X-linked hypophosphatemic rickets: A study (with literature review) of linear growth response to...
15
JOURNAL OF BONE AND MINERAL RESEARCH Volume 7, Number 6, 1992 Mnry Ann Liebert. Inc., Publishem X-Linked Hypophosphatemic Rickets: A Study (with Literature Review) of Linear Growth Response to Calcitriol and Phosphate Therapy DEBORAH J. PETERSEN,'.' ANNE M. BONIFACE,'.'.' FRANCINE W. SCHRANCK,',' RETA C. RUPICH,' and MICHAEL P. WHYTE'.3 ABSTRACT Not all children with X-linked hypophosphatemia (XLH) have demonstrated improved linear growth with calcitriol [1,25-(OH),D,] and inorganic phosphate (Pi) therapy. To assess which factors are associated with a favorable growth response during this treatment, we retrospectively compared demographics and biochemi- cal parameters of bone metabolism to the linear growth patterns of 20 children with XLH who were pre- pubertal and had not required osteotomy. A total of 15 patients had family histories consistent with XLH; 5 appeared to be sporadic cases. During 3 years of therapy, the growth velocities of 12 patients had been at or above the mean for age (good growers) and those of 8 patients had been below the mean (poor growers). Data from the two groups were contrasted. We found no difference between the good growers and poor growers before or after the 3 year period of therapy in mean age, dietary calcium, calcitriol dose or compli- ance, or Pi dose or compliance. Both groups increased their mean fasting serum Pi levels with treatment. The TmP/GFR (x f SEM) of the good growers improved with therapy (1.9 f 0.2 to 2.6 f 0.2 mg/dl, p = 0.01), and their posttreatment value was higher compared to that of the poor growers (2.6 f 0.1 versus 2.2 f 0.1 mg/dl, p = 0.02). However, their enhanced TmP/GFR was not associated with a reduction in serum iPTH levels (before, 693 f 50; after, 688 f 76 pg/ml; p = 0.9). The Z test for binomial proportions showed that the group that grew well contained a disproportionate number of girls (10 of 12, p = 0.04). Our findings suggest that calcitriol may exert a direct effect on the renal tubule to improve Pi reclamation in XLH. The observation that heterozygous girls appear to respond better than hemizygous boys to calcitriol and Pi therapy provides evidence for a gene dosage effect in the expression of this X-linked dominant dis- order. INTRODUCTION -LINKED HYPOPHOSPHATEMU (XLH) is the most com- X mon heritable form of rickets"'; its frequency has been estimated as approximately 1 per 20,000 live births.121 The pattern of disease transmission is X-linked domi- nant.".'] We now know from multilocus linkage studies that the XLH gene is found on the distal short arm of the X chromosome in the Xp22.1-p22.2 region.",61 However, neither the function of the normal gene nor the molecular defect(s) at the XLH locus have been identified. Abnormalities of mineral homeostasis that occur in XLH include selective wasting of inorganic phosphate (Pi) by the kidney, impaired absorption of calcium and Pi by the intestine, and defective mineralization of the skele- ton."] The biochemical expression of these disturbances 'Metabolic Research Unit, Shriners Hospital for Crippled Children, St. Louis, Missouri. 'Division of Pediatric Endocrinology and Metabolism, Department of Pediatrics, St. Louis Children's Hospital, St. Louis, Missouri. 'Division of Bone and Mineral Diseases, Department of Medicine, The Jewish Hospital of St. Louis, and at the Washington Univer- sity Medical Center, St. Louis, Missouri. 583
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of X-linked hypophosphatemic rickets: A study (with literature review) of linear growth response to...

JOURNAL OF BONE AND MINERAL RESEARCH Volume 7, Number 6, 1992 Mnry Ann Liebert. Inc., Publishem
X-Linked Hypophosphatemic Rickets: A Study (with Literature Review) of Linear Growth
Response to Calcitriol and Phosphate Therapy
DEBORAH J. PETERSEN,'.' ANNE M. BONIFACE,'.'.' FRANCINE W. SCHRANCK,',' RETA C. RUPICH,' and MICHAEL P. WHYTE'.3
ABSTRACT
Not all children with X-linked hypophosphatemia (XLH) have demonstrated improved linear growth with calcitriol [1,25-(OH),D,] and inorganic phosphate (Pi) therapy. To assess which factors are associated with a favorable growth response during this treatment, we retrospectively compared demographics and biochemi- cal parameters of bone metabolism to the linear growth patterns of 20 children with XLH who were pre- pubertal and had not required osteotomy. A total of 15 patients had family histories consistent with XLH; 5 appeared to be sporadic cases. During 3 years of therapy, the growth velocities of 12 patients had been at or above the mean for age (good growers) and those of 8 patients had been below the mean (poor growers). Data from the two groups were contrasted. We found no difference between the good growers and poor growers before or after the 3 year period of therapy in mean age, dietary calcium, calcitriol dose or compli- ance, or Pi dose or compliance. Both groups increased their mean fasting serum Pi levels with treatment. The TmP/GFR ( x f SEM) of the good growers improved with therapy (1.9 f 0.2 to 2.6 f 0.2 mg/dl, p = 0.01), and their posttreatment value was higher compared to that of the poor growers (2.6 f 0.1 versus 2.2 f 0.1 mg/dl, p = 0.02). However, their enhanced TmP/GFR was not associated with a reduction in serum iPTH levels (before, 693 f 50; after, 688 f 76 pg/ml; p = 0.9). The Z test for binomial proportions showed that the group that grew well contained a disproportionate number of girls (10 of 12, p = 0.04). Our findings suggest that calcitriol may exert a direct effect on the renal tubule to improve Pi reclamation in XLH. The observation that heterozygous girls appear to respond better than hemizygous boys to calcitriol and Pi therapy provides evidence for a gene dosage effect in the expression of this X-linked dominant dis- order.
INTRODUCTION
-LINKED HYPOPHOSPHATEMU (XLH) is the most com- X mon heritable form of rickets"'; its frequency has been estimated as approximately 1 per 20,000 live births.121 The pattern of disease transmission is X-linked domi- nant.".'] We now know from multilocus linkage studies that the XLH gene is found on the distal short arm of the
X chromosome in the Xp22.1-p22.2 region.",61 However, neither the function of the normal gene nor the molecular defect(s) at the XLH locus have been identified.
Abnormalities of mineral homeostasis that occur in XLH include selective wasting of inorganic phosphate (Pi) by the kidney, impaired absorption of calcium and Pi by the intestine, and defective mineralization of the skele- ton."] The biochemical expression of these disturbances
'Metabolic Research Unit, Shriners Hospital for Crippled Children, St. Louis, Missouri. 'Division of Pediatric Endocrinology and Metabolism, Department of Pediatrics, St. Louis Children's Hospital, St. Louis, Missouri. 'Division of Bone and Mineral Diseases, Department of Medicine, The Jewish Hospital of St. Louis, and at the Washington Univer-
sity Medical Center, St. Louis, Missouri.
583
584 PETERSEN ET AL.
includes hypophosphatemia, elevated serum alkaline phos- phatase activity, and serum 1,25-dihydroxyvitamin D [ 1 ,25-(OH)ID] levels that are inappropriately normal in the presence of hypophosphatemia, which acts to stimulate renal 25-OHD la-hydroxylase activity.(7-131 Affected indi- viduals, however, are generally normocalcemic and have normal serum parathyroid hormone (PTH) levels. Typical clinical manifestations of XLH in children are short stature and lower extremity deformity, predominantly bowing, which may require surgical correction. 13.4.14.15) Af- fected adults are primarily troubled with dental disease, osteoarthritis, and painful pseudofractures.[lS1
Calcitriol [1,25-(OH)ID3] and Pi therapy for XLH has been shown to be capable of healing rachitic changes evi- dent radiologi~ally~~~~~~~~~’~~ and improving defective bone mineralization as demonstrated by iliac crest bone biopsy in a small number of children.(o-lo.lal Nevertheless, there is a striking lack of information in the literature regarding the impact of this medical regimen on lower limb deformi- ties, and its effect on linear growth remains equivocal. Some investigators have described patients with XLH who grew better with calcitriol and Pi treatment,~1n~17~1P~10~ but this response has not been consistent.(lll Since XLH oc- curs infrequently, most of the growth studies understand- ably describe results with small numbers of children of variable ages. However, these investigations often provide only incomplete information regarding the pubertal status and previous lower extremity orthopedic surgeries of the study subjects. Additionally, the duration of medical treat- ment is variable within and between studies, most do not report medication doses corrected for body weight, and none cite drug compliance data.
To assess the factors associated with a favorable growth response to calcitriol and Pi treatment in XLH, we retro- spectively compared demographic factors and biochemical parameters of bone metabolism to linear growth patterns of 20 prepubertal and nonsurgically treated children with XLH during 3 years of treatment.
PATIENTS AND METHODS
When this retrospective study was begun, a total of 70 children with XLH had been treated for varying periods of time with calcitriol and Pi supplementation at the Meta- bolic Research Unit (MRU), Shriners Hospital for Crip- pled Children in St. Louis. The diagnosis of XLH from among various types of rickets encountered at the MRU was based on a consistent medical history and physical ex- amination, radiologic evidence of rickets, hypophospha- temia due to selective renal Pi wasting for which no other cause was found, and a family history consistent with XLH or sporadic occurrence. The study protocol, which included informed parental consent and, when appropri- ate, patient consent, was approved by the Human Studies Committee of the Washington University School of Medi- cine. Patients were admitted to the MRU for 5 days of baseline evaluation before initiation of calcitriol and Pi therapy and at least yearly thereafter for follow-up studies. During hospitalizations, they were fed “constant” or “con-
trolled” diets(111 that replicated their ad libitum calcium and phosphorus intakes as calculated by the MRU research dietitian. Three 24 h urine collections were used to assess calcium, phosphorus, and creatinine excretion. Two con- secutive, fasting, well-hydrated, 2 h urine collections with midpoint serum specimens were used to determine average values of creatinine clearance and tubular maximum of phosphate/glomerular filtration rate (TmP/GFR). Serum obtained after an overnight fast was assayed for total and ionized calcium, Pi, creatinine, electrolyte, alkaline phos- phatase, immunoreactive PTH (iPTH), and osteocalcin levels. Radiographs of the knees and wrists were used to evaluate rachitic changes. Recorded height was the average of three measurements obtained with a fixed Harpenden stadiometer (Holtain, Ltd., Crymmych, Great Britain).
Calcitriol (Rocaltrol; Hoffmann-La Roche, Inc., Nut- ley, NJ) and Pi (K-Phos Neutral; Beach Pharmaceuticals, Tampa, FL) therapy was begun after the completion of the initial hospitalization. Pi doses were gradually increased to three to four times throughout the waking hours and to the maximum amount tolerated without causing the typical side effect of diarrhea. Calcitriol doses were given once or twice daily and adjusted to maintain a urinary calcium ex- cretion as close to 200 mg calcium per g creatinine as possi- ble, without exceeding this limit. The patients were evalu- ated at least every 3 months as outpatients to assess heights and weights; measure 24 h urine excretion of calcium, phosphorus, and creatinine; assay serum calcium, Pi, crea- tinine, and alkaline phosphatase levels; perform pill counts for calcitriol and Pi compliance calculations; and adjust medication dosages. Throughout subsequent hospitaliza- tions and outpatient visits, patients continued to receive calcitriol and Pi therapy.
Biochemical assays performed in the MRU laboratory included serum total calcium (atomic absorption spectro- photometer model 457; Instrumentation Laboratory, Wil- mington, MA); ionized calcium (Nova 2 analyzer; Nova Biomedical, Newton, MA); Pi (kit 7501-7503; American Monitor Corp., Indianapolis, IN; Beckman spectropho- tometer model DU6; Beckman Instruments, Inc., Fuller- ton. CA); alkaline phosphatase activity measured kinet- ically by the Bowers and McComb method at 30°C (Beck- man spectrophotometer); midregion iPTH (kit P-73; Ramco Laboratories, Inc., Houston, TX; Beckman gamma counter with DP 5500 data reduction); and osteo- calcin (kit 15065; INCSTAR Corporation, Stillwater, MN; Beckman gamma counter with DP 5500 data reduction). Serum samples for iPTH and osteocalcin levels were batched and assayed in three runs, with pretreatment and posttreatment specimens for each patient included in the same run to minimize interassay variation. TMP/GFR was calculated using the Walton-Bijvoct nomogram.”a’ 2 scores for both height and growth velocity were calculated using the Genentech Growth Calculator (Genentech Corp., San Francisco, CA), which is derived from the National Center for Health Statistics growth standards.””
To assess the demographic factors and/or biochemical parameters of bone metabolism that might be associated with a favorable growth response to calcitriol and Pi ther- apy, we eliminated the confounding impact of the pubertal

XLH: RESPONSE TO CALCITRIOL AND PHOSPHATE 585
growth spurt and/or lower limb surgical procedures on growth velocity. This was done by excluding from the 70 patients those who had not received 3 years of calcitriol and Pi therapy before the age of their anticipated growth spurt (age 10 years for girls and 12 years for boys) and those who had undergone surgical correction of lower ex- tremity deformities.
Of our 70 XLH patients, 20 children met the criteria for inclusion in this retrospective study and are the subject of this report. All data are from inpatient evaluations. We compared baseline pretreatment laboratory values and heights with Posttreatment values obtained after 3 years of therapy. However, medication doses, compliance calcula- tions, and posttreatment urinary calcium excretions were the average of the values obtained during all three hospi- talizations after the initiation of therapy.
Of the 20 select patients, 13 were girls and 7 were boys. Two sisters were fraternal twins. One patient was His- panic, and all others were white. A family history consis- tent with XLH was elicited for I5 of the children. The other 5 subjects were presumed to be sporadic cases of XLH, since careful evaluation showed no evidence for other causes of hypophosphatemic rickets. A total of 16 patients had genu vamm and 2 genu vaigum at the initia- tion of therapy; 7 had received ergocalciferol and Pi and 3 had received calcifriol and P, before baseline evaluation on the MRU. The 3 patients with prior calcitriol and 1 subject with prior ergocalciferol treatment discontinued medica- tions several weeks before their initial MRU hospitaliza- tion. The other 6 patients who had been treated with ergo- calciferol discontinued medications at the time of their ini- tial studies.
Sufficient growth data to calculate pretreatment growth velocities for these 20 children were not available. Their pretreatment height standard deviation (SD) scores for age (height Z scores), however, indicated that their growth was impaired. With the exception of one child whose height Z score was -0.6, height Z scores ranged from - 1.2 to -3.7 (mean - I .9 f 0.8 SD) before treatment by the MRU.
For purposes of data analysis, the 20 children were as- signed to one of two groups based upon their growth ve- locity Z scores (not heights) during the 3 years of calcitriol and Pi treatment. A total of 12 children had growth veloc- ity Z scores greater than or equal to 0 (indicating that their growth velocities were above or at the mean for age); they were classified as demonstrating “good growth’’ response to therapy. The other 8 children had growth velocity Z scores less than 0; they were designated the group with “poor growth.”+ Of the 5 presumed sporadic XLH cases, 3 and 2 subjects were found in the group with good and poor growth, respectively.
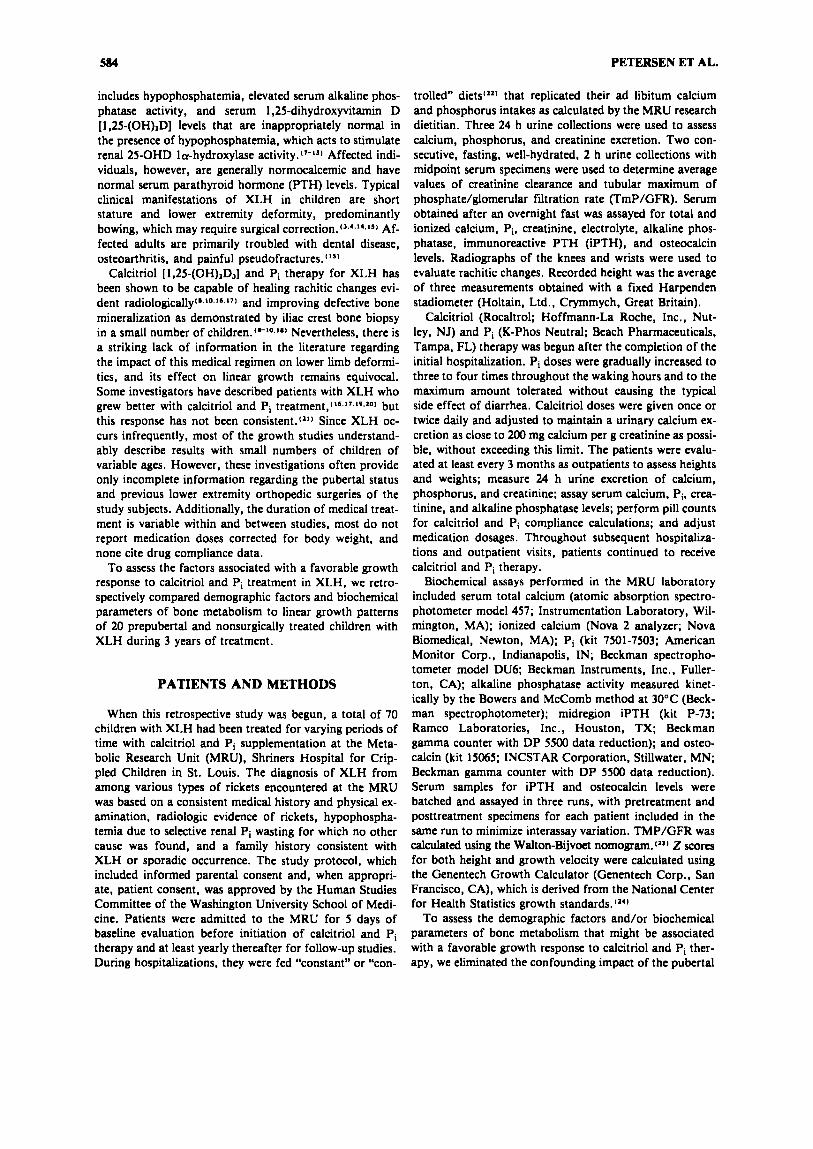
Figure 1 helps to illustrate the two groups from which the data were subsequently analyzed. I t shows the height Z scores (x * SEM) before and after 3 years of therapy for both the group with good growth velocity and the group with poor growth velocity. The mean height Z scores of
*We refer to growth velocity Z scores. not growth velocities. Thus, all the patients were growing children.
HEIGHT (z-score)
- 2 Y GOOD POOR
GROWTH GROWTH Pre Post Pre
l.
- 3 I----’ p=o45
Post
FIG. 1. Mean height Z scores (x f SEM) before and after 3 years of calcitriol and Pi therapy for the group with good growth (growth velocity Z score z 0) and the group with poor growth (growth velocity Z score < 0).
the two groups before initiation of calcitriol and Pi therapy were essentially the same (good growth - 1.92 * 0.24 ver- sus poor growth -2.20 * 0.26, p = 0.45). Thus, the group that would ultimately show a good growth response began with a clinically important degree of short stature that was the same as that of the group that would demon- strate a poor growth response.
As expected from our definitions of the two groups, those with good growth demonstrated an improved mean height Z score with therapy (pretreatment -1.92 f 0.24 versus posttreatment - 1.08 * 0.18). Importantly, how- ever, this improvement was nearly l SD, which represents a change from the 6th to the 18th percentile. Therefore, the improved linear growth velocity led to a clinically im- portant improvement in stature. Also as expected by defi- nition, the group with poor growth showed a decreased mean height Z score despite therapy (pretreatment -2.20 f 0.26 versus posttreatment -2.48 0.27). Thus, the mean height of the poor growers remained below the 4th percentile. The difference in the posttreatment height Z score between the two groups was 1.4 SD and statistically significant (-1.08 0.18 versus -2.48 * 0.27, p = 0.0003). The similar mean heights for the two groups be- fore therapy and the clinically important difference in height observed after treatment indicated to us that the separation of patients into the two groups based on growth velocity Z scores was a valid division for purposes of this study.
RESULTS Demographic and biochemical findings: Good growth versus poor growth
Several major demographic features of the group with good growth response versus poor growth response to cal- citriol and Pi are compared in Table l (top). There was no

586 PETERSEN ET AL.
TABLE 1. DIETARY AND THERAPEUTIC CHARACTERISTICS OF THE X-LINKED HYPOPHOSPHATEMU PATIENT GROUPS~
Dietary calcium Calcitriol Phosphate
Initial age Pretreatment Posttreatment Dose Compliance Dose Compliance (years) (mg/kg/day) (mg/kg/day) (ng/kg/day) (%) (mg/kg/dayl (%)
Good growthb 4.0 f 0.6 56 f 6 43 f 5 31 f 2 86 f 4 49 f 3 79 f 5 (N = 12)
(N = 8) Poor growthc 2.8 f 0.Y 54 f 5 43 f 4 30 f 4 94 f 2 54 f 5 82 f 4
(N = 7)
Girls 3.6 f 0.5 58 f 6 4 6 f 4 30 f 3 86 f 4 49 f 3 77 f 5
Boys 3.2 f 0.4 50 f 5 38 f 7 33 f 4 % f 2= 54 f 4 86 f 4 (N = 13) (N = 12) (N = 12)
(N = 7)
aVaIues are the mean f SEM. P values refer to Student’s unpaired M a t comparison of the group with good growth to the group with
bGrowth velocity Z score L 0. CGrowth velocity Z score < 0. dp = 0.07.
poor growth or of the girls to the boys and are not significant except as indicated.
cp = 0.02.
statistically significant difference between groups for mean age at initiation of therapy, pretreatment or posttreatment ad libitum dietary calcium, mean calcitriol dose, calcitriol compliance, mean Pi dose, or Pi compliance.
All 20 patients demonstrated improvement of rickets on radiographs in response to therapy. Although 90% of the children had lower extremity deformities at the initiation of treatment (1 1 of 12 who grew well and 7 of 8 who grew poorly), only 35% had clinically apparent deformity after 3 years of therapy (3 of 12 who grew well and 4 of 8 who grew poorly). One child from each group began brace ther- apy coincident with initiation of calcitriol and Pi treat- ment; the patient from the group who grew well was able to discontinue the braces after 3 years. However, an addi- tional patient from each group required leg braces during the period of study.
Of the 20 children studied, renal ultrasound examination revealed subradiographic nephrocalcinosis in 2 patients. In 1 boy, this finding was probably present upon referral to us for treatment. In another boy, renal ultrasound exami- nation was first performed 1 year after the data for this study were accumulated and revealed evidence of medul- lary nephrocalcinosis. Thus, while they received treatment from us, subradiographic nephrocalcinosis appeared to have developed in 1 of 19 patients (5.3%).
There was no significant difference in mean pretreat- ment or mean posttreatment urinary calcium excretion be- tween the two groups (Table 2, top). Both groups demon- strated significant, and comparable, increases in mean uri- nary calcium excretion with therapy [good growth, pre- treatment 65 f 9 versus posttreatment 136 f 20 mg Ca per g Cr. p = 0.005; poor growth (n = 7). pretreatment 66 f 16 versus posttreatment 153 f 24 mg Ca per g Cr, p = 0.0121 on paired analysis.
Mean pretreatment and posttreatment serum creatinine levels were normal before therapy and did not differ signif- icantly between the two groups (Table 2, top). Following 3 years of treatment, neither group demonstrated a statis-
tically significant change [good growth ( n = 1 l), pretreat- ment 0.51 f 0.06 versus posttreatment 0.39 f 0.06 mg/ dl, p = 0.18; poor growth (n = 7), pretreatment 0.49 f 0.05 versus posttreatment 0.40 f 0.05 mg/dl, p = 0.321. Furthermore, mean pretreatment and posttreatment creati- nine clearances did not differ significantly between the two groups (Table 2, top), nor did either group demonstrate a statistically significant change with therapy [good growth (n = 9), pretreatment 125 f 26 versus posttreatment 178 f 32 ml/minute per 1.73 m’,p = 0.11; poorgrowth (n = 3), pretreatment 108 f 32 versus posttreatment 165 f 6 ml/minute per 1.73 m2, p = 0.251. Although there is some inaccuracy inherent in using creatinine clearance to assess kidney function, these results are reassuring that renal function was not impaired by the treatment.
Despite pharmacologic doses of calcitriol, the mean serum total calcium level did not differ significantly before and after therapy for either group (good growth, pretreat- ment 9.75 f 0.10 versus posttreatment 9.86 f 0.07 mg/ dl, p = 0.5; poor growth, pretreatment 9.49 f 0.09 versus posttreatment 9.69 f 0.06 mg/dl, p = 0.09) or between the two groups before or after treatment (Table 2, top). Furthermore, mean serum ionized calcium levels did not differ significantly before and after therapy for either group [good growth, pretreatment 4.86 f 0.05 versus posttreatment 4.94 f 0.06 mg/dl, p = 0.3; poor growth (n = 7), pretreatment 4.75 f 0.08 versus posttreatment 4.76 f 0.05 mg/dl, p = 0.91. The mean pretreatment serum ionized calcium level was not significantly different between the good growers and the poor growers (Table 2, top). Although the posttreatment mean ionized calcium value appeared to be slightly higher for the group with good growth, the level only approached statistical signifi- cance (Table 2, top).
All patients demonstrated fasting hypophosphatemia be- fore and after calcitriol and Pi therapy. Figure 2 (top) shows that both groups had significantly higher mean fast- ing serum Pi levels after 3 years of treatment (good

TABL
E 2. BI
OCHE
MICAL FI
ND
IN~S
O
F TH
E X
-LIN
KED
HY
POPH
OSP
HA
TEM
U
PATI
ENT G
RO
UP
S~
X
r z
Cre
atin
ine
clea
ranc
e U
rina
ry c
alci
um
Seru
m c
reat
inin
e (7
9-18
7 m
l/min
ute/
Se
rum
tot
al c
alci
um
(~
22
0
mg
Ca/
g C
r)
(0.5
-1.4
mg/
dU
1.73
ma)
(8
.5-1
0.4
mg/
dl)
Pret
reat
men
t Po
sttr
eatm
ent
Pret
reat
men
t Po
sttr
eatm
ent
Pret
reat
men
t Po
sttr
eatm
ent
Pret
reat
men
t Po
sttr
eatm
ent
Goo
d gr
owth
d
Poor g
row
the
(n =
12)
(n =
8)
65 f 9
136 f 20
0.51 f 0.06
0.40 f 0.06
66 f 16
146
+ 22
0.49 f 0.05
0.40 f 0.05
(n =
7)
(n =
8)
(n =
7)
(n =
8)
(n =
11)
(n
= 12)
Girl
s
Boy
s (n
= 13)
(n =
7)
__
__
~
66 f 10
150
+ 20
0.50 f 0.05
0.37 f 0.05
65 f 15
120 f 17
0.51 +
0.06
0.46 f 0.08
(n =
6)
(n =
7)
(n =
6)
(n =
7)
(n =
12)
(n =
13)
125 f 26
(n =
9)
108 f 32
(n =
3)
148
+ 27
(n =
7)
82 f 23
(n =
5)
168 f 27
9.75 f 0.10
9.86 +
0.07
(n =
11)
144
+ 12
9.49 *
0.09
9.69 f 0.06
(n =
8)
169 f 23
9.68 f 0.10
9.80 f 0.07
(n =
12)
140 f 16
9.59 f 0.11
9.77 f 0.06
(n =
7)
Seru
m io
nize
d ca
lciu
m
Alk
alin
e ph
osph
atas
e O
steo
calc
in
(4.2
-5.4
mg
/dl)
(8
0-34
2 IU
/lite
r)b
(7.7
-15.
3 m
g/dl
)c
Pret
reat
men
t Po
sttr
eatm
ent
Pret
reat
men
t Po
sttr
eatm
ent
Pret
reat
men
t Po
sttr
eatm
ent
Good g
row
thd
4.86 +
0.05
4.94 +
0.06
388
+ 25
318 f 16
7.8
+ 0.7
10.6 f 0.7
9.0 f 1.6
11.9 f 0.5
Poor
gro
wth
C
4.75 f 0.08
4.76 f 0.05'
359 f 25
276 f 32
(n =
12)
(n =
8)
(n =
7)
(n =
8)
(n =
6)
(n =
8)
11.3 f 0.5
Girl
s 4.82 f 0.06
4.92 f 0.06
400 f 21
332 f 19
8.2 f 0.9
(n =
13)
Boy
s 4.81 f 0.06
4.76 +
0.0
48
332
+ 28h
243
+ 13'
8.3
+ 1.4
10.9 f 1.0
(n =
7)
(n =
6)
(n =
7)
(n =
5)
(n =
7)
A 0
PUnl
ess
mar
ked
othe
rwis
e, n
orm
al r
ange
s ( f 2 SD
mea
n) s
how
n in
par
enth
eses
are
bas
ed on
spec
imen
s fr
om 20
heal
thy
adul
ts. V
alue
s ar
e th
e m
ean
+ SE
M. P
val
ues
refe
r to
Stu
dent
's un
paire
d t-t
est c
ompa
riso
n of
the
gro
up w
ith g
ood
grow
th t
o th
e gr
oup
with
poo
r gr
owth
or o
f the
girl
s to
the
boys
, and
are
no
t sig
nific
ant e
xcep
t as
indi
cate
d.
bFro
m 10
norm
al c
hild
ren.
CK
ruse
K, K
rach
t U 1986 E
valu
atio
n of
ser
um o
steo
calc
in as
an in
dex
of a
ltere
d bo
ne m
etab
olis
m. A
m J
Ped
iatr
245:27-33.
dGro
wth
vel
ocity
Z sc
ore 2 0
. G
row
th v
eloc
ity Z
sco
re <
0.
'p =
0.05.
Bp
= 0.09.
hp =
0.07.
'p =
0.005.

588 PETERSEN ET AL.
p = 0.053 r -
Pre Post Pre Post GOOD POOR
GROWTH GROWTH p = o . o 2 p-0.w
FIG. 2. Mean fasting serum Pi levels before and after 3 years of calcitriol and Pi therapy for the group with good growth and the group with poor growth. Both groups had significantly higher Pi levels after therapy. The mean pre- treatment Pi level was higher in the group with good growth at p = 0.053. The posttreatment Pi levels were not significantly different between the two groups (normal MRU range, * 2 SD mean, 4.8-6.4 mg/dl in eight children).
growth, pretreatment 2.90 * 0.09 versus posttreatment 3.17 0.15 mg/dl, p = 0.02; poor growth, pretreatment 2.54 0.16 versus posttreatment 3.05 f 0.1 1 mg/dl, p = 0.04). The difference in mean pretreatment levels (higher in the good growers) approached statistical significance (good growth, 2.90 f 0.09 versus poor growth, 2.54 0.16 mg/dl; p = 0.053). However, the mean posttreatment fasting serum Pi levels were not significantly different be- tween the two groups (good growth, 3.17 * 0.15 versus poor growth, 3.05 f 0.11 mg/dl; p = 0.57). Thus, al- though there was the suggestion that pretreatment fasting serum Pi levels might predict those patients who would have a good growth response to therapy, posttreatment values did not.
Because of the inability of the youngest children to CO-
operate with timed urine collections, TmP/GFR ratio mea- surements were available pretreatment for 9 of the 12 pa- tients who grew well but for only 3 of the 8 children who grew poorly (Fig. 3A). The data available from the group with good growth revealed that they had a statistically sig- nificant increment in mean TmP/GFR with treatment [pretreatment ( n = 9), 1.94 * 0.22 versus posttreatment (n = 9), 2.57 f 0.19 mg/dl; p = 0.011). Although the group with poor growth also demonstrated a trend toward an increased TmP/GFR with therapy [pretreatment ( n = 3), 1.38 * 0.08 versus posttreatment ( n = 3). 1.89 f 0.25 mg/dl], there were only three paired measurements avail-
3.0r
I * T
T
Pre Post GOOD
GROWTH p = 0.07
Pre Post POOR
GROWTH p > 0. 1(NS)
3.01 B
- Good Poor Growth Growth
POST TREATMENT p=o.m
FIG. 3. (A) Paired t-test shows that the group with good growth had a significant increment in mean TmP/GFR after 3 years of calcitriol and Pi therapy (p = 0.01). The group with poor growth also demonstrated an increase in TmP/GFR, but paired measurements were available for only three patients. (B) With more posttreatment measurements available for both groups, nonpaired 1-test comparison shows that the group with good growth had a significantly higher mean posttreatment TmP/GFR than the group with poor growth (p = 0.02).

XLH: RESPONSE TO CALCITRIOL AND PHOSPHATE 589
able for comparison for this group. However, since the pa- tients were 3 years older at the end of the study and better able to cooperate with timed urine collections, TmP/GFR ratios were available for 1 1 of the 12 patients who grew well and for all 8 patients who grew poorly (Fig. 3B). The group with good growth had a significantly higher post- treatment TmP/GFR than the group with poor growth [good growth (n = 1 l), 2.64 f 0.13 versus poor growth (n = 8), 2.18 * 0.13 mg/dl; p = 0.023). Neither group, however, reached the normal range for children of about 4.0-6.0 mg/dl with therapy.
Figure 4 shows that mean pretreatment and posttreatment serum iPTH levels did not differ significantly between the two groups [good growth pretreatment, 693 * 50 versus poor growth (n = 7), 727 * 51 pg/ml, p = 0.66; good growth posttreatment, 688 76 versus poor growth (n = 8), 587 39 pg/ml, p = 0.251. The mean serum iPTH level in the group with good growth did not change signifi- cantly with therapy (pretreatment, 693 * 50 versus post- treatment, 688 * 76 pg/ml; p = 0.92), whereas the mean iPTH level of the group with poor growth decreased signif- icantly [pretreatment (n = 7), 727 + 51 versus posttreat- ment (n = 7), 5% f 44 pg/ml; p = 0.0231. All mean serum iPTH values were within the normal range of 457- 751 pg/ml for our laboratory as determined with 20 nor- mal young or middle-aged adults (* 2 SD mean). Addi- tionally, linear regression analysis for all patients revealed a nonsignificant correlation between posttreatment iPTH and TmP/GFR ( r = -0.11, p = 0.64).
Mean pretreatment and posttreatment serum alkaline phosphatase (ALP) activity did not differ significantly be- tween the two groups (Table 2, top). Both groups had sig-
I PTH (w
800 r 1
I I I 1 Normal i Range I I A
- " Pre Post Pre Post
GOOD POOR GROWTH GROWTH p > 0.1 (NS) p = 0.02
FIG. 4. Mean pretreatment and posttreatment serum iPTH levels did not differ significantly between the two groups. The mean serum iPTH of the group with good growth did not change after 3 years of calcitriol and Pi therapy. However, it decreased significantly in the group with poor growth (p = 0.02) (normal MRU range, mean * 2 SD, 457-751 p u m l in 20 adults).
nificantly lower mean serum ALP activity after 3 years of therapy (good growth, pretreatment 388 * 25 versus post- treatment 318 * 16 U/liter, p = 0.013; poor growth, pre- treatment 359 25 versus posttreatment 276 f 32 U/liter, p = 0.024).
Mean pretreatment and posttreatment serum osteocalcin levels did not differ significantly between the two groups (Table 2, top). After 3 years of therapy, there was a statis- tically significant increase for the good growers (pretreat- ment, 7.8 * 0.7 versus posttreatment, 10.6 * 0.7 ng/ml; p = 0.011) but not for the poor growers [pretreatment (n = 6), 9.0 f 1.6 versus posttreatment (n = 6), 11.7 * 0.5 ng/ml; p = 0.17).
Demographic and biochemical findings: Girls versus boys
During our analysis of these data, it became apparent that the group of children who grew well was comprised predominantly of girls, whereas the group who grew poorly was primarily boys. When analyzed by the Z test for binomial proportion^^^^^ 10 girls of 12 children in the group with good growth were found to be a disproportion- ately large ratio of females that did not occur by chance (p = 0.04). Accordingly, we reanalyzed our data according to patient gender.
Comparison of the mean height Z scores of girls to boys (Fig. 5) shows that stature was not different at the initia- tion of therapy (girls -2.05 * 0.23 versus boys - l .98 * 0.31; p = 0.86). After therapy, the girls' mean height Z score had improved significantly, but the boys' mean value was unchanged (girls pretreatment -2.05 * 0.23 versus posttreatment - 1.40 * 0.24, p = 0.005; boys pretreat- ment -1.98 * 0.31 versus posttreatment -2.09 * 0.40, p
C
- I HEIGHT (2-score)
-2
p = 0.005 p 0.1 (NS)
GIRLS BOYS Pre Post Pre Post
1 p = 0.13
- 3
FIG. 5. Mean height Z scores were the same for the boys and the girls at the initiation of calcitriol and Pi therapy. The girls' mean height Z score improved significantly (p = 0.005), but the boys' mean was unchanged after 3 years of therapy.

590 PETERSEN ET AL.
= 0.6). A comparison of the height Z scores of boys ver- sus girls at the end of therapy was problematic because of increased variance and did not demonstrate a significant difference (p = 0.13).
Table 1 (bottom) shows that there was no statistically significant difference between mean values for the girls versus the boys for age at initiation of therapy, pretreat- ment or posttreatment ad libitum dietary calcium, calcit- riol dose, Pi dose, or Pi compliance. There was a statis- tically significant difference for the mean calcitriol compli- ance, but it was the poorly growing boys who took this drug more reliably.
Of the 18 children who had lower extremity deformities at the start of therapy, 7 patients (39Vo) demonstrated re- sidual deformity after 3 years of therapy. There was a simi- lar incidence of persistent deformity for boys (2 of 6 or 33%) and girls (5 of 12 or 42%); 2 girls started brace ther- apy coincident with initiation of treatment, and 1 was able to discontinue braces after 3 years. Another 2 children (1 boy, 1 girl) required leg braces during the period of the study.
There was no significant difference in mean pretreat- ment or posttreatment urinary calcium excretion between the sexes (Table 2, bottom). Both groups, however, dem- onstrated significant increases with therapy [girls, pretreat- ment 66 * 10 versus posttreatment 150 * 20 mg Ca per g Cr, p = 0.001; boys ( n = a), pretreatment 65 f 15 versus posttreatment 123 f 20 mg Ca per g Cr, p = 0.051.
Mean pretreatment and posttreatment serum creatinine levels and creatinine clearances did not differ significantly between the sexes (Table 2, bottom).
Mean serum total calcium level did not differ signifi- cantly before and after therapy for either group (girls, pre- treatment 9.68 f 0.10 versus posttreatment 9.80 f 0.07 mg/dl, p = 0.40; boys, pretreatment 9.59 * 0.11 versus posttreatment 9.77 f 0.06 mg/dl, p = 0.13) or between the two groups before or after therapy (Table 2, bottom).
Mean serum ionized calcium level did not differ signifi- cantly before and after therapy for either group [girls, pre- treatment 4.82 f 0.06 versus posttreatment 4.92 + 0.06 mg/dl, p = 0.20; boys ( n = a), pretreatment 4.81 f 0.06 versus posttreatment 4.76 f 0.04 mg/dl, p = 0.561 or be- tween the two groups before or after therapy (Table 2, bottom).
Figure 6 shows that mean pretreatment and posttreat- ment fasting serum Pi did not differ between the sexes (girls pretreatment, 2.73 f 0.13 versus boys 2.81 f 0.08 mg/dl, p = 0.61; girls posttreatment, 3.20 f 0.14 versus boys 2.97 f 0.12 mg/dl, p = 0.28). The girls demon- strated a significant increase in fasting serum Pi with ther- apy, but the boys did not (girls, pretreatment 2.73 * 0.13 versus posttreatment 3.20 f 0.14 mg/dl, p = 0.003; boys, Pretreatment 2.81 f 0.08 versus posttreatment 2.97 f 0.12 mg/dl, p = 0.27) on paired analysis.
Both sexes showed statistically significantly increased mean TmP/GFR with therapy [Fig. 7A; girls ( n = 7), pre- treatment 2.07 * 0.19 versus posttreatment 2.61 f 0.16 mg/dl, p = 0.05; boys ( n = S), pretreatment 1.41 f 0.27 versus posttreatment 2.10 f 0.23 mg/dl, p = 0.041. Al- though the values for the mean pretreatment TmP/GFR
r -I-
I .o I: n
T
Pre Post
p > O.l(NS)
U Pre Post
GIRLS BOYS p = 0.003
FIG. 6. Mean Pretreatment and posttreatment fasting serum Pi levels did not differ between the girls and the boys. The girls demonstrated a significant increase in mean fasting serum Pi level after 3 years of calcitriol and Pi ther- apy (p = 0.003), whereas the boys did not (normal range per Fig. 2).
was higher for the girls, the difference only approached statistical significance [girls ( n = 7), 2.07 f 0.19 versus boys ( n = 5). 1.41 f 0.27 mg/dl; p = 0.071. However, the posttreatment TmP/GFR was statistically significantly higher [Fig. 7B; girls ( n = 12), 2.62 f 0.1 1 versus boys ( n = 7), 2.15 f 0.16 mg/dl; p = 0.02).
Figure 8 shows that mean serum iPTH level did not change significantly with therapy for the girls (pretreat- ment 736 * 38 versus posttreatment 710 * 65 pg/ml; p = 0.53) or for the boys ( n = 6; pretreatment 638 * 77 ver- sus posttreatment 536 * 60 pg/ml, p = 0.09). There was no statistically significant posttreatment difference [girls, 710 f 65 versus boys ( n = 7), 533 f 51 pg/ml; p = 0.081.
Both sexes had significantly lower mean serum ALP ac- tivity after therapy (girls, pretreatment 400 f 21 versus posttreatment 332 f 19 U/liter, p = 0.01; boys, pretreat- ment 332 * 28 versus posttreatment 243 * 13 U/liter, p = 0.03). Mean pretreatment serum ALP activity did not differ significantly between the sexes, but the boys had sta- tistically significantly lower posttreatment mean serum ALP activity (Table 2, bottom).
Mean pretreatment and posttreatment serum osteocalcin levels did not differ significantly between the sexes (Table 2, bottom). Both groups had higher osteocalcin levels after therapy. The increase was statistically significant for the girls (pretreatment 8.2 f 0.9 versus posttreatment 11.3 * 0.5 ng/ml; p = 0.005) but not for the boys ( n = 5; pre- treatment 8.3 * 1.4 versus posttreatment 10.3 f 1.3 ng/ ml, p = 0.33) on paired analysis.

XLH: RESPONSE TO CALCITRIOL AND PHOSPHATE 591
p = 0.07 (NS) 71 '"1 A T
-
2.0 -
-
1.0 -
U Pre Post
GIRLS p = 0.05
T
Pre Post BOYS p=o.o4
2.0 -
1.0 -
b
-0- Girls Boys POST TREATMENT
p=o.o2
FIG. 7. (A) Both girls and boys demonstrated significantly increased mean TmP/GFR after 3 years of calcitriol and Pi therapy. The girls' mean pretreatment TmP/GFR was higher than that of the boys', but the difference only approached significance (p = 0.07). (B) The girls' mean posttreatment TmP/GFR was significantly higher than that of the boys' (p = 0.02).
DISCUSSION
p = 0 08 (NS) f 1
800
600
400
200
O Pre post Pre Post GIRLS BOYS
p > O.l(NS) p = 0.09 (NS)
FIG. 8. The mean serum iPTH level of the girls did not change significantly after 3 years of calcitriol and Pi ther- apy. The mean serum iPTH of the boys decreased with therapy, but the change was not significant and did not re- sult in a significant posttreatment difference between the two groups (normal range per Fig. 4).
After briefly reviewing the early attempts at medical therapy of XLH, we discuss our results with regard to medical literature reports concerning the affects of calcit- riol and Pi treatment on alterations in patient growth and changes in renal reclamation of Pi. We then focus on the influence of gender on both parameters.
Background
Several medical regimens have been used to treat XLH since it was first described as "rickets resistant to vitamin D by Albright and his colleagues in 1937.fZn' In their case report, a boy whose bone disease was refractory to doses of vitamin D sufficient to heal vitamin D deficiency rickets improved radiographically in response to massive doses (up to 1,500,000 U/day). Subsequently, a number of simi- lar cases were also found to benefit from high-dose vita- min D, therapy. The rickets evident on radiographs im- proved in most patients, and lower limb deformities les- sened in some, but biochemical and growth abnormalities were rarely corrected. (27-311 Additionally, it was recognized early that at the large doses necessary to heal XLH rickets, vitamin D, has a small "therapeutic window." The medical literature thoroughly documents vitamin D intoxication during treatment of XLH(27-*9,31-33) that sometimes pro- gressed to renal failure. f29,3'-361

592 PETERSEN ET AL.
In the mid-I960s, as attention focused on the hypophos- phatemic aspect of XLH. the impact of Pi supplementa- tion alone or in combination with vitamin D, was evalu- ated. Although there are a few early reports of radio- graphic improvement of rickets and better growth with Pi therapy alone, 'l') typically this was not the outcome. (11.3g)
Furthermore, secondary hyperparathyroidism was recog- nized as a complication of Pi administrati~n.(~~~~~'~] Ac- cordingly, Pi supplementation was combined with vitamin D, to increase absorption of dietary calcium to negate Pi- induced hyperparathyroidism. This combined regimen par- tially healed the rickets evident on x-rays, '11"1~17.'1-'') de- creased the adverse effects of either agent when used alone,'121 and improved the growth of some pa- tient~. '~'~'~-' '~ However, growth acceleration did not occur consistently, i'l-'dl osteomalacia remained unchanged on bone biopsy, [l','lm and hypercalcemia and/or secondary hyperparathyroidism continued to occur. r13.1'.a~'1-451 AI- though there have been few studies, the experience with calcidiol (25-OHD1) and Pi therapy has generally been sim-
Beginning in the 1970s, several groups measured serum 1,25-(OH),D levels in untreated patients with XLH. The findings were variable. Delvin and Glorieux'lll reported a high mean 1,25-(0H)1D level in 16 children, although all but one of the individual values were within the control range. Balsan and Tiederilll found a high level in 1 child and low-normal levels in 6 children. Mason et al.,'"] Glorieux et al.,In1 and Drezner et al.cgr described normal serum levels of 1,2S-(OH),D in 8, 6, and 2 children, re- spectively; however, 14 of these values were in the low-nor- mal range. Lyles and coworkers'"' reported a normal mean level in 17 adults and a low mean level in 9 children. However, it was subsequently recognized that a "normal" serum 1 ,25-(OH),D level is inappropriately low in the pres- ence of hypophosphatemia.~7.g.11.11' Accordingly, the ma- jority of XLH patients appear to have relatively, if not ab- solutely, low 1 ,25-(OH),D levels in serum.
Since 1,25-(OH),D is the most physiologically active metabolite of vitamin D, trials of calcitriol [ 1,25-(OH),Dl] for treatment of XLH were instituted soon after synthetic material became available during the 1970s. During short courses (4-12 days) of calcitriol and Pi, mineral balance studies performed by Russell et al.'sl' and Chan et al.'16.171 on a small number of adults and adolescents with XLH demonstrated enhanced positive calcium balance and con- version to positive Pi balance due to increased intestinal absorption of the minerals. Drezner and colleague^'^^ per- formed mineral balance studies on two adolescents and two adults with XLH, before and after 6 months of calcit- riol therapy alone, and found an approximate doubling of gastrointestinal Pi absorption and conversion to positive Pi balance. Gut calcium absorption and positive calcium bal- ance were also increased.
Histologic examinations have consistently demonstrated improvement in skeletal mineralization when calcitriol therapy is used for XLH. Histomorphometry of nondecal- cified iliac crest specimens from 11 XLH children was per- formed by Glorieux asnd colleaguesin1 to assess various treatment regimens (Pi alone, ergocalciferol with Pi, and
ilar. (47-101
calcitriol with Pi). Among their 11 patients, 6 girls (ages 4-12 years) were studied before and after 0.5-19 months of calcitriol and Pi therapy (mean 6.7 months). All showed improvement in their osteomalacia. Drezner et al.lP1 stud- ied 2 adolescents and 1 adult with XLH and demonstrated normalization of their mineralization front activity (with diminished osteoid accumulation) after 6 months of calcit- riol therapy alone. Additionally, they found a positive lin- ear relationship between serum 1,25-(OH),D levels and mineralization front activity. Costa and coworkersi10' also demonstrated improved mineralization and decreased oste- oid accumulation in 5 prepubertal and 5 postpubertal XLH patients who were treated with calcitriol and Pi for 6-8 months. Harrell et al.'lnl studied nondecalcified iliac crest biopsies of 1 child, 2 adolescents, and 2 adults after 8-1 1 months of "high-dose" and again after 19-24 months of "low-dose" calcitriol and Pi therapy. The patients dem- onstrated decreased mean osteoid seam width and normal- ization of mean relative osteoid volume, osteoid surface, mineralization front activity, and rate of mineral apposi- tion.
Growth
Reports of the effect of calcitriol and Pi therapy on the two major clinical sequelae of XLH during childhood, lower limb deformity and impaired linear growth, are few and suffer from several shortcomings. Because of the in- frequent occurrence of XLH, most of the studies describe the growth data of small numbers of children of variable ages. Apparently, the investigators could not control for pubertal status or prior orthopedic surgery, but medication doses corrected for body weight, duration of therapy, or compliance with the treatment regimen also typically were not reported.
Chan and Bartter[161 described a boy with XLH who maintained a growth velocity of 5-7 cm/year between the ages of 6 and 16 years while taking ergocalciferol and Pi. He began puberty at 13 years of age. Between the ages of 16 and 17 years, when he was treated with calcitriol and Pi, he demonstrated an accelerated growth velocity of 14 cm/ year. Later, Chan et al.l1'] reported the growth velocities of four XLH patients before their growth was complete. Each patient had had a stable or declining growth velocity during several years of ergocalciferol and Pi or calcidiol and Pi treatment. During subsequent calcitriol and Pi ther- apy, however, the growth velocity of each of the four pa- tients increased impressively. Unfortunately, there is not enough information in their report to be certain that the improved growth velocity of one of the boys was not due to his pubertal growth spurt.
Chesney et al."g' compared the growth of seven children (ages 2-13 years) during three different consecutive treat- ment regimens: at least 12 months of no therapy or ergo- calciferol alone; at least 12 months of ergocalciferol and Pi (with the exception of one girl who was treated for only 1 month); and at least 12 months of calcitriol and Pi ther- apy. The mean height Z score was significantly increased from baseline (-2.3) after ergocalciferol with Pi (- 1.8) and further increased with calcitriol with Pi (-1.4). Al-

XLH: RESPONSE TO CALCITRIOL AND PHOSPHATE 593
though the mean height Z score was less negative after cal- citriol and Pi treatment than after ergocalciferol and Pi therapy, the differences between the mean height Z scores and the mean growth velocities of these two treatment phases were not statistically significant. Of interest, at least six and possibly all seven of these children were girls (see Gender Effects below).
Tsuru et a l .ol l studied the growth of 9 girls and 10 boys (mean age 12 years) with XLH who had received at least 1 year of calcitriol (mean dose 58 ng/kg/day) and Pi ther- apy. They reported a significant increase in mean growth velocity index (actual growth velocity/normal growth ve- locity x 100) from 62% at age 2 years to 101% at age 11 years. They also found that the mean height Z score of the patients improved, but the change was of borderline signif- icance (-2.7 at age 2 years versus -2.4 at age 12 years). By comparing the growth of their patients at age 2 years to that at age 12 years, however, and after a mean duration of only 42 months total of calcitriol and Pi therapy, their data were likely confounded by the effects of other treat- ment regimens used before the initiation of calcitriol treat- ment. Furthermore, these investigators did not provide in- formation regarding the pubertal status of their patients.
Saggese et aI.lzoL compared the effect of what they re- ferred to as “supraphysiologic” doses (2-3 p/day) to that of “physiologic” doses (0.5-1 &day) of calcitriol on growth of nine XLH patients (ages 3-11 years). Both groups demonstrated a significant improvement in their mean height Z scores after 12 months of therapy, but the improvement was greater in the group who received the higher dose of calcitriol (+0.77 SD versus +0.39 SD). However, since four of the five patients who received “supraphysiologic” calcitriol doses were girls and three of the four patients who received “physiologic” doses were boys. we believe that the differing growth responses could have been due to the different gender compositions of the two groups (see Gender Effects below).
Our experience since 1983, based upon data from a select group of 20 patients from among the relatively large number of children with XLH followed at our facility (n = 70), suggested that there is a subgroup of children who grow well in response to calcitriol and Pi treatment (in doses approximately 30 ng/kg/day and 50 mg/kg/day as P , respectively), and a subgroup of children who d o not. Analysis of this information revealed no difference in mean age, dietary calcium, calcitriol dose or compliance, Pi dose or compliance, creatinine clearance, or pretreat- ment height Z score between the two subgroups. Those who grew well had a significantly higher fasting serum Pi level before treatment, but both groups demonstrated sig- nificantly increased fasting serum Pi levels with therapy, resulting in comparable posttreatment levels. By itself, an increase in fasting serum Pi was not necessarily associated with improved growth, since the change was actually great- est for the group with poor growth. The increment in fast- ing serum Pi appeared to be at least partially mediated through improved renal tubular reabsorption, that is, in- creased posttreatment TmP/GFR for both groups. The group with good growth response had a statistically signifi- cantly (p = 0.02) higher posttreatment TmP/GFR than
the group with poor growth response. Since pretreatment TmP/GFR measurements were available for only 3 of the 8 children who grew poorly, comparison of pretreatment and posttreatment values for that group was somewhat tenuous.
Renal phosphate reclamation
The reported effect of calcitriol and Pi treatment on renal Pi reclamation in XLH has been variable. Glorieux et al.[531 found that tubular reabsorption of phosphorus (TRP) increased 13% within 30 minutes of a single intra- venous dose of calcitriol given to one previously untreated boy. However, his TRP remained low and unchanged from baseline with additional calcitriol treatment adminis- tered as five daily intravenous doses followed by four daily oral doses. Brickman et a1.‘541 studied one child, one ado- lescent, and two adults during 7 days of calcitriol and Pi therapy. The two younger subjects had increases in TRP that were accompanied by decreases in urinary CAMP ex- cretion and serum iPTH levels, but the two adults demon- strated no change. Balsan and G a r a b e d i a ~ ~ ~ ~ ~ ] reported that TRP increased from 36% before therapy to 61% after 5 days of calcitriol and Pi supplementation in one child with XLH, but serum iPTH was not measured.
The TmP/GFR is a more accurate means of assessing re- absorption of Pi by the kidney. TmP/GFR, unlike TRP, is independent of factors that alter plasma Pi concentration, such as GFR and Pi inflow to the extracellular space.‘”] The reported effect of short-term calcitriol therapy on TmP/GFR in XLH patients has also been variable. Russell et studied the TmP/GFR of three adults during 4-12 days of calcitriol therapy alone and found that it did not change. Alon and char^'"^ examined the effect of 6 days of calcitriol treatment on eight patients: four received Pi supplementation and four did not. With calcitriol treat- ment, the entire group demonstrated a significant increase in TmP/GFR from 1.4 to 1.9 mg/dl and a significant de- crease in serum iPTH. They noted an inverse linear corre- lation between TmP/GFR and serum iPTH before and after therapy ( r = -0.95). When the subgroup who re- ceived calcitriol and Pi supplementation was compared to the subgroup who received calcitriol alone, the former group demonstrated significantly greater increments in “fasting” serum Pi levels (+ 1.2 versus +0.2 mg/dl) and TmP/GFR (+0.7 versus +0.3 mg/dl). However, all deter- minations were made 2 h after morning medications were taken. Although the change was not statistically signifi- cant, the group who received calcitriol with Pi supplemen- tation also demonstrated a greater decrement in serum iPTH than the group who received calcitriol alone. Alon and Chan concluded that the increase in TmP/GFR that occurred with calcitriol therapy was mediated through the reduction of PTH and that the latter was accentuated by Pi supplementation.
Studies of the effect of long-term calcitriol therapy on TmP/GFR in XLH patients have also shown variable re- sults. The 2 adolescents and 2 adults treated with calcitriol alone for 6 months by Drezner et al.[gl demonstrated a sig- nificant increase in mean TMPIGFR from 2.1 to 2.4 mg/

594 PETERSEN ET AL.
dl and a decrease in serum iPTH levels (measured by four radioimmunoassays with different antigenic specificity). They concluded that the effect of calcitriol on TmP/GFR may be partially modulated by suppression of circulating PTH levels. One child, 2 adolescents, and 2 adults studied by Harrell et a1.‘la1 had increased mean TmP/GFR from 2.1 to 3.2 mg/dl with Pi supplementation but with doses of calcitriol that were high enough to cause hypercalciuria in three and hypercalcemia in one of their five patients. How- ever, the mean TmP/GFR decreased to below baseline (1.7 mg/dl) when calcitriol doses were lowered to maintain nor- mocalciuria and normocalcemia. Although they demon- strated no significant change in serum iPTH levels as mea- sured by carboxy-terminal and intact molecule assays, serum iPTH levels measured by midmolecule assay in- creased significantly with calcitriol treatment at the higher dose. Glorieux et al.ial reported no change in TmP/GFR of 10 girls and 1 boy with XLH who were treated with cal- citriol and Pi for 0.5-17 months (mean 8.5 months). Costa et aI.“O1 treated 5 prepubertal and 6 postpubertal patients with calcitriol and Pi for 6-8 months and noted no signifi- cant changes in mean TmP/GFR or serum iPTH levels. Tsuru et al.ia1] studied 19 XLH patients after a minimum of 12 months of calcitriol and Pi therapy (mean 42 months) and demonstrated no significant change in TmP/GFR (1.7-2.0 mg/dl) or serum iPTH levels with treatment.
Thus, the results of clinical studies of XLH in which the effect of calcitriol on renal Pi reclamation is investigated are clearly not consistent; increased TmP/GFR is reported by some i n v e ~ t i g a t o r s ‘ ~ . ~ ~ . ~ ’ ~ but not by others. 1a .10 .21 ,52 )
The variable findings may be due to the relatively small number of patients examined and the heterogeneity of the study designs, treatment regimens and doses, patient popu- lations, and medical compliance.
Our patients whose growth velocities improved with cal- citriol and Pi therapy demonstrated an improved TmP/GFR to a level that was significantly higher than for those subjects whose growth velocities did not improve. The improved TmP/GFR was not associated with suppres- sion of circulating iPTH levels using our midregion assay. Our observation is consistent with a direct effect of calcit- riol on the renal tubule to improve Pi reclamation. Indeed, recent studies of renal brush-border membrane vesicles by Kurnik and colleagues suggest that calcitriol may directly stimulate Na’-dependent Pi transport by altering the lipid composition of kidney tubule membranes. ‘Sa3Q)
Gender effects
In our study, the majority of good growers were girls. Thus, we also compared our data according to gender. The findings were similar to the results when growth velocity per se was examined (see Growth earlier). The baseline mean height Z scores of the girls and boys were essentially the same, but the girls’ score improved significantly with treatment. whereas the boys’ did not. Mean pretreatment and posttreatment fasting serum Pi levels did not differ be- tween the groups, but the girls’ level increased significantly with therapy but the boys’ did not. Both groups had sig- nificant increases in mean TmP/GFR with therapy, but the
girls’ posttreatment TmP/GFR was statistically signifi- cantly higher than that of the boys’. The girls’ improved TmP/GFR was not associated with a reduction in serum iPTH levels.
The earliest studies of XLH kindreds alleged that skele- tal disease and resultant deformities were more severe and serum Pi levels were lower in affected males than in af- fected females. [3,4,14’ Additionally, these reports described asymptomatic carriers who had hypophosphatemia with- out clinically or radiologically detectable skeletal disease. These individuals were most often females. It has been speculated that presence of a normal allele in heterozygous females with XLH may somehow modify the severity of d i~ease , ‘~ . ’~’ that one of the X chromosomes in females is inactivated leading to variable expression due to mosai- cism,I4’ or that an unidentified internal or environmental factor is responsible for the sex difference.[3’ Although studies of the HYP mouse. a murine model for XLH, show that males have more severe skeletal abnormalities than females,“’ sex differences in the severity of expres- sion of XLH have not been as well documented in hu- mans. Two notable exceptions in the recent literature de- scribed a gender difference in human XLH.
Shields et al.cwl studied mineralization of primary and secondary dentin in 8 male and 11 female XLH patients who had been treated with vitamin D and Pi or calcitriol and Pi. Mineralization was assessed using the dental pulp profile area (PRATIO, pulp area/tooth area), which is in- versely proportional to dental mineralization. Serum Pi levels and PRATIO values for teeth forming primary den- tin were comparable for boys and girls below 15 years of age. However, females aged 15-25 years demonstrated mean PRATIO values in teeth forming secondary dentin that were significantly lower than those of the age-matched males yet higher than those of controls. The findings were interpreted as evidence for a gene dosage effect in older XLH patients. Although they reported that the mean age of initiation of therapy was comparable in males and fe- males and that treatment was similar in all patients, it is unclear how well matched the groups were for treatment regimens, medication doses, and duration of therapy.
Balsan and TiederI1,’ compared the effect of various treatment regimens (Pi in combination with ergocalciferol, calcidiol, or la-hydroxyvitamin D,) and the influence of parental midheights on the final adult heights of 40 chil- dren with XLH. They concluded that regardless of the treatment regimen, the girls in their study attained a better height Z score than did the boys. However, 16 of the chil- dren had not reached final heights, and “predicted” adult heights of these patients were estimated values used in the calculations. Furthermore, the Bayley-Pinneau method used in their study is based on growth and skeletal matura- tion of normal children and cannot be assumed to apply to growth of children with a disease that impairs
If the predicted heights of these 16 children are disregarded, there still appears to be a trend for girls to achieve a better adult height Z score than boys. However, the number of boys who actually reached final adult heights in their study is probably too small to enable statis- tical comparisons with the girls. The authors also con-

XLH: RESPONSE TO CALCITRIOL AND PHOSPHATE 5%
cluded that there is a positive correlation between parental midheights and final adult heights of the girls but that there is no influence of parental midheights on final adult heights of the boys. The utility of parental midheights when either parent has a disease that impairs growth is questionable. However, their data suggest that the parental midheights of the girls were lower than those for the boys. Since XLH is an X-linked dominant condition, affected boys have only affected mothers. Whereas, affected girls have either affected mothers or fathers. If XLH men truly are more severely affected than women, fathers with XLH would lower the parental midheight more significantly than would XLH mothers. The result would be a more im- paired mean parental midheight for the girls than the boys. This appears to be the case in their study.
Our finding that under carefully controlled calcitriol and Pi therapy heterozygous girls have a better growth re- sponse than hemizygous boys provides evidence for a gene dosage effect in the expression of XLH. It also suggests that satisfactory growth may be achieved by most girls with lower doses than required by boys. Accordingly, po- tential complications of therapy (e.g., nephrocalcinosis or secondary hyperparathyroidism) might be easier to avoid in girls. Conversely, more vigorous or alternative therapies may be necessary for boys with XLH if improved growth is to be achieved. We are aware that our findings may have been more striking if we had studied the XLH population at large. A possible bias exists in our study in the way pa- tients are recruited for therapy. They are primarily referred to us for treatment of overt skeletal disease. Consequently, relatively mildly affected girls are less likely to be available for study.
I t is also important to note that the majority of the pa- tients in our study, both boys and girls, demonstrated reso- lution of lower limb deformities with this medical regimen. This observation provides a compelling reason to treat XLH children with calcitriol and Pi supplementation, since this therapy can obviate the need for corrective operative procedures. Of course, careful monitoring (especially for nephrocalcinosis and secondary hyperparathyroidism) is essential to avoid potential complications of these medica- tions.
ADDENDUM
Since this paper was accepted for publication, a report by Verge and coworkers (N Engl J Med 325:1843-1848, 1991) describes a “slight beneficial effect” on the height of 13 children with XLH who received at least 2 years of cal- citriol and Pi therapy before puberty, and a 79% incidence of nephrocalcinosis detected by renal ultrasound in their total XLH population of 24 subjects who received medical treatment.
A pilot investigation by Wilson and coworkers of 11 pediatric patients with XLH who received biosynthetic growth hormone in addition to calcitriol and Pi therapy in- dicated improved growth rate Z scores (Am J Dis Child 1451 165-1 170, 1991).
ACKNOWLEDGMENTS
We are grateful to the nursing, dietary, and laboratory staffs of the Metabolic Research Unit, Shriners Hospital for Crippled Children, St. Louis, MO, for making this study possible; to Hoffmann-La Roche, Inc. and Beach Pharmaceuticals, Inc. for their generous gifts of Rocaltrol (calcitriol) and K-Phos Neutral (inorganic phosphate), re- spectively; and to Louise Feager for expert secretarial help. Supported by Grant 15958 from the Shriners Hospitals for Crippled Children and NIH Training Grant 5T32AR07033. Dr. Petersen is the recipient of a Research Fellowship from the Shriners Hospitals for Crippled Children. Presented in part at the 12th Annual Scientific Meeting of the American Society for Bone and Mineral Research, August 28-31, 1990, Atlanta, GA. (J Bone Miner Res 55171, 1990).
REFERENCES
1. Rasmussen H, Anast C 1983 Familial hypophosphatemic rickets and vitamin D-dependent rickets. In: Stanbury JB, Wyngaarden JB, Frederickson DS, Goldstein JL, Brown MS (eds), The Metabolic Basis of Inherited Disease, 5th ed. Mc- Graw-Hill. New York, pp. 1743-1773.
2. Scriver CR, Beaudet AL, Sly WS, Valle D (eds) 1989 The Metabolic Basis of Inherited Disease, 6th ed. McGraw-Hill, New York. p. 154.
3. Winters RW, Graham JB. William TF, McFalls WV, Burnett CH 1958 A genetic study of familial hypophosphatemia and vitamin D-resistant rickets with a review of the literature. Medicine (Baltimore) 37:97-142.
4. Burnett CH, Dent CD. Harper C, Warland BJ 1964 Vitamin D resistant rickets: Analysis of twenty-four pedigrees with hereditary and sporadic cases. Am J Med 36:222-232.
5. Machler M, Frey D, Gal A, et al. 1986 X-linked dominant hypophosphatemia is closely linked to DNA markers DXS41 and DXS43 at Xp22. Hum Genet 73:271-275.
6. Thakker RV, Read AP, Davies KE, Whyte MP, et al. 1987 Bridging markers defining the map position of X-linked hy- pophosphatemic rickets. J Med Genet ?A:756-760.
7. Scriver CR, Reade TM, DeLuca HF, Hamstra AJ 1978 Serum 1.25-dihydroxyvitamin D levels in normal subjects and in patients with hereditary rickets or bone disease. N Engl J Med 299:976-979.
8. Glorieux FH, Marie PJ, Pettifor JM, Delvin EE 1980 Bone response to phosphate salts, ergocalciferol, and calcitriol in hypophosphatemic vitamin D-resistant rickets. N Engl J Med
9. Drezner MK, Lyles KW, Haussler MR, Harrelson JM 1980 Evaluation of a role for 1.25-dihydroxyvitamin D, in the pathogenesis and treatment of X-linked hypophosphatemic rickets and osteomalacia. J Clin Invest 66:1020-1032.
10. Costa T, Marie PJ, Scriver CR, et al. 1981 X-linked hypo- phosphatemia: Effect of calcitriol on renal handling of phos- phate, serum phosphate, and bone mineralization. J Clin Endocrinol Metab 52:463-472.
11. Mason RS, Rohl PG, Lissner D, Posen S 1982 Vitamin D metabolism in hypophosphatemic rickets. Am J Dis Child 136:909-913.
12. Lyles KW, Clark AG, Drezner MK 1982 Serum 1,25-dihy- droxyvitamin D levels in subjects with X-linked hypophos- phatemic rickets and osteomalacia. Calcif Tissue Int 34:125- 130.
303: 1023- 103 1 .

5% PETERSEN ET AL.
13. Balsan S, Tieder M 1990 Linear growth in patients with hypophosphatemic vitamin D-resistant rickets: Influence of treatment regimen and parental height. J Pediatr 116:365- 371.
14. Graham JB, McFalls VW, Winters RW 1959 Familial hypo- phosphatemia with vitamin D-resistant rickets. 11. Three ad- ditional kindreds of a sex-linked dominant type with a ge- netic analysis of four such families. Am J Hum Genet 11:
15. Reid IR, Hardy DC, Murphy WA, Teitelbaum SL, Bergfeld MA, Whyte MP 1989 X-linked hypophosphatemia: A clini- cal, biochemical, and histopathologic assessment of morbid- ity in adults. (Baltimore) Medicine 68:336-352.
16. Chan JCM, Bartter FC 1979 Hypophosphatemic rickets: Ef- fect of 1,25-dihydroxyvitamin D, on growth and mineral me- tabolism. Pediatrics 64:488-495.
17. Chan JCM, Lovinger RD, Mamunes P 1980 Renal hypo- phosphatemic rickets: Growth acceleration after long-term treatment with 1,25-dihydroxyvitamin-D,. Pediatrics 66:445- 454.
18. Harrell RM, Lyles KW, Harrelson JM, Friedman NE, Drez- ner MK 1985 Healing of bone disease in X-linked hypophos- phatemic rickets/osteomalacia. Induction and maintenance with phosphorus and calcitriol. J Clin Invest 75:1858-1868.
19. Chesney RW, Mazess RB, Rose P. Hamstra AJ, DeLuca HF, Breed AL 1983 Long-term influence of calcitriol (1.25- dihydroxyvitamin D) and supplemental phosphate in X- linked hypophosphatemic rickets. Pediatrics 71559-567.
20. Saggese G, Baroncelli GI. Bcrtelloni S, Buggiani B, Gualtieri M 1989 Growth delay in renal hypophosphatemic rickets: Ef- fects of 1,25(OH),D, at supraphysiological doses. In: Bierich JR, Calliari E. Raiti S (eds) Growth Abnormalities. Serono Symposia Publications from Raven Press, New York. 56:
21. Tsuru N, Chan JCM, Chinchilli VM 1987 Renal hypophos- phatemic rickets. Growth and mineral metabolism after treatment with calcitriol (1.25-dihydroxyvitamin D,) and phosphate supplementation. Am J Dis Child 141:lOE-110.
22. de St. Jeor ST, Bryan GT 1973 Clinical research diets: Dcfi- nitions of terms. J Am Diet 6247-51.
23. Walton RJ, Bijvoct OLM 1975 Nomogram for derivation of renal threshold phosphate concentration. Lancet 2309-310.
24. U.S. Department of Health, Education and Welfare. Na- tional Center for Health Statistics growth curves for U.S. children-birth to 18 years. Vital and Health Statistics 1977. Series 11. 165:l-73.
25. Cohen L, Holliday M 1982 Choosing an appropriate test. In: Cohen L. Holliday M (eds) Statistics for Social Scientists, Harper and Row, London, pp 137-138.
26. Albright F. Butler AM, Bloombcrg E 1937 Rickets resistant to vitamin D therapy. Am J Dis Child 54529-547.
27. Tapia J. Stearn SG, Ponseti I 1964 Vitamin-D resistant rickets: A long-term clinical study of eleven patients. J Bone Joint Surg [Am edition] 46(5):935-958.
28. Stamp WG. Whitesides TE, Field MH. Schccr GE 1964 Treatment of vitamin-D resistant rickets: A long-term evalu- ation of its effectiveness. J Bone Joint Surg [Am edition] 46 (5):965-977.
29. Pierce DS, Wallace WM, Herndon CH 1964 Long-term treatment of vitamin-D resistant rickets. J Bone Joint Surg 46(5):979-997.
30. Earp HS. Ney RL. Gitelman HJ, Richman R, DcLuca HF 1970 Effects of 25-hydroxycholccalciferol in patients with fa- milial hypophosphatemia and vitamin-D-resistant rickets. N Engl J Med 2113:627-630.
31. Schocn EJ, Reynolds JB 1970 Severe familial hypophospha-
31 1-326.
413-423.
temic rickets: Normal growth following early treatment. Am J Dis Child 120:58-61.
32. West CD, Blanton JC. Silverman FN, Holland NH 1964 Use of phosphate salts as an adjunct to vitamin D in the treat- ment of hypophosphatemic vitamin D refractory rickets. J Pediatr 64:469-477.
33. Menking M, Sotos JF 1969 Effect of administration of oral neutral phosphate in hypophosphatemic rickets. J Pediatr
34. Robinson HW, Nelson WE 1945 Phosphorus clearance in children with vitamin D-resistant rickets. Am J Dis Child 69: 323.
35. Nigrin G, Cochrane WA. Jannigan D. Ernst A 1962 Results of calcium infusion and renal biopsy results in refractory rickets. Am J Dis Child 104:478-801.
36. Paunier L, Kooh SW, Conen PE, Gibson AAM, Frascr D 1968 Renal function and histology after long-term vitamin D therapy of vitamin D refractory rickets. J Pediatr 73:833- 844.
37. Glorieux FH. Bordier PJ, Marie P. Dclvin EE. Travers R 1978 Inadquate bone response to phosphate and vitamin D in familial hypophosphatemic rickets. Adv Exp Med Biol
38. Frame B, Smith RW, Fleming JL, Manson G 1963 Oral phosphates in vitamin D-refractory rickets and ostcomalacia. Am J Dis Child 1W147-153.
39. Stickler GB, Hayles AB, Roscvear JW 1965 Familial hypo- phosphatemic vitamin D resistant rickets: Effcct of increased oral calcium and phosphorus intake without high doscs of vitamin D. Am J Dis Child 110:664-667.
40. Arnaud C, Glorieux F, Scriver C 1971 Serum parathyroid hormone in X-linked hypophosphatemia. Science 173:845- 847.
41. Krohn HP, Offermann G, Brandis M, Brcdehl J. Hanke K, Offner G 1977 Occurrence of hypcrparathyroidism in chil- dren with X-linked hypophosphatemia under treatment with vitamin D and phosphate. Adv Exp Med Biol 81:345-351.
42. Moncrieff MW, Chance GW 1969 Nephrotoxic effect of vita- min D therapy in vitamin D refractory rickets. Arch Dis Child 44571-579.
43. McEnery PT. Silverman FN, West CD 1972 Acceleration of growth with combined vitamin D-phosphate therapy of hy- pophosphatemic resistant rickets. J Pediatr M):763-774.
44. Glorieux FH. Scriver CR, Reade TM. Goldman H, Rose- borough A 1972 Use of phosphate and vitamin D to prevent dwarfism and rickets in X-linked hypophosphatemic. N Engl
45. Alon U, Newsome H Jr. Chan JCM 1984 Hyperparathyroid- ism patients with X-linked dominant hypophosphatemic rickets-application of the calcium infusion test as an indica- tor for parathyroidectomy. Int J Pediatr Nephrol 5:39-43.
46. Lyles KW, Harrelson JM, Drezner MK 1982 The efficacy of vitamin D, and oral phosphorus therapy in X-linked hypo- phosphatemic rickets and ostcomalacia. J Clin Endocrinol Metab 54.307-315.
47. Cohanin M, DcLuca HF, Yendt ER 1972 Effects of pro- longed treatment with 25-hydroxycholccalciferol in hypo- phosphatemic (vitamin D refractory) rickets and ostcoma- lacia. Johns Hopkins Med J 131:118-132.
48. Pak CY, DcLuca HF, Bartter FC, et al. 1972 Treatment of vitamin D-resistant rickets with 25-hydroxycholecalciferol. Arch Intern Med 129:894-899.
49. Balsan S, Garabcdian M 1972 25-Hydroxycholecalciferol: A comparative study in deficiency rickets and different types of resistant rickets. J Clin Invest 51:749-759.
50. Puschett JB, Gene1 M. Rastegar A. Anast C, DcLuca HF,
75: 1001 - 1007.
103:227-232.
J Med 287:481-487.

XLH: RESPONSE TO CALCITRIOL AND PHOSPHATE 597
Friedman A 1975 Long-term therapy of vitamin D-resistant rickets with 25-hydroxycholecalciferol. Clin Pharmacol Ther
51. Delvin EE, Glorieux FH 1981 Serum 1,25-dihydroxyvitamin D concentration in hypophosphatemic vitamin D-resistant rickets. Calcif Tissue Int 33:173-175.
52. Russell RGG. Smith R. Preston C, et al. 1975 The effect of 1.25dihydroxycholecalciferol on renal tubular reabsorption of phosphate, intestinal absorption of calcium and bone his- tology in hypophosphatemic renal tubular rickets. Clin Sci Mol Med 48:177-186.
53. Glorieux FH, Holick MF, Scriver CR, DeLuca HF 1973 X- linked hypophosphatemic rickets: Inadequate therapeutic re- sponse to 1.25dihydroxycholecalcifero1. Lancet 2287-289.
54. Brickman AS, Coburn JW, Kurokawa K, Bethune JE. Harri- son HE, Norman AW 1973 Actions of 1,25-dihydroxychole- calciferol in patients with hypophosphatemic, vitamin-D-re- sistant rickets. N Engl J Med ZW495-498.
55. Balsan S. Garabedian M 1975 1.25-Dihydroxyvitamin D, and 1-alpha hydroxyvitamin D, in children: Biologic and thera- peutic effects in nutritional rickets and different types of vitamin D resistance. Pediatr Res 9:586593.
56. Bijvoet OLM 1980 Indices for the measurement of the renal handling of phosphate. In: Massry SG. Fleisch H (eds) Renal Handling of Phosphate. Plenum, New York, pp 1-37.
57. Alon U, Chan JCM 1984 Effects of parathyroid hormone and 1,25-dihydroxyvitamin D, on tubular handling of phos- phate in hypophosphatcmic rickets. J Clin Endocrinol Metab 58:67 1-675.
58. Kurnik BRC. Hruska KA 1985 Mechanism of stimulation of
171202-21 1.
renal phosphate transport by 1,25-dihydroxycholecaIciferol. Biochim Biophys Acta 817:42-50.
59. Kurnik BRC, Huskey M, Hruska KA 1987 1,25-Dihydroxy- cholccalciferol stimulates renal phosphate transport by di- rectly altering membrane phosphatidylcholine composition. Biochim Biophys Acta 917:81-85.
60. Shields ED, Scrivcr CR, Reade T, et al. 1990 X-linked hypo- phosphatemia: The mutant gene is expressed in teeth as well as in kidney. Am J Hum Genet 46:434-442.
61. Bayley N, Pinneau S 1952 Tables for predicting adult height from skeletal age. J Pediatr 40:423-441.
62. Greulich WW, Pyle SI. Radiographic Atlas of Skeletal De- velopment of the Hand and Wrist, 2nd ed. Stanford Univer- sity Press, Stanford, CA, 1959.
63. Zachmann M, Sobradillo B. Frank M, Frisch H, Prader A 1978 Bayley-Pinncau, Roche-Wainer-Thissen. and Tanner height predictions in normal children and in patients with various pathologic conditions. J Pediatr 93749-755.
Address reprint requests to: Michael P. Whyte, M.D. Metabolic Research Unit
Shriners Hospital for Crippled Children 2eOl South Lindbergh Boulevard
St. Louis, MO 63131
Received for publication July 16. 1990; in revised form January 9, 1992; accepted January 15, 1992.