
A Diet Containing Whey Protein, Free Glutamine, and Transforming Growth Factor Ameliorates...
7
The Journal of Nutrition Nutrition and Disease A Diet Containing Whey Protein, Free Glutamine, and Transforming Growth Factor-b Ameliorates Nutritional Outcome and Intestinal Mucositis during Repeated Chemotherapeutic Challenges in Rats 1–3 Nabile Boukhettala, 4 Ayman Ibrahim, 4 Moutaz Aziz, 5 Jacques Vuichoud, 6 Kim-Yen Saudan, 6 Ste ´phanie Blum, 6 Pierre De ´chelotte, 4 * Denis Breuille ´, 6 and Moı¨se Coe ¨ffier 4 4 Nutrition Unit, Rouen University Hospital, Rouen, France and ADEN–EA4311, Institute for Biomedical Research and European Institute for Peptide Research, Rouen University, Rouen F-76183, France; 5 Laboratory of Anatomo-Pathology, Rouen University Hospital, Rouen, France; and 6 Nestle ´ Research Center, Nutrition and Health Department, Lausanne CH-1000, Switzerland Abstract Anticancer chemotherapy often induces side effects such as mucositis. Recent data suggest that a diet, Clinutren Protect (CP), containing whey proteins, glutamine, and transforming growth factor-b (TGFb)-rich casein limits intestinal mucositis and improves recovery after a single methotrexate (MTX) challenge in rats. Chemotherapy consists of alternating periods of treatment and rest. Thus, our study evaluated the effects of CP on nutritional outcome and intestinal mucositis in rats receiving repeated chemotherapeutic challenges. Thirty-six Sprague-Dawley rats received 3 cycles of MTX at 8-d intervals. Rats had free access to CP or control diet (Co) from 7 d before the first MTX injection until the end of the experiment at d 27. In Co, whey proteins and TGFb-rich casein were replaced by TGFb-free casein. L-Glutamine was replaced by L-alanine. Body composition was assessed by dual energy X-ray absorptiometry. Before MTX challenges, food intake and body weight were similar in both groups but became higher during MTX challenges in CP (P , 0.05). Fat mass decreased similarly in both groups. In contrast, the decrease of fat free mass between d 21 and d 27 was less pronounced in the CP group (29.5 g) than in the Co group (257.2 g) (P , 0.05). The intestinal damage score was lower in the CP group (0.6 6 0.3 vs. 2.1 6 0.6; P , 0.05). Fecal IgA increased over time in the CP group (P , 0.05) but not in the Co group. A diet containing whey proteins, glutamine, and TGFb improves nutritional outcome by limiting the reduction of fat free mass and reduces intestinal mucositis during repeated chemotherapeutic challenges in rats. J. Nutr. 140: 799–805, 2010. Introduction Cancer patients are at a high risk for malnutrition due to malignancy-induced cachexia and dysphagia and to the effects of chemoradiation. Chemotherapy, which is often used to treat cancer patients, alternates periods of treatment and rest. The periods of rest between the periods of chemotherapeutic challenge are needed to allow the organism to recover from possible side effects. Among them, mucositis is frequent and is related to many chemotherapeutic agents such as methotrexate (MTX). 7 The onset of mucositis leads to the limitation or even cessation of chemotherapy (1,2). The pathophysiology of intestinal mucositis involves hypoproliferation, apoptosis, in- flammatory response, and intestinal barrier disruption (3). We previously reported that MTX treatment also induces an alteration of protein metabolism (4). Indeed, MTX treatment is associated with a decrease of protein synthesis and an increase of proteolysis and particularly of the lysosomal pathway in jejunal mucosa in rats (5). To limit chemotherapy-induced mucositis, nutritional inter- ventions may be beneficial. A new diet, Clinutren Protect (CP), tailored to alleviate intestinal mucositis, has been designed. It contains whey proteins, transforming growth factor-b (TGFb)- 7 Abbreviations used: Co, control group; CP, Clinutren Protect; GSH, glutathione; MTX, methotrexate; TGFb, transforming growth factor-b. 1 Supported by Nestle ´ Research Center, Nutrition and Health Department, Lausanne, Switzerland. 2 Author disclosures: P. De ´ chelotte received honoraries for lectures by Nestle ´ Nutrition. J. Vuichoud, K-Y. Saudan, S. Blum, and D. Breuille ´ are employees of Nestle ´ . N. Boukhettala, A. Ibrahim, M. Aziz, S. Blum, and M. Coe ¨ ffier, no conflicts of interest. 3 Supplemental Figure 1 is available with the online posting of this paper at jn. nutrition.org. * To whom correspondence should be addressed. E-mail: pierre.dechelotte@ univ-rouen.fr. 0022-3166/08 $8.00 ã 2010 American Society for Nutrition. Manuscript received November 19, 2009. Initial review completed December 15, 2009. Revision accepted January 30, 2010. 799 First published online February 24, 2010; doi:10.3945/jn.109.119222. by guest on February 5, 2013 jn.nutrition.org Downloaded from 2.DC1.html http://jn.nutrition.org/content/suppl/2010/03/19/jn.109.11922 Supplemental Material can be found at:
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of A Diet Containing Whey Protein, Free Glutamine, and Transforming Growth Factor Ameliorates...

The Journal of Nutrition
Nutrition and Disease
A Diet Containing Whey Protein, FreeGlutamine, and Transforming GrowthFactor-b Ameliorates Nutritional Outcomeand Intestinal Mucositis during RepeatedChemotherapeutic Challenges in Rats1–3
Nabile Boukhettala,4 Ayman Ibrahim,4 Moutaz Aziz,5 Jacques Vuichoud,6 Kim-Yen Saudan,6
Stephanie Blum,6 Pierre Dechelotte,4* Denis Breuille,6 and Moıse Coeffier4
4Nutrition Unit, Rouen University Hospital, Rouen, France and ADEN–EA4311, Institute for Biomedical Research and European
Institute for Peptide Research, Rouen University, Rouen F-76183, France; 5Laboratory of Anatomo-Pathology, Rouen University
Hospital, Rouen, France; and 6Nestle Research Center, Nutrition and Health Department, Lausanne CH-1000, Switzerland
Abstract
Anticancer chemotherapy often induces side effects such as mucositis. Recent data suggest that a diet, Clinutren
Protect (CP), containing whey proteins, glutamine, and transforming growth factor-b (TGFb)-rich casein limits intestinal
mucositis and improves recovery after a single methotrexate (MTX) challenge in rats. Chemotherapy consists of
alternating periods of treatment and rest. Thus, our study evaluated the effects of CP on nutritional outcome and
intestinal mucositis in rats receiving repeated chemotherapeutic challenges. Thirty-six Sprague-Dawley rats received
3 cycles of MTX at 8-d intervals. Rats had free access to CP or control diet (Co) from 7 d before the first MTX injection
until the end of the experiment at d 27. In Co, whey proteins and TGFb-rich casein were replaced by TGFb-free casein.
L-Glutamine was replaced by L-alanine. Body composition was assessed by dual energy X-ray absorptiometry. Before
MTX challenges, food intake and body weight were similar in both groups but became higher during MTX challenges in
CP (P , 0.05). Fat mass decreased similarly in both groups. In contrast, the decrease of fat free mass between d 21
and d 27 was less pronounced in the CP group (29.5 g) than in the Co group (257.2 g) (P, 0.05). The intestinal damage
score was lower in the CP group (0.6 6 0.3 vs. 2.16 0.6; P, 0.05). Fecal IgA increased over time in the CP group (P,
0.05) but not in the Co group. A diet containing whey proteins, glutamine, and TGFb improves nutritional outcome by
limiting the reduction of fat free mass and reduces intestinal mucositis during repeated chemotherapeutic challenges in
rats. J. Nutr. 140: 799–805, 2010.
Introduction
Cancer patients are at a high risk for malnutrition due tomalignancy-induced cachexia and dysphagia and to the effectsof chemoradiation. Chemotherapy, which is often used to treatcancer patients, alternates periods of treatment and rest. Theperiods of rest between the periods of chemotherapeuticchallenge are needed to allow the organism to recover frompossible side effects. Among them, mucositis is frequent and is
related to many chemotherapeutic agents such as methotrexate(MTX).7 The onset of mucositis leads to the limitation or evencessation of chemotherapy (1,2). The pathophysiology ofintestinal mucositis involves hypoproliferation, apoptosis, in-flammatory response, and intestinal barrier disruption (3). Wepreviously reported that MTX treatment also induces analteration of protein metabolism (4). Indeed, MTX treatmentis associated with a decrease of protein synthesis and an increaseof proteolysis and particularly of the lysosomal pathway injejunal mucosa in rats (5).
To limit chemotherapy-induced mucositis, nutritional inter-ventions may be beneficial. A new diet, Clinutren Protect (CP),tailored to alleviate intestinal mucositis, has been designed. Itcontains whey proteins, transforming growth factor-b (TGFb)-
7 Abbreviations used: Co, control group; CP, Clinutren Protect; GSH, glutathione;
MTX, methotrexate; TGFb, transforming growth factor-b.
1 Supported by Nestle Research Center, Nutrition and Health Department,
Lausanne, Switzerland.2 Author disclosures: P. Dechelotte received honoraries for lectures by Nestle
Nutrition. J. Vuichoud, K-Y. Saudan, S. Blum, and D. Breuille are employees of
Nestle. N. Boukhettala, A. Ibrahim, M. Aziz, S. Blum, and M. Coeffier, no
conflicts of interest.3 Supplemental Figure 1 is available with the online posting of this paper at jn.
nutrition.org.
* To whom correspondence should be addressed. E-mail: pierre.dechelotte@
univ-rouen.fr.
0022-3166/08 $8.00 ã 2010 American Society for Nutrition.
Manuscript received November 19, 2009. Initial review completed December 15, 2009. Revision accepted January 30, 2010. 799First published online February 24, 2010; doi:10.3945/jn.109.119222.
by guest on February 5, 2013
jn.nutrition.orgD
ownloaded from
2.DC1.html http://jn.nutrition.org/content/suppl/2010/03/19/jn.109.11922Supplemental Material can be found at:
rich casein, and free glutamine. These nutrients have been shownto exhibit beneficial effects in various pathological conditions. Incolon cancer models in rats, whey protein concentrate had aprotective role (6) associated with an increase in the intracellularlevels of glutathione (GSH) (7), a major cellular antioxidant (8).In addition, whey protein is rich in branched-chain amino acidsthat can stimulate protein synthesis (9). Glutamine is a condi-tionally essential amino acid during various conditions of stress(10). Glutamine is depleted in cancer patients (11) and thecontent of glutamine is reduced during intestinal inflammation(12). Glutamine prevents atrophy of the intestinal mucosa inpatients receiving total parenteral nutrition (13) and modulatesintestinal inflammatory and antioxidant responses (14). TGFb isan immunomodulatory cytokine that plays an important role inimmune function. TGFb can stimulate the IgA production inthe intestine (15), plays a central role in the maintenance ofintestinal epithelial homeostasis (16), and enhances epithelialrestitution (17). We have recently reported that CP reducesintestinal damage in the acute phase of MTX-induced mucositisin rats and improves recovery after a single MTX challenge (18).
Thus, the aim of the present study was to evaluate the effectsof a specific diet containing whey proteins, glutamine, and TGFbon intestinal mucositis and nutritional outcome in rats receivingrepeated chemotherapeutic challenges mimicking chemothera-peutic cycles in cancer patients.
Materials and Methods
Rats, housing, diet, and MTX injections. Animal care and experi-
mentation complied with both French and European Communityregulations (Official Journal of the European Community L 358, 18/
12/1986) and M.C. is authorized by the French government to use
animal models (authorization no. 76–107). Male Sprague-Dawley rats(350–400 g, Elevage Janvier) were acclimatized at 258C with a 12-h-
light/-dark cycle. Rats were individually housed in metabolic cages.
Rats were given free access to water and standard diet until d 27, with
d 0 being the first day of the first cycle of MTX treatment. From d27 tod 27, rats received CP or isonitrogenous and isocaloric control (Co)
diets. In the Co diet, whey proteins and TGFb-rich casein were replaced
by TGFb-free casein. Free L-glutamine was replaced by free L-alanine
(Table 1). TGFb-free casein contained a standard amount of TGFb(~0.06 mg×g proteins21), whereas TGFb-rich casein contained a high
amount of TGFb (~0.29 mg×g proteins21). A chemotherapeutic model
was induced by 3 cycles of subcutaneous injections of 2.5 mg×kg21MTX(Teva Pharma). The 3 cycles were applied at 8-d intervals between d 0
and 20 (Supplemental Fig. 1). Rats were divided into 2 groups: 1) the Cogroup received MTX injections and had free access to the control diet;
and 2) the CP group received MTX injections and had free access to theCP diet.
Daily clinical state monitoring. From d 27 until the end of the
experiment (d 27), body weight and food intake were monitored at 24-hintervals.
Killing and tissue sampling. Fresh fecal samples were collected rightafter emission at d 27, d 0, 9, 18, and 27 and frozen until IgA analysis.
Blood was withdrawn with a capillary in the retro-orbital sinus in rats
under anesthesia at d 28, 21, 8, 17, and 27 for measurement of
orosomucoid and a2-macroglobulin. At d 27, rats were decapitated aftercarbon dioxide inhalation and blood samples were collected, frozen, and
stored at2208C. The jejunum was quickly removed and rinsed with ice-
cold PBS (140 mmol×L21 NaCl, 3 mmol×L21 KCl, 8 mmol×L21
Na2HPO4, 1.5 mmol×L21 KH2PO4). For histological and immunohis-tochemistry assessments, proximal samples of jejunum (1 cm long each)
were fixed in formalin (10%). Middle pieces (1 cm long) were removed
for assessment of the GSH concentration. Samples were immediately
frozen in liquid nitrogen and stored at 2808C.
Histology. For histological and immunohistochemistry assessments,
jejunal samples were fixed in formalin (10%) and treated as previously
described (4,5). Briefly, sections were scored by the same pathologist(M.A.) whowas unaware of the treatment allocation. Epithelial necrosis,
inflammatory cell infiltration, and exocytosis were assessed using
semiquantitative scores that ranged from 0 (no damage) to 3 (severedamage) for each marker: villus atrophy, necrosis, inflammation, and
exocytosis. Villus height was measured on 10 well-oriented villi
from each rodent using the analysis software Leica QWin (Leica
Microsystems).
Intestinal GSH concentration. The GSH concentration was assessed in
the jejunum by a standardized spectrophotometric assay as previously
described (4,19). GSH concentration was expressed as mmol×g tissue21.
IgA content. Frozen fresh feces collected at d 27, 0, 9, 18, and 27 were
homogenized with 1 mL extraction buffer (30 mmol×L21 EDTA, 105
mg×L21 soybean trypsin inhibitor in PBS). Supernatants were collectedafter centrifugation at 11,0003 g for 15 min at 48C and used for analysis
of protein content by BCA protein assays and the IgA level, which was
measured by ELISA with a commercial kit according to supplierinstructions (Bethyl Laboratories) and normalized to the protein content
of each fecal extract.
Intestinal permeability. Intestinal permeability was determined at 2time points: d 12 and d 21. A bolus dose of 5 mL×kg-1×d21 Iodixanol (320 g
iodine×L21 Visipaque; AmershamHealth)was administered by oral gavage
at d 11 and 20, respectively (4,20). Urine samples were collected over the
following 24 h and frozen at 2208C. Iodixanol was assessed in urine byHPLC (20) and the results were expressed as the total amount of iodixanol
excreted in urine per day.
Orosomucoid and a2-macroglobulin levels. Orosomucoid and a2-
macroglobulin levels were evaluated using a rat orosomucoid ELISA
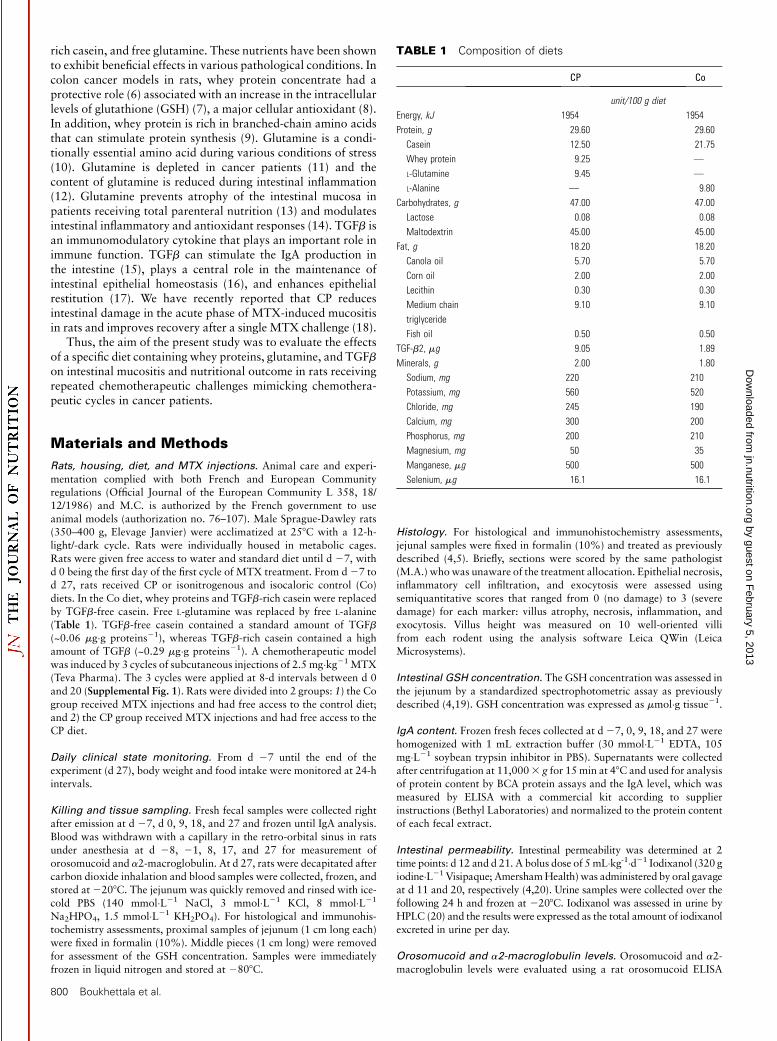
TABLE 1 Composition of diets
CP Co
unit/100 g diet
Energy, kJ 1954 1954
Protein, g 29.60 29.60
Casein 12.50 21.75
Whey protein 9.25 —
L-Glutamine 9.45 —
L-Alanine — 9.80
Carbohydrates, g 47.00 47.00
Lactose 0.08 0.08
Maltodextrin 45.00 45.00
Fat, g 18.20 18.20
Canola oil 5.70 5.70
Corn oil 2.00 2.00
Lecithin 0.30 0.30
Medium chain
triglyceride
9.10 9.10
Fish oil 0.50 0.50
TGF-b2, mg 9.05 1.89
Minerals, g 2.00 1.80
Sodium, mg 220 210
Potassium, mg 560 520
Chloride, mg 245 190
Calcium, mg 300 200
Phosphorus, mg 200 210
Magnesium, mg 50 35
Manganese, mg 500 500
Selenium, mg 16.1 16.1
800 Boukhettala et al.
by guest on February 5, 2013
jn.nutrition.orgD
ownloaded from
quantitation kit and rat a2-macroglobulin ELISA quantitation kit
(GenWay Biotech) at d 28, 21, 8, 17, and 27. The results were
expressed in mg×L21.
Body composition. The measurement of the body composition of the
rats (fat mass and fat free mass) was determined by dual energy X-ray
absorptiometry using the Lunar Prodigy Equipment DPX-IQ (GEHealthcare) in conjunction with the Lunar Software version 4.7E. The
acquisition time at high resolution (0.1 g×cm-2) was ~20 min. The rats
were anesthetized with a mixture of ketamine (40 mg×kg21, Panpharma)
and largactil (1 mg×kg21, Sanofi Aventis). This measure was carried outat d28,21, 8, 17, and 27. All measurements were performed by a single
operator (N.B.).
Calculation methods and statistical analysis. Statistical analysis was
performed using GraphPad Prism 5.01 (GraphPad Software). For
variables evaluated throughout the study in the same rats, statistical
analysis consisted of a 2-way ANOVA for repeated measures. Bonferronipost hoc tests were performed when the P-value for interaction was
, 0.05. For variables evaluated at one time, a t test was performed when
variances were homogeneous as assessed by Bartlett’s test. In other cases,
a nonparametric Mann-Whitney test was used. Survival curves werecompared using the logrank test of Mantel-Cox. For all, P , 0.05 was
considered significant. Values in the text are means 6 SE.
Results
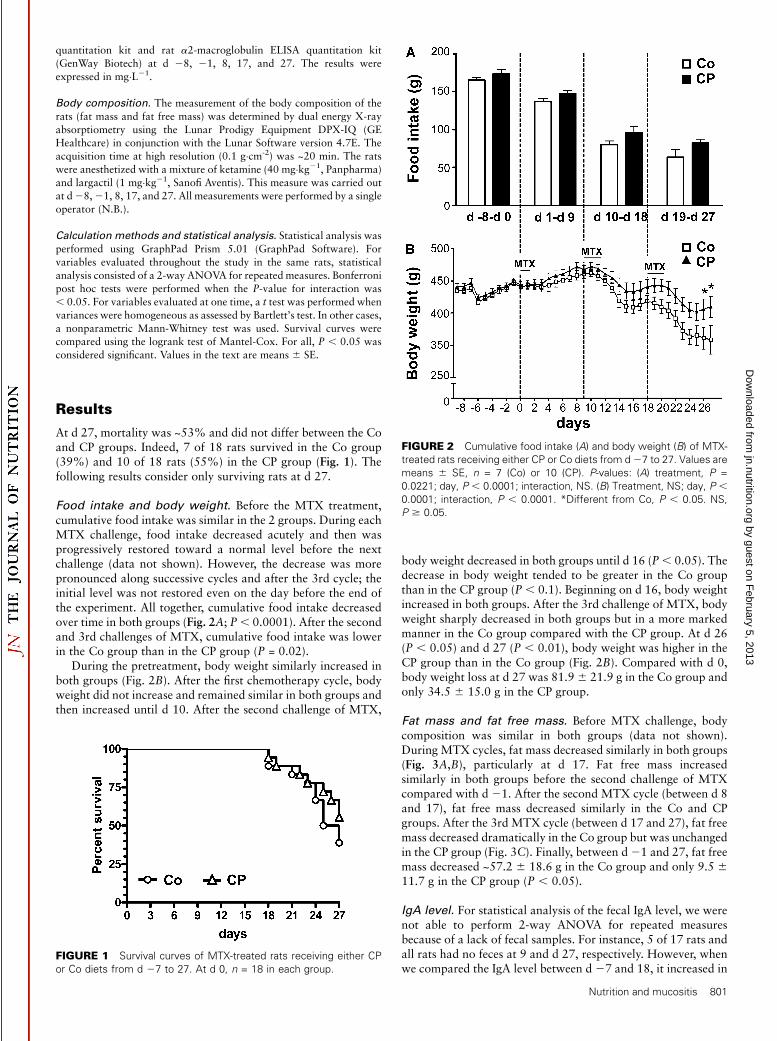
At d 27, mortality was ~53% and did not differ between the Coand CP groups. Indeed, 7 of 18 rats survived in the Co group(39%) and 10 of 18 rats (55%) in the CP group (Fig. 1). Thefollowing results consider only surviving rats at d 27.
Food intake and body weight. Before the MTX treatment,cumulative food intake was similar in the 2 groups. During eachMTX challenge, food intake decreased acutely and then wasprogressively restored toward a normal level before the nextchallenge (data not shown). However, the decrease was morepronounced along successive cycles and after the 3rd cycle; theinitial level was not restored even on the day before the end ofthe experiment. All together, cumulative food intake decreasedover time in both groups (Fig. 2A; P, 0.0001). After the secondand 3rd challenges of MTX, cumulative food intake was lowerin the Co group than in the CP group (P = 0.02).
During the pretreatment, body weight similarly increased inboth groups (Fig. 2B). After the first chemotherapy cycle, bodyweight did not increase and remained similar in both groups andthen increased until d 10. After the second challenge of MTX,
body weight decreased in both groups until d 16 (P, 0.05). Thedecrease in body weight tended to be greater in the Co groupthan in the CP group (P , 0.1). Beginning on d 16, body weightincreased in both groups. After the 3rd challenge of MTX, bodyweight sharply decreased in both groups but in a more markedmanner in the Co group compared with the CP group. At d 26(P , 0.05) and d 27 (P , 0.01), body weight was higher in theCP group than in the Co group (Fig. 2B). Compared with d 0,body weight loss at d 27 was 81.9 6 21.9 g in the Co group andonly 34.5 6 15.0 g in the CP group.
Fat mass and fat free mass. Before MTX challenge, bodycomposition was similar in both groups (data not shown).During MTX cycles, fat mass decreased similarly in both groups(Fig. 3A,B), particularly at d 17. Fat free mass increasedsimilarly in both groups before the second challenge of MTXcompared with d 21. After the second MTX cycle (between d 8and 17), fat free mass decreased similarly in the Co and CPgroups. After the 3rd MTX cycle (between d 17 and 27), fat freemass decreased dramatically in the Co group but was unchangedin the CP group (Fig. 3C). Finally, between d21 and 27, fat freemass decreased ~57.2 6 18.6 g in the Co group and only 9.5 611.7 g in the CP group (P , 0.05).
IgA level. For statistical analysis of the fecal IgA level, we werenot able to perform 2-way ANOVA for repeated measuresbecause of a lack of fecal samples. For instance, 5 of 17 rats andall rats had no feces at 9 and d 27, respectively. However, whenwe compared the IgA level between d 27 and 18, it increased in
FIGURE 1 Survival curves of MTX-treated rats receiving either CP
or Co diets from d 27 to 27. At d 0, n = 18 in each group.
FIGURE 2 Cumulative food intake (A) and body weight (B) of MTX-
treated rats receiving either CP or Co diets from d27 to 27. Values are
means 6 SE, n = 7 (Co) or 10 (CP). P-values: (A) treatment, P =
0.0221; day, P , 0.0001; interaction, NS. (B) Treatment, NS; day, P ,0.0001; interaction, P , 0.0001. *Different from Co, P , 0.05. NS,
P $ 0.05.
Nutrition and mucositis 801
by guest on February 5, 2013
jn.nutrition.orgD
ownloaded from
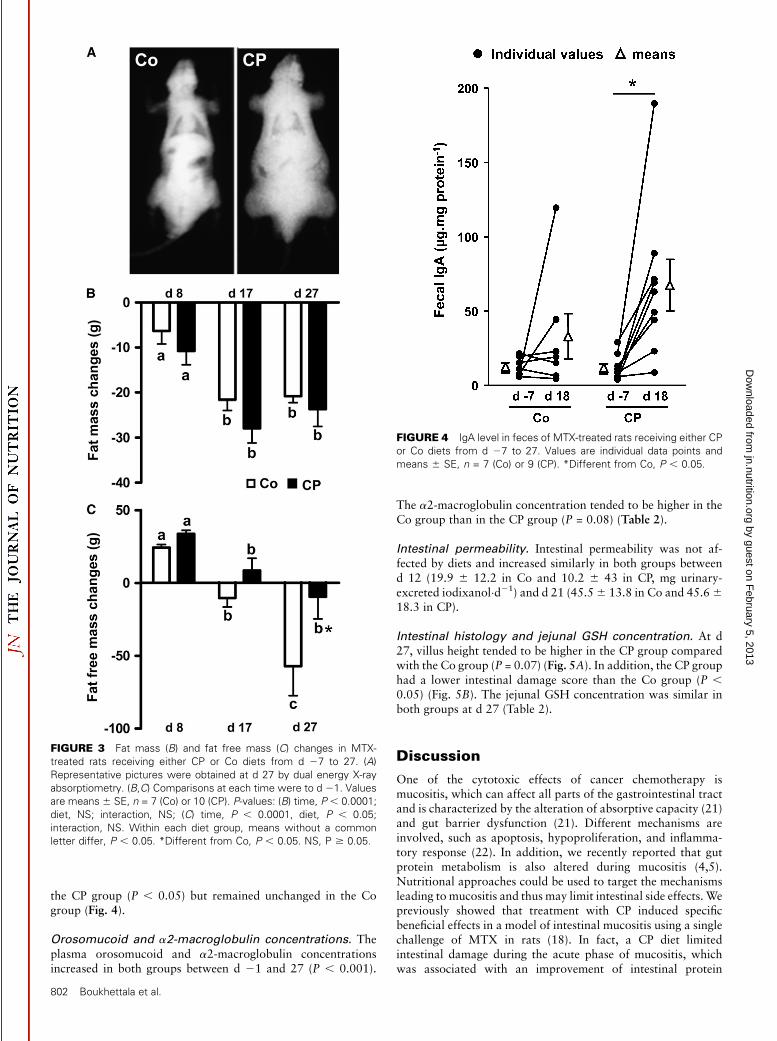
the CP group (P , 0.05) but remained unchanged in the Cogroup (Fig. 4).
Orosomucoid and a2-macroglobulin concentrations. Theplasma orosomucoid and a2-macroglobulin concentrationsincreased in both groups between d 21 and 27 (P , 0.001).
The a2-macroglobulin concentration tended to be higher in theCo group than in the CP group (P = 0.08) (Table 2).
Intestinal permeability. Intestinal permeability was not af-fected by diets and increased similarly in both groups betweend 12 (19.9 6 12.2 in Co and 10.2 6 43 in CP, mg urinary-excreted iodixanol×d21) and d 21 (45.56 13.8 in Co and 45.6618.3 in CP).
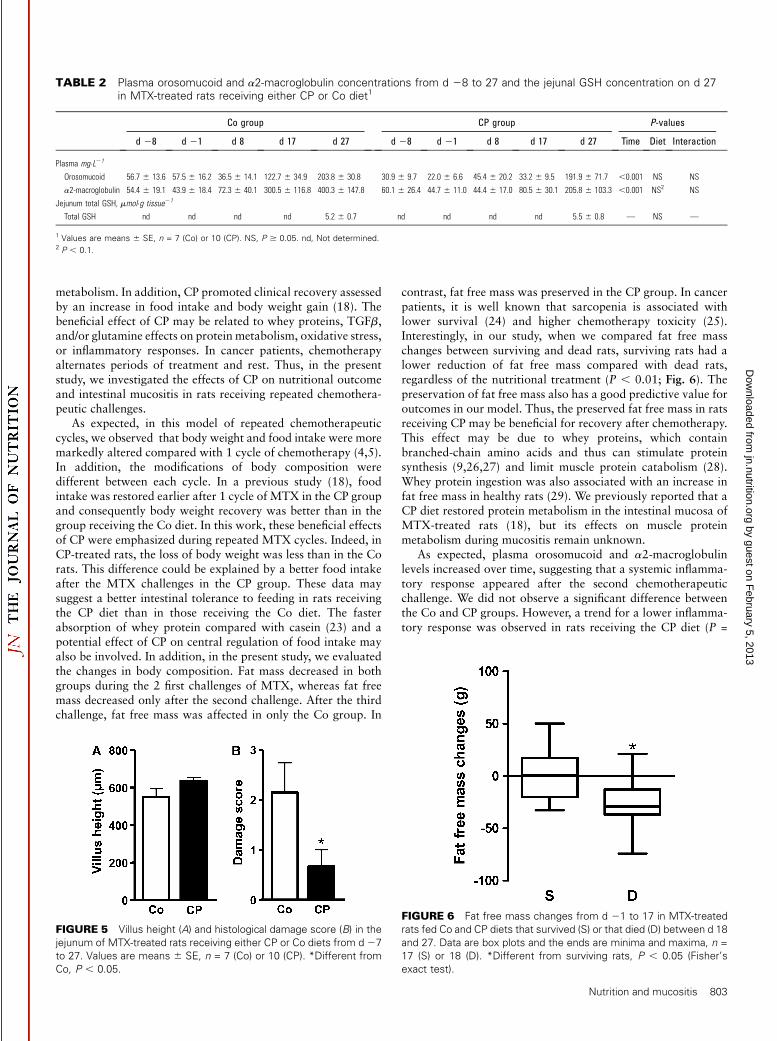
Intestinal histology and jejunal GSH concentration. At d27, villus height tended to be higher in the CP group comparedwith the Co group (P = 0.07) (Fig. 5A). In addition, the CP grouphad a lower intestinal damage score than the Co group (P ,0.05) (Fig. 5B). The jejunal GSH concentration was similar inboth groups at d 27 (Table 2).
Discussion
One of the cytotoxic effects of cancer chemotherapy ismucositis, which can affect all parts of the gastrointestinal tractand is characterized by the alteration of absorptive capacity (21)and gut barrier dysfunction (21). Different mechanisms areinvolved, such as apoptosis, hypoproliferation, and inflamma-tory response (22). In addition, we recently reported that gutprotein metabolism is also altered during mucositis (4,5).Nutritional approaches could be used to target the mechanismsleading to mucositis and thus may limit intestinal side effects.Wepreviously showed that treatment with CP induced specificbeneficial effects in a model of intestinal mucositis using a singlechallenge of MTX in rats (18). In fact, a CP diet limitedintestinal damage during the acute phase of mucositis, whichwas associated with an improvement of intestinal protein
FIGURE 3 Fat mass (B) and fat free mass (C) changes in MTX-
treated rats receiving either CP or Co diets from d 27 to 27. (A)
Representative pictures were obtained at d 27 by dual energy X-ray
absorptiometry. (B,C) Comparisons at each time were to d 21. Values
are means 6 SE, n = 7 (Co) or 10 (CP). P-values: (B) time, P , 0.0001;
diet, NS; interaction, NS; (C) time, P , 0.0001, diet, P , 0.05;
interaction, NS. Within each diet group, means without a common
letter differ, P , 0.05. *Different from Co, P , 0.05. NS, P $ 0.05.
FIGURE 4 IgA level in feces of MTX-treated rats receiving either CP
or Co diets from d 27 to 27. Values are individual data points and
means 6 SE, n = 7 (Co) or 9 (CP). *Different from Co, P , 0.05.
802 Boukhettala et al.
by guest on February 5, 2013
jn.nutrition.orgD
ownloaded from
metabolism. In addition, CP promoted clinical recovery assessedby an increase in food intake and body weight gain (18). Thebeneficial effect of CP may be related to whey proteins, TGFb,and/or glutamine effects on protein metabolism, oxidative stress,or inflammatory responses. In cancer patients, chemotherapyalternates periods of treatment and rest. Thus, in the presentstudy, we investigated the effects of CP on nutritional outcomeand intestinal mucositis in rats receiving repeated chemothera-peutic challenges.
As expected, in this model of repeated chemotherapeuticcycles, we observed that body weight and food intake were moremarkedly altered compared with 1 cycle of chemotherapy (4,5).In addition, the modifications of body composition weredifferent between each cycle. In a previous study (18), foodintake was restored earlier after 1 cycle of MTX in the CP groupand consequently body weight recovery was better than in thegroup receiving the Co diet. In this work, these beneficial effectsof CP were emphasized during repeated MTX cycles. Indeed, inCP-treated rats, the loss of body weight was less than in the Corats. This difference could be explained by a better food intakeafter the MTX challenges in the CP group. These data maysuggest a better intestinal tolerance to feeding in rats receivingthe CP diet than in those receiving the Co diet. The fasterabsorption of whey protein compared with casein (23) and apotential effect of CP on central regulation of food intake mayalso be involved. In addition, in the present study, we evaluatedthe changes in body composition. Fat mass decreased in bothgroups during the 2 first challenges of MTX, whereas fat freemass decreased only after the second challenge. After the thirdchallenge, fat free mass was affected in only the Co group. In
contrast, fat free mass was preserved in the CP group. In cancerpatients, it is well known that sarcopenia is associated withlower survival (24) and higher chemotherapy toxicity (25).Interestingly, in our study, when we compared fat free masschanges between surviving and dead rats, surviving rats had alower reduction of fat free mass compared with dead rats,regardless of the nutritional treatment (P , 0.01; Fig. 6). Thepreservation of fat free mass also has a good predictive value foroutcomes in our model. Thus, the preserved fat free mass in ratsreceiving CP may be beneficial for recovery after chemotherapy.This effect may be due to whey proteins, which containbranched-chain amino acids and thus can stimulate proteinsynthesis (9,26,27) and limit muscle protein catabolism (28).Whey protein ingestion was also associated with an increase infat free mass in healthy rats (29). We previously reported that aCP diet restored protein metabolism in the intestinal mucosa ofMTX-treated rats (18), but its effects on muscle proteinmetabolism during mucositis remain unknown.
As expected, plasma orosomucoid and a2-macroglobulinlevels increased over time, suggesting that a systemic inflamma-tory response appeared after the second chemotherapeuticchallenge. We did not observe a significant difference betweenthe Co and CP groups. However, a trend for a lower inflamma-tory response was observed in rats receiving the CP diet (P =
TABLE 2 Plasma orosomucoid and a2-macroglobulin concentrations from d 28 to 27 and the jejunal GSH concentration on d 27in MTX-treated rats receiving either CP or Co diet1
Co group CP group P-values
d 28 d 21 d 8 d 17 d 27 d 28 d 21 d 8 d 17 d 27 Time Diet Interaction
Plasma mg�L21
Orosomucoid 56.7 6 13.6 57.5 6 16.2 36.5 6 14.1 122.7 6 34.9 203.8 6 30.8 30.9 6 9.7 22.0 6 6.6 45.4 6 20.2 33.2 6 9.5 191.9 6 71.7 ,0.001 NS NS
a2-macroglobulin 54.4 6 19.1 43.9 6 18.4 72.3 6 40.1 300.5 6 116.8 400.3 6 147.8 60.1 6 26.4 44.7 6 11.0 44.4 6 17.0 80.5 6 30.1 205.8 6 103.3 ,0.001 NS2 NS
Jejunum total GSH, mmol�g tissue21
Total GSH nd nd nd nd 5.2 6 0.7 nd nd nd nd 5.5 6 0.8 — NS —
1 Values are means 6 SE, n = 7 (Co) or 10 (CP). NS, P $ 0.05. nd, Not determined.2 P , 0.1.
FIGURE 5 Villus height (A) and histological damage score (B) in the
jejunum of MTX-treated rats receiving either CP or Co diets from d 27
to 27. Values are means 6 SE, n = 7 (Co) or 10 (CP). *Different from
Co, P , 0.05.
FIGURE 6 Fat free mass changes from d 21 to 17 in MTX-treated
rats fed Co and CP diets that survived (S) or that died (D) between d 18
and 27. Data are box plots and the ends are minima and maxima, n =
17 (S) or 18 (D). *Different from surviving rats, P , 0.05 (Fisher’s
exact test).
Nutrition and mucositis 803
by guest on February 5, 2013
jn.nutrition.orgD
ownloaded from

0.08) that could be a consequence of an improved intestinalbarrier function. Intestinal permeability, which was evaluated byiodixanol urinary excretion as previously described (4), in-creased similarly over time in both groups. GSH plays a key rolein the antioxidant system. In the present study, the jejunal GSHconcentration was similar in the CP and Co groups. In ourprevious study, the GSH concentration increased during theacute phase of mucositis after a single MTX challenge in ratsreceiving CP but not during the recovery phase (18). In thepresent study, the GSH concentration was assessed at only therecovery phase. Thus, a potential benefit may have occurredearlier along each chemotherapy cycle and may have disap-peared 1 wk after the last MTX treatment.
We also evaluated the fecal IgA level. Secretory IgA plays amajor role in intestinal barrier function by surveillance ofcommensal bacteria and exclusion of pathogens. In addition,secretory IgA enhances innate immune defenses in the intestinalepithelium (30). In the CP group, the IgA level increased overtime, whereas it remained unchanged in the Co group. Thisdifference may contribute to enhancing intestinal defensesagainst pathogens and to limiting infections. Unfortunately, wewere not able to analyze IgA at d 27 because of a lack of feces.Thus, the benefit observed for the IgA level change ocurredbetween d 7 and 18. An extrapolation of the beneficial effects onother variables such as body weight change, body composition,and inflammation, which increased from one cycle to the next,suggests that the difference in the IgA level between the 2 groupscould be higher at d 27 and contributes to the overall protectiveeffect on the intestinal mucosa. Whey protein may be respon-sible for this increase in IgA because it contains Ig (31), but theCP diet also contained TGFb, which plays a pivotal role in thestimulation of IgA at mucosal sites (32). Indeed, Borsutzky et al.(32) showed that IgA production in intestinal mucosa was lowerin knockout mice for the receptor of TGFb (32). Glutamine mayalso enhance IgA production, as previously reported in paren-terally fed rats (33). Further studies are needed to evaluate whichnutrient contributed to the CP effects on the fecal IgA level.
We also observed that intestinal damage was lower in the CPgroup than in the Co group. Indeed, we observed a trend forhigher villus height but especially a strong decrease in damagescore in the CP group. We were not able to determine whichnutrient is responsible for these effects, but previous studiesreported beneficial effects of each active nutrient included in theCP diet. Indeed, whey proteins reduced MTX-induced damagein the small bowel (34) and improved gut permeability (35).Similarly, it was reported that TGFb reduced the severity of oralmucositis after 5-fluorouracil treatment in hamsters (36).Finally, several studies showed that glutamine improved intes-tinal damage during chemotherapy-induced mucositis (37–40).However, the present study is the first to our knowledge to showthat an integrated diet can improve intestinal damage aftersuccessive cycles of chemotherapeutic treatment and rest.
In conclusion, a specific diet containing whey proteins,glutamine, and TGFb has protective effects in rats receivingrepeated chemotherapeutic cycles by improving nutritionaloutcome and decreasing intestinal damage. Although we werenot able to determine in the present study which nutrients areresponsible for these effects, these observations should beconsolidated in a tumor-bearing model, and more importantly,in a clinical study in cancer patients.
AcknowledgmentsS.B., D.B., P.D., and M.C. designed research; N.B., A.I.,M.A., J.V., K-Y.S., and M.C. conducted research; N.B., D.B.,
and M.C. analyzed data; N.B. and M.C. performed statisticalanalysis; N.B., D.B., and M.C. wrote the paper; and M.C. hadprimary responsibility for final content. All authors read andapproved the final manuscript.
Literature Cited
1. Keefe DM. Intestinal mucositis: mechanisms and management. CurrOpin Oncol. 2007;19:323–7.
2. Gibson RJ, Bowen JM, Keefe DM. Technological advances in mucositisresearch: new insights and new issues. Cancer Treat Rev. 2008;34:476–82.
3. Logan RM, Stringer AM, Bowen JM, Yeoh AS, Gibson RJ, Sonis ST,Keefe DM. The role of pro-inflammatory cytokines in cancer treatment-induced alimentary tract mucositis: pathobiology, animal models andcytotoxic drugs. Cancer Treat Rev. 2007;33:448–60.
4. Leblond J, Le Pessot F, Hubert-Buron A, Duclos C, Vuichoud J, FaureM, Breuille D, Dechelotte P, Coeffier M. Chemotherapy-inducedmucositis is associated with changes in proteolytic pathways. Exp BiolMed (Maywood). 2008;233:219–28.
5. Boukhettala N, Leblond J, Claeyssens S, Faure M, Le Pessot F, Bole-Feysot C, Hassan A, Mettraux C, Vuichoud J, et al. Methotrexateinduces intestinal mucositis and alters gut protein metabolism indepen-dently of reduced food intake. Am J Physiol Endocrinol Metab.2009;296:E182–90.
6. McIntosh GH. Colon cancer: dietary modifications required for abalanced protective diet. Prev Med. 1993;22:767–74.
7. McIntosh GH, Regester GO, Le Leu RK, Royle PJ, Smithers GW. Dairyproteins protect against dimethylhydrazine-induced intestinal cancers inrats. J Nutr. 1995;125:809–16.
8. Meister A. Glutathione, ascorbate, and cellular protection. Cancer Res.1994;54:s1969–75.
9. Dardevet D, Sornet C, Balage M, Grizard J. Stimulation of in vitro ratmuscle protein synthesis by leucine decreases with age. J Nutr. 2000;130:2630–5.
10. Lacey JM, Wilmore DW. Is glutamine a conditionally essential aminoacid? Nutr Rev. 1990;48:297–309.
11. Klimberg VS, Souba WW, Salloum RM, Plumley DA, Cohen FS, DolsonDJ, Bland KI, Copeland EM III. Glutamine-enriched diets supportmuscle glutamine metabolism without stimulating tumor growth. J SurgRes. 1990;48:319–23.
12. Sido B, Seel C, Hochlehnert A, Breitkreutz R, Droge W. Low intestinalglutamine level and low glutaminase activity in Crohn’s disease: arational for glutamine supplementation? Dig Dis Sci. 2006;51:2170–9.
13. van der Hulst RR, van Kreel BK, von Meyenfeldt MF, Brummer RJ,Arends JW, Deutz NE, Soeters PB. Glutamine and the preservation ofgut integrity. Lancet. 1993;341:1363–5.
14. Coeffier M, Dechelotte P. The role of glutamine in intensive care unitpatients: mechanisms of action and clinical outcome. Nutr Rev.2005;63:65–9.
15. Cross D, Cambier JC. Transforming growth factor beta 1 has differ-ential effects on B cell proliferation and activation antigen expression.J Immunol. 1990;144:432–9.
16. Dignass AU, Podolsky DK. Cytokine modulation of intestinal epithelialcell restitution: central role of transforming growth factor beta.Gastroenterology. 1993;105:1323–32.
17. McKaig BC, Makh SS, Hawkey CJ, Podolsky DK, Mahida YR. Normalhuman colonic subepithelial myofibroblasts enhance epithelial migra-tion (restitution) via TGF-beta3. Am J Physiol. 1999;276:G1087–93.
18. Boukhettala N, Ibrahim A, Claeyssens S, Faure M, Le Pessot F,Vuichoud J, Lavoinne A, Breuille D, Dechelotte P, et al. A dietcontaining whey protein, glutamine and TGFb modulates gut proteinmetabolism during chemotherapy-induced mucositis in rats. Dig Dis Sci.Epub 2009 Nov 13.
19. Baker MA, Cerniglia GJ, Zaman A. Microtiter plate assay for themeasurement of glutathione and glutathione disulfide in large numbersof biological samples. Anal Biochem. 1990;190:360–5.
20. Kerr SW, Wolyniec WW, Filipovic Z, Nodop SG, Braza F, Winquist RJ,Noonan TC. Repeated measurement of intestinal permeability as anassessment of colitis severity in HLA-B27 transgenic rats. J PharmacolExp Ther. 1999;291:903–10.
21. Carneiro-Filho BA, Lima IP, Araujo DH, Cavalcante MC, CarvalhoGH, Brito GA, Lima V, Monteiro SM, Santos FN, et al. Intestinal
804 Boukhettala et al.
by guest on February 5, 2013
jn.nutrition.orgD
ownloaded from

barrier function and secretion in methotrexate-induced rat intestinalmucositis. Dig Dis Sci. 2004;49:65–72.
22. Logan RM, Stringer AM, Bowen JM, Gibson RJ, Sonis ST, Keefe DM. Isthe pathobiology of chemotherapy-induced alimentary tract mucositisinfluenced by the type of mucotoxic drug administered? CancerChemother Pharmacol. 2009;63:239–51.
23. Beaufrere B, Dangin M, Boirie Y. The ’fast’ and ’slow’ protein concept.Nestle Nutr Workshop Ser Clin Perform Programme. 2000;3:121–31,discussion 31–3.
24. Prado CM, Lieffers JR, McCargar LJ, Reiman T, Sawyer MB, Martin L,Baracos VE. Prevalence and clinical implications of sarcopenic obesityin patients with solid tumours of the respiratory and gastrointestinaltracts: a population-based study. Lancet Oncol. 2008;9:629–35.
25. Prado CM, Baracos VE, McCargar LJ, Reiman T, Mourtzakis M,Tonkin K, Mackey JR, Koski S, Pituskin E, et al. Sarcopenia as adeterminant of chemotherapy toxicity and time to tumor progression inmetastatic breast cancer patients receiving capecitabine treatment. ClinCancer Res. 2009;15:2920–6.
26. Rieu I, Balage M, Sornet C, Debras E, Ripes S, Rochon-Bonhomme C,Pouyet C, Grizard J, Dardevet D. Increased availability of leucine withleucine-rich whey proteins improves postprandial muscle proteinsynthesis in aging rats. Nutrition. 2007;23:323–31.
27. Hayes A, Cribb PJ. Effect of whey protein isolate on strength, bodycomposition and muscle hypertrophy during resistance training. CurrOpin Clin Nutr Metab Care. 2008;11:40–4.
28. Combaret L, Dardevet D, Rieu I, Pouch MN, Bechet D, Taillandier D,Grizard J, Attaix D. A leucine-supplemented diet restores the defectivepostprandial inhibition of proteasome-dependent proteolysis in aged ratskeletal muscle. J Physiol. 2005;569:489–99.
29. Siddiqui SM, Chang E, Li J, Burlage C, Zou M, Buhman KK, Koser S,Donkin SS, Teegarden D. Dietary intervention with vitamin D, calcium,and whey protein reduced fat mass and increased lean mass in rats. NutrRes. 2008;28:783–90.
30. Corthesy B. Roundtrip ticket for secretory IgA: role in mucosalhomeostasis? J Immunol. 2007;178:27–32.
31. Marshall K. Therapeutic applications of whey protein. Altern Med Rev.2004;9:136–56.
32. Borsutzky S, Cazac BB, Roes J, Guzman CA. TGF-beta receptorsignaling is critical for mucosal IgA responses. J Immunol. 2004;173:3305–9.
33. Kudsk KA. Current aspects of mucosal immunology and its influence bynutrition. Am J Surg. 2002;183:390–8.
34. Howarth GS, Francis GL, Cool JC, Xu X, Byard RW, Read LC. Milkgrowth factors enriched from cheese whey ameliorate intestinal damageby methotrexate when administered orally to rats. J Nutr. 1996;126:2519–30.
35. Tran CD, Howarth GS, Coyle P, Philcox JC, Rofe AM, Butler RN.Dietary supplementation with zinc and a growth factor extract derivedfrom bovine cheese whey improves methotrexate-damaged rat intestine.Am J Clin Nutr. 2003;77:1296–303.
36. Sonis S, Koplowsky A, Mitus J, Rosenthal D, Brand M. Relationship ofchemotherapy-induced mucositis and myelosuppression in hamsters.Eur J Cancer B Oral Oncol. 1992;28B:43.
37. Rubio IT, Cao Y, Hutchins LF, Westbrook KC, Klimberg VS. Effect ofglutamine on methotrexate efficacy and toxicity. Ann Surg. 1998;227:772–8, discussion 8–80.
38. Fox AD, Kripke SA, De Paula J, Berman JM, Settle RG, Rombeau JL.Effect of a glutamine-supplemented enteral diet on methotrexate-induced enterocolitis. JPEN J Parenter Enteral Nutr. 1988;12:325–31.
39. Amara S. Oral glutamine for the prevention of chemotherapy-inducedperipheral neuropathy. Ann Pharmacother. 2008;42:1481–5.
40. Sukhotnik I, Mogilner JG, Karry R, Shamian B, Lurie M, KokhanovskyN, Ure BM, Coran AG. Effect of oral glutamine on enterocyte turnoverduring methotrexate-induced mucositis in rats. Digestion. 2009;79:5–13.
Nutrition and mucositis 805
by guest on February 5, 2013
jn.nutrition.orgD
ownloaded from




















