Tugas THT Ifa

of 4
-
Upload
rifa-ben-bella -
Category
Documents
-
view
217 -
download
0
Transcript of Tugas THT Ifa
-
7/28/2019 Tugas THT Ifa
1/4
Hal 202
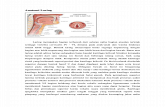
the normal mucosa in the middle ear, particularly in the mastoid, has morphological features
advantageous for the gas exchange. just underneath the single-layer simple squamous ephithelium, rich
distribution of capillaries is observed and there is little interstitial tissue between them (fig.6).
furthermore, observations of the mastoid mucosa by electron microscope reveal that, between themucosal ephithelial cells, there is a wide space where capillaries are almost exposed to the mastoid air
space. This structure is similar to that observed in the alveole in the lung, and looks advantageous for
the efficient gas exchange between the middle ear cavity and capillaries.
More recently, this transmucosal gas-exchange function has been investigated more in detail.
Hergirls et al. by directly measuring the middle ear gas composition by a mass spectrometry, reported
that the partial pressure of nitrogen in the middle ear exceeded that of the blood by approximately 50
mmHg, indicating that gradient may drive the middle ear pressure to profoundly negative level. Doyle et
al., addressing middle ear gas exchange of nitrogen by measuring the nitrous oxide time constant for
middle ear transmucosal gas exchange in monkeys, and using a mathematical model, concluded that
there is an asymmetric rate of nitrous oxide and by extension, nitrogen exchange for the middle ear.
Kania et al., employing similar methods and animal model, as well as a mathematical model, concluded
that transmucosal gas absorption in the middle ear during steady state conditions is governed mainly by
diffusive N2 exchange between the middle ear and its mucosal blood circulation.
Although the ET functions have been examined by various methods over the
Hal 203
Past several decades, there has never been a consistent method to clinicali assess this
transmucosal gas-exchange function in the ME. A method using nitrous oxide during general anasthesithat we developed is one of the versatile measures to assess the function. When nitrous oxide is
inhaled, as is well known, it moves quickly from the lung to the blood and from the blood to any aitr
space within the body such as ME cavity, because nitous oxide has great diffusibility. At that time, the
other gases tend to move in the opposite direction according to the partial pressure gradients caused by
the decreaseof there partial pressure in the blood due to the influx of nitrous oxide, but the velocity of
their movement is slower than that of nitrous oxide. As a result, the ME pressure increases temporarily.
The presence or absence of the increase in the ME pressure by inhalation of nitrous oxide instantly
indicates the permeability of any gas through the ME mucosa, that is, in other word, the transmucosal
gas-exchange function.
Practically, general anesthesia is induce by the mixed gas constaining 67% of room air, 33% of
oxygen and enflurane, than 67% of room air is replaced by nitrous oxide after starting the monitoring of
the middle-earr pressure by the tympanogram or a pressure sensor (Fig. 7).
We first examined 44 normal ears with this method under general anesthesia during various
surgeries other than those on ears, and found that ME pressure increased in all the ears except one: this
indicated that transmucosal gas exchange is working in almost all normal ears. However, the pressure-
-
7/28/2019 Tugas THT Ifa
2/4
increase rate was quite variable ranging from 1.9 to 95 mmH2O per minute (Fig. 8). Correlating the
pressure-increase rate in each ear with the ize of their mastoid(mastoid area on schullers X-ray view),
we found that they were rather inversely
Hal 204
proportional: ear with bigger mastoid had rather smaller pressure-increase rate in vice versa (Fig. 9). It
was contrary to out expectation that an ear with a bigger mastoid would have a grater pressure-increase
rate. Although further studies using subject with more uniform condition as for age or lung condition,
etc. is recurred to regonize it as an absolute phenomenon, this is probably because the gas exchange
taking place on the mucosal surface in the mastoid would be proportional to the mastoid surface area
(twodimensional factor),
Hal 205
Whereas the pressure increase would be inversely proportional to the mastoid volume (three-
dimensional factor). Therefore, if the gas-exchange function by mastoid surface area is the same, the
pressure-increase rate is considered to be rather smaller in an ear with a bigger mastoid. Thus, the
pressure-increase rate does not necessarily indicate a quantitative index of the gas-exchange function in
each individual ear, and we knew that only the presence or absence of the pressure increase should be
interpreted in this examination. The volume-increase rate due to nitrous oxide which should be a true
index of the gas-exchange function in the middle ear, can be calculated from the pressure-increase rate
and the volume of the middle ear. The middle ear volume was logically calculated from the area of the
mastoid on schullers view using a formula that we previosly developed. We then correlated it with the
mastoid size, and found that a bigger mastoid had greater gas-exchange function (fig 10). Thus, as weexpected, a well-developed mastoid appears to be important for the ventilation and pressure regulation
of the middle ear.
Looking at the relationship between the gas-exchange function and the age, an interesting
tendency can be seen (fig 11): the pressure-increase rates in children under the age of fifteen are all
greater than the regression line calculated from the values of adults, regardless of the mastoid size.
Although in general a more rapid nitrous oxide blood saturation may be obtained in children than in
adults, this may indicate that the gas-exchange function is more active in children than in adults. This
may be explained by the fact that the mastoid mucosa has a richer blood supply in children than in
adults. This also accounts for the fact that mastoid aeration tends to recover better in children than in
adults after mastoid surgery.
Hal 206
acute immplamation in the middle ear cleft
negative ME pressure manifested by retraction of the eardrum is often seen in patients with
otitis media, and various causes have been considered related to production of the negative pressure .
-
7/28/2019 Tugas THT Ifa
3/4
we will discuss about possibility to produce the negative ME pressure from the viewpoint of
pathophysiology of the transmucosal gas-exchange function during otitis media.
Kania et al. utilized a rat experimental model to study transmucosal gas-exchange by measuring
volume change in the ME. ME gas exchange was recorded after resolution of effusion caused by LPS
inoculation. The ME gas volume decreased significantly steeper with time in inflamed ears compared tothe normal control. Mucosal thickness was significantly greater in the inflamed ears. These changes are
consistent with increased mucosal blood flow. Ar et al. compared the mucosal blood flow in normal and
inflamaed ears, concluding, that the increased gas exchange, despite yhe doubling of the mucosal
thickness may be explained by doubling the mucosal blood flow. ME-gas loss was assessed when its
mucosa was inflamed in the rat, and from a mathematical model,. Concluded that the model predicts
that the increased gas loss may be explained by increased blood flow rate. Demonstrated that nasal
inflammation created with bradykinin and prostaglandin D2 challenge increased the inert gas exchange
rate, indicating that persistent nasal inflammation would increase yhe demand on the ET for the gas
supply , and may result in OME when this demand is not met. These data may indicate that, in
Hal 207
An abnormal condition of inflammation, transmucosal gas-exchange function works for gas
absorption rather than pressure regulation in the middle ear.
As another possible cause of negative middle ear pressure production during otiitis media, we
recently hypothesized that, only when there is infection in the middle ear (otitis media), the oxygen
consumption by bacteria or inflammatory cells might produce progessive negative middle ear pressure,
and we examined in vitro whether or not gas absorption comes from bacteria, streptococcuspneumoniae, which in one of the most popular bacteria of the otitis media. (fig 12). Each 1-ml sample of
a bacterial suspension containing the bacteria and controls containing only culture medium were
hermetically sealed in tubes and were kept in the 37 C bath, and then the air pressure in the tube was
monitored. Three hours later, pressure of the majority of samples with bacteria were observed to
decrease progressively to be -174 mmH2O on average, while those of the control group did not
significantly change (mean 1.35 mmH2O). more recently, we added gas analysis of the samples to this
experiment, which revealed apparent decrease in oxygen partial pressure in the bacterial samples while
no distinct change in the control samples (). Thus, consumption of oxygen by bacteria was considered as
one of the possible causes of production of middle ear negative pressure specifically in cases with
bacterial infection.
At this stage, an important problem is ET function of those ears. It is well knows that patients
with OME have ET with poor ventilatory function , namely almost all of them cannot equalize negative
middle ear pressure. This characteristic feature of the ET in OME patients seems a kind of their
predisposition, because this inability to equalize the negative middle ear pressure did not improve even
in the convalescent stage of OME (fig 13).
-
7/28/2019 Tugas THT Ifa
4/4
Then, how is the Eustachian tube function in normal? Normal individuals have ability to reduce
more than half of the applied positive middle ear pressure, and ability to reduce any degree of the
applied negative middle ear pressure afteer several swallowings. These facts suggest that the ET has a
one-way-valve structure where air goes more readily from the middle ear to the pharynx than in the
opposite
Hal 208
Direction. This may be also the reason why the ET function tends to be easily impaired once it
develops a pathological condition. For example, even a normal individual, who is not otitis-prone ,
sometimes has ET dysfunction with upper respiratory tract infection ands need several weeks to recover
from it (fig 14). We are sometimes aware that we feel ear fullness when we have an upper respiratory
tract infection , and that we cannot release it by various tasks like swallowing. In the ET of ears with
OME , which is regarded as one of the representative middle ear diseases in which failure of the middle
ear ventilation is most related to its pathogenesis, the above-mentioned aerodynamic character of the
one-way-valve generally becomes more prominent despite rare organic stenosis or obstruction . this is
also a good example of the high vulnerability of ET function.
Hal 209
Hal 210
Hal 213
Hal 214