Atmospheric pressure plasma in dermatology: Ulcus treatment and much more
6
Invited paper Atmospheric pressure plasma in dermatology: Ulcus treatment and much more Steffen Emmert a,n , Franziska Brehmer a , Holger H¨ anßle a , Andreas Helmke b , Nina Mertens b , Raees Ahmed c , Dirk Simon c , Dirk Wandke d , Wolfgang Maus-Friedrichs e , Georg D¨ aschlein f , Michael P. Sch ¨ on a , Wolfgang Vi ¨ ol b,g a Department of Dermatology, Venerology and Allergology, University Medical Center G¨ ottingen, Georg-August-University G¨ ottingen, Robert-Koch-Str. 40, 37075 G¨ ottingen, Germany b Department of Sciences and Technology, HAWK University of Applied Sciences and Arts, Von-Ossietzky-Str. 99, 37085 G¨ ottingen, Germany c Institute for Applied Research and Clinical Studies (IFS GmbH), Von-Bar-Strasse 2/4, 37075 G¨ ottingen, Germany d CINOGY GmbH, Max-N¨ ader-Str. 15, 37114 Duderstadt, Germany e Institute for Energy Research and Physical Technologies, Technical University Clausthal, Leibnizstrasse 4, 38678 Clausthal-Zellerfeld, Germany f Department of Dermatology of the Ernst-Moritz-Arndt-University Greifswald, Sauerbruchstrasse, 17489 Greifswald, Germany g Application Center for Atmospheric Pressure Plasma, Fraunhofer Institute for Surface Engineering and Thin Films IST, Von-Ossietzky-Str. 99, 37085 G¨ ottingen, Germany article info Article history: Received 12 July 2012 Received in revised form 6 November 2012 Accepted 22 November 2012 Available online 2 January 2013 Keywords: Cold atmospheric pressure plasma (CAP) Ultraviolet radiation Reactive gas species Electric current Chronic wounds Superinfected eczema abstract Plasma in the sense of ionized gas can be referred to as the fourth state of matter following solids, liquids, and gases in view of their energy content. Application of high voltages across small gas filled spaces results in ionization of the air. Generally, two types of cold plasma can be discerned: direct plasma (e.g. dielectric barrier discharge—DBD) and indirect plasma (plasma torch, plasma jet). In indirect plasma treatment, the plasma is produced in a remote cavity and ejected by gas flow onto the skin in the form of an effluent. In direct plasma treatment, the skin itself acts as the counter electrode. Advantageous features of direct plasma treatment include the higher plasma density as well as the induced high frequency electric current onto the skin. In plasma treatment antiinflammatory, antipruritic, antimicrobial, tissue stimulation, stimulation of microcirculation, and other therapeutic effects are achieved in a single treatment due to the combined action of ultraviolet radiation, reactive oxygen species (e.g. ozone), reactive nitrogen species, and electric fields. In line with other reports, we have already demonstrated the use of direct plasma treatment in skin disinfection, in atopic eczema (superinfected dermatitis), in modulating the epidermal barrier, as well as in chronic wound treatment. We as well as others did not notice any side effects of plasma treatment so far. In summary, cold atmospheric pressure plasma constitutes a new and innovative treatment option especially for superinfected skin diseases. These promising relatively new clinical applications warrant further carefully conducted translational research to delineate the modes of actions of plasma as well as potential long term side effects. This should lead to norms for the technical devices to allow a standardized treatment of given diseases in the mid-term. & 2012 Elsevier GmbH. All rights reserved. 1. Cold atmospheric pressure plasma Plasma was first described by Sir William Crookes, a British chemist, in 1879 as radiant matter [1]. In 1928 the term plasma was introduced by Irving Langmuir due to the composition of the ionized gas. Since then the term plasma indicates an ionized gas in a wide range of parameters such as density and temperature and must not be confused with blood plasma. As the fourth and highest energy state of matter following solids, liquids, and gases, plasma is the by far dominant state of matter in the universe, e.g. solar corona, solar winds. On Earth plasma can be generated technically by electric gas discharges. Due to the energy gained from strong electric fields, air (or any other gas) can be trans- formed into the plasma state. A complex mixture of inter-reacting and quite short-lived free electrons, ions, atoms, excited species, and photons is generated [2,3]. Low-pressure, high-pressure, and atmospheric pressure plasmas can be discerned. At atmospheric pressure, plasma in the easiest configuration of two metallic electrodes developed in the form of arcs. The drawback of arc plasmas characterized by high current densities and high collision frequencies is a thermal equilibrium resulting in gas temperatures of hundreds or several thousand Contents lists available at SciVerse ScienceDirect journal homepage: www.elsevier.com/locate/cpme Clinical Plasma Medicine 2212-8166/$ - see front matter & 2012 Elsevier GmbH. All rights reserved. http://dx.doi.org/10.1016/j.cpme.2012.11.002 n Corresponding author. Tel.: þ49 551 396 410; fax: þ49 551 398 983. E-mail address: [email protected] (S. Emmert). Clinical Plasma Medicine 1 (2013) 24–29
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Atmospheric pressure plasma in dermatology: Ulcus treatment and much more

Clinical Plasma Medicine 1 (2013) 24–29
Contents lists available at SciVerse ScienceDirect
Clinical Plasma Medicine
2212-81
http://d
n Corr
E-m
journal homepage: www.elsevier.com/locate/cpme
Invited paper
Atmospheric pressure plasma in dermatology: Ulcus treatmentand much more
Steffen Emmert a,n, Franziska Brehmer a, Holger Hanßle a, Andreas Helmke b,Nina Mertens b, Raees Ahmed c, Dirk Simon c, Dirk Wandke d, Wolfgang Maus-Friedrichs e,Georg Daschlein f, Michael P. Schon a, Wolfgang Viol b,g
a Department of Dermatology, Venerology and Allergology, University Medical Center Gottingen, Georg-August-University Gottingen, Robert-Koch-Str. 40,
37075 Gottingen, Germanyb Department of Sciences and Technology, HAWK University of Applied Sciences and Arts, Von-Ossietzky-Str. 99, 37085 Gottingen, Germanyc Institute for Applied Research and Clinical Studies (IFS GmbH), Von-Bar-Strasse 2/4, 37075 Gottingen, Germanyd CINOGY GmbH, Max-Nader-Str. 15, 37114 Duderstadt, Germanye Institute for Energy Research and Physical Technologies, Technical University Clausthal, Leibnizstrasse 4, 38678 Clausthal-Zellerfeld, Germanyf Department of Dermatology of the Ernst-Moritz-Arndt-University Greifswald, Sauerbruchstrasse, 17489 Greifswald, Germanyg Application Center for Atmospheric Pressure Plasma, Fraunhofer Institute for Surface Engineering and Thin Films IST, Von-Ossietzky-Str. 99, 37085
Gottingen, Germany
a r t i c l e i n f o
Article history:
Received 12 July 2012
Received in revised form
6 November 2012
Accepted 22 November 2012Available online 2 January 2013
Keywords:
Cold atmospheric pressure plasma (CAP)
Ultraviolet radiation
Reactive gas species
Electric current
Chronic wounds
Superinfected eczema
66/$ - see front matter & 2012 Elsevier Gmb
x.doi.org/10.1016/j.cpme.2012.11.002
esponding author. Tel.: þ49 551 396 410; fax
ail address: [email protected] (S. Emmert).
a b s t r a c t
Plasma in the sense of ionized gas can be referred to as the fourth state of matter following solids,
liquids, and gases in view of their energy content. Application of high voltages across small gas filled
spaces results in ionization of the air. Generally, two types of cold plasma can be discerned: direct
plasma (e.g. dielectric barrier discharge—DBD) and indirect plasma (plasma torch, plasma jet).
In indirect plasma treatment, the plasma is produced in a remote cavity and ejected by gas flow onto
the skin in the form of an effluent. In direct plasma treatment, the skin itself acts as the counter
electrode. Advantageous features of direct plasma treatment include the higher plasma density as well
as the induced high frequency electric current onto the skin. In plasma treatment antiinflammatory,
antipruritic, antimicrobial, tissue stimulation, stimulation of microcirculation, and other therapeutic
effects are achieved in a single treatment due to the combined action of ultraviolet radiation, reactive
oxygen species (e.g. ozone), reactive nitrogen species, and electric fields. In line with other reports, we
have already demonstrated the use of direct plasma treatment in skin disinfection, in atopic eczema
(superinfected dermatitis), in modulating the epidermal barrier, as well as in chronic wound treatment.
We as well as others did not notice any side effects of plasma treatment so far. In summary, cold
atmospheric pressure plasma constitutes a new and innovative treatment option especially for
superinfected skin diseases. These promising relatively new clinical applications warrant further
carefully conducted translational research to delineate the modes of actions of plasma as well as
potential long term side effects. This should lead to norms for the technical devices to allow a
standardized treatment of given diseases in the mid-term.
& 2012 Elsevier GmbH. All rights reserved.
1. Cold atmospheric pressure plasma
Plasma was first described by Sir William Crookes, a Britishchemist, in 1879 as radiant matter [1]. In 1928 the term plasmawas introduced by Irving Langmuir due to the composition of theionized gas. Since then the term plasma indicates an ionized gasin a wide range of parameters such as density and temperatureand must not be confused with blood plasma. As the fourth andhighest energy state of matter following solids, liquids, and gases,
H. All rights reserved.
: þ49 551 398 983.
plasma is the by far dominant state of matter in the universe, e.g.solar corona, solar winds. On Earth plasma can be generatedtechnically by electric gas discharges. Due to the energy gainedfrom strong electric fields, air (or any other gas) can be trans-formed into the plasma state. A complex mixture of inter-reactingand quite short-lived free electrons, ions, atoms, excited species,and photons is generated [2,3].
Low-pressure, high-pressure, and atmospheric pressure plasmascan be discerned. At atmospheric pressure, plasma in the easiestconfiguration of two metallic electrodes developed in the form ofarcs. The drawback of arc plasmas characterized by high currentdensities and high collision frequencies is a thermal equilibriumresulting in gas temperatures of hundreds or several thousand

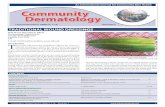
Fig. 1. Random distribution of microdischarges over the electrode area.
S. Emmert et al. / Clinical Plasma Medicine 1 (2013) 24–29 25
degrees Celsius [4,5]. Such thermal plasmas cannot be applied toliving tissue like the skin without causing necrosis of cells.However, the thermal plasma energy can be medically used forsterilization or tissue removal, cutting, or cauterization [6–10].In contrast, electrical gas discharges at atmospheric pressure canbe utilized for the generation of low-temperature plasmas byparticular constructive measures and appropriate electrical cir-cuits. Such non-thermal or non-equilibrium plasmas do not exceedbody temperature and may be applied to the skin as a coldatmospheric pressure plasma treatment.
Generally, two types of cold atmospheric pressure plasmas canbe discerned: direct plasma (dielectric barrier discharge—DBD,corona discharge) and indirect plasma (plasma torch, plasma jet).Indirect plasmas are produced between two electrodes and thentransported onto the skin via a constant gas flow. The skin is notused as the counter electrode [11,12]. Direct cold atmosphericpressure plasma production applying the DBD technique wasdescribed as early as 1857 by von Siemens for the generation ofozone [13]. While dielectric barrier discharge (DBD) plasmatreatment of technical surfaces is a standard method since years,the DBD plasma treatment of biological tissue is quite novel [14].Operated at appropriate parameters, DBD generates a low tem-perature plasma under atmospheric pressure and, thus, is asuitable instrument for a non-destructive treatment of biologicalmaterial [15]. Advantages of direct compared to indirect plasmageneration may include a higher plasma density at the treatedsurface and the electrical current induced in the counter electrodeskin (Table 1).
For our investigations, a non-equilibrium, weakly ionizedphysical plasma is generated by the application of alternatingvoltage pulses with amplitudes410 kV across air gaps in the lowmm range, whereas the high voltage electrode is covered by adielectric. This non-conducting barrier, which is essential in DBDsettings, avoids the transition of the gas discharge into a hot arcby limiting the current. The biological tissue itself (i.e. skin) actsas the counter electrode. The plasma usually propagates in tinybreakdown channels, the so called microdischarges. These are ofcylindrical shape (radius of 10�4 m) and appear stochasticallydistributed over the electrode area (Fig. 1). Only electrons gainnameable kinetic energies in the strong oscillating electric fieldbetween two electrodes. A reactive mix of excited atoms andmolecules, UV photons, charged particles as well as reactiveoxygen species (ROS) and reactive nitrogen species (RNS) isformed in the microdischarges. Typical species in air-plasmas areO3, OH, NxOx, and HNOx. The composition of species can bemodulated depending on the plasma parameters, e.g. processgas composition, humidity, gas temperature, energy density andlocal electric fields [16]. Our DBD cold atmospheric pressureplasma device is depicted in Fig. 2 (CINOGY GmbH Duderstadt).The control unit (Fig. 2a) ensures defined physical parameters.Only one ‘‘on’’ button allows the start of treatment for exactly 45 s(timer in the display). Then the device switches off automaticallyand needs to be re-started. The hand held applicator (Fig. 2b) is
Table 1Comparison of direct and indirect cold atmospheric pressure plasma generation.
Direct plasma
Mode of generation Dielectric barrier discharge against the skin
Gas ionized Ambient air
Plasma density on skin High
Distance to skin Millimetre
Gas temperature Room temperature
Ultraviolet radiation Weak, predominately UVA and some UVB
Electrical current Yes
Reactive gas species Produced in the plasma
connected to the control unit and carries the DBD electrodecovered by a dielectric (1 cm in diameter). A specially constructedspacer (sterile, ready to use) ensures a contact-free plasmaapplication as well as a constant distance of the DBD electrodeto the skin. Direct skin contact of the DBD electrode is harmlessexcept that the discharge stops and, thus, the plasma generationabove the skin.
2. Effective components of plasma skin treatment
The skin comprises the biggest human organ. Its size is about1.5–2 m2. Without the skin life would not be possible. Generally,the skin consists of three layers, the epidermis, the dermis(or cutis), and the subcutaneous fat tissue (Fig. 3). The maincomponents of the dermis are collagen and elastic fibres givingskin elasticity and, if damaged, wrinkle formation and skin ageing.Other components of skin are nerve ends, sweat glands, and hairfollicles. A sebaceous gland empties into each hair follicle and asmall erector pili muscle connected to the hair follicle results in‘‘goose skin’’, if contracted. In the top of the dermis just below the
Indirect plasma
Discharge in a device and plasma efflux onto skin via gas flow
Noble gas and/or ambient air
Low
Millimetre–Centimetre
Hot at the efflux site
Strong in all UV ranges (UVA–UVC) [57]
No
Produced by mixing plasma with ambient air

Fig. 2. PlasmaDerms VU-2010 device constructed by CINOGY GmbH, Duderstadt,
Germany. Control unit with start button and timer display (a); hand-held plasma
applicator with electrode covered by a dielectric (M) and specially designed spacer
(N) (b).
Fig. 3. Histologic skin section (H&E stain). The different layers of the epidermis
consisting of differentiated keratinocytes (epidermal barrier) as well as the dermis
with its collagen and elastic fibres (red structures) are depicted.
Table 2Modes of action of DBD plasma and clinical effects.
Modes of action Clinical effects
Ultraviolet radiation
(UVA4UVB)
Antiinflammation, antiitch, germicidal
Electric current Iontophoretic, transdermal resorption, anti-hydrotic,
antiitch, tissue stimulation
Reactive oxygen
species/ozone
Germicidal, tissue stimulation, others
Reactive nitrogen
species
Stimulation of cell proliferation and blood
microcirculation, acidification, others
S. Emmert et al. / Clinical Plasma Medicine 1 (2013) 24–2926
basal membrane a horizontal capillary network exists whichnourishes the cells in the epidermis per diffusion. No blood orlymph vessels exist in the epidermis. A second important functionof this capillary network is thermoregulation. The epidermisconsists of four layers all formed by a sequencial differentiationof keratinocytes. It takes about 4 weeks for a keratinocyte tomigrate from the stratum basale to the stratum corneum.The main function of the epidermis lies in the mechanicaldefence. In the stratum corneum the keratinocytes have expelledtheir organellae and form the bricks held together by a lipid-richsubstance. This epidermal barrier prevents from water loss.Further, the epidermis can be viewed as an immunologic organpreventing germ invasion. If this labile balance is disturbed, skindiseases like eczema (inflammation), infections or superinfections, dryskin (ichthyoses) or skin defects (wounds) may occur [17].
In cold atmospheric pressure plasma medicine antiinflamma-tory, antipruritic, antimicrobial, tissue stimulation, stimulation ofmicrocirculation, and other therapeutic modalities are combinedwithin one application due to the combined action of ultravioletradiation, electric fields, reactive oxygen species (ozone), reactivenitrogen species, and possibly others, yet unknown (Table 2) [2,3].
2.1. Ultraviolet radiation (UV)
Photodermatology is a unique dermatological subspecialty [18].The therapeutic use of UV irradiation dates back as long as to ancientEgypt where photochemotherapy was already practiced. Today, theanti-inflammatory, anti-pruritic, and anti-fibrotic properties of dif-ferent UV wavelengths are well established [19]. UV radiation inmedicine is divided into UVA (UVA2: 320–340 nm; UVA1: 340–400 nm), UVB (320–280 nm), and UVC (below 280 nm). UVA isadjacent to the visible light spectrum (blue: 400 nm–red: 800 nm).UVA, especially UVA1, exerts anti-pruritic and anti-fibrotic proper-ties as it penetrates deeper into the dermis whereas UVB, especiallymonochromatic UVB 311 nm, exerts anti-inflammatory properties.On the other side of the chart, UV light also has considerable, dose-dependent side effects. Acute over-dosage results in sunburn (der-matitis solaris). Chronic UV exposure may result in accelerated skinageing and wrinkle formation (predominately UVA-induced) as wellas in skin carcinogenesis (predominately UVB-induced) [18,20]. Ourcold plasma generator produces emission from excited molecularnitrogen (Second Positive System). Minor UVB (295–297 nm and311–315 nm peaks) and predominately UVA (337, 358, 375 and380 nm peaks) radiation at effective irradiances of up toEeff¼0.4 mW/m2 between 200 nm and 850 nm. This value is spec-trally weighted according to weigthing factors proposed by theInternational Comission on Non-Ionizing Radiation Protection(ICNIRP) to indicate the approximate relative erythemal efficacyand is thereby well below the minimal erythemal doses of Heff¼30 J/m2 (sunburn as an acute UV side effect) for skin treatment of up to20 h per day [21,22].
2.2. Electric current
The plasma device produces an alternating, pulsed currentwith pulse repetition rate of about fp¼300 Hz and a pulse lengthof tp¼3 ms [21]. This excludes current conduction to inner organse.g. via nerves, as the nerve conduction velocity is much slower(30–50 ms). In-vivo investigations revealed a skin current withinstantaneous amplitude values of up to 420 mA [21]. Yet, theserather high current amplitudes are extremely transient eventsand only last for some 10�9–10�8 s during one pulse lengthwhereby the energy transfer per current pulse is inherentlyrestricted. Briefly said, short-term high currents in combinationwith actually now current flow until the subsequent initiation of a

S. Emmert et al. / Clinical Plasma Medicine 1 (2013) 24–29 27
current pulse (after�10�3 s) results in very low rms (root meansquare) values in the range of 100 mA.
Electrical fields can stimulate and act on biological tissue. Indermatology, iontophoresis is applied to treat hyperhidrosis ofthe palms and soles [23,24]. Patients wet their hands or feet inwater for several minutes daily. A constant electric current of5–10 mA runs through the water, reduces sweat production, andis well tolerated. Other dermatological applications of electriccurrent are iontophoretic transdermal systems (ITS). Here, aconstant current of about 170 mA can deliver a medication intothe body via the skin. For example, 40 mg Fentanyl (anaesthetic)can be delivered transdermally within 10 min [25]. These estab-lished medical applications indicate that a plasma applicationcreating an average of 100 mA (rms value) can be considered safe.
2.3. Reactive oxygen species (ozone)
It is well established that plasmas operated in air induce reactiveoxygen species on the surface of living tissue [26]. A majorcomponent of the reactive gas species produced by the device isozone. The TRK (technical relevant concentration) value for ozoneis 200 mg/m3 for 8 h. The MIK (max inhalative concentration) valueis 120 mg/m3 for 30 min. The ozone concentration measured at adistance of 5 mm from the electrode is o100 mg/m3 [21]. Ozone isused for 80 years for wound disinfection and immunomodulation inmedicine (60 mg/l ozone for 1 h) [27]. Ozone skin disinfection andantimicrobial surface ozone treatment is already in use [28].In addition, positive effects of ozone on wound healing, e.g. ondiabetic wounds at concentrations of 60 g/m3 applied for 1 hfollowed by a coverage of the lesion with an ozone containingemulsion, were reported [29]. The authors found no side effects atthese relatively high ozone concentrations.
2.4. Reactive nitrogen species
Plasma also induces a variety of reactive nitrogen species onthe treatment surface. For example, we measured the generationof nitrate (NO3�) and nitrite (NO2�) on human lipid surfaces withour DBD device [14]. Such nitrogen species probably relate to skinacidification, an effect mediating disinfection as well as properwound healing. We already found in a basic research-relatedproject that plasma treatment leads to considerable changes inthe human skin lipid barrier [30]. By using the latest X-RayPhotoelectron Spectroscopy (XPS) technology we investigatedthe physiological skin lipid composition of human skin and theeffects of plasma treatment on the lipid composition. Skin lipidswere stripped off over the forearms of healthy volunteers usingthe cyanoacrylate glue technique, plasma treated or not, and thensubjected to detailed XPS analysis. We found that the human lipidskin barrier consisted of 84.4% carbon (þ0.2 sem%), 10.8% oxygen(þ0.3 sem%) and 4.8% nitrogen (þ0.5 sem%). The compositions ofphysiological skin lipids were not different in males and females.Plasma treatment resulted in significant changes in skin barrierlipid stoichiometry. The total carbon amount was reduced to76.7% and the oxygen amount increased to 16.5%. There was alsoa slight increase in nitrogen to 6.8%. These changes could beattributed to reduced C–C bonds and increased C–O, CQO, C–N,and N–C–O bonds. The moderate increase in nitrogen was causedby an increase in C–N and N–C–O bonds. Our proof of principleinvestigations established the technical means to analyse, ifplasma-induced skin lipid barrier changes may be beneficial inthe treatment of ichthyotic or eczematous skin. In addition,nitrogen species-containing therapies have been applied in thepast to treat lung diseases [31].
2.5. Side effects
Up to now there is no indication that there are DBD plasmatreatment-related side effects on the skin. In-vitro experimentson human cells and ex-vivo skin models as well in-vivo experi-ments on mouse skin revealed no cellular toxicity, e.g. necrosis[21,32]. Using human skin biopsies DBD plasma treatment of upto 400 Hz and 120 s revealed no cellular damage or damage of thecell nucleus [33,34]. In addition, in-vivo two photon microscopyrevealed no human epidermal skin alterations on the cellularlevel after 120 s of DBD plasma treatment. Histological evalua-tions of mouse skin after 2 min DBD plasma treatment alsoshowed no alterations at all [35,36].
3. Treatment of skin infections/disinfection
The disinfective properties of plasma and its use in thetreatment of superinfected skin appears to be the best evaluatedindication for cold atmospheric plasma usage today, as shown byseveral groups independently. Several in-vitro and in-vivo studiesdemonstrated the bactericidal effects of plasma. Daschlein et al.showed that plasma is active against most germs on woundedskin [37]. We also detected a germicidal action of the plasmadevice [38,39]. We found that the antibacterial effect correlateswith a decrease in pH and is mediated by bacterial membranedamage [39]. Other groups showed the disinfective properties ofplasma treatment in-vivo, e.g. in reduction of bacterial coloniza-tion of chronic wounds [40].
4. Treatment of eczema
Atopic eczema is a very common chronic medical conditionthroughout the population (3–5%). Predisposition sites includethe great flexures on the arms and legs. Usually a combinatorytreatment of eczema is performed including a moisturizingtreatment as a basic treatment, followed by topical antiinflam-matory (e.g. corticosteroids) and antimicrobic treatments.Due to therapeutic resistance this is often combined with UV-phototherapy. The long-term adequate combination of thesedifferent topical treatments is often difficult to pursue for thepatient at home and the combination of several treatments perday is laborious [41].
We treated an adult patient with atopic eczema for 30 daysand for 1 min/d with the DBD device on a defined area on theexternal aspect of the left upper arm. The right side served as acontrol. A moisturizing basic emollient treatment was allowed forboth sides. After plasma treatment itch was reduced for 4 h andafter 30 days itch was overall reduced from 8 to 3 on a 10-pointscale (0: No itch; 10: Worst itch). Agar plates pressed onto theskin showed a more than 10-fold reduction in bacterial coloniza-tion (Staphylococcus aureus). In addition, an overall improvementof the eczema (skin redness) was observed [42]. The reduction ofbacterial colonization is in line with another study from Daes-chlein et al. [37] who found an eradication of Staphylococcus
aureus after cold plasma treatment on colonized skin. Protectivephysiological flora (Staphylococcus epidermidis) was mobilizedfrom deeper skin to the surface and was still present.
Recently, Isbary et al. [43] reported the successful treatment ofHailey–Hailey disease, another superinfected dermatitis, withcold atmospheric plasma. This genetic disease is caused by adefect in the ATP2C1 gene resulting in skin erosions, inflammationand bacterial superinfection predominately in the axillae andgroins. Daily cold plasma treatments for 5 min were performed

S. Emmert et al. / Clinical Plasma Medicine 1 (2013) 24–2928
and led to significant improvement of the disease after 11treatments.
5. Treatment of chronic wounds
Chronic wounds comprise skin tissue defects in diseased skin.Ulcers on the lower legs (ulcus cruris) and feet are the mostcommon wounds from which especially elderly suffer. Varicosisand other venous diseases are the underlying cause in 80% ofpatients with ulcus cruris [44]. Arterial diseases (10%) and diabetes(4%) constitute the two other common causes for wounds on thelegs or feet. The prevalence of ulcus cruris is estimated between0.3 and 1.0%. In Germany 240,000–800,000 patients suffer fromulcus cruris [45]. The risk for venous ulcers increases with age andmost patients are within their 60s to 80s [46]. The lifelong risk todevelop a leg ulcer is 2% [44].
Due to the chronicity and high prevalence venous ulcersconstitute a considerable socioeconomic burden. It is estimatedthat 1–2% of the health care budget is consumed by the treatmentof venous ulcers which is 600–900 million Euros in the countriesof Western Europe [47]. Mean costs per patient are estimated at9.560 Euro per patient per year [48]. This does not includeindirect costs for early retirement or reduced quality of life.
Basically, wound healing can be divided into three phases: acleaning phase, a granulation phase, and an epithelialisationphase [49]. A plethora of different processes is active in thesephases and include blood coagulation, inflammation, matrixsynthesis, angiogenesis, fibrosis, cell proliferation, and remodel-ling [50]. During the first phase the wound is cleaned from celldetritus, dirt, and bacteria. Then angiogenesis and granulation ofdermal tissue occurs closing the wound from the depth. Duringthe final phase keratinocytes from the epidermis proliferate overthe granulation tissue and finally close the wound. Delayedhealing processes can occur in any phase and often includemultiple processes in multiple phases. These processes are farfrom being understood and are intensively investigated.
As the exact molecular mechanisms of wound healing arelargely unknown, therapeutic strategies to treat venous ulcers arelargely symptomatic. Modern wound care of venous ulcersincludes compression therapy. The use of elastic bandages orstockings is suggested to support the venous blood flow anddecrease venous stasis. Second, adequate wound dressings arerecommended. The paradigm is to keep the wound moist, yet thedressing should have the capacity to take on wound exudates toallow a change of the dressing only every 2–4 days. Modernwound dressings should allow air exchange, reduce pain, controlbacterial colonisation, and protect the wound against mechanicalstress. Moreover, the material of the wound dressing should behypoallergenic and non-irritative. Ease of handling is anotherprerequisite as the patients often change the dressings them-selves. Additional procedures like surgical debridement may beindicated [51].
As outlined above the disinfective property of cold atmo-spheric plasma treatment has been demonstrated in several in-vitro as well as in-vivo studies. The control against bacterialsupercolonisation is one goal in modern wound healing strategiesas bacterial colonisation delays wound healing and fosterschronic wounds [52]. Secondly, cold plasma leads to proliferationof endothelial cells via the stimulation of growth factors forangiogenesis [53]. This constitutes another important mechanismin wound healing. Third, we and others found that plasmadecreases the pH leading to wound acidification [14,54]. Ther-apeutically induced wound acidification can positively affect thehealing process [55]. Thus, our cold plasma device combines
several single positive effects on wound healing within oneapplication (Table 2).
Due to these reasons we are currently conducting a clinicaltrial to investigate the safety, efficacy, and applicability of DBDplasma treatment of chronic venous wounds. We strictly selectedinclusion and exclusion criteria. The trial is certified according toactual legislation in Germany by all necessary authorities. It is thevery first clinical trial applying direct cold atmospheric plasma(PlasmaDerms VU-2010 device) in wound treatment officiallylisted in trial databases (e.g. NCT01415622 in clinical trials.gov)world-wide. We envisage that our results obtained in this trial forthe plasma treatment of chronic venous leg ulcers may also betransferred for wound plasma treatment of arterial or diabeticcauses as pathomechanisms appear similar [56].
6. Conclusions
Cold atmospheric pressure plasma appears as a novel andpromising new therapeutic strategy in medicine as several modesof action are combined within one treatment application.UV irradiation, electric current, reactive oxygen species, ozone,and reactive nitrogen species confer antiinflammatory, antiitch,antimicrobic, tissue stimulation, stimulation of microcirculation,and potentially other therapeutic properties. The germicidalproperty of plasma is clearly established and first clinical reportsshow positive results in the treatment of superinfected wounds orsuperinfected dermatitis of different causes. So far, no side effectsof plasma treatment were reported. These results should fosterbroader translesional research efforts to further the understand-ing of plasma treatment benefits as well as potential side effects.With this respect the mid-term goal would be to standardizetechnical parameters for the treatment of a given disease.
Acknowledgements
We thank Petra Laspe, Dept. of Dermatology in Gottingen, forinvaluable technical assistance. Financial support by the DeutscheForschungsgemeinschaft Ma 1893/20-1, VI 359/10-1 and EM63/8-1 is gratefully acknowledged.
References
[1] Crookes W. On radiant matter spectroscopy: a new method of spectrumanalysis. Proceedings of the Royal Society 1983;35:262–71.
[2] Heinlin J, Morfill G, Landthaler M, Stolz W, Isbary G, Zimmermann JL, et al.Plasma medicine: possible applications in dermatology. Journal derDeutschen Dermatologischen Gesellschaft 2010;8:968–76.
[3] Heinlin J, Isbary G, Stolz W, Morfill G, Landthaler M, Shimizu T, et al. Plasmaapplications in medicine with a special focus on dermatology. Journal of theEuropean Academy of Dermatology and Venereology 2011;25:1–11.
[4] Ramakrishnan S, Rogozinski MW. Properties of electric arc plasma for metalcutting. Journal of Physics D: Applied Physics 1997;30:636–44.
[5] Semenov S, Cetegen B. Spectroscopic temperature measurements in directcurrent arc plasma jets used in thermal spray processing of materials. Journalof Thermal Spray Technology 2001;10:326–36.
[6] Bogle MA, Arndt KA, Dover JS. Evaluation of plasma skin regenerationtechnology in low-energy full-facial rejuvenation. Archives of Dermatology2007;143:168–74.
[7] Elsaie ML, Kammer JN. Evaluation of plasma skin regeneration technology forcutaneous remodeling. Journal of Cosmetic Dermatology 2008;7:309–11.
[8] Foster KW, Moy RL, Fincher EF. Advances in plasma skin regeneration. Journalof Cosmetic Dermatology 2008;7:169–79.
[9] Kilmer S, Fitzpatrick R, Bernstein E, Brown D. Long term follow-up on the useof plasma skin regeneration (PSR) in full facial rejuvenation procedures.Lasers in Surgery and Medicine 2005;36:22.
[10] Kilmer S, Semchyshyn N, Shah G, Fitzpatrick R. A pilot study on the use of aplasma skin regeneration device (Portrait PSR3) in full facial rejuvenationprocedures. Lasers in Medical Science 2007;22:101–9.
[11] Shimizu T, Steffes B, Pompl R, Jamitzky F, Bunk W, Ramrath K, et al.Characterization of microwave plasma torch for decontamination. PlasmaProcesses and Polymers 2008;5:577–82.

S. Emmert et al. / Clinical Plasma Medicine 1 (2013) 24–29 29
[12] Sladek RE, Stoffels E. Deactivation of Escherichia coli by the plasma needle.Journal of Physics D: Applied Physics 2005;38:1716–21.
[13] von Siemens W. Ozone production in an atmospheric-pressure dielectricbarrier discharge. Poggendorfs Annale 1857;102:66–122.
[14] Helmke A, Hoffmeister D, Mertens N, Emmert S, Schuette J, Vioel W. Theacidification of lipid film surfaces by non-thermal DBD at atmosphericpressure in air. New Journal of Physics 2009;11:115–25.
[15] Gesche R, Awakowicz P, Bibinov N, Born M, Niemann U, Busse B, et al.Biological stimulation of the human skin applying health-promoting lightand plasma sources. Contributions to Plasma Physics 2009;49:641–7.
[16] Helmke A, Gruening P, Fritz U, Wandke D, Emmert S, Petersen K, et al. Low-temperature plasma—a prospective microbicidal tool. Recent Patents onAnti-infective Drug Discovery. British Journal of Dermatology 2012 June 21[Epub ahead of print].
[17] Fritsch P. Dermatologie und venerologie. Berlin: Springer; 1998.[18] Holzle E, Honigsmann H, Rocken M, Ghoreschi K, Lehmann P. Empfehlungen
zur Phototherapie und Photochemotherapie. Journal Der Deutschen Derma-tologischen Gesellschaft 2003;1:985–97.
[19] Leung DYM, Boguniewicz M, Howell MD, Nomura I, Hamid QA. New insightsinto atopic dermatitis. Journal of Clinical Investigation 2004;113:651–7.
[20] ICNIRP. Guidelines on limits of exposure to ultraviolet radiation of wave-lengths between 180 nm and 400 nm (incoherent optical radiation). HealthPhysics 2004;87:171–86.
[21] Tummel S, Mertens N, Wang J, Viol W. Low temperature plasma treatment ofliving human cells. Plasma Processes and Polymers 2007;4:465–9.
[22] Wandke D. Medizinisch nutzbare Effekte durch eine dielektrisch behinderteEntladung (DBD): Untersuchungen zu Anwendungssicherheit und Therapieop-tionen. Ernst-Moritz-Arndt-Universitat Greifswald: URN:NBN:DE:GBV:9-001217-2; 2011.
[23] Kreyden OP. Iontophoresis for palmoplantar hyperhidrosis. Journal of Cos-metic Dermatology 2004;3:211–4.
[24] Vorkamp T, Foo FJ, Khan S, Schmitto JD, Wilson P. Hyperhydrosis: evolvingconcepts and a comprehensive review. The Surgeon 2010;8:287–92.
[25] Power I. Fentanyl HCl iontophoretic transdermal system (ITS): clinicalapplication of iontophoretic technology in the management of acute post-operative pain. British Journal of Anaesthesia 2007;98:4–11.
[26] Rajasekaran P, Mertmann P, Bibinov N, Wandke D, Viol W, Awakowicz P. DBDplasma source operated in single-filamentary mode for therapeutic use indermatology. Journal of Physics D: Applied Physics 2009;42:1–8.
[27] Valacchi G, Fortino V, Bocci V. The dual action of ozone in the skin. BritishJournal of Dermatology 2005;153:1096–100.
[28] Skomro P, Opalko K, Gadomska-Krasny J, Lietz-Kijak D, Perzanowska-Stefanska M. Ozone therapy with the OzonyTron apaaratus. Annales Acade-miae Medicae Stetinensis 2005;51:39–42.
[29] Martinez-Sanchez G, Al-Dalain AM, Menendez S, Re L, Giuliani A, Candelario-Jalil E, et al. Therapeutic efficacy of ozone on patients with diabetic foot.European Journal of Pharmacology 2005;253:151–61.
[30] Marschewski M, Hirschberg J, Omairi T, Hofft O, Viol W, Emmert S, et al.Electron spectroscopic analysis of the human lipid skin barrier: plasma-induced changes in lipid composition. Experimental Dermatology 2012;21(12):921–5, http://dx.doi.org/10.1111/exd.12043.
[31] Rossaint R, Falke KJ, Lopes F, Slama K, Pison U, Zapol WM. Inhaled nitric oxidefor the adult respiratory distress syndrome. New England Journal of Medicine1993;328:399–405.
[32] Fridman G, Friedman G, Gutsol A, Shekhter AB, Vasilets VN, Fridman A.Applied plasma medicine. Plasma Processes and Polymers 2008;5:503–33.
[33] Abschlussbericht BioLip HHUD: /http://opac.tib.uni-hannover.de/DB=1/SET=3/TTL=1/SHW?FRST=8(08.09.2010)S.
[34] Awakowicz P, Bibinov N, Born M, Busse B, Gesche R, Helmke H, et al.Biological stimulation of the human skin applying health-promoting lightand plasma sources. Contributions to Plasma Physics 2009;49:641–7.
[35] Abschlussbericht BioLip Cinogy GmbH: /http://opac.tib.uni-hannover.de/DB=1/SET=3/TTL=8/CMD?ACT=SRCHA&IKT=1016&SRT=YOP&TRM=biolipþcinogy (08.09.2010)S.
[36] Rajasekaran P, Oplander C, Hoffmeister D, Bibinov N, Suschek C, Wandke D,et al. Characterization of Dielectric Barrier Discharge (DBD) on mouse and
histological evaluation of the plasma-treated tissue. Plasma Processes andPolymers 2011;8:246–55.
[37] Daeschlein G, von Woedtke T, Kindel E, Brandenburg R, Weltmann KD, JungerM. Antibacterial activity of an atmospheric pressure plasma jet againstrelevant wound pathogens in vitro on a simulated wound environment.Plasma Processes and Polymers 2010;7:224–30.
[38] Daeschlein G, Scholz S, Arnold A, von Podewils S, Haase H, Emmert S, et al. Invitro susceptibility of important skin and wound pathogens against lowtemperature atmospheric pressure plasma jet (APPJ) and dielectric barrierdischarge plasma (DBD). Plasma Processes and Polymers 2012;9:380–9.
[39] Helmke A, Hoffmeister D, Berge F, Emmert S, Laspe P, Mertens N, et al.Physical and microbiological characterization of Staphylococcus epidermidis
inactivation by dielectric barrier discharge. Plasma Processes and Polymers2011;8:278–86.
[40] Isbary G, Heinlin J, Shimizu T, Zimmermann JL, Morfill G, Schmidt HU, et al.Successful and safe use of 2 min cold atmospheric argon plasma in chronicwounds: results of a randomized controlled trial. British Journal of Dermatology2012;167(2):404–10, http://dx.doi.org/10.1111/j.1365-2133.2012.10923.x [Epub2012 July 10].
[41] Werfel T on behalf of the AWMF guideline group. Atopic eczema (Neuro-dermitis). AWMF guideline register no.: 013/027; 2008.
[42] Mertens N, Helmke A, Goppold A, Emmert S, Kaemling A, Wandke D, et al.Low temperature plasma treatment of human tissue. In: Proceedings of thesecond international conference on plasma medicine. San Antonio Texas:USA; 2009.
[43] Isbary G, Morfill G, Zimmermann J, Shimizu T, Stolz W. Cold atmosphericplasma: a successful treatment of lesions in Hailey–Hailey disease. Archivesof Dermatology 2011;147:388–90.
[44] Valencia IC, Falabella A, Kirsner RS, Eaglstein WH. Chronic venous insuffi-ciency and venous leg ulceration. Journal of the American Academy ofDermatology 2001;44:401–21.
[45] Nord M. Kosteneffektivitat in der Wundbehandlung. Zentralblatt fur Chir-urgie 2006;131:185–8.
[46] de Araujo T, Valencia I, Federman DG, Kirsner RS. Managing the patient withvenous ulcers. Annals of Internal Medicine 2003;138:326–34.
[47] Deutsche Gesellschaft fur Phlebologie. Leitlinien zur Diagnostik und Therapiedes Ulcus cruris venosum, AWMF-Guideline-Register 037/009; 2008.
[48] Purwins S, Herberger K, Debus ES, Rustenbach SJ, Pelzer P, Rabe E, et al. Cost-of-illness of chronic leg ulcers in Germany. International Wound Journal2010;7:97–102.
[49] Karrer S. Topische Ulkustherapie. Hautarzt 2005;56:1165–79.[50] Robson MC. Wound infection: a failure of wound healing caused by an
imbalance of bacteria. Surgical Clinics of North America 1997;77:637–50.[51] Robson MC, Cooper DM, Aslam R, Gould LJ, Harding KG, Margolis DJ, et al.
Guidelines for the treatment of venous ulcers. Wound Repair and Regenera-tion 2006;14:649–62.
[52] Edwards R, Harding KG. Bacteria and wound healing. Current Opinion inInfectious Diseases 2004;17:91–6.
[53] Kalghatgi S, Fridman G, Fridman A, Friedman G, Clyne AM. Non-thermaldielectric barrier discharge plasma treatment of endothelial cells. IEEEEngineering in Medicine and Biology Society 2008;2:3578–81.
[54] Fridman G, Shereshevsky A, Jost M, Brooks A, Fridman A, Gutsol A, et al.Floating electrode dielectric barrier discharge plasma in air promotingapoptotic behavior in melanoma skin cancer cell lines. Plasma Chemistryand Plasma Processing 2007;27:163–78.
[55] Schneider LA, Korber A, Grabbe S, Dissemond J. Review. influence of pH onwound-healing: a new perspective for wound-therapy? Archives of Derma-tological Research 2007;298:413–20.
[56] Chen WYJ, Rogers AA. Recent insights into the causes of chronic legulceration in venous diseases and implications on other types of chronicwounds. Wound Repair and Regeneration 2007;15:434–49.
[57] Metelmann HR, von Woedtke T, Bussiahn R, Weltmann KD, Rieck M, Khalili R,et al. Experimental recovery of CO2-laser skin lesions by plasma stimulation.American Journal of Cosmetic Surgery 2012;29:52–6.