GIT Pemicu 1

of 49
-
Upload
ryan-putra-tantrajaya -
Category
Documents
-
view
246 -
download
0
Transcript of GIT Pemicu 1
-
7/30/2019 GIT Pemicu 1
1/49
Gastrointestinal System
Problem 1 B
Please Dont Remove The Baby
Ryan Putra405080212
-
7/30/2019 GIT Pemicu 1
2/49
Histology
-
7/30/2019 GIT Pemicu 1
3/49
-
7/30/2019 GIT Pemicu 1
4/49
Oral Mucosa:
All of the oral mucosa is made up of a thick stratified squamousepithelium, supported by a lamina propria. The epithelium is thickbecause the epithelial lining of the oral cavity is subject to a lot ofwear and tear.
In mobile areas, such as the soft palate, underside of the tongue,floor of the mouth, and mucosal surfaces of the cheeks and lips, theepithelium is not keratinised.
In other areas, such as the gums (gingivae), hard palate, and mostof the upper surface of the tongue, the epithelium is keratinised.
Underneath the oral mucosa, there is a tough collagenoussubmucosal layer, with accessory salivary glands, except where theoral mucosa lies over bone, where the submucosa is thin.
-
7/30/2019 GIT Pemicu 1
5/49
-
7/30/2019 GIT Pemicu 1
6/49
-
7/30/2019 GIT Pemicu 1
7/49
-
7/30/2019 GIT Pemicu 1
8/49
-
7/30/2019 GIT Pemicu 1
9/49
-
7/30/2019 GIT Pemicu 1
10/49
-
7/30/2019 GIT Pemicu 1
11/49
-
7/30/2019 GIT Pemicu 1
12/49
Anatomy
-
7/30/2019 GIT Pemicu 1
13/49
-
7/30/2019 GIT Pemicu 1
14/49
-
7/30/2019 GIT Pemicu 1
15/49
-
7/30/2019 GIT Pemicu 1
16/49
-
7/30/2019 GIT Pemicu 1
17/49
Physiology
-
7/30/2019 GIT Pemicu 1
18/49
Physiology
First step in the process of digestion is chewing ormastication. Mouth motility that involving cutting,ripping, grinding, and mixing food by the teeth. Upperteeth and lower teeth usually fix each other if we close
our mouth. This Occlusion allows food milled andcrushed by both surfaces. If teeth dont fix each otherfood cant be milled and crushed perfectly. Thismalocclusion caused by abnormality of the teethposition.
Purposes of chewing are : (1) Grind and crush food intolittle pieces so its easier to swallow; (2) to mix foodwith saliva; and (3) to stimulate taste bud.
-
7/30/2019 GIT Pemicu 1
19/49
The last purpose not only generate a sensationof taste, but also by reflex, trigger saliva,gaster, pancreas, and bile excretion as
preparation to welcome incoming food.Chewing could be volunteer, but most of the
process are rythmic reflex that generated bythe activation of jaw, lips, cheek, and toungeskeletal muscles as a response to the foodpreasure to the mouth tissue.
-
7/30/2019 GIT Pemicu 1
20/49
Saliva, secretion that related to the mouth, producted by three pair ofprimary saliva glands ( sublinguale, submandibulae and parotic )that located outside the mouth cavity and channeling saliva throughshort ducts to the mouth. Saliva consists of 99,5% H2O, 0,5%proteins, and electrolite. The most important saliva proteins areamilase, mucus, and lyzosime.
Although saliva has so many functions, saliva is not essential for properdigestion and food absorption, because pancreas and smallintestines enzymes could finish food digestion without thesecretion of saliva and stomach.
Saliva secretion is spontaneous and continuous, even without
stimulation, caused by low constant stimulation by parasympatheticnerve endings that ends in the salivary glands. This basal secretionis important to keep mouth and throat wet all the time.
-
7/30/2019 GIT Pemicu 1
21/49
Saliva secretion is the only one digest secretion thatentirely occured under nerve control. All otherdigest secretions controled by reflex of nervesystem and hormones.
Digestion in the mouth involves hydrolysis ofpolysaccharide into disaccharide by amilase. But,most of digestion by this enzyme occur in thecorpus of stomach after food and saliva have
been swallowed. Acid makes this enzymeinactive.
In the mouth, absorption doesnt happen.
-
7/30/2019 GIT Pemicu 1
22/49
Motility that associated to Pharynx and Oesophagus isswallow or deglutition. Swallow starts when a bolus orfood ball, volunteerly pushed by tounge to the back ofthe mouth into the pharynx. Bolus pressure on pharynx
stimulate pressure receptor in the pharynx which thensend an aferen impulse to swallowing center in themedulla.
Swallowing center then by reflex generate the activationof muscles that involve in the process of swallowing.
Swallow is an all-or-none reflex. Swallow starts as avolunteer process, but after it has been started, itcould not stop.
-
7/30/2019 GIT Pemicu 1
23/49
Swallow difined into two stages: Oropharynx stageand Oesophagus stage.
Oropharynx stage takes time about one second andform of bolus transfer from the mouth throughpharynx and into oesophagus.
Oesophagus is a muscled-channel that straight andrunning lengthwise between the pharynx andstomach. Sphincters guard both ends of
oesophagus. Sphincters are muscled structureformed like rings that if its closed, it preventobjects pass through what its guarding.
-
7/30/2019 GIT Pemicu 1
24/49
Swallowing center starts primary peristaltic wave from the base ofoesophagus to the end, pushing bolus in front of it throughoesophagus to the stomach. Thus, food pushing throughoesophagus is an active process that not depend on gravitation.Peristaltic take time around 5 to 9 seconds to reach the end ofoesophagus. This movement is controled by the swallowing center,via the vagus innervation.
Except when swallowing, Gastroesophagus sphincter keeps oncontraction to maintain barrier between oesopahgus and stomach,that reduce the chance to reflux of the acid gastric contents to theoesophagus.
Gastroesophagus sphincter weakened by reflex when peristaltic wavereach the bottom of oesophagus so bolus could enter the stomach,after which it will contract again.
-
7/30/2019 GIT Pemicu 1
25/49
Stomach performs some function. The most important isto keep foods until it transfer to the small intestinewith appropriate speed for digestion and optimalabsorption. Because of small intestine is the major site
of digestion and absorption, stomach has to keep foodand transfer it little by little to the duodenum withspeed that not beyond the intestines capacity.
Second function of stomach is to secret hydrochloric acid(HCl) and enzymes that start proteins digestion. Finally,
through mixing movement of the stomach, the foodmashed and mixed with stomach secretion to produceviscous mixture called kimus.
-
7/30/2019 GIT Pemicu 1
26/49
There are four aspect of stomach motility:
1. Gastric filling
2. Gastric storage3. Gastric mixing
4. Gastric emptying
-
7/30/2019 GIT Pemicu 1
27/49
Gastric filling, if empty, stomach has capacity around50mL, but this organ could expand until its capacityreach 1L while eating. There are 2 factor that maintainthe expandable of the stomach, there are: (1) plasticity
of stomachs smooth muscle and (2) reseptiverelaxation of the stomach while it filled.
Plasticity point at the ability of smooth muscle tomaintain the constant tension. Basicly, smooth musclestrengthened by the relaxation of stomach reflex while
filled. Stomachs interior form folds, known as rugae.While eating these folds are shrinking and flattenedout when stomach little by little relax because of filled.This reflex called reseptive reflex.
-
7/30/2019 GIT Pemicu 1
28/49
Gastric storage, remember, partly of the smooth muscle areable to partial depolarization which is autonomous andrhytmic. One of this group located in the upper fundus.These cells produce slow potential waves which swipe tothe bottom along the stomach to the sphincter pilorus
three times in one second.After it has been started, peristaltic wave spread to the whole
fundus and corpus then go to the antrum and sphincterpilorus. Because of fundus and corpus muscular layerwere thin, peristaltic contraction in these both side are very
weak. While reaching antrum, waves become stronger.Because fundus and corpus have weak contraction, food
which came into the stomach stored quietly without havingmix. Fundus area usually doesnt store food, its only gas.
-
7/30/2019 GIT Pemicu 1
29/49
Gastric mixing, strong peristaltic movement of thestomach is the main cause of mixing of food withstomach secretion that produce kimus. Every antrumperistaltic movement, it push the food to the sphincter
pilorus. Normal sphincter contraction keeps it but notcompletely closed. There is a gap for water and liquidto pass. The biggest part of the antrum kimus thatpushed towards but couldnt transfered to theduodenum, suddenly stop by theclosing of sphincter
pilorus and reflected back to the antrum,thismovement called retropulsion, which made kimusmixed well in the antrum.
-
7/30/2019 GIT Pemicu 1
30/49
Gastric emptying, stomach factor that related to thecontraction is the number of kimus. If this thingbalance, stomach empty its contain with speedequally to the number of kimus every time.Stomach expand stimulate motility to increasethrough direct expand effect on smooth muscleand also through plexus intrinsic, vagus nerve,
and stomach hormone gastrin.Beside that, the fluidity of kimus inside the stomach
also related to the process of gastric emptying.
-
7/30/2019 GIT Pemicu 1
31/49
Vomitting
Most of the time, vomiting in children is caused bygastroenteritis, usually due to a virus infecting thegastrointestinal tract. (Gastroenteritis is sometimes calledthe "stomach flu," which can also cause nausea anddiarrhea.)
These infections usually don't last long and are moredisruptive than dangerous. However, kids (especiallyinfants) who are unable to take in enough fluids and alsohave diarrhea could become dehydrated.
Vomiting is frightening for young children (and parents,too) and exhausting for kids of all ages. Offering plenty ofreassurance to your child and taking measures to preventdehydration are key for a quick recovery.
-
7/30/2019 GIT Pemicu 1
32/49
For Infants Under 6 Months
Avoid giving plain water to a young infant unless your doctor directlyspecifies an amount.
Offer your infant small but frequent amounts about 2 to 3 teaspoons,or up to ounce (about 20 milliliters) of an oral electrolyte solutionevery 15 to 20 minutes with a spoon or an oral syringe. Oral electrolytesolutions (available at most supermarkets or pharmacies and also called
oral electrolyte maintenance solutions) are balanced with salts to replacewhat's lost with vomiting or diarrhea, and they also contain some sugar.It's especially important for young infants that any fluids given have thecorrect salt balance (unflavored electrolyte solutions are best for youngerinfants).
Gradually increase the amount of solution you're giving if your infant is
able to keep it down for more than a couple of hours without vomiting.For instance, if your little one takes 4 ounces (or about 120 milliliters)normally per feed, slowly work up to giving this amount of oral electrolytesolution over the course of the day.
-
7/30/2019 GIT Pemicu 1
33/49
Do not give more solution at a time than your infant would normally eat this will overfill an already irritated tummy and will likely cause morevomiting.
After your infant goes for a period of time (more than about 8 hours)without vomiting, reintroduce formula slowly if your infant is formula-fed.Start with small ( to 1 ounce, or about 20 to 30 milliliters), more frequent
feeds and slowly work up to the normal feeding routine. If your infantalready eats baby cereal, it's OK to start solid feedings in small amountsagain.
If your infant is exclusively breastfeeding and vomits (not just spits up, butvomits what seems like the entire feed) more than once, then breastfeedfor a total of 5-10 minutes every 2 hours. If your infant is still vomiting,
then call your doctor. After 8 hours without vomiting, you can resumebreastfeeding normally.
If your infant is under 1 month old and vomiting all feeds (not just spittingup), call your doctor immediately.
-
7/30/2019 GIT Pemicu 1
34/49
Mild to moderate dehydration:
dry mouth
few or no tears when crying
fussy behavior in infants
fewer than four wet diapers per day in an infant (more than 4 to 6 hours without a wet diaper in a younger infantunder 6 months of age)
no urination for 6 to 8 hours in children
soft spot on an infant's head that looks flatter than usual or somewhat sunken
Severe dehydration:
very dry mouth (looks "sticky" inside)
dry, wrinkled, or doughy skin (especially on the belly and upper arms and legs)
inactivity or decreased alertness
appears weak or limp
sunken eyes
sunken soft spot in an infant
excessive sleepiness or disorientation
deep, rapid breathing
no urination for more than 6 to 8 hours in infants
no urination for more than 8 to 10 hours in children
fast or weakened pulse
-
7/30/2019 GIT Pemicu 1
35/49
Regurgitation
"Spitting up", or regurgitation, is very commonduring a baby's first few months of life. About40% of normal, healthy babies spit up, usuallyright after feeding. The liquid your baby
regurgitates may look very similar to the milk sheor he was just fed; or, if it has been partiallydigested, it may appear curdled and smell likesour milk. Though it may seem like your baby is
spitting up a lot of milk, that's not likely to be thecase. The liquid spit up during regurgitation isusually made up mostly of saliva and gastric
juices, and only a small amount of milk.
-
7/30/2019 GIT Pemicu 1
36/49
In older children and adults, an elastic-like muscle at the entryto the stomach closes like a valve to prevent liquids frombeing pushed back up. In babies, however, this valve orsphincter isn't fully effective until between 6 and 12months of age. Since it isn't fully developed yet, the valve is
easily pushed back by the contents of the stomach -resulting in regurgitation or spitting up. Regurgitation oftenoccurs after overfeeding, or in combination with burping.Consequently, breastfed babies tend to spit up less thanbottle-fed babies, because they usually take in only as
much milk as they need, and because they tend to swallowless air. Regurgitation is not caused by allergy or foodintolerance, and shouldn't be confused with vomiting.
-
7/30/2019 GIT Pemicu 1
37/49
Vommiting / Regurgitation
Unlike spitting up, vomiting is characterized by the forceful expulsionof the contents of the stomach. It's important to know thedifference between vomiting and spitting up because repeatedvomiting can be a signal of a more serious illness, and because itcan easily lead to dehydration. Dehydration is a dangerouscondition in which excessive loss of body fluids results in apotentially life-threatening imbalance of water and essential bodysalts. If vomiting is persistent, accompanied by very hightemperatures and/or increasing lethargy, or if vomit contains blood,medical attention should be sought immediately. Occasionalvomiting, if unaccompanied by other symptoms, may not be acause for concern but should be discussed with a doctor.
-
7/30/2019 GIT Pemicu 1
38/49
Treatment
Your baby's stomach and undeveloped sphincter are like abottle with a cap that isn't fully closed. If the bottle is filledto the brim with any type of liquid, be it water, milk or
juice, it will overflow through the partially closed cap. If it ismoved or tilted, it will also overflow or spill. Understanding
this comparison will help you better understandregurgitation and what you can do to minimize it. It'simportant not to overload your baby's stomach, or it will"spill" its contents, causing your baby to spit up. Instead,give your baby less to drink during a feeding, but feed him
or her more frequently. And don't move your baby abouttoo vigorously after a feeding.
-
7/30/2019 GIT Pemicu 1
39/49
In addition, how you position yourbaby during the twenty minutes aftera feeding is important. Any uprightposition, such as holding your babyto your shoulder (as you would toburp him or her), will help reduceregurgitation.
However, placing the baby in aninfant seat can make matters worseand should be avoided, especiallyimmediately after a feeding. Thebaby's slouching position in this kindof seat puts pressure on the stomach
that can result in regurgitation. Besure to consult your doctor beforemaking any changes in your baby'sposition or diet.
-
7/30/2019 GIT Pemicu 1
40/49
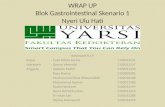
Gastroesophageal Reflux Disease
Gastroesophageal reflux disease (GERD) is a
condition in which the stomach contents (food
or liquid) leak backwards from the stomach
into the esophagus (the tube from the mouthto the stomach). This action can irritate the
esophagus, causing heartburn and other
symptoms.
-
7/30/2019 GIT Pemicu 1
41/49
Causes
When you eat, food passes from the throat to the stomach through the esophagus (also called the foodpipe or swallowing tube). Once food is in the stomach, a ring of muscle fibers prevents food frommoving backward into the esophagus. These muscle fibers are called the lower esophagealsphincter, or LES.
If this sphincter muscle doesn't close well, food, liquid, and stomach acid can leak back into theesophagus. This is called reflux or gastroesophageal reflux. This reflux may cause symptoms, or caneven damage the esophagus.
The risk factors for reflux include hiatal hernia (a condition in which part of the stomach moves above
the diaphragm, which is the muscle that separates the chest and abdominal cavities), pregnancy,and scleroderma.
Obesity, cigarettes, and possibly alcohol also increase the chance of GERD.
Heartburn and gastroesophageal reflux can be brought on or worsened by pregnancy and manydifferent medications. Such drugs include:
Anticholinergics (e.g., for seasickness)
Beta-blockers for high blood pressure or heart disease
Bronchodilators for asthma
Calcium channel blockers for high blood pressure
Dopamine-active drugs for Parkinson's disease
Progestin for abnormal menstrual bleeding or birth control
Sedatives for insomnia or anxiety
Tricyclic antidepressants
-
7/30/2019 GIT Pemicu 1
42/49
Symptoms
More common symptoms are: Feeling that food may be left trapped behind the breastbone
Heartburn or a burning pain in the chest (under the breastbone) Increased by bending, stooping, lying down, or eating
More likely or worse at night
Relieved by antacids Nausea after eating
Less common symptoms are:
Cough or wheezing
Difficulty swallowing
Hiccups
Hoarseness or change in voice
Regurgitation of food
Sore throat
-
7/30/2019 GIT Pemicu 1
43/49
Test
You may not need any tests if your symptoms are not severe.If your symptoms are severe or they come back after you have been
treated, one or more tests may help diagnose reflux or anycomplications:
Esophagogastroduodenoscopy (EGD) is often used to identify the
cause and examine the esophagus (swallowing tube) for damage.The doctor inserts a thin tube with a camera on the end throughyour mouth. The tube is then passed into your esophagus, stomach,and small intestine.
Barium swallow
Continuous esophageal pH monitoring
Esophageal manometry
A positive stool occult blood test may diagnose bleeding from theirritation in the esophagus.
-
7/30/2019 GIT Pemicu 1
44/49
Treatment
To prevent heartburn, avoid foods and beverages that may trigger yoursymptoms. For many people, these include:
Alcohol
Caffeine
Carbonated beverages
Chocolate Citrus fruits and juices
Tomatoes
Tomato sauces
Spicy or fatty foods
Full-fat dairy products
Peppermint
Spearmint
-
7/30/2019 GIT Pemicu 1
45/49
Also, try the following changes to your eating habits and lifestyle: Avoid bending over or exercising just after eating
Avoid garments or belts that fit tightly around your waist
Do not lie down with a full stomach. For example, avoid eatingwithin 2 - 3 hours of bedtime.
Do not smoke. Eat smaller meals.
Lose weight if you are overweight.
Reduce stress.
Sleep with your head raised about 6 inches. Do this by tilting yourentire bed, or by using a wedge under your body, not just withnormal pillows.
-
7/30/2019 GIT Pemicu 1
46/49
Over-the-counter antacids may be used after meals and at bedtime, although they donot last very long. Common side effects of antacids include diarrhea orconstipation.
Other over-the-counter and prescription drugs can treat GERD. They work more slowlythan antacids but give you longer relief. Your doctor or nurse can tell you how totake these drugs.
Proton pump inhibitors (PPIs) are the most potent acid inhibitors: omeprazole(Prilosec), esomeprazole (Nexium), iansoprazole (Prevacid), rabeprazole (AcipHex),and pantoprazole (Protonix)
H2 antagonists: famotidine (Pepsid), cimetidine (Tagamet), ranitidine (Zantac), andnizatidine (Axid)
Promotility agents: metoclopramide (Reglan)
Anti-reflux operations (Nissen fundoplication and others) may be an option for
patients whose symptoms do not go away with lifestyle changes and drugs.Heartburn and other symptoms should improve after surgery, but you may stillneed to take drugs for your heartburn. There are also new therapies for reflux thatcan be performed through an endoscope (a flexible tube passed through themouth into the stomach).
-
7/30/2019 GIT Pemicu 1
47/49
Prognosis
Most people respond to nonsurgical measures,
with lifestyle changes and medications.
However, many patients need to continue
taking drugs to control their symptoms.
-
7/30/2019 GIT Pemicu 1
48/49
Complication
Barrett's esophagus (a change in the lining of theesophagus that can increase the risk of cancer)
Bronchospasm (irritation and spasm of theairways due to acid)
Chronic cough or hoarseness
Dental problems
Esophageal ulcer
Inflammation of the esophagus Stricture (a narrowing of the esophagus due to
scarring from the inflammation)
-
7/30/2019 GIT Pemicu 1
49/49
Prevention
Heartburn prevention techniques
Looking at the esophagus with an endoscope
and obtaining a sample of esophagus tissue
for examination (esophagoscopy with biopsy)
may be recommended to diagnose Barrett's
esophagus.
Follow-up endoscopy to look for dysplasia orcancer is often advised.