
Biomechanical Performance Factors in the Track and Field ...

rr
Biomechanical Evaluation of Margin Convergence
Augustus D. Mazzocca, M.S., M.D., Matthew Bollier, M.D., Drew Fehsenfeld, M.D.,Anthony Romeo, M.D., Kelly Stephens, B.S., Olga Solovyoya, B.S., Elifho Obopilwe, M.S.,
Angelo Ciminiello, M.D., Michael D. Nowak, D.Sc., and Robert Arciero, M.D.
Purpose: The aim of this study was to examine rotator cuff strain and gap size after marginconvergence was performed for a large retracted rotator cuff tear. Methods: We tested 20 cadavericshoulders using a custom shoulder testing system. A large retracted rotator cuff tear was created byremoving the supraspinatus muscle-tendon unit to provide a reproducible model. Margin conver-gence was performed and strain was measured by use of differential variable reluctance transducersin the intact state, after a massive rotator cuff tear was created, and after each of 5 marginconvergence sutures were placed. Data were obtained at 0° and 60° of abduction and with internaland external rotational torques applied to the humerus. Gap size was measured before and aftermargin convergence sutures were placed. Results: Strain was significantly reduced at all degrees ofrotation in 0° of abduction after margin convergence sutures were placed (P � .05). There was asignificantly significant decrease in gap size with each suture: 50% with the first suture, 60% with thesecond suture, 67% with the third suture, and 75% with the fourth suture (P � .05). There was onlyminimal intrinsic rotator cuff tension during knot tying, with each subsequent suture having less ofan effect than the previous. Four margin convergence sutures resulted in a mean of 5 mm of anteriorhumeral head translation. Conclusions: There was a significant decrease in rotator cuff strain and gapsize after margin convergence was performed for a large retracted tear. The first margin convergencesuture caused the greatest increase in intrinsic rotator cuff tension, with each subsequent suturehaving a similar but less dramatic effect. Clinical Relevance: Biomechanical rationale exists for theuse of margin convergence in large retracted rotator cuff tears.
f
trhttttc
The treatment of large and massive rotator cufftears has been challenging. Significant tendon
etraction, muscle atrophy, and scarring prevent easyeduction of the free tendon edge to the rotator cuff
From the Department of Orthopaedic Surgery, University of Con-necticut (A.D.M., K.S., O.S., E.O., M.D.N., R.A.), Hartford, Connect-icut; Department of Orthopaedic Surgery, University of Iowa Hospi-tals and Clinics (M.B.), Iowa City, Iowa; Advanced Orthopaedics andSports Medicine (D.F.), Houston, Texas; Department of Orthopae-dics, Rush University (A.R.), Chicago, Illinois; and Danbury Ortho-paedic Associates (A.C.), Danbury, Connecticut, U.S.A.
A.D.M. and R.A. received support exceeding $500) related tothis research from Arthrex, Naples, Florida.
Received February 22, 2010; accepted September 1, 2010.Address correspondence and reprint requests to Matthew Bol-
lier, M.D., Department of Orthopaedic Surgery, University of IowaHospitals and Clinics, 200 Hawkins Dr, 01008 JPP, Iowa City, IA52242, U.S.A. E-mail: [email protected]
© 2011 by the Arthroscopy Association of North America
b0749-8063/10121/$36.00doi:10.1016/j.arthro.2010.09.003
330 Arthroscopy: The Journal of Arthroscopic and Related S
ootprint.1-4 Arthroscopic advances have allowed im-proved visualization, recognition, and mobilization ofthese tears.5-13 Crescent-shaped tears have a largeranterior-to-posterior width than medial-to-laterallength. They usually have adequate excursion whenpulled laterally and can often be repaired by securingtendon to bone under low tension.5,6,9,14 However,longitudinal-type tears (U shaped and L shaped) ex-hibit a long and narrow pattern with increased medial-to-lateral length.5,14 Traditional techniques involveranslation of the retracted cuff from medial to lateral,esulting in significant strain at the site of repair andigh rates of failure.4,15-19 Burkhart et al.20 coined theerm “margin convergence” to describe an initial side-o-side repair of a large or massive longitudinal-typeear. Instead of pulling a large U-shaped rotator cuffear back to the footprint, the surgeon first repairs theuff side to side, starting at the apex medially. It has
een proposed that margin convergence decreases theurgery, Vol 27, No 3 (March), 2011: pp 330-338

tthsepsphight
aicsmtmwaifpammes�
331MARGIN CONVERGENCE
tear gap, provides easier control of the free edge of thetear, and reduces tension at the tendon-bone junc-tion.8,20-22
Burkhart et al.8 reported that U-shaped tears directlyrepaired to bone after margin convergence had similarclinical outcomes to crescent-shaped tears with ten-don-to-bone fixation. Wolf et al.10 showed 98% goodo excellent results with side-to-side repair of largeears. Although the technique of margin convergenceas been discussed from a theoretic and clinical per-pective, no studies have evaluated the biomechanicalffect of margin convergence on the rotator cuff. Theurpose of this study was to examine rotator cufftrain and gap size after margin convergence waserformed in a large retracted rotator cuff tear. Ourypothesis is that margin convergence will reducenfraspinatus and subscapularis strain and decreaseap size in a large retracted rotator cuff tear whileaving only minimal effect on glenohumeral transla-ion and intrinsic tendon strain during knot tying.
METHODS
Twenty fresh-frozen cadaveric shoulders (meange, 66.1 � 9.3 years) were used. Exclusion criteriancluded glenohumeral arthritic changes, prior rotatoruff tear, and prior shoulder surgery. No cadaverichoulder was excluded. The deltoid muscle was re-oved from the acromion, providing complete access
o the coracoacromial arch, rotator cuff, and glenohu-eral joint. The supraspinatus tendon and muscleere sharply elevated from the supraspinatus fossa,
nd the glenohumeral joint capsule was left intact. Thendividual muscles of the rotator cuff were dissectedree from the joint capsule. The circumference andennation angle (angle between the muscle fibersnd most centrally located tendon of insertion) wereeasured for each rotator cuff muscle. The maxi-um torque was calculated by use of the following
quation: Maximum torque (Tmax) � (Muscle cross-ection area cos pennation angle � Specific tension)
Moment arm.23 This allowed us to calculate theactual moment of each rotator cuff muscle so that theshoulder would be balanced and have physiologicloads during testing.
The medial aspects of the supraspinatus, subscapu-laris, and infraspinatus muscle bellies were individu-ally secured with nylon strapping for individual load-ing. The scapula was potted with plaster of Paris in acustom aluminum box with the glenoid fixed perpen-dicularly to the top of the scapular potting box. The
humerus was cut 20 cm from the joint, centered in a Dpolyvinyl chloride pipe, and potted with plaster ofParis. On the basis of previous models, the pottedcadaveric specimen was then mounted on a customshoulder testing apparatus.24,25 To center the humeralhead in the glenoid, a compressive load of 22 N wasapplied to the glenohumeral joint by applying a hang-ing weight at the end of each lever arm underneath thescapular box (11 N for the supraspinatus, 5.5 N forthe subscapularis, and 5.5 N for the infraspinatus).26
The humerus was centered in a cylinder attached tothe jig that allowed multiple positions of rotation andabduction (Fig 1). A goniometer was used to ensureneutral humeral rotation and 0° of abduction.
Two differential variable reluctance transducers(DVRTs) (Microstrain, Burlington, VT) were placed 5mm from the leading edges of the subscapularis andthe infraspinatus (Fig 1). Two additional transducerswere placed 15 mm from the tubercular groove of thesubscapularis and 15 mm from the medial aspect ofthe infraspinatus footprint. A No. 15 blade scalpel wasused to remove the supraspinatus muscle and tendon.The entire supraspinatus was excised to create a largeretracted rotator cuff tear (Fig 2). Our pilot testsshowed that by removing the entire supraspinatusmuscle-tendon unit, we could obtain a consistentlyreproducible model to reliably measure strain.
The supraspinatus footprint area was then quantifiedby use of a MicroScribe digitizer (Immersion, SanJose, CA). Margin convergence was then performedby placing simple sutures 5 mm apart beginning at theglenoid rim medially and proceeding laterally (Fig 3).No. 2 FiberWire suture (Arthrex, Naples, FL) was
FIGURE 1. Biomechanical setup showing position of shoulder jig,
VRT position, and forces on each rotator cuff muscle.
m
msMvcttd
S
tsp
i
332 A. D. MAZZOCCA ET AL.
used. Sutures were placed at the edge of the subscap-ularis and infraspinatus tendon and tied by use of asliding-locking arthroscopic knot backed up with 3alternating half-hitch sutures. Margin convergencewas performed in an open fashion, not arthroscopi-cally. There were no failures during suture passage,knot tying, or testing. After each convergence suturewas placed, the gap area was quantified by use of theMicroScribe digitizer.
Infraspinatus and subscapularis strain was measuredfor each specimen in the intact state, after supraspi-natus removal, and after each convergence suture wasplaced. In addition, strain was calculated after every10° of rotation at 0° and 60° of abduction with aninternal and external rotation torque of 3.5 Nm appliedto the humerus. This torque was based on a pilot studyconducted to determine the average applied torquenecessary to achieve the end point of the range ofmotion without damaging the capsular tissue. Therotational range of motion was quantified with the useof a 360° goniometer that was secured to the base ofthe custom shoulder testing jig. The maximum angleat which the DVRTs successfully cleared the acro-mion was 60°. Displacement data recorded for straincalculations were recorded according to the formula�L/L, where �L represents the displacement of the
uscle upon internal and external rotation and L is theoriginal length before displacement. The distance be-tween the 2 anchoring barbs of the DVRT was mea-sured for each specimen and used as the originallength.
Testing was conducted to calculate glenohumeraljoint translation and to measure tension in the rotatorcuff itself during knot tying and gap closure. Two
FIGURE 2. Massive U-shaped rotator cuff tear created by remov-ng supraspinatus muscle.
methods of displacement tracking were used to mon-
itor the movement of the humerus with respect to theglenoid during margin convergence knot tying. First,a predetermined point of the baseplate of the cus-tom shoulder testing jig was measured with theMicroScribe digitizer in the neutral position to estab-lish an initial reference position. The suture was thentied, and movement of the baseplate was measured.27
Our alternate method of tracking glenohumeral trans-lation used 2 surface markers, 1 placed on the glenoidand 1 placed directly opposite, on the humerus.28 The
arkers were tracked by video camera during alluture ties. This video was then analyzed by use ofaxTraq software (Innovisions Systems, Columbia-
ille, MI). In addition, the DVRTs were used to cal-ulate strain in the infraspinatus and subscapularisendons because each margin convergence suture wasied to examine what was occurring in the rotator cuffuring knot tying and gap closure.
tatistical Analysis
Power analysis to determine sample size showedhat 20 shoulders were needed to detect a clinicallyignificant strain of 1.5%29 (SD, 0.3%) with 80%ower and � equal to 0.05.The effect of margin convergence sutures at differ-
ent degrees of rotation and abduction was evaluatedwith random-intercept, mixed-effects regression mod-els by use of SAS software, version 9.2 (SAS, Cary,NC). This method properly accounted for the repeatedmeasures and allowed the most efficient use of thedata. Separate models were fitted for strain in theinfraspinatus and subscapularis. Rotation was treatedas a series of categorical variables because its relation
FIGURE 3. Margin convergence sutures placed 5 mm apart start-ing medially at glenoid and moving laterally. Suture is placed
through the leading edge of the subscapularis and infraspinatustendons.
swtw
f
8matcsssrhlat
rcwiafgvwgsbft
rMsg
333MARGIN CONVERGENCE
to strain was found to be nonlinear. The models werestratified by abduction angle and included interactionterms for rotation � state. Model performance wasassessed by use of the likelihood ratio test and byplotting the observed versus predicted values to checkfor lack of fit. Predicted values were identical with andwithout the main effects terms, so only the interactionterms were included in the final models for ease ofinterpretation.
RESULTS
Margin convergence caused a progressive closureof the rotator tear, from a large U-shaped tear to asmall crescent-shaped tear (Fig 4). The coverage ofthe humeral head appeared to be caused mainly by ashift of the infraspinatus tendon. The mean tear gapwas 661.55 mm2 (SD, 201.64) before margin conver-gence sutures. After the first suture was placed medi-ally, the gap was 450.02 mm2 (SD, 138.02). After thesecond suture, the gap was 327.76 mm2 (SD, 137.87).The gap was 258.72 mm2 (SD, 110.00) after the thirdsuture and 218.52 mm2 (SD, 84.43) after the fourthuture. There was a statistically significant gap closureith each suture: 50% with the first suture, 60% with
he second suture, 67% with the third suture, and 75%ith the fourth suture (P � .05).With an intact rotator cuff, the humerus rotated
rom a mean of 69° � 8.5° external rotation to 66° �
FIGURE 4. Quantification ofotator cuff tear closure with
icroScribe digitizer and mea-urement of gap size after mar-in convergence suture placement.
.8° internal rotation. After supraspinatus removal andargin convergence suture placement, mean internal
nd external range of motion did not change. In neu-ral abduction, functional testing of the intact rotatoruff showed progressively increasing strain in theubscapularis with external rotation and decreasingtrain with internal rotation (Fig 5A). Conversely, thetrain decreased in the infraspinatus with externalotation and increased with internal rotation. As theumerus was abducted to 60°, the overall strain wasower at all degrees of rotation compared with 0° ofbduction, but internal and external rotation strainrends remained the same (Fig 5B).
After removal of the supraspinatus to create a largeetracted rotator cuff tear, there was minimally in-reased strain in the infraspinatus or subscapularishen compared with the intact state. When comparing
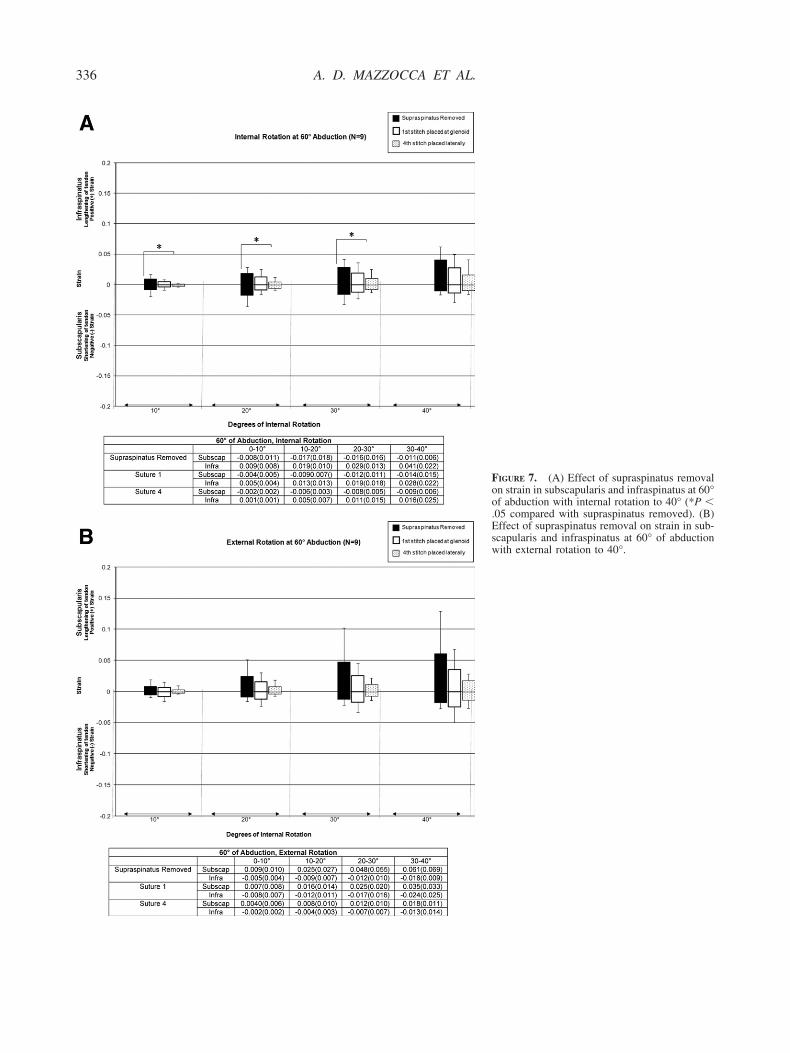
nfraspinatus strain and subscapularis strain beforend after margin convergence was performed, weound that strain was significantly reduced at all de-rees of rotation in 0° of abduction after margin con-ergence sutures were placed (P � .05) (Fig 6). Thereas up to a 58% strain reduction after margin conver-ence. As abduction was increased to 60°, the ab-olute strain values for all positions were reducedut not statistically significant except in the in-raspinatus after the fourth margin convergence su-ure (P � .05) (Fig 7).

334 A. D. MAZZOCCA ET AL.
There was minimal tension and stress in the rotatorcuff during knot tying. Infraspinatus and subscapularisstrain increased slightly as the tendons were pulledtogether during knot tying. After the first margin con-vergence suture was tied medially, strain was 1.06 �
1.6 in the subscapularis and 1.5 � 2.0 in the infraspi- snatus. This was the greatest increase in strain. Eachsubsequent suture produced a similar but less dramaticincrease in strain. The subscapularis showed a meanstrain of 0.25 � 0.3 for the second suture, 0.29 � 0.5for the third suture, and 0.19 � 0.3 for the fourth
FIGURE 5. (A) Effect of inter-nal and external rotation onsubscapularis and infraspinatusstrain at 0° of abduction withintact rotator cuff. (B) Effectsof internal and external rotationon strain in subscapularis andinfraspinatus muscle at 60° ofabduction with intact rotatorcuff.
uture. The infraspinatus showed strain changes al-

335MARGIN CONVERGENCE
FIGURE 6. (A) Effect of supraspinatus removalon strain in subscapularis and infraspinatus at 0°of abduction with internal rotation to 40° (*P �.05 compared with supraspinatus removed). (B)Effect of supraspinatus removal on strain in sub-scapularis and infraspinatus at 0° abduction withexternal rotation to 40° (*P � .05 compared withsupraspinatus removed; **P � .01 comparedwith supraspinatus removed).
336 A. D. MAZZOCCA ET AL.
FIGURE 7. (A) Effect of supraspinatus removalon strain in subscapularis and infraspinatus at 60°of abduction with internal rotation to 40° (*P �.05 compared with supraspinatus removed). (B)Effect of supraspinatus removal on strain in sub-scapularis and infraspinatus at 60° of abductionwith external rotation to 40°.

tcbfmidraesgsbp
gSsvap
otcsdtstlhitiaswc
gsiimorts
337MARGIN CONVERGENCE
most double that of the subscapularis: 0.41 � 0.6 forthe second suture, 0.45 � 0.7 for the third suture, and0.13 � 0.1 for the fourth suture. Although there wasan increase in tendon strain during knot tying, the newbaseline strain remained constant throughout func-tional testing.
Mean humeral head anterior translation with 4 mar-gin convergence sutures was 4.97 mm. Margin con-vergence caused 1.68 � 1.7 mm of anterior humeralhead translation as suture 1 was tied. Suture 2 pro-duced 0.93 � 0.7 mm of anterior translation, suture 3resulted in 0.66 � 0.6 mm, and suture 4 resulted in1.70 � 1.5 mm.
DISCUSSION
Although margin convergence has been proposed toreduce the gap size of a large retracted rotator cufftear, there have been no biomechanical studies exam-ining its role in rotator cuff repair. Our purpose was toexamine the strain behavior of the subscapularis andinfraspinatus after margin convergence sutures wereplaced. We hypothesized that margin convergencewould decrease the size of the tear gap and reducestrain with minimal effect on glenohumeral translationand intrinsic tendon strain during knot tying. Ourresults support our hypothesis.
Recent biomechanical studies have shown that en-largement of rotator cuff tears is caused by increasedstrain at the torn edge.30 Repairing a large U-shapedear by securing the tendon to bone with suture an-hors alone will result in high tension at the tendon-one interface with higher rates of failure.31,32 If theree tendon edge is repaired to the bony footprint afterargin convergence, it has been suggested that there
s less tension at the tendon-bone interface.8,20,21 Ourata suggest that margin convergence causes markededuction in overall strain (up to 58%). We also found
statistically significant decrease in gap size withach margin convergence suture. This causes a lateralhift of the free margin of the tendon edge toward thereater tuberosity and also reduces tendon-bone ten-ion. Even if the tendon is not directly repaired toone, a side-to-side repair with strain reduction canrotect against tear propagation.20,21 It has been sug-
gested that decreased strain after side-to-side repaircan improve function indirectly by allowing less cuffdeformation and decreased mechanical activation ofpain receptors in the rotator cuff.20
Arthroscopic observations of large rotator cuff tearsshow a large defect that is bordered medially by the
glenoid, anteriorly by the subscapularis, and posteri- dorly by the infraspinatus. As we designed our biome-chanical model, we wanted to re-create a large tearthat mimics what is seen at the time of arthroscopy. Itwas important to create a tear in a reproducible way sothat there would be no variability between specimens.Our pilot tests showed that by removing the entiresupraspinatus muscle-tendon unit, we could obtain aconsistently reproducible biomechanical model thatappeared similar to a large retracted tear during ar-throscopy. Removing the supraspinatus caused a de-crease in the strain of the infraspinatus with littleeffect on the subscapularis. Anatomic studies haveshown that the infraspinatus and supraspinatus areintrinsically related at their insertion on the hu-merus.33,34 Reduced strain in the infraspinatus sug-ests that it shares the load of the supraspinatus.upraspinatus removal had a limited effect on theubscapularis. This may indicate that the rotator inter-al tissue serves as a buffer between the subscapularisnd supraspinatus, allowing these tendons to act inde-endently of one another.Translation of the subscapularis and infraspinatus
ver the humeral head restores the force couple abouthe glenohumeral joint. We chose to place the marginonvergence sutures in the leading edge of the sub-capularis and infraspinatus tendons to create a repro-ucible technique. Our study showed that the size ofhe tear was reduced with each margin convergenceuture shifting the subscapularis and infraspinatus intohe gap. The infraspinatus was more mobile and trans-ated more than the subscapularis to cover the humeralead. With shoulder external rotation, strain increasedn the subscapularis as it was placed under increasingension and strain decreased in the infraspinatus. Withnternal rotation, strain increased in the infraspinatuss it stretched whereas strain decreased in the sub-capularis. Intrinsic rotator cuff tension associatedith closure of the gap was minimal, and each suc-
essive suture had even less effect than the previous.There were several limitations to this study. Despite
ood reproducibility within an individual specimen, aignificant amount of variability existed between spec-mens, which could not be standardized. This resultedn large standard deviations that may have underesti-ated or overestimated the effects on strain. Second,
ur massive U-shaped rotator cuff tear was created byemoving the entire supraspinatus muscle. Althoughhis is not what is typically observed clinically, itimulated the worst-case scenario and created a repro-
ucible model for testing.
gra
338 A. D. MAZZOCCA ET AL.
CONCLUSIONS
There was a significant decrease in rotator cuff strainand gap size after margin convergence was performedfor a large retracted tear. When comparing strain beforeand after margin convergence was performed, we foundthat strain was significantly reduced at all degrees ofrotation in 0° of abduction after margin convergencesutures were placed (P � .05). The first margin conver-ence suture caused the greatest increase in intrinsicotator cuff tension, with each subsequent suture havingsimilar but less dramatic effect.
REFERENCES
1. Kasten P, Loew M, Rickert M. Repair of large supraspinatusrotator-cuff defects by infraspinatus and subscapularis tendontransfers in a cadaver model. Int Orthop 2007;31:11-15.
2. Zumstein MA, Jost B, Hempel J, Hodler J, Gerber C. Theclinical and structural long-term results of open repair ofmassive tears of the rotator cuff. J Bone Joint Surg Am 2008;90:2423-2431.
3. Hanusch BC, Goodchild L, Finn P, Rangan A. Large andmassive tears of the rotator cuff: Functional outcome andintegrity of the repair after a mini-open procedure. J BoneJoint Surg Br 2009;91:201-205.
4. Yoo JC, Ahn JH, Koh KH, Lim KS. Rotator cuff integrity afterarthroscopic repair for large tears with less-than-optimal foot-print coverage. Arthroscopy 2009;25:1093-1100.
5. Burkhart SS. A stepwise approach to arthroscopic rotator cuffrepair based on biomechanical principles. Arthroscopy 2000;16:82-90.
6. Lo IK, Burkhart SS. The interval slide in continuity: A methodof mobilizing the anterosuperior rotator cuff without disrupt-ing the tear margins. Arthroscopy 2004;20:435-441.
7. Lo IK, Burkhart SS. Double-row arthroscopic rotator cuffrepair: Re-establishing the footprint of the rotator cuff. Ar-throscopy 2003;19:1035-1042.
8. Burkhart SS, Danaceau SM, Pearce CE Jr. Arthroscopic rota-tor cuff repair: Analysis of results by tear size and by repairtechnique-margin convergence versus direct tendon-to-bonerepair. Arthroscopy 2001;17:905-912.
9. Lo IK, Burkhart SS. Arthroscopic repair of massive, con-tracted, immobile rotator cuff tears using single and doubleinterval slides: Technique and preliminary results. Arthroscopy2004;20:22-33.
10. Wolf EM, Pennington W, Agrawal V. Arthroscopic side-to-side rotator cuff repair. Arthroscopy 2005;21:881-887.
11. Ahmad CS, Stewart AM, Izquierdo R, Bigliani LU. Tendon-bone interface motion in transosseous suture and suture anchorrotator cuff repair techniques. Am J Sports Med 2005;33:1667-1671.
12. Dines JS, Bedi A, Elattrache NS, Dines DM. Single-rowversus double-row rotator cuff repair: Techniques and out-comes. J Am Acad Orthop Surg 2010;18:83-93.
13. Waltrip RL, Zheng N, Dugas JR, Andrews JR. Rotator cuffrepair. A biomechanical comparison of three techniques. Am JSports Med 2003;31:493-497.
14. Davidson JF, Burkhart SS, Richards DP, Campbell SE. Use ofpreoperative magnetic resonance imaging to predict rotatorcuff tear pattern and method of repair. Arthroscopy 2005;21:1428.
15. Domb BG, Glousman RE, Brooks A, Hansen M, Lee TQ,ElAttrache NS. High-tension double-row footprint repair
compared with reduced-tension single-row repair formassive rotator cuff tears. J Bone Joint Surg Am 2008;90:35-39 (Suppl 4).
16. Hansen ML, Otis JC, Johnson JS, Cordasco FA, Craig EV,Warren RF. Biomechanics of massive rotator cuff tears: Im-plications for treatment. J Bone Joint Surg Am 2008;90:316-325.
17. Worland RL, Arredondo J, Angles F, Lopez-Jimenez F. Repairof massive rotator cuff tears in patients older than 70 years. JShoulder Elbow Surg 1999;8:26-30.
18. Gazielly DF, Gleyze P, Montagnon C. Functional and anatom-ical results after rotator cuff repair. Clin Orthop Relat Res1994:43-53.
19. Galatz LM, Ball CM, Teefey SA, Middleton WD, YamaguchiK. The outcome and repair integrity of completely arthroscopi-cally repaired large and massive rotator cuff tears. J Bone JointSurg Am 2004;86:219-224.
20. Burkhart SS, Athanasiou KA, Wirth MA. Margin conver-gence: A method of reducing strain in massive rotator cufftears. Arthroscopy 1996;12:335-338.
21. Burkhart SS. The principle of margin convergence in rotatorcuff repair as a means of strain reduction at the tear margin.Ann Biomed Eng 2004;32:166-170.
22. Burkhart SS. Arthroscopic treatment of massive rotator cufftears. Clin Orthop Relat Res 2001:107-118.
23. Juul-Kristensen B, Bojsen-Moller F, Finsen L, et al. Musclesizes and moment arms of rotator cuff muscles determined bymagnetic resonance imaging. Cells Tissues Organs 2000;167:214-222.
24. Remia LF, Ravalin RV, Lemly KS, McGarry MH, Kvitne RS,Lee TQ. Biomechanical evaluation of multidirectional gleno-humeral instability and repair. Clin Orthop Relat Res 2003:225-236.
25. Schneider DJ, Tibone JE, McGarry MH, Grossman MG,Veneziani S, Lee TQ. Biomechanical evaluation after five andten millimeter anterior glenohumeral capsulorrhaphy using anovel shoulder model of increased laxity. J Shoulder ElbowSurg 2005;14:318-323.
26. Halder AM, O’Driscoll SW, Heers G, et al. Biomechanicalcomparison of effects of supraspinatus tendon detachments,tendon defects, and muscle retractions. J Bone Joint Surg Am2002;84:780-785.
27. Shafer BL, Mihata T, McGarry MH, Tibone JE, Lee TQ.Effects of capsular plication and rotator interval closure insimulated multidirectional shoulder instability. J Bone JointSurg Am 2008;90:136-144.
28. Ludewig PM, Cook TM. Translations of the humerus in per-sons with shoulder impingement symptoms. J Orthop SportsPhys Ther 2002;32:248-259.
29. Mazzocca AD, Rincon LM, O’Connor RW, et al. Intra-artic-ular partial-thickness rotator cuff tears. Am J Sports Med2008;36:110-116.
30. Andarawis-Puri N, Ricchetti ET, Soslowsky LJ. Rotator cufftendon strain correlates with tear propagation. J Biomech2009;42:158-163.
31. Burkhart SS, Johnson TC, Wirth MA, Athanasiou KA. Cyclicloading of transosseous rotator cuff repairs: Tension overloadas a possible cause of failure. Arthroscopy 1997;13:172-176.
32. Burkhart SS, Diaz Pagan JL, Wirth MA, Athanasiou KA.Cyclic loading of anchor-based rotator cuff repairs: Confirma-tion of the tension overload phenomenon and comparison ofsuture anchor fixation with transosseous fixation. Arthroscopy1997;13:720-724.
33. Clark JM, Harryman DT II. Tendons, ligaments, and capsuleof the rotator cuff. Gross and microscopic anatomy. J BoneJoint Surg Am 1992;74:713-725.
34. Sonnabend DH, Young AA. Comparative anatomy of the
rotator cuff. J Bone Joint Surg Br 2009;91:1632-1637.Copyright © 2022 FDOKUMEN




















