
veterinary - journal - CiteSeerX
98
THE JOURNAL OF THE AUSTRALIAN VETERINARY ASSOCIATION LTD ACN 008 522 852 ISSN 0005-0423 JANUARY/FEBRUARY 2003 VOLUME 81 Nos 1 & 2 Australian VETERINARY JOURNAL • Canberra fires bring out AVA spirit • AVA’s new CEO, Margaret Conley • Three honoured on Australia Day • AVA/Pfizer Practices of Excellence • Nominations called for AVA Board • Canine Hyperadrenocorticism • Mosquito borne viruses of horses • Ovine footrot • Bovine pregnancy detection • Mating behaviour in alpacas • Sciatic nerve tumours in dogs
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of veterinary - journal - CiteSeerX
THE JOURNAL OF
THE AUSTRALIAN
VETERINARY
ASSOCIATION LTD
ACN 008 522 852 ISSN 0005-0423
JANUARY/FEBRUARY 2003 VOLUME 81 Nos 1 & 2
Australian
VETERINARYJOURNAL
• Canberra fires bring out AVA spirit• AVA’s new CEO, Margaret Conley• Three honoured on Australia Day• AVA/Pfizer Practices of Excellence• Nominations called for AVA Board• Canine Hyperadrenocorticism• Mosquito borne viruses of horses • Ovine footrot• Bovine pregnancy detection• Mating behaviour in alpacas• Sciatic nerve tumours in dogs

AVA family pulls together after Canberra firestorm ................... 5
PetPEP competition winners are all smiles ................................. 6
Three vets named in Australia Day honours .............................. 6
AVA Members HR Advisory Service reports on first year .......... 8
CSIRO researchers moot antibiotics alternative for poultry ..... 10
DPI’s VetMed CD offers data on registered medicines ............ 10
Era passes with death of Dr Will Chamberlin ......................... 10
Notice of 2003 Annual General Meeting ................................ 10
A message from AVA’s new CEO, Margaret Conley ................ 11
AVA boosts national marketing and communications .............. 11
Report: Codex committee confers in Adelaide ......................... 12
VIEWPOINTJo Toia ...................................................................................... 13
AVA/Pfizer Vet Practices of Excellence profiled ........................ 14
Online resource gives latest on treatment of wounds ............... 14......................................................................................................Media Update: AVA’s communications this month .................. 15
Exotic Animal Diseases Bulletin .............................................. 16
WORLDWATCHGardner Murray ....................................................................... 18
Tributes flow upon retirement of Dr Lyndal Scott ................... 18
Cairns 2003 – the social agenda .............................................. 19
NSW launches campaign to reduce feral pig numbers ............. 19
Nominations invited for two Board positions .......................... 19
Letters to the Editor ................................................................ 22
Ex-WVA chief Jim Edwards wins NZ award for service .......... 24
VIEWPOINTS IN CANINE HYPERADRENOCORTICISM
Diagnosis of hyperadrenocorticism in the dogJA Braddock ...............................................................................25
Ultrasonographical examination in canine hyperadrenocorticismKL Hoffmann.............................................................................27
Medical treatment of hyperadrenocorticism in the dogJA Braddock ...............................................................................31
Surgery in the treatment of canine hyperadrenocorticism -1. AdrenalectomyJ Culvenor ..................................................................................34
Surgery in the treatment of hyperadrenocorticism -2. HypophysectomyGB Hunt....................................................................................35
ARTICLES
Cytological examination and physical characteristics of the analsacs in 17 clinically normal dogsDC Robson, GG Burton, MF Lorimer .........................................36
Diagnosis of sciatic nerve tumour in two dogs byelectromyography and magnetic resonance imagingLA Abraham, RW Mitten, C Beck, JA Charlesand SA Holloway ........................................................................42
A severe hepatic disorder with myelodysplastic syndrome,treated with cytarabine ocfosfate in a dogK Ide, Y Monoi, M Minegishi, M Sekiguchi, K Konno,and T Iwasaki ............................................................................47
Transposition of first digital pad for reconstruction of apalmar antebrachial soft tissue defect in a catSM Fearnside and RC Straw .......................................................50
BOOK REVIEWSSkin Diseases of the Dog ..............................................................41
Skin Diseases of the Cat...............................................................41
Alternative Pets from Budgies and Yabbies to Rabbits and Rats ......54
Mechanisms of Disease: A Textbook of Comparative GeneralPathology....................................................................................54
Veterinary Microbiology and Microbial Disease ............................55
Hand-Rearing Wild and Domestic Mammals ...............................55
Equine Dentistry.........................................................................55
EDITORIAL
West Nile virus revisited and other mosquito borne virusesof horses in AustraliaMJ Studdert ............................................................................. 56
ORIGINAL ARTICLES
Failure to eradicate ovine footrot associated with Dichelobacternodosus strain A198 by repeated daily footbathing in zincsulphate with surfactantPD Jelinek and LJ Depiazzi ........................................................58
Accuracy of bovine pregnancy detection using transrectalultrasonography at 28 to 35 days after inseminationDP Nation, J Malmo, GM Davis and KL Macmillan ..................63
S C I E N T I F I C
C L I N I C A L
N E W S
Volume 81 Nos.1 & 2 January/February 2003
C O N T E N T S
Australian
VETERINARYJOURNAL

Aust Vet J Vol 81, Nos 1 & 2, January, February 20034
News
Trial introduction of the Willis dropped ovary technique forspaying cattle in northern AustraliaTF Jubb, G Fordyce, MJ Bolam, DJ Hadden, NJ Cooper,TR Whyte, LA Fitzpatrick, F Hill and MJ D’Occhio....................66
Specificity of absorbed ELISA and agar gel immuno-diffusiontests for paratuberculosis in goats with observations aboutuse of these tests in infected goats RJ Whittington, GJ Eamens and DV Cousins ...............................71
Polymerase chain reaction tests for the identification of RossRiver, Kunjin and Murray Valley encephalitis virus infectionsin horsesMJ Studdert, JK Azuolas, JR Vasey, RA Hall, N Ficorilliand J-A Huang ...........................................................................76
Echinococcus granulosus in wildlife in and around theKosciuszko National Park, south-eastern AustraliaDJ Jenkins and B Morris .............................................................81
Effects of mating behaviour and the ovarian follicular state offemale alpacas on conceptionJL Vaughan, KL Macmillan, GA Anderson and MJ D’Occhio.......86
Prevalence of caseous lymphadenitis and usage of caseouslymphadenitis vaccines in sheep flocksMW Paton, SB Walker, IR Rose, and GF Watt .............................91
SHORT CONTRIBUTION
Infectious coryza due to Haemophilus paragallinarum serovarB in ChinaP-J Zhang, M Miao, H Sun, Y Gong and PJ Blackall ..................96
Graduates in Veterinary Science 2002 .................................... 85
Acknowledgment of referees .....................................................98
Statistical Guidelines for Authors .............................................99
Instructions for Authors .........................................................100
BOOK REVIEWS
Parasitic Diseases of Wild Mammals.............................................80
ABSTRACTS FROM OTHER JOURNALS
Principles of ethical decision-making in veterinary practice .......46
Revalidation and virtual patients: a vision of the future?............53
Examination of the horse with colic: is it medical or surgical? ..53
The dynamics, prevalence and impact of nematode infectionsin organically raised sheep in Sweden ........................................57
Polysaccharide storage myopathy in the M longissimus lumborumof showjumpers and dressage horses with back pain ..................95
The use and abuse of Aesculapian authority in veterinarymedicine ....................................................................................97
WOULD YOU RECOMMEND YOUR INSURER TO A COLLEAGUE?
In a recent client survey, 98.8% of respondents said they would recommend Guild Insurance.
Guild Insurance in conjunction with the Australian Veterinary Association, has developed an insurance program specifically tailored for veterinarians.
With 40 years experience in providing quality insurance services to healthcare professionals around Australia, Guild Insurance is renowned for delivering an unparalleled level of customer service to it's clients.
Veterinarians can benefit from Guild's unique product features which include:Combined Professional Indemnity, Public and Products Liability cover.Full accidental damage cover and replacement cost cover on your building and business contents.Full value burglary cover and automatic flood cover.A national 24 hour Freecall emergency service.
For further information Freecall 1800 810 213 or visit www.guildifs.com.au
Guild Insurance Limited ABN 55004 538 863Your association may receive a referral fee for any insurance you take out with Guild Insurance.

5
News
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Bushfires in Canberra on the weekendof January 18-19 turned into adevastating firestorm that left four
people dead, 300 people injured, anddestroyed more than 500 houses.Hundreds of horses, and thousands ofsheep and wildlife were killed in one of themost damaging fires seen in Australia sincethe Ash Wednesday fires of 1983, or theBlack Tuesday fires of 1967.Although, thankfully, the loss of humanlife was much less than some previousconflagrations, the death toll amonganimals was immense. In NSW alone, thefires claimed 5,300 sheep and 40 cattle,plus uncounted numbers of wild animals.One of the most heartbreaking losses of alloccurred when the Weston Woden AnimalHospital (also known as the ACT AnimalHospital and Clinic) was burned down.Given thirty minutes to get out, the twovets and two nurses at the hospital movedthe animals from the fibro stables to theapparently more robust besser-blockhospital, on the natural assumption thatthis would be safer. The fire arrived in lessthan 15 minutes and burnt out thehospital building killing all 48 animals –but left the stables intact. The AVA Benevolent Fund was quickly intouch with the Hospital’s vets, and DrRandall Lemin, a local practitioner andChairperson of the Fund offered themconsulting rooms at his nearby clinic. DrLemin received many offers from AVAmembers of equipment to help. When arequest for a consulting table was broadcastnationally by AVA, it was swiftly fulfilled.Six days after the fire struck, severalhundred people attended a memorialservice for all animals that had died onJanuary 18, and in particular for thoseanimals lost at Weston Woden AnimalHospital. This ceremony brought togetherveterinarians, animal owners – manybereaved – supporters and sympatheticbystanders in an atmosphere mixed withsadness, sympathy, hope and mutualsupport. Bouquets of flowers were laid atthe site of the Hospital, and during theservice a dozen homing pigeons werereleased. Veterinary supplies company (and AVAsponsor) Provet swung into action early inthe piece to do whatever it could to assistCanberra’s vets in the immediate aftermathof the bushfires. Tony Thelander and
Robert Menrath from Provet contacted theAVA with regard to setting up a system tocollect resources for ACT practitioners, asthey felt there could be many people withinjured pets, or wildlife, needingtreatment. Provet mobilised its branches ascollection centres for any donations ofpharmaceuticals or supplies, aiming totransport these to the ACT from theircentres in Wagga and Sydney. AVA ACTDivision secretary Dr Michael Haywardacted as the AVA contact point for thendistributing the material from there. DrHayward said that many offers ofassistance were received, from theVeterinary Science Foundation at theUniversity of Sydney, as well as from AVANational and Provet. On behalf of the AVA, Dr Hayward also
notified the RSPCA in Canberra that AVAvets in the ACT were available to assistwith companion animals or with injuredwildlife. (The RSPCA itself lost itsadministrative offices in the fires.) AVAvets also acted swiftly to assist in treatingsome of the many sheep that were burntand distressed by the fires.Sadly, AVA member Dr Tim Buick, whoworks for AFFA, lost his home inChapman when the fires struck. The AVABenevolent Fund moved to do what itcould to help Dr Buick.AVA President Dr Jo Toia expressed herappreciation to everyone who helped, andin particular to the members of ACTDivision who stepped in so quickly and soeffectively at this tragic time (Viewpoint,page 13).
Canberra fires see AVAvets pull together
ABOVE: Some of thecages in which animals atWeston Woden AnimalHospital died, with atreatment bench andanaesthetic machine in theleft foreground, andoperating table in thebackground.(Photo courtesy of Dr. M.Hayward)
LEFT: Mourners gather atthe memorial service foranimals killed by the firesat Weston Woden AnimalHospital (Photo courtesyof Dr. P. Boland).

Aust Vet J Vol 81, Nos 1 & 2, January, February 20036
News
MANAGING EDITOR STEVE IRELAND
SCIENTIFIC EDITORCOLIN WILKS
CLINICAL EDITORMAUREEN REVINGTON
DESIGNNEWS MANAGEMENT
NATIONAL ADVERTISING MANAGERTONKIN MEDIA
PROFESSIONAL ADVERTISEMENTS CO-ORDINATOR
ANGELA JACKSON
BOARD MEMBER RESPONSIBLE FOR PUBLICATIONS
JOANNE SILLINCE
AUSTRALIAN VETERINARY ASSOCIATION
CHIEF EXECUTIVE OFFICERMARGARET CONLEY
AVA BOARDPRESIDENT JO TOIA, VICE-PRESIDENT
ROBERT BAKER, PRESIDENT-ELECT JO SILLINCE, BOARD MEMBERS NORM BLACKMAN, DAVID LOVELL,
MALCOLM MCLENNAN, BOB RHEINBERGER, LYNDY SCOTTAND DIANE SHEEHAN.
The Australian Veterinary Journal (AVJ) is the official journal of theAustralian Veterinary Association. It is produced each month and isdistributed to members of the AVA and to subscribers. The publisher,The Australian Veterinary Association, does not hold itself responsiblefor the statements made in the AVJ. Unless so stated, material in theAVJ does not reflect the endorsement, official attitude or position of theAustralian Veterinary Association or the Editors. Advertisers areresponsible for complying with the Trade Practices Act 1974, asamended.
CONTRIBUTIONSNews and general correspondenceNews items and general correspondence should be submitted to theManaging Editor, AVA House, 134-136 Hampden Rd, Artarmon NSW2064, Australia or PO Box 371 Artarmon NSW 1570 Australia.Telephone (02) 9411 2733, fax (02) 9411 5089, [email protected] Web address www.ava.com.au
Scientific sectionArticles for the Scientific Reports section of the AVJ shouldbe submitted to The Scientific Editor, AVA House, 272 BrunswickRoad, Brunswick Victoria 3056. Telephone (03) 9387 2982,fax (03) 9388 0112, email [email protected]
Clinical section:Articles for the Clinical Section should be submitted to The Editor,Clinical Section, AVA House, 272 Brunswick Rd, Brunswick Victoria3056. Telephone (03) 9387 2982, fax (03) 9388 0112, [email protected]
Non-member subscriptionsNon-members pay $341 (incl GST) a year for subscription to the AVJ.Contact Debbie Dresner at the AVA National Office.
AdvertisingSydney: Tonkin Media, PO Box 101, Avoca Beach NSW 2251, telephone (02) 4385 1746, fax (02) 4385 2017.
Australian
VETERINARYJOURNAL
This month’s coverphotograph shows Shabani,a six year old WesternLowlands male Gorilla(Gorilla gorilla gorilla).Shabani was cooling off atSydney’s Taronga Zoo on 8January 2003, during thecity’s extremely warmweather. (AAP Image/MickTsikas).
Three distinguished veterinarians –Percy Sykes, John Aubrey andTrevor Heath – were honoured in
this year’s Australia Day honours list.Sydney veterinarian Dr Percy Sykes wasnamed a Member of the Order of Australia(AM), his citation reading: “For service toveterinary science, particularly equinehealth, and to the thoroughbredhorseracing industry.”Dr John Aubrey, of Mundingburra in
Queensland, received the Medal of theOrder of Australia (OAM) for “service toveterinary science, and to the communityof Townsville”.Fellow Queenslander, Emeritus ProfessorTrevor Heath, also was awarded the Medalof the Order of Australia. Professor Heath’scitation noted his “service to the veterinaryprofession, particularly as an educator,mentor and administrator”.
Australia Day Honours for three vets
The AVA’s PetPEP program has hadamazing growth over the past fewyears, with growing support from
many fields such as the RSPCA, DPI andlocal councils.As an AVA initiative, the veterinaryindustry’s financial and in-kind supportis highly regarded and certainly veryhighly valued. All AVA members wouldrecently have received their membershiprenewal for 2003. As members would
probably be aware, PetPEP is featured onthe renewal form with a $20 VoluntaryLevy Box.Last year, PetPEP had its largest evernumber of voluntary levy contributionsto date (almost 1600 nationally) and theteam is hoping to beat this record thisyear.Please show your support by activelyticking the $20 PetPEP box, and thankyou for supporting an extremelyworthwhile program.
A PetPEP message: support for 2003
Cody Lee (12), Steven Piper (8),and Maddison Kraus (6) – thethree primary school students
who won the Australian VeterinaryAssociation’s PetPEP ‘Me and My Pet’National Schools Competition – posewith AVA President Jo Toia, celebrity vetDr Katrina Warren and her dog Toby,and the whole PetPEP team from aroundAustralia. The lunch was held at the Centennial
Parklands Restaurant in Sydney onDecember 9, and was attended by thethree winners, members of the winners’families, AVA Board members, sponsors,local and national media, and PetPEPand AVA staff.The AVA launched the ‘Me and My Pet’competition during Pet Week inNovember as its biggest-ever campaignto generate awareness of responsibleanimal ownership among school children
across Australia. Almost 8,000 primary schoolsreceived a Competition Kit, whichinvited students to submit a drawing,poem or short story entitled ‘Caringfor My Favourite Pet’, and nearly10,000 students from all over thecountry took part in the competition.Local veterinarians from aroundAustralia participated in thecompetition by offering their time forpromotion, judging and presentationof Certificates of Merit to participants.
PetPEP competition winners all smiles
Aust Vet J Vol 81, Nos 1 & 2, January, February 20038
News
By Michelle Gilliver-Smith*
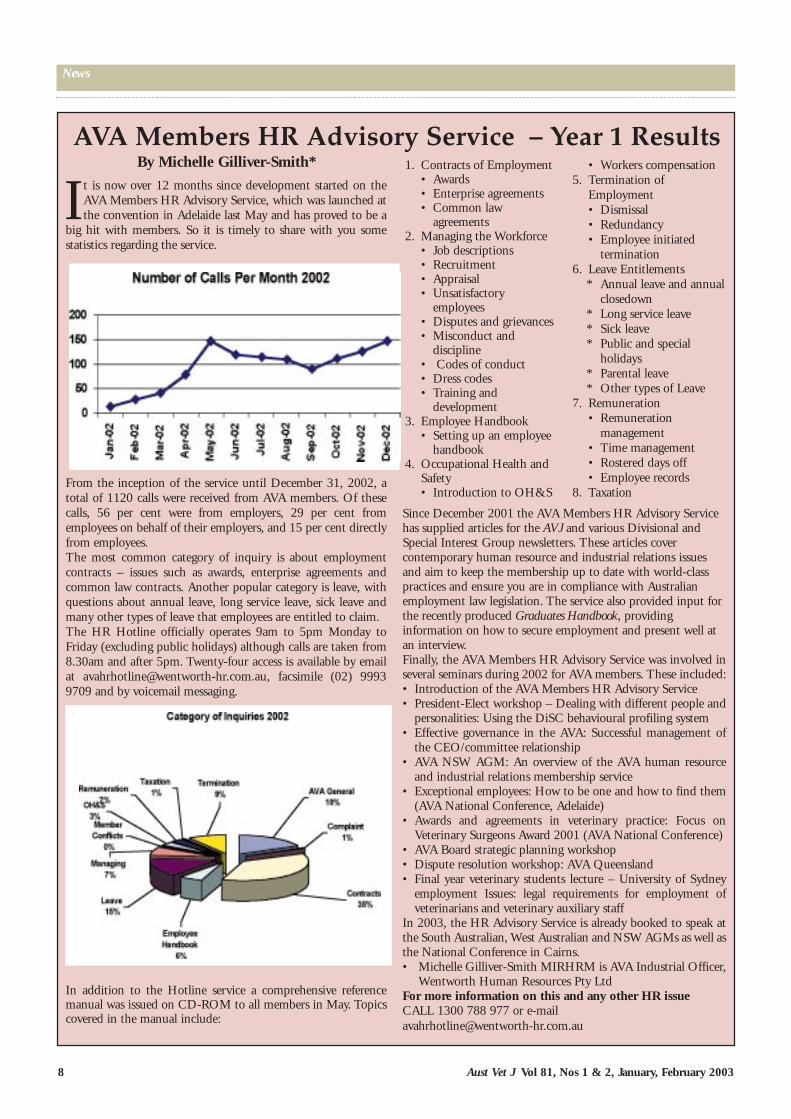
It is now over 12 months since development started on theAVA Members HR Advisory Service, which was launched atthe convention in Adelaide last May and has proved to be a
big hit with members. So it is timely to share with you somestatistics regarding the service.
From the inception of the service until December 31, 2002, atotal of 1120 calls were received from AVA members. Of thesecalls, 56 per cent were from employers, 29 per cent fromemployees on behalf of their employers, and 15 per cent directlyfrom employees.The most common category of inquiry is about employmentcontracts – issues such as awards, enterprise agreements andcommon law contracts. Another popular category is leave, withquestions about annual leave, long service leave, sick leave andmany other types of leave that employees are entitled to claim. The HR Hotline officially operates 9am to 5pm Monday toFriday (excluding public holidays) although calls are taken from8.30am and after 5pm. Twenty-four access is available by emailat [email protected], facsimile (02) 99939709 and by voicemail messaging.
In addition to the Hotline service a comprehensive referencemanual was issued on CD-ROM to all members in May. Topicscovered in the manual include:
AVA Members HR Advisory Service – Year 1 Results1. Contracts of Employment
• Awards• Enterprise agreements• Common law
agreements2. Managing the Workforce
• Job descriptions• Recruitment• Appraisal• Unsatisfactory
employees• Disputes and grievances• Misconduct and
discipline• Codes of conduct• Dress codes• Training and
development3. Employee Handbook
• Setting up an employeehandbook
4. Occupational Health andSafety• Introduction to OH&S
• Workers compensation5. Termination of
Employment• Dismissal• Redundancy• Employee initiated
termination6. Leave Entitlements
* Annual leave and annualclosedown
* Long service leave* Sick leave* Public and special
holidays* Parental leave* Other types of Leave
7. Remuneration• Remuneration
management• Time management• Rostered days off• Employee records
8. Taxation
Since December 2001 the AVA Members HR Advisory Servicehas supplied articles for the AVJ and various Divisional andSpecial Interest Group newsletters. These articles covercontemporary human resource and industrial relations issuesand aim to keep the membership up to date with world-classpractices and ensure you are in compliance with Australianemployment law legislation. The service also provided input forthe recently produced Graduates Handbook, providinginformation on how to secure employment and present well atan interview.Finally, the AVA Members HR Advisory Service was involved inseveral seminars during 2002 for AVA members. These included:• Introduction of the AVA Members HR Advisory Service• President-Elect workshop – Dealing with different people and
personalities: Using the DiSC behavioural profiling system• Effective governance in the AVA: Successful management of
the CEO/committee relationship• AVA NSW AGM: An overview of the AVA human resource
and industrial relations membership service• Exceptional employees: How to be one and how to find them
(AVA National Conference, Adelaide)• Awards and agreements in veterinary practice: Focus on
Veterinary Surgeons Award 2001 (AVA National Conference)• AVA Board strategic planning workshop• Dispute resolution workshop: AVA Queensland• Final year veterinary students lecture – University of Sydney
employment Issues: legal requirements for employment ofveterinarians and veterinary auxiliary staff
In 2003, the HR Advisory Service is already booked to speak atthe South Australian, West Australian and NSW AGMs as well asthe National Conference in Cairns.• Michelle Gilliver-Smith MIRHRM is AVA Industrial Officer,
Wentworth Human Resources Pty LtdFor more information on this and any other HR issueCALL 1300 788 977 or e-mail [email protected]

BOARD OF DIRECTORS NOMINATIONSNOMINATIONS are invited for the following positions on the Board of Directors ofThe AVA Ltd to take office in May 2003.• President-elect to take office as President in 2004.• One Director to take office for a three year term.
Who may nominate?In accordance with Article 68(7) of the Articles of Association, any ordinary member, fellow, life member,life fellow, retired member or retired fellow of the Association may be nominated for election to the offices,provided that some other member proposing the candidate does so at least 60 days before the annual generalmeeting of the Association.
Nominations may be made in writing on the form below. A citation not exceeding 100 words must accompanythe nomination. The citation should provide information that will indicate to the members that the candidatehas the skills and qualities required to lead and serve the profession for the next three years. This citation willbe printed on the ballot papers. A passport size colour photograph should also accompany your nominationform.
Postal ballotA postal ballot for each position will (if necessary) be conducted and nominations together with a citation foreach candidate will be mailed to all eligible voting members at least 21 days before the annual generalmeeting.
Nomination for election of Directors of The AVA Ltd2003-04.Part AProposer
I, ...................................................................................................................................................... (full name)
(signature) ......................................................................... of ................................................. (AVA Division)
wish to nominate .............................................................................................................................. (nominee)for election to the AVA Board of Directors for the position of:-(a) President-elect(b) Director on the BoardPlease delete any position/s not nominated for this election.
Part BCandidate
I, ...................................................................................................................................................... (full name)
of ........................................................................................................................................................................
............................................................................................................................................................. (address)
accept nomination for the position/s of .............................................................................................................
.......................................................................................................................................................... (signature)
Nominations should reach the Chief Executive Officer by no later than Friday, 7 March 2003, PO Box371, Artarmon, NSW, 1570, Fax (02) 9411 5089.
Nominees will be notified of receipt of their nomination in writing. If you have not receivednotification of the receipt of your nomination by the closing date, please contact the CompanySecretary on (02) 9411 2733.
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 9
Aust Vet J Vol 81, Nos 1 & 2, January, February 200310
News
Era passes with death ofWill Chamberlin
Dr Will Chamberlin, the AVA’s oldestmember, passed away peacefully onSunday 19 January. He was 102
years old. Born on 22 October 1900 in Malvern,Victoria, Dr Chamberlin earned his BVScdegree at Melbourne University in the late1920’s, and an MVSc degree in 1931. Afterworking at the Veterinary Research Station,Glenfield, under Dr HR Seddon, he movedto Launceston in 1933 as VeterinaryPathologist and CSIR research officer,before commencing private practice inLaunceston in 1937. Returning in his early60’s to Victoria, he subsequently practiseduntil the age of 80.A life member of the AVA, Dr Chamberlinwas involved with the AVA since the 1920s,holding office in three states and beinginstrumental in the resurrection of theTasmanian division in 1933. He was alsoinvolved in the early stages of successfulprograms to eradicate two diseases of publichealth significance – brucellosis andhydatids. A formal obituary is in preparation for theAVJ.
The 80th Annual GeneralMeeting of the AVA will beconducted on Wednesday, 28
May 2003 at the AVA NationalConference in Cairns.Members who wish to submitagenda items should send these inwriting to the Company Secretary,Lauretta Stace, at the NationalOffice by Friday, 14 February. A
formal notice of the AGM and thebusiness to be conducted will beissued to members in April.Following is a list of DivisionalAGMs: Tasmania (1-2 March),South Australia (15-16 March), NT(16 March), Queensland (21-23March), ACT (22-23 March), NSW(2-3 May), Victoria (TBA) andWestern Australia (TBA).
Cytokines promise alternative to antibiotics for poultry
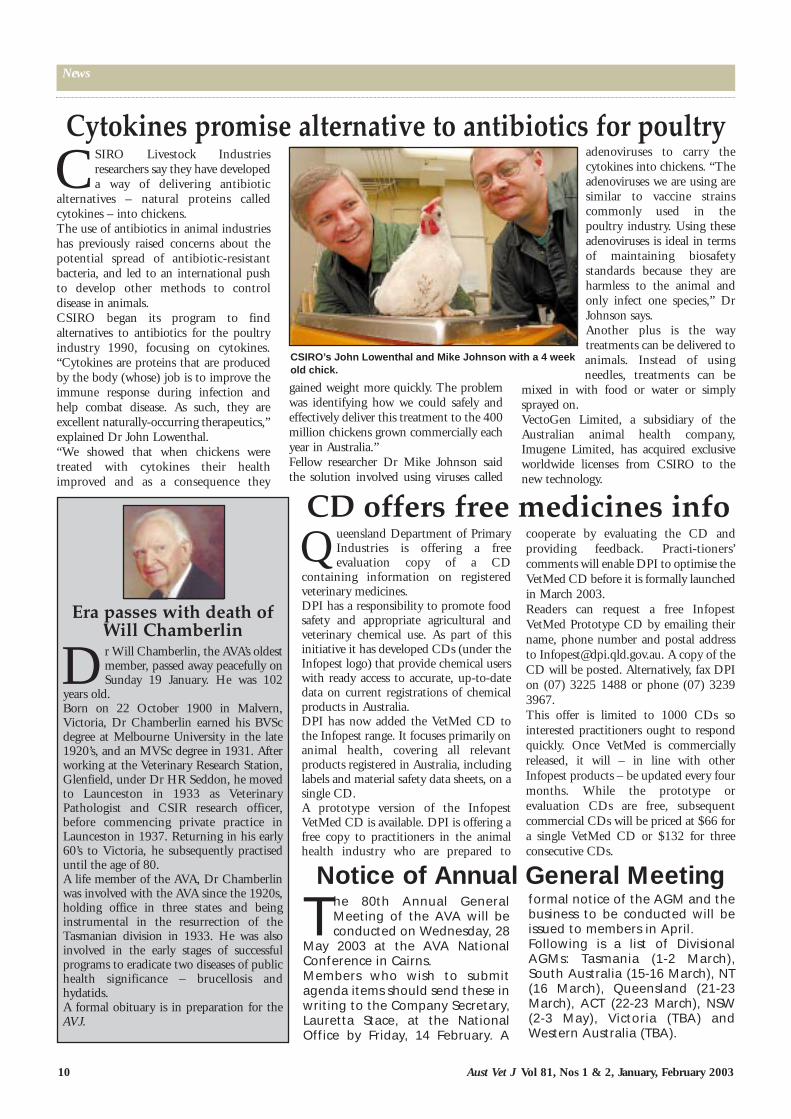
CSIRO Livestock Industriesresearchers say they have developeda way of delivering antibiotic
alternatives – natural proteins calledcytokines – into chickens.The use of antibiotics in animal industrieshas previously raised concerns about thepotential spread of antibiotic-resistantbacteria, and led to an international pushto develop other methods to controldisease in animals.CSIRO began its program to findalternatives to antibiotics for the poultryindustry 1990, focusing on cytokines.“Cytokines are proteins that are producedby the body (whose) job is to improve theimmune response during infection andhelp combat disease. As such, they areexcellent naturally-occurring therapeutics,”explained Dr John Lowenthal.“We showed that when chickens weretreated with cytokines their healthimproved and as a consequence they
gained weight more quickly. The problemwas identifying how we could safely andeffectively deliver this treatment to the 400million chickens grown commercially eachyear in Australia.”Fellow researcher Dr Mike Johnson saidthe solution involved using viruses called
adenoviruses to carry thecytokines into chickens. “Theadenoviruses we are using aresimilar to vaccine strainscommonly used in thepoultry industry. Using theseadenoviruses is ideal in termsof maintaining biosafetystandards because they areharmless to the animal andonly infect one species,” DrJohnson says.Another plus is the waytreatments can be delivered toanimals. Instead of usingneedles, treatments can be
mixed in with food or water or simplysprayed on.VectoGen Limited, a subsidiary of theAustralian animal health company,Imugene Limited, has acquired exclusiveworldwide licenses from CSIRO to thenew technology.
CSIRO’s John Lowenthal and Mike Johnson with a 4 weekold chick.
Queensland Department of PrimaryIndustries is offering a freeevaluation copy of a CD
containing information on registeredveterinary medicines.DPI has a responsibility to promote foodsafety and appropriate agricultural andveterinary chemical use. As part of thisinitiative it has developed CDs (under theInfopest logo) that provide chemical userswith ready access to accurate, up-to-datedata on current registrations of chemicalproducts in Australia.DPI has now added the VetMed CD tothe Infopest range. It focuses primarily onanimal health, covering all relevantproducts registered in Australia, includinglabels and material safety data sheets, on asingle CD.A prototype version of the InfopestVetMed CD is available. DPI is offering afree copy to practitioners in the animalhealth industry who are prepared to
cooperate by evaluating the CD andproviding feedback. Practi-tioners’comments will enable DPI to optimise theVetMed CD before it is formally launchedin March 2003.Readers can request a free InfopestVetMed Prototype CD by emailing theirname, phone number and postal addressto [email protected]. A copy of theCD will be posted. Alternatively, fax DPIon (07) 3225 1488 or phone (07) 32393967. This offer is limited to 1000 CDs sointerested practitioners ought to respondquickly. Once VetMed is commerciallyreleased, it will – in line with otherInfopest products – be updated every fourmonths. While the prototype orevaluation CDs are free, subsequentcommercial CDs will be priced at $66 fora single VetMed CD or $132 for threeconsecutive CDs.
CD offers free medicines info
Notice of Annual General Meeting
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 11
News
Since I took up the position ofyour Chief Executive Officerjust three weeks ago I have
reflected on my good fortune tonow be a part of this organisation.I have previously worked inradiography, small business,association management andpublic health policy roles andthought public health interestswere diverse, but I am fastlearning that veterinarians’interests are even more diverse.My focus will be to realise theobjectives of the strategic planand in particular to retain and expand membership. I also have apassion for improving AVA’s public profile, exploring the forms ofcontinuing professional education (CPE) that can work for AVA,and building alliances within AVA and with other organisations.But first my role is to listen. One listening post will be the surveyof members and lapsed members and we expect that report to bewith us very soon. The other listening posts are the traditionalones - meeting you face to face, the phone (02 9411 2733) andthe email [email protected] look forward to hearing from you. ❞
Meet Margaret Conley,AVA’s new Chief Exec
New AVA CEO, MargaretConley
Eddie Ripard is the recentlyappointed National Market-ing and Communications
Manager for the AVA. With previous experience inmarketing and membershipmanagement capacities with severalmember-based organisations,including the UTS AlumniAssociation, the AustralianInstitute of Management and theInstitute of Chartered Accountantsin Australia, Eddie says there isgreat potential for the AVA to raiseits profile in the community.“I’ve only been here for two and ahalf weeks and it’s been hectic,” he said. “Amongst other things,we’ve commented in the media on two separate animal welfareissues, we’ve assisted ACT members and responded to theCanberra bushfire crisis, and together with Animal HealthAustralia we are about to launch the Protect Australian LivestockCampaign.“I have been very impressed with the concern and offers ofassistance that veterinarians have made to their fellow membersafter the Canberra fires. I look forward to harnessing this kindredspirit and raising the profile of the profession and the Associationin the general community.”
AVA marketing boostedwith new appointment
AVA’s new NationalMarketing andCommunications Manager,Eddie Ripard
❝

News
Aust Vet J Vol 81, Nos 1 & 2, January, February 200312
AVA’s National Veterinarian Dr Kevin Doyle recently attended the11th session of the Codex Committee on Food Import and ExportInspection and Certification Systems (CCFICS), on behalf of theAVA as representative of the World Veterinary Association. The work of the CCFICS is extremely important because Australiaexports a large proportion of its agricultural production, includinganimal production.World Veterinary Association participation on Codex Alimentariusand other international organisations, such as the OfficeInternational des Epizooties reflects the revamped mission androle of the WVA, recognising the fact that veterinarians participatein animal production and food safety at all levels: local, national,regional, and world. WVA takes part via representation throughthe veterinary association of the countries in which meetings areheld.Codex work on food standards is of value to Australia given theimportance of international harmonisation of rules for world trade.Food safety is of prime concern to veterinarians in practice and ininspection and certification at government and non-governmentlevels.The eleventh session of CCFICS met in Adelaide 2 - 6thDecember 2002. The Committee considered matters referredfrom the Executive Committee of the Codex AlimentariusCommission and other Codex committees. This committee ishosted by, and held in, Australia. Codex committees are hostedby countries throughout the world.
Major issues on the agenda included:1) Draft guidelines on the Judgement of Equivalence of Sanitary
Measures Associated with Food Inspection and CertificationSystems.
A drafting group led by New Zealand had prepared a revisedversion of the draft guidelines, which include guidance onpossible information to be provided for the establishment of anobjective basis of comparison of sanitary measures. The committee considered the draft and forwarded the guidelinesfor consideration at the 26th Section of the Codex AlimentariusCommission for final adoption.This issue is important because of the requirement that nationsaccept equivalent methods of inspection and certification underthe Sanitary and Phyto-sanitary Agreement of the World TradeOrganisation.
2) Draft Guidelines for the Utilisation and Promotion of QualityAssurance Systems to Meet Requirements in Relation toFood.
CCFICS considered proposed guidelines developed by a draftinggroup convened by Australia. The document is complementary tothe work being done by ISO in that it is primarily intended forgovernments while the ISO work is primarily directed towardsindustry. The document also emphasised the importance ofHACCP systems in quality assurance. The veterinarian plays apart in building in quality from inside the farm gate through themanufacturing process and inspection and certification to deliveryto the consumer. It was decided that further work on this topicwould be picked up in the context of Codex texts on GeneralPrinciples of Food Hygiene and HACCP; Principles for FoodImport and Export Inspection and Certification; and in theGuidelines for the Design Operation Assessment andAccreditation of Food Import and Export Inspection andCertification Systems.
3) Proposed Draft Revision of the Codex Guidelines for theExchange of Information in Food Control EmergencySituations.
Food emergencies must be managed by veterinarians and otherswho rely greatly on receipt of essential information. The guidelinesare in progress and will consider:
• Development of food emergency control plans • Difficulty in implementing risk management risk
communication practices• Need to expand risk communication including a framework for
feed back• Differences and similarities between importing and exporting
countries• Final disposition of food products including traceability and
third country exports• A revised version for food emergency situations.Australia will convene a drafting group to revise the text forconsideration at the next meeting of CCFICS.
4) Discussion Paper on the Judgement of Equivalence ofTechnical Regulations associated with Food Inspection andCertification Systems.
CCFICS considered a document prepared by a drafting group ledby Australia. The Committee decided that in view of the lack ofspecific or theoretical examples of trade that could be facilitatedby the application of equivalence and technical regulations thatthese matters could be best handled bilaterally. The workinggroup will revise the document in the light of extensive discussionand return it for the next meeting and broadcast a request forexamples of the problems. This also relates to the equivalenceprovision of SPS Agreement of the WTO.
5) Discussion Paper on Traceability in the Context of FoodInspection and Certification Systems.
The concept of traceability is being discussed generally by theExecutive Committee of the Codex Alimentarius Commission.Traceability is important as a risk management option for riskanalysis. The Committee considered a discussion paper preparedby Switzerland. It was noted that responsibility was shared withseveral Codex committees. It was decided that the working groupwould reconvene and consider the paper in the context of theextensive discussions held at the meeting.
Other WorkThe International Atomic Energy Agency (IAEA) informed thecommittee of the Revised Guidelines for Certification of Foodirradiated for non-phyto sanitary purposes developed by the jointFAO/WHO/IAEA International Consultative Group on FoodIrradiation would be on the consultative group’s web site shortly.CCFICS noted the comments of Consumers Internationalsuggesting development of three appendices or references toGuidelines on the Judgement of Equivalence of SanitaryMeasures Associated with Food Inspection and CertificationSystems, i.e. requirements for the submission of a request forjudgement for equivalence, terms for on-site visits by importingauthorities to verify inspection and certification systems andtechnical assistance to be provided by importing countries toexporting developing countries. This was noted because work isbeing done by FAO and WHO. This is important to in food safety,especially to Australia because the countries to which Australiaexports regularly visit to examine Australia’s inspection andcertification systems.
A report is provided to the World Veterinary Association which isplaced on its web site with due recognition of the work done bythe national association involved, i.e. AVA.
Dr Kevin DoyleNational Veterinarian
December 2002
Codex Alimentarius Committee on Food Import AndExport Inspection And Certification Systems
R E P O R TCodex committee confers in Adelaide

Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 13
News
There are no words that canadequately describe thedevastation of the fires that
ravaged Canberra with lives lost, morethan 500 homes destroyed (including thehome of a member of the AVA), extensivedamage to the RSPCA reception areas,and the loss of Woden Animal Hospital. Board member Lyndy Scott, ACTDivision members and AVA staff locatedin Canberra have kept us informed on theeffects of the fires and members requiringsupport. I applaud the ACT Division,particularly Michael Hayward and PatBoland, and members of the VeterinaryBenevolent Fund who have been tirelessin their efforts to assist those affected bythis disaster. The assistance from ACT veterinariansand members throughout Australia hasbeen outstanding. Within 24 hours therewere offers of equipment and resources to
practitioners in Canberra who may becalled on to care for injured pets, bothstrays and animals whose owners areunable to pay for their services.PROVET offered to collect and transport
donations of emergency supplies toCanberra, where Michael Hayward wasthe contact and distribution point forthese and other donations. Othermanufacturers and companies also offeredassistance and donations. With regard toassistance to Woden Animal Hospital,neighbouring practice Weston CreekVeterinary Hospital, through its principalRandall Lemin, offered the use ofconsulting rooms. There was also a floodof offers of equipment and resources toassist in re-establishment of the practice.Contact was made with the RSPCA todetermine areas of need and offerassistance where required. At this timethere were also a number of seriousbushfires in Victoria and Tasmania withhomes lost. At time of writing,communication with Division Presidentswas continuing to establish supportrequired in these areas.
AVA President Jo Toia
v i e w p o i n t
Fires bring out the real AVA spirit
New staff welcomed
The appointment of two new staffmembers was finalised in earlyDecember and both officially took up
duty on January 6. I have great pleasure inintroducing Margaret Conley as our newCEO while Eddie Ripard fills the newposition of Marketing and CommunicationsManager. Those involved at Division andSIG levels will already have received somecommunication from Eddie as he takes onthis challenging role. He joins us with animpressive background of qualificationsand experience in marketing andcommunications.Margaret Conley brings to the AVA a highlevel of skills and organisational management,having 13 years’ experience at CEO level inthe not-for-profit sector, including the AlliedHealth Professions Association which issimilar in structure to the AVA with adiversity of SIGS and branches. An addedstrength is Margaret’s experience in Canberraat Federal Government level and her insightinto government procedures and effectivelobbying.To say she hit the ground running would bean understatement, as she quickly came togrips with a range of issues in the first weekand rounded it off by attending theQueensland Division strategic planningweekend. Thank you, Queensland, forthe invitation to a valuable and productiveweekend for the Division and theAssociation.
Early January saw the finalisationof responses to the VeterinaryReview and draft recommen-
dations designed to strengthen ruralveterinary practice, its capability torespond to emergency diseaseoutbreaks and to perform surveillance.The AVA continues to press for theinclusion of a range of findings fromthe review which were not included inthe draft recommendations. Theseinclude:• adoption of the National Livestock
Identifications Scheme for traceback and forward
• research into new models of practiceand promotion of servicesveterinarians can provide, andproducer awareness thereof
• farm biosecurity issues and qualityassurance schemes such as Cattlecare
• establishment of the AustralianVeterinary Reserve to be clearlyidentified in the recommendationsand allocation of priority for
funding• postgraduate training in farm animal
production• national veterinary registration to
facilitate movement betweenjurisdictions in emergencies andwhere special skills are required
• endemic disease control andsurveillance (not all such activity isdirected to exotic or emergencydiseases)
• Australia needs to maintain a stronginfluence and input into OIEmatters, especially within the region,which is particularly importantbecause of our reliance oninternational trade
Thank you once again to all whocontributed to this response,particularly AVA National VeterinarianKevin Doyle and Vice-PresidentRobert Baker who collated theresponses and finalised the reply onbehalf of the AVA.
AVA presses Reviewto include its findings
Sad newsSadly the AVA’s oldest veterinarian, 102-year-old Will Chamberlin,passed away on January 19. Dr Chamberlin joined the AVA in the1920s and enjoyed a long and distinguished career. I wasprivileged to spend some time with him on his 102nd birthday.

Aust Vet J Vol 81, Nos 1 & 2, January, February 200314
News
Wounds resourceis an online first
An online resource thatgives healthcare providersthe latest information on
how to best manage patients withwounds was launched at MonashUniversity in December.The Online Wound CareProgram (at www.pharmace.vic.edu.au) issaid to be the first of its kind inAustralia and is freely available togeneral practitioners, veteri-narians, pharmacists, podiatrists,nurses and allied healthprofessionals who want to furtherdevelop their knowledge andskills in wound care.The program should benefitveterinarians who treat acute andchronic wounds in companionanimals and thoroughbred andexotic animals housed in zoosaround Australia.Dr Helen McCracken, seniorveterinarian with Zoos Victoria,said the wound managementprogram would help vets betterunderstand how to treat wounds,aiding wound healing andanimals’ return to function."Our zoo animals may be quicklyreturned to their family groupsand naturalistic displays, andinjured wildlife rapidly releasedback into the wild as a result ofapplying advanced woundmanagement techniques," shesaid.Content for the website wasdeveloped by the MonashWound Care Consortium whichinvolves Monash University, theWound Foundation of Australia,the National Ageing ResearchInstitute, the University ofMelbourne and La TrobeUniversity.Information on the websitecurrently covers wound healingand repair, phases of woundhealing and factors affectingwound healing. Over the nexttwo years information on woundassessment, wound products,management of burns, scars andacute and chronic wounds,dermatology and reconstructivesurgery will be added.
Clients – and pets – justlove to visit Karingal
AVA/Pfizer Practice of Excellencewinner Karingal Veterinary Hospital,50km south of Melbourne in the
bayside suburb of Frankston, opened its doorsin 1971.At first it operated from the original displayhome of the new Karingal housing estate butin September 2000 a purpose-built facilitywas completed, making it the biggestveterinary facility in Frankston and theMornington Peninsula. Initially a single-person mixedpractice, Karingal VeterinaryHospital has expanded to employfive full-time veterinarians and14 support staff (six full-timeand a part-time nurse, fivecasuals, an office manager and akennel hand). The hospital is now exclusively smallanimal, catering predominantly for dogs(61 per cent) and cats (29 per cent), with anincreasing number of exotic pets such asrabbits, guinea pigs and reptiles.Strong marketing and branding of thepractice, in addition to the hospital’s high-exposure location (on the corner of two busyroads, opposite a medium-sized shoppingcentre and well known fast food restaurant)has resulted in high growth over the past twoyears. As befits an ASAVA-accredited hospital,Karingal has high standards. It is wellequipped with ultrasound, endoscope,cryosurgery, in-house pathology, ICU ward,isolation ward, MedRex Vetscope, digitalcamera, infusion pumps, pulse oximetry,ECG and blood pressure monitoring. A DIYhydro bath is available as is a 24-houremergency service.
“The waiting room and reception area ishome to the hospital resident pets – green treefrogs, central bearded dragons and a children’spython,” said Pfizer territory manager SharonCini.“These provide a welcome distraction for theclients from the stress of being at the vet’s. Aphoto album in the waiting room entitled ‘ATrip To The Vet: A Dog’s Perspective’ hasmany photos of the hospital from a dog’s eye
view.”Karingal’s vision statement is “to
provide unequalled excellence ineducating, celebrating andpromoting the wealth in thehuman-animal-veterinarybond”. This vision is achievedthrough an effort to make every
visit to the hospital a positiveone. Customer service is ingrained
into the culture. Weekly customerservice meetings evaluate staff performanceand highlight potential improvements. Staffare recognised by peers for excellent customerservice. A set of standards of excellenceprovides the framework for how clients areserviced at the hospital. This handbook is adocument into which all staff have input.
Other ancillary services include PuppySchool, a weight loss clinic called Kilo Club,and wellness monitoring for animals on long-term medications or with chronic conditions.All discharged patients are fitted with abandanna.Each year Karingal raises money andpromotes national bandanna day by usingCanteen – Kids with Cancer bandannas. Amedical flavouring system allows greaterclient compliance when giving medications to
pets. A website atwww.kvh.com.au and amonthly e-mail newsletterinform clients of changes,offers and informationavailable at Karingal.Continuing staffeducation is promoted.Veterinarians regularlyattend conferences inAustralia, North Americaand Europe. Education ofclients is just asimportant. Staff areencouraged to showclients through thehospital and give theminsights into what thehospital can do for themand their pets.
Dr. Scott Tinson and staff of Karingal Veterinary Hospital with PfizerTerritory Manager Sharon Cini.
VET
PRACTICES OF EXCELLEN
CE

Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 15
News
AVA/Pfizer Practice of Excellence winner GuildfordVeterinary Hospital in the western suburbs of Sydneysums up its philosophy in the motto “health through
science and compassion”.Established more than 50 years ago, it is a four-veterinarian,small animal practice with four veterinary nurses, two kennelhands, a receptionist, office manager and three after-hours staff.One of Guildford’s most innovative ideas is a customer advisorycommittee. Vets wanted to know what their customers’expectations were so they could deliver what was wanted ratherthan what they thought was wanted. Staff are involved in selecting 10 clients to be invited to serve onthis committee for a year. Quarterly meetings are held over ameal to discuss what the practice does well and where it canimprove. One of the key findings has been not to restrictmembership to the “best” clients, as it is difficult to extractcriticism from happy customers.Staff training focuses on customer service, with softwareprograms to manage relationships and telephone technique usedas key tools. Customer service is a prominent discussion point atstaff meetings, as is rewarding employees. An underpinningprinciple is recognition that when staff are well treated this willreflect in the way they treat clients. Staff can deal with customercomplaints without reference to practice partners. They are alsoencouraged to attend conferences and drug company lectures. Community involvement is high, with participation in theannual Guildford Festival, sponsorship of Delta Dogs in localnursing homes, representation on the local council’s companionanimal advisory committee, and free treatment of guide dogs andwildlife.One of the practice partners has completed a graduate certificatein management, a small business management course at TAFE,and is a qualified workplace assessor. Pfizer territory managerBronwyn Viney said Guildford Veterinary Hospital always has awarm ambience that makes visitors feel welcome. “Although the clinic maintains an exceptional level ofprofessionalism it also manages to provide a relaxed atmosphere,”Bronwyn said. The clinic has always encouraged staff to excel.Caroline Outred last year received an Employers First employeeof the year award.
Guildford vets takea lead from clients
Dr Neil Hannan and Dr Deborah Neutze of Guildford VeterinaryHospital with Pfizer’s Bronwyn Viney
The AVA publicly en-dorsed the AustralianQuarantine Inspection
Service’s decision in January tosuspend livestock exports by aWest Australian-based com-pany until a comprehensivereview of its quality assuranceprogram was completed.“The AVA is pleased that thisdecision has been taken as wehave had concerns for sometime now about the state of thelivestock export industry”, saidAVA President Dr Jo Toia.On several occasions last year,the AVA expressed graveconcern to Minister forAgriculture, Fisheries andForestry, Warren Truss, aboutthe large number of cattle and
sheep deaths on export voyagesfrom Australia, Dr Toia noted:“In November we welcomedthe cancellation of anothercompany’s livestock exportlicence and it is encouraging tosee AQIS and the Ministermaintaining their hard line toprotect this billion-dollarindustry. However it isregrettable that it has taken thedeaths of thousands of sheepand cattle for animal health andwelfare to be improved.”“These changes havesignificantly improved animalwelfare,” Dr Toia concluded.“After last year’s tragedy the MVBecrux has made several voyageswith low mortality rates and weapplaud this improvement.”
AVA media releases in January
MEDIAUPDATE
Australians should takespecial care of their pets
during any Australia Dayfireworks displays in their localareas, according to an AVArelease sent to media outletsbefore the celebrations.President Dr Jo Toia, who wasinterviewed on the subjectseveral times, said the AVA wasa supporter of the Australia Daycelebrations and appreciatedthat fireworks displays are amajor part of many local events.But, she added, the AVA alsohad a role in alerting pet ownersto the best methods ofalleviating the fear and distresscaused to many animals by thesounds, smells and bursts ofbright light that fireworksproduce:“Our recommendation is thatpets be kept indoors in a safe,quiet place. Try to keep theanimals feeling secure andminimise the impact the
fireworks might have on them.Moving their regular beddinginside may help to minimiseproblems.”“If your animal is showing signsof severe stress - or has a historyof serious problems in theaftermath of fireworks displays -you might consider consultingyour veterinarian for specificadvice or treatment.”“We also need to give somestrong advice from our animalbehaviour experts - advice thatmay sound harsh or uncaring,but which is absolutely aimed atthe welfare of the animals.”“That advice is to move youranimal to a secure place andNOT to cuddle and pet youranimals while they exhibit signsof actual distress from thefireworks. And owners shouldjust talk normally and not talkunusually quietly to the animalin an effort to make it feel safe.”
January 24: AVA calls on pet owners to protectanimals during Australia Day fireworks
January 10: AVA applauds decision to suspendexporter’s livestock shipments

News
IMPORT RISK ANALYSIS FOR PSITTACINE BIRDS
An import risk analysis (IRA) is nearing completion for live psittacinebirds (members of the Order Psittaciformes, which includes parrotsand related species). In 1949, Australia banned imports of all birds andavian genetic material from all countries except New Zealand, and in1972 this was extended to include New Zealand. As a result ofconcerns with bird smuggling into Australia, and the associatedpotential for introducing exotic avian diseases, imports of live birdsrecommenced in 1990 under new protocols. However, a routine reviewof the live bird import program in the early 1990s raised someconcerns regarding the risk of introducing particular exotic diseases ofpsittacine birds. Imports of live psittacine birds were suspended in1995 in light of the incomplete knowledge and lack of definitivediagnostic methods for specific psittacine diseases.
The IRA was initiated in response to a number of factors. Aviculturalorganisations have been actively pursuing a review of importconditions to ease the current suspension of imports. Australiancustoms and quarantine officers continue to detect periodic attemptsto import psittacine birds or their eggs illegally, indicating that theincentive for smuggling still exists. Such illegal trade poses a very realexotic disease risk. The introduction of an exotic pathogen in importedpsittacine birds has the potential to affect not only the aviculturalindustry but also pet-bird owners, the commercial poultry industry,human health, native bird populations and the Australian environment.Allowing controlled imports of psittacine birds should decrease theincentive for smuggling.
In 1999, a technical issues paper for this IRA was released for publiccomment. The paper identified those diseases that are of potentialquarantine concern in relation to imports of psittacine birds, from anycountry, to Australia. Scientific data on several diseases of relevanceare very limited, reflecting their relatively recent recognition. Thescientific information contained in the issues paper was derived froma number of sources including peer-reviewed journals, a 1995 reviewby W.A. Snowdon, unpublished reports, and personal communicationwith relevant experts worldwide.
The issues paper concentrated on significant risks to animal healththat might be posed by imports of live psittacine birds. The aviandisease agents of concern include those Office International desEpizooties (OIE) List A and List B diseases of poultry and other birdsthat are exotic to Australia and that can be transmitted by psittacinebirds. In addition to the diseases listed by OIE, the paper considers anumber of other exotic diseases specific to psittacine birds that couldpose a risk to Australia’s large and unique psittacine population.
An expert Risk Analysis Panel was established to consider thediseases identified in the technical issues paper as posing a potentialrisk and to review stakeholders’ comments on the paper. The panelalso considered a number of other avian diseases raised bystakeholders as being of potential biosecurity significance. The finallist of diseases that are considered to be of concern and that requirefurther assessment includes:
* highly pathogenic avian influenza;* Newcastle disease;* avian paramyxovirus serogroups 2 and 3 (A/PMV 2 and A/PMV 3);* fowl typhoid (Salmonella Gallinarum);* pullorum disease (Salmonella Pullorum);* Salmonella Enteritidis;* Eastern, Western and Venezuelan equine viral encephalomyelitis;* West Nile virus;* Mycoplasma iowae;* Pacheco’s disease;* Amazon tracheitis;* budgerigar herpesvirus;* poxvirus infection in parrots;* reovirus infection in parrots;* internal papillomatous disease; and* psittacine proventricular dilatation syndrome.
The panel’s findings will be reported in the draft IRA, which should becompleted by March 2003. Possible risk management measures andtheir effect on the overall risk of introduction of exotic disease will beincluded in the draft IRA. Following consideration of stakeholders’comments received during a 60-day comment period, the panelshould be able to finalise the IRA. It is beyond the scope of the currentIRA to address either issues related to the Wildlife Protection(Regulation of Imports and Exports) Act 1982 or the potential risk ofimported psittacine birds establishing as feral pests.
A joint meeting between the panel developing the psittacine IRA anda panel developing an IRA for uncooked chicken meat is planned toensure a consistent approach. As a member of the World TradeOrganization and a signatory to the Agreement on the Application ofSanitary and Phytosanitary Measures (the SPS Agreement), Australiahas an obligation to ensure that quarantine conditions are are basedon sound science and are applied only to the extent necessary toprotect human, animal or plant life or health. The SPS Agreement alsorequires that import conditions applicable in one situation areconsistent with those applicable under other similar situations. This
Exotic Animal Diseases Bullet inJ a n u a r y / F e b r u a r y 2 0 0 3 N o . 8 3
The Exotic Animal Diseases Bulletin is produced by Agriculture, Fisheries and Forestry – Australia (AFFA). For details contact: Officeof the Chief Veterinary Officer; Agriculture, Fisheries and Forestry – Australia; GPO Box 858; Canberra ACT, 2601.
BSE causesvacuolation(spongiformchange) in thebrain (Source:AFFA)
The IRA aims toaddress issuesassociated withimporting livepsittacine birds(Source:BiosecurityAustralia)

Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 17
News
means that any conditions that may be developed for importingpsittacine birds should be consistent with conditions for imports ofother avian species or their products.
It was originally expected that the draft IRA would have been releasedsome time ago. However, the panel has devoted considerable time toa careful consideration of the methods for evaluating the pest anddisease risks, including both the release and exposure pathways. Thepanel has also focused on making sure the analysis is soundly basedand well-documented. The IRA follows the IRA Guidelines, a templatefor developing IRA reports established by Biosecurity Australia. Thepsittacine birds’ panel is one of the first groups to conduct an IRAusing this template, which is available online available fromBiosecurity Australia’s website (www.affa.gov.au/biosecurityaustralia –follow the links to ‘IRAs’ and then ‘review of IRA process’). Papersassociated with the IRA are also available from this website.
ANALYTICAL TESTS TO SUPPORT TSE PREVENTIVE MEASURES
Australia remains free of transmissible spongiform encephalopathies(TSEs) affecting animals, including bovine spongiform encephalopathy(BSE) and scrapie. This status protects animal health, public healthand export trade. It is supported by measures to prevent theintroduction of these diseases to Australia, and to prevent theirdissemination and amplification should they occur here. Thesemeasures were summarised in the Exotic Animal Diseases Bulletin No.76 (February 2001). An update on international developments onTSEs, including the spread of BSE to affect more European countriesand its occurrence in Japan, was also provided in the Exotic AnimalDiseases Bulletin No. 78 (November 2001).
This article highlights recent progress with analytical methods tosupport two key aspects of Australia’s animal TSE controls – rapidpost mortem TSE diagnostic tests used for disease surveillance and apolymerase chain reaction (PCR) test for detecting ruminantdeoxyribonucleic acid (DNA) in stockfeeds.
Rapid post mortem TSE tests
The National TSE Surveillance Program (NTSESP) is an active,targeted surveillance program introduced in 1998. It meets therequirements of the Office International des Epizooties (OIE)International Animal Health Code to test a minimum number ofsamples nationally for BSE and scrapie. For Australia, the number ofsamples required by the Code is a minimum of 400 cattle and 450sheep each year. The animals tested must meet specific casedefinitions related to neurological signs and age.
In recent years, a number of countries in Europe have adopted TSEsurveillance programs based on new rapid BSE post mortem tests onlarge numbers of samples from livestock sub-populations consideredto be of higher TSE-risk (i.e. slaughtered cattle over 30 months old,emergency slaughter animals, and dead-on-farm animals). InAustralia, a national working group reviewed three new rapid BSE postmortem tests that had been approved for use in the European Union(EU) in July 1999. It recommended that the Prionics(r) CheckImmunoblot test, which is a modified Western blot test, be trialledunder Australian conditions to assess its suitability for possible use forsurveillance or other testing purposes. This work was progressed as a
research and development (R&D) project at the CSIRO AustralianAnimal Health Laboratory (AAHL) at Geelong.
Staff from AAHL were trained in test methodology at the mainPrionics’ laboratory in Switzerland. Field staff from the AustralianQuarantine and Inspection Service and the Victorian Department ofNatural Resources and Environment were also trained in collectingbrainstem samples using a modified spoon inserted through theforamen magnum. A total of 2400 tests were conducted in a field trialon targeted sub-populations of cattle and sheep such as aged dairycattle, knackery cattle, emergency slaughter or suspect cattle andaged sheep. Bos indicus cattle were also specifically selectedbecause this test had previously only been validated for use on Bostaurus stock. The trial yielded negative results for all tests conducted,provided valuable additional surveillance data, and validated the useof the test under Australian conditions.
Japan has recently commenced screening all cattle at slaughter usingother approved rapid BSE tests – the Enfer(r) and Biorad Platelia(r) tests,which are both based on enzyme-linked immunosorbant assay (ELISA)technology. As a result, R&D funding is also being used for AAHL toacquire the capability to perform these rapid screening tests. NewZealand, the United States and Canada have also recently announcedrapid screening programs to increase the number of animals tested forTSEs above their existing programs, which are designed to meet therequirements of the OIE Code. Some European countries have alsosignificantly increased testing of adult sheep and goats.
Future R&D work in Australia could focus on improving the design andexpanding the scope of the surveillance program using rapid TSE postmortem tests on livestock sub-populations such as dead-on-farm anddowner animals that have demonstrated a higher prevalence of TSEsoverseas. This would enhance Australia’s preparedness in the eventthat use of these rapid tests was required on a larger scale in thefuture. In addition, work could be undertaken to determine therequirements to transfer this technology from AAHL to State andTerritory veterinary laboratories at short notice if a larger number oftests were required.
This strategy should ensure that Australia has ready access to anappropriate range of analytical tests for animal TSEs. It should alsomake it easier to respond quickly to any changes to the TSEsurveillance requirements of the OIE International Animal Health Codeor to changes in conditions imposed by countries that importAustralian livestock and livestock products.
PCR test for ruminant DNA in stockfeeds
Australia has in place a legislated ban on the feeding to ruminants ofmeat-and-bone meal derived from all vertebrates, including fish andbirds. This acts as a failsafe control measure to rule out the possibilitythat supplementary feeding of ruminants could amplify the BSE agentif it were to occur in Australia.
The Australian Government Analytical Laboratories (AGAL) havedeveloped and validated a polymerase chain reaction (PCR) test todetect small amounts of ruminant DNA in stockfeeds. A trial thatexamined the usefulness of this test under field conditions was recentlycompleted. The trial established that the PCR test could be used as aconfirmatory test to support regulatory audits of domestic stockfeedmanufacturers. Biosecurity Australia has recently released a policy touse the PCR test on imported plant-based stockfeeds at port-of-entry,to test them for contamination with animal materials. This test shouldform one part of a comprehensive, risk-based approach to ensuringcompliance with the ruminant feed ban in Australia.
However, further R&D work is needed to evaluate a more cost-efficient, rapid screening test for animal material in stockfeed thatwould compliment the confirmatory PCR test. Additional work is alsoneeded to assess the effect of permitted animal-derived stockfeedingredients such as tallow, gelatin and milk powder on screening andconfirmatory tests.
There will be a need to continue to modify preventive and surveillancemeasures for animal TSEs in light of ongoing scientific developments,such as new diagnostic tests and a better understanding of theepidemiology of TSEs, to ensure that Australia remains free of thesediseases.
Exotic Animal Diseases Bullet inJ a n u a r y / F e b r u a r y 2 0 0 3 N o . 8 3
AAHL laboratory technician preparing a specimen for TSEtesting (Source: CSIRO Livestock Industries)

Aust Vet J Vol 81, Nos 1 & 2, January, February 200318
News
Drought feeding raisesresidues concerns
SAFEMEAT – a partnership between the Australian meat andlivestock industry, the Commonwealth Government andState/Territory governments – recognises that during the
drought, alternative and novel feedstuffs are being used to keep stockalive. The risk is that some of these feeds may have been treated withpesticides, which could lead to concerns with residues of agriculturalchemicals in livestock above regulatory limits.A recent publicity campaign has urged livestock producers to adoptsafe practices when sourcing fodder, especially when feed is scarce.Products such as cotton trash and other feedstuffs treated withagricultural chemicals, particularly in the period leading up to harvest,should be avoided as sources of drought feed. As a general precaution,producers should request details of the chemical residue status offodder by asking the seller to provide a commodity vendordeclaration. They should also ensure that withholding periods are met
if livestock graze the stubble ofcrops treated with agriculturalchemicals.SAFEMEAT recently reaffirmedits position against feeding plantbyproducts or waste to livestock,particularly if the crop was likelyto have been treated with achemical that carried a labeldirection prohibiting its use in oron feed. Given the severe drought,SAFEMEAT has implemented amanagement strategy to mitigateany associated potential risks ofchemical residues to the cattle andsheep industries. The strategyincludes additional random
background residue testing of carcasses and increased audits ofnational vendor declarations provided for cattle at sale to ensure thataccurate statements are provided on chemical residue risk.
Links with Europe
In November last year I provided debriefing on Australia’s foot-and-mouth disease (FMD) simulation (Exercise Minotaur) in Brusselsfor representatives of member States of the European Union and
their respective industries. Trevor Roche, from EmergencyManagement Australia’s training institute at Mount Macedon, alsooutlined the design and execution of the simulation, and its place innational emergency preparedness operations. We also gained someinsight into the way Europe is responding to the risk of FMD.In late December, Neil Tweddle returned to Agriculture, Fisheries andForestry – Australia after spending six months with the Department ofEnvironment, Food and Rural Affairs (DEFRA) in the UnitedKingdom. DEFRA requested the secondment to provide independentinput to a range of emergency animal disease contingency planningissues it is addressing following the 2001 FMD epidemic. Neilprovided high-level policy advice on a range of issues related to diseasepreparedness and response, including compensation, cost-sharingarrangements and movement controls. He also assisted with a reviewof the FMD International Vaccine Bank. This secondment reflects anincreasing trend towards international collaboration on animal healthmatters.
World Watch
Commonwealth ChiefVeterinary OfficerGardner Murray
At the recent November Dinner Meeting of theCentral Branch of the AVA’s Victorian Division,colleagues noted the retirement of Dr Lyndal Scott
from being the first person to hold the position of AnimalWelfare Officer at the University of Melbourne. BranchPresident Dr Andrew Turner paid warm tribute to Dr Scottas follows:“It would be difficult to find an individual who has donemore to advance laboratory animal science and welfare inMelbourne than Lyn Scott.Lyn’s involvement with research commenced at RoyalMelbourne Hospital in 1964/65. This experience wasinvaluable for her teaching position at Footscray TAFEwhere she was employed (1975-1986) soon after newtraining courses for animal technicians were established in1973 by TAFE in Victoria. Lyn played an active role in thedevelopment of the Applied Science (Animal Technician)Certificate training course, contributing as Course Co-ordinator, Head of Study Area for all TAFE Animal BasedCourses in Victoria, and chief protagonist for a NationalCore Curriculum. She also served as Chairman of theIndustry Advisory Committee after her appointment to TheUniversity of Melbourne. Lyn was the first Animal WelfareOfficer appointed to the University of Melbourne (1986)and the second in the State – the other universities soonfollowed.As a pioneer in animal welfare in a major research institutionLyn was the ideal person to undertake the major shifts inattitude required to conform to the legislation and indeedrecognise that good animal welfare is good science. Who elsecould take on those university dinosaurs and win. Herconfidence, conviction and charm enabled this to happen.As well, Lyn possessed good political instincts – absolutelyessential in the university environment.Lyn has maintained an optimistic and enthusiastic approachto her work. This has resulted in numerous useful teachingitems - her anaesthetic video still has the best view ofendotracheal intubation, and the animated diagrams musthave driven the educational technology buffs crazy! Thesuccess of this production lead to Careful how you hold mevideos 1 and 2 (1986/7) - starring Lyn’s dog modellingeuthanasia (a university best seller) - and later the CD (2000)by the same name. Lyn also edited and contributed toMouse Management - A Practical Guide to the Care ofLaboratory Mice (1991), provided the major portion of thepublication on Alternatives to the Use of Animal inUndergraduate Teaching in Australia and NZ (1993) andproduced a suppliers Register for the laboratory animalindustry. Lyn’s energy in organising people has benefited Melbournewith speakers, conferences, seminars, articles, and trainingprograms to promote laboratory animal science and welfare.She has been highly visible in ANZCCART, ANZLAS, AVA(both AVERT and Central Branch, Vic Div) and the AATA,serving terms as president of each of the last three.Her generosity in supporting animal technicians, animalhouse managers and veterinarians involved in the field arelegend. Many have benefited by Lyn’s mentoring. All those involved in laboratory animal science have beenenriched by her work and her many colleagues wish her along, happy and fruitful retirement.
Tributes flow on retirementof Victoria’s Dr Lyndal Scott

Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 19
News
A truly portable, rugged wideview sector system for pregnancy detection in cattle
FREEPHONE 1800 001 599www.bcfultrasound.co.nzemail: [email protected] Sheffield Crescent, Christchurch, NZ
Providing the solutions you require in animal diagnostic ultrasound
DuoscanNSW’s WesternDivision LandsProtection Boards has
begun a million dollar controlcampaign aimed at significantlyreducing feral pig and foxpopulations. The programstarted on December 16 andinvolves the strategiccoordination of aerial shooting,baiting and trapping programsacross the Western Division ofNSW.“The Boards are takingadvantage of the currentdrought conditions which haveforced pests to congregate inareas with access to feed andwater,” said Minister forAgriculture Richard Amery.“In collaboration with NSW
Agriculture, Western DivisionBoards have prepared detailedcontrol programs that integratewith current local and regionalpest control strategies carriedout by landholders and the
National Parks and WildlifeService.”“Feral pig and fox distributionand densities will be monitoredthroughout the campaign toassess the effectiveness andefficiency of the programsimplements.”Amery noted that pest animalscontributed significantly tostock predation, compete withlivestock and native animalspecies for water and food, andcan potentially host and spreadendemic and exotic diseases.At its 2002 AnnualConference, the AVA called fora national program to containand ultimately eradicate feralpigs for precisely these reasons.Meanwhile in WA, the StateGovernment has set up a panelto review current methods ofcontrolling the increasingnumbers of wild dogs, with aview to seeing whether anychanges are needed.
NSW commences campaignto reduce feral pig numbers
Nominations are invited for thefollowing positions on the Board ofDirectors of AVA Ltd to take office in
May 2003:• President-Elect to take office as President
in 2004• One Director to take office for a three-
year termCLOSING DATE FOR NOMINATIONS IS
FRIDAY, 7 MARCH 2003 AT 5 PM.Notes for candidatesA citation not exceeding 100 words and apassport-size colour photograph shouldaccompany your nomination form. Thenomination form can be found in thisedition of the AVJ and is also available fromthe AVA National Office or the AVA website.The citation will be printed on the ballotpapers.Nominees should also start preparing their300-word “why you should vote for me”statements to maximise their chances ofsuccess. These statements, along withphotographs of candidates, will bepublished in the April edition of the AVJ toassist members in casting their votes.These statements should be submitted tothe Managing Editor of the AVJ at the AVANational Office by the close of nominations.
Nominations soughtfor Board positions
There will be a plethora of touring,sporting and cultural oppor-tunities available to delegates to
the AVA’s Annual Conference in Cairns,25-30 May.Delegates who arrive early will have thechance to take a trip out to the Reef,which is being organised for Sunday, 24thMay. More detail on the reef trip willfollow in the conference Handbook.The Cairns ‘Welcome’ will be hostedwithin the Industry Exhibit in theConvention Centre on the Sundayevening commencing at 6.30pm. Thiswill be a time to “refresh & refocus” at theend of the day.The Tuesday evening dinner will be at theTjapukai Aboriginal Cultural Park wheredelegates will enter a magical, mysticalworld. The entire park has been dedicatedto preserving and presenting authenticAboriginal culture with the aid of themost modern technology. This promisesto be a wonderful night’s entertainment.A conference golf day is planned forWednesday at one of the region’s most
renowned resort courses, Paradise Palms.Set amongst the rainforest, the views arespectacular and the course is magnificent.The AVA Annual Conference Dinner willbe held on Thursday evening at theCairns Convention Centre. Many of theSIG’s will host separate social functionsduring the course of the week. Moredetail on these will be available in theconference Handbook.Accompanying guests are most welcomeat the conference. A hospitality loungewill be set up to act as a meeting area forguests wishing to go on the many daytours on offer in the region. For just$93.50, accompanying guests can registerand receive unlimited access to theIndustry Exhibit area over the week.** Early Bird Registration **If you register early for Cairns 2003 thenyou will be placed in a draw with achance to WIN a return airfare to Cairnsfrom Brisbane, Sydney, Melbourne orAdelaide!Early Bird closes 21 March 2003.Register now!
Cairns 2003 – the social side

Aust Vet J Vol 81, Nos 1 & 2, January, February 200322
News
In 1985, the Australian Small Animal Veterinary Association(ASAVA) established the Australian Companion Animal Health
Foundation as a charitable research trust of the AVA. ACAHFfunds scientific research at universities into the clinical diseases ofcompanion animals. It is one of the few institutions funding thistype of research and depends entirely upon donations fromveterinarians and members of the public for supportAVA members, it is your foundation and it is your help that makesits work possible. Each year we ask members of the AVA to makea voluntary donation to several charities when they make theirannual subscription. Last year members contributed only $2752 tothe ACAHF. I know members can do a lot better and have givenmore generously in the past. On the subscription form there are three main AVA charities toconsider: ACAHF, the Benevolent Fund, and now the AVAAnimal Welfare Trust. I support them all and all are worthy of yoursupport. If each AVA member gave $20 to each charity this wouldboost the funds available by at least $80,000 per charity per year.This is not a lot to ask and would help a great deal. If funds aretight, I am sure members can all afford to donate something to atleast one of these charities each year.Please consider these worthwhile causes seriously. This is a way ofmaking your AVA work for you. Donations to the ACAHF arefully tax-deductible and your gift could help to fund valuableresearch in universities and keep veterinary skills here in Australia.
Roger ClarkeChairman
ASAVA Companion Animal Health Foundation Trust
Dr Ben David’s December AVJ letter (Aust Vet J 80 12 p738)sounds like sour grapes. He opposes all hunting activities
with the usual transparent and faded distortions of facts andemotive language that is no longer acceptable in an educatedworld.Unless Dr Ben David has participated in a particular type of
hunting he is not in a position to objectively criticise what he callsthis “barbaric activity”. How hypocritical. That he is ill-informedis patently obvious. Fishing is undeniably a form of hunting, andwhen we kill and bleed a fish for food it is no less of a blood sportthan hunting mammals, yet he condones fishing. Consider beinghauled up from five fathoms with a hook through your cheek. Isthat really humane?However, it is undeniably thrilling to have a hard-fighting fish ona rod and line, hence its general popularity. And so what is wrongwith owning a gun to kill animals? It is all permitted under Statelegislation so AVA must in essence endorse such activity. Also theAVA has nothing to hide in this and is not accountable just toschoolteachers, who as a whole are among the worst informedpublic groups when it comes to hunting.Being shot and instantly dead while grazing in a meadow is not acruel death. Here the thrill for the hunter is in the approach andnot the kill. All those people out there who pay someone else tokill their meat unwittingly subject their victim to the trauma of atrip to and through an abattoir. How humane is that? And for thevegans out there, how many of you wear leather shoes? Get real.There is nothing wrong with hunting if it is conducted properly.Most hunters are responsible people, just as fishermen are, as Onnalready admits. I have put my money where my mouth is andgiven up 13 years of spare time to hunter education because it wasneeded. As a veterinarian I must be concerned about the humaneaspects of hunting.
Hunting is an age-old traditional activity of Europeans as wellindigenous people. Hunting is about the acquisition of the preyspecies, followed by its conversion to food. Such game meats areoften only obtainable this way and are thus seen as prized fooditems. Shooting for pest or population control is highly selectivewhen compared with other control measures such as poisoning,and is the most cost-effective alternative. Some of these pests areutilised for food, the showcase being the NSW kangarooharvesting program which is a multi-million dollar export industryrun on internationally recognised humane principles. The AVAhad input into the shooter protocol.The new Game Council will address ALL the concerns that OnnBen David has and AVA will get the chance to control andmonitor policy on welfare and hunting within this body. Thehunters themselves have everything at stake, so are continually andceaselessly working to rid hunting of the irresponsible minorityand has made enormous progress. Consider the introduction ofthe waterfowl identification test as an example. Only thosededicated enough to do so sat for this test, the marking standardsof which are very severe. Shooter behaviour improved dramaticallyand the number of licensed duck hunters was reduced to thosewho cared about their traditional activities.It is because the AVA has such notable people as Dr Tony Englishon their Policy Council that AVA policies do not get hijacked bythe Onn Ben Davids for their own private agendas.
Dr Matt DraismaWarragul, West Gippsland, VIC
The problem of excessive or nuisance barking will be presentedto veterinarians in small animal practice on a regular basis.
The time constraints placed on practitioners can make it temptingto reach for a quick fix for owners who are distressed about thisissue. While electronic devices for barking dogs may reduce therisk of the dog being debarked, I believe there are more humane,effective and long-lasting treatments available. The reasons for barking are many and varied. Attempting to useone treatment plan for an excessive barker could be compared tousing the same plan for any vomiting dog. For instance, the use oftechniques that punish barking are of major concern if applied todogs that bark due to, say, separation anxiety. While it may stopthe barking, it does nothing to address the underlying cause.Punishing this group of barkers is likely to make the problemworse and must raise concerns about the welfare of the dog.Veterinarians need to educate clients that merely reducing barkingis not always a successful outcome. We need to take the time to
Editor’s note: The AVJ welcomes letters from members inall areas of the profession on matters of importance to you.Please keep them brief - to meet our space constraints.Letters will be subject to minimal editing procedures.Subject to letters complying with the AVJ’s legalresponsibilities, they will not be censored. Nor willindividuals or groups waging ‘campaigns’ be permitted toabuse these pages. If submitting a letter intended forpublication, kindly identify it as such. Letters to the Editorcan be sent by mail, fax or e-mail at the contact pointslisted at the start of the News Section. Writers may use apseudonym to protect their identities - but must supply theEditor with verifiable names and points of contact.
L e t t e r s

Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 23
News
gather a proper history and devise an individual treatment plan inthe best interests of the dog, as well as the client. It is important tolook beyond the bark to the welfare of the dog.Dr Perkins (Aust Vet J 80 11 p670) suggests that veterinarians
should not perform debarking before recommending an electronicno-bark collar. In my opinion, no veterinarian should reach for anelectronic no-bark collar without exploring less aversive methodoptions first.
Dr Debbie CalnonBehaviour Counselling Service
Melbourne VIC
Iwish to comment on the AVA draft policy for use of behaviourmodifying collars (Aust Vet J 80 11 p660). I have used both the
citronella and electronic collars. I have found the electronic collarsfar superior in terms of results, reliability, price and humaneness. Iam therefore surprised at the policy relegating electronic collars foruse only as an alternative to euthanasia, and recommending theuse of citronella collars.It is common for working breeds to beat the citronella bark controlcollar, and working breeds are most commonly the problembarkers. Typically, the citronella bark control collar works for up totwo weeks. Then the working dog learns it can simply bark untilthe citronella runs out, resulting in more barking. I believe theylearn this relatively easily because, once squirted with citronella,they don’t care how many times they are squirted. The electroniccollar is not prone to this failure because the stimulus is equallyaversive each time it is applied. Also, it is designed for use whenthe owner is not home because it does not run out of stimulatingsubstance.I also believe citronella collars operate by socially humiliating the
dog. Scent is a dog’s primary sense. That dogs loathe to smell niceby human standards is legendary. We all know the first thing anyself-respecting dog does after a shampoo is seek the foulestsmelling substance to roll in. Dogs prefer to be perfumed with analgland secretion, the most repugnant of all odours by humanstandards. Humans like the smell of citronella and consider it abenign substance; Not so from a canine viewpoint. To smell ofcitronella is the equivalent of making a dog look bad to its friends.It is humiliating and this form of punishment is outdated. I shall lupomorphise (make people into dogs) to illustrate. Inanother world, where people are kept as pets (see “The CultureClash”, by Jean Donaldson) and owners think anal gland secretionis benign and sweet smelling, people are squirted in the face withanal gland secretion for talking too much. Which would youconsider more humane, if you were a pet on the planet Gorn? Tobe squirted in the face with anal gland secretion, or given a mildstatic discharge just like pulling a jumper over your head on a dryday? I am concerned that the draft policy reflects anthropomorphicstandards in recommending citronella as a benign substance over amild static discharge, since citronella is benign to humans but notto dogs. Furthermore it is an irrational human fear of a mild staticdischarge driving the anti-electronic collar campaign. Dogs do notshare this irrational fear. Let the AVA present a scientific andrational policy. The current draft policy lacks objectivity and needsto be redrawn.
Dr Jacqueline PerkinsGood Dog Vet and Training Solutions
Brisbane QLD
Regarding my own experience with electronic collars, Ipurchased a golden retriever pup and attempted to train her
with the usual techniques I’ve used on previous dogs successfully.I had only limited success with her. When I let her off the lead shewould only reluctantly respond. I was advised to get an electroniccollar. I was reluctant to use and only used it in desperation afterwatching the video instructions with the help of two grandsons.Within half an hour and using the lowest voltage of the fourstrengths only twice the dog was beautifully obedient.Occasionally I have had to use the button, which makes noise onlyto warn the dog that if she doesn’t obey she will get a shock. If Ihad not used the collar I have no doubt I would still have adisobedient dog, or no dog at all. I think it is about time the AVAtook a practical stance against the bleeding hearts. Next thing theywill ban electric fences for cattle and horses.The law since March 1, 2002, has us muzzling pig dogs. Pig dogsare trained to only chase feral pigs, and if they are no good at thisthey are used as pets or guard dogs, and if unsuitable for any ofthese purposes are put down. A big proportion of the freezer boxexport pig trade to Europe (a $30 million export earner) is caughtby unmuzzled pig dogs. Why doesn’t the AVA take a video of aboar pig waiting beside a ewe lambing, and the pig then eating thelamb alive, and show that on TV? On the local common here inTownsville, ground nesting birds are disappearing because the wildpig population is in plague proportions, eating the eggs and younghatchlings. The 1080 poisoning and trapping campaigns are notworking. When – not if – foot and mouth disease gets here we canonly imagine how devastating it will be with feral pigs acting as theperfect carriers.The law also has local anaesthetic for beasts over six months forcastrating. It was proven years ago that the beast suffers muchmore distress while being held down for a local anaesthetic,waiting for it to work, than two swift cuts.It will be very hard to get the politicians to act as the would-be do-gooders have the balance of power. But we should at least try to getback to practical solutions to these problems.
Dr John Aubrey OAMMundingburra QLD
Many Australian veterinarians have recently temporarilydeparted Australia for the United Kingdom to work on the
foot and mouth project. Under advice from their UK accountants,some have established private companies through which theyprovided services via local veterinary clinics. Typically, it appears,the veterinarians then received a fairly nominal salary from theirown company which was largely non-taxable in the UK.The additional monies required to live on were taken by the vetsfrom their companies as dividends throughout the year, suchdividend income not being taxable to them individually in the UKafter credits were allowed to them for the tax paid by the companyon the profits giving rise to the dividends (at a lower rate than theywould otherwise have paid if they had received the professionalincome personally).The concern here is that most vets who are born and educated inAustralia, and plan to return to Australia to live and work after asojourn in the UK, will be deemed to be residents of Australia fortax purposes, including during the period abroad.Broadly, Australian tax residents are taxed on their worldwide
incomes, with the notable exception under S.23 AG of the Income
L e t t e r s

Aust Vet J Vol 81, Nos 1 & 2, January, February 200324
News
Tax Assessment Act (1936) only applying to salary received over acontinuous period of foreign service of more than 91 days (inwhich case it is still included in determining the rate of tax toapply to Australian domestic income during that financial year).That is, dividends received from a foreign company are not exemptfrom tax in Australia.Pursuant to Article 8 of the Australian/United Kingdom DoubleTax Agreement, the gross dividend from the UK company(including the full UK company tax paid before arriving at the netamount available for distribution as a cash dividend) will betaxable in Australia with only a 10 per cent credit for UK tax as anoffset. Depending on the vet’s other Australian income during theyear (including reference to the S.23 AG exempt UK salary), theAustralian vet may well have an Australian tax ratedifferential/shortfall of say 30 per cent on a sizeable UK dividendtotal for the year (particularly if they worked for say half a year inAustralia prior to leaving for or returning from, the UK).It should be noted that even abstinence from drawing dividendsout of the company would not seem to overcome the exposuresince the Brewing Investments Case (2000) held that Australianresident shareholders in private UK companies are required tosimulate Australian liquidation conditions on the liquidation ofthe UK companies for tax purposes, thus causing thesuperimposition of S.46 (of the Australian Tax Act) dividendsupon liquidation into the individual’s Australian tax return.Any potential exposure to additional tax or penalties being assessedby the Australian authorities as a result of such practices havingbeen engaged in, even in good faith, are particularly concerning insituations where the veterinarian has returned from abroad withplans to buy into a practice and/or house, but with a stillsubstantial HECS and/or SLS liability awaiting them. Anyone so affected should immediately seek advice from anadviser specialising in such personal international tax issues.
Basil Brock (CA) and Frederick Mahar (CPA)Sinclair Wilson
Warrnambool VIC
Thank you for publishing our letter requesting support forTimor-Leste veterinary student Alipio De Almeida
(Aust Vet J 80 12 p738). We have already had a good response tothe request, and with the Commonweath Veterinary Associationpledge, we have close to half the amount of money required forAlipio to return to his studies. Our only problem with the letterwas the lack of contact details for us: most of our donations to datehave been from personal acquaintances. I was wondering if youcould publish some contact details in this month’s journal? The main contact point for people wishing to donate is:Emma Watkinsph: 08 8999 2351mob: 0417 662 371email: [email protected]
Emma Watkins,Veterinary Officer, AQIS East Timor Program,
Northern Australia Quarantine Strategy,Darwin NT
The Victorian Division of the AVA is disappointed that, at theOctober 2002 meeting of Policy Council, the procedures
introduced to ensure proper review of the Association’s policieswere not followed. The draft Policy on Hunting adopted by thecouncil was very significantly different to the one circulated priorto the meeting. The considerable redrafting that was undertaken
during the meeting including the addition of fishing as a form ofhunting, resulted in a gross change to the original policy. Thisshould have led to no further discussion and definitely no decision.Rather than returning the new policy draft to Divisions and SIGsfor review and comment, the new draft was accepted and rushedinto press in the Australian Veterinary Journal.Such an action negates and diminishes the role of Divisions andSIGs in the formulation of policies. It is particularly disturbingthat this subversion of the process of policy formulation wasapplied to a policy that is of particular ethical concern to manymembers of the AVA, and a policy to which several Divisions andSIGs, including the Victorian Division, were opposed. It took several years to develop the procedure for the processing ofpolicy development by the AVA. The procedures were aimed toensure that draft policies were properly developed prior topublication or endorsement. If the argument for altering thisprocedure without consultation is the urgency of finalising apolicy, it would be more appropriate to review the entire process ofdevelopment of policy, rather than subvert it for a controversialpolicy.We urge other Divisions and SIGs to comment on their concernswith the development of AVA policies.
Matthew R MakinPresident, AVA Victorian Division
L e t t e r s
Dr Jim Edwards, outgoing President of the WorldVeterinary Association, recently received the New ZealandVeterinary Association’s Outstanding Service Award.
The Award, which recognises long and valued services to theaffairs of NZVA, was presented to Edwards by NZVA presidentLewis Griffiths in Wellington. It is only the second time thenewly instituted award has been made. “Jim Edwards has given the New Zealand veterinary professiona high profile overseas and the initiatives taken during his termhave provided the world association with a sound base to facethe future,” says Griffiths. Under his leadership, the WorldVeterinary Association underwent significant restructuring andintroduced initiatives such as World Veterinary Day, Griffithsadded. A long time employee of the NZ Ministry of Agriculture andFisheries’ Biosecurity Authority, Dr Edwards recently establishedhis own international veterinary consultancy business, WorldVeterinary Consultants Ltd(www.worldveterinaryconsultants.com).
Service award goes toex-WVA chief
Jim Edwards (R) receives the award from NZVA president LewisGriffiths

25
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
EDITORMAUREEN REVINGTON
ADVISORY COMMITTEE
ANAESTHESIALEN CULLEN
AVIAN MEDICINE AND SURGERYGARRY CROSS
EQUINE MEDICINE AND SURGERYJOHN BOLTON
LABORATORY ANIMAL MEDICINEMALCOLM FRANCE
OPHTHALMOLOGYJEFF SMITH
PATHOLOGYCLIVE HUXTABLE
PHARMACOLOGY / THERAPEUTICSSTEPHEN PAGE
PRODUCTION ANIMAL MEDICINE JAKOB MALMO
RADIOLOGYROBERT NICOLL
REPRODUCTIONPHILIP THOMAS
SMALL ANIMAL MEDICINEBRIAN FARROWDAVID WATSON
SMALL ANIMAL SURGERYGEOFF ROBINS
GERALDINE HUNT
WILDLIFE / EXOTIC ANIMALSLARRY VOGELNEST
EDITORIAL ASSISTANT AND DESKTOP PUBLISHING
ANNA GALLO
CONTRIBUTIONS INVITED
Practising veterinarians and others are
invited to contribute clinical articles to the
Australian Veterinary Journal. We will
consider material in a variety of formats,
including clinically orientated reviews, reports
of case series, individual case studies, diag-
nostic exercises, and letters containing
comments or queries. Practitioners are also
invited to contribute to the case notes
feature, where accepted articles are not peer
reviewed but are edited for publication.
Contributors should consult instructions to
authors and recent issues of the journal for
guidelines as to formatting. Over referencing
should be avoided: authors should preferably
quote only those articles they feel are most
likely to be of interest and benefit to readers.
Send all contributions to:
Editor, AVJ Clinical Section
AVA House, 272 Brunswick Road,
Brunswick, Vic. 3056,
Phone: (03) 9387 2982
Fax: (03) 9388 0112
Email: [email protected]
Australian
VETERINARYJOURNAL
C L I N I C A L S E C T I O N
Hyperadrenocorticism is a common endocrine disease of the dog, and isthought to be the most commonly diagnosed endocrine disorder of the geri-atric age group.1
The diagnosis of hyperadrenocorticism requires an understanding of the clinicalmanifestations of the disease, an ability to interpret endocrine test results in the contextof the clinical setting, an appreciation of the various tests’ limitations, and considera-tion of factors that may influence endocrine testing.
Being a clinical syndrome rather than a laboratory diagnosis, it is vital that the veteri-narian maintains a high index of suspicion for this disease. Rather than the ‘textbook’history of polydipsia, polyuria, polyphagia, alopecia and conformation changes, theowner may simply report that the pet has noticeably ‘aged’ recently, or may present itfor perceived exercise intolerance. The astute veterinarian will include hyperadrenocor-ticism on a list of potential diagnoses, rather than dismiss these complaints as the onsetof old age.
With the increasing popularity of bench-top biochemistry analysers in general prac-tice, practitioners are frequently performing pre-anaesthetic or routine screeningbiochemical tests on veterinary patients. A finding of increased plasma ALP concentra-tion, hypercholesterolaemia and lipaemia will often lead to the pursuit of hyperadreno-corticism as the cause. Without concordant clinical history and physical changes,however, the diagnosis cannot be made. Other disease states or drug administrationshould also be considered as possible causes for such findings.
Dynamic endocrine testing remains the definitive test for the diagnosis of hypera-drenocorticism in dogs. The aim of such tests is to demonstrate either an abnormalhypothalamo-hypophyseal-adrenal axis or excessive functional adrenocortical reserve.
Tests for Hyperadrenocorticism LDDST
Many, including the author, consider the LDDST to be the benchmark test for diag-nosis of hyperadrenocorticism. Though it is highly sensitive2-4 it lacks specificity3,4 andthe veterinarian must be vigilant in identifying other causes of hypercortisolaemia, suchas physiological or psychological stressors, or administration of exogenous corticos-teroids that cross react with endogenous corticosteroids in the corticoid assay. It is oftenforgotten that hospitalisation or boarding, sedation and diagnostic procedures, as wellas general anaesthesia within several days of the LDDST, can lead to false diagnoses. An
Diagnosis of hyperadrenocorticismin the dog
Viewpoints in canine hyperadrenocorticism
JA BRADDOCKFaculty of Veterinary Science, The University of Sydney, New South Wales 2006E-mail: [email protected]
Aust Vet J 2003;81:25-27
ACTH Adrenocorticotropic hormoneAT Adrenal tumourALP Alkaline phosphataseHDDST High-dose dexamethasone suppression testLDDST Low-dose dexamethasone suppression testOHP 17-hydroxyprogesteronePDH Pituitary-dependent hyperadrenocorticism UCCR Urinary corticoid:creatinine ratioUVCS University Veterinary Centre, Sydney

Endogenous ACTH measurementEndogenous ACTH measurement can be very useful. The
reference range for normal dogs is 10 to 100 ng/L, with mean of45 ng/L.7 A measured ACTH concentration below the refer-ence range would clearly suggest adrenal tumour as the cause ofhyperadrenocorticism. Other references cite a value of < 20ng/L as diagnostic for adrenal tumour disease.11
If the ACTH concentration is > 45 ng/L then pituitarydependent disease or ‘stress’ is implicated.7 ACTH concentra-tion measurements of 20 to 45 ng/L are not definitively diag-nostic: repeated ACTH measurement or alternative testingprocedures are recommended to clarify the diagnosis. Repeatedmeasurement of ACTH concentration can give diagnostic accu-racy of 98%.11
An important limitation to this test is the necessity of carefuland prompt handling of the sample, with collection into plasticor silicone tubes only, and immediate separation and freezing ofthe plasma. Samples should be submitted frozen to the labo-ratory.
Diagnostic imagingAbdominal ultrasound examination is the author’s preferred
diagnostic tool for differentiation of adrenal and pituitary-dependent disease if a single test is to be used. In experiencedhands it is extremely reliable [see Karon Hoffmann viewpoint].Difficulties in interpretation can arise when nodular hyperplasiaoccurs, as this may initially resemble an adrenal mass. It mustalso be remembered that an adrenal mass is not necessarily afunctional adrenocortical tumour, and endocrine testing isalways necessary to confirm this. Both adrenal glands must beimaged if this is the sole differentiation method used because asingle normal adrenal gland does not rule out the possibility of acontralateral adrenal tumour. Similarly, bilateral adrenaltumours occur, and must be identified prior to effective surgicalintervention.12
Imaging should not be used alone to identify the cause ofhyperadrenocorticism because of the potential occurrence of anincidental or non-functional adrenal tumour with concurrentPDH,13 or of concurrent functional adrenal tumour andPDH.14
Abdominal imaging has the benefit in the geriatric age-group,of also allowing detection of clinically silent abdominal disease.
Other modes of imaging (computed tomography andmagnetic resonance imaging) have been used to assess theadrenal glands and pituitary gland but are not readily accessibleto most practitioners. They have potential, though, for identifi-cation of pituitary macroadenomas in dogs with neurologicalsigns.
Treatment TrialSome clinicians rely on a treatment trial for confirmation of
PDH: if a dog requires a cumulative dose of mitotane of ≤ 550mg/kg for satisfactory induction, and ≤ 60 mg/kg weekly main-tenance dose it is considered to have PDH,10 while failure toinduce and maintain on this protocol is a non-specific findingthat requires further investigation.
It is clear that all of the many diagnostic tests available havesome limitations and results should be interpreted always in thecontext of the historical and clinical findings, recognising thepossible effects of concurrent disease and exogenous steroidadministration.
intravenous dose of 0.01 mg/kg of dexamethasone shouldsuppress endogenous cortisol production 2 to 3 h post dexam-ethasone administration, and maintain suppression for at least 8h in a dog with a normal hypothalamo-hypophyseal-adrenalaxis.5 Experience at UVCS indicates values < 20 nmol/L forboth 4- and 8-hour plasma cortisol concentrations indicatenormal pituitary and adrenal suppression (DB Church, unpub-lished).
ACTH Stimulation TestThe ACTH stimulation test is used to demonstrate excessive
adrenocortical reserve, caused by adrenal hypertrophy due tochronic overstimulation by ACTH (PDH) or functional AT. Ithas the advantage of requiring only 1 hour to perform and maybe more specific than the LDDST in identifying hyperadreno-corticism.3,4 It is the author’s clinical experience that this test isless sensitive than the LDDST, a view shared by others.2-4,6 Testprotocols and reference values have been published.7 In theUVCS 5 µg/kg tetracosactrin/cosyntropin (Synacthen®) is usedfor adrenocortical stimulation and baseline and 1 h cortisolconcentrations are measured.
Similar limitations apply to the ACTH stimulation test, as forthe LDDST, with respect to false positive diagnoses in animalswith physiological hypersecretion of cortisol.
UCCRThe UCCR is generally reserved as a screening test for hyper-
adrenocorticism because of its very high sensitivity but lowspecificity. It is essential to use a home-collected urine sample asany stressor (even a car trip to the veterinary clinic) can increaseurinary cortisol clearance sufficiently to give a false result. Thefinding of an elevated UCCR must always be validated byfurther endocrine testing (LDDST or ACTH stimulation test).
Other TestsThere are other reported tests for the diagnosis of canine
hyperadrenocorticism, generally adapted from human tech-niques. These have not been widely used and are generally lessreliable than the tests discussed here. Recent studies havedemonstrated a subgroup of ‘atypical’ hyperadrenocorticoiddogs that produce excessive quantities of 17-hydroxyproges-terone (OHP) but not cortisol, unlike typical hyperadrenocorti-coid dogs that produces excessive quantities of both.8 Routineendocrine testing fails to diagnose these dogs but assays specificfor OHP will. OHP responses to LDDST and ACTH stimula-tion test parallel those of cortisol in ‘typical’ dogs.
Differentiation of PDH and ATHDDST
The HDDST is performed in the same way as the LDDSTbut with 0.1 mg/kg dexamethasone administered intravenously.It relies on the fact that adrenal tumours secrete cortisolautonomously and continuously without susceptibility tosuppression by glucocorticoids or higher centres. No amount ofdexamethasone will normally suppress adrenal tumour secre-tion. In contrast, pituitary tumours or a physiologically hyper-secretory pituitary gland usually retain some responsiveness toglucocorticoid suppression and 75% will suppress eventually ifenough glucocorticoids are administered.7,9,10 Unfortunately,this test will not distinguish between the 25% of glucocorti-coid-resistant pituitary tumours and functional adrenocorticaltumours, so further diagnostics are recommended in thesepatients.
26
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003

References1. Bruyette DS, Ruehl WW, Entriken TL, Darling LA, Griffin DW. Treating caninepituitary-dependent hyperadrenocorticism with L-deprenyl. Vet Med1997;92:711-727.2. Herrtage ME. The adrenal glands. In: Manual of Small Animal Endocrinology.British Small Animal Veterinary Association, Cheltenham, 1990:73-104. 3. Kaplan AJ, Peterson ME, Kemppainen RJ. The effects of disease on theresults of diagnostic tests for use in detecting hyperadrenocorticism in dogs. JAm Vet Med Assoc 1995;207:445-451.4. van Liew CH, Greco DS, Salman MD. Comparison of results of adrenocorti-cotropic hormone stimulation and low-dose dexamethasone suppression testswith necropsy findings in dogs: 81 cases (1985-1995). J Am Vet Med Assoc1997:211:322-325 5. Toutain PL, Alvinerie M, Ruckebusch Y. Pharmacokinetics of dexametha-sone and its effect on adrenal gland function in the dog. Am J Vet Res1983;44:212-217. 6. Feldman EC. Comparison of the ACTH response and dexamethasonesuppression as screening tests in canine hyperadrenocorticism. J Am Vet MedAssoc 1983;182:506-510.7. Feldman EC, Nelson RW. Hyperadrenocorticism (Cushing’s syndrome). In:Canine and Feline Endocrinology and Reproduction, 2nd edn. Saunders,Philadelphia, 1996:187-265.
8. Ristic JME, Evans H, Herrtage ME. Plasma 17-hydroxyprogesterone concen-trations in the diagnosis of canine hyperadrenocorticism [abstract]. J Vet InternMed 2001;15:298 9. Feldman EC, Nelson RW, Feldman MS. Use of low- and high-dose dexam-ethasone tests for distinguishing pituitary-dependent from adrenal tumourhyperadrenocorticism in dogs. J Am Vet Med Assoc 1996;209:772-775. 10. Gould SM, Baines EA, Mannion PA, Evans H, Herrtage ME. Use of endoge-nous ACTH concentration and adrenal ultrasonography to distinguish the causeof canine hyperadrenocorticism. J Small Anim Pract 2001;42:113-121. 11. Feldman EC. Distinguishing dogs with functioning adrenocortical tumoursfrom dogs with pituitary-dependent hyperadrenocorticism. J Am Vet Med Assoc1983;183:195-200.12. Hoerauf A, Reusch C. Ultrasonographic characteristics of both adrenalglands in 15 dogs with functional adrenocortical tumors. J Am Anim Hosp Assoc1999;35:193-199.13. von Dehn BJ, Nelson RW, Feldman EC, Griffey SM. Pheochromocytomaand hyperadrenocorticism in dogs: six cases (1982-1992). J Am Vet Med Assoc1995;207:322-324.14. Greco DS, Peterson ME, Davidson AP, Feldman EC, Komurek K.Concurrent pituitary and adrenal tumors in dogs with hyperadrenocorticism: 17cases (1978-1995). J Am Vet Med Assoc 1999;214:1349-1353.
27
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Ultrasonographical examination in canine hyperadreno-corticism
Radiography and ultrasonography are readily available tomost practitioners, and are now considered part of thework up for any dog suspected of HA. Sonography has
been used increasingly over the last decade to help differentiatepituitary from adrenal dependent HA. The purpose of thisviewpoint article is to outline the use of sonography in the diag-nostic investigation of cases where adrenocortical disease issuspected or may be a possible cause of presenting clinical signs.
Patient preparationFactors which make evaluation of the abdomen, and in
particular the adrenal glands, more difficult include pyloric gas,intestinal gas, and deep-chested body conformation or largebody size.1 Therefore preparation of the animal to reduceaerophagia secondary to anxiety and to reduce gastrointestinalingesta and gas is desirable. I try to have the dog fastedovernight (if not diabetic), keep the dog quiet (not barking),and sedate prior to removing the hair coat over both sides of theentire abdomen and last three intercostal spaces.
Sonographic technique for imaging adrenal glandsImaging the adrenal glands requires some practice. The
following is the technique I use as part of the abdominal sono-graphic examination: Ideally the transducer selected will have a
small contact ‘foot print’ so as to easily angle the face of thetransducer under the costal arch as needed. The frequencychosen should be the highest frequency that will still penetrateto the depth required in the individual animal.
With the dog in right lateral recumbency, the left adrenalgland can be imaged by placing the transducer in theparalumbar fossa in the dorsal plane (along the body lengthparallel to the dorsum of the dog) and locating the aorta andcaudal vena cava in long axis. Then slide the transducer craniadalong to the level of the left kidney keeping the aorta in viewand locate the left renal artery and vein. Rotate the transducer45 degrees clockwise and gently sweep cranial to the renal arteryand vein to locate the left adrenal gland in long axis. The aortaand left kidney are not usually in the field of view when theadrenal gland is imaged.
For location of the right adrenal gland place the dog in leftlateral recumbency. The transducer is placed over theparalumbar fossa and the great vessels are again located in longaxis in the dorsal plane. Slide the transducer cranially, keepingthe caudal vena cava in view. Put gentle but firm pressure on thetransducer so that images can be made at the level of the cranialextremity of the right kidney and the celiac and cranial mesen-teric arteries branching from the aorta. At this level, carefullysearch for the right adrenal gland along side and dorsal to thecaudal vena cava. Once located rotate the transducer 30 to 45degrees anti-clockwise to bring the gland into long axis view.From this location the left adrenal may also be imaged, if thetransducer is redirected dorsally and slightly caudally.
KL.HOFFMANNVeterinary Diagnostic Ultrasound Consultant, Animal Ultrasound Services Pty Ltd, PO Box 3055 Putney, New South Wales 2112Email: [email protected]
Aust Vet J 2003;81:27-30
CT Computed x-ray tomographyHA Hyperadrenocorticism MRI Magnetic resonance imaging

Animals with severe illnesses may have physiological adreno-cortical hyperplasia, the appearance of which can overlap withearly signs of PDH. Therefore evaluation of adrenal size shouldbe repeated after resolution of any concurrent illness.Physiological adrenocortical hyperplasia, in my experience, willincrease adrenal thickness by only 1 to 2 mm during the periodof illness.
When HA is adrenal-dependent (cortical adenoma, corticaladenocarcinoma), there will be a nodule or mass associated withone or both glands (Figures 2c, 2d). Conventional wisdomsuggests that with a functional adrenocortical tumour, thecontralateral cortex will atrophy and be smaller than normal.6
Although this occurs histologically, the adrenal medulla alsoappears to expand.7 This may explain the sonographic observa-tion that the opposite gland is often normally imaged.8 Novicesonographers failing to identify the contralateral adrenal glandshould take care not to reach the false conclusion that theadrenomegaly is unilateral and therefore more consistent with afunctional adrenocortical tumour.
Unfortunately, both PDH and adrenal tumours can alsocoexist in dogs with HA, resulting in a confusing mixture ofsonographic findings and test results9 to challenge the investi-gator. Cortical adenocarcinomas may have local extension intosurrounding tissue and caudal vena cava and may create tumourthrombi.
LiverThe associated “steroid hepatopathy” may be represented
sonographically by an increase in size of the liver, rounding of
Normal adrenal anatomyAnatomically, the adrenals are asymmetrical in both shape
and position (Figure 1). The left adrenal gland is medial to thecranial extremity of the left kidney and lies along side the aortabetween the roots of the left renal artery and the cranial mesen-teric artery. The normal left canine adrenal gland is bilobed witha central constriction where the phrenicoabdominal vessels arelocated, the cranial extremity is broad and flattened and thecaudal extremity is more oval in cross section 2
The right adrenal gland lies between the medial surface of thecranial extremity of the right kidney and the lateral aspect of thecaudal vena cava. A portion of the cranial extremity of the rightadrenal gland is directed sharply lateral and caudad, giving adistinct hook shape.2
Normal adrenal sonographic findingsWide variations in measurements of length, width and thick-
ness have been reported in normal dogs weighing from 1.8 kg to72 kg. There was a strong linear correlation between adrenalgland length and body weight.3 That is, the larger the dog thegreater the length of the gland. A more accurate means of evalu-ating adrenal size has been reported by measuring maximumthickness (dorsal to ventral measurement).4 In my experience,most dogs with normal glands range in thickness from 3 to5mm and up to 7 mm in large dogs. The shape of the normalgland has been described above. The echogenicity of normaladrenal glands is less than that of the renal cortex 5 and theperirenal adipose tissue. The normal echotexture is uniform andoccasionally the adrenal cortex and medulla can be differenti-ated (Figure 1).
Sonographic abnormalities in cases of hyperadreno-corticism
The degree of structural adrenal changes imaged will dependon the stage of the clinical course of the disease. Sonologistsmay increase their diagnostic confidence with experience and bylooking for supporting changes in other organs.
Adrenal glandsAdrenal pathology in cases of HA generally consists of diffuse
hyperplasia, nodular hyperplasia or neoplasia. Adrenal masslesions not associated with HA such as pheochromocytomas,neuroblastomas, and metastastic lymphosarcoma or mammarycarcinomas may also occur but will not be discussed here.
The adrenal glands are examined for changes in size, shape,margins, relative echogenicity and echotexture from theexpected normal for the dog. In my case population adrenalenlargement is noted when the thickness is greater than 7.5 mmin medium to large dogs and greater than 5mm in small dogs.
With PDH both adrenal glands may be uniformly enlargedand hypoechoic with a homogeneous echotexture and smoothmargins (Figure 2b). The echogenicity of the adrenal glandsmaybe normal, that is less than that of the renal cortex.5 Insome cases with PDH, the adrenal glands may appear to bewithin normal sonographic limits. In cases with associatednodular cortical hyperplasia, the echogenicity may be heteroge-neous and the glands may be irregular and asymmetric (Figure2c). These cases can require ultrasound guided fine needle aspi-rate or biopsy for cytological or histological examination to helpdifferentiate nodular hyperplasia from primary adrenocorticalneoplasia.
28
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Figure 1. Line drawing of the anatomic landmarks for adrenalimaging. Key: Cd = caudal. Cr = cranial, L = left, R =right, a = leftadrenal gland, b= right adrenal gland, c = caudal vena cava, d =aorta, e = celiac artery, f = cranial mesenteric artery, g = rightkidney, h = left kidney, i = ureter, j = right renal vein, k = left renalvein, l = right renal artery, m = left renal artery.

the liver margins, homogenous hyperechoic echotexture withincreased acoustic attenuation or hyperattentuation.Attenuation or the decrease in amplitude and intensity of soundas it travels through tissue is a subjective evaluation and can beprone to error. Comparisons should always be made to othertissues within the same animal during the same examinationtaking care not to alter the equipment settings (gain, time gaincompensation, decreasing dynamic range, changing the focalzone) or the transducer frequency. The higher the transducerfrequency the greater the attenuation of sound.
Focal liver lesions may also be present. Regenerative nodulesor hepatomas in the liver may become more apparent as thesurrounding parenchyma brightens. Secondary metastaticneoplasia from malignant adrenocortical neoplasms may beimaged in the liver. While sonography can be used to locate afocal liver lesion, cytological or histopathological examination isneeded to confirm which cell process is involved.
Dogs receiving exogenous steroids may also have sonographichepatic and/or pancreatic changes with bilaterally small adrenalglands. Dogs receiving mitotane have a variable and oftencoarse hepatic echotexture, and, depending on the duration oftreatment, may have bilaterally small adrenal glands.
PancreasIt is not uncommon in the author’s experience for HA cases
with structural adrenal changes suggestive of PDH or a func-tional adrenocortical tumour to have concurrent pancreatitiswith surrounding inflammed hyperechoic peri-pancreaticmesenteric fat.
KidneysSmall dilation of the renal pelves with fluid is often imaged in
dogs with polyuria. This observation is a non-specific sono-graphic sign, as it may also occur in cases with renal failure,
29
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Figure 2: Sonographic images of left adrenal gland. Cranial is to the left and medial is to the base of each image. There is a centimetrescale to the right side of each image.a. Sonographic image of a normal left adrenal gland in a 5 kg 6-year-old Maltese Terrier. The image was made with a broadband linear 10-5 MHz transducer. Note the increased echogenicity of the adrenal medulla relative to the adrenal cortex. The cranial extremity measures0.30 cm and the caudal extremity measures 0.29 cm in thickness.b. Sonographic image of a hyperplastic left adrenal gland in a 13-year-old Terrier crossbred with pituitary dependent hyperadrenocorti-cism. The image was made with a broadband linear 10-5 MHz transducer. The cranial extremity measures 1.18 cm and the caudal extremity1.07 cm in diameter. The right adrenal gland was also enlarged.c. Sonographic image of an enlarged caudal extremity of the left adrenal gland in a 13-year-old Fox Terrier. The image was made with abroadband curvilinear 7 – 4 MHz transducer. The mass has equivalent echogenicity to the renal cortex. The cranial extremity measures0.47 cm and the caudal extremity 1.24 cm in diameter. Differential diagnoses include nodular hyperplasia or adrenal neoplasia. A fineneedle aspirate would be performed to confirm.d. Sonographic image of a left adrenal mass in an aged Australian Terrier. The image was made with a broadband curvilinear 7 – 4 MHztransducer. The adrenal gland (between white arrows) is grossly enlarged (4.83 x 3.29 cm), has irregular margins and is hypoechoic to thesurrounding peri-renal adipose tissue. As part of this examination the surrounding vessels would be investigated carefully for evidence oftumour invasion.

ultrasound examination may be performed early in the work upand before the results of other laboratory tests are known.Therefore the sonologist must be methodical so as not to over-look vital clues to the syndrome. Sonography has becomealmost mandatory in the assessment of dogs suspected of havingHA by specialists of small animal medicine. Sonographicchanges in the adrenal glands are frequently used to determinewhether chemotherapy or surgery is the appropriate treatmentfor affected patients. As many animals investigated for HA haveconcurrent disease, it is only with a thorough approach tosonography can it truly become a useful “diagnostic aid”.
References1. Grooters AM, Biller DS, Miyabayashi T, Leveille R. Evaluation of routineabdominal ultrasonography as a technique for imaging the canine adrenalglands. J Am Anim Hosp Assoc 1994;30:457-462.2. Smithcors JF. The endocrine system. In: Miller M, editor. The Anatomy of theDog. Saunders, Philadelphia, 1964: 826-829.3. Douglass JP, Berry CR, James S. Ultrasonographic adrenal gland measure-ments in dogs without evidence of adrenal disease. Vet Radiol Ultrasound1997;38:124-130.4. Barthez PY, Nyland TG, Feldman EC. Ultrasonographic evaluation of theadrenal glands in dogs. J Am Vet Med Assoc 1995;207:1180-1183.5. Grooters AM, Biller DS, Merryman J. Ultrasonographic parameters of normalcanine adrenal glands: comparison to necropsy findings. Vet Radiol1995;36:126-130.6. Schelling CG. Ultrasonography of the adrenal gland. Probl Vet Med1991;3:604-617.7. Capen CC. The Endocrine Glands. In: Jubb KVF, Kennedy PC, Palmer N,editors. Pathology of Domestic Animals. 3rd edn. Academic Press, San Diego,1985:238-297.8. Hoerauf A, Reusch C. Ultrasonographic characteristics of both adrenalglands in 15 dogs with functional adrenocortical tumors. J Am Anim Hosp Assoc1999;35:193-199.9. Greco DS, Peterson ME, Davidson AP, Feldman EC, Komurek K. Concurrentpituitary and adrenal tumors in dogs with hyperadrenocorticism: 17 cases(1978-1995). J Am Vet Med Assoc 1999;214:1349-1353.10. Widmer WR, Guptill L. Imaging techniques for facilitating diagnosis ofhyperadrenocorticism in dogs and cats. J Am Vet Med Assoc 1995;206:1857-1864.11. Penninck DG, Feldman EC, Nyland NG. Radiographic features of caninehyperadrenocorticism caused by autonomously functioning adrenocorticaltumors 23 cases:(1978-1986). J Am Vet Med Assoc 1988;192:1604-1608.12. Bertoy EH, Feldman E, Nelson RW, Dublin AB et al. One-year follow -upevaluation of magnetic resonance imaging of the brain in dogs with pituitary-dependent hyperadrenocorticism. J Am Vet Med Assoc 1996;208:1268-1273.
pyelonephritis, early urinary tract obstruction and animalsadministered diuretics or intravenous fluids. Other urinary tactchanges associated with HA include renal and cystic calculi,cystitis and metastatic mineralisation of soft tissues particularlythe renal pelvic diverticuli.
Further imagingRadiographic changes commonly observed with HA are
hepatomegaly, osteopenia, abdominal enlargement, and disten-sion of the urinary bladder and metastatic mineralisation.Adrenocortical neoplasms may occasionally be large enough tobe seen on conventional abdominal radiographs. To detectadrenal neoplasms there must be sufficient fat surrounding theadrenal gland to provide radiographic contrast.10 Adrenalmineralisation has been reported in half of the dogs withadrenal adenomas and carcinomas,11 however, mineralisationalso occurs in non- neoplastic adrenal glands.
The adrenal glands can also be imaged by CT or MRI, avail-able through most large referral centres. When investigatingPDH, MRI is a reliable non-invasive means of evaluating thepituitary gland area in dogs with PDH and is capable ofdetecting pituitary masses as small as 3mm.12 These modalitiesare usually more expensive, time consuming and require generalanaesthesia to perform and are often performed only on moredifficult cases.
Sonography on the other hand is widely available and rela-tively affordable, can be performed in the conscious patient,often without sedation, provides a means of determining treat-ment options (chemotherapy or surgery), and can identifyconcurrent (related or unrelated) disease processes, thus makingit a practical diagnostic tool. However, the disadvantages ofdiagnostic ultrasound examinations are that they require anoperator with an appropriate level of skill, high resolution sono-graphic equipment and there are difficulties in the differentia-tion of some diseases such as nodular hyperplasia and neoplasia.
ConclusionsDiagnostic imaging provides an additional layer of informa-
tion to endocrine testing in cases with HA. In many cases, an
30
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003

31
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Medical treatment of hyperadrenocorticism in the dog
JA BRADDOCK Faculty of Veterinary Science, The University of Sydney, New South Wales, 2006. E-mail: [email protected]
Aust Vet J 2003;81:31-33
The aim of most medical treatments of hyperadrenocorti-cism (mitotane, ketoconazole, trilostane) is to suppressadrenal production of cortisol to a relative hypoadreno-
corticoid state, leaving the animal with enough cortisol produc-tion for day-to-day existence but abolishing adrenal reserve,thus limiting adrenal responsiveness to excessive ACTH secre-tion or suppressing cortisol production by tumour cells.
The centrally acting medical treatments (for example selegi-line, cyproheptadine and bromocriptine) are believed to influ-ence pituitary production of ACTH, and their use (if any) isrestricted to PDH.
Mitotane Mitotane is the most commonly used treatment for PDH and
it is generally accepted as the most efficacious.Mitotane is administered orally and should be given with
food to optimise absorption.1 It is metabolised to its activemetabolite in the adrenal cortex2 where its main action is tobind to mitochondrial macromolecules and destroy them,leading to cell death and thus destruction of the affected tissues.The adrenal gland zonae reticularis and fasciculata are selec-tively affected, generally sparing the zona glomerulosa unlessdestruction is very extensive.3
There are two widely practised protocols utilising mitotane.4-7
Generally, it is either administered daily for an induction periodof 5 to 14 days to induce controlled partial destruction of theadrenal cortex, followed by weekly maintenance treatment(‘standard protocol’), or it is administered for a longer inductionperiod until the adrenal cortex has been chemically ablated, andthen administration ceases (‘alternative protocol’). In eitherprotocol glucocorticoid supplementation may be used in theinduction period to ameliorate signs of rapidly decliningcortisol concentrations, and in the latter protocol, both gluco-corticoid and mineralocorticoid should be administered toprevent signs from iatrogenic hypoadrenocorticism as adrenalablation is achieved.
Up to 25% of dogs have adverse affects during the inductionperiod and up to 30% have adverse effects during maintenancetherapy.4 Most of these adverse effects are attributable toabsolute or relative hypoadrenocorticism. Other adverse effectsare neurological signs and gastrointestinal disturbances.Relapses requiring further induction are not uncommon, and anumber of animals will develop permanent iatrogenic hypoad-renocorticism.
The ‘alternative’ treatment protocol of chemical ablation ofthe adrenal cortex5 seems to have the advantage of fewer relapsesin the first 12 months of treatment (27% compared to 58%)and lower costs because less mitotane is used, but the prevalenceof side effects during induction is comparable.
The author’s preference is to use the standard protocolinitially, usually giving the induction dose of mitotane for 5days, then performing an ACTH stimulation test to assessresponse to treatment before proceeding with further inductionor maintenance dosing. ACTH response testing is performed48 hours after the last mitotane dose is administered to assessthe maximal effect of the mitotane dose on the adrenal gland asfull cytotoxic effect is not attained until this time. If an animalproves very difficult to control on the standard mitotaneprotocol, then the ‘alternative protocol’ or, more often, surgicaladrenalectomy is considered.
Mitotane can be used as a chemotherapeutic option for dogswith adrenal tumours. It is palliative only, and reserved for casesin which the tumour is inoperable, has metastasised, or inwhich surgical treatment is declined. The induction periodrequired to suppress adrenal cortisol production satisfactorily isgenerally longer than that needed for PDH dogs, and the main-tenance dose higher.
KetoconazoleKetoconazole is used much less frequently than mitotane, but iscurrently the main alternative medical treatment for PDH. Itreduces cortisol production principally by inhibition of enzymesystems integral to mammalian steroidogenesis.8,9
Ketoconazole has been shown to be effective in controllinghypercortisolaemia in dogs with PDH.10 It needs to be adminis-tered twice daily and up to 20 to 25% of dogs will not respondto ketoconazole,7 due to poor intestinal drug absorption orother undefined reasons. Side effects are generally caused byinadequate circulating cortisol concentrations due to overdose.Gastrointestinal signs such as anorexia and vomiting arereported, as well as altered coat colour and temporary increaseof plasma enzymes of hepatic origin, though this usuallyreverses on withdrawal of the drug.11 The most serious toxicityreported in people is idiosyncratic hepatic necrosis12 at thera-peutic drug doses.
Ketoconazole can also be used for symptomatic treatment ofadrenal tumour disease when surgical treatment is not possible.
EtomidateEtomidate, an anaesthetic agent, is another imidazole derivative
and is the most powerful adrenal enzyme inhibitor known.13,14
While this drug has a place in human endocrine therapy foracute treatment of endocrinopathic psychoses or severe hypera-drenocorticoid complications, its brief effect and parenteraladministration limit its usefulness in veterinary patients.
ACTH Adrenocorticotropic hormoneLDDST Low-dose dexamethasone suppression testPDH Pituitary-dependent hyperadrenocorticism OR
pituitary-dependent hyperadrenocorticoidUVCS University Veterinary Centre, Sydney

a
32
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
inhibitor of almost all steroid hormone production includingadrenal, gonadal and placental sources. Inhibition of adrenalsteroidogenesis has been shown to occur at lower doses thanthat inhibiting steroidogenesis in other organs.24,25
There are three published abstracts reporting trilostane use inthe dog26-28 with variable results. A recent 2-year clinical trialconducted by the author at UVCS,29 found this drug to be avery successful treatment for medical management of PDH in30 dogs, although dose rates and frequency varied considerablybetween dogs. No adverse side effects were observed. Figures 1aand 1b show one of the dogs in the UVCS trial before, and aftertreatment with trilostane.
The author’s experience in treating a single dog with adrenaltumour has been similarly successful.
Trilostane is not currently available in Australia, and if it doesbecome available, cost will be a major impediment to its routineuse for treating hyperadrenocorticism in dogs. The cost ofmedical treatment with trilostane is likely to be triple that ofmaintaining a dog on mitotane treatment.
SelegilineSelegiline (L-deprenyl) is a monoamine oxidase B inhibitor
that acts centrally as a dopamine agonist. In dogs it has beenreported as useful for geriatric canine cognitive disorder30 butrecent interest has largely been focussed on its role in treatingexcessive ACTH secretion in PDH dogs. The rationale for suchuse is based on the belief that dopamine secretion from highercentres regulates ACTH secretion from the pituitary, howeverexperimental data is conflicting regarding both the influence ofdopamine on ACTH secretion, and the effect of selegiline ondopamine concentrations in the central nervous system andpituitary.
There have been two published clinical studies examining theeffects of selegiline in PDH patients, with conflicting results.The first31,32 was the basis for national registration of this drugin Canada for treatment of PDH in dogs. Response to treat-ment was judged primarily on subjective assessment by theowner and physical examination by a veterinarian. LDDSTs,haematological examinations and biochemical tests wereperformed monthly to assess endocrine changes. Fifteen percentof patients achieved ‘normalisation’ of their LDDST, and meanplasma cortisol measurements decreased sufficiently to be statis-tically significant. The drug was assessed to be an effective treat-ment in some dogs with PDH.
AminoglutethimideAminoglutethimide is a non-selective blocker of adrenal
steroid synthesis affecting cortisol, aldosterone and adrenalandrogen production. This drug causes only partial blockade,and excessive secretion of ACTH eventually over-rides theblockade and causes return of cortisol concentrations to pre-treatment values within days.15 For this reason, when used forpituitary dependent disease in people, it is combined with othertreatments such as metyrapone (which exerts a synergisticeffect) or pituitary irradiation. Side-effects in people arefrequent and include anorexia, nausea, vomiting, lethargy, seda-tion, blurred vision, headache and myalgia. A transient skinrash is common and hypothyroidism is thought to occur in 5%of patients.16
Little is known about aminoglutethimide use for treatment ofhyperadrenocorticism in dogs. It has been shown to reducecirculating cortisol concentrations in normal dogs withoutadverse side-effects.17 The drug has been used in 12 dogs withPDH and was reported to have induced clinical remission and‘tendency toward normalisation’ of a number of laboratory vari-ables including blood cortisol concentrations.18
Metyrapone Like aminoglutethimide, metyrapone is an enzyme blocker
that works at the level of the adrenal gland. It has a more selec-tive effect, acting to block transformation of 11-deoxycortisol tocortisol.19 As a result of this, large amounts of precursor steroidswith mineralocorticoid effect accumulate, and hypertension andhypokalaemia can result. Nausea, vomiting and dizziness arecommon side effects in people and, because of this and the costof the drug, it has been relegated largely to combination therapy(often with aminoglutethimide).20 As with aminoglutethimide,ACTH secretion in PDH can eventually overcome the incom-plete enzyme blockade but metyrapone can be very useful tocontrol hypercortisolaemia in the short-term.21 To the author’sknowledge, there are no reports of use of metyrapone for treat-ment of canine PDH, but it has been used successfully in twoaffected cats for stabilisation and alleviation of signs prior tobilateral adrenalectomy.22,23
Trilostane Trilostane (WIN 24,450) is a synthetic, hormonally inactive
steroid that competes with pregnenolone as a substrate for 3-β-hydroxysteroid dehydrogenase and thus inhibits pregnenoloneconversion to progesterone.24 It is therefore a non-selective
aFigure 1. Dog in UVCS trilostane treatment trial before (a) and after (b) successful treatment with trilostane.
b

33
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
The second selegiline study33 concluded that selegiline couldnot be recommended for treatment of PDH in dogs due to lackof consistent improvement in clinical signs and endocrineabnormalities.
In a clinical trial with 11 dogs, this author found the drug tohave no appreciable effect on clinical signs or endocrine testingin PDH patients during 3 months treatment,34 and the conclu-sion was that this drug could not be recommended for treat-ment of canine PDH.
Bromocriptine and cyproheptadineBromocriptine and cyproheptadine are two other centrally
acting drugs proposed to act by suppression of ACTH produc-tion by the pituitary. Both have been shown to be ineffective inthe treatment of PDH in dogs35,36 and bromocriptine wasfound to have unacceptable side-effects.36
ConclusionFrom the above discussion it can be seen that there are a
number of medical therapies and protocols for the treatment ofhyperadrenocorticism in the dog, and in combination withsurgical options, these provide some scope to individualise treat-ment and select that which best suits the needs of a particularpatient.
In discussion of treatment options with owners, it is impor-tant to make them aware of possible deleterious effects as well asbenefits to the various treatment options. One aspect of long-term treatment that is often neglected in discussions is cost.Maintenance treatment for a 20 kg dog treated with mitotanewill cost approximately $2000 per annum, including drug costsand 3-monthly consultation and ACTH stimulation testing.This is often not appreciated by owners until long after the deci-sion has been made to treat their dog.
References1. Watson ADJ, Rijnberk A, Moolenaar AJ. Systemic availability of o,p’-DDD innormal dogs, fasted and fed, and in dogs with hyperadrenocorticism. Res VetSci 1987;43:160-165. 2. Cai W, Counsell RE, Djanegara T et al. Metabolic activation and binding ofmitotane in adrenal cortex homogenates. J Pharm Sci 1995;84:134-138. 3. Hart MM, Reagan RL, Adamson RH. The effect of isomers of DDD on theACTH-induced steroid output, histology, and ultrastructure of the dog adrenalcortex. Toxicol Appl Pharmacol 1973;24:101-113. 4. Kintzer PP, Peterson ME. Mitotane (o,p’-DDD) treatment of 200 dogs withpituitary-dependent hyperadrenocorticism. J Vet Intern Med 1991;5:182-190. 5. Rijnberk A, Belshaw BE. An alternative protocol for the management ofcanine pituitary-dependent hyperadrenocorticism. Vet Rec 1988;122:486-488. 6. Peterson ME, Kintzer PP. Medical treatment of pituitary-dependent hypera-drenocorticism. Mitotane. Vet Clin N Am 1997;27:255-272. 7. Feldman EC, Nelson RW. Hyperadrenocorticism (Cushing’s syndrome). In:Canine and Feline Endocrinology and Reproduction, 2nd edn. Saunders,Philadelphia, 1996:187-265. 8. Loose DS, Kan PB, Hirst MA, Marcus RA, Feldman D. Ketoconazole blocksadrenal steroidogenesis by inhibiting cytochrome P450-dependent enzymes. JClin Invest 1983;71:1495-1499. 9. Nagai K, Miyamori I, Ikeda M et al. Effect of ketoconazole (an imidazoleantimycotic agent) and other inhibitors of steroidogenesis on cytochrome P450-catalysed reactions. J Steroid Biochem 1986;24:321-323. 10. Feldman EC, Bruyette DS, Nelson RW, Farver TB. Plasma cortisolresponse to ketoconazole administration in dogs with hyperadrenocorticism. JAm Vet Med Assoc 1990;197:71-78.
11. Legendre AM, Selcer BA, Edwards DF, Stevens R. Treatment of canineblastomycosis with amphotericin B and ketoconazole. J Am Vet Med Assoc1984;184:1249-1254. 12. Janssen PA, Symoens JE. Hepatic reactions during ketoconazole treat-ment. Am J Med 1983;74:80-85. 13. Schulte HM, Benker G, Reinwein D, Sippell WG, Allolio B. Infusion of lowdose etomidate: correction of hypercortisolaemia in patients with Cushing’ssyndrome and dose-response relationship in normal subjects. J Clin EndocrinolMetab 1990;70:1426-1430. 14. Lambert A, Mitchell R, Frost J, Ratcliffe JG, Robertson WR. Direct in vitroinhibition of adrenal steroidogenesis by etomidate. Lancet 1983;11:1085-1086. 15. Schteingart DE, Conn JW. Effects of aminoglutethimide upon adrenal func-tion and cortisol metabolism in Cushing’s syndrome. J Clin Endocrinol Metab1967;27:1657-1666.16. Schteingart DE. Cushing syndrome. In: Principles and Practice ofEndocrinology and Metabolism, 2nd edn. JB Lippincott Company, Philadelphia.1995;667-682. 17. Lacoste D, Caron S, Belanger A, Labrie F. Effect of 3-week treatment with[D-Trp6, des-Gly-NH2
10] LHRH ethylamide, aminoglutethimide, ketoconazole, orflutamide alone or in combination on testicular, serum, adrenal and prostaticsteroid levels in the dog. J Steroid Biochem 1989;33:233-242. 18. Castill V, Lalia J, Casal J et al. Aminoglutethimide: Therapeutic alternative incanines with Cushing’s disease (hypophysis dependent). [Spanish]. Avan CiencVet 1996;11:93-96. 19. Thoren M, Adamson U, Sjöberg HE. Aminoglutethimide and metyrapone inthe management of Cushing’s syndrome. Acta Endocrinol 1985;109:451-457. 20. Orth DN, Kovacs WJ. Hyperfunction. Glucocorticoids: hypercortisolism(Cushing’s syndrome). In: Williams textbook of endocrinology, 9th edn.Saunders, Philadelphia. 1998:565-595. 21. Verheist JA, Trainer PJ, Howlett TA et al. Short and long-term responses tometyrapone in the medical management of 91 patients with Cushing’ssyndrome. Clin Endocrinol 1991;35:169-178. 22. Daley CA, Zerbe CA, Schick RO, Powers RD. Use of metyrapone to treatpituitary-dependent hyperadrenocorticism in a cat with large cutaneouswounds. J Am Vet Med Assoc 1993;202:956-960. 23. Moore LE, Biller DS, Olsen DE. Hyperadrenocorticism treated withmetyrapone followed by bilateral adrenalectomy in a cat. J Am Vet Med Assoc2000;217:691-694.24. Potts GO, Creange JE, Harding HR, Schane HP. Trilostane, an orally activeinhibitor of steroid biosynthesis. Steroids 1978;32:257-267. 25. Schane HP, Potts GO, Creange JE. Inhibition of ovarian placental andadrenal steroidogenesis in the rhesus monkey by trilostane. Fertil Steril1979;32:464-467.26. Hurley K, Sturgess K, Cauvin A, Kuipers R. The use of trilostane for thetreatment of hyperadrenocorticism in dogs [abstract]. J Vet Intern Med1998;12:210. 27. Ramsey IK, Hurley K. Use of trilostane in hyperadrenocorticism [abstract]. JSmall Anim Pract 2000;41:373. 28. Neiger R, Hurley K. 24-hour cortisol values in dogs with hyperadrenocorti-cism on trilostane [abstract]. J Small Anim Pract 2001;42:376. 29. Braddock JA, Church DB, Robertson ID, Watson ADJ. Trilostane treatmentin dogs with pituitary-dependent hyperadrenocorticism, submitted for publication.30. Campbell S, Trettien A, Kozan B. A noncomparative open-label study evalu-ating the effect of selegiline hydrochloride in a clinical setting. Vet Therap2001;2:24-39.31. Bruyette DS, Ruehl WW, Entriken T, Griffin D, Darling L. Management ofcanine pituitary-dependent hyperadrenocorticism with l-deprenyl (Anipryl). VetClin N Am 1997;27:273-286.32. Bruyette DS, Ruehl WW, Entriken TL, Darling LA, Griffin DW. Treatingcanine pituitary-dependent hyperadrenocorticism with L-deprenyl. Vet Med1997;92:711-727. 33. Reusch CE, Steffen T, Hoerauf A. The Efficacy of L-deprenyl in dogs withpituitary-dependent hyperadrenocorticism. J Vet Intern Med 1999;13: 291-301. 34. Braddock JA, Church DB, Robertson ID, Watson ADJ. Selegiline treatmentin dogs with pituitary-dependent hyperadrenocorticism, submitted for publication.35. Stolp R, Croughs RJM, Rijnberk A. Results of cyproheptadine treatment indogs with pituitary-dependent hyperadrenocorticism. J Endocrinol1984;101:311-314. 36. Rijnberk A, van Wees A, Mol JA. Assessment of two tests for the diagnosisof canine hyperadrenocorticism. Vet Rec 1988;122:178-180.

midline approach to the right adrenal may be difficult in obesepatients. Paracostal incisions have the advantage of requiringless retraction of viscera, and less chance of postoperativewound dehiscence.6 The disadvantage of paracostal incisions isthat access to only one adrenal is possible and there is limitedscope for examination of other abdominal organs. Bilateraladrenalectomy requires bilateral flank approaches.
Careful dissection and haemostasis is crucial in adrenalec-tomy. This is facilitated by the use of haemostatic clips andgood retraction. A range of retractors, especially malleableretractors, and an assistant, are imperative.
Adrenalectomy of a unilateral functional cortisol producingadrenal tumour will leave the patient with only the hypotrophicipsilateral adrenal gland and hence deficient in glucocorticoidsand possibly mineralocorticoids for some time. Various regimesof replacement therapy have been suggested. The preferred is aninfusion of hydrocortisone commenced intra-operatively at 0.5to 1.0 mg/kg/hr10 and tapered for 2 to 3 days, and then hydro-cortisone commenced orally for 1 to 2 weeks. At this time it isassumed the remaining adrenal gland will have been able toresume cortisol production, although the time scale will varybetween individuals. Patients undergoing bilateral adrenalec-tomy will require lifelong supplementation with glucocorticoidand mineralocorticoid.
Pulmonary thromboembolism is potentially a serious post-operative complication especially in the presence of vena cavalinvasion.12 Pretreatment with aspirin and heparin has beensuggested to decrease the incidence of thromboembolism.13
Acute pancreatitis with peritonitis was responsible for 25%mortality in one study.14 Although demanding both peri-opera-tively and intra-operatively, surgery of the adrenal gland can bevery rewarding. Most patients will require the care of a referralcentre with the combined input of medical and surgical special-ists as well as 24 hr monitoring for the first few postoperativedays.
Hyperadrenocorticism or canine Cushings disease is acommon endocrinopathy in middle aged and olderdogs. Approximately 85% of cases with CCD are due
to pituitary dependent hyperadrenocorticism and this iscommonly treated medically.1 The remainder have increasedglucocorticoid levels due to a functional adrenocortical tumourand surgical removal of the affected gland is the treatment ofchoice1. Although uncommon clinically, pheochromocytoma (afunctional tumour of the adrenal medulla) is another indicationfor adrenalectomy.2-4 A recent report presents some cases ofserious spontaneous haemorrhage from adrenal tumours neces-sitating emergency exploration and adrenalectomy.5
Bilateral adrenalectomy was the treatment of choice for CCDprior to the introduction of mitotane therapy6 and is still occa-sionally used in large dogs for PDH to avoid the expense ofmitotane, or in dogs that respond poorly to mitotane.
Ultrasonography has facilitated the diagnosis and evaluationof adrenal tumours being able to determine the size and sideaffected.7 Size measurements can differentiate the usuallyunilateral tumours from the bilateral hypertrophy seen in PDH,although there are a few reported cases of bilateral tumours.8-10
Ultrasonography may also often detect the presence of tumourinvasion of the caudal vena cava, seen in approximately 20% ofadrenal tumours and more common on the right hand side dueto the close proximity of the gland to the caudal vena cava(Figure 1). If there is significant caval invasion there may becongestion of caudal veins, which can be noted as engorgementof the caudal epigastric veins on the belly and flanks. Extensivevenous thrombosis has been reported.11
Patients with CCD due to adrenal tumours require carefulperi-operative management. A full medical evaluation isinevitably part of the diagnostic process. These patients areusually obese, unfit and may be affected concurrently withdiabetes mellitus.12 During surgery liver enlargement andobesity limit diaphragmatic movements and complicate thesurgical approach. Blood pressure should be monitored as thereis a significant risk of intra-operative bleeding during adrenal-ectomy. Functional pheochromocytoma may release cate-cholamines during manipulation, which could lead to hyperten-sion and arrhythmias.3 Electrocardiogram should be monitoredroutinely to detect arrhythmias.
Blood should be available for infusion during surgery espe-cially if vena caval invasion is evident on ultrasonography andresection of the wall of the vena cava is anticipated. In thisinstance, temporary occlusion of the caudal cava cranial andcaudal to the site may be required. The caudal vena cava may berepaired by direct suturing or patched using autogenous tissuesuch as pericardium or internal rectus sheath.13
The adrenal glands can be approached via either a midlinelaparotomy or paracostal incisions into the retroperitonealspace. Midline incisions enable visualisation of both adrenalsand thorough exploration of the abdominal cavity.14 The
34
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Figure 1. Right adrenal tumour (arrow) which has invaded thevena cava in a dog.
Surgery in the treatment of canine hyperadrenocorticism1. AdrenalectomyJ CULVENORNorth Shore Veterinary Hospital, 64 Atchinson Street, Crows Nest, New South Wales 2069
Aust Vet J 2003;81:34-35
CCD Canine Cushings diseasePDH Pituitary dependent hyperadronicoticism

Some adrenal tumours are locally aggressive and completeexcision is not always possible. The tumours can spread locallyor via the blood vessels. In a series of 36 cases two patients hadnon-resectable tumours and metastases were found in the lungand liver of some at subsequent necropsy examination.14
Twenty-two cases showed microscopic expansion of neoplastictissue into blood vessels. Regrowth is often very slow and recur-rence of clinical problems may take years. Mitotane at highdosages is of some use in the treatment of adrenal tumourseither not amenable to surgery16 or recurring postoperatively.17
References1. Feldman EC, Nelson RW, Hyperadrenocorticism. In: Canine and felineendocrinology. Saunders Co. Philadelphia. 1987;137-186.2. Gilson SD, Withrow SJ, Wheeler SL, Twedt DC. Pheochromocytoma in 50dogs. J Vet Intern Med 1994;8:228-232.3. Gilson SD, Withrow SJ, Orton EC. Surgical treatment of pheochromocytoma:technique, complications, and results in six dogs. Vet Surg 1994;23:195-200.4. von Dehn BJ, Nelson RW, Feldman EC, Griffey SM. Pheochromocytoma andhyperadrenocorticism in dogs: six cases (1982-1992). J Am Vet Med Assoc1995;207:322-324.5. Whittemore JC, Preston CA, Kyles AE, Hardie EM Feldman EC.Nontraumatic rupture of an adrenal gland tumor causing intra-abdominal orretroperitoneal hemorrhage in four dogs. J Am Vet Med Assoc 2001;219,329-324.6. Johnston DE. Adrenalectomy via retroperitoneal approach in dogs. J Am VetMed Assoc 1977;170:1092-1095.
7. Grooters AM, Biller DS, Miyabayshi T, Leveille R. Evaluation of routineabdominal ultrasonography as a technique for imaging the canine adrenalglands. J Am Anim Hosp Assoc 1994;30:457-462.8. Ford SL, Feldman EC, Nelson RW. Hyperadrenocorticism caused by bilateraladrenocortical neoplasia in dogs: four cases (1983-1988) J Am Vet Med Assoc1993;202:789-792.9. Thuroczy J, van Sluijs FJ, Kooistra HS et al. Multiple enodocrine neoplasiasin a dog: corticotrophic tumour, bilateral adrenaocortical tumours, andpheochromocytoma. Vet Q. 1998;20:56-61.10. Hoerauf A, Reusch C. Ultrasonographic characteristics of both adrenalglands in 15 dogs with functional adrenocortical tumors. J Am Anim Hosp Assoc1999;35:193-19911. Church DB, Lamb WA, Emslie DR. Plasma cortisol concentrations in normaldogs given hydrocortisone sodium succinate. Aust Vet J. 1999;77:316-317.12. Jaffe MH, Grooters AM, Partington BP, Camus AC, Hosgood G. Extensivevenous thrombosis and hind-limb edema associated with adrenocortical cari-noma in dog. J Am Anim Hosp Assoc 1999;35:306-310.13. Nichols R. Complicaitons and concurrent disease associated with caninehyperadrenocorticism. Vet Clin N Am Sm Anim Prac 1997,27:309-320.14. Scavelli TD, Peterson ME, Mathieson DT. Results of surgical treatment forhyperadrenocorticism caused by adrenocortical neopalsia in the dog: 25 cases(1980-1984). J Am Vet Med Assoc 1986;189:1360-1364.15. van Sluijs FJ, Sjollema BE, Voohout G, van den Ingh TS, Rijnberk A.Results of adrenalectomy in 36 dogs with hyperadrenocorticism caused byadreno-cortical tumour. Vet Q 1995;17:113-116.16. Kintzer PP, Peterson ME, Mitotane treament of 32 dogs with cortisol-secreting adrenocortical neoplasms. J Am Vet Med Assoc 1994;205:54-61.17. Keiser M, Fluckiger M, Gardelle O, Reusch C. Mitotane treatment in a dogwith a recurring adrenocortical carcinoma-a case report. Schweiz ArchTierheilkd. 1999;141:279-285.
35
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
2. HypophysectomyGB HUNTFaculty of Veterinary Science, The University of Sydney, New South Wales 2006
Aust Vet J 2003;81:35
survival rate was 80%. Remission of hyperadrenocorticismoccurred in 43 dogs, and was sustained in 38. Complicationsincluded keratoconjunctivitis sicca (as a result of damage to themajor petrosal nerves) that resolved in all but one case within 10weeks of surgery. Diabetes insipidus necessitated administrationof desmopressin eyedrops, although this was eventually discon-tinued in all but 5 dogs. Life-long treatment with cortisone andl-thyroxine was required in all dogs.
Trans-sphenoidal hypophysectomy is now the standard treat-ment for PDH at the University of Utrecht; almost 150 caseshave been performed in dogs, and a much smaller number incats,8 with a substantial reduction in morbidity since the orig-inal report.
References1. Kawamata T, Iseki H, Ishizaki R, Hori T.Minimally invasive endoscope-assistedendonasal trans-sphenoidal microsurgery for pituitary tumors: experience with215 cases comparing with sublabial trans-sphenoidal approach. NeurologicalResearch 2002;24:259-265.2. Feldman EC, Nelson RW. Hyperadrenocorticism. In: Canine and felineendocrinology. Saunders, Philadelphia. 1987:137-186.3. Yada T, Azuma T. Hypophysectomy depresses immune functions in rainbowtrout. Comp Biochem Physiol Part C Pharmacol Toxicol Endocrinol 2002;131:93-100.4. Anderson LL, Hard DL, Trenkle AH, Cho SangJoon. Long-term growth afterhypophyseal stalk transection and hypophysectomy of beef calves. Endocrinology1999;140: 2405-2414.5. Meij BP. Hypophysectomy as a treatment for canine and feline Cushing’sdisease. Veterinary Clinics of North America - Small Animal Practice2001;31:1015-1041.6. Niebauer G, Evans SM. Transsphenoidal hypophysectomy in the dog. A newtechnique. Vet Surg 1988;17:296-303.7. Meij BP, Voorhout G, Ingh TSGAM van den et al. Results of transsphenoidalhypophysectomy in 52 dogs with pituitary-dependent hyperadrenocorticism. Vet Surg1998;27:246-261.8. Meij BP, Voorhout G, Ingh TSGAM van den, Rijnberk A. Hyp Transsphenoidalhypophysectomy for treatment of pituitary-dependent hyperadrenocorticism in 7 cats.Vet Surg 2001;30:72-86.
The emphasis on surgical treatment of hyperadrenocorti-cism in dogs has historically comprised removal of func-tional adrenal tumours. Bilateral adrenalectomy for
animals with PDH that is poorly responsive to medical manage-ment has also been performed in a number of clinical cases atthe University Veterinary Centre, Sydney, with low operativemorbidity and good long-term clinical results.
However, despite the fact that surgical removal of pituitarytumours is considered the treatment of choice in man,1 andexcision plays a major role in treatment of most neoplasia inanimals,2 dogs with pituitary neoplasia have not generally beenconsidered feasible candidates for surgery. Experimentalhypophysectomy is performed routinely in experimentalanimals from fish to bovines with good survival rates.3,4 Thetrans-sphenoidal approach is the most direct for hypophysec-tomy in dogs.5 Because of major conformational differencesbetween breeds, and an inconsistent anatomical relationshipbetween the pituitary and surgical landmarks such as thehamular processes and intersphenoid suture, trans-sphenoidalhypophysectomy was historically extremely difficult in theabsence of advanced imaging. A technique for localising thepituitary using cranial sinus venography was reported byNiebauer and others in 1988.6 With improved access to CT andMRI, however, it became much easier to determine landmarksfor trans-sphenoidal hypophysectomy for individual cases.
In 1998, Bjorn Meij reported results of CT-guided trans-sphenoidal hypophysectomy in 52 dogs with PDH.7 The peri-operative mortality rate was 10%, and the 2 year estimated
CT Computed tomographyMRI Magnetic resonance imagingPDH Pituitary dependent hyperadrenocorticism

36
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Cytological examination and physical characteristics ofthe anal sacs in 17 clinically normal dogs
DC ROBSONa, GG BURTONa, MF LORIMERb
Objective To quantify numbers of leucocytes, keratinocytesand microorganisms in, as well as the turgidity, colour andconsistency of, anal sac exudates in clinically normal dogs.
Design Selection criteria were formed based on theabsence of clinical signs associated with anal sac disease,and the absence of factors potentially affecting colonic flora.Anal sacs were palpated for turgidity then expressed onto aswab, where colour and consistency were noted. A squashpreparation made from any exudate was heat fixed andstained with modified Wright’s stain. Eight representative1000x oil immersion fields from each were examined for leuco-cytes, erythrocytes, keratinocytes, bacteria and yeast. Resultswere summarised, and cytological counts grouped into quar-tiles (minimal, few, moderate, numerous). Due to the multi-variate nature of the study and limited subject numbers, furthersignificant statistical analysis could not be performed.
Results Seventeen dogs satisfied the selection criteria. Thephysical characteristics of the exudate and sac varied, though31/34 sacs were empty or soft, 22/27 exudates were light ordark brown and 19/27 exudates were a thin liquid. Total leuco-cyte, keratinocyte and bacilli counts were extremely variable.Yeasts were present in 26/208 microscopic fields examinedcytologically. Only 5/208 fields showed numerous cocci. Asingle instance of intracellular bacteria and a single erythro-cyte were noted following examination of all fields.
Conclusion In this study, the characteristics of normal analsacs and their exudate varied but greater than 70% showedsimilar features. Exudate cytology was highly variable, thoughyeasts were uncommon, and intracellular cocci and erythro-cytes extremely rare. Aust Vet J 2003;81:36-41
OIF 1000x magnification oil-immersion fieldpOIF Partial (78.2%) 1000x magnification oil-immersion field
Non-neoplastic anal sac disease (including anal sacimpaction, infection and abscessation) has beenreported to account for 12.5%1 and 1.3%2 of cases
presenting to first opinion practices. The criteria used for thediagnosis of anal sac disease in these studies were subjective. Inone study2 the diagnosis was based on “those showing clinicalsigns and physical examination findings associated with anal sacdisease” and in the other1 it was based on a wide variety ofbehavioural signs, certain concomitant clinical signs, the char-acter of the exudate, ‘abnormal’ bacterial flora and enlargementof anal sacs.
A definitive diagnosis of anal sac impaction or anal sac infec-tion is problematic.3 The clinical symptoms of anal sac diseaseare non-specific and may be associated with many other diseases
including hypersensitivities, ano-rectal neoplasia, rectal foreignbodies, perianal fistulae, perineal candidiasis, vaginitis, proctitisand endoparasitosis.4-6 The character of the exudates and thebacterial species present may not be helpful in confirming analsac disease due to wide individual variation and overlap between‘normal’ and ‘diseased’ sacs7-9 (Tables 1 and 2). Anal sac absces-sation is the least difficult disorder to diagnose of the non-neoplastic anal sac diseases because of its more typical clinicalpresentation.3
Cytology may be a useful diagnostic tool in the diagnosis ofanal sac disease. Dogs clinically diagnosed with enlarged andinfected anal sacs were reported to yield a plentiful population ofleucocytes and numerous cocci and bacilli on cytological exami-nation, while an undisclosed number of apparently normal dogsrevealed cellular debris and few leucocytes.7
A second, more recent qualitative study9 revealed the anal sacsof 20 normal dogs to contain neutrophils (12.5% of normaldogs), Malassezia sp. yeast (13% of normal dogs) and rare intra-cellular bacteria (2.5% of normal dogs).
Van Duijiken,5 in a critical literature review of anal sacdisease, concluded that further research on normal anal sacs wasnecessary to find better criteria for diagnosis of anal sac diseasethrough investigation of morphological, physical and biochem-ical aspects of anal sacs and their secretions in healthy dogs.
The objectives of this study were to quantify numbers ofleucocytes, keratinocytes and microorganisms in, as well as theturgidity, colour and consistency of, anal sac exudates in clini-cally normal dogs using a technique that would be practical inclinical practice.
Materials and methodsSourcing of material — Cases were sourced from a first-
opinion veterinary clinic in Melbourne, Australia. Selection wasbased on a 10-question true/false client questionnaire, evaluation ofpast medical records and complete physical examination. Only dogswith none of the clinical signs previously reported 3-7,11,12,14,16-18 asassociated with anal sac disease, and no factors potentiallyaffecting colonic flora (Table 3) were used in the study.Exclusions criteria thus included any dogs with evidence ofdermatological, gastrointestinal or moderate to severe dentaldisease, as well as dogs that had received antimicrobials withinthe last 7 days. Client permission was obtained for admissioninto the study.
Collection and clinical evaluation — Three operators wereinvolved with sample collection and initial evaluation. Thesignalment and weight of the dogs were recorded, and each dogwas condition scored using standard criteria.10 The external anuswas cleaned with a sterile saline soaked gauze swab to removecontaminants. A gloved, lubricated index finger was insertedinto the anus. Turgidity was assessed, and manual evacuation ofthe sac was achieved by gentle pressure between index finger andthumb. Anal sac turgidity was measured subjectively on a scale of 1
aAnimal Skin and Allergy Service, Melbourne Veterinary Specialist Centre, 70Blackburn Road, Glen Waverley, Victoria 3150bBiometricsSA, University of Adelaide, PMB 1, Glen Osmond, South Australia 5064

37
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
(empty), 2 (soft) or 3 (firm). The secretion was then collected ina 10cmx10cm cotton gauze swab held adjacent to the exit of theanal sac duct. The external rectum was again swabbed withsaline and the process repeated with the contralateral sac.
The colour of the exudate was assessed against standardcolour cards (Table 4). Determination of the red:green:bluevalues of the colour cards was achieved using a scanner (ScanJet3400C, Hewlett-Packard) and image editing software (PicturePublisher 7, Micrografx). After the colour was recorded, thepresence of flecks was noted and the consistency of the exudatewas subjectively recorded as thin liquid, thick liquid, or dry oroily paste. The swab was pressed against a microscope slide toachieve an impression smear, then smeared using a squash tech-nique to create a monolayer. The slide was labelled, heat fixedusing a lighter and stored for up to 7 days before staining. Thiswas repeated for both anal sac samples.
Staining was performed using a modified Wright’s stain(Rapid Diff Stain, Australian Biostain Pty Ltd), and, followingdrying, was preserved using mounting medium (Biomount-XT,Biochroma) under a 50 mm cover slip.
Cytological evaluation — Slide preparations were examinedunder 1000 x oil immersion magnification over eight represen-tative fields, and all leucocytes, keratinocytes, erythrocytes andmicroorganisms were counted and recorded. For bacterialcounts, 78.2% of each oil immersion field was digitallyphotographed (Coolpix 990, Nikon) and counts performed onthe enlarged image. These latter counts were facilitated by asuperimposed grid that divided each field into sixteen smallerareas. This was done in a single blinded fashion by the principalinvestigator, who was not involved in collection of the samples.
Table 1. Previously reported physical parameters of normal anal sac exudate.
Physical parameter Reference
Colour
Black to black-brown, dark red-brown, light red-brown, 8dark grey, light grey and yellowish grey
Brown 4, 11, 16
Pale yellow, pale yellow-brown, straw 7, 14, 11
Greyish-brown 15
Variety of colours 9
Consistency
Watery / thin liquid 8, 16, 17
Viscous 4, 8
Pasty 8, 15
Mucous 15
Variety of consistencies 9
Translucency
Clear 7, 11
Translucent 7
Flecks
Slightly granular 4
Small flecks 16, 17
Table 2. Previously reported physical and cytological criteria for diagnosis of non-neoplastic anal sac disease.
Criteria Reference
Anal sac impaction
Palpable enlargement of sacs 11
- may be present also in normal dogs 3
Thick pasty dark brown or greyish brown secretion 11, 14, 4, 3
- may extrude as a thin ribbon with pressure 14, 4, 3
- may also be present in normal dogs 3
Clay coloured dry paste 17
Black coloured dry or thick liquid 17
Anal sac infection
Sometimes enlarged anal sac 3, 4, 7
- thick sac wall if chronic disease 4
Greenish-yellow to purulent discharge 3, 4, 7, 11, 17, 18
- sometimes blood tinged 4, 7, 11, 18
Thin discoloured secretions with flecks of 4, 11debris or blood
Red oily thick paste 17
Pale yellow, ochre or light to dark brown 7
Consistency always turbid from honey-like to pasty 7± pale flecks
Exudate always opaque 7
Cytology shows numerous bacteria and numerous 3, 7
leucocytes / neutrophils
Cytology shows inflammatory cells with intracellular 17
bacteriaTable 3. Selection criteria.
1. No history of previously diagnosed anal sac disease.
2. No sign of the following for at least 12 months:
Behavioural History
- tenesmus
- perineal pruritus
- pruritus of flank or lumbosacral region
- discomfort sitting
- back rubbing
- tail chasing
- skin rash
- epicritic (as if suddenly bitten by something) pruritus and rump staring
- odour unrelated to washing
Medical History
- dermatologic abnormalities (including otitis, interdigital skin inflammation, pruritus)
- gastrointestinal abnormalities (including normal appetite,no other acute diseases which affected appetite, diarrhoea)
- moderate – severe dental calculus, plaque or periodontal disease
- any chronic illnesses which may affect immune function or appetite
Clinical Examination
- dermatological abnormalities (including lichenification, acute moistdermatitis, pyoderma, otitis, pododermatitis, periorbital dermatitis)
- moderate to severe dental abnormalities (as mouth flora largelydictates colonic flora)19
- periocular skin abnormalities
- evidence for illnesses which may affect immune function or appetite
- smell not related to the coat
3. No antibiotic therapy in the last 7 days.

38
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Due to the multivariate nature of the study and limitedsubject numbers, further significant statistical analysis could notbe performed.
ResultsSeventeen dogs, including five entire male, five entire female,
four desexed male and three desexed female dogs satisfied selec-tion criteria. There were fifteen breeds represented, and dogsranged in age from 6 months to 12 years (median 19 months),in weight from 2.5 to 54.6 kg (median 16.8 kg) and in condi-tion score from 2 to 4 (mean 2.7). As seven anal sacs containedno palpable exudate, the physical characteristics of 27 exudatescould be assessed. A further sample was damaged duringprocessing, leaving 26 samples that were assessed cytologically.
Physical parameters — The physical characteristics of theexudate and anal sacs varied between individuals (Table 4),though there were some trends apparent.
Thirty-one of 34 sacs palpated were subjectively assessed aseither empty or soft, and 19/27 sacs contained a thin liquidexudate. There was no obvious trend between turgidity of thesac and consistency of the exudate: two of the three sacs gradedfirm had liquid exudate, though the third firm sac did contain apasty exudate. Twenty-one of 27 sacs showed a light or darkbrown exudate. Within individuals, there was similarity in theconsistency and colour of exudate from left and right anal sacswith 10 of 11 the same consistency and 9 of 11 the same colour.Comparison was not possible in six dogs because one or bothsacs were empty.
Other physical characteristics were more variable. Exudatefrom 14 sacs was graded translucent and in 12 was gradedopaque. Eighteen had noticeable flecks of more solid matterpresent in the exudate.
Cytology — Processing of the specimens was difficult in somecases, with some of the sample flaking off in the course ofstaining and rinsing. This was not a consistent finding buttended to occur with samples of thicker consistency. In sampleswhere this occurred, the affected regions were not included incytological analyses. Two hundred and eight oil immersionfields (26 samples and 8 fields examined per sample) wereincluded for analysis. The summary statistics did not considerpossible associations in data between anal sacs within a dog andbetween the eight fields of view.
Keratinocytes were found in all but two anal sac exudatesamples. The degree of variability in counts between sacs wasvery high (Table 5), ranging from 0 to 44 keratinocytes/OIF.Nucleated keratinocytes were present in 6 of 24 sacs thatcontained keratinocytes, and ranged from 1 to 10 per OIF. Thisrepresented from less than 1% to over 68% of the totalkeratinocyte counts in these sacs.
Leucocytes were found in all sacs, though the total countswere highly variable (Table 5) ranging from 0 to 56 leucocytesper OIF. Seventy-five point three % of leucocytes were degen-erate, with loss of cellular architecture (see Figure 1) precludingdifferentiation as to the type. Of the remaining identifiable24.7% of leucocytes, 69.3% were degenerate neutrophils andthe remainder were macrophages and lymphocytes. Only twoeosinophils were observed in all the fields examined, and thesewere present in the exudate from only a single sac. It was notpossible to group leucocyte counts semi-quantitatively because anear maximum number was not reached.
Erythrocytes were a very uncommon finding and were foundonly in one sac of one dog.
Statistical analysis — Cytological results were summarised,and where possible grouped semi-quantitatively into quartiles(minimal, few, moderate, numerous) based on the five-numbersummary (minimum, first quartile, median, 3rd quartile andmaximum) to attempt to identify normal ranges, and to try andprovide clinical relevance of the results. Relevant semi-quantita-tive grouping for each cell type was dependent on the maximumnumber attaining, or nearly attaining complete coverage of anOIF (that is, a number beyond which no more of that cell typemay have fit on the microscopic field).
Table 4. Physical parameters of anal sacs and their exudates.
Anal sac turgidity (n = 34) No. of anal sacs
Empty 7
Soft 24
Firm 3
Same left/right 11/17 dogs
Exudate consistency (n = 27)
Thin Liquid 19
Thick Liquid 6
Pasty 2
Same left/right 10/11 dogs
Exudate colour (n = 27)
Off White (202:184:150)a 4
Straw (242:211:91) 0
Greenish-Yellow (193:193:121) 0
Light Brown (132:105:73) 11
Dark Brown (85:62:53) 10
Red-Brown (122:61:51) 0
Black (56:61:69) 2
Same left/right 9/11 dogsaBracketed numbers are red:green:blue colour values (0-255)
Exudate translucency (n = 27)
Clear 1
Translucent 14
Opaque 12
Same left/right 6/11 dogs
Flecks in exudate (n = 27)
Present 18
Not Present 9
Same left/right 6/11 dogs
Table 5. Leucocyte and keratinocyte counts in anal sac exudates per OIF.
Leucocytes Keratinocytes
Observations n = 208 n = 208
Minimum 0 0
1st Quartile 1 2
Median 3 9
3rd Quartile 10 23
Maximum 56 44
Mean 7.93 12.61
Standard Deviation 10.69 11.66

39
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Bacteria were seen in all samples, and though the numberswere generally low, the exudate from several sacs containedextremely high numbers (see Table 6). Semi-quantitativegrouping combining all bacterial types was possible because anear complete coverage of the OIF was achieved with theselatter samples.
Rods were especially variable in number. Coccal counts werelower, with 162/208 (77.9%) fields containing cocci havingminimal to few (0 to 97) cocci, and only 5/208 (2.4%) fieldsshowing numerous (319 or more) cocci (Figure 2). Only asingle instance of intracellular bacteria (cocci) was notedfollowing examination of all fields. The only other morphologi-cally different bacteria observed in this study were spirochetes,which were seen in 4/26 sacs and in very low numbers (three orless per pOIF).
Only 26/208 fields (contained within 8/26 sacs) wereobserved to contain any yeasts. All except one showed three orfewer yeasts/OIF, and no fields contained > 10 yeasts/OIF.
DiscussionInterpretation of some of the previously published studies
regarding the properties of normal anal sac secretions is madedifficult by the variable or loose definition of ‘normal’. Theinclusion and exclusion criteria used in this study may havelimited the number of cases investigated, but ensured that theanimals included did not have anal sac disease, as currentlydefined in the veterinary literature.3-7,11,12,14,16-18
Physical characteristics — The colour and consistency of analsac exudate in this study were similar to, but showed less varia-tion than, previous studies of normal anal sac exudate.8,9
Greater than 70% of all anal sacs were empty or soft to palpate,exudates were a light or dark brown liquid, and dogs had similarcolour and consistency of exudate in both sacs where present.This comparatively reduced variation may have been a conse-quence of the strict selection criteria, or a limitation of the sizeof the study. If the former, then these findings above may repre-sent the typical gross characteristics of anal sacs and theirexudates in the absence of anal sac disease.
Most of the previously described assessments of normal analsac characteristics (Table 1) fit the ranges found in this study,with the exception of one11 that suggested that the presence offlocculation, turbidity and granular material was abnormal.None of the previously described gross characteristics of anal sac
Figure 1. Micrographs of four pOIFs showing bacterial numbers represen-tative of each of the four quartiles. Field 1a contains 22 bacteria (minimal),field 1b contains 61 bacteria (few), field 1c contains 212 bacteria(moderate) and field 1d contains 1209 bacteria (numerous). Note also theunidentifiable degenerate leucocytes (black arrows) and degenerateneutrophils (white arrows). Photographic density has been altered digitally.
CocciRods
140
120
100
90
60
40
20
0
Nu
mb
er o
f F
ield
s
Minimal Few Moderate Numerous(0-43) (44-97) (98-318) 319+
Number of Bacteria
Figure 2. Bacterial counts / pOIF over 208 fields.
a
b
c
d

40
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
The presence of leucocytes appeared to be normal, beingfound in most exudates, and sometimes in large numbers.Neutrophils were the most commonly identified inflammatorycell present, though there was a high proportion of undifferenti-atable markedly degenerate leucocytes in this study. This mayhave been due to fixation artefact, the delay between collectionand staining or a true finding. In several freshly stained andexamined samples taken by one author from dogs following thecompletion of this study degenerate leucocytes were commonlyfound, but marked degeneration was less commonly found(data not included), suggesting that the extreme degenerationfound in the study may have been partly artefactual, possiblydue to the drying process or the prolonged storage time in somecases.
Very few erythrocytes were found suggesting that, wherepresent, large numbers may be abnormal. Potential causes oferythrocytosis in anal sac exudate include trauma prior to or atcollection, anal sac inflammation, anal sac neoplasia and coagulo-pathies.
Although the presence of low numbers of bacilli predomi-nated, the finding of extreme numbers in several samplessuggested there is a wide range of normality, and the number ofbacilli alone is unlikely to be a useful criterion for disease. Faecalcontamination of some of the samples cannot be ruled out,however was most unlikely because of the measures taken toavoid it. The variation in numbers of coccoid bacteria was not asgreat. Large numbers of coccoid bacteria may be abnormal,although further study is required to substantiate this. Themicroscopic appearance of numerous bacteria (as defined in thisstudy) is shown in Figure 3.
Spirochetes, a few of which were found in three anal sacexudates, have not been previously documented as part ofnormal anal sac flora.
Most of these cytological findings were consistent withPappalardo et al,9 with the exception of leucocytes, which weremore frequently found in this study.
Relevance to diagnosis of disease — The findings of this studycontrast with those of Halnan,7 the only study to examineexudate cytology from both apparently normal and inflamedanal sacs. While the exudate from several cases in this study didshow cellular debris and few leucocytes consistent with normalanal sacs according to Halnan,7 at least 7/17 cases would havebeen consistent with cytological characteristics that Halnan7
ascribed to dogs with anal sacculitis. Several species of bacteria have been isolated from inflamed
anal sacs in previous studies (Table 7), and instillation of a bacte-rial broth into anal sacs has experimentally reproduced analsacculitis.12 In this study, however, gross numbers of bacteriaalone, especially bacilli, did not seem to be diagnostically rele-vant. Potentially of more importance was that only a singleinstance of intracellular bacteria was seen in all fields examined,suggesting that this is a rare event in normal anal sacs. However,it cannot be ruled out that further instances of intracellularbacteria were not observed in this study due to the dense chro-matin of the degenerate leucocytes, though this was consideredunlikely because the bacteria stained a deeper colour than thenuclei of the cells and should still have been visible if present(Figure 1).
Yeast (Malassezia pachydermatis, previously Pityrosporum canis)have also been cultured from dogs diagnosed with impactionand infection of the anal sacs.13 They were, however, isolatedwith a variety of other bacteria and their role in the pathogenesis
exudate associated with anal sacculitis were found in this study,again with the exception of one report.7 It is interesting to notethat one sac in this study would have fit several reports’ criteria4,
11,14,17 for anal sac impaction. In contrast to this, some of the samples from Doty and
Dunbar,8 where a wider variety of exudate colour was foundcompared with this study, would have satisfied some reportedcriteria4,7,17,18 for anal sacculitis. Variations in the physical char-acteristics of anal sac exudates, however, may be partlyexplained by different proportions of the glandular secretions inthe sac5 and exudate described as grossly purulent may be aproduct of predominantly holocrine secretion (which is moreviscid and yellow) of sebaceous glands located in the duct of theanal sac.
Cytology — Keratinocytes appeared to be a normal finding inmost anal sac exudates though there was wide variation innumbers present, suggesting that this characteristic alone isunlikely to be useful diagnostically. The significance of thenucleated keratinocytes seen in some samples is unknown andwas not consistently associated with any other cytological findings.
Table 6. Bacterial counts in anal sac exudates per pOIF (n = 208).
Cocci Bacilli Total
Minimum 0 0 0
1st Quartile 14.75 23.5 43
Median 32.5 60 97
3rd Quartile 83.75 184 318
Maximum 763 2368 2457
Mean 67.39 223.49 290.88
Standard Deviation 98.02 410.90 452.61
Table 7. Bacterial species isolated fromnormal and diseased anal sacs.
Normal Anal Sacs7,9
Micrococci7
E coli7,9
Streptococcus faecalis7
Staphylococcus sp7
Staphylococcus intermedius9
Proteus mirabilis9
β-haemolytic streptococci9
Bacillus sp9
Pseudomonas aeruginosa9
Diseased Anal Sacs7
Micrococci
E coli
Streptococcus faecalis
Staphylococcus sp
Diphtheroids
Clostridium welchii
Bold typeface indicates species isolated fromboth normal and apparently diseased analsacs.

41
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
of the disease in these cases was questioned. It seems plausiblethat the role of yeast in the anal sac is similar to that in the earcanal, where small numbers can be part of the normal flora.17 Inthat case it may also be possible that large numbers may beabnormal, and potentially pathogenic.
ConclusionAlthough the definitive diagnosis of anal sac disease remains
difficult, the results of this study suggest that assessment ofphysical characteristics of the anal sac and its exudate, and espe-cially cytology of the exudate, may represent clinically usefuldiagnostic aids when trying to differentiate normal anal sacsfrom anal sacculitis. The finding of large numbers of non-degenerative neutrophils, intracellular bacteria, erythrocytosisand large numbers of cocci, spirochaetes or yeast would appearto be abnormal. Further study is required to confirm these find-ings in normal dogs, and characterise findings in both diseasedanal sacs, and dogs with dermatologic disease but no evidence ofanal sac disease.
AcknowledgmentsThe authors would like to thank all the staff from Rowville
Veterinary Clinic for their assistance in the case work, and theMelbourne Veterinary Referral Centre research fund for finan-cial assistance with the statistical analysis.
References1. Halnan CR. The frequency of occurrence of anal sacculitis in the dog. J SmallAnim Pract 1976;17:537-541.2. Harvey CE. Incidence and distribution of anal sac disease in the dog. J AmAnim Hosp Assoc 1974;10:573.3. Thomson MS. Diseases of the anal sacs. In: Kirk RW, editor. CurrentVeterinary Therapy XIII. Saunders, Philadelphia, 2000:591-593.4. Anderson RK. Anal sac disease and its related dermatoses. Compend ContinEduc 1984;6:829.
5. van Duijkeren E. Disease conditions of canine anal sacs. J Small Anim Pract1995;36:12-16.6. DeNovo RC, Bright RM. Recto-anal disease. In: Ettinger SJ and FeldmanEC, editors. Textbook of Veterinary Internal Medicine. 5th edn. Saunders,Philadelphia, 2000:1266-1267.7. Halnan CR. The diagnosis of anal sacculitis in the dog. J Small Anim Pract1976;17:527-535.8. Doty RL, Dunbar I. Color, odor, consistency, and secretion rate of anal sacsecretions in male, female and early-androgenized female beagles. Am J VetRes 1974;35:729-731.9. Pappalardo E, Martino P, Noli C. Clinical, cytological and bacteriological eval-uation of anal sacs of normal dogs and of dogs with pyoderma, Malasseziainfection or atopic dermatitis. (Abstr) In: Proceedings 17th Annual MembersMeeting of the American Academy of Veterinary Dermatology and AmericanCollege of Veterinary Dermatology. American Academy of VeterinaryDermatology and American College of Veterinary Dermatology, April 2002.10. Pantalo J. Body conditioning scoring. In: Nutritional Management of Obesity(informational monograph), Iams Company, Dayton.11. Greiner TP, Greene RW, Archibald J. Large intestine and anus. In:Archibald J and Catcott EJ, editors. Canine and Feline Surgery. 1st edn.American Veterinary Publications, Santa Barbara, 1984:216-218.12. Halnan CR. The experimental reproduction of anal sacculitis. J Small AnimPract 1976;17:693-697.13. Hajsig M, Lukman P. Pityrosporum pachydermatis (P. canis) in the inflamedcanine anal sacs. Vet Archiv 1980;50:43.14. Burrows CF, Ellison GV. Recto-anal disease. In: Ettinger SJ, editor.Textbook of Veterinary Internal Medicine. 3rd edn. Saunders, Philadelphia,1989:1570-1572.15. Neurand K, Meyer W. Die Drüsen der Analregion des Hundes. TierärztlichePraxis 1982;10:243-252.16. Baker E. Diseases and therapy of the anal sacs of the dog J Am Med VetAssoc 1962;141:1347-1350.17. Scott DW, Miller WH, Griffin CE. Diseases of eyelids, claws, anal sacs andear canals. In: Muller and Kirk’s Small Animal Dermatology. 5th edn. Saunders,Philadelphia, 2001:1200-1203,1214.18. Burrows CF, Sherding RG. Constipation and Dyschezia. In: Anderson et al,editors. Veterinary Gastroenterology. 2nd edn. Lee & Febiger, Philadelphia,1992:484-503.19. Strombeck DR. Microflora of the Gastrointestinal Tract and its SymbioticRelationship with the Host. In: Guilford WG et al, editors. Strombeck’s SmallAnimal Gastroenterology. 3rd edn. Saunders, Philadelphia, 1996:14-18.
(Accepted for publication 14 October 2002)
BOOK REVIEW
Skin Diseases of the Dog. Paterson S. Blackwell Science Asia, Carlton, 2002, 309 pages. Price $137.90. ISBN 0632048085.
Skin Diseases of the Cat. Paterson S. Blackwell Science Asia, Carlton, 2002, 270 pages. Price $137.90. ISBN 0632048050.
These companion soft-backed reference handbooks are produced for use in the clinical situation. Designed for use by practitioners toassist in establishing a diagnosis or to recognise when referral is indicated, the books should also prove invaluable to students as the
content appears to be comprehensive.While the Introductions have minor differences because of species characteristics, the two books follow identical composition, describing
skin structure, history taking, skin examination and various diagnostic tests that can be utilised.Subsequent chapters are individually devoted to the various types of skin disease, ranging from bacterial, fungal and viral, through para-
sitic, endocrinal, neoplastic and keratinisation defects, ultimately covering the total spectrum of present knowledge. One chapter unique tothe ‘Dog’ volume concerns otitis externa, whereas that of the ‘Cat’ gains a chapter on the eosinophilic allergic syndrome.
The text structure for each skin condition is identical: cause and pathogenesis, clinical signs, differential diagnosis, diagnosis and treat-ment. Each of these sections is in bold type and is spaced to allow easy reading of the text. The title of the chapter is printed at the top ofeach page alongside the page number. This is a readily readable format; a comprehensive index results in a functional reference book.
The author, who is a specialist veterinary dermatologist, has wisely chosen to separate consideration of the skin diseases of the twospecies into distinct volumes, each of which has gained from this decision.
My single reservation, and it is a serious one, concerns the poor quality and unsuitability of a large number of the photographs in the twobooks; they detract from the high standard of the text. Informative value in dermatological photos demands good light, sharp focus andadequate depth of field, particularly in close-ups; this is exemplified in pharmaceutical company advertisements. Had the photographsmatched the quality of the text these volumes would have been much improved.
Nevertheless, the large increase in knowledge of veterinary dermatology over the last several years is presented here in a very practicalform for application by the practitioner, and both volumes are suitable for inclusion in the practice library.
A Lawther
Dr Alan Lawther is a retired Melbourne practitioner.

42
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
semimembranosus), gastrocnemius and cranial tibial muscles.There was pain on extension of the left coxofemoral joint andalso on palpation of soft tissue surrounding the joint. There wasno pain associated with manipulation of the thoracolumbarspine. A large, bilateral, nodular mass was palpable through thedorsolateral rectal wall. Conscious proprioception was absent inthe left hind limb, the patellar reflex was exaggerated and with-drawal was reduced. Sensation in the left hind foot was reduced.Both fore limbs and the right hind limb were neurologicallynormal at this stage.
Haematological and serum biochemical analyses were withinnormal limits. Survey radiographs of the pelvis and lumbarspine were consistent with mild bilateral hip dysplasia and milddegenerative changes at the lumbosacral junction. Thesechanges were not considered to account for the clinical signsand both EMG and MRI were recommended.
EMG demonstrated spontaneous depolarisations and positiveSharp waves in the left proximal semitendinosus and left glutealmuscles. The conduction velocity of the left sciatic nerve was 35msec-1. The conduction velocity of the right sciatic nerve wasthe same and this was considered normal for a dog of this age.The EMG findings were consistent with denervation of muscleinnervated by the sciatic nerve. A presumptive diagnosis ofsciatic nerve sheath tumour was made.
MRI demonstrated an extensive mass lesion. On T1-weightedsagittal images there was a large clearly marginated mass ventralto the vertebral column (Figure 1A). The mass extended fromthe caudal aspect of L7 to caudal S3. Within the mass were ill-defined circular regions of hyperintensity. The mass displacedthe colon ventrally. On T2-weighted images, the mass wasmoderately heterogeneous. On T1-weighted images postadministration of gadolinium-based contrast medium, therewas heterogeneous contrast enhancement with multiple regionsof contrast void throughout the mass (Figure 1B). On transverseT2-weighting, the mass could be seen extending through thevertebral foramen on the left side at L7-S1 with a mild loss ofepidural fat laterally. The mass extended medially to the rightventral aspect of the sacrum. There was alteration of the corticalmargin of the medial aspect of the ischium on the left side(Figure 2).
During the investigation, the bilateral nature of the tumourbecame apparent and the dog exhibited signs in the right hindlimb associated with reduced sciatic function. Given the exten-sive and bilateral nature of the tumour, surgery was not recom-mended and the dog was sent home with continued palliativetreatment (Meloxicam). The dog was euthanased by the refer-ring veterinarian 3 months later and tissue from the mass wascollected postmortem and fixed in formalin.
Histological examination revealed a high density sarcoma inwhich the tumour cells were forming irregularly shaped nodulesthat were haphazardly dissected by thick bands of hypocellularcollagen. The tumour cells were spindloid with bipolar cyto-
Sciatic nerve tumour was diagnosed in a Staffordshire BullTerrier cross-bred and a Bichon Frise, both presenting withchronic left hind limb lameness. Neurological examination ineach case was consistent with left sciatic nerve deficits andthis was confirmed by EMG studies. Rectal examination ofboth dogs revealed a palpable intrapelvic mass that was notapparent on survey radiographs. A sciatic nerve tumour wasidentified using MRI in each case. Histological examination oftissue taken from the Staffordshire Bull Terrier cross-bred wasconsistent with a malignant peripheral nerve sheath tumour.Aust Vet J 2003;81:42-46
CSF Cerebrospinal fluidCT Computerised tomographyEM Electron microscopyEMG ElectromyographyMRI Magnetic resonance imagingPCV Packed cell volume
Peripheral nerve sheath tumours most commonly arisefrom the cervical nerves and nerves of the brachialplexus.1-18 Peripheral nerve sheath tumours of the cranial
nerves, thoracic, thoracolumbar, lumbar and lumbosacralnerves, cheek subcutis and oral submucosa, phrenic nerve anddiaphragm, and vagosympathetic trunk have also beenreported.6,7,13,14,19-26 The majority of peripheral nerve sheathtumours manifest clinically as chronic lameness with muscleatrophy or as acute, progressive spinal cord compression.12
Treatment is usually surgical and early diagnosis maximises thepossibility of complete resection.13,23 Early diagnosis may bedifficult due to the initial clinical signs mimicking those ofmusculoskeletal disease.5,6,27 Ancillary tests used for diagnosis ofperipheral nerve sheath tumours include plain radiography,myelography, EMG, CSF analysis, CT and MRI. In both dogsdescribed in this case report, neurological and rectal examina-tion led to a presumptive diagnosis of sciatic nerve sheathtumour. Sciatic nerve dysfunction was confirmed by EMG, andMRI was then used to image lesions that were not apparent onsurvey radiographs.
Case reportsCase 1
A 10-year-old neutered female Staffordshire Bull Terriercross-bred (20 kg) was presented with a 6 week history of lefthind limb lameness. The dog appeared to experience severe painat the onset of the lameness. Initially there had been a partialresponse to non-steroidal anti-inflammatory drugs (Meloxicam,Boehringer Mannheim) but the dog was non-weight bearingwhen presented for examination.
On examination, non-weight bearing lameness of the lefthind limb was accompanied by marked muscle atrophy of thecaudal thigh musculature (biceps femoris, semitendinosus,
Diagnosis of sciatic nerve tumour in two dogs by electromyography and magnetic resonance imaging
LA ABRAHAM, RW MITTEN, C BECK, JA CHARLES and SA HOLLOWAYUniversity of Melbourne, Department of Veterinary Science, 250 Princes Highway, Werribee, Victoria 3030

43
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
plasmic tails. Nuclei were centrally positioned, hyperchromatic,with tapered ends. There was a high mitotic index with manyabnormal mitoses. The tumour cells were arranged into tightlyinterwoven fascicles, with serpentine nuclear profiles in someareas. At low power, a distinctive feature was palisading oftumour cells to form pseudorosettes centred on hyalinisedeosinophilic material. There was widespread osteoid synthesisthroughout the tumour with variable mineralisation of thesmall deposits. Multifocal ischaemic necrosis and mild chronichaemorrhage with haemosiderosis were also present throughoutthe mass. Older regions of necrosis had been replaced by maturecollagen that was irregularly mineralised. There was multifocalevidence of tumour invasion of stromal lymphatics or thinwalled veins.
The morphology of the tumour was most consistent with amalignant peripheral nerve sheath tumour although anosteosarcoma could not be discounted. EM and immunohisto-chemistry were performed on formalin fixed tissue in anattempt to confirm the cellular origin of the tumour. Cellpreservation, however, was insufficient for EM and it was notpossible to differentiate between a nerve sheath tumour and
osteosarcoma by this technique. Immunohistochemistry wasperformed using S-100 antibody and the result was inconclusive(again most likely due to poor preservation of the tissue). Thetissue was also examined using antibodies against smoothmuscle actin and vimentin. The tumour was negative forsmooth muscle actin. There was uniformly positive staining forvimentin. Based on the immunohistochemical screening, thetumour may be classified as a peripheral nerve sheath tumour,spindle cell tumour of connective tissue origin or a haeman-
Figure 1. Sagittal T1-weighted images of the lumbosacral regionof a 10-year-old Staffordshire Bull Terrier with left hind linb lame-ness (Case 1) before (A) and after (B) administration ofgadolinium-based contrast medium. (A) There is a large mass(m) ventral to the vertebral column. Within the mass, there are ill-defined regions of hyperintensity. (B) There is heterogeneouscontrast enhancement of the mass.
Figure 2. Transverse plane T2-weighted image of the lumbarregion of Case 1 with the dog positioned in dorsal recumbency.The mass (m) extends medially to the right ventral aspect of thesacrum and can be seen extending into the left intervertebralforamen.
Figure 3. Dorsal plane T1-weighted image of the pelvic andlumbosacral region of a 7-year-old Bichon Frise with left hindlimb lameness (Case 2) post administration of gadolinium-basedcontrast medium. The mass (arrow heads) extends laterallyaround the caudal aspect of the ischium. There is hetero-geneous contrast enhancement.

44
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Peripheral nerve sheath tumours arise most commonly fromthe spinal roots of the cervical nerves and nerves of the brachialplexus.1-18 Peripheral nerve sheath tumours of the skin, cranialnerves, thoracic, thoracolumbar, lumbar and lumbosacralnerves, cheek subcutis and oral submucosa, phrenic nerve anddiaphragm, vagosympathetic trunk, testis, skeleton, thoracicand abdominal cavity have also been reported.6,7,11,13,14,18-
26,30,31.Since the majority of peripheral nerve sheath tumours affect
the cervical nerve roots and nerves contributing to the brachialplexus, chronic fore limb lameness is the most commonpresenting clinical sign. A palpable mass, pain and hyperaes-thesia are inconsistent features, although marked muscleatrophy is usually present.1,2,4-6,8,9,12,13,16,32 In the two casesreported here, chronic lameness with marked muscle atrophyand pain on palpation in the region of the left coxofemoral jointwere present. These findings were similar to other cases ofperipheral nerve sheath tumours arising from lumbar orlumbosacral nerves.13,23 Rectal examination demonstrated apalpable mass in both of our cases and has been reported previ-ously with a lumbosacral nerve sheath tumour.23 The presenceof a rectal mass and the distribution of the neurological deficitsled to a presumptive diagnosis of a sciatic nerve tumour andfurther tests were recommended.
Ancillary diagnostic tests used to confirm a diagnosis ofperipheral nerve sheath tumour include plain radiography,myelography, EMG, CSF analysis, CT, MRI and histologicalstudies. Ultrasound (with ultrasound guided biopsy) and onco-logical scintigraphy have also been used more recently in thediagnosis of peripheral nerve sheath tumours23,26,33 but werenot employed in our dogs.
Survey radiographs are of limited use in the diagnosis ofperipheral nerve sheath tumours since abnormalities are onlydetected when masses attain a palpable size.4,5 When abnormal-ities are present on survey radiographs, they may include miner-alised mass lesions, bony erosion and disuse osteo-porosis.4,5,12,13,31 Survey radiographs of the pelvis and lumbarspine were consistent with mild bilateral hip dysplasia and milddegenerative changes at the lumbosacral junction in the first ofthe cases reported here and were normal in the second case. Theradio-graphical findings in both dogs failed to explain the clin-ical signs and EMG was therefore performed to confirm thatthe neurological deficits were confined to the sciatic nerve.
EMG historically has been shown to be the most reliableancillary test in the diagnostic evaluation of peripheral nervesheath tumours.5,9,12,13,16,17,20,26,32,34 EMG abnormalities maybe observed with damage to peripheral nerves but are notspecific for peripheral nerve sheath tumours. Denervationpotentials are detected in muscle as soon as 5 days after denerva-tion injury and correct localisation of lesions by EMG has beenconfirmed at necropsy.35 EMG or nerve conduction velocitywas abnormal in the cases reported here, with denervationpotentials present in our first case. Delayed conduction velocityin our second case indicated demyelination or axonal injury.EMG was accurate in the localisation of the lesions of bothdogs. Detection of spontaneous activity in the gluteal musclessuggested injury to the lumbosacral trunk in the first case,although it was not possible to determine whether the lesionextended into the spinal cord by EMG studies.
Myelography has been used to detect spinal invasion ofperipheral nerve sheath tumours, although myelographic find-ings may be normal despite such extension.5,9,12,13,32 Given that
giopericytoma.15,18,19,26,28,29 A peripheral nerve sheath tumourwas considered most likely.
Case 2A 7-year-old neutered male Bichon Frise was presented with a
7 month history of progressive left hind limb lameness. Therehad been no response to non-steroidal anti-inflammatory drugs(Carprofen, Pfizer) and the dog was non-weight bearing whenpresented for examination. Blood samples taken prior to referralhad demonstrated mild anaemia (PCV 0.33 L/L, red blood cellcount 4.81 x 1012/L and haemoglobin 111 g/L; reference range0.37 to 0.55 L/L, 5.5 to 8.5 x 1012/L and 120 to 180 g/Lrespectively), eosinophilia (2.51 x 109/L; reference range 0.1 to1.25 x109/L), hypoglycaemia (3.0 mmol/L; reference range 3.3to 7.8 mmol/L) and decreased urea (3.0 mmol/L; referencerange 3.6 to 8.9 mmol/L).
On examination, there was left hind limb lameness with paindorsal and cranial to the left coxofemoral joint. Muscle atrophywas more severe than in case 1 but the distribution was iden-tical. There was no pain associated with manipulation of thethoracolumbar or lumbosacral spine. A firm mass was palpablethrough the left lateral rectal wall. Neurological deficits weresimilar to the first case and consistent with left sciatic nervedysfunction. Haematological and serum biochemical analyseswere normal. Survey radiographs of the pelvis and lumbar spinewere normal and both EMG and MRI were recommended.
Given the severe muscle atrophy, it was not possible to assessspontaneous muscle activity (by insertion of the electrode) ofmuscles innervated by the left sciatic nerve. The conductionvelocity of the left sciatic nerve was delayed (40 msec-1) whencompared with the conduction velocity of the right sciatic nerve(60 msec-1). A presumptive diagnosis of sciatic nerve sheathtumour was made based on the reduced conduction velocity,pattern of muscle atrophy and palpable rectal mass.
MRI demonstrated severe muscle atrophy involving the entireleft hind limb. Within the pelvic canal on the left side, dorsal tothe urinary bladder and lateral to the colon, was a heteroge-neous mass that was hyperintense on T2-weighted images. Themass was clearly marginated and extended laterally around thecaudal aspect of the ischium (Figure 3). The mass demonstratedheterogeneous contrast enhancement post administration ofgadolinium-based contrast medium. Following contrastenhancement, the mass could be seen extending laterally to thelevel of the gluteal muscles, which were severely atrophied, andmedially into the vertebral foramen at L7-S1.
Surgery was declined and the dog was sent home with non-steroidal anti-inflammatory drugs for palliation. The dog hasremained well, but lame, to date.
DiscussionPeripheral nerve sheath tumours arise from the cells
surrounding the axons of peripheral nerves. These tumours havebeen classified as schwannomas, neurinomas, neurilemmomas,neurofibromas and neurofibrosarcoma.6,11-13 The Schwann cellis the presumed cell of origin of those neoplasms involvingperipheral nerves and nerve roots.6,11-13 In man, clinical andmorphological distinctions are recognised between schwan-noma, neurofibroma and malignant peripheral nerve sheathtumour.18 The same differentiation is currently less recognisedin veterinary literature and tumours of the peripheral nervoussystem are therefore classified as peripheral nerve sheathtumours.

45
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
a rectal mass was palpated in both of the cases reported here,MRI was selected because this imaging modality is capable ofdetermining the full extent of the tumour both within thecentral nervous system and peripherally. Ultrasound was alsoconsidered since it is possible to biopsy the mass with directvisualisation.23 Ultrasound does, however, image the full extentof the mass within the pelvic canal or central nervous system.
The MRI appearance of peripheral nerve sheath tumours hasbeen described in dogs.17,20,36 The tumours are isointense onT1-weighted imaging and isointense or hyperintense on T2-weighted imaging. Contrast enhancement has been noted in allreported cases. Contrast enhancement was mostly uniform,with the exception of one case in which a spherical, hypointensecentral region was visualised.17 In contrast to the previousreports, T1- and T2-weighted images of our cases revealedheterogeneous mass lesions with heterogeneous contrastenhancement. These observed differences suggest that the histo-logical tumour type cannot be predicted by the MRI appearanceof the lesion in cases of peripheral nerve sheath tumours. Inhuman studies, MRI cannot differentiate between neurilem-momas, neurofibromas and malignant nerve sheath tumours.37
However, MRI can be helpful for planning surgery based on theextent of the lesion. Exploratory surgery and histological exami-nation may ultimately be required to determine the true extentof the lesion, since it has been suggested that MRI may overesti-mate invasion into the spinal cord.36 Surgery was declined inboth our cases given the extent of the tumour invasion and like-lihood of incomplete excision. The full extent of the tumouranatomically was not documented in the first case and thesecond dog was alive at the time of writing. It is thereforeimpossible to comment on the reliability of MRI in assessmentof central nervous system invasion in our cases.
Tumours arising from peripheral nerve sheath or showingnerve sheath differentiation are defined as peripheral nervesheath tumours.38,39 These tumours may be high grade malig-nant, low grade malignant or benign.38,39 These tumours areremarkably heterogeneous in their histological appearance.11,40
The benign forms are well differentiated and cells may bearranged in two patterns within the tumour. Antoni A arrange-ments are characterised by repetitive fusiform cells arranged inbands, herringbones, whorls or palisades. Antoni B arrange-ments are degenerative in nature and the spindle cells aredistributed amongst loose, myxoid or hyalinised tissue.11
Mixtures of cell types may be present within a single tumour40
and focal malignant transformation can occur.38 Microscopicfeatures of highly malignant peripheral nerve sheath tumoursare varied. The tumours are highly cellular, comprising undiffer-entiated spindloid cells with readily identifiable mitoses.Cartilaginous and osseous elements may be found infrequentlyin benign tumours4,11,25 and have been reported in less than15% of malignant peripheral nerve sheath tumours in man.38,39
Rhabdomyoblastic, epithelial glandular, squamous or neuroen-docrine differentiation have also been described. Melanotic,epithelioid and combined osseous and glandular differentiationhave been reported in the dog.19,22,41 In our first case, there wasosseous differentiation. Peripheral nerve sheath tumours may bedifficult to diagnose by histopathology alone given their diverseappearance, and alternative techniques (such as EM orimmunohistochemistry) may be required to characterise theorigin of the tissue.
Ultrastructural features of schwannomas in the dog have beendocumented by EM.22,30 They include cytoplasmic processes
and an external lamina surrounding the spindle shaped cells. Ithas been proposed that scanning electron microscopy can differ-entiate between schwannomas and neurofibromas.21
Schwannomas contain proliferations of smooth tube-formingcells; the inner tubular surface contains uneven linear projec-tions whereas the outer surface is smooth. Neurofibromascontain extensive laminations of collagen with scattered fibrob-last-like cells.21 Malignant peripheral nerve tumours are poorlydifferentiated and exhibit few characteristic features on EM.Histologically similar sarcomas may, however, be excluded byEM.39 The tissue taken from our first case was too poorlypreserved to enable ultrastructural evaluation.
Immunohistochemistry has been used to determine thecellular origin of peripheral nerve sheath tumours. Expression ofS-100 protein, vimentin, smooth muscle actin and glial fibril-lary acidic protein has been investigated.10,15,18,24,26,29,40
Positive staining for S-100 has been reported in schwannomasalthough expression of S-100 is not exclusive to this type oftumour, limiting the value of this tissue marker.29 The majorityof peripheral nerve sheath tumours examined in the dog,however, express S-100 protein. It has been suggested that nega-tive expression of S-100 by peripheral nerve sheath tumoursmay correlate with increased malignancy.28,38,42 The fascicles ofaxon-Schwann cell units are surrounded by perineurium andperineurium arises from fibroblasts.43 Nerve sheath tumoursmay therefore arise from Schwann cells or from fibroblasts ofthe perineurium. Tumours that have originated from fibroblastswould not be expected to express S-100 and it is possible thatthe negative staining in our first case was due to a fibroblasticorigin of the tumour in contrast to a Schwann cell origin. Thehistological appearance of the tumour, however, was stronglysuggestive of a Schwann cell origin. In a recent study of animalperipheral nerve tumours, two tumours that were negative forS-100 were found to express a mutation of the neu oncogene(neu oncogene mutation is not exclusive to S-100 negativetumours).18 Similarly, rodent trigeminal schwannoma inducedby ethyl nitrosurea does not express S-100 protein28 andexhibits mutation of the neu oncogene.44 It would therefore beworthwhile investigating the possibility of a neu mutation inour first case since the S-100 antibody staining was negative. Analternative explanation for the negative result would be that thetissue examined was inadequately preserved for the immunohis-tochemistry to be reliable. Despite a negative S-100 staining,this tumour was classified as a malignant peripheral nervesheath tumour based on the anatomical location, tissue infiltra-tion and histological appearance.
AcknowledgmentsThe authors would like to thank Dr D Gust for referral of the
second case and Dr B McMeekin for referral of the first case andsubsequent collection of tissue. The authors would also like tothank Liliana Tatarczuch for EM studies and Professor RFSlocombe for immunohistochemical screening.
References1. Strafuss AC, Martin CE, Blauch B, Guffy M. Schwannoma in a dog. J Am VetMed Assoc 1973;163:245-247.2. Boring JG, Swaim SF. Malignant schwannoma (neurilemmona): anextramedullary-intradural tumor causing cervical cord compression in a dog. JAm Anim Hosp Assoc,1973;9:342-345.3. Goedegebuure SA. A case of neurofibromatosis in the dog. J Small AnimPract, 1975;16:329-335.4. Jones BR, Williams OJ. Malignant schwannoma of the brachial plexus in adog. Aust Vet J 1975;51:40-42.

46
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
26. Ruppert C, Hartmann K, Fischer A et al. Cervical neoplasia originating fromthe vagus nerve in a dog. J Small Anim Pract 2000;41:119-122.27. Prata RG. Diagnosis of spinal cord tumors in the dog. Vet Clin N Am SmallAnim Pract, 1977;7:165-185.28. Yoshida M. Malignant schwannoma arising from the trigeminal nerve in arat. J Comp Pathol, 1992;106:315-318.29. Perez J, Bautista MJ, Rollon E et al. Immunohistochemical characterizationof hemangiopericytomas and other spindle cell tumors in the dog. VetPathol,1996;33:391-397.30. Rothwell TL, Papadimitriou JM, Xu FN, Middleton DJ. Schwannoma in thetestis of a dog. Vet Pathol 1986;23:629-631.31. Wright JA, Clayton Jones D. Diffuse skeletal schwannoma in a dog. Vet Rec1986;118:428-429.32. Vandevelde M, Higgins RJ, Greene CE. Neoplasms of mesenchymal originin the spinal cord and nerve roots of three dogs. Vet Pathol 1976;13:47-58.33. Balogh L, Andocs G, Perge E et al. Oncological scintigraphy in dogs with99mTechnetium MIBI and DMSA(V)—two case reports. Vet Q, 2001;23:52-56.34.Saunders JH, Poncelet L, Clercx C et al. Probable trigeminal nerve schwan-noma in a dog. Vet Radiol Ultrasound 1998;39:539-542.35. Chrisman CL. Electromyography in the localization of spinal cord and nerveroot neoplasia in dogs and cats. J Am Vet Med Assoc 1975;166:1074-1079.36. Kippenes H, Gavin PR, Bagley RS et al. Magnetic resonance imagingfeatures of tumors of the spine and spinal cord in dogs. Vet RadiolUltrasound,1999;40:627-633.37. Hems TEJ, Burge PD, Wilson DJ. The role of magnetic resonance imagingin the management of peripheral nerve tumours. J Hand Surg Br 1997;22B:57-60.38. Scheithauer BW, Woodruff JM, Erlandson RA. Primary malignant tumors ofperipheral nerve. In: Scheithauer BW, Woodruff JM, Erlandson RA, editors.Atlas of Tumor Pathology. Tumors of the peripheral nervous system. ArmedForces Institute of Pathology, Washington, DC, 1999;303-372.39. Woodruff JM, Kourea HP, Loius DN, Scheithauer BW. Malignant peripheralnerve sheath tumour (MPNST). In: Kleihues P, Cavenee WK. Pathology andgenetics of tumours of the nervous system, IARC press, Lyon, 2000;172-175.40. Summers BA, Valentine B, Van Winkle T, Cooper B. Divergent differentia-tion in canine malignant peripheral nerve sheath tumors. Vet Pathol (Abstr)1992;5:447.41. Patnaik AK, Zachos TA, Sams AE, Aitken ML. Malignant nerve-sheathtumor with divergent and glandular differentiation in a dog: a case report. VetPathol 2002;39:406-410.42. Takeuchi A, Ushigome S. Diverse differentiation in malignant peripheralnerve sheath tumours associated with neurofibromatosis-1: an immunohisto-chemical and ultrastructural study. Histopathology 2001;39:298-309.43. Bunge MB, Wood PM, Tynan LB et al. Perineurium originates from fibroblasts:demonstration in vitro with a retroviral marker. Science 1989;243:229-231.44. Kindler-Rohrborn A, Kolsch BU, Fischer C et al. Ethylnitrosourea-induceddevelopment of malignant schwannomas in the rat: two distinct loci on chromo-some 10 involved in tumor susceptibility and oncogenesis. Cancer Res1999;59:1109-1114.
(Accepted for publication 21 October 2002)
5. Carmichael S, Griffiths IR. Tumours involving the brachial plexus in sevendogs. Vet Rec 1981;108:435-437.6. Bradley RL, Withrow SJ, Snyder SP. Nerve sheath tumors in the dog. J AmAnim Hosp Assoc 1982;18:915-921.7. Wright JA. The pathological features associated with spinal tumours in 29dogs. J Comp Pathol 1985;95:549-557.8. Bradney IW, Forsyth WM. A schwannoma causing cervical spinal cordcompression in a dog. Aust Vet J 1986;63:374-375.9. Bailey CS. Long-term survival after surgical excision of a schwannoma of thesixth cervical spinal nerve in a dog. J Am Vet Med Assoc, 1990;196:754-756.10. Uchida K, Nakayama H, Sasaki N et al. Malignant schwannoma in thespinal root of a dog. J Vet Med Sci 1992;54:809-811.11. Jubb KVF, Huxtable CR. The nervous system. In: Jubb KVF, Kennedy PC,Palmer N, editors. Pathology of Domestic Animals, Volume 1. 4th edn.Academic Press, San Diego 1992;429-439.12. Targett MP, Dyce J, Houlton JEF. Tumours involving the nerve sheaths ofthe forelimb in dogs. J Small Anim Pract, 1993;34:221-225.13. Brehm DM, Vite CH, Steinberg HS et al. A retrospective evaluation of 51cases of peripheral nerve sheath tumors in the dog. J Am Anim Hosp Assoc1995;31:349-359.14. Levy MS, Kapatkin AS, Patnaik AK et al. Spinal tumors in 37 dogs: clinicaloutcome and long-term survival (1987-1994). J Am Anim Hosp Assoc1997;33:307-312.15. Kuwamura M, Yamate J, Kotani T et al. Canine peripheral nerve sheathtumor with eosinophilic cytoplasmic globules. Vet Pathol 1998;35:223-226.16. Simpson DJ, Beck JA, Allan GS, Culvenor JA. Diagnosis and excision of abrachial plexus nerve sheath tumour in a dog. Aust Vet J 1999;77:222-224.17. Platt SR, Graham J, Chrisman CL et al. Magnetic resonance imaging andultrasonography in the diagnosis of a malignant peripheral nerve sheath tumorin a dog. Vet Radiol Ultrasound, 1999;40:367-371.18. Stoica G, Tasca SI, Kim HT. Point mutation of neu oncogene in animalperipheral nerve sheath tumors. Vet Pathol 2001;38:679-688.19. Pumarola M, Anor S, Borras D, Ferrer I. Malignant epithelioid schwannomaaffecting the trigeminal nerve of a dog. Vet Pathol 1996;33:434-436.20. Bagley RS, Wheeler SJ, Klopp L et al. Clinical features of trigeminal nerve-sheath tumor in 10 dogs. J Am Anim Hosp Assoc 1998;34:19-25.21. Jones SA, Strafuss AC. Scanning electron microscopy of nerve sheathneoplasms. Am J Vet Res, 1978;39:1069-1072.22. Patnaik AK, Erlandson RA, Lieberman PH. Canine malignant melanoticschwannomas: a light and electron microscopic study of two cases. Vet Pathol1984;21:483-488.23. Niles JD, Dyce J, Mattoon JS. Computed tomography for the diagnosis of alumbosacral nerve sheath tumour and management by hemipelvectomy. JSmall Anim Pract 2001;42:248-252.24. Sawamoto O, Yamate J, Kuwamura M et al. A canine peripheral nervesheath tumor including peripheral nerve fibers. J Vet Med Sci 1999;61:1335-1338.25. Anderson GM, Dallaire A, Miller LM, Miller CW. Peripheral nerve sheathtumor of the diaphragm with osseous differentiation in a one-year-old dog. J AmAnim Hosp Assoc 1999;35:319-322.
Principles of ethical decision-making in veterinary practice
The adoption of any veterinary treatment requires consideration of ethical principles as well as technical aspects of health andwelfare management. Veterinary ethical dilemmas centre around the effect upon welfare that any decision regarding an animal may
produce. Increasing owner and media scrutiny challenges the argument that professional training and self-regulation sufficiently guar-antees ethical conduct.
In this article the authors describe a framework upon which the process of ethical decision-making in practice may be based. Theyrecommend open discussion among staff members to address varying moral positions, and provide examples of ethical issues thatmay be formally incorporated into a practice protocol.
The two main ethical theories guiding the majority of actions are ‘utilitarianism’ and ‘deontology’ and these are discussed here, withinclusion of the four main principles that the medical profession has developed from these theories.
● In consideration of animal welfare they cite the ‘five freedoms’ proposed in 1965 (freedom from hunger and thirst, from pain andinjury, from fear and distress, from physical discomfort and freedom to participate in most forms of normal behaviour).
● Once the decision regarding the action to be undertaken has been made, the authors suggest that further refinement may benecessary to reduce the impact upon individual animals, including improved analgesic regimen, environmental enrichment,using drugs with fewer side effects and restricting the numbers of animals involved.
Mullan S et al. In Practice 2001; 23:394-401.

47
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
A severe hepatic disorder with myelodysplasticsyndrome, treated with cytarabine ocfosfate, in a dog
K IDE, Y MOMOI, M MINEGISHI, M SEKIGUCHI, K KONNO, and T IWASAKIa
Department of Veterinary Internal Medicine, Faculty of Agriculture, Tokyo University of Agriculture and Technology,3-5-8 Saiwai-cho, Fuchu, Tokyo 183-8509, Japan
An 8-year-old female Shih Tzu was presented with weightloss and vomiting. Alanine aminotransferase was high andabdominal radiographs revealed hepato- and splenomegaly.Mild anaemia, neutrophilia with left shift, eosinophilia, andthrombocytosis with dysplastic features of eosinophils andplatelets, were detected. The animal was initially consideredto have hepatitis and was treated accordingly, but clinicalsigns persisted. Histological examination of liver biopsysamples showed disruption of the hepatic lobule, with exten-sive infiltration by haemopoietic cells. Further investigation ofthe bone marrow suggested a diagnosis of myelodysplasticsyndrome. The animal was treated with cytarabine ocfosfate,a prodrug of cytosine arabinoside, and appeared to recover. Aust Vet J 2003;81:47-49
ALT Alanine aminotransferaseAML Acute myelogenous leukaemiaANC All nucleated cellsBID Twice a dayCRP C-reactive proteinFAB French-American-BritishMDS Myelodysplastic syndromeMDS-RA Myelodysplastic syndrome-refractory anaemiaPCV Packed cell volumePO Per osSC SubcutaneouslySID Once a day.
Myelodysplastic syndrome (MDS) is a haematologicaldisorder characterised by cytopenias, dysplasticchanges in more than two cell lines, and a high rate of
transformation into AML.1 Diagnosis of MDS is based on theFAB classification in humans, which is also applied in theveterinary field.1-4 While MDS is fairly common in cats due toFeLV infection, it is extremely rare in dogs,1 and little is knownabout the aetiology, diagnosis, treatment and prognosis ofcanine MDS.
Case reportAn 8-year-old female Shih Tzu was presented with anorexia,
seizures and vomiting. At the initial admission, the dog’s generalcondition was good, although she was slightly underweight. Acardiac murmur of Levine II / VI was auscultated. Results ofhaematological and serum biochemical analyses are shown inTable 1. Mild anaemia, neutrophilia with left shift, eosinophilia,thrombocytosis, elevated ALT (1008 U/L) and total bile acids(131.6 µmol/L) were observed. CRP was positive. A bloodsmear revealed several dysplastic features: promyelocyte-likecells, eosinophils with abnormally large eosinophilic granules,giant platelets and hypersegmented neutrophils (Figure 1).Abdominal radiographs showed hepatomegaly and
aAuthor for correspondence. E-mail: [email protected]
Figure 2. Diff-Quik stain of the liver biopsy sample stamp smear.(a) Degenerate hepatocyte, (b) Mitosis of megakaryocyte, (c)rubriblast, and (d) myelocyte. (x 1000)
Figure 1. Diff-Quik stain of a peripheral blood smear of an 8-year-old Shi Tzu with myelodysplastic syndrome. (a) Myeloblast-likecell, (b) giant platelet, (c) eosinophil with large granules, and (d)hypersegmented neutrophil. (x 1000)

48
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
splenomegaly. Despite the dysplastic features of some blood celllines, we suspected suppurative hepatitis on the basis ofneutrophilia, hepatomegaly and high ALT, and initiated treat-ment with glutathione 10 mg/kg BID and cephalexin 25 mg/kgBID. This treatment was maintained for 60 days starting on theday of the first visit.
In spite of medication, anorexia and weight loss, as well ashigh ALT and neutrophilia, continued. Liver biopsy via alaparotomy was carried out on day 61 from first admission. Theliver was normal macroscopically, although was moderatelyenlarged. An impression smear of the liver biopsy sampleshowed some degenerate hepatocytes along with manyeosinophilic myelocytes, neutrophilic myelocytes, prorubri-blasts, rubriblasts and mitotic megakaryocytes (Figure 2),suggesting an active extramedullary haematopoiesis or a myelo-proliferative disorder. Histologically, the architecture of the liverwas disrupted, and haematopoietic cells had infiltrated aroundthe portal triad and central vein (Figure 3). Enlarged lymphnodes were apparent on palpation, and the right popliteallymph node was removed for histological examination at thetime of the liver biopsy. As in the liver, erythroid andneutrophilic myeloid cells, some in mitosis, were seen, alongwith many eosinophils. Based on these additional findings, weconcluded that the dog had a myeloproliferative disorder, withinfiltration of haematopoietic cells into the liver.
Treatment with glutathione and cephalexin was continued,but severe anaemia (PCV 15%) became apparent on day 167.
Table 2. Myelogram of an 8-year-old Shi Tzu with myelodysplastic syndrome, on day 181 of treatment.
Cell type Percentage (%) Reference range
Rubriblast 0.21 0.04 - 0.22
Prorubricyte 0 0.18 - 0.40
Rubricyte 1.47 3.10 - 5.02
Metarubricyte 2.62 1.84 - 3.28
Myeloblast 0.1 0.08 - 0.22
Promyelocyte 0.63 0.22 - 0.46
Myelocyte 0.63 0.62 - 1.22
Metamyelocyte 0.73 1.06 - 1.76
Band neutrophil 5.67 2.54 - 3.44
Segmented neutrophil 58.8 2.76 - 4.84
Band eosinophil 0.1 0.36 - 1.12
Segmented eosinophil 5.67
Band basophil 2.10 (0 - 0.16)
Segmented basophil 6.41
Lymphocyte 14.8 0.34 - 0.98
Plasmocyte 0 0.12 - 0.48
Monoblast 0 0.08 - 0.4
Monocyte 0
M/E ratio 18.78 (1.8 - 2.52)
EBL: ANC 5.06
Blast ratioANC 1.85
NEC 1.95
Figure 3. Liver biopsy showing infiltration of haemopoietic cellsaround portal triad and central vein, and disruption of hepaticlobules. (Haematoxylin & eosin, x 25)
Table 1. Results of haematological examination of an 8-year-old Shi Tzudog with myelodysplastic syndrome, at first admission.
Variable Patient Reference
RBC (1012/L) 5.0 5.5 - 8.5
Hb (g/L) 113 120 - 180
PCV (L/L) 0.32 0.37 - 0.55
WBC (109/L) 30.7 6.0 - 17.0
Band neutrophil (109/L) 3.4 0 - 0.03
Segmented neutrophil (109/L) 17.0 3.0 - 11.5
Lymphocyte (109/L) 5.2 1.0 - 4.8
Monocyte (109/L) 1.80 0.18 - 1.35
Eosinophil (109/L) 2.10 0.10 - 1.25
Platelet (1012/L) 0.8 0.2 - 0.5
ALP (U/L) 229 10 - 150
ALT (U/L) 1008 5 - 60
AST (U/L) 194 5 - 55
Total protein (g/L) 84 50 - 80
NH3 (µmol/L) 56.4 11.2 - 70.5
BUN (mmol/L) 6.8 2.5 - 9.6
Creatinine (µmol/L) 53 35 - 159
Total bilirubin (µmol/L) 7 0 - 7
Total bile acid (µmol/L) 131.6 < 61.3
CRP ++

49
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
cell lines and a blast rate under 30%. We concluded that MDStriggered the cell infiltration into the liver, a unique aspect ofthis case, and responsible for the clinical signs.
Treatment for canine MDS is not well-established, because sofew cases have been reported.9-12 In human and feline patients,MDS is generally treated with chemotherapeutic drugs toprevent cytopenia and to delay its progress into AML, possiblyby inducing differentiation of haemopoietic cells, and/orreducing the number of blasts.1 Cytarabine ocfosfate is a deriva-tive of cytosine arabinoside and can be administered orally.5-9 Ithas been approved as a medication for MDS in humans andalso for mild chemotherapy in elderly leukaemia patients.5 Thisdrug was chosen because the patient’s owner preferred an oralmedication that could be given at home. Cytarabine ocfosfatehas been used for human MDS at doses from 150 to 300mg/m2/day, which corresponds to low-dose cytarabinetherapy.6,8 However, our starting dose of 200 mg/m2/day wasapparently excessive, because bone marrow suppression ofleukocytes was seen, and the owner complained of the dog’s lossof vigour after medication. Though bone marrow suppressionmay have been associated with this patient’s reduced hepaticfunction, frequent monitoring of the WBC count was necessaryto evaluate the dose of cytarabine ocfosfate.
This report outlines the successful treatment of a case ofcanine MDS with cytarabine ocfosfate.
References1. Blue JT. Myelodysplastic syndromes and myelofibrosis. In: Feldman BF,Zinkl JG, Jain NC, editors. Schalm’s Veterinary Hematology. 5th edn.Lippincott, Williams & Wilkins, Maryland, 2000:682-688, 708-709. 2. Raskin RE. Myelopoiesis and myeloproliferative disorders. Vet Clin N AmSmall Anim Pract 1996;26:1023-1042.3. Jain NC, Blue JT, Grindem CB et al. Proposed criteria for classification ofacute myeloid leukemia in dogs and cats. Vet Clin Pathol 1991;20:63-82.4. Bennett JM, Catovsky D, Daniel MT et al. Proposals for the classification ofthe myelodysplastic syndromes. Br J Haematol 1982;51:189-199.5. Okumura H, Yoshida T, Takamatsu H et al. Treatment of acute myeloidleukemia and myelodysplastic syndrome with orally administered cytarabineocfosfate and granulocyte colony-stimulating factor. Int J Hematol 1997;65:263-268.6. Braess J, Freund M, Hanauske A et al. Oral cytarabine ocfosfate in acutemyeloid leukemia and non-Hodgkin’s lymphoma - phase I/II studies and phar-macokinetics. Leukemia 1998;12:1618-1626.7. Ohno R, Tatsumi N, Hirano M et al. Treatment of myelodysplastic syndromeswith orally administered 1-beta-D-arabinofuranosylcytosine-5’-stearylphos-phate. Oncology 1991;48: 451-455.8. Nishi T, Funasako M, Hata N et al. Five cases of myelodysplastic syndrometreated with cytarabine ocfosfate. Gan To Kagaku Ryoho 1996;23:1331-1334(in Japanese)9. Tricot G, Dekker AW, Boogaerts MA et al. Low dose bytosine arabinoside(Ara C) in myelodysplastic syndromes. Br J Haematol 1984;58:231-240.10. Weiss DJ, Smith SA. Primary myelodysplastic syndromes of dogs: a reportof 12 cases. J Vet Intern Med 2000;14:491-494.11. Miyamoto T, Horie T, Shimada T, Kuwamura M, Baba E. Long-term casestudy of myelodysplastic syndrome in a dog. J Am Anim Hosp Assoc1999;35:475-481.12. Weiss DJ, Raskin R, Zerbe C. Myelodysplastic syndrome in two dogs. J AmVet Med Assoc 1985;187:1038-1040.
(Accepted for publication 25 September 2002
Erythropoietin was discontinued after administration of 200U/kg SC every other day for 6 days, due to the lack of ahaemopoietic response. On day 181, with the PCV down to12%, a whole blood transfusion was given, and a sample ofbone marrow was aspirated under general anaesthesia. Themyelogram is shown in Table 2. The blasts in the bone marrowcomprised 1.85% of ANC, which, based on the FAB classifica-tion, suggested a diagnosis of MDS-RA.1-4 Prednisolone 2mg/kg PO SID and chemotherapy with cytarabine ocfosfate(Starasid; Nihon-Kayaku, Tokyo, Japan), 200 mg/m2/day POSID, was instituted. Since there were no reports of using thisdrug in dogs, we adapted the dose used for humans, 200mg/m2/day PO SID, equivalent to low-dose cytosine arabi-noside therapy.6,8,9
One week after the first blood transfusion and initiation ofcytarabine ocfosfate therapy, the patient’s general conditionimproved. The PCV had increased, and morphological featuressuggested regeneration of RBC in the peripheral blood smear.The WBC count was 8.5 x 109/L, apparently indicating mildbone marrow suppression as a result of cytarabine ocfosfateadministration. Two weeks after starting the medication, theWBC count had fallen to 6.2 x 109/L, and cytarabine ocfosfatewas discontinued for a week. The WBC count recovered (13.4 x109/L), and cytarabine ocfosfate therapy was re-introduced at adose of 200 mg/m2/day PO on 3 consecutive days per week.This regimen was continued for the next 55 days. PCV wasmaintained in the range 25 to 30%, with a reduction ofdysplastic features of the cells. Although still elevated, ALT waslower than on initial presentation. On day 265, the dog showednasal haemorrhage as a sign of coagulopathy originating fromimpaired hepatic function. Administration of vitamin K12 mg/kg/day PO resolved this clinical sign.
Currently, over a year since first presented, the dog’s condi-tion is controlled by a combination of cephalexin (20 mg/kgBID), glutathione (8.3 mg/kg BID), prednisolone (1 mg/kgSID), vitamin K1 (2 mg/kg/day), and cytarabine ocfosfate (200mg/m2/day, 3 days per week). WBC count is in the normalrange, and, though the dog is still mildly anaemic, no furtherblood transfusions have been necessary. However, the existenceof hepatopathy (ALT >1000 IU/L) and lymphadenopathy (onpalpation) are still apparent.
DiscussionThis dog was initially suspected as suffering from suppurative
hepatitis, on the basis of marked neutrophilia with left shift.However, a myeloproliferative disorder with infiltration ofhaemopoietic cells into the liver was considered a more likelydiagnosis following further investigation. Anaemia, dysplasticchanges in two cell lines (eosinophils and platelets), and thedetection of myeloblasts on examination of peripheral blood,suggested MDS. This diagnosis was supported by examinationof a bone marrow aspirate, showing dysplastic features in two

50
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Transposition of first digital pad for reconstruction of apalmar antebrachial soft tissue defect in a cat
SM FEARNSIDEa and RC STRAWb
An 8-year-old female neutered Siamese cat was presentedwith a recent history of incomplete excision of an apocrinegland adenocarcinoma from the palmar aspect of the rightantebrachium, just proximal to the carpal joint. There was noevidence of metastasis. Wide surgical excision of the previoussurgery site was performed resulting in a soft tissue defect.Partial reconstruction was achieved using digital pad transpo-sition of the first digit (dewclaw), forming a local axial patternflap that was transposed into the adjacent defect. Theremaining defect was closed by primary apposition. The skinflap healed successfully. Some breakdown of the skin closedby primary apposition necessitated open wound manage-ment. The cosmetic and functional result of the first digital padtransposition was considered excellent, rendering it a usefulmeans to reconstruct soft tissue defects in the carpal region. Aust Vet J 2003;81:50-53
Defects of the skin in the distal limbs of dogs and catsmay result from physical, chemical or thermal trauma,neoplasia, or infectious agents.1,2 The type of recon-
struction required depends on the extent and position of thedefect. Reported means of reconstruction have includedprimary closure using local tension-relieving techniques such asundermining and fenestration of adjacent skin,1,3 delayedprimary closure,1 healing by second intention through contrac-tion and epithelialisation,1,4 skin flaps1,2,5 or skin grafts.1,2,5,6
The digital pad transposition technique involves creation of alocal axial pattern flap by removal of the proximal, middle anddistal phalanges whilst preserving the vascular supply to theskin. It has been used for repair of defects in the metacarpal andmetatarsal footpads,2,5-11 as well as for digital or dorsal footresurfacing in dogs and cats.5 The latter techniques are indicatedin cases where there has been osseous damage to the digits or wherethere is a severe skin deficit to the dorsum of the paw, or both.5
For replacement of defects to the metacarpal or metatarsal pads,the closest digit to the defect, usually the second or fifth digit, ischosen for the digital pad transposition procedure.5,6
The aim of this report is to describe the use of the digital padtransposition technique of the first digit to form a local axialpattern flap for reconstruction of a soft tissue defect on thepalmar aspect of the distal antebrachium. To the author’sknowledge, this is the first report of this technique for recon-struction of soft tissue defects of the antebrachium in dogs orcats.
Case reportAn 8-year-old female neutered Siamese cat was presented for
assessment following excision of a mass from the palmar aspectof the right carpus. Histological examination of the excised
tissue from the initial surgery led to diagnosis of an apocrineadenocarcinoma. Neoplastic cells extended to the margins ofthe excision and were also noted in local lymphatic channels.The length of the surgical scar was 17 mm (Figure 1). It wassituated between the carpal pad and the dewclaw of the rightthoracic limb. Local lymph nodes were not palpable. Theremainder of the physical examination was unremarkable. Amild generalised increase in broncho-interstitial markings wasnoted on thoracic radiography. There was no evidence ofpulmonary metastasis.
Surgery in an attempt to remove any remaining neoplastictissue with appropriate soft tissue reconstruction of the resultingdefect was elected. General anaesthesia was induced using intra-venous propofol (6 mg/kg), following premedication withmorphine (0.1 mg/kg) and acepromazine (0.05 mg/kg) subcu-taneously. An endotracheal tube was placed and anaesthesiamaintained with halothane and oxygen. The cat was placed inright lateral recumbency for surgery. The right thoracic limbwas draped and the paw was covered in sterile elasticisedbandage material, that was also used to create an Esmarch’sbandage. An elliptical shaped incision was made around theprevious scar, with a skin margin of approximately 10 mm, thatincluded the carpal pad. The dissection was continued deep tothe previous surgery site, beyond the fascia surrounding themusculature on the palmar aspect of the antebrachium (Figure2). The Esmarch’s bandage was then released (total tourniquettime 15 min). Local haemorrhage was controlled usingmonopolar electrocautery. Direct closure of the wound was notpossible without undue tension. Due to its close proximity tothe defect, an axial pattern flap created by transposition of thefirst digit was elected.
An incision was made around the claw of the first digit. Theincision was continued along the palmar-medial aspect of thedigit and extended to communicate with the surgical excisionsite. Dissection to remove the second and third phalanges wasperformed, taking care to dissect as close to the bone as possibleto avoid damage to the vascular supply of the overlying softtissue. Removal of the second and third phalanges enabledcreation of a local axial pattern flap (Figure 3). The skin flap wasrotated through 180 degrees into the adjacent defect (Figure 4).The flap was secured using 4-0 polyglyconate subcuticularsimple interrupted sutures. A short proximal extension of thedefect was closed with primary apposition using simple inter-rupted sutures of 4-0 polyglyconate. The pad of the dewclawwas positioned to simulate the carpal pad. The margins of theexcised tissue were inked using tissue marking ink (TissueMarking Dye, Shandon; USA) and submitted for histologicalexamination.
The limb was supported in a soft padded bandage postopera-tively. The bandage was changed 48 hours later after it becamedislodged when the cat jumped from a window. The flapremained intact, however the short proximal segment of thedefect, which had been closed by primary apposition, had
aWest Chermside Veterinary Clinic, 263 Appleby Road, Stafford Heights,Queensland 4059bAnimal Cancer Care, Veterinary Teaching Hospital, School of VeterinaryScience, University of Queensland, Brisbane, Queensland 4072.

51
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
dehisced. This wound was treated as an open wound andallowed to heal by second intention. Dressings were changeddaily for the first week, followed by once every third or fourthday for 2 weeks. The flap healed without complication and theproximal open wound healed successfully by second intention.
Histological examination of the excised tissue revealedsections comprised of normal epithelium and overlying dermis,containing extensive fibrous tissue. There was no evidence ofneoplastic tissue in the sections examined.
At 12 months following surgery, the cat had normal functionin the limb, no wound complications and no evidence of localor systemic tumour recurrence.
DiscussionApocrine sweat gland tumours in cats account for between
3.6 and 9.0% of feline skin tumours, with adenocarcinomaspredominating over the more benign adenomas.12 Widesurgical excision is the treatment of choice for apocrine glandtumours, with a guarded prognosis for adenocarinoma.12 In the
cat in this report, extension of neoplastic cells to the margins ofthe initial excision prompted wide surgical excision of theprevious scar and entire wound bed in an attempt to effectcomplete removal of the neoplastic tissue. This left a large softtissue defect on the palmar aspect of the antebrachium at thelevel of the carpus.
The digital pad transposition technique, via a palmarapproach, provided a successful one step procedure for recon-struction of the soft tissue defect. A palmar dissection techniqueand a dorsal dissection technique for digital pad transpositionhave been used in dogs and cats,1,2,5,7,11 with the palmarapproach having the advantage of being a one step procedure.The digit is however more difficult to dissect from thisapproach due to the increased risk of damage to its vascularsupply.5,11 The dorsal approach has the advantage of beingsimpler, with reduced potential for damage to the blood supplyto the digit, however it has the disadvantage of being a two-stage procedure.2,5,11 In this approach, the digit is dissected via asingle longitudinal incision on the dorsum of the digit. The
Figure 1. Pre-operative view of the surgical site on the palmarsurface of the distal antebrachium in an 8-year-old femaleneutered Siamese cat which had an apocrine gland adenocarci-noma removed with incomplete margins previously. Note thepresence of the surgical scar from the previous surgery (arrow).
Figure 2. Intra-operative view following complete excision of theprevious surgical site, creating a large soft tissue defect on thepalmar surface of the distal antebrachium.
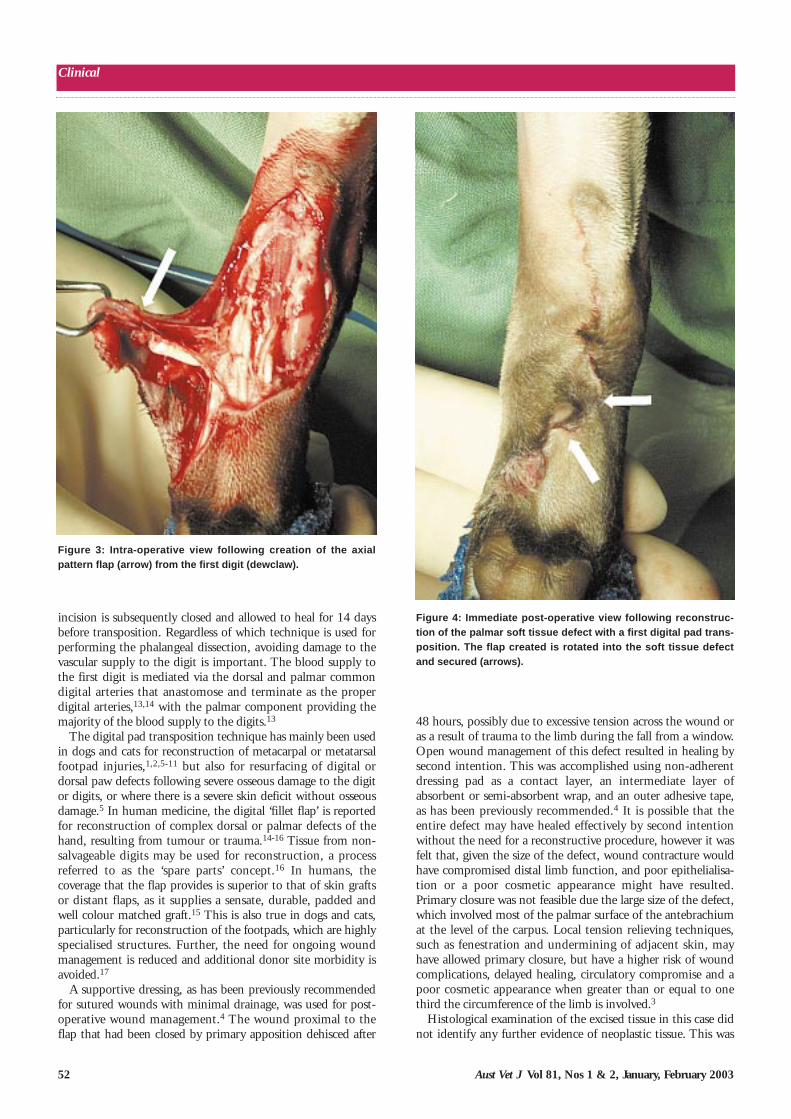
52
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
48 hours, possibly due to excessive tension across the wound oras a result of trauma to the limb during the fall from a window.Open wound management of this defect resulted in healing bysecond intention. This was accomplished using non-adherentdressing pad as a contact layer, an intermediate layer ofabsorbent or semi-absorbent wrap, and an outer adhesive tape,as has been previously recommended.4 It is possible that theentire defect may have healed effectively by second intentionwithout the need for a reconstructive procedure, however it wasfelt that, given the size of the defect, wound contracture wouldhave compromised distal limb function, and poor epithelialisa-tion or a poor cosmetic appearance might have resulted.Primary closure was not feasible due the large size of the defect,which involved most of the palmar surface of the antebrachiumat the level of the carpus. Local tension relieving techniques,such as fenestration and undermining of adjacent skin, mayhave allowed primary closure, but have a higher risk of woundcomplications, delayed healing, circulatory compromise and apoor cosmetic appearance when greater than or equal to onethird the circumference of the limb is involved.3
Histological examination of the excised tissue in this case didnot identify any further evidence of neoplastic tissue. This was
incision is subsequently closed and allowed to heal for 14 daysbefore transposition. Regardless of which technique is used forperforming the phalangeal dissection, avoiding damage to thevascular supply to the digit is important. The blood supply tothe first digit is mediated via the dorsal and palmar commondigital arteries that anastomose and terminate as the properdigital arteries,13,14 with the palmar component providing themajority of the blood supply to the digits.13
The digital pad transposition technique has mainly been usedin dogs and cats for reconstruction of metacarpal or metatarsalfootpad injuries,1,2,5-11 but also for resurfacing of digital ordorsal paw defects following severe osseous damage to the digitor digits, or where there is a severe skin deficit without osseousdamage.5 In human medicine, the digital ‘fillet flap’ is reportedfor reconstruction of complex dorsal or palmar defects of thehand, resulting from tumour or trauma.14-16 Tissue from non-salvageable digits may be used for reconstruction, a processreferred to as the ‘spare parts’ concept.16 In humans, thecoverage that the flap provides is superior to that of skin graftsor distant flaps, as it supplies a sensate, durable, padded andwell colour matched graft.15 This is also true in dogs and cats,particularly for reconstruction of the footpads, which are highlyspecialised structures. Further, the need for ongoing woundmanagement is reduced and additional donor site morbidity isavoided.17
A supportive dressing, as has been previously recommendedfor sutured wounds with minimal drainage, was used for post-operative wound management.4 The wound proximal to theflap that had been closed by primary apposition dehisced after
Figure 3: Intra-operative view following creation of the axialpattern flap (arrow) from the first digit (dewclaw).
Figure 4: Immediate post-operative view following reconstruc-tion of the palmar soft tissue defect with a first digital pad trans-position. The flap created is rotated into the soft tissue defectand secured (arrows).

53
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
for paw salvage: A case report. J Am Anim Hosp Assoc 1993;29:427-433.7. Pavletic MM. Foot pad reconstruction. In: Atlas of small animal reconstructivesurgery. 2nd edn. Saunders, Philadelphia, 1999:365-380. 8. Waldron DR, Trevor P. Management of superficial skin wounds. In: Slatter D,editor. Textbook of small animal surgery. 2nd edn. Saunders, Philadelphia,1993:269-280.9. Hedlund CS. Surgery of the integumentary system. In: Fossum TW, editor.Small animal surgery. Mosby, St Louis, 1997:91-152.10. Olsen D, Straw RC, Withrow SJ, Basher AWP. Digital pad transposition forreplacement of the metacarpal or metatarsal pad in dogs. J Am Anim HospAssoc 1997;33:337-341.11. Swaim SF, Scardino MS. Paw and distal limb salvage and reconstructivetechniques. In: Bojrab MJ, editor. Current techniques in small animal surgery.4th edn. Williams and Wilkins, Baltimore, 1998:625-639.12. Vail DM, Withrow SJ. Tumours of the skin and subcutaneous tissues. In:Withrow SJ, MacEwan EG, editors. Small animal clinical oncology. 3rd edn.Saunders, Philadelphia, 2001:233-260. 13. Dyce KM, Sack WO, Wensing CJG. The cardiovascular system. In:Textbook of veterinary anatomy. Saunders, Philadelphia, 1987:212-254.14. Evans HE. The heart and arteries. In: Evans HE, editor. Miller’s Anatomy ofthe dog. 3rd edn. Saunders, Philadelphia, 1993:586-681.15. Koegel AM, Banducci DR, Kahler SH, Hauck RM, Manders EK. Sensibilityof finger fillet flaps on late follow up evaluation. J Hand Surg 1995;20A:679-682.16. Al-Qattan MM. Lengthening of the finger fillet flap to cover dorsal wristdefects. J Hand Surg 1997;22A:551. 17. Kuntscher MV, Erdman D, Homann HH et al. The concept of fillet flaps:Classification, indications, and analysis of their clinical value. Plast ReconstrSurg 2001;108:885-895.
(Accepted for publication 14 October 2002)
not unexpected since surgery had been performed recently,leaving only microscopic residual disease. Since there was noevidence of lymph node or pulmonary metastases on clinicalstaging, a cautiously optimistic prognosis was given. At 12months postoperatively, there was no evidence of local orsystemic recurrence, and the cosmetic and functional result ofthe flap remains excellent. Adaptation of transposition ofphalangeal flaps from previously reported uses in dogs and catsfor metacarpal or metatarsal foot pad reconstruction should beconsidered for soft tissue defects of the paw or distal ante-brachium that are adjacent to the dew claw.
References1. Basher A. Foot injuries in dogs and cats. Comp Cont Educ Pract Vet1994;16:1159-1176.2. Swaim SF, Garrett PD. Foot salvage techniques in dogs and cats: Options,“do’s” and “don’ts”. J Am Anim Hosp Assoc 1985;21:511-519.3. Vig MM. Management of integumentary wounds of extremities in dogs: Anexperimental study. J Am Anim Hosp Assoc 1985;21:187-192.4. Swaim SF. Management and bandaging of soft tissue injuries of dog and catfeet. J Am Anim Hosp Assoc 1985;21:329-340.5. Swaim SF, Henderson RA. Wounds on limbs. In: Small animal woundmanagement. 2nd edn. Williams and Wilkins, Baltimore, 1997:305-357.6. Bradley DM, Shealy PM, Swaim SF. Meshed skin graft and phalangeal fillet
Revalidation and virtual patients: a vision of the future?
Appraising the situation in the UK, this article notes the important distinction between competence (know-how) and performance(delivery) and the problems of assessing the latter. While one year ago members of the UK medical profession were 'in revolt'
over plans to force them to prove their fitness to continue practising, the General Medical Council now expects 'regular demonstrationthat they remain fit to practise in their chosen field'. This fitness is based upon Continuing Professional Development programs,annual appraisals, and a career development portfolio assessed every 5 years.
Society increasingly expects revalidation of performance by members of any self-regulating profession. The difficulties of estab-lishing a satisfactory revalidation system for the veterinary profession are discussed; comparisons are made with the medical profes-sion and pilots in the aviation industry, where revalidation has been compulsory for decades.
The author concludes that because of the increasing complexity of our field, political hostility to professions and 'litigious gluttony'the profession must address this problem now as he considers revalidation is inevitable.
Michell R. In Practice 2002;24:221-223.
Examination of the horse with colic: is it medical or surgical?
Aproblem commonly faced by practitioners is addressed in this tutorial article. Stating that approximately 7% of colic cases requiresurgical intervention, they stress that early decisions increase the chances of good surgical outcomes.
Choice on the method of treatment is based upon clinical examination and evaluation of diagnostic tests covering pain, cardiovas-cular status, rectal palpation, presence of nasogastric reflux and abdominal paracentesis. Each of these items is separately describedand additional diagnostic tools such as ultrasonography, radiography and radiology also are discussed. It is suggested that while inmost cases comprehensive investigation will determine the path to be taken, revisiting the situation and careful evaluation of theresponse to analgesic administration may be required before the ultimate course of action is decided upon.
Singer ER et al. Equine Vet Educ 2002;14: 87-96.

To be expected, Chapter 4, ‘Inflammation and repair of tissue’ hasbeen markedly revised and rewritten although the basic organisationof the chapter has remained the same as previous editions. Newinformation includes discussion of the contents of azurophil, specificand tertiary granules of neutrophils together with a concise summaryof leucocyte proteinases. Recently leucocyte adhesion moleculeshave emerged as an important area of research and this is well, ifonly briefly, covered together with mechanisms of leucocyte emigra-tion and chemotaxis. An important addition is the inclusion of theorigins and functions of nitric oxide. The explosion of knowledge ofchemokines, arachidonic acid, acute phase proteins and complementmeans these areas have been thoroughly revised and excellentsummary tables are included.
The organisation of Chapter 5, ‘Immunopathology’ has beenrevised. New information on the structure and function of T cell recep-tors has been added. Updated information on T, B, NK cells,macrophages, dendritic cells, cytokines and their receptors has alsobeen included. Mechanisms of immune mediated disease, immuno-deficiency and autoimmune disease have been updated.
Chapter 6, ‘Disorders of Cell Growth and Cancer Biology’ has beenthoroughly revised and reorganised. There is new information on thecell cycle and its regulators. There has also been a marked expansionand introduction of new material on oncogenes, including proteinkinases, GTP binding proteins, growth factors, nuclear proteins andapoptosis regulators, however, more discussion of the molecularmechanisms of p53, Rb, ras and their role in carcinogenesis couldhave been included. The topics of anti-oncogenes and tumourimmunology have been updated and expanded. Brief synopses ofneoplasia caused by Marek’s disease virus, feline leukaemia virusand bovine leukaemia virus and several case studies give a clinicalperspective that is often welcomed by veterinary students.
Chapter 7, ‘The Nature and Causes of Disease’ has been reorgan-ised, discussing Koch’s postulates, various types of infectious organ-isms and, all too briefly, molecular tools for diagnosis. More time couldhave been spent devoted to the latter. New information has beenadded on the mechanisms that pathogens use to escape immunesurveillance through frustrated phagocytosis, confusing complementand molecular mimicry.
The book is written in a clear and concise style that is informativewithout being dull and without suffering from style differencescommon to multi-authored texts. There are abundant photographs ofgross specimens and photomicrographs, all of high quality and a halfpage in size; this is one of the strengths of the book. Diagrams andillustrations supplement the text and are generally informative andsummarise information given in the text. However, the vast majority ofphotographs, photomicrographs, illustrations, diagrams and tableshave been taken from the second edition.
This book is a good resource for the teaching or learning of generalpathology. It is suitable for use by veterinary and postgraduatepathology students. The book would also be of considerable valueand a compact review for those studying towards Membership of theAustralian College of Veterinary Scientists in pathology.
MM Williamson
Dr Mark Williamson is a Veterinary Pathologist at the Victorian Institute ofAnimal Science, Attwood, Victoria.
BOOK REVIEWSAlternative Pets from Budgies and Yabbies to Rabbits and Rats.Stewart R, Hyland House Publishing, Flemington, 2002, 152 pages. Price S19.95. ISBN 1 86447 052 6.
There is a distinct lack of accurate, informative general texts on thecare of unusual pets. I am always on the look out for publications
on these animals that can be recommended to my clients. This publi-cation, is promoted to “… provide invaluable advice on pet selectionand on keeping pets healthy and happy, including information onfeeding and on building them a suitable home”.
This soft back production of over 150 pages is colourful, easy toread, well formatted with numerous photographs, tables and breakouttext boxes. It is arranged into five sections: Animals, Wild and as Pets;Furry Friends; Feathery Friends; Watery Friends; and Some other(Terrarium) Friends. Each section has chapters providing informationregarding the care of various groups or type of animal, such as guineapigs, ferrets, goldfish, axolotls or hermit crabs. The last chapter in eachsection (except section 1) provides information on health problems.
A quick browse through this book revealed some interesting quota-tions and advice. For example: “Now you have trained your goldfish toswim through a hoop when you ring a bell” and “Pam has one specialblue-tongue that licks her nose when she says ‘Give me a kiss’...”.Unfortunately a fair amount of advice is far from accurate, such as “Ifyou have set up your aquarium properly and have situated it correctlyit should never need to be cleaned… Top it up with fresh water everyfew weeks”. The nitrogen cycle will necessitate at least partial waterchanges in all aquariums due to a build of nitrite/nitrate. Or thecomment that wild possums “... love fruit cake, bread and jam..”, thuspromoting the feeding of these type of foods. The health care sectionsare also lacking in accurate information. For example, no mention ismade of the importance of spaying female rabbits to prevent the highincidence of uterine adenocarcinoma present in this species; recom-mendations are made to descent ferrets (rarely needed as desexingmarkedly reduces odour); and advice such as “avoid feeding lettuceto rabbits, as it tends to make them very sleepy and may even killsome breeds” are just some examples.
The inaccuracies, together with the lack of current husbandry anddisease information for ‘alternative’ pets, does not allow me to recom-mend this as a resource for clients, notwithstanding the pleasantformat and novel training techniques! The search continues.
BP Carmel
Dr Carmel owns a primary accession and referral small animal practice inWarranwood, Victoria and has a special interest in Unusual & Exotic Pets.
54
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Mechanisms of Disease: A Textbook of Comparative GeneralPathology. 3rd edn. Slauson DO and Cooper BJ, Mosby, St Louis,2001,445 pages. Price US$ 65.00. ISBN 0323002285.
The third edition of this text is a timely update of the 1990 secondedition. The book is intended as an introduction to pathology for
veterinary science students and graduate students in pathology, andserves these purposes well. The third edition has retained the sevenchapter format of the previous edition together with similar subhead-ings within each chapter. However, in the 12 years since the previousedition there have been significant advances in the understanding ofthe mechanisms of disease. Consequently there are many newlyadded concepts in Chapters 4 to 7, with four new coauthors.
The content and text of Chapters 1 to 3 remain similar if not iden-tical to the second edition. The first chapter describes what pathologyis, what pathologists do and how pathology is studied. Chapter 2describes cell injury, necrosis, apoptosis and pigments. The thirdchapter covers circulatory disturbances and thrombosis.

55
Clinical
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Equine Dentistry: A Practical Guide. Pence P, Lippincott Williams &Wilkins, Baltimore, 2002, 275 pages. Price US$ 59.00. ISBN 0 68330403 8.
This book is very basic though concise and well written with a largenumber of clear photos and diagrams. There are several errors in
the chapter on Dental Anatomy. The text covers most areas of basic equine dentistry in its 12 chap-
ters. Unfortunately, the book is obviously written for the ‘lay’ horsedentist with very detailed explanations on drug doses especially thesection on the use of sedatives. The use of ‘Key Points’ highlights this,for example, “Wait 5 minutes for the sedative to take effect beforeputting in the speculum. Use a kitchen or laboratory timer to ensurethat you wait the full 5 minutes.”
Most veterinarians will find little use for this book due to its basicnature. Some students and those veterinarians with little or no experi-ence in equine dentistry may find it helpful as a staring point and tounderstand some of the terminology and techniques used by lay horsedentists.
GJ Wilson
Dr Gary Wilson is a consultant in veterinary dentistry to the Veterinary TeachingHospital, University of Queensland and lectures undergraduate students inequine dentistry.
Veterinary Microbiology and Microbial Disease. Quinn PJ, MarkeyBK, Carter ME, Donnelly WJ, Leonard FC, Blackwell Science, Carlton,2002, 536 pages. Price $191.40. ISBN 0 63205 525 1.
This new book is primarily aimed at veterinary students in their para-clinical years. It is a soft-covered, 22 x 27 cm book containing just
over 500 pages of text. The text is black and white and there are nocolour illustrations. The book is divided into six sections. Sections I-IIIcover veterinary bacteriology and mycology and sections IV and Vcover viruses and prions. Section VI completes the book with informa-tive chapters on the host-parasite relationship using a body systemsapproach.
Sections I and IV are introductory sections that provide the basicprinciples for understanding veterinary bacteriology and virologyincluding structure, propagation, genetics, laboratory diagnosis, treat-ment and basic pathogenesis.
Sections II, III and V systematically cover the major groups ofbacteria, fungi, viruses and prions of veterinary significance. Eachchapter is devoted to a taxonomic group of organisms and representsan introduction to the group, followed by concise text generally writtenunder the headings of habitat, differentiation, pathogenesis and patho-genicity, diagnostic procedures and clinical infections. Each of themajor diseases caused by the subject is then discussed in more detailunder the headings of epidemiology, pathogenesis, clinical signs,diagnostic procedures and treatment and control.
Section VI then ties microbiology and pathogenesis together bysummarising how pathogenic micro-organisms interact with each ofthe major body systems. Chapters that are covered include thenervous system, reproductive tract, intestinal tract, respiratory tract,bovine mastitis and foot infections. Two chapters at the end of thissection cover disinfection and infection and immunity.
The field of Veterinary Microbiology is rapidly evolving with constantchanges in taxonomy and nomenclature, rapid advances in molecularbiology, and new and emerging diseases. Veterinary Microbiology andMicrobial Disease manages to keep abreast of these changes withoutlosing its clinical focus. It is certainly a major improvement on previoustexts aimed at the veterinary undergraduate and the authors are to becongratulated on their holistic and integrative approach. The chaptersare easy to read, logical and provide up to date information on thevarious reclassifications and newly identified diseases, together withexcellent references and further reading lists.
The section on veterinary mycology and veterinary virology areparticularly informative and are a much-needed improvement on othertextbooks that attempt to integrate veterinary bacteriology andvirology. The discussion of the host-parasite relationship in variousbody systems in Section VI is to be commended and is reflective of thecurrent way in which veterinary microbiology is being taught in veteri-nary schools. Antimicrobial resistance receives little attention in itsown right and should be the subject of a complete chapter. The twochapters at the end of this section on infection and immunity and disin-fection appear out of place in the current version. The inclusion ofthese two chapters together with chapters on antimicrobial resistanceand biosecurity and biocontainment into a separate section wouldstrengthen future editions.
Numerous tables and illustrations add interest to the chapters,although the black and white figures illustrating the microscopicappearance of bacterial smears are too simplified and bear littleresemblance to actual smears from clinical material or pure cultures.A suggested improvement for future editions would be the addition oftextboxes providing a summary of an interesting paper on current topicsthat are relevant to the chapter in question. Finally, it should also be notedthat none of the authors specialise entirely in veterinary virology.
In summary, Veterinary Microbiology and Microbial Disease shouldbecome the recommended textbook for veterinary undergraduates. Itsnew approach covering both systematics and host-parasite relationshipsin body systems is refreshing and will make the subject of veterinarymicrobiology much more enjoyable and easier to comprehend.
DJ Trott
Dr Darren Trott teaches veterinary bacteriology and mycology at The Universityof Queensland.
Hand-Rearing Wild and Domestic Mammals, Gage LJ. Iowa StatePress, Ames, 2002, 304 pages. Price US$59.99. ISBN 0 8138 2683 7.
This book is a handy reference with widespread application. Thefirst seven chapters focus on hand rearing domestic animals: rabbits,dogs, cats, horses, pigs, goats and South American camelids. Theremainder of the book covers a wide range of exotic mammals.Australian fauna is represented by sections on sugar gliders andmacropods with chapters on insectivorous bats and marine mammalsalso being relevant. The other chapters focus on a variety of speciesincluding primates, sloths, squirrels, exotic carnivores, ungulates, andelephants and provide useful information for hand-rearing thesegroups in the zoo setting.
Multi-author books often run the risk of inconsistency betweenchapters. This has been successfully addressed by having everychapter conform to the same series of headings and format. Eachchapter contains specific information on natural history, recordkeeping, equipment, criteria for intervention (particularly important),initial care, what to feed, daily routine, hygiene, housing, tips forweaning, common medical problems and release. The reader is takenstep by step through the process of handraising. There are valuablecharts detailing expected weight gains, useful tips on feeding tech-niques and an appendix listing addresses of suppliers.
The book does assume some basic knowledge and is probably tooadvanced for absolute beginners. Other books that cover a widerrange of specifically Australian species are available and would bebetter suited for wildlife carers. The book would be most useful in thediverse zoo environment and represents good value for money ifapplied to this setting. The domestic animal chapters make it applic-able to private practice but, again it would be more efficient to select abook focusing solely on puppies or kittens without worrying about howto raise a walrus.
PH HoIz
Dr HoIz is a veterinarian at Healesville Sanctuary, Victoria

56 Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Scientific
An editorial in these pages1 summarised some of the circumstances and conse-quences surrounding the introduction of West Nile virus (WNV) into New York
City beginning in July 1999. It remains unclear how WNV reached New York but ifinadvertent, it presumably was carried in via a mosquito on a vessel, a wild or domesticbird or possibly a human infected shortly before embarkation and with sufficientviraemia to infect a mosquito. The latter is unlikely since mammals, unlike avianspecies, are considered ‘dead end’ hosts for these viruses that is, the level of viraemiaattained is insufficient for a mosquito, during a blood meal, to acquire the virus. Uponarrival, the virus entered the New York bird population via mosquitoes, notablyinfecting and killing crows (Corvus spp) in the precinct and environs of the Bronx Zooand the epidemic ensued.
WNV is a member of the family Flaviviridae. It was originally isolated in Uganda in1937 and has hitherto been distributed predominantly in the Eastern Hemisphereincluding Africa, the Middle East, the southern nations of the former USSR, theIndian subcontinent and Southwest Asia including Indonesia. Culex pipiens is promi-nent as a vector for WNV but other Culex, Aedes and Anopheles spp mosquitoes are alsorecognised as vectors depending on locale. By sequence analysis the virus that enteredNew York is almost identical ( > 99.97% nucleotide identity) to a strain of WNVisolated from a dead goose in Israel in 1998.2,3
One of the questions when the first frosts came in the fall of 1999 was whether the viruswould over winter in the United States, become endemic and spread beyond New Yorkand the few nearby states in which it occurred in 1999. In January-February 2000 thevirus was identified in three pools of Culex spp mosquitoes collected in New York.
For 1999 final case numbers were: 25 equine cases of which 8 (32%) died or wereeuthanased and 60 human cases with 7 (10%) deaths. Corresponding figures forsubsequent years were: 2000, 60 equine cases, 23 (38%) died or were euthanased and21 human cases with 1 (4%) death; 2001, 738 equine cases and of 470 of these forwhich the outcome was known 156 (33.2%) died or were euthanased. During 2002WNV was detected in 44 states including all of the states east of the Rocky Mountainsand also in California, Idaho and Washington State (Figure 1) and in five provinces inCanada. For 2002 there were 14,717 equine cases with case fatality rates and attackrates yet to be recorded; the weekly rate of equine cases reported by the United StatesDepartment of Agriculture, National Veterinary Services Laboratory peaked at 1093for the week ending 8 September. For 2002 there were 3873 human cases of which284 (6.4%) were fatal. Most human infections with WNV are either subclinical orresult in mild febrile illness lasting a few days; the serious human cases are mostly inindividuals > 50 years of age and all human infections correlate with time spentoutdoors. In one alarming incident four of four human patients that received organsfrom a single donor were infected with WNV and one of them died. The donor was amotorcar accident victim that received multiple blood transfusions before death. Theblood of one of the transfusions was considered the source of the virus.
The number of North American avian species known to be infected with WNV hascontinued to increase and is now > 110. In many instances these infections are accom-panied by severe illness and a fatal outcome.
West Nile virus revisited and othermosquito borne viruses of horses inAustralia
EDITOR COLIN WILKS
ASSOCIATE EDITOR KEITH HUGHES
EDITORIAL COMMITTEENORMAN ANDERSON, GLENN BROWNING,
COLIN CHAPMAN, ROBIN CONDRON,TREVOR FARAGHER, STEVEN HOLLOWAY,
KEITH HUGHES, TONY LEPPER,JOCK MCLEAN, CARL PETERSON,ANDREW TURNER, COLIN WILKS
JOURNAL ABSTRACTSALAN LAWTHER
EDITORIAL ASSISTANT ANDDESKTOP PUBLISHING
ANNA GALLO
The Australian Veterinary Journal welcomes
original contributions on all aspects of
veterinary science.
Submission of a manuscript for publication
will be held to imply that it is a record of
unpublished original work of the author(s)
and, if accepted will not be published else-
where in whole or part without permission.
The Journal reserves the right to reject any
manuscript.
Send contributions to the Scientific Section
of the AVJ to:
Editor,
AVA House, 272 Brunswick Road,
Brunswick, Victoria 3056.
Telephone: (03) 9387 2982, 9387 8808.
International -61 3 9387 8808
Telefax: (03) 9388 0112,
International +61 3 9388 0112.
Email: [email protected].
‘Instructions for authors’ and ‘Statistical
guidelines for authors’ are published in this
issue. Both are available on
http://www.ava.com.au
S C I E N T I F I C S E C T I O N
Australian
VETERINARYJOURNAL
MJ STUDDERTCentre for Equine Virology, School of Veterinary Science, The University ofMelbourne, Parkville, Victoria 3010
EDITORIAL

Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 57
Scientific
flight to Australia. Beginning day 5 after arrival the stalliondeveloped severe, life threatening, illness characterised by fever,incoordination and muscle tremors. Euthanasia was consideredimminent but a recovery to full soundness and release fromquarantine followed. Unlike the mosquitoes and avian speciesrecovered mammalian species do not remain carriers of WNV.A serological diagnosis of WNV infection was made atWestmead Hospital, Sydney in collaboration with ElizabethMacarthur Agriculture Institute, Camden.
As part of an effort to establish a comprehensive set of testsfor the diagnosis of all endemic equine virus diseases inAustralia we have, in addition to using established diagnostictests, developed a range of rapid (< 24 h) tests based on poly-merase chain reaction (PCR).5,6 As an extension of these efforts,beginning in May 1999 we set out to develop PCR tests forthree mosquito borne viruses (Ross River virus, West Nile virus[Kunjin virus] and Murray Valley encephalitis virus) that areendemic in Australia and are sometimes, and usually uncer-tainly, linked to disease in horses. The results of these studies arereported in this issue.4
There are obviously important differences between the WNVthat is endemic in Australia and the strain that entered andbecame endemic in the USA.3 Genetic markers that confer thehigh human, equine and avian pathogenicity on the USA virushave not been identified. For Australia the threats posed by theintroduction and establishment of the USA strain of WNV aresignificant for human public health, the equine industry andthe environment through its impact on native avian andmammalian species.
References1. Studdert MJ. West Nile virus finds a new ecological niche in Queens, NewYork. Aust Vet J 2000;78:400-401.2. Jia XY, Briese T, Jordan I et al. Genetic analysis of West Nile New York 1999encephalitis virus. Lancet 1999;354:1971-1972.3. Lanciotti RS, Ebel GD, Deubel V et al. Complete genome sequences andphylogenetic analysis of West Nile virus strains isolated from the United States,Europe, and the Middle East. Virology 2002;298:96-105.4. Studdert MJ, Azuolas JK, Ficorilli N et al. Polymerase chain reaction tests forthe identification of Ross River, Kunjin and Murray Valley encephalitis virusinfections in horses. Aust vet J 2003;81:76-80.5. Varrasso A, Dynon K, Ficorilli N, et al. Identification of equine herpesviruses1 and 4 by polymerase chain reaction. Aust Vet J 2001;79:563-569.6. Dynon K, Varrasso A, Ficorilli N et al. Identification of equine herpesvirus 3(equine coital exanthema virus), equine gammaherpesviruses 2 and 5, equineadenoviruses 1 and 2, equine arteritis virus and equine rhinitis A virus by poly-merase chain reaction. Aust Vet J 2001;79:695-702.
What is the relevance to Australia of the USA experience withWNV? We do have a strain of WNV endemic in Australiacalled Kunjin virus. Kunjin virus is considered nonpathogenicfor humans although it has been isolated from two fatal equinecases.4 By sequence analysis Kunjin virus forms a distinct clade,one of three, within lineage 1, one of two, that encompasses allWNV isolates.3 The endemicity of a WNV in Australia under-scores the fact that we also have bird species and competentmosquito vectors that would almost certainly confer endemicityon the USA strain of WNV should it enter Australia. It ispossible that prior infection with Kunjin virus of various avianspecies and its established presence in Australian mosquitopopulations would modify the epidemiological pattern of infec-tions if the USA WNV was to be introduced and gain afoothold.
On 12 August 2002 a Standardbred shuttle stallion infectedwith WNV was imported into the Eastern Creek, New SouthWales animal quarantine facility. The stallion originated fromPort Pierre, near Toronto, Canada and was one of 49 shuttlestallions in a consignment. The stallion travelled by road fromPort Pierre to Chicago where it joined the other stallions for the
Figure 1. West Nile virus in the United States 2002. Statesreporting laboratory-positive cases of WNV infection in birds,mosquitoes, animals or humans in 2002. Reproduced withpermission. (Centers for Disease Control and Prevention.www.cdc.gov/ncidod/dvbid/westnile/surv&control.htm. 17 December2002. Retrieved 14 January 2003.)
Verified avian, animal, and mosquito infections during 2002, as ofDecember 11, 2002
Indicates human case(s) verified as of December 11, 2002
The dynamics, prevalence and impact of nematode infections in organically raised sheep in Sweden.
A3-year survey (1997-99) was carried out on organically reared sheep flocks throughout Sweden as a result of anecdotal reports that thesemethods of farming increased the difficulties associated with nematode infection, which is recognised as the most important infectious disease
problem within the Swedish sheep industry.Scandinavian countries are moving toward organic agricultural production because of consumer demand and government policy, which is aiming
at 10% of all lamb meat produced in Sweden by 2005 being organically raised. Regulations include the prohibition of prophylactic anthelmintics. Sweden's 440,000 sheep are found mostly in the southern parts of the country, and farms with organically reared flocks are distributed throughout
these sheep rearing areas; their main enterprise is the production of prime lambs for the domestic market. Spring lambing (April/May) is practisedwith an autumn (October) target live weight of 40 kg; significant numbers of lambs do not reach this weight and are winter-housed until the nextspring.
Fecal samples from the ewes and lambs of 152 organic flocks were taken at lambing and during the grazing period. The resulting nematode fecalegg counts were used to compare different management practices. The authors conclude that whereas parasite burdens in organically farmedlambing ewes may be considered moderate, they do prime the process of parasite build-up in the forthcoming grazing season, resulting in significantproductivity penalties for the offspring. They also note that that the control of these diseases on organic farms also implies serious animal welfareissues even low infection levels can incur distress.
Lindqvist A et al. Acta Vet.Scand.2001;42:377-389.

58
Scientific
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Failure to eradicate ovine footrot associated withDichelobacter nodosus strain A198 by repeated daily footbathing in zinc sulphate with surfactant
PD JELINEK and LJ DEPIAZZIDepartment of Agriculture, PO Box 1231, Bunbury, Western Australia 6230.
Objective To investigate the effect of repeated daily foot-bathing in zinc sulphate on virulent ovine footrot associatedwith S1, U1 and U5 zymogram types of Dichelobacternodosus, including the highly virulent S1 strain A198.
Design A field trial with experimentally infected sheep.
Procedure At week 0, 50 sheep were infected with Dnodosus strains A198 (S1), C305 (U1), BC3993 (U5) andBC3995 (U5). At weeks 1 and 47, respectively, 169 and 235uninfected sheep were added. At week 60, sheep were allo-cated to control and treatment groups each containing 220sheep. Every 2 or 4 weeks to week 113, feet were inspected,and lesions were scored and sampled. Treatment sheep werefootbathed in 15 to 18% (w/v) zinc sulphate with surfactant for5 consecutive days (10 min per day) during week 61. Duringweek 110, the footbathing protocol was applied again, thistime to all surviving treatment and control sheep.
Results BC3993 and A198 were isolated from 57% (162 of285) and 20% (58 of 285), respectively, of new lesionssampled between weeks 3 and 13, and 21% (57 of 271) and50% (136 of 271) between weeks 49 and 59. Percentages ofnew lesions associated with C305 and BC3995 remainedconstant. During the initial 17 weeks after footbathing at week61, 90% (75 of 83) and 19% (95 of 490) of lesions in treatmentand control sheep, respectively, were score 4 or 5, and 94%(47 of 50) and 38% (33 of 87) of those were associated withA198.
Conclusions Repeated daily footbathing did not eradicatevirulent ovine footrot because strain A198 produced deep,covert lesions that facilitated the survival of D nodosus.Aust Vet J 2003;81:58-62
S Thermostable protease strainU Thermounstable protease strainPCR Polymerase chain reactionTASH Trypticase/arginine/serine/hoof horn agarDNA Deoxyribonucleic acid
Dichelobacter nodosus is the infectious agent of footrot, acontagious disease of ruminants in high rainfall areas.1
In a recent study, virulent ovine footrot associated withS1,2 U12 and T3 zymogram types of D nodosus was eradicatedby repeated daily footbathing (10 min each day for 5 consecu-tive days) in a 15 to 18% (w/v) solution of zinc sulphate withsurfactant, followed by prolonged exposure of the sheep to a dryenvironment.4 In that study, sheep had chronic, underrunningfootrot lesions, a small percentage had score 4 or 5 lesions justprior to footbathing, and feet were not pared. In previous zincsulphate footbathing experiments, neither single treatments,5,6
nor multiple treatments in which the interval between treat-
ments was greater than 1 day,1, 7-14 nor repeated daily, walk-through treatments,15 eradicated virulent ovine footrot evenwhen feet were pared.
This paper reports the results of an experiment designed tovalidate the findings of the previous study,4 by the inclusion of ahighly virulent strain of D nodosus in a multi-strain, experi-mental infection. In this experiment, sheep were infected withS1, U1 and U5 zymogram types of D nodosus, including thehighly virulent S1 strain A198. Before the sheep were foot-bathed, the occurrence of different strains of D nodosus in newclinical lesions was investigated.
Materials and methodsA standard scoring system16 was used to grade the severity of
footrot lesions. Feet scored as 0 had no evidence of necrosis,inflammation or cleavage of horn. Lesions scored as 1 or 2 wereconfined to the interdigital skin (interdigital lesions), whilethose scored as 3a, 3b, 3c, 4 or 5 involved progressive separationof horn from the underlying laminae (underrunning lesions).
SheepThe sheep were mixed-age, mixed-sex Merinos from multiple
genetic lines and were obtained from properties with no historyof footrot. Initially, the sheep were grazed at Wokalup ResearchStation, Western Australia, on unirrigated paddocks dominatedby ryegrass and kikuyu, and thereafter at Vasse Research Station,Western Australia, on unirrigated paddocks dominated byryegrass and clover, at stocking rates of between 20 to 30sheep/ha. There was no clinical evidence of footrot in any ofthese sheep before they were included in the experiment.
Inoculating strains of D nodosusFour strains of D nodosus were used to inoculate sheep, with
each strain uniquely identifiable by its zymogram type andhybridisation pattern with 1 or more of the recombinant plas-mids pJIR318L,17 pJIR318H,17 pJIR314B17 and pB645-335.18
Strain A198 was zymogram type S1 and hybridised withpJIR318L and pJIR314B. This standard virulent strain of Dnodosus was obtained from CSIRO, Victoria. Strain C305 waszymogram type U1 and hybridised with pJIR318L and pB645-335. This standard benign strain of D nodosus was obtainedfrom CSIRO, Victoria. Strain BC3993 was zymogram type U5and hybridised with pB645-335, and was isolated from sheepwith clinically virulent footrot in Western Australia (data notshown). Strain BC3995 was zymogram type U5 and hybridisedwith pJIR318H, pJIR314B and pB645-335, and was isolatedfrom sheep with clinically benign footrot in Western Australia(data not shown).
Throughout the experiment, a combination of zymogramtype and plasmid hybridisation pattern was used to identify eachre-isolate of D nodosus strains A198, C305, BC3993 and BC3995.

Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 59
Scientific
At week 81 (10 April 2000), and every 4 weeks to week 109(23 October 2000), the feet of all sheep were inspected. At eachinspection, lesion scores were recorded and samples of lesionmaterial were taken from up to 30 lesions selected randomlyfrom treatment sheep, and up to 60 lesions selected randomlyfrom control sheep. At each inspection between weeks 81 and101 (28 August 2000), inclusive, sheep detected with footrotlesions of score 1 or greater in either of groups B or D were relo-cated to groups A or C, respectively, to investigate if any of theremaining sheep still had footrot. There was no further segrega-tion of sheep after week 101.
On the first day of week 110 (30 October 2000), all survivingsheep in each of the groups were combined. These sheep werefootbathed on each of the 5 days of that week using the sameprotocol as the one applied during week 60. At week 113 (20November 2000), sheep were inspected and lesion scores wererecorded. If available, samples of lesion material were taken forlaboratory tests.
Laboratory testsSamples of lesion material were taken by scraping each lesion
with a clean, stainless steel spatula. Samples were embedded inthe upper 5 mm layer of Stuart’s modified transport medium(Oxoid, Australia). Bottles of inoculated media were sent byovernight courier to the National Footrot Reference Laboratoryin Albany, Western Australia, for D nodosus isolation 20 andprotease testing (gelatin gel and protease zymogram).2 PCRtests to detect gene sequences homologous to pJIR318L,pJIR318H, pJIR314B and pB645-335 were performed onwhole cell extracts from 2- to 4-day-old, TASH agar platecultures of D nodosus at the Department of Agriculture inBunbury, Western Australia.
Statistical analysisPrevalence of footrot at each inspection after footbathing was
calculated using the number of sheep detected with lesions ofscore 1 or greater expressed as a percentage of the total numberof sheep inspected. Severity of footrot lesions in control andtreatment sheep was estimated using mean total weighted footscores.21 Frequencies of isolation of different strains of Dnodosus from lesions were compared using Chi-square analysis(Pearson method).
Results Twelve sheep died before they could be footbathed at week
60. Eleven control sheep and 13 treatment sheep died betweenweeks 60 and 113. In each case, the cause of death was notestablished.
New clinical lesionsFigure 1 shows numbers of feet of sheep detected with new
clinical lesions associated with D nodosus strains A198, C305,BC3993 and BC3995 at each inspection between weeks 3 and59. Table 1 shows percentages of new clinical lesions associatedwith D nodosus strains A198, C305, BC3993 and BC3995detected between weeks 3 and 13 in the initial 219 sheep, andbetween weeks 49 and 59 in the 235 sheep added to this flockat week 47. Strain BC3993 was isolated from more lesionsdetected between weeks 3 and 13 than between weeks 49 and59 (χ2 = 74.61, P < 0.001). Strain A198 was isolated from morelesions detected between weeks 49 and 59 than between weeks3 and 13 (χ2 = 54.42, P < 0.001).
Inoculation of sheepAt week 0 (18 September 1998), the left front and right hind
feet of 40 sheep were inoculated with D nodosus strains A198,C305, BC3993 or BC3995 (10 sheep per strain) at WokalupResearch Station. In another 10 sheep, the left front and righthind feet were inoculated with all 4 strains to expedite the estab-lishment of multi-strain infections.
The technique used to inoculate sheep has been describedpreviously.19 Briefly, blocks of TASH agar containing 72 hcultures of D nodosus20 were placed on lightly scarified, interdig-ital skin of feet, that were wrapped with gauze bandage thensurgical tape to secure the agar blocks. Bandages were removedat week 1 (25 September 1998), and 169 clean sheep wereadded to the infected sheep.
New clinical lesionsAt week 3 (12 October 1998), and fortnightly to week 47 (16
August 1999), the feet of all 219 sheep were inspected, lesionscores were recorded and samples of lesion material were takenfrom all new clinical lesions. These were defined as lesions ofscore 1 or greater in feet that had not been inoculated initially,and from which D nodosus had not been previously isolated.
After inspection at week 47, a flock of 235 clean sheep wasadded to the infected flock. At week 49 (30 August 1999), andfortnightly to week 59 (8 November 1999), the feet of all 235sheep added at week 47 were inspected, lesion scores wererecorded, and samples of lesion material were taken from all newclinical lesions. The original flock of 219 sheep was not inspectedbetween weeks 49 and 57, but they were inspected at week 59.
FootbathingThe infected sheep were transported to Vasse Research
Station immediately after the final inspection before foot-bathing (week 59), which was in late spring when pasture wasbeginning to dry off. On the same day, the sheep were allocatedto control and treatment groups of 220 sheep each according tomethodology described previously,4 based on data collectedduring fortnightly inspections between weeks 0 and 59.
On each of the first 5 days of week 60 (15 November 1999),treatment sheep were footbathed for 10 min using a 15 to 18%(w/v) solution of Footrite® (Hardman Australia Pty Ltd), acommercial preparation of zinc sulphate with surfactant, using amethod described previously.4 During week 60, there was norainfall, the ground was dry, and there was no spread of footrotin control sheep (data not shown). Feet were not pared beforetreatment. Control sheep were not footbathed.
At week 61 (22 November 1999), and every 4 weeks to week77 (13 March 2000), the feet of all sheep were inspected. Ateach inspection, lesion scores were recorded and samples oflesion material were taken from up to 60 lesions selectedrandomly from sheep in each group.
Segregation of sheepAt week 77, all remaining control and treatment sheep were
segregated into 4 separate groups, groups A, B, C and D, toinvestigate if sheep with no clinical signs of footrot at that timestill had the disease. Group A comprised 43 control sheep eachwith at least 1 lesion of score 1 or greater. Group B comprised169 control sheep with no detectable footrot lesions. Group Ccomprised 33 treatment sheep each with at least 1 lesion ofscore 1 or greater. Group D comprised 183 treatment sheepwith no detectable footrot lesions.

60 Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Scientific
FootbathingIn the 59 weeks before footbathing, 41% (90 of 220) and
43% (95 of 220) of control and treatment sheep, respectively,were each detected with at least 1 lesion that was score 4 or 5. Atweek 59, the percentages of sheep each detected with at least 1lesion that was score 1 or greater in control and treatmentgroups were 69.5% (153 of 220) and 66.8% (147 of 220),respectively, and the mean total weighted foot scores in thesegroups were 16.8 and 15.9, respectively. Eleven treatment sheepwere each detected with at least 1 lesion that was score 4 or 5 atweek 59. Table 2 shows percentages of feet of control and treat-ment sheep detected with different lesion scores during fort-nightly inspections between weeks 0 and 59.
Figure 2 shows percentages of sheep detected with lesions ofscore 1 or greater, and mean total weighted foot scores, incontrol and treatment groups at each inspection after foot-bathing (weeks 61 to 113). Between weeks 61 and 77, score 4 or5 lesions comprised 19.4% (95 of 490) and 90.4% (75 of 83) ofall lesions detected in control and treatment sheep, respectively.Score 4 or 5 lesions were the first clinical signs of footrot in95.5% (42 of 44) of feet of treatment sheep that were detected withfootrot lesions over the same period. In 8 of these feet, therewere no clinical signs of footrot at any previous inspection.
Table 1 shows percentages of lesions associated with Dnodosus strains A198, C305, BC3993 and BC3995 detected incontrol and treatment sheep between weeks 61 and 77. Duringthat time, strain A198 was isolated from more lesions in treat-ment sheep than control sheep (χ2 = 41.09, P < 0.001), andfrom more lesions in treatment sheep than was any other strainof D nodosus (χ2 = 135.54, P < 0.001). Strain A198 was isolatedfrom all 8 lesions that were score 4 or 5 in treatment sheep thathad no clinical signs of footrot at any previous inspection.
Segregation of sheepTable 1 shows percentages of lesions associated with D
nodosus strains A198, C305, BC3993 and BC3995 detected insheep in groups B and D between weeks 81 and 109. Duringthat time, strain A198 was isolated from more lesions in sheepin group D than group B (χ2 = 52.29, P < 0.001). Lesions weredetected in sheep in group B (1 lesion per sheep) at weeks 81 (4lesions), 85 (1 lesion), 89 (4 lesions) and 93 (1 lesion). Eight ofthese lesions were score 4 or 5, and 4 were sampled. Strain A198was isolated from all 4 lesions sampled.
Table 1 shows percentages of lesions associated with D nodosusstrains A198, C305, BC3993 and BC3995 detected in sheep atthe final inspection at week 113, after sheep in each of the 4groups were combined and footbathed at week 110. At the finalinspection, 10 lesions were detected, 8 of which were score 4 or5 and each was sampled. Strain A198 was isolated from all 8lesions sampled.
Table 3 shows percentages of 1661 lesions associated witheach unique strain of D nodosus detected between weeks 1 and113. Strain A198 was isolated from more lesions during thattime than was either BC3993 (χ2 = 23.08, P < 0.001), BC3995(χ2 = 44.82, P < 0.001) or C305 (χ2 = 765.04, P < 0.001).
D nodosus that hybridised in a novel pattern with pJIR318L,pJIR314B and pB645-335 was isolated from newly infectedsheep between weeks 3 and 13 (5 lesions), and between weeks49 and 59 (8 lesions), and from control sheep at weeks 77 (1lesion), 81 (2 lesions) and 105 (1 lesion). Initial testing of theseisolates showed that they all contained the 5 major proteaseisoenzymes shared by S1 and U5 zymogram types, suggestingthat the isolates were not clonal. This was verified by repeatedsubculturing, which eventually yielded either strain A198 orBC3993 (data not shown).
The U62 zymogram type of D nodosus that hybridised in anovel pattern with pJIR318L and pJIR314B was isolated fromtreatment sheep at weeks 81 (1 lesion), 89 (2 lesions) and 105(1 lesion). These U6 isolates had genetic similarities to strainA198 in terms of their hybridisation patterns (see Table 3) andtheir pulsed-field gel electrophoresis patterns when DNA wasdigested with the restriction endonuclease Apa1 (NB Buller,unpublished data).
The U5 zymogram type of D nodosus that hybridised in anovel pattern with pJIR318H and pB645-335 was isolated froma single lesion at week 37 (7 June 1999).
DiscussionIn this experiment, repeated daily footbathing in a solution of
zinc sulphate with surfactant did not eradicate virulent ovinefootrot. The detection of footrot lesions in treatment sheep theweek after footbathing, and the isolation of D nodosus fromlesions 4 weeks later, demonstrated that D nodosus had survivedthe treatment. There was evidence that the treatment failedbecause strain A198 produced deep, covert lesions that facili-tated the survival of D nodosus.
Figure 1. Numbers of feet of sheep detected with new clinicallesions associated with D nodosus strains A198 (××), C305 (❍),BC3993(❑) and BC3995 (∆∆) at each inspection between weeks 3and 59.
Figure 2. Percentages of sheep detected with lesions of score 1or greater, and mean total weighted foot scores, in control (××))and treatment (∆∆) groups at each inspection between weeks 61and 113. Mean total weighted foot scores = numbers.

Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 61
Scientific
Although the failure to eradicate footrot in this experimentwas consistent with the results of a number of previous reportsdescribing the efficacy of zinc sulphate preparations as topicaltreatments for footrot,1,7-15 it was in stark contrast to thesuccessful eradication of virulent ovine footrot in a more recentexperiment.4 In that experiment, like the current one, feet ofsheep were bathed for 10 min each day for 5 consecutive days atthe end of spring, resulting in the exposure of footbathed sheepto the bactericidal effects of zinc sulphate over 5 days followedby prolonged drought conditions after footbathing. Also, sheepin both experiments had histories of underrunning footrotlesions, a small percentage had score 4 or 5 lesions just beforefootbathing, and feet were not pared. A notable difference,however, was that at no stage during the previous experimentwas there any evidence of atypical score 4 or 5 lesions in the feetof sheep, suggesting that eradication was achieved in that exper-iment because none of the infecting strains of D nodosus had thevirulence of A198.
A198 has been shown to be a highly virulent strain of Dnodosus in standard pen experiments.23 In the current experi-ment, the observation that only 1.7% of lesions detected beforefootbathing were score 4 or 5 was probably a reflection of anenvironment that unlike standard pen conditions, was notconducive to the full expression of the potential virulence ofstrain A198. For example, there was a rapid reduction in thenumber of new clinical lesions detected between weeks 3 and 11due to premature onset of dry weather. In the ensuing 36 weeks,there were no new lesions detected in inoculated sheep. Thesedata were consistent with the results of a previous experimentthat demonstrated widely varying lesion scores in sheep infectedwith a single, S1 strain of D nodosus at 5 geographical sites.24
Before footbathing, the prevalences of new clinical lesionsassociated with D nodosus strains C305 and BC3995 betweenweeks 3 and 13 were not significantly different to those betweenweeks 49 and 59. These data were consistent with the results ofa previous study,3 in which percentages of new clinical lesionsassociated with S1, U1 and T zymogram types of D nodosusremained constant during 12 months of fortnightly inspections,despite seasonal changes in temperature and rainfall, geneticvariation in the population of S1 types, and host resistance tofootrot. It was unclear why strain A198 was isolated from morenew clinical lesions between weeks 49 and 59 (50.2%) thanbetween weeks 3 and 13 (20.4%), why the reverse was the casefor strain BC3993 (21.0% and 56.8%), and why the percentageof new clinical lesions associated with only one U5 zymogramtype of D nodosus were constant before footbathing. Both U5zymogram types of D nodosus behaved similarly in that theysurvived the footbathing treatment, they were not isolated againfrom footrot lesions in treatment sheep until 17 weeks afterfootbathing, and they were isolated only sporadically from treat-ment sheep thereafter.
The origin of the U6 zymogram type of D nodosus detected in4 lesions in footbathed sheep was not established. Whilst it waspossible that some sheep in the original flock had been carryingthe U6 type, this was unlikely given the time that had elapsedbefore it was detected. Also, all sheep were obtained from aproperty that had no history of footrot, and there were no clin-ical signs of footrot before the sheep were inoculated. It was alsopossible that the U6 type was a genetic recombinant of Dnodosus,25 although there was no evidence of this based onprotein isoenzyme and plasmid hybridisation profiles of theinoculating strains. A plausible explanation for the appearance
During the first 17 weeks after footbathing, there was negli-gible spread of footrot due to the prevailing drought condi-tions.22 During that time, score 4 or 5 lesions were the first clin-ical signs of disease in 96% of feet of treatment sheep detectedwith footrot. Most of these lesions were atypical, characterisedby extensive necrosis of the hoof that was visible at the sole, butwith no concurrent interdigital necrosis or separation of hornfrom the underlying laminae. Significantly fewer atypical, score4 or 5 lesions were detected in feet of control sheep (19%) rela-tive to treatment sheep (90%) during that same period.
During the first 17 weeks after footbathing, D nodosus strainA198 was isolated from all score 4 or 5 lesions detected in treat-ment sheep, and from significantly more lesions in treatmentsheep (94%) than control sheep (38%). Thereafter, strain A198was isolated from all score 4 or 5 lesions sampled both in treat-ment sheep with no previous clinical signs of footrot, and intreatment sheep with no clinical signs of footrot when they weresegregated from clinically affected sheep at the end of summer.Strain A198 was also isolated from all 10 lesions, 8 of whichwere score 4 or 5, detected after the second footbathing.
Table 2. Percentages of feet of control and treatment sheep detectedwith different lesion scores during fortnightly inspections betweenweeks 0 and 59.
Group Number of Lesion score
observations 0 1 2 3a 3b 3c 4 5
Control 13116 77.2 13.5 5.2 1.4 0.5 0.5 1.4 0.3
Treatment 13084 77.2 13.1 5.6 1.5 0.7 0.5 1.2 0.5
Table 1. Percentages of lesions associated with D nodosus strains A198,C305, BC3993 and BC3995 detected at different time intervals betweenweeks 3 and 113.
Week Sheep sampled Number Strain of D nodosus (%)of lesions A198 C305 BC3993 BC3995
3 to 13 Original flock (219) 285 20.4 1.8 56.8 19.3
49 to 59 Added at week 47 (235) 271 50.2 0.0 21.0 25.8
61 to 77 Control group 150 37.9 0.0 32.2 28.7
61 to 77 Treatment group 83 94.0 0.0 2.0 2.0
81 to 109 Group B 183 52.5 0.0 19.7 26.2
81 to 109 Group D 173 87.8 0.0 3.5 6.4
113 All 10 100.0 0.0 0.0 0.0
Table 3. Percentages of 1661 lesions associated with each unique strainof D nodosus detected between weeks 1 and 113.
Strain Zymogram Plasmid hybridisation pattern: Percentagetype
pJIR318H PJIR318L pJIR314B pB645-335
A198 S1 - + + - 38.9
BC3993 U5 - - - + 30.9
BC3995 U5 + - + + 27.9
C305 U1 - + - + 0.7
Unknown S1/U5 - + + + 1.3
Unknown U6 - + + - 0.2
Unknown U5 + - - + 0.1

62 Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Scientific
of the U6 type, based on both clinical and laboratory data, wasthat it was a deletion mutant of strain A198. This was consis-tent with the results of a previous experiment in which U6 typeswere isolated from sheep that were experimentally infected witha single, S1 strain of D nodosus.24
By the end of the experiment, D nodosus strain A198 hadbeen the most, and C305 the least, prevalent strain of D nodosusisolated from lesions in sheep. Strain A198 was isolated fromthe majority of lesions in both control and treatment sheep afterfootbathing compared to either BC3992 or BC3995. StrainC305 was not detected at any inspection after week 7. Thesedata were consistent with other reports that S strains of Dnodosus were more prevalent than U strains in footrot lesions insheep.3,20,26 The high rate of isolation of strains of D nodosuswith laboratory characteristics comparable to the inoculatingstrains (99.7% of 1661 isolates) suggested that each strain wasmost probably a clonal, rather than a mixed, culture of Dnodosus.
In conclusion, the data suggested that repeated daily foot-bathing did not eradicate virulent ovine footrot in this experi-ment because strain A198 produced lesions that in some feetprotected D nodosus from exposure to the zinc sulphate solu-tion. This treatment protocol might have a role in the eradica-tion of footrot associated with strains of D nodosus that are notas virulent as A198. Some of these can be difficult to detect ineradication programs,27,28 particularly in environments that areprone to drought.
AcknowledgmentsThe authors would like to acknowledge Mike Palmer and
David Pitman for their laboratory support, including culturingof D nodosus isolates and protease testing, Ian Spicer for histechnical and field assistance, and the staff at Vasse ResearchStation, including Frank Coupar and Andrew Lindsay. Thesupport of the Western Australian Footrot EradicationCampaign Advisory Committee is acknowledged.
References1. Beveridge WIB. Footrot in sheep: a transmissible disease due to infectionwith Fusiformis nodosus (n sp). Bull Counc Sci Ind Res (Melbourne) 1941;No140.2. Palmer MA. A gelatin gel test to detect activity and stability of proteasesproduced by Dichelobacter (Bacteroides) nodosus. Vet Micro 1993;36:113-122.3 .Jelinek PD, Depiazzi LJ, Galvin DA et al. Occurrence of different strains ofDichelobacter nodosus in new clinical lesions in sheep exposed to footrot asso-ciated with multi-strain infections. Aust Vet J 2000;78:273-276.4. Jelinek PD, Depiazzi LJ, Galvin DA et al. Eradication of ovine footrot byrepeated daily footbathing in a solution of zinc sulphate with surfactant. Aust VetJ 2001;79:431-434.5. Cross F. Response of sheep to various topical, oral, and parenteral treat-ments for foot rot. J am Vet Med Assoc 1978;173:1569-1570.6. Lambell RG, Atkins JW, Brightling A. The use of a zinc sulphate formulationfor the eradication of footrot during a period unfavourable for the spread of the
disease. In: Stewart DJ, Peterson JE, McKern NM, Emery DL, editors. Footrotin Ruminants, Proceedings of a Workshop. AWC Technical Publication,Melbourne, 1985;47-49.7. Malecki J, McCausland I, Lambell R. A new topical treatment for footrot. In:Sheep Production and Preventive Medicine, Proceedings No. 67. TheUniversity of Sydney Post-Graduate Committee in Veterinary Science, Sydney1983;63-70.8. Skerman TM, Green RS, Hughes JM et al. Comparison of footbathing treat-ments for ovine footrot using formalin or zinc sulphate. NZ Vet J 1983;31:91-95.9. Skerman TM, Moorhouse SR, Green RS. Further investigations of zincsulphate footbathing for the prevention and treatment of ovine footrot. NZ Vet J1983;31:100-102.10. Atkins JW. The use of zinc sulphate formulation for the eradication of footrotduring a period favouring spread of the disease. In: Stewart DJ, Peterson JE,McKern NM, Emery DL, editors. Footrot in Ruminants, Proceedings of aWorkshop. AWC Technical Publication, Melbourne, 1985;43-45.11. Plant JW, Claxton PD. Efficacy of paring, footbathing and vaccination in thetreatment of footrot. In: Stewart DJ, Peterson JE, McKern NM, Emery DL,editors. Footrot in Ruminants, Proceedings of a Workshop. AWC TechnicalPublication, Melbourne, 1985;57-61.12. Malecki JC, Coffey L. Treatment of virulent ovine footrot with zincsulphate/sodium lauryl sulphate footbathing. Aust Vet J 1987;64:301-304.13. Casey RH, Martin PAJ. Effect of foot paring of sheep affected with footrot onresponse to zinc sulphate/sodium lauryl sulphate foot bathing treatment. AustVet J 1988;65:258-259.14. Hinton DG. Eradication of actively spreading ovine footrot. Aust Vet J1991;68:118-119.15. Bulgin MS, Lincoln SD, Lane MV et al. Comparison of treatment methodsfor the control of contagious ovine footrot. J am Vet Med Assoc 1986;189:194-196.16. Stewart DJ, Claxton PD. Ovine footrot: Clinical diagnosis and bacteriology.In: Corner LA and Bagust TJ, editors. Australian Standard DiagnosticTechniques for Animal Diseases 1993;1-27.17. Rood JI, Howarth PA, Haring V, et al. Comparison of gene probe andconventional methods for the differentiation of ovine footrot isolates ofDichelobacter nodosus. Vet Micro 1996;52:127-141.18. Liu D, Webber J. A polymerase chain reaction assay for improved determi-nation of virulence of Dichelobacter nodosus, the specific causative pathogenfor ovine footrot. Vet Micro 1995;43:197-207.19. Depiazzi LJ, Richards RB. Motility in relation to virulence of Bacteroidesnodosus. Vet Micro 1985:10:107-116.20.Pitman DR, Palmer MA, Depiazzi LJ. The laboratory culture of Dichelobacternodosus in a footrot eradication program. Aust Vet J 1994;71:109-112.21. Whittington RJ, Nicholls PJ. Grading the lesions of ovine footrot. Res VetSci 1995;58:26-34.22. Egerton JR. Footrot control in drought. Aust Vet J 1983;60:315.23. Stewart DJ. Validation and implementation of new technologies for the rapidand precise diagnosis of ovine footrot: Final Report on Woolmark ProjectCHP94 1996.Depiazzi LJ, Roberts WD, Hawkins CD et al. Severity and persistence of footrotin Merino sheep experimentally infected with a protease thermostable strain ofDichelobacter nodosus at five sites. Aust Vet J 1998;76 (1):32-38.25. Ghimire SC, Egerton JR. PCR-RFLP of outer membrane proteins gene ofDichelobacter nodosus: a new tool in the epidemiology of footrot. EpidemiolInfect 1999;122:521-528.26. Depiazzi LJ, Richards RB, Henderson J et al. Characterisation of virulentand benign strains of Bacteroides nodosus. Vet Micro 1991;26:151-160.27. Egerton JR, Raadsma HW. Unresolved questions about footrot eradication.Wool Tech Sheep Breed 1993;41:99-107.28. Allworth MB, Egerton JR. The eradicability of strains of Dichelobacternodosus from benign, intermediate and virulent footrot. In: Proceedings of theAustralian Sheep Veterinary Society, Melbourne 1995;37-41.
(Accepted for publication 15 May 2002)

63
Scientific
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Accuracy of bovine pregnancy detection using transrectalultrasonography at 28 to 35 days after insemination
DP NATIONa, J MALMOb, GM DAVISb and KL MACMILLANa
Objective To estimate the accuracy of real-time ultrasonog-raphy to detect pregnancy in dairy cows at 28 to 35 days afterinsemination.
Methods Cows that did not return to oestrus between 18and 24 days after a first insemination (n = 526) were exam-ined by transrectal ultrasonography from 28 to 35 days afterinsemination. Pregnancy was confirmed by the observation ofa foetus, but fluid in the uterine horn and the presence ofembryonic membranes were also noted. When pregnancywas not confirmed by the observation of a foetus, a secondexamination 7 days later, confirmed these remaining cows aspregnant or not pregnant to the first insemination. Detection ofpregnancy at this early examination was compared withmanual transrectal pregnancy examination performed 10 to13 weeks after insemination (13-week examination).
Results There were 44% of cows that were pregnant to thefirst service, 34% that had returned for a second service 18 to24 days after the first insemination, and 20% of cows thatwere not pregnant, and had not returned normally for asecond service (non-pregnant, non-return) within 24 days oftheir initial insemination. The presence of a foetus at 28 to 35days after insemination was accurately predicted by a simpli-fied method where uterine fluid accumulation and embryonicmembranes were observed. Foetal loss between the earlydetection and the 13-week examination (9% of pregnancies)indicated that 28 to 35 days post insemination was too early toreliably detect pregnancy.
Conclusion Early examination of pregnancy with trans-rectal ultrasonography is an accurate method to identify non-pregnant, non-return cows. The examination can be simplifiedby the observation of uterine fluid accumulation and embry-onic membranes, as opposed to the more involved process ofobserving the foetus.Aust Vet J 2003;81:63-65
CL Corpus luteumMSD Mating Start Date
Although there have been many reports of ultrasound usefor early pregnancy diagnosis in Europe and the USA,1-5
the uptake of this technology has been limited inAustralia. The uptake of such a service might be improved if anindirect form of pregnancy detection, namely the observation ofuterine fluid accumulation and embryonic membranes, couldbe substituted for the requirement to observe a foetus. Theobservation of uterine fluid and embryonic membranes wouldtake substantially less time than observation of the embryoitself, and require less interference with the uterine horns. Thisshould be less traumatic for the cow and more efficient for theveterinarian.
It would be expected that a diagnosis based on direct foetalobservation would be more definitive, and the simplified diag-nosis compromised by the occasional presence of a uterineinfection. A similar comparison has been made where the directobservation of a foetus was described more accurately thanassays for the presence of pregnancy specific proteins in plasma,but resulted in more false negative diagnoses. 6
The ability to detect pregnancy as early as possible after aninsemination is of importance due to the significant populationof modern Holstein-Friesian dairy cows, which are not pregnantto the first insemination and do not return for a subsequentservice within 24 days. Non-pregnant, non-return cowscomprised 19% of a recent study population in some Australiandairy herds. 7
This study serially observed inseminated cows from 28 daysafter insemination using transrectal ultrasonography. A simpli-fied pregnancy diagnosis, as defined by the presence of uterinefluid accumulation and the presence of embryonic membranesat a single ultrasonographic observation, was compared againstthe standards of either a) the observation of a foetus from serialultrasonographic observations; and b) manual palpation ofuterine contents from 10 to 13 weeks after insemination.
Materials and methodsAnimals
A sub-population was selected from four dairy herds in theMacalister region, Victoria. Cows (n = 777; ranging from n =169 to n = 240 cows per herd) were randomly selected from thewhole herd, balanced for age as well as the interval from calvingto the MSD. Those that had not returned to oestrus 18 to 24days after insemination (n = 526) were selected for serial exami-nation for pregnancy. Every cow in each of the four herds wasexamined from 10 to 13 weeks after insemination, using rectalpalpation of uterine contents, to detect pregnancy (13-weekexamination). The proportion of herdmates that were pregnantfrom three of the four herds was compared with the study popu-lation at this time.
Early pregnancy detectionAn Aloka 500 ultrasound unit with a 7.5 MHz probe was
used to visualise the entire length of both uterine horns and,when necessary, ovarian structures. The ultrasound probe wascarried into the rectum by the operator and moved over bothuterine horns so that the appropriate structures could be visu-alised. The ultrasound image was observed by both the seniorauthor of the paper and by the ultrasound operator and theconfirmation of a foetus was only made with agreementbetween both observers.
Each herd was visited weekly to examine groups of cows thathad been inseminated from 28 to 35 days previously.Observation of each uterine horn was described by the site offluid accumulation, the maximum observed diameter of uterinefluid (lumen diameter in 5 mm intervals), the visible presenceof embryonic membranes, the maximum length of a visible
aDepartment of Veterinary Science, University of Melbourne, Werribee, Victoria 3030bMaffra Veterinary Centre, Maffra, Victoria 3860

64 Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Scientific
foetus, and the presence of an observable heartbeat. Abnormalpalpable structures which were noted included ovarian enlarge-ment due to a follicle ≥ 25 mm in diameter (Cystic Ovary),uterine adhesions (Adhesions), and open pyometra diagnosed asa grainy image of fluid in the uterine lumen as well as pusmanually removed from the vagina (Pyometra).
Pregnancy detection was definitive when an abnormality wasrecorded or a foetus was observed. Those cows in which a foetuswas not observed, and when no other abnormality was detected,were re-examined at the next weekly visit to confirm pregnancyof the cow. Serial observations also allowed additional abnormalcategories to be classified including: a) the abnormally small sizeof the foetus or the uterine lumen, with no heartbeat evident(Small Foetus); and b) evidence of a lost pregnancy withsubstantial cloudy uterine fluid, flaccid membrane-like struc-tures, and occasionally a white echogenic body (LostPregnancy?).
Statistical analysisCows were classified according to the range of observations
during the serial ultrasonographic examinations. Cows classifiedas Cystic Ovary, Adhesions, Pyometra, Small Foetus or LostPregnancy? were excluded from further analyses. Individualswere categorised according to whether or not they were preg-nant on the basis of detection of uterine fluid and embryonicmembranes at the first examination (Simplified pregnancy diag-nosis) and compared with: a) the observation of a foetus fromserial diagnoses (Foetal observation); or b) the manual diagnosisof pregnancy at 13 weeks (13-week examination).
Categorical data were analysed with a Chi-square test.Significant differences where reported where P < 0.05.
ResultsCategories from serial ultrasonographic pregnancy diagnoses
are presented in Table 1. Within the study population of 777cows, 44% were pregnant to the first service, 3% had observedabnormalities, 34% returned for a second service within 24 daysof the first service, and the remaining 20% were not diagnosedpregnant and had not returned to service within 24 days.
A comparison between a simplified diagnosis and foetalobservation is presented in Table 2. All accuracy parameterswere over 90%, with the least accuracy in the negative predic-tive value (92%).
Both the Simplified pregnancy diagnosis and FoetalObservation have similar accuracy when compared to the 13-week examination (Table 3). Both methods have reduced accu-racy due to the pregnancy loss between the early examinationand the 13-week examination (31 cases, or 9% pregnancy loss).There were also two cases where cows were reclassified from notpregnant to pregnant that could be attributed to an error inmanual palpation or a missed ultrasound detection (1% error).
The conception rate to first service, as calculated from the 13-week examination, did not differ between the study populationand their herdmates (P > 0.05; Table 4). This indicates thatultrasonographic examination had no effect on the establish-ment of pregnancy.
Among those cows diagnosed pregnant with serial ultra-sonography, 58% of conceptuses were in the right uterine horn.The changes in embryo size, uterine horn diameter and thepresence of a heartbeat are described in Figure 1. The length ofthe embryo increased from an average of 6.9 ± 0.20 mm (sem)at 28 days after insemination to 13.5 ± 0.34 mm at 35 days
Table 1. Classification of ovarian and uterine descriptions from serialultrasonography commencing from 28 to 35 days after insemination.
Description No. of cases
Foetus and embryonic membranes observed at 1st observation 289
Uterine fluid and embryonic membranes observed at 1st diagnoses, pregnancy confirmed from subsequentobservation of foetus 40
No evidence of gravid structures at the 1st diagnoses,but a foetus was observed at a subsequent diagnoses 13
Uterine fluid and embryonic membranes observed at1st diagnoses, no foetus was observed at subsequent diagnoses 4
No evidence of gravid structures at two consecutive diagnoses 151
*Abnormal embryo observed 2
*Lost Pregnancy? 11
*Cystic ovary 9
*Pyometra 6
*Adhesions 1
*excluded from further comparisons.
Table 2. Accuracy of a Simplified pregnancy diagnosis (the observationof ≥≥ 15 mm fluid in the uterine lumen and embryonic membranes at asingle examination) compared with Foetal observation (observation of afoetus during serial ultrasonographic examination).
Classification No. of cases
Correct Positive (a) 329
Correct Negative (b) 151
False Positive (c) 4
False Negative (d) 13
Sensitivity (a / a + d) 96%
Specificity (b / b + c) 97%
Positive Predictive Value (a / a + c) 99%
Negative Predictive Value (b / b + d) 92%
Table 3. Accuracy of individual comparisons of either a Simplified preg-nancy diagnosis (the observation of ≥≥ 15 mm fluid in the uterine lumenand embryonic membranes at a single examination) or Foetal observa-tion (observation of a foetus during serial ultrasonographic examina-tions) with a 13-week examination.
Classification Simplified Foetaldiagnoses observation
Correct Positive (a) 301 305
Correct Negative (b) 151 155
False Positive (c) 31 26
False Negative (d) 14 11
Sensitivity (a / a + d) 96% 97%
Specificity (b / b + c) 83% 86%
Positive Predictive Value (a / a + c) 91% 92%
Negative Predictive Value (b / b + d) 92% 93%

Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 65
Scientific
predictor of pregnancy at mid-gestation, and thus at term. Theapplication of such an early technique should be limited to thediagnosis of non-pregnancy. However, this has considerablemerit for the more rapid identification of cows that are notpregnant to the first service and may not naturally return for asecond service within 24 days.
References1. White IR, Russel AJF, Wright IA, Whyte TK. Real-time ultrasonic scanning inthe diagnosis of pregnancy and the estimation of gestational age in cattle. VetRec 1985;117:5-8. 2. Curran S, Pierson RA, Ginther OJ. Ultrasonographic appearance of thebovine conceptus from days 10 through 20. J Am Vet Med Ass 1986;189:1289-1294.3. Hughes EA, Davies DAR. Practical uses of ultrasound in early pregnancy incattle. Vet Rec 1989;124:456-458.4. Boyd JS, Omran SN, Ayliffe TR. Evaluation of real time B-mode ultrasoundscanning for detecting early pregnancy in cows. Vet Rec 1990;127:350-352. 5. Scenzi O, Gyulai G, Nagy P et al. Effect of uterus position relative to thepelvic inlet on the accuracy of early bovine pregnancy diagnosis by means ofultrasonography. Vet Quart 1995;17:37-39.6. Szenci O, Beckers JF, Humblot P et al. Comparison of ultrasonography,bovine pregnancy-specific protein B, and pregnancy assisted glycoprotein 1tests for pregnancy detection in dairy cows. Theriogenology 1998;50:77-88.7. Nation DP, Morton J, Cavalieri J, Macmillan KL. Phantom Cows: A majorcause of late pregnancies and reproductive wastage in Australian dairy herds.NZ Soc Anim Prod 2001;61:180-183.8. Boyd H, Reed HCB. Investigations into the incidence and causes of infertilityin dairy cattle – fertility variations. Brit Vet J 1961;117:18-36.9. Baxter SJ, Ward WR. Incidence of fetal loss in dairy cattle after pregnancydiagnosis using an ultrasound scanner. Vet Rec 1997;140:287-288.10. Dunne LD, Diskin MG, Sreenan JM. Embryo and foetal loss in beef heifersbetween day 14 of gestation and full term. Anim Reprod Sci 2000;58:39-44.
(Accepted for publication 8 April 2002)
after insemination (Figure 1a). The proportion of pregnantcows with a lumen diameter ≥ 25 mm increased from 0% to85% over this period (Figure 1b), and the proportion ofembryos with an observed heartbeat increased from 67% to100% (Figure 1c).
DiscussionThe use of a simplified method to detect pregnancy, based on
the observation of fluid in the uterine horn (a lumen diameterof at least 15 mm) as well as embryonic membranes, was anaccurate estimation of the presence of an embryo at the time ofobservation. However, there was a substantial loss of pregnan-cies between the early ultrasonographic observation and the 13-week examination, resulting in the simplified method being aless reliable predictor of pregnancy at 13-weeks.
These observations are reliant on the systematic observationof the entire length of both uterine horns. The conclusionsmade are dependent on operator ability. In some cases, persis-tence was required to follow the uterine horn through contor-tions and also sometimes where it protruded cranial to thepelvic floor. The identification of fluid and membranes is amore efficient process than the time required to find an embryoas small as 6 mm in a convoluted uterine horn. This simplifiedmethod of pregnancy detection provided a rapid gain in effi-ciency at this early stage.
The 31 cases where there was an observed loss of pregnancybetween 5 weeks and 13 weeks gestation equates to an occur-rence of 3.5% of all cows in the study. This is similar to previousreports of losses between 30 days and term of 4% to 6%. 8-10
Similar 13-week pregnancy rates for both the study populationand their herdmates suggested that early pregnancy examinationdid not affect subsequent pregnancy rates as has been previouslyreported. 9
The simplified early pregnancy examination had a negativepredictive value of 92 and 92% as compared to the FoetalObservation and the 13-week observation, respectively. Thismethod therefore could identify a significant proportion ofcows that could be treated with a progesterone-based synchronyprotocol. The 8% inaccuracy may contraindicate the use ofprostaglandin in such a protocol due to the chance of a falseclassification of non-pregnancy.
In conclusion, early pregnancy detection from 28 to 35 daysafter insemination was possible with dairy cows in commercialAustralian herds. A simplified examination when substantialuterine fluid and embryonic membranes were observed is a suit-able compromise to the effort required to observe a foetus.However, as approximately 9% of foetuses may be lost betweenthe early and the 13-week examinations, it is a less reliable
Figure 1. Relationship between time after insemination (28 to 35days) and a) the length of the foetus (average ± sem); b) theproportion of the pregnant population with a uterine horn diam-eter greater than 15, 20 or 25 mm; and, c) the proportion offoetuses observed with a heartbeat.
Table 4. Comparison of conception rate to first service (when the firstservice occurred in the 3 weeks following MSD) for the study populationand their contemporary herdmates at the 13-week examination.
Number (%) of cows pregnant
Herd No. Study population Herdmates(n = 628) (n = 1125)
1 71 (39%) 120 (37%)
2 70 (35%) 146 (38%)
3 129 (57%) 178 (46%)
Overall 270 (43%) 455 (40%)

66
Scientific
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Trial introduction of the Willis dropped ovary techniquefor spaying cattle in northern Australia
TF JUBBab, G FORDYCEc, MJ BOLAMa, DJ HADDENa, NJ COOPERc, TR WHYTEd, LA FITZPATRICKe, F HILLf andMJ D’OCCHIOd
Objective To compare the Willis dropped ovary techniquewith traditional spaying methods in extensive beef cattle herdsin northern Australia.
Procedure Three field trials were conducted simultane-ously at different sites in northern Australia in 1996-97.Brahman and Brahman-Shorthorn cross heifers (n = 219, 2years, 250 to 378 kg) and cows (n = 211, 3 to 16 years, 256 to540 kg) were allocated by stratified randomisation to threetreatments: spaying using the Willis dropped ovary technique(WDOT); spaying using traditional paralumbar and vaginalmethods; and unspayed. Following these procedures, thesenonpregnant, nonlactating cattle were then exposed to bulls(4 per 100 females) under extensive rangeland conditions for12 months during which time weight, body condition, preg-nancy and ovarian function were monitored and compared.
Results Pregnancy rates varied from 60 to 90% for entireheifers and 80 to 100% for entire cows depending on site.The traditional spay methods were 100% successful inpreventing pregnancy; the WDOT was 92 to 97% effective,depending on operator experience. The number of deathswas the same or higher in Willis spayed animals than othergroups. Weight changes were similar in all groups at the threesites over the trial period. The time taken to spay using theWDOT was similar to or less than that required for the tradi-tional methods. Uterine abnormalities were not observed inanimals spayed with the WDOT, there were however 30(12.4%) animals where excision of the ovary was incomplete;the still-attached ovarian remnant presumably accounting forthe three pregnant animals in this group.
Conclusion The WDOT suffers from requiring a highdegree of skill in transrectal ovarian manipulation. There weremore deaths and more pregnancies than with traditional spaymethods. More experienced operators can be expected toachieve lower mortalities, better contraception and higherprocessing rates. Pregnancy will occur as a consequence ofovarian remnants unless care is taken to ensure removal ofthe entire ovary. Aust Vet J 2003;81:66-70
For reasons of animal welfare, land rehabilitation andindustry economics, there is an imperative to controlpregnancy in northern Australian cattle herds; preventing
pregnancies in selected females by spaying (ovariectomy) is theonly practicable method to achieve this.1-4
The Willis dropped-ovary technique (WDOT) is a vaginalmethod of spaying using the Willis ovariotome.5,6 The spayingtechnique is so-named because the ovaries are dropped and leftinside the abdomen. It was introduced into northern Australiain 19967 where the uptake by the cattle industry and spayingcontractors was rapid.8,9 The technique offers numerous poten-tial advantages for the Australian cattle industry4,7-9, in partic-ular, the aesthetics of the procedure are far superior to tradi-tional paralumbar and vaginal spaying methods because itsoutward appearance is more like a combination of pregnancy
testing and artificial insemination and appears not to generatemore discomfort than is normally associated with these twoprocedures.
The technique had been evaluated under North Americanconditions5,6,10 involving more intensive systems and with Bostaurus heifers. These conditions are much different from theextensive systems in northern Australia where the Bos indicusbreed and its crosses dominate, cattle walk long distances to feedand water, parasites and seasonal undernutrition can haveprofound effects on animal performance, and cows as well asheifers are spayed. As part of a larger study examining oestrouscontrol and pregnancy prevention in extensive beef herds, theefficacy of the WDOT as a suitable alternative to traditionalspaying methods was studied using Brahman and Brahman-Shorthorn cross cattle in extensively-managed beef herds atthree sites in northern Australia.
Materials and methodsAnimals and location
Brahman and Brahman-Shorthorn cross females were selectedand maintained as one group on each of three northernAustralian cattle stations (Table 1). Potential trial animals,nonpregnant on palpation, were given a luteolytic intramus-cular injection of 500 mg cloprostenol (estroPLAN; ParnellLaboratories, Alexandria). Bulls were excluded until allocationto treatments about 1 month later. More than 90% of the cowshad recently weaned a calf at Site 1 and Site 3 and only 50%had at Site 2. An ultrasound scanner (Aloka 500) fitted with a7.5 MHz transducer was used to identify corpora lutea or folli-cles to ascertain ovarian activity in subgroups of 50 heifers and50 cows at Sites 1 and 2. Oestrus detection devices (BullingBeacon; Beacon Marketing Pty Ltd, Scone) were applied to theskin over the sacrum of all selected animals to provide a furtherindication of cyclicity before treatments were allocated.
Allocation to treatmentsDetails of site locations and the timing of key events are
shown in Table 1. Allocation of animals to the study occurred inApril-June of 1997(early to mid dry season) when the cattlewere weighed, scored for body condition, and ear tagged.Allocation to treatment was by stratified randomisation on age(heifer, cow), frame size and body condition. Treatments were;surgical spaying using the flank or passage methods (SPAY),
aAgriculture Western Australia, PO Box 19, Kununurra, WA 6743bCurrent address and author for correspondence: Box 2500, Bendigo DeliveryCentre, Victoria 3554cQueensland Beef Industry Institute, Department of Primary Industries, SwansLagoon Beef Cattle Research Station, Millaroo, Qld 4807dPrimary Industries Research Centre, Central Queensland University, NorthRockhampton, Qld 4702eAustralian Institute of Tropical Veterinary and Animal Science, James CookUniversity, Townsville, Qld, 4811 fDepartment of Primary Industries, Queensland Beef Institute, PO Box 53,Cloncurry, Qld 4824

Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 67
Scientific
spaying with the Willis ovariotome(WDOT), and no treatment (ENT0).Treatment times, success of ovariectomy ofone or both ovaries, and problems encoun-tered were recorded for each animal.Animals were maintained as one groupunder extensive rangeland conditions oneach station. Bulls (4 per 100 females) wereadded to trial groups within 15 days of treat-ment. Between 6 and 10 months after treat-ment, a further 50 untreated, non-pregnantanimals (ENT6) were added to each trialgroup to check the fertility of bulls andcyclicity of untreated animals in the latterstages of the trial.
Once weekly paddock observations ofcattle were made by station staff. Every twomonths, the cattle were weighed, scored forbody condition, and rectally palpated. Atthe end of the trial, about 12 months aftertreatment, the remaining nonpregnant andsome pregnant heifers and cows not wantedfor breeding were slaughtered. Reproductivetracts were examined and ovarian structures,uterine dimensions and abnormalitiesrecorded.
Spaying proceduresAll animals were fasted overnight before
the treatments were performed. After eachanimal was spayed, the instruments wererinsed and immersed in a 0.8 g/L chlorhexi-dine solution (Hibitaine Disinfectant;Mallinckrodt Veterinary, North Ryde)before next use. Spaying of SPAY heifersand cows was by flank and passagemethods, respectively.
All spaying procedures at Site 3 wereperformed by an operator (TFJ) skilled inflank and passage methods described byFordyce et al 11 but with moderate experi-ence (about 300 cattle) with the WDOT.Another skilled operator (NJC) conductedflank and passage spaying at Sites 1 and 2. Afurther operator (GF), who had excellentpalpation skills as judged by his peers, andwho had received training in the techniquefrom a visiting Canadian exponent of thetechnique (Norman Habermehl), but wasinexperienced (less than 30 cattle),performed the WDOT at Sites 1 and 2.
Spaying of WDOT heifers and cows wasperformed using the Willis ovariotome(DLC Australia Pty Ltd, Hoppers Crossing)(Figure 1). The ovariotome is a stainlesssteel rod about 48 cm long (varies fordifferent age and size animals) with a 6 mm-diameter shaft; it has a T-bar handle and aflattened spear head with a tear drop-shapedhole and slit cut in it. The forward end ofthe slit is sharpened to form a concealedblade that is used to cut the ovarian vascula-
Table 2. Growth rates (kg per day) of cattle that were untreated (ENT0), spayed using traditionalmethods (SPAY), or spayed using the Willis dropped ovary technique (WDOT).
Growth period Age Treatment(Months aftertreatment)
ENT0 SPAY WDOT Standard P-valueError
(average)
0 - 2 Heifers 0.01C - 0.11A - 0.05B 0.07 0.002
Cows - 0.04B - 0.20A - 0.09B 0.06 0.004
2 - 4 Heifers 0.06 0.08 0.07 0.16 0.8
Cows - 0.05A 0.13b - 0.02A 0.19 < 0.001
4 - 6 Heifers - 0.34 -0.33 -0.35 0.17 0.7
Cows - 0.38 - 0.40 - 0.46 0.19 0.4
6 – 8 Heifers 0.68B 0.52A 0.53A 0.18 0.02
Cows 0.43 0.53 0.52 0.25 0.7
8 – 10a Heifers 0.61 0.56 0.55 0.15 0.7
Cows - 0.53 0.52 0.24 0.9
10 – 12b Heifers 0.32 0.30 0.32 0.05 0.9
Cows - 0.33 0.28 0.04 0.5
8 – 12c Heifers - 0.75 0.74 0.02 0.6
Cows - 0.56 0.56 0.04 0.9
aHavilah and Flora Valley only; bFlora Valley only; cCanobie only.Data included only for animals non-pregnant at start of growth period and where the treatment wassuccessful.Treatment means within growth period not sharing a common superscript letter differ significantly (P < 0.05).
Table 1. Locations and selection, treatment, and measurement dates in a trial comparing the Willisdropped ovary technique and traditional spaying methods.
Procedures Site
1 2 3Havilah Station Canobie Station, Flora Valley Station,Collinsville, Qld Julia Creek, Qld Halls Creek, WA
Location 147°49’E 20°49’S 140°37’E 19°44’S 128°33’E 18°17’S
Trial paddock area ~2,000 ha ~4,000 ha ~5,000 ha
End of dry season Early Oct 97 Early Dec 97 Late January 98
Animal selection 26 Mar 97 14 Apr 97 10 May 97
Allocation to treatment 21 Apr 97 14 May 97 04 Jun 97
WDOT treatment pm:21 April 97 am: 22 April 97 pm: 15 May 97 pm: 5 Jun 97
SPAY treatment pm: 21 April 97 am: 16 May 97 pm: 5 Jun 97 (Heifers)am: 6 Jun 97 (Cows)
ENT6 added 08 Jan 98 19 Nov 97 23 Mar 98
Bulls added 7 May 97 19 May 97 9 Jun 97
2-month measurement 12 Jun 97 15 Jul 97 04 Aug 97
4-month measurement 12 Aug 97 18 Sep 97 07 Oct 97
6-month measurement 21 Oct 97 19 Nov 97 02 Dec 97
8-month measurement 09 Dec 97 21 Jan 98 03 Feb 98
10-month measurement 05 Mar 98 Nil: Too wet 08 Apr 98
12-month measurement 21 Apr 98 30 Apr 98 10 Jun 98
Slaughter 14 May 98 12 Jun 98 15 Jun 98

68 Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Scientific
ture and ligaments. The vulvar area immediately around thevaginal opening was wiped clean with paper towel before theinstrument was introduced into the vagina. The anterior vaginalwall, dorsal to the cervix was pierced with the spear head end ofthe ovariotome. By rectal manipulation each ovary was passedthrough the spear head of the ovariotome and attachmentssevered by retracting the instrument, so that the ovariesdropped into the abdominal cavity. 5
Animal welfareAll studies were approved under the guidelines of the
‘Australian Code of Practice for the Care and Use of Animals forScientific Purposes’. Agriculture Western Australia Animal
Experimentation Ethics Committee approved studies at Site 3:Approval 06-96-30. The Tropical Beef Centre AnimalExperimentation Ethics Committee approved studies at Sites 1and 2: Ethical Clearance Certificate Number TBC87.
Statistical analysesData for heifers and cows were analysed separately. Treatment
effects on growth rates calculated for each 2-month periodbetween allocation and slaughter were estimated using REML(GenStat, GenStat Committee, 2000). Random effects in theanalysis were animal within site and the fixed effect was treat-ment. Significance of random effects was assessed by use of theSUBMODEL option. This allows the calculation of a likeli-hood-based test by comparing the difference in deviancebetween the full model (Constant + Treatment) with that of thesub-model (Constant only). Data were included only forsuccessfully-treated animals. Treatment groups were excludedfrom analysis where this restriction left only one datum. Arepeated-measures analysis of growth rates was inappropriate forthe full 12 months as few data were available for ENT0 animalsin the latter half of the experiment.
For each site and for heifers and cows, the proportion ofanimals pregnant in each treatment group at each muster wascompared to other groups using Chi-square test of goodness of fit.
ResultsGrowth and body condition
In the 2 months following treatment WDOT heifers lost lessweight than SPAY heifers but more than ENT0 heifers. WDOTcows lost weight at a similar rate to ENT0 cows but moreslowly than SPAY cows (Table 2). In the subsequent 2 months,SPAY cows grew faster than ENT0 and WDOT cows, andSPAY heifers grew similarly to ENT0 and WDOT heifers. Notreatment effects on growth occurred beyond 4 months aftertreatment except 6 to 8 months when growth of ENT0 heiferswas greater than other treatments in a period of rapid weightgain. After 8 months there were too few ENT0 animalsremaining nonpregnant to compare growth rates with WDOTand SPAY animals. By the end of the trial there were no differ-ences in growth between SPAY and WDOT animals.
Over the study, body condition increased by 1.2, 0.6, and 1.6units at Sites 3, 2 and 1, respectively, with no treatment effect.Average body condition of the Site 1 cattle steadily improvedover the trial, but suffered declines of 2.5 and 0.7 units in cattleat Sites 3 and 2, respectively, during the dry season.
Treatment duration and successThe average treatment times for SPAY heifers and cows were
4.0 min and 4.5 min (15 and 13 / h), respectively, with no sitedifferences. Procedures were completed without complication.
WDOT spaying at Site 3 was at approximately 30 animalsper hour. At Site 3 only, less time was taken to use the WDOTon heifers than cows (68 v 76 s; P < 0.05). Fatigue of the oper-ator’s hand and forearm muscles and delays while restraininganimals with poor temperament, were the main problemsencountered at all sites.
At the time of spaying, the WDOT was considered successfulin ovariectomising all Site 3 animals submitted for this treat-ment. At Sites 1 and 2, bilateral ovariectomy was not achievedin some animals because of operator fatigue or poor tempera-ment of the animal (Table 3).
Figure 1. A Willis ovariotome.
Figure 2. Cumulative pregnancies in ENT0, ENT6, SPAY andWDOT treatment groups.

Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 69
Scientific
Ovarian functionIn the subset of 50 animals selected for the trial
at Sites 1 and 2, ultrasound examination 1 monthprior to allocation to treatments revealed that 60to 90% had a corpus luteum with the balancehaving at least one large follicle, indicating that themajority of the cattle were cycling. However, atSite 3, up to 30% of cattle may not have beencycling at allocation based on the number ofnontriggered oestrus detection devices. A similarresult was recorded in heifers at Site 2.
PregnancyConceptions in the ENT0 and ENT6 animals at
the three sites demonstrated that when untreated,environment and bulls were not limiting factors(Figure 2). Pregnancy was not recorded in theSPAY animals at any site. Pregnancy rates forentire heifers and cows ranged from 60 to 90%and 80 to 100% respectively, between the proper-ties.
Two WDOT animals conceived at Site 3 duringthe trial. Pregnancy was detected by rectal palpa-tion. Each had what felt like a small ovary with acorpus luteum present, presumably as a result ofthe ovariotome cutting through the base of theovary rather than the intended ovarian ligament.Within WDOT animals at Sites 1 and 2, preg-nancy occurred in 10 of the 16 animals in whichone or both ovaries could not be removed (Table2), but in only 1 of the 15 animals in which therewas an ovarian remnant.
Examination after slaughter At slaughter, there were no ovarian remnants
recorded in reproductive tracts from SPAYanimals. Localised scarring and small adhesions ofthe oviduct around the site of ovarian removalwere recorded in four (12%) cows.
In WDOT animals, sites of ovary excision occa-sionally had localised fibrosis usually in the form of a small (3mm diameter) nodule and occasionally oviducts were distendedwith fluid where scarring or adhesions had caused strictures. Anobvious ovarian remnant was present in 30 of 242 (12.4%)animals examined, three of these animals were affected bilater-ally. Most remnants (67%) presented as a fluid filled cyst (up to15 mm diameter) growing from a small nodule (1 to 2 mmdiameter). In three animals the ovarian remnant was large (10mm diameter). In five animals, the small ovarian remnant had acorpus luteum present and two of these animals were in earlygestation.
No evidence of any localised infection or inflammation at thevaginal fornix penetration sites was found. The penetration siteswere marked by a slight depression in the serosal surface.
DiscussionProcessing rates and success of the WDOT procedure will be
influenced by animal temperament, ability to restrain theanimal and the amount of assistance available and how theyinteract with experience of the operator. The WDOT, whenused by the more experienced operator in this study at Site 3,achieved a high processing rate, low morbidity and minor
Morbidity and mortalityPostoperatively at all sites, an estimated 5 to 10% of SPAY
animals were reluctant to move, hung their heads, and weredull and poorly responsive. The animals spayed using theWDOT moved freely, were bright and alert and appearedlargely unaffected. All skin wounds in the flank-spayed heiferswere healed 2 months after surgery. No adhesions were palpablein the SPAY heifers during the study at any site. Six SPAY cowshad palpable adhesions, three of these at 2 months, and oneeach at 4, 6, and 12 months after surgery.
At Site 1, one WDOT heifer died within 48 hours of treat-ment and was not necropsied. One WDOT cow subsequentlywas missing presumed dead, resulting in a mortality rate of 2out of 76 WDOT animals at Site 1.
At Site 2, one cow in the WDOT group died within 2 hoursof treatment and another 3 died within 48 hours. They werenot necropsied. A further WDOT heifer was recorded asmissing, resulting in a mortality rate of 5 out of 99 WDOTanimals. One SPAY cow also went missing at Site 2.
At Site 3, two animals, one each from the SPAY and WDOTgroups, did not appear at subsequent musters. Though theircarcasses were not found, they were considered mortalities inthis study.
Table 3. Comparison of treatment failures between the Willis dropped ovary technique andtraditional spaying methods.
Cows Heifers
ENT0 ENT6 SPAY WDOT ENT0 ENT6 SPAY WDOT
Havilah
Allocated 10 15 36 10 10 20 40
Died within 48 h 0 0 0 1
Missing presumed dead 0 1 0 0
One or both ovaries not 10 0 4 10 10 0 5 removed
Pregnant if one or more 10 0 3 10 6 0 3 ovaries remain
Ovarian remnants left 0 4 0 1
Pregnant if ovarian remnants 0 0 0 0
Canobie
Allocated 10 10 19 49 10 10 21 51
Died within 48 h 0 4 0 0
Missing presumed dead 1 0 0 1
One or both ovaries not 10 10 0 3 10 10 0 4removed
Pregnant if one or more 8 8 0 2 9 8 0 2 ovaries remain
Ovarian remnants left 0 4 0 6
Pregnant if ovarian remnants 0 0 0 1
Flora Valley
Allocated 11 15 46 8 20 15 44
Died within 48 h 0 0 0
Missing presumed dead 1 1 0 0
One or both ovaries not 11 0 8 20 0 0 removed
Pregnant if one or more 11 0 4 8 0 0ovaries remain
Ovarian remnants left 0 9 0 6
Pregnant if ovarian remnants 0 2 0 0
ENT0 = Non pregnant heifers and cows at trial start that were not spayedENT6 = Non pregnant heifers and cows introduced 6 months into the trial that were not spayed.SPAY = Heifers were flank spayed, cows were passage spayedWDOT = Spayed with the Willis dropped ovary technique

70 Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Scientific
temporary effects on growth of animals. The two pregnanciesand one death that occurred at Site 3 show that the techniquedoes not guarantee contraception and is not free of risk. Thedifficulties and complications encountered by the less experi-enced operator at Sites 1 and 2 show that the technique can bedifficult to master, even by someone experienced in palpation ofthe reproductive tract.
Low morbidity and mortality rates are achievable; two NorthAmerican studies 6,10 using the WDOT on Bos taurus heifersfound mild stiffness and straining for a few hours post surgerywith a few animals walking stiffly the next day. Mortality ratesof 0/54, 1/522 and 10/3400 were recorded.
The mortalities associated with the WDOT in the presentstudy were probably caused by intestinal trapping, or internalbleeding from the ovariectomy site. These complications andmethods to prevent them have been described previously. 9
Failure to conceive was due to the treatment as indicated bythe high pregnancy rates in entire and incompletely spayedanimals. The ovarian remnants observed at slaughter in animalsspayed using the WDOT and the pregnancies observed post-spaying indicate that the WDOT is not always effective atremoving all ovarian tissue. Other studies5,10 have also foundhypertrophied ovarian remnants in 2 of 15 (13%) and 2 of 54(4%) heifers, respectively, that were spayed using the WDOT.Pregnancy will occur as a consequence of ovarian remnantsunless care is taken to ensure removal of the entire ovary. Thisproblem should be easily overcome by pushing the ovary furtherthrough the cutting hole in the ovariotome to ensure that theligament is cut, not the base of the ovary.
The time required to perform procedures, such as spaying,under extensive management systems, must be kept to aminimum to make these procedures commercially viable.Traditional procedures such as the flank and passage techniquesare commonly completed at rates of 10 to 25 / h, the higherrates being achieved only if facilities, persons assisting, andanimal temperament are good. The rate in excess of 30 /h at Site3 would be an acceptable commercial rate.
The lack of overt discomfort exhibited in the postoperativeperiod and no requirement for major wound healing means thatWDOT animals can be marketed sooner than animals spayedusing the traditional methods. The absence of internal adhe-sions in WDOT animals at slaughter means that the hygiene ofthe procedure is acceptable under the difficult and dusty condi-tions of northern Australian cattle yards.
All females in this study exhibited live weight changes typicalof grazing cattle in northern Australia. 12 Site 1 is located in arelatively high nutrition region and females tended to be heavierand maintained live weight over the dry season. This contrastswith the harsher environment and longer dry season at Site 3where considerable loss of body condition was observed in cowsover this period. Conditions at Site 2 were intermediate.
There were no differences in weight changes by the end of thetrial period for animals spayed using either the traditionalmethods or the WDOT. The three spaying methods shouldhave a similar affect on weight change if performed correctlyalthough the animals in the SPAY groups that grew more slowlythan WDOT heifers in the 2 months following treatment mayhave done so because of increased stress and trauma associatedwith the more invasive surgery associated with these procedures.The absence of weight changes observed between spayed and
entire animals by the time meaningful comparative measure-ments ceased, contrasts with the findings from temperate envi-ronments where it is generally considered that spayed animalsmust receive growth-promoting hormonal implants to over-come the growth retarding effects of spaying.13
AcknowledgmentsThis research was funded by Meat and Livestock Australia,
Agriculture Western Australia, Queensland Department ofPrimary Industries, Central Queensland University, and JamesCook University. Angela Reid of Queensland Department ofPrimary Industries performed the statistical analyses.
We gratefully acknowledge the support from the following:Bob Hall, James Mitchell and their staff of Stanbroke PastoralCompany’s, Havilah Station, Collinsville, who provided andmanaged an experimental group; Bob McLelland, Mick Tasker,Anne Moody and their staff of the Australian AgriculturalCompany’s Canobie Station, Julia Creek, who provided andmanaged an experimental group; Wayne Bean, Steve Petty andtheir staff of Heytesbury Beef ’s, Flora Valley Station, HallsCreek, who provided and managed an experimental group;Neville Beard of DLC Australia Pty Ltd who supplied the Willisinstruments; Dennis Peters, Lance Loveday, John Payne, andthe staff of Australian Meat Holdings; Paul Herrod and the staffof Consolidated Meat Group’s Katherine Meatworks and BoydUnger and Paul Graves of the Australian Quarantine InspectionService who collaborated in the collection of slaughter data.
References1. Jubb TF, Kerr JW, Bolam MJ. Problem definition for veterinarians workingwith extensive beef herds. Proc Aust Soc Cattle Vet 1997:163-169.2. Armstrong J, Henderson AG, Lang DR, Robinson DW and Suijendorp H.Preliminary observations on productivity of female cattle in the Kimberley regionof north-western Australia, Aust Vet J 1968;44:357-363.3. Jubb TF, Vassallo RL, Annand TE. Estimating deaths in breeder age femalecattle in the Kimberley region of Western Australia. Aust Vet J 1996;73:152-153.4. Jubb TF, Letchford PJ. Cattle spaying and electroimmobilisers - their use inextensive beef cattle herds in the Kimberley region. Proc Aust Assoc Cattle Vet1997:31-35.5. Johnson S, Hudson D, Clanton D, Johnson J. Evaluation of spaying tech-niques for heifers. Mod Vet Prac 1987;68:98-101.6. Habermehl NL. Heifer ovariectomy using the Willis spay instrument:Technique, morbidity and mortality. Can Vet J 1993;34:664-667.7. Jubb TF, Bolam M, Letchford P, Fordyce G. Evaluation of the Willis spayinstrument, Project NAP3.102, A Report to the Meat Research Corporation.1997.8. Jubb TJ, Bolam MJ, Kerr J. Introduction of the Willis dropped ovary techniquefor oestrus control in cattle in northern Australia. In: Blakeley S, editor. TheNorth Australia Program, 1998 Review of Reproduction and Genetics. NAPOccasional Publication No 8, Meat and Livestock Australia, Brisbane, 1999:83-86.9. Jubb TF, De Witte KW, Smith GI. The use of the Willis dropped ovary tech-nique in extensive beef herds in northern Australia, Proceedings of the XXthWorld Association for Buiatrics Congress, Sydney, New South Wales. July,1998; p 507-510. 10. Garber MJ, Roeder RA, Combs JJ. Efficacy of vaginal spaying and anabolicimplants on growth and carcass characteristics in beef heifers. J Anim Sci1990;68:1469-1475.11. Fordyce G, Jubb TF, Fitzpatrick LA et al. Efficacy of an intra-uterine devicein reproductive management of Brahman cattle. Anim Reprod Sci 2001;65:193-204.12. McLennan SR, Hendricksen RE, Beale IF et al. The Nutritive Value ofNative Pastures. In: Burrows WH, Scanlan JC, Rutherford MT, editors, NativePastures in Queensland: The resources and their management, Department ofPrimary Industries, Queensland Government, Brisbane 1988,125-159.13. Rupp GP, Hamilton ED, Management of spayed heifers. Compend ContinEd Pract Vet, Food Animal Supp, August 1995; 17: S42-S47, S56.
(Accepted for publication 15 May 2002)

71
Scientific
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Specificity of absorbed ELISA and agar gel immuno-diffusion tests for paratuberculosis in goats with observations about use of these tests in infected goats
RJ WHITTINGTONab, GJ EAMENSa and DV COUSINSc
Objective To determine the specificity of serological teststhat are currently used in veterinary diagnostic laboratories inAustralia for detection of Mycobacterium avium subsp para-tuberculosis infection in goats.
Design A laboratory study.
Procedure Four tests were studied, comprising AGID withM a paratuberculosis antigen derived from cattle isolates ofcaprine or bovine origin, the EMAI caprine Johne’s diseaseabsorbed ELISA and the CSL PARACHEK Johne’s absorbedEIA. The specificities of AGID and ELISA for paratuberculosis(Johne’s disease) were estimated after examining a panel of1000 serum samples collected from goats in WesternAustralia, a region free of paratuberculosis. In addition acomparison was made of test performance in a small numberof paratuberculous goats from New South Wales using serafrom two archival collections.
Results The specificity of the AGID tests was 100% whilethe specificities of the two absorbed ELISA were 99.7 to99.8% at appropriate positive-negative cut-offs. Based ontesting the small sample of sera from infected goats, theabsorbed ELISA tests detected about twice as many goatswith Johne’s disease as the AGID. Each test detected para-tuberculous animals regardless of whether infection wascaused by cattle or sheep strains of M a paratuberculosis.
Conclusions Both ELISA and AGID tests for paratubercu-losis have high specificity and can be used in a market assur-ance program without risk of generating large proportions offalse positive test results. However, the results suggested theELISA is more sensitive for detection of infected goats andshould be used in preference to the AGID. The two formats ofELISA evaluated in this study have similar characteristics andcould be used in paratuberculosis control programs for thegoat industries, but further data on sensitivity would increaseconfidence in their application.Aust Vet J 2003;81:71-75
Paratuberculosis or Johne’s disease was first reported ingoats in Australia in 1977.1 For almost two decades itappeared to be confined to dairy breeds and was due to
infection with cattle [C] strains of Mycobacterium avium subspparatuberculosis. Coincident with increased surveillance, paratu-berculosis caused by sheep [S] strains of M a paratuberculosiswas detected in fibre goats in 1995.2 Paratuberculosis in goatsresembles clinically and pathologically the condition in otherspecies, being a chronic progressive enteropathy with weight
loss, sometimes diarrhoea and eventually death. However, thedisease appeared to be less fulminant in fibre goats infected withS strain than in sheep infected with the same strain or in dairygoats infected with C strain.2
The serological tests currently used in veterinary diagnosticlaboratories in Australia to detect paratuberculosis in goatscomprise the AGID or gel test and the absorbed ELISA. TheAGID test is available in two formats, known colloquially as thecaprine AGID test and the ovine AGID test. These tests differonly in the nature and concentration of the antigen and in thereference sera used as controls. The ovine AGID utilises anantigen derived from a laboratory adapted bovine isolate of M aparatuberculosis whereas the caprine AGID utilises a clinicalisolate from a goat, which is also a bovine strain. The absorbedELISA currently is available in two formats in Australia; theEMAI caprine Johne’s disease absorbed ELISA and the CSLPARACHEK Johne’s absorbed EIA. The latter is commerciallyavailable in kit form but has not been marketed for use in goatsbecause of lack of supportive data. The former is supplied fromEMAI as reagents with a protocol. The AGID and absorbedELISA tests are based on the principle that antibodies producedby an infected goat in response to infection with M a paratuber-culosis will react with antigenic components of this bacteriumand produce a detectable response. The AGID test is a verysimple test requiring minimal apparatus and results are subjec-tively interpreted by eye, whereas the absorbed ELISA is a morecomplex, multi-step test requiring specific instrumentation toperform and measure the end point. However, economies ofscale are possible with the ELISA so that the costs of the twotypes of test are similar.
There is considerable interest among the goat industries inefficient diagnosis of paratuberculosis as well as in a marketassurance program to provide increased confidence that herdsare free of the infection.3 Laboratory tests are required for bothpurposes. A market assurance program was recently introducedfor goats and is based on herd screening with serological tests.These tests have not been formally validated but are believed toperform in a similar fashion to those in use for detection ofparatuberculosis in cattle. Ideally, use of these tests for diagnosisor in a market assurance program would require independentestimates of test performance in goats. However, there has beenlittle opportunity to study caprine paratuberculosis in Australiabecause the disease is still relatively uncommon and insufficientfunds have been available. Similarly in other countries there
aNSW Agriculture, Elizabeth Macarthur Agricultural Institute, Camden, NewSouth Wales 2570bPresent address: Faculty of Veterinary Science, University of Sydney,Camden, New South Wales 2570.cDepartment of Agriculture, Animal Health Laboratories, South Perth, WesternAustralia 6151
AGID Agar gel immunodiffusion testEMAI Elizabeth Macarthur Agricultural InstituteELISA/EIA Enzyme-linked immunosorbent assayPBS Phosphate buffered saline pH 7.2 PBSTG PBS with 0.025% v/v Tween 80, 0.05% w/v gelatinOD Optical density

72 Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Scientific
have been few detailed studies of the specificity of ELISA forparatuberculosis in goats and data on sensitivity are scantcompared to the situation with cattle.4-7 These studies are char-acterised by small sample sizes and limited geographic origins oflivestock, which can compromise estimates of both specificityand sensitivity.
The aim of this project was to determine the specificities ofthe AGID and ELISA tests for caprine paratuberculosis that arecurrently used routinely in Australia by studying a diverse popu-lation of goats from a paratuberculosis-free region of Australia.A secondary aim was to determine how these tests performedrelative to each other in detecting infection in a small number ofgoats known to be infected with either cattle or sheep strains ofM a paratuberculosis.
Materials and methodsSpecificity was defined as the proportion of disease free
animals yielding a negative result in the test. As ruminants inWestern Australia are considered to be free of paratuberculosis,8
blood samples were collected from 1000 goats from a range ofgeographic locations in Western Australia and were defined assamples from animals free of paratuberculosis. The animalsranged from 1 to 5 years of age, most were female and breedsincluded dairy, Boer, cashmere, Angora and feral. Serum washarvested from each sample, divided into two aliquots andplaced in storage at -20°C. One aliquot of each serum samplewas shipped to EMAI and placed in storage at -20°C until used.Each sample was tested in the CSL PARACHEK Johne’sabsorbed EIA kit at both participating laboratories, in theEMAI caprine Johne’s disease absorbed ELISA at the EMAIlaboratory and in the caprine and ovine AGID tests at theEMAI laboratory. The results of ELISA are expressed on acontinuous scale; a positive-negative cut-off point is chosen sothat sensitivity and specificity are optimised. Therefore thespecificity of each ELISA was calculated at a number of posi-tive-negative cut-offs. The AGID test provides dichotomousresults so that choice of cut-off was not an issue.
True sensitivity could not be determined in this study becauseanimals were subjected to histopathology and culture usuallyafter selection from flocks based on the results of either clinicalexamination or these blood tests. However, two sources of datawere used to compare the performance of the tests in infectedgoats. The first source was existing serological results from 47goats with paratuberculosis, obtained from laboratory records(that is the sera were not tested again). In this case only theEMAI caprine Johne’s disease absorbed ELISA and the caprineAGID test had been used, both at the EMAI laboratory. Thepresence of disease in individual goats had been confirmed byhistopathology and/or the culture of M a paratuberculosis fromfaeces and/or intestinal wall and/or mesenteric lymph node.Each goat was classified into one of two groups based on clinicaland laboratory findings: clinical, where there were clinical signsconsistent with paratuberculosis plus histological and/orcultural (tissue and/or faecal) evidence of M a paratuberculosisinfection, or; subclinical, where there were no clinical signs ofparatuberculosis but where there was histological and/orcultural (tissue and/or faecal) evidence of M a paratuberculosisinfection.
The second source was a collection of sera from 19 goats withparatuberculosis that had been confirmed by culture and/orhistopathology and faecal smear. The sera were obtained fromlaboratory submissions between 1994 and 1997 and were stored
at -20°C; 7 sera were from goats that were also present in thefirst data source. The genotype of the infecting strain of M aparatuberculosis was determined for each case. This was based onthe cultural characteristics of isolates of M a paratuberculosis,9
restriction fragment length polymorphism analysis and/orIS1311 polymorphism analysis,10,11 or based on epidemiolog-ical criteria where the case was detected by tracing back from aproperty where strain typing had already been conducted.Twelve sera were derived from goats infected with cattle strainsof M a paratuberculosis on five farms while seven were derivedfrom goats infected with sheep strains of M a paratuberculosis onthree farms. The samples were tested in the CSL PARACHEKJohne’s absorbed EIA kit at both participating laboratories andin the other tests at the EMAI laboratory.
EMAI caprine paratuberculosis absorbed ELISAThe method was based on that of Yokomizo et al.12,13 In
brief, test sera diluted 1:100 in PBSTG were absorbed with heatkilled M phlei cells overnight at 5oC with constant rotation,then centrifuged to remove particulate matter. Flat-bottomedELISA plates were coated overnight at 5oC with antigen derivedfrom mechanically-disrupted M a paratuberculosis strain 316V.After washing, aliquots of 100 µL of diluted test serum wereadded to each well and incubated for 90 min at room tempera-ture (RT). Plates were washed four times with PBS, 0.05% v/vTween 20 using an automatic 96-well ELISA washer. 100 µL ofrabbit anti-goat IgG conjugated to horse radish peroxidase(KPL Laboratories) diluted in PBSTG was added to each welland incubated for 45 min at RT. After washing, 100 µL of chro-mogenic substrate (2,2’-azino-bis(3-ethyl-benzthiazoline-6-sulphonic acid)) (ABTS) with hydrogen peroxide was added toeach well and incubated at RT for 20 to 45 min. OD at 414 nmwas read after shaking, using an ELISA plate reader. Each testserum was evaluated in two adjacent wells. Positive and negativecontrol sera were each included in six wells on each plate. ODwere determined for each plate when the positive control serumhad a mean OD in the range 0.6 to 0.7 and the negative controlserum had a mean OD in the range 0.06 to 0.10. Results wereexpressed as an ELISA ratio, being the mean OD of the testserum divided by the mean OD of the six wells containing thenegative control serum. All sera with an initial mean ELISAratio of 1.5 or higher were retested to ensure that consistentresults were obtained. The final ELISA ratio of such sampleswas determined as the mean result of testing in at least two testson separate days. In addition, where an individual well in a pairof duplicates returned an ELISA ratio above 2, the sample wasretested; if the result of the retest indicated that the single orig-inal high figure was an artefact then the second result wasaccepted. Results for this test and the bovine test upon which itis based have been classified historically as follows: ELISA ratio< 1.5 = negative; > 1.5 to < 2 = inconclusive; > 2 = positive. Thisinterpretation was retained in the present study.
CSL PARACHEK Johne’s absorbed EIAThis is a kit test. The method was based on that of Yokomizo
et al,13 but modified and evaluated for use in cattle by otherworkers.14-16 The test was conducted at both participating labo-ratories according to the manufacturer’s instructions using thebovine controls supplied. Samples were tested in single wells atthe Western Australian laboratory and any samples with reac-tions greater than the OD of the negative control + 0.1 wereretested in duplicate. The mean OD of the duplicates of the
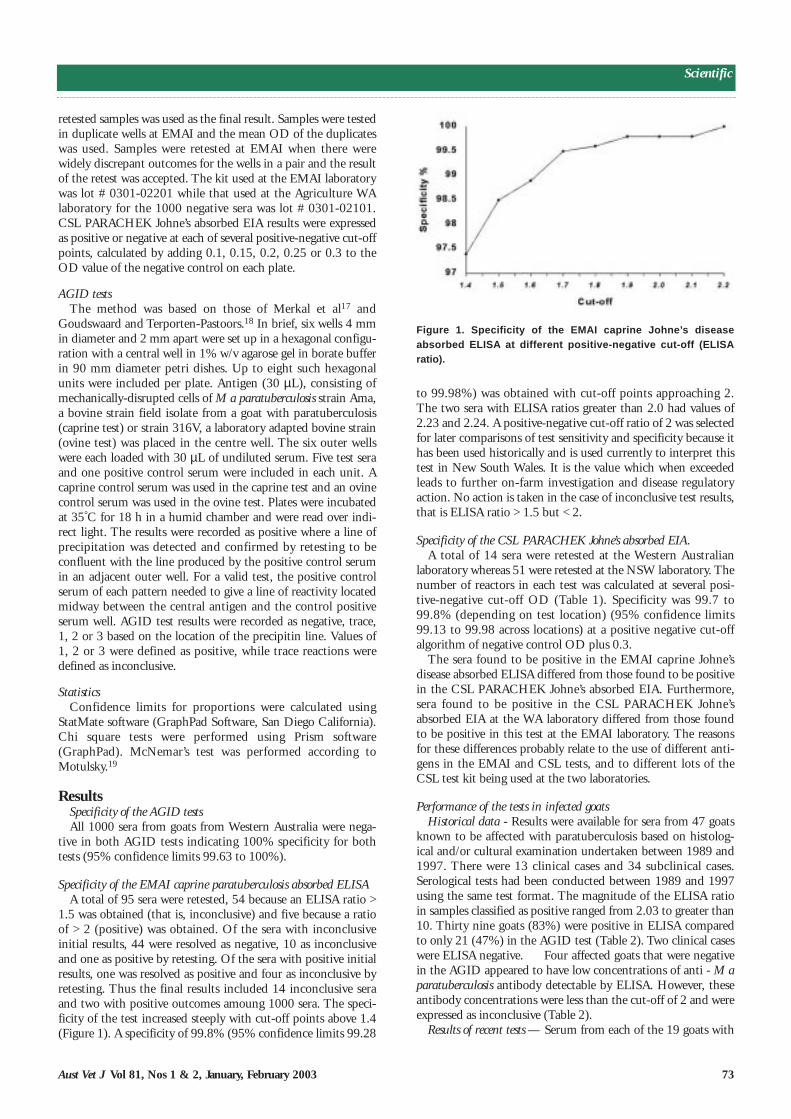
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 73
Scientific
to 99.98%) was obtained with cut-off points approaching 2.The two sera with ELISA ratios greater than 2.0 had values of2.23 and 2.24. A positive-negative cut-off ratio of 2 was selectedfor later comparisons of test sensitivity and specificity because ithas been used historically and is used currently to interpret thistest in New South Wales. It is the value which when exceededleads to further on-farm investigation and disease regulatoryaction. No action is taken in the case of inconclusive test results,that is ELISA ratio > 1.5 but < 2.
Specificity of the CSL PARACHEK Johne’s absorbed EIA.A total of 14 sera were retested at the Western Australian
laboratory whereas 51 were retested at the NSW laboratory. Thenumber of reactors in each test was calculated at several posi-tive-negative cut-off OD (Table 1). Specificity was 99.7 to99.8% (depending on test location) (95% confidence limits99.13 to 99.98 across locations) at a positive negative cut-offalgorithm of negative control OD plus 0.3.
The sera found to be positive in the EMAI caprine Johne’sdisease absorbed ELISA differed from those found to be positivein the CSL PARACHEK Johne’s absorbed EIA. Furthermore,sera found to be positive in the CSL PARACHEK Johne’sabsorbed EIA at the WA laboratory differed from those foundto be positive in this test at the EMAI laboratory. The reasonsfor these differences probably relate to the use of different anti-gens in the EMAI and CSL tests, and to different lots of theCSL test kit being used at the two laboratories.
Performance of the tests in infected goatsHistorical data - Results were available for sera from 47 goats
known to be affected with paratuberculosis based on histolog-ical and/or cultural examination undertaken between 1989 and1997. There were 13 clinical cases and 34 subclinical cases.Serological tests had been conducted between 1989 and 1997using the same test format. The magnitude of the ELISA ratioin samples classified as positive ranged from 2.03 to greater than10. Thirty nine goats (83%) were positive in ELISA comparedto only 21 (47%) in the AGID test (Table 2). Two clinical caseswere ELISA negative. Four affected goats that were negativein the AGID appeared to have low concentrations of anti - M aparatuberculosis antibody detectable by ELISA. However, theseantibody concentrations were less than the cut-off of 2 and wereexpressed as inconclusive (Table 2).
Results of recent tests — Serum from each of the 19 goats with
retested samples was used as the final result. Samples were testedin duplicate wells at EMAI and the mean OD of the duplicateswas used. Samples were retested at EMAI when there werewidely discrepant outcomes for the wells in a pair and the resultof the retest was accepted. The kit used at the EMAI laboratorywas lot # 0301-02201 while that used at the Agriculture WAlaboratory for the 1000 negative sera was lot # 0301-02101.CSL PARACHEK Johne’s absorbed EIA results were expressedas positive or negative at each of several positive-negative cut-offpoints, calculated by adding 0.1, 0.15, 0.2, 0.25 or 0.3 to theOD value of the negative control on each plate.
AGID testsThe method was based on those of Merkal et al17 and
Goudswaard and Terporten-Pastoors.18 In brief, six wells 4 mmin diameter and 2 mm apart were set up in a hexagonal configu-ration with a central well in 1% w/v agarose gel in borate bufferin 90 mm diameter petri dishes. Up to eight such hexagonalunits were included per plate. Antigen (30 µL), consisting ofmechanically-disrupted cells of M a paratuberculosis strain Ama,a bovine strain field isolate from a goat with paratuberculosis(caprine test) or strain 316V, a laboratory adapted bovine strain(ovine test) was placed in the centre well. The six outer wellswere each loaded with 30 µL of undiluted serum. Five test seraand one positive control serum were included in each unit. Acaprine control serum was used in the caprine test and an ovinecontrol serum was used in the ovine test. Plates were incubatedat 35°C for 18 h in a humid chamber and were read over indi-rect light. The results were recorded as positive where a line ofprecipitation was detected and confirmed by retesting to beconfluent with the line produced by the positive control serumin an adjacent outer well. For a valid test, the positive controlserum of each pattern needed to give a line of reactivity locatedmidway between the central antigen and the control positiveserum well. AGID test results were recorded as negative, trace,1, 2 or 3 based on the location of the precipitin line. Values of1, 2 or 3 were defined as positive, while trace reactions weredefined as inconclusive.
StatisticsConfidence limits for proportions were calculated using
StatMate software (GraphPad Software, San Diego California).Chi square tests were performed using Prism software(GraphPad). McNemar’s test was performed according toMotulsky.19
ResultsSpecificity of the AGID testsAll 1000 sera from goats from Western Australia were nega-
tive in both AGID tests indicating 100% specificity for bothtests (95% confidence limits 99.63 to 100%).
Specificity of the EMAI caprine paratuberculosis absorbed ELISAA total of 95 sera were retested, 54 because an ELISA ratio >
1.5 was obtained (that is, inconclusive) and five because a ratioof > 2 (positive) was obtained. Of the sera with inconclusiveinitial results, 44 were resolved as negative, 10 as inconclusiveand one as positive by retesting. Of the sera with positive initialresults, one was resolved as positive and four as inconclusive byretesting. Thus the final results included 14 inconclusive seraand two with positive outcomes amoung 1000 sera. The speci-ficity of the test increased steeply with cut-off points above 1.4(Figure 1). A specificity of 99.8% (95% confidence limits 99.28
Figure 1. Specificity of the EMAI caprine Johne’s diseaseabsorbed ELISA at different positive-negative cut-off (ELISAratio).

74 Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Scientific
infection confirmed by cultureand/or histopathology fromsource 2 was tested in each ofthe tests in late 1998 or early1999, except for three sampleswhere there was insufficientserum to enable testing in theCSL PARACHEK Johne’sabsorbed EIA at the WA labo-ratory (Table 3). Of the 19goats, 17 were positive andtwo were negative in ELISA.Both the EMAI and CSLassays (at both testing loca-tions) identified the same indi-viduals as positive. ELISAratios for positive sera in theEMAI assay ranged from 2.6 to 7.6 while OD in the CSL testranged from 0.34 to 3.45. In comparison to ELISA, only eightgoats were detected as positive in the ovine AGID, and five inthe caprine AGID. A statistical comparison was made betweenthe ovine AGID test and ELISA assuming that inconclusiveresults in both tests were negative, as this is how the test resultsare used in disease control programs. The AGID detected fewerinfected goats than the ELISA (P < 0.05, McNemar’s test, Chisquare = 4.90). The ovine AGID test detected a greater numberof infected goats compared to the caprine AGID test but thedifference was not statistically significant (assuming inconclu-sive results were negative) (P > 0.05, McNemar’s test, Chisquare = 0.25). The two goats with negative results in ELISAwere infected with cattle strains but each of the tests was capableof detecting goats infected with cattle or sheep strains of M aparatuberculosis.
DiscussionThe EMAI caprine Johne’s disease absorbed ELISA at a posi-
tive-negative cut-off ratio of 2.0 and the CSL PARACHEKJohne’s absorbed EIA at a positive-negative cut-off algorithm ofnegative OD + 0.25 or 0.3 are both highly specific tests. Basedon this criterion they appear suitable for use in a market assur-ance program because they are unlikely to produce a significantproportion of false positive test outcomes. False positive reac-tions trigger expensive and time consuming follow-up testingusing serology, faecal culture or necropsy and undermineproducer and industry confidence in such programs. Althoughthe AGID tests were also highly specific, the limited data forinfected goats provided in this study suggest that the ELISAtests may be more sensitive and therefore should be used inpreference to the AGID test in a market assurance program.The AGID may still be required in certain situations, forexample where export testing requirements specify the use ofthis test, or where it is desired to use a test with higher speci-ficity in series with ELISA.20
The estimates of specificity of ELISA obtained in this studycompare favourably with those from smaller studies conductedin other countries. Values of 93.6 to- 95.2% were reportedwhen comparing antigens for ELISA using sera from 63 disease-free goats in Spain whereas an estimate of 100% was obtainedfor an ELISA applied to samples from 123 goats tested from 10herds believed free of paratuberculosis in the USA.4,6
Sensitivity estimates for ELISA are also scarce. Molina et al4
found a sensitivity of 87.5 to 88.2% for various antigens using
sera from 17 affected goats. A sensitivity of 87% was found foran ELISA in a study with 26 goats with clinical paratubercu-losis,5 and in another study an estimate of 54% was obtainedfrom 35 goats shown to have M a paratuberculosis in faeces byPCR. 6 A meaningful estimate of the sensitivity of serology fordetection of paratuberculosis in goats was not determined in thepresent study due to lack of funding for an unbiased survey, lackof suitable case material and lack of an independent means ofselection of goats for inclusion in the study. However, someuseful results were obtained on the comparative sensitivity ofELISA and AGID tests in infected goats. Based on the samplestested in this study it appears that the ELISA is likely to detectabout twice as many goats with paratuberculosis as the AGIDtests. ELISA also appeared to be more sensitive than AGID inan earlier Australian study.5 This would be expected intuitively
Table 1. Specificity of the CSL PARACHEK Johne’s absorbed EIA based on the results of testing 1000 sera fromgoats from Western Australia.
Positive-negative cut-off algorithm for the CSL PARACHEK EIA
Plus 0.1 Plus 0.15 Plus 0.2 Plus 0.25 Plus 0.3
Tested at EMAI
No. reactors 26 11 7 4 3
Specificity % 97.4 98.9 99.3 99.6 99.7
95% confidence limits 96.2 - 98.3 98.0 - 99.5 98.6 - 99.7 99.0 - 99.9 99.1 - 99.9
Tested at Ag WA
No. reactors 6 4 2 2 2
Specificity % 99.4 99.6 99.8 99.8 99.8
95% confidence limits 98.7 - 99.8 99.0 - 99.9 99.3 - 100 99.3 - 100 99.3 - 100
Table 2. EMAI ELISA and caprine AGID test results for 47 paratuberculousgoats categorised by stage of disease. ELISA ratio < 1.5 = negative; ≥≥ 1.5to < 2 = inconclusive; ≥≥ 2 = positive.
Stage of disease AGID test EMAI ELISA
Positive Inconclusive Negative
Clinical positive 7 - -(n = 13)
negative 4 - -
not tested - - 2
Subclinical positive 14 - -(n = 34)
negative 14 4 2
TOTAL 39 4 4
Table 3. Relative sensitivities of the AGID tests and ELISA tests basedon results from 19 goats with paratuberculosis.
Test Positive Inconclusive Negative Not tested
Caprine AGID test 5 - 14 -
Ovine AGID test 8 4 7 -
EMAI ELISA 17 2 - -
CSL EIA at EMAI 17 - 2 -
CSL EIA at AgWA 15 - 1 3a
ainsufficient sera; note that these were all positive in the CSL test at the EMAIlaboratory

Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 75
Scientific
Gonsalves and Ann-Michele Whittington (EMAI) and BobLove, Paul Matson, Geoff Eliot, Leo Hustas and Brett Carson(Department of Agriculture WA).
References1. Lenghaus C, Badman RT, Gillick JC. Johne’s disease in goats. Aust Vet J1977;53:460.2. Whittington RJ, Taragel CA. Cross Species Transmission of Ovine Johne’sDisease - Phase 1. Final Report to Meat and Livestock Australia. NSWAgriculture, Camden, 2000.3. Whittington RJ, Sergeant ESG. Progress towards understanding the spread,detection and control of Mycobacterium avium subsp. paratuberculosis inanimal populations. Aust Vet J 2001;79:267-278.4. Molina A, Morera L, Llanes D. Enzyme-linked immunosorbent assay fordetection of antibodies against Mycobacterium paratuberculosis in goats. Am JVet Res 1991;52:863-868.5. Milner AR, Mack WN, Coates KJ. A modified ELISA for the detection of goatsinfected with Mycobacterium paratuberculosis. Aust Vet J 1989;66:305-306.6. Burnside DM, Rowley BO. Evaluation of an enzyme-linked immunosorbentassay for diagnosis of paratuberculosis in goats. Am J Vet Res 1994;55:465-466.7. Reviriego FJ. Diagnosis of caprine paratuberculolsis by enzymeimmunoassay. Preliminary study. Revista de Salud Animal 1996;18:69-76.8. Ellis TM, Norris RT, Martin PAJ et al. Evidence for freedom from Johne’sdisease in cattle and goats in Western Australia. Aust Vet J 1998;76:630-633.9. Whittington RJ, Marsh I, McAllister S et al. Evaluation of modified BACTEC12B radiometric medium and solid media for the culture of Mycobacteriumavium subsp. paratuberculosis from sheep. J Clin Microbiol 1999;37:1077-1083.10. Whittington RJ, Hope AF, Marshall DJ et al. Molecular epidemiology ofMycobacterium avium subsp. paratuberculosis: IS900 restriction fragmentlength polymorphism and IS1311 polymorphism analyses of isolates fromanimals and a human in Australia. J Clin Microbiol 2000;38:3240-3248.11. Marsh I, Whittington R, Cousins D. PCR-restriction endonuclease analysisfor identification and strain typing of Mycobacterium avium subsp. paratubercu-losis and M. avium subsp. avium based on polymorphisms in IS1311. Molecularand Cellular Probes 1999;13:115-126.12. Yokomizo Y, Merkal RS, Lyle PAS. Enzyme-linked immunosorbent assayfor detection of bovine immunoglobulin G1 antibody to a protoplasmic antigen ofMycobacterium paratuberculosis. Am J Vet Res 1983;44:2205-2207.13. Yokomizo Y, Yugi H, Merkal RS. A method for avoiding false-positive reac-tions in an enzyme-linked immunosorbent assay (ELISA) for the diagnosis ofbovine paratuberculosis. Jap J Vet Sci 1985;47:111-119.14. Milner AR, Mack WN, Coates KJ et al. The sensitivity and specificity of amodified ELISA for the diagnosis of Johne’s disease from a field trial in cattle.Vet Microbiol 1990;25:193-198.15. Collins MT, Sockett DC, Ridge S et al. Evaluation of a commercial enzyme-linked immunosorbent assay for Johne’s disease. J Clin Microbiol 1991;29:272-276.16. Cox JC, Drane DP, Jones SL et al. Development and evaluation of a rapidabsorbed enzyme immunoassay test for the diagnosis of Johne’s disease incattle. Aust Vet J 1991;68:157-160.17. Merkal RS, Larsen AB, Kopecky KE et al. Experimental paratuberculosis insheep after oral, intratracheal, or intravenous inoculation: serologic and intra-dermal tests. Am J Vet Res 1968;29:963-969.18. Goudswaard J, Terportenpastoors WWM. Johne’s disease in goats;comparison of serological tests. Neth J Vet Sci 1972;4:93-114.19. Motulsky H. Intuitive Biostatistics. Oxford University Press, Oxford, 1995.20. Eamens GJ. Johne’s disease in goats. In: Milnar AR, Wood PR, editors.Johne’s disease: current trends in research, diagnosis and management.CSIRO Publications, Melbourne, 1989:105-112.21. Lyle PAS, Merkal RS. Comparison of ELISA and gel diffusion precipitin testsfor paratuberculosis in cattle, sheep and goats. In: Merkal RS, editor.Proceedings of the International Colloquium on Research in Paratuberculosis,June 16-18. National Animal Disease Centre, Ames, Iowa, 1983:109-112.
(Accepted for publication 15 May 2002)
because ELISA is a primary antigen-antibody binding assay inwhich results follow directly from this interaction whereas theAGID is a secondary binding assay requiring an antigen-anti-body reaction and then cross-linking of the combination toform visible precipitates. However, it is known from studies insheep with paratuberculosis in Australia that overlapping butslightly different populations of animals are detected by AGIDand ELISA from within an infected flock (unpublished data).Since infected goats in this study were selected from infectedflocks based on factors including their reactions in a serologicaltest it is possible that the results are biased in favour of eitherELISA or AGID, but we were unable to assess this retrospec-tively. If larger studies of infected goats become feasible inAustralia in the future it would be desirable to test all goats inan infected population using a range of tests and then deter-mine the sensitivity of each test.
An interesting finding in this study was the tendency for theovine AGID test to detect more infected goats than the caprineAGID test. The reasons for this are unclear. Although both testsutilise antigen derived from cattle strains of M a paratuberculosisthere may be subtle differences in the composition of the anti-gens; the concentration of the antigen used in each test differs asdo the control sera. Therefore the precipitin lines regarded aslines of identity probably differ between the two tests. Thisrequires further investigation.
Diagnosis of paratuberculosis using serological tests is notlimited by the strain of M a paratuberculosis. Both cattle andsheep strains stimulated antibody mediated immunity detectedin each of the tests. As each test includes antigen derived from acattle strain of M a paratuberculosis, antigenic cross reactionbetween cattle and sheep strains is clearly evident. It is notknown whether use of a sheep strain would improve the detec-tion of paratuberculosis due to the sheep strain in goats.
Although favourable data have now been obtained to supportthe high specificity of serological tests for paratuberculosis ingoats it is important to recognise that serology is unlikely to bemore sensitive in goats than in other species and is likely to beless sensitive than faecal culture. This is the case in cattle andsheep.3,21 In these species serology is thought to have sensitivityof only 25 to 35% across a herd or flock.3 Consequently the useof serology in market assurance program tests in the goat indus-tries must be based on statistically valid sampling of animalsfrom a herd, and this requires large sample sizes to compensatefor low test sensitivity.3
AcknowledgmentsThis project was funded by NSW Agriculture, Agriculture
WA and Rural Industries Research and DevelopmentCorporation. Stephen Jones of CSL kindly supported thetesting of samples in Western Australia through financial contri-bution and provided test kits for use in New South Wales. Thefollowing staff provided skilled assistance during this study:Mark Turner, Deneane Coogan, Kirstina Lamont, Jocelyn

76
Scientific
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Polymerase chain reaction tests for the identification ofRoss River, Kunjin and Murray Valley encephalitis virusinfections in horses
MJ STUDDERTa, JK AZUOLASb, JR VASEYc, RA HALLd N FICORILLIa, AND J-A HUANGa
Objective To develop and validate specific, sensitive andrapid diagnostic tests using RT-PCR for the detection of RossRiver virus (RRV), Kunjin virus (KV) and Murray Valleyencephalitis virus (MVEV) infections in horses.
Methods Primer sets based on nucleotide sequenceencoding the envelope glycoprotein E2 of RRV and on thenonstructural protein 5 (NS5) of KV and MVEV were designedand used in single round PCRs to test for the respectiveviruses in infected cell cultures and, in the case of RRV, insamples of horse blood and synovial fluid.
Results The primer pairs designed for each of the threeviruses amplified a product of expected size from prototypeviruses that were grown in cell culture. The identity of each ofthe products was confirmed by nucleotide sequencing indi-cating that in the context used the RT-PCRs were specific.RRV was detected in serums from 8 horses for which therewere clinical signs consistent with RRV infection such that anacute-phase serum sample was taken and submitted for RRVserology testing. The RRV RT-PCR was analytically sensitivein that it was estimated to detect as little as 50 TCID50 of RRVper mL of serum and was specific in that the primer pairs didnot amplify other products from the 8 serum samples. TheRRV primers also detected virus in three independentmosquito pools known to contain RRV by virus isolation in cellculture. Samples from horses suspected to be infected with KVand MVEV were not available.
Conclusion Despite much anecdotal and serologicalevidence for infection of horses with RRV actual infection andassociated clinical disease are infrequently confirmed. Theavailability of a specific and analytically sensitive RT-PCR forthe detection of RRV provides additional opportunities toconfirm the presence of this virus in clinical samples. The RT-PCR primers for the diagnosis of KV and MVEV infectionswere shown to be specific for cell culture grown viruses butthe further validation of these tests requires the availability ofappropriate clinical samples from infected horses.Aust Vet J 2003;81:76-80
RRV is a member of the family Togaviridae, genusAlphavirus. MVEV and KV are both members of the family
Flaviviridae, genus Flavivirus. These three arthropod borneviruses are known to infect horses in Australia based on serolog-ical data and, in the case of RRV and KV, on virus isolation.RRV has been isolated from horses in Australia on at least fouroccasions.1-3 RRV is believed to be maintained in marsupial,possibly flying fox, hosts and when seasonal conditions are
favourable for the mosquito vectors the virus is transmitted toother hosts notably to humans and horses.1 There are consider-able serological data to show that horses are frequently infectedwith RRV and that there is a temporal association with a gener-alised disease in horses often including arthropathy and theoccurrence of specific antibody in serum.2 For example betweenJanuary and April 1984 veterinary practitioners in northernVictoria attended many horses with locomotor disturbancesincluding disinclination to move, incoordination, staggering,cutaneous hyperaesthesia and fasciculation of limb muscles withrecovery occurring within 2 to 5 days.3 In the Murray Darlingbasin and regions of central Victoria there is a backgroundprevalence of RRV antibody in horses of about 30%, that intimes of high virus activity can rise to 60%.2 McConnell(1996)4 described an outbreak of disease, attributed to RRVinfection, affecting 20 horses near Hobart during March andApril 1996 in which horses showed reluctance to move, pyrexia,swollen legs, abdominal discomfort or mild colic, inappetenceand shifting lameness; in several of these cases serial bloodsamples taken 2 weeks apart, confirmed a rising IgG ELISAantibody titre to RRV.
As a consequence of efforts to isolate RRV from clinicallyaffected horses Badman et al3 described 2 yearlings with severenervous signs that required euthanasia; both horses initiallyshowed signs of colic and within 12 hours developed posteriorparalysis followed by lateral recumbency, cutaneous anaesthesia,marked dullness and convulsions. At necropsy a severe nonsup-purative encephalomyelitis was present with lesions predomi-nantly in the thalamus, mid brain and medulla. KV was isolatedfrom the spinal cord of one of the horses; this horse had a titreof 80 to Sindbis virus and 640 to KV and MVEV and was nega-tive for RRV antibody. There is considerable anecdotal evidencethat, in those occasional years when MVEV causes epidemicdisease in humans in northern Victoria, there is an increasednumber of reports of neurological disease in horses. MVEVantibody was reported in 13 horses in a limited study under-
aCentre for Equine Virology, School of Veterinary Science, The University ofMelbourne, Parkville, Victoria 3010bVictorian Institute of Animal Science, Department of National Resources andEnvironment, Attwood, Victoria 3049cGoulburn Valley Equine Hospital, Shepparton, Victoria 3630dDepartment of Microbiology and Parasitology, University of Queensland,Brisbane, Queensland 4072
CEV Centre for Equine VirologycDNA Complementary DNAE2 Glycoprotein E2ELISA Enzyme linked immunosorbent assayIgG Immunoglobulin GIgM Immunoglobulin MPCR Polymerase chain reactionKV Kunjin virusMVEV Murray Valley encephalitis virusNS5 Nonstructural protein 5 RRV Ross River virusRT-PCR Reverse transcriptase-polymerase chain reactionTCID50 50% tissue culture infectious doseVIAS Victorian Institute of Animal ScienceWNV West Nile virus

Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 77
Scientific
recorded as negative for RRV IgM because the titre was < 5120but when retested using a revised cut off value of > 2560 thesample was positive (Azuolas et al unpublished). A second bloodsample from horse 6 taken 2 weeks after the first, was obtainedand this had a reduced IgM titre (81,920 to 10,000) and a posi-tive IgG titre (2500); a third blood sample taken 4 weeks afterthe first had an IgM titre of 0 and an IgG titre of 81,920. 8 ofthe 13 horse serum samples were tested for the presence of RRVby RT-PCR. We also had available three pools of Ochlerotatuscamptorhynchus mosquitoes each comprising about 25 mosqui-toes that were trapped in Gippsland, Victoria in the years 1986,1988 and 1989 respectively and a fourth pool of Oc globocoxitustrapped in Mildura, Victoria in 2000, that were known to bepositive for RRV by virus isolation in C6/36 mosquito (Culexalbopictus) cell cultures. These mosquito pools were obtained ashomogenised suspensions in cell culture medium and were useddirectly in the RT-PCR.
KV.Boort, isolated from the spinal cord of a yearling horsethat had neurological disease,3 and KV.35911, isolated from abrain of a horse that died in the Hunter Valley, NSW in 198410
were obtained as suspensions of infected Vero cell cultures.MVEV.FD5 was obtained as a second passage mouse brainsuspension, which was passaged once in C6/36 cells and the cellculture supernatants used in the RT-PCR.
Virus RNA from all samples was prepared using a QIAampviral RNA mini kit (Qiagen, Clifton Hill, Victoria) according tothe manufacturer’s instructions.
Primers were designed based on the available sequences of
taken in 1974, an epidemic year for MVE5 and it has beenestablished that horses can be experimentally infected followingthe bite of infected mosquitos.6
We report initial studies in developing RT-PCRs for RRV,KV and MVEV, which have the capacity to serve as adjunct toexisting tests, which include serology and virus isolation, for theidentification of these virus infections in horses.
Materials and methodsThe viruses used in the study are listed in Table 1. RRV.T487
was grown in Vero cells. A second RRV isolate, designated762/84, was coincidentally isolated from cell cultures preparedfrom equine synovial membranes obtained from the joints of ahorse collected at a Melbourne knackery.8 Two blood samplescollected into lithium-heparin tubes from wild horses nearKatherin, Nothern Territory in 1984 from which RRV wasisolated 9 were available; these samples had been stored at 4°C.Synovial fluids collected from a fetlock joint and a tendonsheath of a filly with synovitis near Shepparton in March 1999were examined for the presence of RRV. Serum collected fromthe filly at the time had a RRV IgG ELISA antibody titre of >81,920. We also had available 13 serum samples collected fromhorses showing signs consistent with a clinical diagnosis of RRVinfection such that a blood sample was taken and submitted toVIAS for RRV antibody testing. These serums were tested inELISAs for RRV IgM and IgG. All were positive for IgM butnegative for IgG. One of the horses (horse 6) was initially
Table 1. Viruses used in this study.
Virus Year of Place of origin Reference PCR amplification Most closely related virus and isolation GenBank accession number
RRV.T48 1939 Townsville, Qld Doherty et al17 Yes RRV.T48 (M23708)
RRV.762/84 1984 Melbourne, Vic Fraser8 Yes RRV.T48 (M23708)
RRV.G88/25 1988 Gippsland, Vic This study Yes RRV.NB1053 (L40563)
RRV.G86/26 1986 Gippsland, Vic This study Yes RRV.NB5092 (NC_001544)
RRV.G89/140 1989 Gippsland, Vic This study No Not applicable
RRV.449/00 2000 Mildura, Vic This study Yes RRV.T48 (M23708)
Kunjin.Boort 1984 Boort, Vic Badman3 Yes Kunjin.Boort (AF297840)
Kunjin.35911 1984 Hunter Valley, NSW Scherret et al10 Yes Kunjin.MRM16 (L48979)
MVE.FD 1951 Mooroopna, Vic Marshall et al7 Yes MVE-1-51 (NC_000943)
Table 2. Ross River, Kunjin and Murray Valley encephalitis virus primer pairs used for RT-PCR.
Primer Target Primer sequence Priming GenBank Expected sequence positionsa Accession product size
No. of referencevirus
RRVFP Envelope E2 5’-AGTCTCCGCCCAAATAGGTCTG-3’ 8713-8734 glycoprotein M20162 505 bp
RRVRP (C terminus) 5’-GATGGTCTTGTCAGTACTGGTAG-3’ (R/C) 9195-9217
KUNFP Non structural 5’-GGAAAACGAGAGGACATCTGGTGTGG-3’ 10213-10238 AF196835 415 bpb
KUNRP protein NS5 5’-CGAGACGGTTCTGAGGGCTTAC-3’ (R/C) 10606-10627
MVEFP Non structural 5’-GCTTAGCAAAAGCATATGCACAGA-3’ 9955-9978 MVERP protein NS5 5’TGGTAACCCAGTCCTCCTGGGGTTG-3’ (R/C)c 10550-10575
AF161266 621 bpb
aThe priming position is based on the reference sequence. bThe size of the expected PCR product may vary between strains of flaviviruses. cR/C = reversed and complemented.

78 Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Scientific
each virus in GenBank using a set of programs from theAustralian National Genomic Information Service (ANGIS).Details of the primers used are shown in Table 2. Primers forRRV were similar to those used by Sellner et al 1992.11
Extracted virus RNA was used as template to synthesise acomplementary DNA (cDNA) using SuperScript II reversetranscriptase (Invitrogen, Mulgrave, Victoria) according to themanufacturer’s instructions. PCR amplification was performedin a thermal cycler (Hybaid, Ashford, UK) using the followingconditions: 95°C for 5 min followed by 35 cycles of 30 s at94°C, 30 s at 57°C and 1 min at 72°C. At the completion ofthe PCR, 2 µL of the reaction mix was analysed by elec-trophoresis in a 1% agarose gel containing 0.5 µg/mL ethidiumbromide and the amplified products visualised by UV transillu-mination.
For nucleotide sequencing the PCR products were separatedin a 1% agarose gel and the band of the expected size was cutfrom agarose gel, purified using the Gel Extraction Kit (Qiagen)and ligated into pGEM-T plasmid (Promega, Annandale,NSW) as described previously.12 Plasmids containing each ofthe PCR products were sequenced to confirm the identity of theviral inserts and accordingly the specificity of the RT-PCR. Thenucleotide sequences of the RRV PCR products were deter-mined by direct sequencing of the product and compared. The
sensitivity of the RRV RT-PCR was assessed as follows. Startingwith 140 µL of RRV infected cell culture lysate that contained1x108 TCID50 per mL, 60 uL of a solution containing RRVRNA was obtained. 2uL of this RNA-containing solution(~4.7x105 TCID50 RRV equivalent) was used in a cDNAsynthesis reaction of 20 uL. The resultant cDNA was seriallydiluted to 10-6 and 1 uL of the cDNA solutions (from 100 to 10-6)was used for the PCR. Nucleotide sequences of the two KVisolates were also determined and compared.
ResultsEach of the primer pairs amplified a product of the expected
size from cDNA prepared from prototype virus strains of RRV,KV and MVEV (Figure 1). For RRV a product of the expectedsize was also obtained from RRV.762/84 and from acute phaseserum samples taken from 8 of the 13 horses that were tested(Figure 1). RRV was also isolated in cell culture from the 13horse serum samples (Azuolas et al unpublished) and when 3 of5 first passage cell culture lysates were tested by RT-PCR aproduct of expected size and sequence was obtained. The 2blood samples from which RRV was isolated in 19849 and thefluids from the fetlock and tendon sheath of the filly were nega-tive by RT-PCR for RRV. Two out of the three Oc camp-torhynchus mosquito pools and the Oc globocoxitus pool eachyielded a RRV product of expected size. The nucleotidesequence of the 504 base pair RT-PCR products of the RRVamplified during the study showed that all were very closelyrelated. An alignment of the deduced amino acid sequence ofthe RT-PCR products is shown in Figure 2. The nucleotidesequence and deduced amino acid sequence of 7 of the 8 RRVPCR products derived from the equine samples were identicalto each other and to the sequence of the RRV product amplifiedfrom the Oc globocoxitus mosquito pool (Figure 2). In assessingthe sensitivity of the RRV RT-PCR in detecting cell culturegrown virus it was found that the assay detected a product ofthe expected size at a dilution of 10-5 but not at 10-6, which isthe equivalent of a detection sensitivity of 0.5 TCID50 per mLRRV in the starting cell culture lysate. The sensitivity of theRRV RT-PCR in detecting RRV in horse serum samples wassimilarly examined and it was estimated that each of 2 serumstested contained > 108 genome copies of RRV per mL (data notshown).
DiscussionFrom their studies of RRV infection of horses Kay et al6
concluded that, “such experimental studies (as they had under-taken), not only of RRV but other arthropod borne virusdiseases in horses, are likely to be less rewarding in incrimi-nating these viruses in disease in horses than identification ofthese viruses in clinical samples”. The identification of RRV in8 serum samples from horses with a provisional clinical diag-nosis of RRV infection obtained from widely scattered regionsin Australia appears to be a fulfilment of this prediction. It is ofinterest that in their studies of experimental infection of horseswith RRV Kay et al observed one horse that developed aviraemia, detectable by mouse brain inoculation, which lasted 4days with a peak virus tire of 106.5 infectious doses per mL.6 Weestimated that acute phase horse serum may contain > 108
TCID50 per mL of RRV. These concentrations of virus aresomewhat higher than that expected in other togavirus infec-tions of horses and suggest that the horse may not necessarily be
Figure 1. (A) Detection of Ross River virus by RT-PCR. Theprimers detected the cell culture grown RRV isolates (T48 and762/84) and identified RRV in the serum of eight horses (Nos. 6-13) with a clinical diagnosis of RRV disease. The samples fromhorses (460, 461, tendon and fetlock) were negative for RRV.RRV was identified in three of four pools of mosquitoes (G88/25,G86/26 and 449/00). λλ is bacteriophage λλ DNA cut with HindIII,included as a base pair marker.(B) Detection of Kunjin and Murray Valley encephalitis viruses byRT-PCR. The two Kunjin viruses, isolated in cell culture fromcentral nervous tissues of horses, were both detected with theprimers used. The plasmid pUC18 DNA cut with MspI and λλphage DNA cut with HindIII were included as a base pair marker.
T48
762/
84
Hor
se-6
Hor
se-7
Hor
se-8
Hor
se-9
Hor
se-1
0
Hor
se-1
1
Hor
se-1
2
Hor
se-1
3
460
461
Ten
don
Fetlo
ck
λD
NA
/Hin
dIII
449/
00
G88
/25
G86
/26
G89
/140
Neg
ativ
e co
ntro
l
B.
pUC
12/M
spI
Kun
jin.B
oort
Kun
jin. 3
59II
Neg
ativ
e co
ntro
l
λD
NA
/Hin
dIII
MV
E.F
D
Neg
ativ
e co
ntro
l
564 bp
564 bp502 bp
A.

Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 79
Scientific
and caused the death of many thousands of birds, serious illnessin 56 humans of which seven died and the death or euthanasiaof 24 horses that developed encephalomyelitis (and death oreuthanasia of 37 of 60 infected horses in 2000) is of the samegenetic lineage as KV (Lineage I).15 In the Australian context itis important to recognise that the phylogenetic analysis ofWNV isolates that constitute the total quasispecies, is complexand that a close phylogenetic relationship may not necessarilycorrelate with pathogenicity of a particular topotype.
It has been a major theme of the CEV research programduring the past several years to have in place PCR tests for allendemic equine virus diseases in Australia and in large measurethis has been achieved.12,16 The present report deals with threemosquito borne viruses that have not been the subject of anymajor study at the CEV but the development of a PCR test foreach virus is a natural extension of the overall effort to haveavailable PCR tests for all endemic equine viruses. For manydecades there has been much anecdotal evidence that, particu-larly in regional and rural areas, these mosquito borne virusesare a cause of significant morbidity and disease including deathin horses. It also seems evident that, despite considerableepidemiological surveillance work based on serology and samplesubmission, present resources including available tests princi-pally because of cost and timing of sample collection, have notresolved in satisfactory ways the role of these viruses in thedisease outbreaks with which they are associated. The avail-ability of PCR for RRV, KV and MVEV should encourage prac-titioners to submit blood samples and other tissue or joint fluidsamples taken during the acute phase of disease for confirma-tion of a specific virus diagnosis by PCR. These PCRs will be animportant adjunct to serology, particularly differential IgM/IgG
a dead end host for RRV but may serve as asource of virus for infection of mosquitoesduring a blood meal and play a role as a trans-mitting host in the rise of an epidemic. Thefailure to detect RRV RNA in the 2 bloodsamples collected from horses near AliceSprings in 1984 and which had been storedsince then at 4oC was not surprising since it isunlikely that RRV would survive such longterm storage at 4oC; the storage conditionsused are suitable for the long term storage oforbiviruses which were also a focus of thesurveillance study.9 Also it is perhaps notsurprising that the fetlock and tendon sheathfluid samples did not yield RRV RNA giventhe long standing nature of the clinical disease(synovitis) and the observation that RRV IgGELISA antibody titre at the time the sampleswere collected was > 81,920; both of thesefindings would suggest that the primaryviraemia may have occurred before the sampleswere taken. It is recognised that antibody titresas low as 40 are sufficient to block detection ofvirus by PCR, an observation that highlightsthe need for very early (< 72 hours) collectionof samples after the first sign of clinical disease.Samples from some of 11 horses that had beenexperimentally infected with RRV and whichbecame viraemic6 were sought but were nolonger available.
Failure to amplify a PCR product from oneof the three Oc camptorhynchus mosquito pools that was positiveon virus isolation, may have been due to the degradation of theviral RNA, the presence of inhibitors or, less likely, mutations inthe priming sites.
The high sequence identity among the 12 RRV PCR prod-ucts is not unexpected in that the primers were based on aknown highly conserved region of the genome.13 The sequenceof RRV.762/84 isolated from the synovial membrane of a horse8 indicated that this virus, although closely related, was distinctfrom RRV.T48.
Initially several different primer pairs were designed for bothKV and MVE. When used on templates prepared from virusespassaged twice in mouse brain, it was found that there wasconsiderable nonspecific amplification, presumably repre-senting cellular DNA or RNA, including some bands thatapproximated the expected PCR product size from the viruses.However, when sequenced, these were shown not to be virusspecific products. It was found necessary to passage MVE inC6/36 cells and to prepare the cDNA from cell culture grownvirus in order to obtain an authentic PCR product. It was estab-lished that the PCR primer sets for both KV and MVE ampli-fied a product of expected size from prototype viruses and thatthe products were confirmed to be viral specific by sequenceanalysis (data not shown). Further validation of PCRs for MVEand KV on clinical samples is required.
Although originally isolated in Australia and named Kunjinvirus and designated a distinct virus species, it is clear fromsequence analysis that KV is a subtype (topotype) of WNV andthe International Committee for the Taxonomy of Viruses hasindicated that KV shall be listed as WNV.14 It is of interest thatthe strain of WNV that emerged in New York state in mid 1999
Figure 2. Alignment of the deduced amino acidsequence of the twelve RRV isolates that weredetected by RT-PCR. Ref T48 is published sequenceof the reference strain. RRV.762/84 is a cell culturegrown isolate. The prototype virus T48 was rese-quenced as part of this study. 449/00, G88/25 andG86/26 are from pools of mosquitoes. Horses 6 to 13are RRV identified in horse serum samples.

80 Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Scientific
ELISA (Azuolas et al unpublished), and virus isolation for thediagnosis of these infections in horses.
AcknowledgmentsFunding for this project was provided by a Special Virology
Fund and by Racing Victoria. We thank JRE Fraser for the RRVisolate 762/84, LF Melvile, Division of Primary Production,Darwin NT, for RRV samples and Cynthia Brown for technicalhelp.
References1. McKenzie JS, Smith DW, Ellis TM et al. Human and animal arboviraldiseases in Australia. Recent Advances in Microbiology. 1994;2:1-91.2. Azuolas JK. Ross River virus disease in horses. Aust Equine Vet.1998;16:56-58.3. Badman R, Campbell, J, Aldred, J. Arbovirus infections in horses. CommunDis Intell. 1984;17:5-6.4. McConnell A. Ross River virus. Animal Health Surveillance Bulletin.1996;4:8.5. Marshall I. Murray Valley and Kunjin encephalititis. In: Monath T, editor. TheArboviruses: Epidemiology and Ecology. Vol III. CRC Press, Boca Raton1988:151-189.6. Kay BH, Pollitt CC, Fanning ID, Hall RA. The experimental infection of horseswith Murray Valley encephalitis and Ross River viruses. Aust Vet J 1987;64:52-55.
7. Marshall ID, Miles JAR. Ross River virus and epidemic polyarthritis. CurrTopics Virus Res 1984;3:31.8. Fraser JRE. Epidemic polyarthritis and Ross River virus disease. ClinRheumatol Dis. 1986;12:369-388.9. Gard GP, Shorthose JE, Weir RP, Walsh SJ, Melville LF. Arboviruses recov-ered from sentinel livestock in northern Australia. Vet Microbiol 1988;18:109-118.10. Scherret JH, Poidinger M, Mackenzie JS, et al. The relationships betweenWest Nile and Kunjin viruses. Emerg Infect Dis. 2001;7:697-705.11. Sellner LN, Coelen RJ, Mackenzie JS. A one-tube, one manipulation RT-PCR reaction for detection of Ross River virus. J Virol Methods. 1992;40:255-263.12. Varrasso A, Dynon K, Ficorilli N, Hartley CA, Studdert MJ, Drummer HE.Identification of equine herpesviruses 1 and 4 by polymerase chain reaction.Aust Vet J. 2001;79:563-569.13. Sammels LM, Coelen RJ, Lindsay MD, Mackenzie JS Geographic distribu-tion and evolution of Ross River virus in Australia and the Pacific Islands.Virology. 1995;212:20-29.14. Fauquet CM, Pringle CR. Abbreviations for vertebrate virus species names.Arch Virol 1999;144:1865-1880.15. Studdert MJ. West Nile virus finds a new ecological niche in Queens, NewYork [editorial]. Aust Vet J 2000;78:400-401.16. Dynon K, Varrasso A, Ficorilli N, et al. Diagnosis of equine herpesvirus 3(equine coital exanthema virus), equine gammaherpesviruses 2 and 5, equineadenoviruses 1 and 2, equine arteritis virus and equine rhinitis A virus by poly-merase chain reaction. Aust Vet J 2001;79:695-702.17. Doherty R, Whitehead RH, Gorman BM, O’Gower AK. The isolation of athird group A arbovirus in Australia, with preliminary observations on its relation-ship to epidemic polyarthritis. Aust J Sci 1963;26:183-188.
(Accepted for publication 6 September 2002)
BOOK REVIEWParasitic Diseases of Wild Mammals, 2nd edn. Edited by Samuel WM, Pybus MJ, and Kocan AA , Iowa State University Press, Ames, 2001, 569pages. Price US$94.95.ISBN 0 8138 2978-X.
This book is an update of a volume by the same name edited by JW Davis and first published in 1971. Needless to say after 30 years, there havebeen tremendous advances in the field of wild mammal parasitology and this edition was long overdue. Indeed the first volume, for the most part,
was limited to documenting the occurrence of approximately 17 parasites, or parasite groups, and their respective hosts. The new volume expandson the information provided on those parasites and includes chapters on parasites not covered in the first edition. There are 30 contributing authorsthe majority of whom work in North America and the content of the volume reflects this bias. However, there are five contributors from Europeancountries and two from Australia, DM Spratt and GR Singleton both from CSIRO, Wildlife and Ecology, Canberra, who have co-authored a chapter onhepatic capillariasis. Each chapter is a current review and synthesis of the literature following a generally uniform layout that includes an introduction,notes on taxonomy, life history, epidemiology, clinical signs and pathology, immunology, diagnosis, control, human health implications, and risks todomestic animals. The topics reflect the dramatic increase in the depth of wildlife parasitology research in recent years particularly in the areas ofecology/epidemiology and the role of parasitic diseases in population dynamics and conservation biology. In early studies parasites of free rangingmammals were generally regarded as host-adapted and seldom the cause of significant disease. More recent research has shown the complexity ofthe host-parasite relationship and revealed that some parasites are able to cause severe disease and death of hosts and may in some circumstancespose a risk to a species or population. A good close-to-home example of this is the impact of Sarcoptes scabei var wombati epidemics on remnantwombat populations. Such insights make this volume a more interesting text for wildlife veterinarians or biologists and broaden its appeal beyond theparasitology fraternity. The new or greatly expanded sections on immunology and mechanisms of pathogenesis are also a reflection of the depth ofmolecular research currently undertaken on many of these parasites.
The parasites and parasite groups covered in this volume include five groups of ectoparasites (lice, biting flies, bot flies, ticks, and mange mites),ten groups of helminthes (liver flukes, taeniid tapeworms, gastrointestinal nematodes, lungworms, Baylisascaris sp, filaroid nematodes, kidneyworms, hepatic nematodes, and Trichinella sp), and nine groups of protozoa including enteric forms (Amoeba, Giardia, and coccidia), and tissue-invasive forms (amoebae, hepatozoons, Besnoitia, Toxoplasma, Sarcocystis and Neospora), and blood parasites (trypanosomes and relatives, piro-plasms). The coverage of selected topics is detailed and current and most authors review the international literature on parasite occurrence. The textis generally supplemented by tables and less frequently by black and white graphs, figures, or distribution maps. Some chapters are illustrated byblack and white photographs, and/or light micrographs or electron micrographs. Excellent examples are the chapter by JP Dubey on toxoplasmosis,and the chapter on bot flies and warble flies by DD Colwell. However, the quality of some gross lesion photographs is poor and future editions woulddo well to use colour photographs instead.
A criticism of the volume is that only selected parasite groups or host groups have been covered and the emphasis is strongly North American,limiting the appeal of this book to antipodeans especially given its US$94 recommended retail price. The comparatively poor coverage of parasites ofAustralian marsupial fauna is noticeable. Indeed one author seems to suggest that marsupials are not classed as mammals (p 109). An example ofthe selective coverage is the chapter on ticks that is limited to the species found in North America north of the Mexican border. Similarly the onlygastrointestinal nematodes covered are those of ruminants while the only lungworms treated are those of marine mammals and deer. A potentialreader with a particular interest in a parasite group, geographical region, or host would be advised to peruse the volume before purchase.
On balance, this volume will serve as a good reference text for selected parasite groups and hosts. It is current, well written, consistently edited,and well referenced. It will be most useful for veterinary students or practitioners with an interest in wildlife diseases. It will also serve as a usefulreference for parasitologists, academics, and wildlife biologists. The Australasian content could be greater and the volume does not really do justiceto the excellent wildlife parasitology research carried out down under in the past three decades. For that reason, those who may wish to purchasethis book to learn more about parasites of Australian native fauna may be disappointed.
PJ Duignan
Dr Duignan is Senior Lecturer in Comparative Pathology at Massey University and director of the NZ Wildlife Heatlh Centre.

81
Scientific
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Echinococcus granulosus in wildlife in and around theKosciuszko National Park, south-eastern Australia
DJ JENKINSa and B MORRISb
Objective To investigate the distribution of Echinococcusgranulosus in wild dogs and foxes and hydatidosis in wildlifecoexisting with foxes and wild dogs in and around KosciuszkoNational Park.
Design Prospective and ad hoc surveys by necropsy ofdefinitive and intermediate hosts.
Procedure Wild dogs and foxes were trapped at one loca-tion in the Kosciuszko National Park and at 7 locations aroundthe periphery of the Park. Feral pigs, macropodid marsupials,wombats, and feral goats were collected at some of the samelocations. The animals were humanely killed, their smallintestines removed in the field, the contents collected,preserved and examined microscopically. All internal organsof intermediate hosts were examined for hydatid cysts.Unidentified lesions were examined histologically.
Results Echinococcus granulosus tapeworms were foundin wild dogs from all locations. Prevalence ranged up to 100%with worm burdens up to 300,000 worms.
Prevalence in foxes ranged up to 50% in animals recoveredfrom 5 locations. The worm burdens were usually less than 50E granulosus per fox. Hydatid cysts were found in all macrop-odid species. Prevalence (69%) and cyst fertility (100%) werehighest in swamp wallabies (Wallabia bicolour). Prevalence ofcysts in feral pigs ranged up to 49%. Less than 22% of thecysts were fertile. No cysts were found in any of the wombatsor feral goats.
Conclusion Echinococcus granulosus occurs commonly inwildlife in and around the Kosciuszko National Park. Highnumbers of fertile cysts in swamp wallabies, a favoureddietary item for wild dogs in this region, suggests swampwallabies are pivotal in maintaining transmission. Physicalcontact with wild dogs and foxes or accidental contact withwild canid faeces is a public health risk.Aust Vet J 2003;81:81-85
The genus Echinococcus comprises 4 species of cyclo-phylidean cestodes, all of which may cause the zoonosishydatidosis.1 Echinococcus granulosus is the only member
of the genus Echinococcus to occur in Australia. Although stillcontroversial, it is likely that E granulosus was introduced ontothe mainland of Australia with dogs and sheep during Europeansettlement.
The key to the introduction and establishment of E granu-losus into the wildlife of south-eastern Australia was largely dueto the presence of dingoes, hydatid-susceptible macropodidmarsupials and transhumant grazing.2 Transhumant grazingbrought domestic animals infected with E granulosus into closecontact with native wildlife in alpine south–eastern Australia,annually, for almost 150 years. The last alpine grazing lease was
revoked in 1976. The distribution of E granulosus in easternAustralia is largely dictated by rainfall. Optimal transmission ofE granulosus occurs in regions with temperatures below 30oCand rainfall of more than 25 mm/month for 6 months of theyear.3 These conditions restrict the presence of E granulosusmainly to areas in the Great Dividing Range.1
Apart from transmission between domestic dogs and live-stock, transmission in wildlife is maintained through apredator/prey interaction between wild dogs (dingoes [Canislupus dingo]4 and dingo/domestic dog hybrids) and less impor-tantly foxes (Vulpes vulpes) and mainly macropodid marsupials,but also feral pigs (Sus scrofa)5 and wombats (Vombatus ursinus)6.
Formerly, it was thought that E granulosus from wildlife anddomestic animals were distinct strains, but recent studies haveshown no detectable genetic differences between E granulosusfrom either origin.7 Observations in the field and data fromexperimental infections indicate that there is no impediment totransmission of E granulosus between wildlife and domesticanimal hosts or humans.7
Wildlife populations in several parts of south-easternAustralia have been shown to be reservoirs for E granulosusproviding a potentially important source of hydatid infectionfor domestic livestock and humans.6,8 Crown Land (nationalparks and state forests) incorporate large tracts of south-easternNew South Wales and the Australian Capital Territory, impor-tant areas of wildlife refuge and popular centres for out-doorrecreation for humans. The Koscuiszko National Park currentlycomprises approximately 790,000 hectares. This area representsa major wildlife refuge for the region with resident populations ofwild dogs, foxes, macropodid marsupials, wombats, feral pigs andferal goats. In this paper, we present data on the occurrence of Egranulosus in wildlife intermediate and definitive host popula-tions, collected in and around the Kosciuszko National Park.
Materials and methodsDescription of the study area
Eight collection sites were located on the Tablelands of south-eastern New South Wales (Figure 1). The area ranges in altitudefrom approximately 600 to 2229 metres (Mount Kosciuszko),and consists of national park, state forest (both native hardwood and commercial pine forest), and sheep and cattle grazingproperties. Much of the area is subject to severe winter weatherwith snow and icy conditions, usually from about the middle ofMay to the middle of August. The average rainfall ranges from558 to 2343 mm and the mean daily temperatures in summerrange from 2.4 to 29.7oC and in winter from -5.6 to 11.1oC.9
The fauna of the region that may act as intermediate hosts forE granulosus includes, eastern grey kangaroos (Macropusgigantea), red necked wallabies (Macropus rufogriseus) andswamp wallabies (Wallabia bicolour), wombats, feral pigs andferal goats (Capra hircus). Carnivores are wild dogs, foxes andferal European domestic cats (Felis domesticus).
aAustralian Hydatid Control and Epidemiology Program,12 Mildura Street,Fyshwick, Australian Capital Territory 2609bRural Lands Protection Board, PO Box 10, Yass, New South Wales 2582

82 Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Scientific
losus as above.Intermediate hosts — Internal organs were examined in the
field for hydatid cysts that were opened and examined for thepresence of protoscoleces. Any small lesions that could not beidentified were preserved in 10% formalin for histologicalexamination.
The feral pigs were caught mainly by pig hunters usingtrained dogs; some were caught in pig traps set by feral animal;control officers of the Rural Lands Protection Boards (RLPB)and some were caught accidentally in traps set to catch wilddogs. The pigs were shot.
The macropodid marsupials were either shot under licencefrom the New South Wales National Parks and Wildlife Service,found dead on roads following collisions with motor vehicles orshot after being injured following accidental capture in traps setto catch wild dogs.
Feral goats were shot by Officers of the RLPB during thenormal course of their duties.
Four wombats (Vombatus ursinus) killed by vehicles on bushroads in Bondo State Forest were examined.
Determination of cyst fertility — Hydatid cysts were removedfrom the host, placed in a black plastic dish, cut open andexamined for the presence or absence of protoscoleces. Cystswith protoscoleces were considered fertile.
ResultsThe data are summarised in Tables 1 and 2. The numbers of
E granulosus in wild dogs were commonly several thousand; over300,000 were found in two males, over 200,000 in one femaleand over 100,000 in two males and one female. All the wilddogs with over 100,000 worms came from Bondo State Forest(Location 2). Small numbers of infected foxes were found infive of the locations (Table 1). The worm burden in foxes rarelyexceeded 50 worms. None of 23 feral cats was infected with Egranulosus.
Hydatid cysts in macropodids occurred mostly in the lungs,although cysts were present occasionally in the liver in easterngrey kangaroos. The number of fertile cysts was highest (100%)in both species of wallaby with volumes of protoscoleces from asingle cyst in swamp wallabies measuring up to 2 mLs. Hydatidinfection in swamp wallabies was often massive with cysts infil-trating large areas of pulmonary tissue and filling much of thethoracic cavity (Figure 2). In eastern grey kangaroos fromBondo Forest the proportion of fertile cysts was 75%. Somecysts were calcified or caseous.
Daughter cysts were not found in hydatids removed from anyof the macropodid species. Hydatid-infected feral pigs wererecovered in five localities. Hydatid cysts were found mostfrequently in the lungs although hepatic infection was also seenregularly and a single cyst was found in a kidney of one pig. Theproportion of fertile cysts recovered from feral pigs was low (15 to22%) compared to those from macropodids. Daughter cysts werepresent in lung cysts from two individuals. Hydatid infectionwas not found in any of the feral goats or wombats examined.
DiscussionThe data show that E granulosus infection occurs commonly
in wild dogs over a wide area in and around the KosciuszkoNational Park. The data also confirm previous studies fromother areas of Australia that the worm burdens in wild dogs arecommonly high (eastern Queensland,12 north-eastern
The area is a major tourist destination for snow sports in thewinter and other outdoor activities such as camping, hiking,horse riding and fishing from spring to autumn. In additionrecreational pig hunting is widespread in the area includingillegal pig hunting in the Kosciuszko National Park. Control offeral pigs, wild dogs and foxes is undertaken in some areas of theKosciuszko National Park, in adjacent state forest and on adja-cent privately owned farming country.
Collection and examination of hostsDefinitive hosts — Wild dogs, foxes and feral cats were caught
using leg-hold traps in which the inner holding surfaces of thetrap jaws were lined with rubber sleeves to minimise injuries tothe trapped animals10 in accordance with current animal welfarelegislation. Traps were visited daily and wild dogs or foxes wereshot while in the trap, all other species that were accidentallytrapped were released. Carcases of wild dogs, foxes and cats werekept cool and examined within 12 h. Parasite collection hasbeen described previously.11
Estimation of the worm burdens in wild dogs and foxes.The sieved intestinal contents of wild dogs were adjusted to 1 L
in a beaker. All E granulosus in each of two 50 mL sub-sampleswere counted separately in small volumes in a Petri dish using adissecting microscope. The intestinal contents of foxes werediluted to 500 mL and the whole volume examined for E granu-
Figure 1. Map of the study area indicating the survey locations(1-8). ACT = Australian Captial Territory; KNP = KosciuszkoNational Park.
6

Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 83
Scientific
Victoria6,8). The worm burdens of six of the wilddogs examined in this study were unusually largebeing in excess of 100,000 worms; all were fromBondo Forest (Location 2). The reasons for thisare unclear. Wild dogs from Crown Land arelikely to hunt across adjacent farms, predate onsheep and defecate in the paddocks. These wilddogs may be acting as a more important sourceof transmission of E granulosus to livestock andhumans in the region than is currently realised.
Foxes infected with E granulosus were recov-ered from five areas. The source of infection offoxes is likely to have been the result ofsecondary scavenging of macropodids killed bywild dogs, but foxes are able to kill smallermacropodid species for themselves.13 The smallnumbers of E granulosus in bush-dwelling foxesexamined in our study and in previousstudies6,14,15 indicate that the contribution offoxes with respect to contaminating the environ-ment with eggs of E granulosus is of little impor-tance. However, a study in 19948 reportedburdens of several thousand worms in each oftwo foxes from the Tallangatta area of north-eastern Victoria.
The presence of calcified and/or caseous cysts insome kangaroos indicates that the immune system ofthese individuals had been able to overwhelm the invading E gran-ulosus. No such indication was evident in any of either species ofwallaby examined.
The high prevalence of hydatid infection observed in swampwallabies suggests these animals may be particularly susceptibleto infection with E granulosus. Alternatively, there may be somebehavioural trait of swamp wallabies, not shared by otherspecies of macropodid marsupial that results in swamp wallabieshaving frequent exposure to eggs of E granulosus. Anecdotalreports from trappers of wild dogs, and other experiencesupported by limited documented data (Jenkins unpublished),suggest that swamp wallabies are attracted to the smell of dogfaeces. Trappers commonly use a lure containing dog faeces ontheir traps. Of the other species caught in dog traps throughout
eastern Victoria and south-eastern New South Wales.16 swampwallabies were the most commonly caught macropodid.
The site of predilection of hydatid cysts in wallabies, andcommonly in kangaroos, is the lungs, which may renderinfected hosts, particularly those with massive infection, moresusceptible to predation, through compromised lung function,see Figure 2. In Canada wolves catch a disproportionately largenumber of moose infected with pulmonary hydatidosis.17 Wilddogs have a strong dietary preference for swamp wallabies.18
This preference together with a high occurrence of hydatidinfection in swamp wallabies and the increased susceptibility ofhydatid-infected swamp wallabies to predation by wild dogs,strongly suggest that swamp wallabies are pivotal for main-taining E granulosus in wildlife in this region of Australia.
Table 1. Echinococcus granulosus recovered from naturally infected definitive and intermediate hosts collected from 8 locations in south-eastern NewSouth Wales.
Location Species
Wild dogs Foxes Feral Cats RNWa SWa EGKa Feral pigs
1) Wee Jasper/Burrinjuk 2/8b 0/46 0/5 ne 0/2 1/3 5/58
2) Bondo State Forest 64/73 11/24 0/9 7/23 20/29 4/15 23/47
3) N. Kosciuszko: 17/21 6/17 0/3 ne ne ne 20/70Peppercorn/Tantangarra
4) S. Kosciuszko: 2/4 ne ne ne 0/1 ne 0/2Saw Pit Creek
5) Brindabella Valley 12/21 3/14 0/6 0/2 1/3 1/1 1/3
6) Shannon’s Flat/Yaouk 18/63 1/22 ne 0/2 0/2 ne 3/24
7) Delegate 13/16 ne ne ne ne ne ne
8) Tumbarrumba 15/15 3/6 ne ne ne ne ne
Regional totals 143/221 24/129 0/23 7/27 21/37 6/19 52/204
aRNW = red necked wallaby; SW= swamp wallaby; EGK = eastern grey kangaroobnumber infected/number examined ne = not examined
Table 2. Worm burdens of Echinococcus granulosus in naturally infected wild dogs andfoxes from 8 locations in south-eastern New South Wales.
Location Species
Wild dogs Foxes
Male Female Male Female
1. Wee Jasper/Burrinjuk 2a 0 0 0150-1,670b
2. Bondo state Forest 22 42 4 7
150-309,750 10-302,580 2-33 1-42
3. N.Kosciuszko: 8 9 4 2 Peppercorn/Tantangara 10-7,073 10-45,000 2-24 10-45
4. S. Kosciuszko: 2 0 0 0Saw Pit Creek 1,820-7,200
5. Brindabella Valley 7 5 2 150-6,490 40-6,000 6-23 3
6. Shannon’s Flat/Yaouk 8 10 0 110-36,000 10-9,600 31
7. Delegate 9 4 0 020-17,685 800-18,413
8. Tumbarumba 6 9 1 2 910-27,200 40-69,200 2 6-54
anumber of animals examined.bworm burden range.

84 Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Scientific
ously. Other reports of human hydatidosis associated withwildlife include a case thought to have occurred via domesticdogs fed offal of kangaroos5 and a dingo trapper who wasthought to have become infected through handling the carcassesof dingoes infected with E granulosus.21 Other anecdotal reportsof hydatid infection in dingo trappers from eastern Victoriahave been mentioned in the literature.22
The Kosciuszko National Park is a major destination forpublic recreation and the high prevalence of E granulosus infec-tion in the wild canids resident in the Park constitutes a poten-tially important public health risk for visitors, Park staff andwildlife researchers. Direct physical contact with wild dogs andfoxes for visitors and Park staff is likely to be rare, but accidentalcontact with wild dog and/or fox faeces containing the infectiveeggs of E granulosus is much more likely, because wild dogs andfoxes frequently defecate on bush tracks and aroundpicnic/camping sites that are used by visitors and/or Park staff.The role of coprophagous flies in the transmission of eggs of Egranulosus from wild dog or fox faeces to humans has yet to beassessed. Flies have been shown capable of ingesting eggs oftaeniid cestodes and the eggs maintain their infectivityfollowing passage through flies.23
The eradication of E granulosus from the mainland ofAustralia is unlikely because of the extent of infection in wildlifethat are often in relatively inaccessible areas. A study inGermany, where meat baits containing praziquantel weredropped from aeroplanes over a defined area, demonstrated thatE multilocularis can be controlled in wild canid (fox) popula-tions.24 Although impractical over large areas, baiting of wilddogs and foxes with praziquantel in Australia in defined areas incertain national parks may be a useful control option.
The most important point for controlling transmission of Egranulosus to humans is in domestic situations. This is achievedmost efficiently through public education, regular worming ofdomestic dogs, restricting access of domestic dogs to raw offaland good personal hygiene.
AcknowledgmentsThe authors gratefully acknowledge the support and coopera-
tion of the New South Wales National Parks and WildlifeService and the Rural Lands Protection Boards of Bombala,Cooma and Yass throughout the study. Sincere thanks are alsoexpressed to Bill Osmond, John Coman, Michael Davis, NealSeagrim and Tim Russell for providing many of the specimensfor examination. Thanks to Australian National UniversityPhotography for preparing Figures 1 and 2. The financialsupport for part of this study was provided by the NationalHealth and Medical Research Council of Australia.
References1. Thompson RCA. Biology and systematics of Echinococcus In: ThompsonRCA, Lymbery AJ, editors. Echinococcus and Hydatid Disease. CABInternational, Wallingford, 1995:1-50.2. King HWH. Transhumant grazing in the snow belt of New South Wales. AustGeogr 1959;7:129-140.3. Gemmell MA. Hydatid disease in Australia III. Observations on the incidenceand geographical distribution of hydatidosis in sheep in New South Wales. AustVet J 1958;34:269-280.4. Corbett L. The Dingo in Australia and Asia. University of New South WalesPress, Sydney, 1995.5. Schantz PM, Chai J et al. Epidemiology and control of hydatid disease In:Thompson RCA, Lymbery AJ, editors. Echinococcus and Hydatid Disease.CAB International, Wallingford, 1995;233-331.6. Grainger HJ, Jenkins DJ. Transmission of hydatid disease to sheep from wilddogs in Victoria, Australia. Int J Parasitol 1996;26:1263-1270.
Our study found hydatid infection in feral pigs to be wide-spread (Table 1) with the highest prevalence in pigs from BondoState Forest (Area 2) and the northern end of the KosciuszkoNational Park (Area 3), areas with a high prevalence of E granu-losus infection in the wild dogs. In south–eastern Australia, wilddogs prey on pigs that are mainly less than one year old.16 Thispreference and the small number of adult pigs with fertile cystsindicates that the contribution of feral pigs to the transmissionof E granulosus in south-eastern Australia is likely to be small.However, in northern Queensland the contribution of pigs totransmission of E granulosus may be greater. In one study in thearea of Charters Towers, 31% were found infected and 70.1%of the cysts were fertile.19
Human hydatid disease still occurs regularly in easternAustralia.20 Data collected by the Australian Institute of Healthand Welfare (AIHW) recorded 89 new cases of human hydati-dosis, nationally, in 1996-7 (AIHW unpublished). In view ofthe amount of infection found in wildlife it is not unreasonableto speculate that a proportion of human cases occurring inAustralia are derived from wild dogs. Directly linking cases ofhuman hydatidosis to contact with wildlife is difficult. There isa long latent period from the time of infection to the time ofdiagnosis and human cyst material is genetically indistinguish-able from E granulosus cyst and adult worm tissue fromwildlife.7 In two cases of human hydatidosis investigated inQueensland,7 one person had had contact for 9 years withdomestic dogs fed offal from macropodids, whereas the otherhad had contact with a wild-caught dingo pup 5 years previ-
Figure 2. The lungs and liver from a swamp wallaby withpulmonary hydatidosis (note cysts also attached to the dorsalsurface of the diaphram). Bar = 1.5 cm.

Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 85
Scientific
7. Hope M, Bowles J, Prociv P, McManus DP. A genetic comparison of humanand wildlife isolates of Echinococcus granulosus in Queensland: public healthimplications. Med J Aust 1992;156:27-30. 8. Reichel MP, Lyford RA, Gasser RB. Hyperendemic focus of Echinococcus innorth-eastern Victoria. Med J Aust 1994;160:499-501.9. Annon. Climatic Averages. Metric edition. Australian Bureau of Meteorology,1975. 10. Meek PD, Jenkins DJ, Morris B, Ardler A, Hawksby R. Use of two leg-holdtraps for catching pest species. Wldl Res 1995;22:733-739.11. Jenkins DJ, Craig NA. The role of foxes (Vulpes vulpes) in the epidemiologyof Echinococcus granulosus in urban environments. Med J Aust 1992;157:754-756.12. Baldock FC, Thompson RCA, Kumartilake LM, Shield J. Echinococcusgranulosus in farm dogs and dingoes in south-eastern Queensland. Aust Vet J1985;62:335-337.13. Hornsby PE. Predation of the euro Macropus robustus (Marsupilia:Macropodidae) by European fox Vulpes vulpes (Placentalia; Candidae). AustMammal 1982;5:225-227.14. Thompson RCA, Nicholas WL, Howell MJ, Kumaritlake LM. Echinococcusin a fox. Aust Vet J 1985;62:200-201.15. Obendorf DL, Matheson MJ, Thompson RCA. Echinococcus granulosusinfection in foxes in south-eastern New South Wales. Aust Vet J 1989;66:123.16. Newsome AE, Corbett LK, Catling PC, Burt RJ. The feeding ecology of the
dingo 1. Stomach contents from trapping in south eastern Australia, and thenon-target wildlife also caught in dingo traps. Aust Wldl Res 1983;1:477-486.17. Mech LD. The Wolves of Isle Royale, Fauna of the National Parks of theUSA. Fauna Series 7. US Government Printing Office, Washington DC, 1966. 18. Robertshaw JD, Harden RH. The ecology of the dingo in north-eastern NewSouth Wales IV. Prey selection by dingoes, and its effect on the major preyspecies, the swamp wallaby, Wallabia bicolour (Desmarest). Aust Wldl Res1986;13:141-163.19. Lidetu D. Epidemiological, serological and histopathological studies onsylvatic hydatid disease in north Queensland. [MVSc Thesis]. James CookUniversity of North Queensland,1992.20. Jenkins DJ, Power K. Human hydatidosis in New South Wales and theAustralian Capital Territory, 1987- 1992. Med J Aust 1996;164:18-21.21. Taylor K. Hydatids in 1992: public health lesson. Update. Department ofHealth and community services, Victoria, 1993;2:63-64.22. Coman BJ. A sylvatic cycle for the hydatid tapeworm (Echinococcus granu-losus) in remote areas of eastern Victoria. Aust Vet J 1972b;48:552-553.23. Lawson R, Gemmell MA. The potential role of blowflies in the transmissionof taeniid tapeworm eggs. Parasitology 1985;91:129-143.24. Schelling U, Frank W, Will R, Romig T, Lucius R. Chemotherapy with prazi-quantel has the potential to reduce the prevalence of Echinococcus multilo-cularis in wild foxes (Vulpes vulpes). Ann Trop Med Parasit 1997;91:179-186.
(Accepted for publication 22 April 2002)
The University of MelbourneAllan K, Altmann JL, Appan A, Baird HL, Ballis P, Bennett MD,Bergfeld J, Blaszak JDH, Brettingham-Moore WE, Bruton AN,Chan FFL, Chan MW, Chow S, Crea DL, Enzinger KR, GleesonCJ, Golaszewski K, Grice JB, Hambrook LE, Hanlon CM, HayatPQ, Haynes SM, Hill MA, Ho AK, Holland JA, Innes SN, Ivens SN,Lau JMC, Llewelyn A, Maguire AK, Manning S, Meehan MC,Milne OJ, Mitchell DJ, Moore AJ, Narayan A, Niedzwiedzki ME,Oon KBB, Parker KI, Parkin G, Peacock RE, Pearce FL, PinfoldLD, Radihephi B, Reid SN, Remington SJ, Rich TC, Robson NM,Rostron AJ, Saunders LM, Siegel D, Simic T, Smithard RM,Sotirakopoulos AJ, Spencer TH, Stefani AJ, Stockil VW, StuckeyGI, Swietlik NH, Tepper KN, Thom LK, Torode JT, Tudor AB,Walker AL, Watts NJ, Way ASC, Wise IK, Woodruff MJ.
The University of QueenslandAhern BJ, Andrews JB, Atkinson LJ, Austin RS, Baldwin GI,Barbuto MA, Batten IJ, Beckett JB, Berger A, Berkeley YL, BriggRM, Brownhalls ST, Bucher AM, Cameron CM, Child V, ClaridgeSL, Cochrane JS, Cochrane LA, Conwell SA, Cook TR, CrotonCD, Davis AM, Delisser PJ, Dieu W, Duigan SA, Eyssens DJM,Ferrier-Watson SM, Fitzgerald CJ, Frasca ZE, Fredericks GC,Galloway KP, Gartrell WBM, Gates AV, Gotley BM, Grenfell JL,Hitchcock NKH, Hockey CD, Holmes MJ, Horne KL, Hourigan SE,Jackson KV, Johnston JL, Kemp EB, Kibbe JM, Kim DK, KocsisA, Lang JD, Martyn AK, Mashruwala U, McDonald KA, McGarryM, McIntosh KE, McKinnon XT, Miller J, Nalliah JR, Neale KL,Nicholson LJ, Norton CT, Ong EYH, Palmer IK, Palmer MJ, PercyCS, Reinders BG, Reineke LJ, Rourke AK, Schneider A, See AM,Serbanescu SO, Sharpe RM, Shearer DS, Shepherd DM,Silverstein MD, Simmons TJ, Smith J, Smith JA, Sutherland L,Swift IM, Szokolai KH, Thompson GMB, Thrower HR, Trezise CL,Wake KJ, Waldron CN, Ward JL, Watkins SD, White AJ, WilliamsNS, Wittwer CJ, Zondagh MG.
Murdoch University Applied Veterinary Medicineand SurgeryAnderson JM, Bentley TD, Beveridge HM, Bota KB, Bray NL,Briggs AE, Brodie AE, Castle RD, Cusworth WA, Dann SE, DaveyJS, De Carbonnieres J, Dow PA, Drury PJ, Edwards BG,Finkelstein J, Float CR, Goodall RT, Hanson JL, Henry JA,Jackson RL, Jones DR, Jones MJ, Kagan P, Keen ME, KeenihanEK, Kelman KR, Lang C, Lee JL, Lillis SM, Lim R, Linstead GG,Manickavasagar P, Mardell CH, Masterton TA, McGregor CC,Nanscawen ML, Neretti PM, Norman I, Olding NJ, Palmer CS,Prakash N, Roach EM, Rutland BE, Sceales LC, Seet DT, SextonSJ, Sharp CR, Spanoghe JJ, Stump HD, Thian LLA, Timmer T,Vaughan RJ, Warne FE, Wereszka MM, Williams ME, Wong S,Woolford L, Yap BMK.
The University of SydneyAhern TJ, Alexander MH, Andrews JP, Arnold CM, Bailey SP,Barfield DM, Barker DM, Bastian FA, Berman JDS, BlackshawJN, Bousaleh T, Bowland CL, Bramley EJ, Brown AL, CampbellGC, Colantonio D, Corbett J, Coyle CL, Drew MG, Drynan EA,Dwyer RL, Etel J, Fletcher AJ, Floyd TJ, Gerhardt AJ, Gidley BairdSE, Gleeson BL, Goh SSC, Grant JP, Greenwell CM, Haebich BL,Hales BM, Higgins KA, Ho GCK, Hogan AL, Hoshina S, Hsu ZM,Hynes CE, Ireland KA, Iwata DD, James CS, James DR, JamesK, Jang RM, Jol KAH, Jones LC, Kenny PJ, King YB, Knight GC,Larmor KE, Lawler MA, Lubans SR, Lutrell MJ, Lynch TA, MaherIE, Mason TE, Mazwiduma M, Ng CC, Norris JT, O’Connell A,Philipzen RK, Poon PSP, Reis SJ, Rich DS, Roberts DC,Robertson SM, Russell HC, Ruszczyk JM, Santos De Oliveira P,Smith BN, Smith JM, Smith WM, Soo T, Stanislaus CJ, Stayt J,Stead M, Streckfuss EM, Strinic D, Tarszisz E, Toyer CGJ, TsangMMW, Wearne CG, Woodward DJ, Yan EWL, Yeom WJ, Zylan K.
Graduates in Veterinary Science 2002

86
Scientific
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Effects of mating behaviour and the ovarian follicularstate of female alpacas on conception
JL VAUGHANa, KL MACMILLANb, GA ANDERSONb and MJ D’OCCHIOa
Objective To determine relationships between matingbehaviour, ovarian follicular state and successful conceptionin receptive female alpacas.
Procedure Seventy pen matings were observed at acommercial alpaca stud in south-western Victoria. The behav-iours observed included time taken to assume sternal recum-bency, mating duration, and evidence of nonreceptive behav-iour such as spitting, kicking and vocalisation. Ovarian follic-ular state was determined by ultrasonography, which wascomplemented by measuring plasma concentrations ofoestradiol and progesterone. Pregnancies were confirmed bytransabdominal ultrasonography between days 45 and 80after mating.
Results There were no significant differences betweenreceptive females that conceived and those that failed toconceive in the time taken to adopt the copulation position ofsternal recumbency, mating duration, or maximum folliclediameter. There was no significant relationship between timetaken to assume sternal recumbency (log10) and maximumfollicle diameter or plasma oestradiol (log10). However, therewas a significant quadratic relationship between plasmaoestradiol concentration (log10) and follicle diameter, and theprobability of pregnancy increased as the plasma concentra-tion of oestradiol (log10) at the time of mating increased.Females were sexually receptive most of the time in theabsence of a corpus luteum, and regardless of size of thelargest follicle or plasma concentration of oestradiol. Breed(Huacaya vs Suri), site of the dominant follicle (left or rightovary), lactation state, number of matings by the male (1 or 2),or interval between parturition and mating, did not affect preg-nancy outcome. Follicles with a diameter less than 7 mm wereable to ovulate in response to mating. This was smaller thanpreviously reported. Thirty-four pregnancies (49% pregnancyrate) resulted in 30 (88%) births with a gestation length of 343days (SEM ± 2, range 316-367 days). There were 4 (12%)abortions between days 45 and 80 of gestation and full term.
Conclusion It was not possible to correlate mating behav-iour and ovarian state with conception. To optimise pregnancyrates in receptive alpacas, matings need to occur in the pres-ence of an oestrogenic follicle that is capable of ovulation inresponse to mating. A simple method of detecting alpacaswith follicles in this state is not currently available and treat-ments that control ovarian follicular growth should thereforebe investigated.Aust Vet J 2003;81:86-90
The Australian alpaca industry relies almost exclusively onsingle-sire pen matings for breeding and geneticimprovement in the national herd. However, there is a
lack of information on the relationships between the matingbehaviour of females during pen matings and their underlying
reproductive state including stage of ovarian follicular growthand regression.1-3 Female alpacas are induced ovulators and donot have regular oestrous cycles that are typical of spontaneousovulators. Hence, alpacas do not exhibit distinct periods ofovert oestrus as do spontaneous ovulators such as cattle andsheep. The receptivity or nonreceptivity of a female alpaca to amale is therefore used to determine the appropriate time ofmating. This strategy is supported by reports that a minimumfollicle diameter of 7 mm is required for the induction of ovula-tion in alpacas,4 and that a follicle(s) of 6 to 7 mm is typicallypresent on at least one ovary at most times during successiveovarian follicular waves.5 This may explain why nonpregnantfemale alpacas appear receptive to males on most occasionswhen a male is introduced in a controlled mating situation.
Alpacas and closely related llamas without a corpus luteumwere found to show variability in sexual receptivity, regardless ofthe size of the largest follicle present on either ovary.4-9 Sumarand coworkers8 reported that alpacas with follicles of 5 to 6 mmdiameter were sexually receptive, but did not ovulate inresponse to mating. Some alpacas with follicles of 8 to 12 mmdiameter were nonreceptive, or relatively slow to mate. A lowcorrelation was found between plasma concentrations of oestra-diol, which was used as an index of follicle state, and sexualreceptivity in llamas.10 Similarly, there was no apparent relation-ship between urinary oestrone sulphate and sexual receptivity inllamas, even though oestrone sulphate accurately reflectedovarian follicular development.11
The objectives in the present study were to record the sexualreceptivity of female alpacas during pen matings typical of thealpaca industry in Australia and to establish relationshipsbetween mating behaviour, ovarian structures and plasmaconcentrations of oestradiol, with successful conception inreceptive females. The demonstration of relationships betweensexual receptivity, ovarian follicular state and conception, couldlead to the development of a test to determine the optimal timefor mating in female alpacas.
Materials and methodsThe experimental animals were mixed-age Huacaya and Suri
alpacas at a commercial establishment in south-west Victoria,Australia. All decisions on matings were determined by themanager to avoid bias of animal selection for the study.
Observations were made approximately weekly for a 12-month period from December 1998 to December 1999. Alpacaidentification, breed, lactation state, date, time of day, ambienttemperature, date of parturition and number of matings sinceparturition were recorded for each female. Information on ageand parity was not available for all animals. Each female wasobserved for the time (seconds) between when a male was intro-
aAnimal Sciences and Production Group, Central Queensland University,Rockhampton, Queensland 4702bVeterinary Clinical Centre, Department of Veterinary Science, University ofMelbourne, Werribee, Victoria 3030
17b-oestradiol OestradiolSITTIME Time taken by female to adopt sternal
recumbency

Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 87
Scientific
duced into the mating pen and when the female assumed thecopulation position of sternal recumbency. Females that did notassume sternal recumbency within 2 min were classified asnonreceptive. It was reported that failure to show receptivityafter 4 min usually resulted in a lack of mating.12 However, 2min was the limit used by management in the present study tominimise stress on females. Nonreceptive behaviour was charac-terised by spitting, kicking and vocalisation, sometimes withattempts to leave the mating pen.
Each male used for individual pen mating was identified. Theduration of copulation was defined as the time (min) elapsingfrom when the male and female first assumed the copulationposition until the male was standing again at the completion ofmating.
UltrasonographyWithin 2 h of mating the ovaries of each female were exam-
ined by transrectal ultrasound using an Aloka 500 (Aloka Co,Japan) ultrasonography machine with a 7.5 MHz linear arraytransducer. The size and relative position of follicles and corporalutea 3 mm diameter or greater were recorded. Ovaries withstructures less than 3 mm were recorded as ‘no visible structures’and were given a numerical value of 2 mm. The follicular dataare presented as the maximum vertical diameter (mm) of thelargest follicle observed for both ovaries, or for each ovary.Where possible, the transducer was placed adjacent to the ovarytransrectally directly by hand. In cases where the pelvic canalwas too narrow, the transducer was secured into a rigid plasticextension for transrectal ovarian examination. Nonreceptivefemales were not examined by ultrasonography if they had arecent mating history to avoid the risk of inducing embryonicmortality.
Pregnancy was diagnosed between days 45 and 80 aftermating by transabdominal ultrasound using a Pie Medical 200(Pie Medical, Japan) and subsequent parturition date recorded.
Blood sampling and hormone assaysA 10 mL blood sample was collected from the right jugular
vein of each animal included in the study into a heparinisedblood tube and placed immediately in crushed ice. Sampleswere centrifuged within 2 h and plasma removed and stored at -20°C until required for oestradiol and progesterone analyses.The blood sample was taken after ovarian ultrasonography. Asmall group of females was bled at the start of mating and thenagain after ultrasonography to determine whether there wereany significant changes in plasma oestradiol concentrations overthis period.
Plasma concentrations of oestradiol were measured using theEstradiol Maia RIA Kit® (Biochem Immunosystems, Italy). Alog-logit transformation was used to calculate oestradiolconcentrations.13 The sensitivity of the assay was 0.13 pg/mLand the intra-assay coefficient of variation was less than 20%over the range of 0.41 ± 0.03 to 19.5 ± 3.2 pg/mL. The inter-assay coefficients of variation for internal standard plasmasamples of 0.96, 3.17 and 6.29 pg/mL were 20, 11 and 11%,respectively.
Plasma concentrations of progesterone were measured in asingle assay using the Coat-A-Count RIA Progesterone® kit(Diagnostic Products Corporation, USA). The progesteroneconcentrations and quality control data were calculated usingthe computer program of Burger et al.13 The sensitivity was0.02 ng/mL and the intra-assay coefficient of variation was lessthan 20% over the range of 0.07 to 31.20 ng/mL.
Statistical analysesDescriptive statistics were obtained using Minitab® for
Windows Release 12.1 and Microsoft® Excel 97. Data weregenerally considered to be normally distributed, but were log10transformed when descriptive statistics indicated otherwise.Two sample t-tests were used to identify differences between themeans of the following variables: (a) SITTIME and pregnancystate; (b) mating duration and pregnancy state; (c) follicle diam-eter and pregnancy state; (d) plasma oestradiol and pregnancystate; (e) ambient temperature and pregnancy state; and (f )gestation length and breed.
A paired t-test was performed on premating and postmatingplasma concentrations of oestradiol. A Mann-Whitney test wasused to identify differences between the medians of days openand pregnancy state. Logistic regression14 and the likelihoodratio test were performed to determine the statistical signifi-cance of log10 oestradiol on the probability of pregnancy.
A quadratic regression was performed on log10 oestradiol (y)vs follicle diameter (x). Linear regressions were performed on:(a) log10 oestradiol vs log10 SITTIME; (b) follicle diameter vslog10 SITTIME; and, (c) postmating oestradiol vs prematingoestradiol. Because the plot of plasma oestradiol concentrationvs follicle diameter exhibited heterogeneity of variance, theconcentration data were log10-transformed. Regression equa-tions contain standard errors in parentheses.
Fisher’s exact test, as implemented by Stata® StatisticalSoftware Release 6.0, was used to compare categorical data: (a)follicle diameter less than or at least 10 mm and pregnancystate; (b) season and pregnancy state; (c) site of largest follicleand pregnancy state; (d) lactation state and pregnancy state;and, (e) breed and pregnancy state.
Statistical significance was set at P < 0.05 and results arepresented as mean ± SEM.
ResultsSeventy mating attempts were observed during the 12-month
period. There were 59 successful copulations involving the firstmating after parturition and 11 successful copulations involvingthe second mating after parturition when no information wasavailable on the first mating.
The linear regression of postmating (y) vs premating (x)plasma concentrations of oestradiol showed a positive associa-tion [y = – 0.01(SE 0.75) + 1.07(SE 0.15)x; r = 0.92; P < 0.001;n = 11]. Mean premating oestradiol concentration was 4.32 ±0.87 pg/mL and mean postmating oestradiol concentration was4.59 ± 1.0 pg/mL (difference = 0.28 ± 0.39; n = 11 pairs; P =0.49). The oestradiol concentrations of blood samples collectedat the time of ultrasonography were not significantly differentto those collected at the time of mating.
SITTIME, mating time and maximum follicle diameter forfemales that did or did not conceive were not significantlydifferent (Table 1).
The probability of pregnancy increased as plasma oestradiolconcentration increased
[logit of pregnancy = – 0.846(SE 0.423) + 1.883(SE0.800)x;
where x = log10 oestradiol; likelihood ratio statistic = 6.246; df =1; P = 0.012; area under receiver operating characteristic curve =0.65]. The sensitivity was 50 % (17/34) and the specificity was56 % (20/36) using a cut-off probability of pregnancy of 0.5.No pregnancies resulted from the seven matings that occurredwhen plasma oestradiol was less than 1 pg/mL.

88 Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Scientific
2), with a range of 316 to 367 days. Suri and Huacaya femaleshad similar conception rates followed by pregnancies of similargestation length (Table 5). The overall parturition rate was30/70 (43%).
During this study only seven females refused to mate with amale when the plasma progesterone was less than 1 ng/mL.Three of these females were maidens. The predominant signs ofrefusal were spitting and attempts to escape from the matingpen, while some females kicked. Among these seven femalesthere was no corpus luteum present on either ovary, the meanplasma concentration of oestradiol was 1.64 (SEM ± 0.67)and ranged from 0.42 to 5.48 pg/mL and maximum follic-
After adjusting for imbal-ances in temperature andfollicle diameter usinglogistic regression, log10oestradiol was still a signifi-cant predictor of pregnancy[logit of pregnancy = –2.370(SE 1.672) + 3.404(SE1.136; P = 0.003)log10oestradiol – 0.375(SE 0.150;P = 0.012)follicle diameter +0.207(SE 0.100; P =0.038)ambient temperature;area under receiver operatingcharacteristic curve = 0.77].
Thirty-four of 61 femaleswith a maximum folliclediameter < 10 mm becamepregnant whereas none of 9females with a maximumfollicle diameter of at least 10mm conceived (P = 0.0023;Table 2). If these 9 femaleswere excluded, the maximumfollicle diameter for pregnant(6.2 ± 0.4 mm) and non-pregnant (5.6 ± 0.4 mm)alpacas still did not differ (P= 0.27).
The average ambienttemperature was higher forthose alpacas that becamepregnant compared withthose that did not becomepregnant (Table 1). This wasassociated with a trend forhigher pregnancy rates insummer (Table 3). Theorigin of the oocyte from theleft or right ovary had no effect on the likelihood of pregnancy(P = 0.61). Sixteen of 29 (55%), 13 of 31 (42%) and 5 of 10(50%) pregnancies were associated with dominant follicles thatovulated from the left, the right or both ovaries, respectively.
The average pregnancy rate to a single mating was 34 of 70(49%) matings. There was no effect of lactation state at matingon pregnancy (P = 0.57). Nine of 16 (56 %) non-lactatingfemales and 25 of 54 (46 %) lactating females became pregnant.There was also no effect of the interval between parturition andmating on pregnancy rate (Table 4).
The quadratic regression of log10 plasma oestradiol concen-tration (y) and follicle diameter (x) was significant
(y = – 0.365(SE 0.168) + 0.202(SE 0.053)x – 0.011(SE0.004)x2, R2 = 0.30, P = 0.008, n = 70; Figure 1). The regres-sion predicted a maximum log10 plasma oestradiol concentra-tion of 0.563 (3.65 pg/mL oestradiol) when follicle diameterwas 9.2 mm. The linear regression coefficients for follicle diam-eter vs log10 SITTIME, and log10 plasma oestradiol vs log10SITTIME both approached zero.
Of the 34 alpacas found pregnant by transabdominal ultra-sonography between days 45 and 80 of gestation, 30 (88%)gave birth and four (12%) subsequently aborted at an unknownstage of gestation. The gestation length was 343 days (SEM ±
Table 1. Means (± SEM) and ranges of selected variables in females that either failed to become pregnant orbecame pregnant.
Variable Unit Non-pregnant Range Pregnant Range P-value(n = 36) (n = 34)
SITTIMEa sec 14.6 ± 2.7 1-76 17.9 ± 4.6 1-110 0.54
Log10 SITTIME log10 sec 0.86 ± 0.10 0.75 ± 0.12 0.57
Mating duration min 20.1 ± 1.4 6-46 20.2 ± 1.3 8-36 0.97
Follicle diameter mm 6.8 ± 0.5 < 3-13 6.2 ± 0.4 < -9 0.30
Plasma oestradiol pg/mL 2.84 ± 0.36 0.32-8.43 3.98 ± 0.45 1.26-9.96 0.05
Log10 oestradiol log10 pg/mL 0.32 ± 0.06 0.51 ± 0.05 0.01
Ambient temperature °C 15.2 ± 0.5 10-21 16.8 ± 0.6 11-24 0.03
aTime taken for female to adopt sternal recumbency after introduction of male.
Table 2. Maximum follicle diameters (mm) and plasma oestradiol concentrations (pg/mL, mean ± SEM) at the time ofmating in alpacas that did or did not become pregnant.
Follicle Non-pregnant (n = 36) Pregnant (n = 34) Pregnant
diametern Oestradiol Range n Oestradiol Range
(%)
< 3 5 0.71 ± 0.20 0.32 - 1.43 4 2.80 ± 1.20 1.38 - 6.42 44
3 2 1.34 ± 0.12 1.22 - 1.46 0 - - 0
4 0 - - 2 1.51 ± 0.26 1.26 - 1.77 100
5 4 1.70 ± 0.80 0.58 - 4.03 4 4.24 ± 1.40 2.09 - 8.27 50
6 5 3.67 ± 1.10 1.19 - 7.65 10 2.41 ± 0.22 1.47 - 3.51 67
7 4 2.70 ± 0.71 1.20 - 4.62 3 6.37 ± 2.10 2.78 - 9.96 43
8 7 3.72 ± 0.74 1.04 - 6.15 6 5.34 ± 1.40 1.81 - 9.82 46
9 0 - - 5 5.74 ± 0.83 3.65 - 8.42 100
10 6 4.69 ± 1.00 1.27 - 8.43 0 - - 0
11 1 0.82 - 0 - - 0
12 1 1.54 - 0 - - 0
13 1 3.66 - 0 - - 0
Table 3. Effect of season on pregnancy after a single mating in alpacas.
Season Non-pregnant Pregnant Pregnant(n = 36) (n = 34) (%)
Summer 5 13 72
Autumn 9 8 47
Winter 12 5 29
Spring 10 8 44
Fisher’s exact test P = 0.087

Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 89
Scientific
ular diameter was 3.6(SEM ± 0.8) and rangedfrom 2 to 7 mm.
DiscussionFemales that conceived
adopted the mating posi-tion of sternal recum-bency after a similar time to those that failed toconceive. Time taken to adopt sternal recumbencywas not a reliable indicator of either plasma oestradiolconcentration or maximum ovarian follicular diam-eter. Sternal recumbency was adopted and matingachieved in females with follicles ranging from < 3 to13 mm diameter and plasma oestradiol concentra-tions from 0.32 to 9.96 pg/mL. These findings are inaccordance with the observations made by someauthors that female alpacas are sexually receptivemost of the time in the absence of a corpus luteum8
and that there is no association between follicle diam-eter or plasma oestradiol concentration and recep-tivity.2,4,11 In contrast, other authors reported a rela-tionship between ovarian follicular growth andbehavioural receptivity in alpacas and llamas.5,6,9,10
The variability in sexual behaviour of female alpacashas been attributed to differences in geographic loca-tion, degree of domestication and social structure ofthe herd.15
Pregnancy in this study was associated with follicles< 10 mm diameter and plasma oestradiol concentra-tions greater than 1 pg/mL. The probability of preg-nancy increased as log10 oestradiol also increased.These findings suggest that the presence of an oestro-genic ovulatory follicle is required at the time of mating to opti-mise successful conceptions. Unfortunately, a single ultrasono-graphic examination of the ovaries could not be used to deter-mine optimum time of mating because it was impossible todetect whether the largest follicle was growing or regressing, orwhether it was producing oestrogen. This was supported by therelatively low correlation between log10 plasma oestradiolconcentration and follicle diameter (R = 0.47). The mean diam-eter of the largest ovarian follicle at mating in alpacas thatconceived was similar to the diameter in those that did notconceive (6 to 7 mm).
Peak oestradiol levels in the present study were predicted tooccur using quadratic regression when follicles were 9.2 mmdiameter. Alpacas with follicles of 11 to 13 mm diameter hadrelatively low plasma oestradiol. Other researchers observedpeak plasma concentrations of oestradiol occur when folliclesreach 7 to 8 mm diameter in alpacas, and follicles did notsecrete more oestradiol when 9 to 12 mm diameter.16 Folliclesgreater than 12 mm diameter lose their ability to secrete oestra-diol and may be regarded as cystic.17 In the current study, 10mm follicles still had an ability to secrete oestradiol but theymay have contained compromised oocytes as no pregnanciesresulted from matings in the presence of these follicles.Pregnancy rates in cattle have been shown to be reduced whenoocytes ovulated from follicles that exhibited a period of domi-nance longer than 9 days18 as oestradiol exerted an atretogeniceffect directly on the follicle.19
Bravo and coworkers4 reported that the minimum diameterat which follicles ovulated in response to mating in alpacas and
llamas was 7 mm. Observations in the present study suggestedthat follicles of < 3 to 9 mm diameter were capable of ovulation.There are at least two possible explanations for this discrepancy.Firstly, ultrasonographic data collection in the present study wasinaccurate despite efforts to optimise accuracy. Poor agreementwas reported within and between observers when examiningfollicles of less than 10 mm diameter using a 5 MHz linear arrayprobe in cattle.20 A single operator experienced with ovarianultrasonography in alpacas used a 7.5 MHz probe in the presentstudy in an attempt to minimise this problem. However, theremay have been a failure to measure the maximal cross-sectionalplane of some follicles as noted by Ginther,21 or some dominantfollicles may have been missed completely. When ultrasoundfollicular diameter measured in situ in ewes was compared withdissected diameters, one 5 mm and one 6 mm follicle weremissed using ultrasound in 11 ewes examined.22 Secondly,
Table 4. Median interval and ranges from parturition to day of first or second matings according to pregnancy outcomes.
Non-pregnant PregnantMating
n (days) Range n (days) Range P-value
First 29 52.0 17 - 190 30 50.5 21 - 366 0.77
Second 7 92.0 46 - 366 4 122.0 44 - 260 0.92
Table 5. Breed of female alpaca, outcome of matings and gestationlengths (mean ± SEM).
Breed Non-pregnant Pregnant Pregnant Gestation(%) days (n)
Suri 9 6 40a 343 ± 6 (5)b
Huacaya 27 28 51 343 ± 2 (25)
Total 36 34 49 343 ± 2 (30)
aFisher’s exact test was used to compare pregnancy rates between breeds,P = 0.56.bt-test was used to compare gestation lengths between breeds, P = 1.0.
Figure 1. Quadratic regression of log10 oestradiol and follicle diameter foralpacas that conceived (●) and alpacas failed to conceive (❍). y = -0.365(SE0.168) + 0.202(SE 0.053)x -0.011(SE 0.0004)x2, R2 = 0.30, P = 0.008, n = 70.

90 Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Scientific
References1. San-Martin M, Copaira M, Zuniga J et al. Aspects of reproduction in thealpaca. J Reprod Fertil 1968;16:395-399.2. Fernandez-Baca S, Madden DHL, Novoa C. Effect of different mating stimulion induction of ovulation in the alpaca. J Reprod Fertil 1970;22:261-267.3. Adams GP, Griffin PG, Ginther OJ. In situ morphologic dynamics of ovaries,uterus and cervix in llamas. Biol Reprod 1989;41:551-558. 4. Bravo PW, Stabenfeldt GH, Lasley BL, Fowler ME. The effect of ovarianfollicular size on pituitary and ovarian responses to copulation in domesticatedSouth American camelids. Biol Reprod 1991;45:553-559.5. Adams GP, Sumar J, Ginther OJ. Effects of lactational and reproductivestatus on ovarian follicular waves in llamas (Lama glama). J Reprod Fertil1990;90:535-545.6. Bravo PW, Sumar J. Laparoscopic examination of the ovarian activity inalpacas. Anim Reprod Sci 1989;21: 271-281.7. Bravo PW, Fowler ME, Lasley BL. The post-partum llama: Fertility after partu-rition. Biol Reprod 1994;51:1084-1087.8. Sumar J, Bravo PW, Foote WC. Sexual receptivity and time of ovulation inalpacas. Small Rumin Res 1993;11:143-150.9. Sumar JB, Adams GP. Reproductive anatomy and physiology of the femalellama. In: Youngquist RS (editor) Current therapy in large animal theri-ogenology. Saunders, Philadelphia, 1997:792-798.10. Leon JB, Smith BB, Timm KI. Correlation of hormonal and vaginal cytologychanges in the llama (Lama glama). In: 12th Int Congr Anim Reprod, TheNetherlands, 1992:972-974.11. Bravo PW, Stabenfeldt GH, Fowler ME, Lasley BL. Urinary steroids in theperiparturient and postpartum periods through early pregnancy in llamas.Theriogenology 1991;36:267-278.12. England BG, Foote WC, Cardozo AG, Matthews DH and Riera S. Oestrusand mating behaviour in the llama (Lama glama). Anim Behav 1971;19:722-726.13. Burger HG, Lee VWK, Rennie GC. A generalised computer program for thetreatment of data from competitive protein binding assays including radioim-munoassays. J Lab Clin Med 1972;80:302-312.14. Hosmer DW, Lemeshow S. Applied logistic regression. 2nd edition, Wiley,New York, 2000.15. Novoa C. Reproduction in Camelidae (Review). J Reprod Fertil 1970;22:3-20.16. Bravo PW, Pezo D, Alarcon V. Evaluation of early reproductive performancein the postpartum alpaca by progesterone concentrations. Anim Reprod Sci1995;39:71-77.17. Bravo PW, Stabenfeldt GH, Fowler ME, Lasley BL. Ovarian and endocrinepatterns associated with reproductive abnormalities in llamas and alpacas. JAm Vet Med Assoc 1993;202:268-272.18. Mihm M, Curran N, Hyttel P et al. Effect of dominant follicle persistence onfollicular fluid oestradiol and inhibin and on oocyte maturation in heifers. JReprod Fertil 1999;116:293-304.19. Dierschke DJ, Chaffin CL, Hutz RJ. Role and site of estrogen action in follic-ular atresia. Trends Endocrinol Metab 1994;5:215-219.20. Lean IJ, Abe N, Duggan S, Kingsford N. Within and between observeragreements on ultrasonic evaluation of bovine ovarian structures. Aust Vet J1992;69:279-282.21. Ginther OJ. Ultrasonic Imaging and Animal Reproduction: Cattle. Book 3.Equiservices Publishing, Cross Plains, WI, 1998:29-58.22. Evans ACO, Duffy P, Hynes N, Boland MP. Waves of follicle developmentduring the estrous cycle in sheep. Theriogenology 2000;53:699-715.23. Davis GH, Dodds KG, Moore GH, Bruce GD. Seasonal effects on gesta-tional length and birth weights in alpacas. Anim Reprod Sci 1997;46:297-303.24. Fernandez-Baca S, Novoa C, Sumar J. Actividad reproductiva an la alpacamantenida en separacion del macho. Mem ALPA 1972;7:7-18.25. Bravo PW, Varela MH. Prenatal development of the alpaca (Lama pacos).Anim Reprod Sci 1993;32:245-252.26. Aguero A, Miragaya MH, Ferrer MS, Capdevielle EF, Chaves MG, Rutter B.Follicular dynamics in Vicugna vicugna. Theriogenology 2001;55:379.27. Adams GP. Pregnancy Diagnosis in the Llama. In: Youngquist RS (editor)Current therapy in large animal theriogenology. Saunders, Philadelphia, 1997808-812.
(Accepted for publication 29 May 2002)
alpaca follicles may have the ability to ovulate at a smaller diam-eter than 7 mm. Pregnancies resulting from < 7 mm diameterfollicles in this study indicated that further investigation intothe ovulatory diameter of follicles is warranted.
The average ambient temperature was higher on those dayswhen females conceived. When the conception outcome wascategorised by season, the pregnancy rate was higher in summerthan in spring and autumn, and least in winter. A larger samplesize would need to be studied to make any conclusionsregarding effects of temperature on conception. Parturitionrates of 55/93 (59%) in spring (as a result of spring/summermatings) and of 97/146 (66%) in autumn have been reportedin New Zealand23 but summer and winter matings were notdiscussed. Although alpacas are considered non-seasonalbreeders when nutrition is adequate,24 they still tend to havemore follicles during the breeding season from January toMarch (summer to early autumn) in South America.6
Factors which did not affect pregnancy outcome in this studyincluded origin of the dominant follicle (left or right ovary),lactation state, breed and time taken to assume sternal recum-bency if less than 2 min. Pregnancies only occurred when thefemale was mated more than 20 days postpartum for at least 8min. Conceptions were evenly distributed between oocytes orig-inating from the left and right ovary. This agrees with previousfindings of ovulation frequency being equal from both ovaries1,6
even though 98% of pregnancies are situated in the left uterinehorn.25 Ten of 70 females (14%) exhibited follicles of the samediameter on both ovaries at the time of examination, almost halfthe frequency of ‘double dominant’ follicles observed in vicunas(8/32, 25%)26 and despite the rare event of twinning inalpacas.27
In summary, pregnancy in alpacas most often occurred whenmating of a receptive female coincided with the presence of anoestrogenic follicle. Simple detection of animals with follicles inthis state unfortunately is not currently possible. It wouldappear, however, that alpacas may have developed a mechanismto maximise the likelihood of follicles in this state as an overallpregnancy rate of 49% was achieved with single matings. Itmight be possible to further increase pregnancy rates to a singlemating in alpacas by controlling ovarian follicular growth so asto ensure the presence of an oestrogenic follicle at the time ofmating.
AcknowledgmentsThis research was supported by funding from the Rural
Industries Research and Development Corporation andResearch Services Office of Central Queensland University. Theauthors thank Ms Jude Anderson and Mr Alan Cousill (PucaraAlpaca Stud) for access to alpacas and assistance with observa-tions, Drs Denis Ryan and Mark Duncan (Torquay AnimalHouse Veterinary Clinic and Hospital) for expert technicaladvice and Mrs Fiona Amour (University of Melbourne) forassistance with hormone analyses.

91
Scientific
Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Prevalence of caseous lymphadenitis and usage ofcaseous lymphadenitis vaccines in sheep flocks
MW PATONa, SB WALKERb, IR ROSEa, and GF WATTc
Objective To estimate the prevalence of caseouslymphadenitis (CLA), determine the current usage of vaccinesagainst CLA and to measure the effectiveness of thesevaccines on sheep farms.
Design and population A survey was undertaken on 223sheep flocks in New South Wales, Victoria and WesternAustralia.
Method The prevalence of CLA was measured by conven-tional inspection techniques at abattoirs in lines of sheep thatcould be traced back to a farm. Managers of the flocks weresent a questionnaire about their vaccine practices, manage-ment practices and knowledge of CLA.
Results The average prevalence of CLA in adult sheep inthese flocks was 26% and varied from 20% in WesternAustralia to 29% in New South Wales. About 43% of sheepproducers used CLA vaccines; only 12% used them asrecommended. Awareness of CLA was highest in WesternAustralia. More producers would use CLA vaccine if theyknew the prevalence of CLA in their flock and producersobtained most information about CLA from vaccine resellers.
Conclusions Only 10 to 15% of producers are currentlyachieving effective CLA control through the use of recom-mended CLA vaccination programs. In Western Australianflocks more than 25% of effectively vaccinated ewes will besent to abattoirs in the 2 to 3 years after this study. However,large decreases in the prevalence of CLA can be achieved byabout 70% of producers by either making adjustments to theirvaccination programs or buying a vaccine with a CLA compo-nent. Two or three key facts on effective CLA vaccinationcould be made available at the point of sale of vaccines andfrom abattoirs that reported the prevalence of CLA to farmers.Aust Vet J 2003;81:91-95
CLA Caseous lymphadenitisAQIS Australian Quarantine and Inspection ServiceNSW New South WalesVIC VictoriaWA Western Australia.
CLA is a chronic disease of sheep and goats caused byCorynebacterium pseudotuberculosis. The disease causesabscesses in lymph nodes, lung tissue, and occasionally
other organs. It causes a 4 to 7% decrease in clean wool produc-tion in the year of infection,1 which results in an annual cost ofapproximately $15 million to the sheep industry.
The most direct cost of CLA is the total condemnation ofseverely affected sheep carcases. Other costs of meat inspectionand trimming of CLA affected carcases bring the total losses atabattoirs to $12 to 15 million annually.7
The average prevalence of CLA in Western Australian adultsheep has decreased since it was first measured in 1973 at 58%2
and in 1984 at 53%3 to about 27% in 1993.4 Although thisappears to be a pleasing decrease, the most recent study4 alsofound that the prevalence of CLA in flocks in which vaccinationwas not used had decreased to approximately 35%. This indi-cates that the decreases in the prevalence of CLA in vaccinatedflocks are not entirely due to vaccination.
The study of the prevalence of CLA in 19934 also indicatedthat only vaccination programs that followed the manufacturer’srecommendations produced low prevalence of CLA. A recom-mended CLA vaccination program constitutes two primingdoses (without being specific about their timing) to lambs andyearly boosters to adult sheep throughout their life.
This study was carried out to assess the adoption of vaccina-tion programs to control CLA in sheep killed at selected abat-toirs in three Australian States. The study compared the preva-lence of CLA in lines of adult sheep from flocks in some ofwhich different vaccination programs to control CLA wereused. It also assessed the producers’ knowledge of CLA, thesource of and application of this knowledge and sought infor-mation about management factors on the farms associated withthe prevalence of CLA.
Materials and methodsParticipants in the study were those who responded to a ques-
tionnaire sent to managers of lines of adult sheep inspected atselected abattoirs. These lines were examined in four abattoirs inNSW, (Dubbo, Goulburn, Blayney and Mudgee) one in VIC(Ararat) and two in WA (Lindley Valley and Katanning boththen operated by Metro Meats). The NSW abattoirs are the twolargest export mutton works and two of the smaller operations.The WA abattoirs were the only ones with export muttonlicences at the time of the study. The Ararat abattoir in VICmay not have been as representative as other abattoirs but linesinspected were from the main sheep growing areas in VIC.AQIS Veterinarians identified lines of more than 50 adultsheep. Fifty sequential carcases in each line were then assessedby standard AQIS techniques (Export Meat Manual Volume 3,Australian Quarantine and Inspection Service). The number ofinfected carcases was recorded and an estimate of the prevalenceof CLA in the flock of origin and the 95% confidence intervalwas calculated.
Questionnaires were mailed to the owner or manager of eachof the lines of sheep. These questionnaires had 34 questionsabout vaccination practices, producer knowledge and manage-ment practices relating to CLA. The questionnaire is availablefrom the senior author (Paton). The producers were informedthat they would be given the prevalence of CLA recorded intheir flock, upon receipt of the completed questionnaire.
The mean and confidence intervals for the average prevalenceof CLA in each state were calculated using @Risk (Version 3.5.2Palisade Corp. Newfield, NY USA) using the number of sheepper line and the number of lines assessed. Numerical results
aExotic Disease Preparedness & Animal Welfare, Western AustraliaDepartment of Agriculture, Locked Bag 4, Bentley Delivery Centre, WesternAustralia 6983bNSW Agriculture, PO 546, Gunnedah, New South Wales 2380cDepartment of Natural Resources and Environment, State GovernmentOffices, Ballarat, Victoria 3350

92 Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Scientific
such as prevalence comparisonswere analysed using one-wayanalysis of variance.
ResultsCharacteristics of the population
One hundred and forty-fourquestionnaires from NSW, 45 fromVIC and 34 from WA wereincluded in the study (Table 1).The response to the questionnaireswas 63, 85 and 71% in NSW, VICand WA respectively. The averageprevalence of CLA of lines recordedat abattoirs compared to that onfarms from which a questionnairewas returned did not vary by morethan 1%. The prevalence of CLA inlines recorded at abattoirs was 31%in NSW, 23% in VIC and 21% inWA whereas that on farms fromwhich questionnaires were returnedwas 32% in NSW, 22% in VIC and20% in WA.
Of the 223 flocks in this study,95% had at least one CLA affectedsheep in the line that was inspected(NSW 97%, VIC 91% and WA88%). Of the lines inspected, 60%of sheep were 5 years or older, 20%were mixed ages, 15% 4 years oldand 5% were 3 years or younger. The only marked differencebetween States in this age pattern was that 44% of lines fromWA were mixed ages. The type of sheep was recorded as ewes,wethers or mixed lines. In WA all lines were ewes. At the fourabattoirs in NSW 51% were wethers, 31% ewes and 18%mixed lines whereas at the one in VIC, 62% were wethers, 32%ewes and 6% mixed lines. The percentage of sheep bred on theproperty was highest in lines from the Victorian abattoir, wherethere were 80% in this category. In WA and NSW 59% of thesheep were bred on the property of origin.
Vaccine usageIn the questionnaire, producers were asked whether they used
any one of three types of vaccine to control CLA and/orclostridial infections. These were 3-in-1, vaccines that protectagainst enterotoxaemia, tetanus and CLA, 5-in-1 that protectagainst enterotoxaemia, tetanus, infectious necrotic hepatitis,malignant oedema and blackleg and 6-in-1 that protects againstthese five diseases and CLA. Table 2 shows the percentage ofproducers using different vaccines or using no vaccine. Of thelines of sheep inspected at abattoirs, 31, 29 and 38% in NSW,VIC and WA respectively, had ever been vaccinated with anyCLA vaccine. However in 43% of all flocks, CLA vaccine wasbeing used. Some of these vaccinated sheep had not yet reachedslaughter age (Table 2).
The percentage of CLA vaccine users that had the recom-mended vaccination program in place for ewes was muchsmaller and even less for wethers. Only 6% of farms arecurrently turning off sheep vaccinated according to the manu-facturer’s recommendations (Table 2).
The percentage of producers using different elements of good
vaccination programs for ewes or wethers was examined.Overall, 58% of farms were giving two doses of vaccine tolambs (NSW 56%, VIC 59%, WA 70%). The percentage ofproducers giving yearly boosters to ewes was 50% (NSW 50%,VIC 35%, WA 65%) whereas only 38% administered yearlyboosters to wethers (NSW 38%, VIC 35%, WA 40%).
Producers supplying the four abattoirs in NSW had differentusage schedules for CLA vaccination. The percentages of flocksin which CLA vaccination was used were 42 and 50% forDubbo and Goulburn and 35 and 29% for Blayney andMudgee respectively. The percentage of flocks using recom-mended CLA vaccination programs was 7 and 8% for Dubboand Goulburn and zero for both Blayney and Mudgee.
The timing of yearly booster vaccinations was also examined.For ewes, 34% of flocks were given boosters at or immediatelybefore shearing, 33% in the 3 week to 6 month period before
Table 3. Average prevalence of CLA in lines of sheep from flocks inwhich different CLA vaccination programs are used.
Vaccination program Average prevalenceof CLA (%)
Sheep not given any CLA vaccination 29
Sheep given one dose as lambs with no boosters 31
Sheep given two doses as lambs with no boosters 22
Sheep given one dose as lambs with boosters 33
Sheep given two doses as lambs with boosters 3
Table 2. Percentage of producers in three States using different vaccines against sheep diseases and thepercentage of flocks that use CLA vaccine, those sending sheep vaccinated with a recommended CLAprogram to abattoirs during the study and those with recommended CLA vaccination programs for ewesand for wethers.
State Type of Vaccine used (%) Percentage of flocks vaccinated against CLA
Nil 3-in-1a 5-in-1b 6-in-1c Total Recommended program Recommended programin sheep inspected commenced
at abattoir
Ewes Wethers
WA 41 47 3 9 56 9 27 15
NSW 29 3 28 40 43 6 10 8
VIC 9 2 53 36 38 4 13 9
Overall 22 10 32 36 43 6 14 9
a3 in 1 vaccines control CLA, tetanus and enterotoxaemia.b5 in 1 vaccines control enterotoxaemia, tetanus, infectious necrotic hepatitis, malignant oedema and blackleg.c6 in 1 vaccines control CLA, enterotoxaemia, tetanus, infectious necrotic hepatitis, malignant oedema and blackleg.
Table 1. Average prevalence of CLA in all flocks, flocks no using CLA vaccination and flocks with non-recommended and recommended CLA vaccination programs.
State No. of Flocks Average prevalence of CLA (%)
All flocks Flocks with no CLA Flocks with non- Flocks withvaccination programs recommended CLA recommended CLA
vaccination programs vaccination programs
WA 34 20 24 22 1
NSW 144 29 32 31 4
VIC 45 23 22 23 5
Overall 26 29 28 3

Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 93
Scientific
When asked, to what extent CLA affects the profitability oftheir flock, 60% thought it was of little or no significance(NSW 66%, VIC 70% and WA 30%). Thirty-four percent saidit caused slight production loss (NSW 28%, VIC 30% and WA57%). Only 4% of producers (NSW 5%, VIC 0% and WA9%) thought it caused moderate production losses, whereas 1NSW producer thought it caused serious production losses.
Producers were asked about their awareness of the effects ofCLA on the their enterprises. When asked if they were awarethat CLA reduces wool production, 58% replied “yes” (NSW56%, VIC 52% and WA 74%). Seventy-nine percent said theywere aware that CLA was a cause of condemnation of sheepcarcases (NSW 77%, VIC 72% and WA 97%). Only 38% wereaware that CLA causes about $3M loss in carcase trimming(NSW producers were not asked this question and 24% of VICand 53% of WA producers were aware). Only 12% of farmerswere aware of the abattoir inspection cost due to CLA (VIC 7%and WA 18%). This question not asked in NSW. Forty-fourpercent of producers were aware that estimated losses due toCLA were averaged over all prices offered for adult sheep (50%NSW, 20% VIC and 50% WA).
When producers were asked what information would be mostlikely to persuade them to change to an effective CLA vaccina-tion program, producers ranked the issues according to the listshown in Table 6. The importance producers placed on theseissues did not vary markedly between VIC and WA (NSWproducers were not asked this question).
Less than a third of producers had sought advice on CLA inthe past 3 years (NSW 31%, VIC 32% and WA 27%).Producers sought this advice from the sources shown in Table 7.
Seventy-seven percent of producers did not seek advice onCLA because they saw no need to vaccinate.
DiscussionThe most significant finding of this study was that although
43% of producers use vaccination to control CLA in their sheep,only about 12% have recommended CLA vaccination programs
shearing and 33% in the 6 months after shearing. For wethers,24% were vaccinated just before or at shearing, 29% in the 3weeks to 6 months before shearing and 48% in the 6 monthsafter shearing.
Prevalence of CLATable 1 shows the overall and State average prevalence of CLA
for all sheep flocks, those in which no CLA vaccination is used,those in which non-recommended CLA vaccination programshad been used and those in which recommended CLA vaccina-tion programs had been used. The average prevalence of CLA inflocks in which some different vaccination program optionswere combined, is shown in Table 3. The 95% confidence inter-vals of the average prevalence of CLA from the selected abattoirsin each state were 28.2 to 30.0 (NSW), 21.1 to 24.0 (VIC) and18.5 to 21.6 (WA).
On farms where recommended CLA vaccination programswere used, sheep given CLA boosters in the 6 months beforeshearing had an average prevalence of CLA of 5%. Sheep vacci-nated at shearing or in the 6 months after shearing had anaverage prevalence of CLA of 15%. However these averageswere not significantly different (P = 0.15).
The prevalence of CLA in different classes of sheep thatreceived no CLA vaccine was similar. There was an averageprevalence of 29% among ewes and 28% among wethers. InNSW the sample size was sufficiently large to show differencesin the prevalences measured at the four abattoirs. Producerssupplying these abattoirs had different usage schedules of CLAvaccination and different average prevalence of CLA. Linessupplied to the Dubbo and Goulburn abattoirs both had anaverage prevalence of CLA of 22% whereas those supplied toBlayney and Mudgee abattoirs had average prevalence of CLAof 50 and 43% respectively. When flocks using no CLA vaccinewere examined, Dubbo and Goulburn abattoirs also had loweraverage prevalences of CLA (25 and 27% respectively) thanBlayney and Mudgee (53 and 44% respectively).
Because CLA is spread by dipping,5 the control practices forlice were also examined. A summary of these practices and theaverage prevalences of CLA associated with them are in Table 4.Flocks in which no lice control was used had approximately halfthe prevalence of CLA of flocks using any form of lice control.
Producer knowledge and beliefsThe reasons why producers do not use CLA vaccine are
summarised in Table 5. Producers were also asked about theirawareness of CLA and issues associated with this disease. Forty-seven percent of producers had read literature produced by theState agricultural agency on CLA (NSW 37%, VIC 45% andWA 85%). Sixty-four percent of producers had read literaturefrom vaccine companies on CLA (NSW 65%, VIC 55% andWA 71%).
Seventy-one percent of producers (NSW 68%, VIC 71% andWA 76%) thought CLA was present in their flock, whereas20% of WA producers were prepared to admit they did notknow. Of those who thought CLA was not present, only 14%were correct and of the producers who thought their flock hadCLA, only 3% did not. The average prevalence of CLA in flocksin which producers believed they did not have CLA was 20%whereas the average in those flocks owned by producers whobelieved they did have it was 28%. Of the 223 flocks in thisstudy, 95% had CLA in the inspected sheep (NSW 97%, VIC91% and WA 88%).
Table 4. Prevalence of CLA in flocks with different practices for lice control.
Lice control Percentage of producers Average prevalencemethod using this method of CLA (%)
None 6 14
Plunge dip 37 29
Shower dip 39 31
Backline 22 27
Table 5. Reasons why producers in NSW, VIC and WA do not use avaccine against CLA.
Percentage of producers choosing this reason
Reason NSW VIC WA Overall
Never see CLA in this class of sheep 17 22 9 17
See CLA, but don’t believe it causes a 14 11 12 13significant loss
Extra cost of CLA component in the vaccine 8 16 0 9
Already using 5-in-1 for cattle 6 2 3 5
Prevalence CLA is known to be low from 2 0 0 1abattoir data

94 Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Scientific
that will decrease their prevalence of CLA. The finding thatonly 9% of producers were sending effectively vaccinated sheepto abattoirs at the time of the survey was disappointing.However, it was more encouraging that this can be expected toincrease to 14% overall and nearly double from 15 to 27% inWA 2 to 4 years after the study when ewes vaccinated accordingto recommended CLA programs are culled for age.
The inferences drawn from the prevalence of CLA in lines ofsheep inspected in this study can be shown to be a reasonablerepresentation of the Australian sheep flock. The 95% confi-dence intervals for the average prevalence for each state werewithin 2% in NSW and within 3 % in the other States. Thisprovides a measure of the accuracy of the estimated prevalencein adult sheep only, because all but 5% were older than 3 years.CLA spreads mostly at the second and third shearing6 so theprevalence of CLA is fairly constant as the age of sheep increasesfrom 3 to 6 years old and does not vary markedly betweenyears.7
There were some important differences between States andabattoirs in this study. Of lines of sheep killed at selected abat-toirs in NSW and VIC, more than 50% were wethers, whereasin WA no wether lines were assessed. This is largely due to thepurchase of wethers for export as live animals from WA. Thecomparison of the prevalence of CLA between ewes and wethersmay be biased to some extent because of the over-representationof data from the Dubbo abattoir in this study. Dubbo abattoirseeks to buy wethers from flocks with no record of lines with ahigh prevalence of CLA (R Fletcher, Fletcher International,personal communication). This is partly borne out by the loweraverage prevalence of CLA of lines from Dubbo compared toBlayney and Mudgee, even in unvaccinated sheep. These differ-ences may also be a reflection of the abattoir’s policy ofeducating producers about CLA control. This may also indicatethe possibility of some bias in the data from WA and VIC. Thelines of sheep in these States came from either one abattoir, in thecase of VIC, or two abattoirs owned by one company in WA.
A potential problem in assessing and assuring the applicationof recommended vaccination programs for CLA was that 59%
of lines in NSW and WA were not bred on the property oforigin. The high proportions of sheep not given two doses aslambs (mentioned earlier) indicate that starting a CLA vaccina-tion program in sheep, after they are purchased, is unlikely toresult in a low prevalence of CLA. This is particularly relevant ifno vaccination history of purchased sheep is known, given thelow proportion of effectively vaccinated sheep in the popula-tion.
One encouraging aspect of this study is that a high propor-tion of producers use vaccine against CLA. If the informationabout effective CLA vaccination is available from agents whosell vaccine, sheep producers can adopt the recommended vacci-nation programs. Forty-three percent of producers already buyproduct that can control CLA and an additional 30% buy avaccine that does not protect against CLA (5-in-1). Only 27%of producers (NSW 29%, VIC 9% and WA 41%) do not vacci-nate their sheep and would therefore need to be informed aboutCLA control from a source other than vaccine sellers to inducethem to start to use vaccination against CLA.
The deficiencies identified in vaccination programs indifferent States can be used to improve extension programs inthese areas. For example a small proportion of producers gaveyearly boosters in VIC. Giving yearly boosters to wethers is alsoan issue that could be the subject of improved extension.
An important finding of this study is that only when twodoses are given to lambs and then yearly boosters are given toadult sheep is the prevalence of CLA reduced. The best resultobtained with an non-recommended vaccination program was areduction in the prevalence of CLA from 29% in unvaccinatedsheep to 22% in sheep that received two doses of vaccine aslambs but no yearly boosters. This difference was not significant(P = 0.66). In comparison to an average reduction in CLAprevalence from 29% to 3% was achieved for a recommendedprogram.
The effect of timing for yearly boosters could be important,because of the high proportion of flocks giving boosters atshearing or more than 6 months before shearing. Evidence of ahigher prevalence of CLA in one research station flock4
supports the suggestion that this practice decreases the effi-ciency of CLA control. The average prevalence of 5% for flocksin which boosters were given in the 6 months before shearingwas one third of the 15% average in flocks in which boosterswere given at or more than 6 months before shearing. This indi-cates that this aspect of effective CLA control should beincluded in extension programs.
The finding that flocks not dipped for lice had lower averageprevalence of CLA was consistent with other studies5 but it issomewhat surprising that flocks treated with backlines hadhigher prevalence of CLA. This may arise because backlinetreatment is more likely to be applied immediately aftershearing, which necessitates sheep being kept together longerafter shearing. This would give a greater opportunity for CLAspread via sheep coughing infected material onto shearing cutsof uninfected sheep.6
The awareness of CLA as a problem seems to be higheramong producers in WA, coinciding with the lower averageprevalence there. More producers in WA have read literature onCLA. Over half of WA producers thought CLA caused slightproduction loss compared with 28 and 30% in NSW and VICrespectively. Approximately 20% more WA producers wereaware of most losses during meat processing due to CLAcompared with other States. The exception to this was that 50%
Table 6. Issues or information that sheep producers consider most likelyto persuade them to adopt effective vaccination against CLA.
Issue Ranked first (%)
Prevalence of CLA in their flock 29
Buyers pay more for sheep without CLA 26
Economic losses and their prevalence of CLA 21
Detail of economic losses caused by CLA 16
Average CLA prevalence in the area 8
Table 7. Percentage of producers using different sources of informationon the control CLA, in three States.
Source of information Percentage of producers
Overall NSW VIC WA
Merchandise agent/ vaccine retailer 40 29 55 70
Vaccine manufacturer’s representative 20 22 20 10
State agricultural agency veterinarian 20 27 10 -
Private veterinarian 14 16 5 20
Other producer 6 5 10 -

Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 95
Scientific
three key facts on effective CLA vaccination could be availableat the point of sale of vaccines and from abattoirs along withinformation on the prevalence of CLA. This information canimprove producers’ motivation and knowledge for controllingCLA. The prevalence of CLA could then decrease dramaticallyin the next 5 years and the investments made in vaccines wouldbe returned to producers and processors.
AcknowledgmentsWe acknowledge the generous support of the Meat Research
Corporation for funding this research. We thank the manage-ment of all the abattoirs where data was collected during thisproject and the producers who took the time to fill out thequestionnaires. We also thank the meat inspectors and otherAustralian Quarantine and Inspection Service staff for recordingthe data used for this project.
References1. Paton MW, Rose IR, Hart RA et al. New infection with Corynebacteriumpseudotuberculosis reduces wool production. Aust Vet J 1994;71:47-49.2. Robertson JP Studies on diagnosis, epidemiology and immunity ofCorynebacterium pseudotuberculosis infection in sheep [MPhil thesis]. MurdochUniversity, Western Australia,1980.3. Batey RG. Frequency and consequence of caseous lymphadenitis in sheepand lambs slaughtered at a Western Australian abattoir. Am J Vet Res1986;47:482-485.4. Paton MW, Sutherland SS, Ellis TM, Mercy AR. Extending CLA control toAustralian sheep farmers. In: Proceedings of Australia Sheep VeterinarySociety, Australian Veterinary Association Conference, Canberra. AustralianVeterinary Association, 1994;34-36.5. Paton MW, Rose IR, Hart RA et al. T.M. Post- shearing management effectsthe seroincidence of infection with Corynebacterium pseudotuberculosis. PrevVet Med 1996;26:275-284.6. Paton MW, Rose IR, Hart RA et al. The spread of Corynebacterium pseudo-tuberculosis infection to unvaccinated and vaccinated sheep. Aust Vet J1995;72:266-269.7. Paton MW, Mercy AR, Sutherland SS et al. Vaccination and post-shearingmanagement to control CLA. In: Proceedings of the Australian SheepVeterinary Society, Australian Veterinary Association Conference, Gold Coast,Australian Veterinary Association, 1993;101-106.
(Accepted for publication 10 July 2003)
of both NSW and WA producers were aware that assumedlosses due to CLA were included in mutton prices comparedwith a 20% awareness of this in VIC. This higher awareness inNSW may be due to extension programs about meat qualityissues provided to producers by the operators of Dubbo andGoulburn abattoirs.
Producers who did not use CLA vaccine failed to do somostly because they never see CLA in their sheep. This is notsurprising because producers seldom visit abattoirs where CLAis seen as a problem. However, the reasons vary betweenproducers in different States. More WA producers are aware ofCLA even though some are still unaware of its economic effects.Producers in VIC were more concerned by the small extra costof CLA vaccine than those in NSW. This is not an issue in WAbecause only a negligible amount of vaccine without a CLAcomponent (5-in-1) is available to sheep producers. The lowpercentage of producers who correctly thought they did nothave CLA emphasises the problem of awareness associated withthe lack of clinical signs of CLA.
Of producers who did not use CLA vaccine, there are morethat would be persuaded to start an effective program if theirprevalence of CLA was communicated to them. This indicatesthat simple and effective transfer of information can affectproducers’ attitude to controlling this problem. The next mostpopular incentive to change to CLA vaccination would be ifbuyers paid more for sheep with a low prevalence of CLA. Ifprocessors collected information on the prevalence of CLA toconvey to producers, then they could pay more to producerswith flocks with low CLA prevalence.
Retailers who sell vaccine are the most popular source ofinformation on CLA control by a factor of two. It is probablethat these retailers have the least knowledge of CLA vaccinationissues, so improving their knowledge would increase the use ofvaccination against CLA.
Large decreases in the prevalence of CLA could be achievedby about 70% of producers by either making adjustments totheir vaccination programs or using a different vaccine. Two or
Polysaccharide storage myopathy in the M longissimus lumborum of showjumpers and dressage horseswith back pain.
Designed to investigate whether horses with clinical signs of back pain due to suspected soft tissue injuries were affected bypolysaccharide storage myopathy (PSSM), this study of muscle biopsies from the M longissimus lumborum of 5
showjumpers and 4 dressage horses with back pain is reported. Histopathological and electron microspical examinations werecompared with the results of M gluteus biopsies from the same horses. Further comparison was made with M g3luteus biopsiesof 6 Standardbreds with recurrent exertional rhabdomyolysis and from 6 healthy trotters. M longissimus biopsies from horseswith back pain showed pathognomonic signs of PSSM involving high glycogen and/or abnormal complex amylase-resistant poly-saccharide deposits. The M gluteus biopsies from the same horses also showed similar features. The biopsies from horses withrhabdomyolysis displayed increased PAS stain compared to healthy horses but did not show amylase-resistant material.
The authors conclude that epaxial muscle biopsy is an option in the aetiological investigation of this condition in horsesengaged in these activities when clinical examination and imaging techniques have failed to produce a precise diagnosis.
Quiroz-Rothe E et al. Equine Vet J 2002;43:171-176.

96 Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Scientific
Infectious coryza due to Haemophilusparagallinarum serovar B in China
P-J ZHANG Institute for Animal HusbandryM MIAO and Veterinary Science,H SUN Beijing Academy of AgriculturalY GONG and Forestry Sciences,
Beijing, China
PJ BLACKALL Agency for Food and Fibre Sciences,Queensland Department of Primary Industries,Animal Research Institute,Yeerongpilly, Queensland 4105
Aust Vet J 2003;81:96-97
Infectious coryza, a disease of the upper respiratory tract ofchickens, is caused by Haemophilus paragallinarum.1 The clin-
ical signs of the disease include nasal discharge, facial swellingand a reduction in feed and water consumption.1 Infectiouscoryza in poultry is a disease of economic significance in manyparts of the world with the greatest economic losses resultingfrom an increased number of culls and marked reduction (10 to40%) in egg production.1 The most widely used serological clas-sification scheme for H paragallinarum is the Page scheme,which recognises three different serovars, termed A, B and C.2
The importance of the Page scheme is that inactivated vaccinesprotect only against those serovars present in the vaccine.1
There have been few studies performed in China on the sero-logical characterisation of H paragallinarum isolates. All 29Chinese isolates of H paragallinarum that have been examinedto date have been shown to be serovar A.3-5 We report the firstisolation of H paragallinarum serovar B from an outbreak ofinfectious coryza in China.
A large 100,000 layer flock located in Liaoning Province hada history of outbreaks of a respiratory disease in successiveflocks. The clinical signs of swollen sinuses, nasal and oculardischarge were suggestive of infectious coryza. A number ofdifferent, commercial infectious coryza vaccines were tried withno obvious effect on the disease. In 2001, the flock suffered anoutbreak in which 50% of the 100,000 birds (130 to 300 daysold) showed the typical clinical signs. The mortality associatedwith the outbreak was estimated to be between 2 to 5%. Theoutbreak caused an average 10% drop in egg production.
A satellitic non-haemolytic isolate was obtained in pureculture from the sinus of each of three chickens. The isolaterequired increased CO2 for growth. The isolate was a Gram-negative short rod or coccobacillus that was catalase negative.The organism was confirmed as H paragallinarum by using aPCR test known to be specific for H paragallinarum.6 The testwas performed using a colony preparation as previouslydescribed.6 Only one of the three isolates could be maintainedin subculture. This isolate was transferred to the AnimalResearch Institute, Queensland and was shown to be Pageserovar B using a haemagglutination–inhibition test.7
The pathogenicity of the isolate that was typed as serovar Bwas examined, in China, using 60-day-old commercial layerchickens from a farm with no history of infectious coryza, nouse of infectious coryza vaccine and which was regularly tested
as negative in the H paragallinarum serovar A and serovar Cblocking ELISA.8 Each of the four chickens used was inocu-lated, via the infra-orbital sinus, with 0.2 mL of an overnightbroth culture corresponding to a dose of around 8 x 106 colonyforming units per chicken. Two days after the challenge, all fourchickens showed the typical clinical signs of infectiouscoryza. Three days after challenge, the nasal exudate from eachchicken was tested using the species-specific H paragallinarumPCR test as previously described.6 As well, the nasal exudate wascultured onto the medium described by Kume et al,9 which wasincubated in a candle jar for up to 48 h. Suspect H paragalli-narum-like colonies from the Kume medium were confirmed bythe species-specific H paragallinarum PCR. All four chickenswere positive in the nasal swab examined directly by PCR andall four chickens yielded H paragallinarum colonies that wereconfirmed by PCR.
This isolate of H paragallinarum is the first reported occur-rence of serovar B in China. The only previous serological char-acterisations of Chinese isolates of H paragallinarum reportedthe presence of serovar A only.3-5 Our finding of serovar B hasseveral important practical implications for the Chinese poultryindustry. Page serovar B isolates show little cross-immunity withserovars A and C.10 Hence, infectious coryza vaccines based onserovar A and/or C have little chance of providing protectionagainst a Page serovar B challenge. A further complication isthat, within Page serovar B, some isolates show limited cross-protection.10 Hence, the presence of serovar B in a largecommercial layer chicken farm in China indicates that there is aneed for careful selection of the seed strains used to produceinfectious coryza vaccines for use in China. In particular, unlessthere is specific knowledge of the serovars present in the targetpopulation, the use of bivalent vaccines that contain only Pageserovars A and C cannot be recommended in China. We esti-mate that the majority of infectious coryza vaccines in use inChina are based on serovar A alone or serovars A and C. As anexample, our isolate was obtained from a farm with a repeatedhistory of infectious coryza-like outbreaks despite regular use ofinactivated infectious coryza vaccines based on serovars A andC. Clearly, the strains to be included in infectious coryzavaccines used on poultry farms in China need to be carefullyconsidered.
There is a report that the reference strain H paragallinarumfor serovar B, 0222, is non-pathogenic.11 We have found thatour field isolate of Page serovar B is fully pathogenic; a similarfinding has been reported for other Page serovar B isolates.12,13
Other than the single report of the lack of pathogenicity ofstrain 0222, a laboratory strain that has been extensivelypassaged in vitro, by Kume et al11 there is no other evidencethat serovar B isolates are non-pathogenic. Indeed, all the avail-able evidence is the opposite; isolates of H paragallinarumserovar B are as pathogenic as any other serovar.12,13 Hence,until there is further evidence, the isolates of H paragallinarumserovar B from clinical cases of infectious coryza should beaccepted as pathogenic without need for pathogenicity testing.
While we were only able to serotype one isolate from thisoutbreak, there has never been a report of multiple serovars inan outbreak of infectious coryza. Absence of reports of multipleserovars in a single outbreak is not strong evidence because theability to serotype H paragallinarum is not widely available.Hence, there are few reports on the serotyping of multipleisolates of H paragallinarum from a single outbreak. In one ofthe few such investigations, an Australian based study found no

Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 97
Scientific
5. Miflin JK, Chen X, Blackall PJ. Molecular characterisation of isolates ofHaemophilus paragallinarum from China by ribotyping. Avian Pathol1997;27:119-127.6. Chen X, Miflin JK, Zhang P, Blackall PJ. Development and application ofDNA probes and PCR tests for Haemophilus paragallinarum. Avian Dis1996;40:398-407.7. Blackall PJ, Eaves LE, Aus G. Serotyping of Haemophilus paragallinarum bythe Page scheme: comparison of the use of agglutination and hemagglutina-tion-inhibition tests. Avian Dis 1990;34:643-645.8. Zhang P, Blackall PJ, Yamaguchi T, Iritani Y. A monclonal antibody blockingELISA for the detection of serovar-specific antibodies to Haemophilus paragalli-narum. Avian Dis 1999;43:75-82.9. Kume K, Sawata A, Nakase Y. Haemophilus infections in chickens. 1.Characterization of Haemophilus paragallinarum isolated from chickensaffected with coryza. Jpn J Vet Sci 1978;40:65-73.10. Yamaguchi T, Blackall PJ, Takigami S, Iritani Y, Hayashi Y. Immunogenicityof Haemophilus paragallinarum serovar B strains. Avian Dis 1991;35:965-968.11. Kume K, Sawata A, Nakase Y. Immunological relationship between Page’sand Sawata’s serotype strains of Haemophilus paragallinarum. Am J Vet Res1980;41:757-760.12. Yamaguchi T, Blackall PJ, Takigami S, Iritani Y, Hayashi Y. Pathogenicityand serovar-specific hemagglutinating antigens of Haemophilus paragallinarumserovar B strains. Avian Dis 1990;34:964-968.13. Terzolo HR, Sandoval VE, Gonzalez Pondal F. Evaluation of inactivatedinfectious coryza vaccines in chickens challenged by serovar B strains ofHaemophilus paragallinarum. Avian Pathol 1997;26:365-376.14. Blackall PJ, Morrow CJ, McInnes A, Eaves LE, Rogers DG. Epidemiologicstudies on infectious coryza outbreaks in northern New South Wales, Australia,using serotyping, biotyping, and chromosomal DNA restriction endonucleaseanalysis. Avian Dis 1990;34:267-276.15. Bland MP, Bickford AA, Charlton BR, Cooper GC, Sommer F, Cutler GCase Report: A severe infectious coryza infection in a multi-age layer complexin central California. In: Proceedings 51st Western Poultry DiseaseConference/ANECA, Peurto Vallajarta, México, 2002.16. Poernomo S, Sutarma, Rafiee M, Blackall PJ. Characterisation of isolates ofHaemophilus paragallinarum from Indonesia. Aust Vet J 2000;78:759-762.17. Nagaoka K, De Mayo A, Takagi M, Ohta S. Characterization ofHaemophilus paragallinarum isolated in the Philippines. J Vet Med Sci1994;56:1017-1019.18. Thornton AM, Blackall PJ. Serological classification of Australian isolates ofHaemophilus paragallinarum. Aust Vet J 1984;61:251-253.19. Blackall PJ, Eaves LE. Serological classification of Australian and SouthAfrican isolates of Haemophilus paragallinarum. Aust Vet J 1988;65:362-363.20. Eaves LE, Rogers DG, Blackall PJ. Comparison of hemagglutinin andagglutinin schemes for the serological classification of Haemophilus paragalli-narum and proposal of a new hemagglutinin serovar. J Clin Microbiol1989;27:1510-1513.21. Blackall PJ, Eaves LE, Rogers DG. Proposal of a new serovar and alterednomenclature for Haemophilus paragallinarum in the Kume hemagglutininscheme. J Clin Microbiol 1990;28:1185-1187.
(Accepted for publication 1 July 2002)
evidence of multiple serovars within a series of epidemiologi-cally connected outbreaks in which a total of 11 isolates fromthe single outbreak involving six farms were examined.14 Afurther difficulty in serotyping multiple isolates of H paragalli-narum from outbreaks of infectious coryza is that the isolationand maintenance of H paragallinarum is a challenging task formany diagnostic laboratories. Even in the best equipped labora-tories there can be great difficulties in working with H paragalli-narum. As an example, there has been a recent report of a verylarge outbreak of infectious coryza on a multi-age layer farm inCalifornia.15 This outbreak was associated with nearly 50%mortality and almost 60% decrease in egg production.15
Despite the best efforts of the diagnostic laboratory involved, noisolate of H paragallinarum could be maintained long enoughfor transfer to a laboratory that could perform serotyping.15
This report now means that serovar B has been reported in anumber of Asian countries – China, Indonesia16 and thePhilippines.17 To date, H paragallinarum serovar B has neverbeen encountered in the studies of Australian H paragallinarumisolates.18-21 Hence, as we have suggested earlier, H paragalli-narum serovar B can be regarded as exotic to Australia.16 As thecurrently available infectious coryza vaccines for use in Australiacontain only serovars A and C, any entry of H paragallinarumserovar B would result in vaccine failures. The chicken is theonly host for H paragallinarum,1 meaning that the main entrypoint for serovar B into Australia would be via live chickens thatare carriers of the organism. Since we have shown that H para-gallinarum serovar B is present in village chickens inIndonesia,16 the threat of entry of serovar B is via both any legallive chicken import as well as via illegal entries in the northernregions of Australia.
References1. Blackall PJ, Matsumoto M, Yamamoto R. Infectious coryza. In: Calnek BW,Barnes HJ, Beard CW, McDougald LR, Saif YM, editors. Diseases of Poultry.Iowa State University Press, Ames, 1997:179-190.2. Page LA. Haemophilus infections in chickens. 1. Characteristics of 12Haemophilus isolates recovered from diseased chickens. Am J Vet Res1962;23:85-95.3. Feng W. Isolation and identification of the infectious coryza pathogen inBeijing (in Chinese). Microbiol (China) 1987;5:216-219.4. Chen X, Zhang P, Blackall PJ, Feng W. Characterization of Haemophilusparagallinarum isolates from China. Avian Dis 1993;37:574-576.
The use and abuse of Aesculapian authority in veterinary medicine.
Aesculapian authority is the unique authority vested in those that society sees as healers and originated when medicine was insepa-rable from magic and religion. While implicitly recognised in human medicine, it has not been applied to veterinary medicine. The
author of this article considers this situation may be changing with the increasing role of companion animal practice in the veterinaryindustry and as society begins placing more than market value on pets.
Increasingly owners consider these animals as family, and veterinarians are moving from the role of 'mechanic' (in treatment on apurely commercial basis) to that of the 'paediatrician'. With this change comes a growing relevance of the concept of Aesculapianauthority to companion animal practice - and the resultant question of potential abuse of that authority.
The author compares the application of this authority between human and veterinary fields, covering the issues of informed consent,the conflict between personal gain and ethical treatment, and the problems associated with alternative medicine. Deliberations involvingthe consideration of euthanasia are scrutinised from the veterinary point of view. Rolling BE. J Am Vet Med Assoc 2002;220:1144-1149.
98 Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Scientific
Adams DBAinsworth DAllen JGAnderson BHAnderson DEAnderson GAAnderson NAtkinson SBagust TJBarrs VRBennett PFBesier RBBlack HBlackall PJBlackshaw JKBlyde DJBolton JRBourke CABrightling ABrown TT JrBrowning GFBurgess GWCameron ACameron RDACanfield PJCaple IWCaporn TCappai RCarmel BPCarmichael IHChadwick BChapman CBChappel RJCharles JAChild GChurch SChurcher RKClarke AClarke RECoghlan SCondron RJ
Cook RWCousins DVCrane MCribb THCross GMCullen LKCutler RSDaniel RCWDart AJDart CMDavies ASDavies PRde Lisle GWDemirkan IDennis JADepiazzi LJDoneley RJTDorling PEamens GJEger CEEllis JTEmms SGFaragher JTFarrow BRHFenwick SFinnie JWFoster SFFrance MPFreestone JFubini SLGalloway DBGavaghan BJGibson KTGibson NRGleeson LJGould ARHemsworth PMHendriks WHiggins DAHill AHolloway SA
Holmes RJHolz PHHorner GWHughes KLHunt GBHusband AJHutchison J Huxtable CRRHyland JHIrwin PJJackson CAWJohnson PWJohnston REJohnstone AJolly RDJonsson NNKelly WRKing TKirkland PDKluver PFKnox MRLancaster MLarsen JWALawther WALenghaus CLepper AWDLew ALewis ILloyd LLohr JLoneragan GHLove RJMachon RMackay BMMacwhirther PJMadie PMalik RMalmo JManefield GWManktelow BWMcCance I
McConnell MFMcDonald BMcGregor BMcKenzie JAMcLean JGMcMeniman NPMcNeil JMcOrist SMellor DJMills JNMitten RWMoise SMoore ASMoses PAMunday BLMurray NNicoll RGO’Donoghue PJOlsson ARPage SParkinson GParkinson TJPass DAPenhale WJPeterson JEPointon AMPost LRacklyeft DJRaidal SRRead RAReece RLReichel MPRevington MLRobins GSangster NCScheerlinck J-PSchramme MScott PCSergeant ESGSimpson KWSlocombe RF
Smith JSSmith KRSommers BStafford KJStanislawek WLStanley RGSteel.CMStewart MStraw RCSutton RHTaylor EThacker ELThomas JThomas PGAThompson KGTulloch JDTurnbull PTurner AJ Vaughan JLVerkerk GVogelnest LVogelnest LJWalsh TWansborough RKWatson ADJWebster AJFWest DMWestbury HAWestwood CWhittington RJWilcox GWilesmith JWWilks CRWilliamson MWilliamson NBWilson GWindsor PAWright JDYoumans KRYoung PL
Acknowledgment of refereesThe Australian Veterinary Journal acknowledges the invaluable contribution of the referees. They have generously
given their time and expertise to ensure that the scientific standards of the Journal are maintained. Those who reviewedmanuscripts in 2002 are listed below.

Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 99
Scientific
Australian Veterinary Journal
Statistical guidelines for authorsRemember that repeated observations on the same subject shouldnot be used in any calculation of the SE.
PresentationInclusion of data: do not omit data referred to in Methods. It is
obviously impossible to include all raw data, but in general the readershould have enough information to verify the main conclusions.
Inclusion of information about testing: the reader’s full under-standing of the analysis depends on the precise description of themethods used. Indicate whether a t test was paired or not, and/orthe type of analysis of variance employed, including the number offactors involved, the interactions examined and the error termsused. If the analysis is complex it should be explained in terms thatare intelligible to non-statistical readers and should be referenced. Ifa computer statistics package is used to execute the analysis, then itsname, version and vendor should be given.
SD and SE: include SD when describing observations, SE wherethe objective is estimation or to test a hypothesis. Always includethe n on which statistics are based. It is important that the SEsshown should be relevant to any comparisons tested – thus wherethe paired t test is used the SEs of the means are not relevant to testingthe differences between them – the SEs of the mean of the differ-ences should be quoted. Where SEs have been calculated fromanalysis of variance it is likely that they will be based on the sameresidual mean square, so that it is not necessary to show individualSEs.
P values: prefer to show actual P values rather than stating ‘signi-ficant’ or ‘not significant’ (terms that need to be defined). Ingeneral, it is appropriate to state P < 0.001 for values that aresmaller. This is particularly important where the null hypothesis isnot rejected and there is a possibility of a type II error, the failure todetect a real effect.
Confidence intervals: confidence intervals are used to indicate therange of values within which a parameter will be found at a speci-fied probability. In many cases presentation of a CI is more infor-mative than the yes/no result of a test of significance or an actual P-value.
Precision: Avoid the spurious suggestions of precision that areproduced by including too many digits. In most cases two or threesignificant figures are sufficient.
ConclusionsConclusions should be justified by the results of the analysis. The Null Hypothesis (NH): (i) failure to reject the NH, that is the
finding that the effects tested are ‘not significant’, does not provethat the NH is true. Calculation of CI for the effect may afford abasis for concluding that any effect is inconsequential. (ii) rejectionof NH, that is the finding ‘statistically significant’, is prima facieevidence for the existence of the effect investigated but bias as apossible reason for the difference must also be examined. Theproportion that it is biologically unimportant should also besupported by argument from CI.
Discrepancies: internal inconsistencies, as for example in the levelof the end-measure between one part of the experiment and another,should be addressed in discussion.
References1. Ludbrook J. On making multiple comparisons in clinical and experimentalpharmacology and physiology. Clin Exp Pharmacol Physiol 1991;18:379-392.2. Ludbrook J. Repeated measurements and multiple comparisons in cardio-vascular research. Cardiovasc Res 1994;28:303-311.3. Rowell JG, Walters DE. Analyzing data with repeated observations on eachexperimental unit. J Agric Sci 1976;87:423-432.
DesignConsultation with a biometrician is recommended before
commencement of an experiment, since decisions made at thedesign stage are critical for a successful outcome.
Experiments should be designed to test specific hypotheses. Thedesign constitutes the best way to set up and perform the experi-ment in order to test the hypotheses.
The number of subjects: the experiment should be neither toosmall nor too large. Where feasible a pre-study ‘power’ calculationshould be carried out to estimate the numbers required.
Method of analysis: the method of analysis should be clearly spec-ified. Although in most cases standard methods of analysis will besufficient, complex analyses are readily available in computer pack-ages. Experimenters should be satisfied that the output of a packageis both appropriate and intelligible.
Randomisation: an appropriate physical method should be usedto allocate subjects to treatments, and should be briefly mentionedin the text. If some other variable, such as body weight, is takeninto account in the allocation, it should be included in the analysisas a covariate or a blocking factor.
Surveys should be designed so that the parameters to be estimated,for example, the prevalence of a particular disorder, can be estimatedwith appropriate precision. Possible sources of bias, as for exampleintroduced by structuring or incomplete returning of a question-naire, should be discussed.
AnalysisErrors in calculation: rigorous checking should be used to avoid
computational errors, including those of data entry and selection ofoptions when using a package. Any seeming discrepancy between Pvalues and intuition should be viewed with suspicion.
Appropriate analysis: the analysis used should be appropriate tothe design. Take account of blocking if this has been used in alloca-tion, and of trend if an explanatory variable (for example, dose atdifferent levels) is included.
Appropriate test: statistical tests used should be appropriate.Remember that there are restrictions on the use of the commonertests – for example the t test and analysis of variance require thatthe data are reasonably consistent with a normal distribution andthat the variances to be pooled are compatible. If such assumptionsare untenable, the variable can be transformed or non-parametrictechniques can be applied. The χ2 test is not recommended ifexpected values are low, in which case an alternative test should beadopted.
Direction of testing and level of significance: use two-sidedtesting unless a very clear case is made out for one-sided. The mostcommonly used level of significance (α) is 0.05. This may be varieddepending on the relative weights to be given to type I and type IIerrors, but the case should be argued by the authors, especially forα = 0.1.
Multiple testing: Tests should be made on comparisons appropriateto the aims of the experiment, not just suggested by the data. Ifmultiple applications of significance testing are necessary, signifi-cance levels should be protected using methods such as describedby Ludbrook.1
Repeated measures: where observations on the same subjects arerepeated over time, it is important to recognise that the observa-tions are correlated. Apply corrections, such as described byLudbrook,2 select a single end-measure such as the area under theindividual time-response curve, or fit a function to it.3 Ensure thatinclusion of ‘repeated measures’ in the repertoire of a computerpackage means more than its ability to handle the paired t test.

100 Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Scientific
AuthorshipEligibility for authorship should be based only on substantial
contributions (a) to conception and design, or analysis andinterpretation of data; (b) to drafting the article or revising it crit-ically for important intellectual content; and (c) on finalapproval of the version to be published. Conditions (a), (b) and(c) must all be met. Each author must have participated suffi-ciently in the work to take public responsibility for the article.General supervision of the research group or participation inthe acquisition of funding or the collection of data do not inthemselves justify authorship.
ManuscriptSubmit the manuscript in triplicate. Type it on one side of A4
paper, with 10 cpi font, leaving a left-hand margin of 3 cm andnumbering every fifth line. Use double spacing throughout,including title page, abstract, text, acknowledgments, refer-ences, tables and legends for illustrations. Do not underlineanything. Number all pages. Keep copies of everything sub-mitted.
Once the Journal has accepted and edited the manuscript,the author will be required to send a copy of the finalised man-uscript as an email attachment to [email protected](Scientific) or [email protected] (Clinical). Alternatively aversion can be provided on a computer diskette, preferably inPC format. Acceptable word processing programs areWordPerfect and MS Word. If you use a Macintosh send yourmanuscript as an email attachment or on a PC formatted disc.
LanguageUse concise English without jargon or colloquialisms. Avoid
repetitive use of long sentences and the passive tense.Reading the text aloud helps with punctuation and finding theright syntax. The spelling should conform to that of the ConciseOxford Dictionary. It is recommended that the text be runthrough computer spelling and grammar programs. Pay atten-tion to the readability index available in word processing pro-grams. It is important to have the manuscript critically read bya senior colleague, who is not directly involved in the study,before submitting it to the Journal. Poorly presented manu-scripts reflect badly on the submitter and their host institution.
TitleThe title should be short, specific and informative but should
not make an assertive claim about the conclusions of thestudy. Avoid including locations unless they are of epidemio-logical significance. Type the title in bold letters at the head ofthe first page with only the initial letter capitalised.
Authors’ names and addressesGive initials and surnames in capitals without stops. Separate
the authors’ names with a comma, except the names of thepenultimate and ultimate author, which are separated with ‘and’in lower case letters. Type a single full postal address below theauthors’ names. If there is more than one address, provide all asfootnotes. An address for reprint requests may be given as a foot-note. Footnotes are separated from the text with a horizontal lineand marked with superscript lower case letters.
The Australian Veterinary Journal publishes original arti-cles, case reports, short contributions and review articles.Please contact the Editors if you plan to write a review.
Send manuscripts for the Scientific Section to:
Professor Colin Wilks, Scientific Editor, AVA House,272 Brunswick Road, Brunswick Vic 3056.
Send articles for the Clinical Section to:
Dr Maureen Revington, Clinical Editor, AVA House, 272 Brunswick Road, Brunswick Vic 3056.
In cases where it is not clear in which Section the articlewould be best placed, the Editors will decide after consideringthe authors’ preference. A non-refundable handling charge of$33 (including GST) must accompany all manuscripts.
All submissions are peer-reviewed. The Journal reservesthe right to reject any manuscript.
Covering letterManuscripts must be accompanied by a letter to the Editor,
signed by all coauthors. It must include:
● information on prior or duplicate publication or submissionelsewhere of any part of the paper;
● a statement of financial or other relationships that mightlead to a conflict of interests;
● a statement that the manuscript has been read andapproved by all authors; and
● the name of and contact information for the correspondingauthor, who is responsible for communicating with theother authors about revisions and final approval of theproofs.
The letter should give any additional information that maybe helpful to the Editor, such as the number of words andwhich one of the four types of article is intended.
CopyrightSubmission of a manuscript will be held to imply that it is the
unpublished original work of the author(s) and, if accepted,will not be published elsewhere in whole or in part withoutpermission. It will also be held to imply that all authors haveread the manuscript and have consented to its submission forpublication. Copyright, including the right to reproduce thearticle in all forms and media, is assigned exclusively to theAustralian Veterinary Journal. The Editors will not refuse anyreasonable request by the author(s) seeking to reproduce partor all of any article, provided that the source is appropriatelyacknowledged.
Animal welfareThe handling and use of animals in experiments must
conform to the Australian code of practice for the care anduse of animals for scientific purposes, 6th edn, NationalHealth and Medical Research Council, 1997.
Australian Veterinary Journal
INSTRUCTIONS FOR AUTHORS

Aust Vet J Vol 81, Nos 1 & 2, January, February 2003 101
Scientific
LayoutRefer to specific instructions for each type of article. Do not
number subheadings, paragraphs or itemised lists in the text.Do not end headings with stops. Headings are typed in bold.Subheadings should be brief. Only the first letter is capi-talised. First-order subheadings are typed on a separate line.They are positioned at the left margin and italicised. Second-order subheadings are indented, italicised and followed by adash to separate them from the text, which follows on thesame line. Mention the manufacturer and the essential infor-mation on drugs, reagents and equipment in parentheseswithin the text. Details on commonly used and well-knownmaterials may not be necessary.
TablesType each table on a separate page double-spaced.
Number tables in Arabic in the order they are referred to in thetext. Each table should have a brief title that describes itscontent adequately. Information in the table must not berepeated in detail in the text. Tables should contain sufficientinformation to be understood without reference to the text.
Do not use vertical lines. Use horizontal lines to separatethe table from the title, and footnotes and headings from data.Type the electronic presentation of data across the rows, notdown the columns. Capitalise only the initial letter of columnand line headings. Use superscript lower case letters to markfootnotes and superscript capital letters to mark statisticalsignificance.
FiguresBoth black and white and colour photographs are accept-
able. Colour illustrations are produced at no cost to the author.Figures, including graphs, drawings and photographs may beprovided as directly reproducible glossy prints or colour trans-parencies. Prints should be vertically orientated and in singleor double column widths. Standard widths are 85 and 177mm. Submit figures in duplicate, except slides. Enclose twoprint copies of each slide.
Figures can be submitted in digital form as separate files.They should be saved as TIFF, JPEG or EPS files in at least300 dpi density. Enclose two paper copies of each figure.
Use a consistent style of lay-out, lettering, symbols andthickness of lines. Lettering should be sans-serif, preferablyHelvetica. Include photographs if they are informative andnecessary for the understanding of the text. Magnificationmay be shown by a scale bar. Mark the name of the authorand the number and orientation of the figure on the back usinga self-adhesive label.Write legends for figures and explana-tions of symbols on a separate page. Legends should containenough information to make the figure comprehensiblewithout reference to the text.
Digital manipulation of an image is only acceptable if it isdone to enhance photographic density or to eliminate arte-facts. Any digital manipulation must be mentioned in thelegend of the figure. The author(s) must also state in thecovering letter that the scientific content of the image has notbeen altered. The Journal may need to examine the originalimage.
ReferencesPlease use references judiciously. Cite only those publica-
tions that are essential for the understanding of the study. It isoften practical to cite a review, instead of listing several publi-cations with similar findings. Ten references should suffice fora short study. Usually only a review article needs to contain
more than 25 references. Number text references consecu-tively, in the order in which they are mentioned, by superscriptArabic numerals. References cited only in tables or in figurelegends are numbered according to the first identification ofthe table or figure in the text. Write and number the referencelist in the sequence of the references in the text. Referencesto journals, books, conference proceedings, organisationalpapers, anonymous editorials, foreign language articles andinternet web sites, respectively, are written as follows:
1. Gibson KT, Hodge H, Whittem T. Inflammatory mediators in equinesynovial fluid. Aust Vet J 1996;73:148-151.2. Peterson ME, Randolph JF, Mooney CT. Endocrine diseases. In:Sherding RG, editor. The cat: diseases and management. 2nd edn.Churchill Livingstone, New York, 1994:1403-1506.3. Rhodes AP. Infectious bovine keratoconjunctivitis vaccination. In:Proceedings of the 23rd Seminar, Sheep and Beef Cattle Society,New Zealand Veterinary Association, June 1993.4. Australian Veterinary Association. Tethering of sows and sow stalls.In: Greenwood PE, editor. Members’ directory and policycompendium. 1997:B5.5. Where do we stand on manpower? [editorial] Vet Rec 1995;137:1.6. Homberger FR. Mäusehepatitis-Virus. Schweiz Arch Tierheilkd1996;138:183-188.7. Council of Docked Breeds. The case for docking.http://www.cdb.org. 1992. Retrieved 15 October 2001.
List all authors if there are five or fewer. When there aremore than five authors, list only the first three and add ‘et al’.Write titles of books, journals and other publications in italics.Capitalise only the first letter of the book titles. Do not under-line or use bold letters.
The abbreviation of journals follows that of Serial sourcesfor the BIOSIS previews database. Cite references to unpub-lished work only in the text, with a notation of (personalcommunication) or (unpublished). Please send a copy of anycited work that is included in the reference list as ‘in press’. Itis the authors’ responsibility to check the accuracy of refer-ence citations.
Units and numbersUse SI units.Write dates in the form 10 April 1996.Spell out one-digit numbers if they are used for counting
(three sheep, five paddocks) but not those used with a SI (5mL, 9 m) or time unit (5 days, 7 weeks) or as an attribute(farms 7 and 9). If you start a sentence with a number, spell itout.
AcknowledgmentsAcknowledge significant intellectual, technical and financial
contributions. A short work warrants short acknowledgments.
Types of articlesOriginal articles
Original articles for both the Scientific and Clinical sectionsshould have a structured abstract of no more than 250 words.The subdivision is up to the author, but should encompass theObjective, Design, Procedure, Results and Conclusion. Writesubheadings in lower case bold letters, followed by the text onthe same line. List nonstandard abbreviations and theirexplanations after the abstract. Use only the abbreviated formin the text. Avoid use of abbreviations in the abstract.
The main headings, following an untitled introduction, areMaterials and methods, Results, Discussion,Acknowledgments and References. The introduction should

102 Aust Vet J Vol 81, Nos 1 & 2, January, February 2003
Scientific
ours. Students are advised to consult with all clinicians whohave responsibility for the case during its time in the universityclinic and those staff who contributed in any significant way tocase management.
Review articlesReviews on a specific topic are either invited or offered by an
author or a group of authors. In the latter case we recommendthat the author(s) contact the editor to inquire if the topic is ofinterest to the Journal and often request a synopsis of thereview to be sent for scrutiny before the author(s) undertakewriting the full version.
A review article may be a critical review, where the author(s)draw totally new conclusions on the basis of previously pub-lished information, a state-of-the-art review, where current liter-ature on a topic is surveyed and analysed, or a combination ofthe two.
A review should articulate a clear question or a set of ques-tions. Pertinent published (sometimes unpublished) evidenceshould be found, selected and presented in an unbiased andreproducible way. If pooling of data is possible and needed, itshould be determined if there is enough consistency in the stud-ies to warrant such an approach. Characterise findings in a waythat is statistically valid and present a conclusion that readerscan verify for themselves. Thus the reviewer should adhere tothe same scientific principles in summarising studies that arerequired of authors of original papers. A review should includethe following information: objective, data sources, data extrac-tion (methods of assessing the quality, validity and application ofthe data), data synthesis (main results) and conclusions.
A review should be written mainly in the present tense sinceit predominantly surveys published, and therefore established,information.
Short contributionsThe length of a short contribution should not exceed one
printed page (about 1350 words) including any figures andtables. Short contributions do not have an abstract orsubheadings, except References. Short contributions may besubmitted to either the Scientific or Clinical sections. They areappropriate for reporting prospective studies or case reportsin which the scope of the study does not justify a full article.The concise nature of short contributions may enable fasterpublication following acceptance.
Invited contributionsEditors will from time to time invite and provide specific
guidelines for contributions to the following:
Editorials
Leading articles
Viewpoints
Diagnosis and therapy
Book reviews
state the purpose of the study. The contents of Materials andmethods should enable others to reproduce the work. Presentthe findings in Results concisely and logically. Evaluate andinterpret the findings in the Discussion, but do not presentnew data. If possible, write the main conclusions at the end ofthe Discussion. Headings may vary from standard if the varia-tion makes the article more informative.
Case reportsProvide a concise, unstructured summary of no more than
200 words. The main headings, following an untitled introduc-tion, are Case report, Discussion, Acknowledgments andReferences.
An untitled introduction should indicate the importance ofthe case and why it is worth reporting. This rationale of what isinteresting and relevant may contain some evidence frompublished articles to substantiate the claim that the case isimportant, however a full review of the literature is notwarranted.
A description of the case should include:
- History and description of animals- Clinical features- Diagnosis- Interventions and procedures- OutcomeDescription should be adequate, brief and clear. The clinical
features should be only those needed to convince readersthat the case is what it is claimed to be and that other plau-sible diagnoses have been excluded. Normal range of valuesfor any laboratory tests conducted must be included.
The case should be discussed in the light of relevantpublished work. The width and depth of the search of publica-tions should be described but only findings that are relevant tothe case should be discussed. If authors think a full review isnecessary, then they should consider two manuscripts — acase report and a review. However, initial submission of asynopsis of a review is required.
Authors should discuss:
- The evidence that the case is what they believe it to be
- How their observations and the results of tests supporttheir diagnosis, treatment and recommendations
- Are other plausible explanations considered andrefuted?
- Are other contradictory observations or evidenceexplained?
- Implications and relevance of the case
- Lessons learnt from the case for investigation ormanagement of similar cases.
Submissions will be subject to the Journal’s usual peerreview and editorial process. A submission by a student whois the sole author of a case report should be accompanied bya letter from the Head of Department or Dean, who verifiesthat the report has been generated by the student’s endeav-




















