
Inosine Pranobex Significantly Decreased the Case-Fatality ...

European Journal of Pharmacology 649 (2010) 376–381
Contents lists available at ScienceDirect
European Journal of Pharmacology
j ourna l homepage: www.e lsev ie r.com/ locate /e jphar
Immunopharmacology and Inflammation
Adenosine A2A receptors and uric acid mediate protective effects of inosine againstTNBS-induced colitis in rats
Reza Rahimian a, Gohar Fakhfouri b, Ali Daneshmand c, Hamed Mohammadi a, Arash Bahremand a,Mohammad Reza Rasouli a, Kazem Mousavizadeh d, Ahmad Reza Dehpour a,⁎a Department of Pharmacology, School of Medicine, Tehran University of Medical Sciences, Tehran, Iranb Department of Pharmacology, School of Medicine, Shahid Beheshti University of Medical Sciences, Tehran, Iranc Interdisciplinary Neuroscience Research Program (INRP), Tehran University of Medical Sciences, Tehran, Irand Department of Basic Sciences and Cellular and Molecular Research Center and Oncopathology research center, Iran University of Medical Sciences, Tehran, Iran
⁎ Corresponding author. Tel.: +98 21 8897 3652; faxE-mail address: [email protected] (A.R. Dehpour
0014-2999/$ – see front matter © 2010 Elsevier B.V. Adoi:10.1016/j.ejphar.2010.09.044
a b s t r a c t
a r t i c l e i n f oArticle history:Received 29 May 2010Received in revised form 28 August 2010Accepted 7 September 2010Available online 22 September 2010
Keywords:InosineUric acidAdenosine receptorInflammatory bowel disease
Inflammatory bowel disease comprises chronic recurrent inflammation of gastrointestinal tract. This studywas conducted to investigate inosine, a potent immunomodulator, in 2,4,6-trinitrobenzene sulphonic acid(TNBS)-induced chronic model of experimental colitis, and contribution of adenosine A2A receptors and themetabolite uric acid as possible underlying mechanisms. Experimental colitis was rendered in rats by a singlecolonic administration of 10 mg of TNBS. Inosine, potassium oxonate (a hepatic uricase inhibitor), SCH-442416 (a selective adenosine A2A receptor antagonist), inosine+potassium oxonate, or inosine+SCH-442416 were given twice daily for 7 successive days. At the end of experiment, macroscopic andhistopathologic scores, colonic malondialdehyde (MDA), Tumor Necrosis Factor-alpha (TNF-α) andInterleukin-1beta (IL-1β) levels, and myeloperoxidase (MPO) activity were assessed. Plasma uric acid levelwas measured throughout the experiment. Both macroscopic and histological features of colonic injury weremarkedly ameliorated by either inosine, oxonate or inosine+oxonate. Likewise, the elevated amounts ofMPO and MDA abated as well as those of TNF-α and IL-1β (Pb0.05). SCH-442416 partially reversed the effectof inosine on theses markers, while inosine+oxonate showed a higher degree of protection than eachtreatment alone (Pb .0.05). No significant difference was observed between TNBS and SCH-442416 groups.Uric acid levels were significantly higher in inosine or oxonate groups compared to control. Inosine+oxonateresulted in an even more elvelated uric acid level than each treatment alone (Pb0.05). Inosine elicits notableanti-inflammatory effects on TNBS-induced colitis in rats. Uric acid and adenosine A2A receptors contribute tothese salutary properties.
: +98 21 66402569.).
ll rights reserved.
© 2010 Elsevier B.V. All rights reserved.
1. Introduction
Ulcerative colitis and Crohn's disease, collectively termed inflam-matory bowel disease, have received enormous attention in recentyears. Inflammatory bowel disease is characterized by recurrentinflammation and disruption of gut wall resulting from leukocyteinfiltration and excessive generation of inflammatory mediators andoxidants. The aetiology is still unclear and presumed to encompassgenetic, environmental and immunologic factors (Podolsky, 2002).Reactive oxygen species such as hydrogen peroxide, superoxide anionor hydroxyl radicals, and specially, reactive nitrogen species such asperoxynitrite, are implicated in pathogenesis of inflammatory boweldisease (Fillmann et al., 2007; Pavlick et al., 2002; Yoshida et al.,1999). The pro-inflammatory roles of these reactive species include
recruitment of more neutrophils at the site of inflammation,formation of chemotactic factors, lipid peroxidation, and release ofcytokines, such as Interleukine-1beta (IL-1β) and Tumor NecrosisFactor-alpha (TNF-α) (Mazzon et al., 2006). Interestingly, mucosalantioxidant components, such as glutathione, urate and alpha-tocopherol are depleted in human inflammatory bowel disease.Such deficit in antioxidant defence leaves the space for oxidizingagents to inflict damage on the compromised mucosa and hampersrecovery of its intact architecture (Buffinton and Doe, 1995). Atpresent, the management of inflammatory bowel disease is based ontwo classes of drugs; aminosalicylates and corticosteroids. Theseagents reduce inflammation and ameliorate the expression of pro-inflammatory mediators but their untoward effects have constrainedtheir long-term use (Baumgart and Sandborn, 2007). It is thereforenecessary to investigate new agents as an alternative therapy ininflammatory bowel disease.
Inosine has been used traditionally as an energy supplement andperformance enhancer (Starling et al., 1996). Ample evidence has

377R. Rahimian et al. / European Journal of Pharmacology 649 (2010) 376–381
linked inosine with modulation of inflammatory phenomena. Inosineprotects against the development of disease in several murine modelsof autoimmune conditions (Hasko et al., 2004). Inosine's anti-inflammatory effects are said to be partially mediated by activationof adenosine receptors (Hasko et al., 2000). It is possible that inosineproduces its inhibitory effects on cytokine production via binding toadenosine A2 receptors, a subtype shown to be present on immunecells (Mabley et al., 2003a). Inosine breakdown yields uric acid, theend product of purine metabolism and a strong reactive nitrogenspecies scavenger. This powerful endogenous antioxidant has provedpromising in experimentally and clinically inflammatory conditionssuch as multiple sclerosis, bacterial meningitis and spinal cord injury(Kastenbauer et al., 2001; Scott et al., 2002, 2005).
In the present study, we investigated effects of inosine on TNBS-induced chronic model of experimental colitis, and possible contri-bution of adenosine A2A receptors and the metabolite uric acid.
2. Materials and Methods
2.1. Ethics
The whole study was conducted in accordance with TehranUniversity of Medical Sciences guidelines for the care and use oflaboratory animals.
2.2. Animals
Male Sprague-Dawley rats weighing 200-250 g were used in thisstudy. Animals were kept under a 12-hour light/12-hour dark cycle at22-24 °C and had free access to peleted chow and water.
2.3. Induction of experimental inflammatory bowel disease
All rats were fasted for 24 hours prior to induction of inflammatorybowel disease. Rats were anesthetized intraperitoneally (i.p.) withPentobarbital (45 mg/kg). Experimental inflammatory bowel diseasewas rendered in rats by a single colonic administration of 10 mg of2,4,6-trinitrobenzene sulphonic acid (TNBS; Sigma, USA) dissolved in50% ethanol (total volume, 0.25 ml) using a rubber catheter inserted8 cm via the anus (Morris et al., 1989). Drugs were administered tothe rats for 7 successive days, starting from the colitis induction day(day one) asmentioned below. On the 8th day, animals were sacrificedusing an overdose of ether inhalation, then the abdomen was openedand the colon removed. In an ice bath, colons were cut open, cleansedgently with normal saline and macroscopic scores were determinedfor each. Subsequently, colons were weighed, and cut into 2 samepieces, one for histopathologic assessment (kept in 5 ml of 10%formalin) and the other for analysis of biochemical markers. The latterwas weighed again and homogenized in potassium phosphate buffer(pH 7.4). Afterwards, homogenates were centrifuged and super-natants were separated, aliquoted, and kept at -80 °C until analysis.
2.4. Experimental groups
Rats were randomized into the 7 following groups each compris-ing 6 animals.
1- Sham group, receiving normal saline instead of TNBS.2- Control group (TNBS-induced colitis), receiving no treatment.3- Inosine (5´-monophosphate, disodium salt, Sigma, USA) group,
receiving 500 mg/kg inosine i.p. twice daily, starting from 2 h priorto induction of inflammatory bowel disease and continued for7 days thereafter.
4- Oxonic acid group, receiving 250 mg/kg potassium oxonate(Sigma, USA) i.p. twice daily, starting from 2 h prior to induction
of inflammatory bowel disease and continued for 7 daysthereafter.
5- Inosine plus oxonic acid group, where a combination of inosineand potassium oxonate was given in the same fashion as describedearlier for each medication.
6- SCH-442416, (2-Furanyl)-7-[3-(4-methoxyphenyl)propyl]-7H-pyrazolo[4,3-e][1,2,4]triazolo[1,5-c]pyrimidin-5-amine, group, re-ceiving 0.17 mg/kg SCH-442416 (Cayman chemical, USA), anadenosine A2A receptor selective antagonist, i.p. twice daily,starting from 3 h prior to induction of inflammatory bowel diseaseand continued for 7 days thereafter.
7- Inosine plus SCH-442416 group, receiving the first dose of SCH-442416 1 h before inosine administration and that of inosine 2 hprior to inflammatory bowel disease induction. Administration ofinosine and SCH-442416 twice daily continued for 7 successivedays such that inosine was always injected 1 h after SCH-442416.
2.5. Weight loss
Body weights were recorded on the day of colitis induction (dayone) and day of sacrifice (day 8) and wasting disease was determinedby percentage of weight loss from initial body weight (Neurath et al.,1996).
2.6. Macroscopic assessment of severity of inflammatory bowel disease
7 days following induction of experimental inflammatory boweldisease, animals were euthanized by ether and distal colon was cutout, opened longitudinally along its mesenteric border and cleaned bya gentle flushing with saline. The wet weight of the distal 6 cm ofcolon was measured and used as an index of disease-related intestinalwall edema. Subsequently, each colon was divided longitudinally intotwo parts: one for histology, the other was snap-frozen in liquidnitrogen and stored at -80 °C for cytokine measurement Macroscopicscoring was done under a magnifying glass by an independentobserver based on the criteria as follows: 0, no damage; 1, localizedhyperaemia without ulcers; 2, linear ulcers with no significantinflammation; 3, linear ulcers with inflammation at one site; 4, twoor more major sites of inflammation and ulceration extending N1 cmalong the length of the colon; and 5-8, one point is added for eachcentimeter of ulceration beyond an initial 2 cm (Wallace et al., 1992).
2.7. Microscopic assessment of inflammatory bowel disease
5-μm thick formalin-fixed sections, stained with eosin andhematoxilin, were scored randomly by a blind pathologist (5 ormore longitudinal sections per colon) using the following criteria: 0,no damage; 1 (mild), focal epithelial edema and necrosis; 2(moderate), diffuse swelling and necrosis of the villi; 3 (severe),necrosis with presence of neutrophil infiltrate in the submucosa; 4(highly severe), widespread necrosis with massive neutrophilinfiltrate and haemorrhage (Cuzzocrea et al., 2003).
2.8. Biochemical assays
2.8.1. Myeloperoxidase activityMyeloperoxidase (MPO) is generally considered as a biochemical
indicator of granulocyte, in particular neutrophil infiltration intogastrointestinal tissues. MPO activity was measured as previouslydescribed (Bradley et al., 1982). Seven days after intra-colonicinjection of TNBS the colon was removed and specimens of distalcolon were homogenized in 10 mM potassium phosphate buffer, pH7.0 containing 0.5% hexadecyl trimethyl ammonium bromide andcentrifuged at 20,000×g for 30 min at 4 °C. A solution of 1.6 mMtetramethyl benzidine and 0.1 mM H2O2 was added and reacted to analiquot of the supernatant. The rate of change in optical density was
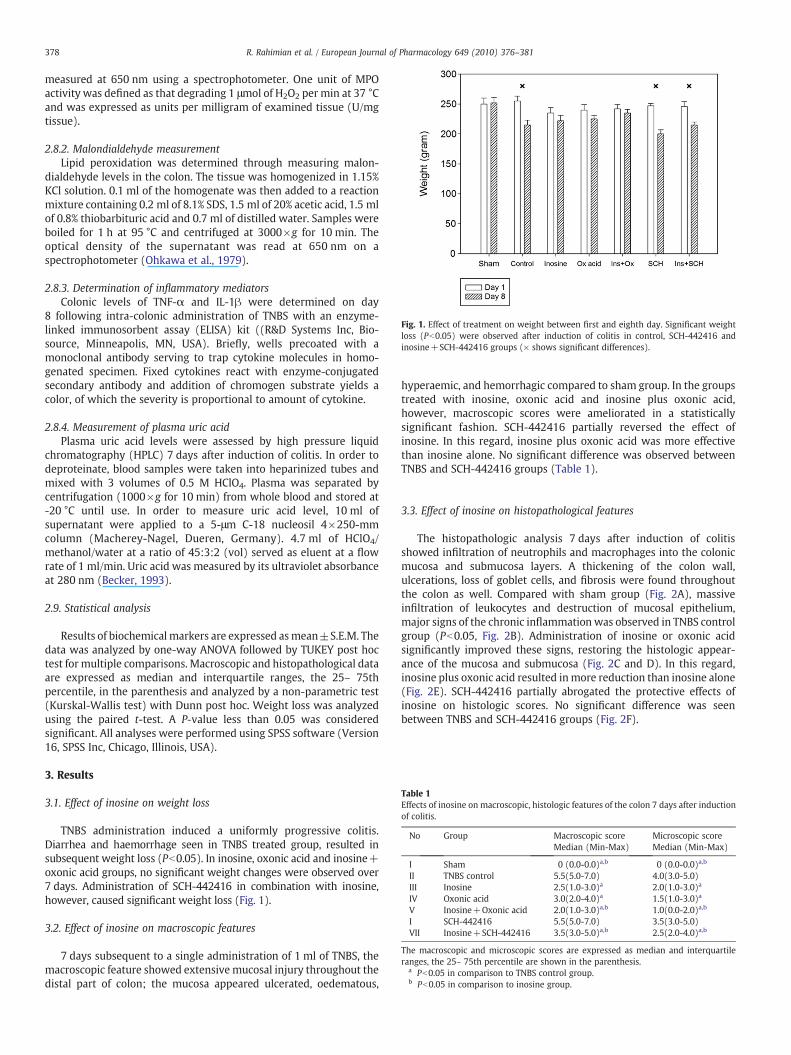
Fig. 1. Effect of treatment on weight between first and eighth day. Significant weightloss (Pb0.05) were observed after induction of colitis in control, SCH-442416 andinosine+SCH-442416 groups (× shows significant differences).
Table 1Effects of inosine on macroscopic, histologic features of the colon 7 days after inductionof colitis.
No Group Macroscopic scoreMedian (Min-Max)
Microscopic scoreMedian (Min-Max)
I Sham 0 (0.0-0.0)a,b 0 (0.0-0.0)a,b
II TNBS control 5.5(5.0-7.0) 4.0(3.0-5.0)III Inosine 2.5(1.0-3.0)a 2.0(1.0-3.0)a
IV Oxonic acid 3.0(2.0-4.0)a 1.5(1.0-3.0)a
V Inosine+Oxonic acid 2.0(1.0-3.0)a,b 1.0(0.0-2.0)a,b
I SCH-442416 5.5(5.0-7.0) 3.5(3.0-5.0)VII Inosine+SCH-442416 3.5(3.0-5.0)a,b 2.5(2.0-4.0)a,b
The macroscopic and microscopic scores are expressed as median and interquartileranges, the 25– 75th percentile are shown in the parenthesis.
a Pb0.05 in comparison to TNBS control group.b Pb0.05 in comparison to inosine group.
378 R. Rahimian et al. / European Journal of Pharmacology 649 (2010) 376–381
measured at 650 nm using a spectrophotometer. One unit of MPOactivity was defined as that degrading 1 μmol of H2O2 per min at 37 °Cand was expressed as units per milligram of examined tissue (U/mgtissue).
2.8.2. Malondialdehyde measurementLipid peroxidation was determined through measuring malon-
dialdehyde levels in the colon. The tissue was homogenized in 1.15%KCl solution. 0.1 ml of the homogenate was then added to a reactionmixture containing 0.2 ml of 8.1% SDS, 1.5 ml of 20% acetic acid, 1.5 mlof 0.8% thiobarbituric acid and 0.7 ml of distilled water. Samples wereboiled for 1 h at 95 °C and centrifuged at 3000×g for 10 min. Theoptical density of the supernatant was read at 650 nm on aspectrophotometer (Ohkawa et al., 1979).
2.8.3. Determination of inflammatory mediatorsColonic levels of TNF-α and IL-1β were determined on day
8 following intra-colonic administration of TNBS with an enzyme-linked immunosorbent assay (ELISA) kit ((R&D Systems Inc, Bio-source, Minneapolis, MN, USA). Briefly, wells precoated with amonoclonal antibody serving to trap cytokine molecules in homo-genated specimen. Fixed cytokines react with enzyme-conjugatedsecondary antibody and addition of chromogen substrate yields acolor, of which the severity is proportional to amount of cytokine.
2.8.4. Measurement of plasma uric acidPlasma uric acid levels were assessed by high pressure liquid
chromatography (HPLC) 7 days after induction of colitis. In order todeproteinate, blood samples were taken into heparinized tubes andmixed with 3 volumes of 0.5 M HClO4. Plasma was separated bycentrifugation (1000×g for 10 min) from whole blood and stored at-20 °C until use. In order to measure uric acid level, 10 ml ofsupernatant were applied to a 5-μm C-18 nucleosil 4×250-mmcolumn (Macherey-Nagel, Dueren, Germany). 4.7 ml of HClO4/methanol/water at a ratio of 45:3:2 (vol) served as eluent at a flowrate of 1 ml/min. Uric acid was measured by its ultraviolet absorbanceat 280 nm (Becker, 1993).
2.9. Statistical analysis
Results of biochemical markers are expressed asmean±S.E.M. Thedata was analyzed by one-way ANOVA followed by TUKEY post hoctest for multiple comparisons. Macroscopic and histopathological dataare expressed as median and interquartile ranges, the 25– 75thpercentile, in the parenthesis and analyzed by a non-parametric test(Kurskal-Wallis test) with Dunn post hoc. Weight loss was analyzedusing the paired t-test. A P-value less than 0.05 was consideredsignificant. All analyses were performed using SPSS software (Version16, SPSS Inc, Chicago, Illinois, USA).
3. Results
3.1. Effect of inosine on weight loss
TNBS administration induced a uniformly progressive colitis.Diarrhea and haemorrhage seen in TNBS treated group, resulted insubsequent weight loss (Pb0.05). In inosine, oxonic acid and inosine+oxonic acid groups, no significant weight changes were observed over7 days. Administration of SCH-442416 in combination with inosine,however, caused significant weight loss (Fig. 1).
3.2. Effect of inosine on macroscopic features
7 days subsequent to a single administration of 1 ml of TNBS, themacroscopic feature showed extensivemucosal injury throughout thedistal part of colon; the mucosa appeared ulcerated, oedematous,
hyperaemic, and hemorrhagic compared to sham group. In the groupstreated with inosine, oxonic acid and inosine plus oxonic acid,however, macroscopic scores were ameliorated in a statisticallysignificant fashion. SCH-442416 partially reversed the effect ofinosine. In this regard, inosine plus oxonic acid was more effectivethan inosine alone. No significant difference was observed betweenTNBS and SCH-442416 groups (Table 1).
3.3. Effect of inosine on histopathological features
The histopathologic analysis 7 days after induction of colitisshowed infiltration of neutrophils and macrophages into the colonicmucosa and submucosa layers. A thickening of the colon wall,ulcerations, loss of goblet cells, and fibrosis were found throughoutthe colon as well. Compared with sham group (Fig. 2A), massiveinfiltration of leukocytes and destruction of mucosal epithelium,major signs of the chronic inflammation was observed in TNBS controlgroup (Pb0.05, Fig. 2B). Administration of inosine or oxonic acidsignificantly improved these signs, restoring the histologic appear-ance of the mucosa and submucosa (Fig. 2C and D). In this regard,inosine plus oxonic acid resulted inmore reduction than inosine alone(Fig. 2E). SCH-442416 partially abrogated the protective effects ofinosine on histologic scores. No significant difference was seenbetween TNBS and SCH-442416 groups (Fig. 2F).

Fig. 2.Histological appearances of colonic tissues. Photomicrographs of haematoxylin and eosin stained paraffin sections of rat colonic tissues. (A) Normal intact mucosa from normalsham animals showed intact epithelial surface; magnification×100. (B) TNBS-induced colitis showed massive necrotic destruction of epithelium , fibrosis or hemorrhage;magnification×100. (C and D) Treatment with Inosine (500 mg/Kg) and Oxonic acid (250 mg/Kg), respectively, attenuated the extent and severity of the histological signs of celldamage; magnification×100. (E) Inosnie+Oxonic acid nearly reversed the infiltration caused by TNBS administration;magnification×100. (F) Concurrent administration of inosineand SCH-442416 caused epithelial destruction, hemorrhage and fibrosis; magnification×100.
379R. Rahimian et al. / European Journal of Pharmacology 649 (2010) 376–381
3.4. Effects of inosine on biochemical markers
3.4.1. Effect of inosine on myeloperoxidase and malondialdehyde levelsTissue MPO activity in the inosine, oxonic acid and inosine plus
oxonic acid groups was significantly decreased (Pb0.05, Fig. 3A) on dayeight, compared to the TNBS control group. MDA activity was alsomeasured as a marker of lipid peroxidation. MDA activity attained itsmaximal levels in TNBS treated group, while it was minimal in shamgroup. MDA levels were lower in inosine, oxonic acid and inosine plusoxonic acid treated groups, whichwere statistically significant (Pb0.05,Fig. 3B). As compared with inosine alone, inosine plus oxonic acidtreatment causedmore reduction in the elevatedMPO activity andMDAlevel. SCH-442416 partially compromised the effect of inosine on bothMDA level and MPO activity. No significant difference was observedbetween TNBS and SCH-442416 groups.
3.4.2. Effect of inosine on cytokine productionSeven days after colitis induction by TNBS administration, tissue
concentrations of TNF-α and IL-1β, in TNBS given ratswere significantlyhigher than those of the sham treated rats (Pb0.05). TNBS-inducedincrease in TNF-α and IL-1β concentrations in the colonic tissue wassignificantly suppressed (Pb0.05) by the administration of eitherinosine, oxonic acid, or inosine plus oxonic acid (Fig. 4A and B). In
animals receiving inosine plus oxonic acid, more diminution wasobserved in proinflammatory cytokines compared with those receivinginosine alone. In presence of SCH-442416, inosine failed to elicit itsmaximal inhibitory effect on cytokine level. No significant differencewas observed between TNBS and SCH-442416 groups.
3.4.3. Plasma levels of uric acid7 days after induction of colitis, serum uric acid level was
measured in control, inosine, oxoninc acid and inosine+oxonic acidgroups. Baseline uric acid levels averaged 1.1 mg/dl in control group.Oxonic acid, as well as inosine, induced a moderate hyperuricemia incomparison with control (Pb0.05). Inosine+oxonic acid-treatedgroup showed higher plasma uric acid levels, as compared withinosine or oxonic acid group (Pb0.05) (Fig. 5).
4. Discussion
Results of this study indicate the beneficial effects of inosine onTNBS-induced colitis in rats. Bothmacroscopic and histological featuresof colonic injury were markedly ameliorated by either inosine, oxonicacid or inosine plus oxonic acid. Likewise, the elevated amounts ofmarkers of neutrophil infiltration and lipid peroxidation, respectivelyMPO and MDA, abated as well as those of TNF-α and IL-1β.
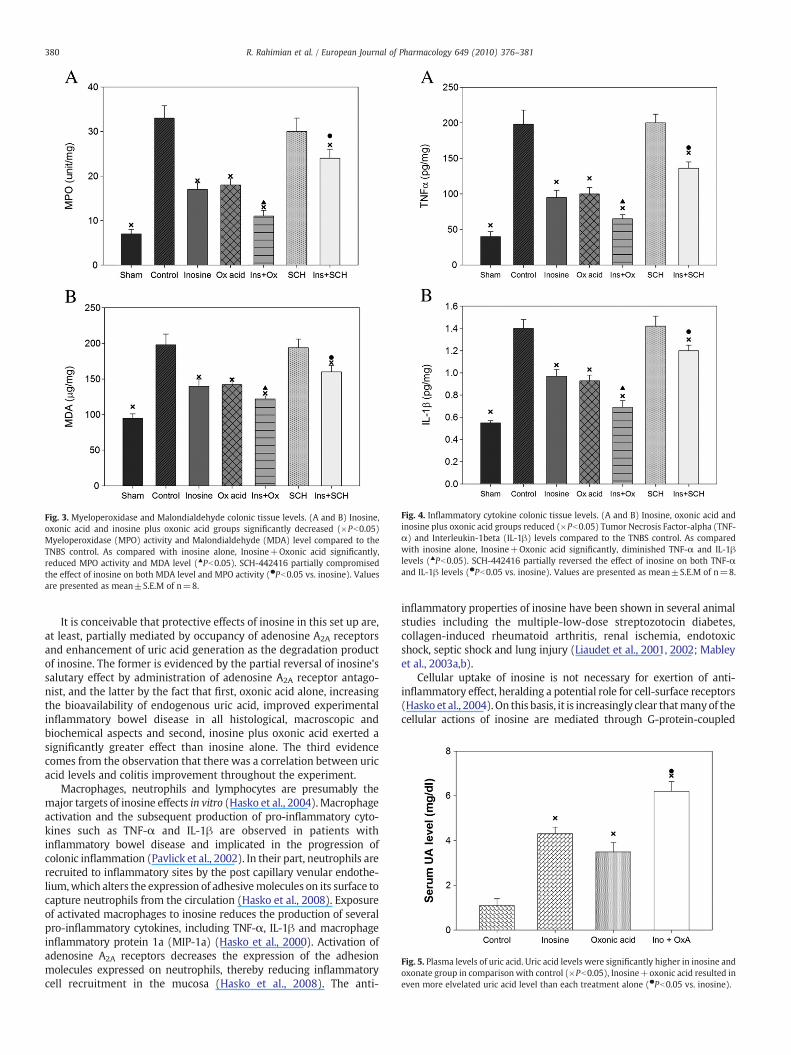
Fig. 3. Myeloperoxidase and Malondialdehyde colonic tissue levels. (A and B) Inosine,oxonic acid and inosine plus oxonic acid groups significantly decreased (×Pb0.05)Myeloperoxidase (MPO) activity and Malondialdehyde (MDA) level compared to theTNBS control. As compared with inosine alone, Inosine+Oxonic acid significantly,reduced MPO activity and MDA level (▲Pb0.05). SCH-442416 partially compromisedthe effect of inosine on both MDA level and MPO activity (●Pb0.05 vs. inosine). Valuesare presented as mean±S.E.M of n=8.
Fig. 4. Inflammatory cytokine colonic tissue levels. (A and B) Inosine, oxonic acid andinosine plus oxonic acid groups reduced (×Pb0.05) Tumor Necrosis Factor-alpha (TNF-α) and Interleukin-1beta (IL-1β) levels compared to the TNBS control. As comparedwith inosine alone, Inosine+Oxonic acid significantly, diminished TNF-α and IL-1βlevels (▲Pb0.05). SCH-442416 partially reversed the effect of inosine on both TNF-αand IL-1β levels (●Pb0.05 vs. inosine). Values are presented as mean±S.E.M of n=8.
Fig. 5. Plasma levels of uric acid. Uric acid levels were significantly higher in inosine andoxonate group in comparison with control (×Pb0.05), Inosine+oxonic acid resulted ineven more elvelated uric acid level than each treatment alone (●Pb0.05 vs. inosine).
380 R. Rahimian et al. / European Journal of Pharmacology 649 (2010) 376–381
It is conceivable that protective effects of inosine in this set up are,at least, partially mediated by occupancy of adenosine A2A receptorsand enhancement of uric acid generation as the degradation productof inosine. The former is evidenced by the partial reversal of inosine'ssalutary effect by administration of adenosine A2A receptor antago-nist, and the latter by the fact that first, oxonic acid alone, increasingthe bioavailability of endogenous uric acid, improved experimentalinflammatory bowel disease in all histological, macroscopic andbiochemical aspects and second, inosine plus oxonic acid exerted asignificantly greater effect than inosine alone. The third evidencecomes from the observation that there was a correlation between uricacid levels and colitis improvement throughout the experiment.
Macrophages, neutrophils and lymphocytes are presumably themajor targets of inosine effects in vitro (Hasko et al., 2004). Macrophageactivation and the subsequent production of pro-inflammatory cyto-kines such as TNF-α and IL-1β are observed in patients withinflammatory bowel disease and implicated in the progression ofcolonic inflammation (Pavlick et al., 2002). In their part, neutrophils arerecruited to inflammatory sites by the post capillary venular endothe-lium,which alters the expression of adhesivemolecules on its surface tocapture neutrophils from the circulation (Hasko et al., 2008). Exposureof activated macrophages to inosine reduces the production of severalpro-inflammatory cytokines, including TNF-α, IL-1β and macrophageinflammatory protein 1a (MIP-1a) (Hasko et al., 2000). Activation ofadenosine A2A receptors decreases the expression of the adhesionmolecules expressed on neutrophils, thereby reducing inflammatorycell recruitment in the mucosa (Hasko et al., 2008). The anti-
inflammatory properties of inosine have been shown in several animalstudies including the multiple-low-dose streptozotocin diabetes,collagen-induced rheumatoid arthritis, renal ischemia, endotoxicshock, septic shock and lung injury (Liaudet et al., 2001, 2002; Mableyet al., 2003a,b).
Cellular uptake of inosine is not necessary for exertion of anti-inflammatory effect, heralding a potential role for cell-surface receptors(Hasko et al., 2004).On this basis, it is increasingly clear thatmanyof thecellular actions of inosine are mediated through G-protein-coupled

381R. Rahimian et al. / European Journal of Pharmacology 649 (2010) 376–381
adenosine receptors, all ofwhich are expressed on immune cells (Haskoet al., 2004; Ye and Rajendran, 2009). Among them, adenosine A2A
receptors are unique in that they induce anti-inflammatory signals(Naganuma et al., 2006; Odashima et al., 2005). In our study, inosineattenuated TNBS-provoked chronic intestinal inflammation asevidenced by a significant reduction in colonic levels of TNF-α, IL-1β,MDA, and MPO. As the selective adenosine A2A receptor antagonistpartially abolished inosine-induced intestinal protection, this receptorsubtype most likely plays a role in colitis attenuation. Therefore,adenosine A2A receptor activation by inosine may be of therapeuticbenefit in chronic bowel inflammation (Ye and Rajendran, 2009).
To investigate whether uric acid also plays a role in inosineprotection, oxonic acid, an inhibitor of uricase, was employed eitheralone or in combination with inosine. Uricase is responsible for uricacid breakdown to allantoin in rats; therefore, its inhibition helpedmaintain higher serum uric acid levels (Mousavizadeh et al., 2003). Inhumans, uric acid is the main aqueous antioxidant accounting fortwo-third of all free radical scavenging capacity in plasma. It isparticularly effective in neutralizing hydroxyl, superoxide andperoxynitrite radicals, and may serve a protective physiological roleby preventing lipid peroxidation (Waring, 2002). Our results showthat inosine+oxonic acid administration was associated with a morereduction than inosine alone in MPO activity, MDA levels and pro-inflammatory cytokines profile. This finding, along with a similareffect seenwith oxonic acid alone, emphasizes the contribution of uricacid in inosine-mediated amelioration of colitis. It appears that oxonicacid or inosine-induced uric acid elevationmight replenish urate pool,which is reportedly depleted in inflammatory bowel disease patients,leading to mucosal defense system restoration (Tuzun et al., 2002).
It has been suggested that inflammation of mucosa impairsantioxidant defense mechanisms and exposes tissue to oxidative insultinflicted by infiltrating macrophages and neutrophils. Increased oxida-tive and nitrosative stress and decreased antioxidant defenses arereported in colonic mucosal biopsies of patients with inflammatorybowel disease (McCafferty, 2000). Reactive oxygen species releasedfrom these cells along with reactive nitrogen species disrupt cellularmembrane stability, alter normal function of proteins and promote celldeath by leading lipid peroxidation (Hooper et al., 2000). Moreover,some free radicals influence the activation state of nuclear transcriptionfactors, notably Nuclear Factor-kappa B (NF-kB), thereby modulatingcytokines and adhesion molecules involved in inflammatory andimmune responses (Maunder, 2000). In this respect, the ability ofurate sparing interventions, i.e. inosine, oxonic acid and inosine+oxonicacid, to suppress pro-inflammatory cytokines TNF-α and IL-1β, and todecrease neutrophil infiltration can lie in their antioxidant capacity.
In summary, our results show the notable anti-inflammatory effectsof inosine in a valid chronic experimental inflammatory bowel diseaseand the contribution of uric acid as well as adenosine A2A receptors tothese salutary properties. Nevertheless, more investigations should beassigned to clarify additional mechanisms underlying the protectiveeffects of inosine. Regarding the prominent anti-inflammatory proper-ties of inosine, it is plausible that such widely used dietary supplementbe investigated in patients with inflammatory bowel disease.
References
Baumgart, D.C., Sandborn, W.J., 2007. Inflammatory bowel disease: clinical aspects andestablished and evolving therapies. Lancet 369, 1641–1657.
Becker, B.F., 1993. Towards the physiological function of uric acid. Free Radic. Biol. Med.14, 615–631.
Bradley, P.P., Priebat, D.A., Christensen, R.D., Rothstein, G., 1982. Measurement ofcutaneous inflammation: estimation of neutrophil content with an enzymemarker.J. Invest. Dermatol. 78, 206–209.
Buffinton, G.D., Doe, W.F., 1995. Depleted mucosal antioxidant defences in inflamma-tory bowel disease. Free Radic. Biol. Med. 19, 911–918.
Cuzzocrea, S., Ianaro, A., Wayman, N.S., Mazzon, E., Pisano, B., Dugo, L., Serraino, I., DiPaola, R., Chatterjee, P.K., Di Rosa, M., Caputi, A.P., Thiemermann, C., 2003. Thecyclopentenone prostaglandin 15-deoxy-delta(12, 14)- PGJ2 attenuates the
development of colon injury caused by dinitrobenzene sulphonic acid in the rat.Br. J. Pharmacol. 138, 678–688.
Fillmann, H., Kretzmann, N.A., San-Miguel, B., Llesuy, S., Marroni, N., Gonzalez-Gallego,J., Tunon,M.J., 2007. Glutamine inhibits over-expression of pro-inflammatory genesand down-regulates the nuclear factor kappaB pathway in an experimental modelof colitis in the rat. Toxicology 236, 217–226.
Hasko, G., Kuhel, D.G., Nemeth, Z.H., Mabley, J.G., Stachlewitz, R.F., Virag, L., Lohinai, Z.,Southan, G.J., Salzman, A.L., Szabo, C., 2000. Inosine inhibits inflammatory cytokineproduction by a posttranscriptional mechanism and protects against endotoxin-induced shock. J. Immunol. 164, 1013–1019.
Hasko, G., Sitkovsky, M.V., Szabo, C., 2004. Immunomodulatory and neuroprotectiveeffects of inosine. Trends Pharmacol. Sci. 25, 152–157.
Hasko, G., Linden, J., Cronstein, B., Pacher, P., 2008. Adenosine receptors: therapeuticaspects for inflammatory and immune diseases. Nat. Rev. Drug Discov. 7, 759–770.
Hooper, D.C., Scott, G.S., Zborek, A., Mikheeva, T., Kean, R.B., Koprowski, H., Spitsin, S.V.,2000. Uric acid, a peroxynitrite scavenger, inhibits CNS inflammation, blood-CNSbarrier permeability changes, and tissue damage in a mouse model of multiplesclerosis. FASEB J. 14, 691–698.
Kastenbauer, S., Koedel, U., Becker, B.F., Pfister, H.W., 2001. Experimental meningitis inthe rat: protection by uric acid at human physiological blood concentrations. Eur. J.Pharmacol. 425, 149–152.
Liaudet, L., Mabley, J.G., Soriano, F.G., Pacher, P., Marton, A., Hasko, G., Szabo, C., 2001.Inosine reduces systemic inflammation and improves survival in septic shockinduced by cecal ligation and puncture. Am. J. Respir. Crit. Care Med. 164,1213–1220.
Liaudet, L., Mabley, J.G., Pacher, P., Virag, L., Soriano, F.G., Marton, A., Hasko, G., Deitch, E.A., Szabo, C., 2002. Inosine exerts a broad range of antiinflammatory effects in amurine model of acute lung injury. Ann. Surg. 235, 568–578.
Mabley, J.G., Pacher, P., Liaudet, L., Soriano, F.G., Hasko, G., Marton, A., Szabo, C.,Salzman, A.L., 2003a. Inosine reduces inflammation and improves survival in amurine model of colitis. Am. J. Physiol. Gastrointest. Liver Physiol. 284, G138–G144.
Mabley, J.G., Rabinovitch, A., Suarez-Pinzon, W., Hasko, G., Pacher, P., Power, R.,Southan, G., Salzman, A., Szabo, C., 2003b. Inosine protects against the developmentof diabetes in multiple-low-dose streptozotocin and nonobese diabetic mousemodels of type 1 diabetes. Mol. Med. 9, 96–104.
Maunder, R., 2000. Mediators of stress effects in inflammatory bowel disease: not theusual suspects. J. Psychosom. Res. 48, 569–577.
Mazzon, E., Esposito, E., Crisafulli, C., Riccardi, L., Muia, C., Di Bella, P., Meli, R., Cuzzocrea,S., 2006. Melatonin modulates signal transduction pathways and apoptosis inexperimental colitis. J. Pineal Res. 41, 363–373.
McCafferty, D.M., 2000. Peroxynitrite and inflammatory bowel disease. Gut 46,436–439.
Morris, G.P., Beck, P.L., Herridge, M.S., Depew, W.T., Szewczuk, M.R., Wallace, J.L., 1989.Hapten-induced model of chronic inflammation and ulceration in the rat colon.Gastroenterology 96, 795–803.
Mousavizadeh, K., Dehpour, A.R., Minagar, A., Ghafourifar, P., 2003. Uric acid: a noveltreatment strategy for multiple sclerosis. Trends Pharmacol. Sci. 24, 563–564author reply 564-565.
Naganuma, M.,Wiznerowicz, E.B., Lappas, C.M., Linden, J., Worthington, M.T., Ernst, P.B.,2006. Cutting edge: Critical role for A2A adenosine receptors in the T cell-mediatedregulation of colitis. J. Immunol. 177, 2765–2769.
Neurath, M.F., Fuss, I., Kelsall, B., Meyer zum Buschenfelde, K.H., Strober, W., 1996.Effect of IL-12 and antibodies to IL-12 on established granulomatous colitis in mice.Ann. NY Acad. Sci. 795, 368–370.
Odashima, M., Bamias, G., Rivera-Nieves, J., Linden, J., Nast, C.C., Moskaluk, C.A., Marini,M., Sugawara, K., Kozaiwa, K., Otaka, M., Watanabe, S., Cominelli, F., 2005.Activation of A2A adenosine receptor attenuates intestinal inflammation in animalmodels of inflammatory bowel disease. Gastroenterology 129, 26–33.
Ohkawa, H., Ohishi, N., Yagi, K., 1979. Assay for lipid peroxides in animal tissues bythiobarbituric acid reaction. Anal. Biochem. 95, 351–358.
Pavlick, K.P., Laroux, F.S., Fuseler, J., Wolf, R.E., Gray, L., Hoffman, J., Grisham, M.B., 2002.Role of reactive metabolites of oxygen and nitrogen in inflammatory bowel disease.Free Radic. Biol. Med. 33, 311–322.
Podolsky, D.K., 2002. Inflammatory bowel disease. N Engl J. Med. 347, 417–429.Scott, G.S., Spitsin, S.V., Kean, R.B., Mikheeva, T., Koprowski, H., Hooper, D.C., 2002.
Therapeutic intervention in experimental allergic encephalomyelitis by adminis-tration of uric acid precursors. Proc. Natl Acad. Sci. USA 99, 16303–16308.
Scott, G.S., Cuzzocrea, S., Genovese, T., Koprowski, H., Hooper, D.C., 2005. Uric acidprotects against secondary damage after spinal cord injury. Proc. Natl Acad. Sci. USA102, 3483–3488.
Starling, R.D., Trappe, T.A., Short, K.R., Sheffield-Moore, M., Jozsi, A.C., Fink, W.J., Costill,D.L., 1996. Effect of inosine supplementation on aerobic and anaerobic cyclingperformance. Med. Sci. Sports Exerc. 28, 1193–1198.
Tuzun, A., Erdil, A., Inal, V., Aydin, A., Bagci, S., Yesilova, Z., Sayal, A., Karaeren, N., Dagalp,K., 2002. Oxidative stress and antioxidant capacity in patients with inflammatorybowel disease. Clin. Biochem. 35, 569–572.
Wallace, J.L., Keenan, C.M., Gale, D., Shoupe, T.S., 1992. Exacerbation of experimentalcolitis by nonsteroidal anti-inflammatory drugs is not related to elevatedleukotriene B4 synthesis. Gastroenterology 102, 18–27.
Waring, W.S., 2002. Uric acid: an important antioxidant in acute ischaemic stroke. QJM95, 691–693.
Ye, J.H., Rajendran, V.M., 2009. Adenosine: an immune modulator of inflammatorybowel diseases. World J. Gastroenterol. 15, 4491–4498.
Yoshida, N., Yoshikawa, T., Yamaguchi, T., Naito, Y., Tanigawa, T., Murase, H., Kondo, M.,1999. A novel water-soluble vitamin E derivative protects against experimentalcolitis in rats. Antioxid. Redox Signal. 1, 555–562.
Copyright © 2022 FDOKUMEN





![An amperometric uric acid biosensor based on Bis[sulfosuccinimidyl] suberate crosslinker/3-aminopropyltriethoxysilane surface modified ITO glass electrode](https://static.fdokumen.com/doc/165x107/63129cf1fc260b71020eb9f6/an-amperometric-uric-acid-biosensor-based-on-bissulfosuccinimidyl-suberate-crosslinker3-aminopropyltriethoxysilane.jpg)














