Trauma Pelvis Ppt
61
TRAUMA PELVIS Humaryanto
Transcript of Trauma Pelvis Ppt
TRAUMA PELVIS Humaryanto
Tujuan
Mengetahui jenis-jenis
fraktur pelvis dan
penatalaksanaannya
Mengetahui indikasi dan
tehnik pemasangan c-
clamp
Pelvis
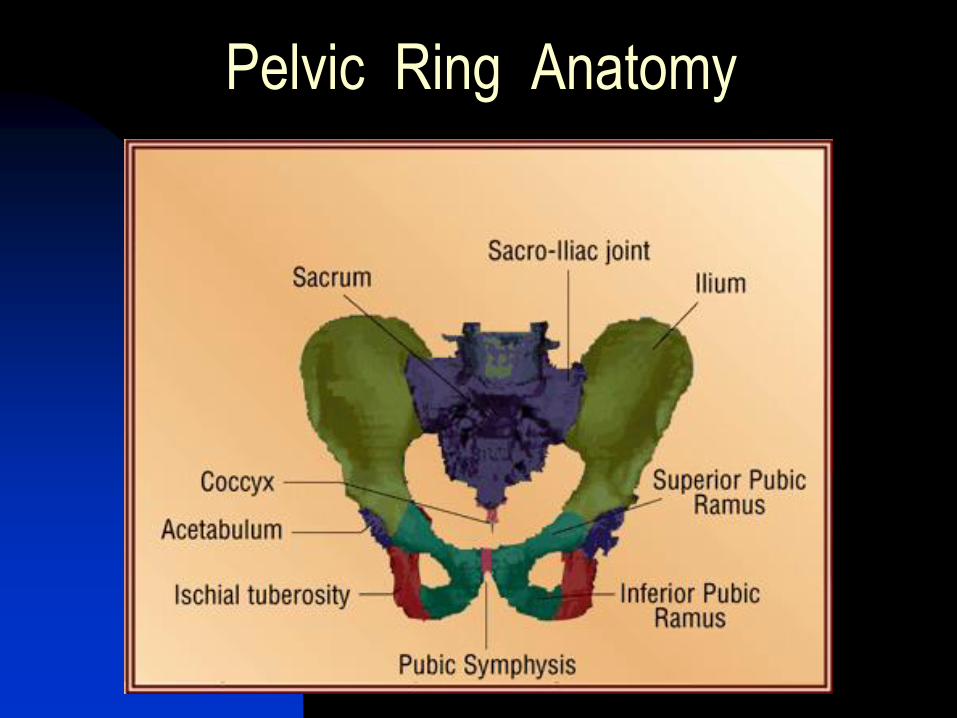
Anatomi pelvis :
Berbentuk cincin, terdiri dari tulang ilium, ischium, pubis dan sacrum
Di bagian anterior berartikulasi pada simfisis pubis dan di posterior pada sendi sakroiliac
Di rongga pelvis banyak terdapat organ penting : saraf, pemb.darah, buli-buli dll
Pelvis Stabilitas pelvis tergantung dari integritas
ligamen dan tulang
Ligamen yang terpenting dan terkuat
adalah ligamen pada bagian posterior
yaitu lig. sacroiliac dan iliolumbar
Pada trauma pelvis yang tidak stabil
dapat terjadi kehilangan darah yang
sangat besar dan dapat terjadi
komplikasi pada organ viscera pada
rongga pelvis
Fraktur pelvis
Fraktur pelvis menyebabkan terbukanya
cincin pelvis dan dapat mengakibatkan
ketidakstabilan
Derajat ketidakstabilan tergantung dari
cincin bagian mana yang terputus
Ketidakstabilan secara mekanik dapat
mengakibatkan ketidakstabilan
hemodinamik bila disertai dengan
kerusakan vaskuler dalam rongga pelvis
syok
Fraktur pelvis
Mortalitas akibat fraktur
pelvis
3% pada pasien yang MRS
dengan hemodinamik stabil
38% pada pasien dengan
hemodinamik tidak stabil
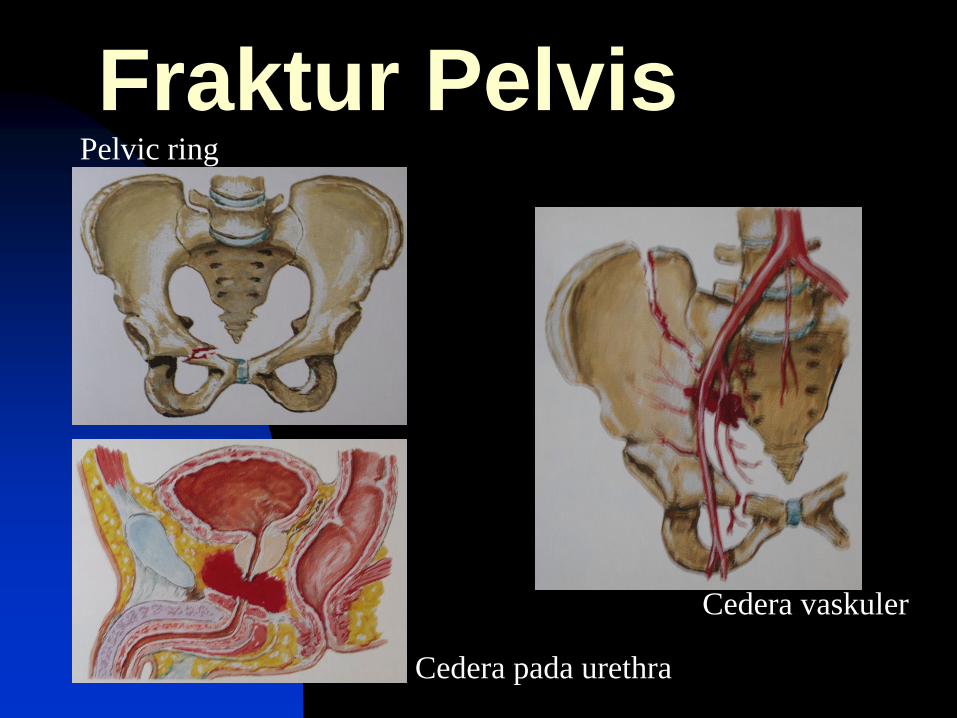
Fraktur Pelvis Pelvic ring
Cedera pada urethra
Cedera vaskuler
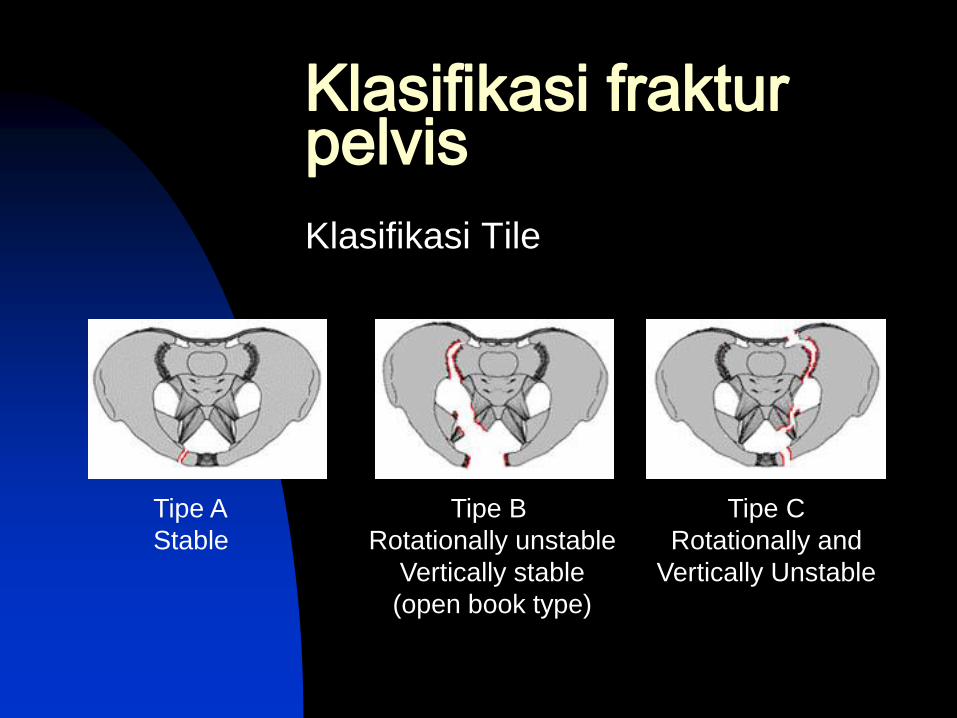
Klasifikasi fraktur pelvis
Klasifikasi Tile
Tipe A
Stable
Tipe B
Rotationally unstable
Vertically stable
(open book type)
Tipe C
Rotationally and
Vertically Unstable
Young and Burgess
proposed a different
modification of the
original Pennal
classification, adding a
new category for
combined mechanism
injuries
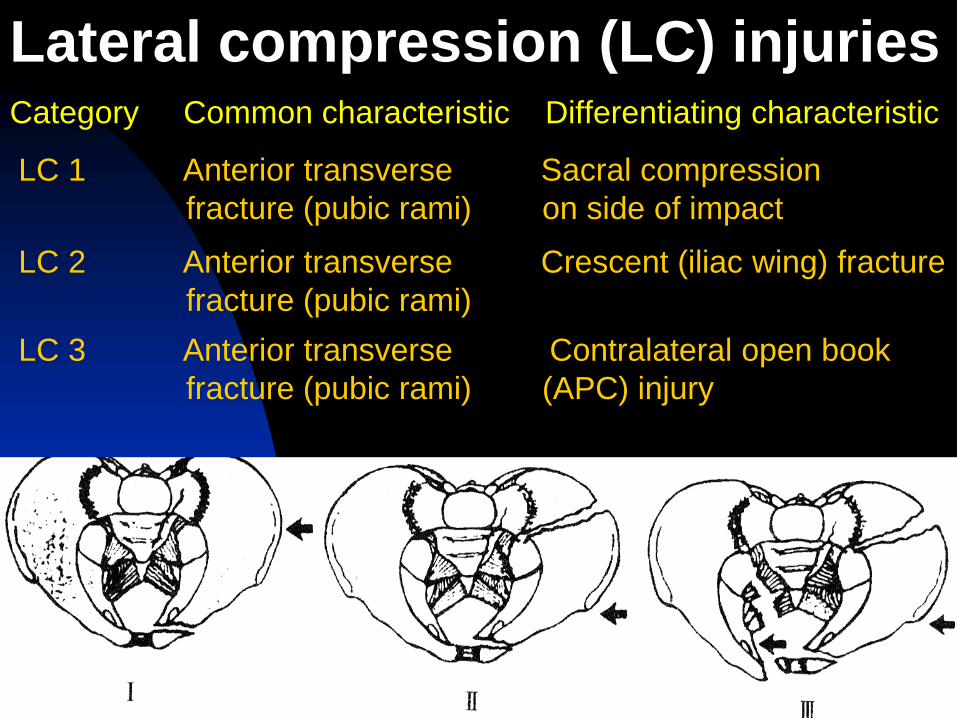
Category Common characteristic Differentiating characteristic LC 1 Anterior transverse Sacral compression
fracture (pubic rami) on side of impact LC 2 Anterior transverse Crescent (iliac wing) fracture
fracture (pubic rami) LC 3 Anterior transverse Contralateral open book
fracture (pubic rami) (APC) injury
Lateral compression (LC) injuries
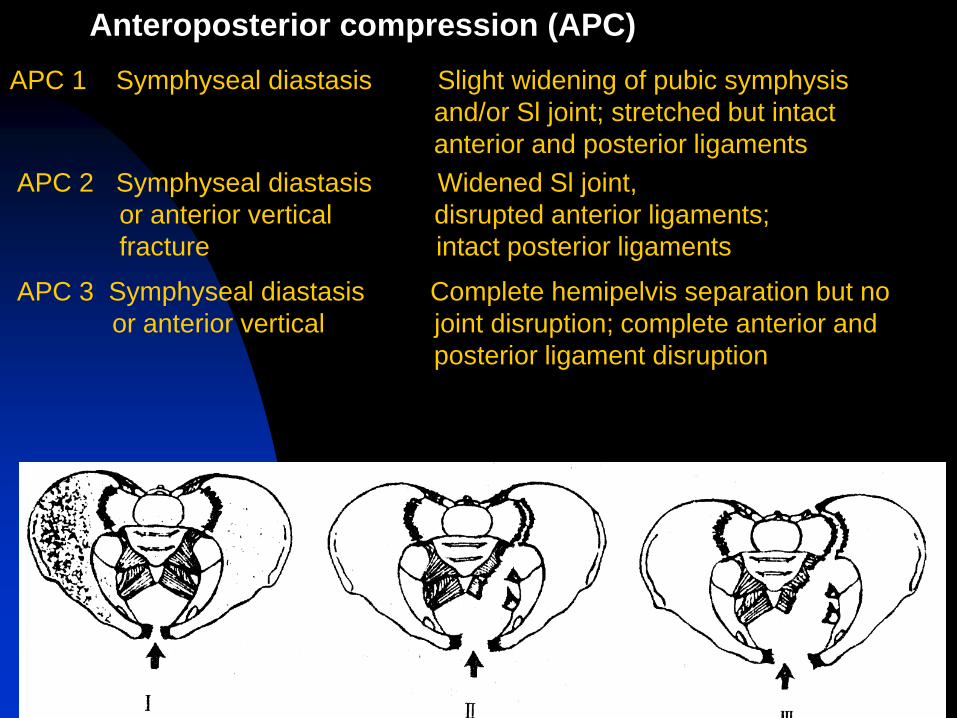
APC 1 Symphyseal diastasis Slight widening of pubic symphysis
and/or Sl joint; stretched but intact
anterior and posterior ligaments APC 2 Symphyseal diastasis Widened Sl joint,
or anterior vertical disrupted anterior ligaments;
fracture intact posterior ligaments
APC 3 Symphyseal diastasis Complete hemipelvis separation but no
or anterior vertical joint disruption; complete anterior and
posterior ligament disruption
Anteroposterior compression (APC)
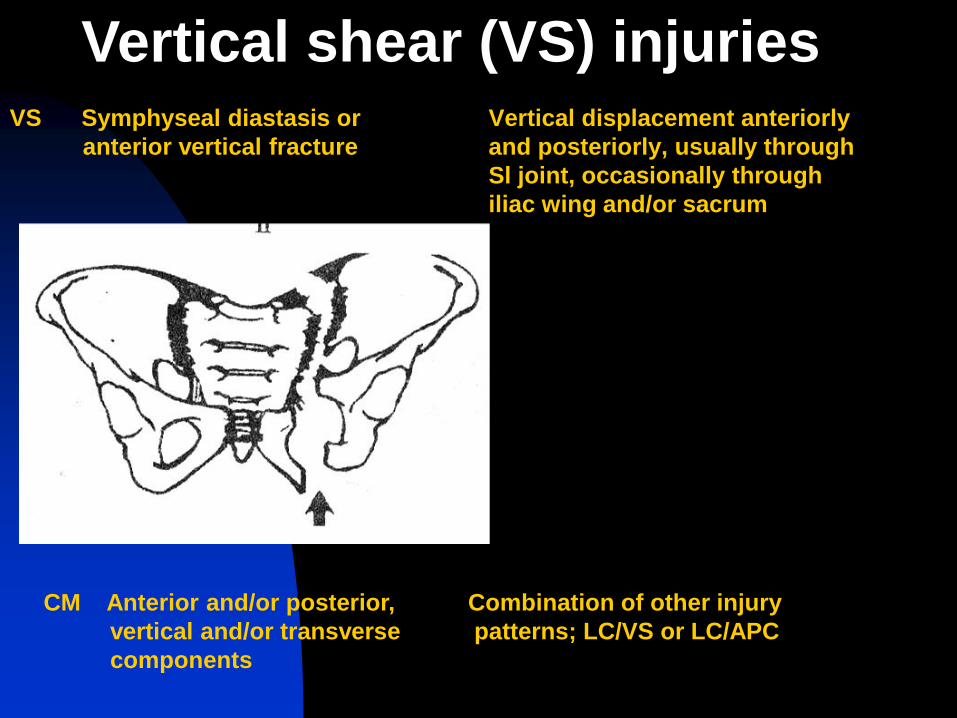
VS Symphyseal diastasis or Vertical displacement anteriorly
anterior vertical fracture and posteriorly, usually through
Sl joint, occasionally through
iliac wing and/or sacrum
Vertical shear (VS) injuries
CM Anterior and/or posterior, Combination of other injury
vertical and/or transverse patterns; LC/VS or LC/APC
components
In a subsequent series, lateral compression (LC)
injuries were the most common injury pattern,
accounting for 41% of the patients, followed by
anteroposterior compression (APC) injuries
(26%), acetabular fractures (18%), combined
mechanism (CM) injuries (10%), and vertical
shear (VS) injuries (5%). Hypovolemic shock
and large blood requirements were more
common in patients with vertically unstable
APC type 3 injuries than in those with vertically
stable anteroposterior or lateral compression
injuries.
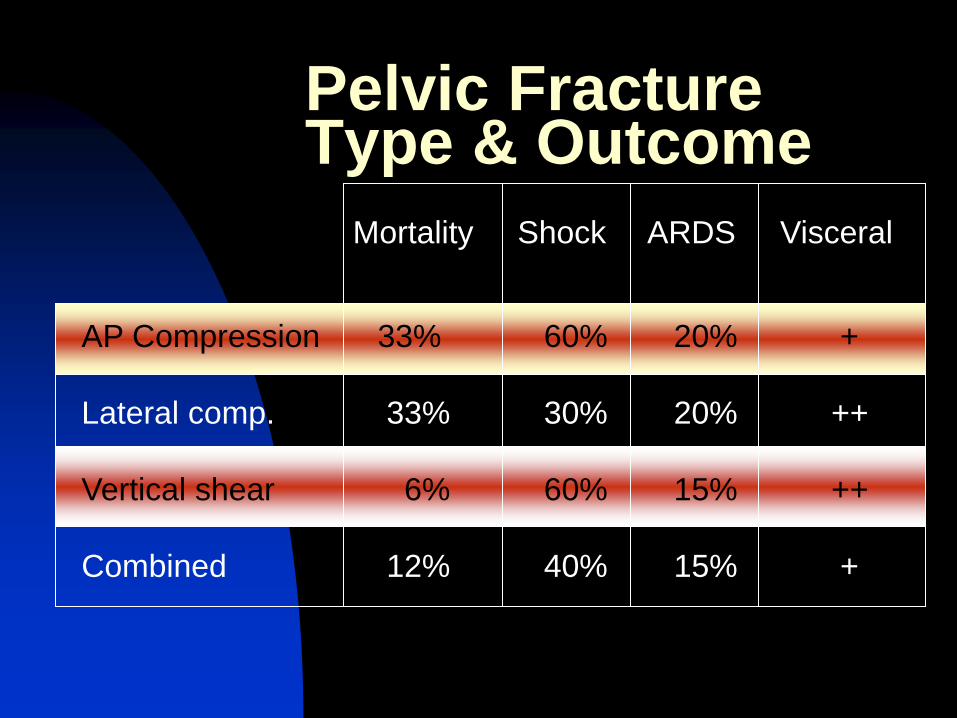
Pelvic Fracture Type & Outcome
Mortality Shock ARDS Visceral
AP Compression 33% 60% 20% +
Lateral comp. 33% 30% 20% ++
Vertical shear 6% 60% 15% ++
Combined 12% 40% 15% +

Pelvic trauma
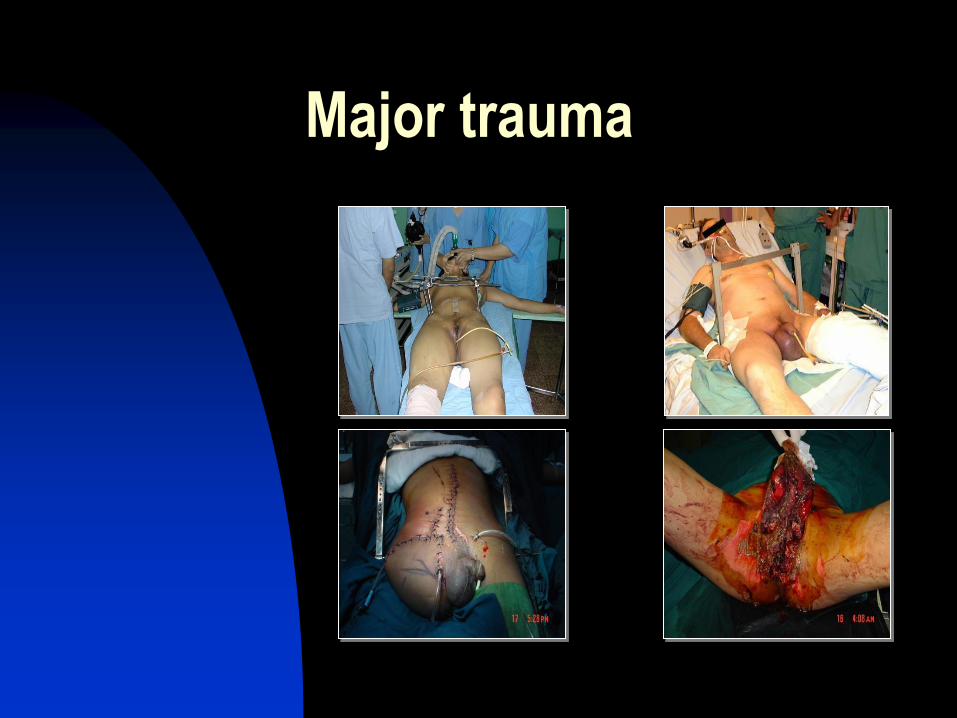
Major trauma
Polytrauma patients
Life threatening
Haemorrhagic shock
Traffic accident
Injuries
Major trauma
Polytrauma
Head
Chest
Abdomen
Spine
Pelvis
Extremities
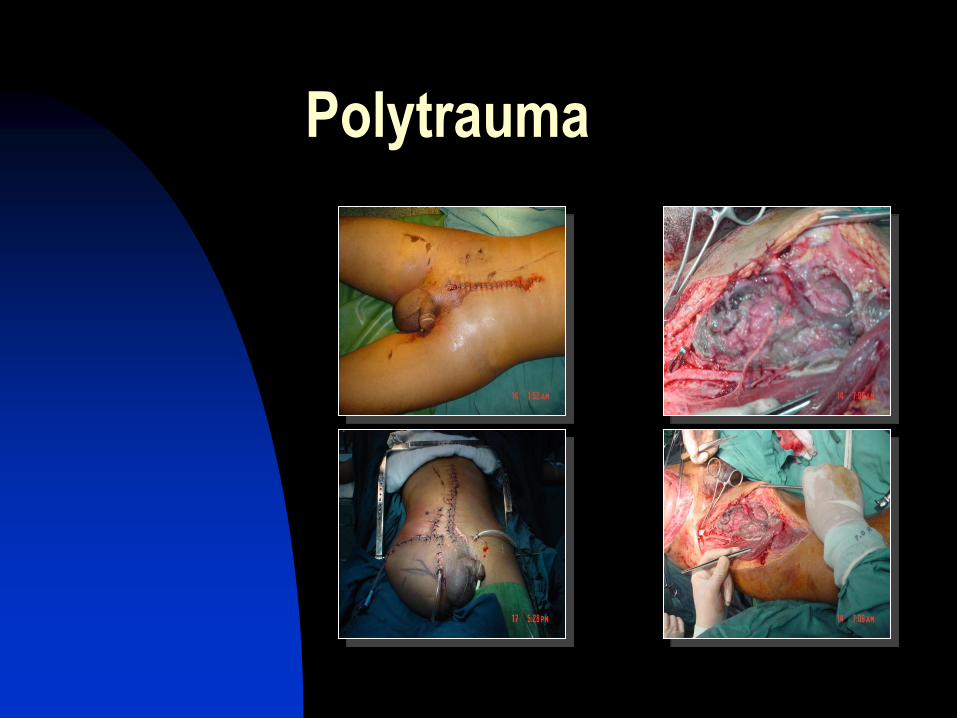
Polytrauma
Anatomy
Bones
Ligaments
Vessels
Nerves
Visceras
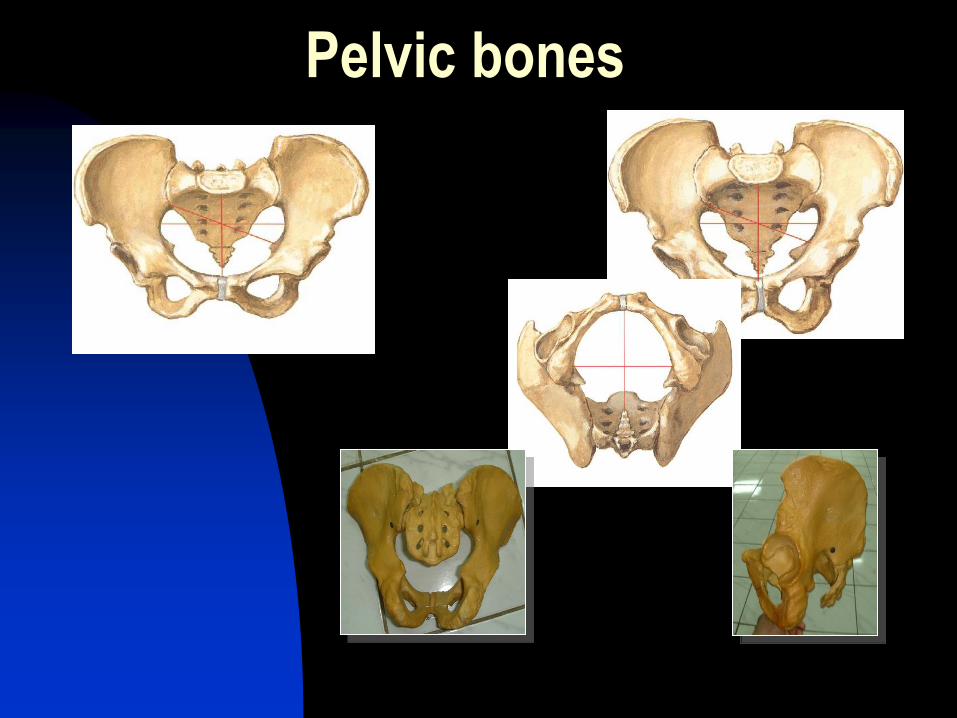
Pelvic bones
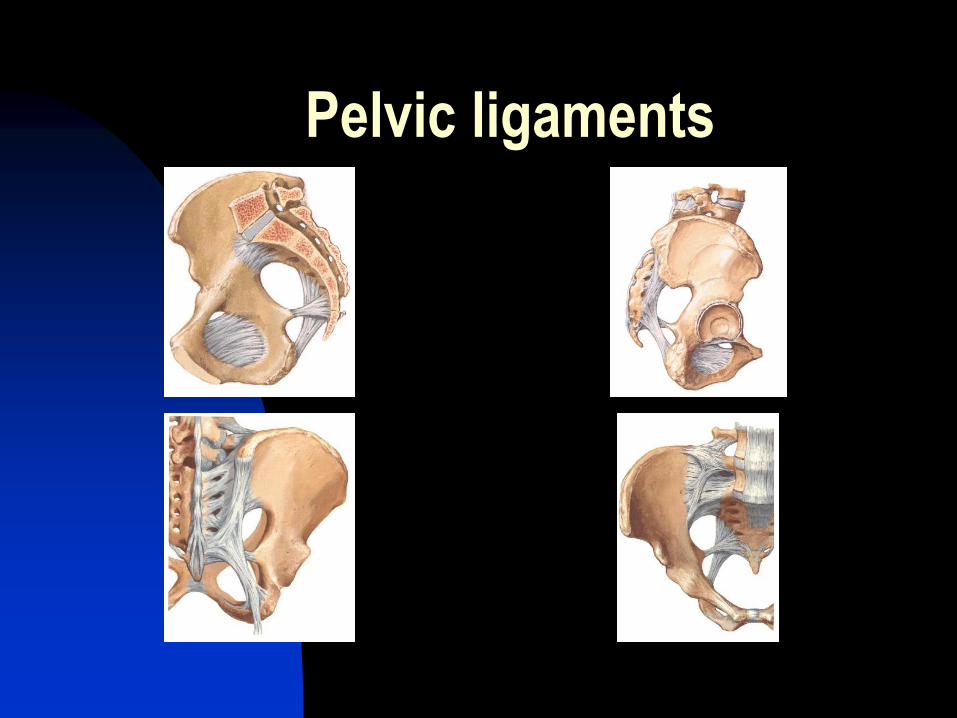
Pelvic ligaments
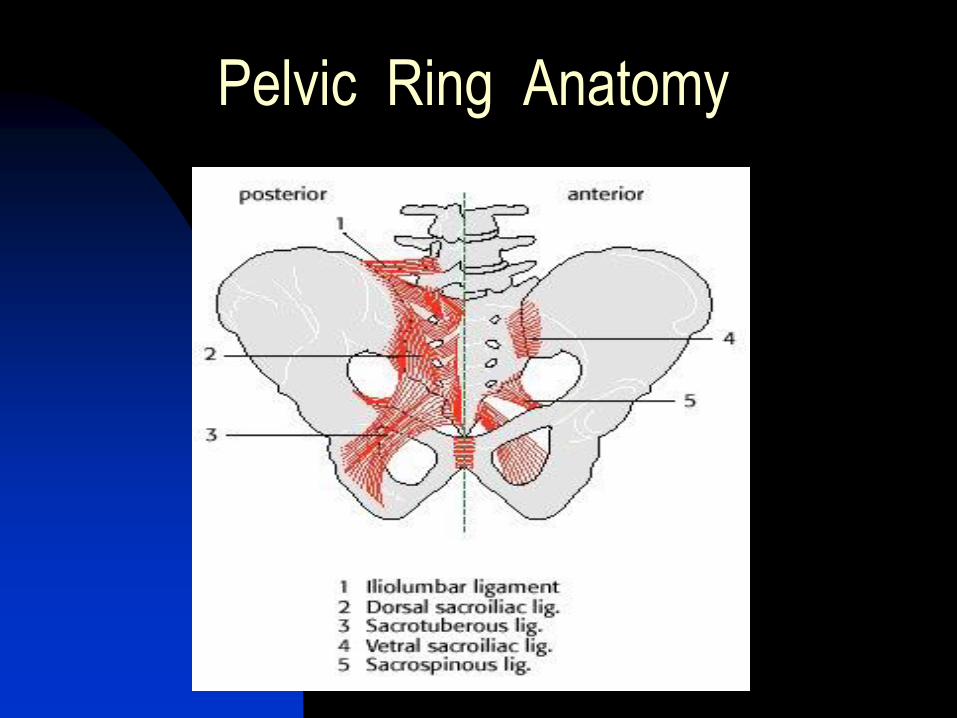
Pelvic Ring Anatomy
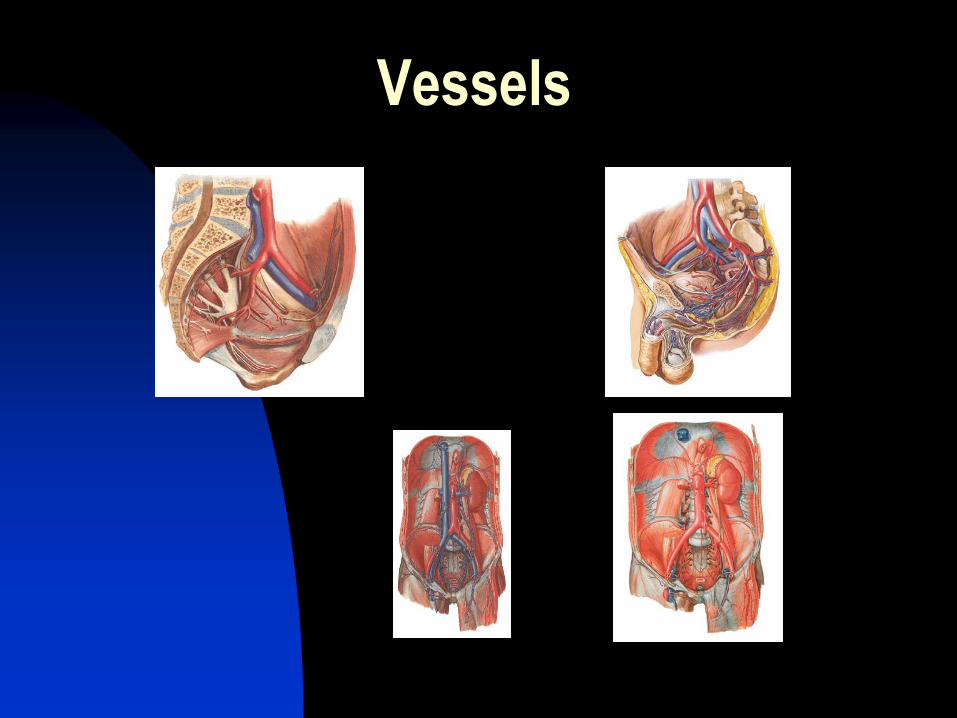
Vessels
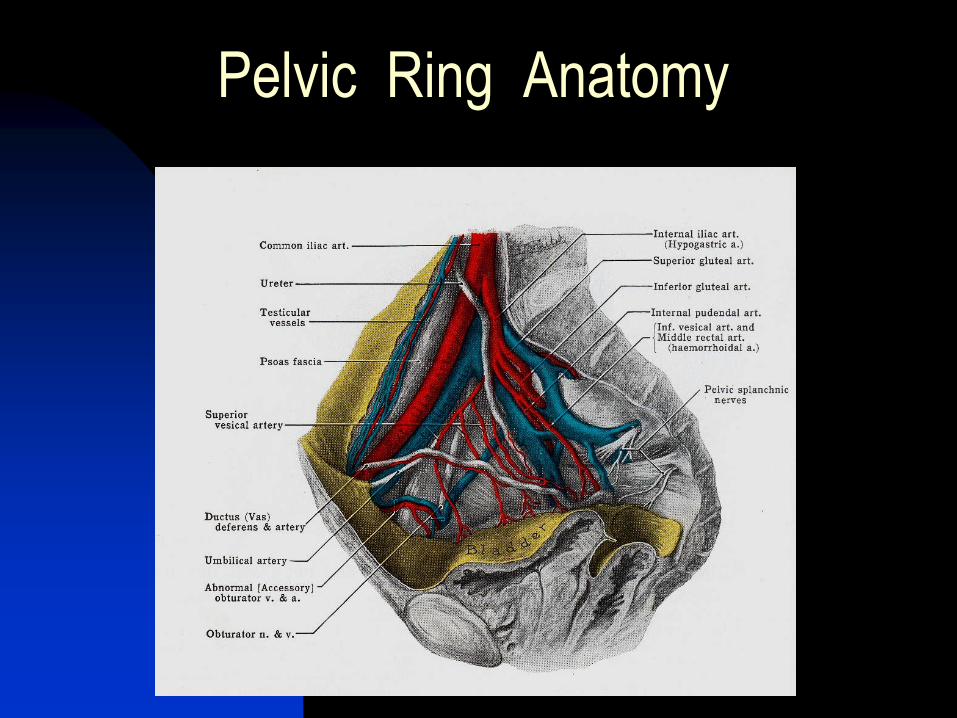
Pelvic Ring Anatomy
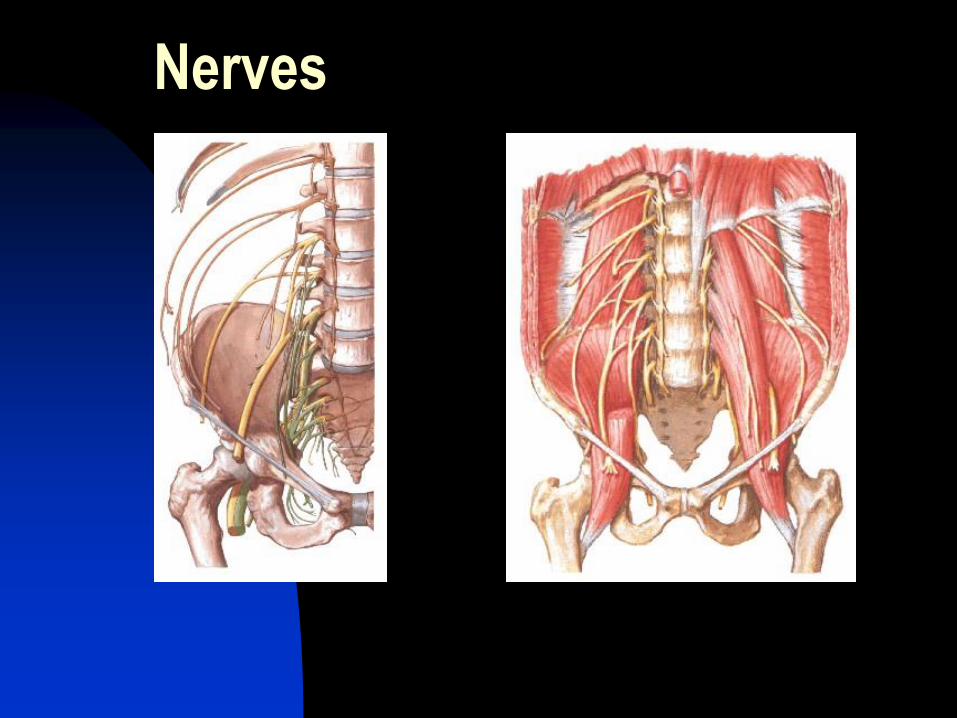
Nerves
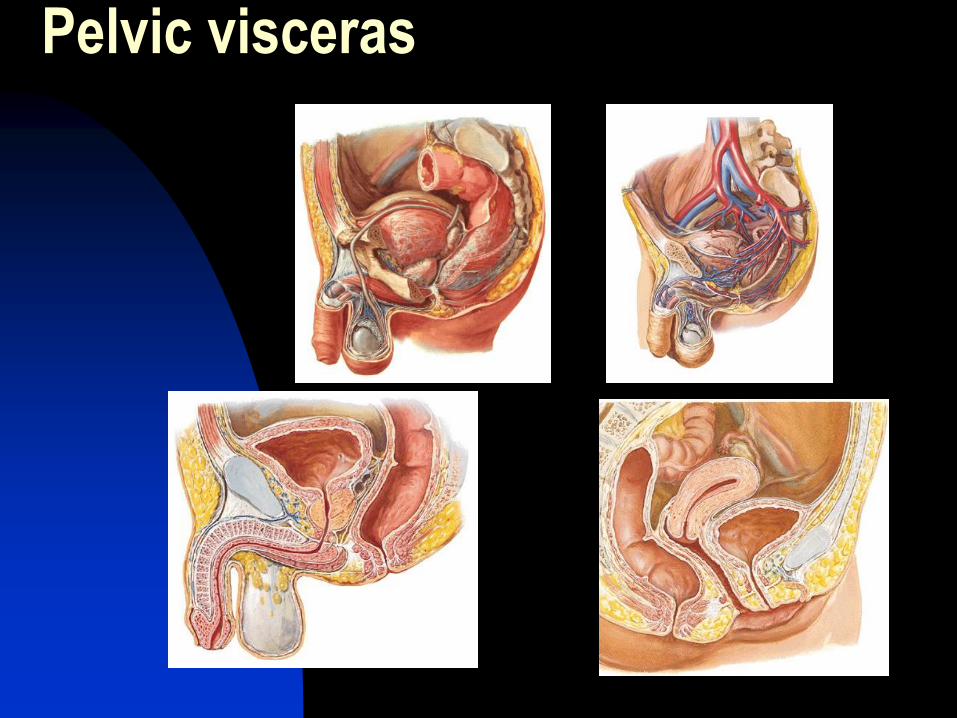
Pelvic visceras
Diagnosis Pada setiap trauma abdomen bawah dan tungkai selalu pikirkan kemungkinan fraktur pelvis
Perhatikan mekanisme cedera
Pemeriksaan klinis :
Jejas pada pelvis/abdomen bagian bawah
Nyeri tekan pada pelvis
Ketidakstabilan pada perabaan
Perbedaan panjang kedua tungkai
Rectal examination & darah pada mue
Hipotensi & tachycardia (bila disertai gangguan hemodinamik)
Radiologis : foto pelvis AP, CT scan
Diagnosis
History
Physical examination
Radiographic examination
Mechanisms of Injury
low-energy fractures: generally
resulting in isolated fractures of
individual bones
do not damage the true integrity of
the ring structure
domestic falls: "straddle" injury
from a fall in the bathtub, an
etiology frequently found in the
elderly population
avulsion injuries of the muscle
apophyses in skeletally immature
patients.
Mechanisms of Injury
high-energy fractures: generally producing pelvic ring disruption
motor vehicle, 57%; pedestrian, 18%; motorcycle, 9%; falls from heights, 9%; and crush, 4%
often result in two or more fractures of the pelvic ring
AP force, lateral impacts, vertical shear
Penetrating mechanisms: associated visceral and neurovascular injuries

History of trauma
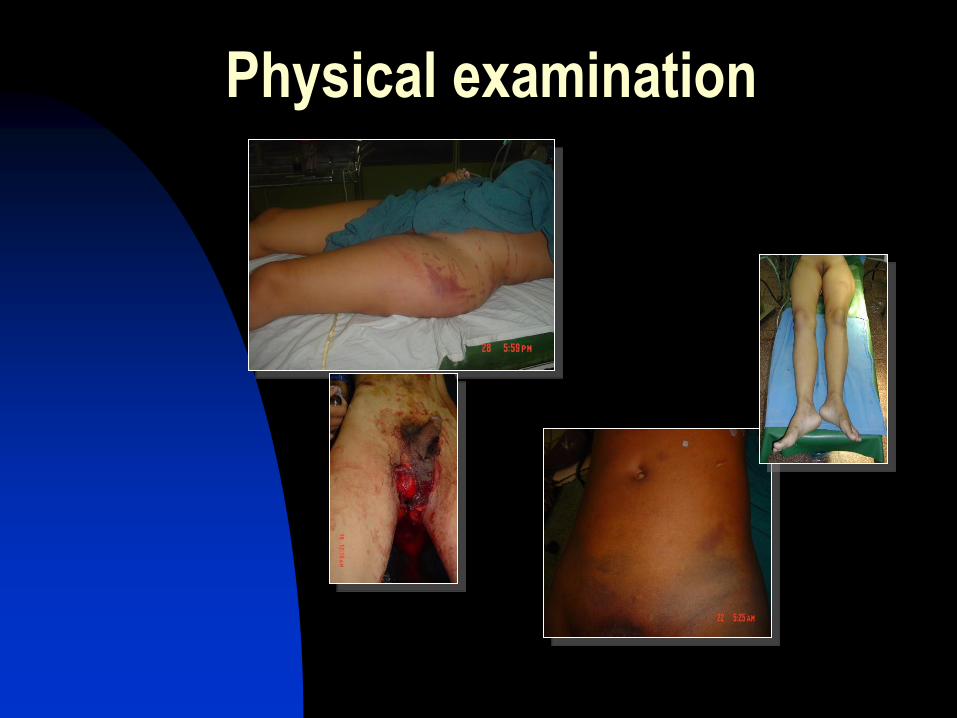
Physical examination
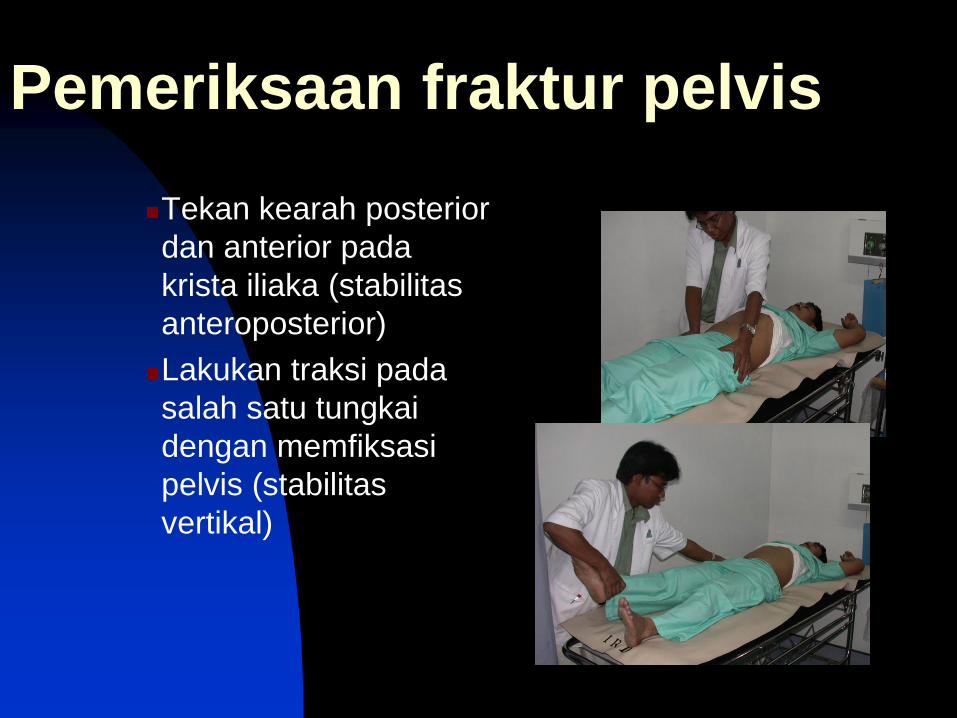
Pemeriksaan fraktur pelvis
Tekan kearah posterior
dan anterior pada
krista iliaka (stabilitas
anteroposterior)
Lakukan traksi pada
salah satu tungkai
dengan memfiksasi
pelvis (stabilitas
vertikal)
Pemeriksaan radiologis
Bila keadaan pasien memungkinkan
segera dilakukan pemeriksaan foto
pelvis AP
CT scan
3 dimensional CT
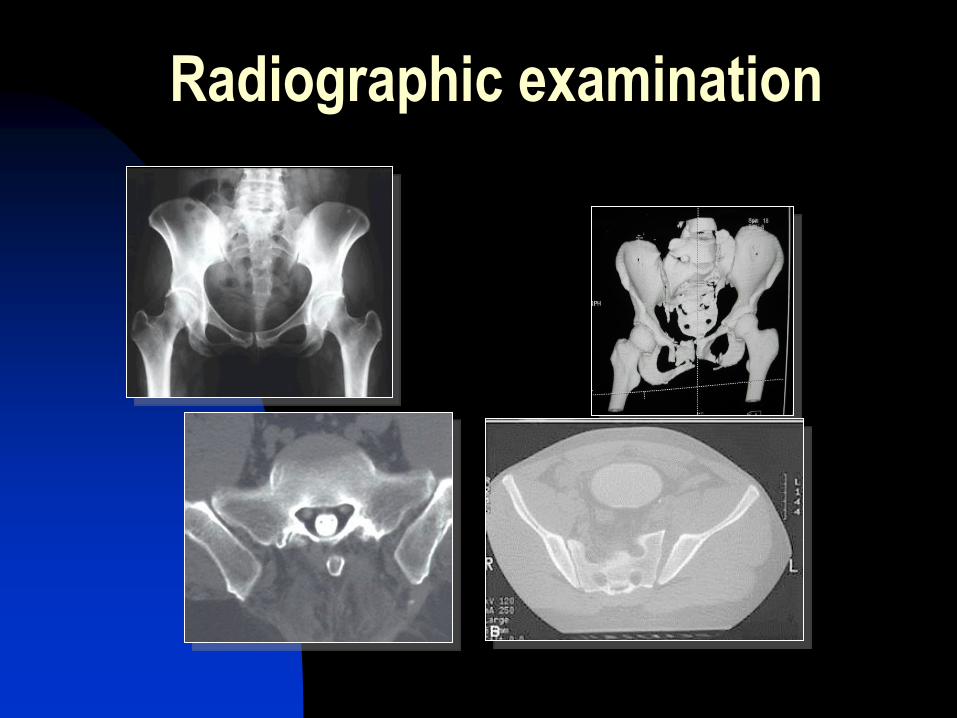
Radiographic examination
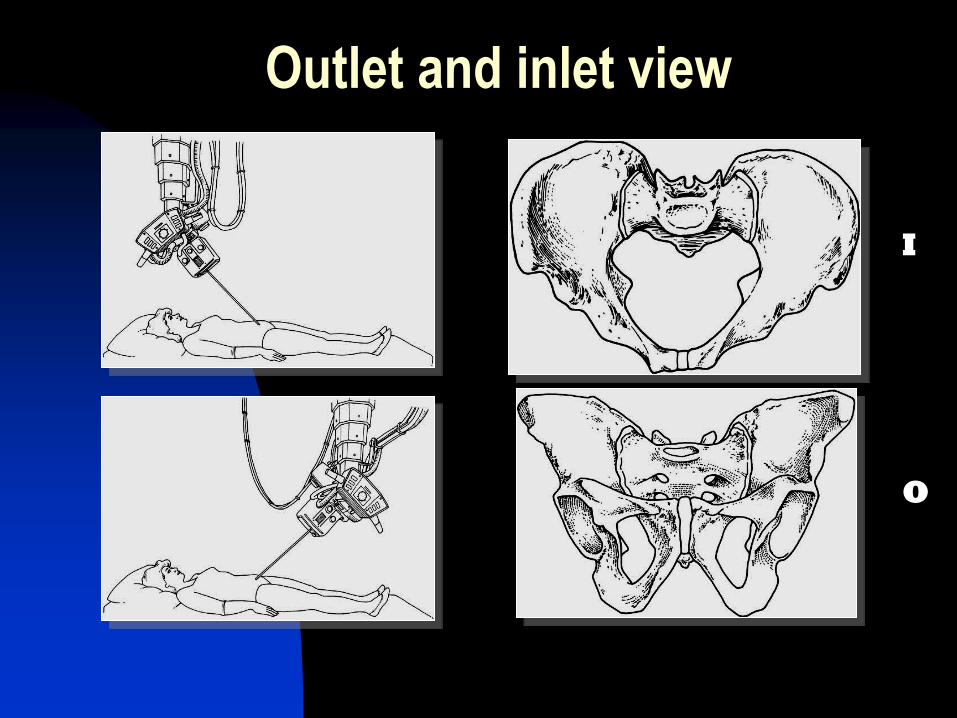
Outlet and inlet view
I
O
Emergency management
Comprehensive
Evaluation
Treatment
Priorities
Other life threatening
injuries
Retroperitoneal
bleeding
Retroperitoneal bleeding
Fracture stabilization
Pelvic volume
Angiography + embolization
Exploration + packing
Pelvic volume
Pneumatic antishock garment
Pelvic sling
External fixation
Pelvic C clamp

Fraktur Pelvis - terapi konservatif
Pelvic sling
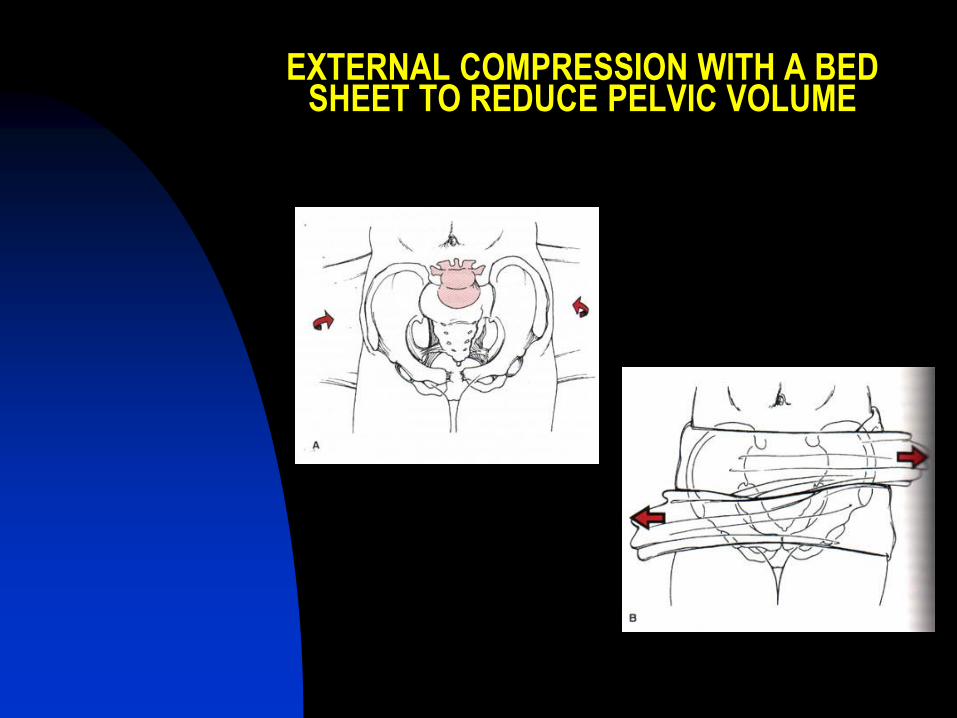
EXTERNAL COMPRESSION WITH A BED SHEET TO REDUCE PELVIC VOLUME
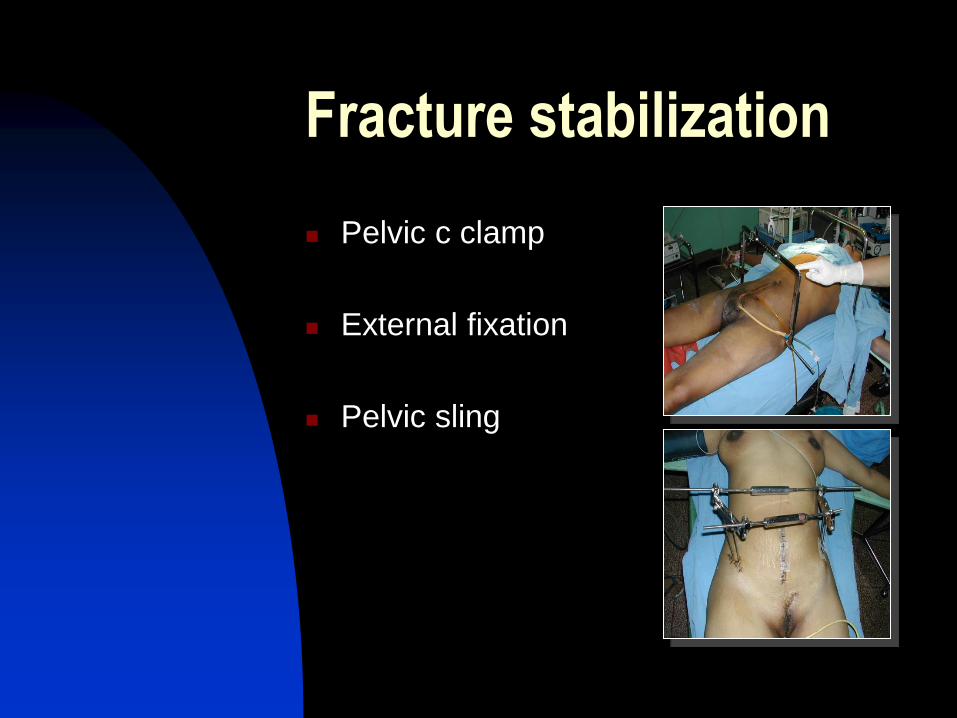
Fracture stabilization
Pelvic c clamp
External fixation
Pelvic sling
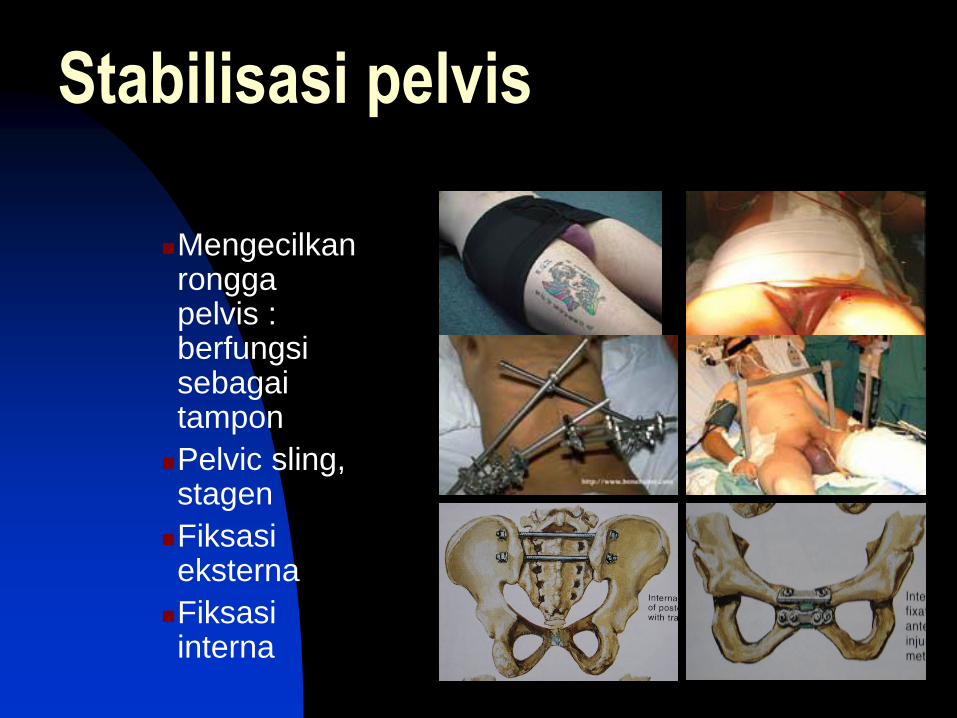
Stabilisasi pelvis
Mengecilkan rongga pelvis : berfungsi sebagai tampon
Pelvic sling, stagen
Fiksasi eksterna
Fiksasi interna
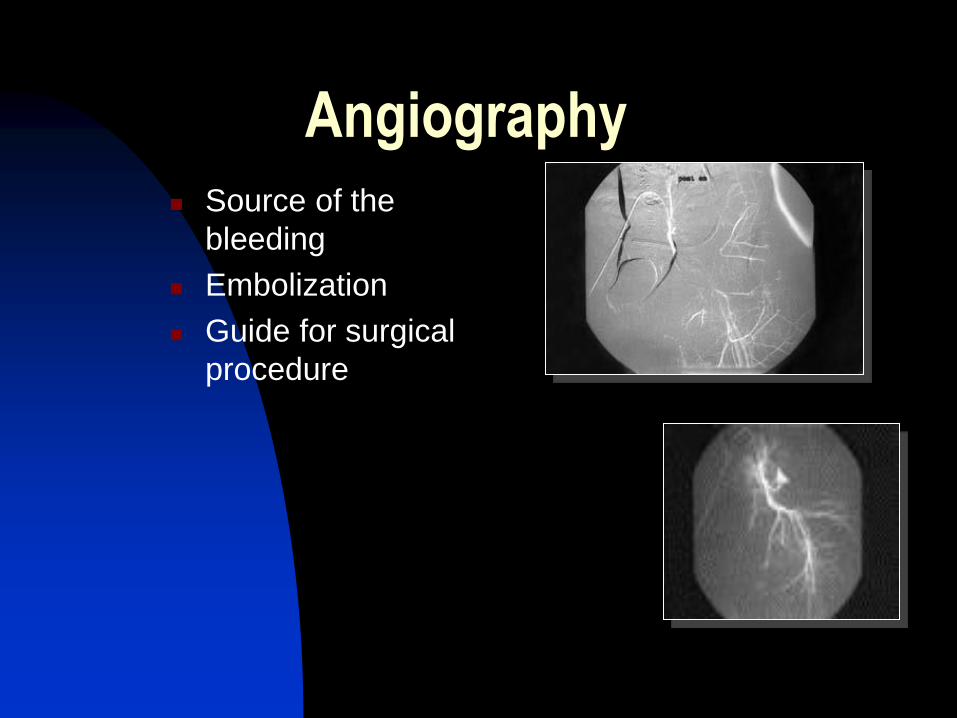
Angiography Source of the
bleeding
Embolization
Guide for surgical
procedure
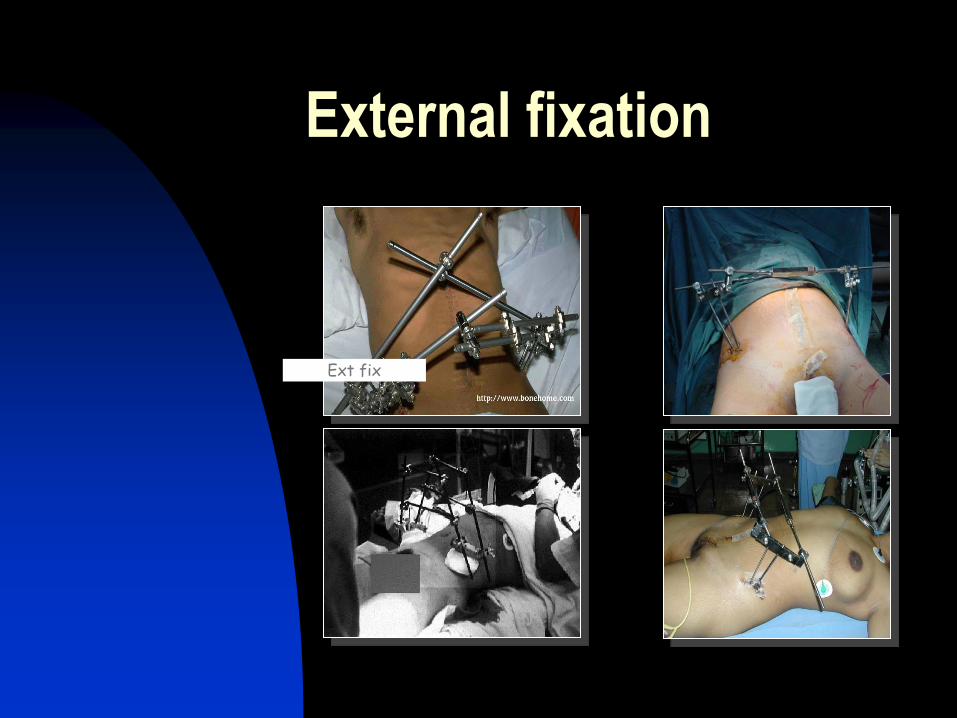
External fixation
Ext fix
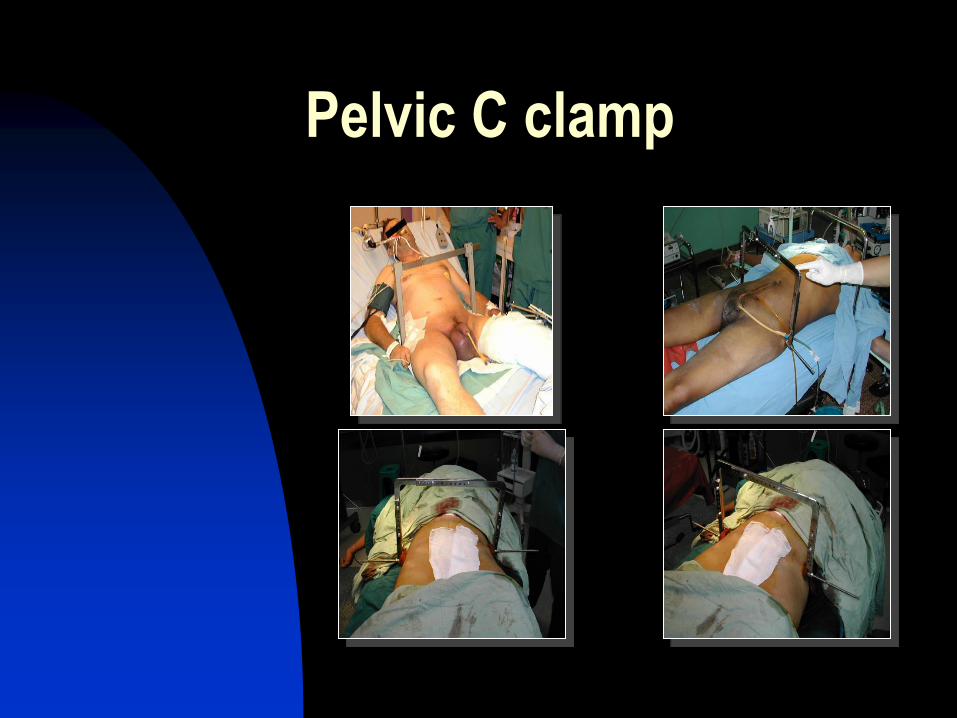
Pelvic C clamp

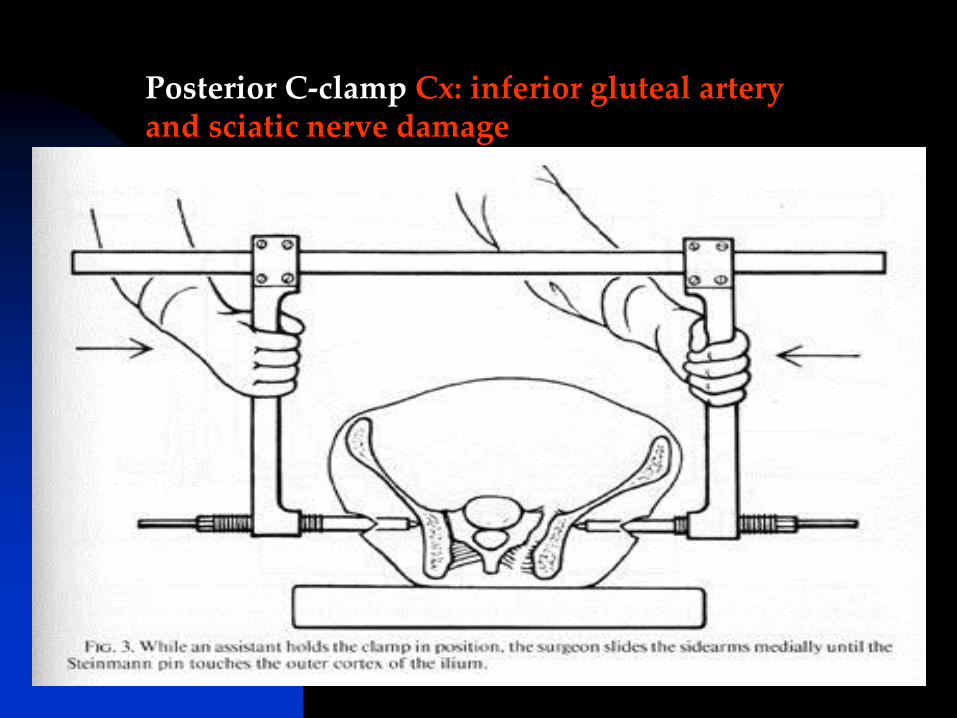
Posterior C-clamp Cx: inferior gluteal artery and sciatic nerve damage
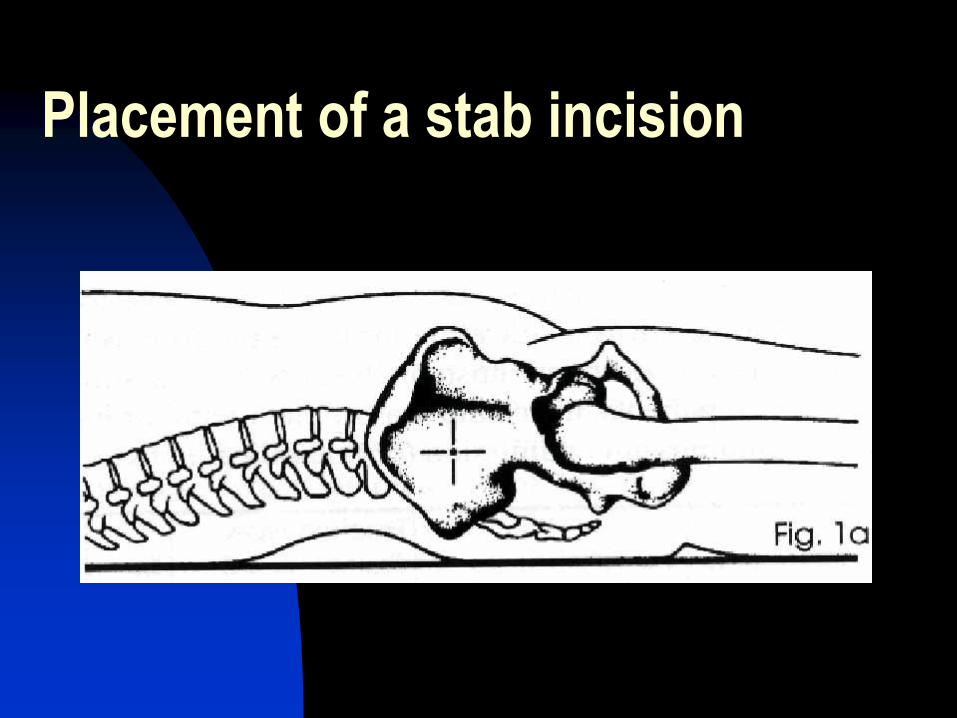
Placement of a stab incision
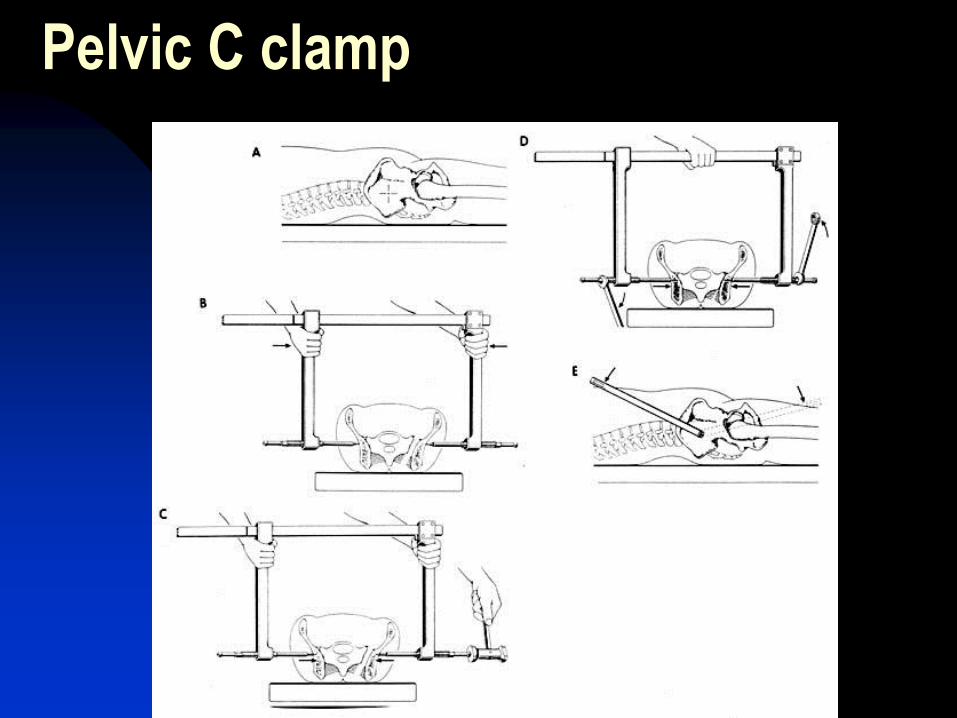
Pelvic C clamp
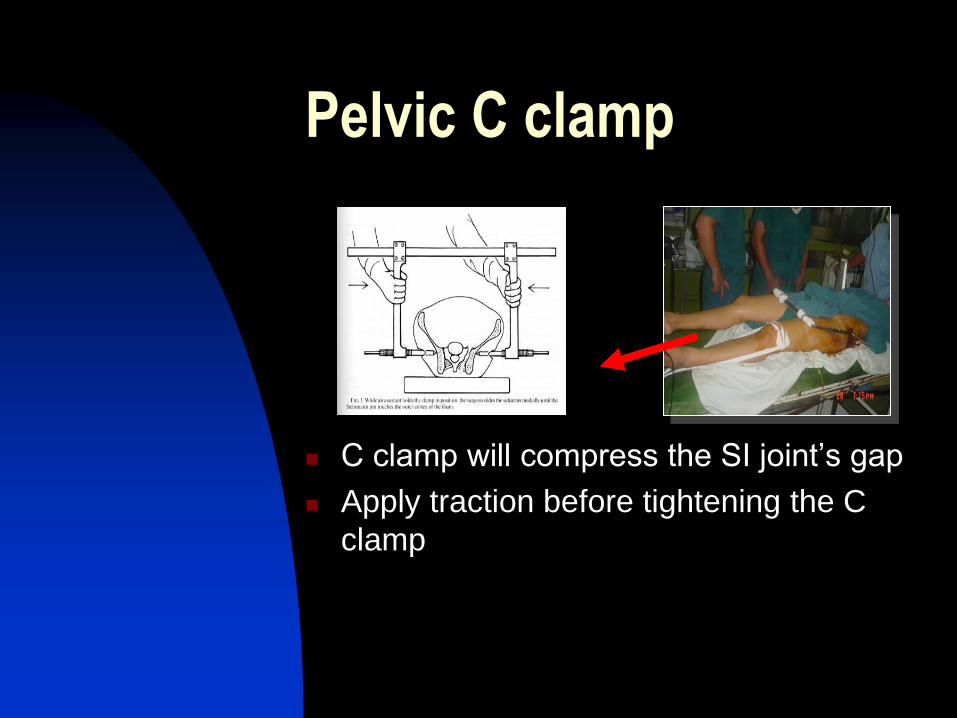
Pelvic C clamp
C clamp will compress the SI joint’s gap
Apply traction before tightening the C
clamp
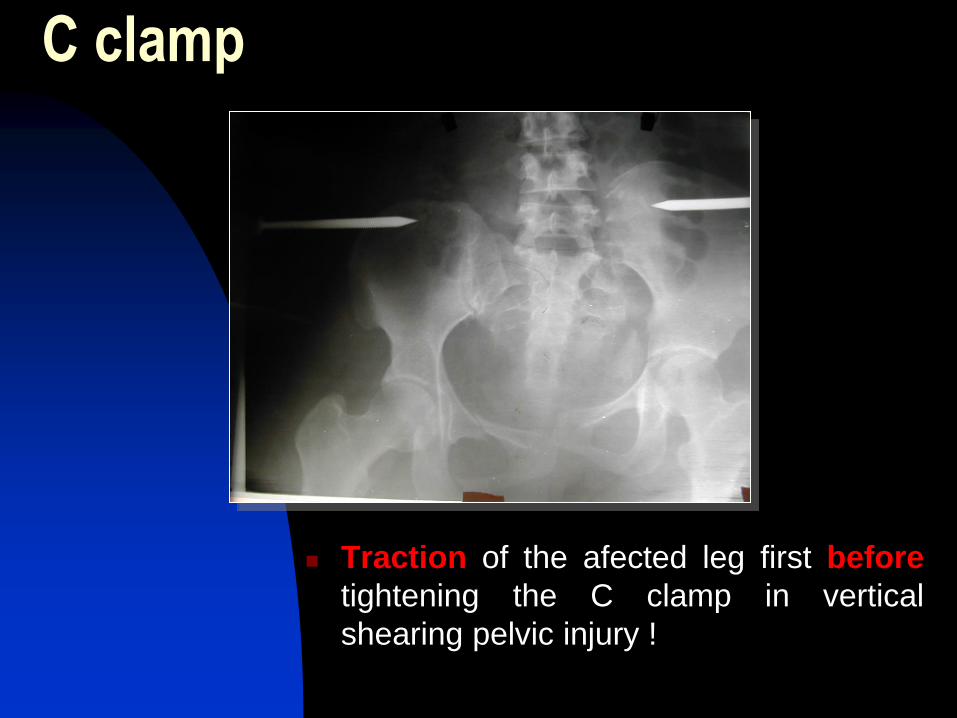
C clamp
Traction of the afected leg first before
tightening the C clamp in vertical
shearing pelvic injury !
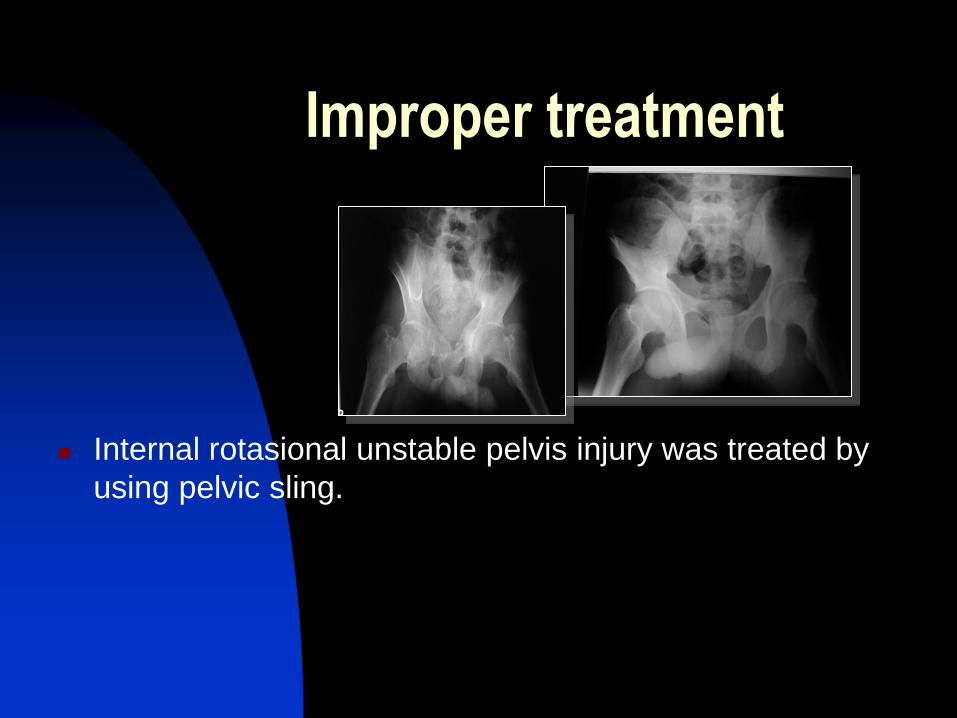
Improper treatment
Internal rotasional unstable pelvis injury was treated by
using pelvic sling.
Patient with c clamp
Check the c clamp’s position
radiographically
Use a firm bed for easier mobilization
Check the tightness of the c clamp’s
bolt and it’s attachment to the pelvic
bone.
Check the wound at the pin insertion.
C clamp removal
Stable haemodynamic condition.
Planning for definitive treatment of
the pelvic injury.
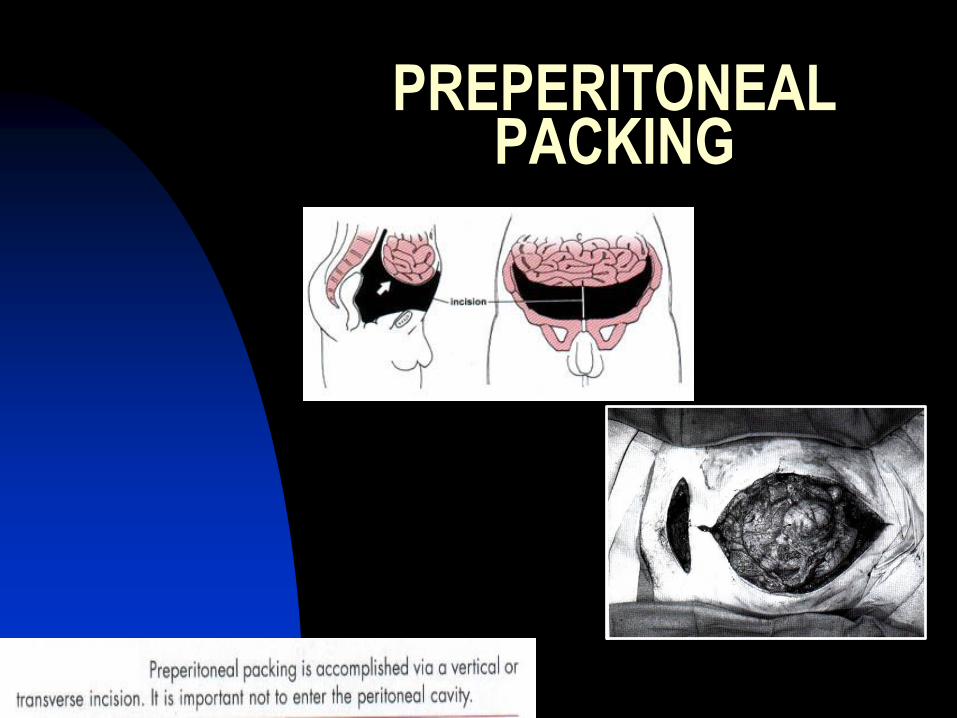
PREPERITONEAL PACKING
Conclusion
A major, life threatening pelvic injury should be treated comprehensively, with priority to manage the dangerous associated injuries and to achieve pelvic stability that provide tamponade mechanism to stop the bleeding so haemorrhagic shock can be prevented.
Choose the methods and instruments to treat the pelvic injury based on proper evaluation and diagnosis.
The procedure to treat the pelvic injuries should be done correctly to achieve a good result and to prevent complications.