Synthesis of nano‑fibers containing nano‑curcumin in zein ...
Upload
khangminh22Category
view
2download
0
Prevalence of Atypical Radiographic Findings inBitewings of Class II Composite Restorations:
Detection and Assessment of Radiolucent Areas
Item Type dissertation
Authors Bazerbashi, Jood
Publication Date 2020
Abstract This retrospective study aimed to describe the prevalence ofradiographic abnormalities in bitewing radiographs of proximalclass II composite restorations. Bitewing radiographs of proximalcomposite restorations of adult patients who underwent resto...
Keywords dental adhesives; radiographs; radiolucency; Composite Resins;Dental Bonding; Dental Cements
Download date 15/09/2022 22:00:20
Link to Item http://hdl.handle.net/10713/13006

Curriculum Vitae
Name: Jood Bazerbashi, DDS
Email address: [email protected]
EDUCATION
Degree And Date To Be Conferred:
Masters in Dental Biomedical Science May 2020
AEGD Certificate June 2020
University of Maryland School of Dentistry, Advanced Education in
General Dentistry, Baltimore, Maryland, USA
Major:
Doctor of Dental Medicine July 2014
Near East University Faculty of Dentistry, Lefkoşia, Cyprus
CLINICAL EXPERIENCE
Trainee at North Jeddah Specialty Dental Clinics Jan. 2018 – March 2018
North Jeddah Specialty Dental Clinics, Jeddah, Saudi Arabia
Shadowing at Dr. Mohammad H. Shahegh Clinic November 2017
Dr. Mohammad Shahegh Clinic, Clarksville, Maryland, USA
General Dentist Oct. 2016 – May 2017
Dental Pearl Clinic, Jeddah, Saudi Arabia
Shadowing at iSmile Specialists June 2016 – Aug.2016
iSmile Specialists, Houston, Texas, USA
COMMUNITY SERVICE
Volunteer Resident Sept.14, 2019
Mid- Maryland Mission of Mercy, College Park, Maryland, USA
Volunteer Resident April 6, 2019
Eastern Shore Mission of Marcy, Salisbury, Maryland, USA

Volunteer Resident July 28, 2018
Southern Maryland Mission of Mercy, Waldorf, Maryland, USA
Volunteer Dentist Feb.2016- May 2016
L- Medical Specialists Polyclinic Charity Clinic, Jeddah, Saudi Arabia
Volunteer at NEU Dental Public Health Program Feb. 2014 –May 2014
NEU Dental Public Health Program, Lefkoşia, Cyprus
Participant in NEU World Events Jan. 2013 - May 2014
Near East University World, cultural exchange event, Lefkoşia, Cyprus
Fundraiser coordinator Novmber 2010
Syrian Orphanage Charity Organization, Aleppo Syria
PROFESSIONAL LICENSE
Saudi Professional General Dentist License

ABSTRACT
Prevalence of Atypical Radiographic Findings in Bitewings of Class II Composite
Restorations: Detection and Assessment of Radiolucent Areas.
Jood Bazerbashi, General Dentist, 2020
Thesis directed by : Mary Anne S. Melo, Director of Operative Dentistry, Department of
General Dentistry
This retrospective study aimed to describe the prevalence of radiographic abnormalities
in bitewing radiographs of proximal class II composite restorations. Bitewing radiographs
of proximal composite restorations of adult patients who underwent restorative care at
predoctoral clinics at the University of Maryland School of Dentistry from August 2014
to July 2016 were identified. Atypical radiographic features were categorized by type of
material and location. The information recorded for patients included age, sex, tooth, and
restored surface. Out of the 669 examined restorations, 16.5% radiographs showed no
atypical radiographic findings and 83.5% restorations had unusual radiographic signs.
The types of atypical radiographic findings were distributed as 16.5% internal voids, 3%
overhang, 7.8% interlayer lines, 12.6% secondary caries, 20.7% interfacial gaps and
23.1% had multiple atypical findings. There is high prevalence of atypical radiographic
findings in class II composite restorations, particularly in the body of the composite,
premolars, and disto-occlusal restorations.

Prevalence of Atypical Radiographic Findings in Bitewings of Class II Composite
Restorations: Detection and Assessment of Radiolucent Areas
by
Jood Bazerbashi
A thesis submitted to the Faculty of the Graduate School of the
University of Maryland, Baltimore in partial fulfillment
of the requirements for the degree of
Master of Science
2020

©Copyright 2020 by Jood Bazerbashi
All rights Reserved.

iii
Acknowledgments
The authors thank the staff of the IT at the University of Maryland School of Dentistry on
behalf of Christine Livesay for her assistance with the database settings.

iv
Table of Contents
Chapter Page
Acknowledgments …………………………………………………………………… iii
List of Tables ……………………………………………………………………..……v
List of Figures …………………………………………………………………….......vi
List of Abbreviations …………………………………………...................................vii
1. Introduction …………………………………………………………...………1
2. Methodology…………………………………………………………...............3
2.1 Study Design…………………………………………………………. 3
2.2 Eligibility Criteria……………………………………………………..4
2.3 Radiographic Assessment……………………………………………..7
2.4 Categorization of the Radiographic Findings…………………………7
2.5 Statistical Analysis…………………………………………………….8
3. Results ...……………………………………………………………………….11
4. Discussion ……………………………………………………………..............18
5. Conclusion.…………………………………………………………………….29
6. References.…………………………………………………………………….30

v
List of Tables
Table 1. Inclusion and Exclusion criteria applied to the selection of
radiograph images …………………………………………………………………….… 5
Table 2. Description of the categories for classification of findings……........................10
Table 3. The prevalence of radiographic abnormalities found in class II
composites restorations………………………………………………………………….13
Table 4. The prevalence of radiographic abnormalities found in class II
composites restorations with secondary caries………………………………………….14
Table 5. The prevalence of radiographic abnormalities found in class II
composites restorations among genders, age groups, tooth, and restoration surfaces…..15
Table 6. The prevalence of interface gap locations showing frequencies and
percentage among genders, age groups, tooth, and restoration surfaces……………….16
Table 7. The prevalence of secondary caries in class II expressed by frequencies
and percentage among genders, age groups, tooth, and restoration surfaces…………..16
Table 8. The prevalence of atypical radiographic findings with multiple
radiographic findings showing frequencies and percentages among genders, age
groups, teeth, and restoration surfaces………………………………………………….17

vi
List of Figures
Figure 1. Flow chart showing the selection criteria and categorization of the findings
used in this study………………………………………………………………………...6
Figure 2. Illustrative scheme of the classification criteria for radiographic findings
in class II composite restorations………………………………………………………..9
Figure 3. Radiographic image illustrating voids within the body of a composite of
the right maxillary second premolar………………………………………………….....19
Figure 4. Radiographic image showing interlayer lines within the body of composite
in the DO restoration of left maxillary first premolar…………………………………..20
Figure 5. A radiographic image representing overhang in the DO restoration first of
left maxillary premolar………………………………………………………………….21
Figure 6. Radiographic image showing an external bond interface gap in the DO
restoration of left mandibular premolar………………………………………………....22
Figure 7. Radiographic image illustrating internal interface gap in the DO restoration
of left maxillary premolar…………………………………………………………….....23
Figure 8. Radiographic image illustrating secondary caries MO restoration of right
maxillary premolar……………………………………………………………………...25
Figure 9. A radiographic image representing multiple radiolucent findings of body
void and external bond interface gap in the DO restoration of left maxillary premolar..27
Figure 10. Radiographic image illustrating various radiolucent findings of body
interlayer gap and external bond interface gap in the DO restoration of mandibular
right premolar…………………………………………………………………………...27
vii
List of Abbreviations:
BW Bitewing
F Female
M Male
PM Premolar
MO Mesio-occlusal
DO Disto-occlusal
MOD Mesio-occluso-distal
1
INTRODUCTION
About half of all restorations placed in adults in general dental practice are
replacements 1. Replacement restorations take up a substantial part of the tooth structure
as compared to the initial restorative treatment for the primary carious lesion. They are
very cost-intensive for patients and the health system 2, 3
. In addition to the financial burden
imposed on the patient, there are other reasons to avoid replacement, such as the risk of
pulp exposure and pulp irritation 4. Atypical radiographic findings such as voids and gaps
in the composite may result from several operator-related factors, such as poor placement
technique and entrapment of air within the composite or material-related factors such as
polymerization stress or radiopacity of the materials 5–7
.
From a functional perspective, the presence of voids within restorations may
negatively affect the mechanical properties of the material over time 8. Reduced resistance
to fatigue and wear, due to their contribution to the initiation and propagation of cracks,
may lead to premature failure of the restoration when subjected to mechanical and external
loads 9, 10
. The presence of voids in the body of composite restorations has also been
reported as a detrimental factor for the clinical longevity of posterior composites 11
.
Secondary carious lesions are reported to be the most common reason to replace or
repair a defective dental restoration in general practice 1. If these gaps or voids are at the
margin, the risk of leakage and secondary caries is present. The detection of secondary
carious lesions or gaps at margins detected by explorer as well as pain and sensitivity
symptoms reported by patients led to a more precise diagnosis and decision to replace the

2
restoration12
. However, in the absence of clinical findings and the presence of atypical
radiographic findings, the diagnosis of caries can pose a challenge 13, 14
, leading to
uncertainty regarding the need to replace or repair existing restorations. Along with the
assessment of a patient’s caries risk status, radiographic interpretations are critical for new
patients who have received comprehensive treatment by another provider and are now
under periodic evaluation.
The American Dental Association (ADA) recommends posterior bitewing (BW)
exam for adults with high caries risk every six to 12 months, whereas for adults with low
caries risk exam can be done every two to three years 15–17
. From a radiographic point of
view, successful restorative treatment can be measured by the absence of radiographic
signs suggestive of underlining carious lesions, open margins, voids, or overhang 18, 19
.
However, when these radiolucent areas are mistakenly suspected to be caused by secondary
caries, there is a high likelihood that no lesion will be found after restoration removal. This
misdiagnosis leads to overtreatment and unnecessary replacement of the restoration.
Most of the atypical radiographic findings in the region of the bonding interface
between the restoration and the cavity walls directly influence secondary caries
formation20, 21
. Moreover, increased adhesive thickness layer or low adhesive opacity may
impose some difficulties in diagnosis 2, 22
. Another factor affecting radiographic evaluation
is the concentration of radiopacifiers in the composite. Low radiopacity constituents in the
resin-based material makes it hard to discriminate between composite and tooth structure
22.

3
The potential influence of recall BW findings related to class II composites on
outcomes of replacement remains controversial. This suggests that although significant
investigational and clinical, educational efforts are currently underway, mainstream
awareness and thorough quantification of these findings are still lacking. The purpose of
this study is to begin establishing a foundation of knowledge for the greater understanding
of influencing factors on the decision of replacement by identifying the prevalence of
radiographic abnormalities in class II composite restorations. F
MATERIALS AND METHODS
2.1. Study Design
This is a retrospective patient chart cohort study using charts for patients seen at the
predoctoral clinic at the University of Maryland, Baltimore, School of Dentistry. Bitewing
radiographs with Class II restorations were selected to quantify the prevalence of atypical
radiographic findings in composite restorations. The study was approved by the respective
Institutional Review Board (IRB) (HP-00084713).
A digital search was utilized using the Axium (Exan Group, Las Vegas, NV, USA)
Electronic Health Record (EHR). The search filtered patients between the ages 18-84 that
would qualify for the two following categories: 1) patients who had two or more surface
resin-based restorations placed by third and fourth year dental students on posterior teeth
from August 2014 to July 2016; 2) patients who had single, two- or four- horizontal or
vertical BW taken from August 2016 to July 2017. Data were extracted into a Microsoft ®
Excel file (Microsoft, Redmond, WA, USA).

4
2.2 Eligibility Criteria
Inclusion criteria included men and women between the ages of 18- 84 who
underwent Class II restorative treatment from August 2014 to July 2016 with BW
radiographs taken from August 2016 to July 2017. Only BW radiographs exposed with
XDR ® (XDR Radiology, Los Angeles, CA, USA) sensors, the available direct digital
sensor system at the university, were included.
The exclusion criteria included posterior BW radiographs showing
superimpositions on the restoration, poor image quality, or the use of different restorative
material other than composite resin. At the predoctoral clinic of the University of Maryland
School of Dentistry, in the lack of suspicion of caries, overlap less than one-third the width
of interproximal enamel would categorize as clinically acceptable BW. However, in this
study, BWs with any overlap of the restoration were excluded.
Excluded radiographs displaying objects or restoration interfered with the
visualization of the Class II composite restoration, such as orthodontic brackets, Class V
restoration, or crown. Also, radiographs that did not show the assigned tooth due to
extraction or BWs that show the teeth on the contralateral side were excluded (Table 1).
5
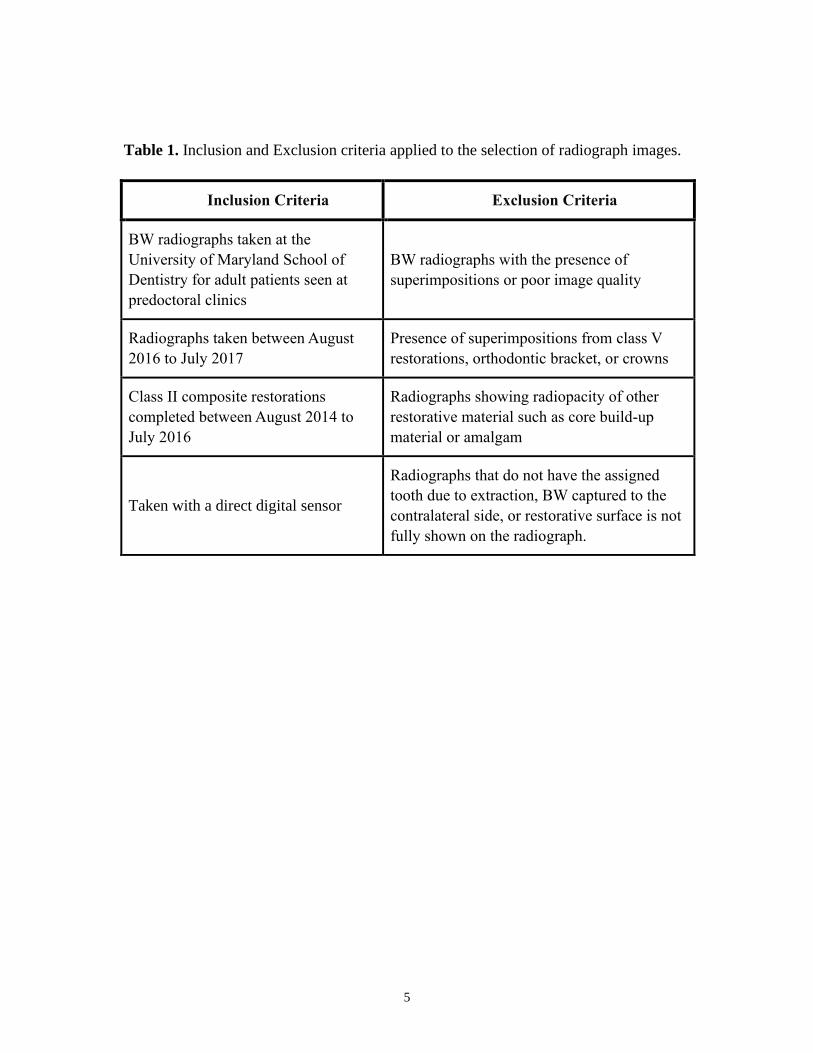
Table 1. Inclusion and Exclusion criteria applied to the selection of radiograph images.
Inclusion Criteria Exclusion Criteria
BW radiographs taken at the
University of Maryland School of
Dentistry for adult patients seen at
predoctoral clinics
BW radiographs with the presence of
superimpositions or poor image quality
Radiographs taken between August
2016 to July 2017
Presence of superimpositions from class V
restorations, orthodontic bracket, or crowns
Class II composite restorations
completed between August 2014 to
July 2016
Radiographs showing radiopacity of other
restorative material such as core build-up
material or amalgam
Taken with a direct digital sensor
Radiographs that do not have the assigned
tooth due to extraction, BW captured to the
contralateral side, or restorative surface is not
fully shown on the radiograph.

6
Figure 1. Flow chart showing the selection criteria and categorization of the findings used
in this study

7
2.3 Radiographic Assessment
Digital radiographs were assessed by two examiners (general dentists). In cases of
disagreement, a consensus was obtained. Reliability tests were performed for the
radiographic assessment (kappa= 0.72). After three months, approximately 50% of the
radiographs were re-evaluated under the same settings to calculate the intra-examiner
reproducibility.
Six hundred sixty-nine images from 351 patients were assessed using MiPACS
software (Medicare Imaging, Charlotte, NC, USA) displayed on ViewSonic VX3276-
MHD 32” high definition light-emitting diode backlit display monitor (native resolution
1535x2048) in a view distance of 70 cm in dim lighting. Radiographic filters were applied
to adjust sharpness and brightness. Three hundred thirty-five radiographs were excluded
following the exclusion criteria ( Figure 1).
2.4 Categorization of the Radiographic Findings
Three hundred thirty-four included images were transferred to PowerPoint
(Microsoft) on slides with a black background. Slides were labeled with the sample
number, tooth number, and restoration surface. PowerPoint slides and Excel spreadsheets
were both linked with a numeric coding system for each sample. A classification was
designed to codify the radiographic findings and used for screening. The classification
consists of a written description of each category intended to reduce ambiguity. Figure 2
illustrates the description used for classification in a radiographic image.

8
From the pool of 334 included x-rays, 55 BWs showed no atypical radiographic
findings, and 279 BWs demonstrated atypical radiolucency/radiopacity findings. This set
of radiographs provides examples of appearances classifiable as standard and normal. This
category refers to radiographs, where there are no large areas of radiolucency. Those
divisions are defined by the standard radiographs, together with the written description.
For assessment of the bonding interface, the presence or absence of a radiolucent halo
adjacent to the gingival, mesial, distal, and pulpal walls was considered.
The 279 BWs were categorized according to the type of material (composite or
adhesive) and location (internal or external) (Table 2). The information recorded for each
patient included age, sex, tooth, and restored surface.
Guidelines were placed to avoid misinterpretation of bond interface radiolucency
and secondary caries. Radiolucent areas that are detected at the cavity preparation walls
were considered as interfacial gaps. Large radiolucent regions that are not bound to the
preparation structure and are extending into the dentine were interpreted as secondary
caries.
2.5 Statistical Analysis
The radiographic prevalence of atypical findings was presented as frequencies and
percentages, whereas demographic variables were presented as frequencies and
percentages, when appropriate.

9
Figure 2. Illustrative scheme of the classification criteria for radiographic findings in class
II composite restorations.

10
Table 2. Description of the categories for classification of findings.
LOCATION CATEGORY DESCRIPTION
No atypical
radiographic
finding
No radiolucent or radiopaque results
suggesting atypical radiographic findings
in composite restoration
BODY OF THE
RESTORATION
Mass of composite
constituting the
restoration
Internal
Void/Porous
Void =pore Circular volumetric (2D)
empty radiolucent spaces located at the
body
Interlayer line Lack of continuity between the
composite layers characterized by a thin
radiolucent line
Overhang Excess radiopaque composite in the
interproximal area
BONDING
INTERFACE
Surface (Line)
between tooth and
composite
Internal gap–not
gingival margin
Lack of continuity, radiolucency between
the composite and tooth NOT involving
gingival margins
External gap –at
the gingival
margin
Radiolucency, lack of continuity between
the composite and tooth involving
gingival margins: usually “notch” shape.
Secondary caries Presence of radiolucency in dentine
indicating recurrent caries
Other More than one radiographic finding
indicating multicategory

11
RESULTS
Table 3 summarizes the results of the radiographic findings. Out of 669 BW
radiographs, 335 were excluded for meeting the exclusion criteria; therefore, 334 BWs
were used in the current study. A total of 55 (16.5%) BW did not show any atypical
radiographic findings. 279 (83.5%) radiographs showed radiolucent or radiopaque areas in
the restoration, suggesting atypical radiographic findings.
There were 91 of 279 (27.2%) restorations that had at least one atypical finding in the
body of the composite recorded and were classified as follows: 55 (16.5%) presented with
internal body voids, 26 (7.8%) interlayer lines, 10 (3%) demonstrated radiopacity
suggesting overhang.
Sixty-nine (20.7%) restorations showed a discontinuity in the adhesive bond area,
leaving a gap between the tooth structure and the composite. Thirty-seven (53.6%) of these
restorations had a notch-like appearance suggesting a noticeable gap at or around the
gingival margin, and 32 (46.4%) out of the 69 had an internal inconsistency between tooth
structure and resin-base material not involved with the exogenous seal of the restoration.
Secondary carious lesions were in a total of 42 (12.6%) restorations. Out of the 42
restorations suggesting secondary caries, 20 (47.6%) had other radiographic findings, and
22 (52.4%) did not present with any additional radiographic finding other than secondary
caries (Table 4).

12
Furthermore, 77 (23.1%) of restorations presented with multiple radiolucencies or
mixed radiolucency and radiopacity abnormal radiographic findings. 11(3.3%) BW’s
indicate the tooth bond interface gap and interlayer gaps between the body of composite
layers. Remaining BW radiographs with multiple radiolucent findings were classified as
follows: 58 (17.4%) restorations presented with voids within the composite and bonding
interface, 2 (0.6%) restorations had void interlayer radiolucencies, and 3 (0.9%) BW’s
revealed radiolucencies of interlayer lines and voids within composite with the interface.
Three BWs presented heterogenous radiographic findings composing radiopaque
and radiolucency areas. Out of the three, 1 (0.3%) restoration had radiolucent composite
body pore and radiopaque excess composite, indicating overhang on the gingival margin.
The other 2 (0.6%) BW’s showed radiolucent lines withing the composite body and
radiopaque overhang. Table 5-8 explains the information recorded for each patient
included age, sex, tooth, and restored surface.

13
Table 3. The prevalence of radiographic abnormalities found in class II composites
restorations.
Radiographic Finding Frequency/ total Percentage %
No atypical findings 55/334 16.5%
Atypical findings 279/334 83.5%
Bonding interface 69/334 20.7%
External bonding interface 37/334 11.1%
Internal bonding interface 32/334 9.6%
Body of composite 91/334 27.2%
Internal Void 55/334 16.5%
Interlayer lines 26/334 7.8%
Overhang 10/334 2.9%
Secondary caries 42/334 12.6%
With other radiographic findings 20/334 6.0%
Without other findings 22/334 6.6%
Other findings 77/334 23.1%
Interlayer/ interface 11/334 3.3%
Void/ interface 58/334 17.4%
Void/ overhang 1/334 0.3%
Void/ interlayer 2/334 0.6%
Void/interlayer/ interface 3/334 0.9%
Interlayer/ overhang 2/334 0.6%
14
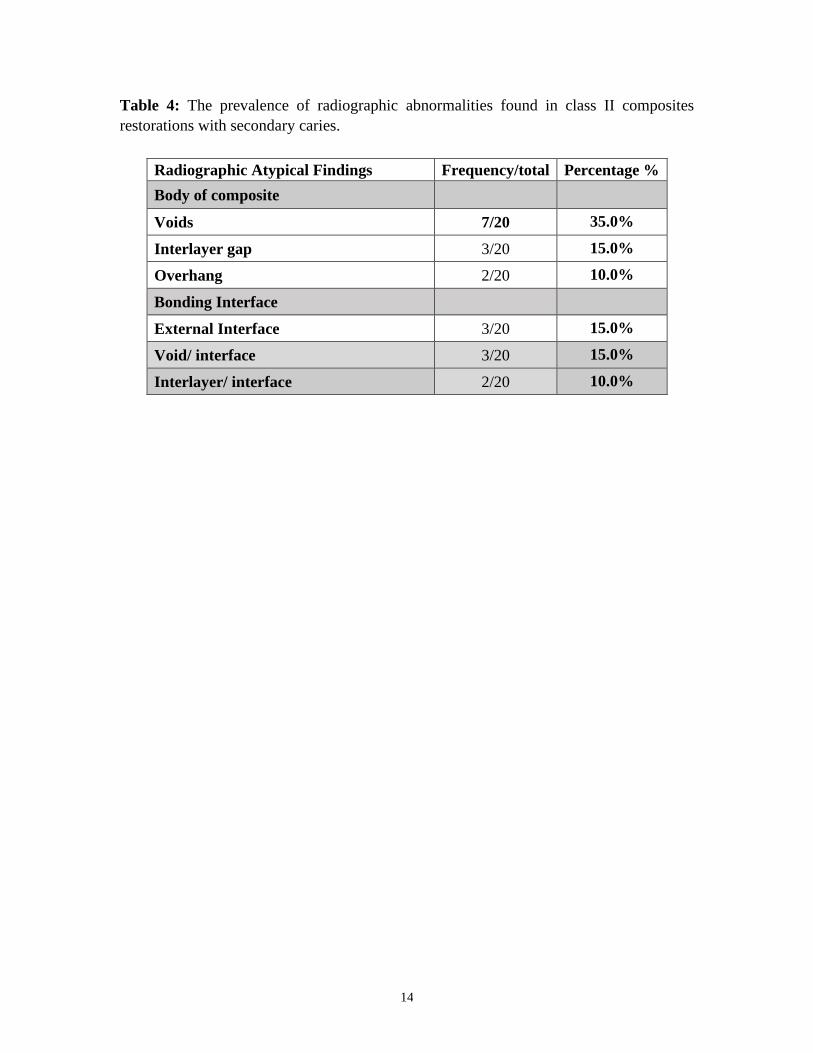
Table 4: The prevalence of radiographic abnormalities found in class II composites
restorations with secondary caries.
Radiographic Atypical Findings Frequency/total Percentage %
Body of composite
Voids 7/20 35.0%
Interlayer gap 3/20 15.0%
Overhang 2/20 10.0%
Bonding Interface
External Interface 3/20 15.0%
Void/ interface 3/20 15.0%
Interlayer/ interface 2/20 10.0%

15
Table 5: The prevalence of radiographic abnormalities found in class II composites
restorations among genders, age groups, tooth, and restoration surfaces

16
Table 6: The prevalence of interface gap locations showing frequencies and percentage among
genders, age groups, tooth, and restoration surfaces.
Table 7: The prevalence of restorations suggesting secondary caries in class II showing
frequencies and percentage among genders, age groups, tooth, and restoration surfaces

17
Table 8: The prevalence of atypical radiographic findings presenting multiple radiographic
findings expressed by frequencies and percentages among genders, age groups, teeth, and
restoration surfaces.

18
DISCUSSION
The goal of this study was to establish the previously undefined prevalence of
radiographic abnormalities in class II composite restorations. The prevalence rates and data
obtained in this radiographic analysis dramatically illustrates that the prior comprehended
notion that radiographic assessment, class II composite, in particular, continues to be
underrecognized. The prevalence rates of radiographic abnormalities were significantly
higher than anticipated by the authors.
Voids within the body of the restoration are also referred to as porosities or bubbles.
Here, referred to as internal voids, they represented a large subset of these atypical findings,
affecting 16.5% (55/334) of performed restorations (Figure3) (Table 3). These results are
less compared to the 70% voids found in the examined samples in the light microscope in
vitro study 5. However, the higher incidence of voids results in the current study brings into
question the causes of these alterations. Voids are caused by air entrapment and can be
incorporated into composites during their manipulation when performing a restorative
procedure or even while being manufactured 23. Here, all the restorations were assumed to
be performed by an incremental technique using low-viscosity or high viscosity universal
hybrid composites TPH Spectra ST (Dentsply, Milford, DE, USA) since this the employed
restorative method and the material available in the predoctoral clinics. However, definitive
conclusions cannot be made, as this information was not collected in our study.

19
Figure 3. Radiographic image illustrating voids within the body of a composite of the
right maxillary second premolar
Since, in the present study, all the restorations were placed by the provider under
training (juniors and senior dental students), the operator’s ability may have influenced this
outcome. Sixty-five percentage of voids were found in restored premolars, and 69% were
accounted by two-surface (disto-occlusal) restorations (Table 5). Cavity preparations in
premolars are very often conservative and represented by slot preparations compromising
the proximal lesions and occlusal access. This type of preparation may offer challenges for
incremental placement of the composite. Furthermore, in certain clinical scenarios, the
distal box of the preparation can be more difficult for visualization and adaptation of the
material.
Voids between the layers of class II composite was another subset from our study
(Figure 4). In the previously mentioned in vitro study, nearly 63% of the examined samples
had voids between the layers 5. These results were substantially higher compared to 7.8%

20
examined radiographically in the present study (Table 3). Premolars and disto-occlusal
restorations had a high rate in this radiographic condition (Table 5). The appearance of
interlayer gaps is frequent in incremental techniques if the layers were not adapted properly
24. These interlayer gaps affect the physical properties of the restoration 5.
Figure 4. Radiogr aphic image showing interlayer lines within the body of composite in
the DO restoration of left maxillary first premolar
Three percent of the examined restorations had an overhang (Figure 5). Sixty
percent of overhangs were identified in restored premolars and (mesio-occlusal)
restorations (Table 5). A previous study found similar rates of 4% of prevalence overhang
25. The positive ledge at the margins is an iatrogenic factor for gingivitis through
mechanical irritation. Studies have shown that there is higher radiographic attachment loss
with the presence of marginal overhangs in periodontally involved patients 26. In addition
to the contribution in degrading local periodontal health, it also promotes secondary caries

21
formation 27. The irregular rough surface of overhang acts as the perfect area for bacterial
plaque accumulation.
The presence of overhang is mainly caused by incorrect proximal matrix placement.
Prior studies have pointed out that the application of low viscosity composites may increase
the presence of an overhang 28. Proximal restorations involve restoring the anatomical
structure of the tooth, which could be challenging for students. The correct matrix system
should be adapted to restore the unique anatomy of every tooth, which varies from case to
case.
Figure 5. A radiographic image representing overhang in the DO restoration first of left
maxillary premolar
Twenty-one percent of the radiographs examined had an abnormal adhesive
interface, implying the presence of radiolucent areas between the restoration and tooth
structure (Table 3). 11.1% of this radiographic condition is present as an external bonding
interface and 9.6% as an internal interface gap. This result is consistent with previously

22
published findings for a 14% (111/770) bond layer interface and 11.8% (91/770) lack of
adaptation, which includes both external interface gap and overhang 29.
Our data indicated that there is a higher prevalence of external gap at the gingival margin
11.1% represented by radiolucency between the composite and tooth involving gingival
margins, usually “notch” shape (Figure 6). This result is less, compared to other studies
of 33 % underfilled restorations 25. Gaps at the gingival margins are a dilemma for class
II composites. The presence of gingival interfacial gap at the enamel level suggests
weaker bonds and higher microleakage potential at the dentine level 30. The gingival
interface is the most common zone for secondary caries development. Several studies
showed that there is a correlation between the depth of the ditched margins and the
demineralization process 31, 32.
Figure 6. Radiographic image showing an external bond interface gap in the DO
restoration of left mandibular premolar

23
Internal interface gaps can be caused by moisture contamination that reduces the
adaptability of material on the prepared tooth surface (Figure 7). This contamination would
manifest as post-operative pain sensitivity due to fluid and bacterial movement 20.
Figure 7. Radiographic image illustrating internal interface gap in the DO restoration of
left maxillary premolar
Every so often, this interface can be generated by the adhesive layer. The
insufficient radiopacity of bonding agents can assist in radiographic misdiagnosis of the
tooth- restoration interface 17. Replacement decisions based on radiographic assessment
can be commonly affected by the composition of the adhesive system.
Other technique related factors can create radiolucent halos 33. Thick adhesive layer
functions as elastic buffer underneath the restoration, absorbing stress 34. Therefore
applying a thicker adhesive layer contributes to a more apparent radiolucent zone that gives
rise to the misdiagnosis and retreatment 2.

24
The most used adhesive system at the predoctoral clinic is OptiBond® Solo Plus™
(Kerr, Orange, CA, USA). In a study comparing adhesive systems and their radiopacity,
OptiBond Solo Plus shows the most radiopaque effect 35. However, the enamel is more
radiopaque than OptiBond Solo Plus. Different radiodensity can influence the diagnosis of
secondary caries 36. In addition to this, the application of the adhesive system is technique
sensitive and, if not appropriately blown after application, will exhibit pooling. Although
this acts in return as an elastic buffer, it also contributes to a high number of false
replacement decisions 34.
Both gaps at the gingival margin and the internal interface showed similar results
toward pre-molars, 65% and 63% consequently. However, there was a higher rate of
prevalence, according to restoration surfaces. Seventy percent of the external interface gaps
were in disto-occlusal restorations, and fifty percent of the internal interface gaps were in
mesio- occlusal restorations (Table 6).
Secondary caries was detected in the screened BWs at 12.6 % (Table 3) (Figure 8).
A study evaluating radiographs had consistent findings of 15% (119/770) 29. In another
study, secondary caries was diagnosed radiographically in 14% of restoration 37.
Examination of BWs for radiolucent secondary caries is a diagnostic challenge.
Many different factors can influence the ability to detect these alterations accurately. These
may be exposure parameters, type of image receptor, image processing, display system,
viewing conditions, and ultimately, the training and experience of the clinician. Moreover,
various morphologic phenomena, such as pits and fissures, cervical burnout, mach band
effect, and dental anomalies, such as hypoplastic pits and concavities, can mimic the

25
appearance of a carious lesion. The radiolucent thick adhesive material and residual caries
underneath the restoration cause a halo mimicking caries, which makes it tricky to diagnose
32.
Figure 8. Radiographic image illustrating secondary caries MO restoration of right
maxillary premolar
Furthermore, the illusory optical effect of each band appears when there is a vast
difference between the radiopacity of the tooth structure and restorative material 38. The
mach band effect causes a dilemma on the misdiagnosis and, consequently, false-positive
retreatment 39. In the present study, we have managed to cover up the restoration (less
radiopacity) with a black square filter on MiPacs during radiographic evaluation to inhibit
the false effect on optical receptors.

26
About forty-seven percent of restorations that are suggesting secondary carious
presented with other radiographic conditions. Eight out of twenty of these restorations
exhibit an external interfacial gap as one of the other radiographic findings (Table 4). The
exposed margins of the external interface may explain the reason for the secondary caries
progression. The other radiographic conditions associated with secondary caries were
found within the body of composite.
It is also worth mentioning that a higher rate of secondary caries was found in class
II distal restorations (Table 5) (Table 7). This leads to the question if caries excavation
was completed properly or the patient’s oral hygiene is the reason behind these results.
Cavity preparation in a distal box and indirect vision through the mirror are both a
challenge to providers that would affect caries excavation. A patient’s oral hygiene is the
primary factor that determines the progression of secondary caries. Although flossing is
important, many patients find it difficult to access posterior interproximal surfaces. The
difficulty of access to some interproximal areas facilitates plaque accumulation and
consequent secondary caries progression.
As a combination of the previously discussed finding, multiple radiographic
findings detected in the examined sample at 23.1% (Table 3) (Figure9) (Figure 10). This
category was further assessed in detail in Table 6. Some of these conditions can be
interpreted as imperfections that genuinely affects the longevity of the restorations. To also
determine the diagnosis of repair versus replacement, minor imperfections should not be
the reason to intervene. The difference between genders is not well understood at this time.
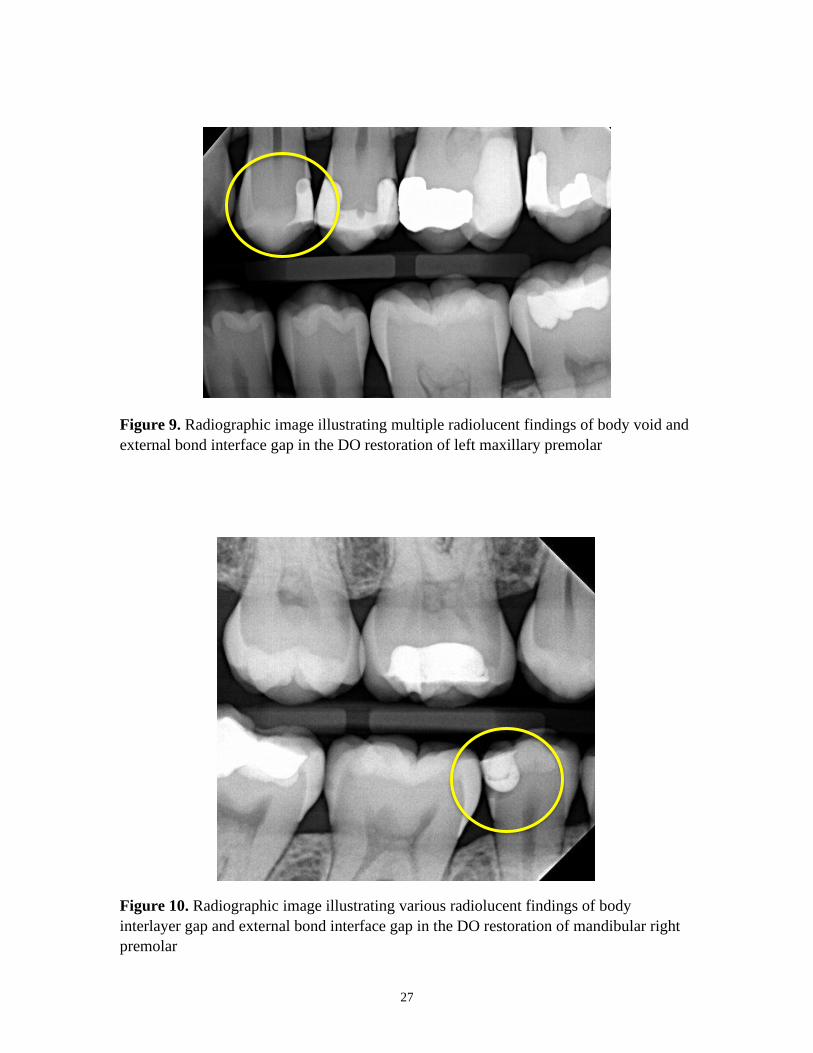
27
Figure 9. Radiographic image illustrating multiple radiolucent findings of body void and
external bond interface gap in the DO restoration of left maxillary premolar
Figure 10. Radiographic image illustrating various radiolucent findings of body
interlayer gap and external bond interface gap in the DO restoration of mandibular right
premolar
28
Limitations
We acknowledge several limitations of our study. First, it is a database review and
was limited by the number of patients with adequate radiographs. The radiographs that
were excluded were not indicative of clinically unacceptable radiographs. The BW
radiographs exclusion was based on parameters that would affect the accurate detection
and calculation of the prevalence of atypical radiographic abnormalities. The 83.5%
prevalence of atypical findings is an aggressive estimate of the restorative practice because
this percentage was based on patients who had restorative treatment provided by dental
students. Dental students are providers under training, and their performance may differ
from general dentists with years of experience. Published results in the previous study
showed that there is a difference in the resulting restorations between operators5. Many
studies discussed the presence of atypical radiographic findings in BWs. However, these
variables were discussed separately, and there was limited research on the prevalence of
radiographic interlayer gaps 5, 25, 29, 37.
Second is the subject-defined parameters for assessing the adhesive interface. We have
not measured the thickness of adhesive space and did not include a quantitative reference
for it. Thus, we may have underestimated the number of adhesive interfaces that are
atypical. Likewise, not much information was provided in records to know if there were
any liners applied underneath the restoration. Liners would contribute to the
radiolucency. Third, our study does not include clinical data such as the presence of the
pain or sensitivity on oral examination, analysis of the interpretation of radiographs by
oral care providers, or assessment patients’ restoration complaints.

29
CONCLUSION
The prevalence of atypical radiographic findings in class II composite restorations
is considerable, particularly in the body of the composite followed by the bonding interface.
Within the body of composite internal voids were in the highest percentage. The overall
results have shown a higher prevalence of abnormal radiographic findings in both pre-
molars and (disto-occlusal) restorations. Dental practitioners should be aware of the
inadequate bonding, and inappropriate placement of posterior restorations could impart
increased premature composite replacement.

30
REFERENCES
1. Eltahlah D, Lynch CD, Chadwick BL, Blum IR, & Wilson NHF (2018) An update
on the reasons for placement and replacement of direct restorations J Dent 72 1–7,
https://doi.org/10.1016/j.jdent.2018.03.001.
2. Fröhlich TT, Nicoloso GF, Lenzi TL, Soares FZM, & De Oliveira Rocha R (2017)
The Thickness of the Adhesive Layer Increases the Misdiagnosing of the
Radiolucent Zones and Restoration Replacement Indication J Esthet Restor Dent
29(3) 193–200, https://doi.org/10.1111/jerd.12297.
3. Gordan VV, Garvan CW, Richman JS, Fellows JL, Rindal DB, Qvist V, Heft MW,
Williams OD, Gilbert GH, & DPBRN Collaborative Group (2009) How dentists
diagnose and treat defective restorations: evidence from the dental practice-based
research network Oper Dent 34(6) 664–673, https://doi.org/10.2341/08-131-C.
4. Wilson N, Lynch CD, Brunton PA, Hickel R, Meyer-Lueckel H, Gurgan S, Pallesen
U, Shearer AC, Tarle Z, Cotti E, Vanherle G, & Opdam N (2016) Criteria for the
Replacement of Restorations: Academy of Operative Dentistry European Section
Oper Dent 41(S7) S48–S57, https://doi.org/10.2341/15-058-O.
5. Opdam NJM, Roeters JJM, Joosten M, & Veeke O vd (2002) Porosities and voids in
Class I restorations placed by six operators using a packable or syringable
composite Dent Mater 18(1) 58–63, https://doi.org/10.1016/s0109-5641(01)00020-
3.
6. Ferracane JL (2005) Developing a more complete understanding of stresses
produced in dental composites during polymerization Dent Mater 21(1) 36–42,
https://doi.org/10.1016/j.dental.2004.10.004.
7. de Moraes Porto ICC, Honório NC, Amorim DAN, de Melo Franco AV, Penteado
LAM, & Parolia A (2014) Comparative radiopacity of six current adhesive systems
J Conserv Dent 17(1) 65–69, https://doi.org/10.4103/0972-0707.124151.
8. Pardo Díaz CA, Shimokawa C, Sampaio CS, Freitas AZ, & Turbino ML (2020)
Characterization and Comparative Analysis of Voids in Class II Composite Resin
Restorations by Optical Coherence Tomography Oper Dent 45(1) 71–79,
https://doi.org/10.2341/18-290-L.
9. Liedke GS, Spin-Neto R, da Silveira HED, & Wenzel A (2014) Radiographic
diagnosis of dental restoration misfit: a systematic review J Oral Rehabil 41(12)
957–967, https://doi.org/10.1111/joor.12215.

31
10. Francio LA, Silva FE, Valerio CS, Cardoso CA e A, Jansen WC, & Manzi FR
(2018) Accuracy of various imaging methods for detecting misfit at the tooth-
restoration interface in posterior teeth Imaging Sci Dent 48(2) 87–96,
https://doi.org/10.5624/isd.2018.48.2.87.
11. Soares CJ, Rosatto C, Carvalho VF, Bicalho AA, Henriques J, & Faria-E-Silva AL
(2017) Radiopacity and Porosity of Bulk-fill and Conventional Composite Posterior
Restorations-Digital X-ray Analysis Oper Dent 42(6) 616–625,
https://doi.org/10.2341/16-146-L.
12. Kirsch J, Tchorz J, Hellwig E, Tauböck TT, Attin T, & Hannig C (2016) Decision
criteria for replacement of fillings: a retrospective study Clin Exp Dent Res 2(2)
121–128, https://doi.org/10.1002/cre2.30.
13. Lynch CD, McConnell RJ, & Wilson NHF (2006) Teaching the placement of
posterior resin-based composite restorations in US dental schools J Am Dent Assoc
137(5) 619–625, https://doi.org/10.14219/jada.archive.2006.0257.
14. Hayashi J, Shimada Y, Tagami J, Sumi Y, & Sadr A (2017) Real-Time Imaging of
Gap Progress during and after Composite Polymerization J Dent Res 96(9) 992–
998, https://doi.org/10.1177/0022034517709005.
15. Wenzel A (2006) A review of dentists’ use of digital radiography and caries
diagnosis with digital systems Dentomaxillofac Radiol 35(5) 307–314,
https://doi.org/10.1259/dmfr/64693712.
16. Akarslan ZZ, Akdevelioğlu M, Güngör K, & Erten H (2008) A comparison of the
diagnostic accuracy of bitewing, periapical, unfiltered and filtered digital panoramic
images for approximal caries detection in posterior teeth Dentomaxillofac Radiol
37(8) 458–463, https://doi.org/10.1259/dmfr/84698143.
17. Atchison KA, White SC, Flack VF, & Hewlett ER (1995) Assessing the FDA
guidelines for ordering dental radiographs J Am Dent Assoc 126(10) 1372–1383,
https://doi.org/10.14219/jada.archive.1995.0048.
18. Haak R, Wicht MJ, Hellmich M, & Noack MJ (2002) Detection of marginal defects
of composite restorations with conventional and digital radiographs European
Journal of Oral Sciences 110(4) 282–286, https://doi.org/10.1034/j.1600-
0722.2002.21271.x.
19. Wenzel A (2004) Bitewing and digital bitewing radiography for detection of caries
lesions J Dent Res 83 Spec No C C72-75,
https://doi.org/10.1177/154405910408301s14.

32
20. Purk JH, Dusevich V, Glaros A, & Eick JD (2007) Adhesive analysis of voids in
Class II composite resin restorations at the axial and gingival cavity walls restored
under in vivo versus in vitro conditions Dent Mater 23(7) 871–877,
https://doi.org/10.1016/j.dental.2006.07.001.
21. Chuang SF, Liu JK, Chao CC, Liao FP, & Chen YH (2001) Effects of flowable
composite lining and operator experience on microleakage and internal voids in
class II composite restorations J Prosthet Dent 85(2) 177–183,
https://doi.org/10.1067/mpr.2001.113780.
22. Kurşun Ş, Dinç G, Oztaş B, Yüksel S, & Kamburoğlu K (2012) The visibility of
secondary caries under bonding agents with two different imaging modalities Dent
Mater J 31(6) 975–979, https://doi.org/10.4012/dmj.2012-062.
23. Sarrett DC (2005) Clinical challenges and the relevance of materials testing for
posterior composite restorations Dent Mater 21(1) 9–20,
https://doi.org/10.1016/j.dental.2004.10.001.
24. Samet N, Kwon K-R, Good P, & Weber H-P (2006) Voids and interlayer gaps in
Class 1 posterior composite restorations: a comparison between a microlayer and a
2-layer technique Quintessence Int 37(10) 803–809.
25. Opdam NJ, Roeters FJ, Feilzer AJ, & Smale I (1998) A radiographic and scanning
electron microscopic study of approximal margins of Class II resin composite
restorations placed in vivo J Dent 26(4) 319–327, https://doi.org/10.1016/s0300-
5712(97)00024-9.
26. Jansson L, Ehnevid H, Lindskog S, & Blomlöf L (1994) Proximal restorations and
periodontal status J Clin Periodontol 21(9) 577–582, https://doi.org/10.1111/j.1600-
051x.1994.tb00746.x.
27. Reeves J (2014) Periodontal health--challenges in restorative dentistry Prim Dent J
3(2) 73–76, https://doi.org/10.1308/205016814812144049.
28. Frankenberger R, Krämer N, Pelka M, & Petschelt A (1999) Internal adaptation and
overhang formation of direct Class II resin composite restorations Clin Oral Investig
3(4) 208–215, https://doi.org/10.1007/s007840050103.
29. Signori C, Laske M, Mendes FM, Huysmans M-CDNJM, Cenci MS, & Opdam
NJM (2018) Decision-making of general practitioners on interventions at
restorations based on bitewing radiographs J Dent 76 109–116,
https://doi.org/10.1016/j.jdent.2018.07.003.

33
30. Araujo F de O, Vieira LCC, & Monteiro Junior S (2006) Influence of resin
composite shade and location of the gingival margin on the microleakage of
posterior restorations Oper Dent 31(5) 556–561, https://doi.org/10.2341/05-94.
31. Cenci MS, Pereira-Cenci T, Cury JA, & Ten Cate JM (2009) Relationship between
gap size and dentine secondary caries formation assessed in a microcosm biofilm
model Caries Res 43(2) 97–102, https://doi.org/10.1159/000209341.
32. Turkistani A, Nakashima S, Shimada Y, Tagami J, & Sadr A (2015) Microgaps and
Demineralization Progress around Composite Restorations J Dent Res 94(8) 1070–
1077, https://doi.org/10.1177/0022034515589713.
33. Hotta M, & Yamamoto K (2009) Comparative radiopacity of bonding agents J
Adhes Dent 11(3) 207–212.
34. Pamir T, Kaya AD, Baksi BG, Sen BH, & Boyacioglu H (2010) The influence of
bonding agents on the decision to replace composite restorations Oper Dent 35(5)
572–578, https://doi.org/10.2341/10-097-L.
35. Oztas B, Kursun S, Dinc G, & Kamburoglu K (2012) Radiopacity evaluation of
composite restorative resins and bonding agents using digital and film x-ray systems
Eur J Dent 6(2) 115–122.
36. pubmeddev, & al MG et Effects of adding barium-borosilicate glass to a simplified
etch-and-rinse adhesive on radiopacity and selected properties. - PubMed - NCBI
Retrieved online April 5, 2020 from: https://www-ncbi-nlm-nih-gov.proxy-
hs.researchport.umd.edu/pubmed/?term=effect+of+adding+barium-borosilicate.
37. Hewlett ER, Atchison KA, White SC, & Flack V (1993) Radiographic secondary
caries prevalence in teeth with clinically defective restorations J Dent Res 72(12)
1604–1608, https://doi.org/10.1177/00220345930720121301.
38. Diagnostic Challange: Instances Mimicking a Proximal Carious LesionDetected by
Bitewing Radiography | Semantic Scholar Retrieved online April 2, 2020 from:
https://www.semanticscholar.org/paper/Diagnostic-Challange%3A-Instances-
Mimicking-a-Carious-Secgin-
Gulsahi/c8b5532771386f955999b752bfa01fb7edf4f796.
39. Mua B, Barbachan E Silva B, Fontanella VRC, Giongo FCMDS, & Maltz M (2015)
Radiolucent halos beneath composite restorations do not justify restoration
replacement Am J Dent 28(4) 209–213.
Copyright © 2022 FDOKUMEN