A polymorphism in the major gene regulating serum uric acid associates with clinic SBP and the...
8
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. A polymorphism in the major gene regulating serum uric acid associates with clinic SBP and the white-coat effect in a family-based study Francesca Mallamaci a,b , Alessandra Testa a , Daniela Leonardis a , Rocco Tripepi a , Anna Pisano a , Belinda Spoto a , Maria Cristina Sanguedolce a , Rosa Maria Parlongo a , Giovanni Tripepi a , and Carmine Zoccali a,b Objectives: Hyperuricemia associates with hypertension, but it is uncertain whether this relationship is causal in nature. Glucose transporter 9 (GLUT9) gene is a major genetic determinant of plasma uric acid levels in humans. Since polymorphisms are randomly distributed at mating (Mendelian randomization), studies based on GLUT9 polymorphisms may provide unconfounded assessment of the nature of the link between uric acid and hypertension. Methods: We tested the association between uric acid, the rs734555 polymorphism of the GLUT9 gene and arterial pressure in a family-based study including 449 individuals in a genetically homogenous population in Southern Italy. Results: Serum uric acid levels were strongly associated (P < 0.001) with all components of clinic and 24-h ambulatory blood pressures (BPs). However, only clinic SBP and the white-coat effect (the difference in clinic systolic and daytime systolic ambulatory blood pressure monitoring) associations remained significant after adjustment for classical risk factor and the estimated glomerular filtration rate. Serum uric acid was strongly associated with the risk allele (T) of the rs734555 polymorphism (P < 0.001). Furthermore, TT individuals showed higher clinic SBP (129 þ SEM 1 mmHg) than GT (125 þ 1 mmHg) and GG individuals (122 þ 3 mmHg), as well as a higher white-coat effect (P ¼ 0.02), confirming that the association between uric acid and these BP components is unconfounded by environmental risk factors. Conclusion: Results in this family-based study are compatible with the hypothesis that uric acid is a causal risk factor for hypertension. Trials testing uric acid-lowering interventions are needed to definitively establish the causal implication of hyperuricemia in human hypertension. Keywords: genetic analysis, GLUT9 gene, hypertension, uric acid Abbreviations: ABPM, ambulatory blood pressure monitoring; BP, blood pressure; eGFR, estimated glomerular filtration rate; GLUT9, glucose transporter 9; PRA, plasma renin activity; SNP, single-nucleotide polymorphism INTRODUCTION H yperuricemia is perhaps one of the very first risk factors which was suspected to be causally associ- ated to hypertension, but notwithstanding inten- sive past and recent clinical research (reviewed in ref. [1]), the issue remains highly controversial [2]. In general, the strong link between uric acid and blood pressure (BP) demonstrated in several observational studies is considered in large part, if not entirely, attributable to confounding by other major risk factors for hypertension [1]. Establishing whether high uric acid levels may cause hypertension is a question with major clinical and public health implications because the prevalence of hyperuricemia and gout has shown a steady rise over the past decades, and such an increase has paralleled the surge of hypertension, over- weight and obesity, diabetes and hyperlipidaemia [3]. The concentration of uric acid in plasma has an important genetic control. Because genes are transmitted randomly (Mendelian randomization), polymorphisms in the genes that control uric acid levels may therefore represent an instrumental variable to further explore the link between uric acid and hypertension in human studies [4]. In this respect, very large case-control studies in various ethnicities have already shown that polymorphisms in genes that determine prevailing serum uric acid levels associate with the risk for gout, but not for hypertension [5 – 7], supporting the view that the link between hyperuricemia and hyper- tension is attributable to confounding by risk factors associ- ated with hyperuricemia. However, combining a large number of heterogeneous populations in disparate, uncon- trolled settings may limit rather than enhance the power of association studies aimed at investigating the BP–uric acid Journal of Hypertension 2014, 32:1621–1628 a CNR-IBIM, Reggio Calabria and b Unita ` Operativa di Nefrologia, Ipertensione e Trapianto Renale Ospedali Riuniti, Reggio Calabria, Italy Correspondence to Professor Carmine Zoccali, CNR-IBIM & Divisione di Nefrologia e Dialisi, c/o euroline di barilla’ francesca, Via Vallone Petrara 55–57, 89124 Reggio Calabria, Italy. Tel: +39 0965 397010; fax: +39 0965 26879; e-mail: carmine.zoccali @tin.it Received 27 December 2013 Revised 26 March 2014 Accepted 26 March 2014 J Hypertens 32:1621–1628 ß 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. DOI:10.1097/HJH.0000000000000224 Journal of Hypertension www.jhypertension.com 1621 Original Article
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of A polymorphism in the major gene regulating serum uric acid associates with clinic SBP and the...

Original Article
Apolymorphism in themajor gene regulating serumuric acid associates with clinic SBPand thewhite-coateffect in a family-based study
Francesca Mallamacia,b, Alessandra Testaa, Daniela Leonardisa, Rocco Tripepia, Anna Pisanoa,Belinda Spotoa, Maria Cristina Sanguedolcea, Rosa Maria Parlongoa, Giovanni Tripepia, andCarmine Zoccalia,b
Journal of Hypertension 2014, 32:1621–1628aCNR-IBIM, Reggio Calabria and bUnita Operativa di Nefrologia, Ipertensione eTrapianto Renale Ospedali Riuniti, Reggio Calabria, Italy
Correspondence to Professor Carmine Zoccali, CNR-IBIM & Divisione di Nefrologia eDialisi, c/o euroline di barilla’ francesca, Via Vallone Petrara 55–57, 89124 ReggioCalabria, Italy. Tel: +39 0965 397010; fax: +39 0965 26879; e-mail: [email protected]
Received 27 December 2013 Revised 26 March 2014 Accepted 26 March 2014
J Hypertens 32:1621–1628 � 2014 Wolters Kluwer Health | Lippincott Williams &Wilkins.
Objectives: Hyperuricemia associates with hypertension,but it is uncertain whether this relationship is causal innature. Glucose transporter 9 (GLUT9) gene is a majorgenetic determinant of plasma uric acid levels in humans.Since polymorphisms are randomly distributed at mating(Mendelian randomization), studies based on GLUT9polymorphisms may provide unconfounded assessment ofthe nature of the link between uric acid and hypertension.
Methods: We tested the association between uric acid,the rs734555 polymorphism of the GLUT9 gene andarterial pressure in a family-based study including 449individuals in a genetically homogenous population inSouthern Italy.
Results: Serum uric acid levels were strongly associated(P<0.001) with all components of clinic and 24-hambulatory blood pressures (BPs). However, only clinic SBPand the white-coat effect (the difference in clinic systolicand daytime systolic ambulatory blood pressuremonitoring) associations remained significant afteradjustment for classical risk factor and the estimatedglomerular filtration rate. Serum uric acid was stronglyassociated with the risk allele (T) of the rs734555polymorphism (P<0.001). Furthermore, TT individualsshowed higher clinic SBP (129þ SEM 1 mmHg) than GT(125þ1 mmHg) and GG individuals (122þ 3 mmHg), aswell as a higher white-coat effect (P¼ 0.02), confirmingthat the association between uric acid and these BPcomponents is unconfounded by environmental riskfactors.
Conclusion: Results in this family-based study arecompatible with the hypothesis that uric acid is a causalrisk factor for hypertension. Trials testing uric acid-loweringinterventions are needed to definitively establish the causalimplication of hyperuricemia in human hypertension.
Keywords: genetic analysis, GLUT9 gene, hypertension,uric acid
Abbreviations: ABPM, ambulatory blood pressuremonitoring; BP, blood pressure; eGFR, estimatedglomerular filtration rate; GLUT9, glucose transporter 9;PRA, plasma renin activity; SNP, single-nucleotidepolymorphism
Copyright © Lippincott Williams & Wilkins. UnauthJournal of Hypertension
INTRODUCTION
Hyperuricemia is perhaps one of the very first riskfactors which was suspected to be causally associ-ated to hypertension, but notwithstanding inten-
sive past and recent clinical research (reviewed in ref. [1]),the issue remains highly controversial [2]. In general, thestrong link between uric acid and blood pressure (BP)demonstrated in several observational studies is consideredin large part, if not entirely, attributable to confounding byother major risk factors for hypertension [1]. Establishingwhether high uric acid levels may cause hypertension is aquestion with major clinical and public health implicationsbecause the prevalence of hyperuricemia and gout hasshown a steady rise over the past decades, and such anincrease has paralleled the surge of hypertension, over-weight and obesity, diabetes and hyperlipidaemia [3]. Theconcentration of uric acid in plasma has an importantgenetic control. Because genes are transmitted randomly(Mendelian randomization), polymorphisms in the genesthat control uric acid levels may therefore represent aninstrumental variable to further explore the link betweenuric acid and hypertension in human studies [4]. In thisrespect, very large case-control studies in various ethnicitieshave already shown that polymorphisms in genes thatdetermine prevailing serum uric acid levels associate withthe risk for gout, but not for hypertension [5–7], supportingthe view that the link between hyperuricemia and hyper-tension is attributable to confounding by risk factors associ-ated with hyperuricemia. However, combining a largenumber of heterogeneous populations in disparate, uncon-trolled settings may limit rather than enhance the power ofassociation studies aimed at investigating the BP–uric acid
orized reproduction of this article is prohibited.
DOI:10.1097/HJH.0000000000000224
www.jhypertension.com 1621

Mallamaci et al.
link. Studies based on families in homogenous popu-lations may provide important information about geneticassociations because these communities are also morehomogeneous for exposure to environmental factors [8].In this respect, it is worth noting that in the sole family-based study, a survey in the Amish community [9], lookingat the association between uric acid and BP in a researchsetting applying 24-h ambulatory blood pressure monitor-ing (24ABPM) and fixed sodium intake, a polymorphismin the glucose transporter 9 (GLUT9) transporter geneassociated strongly with BP. Confirmation of the uricacid–BP association in a family-based study in a differentcommunity is important to test the relevance of thisgenetic link revealed by seminal observations in theAmish population. With this background in mind, wehave therefore attempted to replicate findings in thiscommunity by investigating the association between uricacid levels and the rs734553 polymorphism in the GLUT9gene – that is, the strongest genetic determinant of uricacid levels in a large meta-analysis [10], with clinic BP and24ABPM in a cardiovascular complication-free populationin Southern Italy characterized by a homogeneous geneticbackground [11] and shared nutritional habits [12] whichwas recruited in the framework of a national projectaimed at studying the genetic factors in human hyperten-sion [13].
METHODS
Study protocolThe protocol was in conformity with the ethical guidelinesof our institution and informed consent was obtained byeach participant.
Study populationWe enrolled 459 cardiovascular complication-free indivi-duals who participated in a health screening offered to 107families in the Reggio Calabria Province. This screeningwas undertaken as a part of a national project promotedand supported by the Italian Society of Hypertension toinvestigate genetic factors of human hypertension [13].These families were part of a Southern Italian population,that is a population with shared genetic background [11]and nutritional habits characterized by relatively highintakes of vitamin E and monounsaturated fatty acids[12]. The diagnosis of primary hypertension was basedon the diagnostic protocol routinely applied at our hyper-tension centre, which includes routine biochemical tests,the measurement of 24-h catecholamines, supine and erectplasma renin activity (PRA) and plasma aldosterone,captopril renography and/or digital subtraction angio-graphy and eco-colour Doppler of renal arteries.
Standardized blood pressure in the clinic and24-h ambulatory blood pressure monitoringIn each individual, somatometric and BP measurementswere assessed in the day of the study. Measurements in theclinic were standardized and taken bias-free by the ambu-latory BP monitor. These measurements were made after a10–20-min period of quiet resting in a semi-recumbentposition after which BP was measured three times with
Copyright © Lippincott Williams & Wilkins. Unaut1622 www.jhypertension.com
an interval of 1–2 min, and the average of these threemeasurements was recorded. Twenty-four-hour ABPM wasperformed by using a device conforming to the Associationfor the Advancement of Medical Instrumentation recom-mendations (Spacelabs 90207, Redmond, Washington,USA). All 24ABPM recordings were carried out every15min both during the day (0700–2200 h) and duringthe night (2200–0700 h). Patients were instructed to main-tain their usual level of activity. Twenty-four-hour ABPMdata were stored on personal computers. BP readings wereprinted out for direct inspection and edited according torecommendations of the European Society of Hypertension[14]. The difference between clinic and daytime ABPMsystolic pressure was taken as a surrogate of the white-coat effect.
Laboratory measurementsA fasting blood sampling was undertaken and plasma wasstored at �808C until analysis. Serum uric acid, creatinine,lipids, albumin and haemoglobin were measured by stand-ard methods in the routine clinical laboratory. Estimatedglomerular filtration rate (eGFR) was calculated by usingthe four-variable Modification of Diet in Renal Diseasestudy equation [15].
Genotyping analysisGenomic DNA was extracted from peripheral bloodleucocytes by the standard salting-out technique. Theparticipants were genotyped for the rs734553 GLUT9 poly-morphism (SLC2A9). This polymorphism was studied by avalidated TaqMan single-nucleotide polymorphism (SNP)genotyping assay. SNP genotyping was performed by ABIPRISM 7900HT according to the manufacturer’s recommen-dations (Life Technologies, Carlsbad, California, USA). Theassays mix (including unlabeled PCR primers, FAM and VICdye-labelled TaqMan MGB probes) was designed by LifeTechnologies. The reaction system contained 1–5 ng ofgenomic DNA, 12.5 ml of TaqMan Universal PCR MasterMix, 2�No AmpErase UNG, 1.25 ml 40� assay mix and wasadjusted with H2O for a total volume of 25 ml. Alleles werescored using the allelic discrimination software SequenceDetection System v2.2 (Life Technologies). A random 5% ofsamples were independently repeated to confirm genotyp-ing results. The genotype results for these samples werecompletely consistent.
Study power and statistical analysisIn a previous study including never-treated patients withuncomplicated essential hypertension, all resident in thesame geographical area of the study population (Calabriaregion), the SD of 24-h SBP was reported to be 8mmHg [16].We hypothesized theBP increase portended by TT genotype(as compared to GG genotype) be higher than the spon-taneous variability of 24-h SBP (i.e. >8mmHg). Because ofthe presence in our study population of normotensive indi-viduals (a condition which could increase the variability ofthe hypothesized effect) and by considering a TT/GGpatients ratio of 6 in our study sample, we assumed theSD of the hypothesized effect be two times higher than thescheduled point estimate (i.e. 8� 16mmHg). By adoptingthis conservative approach, we calculated that a sample size
horized reproduction of this article is prohibited.Volume 32 � Number 8 � August 2014

Glucose transporter 9 polymorphism and SBP
of at least 400 individualswould have an 80%power todetectas significant (a error¼ 0.01) the hypothesized difference in24-h SBP between TT and GG individuals.
Normally distributed data are summarized as mean� SEM (standard error) and non-normally distributed dataas median and inter-quartile range. Comparisons amonggroups were made by P for linear trend. The associationbetween continuous variables considered simultaneouslywas analysed by the Pearson product moment correlationcoefficient (r) and P value. The genotypic distributionswere investigated by testing the Hardy–Weinberg equi-librium. In multivariate models (with BP components asdependent variables), we included uric acid as well as aseries of potential confounders, that is age, sex, diabetes,waist circumference, low-density lipoprotein (LDL) choles-terol, triglycerides and eGFR, as well as the use of thiazidesand the alcohol habit. By this strategy, we constructedmodels of adequate statistical power (at least 50 patientsfor each variable into the model). The relationship betweenBP and uric acid levels as derived by multiple regressionmodels was shown graphically by plotting individual uricacid level (as adjusted for potential confounders) and all BPcomponents, and the strength of these associations wasexpressed as standardized regression coefficients (b) and Pvalue. All calculations were done using a standard statisticalpackage (SPSS for Windows Version 9.0.1, 1999; Chicago,Illinois, USA).
RESULTSAmong 449 individuals in 107 siblings, 195 individuals werehypertensive (43%) and the remaining 254 (57%) werenormotensive. No individual had suffered myocardial
Copyright © Lippincott Williams & Wilkins. Unauth
rs73GG G
GG GT TT
6.0
5.0
4.0
3.0
Uric acid(mg/dl)
Uric acid(mg/dl)
P =
P = 8x10-5
Whole stud
6.0
5.0
4.0
3.0
Normotensives
rs734553
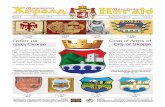
FIGURE 1 Association between uric acid levels and SLC2A9 polymorphism in the wholeare mean� SEM.
Journal of Hypertension
infarction or stroke, or presented symptoms of coronaryheart disease or peripheral artery disease at the time of thestudy. One hundred and forty-five patients were treatedwith various antihypertensive drugs (32%), includingangiotensin-converting enzyme inhibitors or angiotensinII blockers (n¼ 89; 20%), calcium antagonists (n¼ 62;14%), sympathetic blockers (n¼ 44; 10%), thiazides(n¼ 32; 7%) and vasodilators (n¼ 4; 1%). GFR was onaverage (98� 1ml/min per 1.73 m2) and was below60ml/min per 1.73 m2 only in 10 individuals (2%). Albu-minuria was on average 19 mg/24 h. and the majority (86%)had albuminuria below 20mg/24 h. The prevalence rates ofdiabetic patients and smokers were 6 and 22%, respectively.Twenty-four-hour urinary sodium in this population was178� 75mmol/day.
Uric acid and the rs734553 polymorphismAlleles in the rs734553 polymorphism were in Hardy–Weinberg equilibrium (GG: 8%; GT: 44%; TT: 48%,x2¼ 1.5, P¼ 0.22). Serum uric acid levels co-segregatedwith the T allele (risk allele) of SLC2A9 polymorphism(Fig. 1, upper panel) specifically confirming in our popu-lation that this polymorphism is strongly associated withprevailing uric acid levels. Separate analyses in normoten-sive and hypertensive individuals fully confirmed the con-sistency of this association (Fig. 1, bottom panels).
Association of uric acid levels withstandardized clinic blood pressure andambulatory blood pressure monitoringSerum uric acid was directly related with both clinic (Fig. 2,left panels) and 24-h ambulatory SBP and DBP (Fig. 3, left
orized reproduction of this article is prohibited.
4553T TT
GG GT TT
8x10-6
P = 3x10-3
y population
6.0
5.0
4.0
3.0
Hypertensives
rs734553
study population and separately in normotensive and hypertensive individuals. Data
www.jhypertension.com 1623

200r = 0.34, P < 0.001
180
160
140
120
Sta
ndar
dize
d c
linic
SB
P (
mm
Hg
)100
80
600 2 4
Uric acid (mg/dl)
Unadjusted
6 8 10
r = 0.31, P < 0.001120
110
100
90
Sta
ndar
dize
d c
linic
DB
P (
mm
Hg
)
80
70
60
5040
0 2 4
Uric acid (mg/dl)6 8 10
β = 0.03, P = 0.62120
110
100
90
Sta
ndar
dize
d c
linic
DB
P (
mm
Hg
)
80
70
60
5040
0 2 4
Uric acid (mg/dl)6 8 10
200β = 0.14, P = 0.01
180
160
140
120
Sta
ndar
dize
d c
linic
SB
P (
mm
Hg
)
100
80
600 2 4
Uric acid (mg/dl)
Adjusted
6 8 10
FIGURE 2 Unadjusted (left panels) and adjusted (right panels) relationships between uric acid levels and standardized clinic SBP and DBP. Data are expressed as Pearsonproduct moment correlation coefficients, standardized regression coefficients (beta) and P values. See also text for more details.
Mallamaci et al.
panels) and inversely with eGFR (r¼�0.38, P< 0.001),and similar associations existed with other traditionalrisk factors, including age (r¼ 0.30, P< 0.001), male sex(point bi-serial correlation coefficient¼ 0.57, P< 0.001),
Copyright © Lippincott Williams & Wilkins. Unaut
160 r = 0.31, P < 0.001
Unadjusted
24h
DB
P (
mm
Hg
)24
h D
BP
(m
mH
g)
Wh
ite-
coat
eff
ect (
mm
Hg
)(D
ayti
me
SB
P-c
linic
SB
P)
150
140
130
120
110
100
900 2 4
Uric acid (mg/dl)6 8 10
r = 0.21, P < 0.001
0 2 4Uric acid (mg/dl)
6 8 10
r = 0.14, P < 0.009
0 2 4Uric acid (mg/dl)
6 8 10
110
100
90
80
70
60
50
80
60
40
20
–20
–40
0
FIGURE 3 Unadjusted (left panels) and adjusted (right panels) relationships betweenSBP� clinic BP). Data are expressed as Pearson product moment correlation coefficients,details.
1624 www.jhypertension.com
antihypertensive treatment (point bi-serial correlationcoefficient¼ 0.30, P< 0.001), BMI (r¼ 0.27, P< 0.001),waist circumference (r¼ 0.46, P< 0.001), serum glucose(r¼ 0.16, P¼ 0.001), triglycerides (r¼ 0.35, P< 0.001),
horized reproduction of this article is prohibited.
160 β = 0.02, P = 0.78
β = 0.06, P = 0.35
β = 0.14, P = 0.02
Adjusted
24h
DB
P (
mm
Hg
) 150
140
130
120
110
100
900 2 4
Uric acid (mg/dl)6 8 10
Wh
ite-
coat
eff
ect (
mm
Hg
)(D
ayti
me
SB
P-c
linic
SB
P)
0 2 4Uric acid (mg/dl)
6 8 10
80
60
40
20
–20
–40
0
24h
DB
P (
mm
Hg
)
0 2 4Uric acid (mg/dl)
6 8 10
110
100
90
80
70
60
50
uric acid levels, 24-h SBP and DBP and white-coat effect (calculated as daytimestandardized regression coefficients (beta) and P values. See also text for more
Volume 32 � Number 8 � August 2014

Glucose transporter 9 polymorphism and SBP
high-density lipoprotein (HDL) (r¼�0.27, P< 0.001) andLDL cholesterol (r¼ 0.15, P¼ 0.005). These multiple associ-ations of uric acid with traditional risk factors warnedagainst cause-and-effect interpretation of the associationof uric acid with BP because these and other unknownassociations may confound the interpretation of theBP–uric acid relationship. Indeed, in analyses adjustingfor potential confounders (age, sex, diabetes, waist circum-ference, LDL cholesterol, triglycerides and eGFR), as well asfor the use of thiazides and the alcohol habit, the associ-ation of uric acid with 24-h SBP and DBP (Fig. 3, rightpanels), as well as with all components of 24 ABPM (day-time and night-time BPs values) lost statistical strength andbecame largely non-significant (b ranging from �0.06 to0.02, P ranging from 0.32 to 0.91). However, the uric acid–clinic SBP link (b¼ 0.14, P¼ 0.01) remained significant alsoafter data adjustment for the same variables (Fig. 2, rightpanels). A sensitivity analysis carried out by excludingpatients assuming diuretics (n¼ 32) provided almost iden-tical results (b¼ 0.12, P¼ 0.02).
The association of uric acid levels with clinic systolic butnot with daytime or 24ABPM systolic pressure implied anunderlying relationship with the white-coat effect. In linewith this hypothesis, the clinic–daytime SBP difference (ametric of the white-coat effect) associated directly withserum uric acid (r¼ 0.14, P¼ 0.009) (Fig. 3, left panel)and such an association remained substantially unmodifiedin an analysis adjusting for all potential confounders listedabove (b¼ 0.14, P¼ 0.02) (Fig. 3, right panel). The relation-ship between uric acid levels and clinic–daytime SBP
Copyright © Lippincott Williams & Wilkins. Unauth
TABLE 1. Clinical and biochemical data in the study population
GG (n¼34)
Age (years) 45�3
Men (%) 38%
Diabetes (%) 3%
Smokers (%) 24%
Alcohol users (%) 12%
BMI (kg/m2) 27.5�1.1
Waist circumference (cm) 89�3
On antihypertensive treatment (%) 39%
On diuretics (%) 18%
Glucose (mg/dl) 92�3
Triglycerides (mg/dl) 78 (48–104)
HDL cholesterol (mg/dl) 48�3
LDL cholesterol (mg/dl) 102�7
CRP (mg/l) 3.2 (1.6–3.8)
eGFR MDRD186 (ml/min per 1.73 m2) 95�4
Microalbuminuria (mg/24 h) 11.9 (9.3–18.6)
Standardized clinic SBP (mmHg) 122�3
Standardized clinic DBP (mmHg) 78�2
24-h SBP (mmHg) 120�2
24-h DBP (mmHg) 74�2
Daytime SBP (mmHg) 124�3
Daytime DBP (mmHg) 78�2
White-coat SBP (mmHg) 0.6�2.5
Night-time SBP (mmHg) 112�2
Night-time DBP (mmHg) 67�2
Data are expressed as mean� SE, median (inter-quartile range) or as percentage frequency, asglucose transporter 9; HDL, high-density lipoprotein; LDL, low-density lipoprotein; MDRD, Modi�P¼0.02.��P¼0.01.
Journal of Hypertension
difference held true also in an analysis restricted to patientsnot assuming diuretics (crude relationship: r¼ 0.12,P¼ 0.02; adjusted relationship: b¼ 0.12, P< 0.05).
Association of SLC2A9 with standardized clinicblood pressure and 24-hour ambulatory bloodpressure monitoringIn line with the Mendelian randomization principle,risk factors appeared to be randomly distributed acrossrs734553 genotypes. The proportion of diabetics, LDLcholesterol, and waist circumference tended to be higherin patients with TT genotype than in those with GT andGG genotypes, but these differences failed to reach formalstatistical significance (Table 1). Age and the proportionof patients on antihypertensive treatment and the GFRhad an erratic trend across genotypes (Table 1). Nosignificant differences were found among the threegenotypes as for the remaining demographic and clinicalcharacteristics, as well as for the use of thiazides and thealcohol habit.
Patients having the TT genotype had a higher clinic SBP(Fig. 4, upper panel) when compared to those with GTand GG genotypes (see also Table 1), and this was alsotrue after the exclusion of patients treated by diuretics(n¼ 32) from the analysis (GG patients, SBP:122� 18mmHg; GT: 125� 18mmHg; TT: 128� 19mmHg,P¼ 0.05). In contrast, 24-h night-time and daytime systolicand diastolic ABPM were very similar across GG, GT andTT individuals (Table 1), again implying that this linkmay underlie a relationship between the same risk allele
orized reproduction of this article is prohibited.
GLUT9 polymorphism
GT (n¼198) TT (n¼217)
39�1 44�1
51% 43%
4% 9%
24% 20%
22% 23%
27.2�0.4 28.0�0.4
89�1 91�1
25% 39%
3% 9%
94�2 97�2
82 (56–115) 84 (60–114)
48�1 47�1
106�3 112�2
2.0 (0.9–3.3) 2.2 (1.2–3.3)
102�1 94�1
9.4 (5.7–15.4) 9.0 (5.9–15.6)
125�1 129�1�
82�1 82�1
121�1 121�1
74�1 72�1
126�1 125�1
78�1 77�1
�0.8�1.1 3.9�1.1��
114�1 113�1
67�1 66�1
appropriate. CRP, C reactive protein; eGFR, estimated glomerular filtration rate; GLUT9,fication of Diet in Renal Disease.
www.jhypertension.com 1625

P = 0.02
P = 0.01
Standardized clinicSBP (mmHg)
White-coateffect (mmHg)
6
3
0
–3
140
130
120
110
rs734553
GG GT TT
rs734553
GG GT TT
FIGURE 4 Association between the rs734553 polymorphism in the GLUT9 gene,standardized clinic SBP and white-coat effect. Data are mean� SEM. GLUT9,glucose transporter 9.
Mallamaci et al.
with the white-coat effect. Indeed, clinic SBP�daytime SBPdifference was minimal in GG and GT heterozygote indi-viduals and maximal in TT homozygote individuals (Fig. 4,bottom panel), and again an analysis excluding patientsassuming diuretics provided identical results (GG patients,clinic SBP�daytime SBP difference: �1� 11mmHg; GT:�0.9� 15mmHg; TT: 4� 15mmHg, P¼ 0.005). Data adjust-ment for the use of thiazides (clinic SBP: P¼ 0.02; white-coateffect: P¼ 0.007) and other antihypertensive drugs (clinicSBP: P ranging from 0.008 to 0.031; white-coat effect: Pranging from 0.003 to 0.017), as well as adjustment for24-h urine sodium excretion (clinic SBP: P¼ 0.02; white-coateffect: P¼ 0.008) and alcohol habit (clinic SBP: P¼ 0.02;white-coat effect: P¼ 0.01) did not materially change thestrength of these associations. Accordingly, there was noeffect modification by diuretics or alcohol habit on therelationship between uric acid levels (P¼ 0.50 andP¼ 0.69) or the genetic polymorphism rs734553 (P¼ 0.34
Copyright © Lippincott Williams & Wilkins. Unaut1626 www.jhypertension.com
and P¼ 0.44) with SBP (clinic), indicating that the SBP–uricacid (or rs734553polymorphism) links are largely unaffectedby these factors.
DISCUSSIONIn this study, in a population with a homogeneous geneticbackground and shared nutritional habits, serum uric acidlevels and the T allele of the rs734553 polymorphism in thegene encoding the GLUT9 transporter, a genetic polymor-phism predisposing to hyperuricemia, were independentlyassociated with clinic SBP as well as with the white-coateffect.
Whether hyperuricemia is a causal risk factor for hyper-tension is a long-standing, controversial issue in cardiovas-cular medicine. Observational studies of various designsincluding cross-sectional, follow-up and longitudinal stud-ies in the young and middle-aged populations have almostinvariably documented an association between high uricacid levels and the risk for hypertension (reviewed in [1]).Such a link was once again confirmed in a very recent,population-based study in middle-aged individuals byCicero et al. [17]. Other observational studies, particularlystudies in elderly populations negated that the uric acid–BPlink, are causal in nature and attributed the apparentassociation between hypertension and hyperuricemia toconfounding by classical risk factors including abdominalobesity, dyslipidaemia and diabetes. The randomizedclinical trial is the undisputable standard for establishingcausality in clinical medicine, and the issue whether uricacid is a cause of hypertension can only be solved by a wellpowered double-blinded, randomized study testing theeffect of an uric acid-lowering intervention in hypertensivepatients. In this respect, uncontrolled or quasi experimentaltrials in children and in young individuals would supportthe tenet that hyperuricemia per se is a hypertension trigger(reviewed in ref. (1)]. However, these studies were eithersmall or methodologically suboptimal to form the basis fortreatment recommendations and the need of performingsuch a large trial in adults is perceived as a public healthpriority in the quest to prevent hypertension by interveningon this metabolic risk factor. Genetic variations in theenzyme that regulates the synthesis of uric acid havealready been associated to hypertension, atherosclerosisand chronic kidney disease in a community study in Japan[18].
Uric acid is mainly excreted by renal route (70%). GLUT9is a major urate transporter [19,20] whose correspondinggene is located in chromosome 4. Loss-of-functionmutations in this gene determine marked hypouricemiain vivo in humans [21]. On the contrary, various GLUT9polymorphisms have been linked with hyperuricemia inhumans and the T allele of the rs734553 polymorphismemerged as the genetic variant most strongly and consist-ently associated with hyperuricemia (P¼ 10–201) in a largemeta-analysis including over 28 000 participants encom-passing individuals in the general population and patientswith hypertension and metabolic syndrome [10]. Becausetransmission of the rs734553 allele responsible for hyper-uricemia (the T allele) occurs randomly at gamete formation(Mendelian randomization), this genetic marker may be
horized reproduction of this article is prohibited.Volume 32 � Number 8 � August 2014

Glucose transporter 9 polymorphism and SBP
useful for testing the hypothesis that hyperuricemia iscausally implicated in hypertension. Like in the abovementioned meta-analysis [10], in our family-based study[12], the T allele of GLUT9 gene was strongly and dose-dependently associated with serum acid levels. Whereasthe link of such an allele with uric acid levels is very robustacross populations [10] and in our study as well, the precisemechanism whereby it interferes with the renal handling ofurate has not been established as yet. This SNP mayunderlie a gain of function in urate transport, favouringtubular re-absorption of this anion or this polymorphism initself may not be the cause of hyperuricemia, but simply amarker of an effect on serum uric acid levels mediated byanother gene in linkage disequilibrium with the rs734553polymorphism. Nonetheless, from a methodological pointof view [4], it is legitimate using this genetic marker as anunbiased surrogate of life-time exposure to uric acid.
The hypothesis that uric acid is a causal risk factor forhypertension emerged in a study that tested another poly-morphism in the GLUT 9 gene in the Amish community [9].Given the peculiarity of genetic studies in homogenouspopulation, the issue of confirming observations in theAmish community is of obvious scientific relevance.
In line with some previous observational studies, wefound that the association of uric acid with DBP (Fig. 2) and24ABPM systolic and diastolic pressure (Fig. 3) was largelyconfounded by traditional risk factors, whereas the inde-pendent link between clinic BP and the white-coat effectand uric acid remained significant. Yet, the possibilityremains that these associations be an expression of residualconfounding, that is, confounding by variables not con-sidered in the analysis and/or because confoundingvariables were not measured with sufficient precision.However, exactly the same BP components – clinic SBPand the systolic white-coat effect – remained significantlyassociated with the risk allele for hyperuricemia in thers734553 polymorphism of the gene encoding GLUT9 trans-porter. As opposed to the easily confoundable associationbetween uric acid and BP, the association between thegenetic marker of hyperuricemia and BP is environmentallyunconfounded. Indeed, as expected from Mendelianrandomization, the rs734553 polymorphism was not associ-ated with Framingham risk factors, BMI and waist circum-ference, and other potential confounders. These findingssupport the interpretation that the independent link of SBPand the white-coat effect with uric acid levels underlies atrue causal association. The white-coat effect measure-ments applied in this study is an inherently imperfectmeasure of the true white-coat effect [22]. However, thissurrogate associates with organ damage and current guide-lines recommend to consider drug treatment in addition tolifestyle changes in white-coat hypertensive patients with ahigher cardiovascular risk because of metabolic derange-ments or asymptomatic organ damage [23]. The white-coatresponse accompanying BP measurement in the clinicunderlies increased sympathetic nerve activity in the skinand inhibition of sympathetic outflow to the skeletal muscle[24]. Rats made hyperuricemic by oxonic acid (an uricaseinhibitor) exhibit an amplified BP response to stressfulenvironmental stimuli like changes in salt intake [24] andsuch an amplification is prevented by lowering the uric acid
Copyright © Lippincott Williams & Wilkins. UnauthJournal of Hypertension
levels with allopurinol (a xanthine oxidase inhibitor) orwith benziodarone (an uricosuric agent) [25]. The white-coat effect is common in a syndrome characterized byhyperuricemia like the metabolic syndrome [26,27] andpatients with this syndrome display high sympatheticactivity [28] and are frequently salt-sensitive [29]. Further-more, both high uric acid levels and high norepinephrinepredict future hypertension in young, non-obese, normo-tensive men [30].
Some limitations of our study deserve comment. Thesample size of our study was limited to 449 participants.However, our family-based study was precisely set toconfirm observations in a previous study in a homogenouscommunity like the Amish population, and the powercalculation was based on available information on clinicand 24ABPM in the population of our region. Furthermore,we specifically confirmed in our population the consistentstrong linear association of the rs734553 GLUT9 SNPswith uric acid levels previously established across numer-ous cohorts and ethnicities [10]. We believe that findingsin the study in the Amish community and our confirmatorystudy in a genetically homogenous population in SouthernItaly support the contention that the uric-hypertensionlink is causal in nature. Well powered clinical trials testingthe effect uric acid lowering interventions for preventingand treating hypertension at an early phase of the hyper-tensive process [31] are needed to definitely test thehypothesis that the relationships we described underliesa causal link.
ACKNOWLEDGEMENTSFilippo Catalano helped with data management and AngelaMafrica provided valuable nursing assistance during theperformance of this study.
Funding: The study was supported by grants of theNational Research Council of Italy (CNR) and RegioneCalabria, Department of Health.
Conflicts of interestThere are no conflicts of interest.
REFERENCES1. Feig DI. Hyperuricemia and hypertension. Adv Chronic Kidney Dis
2012; 19:377–385.2. Johnson RJ, Sanchez-Lozada LG, Mazzali M, Feig DI, Kanbay M, Sautin
YY. What are the key arguments against uric acid as a true risk factor forhypertension? Hypertension 2013; 61:948–951.
3. Zhu Y, Pandya BJ, Choi HK. Prevalence of gout and hyperuricemia inthe US general population: the National Health and Nutrition Exam-ination Survey 2007–2008. Arthritis Rheum 2011; 63:3136–3141.
4. Smith GD, Ebrahim S. Mendelian randomization: prospects, potentials,and limitations. Int J Epidemiol 2004; 33:30–42.
5. Caulfield MJ, Munroe PB, O’Neill D, Witkowska K, Charchar FJ,Doblado M, et al. SLC2A9 is a high-capacity urate transporter inhumans. PLoS Med 2008; 5:e197.
6. Yang Q, Kottgen A, Dehghan A, Smith AV, Glazer NL, Chen MH, et al.Multiple genetic loci influence serum urate levels and their relationshipwith gout and cardiovascular disease risk factors. Circ CardiovascGenet 2010; 3:523–530.
7. Kottgen A, Albrecht E, Teumer A, Vitart V, Krumsiek J, Hundertmark C,et al. Genome-wide association analyses identify 18 new loci associ-ated with serum urate concentrations. Nat Genet 2013; 45:145–154.
8. Benyamin B, Visscher PM, McRae AF. Family-based genome-wideassociation studies. Pharmacogenomics 2009; 10:181–190.
orized reproduction of this article is prohibited.www.jhypertension.com 1627

Mallamaci et al.
9. Parsa A, Brown E, Weir MR, Fink JC, Shuldiner AR, Mitchell BD, et al.Genotype-based changes in serum uric acid affect blood pressure.Kidney Int 2012; 81:502–507.
10. Kolz M, Johnson T, Sanna S, Teumer A, Vitart V, Perola M, et al. Meta-analysis of 28,141 individuals identifies common variants within fivenew loci that influence uric acid concentrations. PLoS Genet 2009;5:e1000504.
11. Di Gaetano C, Voglino F, Guarrera S, Fiorito G, Rosa F, Di Blasio AM,et al. An overview of the genetic structure within the Italian populationfrom genome-wide data. PLoS One 2012; 7:e43759.
12. Freisling H, Fahey MT, Moskal A, Ocke MC, Ferrari P, Jenab M, et al.Region-specific nutrient intake patterns exhibit a geographical gradientwithin and between European countries. J Nutr 2010; 140:1280–1286.
13. Castellano M, Glorioso N, Cusi D, Sarzani R, Fabris B, Opocher G, et al.Genetic polymorphism of the renin-angiotensin-aldosterone systemand arterial hypertension in the Italian population: the GENIPERProject. J Hypertens 2003; 21:1853–1860.
14. O’Brien E, Asmar R, Beilin L, Imai Y, Mallion JM, Mancia G, et al.European Society of Hypertension recommendations for conventional,ambulatory and home blood pressure measurement. J Hypertens 2003;21:821–848.
15. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A moreaccurate method to estimate glomerular filtration rate from serumcreatinine: a new prediction equation. Modification of Diet in RenalDisease Study Group. Ann Intern Med 1999; 130:461–470.
16. Perticone F, Maio R, Tripepi G, Sciacqua A, Mallamaci F, Zoccali C.Microalbuminuria, endothelial dysfunction and inflammation inprimary hypertension. J Nephrol 2007; 20 (Suppl 12):s56–s62.
17. Cicero AF, Salvi P, D’Addato S, Rosticci M, Borghi C, Brisighella HeartStudy group. Association between serum uric acid, hypertension,vascular stiffness and subclinical atherosclerosis: data from theBrisighella Heart Study. J Hypertens 2014; 32:57–64.
18. Yang J, Kamide K, Kokubo Y, Takiuchi S, Horio T, Matayoshi T, et al.Association of hypertension and its complications with variations of thexanthine dehydrogenase gene. Hypertens Res 2008; 31:931–940.
19. Sakurai H. Urate transporters in the genomic era. Curr Opin NephrolHypertens 2013; 22:545–550.
Copyright © Lippincott Williams & Wilkins. Unaut1628 www.jhypertension.com
20. Bobulescu IA, Moe OW. Renal transport of uric acid: evolving conceptsand uncertainties. Adv Chronic Kidney Dis 2012; 19:358–371.
21. Matsuo H, Chiba T, Nagamori S, Nakayama A, Domoto H, Phetdee K,et al. Mutations in glucose transporter 9 gene SLC2A9 cause renalhypouricemia. Am J Hum Genet 2008; 83:744–751.
22. Parati G, Mancia G. Assessing the white-coat effect: which bloodpressure measurement should be considered? J Hypertens 2006;24:29–31.
23. Mancia G, Fagard R, Narkiewicz K, Redan J, Zanchetti A, Bohm M, et al.2013 Practice guidelines for the management of arterial hypertension ofthe European Society of Hypertension (ESH) and the European Societyof Cardiology (ESC): ESH/ESC Task Force for the Management ofArterial Hypertension. J Hypertens 2013; 31:1925–1938.
24. Grassi G, Turri C, Vailati S, Dell’Oro R, Mancia G. Muscle and skinsympathetic nerve traffic during the ‘white-coat’ effect. Circulation1999; 100:222–225.
25. Mazzali M, Hughes J, Kim YG, Jefferson JA, Kang DH, Gordon KL, et al.Elevated uric acid increases blood pressure in the rat by a novel crystal-independent mechanism. Hypertension 2001; 38:1101–1106.
26. Muldoon MF. White-coat hypertension and carotid artery atherosclero-sis: a matching study. Arch Intern Med 2000; 160:1507–1512.
27. Afsar B. Comparison of demographic, clinical, and laboratoryparameters between patients with sustained normotension, white coathypertension, masked hypertension, and sustained hypertension.J Cardiol 2013; 61:222–621.
28. Grassi G. Sympathetic overdrive and cardiovascular risk in the meta-bolic syndrome. Hypertens Res 2006; 29:839–847.
29. Chen J, Gu D, Huang J, Rao DC, Jaquish CE, Hixson JE, et al., GenSaltCollaborative Research Group. Metabolic syndrome and salt sensitivityof blood pressure in nondiabetic people in China: a dietary interven-tion study. Lancet 2009; 373:829–835.
30. Masuo K, Kawaguchi H, Mikami H, Ogihara T, Tuck ML. Serum uric acidand plasma norepinephrine concentrations predict subsequent weightgain and blood pressure elevation. Hypertension 2003; 42:474–480.
31. Watanabe S, Kang DH, Feng L, Nakagawa T, Kanellis J, Lan H, et al. Uricacid, hominoid evolution, and the pathogenesis of salt-sensitivity.Hypertension 2002; 40:355–360.
Reviewers’ Summary Evaluations
Reviewer 1The strength of the paper is the demonstration that therelationship between serum uric acid and blood pressurecan be genetically determined and this might explain thesusceptibility to blood pressure increase at a young age. Inaddition, the manuscript excludes the possibility of somedegree of interference between serum uric acid, diuretictreatment and blood pressure control, thereby emphasizingthe primary role of genetic predisposition. The only weak-ness is the fact that the observation is limited to a singlepopulation and should be replicated on a larger basis, in a
different population of subjects and under different clinicalexpressions of the hypertensive disease.
Reviewer 2Strength: This study firstly demonstrated that the geneticinfluence of gene, GLUT9, related to uric acid metabolismmight affect blood pressure (BP) regulation. BP evaluationwas performed by both office and ambulatory measure-ments in this study.
Weaknesses: Study subjects are relatively few for thegenetic analysis. There are no mechanistic and basicresearch considerations for interpreting the results.
horized reproduction of this article is prohibited.Volume 32 � Number 8 � August 2014




















