Amniotic mesenchymal cells autotransplanted in a porcine model of cardiac ischemia do not...
8
Amniotic mesenchymal cells autotransplanted in a porcine model of cardiac ischemia do not differentiate to cardiogenic phenotypes Saverio Sartore a, * , Maddalena Lenzi a , Annalisa Angelini b , Angela Chiavegato a , Lisa Gasparotto a , Paolo De Coppi c , Roberto Bianco d , Gino Gerosa d a Department of Biomedical Sciences, University of Padua, Viale G. Colombo, 3, I-35121 Padua, Italy b Institute of Pathologic Anatomy, University of Padua, Padua, Italy c Department of Pediatrics, University of Padua, Padua, Italy d Department of Cardiological, Thoracic and Vascular Sciences, University of Padua, Padua, Italy Received 17 June 2005; received in revised form 25 July 2005; accepted 27 July 2005; Available online 26 September 2005 Abstract Objective: Transplantation of stem cells in the acute ischemic myocardium (AMI) may play a role in the recovery of cardiac function. Here, we investigated the ability of amniotic fluid-derived mesenchymal cells (AFC) for phenotypic conversion to vascular cells and cardiomyocytes (CM) when autotransplanted in a porcine model of AMI. Methods: Single AFC preparations were taken from 12 fetuses 3 days before normal delivery. AFC were expanded in vitro and stored separately until animals of the original litter weighed 22—25 kg. A new model of AMI, i.e. 45-min circumflex coronary occlusion followed by wall dissection, was used to assess AFC differentiation potential. CMFDA-labeled AFC were autogenically transplanted in the ischemic area 1 week after AMI induction. Thirty days later, pigs were sacrificed and the phenotypic profile of transplanted AFC was assessed and compared to the corresponding pre-injection pattern. Results: AFC showed in vitro to be of mesenchymal type also expressing markers of ‘embryonic stem’ cells (SSEA4 and Oct-4), as well as endothelial (von Willebrand factor, VE-cadherin) and smooth muscle (SM a-actin, SM22) cells. Thirty days after transplantation, in the survived AFC (5 1%) ‘embryonic stem’ cell markers disappeared and mesenchymal cell markers were down regulated with the exception of smooth muscle and endothelial antigens. No evidence for expression of cardiac troponin I was found.Conclusions: In the conditions used in this study, AFC were able to transdifferentiate to cells of vascular cell lineages but not to CM. Thus, porcine AFC may require further ex vivo re-programming to be suitable for therapeutic use in AMI. # 2005 Elsevier B.V. All rights reserved. Keywords: Cell transplantation; Ischemia; Myocardial infarction; Tissue engineering. 1. Introduction Stem cells, directly transplanted or mobilized from cardiac or extra-cardiac derived compartments, have been proposed as innovative and efficacious strategies to replace damaged myocardium and vessels or to limit remodeling of the post-ischemic heart [1]. It has been hypothesized that cells of the cardiogenic lineages can be produced via a transdifferentiation (a phenotypic conversion from an ontogenically distinct cell type to another), fusion (with a differentiated resident cell), growth factor/cytokine stimu- lation (released from transplanted or resident stem cells) or, perhaps, a combination of these processes [1]. Newly formed CM, vascular smooth muscle or endothelial cells in the ischemic heart can be obtained by transplantation of embryonic or adult (bone marrow-derived or circulating) stem cells, resulting in functional improvement with partial recovery of contractility or reduced cardiac remodeling [2]. Embryonic stem cells seem to be potentially a better tool than the adult counterpart [2] in terms of cell plasticity and, hence, differentiation potential. In contrast, the use of these cells is hampered by ethical reasons. Thus, other sources of stem cells not sharing these problems, such as cord blood stem cells [3] or cells of the amniotic fluid [4], could be potentially of interest for clinical applications provided that they are able to give structural and functional benefits to the damaged heart once transplanted. Human amniotic fluid cells are endowed with some interesting properties such as: (1) in vitro expression of ‘stemness’ markers [5] as well as mesenchymal and neuroglial markers [4—6], (2) a tolerant-type histocompatibility antigen profile [7], (3) the capacity to switch to CM-like cells in vitro after stimulation with FGF-2, activin A or coculture with rat neonatal CM [8], and (4) the ability of correcting genetically based enzymatic defects once transplanted in injured brain [9]. Before moving on to functional studies, it is preliminarily important to assess the differentiation potential of AFC in vivo, possibly using a model of AMI of clinical relevance. The porcine model appears to be particularly suitable in this www.elsevier.com/locate/ejcts European Journal of Cardio-thoracic Surgery 28 (2005) 677—684 * Corresponding author. Tel.: þ39 049 827 6032; fax: þ39 049 827 6040. E-mail address: [email protected] (S. Sartore). 1010-7940/$ — see front matter # 2005 Elsevier B.V. All rights reserved. doi:10.1016/j.ejcts.2005.07.019
Transcript of Amniotic mesenchymal cells autotransplanted in a porcine model of cardiac ischemia do not...

Amniotic mesenchymal cells autotransplanted in a porcine model of cardiacischemia do not differentiate to cardiogenic phenotypes
Saverio Sartore a,*, Maddalena Lenzi a, Annalisa Angelini b, Angela Chiavegato a,Lisa Gasparotto a, Paolo De Coppi c, Roberto Bianco d, Gino Gerosa d
aDepartment of Biomedical Sciences, University of Padua, Viale G. Colombo, 3, I-35121 Padua, Italyb Institute of Pathologic Anatomy, University of Padua, Padua, Italy
cDepartment of Pediatrics, University of Padua, Padua, ItalydDepartment of Cardiological, Thoracic and Vascular Sciences, University of Padua, Padua, Italy
Received 17 June 2005; received in revised form 25 July 2005; accepted 27 July 2005; Available online 26 September 2005
Abstract
Objective: Transplantation of stem cells in the acute ischemic myocardium (AMI) may play a role in the recovery of cardiac function. Here, weinvestigated the ability of amniotic fluid-derived mesenchymal cells (AFC) for phenotypic conversion to vascular cells and cardiomyocytes (CM)when autotransplanted in a porcine model of AMI. Methods: Single AFC preparations were taken from 12 fetuses 3 days before normal delivery.AFC were expanded in vitro and stored separately until animals of the original litter weighed 22—25 kg. A new model of AMI, i.e. 45-mincircumflex coronary occlusion followed by wall dissection, was used to assess AFC differentiation potential. CMFDA-labeled AFC wereautogenically transplanted in the ischemic area 1 week after AMI induction. Thirty days later, pigs were sacrificed and the phenotypic profile oftransplanted AFC was assessed and compared to the corresponding pre-injection pattern. Results: AFC showed in vitro to be of mesenchymaltype also expressing markers of ‘embryonic stem’ cells (SSEA4 and Oct-4), as well as endothelial (von Willebrand factor, VE-cadherin) andsmooth muscle (SM a-actin, SM22) cells. Thirty days after transplantation, in the survived AFC (5 � 1%) ‘embryonic stem’ cell markersdisappeared and mesenchymal cell markers were down regulated with the exception of smooth muscle and endothelial antigens. No evidencefor expression of cardiac troponin I was found.Conclusions: In the conditions used in this study, AFC were able to transdifferentiate to cells ofvascular cell lineages but not to CM. Thus, porcine AFC may require further ex vivo re-programming to be suitable for therapeutic use in AMI.# 2005 Elsevier B.V. All rights reserved.
Keywords: Cell transplantation; Ischemia; Myocardial infarction; Tissue engineering.
www.elsevier.com/locate/ejctsEuropean Journal of Cardio-thoracic Surgery 28 (2005) 677—684
1. Introduction
Stem cells, directly transplanted or mobilized fromcardiac or extra-cardiac derived compartments, have beenproposed as innovative and efficacious strategies to replacedamaged myocardium and vessels or to limit remodeling ofthe post-ischemic heart [1]. It has been hypothesized thatcells of the cardiogenic lineages can be produced via atransdifferentiation (a phenotypic conversion from anontogenically distinct cell type to another), fusion (with adifferentiated resident cell), growth factor/cytokine stimu-lation (released from transplanted or resident stem cells) or,perhaps, a combination of these processes [1]. Newly formedCM, vascular smooth muscle or endothelial cells in theischemic heart can be obtained by transplantation ofembryonic or adult (bone marrow-derived or circulating)stem cells, resulting in functional improvement with partialrecovery of contractility or reduced cardiac remodeling [2].
* Corresponding author. Tel.: þ39 049 827 6032; fax: þ39 049 827 6040.E-mail address: [email protected] (S. Sartore).
1010-7940/$ — see front matter # 2005 Elsevier B.V. All rights reserved.doi:10.1016/j.ejcts.2005.07.019
Embryonic stem cells seem to be potentially a better toolthan the adult counterpart [2] in terms of cell plasticity and,hence, differentiation potential. In contrast, the use ofthese cells is hampered by ethical reasons. Thus, othersources of stem cells not sharing these problems, such ascord blood stem cells [3] or cells of the amniotic fluid [4],could be potentially of interest for clinical applicationsprovided that they are able to give structural and functionalbenefits to the damaged heart once transplanted. Humanamniotic fluid cells are endowed with some interestingproperties such as: (1) in vitro expression of ‘stemness’markers [5] as well as mesenchymal and neuroglial markers[4—6], (2) a tolerant-type histocompatibility antigen profile[7], (3) the capacity to switch to CM-like cells in vitro afterstimulation with FGF-2, activin A or coculture with ratneonatal CM [8], and (4) the ability of correcting geneticallybased enzymatic defects once transplanted in injured brain[9]. Beforemoving on to functional studies, it is preliminarilyimportant to assess the differentiation potential of AFCin vivo, possibly using a model of AMI of clinical relevance.The porcine model appears to be particularly suitable in this

S. Sartore et al. / European Journal of Cardio-thoracic Surgery 28 (2005) 677—684678
respect inasmuch as other transplantation studies with stemand non-stem cells were performed [10—18]. In addition,such a model could allow, in perspective, the use of imagingmodalities that are clinically important and can validate theputative structural changes inherent to cell transplantation.The aim of this study was to ascertain the ability of AFC todifferentiate to vascular cells and CM once transplanted intothe infarcted myocardium of a porcine model. Since theamniotic fluid contains a mixture of different cell popula-tions, we have selected a plastic-adherent cell fraction,potentially comparable to the bone marrow MSC alreadyused in other experiments [15,16].
Fig. 1. Experimental design of the in vivo protocol.
2. Material and methods
2.1. Cesarean section and collection of amniotic fluid
A pregnant Large White sow underwent a cesareansection three days before term. All procedures wereapproved by the Italian Ministry of Public Health andperformed in accordance with the ‘Guide for the Care andUse of Laboratory Animals’ prepared by the Institute ofLaboratory Animal Resources, National Research Council(published by the National Academy Press, revised 1966).The pig used in this study originated from a colony in whichMHC class II antigen, as determined by indirect immuno-fluorescence with a specific anti-porcine antibody (Serotec,Oxford, UK), is expressed in 100% of bone marrow-derivedMSC.
The pig was pre-medicated with azaperone, midazolaneand ketamine hydrochloride. Anesthesia was induced with aventilation mask using 4.0% isofluorane. The animal wasintubated with a cuffed endotracheal tube and ventilatedwith 100% oxygen. Anesthesia was maintained with 1.5%isofluorane. Electrocardiogram and respiration were mon-itored by a multiple channel recorder. By abdominalhysterectomy, 15 fetuses and the respective amniotic fluids(about 50 ml) were rapidly collected. All piglets werereanimated and kept in a controlled environment for a fewhours and then transferred to a foster-mother in the animalfacility where they were kept for 3 months.
2.2. Induction of AMI
Cesarean-born animals enrolled in this experiment,weighing about 22—25 kg, were subjected to AMI. Pre-medication and anesthesia were given as described above.Antibiotics (Cefazolin, 35 mg/kg) were given the daybefore surgery and continued up to 5 days post-surgery.AMI was obtained by a percutaneous procedure involvingan intraluminal thrombotic occlusion of the 3rd lateralbranch of circumflex coronary artery. In this procedure,the left femoral artery was isolated and cannulated withan introduction sheath (percutaneously accessed byneedle puncture, in which a flexible guide wire wasadvanced, then the needle was withdrawn and theintroducing sheath placed over the guide wire). Throughthe sheath, a JR 3.5 6F guiding catheter was used tocannulate the left main stem under fluoroscopic guidance.Once the circumflex branch of choice became visible by
angiography, a guide wire was positioned in it and aballoon (Opensail, 2.5 mm of diameter) was advanced inthe lumen. Occlusion of this vessel branch was achievedby increasing the intraluminal pressure to 8 atm andconfirmed by angiography. After 45 min of occlusion, thepressure was further increased to 20 atm to induce walldissection and subsequent thrombosis. Electrocardio-graphic monitoring showed ST-segment change andocclusion of the vessel was confirmed by angiography.Episodes of ventricular tachycardia and fibrillation wereterminated with lidocaine and external defibrillation.Finally, a 6-Fr pigtail catheter was retrogradely advancedinto the left ventricle and a cardiac ventriculography wasobtained to confirm the segmental dysfunction of the leftventricular wall caused by coronary artery occlusion.After intervention, pigs received analgesics (Buprenex,0.03 mg/kg) and cortisone (1 mg/kg) before returning tothe animal facility.
One of the operated animals was sacrificed 2 h afterinjection to identify the AFC distribution with respect to theischemic region and to evaluate the surviving level ofCMFDA-labeled AFC 30 days after transplantation (seeFig. 1). Two animals were injected with aMEM solutiononly. Two pigs were sacrificed 7 and 37 days, respectively,after induction of AMI to study the time-course of infarctionin absence of AFC transplant. Two AFC preparations werealso delivered in an autogenic manner, to the heart of intactanimals.
2.3. Preparation of AFC
Samples of amniotic fluids taken from the differentfetuses were diluted with PBS pH 7.2 (1:2, v/v) and thenspun down at 1000 rpm in Eppendorf 5804R Centrifuge.Pellets were resuspended in the Amniotic Culture Medium(ACM; 63% aMEM (Life Technology, Gaithersburg, MD), 20% ofChang Medium (Chang B plus Chang C; Irvine Scientific,Santa Ana, CA), 15% of fetal bovine serum (FBS) containingstreptomycin, penicillin and L-glutamine. Cell seeding wasperformed on Falcon petri dishes (Becton Dickinson, LosAngeles, Ca) at a density of 4.5�102 cells/cm2. After 3 days,non-adherent cells and debris were discharged and theadherent cells cultivated until preconfluency. Adherentcells were detached from the plastic substrate using 0.05%trypsin and 0.02% sodium-EDTA (Life Tech). Cells grown in anincubator at 378C with 95% air and 5% carbon dioxide were

S. Sartore et al. / European Journal of Cardio-thoracic Surgery 28 (2005) 677—684 679
Table 1Immunophenotypic characterization of AFC as determined in vitro (tissuecultures and cytospins) and in vivo (CMFDA-positive transplanted cells inthe ischemic myocardium)
Antigens Cell cultures Cytospins CMFDAþ-transplantedcells
CD34 — — —CD45 — — —CD117/c-kit — — —Sca-1 — — —SSEA4 þ þ —Oct4 þ þ —Vimentin þþþ þþþ —CD105/Endoglin — þþ þThy-1/CD90 þþþ þþþ þDesmin n.d. — n.d.CardiacTnI — — —SM a-actin þ þþ þSM22 þþþ þþ —SM myosin n.d. — —CD31/PECAM þ þ þvon Willebrand factor þþþ þþ þVE-cadherin þ þþ þ
n.d., Not determined; —, no cell labelled; þ, up to 30% labelled cells; þþ,from 30 to 60% of cells are labelled; þþþ, 60—90% of cells are labeled. Notethat the expression of antigenic markers in AFC reported in the Cell Culturescolumn was evaluated after 15 days in cultures, keeping AFC on confluentconditions and in the presence of ACM.
passaged until approximately 10—12 million of AFC for eachanimal were collected (5—6 passages).
2.4. In vitro phenotypic profile of AFC
Stability of antigenic marker expression in ACM wasassayed by culturing AFC at each passage onto 1% gelatin-coated glass coverslips for 5 days. Propensity of AFC tovascular cell phenotypic conversion was evaluated by seedingcells (3�103 cells/cm2) in Endothelial Growth Medium(Promocell, Heidelberg, Germany), containing 20% FBS (forendothelial cells), or in Smooth Muscle Cell Medium,containing DMEM and 10% FBS (for smooth muscle cells) ongelatin-coated Falcon petri dishes. Cells were fixed after7 days of culture. Coverslips with AFC grown in ACM or in thetwo differentiating media were fixed in 1.5% p-formaldehydein PBS and tested in single or double immunofluorescenceusing anti-PECAM/CD31 (Chemicon, Temecula, Ca), anti-VE-cadherin (Santa Cruz Biotech, Santa Cruz, Ca), anti-Oct4(Chemicon), anti-SM a-actin (Sigma, St Louis, Mo) and SM-E7anti-SM myosin [19] and IgG anti-mouse or anti-rabbitrhodaminated or fluoresceinated secondary antibodies (Che-micon). Distribution of antigens was studied using a ZeissAxioplan epifluorescence microscope (Zeiss, Oberkochen,Germany), and images were acquired using a Leica DC300Fdigital videocamera (Leica, Wetzlar, Germany).
2.5. Labeling and injection of AFC
To identify the transplanted cells in the recipientmyocardium, AFC were labeled with CMFDA (chloromethyl-fluorescein diacetate) following the instructions furnished bythe manufacturer (Molecular Probes, Eugene, Or). Fortransplantation, cells taken from cultures at confluentconditions were dissociated from the petri dishes using0.025% trypsin-EDTA and spun at 1050 rpm for 10 min toremove the enzyme. The pellet was rinsed twice in PBS andcells suspended in alpha MEM medium at a concentration of7.5�106 cells/ml. Trypan blue staining of CMFDA-labeledcells showed that >90% of AFC were viable. One week afterAMI induction (see Fig. 1), pigs destined to receive AFCtransplants were examined by echocardiography and ven-triculography to confirm and localize the infarcted region.Subsequently, with the animals under general anesthesia, theinfarcted area was exposed through a left thoracotomy. Thevarious cell suspensions were autogenic injected in theborder zone of ischemic region (1 ml, 7.5�106 cells,distributed in 3—4 sites) of the corresponding animals usingan insulin syringe and a 27-gauge needle. Culture medium(aMEM) was used as control.
Area of cell transplantation or culture medium injectionwas marked with a Prolene suture for subsequent identifica-tion at the time of sacrifice. Then, the chest was closedleaving the pericardial wound open and the air evacuatedfrom the cardiac cavity. After intervention, pigs receivedanalgesics (Buprenex, 0.03 mg/kg) and cortisone (1 mg/kg)before returning to the animal facility. AMI pigs withtransplanted AFC were euthanized after 30 days from cellinjection. Score of survived CMFDA-stained AFC in AMI heartswas performed by counting positive cells in four randomlyselected high-power fields taken from 10 cryosections per
tissue blocks of animals sacrificed 2 h vs. 30 days from AFCtransplantation.
2.6. Immunocytochemical analysis of AMI lesion
Cardiac cryosections from AMI hearts were fixed in 1.5% p-formaldehyde in PBS pH 7.2 and then incubated with theprimary antibody for 30 min at 37 8C. After two rinses in PBS,cells were incubated with peroxidase-labeled secondaryantibody (Dako, Glostrup, Denmark) to the monoclonalprimary antibody according to Chiavegato et al. [19]. Theprimary antibodies were the followings: anti-cardiac tropo-nin I [20]; anti-EIIIA fibronectin (a generous gift of Dr LucianoZardi, Genoa, Italy); anti-desmin (Chemicon); anti-procolla-gen I (Iowa Hybridoma Bank; Iowa City); anti-SM a-actin(Sigma); anti-von Willebrand factor (Dako), anti-CD45(Serotec); 1B8 anti-SM22 [19]. Optical images were acquiredby a Leica DMR microscope connected to a Leica DC300videocamera (Leica, Wetzlar, Germany).
2.7. Immunocytochemical analysis of AFC before andafter transplantation
AFC to be used in cell transplantation were enzymaticallydetached from petri dishes and studied for their immuno-phenotypic properties by cytospin preparations obtainedwith a Shandon Cytospin 4 centrifuge. Cytospin-obtainedcells were fixed in 1.5% p-formaldehyde in PBS pH 7.2 andthen incubated with the primary antibody (antigens of thecardiogenic and non-cardiogenic cell lineages as wellembryonic and hematopoietic antigens; see Table 1) for30 min at 37 8C. Cells were incubated with rhodaminatedsecondary antibody (Chemicon) to the monoclonal orpolyclonal primary antibodies. CMFDA-labeled cells in thetransplants were detected by FITC-conjugated rabbit

S. Sartore et al. / European Journal of Cardio-thoracic Surgery 28 (2005) 677—684680
anti-CMFDA antibody (Molecular Probes) in double labelingexperiments [19]. The primary antibodies used in theimmunofluorescence experiments were the following:anti-CD34 (Becton Dickinson); anti-CD45 (Serotec); anti-c-kit/CD117 (Dako); anti-Oct4 (Chemicon); anti-SSEA4 (Che-micon); anti-Sca-1 (Cedarlane, Hornby, Ont., Canada); anti-Thy-1/CD90 (Cymbus, Chandlers Ford, UK); 1B8 anti-SM22[19]; anti-SM a-actin (Sigma); SM-E7 anti-SM myosin [19];anti-PECAM/CD31 (Chemicon); anti-VE-cadherin (SantaCruz); anti-von Willebrand factor (Dako); anti-vimentin(Dako); anti-desmin (Chemicon); anti-endoglin/CD105(Cymbus). Immunofluorescence observations were carriedout using a Zeiss Axioplan epifluorescence microscope andresults obtained re-evaluated by Leica SPS2SL confocalmicroscope.
Semiquantitative evaluation of antigenic expressionprofile in cytospins, cell cultures and transplants of AFC(Table 1) was carried out by manually counting positive cellswith respect to Hoechst-stained nuclei by two independentoperators. Cells in four randomly selected high-power fields,five cytospin preparations or cryosections, were averaged.There was a total of at least 100 cells in each field.
3. Results
3.1. Animal data
Three out of the 15 animals obtained by cesarean sectiondied within a few days after birth (Fig. 1). The 12 survivinganimals were operated via the percutaneous procedurewhich, in our hands, was not life-threatening and allowed fora clear cut recognition of the ischemic area and a safepositioning of AFC injections in the border zone. Six pigs of
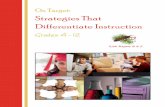
Fig. 2. Results of percutaneous catheterism on circumflex coronary artery atday 37 after intervention. (A) Control vessel; (B) obliterated vessel (arrow-head); hematoxylin—eosin (C) and Azan Mallory (D) staining of the vesselshowed in B, in which a thrombus completely occludes the lumen (arrow-heads). (E) Lateral view of the heart showing the ischemic region (rectangle).(F) Cross-section of the heart showing localization of the ischemic region andthinning of the cardiac wall (arrowhead).
the original litter were randomly selected as candidates ofautogenic cell transplantation with their own CMFDA-labeledAFC preparations after induction of AMI.
3.2. Characterization of AMI model
The transient blood flow obstruction followed by walldissection applied to induce the AMI model in pig gave riseto a thrombus formation (Fig. 2B—D) and a reproducibleischemic lesion which involved the lateral region of theleft ventricle showing a marked wall thinning out (Fig. 2Eand F). Cross-sections of the ventricular wall at day 7 post-ischemic time revealed that the infarction is predomi-nantly transmural (not shown). Histological staining withhematoxylin—eosin showed that the ischemic region ischaracterized by the absence of CM (no immunoreactivityfor cardiac troponin I and desmin), presence of granulationtissue (i.e. myofibroblasts identified by immunoreactivityfor SM a-actin and SM22; neoangiogenesis identified byimmunoreactivity for von Willebrand factor; fibrous tissueidentified by immunoreactivity for fibronectin EIIIA isoform
Fig. 3. Immunocytochemical patterns of cardiac cryosections from day 7 post-AMI stained with antibodies to cardiac troponin I (cTnI; A), desmin (B), SM a-actin (C), SM22 (D), von Willebrand factor (vWf; E), fibrionectin isoform EIIIA(F), procollagen I (G) and CD45 (H). Asterisks indicate the ischemic region.Note that CM have almost disappeared and a granulation tissue is now visible. Afew inflammatory cells are detectable in H. Bar, 150 mm.

S. Sartore et al. / European Journal of Cardio-thoracic Surgery 28 (2005) 677—684 681
Fig. 5. Immunofluorescence patterns of cytospin-plated porcine AFC stainedwith antibodies to vimentin (A), cardiac troponin I (cTnI; B), SM a-actin (C),SM22 (D), von Willebrand factor (vWf; E), and VE-cadherin (F). Note that nocells are reactive for cTnI. Arrowheads indicate cells with double-nucleicontent. Nuclei are in blue. Bars, 50 mm (A, C—H) and 80 mm (B).
and procolloagen I) and a few inflammatory, mainly CD45-positive, cells (see Fig. 3). Histological examination ofcryosections after 37 days of ischemia showed the presenceof some vessels and myofibroblasts embedded into anorganizing fibrous tissue (not shown).
3.3. Immunophenotyping of AFC before transplantation
Fifteen days after the initial plating, two majormorphologically distinguishable AFC populations appearedin vitro: one is of spindle-shape and the other is a polygonal-type (Fig. 4B). The polygonal-type cells, often grouped inclusters, are predominantly expressed in confluent cultures(Fig. 4C). There was no difference in the relative proportionof the two populations after passaging, but some AFCpreparations from different animals presented almostexclusively spindle-shaped cells.
Immunophenotyping of cultured, confluent AFC in ACM didnot show any correlation between antigenic marker dis-tribution (at least for the markers shown in Table 1) andmorphological features. Interestingly, some markers (e.g.CD105/endoglin) disappeared when AFC were cultured on adifferent substrate (non-tissue culture Petri dishes vs. glasscoverslips; not shown).
When the AFC were grown in differentiating media, e.g.Endothelial Growth Medium or Smooth Muscle Cell Medium,both in sub- and confluent conditions, the expression ofvascular cell markers is enhanced and occurs earlier than in
Fig. 4. Phase contrast aspects of in vitro grown AFC as seen at 7 (A), 15 (B) and20 (C) days of culture in Amniotic Culture Medium. In panel A, black arrowheadin A shows a cell with a neuron-like morphology whereas white arrowheadindicates a spindle-shaped cell. Arrows in B and C indicate clusters of poly-gonal-shaped cells particularly abundant in confluent cultures (C). Phasecontrast (D and G) and immunofluorescence staining (E and F;H and I) of 7-day cultured porcine AFC in Endothelial Growth Medium (D—F) or SmoothMuscle Cell Medium (G—I). Note the different morphology of AFC when grownin the two different media. AFC grown in Endothelial Growth Mediumwhere allOct4 and PECAM positive (E) whereas VE-cadherin (F) is heterogeneouslyexpressed (red arrowhead in F indicates a negative cell for this marker). InSmooth Muscle Cell Medium, a minority of AFC shows to be positive for SM a-actin (blue arrowhead in H indicates a negative cells for this marker) and all areOct4þ (H) SM myosin is, however, undetectable (I). Bars, 90 mm (A—C), 60 mm(D—G) and 70 mm (E and F, H and I). Hst, Hoechst staining. (For interpretationof the reference to color in this legend, the reader is referred to the webversion of this article.)
ACM. Fig. 4E and F shows that all AFC are now labeled withanti-PECAM and most of them are also positive with anti-VE-cadherin. Similarly, the majority (about 60%) of AFC grown inthe presence of Smooth Muscle Cell Medium are now SM a-actinþ but a complete differentiation is not achievedinasmuch as these cells are SM myosin� (Fig. 4H and I). AllAFC in either cell cultures were Oct4þ (Fig. 4E and H).
In cytospinpreparations, all cells (obtained fromAFCgrownin ACM, just before transplantation) appeared to be ofmesenchymal type inasmuch as they are vimentin-positive(Fig. 5; Table 1). Part of them was also reactive for themesenchymal cell markers CD105/endoglin and Thy-1/CD90(Table 1). They did not express hematopoietic cell markers,such as CD34 and c-kit, but they were variably positive formarkers of smooth muscle (SM a-actin and SM22), andendothelial (von Willebrand factor, VE-cadherin, PECAM) celllineages. Interestingly, minority of cells were also stained forthe ‘embryonicmarkers’ SSEA4andOct4 (Table 1). Noticeably,about one-third of AFC collected and examined via cytospins(Fig. 5A and D) or glass coverslips (not shown) displayed adouble-nuclei content. This ratio did not change with CMFDAlabeling or with the duration of cell culturing.
3.4. Immunophenotyping of AFC after transplantation
Before transplanting CMFDA-labeled AFC in the intact orAMI hearts we tested in vitro whether the immunofluores-cence signal was still detectable with cell proliferation. AFClabeled with CMFDA were grown in pre-confluent conditionsand subjected to repeated passages. After three passages,the immunofluorescence staining was still evident. From thefourth up to the eight passage, the presence of CMFDA in theAFC was detectable only using a FITC-labeled anti-CMFDAantibody (not shown).

S. Sartore et al. / European Journal of Cardio-thoracic Surgery 28 (2005) 677—684682
Fig. 6. Cell tracking at 2 h (A) and 30 days (B) of CMFDA-labeled AFCtransplanted in ischemic porcine hearts by immunofluorescence. Long rowsof transplanted cells are particularly visible in B whereas in A they aredispersed among cardiac tissues. In panel B is shown an example of CMFDAþ
cells studied for the expression of differentiation markers and identified bysmall lettered boxes. Vital CMFDA transplanted AFC are in green and anapoptotic cell in yellow (identified by a yellow arrowhead in panel B). Bars,110 (A) and 80 mm (B). (For interpretation of the reference to color in thislegend, the reader is referred to the web version of this article.)
Fig. 7. Phenotypic expression of mesenchymal (A—C), myocardial (D—F),smooth muscle (G—O) and endothelial (P—R) cell markers in CMFDA-labeledAFC transplanted in ischemic porcine hearts 30 days after injection. A—C,Vimentin; D—F, cardiac troponin I (cTnI); H and I, SM a-actin; J—L, SMmyosin;M—O, SM22; P—R, PECAM. Green arrowheads indicate transplanted AFCexclusively positive for CMFDA whereas yellow arrowheads identify trans-planted CMFDA-labeled AFC and also reactive with other antibodies. Nucleiare stained blue by Hoechst staining. Bar, 80 mm. (For interpretation of thereference to color in this legend, the reader is referred to the web version ofthis article.)
There was a considerable number of CMFDA-labeled cells2 h after transplantation in the border zone of the ischemicregion (Fig. 6A) whereas AFC were not found in cardiacregions remote from the injection sites. A large number ofcells, morphologically identified as apoptotic cells, and fewCMFDA-labeled cells could be detected when AFC wereinjected in the intact heart (not shown).
As a general rule, AFC at day 30 post-implantation timewere mostly found grouped in long rows in close vicinity ofnewly formed fibrous tissue (Fig. 6B) and very rarely seenapposed to the survived myocardial tissue of the borderzone. CMFDA-positive cell aggregates were frequentlyobserved, but without any evidence for organized tissuestructures such as blood or lymphatic vessels. About 5 � 1%of the CMFDA-labeled cells present 2 h after transplantationin AMI hearts were still detectable 30 days later.
Results of double immunofluorescence experiments ofimmunophenotyping of tracked AFC using the panel ofantibodies as differentiation markers are shown in Fig. 7 andsummarized in Table 1. Noticeably, the ‘embryonic stem’cellmarkers SSEA4 andOct4 completely disappeared and themesenchymal markers vimentin (Fig. 7A—C), CD105/endo-glin and Thy-1/CD90 (Table 1) were lost or decreased. AFCimmunoreactive for cardiogenic cell lineagemarkerswere ingeneral less numerous with respect to the correspondingcells examined in cytospins or in tissue culture. In particular,the CMFDA-tracked cells did not develop any immunostain-ing for themyocardial marker cardiac troponin I (Fig. 7D—F).As to the endothelial (PECAM, von Willebrand factor, VE-cadherin) and smooth muscle (SM22 and SM myosin) celllineage markers, we observed a loss/decrease of reactivitywith the corresponding antibodies. The only exception isrepresented by SM a-actin, which is still detectable(Fig. 7G—I). Altogether, the CMFDA-positive cells alsoreactive for the vascular cell markers shown in Fig. 7 areless than 2%. AMI pigs injected with aMEM showed aimmunophenotypic pattern very similar to the day 30ischemic heart (not shown). AFC injected in the non-ischemic control heart gave an immunophenotypic profilesimilar to that of AFC-transplanted ischemic hearts (notshown).
4. Discussion
In this study, we investigated the differentiationpotential of porcine AFC in vitro and in an in vivo modelof AMI with the aim to evaluate the possible use of theseimmature stem cells for cellular therapy of myocardialischemia. We selected the plastic-adherent AFC andautotransplanted these cells labeled with the cell trackerCMFDA in a novel model of AMI.
Different porcine models of ischemic injury have beenpreviously described to study the structural and functionalconsequences of CM/stem cell transplantation, namelysurgical [13,15,16], microcoil embolization [21], interlum-inal coil occlusion and Gelfoam gelatine embolization [12],and ameroid constrictor implantation [14,17,18]. This

S. Sartore et al. / European Journal of Cardio-thoracic Surgery 28 (2005) 677—684 683
protocol is safe, reproducible and gives almost no pericardialadherence formation and contrary to the coronary arteryligature does not form tenacious adherences and does notgive rise to uncontrolled arrhythmias [21].
In vitro, the selected porcine AFC grown in ACM and inconfluent conditions displayed mostly the immunopheno-typic profile of the ‘classical’ bone marrow-derivedmesenchymal stem cells (MSC), i.e. reactivity for vimentin,CD105/endoglin and CD90/Thy-1 [2] whereas the hemato-poietic antigens CD34, Sca-1 and CD117/c-kit were absent[6]. Interestingly, markers of endothelial (von Willebrandfactor, VE-cadherin, CD31/PECAM) and smooth muscle (SMa-actin, SM22) cell lineages are also expressed. None of thedifferentiation antigens, however, are entirely shared by thewhole AFC population, which is also morphologicallyheterogeneous (Fig. 4 and [22]). The presence of the‘embryonic stem’ cell associated cell surface marker SSEA4along with Oct4 transcription factor suggests that porcineAFC closely resemble the human multipotent AFC [5,23].This is confirmed by the in vitro experiments performed withEndothelial Growth Medium and Smooth Muscle CellMedium: AFC are capable of giving rise to an endothelial-and smooth muscle cell-like phenotypic conversion in thepresence of Oct4. We do not say whether: (1) prolongedcultivation of AFC in these media can complete thedifferentation-maturation process that characterizes thevascular cell lineages, and (2) this event is accompanied bydown regulation of Oct4 expression.
The results of the in vivo study (obtained with AFCpreviously grown in ACM) suggest that these cells did notshow a particular tendency to differentiate giving rise to cellsof the cardiogenic lineages. In fact, after 30 days of tran-splantation in the ischemic myocardium, ‘embryonic stem’cell and mesenchymal cell markers were absent or reduced,expression of differentiation markers of endothelial andsmooth muscle cell lineages was diminished (Table 1). Int-erestingly, Oct4 and SSEA4 immunoreactivity was undetect-able in all survived, transplanted cells. This may suggest thattransplanted AFC not expressing originally these markers areunsuitable for phenotypic conversion to vascular cells.Alternatively, the original Oct4-positive AFC may have downregulated the expression of thesemarkers as a consequence ofvascular cell commitment induced by the myocardial micro-environment and, perhaps, they are differentiating cells.
To sum up, contrary to the porcine bone marrow-derivedMSC [13,14, and our own unpublished results], porcine AFCcould not increment vascular structures in the ischemic/post-ischemic environment. As to AFC transdifferentiation to CM,our data suggest a different scenario with respect to porcineMSC [15,16] or human AFC [8]. In fact, we were unable todetect any antigenic expression of cardiac troponin I (cardiactroponin Tor connexin43; not shown) in transplanted porcineAFC, at least after 30 days of transplantation.
Though possible, it seems unlikely that the post-ischemicenvironment can influence the potential stem cell progres-sion to the vascular and/or CM phenotypes. We took intoaccount the suggestions raised by Lee and Makkar [24] aboutthe benefits that could be attained when stem celltransplantation in AMI is carried out between days 7 and14 post-injury time, i.e. when the inflammatory response isdeclining and reparative process is at its beginning. Our
immunocytochemical data (Fig. 3) confirm that at the 7th daypost-injury, when the AFC were transplanted, granulationtissue was particularly evident. It is well known that fromthis, tissue growth factors and cytokines are abundantlyreleased and, hence, possibly sustaining transplanted cellgrowth/survival. In our model, however, these factors seemunable to induce a further differentiation of AFC. That thepost-ischemic microenvironment is unable to influence thephenotypic potential of AFC is also demonstrated by thesubstantial similarity of the differentiation patterns of thesecells in the ischemic vs. non-ischemic heart.
Our data are apparently in contrast to those of Zhao et al.[8] who used freshly isolated ‘human amniotic mesenchymalcells’ injected in the ischemic rat heart and found that 1 or2 months after xenotransplantation, these cells improvedtheir myocardial commitment by expressing two markers ofdifferentiated CM, i.e. atrial natriuretic protein and b-myosin heavy chains. This discrepancy could be explained bythe inherent structural characteristics of mesenchymal cellsobtained from the amniotic fluid (this study) and theplacenta [8]. In fact, placental-derived mesenchymal cells,prepared by enzymatic digestion, express the cardiomyo-genic transcription factors GATA-4 and Nkx2.5 [25], whichcan switch on these cells a peculiar propensity todifferentiate along this lineage. We cannot exclude,however, that AFC may be phenotypically unstable and cellpassaging to obtain enough cells for transplantation maycompromise their capacity for engrafting and differentiateto cardiogenic cell lineages as might be inferred from thedifferent phenotypic patterns observed in cytospins vs. cellcultures. Obviously, the incapability of AFC to be phenoty-pically converted to CM in our model (at least at the timepoint used in this study) does not deny the possibility thatparacrine effects produced by transplanted AFC areindirectly able to influence the functional recovery ofpost-ischemic lesion [12].
In conclusion, our results indicate that despite the highexpansion capacity of AFC these cells, at least in the swineand in naıve, non-manipulated conditions are inadequate tosupport regeneration of cardiogenic cells. AFC do not seem tosurvive long enough in the periphery of the ischemic lesionand to give rise to a target-specific, committed progeny.Further ex vivo genetic and epigenetic manipulations mightbe needed to implement the surviving and differentiationpotential of AFC.
Acknowledgements
We wish to thank Prof. R. Busetto and Dr A. Ramondo forsetting up the AMI model in pig. We are indebted to DrGiovanni Gaudenzi for staff organization. Dr Paolo De Coppihas been supported by ‘Fondazione Citta della Speranza’.This project was funded by a grant from Istituto Superiore diSanita, Programma sulle Cellule Staminali, Convenzione n.CS 18 to S. Sartore.
References
[1] Orlic D, Hill JM, Arai AE. Stem cells for myocardial regeneration. Circ Res2002;91:1092—102.

S. Sartore et al. / European Journal of Cardio-thoracic Surgery 28 (2005) 677—684684
[2] Pittenger MF, Martin BJ. Mesenchymal stem cells and their potential ascardiac therapeutics. Circ Res 2004;95:9—20.
[3] Huss R. Isolation of primary and immortalized CD34-hematopoietic andmesenchymal stem cells from various sources. Stem Cells 2000;18:1—9.
[4] Kaviani A, Guleserian K, Perry TE, Jennings RW, Ziegler MM, Fauza DO.Fetal tissue engineering from amniotic fluid. J Am Coll Surg 2003;196:592—7.
[5] Prusa A-R, Marton E, Rosner M, Rosner M, Bernaschek G, HengstschlagerM. Oct-4- expressing cells in human amniotic fluid: a new source for stemcell research? Hum Reprod 2003;18:1489—93.
[6] in’tAnker PS, Scherjon SA, Kleijburg-van der Keur C, Noort WA, Claas FHJ,Willemze R, Fibbe WE, Kanhai HHH. Amniotic fluid as a novel source ofmesenchymal stem cells for therapeutic transplantation. Blood 2003;102:1548—9.
[7] Szekeres-Bartho J. Immunological relationship between the mother andthe fetus. Int Rev Immunol 2002;21:471—95.
[8] Zhao P, Ise H, Hongo M, Ota M, Konishi I, Nikaido T. Human amnioticmesenchymal stem cells have some characteristics of cardiomyocytes.Transplantation 2005;79:528—35.
[9] Kosuga M, Sasaki K, Tanabe A, Li XK, Okawa H, Ogino I, Okuda O, Arai H,Sakuragawa N, Kamata Y, Azuma N, Suzuki S, Yamada M, Okuyama T.Engraftment of genetically engineered amniotic epithelial cells correctslysosomal storage in multiple areas of the brain in mucopolysaccharidosistype VII mice. Mol Ther 2001;3:139—48.
[10] Van Meter CH, Claycomb WC, Delcarpio JB, Smith DM, deGruiter H, SmartF, Ochsner JL. Myoblast transplantation in the porcine model: a potentialtechnique for myocardial repair. J Thorac Cardiovasc Surg 1995;110:1442—8.
[11] Li R-K, Weisel RD, Mickle DAG, Jia ZQ, Kim EJ, Sakai T, Tomita S, SchwartzL, Iwanochko M, Husain M, Cusimano RJ, Burns RJ, Yau TM. Autologousporcine heart cell transplantation improved heart function after a myo-cardial infarction. J Thorac Cardiovasc Surg 2000;119:62—8.
[12] Kamihata H, Matsubara H, Nishiue T, Fujiyama S, Tsutsumi Y, Ozono R,Masaki H, Mori Y, Iba E, Tateishi E, Kosaki A, Shintani S, Murohara T,Imaizumi T, Iwasaka T. Implantation of bone marrow mononuclear cellsinto ischemic myocardium enhances collateral perfusion and regionalfunction via side supply of angioblasts, angiogenic ligands, and cytokines.Circulation 2001;104:1046—52.
[13] Fuchs S, Baffour R, Zhou YF, Shou M, Pierre A, Tio FO, Weissman NJ, LeonMB, Epstein SE, Kornowski R. Transendocardial delivery of autologousbone marrow enhances collateral perfusion and regional function in pigswith chronic experimental myocardial ischemia. J Am Coll Cardiol 2001;37:1726—32.
[14] Min J-Y, Sullivan MF, Yang Y, Zhang JP, Converso KL, Morgan JP, Xiao YF.Significant improvement of heart function by cotransplantation of humanmesenchymal stem cells and fetal cardiomyocytes in postinfarcted pigs.Ann Thorac Surg 2002;74:1568—75.
[15] Shake JG, Gruber PJ, Baumgartner WA, Senechal G, Meyers J, RedmondJM, Pittenger MF, Martin BJ. Mesenchymal stem cell implantation in aswine myocardial infarct model: engraftment and functional effects. AnnThorac Surg 2002;73:1919—26.
[16] Tomita S, Mickle DAG, Weisel RD, Jia ZQ, Tumiati LC, Allidina Y, Liu P, LiRK. Improved heart function with myogenesis and angiogenesis afterautologous porcine bone marrow stromal cell transplantation. J ThoracCardiovasc Surg 2002;123:1132—40.
[17] Kamihata H, Matsubara H, Nishiue T, Nishiue T, Fujiyama S, Amano K, IbaO, Imada T, Iwasaka T. Improvement of collateral perfusion and regionalfunction by implantation of peripheral blood mononuclear cells intoischemic myocardium. Arterioscler Thromb Vasc Biol 2002;22:1804—10.
[18] Kawamoto A, Tkebuchava T, Yamaguchi JI, Nishimura H, Yoon YS, MillikenC, Uchida S, Masuo O, Iwaguro H, Ma H, Hanley A, Silver M, Kearney M,Losordo DW, Isner JM, Asahara T. Intramyocardial transplantation ofautologous endothelial progenitor cells for therapeutic neovasculariza-tion of myocardial ischemia. Circulation 2003;107:461—8.
[19] Chiavegato A, Roelofs M, Franch R, Castellucci E, Sarinella F, Sartore S.Differential expression of SM22 isoforms in myofibroblasts and smoothmuscle cells from rabbit bladder. J Muscle Res Cell Motil 1999;20:133—46.
[20] Gorza L, Ausoni S, Merciai N, Hastings KE, Schiaffino S. Regional differ-ences in troponin I isoform switching during rat heart development. DevBiol 1993;156:253—64.
[21] Pak H-N, Qayyum M, Kim DT, Hamabe A, Miyauchi Y, Lill MC, Frantzen M,Takizawa K, Chen LS, Fishbein MC, Sharifi BG, Chen PS, Makkar R.Mesenchymal stem cell injection induces cardiac nerve sprouting andincreased tenascin expression in a swine model of myocardial ischemia. JCardiovasc Electrophysiol 2003;14:841—8.
[22] Hoehn H, Salk D. Morphological and biochemical heterogeneity of amnio-tic fluid cells in culture. Methods Cell Biol 1982;26:11—34.
[23] in’tAnker PS, Scherjon SA, Kleijburg-van der Keur C, De Groot-SwingsGMJS, Claas FHJ, Fibbe WE, Kanhai HHH. Isolation of mesenchymal stemcells of fetal or maternal origin from human placenta. Stem Cells 2004;22:1338—45.
[24] Lee MS, Makkar RR. Stem-cell transplantation in myocardial infarction: astatus report. Ann Intern Med 2004;140:729—37.
[25] Fukuchi Y, Nakayama H, Sugiyama D, Hirose I, Kitamura T, Tsuji K. Humanplacenta- derived-cells have mesenchymal stem/progenitor cell poten-tial. Stem Cells 2004;22:649—58.