
A phase II trial of vaccination with autologous, tumor-derived heat-shock protein peptide complexes...
10
Cancer Immunol Immuoother (2006) 55: 958-968 DO1 10.1007/~00262-005-0084-8 Lorenzo Pilla Roberto Patuzzo Licia Rivoltini Michele Maio Elisabetta Pennacchioli - Elda Lamaj Andrea Maurichi Samuele Massarut Alfonso Marchianò Cristina Santantonio Diego Tosi Flavio Arienti Agata Cova Gloria Sovena Adriano Piris Daisuke Nonaka Nana Bersani Annabella Di Florio Mariani Luigi Pramod K. Srivastava Axel Hoos - Mario Santinami Giorgio Parmiani A phase Il trial of vaccinatian with awtologous, tum keat-s hock protein peptide corn plexes Gp96, in coni bination F and interferon-cr in metastatic melanoma patients Received: 3 Aiigust 2005 / Accepted: 27 August 2005 /Published online: 8 October 2005 O Springer-Verlag 2005 Abstract The aim of this study was to determine the iilimunogenicity and antitumor activity of autologous, tumor-derived heat shock protein gp96-peptide complex vaccine (HSPPC-96; OncophageB) given with GM-CSF and IFN-a in prc-ireated metastatic (AJCC stage IV) melanoma patients. Patients underwent surgical resec- tlon of metastatic lesions for HSPPC-96 production. HSPPC-96 was administered subcutaneously (s.c.) in four weekly iiitervals (first cycle). Patients with inore avaijable vaccine and abseuce of progressive disease re- ceived four additional injections in 2-week intervals (second cycle) or more. GM-CSF was given s.c. at the sarmie site at days -1, O and + 1, wlule IFN-a (3 MU) was L.P. and R.P. have equally contributed to the work. L. Pilla . L. Rivoltini . D. Tosi - A Cova . G. Sovena I. Bersani . A. D Florio G. Parmiani (€3) Unit of Immunotherapy of Human Tumors, Istituto Nazionale per Io Studio e la Cura dei Tumori, Via Veiiezian 1, 20133 Milan, Italy E-inail: ;[email protected] R. Paiuz~o . E. Pennacchioli . A. Maurichi - M. Saiitinami Unit of Melanoma and Sarcoma Surgery, Istituto Nazionale per lo Studio e ia Cura dei Tumori, Milan, Italy M. Maio . E. Lamaj . S. Massarut . C. Santantonio Centro di Riferimento Oncologico, Aviano, Italy A. Marcliianò Unit of Radiology, Istituto Nazionale per lo Studio e la Cura dei Tuniori, Milan, ILaly F. Arienti Unit of Immunohematology, Istituto Nazionale per lo Studio e la Cura dei Tuniori, Milan, Italy admiiiistered s.c. at a different site at days + 4 and + 6. Antigen-specific anti-ineIanoma T and NK lymphocy~e response was assessed by enzyme-Iinked irnmui~ospot assay on peripheral blood mononuclear cells obt.dined before and after vaccination. Thirty-eight patients were enrolled, 20 received at least four injectioas (ane cycle) of HSPPC-96 and were considered assessable, Toxicity was mild and most treatment-related adveme events were local erythema and induration at the injqtion site. Patiexits receiving at least four injections of HSPPC-96 showed stable disease @D). The ELI A. Piris - D. Nonaka Unit of Pathology, Istituto Nazionale per lo Studio e la Cura dei Tuniori. Miian, Italy M. Luigi TJnit of Medical Statistics and Biometry, Istituto Nazionale per lo Studio e la Cura dei Tumori, Milan, Italy i P. K. Srivastava Department of Microbiology and Iminunol University of Connecticut, Farmington, CT, USA A. Hoos Antigenics Inc., Lexington, MA, USA ' l Presenr address: M Maio Unit of Medical Oncologic and ~mrndnothera~y, Department of Oncology, Azienda Ospedaliera Universitana Senese, Siena, Italy
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of A phase II trial of vaccination with autologous, tumor-derived heat-shock protein peptide complexes...

Cancer Immunol Immuoother (2006) 55: 958-968 DO1 10.1007/~00262-005-0084-8
Lorenzo Pilla Roberto Patuzzo Licia Rivoltini Michele Maio Elisabetta Pennacchioli - Elda Lamaj Andrea Maurichi Samuele Massarut Alfonso Marchianò Cristina Santantonio Diego Tosi Flavio Arienti Agata Cova Gloria Sovena Adriano Piris Daisuke Nonaka Nana Bersani Annabella Di Florio Mariani Luigi Pramod K. Srivastava Axel Hoos - Mario Santinami Giorgio Parmiani
A phase Il trial of vaccinatian with awtologous, tum keat-s hock protein peptide corn plexes Gp96, in coni bination F and interferon-cr in metastatic melanoma patients
Received: 3 Aiigust 2005 / Accepted: 27 August 2005 /Published online: 8 October 2005 O Springer-Verlag 2005
Abstract The aim of this study was to determine the iilimunogenicity and antitumor activity of autologous, tumor-derived heat shock protein gp96-peptide complex vaccine (HSPPC-96; OncophageB) given with GM-CSF and IFN-a in prc-ireated metastatic (AJCC stage IV) melanoma patients. Patients underwent surgical resec- tlon of metastatic lesions for HSPPC-96 production. HSPPC-96 was administered subcutaneously (s.c.) in four weekly iiitervals (first cycle). Patients with inore avaijable vaccine and abseuce of progressive disease re- ceived four additional injections in 2-week intervals (second cycle) or more. GM-CSF was given s.c. at the sarmie site at days -1, O and + 1 , wlule IFN-a (3 MU) was
L.P. and R.P. have equally contributed to the work.
L. Pilla . L. Rivoltini . D. Tosi - A Cova . G. Sovena I. Bersani . A. D Florio G. Parmiani (€3) Unit of Immunotherapy of Human Tumors, Istituto Nazionale per Io Studio e la Cura dei Tumori, Via Veiiezian 1, 20133 Milan, Italy E-inail: ;[email protected]
R. Pa iuz~o . E. Pennacchioli . A. Maurichi - M. Saiitinami Unit of Melanoma and Sarcoma Surgery, Istituto Nazionale per lo Studio e ia Cura dei Tumori, Milan, Italy
M. Maio . E. Lamaj . S. Massarut . C . Santantonio Centro di Riferimento Oncologico, Aviano, Italy
A. Marcliianò Unit of Radiology, Istituto Nazionale per lo Studio e la Cura dei Tuniori, Milan, ILaly
F. Arienti Unit of Immunohematology, Istituto Nazionale per lo Studio e la Cura dei Tuniori, Milan, Italy
admiiiistered s.c. at a different site at days + 4 and + 6. Antigen-specific anti-ineIanoma T and NK lymphocy~e response was assessed by enzyme-Iinked irnmui~ospot assay on peripheral blood mononuclear cells obt.dined before and after vaccination. Thirty-eight patients were enrolled, 20 received at least four injectioas (ane cycle) of HSPPC-96 and were considered assessable, Toxicity was mild and most treatment-related adveme events were local erythema and induration at the injqtion site. Patiexits receiving at least four injections of HSPPC-96
showed stable disease @D). The ELI
A. Piris - D. Nonaka Unit of Pathology, Istituto Nazionale per lo Studio e la Cura dei Tuniori. Miian, Italy
M. Luigi TJnit of Medical Statistics and Biometry, Istituto Nazionale per lo Studio e la Cura dei Tumori, Milan, Italy i
P. K. Srivastava Department of Microbiology and Iminunol University of Connecticut, Farmington, CT, USA
A. Hoos Antigenics Inc., Lexington, MA, USA ' l
Presenr address: M Maio Unit of Medical Oncologic and ~mrndnothera~y, Department of Oncology, Azienda Ospedaliera Universitana Senese, Siena, Italy
revealed an increased class I HLA-restricted T and NK cell-mediated post-vaccination response in 5 out of 17 and 12 out of the 18 patients tested, respectively. Four of the five class I HLA-restricted T ce11 fesponses fa11 in the group of SD patients. Vaccination with autologous HSPPC-96 together with GM-CSF and IFN-a is feasible and accompanied by mild local and systemic toxicity. Both tunior-specific T cell-mediated and NK ce11 re- spoiises were generated in a proportion of patients. Clinical activity was limited to SD. However, both immunological and clinical responses were not improved as compared with those recorded in a previous study investigating HSPPC-96 monotherapy.
Keywords Vaccination - Metastatic rnelanoma - Heat sliock proteins GM-CSF . IFN-a - Phase I1 trial
Abbreviations AEs: adverse events . DTH: delayed-type hypersensitivity - ELISPOT enzyrne-linked iminunospot - GM-CSF: granulocyte/inacrophage- colony stimulating factor - HSP: heat shock proteins - HSPPC-96: heat shock proteins peptide complexes gp96 IFN: iiiterferon . IHC: irnmunohistoclieinistry - IL: interleukiii - NK: natura1 killer - PBNC: penpheral blood rnononuclear cells . RECIST: response evaluation criteria in solid tuniors . s.c.: subcutaneously
We have previously shown that approxiinately 50% of therapy refractory stage IV (American Joint Commis- sioii on Cancer, AJCC) metastatic rnelanoma patients vaccinated after surgery with autologous tumor-derived heat sliock protein peptide complexes gp96 (HSPPC- 96)$ develol-ied class I HLA-restricted tumor-specific T ce11 immunity. Clinical responses and long-term disease stabilization were noted in this study [l]. Results of this and other similar studies have been recently discussed P].
Siiice the local administration of GM-CSF has beeii reported to recruit inflammatory-like cells, to activate dendritic cells and to increase the immunogenicity of vaccines both in aniinal models and humans 13-51, in an attemp t to potentially enhance the imnune and cliiiical response of the HSPPC-96 vaccine, we designed this protocol in which GM-CSF was given at the site of the HSPPC-96 injection. Moreover, in order to up-regulate the expression of the target HLAlpeptide complex rec- ognizable by T cells, which is often down-regulated in metastatic melanoma cells [6], patients also received low dose IFN-a mice a week after vaccine administration. Such a dose has been previously shown to up-regulate tlie expression of class I HLA in peripheral blood cells of melanoma patients [7].
Here we report the results of this trial which confirms the in vivo imniunogenicity of HSPPC-96 even in com-
bination with GM-CSF and IFN-a at least in a fraction of patients with advanced melanoma and suggests a clinical effect in ternis of disease stabilization. However, this study fails to deinoiistrate a noticeable improveinent in the freqiiency and intensity of both immunologic and clinical responses as compared witli our previous stiidy of vaccination of clinically siinilar patients receiving HSPPC-96 monotherapy [l].
Patients and treatments
Between March 2002 and February 2003, 38 pre-treated stage IV AJCC inetastatic melanoina patients were en- rolled in the study and had surgical resection of tumor tissue for vaccine p r o d e o n . Patients were enrolled at two Italian centers: mz%tituto Nazioiiale Tumori (n = 3 1) and the Regiond Oncology Center of Aviano (n=7). Of these patients, 27 started treatment and 70 received at least one cycle of four vaccinations aiid were considered assessable. Eligibility criteria for study par- ticipation included the following: (I) histologically ver- ified melanoma with resectability of at least one lesion that provided the necessary amount of non-necrotic neoplastic tissue (5 g. four of which to be used for vac- ciiie preparation and one for immunological assays); (2) performance status (Zubrod) of two or less; (3) lifc expectancy of at least 5 months; (4) normal WBC and platelets counts, and hernoglobin leve1 greater than 10 g/ 1: (5) bilirubin less than 1.5 times normal, ALT less tlian four times normal. and adequate renal function with serum creatinine less than m-ice nomi; (6) fully recovered froiii prior anticancer therapy with at least a 4-week intemal from the last rrdministrathn of piior anticancer treatnient.
Al1 patients underwent clinical and staging before treatment. Patients were the study if they had active brain metasta coniitant autoimmune or maligiiant di receiving coiicurrent anticancer ther immunosuppressive driigs, or had a history bf serious intercurrent medica1 illness. Women of cdldbearing potential had a negative seruiii yregnancy test before entry into tlie study and agreed to use aa eiTective method of contraception while oli treatinen&. Al1 pa- tients gave written inforilied consent t study.
The cliiiical protocol was approv Scientific Review Board and by the I Committee of the Istituto Nazionale and of the other participating center. cinated with aritologous HSPPC-96 star&@$- 5-8 weeks after resection of tumor metastasei: they reaeived 25 pg of vaccine giveii subcutaneously (s.c,) at weekly intervals for 4 weeks (first cycle). After 4 weeks of rest and if no progression occurred, patients received four additional injectioiis every 2 weeks (second cycle) if the vaccine was available. Siinilarly, additional vaccinations were given after two cycles wliere available. The cytokine GM-CSF

(Leukomax, Novartis Farma, Origgio, VA, Italy) was administered S.C. in the amount of 75 pg the day before, the same day of the vaccination and the following day during the first two vaccinations of the first and second cycle, and at the same site like HSPPC-96 vaccinations. During the other vaccinations, GM-CSF was adminis- tered only once, along with HSPPC-96. IFN-a 2b (Schering-Plough, Milan, Italy) was given as 3 MU S.C. twice weekly, 1 and 3 days after the last administration of GM-CSF during the first cycle and at a site different from that of GM-CSF. During the second cycle, IFN-r: was given three tiines a week duiiiig the weeks in between the vaccination weeks (see Figure 1).
Patients were monitored for toxicity, including com- plete clinica1 evaluation, standard blood tests including ciinerential blood counts, serum chemistry, urinalysis, cardiac, liver and renal functions, and autoiminune reactions (anti-microsoinal and anti-thyroglobulin anti- bodies, T3, free T4, and anti-nucleoprotein antibodies). Ophthalmologic examinations were carried out at 4, 8 and 12 weeks to assess possible autoimmune reactions caused by melanoma/retina cross-reacting differentia- tion antigens.
Tuinor evaluation was perfoimed before resection of metastatic melanoma, at pre-treatment visits 1 or 2 (V1 or V2) (baseline evaluation), at week 4 (V6) of the study, and thereafter every 3 months and as clinically indicated. Al1 time points of response were recorded from the time of surgery. This was done by the same sequential diatgnostic imaging method. The size of tumor lesion was evaluated as the sum of the longest perpendicular diameters of the relevant target lesions and recorded. Clinica1 responses were defined accoi-ding to (RECIST) response evaluation criteria iil solid tumors [8]. Time to progression (TTP) was calculated from the day of surgery until first docu- mented progressi011 or last documented evaluation without progression. Overall survival was calculated from the day of surgery until the last contact date or the date of deatla. Skin punch biopsies were carried out al the site of vaccination whenever possible.
vaccination (V1 or 2) and at V6 (fourth vaccination), V7 (fifth vaccination, 4 weeks afterward) and at V10 (eighth vaccination). In the case of patients who i-eceived addi- tional vaccinations, blood was obtained also during the subsequent follow-up visit at V1 1 or V12. PBMCs were isolated by Eicoll gradient centrifugation and frozen in aliquots in liquid nitrogen. The immune tests (see below) were al1 performed at the Istituto Nazionale Tumori to assess the patients' anti-melailoma immune response. Peripheral blood mononuclear cells (PBMCs) of 17 out of 19 evaluable subjects could be analyzed; patient 01- 022 was not assessed since he was found positive for HCV.
Preparation of vaccine
HSPPC-96 vaccine was manufactured from autologous tumor samples of each patient by Antigenics Inc. (Lex- ington, MA, USA) as reported previously [l] with minor modifications. After dissection and freezing, each sample was shipped to Antigenics facili0 in Lexington, MA, and processed under good manufacturing practice con- ditions.
Evaluation of the immune response
HLA tjying
Serological typing for HLA-A, -B, -C was performed by the standard two-stage complement-dependwt micro- cytotoxicity assay. For molecular typing, genomic DNA was purified from protease-treated PBMCs with QIArnp DNA (Qiagen, Hilden, Germany), and HLA t w g was performed by amplification with se primers (Dynal, Bromborough, UK).
Skin reactions at the site of vaccination were a&essed lmn~unological evaluation 1 h after every injection of the vaccine and/or GM-CSF
by the atteading physician, and after 24 and 48 h by the Eighty to l00 m1 of heparinized blood was obtained by physician or the instructed patient. DTH was carrqid out preparation of a buffy-coat from each patieiit before by injection of 5x10~ irradiateci (100 Gy) a ~ t + ~ o u s
i
Fig. 1 Scheme of treatment and of tiine of blood wit]idrawal of vacane (25 ug) injected s.c. GM-CCF (75ug) injected S.C. 100 mi b~ood withdmwal * IFN i d d s.c. staze IV melanoma patients
B * * * * * 1 49---4 ------ ?2bd?',*l *
1 i I
melanoma cells (when available) derived from mela- noina lesions by mechanical processing from patieiits 01 - 001 Lo 01-0019 and of 1x10~ from patients 01-020 to 01- 003 1 because or lack of positive DTH reaction with the lower dose. These cells were tested for sterility by routine rnicrobiological assays. Cells were suspended in 10% humaii AB serum, aliquoted, stored in liquid nitrogen and thawed before injection. Autologous irradiated (30 Gy) PBMCs, obtained from blood by Fico11 gradient (Pharmacia Biosystern, Uppsala, Sweden) centrifuga- tion, were also injected as negative contro1 immediately before the first, fourth and fifth vaccination. All injec- tions were done in 0.5 m1 volume intra-dermally at sites distant froin that of vaccine and cytokine administra- tion.
after vaccination, was performed by using the Student's t test for unpaired samples. Standard deviatioii was evaluated in three or six well replicates. A Pc0.05 was considered statistically significant.
Melanoma nnd other cell lirtes
Tumor celi suspensions were obtained by mechanical processing of melanoma lesions after surgery; in some cases enzymatic digestion was also used (see Ref. [l]. Ttimor eells were then aliquoted, frozen, and stored in liquid nitrogen). The melanoma line 501mel and 624.38mel were used as HLA-A2*0201 target cells [14]. T2 is a TAP-deficient lyrnphoma line that can express pulsed HLA-A"0201-feptsicted peptides and present them to T l y m p h o c y t e s . ~ ~ ~ ~ ce11 lines were maintained in RPMI 1640 with 10% FCS unless otherwise indicated.
This assay allows for the direct testing of antigeil rec- ognition by patieiit lymphocytes (T or NK) and has been In~~nui~opntholog of resected melanonza nretastases
used in severa1 trials of vaccination, including those with HSPPC-96 [l, 9-13]. The enzyme-linked immunospot (ELISPOT) assay was carried out as recently described [l. 131. Briefly, 96-well nitrocellulose plates (Mlititer, Millipore, Redford, MA, USA) were coated with 50 p1/ well of inouse anti-human IFN-y mAb (Mabtech, Na- cka, Sweden) in sterile buffer and incubated overnight at 4°C then washed to remove unbound antibody. Previ- ously thawed PBMCs were suspended in 10% FCS RPMI and added to the plates at the concentration of P-67x10' per well (in three or six replicates for each target) in 100 pl/well volume. After 30 min incubation at 37"C, targets were added at the concentration of 1 . 6 7 ~ 1 0 ~ per well. Non-specific total control release of IFN-.I was obtained by pokeweed mitogen (1 pg/ml, Sigma, Munich. Germany) stimulation. Blocking experirnents were perfomed by pre-incubating target cells for 30 rnin at 37°C with the anti-class 1 or anti-class TI mAb W6.32 or L243, respectively. To control the ELISPOT assay, the anti-Melan-A/MART- l T celi clone A42 in the presence or abseiice of the cognate antigen (T2 cells pulsed with M ~ ~ ~ I I - A / M A R T - ~ ~ , - ~ ~ peptide 01- the Melan-A/MART-l+ melanoma 501) were always included at the concentration of 400 ceIls/ well. After 20 11 of incubation at 3 7 T , the plates were washed and wells incubated for 2 h at room temperature with 100 pl/well of biotinylated anti-human IFN-p mAb (Mabtech). Aftenvard, wells were washed again and 50 pl/well of streptavidin alkaliiie phosphatase (Mab- tech) added. After 1 li incubation at room temperature, plates were washed extensively and added to 100 pi/well of the substrate (Biorad Laboratories, Hercules, CA, USA). Color development was stopped by washing in tap waler when dark spots emerged. Plates were then left to dry overnight and spots counted by a computer-as- sisted ELISPOT reader (Bioline, ALD, TurBn, Italy). Statistica1 analysis of the differente in ELISPOT data (after background subtraction) obtained before and
Routine histologic diagnosis and immunohistochemistry (IHC) evaluation were performed for al1 tumor samples used for vaccine production and for some recurrent le- sions detected during treatment. Classification of the metastatic foci on the basis of the "brisk/non-brisk" system for tumor-infiitrating lymphocytes [l51 was per- formed on routine Iiematoxylin and eosin-stained slides. In addition, this was correlated with IHC analysis using the routiiie imlluiioperoxidase technique. Tissue sec- tions were stained with the following antibodies: CD3 and CD4 (Novocastra Labs, Newcastle on Tyne, UK), CD8 (DAKO A/S, Glostrup, Denmarkj, CD45RO (DAKO A/S), CD56 N M (Sigma), HM84 S), S-100 (DAKO A/S), Melan-A/MA A103, Novocastra Labs), HLA-DR (clone AG, Dreieich, Germany), anti-HLA-A,-B,- rnAb HC-10 (kindly provided by Dr Sold Buffalo, USA). Previously well-document cases were used as positive controls for antigens. If al1 tumor-iiifiltrating lyinphocytes *ere of T phenotype, the CD3 population was consideed to be 100%. This was used as a baseline for a seini$uantita- tive couiit of CD4, CD8 and CD45 cells that &ere esti- mated as a percentage of the CD3 coun A, -B, -C and melanoina antigens (gp100 a MART-I) were arbitrarily considered as do when less than 20% of the tumor cells highly expressed when at least 50%, the. %<ere positive after staining witli the given . "
Resuh
Patients and vaccination
Of the 38 patieiits (see Table 1 for demographics and cliiiical data) who underwent surgery for renioval of
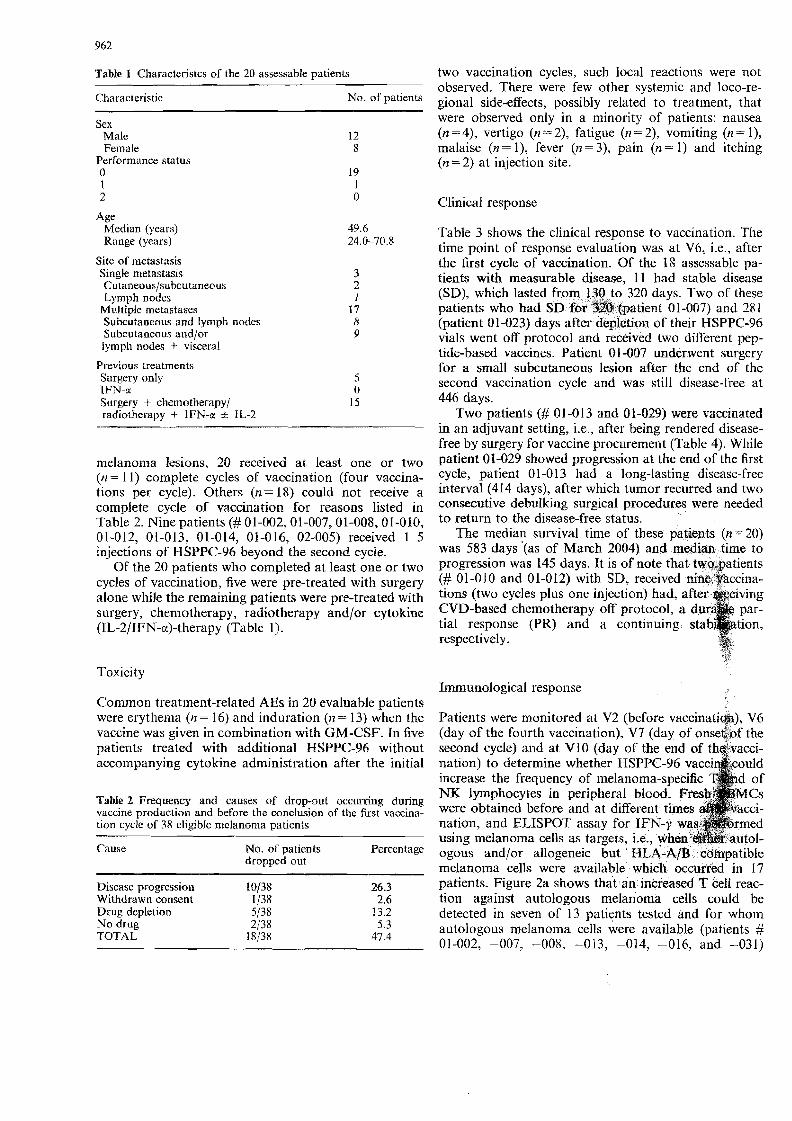
Table 1 Characieristcs of the 20 assessable patients
Characteristic No. of patieilts
Sex Male 12 Female 8
Performance status O 19 1 I 2 o
Age Median (years) Ratige (years)
Site of nletiistasis Single metastasis Cu~aileous/subcutaneous Lymph nodes
Multiple metastases Suhcutaneous and lyniph nodes Subcutaneous aild/or lympli iiodes + visceral
Previous treatinents Surgery only 5 IFN-a O Surgery + chemo therapy/ 15 radioihei-apy t IFN-x z t IL-2
melanoma lesions, 20 received at least one or two (n- l l) complete cycles of vaccinaiion (four vaccina- tions per cycle). Others (I%= 18) could not receive a coinpiete cycle of vaccination for reasons listed in Table 2. Nine patients (# 01-002, 01-007,Ol-008, 01-010, 0 1-0 1 2, 0 1-0 13, 0 1-0 14, 0 1-0 16, 02-005) received 1-5 injections of HSPPC-96 beyond the second cycle.
Of the 20 patients who completed at least one or two cycles of vaccination, five were pre-treated witli surgery alone while the reinaining patients were pre-treated with surgery, chemotherapy, radiotherapy and/or cytokine (IL-2/IFN-cc)-therupy (Sable 1).
two vaccination cycles, such local reactions were not observed. There were few otber systemic and loco-re- gional side-effects, possibly related to treatinent, that were observed only in a minority of patients: nausea (n = 4), vertigo (n = 2), fatigue (i? = 2), vomiting (n = l), malaise (n = l), fever (n = 3), pain (n = l) and itching (n = 2) at injectioii site.
Clinica1 response
Table 3 shows the clinica1 response to vaccination. Slie time point of response evaluation was at V6, Le., after the ikst cycle of vacciiiation. Of the 18 assessable pa- tients with measurable disease, 11 had stable disease (SD), which lasted from 130 to 320 days. Two of these patients who had SD fu9 3BQ batient 01-007) and 781 (patient 01-023) days after depletion of their HSPPC-96 vials went off protocol and received two diiTerent pep- tide-based vaccines. Patient 01-007 underwent surgery for a small subcutaneous lesion after the end of the second vaccination cycle and was still disease-free at 446 days.
Two patients (# 01-013 and 01-029) E r e vaccinated in an adjuvant setting, Le., after being rendered disease- free by surgery for vaccine procuremeiit (Table 4). Wliile patient 01-029 shohved progression at the etid of the first cycle, patient 01-013 liad a long-lasting disease-iree intemal (414 days), after which tumor recurred and two consecutive debulkiiig surgical procedures were needed to ieturn to the disease-free status.
The mediai1 survival time of these patients (n =20) was 583 days '(as of March 2004) and median time to progression was 145 days. It is of note that twogatients (# 01-01 0 and 01-012) with SD, received ninq $accina- tions (two cycles plus one injection) had, CVD-based cliemotherapy off protocol, a d tial response (PR) and a continuing respectively.
Toxici ty Immunological respoilse
Coirimon treatment-related AEs in 20 evaluable patients were erythema (11 = 16) and induration (n = 13) when the vaccine was given in combination with GM-CSF. In five patients treated with additional HSPPC-96 without accoinpanying cytokine administration after the initial
Table L Frequency and causes of drop-out occurring dunng vaccine production and before the conclusion of the first vaccina- tion cycle of 38 eligible melanon~a patjents
Cause No. of patients Percentage dropped out
Disease progression 10/38 26.3 Withdrawii consent 1/38 2.6 Dmg depletion 5/38 13.2 No drug 2/38 5.3 TOTAL 18/38 47.4
Patients were monitored at V2 (before vaccinati@), V6 (day of the fourtli vaccination). V7 (day of onseaof the second cycle) and at V10 (day of the e
NX lymphocytes
using melanoma celIs as targets, ie., when ogous and/or ailogeneic but HLA-A/B cmpatible melanoma cells were available which occurred in 17 patients. Figure 2a shows that ,an inkreased T ceII reac- tion against autologous melanoma ceIls could be detected in seven of 13 patients tested aild far whoin autologous melanoma cells were available (patients # 01-002, -007, -008, -013, -014, -016, and -031)
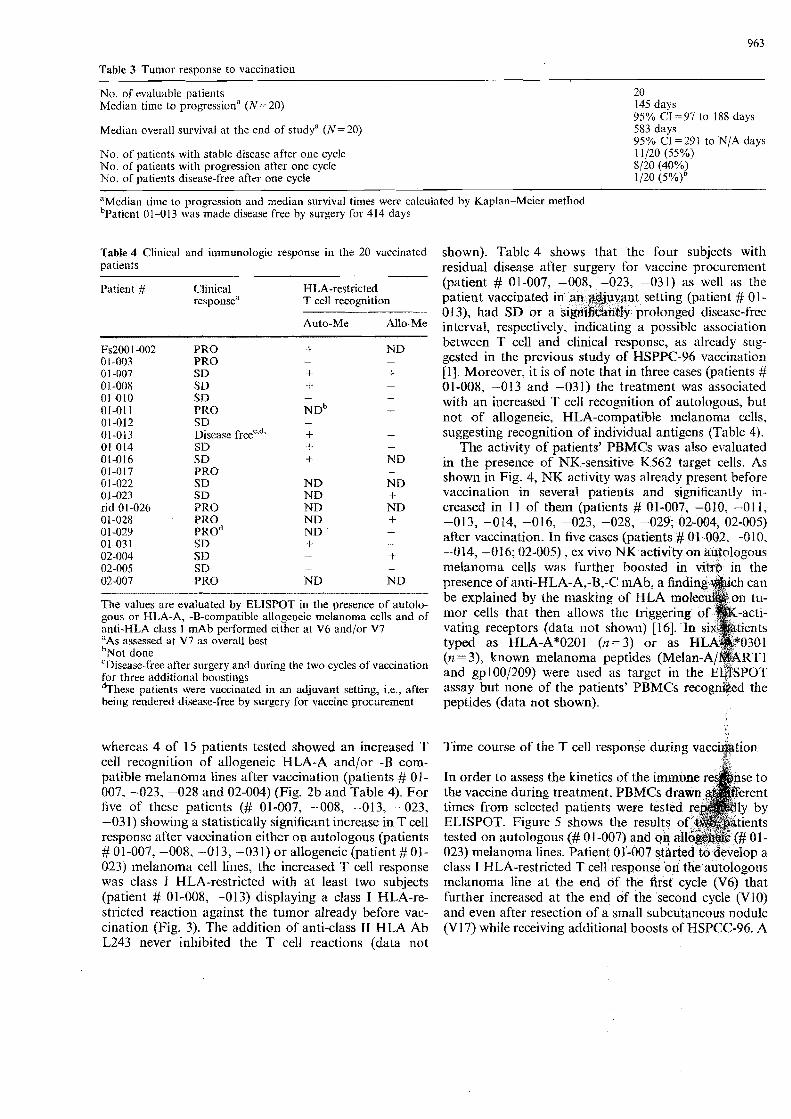
Table 3 Tun~or response to vaccination
No. of evaluable patients 20 Median tiine to progressiona (N = 20) 145 days
95% CI = 97 to 188 days Median overall survival at the ead of studya (N=20) 583 days
95% CI = 29 l to N/A days No. of patients with stable disease after one cycle 11/20 (55%) No. o€ patients with progression after one cycle SI20 (40%) No. of patients disease-free after one cycle 1/20 (5%lb
"Median tiiiie Lo progression aiid mediali survival times were calculated by Kaplan-Meier metliod "~at ient 01-013 was made disease free by surgery for 414 days
Table 4 Clinica1 2nd iinmunologic response in the 20 vaccinated patients
Patient # Clinica1 HLA-restricted response" T cell rezognition
Auto-Me Allo-Me
PRO PRO SD SD SD PRO SD Discase ~ r e e ~ ' ~ ~ SD SD PRO SD SD PRO PRO PRO^ SD SD SD PRO
The values are evaluated by ELISPOT in the presence of autoio- gous or HLA-A, -B-compatible allogeneic melanoina cells and of anti-HLA class I inAb performed either at V6 and/or V7 "As assessed at V7 as overall best " ~ o t done CDisease-frcc after surgery and during the two cycles of vaccination €or three addiiional boostinys * ~ h e s c patients were vaccinated in an adjuvant setting, i.e., after being rendered disease-free by surgery for vaccine procurement
whereas 4 of 15 patients tested showed an increased T ce11 recogiiition of allogeneic HLA-A and/or -B com- patible melanoma lines after vaccination @atients # 01- 007. -023, -028 and 02-004) (Fig. 2b and Table 4). For five of tliese patients (# 01-007, -008, -013, -023, --031) showing a statistically significant increase in T ce11 responsc after vaccinaiion either on antologous (patients # 01 -007, -008, -013, -03 1) or allogeneic (patient # 01- 023) inelanoma ce11 lines, the increased T ce11 response was class I HLA-restricted with at least two subjects (patient # 01-008, -013) displaying a class I HLA-re- sti-icted reactioii against the tuinor already before vac- cinatioii (Fig. 3). The addition of anti-class I1 HLA Ab L243 never inhibited the T ce11 reactions (data not
shown). Table 4 shows that the four subjects witli residua1 disease after surgery for vaccine procureineiit (patient # 01-007, -008, -023, -031) as well as tlie patient vaccinated in an adjuvant setting (patient # 01 - 013), had SD or a sign1i6&nty prolonged disease-free iiiterval, respectively, indicating a possible association between T ce11 and clinica1 respoiise, as already sug- gested in tlie previous study of HSPPC-96 vaccination [l]. Moreover, it is of note tliat in three cases (patients # 01-008, -013 and -031) the treatment was associated with an increased T ce11 recognition of autologous, but not of allogeneic, HLA-compatible melanoma cells. suggesiing recognition of individua1 antigens (Table 4).
The activity of patients' PBMCs was also evaluated in the preseilce of NK-sensitive K562 target cells. As showii in Fig. 4, NK activity was already present before vaccination in severa1 patients and significantly in- creased in 11 of them (patients # 01-007, -010, -011, -013, -014, -016, -023, -028, -029; 02-004, 02-005) after vaccination. In five cases (patients # 01-002, -010, -014, -016; 02-005) . ex vivo NK activity on au%ologous melanoma cells was further boosted in vitrp in the presence of aiiti-HLA-A,-B,-C niAb. a find be explained by the rnasking of HLA m mor cells that then allows the triggering vatii~g receptors (data not showii) [16]. In typed as HLA-A*0201 ( 1 2 = 3 ) or as (12 = 3), known melanonia peptides (Me1 aiid gp100/209) were used as target in assay b i ~ t none of the patients' PBMCs recogniked the peptides (data not showii).
Time course of the T ce11 respoiise during vacci@tion 4
In order to assess the kinetics of the i the vaccine during treatrnent, PBM times from selected patients were t ELISPOT. Figure 5 shows the results of tested on autolapous (# 0 1-007) and 023) melanoma lines. Patient 01-007 started to develop a class I HLA-restricted T ce11 response on the autologous melanoma line at the end ofi the first cycle (V6) that further increased at the end of the second cycle (V10) and even after resectioii of a small subcutaneous nodule (V17) while receiving additioral boosts of HSPCC-96. A
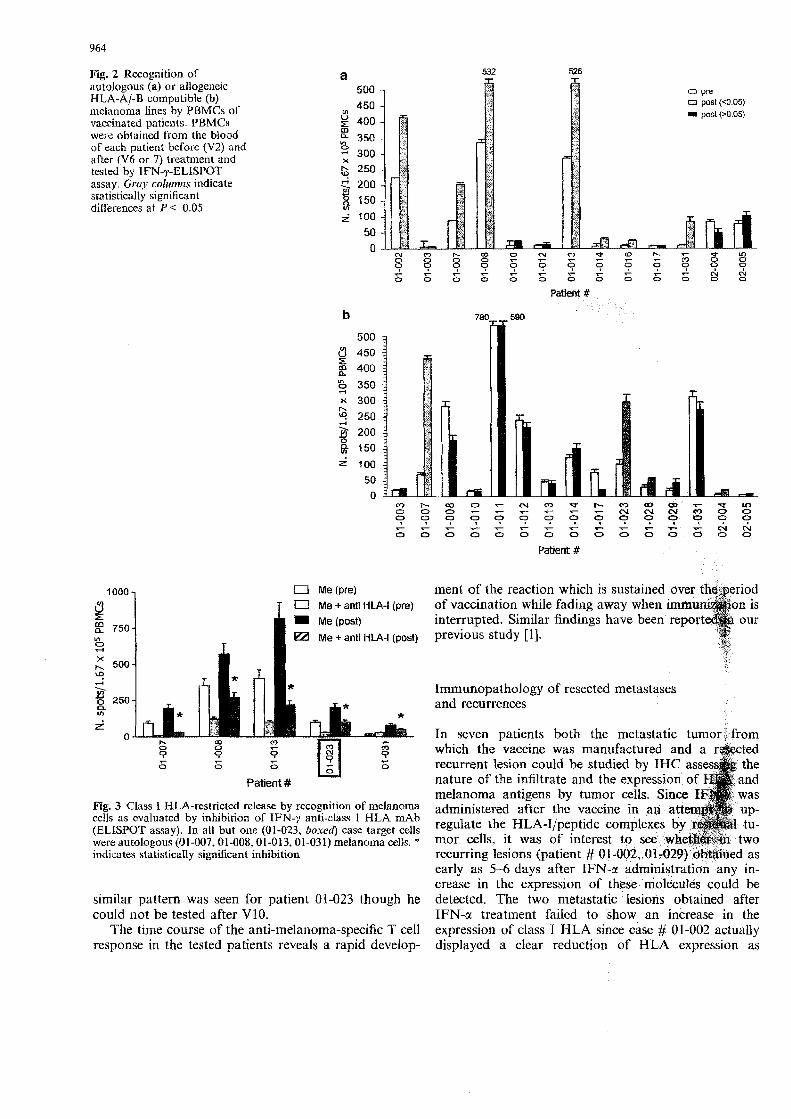
Fig. 2 Recognibon of autologous (a) or allogeneic HLA-A/-B coinpatible (b) il~elanoina lines by PBMCs of vaccinated patieiits. PBMCs were obtaincd froin the biood of each patient before (V2) and after (V6 or 7) treatment and tested by IFN-yELISPOT assay. Giwy coittriins indicate statistically significant differences at P < 0.05
o pre o post (-4.05) i posl p0.05)
17 Me + anti HLA-l (pre)
Me + anti HLA-l (post)
Patient #
Fig. 3 Class I HLA-restricted release by recognition of melanoma cells as evaluated by inhibition of IFN-7 anti-class I HLA mAb (ELISPOT assay). In ali but one (01-023, boxe4 case target cells were autologous (01-007,Ol-008,OI-013,01431) melanoma cells. ' indic~tes statisticaIly significnnt inhibition
similar pattern was seen for patient 01-023 though he could iiot be tested after V10.
The time course of the anti-melanoma-specific T ce11 vesponse in the tested patients reveals a rapid develop-
ment of the reaction which is sustained o of vaccination while fading away when i interrupted. Similar findings have been previous study [l].
Immunopathology of resected metastases and recumences
In seven patients both the metastatic tumorj from which the vaccine was rnanufactured and a recurrent lesion could be studied by IHC ass nature of the infiltrate and the expression of melanoma antigens by tumor cells. Since I administeved after tlie vaccine in an att regulate the HLA-I/peptide complexes by mor cells. it was of interest to see whe recurring Iesions (patient # 0 1-002, 0 1-029) obained as early as 5 -6 days after IFN-a administi-atio'n any in- crease in the expression of these dolecutes could be detected. The two metastatic lesions obtained after IFN-o! treatment failed to show an increase in the expression of class I HLA since case # 01-002 actually displayed a clear reduction of HLA expression as
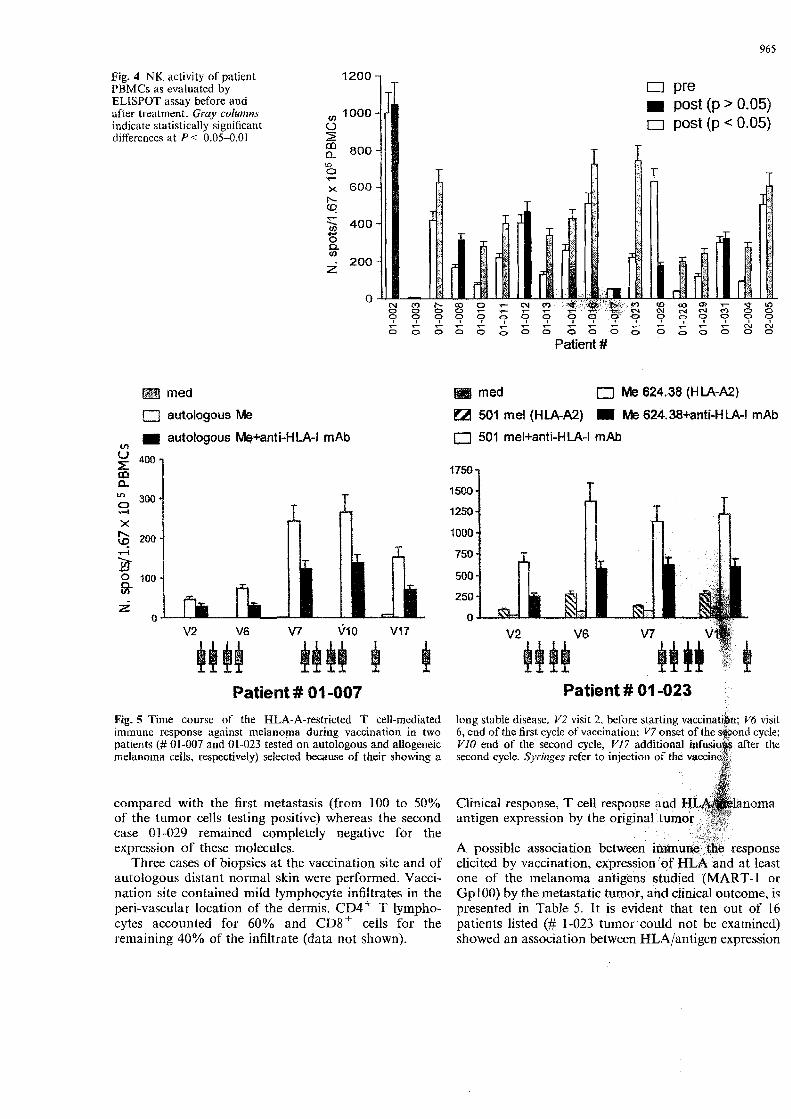
Fig. 4 NK activity of patient PBMCs as evaliiated by EIJSPOT assay before and after treatment. Graj? cofu??zn.s indicate statistically significant differences at P< 0.05-0.01
i post (p > 0.05) n post (p < 0.05)
4 9 4 4 9 9 g 4 . - . - . - . - T - . - 7 4 0 4 P ? 4 4 ? 0 .- - ? - - . - . - . - . - 0 0 0 0 0 ~ 0 0 O 0 0 0 0 0 0 0 1 : 0
Patient #
med med n Me 624.38 (H LA-N)
n autologous Me 501 me1 (HLA-A2) m Me 624.38+anti-H LA-! mAb
V) autologous W+anti-HLA-l mAb a 501 mel+anti-HLA-l mAb
$ 400 t750 n
1500 g 300 ,-I 1 250 X
Q mQ 1000
5 750
Bi 'O0 500
250 z o o
V2 V6 V7 V1 O V17
Patient # 01-007 Patient # 01 -023
Fig. 5 Time course of the HLA-A-restricted T cell-rnediated long stable disease. V 2 visit 2, before startiiig vaccinatibn; 1% visit irn~nune response against nela ano ma duriiig vaccination in two 6 , end of the first cycle of vaccinatioii; V7 onset ond cycle; patients (# 0 1-007 and 0 1-023 tested on autologous and aiiogeneic V I 0 end of the second cycle, 1/17 additional after tlie rnelanoina cells, respcctively) selected because of their shoiving a second cycle. Syringes refer to injectioii of the
cornpai-ed with the h s t metastasis (from 100 to 50% of the tumor cells testiiig positive) whereas the second case 01-029 reinained completely negative for the expression of these molecules.
Three cases of biopsies at the vaccination site and of autologous distant norma1 skin were performed. Vacci- nationi site contained rnild lymphocyte infìitrates in the peri-vascular location of the derrnis. C D ~ + T lympho- cytes accounted for 60% and C D ~ ' cells for the remaining 40% of the infiltrate (data not shown).
Clinica1 response, T ce11 respoirse antigen expression by the original
A possible associatican between elicited by vaccination, expressio one of the inelanoma antigeos Gp100) by the inetastatic tumor, and clinica1 outcome, is presented in Table 5. It is evident that ten out of 16 patients listed (# 1-033 tuinor could not be exainined) showed an association between HLAIantigen expression

and clinical outcome (7116 a positive association, i.e. high HLA/antigen and SD, and 3/16 a negative associ- ation, i.e., low HLA/antigen and PRO). In two cases (# 1-022, 1-023), SD was associated either to high HLA/ antigen or to T ce11 response only, due to the lack of T ce11 response and HLAlantigen evaluation, respectively. Considering the two groups of responders (ten SD) and progressors (seven patients), there was no correlation between HLA class I expression and T ce11 response. However, a clear correlation is evident between clinical outcome and T ce11 response since, among the ten SD patients, seven had developed a T ce11 reaction while only oile of six progressors did so.
In this trial stage IV, pre-treated inelanoma patients received autologous tuinor-derived HSPPC-96 along with GM-CSF and IFN-a in an attempt to potentially eiihance the iminunologic aiid ciiilical response obtained in a previous phase 11 study conducted with similar subjects receiving HSPPC-96 monotherapy [l]. The coinbination treatment in this study was well tolerated with fev, episodes of low-grade locai or systemic toxicity caused by the administered cytokines. However, the clinical response was limited to a high frequency of SD (11 out of 20 patients treated) though three patients experienced a prolonged clinical benefit after HSPPC-96 vaccination. One patient (# 0 1 -013), vaccinated without evideiice of disease, had a long lasting disease-free interval (414 days). Two additional patients (# 01-010 and 0 1-0 12) who received chemotherapy off protocol after HSPPC-96 vaccination, showed one (# 01-010) had a long-lasting (602 days) PR, while the other (# 01-012) had a long-term stabilization of the disease.
Tliis work shows that tlie HSPPC-96 autologous vaccine adrniiiistered with GM-CSF could elicit an anti- melanoma, cIass I HLA-restricted T cell-mediated im- mune rcaction in a proportion of patieiits treated but
Table 5 Association between clinical response, T cell response and HLA/rnelailoma antigen expression by the original tuinor
"Only HLA class I-i-estricted T ce11 responses were considered, including tllose directed againsi autologous and/or alloge- neic niekinom:i cells (see Table 4) h ~ s evaluated by irnmunohis- tochemistry 'Correlation between clinical response and HLAJMAA expression
that neither the frequency of responding subjects (5 out of 13) nor the strength of the reaction was noticeably higher than that obtained in a previous study of similar patients vacciilated with the HSPPC-96 moilotherapy [il.
Of some interest is the observation made in the present study, but not in the previous one, that three patients developed an increase in class I HLA-restricted recognition of autologous but not of allogeneic class I HLA-compatible melanoma cells, suggesting a recogni- tion of individua1 type of tumor antigens as described in animal models [17].
As for the effect of HSPPC-96 on the NK activity, we found that 12 of 18 patieilts that could be tested devel- oped a statisticaliy significant increased reaction against K562 after vaccination, a indicating the ability of the vaccine to stimulate s componeiit of Lhe in- nate immune system. We cannot exclude that IFN-a may have contribiited to such an increase of NK activity though in a previous trial in patients with liver metas- lases of colorectal carcinoma given HSPPC-96 nlono- therapy a siniilar in vivo activation of NK activity was observed [9]. Moreover, this has been previously re- ported in anima1 models where NK cells were shown to be required for therapeutic anti-tumor activity mediated by HSPs [l81 and in a small group of cancer patieiits as well [19]. It is of interest also that HSPs expressed on the tumor ce11 surface may stimulate not only the cytolytic activity of NK cells but also their chemotaxis 1201. We have found that even gp96 can stimulate in vitro human NK cells to release cytokine and to kill tumor lines thus potentially explaining their increased activity upon HSPPC-96 vaccination [l81 though the role of NK in anti-tuinor activity in our clinica1 setting rem@ns to be determined.
It is of interest that the observations study do not indicate a positive effect of IFN-a at the regirnen given on the immun clinical activity in this patient group studie lias been described to possibly iiicrease the i
Patient # Clinica1 response T ce11 responseJ Percentage of ce11 e~~i-essin&~
MARTI Gp100 , HLA-f
PRO SD SD SD PRO SD DF SD SD PRO
022' SD ND 90 20 l O0 023 SD f ND I ND ND 026 PRO ND 1 O0 I 00 1 O0 028" PRO f 70 1 O0 20 029" PRO 1 00 1 O0 0 031' SD + 1 00 60 1 O0
1.4. Kawakan~i Y, Eliyahu S, Delgado CH, Robbins PF, Rivoltini L, Topaliaii SL, Miki T, Rosenbergs SA (1994) Cloning of the gene coding for a shared human melanoma antigen recognized by autologous T cells infiltrating into tumor. Proc Natl Acad Sci USA 91:3515-3519
15. Mihm M C Jr, Clemente CG, Cascinelii N (1996) Tumor infil- trating lymphocytes in lymph ilode melanoma metastases: a histopathologic progiiostic indicator and an expression of local immune response. Lab Invest 74:43-47
16. Moretta L, Bottino C, Pende D, Miilgari MC, Biassoni R, Moretta A (2002) Human natura1 killer cells: their origin, receptors and function. Eur J Immunol 32:1205-1211
17. Tamura Y7 Peng P, Liu K, Srivastava PK (1997) Immuno- therupy of tumors with autologous tumor-detived heat shoqk protein preparations. Science 278: 1 17-120
18. Pilla L, Squarcina P, Coppa J, Mazzaferro V, Huber V, Pende D, Maccalli C, Sovena G, Mariani L, Castelli C, Parmiani G, Rivoltini L (2005) Natura1 killer and NK-Like T-cell activation in colorectal carcinoma patients treated with autologous tu- mor-derived heat shock protein 96. Cancer Res 65:3942-3949
19. Jrinetzki S, Palla D, Rosenhauer V, Lochc H, Lewis JJ, Sri- vastava PK (2000) Iinmunization of cancer patients with autologous cancer-derived heat sliock protein m96 prepara- tioiis: a pilot study. Int J Cailcer 88:232-238
20. Gastpar R, Gross C, Rossbacher L, Ellwart J, Riegger J, Multhoff G (2004) The cell surface-localized heat shock protein 70 epitope TKD induces nligration and cytolytic activity selectively in human NK ceils. J Immunol 172:972-980
21. Scheibenbogen CI Schmittel A, Keilhjolz U, Allgauer T, Hof- mani1 U, Max R, Thiel E, Schadendorf D (2000) Phase 2 trial of vaecination with tyrosiiiase peptides and granulocyte-mac- rophage colony-siimulating factor in patients with metastatic melanoma. J Immunother 23:275-281
22. Slingluff CL, Petroni GR, Yamshikov GW, Barnd DL, Eas- tham S. Galavotti H, Patterson JW, Deacon DH, Hibbitts S, Teates D, Neese PY. Grosh WW et al (2003) Clinica1 and immunological results of a randomized pliase 11 trial of vaccination using four melanoma peptides eitlier adininis- tered in granulocyte-macrophage colony stimulating hctor in adjuvant or pulsed on deudritic cells. J Clin Oncol 21:4016- 402 6
23. Ullenhag GJ, Frodin J-E, Mosolitis S. Kiaii S, Hassan M, Bonnet MC, Moingeon P, Mellstedt H, Rabbani R (2003) Immunization of colorectal carciaoma patients with a re- combinant canarypox virus expressing tbe tiiinpr antigen Ep- CAMIKSA (ALVAC-KSA) and granulocyte inncropliage col- ony-stimulating factor induced a tumor-specific cellular iin- mune response. Clin Cancer Res 93447-2456
24. Von Meheren M, Arlen P, Culley J, Rogatko A. Cooper HS, Meropol NJ, Alpaugh RK, Davey M, McLaughlin S. Beard MT, Tsang KY, Schlom J, Weiner LM (2001) The influente of granulocyte macrophage coloi~y-stiniulaiing factor and prior chemotherapy on e - m * o l o g i c a l response to a vaccine (ALVAC-CEA B7.1) in p&&&~b with metastatic carcinoma. Clin Cancer Res 7:1181-1191
25. Dillrnsn RO, Wiemann M, Nayak SK, deLeon C. Hood K, DePriest C (2003) Interferon-gamma or granuloeyte-macro- phage colony-stimulating factor administeced as ridjirvanis with a vaccine of irradiated autologous tumor cells from short-tenn cell liiie cultures: a randomized pliase 2 trial of the cancer biotherapy research group. J Immunnthcr 35367- 373
26. Pansky A, Hildebrand P, Fasler-Kan E, Beglinger C, Heiin MH (2000) Defective JAK-STAT signal transduction pathway in inelanon~d ce11 resistent to growth inhibition by interferon-x. Int J Cancer 85:720-725




















