
A MODEL FOR COMPUTED TOMOGRAPHY CAPACITY ...
126
A MODEL FOR COMPUTED TOMOGRAPHY CAPACITY PLANNING AND IDENTIFYING OPPORTUNITIES TO IMPROVE UTILIZATION AND PATIENT ACCESS by Sabrina Kun Tang A thesis submitted in conformity with the requirements for the degree of Master of Health Sciences in Clinical Engineering Institute of Biomaterials & Biomedical Engineering University of Toronto © Copyright by Sabrina Kun Tang 2015
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of A MODEL FOR COMPUTED TOMOGRAPHY CAPACITY ...

A MODEL FOR COMPUTED TOMOGRAPHY CAPACITY
PLANNING AND IDENTIFYING OPPORTUNITIES TO
IMPROVE UTILIZATION AND PATIENT ACCESS
by
Sabrina Kun Tang
A thesis submitted in conformity with the requirements
for the degree of Master of Health Sciences in Clinical Engineering
Institute of Biomaterials & Biomedical Engineering
University of Toronto
© Copyright by Sabrina Kun Tang 2015

ii
Abstract
A Model for Computed Tomography Capacity Planning and Identifying Opportunities to Improve
Utilization and Patient Access
Sabrina Kun Tang
Master of Health Sciences in Clinical Engineering
Institute of Biomaterials & Biomedical Engineering
University of Toronto
2015
A capacity planning model was developed to improve decision making around CT facilities and
ultimately, increase patient access to CT services. The capacity planning model is used to
determine where and when CT scanners should be located, how many CT scanners are
needed, and how many shifts should be staffed to achieve a minimum percent of demand
served within a catchment area while minimizing cost. Saskatchewan is used as a case study.
Utilization and access metrics are calculated to evaluate the current situation at Saskatchewan’s
CT facilities and for their patients. These metrics were used to estimate model parameters and
the model was run for scenarios to evaluate the cost and access trade-offs. The results indicate
one new CT facility need to be implemented now to reach 90% of demand in 2 hours and a
second facility is needed by 2026.

iii
Acknowledgments
I would like to express my sincere thanks to Professor Michael Carter and Professor Sonia
Vanderby, Professor Tony Easty, and Professor Timothy Chan for all your genuine support,
expertise, and mentorship through the highs and lows. I will do my best to remember Mike’s
advice to “think twice, cut once”.
To Dr. Paul Babyn, Brenda Downing, and all the people I have conversed with in
Saskatchewan, thank you for answering my questions and providing the data to make this
research possible.
To all my friends in Massey College, clinical engineering, Applied Optimization Laboratory and
Centre for Research in Healthcare Engineering, thank you for your encouragement and for
giving me the strength to complete this thesis.
Finally, thank you to my parents for being there for me every step along the way.
The research conducted in this thesis was supported by the Saskatchewan Health Research
Foundation Establishment Grant, a Canadian Institutes of Health Research Master’s Award
(CGS-M) Frederick Banting and Charles Best Canada Graduate Scholarship, and an Ontario
Graduate Scholarship Master’s Level (OGS-M) award from the Ontario Ministry of Training,
Colleges, and Universities.

iv
Table of Contents
Acknowledgments ......................................................................................................................... iii
Table of Contents ......................................................................................................................... iv
List of Tables ................................................................................................................................ vii
List of Figures .............................................................................................................................. ix
List of Appendices ........................................................................................................................ xi
Acronyms ..................................................................................................................................... xii
Chapter 1. Introduction ................................................................................................................. 1
1.1. Contributions ...................................................................................................................... 3
1.2. Organization ....................................................................................................................... 4
Chapter 2. Literature Review ........................................................................................................ 5
2.1. CT Utilization and Access .................................................................................................. 5
2.1.1. Trends in Computed Tomography Usage .................................................................... 5
2.1.2. Geographic Variation and Access issues .................................................................... 7
2.2. Capacity Planning Methods ................................................................................................ 9
2.2.1. Capacity Planning in Medical Imaging ......................................................................... 9
2.2.2. Geographical Methods ............................................................................................... 10
2.2.3. Facility Location Modelling in Operations Research .................................................. 11
Chapter 3. Methods .................................................................................................................... 14
3.1. Data Acquisition and Processing ...................................................................................... 14
3.1.1. Regional Health Authorities ....................................................................................... 14
3.1.2. CT Facilities ............................................................................................................... 17
3.1.3. Saskatchewan’s Ministry of Health ............................................................................ 18
3.1.4. Statistics Canada ....................................................................................................... 19
3.1.5. Key Calculations ........................................................................................................ 21

v
3.2. Metrics and Current Situation ........................................................................................... 23
3.2.1. CT Provision .............................................................................................................. 23
3.2.2. CT Utilization ............................................................................................................. 24
3.2.3. Patient Utilization ....................................................................................................... 25
3.2.4. Patient Access ........................................................................................................... 26
3.2.5. Expected Demand ..................................................................................................... 26
3.3. Capacity Planning Model .................................................................................................. 27
Chapter 4. Current Situation of CT Utilization and Patient Access in Saskatchewan ................. 28
4.1. CT Provision ..................................................................................................................... 28
4.1.1. Operating Hours ........................................................................................................ 29
4.2. CT Utilization .................................................................................................................... 30
4.3. Demographics .................................................................................................................. 34
4.4. Patient Utilization .............................................................................................................. 37
4.5. Patient Access .................................................................................................................. 40
4.5.1. Patient Travel ............................................................................................................. 40
4.5.2. Wait Times ................................................................................................................. 43
4.6. Expected Demand ............................................................................................................ 44
4.7. Discussion ........................................................................................................................ 46
Chapter 5. Capacity Planning Model for CT scanners ................................................................ 50
5.1. The Problem ..................................................................................................................... 50
5.2. Model Development ......................................................................................................... 51
5.2.1. Formulation ................................................................................................................ 54
5.3. Model Inputs for Saskatchewan’s CT Capacity Plan ........................................................ 59
5.3.1. Input Data Calculations .............................................................................................. 59
5.3.2. Resulting Input Data .................................................................................................. 63
5.4. Solution Approach ............................................................................................................ 64
5.5. Scenarios and Sensitivity Analysis ................................................................................... 64
vi
5.5.1. Saskatchewan’s Coverage Limits .............................................................................. 65
5.5.2. Main Scenarios .......................................................................................................... 65
5.5.3. Sensitivity Analysis .................................................................................................... 67
5.6. Results ............................................................................................................................. 69
5.6.1. Scenario 1: Cost and access trade-offs ..................................................................... 69
5.6.2. Scenario 2: Covering all provincial demand .............................................................. 73
5.6.3. Scenario 3: Green Field ............................................................................................. 74
5.6.4. Sensitivity Analysis .................................................................................................... 76
5.7. Discussion of Model ......................................................................................................... 78
5.8. Recommendations for Saskatchewan .............................................................................. 80
Chapter 6. Conclusions ............................................................................................................... 85
References .................................................................................................................................. 87
vii
List of Tables
Table 1: Date ranges and number of records for the exam-level data from RIS from each health authority
with a CT scanner. .............................................................................................................................. 15 Table 2: Common RIS data fields for retrospective exam-level data from each health authority. .............. 15 Table 3: CT installation year, CT replacement year, and RIS implementation year for each CT facility. ... 17 Table 4: NACRS data date ranges by CT facility ....................................................................................... 18 Table 5: Number of CTs per million population in Saskatchewan for each census year ........................... 28 Table 6: Operating Hours for each CT facility. ........................................................................................... 29 Table 7: Provincial statistics for rectilinear travel distance (km) in 2011 by population centre and rural area
classification based on the patient’s residential postal code. ............................................................. 40 Table 8: Estimated maximum wait time by number of days from day of referral to day of appointment
scheduling on December 31, 2011. .................................................................................................... 43 Table 9: Wait time by number of days from referral to appointment scheduling on December 31, 2011 for
RQHR and Saskatoon Heath Region. ................................................................................................ 43 Table 10: Maximum percent of demand in 2012 within catchment areas by maximum patient travel time.
............................................................................................................................................................ 65 Table 11: Opened facilities for each travel time and minimum coverage scenario. Unless otherwise
specified, facilities were opened in 2013. ........................................................................................... 71 Table 12: Summary of sensitivity analysis scenarios ................................................................................. 77 Table 13: Current operating hours in comparison to average operating hours in model using base
scenario (90% coverage and 2 hour travel time) by facility ................................................................ 81 Table 14: Data fields provided by health region ......................................................................................... 95 Table 15: Population projection based on sex and age group with growth scenario M1. .......................... 97 Table 16: Population projection based on sex and age group with growth scenario L. ............................. 97 Table 17: Population projection based on sex and age group with growth scenario H. ............................. 98 Table 18: CT exam data map based on postal code. ............................................................................... 100 Table 19: Number of data points by facility and year ............................................................................... 100 Table 20: Number of data points by priority level and facility in 2011 ...................................................... 101 Table 21: Number of data points by patient type and facility in 2011 ....................................................... 101 Table 22: Number of data points which have exam time by facility in 2011. ............................................ 102 Table 23: Number of data points by procedure group and facility in 2011 ............................................... 102 Table 24: Number of data points with report turnaround time by facility in 2011 ..................................... 103 Table 25: Number of visits in 2011 by facility. .......................................................................................... 103 Table 26: Number of visits by population centre and rural area classification in 2011 ............................. 104 Table 27: Number of visits by patient health region and CT facility in 2011. ............................................ 104 Table 28: Percentage of patient’s by health region of origin for each CT Facility in 2011 ....................... 110

viii
Table 29: Percent of outpatient visits that went to each CT facility from each health region in 2011 based
on the patient’s residential postal code. ........................................................................................... 111 Table 30: Proportion of each procedure group by facility ......................................................................... 112 Table 31: List of potential facilities ........................................................................................................... 113
ix
List of Figures
Figure 1: Comparison of CT exams per 1000 population by OECD [2]. ...................................................... 1 Figure 2: Comparison of the number of CT scanners per million population as a common measure of
supply [2]. ............................................................................................................................................. 2 Figure 3: Map of all Saskatchewan health regions with the CT scanner locations marked by the city they
are in and the number of CT scanners in brackets. [4] ........................................................................ 3 Figure 4: Boundaries of the One Arrow 95 CSD, neighbouring CSDs, and postal codes. ......................... 20 Figure 5: Number of exams completed in 2011 by CT facility. ................................................................... 30 Figure 6: Average number of exams per CT scanner by hospital. ............................................................. 30 Figure 7: Proportions of patient type by CT facility in 2011 ....................................................................... 31 Figure 8: Estimated exams per operating hour by CT facility and year which includes on-call exams. ..... 32 Figure 9: Number of exams per operating hour by CT facility and year ..................................................... 33 Figure 10: Proportion of patients by priority levels and CT facility in 2011. ................................................ 34 Figure 11: Proportion of exams by procedure group in 2011. .................................................................... 34 Figure 12: Size of the insured population by Saskatchewan’s Ministry of Health in 2011 by health region.
............................................................................................................................................................ 35 Figure 13: Age distribution of CT patients compared to the insured population in Saskatchewan in 2011.
............................................................................................................................................................ 35 Figure 14: Mean CT patient age in Saskatchewan based on data from the RIS. ...................................... 36 Figure 15: Mean CT patient age in 2011 for each health region. ............................................................... 36 Figure 16: Histogram of exams per 1000 population for CSDs with a non-zero population in 2011. ......... 37 Figure 17: Histogram with non-zero exams per 1000 population by CSD with a non-zero population in
2011.................................................................................................................................................... 37 Figure 18: Number of exams per 1000 population by 20-year age cohorts and sex in 2011. .................... 38 Figure 19: Exams per 1000 inpatient visits by facility ................................................................................. 38 Figure 20: Histogram of the number of exams per patient in 2011 for all health regions ........................... 39 Figure 21: Mean travel time to the health facility where CT exam was performed in 2011 from the patient’s
residential postal code. ....................................................................................................................... 41 Figure 22: Proportion of outpatient visits from each health region that went to a CT facility outside their
health region and went to the closest CT scanner in 2011. ............................................................... 42 Figure 23: Current number of exams per CSD in 2011 .............................................................................. 44 Figure 24: Expected demand (number of exams) per CSD in 2011 .......................................................... 45 Figure 25: Number of CT scanners per million population in 2011 by OECD countries in comparison to
Saskatchewan. [2] .............................................................................................................................. 47 Figure 26: Average number of exams per hospital CT scanner in 2011 by OECD countries in comparison
to Saskatchewan. [2] .......................................................................................................................... 47

x
Figure 27: Number of exams per 1000 population in 2011 by OECD countries in comparison to
Saskatchewan. [2] .............................................................................................................................. 48 Figure 28: Cost of tradeoffs between minimum coverage percentage and maximum travel time for
assigned exams. ................................................................................................................................ 69 Figure 29: Weekly operating hours until 2030 by facility with a maximum travel time of 2.5 hrs and 95%
coverage level. ................................................................................................................................... 70 Figure 30: Weekly operating hours until 2030 by facility with a maximum travel time of 2 hrs and 90%
coverage level. ................................................................................................................................... 71 Figure 31: Map of Scenario 1 with a 95% coverage level and 2.5-hour travel time. .................................. 72 Figure 32: Map of Scenario 1 with 90% coverage level and 2-hour travel time ......................................... 72 Figure 33: Map of Scenario 1 with 90% coverage level and 1.5-hour travel time. ..................................... 73 Figure 35: Weekly operating hours for all CT facilities for Scenario 2. ....................................................... 74 Figure 36: Weekly operating hours for all CT facilities for Scenario 3. ....................................................... 75 Figure 37: Map of chosen facilities and 2-hr catchment areas for the green field scenario. ...................... 75 Figure 38: Sensitivity analysis for exams per operating hour ..................................................................... 76 Figure 39: Proportions of patient type by health region in 2011. .............................................................. 111

xi
List of Appendices
Appendix A : Data Fields Provided ............................................................................................. 95
Appendix B : Population Growth Rates ....................................................................................... 97
Appendix C : Data Map ............................................................................................................. 100
Appendix D : AMPL Files .......................................................................................................... 106
Appendix E : Metrics ................................................................................................................. 110
Appendix F : Potential Facilities ................................................................................................ 113
xii
Acronyms
BUH – Battlefords Union Hospital in Prairie North RHA
CIHI - Canadian Institute for Health Information
CRH – Cypress Regional Hospital in Cypress RHA
CSD – Census Sub-division
CT – Computed Tomography
DAD – Discharge Abstract Database
HR - Hour
ICES – Institute for Clinical Evaluative Studies
KM – Kilometre
LH – Lloydminster Hospital in Prairie North RHA
LHIN – Local Health Integration Network
Max – Maximum
MCR - Mamawetan Churchill River Health Region
MIP – Mixed Integer Problem
MJU/MJUH – Moose Jaw Union Hospital in Five Hills RHA
MRI – Magnetic Resonance Imaging
NACRS – National Ambulatory Care Reporting System
OECD - Organisation for Economic Co-operation and Development
PAPHR – Prince Albert Parkland Health Region
PH – Pasqua Hospital in Regina Qu’Appelle Health Region

xiii
POP - Population
RGH – Regina General Hospital in Regina Qu’Appelle Health Region
RHA – Regional Health Authority (Health Region)
RIS - Radiology Information System
RQHR – Regina Qu’Appelle Health Region
RUH – Royal University Hospital in Saskatoon Health Region
SCH – Saskatoon City Hospital in Saskatoon Health Region
SPH – St. Paul's Hospital in Saskatoon Health Region
USA – United States of America
VH – Victoria Hospital in Prince Albert Parkland Health Region
WK – Week
YRH/YRHC – Yorkton Regional Health Centre in Sunrise Health Region

1
Chapter 1. Introduction
Computed tomography (CT) is a medical imaging modality that helps diagnose many conditions
by producing 2-dimensional and 3-dimensional images of soft tissue and bone [1]. Demand for
CT exams is increasing in Canada (Figure 1) and supply has been increasing as well [2] (Figure
2) according to the Organisation for Economic Co-operation and Development (OECD). Due to
lengthy wait times, it was a priority area for the First Ministers in 2004 [3]. CT equipment is
costly to purchase and CT facilities have the second highest operating costs among medical
imaging modalities since they require highly skilled technologists to operate them [1]. CT
capacity planning is important to reduce wait times while being cost effective.
*Data for Canada in 2007 was interpolated
Figure 1: Comparison of CT exams per 1000 population by OECD [2].
0
20
40
60
80
100
120
140
2003 2004 2005 2006 2007* 2008 2009 2010
CT exams p
er 1000 po
p.
OECD Average Canada (OECD)
2
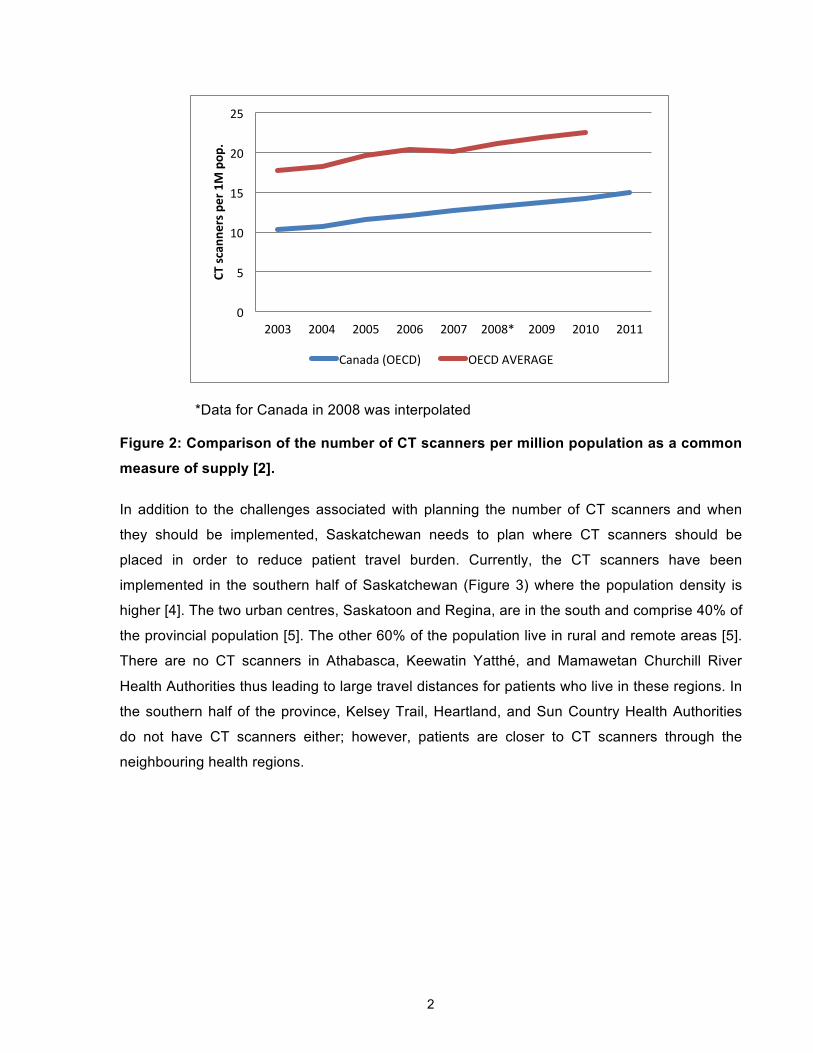
*Data for Canada in 2008 was interpolated
Figure 2: Comparison of the number of CT scanners per million population as a common
measure of supply [2].
In addition to the challenges associated with planning the number of CT scanners and when
they should be implemented, Saskatchewan needs to plan where CT scanners should be
placed in order to reduce patient travel burden. Currently, the CT scanners have been
implemented in the southern half of Saskatchewan (Figure 3) where the population density is
higher [4]. The two urban centres, Saskatoon and Regina, are in the south and comprise 40% of
the provincial population [5]. The other 60% of the population live in rural and remote areas [5].
There are no CT scanners in Athabasca, Keewatin Yatthé, and Mamawetan Churchill River
Health Authorities thus leading to large travel distances for patients who live in these regions. In
the southern half of the province, Kelsey Trail, Heartland, and Sun Country Health Authorities
do not have CT scanners either; however, patients are closer to CT scanners through the
neighbouring health regions.
0
5
10
15
20
25
2003 2004 2005 2006 2007 2008* 2009 2010 2011
CT sc
anne
rs per 1M pop
.
Canada (OECD) OECD AVERAGE

3
Figure 3: Map of all Saskatchewan health regions with the CT scanner locations marked
by the city they are in and the number of CT scanners in brackets. [4]
To reduce the inequities in access while balancing supply and demand, this thesis will propose
a capacity planning model and use the province of Saskatchewan as a case study. This will aid
policy makers in knowing when and where CT scanners should be implemented. Although the
thesis is focused on Saskatchewan, we expect the work to be widely applicable for CT capacity
planning.
1.1. Contributions
There are three main areas of contribution from this thesis.
First, utilization and access metrics are presented based on data from all CT-equipped health
regions in Saskatchewan to understand the current situation. While previous papers have
discussed utilization and access in the United States, Norway, and Canada, this is the first

4
analysis for Saskatchewan. The key metrics are the number of exams per operating hour,
number of exams per 1000 population, and patient travel time.
Second, the capacity planning model is a mixed-integer optimization model. It is based on
choosing appropriate CT facilities to achieve patient access standards and understanding how
much regular operating capacity is needed at each facility. Saskatchewan’s utilization metrics
are used to estimate the parameters for the model.
Third, recommendations for capacity planning in Saskatchewan are discussed based on the
model results.
1.2. Organization
This thesis is organized as follows.
Chapter 2 reviews the literature relevant to CT scanner utilization and access to health care
services with a focus on geographic variations between urban and rural populations. For
capacity planning, it describes possible approaches from geography and operations research to
capacity planning for minimizing cost and travel burden. Chapter 3 presents the methods and
data used to understand the current CT scanner situation in Saskatchewan and to develop the
capacity planning model. Chapter 4 shows the results of the current situation in Saskatchewan
with respect to CT scanner utilization and access. Chapter 5 describes the capacity planning
model design and results. The design of the model and the scenarios are outlined in detail. The
aim is to understand the trade-offs between access and cost as well as the capacity necessary
to meet the demand in Saskatchewan. Chapter 6 presents practical recommendations and
ideas for future work.
5
Chapter 2. Literature Review
This chapter provides an overview of the existing trends in computed tomography utilization and
access as well as different types of capacity planning models.
2.1. CT Utilization and Access This section reviews the literature related trends in CT scanner usage in different jurisdictions
and the factors that affect access. This understanding feeds into CT scanner capacity planning.
2.1.1. Trends in Computed Tomography Usage
The motivation behind this research lies in the recent trends in diagnostic CT scanning in terms
of increases in supply, and utilization.
CT utilization is commonly measured by number of exams per a given population or percentage
of the population that have had a CT exam. Specific populations have been analyzed such as
inpatient, outpatient, emergency department patients [6], Medicare [7, 8], and health system
enrollees [9]. From the OECD Health Data in 2011 [2], Canadians receive 127 CT exams per
thousand population which is almost equal the OECD average of 127.9. In the United States,
there are many methods of calculating patient utilization based on specific populations including
enrollees [10], Medicare beneficiaries [7, 8], and case-mix adjusted patient admissions [11, 12].
This led to a large range in CT utilization values; however, the overall trend was that utilization
had increased over the past decade and that there was substantial regional variation. Due to the
healthcare funding models in the USA, each study focuses separately on a particular population
within the country and it is difficult to obtain data for the entire country, which also makes
international comparisons challenging. The USA has a high prevalence of self-referral, which is
when a physician refers a patient to a CT facility where they receive financial compensation
[13]. It is also common to have an additional technical fee, which is paid to the health facility
where the CT scanner is located [14]. Both the self-referral and technical fee change the
incentives for CT supply and utilization in the USA [13, 14]. Furthermore, physicians who refer
patients to physicians of the same specialty for diagnostic imaging, tend to use diagnostic
imaging more frequently than physicians who refer to radiologists [15].
Utilization has also been analyzed based on body region [8,15,16] but different categorizations
of body regions make it difficult to compare. In 2007, Parker et al. [8] analyzed the national
Medicare data in the USA and the most common CT exams by body region in descending order

6
were CT body, spine, head, musculoskeletal, vascular, and cardiac. Lee et al. [15] also
analyzed data from 2001 to 2007 for an adult emergency department at an urban academic
hospital in New York City. They found that out of all CT scans, 56% were head scans and 28%
were abdomen/pelvis scans. Although there were low percentages of chest (4%) and neck (8%)
scans overall, they had the largest increase of 600% and 500% respectively from 2001 to 2007.
Similarly in Korea, Oh et al. [16] analyzed data from 2001 to 2010 and the body regions with the
most exams were head (67.5%), abdomen (14.8%), chest (8.1%), and facial bones (6.6%),
miscellaneous CTs (2.4%) and cervical CTs (0.6%).
CT supply can be compared using number of CT scanners per million population. In the 2011
OECD Health Data [2], Canada was below the OECD average (23.2/million population) with
14.6 CT scanners per million population. In comparison, the supply ranged from 8.9 (United
Kingdom) to 50.6 (Australia). Taiwan had 3.71 per million population in 2001 [9].
For CT utilization and workload, the Canadian Institute for Health Information (CIHI) [1]
analyzed the number of exams per scanner per year and number of operating hours per
scanner per week in 2007. Facilities submit their data online and follow Management
Information System Standards. Compared with several European countries and the United
States, Canada’s CT utilization level is higher using the measure of exams per scanner per year
at 8,735, but the average number of exams and average number of hours in operation per CT
scanner suggests that CT scanners are underutilized [1]. On average, Saskatchewan’s CT
facilities operate 59 hours per week compared to the national average of 60 hours per week,
indicating that there may be an opportunity to increase utilization. However, several factors
need to be taken into consideration such as funding level, staff availability, and population
density [1].
When CIHI [17] released data from 2011-2012, Saskatchewan was above the national average
with 144.9 CT exams per thousand population and 15 CT scanners per million population.
When one looks at provincial statistics, there are substantial variations due to factors such as
population density, so the average national statistic can be misleading. The next section will
discuss geographic variations in CT utilization, supply, and access.

7
2.1.2. Geographic Variation and Access issues
While country comparisons are useful, there can also be substantial variations in utilization
between different regions within a country. This may be due to varying levels of CT accessibility
in each region.
Healthcare Access in General
An American survey in North Carolina revealed that the key determinant of health service
utilization is access to transportation resources such as a family member with a driver’s license
and car [18]. For mental health services, the more severe the diagnosis, the farther people were
willing to travel [19]. Nemet and Bailey [20] wrote that for the elderly, service utilization is also
dependent on where their other activities occur such as grocery shopping. These areas are
called their activity spaces. The closer the service is to their activity spaces, the higher the rates
of service utilization.
A study on USA Medicare claims data in 2008 [21] was adjusted for health status and found no
significant difference between urban and rural service utilization despite differences between
states. However, in another study, several states were selected in 1998 [22] and when their
claims data were analyzed, the population was stratified into urban, large rural, small rural, and
isolated rural populations. It showed that for general services, the travel burden difference
between urban and rural populations was not large, but was significant for specialized services.
Access in Radiology
Radiology studies in the USA [8, 23, 24] and Norway [25] show substantial geographic variation
in utilization and access to imaging services. While the American studies [8, 23, 24] noted that
there were differences between regions, the reasons for this variation were unknown. The
Norwegian study [25] ran correlations between radiological services, examinations rates, and
population and their differences were statistically significant between regions. However, when
the main urban centre, Oslo, was removed, the correlation was not significant between the non-
urban regions. The researchers found that accessibility was the main cause for variation
between populations and also found that socioeconomic factors, mainly education, led to
increased examination rates. Oslo had the highest education levels in Norway and had access
to private clinics. People with high education levels were more likely to pressure their physicians

8
for a referral. If physicians did not think the CT exam was medically necessary, they would refer
the patient to a private clinic instead of a publicly funded hospital.
In 2001, a Taiwanese study [9] analyzed national claims data from the universal and
comprehensive health insurance and found that increased CT utilization was correlated with the
percentage of females in the population, number of hospital physicians, and percentage of
children in the population. In general, females cost the healthcare system more and hospital
physicians drive healthcare costs. Children would receive more scans due to the disease
patterns in children and the population was more willing to spend healthcare resources on
children than elderly people. The percentage of elderly and income levels in Taiwan did not
correlate with increased utilization.
Access in Ontario
The Institute for Clinical Evaluative Studies (ICES) [26, 27] analyzed Ontario’s health insurance
claims for CT scans and found that CT scan rates increased 12% between 2003/2004 and
2004/2005. The replacement of old CT scanners with newer and faster machines was one
reason for the increase since more CT scans could potentially be done in the same amount of
time. When compared between Local Health Integration Networks (LHINs), the rural North
Simcoe Muskoka LHIN had the highest CT scanning rate which was 1.5 times higher than the
urban Hamilton Niagara Haldimand Brant LHIN with the lowest rate. Neighbourhood income did
not seem to have an impact on utilization rates. According to the ICES report in 2005, elderly
patients had higher rates of CT scanning and men aged 65 and older had higher scanning rates
than women in their age group. However, under age 65, men and women had similar CT
scanning rates.
While there has been a substantial amount of literature on CT utilization and health services
access in general, there has been no research that analyzes CT utilization, patient utilization,
and access to CT scanners in Saskatchewan.

9
2.2. Capacity Planning Methods Demand for CT exams is rising and reducing patient travel distance is important for service
access. Therefore, capacity planning for CT scanners in Saskatchewan needs to take the
following factors into consideration:
• Allowing multiple CT scanners at the same location
• Reducing patient travelling time to improve accessibility
• Minimizing the overall cost to the system
• Incorporating flexibility for different service levels (e.g. distances travelled, percentage of
demand serviced) since serving all patients equally may not be economically feasible
• Allowing a long planning horizon (e.g., 20 years) is useful for understanding how to
match demand as the population size and demography in each area changes.
To understand how these factors have been incorporated in the literature, this section will delve
into the capacity planning methods in medical imaging, geographical planning, and operations
research.
2.2.1. Capacity Planning in Medical Imaging
Although there have been many capacity planning models done in healthcare, few of them are
specific to medical imaging. Within medical imaging, there are general management articles
[27], heuristic methods [28], and a linear program [29] which consider patient travel times and
costs.
Szcepura and Clark [27] published a discussion on strategic management of magnetic
resonance imaging (MRI) in the United Kingdom’s National Health Service Trusts. While several
suggestions pertained to the organizational structure, their overall approach is to use population
projections and utilization rates to predict future demand. First, the total number of new MRIs
required for the United Kingdom was estimated. Although the exact estimation process is not
stated, the locations were then decided by the decision makers on the basis of patient travel
costs, equitable distribution of services, and gaining economies of scope. By tracking utilization
in each area over a period of time, they will assess when it will be appropriate to add a new MRI
and how the wait lists decrease in response. As wait lists decrease, they expect a slight
increase in MRI referrals, but are unsure of the relationship between waitlists and referrals. For

10
example, there could be a substantial jump in referrals if the waitlist drops to zero days.
Therefore, the implementation of MRIs will be an ongoing assessment based on utilization,
waitlists, and referrals.
In Germany, Bach and Hoberg [28] presented a model where combinations of alternative CT
scanner locations were chosen and then decision criteria were calculated such as total cost,
patient transportation cost, utilization level, maximum distance travelled, and number of CT
scanners implemented. By recognizing fixed threshold costs after a certain threshold capacity, a
second shift of staff would need to be employed to increase the capacity of the scanner.
Although it was presented in a similar manner to a linear program, they believe it is a more
practical approach for decision makers to look at various CT facility combinations and then
make a decision based on the differences in decision criteria results. From the results of the
alternatives, they developed a sequential process to add new CT scanners.
Greenwald et al [29] developed a static linear programming model for a 10-year planning
horizon to minimize CT facility costs, transportation costs, and opportunity costs of patient travel
times subject to capacity constraints and to satisfy all of the expected demand. The paper
focuses on patient travel cost estimates and opportunity costs by including hospital shuttle
costs, public transit, and wages lost due to time away from work. Assumptions of utilization level
and transportation costs were varied and the decision maker could choose the option given the
factors which were most important to them.
2.2.2. Geographical Methods
Geographical methods have also been used to estimate travel time and aid in capacity planning.
They incorporate road network usage and travel time estimates based on road speed limits. The
common software is ArcGIS for calculations and visual representation.
In Chicago [30], Wang and Luo calculated spatial accessibility for primary care physicians using
a two-step floating catchment area based on a threshold travel time between the population and
physicians. In rural British Columbia [31], hospital catchment areas were analyzed to look at the
percentage of the population they could serve within different travel times. For example, the
percentage of the rural population that can access the service within 15 minutes, 30 minutes,
and an hour. What-if scenarios allowed the policy maker to see the impact on the population

11
when a service is removed since it means that a certain percentage of the population may have
to travel four hours instead of two hours.
2.2.3. Facility Location Modelling in Operations Research
The concept of ensuring demand can be serviced while minimizing cost and improving access
has been approached from several different objectives.
• Minimize distance travelled by customers
• Minimize number of facilities
• Minimize total cost
Minimizing distance travelled or the number of facilities available is often used as a proxy for
minimizing cost and covering models are used especially for public services [32]. Location-
allocation and plant location problem models are used for the private sector since their objective
is to minimize total costs [32].
In covering models [33, 34], the three main types are set covering, p-median, and maximum
covering. In the set covering location problem, the total number of facilities assigned is
minimized to reduce cost. In p-median, the travel distance to the closest facility is minimized to
improve access by giving a specified number of new facilities to control cost. Similarly, the
maximum covering location problem sets a maximum travel distance allowed and locates a
specified number of facilities such that the most demand possible is within the maximum travel
distance.
For emergency services, Toregas et al. [35] used simple set covering and p-median models.
The simple covering models have also been built into a decision support tool in India for
neighbourhood planning of public services such as schools and health centres [36]. The models
have been expanded to take facility capacity into consideration with both maximum coverage
and partial coverage. The maximum coverage model views demand beyond a threshold
distance is not covered. For partial coverage, there is the first zone with full coverage and a
second threshold distance. Demand is partially covered if it is between the first zone and the
second threshold distance. This allows for a demand assignment that is less desirable, but is
still acceptable to reduce the number of facilities required. Distance is often used as a proxy for

12
time. This has been applied to locating shelters in preparation for disasters [37]. Storage
location modelling for emergency response used threshold travel time instead of distance and
each facility had different capacity levels [38].
Dynamic covering models have been used for long term planning [39]. A dynamic maximum
covering location problem was used for emergency services with multiple objectives [40]. A
stochastic model was developed with weighted scenarios, a specified number of facilities, and a
budget constraint. To locate medical services for large scale emergencies [41], a minimum
number of facilities were assigned to large demand points to ensure a minimum level of
coverage and scenarios were given different weights. The problem was solved with several
models including the maximum covering location problem, p-median, and p-centre model. The
p-centre model minimizes the maximum travel distance.
In location-allocation models and the plant location problem, the goal is to minimize the total
cost to meet all the demand [42]. For location-allocation models, there are fixed facility costs,
assignment costs, and variable costs [42]. For the plant location problem, the cost elements are
similar except that the assignment cost is generally a transportation cost [43]. There have also
been dynamic location problems which minimize total costs over a planning horizon [42].
Wesolowsky and Truscott [44] proposed the dynamic location-allocation problem which
minimized total costs including assignment costs and relocation costs over a planning horizon. It
has also been expanded to include minimum and maximum capacities to ensure manufacturing
efficiency and all demand must be satisfied. Decision rules for small scale public facilities have
also been derived using the location-allocation model [45]. For daycares [46], the location-
allocation algorithm was applied to maximize the number of people who can access the day
care within a threshold distance. A maximum travel restriction was placed with a decay function
since fewer people were expected to use the day care the farther they needed to travel.
Other facility location models have been developed for similar facility types including goal
programming and fuzzy goals. For locating plants while taking employee needs into
consideration [47], a goal programming model was developed to incorporate cost, air quality,
and quality of life. Quality of life included education, health, and community planning scores
which were out of 100. Capacity planning for libraries [48] in the Columbus, Ohio area was used
as a case study for a multi-objective dynamic location model with a fuzzy goal to take social
factors into consideration. The objective was to minimize the maximum deviation from the fuzzy
goal subject to budget constraints and accessibility measures (e.g. highway access, public
transportation, parking lots). Luss [49] wrote a large overview of capacity expansion problems in

13
operations research, including continuous and discrete models. While many papers looked at
continuous expansion sizes or discrete incrementing capacity sizes, having multiple facilities at
the same site had not been well explored.
Multiple facilities at the same site
Despite the substantial amount of research on facility location modelling, capacity planning
models to address our problem with multiple facilities at the same site are not well researched.
ReVelle and Laporte [43] identified this gap in the literature and proposed a static formulation for
the single product capacitated machine siting problem. It minimized total costs for new sites,
new machines at each site, product delivery, and product manufacturing. All demand had to be
satisfied and there were no delivery time or distance limitations.
Several papers had a p-median formulation based on having multiple facilities in each area and
then the model was re-run for each area [50 - 52]. Each area had a maximum number of
facilities it could implement to control costs. In this situation, the borders of each area were strict
– demand could only be fulfilled by a facility in its area. This was applied to electoral polling
stations in Italy [51].
The static capacitated facility location problem was expanded to include multiple facilities of
different types at each site [53]. Set-up costs were divided into opening the site and
implementing new facilities at the site. Like the plant location problem, a lower connection cost
was used to help assign demand to the appropriate facility. However, there were no delivery
time or distance limitations.
While the studies mentioned above include relevant pieces, our problem is not completely
represented by any of them.

14
Chapter 3. Methods
To develop a capacity planning model, an understanding of the current situation in
Saskatchewan with respect to CT utilization and access is needed. The province was used as a
case study. The three main stages are:
1. Data Acquisition and Processing
2. Metrics and Current Situation
3. Capacity Planning Model
The collected data were obtained from various sources. Metrics were calculated to extract a
better understanding of the current situation. Different scenarios were run on an optimization
model to illustrate a method for capacity planning, using the metrics to inform the model
parameters.
3.1. Data Acquisition and Processing
Data were obtained from the Regional Health Authorities (RHA), CT facilities, Statistics Canada,
and Saskatchewan’s Ministry of Health.
3.1.1. Regional Health Authorities
We requested anonymous patient-level data from each Regional Health Authority (RHA) with a
CT scanner for each CT exam for all the years within the Radiology Information System (RIS).
All RHAs provided data from different time periods as listed in Table 1 and common data fields
are listed in Table 2. To provide comparisons between RHAs, only complete years of data were
used starting in January. Although the data from each of the RHAs spans a few years, only
2011 data overlaps with all RHAs. This limited the analysis of the province since province-wide
exam data are not available for any other year.

15
Table 1: Date ranges and number of records for the exam-level data from RIS from each
health authority with a CT scanner.
Regional Health Authorities Data Date Range Number of Exams
Cypress 2007 November to 2013 April 21,976
Prince Albert Parkland 2010 April to 2013 December 41,531
Prairie North
2009 February to 2013 March
BUH: 2009 February to 2013 March
LH: 2009 April to 2013 March
34,497 total
BUH: 18,591
LH: 15,906
Sunrise 2010 November to 2013 October 15,883
Five Hills 2009 November to 2013 April 21,272
Saskatoon
2000 January to 2012 May
RUH – 2000 January to 2012 May
SPH – 2004 February to 2012 May
SCH – 2003 November to 2012 May
355,418 total
RUH: 184,643
SPH: 87,121
SCH: 83,654
Regina Qu’Appelle
2003 April to 2012 September
RGH – 2003 April to 2012 September
Pasqua – 2003 April to 2012 March
119,210 total
RGH: 97,472
Pasqua: 21,738
Table 2: Common RIS data fields for retrospective exam-level data from each health
authority.
Patient Data Imaging Data
Anonymous patient identifier/ visit identifier
Age
Sex
Postal Code
Patient Type (outpatient, inpatient, emergency)
Hospital/Facility
Exam date
Final report date (All except RQHR)
Order procedure
For the data fields provided by each RHA, see Appendix A

16
Due to different RIS programs, there are inconsistencies in how CT exams are recorded. For
example, RQHR records some emergency patients as inpatients. Order procedure and patient
type were re-categorized to make the data more consistent. Even among facilities with the same
RIS program there may be slight differences in how each staff member enters the information.
Furthermore, the dataset includes false starts and cancelled exams. The inconsistencies
negatively impact the quality of the data; however, the results will still provide a good
understanding of the general situation.
Order Procedure to Procedure group
All RHAs provided order procedure names indicating what type of CT exam was performed on
the patient which included details such as body location and whether contrast was used.
Procedure groups were based on body location (head, spine, thorax, abdomen/pelvis, lower
extremities, upper extremities, vascular, and miscellaneous). In total, there were 508 different
order procedures which were matched to the eight procedure groups. If an order procedure
contained multiple body locations then it was matched with multiple procedure groups.
Patient Type
Patient type (emergency, inpatient, outpatient) was recorded differently in each RHA’s dataset.
For each RHA, the different descriptors for patient type were matched as emergency, inpatient,
or outpatient. For example, “Orthopaedic Clinic” in Cypress RHA was re-categorized as
outpatient.
Cost Data
Saskatoon Health Region provided cost data from April 2011 to March 2013 with categories
such as salaries, drugs, and supplies. This allowed us to calculate an estimated cost per exam.
17
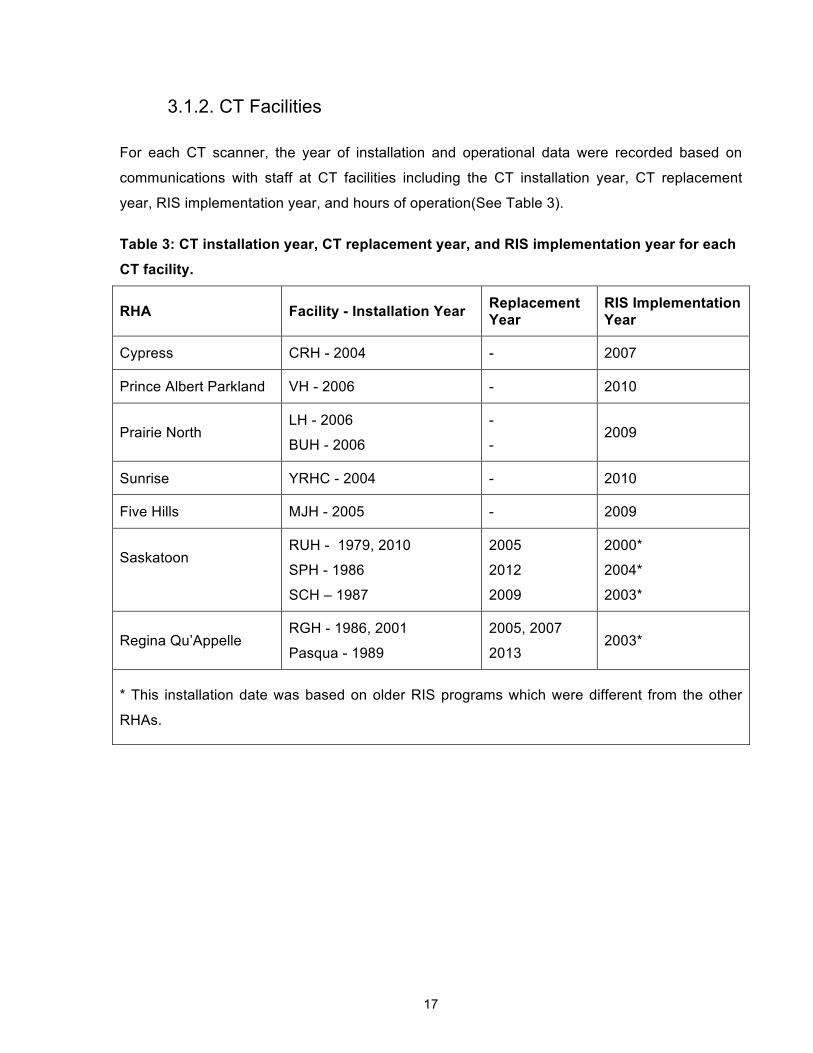
3.1.2. CT Facilities
For each CT scanner, the year of installation and operational data were recorded based on
communications with staff at CT facilities including the CT installation year, CT replacement
year, RIS implementation year, and hours of operation(See Table 3).
Table 3: CT installation year, CT replacement year, and RIS implementation year for each
CT facility.
RHA Facility - Installation Year Replacement Year
RIS Implementation Year
Cypress CRH - 2004 - 2007
Prince Albert Parkland VH - 2006 - 2010
Prairie North LH - 2006
BUH - 2006
-
- 2009
Sunrise YRHC - 2004 - 2010
Five Hills MJH - 2005 - 2009
Saskatoon
RUH - 1979, 2010
SPH - 1986
SCH – 1987
2005
2012
2009
2000*
2004*
2003*
Regina Qu’Appelle RGH - 1986, 2001
Pasqua - 1989
2005, 2007
2013 2003*
* This installation date was based on older RIS programs which were different from the other
RHAs.

18
3.1.3. Saskatchewan’s Ministry of Health
Saskatchewan’s Ministry of Health provided wait times by health region and data for emergency
and inpatients including those who did not receive a CT exam as outlined below.
Discharge Abstract Database (DAD)
The DAD provided general inpatient admissions and discharge data for all CT-equipped
hospitals from January 2000 to March 2013. Twelve years of data (2000 – 2012) were used in
the analysis since it was restricted to complete years of data. This decreases the seasonality
bias since each month was incorporated the same number of times. Data fields included were
admission date, sex, hospital, 5-year age cohorts, total length of stay, and unique patient
identifier. The unique patient identifier was a number assigned to a patient’s account and allows
multiple records to be linked to a patient while keeping the patient anonymous.
National Ambulatory Care Reporting System (NACRS)
NACRS provided emergency patient data for select hospitals from April 2011 to December 2012
(Table 4). This did not include all CT-equipped hospitals. Information was only provided for five
facilities because the data collection tool has not been implemented in the other CT facilities.
Data fields included were unique patient identifier, registration date, sex, hospital, 5-year age
cohorts, length of stay, and triage level.
Table 4: NACRS data date ranges by CT facility
CT Facility Data Date Range
RUH 2011 April to 2012 December
SPH 2011 April to 2012 December
SCH 2011 April to 2012 December
Pasqua 2012 April to 2012 September
RGH 2012 April to 2012 September

19
Wait Times
CT wait times as of December 31, 2011 were provided by the Ministry of Health and were
reported by priority level for each health region. Priority level is on a scale of 1 to 4 from
emergent to non-urgent. The wait time was defined as the number of days between the date a
CT facility receives the examination request and the date of the scheduled exam. There were
two methods for calculating wait time. Saskatoon and Regina Qu’Appelle Health Region used
the new reporting method which was based on days waited for exams which were completed.
The median and 90th percentile wait time in days was provided. The rest of the health regions
used an estimated maximum wait time based on the next available appointment in the schedule
and not the actual date of the scheduled exam.
3.1.4. Statistics Canada
Statistics Canada provides population and demographic data for census sub-divisions (CSD) as
well as population estimates and projections for the province. Furthermore, it provided the
postal code conversation file which links postal codes with CSDs.
Census 2011
From the national census in 2011, the population by age and sex was reported by CSD. Median
age and population density were additional fields.
National Household Survey 2011
From the National Household Survey in 2011, the data provided the size of the Aboriginal
population by CSD.
Population Estimates
The population of Saskatchewan was estimated from 2011 to 2014 to reflect the current
demographics by 5-year age cohorts and sex at the provincial level.
Population Projections
Statistics Canada publishes six scenarios for population projections [54]. They provided
provincial population projections by 5-year age cohorts and sex from 2014 to 2030 based on
provincial growth rates for the total population which assume medium growth and historical
migration trends (constant fertility rate of 1.7 births per woman, life expectancy of 80.4 years for

20
males and 87.3 years for females by 2036, constant national immigration rate of 0.75%, and
interprovincial migration rates based on 1981 to 2008). This set of growth assumptions is called
M1.
There were six possible scenarios; however, M1 was chosen out of four medium growth
scenarios since it was closest to the average in total population increase. Scenarios H and L for
high and low population growth respectively were also used to better understand the range of
population changes.
Postal Code Conversion File
The postal code conversion file [55] allows for matching between postal codes and Statistics
Canada administrative areas (e.g. dissemination areas, census sub-divisions, etc.). Additional
fields include the population centre and rural area classification and the latitude/longitude
coordinates for the CSD. The population centre and rural area classification distinguish between
urban and rural CSDs by population size. The latitude and longitude coordinates are based on
each CSD’s representative point which is weighted by the number of households.
Since postal codes can span multiple CSDs, a single link indicator provides a one-to-one match
between postal codes and dissemination areas based on the most number of households. An
example of how multiple CSDs and postal code borders do not align is in Figure 4. While the
single link indicator provided the most likely match, this can convert records from a postal code
to a CSD where the person does not live.
Figure 4: Boundaries of the One Arrow 95 CSD, neighbouring CSDs, and postal codes.

21
3.1.5. Key Calculations
Number of Exams
The number of exams is the number of times procedure groups are scanned in a visit. The
number of times an order procedure was executed in a visit is converted into the number of
procedure groups multiplied by the number of times it was executed. For example, if an order
procedure corresponded with two procedure groups and the order procedure was executed
twice, then this would count as four exams.
Travel Distance
The travel distance is the distance between a patient’s CSD (derived from their residential
postal code) to a CT facility. To calculate travel distance between a CSD and a CT facility, the
latitude and longitude coordinates of the representative point from the postal code conversion
file are converted into Universal Transverse Mercator (UTM) [56] in ArcGIS Desktop v10.2 [57].
UTM is a coordinate system based in metres. The Pythagoras Theorem is used to calculate the
rectilinear distance between a CSD’s representative point and a CT facility since this is a good
estimation of highway distances [58]
Travel Time
The travel time is the estimated driving time from the patient’s CSD centroid to CT facilities
using the road network. The ArcGIS’s Origin-Destination Cost Matrix tool in ArcGIS’s Network
Analyst toolbox was used to calculate the travel time using the road network from CanMap
RouteLogistics Saskatchewan v2013.3, population-weighted representative point coordinates,
and CT facility coordinates. The tool calculates the travel times by adding up the road segments
which create the shortest route and estimating times for each road segment using the posted
speed limits. If the representative point was farther than 5 km from the closest road segment,
ArcGIS could not calculate accurate travel times since the centroids were not close enough to
the road network. Thirteen of the CSDs had centroids where this was the case and their travel
times were estimated based on the rectilinear distance from the UTM coordinates for the
centroids and CT facilities. From there, the rectilinear distance was used to approximate travel
times assuming a speed of 100km/hour.

22
Matching Regional Health Authorities to Postal Codes
Using ArcGIS, the boundaries of postal codes and RHAs were matched to indicate which postal
codes overlapped the respective RHA. Postal codes could overlap with multiple RHAs and
contain many postal code areas. Since the number of postal code areas is based on the number
of addresses, it is an indication of population density. Therefore, the best match of a postal
code to a RHA is based on the highest number of postal code areas.
Populations Projections by Census Sub-Division until 2030
Saskatchewan’s population estimates and population projections were only provided at the
provincial level and not by CSD by 5-year age cohort and sex. To estimate population growth
each year at the provincial level, a year’s population is divided by last year’s population for each
20-year age cohort and sex at the provincial level. The 5-year age cohorts are combined to 20-
year age cohorts to match the 20-year age cohorts in the patient utilization data. For example, if
the population of female 0 to 19 year olds is 100 in 2011 and 150 in 2012, then the population
growth rate is 1.5. The population growth rates for each 20-year age cohort and sex and applied
to all CSDs each year until 2030 based on their 20-year age cohort and sex distribution in the
2011 census. For example, if the growth rate for 0 to 19 year olds is 1.5 in 2012, then a CSD
with 10 females aged 0 to 19 years old in 2011 would be calculated to have 15 people in that
population group. See Appendix B for population growth rates

23
3.2. Metrics and Current Situation
To understand the current situation with respect to CT scanners in Saskatchewan, metrics were
calculated to compare the different health regions and to estimate parameters for a capacity
planning model. The main dimensions for the metrics were CT provision, CT utilization, patient
utilization, and patient access. These calculations were performed in SPSS v.22. For simplicity,
it is assumed that all CT scanners can perform all exam types, although facilities have different
types of CT scanners depending on the physician specialists at the hospital. See Appendix C for
the number of records depending on how the data was segmented.
Due to the unavailability of critical data elements such as staffing levels and human resource
costs, not all desired metrics could be calculated. These include number of exams per human
resource working hour, number of CT operating hours per week per human resource type, cost
per exam, and cost per patient.
3.2.1. CT Provision
Understanding the amount of supply in a system is crucial. The two main metrics were the
number of CT scanners per million population and CT scanner operating hours per week.
Number of CT scanners per million population
The number of CT scanners in Saskatchewan was divided by the provincial population. This
allowed Saskatchewan to be compared to jurisdictions internationally.
𝑁𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝐶𝑇 𝑠𝑐𝑎𝑛𝑛𝑒𝑟𝑠 𝑝𝑒𝑟 𝑚𝑖𝑙𝑙𝑖𝑜𝑛 𝑝𝑜𝑝𝑢𝑙𝑎𝑡𝑖𝑜𝑛 = 𝑁𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝐶𝑇 𝑠𝑐𝑎𝑛𝑛𝑒𝑟𝑠 𝑖𝑛 𝑝𝑟𝑜𝑣𝑖𝑛𝑐𝑒
𝑝𝑟𝑜𝑣𝑖𝑛𝑐𝑖𝑎𝑙 𝑝𝑜𝑝𝑢𝑙𝑎𝑡𝑖𝑜𝑛∗ 1𝑀
CT scanner operating hours per week
Within each CT facility, CT scanners require specially trained staff who are available during
operating hours. By increasing the number of hours per week, the CT scanner should be able to
perform more exams thereby increasing capacity in the system.

24
3.2.2. CT Utilization
In addition to the amount of supply in the system, the extent to which these resources were
used is of interest. The key metrics were the number of exams per CT scanner and the number
of exams per hour. All calculations were based on a 52-week year, which does not account for
holidays and slightly overestimates the number of operating hours each year. Furthermore, the
calculations assume that exams were equally distributed between multiple CT scanners at the
same facility
Number of exams per CT scanner per year
This metric measured how many exams were completed by each CT scanner in a year. Using
the data from the RHAs for each CT exam completed, the total number of exams each year is
calculated and divided by the number of CT scanners at the facility. This metric is segmented by
procedure group, patient type, and priority level.
𝑁𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑒𝑥𝑎𝑚𝑠 𝑝𝑒𝑟 𝐶𝑇 𝑠𝑐𝑎𝑛𝑛𝑒𝑟𝑠 𝑝𝑒𝑟 𝑦𝑒𝑎𝑟 = 𝑁𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑒𝑥𝑎𝑚𝑠 𝑎𝑡 𝑎 𝑓𝑎𝑐𝑖𝑙𝑖𝑡𝑦 𝑖𝑛 𝑜𝑛𝑒 𝑦𝑒𝑎𝑟𝑁𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝐶𝑇 𝑠𝑐𝑎𝑛𝑛𝑒𝑟𝑠 𝑎𝑡 𝑡ℎ𝑒 𝑓𝑎𝑐𝑖𝑙𝑖𝑡𝑦
Number of estimated exams per machine operating hour
The number of exams which can be fulfilled by a CT scanner is affected by the number of
operating hours. To adjust for the different operating hours at each CT facility, the total number
of exams is divided by the number of operating hours in a year. This included exams completed
outside of operating hours since the time of exam was not provided.
𝑁𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑒𝑥𝑎𝑚𝑠 𝑝𝑒𝑟 𝑚𝑎𝑐ℎ𝑖𝑛𝑒 𝑜𝑝𝑒𝑟𝑎𝑡𝑖𝑛𝑔 ℎ𝑜𝑢𝑟
= 𝑁𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑒𝑥𝑎𝑚𝑠 𝑎𝑡 𝑎 𝑓𝑎𝑐𝑖𝑙𝑖𝑡𝑦 𝑖𝑛 𝑜𝑛𝑒 𝑦𝑒𝑎𝑟
𝑁𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑚𝑎𝑐ℎ𝑖𝑛𝑒 𝑜𝑝𝑒𝑟𝑎𝑡𝑖𝑛𝑔 ℎ𝑜𝑢𝑟𝑠 𝑎𝑡 𝑡ℎ𝑒 𝑓𝑎𝑐𝑖𝑙𝑖𝑡𝑦 𝑖𝑛 𝑜𝑛𝑒 𝑦𝑒𝑎𝑟
Number of exams per machine operating hour
For facilities that provided the exam time, a more accurate exams per operating hour can be
calculated.
𝑁𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑒𝑥𝑎𝑚𝑠 𝑝𝑒𝑟 𝑚𝑎𝑐ℎ𝑖𝑛𝑒 𝑜𝑝𝑒𝑟𝑎𝑡𝑖𝑛𝑔 ℎ𝑜𝑢𝑟
= 𝑁𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑒𝑥𝑎𝑚𝑠 𝑑𝑢𝑟𝑖𝑛𝑔 𝑜𝑝𝑒𝑟𝑎𝑡𝑖𝑛𝑔 ℎ𝑜𝑢𝑟𝑠 𝑎𝑡 𝑎 𝑓𝑎𝑐𝑖𝑙𝑖𝑡𝑦 𝑖𝑛 𝑜𝑛𝑒 𝑦𝑒𝑎𝑟𝑁𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑚𝑎𝑐ℎ𝑖𝑛𝑒 𝑜𝑝𝑒𝑟𝑎𝑡𝑖𝑛𝑔 ℎ𝑜𝑢𝑟𝑠 𝑎𝑡 𝑡ℎ𝑒 𝑓𝑎𝑐𝑖𝑙𝑖𝑡𝑦 𝑖𝑛 𝑜𝑛𝑒 𝑦𝑒𝑎𝑟

25
3.2.3. Patient Utilization
To understand where current utilization was coming from, patient utilization was analyzed in
terms of the general population, inpatient population, and emergency patients.
Number of exams per 1000 population per year
Using the exam data from RHAs the patient’s postal code was matched to a CSD with Statistics
Canada’s Postal Code Conversation File. The number of exams completed on patients from
each CSD was divided by the population of the CSD in order to understand the variability in
utilization among CSDs. It was also calculated by 20-year age cohorts and sex. Due to the
limitations of the single link indicator in the Postal Code Conversion File, some CSDs will have
more exams attributed to them than in actuality and some will have less.
𝑁𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑒𝑥𝑎𝑚𝑠 𝑝𝑒𝑟 1000 𝑝𝑜𝑝𝑢𝑙𝑎𝑡𝑖𝑜𝑛 𝑝𝑒𝑟 𝑦𝑒𝑎𝑟
= 𝑁𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑒𝑥𝑎𝑚𝑠 𝑝𝑒𝑟𝑓𝑜𝑟𝑚𝑒𝑑 𝑜𝑛 𝑝𝑎𝑡𝑖𝑒𝑛𝑡𝑠 𝑓𝑟𝑜𝑚 𝑡ℎ𝑎𝑡 𝑎𝑟𝑒𝑎 𝑖𝑛 𝑜𝑛𝑒 𝑦𝑒𝑎𝑟
𝑃𝑜𝑝𝑢𝑙𝑎𝑡𝑖𝑜𝑛 𝑜𝑓 𝑡ℎ𝑎𝑡 𝑎𝑟𝑒𝑎∗ 1000
Number of exams per 1000 inpatient visits per year
The number of inpatient exams from RHA data was divided by the number of inpatients at each
CT-equipped hospital from the DAD. This provided a better understanding of how inpatients use
CT scanners at different rates than the general population and between different CT facilities.
𝑁𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑒𝑥𝑎𝑚𝑠 𝑝𝑒𝑟 1000 𝑖𝑛𝑝𝑎𝑡𝑖𝑒𝑛𝑡𝑠 𝑝𝑒𝑟 𝑦𝑒𝑎𝑟
= 𝑁𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑒𝑥𝑎𝑚𝑠 𝑝𝑒𝑟𝑓𝑜𝑟𝑚𝑒𝑑 𝑜𝑛 𝑖𝑛𝑝𝑎𝑡𝑖𝑒𝑛𝑡𝑠 𝑖𝑛 𝑜𝑛𝑒 𝑦𝑒𝑎𝑟
𝑁𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑖𝑛𝑝𝑎𝑡𝑖𝑒𝑛𝑡 𝑣𝑖𝑠𝑖𝑡𝑠 𝑖𝑛 𝑜𝑛𝑒 𝑦𝑒𝑎𝑟 ∗ 1000
Number of exams per 1000 emergency visits per year
The number of emergency exams from the RHA data was divided by the number of emergency
patients at certain hospitals from the NACRS. The aim was to understand the rate of utilization
by emergency patients. Data was taken from April 2011 to March 2012 for Saskatoon Health
Region.
𝑁𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑒𝑥𝑎𝑚𝑠 𝑝𝑒𝑟 1000 𝑒𝑚𝑒𝑟𝑔𝑒𝑛𝑐𝑦 𝑣𝑖𝑠𝑖𝑡𝑠 𝑝𝑒𝑟 𝑦𝑒𝑎𝑟
= 𝑁𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑒𝑥𝑎𝑚𝑠 𝑝𝑒𝑟𝑓𝑜𝑟𝑚𝑒𝑑 𝑜𝑛 𝑒𝑚𝑒𝑟𝑔𝑒𝑛𝑐𝑦 𝑝𝑎𝑡𝑖𝑒𝑛𝑡𝑠 𝑖𝑛 𝑜𝑛𝑒 𝑦𝑒𝑎𝑟
𝑁𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑒𝑚𝑒𝑟𝑔𝑒𝑛𝑐𝑦 𝑣𝑖𝑠𝑖𝑡𝑠 𝑖𝑛 𝑜𝑛𝑒 𝑦𝑒𝑎𝑟 ∗ 1000

26
3.2.4. Patient Access
One of the key factors in patient utilization is the ease of access. Access was measured by
patient travel distance, estimated travel time, wait time, and report turnaround time.
Rectilinear patient travel distance
As described in Section 0, the travel distance is the number of kilometers from the centroid of
the patient’s residential CSD to a CT facility where the exam was completed. The patient’s
residential CSD was determined from their postal code in the RHA data. To estimate the
distance travelled on the street grid, the rectilinear distance between the CSD’s centroid and CT
facility was used.
Wait times
Data from the RHA’s were insufficient for calculating wait time since the exam referral date was
not provided. Therefore, the publicly reported wait times were obtained from Saskatchewan’s
Ministry of Health. The wait time is defined as the number of days between the date a facility
receives the examination request and the date set for the scheduled exam.
3.2.5. Expected Demand
Provincial patient utilization rates (exams per 1000 population) from 2011 for 20-year age
cohorts and sex were multiplied by to the age cohort and sex distribution of each CSD in 2011
to calculate an expected demand for CT exams. This was calculated to visually identify the
difference between current utilization rates in a CSD and then adjust this for the demographics
in each CSD since there are potentially lower utilization rates in CSDs located farther from CT
facilities among other factors [19].

27
3.3. Capacity Planning Model
A capacity planning model was developed based on a combination of covering models and
capacitated plant location models. The aim was to account for the dynamics in supply and
demand while adhering to patient access standards such as a maximum travel time and percent
of the population within the facility catchment areas. As demand changes over time, candidate
facilities locations are assigned shifts and charged overtime to fulfill demand while minimizing
the capital costs, equipment costs, and exam costs. Parameters were estimated based on
Saskatchewan’s metrics and the literature.
To obtain results, AMPL model files (.mod) and data files (.dat) were created using MATLAB
v.7.12.0.635 (R2011a). In AMPL v.20140331, the CPLEX solver was called to obtain results.
See Appendix D for the AMPL code.
Scenarios were run to assess the trade-off between cost, coverage, and patient travel time in
terms of magnitude and timing. Scenario 1 started with existing CT facilities in place. In
Scenario 2, the travel time restriction was removed and the model was set to cover all provincial
demand with the existing CT facilities at the start. Scenario 3 is the green field scenario where
there are no existing CT facilities, which provides insight into the minimum number of facilities
required to service the province based on how demand is distributed. Different parameter
ranges were tested to determine the sensitivity of the model results for demand, cost of opening
a CT facility, cost of a CT scanner, exam cost, extra overtime costs, and exam rates.

28
Chapter 4. Current Situation of CT Utilization and Patient
Access in Saskatchewan
An analysis of the current situation was conducted by calculating metrics on current levels of CT
supply and patient utilization as well as the accessibility of the services. Supply is split into CT
provision and CT utilization. These metrics for CT provision are measures of the system’s
available capacity. For CT utilization, metrics provide a picture of how much output is produced
given the available capacity. Patient utilization provides an understanding of the utilization rate
variation between different geographic areas and hospitals in Saskatchewan based on the
patient’s residential postal code and provides insight into demand, albeit imperfectly as unmet
demand is not captured. The accessibility of services for patients is estimated through analysis
of patient travel distances to the CT facilities and overall statistics on where patients are
travelling. Understanding these factors can assist with interpreting results of the capacity
planning model and the limitations based on the estimation of parameters. Furthermore, using
calculated exam rates by age cohort and sex, an expected demand is calculated to identify
potential areas of unmet demand.
This chapter outlines the results for each metric and the expected demand calculation.
4.1. CT Provision
Saskatchewan has 13 CT scanners at 11 facilities. In Table 5, the number of CT scanners per
million population has increased substantially in the past ten years with a slight dip in 2011 due
to the increase in population. The number of CT scanners in the province has increased from
five to thirteen from 2001 to 2011. The census population has decreased slightly in 2006 and
then increased in 2011.
Table 5: Number of CTs per million population in Saskatchewan for each census year
Year Provincial Population
Number of CT scanners
CT per million population
2001 978,933 5 5.12
2006 968,157 12 12.39
2011 1,066,300 13 12.19

29
4.1.1. Operating Hours
Each CT facility has different weekly operating hours for each CT scanner, which are listed in
Table 6. The provincial average operating hours per CT scanner is 58.64 hours per week. For
CT facilities indicated with an asterisk in Table 6, the daily operating hours are an extra 30
minutes long. For example, Cypress Region Hospital starts at 7:30am instead of 8:00am and
runs for 8.5 hours per weekday instead of 8 hours per weekday. This allows for a bank day,
which is when the CT scanners are maintained for a day every three weeks.
Table 6: Operating Hours for each CT facility.
CT Facility (Region – Facility) Weekdays (Mon. - Fri.)
Weekends (Sat. - Sun.)
Average Hours/Wk
Cypress - Cypress Regional Hospital* 7:30 - 16:00 - 40
Five Hills - Moose Jaw Union Hospital* 8:00 - 16:30 - 40
Prince Albert Parkland - Victoria Hospital* 8:00 - 16:30 8:00 - 16:30** 40 or 54**
Prairie North - Battlefords Union Hospital* 8:00 - 16:30 - 40
Prairie North - Lloydminster Hospital* 8:00 - 16:30 - 40
Regina Qu'Appelle - Pasqua Hospital* 7:00 - 0:30 7:00 - 0:30 119
Regina Qu'Appelle - Regina General Hospital
CT 1: 7:00 - 23:00 CT 2: 7:00 - 17:00
CT 1: 7:00 - 23:00 CT 2: 7:00 - 17:00 182
Saskatoon - Royal University Hospital* CT 1: 9:30 - 16:00 CT 2: 7:30 - 22:30
CT 1: -- CT 2: 8:00 - 0:00 137
Saskatoon - Saskatoon City Hospital * 7:30 - 17:30 9:15 - 15:30 *** 62.5***
Saskatoon - St. Paul's Hospital* 7:30 - 17:00 - 50
Sunrise - Yorkton Regional Health Centre* 8:00 - 16:30 - 40
*There is an extra half hour in the schedule for “bank days”, so hours per week is the average
weekly hours including the bank days.
**These weekend operating hours started in January 2013 which increased the average hours
per week from 40 to 54.
***These weekend operating hours started in January 2010 and the average hours per week
include the weekend hours.
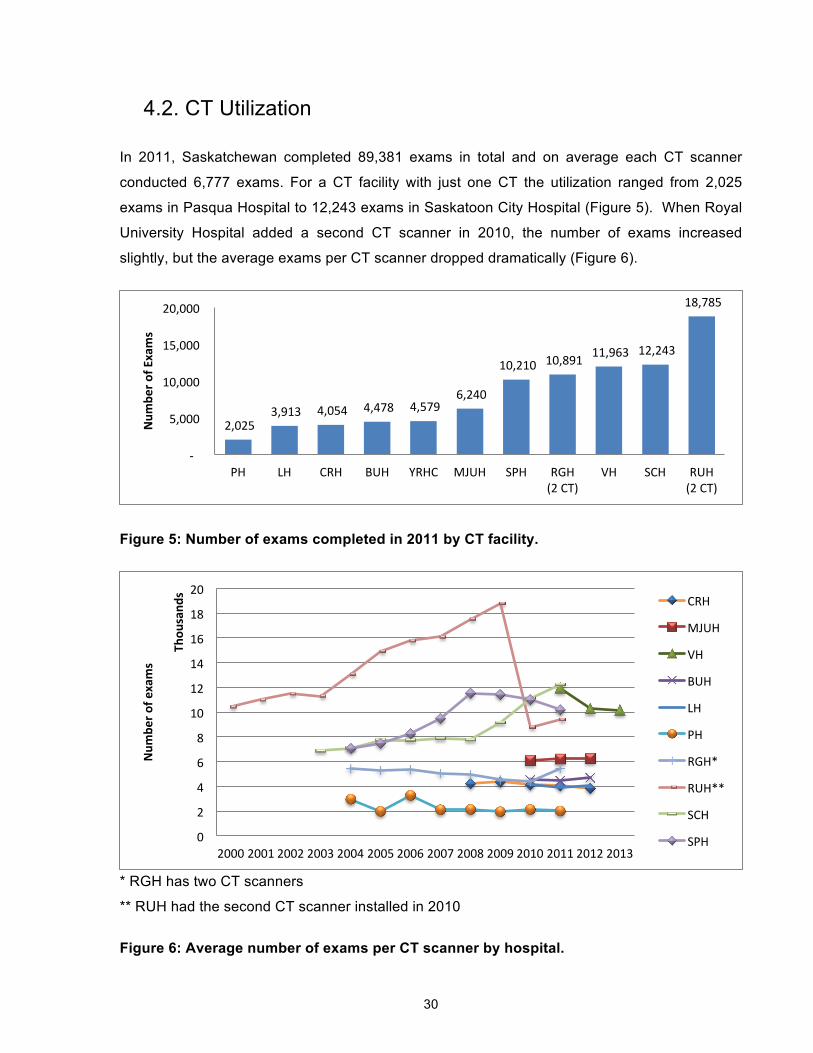
30
4.2. CT Utilization
In 2011, Saskatchewan completed 89,381 exams in total and on average each CT scanner
conducted 6,777 exams. For a CT facility with just one CT the utilization ranged from 2,025
exams in Pasqua Hospital to 12,243 exams in Saskatoon City Hospital (Figure 5). When Royal
University Hospital added a second CT scanner in 2010, the number of exams increased
slightly, but the average exams per CT scanner dropped dramatically (Figure 6).
Figure 5: Number of exams completed in 2011 by CT facility.
* RGH has two CT scanners
** RUH had the second CT scanner installed in 2010
Figure 6: Average number of exams per CT scanner by hospital.
2,025 3,913 4,054 4,478 4,579
6,240
10,210 10,891 11,963 12,243
18,785
-‐
5,000
10,000
15,000
20,000
PH LH CRH BUH YRHC MJUH SPH RGH (2 CT)
VH SCH RUH (2 CT)
Num
ber o
f Exams
0
2
4
6
8
10
12
14
16
18
20
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Num
ber o
f exams
Thou
sand
s CRH
MJUH
VH
BUH
LH
PH
RGH*
RUH**
SCH
SPH
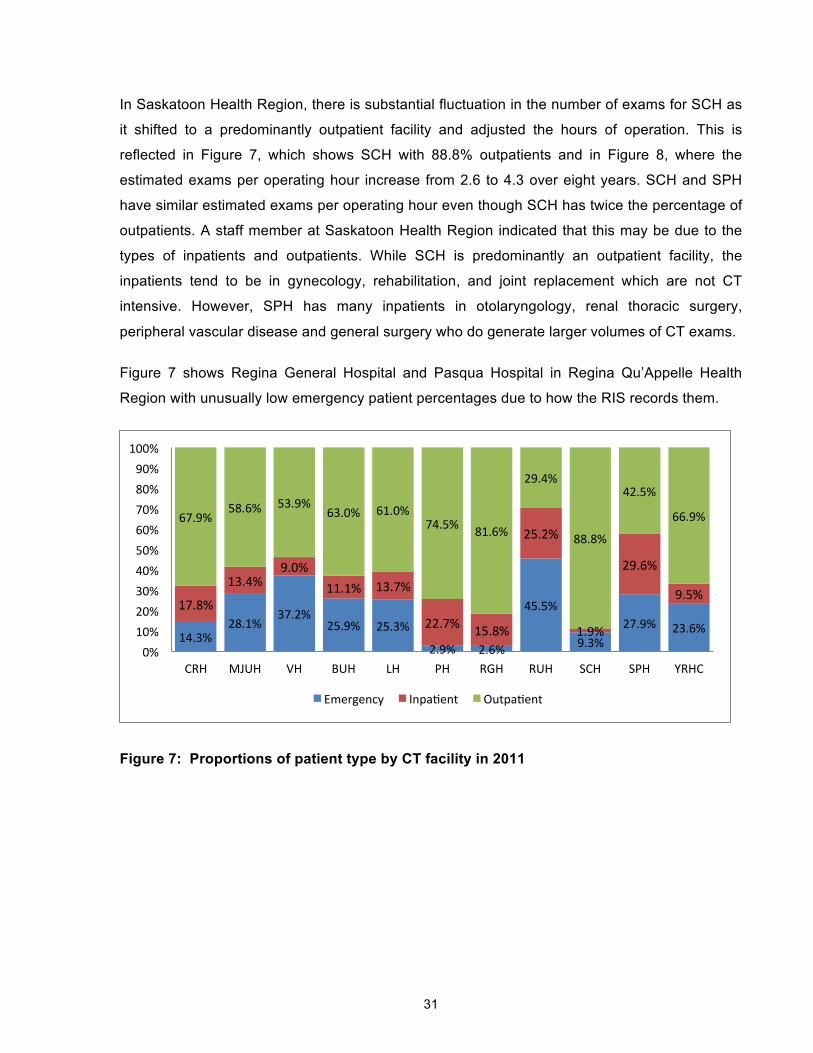
31
In Saskatoon Health Region, there is substantial fluctuation in the number of exams for SCH as
it shifted to a predominantly outpatient facility and adjusted the hours of operation. This is
reflected in Figure 7, which shows SCH with 88.8% outpatients and in Figure 8, where the
estimated exams per operating hour increase from 2.6 to 4.3 over eight years. SCH and SPH
have similar estimated exams per operating hour even though SCH has twice the percentage of
outpatients. A staff member at Saskatoon Health Region indicated that this may be due to the
types of inpatients and outpatients. While SCH is predominantly an outpatient facility, the
inpatients tend to be in gynecology, rehabilitation, and joint replacement which are not CT
intensive. However, SPH has many inpatients in otolaryngology, renal thoracic surgery,
peripheral vascular disease and general surgery who do generate larger volumes of CT exams.
Figure 7 shows Regina General Hospital and Pasqua Hospital in Regina Qu’Appelle Health
Region with unusually low emergency patient percentages due to how the RIS records them.
Figure 7: Proportions of patient type by CT facility in 2011
14.3% 28.1%
37.2% 25.9% 25.3%
2.9% 2.6%
45.5%
9.3% 27.9% 23.6%
17.8%
13.4% 9.0%
11.1% 13.7%
22.7% 15.8%
25.2%
1.9%
29.6%
9.5%
67.9% 58.6% 53.9%
63.0% 61.0% 74.5% 81.6%
29.4%
88.8%
42.5%
66.9%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
100%
CRH MJUH VH BUH LH PH RGH RUH SCH SPH YRHC
Emergency InpaQent OutpaQent

32
Figure 8: Estimated exams per operating hour by CT facility and year which includes on-
call exams.
The new RIS system records the time of the CT exam, which allows for the removal of exams
that occur outside the main operating hours. Most of the exams per operating hour ranged from
1.4 to 2.3 and remained stable (Figure 9). However, over three years Victoria Hospital in Prince
Albert Parkland Health Region the number of exams per operating hour decreased from 4.2 to
2.6. Part of this is due to increased operating hours in 2013. However, Victoria Hospital’s 2.6
exams per operating hour is still higher than the other CT facilities. When comparing the
difference between estimated exams per hour with the number of exams per hour, the average
difference is 0.74 exams more per hour. This makes sense since estimated exams per hour
includes exams completed outside of operating hours. However, the end time of the exam was
not known.
0
1
2
3
4
5
6
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Es9m
ated
num
ber o
f exm
as
CRH
MJUH
VH
BUH
LH
PH
RGH
RUH
SCH
SPH
YRHC
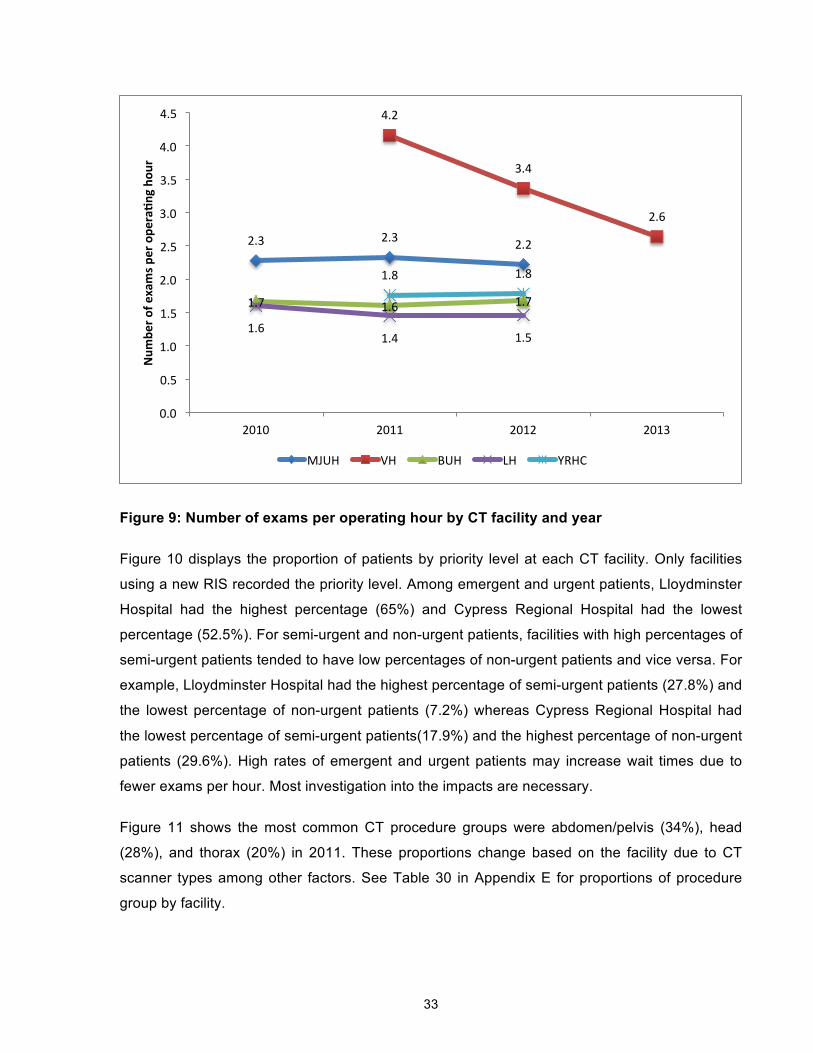
33
Figure 9: Number of exams per operating hour by CT facility and year
Figure 10 displays the proportion of patients by priority level at each CT facility. Only facilities
using a new RIS recorded the priority level. Among emergent and urgent patients, Lloydminster
Hospital had the highest percentage (65%) and Cypress Regional Hospital had the lowest
percentage (52.5%). For semi-urgent and non-urgent patients, facilities with high percentages of
semi-urgent patients tended to have low percentages of non-urgent patients and vice versa. For
example, Lloydminster Hospital had the highest percentage of semi-urgent patients (27.8%) and
the lowest percentage of non-urgent patients (7.2%) whereas Cypress Regional Hospital had
the lowest percentage of semi-urgent patients(17.9%) and the highest percentage of non-urgent
patients (29.6%). High rates of emergent and urgent patients may increase wait times due to
fewer exams per hour. Most investigation into the impacts are necessary.
Figure 11 shows the most common CT procedure groups were abdomen/pelvis (34%), head
(28%), and thorax (20%) in 2011. These proportions change based on the facility due to CT
scanner types among other factors. See Table 30 in Appendix E for proportions of procedure
group by facility.
2.3 2.3 2.2
4.2
3.4
2.6
1.7 1.6 1.7
1.6 1.4 1.5
1.8 1.8
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
2010 2011 2012 2013
Num
ber o
f exams p
er ope
ra9n
g ho
ur
MJUH VH BUH LH YRHC

34
Figure 10: Proportion of patients by priority levels and CT facility in 2011.
Figure 11: Proportion of exams by procedure group in 2011.
4.3. Demographics
Saskatchewan has an insured population of 1,122,537 people and there were 78,687 in-
province CT patients in 2011. The insured population is the number of people which have a
current health card number in Saskatchewan and who therefore have health coverage. Figure
12 provides a breakdown of the size of the insured population for each health region. The
insured population is actually larger than the population of 1,066,300 people reported in the
2011 census by Statistics Canada. This is an ongoing trend due to fraud, death, and migration
outward among other possible factors. Every three years health cards are renewed and the
provincial health registry is updated. After the updates, the insured population more closely
matches Statistics Canada population estimates. [59]
34.5% 45.2% 47.3% 35.4% 36.3% 42.9%
18.1% 12.9% 15.9% 28.3% 28.8% 19.9%
17.9% 23.3%
25.2% 26.4% 27.8% 22.5% 29.6% 18.6% 11.6% 9.9% 7.2% 14.7%
0%
20%
40%
60%
80%
100%
CRH MJUH VH BUH LH YRHC
1 (Emergent) 2 (Urgent) 3 (Semi-‐Urgent) 4 (Non-‐Urgent)
0.5% 1.4% 2.0% 6.4% 7.1%
20.4% 28.4%
33.8%
0% 5%
10% 15% 20% 25% 30% 35% 40%
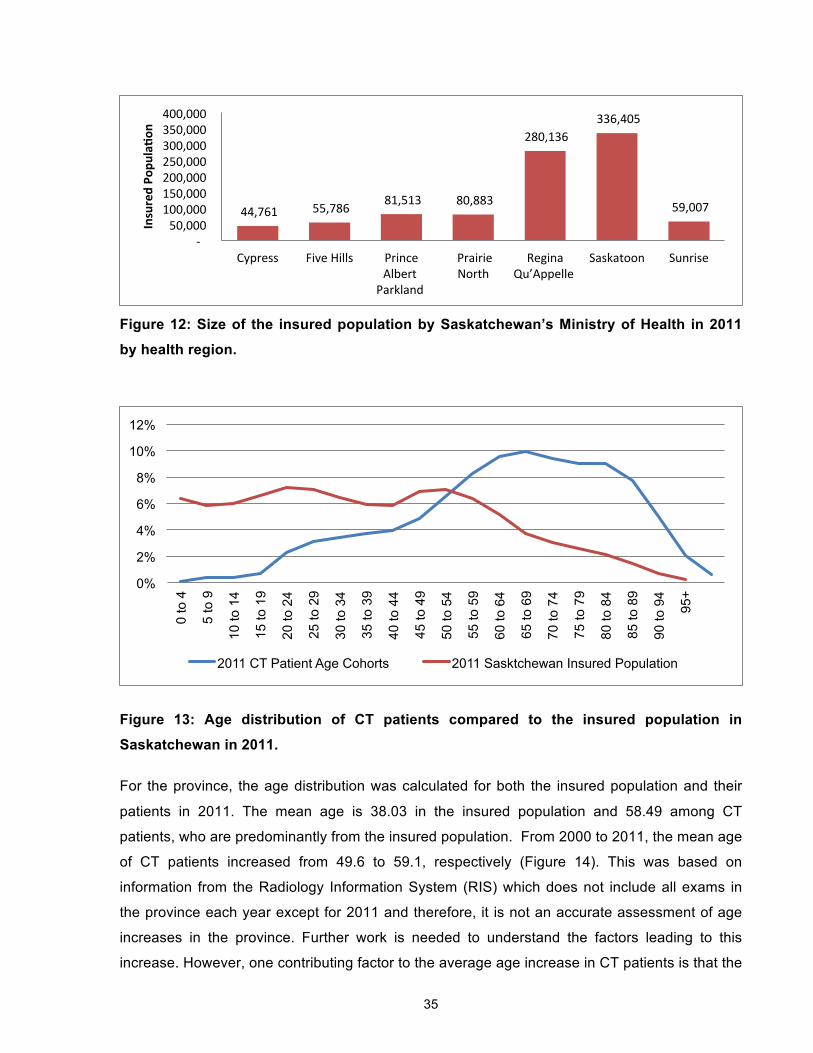
35
Figure 12: Size of the insured population by Saskatchewan’s Ministry of Health in 2011
by health region.
Figure 13: Age distribution of CT patients compared to the insured population in
Saskatchewan in 2011.
For the province, the age distribution was calculated for both the insured population and their
patients in 2011. The mean age is 38.03 in the insured population and 58.49 among CT
patients, who are predominantly from the insured population. From 2000 to 2011, the mean age
of CT patients increased from 49.6 to 59.1, respectively (Figure 14). This was based on
information from the Radiology Information System (RIS) which does not include all exams in
the province each year except for 2011 and therefore, it is not an accurate assessment of age
increases in the province. Further work is needed to understand the factors leading to this
increase. However, one contributing factor to the average age increase in CT patients is that the
44,761 55,786 81,513 80,883
280,136 336,405
59,007
-‐ 50,000 100,000 150,000 200,000 250,000 300,000 350,000 400,000
Cypress Five Hills Prince Albert
Parkland
Prairie North
Regina Qu’Appelle
Saskatoon Sunrise
Insured Po
pula9o
n
0%
2%
4%
6%
8%
10%
12%
0 to
4
5 to
9
10 to
14
15 to
19
20 to
24
25 to
29
30 to
34
35 to
39
40 to
44
45 to
49
50 to
54
55 to
59
60 to
64
65 to
69
70 to
74
75 to
79
80 to
84
85 to
89
90 to
94
95+
2011 CT Patient Age Cohorts 2011 Sasktchewan Insured Population

36
number of people aged 65 and older has increased substantially from 147,570 in 2001, to
216,160 in 2011 [60]. Since elderly patients have higher exam rates (Figure 18), this increases
the average age of CT patients. A higher average age could indicate an increase in the number
of exams needed for the province.
Between the health regions in 2011, Prairie North Health Region had the lowest mean patient
age of 55.5 year old and Sunrise Health Region had the oldest with a mean age of 62.9 years
old (Figure 15). In 2011, the sex distribution was 50.3% female and 49.7% male.
Figure 14: Mean CT patient age in Saskatchewan based on data from the RIS.
Figure 15: Mean CT patient age in 2011 for each health region.
49.6 50.3 50.5 53.5 56.5 56.9 57.1 57.3 57.5 57.6 57.9 58.5 59.1
0 10 20 30 40 50 60 70
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Year
Mea
n Pa
tient
Age
61 61.3 58.8 55.5 59.4 57.7 62.9
0 10 20 30 40 50 60 70
Cypress Five Hills Prince Albert Parkland
Prairie North Regina Qu’Appelle
Saskatoon Sunrise
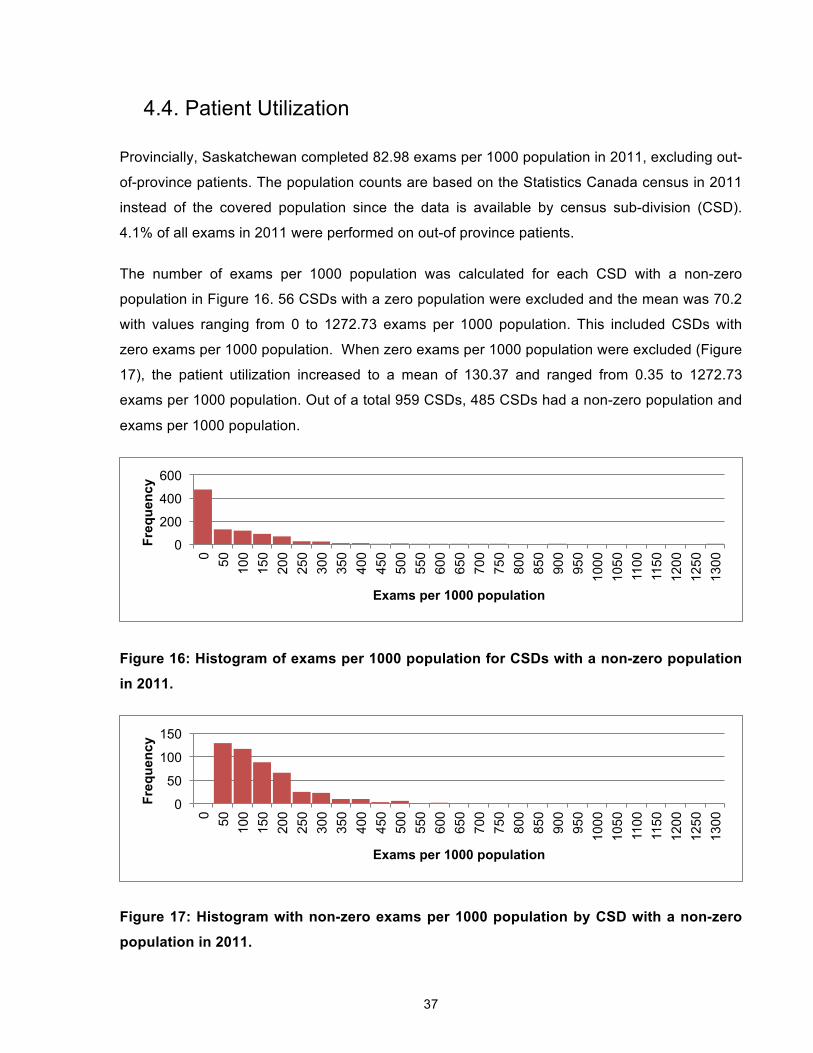
37
4.4. Patient Utilization
Provincially, Saskatchewan completed 82.98 exams per 1000 population in 2011, excluding out-
of-province patients. The population counts are based on the Statistics Canada census in 2011
instead of the covered population since the data is available by census sub-division (CSD).
4.1% of all exams in 2011 were performed on out-of province patients.
The number of exams per 1000 population was calculated for each CSD with a non-zero
population in Figure 16. 56 CSDs with a zero population were excluded and the mean was 70.2
with values ranging from 0 to 1272.73 exams per 1000 population. This included CSDs with
zero exams per 1000 population. When zero exams per 1000 population were excluded (Figure
17), the patient utilization increased to a mean of 130.37 and ranged from 0.35 to 1272.73
exams per 1000 population. Out of a total 959 CSDs, 485 CSDs had a non-zero population and
exams per 1000 population.
Figure 16: Histogram of exams per 1000 population for CSDs with a non-zero population
in 2011.
Figure 17: Histogram with non-zero exams per 1000 population by CSD with a non-zero
population in 2011.
0
200
400
600
0 50
100
150
200
250
300
350
400
450
500
550
600
650
700
750
800
850
900
950
1000
10
50
1100
11
50
1200
12
50
1300
Freq
uenc
y
Exams per 1000 population
0
50
100
150
0 50
100
150
200
250
300
350
400
450
500
550
600
650
700
750
800
850
900
950
1000
10
50
1100
11
50
1200
12
50
1300
Freq
uenc
y
Exams per 1000 population

38
Patient utilization rates were calculated by 20-year age cohorts and sex (Figure 18). Utilization
increased as patients became older, ranging from 11 to 235.8 exams per 1000 population for
females and 13.6 to 335.3 for males in 2011.
Figure 18: Number of exams per 1000 population by 20-year age cohorts and sex in 2011.
Patient utilization was also calculated for inpatients and emergency patients. Provincially,
inpatients had an imaging rate of 167.09 exams per 1000 inpatient visits in 2011 ranging from
43.79 to 319.85 in Saskatoon City Hospital and St. Paul’s Hospital respectively (Figure 19). The
factors which contribute to this difference are discussed in Section 4.2.
Figure 19: Exams per 1000 inpatient visits by facility
For emergency patients, the imaging rate from April 2011 to March 2012 was 156.71, 66.617,
and 69.541 exams per 1000 emergency visits for RUH, SCH, and SPH respectively. Emergency
imaging rates could not be calculated for other hospitals due to lack of data.
11.0 45.5
93.0
187.6 235.8
13.6 46.0
84.5
272.0 335.3
0
100
200
300
400
0-‐19 20-‐39 40-‐59 60-‐79 80+
Exam
s per 1000 po
p.
Age Cohorts
Female Male
43.5 43.8 68.0
93.4 108.1 118.5 121.8 129.8 169.1 188.9
319.8
0 50
100 150 200 250 300 350
RGH SCH PH YRHC VH BUH LH MJUH CRH RUH SPH
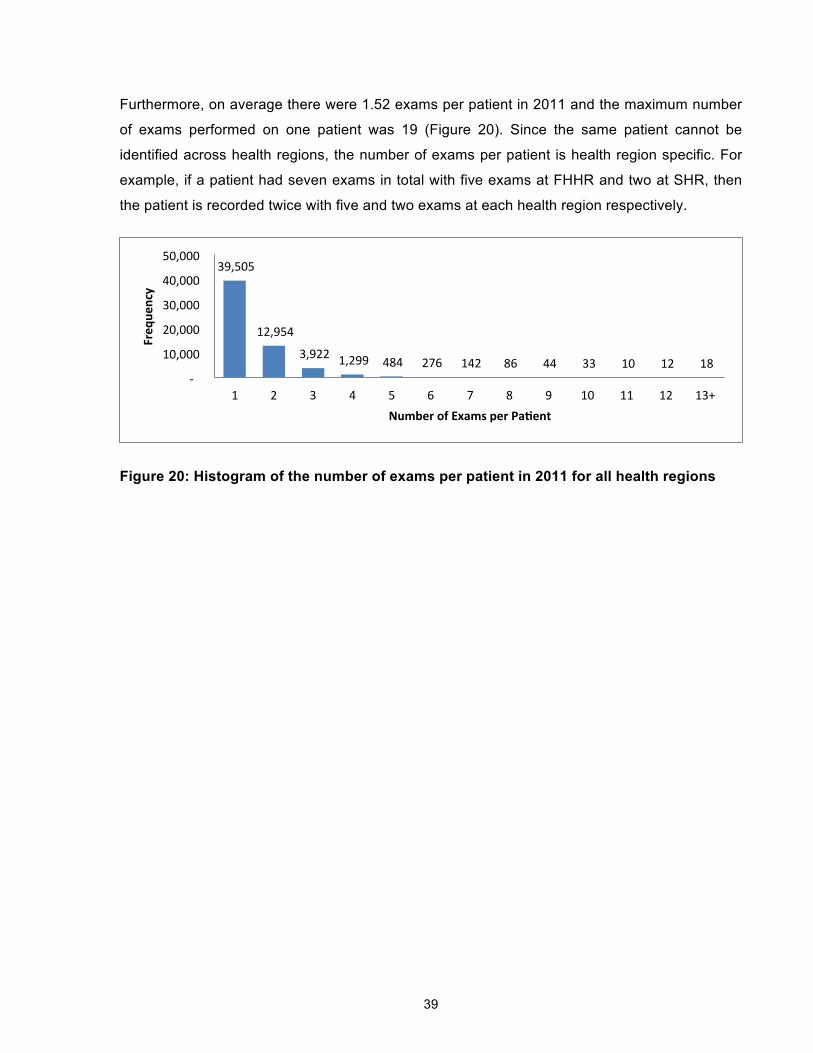
39
Furthermore, on average there were 1.52 exams per patient in 2011 and the maximum number
of exams performed on one patient was 19 (Figure 20). Since the same patient cannot be
identified across health regions, the number of exams per patient is health region specific. For
example, if a patient had seven exams in total with five exams at FHHR and two at SHR, then
the patient is recorded twice with five and two exams at each health region respectively.
Figure 20: Histogram of the number of exams per patient in 2011 for all health regions
39,505
12,954
3,922 1,299 484 276 142 86 44 33 10 12 18 -‐
10,000
20,000
30,000
40,000
50,000
1 2 3 4 5 6 7 8 9 10 11 12 13+
Freq
uency
Number of Exams per Pa9ent

40
4.5. Patient Access
Patient access was analyzed in terms of patient travel and wait times.
4.5.1. Patient Travel
Travel distances were estimated based on the patient’s postal code and CT facility. The
rectilinear distance was used to mimic driving on a street grid and calculations were made
based on each visit instead of number of exams. The mean travel distance for outpatients was
130.28 km whereas the median was 37.51 km (Table 7). The mean travel time for outpatients
was 52.7 minutes.
For urban CSDs, the median travel distance was 5.5km and for rural CSDs, the median travel
distance was 176.4km (Table 7). Similarly, rural and small CSDs had a much higher mean
travel time than medium and urban CSDs (Figure 21). Urban and rural CSD classifications were
determined by Statistics Canada [61].
Table 7: Provincial statistics for rectilinear travel distance (km) in 2011 by population
centre and rural area classification based on the patient’s residential postal code.
Population centre and rural area classification Mean Median 75th Percentile 95th Percentile
Rural Area 212.45 176.4 353.64 478.13
Small (1,000 – 29,999 pop.) 188.57 139.4 369.33 423.49
Medium (30,000 - 99,999 pop.) 24.23 3.71 5.9 180.81
Large Urban (100,000 or greater) 8.27 5.5 7.2 10.23
Overall Rectilinear Travel Distance (km) 130.28 37.51 183.65 447.43

41
Figure 21: Mean travel time to the health facility where CT exam was performed in 2011
from the patient’s residential postal code.
For outpatients from health regions without a CT facility, the majority did not go to the closest
CT facility. The outpatient’s health region of origin was based on their residential postal code.
Figure 22 shows that the majority of outpatients in health regions with a CT scanner went to the
CT facility in their health region. Saskatoon Health Region had the lowest proportion of
outpatients going out-of–region (2%). Prince Albert Parkland Health Region had the highest with
28.2% of outpatients going outside their health region for a CT exam in 2011. More research
needs to be done to understand why, but contributing factors include the teaching affiliations,
reputation, and physician referral patterns [62].
Overall, high percentages of outpatients from health regions without a CT facility went to Royal
University Hospital and to a lesser extent Saskatoon City Hospital and St. Paul’s Hospital with
the exception of outpatients from Sun Country RHA who are close to Pasqua Hospital in RQHR
(See Table 29 in Appendix E). Outpatients from Athabasca RHA went to Victoria Hospital
(63.3%) in Prince Albert Parkland Heath Region and Royal University Hospital (18.3%),
Saskatoon City Hospital (13.3%) and St. Paul’s Hospital (3.3%) in Saskatoon Health Region.
Mamawetan Churchill River Health Region and Kelsey Trial RHA have a similar pattern to
Athabasca. Outpatients from Keewatin Yatthé RHA primarily go to Lloydminster Hospital
(60.5%) in Prairie North RHA; Victoria Hospital (8.3%) in Prince Albert Parkland Health Region;
and Royal University Hospital (12.4%), Saskatoon City Hospital (13.6%) and St. Paul’s Hospital
(5.2%) in Saskatoon Health Region. Heartland RHA is surrounded by several health regions
with CT facilities and while outpatients go to all bordering health regions, 63% go to Saskatoon
Health Region.
112.0
81.7
33.6 35.4
0
20
40
60
80
100
120
Rural Area Small (1,000 – 29,999 pop.)
Medium (30,000 -‐ 99,999 pop.)
Large Urban (100,000 or greater)
Travel Tim
e (m
inutes)

42
Figure 22: Proportion of outpatient visits from each health region that went to a CT
facility outside their health region and went to the closest CT scanner in 2011.
36.7%
11.9% 12.6%
84.1%
48.3% 51.8% 39.1%
21.7% 27.8%
4.9% 1.3%
42.3% 20.0%
63.3%
0.0% 0.4%
15.9%
51.7% 48.2% 60.9%
0.0% 0.4%
1.4% 0.7%
57.7%
0.0%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
100%
Patient Health Region
Out-of-Region & Not Closest CT Out-of-Region & Closest CT

43
4.5.2. Wait Times
Patients have different target wait times depending on the urgency. Level 1 (Emergent) patients
have a target wait time of within 24 hours and are therefore not included in the wait time metrics.
In Table 8, LH and BUH in Prairie North RHA have the shortest wait times while CRH and
MJUH in FHHR have the highest wait times for non-urgent patients at 63 days and 48 days
respectively. All the estimated maximum wait times are within the targets. RQHR and SHR
report the wait times by 50th and 90th percentiles in Table 9. RQHR is not within targets for Level
2 and the 90th percentile for Level 3 patients exceeds the 30 day target. SHR also has longer
wait times for Level 2 patients in the 90th percentile.
Table 8: Estimated maximum wait time by number of days from day of referral to day of
appointment scheduling on December 31, 2011.
Facility Level 2 (Urgent) Level 3 (Semi-Urgent) Level 4 (Non-Urgent)
LH 0 0 7
MJU 1 7 48
BUH 2 2 7
VH 7 17 63
CRH 0 11 18
YRHC 4 15 40
Targeted Wait Time Within 7 days Within 30 days Within 90 days
Table 9: Wait time by number of days from referral to appointment scheduling on
December 31, 2011 for RQHR and Saskatoon Heath Region.
Locations Level 2 (Urgent)
Level 3 (Semi-Urgent)
Level 4 (Non-Urgent)
Regina Qu’Appelle 50% completed within (median) 9 22 24
90% completed within 28 36 46
Saskatoon 50% completed within (median) 5 8 15
90% completed within 9 17 19 Provincial Hospitals (RGH and RUH)
50% completed within (median) 6 14 23
90% completed within 21 30 45 Targeted Wait Time Within 7 days Within 30 days Within 90 days
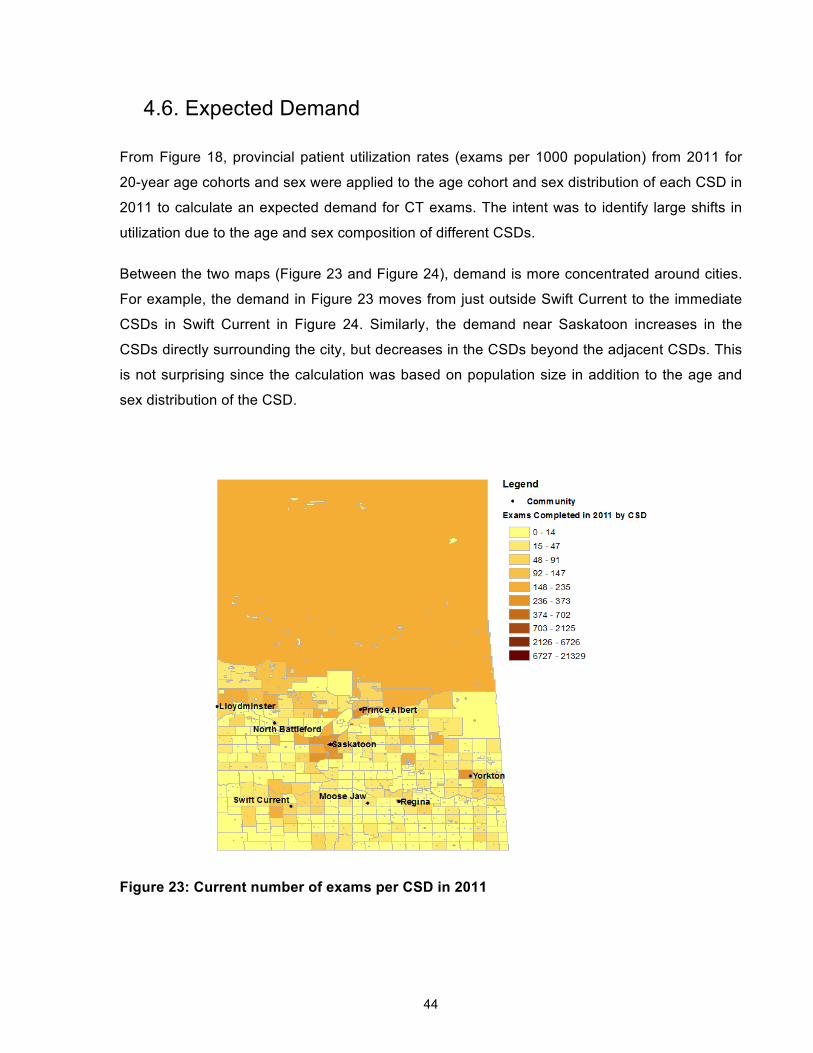
44
4.6. Expected Demand
From Figure 18, provincial patient utilization rates (exams per 1000 population) from 2011 for
20-year age cohorts and sex were applied to the age cohort and sex distribution of each CSD in
2011 to calculate an expected demand for CT exams. The intent was to identify large shifts in
utilization due to the age and sex composition of different CSDs.
Between the two maps (Figure 23 and Figure 24), demand is more concentrated around cities.
For example, the demand in Figure 23 moves from just outside Swift Current to the immediate
CSDs in Swift Current in Figure 24. Similarly, the demand near Saskatoon increases in the
CSDs directly surrounding the city, but decreases in the CSDs beyond the adjacent CSDs. This
is not surprising since the calculation was based on population size in addition to the age and
sex distribution of the CSD.
Figure 23: Current number of exams per CSD in 2011

45
Figure 24: Expected demand (number of exams) per CSD in 2011

46
4.7. Discussion
The results are discussed in comparison to other jurisdictions, how the different metrics relate to
each other, and the factors in projecting supply and utilization.
Comparing Saskatchewan to other jurisdictions
The provincial average operating hours per CT scanner are 58.64 hours per week. This is
slightly below the rest of Canada which operates for 60 hours per week on average [1].
However, in terms of CT provision by number of CT scanners per million population,
Saskatchewan is lower than Canada and the OECD average (Figure 25). From Figure 26, the
average CT scanner in Saskatchewan (6,777 exams/scanner) is performing slightly more
exams than the OECD average (6,312 exams/scanner) and far fewer than the Canadian
average (9,017 exams/scanner). The average CT scanner in Canada is performing 42.9% more
exams each year despite only running for 2.3% more operating hours than in Saskatchewan.
Given the variance in average exams per CT scanner (Figure 5) and exams per operating hour
(Figure 8) within Saskatchewan, this indicates that there is remaining capacity in the existing
system either through unused capacity or improving efficiency. In Figure 27, Saskatchewan also
has a patient utilization which is much lower than Canada’s and OECD average. This suggests
that although Saskatchewan’s existing system can perform more exams with similar operating
hours per year, there are also areas which are currently under-serviced. Variations in patient
utilizations have been found in Norway for CT exams by Lysdahl and Borretzen [25] due to
accessibility and socioeconomic factors. In 2002, patient utilization ranged from 56 exams per
1000 population in a rural area to 216 exams per 1000 population in Oslo, the largest city. The
average utilization was 108 exams per 1000 population.
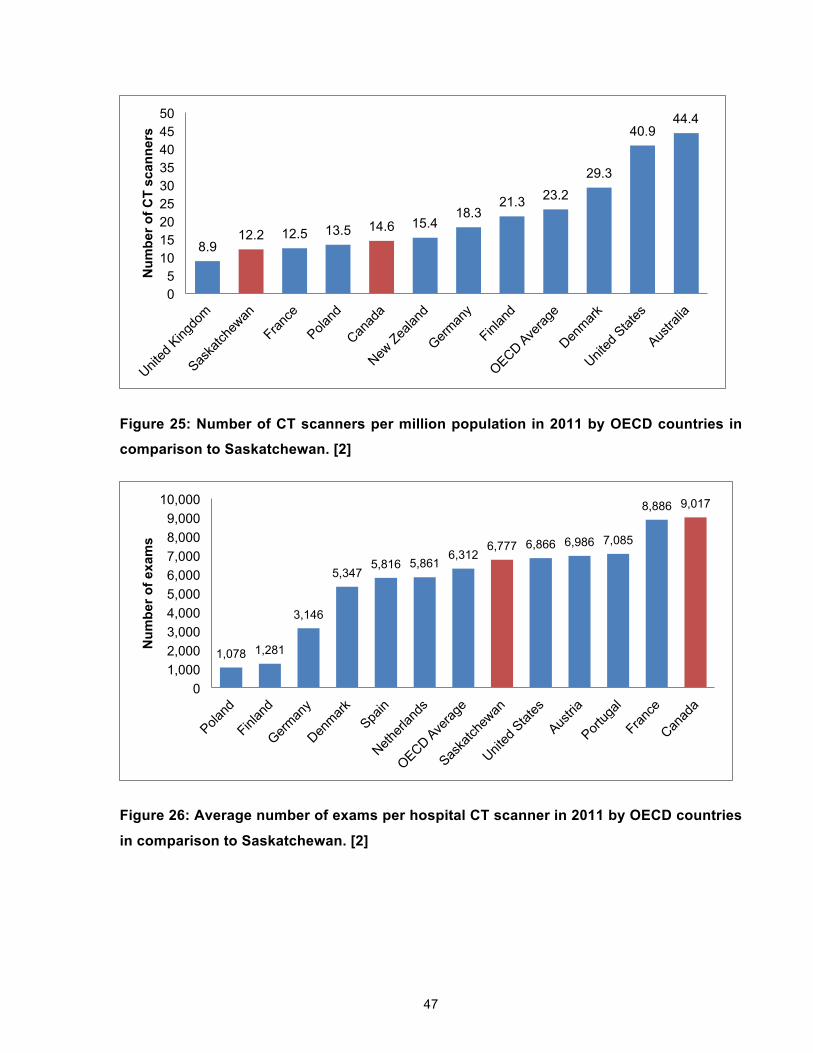
47
Figure 25: Number of CT scanners per million population in 2011 by OECD countries in
comparison to Saskatchewan. [2]
Figure 26: Average number of exams per hospital CT scanner in 2011 by OECD countries
in comparison to Saskatchewan. [2]
8.9 12.2 12.5 13.5 14.6 15.4
18.3 21.3 23.2
29.3
40.9 44.4
0 5
10 15 20 25 30 35 40 45 50
Num
ber o
f CT
scan
ners
1,078 1,281
3,146
5,347 5,816 5,861
6,312 6,777 6,866 6,986 7,085
8,886 9,017
0 1,000 2,000 3,000 4,000 5,000 6,000 7,000 8,000 9,000
10,000
Num
ber o
f exa
ms

48
Figure 27: Number of exams per 1000 population in 2011 by OECD countries in
comparison to Saskatchewan. [2]
CT utilization with patient utilization
In terms of exams per operating hour and proportions of patient types, there does not appear to
be a clear relationship when comparing Figure 7 and Figure 8. For example, even within the
same health region, Saskatoon City Hospital (SCH) and St. Paul’s Hospital (SPH) have similar
estimated exams per operating hour even though SCH has twice the percentage of outpatients
due to different patient populations. SPH has an exam rate of 319.8 exams per 1000 inpatients
in contrast to SCH that has only 43.8. SPH also has more emergency patients than SCH
(27.9% vs. 9.3%). From the literature, emergency departments have high CT exam rates such
as 705 and 394 scans per 1000 ED visits for patients 21 to 30 years old and 61 to 70 years old
respectively [63]. However, the emergency patient exam rate is 66.617 for SCH and 69.541 for
SPH. Furthermore, varying levels of patient complexity at different facilities may impact how
many exams can be done each hour.
29.1 37.3
70.8 83 90.4
104.1 128.2 129.3 130.1
172.1 178.5 180.3
256.8
0.0
50.0
100.0
150.0
200.0
250.0
300.0
Num
ber o
f exa
ms
per 1
000
pop.

49
CT utilization with patient access
BUH and YRHC have the same operating hours; they perform a similar number of exams per
year; and they have similar proportions of patient type and priority level. However, the wait times
at YRHC are much longer. A more detailed analysis of their processes and patients is needed to
understand the differences between the two facilities.
In terms of distance travelled by outpatients, 8 out of 13 health regions had 7% or more
outpatients go to Saskatoon Health Region which is expected because Royal University
Hospital is a tertiary hospital. Health regions with a CT facility also send patients to Saskatoon
City Hospital and St. Paul’s Hospital for outpatient CT exams. This may be due to referral
patterns or wait times in their facilities. For example, Victoria Hospital (PAPHR) has wait times
which are much longer than at neighbouring Battlefords Union Hospital and Prince Albert
Parkland Health Region has 17.9% of their patients going to SCH and SPH. More research
needs to be done in terms of why patients are being referred to specific institutions.
Projecting CT supply and utilization
From the metrics and discussion, it is clear that there are many factors that contribute to large
differences in exams performed at separate facilities beyond simply the number of operating
hours. Factors include, but are not limited to, the proportions of patient type, the patient
illnesses within each of those patient types, and referral practices [9].
For the expected demand calculation, only age and sex were used to adjust the utilization rates
for each CSD. However, the literature is clear that geographic factors impact patient utilization,
in particular, proximity to a CT scanner [25]. Furthermore, with the increase in the aging
population [60] and potential changes in migration and overall growth the demand may change
substantially. A more thorough analysis on socio-demographic and geographic factors,
including proportions of First Nations per CSD, should be done to improve demand projections.

50
Chapter 5. Capacity Planning Model for CT scanners
The previous chapter described the current situation with respect to CT supply, patient
utilization, and patient access. In this chapter, the metrics are used to inform the parameters of
the model and provide context to the results. This chapter begins with a description of the
problem specific to CT scanner capacity planning and then describes the model assumptions
and formulation. Calculations for the model’s input data are discussed followed by descriptions
of the model scenarios. Scenarios results are presented to understand cost and access trade-
offs and the sensitivity of the results.
5.1. The Problem
The goal of the proposed model is to determine for a specified planning horizon: 1) where CT
scanners should be located, and for each location, 2) how many CT scanners are needed,
3) how many operating hours are necessary, and 4) when capacity changes are needed while
achieving targets for covering demand within facility catchment areas and minimizing cost. The
size of the catchment area is determined by the maximum patient travel time.
In the model we assume that a proportion of demand from each location (e.g., community,
census subdivision) will be assigned to a facility if the demand is within the facility’s catchment
area and capacity is available at the facility. The minimum coverage percentage determines the
amount of assigned demand. However, all demand must be met. In the case that demand is not
assigned to a specific facility, then the unassigned demand has no patient travel time restriction.
It is assumed that any facility can fulfill unassigned demand which leads to longer travel times
for the remaining percent of demand. Any unused capacity at existing facilities can be used to
meet the unassigned demand. If there is insufficient capacity, then more capacity needs to be
added to the system through adding capacity to the existing facilities or opening a new facility.
The set of potential CT facilities is predetermined to ensure suitability.
To identify overtime utilization and leftover capacity, a week is segmented into smaller units
based on shift work. Each segment is called a shift and is considered part of regular time. We
made the simplifying assumption that a shift is 40 hours. The sum of shifts for each facility
constitute the total number of regular operating hours per week and the model does not
determine how the hours are spread during the week. There are two ways to add capacity to
existing facilities: staff another shift and add a new CT scanner. An open facility can have
multiple CT scanners, which each need to be staffed for at least one shift and can be operated
51
for a specified maximum number of shifts (e.g. 3 shifts for a total of 24 hours per day). When
there are multiple shifts at the same facility, the assumption is that shifts are running in series on
the same CT scanner. If there is more than one CT scanner at a facility, then shifts can run in
parallel. There is no limit on the number of CT scanners a facility can hold. When demand
assigned to a facility exceeds the capacity of a shift, then it will be charged at an overtime rate.
When the cost of overtime exams exceeds the cost of a shift, then another shift is added to the
facility to increase the regular operating hours. Shifts are removed from a facility at a dummy
cost called a shift removal cost. Another CT scanner is added to the facility in two situations: 1)
when the number of shifts required exceeds the maximum number of shifts and the cost of
overtime exams is more than the cost of both a CT scanner and one shift or 2) the assigned
demand exceeds the maximum capacity of the CT scanners.
In order to build a new CT facility, the catchment area of existing facilities must need the new
CT facility to reach the minimum percentage of covered demand. To reach more demand within
the maximum travel time, another CT facility is built at the cost of opening and purchasing a CT
scanner. To ensure a balance between cost and access, many health care systems will have
existing CT scanners which should be incorporated into the capacity plan. Therefore, the
opening cost is only incurred when there is no pre-existing facility.
5.2. Model Development
To develop the model formulation, the following assumptions are made:
Assumption 1: A minimum percentage of patient demand must be able to reach a CT scanner
within specified travel time radius.
Assumption 1 may not hold because of possible referral patterns, central appointment booking,
and patient activity spaces may bring patients outside of the specified travel radius [20]. If
central appointment booking were implemented, it may give patients earlier appointments at the
expense of longer travel times. Patients may also prefer different locations depending on where
their other life activities occur [20]. However, this assumption matches rural access standards
for healthcare services set by British Columbia [64] and Ontario [65].

52
Assumption 2: New CT scanners could be placed at a specific set of candidate locations.
Assumption 2 acknowledges that there are many factors which contribute to a CT facility
candidate such as existing hospitals, human resources and road infrastructure.
Assumption 3: CT scanners cannot be relocated or closed.
Assumptions 3 may not hold when CT scanners get old and need to be replaced. In addition to
a large capital investment, CT scanners require substantial human resources and are in high
demand for diagnostics, especially for emergency and inpatients. While it may be possible for a
CT scanner to be relocated, it is unlikely.
Assumption 4a: The maximum number of exams a CT scanner can complete each year will
remain constant in each time period in the planning horizon.
Assumption 4b: The duration of CT exams does not change.
Assumptions 4a and 4b imply that there will not be improvements which make CT scanners
more efficient. Over a 20-year planning horizon it is possible for new technology to be invented
that dramatically impacts utilization rates by allowing more CT scans to be done each day.
However, when technology improves, more images tend to be ordered per exam [66]. This
suggests that exam duration may not change substantially. Furthermore, although different
types of exams take various lengths of time, the aggregate exam time in a year may vary less
than specific exam types.
Assumption 6: Costs do not differ depending on the geographic location or facility type.
Costs associated with CT scanners will not change (exams, supplies, technologists) depending
on where CT exams are provided. This may not hold due to transportation costs and incentives
to practice in less popular locations.
Assumption 7: The real cost of goods and services does not change.
As the cost of goods and services will increase with inflation, the real cost to the system does
not change. Furthermore, the increase in cost of a CT scanner and facility due to inflation is
negligible compared to the overall cost of the CT scanner system.

53
Assumption 8: One CT scanner at each candidate location can be added in each time period.
This assumption may hold when the demand within a candidate location’s catchment area does
not increase dramatically. For example, if the unused overtime capacity for a CT scanner is
18,837 exams and the demand rate is 83 exams per 1000 population, then the population would
need to increase by more than 226,952 people to require a second CT scanner in the same
time period at the same facility. This assumption was made to improve the solvability of the
model. If more than one CT scanner can be added to each candidate location in each time
period, this will add complexity to the model.
Assumption 9: It costs less to add a new CT scanner at an existing facility than open a new
facility with a new CT scanner.
According to the CIHI report [1], in general it was less expensive to add CT scanners to existing
facilities than to build a new CT facility. However, the costs of renovating the rooms and
buildings for CT scanners are in the range of $400K to $1.8M. There may be certain
circumstances where this assumption does not hold.
Assumption 10: All CT scanners can do all types of scans.
Different CT scanners are capable of different types of CT images. For example, a volumetric
computed tomography scanner allows for 3D imaging, but this type of CT scanner is only
available at tertiary hospitals. However, the majority of scans can be completed on just 16-slice
CT scanners [67] and this assumption simplifies the model for most scans.
Assumption 11: Costs during regular operating hours are the same regardless of the number
of exams completed.
The current formulation assumes that the cost of a shift is the same regardless of how much
unused operating capacity is left. According to Saskatoon Health Region’s budget from April
2011 to March 2013, operating and personnel costs comprise of 92.2% of expenses. The
material costs of exams only make up the remaining 7.8%. While this assumption overestimates
the cost of a shift if there is idle time, the additional cost is a small percentage of the overall
costs because of the operating and personnel costs.
54
5.2.1. Formulation
Description: Suppose there is a set of I CT demand locations and a set of J CT facility
locations to be planned for in T time periods. CT demand changes magnitude with time t for
each demand location i. A proportion of demand at location i is covered by an open CT facility in
location j in time t. The province must have the capacity to meet all the demand regardless of
CT catchment areas. When a new CT facility is built, it incurs an opening cost. Additional CT
scanners can be added to the existing CT facilities. Shifts can be added to each CT scanner in
order to increase the normal operating capacity in each time period. Furthermore, when a CT
scanner is assigned more exams than the normal operating capacity, it incurs an overtime
surcharge to the cost per additional exam.
Indices:
i = 1... I: Index of CT demand locations
j = 1... J: Index of CT facility locations
t = 0…T: Index of capacity planning time periods
Parameters:
Demandit = number of CT exams that need to be performed in area i at time t
DemandTotalt = Demand!"!!!!
MinCoverage = minimum percentage of total demand that must be covered with a maximum
patient travel time
aij = { 1 if CT demand in area i is within a maximum patient travel time of location j, 0 otherwise}
CapMax = maximum number of exams for each CT scanner
CapShift = maximum number of exams in a shift
MaxShifts = maximum number of shifts per CT scanner which make up regular operating hours
CostOpen = cost of opening a new CT facility
CostCT = cost of adding a CT scanner to an open facility

55
The cost of opening a new CT facility is separate from the cost of purchasing a CT
scanner. Therefore, to open a new CT facility, the total cost is the cost of opening the
facility plus the cost of the new CT scanner (Total Cost of New CT Facility = Cost Open
+ CostCT).
ExamCost = cost for each exam completed during regular operating hours
OvertimeSurcharge = percent increase in cost per exam that exceeds a CT scanner’s normal
operating capacity
ShiftRemovalCost = cost of removing a shift from a CT facility
To initialize the model: CTTotalj0 = number of current CTs at location j at time 0
Decision Variables:
xijt = fraction of demand covered at location i by a CT at location j at time t
yjt = {1 if a new CT is placed in location j at time t, 0 otherwise}
CTTotaljt = total number of CTs at location j at time t = CTTotal!"!! + y!"
zj = {1 if a new facility is placed at location j in any period, 0 otherwise}
z! ≥ y!" − CTTotal!" ∀ j ∀ t
CToverjt = number of assigned exams exceeding normal operating capacity at location j at time t
CTunderjt= number of exams below the normal operating capacity at location j at time t
Shiftsjt = number of sets of regular operating hours at location j at time t
UnassignedDemandt = number of unassigned exams at time t
UnassignedOverjt = number of unassigned exams completed in overtime at location j at time t
UnassignedUnderjt = unused regular operating capacity at location j at time t (measured in
number of exams)
ShiftRemovedjt = number of shifts removed from a location j at time t

56
ShiftAddedjt = number of shifts added to a location j at time t
Model:
The following is a formulation for the dynamic CT scanner facility location problem.
Minimize CostOpen z! + CostCT y!"!!!!
!!!! !
!!! +
OvertimeSurcharge*ExamCost CTover!"!!!!
!!!! + UnassignedOver!!
!!! +
ExamCost*CapShift Shifts!"!!!!
!!!! + ShiftRemovalCost ShiftRemoved!"
!!!!
!!!!
s.t.
x!"#Demand!"!! ≥ MinCoverage ∗ DemandTotal! ∀ t (1)
Capmax CTTotal!"! ≥ DemandTotal! ∀ t (2)
x!"#Demand!"! = CapShift ∗ Shifts!" + CTover!" − CTunder!" ∀ j,∀t (3)
CTover!" ≤ CapMax ∗ CTTotal!" − CapShift ∗ Shifts!" ∀ j,∀t (4)
x!"# ≤ a!"CTTotal!" ∀ i ∀ j ∀ t (5)
x!"#! ≤ 1 ∀ i ∀ t (6)
z! ≥ y!" − CTTotal!" ∀ j ∀ t (7)
CTTotal!" = CTTotal!"!! + y!" ∀ j ∀ t ≥ 1 (8)
Shifts!" ≤ MaxShifts ∗ CTTotal!" ∀ j ∀ t (9)
Shifts!" ≥ CTTotal!" ∀ j ∀ t (10)
Shifts!"!! − Shifts!" = ShiftRemoved!" − ShiftAdded!"∀ j ∀ t (11)
DemandTotal! − x!"#Demand!"!! = UnassignedDemand! ∀ t (12)
UnassignedDemand! − CTunder!"! = UnassignedOver! − UnassignedUnder! ∀ t (13)

57
y!" binary ∀ j ∀ t (14)
z! binary ∀ j (15)
CTTotal!" ≥ 0 ∀ j ∀ t (16)
CTover!" ≥ 0 ∀ j ∀ t (17)
CTunder!" ≥ 0 ∀ j ∀ t (18)
Shifts!" ≥ 0 integer ∀ j ∀ t (19)
UnassignedDemand! ≥ 0 ∀ t (20)
UnassignedOver! ≥ 0 ∀ t (21)
UnassignedUnder! ≥ 0 ∀ t (22)
ShiftRemoved!" ≥ 0 ∀ j ∀ t (23)
ShiftAdded!" ≥ 0 ∀ j ∀ t (24)
0 ≤ x!"# ≤ 1 ∀ i ∀ j ∀ t (25)
The objective is to minimize the cost of opening new CT facilities, adding new CT scanners,
overtime exams, regular operating hours, and shift removal. The exam cost is multiplied by the
capacity during regular operating hours to account for salaries, operating costs, and materials.
The overtime surcharge incorporates the additional variable costs such as overtime wages paid
to staff.
Constraint (1) ensures that a minimum percentage of the total provincial demand is covered in
each time period. For example, if the minimum coverage is 95% and the maximum travel time is
30 minutes, then a minimum of 95% of demand can reach a CT scanner in 30 minutes.
Constraint (2) ensures that there is enough existing capacity, using the maximum CT capacity,
from all the implemented CT scanners to meet all of the provincial demand each time period.

58
Constraint (3) calculates the assigned demand, the number of shifts required to cover both
assigned and unassigned demand, and the resulting overtime exams and unused exam
capacity for each CT facility in each time period.
Constraint (4) checks that the overtime is within the overtime capacity for each CT facility in
each time period.
Constraint (5) makes sure that the assigned demand to the CT facility is within the maximum
travel time of the CT facility based on the feasibility matrix, aij.
Constraint (6) prevents covered demand from being assigned more than once.
Constraint (7) opens a new CT facility when the initial CT scanner needs to be built and ensures
the opening cost is only incurred for new CT facilities.
Since CT scanners can only be added, Constraint (8) does not allow CT facilities to be closed
and updates the total number of CT scanners at each candidate location in each time period.
For Constraint (9), the number of shifts at each location and time period cannot exceed the
maximum number of shifts allowed for each CT scanner.
Constraint (10) ensures that each CT scanner is run for at least one shift.
Constraint (11) calculates the number of shifts which are added and removed for each CT
facility for each time period.
The amount of unassigned demand in each time period is calculated in Constraint (12).
Constraint (13) calculates the number of unassigned overtime exams and unused exam
capacity in the system for each time period.
z! and y!" are binary decision variables in Constraint (14) and (15) respectively. Since y!" is
binary, it assumes that there will be no more than one CT scanner added each year. For z!, a
facility is either opened or not and for y!", a CT scanner is added to an open facility or not. In
Constraint (16), CTTotal!" is a real number, but only increments by 1 because y!" is binary.
CToverjt, CTunderjt, UnassignedDemandt, UnassignedOvert, UnassignedUndert, ShiftRemovedjt,
and ShiftAddedjt are positive real numbers. Shiftsjt is integer and non-negative since each CT
scanner can have multiple shifts and there cannot be partial shifts. x!"# is the fraction of demand

59
covered by a CT so its values are continuous from 0 to 1. While partial CT exams are not
realistic, having fractional exams does not have a large impact on the model results and
improves computation time.
5.3. Model Inputs for Saskatchewan’s CT Capacity Plan
The capacity planning model will output the number of required CT scanners, the locations they
are placed, the year they should be implemented, and the utilization level in each year. A long
planning horizon of 19 years (until 2030) was based on results from population projections of
Saskatchewan from Statistics Canada. However, population projections and CT scanner
technology will change over time. This will alter demand patterns and capacity levels, which
could have a substantial impact on accuracy of the capacity plan. The model should be re-run
with new information as necessary to create an updated capacity plan. This section explains
the model input data calculations and resulting input data for applying the model to
Saskatchewan.
5.3.1. Input Data Calculations
All the model parameters were calculated from various sources for the model.
Existing CT Facilities
The decision variable, CTTotaljt, was initialized based on the current CT scanner locations in the
province (See Table 6). Data on existing CT facilities were collected from each of the CT-
equipped health regions. The assumption for most of the scenarios is that policy makers would
want to build upon existing resources to reduce costs. It also acknowledges that there are many
reasons why a CT facility is chosen beyond the demand within a certain catchment area. In this
model, existing CT facilities can install additional CT scanners. Therefore, only the cost of the
new CT scanner is incurred for existing CT facilities and not the cost of building a new CT
facility.
Candidate Facility Locations
Potential new CT facilities were the existing hospitals in Saskatchewan due to the impact on
improving care by providing the ability to diagnose inpatients and emergency patients on
premise. Freestanding clinics could be considered for outpatients only; however, they tend to be
more efficient for areas with a high population density and our research focuses on improving

60
access for remote and rural populations [1]. For the purposes of this model, only existing
hospitals were considered candidate facility locations.
Hospitals are given a facility designation based on the types of services they provide according
to The Facility Designation Regulations [68]. Currently, all provincial and regional hospitals have
CT scanners. All district hospitals were chosen as potential CT facilities because they were the
next largest hospital classification. District hospitals are larger than community hospitals, so
from a policy perspective, district hospitals would require less investment in infrastructure to
implement CT scanners than community hospitals. Northern hospitals are a type of community
hospital which is more focused on servicing northern Saskatchewan populations. Due to our
interest in patient access, all three northern hospitals (i.e. La Loche Health Centre, La Ronge
Health Centre, and St. Joseph's Health Centre) were included so there would be potential CT
facilities north of existing facilities.
In summary, hospitals classified as provincial, regional, district, and northern were included in
this model as candidate facility locations.
Patient Travel Time Calculations
As described in the Methods Section 0, travel times between the census subdivision centroid
and all candidate facility locations were estimated in ArcGIS using the road network and
rectilinear travel distances. The maximum travel times form the catchment area of the CT
facilities. A study has shown that as travel burden increases (time increases), patient utilization
and access to mental health services will decrease [19]. For CT specifically, geographic location
may explain lower scanner utilization in a region [1].
The travel times between each census subdivision and CT facility are combined with the
maximum travel time to create the binary aij parameter.
Cost of opening a CT facility
Estimates of the cost to renovate a facility for its first CT scanner was based on previous
implementations across Canada, which separated the renovation cost from CT scanner costs.
Data were obtained from the CIHI report [1] and press releases from the Saskatchewan Ministry
of Health [69 - 73]. Renovation costs ranged substantially from $400K to $1.8M.
The average renovation cost was $1.25M, which is used in the capacity planning model.
61
Cost of a CT scanner
For the estimate on the cost of a single CT scanner, the CIHI report [1] used the value $1.7M
per CT scanner which was based on the average cost of CT scanners in Ontario. This value
was checked against the Emergency Care Research Institute 2012 white paper [74] on CT
scanners which included the average vendor-quoted cost for a CT scanner in addition to the
service cost which was $1.67M for “premium” scanners. Hence, the cost of an additional CT
scanner in the capacity planning model was $1.7M.
Exam cost and overtime surcharge of additional exams
The exam cost and overtime surcharge of additional exams was calculated based on the
average exam cost in Saskatoon Health Region excluding physician remuneration and benefits
in 2011. Each exam costs $62.26 for the technologist, operations cost, and materials. This cost
does not separate the operating costs during regular operating hours from overtime hours since
our cost data does not distinguish between the two times of operation. Therefore, when the
cost of a shift is calculated in the model, it slightly overestimates the cost of a shift if there is
unused exam capacity during regular operating hours.
The overtime surcharge is estimated to be 50% more than the exam cost of a regular exam to
reflect the typical time and a half paid for overtime.
CT scanner capacity
The average number of exams per hour is used to estimate CT scanner capacity. We had
obtained the time the exam began from Moose Jaw Union Hospital, Victoria Hospital,
Battlefords Union Hospital, Lloydminster Hospital and Yorkton Regional Health Centre. This
filters for exams completed within regular operating hours and the average number of exams
per hour was 2.26. The other facilities did not have exam times. Their estimated exams per hour
is 2.61 which is higher due to the inclusion of overtime exams. For calculating the capacity
parameters, 2.26 was used as the average number of exams per hour.
The smaller CT facilities in Saskatchewan run for eight hours a day and five days a week, thus a
shift is defined as 40 hours per week. Hence, the annual CT capacity was 4,700 exams for the
purpose of a regular shift and the maximum annual CT scanner capacity is 19,743 exams per
year based on operating a CT scanner 24 hours a day and 52 weeks a year without holidays.

62
Demand calculations
Demand from 2012 to 2030 for each CSD is estimated using provincial patient utilization rates
based on 20-year age cohorts and sex, provincial population estimates from 2011 to 2014, and
M1 provincial growth rates from 2014 to 2030. 20-year age cohorts were chosen to achieve a
larger sample size and thus more accurate utilization rates. The M1 scenario has a medium
growth rate and historical migration trends. Population projections for each demand area i were
multiplied by 2011’s average utilization rates by sex and age cohort. The yearly provincial
growth rates by age cohort and sex were applied to each census subdivision (Appendix B).
There was no adjustment made for different exam procedure groups and patient types
(emergency, inpatient, outpatient). See Methods Section 3.1.4 and 0 for more details on the
population projection calculations.
As a result, the demand calculations assume that the demand rate will remain constant;
provincial growth by age cohort and sex is the same across all census subdivisions; and
demand rate is independent of proximity to a CT scanner.
The assumption that the demand rate will remain constant in each time period and each
demand location over the planning horizon may not hold since new technology can change
usage patterns by increasing the range of possible diagnosis thereby increasing the need for CT
scans. Furthermore, studies in mental health [19] and radiological services [25] have shown that
areas with less access to medical equipment have lower utilization rates making it unlikely that
the utilization rate in Saskatchewan is independent of proximity to a CT scanner. If there is less
access to care, then low utilization rates are more reflective of low access and may still have a
higher demand rate than the utilization rate suggests.
Maximum Shifts
Given the current operating hours for CT scanners in Saskatchewan (Table 6), each shift is the
equivalent of 40 hours a week with a maximum of 3 shifts each year. While it is possible to run a
4th shift for the remaining hours in the week, none of the existing CT scanners has regular
operating hours 24 hours a day.

63
Shift Removal Cost
This is a dummy cost to prevent the model from moving shifts back and forth between different
facilities. A shift cost of $100K was used with no impact on the objective function (See Section
5.6.4).
5.3.2. Resulting Input Data
Based on the calculations and sources in Section 5.3.1 (Input Data Calculations), the values in
this section were used as parameters in the model unless otherwise noted in the scenario.
For the indices, the set of I demand locations is 959 since each CSD is considered a CT
demand location. All CSDs in Saskatchewan are used for completeness. The set of J candidate
facility locations includes all 23 existing and potential CT facility locations (See Table 31 in
Appendix F). There are 19 time periods T, so that the model runs from 2012 until 2030. The
feasibility matrix, aij,, is adjusted based on the maximum travel time.
The base case parameter values are:
CapMax = 19, 743 exams per year per CT scanner
CapShift = 4,700 exams per year per shift
CTTotalj0 = See Table 6
CostOpen = $1.7M
CostCT = $1.25M
ExamCost = $62.26 per exam
OvertimeSurcharge = 50% extra
MaxShifts = 3 per CT per year
ShiftRemovalCost = $100K

64
5.4. Solution Approach
As described in Methods Section 0, in order to obtain results, AMPL model files (.mod) and data
files (.dat) were created using MATLAB v.7.12.0.635 (R2011a). In AMPL v.20140331, the
CPLEX solver was called to obtain results. The run time was limited to 1 hour.
Limiting the run time to an hour means that the optimal solution was not necessarily found. To
check whether limiting the run time to an hour would result in substantially different results, the
model was run for 2 hours, 30 minutes, 15 minutes, and 10 minutes with a 2-hour travel time
and 90% minimum coverage. The results for all run times were the same except for the run time
of 10 minutes. With a 10 minute run time, the model finds a worse solution. However, run times
of 15 minutes and 2 hours output the same results. Furthermore, the model is trying to find an
optimal solution to a problem where all the model parameters have been estimated. Since a
model’s result is only as accurate as the input data, having an optimal solution is not crucial.
The relative mixed-integer program (MIP) gap is the percent difference between a theoretical
optimal answer from a linear program relaxation and the current best answer. So a difference of
1% suggests that the solution is within 1% of the theoretical optimal answer. If the relative MIP
gap is too high, then it implies that the solution may not be optimal.
5.5. Scenarios and Sensitivity Analysis
The model was used to run several scenarios to analyze the results based on various
parameters. The feasibility of access and cost was assessed analytically. The three main model
scenarios were:
Scenario 1: Trade-off between access and cost
Scenario 2: Covering provincial demand
Scenario 3: Green field
Furthermore, a sensitivity analysis was conducted to understand how the model results would
change if key parameters were modified.
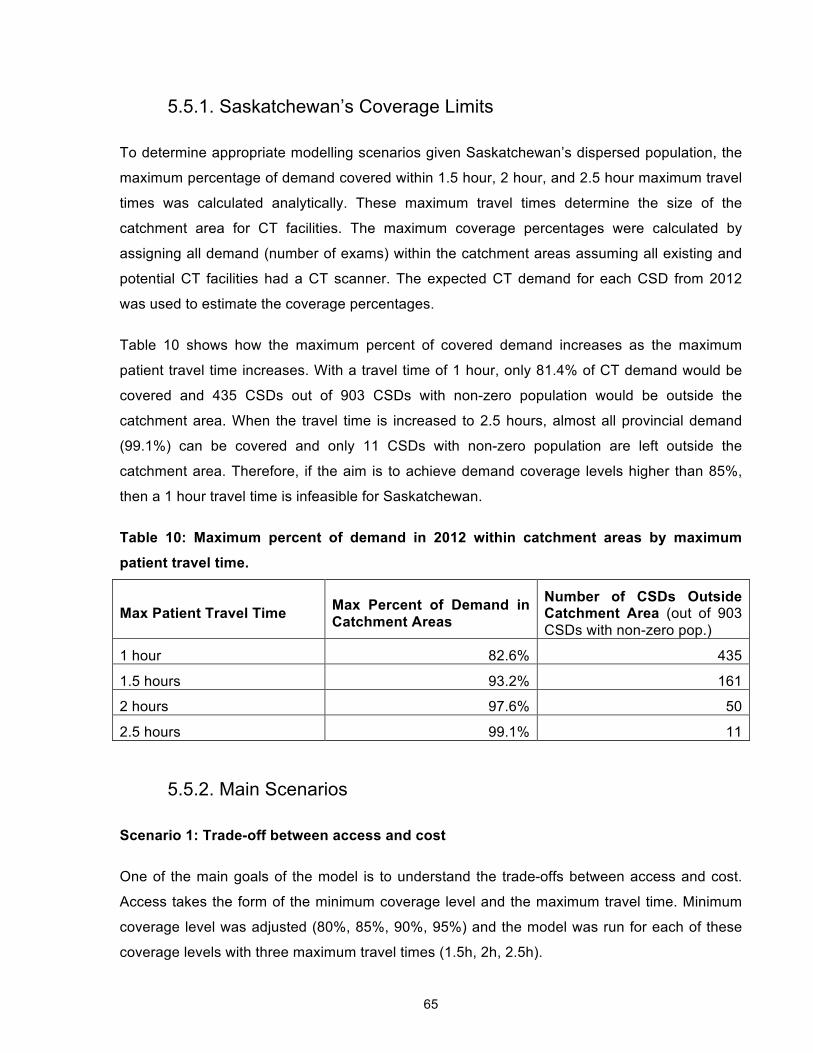
65
5.5.1. Saskatchewan’s Coverage Limits
To determine appropriate modelling scenarios given Saskatchewan’s dispersed population, the
maximum percentage of demand covered within 1.5 hour, 2 hour, and 2.5 hour maximum travel
times was calculated analytically. These maximum travel times determine the size of the
catchment area for CT facilities. The maximum coverage percentages were calculated by
assigning all demand (number of exams) within the catchment areas assuming all existing and
potential CT facilities had a CT scanner. The expected CT demand for each CSD from 2012
was used to estimate the coverage percentages.
Table 10 shows how the maximum percent of covered demand increases as the maximum
patient travel time increases. With a travel time of 1 hour, only 81.4% of CT demand would be
covered and 435 CSDs out of 903 CSDs with non-zero population would be outside the
catchment area. When the travel time is increased to 2.5 hours, almost all provincial demand
(99.1%) can be covered and only 11 CSDs with non-zero population are left outside the
catchment area. Therefore, if the aim is to achieve demand coverage levels higher than 85%,
then a 1 hour travel time is infeasible for Saskatchewan.
Table 10: Maximum percent of demand in 2012 within catchment areas by maximum
patient travel time.
Max Patient Travel Time Max Percent of Demand in Catchment Areas
Number of CSDs Outside Catchment Area (out of 903 CSDs with non-zero pop.)
1 hour 82.6% 435
1.5 hours 93.2% 161
2 hours 97.6% 50
2.5 hours 99.1% 11
5.5.2. Main Scenarios
Scenario 1: Trade-off between access and cost
One of the main goals of the model is to understand the trade-offs between access and cost.
Access takes the form of the minimum coverage level and the maximum travel time. Minimum
coverage level was adjusted (80%, 85%, 90%, 95%) and the model was run for each of these
coverage levels with three maximum travel times (1.5h, 2h, 2.5h).

66
Adjusting travel time and minimum coverage level will lead to differences in the total cost which
can be presented to the decision maker, who can determine which parameter assumptions and
costs are most appropriate. By adjusting coverage percentage, the relative financial impact of
increasing the percentage of the population that are within the maximum travel distance can be
assessed. The maximum travel time defines the travel burden for patients and needs to be
understood relative to the financial impact on the province. This scenario also assumes that the
province will build upon its existing CT facilities.
Scenario 2: Covering provincial demand
To get a better understanding of the capacity and costs if travel time was not a limiting factor,
scenario 2 was run with the minimum coverage level set at 100% and the maximum travel time
20.2 hours since it was the highest travel time for CSDs with demand to a CT facility.
Selecting a base scenario
For sensitivity analysis and green field scenario, the base case was for a minimum coverage
level of 90% and the maximum travel time of 2 hours. From the metrics, the 75th percentile of
patients travelled 183.65 km which would take approximately 2 hours to drive. For basic
inpatient services, guidelines on rural health service provision from British Columbia [64] and
Ontario [65] indicate a maximum travel time of 2 hours at a 95% coverage level and 1 hour at a
90% coverage level, respectively. The next health provision category is tertiary level care with a
maximum travel time of 4 hours for both British Columbia and Ontario. Furthermore, a national
study was conducted on travel time to hospitals for women giving birth [75] and it uses 2 hours
as the travel time threshold, which further suggests that travelling 2 hours is the maximum
appropriate travel time. For the coverage level, there is at least 90% coverage in British
Columbia and Ontario. Given the results in Section 5.5.1, a 95% coverage level may not be
practical for Saskatchewan.
Scenario 3: Green Field
In scenarios 1 and 2, it is assumed that current resources will continue to be open, which
reduces capital costs in the model. In scenario 3, this assumption is removed by starting with no
CT scanners. Using these results, a comparison between the current situation and an
alternative set of facilities can be made. Although this scenario may not be realistic given
emergency care situations and the benefits to hospital inpatients, it provides insight into the
minimum viable facilities needed to meet the access requirements.

67
5.5.3. Sensitivity Analysis
These parameter ranges are based on research from Section 5.3.1 and were verified by a
radiologist. Key parameters are the cost of opening a new facility, cost of a CT scanner, cost of
an exam, overtime surcharge percentage, and number of exams in a shift.
For the cost of a new CT facility, there is a large range of values because each hospital needs
different renovations to support a CT scanner. From the CIHI report [1]and press releases from
the Saskatchewan Ministry of Health [69 - 73], renovation costs ranged from $0.400M to $1.8M.
$0.625M was also run since it is half the value used in the model.
CT scanner costs depend on which scanner is purchased (e.g., 16-slice or 64-slice). From the
CIHI report [1]and press releases from the Saskatchewan Ministry of Health [69 - 73],costs
ranged from $0.850M to $2M. However, the most likely cost range is $1M to $1.5M per CT
scanner.
Exam costs were estimated based on Saskatoon Health Region’s operating budget. However,
each facility will have different exams costs due to efficiency, human resources, and other
factors. Therefore, sensitivity analysis was run on costs from $50 to $90 at $20 intervals.
The overtime surcharge was originally based on human resources costing time and a half.
However, this may not be the case and there may be additional factors contributing to the cost
of a CT exam. Overtime surcharge was set to 100% extra, which doubles the cost of an exam.
Annual shift capacity is a key parameter since it impacts the operating costs and resulting
number of overtime exams and unused exam capacity. To adjust the annual shift capacity, a
sensitivity analysis based on changing the exam rate four times. If the exam rate increased by
10% (2.49 exams per hour), a total of 5179 exams would be completed in one shift. The
estimated exams per operating hour in the province was an average of 2.61 exams in 2011.
Assuming the same number of operating hours a year, the annual shift capacity is 5428. CIHI
[1] reported a different number of exams per operating hour by CT type. The average was 3.1
for 64-slice, 16-slice, and 8-slice CTs combined which resulted in a shift capacity of 6448
exams. SPH had the highest utilization in the province with 3.93 exams per hour in 2011 and an
annual shift capacity of 8174 was used.
A high shift removal cost of $100K was used, so a scenario with a low cost of $20 was run to
show whether this effected how many shifts were removed.

68
High and low demand scenarios were run based on Statistics Canada’s population projections
and their assumptions for Scenario H and L respectively. The increased assumptions for
Scenario H’s high growth are a total fertility rate of 1.9 births per woman and a life expectancy of
85.4 years for males and 88.4 years for females by 2036. Immigration has a constant national
effective of 265,000 immigrants for the first three years and then a constant national immigration
rate of 0.9%. The decreased assumptions for Scenario L’s low growth are a total fertility rate of
1.5 births per woman and a life expectancy of 82.3 years for males and 86.0 years for females
by 2036. Immigration has a constant national effective of 240,000 immigrants for the first three
years and then a constant national immigration rate of 0.9%.
Using the base scenario, the model was run for each of the following values:
! Cost of a new CT facility (CostOpen) = $0.4M, $0.625M, $1.8M
! Cost of a CT scanner (CostCT) = $0.850M, $1M, $1.5M, $2M
! Exam Cost = $50, $70, $90
! Overtime surcharge on exam cost (OvertimeSurcharge) = 100%
! Exams per operating hour (Shift Capacity) =2.49 (5179 exams), 2.61 (5428 exams), 3.1
(6448 exams), 3.93 exams per hour (8174 exams)
! Shift Cost = $20
! Demand = high, low
This sensitivity analysis allows a better understanding of how substantial changes in parameters
could impact the results of the model. This is particularly important since all the parameters are
based on estimates.
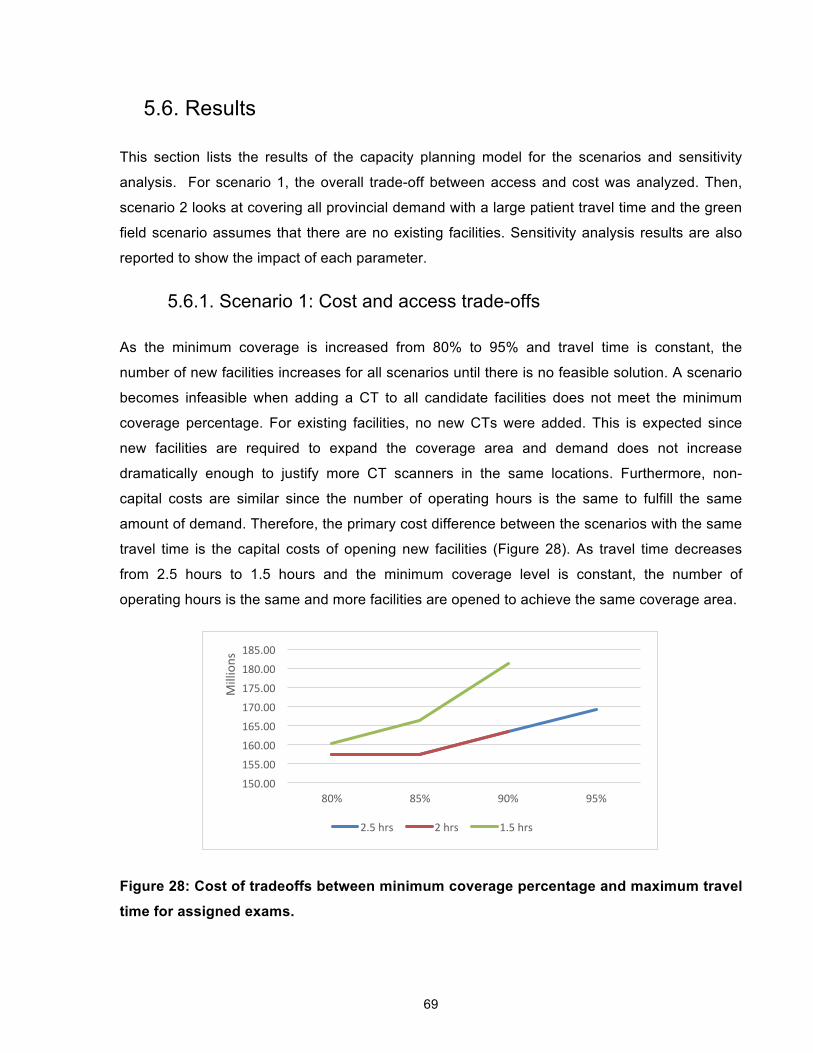
69
5.6. Results
This section lists the results of the capacity planning model for the scenarios and sensitivity
analysis. For scenario 1, the overall trade-off between access and cost was analyzed. Then,
scenario 2 looks at covering all provincial demand with a large patient travel time and the green
field scenario assumes that there are no existing facilities. Sensitivity analysis results are also
reported to show the impact of each parameter.
5.6.1. Scenario 1: Cost and access trade-offs
As the minimum coverage is increased from 80% to 95% and travel time is constant, the
number of new facilities increases for all scenarios until there is no feasible solution. A scenario
becomes infeasible when adding a CT to all candidate facilities does not meet the minimum
coverage percentage. For existing facilities, no new CTs were added. This is expected since
new facilities are required to expand the coverage area and demand does not increase
dramatically enough to justify more CT scanners in the same locations. Furthermore, non-
capital costs are similar since the number of operating hours is the same to fulfill the same
amount of demand. Therefore, the primary cost difference between the scenarios with the same
travel time is the capital costs of opening new facilities (Figure 28). As travel time decreases
from 2.5 hours to 1.5 hours and the minimum coverage level is constant, the number of
operating hours is the same and more facilities are opened to achieve the same coverage area.
Figure 28: Cost of tradeoffs between minimum coverage percentage and maximum travel
time for assigned exams.
150.00
155.00
160.00
165.00
170.00
175.00
180.00
185.00
80% 85% 90% 95%
Millions
2.5 hrs 2 hrs 1.5 hrs

70
Table 11 summaries the new facilities opened for each scenario. With a travel time of 2.5 hours,
no facilities were added until minimum coverage reached 95%. At 95%, four new facilities were
opened. This coverage level was infeasible with a 2 hour and 1.5 hour travel time. With a 2 hour
travel time, no facilities were opened until there was a 90% coverage level, where two new
facilities were opened. These two scenarios increase operating hours in the same years, but
distribute the hours differently between the facilities as shown in Figure 29 and Figure 30. A
travel time of 1.5 hours led to 1, 3, and then 7 facilities being opened for coverage levels of
80%, 85%, and 90% respectively. Facility locations which show up multiple times are Estevan,
Kindersley, Tisdale, and La Ronge which suggests they should be looked at more closely as
potential locations. Figure 31, Figure 32, and Figure 33 shows how the coverage area is
expanded by adding new facilities with different catchment area sizes.
*indicates a new facility
Figure 29: Weekly operating hours until 2030 by facility with a maximum travel time of 2.5
hrs and 95% coverage level.
-‐
200
400
600
800
1,000
1,200
1,400
1,600
2013
2014
2015
2016
2017
2018
2019
2020
2021
2022
2023
2024
2025
2026
2027
2028
2029
2030
Weekly Ope
ra9n
g Ho
urs
Yorkton
Prince Albert
Lloydminster
North Baaleford
Moose Jaw
Swid Current
Saskatoon (SPH)
Saskatoon (SCH)
Saskatoon (RUH)
Regina (RGH)
Regina (PH)
La Ronge *
La Loche*
Estevan*
Nipawin*

71
*indicates a new facility
Figure 30: Weekly operating hours until 2030 by facility with a maximum travel time of 2
hrs and 90% coverage level.
Table 11: Opened facilities for each travel time and minimum coverage scenario. Unless
otherwise specified, facilities were opened in 2013. Minimum Coverage Max Travel Time
80% 85% 90% 95%
2.5 hrs None None None Nipawin Estevan La Loche (2024) La Ronge
2 hrs None None Meadow Lake (2026) Estevan
Infeasible
1.5 hrs Weyburn Kindersley Tisdale Estevan
Kindersley Tisdale Humboldt Estevan Melville Ile a La Crosse La Ronge (2014)
Infeasible
-‐
200
400
600
800
1,000
1,200
1,400
1,600
2013
2014
2015
2016
2017
2018
2019
2020
2021
2022
2023
2024
2025
2026
2027
2028
2029
2030
Weekly Ope
ra9n
g Ho
urs
Yorkton
Prince Albert
Lloydminster
North Baaleford
Moose Jaw
Swid Current
Saskatoon (SPH)
Saskatoon (SCH)
Saskatoon (RUH)
Regina (RGH)
Regina (PH)
Estevan*
Meadow Lake*
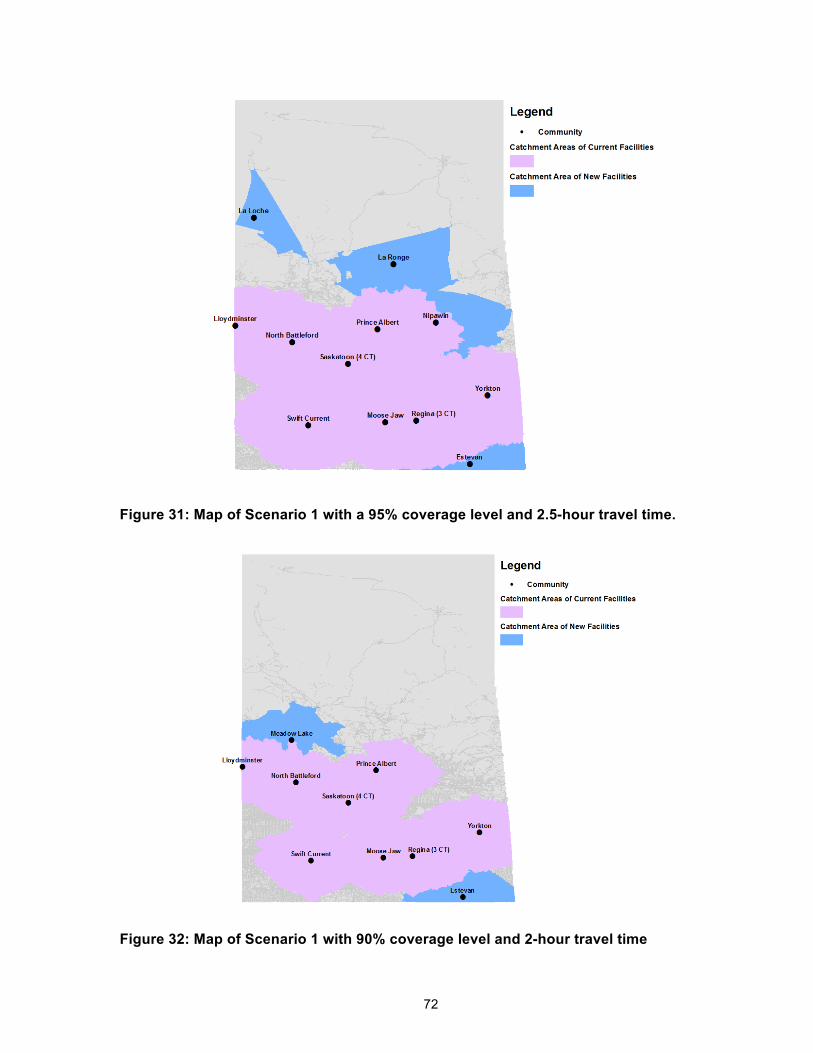
72
Figure 31: Map of Scenario 1 with a 95% coverage level and 2.5-hour travel time.
Figure 32: Map of Scenario 1 with 90% coverage level and 2-hour travel time

73
Figure 33: Map of Scenario 1 with 90% coverage level and 1.5-hour travel time.
5.6.2. Scenario 2: Covering all provincial demand
For scenario 2, the aim was to gain a better understanding of how existing capacity can meet
the entire provincial demand. Therefore, all exams needed to be assigned to a facility and a
high maximum travel time (20.2 hours) allowed all CT resources to be pooled. Existing facilities
were sufficient to meet the provincial demand. See Figure 34 for the distribution of operating
hours. The cost of $157,428,363.50 over the planning horizon is the same as when there is an
85% coverage level with a 2.5 hour or 2 hour catchment area. These scenarios have the same
number of operating hours and have no new facilities or CT scanners, so non-capital costs are
similar and there are no capital costs.

74
Figure 34: Weekly operating hours for all CT facilities for Scenario 2.
5.6.3. Scenario 3: Green Field
For the third scenario, the model was run assuming that there were no existing facilities. In the
first year, the model places nine facilities with one scanner each. Figure 35 shows the nine
chosen facilities and the distribution of operating hours. In 2014, Weyburn and Prince Albert are
each assigned a second CT scanner. See Figure 36 for the reach of catchment areas.
Having 11 CT scanners at 9 facilities is less costly upfront than the current situation of 13 CT
scanners in 11 facilities. However, there are fewer operating hours and increased overtime than
in the base scenario, so the average non-capital costs each year are $60,546.01 more for the
green field scenario.
Therefore, most of the cost difference is due to the capital costs for purchasing the CT scanners
and opening the facilities. With the strategic placement of CT scanners, six fewer shifts are
needed for the same minimum coverage percentage.
-‐
200
400
600
800
1,000
1,200
1,400
1,600
2013
2014
2015
2016
2017
2018
2019
2020
2021
2022
2023
2024
2025
2026
2027
2028
2029
2030
Weekly Ope
ra9n
g Ho
urs
Yorkton
Prince Albert
Lloydminster
North Baaleford
Moose Jaw
Swid Current
Saskatoon (SPH)
Saskatoon (SCH)
Saskatoon (RUH)
Regina (RGH)
Regina (PH)

75
Figure 35: Weekly operating hours for all CT facilities for Scenario 3.
Figure 36: Map of chosen facilities and 2-hr catchment areas for the green field scenario.
-
200
400
600
800
1,000
1,200
1,400
2013
20
14
2015
20
16
2017
20
18
2019
20
20
2021
20
22
2023
20
24
2025
20
26
2027
20
28
2029
20
30
Wee
kly
Ope
ratin
g H
ours
Prince Albert
North Battleford
Moose Jaw
Swift Current
Saskatoon (RUH)
Melville
Weyburn
Meadow Lake
Melfort

76
5.6.4. Sensitivity Analysis
A sensitivity analysis was run on the baseline scenario of 90% minimum coverage and a 2-hour
travel time to assess the impact of parameter changes. In all the scenarios, two facilities were
added except when demand varied; however, the location and opening year of the second
facility varied (Table 12). Overall, the model is not very sensitive to changes to the cost
parameters with similar operating hours. The model was sensitive to demand, overtime
surcharge, and exams per operating hour.
For the scenario of high demand, the shifts increased to 30 one year earlier in 2021 leading to
more shifts in total. For low demand, the increase to 30 shifts occurs one year later in 2023
resulting in fewer shifts in total. The total costs reflect this difference in number of shifts. When
the overtime surcharge is 100%, this changes the break-even point, more shifts are added to
reduce the number of overtime exams, and costs are slightly higher with an overtime surcharge
of 100%. The model is also sensitive to changes in the exams per operating hour. Figure 37
shows that as the number of exams per operating hour increases, fewer shifts are necessary,
but the total cost increases since each shift costs more.
Figure 37: Sensitivity analysis for exams per operating hour
-
100
200
300
400
500
600
163.00
163.20
163.40
163.60
163.80
164.00
164.20
2.49 2.61 3.10 3.93
Tota
l Num
ber o
f Shi
fts
Tota
l Cos
t (M
illio
ns)
Exams per Operating Hour
Total Cost Total Shift Number
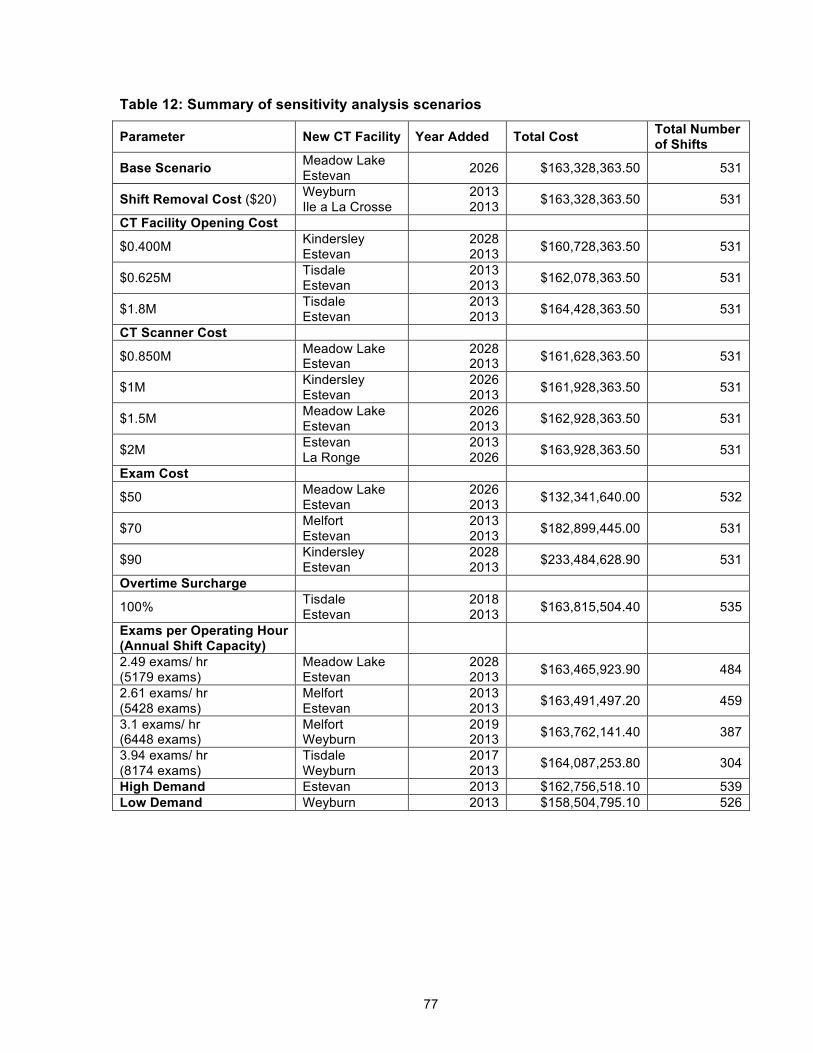
77
Table 12: Summary of sensitivity analysis scenarios
Parameter New CT Facility Year Added Total Cost Total Number of Shifts
Base Scenario Meadow Lake Estevan 2026 $163,328,363.50 531
Shift Removal Cost ($20) Weyburn Ile a La Crosse
2013 2013 $163,328,363.50 531
CT Facility Opening Cost
$0.400M Kindersley Estevan
2028 2013 $160,728,363.50 531
$0.625M Tisdale Estevan
2013 2013 $162,078,363.50 531
$1.8M Tisdale Estevan
2013 2013 $164,428,363.50 531
CT Scanner Cost
$0.850M Meadow Lake Estevan
2028 2013 $161,628,363.50 531
$1M Kindersley Estevan
2026 2013 $161,928,363.50 531
$1.5M Meadow Lake Estevan
2026 2013 $162,928,363.50 531
$2M Estevan La Ronge
2013 2026 $163,928,363.50 531
Exam Cost
$50 Meadow Lake Estevan
2026 2013 $132,341,640.00 532
$70 Melfort Estevan
2013 2013 $182,899,445.00 531
$90 Kindersley Estevan
2028 2013 $233,484,628.90 531
Overtime Surcharge
100% Tisdale Estevan
2018 2013 $163,815,504.40 535
Exams per Operating Hour (Annual Shift Capacity)
2.49 exams/ hr (5179 exams)
Meadow Lake Estevan
2028 2013 $163,465,923.90 484
2.61 exams/ hr (5428 exams)
Melfort Estevan
2013 2013 $163,491,497.20 459
3.1 exams/ hr (6448 exams)
Melfort Weyburn
2019 2013 $163,762,141.40 387
3.94 exams/ hr (8174 exams)
Tisdale Weyburn
2017 2013 $164,087,253.80 304
High Demand Estevan 2013 $162,756,518.10 539 Low Demand Weyburn 2013 $158,504,795.10 526

78
5.7. Discussion of Model
The purpose of the model was to provide some insight into CT capacity planning in order to
improve patient access by aligning CT supply with patient needs. The results of the model are
discussed in terms of increasing demand, increasing patient access, multiple possible
alternatives, and the base scenario.
If the minimum coverage percentage remains the same, but demand increases substantially
within the current catchment areas, then this results in longer operating hours and occasionally
additional CT scanners depending on existing levels of overtime and unused capacity in each
catchment area. This can be seen in the high demand scenario where the operating hours
increased by 1.5%. As the coverage percentage increases, new facilities are added to reach
more demand, raising the total cost. For example, when the travel time was 1.5hrs, the number
of new facilities increased from 1 to 7 as the coverage level rose from 80% to 90%. With the
new facilities came higher total costs.
The maximum travel time defines the hospital catchment areas and therefore is an important
driver in opening a new facility to increase the amount of covered demand. As the maximum
travel time increases from 1.5 hours to 2.5 hours, the cost difference between covering 90% of
the demand is $990,888.58 less on average each year. Most of the cost difference is from the
capital cost of opening new CT facilities since existing facilities do not need additional CT
scanners.
When the overall patient travel time decreases, so do the catchment areas. This reduces the
amount of covered demand and requires more facilities to be opened to meet the minimum
coverage level. More facilities cause the minimum number of required operating hours to
increase to meet the requirement of operating at least one shift per CT scanner. In the results,
the total number of operating hours required to meet all demand remains similar since operating
hours from existing facilities are shifted to the new facilities. However, it is possible that if
demand is more dispersed, many facilities are required to cover the demand. The number of
shifts and resulting capacity increases significantly because each facility must run for at least
one shift.
Furthermore, there are many alternative optimal solutions, which is not surprising given the
significant overlap between catchment areas. This allows decision makers to choose which
alternative optimal solution is most appropriate. The model is also not sensitive to changes in

79
the cost parameters. However, modifications to the demand, overtime surcharge, and exams
per operating hour did have a significant impact on number of new facilities, costs, and
operating hours.
On June 27, 2014, the province announced in a press release that a CT scanner would be
implemented in Estevan at St. Joseph’s Hospital by 2015 [76]. This matches our assumption
that candidate CT facilities should be district hospitals. Furthermore, the base scenario of a 2
hour travel time and 90% coverage level also places the next CT facility in Estevan. This is an
encouraging sign that the model is producing useful results.

80
5.8. Recommendations for Saskatchewan From the results, the main discussion around capacity planning in Saskatchewan centres on
pooling resources, capacity distribution and how the model can be used in the future.
Pooling Resources
The model assumes unassigned demand across the province will have access to any remaining
capacity. However, where patients go for their CT exams often depends on shorter wait times
and the location they are referred to by their physician. Figure 22 shows that a substantial
percentage of patients travel outside their health region for their exams. In 2011, 20% of visits
from Sunrise RHA and 27.8% of visits from Prince Albert Parkland Health Region traveled to
another health region and to a facility further away despite there being a facility in their health
region. By pooling the capacity of the existing system, Saskatchewan could reduce wait times at
some of their facilities.
Capacity Distribution
Capacity can be considered from two standpoints: theoretical maximum capacity and operating
hour capacity. The theoretical maximum capacity is based on how many exams can be done if
the CT scanner could be run and staffed for 24 hours a day, 7 days a week for the entire year.
The operating hour capacity is the number of exams which can be done each year during
regular operating hours.
Based on the theoretical maximum capacity, Saskatchewan has a substantial excess capacity,
because it could add more operating hours to accommodate increases in demand assuming the
human resources could be found. For example, by year 2030 only 25 out of 42 possible shifts of
operating hours (based on 3 shift maximum per CT scanner) are assigned to facilities. When
comparing the current operating hours to the suggested hours from the model, the excess
capacity is concentrated in certain areas.
In total, Saskatchewan currently has 804.5 hours of regular CT capacity per week. Regardless
of coverage percentage and maximum travel times ranging from 1.5 hrs to 2.5 hrs, the model
calculates that in 2013, 1000 operating hours are needed since there are 25 shifts and each
shift is 40 hours per week. This implies that there is currently an undersupply of operating hours
overall. However, the model also assumes that resources will be pooled to service any demand
beyond the minimum coverage percent. The undersupply by 195.5 hours and lack of pooling

81
resources needs to be further investigated to identify whether it is contributing to longer wait
times.
The distribution of the operating hours (Table 13) and additional factors need to be taken into
consideration. For example, in the base scenario, hospitals in Regina have substantially more
operating hours than what is calculated as necessary in the model. However, they also take in
patients from across the province, and out-of-region patients make up a third of the CT visits.
Furthermore, the model increased operating hours or added new facilities at Moose Jaw,
Estevan and Yorkton which have overlapping catchment areas with Regina.
Table 13: Current operating hours in comparison to average operating hours in model
using base scenario (90% coverage and 2 hour travel time) by facility
Health Region Community Hospital
Current Operating Hours per
Week
Model’s Operating Hours per
Week in 2013
Difference (Current -
Model)
Regina Qu'Appelle Regina Pasqua Hospital 119 80 39
Regina Qu'Appelle Regina Regina General
Hospital 182 160 22
Saskatoon Saskatoon Royal University Hospital 137 160 -23
Saskatoon Saskatoon Saskatoon City Hospital 62.5 80 -17.5
Saskatoon Saskatoon St. Paul's Hospital 50 80 -30
Sun Country Estevan St. Joseph's Hospital - 40 -40
Cypress Swift Current Cypress Regional Hospital
40 40 -
Five Hills Moose Jaw Moose Jaw Union Hospital 40 80 -40
Prairie North North Battleford
Battlefords Union Hospital 40 40 -
Prairie North Lloydminster Lloydminster Hospital 40 40 -
Prairie North Meadow Lake
Northwest Health Facility - Meadow Lake Hospital
- 40 -40
Prince Albert Parkland Prince Albert Victoria Hospital 54 120 -66
Sunrise Yorkton Yorkton Regional Health Centre
40 80 -40
Currently, Victoria Hospital in PAPHR has the longest wait times for all patient types (Table 8)
and the model assigns 120 hours per week. BUH and LH had the same number of operating

82
hours in the model and 2011 and they had the shortest wait times. However, Victoria Hospital
also does more exams per operating hour than BUH and LH (Figure 8). This information
suggests that more investigation is needed especially in terms of improved efficiency to avoid
increasing operating hours and staffing levels.
Rural hospitals tend to have staff working on multiple machines in a day such as the CTs and x-
rays. By having dedicated staff, CTs can run for the same number of operating hours, but
perform more exams. This may lower cost per exam since 92.2% of the cost is due to operating
and personnel expenses. However, if staff trained in CT exams are focusing less time on non-
CT exams, then more personnel may need to be hired for less expensive non-CT modalities
such as x-rays. For Victoria Hospital, this may mean that 56 hours per week is sufficient as long
as the staff spend more of their time doing CT exams.
Similarly, if the number of exams per operating hour increases, then this may also lower the
cost per exam since the majority of the costs are due to operations and personnel. In the
sensitivity analysis, it is assumed that the exam costs remain the same when the number of
exams per operating hour is higher so that only one parameter is changed at a time. However,
this overestimates the cost of operating a shift.
Given the potential advantages of pooling resources, a centralized booking system could be
investigated to reduce wait times. However, factors such as different staffing arrangements
need to be considered when looking at capacity.
Using the model
The input parameters for the model are based on many assumptions as detailed in Section
5.3.1. The model should be re-run with more accurate demand projections, which would be
affected by changes in the demand rate estimate. Parameters should also be updated for the
cost of a CT scanner, cost of renovation, and exam cost. From the sensitivity analysis, it is
known that the model results will not fluctuate substantially for these cost parameters, so
estimates can be used to achieve similar results if exact costs are lacking. The model is
intended for long-term planning and not emergency situations.
The model can also be forced to place facilities in certain locations with a specified number of
shifts. For example, the green field scenario did not place a CT scanner in Regina despite it
being one of the two major cities in Saskatchewan. The model does not know that Regina
General Hospital is a tertiary hospital which needs a CT scanner and other political factors.

83
Furthermore, it is beneficial to have more than the minimum number of CT scanners from the
green scenario for the inpatients and emergency patients at the additional hospitals. However,
the model can be forced to place CT scanners at certain facilities in the beginning. By forcing
the number of shifts, operating hours can also be concentrated in tertiary hospitals to reflect
existing patterns and identify the resulting number of operating hours required to meet demand
for the other facilities. Therefore, if the decision maker knows that all tertiary hospitals should
have a CT scanner and a certain number of operating hours, then this can be set in the model.
Being able to choose specific locations to open is also useful since there are multiple alternate
solutions covering similar percentages of demand at the same cost. For the scenario of a 2 hour
travel time and a minimum 90% coverage, there are slight differences in the maximum demand
covered based on 2012 calculations if the second new facility is located in Tisdale (93.5%),
Meadow Lake (93.3%), Melfort (93.3%), or Kindersley (93.1%). 93.3% demand covered is
approximately 1,325,303 people within two hours of a CT facility. This was calculated using the
average exams per 1000 population of 82.98. Since the costs in the model are estimated, it
might also be preferable to open a new facility at a slightly higher cost based on factors outside
the model’s scope. Furthermore, opening new facilities earlier had no cost implications based
on the model results, but improved patient access to CT scanners for more years. Opening new
facilities earlier at no extra cost may not be realistic given the costs associated with
administration and CT scanner replacement among other factors.
Incorporating mobile CT scanners
Improving rural access is one of the main goals of the thesis and all the new facilities selected
by the model are in the southern half of Saskatchewan. One way to reach the northern and
other rural areas is through mobile CT scanners. Saskatchewan previously used mobile CT
scanners in 2000 and it operated between Moose Jaw and Swift Current [77]. The aim was to
reduce travel times to Regina by bringing the CT scanner closer to patients. By 2004 and 2005,
permanent CT scanners were installed for Swift Current and Moose Jaw respectively.
A similar pattern can be used in other parts of Saskatchewan and incorporated into the model. A
set of candidate locations for the mobile scanner would be determined along with the expected
travel path. The model would then determine how much time was needed at each candidate
location (if any) and take into account moving costs each time. The costs associated with the
mobile CT scanner could be incorporated into the model’s objective function so that the capacity
of mobile CTs is taken into consideration when planning the permanent CT facilities.

84
Applying the model to other jurisdictions
This model can also be used outside of Saskatchewan in jurisdictions where planners care
about high population coverage and find the percent of demand within a catchment areas
aligned with their rural access standards. High population coverage tends to matter for areas
where healthcare is treated as a public service. Ontario and British Columbia use similar access
standards and can easily translate the model to their communities since they plan capacity
centrally.
In the United States, healthcare is privately delivered and 46.4% is funded by the government
[79]. However, due to the lack of centralized public planning for health services, the model
would be difficult to apply to the United States.
Although the model was developed for CT capacity planning, the model can be applied to
problems which share the same main characteristics of the high capital costs, high operating
shift costs, multiple machines at the same facility, lengthy planning horizon, and need for access
standards. Magnetic resonance imaging (MRI) facilities are another potential application

85
Chapter 6. Conclusions
The two main approaches for capacity planning research in health care services have been in
geography and operations research. In geography, various scenarios are run to assess the
impact on percent of demand within facility catchment area and resulting travel times. Many
capacitated covering models and plant location models have been developed in operations
research; however, assigning multiple facilities to the same site with shift allocation has not
been well explored. This thesis presents a method that combines an approach from geography
with a capacitated minimum covering model and uses Saskatchewan as a case study.
From Chapter 4, there was substantial variation in CT utilization and patient access metrics
between different CT facilities in Saskatchewan. After metrics were calculated by priority level
and patient type, not all differences between the facilities were explained. For CT utilization, a
more in-depth analysis of the specific facilities would be needed to understand the sources of
the variation. In terms of access, there are clear differences between rural and urban CSDs.
Mean travel times are also three times longer in rural areas than in areas with medium sized
populations. Differences in patient access and patient utilization are likely linked to travel time. A
regression model could be developed to identify which geographic and socio-demographic
factors contribute most to variation in patient utilization.
Through Chapter 5, potential new facilities, trends, and capacity distribution are better
understood. The model determined that Estevan should be the next CT facility in the base
scenario. The Ministry of Health in Saskatchewan [76] also chose Estevan has the next CT
facility and while decisions on where to locate new CT facilities are subject to many factors such
as politics this is an encouraging result. There are many alternative options for the second new
facility and the model can be re-run to determine the potential impact of the preferred locations.
Similarly, the number of shifts and the associated number of operating hours can be set in the
model for preferred locations. Re-running the model will recalculate the necessary number of
operating hours at the remaining facilitates. However, these results assume that the parameters
were accurate and the model should be re-run with when parameter values change.
For capacity, Saskatchewan has slightly less capacity than demand based on the number of
operating hours. Hospitals in Regina and Saskatoon have the most number of operating hours.
For Prince Albert, more work is necessary to determine if operating hours should be expanded,
the percent of time staff dedicate to CT could be increased, or existing processes can be more

86
efficient to prevent the need to expand operating hours. A provincial centralized booking system
could be considered to pool resources from all facilities and reduce wait times.
Furthermore, the model should be used as a tool in the decision making process to explore
different options. For example, a decision maker may want to know the magnitude of impact a
parameter will have on cost to the system. The model can be run multiple times with different
combinations of parameter values to assess the sensitivity of the results and the range of
impact on cost, capacity, and patient access.
To improve the model, a few model extensions could be considered for location-specific
parameters, CT scanner replacement, and closest facility assignment:
• The model assumed that each facility location would have the same opening costs, but
from CIHI [1] and Saskatchewan’s Ministry of Health press releases [69 - 73], the cost to
renovate a facility ranged from $0.400M to $1.8M. Furthermore, depending on the
staffing levels and other factors, facilities will differ in the number of exams per operating
hour. Given that the majority of the cost differences to improve coverage were the result
of capital expenditures and the model was sensitive to the number of exams per
operating hour, having location specific CT facility parameters could substantially
change the model results.
• CT scanners in Saskatchewan have been replaced after a decade or more (Table 3).
The capital costs associated with CT scanner replacement could be added to the model,
which may delay opening a new CT facility to avoid replacement costs.
• In the formulation, only a minimum percent of demand needs to be within a maximum
travel time. The remaining percent of demand is fulfilled, but has no patient travel time
restriction. To further improve rural access to CT scanners, travel time could be limited
by assigning demand to the next closest facility outside the maximum travel time.
The model was developed for CT capacity planning; however, the main characteristics are high
capital costs, high operating shift costs, multiple machines at the same facility, lengthy planning
horizon, and need for access standards. Another potential application is capacity planning for
magnetic resonance imaging facilities. Although this research provides insight into capacity
planning and opportunities for improving patient access and CT utilization, more research is
needed to have a complete understanding of factors affecting utilization and access.

87
References
[1] Canadian Institute for Health Information, "Medical Imaging in Canada ," Canadian Institute
for Health Information, Ottawa, 2008.
[2] Organisation for Economic Co-operation and Development, "OECD Health Data: Key
Tables from OECD," 2013.
[3] Health Canada. (2004) First Minister's Meeting on the Future of Health Care 2004. [Online].
http://www.hc-sc.gc.ca/hcs-sss/delivery-prestation/fptcollab/2004-fmm-rpm/index-eng.php
[4] Saskatchewan Health. (2013, Dec.) Computed Tomography (CT) Wait Times. [Online].
http://www.health.gov.sk.ca/diagnostic-imaging-ct-wait-times
[5] Government of Saskatchewan. (2013, Dec.) Saskatchewan Population Report. [Online].
http://www.stats.gov.sk.ca/stats/population/Censuspop2011.pdf
[6] Larson DB, Johnson LW, Schnell BM, Salisbury SR, Forman HP, "National Trends in CT
Use in the Emergency Department," Radiology, vol. 258, no. 1, pp. 164-173, 2011.
[7] Bhargavan M, Sunshine JH, "Utilization of Radiology Services in the United States: Levels
and Trends in Modalities, Regions, and Populations.," Radiology, vol. 234, pp. 824 – 832,
2005.
[8] Parker L, Levin DC, Frangos A, Rao VM, "Geographic Variation in the Utilization of
Noninvasive Diagnostic Imaging: National Medicare Data, 1998-2007," American Journal of
Roentgenology, vol. 194, no. 4, pp. 1034-1039, 2010.
[9] Kung PT, Tsai WC, Yaung CL, Liao KP, "Determinants of computed tomography and
magnetic resonance imaging utilization in Taiwan," International Journal of Technology
Assessment in Health Care, vol. 21, no. 1, pp. 81-88, 2005.
[10] Smith-Bindman R, Miglioretti DL, Larson EB., "Rising Use of Diagnostic Medical Imaging in
a Large Integrated Health System," Health Affairs, vol. 27, no. 6, pp. 1491-1502, 2008.
88
[11] Agarwal R, Bergey M, Sonnad S, Butowsky H, Bhargavan M, Bleshman MH, "Inpatient CT
and MRI Utilization: Trends in the Academic Hospital Setting," Am Coll Radiol, vol. 7, pp.
949-955, 2010.
[12] Matin A, Bates DW, Sussman A, Ros P, Hanson R, Khorasani R, "Inpatient Radiology
Utilization: Trends over the Past Decade," American Journal of Roentgenology., vol. 186,
pp. 7-11, 2006.
[13] Gazelle GS et al., "Utilization of Diagnostic Medical Imaging: Comparison of Radiologist
Referral versus Same-Specialty Referral," Radiology, vol. 245, no. 2, pp. 517-522 , 2007.
[14] Hillman BJ and Goldsmith J, "Imaging: the self-referral boom and the ongoing search for
effective policies to contain it," Health Affairs, vol. 29, no. 12, pp. 2231-2236, 2010.
[15] Gazelle GS, Halpern EF, Ryan HS, and Tramontano AC , "Utilization of Diagnostic Medical
Imaging: Comparison of Radiologist Referral versus Same-Specialty Referral ," vol. 245,
no. 2, pp. 517-522, 2007.
[16] Lee J, Kirschner J, Pawa S, Wiener DE, Newman DH, Shah K, "Computed Tomography
Use in the Adult Emergency Department of an Academic Urban Hospital From 2001 to
2007," Annals of Emergency Medicine, vol. 56, no. 6, pp. 591 – 596.e1, 2010.
[17] Oh HY, Kim EY, Cho J, Yang HK, Kim KH, Kim HS, Choi HY, "Trends of CT Use in the
Adult Emergency Department in a Tertiary Academic Hospital of Korea during 2001 –
2010," Korean Journal of Radiology, vol. 13, no. 5, pp. 536-540, 2012.
[18] Canadian Institute for Health Information. (2013) Medical Imaging in Canada 2012.
[Online]. http://www.cihi.ca/CIHI-ext-portal/pdf/internet/MIT_SUMMARY_2012_en
[19] Arcury TA, Preissier JS, Gesler WM, Powers JM, "Access to transportation and health care
utilization in a rural region," Journal of Rural Health, vol. 21, no. 1, pp. 31-38, 2005.
[20] Joseph AE, Boeckh JL, "Locational variation in mental health care utilization dependent
upon diagnosis: a Canadian example," Soc. Sci. Med., vol. 15, no. D, pp. 395-404, 1981.
[21] Nemet GF, Bailey AJ, "Distance and health care utilization among the rural elderly," Social

89
Science and Medicine, vol. 50, pp. 1197-1208, 2000.
[22] Stensland J, Akamigbo A, Glass D, Zabinski D, "Rural and urban Medicare beneficiaries
use remarkably similar amounts of health care services.," Health Affairs, vol. 32, no. 11, pp.
2040-2046, 2013.
[23] Chan L, Hart G, Goodman DC, "Geographic access to health care for rural Medicare
beneficiaries," National Rural Health Association, vol. 22, no. 2, pp. 140-146, 2006.
[24] Rao VM, Parker L, Levin DC, Sunshine J, Bushee G, "Use trends and geographic variation
in neuroimaging: Nationwide Medicare data for 1993 and 1998," AJNR Am J Neuroradiol,
vol. 22, pp. 1643-1649, 2001.
[25] Garg PP, Landrum MB, Normand SL, Ayanian JZ, Hauptman PJ, Ryan TJ, McNeil BJ,
Guadagnoli E, "Understanding individual and small area variation in the underuse of
coronary angiography following acute myocardial infarction.," Med Care, vol. 40, no. 7, pp.
614-626, 2002.
[26] Lysdahl KB, Borretzen I, "Geographical variation in radiological services: a nationwide
survey.," BMC Health Services Research, vol. 7, no. 21, 2007.
[27] Laupacis A, Pryzbysz R, Keller MA, "Access to Health Services in Ontario: ICES Atlas - CT
and MRI Scanning," 2005.
[28] Szczepura A, Clark M, "Creating a strategic management plan for magnetic resonance
imaging (MRI) provision.," Health Policy, vol. 53, pp. 91-104, 2000.
[29] Bach L, Hoberg R, "A planning model for regional systems of CT scanners," Socio-Econ
Plan. Sci, vol. 19, no. 3, pp. 189-199, 1985.
[30] Greenwald HP, Woodward JM, Berg DH, "Transportation or CT Scanners: A Theory and
Method of Health Resources Allocation.," Health Services Research, vol. 14, no. 3, pp.
207-219, 1979.
[31] Wang F, Luo W, "Measure of spatial accessibility to health care in a GIS environment:
synthesis and a case study in the Chicago region.," Environment and Planning B: Planning
and Design, vol. 30, pp. 865 - 884, 2003.

90
[32] Schurman N, Fiedler RS, Grzybowski SCW, Grund D, "Defining rational hospital
catchments for non-urban areas based on travel-time," International Journal of Health
Geographics, vol. 5, no. 43, 2006.
[33] ReVelle C, Marks D, Liebman JC, "An analysis of private and public sector location
models," Management Science., vol. 16, no. 11, pp. 692-707, 1970.
[34] Daskin MS, Dean LK, "Location of Health Care Facilities, Chapter 3," in Handbook of
OR/MS in Health Care: A Handbook of Methods and Applications., 2004, pp. 43-76.
[35] Brandeau ML, Chiu SS, "An overview of representative problems in location research.,"
Management Science, vol. 35, no. 6, pp. 645-674, 1989.
[36] Toregas C, Swain R, ReVelle C, Bergman L, "The location of emergency service facilities,"
Operations Research, vol. 19, no. 6, pp. 1363-1373, 1971.
[37] Datta S, Bandyopadhyay R, "An application of OR in micro-level planning in India,"
Computers and Operations Research, vol. 20, no. 2, pp. 121-132, 1993.
[38] Ren X, Chen J, Guo G, Cai W, "The application of the maximal coverage and partial
coverage model in the shelter location problem. Critical issues in transportation systems
planning, development and management," pp. 1472-1478.
[39] Zhu J, Liu D, Huang J, Han J, "Determining storage locations and capacities for emergency
response.," in 9th International Symposium on Operations Research and Its Applications,
Chengdu-Jiushaigou, China., 2010, pp. 262-269.
[40] Owen SH, Daskin MS, "Strategic facility location: A review," European Journal of
Operational Research, vol. 111, no. 3, pp. 423-447, 1998.
[41] Schilling DA, "Dynamic location modelling for public-sector facilities: a multicriteria
approach.," Decision Sciences, vol. 11, pp. 714-724, 1980.
[42] Jia H, Ordonez F, Dessouky MM, "A modeling framework for facility location of medical
services for large-scale emergencies," IIE Transactions, vol. 39, no. 1, pp. 41-55, 2007.

91
[43] Arabani AB, Farahani RZ, "Facility location dynamics: an overview of classifications and
applications," Computers and Industrial Engineering., vol. 62, pp. 408-420, 2012.
[44] ReVelle CS, Laporte G., "The plant location problem: new models and research
prospects.," Operations Research, vol. 44, no. 6, pp. 864-874, 1996.
[45] Wesolowsky GO, Truscott WG, "The multi-period location-allocation problem with
relocation of facilities," Management Science, vol. 22, no. 1, pp. 57-65, 1975.
[46] Rosenberg MW, "Locating small scale public facilities," Socio-Econ Plan. Sci., vol. 18, no.
3, pp. 151-158, 1984.
[47] Holmes J, Williams FB, Brown LA, "Facility location under a maximum travel restriction: An
example using day care facilities," Geographical Analysis, vol. 4, no. 3, pp. 258-266, 1972.
[48] Lee SM, Green GI, Kim CS, "A multiple criteria model for the location-allocation problem,"
Computers and Operations Research, vol. 8, pp. 1-8, 1981.
[49] Min H, "The dynamic expansion and relocation of capacitated public facilities: A multi-
objective approach," Computers and Operations Research, vol. 15, no. 3, pp. 243-252,
1986.
[50] Luss H, "Operations research and capacity expansion problems: A survey.," Operations
Research, vol. 30, no. 5, pp. 907-947, 1982.
[51] Murray AT, Gerrard RA, "Capacitated Service and Regional Constraints in Location-
Allocation Modelling," Location Science, vol. 5, no. 2, pp. 103-118, 1997.
[52] Ghiani G, Guerriero F, Musmanno R, "The capacitated plant location problem with multiple
facilities in the same site," Computers and Operations Research, vol. 29, pp. 1903-1912,
2002.
[53] Church RL, "The regionally constrained p-median problem," Geographical Analysis, vol. 22,
no. 1, pp. 22-32, 1990.
[54] Wu LY, Zhang XS, Zhang JL, "Capacitated facility location problem with general setup

92
cost," Computers & Operations Research, vol. 33, no. 5, pp. 1226-1241, 2006.
[55] Statistics Canada. (2014) Table 052-0005 - Projected population, by projection scenario,
age and sex, as of July 1, Canada, provinces and territories, annual (persons). [Online].
http://www5.statcan.gc.ca/cansim/a26?lang=eng&retrLang=eng&id=0520005&paSer=&patt
ern=&stByVal=1&p1=1&p2=37&tabMode=dataTable&csid=#F1
[56] Statistics Canada. (2006) Postal Code Conversion File.
[57] Esri. (2013) Universal Transverse Mercator. [Online].
http://help.arcgis.com/en/arcgisdesktop/10.0/help/index.html#/Universal_Transverse_Merca
tor/003r00000049000000/
[58] Environmental Systems Research Institute. (2011) ArcGIS Desktop: Release 10.2.
[59] Neuman CDG. (2007) Index of /~cneuman/mgtsc461/Lectures/Lecture 1 Sep 09. [Online].
http://www.ualberta.ca/~cneuman/mgtsc461/Lectures/Lecture%201%20Sep%2009/
[60] Saskatchewan Ministry of Health. (2013) Ministry of Health Covered Population 2013:
Notice to Readers. [Online]. http://population.health.gov.sk.ca/NoticetoReaders2013.htm
[61] Statistics Canada. (2012, May) Census release topics and dates. [Online].
http://www12.statcan.gc.ca/census-recensement/2011/rt-td/index-eng.cfm
[62] Statistics Canada, "Postal Code Conversion File Reference Guide," Catalogue no. 92-154-
G, 2013.
[63] Goel V, Williams JI, Anderson GM, Blackstien-Hirsch P, Fooks C, Naylor CD (eds),
"Patterns of Health Care in Ontario. The ICES Practice Atlas. 2nd edition," Canadian
Medical Association, Ottawa, 1996.
[64] Boone JM, Brunberg JA, "Computed Tomography Use in Tertiary Care University Hospital,"
Am Coll Radiol, vol. 5, pp. 132-138, 2008.
[65] British Columbia's Ministries of Health Services and Health Planning, "Standards of
accessibility and guidelines for provision of sustainable acute care services by health
authorities," 2002.

93
[66] Ontario's Ministry of Health and Long-Term Care, "Rural and Northern Health Care
Framework/Plan - Stage 1 Report," 2011.
[67] Mettler FA et al., "CT scanning: patterns of use and dose," J. Radiol. Prot, vol. 20, pp. 353-
359, 2000.
[68] Goldman LW, "Principles of CT: Multislice CT," Journal of Nuclear Medicine Technology,
vol. 36, pp. 57-68, May 2008.
[69] Government of Saskatchewan. (2011, June) R-8.2 Reg 6 - The Facility Designation
Regulations. [Online]. http://www.publications.gov.sk.ca/details.cfm?p=11559
[70] Government of Saskatchewan. (2006, March) CT scanner opens in Lloydminster. [Online].
http://www.gov.sk.ca/news?newsId=2ded8682-2377-4599-8560-5fd9742038ef
[71] Government of Saskatchewan. (2005, December) CT scanner opens in Saskatoon.
[Online]. http://www.gov.sk.ca/news?newsId=fe3630fb-83be-4dad-8bd3-ee87da700688
[72] Government of Saskatchewan. (2006, March) Prince Albert opens new CT scanner.
[Online]. http://www.gov.sk.ca/news?newsId=e6f4bb90-9e29-4864-b4b8-6284b739bdc5
[73] Government of Saskatchewan. (2005, January) CT service begins in Sunrise Health
Region. [Online]. http://www.gov.sk.ca/news?newsId=9ffd12aa-3dcc-49ab-8838-
a325523103c5
[74] Government of Saskatchewan. (2006, January) CT service officially opens in the
Battlefords. [Online]. http://www.gov.sk.ca/news?newsId=599bdced-4c1a-45da-97ac-
506a4823a1b7
[75] ECRI Institute. (2012) CT Scanning Systems. [Online]. https://www.ecri.org/ctscan
[76] Canadian Institute for Health Information, "Hospital Births in Canada: A Focus on Women
Living in Rural and Remote Areas," 2013.
[77] Government of Saskatchewan. (2014, June) CT Scanner Will Enhance Diagnostic Services
for Southeast Saskatchewan. [Online]. https://www.saskatchewan.ca/government/news-
94
and-media/2014/june/27/ct-scanner-estevan
[78] Government of Saskatchewan. (2000, March) Moose Jaw introduces mobile CT scan.
[Online]. http://www.gov.sk.ca/news?newsId=4807a2b8-c7be-4ab9-bfa4-4af4296ad197
[79] The World Bank. (2014, Nov) 2.15 World Development Indicators: Health Systems.
[Online]. wdi.worldbankorg/table/2.15

95
Appendix A : Data Fields Provided
Table 14: Data fields provided by health region
Health Region Data Fields All Health Regions Facility
Patient Identifier (Visit Identifier for SHR and RQHR) Age Sex Postal Code Exam Date Order procedure
Prairie North RHA Completed Volume Room/Bed Ordered Date and Time (not accurate) Transcribed Date and Time Final Report Date and Time Radiologist Order Physician Priority
Cypress RHA Completed Volume Patient Location Final Report Date and Time Radiologist Order Physician Priority Patient Type
Five Hills RHA Completed Volume Ordered Date and Time (not accurate) Transcribed Date and Time Final Report Date and Time Radiologist Order Physician Priority Patient Type
Sunrise RHA Ordered Date and Time (not accurate) Transcribed Date and Time Final Report Date and Time Radiologist Order Physician Priority Patient Type Detailed Procedure Row Count
Prince Albert Parkland RHA Patient Location Ordered Date and Time (not accurate) Transcribed Date and Time Final Report Date and Time Radiologist Order Physician
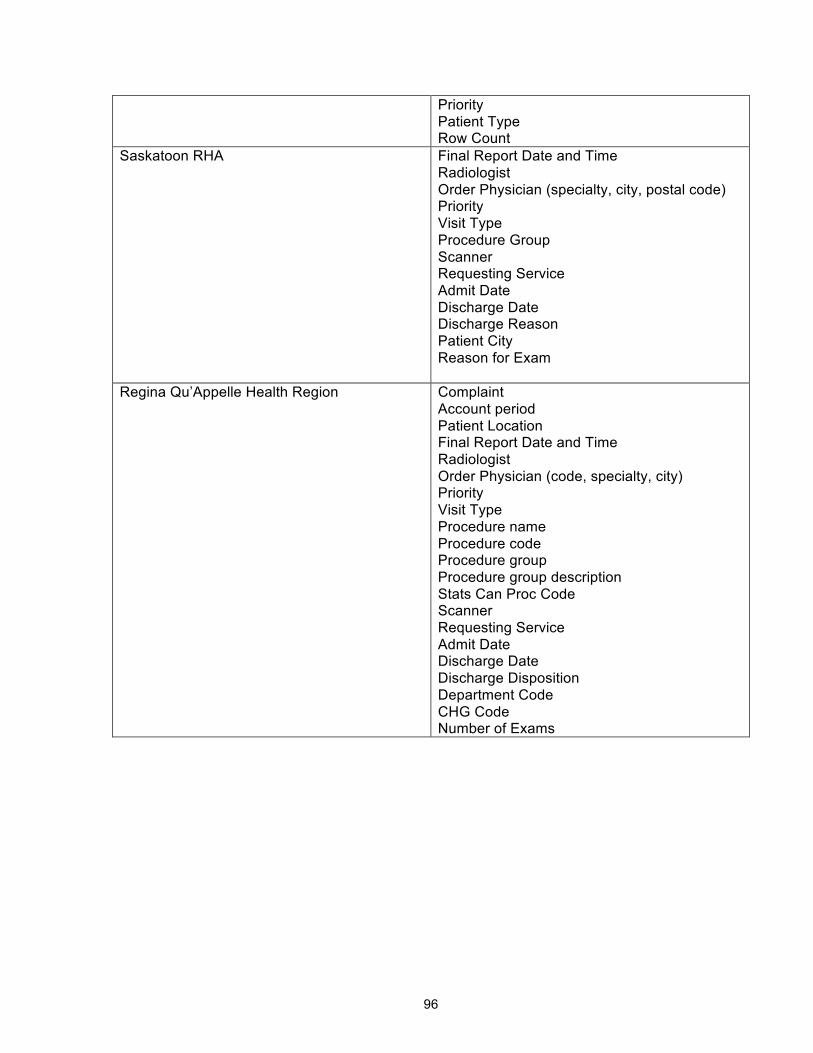
96
Priority Patient Type Row Count
Saskatoon RHA Final Report Date and Time Radiologist Order Physician (specialty, city, postal code) Priority Visit Type Procedure Group Scanner Requesting Service Admit Date Discharge Date Discharge Reason Patient City Reason for Exam
Regina Qu’Appelle Health Region Complaint Account period Patient Location Final Report Date and Time Radiologist Order Physician (code, specialty, city) Priority Visit Type Procedure name Procedure code Procedure group Procedure group description Stats Can Proc Code Scanner Requesting Service Admit Date Discharge Date Discharge Disposition Department Code CHG Code Number of Exams

97
Appendix B : Population Growth Rates
Table 15: Population projection based on sex and age group with growth scenario M1.
Sex Male Female Age Cohort 0-‐19 20-‐39 40-‐59 60-‐79 80+ 0-‐19 20-‐39 40-‐59 60-‐79 80+ Year
2012 1.0122 1.0429 1.0071 1.0320 1.0076 1.0144 1.0325 1.0056 1.0215 1.0027 2013 1.0091 1.0392 1.0027 1.0327 1.0040 1.0125 1.0282 1.0026 1.0267 0.9987 2014 1.0141 1.0313 1.0025 1.0361 1.0022 1.0160 1.0263 0.9997 1.0301 0.9980 2015 1.0083 1.0031 0.9940 1.0414 1.0052 1.0102 1.0053 0.9930 1.0354 0.9935 2016 1.0095 1.0006 0.9960 1.0365 1.0156 1.0122 1.0020 0.9951 1.0363 0.9967 2017 1.0115 0.9994 0.9959 1.0384 1.0000 1.0121 1.0020 0.9958 1.0319 0.9967 2018 1.0134 0.9951 0.9966 1.0380 1.0103 1.0140 1.0007 0.9957 1.0319 1.0000 2019 1.0132 0.9957 0.9966 1.0366 1.0152 1.0131 0.9987 0.9964 1.0329 1.0033 2020 1.0124 0.9950 0.9986 1.0344 1.0100 1.0123 0.9987 0.9964 1.0309 0.9967 2021 1.0129 0.9913 0.9993 1.0332 1.0149 1.0135 0.9961 1.0000 1.0263 1.0033 2022 1.0127 0.9924 1.0021 1.0286 1.0146 1.0126 0.9921 1.0036 1.0265 1.0098 2023 1.0107 0.9924 1.0000 1.0304 1.0288 1.0131 0.9908 1.0043 1.0267 1.0130 2024 1.0093 0.9917 1.0055 1.0236 1.0234 1.0091 0.9920 1.0050 1.0235 1.0096 2025 1.0092 0.9916 1.0075 1.0181 1.0365 1.0096 0.9919 1.0092 1.0197 1.0159 2026 1.0079 0.9929 1.0121 1.0129 1.0352 1.0083 0.9932 1.0134 1.0105 1.0250 2027 1.0054 0.9961 1.0120 1.0048 1.0553 1.0051 0.9959 1.0139 1.0032 1.0396 2028 1.0042 0.9993 1.0112 1.0048 1.0565 1.0038 0.9993 1.0151 1.0024 1.0352 2029 1.0030 1.0007 1.0111 1.0047 1.0496 1.0031 0.9973 1.0121 1.0032 1.0397 2030 1.0018 0.9987 1.0116 1.0024 1.0545 1.0025 1.0000 1.0127 1.0039 1.0381 2031 1.0018 1.0013 1.0089 1.0039 1.0517 1.0025 1.0000 1.0105 1.0016 1.0341 2032 1.0024 1.0020 1.0088 1.0008 1.0492 1.0012 1.0034 1.0085 1.0016 1.0406 2033 1.0018 1.0020 1.0094 1.0000 1.0531 1.0019 1.0041 1.0090 1.0000 1.0439
Table 16: Population projection based on sex and age group with growth scenario L.
Sex Male Female Age Cohort 0-‐19 20-‐39 40-‐59 60-‐79 80+ 0-‐19 20-‐39 40-‐59 60-‐79 80+ Year
2012 1.0122 1.0429 1.0071 1.0320 1.0076 1.0144 1.0325 1.0056 1.0215 1.0027 2013 1.0091 1.0392 1.0027 1.0327 1.0040 1.0125 1.0282 1.0026 1.0267 0.9987 2014 1.0141 1.0313 1.0025 1.0361 1.0022 1.0160 1.0263 0.9997 1.0301 0.9980 2015 1.0048 1.0006 0.9926 1.0414 1.0052 1.0065 1.0033 0.9930 1.0354 0.9903 2016 1.0062 0.9981 0.9960 1.0354 1.0156 1.0101 1.0000 0.9937 1.0342 0.9967 2017 1.0075 0.9969 0.9939 1.0374 0.9949 1.0086 0.9987 0.9950 1.0330 1.0000

98
2018 1.0095 0.9919 0.9952 1.0370 1.0103 1.0071 0.9974 0.9943 1.0300 0.9967 2019 1.0074 0.9931 0.9945 1.0357 1.0051 1.0085 0.9967 0.9943 1.0320 0.9967 2020 1.0066 0.9912 0.9959 1.0335 1.0203 1.0063 0.9954 0.9942 1.0310 1.0000 2021 1.0053 0.9885 0.9972 1.0315 1.0100 1.0076 0.9914 0.9985 1.0264 1.0033 2022 1.0046 0.9897 0.9986 1.0305 1.0148 1.0055 0.9886 0.9993 1.0266 1.0033 2023 1.0046 0.9883 0.9979 1.0279 1.0194 1.0048 0.9864 1.0022 1.0251 1.0099 2024 1.0007 0.9882 1.0021 1.0221 1.0286 1.0020 0.9890 1.0029 1.0219 1.0130 2025 1.0026 0.9880 1.0042 1.0183 1.0231 1.0014 0.9875 1.0058 1.0190 1.0129 2026 1.0000 0.9892 1.0083 1.0098 1.0407 1.0000 0.9887 1.0101 1.0089 1.0190 2027 0.9981 0.9932 1.0082 1.0048 1.0565 0.9980 0.9922 1.0114 1.0032 1.0374 2028 0.9948 0.9959 1.0088 1.0032 1.0453 0.9952 0.9957 1.0099 1.0016 1.0390 2029 0.9948 0.9972 1.0067 1.0024 1.0512 0.9952 0.9942 1.0091 1.0032 1.0347 2030 0.9947 0.9959 1.0067 1.0008 1.0487 0.9938 0.9949 1.0090 1.0008 1.0307 2031 0.9927 0.9972 1.0053 1.0024 1.0464 0.9938 0.9964 1.0068 1.0000 1.0352 2032 0.9940 0.9986 1.0053 1.0000 1.0512 0.9944 1.0000 1.0041 1.0000 1.0366 2033 0.9933 0.9993 1.0046 0.9976 1.0552 0.9930 1.0007 1.0041 0.9976 1.0429
Table 17: Population projection based on sex and age group with growth scenario H.
Sex Male Female Age Cohort 0-‐19 20-‐39 40-‐59 60-‐79 80+ 0-‐19 20-‐39 40-‐59 60-‐79 80+ Year
2012 1.0122 1.0429 1.0071 1.0320 1.0076 1.0144 1.0325 1.0056 1.0215 1.0027 2013 1.0091 1.0392 1.0027 1.0327 1.0040 1.0125 1.0282 1.0026 1.0267 0.9987 2014 1.0141 1.0313 1.0025 1.0361 1.0022 1.0160 1.0263 0.9997 1.0301 0.9980 2015 1.0110 1.0056 0.9953 1.0390 1.0052 1.0116 1.0066 0.9937 1.0365 1.0000 2016 1.0136 1.0025 0.9960 1.0387 1.0156 1.0150 1.0039 0.9958 1.0352 0.9968 2017 1.0147 1.0012 0.9973 1.0383 1.0103 1.0176 1.0026 0.9965 1.0350 0.9967 2018 1.0192 0.9976 0.9980 1.0400 1.0102 1.0180 1.0032 0.9972 1.0308 1.0033 2019 1.0181 0.9975 0.9973 1.0365 1.0151 1.0191 1.0013 0.9964 1.0347 1.0033 2020 1.0191 0.9969 1.0000 1.0361 1.0099 1.0194 1.0013 0.9986 1.0299 1.0000 2021 1.0200 0.9951 1.0020 1.0349 1.0294 1.0203 0.9981 1.0014 1.0290 1.0097 2022 1.0196 0.9963 1.0034 1.0310 1.0190 1.0212 0.9948 1.0043 1.0282 1.0129 2023 1.0192 0.9963 1.0041 1.0301 1.0280 1.0195 0.9948 1.0064 1.0265 1.0190 2024 1.0171 0.9944 1.0074 1.0242 1.0273 1.0173 0.9954 1.0085 1.0250 1.0156 2025 1.0168 0.9956 1.0094 1.0220 1.0354 1.0170 0.9954 1.0112 1.0212 1.0123 2026 1.0154 0.9956 1.0139 1.0136 1.0427 1.0161 0.9961 1.0145 1.0127 1.0242 2027 1.0140 1.0000 1.0150 1.0063 1.0615 1.0129 0.9993 1.0164 1.0047 1.0533 2028 1.0111 1.0019 1.0148 1.0070 1.0618 1.0110 1.0020 1.0168 1.0031 1.0393 2029 1.0104 1.0032 1.0127 1.0054 1.0545 1.0115 1.0013 1.0145 1.0055 1.0405 2030 1.0103 1.0019 1.0144 1.0046 1.0586 1.0102 1.0020 1.0156 1.0047 1.0390

99
2031 1.0102 1.0038 1.0117 1.0054 1.0489 1.0107 1.0033 1.0135 1.0039 1.0425 2032 1.0101 1.0031 1.0116 1.0038 1.0621 1.0094 1.0046 1.0127 1.0023 1.0432 2033 1.0100 1.0050 1.0115 1.0008 1.0585 1.0099 1.0065 1.0106 1.0000 1.0460

100
Appendix C : Data Map
Table 18 through to Table 27 indicate the number of records which were used to calculate the
baseline statistics with different cuts of the data in the rest of the chapter. The number of
records changes due to missing data for certain fields. For certain calculations, the sample size
is dependent on the postal code. Table 18 breaks down the data based on postal code validity
and in-province/out-of-province and provides the total number of data points.
Table 18: CT exam data map based on postal code.
Number of Data Points
Total 586,386
Invalid/Missing postal codes 25
Out-of-province 18,680
In-province, invalid postal code 865
In-province, valid postal code 566,816
Table 19: Number of data points by facility and year
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
CRH 0 0 0 0 0 0 0 318 4244 4232 3758 3643 3457 896
MJU 0 0 0 0 0 0 0 0 0 656 5732 5747 5801 1801
VH 0 0 0 0 0 0 0 0 0 0 4980 6948 7153 8049
BUH 0 0 0 0 0 0 0 0 0 3718 4253 4079 4172 1017
LH 0 0 0 0 0 0 0 0 0 2489 3925 3603 3763 1030
PH 0 0 0 2596 2930 1961 3246 2100 2103 1956 2153 2014 437 0
RGH 0 0 0 8237 10759 10479 10562 9974 9765 8943 8737 10783 8210 0
RUH 10440 10992 11497 11318 13055 14911 15784 16087 17525 18779 17540 18785 7930 0
SCH 0 0 1046 6867 7093 7741 7742 7866 7788 9170 11126 12243 4972 0
SPH 0 0 0 6368 7082 7493 8273 9500 11542 11434 11039 10210 4180 0
YRH 0 0 0 0 0 0 0 0 0 0 477 3992 4006 5084

101
Table 20: Number of data points by priority level and facility in 2011
Priority Level
Facility 1 2 3 4
CRH 1280 647 642 1074
MJU 2597 716 1354 1080
VH 3377 1079 1716 776
BUH 1464 1149 1081 385
LH 1323 1042 988 250
YRHC 1805 765 869 553
Table 21: Number of data points by patient type and facility in 2011
Emergency Inpatient Outpatient
CRH 521 668 2454
MJU 1595 776 3376
VH 2410 669 3868
BUH 1038 474 2566
LH 924 498 2181
PH 58 456 1500
RGH 281 1682 8820
RUH 8539 4729 5517
SCH 1136 237 10870
SPH 2852 3020 4338
YRH 999 391 2602

102
Table 22: Number of data points which have exam time by facility in 2011.
Number of data points
CRH 20548
MJU 19737
VH 27130
BUH 17239
LH 14810
PH 21496
RGH 96449
RUH 184643
SCH 83654
SPH 87121
YRH 13559
Table 23: Number of data points by procedure group and facility in 2011
Head Spine Upper Extremity
Lower Extremity
Thorax Abdomen/ Pelvix
Miscellaneous
Vascular
CRH 1153 536 14 52 754 1155 199 145
MJU 1898 792 17 84 1008 1789 189 463
VH 2779 478 48 96 1305 2287 293 267
BUH 1469 468 22 78 656 1483 176 127
LH 1389 274 16 40 626 1212 84 243
PH 387 51 0 0 489 1025 62 0

103
RGH 2036 539 0 0 3074 4718 416 0
RUH 7244 1556 214 481 2821 4348 1 2120
SCH 2544 241 80 284 3680 4646 0 768
SPH 2117 195 18 98 1808 4102 12 1860
YRH 1234 369 21 42 996 1537 233 147
Table 24: Number of data points with report turnaround time by facility in 2011
Facility Data Points with Report Turnaround Time
CRH 20548
MJU 19737
VH 27130
BUH 17239
LH 14810
PH 21496
RGH 96449
RUH 184643
SCH 83654
SPH 87121
YRH 13559
Table 25: Number of visits in 2011 by facility.
Facility Count
Cypress 2340
FiveHills 3178
PAParkland 3687

104
BUH 2453
LH 2059
PASQUA 893
RGH 5450
RUH 4081
SCH 7349
SPH 3109
Sunrise 2475
Table 26: Number of visits by population centre and rural area classification in 2011
Population centre and rural area classification Number of Visits
Rural Area 1643
Small (1,000 – 29,999 pop.) 7061
Medium (30,000 - 99,999 pop.) 3539
Large Urban (100,000 or greater) 10610
Table 27: Number of visits by patient health region and CT facility in 2011.
CT Facility
Patient Health Region CRH MJUH VH BUH LH PH RGH RUH SCH SPH YRHC Athabasca Health Authority 0 0 1 0 67 0 0 60 10 13 0
Cypress RHA 3310 73 3 3 0 176 58 279 117 103 0
Five Hills RHA 46 5085 6 1 0 578 102 114 65 27 0
Heartland RHA 189 77 418 71 5 8 8 1282 849 645 0
Keewatin YatthÚ RHA 0 0 289 2 72 0 0 353 99 116 2
Kelsey Trail RHA 4 5 3 3 1209 39 6 958 623 581 41 Mamawetan Churchill River RHA 0 1 6 0 515 1 0 411 125 182 0
Prairie North RHA 0 4 3061 1382 12 2 3 1052 531 571 0 Prince Albert Parkland RHA 1 1 158 10 4740 21 7 1139 693 635 1
Regina Qu'Appelle RHA 24 175 10 0 13 7090 1326 227 93 53 75
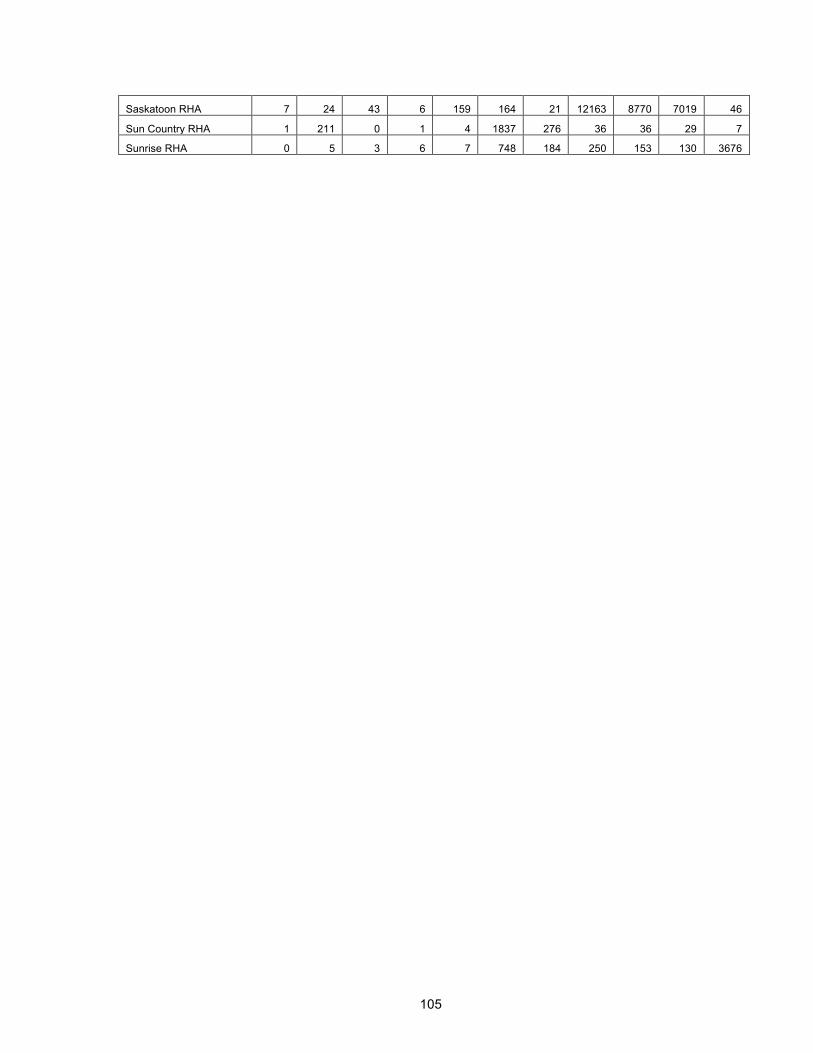
105
Saskatoon RHA 7 24 43 6 159 164 21 12163 8770 7019 46
Sun Country RHA 1 211 0 1 4 1837 276 36 36 29 7
Sunrise RHA 0 5 3 6 7 748 184 250 153 130 3676

106
Appendix D : AMPL Files
AMPL Model Formulation File (.mod) set DEMAND:= 1..959; set CT:= 1..23; set TIME:= 1..19; set TIME_subset within TIME := 1..18; #1 less than TIME set; param Demand{DEMAND,TIME}; #Demandit = number of CT scans in area i in each year t param DemandTotal{TIME}; #DemandTotal param MinCoverage; #= Minimum percentage of total demand in Saskatchewan that must be covered param a{DEMAND,CT}; # = { 1 if CT demand in area i is within patient travel distance radius r of location j, 0 otherwise} param Capmax; #= maximum capacity allowed at a CT param CapShift; #= regular shift hours param CostOpen; #= cost of opening a new CT facility param CostCT; #= cost of adding a CT to an open facility param ExamCost; #= cost of an assigned overtime CT exam param MaxShift;#maximum number of shifts param OvertimeSurcharge; param ShiftRemovalCost; var DemandFraction{DEMAND,CT,TIME}>=0; #xijt = fraction of demand covered at location i by CT at location j at time t var CTDecision{CT,TIME} binary; #yjt = {1 if a new CT is placed in location j at time t, 0 otherwise} var CTTotal{CT,TIME} integer >=0; #Yjt To initialize the model: yj0 = number of current CTs at location j at time 0, Yjt = total number of CTs at location j at time t var CTnew{CT} binary; #zj = {1 if a new facility is placed at location j in any period, 0 otherwise} var CTover{CT,TIME} >=0; #assigned overtime exams var CTunder{CT,TIME} >=0; #assigned undertime exams var Shifts{CT,TIME} integer >=0; #shifts assigned to a facility var ShiftRemoved{CT,TIME} >=0 ; var ShiftAdded{CT,TIME} >=0 ; var AssignedDemand{CT,TIME}>=0; var UnassignedDemand{TIME} >=0; var UnassignedOver{TIME} >=0; #assigned overtime exams var UnassignedUnder{TIME} >=0; #assigned undertime exams #var CapOver{CT,TIME}>=0; minimize Cost: CostOpen*sum{j in CT}CTnew[j] + CostCT*sum{t in TIME_subset}sum{j in CT}CTDecision[j,t+1]+ ExamCost*OvertimeSurcharge*sum{t in TIME_subset}sum{j in CT}CTover[j,t+1] + ExamCost*OvertimeSurcharge*sum{t in TIME_subset}UnassignedOver[t+1]+ ExamCost*CapShift*sum{t in TIME_subset}sum{j in CT}Shifts[j,t+1]+ ShiftRemovalCost*sum{t in TIME_subset}sum{j in CT}ShiftRemoved[j,t+1];; subject to x1 {t in TIME_subset}: sum{i in DEMAND}sum{j in CT}DemandFraction[i,j,t+1]*Demand[i,t+1]>= MinCoverage*DemandTotal[t+1]; subject to x2 {t in TIME_subset}: DemandTotal[t+1]<= Capmax*sum{j in CT}CTTotal[j,t+1];

107
subject to x3 {j in CT, t in TIME_subset}: sum{i in DEMAND}DemandFraction[i,j,t+1]*Demand[i,t+1] = CapShift*Shifts[j,t+1] + CTover[j,t+1] - CTunder[j,t+1] ; subject to x4 {j in CT, t in TIME_subset}: CTover[j,t+1] <= Capmax*CTTotal[j,t+1]- CapShift*Shifts[j,t+1]; subject to x5 {i in DEMAND, j in CT, t in TIME_subset}: DemandFraction[i,j,t+1] <= a[i,j]*CTTotal[j,t+1]; subject to x6 {i in DEMAND, t in TIME_subset}: sum{j in CT}DemandFraction[i,j,t+1] <= 1; subject to x7 {j in CT, t in TIME_subset}: CTnew[j] >= CTDecision[j,t+1] - CTTotal[j,1]; subject to x8 {j in CT, t in TIME_subset}: CTTotal[j,t+1] = CTTotal[j,t] + CTDecision[j,t+1]; #limit to t >= 1 subject to x9 {j in CT, t in TIME_subset}: Shifts[j,t] - Shifts[j,t+1] = ShiftRemoved[j,t+1] - ShiftAdded[j,t+1]; subject to x10:CTTotal[1,1]=0; subject to x11:CTTotal[2,1]=0; subject to x12:CTTotal[3,1]=0; subject to x13:CTTotal[4,1]=0; subject to x14:CTTotal[5,1]=0; subject to x15:CTTotal[6,1]=0; subject to x16:CTTotal[7,1]=0; subject to x17:CTTotal[8,1]=0; subject to x18:CTTotal[9,1]=0; subject to x19:CTTotal[10,1]=0; subject to x20:CTTotal[11,1]=0; subject to x21:CTTotal[12,1]=0; subject to x22:CTTotal[13,1]=1; subject to x23:CTTotal[14,1]=2; subject to x24:CTTotal[15,1]=2; subject to x25:CTTotal[16,1]=1; subject to x26:CTTotal[17,1]=1; subject to x27:CTTotal[18,1]=1; subject to x28:CTTotal[19,1]=1; subject to x29:CTTotal[20,1]=1; subject to x30:CTTotal[21,1]=1; subject to x31:CTTotal[22,1]=1; subject to x32:CTTotal[23,1]=1; subject to x33{j in CT, t in TIME_subset}:Shifts[j,t+1]<= MaxShift*CTTotal[j,t+1]; subject to x34 {t in TIME_subset}:DemandTotal[t+1] - (sum{i in DEMAND}sum{j in CT}DemandFraction[i,j,t+1]*Demand[i,t+1]) = UnassignedDemand[t+1]; subject to x35 {t in TIME_subset}:UnassignedDemand[t+1] - sum{j in CT}CTunder[j,t+1] = UnassignedOver[t+1] - UnassignedUnder[t+1]; subject to x36{j in CT, t in TIME_subset}:Shifts[j,t+1]>= CTTotal[j,t+1]; AMPL Data File (Travel Time 2 hours and 90% coverage) param MinCoverage := 9.000000e-001; param Capmax := 24723; param CapShift := 4700; param CostOpen:= 1250000; param CostCT := 1700000; param ExamCost := 6.226000e+001;

108
param MaxShift := 3; param OvertimeSurcharge := 1.500000e+000; param ShiftRemovalCost:=100000; param Demand := 1 1 3.450769e+001 1 2 3.507199e+001 1 3 3.568170e+001 1 4 3.621902e+001 1 5 3.679340e+001 1 6 3.731274e+001 1 7 3.789408e+001 1 8 3.845858e+001 1 9 3.909870e+001 1 10 3.967275e+001 1 11 4.027297e+001 1 12 4.089807e+001 1 13 4.151963e+001 1 14 4.206922e+001 1 15 4.259477e+001 CONTINUED… param DemandTotal:= 1 1.178736e+005 2 1.197780e+005 3 1.218793e+005 4 1.239983e+005 5 1.263113e+005 6 1.284345e+005 7 1.308426e+005 8 1.334270e+005 9 1.357988e+005 10 1.382672e+005 11 1.407583e+005 12 1.436284e+005 13 1.461050e+005 14 1.486538e+005 15 1.509099e+005 16 1.531696e+005 17 1.554512e+005 18 1.577133e+005 19 1.600728e+005 ; param a default 0 := 364 1 1 385 1 1 386 1 1 387 1 1 388 1 1 389 1 1 390 1 1

109
391 1 1 392 1 1 396 1 1 397 1 1 398 1 1 399 1 1 400 1 1 401 1 1 402 1 1 403 1 1 404 1 1 405 1 1
CONTINUED

110
Appendix E : Metrics
Table 28: Percentage of patient’s by health region of origin for each CT Facility in 2011
Unm
atch
ed
Ath
abas
ca
Cyp
ress
Five
Hill
s
Hea
rtlan
d
Kee
wat
in Y
atth
é
Kel
sey
Trai
l
MC
R
Pra
irie
Nor
th
PA
PH
R
RQ
HR
Sas
kato
on
Sun
Cou
ntry
Sun
rise
CRH 0.77 - 90.3 1.54 6.84 - 0.13 - - - 0.30 0.13 - -
MJUH 0.94 - 1.70 86.0 1.70 - 0.09 - 0.09 0.03 3.87 0.16 5.35 0.06
VH 0.98 1.03 - - 0.05 0.95 25.74 7.21 0.24 61.62 0.08 1.95 0.05 0.08
LH 1.10 0.04 0.04 0.08 14.35 10.35 0.04 0.04 70.97 2.36 - 0.61 - -
BUH 61.00 - - 0.05 2.77 - - - 35.89 0.19 - - - 0.10
PH 1.12 - 1.34 4.37 0.22 - 0.22 - 0.11 0.34 71.11 0.67 11.87 8.62
RGH 0.72 - 1.21 4.59 0.06 - 0.22 0.02 0.02 0.04 70.81 1.43 15.39 5.50
RUH 0.54 0.27 1.47 0.61 7.65 1.27 5.76 1.47 5.46 6.37 0.83 66.67 0.15 1.47
SCH 0.39 0.11 0.83 0.57 7.32 0.78 4.86 0.95 4.12 5.35 0.87 72.25 0.31 1.28
SPH 0.45 0.06 1.00 0.39 7.17 0.71 6.37 1.67 4.79 5.56 0.71 69.73 0.19 1.19
YRHC 2.95 - - - - - 1.09 - - 0.04 2.02 1.05 0.16 92.69

111
Figure 38: Proportions of patient type by health region in 2011.
Table 29: Percent of outpatient visits that went to each CT facility from each health
region in 2011 based on the patient’s residential postal code.
CT HR Cy-
press FH
HR
PAP
HR PNRHA RQHR Saskatoon
Sun-
rise
CT Facility CRH MJU VH LH BUH PH RGH RUH SCH SPH YRH
Patient HR
Athabasca 0.0 0.0 63.3 1.7 0.0 0.0 0.0 18.3 13.3 3.3 0.0
Cypress 88.1 2.3 0.0 0.0 0.0 0.5 2.8 2.5 2.5 1.3 0.0
Five Hills 1.1 87.0 0.0 0.1 0.0 1.2 8.0 0.8 1.3 0.4 0.0
Heartland 9.4 3.2 0.1 20.7 3.3 0.1 0.2 18.3 31.6 13.1 0.0
Keewatin
Yatthé 0.0 0.0 8.3 60.5 0.0 0.0 0.0 12.4 13.6 5.2 0.0
14.3% 28.1%
37.2% 25.6%
2.6%
30.4% 23.6% 25.6%
17.8%
13.4% 9.0%
12.3%
16.9%
19.4%
9.5% 16.0%
67.9% 58.6% 53.9%
62.1%
80.5%
50.3% 66.9%
58.4%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Cypress Five Hills Prince Albert Parkland
Prairie North Regina Qu'Appelle
Saskatoon Sunrise Province
Emergency InpaQent OutpaQent

112
Kelsey Trail 0.2 0.2 53.1 0.1 0.0 0.1 0.7 13.2 20.0 11.1 1.5
MCR 0.0 0.0 59.1 0.2 0.0 0.0 0.2 13.3 15.6 11.6 0.0
Prairie North 0.0 0.1 0.3 54.9 23.3 0.0 0.0 7.0 9.6 4.7 0.0
PAPHR 0.0 0.0 71.7 1.8 0.1 0.1 0.1 8.2 12.4 5.5 0.0
RQHR 0.1 2.6 0.1 0.0 0.0 13.2 80.4 0.7 1.3 0.5 1.0
Saskatoon 0.0 0.0 0.7 0.1 0.0 0.1 0.7 26.2 51.0 20.8 0.2
Sun Country 0.0 14.7 0.2 0.0 0.0 9.2 72.6 0.5 2.0 0.5 0.3
Sunrise 0.0 0.1 0.1 0.0 0.1 2.7 10.5 2.1 3.3 1.3 80.0
Table 30: Proportion of each procedure group by facility
Health Region Facility Head Spine
Upper Extremity
Lower Extremity Thorax
Abdo-men
Pelvis Misc. Vascular Cypress CRH 25.8% 12.6% 0.3% 1.1% 22.3% 30.7% 4.1% 3.2% FHHR MJUH 28.3% 12.3% 0.2% 1.2% 18.8% 29.6% 2.6% 7.1% PAPHR VH
31.7% 5.5% 0.4% 0.8% 20.2% 34.3% 3.0% 4.1% PNRHA BUH 30.7% 10.8% 0.4% 1.5% 17.6% 33.1% 3.3% 2.6%
LH 33.3% 7.0% 0.4% 0.9% 18.9% 31.9% 1.9% 5.9% RQHR PASQUA 19.2% 2.5% 0.0% 0.0% 24.3% 50.9% 3.1% 0.0%
RGH 19.0% 5.1% 0.0% 0.0% 28.5% 43.5% 3.8% 0.0% Saskatoon RUH 38.6% 8.3% 1.1% 2.6% 15.0% 23.1% 0.0% 11.3%
SCH 20.8% 2.0% 0.7% 2.3% 30.1% 37.9% 0.0% 6.3% SPH 20.7% 1.9% 0.2% 1.0% 17.7% 40.2% 0.1% 18.2%
Sunrise YRHC 23.3% 7.3% 0.4% 0.7% 25.9% 35.3% 4.0% 3.0%

113
Appendix F : Potential Facilities Table 31: List of potential facilities
Facility Name Kindersley & District Health Centre Melfort Hospital Tisdale Hospital Nipawin Hospital Northwest Health Facility - Meadow Lake Hospital Humboldt District Hospital St. Joseph's Hospital Weyburn General Hospital St. Peter's Hospital St. Joseph's Health Centre La Loche Health Centre La Ronge Health Centre Pasqua Hospital Regina General Hospital Royal University Hospital Saskatoon City Hospital St. Paul's Hospital Cypress Regional Hospital Moose Jaw Union Hospital Battlefords Union Hospital Lloydminster Hospital Victoria Hospital Yorkton Regional Health Centre




















