MR Imaging of Carotid Plaque Composition During Lipid-Lowering Therapy
Upload
independentCategory
view
0download
0
Eur Radiol (2008) 18: 1710–1719DOI 10.1007/s00330-008-0927-8 NEURO
Fabrice BonnevilleFrédéric BlochEwa KurysSophie Tezenas du MontcelMarie-Laure WelterAnne-Marie BonnetYves AgidDidier DormontJean-Luc Houeto
Received: 19 September 2007Revised: 8 January 2008Accepted: 16 February 2008Published online: 20 March 2008# European Society of Radiology 2008
Camptocormia and Parkinson’s disease:MR imaging
Abstract Camptocormia is charac-terized by an excessive anterior flex-ion of the spine that appears onlywhen standing or walking. The originof this symptom remains unknown,but recent clinical reports of campto-cormia associated with Parkinson’sdisease (PD) suggest cerebral involve-ment in the pathogenesis of campto-cormia. This study was undertaken toinvestigate the hypothesis that camp-tocormia in PD has a central origin.Seventeen PD patients with campto-cormia were prospectively enrolledand were compared to 10 matched PDpatients without camptocormia and 12normal controls. The normalized
volumes of the brain, striatal nuclei,and the cross-sectional areas of themidbrain and pons were measured onthree-dimensional magnetic resonanceimaging. Data were correlated withthe severity of the symptoms. Thenormalized axial surface of the mid-brain was statistically smaller in PDpatients with camptocormia than innormal controls (P=0.01). The nor-malized volumetric data were notstatistically different in PD patientswith camptocormia. There was a sig-nificant negative correlation betweenthe severity of camptocormia and thenormalized brain volume (P<0.009;R=−0.649) and sagittal pons area(P<0.01; R=−0.642). The resultssuggest that PD with camptocormiamay represent a selective form of PDinwhich a specific neuronal dysfunctionpossibly occurs within the brainstem.
Keywords Camptocormia .Parkinson’s disease . Magneticresonance imaging . Brain .Volumetry
Introduction
Camptocormia, derived from the Greek words χαμπτω(campto, “I bend”, and χορμος (cormos, “the trunk”), is arare involuntary posture of the trunk characterized by anextreme forward flexion of the thoracolumbar spineinduced by sitting, standing, or walking that disappearswhen lying supine (Fig. 1) [1]. This bent-spine syndromewas initially attributed to a psychogenic disorder as it had
been first reported in young soldiers who were unable tocope with battle stress [1–3]. It is described with increasingfrequency in association with movement disorders such aspost-encephalitic parkinsonism [4], parkinsonism withmutation of the Parkin gene [5], multiple system atrophy[6, 7], and idiopathic Parkinson’s disease (PD) [8–12].
Camptocormia is associated with a marked atrophy ofthe paraspinal muscles, as observed on computed tomog-raphy [13] or magnetic resonance imaging (MRI) [9]. The
F. Bonneville (*) . E. Kurys .D. DormontService de Neuroradiologie, Hôpital dela Pitié-Salpêtrière, AssistancePublique-Hôpitaux de Paris,47 Boulevard de l’Hôpital,75651 Paris Cedex 13, Francee-mail: [email protected].: +33-1-42163501Fax: +33-1-42163515
F. Bonneville . D. DormontUPR 640 CNRS LENA, Hôpital de laPitié-Salpêtrière, Assistance Publique-Hôpitaux de Paris,Paris, France
F. Bloch . M.-L. Welter .A.-M. Bonnet . Y. Agid . J.-L. HouetoCentre d’Investigation Clinique andINSERM U 289, Hôpital de la Pitié-Salpêtrière, Assistance Publique-Hôpitaux de Paris,Paris, France
S. T. du MontcelService de Biostatistique, Hôpital de laPitié-Salpêtrière, Assistance Publique-Hôpitaux de Paris,Paris, France
J.-L. HouetoService de Neurologie,CHU la Milétrie,Poitiers, France

severity of this paraspinal muscular atrophy has, however,not been compared in PD patients with and withoutcamptocormia. Even though the primary or secondaryorigin of the muscular disorder has still not been elucidated[12, 14, 15], several authors regard camptocormia as anunusual type of action dystonia of the trunk or even asubclass of PD [8, 9, 12, 14, 16–21]. The improvements ofthis abnormal posture after high-frequency deep brainstimulation of bilateral subthalamic nuclei [16] or globuspallidus [19, 21] support the notion that camptocormia isunder the control of brain structures.
Although the exact location of these cerebral alterationsis still unknown, reports of camptocormia caused bylenticular ischemic lesions [22] support the idea thatdysfunction of the basal ganglia plays a role in itspathogenesis. Except in these sporadic observations, inwhich MRI depicted foci of T2 high signal intensity in theputamen or caudate nuclei [9, 10, 22], conventional MRI ofthe brain has not revealed any significant abnormalities inpatients with camptocormia associated with PD [12, 17].However, no dedicated MRI study assessed either the loadof cerebral ischemic lesions or the global or segmentedcerebral atrophy in patients with camptocormia. Thecurrent study uses MR-based volumetry to prospectively
investigate a group of PD patients with camptocormia,compared to a matched group of PD patients withoutcamptocormia, as well as normal controls.
Material and methods
Patients
Sixty-three patients with camptocormia and parkinsonismexamined at our institution since 1995 met the prospec-tively specified inclusion criteria for this study: (1)presence of camptocormia, defined as an anterior flexionof the thoracolumbar spine from 15° to 90° appearing afterstanding or walking and disappearing when lying supine,(2) associated with parkinsonism, defined as an akinetic-rigidity syndrome, with or without tremor [23]. Among thepatients, 7 could not be contacted for this study, 4 weredeceased and 17 refused to participate. Eighteen out of theremaining 35 patients were not included because of thepresence of pre-defined exclusion criteria: (1) presence ofknown neurological symptoms suggestive of MSA orprimary or secondary dystonia (n=2), (2) history of spinalsurgery on more than one occasion, more than threedifferent herniated disks diagnosed on a previous imagingstudy, or scoliosis >30° (n=10), (3) past history ofpsychiatric disorders or presence of dementia with MiniMental Status Score <24 (n=6), or (4) contraindication forMRI examination.
Therefore, 17 patients who met stringent selectioncriteria for our clinical study of PD associated withcamptocormia [8] were prospectively enrolled in this MRimaging protocol. They were 11 men and 6 women withmean (± SD) age: 69.3±7.2 years, PD disease duration:12.2±6.9 years, camptocormia duration: 3.8±3.1 years,and mean Hoehn and Yahr “off-drug” score: 3.3±0.9.
Control subjects
To compare the cerebral volumetric features of parkinso-nian patients with and without camptocormia, a controlgroup of 10 levodopa-responsive PD patients withoutcamptocormia (9 men and 1 woman) was matched for age(66.3±8.0 years), PD duration (10.7±4.6 years) andseverity of the parkinsonian syndrome according toHoehn and Yahr off-drug score (3.3±0.9), with the groupof patients with camptocormia. A group of 12 healthyvolunteers (7 men, 5 women) matched for age (66.8±6.2 years) served as normal controls.
All the patients and controls were scanned at ourinstitution after they gave their written informed consent.The protocol was approved by the local institutional reviewboard in compliance with all applicable legal and ethicalstandards. Informed consent was obtained from all subjectsand controls.
Fig. 1 A 71-year-old man with camptocormia. Note the severeforward flexion of the trunk appearing only in a standing position
1711

Clinical evaluation
Clinical tests were performed in the same manner in PDpatients with and without camptocormia and are reported indetail elsewhere [8]. Briefly, the following clinical featureswere evaluated: (1) The severity of the camptocormia wasassessed by the measure of the distance between theseventh cervical vertebra and the wall when standing. (2)The motor disability was assessed by Unified Parkinson’sDisease Rating Scale (UPDRS) parts II and III [24]. Theevaluation of the severity of the camptocormia and motordisability (UPDRS part III) was performed in the “off”state, i.e., after at least a 12-h interruption of antiparkin-sonian medication, and in the best “on-drug” condition. (3)The neuropsychological state was assessed by standardMini Mental Status examination and Mattis dementiarating scale. Table 1 displays the characteristics of all PDpatients with and without camptocormia. Considering theinclusion criteria, there were no differences in patients withand without camptocormia for the UPDRS III off score,modified axial off score, Mini Mental Status examination,and Mattis dementia rating scale scores.
MR imaging technique
Brain
Data acquisition and MRI parameters Four MRIsequences were acquired for all patients utilizing astandard head coil on a 1.5 Tesla General Electric Signamagnet (General Electric Medical Systems, Milwaukee,WI, USA). A T1-weighted volume of the whole brain wasfirst scanned in an axial plane using a 3D inversion-recovery fast spoiled gradient (IR FSPGR) sequence (TR/TE/TI: 15/5/600 ms, field of view: 240 mm, matrix: 256×256, slice thickness: 1.5 mm). Then, a coronal spin-echo
T2-weighted sequence (TR/TE: 2,200/90 ms, field ofview: 28, matrix: 256×192) with a 2-mm slice thicknesswas acquired twice in interleaved slice positions to obtaina T2-weighted volume covering the brainstem and basalganglia. In addition, axial FLAIR sequence (TR/TE/TI:10,000/140/2,200 ms; field of view: 24 cm; matrix: 256×256; slice thickness: 5 mm) and axial fast spin echo T2-weighted sequence (TR/TE: 3,440/90 ms, field of view:22 cm, matrix: 256×256, slice thickness: 2 mm) wereacquired.
Data were transferred to an Advantage workstation(General Electric Medical Systems, Milwaukee, WI, USA)for visual assessment, volume, and cross-sectional areacalculations. The T1-weighted volume was also transferredto a personal computer for automated calculation of thebrain parenchyma volume [25].
Quantitative analysis The volumetric analysis of the brainof PD patients with and without camptocormia, as well asnormal controls, was made by a single observer (EK)blinded to clinical status, using a highly reproducibleautomated and semi-automated MRI-based techniquevalidated and reported in detail elsewhere [25]. Thebrain volume was automatically calculated from the T1-weighted volume: the parenchyma was extracted with asoftware platform that uses a processing sequence ofsegmentation [26], and the total brain volume (i.e., thecerebral hemispheres, the cerebellum, and the brainstem)was then obtained by calculating and converting thenumber of such segmented voxels into cubic millimeters.The caudate nuclei, the putamina, and total intracranialvolumes were manually segmented on contiguous refor-matted millimetric images, and volumes were thenautomatically calculated using Voxtool software (GeneralElectric Medical Systems, Milwaukee, WI, USA) on anAdvantage workstation. Volumes reported for the caudate
Table 1 Characteristics of Parkinson’s disease (PD) patients with and without camptocormia
PD patients with camptocormia (n=17) Control PD patients without camptocormia (n=10) P
Age at onset of parkinsonism (years) 57.0±10.8 56.7±8.4 NS
UPDRS III
Off 36.0±10.6 34.7±15.5 NS
On 25.1±8.9 (30) 13.3±6.1 (58) 0.05
Axial motor score
Off 10.0±3.1 7.5±3.9 NS
On 8.8±5.3 (11) 3.7±1.5 (50) 0.05
MMSE score 27.0±3.2 26.9±2.7 NS
MATTIS score 135.6±7.0 135.7±6.9 NS
Levodopa equivalent (mg/day) 985±551.4 794±253 NS
NS Not significantValues are mean ± standard deviation. Parentheses indicate percentage improvement compared with the “off-drug” condition
1712

nucleus and putamen are the sum of the right and leftvolumes.
As previously described [25], we used the T2-weightedvolume to measure the mesencephalic and pontine cross-sectional areas because of the reproducible contrast offeredon this sequence by the hyperintense signal of thesurrounding cerebrospinal fluid. The axial midbrain sectionwas delineated on a reformatted plane passing through theintercollicular sulcus and the emergence of the third cranialnerves (Fig. 2). The axial pontine area was traced on atransverse image reformatted in a plane perpendicular tothe floor of the fourth ventricle at the level of the mid-height of the pons. On a median reformatted sagittal image,the sagittal cross-sectional areas of the midbrain and ponswere delineated and measured according to the techniquepreviously described and validated by Oba et al. [27].Briefly, the sagittal midbrain area was measured under thethird ventricle, down to a line drawn as to pass throughthe superior pontine notch and the inferior edge of thequadrigeminal plate, while the sagittal pons area wasmeasured under this latter line down to a line drawnparallel to this one, so as to pass through the inferiorpontine notch (Fig. 3).
Qualitative analysis Camptocormia has been reported inassociation with T2 high signal intensities in the striatum,compatible with vascular lacunae [9, 22]. All MRI scansof the PD patients with and without camptocormia wereexamined for any signal abnormalities in the periventric-ular and subcortical white matter at the infra- andsupratentorial levels, in the basal ganglia and the thalami,as well as in the brainstem. Leukoaraiosis corresponded toareas of hyperintense signals on both T2-weighted andFLAIR images, lacunar infarctions appeared as small deeplesions (smaller than 15 mm in diameter) with high signalintensity in T2-weighted images and low signal intensityon FLAIR images with perilesional halo, whereas Virchow-Robin perivascular spaces demonstrated hyperintensesignal on T2-weighted images and hypo- or isointense
signal on FLAIR images without halo. Based on the Kato etal. classification [28], we graded the extent of leukoaraiosisfrom none to severe in four groups (0–3) in each of thesecerebral regions. Thus, for the periventricular and subcor-tical white matter: grade 0 corresponds to no white matterlesions except for small triangular foci surrounding thefrontal horns; in grade 1, hyperintensities surround bothanterior and posterior horns and/or there are discrete patchywhite-matter lesions; for grade 2, extensive patchy white-matter lesions and their early confluence are observed; andin grade 3, white-matter hyperintensities reach confluence,completely surrounding the lateral ventricle.
Spine
Data acquisition and MRI parameters Two MRI sets ofimages were acquired with a phased array coil on the sameMRI scanner for the thoracolumbar spine analysis: asagittal T2-weighted sequence (TR/TE: 4,000/102 ms,field of view: 36 cm, matrix: 320×320, slice thickness:4 mm) and an axial T1-weighted sequence (TR/TE:600/20 ms, field of view: 24 cm, matrix: 320×256, slicethickness: 7 mm) acquired in a strict horizontal plane,from the 12th thoracic vertebra to the 1st sacral vertebra.
Qualitative analysis The presence of lumbar paraspinalmuscle atrophy and degenerative spinal pathology pre-viously described in association with camptocormia wasassessed on lumbar spine MRI and compared in PDpatients with and without camptocormia [9, 15, 17]. Morespecifically, we looked for the extent of fatty degenerationof the paraspinal muscles on the cumulative axial T1-weighted images, with high signal intensity considered asfat present within the usual isointensity of the muscles.The extent was classified in four grades: grade 0=no fattydegeneration, grade 1=mild fatty degeneration, occupyingless than 1/3 of the muscle cuts, grade 2=moderatedegeneration ranging between 1/3 and 2/3 of the muscle
Fig. 2 a Sagittal reformattedT2-weighted image demon-strates the axial plane passingthrough the emergence of thethird cranial nerves and theintercollicular sulcus, on whichthe axial mesencephalon surfaceis manually delineated (b)
1713

cuts, and grade 3=severe degeneration with more than 2/3of the muscle cuts replaced by fat. For statistical analysis,estimated grades of fatty muscle degeneration in theanterior and posterior group of paraspinal muscles weresummed.
For qualitative analysis of the brain and the spine, allscans were reviewed by two independent observers (FB,EK) blinded to clinical data. In case of disagreement, finaldecision was obtained by consensus.
Statistical analysis
For statistical analysis, the SAS 8.1 software (SASInstitute, Cary, NC, USA) was used. To avoid interpatientvariability due to head size and gender, all volumetric datawere normalized by dividing each cerebral structure metricdatum by the total intracranial volume of each patient orcontrol [29]. To test the hypothesis that PD patients with orwithout camptocormia and normal age-matched controlshave different brain volumes, statistical analysis of thevolumetric data of the three groups was performed byKruskal-Wallis test. Brain and spine qualitative data werecompared between PD patients with and without campto-cormia using the paired Wilcoxon rank sum test. Spearmancorrelation coefficient test was used to find correlationsbetween volumetric data and clinical scores of PD patientswith camptocormia.
For each test, the level of statistical significance wasdefined as P<0.05.
Results
Quantitative cerebral study
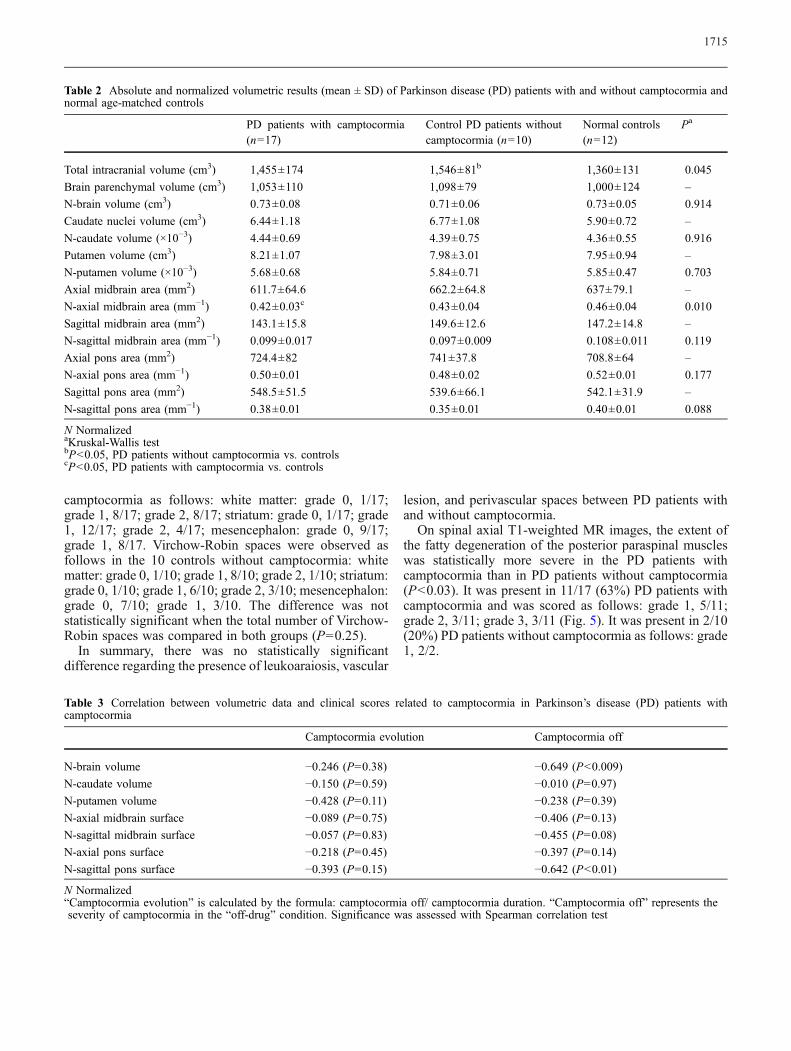
No statistical difference was found between the meannormalized midbrain axial areas of PD patients with andwithout camptocormia. PD patients with camptocormiahad a smaller mean normalized midbrain axial cross-sectional area than normal controls (P=0.01) (Table 2).However, overlap between groups precludes the establish-ment of a diagnostic threshold. Statistical analysis of othernormalized volumes and areas did not reach significantdifference (P>0.05). In particular, there were no significantdifferences of the normalized putamen or caudate volumes.Although mean intracranial volume of PD patients withoutcamptocormia was significantly larger than that of normalage−matched controls (P=0.045) and may be due to a malepredominance in this group, mean normalized brainparenchymal volume was statistically indistinguishable inthe three groups.
Statistical analysis of volumetric data with respect toclinical scores in patients with camptocormia (Table 3)revealed a significant negative correlation between theseverity of camptocormia and the normalized brain volume(P<0.009; R=−0.649) and sagittal pontine area (P<0.01;R=−0.642) (Fig. 4). In other words, the more severe thecamptocormia, the smaller the normalized brain parenchy-ma volume and the sagittal pontine area. There was nosignificant correlation between the normalized midbrainaxial cross-sectional area and the clinical scores. Nosignificant correlation was found between normalizedvolumetric data and age, duration of camptocormia,duration of parkinsonian syndrome, Mattis and Frontaltests results, and modified UPDRS III and axial motorscores (not shown).
Qualitative study
Nine of the 17 PD patients with camptocormia presentedwith leukoaraiosis and vascular lesions scored as follows:periventricular and subcortical white matter: grade 1, 7/17;grade 2, 2/17; pons: grade 1, 4/17; grade 2, 1/17; striatum:grade 1, 1/17. Three of the 10 control PD patients withoutcamptocormia presented with leukoaraiosis grade 1 in thewhite matter. One thalamic vascular lacuna was found ineach PD group with and without camptocormia. Thedifference was not statistically significant when the totalnumber of lesions was compared in the groups (P=0.58).
T2 hyperintense signals and FLAIR iso- or hypointensesignals, corresponding to Virchow-Robin perivascularspaces, were observed in the 17 PD patients with
Fig. 3 Midsagittal reformatted T2-weighted image on which thesagittal midbrain and pons areas are manually delineated
1714
camptocormia as follows: white matter: grade 0, 1/17;grade 1, 8/17; grade 2, 8/17; striatum: grade 0, 1/17; grade1, 12/17; grade 2, 4/17; mesencephalon: grade 0, 9/17;grade 1, 8/17. Virchow-Robin spaces were observed asfollows in the 10 controls without camptocormia: whitematter: grade 0, 1/10; grade 1, 8/10; grade 2, 1/10; striatum:grade 0, 1/10; grade 1, 6/10; grade 2, 3/10; mesencephalon:grade 0, 7/10; grade 1, 3/10. The difference was notstatistically significant when the total number of Virchow-Robin spaces was compared in both groups (P=0.25).
In summary, there was no statistically significantdifference regarding the presence of leukoaraiosis, vascular
lesion, and perivascular spaces between PD patients withand without camptocormia.
On spinal axial T1-weighted MR images, the extent ofthe fatty degeneration of the posterior paraspinal muscleswas statistically more severe in the PD patients withcamptocormia than in PD patients without camptocormia(P<0.03). It was present in 11/17 (63%) PD patients withcamptocormia and was scored as follows: grade 1, 5/11;grade 2, 3/11; grade 3, 3/11 (Fig. 5). It was present in 2/10(20%) PD patients without camptocormia as follows: grade1, 2/2.
Table 3 Correlation between volumetric data and clinical scores related to camptocormia in Parkinson’s disease (PD) patients withcamptocormia
Camptocormia evolution Camptocormia off
N-brain volume −0.246 (P=0.38) −0.649 (P<0.009)
N-caudate volume −0.150 (P=0.59) −0.010 (P=0.97)
N-putamen volume −0.428 (P=0.11) −0.238 (P=0.39)
N-axial midbrain surface −0.089 (P=0.75) −0.406 (P=0.13)
N-sagittal midbrain surface −0.057 (P=0.83) −0.455 (P=0.08)
N-axial pons surface −0.218 (P=0.45) −0.397 (P=0.14)
N-sagittal pons surface −0.393 (P=0.15) −0.642 (P<0.01)
N Normalized“Camptocormia evolution” is calculated by the formula: camptocormia off/ camptocormia duration. “Camptocormia off” represents theseverity of camptocormia in the “off-drug” condition. Significance was assessed with Spearman correlation test
Table 2 Absolute and normalized volumetric results (mean ± SD) of Parkinson disease (PD) patients with and without camptocormia andnormal age-matched controls
PD patients with camptocormia(n=17)
Control PD patients withoutcamptocormia (n=10)
Normal controls(n=12)
Pa
Total intracranial volume (cm3) 1,455±174 1,546±81b 1,360±131 0.045
Brain parenchymal volume (cm3) 1,053±110 1,098±79 1,000±124 –
N-brain volume (cm3) 0.73±0.08 0.71±0.06 0.73±0.05 0.914
Caudate nuclei volume (cm3) 6.44±1.18 6.77±1.08 5.90±0.72 –
N-caudate volume (×10−3) 4.44±0.69 4.39±0.75 4.36±0.55 0.916
Putamen volume (cm3) 8.21±1.07 7.98±3.01 7.95±0.94 –
N-putamen volume (×10−3) 5.68±0.68 5.84±0.71 5.85±0.47 0.703
Axial midbrain area (mm2) 611.7±64.6 662.2±64.8 637±79.1 –
N-axial midbrain area (mm−1) 0.42±0.03c 0.43±0.04 0.46±0.04 0.010
Sagittal midbrain area (mm2) 143.1±15.8 149.6±12.6 147.2±14.8 –
N-sagittal midbrain area (mm−1) 0.099±0.017 0.097±0.009 0.108±0.011 0.119
Axial pons area (mm2) 724.4±82 741±37.8 708.8±64 –
N-axial pons area (mm−1) 0.50±0.01 0.48±0.02 0.52±0.01 0.177
Sagittal pons area (mm2) 548.5±51.5 539.6±66.1 542.1±31.9 –
N-sagittal pons area (mm−1) 0.38±0.01 0.35±0.01 0.40±0.01 0.088
N NormalizedaKruskal-Wallis testbP<0.05, PD patients without camptocormia vs. controlscP<0.05, PD patients with camptocormia vs. controls
1715

A significant correlation was also not found between thedegree of fatty atrophy of the paraspinal muscles and thedifferent cerebral normalized volumetric data.
Degenerative lumbar discs were observed in 14/17patients with camptocormia versus in 3/10 PD patientswithout camptocormia (P<0.03). There was also a trend(P=0.058) for mild scoliosis in patients with camptocormia.Narrowing of the lumbar canal was present in one PDpatient with camptocormia versus two controls (P>0.05).No T2 signal abnormalities were observed in the spinal cordof either the patients or controls.
Discussion
MR-based volumetry is a robust tool that may be used todifferentiate idiopathic PD fromParkinson plus syndromes—
atrophy of the striatum [30] and middle cerebellarpeduncles [31] in multiple system atrophy and severeatrophy of the midbrain in progressive supranuclear palsy[27, 32]—while PD patients demonstrate a rate of globalcerebral atrophy similar to those of healthy age-matchedcontrols [33]. To the best of our knowledge, the currentstudy is the first group-controlled study investigating focalor global differences in brain volumes between PD patientswith camptocormia and PD patients without camptocormia.One limitation of the current study is that it cannot beextrapolated to camptocormia related to other origins.However, the use of rigorous inclusion criteria along with agroup-controlled methodology may strengthen our results.
While no statistical difference was observed between PDpatients with and without camptocormia, nor between PDpatients without camptocormia and normal controls, thenormalized mesencephalon axial cross-sectional area wassignificantly smaller in PD patients with camptocormiathan in normal controls. This finding is consistent withprevious studies suggesting that a neuronal dysfunction oradditional damage to brainstem structures implicated in thecontrol of posture—the pedunculopontine nucleus [8, 34]or the reticulospinal pathway [9]—may account forcamptocormia in PD patients. Though not statisticallydecreased compared to controls, the normalized sagittalsurface of the pons measured on the midline is correlatedwith the severity of camptocormia, while the axial surfaceis not. This further suggests the contribution of apredominant central pons involvement, corresponding tothe location of the reticular formation. Further investigationof these brainstem structures by means of advancedimaging techniques or neuropathology may be of use inelucidating the precise neuroanatomical and pathologicalphenomena underlying camptocormia. Finally, although asample size effect cannot be ruled out, the fact thatbrainstem MR volumetry fails to detect any significantdifferences between PD with and without camptocormia isin agreement with the hypothesis that PD with and withoutcamptocormia may represent a spectrum of the samedisease [8].
Fig. 5 a Axial T1-weightedimage in a Parkinson diseasepatient without camptocormiademonstrates the normal volumeand signal of the posteriorparaspinal muscles. b Axial T1-weighted image in a Parkinsondisease patient with markedcamptocormia demonstrates asevere atrophy with fatty re-placement of nearly all of theposterior paraspinal musculature
Fig. 4 Correlations between the severity of the camptocormia andthe sagittal surface of the pons (P<0.01)
1716

The first report of camptocormia in PD patients [17] andother recent works [7, 12, 16, 19, 21] indicated that adysfunction of the putamen may account for camptocor-mia. Although the absence in this study of significantputaminal atrophy in PD with camptocormia does notsupport this theory, contribution of a putaminal dysfunctionto the pathophysiology of camptocormia cannot be ruledout despite normal putaminal high-resolution MR volu-metry [35]. Moreover, sudden onset of camptocormia hasbeen consistently ascribed to putaminal vascular ischemiclesions [22]. In a recent series of 23 PD patients withcamptocormia, Lepoutre et al. described two patients with alacuna in the head of the caudate nucleus and another witha lacuna in the left putamen [9]. Similarly, Azher et al., whoexplored a heterogeneous group of 16 patients withcamptocormia and neurologic disorders, including PDand dystonia, suggested checking with MR for lesions notonly in the striatum, but also in the thalamus where thetrunk is represented [12]. However, the visual analysis ofthe cerebral MR images of our patients, with specialattention to the striatum and the thalamus, did not revealsignificant T2 signal abnormalities, except for Virchow-Robin spaces which were visible to the same extent as inmatched PD patients without camptocormia.
Similarly, we fail to find any significant difference in thePD patients with or without camptocormia with regard tothe load of leukoaraiosis, in agreement with a previousstudy dealing with typical and atypical parkinsonism onMRI [36]. However, though not statistically different, wefound a trend in the correlation of leukoaraiosis andcamptocormia. Since the severity of camptocormia wasalso strongly correlated with the global normalized brainvolume, this could indicate that diffuse brain insultsbroadly affecting motor circuits, known to be associatedwith motor decline and gait disturbances in elderly people[37], might contribute to camptocormia as well. It should,however, be mentioned that MR in elderly peoplefrequently shows diffuse atrophy and silent infarcts [38]and that cerebral vascular disease and parkinsonismfrequently occur at the same age [39]. Taken together, theabove-mentioned arguments suggest that striatal andthalamic infarct-like lesions along with the leukoaraiosisobserved in PD patients with camptocormia are likely to becoincidental, and therefore should be interpreted withcaution.
Finally, involvement of the paraspinal muscles is thelatest major issue that is still a matter of debate whendealing with camptocormia. Whether or not camptocormiais associated with a parkinsonian syndrome, variable and
sometimes contradictory changes on electromyography,MRI and pathologic findings of the thoracolumbarparaspinal muscles have been described [6, 9, 10, 13, 15,40, 41]. We found significantly more extended and moresevere lumbar paraspinal muscle atrophy and degenerativediscopathies in PD patients with camptocormia than thosewithout camptocormia. This finding is consistent withresults of a previous study in which the most frequentabnormality seen on the MRI of the spine was the atrophyand fatty replacement of the thoracolumbar paraspinalmuscles, mostly associated with degenerative injuries ofthe lumbar spine [9]. However, such abnormalities are alsofound in PD patients without camptocormia [42] or inpatients with dystonia and to some extent, participate in thenormal aging process of the spine [43]. Therefore, wesuggest that—except for the coincidental occurrence ofneuromuscular disease [8, 12]—fatty involution observedin paraspinal muscles of PD patients with camptocormia isnot specific to the disease itself, but its extent to thethoracolumbar spine might be. It could be hypothesizedthat the lack of use of the erector muscles of the spine incamptocormia, possibly due to an excessive activation ofthe rectus abdominis muscles [18, 19], could initiate theirfatty involution. Subsequent spinal instability and defor-mations, together with discopathies and osteophytes, couldcause direct compression of the small spinal nervebranches, which could increase the muscles’ denervationand their fatty replacement [44].
Conclusion
We found (1) that the normalized axial surface of themesencephalon did not significantly differ between PDwith and without camptocormia, but did when comparingcamptocormia patients with controls, and (2) that theseverity of the camptocormia was correlated with thenormalized sagittal surface of the pons and total brainvolume. Our results suggest that PD with camptocormiamay represent a selective form of PD in which a significantadditional neuronal dysfunction possibly occurs within thebrainstem, and in particular within the mesencephalon andthe pons. Further studies and accurate anatomical explora-tions of these brainstem structures are required to bettercharacterize the pathophysiology of this entity.
Acknowledgements We are grateful to the nurses of the Centred’investigation clinique for the patient care and to Dr. DavidSeidenwurm for his constructive review of the manuscript.
1717

References
1. Souques A, Rosanoff-Saloff M (1914)La camptocormie: incurvation du troncconsecutive aux traumatismes du dos etdes lombes; considérations morpholo-giques. Rev Neurol 28:937–939
2. Sandler SA (1945) Camptocormia: afunctional condition of the back inneurotic soldiers. War Med 8:36–45
3. Perez-Sales P (1990) Camptocormia.Br J Psychiatry 157:765–767
4. Onuaguluchi G (1961) Crises in post-encephalitic parkinsonism. Brain84:395–414
5. Inzelberg R, Hattori N, Nisipeanu P etal (2003) Camptocormia, axial dysto-nia, and parkinsonism: phenotypicheterogeneity of a parkin mutation.Neurology 60:1393–1394
6. Diederich NJ, Goebel HH, Dooms G etal (2006) Camptocormia associatedwith focal myositis in multiple-systematrophy. Mov Disord 21:390–394
7. Slawek J, Derejko M, Lass P,Dubaniewicz M (2006) Camptocormiaor Pisa syndrome in multiple systematrophy. Clin Neurol Neurosurg108:699–704
8. Bloch F, Houeto JL, Tezenas duMontcel S et al (2006) Parkinson’sdisease with camptocormia. J NeurolNeurosurg Psychiatry 77:1223–1228
9. Lepoutre AC, Devos D, Blanchard A etal (2006) A specific clinical pattern ofcamptocormia in Parkinson’s disease. JNeurol Neurosurg Psychiatry 77:1229–1234
10. Charpentier P, Dauphin A, Stojkovic Tet al (2005) Parkinson’s disease, pro-gressive lumbar kyphosis and focalparaspinal myositis. Rev Neurol (Paris)161:459–463
11. McCluskey LF (2006) Camptocormia:pathogenesis, classification, and re-sponse to therapy. Neurology 66:1285–1286, author reply 1285–1286
12. Azher SN, Jankovic J (2005) Campto-cormia: pathogenesis, classification,and response to therapy. Neurology65:355–359
13. Delisle MB, Laroche M, Dupont H,Rochaix P, Rumeau JL (1993) Mor-phological analyses of paraspinal mus-cles: comparison of progressive lumbarkyphosis (camptocormia) and narrow-ing of lumbar canal by disc protrusions.Neuromuscul Disord 3:579–582
14. Slawek J, Derejko M (2001) Campto-cormia, a rare form of motor systemdisorders in Parkinson’s disease.Neurol Neurochir Pol 35:1133–1140
15. Laroche M, Delisle MB, Aziza R,Lagarrigue J, Mazieres B (1995) Iscamptocormia a primary muscular dis-ease? Spine 20:1011–1016
16. Yamada K, Goto S, Matsuzaki K et al(2006) Alleviation of camptocormia bybilateral subthalamic nucleus stimula-tion in a patient with Parkinson’sdisease. Parkinsonism Relat Disord12:372–375
17. Djaldetti R, Mosberg-Galili R, SrokaH, Merims D, Melamed E (1999)Camptocormia (bent spine) in patientswith Parkinson’s disease–characteriza-tion and possible pathogenesis of anunusual phenomenon. Mov Disord14:443–447
18. Reichel G, Kirchhofer U, Stenner A(2001) Camptocormia–segmental dys-tonia. Proposal of a new definition foran old disease. Nervenarzt 72:281–285
19. Nandi D, Parkin S, Scott R et al (2002)Camptocormia treated with bilateralpallidal stimulation. J Neurosurg97:461–466
20. Slawek J, Derejko M, Lass P (2003)Camptocormia as a form of dystonia inParkinson’s disease. Eur J Neurol10:107–108
21. Micheli F, Cersosimo MG, PiedimonteF (2005) Camptocormia in a patientwith Parkinson disease: beneficial ef-fects of pallidal deep brain stimulation.Case report. J Neurosurg 103:1081–1083
22. Nieves AV, Miyasaki JM, Lang AE(2001) Acute onset dystonic campto-cormia caused by lenticular lesions.Mov Disord 16:177–180
23. Litvan I, Bhatia KP, Burn DJ et al(2003) Movement Disorders SocietyScientific Issues Committee report: SICTask Force appraisal of clinical diag-nostic criteria for parkinsonian disor-ders. Mov Disord 18:467–486
24. Fahn S, Elton R, Members of theUPDRS Development Committee(1987) Unified Parkinson’s diseaserating scale. Macmillan Healthcare In-formation, Florham Park, NY
25. Bonneville F, Welter ML, Elie C et al(2005) Parkinson disease, brain vol-umes, and subthalamic nucleus stimu-lation. Neurology 64:1598–1604
26. Cointepas Y, Mangin J, Garnero L,Poline J, Benali H (2001) Brain VISA:software platform for visualization andanalysis of multi-modality brain data.Neuroimage 13:S98
27. Oba H, Yagishita A, Terada H et al(2005) New and reliable MRI diagnosisfor progressive supranuclear palsy.Neurology 64:2050–2055
28. Kato H, Izumiyama M, Izumiyama K,Takahashi A, Itoyama Y (2002) Silentcerebral microbleeds on T2*-weightedMRI: correlation with stroke subtype,stroke recurrence, and leukoaraiosis.Stroke 33:1536–1540
29. Whitwell JL, Crum WR, Watt HC, FoxNC (2001) Normalization of cerebralvolumes by use of intracranial volume:implications for longitudinal quantita-tive MR imaging. AJNR Am JNeuroradiol 22:1483–1489
30. Ghaemi M, Hilker R, Rudolf J, SobeskyJ, Heiss WD (2002) Differentiatingmultiple system atrophy fromParkinson’s disease: contribution ofstriatal and midbrain MRI volumetryand multi-tracer PET imaging. J NeurolNeurosurg Psychiatry 73:517–523
31. Nicoletti G, Fera F, Condino F et al(2006) MR imaging of middle cere-bellar peduncle width: differentiation ofmultiple system atrophy fromParkinson disease. Radiology 239:825–830
32. Righini A, Antonini A, De Notaris R etal (2004) MR imaging of the superiorprofile of the midbrain: differentialdiagnosis between progressive supra-nuclear palsy and Parkinson disease.AJNR Am J Neuroradiol 25:927–932
33. Paviour DC, Price SL, Jahanshahi M,Lees AJ, Fox NC (2006) LongitudinalMRI in progressive supranuclear palsyand multiple system atrophy: rates andregions of atrophy. Brain 129:1040–1049
34. Garcia-Rill E, Homma Y, Skinner RD(2004) Arousal mechanisms related toposture and locomotion: 1. Descendingmodulation. Prog Brain Res 143:283–290
35. Black KJ, Ongur D, Perlmutter JS(1998) Putamen volume in idiopathicfocal dystonia. Neurology 51:819–824
36. Hu MT, Chaudhuri KR, Jarosz J,Yaguez L, Brooks DJ (2002) An im-aging study of parkinsonism amongAfrican-Caribbean and Indian Londoncommunities. Mov Disord 17:1321–1328
37. Camicioli R, Moore MM, Sexton G,Howieson DB, Kaye JA (1999) Age-related brain changes associated withmotor function in healthy older people.J Am Geriatr Soc 47:330–334
38. Bryan RN, Cai J, Burke G et al (1999)Prevalence and anatomic characteristicsof infarct-like lesions on MR images ofmiddle-aged adults: the atherosclerosisrisk in communities study. AJNR Am JNeuroradiol 20:1273–1280
1718

39. Sibon I, Fenelon G, Quinn NP, Tison F(2004) Vascular parkinsonism. J Neurol251:513–524
40. Hilliquin P, Menkes CJ, Laoussadi S,Job-Deslandre C, Serratrice G (1992)Camptocormia in the elderly. A newentity by paravertebral muscle in-volvement? Rev Rhum Mal Osteoartic59:169–175
41. Schabitz WR, Glatz K, Schuhan C et al(2003) Severe forward flexion of thetrunk in Parkinson’s disease: focalmyopathy of the paraspinal musclesmimicking camptocormia. Mov Disord18:408–414
42. Babat LB, McLain RF, Bingaman W etal (2004) Spinal surgery in patientswith Parkinson’s disease: constructfailure and progressive deformity.Spine 29:2006–2012
43. Hadar H, Gadoth N, Heifetz M (1983)Fatty replacement of lower paraspinalmuscles: normal and neuromusculardisorders. AJR Am J Roentgenol141:895–898
44. Penisson-Besnier I, Menei P, Dubas F,Bregeon C (1994) Histological de-monstration of the process of paraspinalmuscle denervation in a case of reduc-ible lumbar kyphosis (camptocormia).Rev Rhum Ed Fr 61:868–870
1719
Copyright © 2022 FDOKUMEN