design, ancillary testing, analysis, and fabrication data for the ...
BioMed CentralEnvironmental Health
ss
Open AcceReviewAncillary human health benefits of improved air quality resulting from climate change mitigationMichelle L Bell*1, Devra L Davis2, Luis A Cifuentes3, Alan J Krupnick4, Richard D Morgenstern4 and George D Thurston5Address: 1School of Forestry and Environmental Studies, Yale University, New Haven, CT 06511, USA, 2Graduate School of Public Health, University of Pittsburgh, CNPAV 435, Pittsburgh, PA 15260, USA, 3Industrial and Systems Engineering Department, P. Catholic University of Chile, Engineering School, Santiago, Chile, 4Resources for the Future, Washington, DC 20036, USA and 5School of Medicine, New York University, Tuxedo, NY 10987, USA
Email: Michelle L Bell* - [email protected]; Devra L Davis - [email protected]; Luis A Cifuentes - [email protected]; Alan J Krupnick - [email protected]; Richard D Morgenstern - [email protected]; George D Thurston - [email protected]
* Corresponding author
AbstractBackground: Greenhouse gas (GHG) mitigation policies can provide ancillary benefits in terms ofshort-term improvements in air quality and associated health benefits. Several studies have analyzedthe ancillary impacts of GHG policies for a variety of locations, pollutants, and policies. In this paperwe review the existing evidence on ancillary health benefits relating to air pollution from variousGHG strategies and provide a framework for such analysis.
Methods: We evaluate techniques used in different stages of such research for estimation of: (1)changes in air pollutant concentrations; (2) avoided adverse health endpoints; and (3) economicvaluation of health consequences. The limitations and merits of various methods are examined.Finally, we conclude with recommendations for ancillary benefits analysis and related research gapsin the relevant disciplines.
Results: We found that to date most assessments have focused their analysis more heavily on oneaspect of the framework (e.g., economic analysis). While a wide range of methods was applied tovarious policies and regions, results from multiple studies provide strong evidence that the short-term public health and economic benefits of ancillary benefits related to GHG mitigation strategiesare substantial. Further, results of these analyses are likely to be underestimates because there area number of important unquantified health and economic endpoints.
Conclusion: Remaining challenges include integrating the understanding of the relative toxicity ofparticulate matter by components or sources, developing better estimates of public health andenvironmental impacts on selected sub-populations, and devising new methods for evaluatingheretofore unquantified and non-monetized benefits.
Published: 31 July 2008
Environmental Health 2008, 7:41 doi:10.1186/1476-069X-7-41
Received: 4 April 2008Accepted: 31 July 2008
This article is available from: http://www.ehjournal.net/content/7/1/41
© 2008 Bell et al; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Page 1 of 18(page number not for citation purposes)

Environmental Health 2008, 7:41 http://www.ehjournal.net/content/7/1/41
BackgroundAverting the course of climate change would result inhuman health benefits directly associated with lessenedglobal temperature changes and associated impacts, butwould also bring ancillary health benefits from reducedground-level air pollution in the short-term [1-5]. Manyfossil-fuel combustion processes that generate greenhousegases (GHG) also emit other harmful air pollutants. Sev-eral measures aimed at reducing GHG emissions can alsoimprove local air quality, most commonly particulatematter (PM) and ozone (O3) precursors. Further, whereasthe benefits from climate change mitigation would mate-rialize far in the future, co-benefits, or ancillary benefits,would occur in the short-term.
Figure 1 describes the relationships among the health con-sequences of climate change and air quality policies andthe general framework of how these responses can beassessed. Air quality policies are routinely evaluated interms of the estimated health outcomes avoided and theireconomic impact [6,7]. However, assessment of thehealth impacts of GHG strategies often considers onlyconsequences in the far future (i.e., left side of Figure 1),without integration of the short-term benefits of relatedpolicies [8]. Well-informed public health and environ-mental strategies require full consideration of conse-quences, including co-benefits and potential ancillaryharms.
A broad array of tools to evaluate the health-related ancil-lary costs and benefits of climate change is currently avail-able, and some examples are provided in italics in Figure1. The general structure for most assessments involvesthree key steps: (1) estimating changes in air pollutantconcentrations, comparing levels in response to GHG mit-igation to concentrations under a baseline "business-as-usual" scenario; (2) estimating the adverse health impactsavoided from reduced air pollution; and (3) for somestudies, estimating the monetary benefit from theseaverted health consequences, often with comparison tothe cost of the climate change mitigation measure. Thefirst step is sometimes accomplished through emissionsscenarios and information regarding how emissionstranslate into pollutant concentrations, such as with airquality modeling systems. The second step usually relieson concentration-response functions from existing epide-miological studies on ambient air pollution and health.The third stage utilizes a variety of techniques to translatehealth benefits into monetary terms, such as contingentvaluation (CV). Additional steps include sensitivity analy-sis, such as applying multiple climate change scenarios orconcentration-response functions for health effects.
This paper aims to illuminate the weight of evidence onthe ancillary health benefits of GHG policies, provide a
framework for such analysis, and critique relevant meth-ods. We focus on the effects of air quality; however a fullassessment of the complete ancillary consequences wouldconsider other factors such as the cost of mitigation meas-ures and ecological impacts. We close with recommenda-tions on the appropriate role of ancillary health benefitsand costs in the climate change mitigation debate. As partof these recommendations, we identify a number of pub-lic health and economic related research topics thatrequire clarification in order to promote more effectiveancillary benefits assessments with respect to GHG miti-gation policies.
Studies of ancillary benefitsA variety of studies have been conducted to estimate thehealth and air pollution ancillary benefits from GHGreduction, with a wide range of methods and study areas.Energy scenarios, emission inventories, and global changeand regional air quality modeling systems have beenlinked to estimate the short-term incremental changes inpublic health and the environment that could result fromvarious GHG mitigation policies [9,10].
Recently, the Stern Review [11] addressed a wide range ofglobal benefits and costs associated with climate change,including air pollution co-benefits. Citing a study by theEuropean Environmental Agency, the Review notes thatlimiting global mean temperature increase to 2°C wouldlead to annual savings in the implementation of existingEuropean air pollution control measures of €10 billionand additional avoided annual health costs of €16–46billion. Even larger co-benefits are estimated in develop-ing countries, including via the substitution of modernfuels for biomass. The Stern Review also recognizes someof the trade-offs between climate change objectives andlocal air quality gains. For instance, switching from petrolto diesel reduces carbon dioxide (CO2) emissions butincreases particles with aerodynamic diameter ≤ 10 μm(PM10) and nitrogen oxides (NOx) emissions. Increasingcombustion temperatures of aircraft engines reduces CO2while increasing NOx, as well as water vapor, which canintensify warming effects. Other GHG mitigating actionspresent fewer environmental trade-offs (e.g., reductions inaircraft weight can decrease CO2 emissions and simultane-ously improve local air quality).
A study of three Latin American cities identified signifi-cant health benefits from reducing GHG, including about64,000 cases of avoided premature mortality over a 20-year period [12]. Reducing methane concentrations by20% starting in 2010 was estimated to lower troposphericO3 levels, averting over 30,000 deaths worldwide in 2030alone [13]. Country-wide assessments of GHG mitigationpolicies on public health have been produced for Canada[14] and selected energy sectors in China [15,16], under
Page 2 of 18(page number not for citation purposes)

Environmental Health 2008, 7:41 http://www.ehjournal.net/content/7/1/41
differing baseline assumptions. A synthesis of research onco-benefits and climate change policies in China con-cluded that China's Clean Development Mechanismpotentially could save 3,000–40,000 lives annuallythrough co-benefits of improved air pollution [17]. Sev-eral studies investigated the links between regional airpollution and climate policy in Europe [18-20]. The tablein additional file 1 summarizes key examples of co-bene-fits studies and briefly describes the methods used foreach step of analysis.
Results from co-benefits studies are typically difficult tocompare, even if study area and target year are identical,due to variations in study design. Major differences existin the methodology used to estimate benefits, as demon-strated in the table in additional file 1. Whereas somestudies implement sophisticated modeling systems toestimate altered air quality, capturing regional differencesin pollutant levels [13], others use simple target valueswith uniform pollution reductions across all spatial areas[12]. Likewise, some studies estimate changes in healthimpacts based on a single or small number of concentra-tion-response functions, capturing only a portion of thehealth impacts and at times assuming that concentration-response functions derived from one area are applicable
in others [21], while other analyses select locally devel-oped concentration-response functions where availableand consider a wide range of health impacts [12]. Eachapproach depends on different underlying conjectures.Even with the widely varying methods, results consistentlyindicate significant ancillary health benefits from GHGpolicies. Similarly, estimates of the social cost of air pollu-tion policies were found to be quite insensitive to choicesin the uncertainties of costs and benefits [22].
Estimation of changes in air pollutant concentrationsReductions in local air pollutants resulting from GHGpolicies (step 1 in Figure 1) can be calculated based on theresulting pollutant levels under a baseline and climatemitigation scenarios. Research designs differ not only bythe policy studied but the choice of a baseline "business-as-usual" scenario. Options range from assumptions thatemissions or pollutant concentrations remain at currentlevels, perhaps adjusted for population growth, to aggres-sive air pollution control policies regardless of actionstaken to affect GHGs. A review of studies of ancillary ben-efits concentrating on the energy sector found that choiceof baseline scenario greatly impacted results, especially forstudies assuming lower pollution levels as directed by the1990 Clean Air Act Amendments (CAAA) in comparisonto those omitting the CAAA [23].
Uncertainties in climate change predictions and estima-tion of regional parameters can be considerable, espe-cially for highly disaggregated assessments with long-termprojections [24-26]. However, assessment of ancillarybenefits requires estimates of pollution levels a few yearsinto the future, not several decades, and thus is notmarred by uncertainties that plague many other forms ofclimate-related research. The longest projections for stud-ies in Additional file 1 are about 20 years.
Approaches to estimate changes in air pollution rangefrom complex modeling systems to a simple pollution tar-get, assuming a pollutant's levels will be at a specified con-centration or meet a certain absolute or relative reductionby a given date. Existing emissions inventories and source-receptor matrices can be used to connect changes in emis-sions to changes in specific pollutants [27-31]. Backwardstrajectory modeling has been used to determine pollutantsources and locations [32-36], and this information canthen be used to estimate how changes in pollutant emis-sions will affect concentrations at various locales.Regional air quality modeling systems, such as theUSEPA's Models-3/Community Multi-Scale Air Quality(CMAQ) model in conjunction with meteorological mod-els, link data on meteorology, emissions, and land-use togenerate gridded estimates of pollutants, including O3and PM at various size fractions [37]. Such modeling hasbeen used to estimate how changes in emissions scenarios
Relationship between climate change and air quality policiesFigure 1Relationship between climate change and air quality policies.
Climate change policiesAim: reduce GHG emissions.
Regional, national, andinternational efforts.
(e.g., Carbon tax)
Air quality policiesAim: reduce pollutant levels.Regional and national efforts.
(e.g., changes in public transportation use and
vehicle fleet)
Greenhouse gas levels
Air pollutant levels(e.g., PM, O3,SO2, NO2, etc.)
Human health response(e.g., premature mortality,
frequency of asthma attacks)
Future Short-term
Economic assessmentValuation of avoided
adverse health outcomes, cost of policy implementation
E.g., air quality modeling,
source-receptor matrix
E.g., concentration-response functions from epidemiology
E.g., willingness-to-pay, cost-of-illness
E.g., explicit target,
modeling systems
E.g., Estimate of cost of purchase, installation, and maintenance of
air pollution control
technology
E.g., Evaluation of mitigation
costs by sector
1
2
3
Page 3 of 18(page number not for citation purposes)

Environmental Health 2008, 7:41 http://www.ehjournal.net/content/7/1/41
affect ambient concentrations [38,39] and similarly canbe applied to estimate future changes in ambient pollut-ants from climate change measures [40] and futureimpacts on human health [41].
The choice of method to ascertain future pollutant levelsdepends on what pollutants and regions are consideredand the spatial and temporal resolution desired. Forexample, a recent study [13] applied a sophisticated airquality modeling system to estimate O3 levels across dif-ferent regions of the world, whereas other approaches[12,42] applied uniform reductions assuming equal per-cent reductions in pollutants across all areas. The moreadvanced approach using modeling systems is betterequipped to capture spatial variability and transport ofpollution and precursors; however some pollutants aremore easily modeled than others.
Uncertainties in the translation of a given climate policyto changes in pollutant concentrations vary by themethod used, but include: (1) the choice of "baseline"scenario; (2) translation of a policy into emissionschanges in various sectors; (3) physical transformation ofthe pollutant (e.g., agglomeration of particles to a largersize); (4) chemical transformation of pollutants (e.g.,non-linear transformation of O3 precursors, conversion ofgaseous pollutants such as NOx to particles); and (5) spa-tial and temporal distribution of impacts, as a function ofthe preceding factors. Both the baseline scenario and cli-mate change mitigation policies are assumed to have uni-form or otherwise known spatial and temporaldistribution in pollution levels. This can be particularlyimportant if emissions trading is included, such as SO2cap and trade programs, which set a maximum value foremissions but allow large heterogeneity in emissions thatcan change with time. The level of uncertainty may differby pollutant depending on their spatial heterogeneity. Forexample, within-city gradients have been observed forPM2.5 [43]. While most ancillary studies to date haveexamined policies at the federal level, in theory analysiscould examine the impacts of other mitigation actionssuch as those conducted at the local level [44,45] or evenpersonal choice and household level actions [46,47] thataggregated lead to lower GHG emissions.
Estimation of human health impactsStudies of the health effects potentially avoidable by cli-mate change mitigation strategies have been based almostexclusively on concentration-response functions derivedfrom published epidemiological studies (step 2 of Figure1). Common urban air pollutants likely to be impacted byGHG policy (e.g., PM) have been associated with a widerange of harmful health impacts including increased fre-quency of hospital admissions and increased risk of mor-tality [48]. Table 1 provides the health outcomes and
sources of concentration-response coefficients employedfor the subset of studies in additional file 1 that estimatedhealth impacts. Because mortality dominates benefitsanalyses, additional detail is given on the pollutants andtimeframe of exposure (i.e., acute or chronic) for mortal-ity.
In this context, the method involves applying a mathe-matical relationship between pollution levels associatedwith various types of health endpoints, with an under-standing of the relationships between the health effectand individual (or social) preferences for reducing the riskor incidence of this effect. The use of a concentration-response function without adjustment assumes that theunderlying relationship between air pollution and healthwhen and where the function was derived will hold in thefuture, perhaps in a different location. This integrationinvolves matching as closely as possible the starting pointof the valuation analysis to the endpoint provided byhealth science, that is a measure of pollution (e.g., ambi-ent levels as a surrogate for exposure) to a health response(e.g., increased risk in hospitalization). In addition, theapproach requires knowledge of the population bycohorts that map to the health endpoints (e.g., asthmaticsor those >65 years) and assumptions regarding baselinehealth responses.
Critical differences in this stage of analysis are choice ofpollutants, health effects, time scale (e.g., acute versuschronic), epidemiological studies, and assumptions (e.g.,baseline mortality rate). Almost all studies in Table 1 esti-mated averted mortality for PM, however a variety ofexposure-response coefficients were used, and severalstudies made assumptions regarding conversion of onepollution form to another (e.g., equal toxicity for nitratesand PM10 [23], PM2.5/PM10 = 0.6 [49], PM10/TSP = 0.5[15]).
Criteria for selection of health endpoints and epidemio-logical studies were not consistent across the studies, how-ever common themes were: (1) use of locally conductedstudies where possible; (2) health endpoints with a con-sistent literature demonstrating a relationship with airpollution; and (3) emphasis on peer-reviewed research,although some studies applied non-peer-reviewed work.As the epidemiological literature grows, integrated assess-ments that incorporate these findings also evolve. Forexample, earlier studies estimating averted mortality fromlowered O3 levels were based on epidemiological researchof a single city (e.g., a Los Angeles study [50] applied toLatin America [12,42]), whereas more recent work usesmulti-city epidemiological studies to generate global esti-mates (e.g., a 95-city study [51] applied worldwide [13]).Concentration-response functions derived from numer-ous cities have advantages over single-city studies as they
Page 4 of 18(page number not for citation purposes)

Environmental Health 2008, 7:41 http://www.ehjournal.net/content/7/1/41
are less subject to sample size concerns and city-specificresults can be combined to generate an overall estimateaccounting for within-city and between-city statisticaluncertainty [52]. The choice of location of the epidemio-logical studies used may be based on selecting a city orregion matching or similar to that of the ancillary benefitsassessment. If only non-local single-city studies are avail-able, options are to perform a meta-analysis to generatean average that accounts for the uncertainty of each city-specific relative rate or to select an existing multi-citystudy.
An alternative to identifying epidemiological studiesthrough literature review is to apply an existing databaseor model of concentration-response functions, many ofwhich also include economic valuation tools. The FastEnvironmental Regulatory Evaluation Tool (FERET) is acost-benefit template developed by Carnegie Mellon Uni-versity and the University of Washington to evaluate howpolicy changes affect air-related health outcomes and theirassociated economic impacts [53]. The Benefits Mappingand Analysis Program (BenMAP), developed by USEPA,estimates population-level exposures, changes in healthendpoints, and economic values [54]. The Ozone RiskAssessment Model (ORAM) uses air quality modeling topredict changes in O3 levels and associated healthresponse [55]. These systems can be used to estimatechanges in health and their monetary value, or as a sourceof concentration-response and economic value functions[55-57].
A number of key uncertainties characterizes the use ofpopulation-based research on air pollution and health forancillary benefits studies. These include [58,59]:
CausalityThe precise physiological mechanism(s) by which air pol-lution could cause the health effects indicated in epidemi-ologic studies is not always fully understood. As a resultcausal inferences are generally developed based on con-sistent evidence across multiple epidemiological studiesincluding different areas and study designs, and resultsfrom toxicological and human exposure studies in con-junction with the criteria of biological plausibility.
Other pollutants and pollutant mixturesOften co-pollutants are included in integrated assess-ments separately and their health or economic conse-quences summed. This may underestimate oroverestimate actual damages. The true harmful agent maynot be the pollutant under study but a related pollutant orgroup of pollutants with similar sources and/or formationpathways. For example, O3 can be considered a marker foran array of photochemical pollutants. Nitrates and sul-fates are related to PM as they contribute to secondary par-
ticles. Interaction between multiple pollutants is not wellunderstood, and most results are presented for an individ-ual pollutant, although air pollution is experienced as amixture.
Toxicity relating to PM chemical compositionWhile a substantial literature provides consistent evidencethat particles are detrimental to health and a limitednumber of population-based studies have examined PMeffects by chemical composition [60], the differential tox-icity of various forms of the PM mixture is unidentified.Differential effects have been demonstrated based on par-ticle size, however chemical composition also appears toplay a role as the same size distribution provides differenteffect estimates based on region [61,62]. In current analy-sis of ancillary benefits, all particles of a given size (e.g.,PM2.5) may be treated with equivalent toxicity, however iffor example sulfates are more harmful than other parti-cles, technologies that reduce emissions of particles fromcoal combustion may result in greater health benefits thanother technologies. If, for example, elemental carbon isidentified to be more detrimental to health, transporta-tion technologies may be more effective.
Use of ambient monitorsThe vast majority of epidemiological studies applied inancillary benefits studies use ambient monitoring data asa surrogate for individual or community-level exposure.The relationship between personal exposure and ambientmonitoring data varies by pollutant, typically with bettercorrelation for particles than for O3 [63,64]. Use of ambi-ent monitors increases the possibility of exposure misclas-sification, which if non-differential would generally driveeffect estimates towards the null, resulting in underesti-mates. This issue has particular importance for the extrap-olation of concentration-response functions from onearea to another, as the relationship between ambientmonitors and exposure, and thereby health, is a functionof indoor pollution and indoor/outdoor activity patterns,which may vary widely across populations.
Shape of concentration-response functionsMany concentration-response functions applied in ancil-lary benefits studies assume a log-linear relationshipbetween exposure and risk. If the true shape differs, incor-rect estimates could be obtained. If the assessmentincludes pollutant levels above those used to generate theconcentration-response function, results will be distortedif the log-linear or otherwise assumed function does nothold. If there exists a safe level below which pollutiondoes not adversely impact health, calculations based onfunctions assuming no threshold would be incorrect forpollutant levels below the threshold value. Some studieshave examined the shape of the concentration-responsecurve, however such analysis does not exist for all pollut-
Page 5 of 18(page number not for citation purposes)

Environmental Health 2008, 7:41 http://www.ehjournal.net/content/7/1/41
ants and health outcomes. Several recent US-based studiesfound no evidence of a threshold at typical concentrationsfor the relationship between mortality and O3 [65] or PM[66].
Temporal or spatial extrapolationPollution and health relationships developed in one areamay not be applicable in another location due to differ-
ences in the underlying population and pollutant charac-teristics [67]. Efforts are often made to apply locally-derived studies [49], however concentration-responsefunctions do not exist for many outcomes and pollutantsfor much of the world. Therefore US and European studiesare generally employed, although a growing number ofepidemiological studies are underway in Asia and LatinAmerica [68-71]. Uncertainties introduced by such extrap-
Table 1: Concentration-response functions used in the assessments listed in Additional file 1
Mortality Morbidity
Aaheim et al. 1999 [153]PM: Adult and infant [160] Lung-cancer, acute and chronic respiratory symptoms, pseudo-croup,
asthma [160]
Aunan et al. 2004 [75]PM10 (chronic): modified version of Pope et al. 1995 [160] Outpatient visits, emergency room visits, hospital admissions, work loss
days, acute respiratory symptoms in children and adults, chronic respiratory symptoms in children and adults, asthma attacks [161]
Burtraw et al. 2003 [23]PM10 and nitrates (acute) [162] NOx: respiratory symptoms, eye irritation days, phlegm days [163]
Cifuentes et al. 2001 [12,42]PM10 (acute and chronic): Respiratory hospital admissions [171,172], emergency department visits
[173], chronic adult bronchitis [174], acute bronchitis in children [56], asthma attacks [175], work loss days [176], restricted activity days (RAD) [177-179], respiratory symptom days [180]
Adults [164-169]Infants [84,170]O3 (acute) [50]
Dessus and O'Connor 2003 [155]PM10 (acute): Based on previously conducted literature reviews [181] Respiratory hospital admissions, emergency room visits, RAD, MRAD,
clinic visits for bronchitis for children <15 years, respiratory symptoms for adults and children, chronic bronchitis, chest discomfort, eye irritation, headaches. Based on previously conducted literature reviews [181,182]
Dudek et al. 2003 [156]Did not apply concentration-response functions. Estimated changes in mortality based on baseline burden.
Respiratory disease and neoplasm. Did not apply concentration-response functions. Estimated changes in morbidity based on baseline burden.
Mazzi and Dowlatabadi 2007 [157]PM2.5 (chronic) [167,183,184] Respiratory and cardiovascular (CVD) hospitalizations [185]
McKinley et al. 2005 [49]PM10 (acute and chronic) [167,183,186] O3 (acute) [187] Chronic bronchitis [188], MRAD [176,178], emergency room visits and
hospital admissions: previously conducted review [189]
Wang and Smith 1999 [15]PM (acute and chronic) [190-192] Respiratory hospital admissions [193], emergency room visits [194],
RAD >16 years [177], acute bronchitis <16 years [195], asthma attacks per asthmatic [175,196], respiratory symptoms [180], chronic bronchitis >16 years [174]
West et al. 2006 [13]O3 (acute) [51]
Note: References for health endpoints refer to the concentration-response function applied.
Page 6 of 18(page number not for citation purposes)

Environmental Health 2008, 7:41 http://www.ehjournal.net/content/7/1/41
olation include differences in indoor/outdoor activity pat-terns, population characteristics, household characteris-tics that relate to exposure, and the pollution mixture.Likewise, the study of ancillary benefits involves futuresocieties that may have dissimilar housing, populations,health care systems, and pollutant mixtures compared tothe present day or the timeframe of the epidemiologicalresearch.
Chronic and acute effects and exposuresAir pollution exposure can be categorized as short-term(i.e., a few days) or longer term (i.e., a few months oryears). Health impacts can be classified as those that takeplace immediately or a short time after exposure, or thosethat have a gradual or much-delayed response, such ascancer and neurological disease. Cohort studies of PM,which evaluate long-term exposure, generally providehigher estimates for mortality than do time-series studies,which evaluate short-term exposure [72,73]. Often moreinformation is available regarding health impacts ofshort-term exposure because such exposure estimates aremore readily available. However, the use of only acute-exposure impacts may underestimate the total mortalityburden from air pollution [74]. Co-benefits studies haveused different approaches to address chronic and acutehealth impacts. Whereas one study [75] included esti-mates of chronic mortality, excluding acute mortalityeffects, another [23] incorporated acute mortality only.
Unknown health endpointsWhile air pollution has been quantitatively linked tomany health consequences, there are other health events,including several pediatric and neurological endpoints,for which concentration-response functions have not yetbeen developed. Some of these health responses are lesssevere than the more commonly studied effects. Howeveras a counter example, recent studies elucidated the linkbetween O3 and mortality [51,76-78]. Although lesssevere health endpoints have lower monetary valuationsthan more severe impacts, they often occur in larger num-bers. Thus, the more grave outcomes such as death andhospital admissions are best viewed as indicators of themuch broader spectrum of adverse health effects resultingfrom air pollution.
Degree of mortality displacementThe public health burden of mortality associated with airpollution depends not only on the increased risk of death,but also on the length of life shortening. Several recentstudies provide evidence that short-term mortality dis-placement of a few days or less does not account for theobserved PM mortality effect estimates [79-83]. Past eval-uations of air pollution's effect on life expectancy gener-ally considered only deaths among adults above 30 yearsof age, but some studies [84-86] suggest that infants may
be among the sub-populations particularly affected bylong-term PM exposure, which would indicate a muchlarger reduction in life expectancy. Currently, considera-ble uncertainty remains as to the amount of life-shorten-ing associated with air pollution.
Economic valuation of avoided adverse health outcomesTo help decision-makers assess policies with a wide arrayof consequences, outcomes are often converted into com-parable formats. Several multi-criteria decision-makingtechniques have been applied in the context of climatechange policy [87-90]. Another widely used approach is toconvert health outcomes into economic terms to allowdirect comparison of costs and benefits. Underlying eco-nomic valuation of health is the concept that individualshave preferences that extend over environmental quality,market goods, and other non-market goods. If thisassumption is accepted, in principle it is possible todeduce how individuals tradeoff health by measuringhow much in the way of other services individuals arewilling to forego to enjoy health benefits. Expression ofthese values in monetary terms is used as a surrogate forwhat people are willing to give up in alternative real con-sumption opportunities. The notion that such individualtradeoffs well describe society's interest in environmentalquality is by no means universally accepted, and contro-versy surrounds economic valuation and benefit-costanalysis in particular [91]. For a summary of the economicargument see [92].
Approaches for economic valuation of healthWe identified several approaches for economic valuationof averted health consequences (step 3 of Figure 1): COI;human capital; a variety of WTP methods; and quality-adjusted life year (QALY) approaches.
Cost of illnessThe COI method totals medical and other out-of-pocketexpenditures and has been used for acute and chronichealth endpoints. For instance, separate models of cancerprogression and respiratory disease were used to estimatemedical costs from these diseases over one's lifetime [93].COI incorporates direct medical costs, such as for physi-cians' visits and medications, and indirect costs, includinglost income from work loss days. However the approachdoes not capture other consequences of illness such aspsychological suffering, physical pain, transportation tomedical appointments, dietary restrictions, and expendi-tures for friends or family acting as caretakers. Theapproach can have a welfare theoretic basis, but does notreflect the full damage of illness, hence results usuallyunderestimate costs and should be considered a lowerbound. Some COI studies assign a medical expenditurebased on primary diagnosis [94].
Page 7 of 18(page number not for citation purposes)

Environmental Health 2008, 7:41 http://www.ehjournal.net/content/7/1/41
Human capital approachEarly attempts to value mortality risk reductions appliedthe human capital approach, which estimates the "valueof life" as lost productivity. This method is generally rec-ognized as problematic and not based on modern welfareeconomics, where preferences for reducing death risks arenot captured. Another limitation is incorporation ofracial- or gender-based discrimination in wages. Thismethod assigns value based solely on income, withoutregard to social value, so unpaid positions such as home-maker and lower paid positions such as social workerreceive lower values. Because data are often available forsuperior alternatives, this approach is rarely used in healthbenefit studies.
Willingness to payWTP generates estimates of preferences for improvedhealth that meet the theoretical requirements of neoclas-sical welfare economics, by aiming to measure the mone-tary amount persons would willingly sacrifice to avoidnegative health outcomes. Complications arise in analysisand interpretation because changes in environmentalquality or health often will themselves change the realincome (utility) distribution of society. A valuation proce-dure that sums individual WTP does not capture individ-ual preferences about changes in income distribution.Another complication is that the value of avoided healthrisk may differ by type of health event and age. Forinstance, in one study WTP to reduce cancer was about athird larger than that for a similar chronic, degenerativedisease [95]. VSL estimates can be adjusted based on exist-ing health condition or age, or by the use of a value perlife-year saved [96]. Use of the value of a statistical life year(VSLY) is very controversial, however, because it impliesthat age and WTP are proportionally and inversely related,although the literature does not support this assumption.Estimates for children are very limited; however VSLs aregenerally higher for children [97] and the empirical liter-ature suggests that children's values are approximatelytwice the value for an adult. WTP measures are theoreti-cally superior to the "supply-side" measures of healthdamage because they can capture the complete value ofhealth, including pain and suffering.
The hedonic labor market WTP approach relates wage dif-ferentials to health risk differences across occupations andindustrial/commercial sectors, under the theory that incompetitive labor markets, workers in risky jobs shouldreceive wage premiums equal to the value they place onavoiding health risks [98,99]. Such studies can ask work-ers their perception of health risks to address differencesbetween perceived and actual risk. These studies arenumerous and form the foundation for most VSL esti-mates. However, they are problematic for application tohealth effects of pollution, because of less directly relevant
behavioral contexts and/or the populations. In particular,reducing air pollution may lower some health risks dis-proportionately for older persons who are not in the labormarket. These benefits, furthermore, may be more likelyfor people with chronic heart or lung disease and mayhave a delayed effect, all of which would not be capturedin the labor market studies.
A small literature of consumer preference studies esti-mates WTP to reduce health risks from purchases or otheractual consumer decisions (e.g., purchase of smoke detec-tors [100], driving behavior under different speed limits[101]). These studies typically find lower VSLs than otherapproaches [101]. A difficulty about these studies is statis-tically separating the health risk-reducing attribute fromother valued attributes. A large body of literature applies ahedonic property value approach [102], which provides arevealed WTP for air pollution reductions but is depend-ent on housing market perceptions about pollution andlinks to non-health effects.
The stated preference WTP approaches, of which CV andchoice experiments are most prominent, are survey meth-ods presenting hypothetical choices (e.g., willingness topay some amount or prefer one set of attributes overanother) to recover preferences for health risk reductions.Results can be sensitive to question wording and ordering,and cognition difficulties when understanding smallchanges in probabilities are required. However thesemethods can be molded to a particular population or con-text. Respondents can be tested for their cognition andunderstanding of the survey's concepts.
Some of the best known stated preference studies for mor-tality examine traffic fatalities [103,104] and fewer studiesare available for air pollution contexts [105-108]. A CVsurvey found that WTP was higher when death risk reduc-tion takes place now rather than later in life or if the indi-vidual was mentally healthy [109]. Age had a relativelyminor effect on VSL, and physical health status had noeffect. These results are consistent with those from a studyof adults in the US and Canada, which did not find strongevidence that WTP is lower for older persons or for thosewith chronic heart or lung conditions or cancer [110]. Arecent WTP study of three countries also found that VSL isnot significantly lower for older populations, howeverpersons admitted to the hospital or emergency room forCVD or respiratory causes had higher VSL [111]. The firststudy to investigate WTP for increased life expectancy(one year in expectation) added between ages 75 to 85years found implied VSLs to range from $70,000 to$110,000, but did not provide indication of whetherrespondents understood the complex scenario, andoffered respondents an unrealistically large reduction inrisk [106].
Page 8 of 18(page number not for citation purposes)

Environmental Health 2008, 7:41 http://www.ehjournal.net/content/7/1/41
Two studies applied choice experiments to examine WTPto reduce risks of chronic respiratory disease [112,113].Subjects chose between two cities for residence, both pre-ferred to their present city and differing in risk of develop-ing chronic bronchitis or respiratory disease and in oneother characteristic: the probability of dying in an auto-mobile accident or cost of living. Several studies evaluatedthe WTP to reduce cancer morbidity risks [114,115].
Three of the first CV studies for acute health responsesused bidding procedures to elicit values for respiratory-symptom days, with average estimates from $5 to $25depending on the symptom, its severity, and whether acomplex of symptoms is experienced [116-118]. CV tech-niques have advanced since these studies, however theyoffer consistent ranges of WTP estimates. In one of the fewEuropean studies of this type, over 1,000 Norwegianswere interviewed to ascertain WTP to avoid various ac utehealth effects (e.g., one more day over their usual annualfrequency). The values for avoiding symptoms are slightlysmaller than those found in older US studies, but the asth-matic values are far larger [119]. A survey of 832 Taiwan-ese investigated WTP to avoid participants' most-recentepisode of acute respiratory illness [120]. Statistical tech-niques are used to relate these values to the duration andseverity of the episode and other variables.
Another approach is the averting-behavior method, whichinfers WTP by observing and placing values on behaviorused to avoid adverse health outcomes. For instance, ifsomeone stays indoors with the air conditioner onbecause of high air pollution, the added electricity costsmight relate to WTP to avoid health impacts. Defensibleestimates under this approach require stringent assump-tions, and in practice the method is rarely used, particu-larly in an acute-health context.
Quality-adjusted life yearThe QALY approach attempts to account for the quality oflife lost by adjusting for time "lost" from disease or death.This method is welfare-theoretic only under very restric-tive assumptions, so it is difficult to conceptualize the sig-nificance of any particular QALY score. The estimates maybe very insensitive for distinguishing among differentseverities and types of acute morbidity. See the recentInstitute of Medicine report [121] for a full review of thisapproach as it could be applied in a regulatory, cost-ben-efit analysis setting.
A QALY analysis of USEPA's Heavy Duty Engine/DieselFuel regulations found that for situations in which mor-tality dominates other health outcomes, QALY and WTPmethods can provide similar results [122]. If morbidityand non-health consequences are predominant, resultsfrom QALY and WTP analysis may differ. Another use of
QALYs investigated over 230 WTP estimates, finding thatvariation in WTP values is affected by QALY estimates ofillness severity, illness duration, income, and age [123].There also exists literature providing QALY estimates forchronic diseases, for example for various severities ofasthma [124].
Applications of economic valuationValuations of mortality risk reductions associated withenvironmental policies are usually the largest category ofbenefits, both among health responses and compared toother attributes. For instance, a USEPA analysis of theClean Air Act estimated a value of $100 billion annuallyfor reduced premature mortality out of $120 billion intotal benefits, compared to costs of approximately $20billion [7]. European and Canadian studies similarlyfound that mortality risk dominates analysis of pollutionreductions [125,126]. Next to mortality, reductions in theprobability of developing a chronic respiratory diseasehave been estimated to be the most valued, recognizingthat values for other types of diseases are sparse. Reduc-tions in acute effects are lower valued.
Table 2 provides a sample of values typically used by prac-titioners of health benefits analyses from several majorstudies or models: the USEPA's BenMAP, which is used inRegulatory Impact Analyses of Regulations [7,54]; theExternE model [125], which is used by the EuropeanUnion (EU) in its regulatory analyses, taken from itsClean Air For Europe (CAFÉ) Program (AEA) [127]; theAir Quality Valuation Model (AQVM) for Canada [126];the Australian Bureau of Transport and Regional Econom-ics (BTRE) assessment of transportation-related pollutantsin Australia [128]; and a study of the benefits of environ-mental improvement in New Zealand [129]. Within thetable, health values are converted to common, compara-ble currency using purchasing power parity (PPP) andconstant 2000 dollars. The WTP for reducing risks of mor-tality and chronic morbidity is expressed, for convenience,as VSL and the value of a statistical case (VSC) of chronicdisease. This term is merely shorthand for the WTP for agiven risk reduction divided by that risk reduction. Thisrelationship is useful because VSLs or VSCs can be multi-plied by estimates of the "lives saved" or "chronic casessaved" to obtain benefits.
The table shows a fairly wide range of VSL values, with thehighest in the US. Rank ordering of values across the otherhealth endpoints is very similar across studies, althoughsome different sets of health endpoints are consideredand there are many blank cells (i.e., categories for whichinformation is unknown or not incorporated) outside ofthe US and EU. The relatively close agreement between theUS and EU likely results from reliance on a common poolof studies, results, and interpretations as well as the social
Page 9 of 18(page number not for citation purposes)

Environmental Health 2008, 7:41 http://www.ehjournal.net/content/7/1/41
cost of electricity studies in the US and the ExternE effortin Europe, which benefited from close collaborationbetween the participating researchers in both efforts[130,131]. In addition, the Canadian studies wereinformed by the AQVM developed by researchers active inthe US social costing debate [132].
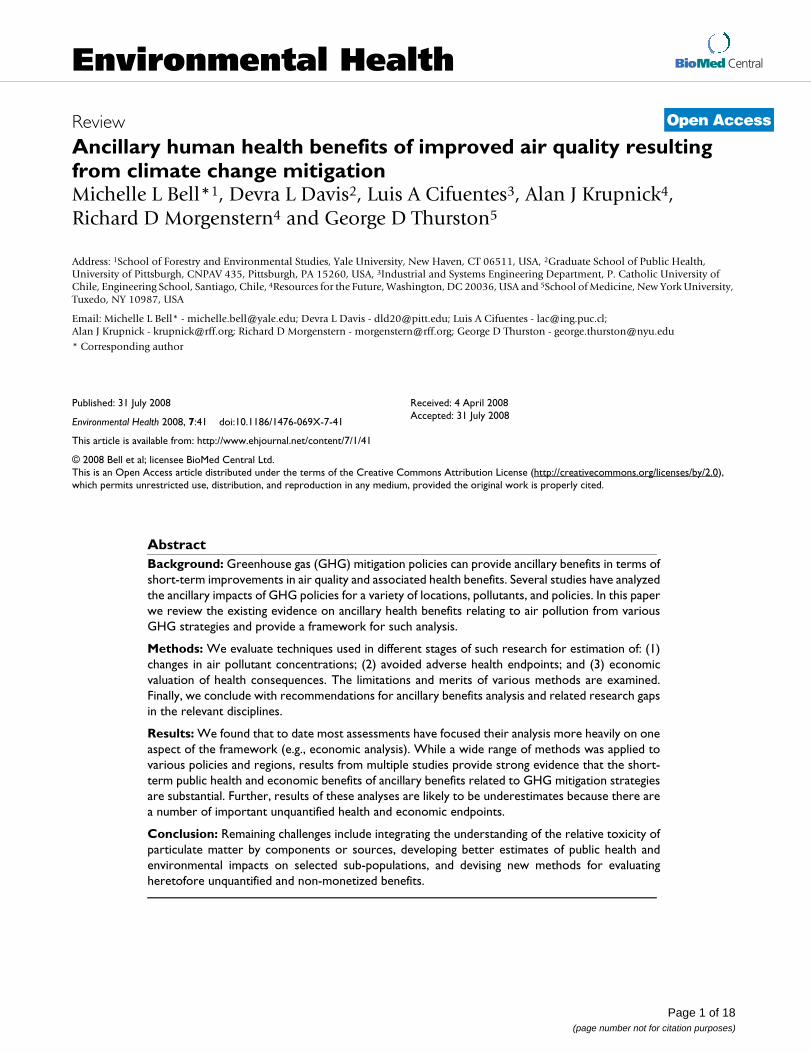
Credibility of economic valuation estimatesWe evaluated economic valuation methods on three crite-ria: (i) the degree to which methods are based on prefer-ences for such health improvements, which we took to bein agreement with welfare economics principles; (ii) thenumber of studies following the technique, which is animperfect measure of degree of consensus and attractive-ness of the technique to researchers; and (iii) additionalmajor limitations, serving to capture other issues, such asdata shortcomings. Based on this admittedly subjectivejudgment, we then rated the reliability of the differentapproaches from A (very reliable) to D (unreliable). Theassessment is intended to provide comparison amongapproaches, rather than an absolute assessment of accu-racy.
As a first step of the evaluation, we compared theoreticalpredictions and empirical results of economic valuation
studies for mortality (Table 3). Under the theoreticalframework, WTP should increase with the size of the riskchange. The life cycle model also implies lower WTP whenrisk change is further in time. Persons facing higher base-line risks should have higher WTP for a given risk reduc-tion (the "dead anyway" effect) [133]. Higher incomes orwealth should relate to higher WTP. With borrowingagainst future earnings, the relationship between WTPand age should be an inverted U-shape according to lifecycle models. Finally, these models do not make a predic-tion regarding health status.
These theoretical predictions are not always matched byempirical results, and Table 3 demonstrates that no sim-ple consistent relationship exists between WTP for mortal-ity and other factors listed, other than income. This couldbe due to differences in the underlying approaches used tosolicit results, or indication of a more complicated system(e.g., age's impact on VSL may further depend on otherfactors). Our subjective evaluation of the valuation meth-ods for mortality, chronic morbidity, and acute morbidityare provided in Tables 4, 5, and 6, respectively. No singlemethod is fully satisfactory. Due to the array of methodsavailable for estimating the economic impact of health
Table 2: Sample of typically used values for PM-related health impacts (mean estimates) ($2000 PPP-adjusted [197])
Health Effects US EU Canada Australia New Zealand
Mortality: 1,042 1,296,552 (premature death) [198]
VSL: Adults 6,300,000 2,247,191 3,480,000 1,439,394 1,717,241 (1,724,138) [198]
VSL: Children 2 × adult 4088764 (infant)VSLY 134,831 70,455 118,621Morbidity: 1929.55 (average cost/
separation) [199]Morbidity: children 2 × adultsChronic bronchitis 340,000 213,483Chronic asthma 39,000Respiratory hospital admission
14,000 2,247 1,032 2,069
CVD hospital admission
21,000 2,247 1,052 2,759
Emergency room visit 300 (asthma) 541 (respiratory) 562 (CVD)
Doctor's visit 60RAD 106 92 (working age) 78
(young, elderly)22 53
MRAD 50 43Acute respiratory symptom
3–24
Use of respiratory medication
1.12
Asthma day 32–74 43 15References: [54] [127] [200] [128]* [129]
Note: *: VSL derived from population-weighted values in the Australian Bureau of Transport and Regional Economics (BTRE) assessment, Table 3 [128]. Population data from the Australian Bureau of Statistic.
Page 10 of 18(page number not for citation purposes)

Environmental Health 2008, 7:41 http://www.ehjournal.net/content/7/1/41
and the limitations of any single approach, we recom-mend the application of multiple methods.
In addition to the issues of credible economic evaluationof the benefits and costs of climate change policies, a cen-tral issue in comparing these values is the discount rateapplied [134]. Selection of the discount rate, whichaccounts for differential value of costs and benefits occur-ring in the far future compared to those taking place in thepresent or near feature, can greatly alter results of cost ben-efit analysis, such as for climate change. In fact, a recentdisagreement regarding climate change policy analysis bytwo leading economists centered largely on the use of adifferent discount rate [11,134]. While some aspects ofbenefit/cost analysis are well-suited to monetary terms,the issue of an appropriate discount rate carries ethicalimplications regarding the relative impacts on variouspopulations.
DiscussionEstimating the ancillary public health consequences ofGHG policies is a challenging task drawing upon expertisein economics, emission inventories, air pollution mode-ling, and public health. However, to date most assess-ments have focused more heavily on one aspect of theframework (i.e., a portion of Figure 1), whether it be esti-mation of changes in air pollutant concentrations, healthresponse, or economic analysis (see Table in additionalfile 1). We have summarized the limitations in the healthand economics estimations, however other uncertaintiesexist for the selection of policy alternatives and estimationof changes in air quality. In spite of differences inapproaches, choice of climate change policy, etc., thewealth of evidence from multiple studies provides a broadconsensus that ancillary health benefits from improvedair quality are substantial, which can be useful informa-tion for the policy debate about the scope, design, andtiming of climate policy.
Results from current ancillary benefits studies may beunderestimates due to unquantified benefits, as only asubset of the health consequences from air pollution haveadequate exposure-response relationships [59,135-137].A USEPA evaluation of the Clean Air Interstate Rule(CAIR) noted numerous unquantified health impactssuch as chronic respiratory damage for O3, pulmonaryfunction for PM, and lung irritation for NOx [135]. Thenature of unquantified effects is continually evolving.Some pollution and health relationships consideredunquantifiable by USEPA in 1999 [7] have since beenidentified, such as for acute O3 exposure and mortality[51,76-78] and air pollution's association with lung can-cer [138,139]. Further some endpoints may be includedin one analysis, but regarded as too uncertain for another,perhaps due to a different study location or differences inresearchers' judgment. One approach to address healthendpoints with uncertain concentration-response func-tions is to include these effects qualitatively in discussionof unquantified benefits. Another is to incorporate theseeffects in sensitivity analysis.
Similarly, some economic costs may not be easily quanti-fiable, even if the health response to air pollution isunderstood. For example, the USEPA's CAIR analysisidentified several unquantifiable costs including employ-ment shifts as workers become reemployed, administra-tion costs in state and federal governments, and somepermitting costs [135]. Only a limited number of studiesare available regarding the value of children's health, suchas several that estimated the cost of children's asthma[140-143]. Valuing reduced mortality risks for newbornsor children is challenging because children are generallynot the key decision-makers over their own health. Tech-niques to transfer adult monetary valuations to childrenhave been explored [144].
This work has focused primarily on health benefits fromimproved air quality resulting from climate change miti-
Table 3: Theoretical predictions and empirical results of studies estimating value of mortality risk reductions. Source: Hammitt and Graham (1999) [103]
Study Size of Risk Change
Future Risk Change
Baseline Risk Income (or proxies)
Age Health Status
Life cycle model: Theory
+, proportional - +a + -b, + then -c indeterminate
Empirical StudiesCompensating Wage + N/A -d + - N/AOther Revealed Preference
+ N/A Unknown + + N/A
CV +, not proportional - Varies + + then -, 0, - No effect, +
a. Small "dead anyway" effect: Higher value to benefits while alive than for a bequest [133].b. With borrowing against future earnings.c. Inverted U with no borrowing.d. Self selection by risk tolerant workers
Page 11 of 18(page number not for citation purposes)

Environmental Health 2008, 7:41 http://www.ehjournal.net/content/7/1/41
gation, however a full assessment of the short-term conse-quences of climate change policies would incorporatetradeoffs that may in fact be negative or for which thedirection of impact is difficult to predict. Policies mightalter unemployment rates and income levels, which havebeen linked to increased suicides [145,146], domestic vio-lence [147,148], depression [149], and mental health[150,151]. The relationships between low income orunemployment and health are not fully understood andsomewhat controversial. Still, changes in employment orincome from climate policies have the potential to intro-duce another set of health-related ancillary benefits orcosts.
As another example, GHG mitigation might incorporatepolicies to deter suburban sprawl, which could reducetransportation-related air emissions and thereby improvehealth in the short-term. However, a fuller understandingof the consequences of such a policy would addresschanges in population-weighted air pollution exposure,which may be higher in urban areas, as well as urbancrime, and other potential impacts from higher popula-
tion density. Other examples are transition to biofuels,which could have implications for nutrition, or the use ofbikes rather than cars for transportation, which wouldlower air pollution emissions but could potentially alsoharm health if biking occurred near major roadways,increasing proximity to high pollution at an increasedventilation rate, or could improve health throughincreased exercise. Thus, while our discussion and mostresearch of ancillary consequences have focused on bene-fits, a full suite of positive and adverse consequencescould exist.
One of the most controversial aspects of ancillary benefitsanalysis is the valuation of health in non-industrializedcountries. Previous Intergovernmental Panel on ClimateChange (IPCC) assessments sparked heated debatebecause they presented non-market values for healthimprovements that some thought unethically devaluedlives in non-industrialized countries. Challenges to eco-nomic valuation of health in these regions are describedelsewhere [152]. Limited data availability, such as forwages, prohibits application of some approaches. Medical
Table 4: Credibility ratings for approaches to valuing changes in the risk of mortality
Criteria
Approach Welfare Theoretic (Y/N) Numbers of Studies (Many/Some/Few)
Other Limitations Rating
Human Capital N M (not recent) Undervalues non-workers DCOI Not usually; in principle could be if
separate estimates available for pain and suffering
M Usually underestimates C
Revealed preference: Hedonic Labor Market; others
Y M Inappropriate commodity/Population sampled
B
CV and choice experiments: health
Y S Hypothetical; hard to understand small probability change
B
QALYs N (except under very restrictive conditions)
M Monetization arbitrary C
Table 5: Credibility ratings for approaches to valuing changes in the risk of chronic morbidity
Criteria
Approach Welfare Theoretic (Y/N) Numbers of Studies (Many/Some/Few)
Other Limitations Rating
COI Not usually; hospitalization; sometimes labor productivity (which is a revealed preference approach)
M: medical cost studies F: labor productivity studies
Pricing medical services can be difficult where medical care is socialized or subsidized
C-B
Revealed preference Y Many on injury/accidents; not on morbidity
C
CV and choice experiments: health
Y F See above B
QALYs Y (under very restrictive conditions) M Arbitrary monetization C
Page 12 of 18(page number not for citation purposes)
Environmental Health 2008, 7:41 http://www.ehjournal.net/content/7/1/41
cost information may not reflect social opportunity costs.Hedonic labor market studies, which presume that laborand goods markets are competitive and workers have rea-sonable information on death and injury risks, may carrymore uncertainties in some regions than others. Valuationof the health of various household members, particularlychildren, may be quite different than in developed coun-tries because of children's more central role in the econ-omy. Rapid economic growth means preferences arechanging as well, raising questions about the applicabilityof indigenous studies several years hence.
A related challenge is differential effects by subpopula-tions. Epidemiological evidence supports the hypothesisthat some segments of the population (e.g., racial orsocio-economic groups) face disproportionate health bur-dens from air pollution. Current ancillary benefit analysisdoes not include separate estimation of health and eco-nomic damages by sub-groups or confront issues of envi-ronmental justice. Further information is needed on therelationship between air pollution and health and eco-nomic valuation methods with respect to subpopulations.
In order to conduct the most robust ancillary benefitsanalyses, we recommend reliance on the most defensible,transparent methods, even if they are recognized as defi-cient. Because a variety of approaches are available, noneof which are ideal, we recommend the application of mul-tiple methods and extensive sensitivity analysis consider-ing a range of changes in air pollution concentrations,spatial distribution of impacts (if considered), health end-points, epidemiological concentration-response func-tions, and economic valuation estimates.
ConclusionOverall, though still a work in progress, the present tech-niques available for the analyses of the ancillary public
health costs and benefits are adequate and appropriate forimplementation by those comparing the relative meritsand overall value of various GHG mitigation policies. Esti-mates of considerable benefits that remain after a varietyof sensitivity analyses can alleviate some concerns regard-ing limitations of individual methods or assumptions.The short-term public health changes associated withGHG mitigation strategies should be considered as a keyfactor in the choice of GHG policies.
List of abbreviationsAQVM Air Quality Valuation Model, BenMAP BenefitsMapping and Analysis Program, BTRE Bureau of Trans-port and Regional Economics, CAAA Clean Air ActAmendments, CAIR Clean Air Interstate Rule, CO2 carbondioxide, COI cost of illness, CV contingent valuation,CVD cardiovascular, EU European Union, GHG green-house gases, MRAD minor restricted activity days, NOxnitrogen oxides, O3 ozone, PM particulate matter, PM10particulate matter with an aerodynamic diameter ≤ 10μm, PM2.5 particulate matter with an aerodynamic diame-ter ≤ 2.5 μm, PPP purchasing power parity, QALY quality-adjusted life year, RAD restricted activity days, SO2 sulfurdioxide, TSP total suspended particles, USEPA US Envi-ronmental Protection Agency, VOCs volatile organic com-pounds, VSC value of a statistical case, VSL value of astatistical life, VSLY value of a statistical life year, WTPwillingness to pay.
Competing interestsThe authors declare that they have no competing interests.
Authors' contributionsAll authors made substantial contributions to the concep-tion and design of this paper, were involved in draftingand revising the manuscript. All authors have approvedthe final version.
Table 6: Credibility ratings for approaches to valuing changes in the risk of acute morbidity
Criteria
Approach Welfare Theoretic (Y/N)
Numbers of Studies (Many/Some/Few)
Other Limitations Rating
COI No M Pricing medical services can be difficult
C
Revealed preference (averting behavior)
Y (under restrictive conditions)
Many for injury and accidents; not for acute respiratory symptoms
C
CV and choice experiments: Health
Y S Old methods/studies; some ad hoc estimates; small samples
B
QALYs Y (under very restrictive conditions)
M Scores insensitive to severity of acute effects
C
Page 13 of 18(page number not for citation purposes)

Environmental Health 2008, 7:41 http://www.ehjournal.net/content/7/1/41
Additional material
References1. Swart R, Amann M, Raes F, Tuinstra W: A good climate for clean
air: linkages between climate change and air pollution: aneditorial essay. Clim Change 2004, 66:263-269.
2. Thurston G: Air pollution, human health, climate change andyou. Thorax 2007, 62:748-749.
3. Walsh MP: Ancillary benefits for climate change mitigationand air pollution control in the world's motor vehicle fleets.Annu Rev Public Health 2008, 29:1-9.
4. Haines A, Smith KR, Anderson D, Epstein PR, McMichael AJ, RobertsI, Wilkinson P, Woodcock J, Woods J: Policies for acceleratingaccess to clean energy, improving health, advancing develop-ment, and mitigating climate change. Lancet 2007,370:1264-1281.
5. Smith KR, Haigler E: Co-benefits of climate mitigation andhealth protection in energy systems: scoping methods. AnnuRev Public Health 2008, 29:11-25.
6. USEPA: The Benefits and Costs of the Clean Air Act 1970 to 1990 Wash-ington, DC: USEPA; 1997.
7. USEPA: The Benefits and Costs of the Clean Air Act 1990 to 2010 Wash-ington, DC: USEPA; 1999. EPA-410-R-99-001
8. Ebi K, Mills DM, Smith JB, Grambsch A: Climate change andhuman health impacts in the United States: an update on theresults of the U.S. National Assessment. Environ Health Perspect2006, 114:1318-1324.
9. Burtraw D, Toman M: The Benefits of Reduced Air Pollutants in the U.S.from Greenhouse Gas Mitigation Policies Washington, DC: Resourcesfor the Future; 1997. Discussion Paper 98-01-REV
10. McCarthy JJ, Canziani OF, Leary NA, Dokken DJ, White KS, eds: Cli-mate Change 2001: Impacts, Adaptation & Vulnerability Contribution ofWorking Group II to the Third Assessment Report of the Intergov-ernmental Panel on Climate Change. Cambridge, UK: Cambridge Uni-versity Press; 2001.
11. Stern N: The Economics of Climate Change: the Stern Review New York,NY: Cambridge University Press; 2007.
12. Cifuentes L, Borja-Aburto VH, Gouveia N, Thurston G, Davis DL:Assessing the health benefits of urban air pollution reduc-tions associated with climate change mitigation (2000–2020): Santiago, São Paulo, Mexico City, and New York City.Environ Health Perspect 2001, 109:S419-S425.
13. West JJ, Fiore AM, Horowitz LW, Mauzerall DL: Global health ben-efits of mitigating ozone pollution with methane emissioncontrols. Proc Natl Acad Sci 2006, 103:3988-3993.
14. Last J, Trouton K, Pengelly D: Taking Our Breath Away: The HealthEffects of Air Pollution and Climate Change Vancouver, Canada: DavidSuzuki Foundation; 1988.
15. Wang X, Smith KR: Near-Term Health Benefits of Greenhouse GasReductions: A Proposed Assessment Method and Application in Two EnergySectors of China Geneva: World Health Organization; 1999. WHO/SDE/PHE/99.1
16. Cao J, Ho MS, Jorgenson DW: "Co-benefits" of Greenhouse Gas Mitiga-tion Policies in China Washington, DC: Resources for the Future; 2008.
17. Vennemo H, Aunan K, Jinghua F, Holtedahl P, Tao H, Seip HM:Domestic environmental benefits of China's energy-relatedCDM potential. Clim Change 2006, 75:215-239.
18. Alcamo J, Mayerhofer P, Gaurdans R, van Harmelen T, van Minnen J,Oningkeit J, Posch M, de Vries B: An integrated assessment ofregional air pollution and climate change in Europe: findingsof the IAR-CLIM project. Environ Sci Pol 2002, 5:257-272.
19. van Harmelen T, Bakker J, de Vries B, van Vuuren D, den Elzen J, May-erhofer P: Long-term reductions in costs of controllingregional air pollution in Europe due to climate policy. EnvironSci Pol 2002, 5:349-365.
20. Working Group on Public Health and Fossil Fuel Combustion: Short-term improvements in public health from global-climatepolicies on fossil-fuel combustion: an interim report. Lancet1997, 350:1341-1349.
21. West JJ, Osnaya P, Laguna I, Martínez J, Fernández A: Co-control ofurban air pollutants and greenhouse gases in Mexico City.Environ Sci Technol 2004, 38:3474-3481.
22. Rabl A, Spadaro JV, Zwaan B van der: Uncertainty of air pollutioncost estimates: to what extent does it matter? Environ Sci Tech-nol 2004, 39:399-408.
23. Burtraw D, Krupnick A, Palmer K, Paul A, Toman M, Bloyd C: Ancil-lary benefits of reduced air pollution in the US from moder-ate greenhouse gas mitigation policies in the electricitysection. J Environ Econ Manage 2003, 45:650-673.
24. Murphy JM, Sexton DMH, Barnett DN, Jones GS, Webb MJ, CollinsM, Stainforth DA: Quantification of modeling uncertainties in alarge ensemble of climate change simulations. Nature 2004,430:768-772.
25. Rotmans J, van Asselt MBA: Uncertainty management in inte-grated assessment modeling: towards a pluralistic approach.Environ Monit Assess 2001, 69:101-130.
26. Allen MR, Stott PA, Mitchell JFB, Schnur R, Delworth TL: Quantify-ing the uncertainty in forecasts of anthropogenic climatechange. Nature 2004, 407:617-620.
27. Chen CL, Tsuang BJ, Pan RC, Tu CY, Liu JH, Huang PL, Bai H, ChengMT: Quantification on source/receptor relationship of pri-mary pollutants and secondary aerosols from groundsources – part I. theory. Atmos Environ 2002, 36:411-419.
28. Hedberg E, Gidhagen L, Johansson C: Source contributions ofPM10 and arsenic concentrations in Central Chile using posi-tive matrix factorization. Atmos Environ 2005, 39:549-561.
29. Calhoun DD, Salmon LG, Schauer JJ, Christoforou CS: PM2.5 char-acterization and source-receptor relations in South Caro-lina. J Environ Eng Sci 2003, 2:441-451.
30. Tsuang BJ, Chen CL, Pan RC, Liu JH: Quantification on source/receptor relationship of primary pollutants and secondaryaerosols from ground sources – part II. model descriptionand case study. Atmos Environ 2002, 36:421-434.
31. Levy JI, Wilson AM, Evans JS, Spengler JD: Estimation of primaryand secondary particulate matter intake fractions for powerplants in Georgia. Environ Sci Technol 2003, 37:5528-5536.
32. Polissar AV, Hopke PK, Poirot RL: Atmospheric aerosol overVermont: chemical composition and sources. Environ Sci Tech-nol 2001, 35:4604-4621.
33. Sapkota A, Symons JM, Kleissl J, Wang L, Parlange MB, Ondov J, Brey-sse PB, Diette G, Eggleston PA, Buckley TJ: Impact of the 2002Canadian forest fires on particulate matter air quality in Bal-timore City. Environ Sci Tech 2005, 39:24-32.
34. Han YJ, Holsen TM, Hopke PK, Yi SM: Comparison betweenback-trajectory based modeling and Lagrangian backwarddispersion modeling for locating sources of reactive gaseousmercury. Environ Sci Technol 2005, 39:1715-1723.
35. Lupu A, Maenhaut W: Application and comparison of two sta-tistical trajectory techniques for identification of sourceregions of atmospheric aerosol species. Atmos Environ 2002,36:5607-5618.
36. Lin YC, Lan YY, Tsuang BJ, Engling G: Long-term spatial distribu-tions and trends of ambient CO concentrations in the cen-tral Taiwan Basin. Atmos Environ 2008, 42:4320-4331.
37. USEPA: Science Algorithms of the EPA Models-3 Community Multiscale AirQuality (CMAQ) Modeling System Research Triangle Park, NC: USEPA;1999. EPA/600/R-99/030
38. Lin CJ, Ho TC, Chu HW, Yang H, Chandru S, Krishnarajanagar N,Chiou P, Hopper JR: Sensitivity analysis of ground-level ozoneconcentration to emission changes in two urban regions ofsoutheast Texas. J Environ Manage 2005, 75:315-323.
39. Bell M, Ellis H: Sensitivity analysis of tropospheric ozone tomodified emissions for the Mid-Atlantic region. Atmos Environ2004, 38:1879-1889.
40. Hogrefe C, Lynn B, Civerolo K, Ku JY, Rosenthal J, Rosenzweig C,Goldberg R, Gaffin S, Knowlton K, Kinney PL: Simulating changesin regional air pollution over the eastern United States due
Additional file 1
Studies investigating the air pollution and health co-benefits from climate change policiesClick here for file[http://www.biomedcentral.com/content/supplementary/1476-069X-7-41-S1.doc]
Page 14 of 18(page number not for citation purposes)
Environmental Health 2008, 7:41 http://www.ehjournal.net/content/7/1/41
to changes in global and regional climate and emissions. JGeophys Res – Atmos 2004, 109:1-13.
41. Knowlton K, Rosenthal JE, Hogrefe C, Lynn B, Gaffin S, Goldberg R,Rosenzweig C, Civerolo K, Ku JY, Kinney PL: Assessing ozone-related health impacts under a changing climate. EnvironHealth Perspect 2004, 112:1557-1563.
42. Cifuentes L, Borja-Aburto VH, Gouveia N, Thurston G, Davis DL:Climate change: hidden health benefits of greenhouse gasmitigation. Science 2001, 293:1257-1259.
43. Jerrett M, Burnett RT, Ma R, Pope CA 3rd, Krewski D, Newbold KB,Thurston G, Shi Y, Finkelstein N, Calle EE, Thun M: Spatial analysisof air pollution and mortality in Los Angeles. Epidemiology2005, 16:727-736.
44. Lutsey N, Sperling D: America's bottom-up climate changemitigation policy. Energy Policy 2008, 36:673-685.
45. Lankao PR: How do local governments in Mexico City manageglobal warming? Local Environ 2007, 12:519-535.
46. Shaw D, Newholm T: Voluntary simplicity and the ethics ofconsumption. Psychol Mark 2002, 19:167-185.
47. Weber CL, Matthews HS: Quantifying the global and distribu-tional aspects of American household carbon footprint. EcolEcon 2008, 66:379-391.
48. Holgate ST, Samet JM, Koren HS, Maynard RL, eds: Air Pollution andHuman Health San Diego, CA: Academic Press; 1999.
49. McKinley G, Zuk M, Höjer M, Avalos M, González I, Iniestra R, LagunaI, Martinez MA, Osnaya P, Reynales LM, Valdés P, Martínez J: Quan-tification of local and global benefits from air pollution con-trol in Mexico City. Environ Sci Technol 2005, 39:1954-1961.
50. Kinney PL, Özkaynak H: Associations of daily mortality and airpollution in Los Angeles County. Environ Res 1991, 54:99-120.
51. Bell ML, McDermott A, Zeger SL, Samet JM, Dominici F: Ozone andshort-term mortality in 95 US urban communities, 1987–2000. J Am Med Assoc 2004, 292:2372-2378.
52. Dominici F: Invited commentary: air pollution and health –what can we learn from a hierarchical approach? Am J Epide-miol 2002, 115:11-15.
53. Farrow RW, Wong E, Ponce RA, Faustman EM, Zerbo RO: Facilitat-ing regulatory design and stakeholder participation: theFERET template with an application to the Clean Air Act. InImproving Regulation: Cases in Environment, Health and Safety Edited by:Fischbeck P, Farrow S. Washington, DC: Resources for the Future;2001.
54. USEPA, Prepared by Abt Associates Inc: Environmental Benefits Map-ping and Analysis Program (BenMAP), Version 2.2 Research TrianglePark, NC: USEPA; 2005.
55. Sanhueza PA, Reed GD, Davis WT, Miller TL: An environmentaldecision-making tool for evaluating ground-level ozone-related health effects. J Air Waste Manage Assoc 2003,53:1448-1459.
56. Hubbell BJ, Hallberg A, McCubbin DR, Post E: Health-related ben-efits of attaining the 8-hr ozone standard. Environ Health Per-spect 2005, 113:73-82.
57. Wong EY, Gohkle J, Griffith WC, Farrow S, Faustman EM: Assessingthe health benefits of air pollution reductions for children.Environ Health Perspect 2004, 112:226-232.
58. Krupnick A, Davis D, Thurston G: The ancillary health benefitsand costs of GHG mitigation: scope, scale, and credibility. InWorkshop on Assessing the Ancillary Benefits and Costs of Greenhouse GasMitigation Strategies Washington, DC: Organization for EconomicCooperation and Development (OECD), Intergovernmental Panel onClimate Change (IPCC); 2000.
59. Committee on Estimating the Health-Risk-Reduction Benefits of Pro-posed Air Pollution Regulations, National Research Council: Estimat-ing the Public Health Benefits of Proposed Air Pollution RegulationsWashington, DC: National Academies Press; 2002.
60. Luttmann-Gibson H, Suh HH, Coull B, Dockery DW, Sarnat SE,Schwartz J, Stone PH, Gold DR: Short-term effects of air pollu-tion on heart rate variability in senior adults in Steubenville,Ohio. J Occup Environ Med 2006, 48:780-788.
61. Dominici F, Peng RD, Bell ML, Pham L, McDermott A, Zeger SL,Samet JM: Fine particulate air pollution and hospital admis-sion for cardiovascular and respiratory diseases. J Am MedAssoc 2006, 295:1127-1134.
62. Peng RD, Dominici F, Pastor-Barriuso R, Zeger SL, Samet JM: Sea-sonal analyses of air pollution and mortality in 100 US cities.Am J Epidemiol 2005, 161:585-594.
63. Sarnat JA, Brown KW, Schwartz J, Coull BA, Koutrakis P: Ambientgas concentrations and personal particulate matter expo-sure. Epidemiology 2005, 16:358-395.
64. Sarnat SE, Coull B, Schwartz J, Gold DR, Suh HH: Factors affectingthe association between ambient concentrations and per-sonal exposures to particles and gases. Environ Health Perspect2006, 114:649-654.
65. Bell ML, Peng RD, Dominici F: The exposure-response curve forozone and risk of mortality and the adequacy of currentozone regulations. Environ Health Perspect 2006, 114:532-536.
66. Daniels MJ, Dominici F, Samet JM, Zeger SL: Estimating particu-late matter-mortality dose-response curves and thresholdlevels: an analysis of daily time-series for the 20 largest UScities. Am J Epidemiol 2000, 152:397-406.
67. Bell ML, Davis D, Cifuentes L, Cohen A, Gouveai N, Grant L, GreenC, Johnson T, Rogat J, Spengler J, Thurston G: International expertworkshop on the analysis of the economic and public healthimpacts of air pollution: workshop summary. Environ HealthPerspect 2002, 110:1163-1168.
68. Zhang Y, Huang W, London SJ, Song G, Chen G, Jiang L, Zhao N,Chen B, Kan H: Ozone and daily mortality in Shanghai, China.Environ Health Perspect 2006, 114:1227-1232.
69. Tsai SS, Cheng MH, Chiu HF, Wu TN, Yang CY: Air pollution andhospital admissions for asthma in a tropical city: Kaohsiung,Taiwan. Inhal Toxicol 2006, 18:549-554.
70. O'Neill MS, Loomis D, Borja-Aburto V, Gold D, Hertz-Picciotto I,Castillejos M: Do associations between airborne particles anddaily mortality in Mexico City differ by measurementmethod, region, or modeling strategy? J Expo Anal Environ Epi-demiol 2004, 14:429-439.
71. Gouveia N, Bremner SA, Novaes HMD: Associations betweenambient air pollution and birth weight in São Paulo, Brazil. JEpidemiol Community Health 2004, 58:11-17.
72. Eftim S, Dominici F: Multisite time-series studies versus cohortstudies: methods, findings, and policy implications. J ToxicolEnvironm Health A 2005, 68:1191-1205.
73. Thomas D: Why do estimates of the acute and chronic effectsof air pollution on mortality differ? J Toxicol Environm Health A2005, 68:1167-1174.
74. Künzli N, Medina S, Kaiser R, Quénel P, Horak FJ Jr, Studnicka M:Assessment of deaths attributable to air pollution: should weuse risk estimates based on time series or on cohort studies?Am J Epidemiol 2001, 153:1050-1055.
75. Aunan K, Fang J, Vennemo H, Oye K, Seip HM: Co-benefits of cli-mate policy-lessons learned from a study in Shanxi, China.Energy Policy 2004, 32:567-581.
76. Bell ML, Dominici F, Samet JM: A meta-analysis of time-seriesstudies of ozone and mortality with comparison to theNational Morbidity, Mortality and Air Pollution Study. Epide-miology 2005, 16:436-445.
77. Ito K, De Leon SF, Lippmann M: Associations between ozone anddaily mortality: analysis and meta-analysis. Epidemiology 2005,16:446-457.
78. Levy JI, Chemerynski S, Sarnat JA: Ozone exposure and mortal-ity: an empiric bayes metaregression analysis. Epidemiology2005, 16:458-468.
79. Fung K, Krewski D, Burnett R, Ramsay T, Chen Y: Testing the har-vesting hypothesis by time-domain regression analysis, II:covariate effects. J Toxicol Environm Health A 2005, 68:1155-1165.
80. Schwartz J: Is there harvesting in the association of airborneparticles with daily deaths and hospital admissions? Epidemi-ology 2001, 12:55-61.
81. Schwartz J: Harvesting and long term exposure effects in therelation between air pollution and mortality. Am J Epidemiol2000, 151:440-448.
82. Zeger SL, Dominici F, Samet J: Harvesting-resistant estimates ofair pollution effects on mortality. Epidemiology 1999,10:171-175.
83. Dominici F, Daniels M, McDermott A, Zeger SL, Samet JM: Shape ofthe exposure-response relation and mortality displacementin the NMMAPS database. In Revised Analyses of Time-Series Stud-ies of Air Pollution and Health Boston, MA: Health Effects Institute;2003.
84. Woodruff TJ, Grillo J, Schoendorf KC: The relationship betweenselected causes of postneonatal infant mortality and partic-
Page 15 of 18(page number not for citation purposes)

Environmental Health 2008, 7:41 http://www.ehjournal.net/content/7/1/41
ulate air pollution in the United States. Environ Health Perspect1997, 105:608-612.
85. Bobak M, Leon DA: Air pollution and infant mortality in theCzech Republic, 1986–88. Lancet 1992, 340:1010-1014.
86. Bobak M, Leon DA: The effect of air pollution on infant mortal-ity appears specific for respiratory causes in the postneona-tal period. Epidemiology 1999, 10:666-670.
87. Bell ML, Hobbs BF, Elliott EM, Ellis H, Robinson Z: An evaluation ofmulti-criteria methods in integrated assessment of climatepolicy. J Multi-Criteria Dec Anal 2001, 10:229-256.
88. Bell ML, Hobbs BF, Ellis H: The use of multi-criteria decision-making methods in integrated assessment of climatechange: implications for IA practitioners. Socioecon Plann Sci2003, 37:289-316.
89. Georgopoulou E, Sarafides Y, Mirasgedis S, Zaimi S, Lalas DP: A mul-tiple criteria decision-aid approach in defining national prior-ities for greenhouse gases emissions reduction in the energysector. Eur J Oper Res 2003, 146:199-215.
90. Borges PC, Villavicencio A: Avoiding academic and decorativeplanning in GHG emissions abatement studies with MCDA:the Peruvian case. Eur J Oper Res 2004, 152:641-654.
91. Shabman L, Stephenson K: Environmental valuation and its eco-nomic critics. J Water Resour Plann Manag 2000, 126:382-388.
92. Freeman AM: The Measurement of Environmental and Resource Values:Theory and Methods Washington, DC: Resources for the Future; 1993.
93. Hartunian NS, Smart CN, Thompson MS: The Incidence and EconomicCosts of Major Health Impairments: a Comparative Analysis of Cancer,Motor Vehicle Injuries, Coronary Heart Disease, and Stroke Lexington,MA: Lexington Books; 1981.
94. Kirchstein R: Disease-Specific Estimates of Direct and Indirect Costs of Ill-ness and NIH Support. Fiscal Year 2000 Update Bethesda, MD: NationalInstitutes of Health; 2000.
95. Hammitt JK, Liu JT: Effects of disease type and latency on thevalue of mortality risk. J Risk Uncertain 2004, 28:73-95.
96. Moore MJ, Vicusi WK: The quality-adjusted value of life. Econ Inq1988, 26:369-388.
97. Leung J, Guria J: Value of statistical life: adults versus children.Accid Anal Prev 2006, 38:1208-1217.
98. Hwang HS, Morgenstern DT, Reed WR: Hedonic wages and labormarket search. J Labor Econ 1998, 16:815-847.
99. Wei X: Estimating British workers' demand for safety. ApplEcon 1999, 31:1265-1271.
100. Dardis R: The value of a life: new evidence from the market-place. Am Econ Rev 1980, 70:1077-1082.
101. Ashenfelter O, Greenstone M: Using Mandated Speed Limits to Measurethe Value of a Statistical Life. IZA Discussion Paper No. 571; FEEM Work-ing Paper No. 65 2002.
102. Smith VK, Huang JC: Hedonic models and air pollution: twenty-five years and counting. Environ Resour Econ 1993, 3:381-394.
103. Hammitt JK, Graham JD: Willingness to pay for health protec-tion: inadequate sensitivity to probability. J Risk Uncertain 1999,181:33-62.
104. Jones-Lee MW, Hammerton M, Phillips PR: The value of safety:results of a national sample survey. Econ J 1985, 95:49-72.
105. Desvousges WH, Johnson FR, Hudson SP, Gable AR, Ruby MC: UsingConjoint Analysis and Health-State Classifications to Estimate the Value ofHealth Effects on Air Pollution: Pilot Test Results and Implications. FinalReport Raleigh, NC: Triangle Economic Research; 1996.
106. Johannesson M, Johannson PO: To be, or not to be, that is thequestion: an empirical study of the WTP for an increased lifeexpectancy at an advanced age. J Risk Uncertain 1996,13:163-174.
107. Hammitt J, Zhou Y: The economic value of air-pollution-related health risks in China: a contingent valuation study.Environ Resour Econ 2006, 33:399-423.
108. Wang H, Mullahy J: Willingness to pay for reducing fatal risk byimproving air quality: a contingent valuation study in Chong-qing, China. Sci Total Environ 2006, 367:50-57.
109. Krupnick A, Alberini A, Cropper M, Simon N, O'Brien B, Goeree R,Heintzelman M: Age, health, and the willingness to pay formortality risk reductions: a contingent valuation survey ofOntario residents. J Risk Uncertain 2002, 24:161-186.
110. Alberini A, Cropper M, Krupnick A, Simon NB: Does the value ofa statistical life vary with age and health status? Evidencefrom the US and Canada. J Environ Econ Manage 2004,48:769-792.
111. Alberini A, Hunt A, Markandya A: Willingness to pay to reducemortality risks: evidence from a three-country contingentvaluation study. Environ Resour Econ 2006, 33:251-264.
112. Krupnick AJ, Cropper ML: The effect of information on healthrisk valuation. J Risk Uncertain 1992, 5:29-48.
113. Viscusi WK, Magat WA, Huber J: Pricing environmental healthrisks: survey assessments of risk-risk and risk-dollar trade-offs for chronic bronchitis. J Environ Econ Manage 1991, 21:32-51.
114. Bateman IJ, Brouwer R: Consistency and construction in statedWTP for health risk reductions: a novel scope-sensitivitytest. Resour Energy Economics 2006, 28:199-214.
115. Leighl NB, Tsao WS, Zawisza DL, Nematollahi M, Shepherd FA: Awillingness-to-pay study of oral epidermal growth factortyrosine kinase inhibitors in advanced non-small cell lungcancer. Lung Cancer 2006, 51:115-121.
116. Dickie M, Gerking SD, Brookshire DS, Coursey DL, Schulze WD,Coulson A, Tashkin D: Improving Accuracy and Reducing Costs of Envi-ronmental Benefit Assessments: Reconciling Averting Behavior and Contin-gent Valuation Benefit Estimates of Reducing Symptoms of OzoneExposure, Draft Washington, DC: USEPA; 1987.
117. Loehman ET, Berg SV, Arroyo AA: Distributional analysis ofregional benefits and cost of air quality control. J Environ EconManage 1979, 6:222-243.
118. Tolley G, Babcock L, Berger M, Bilotti A, Blomquist G, Brien M, FabianR, Fishelson G, Kahn C, Kelly A, Kenkel D, Krumm R, Miller T, Ohs-feldt R, Rosen S, Webb W, Wilson W, Zelder M: Valuation of Reduc-tions in Human Health Symptoms and Risks Washington, DC: USEPA;1986.
119. Navrud S: Valuing health impacts from air pollution inEurope. Environ Res Econ 2001, 20:305-329.
120. Beggs PJ: Impacts of climate change on aeroallergens: pastand future. Clin Exp Allergy 2004, 34:1507-1513.
121. Miller W, Robinson LA, Lawrence RS, eds: Institute of Medicine(IOM) Committee to Evaluate Measures of Health Benefitsfor Environmental, Health, and Safety Regulation. In ValuingHealth for Regulatory Cost-Effectiveness Analysis Washington, DC: Insti-tute of Medicine of the National Academies; 2006.
122. Hubbell BJ: Implementing QALYs in the analysis of air pollu-tion regulations. Environ Resour Econ 2006, 34:365-384.
123. van Houtven G, Powers J, Jessup A, Yang JC: Valuing avoided mor-bidity using meta-regression analysis: what can health statusmeasures and QALYs tell us about WTP? Health Econ 2006,15:775-795.
124. Briggs AH, Bousquet J, Wallace MV, Busse WW, Clark TJH, PedersenSE, Bateman ED: Cost-effectiveness of asthma control: an eco-nomic appraisal of the GOAL study. Allergy 2006, 61:531-536.
125. Bickel P, Friedrich RE: ExternE, Externalities of Energy, Methodology2005 Update Luxemburg: European Commission; 2005.
126. Stratus Consulting: Air Quality Valuation Model Documentation, forHealth Canada Boulder, CO: Stratus Consulting, Inc; 1999.
127. AEA Technology Environment: Methodology for the Cost-Benefit Analysisfor CAFÉ: Uncertainty in the CAFÉ CBA: Methods and First Analysis Volume3. Issue 1 AEAT/ED51014/Methodology; 2005.
128. Australian Department of Transport and Regional Services Bureau ofTransport and Regional Economics (BTRE): Working Paper 63: HealthImpacts of Transport Emissions in Australia: Economic Costs Departmentof Transport and Regional Services, BTRE; 2005.
129. Bicknell K: WTP for the Benefits of Environmental Improvement: A Litera-ture Review and Some Recommendations Prepared for EnvironmentCanterbury. Report No. U01/89; 2001.
130. Lee R: Estimating the Externalities of Electricity Fuel Cycles Washington,DC: McGraw-Hill/Utility Data Institute; 1995.
131. Markandyac A: Economic Valuation in ExternE: Externalities of Energy:Methodology Volume 2. Brussels: Commission of the European Com-munities, DGXII; 1996.
132. Hagler Bailly Consulting Inc: The New York State Externalities Cost StudyDobbs Ferry, NY: Oceana Publications; 1995.
133. Pratt JW, Zeckhauser RJ: Willingness to pay and the distributionof risk and wealth. J Polit Econ 1996, 104:747-763.
134. Broome J: The ethics of climate change. Sci Am 2008,298:96-102.
135. USEPA: Regulatory Impact Analysis for the Final Clean Air Interstate RuleWashington, DC: USEPA; 2005. EPA-452/R-05-002
136. Voorhees AS, Sakai R, Araki S, Sato H, Otsu A: Benefits analysis ofnitrogen dioxide control programmes: a case-study of Chiy-oda-ku, Tokyo. J Environ Plann Manag 2001, 44:149-165.
Page 16 of 18(page number not for citation purposes)

Environmental Health 2008, 7:41 http://www.ehjournal.net/content/7/1/41
137. Voorhees SA: Benefits analysis of particulate matter controlprograms – a case study of Tokyo. J Risk Res 2005, 8:331-329.
138. Filleul L, Rondeau V, Vandentorren S, Le Moual N, Cantagrel A,Annesi-Maesano I, Charpin D, Declercq C, Neukirch F, Paris C, Verv-loet D, Brochard P, Tessier JF, Kauffmann F, Baldi I: Twenty fiveyear mortality and air pollution: results from the FrenchPAARC survey. Occup Environ Med 2005, 62:453-460.
139. Krewski D, Burnett R, Jerrett M, Pope CA, Rainham D, Calle E,Thurston G, Thun M: Mortality and long-term exposure toambient air pollution: ongoing analyses based on the Amer-ican Cancer Society cohort. J Toxicol Environm Health A 2005,68:1093-1109.
140. Gendo K, Sullivan SD, Lozano P, Finkelstein JA, Fuhlbrigge A, WeissKB: Resource costs for asthma-related care among pediatricpatients in managed care. Ann Allergy Asthma Immunol 2003,91:251-287.
141. Stevens CA, Turner D, Kuehni CE, Couriel JM, Silverman M: Theeconomic impact of preschool asthma and wheeze. Eur RespirJ 2003, 21:1000-1006.
142. Ungar WJ, Coyte PC: Prospective study of the patient-levelcost of asthma care in children. Pediatr Pulmonol 2001,32:101-108.
143. Akker-van Marle ME van den, Bruil J, Detmar SB: Evaluation of costof disease: assessing the burden to society of asthma in chil-dren in the European Union. Allergy 2005, 60:140-149.
144. Agee MD, Crocker TD: Transferring measures of adult healthbenefits to children: a review of issues and results. ContempEcon Policy 2004, 22:468-482.
145. Blakely TA, Collings SCD, Atkinson J: Unemployment and sui-cide: evidence for a causal association? J Epidemiol CommunityHealth 2003, 57:594-600.
146. Kposowa AJ: Unemployment and suicide: a cohort analysis ofsocial factors predicting suicide in the US National Longitu-dinal Mortality Study. Psychol Med 2001, 31:127-138.
147. Grande ED, Hickling J, Taylor A, Woollacott T: Domestic violencein South Australia: a population survey of males and females.Aust N Z J Public Health 2003, 27:543-550.
148. Kyriacou DN, Anglin D, Taliferro E, Stone S, Tubb T, Linden JA, Muel-leman R, Barton E, Kraus JF: Risk factors for injury to womenfrom domestic violence. N Engl J Med 1999, 341:1892-1898.
149. Caetano R, Cunradi C: Intimate partner violence and depres-sion among Whites, Blacks and Hispanic. Ann Epidemiol 2003,13:661-665.
150. Artazcoz L, Benach J, Borrell C, Cortès I: Unemployment andmental health: understanding the interactions among gen-der, family roles, and social class. Am J Public Health 2004,94:82-88.
151. Comino EJ, Harris E, Chey T, Manicavasagar V, Penrose Wall J, PowellDavies G, Harris MF: Relationship between mental health dis-orders and unemployment status in Australian adults. Aust NZ J Psychiatry 2003, 37:230-235.
152. Markandya A: The valuation of health impacts in developingcountries. Planejamento e Politicas Publicas 1999, 18:119-154.
153. Aaheim HA, Kristin A, Seip HM: Climate change and local pollu-tion effects – an integrated approach. Mitigation Adapt StrategGlob Chang 1999, 4:61-81.
154. Changhong C, Bingyan W, Qingyan F, Green C, Streets DG: Reduc-tions in emissions of local air pollutants and co-benefits ofChinese energy policy: a Shanghai case study. Energy Policy2006, 34:754-762.
155. Dessus S, O'Connor D: Climate policy without tears: CGE-based ancillary benefits estimates for Chile. Environ Resour Econ2003, 25:287-317.
156. Dudek D, Golub A, Strukova E: Ancillary benefits of reducinggreenhouse gas emissions in transitional economies. WorldDev 2003, 13:1759-1769.
157. Mazzi EA, Dowlatabadi H: Air quality impacts of climate mitiga-tion: UK policy and passenger vehicle choice. Environ Sci Tech-nol 2007, 41:387-392.
158. Syri S, Karvosenoja N, Lehtilä A, Laurila T, Lindfors V, Tuovinen JP:Modeling the impacts of the Finnish climate strategy on airpollution. Atmos Environ 2002, 36:3059-3069.
159. van Vuuren D, Fengqi Z, de Vries B, Kejun J, Graveland C, Yun L:Energy and emission scenarios for China in the 21st century– exploration of baseline development and mitigationoptions. Energy Policy 2003, 31:369-387.
160. Aunan K: Exposure-response functions for health effects of airpollutants based on epidemiological findings. Risk Anal 1996,16:693-709.
161. Aunan K, Fang J, Li G, Seip HM, Vennemo H: Co-Benefits from CO2-emission Reduction Measures in Shanxi, China Oslo: CIERCO; 2000.
162. Schwartz J, Dockery DW: Particulate air pollution and dailymortality in Steubenville, Ohio. Am J Epidemiol 1992, 135:12-19.
163. USEPA: Regulatory Impact Analysis for the Particulate Matter and OzoneNational Ambient Air Quality Standards and Proposed Regional Haze RuleResearch Triangle Park, NC: USEPA; 1997.
164. Pope CA 3rd, Thun MJ, Namboodiri MM, Dockery DW, Evans JS,Speizer FF, Heath CW Jr: Particulate air pollution as a predictorof mortality in a prospective study of U.S. adults. Am J RespirCrit Care Med 1995, 151:669-674.
165. Borja-Aburto V, Loomis DP, Bangdiwala SI, Shy CM, Rascon-PachecoRA: Ozone, suspended particulates, and daily mortality inMexico City. Am J Epidemiol 1997, 145:258-268.
166. Cifuentes LA, Vega J, Köpfer K, Lave L: Effect of the fine fractionof particulate matter versus the coarse mass and other pol-lutants on daily mortality in Santiago, Chile. J Air Waste Man-age Assoc 2000, 50:1287-1298.
167. Dockery DW, Pope CA, Xu X, Spengler JD, Ware JH, Fay ME, FerrisBG Jr, Speizer FE: An association between air pollution andmortality in six U.S. cities. N Engl J Med 1993, 329:1753-1759.
168. Saldiva PH, Pope CA, Schwartz J, Dockery DW, Lichtenfels AJ, SalgeJM, Barone IA, Bohm GM: Air pollution and mortality in elderlypeople: a time-series study in Sao Paulo, Brazil. Arch EnvironHealth 1995, 50:159-163.
169. Gouveia N, Fletcher T: Time series analysis of air pollution andmortality: effects by cause, age, and socioeconomic status. JEpidemiol Community Health 2000, 54:750-755.
170. Loomis D, Castillejos M, Gold DR, McDonnell W, Borja-Aburto VH:Air pollution and infant mortality in Mexico City. Epidemiology1999, 10:118-123.
171. Pope CA, Dockery DW, Spengler JD, Raizenne ME: Respiratoryhealth and PM10 pollution: a daily time series analysis. Am RevRespir Dis 1991, 144:668-674.
172. Thurston GD, Ito K, Kinney PL, Lippmann M: A multi-year studyof air pollution and respiratory hospital admissions in threeNew York State Metropolitan areas: results for 1998 and1989 summers. J Expo Anal Environ Epidemiol 1992, 2:429-450.
173. Barton D, Tets-Grimm K, Kattan M: Emergency room patternsof inner city children for asthma [Abstract]. Am Rev Respir Dis1993, 47:A577.
174. Abbey DE, Petersen F, Mills PK, Beeson WL: Long-term ambientconcentrations of total suspended particulates, ozone andsulfur dioxide and respiratory symptoms in a nonsmokingpopulation. Arch Environ Health 1993, 48:33-46.
175. Whittemore AS, Korn EL: Asthma and air pollution in the LosAngeles area. Am J Public Health 1980, 70:687-696.
176. Ostro BD: Air pollution and morbidity revisited: a specifica-tion test. J Environ Manage 1987, 14:87-98.
177. Ostro BD: Associations between morbidity and alternativemeasures of particulate matter. Risk Anal 1990, 10:421-427.
178. Ostro B, Rothschild S: Air pollution and acute respiratory mor-bidity: an observational study of multiple pollutants. EnvironRes 1989, 50:238-247.
179. Portney PR, Mullahy J: Urban air quality and chronic respiratorydisease. Reg Sci Urban Econ 1990, 20:407-418.
180. Krupnick A, Harrington W, Ostro B: Ambient ozone and acutehealth effects: evidence from daily data. J Environ Econ Manage1990, 18:1-18.
181. World Bank: Chile: Managing Environmental Problems: Economic Analysisof Selected Issues Washington, DC: World Bank; 1994.
182. Ostro BD, Eskeland GS, Sanchez JM, Feyzioglu T: Air pollution andhealth effects: a study of medical visits among children inSantiago, Chile. Environ Health Perspect 1999, 107:69-73.
183. Pope CA, Burnett RT, Thun MJ, Calle EE, Krewski D, Ito K, ThurstonGD: Lung cancer, cardiopulmonary mortality, and long-termexposure to fine particulate air pollution. J Am Med Assoc 2002,287:1132-1141.
184. COMEAP: Quantification of the Effects of Air Pollution on Health in theUnited Kingdom London: The Stationary Office; 1998.
185. Stedman JR, King K, Holland M, Walton H: Quantification of the HealthEffects of Air Pollution in the UK for Revised PM10 Objective Analysis Lon-don: AEA Technology and UK Department of Health; 2002.
Page 17 of 18(page number not for citation purposes)

Environmental Health 2008, 7:41 http://www.ehjournal.net/content/7/1/41
Publish with BioMed Central and every scientist can read your work free of charge
"BioMed Central will be the most significant development for disseminating the results of biomedical research in our lifetime."
Sir Paul Nurse, Cancer Research UK
Your research papers will be:
available free of charge to the entire biomedical community
peer reviewed and published immediately upon acceptance
cited in PubMed and archived on PubMed Central
yours — you keep the copyright
Submit your manuscript here:http://www.biomedcentral.com/info/publishing_adv.asp
BioMedcentral
186. Evans JS, Spengler J, Levy J, Hammitt J, Suh H, Serrano P, Rojas-BrachoL, Santos-Burgoa C, Rojas-Rodriguez H, Caballero-Ramirez M, Cas-tillejos M: Contaminación Atmosférica y Salud Humana en la Ciudad diMéxico La Jolla, CA: MIT-IPURGAP Report No. 10; 2000.
187. Levy JI, Carrothers TJ, Tuomisto JT, Hammitt JK, Evans JS: Assessingthe public health benefits of reduced ozone concentrations.Environ Health Perspect 2001, 109:1215-1226.
188. Abbey DE, Lebowitz MD, Mills PK, Petersen FF, Beeson WL, BurchettRJ: Long-term ambient concentrations of particulates andoxidants and development of chronic disease in a cohort ofnonsmoking California residents. Inhal Toxicol 1995, 7:19-34.
189. Instituto Nacional de Salud Pública: Integrated Environmental Strategies:Health Effects Component Cuernavaca, Mexico: Instituto Nacional deSalud Pública; 2003.
190. Dockery D, Pope CA: Epidemiology of acute health effects:summary of time-series. In Particles in Our Air: Concentrations andHealth Effects Edited by: Wilson R, Spengler J. Cambridge, MA: Har-vard University Press; 1996.
191. Pope C, Dockery D: Epidemiology of chronic health effects:summary of time-series. In Particles in Our Air: Concentrations andHealth Effects Edited by: Wilson R, Spengler J. Cambridge, MA: Har-vard University Press; 1996.
192. Xu X, Gao J, Dockery DW, Chen Y: Air pollution and daily mor-tality in residential areas of Beijing, China. Arch Environ Health1994, 49:216-222.
193. Pope CA: Respiratory hospital admissions associated withPM10 pollution in Utah, Salt Lake and Cache Valleys. ArchEnviron Health 1991, 46:90-97.
194. Samet JM, Bishop Y, Speizer FE, Spengler JD, Ferris BG: The rela-tionship between air pollution and emergency room visits inan industrial community. J Air Pollut Control Assoc 1981,31:236-240.
195. Dockery DW, Speizer FE, Stram DO, Ware JH, Spengler JD, FerrisBG: Effects of inhalable particles on respiratory health of chil-dren. Am Rev Respir Dis 1989, 139:587-594.
196. Ostro BD, Lipsett MJ, Weiner MB, Selner JC: Asthmatic responseto airborne acid aerosols. Am J Public Health 1991, 81:694-702.
197. University of British Columbia: Purchasing Power Parity Exchange Rate2006.
198. New Zealand Ministry for Environment: Proposed National Environmen-tal Standards for Air Quality, Resource Management Act Section 32 2004.
199. Australian Institute of Health and Welfare: Australian Hospital Statistics2000–01, Appendix 8. Health Services Series, Number 19 2002.
200. DSS Management Consultants Inc., RWDI Air Inc., prepared forOntario Ministry of Energy: Cost-Benefit Analysis: Replacing Ontario'sCoal-Fired Electricity Generation 2005.
Page 18 of 18(page number not for citation purposes)
Copyright © 2022 FDOKUMEN