
Analysis of ALK-1 and endoglin in newborns from families with hereditary hemorrhagic telangiectasia...
12
© 2000 Oxford University Press Human Molecular Genetics, 2000, Vol. 9, No. 8 1227–1237 Analysis of ALK-1 and endoglin in newborns from families with hereditary hemorrhagic telangiectasia type 2 Salma A. Abdalla, Nadia Pece-Barbara, Sonia Vera, Esther Tapia 1 , Eduardo Paez 1 , Carmelo Bernabeu 1 and Michelle Letarte + Cancer and Blood Research Programme, The Hospital for Sick Children, and Department of Immunology, University of Toronto, Toronto M5G 1X8, Canada and 1 Centro de Investigaciones Biologicas, Consejo Superior de Investigaciones Cientificas (CSIC), Madrid, Spain Received 28 January 2000; Revised and Accepted 5 March 2000 ALK-1 (activin receptor-like kinase-1), a type I receptor of the transforming growth factor (TGF)-β superfamily, is the gene mutated in hereditary hemorrhagic telangiectasia type 2 (HHT2) while endoglin is mutated in HHT1. Using a novel polyclonal antibody to ALK-1, we measured ALK-1 expression on human umbilical vein endothelial cells (HUVEC) of newborns from HHT families whose affected members had normal endoglin levels. ALK-1 levels were specifically reduced in three HUVEC with ALK-1 missense mutant codons, and normal in two newborns not carrying the missense mutations present in the clinically affected relatives. Levels were also normal in a HUVEC with deletion of S232 in the ATP binding site of ALK-1. Thus HHT2 appears to be associated with a loss of function of the mutant allele due to a reduction in either protein level or activity. We also report three new ALK-1 missense mutations leading to G48E/A49P, C344Y and E407D substitutions. In COS-1 transfected cells, ALK-1 was found in the TGF-β1 and -β3 receptor complexes in association with endoglin and TβRII, but not in activin receptor complexes containing endoglin. In HUVEC, ALK-1 was not detectable in the TGF-β1 or -β3 receptor complexes. However, in the absence of ligand, ALK-1 and endoglin interactions were observed by immuno- precipitation/western blot in HUVEC from normal as well as HHT1 and HHT2 patients. Our data suggest a transient association between these two proteins of the TGF-β superfamily, both required at a critical level to ensure vessel wall integrity. INTRODUCTION Hereditary hemorrhagic telangiectasia (HHT) is an autosomal dominant disorder characterized by multisystemic vascular dysplasia (1). Molecular heterogeneity of the disease has been revealed by genetic linkage studies and identification of two distinct loci. The first locus was mapped to chromosome 9q33 (2,3) and endoglin was recognized as the affected gene in HHT1 (4). The second locus was mapped to chromosome 12q13 (5,6) and ALK-1 (activin receptor-like kinase-1) was identified as the gene mutated in HHT2 (7). The clinical features of the disorder include recurrent nosebleeds, muco- cutaneous telangiectases and arteriovenous malformations (AVMs) in lung, brain and liver (8–11). Families with HHT1 have a higher incidence of pulmonary involvement while HHT2 families tend to have a later onset and milder manifesta- tions of the disease (12–14). Both endoglin and ALK-1 gene products are highly expressed on endothelial cells (15,16) and are associated with the transforming growth factor (TGF)-β superfamily. TGF-β and related factors signal through a heteromeric complex of related Ser/Thr kinase receptors, type I (also known as activin- like kinases, ALKs) and type II (17). ALK-1 was shown to bind TGF-β or activin in COS cells when co-expressed with the corresponding type II receptors (16,18,19) but the natural ALK-1 ligand in vivo remains unknown. For TGF-β, the type II receptor (TβRII) binds ligand, recruits, transphosphorylates and activates the type I receptor (TβRI/ALK-5) (20,21). The type I receptors act on a family of downstream effector proteins known as Smads (22,23). Bone morphogenetic proteins (BMPs) generally signal through Smads 1 and 5 (24,25), whereas activin and TGF-β signal through Smads 2 and 3 (26). In a recent study, a constitutively active form of ALK-1 activated Smad 1 and 5 but not Smad 2 pathways (27), suggesting that ALK-1 functions in regulating BMP signaling. Endoglin, a homodimeric membrane glycoprotein was shown to interact with TGF-β1, TGF-β3, activin-A, BMP-2 and BMP-7, when co-expressed in COS-1 cells with the respective ligand binding kinase receptors (28). ALK-1 shares a high degree of similarity with other type I receptors in the Ser/Thr kinase subdomains, Gly/Ser (GS) rich domain and short C-terminal tail (16,29). There are 10 Cys residues in the extracellular domain, the spacing of which is conserved among type I receptors (17) and is likely to be crit- ical for ligand binding. The intracellular region consists almost entirely of the kinase domain that contains 12 subdomains with conserved amino acids (30). To date, 18 mutations have been + To whom correspondence should be addressed. Tel: +1 416 813 6258; Fax: +1 416 813 6255; Email: [email protected]
-
Upload
philippines -
Category
Documents
-
view
1 -
download
0
Transcript of Analysis of ALK-1 and endoglin in newborns from families with hereditary hemorrhagic telangiectasia...

© 2000 Oxford University Press Human Molecular Genetics, 2000, Vol. 9, No. 8 1227–1237
Analysis of ALK-1 and endoglin in newborns fromfamilies with hereditary hemorrhagic telangiectasiatype 2Salma A. Abdalla, Nadia Pece-Barbara, Sonia Vera, Esther Tapia1, Eduardo Paez1,Carmelo Bernabeu1 and Michelle Letarte+
Cancer and Blood Research Programme, The Hospital for Sick Children, and Department of Immunology,University of Toronto, Toronto M5G 1X8, Canada and 1Centro de Investigaciones Biologicas,Consejo Superior de Investigaciones Cientificas (CSIC), Madrid, Spain
Received 28 January 2000; Revised and Accepted 5 March 2000
ALK-1 (activin receptor-like kinase-1), a type I receptorof the transforming growth factor (TGF)-β superfamily,is the gene mutated in hereditary hemorrhagictelangiectasia type 2 (HHT2) while endoglin is mutatedin HHT1. Using a novel polyclonal antibody to ALK-1,we measured ALK-1 expression on human umbilicalvein endothelial cells (HUVEC) of newborns from HHTfamilies whose affected members had normal endoglinlevels. ALK-1 levels were specifically reduced in threeHUVEC with ALK-1 missense mutant codons, andnormal in two newborns not carrying the missensemutations present in the clinically affected relatives.Levels were also normal in a HUVEC with deletion ofS232 in the ATP binding site of ALK-1. Thus HHT2appears to be associated with a loss of function of themutant allele due to a reduction in either protein level oractivity. We also report three new ALK-1 missensemutations leading to G48E/A49P, C344Y and E407Dsubstitutions. In COS-1 transfected cells, ALK-1 wasfound in the TGF-β1 and -β3 receptor complexes inassociation with endoglin and TβRII, but not in activinreceptor complexes containing endoglin. In HUVEC,ALK-1 was not detectable in the TGF-β1 or -β3 receptorcomplexes. However, in the absence of ligand, ALK-1and endoglin interactions were observed by immuno-precipitation/western blot in HUVEC from normal aswell as HHT1 and HHT2 patients. Our data suggest atransient association between these two proteins of theTGF-β superfamily, both required at a critical level toensure vessel wall integrity.
INTRODUCTION
Hereditary hemorrhagic telangiectasia (HHT) is an autosomaldominant disorder characterized by multisystemic vasculardysplasia (1). Molecular heterogeneity of the disease has beenrevealed by genetic linkage studies and identification of twodistinct loci. The first locus was mapped to chromosome 9q33
(2,3) and endoglin was recognized as the affected gene inHHT1 (4). The second locus was mapped to chromosome12q13 (5,6) and ALK-1 (activin receptor-like kinase-1) wasidentified as the gene mutated in HHT2 (7). The clinicalfeatures of the disorder include recurrent nosebleeds, muco-cutaneous telangiectases and arteriovenous malformations(AVMs) in lung, brain and liver (8–11). Families with HHT1have a higher incidence of pulmonary involvement whileHHT2 families tend to have a later onset and milder manifesta-tions of the disease (12–14).
Both endoglin and ALK-1 gene products are highlyexpressed on endothelial cells (15,16) and are associated withthe transforming growth factor (TGF)-β superfamily. TGF-βand related factors signal through a heteromeric complex ofrelated Ser/Thr kinase receptors, type I (also known as activin-like kinases, ALKs) and type II (17). ALK-1 was shown tobind TGF-β or activin in COS cells when co-expressed withthe corresponding type II receptors (16,18,19) but the naturalALK-1 ligand in vivo remains unknown. For TGF-β, the typeII receptor (TβRII) binds ligand, recruits, transphosphorylatesand activates the type I receptor (TβRI/ALK-5) (20,21). Thetype I receptors act on a family of downstream effectorproteins known as Smads (22,23). Bone morphogeneticproteins (BMPs) generally signal through Smads 1 and 5(24,25), whereas activin and TGF-β signal through Smads 2and 3 (26). In a recent study, a constitutively active form ofALK-1 activated Smad 1 and 5 but not Smad 2 pathways (27),suggesting that ALK-1 functions in regulating BMP signaling.Endoglin, a homodimeric membrane glycoprotein was shownto interact with TGF-β1, TGF-β3, activin-A, BMP-2 andBMP-7, when co-expressed in COS-1 cells with the respectiveligand binding kinase receptors (28).
ALK-1 shares a high degree of similarity with other type Ireceptors in the Ser/Thr kinase subdomains, Gly/Ser (GS) richdomain and short C-terminal tail (16,29). There are 10 Cysresidues in the extracellular domain, the spacing of which isconserved among type I receptors (17) and is likely to be crit-ical for ligand binding. The intracellular region consists almostentirely of the kinase domain that contains 12 subdomains withconserved amino acids (30). To date, 18 mutations have been
+To whom correspondence should be addressed. Tel: +1 416 813 6258; Fax: +1 416 813 6255; Email: [email protected]
1228 Human Molecular Genetics, 2000, Vol. 9, No. 8
reported in the coding region of the ALK-1 gene (7,31,32).These mutations are found in the extracellular, transmembraneand kinase domains of ALK-1 and include small deletions,insertions and nonsense mutations leading to truncatedproteins, as well as missense mutations.
In this study, we describe three new missense mutations inthe coding region of the ALK-1 gene and also identify innewborns, mutations previously published in their affectedfamily members. A novel polyclonal antibody to ALK-1 wasused to measure protein levels on seven human umbilical veinendothelial cells (HUVEC) of newborns from HHT2 families.This allowed us to establish that some mutations in the ALK-1gene, which alter important structural residues, led to reductionor absence of expression of the mutant proteins. However, onemutation in the ATP binding site did not alter the level ofprotein expression but likely inactivated the enzyme. We alsodemonstrate the association of ALK-1 and endoglin inendothelial cells of normal and HHT newborns.
RESULTS
Characterization of a polyclonal antibody to ALK-1
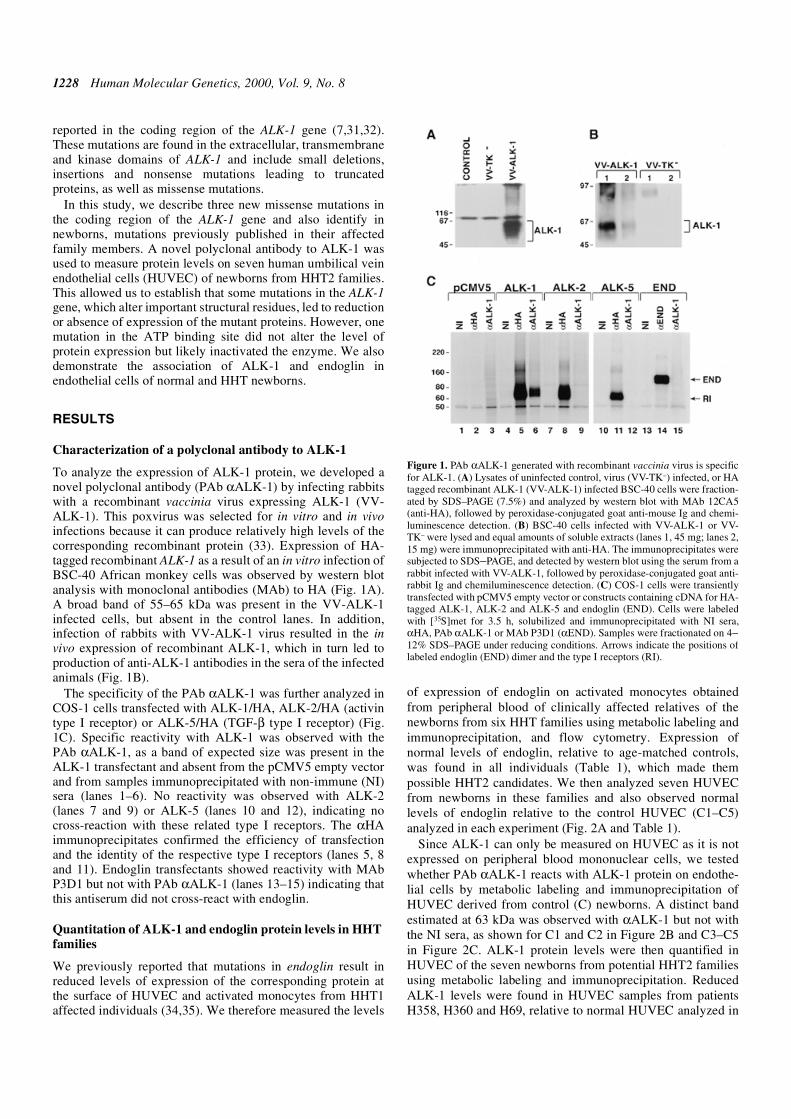
To analyze the expression of ALK-1 protein, we developed anovel polyclonal antibody (PAb αALK-1) by infecting rabbitswith a recombinant vaccinia virus expressing ALK-1 (VV-ALK-1). This poxvirus was selected for in vitro and in vivoinfections because it can produce relatively high levels of thecorresponding recombinant protein (33). Expression of HA-tagged recombinant ALK-1 as a result of an in vitro infection ofBSC-40 African monkey cells was observed by western blotanalysis with monoclonal antibodies (MAb) to HA (Fig. 1A).A broad band of 55–65 kDa was present in the VV-ALK-1infected cells, but absent in the control lanes. In addition,infection of rabbits with VV-ALK-1 virus resulted in the invivo expression of recombinant ALK-1, which in turn led toproduction of anti-ALK-1 antibodies in the sera of the infectedanimals (Fig. 1B).
The specificity of the PAb αALK-1 was further analyzed inCOS-1 cells transfected with ALK-1/HA, ALK-2/HA (activintype I receptor) or ALK-5/HA (TGF-β type I receptor) (Fig.1C). Specific reactivity with ALK-1 was observed with thePAb αALK-1, as a band of expected size was present in theALK-1 transfectant and absent from the pCMV5 empty vectorand from samples immunoprecipitated with non-immune (NI)sera (lanes 1–6). No reactivity was observed with ALK-2(lanes 7 and 9) or ALK-5 (lanes 10 and 12), indicating nocross-reaction with these related type I receptors. The αHAimmunoprecipitates confirmed the efficiency of transfectionand the identity of the respective type I receptors (lanes 5, 8and 11). Endoglin transfectants showed reactivity with MAbP3D1 but not with PAb αALK-1 (lanes 13–15) indicating thatthis antiserum did not cross-react with endoglin.
Quantitation of ALK-1 and endoglin protein levels in HHTfamilies
We previously reported that mutations in endoglin result inreduced levels of expression of the corresponding protein atthe surface of HUVEC and activated monocytes from HHT1affected individuals (34,35). We therefore measured the levels
of expression of endoglin on activated monocytes obtainedfrom peripheral blood of clinically affected relatives of thenewborns from six HHT families using metabolic labeling andimmunoprecipitation, and flow cytometry. Expression ofnormal levels of endoglin, relative to age-matched controls,was found in all individuals (Table 1), which made thempossible HHT2 candidates. We then analyzed seven HUVECfrom newborns in these families and also observed normallevels of endoglin relative to the control HUVEC (C1–C5)analyzed in each experiment (Fig. 2A and Table 1).
Since ALK-1 can only be measured on HUVEC as it is notexpressed on peripheral blood mononuclear cells, we testedwhether PAb αALK-1 reacts with ALK-1 protein on endothe-lial cells by metabolic labeling and immunoprecipitation ofHUVEC derived from control (C) newborns. A distinct bandestimated at 63 kDa was observed with αALK-1 but not withthe NI sera, as shown for C1 and C2 in Figure 2B and C3–C5in Figure 2C. ALK-1 protein levels were then quantified inHUVEC of the seven newborns from potential HHT2 familiesusing metabolic labeling and immunoprecipitation. ReducedALK-1 levels were found in HUVEC samples from patientsH358, H360 and H69, relative to normal HUVEC analyzed in
Figure 1. PAb αALK-1 generated with recombinant vaccinia virus is specificfor ALK-1. (A) Lysates of uninfected control, virus (VV-TK–) infected, or HAtagged recombinant ALK-1 (VV-ALK-1) infected BSC-40 cells were fraction-ated by SDS–PAGE (7.5%) and analyzed by western blot with MAb 12CA5(anti-HA), followed by peroxidase-conjugated goat anti-mouse Ig and chemi-luminescence detection. (B) BSC-40 cells infected with VV-ALK-1 or VV-TK– were lysed and equal amounts of soluble extracts (lanes 1, 45 mg; lanes 2,15 mg) were immunoprecipitated with anti-HA. The immunoprecipitates weresubjected to SDS–PAGE, and detected by western blot using the serum from arabbit infected with VV-ALK-1, followed by peroxidase-conjugated goat anti-rabbit Ig and chemiluminescence detection. (C) COS-1 cells were transientlytransfected with pCMV5 empty vector or constructs containing cDNA for HA-tagged ALK-1, ALK-2 and ALK-5 and endoglin (END). Cells were labeledwith [35S]met for 3.5 h, solubilized and immunoprecipitated with NI sera,αHA, PAb αALK-1 or MAb P3D1 (αEND). Samples were fractionated on 4–12% SDS–PAGE under reducing conditions. Arrows indicate the positions oflabeled endoglin (END) dimer and the type I receptors (RI).

Human Molecular Genetics, 2000, Vol. 9, No. 8 1229
the same experiment (Fig. 2B and Table 1). The remaining fourHUVEC samples (patients H241, H242, H143 and H48)expressed normal levels of ALK-1 (Fig. 2C and Table 1).
Using flow cytometry analysis, >90% of HUVEC werefound to express ALK-1 relative to the NI sera used as a nega-tive control (Fig. 3). This confirmed the specificity of the PAbαALK-1, which was then used to measure the steady stateexpression of ALK-1 at the cell surface of seven HUVEC frompotential HHT2 families. Percentage of positive cells and meanfluorescence intensity were determined for each sample rela-tive to matched control. The expression of ALK-1 was specif-ically reduced on HUVEC from newborns H358, H360 andH69, but was normal on HUVEC from newborns H241, H242,H143 and H48 (Fig. 3 and Table 1). Levels of endoglin, α5β1integrin and CD31 were unchanged on these HUVEC (Fig. 3),confirming the specific reduction of ALK-1 in three of sevenHUVEC, and in agreement with the metabolic labeling studies(Table 1).
Mutation analysis in six HHT2 families
To establish the HHT2 genotype of the families involved in thecurrent study, DNA samples from clinically affected familymembers and newborns were screened for mutations in theALK-1 gene. We confirm that all six families have HHT2 andreport new missense mutations in the coding region of theALK-1 gene in families 109, 48 and 64, respectively (Fig. 4 andTable 2).
In family 109, a complex mutation was observed in exon 3:a G143A substitution, deletion of G145 and insertion of T147(Fig. 4A and Table 2). This mutation was found in DNAsamples obtained from HUVEC and placenta of newbornH358, and peripheral blood lymphocytes from the clinicallyaffected mother H357, but not from the father H386. The muta-tion converts adjacent amino acids G48 to E and A49 to P inthe extracellular domain of ALK-1.
In family 48, the new mutation is a G to A substitution atposition 1031 of exon 7. DNA obtained from both HUVECand placenta of the newborn H143 and from peripheral blood
lymphocytes of the mother H142, who had an uncertain clin-ical diagnosis of HHT, did not exhibit this mutation. It wasfound in the DNA from a clinically affected uncle H167 of thenewborn H143 (Fig. 4B and Table 2). DNA from the non-affected father was normal. This mutation converts C344 to Y.
In family 64, a G to T substitution at position 1221 was iden-tified in exon 8, which corresponds to a region in the ALK-1kinase domain. It was absent from DNA of the fraternal twinsH241 and H242, but present in DNA of the clinically affectedmother H210 and grandfather. This mutation converts E407 toD (Fig. 4C and Table 2).
In family 110, a G150T substitution in exon 3 was identifiedin the DNA samples obtained from HUVEC and placenta ofnewborn H360 and from peripheral blood lymphocytes of theclinically affected mother (Table 2), but not in control DNAfrom the father. This mutation, which was previously reportedin two apparently unrelated families (7,32), converts W50 to Cin the extracellular domain. We could not confirm any relationof family 110 to the previously described families.
We also identified mutations in DNA samples of newbornsfrom HHT2 families 16 and 22 (Table 2). Mutations in thesefamilies were previously published (6,7). In family 16, a CTCdeletion at position 696–698, observed in DNA samples fromnewborn H48, results in the loss of S232 in the kinase domainof the ALK-1 gene (6). In family 22, a G998 to T substitution inexon 7, which results in conversion of S333 to I, was detectedin DNA from newborn H69 (Table 2) (7). We have alsoconfirmed these two mutations by sequencing the cDNA, indi-cating expression of these mutants at the mRNA level.
ALK-1 associates with endoglin in TGF-β1 and -β3 but notin activin-A receptor complexes in COS-1 transfected cells
Since ALK-1 was previously reported to bind TGF-β1 andactivin when overexpressed in COS-1 cells, we tested whetherALK-1 and endoglin could be found in receptor complexes forTGF-β1, -β3 and activin-A. Affinity labeling with[125I]TGF-β1 or -β3 was performed in COS-1 cells transientlytransfected with endoglin or ALK-1 alone, endoglin together
Table 1. Analysis of ALK-1 and endoglin levels in HHT2 families
Levels of ALK-1 and endoglin were measured on HUVEC by metabolic labeling and flow cytometry (FACS) as described in Materials and Methods. Endoglinwas also quantified on activated monocytes from peripheral blood of adults. Protein levels are expressed relative to controls as a mean percentage ± SD.aNovel mutations identified by exon sequencing.bMutation previously published and identified here in a family apparently unrelated to the original families.cKnown mutations for the families, confirmed here in newborns.nd, not done.
Family no. Patient no. ALK-1 levels on HUVEC END levels on HUVEC Affected parent END levels on monocytes
Metabolic labeling FACS Metabolic labeling FACS Metabolic labeling
109 H358a 54 ± 13 52 ± 19 97 ± 27 87 ± 8 Mothera 91 ± 6
110 H360b 67 ± 13 58 ± 25 93 ± 16 109 ± 22 Motherb 124 ± 6
22 H69c 53 ± 6 62 ± 7 104 ± 10 90 ± 2 Motherc nd
64 H241 96 ± 7 114 ± 12 120 ± 25 99 ± 1 Mothera 99 ± 11
H242 95 ± 5 113 ± 12 128 ± 18 121 ± 11 Grandfathera 127 ± 31
48 H143 98 ± 17 109 ± 25 108 ± 12 100 ± 27 Mother 115 ± 31
Unclea 93 ± 16
16 H48c 89 ± 7 85 ± 2 106 ± 7 104 ± 10 Fatherc nd

1230 Human Molecular Genetics, 2000, Vol. 9, No. 8
with ALK-1 and TβRII. No binding was observed when endo-glin and ALK-1 were co-expressed (data not shown).However, cotransfection of TβRII with endoglin and ALK-1led to binding of [125I]TGF-β1 and -β3 to both endoglin andALK-1, as observed from the analysis of total lysates (Fig. 5A,lanes 1, 5 and 9). Specific immunoprecipitation revealed theposition of radiolabeled complexes containing endoglin(compare lanes 3 and 7) and ALK-1 (compare lanes 4 and 8).PAb C16 (αTβRII) co-immunoprecipitated [125I]TGF-β1 or-β3 cross-linked to endoglin/TβRII (lane 2) and to ALK-1/TβRII complexes (lane 6). When ALK-1 was co-expressedwith endoglin and TβRII, both PAb C16 (αTβRII) and MAbP3D1 (αEND) revealed ALK-1 co-precipitation (lanes 10 and11). MAb 12CA5 (αHA) immunoprecipitated the type Ireceptor ALK-1/HA (lane 12) but not the associated TβRII andendoglin.
We next tested binding of activin-A to ALK-1 in COS-1transfectants and examined its association with endoglin inactivin-A receptor complexes. COS-1 cells were transfectedwith endoglin and ALK-1 alone or in combination with ActRIIand were then affinity labeled with activin-A (Fig. 5B). SDS–PAGE analysis of total lysates showed activin-A binding toActRII alone (lane 1), ActRII and endoglin (lane 3), ActRIIand ALK-1 (lanes 4 and 5), whereas ALK-1 and endoglin didnot bind ligand (lane 2). Immunoprecipitation with MAb P3D1(αEND) revealed co-precipitation of endoglin with ActRII inactivin-A complexes, but not when cotransfected with ALK-1(lanes 6 and 7). However, ALK-1 did co-precipitate withActRII as seen using MAb to HA but endoglin was excludedfrom this complex (lanes 8 and 9).
When similar experiments were conducted with ALK-2, atype I receptor that binds activin-A, a complex containingActRII, endoglin and ALK-2 could be precipitated (Fig. 5C).Again, total lysates showed binding of activin-A to ActRII andALK-2 only when ActRII was expressed (lanes 1–5), whereasactivin-A binding to endoglin was only seen by immunopre-cipitation with a MAb to endoglin (lanes 6 and 7) which alsoshowed ActRII association. The high molecular weight bandsseen, particularly in lane 7 (Fig. 5C), likely represent a cross-linked complex of endoglin and ActRII observed underreducing conditions. When ALK-2 was co-expressed with
ActRII and endoglin, ALK-2 also associated with the complexcontaining endoglin, ActRII and radiolabeled activin-A (lanes8 and 9). These results suggest that endoglin interacts withspecific activin-A complexes containing ActRII and ALK-2but not ActRII and ALK-1.
Endogenous ALK-1 is not detectable in TGF-β1 or -β3receptor complexes in HUVEC
Using the characterized PAb αALK-1, we next tested whetherendogenous ALK-1 could be detected in the TGF-β receptorcomplex in HUVEC, as these cells have relatively high levels ofALK-1 (Fig. 6A). HUVEC were incubated with radiolabeledTGF-β1, chemically cross-linked and solubilized with digitonin.This detergent is milder than Triton X-100 (36) and can preserveprotein–protein interactions as previously shown for endoglin–TβRII interactions (28). Immunoprecipitation analysis revealedTGF-β1 binding and effective co-precipitation of endoglin, TβRIIand a trace of a type I receptor, likely to be ALK-5 (lanes 1, 4, 5and 8), as previously reported (28). We could not detect binding ofTGF-β1 to ALK-1, as no product was immunoprecipitated byPAB αALK-1 (lanes 3 and 7).
Similarly, when HUVEC were affinity labeled with TGF-β3(Fig. 6B), analysis of total cell lysates revealed specific cross-linking to TβRII, endoglin dimers (180 kDa) and oligomers(>200 kDa; lanes 1–3). Endoglin dimers were immunoprecipi-tated under non-reducing conditions by MAb P4A4 (αEND,lane 4) while monomers were seen under reducing conditions(lane 8). Anti-TβRII co-precipitated endoglin dimers andoligomers (lane 5) and monomers (lane 9), confirming thatendoglin and TβRII form a complex with TGF-β3. No traces ofALK-1 were observed (lanes 6 and 7, 10 and 11). We were thusunable to identify endogenous ALK-1 in the TGF-β1 or -β3receptor complexes on HUVEC.
ALK-1/endoglin interactions in HUVEC of normal andHHT newborns
Since endoglin can associate with TβRII in the absence ofexogenous ligand (28), we investigated its ability to interactwith TβRII and ALK-1 in HUVEC of normal and HHTnewborns using western blot analysis of specific immuno-
Table 2. Summary of mutation analysis in six HHT2 families
ALK-1 mutation analysis was performed on DNA obtained from HUVEC and placenta of new-borns, and blood lymphocytes of adults as described in Materials and Methods.aNovel mutations identified by sequencing.bPreviously published mutation identified here in a family apparently unrelated to the originalfamilies.cKnown mutation in the family, confirmed here in newborns.dLevels of ALK-1 protein could not be estimated in families 48 and 64, where newborns are non-affected.∆, deletion; +, insertion.
Family no. Exon no. Mutation type cDNA Mutant protein
109a 3 Missense G143A,∆G145,+T147 G48E, A49P; low levels
110b 3 Missense G150T W50C; low levels
22c 7 Missense G998T S333I; low levels
64a 8 Missense G1221T E407D; not testedd
48a 7 Missense G1031A C344Y; not testedd
16c 6 Deletion 3 bp ∆CTC 696–698 ∆S232; normal levels

Human Molecular Genetics, 2000, Vol. 9, No. 8 1231
precipitates. Polyclonal antibodies to endoglin, TβRII andALK-1 were used and the immunoprecipitates were thenprobed with MAb P4A4 to endoglin (Fig. 7A–C). PAb αENDspecifically immunoprecipitated endoglin in all analyzedsamples, as illustrated for controls C6 and C7, and for HUVECfrom non-affected newborn H241 (lanes 1, αEND). Low reac-tivity was observed with the NI sera (NI lanes). PAb C16 toTβRII co-precipitated TβRII and endoglin in HUVEC fromcontrol (C6) as well as from HHT1 (H344) and HHT2 (H48)newborns (Fig. 7A, lanes 3, 5 and 7, respectively), confirmingthat ligand-independent association of these two proteins wasstill occurring in endothelial cells from HHT newborns.
We then tested whether an association between ALK-1 andendoglin could be detected in HUVEC obtained from normaland HHT newborns (Fig. 7B). When extracts were immuno-precipitated with PAb αALK-1 and probed with MAb P4A4under non-reducing conditions, endoglin was found to be asso-ciated with ALK-1 in control HUVEC (lane 3). This interac-tion was also detected in HUVEC from an HHT1 patient
(H344; lane 5) and in three HHT2 HUVEC analyzed (H69,H358 and H360; lanes 7, 9 and 11, respectively).
Because it is known that ALK-1 and endoglin are expressedin placenta, we tested whether their interaction could bedemonstrated in extracts of placental membrane fractionsobtained from control and HHT newborns. Figure 7C showsthat PAb αALK-1 co-precipitated endoglin and ALK-1 insamples from non-affected newborn H241 from HHT2 family64, HHT1 affected newborns H129, H136 (34) and HHT2affected newborn H48 (Fig. 7C, lanes 3, 5, 7 and 9, respec-tively). These results suggest that an interaction between endo-glin and ALK-1 can still be detected, in absence of ligand, inHUVEC and placenta of HHT1 and HHT2 newborns.
DISCUSSION
In this paper, we describe a novel polyclonal antibody thatspecifically detects ALK-1 and we were able to quantify its
Figure 2. Analysis of endoglin and ALK-1 protein expression in newborns fromHHT2 families. HUVEC derived from seven newborns from putative HHT2families and their respective matched controls (C1–C5) were metabolicallylabeled, immunoprecipitated with αEND (MAb P3D1) or αALK-1, fractionatedunder reducing conditions, and quantified as described in Materials and Methods.(A) Endoglin was immunoprecipitated at normal levels as a fully glycosylatedmonomer (E, 90 kDa) and its precursor (P, 80 kDa). (B) ALK-1 was specificallyimmunoprecipitated with αALK-1 versus NI sera, but at reduced levels relative tocontrols, in samples from newborns H358, H360 and H69. (C) ALK-1 wasimmunoprecipitated at normal levels in samples H241, H242, H143 and H48.aNewborns with ALK-1 mutations and reduced levels of ALK-1 protein; bnewbornwith ALK-1 mutation and normal levels of ALK-1 protein. Results from all theexperiments performed are summarized in Table 1.
Figure 3. Analysis of ALK-1 and endoglin expression on HUVEC of newbornsfrom HHT2 families by flow cytometry. HUVEC from newborns of HHT2families (closed histograms) were compared with normal matched controls (openhistograms). Samples were stained with NI and αALK-1 sera, and analyzed asdescribed in Materials and Methods. More than 90% of cells were positive withαALK-1 serum within a defined gate and set with the NI at 5%, except for H360(56%) and H69 (40%). HUVEC were also stained with MAbs to endoglin, α5integrin and CD31. For these antibodies an IgG control was used to define the gatesshown, with <2% of cells within this gate. Ninety-nine percent of cells werepositive in all cases except for endoglin in H69 (70%). The relative meanfluorescence intensity of each patient sample was compared with that of the control(note the logarithmic scale). The mean ALK-1 and endoglin levels estimated fromseveral experiments are summarized in Table 1.

1232 Human Molecular Genetics, 2000, Vol. 9, No. 8
expression on seven HUVEC from six HHT2 families. ALK-1protein levels were reduced in three of the seven HUVEC andALK-1 missense mutations (G48E/A49P, W50C and S333I)were found in all three cases, revealing that these newbornswere affected with HHT2. It is likely that these mutations leadto structural alterations that result in protein misfolding andintracellular degradation, explaining the lack of surfaceexpression of the mutant proteins. The first two mutationsoccur between Cys46 and Cys51, while the third replacesS333. These residues are highly conserved among the type Ireceptors (17,30) and are likely to be critical for proper foldingof the protein. In the case of the S333I substitution, mutantmRNA could be sequenced, confirming expression of themessage and suggesting instability of the mutant protein.
Three other HUVEC, two of which were from fraternaltwins, showed normal levels of ALK-1 protein. Mutation anal-ysis confirmed that these newborns were not affected becausethey did not express the disease-related mutation (C344Y orE407D) found in other affected family members. Thus, in sixof seven families analyzed, levels of ALK-1 correlated withthe presence or absence of a mutant protein.
However, HUVEC from newborn H48 expressed relativelynormal levels of ALK-1 protein, as measured by metaboliclabeling (89%) and flow cytometry (85%), while carrying a 3bp deletion (CTC 696–698) that was previously reported forother affected family members (6). This mutation deletesS232, which is one of two adjacent Ser residues in the ATPbinding site of the kinase domain of ALK-1. These Ser residuesare conserved in most of the type I receptors of the TGF-βsuperfamily (30). This mutation is thus likely to yield a non-functional enzyme. Our results support the hypothesis thatHHT2, like HHT1, is associated with haploinsufficiency aspreviously suggested (7). A loss of ALK-1 expression due tostructural mutations that lead to misfolded and unstableproteins (e.g. as in families 22, 109 and 110), or a loss of func-tion of the mutated allele (as predicted for family 16) are likelyto be the most common mechanisms responsible for HHT2.
We report three novel missense mutations (G48E/A49P,C344Y and E407D) in the coding region of the ALK-1 gene.The first, seen in family 109, consists of substitution, followedby deletion and insertion of single base pairs in exon 3 ofALK-1. The net effect of the mutation is the conversion of adja-cent amino acids G48 to E and A49 to P in the extracellulardomain. In family 48, C344 is replaced by Y, while in family64 the mutation is E407 to D substitution. These two mutationsoccur in exons 7 and 8 of the kinase domain, respectively.
Recent data showed that introducing the W50C mutationinto the extracellular domain of the ALK-1/TβRI chimera ledto abrogation of signaling activity (37). As this mutation isassociated here with reduced expression of ALK-1 in HUVECof newborn H360, the reported loss of signaling activity inCOS-1 cells was likely to be due to low levels of expression ofthe unstable chimeric receptor.
As previously reported by Attisano et al. (16), ALK-1 can befound in the TGF-β1 receptor complex when co-transfected inCOS-1 cells. We now also demonstrate that in COS-1 cells itcan be present in the TGF-β3 receptor complex. This supportsrecent data demonstrating that chimeric ALK-1/TβRI recep-tors can signal for TGF-β1 and -β3, and therefore are capableof binding both of these ligands (37). We also observed that thePAb C16 to TβRII is the most efficient at bringing down the
Figure 4. Analysis of genomic DNA from HHT2 families. ALK-1 exons wereamplified by PCR from DNA isolated from HUVEC and placenta of newborns andperipheral blood lymphocytes of adults. Purified products were sequenced using acycle sequencing protocol and resolved using a Microgeneblaster® automatedsequencer (VGI). The profiles obtained for three families are shown.(A) Substitution of G to A, deletion of G and insertion of T in exon 3 was observedin samples from patients H358 and H357 but not H386 (family 109).(B) Sequencing DNA samples of family 48 revealed a G to A substitution in exon7 of sample H167, but not in H142 and H143. (C) Substitution of G to T in exon 8,was present in sample H210 but absent from fraternal twins H241 and H242(family 64). (Base codes: K = G or T; R = A or G; S = G or C; Y = C or T.)

Human Molecular Genetics, 2000, Vol. 9, No. 8 1233
TGF-β receptor complex containing endoglin and ALK-5 (28)and/or ALK-1 (current study). Our results, that ALK-1 andendoglin are not found in the activin receptor complex inCOS-1 cells despite the fact that ALK-1 can interact withActRII, are in keeping with the observations that the chimericALK-1/ActRI receptor does not signal for activin-A (37). Inour experiments with HUVEC, binding of TGF-β1 and -β3 toendogenous ALK-1 could not be demonstrated. In addition, inthe absence of ligand, we were unable to demonstrate ALK-1interaction with either TβRII or endoglin by surface labeling(data not shown). However, using immunoprecipitation/western blot analysis, we detected an interaction betweenALK-1 and endoglin in HUVEC and placenta in the absence ofligand. This interaction was also observed in samples obtainedfrom HHT1 and HHT2 newborns.
Since the true physiological ligand for ALK-1 is not known,and the type II receptor(s) it interacts with is unclear, it is diffi-cult to establish which ligand binding complexes involve bothendoglin and ALK-1. Endoglin functions in signaling receptorcomplexes of multiple members of the TGF-β superfamily(28). It binds TGF-β1/-β3 via its association with TβRII, andactivin and BMP-7 via ActRII/ActRIIB, regardless of the co-expressed type I receptor. Endoglin also binds BMP-2 via its
Figure 5. ALK-1 and endoglin are detectable in TGF-β1/-β3 but not in activin-Areceptor complexes in COS-1 transfected cells. (A) COS-1 cells were transientlytransfected with the indicated expression constructs containing cDNA for endoglin(END), TβRII and ALK-1/HA (tagged at the N-terminus with influenzahemagglutinin epitope), affinity labeled with 200 pM [125I]TGF-β1 or 250 pM[125I]TGF-β3, cross-linked with DSS and solubilized with 1% Triton X-100 plusinhibitors. Aliquots of lysates containing equivalent total protein were fractionatedunder reducing conditions and analyzed by immunoprecipitation. Shown are totallysates (lanes 1, 5 and 9) and eluates from immunoprecipitates with PAb C16(αTβRII: lanes 2, 6 and 10), MAb P3D1 (αEND: lanes 3, 7 and 11) and with MAb12CA5 (αHA: lanes 4, 8 and 12). Arrows indicate the positions of the affinity-labeled products, endoglin, TβRII and the type I receptor ALK-1. No binding wasobserved when endoglin and ALK-1 were co-expressed (data not shown becauseall lanes were blank). (B) COS-1 cells transiently transfected with the expressionconstructs containing cDNA for endoglin (END), ActRII and ALK-1/HA wereaffinity labeled with 800 pM [125I]activin-A and analyzed as in (A). Total lysatesare fractionated in lanes 1–5, and eluates from immunoprecipitates with MAbsP3D1 (αEND) and 12CA5 (αHA) are shown in lanes 6 and 7, 8 and 9,respectively. Arrows indicate the positions of the affinity-labeled products,endoglin, TβRII and the type I receptor ALK-1. (C) COS-1 cells transientlytransfected with the expression constructs containing cDNA for endoglin (END),ActRII and ALK-2/HA were affinity labeled with [125I]activin-A, and total lysatesand αEND immunoprecipitates analyzed and illustrated as in (B).
Figure 6. Endogenous ALK-1 is not detectable in TGF-β1 or -β3 receptorcomplexes in HUVEC. (A) HUVEC were affinity labeled with 200 pM [125I]TGF-β1, treated with DSS and solubilized with 1% digitonin plus inhibitors. Extractscontaining equal amounts of protein were then immunoprecipitated with MAbP3D1 (αEND) (lanes 1 and 5), NI serum (lanes 2 and 6), PAbs αALK-1 (lanes3 and 7), C16 (αTβRII) (lanes 4 and 8), and fractionated under non-reducing (NR)or reducing (R) conditions. Arrows indicate the affinity-labeled endoglin dimers(END), oligomers (OLIGO), TβRII (RII) and a type I receptor (RI). (B) HUVECwere incubated with 250 pM [125I]TGF-β3, cross-linked with DSS and analyzed asin (A), except total lysates were also fractionated (lane 1). In addition, total lysatesincubated with a 40-fold excess of competing cold ligand (lane 2) and lysatesimmunoprecipitated with an IgG control (lane 3) are shown. Extracts wereimmunoprecipitated with MAb P4A4 (αEND: lanes 4 and 8), PAbs C16 (αTβRII:lanes 5 and 9), NI sera (lanes 6 and 10) and αALK-1 (lanes 7 and 11).

1234 Human Molecular Genetics, 2000, Vol. 9, No. 8
association with the type I receptors ALK-3 and ALK-6. ALK-1 has now been implicated in TGF-β1/-β3 receptor complexesas well as that of an unknown ligand present in serum (37). Aconstitutively active form of ALK-1 was shown to act onSmads 1, 5 and 8, which are involved in BMP signaling(27,38). One of the critical questions that remains to beanswered is whether HHT is associated with modifiedresponses to TGF-β1/-β3 or to an as yet unknown ligand.Endoglin null mice die at mid-gestation due to impairedvascular development (39,40) and ALK-1 null embryos appearto have a similar phenotype (as quoted in 37). Mice deficient inTGF-β1 or TβRII are also embryonic-lethal due to defects inyolk sac vasculogenesis (41,42). These studies suggest thatendoglin and ALK-1 mediate the effects of TGF-β1 in vasculardevelopment. Furthermore, as a loss of function of the mutatedallele of either endoglin or ALK-1 leads to the vasculardisorder HHT, we hypothesize that both endoglin and ALK-1function in a non-classical TGF-β1 pathway that is critical forvascular integrity.
MATERIALS AND METHODS
Clinical samples
Blood samples and medical histories were obtained withinformed consent from all individuals participating in thestudy. In the case of umbilical cord and placenta samples,consent was obtained from the parents in families with a clin-ical diagnosis of HHT. The procedures were reviewed andapproved by the Research Ethics Board of the Research Insti-tute of The Hospital for Sick Children, Toronto, Canada. Allpatients and families were given a number and clinically diag-nosed patients or newborns from HHT families are referred towith a prefix H (for HHT). In total, samples from six familieswith HHT2 were included in the study. In the case of families16 and 22, for which mutations were previously reported(7,31), only samples from newborns were available. Samplesobtained from newborns H129, H136 and H344, all expressingreduced levels of endoglin and with known mutations in endo-glin gene (34), were also analyzed. Mutation in H129 is a 1-bp(A) insertion at position 1470, in exon 11, causing a frameshiftthat leads to a truncated protein terminating at L490. NewbornH136 carries a nonsense mutation in exon 5 of endoglin genecreated by a C to T substitution at position 587, which convertscodon 196 into a stop. The mutation in newborn H344 is aninsertion of G in exon 8 that caused a frameshift and led to astop at position 1112.
HUVEC were derived from umbilical cords of newbornsfrom HHT families and controls from local deliveries(15,34,35). In all assays, experimental and control HUVEC atequivalent cell densities and passage numbers were employed.The mononuclear cells, derived from venous blood of clini-cally affected HHT patients and known non-affected relativesor unrelated volunteers, were used for measurement of endo-glin levels as described previously (34,35,43).
Mammalian expression constructs and transienttransfection
The pCMV5 expression constructs containing cDNAs forendoglin, TβRII, ActRII, ALK-1/HA (tagged at the C-terminus with the influenza hemagglutinin epitope, HA),ALK-2/HA and ALK-5/HA have all been described previously(16,20,22,44–46). All constructs for Ser/Thr kinase receptorswere provided by J. L. Wrana and L. Attisano. COS-1 cellswere maintained and transiently transfected with expressionconstructs using the DEAE–dextran–chloroquine method asreported (22,24). Assays were performed 2 days post-transfec-tion.
Generation of a polyclonal antibody to ALK-1 using arecombinant vaccinia virus construct
BSC-40 African green monkey kidney cells were maintained inDulbecco’s Modified Eagle’s Medium (DMEM) supplementedwith 10% FCS, 2 mM L-glutamine, penicillin (100 U/ml) andstreptomycin (100 µg/ml) in a 5% CO2 atmosphere at 37°C.Culture of the Western reserve strain vaccinia virus and isola-tion of recombinant virus were performed as described (47).The plasmid pCMV5-ALK-1/HA (16) was digested withHindIII and BamHI, and the resulting 1.6 kb fragment wastreated with DNA polymerase I (Klenow fragment) and
Figure 7. ALK-1 associates with endoglin in the absence of added ligand.(A) HUVEC from control C6, HHT1 newborn H344 and HHT2 newborn H48were solubilized with 1% Triton X-100. Extracts were immunoprecipitated withMAb P4A4 (αEND), NI serum and PAb αTβRII, and fractionated by 4–12%SDS–PAGE under non-reducing conditions. Gels were transferred and probedwith MAb P4A4 followed by goat anti-murine IgG-HRP and detected by ECL.(B) HUVEC extracts from control C7, HHT1 newborn H344 and three HHT2newborns (H69, H358 and H360) were immunoprecipitated with PAb αEND, NI,αALK-1 and probed as in (A). (C) Triton X-100 extracts were prepared fromplacental membrane proteins of the unaffected newborn H241, HHT1 newbornsH129 and H136, and from HHT2 newborn H48, and treated as in (B). The amountof protein immunoprecipitated with αALK-1 and NI sera (0.2–0.4 mg) was 10times that used with αEND.

Human Molecular Genetics, 2000, Vol. 9, No. 8 1235
inserted into the SmaI site of vaccinia virus plasmid pSC11.The resulting plasmid vector co-expressed the ALK-1 geneinserted downstream of the vaccinia 7.5 kDa protein promoter,together with the Escherichia coli β-galactosidase gene underthe control of the vaccinia 11 kDa protein late promoter; bothgenes were flanked by viral thymidine kinase (TK) sequences.Thus, upon homologous recombination, both genes wereinserted into the TK locus of the vaccinia virus genomeyielding the VV-ALK-1 virus. Control recombinant TK–
vaccinia virus (VV-TK–) was constructed as described for theother recombinant viruses, using the pSC11 plasmid. NewZealand rabbits were immunized twice with a 4-week intervalwith 109 p.f.u. of either VV-ALK-1 or VV-TK– in PBS. Twoweeks after the last injection, sera were collected and reactivitywith ALK-1 confirmed by western blot.
Antibodies
MAb P3D1 and P4A4 which recognize different epitopes ofthe extracellular domain of human endoglin have beendescribed previously (48). A PAb to human endoglin wasgenerated using recombinant vaccinia virus as described previ-ously (49). MAb 5.6E to CD31 (PECAM-1) was purchasedfrom AMAC and MAb JBS5 to α5β1 integrin was a gift fromDr J. A. Wilkins (University of Manitoba, Winnipeg, Canada).Murine NI IgG1 (Coulter Electronics, Hialeah, FL) was usedas a negative control. PAb C16 to peptide 550–565 of thehighly conserved C-terminal of human TβRII was purchasedfrom Santa Cruz Biotechnology Inc. (Santa Cruz, CA). MAb12CA5 (Boehringer Mannheim, Laval, Canada) to influenzahemagglutinin (αHA) was used for immunoprecipitation ofHA-tagged TGF-β superfamily receptors.
Flow cytometry
HUVEC were released with trypsin–EDTA and washed inCa2+Mg2+-free PBS. Cells (5 × 105) were incubated with therespective MAb or an IgG1 isotype control and FITC-conju-gated F(ab′)2 goat anti-mouse IgG (Tago Inc., Burlingame,CA). For NI and immune anti-ALK-1 sera, FITC-conjugatedF(ab′)2 goat anti-rabbit IgG was used. The HUVEC populationwas defined by forward light scatter versus side scatter, andlive cells were selected with propidium iodide. Percent positivecells within these defined gates and mean fluorescence intensi-ties were determined relative to the respective negative control.In the case of ALK-1, reactivity with NI serum was used todefine the negative gate. Patient HUVEC samples were run inparallel with control HUVEC and their relative mean fluores-cence intensity estimated from at least two experiments. Allsamples were analyzed on the FACScan® (Becton Dickinson,Mountain View, CA).
Metabolic labeling and immunoprecipitation
Control and patient HUVEC at sub-confluence (~90%) weremetabolically labeled as described (34,35,43). Cells were incu-bated with 100 µCi/ml [35S]methionine (met) (Trans35S-label;ICN Pharmaceuticals Ltd, Montreal, Canada) in met-freeDMEM (low glucose; Life Technologies, Rockville, MD) for3.5 h and solubilized in lysis solution containing 1% Triton X-100 or 1% digitonin (Wako, Richmond, VA). After overnight
preclearing with NI sera and Protein A–Sepharose CL-4B(Pharmacia Biotech Inc., Baie d’Urfe, Canada) samples weredivided equally and immunoprecipitated with saturatingamounts of anti-endoglin and anti-ALK-1 antibodies, followedby elution in non-reducing solution (60 mM Tris–HCl, pH 6.8,2% SDS, 10% glycerol, 0.05% bromophenol blue).
To quantitate ALK-1 and endoglin expression and to correctfor the differences in yield between samples and respectivelymatched controls, we measured total protein by TCA precipita-tion in aliquots of total lysates. Equivalent c.p.m. were frac-tionated on 4–12% SDS–PAGE gradient gels (NovexExperimental Technology, San Diego, CA) which were thenfixed, dried and exposed to BioMax MS films in the BioMaxTransScreen LE cassettes (Eastman Kodak, Rochester, NY).Radioactivity in the bands corresponding to ALK-1, run underreducing conditions, or the fully processed form of endoglin(E) was quantified using a PhosphorImager and ImageQuantSoftware (Molecular Dynamics, Sunnyvale, CA). The patientto control pixel value ratios were calculated for each immuno-precipitate and the mean ± SD determined from at least fourvalues. Transfected COS-1 cells and activated monocytes,obtained from peripheral blood of controls and patients, wereprocessed as described above.
DNA preparation
Genomic DNA was isolated from HUVEC, placenta andperipheral blood lymphocytes using DNAZOL® reagent(Gibco BRL, Gaithersburg, MD) or Puregene® DNA IsolationKit (Gentra Systems, Minneapolis, MN) according to manu-facturers’ protocols.
Mutation analysis
Two sets of primers were designed for amplification andsubsequent sequencing of each of the nine coding exons of theALK-1 gene. Each reaction contained 2.5 mM of dNTP,0.2 µM of oligonucleotide primers, optimal concentration ofMgCl2, AmpliTaq polymerase, obtained from Perkin-Elmer(Roche Molecular Systems, Branchburg, NJ) and 300 ng ofDNA. Thermocycling conditions were: initial denaturation for2 min at 94°C followed by 30 cycles of 45 s at 94°C, 45 sannealing at 56°C, 60 s at 72°C and a final extension of 5 minat 72°C. PCR products were purified using QIAquick PCRPurification Kit (Qiagen, Mississauga, Canada) and templateswere sequenced using a cycle sequencing protocol. Thesequencing primers were designed to be at least 5 bp within theamplification primers and were labeled with Cy5.5 fluorescentdye (Visible Genetics Inc., Toronto, Canada). Templates (20–40 ng), 3 pM of Cy5.5 labeled primer, and 4 U of Thermo-Sequenase™ enzyme (Amersham Life Sciences, Cleveland,OH) in ThermoSequenase™ buffer were added to dNTP termi-nators. Cycle sequencing conditions were: 2 min at 94°Cfollowed by 30 cycles of 30 s at 94°C, 30 s at annealingtemperature (56–60°C), 1 min at 70°C and a final extension of2 min at 72°C. Products were resolved on a MicroGeneBlaster™ sequencer at 1300 V and 54°C for 30–40 min andsequences analyzed using the Open Gene™ DNA AnalysisSoftware (Visible Genetics Inc.).

1236 Human Molecular Genetics, 2000, Vol. 9, No. 8
Affinity labeling
TGF-β1 and TGF-β3 were from R&D Systems (Minneapolis,MN); recombinant human activin-A was a generous gift fromY. Eto (Ajinomoto Co. Inc., Kawasaki, Japan). Ligands wereiodinated with [125I]chloramine-T as previously described(46,50,51). HUVEC were incubated with 200 pM [125I]TGF-β1, 250 pM [125I]TGF-β3 or 800 pM [125I]activin-A for 4 h,washed, treated with DSS crosslinker (disuccinimidylsuberate; Pierce, Rockford, IL) and solubilized with lysisbuffer containing 1% digitonin or 1% Triton X-100 andprotease inhibitors (52). Cell lysates containing equivalenttotal protein were immunoprecipitated with control NI IgG,MAb P3D1 and P4A4 (α-endoglin), 12CA5 (αHA), PAb C16(α-TβRII), NI serum and PAb αALK-1. Immune complexeswere collected with Protein G– or Protein A– Sepharose,washed with lysis buffer containing either digitonin or TritonX-100 and eluted in 1% SDS. Cross-linked receptors bound toradiolabeled ligands were visualized by separation on 4–12%gradient gels by SDS–PAGE and autoradiography usingBioMax MS film and the BioMax TransScreen HE intensi-fying screen system (Eastman Kodak).
Western blot analysis
Soluble extracts, obtained by lysing uninfected control,infected recombinant TK– vaccinia virus (VV-TK–) and theHA-tagged ALK-1 recombinant vaccinia virus (VV-ALK-1)infected BSC-40 cells were fractionated by 7.5% SDS–PAGEand transferred to nitrocellulose membranes. These wereblocked with PBS containing 5% milk powder for 1 h, andprobed with MAb 12CA5 (anti-HA), followed by peroxidase-conjugated goat anti-mouse IgG and detected by ECL. Anti-HA immunoprecipitates were subjected to SDS–PAGE, trans-ferred to nitrocellulose and probed with the serum from arabbit infected with VV-ALK-1, followed by peroxidase-conjugated goat anti-rabbit Ig and chemiluminescence detec-tion.
HUVEC at subconfluence were lysed with 1% Triton X-100and immunoprecipitated with PAb αALK-1, NI sera and PAbαEND prior to SDS–PAGE on 4–12% gels under non-reducing conditions. The total amount of protein was estimatedand the amount used for immunoprecipitation with αALK-1(0.2–0.4 mg) was 10 times more than with αEND. After elec-trophoretic transfer to nitrocellulose membranes, the immuno-precipitates were probed with mAb P4A4 followed by goatanti-murine IgG-HRP and detection by ECL. Crude membranefractions, prepared from the placenta by subsequent centrifu-gation at 5000 and 100 000 g were solubilized in 1% Triton X-100 plus inhibitors and analyzed using the same procedure.
ACKNOWLEDGEMENTS
We are grateful to all the patients and their family members whoparticipated in this study and for the support of the HHTFoundation International and to Jamie McDonald from SaltLake City for providing us with patient information. We thankDrs L. Attisano and J.L. Wrana for the type I Ser/Thr kinasereceptor constructs, and Dr J. L. Wrana for the critical review ofthe manuscript. We are grateful to Ursula Cymerman for tech-nical advice on cycle sequencing, Carmen Langa for excellenttechnical assistance and Dr J. Dunn from Visible Genetics Inc.
for the use of the Microgeneblaster®. This work was supportedby grant #NA3434 from the Heart and Stroke Foundation ofOntario, grant #MT6247 from the Medical Research Council ofCanada, grant HHT-FY99-677 from March of Dimes (M.L.),and from Comision Interministerial de Ciencia y Tecnologia(CICYT-SAF97-0034) and Comunidad Autonoma de Madrid(CAM) (C.B.).
REFERENCES
1. Guttmacher, A.E., Marchuk, D.A. and White, R.I.J. (1995) Hereditaryhemorrhagic telangiectasia. N. Engl J. Med., 333, 918–924.
2. McDonald, M.T., Papenberg, K.A., Ghosh, S., Glatfelter, A.A., Biesecker,B.B., Helmbold, E.A., Markel, D.S., Zolotor, A., McKinnon, W.C.,Vanderstoep, J.L. et al. (1994) A disease locus for hereditary haemorrhagictelangiectasia maps to chromosome 9q33-34. Nature Genet., 6, 197–204.
3. Shovlin, C.L., Hughes, J.M.B., Tuddenham, E.G.D., Temperley, I.,Perembelon, Y.F.N., Scott, J., Seidman, C.E. and Seidman, J.G. (1994) Agene for hereditary haemorrhagic telangiectasia maps to chromosome 9q3.Nature Genet., 6, 205–209.
4. McAllister, K.A., Grogg, K.M., Johnson, D.W., Gallione, C.J., Baldwin,M.A., Jackson, C.E., Helmbold, E.A., Markel, D.S., McKinnon, W.C.,Murrell, J. et al. (1994) Endoglin, a TGF-β binding protein of endothelialcells is the gene for hereditary haemorrhagic telangiectasia type 1. NatureGenet., 8, 345–351.
5. Vincent, P., Plauchu, H., Hazan, J., Faure, S., Weissenbach, J. and Godet, J.(1995) A third locus for hereditary haemorrhagic telangiectasia maps tochromosome 12q. Hum. Mol. Genet., 4, 945–949. [Published erratumappears in (1995) Hum. Mol. Genet., 4, 1243.]
6. Johnson, D.W., Berg, J.N., Gallione, C.J., McAllister, K.A., Warner, J.P.,Helmbold, E.A., Markel, D.S., Jackson, C.E., Porteous, M.E. and Marchuk,D.A. (1995) A second locus for hereditary hemorrhagic telangiectasia mapsto chromosome 12. PCR Methods Appl., 5, 21–28.
7. Berg, J.N., Gallione, C.J., Stenzel, T.T., Johnson, D.W., Allen, W.P.,Schwartz, C.E., Jackson, C.E., Porteous, M.E. and Marchuk, D.A. (1997)The activin receptor-like kinase 1 gene: genomic structure and mutations inhereditary hemorrhagic telangiectasia type 2. Am. J. Hum. Genet., 61, 60–67.
8. Plauchu, H., de Chadaverian, J.-P., Bideau, A. and Robert, J.-M. (1989)Age-related clinical profile of hereditary hemorrhagic telangiectasia in anepidemiologically recruited population. Am. J. Med. Genet., 32, 291–297.
9. Shovlin, C.L., Winstock, A.R., Peters, A.M., Jackson, J.E. and Hughes, J.M.(1995) Medical complications of pregnancy in hereditary haemorrhagictelangiectasia. Q. J. Med., 88, 879–887.
10. Shovlin, C. and Letarte, M. (1999) Hereditary hemorrhagic telangiectasiaand pulmonary arteriovenous malformations: issues in clinical managementand review of pathogenic mechanisms. Thorax, 54, 714–729.
11. Kikuchi, K., Kowada, M. and Sasajima, H. (1994) Vascular malformationsof the brain in hereditary hemorrhagic telangiectasia (Rendu-Osler-Weberdisease). Surg. Neurol., 41, 374–380.
12. Heutink, P., Haitjema, T., Breedveld, G.J., Janssen, B., Sandkuijl, L.A.,Bontekoe, C.J.M., Westerman, C.J.J. and Oostra, B.A. (1994) Linkage ofhereditary haemorrhagic telangiectasia to chromosome 9q34 and evidencefor locus heterogeneity. J. Med. Genet., 31, 933–936.
13. McAllister, K.A., Lennon, F., Bowles-Biesecker, B., McKinnon, W.C.,Helmbold, E.A., Markel, D.S., Jackson, C.E., Guttmacher, A.E., Pericak-Vance, M.A. and Marchuk, D.A. (1994) Genetic heterogeneity in hereditaryhaemorrhagic telangiectasia: possible correlation with clinical phenotype. J.Med. Genet., 31, 927–932.
14. Berg, J.N., Guttmacher, A.E., Marchuk, D.A. and Porteous, M.E. (1996)Clinical heterogeneity in hereditary haemorrhagic telangiectasia: arepulmonary arteriovenous malformations more common in families linked toendoglin? J. Med. Genet., 33, 256–257.
15. Gougos, A. and Letarte, M. (1988) Biochemical characterization of the44G4 antigen from the HOON pre-B leukemic cell line. J. Immunol., 141,1934–1940.
16. Attisano, L., Cárcamo, J., Ventura, F., Weis, F.M.B., Massagué, J. andWrana, J.L. (1993) Identification of human activin and TGFβ type Ireceptors that form heteromeric kinase complexes with type II receptors.Cell, 75, 671–680.
17. Massagué, J., Attisano, L. and Wrana, J.L. (1994) The TGF-β family and itscomposite receptors. Trends Cell Biol., 4, 172–178.

Human Molecular Genetics, 2000, Vol. 9, No. 8 1237
18. ten Dijke, P., Yamashita, H., Ichijo, H., Franzen, P., Laiho, M., Miyazono,K. and Heldin, C.-H. (1994) Characterization of the type I receptors fortransforming growth factor-β receptor-like and activin. Science, 264, 101–104.
19. Miyazono, K., ten Dijke, P., Ichijo, H. and Heldin, C.-H. (1994) Receptorsfor transforming growth factor-β. Adv. Immunol., 55, 181–220.
20. Wrana, J.L., Attisano, L., Cárcamo, J., Zentella, A., Doody, J., Laiho, M.,Wang, X.-F. and Massagué, J. (1992) TGF-β signals through a heteromericprotein kinase receptor complex. Cell, 71, 1003–1014.
21. Wrana, J.L., Attisano, L., Wieser, R., Ventura, F. and Massagué, J. (1994)Mechanisms of activation of the TGF-β receptor. Nature, 370, 341–347.
22. Attisano, L., Wrana, J.L., Montalvo, E. and Massagué, J. (1996) Activationof signaling by the activin receptor complex. Mol. Cell. Biol., 16, 1066–1073.
23. Heldin, C.H., Miyazono, K. and ten Dijke, P. (1997) TGF-beta signallingfrom cell membrane to nucleus through SMAD proteins. Nature, 390, 465–471.
24. Hoodless, P.A., Haerry, T., Abdollah, S., Stapleton, M., O’Connor, M.B.,Attisano, L. and Wrana, J.L. (1996) MADR1, a MAD-related protein thatfunctions in BMP2 signaling pathways. Cell, 85, 489–500.
25. Kretzschmar, M., Liu, F., Hata, A., Doody, J. and Massagué, J. (1997) TheTGF-beta family mediator Smad1 is phosphorylated directly and activatedfunctionally by the BMP receptor kinase. Genes Dev., 11, 984–995.
26. Yamashita, H., ten Dijke, P., Huylebroeck, D., Sampath, T.K., Andries, M.,Smith, J.C., Heldin, C.H. and Miyazono, K. (1995) Osteogenic protein-1binds to activin type II receptors and induces certain activin-like effects. J.Cell Biol., 130, 217–226.
27. Macías-Silva, M., Hoodless, P.A., Jun Tang, S., Buchwald, M. and Wrana,J.L. (1998) Specific activation of Smad1 signalling pathways by the BMP7type I receptor ALK2. J. Biol. Chem., 273, 25628–25636.
28. Barbara, N.P., Wrana, J.L. and Letarte, M. (1999) Endoglin is an accessoryprotein that interacts with the signaling receptor complex of multiplemembers of the transforming growth factor-beta superfamily. J. Biol.Chem., 274, 584–594.
29. ten Dijke, P., Ichijo, H., Franzen, P., Schulz, P., Saras, J., Toyoshima, H.,Heldin, C.-H. and Miyazono, K. (1993) Activin receptor-like kinases: anovel subclass of cell surface receptors with predicted serine/threoninekinase activity. Oncogene, 8, 2879–2887.
30. Hanks, S.K., Quinn, A.M. and Hunter, T. (1988) The protein kinase family:conserved features and deduced phylogeny of the catalytic domains.[Review] Science, 241, 42–52.
31. Johnson, D.W., Berg, J.N., Baldwin, M.A., Gallione, C.J., Marondel, I.,Yoon, S.J., Stenzel, T.T., Speer, M., Pericak-Vance, M.A., Diamond, A. etal. (1996) Mutations in the activin receptor-like kinase 1 gene in hereditaryhaemorrhagic telangiectasia type 2. Nature Genet., 13, 189–195.
32. Klaus, D.J., Gallione, C.J., Antony, K., Yeh, E.Y., Yu, J., Lux, A., Johnson,D.W. and Marchuk, D.A. (1998) Novel missense and frameshift mutations inthe activin receptor-like kinase-1 gene in hereditary hemorrhagic telangiectasia.Hum. Mutat., http://journals.wiley.com/1059-7794/mutbr7.htm/
33. Moss, B. and Flexner, C. (1987) Vaccinia virus expression vectors. Annu.Rev. Immunol., 5, 305–324.
34. Cymerman, U., Vera, S., Pece-Barbara, N., Bourdeau, A., White, R.J.,Dunn, J. and Letarte, M. (2000) Identification of hereditary hemorrhagictelangiectasia type 1 in newborns by protein expression and mutationanalysis of endoglin. Pediatr. Res., 47, 24–35.
35. Pece, N., Vera, S., Cymerman, U., White, R.J., Wrana, J.L. and Letarte, M.(1997) Mutant endoglin in hereditary hemorrhagic telangiectasia type 1 istransiently expressed intracellularly and is not a dominant negative. J. Clin.Invest., 100, 2568–2579.
36. Oettgen, H.C., Pettrey, C.L., Maloy, W.L. and Terhorst, C. (1986) T3-likeprotein complex associated with the antigen receptor on murine T cells.Nature, 320, 272–275.
37. Lux, A., Attisano, L. and Marchuk, D.A. (1999) Assignment oftransforming growth factor beta1 and beta3 and a third new ligand to thetype I receptor ALK-1. J. Biol. Chem., 274, 9984–9992.
38. Chen, Y.G. and Massague, J. (1999) Smad1 recognition and activation bythe ALK1 group of transforming growth factor-beta family receptors. J.Biol. Chem., 274, 3672–3677.
39. Li, D.Y., Sorensen, L.K., Brooke, B.S., Urness, L.D., Davis, E.C., Boak,B.B. and Wendel, D.P. (1999) Defective angiogenesis in mice lackingendoglin. Science, 284, 1534–1537.
40. Bourdeau, A., Dumont, D.J. and Letarte, M. (1999) A murine model ofhereditary hemorrhagic telangiectasia. J. Clin. Invest., 104, 1343–1351.
41. Dickson, M.C., Martin, J.S., Cousins, F.M., Kulkarni, A.B., Karlsson, S.and Akhurst, R.J. (1995) Defective haematopoiesis and vasculogenesis intransforming growth factor-β1 knock out mice. Development, 121, 1845–1854.
42. Oshima, M., Oshima, H. and Taketo, M. (1996) TGF-β receptor type IIdeficiency results in defects of yolk sac hematopoiesis and vasculogenesis.Dev. Biol., 179, 297–302.
43. Pece-Barbara, N., Cymerman, U., Vera, S., Marchuk, D.A. and Letarte, M.(1999) Expression analysis of four endoglin missense mutations suggestshaploinsufficiency is the predominant mechanism for hereditaryhemorrhagic telangiectasia type 1. Hum. Mol. Genet., 8, 2171–2181.
44. Bellón, T., Corbi, A., Lastres, P., Calés, C., Cebrián, M., Vera, S., Chefeitz,M., Massagué, J., Letarte, M. and Bernabeu, C. (1993) Identification andexpression of two forms of the human transforming growth factor-β-bindingprotein endoglin with distinct cytoplasmic regions. Eur. J. Immunol., 23,2340–2345.
45. Carcamo, J., Weis, F.M.B., Ventura, F., Wieser, R., Wrana, J.L., Attisano,L. and Massagué, J. (1994) Type I receptors specify growth-inhibitory andtranscriptional responses to transforming growth factor β and activin. Mol.Cell. Biol., 14, 3810–3821.
46. Attisano, L., Wrana, J.L., Cheifetz, S. and Massagué, J. (1992) Novelactivin receptors: distinct genes and alternative mRNA splicing generate arepertoire of serine/threonine kinase receptors. Cell, 68, 97–108.
47. Lopez-Guerrero, J.A., Lopez-Bote, J.P., Ortiz, M.A., Gupta, R.S., Paez, E.and Bernabeu, C. (1993) Modulation of adjuvant arthritis in Lewis rats byrecombinant vaccinia virus expressing the human 60-kilodalton heat shockprotein. Infect. Immun., 61, 4225–4231.
48. Pichuantes, S., Vera, S., Bourdeau, A., Pece, N., Kumar, S., Wayner, E.A.and Letarte, M. (1997) Mapping epitopes to distinct regions of theextracellular domain of endoglin using bacterially expressed recombinantfragments. Tissue Antigens, 50, 265–276.
49. Raab, U., Velasco, B., Lastres, P., Letamendia, A., Cales, C., Langa, C.,Tapia, E., Lopez-Bote, J.P., Paez, E. and Bernabeu, C. (1999) Expression ofnormal and truncated forms of human endoglin. Biochem. J., 339, 579–588.
50. Frolik, C.A., Wakefield, L.M., Smith, D.M. and Sporn, M.B. (1984)Characterization of a membrane receptor for transforming growth factor-βin normal rat kidney fibroblasts. J. Biol. Chem., 259, 10995–11000.
51. Cheifetz, S., Bassols, A., Stanley, K., Ohta, M., Greenberger, J. andMassagué, J. (1988) Heterodimeric transforming growth factor β.Biological properties and interaction with three types of cell surfacereceptors. J. Biol. Chem., 263, 10783–10789.
52. Massagué, J., Czech, M.P., Iwata, K., DeLarco, J.E. and Todaro, G.J. (1982)Affinity labeling of a transforming growth factor receptor that does notinteract with epidermal growth factor. Proc. Natl Acad. Sci. USA, 79, 6822–6826.

1238 Human Molecular Genetics, 2000, Vol. 9, No. 8




















