
A Phase II Study of Plerixafor (AMD3100) plus G-CSF for Autologous Hematopoietic Progenitor Cell...
9
A Phase II Study of Plerixafor (AMD3100) plus G-CSF for Autologous Hematopoietic Progenitor Cell Mobilization in Patients with Hodgkin Lymphoma Amanda Cashen, 1 Sandra Lopez, 1 Feng Gao, 1 Gary Calandra, 2 Ron MacFarland, 2 Karin Badel, 2 John DiPersio 1 Collection of an adequate number of hematopoietic stem cells can be difficult in patients with relapsed or refractory Hodgkin lymphoma (HL) who are candidates for autologous stem cell transplantation (ASCT). Plerixafor (AMD3100), an inhibitor of the interaction between stromal cell-derived factor 1 (SDF-1) and its receptor CXCR4, is an effective hematopoietic stem cell mobilization agent in patients with multiple my- eloma and non-Hodgkin lymphoma (NHL). This study was undertaken to investigate the efficacy and safety of hematopoietic stem cell mobilization with plerixafor in patients with HL. Twenty-two patients with HL who were candidates for ASCT underwent hematopoietic stem cell mobilization with a combination of granulo- cyle-colony stimulating factor (G-CSF), 10 mg/kg daily, and plerixafor, 240 mg/kg subcutaneous, 10-11 hours prior to apheresis. The primary endpoint was the proportion of patients who collected $5 10 6 CD34 1 cells/kg. Outcomes were compared to a historical control population of HL patients mobilized with G-CSF alone. Pharmacokinetic (PK) analysis of plerixafor was performed in a subset of patients. Fifteen patients (68%) collected $5 10 6 CD34 1 cells/kg, and 21 patients (95%) achieved the minimum collection of $2 10 6 CD34 1 cells/kg, in a median 2 apheresis procedures. Both the proportion of patients collecting $5 10 6 CD34 1 cells/kg and the median CD34 1 cells collected in days 1-2 of apheresis were significantly im- proved over historical controls. The PK of plerixafor in this patient population was similar to that previously seen in healthy volunteers. The regimen was generally safe and well tolerated. Biol Blood Marrow Transplant 14: 1253-1261 (2008) Ó 2008 American Society for Blood and Marrow Transplantation KEY WORDS: Hodgkin lymphoma, Hematopoietic stem cell mobilization, AMD3100, Plerixafor INTRODUCTION Autologous stem cell transplantation (ASCT) is in- dicated for patients with Hodgkin lymphoma (HL) who have primary progressive disease or who relapse af- ter a chemotherapy-induced complete remission [1-7]. For these patients, as for other patients undergoing au- tologous transplantation, the number of CD34 1 cells collected is a reliable predictor of neutrophil and platelet engraftment after transplantation. Patients who receive at least 5 10 6 CD34 1 cells/kg have faster recovery of neutrophils and platelets, and the rate of platelet recov- ery may continue to improve with doses .5 10 6 CD34 1 cells/kg [8]. Conversely, if \1-2 10 6 CD34 1 cells/kg cells are transplanted, patients may have delayed engraftment or graft failure. Unfortunately, collection of peripheral blood stem cells (PBSCs) can be difficult in the HL population [9,10], as these patients usually have received multiple prior cytotoxic regimens. Plerixafor (AMD3100) reversibly inhibits the binding of stromal cell-derived factor 1 (SDF-1), con- stitutively expressed on bone marrow stromal cells, to its receptor CXCR4, expressed on CD34 1 cells. After a single subcutaneous dose of plerixafor, rapid mobili- zation of CD34 1 cells has been observed in both nor- mal volunteers [11] and in patients with multiple myeloma (MM) or non-Hodgkin lymphoma (NHL) [12]. Phase III studies have demonstrated that plerixa- for combined with granulocyte-colony stimulating factor (G-CSF) improves PBSC collection compared to mobilization with G-CSF alone in patients with MM or NHL [13,14]. This study was undertaken to determine the effi- cacy and safety of the addition of plerixafor to the From the 1 Washington University School of Medicine, St. Louis, Missouri; and 2 Genzyme Corporation, Cambridge, Massachu- setts Correspondence and reprint requests: Amanda F. Cashen, MD, 660 South Euclid Avenue, Box 8007, St. Louis, MO 63110 (e-mail: [email protected]). Received May 27, 2008; accepted August 24, 2008 1083-8791/08/1411-0001$34.00/0 doi:10.1016/j.bbmt.2008.08.011 1253
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of A Phase II Study of Plerixafor (AMD3100) plus G-CSF for Autologous Hematopoietic Progenitor Cell...

A Phase II Study of Plerixafor (AMD3100) plus G-CSF forAutologous Hematopoietic Progenitor Cell
Mobilization in Patients with Hodgkin Lymphoma
Amanda Cashen,1 Sandra Lopez,1 Feng Gao,1 Gary Calandra,2 Ron MacFarland,2
Karin Badel,2 John DiPersio1
Collection of an adequate number of hematopoietic stem cells can be difficult in patients with relapsed orrefractory Hodgkin lymphoma (HL) who are candidates for autologous stem cell transplantation (ASCT).Plerixafor (AMD3100), an inhibitor of the interaction between stromal cell-derived factor 1 (SDF-1) andits receptor CXCR4, is an effective hematopoietic stem cell mobilization agent in patients with multiple my-eloma and non-Hodgkin lymphoma (NHL). This study was undertaken to investigate the efficacy and safety ofhematopoietic stem cell mobilization with plerixafor in patients with HL. Twenty-two patients with HL whowere candidates for ASCTunderwent hematopoietic stem cell mobilization with a combination of granulo-cyle-colony stimulating factor (G-CSF), 10 mg/kg daily, and plerixafor, 240 mg/kg subcutaneous, 10-11 hoursprior to apheresis. The primary endpoint was the proportion of patients who collected $5 � 106 CD341
cells/kg. Outcomes were compared to a historical control population of HL patients mobilized with G-CSFalone. Pharmacokinetic (PK) analysis of plerixafor was performed in a subset of patients. Fifteen patients(68%) collected $5 � 106 CD341 cells/kg, and 21 patients (95%) achieved the minimum collection of $2� 106 CD341 cells/kg, in a median 2 apheresis procedures. Both the proportion of patients collecting $5� 106 CD341 cells/kg and the median CD341 cells collected in days 1-2 of apheresis were significantly im-proved over historical controls. The PK of plerixafor in this patient population was similar to that previouslyseen in healthy volunteers. The regimen was generally safe and well tolerated.
Biol Blood Marrow Transplant 14: 1253-1261 (2008) � 2008 American Society for Blood and Marrow Transplantation
KEY WORDS: Hodgkin lymphoma, Hematopoietic stem cell mobilization, AMD3100, Plerixafor
INTRODUCTION
Autologous stem cell transplantation (ASCT) is in-dicated for patients with Hodgkin lymphoma (HL)who have primary progressive disease or who relapse af-ter a chemotherapy-induced complete remission [1-7].For these patients, as for other patients undergoing au-tologous transplantation, the number of CD341 cellscollected is a reliable predictor of neutrophil and plateletengraftment after transplantation. Patients who receiveat least 5 � 106 CD341 cells/kg have faster recovery ofneutrophils and platelets, and the rate of platelet recov-
From the 1Washington University School of Medicine, St. Louis,Missouri; and 2Genzyme Corporation, Cambridge, Massachu-setts
Correspondence and reprint requests: Amanda F. Cashen, MD, 660South Euclid Avenue, Box 8007, St. Louis, MO 63110 (e-mail:[email protected]).
Received May 27, 2008; accepted August 24, 20081083-8791/08/1411-0001$34.00/0doi:10.1016/j.bbmt.2008.08.011
ery may continue to improve with doses .5 � 106
CD341 cells/kg [8]. Conversely, if\1-2 � 106 CD341
cells/kg cells are transplanted, patients may have delayedengraftment or graft failure. Unfortunately, collection ofperipheral blood stem cells (PBSCs) can be difficult inthe HL population [9,10], as these patients usuallyhave received multiple prior cytotoxic regimens.
Plerixafor (AMD3100) reversibly inhibits thebinding of stromal cell-derived factor 1 (SDF-1), con-stitutively expressed on bone marrow stromal cells, toits receptor CXCR4, expressed on CD341 cells. Aftera single subcutaneous dose of plerixafor, rapid mobili-zation of CD341 cells has been observed in both nor-mal volunteers [11] and in patients with multiplemyeloma (MM) or non-Hodgkin lymphoma (NHL)[12]. Phase III studies have demonstrated that plerixa-for combined with granulocyte-colony stimulatingfactor (G-CSF) improves PBSC collection comparedto mobilization with G-CSF alone in patients withMM or NHL [13,14].
This study was undertaken to determine the effi-cacy and safety of the addition of plerixafor to the
1253

1254 Biol Blood Marrow Transplant 14:1253-1261, 2008A. Cashen et al.
mobilization regimen of patients undergoing ASCTfor HL. Results were compared with a historical con-trol population composed of 98 consecutive patientswith HL who underwent PBSC collection withG-CSF alone mobilization at Washington UniversitySchool of Medicine from 1998 to 2003. In addition,pharmacokinetic analysis was performed in a subsetof 9 patients following the first dose of plerixafor.
METHODS
Patient Eligibility
Patients with a diagnosis of HL who were candi-dates for autologous PBSC transplantation were eligi-ble for this study. Additional eligibility criteriaincluded: age 18 to 70 years, no more than 3 prior reg-imens of chemotherapy, receipt of last dose of chemo-therapy more than 4 weeks before study entry, EasternCooperative Oncology Group (ECOG) performancestatus of 0 or 1, white blood cell (WBC) count .3.0� 109/L, absolute neutrophil count (ANC) .1.5 �109/L, platelet count .100 � 109/L, serum creatinine#2.2 mg/dL, liver function tests \2 times the upperlimit of normal, adequate cardiac and pulmonary func-tion, negative for HIV infection. Exclusion criteriaincluded: failed previous stem cell collection, residualacute medical condition resulting from prior chemo-therapy, HL involving the central nervous system,acute infection or fever, pregnant or lactating female,actual body weight exceeding 150% of ideal bodyweight, history of ventricular arrhythmias, history ofgrade $2 paresthesias.
The study protocol was approved by the HumanResearch Protection Office at Washington UniversitySchool of Medicine. All patients provided writteninformed consent.
Investigational Drug
Plerixafor was supplied as a solution of 10 mg/mLor 20 mg/mL per 1 mL glass ampule. The amount ofstudy drug administered was calculated based on thepatient’s actual weight. The study drug was stored atroom temperature (15
�C to 25
�C) in a secure location
accessible only by authorized personnel.
PBSC Mobilization and Transplantation
Each patient was given a subcutaneous injection ofG-CSF 10 mg/kg daily in the morning for 4 days priorto the first day of apheresis and continuing each morn-ing just prior to apheresis. On the evening of the fourthday of G-CSF and each evening prior to apheresis(10-11 hours prior to the start of apheresis), plerixafor240 mg/kg was given as a subcutaneous injection.Venous samples for CBC and FACS analysis werecollected immediately prior to each dose of plerixafor
and 10-11 hours after each dose, immediately priorto apheresis. CD341 cells were enumerated usingstandard flow cytometric techniques both in the locallaboratory (Barnes Jewish Hospital, St. Louis, MO)and in a central reference laboratory (Esoterix, Mem-phis, TN). Patients returned daily for a morningdose of G-CSF, the collection of hematopoietic stemcells, and an evening dose of plerixafor for up to 5 con-secutive days or until $5 � 106 CD341 cells/kg hadbeen collected. Patients underwent a standard 3-bloodvolume apheresis procedure on each day of hemato-poietic stem cell collection. At each visit, patientswere asked about toxicities, and their symptoms wererecorded in the nursing record. Patients returned 24hours after the last apheresis procedure for a finallaboratory and toxicity assessment. Toxicity data wascollected from the nursing record and transcribed inthe case report forms.
Patients received myeloablative conditioning fol-lowed by infusion of the G-CSF 1 plerixafor-mobi-lized cells. The choice of conditioning regimen andsupportive care were left to the discretion of the treat-ing physicians. Posttransplantation, patients weremonitored for neutrophil and platelet engraftment.Date of neutrophil engraftment was either the first of3 consecutive days in which the ANC was .500/mLor the first day in which the ANC was .1000/mL,and date of platelet engraftment was the first of 7days in which the platelet count exceeded 20,000/mLwithout transfusion.
Pharmacokinetics
In a subset of 9 patients, blood samples for the de-termination of plerixafor plasma concentrations werecollected at multiple time points over 10 hours follow-ing the first dose of plerixafor, with the 10-hour samplecollected just prior to apheresis. Plerixafor concentra-tions in heparinized plasma were determined usinga validated HPLC-mass spectrometry method (Av-Tech Laboratories, Kalamazoo, MI). In this method,internal standard (deuterated plerixafor, 5 ng) wasadded to plasma (200 mL) followed by the addition ofethylenediamine dihydrochloride (2 mg). Plasma pro-teins were then precipitated by the addition of acetoni-trile acidified with trifluoroacetic acid (TFA), followedby vortexing (5 seconds) and microcentrifugation(�12,000 � g for 5 minutes). Supernatants were trans-ferred to clean tubes, 20 mL ethylene glycol was added,and the samples vortexed, followed by evaporation todryness under a stream of nitrogen. Calibration stan-dards and quality control (QC) samples were preparedby the addition of plerixafor to blank human plasmaand were processed in the same manner as patient sam-ples. Following reconstitution in 0.5% TFA in water,extracts were analyzed by reverse-phase chromatogra-phy (C18 column, acetonitrile:water gradient; total

Biol Blood Marrow Transplant 14:1253-1261, 2008 1255Plerixafor Mobilization for Hodgkin Lymphoma
run duration 5 4 minutes) coupled to MS/MS detec-tion (electrospray interface in positive ion mode).
Validation of this method included assessment oflinearity, within-run and between-run precision andaccuracy, selectivity, long-term (frozen), short-term(room temperature), autosampler, freeze-thaw, andprocessed sample stability, extraction efficiency, carry-over, and the effect of dilution. The validated calibra-tion range was from 5-1000 ng/mL and was selectedbased on linearity (R2 . .95) and accuracy and preci-sion criteria for the validation runs. Acceptance criteriafor patient sample runs were based on results for cali-bration standards and QC samples included in eachrun.
Pharmacokinetic parameters were estimated bynoncompartemental methods using WinNonlinProfessional, version 5.2 (Pharsight Corp., MountainView, CA). The area under the plasma concentrationtime curve (AUC), peak concentration in plasma(Cmax), time to maximum concentration (Tmax), termi-nal elimination half-life (t1/2), apparent total systemicclearance (CL/F, where F represents the fraction ofthe dose absorbed), and apparent volume of distribu-tion (Vz/F) were calculated.
Historical Control Population
The control group is composed of all patients withHL who were mobilized with G-CSF alone at Wash-ington University School of Medicine from 1997 to2003. Information about the control group was col-lected as part of a comprehensive retrospective studyexamining hematopoietic stem cell mobilization out-comes at our center. The control patients underwent20 liter exchanges for each apheresis procedure.
Statistical Analysis
All enrolled patients were analyzed for safety andefficacy. The primary endpoint was the proportion ofpatients who collected $5 � 106 CD341 cells/kg.The secondary endpoints were the proportion of pa-tients who collected $2 � 106 CD341 cells/kg, thesafety of plerixafor in this patient population, the num-ber of days of apheresis required to obtain $5 � 106
CD341 cells/kg, the change in the number ofCD341 cells circulating in the peripheral blood fromtime 0 to 10-11 hours after a dose of plerixafor, thetime to engraftment of neutrophils and platelets, andgraft durability at 3, 6, and 12 months after stem celltransplantation. One patient underwent 2 mobiliza-tions with G-CSF 1 plerixafor because the first hema-topoietic stem cell product was discarded for bacterialcontamination. Only the data from that patient’s firstcollection was included in the evaluation of theprimary and secondary endpoints.
CD341 cells counts as reported by the local labo-ratory were used to calculate the primary and second-
ary endpoints and in comparison with historicalcontrols. Adverse events were categorized as mild(awareness of sign or symptoms, but easily tolerated),moderate (discomfort enough to cause interferencewith usual activity), or severe (incapacitating with in-ability to work or do usual activity). Descriptive statis-tics were used to summarize CD341 cell collections,number of days of apheresis, circulating CD341 cells,and days to neutrophil and platelet engraftment. Apower justification was conducted using c2 test basedon a binomial distribution. Compared with the histor-ical success rate of 15% (percent of patients reaching5 � 106 CD341 cells/kg), a minimum of 16 evaluablepatients would allow us, with 80% power and at a1-sided .05 significance level, to detect a minimal25% improvement in success rate (eg, 15% versus40%). Therefore, our study was adequately powered.
RESULTS
Patient Characteristics
Twenty-two patients with relapsed or refractoryHL were enrolled in this study and underwent hema-topoietic stem cell mobilization with G-CSF 1 plerix-afor. Patient characteristics are summarized in Table1. Ninety-one percent of patients had received 2 ormore prior chemotherapy regimens. Seventy-threepercent of patients were in second complete remission(CR) or partial remission (PR); 14% in first CR or PR;and 14% had active or refractory disease at the time oftransplant.
Response to Plerixafor
CD341 cell collection
Fifteen patients (68%) met the primary endpointand achieved a collection of $5 � 106 CD341 cells/kg, and 21 patients (95%) collected $2 � 106
CD341 cells/kg. The median collection was 6.6 �106 CD341 cells/kg (range: 0.9-10.4 � 106). MeanCD341 cell collection was higher in patients underthe age of 45 years (n 5 16, 7.2 � 106 CD341 cells/kg) than in patients over the age of 45 (n 5 6, 4.3 �106 CD341 cells/kg) (P 5 .01). These results were de-termined using local laboratory data. Apheresis sam-ples from 20 patients were received in the centrallaboratory for CD341 cell enumeration. Based onanalysis from the central laboratory, 13 of 20 patients(65%) achieved a collection of $5 � 106 CD341
cells/kg, 19 of 20 patients (95%) collected $2 � 106
CD341 cells/kg, and the median collection was 6.9� 106 CD341 cells/kg (range: 1.3-15.1 � 106).
The only patient who failed to collect $2 � 106
CD341 cells/kg was a 54-year-old man who hadbeen treated in the 12 months prior to hematopoieticstem cell mobilization with the Stanford 5 regimen,
1256 Biol Blood Marrow Transplant 14:1253-1261, 2008A. Cashen et al.
inverted Y radiation, and dexamethasone, cytarabine,and cisplatin (DHAP). His circulating CD341 cellcount increased from 2 to 6 cells/mL after the firstdose of plerixafor, and he collected a total of 0.94 �106 CD341 cells/kg in 3 apheresis procedures.
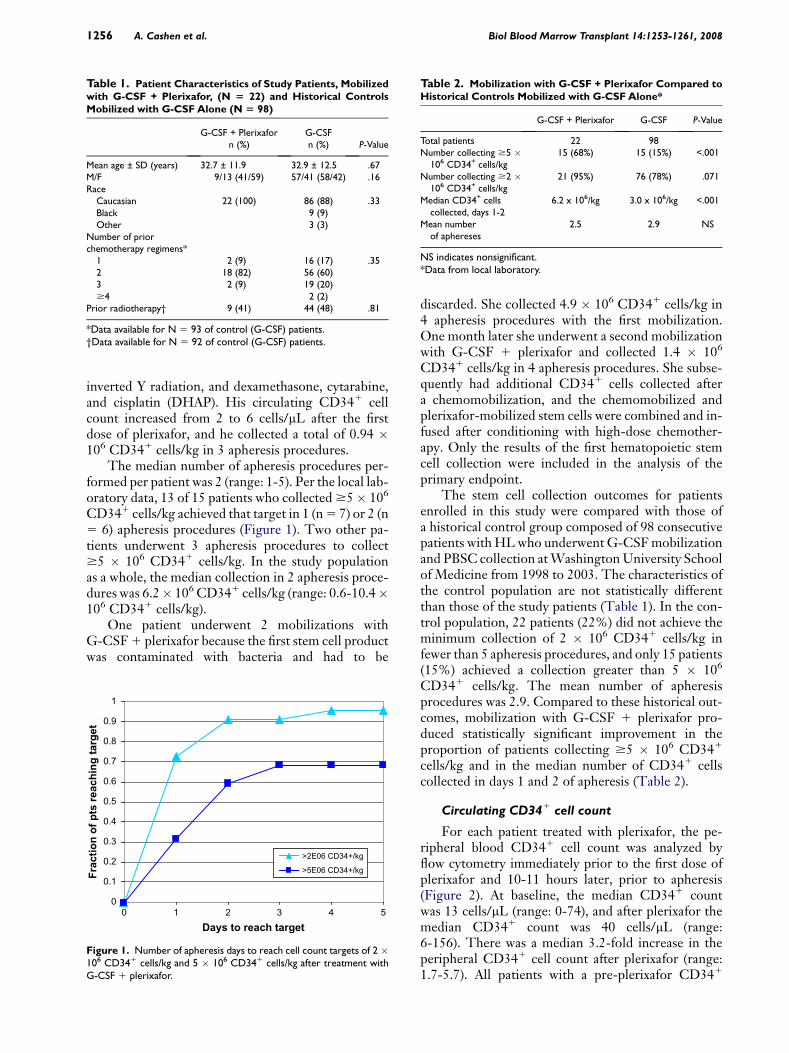
The median number of apheresis procedures per-formed per patient was 2 (range: 1-5). Per the local lab-oratory data, 13 of 15 patients who collected $5� 106
CD341 cells/kg achieved that target in 1 (n 5 7) or 2 (n5 6) apheresis procedures (Figure 1). Two other pa-tients underwent 3 apheresis procedures to collect$5 � 106 CD341 cells/kg. In the study populationas a whole, the median collection in 2 apheresis proce-dures was 6.2� 106 CD341 cells/kg (range: 0.6-10.4�106 CD341 cells/kg).
One patient underwent 2 mobilizations withG-CSF 1 plerixafor because the first stem cell productwas contaminated with bacteria and had to be
Table 1. Patient Characteristics of Study Patients, Mobilizedwith G-CSF + Plerixafor, (N 5 22) and Historical ControlsMobilized with G-CSF Alone (N 5 98)
G-CSF + Plerixaforn (%)
G-CSFn (%) P-Value
Mean age ± SD (years) 32.7 ± 11.9 32.9 ± 12.5 .67M/F 9/13 (41/59) 57/41 (58/42) .16Race
Caucasian 22 (100) 86 (88) .33Black 9 (9)Other 3 (3)
Number of priorchemotherapy regimens*
1 2 (9) 16 (17) .352 18 (82) 56 (60)3 2 (9) 19 (20)$4 2 (2)
Prior radiotherapy† 9 (41) 44 (48) .81
*Data available for N 5 93 of control (G-CSF) patients.†Data available for N 5 92 of control (G-CSF) patients.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 1 2 3 4 5Days to reach target
Fractio
n o
f p
ts reach
in
g targ
et
>2E06 CD34+/kg
>5E06 CD34+/kg
Figure 1. Number of apheresis days to reach cell count targets of 2 �106 CD341 cells/kg and 5 � 106 CD341 cells/kg after treatment withG-CSF 1 plerixafor.
discarded. She collected 4.9 � 106 CD341 cells/kg in4 apheresis procedures with the first mobilization.One month later she underwent a second mobilizationwith G-CSF 1 plerixafor and collected 1.4 � 106
CD341 cells/kg in 4 apheresis procedures. She subse-quently had additional CD341 cells collected aftera chemomobilization, and the chemomobilized andplerixafor-mobilized stem cells were combined and in-fused after conditioning with high-dose chemother-apy. Only the results of the first hematopoietic stemcell collection were included in the analysis of theprimary endpoint.
The stem cell collection outcomes for patientsenrolled in this study were compared with those ofa historical control group composed of 98 consecutivepatients with HL who underwent G-CSF mobilizationand PBSC collection at Washington University Schoolof Medicine from 1998 to 2003. The characteristics ofthe control population are not statistically differentthan those of the study patients (Table 1). In the con-trol population, 22 patients (22%) did not achieve theminimum collection of 2 � 106 CD341 cells/kg infewer than 5 apheresis procedures, and only 15 patients(15%) achieved a collection greater than 5 � 106
CD341 cells/kg. The mean number of apheresisprocedures was 2.9. Compared to these historical out-comes, mobilization with G-CSF 1 plerixafor pro-duced statistically significant improvement in theproportion of patients collecting $5 � 106 CD341
cells/kg and in the median number of CD341 cellscollected in days 1 and 2 of apheresis (Table 2).
Circulating CD341 cell count
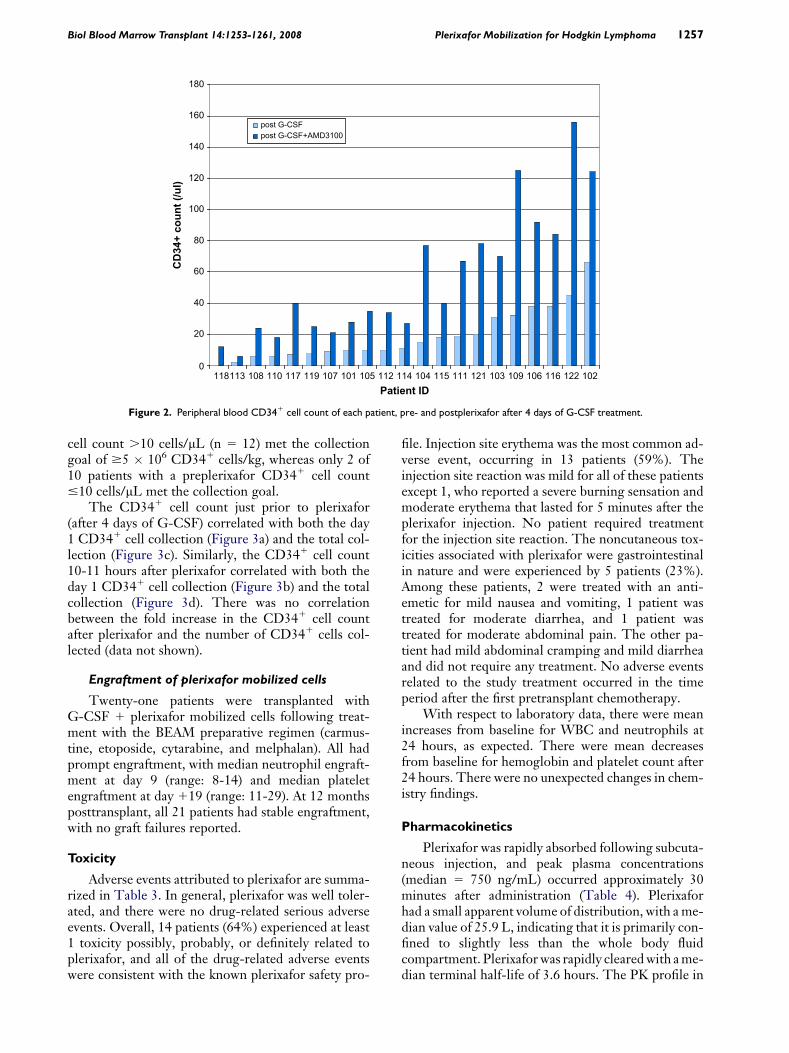
For each patient treated with plerixafor, the pe-ripheral blood CD341 cell count was analyzed byflow cytometry immediately prior to the first dose ofplerixafor and 10-11 hours later, prior to apheresis(Figure 2). At baseline, the median CD341 countwas 13 cells/mL (range: 0-74), and after plerixafor themedian CD341 count was 40 cells/mL (range:6-156). There was a median 3.2-fold increase in theperipheral CD341 cell count after plerixafor (range:1.7-5.7). All patients with a pre-plerixafor CD341
Table 2. Mobilization with G-CSF + Plerixafor Compared toHistorical Controls Mobilized with G-CSF Alone*
G-CSF + Plerixafor G-CSF P-Value
Total patients 22 98Number collecting $5 �
106 CD34+ cells/kg15 (68%) 15 (15%) <.001
Number collecting $2 �106 CD34+ cells/kg
21 (95%) 76 (78%) .071
Median CD34+ cellscollected, days 1-2
6.2 x 106/kg 3.0 x 106/kg <.001
Mean numberof aphereses
2.5 2.9 NS
NS indicates nonsignificant.*Data from local laboratory.
Biol Blood Marrow Transplant 14:1253-1261, 2008 1257Plerixafor Mobilization for Hodgkin Lymphoma
0
20
40
60
80
100
120
140
160
180
118113 108 110 117 119 107 101 105 112 114 104 115 111 121 103 109 106 116 122 102Patient ID
CD
34+
co
un
t (/u
l)
post G-CSFpost G-CSF+AMD3100
Figure 2. Peripheral blood CD341 cell count of each patient, pre- and postplerixafor after 4 days of G-CSF treatment.
cell count .10 cells/mL (n 5 12) met the collectiongoal of $5 � 106 CD341 cells/kg, whereas only 2 of10 patients with a preplerixafor CD341 cell count#10 cells/mL met the collection goal.
The CD341 cell count just prior to plerixafor(after 4 days of G-CSF) correlated with both the day1 CD341 cell collection (Figure 3a) and the total col-lection (Figure 3c). Similarly, the CD341 cell count10-11 hours after plerixafor correlated with both theday 1 CD341 cell collection (Figure 3b) and the totalcollection (Figure 3d). There was no correlationbetween the fold increase in the CD341 cell countafter plerixafor and the number of CD341 cells col-lected (data not shown).
Engraftment of plerixafor mobilized cells
Twenty-one patients were transplanted withG-CSF 1 plerixafor mobilized cells following treat-ment with the BEAM preparative regimen (carmus-tine, etoposide, cytarabine, and melphalan). All hadprompt engraftment, with median neutrophil engraft-ment at day 9 (range: 8-14) and median plateletengraftment at day 119 (range: 11-29). At 12 monthsposttransplant, all 21 patients had stable engraftment,with no graft failures reported.
Toxicity
Adverse events attributed to plerixafor are summa-rized in Table 3. In general, plerixafor was well toler-ated, and there were no drug-related serious adverseevents. Overall, 14 patients (64%) experienced at least1 toxicity possibly, probably, or definitely related toplerixafor, and all of the drug-related adverse eventswere consistent with the known plerixafor safety pro-
file. Injection site erythema was the most common ad-verse event, occurring in 13 patients (59%). Theinjection site reaction was mild for all of these patientsexcept 1, who reported a severe burning sensation andmoderate erythema that lasted for 5 minutes after theplerixafor injection. No patient required treatmentfor the injection site reaction. The noncutaneous tox-icities associated with plerixafor were gastrointestinalin nature and were experienced by 5 patients (23%).Among these patients, 2 were treated with an anti-emetic for mild nausea and vomiting, 1 patient wastreated for moderate diarrhea, and 1 patient wastreated for moderate abdominal pain. The other pa-tient had mild abdominal cramping and mild diarrheaand did not require any treatment. No adverse eventsrelated to the study treatment occurred in the timeperiod after the first pretransplant chemotherapy.
With respect to laboratory data, there were meanincreases from baseline for WBC and neutrophils at24 hours, as expected. There were mean decreasesfrom baseline for hemoglobin and platelet count after24 hours. There were no unexpected changes in chem-istry findings.
Pharmacokinetics
Plerixafor was rapidly absorbed following subcuta-neous injection, and peak plasma concentrations(median 5 750 ng/mL) occurred approximately 30minutes after administration (Table 4). Plerixaforhad a small apparent volume of distribution, with a me-dian value of 25.9 L, indicating that it is primarily con-fined to slightly less than the whole body fluidcompartment. Plerixafor was rapidly cleared with a me-dian terminal half-life of 3.6 hours. The PK profile in

1258 Biol Blood Marrow Transplant 14:1253-1261, 2008A. Cashen et al.
*
*
*
*
*
*
**
*
*
*
**
* *
**
*
*
*
*
0 20 40 60 80 100 0 50 100 150
0 50 100 1500 20 40 60 80 100
0
5
10
15
0
5
10
15
0
5
10
15
0
5
10
15
pre−AMD3100 CD34+ count (/ul)
day
1 C
D34
+ ce
ll co
llect
ion
(1.0
E06/
kg)
Spearman r=0.928p<0.0001
*
*
*
*
*
*
**
*
*
*
**
* *
*
**
*
*
*
*
post−AMD3100 CD34+ count (/ul)
day
1 C
D34
+ ce
ll co
llect
ion
(1.0
E06/
kg)
Spearman r=0.903p<0.0001
*
*
*
*
*
*
**
*
*
*
*
*
* **
*
*
*
***
pre−AMD3100 CD34+ count (/ul)
tota
l CD
34+
cell
colle
ctio
n (1
.0E0
6/kg
)
Spearman r=0.854p<0.0001
*
*
*
*
*
*
**
*
*
*
*
*
* **
*
*
*
***
post−AMD3100 CD34+ count (/ul)
tota
l CD
34+
cell
colle
ctio
n (1
.0E0
6/kg
)
Spearman r=0.873p<0.0001
C D
A B
Figure 3. Correlations between circulating CD341 cell count and CD341 cell collection. (A) CD341 cell count just prior to plerixafor (after 4 days ofG-CSF) versus day 1 CD341 cell collection; (B) CD341 cell count 10-11 hours after plerixafor versus day 1 CD341 cell collection; (C) CD341 cell countjust prior to plerixafor (after 4 days of G-CSF) versus total CD341 cell collection; and (D) CD341 cell count 10-11 hours after plerixafor versus totalCD341 cell collection.
HL patients pretreated with G-CSF (Figure 4) wassimilar to the profiles previously observed in healthyvolunteers who received plerixafor, 240 mg/kg, alone[15] and in NHL and MM patients treated withG-CSF 1 plerixafor [16].
DISCUSSION
G-CSF is currently the agent most commonly usedfor hematopoietic stem cell mobilization, because ofits potency and relative safety. However, a significant
Table 3. Adverse Events Possibly, Probably, or DefinitelyRelated to Plerixafor
Number of Patients (N 5 22)
Adverse Event Mild Moderate Severe
Injection site erythema or irritation 12 0 1Diarrhea 2 1Nausea 2Vomiting 1Abdominal pain or discomfort 1 1
minority of patients fail to collect an adequate numberof hematopoietic stem cells with standard G-CSFmobilization, often resulting from advanced age orextensive prior chemotherapy [17-19]. Plerixafor isa promising new mobilizing agent that has demon-strated efficacy in patients with NHL and MM under-going autologous stem cell mobilization. In a Phase Istudy in 13 patients with MM or NHL, a mean6-fold increase in the peripheral CD341 cell countwas observed 6 hours after an injection of plerixafor,160 or 240 mg/kg [12]. Flomenberg et al. [20] subse-quently used a combination of G-CSF and plerixaforfor autologous stem cell mobilization in 25 patientswith MM or NHL. Each patient underwent 2 mobili-zations: 1 with G-CSF alone and 1 with the plerixaforcombination. In all cases, G-CSF 1 plerixafor mobi-lized more CD341 cells per leukapheresis than didG-CSF alone, and 9 patients who failed to collect $2� 106 CD341 cells/kg with G-CSF did achieve thattarget with G-CSF 1 plerixafor. In addition, G-CSF1 plerixafor mobilization was associated with fewerleukaphereses and a greater likelihood of collecting$5 � 106 CD341 cells/kg. The combination of

Biol Blood Marrow Transplant 14:1253-1261, 2008 1259Plerixafor Mobilization for Hodgkin Lymphoma
Table 4. Pharmacokinetic Parameters after the First Dose of Plerixafor
Cmax (mg/mL) Tmax (h) t1/2 (h) CL/F (L/h) Vz/F (mL) AUC0-10 (ng � h/mL) AUC0-24 (ng � h/mL)
Median 0.75 0.5 3.6 4.9 25.9 3,501 3,884Range 0.62-1.16 0.3-1.3 2.4-4.3 3.0-9.5 10.6-41.7 2646-5042 2877-5307
Cmax indidates maximum concentration; Tmax, time to maximum concentration; t1/2, half-life; CL/F, systemic clearance; Vz/F, volume of distribution; AUC,area under the plasma concentration time curve.
G-CSF and plerixafor also has been demonstrated tomobilize the majority of patients with lymphoma orMM who have failed prior mobilization with cytokinesand/or chemotherapy [21,22].
A Phase III trial randomized 298 patients withNHL to mobilization with G-CSF 1 plerixafor orG-CSF 1 placebo [14]. The primary endpoint, collec-tion of $5� 106 CD341 cells/kg in #4 apheresis days,was achieved by 59% of patients in the plerixaforgroup, versus 20% in the G-CSF alone group (P \.0001). In addition, fewer patients in the plerixaforgroup failed to collect at least 2 � 106 CD341 cells/kg (13% versus 53%, P \ .0001). A randomized, pla-cebo-controlled study in MM patients showed a similarbenefit to the combination of G-CSF and plerixafor[13]. In that trial, 72% of myeloma patients mobilizedwith G-CSF 1 plerixafor collected $6 � 106 CD341
cells/kg in 2 or fewer apheresis compared to 34% ofpatients mobilized with G-CSF alone (P \ .0001).Over half of patients given G-CSF 1 plerixaforreached the target collection in 1 day of apheresis.
Our results expand the clinical experience withplerixafor to include patients with relapsed or refrac-tory HL, for whom ASCT is a potentially curative pro-cedure. In our experience, 20% to 30% of this patientpopulation does not collect sufficient hematopoieticstem cells with G-CSF mobilization to proceed witha stem cell transplant. In addition, only 15% of our his-torical population collected .5� 106 CD341 cells/kg,a target stem cell dose associated with faster platelet re-covery. In contrast, with the combination of G-CSF 1
plerixafor, 21 of 22 patients achieved the minimum he-matopoietic stem cell collection, and 15 of 22 collected$5 � 106 CD341 cells/kg, a significant improvementover the historical control group. Although the meannumber of aphereses performed per patient did notdiffer significantly between the historical controlgroup and the study group mobilized with G-CSF 1
plerixafor, the combination was associated with a statis-tically significant improvement in the number of he-matopoietic stem cells collected in the first 2 days ofapheresis. Collection of more stem cells in fewerapheresis procedures has many potential advantages,including a decrease in procedure-related adverse re-actions, less utilization of costly personnel and bloodbank resources, and improved transplant outcomesfrom infusion of a higher stem cell dose. Potentialdisadvantages of the addition of plerixafor to G-CSFmobilization include the expense of plerixafor, possi-ble side effects, and the inconvenience of giving aninjection the evening prior to apheresis.
This study included measurement of each patient’speripheral CD341 cell count immediately prior to thefirst dose of plerixafor (after 4 days of G-CSF) and10-11 hours after plerixafor. There was marked inter-patient variation in the peripheral CD341 cell countsat both of these time points, with a median 3.2-foldincrease in circulating CD341 cells after plerixafor.Notably, both the pre- and postplerixafor CD341
cell counts correlated significantly with the subsequenthematopoietic stem cell collection, suggesting thatanalysis of the peripheral CD341 cell count prior to
Time (hours)0 2 4 6 8 10
AMD
3100
Con
cent
ratio
n (n
g/m
L)
10
100
1000
10000
Figure 4. Mean plerixafor plasma concentrations over time in HL patients following a subcutaneous 240 mg/kg dose (shown on a semilog scale). Errorbars are standard deviations.

1260 Biol Blood Marrow Transplant 14:1253-1261, 2008A. Cashen et al.
plerixafor or prior to apheresis could predict whethera patient will have a successful stem cell collection afterG-CSF 1 plerixafor mobilization.
Because the CXCR4 receptor on CD341 cellsplays a role in hematopoietic stem cell homing tobone marrow, there has been concern that stem cellsmobilized with plerixafor may exhibit poor engraft-ment. However, studies in animal models have demon-strated that stem cell engraftment is not affected bymobilization with plerixafor [23,24]. In fact, bone mar-row repopulation may actually be improved with pler-ixafor mobilization [25,26]. The reliable engraftmentcapacity of hematopoietic stem cells mobilized withplerixafor has been demonstrated in the clinical trialsreported to date, and our results confirm thosefindings. All of the HL patients transplanted withG-CSF 1 plerixafor mobilized cells had prompt anddurable engraftment.
This study includes the first published report of thepharmacokinetics of plerixafor in cancer patients. Pler-ixafor was rapidly absorbed, with peak plasma concen-trations occurring approximately 30 minutes aftersubcutaneous injection, and had a median eliminationhalf-life of 3.6 hours. The pharmacokinetic profile ofplerixafor reported in this study population is consis-tent with those previously observed in healthy volun-teers in the absence of G-CSF [15] and in patientswith MM and NHL [16].
In conclusion, our study demonstrates that G-CSF1 plerixafor is an effective and well-tolerated mobiliza-tion regimen in patients with HL undergoing autolo-gous stem cell collection. When compared tohistorical outcomes with G-CSF alone mobilization,the combination of G-CSF 1 plerixafor is associatedwith a significant improvement in the proportion ofpatients who collect $5 � 106 CD341 cells/kg and inthe number of CD341 cells collected in the first 2days of apheresis. Importantly, mobilization with pler-ixafor enables more HL patients to collect the mini-mum number of CD341 cells required for stem celltransplantation, increasing the proportion of patientswho can proceed with that potentially curative therapy.
ACKNOWLEGEMENTS
This work was sponsored by Genzyme Corpora-tion. This data was presented in part at the 2005 and2006 annual meetings of the American Society ofHematology.
REFERENCES
1. Andre M, Henry-Amar M, Pico J-L, et al. Comparison of high-dose therapy and autologous stem-cell transplantation withconventional therapy for Hodgkin’s disease induction failure:a case-control study. J Clin Oncol. 1999;17:222-229.
2. Lazarus HM, Loberiza FR, Zhang M-J, et al. Autotransplantsfor Hodgkin’s disease in first relapse or second remission. a re-port from the autologous blood and marrow transplant registry(ABMTR). Bone Marrow Transplant. 2001;27:387-396.
3. Lazarus BHM, Rowlings PA, Zhang M-J, et al. Autotransplantsfor Hodgkin’s disease in patients never achieving remission: a re-port from the Autologous Blood and Marrow Transplant Regis-try. J Clin Oncol. 1999;17:534.
4. Linch DC, Goldstone AH, McMillan A, et al. Dose intensifica-tion with autologous bone-marrow transplantation in relapsedand resistant Hodgkin’s disease: results of a BNLI randomisedtrial. Lancet. 1993;341:1051-1054.
5. Schmitz N, Pfistner B, Sextro M, et al. Aggressive conventionalchemotherapy compared with high-dose chemotherapy withautologous haemopoietic stem-cell transplantation for relapsedchemosensitive Hodgkin’s disease: a randomised trial. Lancet.2002;359:2065-2071.
6. Sureda A, Arranz R, Iriondo A, et al. Autologous stem-cell trans-plantation for Hodgkin’s disease: results and prognostic factorsin 494 patients from the Grupo Espanol de Linfomas/Trans-plante Autologo de Medula Osea Spanish Cooperative Group.J Clin Oncol. 2001;19:1395-1404.
7. Sweetenham JW, Carella AM, Taghipour G, et al. High-dosetherapy and autologous stem-cell transplantation for adult pa-tients with Hodgkin’s disease who do not enter remission afterinduction chemotherapy: results in 175 patients reported tothe European Group for Blood and Marrow Transplantation.J Clin Oncol. 1999;17:3101-3109.
8. Siena S, Schiavo R, Pedrazzoli P, et al. Therapeutic relevance ofCD34 cell dose in blood cell transplantation for cancer therapy.J Clin Oncol. 2000;18:1360-1377.
9. Haas R, Mohle R, Fruhauf S, et al. Patient characteristics asso-ciated with successful mobilizing and autografting of peripheralblood progenitor cells in malignant lymphoma. Blood. 1994;83:3787-3794.
10. Canales M, Fernandez-Jimenez M, Martin A, et al. Identifica-tion of factors associated with poor peripheral blood progenitorcell mobilization in Hodgkin’s disease. Haematologica. 2001;86:494-498.
11. Liles WC, Broxmeyer HE, Rodger E, et al. Mobilization ofhematopoietic progenitor cells in healthy volunteers byAMD3100, a CXCR4 antagonist. Blood. 2003;102:2728-2730.
12. Devine SM, Flomenberg N, Vesole DH, et al. Rapid mobiliza-tion of CD341 cells following administration of the CXCR4antagonist AMD3100 to patients with multiple myeloma andnon-Hodgkin’s lymphoma. J Clin Oncol. 2004;22:1095-1102.
13. DiPersio J, Stadtmauer EA, Nademanee AP, et al. A Phase III,multicenter, randomized, double-blind, placebo-controlled,comparative trial of AMD3100 (Plerixafor)1G-CSF vs. G-CSF1placebo for mobilization in multiple myeloma (MM)patients for autologous hematopoietic stem cell (aHSC) trans-plantation. ASH Annu Meet Abstr. 2007;110:445.
14. DiPersio JF, Micallef I, Stiff PJ, et al. A Phase III, multicenter,randomized, double-blind, placebo controlled, comparative trialof AMD3100 (Plerixafor)1G-CSF vs. placebo1G-CSF in non-Hodgkin’s lymphoma (NHL) patients for autologous hemato-poietic stem cell (aHSC) transplantation. ASH Annu Meet Abstr.2007;110:601.
15. Hubel K, Liles W, Broxmeyer HE, et al. Leukocytosis and mo-bilization of CD341 hematopoietic progenitor cells byAMD3100, a CXCR4 antagonist. Support Cancer Ther. 2004;1:165-172.
16. Douglas S, Smith C, McFarland R, et al. AMD3100 with G-CSFfor autologous peripheral blood progenitor cell (PBPC) mobili-zation in non-Hodgkin’s lymphoma (NHL) and multiple mye-loma (MM): mobilization, engraftment, and pharmacokinetics(PK). ASH Annu Meet Abstr. 2006;108:3383.
17. Morris CL, Siegel E, Barlogie B, et al. Mobilization of CD34cells in elderly patients ($70 years) with multiple myeloma:influence of age, prior therapy, platelet count and mobilizationregimen. Br J Haematol. 2003;120:413-423.

Biol Blood Marrow Transplant 14:1253-1261, 2008 1261Plerixafor Mobilization for Hodgkin Lymphoma
18. Sugrue M, Williams K, Pollock B, et al. Characterization andoutcome of ‘‘hard to mobilize’’ lymphoma patients undergoingASCT. Leuk Lymphoma. 2000;39:509-519.
19. Perea G, Sureda A, Martino R, et al. Predictive factors for a suc-cessful mobilization of peripheral blood CD341 cells in multi-ple myeloma. Ann Hematol. 2001;80:592-597.
20. Flomenberg N, Devine SM, DiPersio JF, et al. The use ofAMD3100 plus G-CSF for autologous hematopoietic progeni-tor cell mobilization is superior to G-CSF alone. Blood. 2005;106:1867-1874.
21. Calandra G, McCarty J, McGuirk J, et al. AMD3100 plusG-CSF can successfully mobilize CD341 cells from non-Hodg-kin’s lymphoma, Hodgkin’s disease and multiple myelomapatients previously failing mobilization with chemotherapyand/or cytokine treatment: compassionate use data. BoneMarrow Transplant. 2008;41:331-338.
22. Micallef I, Stiff PJ, DiPersio JF, et al. Successful stem cell mobi-lization rescue by AMD3100 (Plerixafor)1G-CSF for patients
who failed primary mobilization: results from the Phase III(3101-NHL) study. ASH Annu Meet Abstr. 2007;110:602.
23. Devine SM, Liu F, Holt M, et al. AMD1300-mobilized murinehematopoietic stem cells and T-lymphocytes have identicalcapacity to induce multilineage stem cell engraftment, donorT-cell chimerism and GVHD in mice compared with G-CSFmobilized cells. Blood. 2003;102:938a-939a.
24. Larochelle A, Krouse A, Metzger M, et al. AMD3100 mobilizeshematopoietic stem cells with long-term repopulating capacityin nonhuman primates. Blood. 2006;107:3772-3778.
25. Hess DA, Wirthlin L, Craft TP, et al. Human CD341 cells mo-bilized by AMD3100 demonstrate enhanced NOD/SCID repo-pulating function compared to CD341 cells mobilized bygranulocyte colony stimulating factor. Blood. 2005;106: #1962.
26. Broxmeyer HE, Orschell CM, Clapp DW, et al. Rapid mobili-zation of murine and human hematopoietic stem and progenitorcells with AMD3100, a CXCR4 antagonist. J Exp Med. 2005;201:1307-1318.




















