110-1067 © 2014 The Egyptian Society of Haematology
8
Transcript of 110-1067 © 2014 The Egyptian Society of Haematology


1110-1067 © 2014 The Egyptian Society of Haematology DOI: 10.4103/1110-1067.124843
Original article 25
IntroductionApoptosis is a morphologically distinct form of programmed cell death that plays a major role during development, homeostasis [1]. It is an active death process genetically encoded to eliminate abnormal unwanted cells [2].
Fas (Apo-1/CD95) is a cell surface transmembrane molecule belonging to the tumor necrosis factor/nerve
growth factor receptor superfamily that is characterized by cysteine-rich extracellular domains [3].
Fas antigen is expressed on a variety of human B and T cell lines, on various normal human tissues, and on many different tumor cells [4]. The interaction between Fas receptor (CD95) on the target cell and Fas ligand (FasL) on cytotoxic T-lymphocytes
Fas (CD95) expression as a prognostic marker in acute leukemia and blastic transformation phase in chronic myeloid leukemiaNahla A. Nosaira, Enaam S. Abd EL Bara, Atef M. Tahab, Amr M. Gawalyb
Introduction Fas is expressed on a majority of human leukemic cells. Fas-mediated cell death is involved in drug-induced apoptosis in various cell types. Hence, failure of apoptosis could lead to chemoresistance and may therefore have an impact on clinical outcome. The aim of the present study was to evaluate the percentage of Fas receptor expression on blast cells in patients with adult acute leukemia and blastic transformation phase of chronic myeloid leukemia (CML-BT), and to find out the impact of Fas expression on prognosis.
Subjects and methods The participants of this study were 80 adult acute leukemia patients classified as follows: 40 acute myeloid leukemia (AML) patients, 32 ALL patients, and eight CML-BT patients. In addition, 10 age-matched and sex-matched healthy controls were also included in the study. Patients with acute leukemia were studied at diagnosis and after treatment. The diagnosis of AML, ALL, and CML-BT was assessed by morphological study, cytochemical analysis, and immunophenotyping of peripheral blood (PB) and bone marrow aspirate according to FAB classification. Fas expression on blast cells from bone marrow aspirate or PB samples of the patients or on normal monocytes, granulocytes, and lymphocytes obtained from PB samples of controls was measured using flow cytometry. The correlation between prognostic markers (age, sex, total leukocytic count, serum lactate dehydrogenase (LDH), and cytogenetic risk categories) and Fas expression levels on blast cells of leukemic patients at diagnosis was ascertained. After treatment, patients were followed up for periods ranging from 25 to 31 months.
Results Fas expression was seen to be the highest on control monocytes (31.2 ± 6.95%), followed by granulocytes (24.8 ± 7.61%), whereas lymphocytes expressed the lowest levels (17.1 ± 4.01%) with a highly statistically significant difference (P < 0.001) between variables. The mean value of Fas expression by blast cells from AML patients at diagnosis was 41.72 ± 10.3%. AML patients were divided into the Fas-positive group [29 patients (72.5%)] and the Fas-negative group [11 patients (27.5%)]. The mean values of expression increased significantly from M1 to M5 with the weakest expression in M1 (20.28 ± 5.3%) and the strongest in M5 (52.91 ± 11.3%) with highly significant differences (P < 0.001) between Fas
expression levels in different FAB subtypes of AML. The mean value of Fas expression in ALL patients was 42.87 ± 11.5%. Twenty-three (71.88%) patients were positive for Fas expression, whereas nine (28.12%) were negative. Fas expression was positive in 12/19 (63.2%) precursor B-ALL patients and in 11/13 (84.6%) T-ALL patients. The mean value of Fas expression was significantly higher (P = 0.039) in T-ALL (55.15 ± 7.8%) in comparison with precursor B-ALL (34.47 ± 5.76%). CML-BT patients were all transformed to AML type and expressed Fas with a mean of 31.0 ± 7.63%. Only three of them (37.5%) were Fas negative and the remaining five (62.5%) were Fas positive. The percentage of Fas-positive patients was 0% (0/1) in M1, 50% (2/4) in M2, 100% (1/1) in M4, and 100% (2/2) in M5. No significant differences could be detected between Fas-positive and Fas-negative patients with respect to baseline patient characters (age, sex, total leukocytic count, serum LDH levels, and cytogenetic risk category). Highly significant correlation was found between Fas-positive expression and response to therapy (P < 0.001) in AML and ALL patients. Fas-negative patients in CML-BT were nonresponders to chemotherapy with a significant correlation between low Fas expression and failure to respond to therapy (P = 0.049). Overall survival between Fas-positive and Fas-negative patients was statistically significant in AML, ALL, and CML-BT patients (P = 0.001, 0.002, and 0.002, respectively).
Conclusion The mean value of Fas expression by blast cells from AML, ALL, and CML-BT patients at diagnosis was 41.72 ± 10.3, 42.87 ± 11.5, and 31 ± 7.63%, respectively. We can conclude that Fas receptor expression on blast cells from ALL, AML, and CML-BT patients could serve as an independent prognostic factor and help in monitoring the outcome of chemotherapy. Egyptian Journal of Haematology 39:25–31 © 2014 The Egyptian Journal of Haematology.
Egyptian Journal of Haematology 2014, 39:25–31
Keywords: CD95, chronic myeloid leukemia, Fas
Departments of aClinical Pathology and bInternal Medicine, Tanta University, Tanta, Egypt
Correspondence to Amr M. Gawaly, PhD, MD, Department of Internal Medicine, Tanta University, Tanta, 31111, Egypt Tel: +20 122 179 3033; fax: 040-3407734 e-mail: [email protected]
Received 09 October 2013 Accepted 19 November 2013

26 Egyptian Journal of Haematology 2014, Vol 39 No 1
Immunophenotyping was carried out on PB or BM samples on EDTA using Becton Dickinson FAC Scan flow cytometry (Becton Dickinson, San Jose, California, USA) with panels of monoclonal antibodies (MoAbs) stained with either fluorescin isothiocyanate or phycoerythrin (PE) including B-lymphoid markers (CD10, CD19, CD20, and CD22), T-lymphoid markers (CD2, CD3, CD5, and CD7), myeloid and monocytic markers (CD117,CD13, CD33, CD14, and CD64), nonlineage-specific markers (CD34, HLA-DR), and megakaryoblastic and erythroid markers (CD41, CD61, and glycophorin-A). These markers were supplied by Coulter Immunology (Coulter Corporation, Hialeah, Florida, USA).
Cytogenetic analyses were performed using pretreatment samples from all patients according to standard protocols including conventional cytogenetic analysis using the G-banding technique; chromosomal abnormalities were described according to the International System for Human Cytogenetic Nomenclatures (ISCN) [12], and fluorescence in-situ hybridization analysis using a comprehensive DNA probe set allowed for the detection of most relevant AML-associated and ALL-associated genomic aberrations [13].
The AML patients and CML-BT patients were placed cytogenetically into one of three prognostic groups according to the Criteria for the Medical Research Council [14]. The favorable risk group consisted of t(8;21), t(15;17), t(16;16), or inv(16) abnormalities; the poor risk group consisted of -5/5q-, -7/7q-, or 11q23 abnormalities or complex abnormalities (≥3 abnormalities); and the intermediate risk group included patients with any other abnormalities or normal karyotypes. For ALL patients, poor risk included t(9;22), t(4;11), t(1;19), t(2;8), t(8;14), t(8;22), or hypodiploidy; good risk involved hyperdiploidy or t(12;21); and intermediate risk consisted of other cytogenetic abnormalities or normal karyotypes.
After diagnosis, patients received treatment according to the type of acute leukemia and they were followed up for periods ranging from 25 to 31 months, from June 2010 to January 2013, with special attention to clinical and laboratory markers of remission and relapse, taking care to estimate the date of first complete remission, date of relapse, death, or last seen alive.
AML and CML-BT patients were treated according to the protocols of the German AML Cooperative Group (AMLCG). This comprises double induction
has been shown to be an important mechanism of apoptosis [5].
The deregulation of apoptosis may contribute to the pathogenesis of a number of human malignant disorders [6]. Some researchers demonstrated that Fas was expressed on a majority of human leukemia cells, although the intensity of expression was variable [7].
Chemotherapeutic drugs used for leukemia treatment can kill target cells by several mechanisms, including apoptosis [8]. In addition, Fas-mediated cell death is involved in drug-induced apoptosis in various cell types [9]. Hence, failure in the apoptosis machinery could lead to chemoresistance and may therefore have an impact on clinical outcome [10].
This study was conducted to evaluate the percentage of Fas receptor expression on blast cells of adult patients with acute leukemia and blastic transformation phase of chronic myeloid leukemia (CML-BT) and rule out the impact of Fas expression on prognosis and overall survival.
Participants and methodsThe participants of this study were 80 adult acute leukemia patients: 40 acute myeloid leukemia (AML) patients, 32 ALL patients, and eight CML-BT patients. Ten age-matched and sex-matched healthy individuals were also included in the study as the control group. The age of AML patients ranged from 19 to 75 years and comprised 21 (52.5%) men and 19 (47.5%) women. There were 18 (56.25%) male ALL patients and 14 (43.75%) female ALL patients and their ages ranged from 16 to 62 years.
The eight CML patients were under treatment protocol for CML and were included in the study when the blastic transformation phase was confirmed and the blasts of the eight cases were proved to be of myeloid or monocytic types by morphological, cytochemical, and immunophenotyping analyses. Their ages ranged between 37 and 52 years and comprised five (62.5%) men and three (37.5%) women.
Patients were selected from Hematology/Oncology Unit, Internal Medicine Department, Tanta University Hospitals.
Patients with acute leukemia were studied at first diagnosis and were previously untreated. The diagnosis of AML, ALL, and CML-BT were assessed by morphological study, cytochemistry, and immunophenotyping of peripheral blood (PB) and bone marrow aspirate (BMA) according to the FAB classification of acute leukemia [11].

Fas (CD95) expression Nosair et al. 27
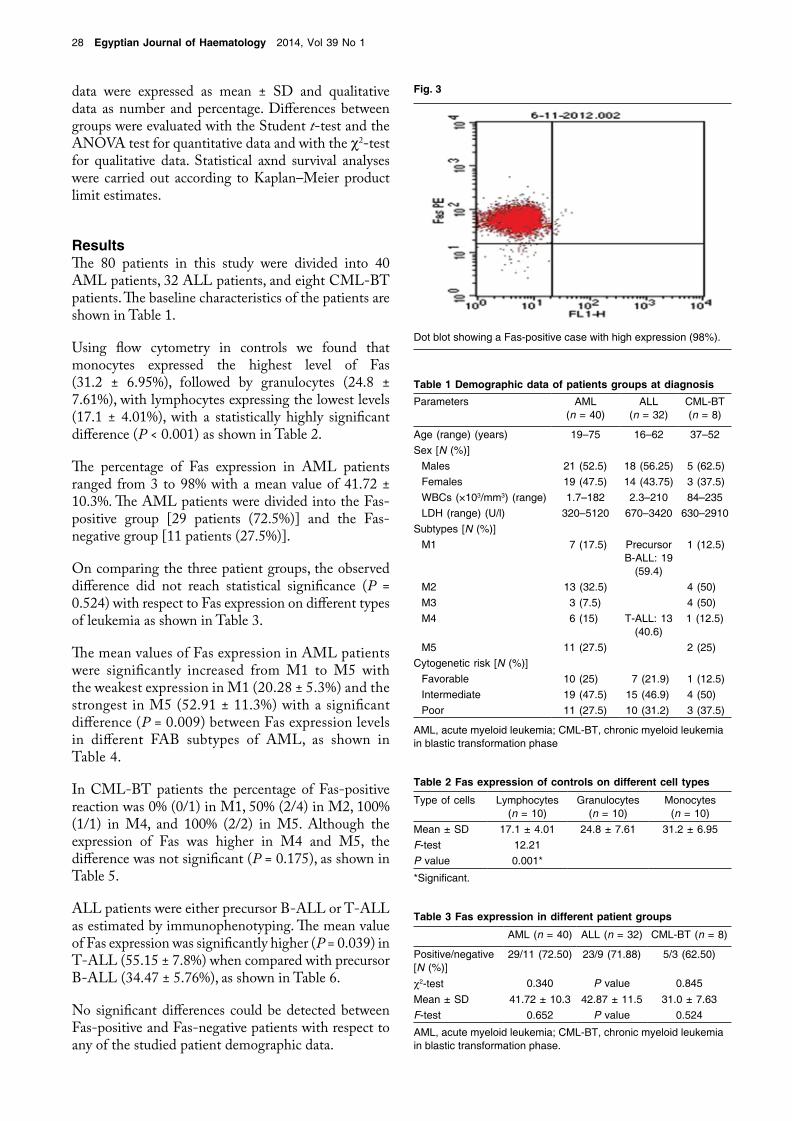
resuspended in 0.3 ml PBS, and then analyzed on a fluorescence-activated cell scanner (FACs Caliber; Becton Dickinson). Data acquisition and analysis was performed using Cell Quest Procount software version 2.1 (Verity Software House, Topsham, ME, USA). A total of 10 000 events were acquired and gating was performed using forward scatter and side scatter and the percentage of positive cells was calculated [18]. Values equal to or greater than 20% were considered positive (Fas positive), whereas values less than 20% were considered negative for Fas expression (Fas negative) (Figs 1–3).
We tried to correlate Fas expression to prognostic factors (age, sex, total leukocyte count, serum LDH, and cytogenetic risk categories) by studying Fas expression levels on blast cells of leukemic patients at diagnosis.
Statistical analysisData were analyzed using SPSS version 16 (IBM Corporation, Armonk, New York, USA). Quantitative
therapy with thioguanine, cytosine arabinoside (AraC), and daunorubicin (TAD), followed by high-dose AraC and mitoxantrone (HAM) [15]. Patients with AML-M3 received all-trans retinoic acid including therapy protocols [16].
Complete remission was determined as achieved when the BM was normocellular, containing less than or equal to 5% blasts, and when neutrophil granulocytes in PB had recovered to 1500/μl and platelets to 100 000/μl. Relapse was diagnosed when the BM contained at least 5% leukemic blasts or when leukemic infiltration occurred at any other site. Criteria for defining a complete remission in AML was revisited, and an analysis was carried out of patients treated in HOVON-SAKK co-operative group studies [17].
After preinduction with steroids for 1 week, phase I induction was given over 4 weeks with vincristine (VCR), daunorubicin (DNR), l-asparaginase (ASP), and prednisolone (PDN). Bone marrow examination was carried out after completion of the phase I induction to assess remission. Phase II induction consisted of cyclophosphamide (Cyclo) and four courses of cytosine (AraC) combined with CNS-directed therapy using intrathecal methotrexate (MTx) and prophylactic cranial radiotherapy. Consolidation consisted of two 5-day courses of AraC (75 mg/m2) and etoposide (50 mg/m2), along with a single dose of intrathecal MTx (12.5 mg). This was followed by reinduction with VCR, DNR, dexamethasone (Dexa), Cyclo, and AraC over a period of 6 weeks. The final maintenance consisted of daily mercaptopurine (6-MP) and weekly oral MTx for 24 months. This maintenance was intensified with monthly pulses of 2 mg VCR, 10 mg/m2 Dexa for 5 days, and 12.5 mg intrathecal MTx once in 3 months [18].
Analysis of Fas expressionExpression of Fas in blast cells from BMA or PB samples of the patients or in normal monocytes, granulocytes, and lymphocytes obtained from PB samples of controls and measured by flow cytometry was studied. Using the whole blood lysis method, 100 μl of fresh EDTA PB or BMA samples was prepared for flow cytometry by adding 10 μl of PE-conjugated anti-human CD95 MoAb (Becton Dickinson). PE-conjugated IgG1 MoAb (0.10 μl) (Becton Dickinson) was used as isotype-matched nonspecific control antibody. Samples were incubated for 30 min at4°C. The erythrocytes were lysed using 1 ml FACs lysis solution (Becton Dickinson) on each tube sample and were incubated for 20 min at 4°C. Cells were washed twice by adding 0.5 ml PBS (pH 7.4) and centrifuged at 3000 rpm for 5 min each. The supernatant was discarded and
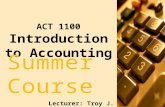
Fig. 1
Gating of blast cell population using forward scatter and side scatter.
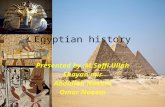
Fig. 2
Dot blot showing negative control.
28 Egyptian Journal of Haematology 2014, Vol 39 No 1
data were expressed as mean ± SD and qualitative data as number and percentage. Differences between groups were evaluated with the Student t-test and the ANOVA test for quantitative data and with the c2-test for qualitative data. Statistical axnd survival analyses were carried out according to Kaplan–Meier product limit estimates.
ResultsThe 80 patients in this study were divided into 40 AML patients, 32 ALL patients, and eight CML-BT patients. The baseline characteristics of the patients are shown in Table 1.
Using flow cytometry in controls we found that monocytes expressed the highest level of Fas (31.2 ± 6.95%), followed by granulocytes (24.8 ± 7.61%), with lymphocytes expressing the lowest levels (17.1 ± 4.01%), with a statistically highly significant difference (P < 0.001) as shown in Table 2.
The percentage of Fas expression in AML patients ranged from 3 to 98% with a mean value of 41.72 ± 10.3%. The AML patients were divided into the Fas-positive group [29 patients (72.5%)] and the Fas-negative group [11 patients (27.5%)].
On comparing the three patient groups, the observed difference did not reach statistical significance (P = 0.524) with respect to Fas expression on different types of leukemia as shown in Table 3.
The mean values of Fas expression in AML patients were significantly increased from M1 to M5 with the weakest expression in M1 (20.28 ± 5.3%) and the strongest in M5 (52.91 ± 11.3%) with a significant difference (P = 0.009) between Fas expression levels in different FAB subtypes of AML, as shown in Table 4.
In CML-BT patients the percentage of Fas-positive reaction was 0% (0/1) in M1, 50% (2/4) in M2, 100% (1/1) in M4, and 100% (2/2) in M5. Although the expression of Fas was higher in M4 and M5, the difference was not significant (P = 0.175), as shown in Table 5.
ALL patients were either precursor B-ALL or T-ALL as estimated by immunophenotyping. The mean value of Fas expression was significantly higher (P = 0.039) in T-ALL (55.15 ± 7.8%) when compared with precursor B-ALL (34.47 ± 5.76%), as shown in Table 6.
No significant differences could be detected between Fas-positive and Fas-negative patients with respect to any of the studied patient demographic data.
Table 1 Demographic data of patients groups at diagnosisParameters AML
(n = 40)ALL
(n = 32)CML-BT (n = 8)
Age (range) (years) 19–75 16–62 37–52Sex [N (%)]
Males 21 (52.5) 18 (56.25) 5 (62.5)Females 19 (47.5) 14 (43.75) 3 (37.5)WBCs (×103/mm3) (range) 1.7–182 2.3–210 84–235LDH (range) (U/l) 320–5120 670–3420 630–2910
Subtypes [N (%)]M1 7 (17.5) Precursor
B-ALL: 19 (59.4)
1 (12.5)
M2 13 (32.5) 4 (50)M3 3 (7.5) 4 (50)M4 6 (15) T-ALL: 13
(40.6)1 (12.5)
M5 11 (27.5) 2 (25)Cytogenetic risk [N (%)]
Favorable 10 (25) 7 (21.9) 1 (12.5)Intermediate 19 (47.5) 15 (46.9) 4 (50)Poor 11 (27.5) 10 (31.2) 3 (37.5)
AML, acute myeloid leukemia; CML-BT, chronic myeloid leukemia in blastic transformation phase
Table 2 Fas expression of controls on different cell types
Type of cells Lymphocytes (n = 10)
Granulocytes (n = 10)
Monocytes (n = 10)
Mean ± SD 17.1 ± 4.01 24.8 ± 7.61 31.2 ± 6.95F-test 12.21P value 0.001*
*Significant.
Table 3 Fas expression in different patient groups
AML (n = 40) ALL (n = 32) CML-BT (n = 8)
Positive/negative [N (%)]
29/11 (72.50) 23/9 (71.88) 5/3 (62.50)
c2-test 0.340 P value 0.845Mean ± SD 41.72 ± 10.3 42.87 ± 11.5 31.0 ± 7.63F-test 0.652 P value 0.524
AML, acute myeloid leukemia; CML-BT, chronic myeloid leukemia in blastic transformation phase.
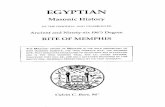
Fig. 3
Dot blot showing a Fas-positive case with high expression (98%).

Fas (CD95) expression Nosair et al. 29
the death-inducing signaling complex. A cascade of caspase activation is initiated in turn, which finally leads to apoptosis of the cell [21].
In the present work, controls showed significant variation in the mean percentage of Fas expression by different normal cells in the PB. Monocytes expressed significantly higher levels of Fas compared with granulocytes, whose expression levels were higher than that of lymphocytes. Many previous studies have found Fas expression on a variety of hematopoietic cell populations, including T and B lymphocytes, monocytes, macrophages, and eosinophils [22,23].
The present study demonstrated that Fas receptors are expressed on a significant proportion of blast cells in adult AML, ALL, and CML-BT patients.
An overall 72.5% of AML patients were positive expressors of Fas (with Fas being expressed by 20% or more of their leukemic cells). AML patients expressed Fas with variable intensity ranging from 3 to 98% of their blast cells. Several studies have reported variable intensities of Fas expression on AML blast cells [24–26], which are in agreement with our results, and may reflect the heterogeneity of AML.
Our study also showed that Fas expression varies significantly between different FAB subtypes of AML, being strongest in M4 and M5 and weakest in M1 with intermediate levels in M2 and M3. In normal hematopoiesis, immature cells do not express a significant level of Fas [27]. Fas expression becomes enhanced with maturation of the myeloid series [28]. Hence, variable expression levels of Fas in different AML subtypes may simply reflect the difference in maturation stage of leukemic cells [25].
It was observed that blast cells of CML-BT patients expressed Fas antigen at levels significantly comparable to those of AML patients, and the expression of Fas by blast cells of monocytic transformation was higher than that of myeloid cells, although the difference was not significant.
Regarding ALL, 71.88% of our patients were positive expressors of Fas, which is similar to the results in previous studies [29,30]. We found that expression of Fas by T-ALL blast cells was significantly higher than that of precursor B-ALL cells. Karawajew et al.
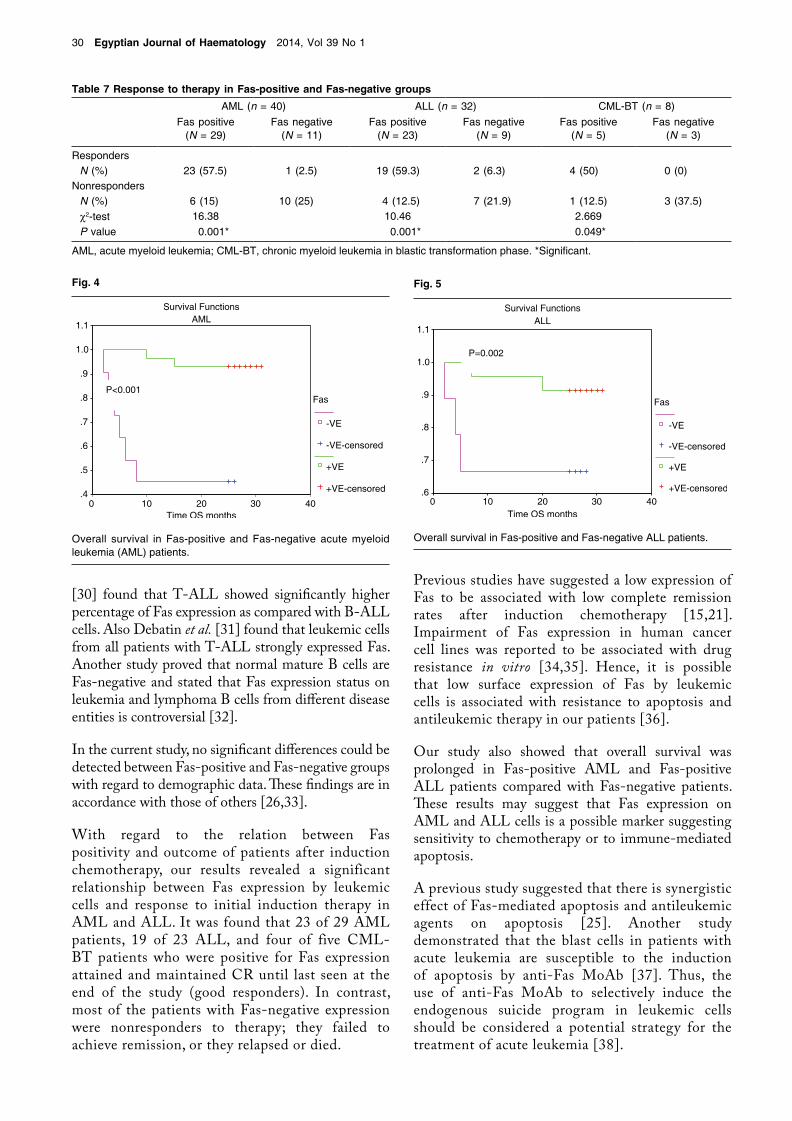
After receiving treatment according to the type of leukemia, follow-up of all the studied patients was carried out for detection of response to therapy and disease outcome. Patients with Fas-positive expression were better responders to therapy (achieved and maintained CR) compared with those with Fas-negative expression, as shown in Table 7.
There was a significant association between Fas-positive expression and response to therapy in AML and ALL patients (P < 0.001). In contrast, in CML-BT patients, all the three Fas-negative patients were nonresponders with a significant association between low Fas expression and failure to respond to therapy (P = 0.049).
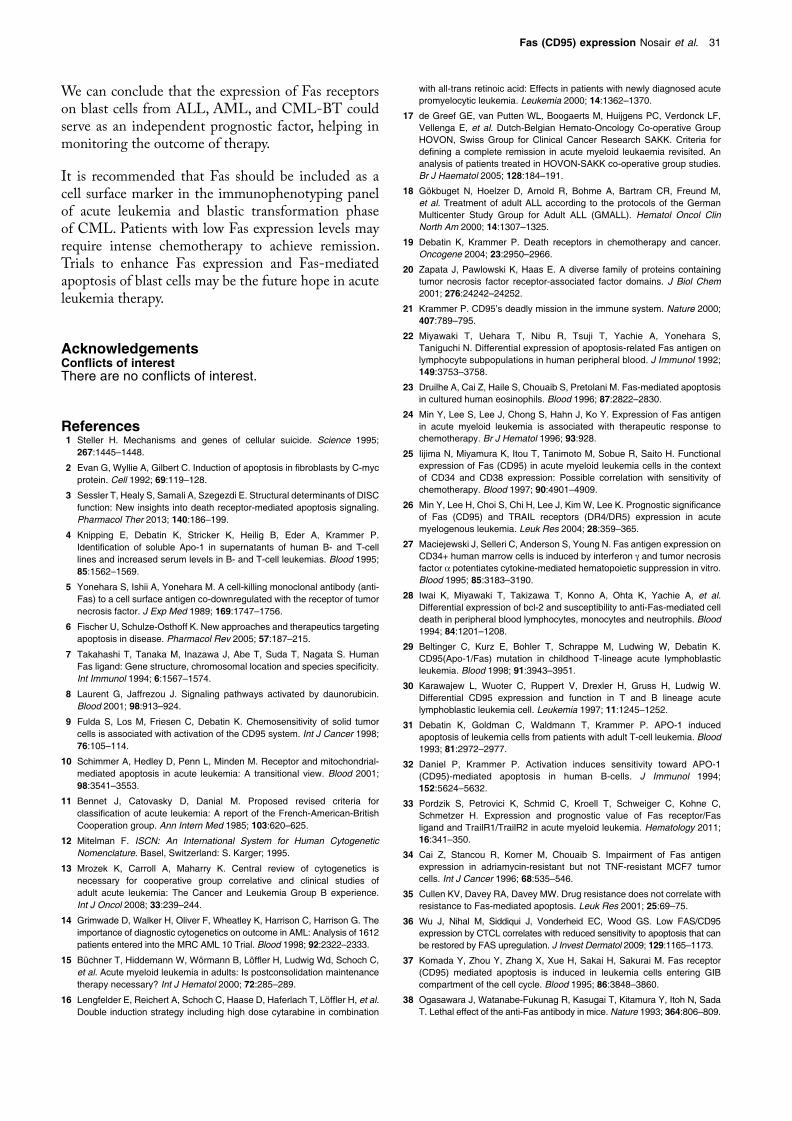
Kaplan–Meier analysis of overall survival as a prognostic test revealed a statistically significant difference in prognosis between Fas-positive and Fas-negative patients (Figs 4 and 5) with significantly higher overall survival in Fas-positive AML and ALL patients as compared with Fas-negative subgroups (P < 0.001 and P = 0.002, respectively).
DiscussionAs an imbalance between apoptosis and proliferation may result in tumor formation, enhancing apoptosis should be a way of killing tumor cells directly and effectively [19]. The two main pathways involved in apoptosis are the extrinsic pathway, which is triggered through the Fas death receptor, and the intrinsic pathway [20]. After being triggered by its natural ligand (FasL), Fas recruits the relative proteins to form
Table 4 Relation between Fas expression and FAB subtypes in AML patientsM1 (n = 7) M2 (n = 13) M3 (n = 3) M4 (n = 6) M5 (n = 11)
Positive Fas [N (%)] 3 (42.9) 9 (69.2) 2 (66.7) 5 (83.3) 10 (90.9)Mean ± SD 20.28 ± 5.3 43.69 ± 8.63 30.67 ± 6.47 49.17 ± 10.77 52.91 ± 11.3c2-test 3.15 P value 0.009*
AML, acute myeloid leukemia. *Significant.
Table 5 Relation between Fas expression and FAB subtypes in CML-BT
M1 (n = 1) M2 (n = 4) M4 (n = 1) M5 (n = 2)Positive Fas [N (%)] 0 (0) 2 (50) 1 (100) 2 (100)c2-test 4.950 P value 0.175
CML-BT, chronic myeloid leukemia in blastic transformation phase.
Table 6 Relation between Fas expression and immunophenotype in ALL patients
Precursor B-ALL (n = 19) T-ALL (n = 13)Positive Fas [N (%)] 12 (63.2) 11 (84.6)Mean ± SD 34.47 ± 5.76 55.15 ± 7.80t-test 4.749P value 0.039*
*Significant.
30 Egyptian Journal of Haematology 2014, Vol 39 No 1
Previous studies have suggested a low expression of Fas to be associated with low complete remission rates after induction chemotherapy [15,21]. Impairment of Fas expression in human cancer cell lines was reported to be associated with drug resistance in vitro [34,35]. Hence, it is possible that low surface expression of Fas by leukemic cells is associated with resistance to apoptosis and antileukemic therapy in our patients [36].
Our study also showed that overall survival was prolonged in Fas-positive AML and Fas-positive ALL patients compared with Fas-negative patients. These results may suggest that Fas expression on AML and ALL cells is a possible marker suggesting sensitivity to chemotherapy or to immune-mediated apoptosis.
A previous study suggested that there is synergistic effect of Fas-mediated apoptosis and antileukemic agents on apoptosis [25]. Another study demonstrated that the blast cells in patients with acute leukemia are susceptible to the induction of apoptosis by anti-Fas MoAb [37]. Thus, the use of anti-Fas MoAb to selectively induce the endogenous suicide program in leukemic cells should be considered a potential strategy for the treatment of acute leukemia [38].
[30] found that T-ALL showed significantly higher percentage of Fas expression as compared with B-ALL cells. Also Debatin et al. [31] found that leukemic cells from all patients with T-ALL strongly expressed Fas. Another study proved that normal mature B cells are Fas-negative and stated that Fas expression status on leukemia and lymphoma B cells from different disease entities is controversial [32].
In the current study, no significant differences could be detected between Fas-positive and Fas-negative groups with regard to demographic data. These findings are in accordance with those of others [26,33].
With regard to the relation between Fas positivity and outcome of patients after induction chemotherapy, our results revealed a significant relationship between Fas expression by leukemic cells and response to initial induction therapy in AML and ALL. It was found that 23 of 29 AML patients, 19 of 23 ALL, and four of five CML-BT patients who were positive for Fas expression attained and maintained CR until last seen at the end of the study (good responders). In contrast, most of the patients with Fas-negative expression were nonresponders to therapy; they failed to achieve remission, or they relapsed or died.
Table 7 Response to therapy in Fas-positive and Fas-negative groupsAML (n = 40) ALL (n = 32) CML-BT (n = 8)
Fas positive (N = 29)
Fas negative (N = 11)
Fas positive (N = 23)
Fas negative (N = 9)
Fas positive (N = 5)
Fas negative (N = 3)
RespondersN (%) 23 (57.5) 1 (2.5) 19 (59.3) 2 (6.3) 4 (50) 0 (0)
NonrespondersN (%) 6 (15) 10 (25) 4 (12.5) 7 (21.9) 1 (12.5) 3 (37.5)c2-test 16.38 10.46 2.669P value 0.001* 0.001* 0.049*
AML, acute myeloid leukemia; CML-BT, chronic myeloid leukemia in blastic transformation phase. *Significant.
Fig. 4
Overall survival in Fas-positive and Fas-negative acute myeloid leukemia (AML) patients.
Fig. 5
Overall survival in Fas-positive and Fas-negative ALL patients.
Fas (CD95) expression Nosair et al. 31
with all-trans retinoic acid: Effects in patients with newly diagnosed acute promyelocytic leukemia. Leukemia 2000; 14:1362–1370.
17 de Greef GE, van Putten WL, Boogaerts M, Huijgens PC, Verdonck LF, Vellenga E, et al. Dutch-Belgian Hemato-Oncology Co-operative Group HOVON, Swiss Group for Clinical Cancer Research SAKK. Criteria for defining a complete remission in acute myeloid leukaemia revisited. An analysis of patients treated in HOVON-SAKK co-operative group studies. Br J Haematol 2005; 128:184–191.
18 Gökbuget N, Hoelzer D, Arnold R, Bohme A, Bartram CR, Freund M, et al. Treatment of adult ALL according to the protocols of the German Multicenter Study Group for Adult ALL (GMALL). Hematol Oncol Clin North Am 2000; 14:1307–1325.
19 Debatin K, Krammer P. Death receptors in chemotherapy and cancer. Oncogene 2004; 23:2950–2966.
20 Zapata J, Pawlowski K, Haas E. A diverse family of proteins containing tumor necrosis factor receptor-associated factor domains. J Biol Chem 2001; 276:24242–24252.
21 Krammer P. CD95’s deadly mission in the immune system. Nature 2000; 407:789–795.
22 Miyawaki T, Uehara T, Nibu R, Tsuji T, Yachie A, Yonehara S, Taniguchi N. Differential expression of apoptosis-related Fas antigen on lymphocyte subpopulations in human peripheral blood. J Immunol 1992; 149:3753–3758.
23 Druilhe A, Cai Z, Haile S, Chouaib S, Pretolani M. Fas-mediated apoptosis in cultured human eosinophils. Blood 1996; 87:2822–2830.
24 Min Y, Lee S, Lee J, Chong S, Hahn J, Ko Y. Expression of Fas antigen in acute myeloid leukemia is associated with therapeutic response to chemotherapy. Br J Hematol 1996; 93:928.
25 Iijima N, Miyamura K, Itou T, Tanimoto M, Sobue R, Saito H. Functional expression of Fas (CD95) in acute myeloid leukemia cells in the context of CD34 and CD38 expression: Possible correlation with sensitivity of chemotherapy. Blood 1997; 90:4901–4909.
26 Min Y, Lee H, Choi S, Chi H, Lee J, Kim W, Lee K. Prognostic significance of Fas (CD95) and TRAIL receptors (DR4/DR5) expression in acute myelogenous leukemia. Leuk Res 2004; 28:359–365.
27 Maciejewski J, Selleri C, Anderson S, Young N. Fas antigen expression on CD34+ human marrow cells is induced by interferon g and tumor necrosis factor a potentiates cytokine-mediated hematopoietic suppression in vitro. Blood 1995; 85:3183–3190.
28 Iwai K, Miyawaki T, Takizawa T, Konno A, Ohta K, Yachie A, et al. Differential expression of bcl-2 and susceptibility to anti-Fas-mediated cell death in peripheral blood lymphocytes, monocytes and neutrophils. Blood 1994; 84:1201–1208.
29 Beltinger C, Kurz E, Bohler T, Schrappe M, Ludwing W, Debatin K. CD95(Apo-1/Fas) mutation in childhood T-lineage acute lymphoblastic leukemia. Blood 1998; 91:3943–3951.
30 Karawajew L, Wuoter C, Ruppert V, Drexler H, Gruss H, Ludwig W. Differential CD95 expression and function in T and B lineage acute lymphoblastic leukemia cell. Leukemia 1997; 11:1245–1252.
31 Debatin K, Goldman C, Waldmann T, Krammer P. APO-1 induced apoptosis of leukemia cells from patients with adult T-cell leukemia. Blood 1993; 81:2972–2977.
32 Daniel P, Krammer P. Activation induces sensitivity toward APO-1 (CD95)-mediated apoptosis in human B-cells. J Immunol 1994; 152:5624–5632.
33 Pordzik S, Petrovici K, Schmid C, Kroell T, Schweiger C, Kohne C, Schmetzer H. Expression and prognostic value of Fas receptor/Fas ligand and TrailR1/TrailR2 in acute myeloid leukemia. Hematology 2011; 16:341–350.
34 Cai Z, Stancou R, Korner M, Chouaib S. Impairment of Fas antigen expression in adriamycin-resistant but not TNF-resistant MCF7 tumor cells. Int J Cancer 1996; 68:535–546.
35 Cullen KV, Davey RA, Davey MW. Drug resistance does not correlate with resistance to Fas-mediated apoptosis. Leuk Res 2001; 25:69–75.
36 Wu J, Nihal M, Siddiqui J, Vonderheid EC, Wood GS. Low FAS/CD95 expression by CTCL correlates with reduced sensitivity to apoptosis that can be restored by FAS upregulation. J Invest Dermatol 2009; 129:1165–1173.
37 Komada Y, Zhou Y, Zhang X, Xue H, Sakai H, Sakurai M. Fas receptor (CD95) mediated apoptosis is induced in leukemia cells entering GIB compartment of the cell cycle. Blood 1995; 86:3848–3860.
38 Ogasawara J, Watanabe-Fukunag R, Kasugai T, Kitamura Y, Itoh N, Sada T. Lethal effect of the anti-Fas antibody in mice. Nature 1993; 364:806–809.
We can conclude that the expression of Fas receptors on blast cells from ALL, AML, and CML-BT could serve as an independent prognostic factor, helping in monitoring the outcome of therapy.
It is recommended that Fas should be included as a cell surface marker in the immunophenotyping panel of acute leukemia and blastic transformation phase of CML. Patients with low Fas expression levels may require intense chemotherapy to achieve remission. Trials to enhance Fas expression and Fas-mediated apoptosis of blast cells may be the future hope in acute leukemia therapy.
AcknowledgementsConflicts of interestThere are no conflicts of interest.
References 1 Steller H. Mechanisms and genes of cellular suicide. Science 1995;
267:1445–1448.
2 Evan G, Wyllie A, Gilbert C. Induction of apoptosis in fibroblasts by C-myc protein. Cell 1992; 69:119–128.
3 Sessler T, Healy S, Samali A, Szegezdi E. Structural determinants of DISC function: New insights into death receptor-mediated apoptosis signaling. Pharmacol Ther 2013; 140:186–199.
4 Knipping E, Debatin K, Stricker K, Heilig B, Eder A, Krammer P. Identification of soluble Apo-1 in supernatants of human B- and T-cell lines and increased serum levels in B- and T-cell leukemias. Blood 1995; 85:1562–1569.
5 Yonehara S, Ishii A, Yonehara M. A cell-killing monoclonal antibody (anti-Fas) to a cell surface antigen co-downregulated with the receptor of tumor necrosis factor. J Exp Med 1989; 169:1747–1756.
6 Fischer U, Schulze-Osthoff K. New approaches and therapeutics targeting apoptosis in disease. Pharmacol Rev 2005; 57:187–215.
7 Takahashi T, Tanaka M, Inazawa J, Abe T, Suda T, Nagata S. Human Fas ligand: Gene structure, chromosomal location and species specificity. Int Immunol 1994; 6:1567–1574.
8 Laurent G, Jaffrezou J. Signaling pathways activated by daunorubicin. Blood 2001; 98:913–924.
9 Fulda S, Los M, Friesen C, Debatin K. Chemosensitivity of solid tumor cells is associated with activation of the CD95 system. Int J Cancer 1998; 76:105–114.
10 Schimmer A, Hedley D, Penn L, Minden M. Receptor and mitochondrial-mediated apoptosis in acute leukemia: A transitional view. Blood 2001; 98:3541–3553.
11 Bennet J, Catovasky D, Danial M. Proposed revised criteria for classification of acute leukemia: A report of the French-American-British Cooperation group. Ann Intern Med 1985; 103:620–625.
12 Mitelman F. ISCN: An International System for Human Cytogenetic Nomenclature. Basel, Switzerland: S. Karger; 1995.
13 Mrozek K, Carroll A, Maharry K. Central review of cytogenetics is necessary for cooperative group correlative and clinical studies of adult acute leukemia: The Cancer and Leukemia Group B experience. Int J Oncol 2008; 33:239–244.
14 Grimwade D, Walker H, Oliver F, Wheatley K, Harrison C, Harrison G. The importance of diagnostic cytogenetics on outcome in AML: Analysis of 1612 patients entered into the MRC AML 10 Trial. Blood 1998; 92:2322–2333.
15 Büchner T, Hiddemann W, Wörmann B, Löffler H, Ludwig Wd, Schoch C, et al. Acute myeloid leukemia in adults: Is postconsolidation maintenance therapy necessary? Int J Hematol 2000; 72:285–289.
16 Lengfelder E, Reichert A, Schoch C, Haase D, Haferlach T, Löffler H, et al. Double induction strategy including high dose cytarabine in combination