
Differential interactions of serum and bronchoalveolar lavage ...
Upload
independentCategory
view
1download
0
Eur Respir J, 1996, 9, 1858–1867DOI: 10.1183/09031936.96.09091858Printed in UK - all rights reserved
Copyright ERS Journals Ltd 1996European Respiratory Journal
ISSN 0903 - 1936
BBrroonncchhooaallvveeoollaarr aanndd ssyysstteemmiicc ccyyttookkiinnee pprrooffiilleess iinn ppaattiieennttss wwiitthh AARRDDSS,,sseevveerree ppnneeuummoonniiaa aanndd ccaarrddiiooggeenniicc ppuullmmoonnaarryy ooeeddeemmaa
H. Schütte, J. Lohmeyer, S. Rosseau, S. Ziegler, C. Siebert, H. Kielisch, H. Pralle, F. Grimminger, H. Morr, W. Seeger
Bronchoalveolar and systemic cytokine profiles in patients with ARDS, severe pneumo-nia and cardiogenic pulmonary oedema. H. Schütte, J. Lohmeyer, S. Rosseau, S. Ziegler,C. Siebert, H. Kielisch, H. Pralle, F. Grimminger, H. Morr, W. Seeger. ERS JournalsLtd 1996.ABSTRACT: The aim of this study was to investigate whether bronchoalveolarlavage (BAL) and serum levels of proinflammatory cytokines discriminate betweendifferent entities of patients with acute respiratory failure.
BAL and circulating concentrations of interleukin-6 (IL-6), interleukin-8 (IL-8)and tumour necrosis factor-α (TNF-α) were measured in 74 mechanically-ventila-ted patients and 17 healthy controls. Patients were classified as cardiogenic pul-monary oedema (CPO), acute respiratory distress syndrome (ARDS), primary severepneumonia (PN) and a combined group (PN+ARDS).
In all patients with ARDS and/or PN, markedly elevated BAL levels of IL-6 andIL-8 were detected, which were significantly greater than levels in CPO and healthycontrols. Absolute quantities and time-course of these cytokines did not differenti-ate between the absence and presence of lung infection, or different categories ofPN. Similarly, circulating IL-6 levels were comparably elevated in patients withARDS and/or PN, whereas circulating IL-8 concentrations were inconsistentlyincreased. TNF-α was rarely detected in BAL samples, but increased serum con-centrations were measured in ARDS and/or PN patients.
Bronchoalveolar lavage levels of interleukin-6 and interleukin-8, but not tumournecrosis factor-α, and serum concentrations of interleukin-6 are consistently ele-vated in acute respiratory distress syndrome and/or severe pneumonia, discrimi-nating these entities from cardiogenic pulmonary oedema. Alveolar and systemiccytokine profiles do not differentiate between acute respiratory distress syndromein the absence of lung infection and states of severe primary or secondary pneu-monia, which evidently present with comparable local and systemic inflammatorysequelae.Eur Respir J., 1996, 9, 1858–1867.
Dept of Internal Medicine, Justus-LiebigUniversity, Klinikstrasse, Giessen, FRG.
Correspondence: W. SeegerDept of Internal MedicineJustus-Liebig UniversityKlinikstrasse 3635385 GiessenFRG
Keywords: Acute respiratory distresssyndromebronchoalveolar lavageinterleukin-5interleukin-8tumour necrosis factor-α
Received: July 6 1995Accepted after revision April 9 1996
Parts of the doctoral theses of S.Z. andC.S. are incorporated in this report.
Cytokines are involved in a variety of inflammatory lungdiseases, but their pathogenetic role and their significanceas diagnostic tools are still controversial. Interleukin-8(IL-8) is important for the recruitment of inflammatorycells into the alveolar space, which is a hallmark of theacute respiratory distress syndrome (ARDS) and severepneumonia (PN). Elevated levels of IL-8 have beenshown in bronchoalveolar lavage (BAL) fluids of ARDSpatients [1–4], as well as under general conditions ofsepsis and multiorgan failure [5–7]. Tumour necrosisfactor-α (TNF-α) is secreted by monocytes or macro-phages, including those of the alveolar space, after expo-sure to bacterial lipopolysaccharides and a variety ofproinflammatory mediators [8, 9]. Together with othercytokines, it appears to orchestrate the response to an in-flammatory stimulus. Many features of septic shock[10–13] and ARDS [14, 15] have been ascribed to TNF-α, but measurements of this cytokine under such clini-cal conditions (serum and lavage fluid) have producedinconsistent results [16–24]. Interleukin-6 (IL-6) is pro-duced by a variety of inflammatory cells in response toother cytokines or bacterial agents. Circulating IL-6 wasfound to be an important marker and mediator of sys-
temic inflammatory responses ("alarm hormone"), par-ticularly in sepsis [5, 17, 22, 25, 26], whereas only a fewstudies have focused on the appearance of this cytokinein the alveolar space [27–30].
In the present study, the incidence of IL-6, IL-8 andTNF-α were investigated in the alveolar and vascularcompartments of a total of 74 patients requiring mechani-cal ventilation due to acute respiratory failure. The datawere compared to healthy controls and to an additional"control" group of patients with cardiogenic pulmonaryoedema, in an attempt to differentiate between the pri-mary sequelae of inflammatory lung injury and secondaryconsequences of severe functional impairment of gasexchange necessitating respirator therapy. Moreover, wefocused particularly on primary and secondary pulmon-ary infections as contributors to lung cytokine gene-ration: despite a recent "uniforming" definition of ARDS[31], the patients were divided into those with ARDS inthe absence of lung infection, those with primary sev-ere PN and those with features of ARDS and PN. Inaddition, we sought possible differences in lung and sys-temic cytokine profiles among different categories ofPN.

CYTOKINE PROFILES IN ACUTE INFLAMMATORY LUNG DISEASE 1859
Methods
Patients included in the study were recruited from theintensive care unit of the Department of Internal Medi-cine, JLU-University Giessen. The project was approvedby the Ethics Committee of the Justus-Liebig-University,and informed consent was obtained either from the pati-ent or closest relatives. All patients were examined byBAL for clinical purposes; the large majority of themwithin 72 h after intubation. In selected patients - depend-ing on the clinical course - bronchoscopy and BAL wererepeated at later time-points. All patients were mechani-cally-ventilated; inspiratory oxygen fraction (FI,O2) andrespirator settings including positive end-expiratorypressure (PEEP) were chosen according to the require-ments of pulmonary insufficiency. General therapeuticapproaches included parenteral nutrition, volume sub-stitution and antibiotic drugs. Vasoactive or inotropicdrugs were administered according to the patients his-tory, and haemodynamic variables as determined by rightheart catheterization.
Definitions of categories
Each patient was classified in one of the four maincategories described below; there was no overlap and nochange of patients between these main categories. Heal-thy volunteers (n=17) without a history of cardiac orpulmonary disease served as the control group. The dis-tribution of age, body weight and sex in patient groupsand controls displayed negligible variations. Generalexclusion criteria for entry into this study were lungcancer, chronic obstructive or interstitial lung disease,and head trauma, stroke or subarachnoidal haemorrhage.
Severe pneumonia (PN). In total, 38 patients with a clini-cal history of primary lung infection were examined(mean age 57 yrs; 31 males and 7 females). Diagnosticcriteria were fever, tachycardia, dyspnoea, typical aus-cultatory findings, characteristic chest roentgenogramsand microbiological identification of pathogens in thelower respiratory tract (bronchoscopy; pathogens listedin table 1). The pulmonary capillary wedge pressure ran-ged <16 mmHg, and there was no history of acute orchronic left heart failure. In this group of patients, basedon radiological criteria according to FRASER et al. [32],subgroups of: bronchopneumonia (patchy peribronchi-ally centred consolidation, n=9); alveolar PN (homo-geneous, sharply demarcated consolidations with airbronchogram, n=14); and aspiration PN (extensive bila-teral airspace consolidation, widespread acinar shadows,irregular opacities, with a history of aspiration of gastriccontents, n=11) were analysed. Four patients could notbe ascribed to a subgroup.
Acute respiratory distress syndrome (ARDS) in the absenceof primary lung infection. In total, 12 patients were exa-mined (mean age 51 yrs; 10 males and 2 females). Fordiagnosis of ARDS, the following general criteria wererequired: 1) An initial, typical underlying catastrophicevent. The predominant event in this group was sepsis(n=7); other causes included shock (n=3), aspiration ofgastric contents with Mendelson's syndrome (n=1), andpancreatitis (n=1); 2) Roentgenographic diffuse and bila-
teral alveolar infiltrates; 3) Pulmonary capillary wedgepressure <16 mmHg and absence of acute or chronic leftheart failure; 4) Absence of microorganisms upon firstbronchoscopy.
ARDS in combination with pneumonia (PN+ARDS). Intotal, 18 patients (mean age 46 yrs; 14 males and 4 fem-ales) were separated into two subcategories. The firstsubgroup (PN→ARDS) was formed by patients with theinitial clinical diagnosis of "severe PN" with circumscriptlung infiltrates, in whom sequential chest radiographsdisplayed rapid, diffuse bilateral spreading of infiltrates,imposing a typical radiographic pattern of ARDS (n=9).The second group (ARDS→PN) consisted of patients ini-tially classified as "ARDS" with underlying events dif-fering from PN, who acquired secondary (nosocomial)PN within <72 h (n=9); underlying causes were sepsis(n=4), aspiration (n=4), and pancreatitis (n=1). PN wasalways confirmed by microbiological identification ofpathogenic microorganisms in BAL fluid.
Cardiogenic pulmonary oedema (CPO). Six patients requi-ring mechanical ventilation due to cardiogenic pulmonaryoedema were enrolled in the study; none of them metthe criteria for ARDS or PN. All of these patients hadclinical and radiographic signs of severe pulmonary con-gestion and alveolar flooding due to left-sided heartfailure, and all of them had pulmonary capillary wedgepressures greater than 18 mmHg. All patients sufferedfrom ischaemic heart disease. Owing to clinical im-provement under therapy, mechanical ventilation in thispatient group was never required for more than 48 h.
For direct comparison of ARDS and PN patients withthe cardiogenic oedema group, all patients with ARDSin the absence or presence of secondary PN were regar-ded as "primary ARDS", and all patients with PN with andwithout secondary ("ARDS-like") bilateral diffuse spread-ing of infiltrates were regarded as "primary PN".
Bronchoalveolar lavage
Flexible fibreoptic bronchoscopy with BAL was per-formed as a routine diagnostic procedure. Ten 20 mLaliquots of sterile saline were infused into one segment
Table 1. – Specific microorganisms detected in the res-piratory tract in patients with pneumonia and those withpneumonia and ARDS
Pathogen PN PN + ARDSn n
Pseudomonas spp. 6 7Haemophilus influenzae 2 1Klebsiella spp. 5 7Escherichia coli 1 -Streptococcus pneumoniae 8 2Other Streptococcus spp. 7 1Staphylococcus aureus 3 3Coagulase(-) Staphylococcus 9 2Anaerobic pathogens 3 -Other Gram(-) pathogens 2 3Other Gram(+) pathogens - -Candida spp. 12 14Aspergillus spp. 2 -Other fungal pathogens - -
PN: pneumonia; ARDS: acute respiratory distress syndrome.

of the lingula or the right middle lobe and removed bygentle suction (recovery 55–70%). In patients with severePN, the lung with predominant infection was examined.Lavage fluids were filtered through sterile gauze, col-lected on ice and immediately centrifuged at 200×g for10 min. Supernatant aliquots were frozen in liquid nitro-gen and stored at -85°C for subsequent measurements.Directly before starting the BAL procedure, samples ofcentral venous blood were collected, allowed to clot for30 min and centrifuged at 1,500×g for 15 min. The serumwas decanted and stored at (-85°C). Endotoxin-free plas-tic materials for collection, centrifugation and storage ofserum and BAL samples were used throughout to avoidsecondary cytokine production due to endotoxin conta-mination [21]. For quantification of alveolar lining fluid,urea was used as an endogenous marker of dilution [33].Blood gas analysis was performed in each patient within30 min before the BAL procedure.
Cytokine assays
IL-6 and IL-8 in serum and BAL fluids were measured bycommercially available assays (IL-6 enzyme-amplified sen-sitivity immunoassay (EASIA) and IL-8 enzyme-linkedimmunosorbent assay (ELISA); Medgenix Diagnostics,Ratingen, Germany). The minimum detectable concen-trations were 3 pg·mL-1 of IL-6 and 11 pg·mL-1 of IL-8,respectively. TNF-α in BAL fluids was measured bymeans of three assay systems. Bioactivity of TNF-α inBAL samples was determined in a cytolytic cell assayin the mouse fibrosarcoma cell line WEHI 164 clone 13(kindly donated by T. Espevik, Institute of Cancer Res-earch, University of Trondheim, Norway), as describedpreviously [34]. The WEHI cells (2×104) were incuba-ted with serial dilutions of BAL fluids in microtitrewells (Nunc). After 18 h, dimethylthiazolyl-dipheny-ltetrazolium-bromide (MTT; 5 mg·mL-1 in phosphate-buffered saline (PBS); 100 µL·well-1) was added. Thereaction was stopped after 4 h by addition of 5% formicacid in 2-propanol, and the content of reduced MTT wasread in a micro-ELISA autoreader (570 nm). The titre ofTNF-α is expressed in units·mL-1 and was chosen as thereciprocal of the dilution necessary to cause 50% cyto-toxi-city. Recombinant human TNF-α (Genzyme,
Rüsselsheim, Germany) served as standard in all assays.The sensitivity of WEHI 164.13 ranged 1–3 pg protein·cytolyt-ic unit-1 in the different tests. Antigenic TNF-α in BAL fluids was determined by two ELISAs (MedgenixDiagnostics, Ra-tingen; and Genzyme, Rüsselsheim,Germany; detection limits 3 pg·mL-1 each). Recovery ofTNF-α in BAL fluids, as determined by addition of recom-binant human TNF-α (Genzyme, Rüsselsheim, Germany)to normal, freshly obtained lavage fluids, ranged 96–107%,as measured by the Genzyme ELISA (n=10 experiments;with BAL fluids from ARDS and PN patients). TNF-αanalysis in serum samples was also performed by meansof the Genzyme ELISA kit.
Data analysis
Differences in cytokine concentrations among patientgroups were analysed by the Kruskal-Wallis H-Test andthe Wilcoxon-Mann-Whitney-Test. Correlations betweenparameters were analysed by calculating the SpearmanRank Correlation Coefficient. P-values of less than 0.05were considered to represent a significant difference orcorrelation. For interpretation of multiple comparisons,the Bonferroni correction was considered. All statisticalprocedures were performed with the Statistical Packagefor the Social Sciences (SPSS)™ for MS Windows™analysis system. "Survival" of patients was defined asbeing alive 4 weeks after onset of mechanical ventila-tion.
Results
Basic data
All four groups of patients (ARDS, PN, PN + ARDS,CPO) displayed a comparable degree of respiratory fail-ure, as reflected by arterial oxygen tension (Pa,O2)/FI,O2
ratios (table 2). Polymorphonuclear neutrophils (PMNs)were markedly elevated in BAL fluids of all patientswith ARDS and/or PN (p<0.001 compared to controls),whereas patients with cardiogenic pulmonary oedemadisplayed normal levels of PMNs. In all four groups,BAL protein concentrations and serum C-reactive protein(CRP) levels were significantly higher than in controls
H. SCHÜTTE ET AL.1860
Table 2. – Selected basic variables of patients with: pneumonia (PN); acute respiratory distress syndrome (ARDS);combined forms (PN+ARDS); cardiogenic pulmonary oedema; and healthy controls
CardiogenicPneumonia ARDS PN + ARDS oedema Control
Protein in BAL µg·mL-1 525±129† 671±256† 437±66† 291±81† 73±13.5(313) (174) (257) (207) (49.7)
PMN in BAL % 36.2±4.4† 42.5±7.5† 32.7±6.5† 5.5±1.1 3.3±1.26(26) (44) (14) (5) (2.5)
PMN counts in BAL 22.3±11.1† 16.1±5.8† 5.7±1.2† 0.4±0.11 0.32±0.09106·mL-1 (4.19) (4.49) (2.78) (0.37) (0.28)
Serum CRP mg·L-1 159±15† 235±33† 230±28† 93±25†
(141) (222)† (173) (69) <5Pa,O2/FI,O2 204±17 213±21 196±15 226±20
(171) (235) (186) (243)
Values are presented as mean±SEM and median in brackets for each group. BAL protein values are presented as directly measuredconcentrations without urea-correction for dilution. All patients with ARDS and/or PN and cardiogenic oedema displayed elevat-ed BAL protein concentrations and serum CRP levels (†: p<0.001 each, compared to controls). Significant differences betweenthese groups were not observed for these two variables or for the Pa,O2/FI,O2 ratios. BAL neutrophils were significantly elevatedin all ARDS/PN patients (†: p<0.001 each, compared to controls), but not in patients with cardiogenic pulmonary oedema. BAL:bronchoalveolar lavage; PMN: polymorphonuclear neutrophils; CRP: C-reactive protein; Pa,O2: arterial oxygen tension in mmHg;FI,O2: inspiratory oxygen fraction.

CYTOKINE PROFILES IN ACUTE INFLAMMATORY LUNG DISEASE 1861
(p<0.001) (table 2); values in patients with cardiogenicoedema ranged below those in ARDS and PN patients.
IL-6 in BAL and serum
Highly elevated concentrations of IL-6 were noted inBAL fluids of patients with ARDS and/or PN, as com-pared to control patients (fig. 1). This was true for allsubgroups, namely, bronchopneumonia, alveolar and as-piration pneumonia, septic and nonseptic ARDS, ARDSwith nosocomial pneumonia and pneumonia with secon-dary diffuse spreading of infiltrates (PN→ARDS). Nostatistical difference was noted among the various sub-groups. BAL IL-6 levels remained elevated for more than10 days after intubation in the groups with ARDS andPN, and then significantly decreased in the latter group(fig. 2). In contrast, BAL IL-6 concentrations of patientswith cardiogenic pulmonary oedema were only slightlyelevated as compared to controls, and data ranged sig-nificantly below those of ARDS and PN patients. SerumIL-6 levels were also markedly elevated in all threeARDS/PN groups and subgroups (fig. 3). Again, no sta-tistical difference among the various subgroups was noted.
IL-8 in BAL and serum
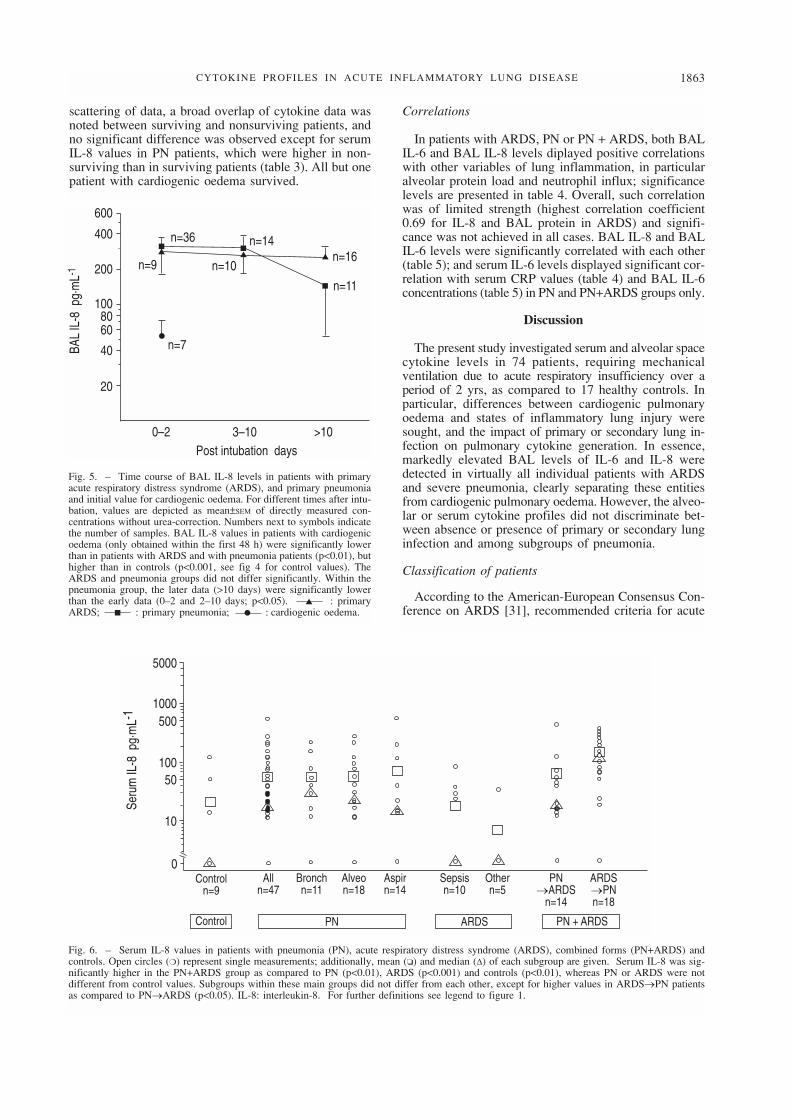
All patients with ARDS and/or PN displayed highlysignificantly elevated BAL levels of IL-8. As detailed infigure 4, this again was true for all subgroups: no sta-tistical difference was noted between or within the threegroups of ARDS and PN. In addition, the kinetics ofBAL IL-8 levels were nearly superimposable for pati-ents with primary ARDS and those with primary PN (fig.5). In analogy with IL-6, marked elevation of the BALconcentrations of this cytokine was observed for morethan 10 days. In contrast, BAL fluids obtained from pati-ents with cardiogenic pulmonary oedema displayed onlyslightly elevated IL-8 levels, which significantly differedfrom the data in the ARDS and PN groups. In serum
samples taken in parallel with the BAL fluids, a broadscattering of data was noted. However, a significant ele-vation in comparison with the control group was onlyfound for the patients suffering from PN + ARDS (fig. 6).
TNF-α in BAL and serum
TNF-α bioactivity was not detected in any BAL fluid,either in PN, ARDS, or cardiogenic pulmonary oedema.
10000050000
100005000
1000500
10050
10
0Bronchn=10
Controln=17
Alln=49
Alveon=19
Aspirn=14
Sepsisn=10
Othern=5
PN→ARDS
n=14
ARDS→PNn=20
Control PN ARDS PN + ARDS
BAL
IL-6
pg·
mL-
1
●●
●
Fig. 1. – BAL IL-6 values in patients with pneumonia (PN), acute respiratory distress syndrome (ARDS), combined forms (PN+ARDS) and con-trols. All values are presented as directly measured concentrations without urea-correction for dilution. Open circles (❍) represent single measure-ments; additionally, mean (❏) and median (∆) of each subgroup are given. PN, ARDS and PN+ARDS were all significantly different from controls(p<0.0001). No differences were observed between these main groups and between subgroups of either main group. Bronch: bronchopneumonia;Alveo: alveolar pneumonia; Aspir: aspiration pneumonia; PN→ARDS: patients initially classified as "severe PN", in whom ARDS developed;ARDS→PN: patients initially classified as "ARDS", who acquired secondary PN.
●
▲
▲
▲■
■
■n=7
n=9
n=37
n=10
n=14 n=16
n=12
10000
5000
1000500
100
50
103–100–2 >10
Post intubation days
BAL
IL-6
pg·
mL-
1
Fig. 2. – Time course of BAL IL-6 levels in patients with primaryacute respiratory distress syndrome (ARDS), and primary pneumoniaand initial value for cardiogenic oedema. For different times after intu-bation, values are depicted as mean±SEM of directly measured con-centrations without urea-correction. Numbers next to symbols indicatethe number of samples. BAL IL-6 values in patients with cardiogenicoedema (only obtained within the first 48 h) were significantly lowerthan in patients with ARDS and with pneumonia (p<0.05), but higherthan in controls (p<0.01, see fig 1 for control values). The ARDS andpneumonia groups did not differ significantly. Within the pneumoniagroup, the later data (>10 days) were significantly lower than the earlydata (0–2 days; p<0.01). ▲ : primary ARDS; ■ : primarypneumonia; ● : cardiogenic oedema. BAL: bronchoalveolar lav-age; IL-6: interleukin-6.

Moreover, in additional measurements with two ELISAtechniques, antigenic TNF-α was very rarely measuredin the BAL samples of these patients (only 4 PN±ARDSpatients, range 66–384 pg·mL-1; no ARDS patient). Incontrast, circulating antigenic TNF-α levels were sig-nificantly elevated in all populations with ARDS, PN orPN + ARDS, as compared to controls (fig. 7). Main groupand subgroup analysis of these values revealed no sig-nificant differences.
Alveolar lining fluid
Correction of single BAL data according to the ureamethod in order to obtain concentrations in the assumed
volume of alveolar lining fluid resulted in ≈10 fold (meanfactor; range 2.5–83 fold) higher cytokine concentrations.Both urea-corrected IL-6 and IL-8 values were substan-tially higher than the corresponding serum levels in eitherpatient group (p≤0.045), indicating local production ofthese cytokines. However, statistical analysis of theseurea-corrected data did not reveal any previously unob-served differences among the various groups and sub-groups of patients.
Survival
Survival rates were 42% for ARDS, 58% for PN and61% for PN+ARDS patients, respectively. Due to the
H. SCHÜTTE ET AL.1862
10000050000
100005000
1000500
10050
10
0Controln=11
Control PN ARDS PN + ARDS
Seru
m IL
-6 p
g·m
L-1
Alln=46
Bronchn=10
Alveon=18
Aspirn=14
Sepsisn=10
Othern=5
PN→ARDS
n=14
ARDS→PNn=18
Fig. 3. – Serum IL-6 values in patients with pneumonia (PN), acute respiratory distress syndrome (ARDS), combined forms (PN+ARDS) andcontrols. Open circles (❍) represent single measurements; additionally, mean (❏) and median (∆) of each subgroup are given. PN, ARDS andPN+ARDS were all significantly different from controls (p<0.0001). No differences were observed between these main groups and between sub-groups of either main group. For definitions see legend to figure 1.
5000
1000500
10050
10
0Controln=17
Control PN ARDS PN + ARDS
BAL
IL-8
pg·
mL-
1
Alln=47
Bronchn=10
Alveon=18
Aspirn=13
Sepsisn=10
Othern=5
PN→ARDS
n=14
ARDS→PNn=20
Fig. 4. – BAL IL-8 values in patients with pneumonia (PN), acute respiratory distress syndrome (ARDS), combined forms (PN+ARDS) and con-trols. All values are presented as directly measured concentrations without urea-correction for dilution. Open circles (❍) represent single mea-surements; additionally, mean (❏) and median (∆) of each subgroup are given. PN, ARDS and PN+ARDS were all significantly different fromcontrols (p<0.0001). No differences were observed between these main groups and between subgroups of either main group. IL-8: interleukin-8.For further definitions see legend to figure 1.
CYTOKINE PROFILES IN ACUTE INFLAMMATORY LUNG DISEASE 1863
●
▲■ ■
■
▲ ▲
n=7
n=9
n=36
n=10
n=14n=16
n=11
600
400
200
10080
40
20
60
3–100–2 >10Post intubation days
BAL
IL-8
pg·
mL-1
5000
1000500
10050
10
0
Control PN ARDS PN + ARDS
Seru
m IL
-8 p
g·m
L-1
Controln=9
Alln=47
Bronchn=11
Alveon=18
Aspirn=14
Sepsisn=10
Othern=5
PN→ARDS
n=14
ARDS→PNn=18
Fig. 5. – Time course of BAL IL-8 levels in patients with primaryacute respiratory distress syndrome (ARDS), and primary pneumoniaand initial value for cardiogenic oedema. For different times after intu-bation, values are depicted as mean±SEM of directly measured con-centrations without urea-correction. Numbers next to symbols indicatethe number of samples. BAL IL-8 values in patients with cardiogenicoedema (only obtained within the first 48 h) were significantly lowerthan in patients with ARDS and with pneumonia patients (p<0.01), buthigher than in controls (p<0.001, see fig 4 for control values). TheARDS and pneumonia groups did not differ significantly. Within thepneumonia group, the later data (>10 days) were significantly lowerthan the early data (0–2 and 2–10 days; p<0.05). ▲ : primaryARDS; ■ : primary pneumonia; ● : cardiogenic oedema.
Fig. 6. – Serum IL-8 values in patients with pneumonia (PN), acute respiratory distress syndrome (ARDS), combined forms (PN+ARDS) andcontrols. Open circles (❍) represent single measurements; additionally, mean (❏) and median (∆) of each subgroup are given. Serum IL-8 was sig-nificantly higher in the PN+ARDS group as compared to PN (p<0.01), ARDS (p<0.001) and controls (p<0.01), whereas PN or ARDS were notdifferent from control values. Subgroups within these main groups did not differ from each other, except for higher values in ARDS→PN patientsas compared to PN→ARDS (p<0.05). IL-8: interleukin-8. For further definitions see legend to figure 1.
scattering of data, a broad overlap of cytokine data wasnoted between surviving and nonsurviving patients, andno significant difference was observed except for serumIL-8 values in PN patients, which were higher in non-surviving than in surviving patients (table 3). All but onepatient with cardiogenic oedema survived.
Correlations
In patients with ARDS, PN or PN + ARDS, both BALIL-6 and BAL IL-8 levels diplayed positive correlationswith other variables of lung inflammation, in particularalveolar protein load and neutrophil influx; significancelevels are presented in table 4. Overall, such correlationwas of limited strength (highest correlation coefficient0.69 for IL-8 and BAL protein in ARDS) and signifi-cance was not achieved in all cases. BAL IL-8 and BALIL-6 levels were significantly correlated with each other(table 5); and serum IL-6 levels displayed significant cor-relation with serum CRP values (table 4) and BAL IL-6concentrations (table 5) in PN and PN+ARDS groups only.
Discussion
The present study investigated serum and alveolar spacecytokine levels in 74 patients, requiring mechanicalventilation due to acute respiratory insufficiency over aperiod of 2 yrs, as compared to 17 healthy controls. Inparticular, differences between cardiogenic pulmonaryoedema and states of inflammatory lung injury weresought, and the impact of primary or secondary lung in-fection on pulmonary cytokine generation. In essence,markedly elevated BAL levels of IL-6 and IL-8 weredetected in virtually all individual patients with ARDSand severe pneumonia, clearly separating these entitiesfrom cardiogenic pulmonary oedema. However, the alveo-lar or serum cytokine profiles did not discriminate bet-ween absence or presence of primary or secondary lunginfection and among subgroups of pneumonia.
Classification of patients
According to the American-European Consensus Con-ference on ARDS [31], recommended criteria for acute

H. SCHÜTTE ET AL.1864
500
100
50
10
0
Control PN ARDS PN + ARDS
Seru
m T
NF-
α p
g·m
L-1
Controln=9
Alln=47
Bronchn=11
Alveon=18
Aspirn=14
Sepsisn=10
Othern=5
PN→ARDS
n=14
ARDS→PNn=18
Fig. 7. – Serum TNF-α values in patients with pneumonia (PN), acute respiratory distress syndrome (ARDS), combined forms (PN+ARDS) andcontrols. Open circles (❍) represent single measurements; additionally, mean (❏) and median (∆) of each subgroup are given. PN, ARDS andPN+ARDS were all significantly different from controls (p<0.01, p<0.001 and p<0.05, respectively). Differences between these main groups andbetween subgroups of either main group were not observed. TNF-α: tumour necrosis factor-α. For further definitions see legend to figure 1.
Table 3. – Cytokine levels in patients with acute respiratory distress syndrome (ARDS), pneumonia (PN), or with acombination of ARDS and PN: comparison of survivors and nonsurvivors
ARDS PN PN + ARDSNon- Non- Non-
Survivors survivors Survivors survivors Survivors survivors
BAL 28.6±88 212±83 258±59 328±87 431±99 323±142IL-8 pg·mL-1 (244.2) (180.8) (189.6) (172.5) (352.9) (153)Serum 6.1±3.8 17±11 34±12 68±20* 110±35 40±16IL-8 pg·mL-1 (0) (0) (13.2) (28) (96.5) (31.1)BAL 3772±2492 705±572 5437±4078 1533±824 1448±567 148±29IL-6 pg·mL-1 (1780) (31) (186) (298) (280) (174)Serum 275±129 600±240 889±432 2907±2438 1785±659 568±317IL-6 pg·mL-1 (96) (252) (281) (306) (366) (202)Serum 31.6±15.4 31.7±13.3 18.3±4.2 51.3±12.7 38.2±11.5 19.2±4.3TNF-α pg·mL-1 (14.2) (10.5) (11.5) (37) (28.6) (18.6)
BAL values are presented as directly measured concentrations without urea-correction for dilution. Values are presented as mean±SEM
and median in brackets for each group. If more than one examination was performed in one single patient, mean values for eachsingle patients were considered. Significant differences between survivors and nonsurvivors were not observed for any cytokine(Wilcoxon-Mann-Whitney test), except for higher serum IL-8 in nonsurviving PN patients (*: p<0.05). IL-8: interleukin-8; IL-6:interleukin-6; TNF-α: tumour necrosis factor-α; BAL: bronchoalveolar lavage.
lung injury (ALI) and ARDS include: timing (acute onset);oxygenation (Pa,O2/FI,O2 <300 mmHg in ALI and <200mmHg in ARDS); radiographic signs (bilateral infiltra-tes) and a capillary wedge pressure <18 mmHg. Therewas controversy regarding diffuse lung infection: "Thequestion is, if a pulmonary infection becomes diffuseand severe enough to meet ARDS criteria, should it beincluded under the ALI/ARDS definitions?" [31]. Theconsensus was that severe pulmonary infection shouldbe considered ALI/ARDS when the physiological crite-ria listed above are met, although "this was not a un-animous decision".
The current study focused on the question, of whetherprimary or secondary lung infection provokes cytokineprofiles that differ from ARDS primarily caused by ex-trapulmonary factors. This issue is worthy of study, assevere PN is assumed to be an increasingly important
antecedent of severe respiratory failure [35]; it was, infact, the quantitatively predominant underlying diseasedemanding mechanical ventilation in this patient groupstudied over 2 yrs. Moreover, secondary pneumoniaacquired during the course of ARDS, although often dif-ficult to diagnose, has been shown to aggravate the dis-ease and to reduce survival rate [36–38]. For the purposeof this study, ARDS primarily caused by extrapulmon-ary factors (mostly sepsis of nonpulmonary origin) was,thus, separated from respiratory failure due to severePN. A third group included patients presenting charac-teristics of both categories: ARDS→PN were patientsthat acquired microbiologically proven pneumonia inthe course of ARDS, and PN→ARDS reflected diffusespreading of lung infiltrates in patients initially present-ing with circumscript (microbiologically classified) pneu-monia. In addition, patients with cardiogenic pulmonary

CYTOKINE PROFILES IN ACUTE INFLAMMATORY LUNG DISEASE 1865
oedema were included as a further "control" group, toprobe the impact of functional lung disturbances oncytokine changes in the absence of primary inflamma-tory disease; the gas exchange abnormalities in thesepatients matched those with ARDS and/or severe PNvery well, but were restricted to the first 48 h after onsetof mechanical ventilation.
Interleukin-8
BAL IL-8 levels were markedly elevated in virtuallyall patients with ARDS and/or PN, and this was true forthe early phase of disease as well as later time periods
(>10 days). Alveolar space IL-8 concentrations were sub-stantially higher than circulating IL-8 levels, which is inaccordance with predominant local generation of this cy-tokine. The data on BAL IL-8 support previous studiesdemonstrating consistently increased lavage IL-8 con-centrations in ARDS patients [3, 4, 39], and in patientsat risk for this disease [2]. This inflammatory cytokineallowed a clear separation of ARDS/PN from cardioge-nic pulmonary oedema, in which only moderately ele-vated levels were noted; previous data for the latter groupare not known to the authors.
In contrast, BAL IL-8 levels did not discriminate bet-ween ARDS and primary or secondary lung infection,and no discrimination within the subgroups of pneumo-nia was achieved. This result differs somewhat frominvestigations by CHOLLET-MARTIN et al. [1], in whichhigher lavage IL-8 levels were noted in ARDS states ascompared to a limited number (n=6) of PN patients.However, this difference may be explained by the factthat, in their study, the ARDS patients displayed moresevere gas exchange disturbances than the PN patients,whereas the degree of functional impairment was com-parable in the current investigation. From experimentaldata, IL-8 is known to be an important chemoattractanteffecting neutrophil recruitment into the alveolar space[40, 41]. In clinical studies in ARDS patients, a signi-ficant correlation between BAL IL-8 levels and alveolarneutrophil numbers was occasionally found [3, 39], butwas also missing in some cases [1]. In the current study,such correlation was evident in patients with ARDS andPN, but - for presently unknown reasons - not for thecombined group (PN + ARDS).
As anticipated from the previously described featuresof IL-8, elevations of serum concentrations of this cyto-kine were less marked than the rise in the levels in thealveolar space in all groups of patients [1, 4]. This find-ing does not refute the hypothesis that under conditionsof a predominance of sepsis and septic shock, substan-tial IL-8 concentrations may appear in the vascularcompartment [5, 7, 42]. Although the BAL IL-8 levelswere greatly increased in all patients with ARDS and/orPN, no association was observed between the level ofthis cytokine and survival rate, either in the ARDS, thePN or the combined (PN + ARDS) group. Such a pre-dictive value of BAL IL-8 for mortality has been sug-gested from preceding studies [1, 3].
Interleukin-6
IL-6 is known to appear in the vascular compartmentin large quantities under conditions of sepsis and septicshock [5, 17, 18, 22, 25, 26]. However, its pathogenicsignificance as being a cause or a consequence in thesedisease states is not exactly known. Persistence of ele-vated serum IL-6 concentrations was described as acharacteristic indicator for the development of multiple-system organ failure [22], and high IL-6 levels werefound to be associated with a poor prognosis in septicshock [5, 25, 26]. We found highly elevated IL-6 con-centrations circulating in all patients with ARDS, andsimilarly in PN, in contrast to patients with cardiogenicpulmonary oedema. This finding suggests that the syste-mic inflammatory response was comparable under condi-tions of ARDS - where it was anticipated - and in states
Table 4. – Correlations between IL-6 and IL-8 concen-trations and selected basic variables in patients with pneu-monia (PN), acute respiratory distress syndrome (ARDS)and combined forms (PN+ARDS)
PN ARDS PN + ARDS
IL-8 BAL 0.164 0.6929 0.3793Protein BAL NS p<0.01 p<0.05
IL-8 BAL 0.5427 0.3879 0.0522% PMN BAL p<0.001 NS NS
IL-8 BAL 0.5054 0.5549 0.0753PMN counts BAL p<0.001 p<0.059 NS
IL-6 BAL 0.5807 0.3324 0.5825Protein BAL p<0.001 NS p<0.001
IL-6 BAL 0.5757 0.58 0.1613% PMN BAL p<0.001 P<0.05 NS
IL-6 BAL 0.5088 0.5805 0.2078PMN counts BAL p<0.001 p<0.05 NS
IL-6 serum 0.4393 0.4196 0.5918CRP p<0.01 NS p<0.001
Nonparametric Spearman's correlation coefficients are given.For calculations, protein and cytokine BAL values were con-sidered as directly measured concentrations without urea-cor-rection for dilution. NS: not significant; PMN: polymorphonuclearneutrophils. CRP: c-reactive protein. For further definitions seelegend to table 2.
Table 5. – Correlations between IL-6 and IL-8 concen-trations in BAL fluids and serum samples in patients withpneumonia (PN), acute respiratory distress syndrome(ARDS) and combined forms (PN+ARDS)
PN ARDS PN + ARDS
IL-8 BAL 0.2745 -0.2658 0.2138IL-8 serum NS NS NS
IL-8 BAL 0.2243 0.1966 0.1527IL-6 serum NS NS NS
IL-8 BAL 0.4558 0.575 0.3679IL-6 BAL p<0.001 p<0.05 p<0.05
IL-6 BAL 0.3066 0.0191 0.3853IL-8 serum p<0.05 NS p<0.05
IL-6 BAL 0.5423 0.3324 0.6793IL-6 serum p<0.001 NS p<0.001
IL-6 serum 0.2567 0.356 0.468IL-8 serum NS NS p<0.01
Nonparametric Spearman's correlation coefficients are given. Forcalculations, cytokine BAL values were considered as directlymeasured concentrations without urea-correction for dilution. NS:not significant. For further definitions see legend to table 2.

of severe PN requiring mechanical ventilation. In accor-dance with this interpretation, the serum CRP levels inPN were only slightly lower than those in ARDS. In con-trast to the previous reports mentioned above [5, 6, 22,26], we again observed no significant differences betweensurvivors and nonsurvivors.
Interestingly, in patients with ARDS and/or PN IL-6levels in BAL and serum were similarly elevated. Giventhe dilution by the lavage fluid the level in the alveolarspace must have been markedly greater than in the intra-vascular space. This finding again signals the predo-minance of local production, as discussed for IL-8.Interestingly, the correlations between BAL cytokinelevels and neutrophil influx, were of similar strength forIL-6 and IL-8. These findings may suggest a local proin-flammatory role for this "alarm hormone", but the datasupporting such a view are much more sparse than thoserelated to IL-8 [27–30].
Tumour necrosis factor
In previous investigations, elevated alveolar space TNF-α levels were found in patients with ARDS [19, 20, 24].In contrast, TNF-α was very rarely detected in the BALfluids either in ARDS or in severe PN in the currentstudy. As this result was puzzling, an attempt was madeto exclude any methodological pitfalls: two differentimmunological tests were employed and the sampleswere analysed in a bioassay system previously reportedby our laboratory to be suitable to quantify TNF-α gen-erated under experimental conditions [43, 44]. Moreover,excellent recovery of recombinant TNF-α was demon-strated when mixed to BAL fluids immediately after per-forming the lavage procedure, thereby excluding thepossibility that TNF-α vanishes due to processing, trans-port or storage procedures. Thus, the present finding ofa near total absence of TNF-α in BAL fluids is well-founded. PARSONS et al. [21] explained discrepancies inTNF-α determinations by differences in the timing ofmeasurement, and this may, indeed, be an important fac-tor with respect to the short half-time of this cytokine(14–18 min [45]). This view has been confirmed by otherinvestigators, who found elevated TNF-α mainly - butnot in all cases - within the early phase after onset ofdisease [19, 24]. We may, thus, have missed early peaksof TNF-α generation due to our lavage protocol dic-tated by clinical necessities. Dilution of the alveolar spaceconcentrations by the lavage fluid may be another im-portant factor to explain the discrepancy between the cur-rent and preceding studies, in which TNF-α was directlyquantified in bronchoalveolar aspirates [20, 24].
In contrast to the analysis of BAL fluids, elevated lev-els of circulating TNF-α were observed in the majorityof the patients with ARDS and/or PN, which is in accor-dance with previous observations [18, 19, 23, 46]. Again,there was no difference between the main categories ofARDS and pneumonia, and among different subgroupsof pneumonia. These findings further support the viewof a major systemic inflammatory response in all of thesepatients, as suggested previously [47].
Alveolar space cytokine sampling by lavage demon-strated rapid onset and persistent local generation ofinterleukin-8 and interleukin-6 in patients with acute res-
piratory distress syndrome and severe pneumonia. Thisprofile clearly separated those patients with inflamma-tory lung injury from healthy controls and from patientswith comparable functional impairment due to cardio-genic pulmonary oedema. However, the alveolar spacecytokines, interleukin-8 and interleukin-6 did not dis-criminate between acute respiratory distress syndromein the absence of lung infection and states of severe pri-mary or secondary pneumonia, as well as among differ-ent subgroups of pneumonia. In addition, circulatinginterleukin-6 and tumour necrosis factor-α and - to lesserextent - interleukin-8 levels suggested systemic inflam-matory responses in association with the lung infection,that were again clearly separate from cardiogenic oede-ma, but comparable for the various entities of acute res-piratory distress syndrome and/or severe pneumonia. Nosingle variable (alveolar or intravascular cytokine) waspredictive for survival. In general, these findings supportsimilarities in local and systemic inflammatory proces-ses between acute respiratory distress syndrome in theabsence of lung infection and states of severe pneumo-nia.
References
1. Chollet-Martin S, Montravers P, Gibert C, et al. Highlevels of interleukin-8 in the blood and alveolar spacesof patients with pneumonia and adult respiratory distresssyndrome. Infect Immun 1993; 61: 4553–4559.
2. Donnelly SC, Strieter RM, Kunkel SL, et al. Interleukin-8 and development of adult respiratory distress syndromein at-risk patient groups. Lancet 1993; 341: 643–647.
3. Miller EJ, Cohen AB, Nagao S, et al. Elevated levels ofNAP-1/interleukin-8 are present in the airspaces of pati-ents with the adult respiratory distress syndrome and areassociated with increased mortality. Am Rev Respir Dis1992; 148: 427–432.
4. Torre D, Zeroli C, Giola M, et al. Levels of interleukin-8 in patients with adult respiratory distress syndrome. JInfect Dis 1993; 167: 505–506.
5. Friedland JS, Supputtamongkol Y, Remick DG, et al.Prolonged elevation of interleukin-8 and interleukin-6concentrations in plasma and of leukocyte interleukin-8mRNA levels during septicemic and localized Pseudomanspseudomallei infection. Infect Immun 1992; 60: 2402–2408.
6. Hack CE, Hart M, Strack van Schijndel RJM, et al.Interleukin-8 in sepsis: relation to shock and inflamma-tory mediators. Infect Immun 1992; 60: 2835–2842.
7. Marty C, Misset B, Tamion F, et al. Circulating inter-leukin-8 concentrations in patients with multiple organfailure of septic and nonseptic origin. Crit Care Med1994; 22: 673.
8. Kelley J. Cytokines of the lung. Am Rev Respir Dis 1990;141: 765–788.
9. Manogue KR, van Deventer SJH, Cerami A. Tumornecrosis factor-alpha or cachectin. The Cytokine Hand-book. Chap. 12. New York, Academic Press Ltd, 1991;pp. 241–256.
10. Cannon JG, Tompkins RG, Gelfand JA, et al. Circula-ting interleukin-1 and tumor necrosis factor in septicshock and experimental endotoxin fever. J Infect Dis1990; 161: 79–84.
11. Cerami A, Beutler B. The role of cachectin/TNF in endo-toxic shock and cachexia. Immunol Today 1988; 9: 28–31.
H. SCHÜTTE ET AL.1866

12. van Deventer SJH, Büller HR, ten Cate JW, et al. Ex-perimental endotoxemia in humans: analysis of cytokinerelease and coagulation fibrinolytic, and complementpathways. Blood 1990; 76: 2520–2526.
13. Tracey KJ, Fong Y, Hesse DG, et al. Anti-cachectin/TNFmonoclonal antibodies prevent septic shock during lethalbacteraemia. Nature 1987; 330: 662–664.
14. Leeper-Woodford SK, Carey PD, Byrne K, et al. Tumornecrosis factor - alpha and beta subtypes appear in cir-culation during onset of sepsis-induced lung injury. AmRev Respir Dis 1991; 143: 1076–1082.
15. Tracey KJ, Beutler B, Lowry SF, et al. Shock and tis-sue injury induced by recombinant human cachectin.Science 1986; 234: 470–474.
16. Debets JMH, Kampneijer R, van der Linden MPMH, etal. Plasma tumor necrosis factor and mortality in criti-cally ill septic patients. Crit Care Med 1989; 17: 489–494.
17. Dofferhoff ASM, Bom VJJ, de Vries-Hospers HG, et al.Patterns of cytokines, plasma endotoxin, plasminogenactivator inhibitor, and acute-phase proteins during thetreatment of severe sepsis in humans. Crit Care Med1992; 20: 185–192.
18. Donnelly TJ, Meade P, Jagels M, et al. Cytokine, com-plement and endotoxin profiles associated with the deve-lopment of the adult respiratory distress syndrome aftersevere injury. Crit Care Med 1994; 22: 768–776.
19. Hyers TM, Tricomi SM, Dettenmeyer PA, et al. Tumornecrosis factor levels in serum and bronchoalveolar lavagefluid of patients with the adult respiratory distress syn-drome. Am Rev Respir Dis 1991; 144: 266–271.
20. Millar AB, Fowley NM, Singer M, et al. Tumor necro-sis factor in bronchopulmonary secretions of patients withadult respiratory distress syndrome. Lancet 1989; 23:712–714.
21. Parsons PE, Moore FA, Moore EE, et al. Studies on therole of tumor necrosis factor in adult respiratory distresssyndrome. Am Rev Respir Dis 1992; 146: 694–700.
22. Pinsky MR, Vincent J-L, Deviere J, et al. Serum cytokinelevels in human septic shock: relation to multiple-sys-tem organ failure and mortality. Chest 1993; 103: 565–575.
23. Roten R, Markert M, Feihl F, et al. Plasma levels of tumornecrosis factor in the adult respiratory distress syndrome.Am Rev Respir Dis 1991; 43: 590–592.
24. Suter PM, Suter S, Girardin E, et al. High bronchoalve-olar levels of tumor necrosis factor and its inhibitors,interleukin-1, interferon and elastase, in patients withadult respiratory distress syndrome after trauma, shockor sepsis. Am Rev Respir Dis 1992; 145: 1016–1022.
25. Hack CE, De Groot ER, Felt-Bersma JF, et al. Increasedplasma levels of interleukin-6 in sepsis. Blood 1989; 74:1704–1710.
26. Waage A, Brandtzaeg P, Halstensen A, et al. The com-plex pattern of cytokines in serum from patients withmeningococcal septic shock. J Exp Med 1989; 169:333–338.
27. Grigg JM, Barber A, Silverman M. Increased levels ofbronchoalveolar lavage fluid interleukin-6 in preterm ven-tilated infants after prolonged rupture of membranes. AmRev Respir Dis 1992; 145: 782–786.
28. Humbert M, Delattre RM, Fattal S, et al. In situ pro-duction of interleukin-6 within human lung allograftsdisplaying rejection or cytomegalovirus pneumonia. Trans-plantation 1993; 56: 623–627.
29. Lindsey HJ, Kisala JM, Ayala A, et al. Pentoxifylline
attenuates oxygen-induced lung injury. J Surg Res 1994;56: 543–548.
30. Trentin L, Garbisa S, Zambello R, et al. Spontaneousproduction of interleukin-6 by alveolar macrophages fromhuman immunodeficiency virus type-1-infected patients.J Infect Dis 1992; 166: 731.
31. Bernard GR, Artigas A, Brigham KL, et al. The American-European Consensus Conference on ARDS. Am J RespirCrit Care Med 1994; 149: 818–824.
32. Fraser RG (Ed), Paré JAP, Paré PD, et al. Diagnosis ofdiseases of the chest. 3rd edn. Philadelphia, W.B. SaundersCo., 1989.
33. Rennard SI, Basset G, Lecossier D, et al. Estimation ofvolume of epithelial lining fluid recovered by lavageusing urea as marker of dilution. J Appl Physiol 1986;60: 532–538.
34. Espevik T, Nissen-Meyer J. A highly sensitive cell line,WEHI 164 clone 13, for measuring cytotoxic factor/tumornecrosis factor from human monocytes. J Immunol Meth1986; 95: 99.
35. Sloane PJ, Gee MH, Gottlieb JE, et al. A multicenterregistry of patients with acute respiratory distress syn-drome. Am Rev Respir Dis 1992; 146: 419–426.
36. Campbell GD, Coalson JJ, Johanson WG. The effect ofbacterial superinfection on lung function after diffusealveolar damage. Am Rev Respir Dis 1984; 129: 974–978.
37. Hyers TM, Fowler AA. Adult respiratory distress syn-drome: causes, morbidity and mortality. Fed Proc 1986;45: 25–29.
38. Seidenfeld JJ, Pohl DF, Bell RC, et al. Incidence, siteand outcome of infections in patients with the adult res-piratory distress syndrome. Am Rev Respir Dis 1986;134: 12–16.
39. Jorens PG, Van Damme J, De Backer W, et al. Interleukin8 (IL-8) in the bronchoalveolar lavage fluid from pati-ents with the adult respiratory distress syndrome (ARDS)and patients at risk for ARDS. Cytokine 1992; 4: 592–597.
40. Kunkel SL, Standiford T, Kasahara K, et al. Interleukin-8 (IL-8): the major neutrophil chemotactic factor in thelung. Exp Lung Res 1991; 17: 17–23.
41. Van Damme J. Interleukin-8 and related molecules. In:Thomson AW, ed. The Cytokine Handbook: Immunologyand Molecular Biology of Cytokines. New York, AcademicPress, 1991; pp. 201–214.
42. Van Zee KJ, DeForge LE, Fischer E, et al. IL-8 in sep-tic shock, endotoxemia, and after IL-1 administration. JImmunol 1991; 146: 3478–3482.
43. Walmrath D, Ghofrani AH, Rosseau S, et al. Endotoxin"priming" potentiates lung responsiveness to E. colihemolysin: an example of endo- and exotoxin co-oper-ativity. J Exp Med 1994; 180: 1437–1443.
44. Walmrath D, Griebner M, Kolb B, et al. Endotoxin primesperfused rabbit lungs for enhanced vasoconstrictor res-ponse to staphylococcal α-toxin. Am Rev Respir Dis 1993;148: 1179–1186.
45. Blick M, Sherwin SA, Rosenblum M, et al. Phase I studyof recombinant tumor necrosis factor in cancer patients.Cancer Res 1987; 47: 2986–2989.
46. Chollet-Martin S, Montravers P, Gibert C, et al. Sub-population of hyperresponsive polymorphonuclear neu-trophils in patients with adult respiratory distress syndrome.Am Rev Respir Dis 1992; 146: 990–996.
47. Meduri GU, Headley S, Kohler G, et al. Persistent ele-vation of inflammatory cytokines predicts a poor out-come in ARDS. Chest 1995; 107: 1062–1173.
CYTOKINE PROFILES IN ACUTE INFLAMMATORY LUNG DISEASE 1867
Copyright © 2022 FDOKUMEN




















