
Clinical, Pathologic, and Immunologic Features of Human T-Lymphotrophic Virus Type I–Associated...
9
Clinical, Pathologic and Immunologic Features of Patients With Non-Hodgkin’s Lymphoma in a Leukemic Phase A Retrospective Analysis of 34 Patients ROBERT J. FRAM, MD,” ARTHUR T. SKARIN, MD. DAVID S. ROSENTHAL. MD, GERALDINE PINKUS, MD, AND LEE M. NADLER, MD A retrospective review of 34 patients with non-Hodgkin’s lymphoma and a leukemic phase was un- dertaken. The median survival after onset of a leukemic phase was 30 months for patients with nodular poorly differentiated lymphocytic lymphoma which was significantly longer than 19 months for diffuse poorly differentiated lymphocytic lymphoma, and 2 months for diffuse histiocytic and undifferentiated lymphoma. Clinical features of patients with diffuse histologies that contributed to a poor prognosis included advanced stage of disease as well as age. Underlying lymph node histology also defined features of the leukemic phase which included duration, peak leukocyte count, and in some instances, distinctive morphologic characteristics of circulating malignant cells. Although small sample size did not permit definitive correlations of immunological subtype and survival, heterogeneity was noted, suggesting that clearer stratification of these patients with immunologic techniques may be useful in assessing prognosis in future investigations. Cancer 52:1220-1228, 1983. NEW LEUKEMIC PHASE Of non-Hodgkin’s lym- A phoma (NHL) occurs when malignant cells are present in the peripheral blood. The latter may occur as a transient finding, but with a persistent or progressive leukemic phase, prognosis generally worsens. Peripheral blood involvement as assessed by light microscopy has been reported in 7.6% to 14% of patients.’ Using more sensitive immunologic techniques, small numbers of monoclonal populations of B-lymphocytes have been detected in the peripheral blood of more than 30% of patients with non-Hodgkin’s l y m p h ~ m a ~ . ~ without an overt leukemic phase. The significance of the latter ob- servation with regard to prognosis is not known. Lymph node histology appears important in deter- mining the prognosis of patients with NHL in a leu- kemic phase as assessed by light microscopy! While this From the Departments of Medical Oncology and Tumor Immunology. Dana-Farber Cancer Institute, Hematology and Pathology Divisions, Brigham and Women’s Hospital, Harvard Medical School, Boston. Massachusetts. Supported in part by grant Number R25 CA I7979 from the National Institutes of Health, Public Health Service. and a *Clinical Scholar grant from the American Cancer Society. The authors thank Cyrus R. Mehta, PhD, Department of Biostatistics and Epidemiology, Dana-Farber Cancer Institute. for his advice. and Ms. Adele Joseph for her secretarial assistance. Address for reprints: Arthur T. Skarin, MD, Dana-Farber Cancer Institute, 44 Binney Street, Boston, MA 02 1 15. Accepted for publication July 2, 1982. phase, often called “lymphosarcoma cell leukemia,” has been viewed as a preterminal event?5 more recent stud- ies have emphasized the longer median survival of pa- tients with a nodular histology and lymphosarcoma cell leukemia compared to diffuse histologic types with a leukemic phase.6 In order to further clarify the latter, the clinical course of 34 patients with non-Hodgkin’s lymphoma in a leukemic phase as assessed by light mi- croscopy was reviewed. All patients had histologically documented non-Hodgkin’s lymphoma. Leukemic cells in 20 patients were evaluated with immunologic tech- niques. Major goals were to correlate prognosis with re- spect to histologic and immunologic subtype and to more clearly define clinical features of the leukemic phase. Materials and Methods The clinical records of patients with non-Hodgkin’s lymphoma treated at the Brigham and Women’s Hospital and the Dana-Farber Cancer Institute from 1963 to 1980 and 197 I to 1980, respectively, were reviewed. Forty-four patients with non-Hodgkin’s lymphoma had abnormal lymphoid cells in their peripheral blood. Of the latter, 34 had bone marrow aspirates and biopsies as well as serial complete blood counts with peripheral blood smears available for review. Thirty patients had simultaneous lymph node biopsies. Patients with lymphoblastic lym- OOO8-543X/83/1001/1220 $1.25 Q American Cancer Society 1220
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Clinical, Pathologic, and Immunologic Features of Human T-Lymphotrophic Virus Type I–Associated...
Clinical, Pathologic and Immunologic Features of Patients With Non-Hodgkin’s Lymphoma in a Leukemic Phase
A Retrospective Analysis of 34 Patients
ROBERT J. FRAM, MD,” ARTHUR T. SKARIN, MD. DAVID S. ROSENTHAL. MD, GERALDINE PINKUS, MD, AND LEE M. NADLER, MD
A retrospective review of 34 patients with non-Hodgkin’s lymphoma and a leukemic phase was un- dertaken. The median survival after onset of a leukemic phase was 30 months for patients with nodular poorly differentiated lymphocytic lymphoma which was significantly longer than 19 months for diffuse poorly differentiated lymphocytic lymphoma, and 2 months for diffuse histiocytic and undifferentiated lymphoma. Clinical features of patients with diffuse histologies that contributed to a poor prognosis included advanced stage of disease as well as age. Underlying lymph node histology also defined features of the leukemic phase which included duration, peak leukocyte count, and in some instances, distinctive morphologic characteristics of circulating malignant cells. Although small sample size did not permit definitive correlations of immunological subtype and survival, heterogeneity was noted, suggesting that clearer stratification of these patients with immunologic techniques may be useful in assessing prognosis in future investigations.
Cancer 52:1220-1228, 1983.
NEW LEUKEMIC PHASE Of non-Hodgkin’s lym- A phoma (NHL) occurs when malignant cells are present in the peripheral blood. The latter may occur as a transient finding, but with a persistent or progressive leukemic phase, prognosis generally worsens. Peripheral blood involvement as assessed by light microscopy has been reported in 7.6% to 14% of patients.’ Using more sensitive immunologic techniques, small numbers of monoclonal populations of B-lymphocytes have been detected in the peripheral blood of more than 30% of patients with non-Hodgkin’s l y m p h ~ m a ~ . ~ without an overt leukemic phase. The significance of the latter ob- servation with regard to prognosis is not known.
Lymph node histology appears important in deter- mining the prognosis of patients with NHL in a leu- kemic phase as assessed by light microscopy! While this
From the Departments of Medical Oncology and Tumor Immunology. Dana-Farber Cancer Institute, Hematology and Pathology Divisions, Brigham and Women’s Hospital, Harvard Medical School, Boston. Massachusetts.
Supported in part by grant Number R25 CA I7979 from the National Institutes of Health, Public Health Service. and a *Clinical Scholar grant from the American Cancer Society.
The authors thank Cyrus R. Mehta, PhD, Department of Biostatistics and Epidemiology, Dana-Farber Cancer Institute. for his advice. and Ms. Adele Joseph for her secretarial assistance.
Address for reprints: Arthur T. Skarin, MD, Dana-Farber Cancer Institute, 44 Binney Street, Boston, MA 02 1 15.
Accepted for publication July 2, 1982.
phase, often called “lymphosarcoma cell leukemia,” has been viewed as a preterminal event?5 more recent stud- ies have emphasized the longer median survival of pa- tients with a nodular histology and lymphosarcoma cell leukemia compared to diffuse histologic types with a leukemic phase.6 In order to further clarify the latter, the clinical course of 34 patients with non-Hodgkin’s lymphoma in a leukemic phase as assessed by light mi- croscopy was reviewed. All patients had histologically documented non-Hodgkin’s lymphoma. Leukemic cells in 20 patients were evaluated with immunologic tech- niques. Major goals were to correlate prognosis with re- spect to histologic and immunologic subtype and to more clearly define clinical features of the leukemic phase.
Materials and Methods
The clinical records of patients with non-Hodgkin’s lymphoma treated at the Brigham and Women’s Hospital and the Dana-Farber Cancer Institute from 1963 to 1980 and 197 I to 1980, respectively, were reviewed. Forty-four patients with non-Hodgkin’s lymphoma had abnormal lymphoid cells in their peripheral blood. Of the latter, 34 had bone marrow aspirates and biopsies as well as serial complete blood counts with peripheral blood smears available for review. Thirty patients had simultaneous lymph node biopsies. Patients with lymphoblastic lym-
OOO8-543X/83/1001/1220 $1.25 Q American Cancer Society
1220

No. 7 LEUKEMIC PHASE OF LYMPHOMA - Frum ez a/. 1221
10 20 30 40 50 60 70 80 90 100 110
Time (months)
FIG. I . Survival after onset of a leukemic phase in patients with non-Hodgkin's lymphoma.
phoma and well differentiated lymphocytic lymphoma were excluded from this study.
All patients had routine examinations and laboratory studies. Peripheral smears were stained with Wright- Giemsa and were assessed for the presence of abnormal lymphoid cells defined as follows: cleaved or fissured lymphocytes; medium sized lymphocytes with nucleoli; and large lymphoid cells generally with eccentrically placed nucleoli and vacuolated cytoplasm. The presence of greater than 5% abnormal lymphoid cells on more than one occasion was defined as a leukemic phase. Lymph node biopsies were reviewed by one of the au- thors (G.P.) and categorized according to a modified Rappaport classification as follows: nodular poorly dif- ferentiated lymphocytic lymphoma (NPDL), nodular mixed lymphocytic histiocytic lymphoma (NML), dif- fuse poorly differentiated lymphocytic lymphoma (DPDL) exclusive of lymphoblastic lymphoma, diffuse moderately well differentiated (intermediate) lympho- cytic lymphoma (DMWDLL), diffuse undifferentiated non-Burkitt's lymphoma (DUL) or diffuse histiocytic lymphoma (DHL). Peripheral smears and complete blood counts were routinely obtained at follow-up visits. Repeat bone marrow studies were done in 25 patients and subsequent lymph node biopsies were obtained in 9 patients. Biopsies of other tissues and Shen prepara- tions of pleural fluid and cerebrospinal fluid were carried out in 2 1 patients.' Postmortem examinations were per- formed in 13 patients. Patients were staged by the stan- dard Ann Arbor classification after evaluation of intra- venous pyelogram (IVP), lymphangiogram, or abdom- inal CT scan, and repeat biopsies if clinically appropriate.
lmmunologic studies were performed on 20 patients. Lymphoid cells were obtained from the peripheral blood during the leukemic phase and in some instances from lymph nodes as well. Cells were characterized for surface
immunoglobulin (slg), the intensity of fluorescence of surface immunoglobulin (whether bright, moderate, or faint, Ia, Common ALL Antigen [CALLA]), B,-cell (a B-cell differentiation antigen), and T-cell antigens using monoclonal antisera and the fluorescent activated cell sorter as previously de~cribed.~.~
Patients were treated by a variety of modalities, in- cluding cyclical combination chemotherapy (20 cases), single alkylating agents (9 cases), total nodal irradiation (1 case), total body irradiation (3 cases), and involved field radiotherapy (1 case). Responses to therapy were classified as a complete remission when no evidence of disease was present for at least one month after therapy, or as a partial remission when greater than 50% regres- sion of measurable disease occurred. Patients with either stabilization or progression of disease were classified as having no response.
Survival was evaluated from initial diagnosis as well as after onset of a leukemic phase of lymphoma. Patients were analyzed according to initial histologic diagnosis as well as laboratory and clinical findings at the time of a leukemic phase. Statistical analysis was carried out by life tables and statistical significance was assessed with the chi-square test for comparing survival curves. io9'
Results
Histologic subtype was the most important overall prognostic determinant. The survival of patients in a leukemic phase was significantly longer in patients with NPDL than in those with diffuse histologies. Of patients with NPDL at the time of their leukemic phase, 50% survived 30 months after the onset of a leukemic phase of their lymphoma compared to a median survival of 19 months for patients with DPDL and two months for patients with DUL and DHL (Fig. 1). The latter differ-
I222 CANCER October I 1983 Vol. 52
. = Patient still alive ( ) = Number of patients at risk
(3) _______-____--_---------. I
L -------. I
(2)
I I L,-- NPDL (11
(21 I WDL i (1)
I I I I I I I 1 I 1 : 11 10 20 30 40 50 60 7 0 80 90 100 110
Time (months)
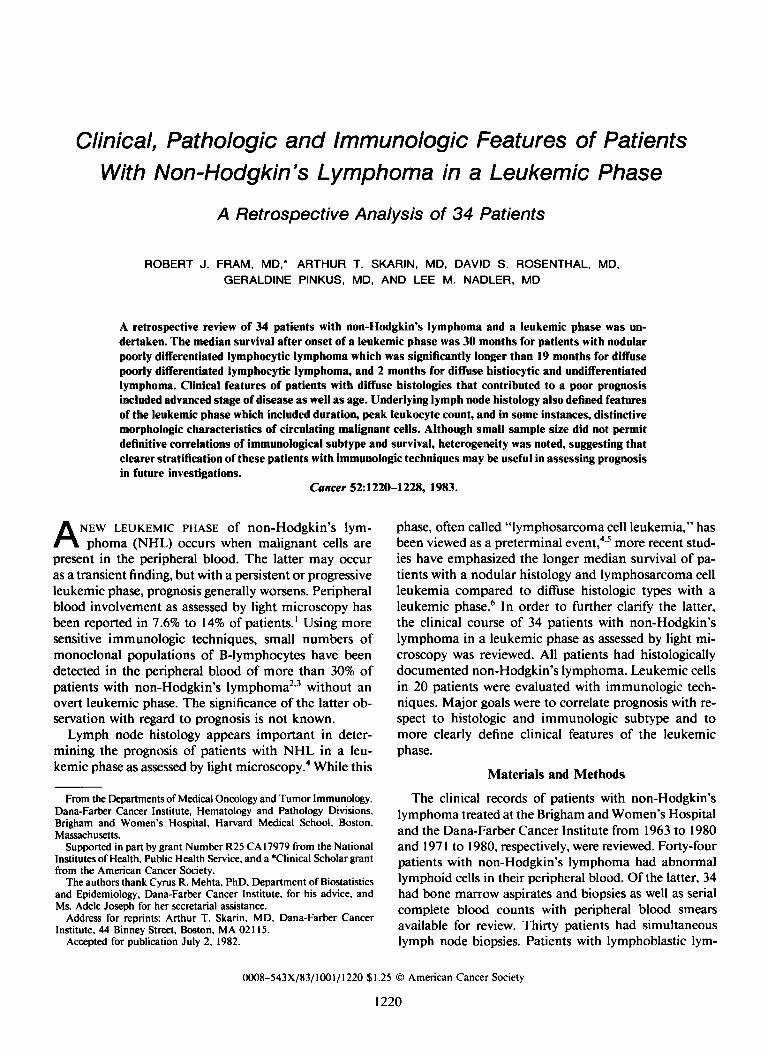
FIG. 2. Survival after diagnosis of non-Hodgkin's lymphoma in patients who had a leukemic phase.
TABLE 1. Clinical Features of Patients
Pathologic diagnosis
NPDL NM DPDL DUL DHL
No. of patients Age
Sex: male/female Stage at diagnosis
Median Range
IV 111
B symptoms during
Lymphadenopathy Hepatomegaly Splenornegal y Extranodal (other than
bone marrow and liver)
involvement
course
Bone marrow
At diagnosis During course
CBC at diagnosis Anemia Leukopenia Thrombocytopenia Onset of leukemic
phase At diagnosis During course Average time until
onset of a leukemic phase (mo)
7 2
53 45 30-72 24-64
513 111
6 2 1 0
I I 7 2 3 1 4 2
20
61
1416
20 0
9 19 6
15
32-12
2 3
44 51 25-62 28-57
111 112
2 3 0 0
1 2 1 2 I 2 0 2
3 1 7 0 3
5 1 20 2 2 I 2 I
I 1 8 2 2 0 0 3 1 2 0 0 7 I I
- -
2 I 14 1 1 5 1 6 1 2
18.7 70 1 1.5 3
NPDL nodular poorly differentiated lymphocytic lymphoma: NML: nodular mixed lymphocytic histiocytic lymphoma: DPDL diffise poorly differentiated lymphocytic lymphoma; D H L diffuse histiocytic lyrn- phoma; DUL diffuse undifferentiated lymphoma: CBC: complete blood count.
ences were highly significant (P > 0.0005). These data were based on histologic diagnosis at the onset of a leu- kemic phase. Thus, patients who initially presented with NPDL (3 patients) or NM ( I patient) and converted to diffuse histologies at the time of their leukemic phase were grouped with patients having diffuse histologic types. Survival of the latter 4 patients reflected an un- favorable lymph node histology and was not appreciably different from that of other patients with similar histo- logic types. Two additional patients showed conversion of histology after onset of a leukemic phase. A patient with NM converted late in her course to DUL and a patient with DPDL was found at autopsy to have DHL.
When survival was evaluated from the time of diag- nosis, histology, as might be anticipated, was also im- portant with regard to prognosis. Among patients with NPDL median survival after diagnosis was 32 months compared to 19 months for patients with DPDL and 6 months among patients with DUL and DHL (P < 0.0005; Fig. 2).
Clinical features contributing to the particularly poor prognosis of patients with diffuse histologies included advanced stage of disease as well as age. Of importance was the presence of Stage IV disease at the time of lym- phoma diagnosis in all patients with diffuse histologies (Table I). Patients with DPDL tended to be older, male, and often had B-symptoms during their clinical course. This group of patients was also characterized by frequent extranodal involvement, organomegaly, and extensive bone marrow involvement at diagnosis (Table 1). As with patients with DPDL, patients with DHL and DUL had extensive disease at presentation and 80% had bone mar- row involvement at diagnosis (Table l). The presence of

No. 7 LEUKEMIC PHASE OF LYMPHOMA - Frum ez a/. 1223
diminished marrow reserve as manifested by anemia, leu- kopenia, and thrombocytopenia as well as the large pro- portion of patients with DPDL who were leukemic at diagnosis (70%) further emphasizes the advanced stage of disease that contributed to the poor prognosis of pa- tients with this histology (Table l).
Characteristics of the Leukemic Phase
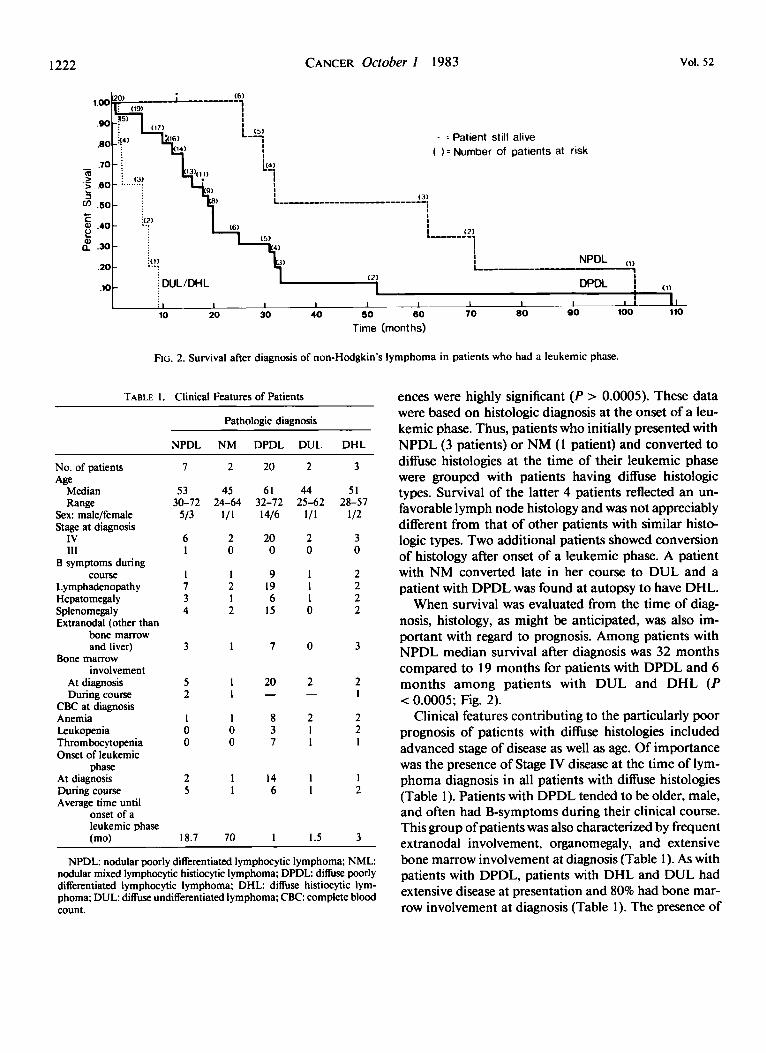
Clinical features of the leukemic phase are summa- rized in Tables 2 and 3. Patients with diffuse histologies tended to have higher numbers of circulating abnormal lymphoid cells compared to nodular histologies. This was particularly evident among patients with DPDL in whom the highest white blood cell counts and percent abnormal cells were observed (Table 2). Of clinical rel- evance among seven patients with DUL or DHL was the presence of a distinct, large lymphoid cell with a prominent nucleolus and vacuolated cytoplasm (Fig. 3). Peripheral blood morphology was not helpful in distin- guishing patients with NPDL from those with DPDL. Cleaved or fissured lymphocytes were the predominant morphologies of abnormal circulating cells in patients with DPDL and NPDL (Table 2 and Figs. 4 and 5) . Greater morphologic heterogeneity was encountered among patients with DPDL who, in addition to cleaved lymphocytes, often had medium sized lymphocytes in- cluding some with nucleoli (Fig. 6). The predominant cell type in the lymph node as well as peripheral blood of a single patient with diffuse moderately well differ- entiated lymphocytic lymphoma was a small round lym- phocyte, although small cleaved lymphocytes were pres- ent as well.
Clearing of abnormal cells from the peripheral blood occurred in patients who attained a complete remission
TABLE 2. Characteristics of a Leukemic Phase
Histologic type at onset of leukemic phase
NPDL NM DPDL DUL/DHL
No. of patients* Duration of leukemic
phase (median in months)
Peak leukocyte count x 1 m / m m 3 (median)
(median) % leukemic cells
No. of patients with: Fissured or cleaved
lymphocytes Medium sized
lymphocytes with nucleoli
Large lymphoid cells
~ ~~
5 I 22
30 56 19
8 7 33
20 17 30
5 I 21
I 1 13 0 0 1
7
2
I 1
25
0
0 7
* One patient had a leukemic phase with NPDL and a second leu- kemic phase after transition to DHL. One patient each changed his- tologically from NPDL to NM to DPDL and entered a leukemic phase after transition to DPDL. An additional patient entered a leukemic phase after transition from NPDL to DUL.
but was transient, lasting at most 3 to 4 months. Two of five patients with NPDL and a leukemic phase had transient clearing of the peripheral blood associated with complete remissions in other disease sites, as did three of 22 patients with DPDL. Partial remissions in two and nine patients with NPDL and DPDL, respectively, were associated with persistence of a leukemic phase.
Immunologic Features
A summary of immunologic data from 20 patients during their leukemic phase is presented in Table 4.
TABLE 3. Characteristics of Patients Who Underwent Conversion Histologically Prior to a Leukemic Phase
Pathologic diagnosis
NPDL -, DPDL - DHL NPDL - DPDL NPDL - NM -- - DHL
No. of patients I 1 1 1 Duration of leukemic
Peak leukocyte count
90 Leukemic cells 5 22 25 64 NO. of patients with:
phase (mos) 3 days I + I 2+
x 1 ~ / m m 3 5.4 26.0 39.4 19.6
Fissured or cleaved
Medium sized lymphocytes 0 I 0 I
lymphocytes with nucleoli 0 0 0 0
Large lymphoid cells I 0 I 0
* The pathologic diagnosis associated with a leukemic phase is underlined.

No. 1 LEUKEMIC PHASE OF LYMPHOMA - Frum d a/. 1225
FIG. 3. Peripheral blood smear from a patient with DHL showing predominantly large immature cells with cytoplasmic vacuoles (Wright- Giemsa Stain, X 1000).
FIG. 4. Peripheral blood smear from a patient with DPDL showing a majority of small fissured or cleaved lymphocytes (Wright-Giemsa Stain. x 1000).
<
While most patients had circulating populations of B- lymphocyte origin (1 5 of 20 patients), significant het- erogeneity is evident. Two patients with NPDL at the onset of a leukemic phase had circulating B-lymphocytes with moderate to bright immunofluorescence. Greater heterogeneity was noted among 12 patients with DPDL. Perhaps of some significance was the poor survival of three patients (Patients 8, 15, and 16) with cells lacking surface immunoglobulin, la, B 1-cell and T-cell antigens. Median survival of the latter patients was 6 months com- pared to 12 months after onset of a leukemic phase in the remainder of the patients with DPDL, and 37 months in a single patient with diffuse moderately well differentiated lymphocytic lymphoma (Patient 3). The intensity of immunofluorescence of surface immuno- globulin, a characteristic that correlates with the quan- tity of surface immunoglobulin,'* varied from bright to
undetectable, emphasizing the biological heterogeneity in patients with DPDL. .
The poor prognosis of patients with DHL in a leu- kemic phase may be related in part to their immuno- logical features. Only one of three patients had circu- lating malignant cells of B-cell origin; cells from the other two patients (Patients 18 and 19) lacked sIg, B1- cell, and T-cell antigens, findings consistent with either a null cell or true histiocytic origin.
Discussion
In this study, histologic subtype was the most impor- tant parameter in assessing the prognosis of patients with non-Hodgkin's lymphoma in a leukemic phase. Prior report^^.^.'^.^^ have emphasized the longer median sur- vival of patients with nodular histologies compared to
FIG. 5. Peripheral blood smear from a patient with NPDL showing medium sized lymphoid cells. some with prominent fissures (Wright- Giemsa stain. X IOOO).

1226 CANCER October I 1983 Vol. 52
FIG. 6. Peripheral blood smear from a patient with DPDL showing a majority of medium-sized lymphoid cells, some containing nucleoli (Wright-Giemsa Stain. X 1000).
that of patients with diffuse histologies in a leukemic phase, and the present study statistically documents this observation.
It has been suggested that marrow or peripheral blood involvement at the time of diagnosis in patients with NPDL does not adversely affect ~urvival. '~ The prog- nosis of patients with NPDL and bone marrow involve- ment did not differ significantly from those without marrow infiltration.'6 Further, the Occurence of a leu- kemic phase in patients with NPDL is consistent with relatively long survival. The survival of patients with a leukemic phase and NPDL versus those with DPDL and a leukemic phase was 19.5 and 9 months, respectively, in an earlier s t ~ d y . ~ In a more recent NCI report' the median survival of patients with NPDL and a leukemic phase was 43 months, which is comparable to 30 months in the current study. In our patients with diffuse large cell lymphoma (DHL) as well as those reported from the National Cancer Institute (NCI); median survival after onset of the leukemic phase was very short (2 and 0.5 months, respectively). The NCI study included other histologic categories (DWDL, NPDL with blastic cyto- logic features, and diffuse lymphoblastic lymphoma) not
considered in the current study. Neither study addressed the poor prognosis of the leukemic phase of Burkitt's lymphoma. I'
Our selected patients with diffuse histologies and a leukemic phase differ in several respects from unselected cases. The presence of Stage 1V disease in all patients contrasts with Stage IV disease in only 45% of unselected patients with DPDL and in 26% to 28% of those with DHL at initial presentation."*19 Also different in our patient population is the uniform occurrence of bone marrow involvement at presentation among patients with DPDL and in 80% of those with DUL and DHL compared to the reported incidence of 45% and 15%, respectively among I70 unselected patients with non- Hodgkin's lymphoma after clinicopathologic staging. l9 In addition to advanced stage of disease, our patients tended to be older and male. While the mean age of 423 consecutively staged patients with non-Hodgkin's lym- phoma was 44 years and 59% were male, the median age of patients with DPDL in this series was 61 years, and 70% were male.'' Advanced stage and age undoubt- edly contributed to the poor prognosis of these patients. Whether the tendency to undergo leukemic conversion

No. 7 LEUKEMIC PHASE OF LYMPHOMA Frum el a/. 1227
TABLE 4. Immunologic Studies on the Peripheral Blood of Patients in a Leukemic Phase of Non-Hodgkin's Lymphoma
Dx at onset of Surface Ig Patient Dx at a leukemic Pattern of no. presentation phase Heavy chain Light chain immunofluorescence la Calla BI
1 NPDL NPDL G x Bright I + 0 I + 2 NPDL NPDL M K Moderate I + 0 2+ 3 DMWDLL DMWDLL IgM, IgD x Faint I + 0 2+
x Bright - - - 4 DPDL DPDL Ig M 5 DPDL DPDL IgM. IgD K Moderate 3+ 0 2+
x 6 DPDL DPDL x Faint I + - 7 DPDL DPDL Ig M
8 DPDL DPDL 0 0 0 0 0 0 9 DPDL DPDL IgM, IgD K Faint I + 0 I +
K 1+ 10 DPDL DPDL IgM. IgD Faint 2+ -
- Faint - - - - 3+
12 DPDL DPDL Ig M 13 DPDL DPDL IgM, IgD x Moderate 3+ 14 NPDL DPDL 0 0 0 1 + 0 3+ 15 NML DPDL 0 0 0 0 0 0 16 DPDL DPDL 0 0 0 0 0 0 17 DUL DUL Ig M K Bright 3+ 0 3+ 18 NPDL DHL 0 0 0 I + 0 0 19 DHL DHL 0 0 0 0 0 0 20 DHL DHL IgM, IgD x Moderate I + 0 I +
- - - - - I +
1 I * DPDL DPDL
* Peripheral blood was evaluated with anti-lg and E-rosettes and revealed 95% B-lymphocytes and 5% T-lymphocytes.
also reflects increased tumor burden or more funda- mental differences in the biology of the circulating ma- lignant cells awaits further investigation. While the more commonly occurring histologies are NPDL and DHL, the current series includes a disproportionate number of patients with DPDL."." The relative paucity of cases with NPDL and DHL is less readily explained and may reflect less tendency for leukemic conversion in these histologies at least as assessed by light microscopy. While DHL represents 58% of all patients with NHL seen at our institutions only 1.4% had a leukemic phase, an incidence comparable to a range of 2.4% to 5.5% re- ported by other ~ t u d i e s . ' ~ * ~ ~
The leukemic phase was characterized by differences in numbers of circulating abnormal lymphoid cells as well as morphology. While the latter did not aid in dif- ferentiating DPDL from NPDL, patients with DPDL tended to have higher numbers of circulating abnormal cells, earlier onset of a leukemic phase and more fre- quent evidence of limited marrow reserve. Of diagnostic importance in patients with DHL and DUL at the time of a leukemic phase was the presence of distinctive large cells usually with an eccentrically placed nucleus, large nucleolus and often vacuolated cytoplasm. This finding was present in seven patients with DHL and DUL at the time of leukemic transition and has been noted in prior reports.'3*'4
Conversion in lymph node histology occurred in 6 of 35 patients (1 7%) simultaneously with the onset of a leukemic phase in 4 patients. The latter is unusual, and was previously reported in only I of 30 patients with
DMWDLL diffuse moderately well differentiated lymphocytic lym- phoma.
non-Hodgkin's lymphoma who underwent histologic conversion.20 Similar to prior reports, the prognosis of patients who undergo histologic transformation was poor.20*2 '
Because of the limited size of the patient population studied, prognosis could not be correlated with immu- nological subtype. Of interest was the presence of cir- culating malignant cells lacking sIg, B 1 -cell, and T-cell antigens among two patients with DHL. This finding differs from the usual predominance of lymphocytes of B-cell origin among patients with DHL and raises the issue of whether such a phenotype may identify a pop- ulation of patients with DHL whose malignant cells are predisposed to ~ i r c u l a t e . ~ ~ . ~ ~ The poor prognosis of all patients lacking evidence of B- or T-cell origin among patients with DPDL may also have prognostic impli- cations although sample size does not permit definitive statistical analysis. Biological heterogeneity was also noted with respect to the intensity of surface immu- noglobulin immunofluorescence. In contrast to a prior report, bright immunofluorescence was rarely present among our patients with DPDL and was, in fact, quite variable.24 No clear prognostic implications with regard to survival were, however, observed.
At the current time, prognosis of the leukemic phase of NHL appears to parallel lymph node histology as defined in this study. Further immunologic investiga- tions on larger numbers of patients, especially with DHL or DUL, may identify those at risk of a leukemic phase. Cytogenetic analysis may also be of diagnostic and prog- nostic value in view of recent studies that demonstrated

1228 CANCER October 1 1983 Vol. 52
specific cytogenetic abnormalities in malignant cells from patients with non-Hodgkin’s lyrnph~ma.’~ More intensive treatment or new therapeutic approaches may then improve the poor prognosis.
REFERENCES
I . Rosenberg SA, Diamond HD, Jaslowitz B, Craver LF. Lympho- sarcoma: A review of I269 cases. Medicine 1964; 40:3 I .
2. Auk KA. Monoclonal lymphocytes in the blood of patients with lymphoma. N Engl J Med 1979; 300:1401-1406.
3. Ligler FS, Smith RG, Kittman JR et ul. Detection of tumor cells in the peripheral blood of nonleukemic patients with B-cell lymphoma: Analysis of “clonal excess.” Blood 1980; 55792-80 I .
4. Schnitzner B, Loesel LS, Reed RE. Lymphosarcoma cell leu- kemia: A clinicopathologic study. Cancer 1970; 26: 1082-1096.
5 . lsaacs R. Lymphosarcoma cell leukemia. Ann Intern Med 1973;
6. Come SE, Jaffe ES, Anderson J C el (11. Non-Hodgkin’s lympho- mas in leukemic phase: Clinicopathologic correlations. Am J Med
7. Shen SC, Homberger F. Studies on effusions: 11. A simple technique for the discovery of cancer cells in neoplastic exudates. Cuncer 1950 3:36-42.
8. Stashenko P, Nadler LM, Nardy R, Schlossman SF. Character- ization of a human lymphocyte antigen. J Imrnunol 1980; 125: 1678- 1685.
9. Nadler LM, Ritz J, Griffin JD, Todd RF 111, Reinherz EL, Schloss- man SF. Diagnosis and treatment of human leukemias and lymphomas utilizing monoclonal antibodies. Prog Hematol 198 1; XII: 187-225.
10. Pet0 R, Pike MC, Armitage P et al. Design and analysis of randomized clinical trials requiring prolonged observation of each patient: 1. Introduction and design. Br J Cuncer 1976; 34585-612.
I I. Pet0 R, Pike MC, Armitage P et al. Design and analysis of ran- domized clinical trials requiring prolonged observation of each patients: 11. Analysis and examples. Br J Cancer 1977; 35:l-37.
12. Cooper AG, Brown MC. Derby MA, Wortis HH. Quantitation
I 1~657-662,
1980; 69~667-674.
of surface membrane and intracellular gamma, and kappa chains of normal and neoplastic human lymphocytes. Clin Exg Imrnunol 1973; I3:487.
13. Alsabati EAK, Aziz MA, Kalidi 02. Leukemic transformation of histimytic lymphoma. J Clin Ifemutol Oncol 1980 1014-24.
14. Schnetzer B, Kass L. Leukemic phase of reticulum cell sarcoma (histiocytic lymphoma): A clinicopathologic and ultrastructural study. Cancer 1973; 31547-559.
15. Dick R, Bloomfield CD, Brunning RD. Incidence, cytology, and histopathology on non-Hodgkin’s lymphomas in the bone mar- row. Cancer 1974; 33:1382.
16. McKenna RW, Bloomfield CD, Brunning RD. Nodular lym- phoma and blood manifestations. Cuncer 1975; 36:428-440.
17. Heideman RL, Falletta JM, Steuber P, Starling KA, Rosenberg HS, Fernbach DJ. Acute leukemia in Burkitt’s lymphoma. Med Pe- diatr Oncol 1976; 2:2 15-222.
18. Dorfman RF, Rosenberg SA, Kaplan MS. Clinical and surgical (laparotomy) evaluation of patients with non-Hodgkin’s lymphomas. Cancer Treat Rep 1977; 61:981-992.
19. Chabner BA, Johnson RE, DeVita VT el (11. Sequential staging in non-Hodgkin’s lymphoma. Cuncer Treat Rep 1977; 61 :993-997.
20. Cullen MH, Lester TA, Brearly RL, Shard WS, Stansfield AG. Histologic transformation of non-Hodgkin’s lymphoma: A prospective study. Cuncer 1979; 44:645-65 I .
21. Young RC, Berard CW, Hubbard SW, Sumon R, DeVita VT. Histologic progression in non-Hodgkin’s lymphoma (NHL). Proceed- ing.s of the American Sociely of Clinical Oncology 1979; 20:353.
22. Jaffe ES, Braylan RC, Nanba K, Frank MM, Berard CW. Func- tional markers: A new perspective on malignant lymphomas. Cancer Treat Rep 1977; 61:953-962.
23. Bloomfield CS, Kersey JM, Bruning RD, Gajl-Peczalska KJ. Prognostic significance of lymphocytic surface markers and histology in adult non-Hodgkin’s lymphoma. Cuncer Treat Reg 1977; 61:963- 970.
24. Aisenberg AC, Wilkes B. Lymphosarcoma cell leukemia: The contribution of cell surface study to diagnosis. Blood 1976; 48:707- 715.
25. Rowley JD, Fukuhara S. Chromosome studies in non-Hodg- kin’s lymphoma. Sernin Oncol 1980; 7:255-266.




















