
A better understanding of urogenital tuberculosis pathophysiology based on radiological findings
12
European Journal of Radiology 76 (2010) 246–257 Contents lists available at ScienceDirect European Journal of Radiology journal homepage: www.elsevier.com/locate/ejrad A better understanding of urogenital tuberculosis pathophysiology based on radiological findings Andre A. Figueiredo a,b,∗ , Antônio M. Lucon b , André N. Arvellos a , Cláudio O.P. Ramos a , Antonio C.T. Toledo a , Renato Falci Jr. b , Cristiano M. Gomes b , Fernando E.Q. Recaverren a , José Murillo B. Netto a , Miguel Srougi b a Department of Morphology and Division of Urology, Federal University of Juiz de Fora, Minas Gerais, Brazil b Division of Urology, Medical School, University of Sao Paulo, Sao Paulo, Brazil article info Article history: Received 12 January 2009 Received in revised form 28 March 2009 Accepted 25 May 2009 Keywords: Bladder tuberculosis Renal tuberculosis Urogenital tuberculosis abstract Purpose: To assess the radiological findings of urogenital tuberculosis (UGT) in patients at different disease stages, for a better understanding of its pathophysiology. Patients and methods: We retrospectively reviewed the radiological exams of 20 men (median age 41 years; range: 28–65) with urogenital tuberculosis diagnosis. The patients were classified in the following groups: (1) bilateral renal tuberculosis with predominantly parenchymatous involvement; (2) unilat- eral renal tuberculosis; (3) unilateral renal tuberculosis with bladder tuberculosis and (4) bilateral renal tuberculosis with bladder tuberculosis. Results: One AIDS patient had multiple bilateral renal tuberculosis abscesses (group 1). Six patients had unilateral renal tuberculosis with hydronephrosis due to stenosis and thickening of the collecting system, without involvement of the bladder or contralateral kidney (group 2). Six patients had bladder tubercu- losis with diffuse thickening of the bladder wall, with one very low or no function kidney while the other kidney was normal (group 3). Seven patients had bladder tuberculosis associated to a very low or no function kidney with the other kidney with high-grade vesicoureteral reflux-associated uretero- hydronephrosis (group 4). In two patients, sequential exams showed evolution of tuberculosis from a unilateral renal and ureteral lesion to contracted bladder and dilatation of the contralateral kidney secondary to high-grade reflux. Conclusions: UGT may have variable radiological presentations. However, in two of our cases we have seen that tuberculosis involvement of the urinary tract may be sequential. Further evidences are necessary to confirm this hypothesis. © 2009 Elsevier Ireland Ltd. All rights reserved. 1. Introduction Tuberculosis is still the main cause of death among the infectious diseases, with estimates pointing to 30% of the world popula- tion (1.7 billion people) harboring Mycobacterium tuberculosis [1]. Although 90–95% of the new cases of tuberculosis occur in devel- oping countries, the association with AIDS has made tuberculosis a global concern [2,3]. AIDS is now the main risk factor for tuberculo- sis development, being the main cause of the disease recrudescence observed in the past three decades [2]. Therefore, tuberculosis is a global public health concern. ∗ Corresponding author at: Rua Irineu Marinho 365, apto 801 – bloco 3, Bom Pastor – Juiz de Fora, MG, CEP: 36021-580, Brazil. Tel.: +55 32 32415370; fax: +55 11 32876922. E-mail address: [email protected] (A.A. Figueiredo). Urogenital tuberculosis (UGT) is the second most common extra- pulmonary presentation of tuberculosis, affecting 8–15% of the patients with pulmonary tuberculosis [4]. From the lungs, the kid- neys are affected through hematogenic dissemination, with subse- quent involvement of the ureters and bladder through descending infection of the collecting system. The genital organs are involved through hematogenic (prostate and epydidimus) or retrograde canalicular dissemination [1,4]. UGT affects all age ranges, but pre- dominates in men in their fourth or fifth decades. Diagnosis is gen- erally delayed, chiefly in developing countries, because of the insid- ious evolution with symptom paucity and inespecificity, along with a lack of physicians’ awareness [5,6]. UGT therefore may become a serious disease leading to end-stage chronic renal failure [4]. In 10% of the cases, a presumptive diagnosis is made based on suggestive clinical, laboratory and radiological data, without micro- biological or histological confirmation [5,7–9]. Imaging exams are around 90% sensitive for UGT diagnosis, with intravenous urog- raphy (IU) and abdominal and pelvic computerized tomography 0720-048X/$ – see front matter © 2009 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ejrad.2009.05.049
Transcript of A better understanding of urogenital tuberculosis pathophysiology based on radiological findings

Ar
AAJa
b
a
ARRA
KBRU
1
dtAogsog
–f
0d
European Journal of Radiology 76 (2010) 246–257
Contents lists available at ScienceDirect
European Journal of Radiology
journa l homepage: www.e lsev ier .com/ locate /e j rad
better understanding of urogenital tuberculosis pathophysiology based onadiological findings
ndre A. Figueiredo a,b,∗, Antônio M. Lucon b, André N. Arvellos a, Cláudio O.P. Ramos a,ntonio C.T. Toledo a, Renato Falci Jr. b, Cristiano M. Gomes b, Fernando E.Q. Recaverren a,
osé Murillo B. Netto a, Miguel Srougi b
Department of Morphology and Division of Urology, Federal University of Juiz de Fora, Minas Gerais, BrazilDivision of Urology, Medical School, University of Sao Paulo, Sao Paulo, Brazil
r t i c l e i n f o
rticle history:eceived 12 January 2009eceived in revised form 28 March 2009ccepted 25 May 2009
eywords:ladder tuberculosisenal tuberculosisrogenital tuberculosis
a b s t r a c t
Purpose: To assess the radiological findings of urogenital tuberculosis (UGT) in patients at different diseasestages, for a better understanding of its pathophysiology.Patients and methods: We retrospectively reviewed the radiological exams of 20 men (median age 41years; range: 28–65) with urogenital tuberculosis diagnosis. The patients were classified in the followinggroups: (1) bilateral renal tuberculosis with predominantly parenchymatous involvement; (2) unilat-eral renal tuberculosis; (3) unilateral renal tuberculosis with bladder tuberculosis and (4) bilateral renaltuberculosis with bladder tuberculosis.Results: One AIDS patient had multiple bilateral renal tuberculosis abscesses (group 1). Six patients hadunilateral renal tuberculosis with hydronephrosis due to stenosis and thickening of the collecting system,without involvement of the bladder or contralateral kidney (group 2). Six patients had bladder tubercu-losis with diffuse thickening of the bladder wall, with one very low or no function kidney while theother kidney was normal (group 3). Seven patients had bladder tuberculosis associated to a very low
or no function kidney with the other kidney with high-grade vesicoureteral reflux-associated uretero-hydronephrosis (group 4). In two patients, sequential exams showed evolution of tuberculosis froma unilateral renal and ureteral lesion to contracted bladder and dilatation of the contralateral kidneysecondary to high-grade reflux.Conclusions: UGT may have variable radiological presentations. However, in two of our cases we have seenthat tuberculosis involvement of the urinary tract may be sequential. Further evidences are necessary to confirm this hypothesis.. Introduction
Tuberculosis is still the main cause of death among the infectiousiseases, with estimates pointing to 30% of the world popula-ion (1.7 billion people) harboring Mycobacterium tuberculosis [1].lthough 90–95% of the new cases of tuberculosis occur in devel-ping countries, the association with AIDS has made tuberculosis alobal concern [2,3]. AIDS is now the main risk factor for tuberculo-
is development, being the main cause of the disease recrudescencebserved in the past three decades [2]. Therefore, tuberculosis is alobal public health concern.∗ Corresponding author at: Rua Irineu Marinho 365, apto 801 – bloco 3, Bom PastorJuiz de Fora, MG, CEP: 36021-580, Brazil. Tel.: +55 32 32415370;
ax: +55 11 32876922.E-mail address: [email protected] (A.A. Figueiredo).
720-048X/$ – see front matter © 2009 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.ejrad.2009.05.049
© 2009 Elsevier Ireland Ltd. All rights reserved.
Urogenital tuberculosis (UGT) is the second most common extra-pulmonary presentation of tuberculosis, affecting 8–15% of thepatients with pulmonary tuberculosis [4]. From the lungs, the kid-neys are affected through hematogenic dissemination, with subse-quent involvement of the ureters and bladder through descendinginfection of the collecting system. The genital organs are involvedthrough hematogenic (prostate and epydidimus) or retrogradecanalicular dissemination [1,4]. UGT affects all age ranges, but pre-dominates in men in their fourth or fifth decades. Diagnosis is gen-erally delayed, chiefly in developing countries, because of the insid-ious evolution with symptom paucity and inespecificity, along witha lack of physicians’ awareness [5,6]. UGT therefore may become aserious disease leading to end-stage chronic renal failure [4].
In 10% of the cases, a presumptive diagnosis is made based onsuggestive clinical, laboratory and radiological data, without micro-biological or histological confirmation [5,7–9]. Imaging exams arearound 90% sensitive for UGT diagnosis, with intravenous urog-raphy (IU) and abdominal and pelvic computerized tomography

ournal
(iaotanskUaacobtfhtoIactc
pp
2
p4tot(rageopbr
Fp(
A.A. Figueiredo et al. / European J
CT) being more used [10]. Typical radiological findings include:rregularity of the caliceal outline (earliest finding); renal mass;utonephrectomy; thickening of the collecting system; calcificationf the urinary tract; stenosis-related dilatation of the collecting sys-em with caliectasis, hydronephrosis or hydroureter; parenchymatrophy and involvement of extraurinary organs such as lymphodes, spleen, liver and vertebrae [10–12]. The findings of multipletenoses of the collecting system or simultaneous involvement ofidneys and bladder are highly suggestive of tuberculosis [10–12].ltrasonography is useful in showing the dilated calyces and antrophic kidney but it has less sensitivity and specificity than IUnd CT in the evaluation of kidney tuberculosis [3]. In most UGTases (70–85%) there is unilateral renal involvement with devel-pment of the changes described above. The pathophysiology ofilateral renal tuberculosis has not been completely understoodhrough [13,14]. Likewise, precise knowledge of disease evolutionrom the initial lesions to the most severe ones is still lacking. Itas recently been postulated, based on analyses of 25 patients withuberculosis-related contracted bladder, that the disease begins inne kidney and progresses to the ipsilateral ureter and bladder.
nvolvement of the contralateral kidney occurs through retrogradescending dissemination secondary to contracted bladder and vesi-oureteral reflux [15]. This concept changes our understanding ofhe disease pathophysiology and management of more advancedases.
This study aims to assess the radiological findings of UGTatients at different disease stages so as to better understand itsathophysiology.
. Patients and methods
Radiological exams of 20 men diagnosed with UGT during theeriod 1989–2008 were retrospectively analyzed. Median age was1 years (range: 28–65). UGT was diagnosed through identifica-ion of Mycobacterium tuberculosis in the urine or histopathologyf resected organs. The patients were investigated with urinaryract ultrasonography (n = 1); abdominal and pelvic CT (n = 6); IUn = 12); urethrocystography (n = 7); abdominal MRI (n = 1) andetrograde pyelography (n = 1). The exams were independentlynalyzed by four physicians: two urologists and two radiolo-ists. The following findings were characterized: functional renal
xclusion; renal parenchyma atrophy; stenosis-related dilatationf the collecting system; thickening of the collecting system wall;redominantly parenchymatous renal involvement; unilateral orilateral renal tuberculosis; contracted bladder and vesicoureteraleflux.ig. 1. Post-contrast phase of abdominal CT in an AIDS patient. (A) Caliceal dilatationarenchyma (arrow). (B) Bilateral renal abscesses and dilatation of the pyelocaliceal sysarrow).
of Radiology 76 (2010) 246–257 247
The patients were classified, according to the radiographic pre-sentation, in the following groups: (1) bilateral renal tuberculosiswith predominantly parenchymatous involvement; (2) unilateralrenal tuberculosis; (3) unilateral renal tuberculosis with bladdertuberculosis and (4) bilateral renal tuberculosis with bladder tuber-culosis. There were sequential exams for three patients, whichallowed for the characterization of the radiological progress of UGTto be made, once none of them had undergone any urological inter-vention.
3. Results
3.1. Bilateral renal tuberculosis with predominantlyparenchymatous involvement
One AIDS patient with a history of fever, bilateral back painand storage symptoms had multiple bilateral renal abscesses withdilatation of the collecting system, atrophy of the renal parenchyma(right upper pole) and retroperitoneal lymph node enlargementwith central necrosis (Fig. 1).
3.2. Unilateral renal tuberculosis
Six patients had unilateral renal involvement without any radio-graphic changes to the bladder or contralateral kidney. Four patientshad a kidney with low or no function, with caliceal dilatationand parenchyma thinning (Fig. 2). In these cases there was norenal pelvis dilatation due to stenosis or contraction. In the othertwo cases, the kidney with tuberculosis had preserved function.In one of them, careful retrospective analysis of the initial IU andCT showed hardening and rectification of the left ureter (Fig. 3A)and thickening of the left renal pelvis and ureter (Fig. 3B and C),respectively. After 8 months, retrograde pyelography showed dis-ease progression with the development of multiple ureteral andintrarenal stenoses, with asymmetric diffuse caliceal dilatation(Fig. 3D and E). In the other patient, initial IU showed diffuse calicealdilatation, mildly dilated renal pelvis and areas of ureteral stenosis(Fig. 4A and B). In a 4-month follow-up exam, there was functionalloss of the upper renal pole, despite the placement of a double Jcatheter and pharmacological treatment (Fig. 4C).
In all these cases, in spite of the absence of radiographic bladderchanges, the patients reported a predominance of storage symp-toms and hematuria.
3.3. Unilateral renal tuberculosis with bladder tuberculosis
In six cases there was bladder tuberculosis with diffuse thick-ening of the bladder walls and reduction of bladder capacity
of the right upper pole, leading to parenchyma atrophy. Abscess in the left renaltem on the right. Retroperitoneal lymph node enlargement with central necrosis

248 A.A. Figueiredo et al. / European Journal of Radiology 76 (2010) 246–257
F nal tubr
aituissn
ig. 2. MRI (A), CT (B and C) and ultrasonography (D) of patients with unilateral reenal parenchyma. There is no dilatation of the renal pelvis.
ssociated to one kidney with low or no function and a radiograph-cally normal contralateral kidney (Figs. 5 and 6). In these cases,he non-functional kidneys had the same findings described for
nilateral tuberculosis, with asymmetric dilatation of the collect-ng system, parenchyma thinning and thickening of the collectingystem on IU and CT (Fig. 5A–C). In these cases, cystographyhowed no or low-grade vesicoureteral reflux to the functional kid-ey.
erculosis, with dilatation of the collecting system (caliectasis) and thinning of the
3.4. Bilateral renal tuberculosis with bladder tuberculosis
In seven cases (Figs. 7–13) bladder tuberculosis with diffuse
thickening of the bladder walls and reduction of bladder capac-ity was associated to a very low or no function kidney withureterohydronephrosis of the contralateral kidney. In all thesecases there was high-grade vesicoureteral reflux to the func-tional kidney. In one of the cases (Fig. 9A and B), CT showed
A.A. Figueiredo et al. / European Journal of Radiology 76 (2010) 246–257 249
Fig. 3. Sequential exams of a patient with unilateral renal tuberculosis. (A) IU with rectification and hardening of the left ureter (retrospective diagnosis) (arrow). (B and C)C gradea
ut(usla(
l
T revealing thickening of the left renal pelvis and ureter (arrows). (D and E) Retrond intrarenal stenoses, with asymmetric diffuse caliectasis.
reterohydronephrosis without thickening of the collecting sys-em or parenchyma changes, suggesting a dilatation mechanismsecondary to reflux) different from that found in the cases ofnilateral tuberculosis described above, in which there was steno-is of the collecting system. In this case, cystography showed
eft high-grade reflux and, apparently, some degree of associ-ted distal ureteral stenosis, once the reflux was not massiveFig. 9D).In two cases there were sequential exams showing the evo-ution of UGT without surgical or pharmacological intervention
pyelography after 8 months, showing infection progression with multiple ureteral
(Figs. 12 and 13). One patient had a non-functional right kid-ney with normal bladder and left kidney on initial IU (Fig. 12A).After a 10-month follow-up period, a new IU showed contractedbladder and the development of left ureterohydronephrosis sec-ondary to high-grade vesicoureteral reflux (Fig. 12B and C). In
another case, there was stenosis of the middle ureter and intrarenalcollecting system, with asymmetric caliectasis on the left, nor-mal bladder and right kidney and no vesicoureteral reflux oninitial evaluation (Fig. 13A and B). After a 6-month follow-upperiod, without any surgical intervention, the left kidney was
250 A.A. Figueiredo et al. / European Journal of Radiology 76 (2010) 246–257
F elay oc te steo h the
nwrr
cu
4
itca
rpaccoaabsm
ig. 4. Sequential exams of a patient with unilateral renal tuberculosis. (A) IU with daliceal system on the left (slight dilatation of the renal pelvis) and extensive discref the renal upper pole and smaller caliectasis in the middle and inferior thirds, wit
on-functional and there was ureterohydronephrosis on the right,ith contracted bladder and grade IV vesicoureteral reflux on the
ight. In both cases the ureterohydronephrosis was secondary toeflux.
In two cases there was prostate tuberculosis associated withontracted bladder with dilatation and irregularity of the prostaticrethra, suggesting autoprostatectomy (Figs. 6B and 9D).
. Discussion
Because it can potentially involve all urogenital organs, the clin-cal and radiological presentation of UGT is polymorphic [4]. Yethis study characterized and classified the most frequent radiologi-al presentations, as well as the natural disease evolution, providingbetter understanding of the pathophysiology.
Starting with primary pulmonary tuberculosis, bacillemia isesponsible for bacillus implant in parenchymatous organs, withossible colonization of the kidneys and prostate. Renal lesionsre then initially bilateral, cortical, glomerular and pericapillary,haracterizing the hematogenous dissemination and being con-omitant with other hematogenic foci in the prostate and otherrgans outside the urogenital system [16]. This phase is usu-
lly asymptomatic, with focus cicatrization and the beginning oflatent period. If any immunological deficiency arises duringacillemia, miliary tuberculosis with systemic symptoms and dis-eminated tuberculosis may supervene [1]. In these cases, UGTay present with either multiple image-silent renal granulo-
f contrast elimination on the left and diffuse caliectasis. (B) IU with dilatation of thenoses of the ipsilateral ureter (arrows). (C) IU after 4 months, with loss of functiondouble J.
mata, only detected through histology, or the development ofmultiple abscess-like renal parenchymatous lesions [17]. Actually,25–62% of the patients with miliary tuberculosis have multiplebilateral renal lesions [16], as happened with our AIDS patient(Fig. 1).
The mean latent period between pulmonary infection and clin-ical UGT is 22 years (range: 1–46), occurring when immunity fallsand granulomata reactivate [13]. Infection reactivation and progres-sion occur from a single focus and in one kidney, with preservationof the contralateral one, accounting for the higher frequency ofunilateral renal tuberculosis [13,14]. This was demonstrated byBarrie et al. [18], who studied 61 kidneys that had been resectedbecause of tuberculosis. These authors demonstrated retraction ofthe collecting system towards a renal pole, the site of the infectionrecrudescence. From the single reactivated granuloma, the pro-cess reaches the papilla and produces bacilluria, with subsequentinfundibular stenosis and stenosis progression to the renal pelvis,ureter and bladder [18]. Descending infection occurs after contigu-ity involvement of the collecting system and consequent bacilluria[16]. Yet this descending spread may occur intramurally (proba-bly through the lymphatics), according to experimental data byWinblad and Duchek [19], who innoculated the bacillus in the kid-neys of pigs and demonstrated the presence of ureteral tuberculosis
even with complete ureteral occlusion. In one of our cases, thicken-ing of the collecting system antedated the occurrence of multiplestenoses, strengthening the hypothesis of intramural spread of theinfection (Fig. 3). Renal tuberculosis has a slow oligosymptomaticprogression, with frequent unilateral functional exclusion on diag-
A.A. Figueiredo et al. / European Journal of Radiology 76 (2010) 246–257 251
Fig. 5. Patient with unilateral renal tuberculosis and contracted bladder: CT showing: (A) middle third of the right kidney with caliectasis and thinning of the renal parenchyma.( ter (art chyma
nb[srtof[
emgrqrtttiNttt
B and C) Parietal thickening of the renal pelvis (arrow) and middle third of the urehe lower pole. Left kidney with preservation of the pyelocaliceal system and paren
osis, chiefly due to obstruction of the collecting system, which maye distal with ureteral stenosis or proximal with intrarenal stenoses20]. In our cases of unilateral tuberculosis there was hydronephro-is due to obstruction of the collecting system and leading to loss ofenal function. In ureteral tuberculosis there are multiple stenoseshroughout the ureter, as found in this study, with a predominancef naturally narrowed sites such as the vesicoureteral junctionollowed by the ureteropyelic junction and the middle ureter21].
In bladder tuberculosis there is acute inflammation with hyper-mia, ulceration and tubercle formation around the ureteraleatus, with subsequent fibrosis of the bladder wall [15]. Pro-
ression of the bladder infection leads to capacity and complianceeduction, with the development of contracted bladder and subse-uent distortion of the ureterovesical junction and vesicoureteraleflux, the latter more commonly to the functional kidney, oncehe ureter primarily affected by tuberculosis develops stenosishat blocks reflux. Reflux to the still functional kidney allowshe collecting system to amplify the contracted bladder capac-
ty with ascending transmission of the intravesical pressure.on-identified and non-treated reflux may damage the kidneyhrough infection or transmission of intravesical pressure, withhe potential to lead to end-stage renal failure [15]. Patients withuberculosis-related renal failure had unilateral reflux, stressing
row). (D) IU showing functional exclusion of the right upper pole and caliectasis of. Bladder volume severely reduced.
the hypothesis of loss of function of one of the kidneys due toreflux and not tuberculosis itself [15]. In two of our cases wecould follow the UGT evolution with unilateral renal and ureterallesion, with progression to contracted bladder and dilatation ofthe contralateral kidney secondary to vesicoureteral reflux. Inthese kidneys, there were no typical tuberculosis lesions such asureteral or intrarenal stenosis, strenghtening the idea that thecause of damage would be reflux nephropathy and not tubercu-losis itself, i.e., damage was caused by the retrograde ascendingway.
In the literature reports of UGT case series, unilateral involve-ment is the most common form, with function preservation onearly diagnosis and with autonephrectomy in more advanced cases,but always with hydronephrosis, thickening and stenosis of thecollecting system [3–5,7–9,11–15]. Although less frequent, bilat-eral renal tuberculosis can occur in up to 30% of he cases, andthis study may contribute to the understanding of such cases[17].
There are three ways through which bilateral renal tuberculosis
can occur:(1) Exacerbation of the hematogenic dissemination period, withmultiple bilateral predominantly parenchymatous foci, some-thing observed in immunodeficient patients with miliary

252 A.A. Figueiredo et al. / European Journal of Radiology 76 (2010) 246–257
Fig. 6. Patients with unilateral renal tuberculosis and contracted bladder with normal contralateral kidney. (A) IU showing a non-functional left kidney and contractedbladder, with dilatation of the right distal ureter due to vesicoureteral reflux. (B) Voiding urethrocystography showing contracted bladder, no vesicoureteral reflux andprostate tuberculosis, with dilatation and irregularities of the prostatic urethra. (C–E) IU of three patients, showing a normal right kidney, contracted bladder and left kidneywith low or no function.

A.A. Figueiredo et al. / European Journal of Radiology 76 (2010) 246–257 253
Fig. 7. Patient with unilateral renal tuberculosis and contracted bladder. (A) IU showing right renal functional exclusion, left ureterohydronephrosis and contracted bladder.(B) Voiding cystography showing contracted bladder and high-grade reflux on the left as a cause of ureterohydronephrosis.
Fig. 8. Patient with unilateral renal tuberculosis and contracted bladder. (A) IU showing left functional renal exclusion, right ureterohydronephrosis and contracted bladder.(B) Voiding cystography showing contracted bladder and high-grade reflux on the right as a cause of ureterohydronephrosis.

254 A.A. Figueiredo et al. / European Journal of Radiology 76 (2010) 246–257
Fig. 9. Patient with previous right nephrectomy due to tuberculosis, showing: (A–C) Abdominal and pelvic CT showing absence of right kidney, left kidney with ureterohy-dronephrosis and dilatation of the whole left ureter (arrow). There is no lesion or atrophy of the renal parenchyma. There is diffuse thickening of the bladder wall. (D) Voidingurethrocystography showing contracted bladder, dilatation of the prostatic urethra due to tuberculosis and left vesicoureteral reflux with a certain degree of stenosis (arrow).
A.A. Figueiredo et al. / European Journal of Radiology 76 (2010) 246–257 255
Fo
(
Fdo
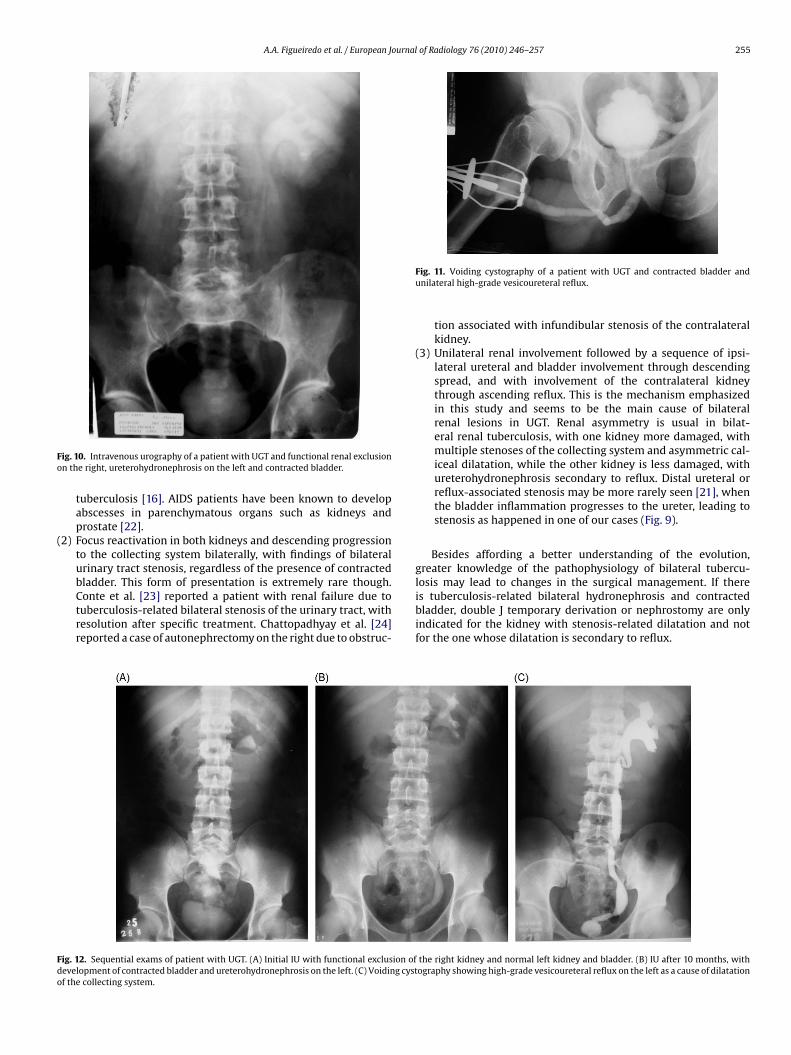
ig. 10. Intravenous urography of a patient with UGT and functional renal exclusionn the right, ureterohydronephrosis on the left and contracted bladder.
tuberculosis [16]. AIDS patients have been known to developabscesses in parenchymatous organs such as kidneys andprostate [22].
2) Focus reactivation in both kidneys and descending progressionto the collecting system bilaterally, with findings of bilateralurinary tract stenosis, regardless of the presence of contracted
bladder. This form of presentation is extremely rare though.Conte et al. [23] reported a patient with renal failure due totuberculosis-related bilateral stenosis of the urinary tract, withresolution after specific treatment. Chattopadhyay et al. [24]reported a case of autonephrectomy on the right due to obstruc-ig. 12. Sequential exams of patient with UGT. (A) Initial IU with functional exclusion ofevelopment of contracted bladder and ureterohydronephrosis on the left. (C) Voiding cystf the collecting system.
Fig. 11. Voiding cystography of a patient with UGT and contracted bladder andunilateral high-grade vesicoureteral reflux.
tion associated with infundibular stenosis of the contralateralkidney.
(3) Unilateral renal involvement followed by a sequence of ipsi-lateral ureteral and bladder involvement through descendingspread, and with involvement of the contralateral kidneythrough ascending reflux. This is the mechanism emphasizedin this study and seems to be the main cause of bilateralrenal lesions in UGT. Renal asymmetry is usual in bilat-eral renal tuberculosis, with one kidney more damaged, withmultiple stenoses of the collecting system and asymmetric cal-iceal dilatation, while the other kidney is less damaged, withureterohydronephrosis secondary to reflux. Distal ureteral orreflux-associated stenosis may be more rarely seen [21], whenthe bladder inflammation progresses to the ureter, leading tostenosis as happened in one of our cases (Fig. 9).
Besides affording a better understanding of the evolution,greater knowledge of the pathophysiology of bilateral tubercu-
losis may lead to changes in the surgical management. If thereis tuberculosis-related bilateral hydronephrosis and contractedbladder, double J temporary derivation or nephrostomy are onlyindicated for the kidney with stenosis-related dilatation and notfor the one whose dilatation is secondary to reflux.the right kidney and normal left kidney and bladder. (B) IU after 10 months, withography showing high-grade vesicoureteral reflux on the left as a cause of dilatation

256 A.A. Figueiredo et al. / European Journal of Radiology 76 (2010) 246–257
Fig. 13. Sequential exams of a patient with UGT. (A) Initial IU with normal right kidney and left kidney with ureterohydronephrosis due to stenosis of the middle ureter (arrow)a ystogr6 onephg
5
tenitdashflht
C
nd intrarenal stenoses without pelvic dilatation (typical tuberculosis feature). (B) Cmonths without treatment, showing functional exclusion on the left, ureterohydr
rade on the right) as a cause of ureterohydronephrosis.
. Conclusions
Urogenital tuberculosis may have variable radiological presen-ations. However, in two of our cases with sequential radiologicalxams we have seen that tuberculosis involvement of the uri-ary tract may be sequential. After unilateral renal and ureteral
nvolvement, with thickening and stenosis of the collecting sys-em with hydronephrosis and renal parenchyma atrophy, bladderamage may follow, with diffuse thickening of the bladder wallnd development of vesicoureteral reflux, usually unilateral to thetill unaffected kidney. High-grade reflux may lead to uretero-ydronephrosis, reflux nephropathy and risk to end-stage renalailure. The present study highlights the possibility of such evo-ution. However, further evidences are necessary to confirm thisypothesis. Early diagnosis, at the early stages, may stop this evolu-
ion and obviate the need for more complex reconstructive surgery.onflicts of interest
There is no conflict of interest.
[
aphy with normal bladder and no reflux. (C and D) IU and voiding cystography afterrosis on the right with contracted bladder and bilateral vesicoureteral reflux (high
References
[1] Leite OHM. Tuberculosis. Prob Gen Surg 2001;18(4):69–78.[2] Havlir DV, Barnes PF. Tuberculosis in patients with human immunodeficiency
virus infection. N Eng J Med 1999;340(5):367–73.[3] Muttarak M, Chiangmai WN, Lojanapiwat B. Tuberculosis of the genitouri-
nary tract: imaging features with pathological correlation. Singapore Med J2005;46(10):568–75.
[4] Wise GJ, Marella VK. Genitourinary manifestations of tuberculosis. Urol Clin NAm 2003;30(1):111–21.
[5] Ferrie BG, Rundle JSH. Genito-urinary tuberculosis in Glasgow 1970 to 1979: areview of 230 patients. Scott Med J 1985;30:30–4.
[6] Schubert GE, Haltaufderheide T, Golz R. Frequency of urogenital tuberculosisin an unselected autopsy series from 1928 to 1949 and 1976 to 1989. Eur Urol1992;21:216–23.
[7] Gokalp A, Gultekin EY, Ozdamar S. Genito-urinary tuberculosis: a review of 83cases. BJCP 1990;44(11):599–600.
[8] Gow JG, Barbosa S. Genitourinary tuberculosis. A study of 1117 cases over aperiod of 34 years. Br J Urol 1984;56:449–55.
[9] Gokce G, Kilicaerslan H, Ayan S, et al. Genitourinary tuberculosis: review of 174cases. Scan J Infect Dis 2002;34:338–40.
10] Hemal AK, Gupta NP, Rajeev TP, Kumar R, Dar L, Seth P. Polymerase chainreaction in clinically suspected genitourinary tuberculosis: comparison withintravenous urography, bladder biopsy, and urine acid fast bacilli culture. Urol-ogy 2000;56(4):570–4.

ournal
[
[
[
[
[
[
[
[
[
[
A.A. Figueiredo et al. / European J
11] Wang LJ, Wu CF, Wong YC, Chuang CK, Chu SH, Chen CJ. Imaging findings ofurinary tuberculosis on excretory urography and computerized tomography. JUrol 2003;169:524–8.
12] Lu P, Li C, Zhou X. Significance of the CT scan in renal tuberculosis. ZhonghuaJie He He Hu Xi Za Zhi 2001;24(7):407–9.
13] Christensen WI. Genitourinary tuberculosis. Review of 102 cases. Medicine(Baltimore) 1974;53(5):377–90.
14] Garcia-Rodríguez JÁ, García Sanchez JE, Munoz Bellido JL. Genitourinary tuber-culosis in Spain: review of 81 cases. Clin Infect Dis 1994;18:557–61.
15] Figueiredo AA, Lucon AM, Srougi M. Bladder augmentation for the treatment of
chronic tuberculous cystitis. Clinical and urodynamic evaluation of 25 patientsafter long term follow-up. Neurourol Urodyn 2006;25:433–40.16] Medlar EM, Spain DM, Holliday RW. Post-mortem compared with clinical diag-nosis of genito-urinary tuberculosis in adult males. J Urol 1949;61(6):1078–88.
17] Matos MJ, Bacelar MT, Pinto P, Ramos I. Genitourinary tuberculosis. Eur J Radiol2005;55:181–7.
[
[
[
of Radiology 76 (2010) 246–257 257
[18] Barrie HJ, Kerr WK, Gale GL. The incidence and pathogenesis of tuberculousstrictures of the renal pyelus. J Urol 1967;98:584–9.
19] Winblad B, Duchek M. Spread of tuberculosis from obstructed andnon-obstructed upper urinary tract. Acta Pathol Microbiol Scand [A]1975;83(2):229–36.
20] Ramanathan R, Kumar A, Kapoor R, Bhandari M. Relief of urinary tract obstruc-tion in tuberculosis to improve renal function. Analysis of predictive factors. BrJ Urol 1998;81(2):199–205.
21] Carl P, Stark L. Indications for surgical management of genitourinary tubercu-losis. World J Surg 1997;21:505–10.
22] Gebo KA. Prostatic tuberculosis in a HIV infected male. Sex Trans Infect2002;78:147–8.
23] Conte G, Iavarone M, Santorelli, De Nicola L. Acute renal failure of unknownorigin. Don’t forget renal tuberculosis. Nephrol Dial Transplant 1997;12:1260–1.
24] Chattopadhyay A, Bhatnagar V, Agarwala S, Mitra DK. Genitourinary tubercu-losis in pediatric surgical practice. J Ped Surg 1997;32(9):1283–6.




















