Wireless EEG with individualized channel layout enables efficient motor imagery training
13
Wireless EEG with individualized channel layout enables efficient motor imagery training Catharina Zich a,⇑ , Maarten De Vos b,c,d , Cornelia Kranczioch a,c , Stefan Debener a,c,d a Neuropsychology Lab, Department of Psychology, European Medical School, Carl von Ossietzky University of Oldenburg, Germany b Methods in Neurocognitive Psychology, Department of Psychology, European Medical School, Carl von Ossietzky University of Oldenburg, Germany c Neurosensory Science Research Group, Carl von Ossietzky University of Oldenburg, Germany d Cluster of Excellence Hearing4all, Carl von Ossietzky University of Oldenburg, Germany article info Article history: Accepted 7 July 2014 Available online xxxx Keywords: Motor imagery Mobile EEG Brain–computer interface Electrode reduction highlights To reduce the number of channels to two bipolar channels a novel reduction method for motor imagery is presented, which outperformed a published procedure and the standard placement. Using an individualized electrode subset, a longitudinal study was performed over four days of motor imagery practice, in which significant learning effects could be observed. On days 2–4 practice took place in an everyday environment using a very user-friendly EEG system consisting of individualized caps and a low-cost wireless hardware. abstract Objective: The study compared two channel-reduction approaches in order to investigate the effects of systematic motor imagery (MI) neurofeedback practice in an everyday environment using a very user- friendly EEG system consisting of individualized caps and highly portable hardware. Methods: Sixteen BCI novices were trained over four consecutive days to imagine left and right hand movements while receiving feedback. The most informative bipolar channels for use on the subsequent days were identified on the first day for each individual based on a high-density online MI recording. Results: Online classification accuracy on the first day was 85.1% on average (range: 64.7–97.7%). Offline an individually-selected bipolar channel pair based on common spatial patterns significantly outper- formed a pair informed by independent component analysis and a standard 10–20 pair. From day 2 to day 4 online MI accuracy increased significantly (day 2: 69.1%; day 4: 73.3%), which was mostly caused by a reduction in ipsilateral event-related desynchronization of sensorimotor rhythms. Conclusion: The present study demonstrates that systematic MI practice in an everyday environment with a user-friendly EEG system results in MI learning effects. Significance: These findings help to bridge the gap between elaborate laboratory studies with healthy participants and efficient home or hospital based MI neurofeedback protocols. Ó 2014 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights reserved. 1. Introduction Motor imagery (MI) electroencephalogram (EEG) neurofeed- back training is a promising therapeutic approach for the recovery of lost motor function. Patients can learn to modulate the ampli- tude of sensorimotor rhythms (SMRs) as recorded with electroen- cephalogram (EEG) and magnetoencephalography (MEG). This may initiate cortical reorganization and thereby support functional recovery (Buch et al., 2008; Caria et al., 2011). However, neurore- habilitation training is in general effortful and a large amount of training over a prolonged period of time seems necessary to facil- itate adaptive cortical reorganization (Langhorne et al., 2009). Since commonly available EEG technology is rather cumbersome and not well suited for frequent use outside of the laboratory, the clinical utility of MI neurofeedback, and in particular the http://dx.doi.org/10.1016/j.clinph.2014.07.007 1388-2457/Ó 2014 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights reserved. ⇑ Corresponding author. Address: Department of Psychology, University of Oldenburg, 26111 Oldenburg, Germany. Tel.: +49 441 798 2172; fax: +49 441 798 5522. E-mail address: [email protected] (C. Zich). Clinical Neurophysiology xxx (2014) xxx–xxx Contents lists available at ScienceDirect Clinical Neurophysiology journal homepage: www.elsevier.com/locate/clinph Please cite this article in press as: Zich C et al. Wireless EEG with individualized channel layout enables efficient motor imagery training. Clin Neurophysiol (2014), http://dx.doi.org/10.1016/j.clinph.2014.07.007
-
Upload
uni-oldenburg -
Category
Documents
-
view
0 -
download
0
Transcript of Wireless EEG with individualized channel layout enables efficient motor imagery training

Clinical Neurophysiology xxx (2014) xxx–xxx
Contents lists available at ScienceDirect
Clinical Neurophysiology
journal homepage: www.elsevier .com/locate /c l inph
Wireless EEG with individualized channel layout enables efficient motorimagery training
http://dx.doi.org/10.1016/j.clinph.2014.07.0071388-2457/� 2014 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights reserved.
⇑ Corresponding author. Address: Department of Psychology, University ofOldenburg, 26111 Oldenburg, Germany. Tel.: +49 441 798 2172; fax: +49 441798 5522.
E-mail address: [email protected] (C. Zich).
Please cite this article in press as: Zich C et al. Wireless EEG with individualized channel layout enables efficient motor imagery training. Clin Neuro(2014), http://dx.doi.org/10.1016/j.clinph.2014.07.007
Catharina Zich a,⇑, Maarten De Vos b,c,d, Cornelia Kranczioch a,c, Stefan Debener a,c,d
a Neuropsychology Lab, Department of Psychology, European Medical School, Carl von Ossietzky University of Oldenburg, Germanyb Methods in Neurocognitive Psychology, Department of Psychology, European Medical School, Carl von Ossietzky University of Oldenburg, Germanyc Neurosensory Science Research Group, Carl von Ossietzky University of Oldenburg, Germanyd Cluster of Excellence Hearing4all, Carl von Ossietzky University of Oldenburg, Germany
a r t i c l e i n f o
Article history:Accepted 7 July 2014Available online xxxx
Keywords:Motor imageryMobile EEGBrain–computer interfaceElectrode reduction
h i g h l i g h t s
� To reduce the number of channels to two bipolar channels a novel reduction method for motorimagery is presented, which outperformed a published procedure and the standard placement.
� Using an individualized electrode subset, a longitudinal study was performed over four days of motorimagery practice, in which significant learning effects could be observed.
� On days 2–4 practice took place in an everyday environment using a very user-friendly EEG systemconsisting of individualized caps and a low-cost wireless hardware.
a b s t r a c t
Objective: The study compared two channel-reduction approaches in order to investigate the effects ofsystematic motor imagery (MI) neurofeedback practice in an everyday environment using a very user-friendly EEG system consisting of individualized caps and highly portable hardware.Methods: Sixteen BCI novices were trained over four consecutive days to imagine left and right handmovements while receiving feedback. The most informative bipolar channels for use on the subsequentdays were identified on the first day for each individual based on a high-density online MI recording.Results: Online classification accuracy on the first day was 85.1% on average (range: 64.7–97.7%). Offlinean individually-selected bipolar channel pair based on common spatial patterns significantly outper-formed a pair informed by independent component analysis and a standard 10–20 pair. From day 2 today 4 online MI accuracy increased significantly (day 2: 69.1%; day 4: 73.3%), which was mostly causedby a reduction in ipsilateral event-related desynchronization of sensorimotor rhythms.Conclusion: The present study demonstrates that systematic MI practice in an everyday environmentwith a user-friendly EEG system results in MI learning effects.Significance: These findings help to bridge the gap between elaborate laboratory studies with healthyparticipants and efficient home or hospital based MI neurofeedback protocols.� 2014 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights
reserved.
1. Introduction tude of sensorimotor rhythms (SMRs) as recorded with electroen-
Motor imagery (MI) electroencephalogram (EEG) neurofeed-back training is a promising therapeutic approach for the recoveryof lost motor function. Patients can learn to modulate the ampli-
cephalogram (EEG) and magnetoencephalography (MEG). This mayinitiate cortical reorganization and thereby support functionalrecovery (Buch et al., 2008; Caria et al., 2011). However, neurore-habilitation training is in general effortful and a large amount oftraining over a prolonged period of time seems necessary to facil-itate adaptive cortical reorganization (Langhorne et al., 2009).Since commonly available EEG technology is rather cumbersomeand not well suited for frequent use outside of the laboratory,the clinical utility of MI neurofeedback, and in particular the
physiol

2 C. Zich et al. / Clinical Neurophysiology xxx (2014) xxx–xxx
potential benefit it may have for motor rehabilitation, remainspoorly understood. By reducing considerably the number of elec-trodes and combining an individualized electrode subset with asmall wireless EEG system the present study aimed to contributeto bridging this gap and to prepare the ground for an MI neurofeed-back system that can efficiently be applied at home or in a rehabil-itation setting.
The neurophysiological basis of motor imagery brain–computerinterfaces (BCIs) are amplitudes of SMRs spanning the 8–30 Hz fre-quency range (Pfurtscheller and Neuper, 2001). The modulation ofSMRs can be induced by voluntary internal drives, such as the exe-cution or imagination of movements (Jasper and Penfield, 1949;Pfurtscheller and Aranibar, 1979; Pfurtscheller et al., 1997, 2006).SMR event-related desynchronization (ERD) patterns seem to bevery similar for executed and imagined movements (McFarlandet al., 2000), which supports the idea that motor imagery involvessimilar neural mechanisms to those operating during real move-ments (Jeannerod, 1995, 2001). Since many individuals can volun-tarily control their SMR amplitude using motor imagery as amental strategy, SMR-based neurofeedback and BCI applicationsare very promising novel neurorehabilitation tools (Prasad et al.,2010; Cincotti et al., 2012; Ortner et al., 2012).
To be useful as neurorehabilitation tools, BCI applicationsshould be suitable for independent domestic application. Thisrequires affordability, short set-up time, reliability, and usabilityof the tools (Sellers et al., 2010; Holz et al., 2013). Achieving theserequirements involves minimizing EEG preparation time. To thisend, the number of EEG channels could be minimized as much aspossible. To achieve and optimize this for a MI neurofeedbackwas the first main objective of the present study. For right- andleft-hand MI paradigms the minimum number of electrodes isthree, supporting one bipolar channel per hemisphere with thesame common midline reference, plus one ground electrode. Herea symmetric electrode layout that includes the standard electrodepositions C3 and C4 or adjacent positions that are approximatelylocated over the primary motor cortex (Wolpaw et al., 2002) anda midline FCz position as reference are common (e.g., Wanget al., 2006, 2007a). However, due to individual differences in brainstructure and function, a ‘‘one cap layout fits all’’ strategy may besuboptimal. Hence, it has been argued that individually deter-mined channel configurations are preferable (Schröder et al.,2005; Lou et al., 2008). An open question however is how to derivethe most optimal electrode sites for each individual. One possibil-ity would be to compare each potential electrode pair, but becauseprocessing demands would be very high approaches that restrictthe search space are favorable. Such approaches are available, yetto the best of our knowledge systematic comparisons or a valida-tion over several days are lacking. We therefore aimed not onlyto reduce the number of electrodes for an MI neurofeedback toan individually selected bipolar channel pair but, importantly, tocompare two selection approaches.
In this comparison we firstly considered the selection approachproposed by Lou et al. (2008) that is based on independent compo-nent analysis (ICA). Secondly, we suggest and consider a novelchannel selection method. This method is based on common spa-tial patterns (CSP), which is currently the state-of-the-art spatialfilter in MI BCIs (Blankertz et al., 2008b). The two selection proce-dures were compared to a standard symmetrical 10–20 channelpair. We used inherently independent data obtained on differentdays in order to verify the individually selected channels whileavoiding circularity. Avoiding circularity is a very important aspectin cognitive neuroscience in general (Kriegeskorte et al., 2009) andthis holds also for the selection of channel subsets for the long-term use of MI BCIs. To achieve independence we applied thetwo channel selection procedures to EEG data collected in a high-density 94-channel laboratory recording session and tested the
Please cite this article in press as: Zich C et al. Wireless EEG with individualized(2014), http://dx.doi.org/10.1016/j.clinph.2014.07.007
selection on independent data from three consecutive daysrecorded outside the laboratory.
The reduction of the number of channels considerably reducesEEG preparation time from about half an hour to five minutesand thus helps to meet the requirements for a BCI-based rehabili-tation tool. Another important aspect of such a tool is the recordinghardware, which should be mobile, affordable and easy to use. Wetherefore not only reduced the number of channels, but also chan-ged from a lab-mounted EEG system to a small, wireless and easyto set up EEG system (Debener et al., 2012; De Vos et al., 2013; DeVos et al., 2014). We also moved out of the laboratory to mimic theenvironment of the end-user, while participants practiced the MItask over three consecutive days. This enabled us to pursue the sec-ond main objective of this study, which was to investigate whetherMI learning takes place given the massive reduction of EEG chan-nels, hardware adaptations, and the weakly controlled environ-ment. Many studies in the MI BCI field are based on smallsample sizes, tend to lack clear protocols, or mix BCI novices andexperienced BCI users. For example Neuper et al. (1999) trainedfour MI and BCI experienced subjects over 5–10 sessions, sched-uled one to three sessions per week, while Guger et al. (2000)examined three BCI experiences subjects over three days andMcFarland et al. (2010) trained four patients, three with and onewithout previous BCI experience, over two to three weeks. How-ever in spite of these shortcomings, a number of studies have dem-onstrated that practicing MI tasks that involve EEG-feedbackresults in significant learning effects (Neuper et al. (1999), Gugeret al. (2000) and Ono et al. (2013); but also see Neuper et al.,2009; Friedrich et al., 2013), and we similarly expected to see MIlearning effects. To demonstrate that MI learning takes place inspite of the number of channels, hardware and recording environ-ment as used in our study is essential for all further efforts toimplement a BCI-based rehabilitation tool.
To summarize EEG-based MI neurofeedback is a promisingtherapeutic approach for the recovery of lost motor function. How-ever, there is a gap in the way in which research on EEG-based MIneurofeedback is conducted and the requirements for an EEG-based MI neurofeedback system that can be efficiently applied athome or in a rehabilitation setting. In order to reduce this gapwe firstly compared two electrode selection approaches for findingoptimal bipolar channels for each individual with a standard chan-nel pair. Secondly, using the selected channels in combination witha low cost, small and mobile EEG system we investigated the fea-sibility of MI learning in an everyday environment.
2. Methods
2.1. Participants
The original sample consisted of 22 individuals (14 females; agerange 18–33 years; mean 25.1 years) with no history of neurolog-ical or psychiatric disorders. All participants were right handedaccording to the Edinburgh handedness inventory (Oldfield,1971) and initially naïve to MI neurofeedback and BCI experi-ments. Written informed consent was obtained from each partici-pant. The study was approved by the local ethics committee. Afterthe first day six participants (3 females, 3 males) were excludedfrom further participation. One did not follow task instructionsand for five participants the bipolar channel selection strategywas not applicable (see section Excluded participants for details).
2.2. Experimental paradigm
N = 16 individuals participated on all four consecutive days.Recording time was kept constant for each participant over the
channel layout enables efficient motor imagery training. Clin Neurophysiol

C. Zich et al. / Clinical Neurophysiology xxx (2014) xxx–xxx 3
four days, to avoid performance fluctuations depending on thetime of day. Every day three experimental sessions (8 min each)were held, one training session and two feedback sessions. Fig. 1illustrates the study design. Between the sessions, there were shortbreaks of 3–5 min. Individual sessions follow the standard Graz-MIprotocol and consisted of 40 trials (20 left and 20 right hand trials)presented in randomized order (Pfurtscheller and Neuper, 2001).Note that the machine learning perspective would recommendmany trials within a single session, as this yields a more stable spa-tial filter and classifier (e.g., Blankertz et al., 2008a). The study washowever designed to accommodate the end-users’ needs, whichare for instance sleepier and suffer from fatigue (Billows et al.,2013). This requires short MI sessions. It has been recommendedfor motor recovery after stroke (Langhorne et al., 2009) and con-firmed in clinical MI studies (Kübler et al., 2005; Buch et al.,2008; McFarland et al., 2010), that motor practice should be repet-itive and high-intensity. In the present study this was accountedfor by testing over four consecutive days. In accordance with thisBlankertz et al. (2008a) could not observe training effects over asingle long practice session, which led them to conclude that oneday of MI practice is not enough to show learning effects.
Each trial started with a fixation cross in the center of thescreen. After 3 s the cross was overlaid for 1.25 s with a red arrowpointing to the right or left, indicating the beginning of the motorimagery period. Participants were instructed to imagine the kines-thetic experience of a sequential finger tapping task (index-mid-dle-ring-little-index-middle-ring-little) from the first-personperspective with either the right or left hand as indicated by thedirection of the arrow (Neuper et al., 2005). After 8 s the trial endedwith a black screen. Inter-trial intervals ranged from 0.5 to 2.5 s. Inthe feedback sessions a light blue horizontal bar varying in lengthwas displayed during the motor imagery interval, representing thereal-time classifier output. The feedback signal was updated at afrequency of 16 Hz. Before the first training and before the firstfeedback session, a few sample trials were presented to the partic-ipants to ensure they understood the task. Stimulus presentationwas controlled with OpenViBE 0.15.0 (Renard et al., 2010) runningon day one on a local computer (screen diagonal: 24 inch; screenresolution 1920 � 1080 pixels; distance: 160 cm) and on days 2–4 on a standard notebook (screen diagonal: 11.6 inch; resolution1366 � 768 pixels; distance: 70 cm).
To evaluate the general ability of motor imagery before the firstand after the last recording session, the German Kinesthetic and
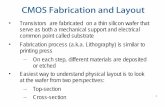
Fig. 1. Experimental paradigm and pictures illustrate the different recording environmesystem while performing the motor imagery task in the laboratory, as on the first day. Ridensity wireless EEG system, as on days 2–4. The amplifier is fixed to the lower edge of tred: ICA-based, highlighted in green: CSP-based) in accordance to the individual scalp d
Please cite this article in press as: Zich C et al. Wireless EEG with individualized(2014), http://dx.doi.org/10.1016/j.clinph.2014.07.007
Visual Imagery Questionnaire (KVIQ-G) was completed (Schusteret al., 2012) twice. This self-assessment questionnaire is a reliableand valid tool to evaluate initial motor imagery abilities and possi-ble changes in motor imagery capacity with practice (Malouinet al., 2007b; Randhawa et al., 2010; Schuster et al., 2012).
2.3. EEG recordings
On the first day, EEG data were acquired from 94 equidistantinfra-cerebral scalp sites with a central fronto-polar site as groundand a nose-tip electrode as reference using a BrainAmp system(BrainProducts GmbH, Gilching, Germany). Data were recordedwith a resolution of 0.1 lV and a sampling rate of 500 Hz (0.1–250 Hz bandpass). In addition, a surface electromyogram (EMG)was recorded from two electrodes per hand, placed on the Oppo-nens Pollicis and First Dorsal Interossei. EMG signals were used toconfirm the absence of target related muscle activity and to ensurethat participants followed task instructions. No participant usedEMG activity systematically to operate the BCI. Due to limitedchannel capacities EMG was recorded from only one hand.
At days 2–4 continuous EEG data were collected with a modi-fied Emotiv (www.emotive.com) system as described previously(Debener et al., 2012). Briefly, the original hardware (128 Hz sam-pling rate; 0.16 and 45 Hz bandpass) was relocated into a smalland light box (49 � 44 � 25 mm; 48 g total weight), which wastightly attached to a state-of-the-art infra-cerebral electrode capfrom Easycap (www.easycap.de) at the back of the head with anelastic band. The electrode caps had exactly the same 94 openingsas the caps used for the laboratory 94-channel recordings. SinteredAg/AgCl electrodes in plastic adaptors were used for the record-ings. Five standard electrodes were fixed to the caps: a midlineoccipital site as ground and a midline frontopolar electrode as ref-erence; close approximations of the 10–20 electrodes C3, C4 andFCz. The positions of a maximum of eight further electrodes weredetermined for each subject individually, after common spatialpattern and ICA analysis of the 94-channel EEG recordings fromthe first day. For all electrodes the same reference was used andbipolar derivations were calculated on- and offline. The resultingchannels are further referred to as bipolar channels. In additionto the scalp channels four EMG electrodes were positioned, twoon the left and two on the right hand. As before EMG data wererecorded for only one hand.
nts and EEG systems. Left: rear view of a participant wearing the high-density EEGght: participant performing the same task in an everyday environment using a low-he EEG cap. Electrodes are placed forming two bipolar channel pairs (highlighted inistribution of the sensory motor rhythm of the participant.
channel layout enables efficient motor imagery training. Clin Neurophysiol

4 C. Zich et al. / Clinical Neurophysiology xxx (2014) xxx–xxx
On all four days electrode impedances where kept below20 kOhm before the recording started using the BrainAmp Soft-ware (BrainProducts GmbH, Gilching, Germany). At the first daydata were acquired in a laboratory environment (i.e., a dimly litand sound shielded room), at the following three days data werecollected in a rather noisy office room. The room was chosen withthe purpose to achieve recording conditions that corresponded clo-sely to an everyday environment: day light could not be controlled,noise from a frequently used adjacent entry hall was clearly audi-ble, and no hardware other than a notebook and the wireless,mobile EEG device was used (see Fig. 1). While, for the laboratoryrecording participants were seated in a comfortable arm chair opti-mized for EEG recordings, for the office recordings participantswere seated on an ordinary chair. All data were recorded withOpenViBE. In all recording sessions participants’ hands rested ontheir lap with palms up. Participants were asked to keep their armsand hands relaxed and to minimize eye movements during therecordings.
2.4. Data analysis
Data were analyzed offline using EEGLAB 10.2.2.4b (Delormeand Makeig, 2004) and BCILAB v1.0 (Delorme et al., 2011), runningunder MATLAB R2011b (Mathworks, Inc., Natick, MA).
2.5. CSP-informed channel selection
Because CSP is computationally efficient and maximizes thevariance of one class while simultaneously minimizes the variancefor the second, CSP has been established as the state-of-the-artspatial filter in MI applications. The outcome of the CSP is a squarematrix W (filter � channels), which contains the unmixing weightsof spatial filter coefficients. As the first and the last rows of thematrix represent the most discriminative filter with respect to var-iance, we used those to select the most discriminative bipolarchannel pair. From each filter one bipolar channel was derived,consisting of the channels with the absolute maximum and mini-mum weight. We reasoned that given the restriction of the numberof channels to two, these two would represent the filter best. Ini-tially raw data were bandpass filtered between 8 and 30 Hz(Müller-Gerking et al., 1999; Blankertz et al., 2008a) and seg-mented from �1.0 s before to 4.0 s after onset of the red arrow.Segments containing large artifacts were rejected (on average 13/120 epochs). The interval from 0.5 to 4.0 s after arrow onset wassubmitted to a CSP implementation following Ramoser et al.(2000). From the unmixing CSP matrix W (filter � channels) thechannel (column) with the absolute minimum weight and thechannel with the absolute maximum weight were determined, ide-ally from the first and the last filter (row). If either the first or thelast filter was clearly distorted by artifact, the next filters (up tofive from the front or back respectively) were evaluated. Each ofthe two bipolar channels consisted of a signal channel (maximum)and reference channel (minimum). Selected channels had to fulfilltwo restrictions. First, each channel should be part of the top/cen-tered 35 channels of the 94-channel layout, and second, a bipolarchannel had to remain within one hemisphere. Midline electrodepositions were considered valid for both hemispheres. Pilot dataindicated that this channel selection procedure returned reason-able results, despite its simplicity. Iterative CSP procedures as pro-posed previously (Farquhar et al., 2006; Popescu et al., 2007; Heet al., 2010) were not applied for the channel selection step, as theyare not designed to identify bipolar channels per hemisphere. Fig. 2displays exemplary for right and left hand MI CSP topographies andthe resulting bipolar channels for two individuals, and the groupaverage maps and frequency maps of the selected electrodes.
Please cite this article in press as: Zich C et al. Wireless EEG with individualized(2014), http://dx.doi.org/10.1016/j.clinph.2014.07.007
2.6. ICA-informed channel selection
For ICA-based electrode selection the EEG raw data were ini-tially filtered between 1 and 40 Hz, segmented into consecutivetime intervals of one second and segments containing large arti-facts were rejected. The remaining data were submitted toextended infomax ICA (Bell and Sejnowski, 1995) as implementedin EEGLAB 10.2.2.4b (Delorme and Makeig, 2004) to estimate theunmixing weights (W) of 60 independent components (ICs) fromthe EEG data. The resulting weights matrix was applied to theraw data (Debener et al., 2010). This strategy provides a reasonabletrade-off between retaining as much variance in the data as possi-ble and protecting ICA against the negative influence of channeldrift and other processes incompatible with the statistical assump-tions of ICA (De Vos et al., 2012). All obtained ICs were back-pro-jected to the sensor level. Note that this included ICs reflectingstereotypical artifact, because the goal was to determine the opti-mal channels for further online application, in the presence ofthose stereotypical artifacts. For further analysis data were againfiltered between 8 and 30 Hz, segmented from 0.5 s before to4.0 s after arrow stimulus onset and segments containing largeartifacts were rejected.
Bipolar channel selection procedure closely followed the oneproposed by Lou et al. (2008), with few exceptions. In their studyinvolving eight MI trained subjects Lou and colleagues acquiredright and left hand MI data from 32 channels (120 trials per class),in order to reduce the number of electrodes to two bipolar channelpairs based on ICA. Therefore the authors first identified one SMRIC for the left and one for the right hemisphere based on threecriteria: (1) the IC activation spectrum had to include a peak inthe l-frequency range (8–13 Hz), (2) the spatial distribution ofthe source (forward matrix W�1) had to have a focus over sensori-motor areas; and (3) the 8–30 Hz band-power of the source had tocorrelate with the site of the imagination task, that is, it wasexpected to show a contralateral power suppression and an ipsilat-eral enhancement. In the present study the SMR ICs were selectedby two independent evaluators (CZ, SD) and criterion 1 was tight-ened as in addition a to a first peak in the l-frequency range a sec-ond one in the b-band had to be present, located approximately attwice the frequency than the first peak. Moreover, while Lou et al.selected three task-unrelated a-ICs to represent noise, we used allICs except for the selected SMR ICs as noise estimator. By this wecould avoid the additional IC selection step. Moreover, we consid-ered our approach of noise estimation more realistic for the subse-quent low-density recordings.
Despite the minor changes regarding the IC selection, during thechannel selection procedure within the defined ICs we closely fol-lowed the method proposed by Lou and colleagues. Specifically, thechannel with the absolute maximum weight in the selected SMR ICwas chosen as signal channel. The corresponding reference channelwas required (1) to have the lowest absolute weight in the selectedSMR IC; and (2) to have a noise level as similar as possible to thenoise level of the selected signal channel. To this end the signal-to-noise ratio (SNR), ratio of task-related power (signal) to noisepower, was calculated for all channels and the channel with thehighest SNR was chosen as the respective reference channel. Thereference channel for the left signal channel L was calculated asfollows:
SNRLðcÞ ¼jðwLL �wcLÞ � PLj
jðwLR þwcRÞ � PRj þPk
i¼1jðwLni�wcni
Þ � Pnij
Here wcn is an element of W�1, where the first index indicates thechannel number and the second the IC number. Ideally, ICA decom-posed the bandpass filtered data in two SMR ICs (L, R) and 58 noiseICs ni, i = 1,. . .,k. The band power P of the ICs was obtained by
channel layout enables efficient motor imagery training. Clin Neurophysiol

Fig. 2. CSP (a, b) and ICA (e, f) SMR topographies for right (a, e) and left (b, f) hand MI of two exemplary subjects and the normalized grand average from N = 16 subjects(bottom row). Middle columns (c, d) displays the selected bipolar channel pairs respectively and the relative frequency of selected channels (bottom row; blue = reference,orange = signal channel).
C. Zich et al. / Clinical Neurophysiology xxx (2014) xxx–xxx 5
bandpass filtering, squaring and averaging all samples in the 3.5 stime window. Similar to the CSP-based channel selection approach,channels were required to be part of the top/centered 35 channels,and a bipolar channel had to stay within one hemisphere. Fig. 2 dis-plays exemplary SMR IC topographies and the selected bipolar chan-nels of two subjects for right and left hand MI, and the normalizedgroup average and relative frequency of the selected channels forall participants.
2.7. Standard channels
The standard bipolar channel pair consisted of close approxima-tions of the 10–20 electrodes C3 and C4, respectively referenced toFCz.
2.8. Classification
OpenViBE was used to calculate the single-trial classificationaccuracies online as well as offline. Band power features were com-puted by first applying a spatial filter. For the first day CSP wasapplied to calculate the appropriate coefficients and for days 2–4the three bipolar channel pairs were used. EEG data were bandpassfiltered (8–30 Hz), segmented into motor imagery intervals cover-ing 0.5 s until 4.0 s after stimulus onset and squared, to obtain thepower. These intervals were subdivided into 40 bins ((3.5–1)/0.0625), resulting in 1 s lasting time windows with an overlap of1–0.0625 s. Samples within one time window were averaged. Theresulting features were submitted to linear discriminant analysiswhere the mean single-trial classification accuracy was deter-mined with a sevenfold cross-validation procedure. To this endeach dataset was divided randomly into seven parts of equal size,then feature selection and classifier training was done on 6/7 ofthe data and obtained predictions compared to the real labels ofthe remaining seventh part.
2.9. ERD
To compute the ERD% time course, the procedure proposed byPfurtscheller and Lopes da Silva (1999) was used, while keepingmost parameter settings as for the single-trial classification in
Please cite this article in press as: Zich C et al. Wireless EEG with individualized(2014), http://dx.doi.org/10.1016/j.clinph.2014.07.007
OpenViBE identical. Specifically, to obtain the power samples of abipolar channel the difference between reference and signal chan-nel of the filtered signal (8–30 Hz) was squared. Task related trialswere extracted by segmenting the data from �3.0 s before until4.0 s after stimulus onset. After averaging the power samplesacross trials, 96 overlapping time windows were generated andthe samples within each time window averaged. ERD% was com-puted as follows: ERD% (t) = (A (t) � R)/R � 100, where R is thepower in the frequency band of 2 s baseline period before stimulusonset, and A the power in the frequency band at time point t, withreference to stimulus onset. By using this equation, ERD% isreflected by negative numbers. For further analysis, left and rightERD% time courses were averaged and only contra- and ipsilateraleffects are reported, because hemispheric differences were notconsidered in this study. For the statistical analysis of ERD% theaverage of the time window from 1.0 to 4.0 s after stimulus onsetwas used.
To verify that changes in ERD% over the three consecutive daysMI practice are caused by narrow-band modulations, the log powerspectra (1–40 Hz) for day 2 and day 4 were calculated from rawdata for the contra- and ipsilateral hemisphere within the MI inter-val. The frequency range of 1–40 Hz was subdivided into fourfrequency bands, namely pre-MI frequency range (1–7 Hz),l- (8–12 Hz) and b- band (13–30 Hz) and post-MI frequency range(31–40 Hz).
2.10. Iterative CSP
Reducing the number of channels to one bipolar channel pairresulted in a very lean system, but the leanest system is only inrare cases the one that performs best for a particular individual.The iterative CSP, as proposed by Popescu et al. (2007) is a channelreduction approach and can be used to find the optimal tradeoffbetween the leanest and the best performing system. The proce-dure works as follows: Once the unmixing CSP matrix W is calcu-lated, the least-discriminative channel (the column with thelowest sum of the absolute values of the first and last filter), isremoved and CSP is applied to the remaining N � 1 channels. Inthe present study this process was repeated until only two chan-nels were left. To do this, Popescu’s approach had to be modified
channel layout enables efficient motor imagery training. Clin Neurophysiol

6 C. Zich et al. / Clinical Neurophysiology xxx (2014) xxx–xxx
such that not the sum of the first and last two filters, but the sum ofthe first and last filter was used to find the least-discriminativechannel. To further explore the relationship between classificationaccuracy and number as well as position of channels for every iter-ation step, the relative importance for any electrode and the accu-racy were determined. Therefore CSP coefficients were calculatedon the training datasets and applied to the two concatenated feed-back sessions. Classification accuracy was again determined usingsevenfold cross-validation. Note that the iterative CSP could not beconsidered in the first place because it does not result in a bipolarchannel pair.
2.11. Statistical analysis
All analysis of variance (ANOVA) models consisted of repeatedmeasurement factors. To analyze if the three sessions recordedwithin one day differed in classification accuracy, a one-wayANOVA with factor session (training, feedback 1, feedback 2) wasconducted on the data obtained on the first day with the 94 chan-nel cap. After channel selection an ANOVA with the factor channelpair (CSP, ICA, standard) was used to statistically test for thehypothesized higher accuracies for individualized compared tostandard channel pairs. To test for learning over days 2–4 and fordifferences between the channel pairs, classification accuraciesand ERD% as dependent variables were analyzed with two separateANOVAs, comprising the factors day (day 2, day 3, day 4) and bipo-lar channel pair (CSP, ICA, standard). Furthermore, one ANOVAwith factors day (day 2, day 3, day 4) and laterality (contra-, ipsi-lateral) was conducted on the ERD% as dependent variable, to sta-tistically check if any increase in ERD% was caused by changeswithin the ipsi- or contralateral hemisphere. To test that changesin ERD% over the practice period are caused by narrow band powermodulations we performed an ANOVA with the factor day (day 2,day 4) and frequency band (1–7 Hz, 8–12 Hz, 13–30 Hz and 31–40 Hz). To estimate the test–retest reliability of single-subjectmeasures Pearson correlations were calculated for classificationaccuracies and ERD% between day 2 and day 4. KVIQ scores wereanalyzed by an ANOVA comprising the factors day (day 1, day 4)and subscale (visual, kinesthetic), to statistically confirm for theassumed stronger increase in scores for the kinesthetic subtestcompared to the visual subtest. For all ANOVAs, Greenhouse–Geis-ser epsilon values were used to account for violations of sphericity.Effect sizes described are g2 (partial eta squared). Paired sample t-tests were conducted to follow up significant main effects andinteraction effects, reported are two-tailed p-values. Single-subjectclassification accuracies were considered significantly abovechance-level if they were above a cut-off value. The cut-off valuedepended on the number of epochs (two feedback sessions with40 trials each) and was defined as chance-level (0.5) plus two stan-dard errors 0:5þ 2 �
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffið0:5 � 0:5Þ=80
p¼ 0:612 (Hill and Schölkopf,
2012). Correlation analyses were performed to explore the possibleassociation of initial KVIQ scores and initial accuracy, change overthe days in KVIQ scores and accuracy as well as change in KVIQscores and change in ERD%.
1 Additional analyses confirmed that no ERD was evident in the pre- (1–7 Hz) andpost-frequency of interest (31–40 Hz) over the three days of MI practice, seeSupplementary Fig. S1.
3. Results
3.1. Day 1 – initial online and offline MI accuracy
On the first day, MI single trial accuracy for the training sessionwas on average 84.2% ranging from 66.7% to 94.8%. This indicatedthat individuals experienced having control over their SMR activ-ity, in the absence of extensive training. Online, the single-trialclassification accuracy was 83.1% (range: 64.7–96.9%) for the firstfeedback session and 87% for the second (range: 69.3–97.7%).
Please cite this article in press as: Zich C et al. Wireless EEG with individualized(2014), http://dx.doi.org/10.1016/j.clinph.2014.07.007
Descriptively, higher accuracies for the second feedback sessionindicated better control and confirmed that participants remainedmotivated over the three recording sessions, but the difference wasnot significant (F2,30 = 1.40, p = .263, g2 = .09). Therefore, for all fur-ther analyses data were collapsed across the two qualitatively sim-ilar feedback sessions. The single-trial classification accuracies foreach individual and group average results are shown in Fig. 3.
After bipolar channel selection the accuracies for every channelpair and all three pairs together were calculated offline. Note thatthis was done for the data of the first day. The single subject andgroup average classification accuracies in Fig. 3 also show the per-formance for each individual channel pair (group average for CSP:71.3% ± 10.1; ICA: 68.3% ± 11; standard: 66.3% ± 10.8) and all threepairs together (group average: 74.4% ± 9.7). Fourteen out of the six-teen participants performed significantly above chance-level wheneither all three pairs together, or just the CSP-based channel pair,was considered. This was the case for ten individuals for the ICA-based and eleven individuals for the standard channel pair. Thethree bipolar channel pairs differed significantly in classificationaccuracy (F2,30 = 7.40, p = .003, g2 = .33). Pairwise comparisonsshowed a significant difference between CSP and standard channelpair (t15 = 3.39, p = .004) as well as between CSP and ICA channelpair (t15 = 2.43, p = .028), indicating that the CSP-informed bipolarchannel pair performed best. No significant difference was foundbetween ICA and standard channel pair (t15 = 1.69, p = .112).
3.2. Day 2 to day 4 – learning effects
The classification accuracies over the three days obtained withthe different bipolar channel pairs were analyzed with a two-way ANOVA with factors day (day 2, 3 and 4) and channel pair(CSP, ICA, standard). A significant main effect of day (F2,30 = 3.62,p = .041, g2 = .19) was found but no significant main effect of chan-nel pair (F2,30 = .01, p = .990, g2 = .001), suggesting similar changesin accuracy over days for all bipolar channel pairs. Therefore, in thefollowing analysis the online accuracies, based on all three channelpairs together, were considered. The group average for day 2–4 ofonline single trial classification accuracies, based on all three bipo-lar channel pairs together, is displayed in Fig. 4. Pairwise compar-ison confirmed that accuracies were significantly higher on day 4than on day 2 (t15 = �3.58, p = .003) indicating learning, in termsof increased accuracies over three days practice. Descriptively,accuracies improved on average from 69.1% on day 2 to 73.3% onday 4. A strong positive correlation between classification accura-cies of the feedback sessions across channel pairs between day 2and day 4 (r = .86, p < .001) confirmed an excellent test–retestreliability.
Confirming previous reports MI caused an ERD prominentabove the contralateral sensorimotor area in the MI specific fre-quency band spanning the 8–30 Hz range.1 Grand average ERD%for the days 2, 3 and 4 are displayed in Fig. 5 for the contra- and ipsi-lateral hemisphere along with the difference between both. TwoANOVAs, one for the contra- and one for the ipsilateral ERD%, withfactors day (day 2, 3 and 4) and channel pair (CSP, ICA, standard)were conducted. Neither for the contralateral nor for the ipsilateralhemisphere a significant difference on ERD% between channel pairswas found (contralateral: F2,30 = 2.85, p = .101, g2 = .16; ipsilateral:F2,30 = 2.80, p = .103, g2 = .16), therefore the following analysis wasbased on the average of all three channel pairs. Changes in the differ-ence of contra- and ipsilateral ERD% over three days of MI trainingwere analyzed by the ANOVA with factor day (day 2, 3 and 4), which
channel layout enables efficient motor imagery training. Clin Neurophysiol

Fig. 3. Single subject and group average EEG single-trial classification results plotted as percent accuracy for: online high-density performance using CSP (blue) and offlinecalculated low-density performance for all channel pairs together (gray), CSP (green), ICA (red) and standard channel pair (black).
Fig. 4. Group average (N = 16) EEG single-trial classification results of all threechannel pairs together plotted as percent accuracy for the training, feedback 1 andfeedback 2 sessions for days 2, 3 and 4.
C. Zich et al. / Clinical Neurophysiology xxx (2014) xxx–xxx 7
revealed a significant effect (F2,30 = 4.64, p = .024, g2 = .24). The dif-ference of contra- and ipsilateral ERD% was significantly higher onday 4 compared to day 2 (t15 = 2.44, p = .028). This indicates learningin terms of more discriminative ERD% of the two hemispheres. Therelative power improved in the motor imagery period from 11.7%on day 2 to 17.0% on day 4. As illustrated, the increase in differencebetween contra- and ipsilateral ERD% over the three days was
Please cite this article in press as: Zich C et al. Wireless EEG with individualized(2014), http://dx.doi.org/10.1016/j.clinph.2014.07.007
related to changes in ERD% of the ipsilateral rather than of the con-tralateral hemisphere. An ANOVA with factors laterality (contra-,ipsilateral) and day (day 2, day 3, day 4) revealed a significant maineffect of laterality (F2,30 = 16.97, p = .001, g2 = .53) and a significantinteraction between day and laterality (F2,30 = 4.64, p = .024,g2 = .24). Within each day the ERD% of the contralateral hemisphere(day 1: �33.2 ± 19.9; day 2: �33.7 ± 18.5; day 3: �33.6 ± 20.6) wassignificantly higher than that of the ipsilateral hemisphere (day 1:�21.2 ± 21.7; day 2: �20.5 ± 21.1; day 3: 16.6 ± 24.8) (all p = .001).Pairwise comparisons on ERD% within the ipsilateral hemisphererevealed a close to significant difference between day 2 and 4(t15 = �2.10, p = .053), which was not observed for the contralateralhemisphere (t15 = �.29, p = .775). This indicates that the reportedchanges in ERD% can be mainly traced back to the ipsilateralhemisphere.
In order to test the frequency-band specificity of the trainingeffect, log power spectra were calculated. Spectra for the two feed-back sessions and the three channel pairs were averaged becausethe learning effect was restricted to the feedback sessions (cf.Fig. 4) and no significant difference between channel pairs wasfound with regard to the learning effect on the three consecutivedays (cf. Fig. 5). Fig. 6 illustrates the difference of contra- and ipsi-lateral hemisphere power at day 2 and day 4 for four frequencybands. An ANOVA with the factors day (day 2, day 4) and frequencyband (1–7 Hz, 8–12 Hz, 13–30 Hz and 31–40 Hz) revealed a signif-icant main effect of frequency band (F3,45 = 7.37, p = .002, g2 = .33),weather factor day failed to reach significance (F1,15 = 4.04,p = .063, g2 = .21). Comparing the power from day 2 and day 4 foreach frequency band, a significant increase could be observed forthe MI relevant frequency bands (l and b), whereas no significantdifference was found for the other frequency bands (1–7 Hz:t15 = �0.91, p = .38; 8–12 Hz: t15 = �2.39, p = .031; 13–30 Hz:t15 = �2.17, p = .046; 31–40 Hz: t15 = �.68, p = .508). This resultwas confirmed when repeating this analysis with a higher spectralresolution with a frequency bin width of 2 Hz (see SupplementaryFig. S2). Thus, the learning effect was frequency-band specific
channel layout enables efficient motor imagery training. Clin Neurophysiol

Fig. 5. Grand average ERD% from N = 16 for every bipolar channel. Straight line indicate contralateral and dotted line ipsilateral bipolar channel, with respect to stimulidirection (a). Differences between contra- and ipsilateral ERD% for all three channel pairs, horizontal line represents the average ERD% for the MI time window (b). Grayshaded area indicate time window of stimulus onset.
Fig. 6. Log power spectra of four frequency bands for days 2 and 4. Shown is thedifference between contra- and ipsilateral hemisphere, with respect to stimulusdirection. The difference is significantly larger on day 4 in the frequency bandscovering the l (8–12 Hz) and b (13–30 Hz) range.
8 C. Zich et al. / Clinical Neurophysiology xxx (2014) xxx–xxx
rather than broadband. Excellent test–retest reliabilities were con-firmed by a strong positive correlation of ERD% across channel
Please cite this article in press as: Zich C et al. Wireless EEG with individualized(2014), http://dx.doi.org/10.1016/j.clinph.2014.07.007
pairs between day 2 and day 4. These correlations were significantfor the contra- and ipsilateral hemisphere as well as for the differ-ence between both (r = .96, p < .001; r = .94, p < 0.001; r = .90,p < .001).
3.3. KVIQ
To explore the relationship between initial KVIQ scores and ini-tial online accuracy, Pearson correlations were calculated, but nei-ther for the total nor for the single subscales a significantcorrelation (total: r = �.16, p = .54; kinesthetic: r < �.01, p = .99;visual: r = �.33, p = .22) was found. Furthermore, KVIQ scores fromthe first and last day were compared in an ANOVA with factors day(day 1, day 4) and subscale (visual, kinesthetic). A significant maineffect for factor subscale (F1,15 = 7.23, p = .017, g2 = .33) and a mar-ginal day � subscale interaction (F1,15 = 4.48, p = .052, g2 = .23) wasfollowed up by t-tests. At the first day scores obtained from thevisual subscale were significantly higher than those obtained fromthe kinesthetic one (t15 = 2.69, p = .017). For the kinesthetic sub-scale, the scores at the last day were significantly higher than onthe first day (t15 = �2.49, p = .025), but no significant effectemerged for the visual subscale (t15 = .20, p = .848). Neither forthe total test nor for one of the subscales the changes betweenthe first and the last day in KVIQ scores correlated significantlywith the changes between day 2 and day 4 in accuracy or in ERD%.
3.4. Post hoc analyses
To explore the relationship between the number of EEG chan-nels and MI accuracy, the data from day 1 were submitted to aniterative CSP approach. Fig. 7 shows the single-trial classification
channel layout enables efficient motor imagery training. Clin Neurophysiol

C. Zich et al. / Clinical Neurophysiology xxx (2014) xxx–xxx 9
accuracies for decreasing number of channels, from all 94 down totwo channels. Topographies illustrate at selective iteration stagesthe relative frequency of non-eliminated channels, considering all16 datasets. In most individuals, the number of channels couldbe reduced to ten, without dropping dramatically in performance.The most important ten channels were located on central scalpsites, very similar to the pattern reported by Popescu et al.(2007). However, individuals differed largely in overall accuracy,as well as in the impact of channel reduction on MI accuracy. Ona single subject level we categorized the datasets into three groups.A first group (01, 05, 10, 11, 12, 15 and 16) delivered a high levelperformance with all channels (>82%) and maintained this leveluntil very few channels were left. A second group (03, 07, 08 and14) performed in the beginning on a lower but still sufficient level,but the performance worsened with decreasing number of chan-nels and to a different degree. The performance of individuals inthe third group (02, 04, 06, 09 and 13) was poor (<75%) with all94 channels and remained low with decreasing number of chan-nels. Topographies illustrating the relative frequencies of theremaining channels across subjects revealed more clearly elec-trodes in proximity to sensorimotor cortex with fewer channels.For the last few iteration stages a pronounced lateralization tothe left hemisphere was observable, presumably reflecting theinclusion of only right-handed participants into this study.
A further post hoc analysis evaluated the role of the number ofchannels for MI performance on days 2–4. This is because theCSP- and ICA-informed channel selection steps were performedindependent from each other. Therefore, in some cases the samechannel was selected twice, which resulted in differences regard-ing the total number of channels (seven to ten) that were usedfor individual subjects days 2–4. This might have caused anartificial increase of the inter-individual differences observed. Toevaluate this, individuals were divided into two groups (group 1:7 or 8 channels, N = 6; group 2: 9 or 10 channels, N = 10). A pair-wise comparison showed no significant difference in MI accuracybetween these two groups (t5 = .31, p = .766).
4. Discussion
The present study investigated effects of systematic multi-dayMI practice in a natural environment using a portable EEG system.To this end, based on an initial high-density recording in the labo-
Fig. 7. Single subject and group average offline classification accuracies fordecreasing number of channels, ranging from all 94 (left) to 2 (right side).Topographies show the relative frequency of remaining channels at selectiveiteration stages considering all subjects.
Please cite this article in press as: Zich C et al. Wireless EEG with individualized(2014), http://dx.doi.org/10.1016/j.clinph.2014.07.007
ratory, the number of channels was reduced to a minimum. Twomethods to obtain an individually selected bipolar channel pairwere used and compared with a standard C3/4 versus FCz bipolarpair. The study reports two important findings: Firstly, individuallyselected channels outperformed the standard channels, and thepair based on CSP performed significantly better than the oneobtained by ICA. Secondly, with the low-density individualizedcap and the wireless EEG system we found an MI learning effect,expressed in higher MI accuracies, ERD% and KVIQ scores afterthree days MI practice in an everyday environment.
Unfortunately only a limited number of previous studies exam-ined the effect of MI practice and a direct comparison of accuraciesand ERD% across studies is difficult for several reasons. Firstly, theparticipants’ level of previous BCI and/or MI experience rangesfrom naïve (Blankertz et al., 2008a; Neuper et al., 2009; Friedrichet al., 2013; Ono et al., 2013), through experienced (Guger et al.,2000; Lou et al., 2008) up to participant selection depending onpreviously achieved performances (Wang et al., 2006, 2007b). Fur-thermore, different class types (Blankertz et al., 2007, 2008a), num-ber of classes (Friedrich et al., 2013), instructions (Neuper et al.,2005; Schuster et al., 2011), frequency bands, channel numbersand applied spatial filters make it even more difficult to comparethe performance obtained in this study with previous findings.
4.1. Day 1 – initial online and offline MI accuracy
Taking the described differences between studies into account,the obtained MI accuracies from the first day using the high-den-sity cap correspond to previous 2-class MI data obtained fromnaïve individuals. Experienced participants, however, like thoseparticipating in the study of Lou et al. (2008), can obtain higheraccuracies. The difference at the low-density level, by comparingthe accuracies obtained with the bipolar channel pair based onICA, is even larger (Lou et al.: mean: 91.1%, range: 69.8–98.3%),despite the fact that the present study closely followed the channelselection procedure by Lou et al. We attribute this difference to thefact that our participants had no previous MI experience, whilethose of Lou et al. were very experienced. Our own results clearlyshow that having practiced MI for only three consecutive days issufficient to improve MI accuracies and ERD%. Since MI practiceleads to more focused SMR topographies (McFarland et al., 2010;Friedrich et al., 2013), the discrepancy in accuracy between expe-rienced and naïve individuals may be inflated at low-density levels.
By comparing the three bipolar channel pairs, our results con-firmed that individually selected channel pairs perform better thanstandard ones. Within the two individually selected bipolar chan-nel pairs the pair based on the spatial filter CSP significantly out-performed the ICA based channel pair. Because not only theunderlying spatial filter differed, but also the selection proceduresand SMR topographies (unmixing, forward) used were differentthis could be due to several reasons. One possibility is that theadvantage is inherent in the CSP algorithm, because the simulta-neous variance maximization of the first class and minimizationof the second class provide better-represented features than ICAcomponents. However, this is not supported by the literature(Naeem et al., 2009; Wang et al., 2012). Moreover, one could arguethat either the channel selection used for determining the CSPchannels and/or the underlying unmixing weights better reflectthe mental state of the participants. Another reason could be thatdespite careful screening of all ICs by two independent evaluators,the optimal SMR components were not found. The manual identi-fication of ICs with the characteristics associated with MI is diffi-cult, especially when more than one possible SMR componentper hemisphere is present. Such a manual identification of ICs issubjective, time consuming and error prone if not enough expertknowledge is available. To overcome these limitations, a future
channel layout enables efficient motor imagery training. Clin Neurophysiol

10 C. Zich et al. / Clinical Neurophysiology xxx (2014) xxx–xxx
goal should be to develop software that automatically identifiesand clusters SMR components, similar to previous software solu-tions, which however were not applicable in the present case(Viola et al., 2009, 2012).
Reducing the number of channels from high-density to bipolarlevel was motivated through issues of practicability and affordabil-ity. Our results support that by increasing the number of channelsat appropriate sites higher accuracies can be achieved. But howmany channels represent the optimal trade-off between a lean sys-tem and acceptable performance is not well understood. Schröderet al. (2005) already showed that this question should be answeredfor each subject individually, as the performance with individualnumber and individual positioning of electrodes revealed betteraccuracies. The iterative CSP approach as proposed by Popescuet al. (2007) and applied in the present study as a post hoc analysisis one approach which could be used to identify the optimal num-ber of channels and channel positions for each individual. Otheriterative procedures based on CSP have been proposed (Farquharet al., 2006; He et al., 2010), but a comparable procedure for ICAis missing. From our iterative CSP results one could conclude that,on average, the number of channels providing a faire trade-offbetween a lean system with a short set-up time and an acceptableperformance is close to ten. However, the number of channelsneeded to perform approximately at the same level as with the full94-channel cap varied strongly between individuals. Therefore, thebest strategy seems to be to define both, optimal low-density chan-nel number and optimal layout for each person separately. Forexcessive longitudinal training studies the extra effort going intoan individualized cap design would pay off quickly.
In addition to the number of electrodes also the type of elec-trodes used is crucial for a practicable EEG system. Without doubtapplicability of regular MI practice would be improved further byreplacing the traditional wet electrodes with high quality dry elec-trodes (Chi et al., 2010; Liao et al., 2012). To the best of our knowl-edge no previous MI study used dry electrodes in a home settingand signal quality issues remain with currently available dry elec-trodes. Therefore we refrained from using dry electrodes in thepresent study.
4.2. Day 2 to day 4 – learning effects
The most crucial aspect of any rehabilitation program is theresulting benefit for the patient. It is likely that the patients’ benefitdepends very often on the ability to perform a rehabilitation taskappropriately, which means in the case of MI training to imaginemoving distinct body parts. The high relevance of the individualability to learn MI is reflected among other things by the attemptsof Blankertz et al. (2008a) to show a learning effect within onepractice session. Despite a large number of trials no significanttrend in accuracy over time was found, therefore the authors con-cluded that one day of MI practice is not enough to show learningeffects. In contrast to this study we kept the recording sessions perday very short (approx. 24 min MI practice per participant perday), in order to sustain attention and keep participants’ compli-ance up over the four consecutive days MI practice, both particu-larly important issues for patients.
Our results show frequency specific MI learning effects over atime range of four consecutive days. Neuper et al. (1999) similarlyobserved learning in terms of improved classification accuraciesand increased differences of contra- and ipsilateral ERD% after 5–10 sessions in all of their four experienced individuals with a fixedbipolar channel pair, and Guger et al. (2000) reported an improve-ment in classification accuracy for three experienced individualsafter three days of MI practice. In spite of these parallels a directcomparison with our results is not possible because firstly, Gugerand colleagues the actual individual learning effect could not be
Please cite this article in press as: Zich C et al. Wireless EEG with individualized(2014), http://dx.doi.org/10.1016/j.clinph.2014.07.007
obtained due to irregular adaptation of spatial filter coefficients,and secondly, our participants were novice BCI users. For naïveindividuals, improved classification accuracies and significantlyincreased ERD% effects were reported by Ono et al. (2013). Theyobserved that practicing MI over five consecutive days inducedprolonged and more robust contralateral ERD% as well as smallerinter-trial variability compared to the initial session. The lateraliza-tion of the learning effect towards the contralateral side is not sup-ported by our study however, as our results provide evidence thatMI practice leads to a decrease of ipsilateral rather than an increasein contralateral ERD%. Our observation of an ipsilateral learningeffect could indicate that MI practice goes along with a higherdegree of decoupling of the hemispheres. Testing this idea willrequire further MEG or high-density EEG studies to obtain detailedspatial and temporal information of the SMRs (Cheyne, 2013).
More complex 2D motor imagery based BCI experiments alsoprovided evidence that participants gradually learned to controltheir SMRs over 21–68 sessions (Wolpaw and McFarland, 2004;McFarland et al., 2010). Royer et al. (2010) reported that theirwell-trained participants learned to successfully navigate a heli-copter continuously in a 3D space with a 4-class motor imageryBCI within 8–11 sessions. In contrast, some MI studies did not finda general improvement of performance or larger contra- versusipsilateral ERD% differences over several days of practice (Neuperet al., 2009; Friedrich et al., 2013). This discrepancy may beexplained by differences in how frequent the classifier wasupdated. The importance of a frequent update of the classifier(Shenoy et al., 2006) and a sufficient number of trials for stability(Blankertz et al., 2008a) has been reported before, and it is conceiv-able that suboptimal settings will hamper MI learning effects.Moreover, in the case of Friedrich et al. (2013) it should be takeninto consideration that a 4-class MI paradigm was used. It is verylikely that learning to operate a 4-class MI paradigm is much moredifficult and thus requires more practice than learning to steer a 2-class paradigm.
To the best of our knowledge the present study is the first todemonstrate MI learning in a comparatively large sample of naïveparticipants in an everyday environment. Learning was reflected inhigher classification accuracies and an increased difference of con-tra- and ipsilateral ERD% after continued practice in an everydayenvironment. The learning effect was likely facilitated by the shortduration of the practice sessions, which helped to avoid exhaustionand boredom. Another probable reason for why we obtained a sig-nificant learning effect despite a relative short practice period isthat our practice schedule was well defined, meaning that everyparticipant practiced on four consecutive days, every day at thesame time, and every day supervised by the same experimenter.The number of sessions was constant every day and known tothe participants. Thus, unlike other studies (Millán et al., 2004;McFarland et al., 2010; Royer et al., 2010), we avoided varyingintervals between practice days and kept as many variables ofthe design as possible constant. But in spite of the overall learningeffect, drops in performance between days were evident in nearlyall participants. Such inconsistency is typical for BCI experimentsand has been reported previously in studies conducted in a labora-tory environment (McFarland et al., 2010). The drops in perfor-mance likely relate to motivational issues or to attentionallapses. It is important to note that even in light of inconsistenciesin the learning curves, a common trend in learning curves is recog-nizable. First, performance improved within one day between ses-sions. Second, this improvement increased over days, that is, on thelast day the improvement from the first to the last session washigher than on the first day. This pattern is also evident in thegroup average of the present data, and it is in line with observa-tions made by Millán et al. (2004). As a final observation, our dataindicate that the learning effect is limited to the feedback sessions
channel layout enables efficient motor imagery training. Clin Neurophysiol

C. Zich et al. / Clinical Neurophysiology xxx (2014) xxx–xxx 11
as performance during the training session was comparable for allfour days. This emphasizes the importance of feedback for MIlearning.
With regard to stroke rehabilitation, at present we can onlyspeculate whether patients would show the same changes in ERDas our healthy volunteers. Neural plasticity after stroke may com-pensate for the loss of motor function. On the other hand, unim-paired motor projections and competitive interaction contributeto maladaptive plasticity, which negatively affects motor recovery.Therefore one reasonable assumption is that patients show pre-training a weaker desynchronization of the lesioned hemisphere,and due to maladaptive plasticity a stronger bilateral activationthan healthy individuals (e.g., Johansen-Berg et al., 2002; Grefkesand Ward, 2014). Training effects could firstly manifest itself inan increase in ERD% in the hemisphere ipsilateral to the impairedlimb, in parallel to the ipsilateral MI learning effect observed inthe present study. This could then be interpreted as minimizationof maladaptive reorganization. The importance of the ipsilateralhemisphere after stroke, as adaptive and compensatory hemi-sphere, has been reported before (Fridman et al., 2004; Buchet al., 2008; Caria et al., 2011). Secondly, we would predict a train-ing-related increase in desynchronization for the lesioned hemi-sphere if motor functions of the lesioned hemisphere recover.Evidently, this prediction can only be investigated in a patient pop-ulation. We believe that alongside these speculations our resultsclearly show that it is important not to neglect the unlesionedhemisphere in neurorehabilitation training protocols. However,as bilateral training may prevent learned nonuse but enhance mal-adaptive plasticity (Takeuchi and Izumi, 2012), the hands shouldbe unilaterally imagined. Consequently, in the case of 2-class par-adigms, right versus left hand imagination is more advisable thanone hand imagination versus rest.
4.3. KVIQ
KVIQ scores obtained on the first day were higher for the visualthan for the kinesthetic subscale, which corresponds to previousfindings (Malouin et al., 2007a). Good test–retest reliabilities ofthe total KVIQ and its subscales have been reported for non-dis-abled individuals (Malouin et al., 2007b) and patients (Malouinet al., 2007b; Randhawa et al., 2010; Schuster et al., 2012), whichallowed for a fair comparison between the KVIQ scores obtainedon the first and last day in our study. Therefore, higher scores forthe kinesthetic but not for the visual subscale on the last day incomparison to the first day indicate improved kinesthetic motorimagery skills after four days of practice.
4.4. Excluded participants
From the initially twenty-two subjects who participated in thestudy, five had to be excluded because the obtained bipolar chan-nels pairs were not suitable. For one participant neither the ICAreveal motor imagery sensitive ICs, nor the CSP result in MI sensi-tive filter. For four participants MI ICs could be selected, but fornone of them did the CSP result in an MI sensitive filter, even ifthe first and last five filters were considered. The mean accuracyfor these four participants using the ICA-based channel pair was53.3%, indicating that their EEGs were not characterized by clearsensorimotor cortex activity. This may explain why the CSPapproach failed. The ICA approach seems less affected by this lackof clear sensorimotor cortex activity, which is also reflected in thefinding that with ICA SMR components can even be obtained fromresting state EEG (Wang et al., 2012). But regardless of spatial filter,the inability of a non-negligible proportion of individuals to suc-cessfully do MI has been reported in many previous studies(Blankertz et al., 2010). Guger et al. (2003) for instance tested 99
Please cite this article in press as: Zich C et al. Wireless EEG with individualized(2014), http://dx.doi.org/10.1016/j.clinph.2014.07.007
naïve participants and found that only approximately half of themreached classification accuracies above 70%. To improve the appli-cability of MI based neurofeedback further studies are clearlyrequired that investigate the relationship between MI BCI perfor-mance and individual differences in the neurophysiological corre-lates of MI.
4.5. Future issues
To conclude, this study demonstrates that MI performance andERD% can be significantly improved after three days MI practice inan everyday environment using individually designed electrodecaps in combination with a wireless EEG system. Furthermore,our results show that MI neurofeedback can be realized with abipolar channel pair and better so by taking individually-selectedsites instead of standard channel sites. If taking this finding a stepfurther then the system best adapted to a user should return thehighest performance. That is, performance can likely be maximizedwhen in addition to the individual selection of channel number andposition, the number of features and the features themselves(Schröder et al., 2003; Fabiani et al., 2004), as well as the frequencyrange (Blankertz et al., 2006, 2007, 2008a) are determined individ-ually. It would be desirable to implement this in an automatic anduser-friendly way, similar to recent advances in P300 speller appli-cation (Kaufmann et al., 2012).
Moreover, our results show that MI practice leads to an increasein the difference between contra- and ipsilateral ERD%. Othersobserved changes in SMR topographies following MI practice(McFarland et al., 2010; Friedrich et al., 2013). It is now importantto evaluate how changes in SMR relate to clinical improvement, forinstance after stroke (Buch et al., 2008). But in the meanwhile ten-tative recommendations for long-term MI based neurorehabilita-tion protocols can be derived. To achieve optimal therapeuticsuccess it seems important to collect high-density reference EEGdata after regular intervals of MI practice and, if necessary, to adaptindividual low-density channel positions.
Acknowledgements
We thank Jeremy Thorne and Martin Bleichner for proofreadingthe manuscript. C.Z. was funded by the PhD program ‘Signals andCognition’ (Niedersächsisches Ministerium für Wissenschaft undKultur). C.K. is supported by grant KR 3433/2-1, German ResearchFoundation (DFG).
Appendix A. Supplementary data
Supplementary data associated with this article can be found, inthe online version, at http://dx.doi.org/10.1016/j.clinph.2014.07.007.
References
Bell AJ, Sejnowski TJ. An information-maximization approach to blind sourceseparation and blind deconvolution. Neural Comput 1995;7:1129–59.
Billows IJ, Khan S, Sterr A. Exploring sleep, sleepiness and fatigue in chronic stroke:A mixed methods study. Int J Stroke 2013;8:73.
Blankertz B, Dornhege G, Krauledat M, Müller KR, Curio G. The non-invasive Berlinbrain–computer interface: fast acquisition of effective performance inuntrained subjects. Neuroimage 2007;37:539–50.
Blankertz B, Dornhege G, Krauledat M, Müller KR, Kunzmann V, Losch F, et al. TheBerlin brain–computer interface: EEG-based communication without subjecttraining. IEEE Trans Neural Syst Rehabil Eng 2006;14:147–52.
Blankertz B, Losch F, Krauledat M, Dornhege G, Curio G, Müller KR. The Berlin brain–computer interface: accurate performance from first-session in BCI-naivesubjects. IEEE Trans Biomed Eng 2008a;55:2452–62.
Blankertz B, Sannelli C, Halder S, Hammer EM, Kübler A, Müller KR, et al.Neurophysiological predictor of SMR-based BCI performance. Neuroimage2010;51:1303–9.
channel layout enables efficient motor imagery training. Clin Neurophysiol

12 C. Zich et al. / Clinical Neurophysiology xxx (2014) xxx–xxx
Blankertz B, Tomioka R, Lemm S, Kawanabe M, Müller KR. Optimizing spatial filtersfor robust EEG single-trial analysis. IEEE Signal Process Mag 2008b;25:41–56.
Buch E, Weber C, Cohen LG, Braun C, Dimyan MA, Ard T, et al. Think to move: aneuromagnetic brain–computer interface (BCI) system for chronic stroke.Stroke 2008;39:910–7.
Caria A, Weber C, Brötz D, Ramos A, Ticini LF, Gharabaghi A, et al. Chronic strokerecovery after combined BCI training and physiotherapy: a case report.Psychophysiology 2011;48:578–82.
Cheyne D. MEG studies of sensorimotor rhythms: a review. Exp Neurol2013;245:27–39.
Chi YM, Jung TP, Cauwenberghs G. Dry-contact and noncontact biopotentialelectrodes: methodological review. IEEE Rev Biomed Eng 2010;3:106–19.
Cincotti F, Pichiorri F, Aricò P, Aloise F, Leotta F, De Vico Fallani F, et al. EEG-basedbrain–computer interface to support post-stroke motor rehabilitation of theupper limb. Conference proceedings – IEEE Eng Med Biol Mag 2012:4112–4115.
De Vos M, Thorne JD, Yovel G, Debener S. Let’s face it, from trial to trial: comparingprocedures for N170 single-trial estimation. Neuroimage 2012;63:1196–202.
De Vos M, Gandras K, Debener S. Towards a truly mobile auditory brain–computerinterface: exploring the P300 to take away. Psychophysiology 2013;91:46–53.
De Vos M, Kroesen M, Emkes R, Debener S. P300 speller BCI with a mobile EEGsystem: comparison to a traditional amplifier. J Neural Eng 2014;11. http://dx.doi.org/10.1088/1741-2560/11/3/036008.
Debener S, Minow F, Emkes R, Gandras K, De Vos M. How about taking a low-cost,small, and wireless EEG for a walk? Psychophysiology 2012;49:1449–53.
Debener S, Thorne JD, Schneider TR, Viola FC. Using ICA for the analysis of multi-channel EEG data. In: Ullsperger M, Debener S, editors. Simultaneous EEG andfMRI: recording, analysis, and application. Oxford University Press; 2010. p.121–33.
Delorme A, Makeig S. EEGLAB: an open source toolbox for analysis of single-trialEEG dynamics including independent component analysis. J Neurosci Methods2004;134:9–21.
Delorme A, Mullen T, Kothe C, Akalin AZ, Bigdely-Shamlo N, Vankov A, et al. Newtools for advanced EEG processing. Comput Intell Neurosci 2011:130714. http://dx.doi.org/10.1155/2011/130714.
Fabiani GE, McFarland DJ, Wolpaw JR, Pfurtscheller G. Conversion of EEG activityinto cursor movement by a brain–computer interface (BCI). IEEE Trans NeuralSyst Rehabil Eng 2004;12:331–8.
Farquhar J, Hill J, Lal TN, Schölkopf B. Regularised CSP for sensor selection in BCI. In:Müller-Putz GR, Brunner C, Scherer R, Schlögl A, Wriessnegger S, Pfurtscheller G,editors. Proceedings of the 3rd international brain–computer interfaceworkshop and training course 2006. Graz; 2006. p. 14–5.
Fridman EA, Hanakawa T, Chung M, Hummel F, Leiguarda RC, Cohen LG.Reorganization of the human ipsilesional premotor cortex after stroke. Brain2004;127:747–58.
Friedrich EVC, Scherer R, Neuper C. Long-term evaluation of a 4-class imagery-based brain–computer interface. Clin Neurophysiol 2013;124:916–27.
Grefkes C, Ward NS. Cortical reorganization after stroke: how much and howfunctional? Neuroscientist 2014;20:56–70.
Guger C, Edlinger G, Harkam W, Niedermayer I, Pfurtscheller G. How many peopleare able to operate an EEG-based brain–computer interface (BCI)? IEEE TransNeural Syst Rehabil Eng 2003;11:145–7.
Guger C, Ramoser H, Pfurtscheller G. Real-time EEG analysis with subject-specificspatial patterns for a brain–computer interface (BCI). IEEE Trans Rehabil Eng2000;8:447–56.
He L, Gu Z, Li Y, Yu Z. Classifying motor imagery EEG signals by iterative channelelimination according to compound weight. In: Wang FL, Deng H, Gao Y, Lei J,editors. Artificial intelligence and computational intelligence. Lecture notes incomputer science. Berlin Heidelberg: Springer; 2010. p. 71–8.
Hill NJ, Schölkopf B. An online brain–computer interface based on shifting attentionto concurrent streams of auditory stimuli. J Neural Eng 2012;9:026011.
Holz EM, Botrel L, Kübler A. Bridging gaps: long-term independent bci home-use bya locked-in end-user. In: Proceedings of the TOBI workshop IV. Sion; 2013. p.35–6.
Jasper H, Penfield W. Electrocorticograms in man: effect of voluntary movementupon the electrical activity of the precentral gyrus. Archiv für Psychiatrie undZeitschrift Neurologie 1949;183:163–74.
Jeannerod M. Mental imagery in the motor cortex. Neuropsychologia1995;33:1419–32.
Jeannerod M. Neural stimulation of action: a unifying mechanism for motorcognition. Neuroimage 2001;14:103–9.
Johansen-Berg H, Rushworth MF, Bogdanovic MD, Kischka U, Wimalaratna S,Matthews PM. The role of ipsilateral premotor cortex in hand movement afterstroke. PNAS 2002;99:14518–23.
Kaufmann T, Völker S, Gunesch L, Kübler A. Spelling is just a click away – a user-centered brain–computer interface including auto-calibration and predictivetext entry. Front Neurosci 2012;6:72.
Kriegeskorte N, Simmons WK, Bellgowan PS, Baker CI. Circular analysis in systemsneuroscience: the danger of double dipping. Nat Neurosci 2009;12:535–40.
Kübler A, Nijboer F, Mellinger J, Vaughan TM, Pawelzik H, Schalk G, et al. Patientswith ALS can use sensorimotor rhythms to operate a brain–computer interface.Neurology 2005;64:1775–7.
Langhorne P, Coupar F, Pollock A. Motor recovery after stroke: a systematic review.Lancet Neurol 2009;8:741–54.
Liao LD, Chen CY, Wang IJ, Chen SF, Li SY, Chen B, et al. Gaming control using awearable and wireless EEG- based brain–computer interface device with noveldry foam-based sensors. J Neuroeng Rehabil 2012;9:5.
Please cite this article in press as: Zich C et al. Wireless EEG with individualized(2014), http://dx.doi.org/10.1016/j.clinph.2014.07.007
Lou B, Hong B, Gao X, Gao S. Bipolar electrode selection for a motor imagery basedbrain–computer interface. J Neural Eng 2008;5:342–9.
Malouin F, Richards CL, Durand A, Doyon J. Clinical assessment of motor imageryafter stroke. Neurorehabil Neural Repair 2007a;22:330–40. http://dx.doi.org/10.1177/1545968307313499.
Malouin F, Richards CL, Jackson PL, Lafleur MF, Durand A, Doyon J. The kinestheticand visual imagery questionnaire (KVIQ) for assessing motor imagery inpersons with physical disabilities: a reliability and construct validity study. JNeurol Phys Ther 2007b;31:20–9.
McFarland DJ, Miner LA, Vaughan TM, Wolpaw JR. Mu and beta rhythmtopographies during motor imagery and actual movements. Brain Topogr2000;12:177–86.
McFarland DJ, Sarnacki WA, Wolpaw JR. Electroencephalographic (EEG) control ofthree-dimensional movement. J Neural Eng 2010;7:252–9.
Millán JR, Renkens F, Mouriño J, Gerstner W. Brain-actuated interaction. Artif Intell2004;159:241–59.
Müller-Gerking J, Pfurtscheller G, Flyvbjerg H. Designing optimal spatial filters forsingle-trial EEG classification in a movement task. Electroenceph ClinNeurophysiol 1999;110:787–98.
Naeem M, Brunner C, Pfurtscheller G. Dimensionality reduction and channelselection of motor imagery electroencephalographic data. Comput IntellNeurosci 2009;1:1–8.
Neuper C, Scherer R, Reiner M, Pfurtscheller G. Imagery of motor actions:differential effects of kinesthetic and visual–motor mode of imagery in single-trial EEG. Cognitive Brain Res 2005;25:668–77.
Neuper C, Scherer R, Wriessnegger S, Pfurtscheller G. Motor imagery and actionobservation: Modulation of sensorimotor brain rhythms during mental controlof a brain–computer interface. Clin Neurophysiol 2009;120:239–47.
Neuper C, Schlögl A, Pfurtscheller G. Enhancement of left-right sensorimotor EEGdifferences during feedback-regulated motor imagery. Electroenceph ClinNeurophysiol 1999;16:373–82.
Oldfield RC. The assessment and analysis of handedness: the Edinburgh inventory.Neuropsychologia 1971;9:97–113.
Ono T, Kimura A, Ushiba J. Daily training with realistic visual feedback improvesreproducibility of event-related desynchronisation following hand motorimagery. Clin Neurophysiol 2013;124:1779–86.
Ortner R, Irimia DC, Scharinger J, Guger C. A motor imagery based brain–computerinterface for stroke rehabilitation. Stud Health Technol Inform2012;181:319–23.
Pfurtscheller G, Aranibar A. Evaluation of event-related desynchronization (ERD)preceding and following voluntary self-paced movement. Electroenceph clinNeurophysiol 1979;46:138–46.
Pfurtscheller G, Brunner C, Schlögl A, Lopes da Silva FH. Mu rhythm(de)synchronization and EEG single-trial classification of different motorimagery tasks. Neuroimage 2006;31:153–9.
Pfurtscheller G, Lopes da Silva GH. Event-related EEG/MEG synchronization anddesynchronization: basic principles. Electroenceph Clin Neurophysiol1999;110:1842–57.
Pfurtscheller G, Neuper C. Motor imagery and direct brain–computercommunication. Proc IEEE 2001;89:1123–34.
Pfurtscheller G, Neuper C, Flotzinger D, Pregenzer M. EEG-based discriminationbetween imagination of right and left hand movement. Electroenceph clinNeurophysiol 1997;103:642–51.
Popescu F, Fazli S, Badower Y, Blankertz B, Müller KR. Single trial classification ofmotor imagination using 6 dry EEG electrodes. PLoS One 2007;2:e637.
Prasad G, Herman P, Coyle D, McDonough S, Crosbie J. Applying a brain–computerinterface to support motor imagery practice in people with stroke for upperlimb recovery: a feasibility study. J Neuroeng Rehabil 2010;7:60.
Ramoser H, Müller-Gerking J, Pfurtscheller G. Optimal spatial filtering of singletrial EEG during imagined hand movement. IEEE Trans Rehabil Eng 2000;8:441–6.
Randhawa B, Harris S, Boyd LA. The kinesthetic and visual imagery questionnaire isa reliable tool for individuals with Parkinson disease. J Neurol Phys Ther2010;34:161–7.
Renard Y, Lotte F, Gibert G, Congedo M, Maby E, Delannoy V, et al. OpenViBE: anopen-source software platform to design, test, and use brain–computerinterfaces in real and virtual environments. Presence 2010;19:35–53.
Royer AS, Doud AJ, Rose ML, He B. EEG control of a virtual helicopter in 3-dimensional space using intelligent control strategies. IEEE Trans Neural SystRehabil Eng 2010;18:581–9.
Schröder M, Bogdan M, Hinterberger T, Birbaumer N. Automated EEG featureselection for brain computer interfaces. In: Proceedings of the 1st internationalIEEE EMBS conference on neural engineering. Capri Island, 2003. p. 626–629.
Schröder M, Lal TN, Hinterberger T, Bogdan M, Hill NJ, Birbaumer N, et al. RobustEEG channel selection across subjects for brain–computer interfaces. EURASIPJASP 2005;2005:3103–12.
Schuster C, Hilfiker R, Amft O, Scheidhauer A, Andrews B, Butler J, et al. Best practicefor motor imagery: a systematic literature review on motor imagery trainingelements in five different disciplines. BMC Med 2011;9:75. <http://www.biomedcentral.com/1741-7015/9/75>.
Schuster C, Lussi A, Wirth B, Ettlin T. Two assessments to evaluate imagery ability:translation, test–retest reliability and concurrent validity of the German KVIQand Imaprax. BMC Med Res Methodol 2012;12:127. <http://www.biomedcentral.com/1471-2288/12/127>.
Sellers EW, Vaughan TM, Wolpaw JR. A brain–computer interface for long-termindependent home use. Amyotroph Lateral Scler 2010;11:449–55.
channel layout enables efficient motor imagery training. Clin Neurophysiol

C. Zich et al. / Clinical Neurophysiology xxx (2014) xxx–xxx 13
Shenoy P, Krauledat M, Blankertz B, Rao RPN, Müller KR. Towards adaptiveclassification for BCI. J Neural Eng 2006;3. http://dx.doi.org/10.1088/1741-2560/3/1/R02.
Takeuchi N, Izumi S. Maladaptive plasticity for motor recovery after stroke:mechanisms and approaches. Neural Plast 2012;2012:359728.
Viola FC, Thorne JD, Edmonds B, Schneider T, Eichele T, Debener S. Semi-automaticidentification of independent components representing EEG artifact. ClinNeurophysiol 2009;120:868–77.
Viola FC, De Vos M, Hine J, Sandmann P, Bleeck S, Eyles S, et al. Semi-automaticattenuation of cochlear implat artifacts for the evaluation of late auditoryevoked potentials. Hear Res 2012;284:6–15.
Wang Y, Hong B, Gao X, Gao S. Phase synchrony measurement in motor cortex forclassifying single-trial EEG during motor imagery. In: engineering in medicineand biology society 2006–28th annual international conference of the IEEE.New York, 2006. p. 75–78.
Please cite this article in press as: Zich C et al. Wireless EEG with individualized(2014), http://dx.doi.org/10.1016/j.clinph.2014.07.007
Wang Y, Hong B, Gao X, Gao S. Design of electrode layout for motor imagery basedbrain–computer interface. Electron Lett 2007a;43:557–8.
Wang Y, Hong B, Gao X, Gao S. Implementation of a brain–computer interface basedon three states of motor imagery. In: Engineering in medicine and biologysociety, 2007–29th annual international conference of the IEEE. Lyon; 2007b. p.5059–62.
Wang Y, Wang YT, Jung TP. Translation of EEG spatial filters from resting to motorimagery using independent component analysis. PLoS One 2012;7:e37665.
Wolpaw JR, Birbaumer N, McFarland DJ, Pfurtscheller G, Vaughan TM. Brain–computer interfaces for communication and control. Clin Neurophysiol2002;113:767–91.
Wolpaw JR, McFarland DJ. Control of a two-dimensional movement signal by anoninvasive brain–computer interface in humans. Proc Natl Acad Sci USA2004;101:17849–54.
channel layout enables efficient motor imagery training. Clin Neurophysiol