Trauma Pelvis Dan Urologi
81
1 Trauma Pelvis dan Trauma Pelvis dan Traktus Urinarius Traktus Urinarius Dr. Adam Suyadi , SpB, MM Dr. Adam Suyadi , SpB, MM Bag Bedah FK UII Yogyakarta Bag Bedah FK UII Yogyakarta
-
Upload
leny-anjani -
Category
Documents
-
view
33 -
download
5
description
trauma pelvis
Transcript of Trauma Pelvis Dan Urologi

1
Trauma Pelvis dan Trauma Pelvis dan Traktus UrinariusTraktus Urinarius
Dr. Adam Suyadi , SpB, MMDr. Adam Suyadi , SpB, MM
Bag Bedah FK UII YogyakartaBag Bedah FK UII Yogyakarta

2
Pendahuluan
• Organ urogenitalia terletak di rongga ekstraperitoneal, kecuali genitalia eksterna
• Terlindung otot dan organ lain• Aman kecuali trauma hebat• Kemungkinan cedera organ sekitarnya

3
Trauma Urogenital
• Trauma Ginjal• Trauma Ureter• Trauma Buli-buli• Trauma Uretra
– Ruptura Uretra Anterior– Ruptura Uretra Posterior
• Trauma Penis

4
TESTISTESTIS
• Pendarahan• Arteri
spermatika• Pleksus
pampiniformis vena spermatika
• 90% varikokel terjadi pada sisi kiri
ANATOMI

5
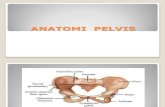
Anatomi Ginjal

6
Trauma Ginjal
• Terjadi karena :1) langsung kena benturan
2) cedera deselerasi• 10% trauma abdomen mengenai ginjal • Dapat karena trauma tumpul, trauma tajam
maupun luka tembak• Guncangan pada ginjal dapat
menyebabkan robeknya capsul ginjal bahkan parenchym

7
Mekanisme Trauma Tumpul

8
Derajat trauma ginjal
• Derajat I : Kontusio ginjal/hematom • Derajat II : Laserasi ginjal pada
cortex• Derajat III : Laserasi sampai medulla• Derajat IV: sampai mengenai calixes• Derajat V : avulsi pedikel ginjal
sampai terbelah

9
Derajat Trauma Ginjal

10
Derajat Trauma Ginjal

11
Diagnosis
• Ada riwayat trauma didaerah pinggang• Ada hematuria• Fractur costa VIII – XII• Trauma tembus abdomen sampai pinggang• Jatuh dari ketinggian• Multiple trauma

12
Penatalaksanaan
• Konservatif• Operatif

13
Trauma Ureter
• Jarang Dijumpai
• Kurang dari 1% kasus cedera urologi:
- trauma tumpul
- trauma tajam
- trauma tembus/tembak (2-3%)
- trauma iatrogenik (terbanyak)

14
PENDAHULUAN
• Cedera ureter jarang terjadi• Kurang dari 1% kasus cedera urologi:
- trauma tumpul- trauma tajam - trauma tembus/tembak (2-3%)- trauma iatrogenik (terbanyak)

15
Kunci keberhasilan penanganan:
- Identifikasi dini
- Kewaspadaan tinggi
- Pengetahuan luas penanganan cedera
Diagnosis yang terlambat:
- morbiditas
- kematian

16
AnatomiUreter

17
ANATOMI

18
FISIOLOGI
• Fungsi Ureter :
Mengalirkan urine dari pelvis ginjal ke kandung kemih
Peristaltik ritmik: lapisan otot longitudinal dan sirkulerTekanan intravesika : Anti RefluksMenyemprotPer menit : 1-5 kali

19
ETIOLOGI & MEKANISME CEDERA
• TRAUMA PEMBEDAHANTersering pada operasi daerah pelvis Histerektomi : 67%Operasi kolorektal : 9%
• Kasus Urologi : 42% dari kasus iatrogenik (Endoskopi 79% ; bedah terbuka 21%)• Mayoritas cedera ureter bagian distal : 87%

20
DERAJAT CEDERA URETER
• Grade I : hematoma tanpa devaskularisasi• Grade II : laserasi terpotong < 50%• Grade III : laserasi terpotong > 50%• Grade IV : laserasi terpotong komplet &
devaskularisasi 2 cm• Grade V : avulsi hilus renalis &
devaskularisasi ren atau > 2 cm

21
Tipe Cedera Ureter

22
Diagnosis Klinis
• Diagnosis Preoperatif Hematuria : 40-70% (+)
- bukan tanda pasti- trauma tajam 23-45% (-)- trauma tumpul 31-67% (-)- trauma iatrogenik : hanya 10-15% (+)
Cek lab : analisa dan kultur urine, DL,
kreatinin serum dan produk drain

23
Kecurigaan Cedera Iatrogenik
DURANTE OPDURANTE OP Lapangan operasi
banyak cairan Hematuria Anuria/Oliguria pada
cedera bilateral
PASCAOPERASIPASCAOPERASI• Demam• Ileus• Nyeri pinggang• Luka operasi basah• Drain jernih dan banyak• Hematuria persisten• Urinoma• Fistula ureterokutan

24
Cedera yang tak teridentifikasi
• Demam dan sepsis (10%)• Massa atau pegal di pinggang (36-90%)• Urinoma, ileus yang lama, gagal ginjal, infeksi
(10%)
Warning : 70-80% cedera iatrogenik terdiagnosis pascaoperasi

25
• Regions of the abdomen• 3 distinct anatomical compartments: peritoneum,
retroperitoneum and pelvis• peritoneal cavity subdivided into:
– intrathoracic segment • covered by bony thorax and includes diaphragm, liver, spleen,
stomach and transverse colon
– abdominal segment

26
• retroperitoneum – aorta, vena cava,
pancreas, kidneys, ureters and portions of duodenum and colon
– injuries to this region notoriously difficult to diagnose because the area is remote from physical examination and is not sampled by peritoneal lavage

27
• pelvic organs – rectum, bladder, iliac
vessels, internal genitalia of women
– injury also difficult to diagnose early because of anatomical location

28
• Fractures of the hip joint include fractures of the proximal femur and acetabular.
• Pelvic fractures also can be included in the category of hip fractures, because pain attributed to the hip region (i.e., buttock, groin, high) can emanate from an injury to the pelvic ring.

29
• most pelvic fractures involve high-energy forces• such as those generated in a motor vehicle
accident, crush accident or fall. • Depending on the direction and degree of the force,
these injuries can be life-threatening

30
• A broken pelvis is painful, often swollen and bruised.
• The individual may try to keep the hip or knee bent in a specific position to avoid aggravating the pain.

31
Pelvic injury• Associated with a mortality
of 13-23% and significant morbidity. In majority of patients massive retroperitoneal haemorrhage is direct cause or a major contributing factor to mortality

32
Mechanism of injury• Significant pelvic
fractures are due to high energy blunt trauma. Usually a RTA, fall or crush injury.

33
Clinical features
• suggested by pain on movement, structural instability, gross haematuria, peripelvic ecchymoses
• rectal examination mandatory to identify rectal injury and prostatic position
• if patient has a stable pelvic fracture hypotension is probably due to haemoperitoneum

34

35

36

37

38

39

40

41

42

43

44

45

46

47

48

49

50

51

52

53

54

55
PELVIC RING FRACTURESFractures of the pelvis involve 1 or more bones of the pelvic ring (i.e., the sacrum and the 2 innominate bones) and may involve the ligamentous structures between these bones

56
classification systems for pelvic ring disruptions
According to the frequently used system proposed by Tile :
• type A pelvic injuries are stable with insignificant displacement,
• type B fractures are rotationally unstable or displaced in the axial plane but are vertically stable,
• type C injuries are vertically (coronally), posteriorly, and rotationally unstable

57

58
ACETABULAR FRACTURES
Acetabular fractures occur primarily in young adults as a result of high-energy trauma. These fractures, by definition, involve the hip joint and may be displaced or nondisplaced. Displaced intraarticular fractures that are allowed to heal in an abnormal position may lead to posttraumatic arthritis

59

60
• Acetabular fractures by Judet and colleagues 1964
• Fractures are divided into 5 simple and 5 associated fracture types. The simple types are fractures of the posterior wall, posterior column, anterior wall, anterior column, and transverse fractures (Figure 4), whereas the associated types are formed by a combination of the simple types

61

62

63

64

65
Complications of comminuted fracture of the pelvis
Acute:• major haemorrhage (leading cause of death);
shock, elevated intra-abdominal pressure • visceral and soft tissue injury: fractures may be
compound into the perineum or vagina, or be associated with lacerations into the rectum or bladder (esp. with lateral compression and vertically unstable injuries).
• urethral injuries common in males. Iinsertion of a urethral urinary catheter contraindicated

66

67
• sacral plexus injury • ileus • pain • fat embolization • acute respiratory distress syndrome: in about 15%
: thoracic injuries, multiple blood transfusions, shock, and fat embolization.
• DVT because of stasis resulting from prolonged bed rest, and prophylaxis is often contraindicated

68
Late:• infection-second most common cause of death • disability/immobility/instability • incontinence • pain

69
• Urinary tract and renal injury• more common after blunt than penetrating injury • identification and treatment of other major injuries
takes precedence • gross haematuria requires investigation (CT is
examination of choice if haemodynamically stable), while microscopic haematuria does not unless there is unexplained shock. Degree of macroscopic haematuria not related to severity of injury

70
• majority of renal injuries can be treated conservatively
• bladder rupture commonly associated with pelvic fractures – >95% have macroscopic haematuria – Retrograde cystography is investigation of choice – Intraperitoneal rupture requires operative repair while
extraperitoneal rupture can be treated conservatively

71

72
Trauma Tractus Urinarius Inferior
• Penanganannya masih kontroversial• Pada kasus multipel trauma, harus diperhatikan:
– monitor urine output dengan DC– Pencegahan eksaserbasi trauma uretra
• Disuspek Ruptur Uretra apabila terdapat:– Darah di Meatus Uretra Eksternus– Laserasi perineum– Prostat melayang pada RT
JANGAN DIPASANG DC

73

74
Management• bleeding is usually bony or venous in origin • if patient is still haemodynamically unstable perform
early open DPL. If grossly positive laparotomy should precede external fixation or angiography. If positive by cell count only risk of major intra-abdominal haemorrhage is low and control of pelvic bleeding becomes main priority
• early stabilization with external fixators helps to minimize bleeding from veins and small arterioles near # sites. Also reduces volume of an open pelvis and thus improves tamponade

75

76
Management
• pelvic angiography with embolization often successful in controlling arterial haemorrhage but logistically difficult
• large vessel bleeding requires surgical control • early operative stabilization of complex pelvic
fractures preferred in ICU: facilitates respiratory care, pain control and early mobilization
• compound fractures involving perineum, rectum or vagina require aggressive surgery to avoid high mortality

77
Pemeriksaan Penunjang• IVP• RPG• Sistografi

78
Treatment is suprapubic drainage and delayed definitive repair

79

80

81
TAMATTAMAT