Polio Miel It Is
13
POLIOMIELITIS Erny FK UWKS
-
Upload
ardi-pratama -
Category
Documents
-
view
19 -
download
0
description
polio
Transcript of Polio Miel It Is

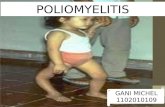
POLIOMIELITIS
Erny FK UWKS

TIU
• Setelah mengikuti kuliah mahasiswa mampu mendiagnosis dengan anamnesa, pemeriksaan fisik dan merujuk penderita ke pusat kesehatan terpadu

Pendahuluan
• Poliomyelitis adalah infeksi enterovirus yang menyebabkan 4 manifestasi klinis :
• infeksi subklinis• Abortive disesase• Poliomyelitis non-paralitik• Poliomyelitis paralisis

Epidemiologi • Sebelum abad 19 : insiden sporadis• Abad 19-20 : epidemi >> dengan puncak
pertengahan 1950• Vaksin polio (1952) (Jonas Salk) : ↓insiden secara
bermakna• Mortalitas : banyak terjadi pada tipe
paralytic poliomyelitis akibat komplikasi respirasi
• Frekuensi : Insiden L = P• Golongan usia : terutama pada anak / individu
dengan gangguan sistim imun• Eradikasi polio hingga dekade terakhir merupakan
prioritas WHO

Virus Polio(RNA Virus)
fecal-oral route
nasofaring & GIT
invasi jaringan limfoid
hematoviremia
Neurotropik padacornu anterior & medula spinalis
destruksi motor neuron Paralisis
Periode inkubasi 5-35
hari

Diagnosis • Riwayat penyakit : 1. Tipe asimptomatik : sebagian besar kasus2. Tipe abortive (5-10%) :
– Anorexia– Vomiting– Nyeri perut– Lama sakit <5 hari
3. Tipe non-paralitik : serupa tipe abortive +gejala iritasi meningeal
4. Tipe paralitik : serupa tipe non-paralitik + manifestasi sistemik (gagal nafas)
• Pemeriksaan fisik neurologis• Pemeriksaan penunjang diagnostik

Pemeriksaan fisik

• Physical• The spectrum of disease varies from inapparent infection to paralytic disease.• In mild cases, the following nonspecific signs and symptoms are observed and
usually resolve within a few days:– Fever– Headache– Nausea– Vomiting– Abdominal pain– Oropharyngeal hyperemia
• Nonparalytic poliomyelitis is characterized by the symptoms described above in addition to the following:– Nuchal rigidity– More severe headache– Back and lower extremity pain– Meningitis with lymphocytic pleocytosis (usually)
• Paralytic poliomyelitis occurs in fewer than 5% of affected patients and is characterized by the following:– Compromise of the motor neurons may be localized or widespread.– More frequently, asymmetric loss of muscle function is observed with involvement of major
muscle groups.– Muscle atrophy is generally observed several weeks after the beginning of symptoms.– Recovery may be complete, partial, or absent.

• Causes• Polioviruses are enteroviruses within the Picornaviridae family.
These viruses are resistant to ether and chloroform but can be inactivated by formaldehyde. They multiply in the GI tract but are particularly neurotropic.
• Documentation suggests that infections with polioviruses can be potentiated by factors such as exercise and tonsillectomy. Additionally, patients who are immunocompromised, such as those with human immunodeficiency virus (HIV) infection, B-cell disfunction, immunoglobulin A (IgA) deficiency, orsevere combined immunodeficiency, are particularly at high risk of developing poliomyelitis when exposed to both wild-type polioviruses and vaccine-attenuated viruses present in the oral poliovirus vaccine.

• Laboratory Studies• Obtain specimens from the cerebrospinal fluid
(CSF), stool, and throat for viral cultures in patients with suspected poliomyelitis infection.
• Obtain acute and convalescent serum for antibody concentrations against the 3 polioviruses.
• A 4-fold increase in the immunoglobulin G (IgG) antibody titers or a positive anti-immunoglobulin M (IgM) titer during the acute stage is diagnostic.

• Medical Care• No antivirals are effective against polioviruses. The treatment of
poliomyelitis is mainly supportive.• Analgesia is indicated in cases of myalgias or headache.• Mechanical ventilation is often needed in patients with bulbar paralysis.• Tracheostomy care is often needed in patients who require long-term
ventilatory support.• Physical therapy is indicated in cases of paralytic disease.
– In paralytic disease, provide frequent mobilization to avoid development of chronic decubitus ulcerations.
– Active and passive motion exercises are indicated during the convalescent stage.
• Fecal impaction is frequent in cases of paralytic disease and can be treated with laxatives as soon as it develops.

• Surgical Care• Total hip arthroplasty is a surgical therapeutic options for patients
with paralytic sequelae of poliomyelitis who develop of hip dysplasia and degenerative disease.[6]
• Consultations• Physical therapist and rehabilitation therapist• Pulmonologist• Neurologist• Immunologist• Infectious diseases specialist• Diet• Because patients with poliomyelitis are prone to develop
constipation, a diet rich in fiber is usually indicated.

• Prognosis• Bulbar paralytic poliomyelitis has been associated with
the highest rate of complications and a mortality rate as high as 60%; spinal poliomyelitis follows. Patients with inapparent or abortive poliomyelitis recover without significant sequelae.
• Patients who have recovered from poliomyelitis occasionally develop a postpoliomyelitis syndrome, in which recurrences of weakness or fatigue are observed and which usually involve groups of muscles that were initially affected. This postpolio syndrome may develop 20-40 years after infection with poliovirus.[5]