Impulse buying and variety seeking: A trait-correlates perspective

A quantitative trait locus (QTL) on chromosome6q influences birth weight in two independentfamily studies
Rector Arya1,4,*, Ellen Demerath5, Christopher P. Jenkinson2, Harald H.H. Goring4,
Sobha Puppala4, Vidya Farook4, Sharon Fowler1, Jennifer Schneider4, Richard Granato1,
Roy G. Resendez4, Thomas D. Dyer4, Shelley A. Cole4, Laura Almasy4, Anthony G. Comuzzie4,
Roger M. Siervogel5, Benjamin Bradshaw3, Ralph A. DeFronzo2, Jean MacCluer4,
Michael P. Stern1, Bradford Towne5, John Blangero4 and Ravindranath Duggirala4
1Division of Clinical Epidemiology, 2Division of Diabetes, Department of Medicine and 3School of Public Health,
University of Texas Health Science Center, 7703 Floyd Curl Drive, San Antonio, TX 78229-3900, USA, 4Department of
Genetics, Southwest Foundation for Biomedical Research, San Antonio, TX 78245, USA and 5The Wright State
University School of Medicine, Kettering, OH 45420, USA
Received January 25, 2006; Revised and Accepted March 22, 2006
Low birth weight is an important cause of infant mortality and morbidity worldwide. Birth weight has beenshown to be inversely correlated with adult complex diseases such as obesity, type-2 diabetes and cardio-vascular disease. However, little is known about the genetic factors influencing variation in birth weight andits association with diseases that occur in later life. We, therefore, have performed a genome-wide search toidentify genes that influence birth weight in Mexican-Americans using the data from the San Antonio FamilyBirth Weight Study participants (n 5 840). Heritability of birth weight was estimated as 72.0+++++ 8.4%(P < 0.0001) after adjusting for the effects of sex and term. Multipoint linkage analysis yielded the strongest evi-dence for linkage of birth weight (LOD 5 3.7) between the markers D6S1053 and D6S1031 on chromosome 6q.This finding has been replicated (LOD 5 2.3) in an independent European-American population. Together,these findings provide substantial evidence (LODadj 5 4.3) for a major locus influencing variation in birthweight. This region harbors positional candidate genes such as chorionic gonadotropin, alpha chain; collagen,type XIX, alpha-1; and protein-tyrosine phosphatase, type 4A, 1 thatmay play a role in fetal growth and develop-ment. In addition, potential evidence for linkage (LOD � 1.2) was found on chromosomes 1q, 2q, 3q, 4q, 9p,19p and 19q with LODs ranging from 1.3 to 2.7. Thus, we have found strong evidence for a major gene onchromosome 6q that influences variation in birth weight in both Mexican- and European-Americans.
INTRODUCTION
Low birth weight (LBW), or small body size at birth, is one ofthe major public health problems in the USA, and an import-ant cause of infant mortality and morbidity worldwide (1). Thepercentage of LBW infants was reported as 6.6 amongnon-Hispanic white mothers, 6.4 among Mexican-Americans(Hispanic) and 13.0 for African-Americans (1). On the basisof socio-demographic characteristics, Mexican-Americanswould be expected to have an elevated risk of adverse
health outcomes including high rates of LBW. Paradoxically,however, MAs have rates of LBW similar to those of non-Hispanic whites, and lower than those of African-Americansof similar socioeconomic status. Given the evidence thatbirth weight is positively associated with weight at laterages, LBW infants who gain weight very rapidly during child-hood (i.e. who experience catch-up growth) may also be atincreased risk of obesity later in life (2,3). There is evidencethat LBW is strongly associated with obesity and type-2 diabetes(T2D) in childhood, two major public health problems, in
# The Author 2006. Published by Oxford University Press. All rights reserved.The online version of this article has been published under an open access model. Users are entitled to use, reproduce, disseminate, or display the open access version ofthis article for non-commercial purposes provided that: the original authorship is properly and fully attributed; the Journal and Oxford University Press are attributed as theoriginal place of publication with the correct citation details given; if an article is subsequently reproduced or disseminated not in its entirety but only in part or as aderivative work this must be clearly indicated. For commercial re-use, please contact: [email protected]
*To whom correspondence should be addressed. Tel: +1 2105675234; Fax: +1 2105676955; Email: [email protected]
Human Molecular Genetics, 2006, Vol. 15, No. 10 1569–1579doi:10.1093/hmg/ddl076Advance Access published on April 12, 2006
by guest on June 9, 2013http://hm
g.oxfordjournals.org/D
ownloaded from

non-European groups such as Mexican-Americans (2–7). LBWhas been considered to be an important marker of variouscomplex diseases in adulthood such as obesity, T2D and coron-ary heart disease (CHD) in adult life in a number of differentpopulations, including western populations (8–15).
The association between birth weight and diseases inlater life has been a much debated topic since Barker andcolleagues proposed the ‘fetal programming’ hypothesis(8,10,11). According to this hypothesis, LBW or small bodysize is a repercussion of malnutrition in early pregnancy,and such fetal states might ‘programme’ tendencies todevelop metabolic disease conditions in adult life (8,13).There is considerable evidence supporting this idea that fetalnutrition deficiencies during critical periods in early life mayhave adverse lifetime consequences (16,17). For example,LBW has been shown to predict the subsequent occurrenceof insulin resistance and related conditions such as T2D,hypertension, dyslipidaemia and CHD (8). Thus, the term‘thrifty phenotype’ has been introduced to refer to maternaland/or fetal nutritional deficiencies as primary environmentalmechanisms that underlie the inverse correlations betweenbirth weight and metabolic diseases in adulthood (18,19).However, some epidemiological studies have reported associ-ations between birth weight (low and high) and T2D and IGT(20–23). Thus, the relationship between birth weight and theprevalence of T2D has been found to be U-shaped, indicatingthat both low and high birth weights are correlated with T2D(22). Interestingly, our recent family-based findings of positivegenetic correlations between birth weight and various com-ponents of the MS are also consistent with the findings fromthe Pima Indian studies (24,25). Although birth weight hasbeen shown to be associated with adult complex diseasessuch as obesity, T2D, the metabolic syndrome and cardio-vascular disease, mechanisms that underlie the correlationbetween birth weight and such diseases that occur later inlife are still not clear and remain controversial (13,17,26–28).
Birth weight is a complex phenotype affected by both geneticand environmental factors, and by their interactions (28–30).Environmental factors such as maternal smoking, intrauterinemalnutrition and placental functioning may lead to LBW(31,32). Family and twin studies have provided ample evidencethat genetic factors also influence birth weight (33,34).Although fetal growth is generally thought to be influencedby genetic factors (31,32), evidence for specific genetic deter-minants of birth weight in humans has been limited. Given theevidence that complex diseases such as T2D, obesity and CHDhave significant genetic determinants, however, there has beenincreasing belief that the link between birth weight and adult-hood diseases might be explained in terms of genetic andenvironmental factors and their interactions (28–30). There-fore, the purpose of this study was to map susceptibilitygenes that influence variation in birth weight used as a continu-ous trait in Mexican-Americans. It should be, however, notedthat LBW is a part of the continuum.
RESULTS
As reported in Table 1, we used birth weight data obtainedfrom birth certificates for 840 participants (449 from
SAFDGS and 391 from SAFHS for whom genotypic datawere available. In the combined data, mean birth weight was3.31 kg and the percentage of LBW was 5.6. The percentageof premature births was 7.6. Mean adult age at clinic examin-ation was 28.2 years.
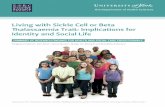
As the SAFDGS families were ascertained on a single T2Dproband, all of our genetic analyses incorporated correctionfor possible ascertainment bias by computing the likelihoodof a pedigree conditional on the birth weight of the proband.After accounting for the effects sex and term (premature:yes or no), the heritability of birth weight analyzed as a con-tinuous trait, was 71.8 + 8.4% which is highly significant(P , 0.0001). Following the estimation of heritability, weperformed multipoint linkage analysis across 22 autosomesfor birth weight with sex and term as covariates. As shownin Table 2 and Figures 1 and 2, we have found significant evi-dence for linkage (LOD ¼ 3.7, nominal P-value ¼ 0.0000175,empirical P-value ¼ 0.00002) between markers D6S1053 andD6S1031 on chromosome 6. The empirical P-value thatcorresponds to our original observed LOD score (3.7) indi-cates that our nominal P-value may not have over-stated theevidence for linkage.
In addition, eight chromosomal regions representing sevenchromosomes across the genome, exhibited modest evidencefor linkage (LOD � 1.2) with birth weight as shown inTable 2 and Figure 1. Genetic regions on chromosomes 2, 4and 9 with suggestive evidence for linkage (LOD � 1.9)appear to harbor genes influencing the variation in birth
Table 1. Characteristics of SAFDGS and SAFHS subjects
Characteristic SAFHS SAFDGS Combinedc
Sample size (females ¼ 57.3%) 391 449 840Mean birth weight (kg) 3.28 3.34 3.31Range (kg) 1.44–5.33 1.59–5.10 1.44–5.332.5 kg (LBW) (%)a 5.9 5.4 5.6.4.0 kg (%) 9.5 8.5 8.9Premature (%)b 6.7 8.4 7.6Mean age at exam (years) 27.1 29.9 28.2
aLBW, less than 2500 g (5 pounds, 8 ounces).bPremature, born before 37 completed weeks of pregnancy.cKurtosis ¼ 0.6405; Skewness ¼ 20.1621.
Table 2. Chromosomal regions linked to birth weight with multipoint LODscores � 1.2a
Marker region Chromosomallocation (cM)b
MaximumLOD score
D1S518–D1S1660 225 (1q31.1-31.3) 1.71D2S1776 187 (2q24.3) 2.66D3S1311 248 (3q29) 1.57D4S1625 159 (4q31.21) 1.92D6S1053–D6S1031 89 (6q12-14.1) 3.72GATA124D09 (D9S925) 30 (9p22.2) 2.28D19S586 38 (19p13.2) 1.47D19S589–D19S418 97 (19q13.42) 1.25
aBirth weight adjusted for sex and term.bLocations in Haldane (cM).
1570 Human Molecular Genetics, 2006, Vol. 15, No. 10
by guest on June 9, 2013http://hm
g.oxfordjournals.org/D
ownloaded from

weight (Fig. 1, Table 2). Thus, our genome-wide linkageanalysis of birth weight implicated multiple regions onchromosomes 1, 2, 4, 6 and 9 with significant and potential/suggestive evidence of linkage with birth weight (Figs 1 and 2).
Importantly, our major linkage finding (LOD ¼ 3.7) on 6qhas been replicated in an independent European-Americanpopulation study, the Fels Longitudinal Study, with a LODof 2.3 between markers D6S460 and D6S1270 (Fig. 3). Asshown in Figure 3, the distance between the study-specificmaximum LOD peaks was about 12 cM. As can be seenfrom the same figure, the combined evidence for linkage
(LODadj ¼ 4.3) occurred at a location between markersD6S1053 and D6S1031. The 1-LOD support interval approxi-mately corresponds to the chromosomal region spanning�16 cM that is flanked by markers D6S1960 and D6S1270.
As multiple linkage peaks with some evidence for linkagewere observed in our genome-wide search, we extended var-iance components linkage analysis to oligogenic models toincorporate two or more loci simultaneously. As shown inTable 3, in a joint two-locus analysis, the two-locus modelyielded a conditional LOD score of 2.9 for the second quanti-tative trait locus (QTL) (P ¼ 0.000127) near D2S1776 marker
Figure 1. Chromosomal regions linked to birth weight in a genome-wide scan (LOD � 1.2).
Human Molecular Genetics, 2006, Vol. 15, No. 10 1571
by guest on June 9, 2013http://hm
g.oxfordjournals.org/D
ownloaded from

on chromosome 2. The three-locus model yielded a con-ditional LOD score of 2.2 for the third QTL (P ¼ 0.000798)near D1S518 marker on chromosome 1. The four-locusmodel yielded a conditional LOD score of 1.4 for the fourthQTL (P ¼ 0.006303) between GATA187D09 and D9S925markers on chromosome 9. Thus, genetic determinants ofbirth weight involve possibly four loci that are found onfour different chromosomes.
DISCUSSION
Knowledge about the genetic basis of variation in birth weightand its association with diseases in adulthood is very limited.Although the available evidence is limited and indirect, itsuggests a significant role for genetic factors in the phenotypicexpression of birth weight. There have been suggestions thatthe variation in birth weight is multifactorially determined,and that the association between birth weight and adulthooddiseases can be explained in terms of genetics and environ-ment and their interactions (33,35,36). Birth weight, beinghighly heritable, showed significant positive genetic corre-lations with various components of the metabolic syndromephenotypes, including fasting insulin (non-diabetics only),BMI, waist circumference and triglycerides, and a negativegenetic correlation with HDL levels (24,25). However, littleis known about the specific chromosomal regions harboringbirth weight susceptibility genes. Also not known is whetherthe already identified susceptibility loci relating to variousmetabolic phenotypes in adults in our study and otherstudies have any common genetic effects on birth weight.
In this study, we utilized the wealth of information from ourtwo family studies for which both phenotypic and genotypicdata are currently available to understand the genetic basisof birth weight. We used previously collected marker data toscan the genome for specific genetic determinants of birthweight in 840 individuals using variance componentslinkage techniques. The significant heritability (72%) of
birth weight estimated in this study indicates that variationin birth weight is highly heritable, which is consistent withthe Fels heritability estimate (h2 ¼ 80%; Demerath et al.,unpublished data). These heritability estimates are higherthan some of those estimates (�50%) reported elsewhere inthe literature (25,37,38). However, it should be noted thatheritability estimates are population-specific, and can beinfluenced by such factors as study population, design,ascertainment criteria and the covariates considered for theanalysis. Such factors could have influenced the differencesin the heritability estimates of birth weight across thepopulations.
To our knowledge, this is the first genome scan linkageanalysis using birth weight as a continuous trait, to find lociwith appreciable influences on birth weight. In particular,the present genome scan in Mexican-Americans providesstrong evidence (LOD ¼ 3.7) for the presence of a novel
Figure 2. Linkage of birth weight to a region on chromosome 6q inMexican-Americans. Figure 3. Linkage of birth weight to chromosome 6q in both SAFBWS and
Fels data sets.
Table 3. Results of the oligogenic analysis of variation in birth weight
Model/QTL region Sequential LOD Conditional LOD(P-value)b
One-locus 3.7a –D6S1053–D6S1031
Two-locus 6.6 2.9 (0.000127)D6S1053–D6S1031D2S1776
Three-locus 8.8 2.2 (0.000798)D6S1053–D6S1031D2S1776D1S518
Four-locus 10.2 1.4 (0.006303)D6S1053–D6S1031D2S1776D1S518GATA187D09–D9S925
aThe largest marginal LOD in the initial linkage analysis.bConditional LODs and P-values obtained from the conditional analysis.
1572 Human Molecular Genetics, 2006, Vol. 15, No. 10
by guest on June 9, 2013http://hm
g.oxfordjournals.org/D
ownloaded from

major locus influencing variation in birth weight on chromo-some 6q12-q14.1 near markers D6S1053–D6S1031. Impor-tantly, our linkage finding in Mexican-Americans has beenreplicated in an independent non-Hispanic white populationwith a LOD of 2.3, given attention to the issues of localiz-ation (39,40). In fact, our combined data yielded substantialevidence for linkage (LODadj ¼ 4.3) of birth weight to thesame chromosomal region. Markers D6S1960 and D6S1270on chromosome 6p12.1 and 6q14.3, respectively, flank the1-LOD support interval surrounding the genetic location,where we found the strongest linkage evidence from the com-bined data. This chromosomal region contains important pos-itional candidate genes: protein-tyrosine phosphatase, type 4A,1 (PTP4A1) also known as phosphatase of regenerating liver 1(PRL-1, 6q12); collagen, type XIX, alpha-1 (COL19A1,6q12-q14); and human chorionic gonadotropin (hCG) or chor-ionic gonadotropin, alpha chain (CGA, 6q12-q21). The proteinproduct of hCG is a placental hormone produced by the tro-phoblast that acts like luteinizing hormone, stimulating thesecretion of the pregnancy-sustaining steroid progesteroneand also acts as a growth factor that facilitates endometrialreceptivity (41,42). hCG plays a major role in the developmentand maintenance of pregnancy and hence it is known as thehormone of pregnancy and development. Col19A gene, witha transient embryonic expression, may be involved inmuscle differentiation and function (43). Furthermore, altera-tions to human type XIX collagen may cause mild cartilagedisorders such as osteoarthritis, mildly short stature and epi-physeal abnormalities (44,45) and modulate several functionsincluding cell–matrix interactions and cell–cell communi-cations (46). PTP4A1 (or PRL-1) is a unique protein tyrosinephosphatase, which is involved in normal cellular growthcontrol, plays a role in liver regeneration and is positivelyassociated with fetal and neoplastic hepatic growth (47,48).
The 6q12-14 region (D6S1053–D6S1031) has also beenreported to be linked to several adult phenotypes such asheight (49), blood pressure (50) and fasting plasma glucose(FPG) (51) with LODs ranging from 1.6 to 3.3 (Table 4).Specifically, this 6q region is concordant with a stronglinkage signal for systolic blood pressure on chromosome 6near marker D6S1031 in a large NHLBI family heart study(50). In another genome scan of blood pressure in familieswith familial combined hyperlipidaemia (FCHL), the samemarker region has been implicated with a LOD of 2.5 fordiastolic blood pressure (52). Thus, our birth weight linkagefinding on chromosome 6q appears to overlap with thepreviously implicated regions influencing variation in height,hypertension and dyslipidaemia. It is worthwhile to notethat, apart from these observations, a number of studiesincluding our own implicated a broad overlapping geneticregion on chromosome 6q16.1-q27 to contain susceptibilitygenes that influence obesity (both childhood and adult) andT2D or their related phenotypes, using the genome scan/linkage approach (53–55). Interestingly, oligogenic analysisyielded two additional linkage regions with improved LODscores on chromosomes 2 and 1 that are similar to thoseobtained in the initial linkage analysis.
Among the other chromosomal regions of interest in ourstudy, the 2q24 region showed evidence for linkage withbirth weight with the second highest LOD, and contains the
activin receptor-like kinase 7 (ALK7) gene, which belongs tothe transforming growth factor-b family. ALK7 and its iso-forms are expressed in human placenta and their expressionis developmentally regulated (56). The 1q chromosomalregion has been shown to be linked to HDL-C (57), metabolicsyndrome phenotypes (58), obesity (59), glycaemic traits (60),dyslipidaemia (61), T2D (62) and FCHL (63). This regionharbors candidate genes such as apolipoprotein A2(APOA2), pyruvate kinase deficiency of erythrocyte (PKLR),LIM homeobox transcription factor 1 (LMX1) andinterleukin-10 (IL-10), which could potentially influencebirth weight and adult disorders such as T2D, metabolic syn-drome and cardiovascular disease. The 9p22 chromosomalregion has also been linked to HDL-C levels inMexican-Americans (61), Finns and Dutch populations (64),and with adiponectin levels, T2D and age of onset of T2D(65–68). Although serum adiponectin levels are inverselyassociated with obesity, T2D and measures of insulin resist-ance, its association with birth weight is unclear. However,in a recent study, Cianfarani et al. (69) indicated that lowadiponectin levels in LBW infants might predict the laterdevelopment of visceral fat and insulin resistance.
The results of this study are consistent with findings fromearlier studies that showed direct or indirect evidence thatgenetic factors may play a significant role in determining vari-ation in birth weight. To our knowledge, there has been onlyone genome scan linkage study of birth weight in PimaIndians (n ¼ 269): in this study, birth weight was analyzedas a discrete phenotype (i.e. LBW) (70). This study found evi-dence for linkage of LBW (LOD ¼ 3.4 at 88 cM) and LBWwith paternal imprinting (LOD ¼ 4.1) on chromosome 11p(70). However, we failed to find any evidence for linkage ofbirth weight at this 11p region in our study. In addition,several genetic variants have been reported to be associatedwith alterations in birth size using animal models andhumans. In animal models, the genes encoding insulin, theinsulin-like growth factors (IGF-1 and IGF-II), their receptorsand their regulatory proteins have been shown to haveprofound effects on fetal growth (71–73).
In humans, studies have been performed to examine theassociation between genetic variants in biologically plausiblecandidate genes, such as insulin, glucokinase and LBW(74,75). It has been shown that mutations in the glucokinasegene (7p15-p13) of the fetus have been associated with bothLBW and subsequent diabetes (74). These mutations couldcause impaired insulin secretion, hence their contributions toimpaired fetal growth and to subsequent diabetes. In contrast,the class III allele of the variable number of tandem repeatlocus in the promoter region of the insulin (INS) gene(11p15.5) has been found to be associated with both increasedbirth weight (76) and with many components of the metabolicsyndrome (77). However, as we failed to identify evidence oflinkage at these chromosomal regions in our present study,these regions may not have a major influence on birthweight in our population.
Some of the limitations of our findings include the follow-ing. We analyzed birth weight as a continuous trait in thisstudy, and that LBW is a part of the continuum. It should,however, be noted that we did not have information oncorrelates of birth weight such as mothers’ behavioral
Human Molecular Genetics, 2006, Vol. 15, No. 10 1573
by guest on June 9, 2013http://hm
g.oxfordjournals.org/D
ownloaded from

Table 4. Correspondence between linkage findings of birth weight and adult phenotypes
Population Phenotype Chromosomalband
Markers Position (cM)a LOD Candidate genes Reference
Mexican-Americans Birth weight 1q31.1-31.3 D1S518–D1S1660 202.2–212.4 1.71 APOA2, PKLR, LMX1, IL 10 Present studyHispanic families MS 1q23-q31 D1S518 202.2 1.6NPL Langefeld et al. (58)Caucasian pedigrees Glycaemic traits 1q D1S1678–D1S3462 218.5–247.2 1.8–2.33 Meigs et al. (60)The DUK2 R UK population T2D 1q24-25 D1S218 191.5 1.46 Wiltshire et al. (62)Finnish population FCHL 1q21-q23 D1S1677 175.6 5.93 Pajukanta et al. (63)Whites of Breda Study Obesity (BMI) 1q31-q42 D1S518–D1S179 202.2–252.1 1.5 Tilburg et al. 2003African population HDL-C 1q25 D1S1660 212.4 2.48 Adeyemo et al. (57)Mexican-American Lipid factor 1q D1S431 182.4 1.9 Arya et al. (88)Mexican-Americans Birth weight 2q24.3 D2S1776 173.0 2.66 ALK7 Present studyItalian families BFIC 2q24 D2S399/D2S2330 169.4 6.29HLOD Malacarne et al. (89)Hong Kong Chinese Triglycerides 2q D2S1391 186.2 1.69 Ng et al. (51)Mexican-Americans Birth weight 3q29 D3S1311 224.9 1.56 MUC4, MUC20, PPP1R2 Present studyFramingham Heart Study
PopulationAtherogenic
dyslipidaemia3q29 D3S2398 209.4 1.95NPL Yip et al. (90)
Austrian families Schizophrenia andbipolar disorder
3q29 D3S1265–D3S3550 222.8/227.6 1.69/1.443.74/3.50NPL
Bailer et al. (91)
Mexican-Americans Birth weight 4q31.21 D4S1625 145.9 1.92 NPY1R, NPY2R, NPY5R,UCP1, CPE
Present study
The Heritage family study Visceral fat 4q31.22 D4S2431 159.5 2.34 Rice et al. (92)Rochester family heart study BMI 4q31.1-q32 D4S1629 157.9 1.89ME Gorlova et al. (93)Mexican-Americans Birth weight 6q12-14.1 D6S1053–D6S1031 80.5–88.6 3.72 HCG, PTP4A, COL19A Present studyDutch sibling pairs Height 6q D6S1053–D6S1031 80.5–88.6 2.32 Willemsen et al. (49)White families Blood pressure 6q D6S1031 88.6 3.3 Hunt et al. (50)Dutch families Blood pressure 6q D6S1031–D6S1056 88.6–102.8 2.5 Allayee et al. (52)Hong Kong Chinese FPG 6q D6S2410–D6S1031 73.1–88.6 1.56 Ng et al. (51)Mexican-Americans Birth weight 9p22.2 GATA187D09–D9S925 32.2 2.28 VLDLR, INF Present studyMexican-Americans T2D, age of
diabetes onset9p24.1 D9S288–D9S925 9.8–32.2 2.06/2.38 Duggirala et al. (65)
Mexican-Americans HDL-C 9p24 D9S925–D9S741 32.2–42.7 3.4 Arya et al. (61)Dutch and Finnish families HDL-C 9p23 D9S921 21.9 2.1 Pajukanta et al. (64)Pima Indians Adiponectin levels 9p D9S168–D9S925 21.9–32.2 3.0/3.5 Lindsay et al. (67)Mexican-Americans Birth weight 19p13.2 D19S586 32.9 1.50 LDLR Present studyPima Indians Total cholesterol 19p D19S1034 20.8 3.89 Imperatore et al. (94)Utah Caucasian families TG-to-HDL ratio 19p D19S247–D19S209 9.8–11.0 2.05/1.9 Elbein and Hasstedt (95)Mexican-Americans Birth weight 19q13.42 D19S589–D19S418 87.7–92.7 1.25 ApoC2/ApoE/ApoC1/
ApoC4, ATF5Present study
Utah Caucasian families Triglycerides 19q13.2 D19S178/ApoC2 68.1–69.5 3.16 Elbein and Hasstedt (95)
Candidate genes: ApoA2, apolipoprotein A2; PKLR, pyruvate kinase deficiency of erythrocyte; LMX1, LIM homeobox transcription factor 1; IL-10, Interleukin 10; ALK7, activin receptor-like kinase 7; PTP4A1, protein-tyrosine phosphate type 4A; PRL-1, phosphatase of regenerating liver-1; MUC4, mucin 4; MUC20, mucin 20; PPP1R2, protein phosphatase inhibitor 2;NPYR, neuropeptide Y receptor 1, 2 and 5; VLDLR, very low-density lipoprotein receptor; LDLR, LDL receptor; INF, interferons; CPE, carboxypeptidase; UCP1, uncoupling protein 1;apolipoproteins–C1 (ApoC1), C2 (ApoC2), 4 (ApoC4) and E (ApoE); ATF5, activating transcription factor 5; BFIC, benign familial infantile convulsions.aFor the purpose of comparison across the studies, we used Marshfield genetic distances. NPL, nonparametric multipoint linkage score; HLOD, heterogeneity LOD; ME, maternal expression.
1574
HumanMolecu
larGenetics,
2006,Vol.15,No.10
by guest on June 9, 2013 http://hmg.oxfordjournals.org/ Downloaded from

attributes (e.g. smoking) or disease conditions (e.g. gestationaldiabetes and obesity) at the time of birth. Although it is inter-esting to note that most of the linked loci are shared byobesity/T2D genome scans, some of these findings could bechance occurrences, whereas some may harbor potential sus-ceptibility genes that have pleiotropic influences on birthweight and adult phenotypes such as obesity and T2D. We,therefore, plan to conduct multivariate analyses to examinewhether birth weight and adult metabolic diseases in our popu-lation have any common genetic influences (i.e. pleiotropy).We also plan to examine potential parent-of-origin effectson genetic variation in birth weight (i.e. imprinting),respectively.
In summary, in this genome-wide linkage study, perhaps forthe first time, we have identified susceptibility loci that influ-ence birth weight in human populations. Our genome-widelinkage analysis in Mexican-Americans yielded severalgenetic regions with significant and suggestive evidence forlinkage to birth weight. In particular, we have identified amajor locus (LOD ¼ 3.7) for birth weight on chromosome 6and this finding has been replicated in an independent studyin European-Americans. In fact, data from these two studiesyielded substantial evidence for linkage (LODadj ¼ 4.3) ofbirth weight on chromosome 6. This locus appears to havesubstantial influence on the phenotypic variation of birthweight. Potential/suggestive evidence for linkage has alsobeen found on chromosomes 1, 2, 4 and 9 indicating potentialmulti-locus influences on birth weight in Mexican-Americans.We plan to follow-up the present findings by fine-mapping our6q region, and screening positional candidate genes in thisregion to examine if the sequence variants in such genescould explain our birth weight linkage findings inMexican-Americans.
MATERIALS AND METHODS
San Antonio Family Birth Weight Study
The San Antonio Family Birth Weight Study (SAFBWS)sought to collect birth weights, gestational ages and relateddata for all individuals who had previously participated asadults in one of the three Mexican-American family studies:the San Antonio Family Diabetes/Gallbladder Study(SAFDGS), the San Antonio Family Heart Study (SAFHS)and the Veterans Administration Genetic EpidemiologyStudy (VAGES). However, to date, both phenotypic and geno-typic data are currently available for SAFDGS and SAFHS.We included 449 subjects for whom birth weight data wereavailable from 910 SAFDGS individuals. The SAFDGSfamilies were ascertained on T2D probands, and the familymembers were distributed across 39 families that participatedin our studies at baseline or recalls for whom genotypes forgenome-wide markers at a 10 cM density, performed by theCenter for Inherited Disease Research (CIDR), was available.In addition, we included 391 individuals with birth weight datafrom 893 individuals distributed across 24 pedigrees from theSAFHS study. These 24 families are part of the original 41Mexican-American families ascertained at random withoutregard to disease status. A detailed description of SAFDGSand SAFHS including subjects, methods and phenotypes and
genome scan data has been presented in previous publications(78–80). Data from these two studies are currently beingexamined for susceptibility genes of various metabolic dis-eases including T2D, obesity, hypertension and metabolicsyndrome-related quantitative traits (e.g. insulin and lipids).Thus, for the present study, birth weight data for 840 individ-uals and genotypic information (a 10 cM map) were used fromcombined SAFDGS and SAFHS data sets as shown in Table 1.
Birth weight phenotype
Birth weight and related information, began late in 1949 to beroutinely recorded on official state birth certificates in SanAntonio and throughout Texas. It was recorded earlier thanthis in some parts of Texas, and in some other states. Ourprimary source of birth weight data for these analyses wasan extensive set of previously microfilmed birth certificatesfrom the San Antonio Metropolitan Health District, for theyears 1949 and later. For participants born outside SanAntonio but within Texas, actual birth weights were availablefrom the Texas Department of Health (TDH) beginning in1964. Participants for whom no birth weight data were avail-able from either of these sources, a letter was sent to the indi-vidual, requesting birth weight documentation from theparticipant himself or herself. Through home visits to thoseparticipants who possessed such documentation, we wereable to obtain data from photocopies of official birth certifi-cates for participants born outside San Antonio or outsideTexas, from hospital birth certificates, or from other materials,such as care instructions, provided by the hospital at the timeof discharge.
We abstracted data from all available records on birthweight and gestational age, along with relevant co-variables,such as maternal and paternal age at the time of birth, andmultiple-birth status. During different time periods, differentmethods were used to record gestational age. In earlieryears, a dichotomous variable (whether the child was at‘term’ or not) was used; later, weeks of gestation wererecorded; and most recently, in a relatively small number ofcases, the date of the last menstrual period of the mother hasbeen recorded. We have therefore included gestational ageas a dichotomized co-variable—whether the child was atterm or not—in these analyses.
We have included in these analyses all individuals forwhom both documented birth weight and gestational agedata were available, on the one hand, and for whom geneticmarker data were available from the full genome scansdescribed earlier. Most individuals who were born beforelate 1949 could not be included in these analyses because ofthe lack of available data either from our microfilm set orfrom their own records. Similarly, most individuals whowere born in Mexico, regardless of age, had to be excludedbecause they did not have copies of their birth certificates;in those few cases in which an individual shared with us acopy of his or her official birth certificate from Mexico, itdid not include birth weight data. These analyses thereforeprimarily included US-born (and particularly San Antonio-and Texas-born) individuals aged 18–52 years at the time oftheir participation in the SAFDGS or the SAFHS. The Insti-tutional Review Board of the University of Texas Health
Human Molecular Genetics, 2006, Vol. 15, No. 10 1575
by guest on June 9, 2013http://hm
g.oxfordjournals.org/D
ownloaded from

Science Center at San Antonio approved all procedures for thedata collection process, and all individuals gave writteninformed consent to participate in the study.
STATISTICAL GENETIC ANALYSIS
Variance components linkage analysis
We used a pedigree-based multipoint variance componentsapproach to test for linkage between marker loci and thebirth weight phenotype using a maximum likelihood method(81,82). In this method, the expected genetic covariancesbetween relatives are specified as a function of the IBDrelationships at a marker locus, which is assumed to beclosely linked to a locus influencing the quantitative trait inquestion. The covariance matrix for a pedigree can bewritten as shown in the following equation:
V ¼Xn
i¼1
Pis2qi þ 2Fs2
g þ Is2e
where V is the covariance matrix for a given pedigree; P, amatrix with elements (pijl) providing the expected proportionof alleles at the specific chromosomal location of the QTL thatindividuals j and l share IBD, which is estimated using geneticmarker data; s2
q the additive genetic variance due to the majorlocus; F the kinship matrix; s2
g the variance due to residualadditive genetic effects; I an identity matrix; and s2
e thevariance due to random environmental effects.
The null hypothesis that the additive genetic variance due toQTL, s2
q, for a given phenotype equals zero (no linkage) canbe tested using the likelihood ratio test. The likelihood of arestricted model in which s2
q is constrained to 0 is comparedwith the likelihood of the general model in which genetic var-iance due to QTL (s2
q) is estimated. The natural logarithm (ln)likelihood values of the general model and restricted modelare then compared using the likelihood ratio test. Twice thedifference between the ln likelihood values of these modelsyields a test statistic that is asymptotically distributed as a1/2:1/2 mixture of a x1
2 and a point mass at 0 (83). The like-lihood value can be converted into a logarithm (base 10) ofodds to obtain a LOD score that is equivalent to the classicalLOD score of linkage analysis. A LOD score of 3.0 and abovewas considered as strong evidence in support of linkage.For the purpose of discussion, other chromosomal regionsacross the genome with LOD scores � 1.2 and LODscores � 1.9 are considered as evidence for potential linkageand suggestive linkage, respectively.
Correction for ascertainment bias
As SAFDGS families were ascertained on a diabetic proband,all of our genetic analyses incorporated correction for ascer-tainment bias by computing the likelihood of a pedigree con-ditional on birth weight of the proband using SOLAR (84).
Multipoint mapping procedure
This method uses information on all available markers separ-ated by known map distances and all possible biological
relationships simultaneously in deciphering the genetic archi-tecture of a given quantitative phenotype. For this study, wecreated a combined genetic map using the marker informationavailable from the two studies (SAFDGS and SAFHS) andcalculated multipoint identical by descent (MIBD) matricesusing Markov Chain Monte Carlo (MCMC) methodsimplemented in Loki (85).
Oligogenic linkage analysis
We also conducted oligogenic linkage analysis which is asequential strategy to identify multiple loci affecting the vari-ation in birth weight. In this approach, the genome wasscanned for linkage and the chromosomal location with thelargest marginal LOD score was retained for further con-ditional analyses. Given the putative location of the firstlocus, we scanned the genome again and examined the result-ing conditional LOD scores. Loci were added to the modelsequentially until no locus met the selected criterion of a con-ditional LOD score of 0.59. In the two-loci model, the positionof the first locus is fixed, and the location of the second locusis allowed to vary through the whole genome. The QTL var-iance (h2
q) for the first locus is re-estimated along with thesecond locus. Similarly, in the three-loci model, the positionsof the first two loci are fixed but the effect sizes arere-estimated along with the third locus. Finally, in the four-loci model, the positions of the first three loci are fixed, butthe effect sizes are re-estimated along with the fourth locus.To obtain a conditional P-value, the likelihood values of thetwo competing models (e.g. one-locus versus two-locusmodels) are compared using the likelihood ratio test. Twicethe difference between the ln likelihood values of thesemodels yields a test statistic that is asymptotically distributedas a 1
2:12
mixture of a x12 and a point mass at 0.
Empirical P-value estimation
We performed simulation analysis to verify our major findingon chromosome 6q by simulating a fully informative markerthat was not linked to the QTL influencing variation in birthweight. For this simulated marker, IBD information was calcu-lated and linkage analysis then conducted. Using simulations,the empirical distribution of the LOD scores under theassumption of multivariate normality was determined basedon information obtained from 100 000 replicates using theSOLAR program (81).
Description of the replication study
The Fels Longitudinal Study (FLS), which was started in1929, is the largest and longest ongoing family study of phys-ical growth and development in the world (86). The Fels studyconsists of over 1200 serial participants, randomly ascertainedfrom the greater Dayton, Ohio area from approximately 200nuclear and multigenerational extended families. Measuredbirth weights are available for all of the Fels study participantswho have been followed from birth. A trained staff membermeasured birth weights of infants in the hospital shortlyafter birth through 1968, after which time-measuredbirth weights were obtained from hospital and birth records.
1576 Human Molecular Genetics, 2006, Vol. 15, No. 10
by guest on June 9, 2013http://hm
g.oxfordjournals.org/D
ownloaded from

For this replication analysis, we used birth weight data for 331individuals (162 males and 169 females), distributed across 57families for whom phenotypic and genotypic data were avail-able. We generated a combined map incorporating the markerinformation from the two studies, SAFBWS and FLS, and cal-culated study-specific MIBDs for chromosome 6 usingMCMC methods implemented in Loki (85). We then per-formed variance components linkage analysis.
Combined evidence for linkage of birth weight onchromosome 6q
After determining the evidence for linkage of birth weight inboth SAFBWS and FLS independently, we combined thelinkage information on chromosome 6 from both studies toobtain combined evidence for linkage of birth weight.However, thus obtained LOD score at a given locationinvolves 2 df; in fact, the test statistic (L) is asymptoticallydistributed as a 1/4:1/2:1/4 mixture of x2
2, x21 and x2
0. Giventhe evidence that birth weight is positively associated withweight at later ages (83). The combined LOD score with 2df can be adjusted to 1 df, denoted as LODadj score, by requir-ing it to provide the same P-value as is provided by the com-bined LOD score (87). Thus, the LODadj score can beconsidered equivalent to the classical univariate LOD score.
WEB RESOURCES
Accession numbers and URLs for data presented herein are asfollows: Center for Medical Genetics, Marshfield MedicalResearch Foundation http://research.marshfieldclinic.org/genetics (for genetic map information used for the purposeof comparison).
Online Mendelian Inheritance in Man (OMIM) http://www.ncbi.nlm.nih.gov/Omim (for hCG, PTP4A1, and COL19A).
UCSC Bioinformatics Site, Human Genome BrowserGateway, May 2004 (hg17) Assembly, http://www.genome.ucsc.edu/cgi-bin/hgGateway (for physical map and cyto-genetic band information regarding microsatellite markersand genes).
ACKNOWLEDGEMENTS
This study was supported by grants from the National Instituteof Health (R01 HD 41111, DK53889, DK42273, P01HL45522, DK47482, MH59490 and M01-RR-01346). Wewarmly thank the participants of SAFBWS subjects for theirenthusiasm and co-operation. We thank Texas Departmentof Health for providing birth weight data for some individuals.We also thank the Center for Inherited Disease Research forproviding a new genome scan using SAFDGS data.
Conflict of Interest statement. None declared.
REFERENCES
1. Guyer, B., Hoyert, D.L., Martin, J.A., Ventura, S.J., MacDorman, M.F.and Strobino, D.M. (1999) Annual summary of vital statistics–1998.Pediatrics, 104, 1229–1246.
2. Parsons, T.J., Power, C., Logan, S. and Summerbell, C.D. (1999)Childhood predictors of adult obesity: a systematic review. Int. J. Obes.Relat. Metab. Disord., 23 (Suppl. 8), S1–S107.
3. Rogers, I. (2003) The influence of birthweight and intrauterineenvironment on adiposity and fat distribution in later life. Int. J. Obes.Relat. Metab. Disord., 27, 755–777.
4. Fagot-Campagna, A. (2000) Emergence of type 2 diabetes mellitus inchildren: epidemiological evidence. J. Pediatr. Endocrinol. Metab., 13(Suppl. 6), 1395–1402.
5. Fagot-Campagna, A., Pettitt, D.J., Engelgau, M.M., Burrows, N.R.,Geiss, L.S., Valdez, R., Beckles, G.L., Saaddine, J., Gregg, E.W.,Williamson, D.F. and Narayan, K.M. (2000) Type 2 diabetes among NorthAmerican children and adolescents: an epidemiologic review and a publichealth perspective. J. Pediatr., 136, 664–672.
6. Farooqi, I.S. and O’Rahilly, S. (2000) Recent advances in the genetics ofsevere childhood obesity. Arch. Dis. Child, 83, 31–34.
7. AL, Rosenbloom (2000) The cause of the epidemic of type 2 diabetes inchildren. Curr. Opin. Endocrinol. Diab., 7, 191–196.
8. Barker, D.J., Winter, P.D., Osmond, C., Margetts, B. and Simmonds, S.J.(1989) Weight in infancy and death from ischaemic heart disease. Lancet,2, 577–580.
9. Barker, D.J., Bull, A.R., Osmond, C. and Simmonds, S.J. (1990) Fetal andplacental size and risk of hypertension in adult life. BMJ, 301, 259–262.
10. Barker, D.J. (1995) Fetal origins of coronary heart disease. BMJ, 311,171–174.
11. Barker, D.J. (1995) The fetal and infant origins of disease. Eur. J. Clin.Invest., 25, 457–463.
12. Burke, J.P., Williams, K., Gaskill, S.P., Hazuda, H.P., Haffner, S.M. andStern, M.P. (1999) Rapid rise in the incidence of type 2 diabetes from1987 to 1996: results from the San Antonio Heart Study. Arch. Intern.Med., 159, 1450–1456.
13. Godfrey, K.M. and Barker, D.J. (2000) Fetal nutrition and adult disease.Am. J. Clin. Nutr., 71, 1344S–1352S.
14. Must, A., Spadano, J., Coakley, E.H., Field, A.E., Colditz, G. andDietz, W.H. (1999) The disease burden associated with overweight andobesity. JAMA, 282, 1523–1529.
15. Sorensen, T.I. (2000) The changing lifestyle in the world. Body weightand what else? Diab. Care, 23 (Suppl. 2), B1–B4.
16. Hoet, J.J. and Hanson, M.A. (1999) Intrauterine nutrition: its importanceduring critical periods for cardiovascular and endocrine development.J. Physiol., 514, 617–627.
17. Waterland, R.A. and Garza, C. (1999) Potential mechanisms of metabolicimprinting that lead to chronic disease. Am. J. Clin. Nutr., 69, 179–197.
18. Hales, C.N. and Barker, D.J. (1992) Type 2 (non-insulin-dependent)diabetes mellitus: the thrifty phenotype hypothesis. Diabetologia, 35,595–601.
19. Hales, C.N. and Barker, D.J. (2001) The thrifty phenotype hypothesis. Br.Med. Bull., 60, 5–20.
20. Carlsson, S., Persson, P.G., Alvarsson, M., Efendic, S., Norman, A.,Svanstrom, L., Ostenson, C.G. and Grill, V. (1999) Low birth weight,family history of diabetes, and glucose intolerance in Swedishmiddle-aged men. Diab. Care, 22, 1043–1047.
21. Hales, C.N., Barker, D.J., Clark, P.M., Cox, L.J., Fall, C., Osmond, C. andWinter, P.D. (1991) Fetal and infant growth and impaired glucosetolerance at age 64. BMJ, 303, 1019–1022.
22. McCance, D.R., Pettitt, D.J., Hanson, R.L., Jacobsson, L.T., Knowler, W.C.and Bennett, P.H. (1994) Birth weight and non-insulin dependent diabetes:thrifty genotype, thrifty phenotype, or surviving small baby genotype?BMJ,308, 942–945.
23. Valdez, R., Athens, M.A., Thompson, G.H., Bradshaw, B.S. and Stern, M.P.(1994) Birthweight and adult health outcomes in a biethnic population in theUSA. Diabetologia, 37, 624–631.
24. Arya, R., Bradshaw, B., Jenkinson, C.P., Schneider, J., Fowler, S.,Puppala, S., Almasy, L., Comuzzie, A.G., MacCluer, J.W., DeFronzo, R.et al. (2004) Genetic Correlations between birth weight and the insulinresistance syndrome-related phenotypes in Mexican-Americans. Diabetes,52 (Suppl. 2), A269.
25. Stern, M.P., Bartley, M., Duggirala, R. and Bradshaw, B. (2000) Birthweight and the metabolic syndrome: thrifty phenotype or thriftygenotype? Diab. Metab. Res. Rev., 16, 88–93.
26. Barker, D.J., Hales, C.N., Fall, C.H., Osmond, C., Phipps, K. andClark, P.M. (1993) Type 2 (non-insulin-dependent) diabetes mellitus,
Human Molecular Genetics, 2006, Vol. 15, No. 10 1577
by guest on June 9, 2013http://hm
g.oxfordjournals.org/D
ownloaded from

hypertension and hyperlipidaemia (syndrome X): relation to reduced fetalgrowth. Diabetologia, 36, 62–67.
27. Fall, C.H., Vijayakumar, M., Barker, D.J., Osmond, C. and Duggleby, S.(1995) Weight in infancy and prevalence of coronary heart disease inadult life. BMJ, 310, 17–19.
28. Jarvelin, M.R. (2000) Fetal and infant markers of adult heart diseases.Heart, 84, 219–226.
29. Hamvas, A. (2000) Disparate outcomes for very low birth weight infants:genetics, environment, or both? J. Pediatr., 136, 427–428.
30. Moran, A. and Sinaiko, A.R. (2000) Influence of intrauterine environmenton development of insulin resistance. J. Pediatr., 136, 567–569.
31. Dar, P. and Gross, S.J. (2000) Macrosomia: a genetic perspective. Clin.Obstet. Gynecol., 43, 298–308.
32. Langer, O. (2000) Fetal macrosomia: etiologic factors. Clin. Obstet.Gynecol., 43, 283–297.
33. Hattersley, A.T. and Tooke, J.E. (1999) The fetal insulin hypothesis: analternative explanation of the association of low birthweight with diabetesand vascular disease. Lancet, 353, 1789–1792.
34. IJzerman, R.G., Stehouwer, C.D. and Boomsma, D.I. (2000) Evidence forgenetic factors explaining the birth weight-blood pressure relation.Analysis in twins. Hypertension, 36, 1008–1012.
35. Frayling, T.M. and Hattersley, A.T. (2001) The role of geneticsusceptibility in the association of low birth weight with type 2 diabetes.Br. Med. Bull., 60, 89–101.
36. Lauren, L., Jarvelin, M.R., Elliott, P., Sovio, U., Spellman, A.,McCarthy, M., Emmett, P., Rogers, I., Hartikainen, A.L., Pouta, A. et al.(2003) Relationship between birthweight and blood lipid concentrations inlater life: evidence from the existing literature. Int. J. Epidemiol., 32,862–876.
37. Clausson, B., Lichtenstein, P. and Cnattingius, S. (2000) Genetic influenceon birthweight and gestational length determined by studies in offspring oftwins. BJOG, 107, 375–381.
38. Magnus, P., Bakketeig, L.S. and Skjaerven, R. (1993) Correlations of birthweight and gestational age across generations. Ann. Hum. Biol., 20,231–238.
39. Hauser, E.R. and Boehnke, M. (1997) Confirmation of linkage results inaffected-sib-pair linkage analysis for complex genetic traits. Am. J. Hum.Genet., 61, A278.
40. Roberts, S.B., MacLean, C.J., Neale, M.C., Eaves, L.J. and Kendler, K.S.(1999) Replication of linkage studies of complex traits: an examination ofvariation in location estimates. Am. J. Hum. Genet., 65, 876–884.
41. Acevedo, H.F. (2002) Human chorionic gonadotropin (hCG), the hormoneof life and death: a review. J. Exp. Ther. Oncol., 2, 133–145.
42. Lustbader, J.W., Lobel, L., Wu, H. and Elliott, M.M. (1998) Structuraland molecular studies of human chorionic gonadotropin and its receptor.Recent Prog. Horm. Res., 53, 395–424.
43. Sumiyoshi, H., Mor, N., Lee, S.Y., Doty, S., Henderson, S., Tanaka, S.,Yoshioka, H., Rattan, S. and Ramirez, F. (2004) Esophageal musclephysiology and morphogenesis require assembly of a collagen XIX-richbasement membrane zone. J. Cell Biol., 166, 591–600.
44. Mundlos, S. and Olsen, B.R. (1997) Heritable diseases of the skeleton.Part II: Molecular insights into skeletal development-matrix componentsand their homeostasis. FASEB J., 11, 227–233.
45. Mundlos, S. and Olsen, B.R. (1997) Heritable diseases of the skeleton.Part I: Molecular insights into skeletal development-transcription factorsand signaling pathways. FASEB J., 11, 125–132.
46. Myers, J.C., Sun, M.J., D’Ippolito, J.A., Jabs, E.W., Neilson, E.G. andDion, A.S. (1993) Human cDNA clones transcribed from an unusuallyhigh-molecular-weight RNA encode a new collagen chain. Gene, 123,211–217.
47. Diamond, R.H., Cressman, D.E., Laz, T.M., Abrams, C.S. and Taub, R.(1994) PRL-1, a unique nuclear protein tyrosine phosphatase, affects cellgrowth. Mol. Cell. Biol., 14, 3752–3762.
48. Diamond, R.H., Peters, C., Jung, S.P., Greenbaum, L.E., Haber, B.A.,Silberg, D.G., Traber, P.G. and Taub, R. (1996) Expression of PRL-1nuclear PTPase is associated with proliferation in liver but withdifferentiation in intestine. Am. J. Physiol., 271, G121–G129.
49. Willemsen, G., Boomsma, D.I., Beem, A.L., Vink, J.M., Slagboom, P.E.and Posthuma, D. (2004) QTLs for height: results of a full genome scan inDutch sibling pairs. Eur. J. Hum. Genet., 12, 820–828.
50. Hunt, S.C., Ellison, R.C., Atwood, L.D., Pankow, J.S., Province, M.A.and Leppert, M.F. (2002) Genome scans for blood pressure and
hypertension: the National Heart, Lung, and Blood Institute FamilyHeart Study. Hypertension, 40, 1–6.
51. Ng, M.C., So, W.Y., Lam, V.K., Cockram, C.S., Bell, G.I., Cox, N.J. andChan, J.C. (2004) Genome-wide scan for metabolic syndrome and relatedquantitative traits in Hong Kong Chinese and confirmation of asusceptibility locus on chromosome 1q21-q25. Diabetes, 53, 2676–2683.
52. Allayee, H., de Bruin, T.W., Michelle, D.K., Cheng, L.S., Ipp, E.,Cantor, R.M., Krass, K.L., Keulen, E.T., Aouizerat, B.E., Lusis, A.J. andRotter, J.I. (2001) Genome scan for blood pressure in Dutch dyslipidemicfamilies reveals linkage to a locus on chromosome 4p. Hypertension, 38,773–778.
53. Duggirala, R., Blangero, J., Almasy, L., Arya, R., Dyer, T.D.,Williams, K.L., Leach, R.J., O’Connell, P. and Stern, M.P. (2001) Amajor locus for fasting insulin concentrations and insulin resistance onchromosome 6q with strong pleiotropic effects on obesity-relatedphenotypes in nondiabetic Mexican-Americans. Am. J. Hum. Genet., 68,1149–1164.
54. Meyre, D., Lecoeur, C., Delplanque, J., Francke, S., Vatin, V., Durand, E.,Weill, J., Dina, C. and Froguel, P. (2004) A genome-wide scan forchildhood obesity-associated traits in French families shows significantlinkage on chromosome 6q22.31-q23.2. Diabetes, 53, 803–811.
55. Meyre, D., Bouatia-Naji, N., Tounian, A., Samson, C., Lecoeur, C.,Vatin, V., Ghoussaini, M., Wachter, C., Hercberg, S., Charpentier, G.et al. (2005) Variants of ENPP1 are associated with childhood and adultobesity and increase the risk of glucose intolerance and type 2 diabetes.Nat. Genet., 37, 863–867.
56. Roberts, H.J., Hu, S., Qiu, Q., Leung, P.C., Caniggia, I., Gruslin, A.,Tsang, B. and Peng, C. (2003) Identification of novel isoforms of activinreceptor-like kinase 7 (ALK7) generated by alternative splicing andexpression of ALK7 and its ligand, Nodal, in human placenta. Biol.Reprod., 68, 1719–1726.
57. Adeyemo, A.A., Johnson, T., Acheampong, J., Oli, J., Okafor, G.,Amoah, A., Owusu, S., Agyenim-Boateng, K., Eghan, B.A., Jr,Abbiyesuku, F. et al. (2005) A genome wide quantitative trait linkageanalysis for serum lipids in type 2 diabetes in an African population.Atherosclerosis, 181, 389–397.
58. Langefeld, C.D., Wagenknecht, L.E., Rotter, J.I., Williams, A.H.,Hokanson, J.E., Saad, M.F., Bowden, D.W., Haffner, S., Norris, J.M.,Rich, S.S. and Mitchell, B.D. (2004) Linkage of the metabolic syndrometo 1q23-q31 in Hispanic families: the Insulin Resistance AtherosclerosisFamily Study. Diabetes, 53, 1170–1174.
59. van Tilburg, J.H., Sandkuijl, L.A., Strengman, E., Pearson, P.L.,van Haeften, T.W. and Wijmenga, C. (2003) Variance-componentanalysis of obesity in type 2 diabetes confirms loci on chromosomes 1qand 11q. Obes. Res., 11, 1290–1294.
60. Meigs, J.B., Panhuysen, C.I., Myers, R.H., Wilson, P.W. andCupples, L.A. (2002) A genome-wide scan for loci linked to plasma levelsof glucose and HbA(1c) in a community-based sample of Caucasianpedigrees: the Framingham Offspring Study. Diabetes, 51, 833–840.
61. Arya, R., Duggirala, R., Almasy, L., Rainwater, D.L., Mahaney, M.C.,Cole, S., Dyer, T.D., Williams, K., Leach, R.J., Hixson, J.E. et al. (2002)Linkage of high-density lipoprotein-cholesterol concentrations to a locuson chromosome 9p in Mexican-Americans. Nat. Genet., 30, 102–105.
62. Wiltshire, S., Hattersley, A.T., Hitman, G.A., Walker, M., Levy, J.C.,Sampson, M., O’Rahilly, S., Frayling, T.M., Bell, J.I., Lathrop, G.M. et al.(2001) A genomewide scan for loci predisposing to type 2 diabetes in aUK population (the Diabetes UK Warren 2 Repository): analysis of 573pedigrees provides independent replication of a susceptibility locus onchromosome 1q. Am. J. Hum. Genet., 69, 553–569.
63. Pajukanta, P., Nuotio, I., Terwilliger, J.D., Porkka, K.V., Ylitalo, K.,Pihlajamaki, J., Suomalainen, A.J., Syvanen, A.C., Lehtimaki, T.,Viikari, J.S. et al. (1998) Linkage of familial combined hyperlipidaemia tochromosome 1q21-q23. Nat. Genet., 18, 369–373.
64. Pajukanta, P., Allayee, H., Krass, K.L., Kuraishy, A., Soro, A., Lilja, H.E.,Mar, R., Taskinen, M.R., Nuotio, I., Laakso, M. et al. (2003) Combinedanalysis of genome scans of dutch and finnish families reveals asusceptibility locus for high-density lipoprotein cholesterol onchromosome 16q. Am. J. Hum. Genet., 72, 903–917.
65. Duggirala, R., Blangero, J., Almasy, L., Dyer, T.D., Williams, K.L.,Leach, R.J., O’Connell, P. and Stern, M.P. (1999) Linkage of type 2diabetes mellitus and of age at onset to a genetic location on chromosome10q in Mexican-Americans. Am. J. Hum. Genet., 64, 1127–1140.
1578 Human Molecular Genetics, 2006, Vol. 15, No. 10
by guest on June 9, 2013http://hm
g.oxfordjournals.org/D
ownloaded from

66. Hanson, R.L., Imperatore, G., Narayan, K.M., Roumain, J.,Fagot-Campagna, A., Pettitt, D.J., Bennett, P.H. and Knowler, W.C.(2001) Family and genetic studies of indices of insulin sensitivity andinsulin secretion in Pima Indians. Diab. Metab. Res. Rev., 17, 296–303.
67. Lindsay, R.S., Funahashi, T., Krakoff, J., Matsuzawa, Y., Tanaka, S.,Kobes, S., Bennett, P.H., Tataranni, P.A., Knowler, W.C. andHanson, R.L. (2003) Genome-wide linkage analysis of serum adiponectinin the Pima Indian population. Diabetes, 52, 2419–2425.
68. Pratley, R.E., Thompson, D.B., Prochazka, M., Baier, L., Mott, D.,Ravussin, E., Sakul, H., Ehm, M.G., Burns, D.K., Foroud, T. et al. (1998)An autosomal genomic scan for loci linked to prediabetic phenotypes inPima Indians. J. Clin. Invest., 101, 1757–1764.
69. Cianfarani, S., Martinez, C., Maiorana, A., Scire, G., Spadoni, G.L. andBoemi, S. (2004) Adiponectin levels are reduced in children born smallfor gestational age and are inversely related to postnatal catch-up growth.J. Clin. Endocrinol. Metab., 89, 1346–1351.
70. Lindsay, R.S., Kobes, S., Knowler, W.C. and Hanson, R.L. (2002)Genome-wide linkage analysis assessing parent-of-origin effects in theinheritance of birth weight. Hum. Genet., 110, 503–509.
71. Baker, J., Liu, J.P., Robertson, E.J. and Efstratiadis, A. (1993) Role ofinsulin-like growth factors in embryonic and postnatal growth. Cell, 75,73–82.
72. Liu, J.P., Baker, J., Perkins, A.S., Robertson, E.J. and Efstratiadis, A.(1993) Mice carrying null mutations of the genes encoding insulin-likegrowth factor I (Igf-1) and type 1 IGF receptor (Igf1r). Cell, 75, 59–72.
73. Tamemoto, H., Kadowaki, T., Tobe, K., Yagi, T., Sakura, H.,Hayakawa, T., Terauchi, Y., Ueki, K., Kaburagi, Y. and Satoh, S. (1994)Insulin resistance and growth retardation in mice lacking insulin receptorsubstrate-1. Nature, 372, 182–186.
74. Hattersley, A.T., Beards, F., Ballantyne, E., Appleton, M., Harvey, R. andEllard, S. (1998) Mutations in the glucokinase gene of the fetus result inreduced birth weight. Nat. Genet., 19, 268–270.
75. Wertheimer, E., Lu, S.P., Backeljauw, P.F., Davenport, M.L. andTaylor, S.I. (1993) Homozygous deletion of the human insulin receptorgene results in leprechaunism. Nat. Genet., 5, 71–73.
76. Dunger, D.B., Ong, K.K., Huxtable, S.J., Sherriff, A., Woods, K.A.,Ahmed, M.L., Golding, J., Pembrey, M.E., Ring, S., Bennett, S.T. andTodd, J.A. (1998) Association of the INS VNTR with size at birth.ALSPAC Study Team. Avon Longitudinal Study of Pregnancy andChildhood. Nat. Genet., 19, 98–100.
77. Ong, K.K., Phillips, D.I., Fall, C., Poulton, J., Bennett, S.T., Golding, J.,Todd, J.A. and Dunger, D.B. (1999) The insulin gene VNTR, type 2diabetes and birth weight. Nat. Genet., 21, 262–263.
78. Hunt, K.J., Lehman, D.M., Arya, R., Fowler, S., Leach, R.J., Goring, H.H.,Almasy, L., Blangero, J., Dyer, T.D., Duggirala, R. and Stern, M.P. (2005)Genome-wide linkage analyses of type 2 diabetes in Mexican-Americans:the San Antonio Family Diabetes/Gallbladder Study. Diabetes, 54,2655–2662.
79. MacCluer, J.W., Stern, M.P., Almasy, L., Atwood, L.A., Blangero, J.,Comuzzie, A.G., Dyke, B., Haffner, S.M., Henkel, R.D., Hixson, J.E.et al. (1999) Genetics of atherosclerosis risk factors inMexican-Americans. Nutr. Rev., 57, S59–S65.
80. Mitchell, B.D., Kammerer, C.M., Blangero, J., Mahaney, M.C.,Rainwater, D.L., Dyke, B., Hixson, J.E., Henkel, R.D., Sharp, R.M.,
Comuzzie, A.G. et al. (1996) Genetic and environmental contributions tocardiovascular risk factors in Mexican-Americans. The San AntonioFamily Heart Study. Circulation, 94, 2159–2170.
81. Almasy, L. and Blangero, J. (1998) Multipoint quantitative-trait linkageanalysis in general pedigrees. Am. J. Hum. Genet., 62, 1198–1211.
82. Amos, C.I. (1994) Robust variance-components approach for assessinggenetic linkage in pedigrees. Am. J. Hum. Genet., 54, 535–543.
83. Self, S.G. and Liang, K.-Y. (1987) Asymptotic properties of maximumlikelihood estimators and likelihood ratio tests under nonstandardconditions. Am. J. Stat. Assoc., 82, 605–610.
84. Boehnke, M. and Lange, K. (1984) Ascertainment and goodness of fit ofvariance component models for pedigree data. Prog. Clin. Biol. Res., 147,173–192.
85. Heath, S.C. (1997) Markov chain Monte Carlo segregation and linkageanalysis for oligogenic models. Am. J. Hum. Genet., 61, 748–760.
86. Roche, A.F. (1992) Growth, Maturation and Body Composition: The FelsLongitudinal Study 1929–1991., Cambridge University Press, Cambridge.
87. Almasy, L., Dyer, T.D. and Blangero, J. (1997) Bivariate quantitative traitlinkage analysis: pleiotropy versus co-incident linkages. Genet.Epidemiol., 14, 953–958.
88. Arya, R., Blangero, J., Williams, K., Almasy, L., Dyer, T.D., Leach, R.J.,O’Connell, P., Stern, M.P. and Duggirala, R. (2002) Factors of insulinresistance syndrome–related phenotypes are linked to genetic locations onchromosomes 6 and 7 in nondiabetic Mexican- Americans. Diabetes, 51,841–847.
89. Malacarne, M., Gennaro, E., Madia, F., Pozzi, S., Vacca, D., Barone, B.,dalla, B.B., Bianchi, A., Bonanni, P., De Marco, P. et al. (2001) Benignfamilial infantile convulsions: mapping of a novel locus on chromosome2q24 and evidence for genetic heterogeneity. Am. J. Hum. Genet., 68,1521–1526.
90. Yip, A.G., Ma, Q., Wilcox, M., Panhuysen, C.I., Farrell, J., Farrar, L.A.and Wyszynski, D.F. (2003) Search for genetic factors predisposing toatherogenic dyslipidemia. BMC Genet., 4 (Suppl. 1), S100.
91. Bailer, U., Leisch, F., Meszaros, K., Lenzinger, E., Willinger, U.,Strobl, R., Heiden, A., Gebhardt, C., Doge, E., Fuchs, K. et al. (2002)Genome scan for susceptibility loci for schizophrenia and bipolardisorder. Biol. Psychiat., 52, 40–52.
92. Rice, T., Rankinen, T., Chagnon, Y.C., Province, M.A., Perusse, L.,Leon, A.S., Skinner, J.S., Wilmore, J.H., Bouchard, C. and Rao, D.C.(2002) Genomewide linkage scan of resting blood pressure: HERITAGEFamily Study. Health, risk factors, exercise training, and genetics.Hypertension, 39, 1037–1043.
93. Gorlova, O.Y., Amos, C.I., Wang, N.W., Shete, S., Turner, S.T. andBoerwinkle, E. (2003) Genetic linkage and imprinting effects on bodymass index in children and young adults. Eur. J. Hum. Genet., 11,425–432.
94. Imperatore, G., Knowler, W.C., Pettitt, D.J., Kobes, S., Fuller, J.H.,Bennett, P.H. and Hanson, R.L. (2000) A locus influencing total serumcholesterol on chromosome 19p: results from an autosomal genomic scanof serum lipid concentrations in Pima Indians. Arterioscler. Thromb. Vasc.Biol., 20, 2651–2656.
95. Elbein, S.C. and Hasstedt, S.J. (2002) Quantitative trait linkage analysis oflipid-related traits in familial type 2 diabetes: evidence for linkage oftriglyceride levels to chromosome 19q. Diabetes, 51, 528–535.
Human Molecular Genetics, 2006, Vol. 15, No. 10 1579
by guest on June 9, 2013http://hm
g.oxfordjournals.org/D
ownloaded from
Copyright © 2022 FDOKUMEN