
A viable approach to key performance indicators delivery process in Universiti Teknologi Malaysia
66
CHAPTER ONE INTRODUCTION Hepatitis C virus (HCV) was discovered in 1989 and the first blood test was available in May; 1990 (Jean-Jacquces et al., 2004). Hepatitis C is a spherical, enveloped, single stranded RNA virus of the family Flaviviridae, Genus Hepacivirus (Kapoor et al., 2011). It is spread primarily through direct contact with blood or body fluids of infected individuals. It is also genetically diverse and divided into at least six different clones (1 to 6) which include eleven types and numerous subtypes (Jean-Jacquces et al., 2004). The diversity depends on mutation on the genome of the virus. The N terminus of E2 protein, the first hyper variable region (HVR), has the highest diversity in studies of chronically infected adults. Higher diversity of this region has been associated with progression of liver disease (Zhi et al., 2004). Hepatitis C virus is an intracellular pathogen that takes over replication machinery within an infected cell (mostly hepatocytes), effectively turning the cell into a factory. People who control HCV before it becomes chronic mount a vigorous T-cell response. But while most people’s T-cell can recognize and attack HCV infected cells, this response is usually not enough to keep up with HCV replication and 1
Transcript of A viable approach to key performance indicators delivery process in Universiti Teknologi Malaysia
CHAPTER ONE
INTRODUCTION
Hepatitis C virus (HCV) was discovered in 1989 and the first
blood test was available in May; 1990 (Jean-Jacquces et al.,
2004). Hepatitis C is a spherical, enveloped, single
stranded RNA virus of the family Flaviviridae, Genus Hepacivirus
(Kapoor et al., 2011). It is spread primarily through direct
contact with blood or body fluids of infected individuals.
It is also genetically diverse and divided into at least six
different clones (1 to 6) which include eleven types and
numerous subtypes (Jean-Jacquces et al., 2004). The diversity
depends on mutation on the genome of the virus. The N
terminus of E2 protein, the first hyper variable region
(HVR), has the highest diversity in studies of chronically
infected adults. Higher diversity of this region has been
associated with progression of liver disease (Zhi et al.,
2004).
Hepatitis C virus is an intracellular pathogen that takes
over replication machinery within an infected cell (mostly
hepatocytes), effectively turning the cell into a factory.
People who control HCV before it becomes chronic mount a
vigorous T-cell response. But while most people’s T-cell can
recognize and attack HCV infected cells, this response is
usually not enough to keep up with HCV replication and
1
protect other liver cells from being infected (Jeffery et al.,
2003).
Antibody response appears to be less important. Studies have
shown that neutralizing antibodies are produced during HCV
infection, but do not appear to be protective against re-
infection in human or in chimpanzees (Jeffery et al., 2003).
If the initial immune response following infection is not
sufficiently strong, persistent viral replication leads to
mutant strains, which are no longer detected by the immune
cells (San Diego, 1999). The possible strategies for HCV to
escape immune elimination may include decrease in visibility
to the immune system, decrease in the effectiveness of
antiviral cytokines, infection of immunologically privileged
sites, induction of immunologic tolerance and immunologic
evasion (Jeffery et al., 2003).
Hepatitis caused by the HCV is a leading cause of liver
failure and liver transplantation in adults (Karen et al.,
2003). The typically newly diagnosed patient is usually
young, healthy and has few or no symptoms that can be
attributed to the HCV infection. Because of these some
doctors and many patients do not consider Hepatitis C to be
a very serious illness (Karen et al., 2003). Clearly Hepatitis
C is a progressive liver disease which eventually leads to
cirrhosis with its attendant risks of liver cancer
(hepatocellular carcinoma), liver transplantation and death
2
(Dale et al., 2004 and Michael and Alexander, 2004). HCV may
take years in some persons to severely damage the liver. The
younger the person when the infection is acquired, the
higher it is likely that progression to cirrhosis may occur
during the person’s life time.
While the primary site of clinical infection with HCV is the
liver, a significant number of people develop disease
symptoms at sites other than the liver, referred to as extra
hepatic manifestations of chronic hepatitis C virus
infection. These include arthralgia, paresthesia, myalgia, pruritia and
sicca syndrome (Jeffery-Schouten, 2000).
The main risk factors for HCV transmission are maternal
infection and transfusion of blood products. Other risk
factors for hepatitis C virus infection include, intravenous
drug use, exposure, intranasal drugs use, multi-sexual
partners, history of sexually transmitted disease,
tattooing, hemodialysis, working in patient care or a
clinical laboratory, and low socioeconomic level (Ala et al.,
1996 and Karen et al., 2003). In 1970s and 1980s post
transfusion non A, non B hepatitis and HCV is the primary
etiologic agent of parenterally transmitted non A, non B,
hepatitis worldwide (Giancarlo et al., 2001 and Maria et al.,
2004).
Currently, unlike Hepatitis A and Hepatitis B, there is no
vaccine to protect people from Hepatitis C as little is
3
known about the variability of HCV genome and how the immune
system interacts with the virus (Maria et al., 2004).
The key to the early diagnosis of HCV infections is to
identify and test those individuals at risks for having
hepatitis C or when liver enzymes (e.g. alanin amino
transferees) are found to be elevated on routine testing
(Dale et al., 2004.). Detection of HCV requires not only the
measurement of levels of liver enzymes, but also testing for
the hepatitis C antibodies in the blood and testing for the
viral genome as some people with hepatitis C infection may
have normal levels of liver enzymes (Dale et al., 2004).
Antibody to hepatitis is detected by the use of 3rd or 4th
generation recombinant enzyme linked immune sorbent assay
(ELISA) which is found to have high sensitivity and
specificity (Dale et al., 2004). Both quantitative and
qualitative RNA tests are used to detect viral genome in the
blood to access therapeutic effectiveness and management of
patient with hepatitis C (Linda et al., 2004). Viral
eradication, however, should not be the only end point in
all HCV patients. Achieving significant reductions in viral
load usually results in marked improvement of the liver
inflammation and will retard progression to more severe
liver damage (Linda et al., 2004). The cornerstone of
hepatitis C treatment is the use of interferon. Interferons
are proteins normally produced by the body’s immune system
in response to a viral infection and the human body produces
4
over 20 different types of interferons. There are four types
of interferons licensed in the USA for the treatment of HCV
namely, interferon alfa2b (intron -A) interferon alfa2a
(Roferon-A), consensus interferon (intergen) and interferon
alpha n-1 (ellferon) (Ala et al., 1996). Studies have shown
the efficiency of the combination of paginated interferon
and ribavirin in the treatment of patients with chronic
Hepatitis C (Jean-Jacque et al., 2004).
Preventive measures are used to reduce the burden of HCV
infection. These measures include primary prevention
activities that reduce risks for contracting HCV infection
and secondary prevention activities that reduce risks for
liver and other chronic diseases in HCV infected persons.
The primary preventive activities include, screening and
testing of blood, plasma, organ, tissue and semen donors,
virus inactivation of plasma derived products, risk
reduction counseling and implementation and maintenance of
infection control practices, while secondary prevention
activities include, identification, counseling and testing
of persons at risk and medical management of infected
persons.
1.1 Statement of the Problem
Egah et al (2004) reported Hepatitis C Virus seroprevalence
of 6.0% among blood donors in Jos. Ayolabi et al (2006) in
Lagos reported a HCV seroprevalence of 8.4% all among blood
5
donors. It is estimated that 130–200 million people, or 3%
of the world's population, are living with chronic Hepatitis
C (Gravitz, 2011 and WHO, 2010). About 3–4 million people
are infected per year, and more than 350,000 people die
yearly from Hepatitis C-related diseases (WHO, 2010). HCV
infection may ultimately lead to cirrhosis and
hepatocellular carcinoma (Karen et al., 2003). HCV is the most
important cause of post transfusion non A and B hepatitis
worldwide (Maria et al., 2004).
1.2 Justification
Hepatitis C virus (HCV) poses a significant threat to health
worldwide (Dale et al., 2004). Although the transmission of
Hepatitis C virus through the transfusion of blood and blood
products has nearly disappeared since the introduction of
approved screening measures worldwide among blood donors,
studies have shown its prevalence in some parts of Nigeria,
viz; Lagos (Lesi and Kehinde, 2003) and Jos (Egah et al.,
2004). The prevalence of chronic HCV among blood donors has
also been noted in some West African countries (Jean-
francois et al., 2001) these include Ghana (Wansbrough et al.,
1998), Senegal, Mauritania and Benin (Jean-francois et al.,
2001). In most parts of Nigeria, the screening for Hepatitis
C among blood donors is not practiced despite the fact that
it can lead to serious sequelae. As a result, the actual
burden of the disease is not known. There is therefore the
6
need for studies to check its prevalence especially in this
part of the Country so as to have a clue to its spread which
can help healthcare policy makers and care givers in
providing measures of controlling the disease.
1.3 Aim and Objectives
Aim:
To determine the prevalence of hepatitis C virus among blood
donors attending General Hospital Minna
Objective:
To determine the risk factors associated with HCV
seropositivity.
CHAPTER TWO
LITERATURE REVIEW
2.1 History of Hepatitis C Virus
In the mid-1970s, Harvey J. Alter, Chief of the Infectious
Disease Section in the Department of Transfusion Medicine at
the National Institutes of Health, and his research team
7
demonstrated how most post-transfusion hepatitis cases were
not due to hepatitis A or B viruses. Despite this discovery,
international research efforts to identify the virus,
initially called nonA-non-B hepatitis (NANBH), failed for the
next decade. In 1987, Michael Houghton, Qui-Lim Choo, and
George Kuo at Chiron Corporation, collaborating with Dr.
D.W. Bradley at the Centers for Disease Control and
Prevention, used a novel molecular cloning approach to
identify the unknown organism and develop a diagnostic test
(Boyer, 2001). In 1988, the virus was confirmed by Alter by
verifying its presence in a panel of NANBH specimens. In
April 1989, the discovery of HCV was published in two
articles in the Journal Science (Choo et al., 1989 and Kuo et al.,
1989). The discovery led to significant improvements in
diagnosis and improved antiviral treatment (Boyer, 2001). In
2000, Drs. Alter and Houghton were honored with the Lasker
Award for Clinical Medical Research for pioneering work
leading to the discovery of the virus (Winner, 2008).
2.2 Biology of Hepatitis C Virus: The hepatitis C virus
(HCV) is a small, enveloped, single, positive-sense RNA
virus (Rosen, 2011).
2.2.1 Genome of Hepatitis C Virus:
The HCV genome carries a single long open reading frame
(ORF) encoding a polyprotein that is proteolytically cleaved
into a set of distinct products. Translation of the HCV ORF8

is directed via a ∼340 nucleotide long 5′ non-translated
region (NTR) functioning as an internal ribosome entry site
(IRES) and permitting the direct binding of ribosomes in
close proximity to the start codon of the ORF (Tsukiyama-
Kohara et al., 1992; Wang et al., 1993). The first ∼40
nucleotides of the RNA genome are not required for
translation but, based on analogy with other plus-strand RNA
viruses, are involved most likely in RNA replication (Boyer
& Haenni, 1994). The 3′ NTR was only recently discovered
(Kolykhalov et al., 1996; Tanaka et al., 1995, 1996; Yamada et al.,
1996). It has a tripartite structure composed of a variable
sequence following the stop codon of the ORF, a poly (U)
tract of heterogeneous length and a highly conserved 98
nucleotide sequence essential for replication in vivo (Yanagi
et al., 1999; Kolykhalov et al., 2000).
The HCV polyprotein is cleaved co- and post-translationally
by cellular and viral proteinases into ten different
products, with the structural proteins located in the amino-
terminal one-third and the nonstructural replicative
proteins in the remainder (Bartenschlager, 1999; Reed et al.,
1998). The first cleavage product of the polyprotein is the
highly basic core protein, forming the major constituent of
the nucleocapsid (Yasui et al., 1998). In addition, a number
of other functions like modulation of several cellular
processes or induction of hepatocellular carcinoma in
transgenic mice have been described (Chang et al., 1998; Chen
9
et al., 1997 and Matsumoto et al., 1997). Envelope proteins (E1
and E2) are highly glycosylated type 1 transmembrane
proteins, forming two types of stable heterodimeric
complexes: a disulfide-linked form representing misfolded
aggregates and a non-covalently linked heterodimer
corresponding most likely to the pre-budding complex
(Deleersnyder et al., 1997). In addition, E2 was shown to
interact with the IFN-induced double-stranded RNA-activated
protein kinase PKR. Upon induction by IFN-α, this enzyme
reduces protein synthesis via phosphorylation of translation
initiation factor eIF2-α, but in cells containing E2, PKR is
inhibited, allowing continuation of translation in the
presence of IFN (Taylor et al., 1999). Protein p7, located at
the carboxy terminus of E2, is a highly hydrophobic
polypeptide of unknown function. Most of the nonstructural
(NS) proteins 2–5B (the term indicates that these proteins
are not expected to be constituents of the virus particle)
are required for replication of the viral RNA (Lohmann et al.,
1997). NS2 and the amino-terminal domain of NS3 constitute
the NS2–3 proteinase, catalysing cleavage at the NS2/3 site
(Grakoui et al., 1993). NS3 is a bifunctional molecule
carrying in the amino-terminal ∼180 residues, a serine-type
proteinase responsible for cleavage at the NS3/4A, NS4A/B,
NS4B/5A and NS5A/B sites and, in the carboxy-terminal
remainder, NTPase/helicase activities essential for
translation and replication of the HCV genome (Gwack et al.,
10
1996; Kim et al., 1995; Suzich et al., 1996; Bartenschlager et al.,
1993; Eckart et al., 1993; Grakoui et al., 1993; Tomei et al.,
1993; Kolykhalov et al., 2000). In addition, NS3 may have
other properties involved in interference with host cell
functions like inhibition of protein kinase A-mediated
signal transduction or cell transformation (Borowski et al.,
1996). NS4A is an essential cofactor of the NS3 proteinase
and is required for efficient polyprotein processing
(Bartenschlager et al., 1994; Failla et al., 1994; 1994; Tanji et
al., 1995). The function of the hydrophobic NS4B is so far
unknown. NS5A is a highly phosphorylated protein and, at
least with some HCV isolates, the level of phosphorylation
is influenced by NS4A via direct interaction with NS5A or it
requires the expression of NS5A in the context of a NS3–5A
polyprotein (Asabe et al., 1997; Tanji et al., 1995., Kaneko et
al., 1994; Koch & Bartenschlager, 1999; Neddermann et al.,
1999;). NS5A phosphorylation is mediated by an as yet
unknown cellular kinase (Tanji et al., 1995;Ide et al., 1997;
Reed and Rice, 1999). For the HCV-H isolate the major
phosphorylation site has been mapped to serine residue 2321
of the polyprotein and the proline-rich nature of the
flanking sequence suggests that a proline-directed kinase is
responsible for NS5A phosphorylation (Reed & Rice, 1999).
The role NS5A may play in RNA replication is so far not
known, but based on analogy with other RNA viruses, where
phosphoproteins are important regulators of replication; one
11
could assume that NS5A plays a similar role. Apart from such
a function, NS5A appears to be involved in resistance of the
infected cell to the antiviral effect of IFN. At least for
some HCV isolates NS5A is able to bind to PKR, blocking the
translational reduction in the IFN-treated cell (Gale et al.,
1997, 1998). Interestingly, an alanine substitution for the
major phosphorylation site at serine residue 2321 did not
affect the NS5A: PKR interaction, showing that
phosphorylation at this particular site is not required for
complex formation with PKR (Reed & Rice, 1999). NS5B was
identified as the RNA-dependent RNA polymerase (RdRp) (Al et
al., 1998; Behrens et al., 1996; Lohmann et al., 1997; Yamashita et
al., 1998; Yuan et al., 1997).
2.3 Classification of Hepatitis C Virus (HCV):
HCV has been classified as the sole member of a distinct
genus called Hepacivirus in the family Flaviviridae, which
includes the Flaviviruses, the animal pathogenic
pestivivruses and although this awaits official
confirmation, the recently cloned GB virus A (GBV-A), GBV-B
and GBV-C/ hepatitis G viruses (Ray et al., 2009). There are
seven major genotypes of HCV, which are indicated
numerically from 1-7 (Nakano et al., 2011). In the United
States, about 70% of cases are caused by genotype 1, 20% by
genotype 2, and about 1% by each of the other genotypes
12

(Wilkins et al., 2011). Genotype 1 is also the most common in
South America and Europe (Rosen, 2011).
2.4 Mode of Replication:
HCV nonstructural proteins and viral RNA have been detected
in livers of infected patients or experimentally inoculated
chimpanzees, confirming that the liver is a site of HCV
replication (Blight & Gowans, 1995). Unfortunately, the
amounts of viral proteins and RNA in infected tissues are
very low, necessitating the use of highly sensitive but also
less reliable detection methods. This may in part explain
why the reported number of HCV-positive cells detected in
infected liver tissue is contradictory and estimates vary
between less than 5% and up to 100% (Blight & Gowans, 1995).
Apart from liver cells, there is strong evidence that HCV
can also replicate in peripheral blood mononuclear cells
(PBMCs) both in vivo and ex vivo or in experimentally infected
B- and T-cell lines (see below). Such a lymphotropism may
account for the numerous immunological disorders, in
particular type II and type III cryoglobulinaemia, observed
in more than 50% of chronic hepatitis C patients (Esteban et
al., 1998).
The dynamics of HCV replication can be deduced from the
rapid rates of virus production and emergence of mutants.
13
Owing to the lack of a convenient animal model and an
efficient cell culture system our current understanding of
the molecular mechanisms of HCV replication is based
primarily on analogies to the closely related flavi- and
pestiviruses and on the characterization of recombinant HCV
proteins. Using this limited information the HCV replication
cycle can be summarized as follows:
i. Penetration of the host cell and liberation of the
genomic RNA from the virus particle into the cytoplasm
ii. Translation of the input RNA, processing of the
polyprotein and formation of a replicase complex associated
with intracellular membranes
iii. Utilization of the input plus-strand for synthesis of a
minus-strand RNA intermediate
iv. Production of new plus-strand RNA molecules which in
turn can be used for synthesis of new minus strands, for
polyprotein expression or packaging into progeny virions
v. Release of virus from the infected cell.
2.5 Life Cycle:
The first step in a virus life-cycle is the attachment of
the infectious particle to the host cell, for which a
specific interaction between a receptor on the cell surface
and a viral attachment protein on the surface of the
particle is required. CD81 was identified as a putative HCV
receptor based on its strong interaction with E2 as well as14
with virus particles in vitro (Pileri et al., 1998). Furthermore,
preincubation of the HCV-containing plasma used for the
binding studies with sera from chimpanzees that were
protected from HCV challenge by vaccination with recombinant
E1 and E2 also blocked in vitro binding of HCV to CD81 (Pileri
et al., 1998). However, whether virus binding to CD81 is
followed by internalization of the virus particle is not
known.
Apart from this route, HCV as well as other members of the
Flaviviridae family may enter the cell by binding to low-
density lipoprotein (LDL) receptors. Based on the
observation that HCV particles are associated with beta-
lipoproteins (Thomssen et al., 1992 and Agnello et al.,1999),
analysed whether endocytosis of HCV is mediated by LDL
receptors. Using in situ hybridization to determine HCV-RNA-
positive cells, a direct correlation between the level of
cell surface-expressed LDL receptor and the number of
positive cells was found. This result and the finding that
HCV does not bind to COS-7 cells unless they have been
transfected with the LDL receptor gene (Monazahian et al.,
1999) suggest that HCV particles associated with LDL bind to
this receptor. Whether interaction with the LDL receptor or
CD81 leads to a productive infection remains to be
determined.
15

While the nature of the HCV receptor is not known currently,
the major envelope glycoprotein E2 is thought to be
responsible for initiating virus attachment to the host cell
because E2-specific antisera can block binding to cells
(Rosa et al., 1996 and Farci et al., 1996). The role of E1 is
less clear but the presence of a stretch of hydrophobic
amino acids tentatively called the E1 fusion peptide,
displaying similarities to the fusion peptides of
Paramyxovirus and Flavivirus suggests that E1 is involved in
membrane fusion (Flint et al., 1999). To study the early steps
in the HCV life-cycle, generated vesicular stomatitis virus
(VSV) pseudotypes. They expressed chimeric envelope proteins
composed of the HCV E1 or E2 ectodomains fused to the
transmembrane and cytoplasmic domains of the VSV G protein.
As indicated by the formation of plaques, a baby hamster
kidney cell line (BHK-21), the human T-cell line MOLT4 and
the human hepatoma cell line HepG2 were susceptible to
infection with the pseudotypes, but the human cervical
carcinoma cell line HeLa and the human embryonic lung cell
line L-132 were not. However, only pseudotypes carrying
either the E1 or the E2 ectodomain were used, not
pseudotypes with both chimeric HCV proteins. This is
surprising, because E2 acts as a chaperone for E1, which in
the absence of E2 forms misfolded aggregates (Michalak et al.,
1999). Furthermore, E1 and E2 form stable heterodimers that
most likely represent the native form found in the HCV
16
envelope (Dubuisson et al., 1994). Finally, studies with
engineered cell surface-expressed E2 glycoproteins folded in
a manner comparable to authentic E2 demonstrated that this
protein alone did not enable cell fusion (Flint et al., 1999).
2.6 Hepatitis C Virus Infection:
HCV is a blood borne liver disease caused by hepatitis C
virus. HCV infection is a leading cause of chronic liver
disease, including cirrhosis of the liver. Chronic hepatitis
C is marked by the persistence of HCV RNA in the blood for
at least six months after onset of acute infection. HCV is
self limiting in only 15% to 25% of patients in whom HCV RNA
in their serum becomes undetectable and the patients possess
normal liver enzymes (Alanine amino transferase (ALT) and
normal liver histology (Michael and Alexander, 2004).
Progression of chronic hepatitis C is slow in the patients
and they can remain asymptomatic for several years. Chronic
HCV infection is caused by many factors including alcohol
abuse, the duration of infection, age at time of infection,
gender, ethnicity, and development of jaundice during acute
infection (Michael and Alexander, 2004).
2.7 MODE OF TRANSMISSION
2.7.1 Intravenous drug use
17
IDU is a major risk factor for hepatitis C in many parts of
the world (Xia et al., 2008). Of 77 countries reviewed 25
(including the United States) were found to have prevalences
of hepatitis C in the intravenous drug user population of
between 60% and 80% ( Nelson et al., 2011 and Xia et al.,
2008).Twelve countries had rates greater than 80% (Nelson et
al., 2011). It is believed that ten million intravenous drug
users are infected with hepatitis C; China (1.6 million),
the United States (1.5 million), and Russia (1.3 million)
have the highest absolute totals (Nelson et al., 2011).
Occurrence of hepatitis C among prison inmates in the United
States is 10 to 20 times that of the occurrence observed in
the general population; this has been attributed to high-
risk behavior in prisons such as IDU and tattooing with
nonsterile equipment (Imperial, 2010 and Vescio, 2008).
2.7.2 Healthcare exposure
Blood transfusion, transfusion of blood products, or organ
transplantation without HCV screening carry significant
risks of infection (Wilkins et al., 2010). The United States
instituted universal screening in 1992 (Marx, 2010), and
Canada instituted universal screening in 1990 (Day et al.,
2009).This decreased the risk from one in 200 units (Marx
and John, 2010) to between one in 10,000 to one in
10,000,000 per unit of blood (Springer Verlag , 2011 and
Ponde, 2010). This low risk remains as there is a period of
18
about 11–70 days between the potential blood donor acquiring
hepatitis C and their blood testing positive depending on
the method (Ponde, 2010). Some countries do not screen for
hepatitis C due to the cost (Alter, 2007).
2.7.3 Sexual intercourse
Whether hepatitis C can be transmitted through sexual
activity is controversial (Tohme, 2010). While there is an
association between high-risk sexual activity and hepatitis
C, it is not known whether transmission of the disease is
due to drug use that has not been admitted to or sex as a
risk factor (|Wilkin et al., 2010).The majority of evidence
supports there being no risk for monogamous heterosexual
couples (Tohme, 2010). Sexual practices that involve higher
levels of trauma to the anogenital mucosa, such as anal
penetrative sex, or that occur when there is a concurrent
sexually transmitted infection, including HIV or genital
ulceration, do present a risk ( Ponde, 2010) .
2.7.4 Body modification
Tattooing is associated with two to threefold increased risk
of hepatitis C (Jafari et al., 2010). This can be due to
either improperly sterilized equipment or contamination of
the dyes being used (Jafari et al., 2010). Tattoos or
19
piercings performed either before the mid-1980s,
"underground," or nonprofessionally are of particular
concern, since sterile techniques in such settings may be
lacking. The risk also appears to be greater for larger
tattoos (Jafari et al., 2010). It is estimated that nearly
half of prison inmates share unsterilized tattooing
equipment (Jafari et al., 2010). It is rare for tattoos in a
licensed facility to be directly associated with HCV
infection (CDC, 2012).
2.7.5 Shared personal items
Personal-care items such as razors, toothbrushes, and
manicuring or pedicuring equipment can be contaminated with
blood. Sharing such items can potentially lead to exposure
to HCV (Lock et al., 2006 and CDC, 2012). Appropriate caution
should be taken regarding any medical condition that results
in bleeding, such as cuts and sores (CDC, 2012). HCV is not
spread through casual contact, such as hugging, kissing, or
sharing eating or cooking utensils (CDC, 2012). Neither is
it transmitted through food or water (Wong and Lee, 2006).
2.7.6 Vertical transmission
Vertical transmission of hepatitis C from an infected mother
to her child occurs in less than 10% of pregnancies (Lam et
20
al., 2010). There are no measures that alter this risk (Lam et
al., 2010). It is not clear when during pregnancy
transmission occurs, but it may occur both during gestation
and at delivery (Ponde, 2011). A long labor is associated
with a greater risk of transmission (Alter, 2007). There is
no evidence that breast-feeding spreads HCV; however, to be
cautious, an infected mother is advised to avoid
breastfeeding if her nipples are cracked and bleeding (Mast,
2004), or her viral loads are high (Ponde, 2011).
2.8 Pathogenesis:
Hepatitis C being a blood borne disease is transmitted
through blood and body fluids. Route of infection vary among
infected individual. They include blood, IVDU, blood
transfusions, sexual activities, among others as discussed
earlier. The virus replicates in the cytoplasm of
hepatocytes but is not directly cytopathic (Lau, et al.,
1995). Persistence infection appears to rely on rapid
production of the virus and continuous cell to cell spread
along with a lack of virgeous T.cell. Immune response to HCV
antigens. The HCV turnover rate can be quite high with
replications ranging from 1010-1212 virions per day and a
product viral half life of 2-3 hours. The rapid viral
replication and lack of error proof reading by the viral RNA
polymerase are reasons why the HCV RNA mutates frequently
(Nahum et al., 2004).
21
2.9 Progression of Liver Fibrosis:
During persistence hepatitis C viremia the rate of
progression of liver fibrosis varies widely (Colina, et al.,
1999). There have been extensive studies focusing on the
natural cause of disease progression from chronic hepatitis
C to cirrhosis, Hepatocellular carcinoma HCC and death.
The liver biopsy is the gold standard for the granding and
staging of chronic hepatitis C (Colina, et al., 1999). The
activity of liver disease or grade is gauged by the number
of mononuclear inflammatory cells present in and around the
portal entry areas, and by the number of dead dying
hepatocytes. The structural liver damage, also known as
Filorosis is variable in chronic HCV infection to cirrhosis.
In mild cases, fibrosis is limited to the portal and
periportal areas.
Multipliers of studies have shown that chronic alcohols use
a major external risk. Factors include gender, co-infection
with HCV and HBV, the degree of inflammation and fibrosis
present on the liver biopsy, and co-morbid conditions such
as immune suppression, insulin resistance, non-alcoholic
steatohepatitis, hemochromatosis and schistosomies.
2.10 Clinical Manifestation:
22
Chronic HCV infection is marked by the persistence of HCV
RNA in the blood for at least 6 months after a set of acute
infection. HCV infection is self-limiting in 15-25% of
patients in whom HCV RNA in serum becomes undetectable and
ALT level return to normal. Approximately 75-85% of infected
individuals do not clear the virus by 6 months and chronic
HCV infection develops (Colina, et al., 1999). The sequence of
chronic HCV infection includes cirrhosis of liver as well as
hepatocellular carcinoma HCC. Chronic HCV infection has been
associated with numerous extra hepatic manifestations
involving multiple organ system including renal,
dermatological, hematological and rheumatological systems
(Colina, et al., 1999). Approximately 1-2% of HCV infected
individuals will develop extra hepatic manifestation (San
Diego, 1999).
2.3 Laboratory Diagnosis
2.3.1 Anti HCV Anti-Body Detection:
The detection of anti-HCV Ab in plasma or serum is based on
the use of third generation EIAS (enzymes immunoassay) that
detect mixtures of Ab directed against various HCV epitopes.
Recombinant antigens are used to capture circulating anti-
HCV antibodies into the wells of a micro-titer plates, micro
beads or specific holder adapted to closed automated
devices.
23
The optical density (OD) ratio of the reaction is
proportional to the amount of Ab in the serum or plasma
sample (Colina et al., 1999). The specificity of third-
generation EIAS for anti-HCV is greater than 99% (Peter et
al., 2003). Their sensitivity is more difficult to determine,
given the lack of a good standard method, but it is
excellent in HCV infected immunocompromised patients.
EIAS can be fully automated and are well adapted to large
volume testing. Immunoblot tests are nowadays clinically
obsolete given the performance of third generation anti-HCV
EIAS (Peter et al., 2003).
2.3.2 Acute Hepatitis C:
Patients with a suspicious acute hepatitis C should be
tested for both anti-HCV Abs by EIA and HCV RNA with a
sensitive techniques, i.e. an HCV RNA assay with a lower
limit of detection of 50 Iuml or less (Colina et al., 1999).
Four marker profiles can be observed according to the
presence of anti-HCV Ab is strongly indicative of acute HCV
infection, which will be confirmed by sera conversion (i.e.
the appearance of anti-HCV Abs) a few day to weeks later.
Acutely infected patients can also have both HCV RNA and
anti-HCV Abs at time of diagnosis. It is difficult in this
case to distinguish acute hepatitis C from an acute
exacerbation of chronic hepatitis C or an acute hepatitis C
cause of another cause in a patient with chronic hepatitis24
C. Acute hepatitis C is very unlikely if both anti-HCV Abs
and HCV RNA are absent. (Christian et al., 2004).
2.4. Signs and Symptoms
2.4.1 Acute infection:
Hepatitis C infection causes acute symptoms in 15% of cases
(Maheshwari et al., 2008). Symptoms are generally mild and
vague, including a decreased appetite, fatigue, nausea,
muscle or joint pains, and weight loss (Wilkins et al., 2010),
and rarely does acute liver failure result(Bailey and
Caittin, 2010). Most cases of acute infection are not
associated with jaundice (Stringer Verlage, 2011). The
infection resolves spontaneously in 10-50% of cases, which
occurs more frequently in individuals who are young and
females (Stringer Verlage, 2011).
2.4.2 Chronic infection
About 80% of those exposed to the virus develop a chronic
infection (Nelson et al., 2011). Most experience minimal or
no symptoms during the initial few decades of the infection,
(Stringer Verlage, 2011), although chronic hepatitis C can
be associated with fatigue (Ray, 2009). Hepatitis C after
many years becomes the primary cause of cirrhosis and liver
cancer (Rosen, 2011). About 10–30% of people develop
cirrhosis over 30 years (Rosen, 2011 and Wilkin et al., 2010).
25
Cirrhosis is more common in those co-infected with hepatitis
B or HIV, alcoholics, and those of male gender (Rosen, 2011
and Wilkin et al., 2010). Those who develop cirrhosis have a
20-fold greater risk of hepatocellular carcinoma, a rate of
1–3% per year, (Rosen, 2011 and Wilkin et al., 2010), and if
this is complicated by excess alcohol the risk becomes 100
fold greater (Mueller et al., 2009). Hepatitis C is the cause
of 27% of cirrhosis cases and 25% of hepatocellular
carcinoma worldwide (Alter, 2007).
Liver cirrhosis may lead to portal hypertension, ascites
(accumulation of fluid in the abdomen), easy bruising or
bleeding, varices (enlarged veins, especially in the stomach
and esophagus), jaundice, and a syndrome of cognitive
impairment known as hepatic encephalopathy. It is a common
cause for requiring a liver transplant (Ozaras and Tahan,
2009).
2.4.3 Extrahepatic
Hepatitis C is also rarely associated with Sjögren's
syndrome (an autoimmune disorder), thrombocytopenia, lichen
planus, diabetes mellitus, and B-cell lymphoproliferative
disorders (Zignego et al., 2007). Thrombocytopenia is
estimated to occur in 0.16% to 45.4% of people with chronic
hepatitis C (Louie et al., 2011). Putative associations with
Hyde's prurigo nodularis (Lee and Shumach, 2005), and
membranoproliferative glomerulonephritis have been reported26

(Ray et al., 2009). Hepatitis C infection is also associated
with a condition called mixed cryoglobulinemia, which is
inflammation of small and medium sized blood vessels (or
vasculitis) caused by deposition of immune complexes
involving cryoglobulins (Iannuzzela et al., 2010).
2.5 Treatment
HCV induces chronic infection in 50–80% of infected persons.
Approximately 40-80% of these clear with treatment (Torresi
et al., 2011 and Ilyas and Vierling, 2011). In rare cases,
infection can clear without treatment (Stringer Verlag,
2011). Those with chronic hepatitis C are advised to avoid
alcohol and medications toxic to the liver, (Wilkins, 2010),
and to be vaccinated for hepatitis A and hepatitis B
(Wilkins, 2010). Ultrasound surveillance for hepatocellular
carcinoma is recommended in those with accompanying
cirrhosis (Wilkins, 2010).
In general, treatment is recommended in those with proven
HCV infection liver abnormalities (Wilkins, 2010). As of
2010, treatments consist of a combination of pegylated
interferon alpha and the antiviral drug ribavirin for a
period of 24 or 48 weeks, depending on HCV genotype
(Wilkins, 2010). When combined with ribavirin, pegylated
interferon-alpha-2a may be superior to pegylated interferon-
alpha-2b, though the evidence is not strong (Awad et al.,
2010). Improved outcomes are seen in 50–60% of people27
(Wilkins, 2010).Combining either boceprevir or telaprevir
with ribavirin and peginterferon alfa improves antiviral
response for hepatitis C genotype 1 (Foote et al., 2011; Smith
et al., 2011 and Ghany et al., 2011). Adverse effects with
treatment are common, with half of people getting flu like
symptoms and a third experiencing emotional problems
(Wilkins, 2010). Treatment during the first six months is
more effective than once hepatitis C has become chronic
(Ozaras and Tahan, 2009). If someone develops a new
infection and it has not cleared after eight to twelve
weeks, 24 weeks of pegylated interferon is recommended
(Ozaras and Tahan, 2009). In people with thalassemia,
ribavirin appears to be useful but increases the need for
transfusion (Alavian and Tabatabaei, 2010).
2.6. Prevention and Control
As of 2011, no vaccine protects against contracting
hepatitis C. However, a number are under development and
some have shown encouraging results (Hagan et al., 2011). A
combination of harm reduction strategies, such as the
provision of new needles and syringes and treatment of
substance use, decrease the risk of hepatitis C in
intravenous drug users by about 75% (Hagan et al., 2011). The
28
screening of blood donors is important at a national level,
as is adhering to universal precautions within healthcare
facilities (Ray et al., 2009). In countries where there is an
insufficient supply of sterile syringes, medications should
be given orally rather than via injection (when possible)
(Alter, 2007). The United States government only recommends
condom use to prevent hepatitis C transmission in the use
with multiple partners (United state department of veteran
affairs).
2.6.1 Primary Prevention Activities
Primary prevention activities reduce potential risk for HCV
transmission from such high risk activities as injecting
drug use, sex with multi-partners and precutaneous exposures
to blood in health care, blood, blood components, plasma
derivatives, tattooing and body piercing (Ala et al., 1996).
Practices that exclude blood, plasma, organ, tissue or serum
from donors who are associated public health policies aimed
at reducing HIV transmission, such as the promotion of
sexual barrier protection and inhabitation of needle
exchange programs are likely to decrease transmission of HCV
in high risk groups (Ala et al., 1996). Counseling and
education to prevent initiation of drug injecting or high
risk sexual practices is important. Persons who inject drug
or who are at risk for STDs should be counseled regarding
what they can do to minimize their risk for infection or
29
transmission to other persons who inject illegal drugs
should be advised to stop using and injecting drugs or never
to re-use or share syringes, needles and to use only sterile
syringe obtained from a reliable source e.g. pharmacies,
clean the injection site with a new alcohol to swab before
inject and to safety dispose syringe after one use.
Health and emergency medical and public safety workers
should be educated on the risk and prevention of blood borne
infection. Standard barrier precautions and engineering
control should be implemented to prevent exposure to blood
(Ala et al., 1996).
As recommended for all healthcare workers those who are HIV
positive should follow strict aseptic techniques and
standard precautions including appropriate use of hand
washing, protective barrier and care in the use and disposal
of needles and other sharp instrument (Ala et al., 1996).
2.6.2 Secondary Prevention Activities
Secondary prevention activities can reduce risks for
chronic disease by identifying HCV infected persons through
diagnostic testing and by providing appropriate medical
management and antiviral therapy. Identification of HCV-
infected persons must be a major focus of currents
prevention programs since their number is significant.
Identification of person at risk for HCV infection provides
30
opportunity for testing to determine their disease status if
infected, and antiviral therapy, if appropriate.
Identification also provides infected persons opportunities
to obtain information concerning how they can be prevented
further to their liver and prevent transmitting HCV to
others.
2.7 Epidemiology:
Hepatitis C Virus (HCV) continues to be a major disease
burden on the world. In 1999 World Health Organization
(WHO), it is estimated that 130–200 million people, or ~3%
of the world's population, are living with chronic hepatitis
C (WHO, 2010 and Gravitz, 2011) About 3–4 million people are
infected per year, and more than 350,000 people die yearly
from hepatitis C-related diseases (WHO, 2010). Rates have
increased substantially in the 20th century due to a
combination of IDU and intravenous medication or poorly
sterilized medical equipment (Alter, 2007).
Among those chronically infected, the risk of cirrhosis
after 20 years varies between studies but has been estimated
at ~10%-15% for men and ~1-5% for women. The reason for this
difference is not known. Once cirrhosis is established, the
rate of developing hepatocellular carcinoma is ~1%-4% per
year (Yu and Chuang, 2002).
31
Between central and south America, a recent community based
study San Juan, Puerto Rocco, should that estimated HCV
prevalence in 2001-2002 was 6.3% (Peter et al., 2003). In
Mexico, the prevalence reported was 1.2% (Nahum et al., 2004).
Among blood donor in Chile and Brazil, prevalence of HCV
antibodies (Abs) was low 0.3% 1.14% respectively (Marshal et
al., 2005 and Munox et al., 1998). Prevalence of HCV antibodies
is 0.87% (1993-1994) in Belgium (Bellentani and Tiribellic,
2001).in U.K, at least 200,000 adult carry HCV (hapetitis C
strategy for England). In Northern Italy prevalence of HCV
Abs was 3.2% (Stroffolini et al., 1995). Three studies in
central and southern Italy showed a higher rate of HCV
(8.4%-22.4%) especially in the order population (Monica et
al., 2003). Among patients of general practitioners in
Lyon, France, the prevalence of HCV was estimated to be
1.3%, very similar to the French population (Peter et al.,
2003) within the Russian army, frequency of anti-HCV was
1.5% among service men and donors with increased prevalence
in the Northern countries, far east and Siberia (3.1-3.8%)
compared to the transikal region (0.70%) (Ogarkov et al.,
2004). Low rates were found in Hungary (0.73% of 15, 864
blood donors) (Egah et al., 2004). Recently, HCV prevalence
studies have come out of Pakistan in the middle east, 751
out of 16,400 patients (4.57%) were found to be positive for
HCV Abs from 1998-2002 (Muhammad and Jan, 2005). Among male
blood donors in Karachi, Pakistan, the seroprovalence of HCV
32
was 1.8% with a trend of increasing proportion of positive
donors from 1998-2002 (Attar et al., 2004) there have been
very high prevalence rates of HCV reported in Egypt in the
past (28%) (Heidi et al., 2003). This was confirmed among 90
blood donors in Cairo, where 14.4% were anti-HCV positive
for RIBA test (Darwish, 1992). Then 26.6% among 188 blood
donors and 22% among 163 donors were positive with both
studies done in Cairo (Bassily et al., 1995 and Darwish et al.,
1993). Rates were lower in Saudi Arabia (1.8%) and semen
(2.1%). Intermediate rates of HCV have been reported out of
Asia from 1995- 2000, 0.49% anti HCV Ab was detected among
3,485,648 blood donors in Japan (Tanak et al., 2004). This was
lower than the 0.98% out of 10,905,489 blood donor reported
in 1992 (Yamaguchi et al., 1994). In China prevalence low with
rate around 1% among blood donor in Beijing and Wuhan (Zhang
et al., 1992 and Wang et al., 1994). However rate may be higher
in certain areas such as the hubei provincs, (30.1%) and
Inner Mongolia autonomous region (31.86%) (Soni et al.,
2004). Low rates have been found in Malaysia (around 1.6%)
and Singapore (0.54%) (Koff, 1997). Higher rate has been
reported in Thailand (3.2-5.6%) (Songsivilar et al., 1997and
Apichartpiyakul et al., 1999) within a smaller community of
103 residences in sherpas, Nepal, only one person had
borderline reaction in 2004 (Chba et al., 2004) in new Delhi,
India, 1.85% of blood donor were positive (Panigrali et al.,
1997). There have been fewer studies out of Africa but lower
33
rate have been reported; 1.6% among blood donors in Ethiopia
and 0.9% in Kenya (Frommel et al., 1993 and Ilako, 1995).
CHAPTER THREE
MATERIALS AND METHODS
3.1 Study Area:
34
The study was conducted at the Laboratory unit of the
General Hospital Minna, in Niger state where patients are
referred for blood donation.
3.2 Study Population:
These include all adult blood donors, aged 18 and above, of
all sexes (male and female) and of all social classes.
3.3 Materials:
These included:
i. Serum from fresh blood samples
ii. Plain blood bottles
iii. One step Hepatitis C virus test strip (Serum/Plasma)
made by Gold Diagnostics for in vitro diagnostics use
only. One package contains 50 strips.
3.4 Methods
i. Blood sample was collected from each subject by vene-
puncture of the median
veins.
ii. The site was cleaned using 70% isopropyl alcohol for
one minute and allowed to
dry.
iii. The blood was allowed to clot.
iv. The clotted blood samples were centrifuged to obtain
serum.
35

v. Using sterile Pasteur pipette, six drops of the serum
were transferred into sterile
plain bottles.
vi. Test for HCV antibodies was carried out using one step
Hepatitis C Virus test
strip (serum/plasma) made by gold diagnostics for
in vitro diagnostics.
vii. Testing was carried out immediately after the transfer.
3.5 Screening of Sera For Anti-HCV Antibodies
3.5.1 Principle of Assay:
The one step HCV test strip (serum/plasma) is a qualitative
membrane based immunoassay for the detection of antibodies
to HCV in serum or plasma. The membrane is coated with
recombinant HCV antigen on the test line region of the
strip. The mixture migrates upwards on the membrane
chromatographically by capillary action to react with the
recombinant HCV antigen on the membrane and generate a
colored line. Presence of this colored line indicates a
positive result. To serve as procedural control, a colored
line would always appear at the control line region
indicating that proper volume specimen has been added and
membrane wicking has occurred (Nahum et al., 2004).
3.6.2 Test Procedure
i. Bring the test kit to room temperature
ii. Cut the foul paper and bring out the test strip
36
iii. Immerse the test strip vertically into the serum
sample with the arrows pointing towards the serum for
fifteen seconds and the test strip not immersed beyond the
line indicated on it.
iv. Immediately after fifteen (15) seconds bring the test
strip out from the sample and allow standing for 25minutes
and observing for red lines each test result was read.
3.7.2 Interpretation of Result
Positive: Test was considered positive when two distinct red
lines appear; one line in the control region and another in
the test region (T). The intensity of the red line on the
test strip varies and this was as a result of concentration
of HCV antibodies presents in the specimen.
Negative: Test was considered negative when only one
distinct red line appeared in the control region © and none
at the test region (T).
Invalid: Test was considered invalid when control line fades
to appear. This may be as a result of insufficient specimen
volume or incorrect procedural techniques.
3.7. Statistical Analysis
The results were subjected to statistical analysis using
graph pad prism software. X2 test was carried out to find
out if there is significant difference between the different
37

age groups and occurrence of Hepatitis C, as well as between
sex and occurrence of Hepatitis C.
38

CHAPTER FOUR
RESULTS
4.1. The results showed that of the 200 samples screened for
Hepatitis C Virus antibodies among Blood donors in General
Hospital, Minna four (4) tested positive giving a prevalence of
2.0%
Table 4.1 shows the seroprevalence of HCV antibodies in relation
to sex of the subjects. The study comprises 181 males and 19
females. Three (1.7%) out of the 181 males were seropositive for
HCV antibodies while 1(5.3%) out of the 19 female blood donors
were seropositive. This is as shown in Table 4.1. The results
showed that females had the higher prevalence of 5.3% for HCV as
compared to the 1.7% for the males. The distribution across sex
is shown in Table 4.1.
Table 4.1 Percentage distribution of HCV by sex of the blood
donors attending General Hospital Minna
Sex No screened No positive %prevalenceMales 181 03 1.7Females 19 01 5.3Total 200 04 2.0
39
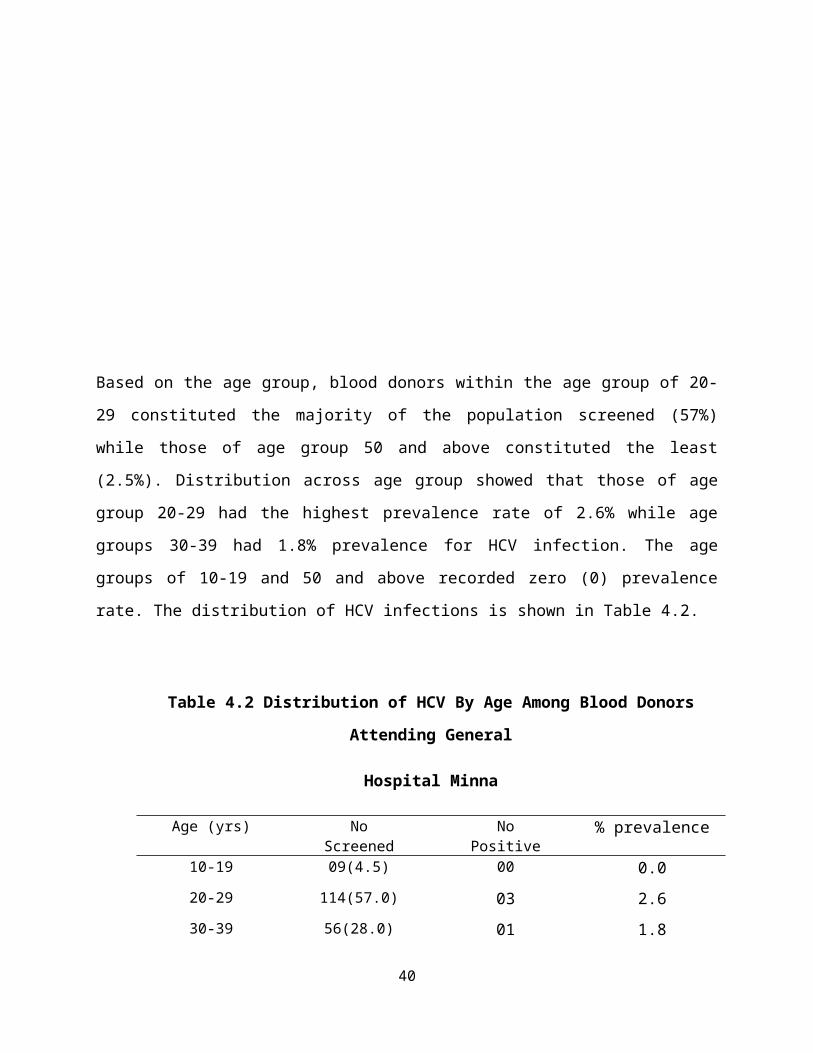
Based on the age group, blood donors within the age group of 20-
29 constituted the majority of the population screened (57%)
while those of age group 50 and above constituted the least
(2.5%). Distribution across age group showed that those of age
group 20-29 had the highest prevalence rate of 2.6% while age
groups 30-39 had 1.8% prevalence for HCV infection. The age
groups of 10-19 and 50 and above recorded zero (0) prevalence
rate. The distribution of HCV infections is shown in Table 4.2.
Table 4.2 Distribution of HCV By Age Among Blood Donors
Attending General
Hospital Minna
Age (yrs) NoScreened
NoPositive
% prevalence
10-19 09(4.5) 00 0.020-29 114(57.0) 03 2.630-39 56(28.0) 01 1.8
40
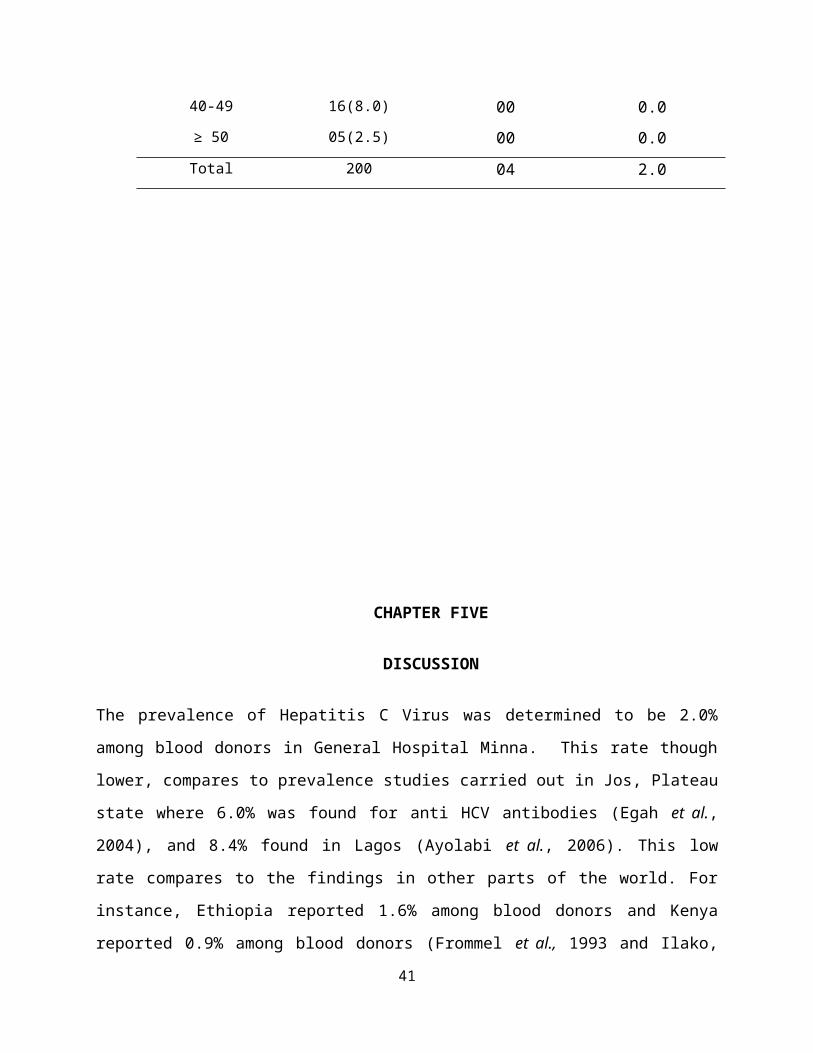
40-49 16(8.0) 00 0.0≥ 50 05(2.5) 00 0.0Total 200 04 2.0
CHAPTER FIVE
DISCUSSION
The prevalence of Hepatitis C Virus was determined to be 2.0%
among blood donors in General Hospital Minna. This rate though
lower, compares to prevalence studies carried out in Jos, Plateau
state where 6.0% was found for anti HCV antibodies (Egah et al.,
2004), and 8.4% found in Lagos (Ayolabi et al., 2006). This low
rate compares to the findings in other parts of the world. For
instance, Ethiopia reported 1.6% among blood donors and Kenya
reported 0.9% among blood donors (Frommel et al., 1993 and Ilako,
41

1995). Nigeria and Africa in general have no well documented
prevalence of Hepatitis C as fewer studies have originated out of
Africa (Janny et al., 2004 and Jordan, 2005).
In Minna General Hospital where this study was conducted, both
male and female donors are received though most are males. This
is corroborated by the study in Jos, Plateau state, in which most
of the donors were males (Egah et al., 2004).
Based on the age group, blood donors within the age group of 20-
29 constituted the majority of the population screened (56%)
while those of age group 50 and above constituted the least
(2.5%). Distribution across age group showed that those of age
group 20-29 had the highest prevalence rate of 2.6% for HCV
infection. They are followed by those of age group 30-39 with
prevalence rate of 1.8% for HCV infection. This may be due to the
sharing of personal-care items such as razors, toothbrushes, and
manicuring or pedicuring equipment which may be common among
members of this age group, and these items can be contaminated
with blood. Sharing such items can potentially lead to exposure
to HCV (Lock et al., 2010 and CDC, 2012). HCV is not spread through
casual contact, such as hugging, kissing, or sharing eating or
cooking utensils (CDC, 2012). Neither is it transmitted through
food or water (Wong and Lee, 2006).
The results showed that sero-prevalence of Hepatitis C Virus
among male Blood donors in General Hospital, Minna was (1.7%) and
42
(5.3%) for females blood donors. This showed that females had
higher prevalence than the males.
In the transfusion setting where the acute onset is best
documented, 70-80% are asymptomatic and only 20-30% develop
symptoms (Chihiro et al., 2004) and this occurs 3-12 weeks after
exposure. In a place like Minna and most probably Nigeria in
general where the awareness of hepatitis is very low, given the
few studies carried out and the little significance given to it
in the transfusion setting, prevalence could be higher than
determined.
Awareness about the disease, its complication and risk factors
among others, should be created mainly among public health
workers in Minna and in Nigeria as a whole in other to reduce the
risk of transmission through transfusion in particular and other
ways in general. Approximately, 75-85% of HCV infected person are
surely going to progress to chronic HCV infection, and are at
risk of developing extra-hepatics manifestation, compensated and
decompensated cirrhosis, and hepatocellular carcinoma (Colina et
al., 1999 and Munox et al., 1998). With most people acutely
infected being asymptomatic and chance of diagnosis in Minna and
Nigeria in general being limited, rate of transmission through
the known risk factors especially sexual inter-course, vertical
transmission, intravenous drug use in particularly among others
is likely to be high.
43
The use of blood donors as prevalence source under-estimates the
real prevalence of the virus because donors are highly selected
population (Alter et al., 1997). In Nigeria social-economic
situation is likely to play important and sometimes positive
roles in checking the prevalence rate of the disease where it is
tested. The incidence or role of commercial donor and free donor
as well come into play. Some hospitals and blood bank centers are
known to offer monetary benefits for blood donation, although it
is known that the knowledge of tests being carried out on blood
before acceptance scares away potential donors.
The Hospital where this study was done, offer such benefits. It
was discovered in the course of this study that regular or well
known blood donors are not regularly tested before bleeding. This
is likely to be a possible risk since blood donated are used
either immediately or sold to other hospitals in need, who are
less likely to re-test the blood on the presumption that it has
already been tested before collection.
Prevalence rate of Hepatitis C across the world has changed with
more countries being aware of transfusion related to Hepatitis C.
The prevalence rate is high as well as intermediate in mainly
developing countries of Asia, where documentation has been
attempted such as Pakistan where rates range from 1.8-4.57%
(Attar et al., 2004), Egypt (22-28%) (Darwish et al., 1992 and
Darwish et al, 1993; Heidi et al., 2003), New delhi, India (1.85%)
(Panigrali et al., 1997).
44
Statistical analysis, however, showed no significant difference
(P=0.299) between the prevalence rates of the male and female
individuals. There was, however, no statistical association (P
=0.299) between age group and prevalence of HCV antibodies. It is
conformity with that of Udeze et al., 2009, who found that there
was no statistically significant difference (P=0.05) between the
different age groups considered in their study. Also, of the two
factors of age and sex considered, there was no association
(P=0.05) between them and occurrence of Hepatitis C. This is also
in line with the finding of Udeze et al., 2009.
5.1 CONCLUSION
The prevalence of Hepatitis C Virus among Blood donors in General
Hospital, Minna was 2.0%. The overall seroprevalence of HCV
antibodies in the study group is 1.7%. Three (1.7%) out of 181
males were female seroprevalence for HCV antibodies while 1 (5.3)
out of 19 females blood donors were seropositive for HCV
antibodies. This showed that females had the higher prevalence of
5.3 % compared to the 1.7% for the males. Based on the age group,
blood donors within the age group of 20-29 constituted the
majority of the population screened (57%) while those of age
group 50 and above constituted the least (2.5%). Distribution
across age group showed that those of age group 20-29 had the
higher prevalence rates of 2.6% while age groups 30-39 1.8% for
HCV infection. The age group of 10-19 and 50 and above recorded
zero (0) prevalence rate. The distribution of HCV
45
infections.Statistical analysis, however, showed no significant
difference (p=0.299) between the prevalence rates of the male and
female individuals. There was, however, no statistical
association (p =0.299) between age group and prevalence of HCV
antibodies.
5.2 Recommendation
Hepatitis C is an emerging disease. There is an urgent need to
introduce HCV screening of blood donors for the disease where it
is not currently practiced, and a radical awareness campaign
about the disease should be introduced to reduce the risk of
transfusion associated with hepatitis C as well as other risk
factors and its complication in Minna and Nigeria in general.
Prevention is the only safeguard against spread of viral
hepatitis infection, thus, careful screening of blood, blood
products, and adequate sterilization of reusable surgical or
dental instruments should be done. Professional and public health
education and implementation of infection control practices in
all health facilities is of utmost importance.
Appropriate caution should be taken regarding any medical
condition that results in bleeding, such as cuts and sores.
Also, appropriate caution should be taken regarding personal-care
items such as razors, toothbrushes, and manicuring or pedicuring
equipment avoid sharing of these items.
46
REFERENCES
Agnello, V., Abel, G., Elfahal, M., Knight, G. B. & Zhang, Q. X.(1999). Hepatitis C Virus and other Flaviviridae virusesenter cells via low density lipoprotein Receptor. Proceedings ofthe National Academy of Sciences, USA 96, 12766-12771.
Al, R. H., Xie, Y. P., Wang, Y. H. & Hagedorn, C. H. (1998).Expression of recombinant Hepatitis C virus non-
47
structural protein 5B in Escherichia coli. Virus Research 53, 141-149.
Ala, I.S., Christine, M.H and Hohn, D.H. (1996). Hepatitis C.annals of internal medicine 125:658-668.
Alavian, S.M and Tabatabaei, S.V. (2010). "Treatment of chronichepatitis C in polytransfused thalassaemicpatients: a meta-analysis". Journal Viral and Hepatology. 17 (4):236–44.
Alter, M.J. (2007). Epidemiology of hepatitis C virus infectionWorld journal of Gastroenterology: WJG 13 (17): 2436–41.
Alter, M.J. (1997). Epidemiology of Hepatitis C. Hepathology.26:62-65
Apichartpiyakul, C., Apichartpiyakul, N.,Urwijitaroon, Y., Gray,J., Natpratan, C., Katayama, Y., Fujii, M and Hotta, H.(1999). Seroprevalence and subtype distribution of HepatitisC Virus among blood donors and intravenous drug users innorthern/ Northeastern Thailand. Journal Public Infest Disease.52:121-123
Asabe, S. I., Tanji, Y., Satoh, S., Kaneko, T., Kimura, K. &Shimotohno, K. (1997). The N- Terminal region of hepatitis Cvirus-encoded NS5A is important for NS4A-Dependentphosphorylation. Journal of Virology 71, 790-796.
Attar, A.K.E., Shamoul, A.M and Shalaby, A.A. (2004). Expressionof Chimeric HCV Petides in Transgentic TobaccoPlants infected with Recombinant Alfalfa Mosaic Virus forDevelopment of a plant- derived Vaccine against HCV. AfricaJournal of Biotechnology. 3 (11):588-594.
Awad, T., Thorlund, K., Hauser, G., Stimac, D., Mabrouk, M andGluud, C. (2010). "Peginterferon alpha-2a is associatedwith higher sustained virological response Thanpeginterferon alfa-2b in chronic hepatitis C: systematicreview of Randomized trials". Hepatology 51 (4): 1176–84.
48
Ayolabi, C.I., M.A. Taiwo, S.A. Omilabu, A.O. Abebisi, O.M.Fatoba, 2006. Seroprevalence of Hepatitis C Virusamong Blood Donors in Lagos, Nigeria. African Journal of.Biotechnology., 5(20): 1944-1946.
Bassily, S., Hyams, R.C., Found, R. A., Samaan, M.D and Hibbs,R.G. (1995). A high risk of Hepatitis C virus infectionamong Egyptian blood donors abuse. America Journal TropicalMedicine and Hygiene 52(6):503-5.
Bailey, B and Caitlin, (2010). Hepatic failure: An Evidence BasedApproach in The Emergency Department Emergencymedicine practice 12 (4).
Bartenschlager, R. (1999). The NS3/4A proteinase of the hepatitisC virus: unraveling Structure and functionof an unusual enzyme and a prime target for antiviralTherapy. Journal of Viral Hepatitis 6, 165-181.
Bartenschlager, R., Ahlborn-Laake, L., Mous, J. & Jacobsen, H.(1993). Nonstructural Protein 3 of the hepatitis Cvirus encodes a serine-type proteinase required For cleavageat the NS3/4 and NS4/5 junctions. Journal of Virology 67, 3835- 3844.
Bartenschlager, R., Ahlborn-Laake, L., Mous, J. & Jacobsen, H.(1994). Kinetic and Structural analyses of hepatitisC virus polyprotein processing. Journal of Virology. 68, 5045-5055.
Bawaaba, A.1. (2010). Highest Rates of Hepatitis C VirusTransmission Found in Egypt. Virology. 1-22
Behrens, S. E., Tomei, L. & De Francesco, R. (1996).Identification and properties of the RNA-dependent RNA polymerase of hepatitis C virus. EMBO Journal 15,12- 22.
Bellentani, S and Tiribellic, C. (2001). The spectrum of liverdisease in the general population: Lesion fromthe Dionysos study, Journal Hepatology. 65:78-79
49

Blight, K. & Gowans, E. (1995). In situ hybridization andimmunohistochemical staining Of hepatitis C virusproducts. Viral Hepatitis Reviews 1, 143-155.
Borowski, P., Heiland, M., Oehlmann, K., Becker, B., Kornetzky,L., Feucht, H. & Laufs, R. (1996). Non-structural protein 3 of hepatitis C virus inhibitsphosphorylation Mediated by cAMP-dependent proteinkinase. European Journal of Biochemistry 237, 611-618.
Boyer, J. C. & Haenni, A. L. (1994). Infectious transcripts and cDNA clones of RNA Viruses. Virology 198, 415-426.
Boyer, J.L. (2001). Liver cirrhosis and its development:proceedings of the Falk Symposium 115. 344.
Centers for Disease Control and Prevention (CDC). (2012)."Hepatitis C FAQs for Health Professionals" 4(1):45.
Chba, H., Takezaki, Neupani, D., Kim, J., Yoshida, S., Mizoguchi,E., Takeuchi, J., Suzuki, J., Tanaka, Y., Ito,K., Kitamura, T., Kurik, K., Wakai, K., Samejima, K.,Sonoda, S and Tajoma, K. (2004). An epidemiological study ofHBV, HCV, and HTLV- 1 In sherpas of Nepal, Asia Pac Journalof cancer prevalence 5(4):370-3.
Chihirio, M., Minjun, C., Kawing, N., Donald, J.B and David, R.G.(2004). Strength and Limitation of commercialtests for HCV RNA Quantification. Journal of Clinical Microbiology.2:421-425.
Christian, G.S., Tana, D and Thomas, D. (2004). Variable Ratio ofHCV RNA to Viral CoreAntigen in patient sera.Journal of Clinical Microbiology 42(5):1977-1981.
Colina, R.C., Azambuja and Uriarte, C. (1999). Evidence ofincreasing Diversification of HCV. Journal of GeneralVirology 80:1377-1382.
50
Choo, Q., Kuo, G., Overby, L.R., Bradley, D.W, and Houghton, M.(1989). Isolation of CDNA clone derived from ablood- born non- A non- B Viral hepatitis genome. Science.244:358-362.
Chang, J., Yang, S. H., Cho, Y. G., Hwang, S. B., Hahn, Y. S. &Sung, Y. C. (1998). Hepatitis C virus core from twodifferent genotypes has an oncogenic potential But is notsufficient for transforming primary rat embryo fibroblastsin Cooperation with the H-ras oncogene. Journal of Virology .72,3060-3065.
Dale, N.M., Qing, N., Xiao-hong, W., Shruit, H.M, and Kanred, N.(2004). Hepatitis C Virus Core Antigen Assay to Detect onGoing HCV infection in Thai injection Drug User. Journal ofClinical Microbiology. 42 (2): 1631-1636.
Darwish, N.M. (1992). Hepatitis C virus infection in blood donorsin Egypt. Journal. Egypt public Health Assoc. 67(3-4):223-36.
Darwish, M.A., Raouf, T.A., Rushdy, P., Constantin, N.T., Rao,M.R and Edelman, R. (1993). Risk factorsassociated with a high seroprevalence of hepatitis C virusinfection in Egyptian blood donors. American Journal TropicalMedicine Hygiene 49 (4): 440.
Day, R.A., Paul, P., Williams, B. (2009). Brunner & Suddarth's textbookof Canadian Medical-surgical nursing (Canadian 2nd Ed.).Philadelphia, PA: Lippincott .1237.
Deleersnyder, V., Pillez, A., Wychowski, C., Blight, K., Xu, J.,Hahn, Y. S., Rice, C. M. & Dubuisson, J. (1997). Formationof native hepatitis C virus glycoprotein Complexes. Journal ofVirology 71, 697-704.
Diener- West, M. (2008). Use of Chi square statistic. Johns Hopkins Bloomberg school of Public Health. 42
Dubuisson, J., Hsu, H. H., Cheung, R. C., Greenberg, H. B.,Russell, D. G. & Rice, C. M. (1994). Formation and
51
intracellular localization of Hepatitis C virus envelopeGlycoprotein complexes expressed by recombinant vaccinia andSindbis viruses. Journal of Virology. 68, 6147-6160.
Eckart, M. R., Selby, M., Masiarz, F., Lee, C., Berger, K.,Crawford, K., Kuo, C., Kuo, G., Houghton, M. &Choo, Q. L. (1993). The hepatitis C virus encodes a serineProtease involved in processing of the putativenonstructural proteins from the Viral polyprotein precursor.Biochemical and Biophysical Research Communications 192, 399-406.
Egah, D.Z., Mandong B.M., Gomwalk, N.E. (2004). Hepatitis C Virusantibodies among Blood Donors in Jos Nigeria.Annals of African Medicine 3(1):35-37.
Esteban, J. I., Cordoba, J. & Sauleda, S. (1998). The Clinicalpicture of acute and chronic Hepatitis C. Journalof virology 102-118.
Failla, C., Tomei, L. & De Francesco, R. (1994). Both NS3 andNS4A are required for proteolytic processing ofhepatitis C virus nonstructural proteins. Journal of Virology. 68,3753-3760.
Farci, P., Shimoda, A., Wong, D., Cabezon, T., Gioannis, D.,Strazzera, A., Shimizu, Y., Shapiro, M., Alter, H.J. & Purcell, R. H. (1996). Prevention of hepatitis C Virusinfectionin chimpanzees by hyperimmune serum against thehypervariable region 1 of the envelope 2 protein. Proceedingsof the National Academy of Sciences, 93, 15394-15399.
Flint, M., Thomas, J., Maidens, C., Shotton, C., Levy, S.,Barclay, W. & McKeating, J. (1999). Functional analysis ofcell surface-expressed hepatitis C virus E2 Glycoprotein.Journal of Virology. 73, 6782-6790.
Foote, B.S., Spooner, L.M and Belliveau, P.P. (2011)."Boceprevir: a protease inhibitor for the Treatment ofchronic hepatitis C". Annal Pharmacother 45 (9): 1085–93.
52
Frommel, D., Tekle- Haimano, R., Berhe, N., Aussel, L., Verdier,M., Preux, P.M and Denis, F.A. (1993). Survey ofantibodies to hepatitis C Virus in Ethiopia. American. JournalTropical Medicine Hygiene 49: 435-439.
Gale, M. J.Jr, Blakely, S. M., Kwieciszewski, B., Tan, S.-L.,Dossett, M., Tang, N. M., Korth, M. J., Polyak, S.J., Gretch, D. R. & Katze, M. G. (1998). Control of PKRProtein kinase by hepatitis C virus nonstructural 5Aprotein: molecular Mechanism of kinase regulation. Molecularand Cellular Biology. 18, 5208-5218.
Gale, M. J., Korth, M. J., Tang, N. M., Tan, S. L., Hopkins, D.A., Dever, T. E., Polyak, S. J., Gretch, D. R. & Katze, M.G. (1997). Evidence that hepatitis C virus resistance tointerferon is mediated through repression of the PKR proteinkinase by the Nonstructural 5A protein. Virology. 230, 217-227.
Ghany, M.G., Nelson, D.R., Thomas, D.L and Seeff, L.B. (2011). Anupdate on Treatment of Genotype 1 Chronichepatitis C Virus infection: practices Guideline by AmericanAssociation for the study of liver Diseases. Hepatology 54(4):1433-44.
Giancarlo, I., Fillipo, A and Blanca, M.B. (2001). Novel Aproachto Reduce the HCV Window period. Journal of Clinical.Microbiology. 39(9):3110-3114.
Graph pad Prism, by Graph Pad Software Inc. 7825 Fay Avenue, Suite 230 La Jolla, CA 92037 ©2014.
Gravitz, L. (2011). A smouldering public- health crisis. Nature474(7350):s2-4.
Grakoui, A., McCourt, D. W., Wychowski, C., Feinstone, S. M. &Rice, C. M. (1993). Characterization of thehepatitis C virus-encoded serine proteinase: DeterminationOf proteinase-dependent polyprotein cleavage sites. Journal ofVirology. 67, 2832-2843.
53
Grakoui, A., McCourt, D. W., Wychowski, C., Feinstone, S. M. &Rice, C. M. (1993). A Second hepatitis C virus-encoded proteinase. Proceedings of the National Academy of Sciences,USA 90, 10583-10587.
Gwack, Y., Kim, D. W., Han, J. H. & Choe, J. (1996).Characterization of RNA binding Activity and RNAhelicase activity of the hepatitis C virus NS3 protein.Biochemical and Biophysical Research Communications 225, 654-659.
Hagan, H., Pouget, E.R. and Des Jarlais, D.C. (2011). Asystematic review and meta analysis ofintraventions to prevention hepatitis C Virus infection inpeople who inject drugs. The Journal of infectious Diseases. 204(1):74-83.
Halim, N.K. and Ajayi, O.I. (2000). Risk factors and seroprevalence hepatitis C antibody in blood donors in Nigeria. East African Medical Journal, 77: 410-12.
Heidi, B., Christune, S and Mohammed, I.A. (2003). CellularBinding of HCV Envelop Glycoprotein E2Requires cell Surface Heparan Sulphate. Journal of BiologyChemistry. 278(42):41003-41012.
Iannuzzella, F., Vaglio, A and Garini, G. (2010). "Management ofhepatitis C virus- related Mixedcryoglobulinemia". American Journal of Medicine. 123 (5): 400–8.
Ide, Y., Tanimoto, A., Sasaguri, Y. & Padmanabhan, R. (1997).Hepatitis C virus NS5A Protein is phosphorylatedin vitro by a stably bound protein kinase from HeLa Cellsand by cAMP-dependent protein kinase A-alpha catalyticsubunit. Gene 201, 151-158.
Ileako, F.M., Mchgeyo, S.O., Riyat, M.S., Lule, G.N., Okoth, F.Aand Kaptich, D. (1995). The Prevalence of hepatitis CVirus antibodies in renal patients, blood donors andPatients with chronic liver disease in kenya. East Africa MedicalJournal. 72:362-364.
54

Ilyas, J.A and Vierling, J.M. (2011). An overview of emergingtherapies for the treatment of Chronic hepatitisC. Clinics in liver disease 15 (3): 515–36.
Imperial, J.C. (2010). Chronic hepatitis C in the state prisonsystem: insights into the Problems and possiblesolutions. Expert review of gastroenterology & hepatology.Journal of Virology 70, 4261-4268.
Jafari, S; Copes R, Baharlou S, Etminan M, Buxton J. (2010)."Tattooing and the risk Of transmission of hepatitis C: asystematic review and meta-analysis". International Journal ofInfectious Diseases.14 (11):928–40.
Jean. Francois, F., Pierre, C., Jacque – Albert, D, and David, P.(2001). Hepatitis C Antibodies among Blood Donors inSenegal. Journal of Emerging Infectious Disease. 9(11):09191. 483.
Jean-Jacques, L., Francois, R and Francois, L. (2004). Expertiseof French and Quantification of Hepatitis C VirusRNA in serum. Journal of Clinical Microbiology 42(5):2027-2030.
Jeffrey, J.G., David, W.M.R and Amber, T. (2003). Evaluation ofTRUGENE HCV 5’ NC Genotyping kit with the new GeneLibrarian Module 3.1.2 for Genotyping of HCV From ClinicalSpecimens. Journal of Clinical Microbiology 41(10):4855-4857.
Jeffrey-Schouten. (2000). Pathogenesis, viral dynamics andimmunologic Response of HCV. The Hepatitis C Report 1-8
Jenny, M., Yoann, M and Slvie, A. (2004). HCV Genotypes inCaribbean land of Martinque. Journal of ClinicalMicrobiology 42(2):784-791.
Karen, F.M., Laura, P.R., Chihiro, M., James, W.M.O, and David,R.G. ( 2003). Prevalence of HCV infection AndRisk factors in an incarcerated Juvenile Population. Pediatrics111(1):153-157.
Kaneko, T., Tanji, Y., Satoh, S., Hijikata, M., Asabe, S.,Kimura, K. & Shimotohno, K. (1994). Production
55
of two phosphoproteins from the NS5A region of the HepatitisC Viral genome. Biochemical and Biophysical Research Communications 205,320-326.
Kapoor, A., Simmods, P., Gerold, G., Qaisar, N., Jain, K.,Henriquez, J.A., Firth, C., Hirschberg, D.L,and Rice C.M. (2011). Characterization of a canine homologof hepatitis C Virus. Proceeding of NationalAcademy of Science 108 (28):11608-11613.
Kim, D. W., Gwack, Y., Han, J. H. & Choe, J. (1995). C-terminaldomain of the hepatitis C Virus NS3 proteincontains an RNA helicase activity. Biochemical and BiophysicalResearch Communications 215, 160-166.
Koff, R.S. (1997). Prevention of HCV infection Clinics in LiverDiseases 1 (3):5-6
Koch, J. O. & Bartenschlager, R. (1999). Modulation of hepatitisC Virus NS5 Ahyperphosphorylation by nonstructural proteinsNS3, NS4A, and NS4B. Journal Of Virology 73, 7138-7146
Kuo, G., Choo, Q.L and Alter H.J et al. (April 1989). "An assayfor circulating antibodies to a major etiologic virus ofhuman non-A, non-B hepatitis". Science 244 (4902):362.
Kolykhalov, A. A., Feinstone, S. M. & Rice, C. M. (1996).Identification of a highly Conserved sequenceelement at the 3′ terminus of Hepatitis C Virus genome RNA.Journal of Virology 70, 3363-3371.
Kolykhalov, A. A., Mihalik, K., Feinstone, S. M. & Rice, C. M.(2000). Hepatitis C Virus Encoded enzymatic activities andconserved RNA elements in the 3′ Nontranslated- region isessential for virus replication in vivo. Journal of Virology 74,2046-2051.
Lam, N.C., Gotsch, P.B and Lagan, R.C. (2010). Caring forpregnant woman and newborns with hepatitis B or C. AmericanFamily Physician 82(10):1225-9.
56
Lau, J.Y., Mizokami, M and Kolberg, J.A. (1995). Application ofsix HCV Genotyping System to sera from ChronicHepatitis C Patients in USA. Journals infectiousDisease.n171:281-289.
Lee, M.R and Shumack, S. (2005). "Prurigo nodularis: a review".The Australian Journal of Dermatology 46 (4): 211–18; quiz 219–20.
Lesi, O.A, and Kehinde, M.O.(2003). Hepatitis C Virus infectionin patients with Sickle Cell Anaemia at thelagos University Hospital. Nigeria postgraduate Medicine Journal. 10(2):79-83.
Linda, C., Ka-wing, N., Arthur, B., Lawrence, C and Keith, R.J.(2004). Use of the magna pure L.C. AutomatedNucleic Acid Extraction System Followed by Real-Time ReverseTranscription PCR for Ultra Sensitive. Quantification of HCVRNA. Journal of Clinical Microbiology 42 (9) 4130-4136.
Lock, G., Dirscherl, M and Obermeier, F. (2006). "Hepatitis Ccontamination of Toothbrushes: myth or reality".Journal of Viral Hepatology. 13 (9): 571–3.
Lohmann, V., Körner, F., Herian, U. & Bartenschlager, R. (1997).Biochemical Properties of hepatitis C virusNS5B RNA-dependent RNA polymerase and Identification ofamino acid sequence motifs essential for enzymatic activity.Journal of Virology 71, 8416-8428.
Louie, K.S., Micallef, J.M., Pimenta, J.M and Forssen, U.M.(2011). Prevalence of Thrombocytopenia amongpatients with chronic hepatitis C: a systematic Review.Journal of viral hepatitis 18 (1): 1–7.
Maheshwari, A., Ray, S and Thuluvath, P.J. (2008). AcuteHepatitis C. Lancet 372 (9635): 321–32.
Marshal, J.G and Roland, B., Berverly, A. (2005). Pilot Study ofLow-dose interleukin-2, Pegyland interferon 2band Ribavirin for the Treatment of HCV infection in Patientswith HIV infection. Journals infectious Disease. 191:686-693.
57

Maria, I.G., Estela, I.T., Saul, G., Maria, C.G, and Maria, V.P.(2004). HCV infection in infants and childrenfrom Argentina. Journal of Clinical Microbiology. 42(3); 1199-1202.
Marx, M and John, M. (2010). Rosen's emergency Medicine: conceptsand clinical practice 7th Edition. Philadelphia, PA:Mosby/Elsevier. 1154.
Mast, E.E. (2004). "Mother-to-infant hepatitis C virustransmission and breastfeeding". Advances inExperimental Medicine and Biology 554: 211–6.
Matsumoto, M., Hsieh, T. Y., Zhu, N., Van Arsdale, T., Hwang, S.B., Jeng, K. S., Gorbalenya, A. E., Lo, S. Y.,Ou, J. H., Ware, C. F. & Lai, M. C. (1997).
Hepatitis C virus core Protein interacts with the cytoplasmictail of lymphotoxin-beta receptor. Journal of Virology 71, 1301-1309.
Michael, L., Maria, E., Sam, P., David, H and Carl, W. (2004).Hepatitis C Genotyping by Denaturing Highperformance Liquid Chromatography. Journal of Microbiology. 42(1): 158-163.
Michael, S. F and Alexander, V. (2004). Verification of an Assayfor Quantification of HCV RNA by use of anAnalyte Specific Reagent and two Different ExtractionMethods. Journal of Clinical Microbiology 42(8): 3581-3588.
Michalak, J.-P., Wychowski, C., Choukhi, A., Meunier, J.-C., Ung,S., Rice, C. M. & Lohmann, V., Körner, F., Koch,J. O., Herian, U., Theilmann, L. & Bartenschlager, R.(1999b). Replication of subgenomic hepatitis C virus RNAs ina hepatoma cell line. Science 285, 110-113.
Mueller, S. Millonig, G and Seitz, H.K. (2009). Alcoholic liverdisease and hepatitis C: a frequentlyunderestimated combination. World Journal of Gastroenterology: WJG15(28):3462-71.
58
Muhammed, N and Jan, M.A. (2005). Frequency of Hepatitis C inBurner. virology15(1):11-14
Munox, G.M., Velasco, V and Thiers, C. (1998). Prevalence andGenotype of HCV in Blood Donors and inPatient with Chronic Liver Disease and HepatocellularCarcinoma in a Chilean Population. Review. Medical Clinical.126:1035-1042.
Monica, A and Juan, J.B. (2003). HCV Model Structure and GenomeOrganization. Accession Information 5:1-2.
Monazahian, M., Bohme, I., Bonk, S., Koch, A., Scholz, C.,Grethe, S. & Thomssen, R. (1999). Lowdensity lipoprotein receptor as a candidate receptor forhepatitis C Virus. Journal of Medical Virology 57, 223-229.
Nahum, M., Daniel, M., Norbertoc.C., Jesus, B., Richardo, C, AndMisael, U. (2004).Prevalenceof HCV infectionAmong Hemodialysis Patient, at a Tertiary Care Hospital inMexico City, Journal of Clinical Microbiology 42(9):4321-4322.
Nakano, T., Lau, G.M and Lau, G.M. (2011). An updated analysis ofhepatitis C Virus genotypes and subtypes based on thecomplete coding region. Liver Intermediate. 32 (2): 339–45.
Neddermann, P., Clementi, A. & De Francesco, R. (1999).Hyperphosphorylation of the Hepatitis C virusNS5A protein requires an active NS3 protease, NS4A, NS4B,and NS5A encoded on the same polyprotein. Journal of Virology 73,9984-9991.
Nelson, P.K., Mathers, B.M., Cowie, B., Hagan, H., Des Jarlais,D., Horyniak, D and Degenhardt, L. (2011).Globalepidemiology of hepatitis B and hepatitis C in People whoinject drugs Virology 571–83.
Ogarkov, P.I., Malyshev, V.V., Tokmakw, V.S and Smirnov, A.V.(2004). Epidemiological Feature of virus
59
hepatitis in the Russian army. Minerva Gastroentrol Dietol.50:165-9.
Ozaras, R and Tahan, V. (2009). "Acute hepatitis C: preventionand treatment". Expert review of anti-infective therapy 7 (3):351–61.
Panigrahi, A.K., Panda, S.K., Dixit, R.K., Rao, K.V., Acharya,S.K., Dasarathy, S and Nanu, A. (1997).Magnitude of hepatitis C Virus infection in india:prevalence in healthy Blood donors, acuts and chronic liverdiseases. Jornal of Medicine Virology.51:167-174.
Peter, J.L., Insil, K., Geoff, A.O and Joseph, D. (2003).Structure of HCV IRES Domain II Determined ByNMR. J.D.P. 10:1004-138.
Pileri, P., Uematsu, Y., Campagnoli, S., Galli, G., Falugi, F.,Petracca, R., Weiner, A. J., Houghton, M.,Rosa, D., Grandi, G. & Abrignani, S. (1998). Binding ofhepatitis C virus to CD81. Science 282, 938-941.
Pondé, R.A. (2011). "Hidden hazards of HCV transmission". Medicalmicrobiology and Immunology 200 (1): 7–11.
Ray, Stuart, C., Thomas, David, L. (2009). "Chapter 154:Hepatitis C". In Mandell, Douglas, and Bennett's principles andpractice of infectious diseases (7th ed.). Philadelphia, PA:Churchill Livingstone.
Reed, K. E., Gorbalenya, A. E. & Rice, C. M. (1998). The NS5A/NS5proteins of viruses from Three genera of the familyFlaviviridae are phosphorylated by associatedSerine/threonine kinases. Journal of Virology 72, 6199-6206.
Reed, K. E. & Rice, C. M. (1999). Identification of the majorphosphorylation site of the Hepatitis C virusH strain NS5A protein as serine 2321. Journal of BiologicalChemistry 274, 28011-28018.
60
Rosa, D., Campagnoli, S., Moretto, C., Guenzi, E., Cousens, L.,Chin, M., Dong, C., Weiner, A. J., Lau, J. Y. N.,Choo, Q. L., Chien, D., Pileri, P., Houghton, M. andAbrignani, S. (1996). A quantitative test to estimateneutralizing Antibodies to the hepatitis C virus:cytofluorimetric assessment of envelope Glycoprotein 2binding to target cells. Proceedings of the National Academy of Sciences93, 1759-1763.
Rosen, H.R. (2011). Clinical practice. Chronic Hepatitis Cinfection. The New England Journal of Medicine 364 (25): 2429–38.
San-Diego (1999). Epidimmune Reports Data which Support thecompany’s Approach to Hepatitis C Vaccine Development.Epimmune inc. Hepatology. 30(4):1088-1098.
Smith, L.S., Nelson, M., Naik, S and Woten, J. (2011).Telaprevir: an NS3/4A protease Inhibitor for thetreatment of chronic hepatitis C. Annal Pharmacother 45 (5):639–48.
Stroffolini, T., Menchineli, M., Dambruoso, V., Menniti lppolito,F., Costantino, A., Rapictetta, M., Lacce, R andTaliani, G. (1995). High prevalence of hepatitis C VirusInfection in a small central Italian town: Lack of evidenceof parenteral exposure. Ital Gastroenterology. 27: 235-8
Springer Verlag. (2011). Chronic Hepatitis C Virus Advances inTreatment. Promise for the Future 103-104.
Songsivilai, S., Jina.thongthai, S., Wongsena, W.,Tiangpitayakon, C and Dharakul, T. (1997). Highprevalence of hepatitis C infection among blood donors innorthastern Thailand. American Journal Tropical Medicine. Hygiene.57:66-69.
Soni, P., Dusheiko, G.M., Dhillon, A.P and Harrison, T.J. (2004).Genetic Diversity of HCV. Journal Lancet 5:562.
61
Suzich, J. A., Tamura, J. K., Palmer, H. F., Warrener, P.,Grakoui, A., Rice, C. M., Tai, C.L., Chi, W. K.,Chen, D. S. & Hwang, L. H. (1996). The helicase activityAssociated with hepatitis C virus nonstructural protein 3(NS3). Journal of Virology 70, 8477-8484.
Tanaka, T., Kato, N., Cho, M. J. & Shimotohno, K. (1995). A novelsequence found at the 3′ terminus of hepatitis C virusgenome. Biochemical and Biophysical Research Communications215, 744-749.
Tanak, J., Kumagai, J., Katayama, Y., Mizui, M., Yamanaka, R.,Suzuki, K., Miyakawa, Y and Yoshizawa, H. (2004).Sex and age- specific carriers of hepatitis B and C Virusesin Japan estimated by the prevalence in the first time blooddonors During 1995-2000. Interivirology. 47(1):32-40.
Tanaka, T., Kato, N., Cho, M. J., Sugiyama, K. & Shimotohno, K.(1996). Structure of the 3′ terminus of the hepatitis Cvirus genome. Journal of Virology 70, 3307-8
Tanji, Y., Kaneko, T., Satoh, S. & Shimotohno, K. (1995b).Phosphorylation of Hepatitis C virus-encoded nonstructuralprotein NS5A. Journal of Virology 69, 3980-
Taylor, D. R., Shi, S. T., Romano, P. R., Barber, G. N. & Lai, M.C. (1999). Inhibition of the Interferon-inducible protein kinase PKR by HCV E2 protein. Science 285,107-110.
Tanji, Y., Hijikata, M., Hirowatari, Y. & Shimotohno, K. (1994).Hepatitis C virus polyprotein Processing:kinetics and mutagenic analysis of serine proteinase-dependent Cleavage. Journal of Virology 68, 8418-8422.
Thomssen, R., Bonk, S., Propfe, C., Heermann, K. H., Köchel, H.G. & Uy, A. (1992). Association of hepatitis Cvirus in human sera with beta-lipoprotein. MedicalMicrobiology and Immunology 181, 293-300.
62
Tomei, L., Failla, C., Santolini, E., De Francesco, R. & LaMonica, N. (1993). NS3 is a Serine protease requiredfor processing of hepatitis C virus polyprotein. Journal ofVirology 67, 4017-4026.
Torresi,J., Johnson, D. and Wedememeyer, H. (2011). Progress inthe development of prevention and therapeuticvaccines for hepatitis C Virus. Journal of hepatology54(6):1273-85.
Tohme, R.A and Holmberg, S.D.(2010). Is sexual contact a majormode of hepatitis C Virus Transmission. Hepatology52 (4): 1497-505.
Tsukiyama-Kohara, K., Iizuka, N., Kohara, M. & Nomoto, A. (1992).Internal ribosome Entry site within hepatitis Cvirus RNA. Journal of Virology 66, 1476-1483.
Udeze, A.O., Okonk, I.O., Donbraye, E., Sule, W.F., Fadeyi, A.and Uche L.N. (2009).Seroprevalence of HepatitisC Antibodies Amongst Blood Donors Ibadan, Southwestern,Nigeria. World Applied Sciences Journal 7 (8): 1023-1028
Vescio, M.F., Longo, B., Babudieri, S., Starnini, G., Carbonara,S., Rezza, G and Monarca, R. (2008). Correlatesof hepatitis C virus seropositivity in prison inmates: aMeta-analysis. Journal of epidemiology and Community Health 62 (4):305–13.
Wang, C., Sarnow, P. & Siddiqui, A. (1993). Translation of humanhepatitis C virus RNA in Cultured cells aremediated by an internal ribosome-binding mechanism. Journal ofVirology 67, 3338-3344.
Wang, Y., Tao, Q.M., Zhao, H.Y., Tsuda, F., Nagayama, R.,Yamamoto, K., Tanaka, T., Tokita, H., Okamoto, Hand Miyakawa, Y. (1994). Hepatitis C Virus RNA andAntibodies among blood donors in Beijing. Journal Hepatology.21:634-640.
63
Wansbrough- Jones, M.H., Frimpong, E., Cant, B., Harris, K.,Evan, M.R., Teo, C.G. (1998). Prevalence andGenotype of HCV- infection in Pregnant Woman and BloodDonors in Ghana.Transfusion Report Social. Tropical MedicineHygiene. 92(5): 496-499.
Winners Albert. (2008).Lasker Award for Clinical MedicalResearch, The Lasker Foundation.
World Health Organization WHO. (2010). Hepatitis C. Wilkins, T.,Malcolm J.K., Raina, D and Schade, R.R. (2010). Hepatitis C:diagnosis and Treatment. American Family Physician 81 (11):1351–7.
Wong, T and Lee, S.S. (2006). Hepatitis C: a review for primarycare physicians. CMAJ 174 (5): 649–59.
Xia, X., Luo, J, Bai, J., Yu, R. (2008). Epidemiology of HCVinfection among injection drug Users in China:systematic review and meta-analysis. Public health 122 (10):990–1003.
Yamada, N., Tanihara, K., Takada, A., Yorihuzi, T., Tsutsumi, M.,Shimomura, H., Tsuji, T. and Date, T. (1996).Genetic organization and diversity of the 3′ noncodingRegion of the hepatitis C Virus genome. Virology 223, 255-261.
Yamaguchi, K., Kiyokawa, H., Machida, J., Obayasbo, A., Nojiri,N., Ueda, S and Takatsuki, K. (1994).Seroepidemiology of Hepatitis C Virus infection in Japan andHCV Infection in haemodialysis Patients. FEMS Microbiology 14:253-258.
Yamashita, T., Kaneko, S., Shirota, Y., Qin, W., Nomura, T.,Kobayashi, K. & Murakami, S. (1998). RNA-dependent RNApolymerase activity of the soluble Recombinant Hepatitis Cvirus NS5B protein truncated at the C-terminal region. Journalof Biological Chemistry 273, 15479-15486.
64

Yanagi, M., St Claire, M., Emerson, S. U., Purcell, R. H. & Bukh,J. (1999). In vivo Analysis of the 3′ untranslatedregion of the Hepatitis C Virus after in vitro Mutagenesisof an infectious cDNA clone. Proceedings of the National Academy ofSciences, USA 96, 2291-2295.
Yasui, K., Wakita, T., Tsukiyama, K. K., Funahashi, S. I.,Ichikawa, M., Kajita, T., Moradpour, D., Wands, J.R. & Kohara, M. (1998). The native form and Maturationprocess of hepatitis C virus core protein. Journal of Virology 72,6048-6055.
Yu, M.L. and Chuang, W.L. (2002). Treatment of chronic hepatitisC in Asia: when East meets west. Journal ofGastroenterology Hepatology 22(3):336-45.
Yuan, Z. H., Kumar, U., Thomas, H. C., Wen, Y. M. & Monjardino,J. (1997). Expression, Purification and partial characterization of HCV RNA polymerase. Biochemical andBiophysical Research Communications 232, 231-235.
Zhi, L., Dale, N.M and Qing M. (2004). Accurate Representation ofthe HCV Quasispecies in 5.2- kilobase Amplicons.Journal of Clinical Microbiology. 42 (9): 4223-4229.
Zignego, A.L., Ferri, C and Pileri, S.A. (2007). "Extrahepaticmanifestations of Hepatitis C Virus infection: a generaloverview and guidelines for a clinical approach". Digestive andLiver Disease 39 (1): 2–17.
Zhang, Y.Y., Hansson, B.G and Widell, A., Nordenfelt, E. (1992).Hepatitis C Virus RNA in chinese blood donors determined byELISA, recombinant immunoblot assay and Polymerase chainreaction APMIS. 100:851-855.
65

66




















