Role of MR imaging in pediatric surgery
16
Role of MR Imaging in Pediatric Surgery Raju Sharma and Shivanand Gamanagatti Department of Radiology, Al India Institute of Medical Sciences, New Delhi, India. Abstract. Magnetic Resonance Imaging is a non-invasive multiplanar imaging modality which does not use ionizing radiation. In recent years major technical advances in this field have led to shorter imaging times and better resolution. This has widened the scope of this modality in pediatric imaging. MRI is already an established technique for the brain and spine and is increasingly being used for musculoskeletal, abdominal and pelvic imaging. In this article the authors provide an update on this exciting modality with stress on applications relevant to pediatric surgeons. [Indian J Pediatr 2004; 71 (12) : 1095-1110] E-mail: raju 152 @yahoo.com Key words : MR/; Pediatric; Craniospial; Body Magnetic resonance imaging (MRI) plays a vital role in the evaluation of many paediatric diseases. It is a non- invasive, multiplanar imaging modality which does not involve the use of ionizing radiation, has excellent contrast resolution, and requires only minimal patient preparation. MR1 has become the modality of choice for many cranio-spinal and musculoskeletal applications and is a useful complementary modality to other cross- sectional modalities such as ultrasound and computed tomography (CT) and a problem solving tool in abdominal and chest imaging. Technical advances in the field of MRI have resulted in improved image quality and shorter scan times, both of which are very relevant to pediatric applications. In paediatric age group the spectrum of diseases is different from adults, with a higher incidence of congenital anomalies, a different group of neoplasms, and a lower incidence of metastatic disorders. The pulse sequences and techniques have to be adapted to the demanding requirements of imaging children, and therefore optimized protocols should be used. TECHNICAL CONSIDERATIONS Surface coils should be used whenever possible for imaging children so that signal-to-noise ratios can be optimized. There is lot of scope for improvisation and either adult head or extremity coils can be used to image the chest or abdomen in infants with excellent results. Faster imaging techniques having short imaging times such as gradient-echo, fast spin-echo (FSE), and echo- planar imaging are particularly advantageous in imaging of children. Newer applications such as diffusion weighted imaging (DWI) and diffusion tensor imaging Correspondence and Reprint requests : Dr. Raju Sharma, Department of Radiology,All India Institute of Medical Sciences, New Delhi 110029. Fax : 91-11-26588641. (DTI), MR angiography (MRA) and MR Cholangiopancreatography (MRCP) have emerged and have been successfully applied to the paediatric population also. 1,2 During the MR study, parents should be encouraged to stay with the children as it helps to reassure them. Apprehensive and uncooperative children frequently require sedation. While sedating, special care should be taken in children with airway compromise, congenital heart disease, or mental retardation because they have a higher incidence of complications. Children requiring sedation should be kept nil by mouth for four to six hours prior to the administration of sedation to minimize the risks of aspiration. General anesthesia may be used if routine sedation fails or in high-risk children. MR contrast agent: Gadolinium chelate contrast agents are useful in the evaluation of mass lesions and vascular malformations. These agents are helpful in defining the borders, characterizing the mass lesion and in identifying its organ of origin2 The standard dose is 0.1mmol/kg and is administered intravenously. Oral MR contrast agents have been developed and have been shown to be both safe and effective in children. 4~ CRANIOSPINAL APPLICATIONS Brain Routine MR imaging sequences: Sagittal Tl-weighted sequence should be performed in all patients, which allows assessment of the midline structures. After obtaining sagittal images, axial T1 and T2 weighted (T2W) images should be obtained in all patients. Three- dimensional gradient echo (GE) techniques using either SPGR or 3D-FLASH can also be used to acquire T1W images. These gradient sequences have the ability to acquire very thin (<1ram) contiguous images in a relatively very short imaging time. Fluid attenuated Indian Journal of Pediatrics, Volume 71--December, 2004 1095
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Role of MR imaging in pediatric surgery

Role of MR Imaging in Pediatric Surgery Raju Sharma and Shivanand Gamanagatti
Department of Radiology, Al India Institute of Medical Sciences, New Delhi, India.
Abstract. Magnetic Resonance Imaging is a non-invasive multiplanar imaging modality which does not use ionizing radiation. In recent years major technical advances in this field have led to shorter imaging times and better resolution. This has widened the scope of this modality in pediatric imaging. MRI is already an established technique for the brain and spine and is increasingly being used for musculoskeletal, abdominal and pelvic imaging. In this article the authors provide an update on this exciting modality with stress on applications relevant to pediatric surgeons. [Indian J Pediatr 2004; 71 (12) : 1095-1110] E-mail: raju 152 @yahoo. com
Key words : MR/; Pediatric; Craniospial; Body
Magnetic resonance imaging (MRI) plays a vital role in the evaluation of many paediatric diseases. It is a non- invasive, multiplanar imaging modality which does not involve the use of ionizing radiation, has excellent contrast resolution, and requires only minimal patient preparation. MR1 has become the modality of choice for many cranio-spinal and musculoskeletal applications and is a useful complementary modality to other cross- sectional modalities such as ultrasound and computed tomography (CT) and a problem solving tool in abdominal and chest imaging. Technical advances in the field of MRI have resulted in improved image quality and shorter scan times, both of which are very relevant to pediatric applications. In paediatric age group the spectrum of diseases is different from adults, with a higher incidence of congenital anomalies, a different group of neoplasms, and a lower incidence of metastatic disorders. The pulse sequences and techniques have to be adapted to the demanding requirements of imaging children, and therefore optimized protocols should be used.
TECHNICAL CONSIDERATIONS
Surface coils should be used whenever possible for imaging children so that signal-to-noise ratios can be optimized. There is lot of scope for improvisation and either adult head or extremity coils can be used to image the chest or abdomen in infants with excellent results. Faster imaging techniques having short imaging times such as gradient-echo, fast spin-echo (FSE), and echo- planar imaging are particularly advantageous in imaging of children. Newer applications such as diffusion weighted imaging (DWI) and diffusion tensor imaging
Correspondence and Reprint requests : Dr. Raju Sharma, Department of Radiology, All India Institute of Medical Sciences, New Delhi 110029. Fax : 91-11-26588641.
(DTI), MR angiography (MRA) and MR Cholangiopancreatography (MRCP) have emerged and have been successfully applied to the paediatric population also. 1,2
During the MR study, parents should be encouraged to stay with the children as it helps to reassure them. Apprehensive and uncooperative children frequently require sedation. While sedating, special care should be taken in children with airway compromise, congenital heart disease, or mental retardation because they have a higher incidence of complications. Children requiring sedation should be kept nil by mouth for four to six hours prior to the administration of sedation to minimize the risks of aspiration. General anesthesia may be used if routine sedation fails or in high-risk children.
MR contrast agent: Gadolinium chelate contrast agents are useful in the evaluation of mass lesions and vascular malformations. These agents are helpful in defining the borders, characterizing the mass lesion and in identifying its organ of origin2 The standard dose is 0.1mmol/kg and is administered intravenously. Oral MR contrast agents have been developed and have been shown to be both safe and effective in children. 4~
CRANIOSPINAL APPLICATIONS
Brain Routine MR imaging sequences: Sagittal Tl-weighted sequence should be performed in all patients, which allows assessment of the midline structures. After obtaining sagittal images, axial T1 and T2 weighted (T2W) images should be obtained in all patients. Three- dimensional gradient echo (GE) techniques using either SPGR or 3D-FLASH can also be used to acquire T1W images. These gradient sequences have the ability to acquire very thin (<1ram) contiguous images in a relatively very short imaging time. Fluid attenuated
Indian Journal of Pediatrics, Volume 71--December, 2004 1095
Raju Sharma and Shivanand Gamanagatti
Fig. 1A Fig. 1B
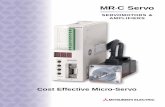
Fig 1. Medulloblastoma A. Axial T1W image shows large hypointense midline mass in the posterior fossa. B. Axial T2W image shows the mass is hyperintense to grey matter. C. Sagittal T2W image shows hyperintense mass arising from cerebellar vermis obstructing the fourth ventricle.
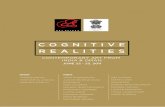
Fig 1. C. Sagittal T2W image shows hyperintense mass arising from cerebellar vermis obstructing the fourth ventricle.
inversion recovery (FLAIR) sequence should be used as a secondary sequence in patients with focal neurological deficits but normal looking standard sequences because of high sensitivity of FLAIR for subtle lesions. After the sagittal and axial images have been obtained, coronal FSE- T2W images may be obtained. T2W GE images are useful in the evaluation of vascular malformations and hemorrhage because they are sensitive to the magnetic suscept ib i l i ty changes and local he t e rogene i ty of magnetic fields. 6
Fig 2. Hamartoma of tuber cinerium A. Sagittal T1W image shows isointense well defined mass
arising from the tuber cinerium.
1096 Indian Journal of Pediatrics, Volume 71--December, 2004
Role of MR Imaging in Paediatric Surgery
usually require scanning in multiple planes with good anatomical delineation. 13-16
Cerebrospinal Fluid Flow Imaging
The multiplanar capabilities of MRI make it the ideal imaging modality to evaluate the level of CSF obstruction in hydrocephalus. Hyperdynamic CSF flow may result from communicating hydrocephalus, causing loss of signal on MR images in the aqueduct and adjacent ventricles? 7-~8 Both qualitative and quantitative CSF flow studies can be acquired by phase contrast (PC) study.
SPECIAL MR TECHNIQUES
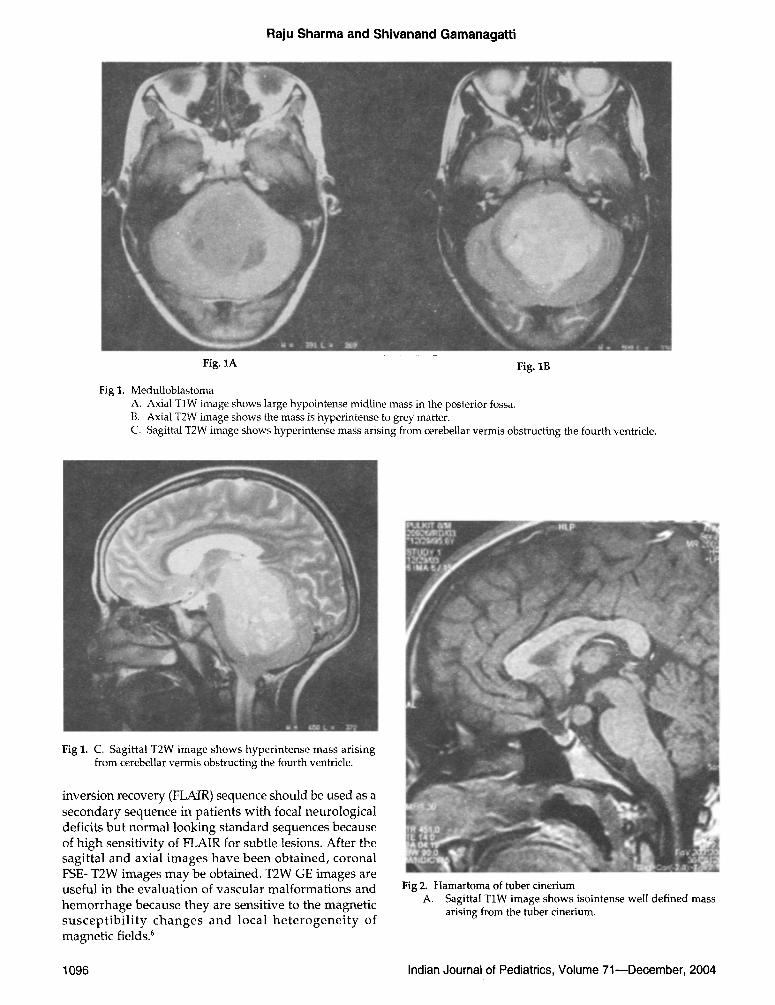
Fig. 2B. Post-gadolinium sagittal TIW image shows no contrast enhancement of the lesion.
Pediatric Brain Tumors
MR[ is the ideal technique for evaluating paediatric brain tumors particularly in the posterior fossa (Fig.l) because of its multiplanar capabilities, high tissue contrast, and ability to show the breakdown of the blood-brain barrier after the administration of gadolinium. 7-1~ MR is also useful in evaluating sellar and suprasellar masses of paediatric age group such as craniopharyngioma and hamartoma of tuber cinerium (Fig. 2).
MRI is useful for showing the secondary effects of brain tumors, including herniation, hydrocephalus, hemorrhage, and infarction.
The increased choline and decreased NAA documented by MR spectroscopy are useful for differentiating brain tumors from other masses in the brain, such as occur in infection, inflammation, and radiation necrosis21-12
Congenital Anomalies
The more common congenital abnormalities of the cerebrum include encephaloceles, meningoceles, agenesis of the corpus callosum, holoprosencephaly (Fig. 3), l issencephaly, gray matter heterotopia, hemimeganencephaly, schizencephaly, and polymicrogyria. The more common congenital abnormalities of the brainstem and cerebellum include the Dandy-Walker malformation, Joubert's syndrome, Chiari I malformation, Chiari II malformation (Fig. 4), and aqueductal stenosis. Congenital brain malformations
MR Angiography and Venography For intracranial vasculature, three-dimensional time of flight (3D TOF) studies using multiple overlapping acquisitions are most useful. After the acquisition is completed, MRAs are created by means of maximum intensity projection technique.
For the studies of cervi'cal carotid and vertebral arteries, two-dimensional Fourier transformed time of flight (2D TOF) images are optimal. Saturation pulses are applied cephalad to axial images to eliminate the signal intensity from the blood flowing across the jugular vein. MIP image are reconstructed in multiple planes.
For obtaining high resolution MRA, contrast enhanced MRA with bolus injection of gadolinium is most useful. Phase contrast images are useful for imaging slow flow and analyzing flow direction.
For imaging dural venous sinuses, contrast enhanced magnetic resonance venograms (MRV) are most useful and are acquired in coronal planes to avoid saturation effects in transverse sinuses secondary to in plane flow.
MRA is useful to diagnose unruptured aneurysms, AVMs, arterial occlusions, and stenoses. MRV is useful to diagnose venous occlusion caused by dural sinus thrombosis. MRA in the paediatric practice is being increasingly used for evaluating vascular patency, vascular topography, flow magnitude and flow direction. It is already established as having a high sensitivity for the detection of intracranial arterio-venous malformations and aneurysms.
MRA has also been applied in evaluation of extra- cranial vascular malformations, renal and peripheral vessel evaluation and for pu lmonary venous abnormalities including hypoplasia, stenosis or abnormal connections. 19-21
Diffusion Weighted Imaging (DWI)
Diffusion imaging is useful in the assessment of brain maturation and to detect the restricted diffusion in acute phase following traumatic, metabolic or toxic injury to brain. Diffusion imaging is performed by using echo planar imaging techniques. The areas with reduced diffusion appear bright. Diffusion weighted imaging is
Indian Journal of Pediatrics, Volume 71--December, 2004 1097
Raju Sharma and Shivanand Gamanagatti
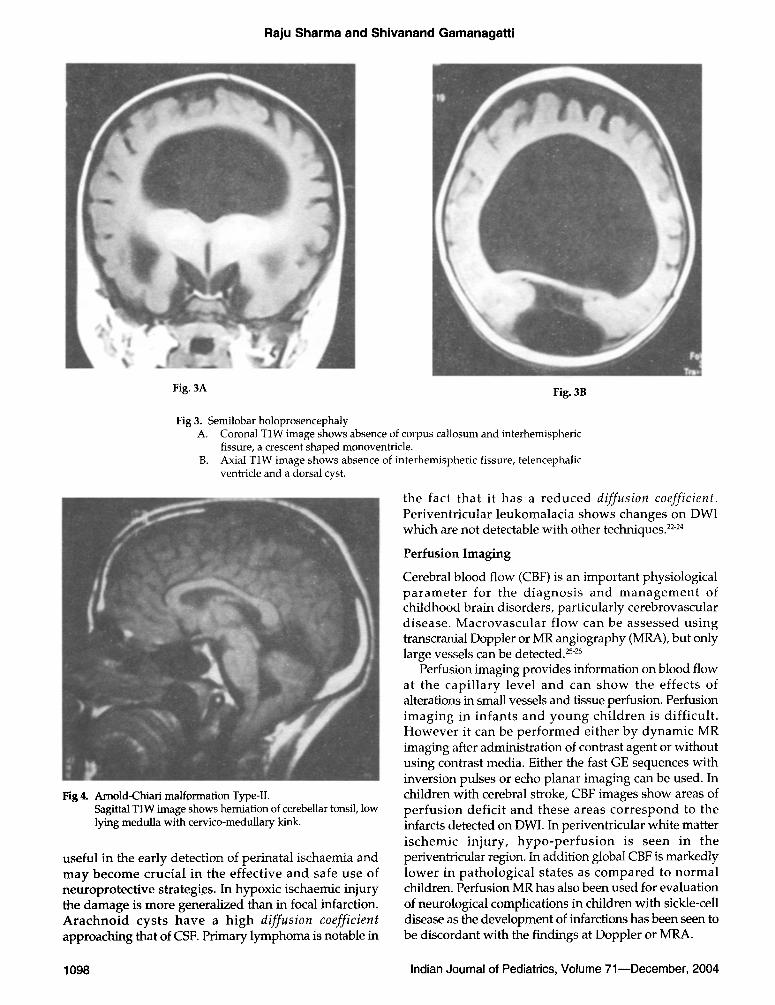
Fig. 3A Fig. 3B
Fig 3. Semilobar holoprosencephaly A. Coronal TIW image shows absence of corpus callosum and interhemispheric
fissure, a crescent shaped monoventricle. B. Axial TIW image shows absence of interhemispheric fissure, telencephalic
ventricle and a dorsal cyst.
Fig 4. Arnold-Chiari malformation Type-II. Sagittal T1W image shows herniation of cerebellar tonsil, low lying medulla with cervico-medullary kink.
useful in the early detection of perinatal ischaemia and may become crucial in the effect ive and safe use of neuroprotect ive strategies. In hypoxic ischaernic injury the damage is more generalized than in focal infarction. A r a c h n o i d cysts have a h igh diffusion coefficient approaching that of CSF. Primary lymphoma is notable in
the fact that it has a r e d u c e d diffusion coefficient. Periventricular leukomalacia shows changes on DWI which are not detectable with other techniques. 22-24
Perfusion Imaging
Cerebral blood flow (CBF) is an important physiological p a r a m e t e r for the d iagnos i s and m a n a g e m e n t of childhood brain disorders, particularly cerebrovascular disease. Macrovascu la r f low can be assessed us ing transcranial Doppler or MR angiography (MRA), but only large vessels can be detected, z5-26
Perfusion imaging provides information on blood flow at the capi l la ry level and can show the effects of alterations in small vessels and tissue perfusion. Perfusion imaging in infants and y o u n g ch i ld ren is diff icult . Howeve r it can be per fo rmed either by dynamic MR imaging after administration of contrast agent or without using contrast media. Either the fast GE sequences with inversion pulses or echo planar imaging can be used. In children with cerebral stroke, CBF images show areas of pe r fus ion deficit and these areas co r r e spond to the infarcts detected on DWI. In periventricular white matter i schemic in jury , h y p o - p e r f u s i o n is seen in the periventricular region, In addition global CBF is markedly lower in pathological states as compared to normal children. Perfusion MR has also been used for evaluation of neurological complications in children with sickle-cell disease as the development of infarctions has been seen to be discordant with the findings at Doppler or MRA.
1098 Indian Journal of Pediatrics, Volume 71--December, 2004
Role of MR Imaging in Paediatric Surgery
Perfusion MR has also been found to be a promising technique for prediction of renal function deterioration and for selection of patients who are likely to benefit from surgical intervention, in the clinical setting of paediatric hydronephrosis.
Functional Imaging
Positron emission tomography (PET) and functional magnetic resonance imaging (fMRI) use the fact that brain cell activity is associated with local changes in oxygen and glucose metabolism and in cerebral blood flow and oxygenation. Focal brain activity leads to observable changes in the MR signal changes due to local changes in blood flow, volume, velocity and oxygenation. These are measured by flow-sensitive sequences, use of intravascular contrast (gadolinium), arterial spin labeling technique and by the BOLD (blood oxygen level d e p e n d a n t ) t e chn ique . 27-29
Fig 6A.
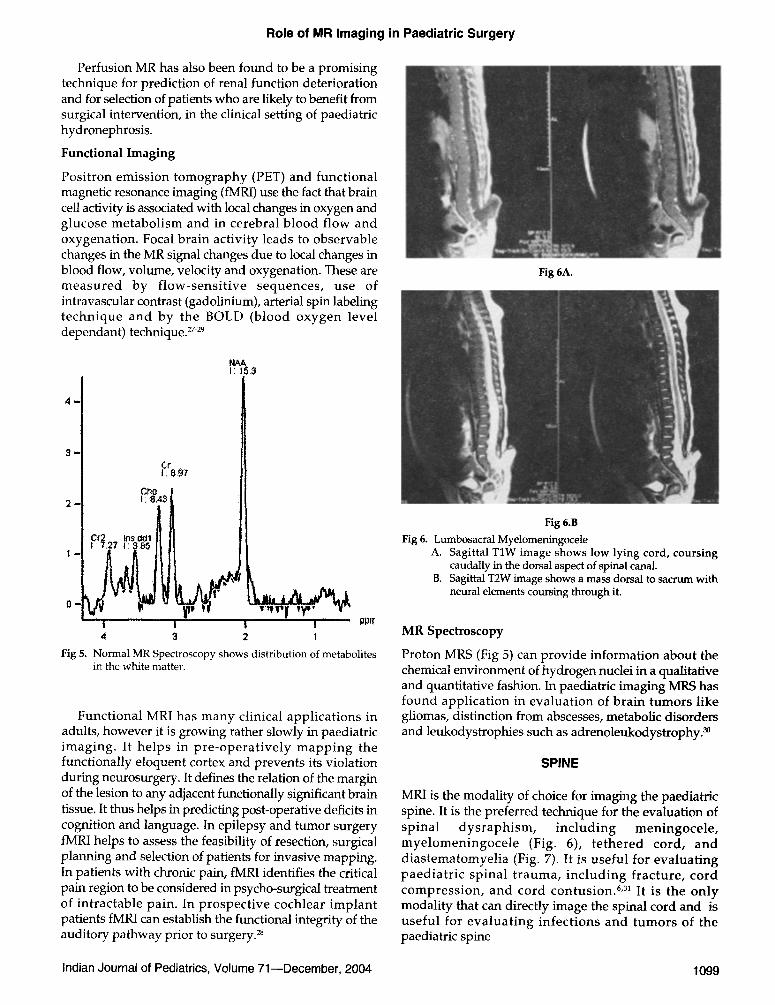
NAA I: 153
Ct �9 ! ; 8 9 7
' 'c'~ t I ICr2 Ins 001 ~ II !
0 - ~j__
I ....... l I I ppn" 4 3 2 t
Fig 5. N o r m a l M R Spectroscopy shows d is t r ibu t ion o f metabo] i tes in the white matter.
Functional MRI has many clinical applications in adults, however it is growing rather slowly in paediatric imaging. It helps in pre-operat ively mapping the functionally eloquent cortex and prevents its violation during neurosurgery. It defines the relation of the margin of the lesion to any adjacent functionally significant brain tissue. It thus helps in predicting post-operative deficits in cognition and language. In epilepsy and tumor surgery fMRI helps to assess the feasibility of resection, surgical planning and selection of patients for invasive mapping. In patients with chronic pain, fMR1 identifies the critical pain region to be considered in psycho-surgical treatment of intractable pain. In prospective cochlear implant patients fMRI can establish the functional integrity of the auditory pathway prior to surgery. 28
Fig 6.B Fig 6. Lumbosacral Myelomeningocele
A. Sagittal TIW image shows low lying cord, coursing caudally in the dorsal aspect of spinal canal.
B. Sagittal T2W image shows a mass dorsal to sacrum with neural elements coursing through it.
MR Spectroscopy
Proton MRS (Fig 5) can provide information about the chemical environment of hydrogen nuclei in a qualitative and quantitative fashion. In paediatric imaging MRS has found application in evaluation of brain tumors like gliomas, distinction from abscesses, metabolic disorders and leukodystrophies such as adrenoleukodystrophy2 ~
SPINE
MRI is the modality of choice for imaging the paediatric spine. It is the preferred technique for the evaluation of spinal dysraphism, including meningocele, myelomeningocele (Fig. 6), te thered cord, and diastematomyelia (Fig. 7). It is useful for evaluating paediatric spinal trauma, including fracture, cord compression, and cord contusion. 6m It is the only modality that can directly image the spinal cord and is useful for evaluating infections and tumors of the paediatric spine
Indian Journal of Pediatrics, Volume 71--December, 2004 1099
Raju Sharma and Shivanand Gamanagatti
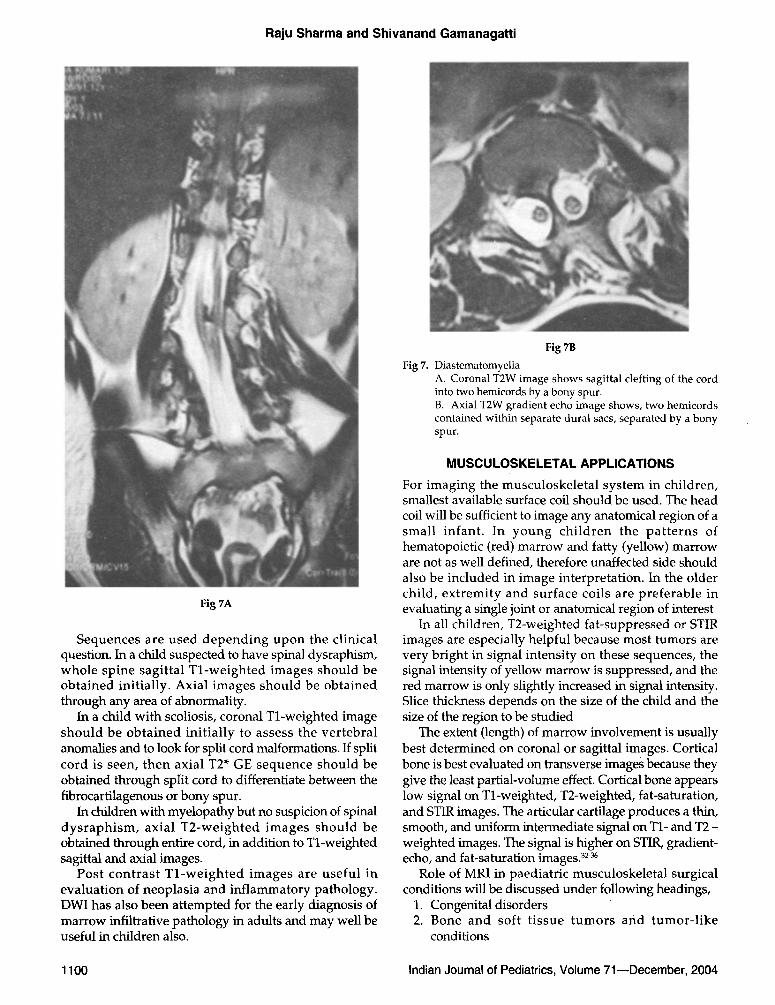
Fig 7A
Sequences are used depending upon the clinical question. In a child suspected to have spinal dysraphism, whole spine sagittal Tl-weighted images should be obtained initially. Axial images should be obtained through any area of abnormality.
In a child with scoliosis, coronal Tl-weighted image should be obtained initially to assess the vertebral anomalies and to look for split cord malformations. If split cord is seen, then axial T2* GE sequence should be obtained through split cord to differentiate between the fibrocartilagenous or bony spur.
In children with myelopathy but no suspicion of spinal dysraphism, axial T2-weighted images should be obtained through entire cord, in addition to Tl-weighted sagittal and axial images.
Post contrast T l -weigh ted images are useful in evaluation of neoplasia and inflammatory pathology. DWI has also been attempted for the early diagnosis of marrow infiltrative pathology in adults and may well be useful in children also.
Fig 7B
Fig 7. Diastematomyelia A. Coronal T2W image shows sagittal clefting of the cord into two hemicords by a bony spur. B. Axial T2W gradient echo image shows, two hemicords contained within separate dural sacs, separated by a bony spur.
MUSCULOSKELETAL APPLICATIONS
For imaging the musculoskeletal system in children, smallest available surface coil should be used. The head coil will be sufficient to image any anatomical region of a small infant. In young children the pat terns of hematopoietic (red) marrow and fatty (yellow) marrow are not as well defined, therefore unaffected side should also be included in image interpretation. In the older child, extremity and surface coils are preferable in evaluating a single joint or anatomical region of interest
In all children, T2-weighted fat-suppressed or STIR images are especially helpful because most tumors are very bright in signal intensity on these sequences, the signal intensity of yellow marrow is suppressed, and the red marrow is only slightly increased in signal intensity. Slice thickness depends on the size of the child and the size of the region to be studied
The extent (length) of marrow involvement is usually best determined on coronal or sagittal images. Cortical bone is best evaluated on transverse images because they give the least partial-volume effect. Cortical bone appears low signal on Tl-weighted, T2-weighted, fat-saturation, and STIR images. The articular cartilage produces a thin, smooth, and uniform intermediate signal on T1- and T2 - weighted images. The signal is higher on STIR, gradient- echo, and fat-saturation images, a2-36
Role of MRI in paediatric musculoskeletal surgical conditions will be discussed under following headings,
1. Congenital disorders 2. Bone and soft t issue tumors and tumor-like
conditions
1100 Indian Journal of Pediatrics, Volume 71mDecember, 2004
Role of MR Imaging in Paediatric Surgery
3. Osteochondral lesions
CONGENITAL DISORDERS
Developmental Dysplasia of the Hip (DDH) Advan tages of MR eva lua t ion of DDH include v i sua l iza t ion of car t i lag inous s t ruc tures (e.g., car t i lag inous femoral epiphysis) , lack of ioniz ing radiation (important in these patients, who are primarily girls), and lack of artifact from spica casts. However, MR[ does not allow dynamic assessment of the hip, and it is un l ike ly to be the most cost-effect ive me thod of evaluation and is reserved for problematic cases. MR[ is superb for delineating the anatomical position of the cartilaginous femoral epiphysis, and perhaps its greatest potential is in defining the causes of failed hip reduction without the need for arthrography.
MR[ may be used to define anatomical structures in a variety of other congenital disorders. Currently, surgical repair of c lubfoot de fo rmi ty (talipes equinovarus) requires the use of the anterior tibialis t endon and musculature. Significant hypoplasia or absence of the anterior tibialis tendon necessitates an alternative surgical approach.
Delayed ossification of cartilaginous structures in congenital disorders such as focal femoral deficiency may also be eva lua ted by MRI. In congeni tal posi t ional abnormalities of the knee (arthrogryposis, congenital anterior subluxation of the knee), MRI can clearly define the anatomical alignment of the joint.
Bone and Soft Tissue Tumors and Tumor-Like Conditions
MRI is superior to computed tomography (CT) in the
evaluation and staging of musculoskeletal tumors and has become the modality of choice for this purpose.
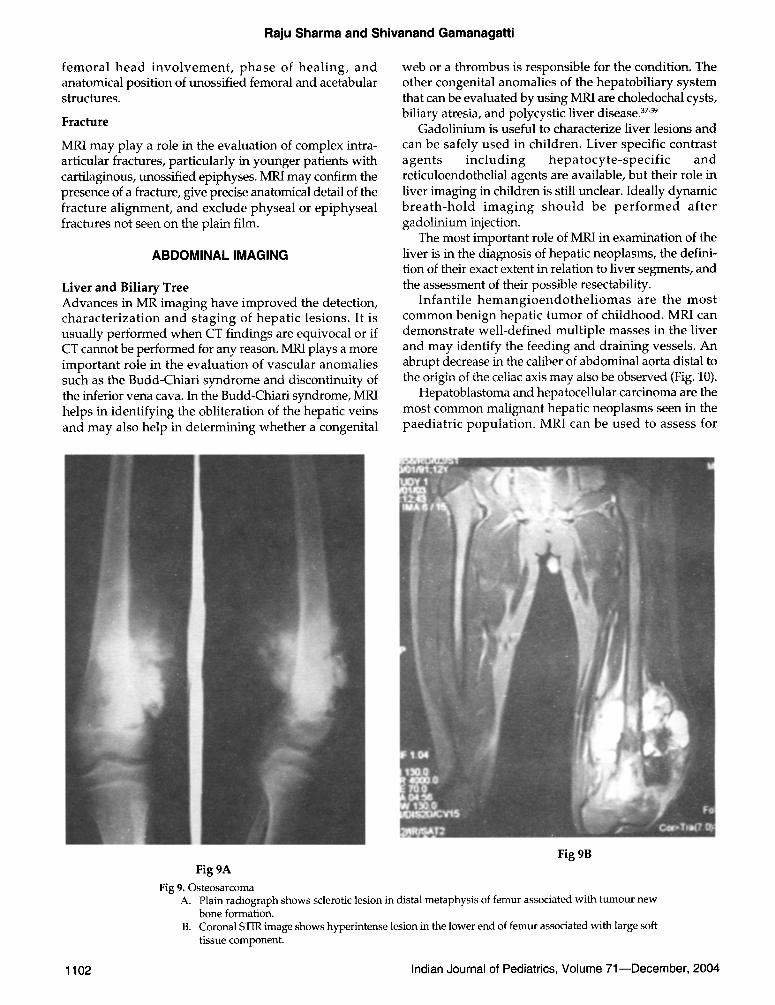
As a rule MR examinations of bone tumors and ~rnor like conditions should not be interpreted without plain film radiographs . Due to advances in neoad juvan t therapy and surgical techniques, 80% of patients with mal ignant bone lesions are treated by limb salvage procedures. MR[ helps in determination of tumor extent, detection of skip lesions, involvement of vital structures such as neurovascular bundle, involvement of adjacent muscle groups, and joint and transphyseal involvement (Fig. 8 and Fig. 9). In addition assessment of successful therapy, complicat ions of surgery and detect ion of recurrent disease can be monitored by MR[.
Contrast should be administered for better delineation of tumor and for distinction between tumor and necrosis in the post treatment setting.
OSTEOCHONDRALLESIONS
Osteochondritis dissecans is an often painful, usually unilateral condition that occurs in young adults and children. This condition is characterized by articular cartilage injury, a subchondral fracture, and an attached fragment of subchondral bone that may become partially or completely separated from the underlying bone. MRI allows accurate assessment of the articular cartilage and subchondral surface of bone.
Perthes Disease
Current indications for MR[ early in the course of Legg- Calve-Pertbes disease include more precise evaluation of
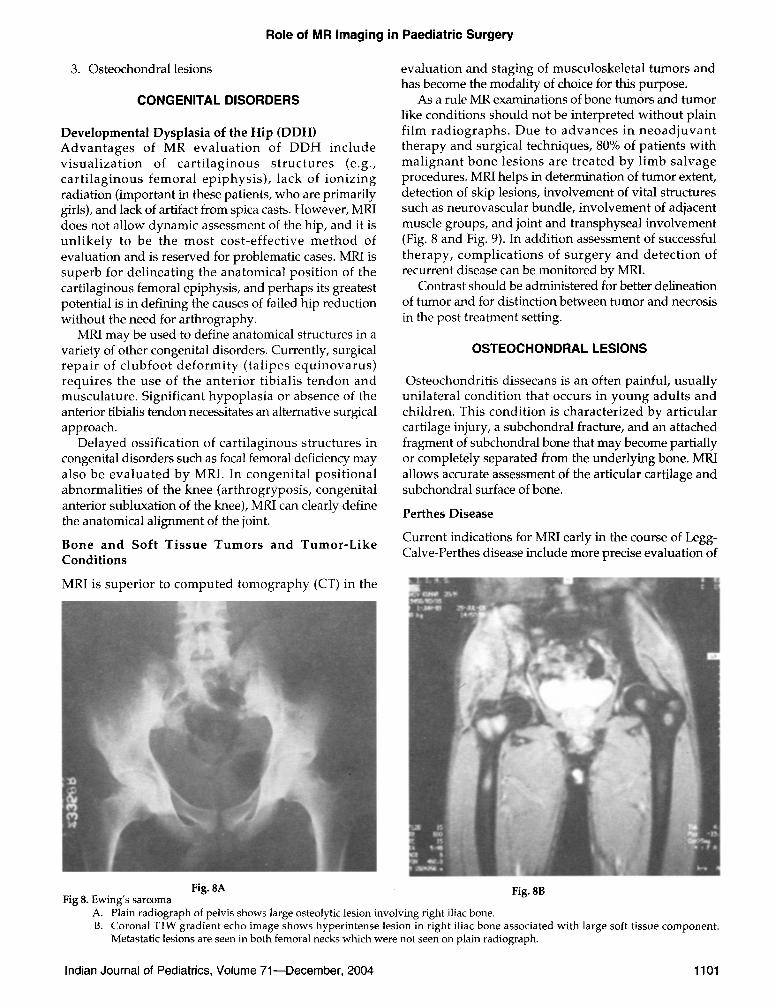
Fig. 8A Fig. 8B Fig 8. Ewing's sarcoma
A. Plain radiograph of pelvis shows large osteolytic lesion involving right iliac bone. B. Coronal TIW gradient echo image shows hyperintense lesion in right iliac bone associated with large soft tissue component.
Metastatic lesions are seen in both femoral necks which were not seen on plain radiograph.
Indian Journal of Pediatrics, Volume 71--December, 2004 1101
Raju Sharma and Shivanand Gamanagatti
f emora l head i n v o l v e m e n t , phase of hea l ing , and anatomical position of unossified femoral and acetabular structures.
Fracture
MRI may play a role in the evaluation of complex intra- articular fractures, particularly in younger patients with cartilaginous, unossified epiphyses. MRI may confirm the presence of a fracture, give precise anatomical detail of the fracture alignment, and exclude physeal or epiphyseal fractures not seen on the plain film.
ABDOMINAL IMAGING
Liver and Biliary Tree Advances in MR imaging have improved the detection, charac ter iza t ion and staging of hepat ic lesions. It is usually performed when CT findings are equivocal or if CT cannot be performed for any reason. MRI plays a more important role in the evaluation of vascular anomalies such as the Budd-Chiari syndrome and discontinuity of the inferior vena cava. In the Budd-Chiari syndrome, MRI helps in identifying the obliteration of the hepatic veins and may also help in determining whether a congenital
web or a thrombus is responsible for the condition. The other congenital anomalies of the hepatobiliary system that can be evaluated by using MRI are choledochal cysts, biliary atresia, and polycystic liver disease. 37-39
Gadolinium is useful to characterize liver lesions and can be safely used in children. Liver specific contrast agents inc lud ing hepa tocy t e - spec i f i c and reticuloendothelial agents are available, but their role in liver imaging in children is still unclear. Ideally dynamic b rea th -ho ld imaging shou ld be p e r f o r m e d af ter gadolinium injection.
The most important role of MRI in examination of the liver is in the diagnosis of hepatic neoplasms, the defini- tion of their exact extent in relation to liver segments, and the assessment of their possible resectability.
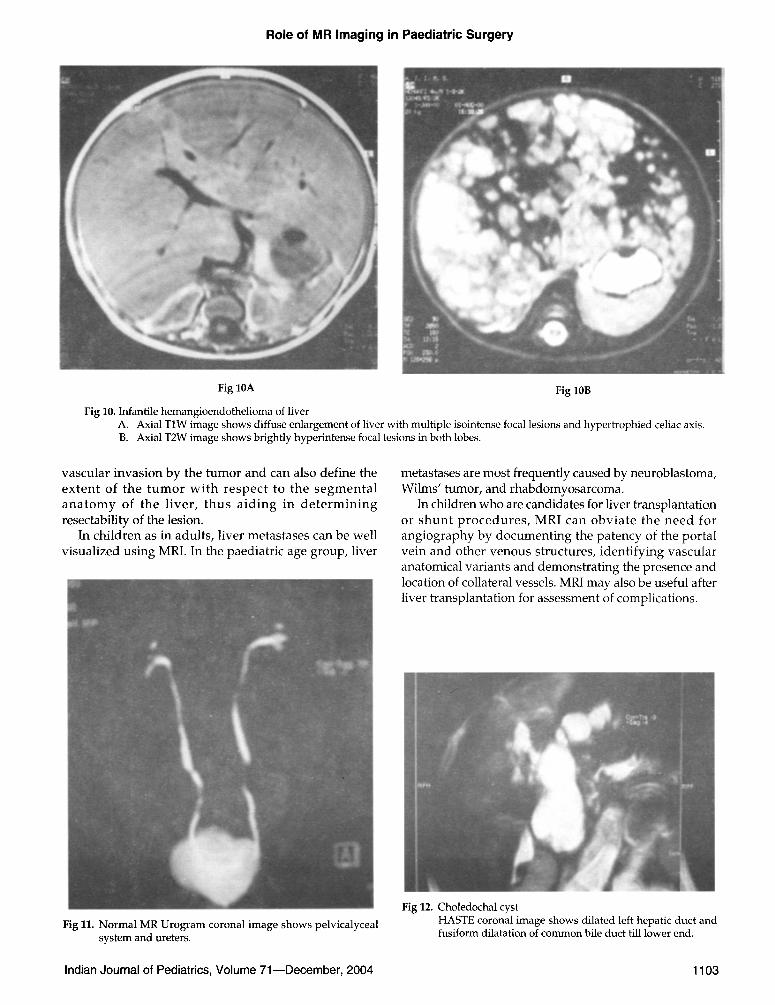
Infant i le h e m a n g i o e n d o t h e l i o m a s are the mos t common benign hepatic tumor of childhood. MRI can demonstrate well-defined multiple masses in the liver and may identify the feeding and draining vessels. An abrupt decrease in the caliber of abdominal aorta distal to the origin of the celiac axis may also be observed (Fig. 10).
Hepatoblastoma and hepatocellular carcinoma are the most common malignant hepatic neoplasms seen in the paediatr ic populat ion. MRI can be used to assess for
Fig 9B Fig 9A
Fig 9. Osteosarcoma A. Plain radiograph shows sclerotic lesion in distal metaphysis of femur associated with tumour new
bone formation. B. Coronal STIR image shows hyperintense lesion in the lower end of femur associated with large soft
tissue component.
1102 Indian Journal of Pediatrics, Volume 71--December, 2004
Role of MR Imaging in Paediatric Surgery
Fig 10A Fig 10B
Fig 10. Infantile hemangioendothelioma of liver A. Axial TIW image shows diffuse enlargement of liver with multiple isointense focal lesions and hypertrophied celiac axis. B. Axial T2W image shows brightly hyperintense focal lesions in both lobes.
vascular invasion by the tumor and can also define the ex ten t of the t u m o r w i th r e spec t to the s e g m e n t a l a n a t o m y of the l iver , thus a id ing in d e t e r m i n i n g resectability of the lesion.
In children as in adults, liver metastases can be well visualized using MRI. In the paediatric age group, liver
metastases are most frequently caused by neuroblastoma, Wilms' tumor, and rhabdomyosarcoma.
In children who are candidates for liver transplantation or shun t p r o c e d u r e s , MRI can obv ia te the need for angiography by documenting the patency of the portal vein and other venous structures, identifying vascular anatomical variants and demonstrating the presence and location of collateral vessels. MRI may also be useful after liver transplantation for assessment of complications.
Fig 11. Normal MR Urogram coronal image shows pelvicalyceal system and ureters.
Fig 12. Choledochal cyst HASTE coronal image shows dilated left hepatic duct and fusiform dilatation of common bile duct till lower end.
Indian Journal of Pediatrics, Volume 71--December, 2004 1103
Raju Sharma and Shivanand Gamanagatti
Magnetic Resonance Cholangiopancreatography (MRCP)
This is a non-invasive method of gett ing cholangio- graphic images, based on heavily T2W sequences such as HASTE, which map the distribution of stationary or slow moving fluid. No contrast medium is injected. The same principle can also be applied to the renal collecting system and ureters to obtain MR urograms (Fig. 11)? o
It has been found to be very useful in the distinction of extra-hepatic biliary atresia from neonatal hepatitis and for the accurate diagnosis of choledochal cyst (Fig. 12). Pancreat ic pa tho logy like chronic pancreat i t is and pancreas divisum are also well delineated.
Kidney
Congenital renal anomalies such as ectopic kidney, horse- shoe kidney and fusion anomalies can be evaluated using MRI obtained in the coronal plane, which provide good anatomical detail 4M2
All of the renal cystic diseases can be demonstrated using MRI, however ul t rasound remains the primary imaging modality for this class of diseases. But MRI is most useful in c lar i fy ing confus ing cases and in demonstrating complications such as hemorrhage.
The renal neoplasms that occur commonly in children include Wilms' tumor and the various forms of leukemia and lymphoma. Less frequently, renal cell carcinoma, teratoma, clear cell sarcoma, and rhabdoid tumor may be seen and in infants, congenital mesoblastic nephroma can also occur.
CT remains the preferred technique for the assessment of children with suspected Wilm's tumor, because it is readily available and the need to evaluate the lungs for metas ta t ic disease. However MRI plays a role in problematic cases such as children with allergies to iodinated contrast materials, vascular extension equivocal on CT, res idual disease or recurrence after par t ia l nephrectomy. 4B
In this region of the body, MRI helps in defining the organ of origin and can often separate renal lesions from those arising in the adjacent liver or adrenal gland. MRI also helps in defining the full extent of the lesion, assess for possible invasion of adjacent organs, and document the presence or absence of associated lymphadenopathy. MRI clearly defines patent vascular structures, and it is extremely useful in demonstrating the presence of tumor thrombus within the renal veins or inferior vena cava, which may be seen in association with Wilms' tumor. The direct ion of d i sp lacement and the pos i t ion of the displaced vessels can be well identified before surgery using MRI, aiding in the planning of the surgical resection of the tumor.
MRI is also a tool for the evaluation of residual or recurrent disease after treatment with chemotherapy or surgical resection. Contrast enhanced MRI is better than contras t enhanced CT for the detect ion of
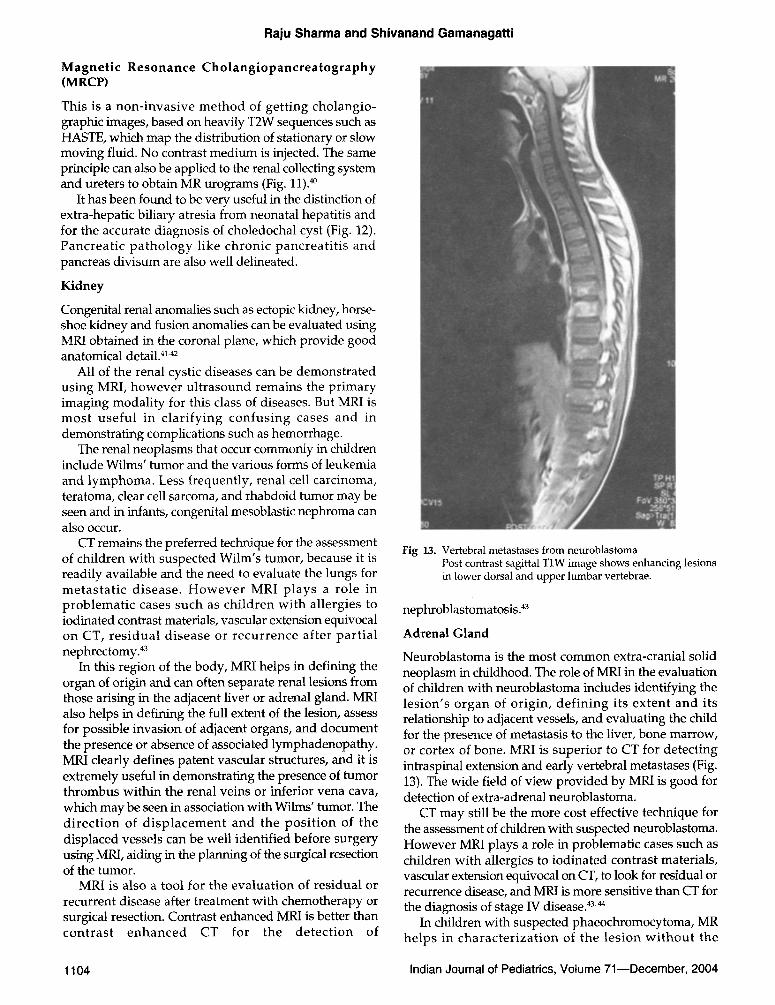
Fig 13. Vertebral metastases from neuroblastoma Post contrast sagittal T1W image shows enhancing lesions in lower dorsal and upper lumbar vertebrae.
nephroblastomatosis ?3
Adrenal Gland
Neuroblastoma is the most common extra-cranial solid neoplasm in childhood. The role of MRI in the evaluation of children with neuroblastoma includes identifying the lesion's organ of origin, def in ing its extent and its relationship to adjacent vessels, and evaluating the child for the presence of metastasis to the liver, bone marrow, or cortex of bone. MRI is superior to CT for detecting intraspinal extension and early vertebral metastases (Fig. 13). The wide field of view provided by MRI is good for detection of extra-adrenal neuroblastoma.
CT may still be the more cost effective technique for the assessment of children with suspected neuroblastoma. However MRI plays a role in problematic cases such as children with allergies to iodinated contrast materials, vascular extension equivocal on CT, to look for residual or recurrence disease, and MRI is more sensitive than CT for the diagnosis of stage IV disease. 43,44
In children with suspected phaeochromocytoma, MR helps in character izat ion of the lesion w i thou t the
1104 Indian Journal of Pediatrics, Volume 71--December, 2004

Role of MR Imaging in Paediatric Surgery
administration of contrast material because of bright signal intensity on T2 weighted images and also helps in defining the extent as well in identifying additional (extradrenal) lesions.
Differentiation of neonatal adrenal hemorrhage from neuroblastoma is crucial. In the majority of cases, differentiation of the two entities using MRI is simple.
Lower Urinary Tract Applications
Multiplanar MR imaging is the most useful in the evaluation of congenital abnormalities of the lower urinary tract in children because it provides superior anatomical resolution and clear depiction of fatty planes. 41
MRI can identify abnormal findings in children with neurogenic bladders. The main role of MRI in these children, however, is to evaluate the lumbosacral spine for possible dysraphic abnormalities or spinal cord tumors that may be the cause of the neurogenic bladder. MR plays important role in the evaluation of children with bladder exstrophy which is associated with complex anomalies of bladder wall, pubic bone, rectus muscle and testes in males and vagina in females.
Cloacal malformations are usually evaluated using a combination of fluoroscopy with contrast injection and ultrasonography. MRI may be useful to accurately demonstrate the relationship of the pelvic organs to one another before surgery. 4s
Urachal anomalies are best evaluated by MRI and sagittal Tl-weighted imaging is able to demonstrate the entire spectrum of anomalies in children with this disorder.
PELVIC APPLICATIONS
Ultrasonography (US) remains the initial imaging study of choice for the evaluation of pelvic abnormality. US does not provide functional information, has limited ability to characterize the lesion and it is inadequate for staging malignancies. If US is suboptimal or suggests a mass, CT is usually the next examination. CT has certain drawbacks such as exposure to ionizing radiation, necessity of oral and intravenous contrast agents. MRI is well suited for characterization and staging of pelvic tumors and also for evaluating congenital anomalies, because of its multiplanar capabilities and higher soft tissue resolution and no risk of exposure to ionizing radiation. ~
Rhabdomyosarcoma arising from the bladder or prostate is the most common tumor of the lower urinary tract in children. The multiplanar capabilities of MRI are extremely useful in the evaluation of children with rhabdomyosarcoma and in defining the extent of lesion.
MRI is useful in defining the extent of sacrococcygeal teratomas as well in distinguishing these tumors from other presacral lesions such as meningocele and lymphomas.
Ovarian tumors are uncommon in the paediatric population. In children, as in adults, the ~_rnors may be of
surface epithelial origin (adenomas and adenocarcinomas), germ cell origin (teratomas, dysgerminomas, and gonadoblastomas), or metastatic origin (lymphomas, leukemia, and neuroblastomas). MRI is not always able to give a definitive diagnosis of the type of ovarian tumor present, but it can identify the lesion as cystic, solid, or mixed in nature, narrowing the differential diagnosis.
Genital Tract
Congenital anomalies of the genital tract in children are divided into disorders of sexual differentiation, mullerian duct anomalies, and aplasia and atresia of the uterus and vagina.
MR images can clearly show the absence or abnormal location of pelvic organs in children with ambiguous genitalia or genetic abnormalities? 7
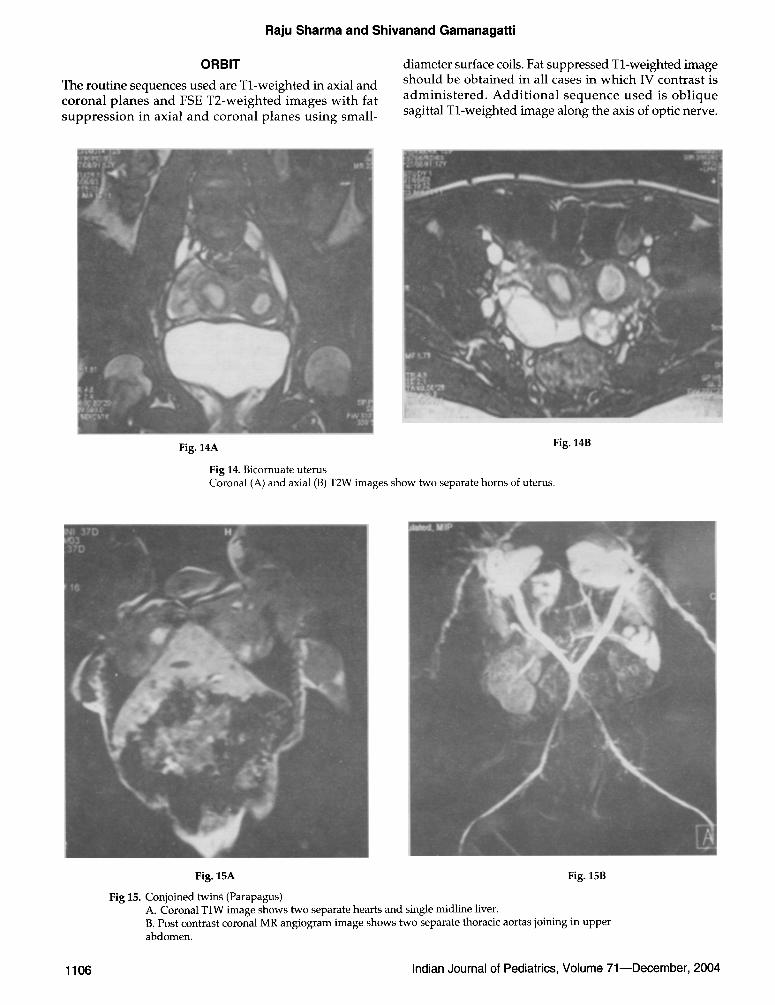
Uterine abnormalities can frequently be diagnosed and differentiated using MRI. MRI is able to differentiate bicomuate (Fig. 14) and septate uteri in postpubertal girls which is crucial if surgical intervention is planned. ~
Absence of both the uterus and the upper vagina is seen in patients with the Mayer-Rokitansky-Kuster- Hauser syndrome. MRI can be used to evaluate the vagina noninvasively; it is the modality of choice for patients with this disorder as well as for patients with isolated vaginal atresia. 49
In hematometrocolpos, MRI can demonstrate blood collection within a markedly dilated upper vagina and uterine cavity.
Undescended Testes: Ultrasonography remains the initial study of choice for locating the undescended testes but if it is unsuccessful or equivocal, then MRI should be performed. 5~
Anorectal Anomalies: Plain-film radiography, contrast fluoroscopy, and ultrasonography have all been helpful in the preoperative evaluation of this group of patients.
MRI can noninvasively give a multiplanar view of the hindgut , the puborectalis sling, and the adjacent structures and has been shown to be extremely useful in the evaluation of continuing or recurrent problems in patients after a repair?l.s2
MRI is less useful in children with rectal stenosis and atresia, in which narrowing or complete closure of the rectum is present with a normally formed anus.
Conjoined Twins
MRI can be extremely useful in the evaluation of complex congenital malformation syndromes such as conjoined twins (Fig. 15). It is a useful modality for planning the feasibility and approach to surgical correction.
HEAD AND NECK APPLICATIONS
Extracranial head and neck masses are a common indication for pediatric MR imaging. Congenital and inflammatory masses are more common than neoplastic lesions. 53
Indian Journal of Pediatrics, Volume 71--December, 2004 1105
Raju Sharma and Shivanand GamanagatU
ORBIT
The routine sequences used are Tl-weighted in axial and coronal planes and FSE T2-weighted images with fat suppress ion in axial and coronal planes using small-
diameter surface coils. Fat suppressed Tl-weighted image should be obtained in all cases in which IV contrast is adminis tered . Addi t iona l sequence used is obl ique sagittal Tl-weighted image along the axis of optic nerve.
Fig. 14A Fig. 14B
Fig 14. Bicornuate uterus Coronal (A) and axial (B) T2W images show two separate horns of uterus.
Fig. 15A Fig. 15B
Fig 15. Conjoined twin~ (Parapagus) A. Coronal TIW image shows two separate hearts and single midline liver. B. Post contrast coronal MR angiogram image shows two separate thoracic aortas joining in upper abdomen.
1106 Indian Journal of Pediatrics, Volume 71--December, 2004

Role of MR Imaging in Paediatric Surgery
Turnouts
Although the diagnosis of ret inoblastoma is made accurately with CT scan, but MRI is superior to CT in the evaluation of retro-ocular extension, cerebrospinal fluid seeding, pineal and suprasellar regions in patients with bilateral retinoblastoma. MR imaging is the modality of choice for imaging optic nerve glioma, enabling the radiologist to evaluate not only the entire optic pathway but also the remainder of the brain.
MR imaging is an important imaging adjunct for imaging rhabdomyosarcoma, especially in patients with parameningeal sites of involvement, to evaluate intracranial extension.
Contrast enhanced MR imaging helps in the evaluation of primary orbital lesion as well intracranial extension in cases of neuroblastoma, leukemia and lymphoma.
MR imaging is ideal to define the orbital, infratemporal fossa and intracranial extension and also the involvement of optic nerve in plexiform neurofibromas.
PARANASAL SINUSES AND SKULL BASE
The routine sequences used are Tl-weighted image in axial and coronal planes, T2-weighted image in axial plane and post gadolinium images in all three planes.
Although CT scan is the most commonly used imaging modali ty in the evaluation of sinonasal cavity, MR imaging better depicts sinus extension, intraosseous extent, intracranial and intra-orbital extension of lesion. Another important advantage of MR imaging is that it provides better differentiation between sinus extension of neoplasm and postobstructive disease.
SOFT TISSUES OF NECK
The routine sequences used are T1 and T2- weighted images with fat suppression in axial plane, Tl-weighted image in coronal plane and post-gadolinium images in axial and coronal planes with fat suppression.
Most neck masses are either inflammatory in origin or related to congenital anomalies such as thyroglossal duct cyst, branchial cleft cyst and lymphatic malformation. The commonest neoplasms include hemangioma, lymphoma, rhabdornyosarcoma, neurofibroma, schwanomma, neuroblastoma and teratoma.
Magnetic resonance imaging is considered the procedure of choice for evaluating suspected neoplasms of the salivary glands. Because a mass of salivary gland origin usually undergoes excisional biopsy, the primary role of MRI is to confirm the location of the mass and determine its relationship to surrounding normal structures. The goal is to determine the relationship of the mass to the facial nerve so that facial nerve function may be preserved.
MRI plays an essential role in the planning of surgery and of precision in radiation therapy by evaluating the size and extent of tumor, and identifying the involvement of adjacent structures. MRI has significant advantages in
the anatomical evaluation of thyroid and parathyroid glands because of its excellent soft tissue contrast and multiplanar capabilities.
THORACIC APPLICATIONS
In the evaluation of the mediastinum, the ability of MRI to easily distinguish vessels containing rapidly flowing blood from adjacent mass lesions without the need for bolus injection of contrast material is useful for dist inguishing congenital cysts (bronchogenic, neurenteric, thymic, duplication, and pericardial) from vascular structures) 1
MRI is particularly useful in the evaluation of lesions arising in the posterior mediastinum because it may noninvasively demonstrate ~he presence br absence of intraspinal extension. These posterior mediastinal masses are most frequently of neurogenic origin and include entities such as neuroblastomas, ganglioneuroma, and neurofibroma. Coronal and axial images are useful in demonstrating any intraspinal extension and in clarifying the relationship of the lesion to adjacent vasculature. 31
Multiplanar MRI may also better define the subcarinal area. MRI may be useful in the evaluation and staging of all types of lymphoma.
MR evaluation of intrathoracic extension of lesions primarily arising from the soft tissues of the neck or thorax can also be useful especially when images are obtained in the coronal and sagittal planes. These masses may arise from any soft tissue component and include lesions such as hemangiomas, lymphangiomas, cystic hygromas, lipomas, and fibromatosis.
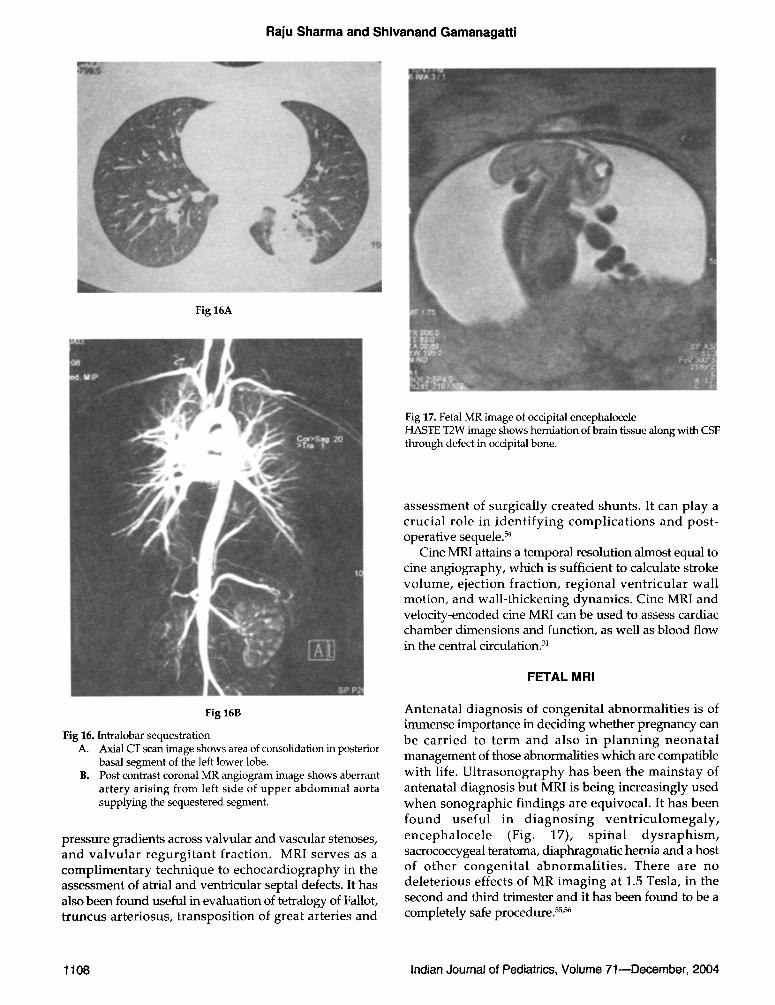
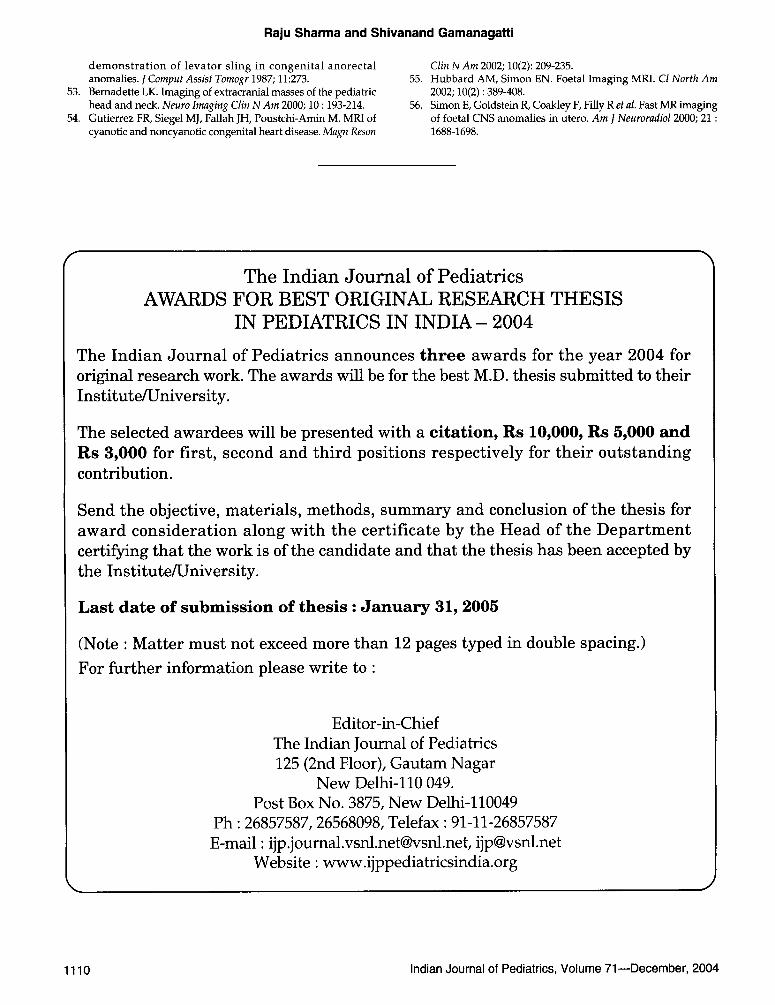
The most common paediatric abnormalities involving the lung include lobar emphysema, cystic adenomatoid malformation and pulmonary sequestration. MRI and MR angiography, can both be very useful in cases of seques- tration because it may be possible to demonstrate the anomalous feeding vessels and draining veins (Fig. 16).
Abnormali t ies of the diaphragm, such as diaphragmatic hernias and eventrations, can also be evaluated using MRI. Coronal and sagittal Tl-weighted images are useful in determining the presence or absence of a portion of the diaphragm as well as identifying if any of the abdominal contents are in the chest.
In patients with defects of the anterior abdominal wall, such as gastroschisis and omphalocele, MRI can be used to determine which abdominal organs have protruded through the defect and to define their position.
CARDIAC APPLICATIONS
MRI is effective for analyzing congenital heart disease (CHD) and is part icularly useful in complex cardiovascular malformations. In addi t ion to the anatomical depiction of CHD, MRI is capable of functional imaging, including measurement of intracardiac shunts, differential pulmonary blood flow,
Indian Journal of Pediatrics, Volume 71--December, 2004 1107
Raju Sharma and Shivanand Gamanagatti
Fig 16A
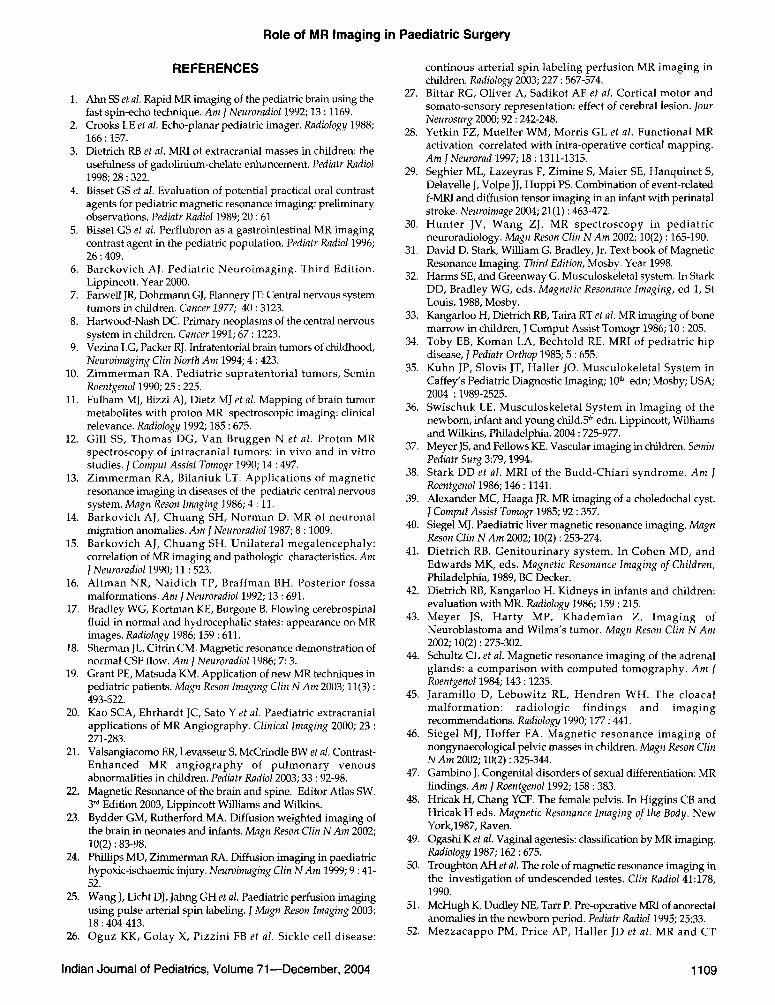
Fig 17. Fetal MR image of occipital encephalocele HASTE T2W image shows herniation of brain tissue along with CSF through defect in occipital bone.
Fig 16B
Fig 16. Intralobar sequestration A. Axial CT scan image shows area of consolidation in posterior
basal segment of the left lower lobe. B. Post contrast coronal MR angiogram image shows aberrant
artery arising from left side of upper abdominal aorta supplying the sequestered segment.
pressure gradients across valvular and vascular stenoses, and va lvu la r r egu rg i t an t fraction. MRI serves as a compl imentary technique to echocardiography in the assessment of atrial and ventricular septal defects. It has also been found useful in evaluation of tetralogy of Fallot, t runcus arteriosus, transposit ion of great arteries and
assessment of surgically created shunts. It can play a crucial role in iden t i fy ing compl ica t ions and post- operative sequele, s4
Cine MRI attains a temporal resolution almost equal to cine angiography, which is sufficient to calculate stroke vo lume, ejection fraction, regional ven t r icu la r wall motion, and wall-thickening dynamics. Cine MRI and velocity-encoded cine MRI can be used to assess cardiac chamber dimensions and function, as well as blood flow in the central circulation? 1
FETAL MRI
Antenatal diagnosis of congenital abnormali t ies is of immense importance in deciding whether pregnancy can be car r ied to t e rm and also in p l ann ing neona ta l management of those abnormalities which are compatible with life. Ul t rasonography has been the mainstay of antenatal diagnosis but MRI is being increasingly used when sonographic findings are equivocal. It has been found usefu l in d i agnos ing v e n t r i c u l o m e g a l y , encepha loce le (Fig. 17), sp ina l d y s r a p h i s m , sacrococcygeal teratoma, diaphragmatic hernia and a host of o the r congeni ta l abnormal i t i e s . There are no deleterious effects of MR imaging at 1.5 Tesla, in the second and third trimester and it has been found to be a completely safe procedure, ss~
1108 Indian Journal of Pediatrics, Volume 71--December, 2004
Role of MR Imaging in Paediatric Surgery
REFERENCES
1. Ahn SS et al. Rapid MR imaging of the pediatric brain using the fast spin-echo technique. Am l Neuroradiol 1992; 13 : 1169.
2. Crooks LE et al. Echo-planar pediatric imager. Radiology 1988; 166 : 157.
3. Dietrich RB et al. MRI of extracranial masses in children: the usefulness of gadolinium-chelate enhancement. Pediatr Radiol 1998; 28 : 322.
4. Bisset GS et al. Evaluation of potential practical oral contrast agents for pediatric magnetic resonance imaging: preliminary observations. Pediatr Radiol 1989; 20 : 61
5. Bisset GS et al. Perflubron as a gastrointestinal MR imaging contrast agent in the pediatric population. Pediatr Radiol 1996; 26 : 409.
6. Barckovich AJ. Pediatric Neuroimaging. Third Edition. Lippincott. Year 2000.
7. Farwell JR, Dohrmann GJ, Flannery JT: Central nervous system tumors in children. Cancer 1977; 40 : 3123.
8. Harwood-Nash DC. Primary neoplasms of the central nervous system in children. Cancer 1991; 67 : 1223.
9. Vezina LG, Packer RJ. Infratentorial brain tumors of childhood, Neuroimaging Clin North Am 1994; 4 : 423.
10. Z immerman RA. Pediatric supratentorial tumors, Semin Roentgenol 1990; 25 : 225.
11. Fulham MJ, Bizzi AJ, Dietz MJ et al. Mapping of brain tumor metabolites with proton MR spectroscopic imaging: clinical relevance. Radiology 1992; 185 : 675.
12. Gill SS, Thomas DG, Van Bruggen N e t al. Proton MR spectroscopy of intracranial tumors: in vivo and in vitro studies. J Comput Assist Tomogr 1990; 14 : 497.
13. Z immerman RA, Bilaniuk LT. Applicat ions of magnetic resonance imaging in diseases of the pediatric central nervous system. Magn Reson Imaging 1986; 4 : 11.
14. Barkovich AJ, Chuang SH, Norman D. MR of neuronal migration anomalies. Am J Neuroradio11987; 8 : 1009.
15. Barkovich AJ, Chuang SH. Unilateral megalencephaly: correlation of MR imaging and pathologic characteristics. Am J Neuroradio11990; 11:523.
16. Al tman NR, Naidich TP, Braffman BH. Posterior fossa malformations. Am J Neuroradiol 1992; 13 : 691.
17. Bradley WG, Kortman KE, Burgone B. Flowing cerebrospinal fluid in normal and hydrocephalic states: appearance on MR images. Radiology 1986; 159 : 611.
18. Sherman JL, Citrin CM. Magnetic resonance demonstration of normal CSF flow. Am J Neuroradiol 1986; 7: 3.
19. Grant PE, Matsuda KM. Application of new MR techniques in pediatric patients. Magn Resort Imaging Clin N Am 2003; 11(3) : 493-522.
20. Kao SCA, Ehrhardt JC, Sato Yet al. Paediatric extracranial applications of MR Angiography. Clinical Imaging 2000; 23 : 271-283.
21. Valsangiacomo ER, Levasseur S, McCrindle BW et al. Contrast- Enhanced MR angiography of pu lmonary venous abnormalities in children. Pediatr Radio12003; 33 : 92-98.
22. Magnetic Resonance of the brain and spine. Editor Atlas SW. 3 rd Edition 2003, Lippincott Williams and Wilkins.
23. Bydder GM, Rutherford MA. Diffusion weighted imaging of the brain in neonates and infants. Magn Reson Clin N Am 2002; 10(2) : 83-98.
24. Phillips MD, Zimmerman RA. Diffusion imaging in paediatric hypoxic-ischaemic injury. Neuroimaging Clin NA m 1999; 9:41- 52.
25. Wang J, Licht DJ, Jahng GH et al. Paediatric perfusion imaging using pulse arterial spin labeling. J Magn Reson Imaging 2003; 18 : 404-413.
26. Oguz KK, Golay X, Pizzini FB et al. Sickle cell disease:
continous arterial spin labeling perfusion MR imaging in children. Radiology 2003; 227 : 567-574.
27. Bittar RG, Oliver A, Sadikot AF et al. Cortical motor and somato-sensory representation: effect of cerebral lesion. Jour Neurosurg 2000; 92 : 242-248.
28. Yetkin FZ, Mueller WM, Morris GL et al. Functional MR activation correlated with intra-operative cortical mapping. Am ]Neurorad 1997; 18 : 1311-1315.
29. Seghier ML, Lazeyras F, Zimine S, Maier SE, Hanquinet S, Delavelle J, Volpe JJ, Huppi PS. Combination of event-related f-MR[ and diffusion tensor imaging in an infant with perinatal stroke. Neuroimage 2004; 21(1) : 463-472.
30. Hunte r JV, Wang ZJ. MR spectroscopy in pediatr ic neuroradiology. Magn Reson Clin N Am 2002; 10(2) : 165-190.
31. David D. Stark, William G. Bradley, Jr. Text book of Magnetic Resonance Imaging. Third Edition, Mosby. Year 1998.
32. Harms SE, and Greenway G. Musculoskeletal system. In Stark DD, Bradley WG, eds. Magnetic Resonance Imaging, ed 1, St Louis, 1988, Mosby.
33. Kangarloo H, Dietrich RB, Taira RT et al. MR imaging of bone marrow in children, J Comput Assist Tomogr 1986; 10 : 205.
34. Toby EB, Koman LA, Bechtold RE. MRI of pediatric hip disease, J Pediatr Orthop 1985; 5 : 655.
35. Kuhn JP, Slovis JT, Haller JO. Musculokeletal System in Caffey's Pediatric Diagnostic Imaging; 10 ~ edn; Mosby; USA; 2004 : 1989-2525.
36. Swischuk LE. Musculoskeletal System in Imaging of the newborn, infant and young child.5 ~ edn. Lippincott, Williams and Wilkins, Philadelphia. 2004 : 725-977.
37. Meyer JS, and Fellows KE. Vascular imaging in children. Semin Pediatr Surg 3:79, 1994.
38. Stark DD et al. MRI of the Budd-Chiari syndrome. Am J Roentgeno11986; 146 : 1141.
39. Alexander MC, Haaga JR. MR imaging of a choledochal cyst. J Comput Assist Tomogr 1985; 92 : 357.
40. Siegel MJ. Paediatric liver magnetic resonance imaging. Magn Reson Clin N Am 2002; 10(2) : 253-274.
41. Dietrich RB. Geni tour inary system. In Cohen MD, and Edwards MK, eds. Magnetic Resonance Imaging of Children, Philadelphia, 1989, BC Decker.
42. Dietrich RB, Kangarloo H. Kidneys in infants and children: evaluation with MR. Radiology 1986; 159 : 215.
43. Meyer JS, Har ty MP, Khademian Z. Imaging of Neuroblastoma and Wilms's tumor. Magn Reson Clin N Am 2002; 10(2) : 275-302.
44. Schultz CL et al. Magnetic resonance imaging of the adrenal glands: a comparison with computed tomography. Am J Roentgenol 1984; 143 : 1235.
45. Jaramillo D, Lebowitz RL, Hendren WH. The cloacal malformat ion: radiologic f indings and imaging recommendations. Radiology 1990; 177 : 441.
46. Siegel MJ, Hoffer FA. Magnet ic resonance imaging of nongynaecological pelvic masses in children. Magn Reson Clin N Am 2002; 10(2) : 325-344.
47. Gambino J. Congenital disorders of sexual differentiation: MR findings. Am ]Roentgenol 1992; 158:383.
48. Hricak H, Chang YCF. The female pelvis. In Higgins CB and Hricak H eds. Magnetic Resonance Imaging of the Body. New York,1987, Raven.
49. Ogashi K et al. Vaginal agenesis: classification by MR imaging. Radiology 1987; 162 : 675.
50. Troughton AH et al. The role of magnetic resonance imaging in the investigation of undescended testes. Clin Radio141:178, 1990.
51. McHugh K, Dudley NE, Tarr P. Pre-operative MRI of anorectal anomalies in the newborn period. Pediatr Radiol 1995; 25:33.
52. Mezzacappo PM, Price AP, Haller JD et al. MR and CT
Indian Journal of Pediatrics, Volume 71--December, 2004 1109
Raju Sharma and Shivanand Gamanagatti
demons t ra t ion of levator sling in congeni ta l anorectal anomalies. J Comput Assist Tomogr 1987; 11:273.
53. Bernadette LK. Imaging of extracranial masses of the pediatric head and neck. Neuro Imaging Clin N Am 2000; 10 : 193-214.
54. Gutierrez FR, Siegel MJ, Fallah JH, Poustchi-Amin M. MRI of cyanotic and noncyanotic congenital heart disease. Magn Reson
Clin N Am 2002; 10(2): 209-235. 55. Hubbard AM, Simon EN. Foetal Imaging MRI. CI North Am
2002; 10(2) : 389-408. 56. Simon E, Goldstein R, Coakley F, Filly R et al. Fast MR imaging
of foetal CNS anomalies in utero. Am J Neuroradiol 2000; 21 : 1688-1698.
The Indian Journal of Pediatrics AWARDS FOR BEST ORIGINAL RESEARCH THESIS
IN PEDIATRICS IN I N D I A - 2004
The Indian Journal of Pediatrics announces t h r e e awards for the year 2004 for original research work. The awards will be for the best M.D. thesis submitted to their Institute/University.
The selected awardees will be presented with a ci tat ion, Rs 10,000, Rs 5,000 a n d Rs 3,000 for first, second and third positions respectively for their outstanding contribution.
Send the objective, materials, methods, summary and conclusion of the thesis for award consideration along with the certificate by the Head of the Department certifying that the work is of the candidate and that the thesis has been accepted by the Institute/University.
Last d a t e o f s u b m i s s i o n o f t h e s i s : J a n u a r y 31, 2005
(Note : Matter must not exceed more than 12 pages typed in double spacing.)
For further information please write to :
Editor-in-Chief The Indian Journal of Pediatrics 125 (2nd Floor), Gautam Nagar
New Delhi-110 049. Post Box No. 3875, New Delhi-110049
Ph : 26857587, 26568098, Telefax :91-11-26857587 E-mail : [email protected], [email protected]
Website : www.ijppediatricsindia.org
1110 Indian Journal of Pediatrics, Volume 71--December, 2004