
The chromosome 9 ALS and FTD locus is probably derived from a single founder

A strabismus susceptibility locus on chromosome 7pVaishali Parikha, Yin Yao Shugartb, Kimberly F. Dohenyc, Jie Zhangc, Lan Lib, John Williamsa, David Haydenc,Brian Craigc, Hilda Capod, Denise Chambleee, Cathy Chend, Mary Collinsf, Stuart Danknerg, Dean Fiergangg,David Guytonh, David Hunterh,i, Marcia Hutcheonj, Marshall Keysk, Nancy Morrisonl, Michelle Munozd, Marshall Parksm,David Plotskyn, Eugene Protzkoo, Michael X. Repkah, Maria Sarubbip, Bruce Schnallq, R. Michael Siatkowskid,Elias Traboulsir, Joanne Waeltermanns, and Jeremy Nathansa,t
aDepartments of Molecular Biology and Genetics, Neuroscience, and Ophthalmology, and Howard Hughes Medical Institute, cCenter for Inherited DiseaseResearch, Institute of Genetic Medicine, and hWilmer Eye Institute, Johns Hopkins University School of Medicine, Baltimore, MD 21205; bDepartment ofEpidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD 21205; dBascom Palmer Eye Institute, University of Miami School ofMedicine, Miami, FL 33101; eSuite 204, 606 Denrigh Boulevard, Newport News, VA 23602; fDepartment of Ophthalmology, Greater Baltimore MedicalCenter Pavillion West, Suite 505, 6569 North Charles Street, Baltimore, MD 21204; gVillage of Cross Keys, Suite 345 West Quadrangle, Baltimore, MD 21210;j19632 Club House Road, Suite 510, Montgomery Village, MD 20886; k121 Congressional Lane, Suite 601, Rockville, MD 20852; l11345 Pembrooke Square,Suite 105, Waldorf, MD 20603; m3400 Massachusetts Avenue Northwest, Washington, DC 20007-1498; n650 Pennsylvania Avenue, Southeast, Suite 270,Washington, DC 20003-2543; o3000 Lyndebrook Court, Fallston, MD 21047; pFoundation for Pediatric Ophthalmology, Colombres 226, 11A Lomasde Zamora (1832), Buenos Aires, Argentina; q1000 White Horse Road, Suite 106, Voorhees, NJ 08043; rCleveland Clinic, 9500 Euclid Avenue, Cleveland,OH 44195; and s1011 Frederick Road, Catonsville, MD 21228-5049
Contributed by Jeremy Nathans, August 8, 2003
Strabismus has been known to have a significant genetic compo-nent, but the mode of inheritance and the identity of the relevantgenes have been enigmatic. This paper reports linkage analysis ofnonsyndromic strabismus. The principal results of this study are:(i) the demonstrated feasibility of identifying and recruiting largefamilies in which multiple members have (or had) strabismus;(ii) the linkage in one large family of a presumptive strabismussusceptibility locus to 7p22.1 with a multipoint logarithm of oddsscore of 4.51 under a model of recessive inheritance; and (iii) thefailure to observe significant linkage to 7p in six other multiplexfamilies, consistent with genetic heterogeneity among families.These findings suggest that it will be possible to localize andultimately identify strabismus susceptibility genes by linkage anal-ysis and mutation screening of candidate genes.
linkage � whole genome scan � complex trait � ophthalmic genetics
S trabismus (misalignment of the eyes; also referred to as‘‘squint’’) is one of the most common ocular disorders in
humans, affecting 1–4% of the population (1). It is frequentlyassociated with amblyopia (uniocular visual neglect), a leadingcause of visual impairment in children and young adults. Thefamilial clustering of strabismus has been recognized sinceantiquity. For example, Hippocrates stated that ‘‘children ofparents having distorted eyes squint also for the most part’’ (1).
Numerous twin and family studies point to a significantgenetic component in the etiology of strabismus (summarized inrefs. 1–4). Summing the data from 11 published twin studiesshows that, among 206 monozygotic and 130 dizygotic twin pairsin which one member of the twin pair had strabismus, 73% ofmonozygotic twin pairs were concordant for strabismus, whereasonly 35% of dizygotic twin pairs were concordant for strabismus.We note that the degree of concordance among dizygotic twinpairs is higher than the �10–15% typically reported for siblings;this may reflect the overall higher incidence of strabismus amongpremature and low-birth-weight infants.
The overall incidence of strabismus and the incidence ofspecific types of strabismus show appreciable differences be-tween racial groups, further supporting the relevance of geneticfactors. Two studies have documented a lower incidence of alltypes of strabismus among Africans or African Americans (0.5%and 0.6%, respectively) relative to Americans of Europeanancestry (2.5%; refs. 5 and 6). Moreover, the majority of African,African American, and Asian strabismics are exotropes, whereasthe majority of Caucasian strabismics are esotropes (5–7).
With respect to overall heritability, the relative risk for firstdegree relatives of an affected individual is estimated to bebetween 3 and 5. Crone and Vezeboer (8) found that 13% of
parents of strabismic probands had strabismus vs. a 3% incidencein the general population. Hu (9) found a 9% incidence amongfirst-degree relatives and a 2.2% incidence among second degreerelatives, versus a population incidence of 0.6%. Richter (10)found that the incidence of strabismus or the various strabismus-associated ocular anomalies among siblings of an affected pro-band was �20% if both parents were unaffected and 30–40% ifone or both parents were also affected, versus a populationfrequency of 4%. To our knowledge, the lowest publishedestimate of relative risk for a sibling is 3 (for esotropia; ref. 11).Strabismus affects males and females equally.
These heritability values are likely to be underestimates for thefollowing three reasons: (i) �15–20% of strabismus is clearlyassociated with nonocular disorders, including low birth weightand global CNS defects (12), which are included in the popula-tion incidence in most studies; (ii) there is incomplete detectionof esophorias and exophorias, microtropias, and the monofix-ation syndrome (reduced stereoacuity to worse than 60 s of arc),all of which occur at higher frequencies in families of strabismicsand probably represent the incompletely penetrant phenotype(13, 14); and (iii) similar or identical subtypes of strabismus tendto cluster within a single family and between monozygotic twinsand this would lead to greater heritability estimates if strabismussubtypes were considered separately (15). As an example of thesecond point, Scott et al. (14) found that the monofixationsyndrome was present in 7.7% of first degree relatives of patientswith infantile esotropia, compared with a prevalence of 1% in thegeneral population.
Ocular alignment relies on complex sensory and motor path-ways in the retina, thalamus, visual cortex, and brainstem, and onthe proper development and functioning of the extraocularmuscles and orbit. In keeping with this multiplicity of compo-nents, current evidence indicates that the inheritance patterns ofthe common forms of strabismus are complex (16–18). Forexample, in a study of 173 pedigrees with infantile nonaccom-modative esotropia, Maumenee and colleagues (18) found thatthe disease best fit a model with either two autosomal dominantgenes with incomplete penetrance or multifactorial inheritance.Not included in this analysis are the many genetic conditions thatare associated with strabismus via their affect on the develop-ment and function of the CNS or the anatomy of the eye andorbit (summarized in ref. 4). These include various chromosomal
Abbreviation: LOD, logarithm of odds.
iPresent address: Children’s Hospital, Boston, MA 02115.
tTo whom correspondence should be addressed. E-mail: [email protected].
© 2003 by The National Academy of Sciences of the USA
www.pnas.org�cgi�doi�10.1073�pnas.2035118100 PNAS � October 14, 2003 � vol. 100 � no. 21 � 12283–12288
GEN
ETIC
S

anomalies, Williams syndrome, Waardenburg syndrome, deLange syndrome, and fragile-X syndrome. A further complica-tion comes from the observation that uncorrected refractiveerror is a risk factor for strabismus. In particular, anisometropiais a general risk factor for strabismus and hypermetropia is a riskfactor specifically for esotropia. As refractive error has a signif-icant heritability (2), genes affecting refraction per se may act asstrabismus susceptibility loci.
Recent progress in understanding genetic mechanisms relevantto ocular motility has come from the study of rare Mendeliandisorders that lead to congenital fibrosis of the extraocular muscles(CFEOM; summarized in ref. 19). The CFEOM syndromes, to-gether with Duane syndrome, most likely reflect primary defects insome combination of cranial nerves III, IV, or VI, with subsequentocular muscle dysfunction and fibrosis. Three CFEOM loci and twoDuane syndrome loci have been mapped, and the gene forCFEOM2 has recently been identified as the ARIX�PHOX2Ahomeobox gene (20), previously implicated in the development ofbrainstem motor nuclei in the mouse (21).
Despite these advances in understanding oculomotor devel-opment, the genetic mechanisms involved in the pathogenesis ofthe common nonsyndromic forms of strabismus and amblyopiaremain little studied and poorly understood (22). To date, therehave been no published reports of systematic, large-scale effortsto map genes that predispose humans to the common forms ofstrabismus. In this paper we describe our initial efforts in thisdirection, including the identification of families with multipleaffected members, the results of whole genome linkage scans inseven of these families, and high-resolution genotyping thatimplicates a recessive locus on chromosome 7p that predisposesto strabismus in one large family.
Materials and MethodsRecruitment of Subjects. Subjects were recruited in accordancewith the guidelines set by The Johns Hopkins University JointCommittee on Clinical Investigation. The vast majority of sub-jects were recruited in the U.S. and most reside in the Mid-Atlantic region. Most appear to be of European ancestry. Patientrecords were surveyed at 15 pediatric ophthalmology practices toidentify families with multiple affected members. Patients (orparents of patients) with a positive family history were informedof the study by letter and invited to contact the study coordi-nator. Respondents were interviewed to identify affected andunaffected relatives, and pedigrees and phenotypes were furtherconfirmed by telephone interviews with multiple family mem-bers, and for some subjects, by retrospective analysis of medicalrecords. Subjects were considered to be affected if they had ahistory of any of the following: (i) readily apparent ocularmisalignment, (ii) ocular surgery to correct a misalignment,(iii) patching of one eye, (iv) orthoptic exercises, or (v) adiagnosis of strabismus or amblyopia. The approximate age ofonset and the type of ocular deviation was recorded when thiswas known, including esotropia vs. exotropia, intermittent vs.constant deviation, and alternate vs. unilateral fixation. Thefollowing were also recorded where possible: age at whichsubjects first began wearing glasses; refractive error and�orvisual acuity; and failure of any vision screening tests at school,in the military, or for driving an automobile. To minimize theeffect of environmental variables and to exclude subjects withsyndromic sources of strabismus, the following were consideredcause for exclusion from the study: strabismus secondary totrauma, craniofacial anomalies, anomalies of the orbit or ex-traocular muscles, mental retardation, CNS infection, chromo-somal anomalies or aneuploidies, prematurity (�35 weeks ges-tation), low birth weight (�1.8 kg), nerve palsies, Duanesyndrome, Williams syndrome, oculocutaneous albinism, orbitalinflammatory disease, strabismus after retinal reattachment
surgery, sensory deprivation strabismus (e.g., secondary to con-genital cataract), and myasthenia gravis.
Genotyping. Blood samples were collected and DNA was pre-pared by proteinase K digestion followed by equilibrium cen-trifugation in CsCl. Genotyping was performed with samplesfrom 133 subjects at the Center for Inherited Disease Researchby using a modification of the Cooperative Human LinkageCenter (CHLC, University of Iowa, Ames) version 9 marker set(386 microsatellite markers; average spacing of 9 cM; andaverage heterozygosity of 0.76). For the whole genome scan,eight masked duplicates of the 133 samples, eight positivecontrols, and two negative controls were genotyped. Allele callswere reviewed by two technicians, masked to family structureand phenotype. Binning of all allele sizes for each marker wasperformed by using the FASTCLUS procedure in SAS. Callsfalling outside of bins and Mendelian inconsistencies (identifiedby using GAS; ref. 23) were reviewed for laboratory error. Familyrelationships were analyzed by using RELCHECK (24). In addition,SIMWALK2 (25) was used to calculate the posterior probability ofa genotyping error for each individual in the data set. Thosegenotypes with a posterior probability of being incorrect of�75% were removed from the analysis, as recommended byDouglas et al. (26). Overall, 2,755 of 54,426 (5.1%) of thegenotypes were not obtained or were judged unusable. Two of2,436 pairs of genotypes from the eight masked duplicatesamples produced different calls, giving an overall error rate of0.04%. The remaining number of Mendelian inconsistencies was83 of 54,426 (0.15%), and these presumably represent a combi-nation of genotyping errors and microsatellite instability. Forhigh-resolution mapping, the 133 subjects were genotyped forfour additional markers on chromosome 7 and two additionalmarkers on chromosome 9. Additional details related to geno-typing methodology can be found at www.cidr.jhmi.edu.
Ten additional tandem repeat markers were developedfor family A by scanning chromosome 7 sequences using theTandem Repeats Finder web site (ref. 27; http:��c3.biomath.mssm.edu�trf). PCR primer sequences and map locations arelisted in Table 3, which is published as supporting information onthe PNAS web site, www.pnas.org.
ResultsIdentification of Strabismus Pedigrees. Most individuals with stra-bismus manifest the trait in infancy or early childhood. There-fore, we focused our recruiting efforts on pediatric ophthalmol-ogy patients. As described in detail in Materials and Methods,phenotyping was largely by history. The success of this approachrests on the efficient detection of ocular misalignment or uni-
Table 1. Number of families and number of affected individualsper family
Number ofaffected subjectsper family
Numberof families
1 132 543 554 305 196 147 108 79 2�10 5Total 209
12284 � www.pnas.org�cgi�doi�10.1073�pnas.2035118100 Parikh et al.

ocular visual dysfunction by family members, childcare andschool personnel, and pediatricians. The limited number ofstrabismus treatment options (surgical realignment, patching ofone eye, and orthoptic exercises) further facilitates the assign-ment of phenotype based on treatment history. Although thismethod of assigning phenotype is efficient and permits theinclusion of relatives who reside in remote locations, it is unlikelyto identify the more subtle manifestations of strabismus such as
microtropia and the monofixation syndrome. To date, we haverecruited 209 families with a median of three to four affectedmembers per family (Table 1).
Seven families were chosen from the first 150 families forwhole genome linkage analysis; the corresponding seven pedi-grees are shown in Fig. 1. Family A is noteworthy for a sibshipin which 8 of 14 individuals are affected. All of the affectedmembers of this sibship were treated by a single clinician (M.P.);
Fig. 1. Seven pedigrees analyzed by whole genome scanning. The assignment of affected individuals (filled symbols) is described in Materials and Methods.Dots indicate those individuals for whom genotypes were obtained. Haplotypes are shown for family A with the 20 high-resolution chromosome 7p markers (Fig.2B and Table 3) arranged in order with the most telomere-proximal marker (D7s3056) at the top and the most centromere-proximal marker (D7s1791) at thebottom, as listed to the left of subject 203. For each individual, the paternal haplotype is on the left and maternal haplotype is on the right. Numbers indicatethe size of the PCR products in bp. The haplotype for individual 203 was reconstructed from the haplotypes of his children; the phase of the markers for individual205 cannot be determined with the available data. The four chromosomes in individuals 203 and 204 are color coded.
Parikh et al. PNAS � October 14, 2003 � vol. 100 � no. 21 � 12285
GEN
ETIC
S
all eight affected individuals developed esotropia in infancy orchildhood, seven of eight had some degree of hypermetropia,and four of eight underwent surgical realignment.
Statistical Analysis of the Whole Genome Scan. Because the mode ofinheritance of strabismus has not been clearly defined, two typesof analyses were performed: the model-dependent logarithm ofodds (LOD) score method using LINKAGE (28, 29) and themodel-free method using GENEHUNTER (25). Allele frequencieswere estimated by using SIB-PAIR (30). Both two point andmultipoint parametric LOD score calculations across the wholegenome were performed under a strong genetic model with aphenocopy rate of 0.0001, penetrance of 0.9, and a frequency ofdisease alleles of 0.001.
Two-point model-based analyses were performed by usingLINKAGE with both recessive and dominant models using theparameters described above. Markers D7S513 and D7S1802gave a maximum single-point LOD score of 2.65 and 1.74,respectively, under the assumption of a recessive mode ofinheritance. In addition, D9S1838 gave a maximum single-pointLOD score of 2.31 under a dominant model.
Multipoint parametric linkage analyses were performed for allchromosomes for the data generated by the genome scan usingGENEHUNTER with the parameters described above. LOD scoresconsidering genetic heterogeneity were also computed. Resultsare presented in Fig. 3, which is published as supporting infor-mation on the PNAS web site. Even though the multipointanalyses did not give any homogeneous LOD scores above 1, theheterogeneity LOD score was 1.21 for D7S513 on chromosome7 (for a recessive model) and 1.35 for D9S1826 on chromosome9 (for a dominant model). Interestingly, the multipoint nonpara-metric analyses supported the location on chromosome 9 andrevealed a new location on chromosome 11. The highest non-parametric LOD scores obtained were 3.87 (P � 0.006) on 9pterwith marker D9S1826 and 3.88 on chromosome 11p with markerD11S2362 (P � 0.006).
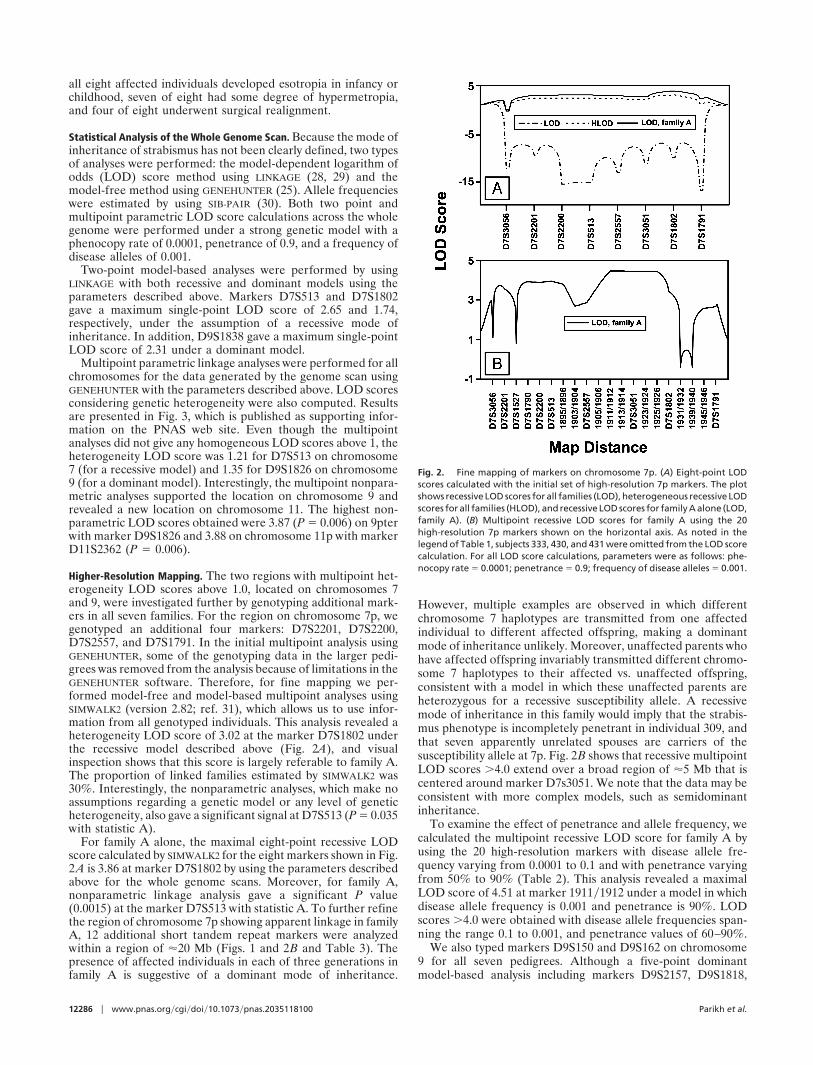
Higher-Resolution Mapping. The two regions with multipoint het-erogeneity LOD scores above 1.0, located on chromosomes 7and 9, were investigated further by genotyping additional mark-ers in all seven families. For the region on chromosome 7p, wegenotyped an additional four markers: D7S2201, D7S2200,D7S2557, and D7S1791. In the initial multipoint analysis usingGENEHUNTER, some of the genotyping data in the larger pedi-grees was removed from the analysis because of limitations in theGENEHUNTER software. Therefore, for fine mapping we per-formed model-free and model-based multipoint analyses usingSIMWALK2 (version 2.82; ref. 31), which allows us to use infor-mation from all genotyped individuals. This analysis revealed aheterogeneity LOD score of 3.02 at the marker D7S1802 underthe recessive model described above (Fig. 2A), and visualinspection shows that this score is largely referable to family A.The proportion of linked families estimated by SIMWALK2 was30%. Interestingly, the nonparametric analyses, which make noassumptions regarding a genetic model or any level of geneticheterogeneity, also gave a significant signal at D7S513 (P � 0.035with statistic A).
For family A alone, the maximal eight-point recessive LODscore calculated by SIMWALK2 for the eight markers shown in Fig.2A is 3.86 at marker D7S1802 by using the parameters describedabove for the whole genome scans. Moreover, for family A,nonparametric linkage analysis gave a significant P value(0.0015) at the marker D7S513 with statistic A. To further refinethe region of chromosome 7p showing apparent linkage in familyA, 12 additional short tandem repeat markers were analyzedwithin a region of �20 Mb (Figs. 1 and 2B and Table 3). Thepresence of affected individuals in each of three generations infamily A is suggestive of a dominant mode of inheritance.
However, multiple examples are observed in which differentchromosome 7 haplotypes are transmitted from one affectedindividual to different affected offspring, making a dominantmode of inheritance unlikely. Moreover, unaffected parents whohave affected offspring invariably transmitted different chromo-some 7 haplotypes to their affected vs. unaffected offspring,consistent with a model in which these unaffected parents areheterozygous for a recessive susceptibility allele. A recessivemode of inheritance in this family would imply that the strabis-mus phenotype is incompletely penetrant in individual 309, andthat seven apparently unrelated spouses are carriers of thesusceptibility allele at 7p. Fig. 2B shows that recessive multipointLOD scores �4.0 extend over a broad region of �5 Mb that iscentered around marker D7s3051. We note that the data may beconsistent with more complex models, such as semidominantinheritance.
To examine the effect of penetrance and allele frequency, wecalculated the multipoint recessive LOD score for family A byusing the 20 high-resolution markers with disease allele fre-quency varying from 0.0001 to 0.1 and with penetrance varyingfrom 50% to 90% (Table 2). This analysis revealed a maximalLOD score of 4.51 at marker 1911�1912 under a model in whichdisease allele frequency is 0.001 and penetrance is 90%. LODscores �4.0 were obtained with disease allele frequencies span-ning the range 0.1 to 0.001, and penetrance values of 60–90%.
We also typed markers D9S150 and D9S162 on chromosome9 for all seven pedigrees. Although a five-point dominantmodel-based analysis including markers D9S2157, D9S1818,
Fig. 2. Fine mapping of markers on chromosome 7p. (A) Eight-point LODscores calculated with the initial set of high-resolution 7p markers. The plotshows recessive LOD scores for all families (LOD), heterogeneous recessive LODscores for all families (HLOD), and recessive LOD scores for family A alone (LOD,family A). (B) Multipoint recessive LOD scores for family A using the 20high-resolution 7p markers shown on the horizontal axis. As noted in thelegend of Table 1, subjects 333, 430, and 431 were omitted from the LOD scorecalculation. For all LOD score calculations, parameters were as follows: phe-nocopy rate � 0.0001; penetrance � 0.9; frequency of disease alleles � 0.001.
12286 � www.pnas.org�cgi�doi�10.1073�pnas.2035118100 Parikh et al.

D9S1826, D9S158, and D9S1838 gave a maximal multipointLOD score of 0.8, pedigree D alone gave a LOD score of 1.70(data not shown). Model-free analyses performed by SIMWALK2gave a significant P value of 0.0017, converted to a minus log(P)of 2.75 for the statistic B, which has been shown to be the mostpowerful statistic for detecting linkage to a dominant trait (32).We have not performed higher-resolution mapping of the can-didate region on chromosome 11p because SIMWALK2 gave onlya marginally significant P value (0.04) with marker D11S2362.
DiscussionThe principal results of this study are: (i) the demonstratedfeasibility of identifying and recruiting large families in whichmultiple members have (or had) strabismus; (ii) the linkage inone large family of a presumptive strabismus susceptibility locusto 7p22.1 with a homogeneous LOD score of 4.51 at marker1911�1912 under a model of recessive inheritance; and (iii) thefailure to observe significant linkage to 7p in six other multiplexfamilies, consistent with genetic heterogeneity among families.These findings suggest that expanded family recruitment andgenotyping efforts are likely to reveal additional strabismussusceptibility loci.
As noted in the Introduction, the common forms of strabismuspresent a number of technical challenges to genetic analysis.However, strabismus also presents a number of attributes thatare technically advantageous for identifying large numbers offamilies with multiple affected individuals, as described below.First, strabismus is common and does not affect viability orfecundity. Second, the phenotype is usually apparent in earlychildhood. Therefore, pedigrees often show multiple genera-tions of affected living subjects. Moreover, relatives who do nothave the major manifestations of strabismus can be readilyidentified because late onset is highly unlikely. Third, in tech-nologically advanced countries, affected individuals are identi-fied efficiently and almost invariably brought to the attention of
an ophthalmologist. A reliable diagnosis can be made by anyophthalmologist using tests that are simple and safe. In untreatedpatients, overt ocular misalignment can also be readily docu-mented by appearance or by examining family photographs.Fourth, both diagnostic and treatment methods have remainedrelatively unchanged over at least 50 years. Therefore, a diag-nosis of strabismus or a history of one of the standard treatmentsis sufficient to establish the phenotype with high confidence.Fifth, in addition to the risk of developing amblyopia, ocularmisalignment is considered a major cosmetic and social handi-cap. As a consequence, the parents of affected children aregenerally motivated to seek treatment, and our experience hasbeen that most families with multiple affected members are alsomotivated to participate in research that might improve diagnosisor treatment. Taken together, these attributes should facilitatethe identification and recruitment of large numbers of familieswith characteristics favorable for linkage analysis.
The experiments reported here represent a first step indefining the genes that predispose to the common forms ofstrabismus. At present, the candidate region on chromosome 7pencompasses 5–10 cM. Therefore, further fine mapping and theidentification of additional families will be required to narrowthe interval. It is hoped that future work will result in theultimate identification of causally relevant genes with a resultingimprovement in the understanding of this disorder.
We thank all of the participating families for their interest and gener-osity. We thank Drs. Patrick Tong and David Valle for helpful advice,Mr. Phil Smallwood for assistance with informatics, Ms. Sharon Black-burn and Terry Stromski for assistance with preparation of the figures,and Dr. Nico Katsanis for helpful comments on the manuscript. Geno-typing services were provided by the Center for Inherited DiseaseResearch (CIDR). CIDR is fully funded through a federal contract withthe National Institutes of Health to The Johns Hopkins University,contract number N01-HG-65403. This work was supported by theHoward Hughes Medical Institute and the National Eye Institute.
1. von Noorden, G. (1996) Binocular Vision and Ocular Motility: Theory andManagement of Strabismus (Mosby, St. Louis), 5th Ed.
2. Francois, J. (1961) in Heredity in Ophthalmology (Mosby, St. Louis), pp. 255–269.3. Mash, A. & Spivey, B. (1973) Doc. Ophthalmol. 34, 285–291.4. Paul, T. O. & Hardage, L. K. (1994) Ophthalmic Genet. 15, 1–18.5. Holm, S. (1939) Acta Ophthalmol. 17, 367–387.6. Gover, M. & Yankey, J. B. (1944) Publ. Health Rep. 59, 1163–1184.7. Ing, M. & Pang, S. W. (1978) in Strabismus: Proceedings of the Third Meeting
of the International Strabismological Association (Grune and Stratton, NewYork), pp. 107–110.
8. Crone, R. A. & Velzeboer, C. M. J. (1956) Arch. Ophthalmol. 55, 455–470.
9. Hu, D.-N. (1987) J. Med. Genet. 24, 584–588.10. Richter, S. (1967) Untersuchungen uber die Hereditat des Strabismus Concom-
itants (VEB Georg Thieme, Leipzig, Germany).11. Podgor, M. J., Remaley, N. A. & Chew, E. (1996) Arch. Ophthalmol. 114,
739–744.12. Nordlow, W. (1964) Acta Ophthalmol. 42, 1015–1037.13. Cantolino, S. J. & von Noorden, G. K. (1969) Arch. Ophthalmol. 81, 753–757.14. Scott, M. H., Noble, A. G., Raymond, W. R. & Parks, M. M. (1994) J. Pediatr.
Ophthalmol. Strabismus 31, 298–301.15. Chimonidou, E., Palimeris, G. & Koliopoulas, V. P. (1977) Br. J. Ophthalmol.
61, 27–29.
Table 2. Multipoint recessive LOD scores for markers on distal 7p for families A–G and forfamily A alone
Disease allele frequency
Penetrance, %
50 60 70 80 90
Families A–G 0.1 2.42 2.50 2.40 2.38 2.780.01 2.63 2.62 2.54 2.64 3.190.001 2.85 2.91 2.92 2.80 3.020.0001 2.47 2.55 2.62 2.65 2.57
Family A 0.1 3.55 3.84 3.99 4.01 3.930.01 3.84 3.98 4.11 4.24 4.350.001 3.93 4.11 4.30 4.47 4.510.0001 3.62 3.75 3.86 3.94 3.91
LOD scores were calculated with SIMWALK2 using a phenocopy rate � 0.0001. For families A–G, the heteroge-neous LOD score calculation is based on the eight markers used in the initial high-resolution map (see Results).For family A alone, the calculation is based on all 20 high-resolution 7p markers (Fig. 1 and Table 3). Subject 333and her children, 430 and 431, were not included in the LOD score calculation for family A alone because subject333, a nonblood relative, is affected.
Parikh et al. PNAS � October 14, 2003 � vol. 100 � no. 21 � 12287
GEN
ETIC
S

16. Schlossman, A. & Priestley, B. S. (1952) Arch. Ophthalmol. 47, 1–20.17. Hegmann, J. P., Mash, A. J. & Spivey, B. E. (1974) Am. J. Hum. Genet. 26,
549–562.18. Maumenee, I. H., Alston, A., Mets, M. B., Flynn, J. T., Mitchell, T. N. & Beatty,
T. H. (1986) Trans. Am. Ophthalmol. Soc. 84, 85–93.19. Engle, E. (2002) Ann. N.Y. Acad. Sci. 956, 55–63.20. Nakano, M., Yamada, K., Fain, J., Sener, E. C., Selleck, C. J., Awad, A. H., Zwaan,
J., Mullaney, P. B., Bosley, T. M. & Engle, E. C. (2001) Nat. Genet. 29, 315–320.21. Morin, X., Cremer, H., Hirsch, M. R., Kapur, R. P., Goridis, C. & Brunet, J. F.
(1997) Neuron 18, 411–423.22. Traboulsi, E. I. (2001) Am. Orthoptic J. 51, 67–74.23. Young, A. (1998) GAS Package (Oxford University, Oxford), Version 2.3.24. Broman, K. W. & Weber, J. L. (1998) Am. J. Hum. Genet. 63, 1563–1564.
25. Kruglyak, L., Daly, M. J., Reeve-Daly, M. P. & Lander, E. S. (1996) Am. J. Hum.Genet. 58, 1347–1363.
26. Douglas, J. A., Boehnke, M. & Lange, K. (2000) Am. J. Hum. Genet. 66,1287–1297.
27. Benson, G. (1999) Nucleic Acids Res. 27, 573–580.28. Ott, J. (1991) Analysis of Human Genetic Linkage (Johns Hopkins Univ. Press,
Baltimore), 2nd Ed.29. Lathrop, G. M., Lalouel, J. M., Julier, C. & Ott, J. (1984) Proc. Natl. Acad. Sci.
USA 81, 3443–3446.30. Duffy, D. L. (1999) SIB-PAIR (Queensland Institute of Medical Research,
Brisbane, Australia), Version 0.99.7.31. Sobel, E. & Lange, K. (1996) Am. J. Hum. Genet. 58, 1323–1337.32. Shugart, Y. Y., Feng, B. J. & Collins, A. (2003) J. Genet. 81, 99–103.
12288 � www.pnas.org�cgi�doi�10.1073�pnas.2035118100 Parikh et al.
Copyright © 2022 FDOKUMEN




















