucleus CRFactivity, alterations in hippocampal function may initiatea feed-forward cascade, whereby increasing damage to thehippocampus would lead to further disinhibiti on of CRFsecretion, leading to further increases in cortisolsecretion, which in tum further damage the hippocampus.Finally, concordant with the notion that CNS CRF regulatesoutflow pathways of the sympathetic nervous system (videsupra), significant positive correlations between plasmacortisol and epinephrine levels have been reported indepressed patients (Rosenbaum et al 1983; Stokes et al1981). Clinical Findings in Anxiety Disorders Stress earlyin life appears to predispose to the development not onlyof depression, but to several anxiety disorders as well.Findings from basic research provide compelling evidencefor a role for CRF in mediating states of anxiety (videsupra). Clinical studies in patients with several anxietydisorders , including panic disorder, generalized anxietydisorder, and obsess ive -compulsive disorder (OCD), arcless conclusive than the findings reviewed previously indepression (see Table I). Patients with panic disorderexhibit normal basal plasma cortisol concentrations;hypereortisolemia is present only if these patients sufferfrom eomorbid depression (Holsboer et al 1987; Roy-Byrne etal 1986). A standard DST results in normal suppression ofcortisol in patients with either panic disorder or socialphobia (Goldstein et al 1987; Roy-Byrne et al 1985; Tancer

1993). Patients with generalized anxiety disorder andpatients with OCD, however, have been reported to exhibitDST nonsuppression, which is not related to eomorbiddepression (Insel et al 1982; Schweizer et al 1986). As indepressed patients, the more sensitive DST/CRF stimulationtest induces an escape from cortisol suppression inpatients with panic disorder, providing evidence for ahyperactive HPA axis (Schreiber et al 1996). Thus, patientswith panic disorder have been shown to demonstrate ablunted ACTH response in a standard CRF stimulation test(Holsboer et al 1987; Roy-Byrne et al 1986). Becauseblunted ACTH responses were also observed in the presenceof basa l eucortisolemia, these findings support pituitaryCRF-receptor downregulation secondary to hypothalamic CRFhypersecretion as underlying this endocrine abnormality inpanic disorder; however, in a recent report, increased ACTHresponses to CRF were observed in patients with panicdisorder, and treatment with alprazolam, reported todecrease hypothalamic CRF activity (Owens et al 1989),normalized pituitary responsiveness (Curt is et al 1997). A
Early 1999;46:I5091522
possible exp lanation for these discrepant findings may be
differences in the HPA axis in panic disorder, depending
on when, in the longitudinal course of the illness, the
patients are studied. Thus, an initial CRF sensitization may
evolve into CRF receptor down-regulation upon long-term
CRF hypersecretion. Although these findings would sug
gest an involvement of CRF systems in panic disorder.
CSF CRF concentrations are unaltered in these patients
(Jolkkonen et al (993). Patients with OCD, in contrast,
have been reponed to exhibit increased CSF CRF concen
trations which normalize upon clinical recovery (Altemus
et aI 1992, 1994). A considerable number of studies inrecent years have
focused on HPA-axis alterations in patients with PTSD. an

anxiety disorder that also is increased in prevalence by
stress early in life (vide supra). Several studies provide
evidence for abnormally low, rather than high, adrenocor
tical activity in PTSD patients, as evidenced by decreased
urinary cortisol excretion and low cortisol concentrations
in single plasma or saliva samples (sec Yehuda 1997). In
a chronobiological study. Vietnam veterans with PTSD
demonstrated a decreased nadir and an increased peak of
con isol release when compared with healthy normal con
trol subjects and depressed patients (Yehuda et al I996a).
Increased GR binding in peripheral mononuclear cells of
Vietnam veterans with PTSD compared with healthy
control subjec ts and other psychiatric patients has been
repon ed (Yehuda et al 1991. 1993a). Although no alter
ations in feedback sensitivity could be detected in the
standard DST, patients with PTSD were shown to exhibit
an exaggerated suppression of cortisol in response to a low
dose of dexamethasone (Yehuda et al 1993b, 1995).
Moreover, dexamethasone induces a more pronounced
decrease in GR binding in patients with PTSD than in
control subjec ts, poss ibly reflecting increased transloca
tion of the activated GR from the cytoplasm to the nucleus
of the cell. Toge ther, these findings suggest thatdecreased
adrenoconical activity and increased negative-feedback
sensitivity occur in PTSD. This neuroendocrine pattern

has been observed in PTSD patients, even in those with
comorbid depression. Interestingly, patients with PTSDdemonstrate increased
ACTH responses to blockade of endogenous con isol
production with the ~-h yd ro x yl a s e inhibitor,metyrapone
(Yehuda et al 1996b). This finding not only supports the
hypothesis of increased feedback inhibition of the HPA
axis in PTSD. but also implies a pronounced increase in
CRF secretion in these patients. Our group has observed
blunted ACTH responses to CRF in Vietnam veterans with
PTSD; both baseline and CRF-stimulated cortisol concen
trations did not differ from control subjects . One half of
the PTSD patients had comorbid major depression (Sm ith
et al 1989). This finding is concordant with downregulationof adenohypophysial CRF receptors secondary to chronicallyincreased CRF secretion, although enhanced feedbacksensitivity of the pituitary gland may contribute to thisfinding. Indeed, CSF CRF concentrations are increased inVietnam veterans with PTSD, lending suppon to hyperactivityof CRF neuronal systems in this disorder (Bremner et al1997). Thus, whereas depression and PTSD are discordant atperipheral HPA axis loci, both disorders sharehypersecretion of CRF in the CNS. As has been repon ed indepression, hippocampal atrophy has also been observed incombat veterans with PTSD (Bremner et al 1995; Gurvits etal 1996), despite the repon ed hypocortisolism, Thishippocampal atrophy may reflect a preexisting risk factorfor the development of stress-related neuropathology;alternatively, it may be due to toxic effects of highcortisol levels at the time of trauma associated withincreased vulnerability of the hippocampus because ofincreased GR function. Patients with PTSD also demonstrateelevated plasma catecholamine concentrations and behavioralsensitization to the selective " , receptor antagonist,yohimbine, which stimulates the central noradrenergicsystem by blockade of presynaptic feedback (Kosten et al

1987; Southwick et al 1993). This hyperreactivity of thecentral noradrenergic system may be due, at least in pan ,to increased CRF release in the locus ceruleu s. Indices ofCRF hypersecretion have been obtained in patients withcenain anxiety disorders. It would appear that in severalanxiety disorders some form of peripheral adaptation occursin response to increased central CRF activity, resulting innormal or decreased adrenocortical activity. Preclinicaland Clinical Findings in Early Life Stress Given therelationship between severe childhood adversity and thedevelopment of mood and anxiety disorders, for which aneurobiological substrate has been posited, preclinical andclinical studies of the neurobiological effects of earlyadverse experiences would appear to provide the bestopportunity to elucidate the precise pathogenesis (seeTable 2). Among rodent models of early life stress arerepeated brief removals of rat pups from their mothersduring the neonatal period. Whereas the mild stress ofearly handling produces a phenotype that is less sensitiveto stress and, thus, better adapted, the more severe stressof prolonged maternal separation results in heightenedstress vulnerability in adulthood (Plotsky and Meaney1993). Thus, adult rats who were repeatedly separated fromtheir mothers for 180 min per day on postnatal days 214demonstrate increased ACTH and corticosterone responses toa variety of stressors in adulthood (Plotsky and
1516 1999;46:1509 -1 522
Table 2. Summary of Long-Term NeuroendocrineChanges inSelected Models of Early Life Stress
Model Species Timing Neuroendocrine changes
Maternal separation
Variable foraging demand
Childhood abuse Rats 180 min/day pod 2-14 ACTH afterpsycholo gical stress CORTafter psychological stress CRF inME and LC CRFreceptor binding in LC CRF mRNA in ME, CeA,BNST 4 6 hlday pod 2-14 ACTH basal and after stress CORTbasal and after stress CRF in ME and PB PituitaryCRFreceptor binding CRFreceptor binding in NR Nonhumanprimates Separated after birth and peer reared ACTH afterstress CORT after stress No nhuman primates 12 weeks(beginnin g at 17 wee ks of age} CSF e RF CSF CO RT HumansBefore the onset of puberty ACTH after psychosocial stressCORTafter psychosocial stress ACTH after CRF challenge ..Without current major depression. 1>With current major

depression. ACTH, adrenocorticotropic hormone; BNST. bednucleus of the stria rcrminalis: CORT, corticosterone or cortisol; CeA . central nucleus of the amygdala; CRF,
corticotropin-releasing factor; LC, locus coruleus; ME.median eminence; mRNA , CRF messenger ribonucleic acid; NR,nucleus raphe; PB, parabrachial nucleus; pnd,
postnatal day.
Meaney 1993). Maternal separation of 4 hours per day on
postnatal days 2-5 and 6 hours per day on postnatal days
6 -20 also results in increased ACTH concentrations in
adulthood (postnatal day 108), both basally and in re
sponse to stress, although corticosterone responses appear
to be normal (Ladd et al 1996). Interestingly , prolonged
maternal separation over 24 hours at postnatal days 3-4
produces normal ACTH and increased corticosteron e re
sponses to stress at postnatal day 20, whereas prolonged
maternal separation at postnatal day 11 -12 produces
blunted ACTH and normal cortico sterone responses to
stress at postnatal day 20 (Workel et al 1997; van Oers et
al 1998). Although these findings contribute only indi
rectly to our knowledge of the long-term neurobiological
consequenc es of early stress, they suggest that there are
critical time window s for the effects of early stress on
neurobiologic al systems. Moreover , with prolonged ma
ternal separation , adrenocortical responsiveness may dis
sociate from pituitary responsiveness. Enhanced pituitaryresponsivene ss seems to be medi
ated by persistenl changes in hypothalamic CRF neurons ,

because increased CRF concentrations in the median
eminence, along with reduced pituitary CRF receptors (as
well as increased CRF mRNA expression in the hypotha
lamic PVN), have been repeatedly demonstr ated in mater
nally separated rats under resting conditions (Ladd et al
1996; Plotsky and Meaney 1993). Increased CRF mRNA
expression in the PVN after stress exposure has also been
observed in these rats relative to rats that had been reared
under normal animal-facility conditions. Remarkably, the
heightened stress responses at all levels of the HPA axisare reversed by treatment of the maternally separated ratswith the selective serotonin reuptake inhibitor ,paroxetine, as well as with the selective norepinephrinereuptake inhibitor, reboxetine (Plotsky et ai, in press) .Increased sensitivity of the HPA axis seems to be limitedto psychological stress (i.e., air puff startle, restraintstress, or novel environment), and is not observed afterphysical stress (i.e., hemorrhage, cold,nitroprussideinduced hypoten sion; Ladd et ai, in press).These findings suggest the involvem ent of corticolimbicpathways in the mediation of the heightened stress response. Interesting in this regard are findings of changes inextrahypothalamic CRF systems as a result of maternalseparation in rats. Indeed , increased CRF concentrationswere also measured in the parabrachial nucleus aftermaternal separation (Ladd et al 1996). Moreover , increasedCRF mRNA expression was observed in the CeA and in theBNST, through which polysynaptic CRF neurons from theamygdala project to the hypothalamus (Plotsky et aI, inpress). In addition, increased CRF concentrations, alongwith increased CRFreceptor binding , were observed in thelocus ceruleus (Plotsky et ai, in press) , which receivesprojections from the amygdala and sends projections to thehypothalamu s. Both of these pathways may be involved inthe modulation of the HPA-axis response to psychologic alstress. Accordingly, increased norepinephrine levels in thePVN of the hypothalamus were measured in maternallyseparated rats after exposure to restraint stress (Liu etaI, in press). In the study by Ladd et al (1996), increasedCRF-receptor binding was observed in the raphe nuclei (the

major origin of forebrain serotonergic pathways) , whichhas been
Early Life Stress, Anxiety,and Depression L 1999:46:15091522
implicated in the pathophysiology of depression and also
PTSD (Con nor and Davidson 1998; Owens and Nemeroff
1994). Concordant with increased extrahypothalamic CRF ac
tivity, matem ally separated rats exhibit marked behavioral
abnormalities. These include anhedonia, i.e., reduced con
sumption of sweetened solution and changes in food
intake. Moreover, these rats exhibit increased anxiety-like
behavior, such as suppressed exploration of a novel
environment, increased freezing in an open field, and
increased startle responses (Caldj i et ai, in press). Manyof
these behavioral changes resemble symptoms of depres
sion and anxiety disorders. It appears that both endocrine
and behavioral long-term consequences of maternal sepa
ration in rats are mediated through changes in maternal
behavior, because cross-fostering of handled and mater
nally separated rats results in reversed changes (Huot et al
1997; Ladd et al, in press). The effec ts of early lifestress have also been studied in
nonhuman primates. Similar to findings in rodents, young
adult nonhuman primates who have been maternally de
prived and reared with peers during infancy exhibit in
creased pituitary -adrenal activation as well as increased
levels of distress vocalizations and pass ive behavior in

response to separation from peers as compared with
primates who have been reared by their mothers for the
first 6 months of life (Suomi 1991). Another paradigm,
which more closely resembles stress experiences of human
infants, consists of exposure of infant nonhum an primates
to diffe rential rearing conditions, in which the mothersare
confronted with different foraging demands. Mothers with
constantly low foraging demand (LVD) can obtain food
without any effort, whereas mothers with constantly high
foraging demand (HVD) have to complete a daily task to
obtain their food. In a variab le foraging demand (VFD)
condition, mothers are exposed to unpredictable condi
tions with respect to food access, resulting in a diminished
perception of security in terms of maternal attachment in
the infants (Rosenblum and Paully 1984). Adult (24
years) bonnet macaques that have been exposed to VFD
over a 12-week period during infancy, beginning at
approx imately 17 weeks of age, demonstrate significan tly
elevated CSF CRF concentrations when compared with
primates reared under LVD or HVD conditions. Cerebro
spinal fluid CRF concent rations did not corre late with CSF
cortisol conce ntrations. Indeed, CSF cortisol concentra
tions were actually lower in the animals exposed to the
variable foraging demand (Coplan et al 1996). The disso
ciation between increased central CRF activity and de
creased adrenal activity parallels our findings in PTSD.
Moreover, VFD-reared nonhuman primates exhibit stable
traits of anxiety along with exagge rated anxiety-like re
sponses to the administration of the selective "',-receptorantagonist , yohimbine (Rosenblum and Paully 1984;Rosenblum et al 1994). Whereas a number of studies havecharacterized the behavioral and neurobiologicalconsequences of early life stress in rodents and nonhumanprimates, only a small number of studies have focused onhuman subjects. Sexually abused girls, many of whomsuffered from dysthymia, exhibit blunted ACTH responses toCRF (DeBellis et al 1994). In another study, abusedchildren who still lived under conditions of ongoing stressand suffered from comorbid PTSD and depression showedincreased ACTH responses to CRF , whereas cortisolresponses were normal (Kaufma n et al 1997), parallelingfindings in rats exposed to prolonged maternal separation(Ladd et al 1996). Our group has obtained preliminaryfindings on stress responsiveness in adult survivors ofchildhood abuse with and without major depression. Uponexposure to standardized psychosocial laboratory stress,women with a history of childhood abuse, with and withoutcurrent major depression, demonstrated markedly increasedACTH responses as compared with healthy control subjectswithout a history of early life stress (Heim et al 1998a).The mean ACTH response was highest in women with a historyof childhood abuse and current major depression . Moreover,women with a history of childhood abuse and current majordepression also showed significantly increased cortisolresponses to psychosocial stress as compared with controlsubjects and abused women without depression. Net ACTH andcortisol responses were positively correlated with thedegree of childhood abuse and the severity of depressionand PTSD. Women with a history of childh ood abuse, withand without depress ion, also demonstrated higher and morepersistent heart rate responses to psychosocial stressrelative to control subjects. Women with a history ofchildhood abuse and current depression suffered more oftenfrom comorb id PTSD and had becn exposed to more recentlife stress when compared with women with a history ofchildhood abuse without depression (Heim et al 1998a).Corticotropin-releasing factor stimulation tests were alsoobtained in these women. Interestingly, women with ahistory of chi ldhood abuse without current majordepression exhibi ted increased ACTE responses along with

normal to decreased cortisol responses (C. Heim et ai,unpublished data, 1999). This finding parallels findings inmaternally deprived rats and abused children (Kaufma n etal 1997; Ladd et al 1996). In contrast, women with ahistory of childhood abuse with comorb id major depressionexhibited blunted ACTH responses , likely due to chronicoverexposure of the pituitary to CRF . Together, thesefindings suggest that there may be an initial sensitizationof the stress hormone system , representing a biologicalvulnerabil ity for the Genetic Vulnerability
1518 1999;46:1509 1522 Development Early AdverseExperience. and • Vulnerable Phenotype: CRFt Figure 3. Therelationship between early life stress, sensitization ofcort icotropin-releasing factor (CRF) neuronal systems, andIhe development of depression and anxiety. HPA,hypothalamic-pituitary-adrenal; ANS, autonomic nervoussystem. Biological Changes HPA Axis and ANS ActivationBehavioral Change. Depression
development of depression and anxiety disorders. This
vulnerability may result in relatively high CRF secretion
whenever these women are stressed, which may then lead
to pituitary receptor down-regulation. The increased
ACTH response to laboratory stress in depressed women
with a history of childhood abuse may reflect the involve
ment of corticolimbic pathways as well as enhanced PVN
CRF activity, overriding the receptor down-regulation.
Interestingly, there are several studies suggesting hip
pocampal atrophy in adult survivors of childhood abuse
(Bremner et al 1997; Stein et al 1997), and an impaired
hippocampus may contribute to the development of an
enhanced HPA-axis response to stress as a consequence of
childhood abuse.
Summary and Future Directions

An interaction of genetic and environmental factors has
long been postulated to determine an individual's vulner
ability to developing affective and anxiety disorders . A
strong relationship between early adverse experiences and
the development of these disorders in adulthood appears
well documented. Both endocrine and behavioral re
sponses to stress are predominantly controlled by CNS
CRF systems. Corticotropin-releasing factor neurons in
limbic and brain stem regions appear to mediate, at least in
part, anxiety. There is evidence for increased CRF activity
in both patients with depression and patients with anxiety
disorders . Preclinical studies suggest that stress during
development may result in persistently increased activity
of one or more CNS CRF systems and a sensitization of
the HPA axis to stress. Our group has suggest ed that stress
early in life results in a persistent sensitization of these
CRF circuits to even mild stress in adulthood, forming the
basis for the development of mood and anxiety disorders(see Figure 3). This hypothesis is supported by our recentclinical study of adult survivors of childhood abuse. Thesefindings have multiple implications for future research.First, genetic factors and the effects of early stressexperiences on neurobiological systems should now becoupled in animal models or human twin studies. Second,central mechanisms underlying increased stress reactivityin human survivors of childhood adversities should beevaluated, particularly with respect to CRFneuronal systemsand functional properties of the amygdala and thehippocampus . Third , the reversibility of this stressvulnerability should be investigated . Potential candidatesfor facilitating this reversal are antidepressants, whichhave been shown to reverse neuroendocrine consequences ofmaternal separation in rats. It would also be of interest

to explore whether various forms of psychotherapy mayprevent or reverse neurobiological consequences of earlylife stress .lfCRF hyperactivity remains, blockade ofcentral CRF effects using select ive CRF I-receptorantagonists may provide an important tool for theprevention and treatment of depression and anxietydisorders. Finally, preclinical and clinical studies havefound that severe early trauma may result in decreasedadrenocortical activity. This abnormality has been observedin several anxiety disorders, even in the case ofcomorbidity with depression . One may thus assume thatthere is a specific traumatic type of mixed anxiety anddepression, which is associated with low adrenocorticalactivity, but central CRF hyperactivity. Similar patternshave been reported for patients with trauma-related bodilydisorders (Heim et al 1998b), and thus reducedpituitaryadrenal activity may have important implicationsfor the physical adaptation of the organism to stress(McEwen 1998). Future studies focusing on these issues mayhave important potential in increasing our knowledge of thepathogenesis of stressDevelopment Development DevelopmentDepression Depression Depression Depression
Early r 1999;46:1509 1522
related di sord er s and may pro vid e novel ap proaches inthe
preventio n a nd treatmen t of suc h di sord er s.
Theauthorsarcsupported by NIHMH·42088, NIH MH·50113, and DFG
He2561t2·1. This work was presented at the scientificsatellite conference, "The
Role of Biological and Psychological Factors on EarlyDevelopmentand
Their Impact on Adult Life," that preceded the AnxietyDisorders
Association of America (ADAA) annual meeting, San Diego,March
1999, The conference was jointly sponsored by the ADAA andthe
National Institute of Mental Health through an unrestrictededucational

grant provided by Wyeth-Ayerst Laboratories.
Altemus M, Pigott T, Kalogeras KT, Demitrack M, Dubbert B,Murphy DL, et al (1992) : Abnormali ties in the regulationof vaspressin and corticotropin-releas ing factor secretionin obses sive-co mpulsive disorder. Arch Gen Psychiatry 49:920.
Altemus M, Swedo SE, Leonard HL, Richter D, Rubinow DR,Potter WZ, et al ( 1994): Changes in cerebrospinal fluidneurochemistry during treatment of obsessive-co mpulsivedisorder with clomipramine. Arch Gen Psychiatry 51:794803.
Amsterdam JD, Winokur A, Abelman E, Lucki I, Rickels K (1983): Cosyntropin (ACTH alpha 1-24) stimulation test indepressed patients and healthy subjects. Am J Psych iatry140:907908.
Amsterdam !D , Maislin G, Winoku A, Berwish N, Kling M,Gold P (1988): The oCRH test before and after clinicalrecovery from depression. J Affect Disord 14:213-222.
Antoni FA, Palkovits T, Makara GB, Linton EA, Lowry PJ,Kiss JZ ( 1983) : Immunoreactive corticotropin-releasinghorm one in the hypothalamoinfundibular tract.Neuroendocrinology 36:415-423.
Arato M, Banki CM, Bisette G, Nemeroff CB (1989): ElevatedCSF CRF in suicide victims. Bioi Psychiatry 25:355-359.
Arborelius L, Owens MJ, Plotsky PM, Nemeroff CB (1999): Therole of cortico tropin-releasing factor in depression andanxiety disorders. J Endocrino/ 160:112.
Axelson DA, Doraiswamy MP, McDonald WM, Boyko OB, TupierLA, Patterson LJ, et al ( 1993): Hypercortisolem ia andhippocampal change s in depress ion. Psychiatry Res47:163173.
Banki CM, Bissette G, Arato M, O' Connor L, Nemeroff CB (1987): Cerebrospinal fluid corticotropin-releasingfactorlike immunoreactivity in depression and schizophrenia. Am J Psychiatry 144:873877.
Banki CM, Karmaksi L, Bissette G, Nemeroff CB ( 1992a):Cerebrospinal fluid neuropeptides in mood disorder anddementia . J Affect Disord 25:39-46.
Banki CM, Karmaksi L, Bissette G, NemeroffCB (1992b): CSFcorticotropin-releas ing hormone and somatostatin in major

depres sion: respons e to antidepressant treatment andrelapse . Eur Neuropharm acoI 2:107-1 13.
Beyer HS. Matta SG, Sharp BM (1988): Regulation of themessenger ribonucleic acid for cortico tropin-releasi ngfactor in the paraventricular nucleus and other brain sitesof the rat. Endocrinology 123:21172123. Board F, Wadeson R,Persky H ( 1957): Depressive affect and endocrine function:Blood levels of adrenal cortex and thyroid horm ones,inpatients suffering from depress ive reactions. Arch NeurolPsychiatry 78:6 12-620. Brady LS, Gold P, Herkenham M, LynnA, Whitfield HJ (1992): The antidepressants fluoxetine,idazoxan, and phenelzine alter cortico tropin-releas inghorm one and tyrosine hydroxylase mRNA levels in rat brain:Therapeutic inplications. Brain Res 572:11 7-125. BremnerJD, Southwick SM, Johnson DR, Yehuda R, Charney DS (1993):Childhood physical abuse and combat-related posttraumaticstress disorder in Vie tnam veterans. Am J Psychia try150:235239. Bremner !D , Randall P, Scott TM, Bronen RA,Seibyl JP, Southwick SM, et al ( 1995): Magnetic resonanceimagingbased measurement of hippocamp al vo lume inpatients with com bat-related posttraumatic stress disorder. Am J Psychiatry 152:973981. Bremner JD, Licino J, DarnellA, Krystal JH, Owens MJ, Southwick SM, et al ( 1997):Elevated CSF corticotropinreleasing factor conc entrationsin PTSD . Am J Psychiatry 154:624-629. Browne A, FinkelhorD (1986): Impact of childhood sexual abuse. Psychol Bull99:6677. Butler PD, Weiss JM, Stout !C, Nemeroff CB (1990):Corticotropin-releas ing factor produces fear-enhancing andbehavioral activating effects followi ng infusion into thelocus coeruleus. J Neurosci 10:176 -1 83. Buwalda B, deBoer SF, van Kalkeren AA, Koolhaas JM (1997): Physiologicaland behavioral effects of of chronic intracerebroventricular infusio n o f corticotropinreleasing factor inthe rat. Psychoneuroendocrino/ogy 22:297-309. Caldji C,Francis D, Sharma S, Plotsky PM. Meaney MJ (in press): Theeffec ts of early rearing environment on the development ofGABA A and central benzodiazepine receptor levels andnovelty-induced fearfulness in the rat. J Neurosci .Carroll BJ, Feinberg M, Greden JF, Tarika J, Albala AA,Haskett RF, et al ( 1981): A specific laboratory test forthe diagnosis of melancholia. Arch Gen Psychia try 38:15-22. Chalmers DT, Lovenberg TW, Grigoriadis DE, Behan DP,Dc Souza EB ( 1996): Corticotropin-releasing factorreceptors: From molecualr biology to drug design. TrendsPharmacol Sci 17:166 -1 72. Chappell PB, Smith MA, KiltsCD, Bissette G, Ritchie JC, Andersen C, et al (1986):Alterati ons in corticotropin-releasing factor-likeimmunoreactivity in disc rete brain regions after acute andchronic stress. J Neurosci 6:290829 14. Connor KM, Davidson

JRT (1998) : The role of serotonin in posttraumatic stressdisorder. e NS Spectrums 3:43-5 1. Coplan Jl), Andrews MW,Rosenblum LA, Owens MJ, Friedman S, Gorman 1M, et al(1996): Persis tent elevations of cerebrospinal flu idconcentrations of corticotropin-releasing factor in adultnonhuman primates exposed to early life stressors:Implications for the pathophysiology of mood and anxietydisorders. Proc Natl Acad Sci U S A 93:1619-1 623. CurtisGC, Abelson JL, Gold PW ( 1997): Adrenocorticotropic andhorm one and cortisol responses to corticotropin-releas ing
1520 1999:46:1509 -1 522 and hormone: Changes in pan icdisorder and effects of alprazolam treatment. BioiPsychiatry 4 1:76 -85 .
Dallman MF, Akana S, Cascio CS , Darlington DN, Jacobson L,Levi n N, et al ( 1987): Regulat ion of ACTH secretion:Variat ions on a theme of B. Rec Prog Horm Res 43 :113-173.
DeBe llis MD , Go ld P, Geracioti TD , Listwak SJ, Kling MA( 1993) : Associat ion of fluoxet ine treatment withreductions in CSF concentrations of corticotropin-releasinghormo ne and arginine vasopression in patients withmajordepression. AmJ Psychiatry 150:656657.
DeBell is MD, Chrousos GP, Dorn LD, Burke L, Helmers K,Kling MA , et al (1994): Hyp othalamic pituitary adrena ldysregulation in sex ually abused girls. J Clin EndocrinolMetab 78:249255.
DeK loet ER, Vreugdenhil E, Oi tzl MS, Joe ls M ( 199 1):Brain corticosteroid receptor balance in health anddisease. Endocr Rev 19:269 30 I.
Dunn AJ, Berrid ge CW ( 1990) : Phys iological andbehavioral responses to co rticot ropin-releas ing factoradministration: Is CRF a mediatorof anxiety or stressresponses? Brain Res Rev 15:71-1 00.
Freud S (1895): General theory on neu roses. In: Freud A,editor . The Standard Edition of the Complete PsychologicalWorks of Sigmund Freud. London : Hogarth .
Geracioti TD, Loosen PT, Orth DN (1997): Low cerebrospina lFluid corticotropin-releas ing hormone concentrations ineuco rtisolemic depression . Bioi Psyc hiatry 42:166 -1 74.
Go ld PW, Chrousos G, Kellner C, Post R, Roy A, Augerin osP, et al ( 1984): Psychiatric implications of basic and

clin ical studies with cortico tropin-releasing factor. AmJ Psychiatry 141:6 19-627 .
Goldstein S, Halbreich U, Asnis G, Endicott J, Al vir J(1987) : The hypothalam ic-p ituit ary-adre nal system inpanic disorder. Am J Psychiatry 144:13201323.
Gray TS, Ca rney M E, Magnuson DJ (1989): Direct projections from the central amyg da loid nucleu s to thehypothalamic paraventricular nucleus: Possible role instress-induced adrenocort icotropin release .Neuroendocrinology 50:433446.
Gurvits TG , Shenton MR , Hokama H, Ohta H, Lasko NB,Gilberson MW , et al ( 1996) : Magnetic resonan ce imagingstudy of hippocampal vo lume in chronic, combat-re latedposttraumatic stress disorder. Bioi Psychiatry 40 :193-199.
Heim C, Graham YP, Heit SC, Bon sall R, Mill er AH,Nemeroff CB ( 1998a) : Increased sensi tivity of thehypotha lamic-pituitary-adrenal axis to psychosocial stressin adult survivors of childhood abuse. Soc Neurosci Abst28:20 1.12.
Heim C, Ehlert U, Hankcr JP, He llhamm er DH ( 1998 b):Abuserelated posttraumatic stress disorder and alterationsof the hypothalamic-pituitary-adrenal axis in women withchronic pelvic pain. Psychosom Med 60:309 -3 18.
Heuser I, Yassouri dis A, Holsboer F (1994): The combineddexamethasone/CR F test: A refined laboratory test forpsychiatri c disorders. J Psychiatr Res 28:341-35 6.
Hitchcock J, Dav is M ( 1996) : Lesio ns of the amyg dala,but not of the cerebellum bloc k co nditioned fear measuredwith the potentiated startle paradigm. Behav Neurosci100:11-22 .
Holsboer F ( 199 \) : The hypothalamic-pituitary-adrenocortical system. In: Paykel ES, ed itor. Handbookof Affec tive Disorders . Livingston: Churchill, 267-287.Holsboer F, Gerken A, Stalla GK, Mueller OA (1985): ACTH,cortisol and corticosterone output after ovinecorticotropinreleasing factor challenge during depressionand after recovery . Bioi Psychiatry 20:276-286. HolsboerF, von Bardeleben U, Buller R, Heuser I, Steiger A ( 1987):Stimulation response to co rticotropin-releas ing hormone(CRH) in patients with depression , alcoho lism and panicdisorder . Horm Metab Res 16:80 88. Huot RL, Smi th M,

Plotsky PM (1997, July): Alterations of maternal-infantinteraction as a result of maternal separation in LongEvans rats and its behavioral and neuroendocrine consequences. Presented at the 28t h Cong ress o f theInternational Society for Psychoneuroendocrinology, SanFrancisco . Insel TR, Kalin NH, Guttmac her LB, Cohen RM,Murph y DL (1982): The dex ame thasone suppress ion test inpatients with primary obsessive compulsive disorder.Psychiatry Res 6:153-160. Jol kkonen J. Lepo la U, Bissette G, Nemeroff CB, Riekki nen ( 1993) : CS Fcorticotropin-reicasing factor is not affected in panic disorde r. Bioi Psychiatry 33: 136 -1 38. Kal in NH (1990):Behavioral and cnd ocrine studies of corticotropin-releasing hormone in primates. In: De Souza EB,Nemeroff CB, editors. Corticotropin-Releasing Factor: Bandand Clinical Studies of a Neuropeptide, Boca Raton, FL: CRCPress, 275 -289. Kaufman J, Birmaher B, Perel J, Dahl RE,Moreci P, Nelson B, et a l (199 7): Th e corticotropin-releasi ng hormo ne challenge in depressed abused,depre ssed nonabused , and normal co ntrol children. BioiPsychiatry 42:669-679. Kendler KS, Kessler RC, Nea le MC,Heath AC, Eaves LJ (1993) : The prediction of majordepression in women: Toward an integrated model. Am JPsychiatry 150:11391148. Kendler KS, Kessler RC, WaltersEE, MacLean C, Nea lc MC, Hea th AC, et al ( 1995) :Stressfu l life events, genetic liability and onset of anepisode of major depression. Am J Psychiatry 152:833842 .Kessler RC ( 1997) : The effec ts o f stressful life events on depression . Annl/ Rev Psychol48:191214. Kessler RC,Mage e WJ (1993): Childhood adve rsit ies and adultdepression: Basic patterns of association in a US nationalsurvey. Psychol Med 23:679-690. Kling MA, Roy A, Doran AR,Calabrese JR , Rubinow DR, Whitfield HJ, et a l (199 1):Cerebrospinal fluid immun oreactive corticotropin-releasinghormone and adrenocorticotropin secretion in Cushing'sdisease and major depression: Potentia l cl inical implications. J Clin Endocrinol Metab 7 1:26027 1. Koob GF, Heinrichs SC, Mc nzaghi F, Pich EM, Britton KT (1994): Corticotropin-releas ing factor, stress and behavior . SeminNeurosci 6:22 1-229 . Kosten TR , Mason JW, Giller EL,Harkn ess L ( 1987): Sustained urinary norepinephrine andepinephrine elevation in posttraumatic stress disorder.Psychoneuroen docrlnology 12:1320. Kr ishnan RR, DoraiswamyPM, Lurie SM , Fig iel GS , Husain MM , Boyko DB, et al (199 1): Pituitary size in depression, J Clin EndocrinolMetab 72:256-259 . Ladd CO, Owens MJ, Nemero ff CB ( 1996): Persistent chang es in corticotropin-releasing factorneuronal systems induced by maternal dep rivation.Endocrinology 137:1212-1 218.

Early 1999:46:l l0 9l l 22
Ladd CO , Huot RL, Thrivikrama n KV, Ne meroff CB, Mean eyMJ, Plotsky PM (in press): Longterm behavioral andneuroendocrine adaptations to adverse early experience. In:Mayer E, Saper C, editors. Progr ess in Brain Research: TheBiological Basis f or Mind Body Interactions . Amsterdam:Elsevier.
LeDoux 1£ (1994): Th e amygdala: Contributions to fear andstress. Semin Neurosci 6:23 1-23 7.
Liang KC, Lee EHY ( 1988): Intra-amygdala injections ofcorticotropin-releasing factor facilitate inhibitoryavoidance learning and redu ce ex ploratory behavior inrats. Psychopharmacology (Berl) 96:232-236.
Liu 0 , Ca ldj i C, Sharma S, Plotsky PM, Meaney MJ (inpress): Influence of neonatal rearing condition onstress-induced hypothalamic-pituitary-adrenal responses andnorepinephrine release in the hypothalamic paraventricu larnucleus. J Neurosci.
McCauley J, Kern DE, Kolodner K, Dill L, Schroeder AF, DeChant, et al ( 1997): Clin ical character istics of womenwith a history of childhoo d abuse. lAMA 277:1362-1 368.
McCranie EW, Hyer LA, Boudewy ns PA , Woods MG (1992) :Negative parenting behavior, combat exposure and PTSDsymptom severity: Test of a person-eve nt interactionmodel. 1 Nerv Ment Dis 180:43 1438.
McEwen BS ( 1998): Pro tective and damaging effe cts ofstress med iators . N Engl 1 Med 338: 171179.
Melia KR, Duman RS ( 1991): Involvement of cort icotropinreleasing factor in chronic stress regulation of the brainnoradrcnergic system. Proc Noll Acad Sci U S A 88:83828386.
Mullen PE, Martin JL, Ande rson JC, Romans SE , Herb isonGP ( 1996): The long-term impact of the physical,emotional, and sexual abu se of children: A co mmunitystudy . Child Ab use Negl 20:7-2 l.
Nemeroff CB , Wider lov E, Bisette G, Walleu s H, Karlss onL, Eklund K, et al ( 1984): Elevated conce ntrations of CSFcorticotropin releasing factor like immunoreactivity indepressed patients. Scien ce 226 :1342-1 344.

Ne meroff CB, Owe ns MJ , Bisette G, Ando m AC, Stanley M(1988): Reduced co rticotropin-re leasi ng factor (CRF)bindin g sites in the frontal cortex of suicide victims.Arch Gen Psy chiat ry 45:577579 .
Nemeroff CB, Bissette G, Aki l H, Fink M ( 1992):Neuropeptide concentrations in the cerebrospinal fluid ofdepressed patients treated with e lectroconvu lsivetherapy. Br 1 Psychiatry 158: 59 63.
Neme roff CB, Kris hnan RR, Reed 0 , Leder R, Beam C, Dunnick NR (1993): Adrena l gland en largeme nt in major depression. Arch Gen Psychiat ry 49 :384 -387 .
Orth ON, Kovacs WJ, deBold CR ( 1992): The ad rena l cortex . In: Wilson 10, Foster OW, editors . Williams rex/boo k ofEndocrino logy . Philade lphia: Saunde rs, 489619.
Owe ns MJ, Ne me rof f CB ( 1991): Physiology and pharmacology of corti co tropin-releasing facto r. Pharmacol Rev43:425473.
Owe ns MJ , Ne meroff CB ( 1994): Role of serotonin in thepathophysio logy o f depr ession: Focus on the serotonintra nsporter. Clin Chem 40 :288 -295.
Owen s MJ, Bissette G, Nemero ff CB (1989): Acute effe ctsof alprazolam on the concentrations of corticotropin-releasing factor in the rat brain. Synapse 4:196202. Pariante CM, Nemeroff CB, Miller AH (1995):Glucocorticoid re ceptors in depr ession . lsr 1 Med Sci31:705-712. Pich EM, Koob OF, Sa ttler SC, Menzag hi F,Heilig M, Heinr ichs SC, et a l (1993): Stress-inducedrelease of corticotropinreleasing factor in the maygdalameasured by in vivo microdialysis. Neuro sci Abstr 18:535.Plot sky PM , Meaney MJ ( 1993): Early, postnatalexperience a lters hypothalam ic cort icotropi n-releasingfactor (CRF) mRNA , med ian eminence CRF content andstress-induced release in adult rats. Mol Brain Res18:195200. Plotsky PM , Thr ivikr aman KV, Caldj i C ,Sharma S, Meaney MJ (in press): The effects of neonatalrearing environment on CRF mRNA and CRF rece ptor levels inadult rat brain . J Neurosci , Portegij s PJM , Jeuken FMH,van der Horst FG , Kraan HF, Knottnerus JA ( 1996): Atroubl ed youth: Relations with somatization, depressionand anxiety in adulthood. Fam Pract 13:1-1 1. Raad sheer Fe, Hoogendijk WJ, Stam FC, Tilders FJ, Swaa b OF ( 1994):Increased numbers of corticotro pin-re leasing hormoneexpressing neurons in the hypothalamic paraventr icularnucleus of dep ressed patients. Neuroendo crinology 60:436

444. Raa dshee r FC, van Heer ikhuize JJ, Luca sse n PJ, Tilders FJ, Swaab OF ( 1995): Corticotropin-re leasinghormone mRN A levels in the paraventricular nucleus ofpatients with Alzheimer' s disease and depression. Am 1Psychia try 152: 13721376. Rosenba um AH, Maru ta T,Schatzberg AF, Ors ulak PJ, Jiang NS , Cole JO, et al (1983): Towa rd a bioc hemical c lassifi cation o fdepressive diso rder s, VII : Urinary free cort isol andurinary MHPG in dep ression . Am 1 Psychia try 140:314 318.Rosenblum SA, Paully GS (1984): The effects of vary ingenvironmental demands on maternal and infant behavior.Child Dev 55:305314. Rosenb lum LA, Cop lan 10, Friedman S,Gonnan JM, Andre ws MW (1994): Adverse early experiencesaffect noradrenergic and sero tonergic functioning in adultprimates. Bioi Psychiatry 35:221227 . Roy-Byrne PP, Biere rLM, Uhde TW ( 1985): The dexam ethasone suppression test inpanic disorder: Comparison with norma l co ntrol. Bio IPsychiatry 20:12371240. Roy-Byrne PP, Uhde TW , Post RM, Gallucci W, Chrousos GP, Go ld PW ( 1986): Thecorticotropin-releas ing hormone stimulation test in patients with panic di sorder. Am 1 Psy chiat ry 143:896899.Saunders BE, Vill oponteaux LA, Lipov sky JA (1992) : Childsexual assault as a risk factor for mental disorders amongwomen: A community survey. J lnterpers Violence 7:189204 .Sch reiber W, Lauer CJ, Krumrey K, Holsboer F, Kr ieg JC(1996): Dysregul at ion of the hypo thalamic-pituitary -adrenal sys tem in panic di sorder . Neuropsychop harmacology 15:715. Schul kin J, McEwen BS , Gold PW (1994) :Allostas is, the amyg dala and anticipatory angst. Neurosci Biobeh Rev 18: 112.
1522 1999;46:1509-1 522 Heim
Sch weizer EE, Swen son CM, Winokur A, Rickels K, Mai slinG (1986); The dexamethasone suppression test in generalizedanxiety disorder. Br J Psychiatry 149:320 -322.
Sheline YI, Wang PW , Gado MH, Csemansky JG, Vanni er MW(1996) ; Hippocampal atroph y in recurrent majordepression. Proc Natl Acad Sci US A 93:39 08 -3913.
Singewald N, Zhou GY, Chen F, Phil ippu A (1996):Corticotropin -releasing factor modulates basal andstress-induced excitatory amino acid release in the locuscoeruleus of conscious rats. Neurosci Lett 204 :45-48.
Skut ella T, Montkowski A, Stohr T , Probst JC, Landgraf R,Holsboer F, et a l (1994) : Cort icotropin-releasing hormone (CRH) antisense oligodeoxynucl eotid e treatment attenuates social-defeat indu ced anxiety in rats. Cell Mol Ne

urobiol 14:579 -588.
Smagin GN, Harri s RBS, Ryan DH (1996): Corticotropinreleasing factor antagonist infused into the locuscoeruleus attenuates immobili zation stress-induceddefensive withdrawal in rats . Neurosci Lett 220 :167-1 70.
Sm ith MA , Dav idson MA , Ritchie JC, Kudle r H, Lipper S,Chappell P, et al (1989): The corticotropin-releasing hormone test in patients with posttrauma tic stress disorder.Bioi Psychiatry 26 :349 -355.
South wick SM , Krystal JH, John son DR , Nag y LM, NicolauA, Heninger GR , et a l (1993) : Abnormal noradrenerg icfunction in posttraumatic stress disorder. Arc h GenPsychiatry 50 : 266 -274.
Ste in MB , Walker JR, Anderson G, Hazen AL, Ross CA,Eldridge G, et al (1996 ): Childhood physical and sexualabuse in patients with anxiety disorders in a co mmunitysample. Am J Psychiatry 153:275277 .
Stein MB , Koverola C. Hanna C, Torchi a MG , McClarty B(199 7): Hippoc amp al volume in women victimized bychildhood sexual abuse. Psy chol Med 27:951-959.
Stokes PE, Frazer A, Casper R (1981 ): Unexpectedneuroendocri ne transmi tter relationships. Psy chopharmacol Bull 17:7275.
Suomi SJ (1991) : Early stress and adult emotional reactivity in rhesu s monk eys. Ciba Found Sy mp 156:171-183 .
Swanson LW , Sawch enko PE, Rivier J, Vale WW (19 83):Organization of ovinc corticotropin-releasingfactorimmunoreactive cells and fibers in the rat brain: Animmunohistochemica l study. Ne uroe ndoc rino logy 36;165186.
Tancer ME (199 3): Neurobiology of social phobia. J ClinPsy chiatry 54:26-30.
Vale W, Spie ss J, Rivier C, Rivier J ( 1981):Characterization of a 41-residue ov ine hypothalamic peptide that stimulates secretion o f corticotropin andbeta-endorphin. Scien ce 213 : 1394 -1397.
Valentino RJ , Foo te SL . Aston-Jones G (1983) : Corticotropinreleasing factor activates noradrenergic neurons

of the locus coeruleus. Brain Res 270 :363-367.
van Bo ck stael e EJ, Colago EEO , Valentino RJ (1996) : Corticotropin-releasin g factor-containing axon terminalssynapse ont o cat ech ol amine dendrites and maypresynapticall y modulate other afferents in the rostra lpole of the nucl eus locus coeruleus in the rat brain . JCa mp Ne ura l 364 :52 3534 . van Oer s HJ, DeKloet ER,Levine S (199 8) : Early versus late maternal depri vationdifferenti ally alte rs the endocrine and hypothal amicrespons es to stre ss. Brain Res I I 1:245-252. Veith RC,Lew is N, Langohr Jl, Murburg MM , Ashleigh EA, Castillo S,et al (1993) ; Effect of desipramin e on cerebrospinalfluid concentrations of corticotropin-releasing factor inhum an subjects . Psychiatry Res 46 : 1-8. von Bardel ebenU, Holsboer F (1989): Corti sol respon se to a combineddexamethasone-human corticotrophin-releasing hormone challeng e in patients with depr ession . J Neuroendocrinol1:485-488. Weiss JM, Stout JC, Aaron M, Owens MJ, NemeroffCB (1994) : Experimental studies of anxiety and depression:Locus coerulcus and corti cotropin-releas ing factor. BrainRes Bull 35: 561-572 . Wid erlo v E. Bissette G, NemeroffCB (198 8): Monoam ine metabolites, corticotropin-releasingfactor and somatostatin as CSF markers in depr essedpatients. J Affect Disord 14;99 -1 07 . Workel 10, OitzlMS, Ledebo er A, DeKlo et ER (199 7): The Brown Nor way ratdisplays enh anced stress-induced ACTH reactivity at day 18after 24 h maternal depr ivation at day 3. Brain Res103:199-203. Yehuda R (1997): Sensitization of thehypothalami c-pituitaryadrenal axis in posttraumatic stressdisorder. Ann N Y Acad Sci 821 :57-75 . Ye huda R, Lowy MT,South wick SM , Shaffer D, Giller EL (1991): Incre asednumber of glucocorticoid receptor in posttraumatic stressdisord er. Am J Psychiatry 148:499 504 . Yehuda R, Boi soneau D, Mason J . Giller EL (I 993 a) : Gl u.cocortico idreceptor number and cortisol excretion in mood , anxiety,and psychotic diso rders. Bioi Psychiat ry 34:18-25. YehudaR, Southwick SM, Krystal m, Bremner DJ , Charney DS, Maso nJW (1993b) : Enhanced suppression of cortisol follo wingdexamethasone administration in postt raumatic stress disorder . Am J Psychiatry 150:8386. Yehuda R, Boisoneau D,Low y MT , Gi ller EL (1995 ): Doserespon se chang es inplasma cortisol and lymph ocyte glucocortico id receptorsfollowing dexamethasone administration in combat veteranswith and without posttraumatic stress disord er. Arch GenPsy chiat ry 52:538 -593. Yehuda R, Leveng ood RA , Schmeidler J, Wilson S, Guo LS, Ge rber D (I 996a) : Increasedpituit ary activation follo wing metyrapone administrationin post-traumatic stress disorder. Psychon euroendocrinology 2I : 1-16. Yehuda R, Teicher RL, Trestm an R,

Siever LJ (1996b): Cortisol regul ation in posttraumaticstress disorder and major depression : A chronobiologicalanalys is. Bioi Psychi atry 40 :79 88. Young EA, AbelsonJL, Curtis GC, Nesse RM ( 1997): Childhood ad versity andvulnerability to mood and anxiety disorders. Depre ss ionAnx 5:66-72. Zaidi LY, Foy DW ( 1993): Childhood abu seexpe riences and combat related PTSD. J Traum Stress7:33-42. Zlotnick C, Ryan CE, Miller IW, Keitn er GI (1995): Childhood abuse and reco very from major depr ession. Child Ab use Negl 19:1513-1 516. ELSEVIER
PERSPECTIVES
The Corticosteroid Receptor Hypothesis
of Depression
Florian Holsboer, M .D ., Ph.D.
Signs and symptoms that are characteristicfor depression
includechanges in the setpoint of the hypothalamic
pituitary-adrenocortical (HPA) system, which in the
majority of these patients result ;'1altered regulation of
corticotropin (ACTH) and cortisol secretoryactivity. More
ref inedanalysis of the HPA system revealedthat
corticosteroid receptor (CR) signaling is impaired in major
depression, resulting among other changes, in increased
production and secretion of corticotropin-releasing hormone
(CRH, alsofrequently abbreviated CRF) in various brain
regions postulated to be involved in the causality of
depression. This articlesumma rizes the clinical and
preclinical data, supporting the concept that impaired CR
KEY WORDS: Corticosteriodreceptors; CRH; HPA; Stress;
Depression; Antidepressants FUNCTIO NAL IM PAIRMENT OFCENTRAL COR TICOSTEROID RECEPTORS

Clinical Evidence
Until now, the serendipitous discovery of antid ep res
sants in the 1950s has profound ly inspired hypotheses
of the pa thogenesis of depression. The well-known
pharmacological effects of antid epr essan ts on presyn
aptic up take transporters and degrad ating enzymes Fromthe Max Planck Institute of Psychia try, Mun ich, Germany.Add ress co rrespondence to: Florian Holsboer, M.D., Ph.D.,Max
Planck Institut e of Psychia try. Kraep eJinstr. 2-10,D-80804 Mun ich,
Germany . Received February 28, 2000; rev ised June 22,2000; accepted June
23.2000.
NEUR Or5 YCHOPHARMACOLOGV 20Q0-VO L 23, NO.5
© 2000 Ame rican College of Neuropsycho pharmaco logy
Published by Els evier Science Inc,
655 Avenue of the Americas. New York. NY 10010 signaling isa key mechanism in the pathogenesis of depression.Mousegenetics, allowingforselective inactivationofgenesrelevantfor HPA regulationand molecularpharmacology, dissecting the intracellularcascade o fCRsignaling, are the most promising future research fields,suitedfor identifying genespredisposing to depression.Focusing On these two research lines may also allow togaininsight into understanding how current antidepressants workandfu rther, how more specifictargets forfutureantidepressant drugs can beidentified.[Neuropsychophann acology 23:477-501, 2000J ©2000AmericanCollegeof Neuropsychophar macology. Published byElsevier ScienceInc. (i.e., MAO) of serotonin and norepinephrine has focused resea rch on causality and treatm entof depression on the metabolism of functional biogenicamines and the capacity of their respective recep tors toalter intracellular signaling pathways that ult imatelyindu ce changes in gene activity. Elevated circulatinglevels of stress hormones among depressives were recognizedeven before antidepressants were discovered, but these

changes were seen as epiphenomena, reflecting the stressfulexperience of depression, although M. Bleuler (1919) already demonstrated that hormones have diverse psychotropiceffects and sugges ted hormone treatments as potentia lantidepressa nts. A vast amount of evidence hasaccumulated, that reject the view that altered stress hormone secretions in depression are epiphenomenal. Dur ing thepast decade, several research groups formul ated ahypothesis relating aberrant stress hormone dysregulationto causa lity of depr ession and submitted thatantidepressants may act through normalisation of these HPAchanges (review: Holsboer and Barden 0893-133X/OO/ keefront ma tter I'll S0893-133X( OO)OOI59-7 478 1996). Thishypothesis was derived from the following clinicalobservations in depressives: 1) the number of ACTH andcortisol secretory pulses is increased which is alsoreflected in elevated urinary cortisol production rates(Rubin et al. 1987); 2) levels of CRH in the CSF areelevated (Nemeroff et al. 1984); 3) the number of CRHsecreting neurons in limbic brain regions is increased(Raadsheer et al. 1994); and 4) the number of CRH bindingsites in the frontal cortex is reduced secondary toincreased CRH concentration (Nemeroff et al. 1988). Thesestudies were complemented by many neuroendocrine functiontests including the suppressibility of ACTH andcorticosteroids by the synthetic glucocorticoiddexamethasone (dexamethasone suppression test, DST). TheDST showed that a high proportion of patients with variousaffective disorders have elevated cortisol levels (Carroll1982), thus escaping the suppressive effect ofdexamethasone. After CRH was discovered and characterizedby Vale and coworkers (1981) initial studies employingovine or human GRH in depressives showed that the ACTHresponse after injection of this neuropeptide wasdecreased, suggesting desensitized pituitary CRH receptorsdue to homologous downregulation by hypersecreted CRH (Goldet al. 1986; Holsboer et al. 1986). The most sensitiveneuroendocrine function test to detect HP A dysregulationcombines the DST and the CRH stimulation test (dex /CRHtest) (von Bardeleben and Holsboer 1989, 1991; Heuser etal. 1994; Rybakowski and Twardowska 1999). In this test,patients are pretreated with a single low dose (1.5 mg) ofdexamethasone at 23:00 h and receive intravenously 100 Il-gCRH at 15:00 h the following day. The amount of ACTH andcortisol subsequently released is much higher amongdepressives. In fact, Heuser and coworkers (1994) concludedfrom their studies that the sensitivity of this test (i.e.,likelihood to differentiate between normal and pathologicalstates) is above 80%, depending on age and gender. WhereasCRH-elicited ACTH response is blunted in depressives,

dexamethasone pretreatment produces the opposite effect andparadoxically enhances ACTH release following CRH .Similarly, CRH-induced cortisol release is much higher indexamethasone-pretreated patients than following achallenge with CRH alone. The interpretation of the abovefindings is as follows: dexamethasone, due to its lowbinding to corticosteroid binding globulin and itsdecreased access to the brain (Meijer et al. 1998), actsprimarily at the pituitary to suppress ACTH. The subsequentdecrease of cortisol and the failure of dexamethasone tocompensate for the decreased cortisol levels in the nervoustissue creates a situation that is sensed by centralregulatory elements of the HPA system as a partial andtransient adrenalectomy. In response to this situation, thesecretion of central neuropeptides which are capable ofactivating ACTH secretion-mainly CRH and vasopressin-isincreased. Vasopressin is known to synergize with CRH,overriding dexamethasone suppression at humancorticotrophs: When vasopressin is infused at a low rateinto dexamethasone pretreated controls, concurrent infusionwith CRH induces an ACTH and cortisol response which issimilar to the hormone secretory profile of depressivesreceiving the combined dex/CRH-test but withoutsimultaneous vasopressin treatment (von Bardeleben et al.1985). This finding led us to postulate that hypothalamicvasopressin is increased in depressives (von Bardeleben andHolsboer 1989). A more recent study by Purba and coworkers(1996) reporting increased numbers ofvasopressin-expressing neurons in the parvocellular part ofthe hypothalamic para ventricular nucleus of depressivesultimately confirmed this view. All three tests (DST, CRHtest, and dex/CRH test) have been frequently administeredto depressed patients by several research groups. SerialDSTs during a variety of antidepressant drug treatmentrevealed that whenever cortisol suppression wasinappropriate, i.e., above a certain threshold,normalization of the neuroendocrine dysreguJation wasnecessary for clinical remission to become manifest. Inaddition, if post-dexamethasone plasma cortisol levelsincreased over time or remained elevated the likelihood foran unfavorable clinical course or nonresponse to treatmentwas high (Holsboer et al. 1982; Greden et al. 1983).Blunted ACTH response to CRH and the normalization ofelevated CRH in the CSF after antidepressantinducedclinical remission has also been reported; these findingsconfirm a close association between HPA dysregulation anddepressive psychopathology (de Bellis et al. 1993). Thecombined dex/CRH test proved particularly useful as apredictor of increased risk for relapse (Holsboer et al.1987; Holsboer-Trachsler et al. 1994; Heuser et al. 1996;

Zobel et al. 1999) . In those patients where theneuroendocrine abnormality persisted, the risk of relapseor resistance to treatment was much higher. Together, allstudies reported so far indicate that reinstatement of a"normal" HPA setpoint is an important prerequisite forclinical improvement and furthermore, if HPA abnormalitiespersist or become more pronounced during drug treatment therespective individual is at increased risk for relapse. Astudy that administered different doses of dexamethasoneprior to CRH showed that ACTH and cortisol suppressionoccurs at higher dexamethasone dosages in the depressivesthan in matched controls. This shift of the dose responsecurve to higher dexamethasone dosages corroborates the viewthat negative feedback mechanisms through glucocorticoidreceptors (GR), to which dexamethasone binds, are impairedin depressives (Modell et al. 1997) . The consequences ofimpaired regulation of cortisol secretion are manifold,ranging from untoward effects in peripheral tissues (e.g.,osteoporosis) to changes in the central nervous system. Thelatter are believed to comprise effects on morphology aswell as on cognitive NO. 5
function . Studies by Sheline et al. (1996, 1998, 1999) and
Bremner et al. (2000) sugges ted that recurrent major de
pression is associated with hipp ocampal volume loss
and that the degr ee of this change is det ermined by the
duration of the illness. Conside ring the finding s that
depressed patients are frequ entl y hypercortisolemic
and that the degree of hipp ocamp al atrophy in aged
humans correlates with the degree of plasma cortisol
increase over time and the current basal corti sol levels
(Lupien et al. 1998). it has been proposed that the neu
roend ocrine chang es in depression may acc ount for the
changes in hippocampal size seen in this disease. Im
portantly , these r eductions in hipp ocampal volume
which are also seen in pati ents with schizophreniaa

disease not particularly associated with endur ing hy
percortisolemia-do not necessarily reflect cell death
(Nelson et al. 1998). Moreover, in post-traum atic stress
disord er, decreased hippocampal volum e is associated
with normal or even r educed plasma and urine gluco
corticoid contents (Bremn er et al. 1999). Studies in ratsand tree shrews showed that psycho
logical stressors may also indu ce atrophy in hippocampal
CA3 pyram idal neur ons wh ich involves reversible
remodeling of apical d endrites, a process where elevated
excitatory amino acids are believed to be a primary cause ,
possibly amplified by increased glucocorticoids (Wa
tanab e et al. 1992;Gould et al. 1997;Magarinos et al. 1996,
1997). That factors -other than glucocorticoids-ac
count for stress-induced reversible or permanent morpho
logical changes in the hippocampu s has also been under
scored by a study in nonhuman primates (Leverenz et al.
1999). Based on works by Land field et al. (1981), Kerr
et al. (1991), and Sapolsky (1992), the study by Lever
enz et al. (1999) administered high doses of glucocorti
coids to aged macaques for 12 months, however, no evi
dence for decreased hipp ocamp al volume, subfield
volumes, subfield neur onal density, and subfield total
neuronal number emerged. This finding is in accor
dance with a report by Muller and coworkers (1998), who
studied postmortem brains of patients with depression

and of patients treated with various synthetic corticoste
roids and failed to observe morphological changes and
signs of cell death und er these clinical conditions. Inthis
context, it is important to note that there is evidence that
primates, unlike rats, have a relative paucity in GR, but a
high density in mineralocorticoid (MR) in the hippocam
pus (sanchez et al. 2000). Since, unlike cortisol, synthetic
corticosteroids bind only poorly to MRs, studies using
synthetic glucocorticoids, e.g., dexamethasone, in humans
produce a situation where MRs remain unliganded in this
brain formation. If it holds true that also in humans MRs
are predominating over GR in hippocampu s, dexametha
sone pretreatment would deprive this brain region from
CRsignaling. As reviewed by McEwen and coworkers (1992), ad
renal steroids can exert a manifold of effects sometimesopp osing on the rat hipp oc ampus, i.e., they can beprotective as well as deleterious. In line with this view,studies by Hassan et al. (1996, 1999) and Almeida et al.(2000) showed that corticosterone and dexamethasone givenat low dosages can exert opposite effects on hippocampalcell viability. It is yet unclear whether these oppos ingeffects are du e to differences in penetration of these twocort icosteroids through the blood brain barrier or whetherthey are du e to differences in relative occupati on of GRand MR. It also seems important to recognize in futur estudies that neurochemical and neuroanat omical effects ofstress hormones can only be studied to a limited extent byexogenous administration of corticosteroids. Produ cingstress-like plasma cortisol concentrations results in avariety of central changes including altered expression ofCRH and neurotroph ins, which in turn may exert neuroprotective and other behavioral effects (Behl et al.1997). Another issue that deserves attention in futur eclinical and preclinical studies relates to the difference

in the effects mediated by GR and MR (reviews: Trapp andHolsboer 1996a; de Kloet et al. 1998). To dissect theirrespective effects on cognition, studies similar to that ofNewcomer et al. (1999), but using selective MR and GR agonists and antagonists, are needed . This is of particularimportance if the provocative study of Sanchez andcoworkers (2000) that reported a relative absence of GR inthe pr imate hipp oc ampus is corroborated. Based on measurement s of GR and MR mRNA, Seckl et al. (1991) showed thatin hum an hipp ocampus both recept ors are highlyexpressed, but also confirmed that differences betweenspecies exist rega rding the subfield distribution of GRand MR. In the past, much emphasis had been put on thepossibility that neurochemical and neuroend ocrine changesassociated with depression account for the morphologicalchanges observed in the CNS of these patients. A recentstudy by Rajkowska et al. (1999) f ound redu ctions indensity and size of neurons and glial cells in thedorsolateral prefrontal cortex of depressed patients andraised the question whether the observed specifichistopathological changes in major depr ession may be du eto a genetic predi sposition for cortical cell changes.Studies that help to resolve this question are awa ited andthey need to include studies on gene networ ks that areinvolved in early brain developm ent . Genetic Studies Thepatient popul ation which would be ideally suited to studyshifted HPA setpoints are subjects with inheritedglucocorticoid resistance. These pat ients may either havea polymorphi sm in the GR gene or other alterations ingenes, whose products are involved in glucocorticoidsignaling. As a consequence of the ubiquitous GRresistance, elevated ACTH and cortisol secretion oc480 curswithout lead ing to symptoms of Cushing's syndrome. Nonethe less, othe r disturbances emerge that are mediated bythose eleva ted adrenocortical hormones that bind to othersteroid recep tors , such as MR or an drogen recep tors .Thus, subjects wi th detected fam ilial GR resistance werediagnosed to have hyp ertension , and among fema les hirsutism, menstru al irregul arities, and acne we re prevalent (Lamb erts et at. 1992, 1996). Because such symp tomsare not apparent in dep ression and becau se of theepisodic co urse of this d isease, it seems un likely atfirst sig ht that the path ology underlying depressioninvolves a major GR gene mutation. Recent data, however,suggest that relative glucocorticoid res istance caused byGR muta tions may not be as infre quent as pr eviouslythought (Koper et al. 1997). Thus, it seems perti nent tostu dy whether psyc hiatric syndromes are mo re preva len tin pat ient s wit h GR resis tance and also whether suchmutations may occu r among psychiatr ic patient s wit h

dysregulation of the HPA sys tem. It is of no te that thepresence of polyme rphisms or mu tatio ns in the GR canno tbe automatically inferre d from glucocorticoid resis tancebecause stru ctur e or asse mbly of cellular co mponents,suc h as chaperones or other tran scr ipt ion factorsinvolved in hormone signaling, may also be defecti ve. Onthe other hand, the episo dic nature of dep ression doesnot reject the possibil ity of GR gene polym orphism sincecompensa tory me chanisms, which help to maint ain stresshormo ne hom eostasis mos t of the time , may be prese nt.One such mecha nism may incl ude interaction of polymorphic GR wi th chaperones, which are responsible for individua l GR-binding prop erties and in coope ration wi thother transcript ion factors can determ ine the activationor repr ession of gene expression t hrough IigandactivatedGRs (see Section III). The capacity of the chaperone/ transcript ion factor assembl y to compe nsate for fun ctionaldeficits du e to allelic GR variants may fluctua te andbecome less effective whenever othe r counteractingnon-genetic factors (e.g., intracellular signals indu cedby enviro nmental stressors) are activated . MunichVulnerability Study. In this light , the data from theMunich Vulne rability Stud y are of in terest as they s howthat subjects who never suffe red from a psychiatric d isorder, but belong to families wit h a high genetic load fordepression may dis play abnorma l respo nses to the dex/CRH test (see Figu re 1). These abnormali ties were foundto be constant over time and 3 250 200 ::r :a E 150 .Eo ~ 0100 U 50 1 0 0 ~ g CRH o -1-1 14.30 14.45 15.00 15.15 15.30Time 15.45 16 00 16.15 16.30 MDE (N=24) HRP (N=75) • CP(N-35) Figure 1. Munich Vulnerability Study. Seventy-fivehealthy probands selected from families with a high geneticload for depression (high risk probands, HRP) received 100tJ.g human CRH (i.v.) at 15:00h after pretreatment with anoral dose of 1.5 mg dexamethasone at 23:00 h the daybefore. The plasma cortisol response (adjusted means ±SEM;adjusted by age and sex) of the HRPs, matched patientswith major depressive episode (MOE) and matched healthycontrols (CP) from families without history for psychiatricmorbidity were found to be significantly (F 2 , ,,. =16.36, P < .001) different. (Adapted from Holsboer et at.1995 and additional data). 50 NO.5
those subjects showing these depression-like HPA
changes were considered to be at risk for developing
depression (Holsboer et al. 1995; Modell et al. 1998).
The possibility that these HPA disturbances are ac

quired and rather reflect the stressful experience of hav
ing a family member suffering from a mood disorder
than a genetic risk can be rejected, as only a fraction of
about 20% of the probands show these alterations. In
terestingly, this figure corresponds well with the calcu
lated risk for developing depression in later life of high
risk probands (Lauer et al. 1998). Whether it proves true
that these individuals are indeed prone to develop de
pression is currently under investigation in longitudi
nal follow-up studies. While it may well be that some ofthe individuals
showing impaired corticosteroid receptor function and
increased risk for depression do have a GR mutation,
e.g., a single amino acid substitution in the ligand bind
ing domain leading to reduced corticosteroid sensitiv
ity, most genetic studies reported so far reject the GR
gene as a possible locus of inherited pathology (Detera
Wadleigh et al. 1992; Morissette et al. 1999). It would
not be surprising, however, if genetic studies of large
kindreds would reveal that GR-regulated genes or
genes whose products are involved in stress hormone
signaling are contributing to genetic susceptibility for
depression.
Preclinical Studies
The CR hypothesis implies that intracellular signaling

of adrenocortical stero ids is impaired in specific areas
of the brain , resulting in a number of changes in gene
activity and neurotransmitter production involved in
causality of depression. Particular emphasis is put on
the interaction of hormone-act ivated GR and the effects
on CRH, which is believed to be a key neuropeptide in
the pathogenesis of depression and other stress-related
disorders (reviews: Owens and Nemeroff 1991; Hols
boer et al. 1992). There is no ' uniform relationship,however, between
activated GRs and CRH secretion, as CRH is differen
tially regulated by GR in different regions of the brain.
In most parts of the hypothalamic paraventricular nu
clei (PVN), glucocorticoids suppress CRH and vaso
pressin as they suppress proopiomelanocortin, the pre
cursor of ACTH of the anterior pituitary (Erkut et al.
1998). In some brain areas that include the central
amygdala expression (Schulkin et al. 1998) and those
nuclei of the PVN that project to the spinal cord ac
counting for CRH content in the cerebrospinal fluid
(Swanson and Simmons 1989), corticosteroids upregu
late CRH gene expression. Positive feedback of gluco
corticoids on CRH synthesis and secretion in many
brain areas is life-sustaining as it keeps the organism re
sponsive to acute stressors under conditions of chronicstress. Elevated CRH in the amygdala , for example, ispertinent to maintaining appropriate emoti onal

responsivity, particularly if stress exposure endures(review: Gray and Bingaman 1996). The effects of CRH aremed iated through specific receptors of which two differentsubtypes (CRH-R1 and CRH-R2) have yet been identified(Chalmers et al. 1995).Their neuroanatomical distributionssuggest that they mediate different effects. Recent studiesusing antisense probes directed against CRH-R1 and CRH-R2mRNA supported this notion as they showed that only reducedCRH·R1 levels produce anxiolytic effects in stressed rats(Liebsch et al. 1999). Reports on mouse mutants where oneof these receptors was genetically inactivated confirmedthat CRH-R1 mediates anxietylike behavior (Timpl et al.1998; Smith et al. 1998). In contrast, two out of threestudies where the CRH-R2 was invalidated noted increasedanxiety-like behavior (Bale et al. 2000; Kishimoto et al.2000; Coste et al. 2000) (see also Section II) GRs arepresent in all rodent brain areas and are most abundant inthe hypothalamus where they repress CRH and vasopressingene activity . Most MRs in the brain are located in thehippocampus where they may be co-express ed with GR by many, but not all neurons. Hippocampal MRs are not selectivefor the prototypic mineralocorticoid aldosterone, but bindthe glucocorticoid corticosterone (or cortisol in primates)with approximately tenfold higher affinity than GRs. This"nonselectivity" of brain MRs is determined by the factthat unlike in peripheral cells, the enzyme1113-hydroxysteroid dehydrogenase (l1I3HSD) does noteffectively exclude corticosterone or cortisol from MR-targets in the hippocampus. For example, in epithelial cells ofthe human kidney containing MR, this enzyme convertscortisol into cortisone , which binds only poorly to MR,allowing electrolyt e homeostasis through aldosteron ealone. In the hippocampus, a different 11I3HSD isoform ispresent, which does not provide such selectivity (vanHaarst et al. 1996a; SeckI1997) . Because of the abouttenfold higher affinity of "nonselective" hippocampal MRsfor corticosterone, these receptors are already almo stcompl etely occupied at basal levels of corticosteroidsecretion. On the other hand, hippocampal GRs are onlyoccupied when corticosteroid levels increase under stressconditions or at the peak of the circadian rhythm ofcorticosteroid secretion. The coexistence of MRs activatedat low corticostero id concentrations, and of GRs activatedonly at high concentrations, allows the brain todifferentiall y respond to the wid e range ofconcentrations over which corticosteroids are secreted .These respons es are extremely diverse and include steroideffects on cell membranes . At low concentrations,corticosterone maintains neuronal excitability which is apredominantly MRgoverned effect, whereas at higher hormone

concentr a482 tions this is oppose d by increasing GRactivation Gaels and de Kloet 1992). Specifically, und erbasal conditions where most of the MRs, bu t only afraction of GRs are occup ied, Ca"" inward currents aresmall in hippocampal n eurons; this result s in a stablefiring rate, thus contributing to the "proactive" role ofcorticosterone in maint aining homeostasis (review: deKloet et al. 1998). Und er stress, more GRs are activatedand there is an associated increase in Ca" influx andrespon sivity to seroton in (S-HT), for example, increases.This conditi on is referred to as the "reactive" mode bywhich corticosteroids prot ect neuro ns throu gh GR and MRby reinstating homeostasis (de Kloet et al. 1998). Thus, itis the ratio of activa ted MR and GR, wh ich determines notonly the effects of corticosteroids on hipp ocampal neuronsthemselves but also in their projection areas, e.g., theamygda la. The effects of the predominant amino acidtransmitters in the brain, glu tama te and 'Y-aminobutyricacid (GABA), which mediate excitatory and inhibitoryeffects on synaptic transmission respectively, are alsocontrolled by the relative occupancy and activation of MRand GR. This is demonstrated by the modul ator y effects ofthese two recep tors on long-term potentiation (LTP), a phenomenon that refers to strengthening of synaptic contactsby repeated stimulation. When glu tamatergic afferent s tothe hipp oc ampus, part icularly the CAl area, arerepeatedly stimulated, prolonged enhancement of synapticresponsivity is observed as a consequ ence. It has beensugges ted that changes in LTP correlate with the capacityto learn and retrieve memorized material. The induction ofLTP has been found to be critically det ermined by thelevel of corticosteroids. As recently argued by de Kloetand cowo rkers (1998, 1999), this effect can be bestexplained by appreciating the specific roles of MRs and GRsand the ratio of ligand activated MR/ GR on neuronalactivity in the hipp oc ampus. Under resting conditions,when corticostero id levels are in the normal range, LTP ismost pronoun ced and the MR /GR ratio is high because MRsbut not GRs are fully occupied . This cond ition isassociated with a facilitated adapt ation to stressfulsitua tions where MR activation accounts for behavio ralreactivity to acute stressors. Under chronic stress, areduced MR/ GR ratio resul ts from increased GR occupationunder increased corticosteroid levels and a grad ualdesensit ization of MRs which precedes GR dese nsitization;the latter changes are associated with reduced LTP. Itseems likely that such changes in synaptic efficiency represent the neural correlate of memory impairment associatedwith hypercortisolism. These cognitive deficits not onlyinclude disruption of memory conso lidation but also

impaired mem ory retrieval (de Quervain et al. 1998). Inthis context, it is important to note that such effects donot solely result from altered corticosteroid effects inthe hippocampus. For example, GR-media ted memory consolidation is also influenced by l3-adrenoceptor stimulation inthe amygdala (Roozend aal et al. 1999). The interactionbetween hippocampal GR and MR also play s a role in HPAregulation of ra t. Studi es using MR antagonists or MRantisense prob es und er trough (morn ing) or stressconditions resulted in exaggerated HPA activity (Oitzl etal. 1994; Reul et al. 1997). interestingly, the GRantagonist mifepri stone (RU 486, also blocking progesterone recept ors) when injected intracerebroventricuiarly (icv)has no effect on basal trough levels because of low GRoccupancy during early daytime hour s. Administration ofthe same dru g in the early evening, when corticosteroidlevels are rising, leads to furth er HPA activity increase.How ever, if RU 486 is injected directly into the hipp ocampus, this results in a decrease of ACTH andcorticosterone secretion (van Haarst et al. 1996b), indicat ing that hipp ocampal GRs, when activated bycorticosterone binding, are oppo sing the inhibitoryeffects of MRs. in other words, MRs medi ate an inhibit orytone on the HPA system which is opp osed by activatedhippocamp al GR. Following icv administra tion, theexcitatory effect of GR antagonism at the hypothalamusoverrides the inhibitory effect of GR antagonism at thehippocampu s. If the balance between MR and GR is intact,then hypothalamic and pituitary GR capacit y is sufficientto maintain adequat e feedba ck upon CRH neurons andcorticotrophic cells. However, if corticosteroid signa lingis defunct, stress-elicited HPA activity is graduallyshifted toward s operating at higher setpoints, resulti ngin continuous HPA hyperdrive with accomp anying behavioraleffects du e to CRH and vasopr essin disinh ibition as wellas the many other sequelae of MR/ GRdysbalance. TheNature-Nurture Conundrum The risk of developing depr essionor other major affective disorders is determined by a complex interpl ay between genetic susceptibility, environmental exposures, and aging. These influences also account forlong-term changes in the regulation of the stress horm onesystem. This is particularly well illustrated by anima lstudies in which stressors were administered preorpostnatally , followed by evaluations of HPA function andemotionality during later life. From these experiments, itwas conclud ed that context and timing are criticaldeterminant s for predicting wh ether early stress exposureresults in hyp oor hyperactive HPA-statu s. For example,Reul and cowor kers (1994) stressed pregnant female ratswith immunostimulants and observed that their pup s had

increased activity throughout adulthood . Since theoriginal rep ort by Levine and Mullins (1966), it has beenrepeatedl y demonstr ated that the effect of postnatal"handling", i.e., a very brief daily separation of motherand pup result s in redu ction of both, emotionality andcorticosterone secre tion. Similarly,
N NO. S
rats that had received norm al maternal care (licking,
grooming) during the first 10 day s of their life had re
duced plasma ACTH and corticosterone response to
stress increased hippocamp al GR and MR mRNA levels
and decreased CRH mRNA when examined as adults.
However, opposite effects were f ound, when these rats
were severely traumatized postnatally by long mother
pup separations alone or in combination with mild foot
shocks (Ladd et al. 1996). These rats showed increased
CRH concentrations in the medi an eminence, decreased
numb er of CRH rec eptors and pituitary ACTH-secret
ing cells, and hypercorticoidism, thus bearing resem
blance to the neuroendocrine state f ound in depres
sives. Of special importance is the observa tion that rats
tha t were postnatally traum atized perform poorly in
learnin g and memor y tests, as oppose d to rats that had
received optimal mat ernal care (Plotsky and Meaney
1993). These findings , which were also confirmed in ex
periment s with non-human primates (Coplan et al.
1996), suggest that early traum a may persistentl y
weaken corticosteroid signa ling, leading to dis inhibited

release of hypothalamic CRH, ACTH, and corticoster
one which, in turn, may have behavioral sequelae that
are related to a number of depressive symptoms. These
data might even be extrapolated to the human situa
tion, explaining wh y ind ividuals who were abu sed dur
ing childhood may be more likely to develop depres
sion in later life (Heirn et al. 2000). A number ofdifferent expe riments, however, dem
onstrates that early trauma does not necessarily result
in HPA disinhibition and cognitive impairm ent. Oitzl et
al. (unpublished result s, cited in de Kloet et al., 1998)
used a different strain of rats than the previous investi
gators and showed that in Brown Norway rats, which
are known for their long and healthy life spans, early
traum a (i.e., long moth er-p up sepa ration) result ed in a
bimodal distribution of cognitive perform ance in later
life. Among animal s that were traumatized as pups,
these inves tigators identified good as well as poor
learners but only a few intermediate learn ers. In the
control group, however, the majority of rats were inter
mediate learners and only few good or poor learners
were observed . The mat ernally-deprived rats had de
creased GR expression in the hyp othalamu s and in the
hipp oc ampus. Among these traumatized rats, the good
performer s had lower plasma ACTH and corticoste rone

concentrations as c ompared to the poor performe rs.
These experiments point to strain-dependent effects
and suggest that it is the ind ividu al geno type that de
termines the consequences of early trauma on the HPA
system and related behaviors. In view of this, the stud
ies by Kendler and coworkers (1999) are important and
have introduced an additional level of complexity as
they show that the genetic endowment interacts with
the environment; indiv idu als with a high genetic risk
for depression are more susceptible to the depressiveepisode-triggering effect of an adverse life event. Inaddition, genetic factors influence not only thesensitivity to potenti ally depressogenic life events , butalso influence the likelihood to expose oneself to such anevent. Hyp othetically then, indi vidu als with aninherited genetic trait that wea kens stress horm oneregulat ion through impaired corticosteroid recept orfunction may be more vulnerable to stressors and inaddition they may select themselves into adve rsivesituations which then trigger the onset of a depr essiveepisode. MOUSE GENETICS AS A TOOL TO PROBE TH E CRHYPOTHESIS Knock-out or Transgenic Manipulation of CRH andCorticosteroid Signaling Mouse mutants with manipulationsof the genes encoding either CRH or its receptors or CRshave been generated . As predicted from studies where CRHwas injected into rodent brains, overexpression of CRH inmice results in an enhancement of anxiety-like behavior(StenzelPoore et al. 1994). Mice with deletions of the CRHgene exhibit normal stress-induced behavior , confirmingthat CRH may not be the only physiologically active ligandof CRH receptors. If CRH is absent, other neuropeptidessuch as urocortin or other yet-to-be identified moleculesacting at CRH1 or CRH2 recept ors (and possibly CRHreceptors yet-to-be discovered) can serve as anxiogenic ordepressogenic signals (Weninger et al. 1999). Studies byLiebsch et al. (1995, 1999), Heinrichs et al. (1997), andSkutella et al. (1998), who used antisense probe s directedagainst the mRNA-encoding CRH-R1 and CRH-R2 in rats, andalso studies involving mouse mutants lacking CRH-R1,suggested that CRH-R1 mediat es anxiety-like behavi or(Timpl et al. 1998; Smith et al. 1998) (Figur e 2). In

contras t, CRH-R2 deficiency was shown to increaseanxiety-like beha vior in some (Bale et al. 2000; Kishimoto et al. 2000) but not all (Coste et al. 2000) stud ies,raising the possibility that the two so far identified CRHrecept ors mediate opposite effects on anxiety-like behavior. Recently, Radulo vic and coworkers (1999) confirmedthat the role of CRH in enha ncing learning andprecipitatin g anxiety-like behavior is brain areaandrecept or type-depend ent and that previous stress fulexperience can also modulate the CRH-mediated behaviors.CRH signaling through CRH receptors is furth er complicatedbecause CRH is b ound to CRHbinding protein (CRH-BP) whichhas an affinity for CRH that is equ al to or greater thanthe respective CRH recept ors (Potter et al. 1991). This37-kDA prot ein bind s 40-90% of total CRH and is presentin most hum an brain regions at tenfold higher concentrations than total CRH, which points to a major role of CRH-BPas regulator of CRH, "buffering" its actions underconditions of excessive release (Behan et al. 1995).

ab l50
Allera A, Wildt L (1992): Glucocortico idrecognizi ng and-effector sites in rat liver plasm a membrane. Kinetics ofcorticosterone upta ke by isolated memb ran e vesicles. I.Bindin g and transport . ) Steroid Bioche m Mol Bioi42:737756
Alme ida OF, Conde GL, Croche mo re C, Demene ix BA, Fischer D, Hassan AH, Meyer M, Hoisboer F, Michaelid is TM(2000): Subtl e shifts in the ratio between proandantiapoptotic molecules after activation of corticosteroidreceptors decid e n euron al fate. FASEB) 14:779-790
Aup han N, Didona to )A, Rosette C, Helmb erg A, K arin M(1995): Immunosu ppression by glucoco rticoids: Inhibi tionof NF-KBactivity through indu ction of IKB syn the sis .Science 270:286-2 90
Bale TI, Gontarino A, S mith GW, Chan R, Gold LH, Sawchenko PE, Koob GF, Vale WW, Lee K-F (2000): Mice deficientfor corticotropin-releasing hormone recept or-2 di spl ayanx iety-like behaviou r and are hypersensitiv e to stress. N ature Genet 24:410-414
Bamberger CM, Bamberger AM, DeCastr o M, C hrousos GP(1995): Glucocorticoid recept or beta, a potenti al endogeno us inhib itor of g lucocortico id action in humans .JClio Invest 95:24352441
Barde n N, Stec 1, Mon tkow ski A, Holsboer F, Reul )MHM(1997): Endocrin e profile and neur oend ocrine cha llengetests in transgenic mice expressing antisense RNA aga instthe glucocorticoid recept or. Neuroe ndoc rinology66:212220
Beato M, Herrlich P, Schu tz G (1995): Steroid hormo nereceptors: Many actors in sea rch of a plot. Cell83:851-857
Beha n D)P, Heinr ichs SC, Troncoso )C, Liu X]. Kawas CH,Ling N, De Souza EB (1995): Displacement of corticotropinreleasing factor from its bindin g p rotein as a possibletreatm ent for Alzheimer 's disease. Na ture 378:284-287
Behl C. Lezoualc'h F, Trap p T, Widm ann M, Skutella T,Hoisboer F (1997): Glucocorticoids enha nce oxida tivestressinduced cell death in hip pocam pal neu ron s illvitro. Endocrinology 138:101106

Berger 5, Bleich M, Schmid W, Cole 1] , Peters l. WatanabeHWK, W arth R, Greger R, Schulz G (1998): Mineralocorticoidreceptor knockout mice: Patho phys iology of sodiummetabolism. Proc Na t! Acad Sci USA 95:9424-9429
Bleuler M (1919): The Intern al Secre tions and the NervousSys tem. (N ervous and Ment al Disease Mon ograph Series,No . 30.) New York, Nervous and Mental Disease Pub l C ompBrad y LS, Whi tfield H) [r, Fox R), Gold PW, Her kenh am M(1991): Long-term antide p ressa nt administr ation alte rscortico trop inreleas ing horm one, tyrosine hyd roxylase,and mineralocorticoid receptor gen e express ion in ratbrain. Therapeu tic imp lications.) Clin Invest 87:831-837Br emner J. Southw ick 5, Charney D (1999): The neurobiology of post-tr aumatic s tress di sorder: An integration of anima l and human research . In Saigh P, Bremn er)(ed s), Post-t raumatic Stress Diso rder: A Co mprehens iveText. Ne edham Height s, MA, Allyn & Cacon, pp 103143 Bremner )D, Na raya n M, Ande rson ER, Staib LH, Miller HL, Charney DS (2000): Hippocampal volum e red uction in major depression . A m) Psychiatry 157:115-117 Burrow s HL, NakajimaM, Lesh )5, Goosens KA, Sa muelson LC, Inu i A, Camper SA,Seasholtz AF (1998): Excess corticotr opin-releasinghormone-binding protein in the hyp otha lamic-pituitaryadren al axis in transgen ic mice. I ClinInvest 101:14391447 Calde nhoven E, Liden I. Wissink 5, Vande Stolpe A, Raaijmakers ), O kret 5, Gus tafsson )-A, Vander Saag PT (1995): Negativ e cross talk b etween RelA andthe gluco co rtico id receptor: A possib le mechanism forthe antiinflammatory action of glucocorticoids . Mol Endocrino l 9:401-412 Calvo N, Martijen a 10, Molin a VA,Volosin M (1998): Metyrapone p retrea tment p reve nts thebeh avioral and n eurochem ical seque lae induced by stress. Brain Res 800:227-235 Carro ll ) (1982): Clinica l applica tions of the dexam eth asone su ppression test for endogenous depr ession . Pharmacopsych ia try 15:19-24 Chalmers DT, Lovenb erg TW, De Souza EB (1995): Localizationof novel co rticotropin-releasing factor recept or (CRF2)mRNA express ion to specific subcortical nucl ei in ratbrain: Compa rison with CRFI recept or mRNA expression. )Neu rosci 15:634(H;350 Chen G, Kolbeck R, Bard e Y-A, Bonhoeffer T, Kossel A (1999): Relative contrib ution of endoge nous neur otrophins in hippocam pal long-termpotentiation . ) Neurosci 19:79837990 C hrousos GP,Renquist D, Brand on D, Eil C, Pugeat M, Vigersky R, CutlerGB [r, Lor iau x DL, Lipsett MB (1982): Glucoco rticoidhorm one resistance d uring p rimate evo lution: receptor-mediated mechan isms . Proc Na tl Acad Sci USA 79:20362040Cole T) (1996): Ste roid recept or knockout s. Curr OpinEndocrino l Diabet 3:363-368 Coplan )D, An drews MW,

Rosenblum LA, Owe ns M), Friedman 5, Gorma n )M, Neme roffCB (1996): Persis tent eleva tions of cerebrospinal fluidconcentrations of corticotrop in-releasing factor in ad ultnon-hum an pr imates exposed to ea rlylife stressors:Implications for the pathoph ysiology of mood and an xietydisor ders. Proc Na tl Acad Sci USA 93:16191623 Coste SC,Kesterson RA, Heldwein KA, Stevens SL, Heard AD, Hollis )H,Murray SE, Hill )K, Pantely GA, Hoh imer AR, Hatt on DC,Phillips T], Finn DA, Low MJ, Rittenb erg MB, Stenze l P,Stenze l-Poore MP (2000): Abno rma l ada p tations to stress and imp air ed card iovascu lar function in micelacking corti cctropin-releasing horm one rec eptor-2. Natu re Genet 24:403-4 09
NEU NO.5
de Bellis MD, Gold, PW, Geracioti TO lr. Listwa k S), KlingMA (1993): Association of fluoxetine treatm ent w ithreductions in CSF concentrations of corticotropinreleasinghormone and arginine vasopressin in patients with majordepression. Am ) Psychiatry 150:656-657
de Kloet ER, Vreugdenhil E, Oitzl MS, [oels M (1998): Braincorticosteroid receptor balance in health and disease.Endocrino l Rev 19:269301
de Kloet ER, Oitzl MS, [oels M (1999): Stress and cognition: Are corticosteroids good or bad guys? Trends Neurosci22:422-426
de Que rvain D)-F, Roozendaal B, McGau gh)L (1998): Stressand glucocorticoids impair ret rieval of long-term spatialmemory. Nature 394:787-790
Deguchi M, Yoshiaki I, Matsu kawa S, Yamaguchi A,Nakagawara G (1998): Useful of metyrap one treatm ent tosuppress cancer metastasis facilitated by surgical stress.Surgery 123:44M 49
Delgad o PL, Cha rney OS, Price LH, Aghajanian GK, LandisH, Hen inger GR (1990): Serotonin func tion and themechanism of antide pressant action: Reversal ofantidepressan t-indu ced remission by rapid depl etion ofplasma trypt ophan . Arch Gen Psychiatry 47:411-4 18
Delgado PL, Price LH, Heninger GR, Cha rney OS (1992):Neuro chemistry of affective disord ers. In Paykel ES (ed),Handbook of Affective Disorders. New York, NY, ChurchillLivingstone, pp 219253

Detera-Wadleigh SO, Berrettin i WH, Goldin LR, Martinez M,Hsieh WT, Hoehe MR, Encio I), Coffman 0 , Rollins DY, Muniec 0 (1992): A sys tema tic search for a bipolar predisposing locus on chro mosome 5. Neu ropsychopharmacology6:219229 .
Dijkstra I, Tilders F)H, Aguilera G, Kiss A, Rabandan-Diehl C, Barden N, Karanth S, Holsboer F, Reul )MHM(1998): Redu ced activity of hypothalamiccorticotropin-releasing horm one neurons in transgenic micewith impaired glucocorticoid receptor function. ] Neurosci18:3909-3918
Dodt C. Kern W, Fehm HL, Born ) (1993):Antirnineralocorticoid canrenoate enhances secretoryactivity of the hypothalamus-pituit ary-adrenocortical(HPA) axis in hum ans. Neuroendocrinology 58:570-574
Drouin ), Sun YL, Cha mberland M, Gau thie r Y, De Lean A,Nemer M, Schmid t T) (1993): Novel glucocorticoid recept orcomplex with DNA element of the hormonerepr essed POMCgene. EMBO ) 12:145-1 56
Drouin J, Maira M, Philips A (1998): Novel mechanism ofaction for Nu r77 and antagonism by glucocorticoids: Aconvergent mechanism for CRH activa tion and glucocorticoidrepression of POMC gene tran scription. ) Steroid BiochemMol Bioi 65:59-63
Duman RS, Hen inger GR, Nestler E) (1997): A molecular andcellular theory of dep ression. Arch Gen Psychiatry54:597-606
Eiring A, Sulser F (1997): An increased syna pticavailability of norepi nephrine is not essential forantidepressant induced increases in hippocampal GR mRNA. INeural Transm 104:12551258
Erkut ZA, Pool C, Swaab OF (1998): Glucocor ticoidssuppress corticotropin-releasing hormone and vasopessinexpress ion in human hypothalam ic neurons. ) Clin Endocrinol Metab 83:2066-2073 Flood )F, Morley )E, Roberts E(1995): Pregnenolone sulfate enhances post-training memoryprocesses when injected in very low doses into limbicsystem structu res; the amygda la is by far the mostsensitive. Proc Nail Acad Sci USA 92:10806-10810 Freedm anLP (1999): Increasing the complexity of coactivation in nuclear receptor signa ling . Cell 97:5-8 Gold PW, Loriau xDL, Roy A, Kling MA, Calabrese )R, Kellner CH, Nieman LK,Post RM, Pickar 0 , Gallucci W, Avgerinos 1', Paul S,

Oldfield EH, Cutler GB [r, Chrou50 S GP (1986): Responsesto corticotropin-releasing hormone in the hypoercortisolism of depr ession and Cushing's disease. N Engl) Med 314:1329-1335 Gould E, McEwen BS, Tanapat 1', GaleaLAM, Fuchs E (1997): Neurogenesis in the dentate gyrus ofthe adult tree shrew is regulated by psychosocial stressand NMDA recept or activation. ) Neurosci 17:2492-2498 GrayTS, Bingaman EW (1996): The amygdala: Corticotropin-releasing factor, steroids, and stress. CriticalRev Neurobiol 10:155-168 Greden F, Gardne r R, King 0 ,Grunha us L, Carroll ), Kronfol Z (1983): Dexameth asonesuppression test in antidepressant treatment ofmelancholia. Arch Gen Psychiatry 40:493-50 0 Hassan AHS,von Rosenstiel 1', Patchev VK, Holsboer F, Almeida OFX(1996): Exacerbation of apoptosis in the dentate gyrus ofthe aged rat by dexamethasone and the prot ective role ofcorticosterone. Exp NeuroI 140:43-52 Hassan AHS, PatchevVK, von Rosenstiel 1', Holsboer F, Almeida OFX (1999):Plasticity of hippoc ampal corticosteroi d receptors duringaging in the rat. FASEB ) 13:11 5-122 Healy DG, Ha rkin A,Cryan )F, Kelly )1', Leonard BE (1999): Metyrapone displays antidepressant-like properties in preclinical pa radigms. Psychopha rmacology 145:303-308 Heck S, Kullmann M,Gast A, Ponta H, Rahmsdorf H), Herrlich 1', Ca to ACB(1994): A distinct modulating domain in glucocorticoidreceptor monomers in the repression of activity of thetranscription factor AP-J. EMBO ) 13:4087-4 095 Heim C,Newp ort OJ, Heit S, Graham YP, Wilcox M, Bonsall R, MillerAH, Nemeroff CB (2000): Increased pituitary-adrenal andautonomic responses to stress in adult women after sexua land physical abuse in childhood . )AMA, In press Heinr ichsSC, Lapsansky J, Lovenberg TW, De Souza EB, Chalmers DT(1997): Corticotropin-releasing factor CRF1, but not CRF2receptors mediat e an xiogenic-like behavior. Regul Peptides 71:1 5-21 Heuser I, Yassouridis A, Holsboer F (1994):The combined dexameth asone/ CRH test: A refined laboratorytest for psychiatr ic d isorders. ] Psychiatric Res28:341356 Heuser I)E, Schw eiger U, Gottha rd t U, Schmider J, Lammers CH, Dettling M, Yassouri d is A, Holsboer F(1996): Pituitary-ad renal-system regulation andpsychopathology du ring amitriptyline treatm en t in elderly dep ressed patients and in normal comparison subjects.Am ) Psychiatr y 153:9399 Holsboer F (1999): The rationalefor corticotropin-releasing hormone recept or (CRH-R)antago nists to treat depression and anxiety. ) PsychiatricRes 33:181214
496
Holsboer F, Barden N (1996): Antidepressants and HPA

regulati on. Endocrinol Rev 17:187-203
Holsboer F, Liebl R, Hofschuster E (1982): Repeateddexamethaso ne su ppression test durin g depr essiveillness. Norma lization of test result compa red withclinical improvement. I Affect Disord 4:93-10 1
Holsboer F, Gerken A, Von Bardeleben U, Grimm W, Beyer H,Muller OA, Stalla GK (1986): Human corticotr opinreleasinghormone (CRH) in patients with depre ssion, alcoholism andpanic disord er . Bioi Psychiatry 21:601611
Holsboer F, Von Bard eleben U, Wi edemann K, Muller OA,Stalla GK (1987): Serial assessm ent ofcorticotropinreleasing hormone response after dexamethasonein depr ession -implications for pathophy siology of DSTnon suppression. Bioi Psychiatr y 22:228-234
Holsboer F, Spengler 0 , Heuse r I (1992): The role ofcorticotropin-releasing hormone in the pathogenesis ofCushing's disease, anorexia ner vosa, alcoholism, affectivedisord ers and dementia. Prog Brain Res 93:385-417
Holsboer F, Lauer C], Schreiber W, Krieg I-C. (1995):Altered hypothalamic-pituitary adrenocortical regulation inhealthy subjects at high familial risk for affectivedisorders. Neuro end ocrinology 62:340-347
Holsboer-Trachsler E, Hemm eter U, Ha lzinger M, SeifritzE, Gerhard U, Hobi V (1994): Sleep deprivation and br ightlight as pot ential augmenters of antidepressant dru gtreatm e nt-neurobiological and psychom etric assessment ofcours e. I Psychiat ric Res 28:381-399
Hope BT, Nye HE, Kelz MB, Self OW, ladarola MI, Nakab eppuY, Dum an RS, Nes tler EI (1994): Indu ction of along-lasting AP-1 complex compose d of altered Fos-likeproteins in brain by chronic cocaine and other chronic treatments. Neu ron 13:1235--1244
Huizenga NATM, Koper IW, de Lange P, Pols HAP, de long FH,Stolk RP, Grobbee DE, Lamberts SWI (1998): Interperson variability, but intraperson r eproducibililty of baselinecortisol concentrations and its relation to the feedbacksensitivity of the hypoth alamo-p ituitary-adr enal axis tolow do se dexamethasone. I Clin End ocrinol Metab 83:4754
[oels M, de Kloet ER (1992): Control of neuronalexcitability by cor ticosteroid hormones. Trend s Neuro sci15:25--30

Kafitz KW, Rose CR, Thoenen H, Konn erth A (1999):Neurotrophin-evoked rapid excitation th rough TrkBreceptors. N ature 401:918-92 1
Kanelakis KC, Mori shima Y, Dittmar KD, Ga ligniana MD,Takayama 5, Reed IC, Pratt WB (1999): Differential effectsof the hsp70-binding protein BAG-1 on glucocorticoidreceptor folding by the hsp9 0-based chap eron e machinery.I Bioi Chem 274:34134-34140
Kang KI, Meng X, Devin-Leclerc I, Bouhouche I, Chadli A,Cadepond F, Baulieu E-E, Catelli M-G (1999): The molecularchaperone hsp90 can negatively regulate the activity of aglucocort icosteroid-d ep endent promoter. Proc Nall AcadSci USA 96:14391444
Karanth 5, Linthorst ACE, Stalla GK, Barden N, Holsboer F,Reul IMHM (1997): Hypoth alamic-pituita ry-adrenocorticalaxis changes in a transgenic mouse with impairedglucocorticoid receptor function. Endocrinology138:34763485 LOGY Karolyi I), Burrows HL, Ramesh TM,Nakajima M, Lesh IS, Seong E, Camper SA, Seasholtz AF(1999): Altered anxiety and weight gain incorticotropin-releasing hormone-bind ing prot ein-deficientmice. Proc Nall Acad Sci USA 96:11595-11600 Kendl er KS,Karkowski LM, Prescott CA (1999): Causal relation ship between stress ful life events and the onset of majordepression. Am I Psychiatry 156:837-8 41 Kerr OS, Campe llLW, Appl egate MD, Brodish A, Landfield PW (1991): Chroni cstress-induced acceleration of electrophysiologic andmorphometric biomarkers of hippocampal aging. I Neuros ci11:1316-1324 Kish imoto T, Radulovic I, R adulovic M, LinCR, Schrick C, Hooshm and F, H ermanson 0 , Rosenfeld MG,Spiess I (2000): Deletion of Crhr2 reveals an anxiolyticrole for corticotropin-releasing hormone receptor-2. NatureGenet 24:415-419 Koper IW, Stolk RP, de Lange P, Hu izengaNATM, Molijn G-I, Pols HAP, Grobbee DE, Karl M, de long FH,Brinkmann AO, Lamberts SWI (1997): Lack of associa tionbetw een five polymo rph isms in the human glucocorticoidreceptor gene and glucocorticoid resistance. Human Genet99:663--{i68 Kor te M, Carroll P, Wolff E, Brem G, ThoenenH, Bonhoe ffer T (1995): Hippocampal long-term potentiation is impaired in mice lacking brain-derived neur otrophi cfactor . Proc Natl Acad Sci USA 92:8856-8860 Korte M,Griesbeck 0 , Grave l C, Carroll P, Staiger V, Thoenen H,Bonh oeffer T (1996): Virus-med iated gene transfer intohippoc ampal CA1 region restores long-term potentiation inbrain-derived neurotrophic factor mutant mice. Proc NallAcad Sci USA 93:1254712552 Lackner C, Daufeldt 5, Wildt L,

Allera A (1998): Glucocorticord-recogniz ing and -effectorsites in rat liver plasma membrane. Kinet ics ofcorticosterone uptake by isolated membrane vesicles. III.Specificity and stereospecificity. I Stero id Biochem MolBioi 64:6982 Ladd CO, Owens M], Nemero ff CB (1996):Persistent changes in corticotropin-releasing factor neuronal systems induced by mat ernal deprivation . Endocrinology 137:1212-1218 Lamber ts SWj, Koper IW, Biemond P,den Holder FH, de long FH (1992): Cortisol receptorresistance: The variability of its clinical presentationand response to treatment. JClin Endocrin ol Metab74:313321 Lamberts SWj, Hui zeng a ATM, de Lange P, de longFH, K oper IW (1996): Clinical aspec ts of glucocorticoidsensitivity. Steroids 61:157160 Landfi eld PW, Baskin RK,Piller TA (1981): Brain aging correlates: Retardation byhorm onal-ph arm acological treatments. Science 214:581-584Lanz RB, McKenna Nj , Ona te SA, Albrecht U, Wong I, TsaiSY, Tsai M-j, O'Malley BW (1999): A steroid receptorcoactivator, SRA, function s as an RNA and is present in anSRC-1 compl ex. Cell 97:17-2 74 Lauer q , Schreiber W,Modell 5, Holsboer F, Krieg I-C (1998): The Muni ch vulnerabilit y study of affective disorde rs. I Psychiatric Res32:393-401 Legradi G, Holzer 0 , Kapcala LP, Lechan RM(1997): Glucocortico ids inhibit st ress-indu ced ph osphorylation of CREB in corticotropin -releas ing h ormoneneurons of
N NO.5 the hypothalamic paraventricular nudeus .Neuroendocrin ology 66:8697
Leveren z )B, Wilkin son CW, Wamble M, Corbin S, Grabber)E, Raskind MA. Peskind ER (1999): Effect of ch ronichigh-d ose exogenous cortiso l on hippocam pa l neurona lnumber in age d nonhuman prima tes . ) Neurosci 19:2356-2361
Levine S, Mullins RF (1966): Hormona l influences on brainorgani zation in infant rats. Scien ce 152:1585-1592
Liebsch G, Landgraf R, Gerstbe rge r R, Probst )C, WotjakCT, Enge lmann M, Ho lsbo er F, M ontkowski A (1995):Chronic infu sion of a CRH, recept or antisense oligodeoxynu deotide into the centra l nudeus of the amygda la reducedanxiety-rela ted behavi or in socially defeated rats. Regul Peptides 59:229239
Liebsch G, Land graf R.Eng elma nn M, Lorscher 1', HolsboerF (1999): Differenti al behavi oural effects of chronicinfusion of CRH, and CRH , receptor antisenseoligodeoxynudeotid es in to the rat brain. ) Psychia tric

Res 33:153163
Linthorst ACE, Flach skamm C, Hopkins S). Hoadley ME, Labeur MS, Holsbo er F, Reu l )MHM (1997): Long -term intraccrebrovcnt ricular infusion of corticotropin-releasinghormone alters neuroend ocrine, neurochemical. autonomic, behavioral, and cytokine responses to a systemic inflammatory cha lleng e. ). Neurosci 17:4448--4460
Linth orst ACE, Kar anth S, Barden N, Holsbo er F, Reul)MHM (1999): Imp air ed glucocorticoid recept or functionevolves in ab err ant ph ysiological responses to bacterial endotoxin . Eu r JNe urosci 11:178-186
Linthorst ACE, Flachsk amm C, Barden N, Ho isboer F, Reul)MHM (2000): Glucoco rticoid recept or impairment altersCNS resp onses to a psychological stressor: An invitromicrodialysis study in transgen ic mice . Eur )Neurosci 12:283291
Liu ], DeFran co DB (1999): Chromatin recyd ing of glucocorticoid rec eptors: Implications for multiple roles of heat shock protein 90. Mol End ocrin ol 13:355-365
Loo H, Saiz-Rui z ], Costa e Silva )A, Anss eau M, He rringto n R, Vaz-Serra A, Dilling H, de Risio S (1999):Efficacy and sa fety of tian eptine in the treatment of depressive diso rde rs in comparison with fluoxetine. ) AffectDisord 56:1 09-118
Lupi en S), de Leon M, d e Santi S, Conv it A, Tarsh ish C,Na ir NI'V , Thaku r M, McEwen BS, Hau ger RL, Mea ney M)(1998): Corti sol levels during human agin g p redic thippoc ampal atrophy and mem or y deficits. Nature Neurosci1:6973
Maga riflos AM, McEwen BS, Fltigge G, Fuchs E (1996):Chronic psycho socia l stress causes apica l de ndriticatrophy of hippocampal CA3 pyramidal ne urons in subo rdinate tree shr ews .) Neurosci 16:3534-3 540
Magariflos AM, Ve rdugo )M, McEwen BS (1997): Ch ronicstress alters syna p tic t erminal structure inhippocampus. Proc Nall Acad Sci USA 94:1400214008
Malkoski SM, Handanos CM, Dron RI (1997): Localiza tion ofa nega tive glucocortic oid response element of the humancorti cotrop in releasing horm one gene . Mol Cell EndocrinoI 127: 189-199

Malkosk i SP, Dorin RI (1999): Co mpos ite glucocorticoidregulat ion at a functionally defined negat iveglucocorticoid or Hyp response element of the humancorticotrop in-releas ing hormone gen e. Mol Endoc rino I13:16291644 Mangelsdorf D), Thummel C, Beato M, Herrlich1', Sch utz G, Umesono K, Blumberg B, Kastn er 1', Mark M,Chambon 1', Evans RM (1995): The nud ear recept or superfamily: The second decade. Cell 83:835-8 39 McEwen BS,Angulo L Cam eron H, Chao HM, Dan iels D, Gannon MN , GouldE, Mendelson S, Sakai R, Spencer R.Woolley C (1992):Paradoxical effects of ad renal steroids on the brain :Protection versus degeneration. Bioi Psychiatry 31:177-19 9Meijer OC, Co le T). Schm id W, Schu tz G, [oe ls M, DeKloet ER (1997): Reg ulati on of hippocampal 5-HTlA receptor mRNA and binding in transgenic mice with a targeteddisruption of the glucocortico id receptor. Mol Brain Res46:290-296 Meijer OC, de Lange ECM, Breimer DD, de Boer AG,Workel )0 , De K10et ER (1998): Penetration ofdexamethasone into brain glucocorti coid targets isenhanced in mdrIAP-glycoprotein knockout mice. Endocrinology 139:1789-1 793 Modell S, Yassouridis A, Hub er ),Hoisboer F (1997): Corticosteroid receptor function isdecreased in depressed pati ents . Neuroendocrinol ogy65:216-222 Mode ll S, Lauer C), Schreiber W, Huber J. Krieg)-C, Holsboer F (1998): Horm onal re sponse pattern in thecombined DEX-CRH test is stable ove r time in subjects athigh familia l risk for affective d isord ers. N europsychopharmac ology 18:253-2 62 Montkowski A, Barden N, WotjakC, Stec I, Ganster I. Mean ey M, Enge lmann M, Reu l )MHM ,Landgraf R, Holsboer F (1995): Longterm antid epressanttreatment reduces behaviou ral deficits in transgenic micewith impaired gluc ocorticoid recep tor fun ction . )NeuroendocrinoI7 :841-845 Mor issett e), Villeneuv e A,Lord eleau L, Rochette D, Laberg e C, Gagn e B, L aprise C,Bouchard G, Plante M, Gobeil L, Shink E, Weiss enba c h).Bard en N (1999): Gen ome-wide sea rch for lin kage ofbipolar affective diso rders in a ve ry large pedig reederived from a homogeneous population in Quebec p oints toa locus of major effect on chromosome 12q23-q24. Am ) MedGene t 88:567-587 Muller MB, Lucassen PI, Yasso u rid is A,Hoogendijk WIG, Holsboer F, Swaab DE (1998): The humanhippocamp us in major d epression or following ad ministration of glucocorticoids: No evidence for major structuralalterations . Soc Neurosci Abstr 24:990 Mu rphy BEl'(1991): Tre atment of major depression with steroidsuppressive drugs. ) Steroid Biochem Mol Bioi 39:239-244Murphy BEl', Filipini D, Ghadirian AM (1993): Poss ible uscof glucoco rticoid receptor an tagonists in the treatmentof major depression: Prelim inary resu lts using RU 486. JPsych iatry Neurosci 18:209213 Murphy El' , Conneely OM

(1997): Neuroend ocrine regulation of the hypotha lam icpituitary ad rena l axis by the nurrl / nu r77 subfamily ofnudear recep tors. Mol End ocrino logy 11:39-4 7 Nelson MD,Saykin A), Flash ma n LA, Ri ordan H) (1998): Hi ppocampalvolume reduction in schizophrenia as asses sed by magneticresonance imaging. A meta-ana lytic study. Arch Gen Psychiatry 55:433-4 40
498
Nemeroff CB, Widerlov E, Bissette G, Walleus H, Karlsson I,Eklund K, Kilts DC, Loosen PT, Vale W (1984): Elevatedconcentrations of CSF corticotropin-releasing factor-likeimmunoreactivi ty in depressed patients. Science226:1342-1344
Nemero ff CB, Owens MI, Bissette G, A ndom AC, Stanley M(1988): Reduced corti cotrop in releasing factor bindingsites in the frontal cortex of suicide victims. Arch GenPsychiatry 45:377-379
Newco mer IW, Selke G, Melson AK, Hershey T, Craft S,Richard s K, Alders on AL (1999): Decreased memoryperformance in health y humans induced by stress-levelcortisol treatment. Arch Gen Psychiatry 56:527-533
Nollen EAA, Brunsting IF, Song I, K ampinga HH, Morimoto RI(2000): Bagl functions in vivo as a negativ e regulator ofhsp70 cha perone activity . Mol Cell Bioi 20:1083-1088
O'Dwyer AM. Lightman SL, Marks M. Cheekley SA (1995):Treatment of major depression with metyrapone and hydrocort isone. J Affect Disord 33:123-128
Oitzl MS, Fluttert M, De Kloet ER (1994): The effect ofcorticosterone on reacitivity to spatial novelty ismediated by central mineralocor ticosteroid recept ors. EurI Neurosci 6:1072-1079
Orchinik M, Murrey TF, Moore FL (1991): A corticosteroidrecept or in n euronal membranes. Science 252:1848-1851
Owens MI, Nem eroff CB (1991): Physiology and pharmacologyof corticotropin-releasing factor. Pha rmacol Rev43:425-473
Pariante CM, Pearce BD, Pisell TL. Owens M). Miller AH(1997): Steroid-independ ent translocation of theglucocorti coid recept or by the antidepressant desip ramine. Mol PharmacoI 52:571581

Patchev VK, Shoaib M, Holsboer F. Almeida OFX (1994): Theneurosteroid tetrahydroprogesterone counteractscorticotropin-releasing hormone-induced anxiety and altersthe release and gene expression of corticotropinreleasinghormone in the rat hyp othalamus. Neuroscience 62:26 5-271
Patchev VK, Hassan AHS, Holsboer F, Almeida OFX (1996): Theneurostero id tetrahydroprogesterone attenua tes theendocrine response to stress and exerts glucocorticoidlikeeffeets on vaso pressin gene transcription in the rathypoth alamu s. Neuropsychopharmacology 15:53 3-540
Patchev VK, Montkowski A, Rouskova D. Koranyi L. HolsboerF, Almeida OFX (1997): Neonatal treatment of rats with theneuroactive steroid tetrahydrodeoxycorticosterone (THDOC)abolishes the behavioral and neuroendocrine consequences ofadverse early life events . J Clin Invest 99:962-966
Paul SM, Purdy RH (1992): Neuroac tive steroids . FASEB I6:2311-2 322
Pepin MC, Pothi er F, Bard en N (1992): Impaired type IIglucocorticoid-receptor functi on in mice bearing antisense RNA transgene. Nature 355:725728
Pfahl M (1993): Nuclear recept or/ AP-l interaction .Endocrinol Rev 14:651-658
Philips A, Maira M. Mullick A, Chamberland M, Lesage S, Hugo P, Drouin I (1997): Antagonism between Nur77 andglucocort icoid receptor for control of tran scription. MolCell Bioi 17:5952-5959 Plotsky P, Meaney M (1993): Early,postnat al experience alters hypothalamiccorticotropin-releasing factor (CRF) mRNA . median eminenceCRF-content and stressindu ced release in adult rats. MolBrain Res 18:195-200 Potter E, Behan DP, Fischer WH, LintonEA, Lowr y PJ, Vale WW (1991): Cloning and characterization of the cDNAs for human and rat corticotropinreleasing factor-bind ing proteins. Natur e 349:423-426Pratt WB, Dittmar KD (1998): Studies with purifi edchaperones ad vance the unde rstanding of the mechanism ofglucocorticoid receptor-hsp 90 heterocompl ex assembly. TEM9:244252 Purb a IS, Hoogendi jk WIG, Hofman MA. Swaab DF(1996): Increased number of vasopressinand oxytocinexpressing neurons in the paraventricular nucleus of thehypothalamus in depression . Arch Gen Psychiatr y 53:137143Raadsh eer FC, Hoogend ijk WIG. Stam FC, Tilders FH). SwaabDF (1994): Increased numbers of corticotropinreleasinghormone expressing neu rons in the hypothalamic paraventri

cula r nucleus of depressed patients. Neur oendocrinology60:433-436 Radul ovic ], Ruhrnann A, Liepold T, Spiess I(1999): Modul ation of learnin g and anxiety bycorticotropin-re leasing factor (CRF) and stre ss:Differential roles of CRF receptors 1 and 2. I Neuro sci19:5016-5025 Rajkows ka G, Miguel -Hid algo jJ, Wei J,Dilley G. Pittman SD, Meltzer HY, Overholser IC, Roth BL,Stockmeie r CA (1999): M orphometric evidence for neuronaland glial prefrontal cell pathology in major depression .Bioi Psychiatry 45:10851098 Reichardt HM, Kaestn er KH,Tuckermann I. Kretz 0 , Wessely 0 , Bock R, Gass P, SchmidW. Herrlich P, Ange l P, Schutz G (1998): DNA binding ofthe glucocorti coid receptor is not essential for survival. Cell 93:531-541 Reynold s PD, Ruan Y,Smith DF, Scammell IG (1999): Glucocorticoid resistance in the squir relmonkeys is associated with overexpr ession of theimmunophilin FKBP51. ) Clin Endoc rinol Metab 84:663-669Reul JMHM, Stec I. SOde r M, Holsboer F (1993): Chronic treatment of rats with the antidepressant amitriptylineattenua tes the activity of the hypothalamic-pituitaryadrenocortical system . Endocrino logy133:312-320 Reul JMHM, Labeur MS, Grigoriad is DE, De SouzaEB, Holsboer F (1994): Hypothalamic-pituit ary-ad renocortical axis changes in the rat after long-term treatm ent withthe reversible monoamine oxidase-A inhibitor moclobemid e.Neuroendoc rinology 60:509-519 Reu l IMHM, Probst IC,Skutella T, Hirschmann M, Stec IS, Montk owski A, Land grafR, Hoisboer F (1997): Increased stress-inducedadrenocorticotropin response after long-term intracerebroventricular treatment of rats with antisensemineralocorticoid receptor oligod eoxynucl eotid es. Neuroendocrinology 65:189-199 Rochford I, Beaulieu S, Rousse I,Glowa I, Barden N (1997): Behavioral reactivity to aversivestimuli in a transgenic mouse mod el of impairedglucocorticoid (type II) receptor function : Effects of diazep am and FG·7142. Psychopharmacology 132:145-152 Romeo E,Strehle A. Spalletta G, d i Michele F, Hermann B, Holsbo erF, Pasini A, Ruppre cht R (1998): Effects of
N NO.5 antide pressa nt treatment on neuroactive steroidsin major dep ression . Am j Psychiatry 155:910-9 13
Rooze ndaal B, Nguyen BT, Power AE, McGaugh jL (1999):Basolateral amygdala noradrenergic influence enablesenhancement of memory conso lida tion induced by hippocampal glucocorticoid recept or activation . Proc Natl Acad SciUSA 96:11642-1 1647
Rossby SP, Nalepa I, Huang M, Burt A, Perr in C, SchmidtDE, Sulser F (1995): Norepinephrine-independ ent regulat

ion of GRII mRNA i" vivo by a tricyclic antide pressant.Brain Res 687:79-8 2
Rossby SP, Man ier DH, Liang S, Na lepa I, Sulser F (1999):Pharm acological actions of the antidepressant venlafaxinebeyo nd am ine rgic receptors. Inti j Neuropsyc hopharmacoI 2:1-8
Rousse I, Beaulieu S, Row e W, Meaney M], Bard en N,Rochford J (1997): Spatial memory in transgeni c mice withimpaired glucoco rticoid receptor function . NeuroReport8:841845
Rubin RT, Poland RE, Lesser 1M, Winston RA, Bl odgett ALN(1987): Neuroend ocrine asp ects of primary endogenousdepression. Arch Gen Psychiatry 44:32S--336
Rupprecht R, Holsboer F (1999): Neuroactive steroids:Mechani sms of action and neuropsyc ho pharmacologicalpersp ectives. Trend s Neu rosci 22:410-4 16
Rupprecht R, Reul jMHM, Trap p T, van Steensel B, Wetzel C,Zieglgansberge r W, Damm K, Holsboer F (1993): Progesteronereceptor medi ated effects of neu roactive steroids . Neuron 11:523-530
Ryba kowski jK, Twardow ska K (1999): Thedexamethasone/corticotropin-releasing hormone test indepression in bip olar and unipolar affective illness . j'Psychiatric Res 33:363370
Sanchez MM, Young Lj, Plotsky PM, Insel TR (1999):Autoradiog rap hic and i" situ hybridization localizationof corticotropin-releasi ng factor 1 and 2 receptors innonhuman prima te brain. j Comp Neur oI408:365-377
Sanchez MM, Young Lj, Plotsky PM, Insel TR (2000): Distribution of corticoste roid receptors in the rhesus brain :Relative absence of glucocor ticoid receptors in the hippoca mpa l f ormation . j Neurosc ience 20:4657-46 68
Sapolsky RM (1992): Stress, the Aging Brain and theMechanism of N euron Death . Londo n, MIT Press
Scha tzberg AF, Roth schild Aj, Lang lais Pj, Bird ED, Coleto (1985): A cor ticosteroid /dopamine hyp othesis forpsycho tic depr ession and related states. j Psychiatri cRes 19:57-64
Schinkel AH, Wagenaar E, Van Deemter L, Mol CAAM, Borst P

(1995): Absence of the mdrla P-glycoprotein in mice affectstissu e distribution and ph arma cokin etics of dexamethasone, d igoxin, and cyclosporin A. j Clin Invest96:16981705
Schneikert J. Hu bner S, Mart in E, Cato ACB (1999): A nuclear action of the eukaryotic cochaperone RAP46 in do wnregulation of glucocorticoid recept or activity. J Cell Bioi146:929940
Schu lkin L Gold PW, McEwen BS (1998): Indu ction ofcorticotropin-releas ing h ormone gene expression by glucocorticoids : Impli cation for und erstanding the states offear and anx iety and allostatic load.Psychoneuroendocrinology 23:219243 Schwaninge r M, SchoelC, Blume R, Rossig L, Knepel W (1995): Inhibiti on byantide pressant drugs of cyclic AMP response element-binding protein / cyclic AMP re sponse clemen t-d irected genetranscripti on . Mol Pharmac oI47:1112-1118 Seash oltz AF,Thompson RC, Doug lass jO (1988): Identi fication of acyclic adenosine mon oph osph ate-resp onsive element inthe rat corticotropin-reieasing IlOr",o"e gene. Mol Endocrino I2 :1311-13 19 Seckl jR (1997): 111l-H ydroxysteroiddehydrogenase in the brain : A neural regulator ofglucocorticoid action? Front N euroendocrin oI1 8:4999Seckl jR, Fink G (1992): Antidepressan ts increaseglucocorticoid and mineralocorticoid receptor mRNAexpression in rat hippocampus ill vivo. Neuroendocrino logy55:621-<;26 Seckl [R, Dickson KL, Yates Co Fink G (1991):Distr ibu tion of glucocorticoid and mineralocorticoidreceptor messenger RNA expression in human postm ort emhipp ocampu s. Brain Res 561:332337 Sheline YI, Wang PW,Gado MH, Hsem ansky JG, Vannier MW (1996): Hippocamp alatro phy in recurr en t major dep ression. Proc Na tl AcadSci USA 93:39083913 Sheline YI, Gado M, Price jL (1998):Amygda la core nuclei vo lumes are decreased in recurrentmajor depress ion . NeuroReport 9:2023-2028 Sheline YI,Sanghav i M, M intun MA, Gado MH (1999): Depr ession duration bu t not age pred icts h ippo campal volume loss inmedically health y women with recur ren t major depr ession. j Neu rosci 19:50345043 Shelton RC, Manier DH, PetersonCS, Truitt CE, Sulser F (1999): Cyclic AMP-de pendent protein kinase in subtyp es of major depression and no rmalvolunteers . Inti j N europsychoph arm acoI 2:187-1 92Shibata H, Spencer TE, Onate SA, jenster G, Tsai SY, TsaiM·J. O' Malley BW (1997): Role of co-activators and corepressors in the mechan ism of steroid / thyroid receptoraction. Rec Progr Horm on e Res 52:141163 Sillaber I, Montkowski A, Landg raf R, Bard en N, Holsboer F, Spanag el R(1998): E nhanced morphine-ind uced beha viou ral effects

and dop amine release in the nucl eus accurnb ens in atransge nic mouse model of impaired glucocorti coid (typeII) receptor function : Influence of long-term treatment with the antidepressant moclobemid e. Neuroscience85:415-425 Siuciak jA, Lewis 0 , Wiegand Sj. Lind say RM(1996): Antidepr essant -like effect of brain-d erived neurotrophic factor . Pharm acol Biochem Behav 56:131137Skutella T, Probst rc. Renner R, Holsboer F, Behl C (1998):Corticotropin-r eleasing horm one receptor (type I)antisense targeting redu ces anxiety . Neu roscience85:795-805 Smith GW, Aubry [-M, Dcllu F, Contarino A,Bilezikjian LM, Gold LH, Hau ser C, Bentl ey CA, SawchenkoPE, Koob GF, Vale W, Lee K-F (1998): Co rticotropinreleasing factor recept or l·deficient mice di splaydecreased anxiety, impaired stress response, and aberrantneuroendocrine developm ent. Neuro n 20:10931103 Sonntag A,Rothe B, Guldner I. Yassouridis A, Holsboer F,
500 Steiger A (1996): Tr imipr amine and im ipramine exertdiff erent effects on the sleep EEG and on nocturnalhormone sec retion du ring treatment of major dep ression.Depr ession 4:1-1 3
Spanage l R, Stohr T, Bard en N, Holsboer F (1996):Morphineinduced locom otor and neurochemic al stimulationis enhanced in transgenic mice with impai red glucocorticoid receptor function . j Neuroend ocrinol 8:93-97
Spencer RL, Kim Pj, Kalman BA, Cole MA (1998):Evidence formineralocorticoid receptor facilitation of glucocorticoidreceptor-depend ent regu lation of hypo thalamic-pituitary-ad renal axis activity. Endocrinology139:2718-2726
Spencer TE, jenster G, Burcin MM, Allis CD, Zhou L MizzenCA, McKenn a Nj , Onate SA, Tsai SY, Tsai M-j, O'Malley BW(1997): Steroid receptor coactivator-l is a histoneacetyltrans ferase . Na tu re 389:194-198
Speng ler 0 , Rup precht R, Phi Van L, Holsboer F (1992):Iden tification and charac terization of a 3',5'-cyclicadenosine mon oph osph ate-responsive element in the humancort icotropin-releasing hormone gen e promo ter. Mol Endocrino I6 :19311941
Stalla GK, Sta lla I. von Werd er K (1989): Nitroimidazolederivates inh ibit anterior pituita ry cell functio napparently by a dir ect effect on the catalytic subunit ofthe ade ny late cyclase holoenzyme. Endoc rinology155:699706

Stec I, Barden N, Reu l jMHM , Holsboer F (1994):Dexamethaso ne nonsu ppression in transgenic mi ce ex pressing antisense RNA to the glucocor ticoid receptor. jPsychia tric Res 28:1-5
Steckler T, Weis C, Sauvage M, Mederer A, Holsboer F(1999): Disrup ted allocentric but preserv ed egocen tricspa tial le arning in transgenic mice w ith impai red glucocorticoid recep tor function. Behav Brain Res 100:77-89
Steckler T, Sa uvage M; Holsboer F (2oo0a): Glucoco rticoidrecept or impa irment enha nces impu lsive respondi ng intransgenic mice performin g on a s imu ltaneous v isual discriminat ion task. Eur J Neu roscience, In press
Steckler T, R ammes G, Sauv age M, van Gaalen MM, Weis C,Zieglgansberger W, Holsboer F (2000b): Effects of themonoamine oxidase A inhibitor moclobemide on hippocampalplasticity in GR-impaired tran sgenic mice. J Psychiatr icRes, In press
Stenze l-Poore MP, Heinrich s SC, Rivest 5, Koob GF, ValeWW (1994): Overprod uction of corticotropin-releasingfactor in transgenic mice: A genetic mod el of anxiogenicbehavior. J Neu rosci 14:25792584
Stoecklin E, Wissler M, Gouilleux F, Groner B (1996):Functional interactions between Sta t5 and the glucocorticoid receptor. Natur e 383:726-728
Stoecklin E, Wissler M, Moriggl R, Groner B (1997):Specific DNA binding of Stat5, bu t not of glucocor ticoidreceptor, is required for their functional co-operation inthe regulation of gene transcription . Mol Cell BioI17:6708-6716
Stre hle A, Poetti g M, Barden N, Holsboer F, Montkowski A(1998): Ageand stimulus-de penden t changes inanxiety-related behaviour of transgenic mice with GRdysfunction . NeuroReport 9:20992102
Stre hle A, Pasini A, Romeo E, Hermann B, Spalletla G, diMichele F, Holsboer F, Rupprecht R (2000) : Fluo xetinedecreases concentrations of 3a,5a -tet rahydrodeoxycor.ticosterone (THDOC) in majo r depression . j PsychiatricRes 34:183-186 Swan son LW, Simmo ns OM (1989): Differential stero id ho rmones and n eural influences on peptidemRNA levels in CRH cells of the para vent ricu lar nucleus: A hybr idizati on hist ochemical study in the rat. j

Comp Neur ol 285:413-435 Thak ore JH, Dinan TG (1995):Cortiso l syn thes is inhibition: A new tr eatment strategyfor the clinical and endoc rine manifestations of depression . Bioi Psychiatry 37:364-368 Timp l P, Spanagel R,Sillaber I, Kresse A, Reul JMHM, Stalla GK, Blanquet V,Steckler T, Holsboer F, Wurst W (1998): Impaired stressresponse and r educed anxiety in mice lacking a functionalcorticotropin-releasing hormone receptor 1. Natu re Genet19:162166 Trapp T, Ruppr echt R, Cas tren M, Reul JMH M,Holsboer F (1994): Hete rodim erization between mineralocorticoid and glucocorticoid recep tor: A new princip le ofglucocorticoid action in the CNS. Neuron 13:14571462 Tr appT, Holsboer F (1996a): Heterodi merization betweenmineralocorticoid and g lucocorticoid receptor increasesthe functional div ersity of cor ticosteroid action. Trendsin Pharmacol Sci 17:14S-149 T rapp T, Holsboer F (1996b):Nuclear orpha n recep tor as a repr essor of glucocorticoid receptor transcriptional activity , j Bioi Chern271:98799882 Tronche R, Kellend onk C, Kretz 0 , Gass P,Anlag K, Orban PC, Bock R, Klein R, Schlitz G (1999): Disruption of the glucocorticoid recep tor gene in thenervous sys tem results in redu ced anxiety . Na tu re GeneI 23:99103 Uhr M, Steckler T, Yassourid is A, Holsboer F(2000): Penetration of amitriptyline, but not fluoxetin e,into brain is enh anced in mice with blood-brain barr ierdeficiency due to mdrla P-glycopr otein gene disruption .Neu ropsych op harm acology 22:38 0-387 Uzunova V, ShelineY, Davis JM, Rasmu sson A, Uzunov DP, Costa E, Gu ido tti A(1998): Increase in the cerebrospinal flu id conten t ofneurosteroids in patients with unip olar major depression who are receiving fluoxetin e or fluvoxa mine. Proc Na tlAcad Sci USA 95:3239-3 244 Vale W, Spiess J, Rivier C,Rivier j (1981): Cha racteriza tion of a 41-residue ovinehypothalamic p eptide that stimulates secretion ofcorticotro pin and (I-endo rphin . Science 213:1394-1397van der Burg B, Liden J, Okret 5, Delaunay F, Wissink 5,van der Saag PT, Gustafsson j-A (1997): Nuclear factor-xbrepression in ant iinflammation and imm unosuppression byglu cocorticoid s. Trends Endoc rinol Metab 8:152157 vanHaarst AD, Welberg LAM, Sut anto W, O itzl MS, De Kloet ER(1996a): l1(1-Hyd roxysteroid dehydroxygenase activity inthe hippocampus: Implica tions for in vivo corticosteron ereceptor binding and ce ll nucl ear retention . j Neuroendocrinol 8:595-600 van Haarst AD, Oitzl MS, Workel [O,Dc Kloet ER (1996b): Chronic brain glucocor ticoid receptor blockad e enhances the rise in circadian andstressinduced pitui tary-ad renal activity, Endoc rinology137:4935-4943 von Barde leben U, Holsboer F (1989): Cortiso l response to a combined dexametha sone-hCRH challenge in patien ts with de press ion. I Ne uroendoc rino l

1:485-488
N
von Bardeleben U, Holsboer F (1991): Effect of age upon thecor tisol response to human CRH in depressed patie nts pretreated with dexamethasone. Bioi Psychia try 29: 10421050
von Bard eleben U, Ho lsboe r F, Stalla GK, Muller OA(1985): Combined administra tion of human corticotropinreleasing factor and lysine vasopr essin induces cortisolescape from dexam ethasone suppression in healthy subjects.Life Sci 37:16131619
Watanabe Y, Gould E, McEwen BS (1992): Stress ind uces atroph y of spa tial den drit es of hippocamp al CA3pyramidal neuron s. Brain Res 588:341-345
Weninge r SC, Dunn A], MugHa L], Dikkes P, Miczek KA,Swiergiel AH, Berrid ge CW, Majzoub jA (1999): Stressinduced beh aviors requi re the cor ticotropin-releasinghormone (CRH) receptor, but not CRH. Proc Nat! Acad Sci USA96:8283-8288
Wissink S, van Heerde EC, van de r Burg B, van der Saag PT(1998): A du al mechan ism med iates repression of NFKBactivity by glucocorticoids . Mol Endocrinol 12:355-363 orWolkowit z OM, Reus VI, Chan T, Manfred i F, Raum W, johnson R, Canick I (1999): Antiglucocorticoid trea tment ofdepression : Doub le-blind ketoconazole. Bioi Psychiatry45:1070-10 74 Young EA, Lopez [F, Murp hy-Weinberg V,Watson SI. Akil H (1998): The role of mineralocorti coidreceptors in hypothalamic-pituitary-adrenal axis regulation in hum ans. j Clin Endocrino! Metab 83:3339-3345Zeiner M, Niyaz Y, Gehring U (1999): The hsp70-associatin gpro tein Hap46 bind s to DNA and stimulates transcription .Proc Nat! Acad Sci USA 96: 10194--10199 Zobel AW, Yassouridis A, Frieboes R-M, Holsboer F (1999): Cortisol responseto the combined dexameth asoneCRH test pred icts medium-term outcome in patients w ith remitted depr ession .Am j Psychiatry 156:949951 Zobel AW, Nickel T, Kunzel HE,Ackl N, Sonntag A, Ising M, HoIsboer F (2000): Effects ofthe high-affinity corticotropin-releasing horm one receptor1 antagonist R121919 in major dep ression: The first 20patients treated. j Psychiat ric Res, 34:171181

A"e A
Sheline et But Not brain and the mechanisms of neuron death, pp 305-3 39. Cambridge, MA :MIT.
Sapo lsky RM, Krey Le , McEwen BS (1983) Corti costeronerecep tors decline in a site-specific manner in the agedrat bra in. Brain Res 289:235-24 0.
Sapolsky RM, Krey LC, McEwen BS (1985) Prolongedglucocorticoid exposure reduces hippocamp al neuron number: implications for aging. J Neurosci 5:12221227.
Sapolsky RM. Krey LC, McEwen as (1986) Th eneuroendocrinology of stress and aging: the glucoco rticoidcascade hypothesis. Endocrinol Rev 7:284301.
Sapolsky RM, Uno H, Rebert CS, Finch CE (1990) Hippocampaldamage associated with prolonged glucoco rticoid exposurein prim ate s. J Neurosci 10:2897-2902.
Sapolsky RM , Zola-Morgan 5, Squire L (1991) Inhibition ofglucoco rticoid secre tion by the hippocampal form at ionin the primate. J Neurosci 11:36953704.
Sheline YI, Wang PW, Gado MH , C sernansky JO . Vannier MW(1996) Hippocampal atrophy in recurrent major depression.Proc Na t! Acad Sci USA 93:3908-3913.
Sheline YI, Gado M, Price JL (1998) Amygdala core nucleivolumes arc: decreased in recurrent major depression.NeuroReport 9:20232028.
Squire LR (1992) Declarati ve and nondeclarative memory:multipl e brain systems supporting learn ing and memory. JCognit Neurosc i 4:232243.
Tierney MC, Szalai J P, Snow WG, Fisher RH, Nores A, NadonG, Dunn E, SI. Geo rge-Hyslop PH (1996) Predict ion ofprobable Alzheime r's disease in memory-impair ed patients:a prospective longitudinal study. Neurology 46:661 -665. Tombaugh GC, Sapolsky RM (1992) Co rticosterone accelerateshypoxiaand cyanide-induced AT P loss in culturedhippocampal astrocytes. Brain Res 588:154158. Watanabe Y,Go uld E, McEwen B5 (1992b) Stress induces atrophy ofapical dendrites of hippocampal CA3 pyramid al neurons.Brain Res 588:341345. West MJ (1993) Regionally specificloss of neurons in the aging human hippocam pus. Neurob iolAging 14:287293. Weehsler 0 (1981) WAIS-R manu al. NewYork: Th e Psychological Co rporation. Wechsler D (1987)

Wechsler Memory Scale-Revised Manu al. San Antonio, TX : The Psychological Cor poration. Whiteford H. Peabody C, Csernansky J, Warner M, Berger P (1987) Elevated baseline andpostdexameth asone cortisol levels. A reflection ofseverity o r endogeneity? J Affective Disord 12:19 9-202.Wong M, Loddi ck S, Bongiorno P, Gold P, Rothwell N,Licinio J (1995) Focal ce rebral ischemia induces CRH mRNAin rat cerebral cortex and amygdala. N euroReport6:17851788. Wooley C, We iland N, McEwen B, Schwartz kroinP (1997) Estradiol increases the sensitivity of hippocampalCAl pyramid al ce lls to NMDA recept or-mediated synapticinput: correlation with dendrit ic spine density. JNeurosci 17:1848-1 859. Young EA , Haskett RF, Murphy-Weinberg V, Watson SJ, Akil H (1991) Loss of glucocorticoidfast feedback in depression. Arch Gen Psychiatry 48:693698.