Orthodontic Journal - CiteSeerX
103
Contents Original articles 97 Validity, reliability and reproducibility of three methods used to measure tooth widths for Bolton analyses Devan Naidu, Justin Scott, Desmond Ong and Christopher T.C. Ho 104 Stresses around a miniscrew. 3-D analysis with the finite element method (FEM) Allahyar Geramy 110 Perception of pain and discomfort during tooth separation Didem Nalbantgil, Derya Germec Cakan, M. Oguz Oztoprak and Tülin Arun 116 Changes in soft tissue profile and electromyographic activity after activator treatment Abdulvahit Erdem, Nihat Kilic and Barçin Eröz 123 Effect of in vivo aging on the shear bond strength of an orthodontic adhesive Evangelia Chatzistavrou, Theodore Eliades, Spiros Zinelis, Athanasios E. Athanasiou and George Eliades 128 Bond failure in clinical practice Mark Ewing 136 Static frictional resistance with the Slide low-friction elastomeric ligature system Steven P. Jones and Saida Ben Bihi 142 Gingival health and relapse tendency: a prospective study of two types of lower fixed retainers Kazem Al-Nimri, Rola Al Habashneh and Mohammed Obeidat 147 Clinical investigation of periodontal ligament distraction osteogenesis for rapid orthodontic canine retraction Priyanka Sethi Kumar, Ruchi Saxena, Sameer Patil, Kanhober M. Keluskar, K. Nagaraj and Sharadindu M. Kotrashetti 153 Changes in shear bond strength of ceramic and stainless steel brackets with different visible light curing times and directions Farzin Heravi and Shahin Bayani 158 Facial asymmetry in subjects with Class III malocclusion Nihat Kilic, Songül Comert Kilic and Gülhan Catal 163 Variations in tooth size and arch dimensions in Malay schoolchildren Khalid W. Hussein, Zainul A. Rajion, Rozita Hassan and Siti Noor Fazliah Mohd. Noor Guest editorial 169 The interaction of function and stability in the dentition James L. Ackerman, Martin R. Kean and William R. Proffit Obituary 173 John F. Reading (1927-2009) General 176 Book reviews 185 Recent publications 189 In appreciation 190 New products 192 Calendar 193 Index Australian Orthodontic Journal Volume 25 Number 2, November 2009 Australian Orthodontic Journal Volume 25 No. 2 November 2009
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Orthodontic Journal - CiteSeerX

ContentsOriginal articles97 Validity, reliability and reproducibility of three methods used to measure tooth widths for Bolton analyses
Devan Naidu, Justin Scott, Desmond Ong and Christopher T.C. Ho
104 Stresses around a miniscrew. 3-D analysis with the finite element method (FEM)Allahyar Geramy
110 Perception of pain and discomfort during tooth separationDidem Nalbantgil, Derya Germec Cakan, M. Oguz Oztoprak and Tülin Arun
116 Changes in soft tissue profile and electromyographic activity after activator treatmentAbdulvahit Erdem, Nihat Kilic and Barçin Eröz
123 Effect of in vivo aging on the shear bond strength of an orthodontic adhesiveEvangelia Chatzistavrou, Theodore Eliades, Spiros Zinelis, Athanasios E. Athanasiou and George Eliades
128 Bond failure in clinical practiceMark Ewing
136 Static frictional resistance with the Slide low-friction elastomeric ligature systemSteven P. Jones and Saida Ben Bihi
142 Gingival health and relapse tendency: a prospective study of two types of lower fixed retainersKazem Al-Nimri, Rola Al Habashneh and Mohammed Obeidat
147 Clinical investigation of periodontal ligament distraction osteogenesis for rapid orthodontic canine retractionPriyanka Sethi Kumar, Ruchi Saxena, Sameer Patil, Kanhober M. Keluskar, K. Nagaraj and SharadinduM. Kotrashetti
153 Changes in shear bond strength of ceramic and stainless steel brackets with different visible light curingtimes and directionsFarzin Heravi and Shahin Bayani
158 Facial asymmetry in subjects with Class III malocclusionNihat Kilic, Songül Comert Kilic and Gülhan Catal
163 Variations in tooth size and arch dimensions in Malay schoolchildrenKhalid W. Hussein, Zainul A. Rajion, Rozita Hassan and Siti Noor Fazliah Mohd. Noor
Guest editorial169 The interaction of function and stability in the dentition
James L. Ackerman, Martin R. Kean and William R. Proffit
Obituary173 John F. Reading (1927-2009)
General176 Book reviews185 Recent publications189 In appreciation190 New products192 Calendar193 Index
AustralianOrthodontic JournalVolume 25 Number 2, November 2009
Australian Orthodontic Journal Volume 25 No. 2 November 2009

Australian Orthodontic Journal Volume 25 No. 2 November 2009
The Australian Orthodontic Journal is published twice a year(May, November) for the Australian Society of OrthodontistsInc. The Journal welcomes articles that contribute to ortho-dontic knowledge from all sources. Material is accepted forpublication on the understanding that it has not been submit-ted or published, in any format, elsewhere. Neither theAustralian Society of Orthodontists Inc. nor the Editor, nor BPAPrint accepts responsibility for the views or statements of theauthors or the advertisers. For studies involving human subjects, or specimens, a brief statement that subjects' rightshave been protected and informed consent was obtained is required. When laboratory animals have been used the appropriate animal use/ethics committee should beacknowledged. These may be given in the covering letter. The Editor reserves the right to edit all contributions for clarityand style. If the Editor requests additional data forming thebasis of the work the authors will make these data availablefor examination. All articles are peer reviewed. All authors ofa manuscript accepted for publication must sign a coveringletter assigning copyright to the Journal in the event that it ispublished. This letter should indicate that the work is originaland has not been published (in any language or format) or isunder consideration for publication elsewhere. It should alsoidentify the corresponding author, and mention any financialsupport or relationships that may pose a conflict of interest.The latter statement has no bearing on the decision to publishan article. When the manuscript is accepted, the author(s) willbe asked to submit an electronic copy of the article.Guidelines for contributors can be downloaded from theJournal website (www.aso.org.au/aoj) or obtained from theJournal office ([email protected])
EDITORDr Michael HarknessPO Box 682, Castlemaine, Vic 3450, AustraliaTel: (+61 3) 5474 3233 Fax: (+61 3) 5474 3006Email: [email protected]
ASSISTANT EDITORDr Craig DreyerDental School, Adelaide UniversityFrome Road, Adelaide SA 5000, AustraliaTel: (+61 8) 8303 3437 Fax: (+61 8) 8303 3444Email: [email protected]
EDITORIAL BOARD Emeritus Professor T. J. Freer (Queensland)Professor A. Darendeliler (New South Wales)Professor O. Kharbanda (India)Professor V. Kokich (USA)Professor W. Sampson (South Australia)Professor K. Takada (Japan)Professor M. Woods (Victoria)Associate Professor K. GodfreyAssociate Professor M. Goonewardene (Western Australia)
Associate Professor C. Ho (Queensland)Dr T. Collett (Victoria)Dr J. Fricker (Australian Capital Territory)Dr D. Fuller (Victoria)Dr W. Weekes (New South Wales)Dr A. Weir (Queensland)
SECTION EDITORSRECENT PUBLICATIONS Dr Craig DreyerDental School, Adelaide UniversityFrome Road, Adelaide SA 5000, AustraliaTel: (+61 8) 8303 3437 Fax: (+61 8) 8303 3444Email: [email protected]
MEETING ABSTRACTS AND CALENDAR Dr Tony Collett7 Dawson Street, Upper Ferntree Gully, Vic 3156, Australia.Tel: (+61 3) 9756 0519 Fax: (+61 3) 9758 6644 Email: [email protected]
EDITORIAL ASSISTANTMrs Dee SansomPO Box 682, Castlemaine, Vic 3450, Australia.Tel: (+61 3) 5474 3233 Fax: (+61 3) 5474 3006 Email: [email protected]
BUSINESS & ADVERTISING MANAGERDr Igor G. LavrinLevel 15, 15 Collins Street, Melbourne, Vic 3000, AustraliaTel: (+61 3) 9650 0037 Fax: (+61 3) 9650 0058 Email: [email protected]
SUBSCRIPTIONSThe annual subscription rate for 2009 for non-member Individualand Institutional subscribers is A$200 (A$100 per issue),including postage and handling. GST is applicable forAustralian subscribers. Postage is by airmail. Payment shouldbe made in Australian dollars, by cheque or Australian bankdraft payable to: The Subscription Manager, AustralianOrthodontic Journal, P.O. Box 576, Crows Nest, NSW 1585,Australia, or by credit card. Tel: (+61 2) 9431 8666Fax: (+61 2) 9431 8677 Email: [email protected]
COPYRIGHT © 2009AUSTRALIAN SOCIETY OF ORTHODONTISTS INC.All rights reserved. No part of this publication may be repro-duced, stored in a retrieval system or transmitted in any formor by any electronic, mechanical photocopying or recordingmeans or otherwise without the prior permission of the copy-right owner. The copyright owner consents that copies of thearticle may be made for personal use only. This consent doesnot extend to other kinds of copying such as copying for general distribution, for advertising and promotional purposes,for creating recollective work or for resale.
The Australian Orthodontic Journal is indexed and abstractedby Science Citation Index Expanded (SciSearch) and JournalCitation Reports/Science Edition.
Australian Orthodontic Journal

Introduction
An important goal in comprehensive orthodontictreatment is to achieve an optimal final occlusionwith an ideal overjet, overbite and buccal segmentrelationships. Factors vital to the success of this goalare the existence of well-proportioned maxillary andmandibular tooth sizes. In 1958 Bolton used cases
with excellent occlusion and proposed desirable toothsize ratios for the anterior teeth and the anterior andposterior teeth, excluding the second and thirdmolars.1 Traditionally, the maximum mesio-distalwidths of the crowns of the teeth, measured withcalipers, have been used in these analyses and calipermeasurements are widely regarded as the 'gold standard'.
© Australian Society of Orthodontists Inc. 2009 Australian Orthodontic Journal Volume 25 No. 2 November 2009 97
Validity, reliability and reproducibility of threemethods used to measure tooth widths for Bolton analyses
Devan Naidu,* Justin Scott,† Desmond Ong* and Christopher T.C. Ho*
School of Dentistry, The University of Queensland, Brisbane,* and The Queensland Institute of Medical Research, Herston,†Queensland, Australia
Background: Vernier calipers have traditionally been used as the ‘gold-standard’ for tooth width measurements. New digitalmethods may prove to be as valid, reliable and reproducible as caliper measurements.Aims: To determine the validity, reliability and reproducibility of mesio-distal crown measurements made with calipers, using the DigiModel method and on digital photographs, and to determine the validity, reliability and reproducibility when the measurements are employed in Bolton tooth size analyses. Methods: Twenty-five consecutive study models were used. The maximum mesio-distal crown widths of 12 teeth in each arch(first molar to first molar) were measured with digital calipers, using the DigiModel software (OrthoProof, Caulfield South,Victoria, Australia) and on standardised digital photographs of the models by eight examiners. One examiner measured allmodels three times using the three measurement methods, two examiners measured all models once using the three measurement methods and five examiners measured all models once using the calipers only. Validity for the widths of individualteeth, the mean tooth width and the Bolton ratios were assessed using a general linear model two-way analysis of varianceand pair-wise comparisons between the two digital methods and the calipers. Reliability was assessed with Cronbach’s alphaand reproducibility with the intra-class correlation coefficient.Results: There were statistically significant differences between the tooth widths measured with DigiModel and the calipers (p < 0.001) and with the calipers and digital photographs (p < 0.001). However these discrepancies were judged not to be clinically significant. The Cronbach’s alpha scores for all methods were classified as 'excellent'. The intra-class correlationcoefficient values exceeded 0.75 for the digital calipers, 0.79 for DigiModel and 0.54 for the digital photographs.Conclusions: The validities of DigiModel and digital photographs for tooth width measurements and Bolton analyses are clinically acceptable. The reliability of both methods is also excellent. However, DigiModel software provided more accurateBolton’s ratios and demonstrated greater reproducibility than the digital photographs.(Aust Orthod J 2009; 25: 97–103)
Received for publication: November 2008Accepted: February 2009
Devan Naidu: [email protected] Scott: [email protected] Ong: [email protected] T.C. Ho: [email protected]

NAIDU ET AL
Australian Orthodontic Journal Volume 25 No. 2 November 200998
Recently, digital methods and 3-D virtual studymodels have been introduced to the profession. Someof the new digital methods scan alginate impressionsand do not require plaster study models. Digital photographs of plaster study models offer an inter-mediate step that may suit many clinicians becausethe technology is readily available, and many clinicians are familiar with the basic equipment.However, no published studies have evaluated thevalidity, reliability and reproducibility of mesio-distalcrown measurements made on 3-D virtual studymodels from a recently developed method that usescomputerised tomography to scan the alginateimpressions, and digital photographs.
The aims of this study were to determine the validity,reliability and reproducibility of mesio-distal crownmeasurements made with calipers, using the Digi-Model method and on digital photographs, and todetermine the validity, reliability and reproducibilityof these measurements in Bolton tooth size analyses.
Materials and methods
Twenty-five consecutive sets of intact pretreatmentstudy models with 12 fully erupted permanent teethin each arch (first molar to first molar) were used.Study models were excluded if a tooth had a largerestoration, an obvious crown deficiency due to cariesor fracture, an impression and/or casting artifact or ifthe digital models had a crown artifact.
The maximum mesio-distal widths of the crownswere measured directly with digital calipers, using theDigiModel software and on digital photographs. Theexaminer was blinded to the identity of the models byassigning new random numbers for each of the threemeasurement methods. The maximum mesio-distalwidth of a tooth was defined as the distance betweenthe anatomical contact areas when the teeth were cor-rectly aligned. In addition, the measurements weremade parallel to the occlusal surface and labial/buccalsurfaces. All mesio-distal widths were measured to thenearest 0.01 mm and the anterior Bolton’s ratio(ABR) and the overall Bolton’s ratio (OBR) were calculated using data from each method.
For the first method, a digital caliper (MitutoyoCorporation, Tokyo, Japan) was used to measure themesio-distal widths directly (Figure 1). The tips of thecalipers were sharpened to permit accurate placementin the interproximal embrasures and the caliper waslinked via a RS-232C interface cable to a personalcomputer. The light source was standardised for alldirect measurements. The second method of meas-urement used the DigiModel software (OrthoProof,Caulfield South, Victoria, Australia). Separate algi-nate impressions of patients were taken and sent tothe OrthoProof laboratory where they were scannedwith computerised tomography (CT) and convertedinto digital models. This data was stored on CDs andreturned to the clinic. The digital models were then
Figure 1. Measurement with Mitutoyo 6”/150 mm Digital Calipers. Figure 2. Measurement with DigiModel.

uploaded onto a computer and opened with theDigiModel software. Tooth widths were measuredusing the DigiModel ‘Measurement tool’ and themagnification, rotation and shifting features wereused as required (Figure 2). The third method ofmeasurement involved measurement of the mesio-distal widths on standardised digital photographs. ACanon EOS 350D digital camera with a 100 mm EFMacro Lens 1:2.8 was used. The camera was mount-ed on a purpose-built stand and adjusted with the aidof two spirit levels attached to the lens so that the sen-sor plane was horizontal (Figure 3). The study modelwas then placed on a surveyor model holder and a tilewith two spirit levels placed on the model, contactingthe incisors and first permanent molars. The survey-or table was then adjusted until the tile was horizon-tal, which averaged out the curves of Spee andMonson, thus equalising image distortion of the teethand ensuring that the sensor and occlusal planes wereparallel. The images were calibrated with a millimetreruler attached to the study model at the level of thecontact areas. An independent ring light was attachedto the camera and three tungsten lamps positionedaround each study cast to prevent shadows falling onthe teeth. The digital photographs were transferred toa computer and the mesio-distal widths measuredwith the image measurement software (ImageMeasurement, School of Dentistry, University ofQueensland, Brisbane, Australia) (Figure 4).Eight independent examiners (A, B, C, D, E, F, G, andH) participated in the study. Examiner A measured
all models three times using the three measurementmethods. Replications were separated by a period oftwo weeks. Examiners B and C measured all modelsonce using the three measurement methods andExaminers D, E, F, G, and H measured all modelsonce using the calipers only.Validity is defined as the extent to which a measure-ment obtained represents the object of interest.2 Theterm 'accuracy' is often used to describe validity.2 Inthe present study, validity was considered to be theextent to which measurements from the two digitalmethods agreed with the caliper measurements.Measurements made by the calipers were taken as the‘true’ values or the ‘gold standard’. Thus, accuracy wasjudged as the closeness of the digital values to thecaliper measurements. Reliability was considered asthe extent to which the measurements were repeat-able under identical conditions,3 and reproducibilitywas the closeness of agreement between independentresults obtained with the same method on identicaltest material, but under different conditions.4 It refersto the ability of a measurement technique to be accurately reproduced by another examiner.4
Statistical analysisThe data were analysed using the statistical softwarepackages SAS version 9.1 and SPSS version 15.0.Measurements from Examiner A were used to inves-tigate validity and reliability. Validity was assessedusing a general linear model (GLM) two-way analysisof variance (ANOVA) and pair-wise comparisons(Tukey's test) between the two digital methods andthe calipers.5,6 This was done for each individual
VALIDITY, RELIABILITY AND REPRODUCIBLITY OF TOOTH WIDTH MEASUREMENTS
Australian Orthodontic Journal Volume 25 No. 2 November 2009 99
Figure 3. A Canon EOS 350D digital camera mounted on a specialisedwork station.
Figure 4. Measurement with digital photos.

NAIDU ET AL
Australian Orthodontic Journal Volume 25 No. 2 November 2009100
tooth width, the average tooth width, the OBR andthe ABR. A significance level of 0.05 was selected.Reliability was assessed with Cronbach’s alpha.7 ACronbach’s alpha score was derived to examine theassociation between the three replicate measurements.Measurements from Examiners A, B, and C wereused to investigate the reproducibility of the Digi-Model and digital photographic measurements.Measurements from all eight examiners were used toinvestigate the reproducibility of the caliper measure-ments. Reproducibility was tested with the intra-classcorrelation coefficient (ICC).8
ResultsDigital calipersCronbach’s alpha scores for the digital calipers were:mesio-distal widths 0.99; OBR 0.98; ABR 0.99. The data were in close agreement when the caliper measurements for the eight examiners were compared. The ICC values for the digital calipersexceeded 0.75 (Table I).
DigiModel vs digital calipersThere was a statistically significant difference betweenthe mean tooth widths obtained with DigiModelsoftware and the calipers (p < 0.001). Tooth widthsmeasured with the DigiModel software were, on average, 0.08 mm less than those measured with thecalipers (95% CI: 0.05, 0.12 mm) (Table II). Therewere no statistically significant differences betweenthe mean Bolton’s ratios obtained with theDigiModel method and the calipers (OBR: p = 0.75;ABR: p = 0.28). The OBRs obtained with DigiModelwere, on average, 0.18 per cent greater than thoseobtained with the calipers (95% CI: –0.42, 0.78%),and the ABRs were, on average, 0.43 per cent less
than those obtained with the calipers (95% CI:–1.11, 0.25%) (Table III). The Cronbach’s alphascores for the DigiModel software were 0.99 for tooth widths, and 0.97 for the OBR and ABR. Inter-examiner measurements with the software werehighly correlated with ICC values exceeding 0.79(Table I).
Digital photographs vs digital calipersWhen measurements taken from the digital photo-graphs were compared with the caliper measure-ments, a statistically significant difference was detectedbetween the mean mesio-distal widths (p < 0.001).Tooth width measurements from the digital photo-graphs were, on average, 0.07 mm larger than thosefrom the calipers (95% CI: 0.03, 0.10 mm) (TableII). Highly significant differences were evident formeasurements of the lower incisor teeth (p < 0.001).There was no statistically significant differencebetween the mean OBRs from measurements takenfrom the digital photographs and the calipers (p = 0.06), but there was a statistically significant dif-ference between the mean ABRs (p = 0.02). TheOBRs and ABRs calculated from data obtained fromthe digital photographs were, on average, 0.59 percent (95% CI: –0.01, 1.19%) and 0.82 per cent(95% CI: 0.14, 1.50%) greater, respectively, than theOBRs and ABRs obtained using the caliper measure-ments (Table III). The Cronbach’s alpha scores for thedigital photographs were 0.99 for measuring toothwidths, 0.99 for the OBR and 0.98 for the ABR. TheICC values exceeded 0.54 (Table I).
Discussion
This study is the first to evaluate the validity, reliabil-ity and reproducibility of crown width measurements
Table I. Inter-examiner reproducibility.
Examiners ExaminersA,B,C,D,E,F,G,H A,B,C
Digital caliper DigiModel Digital photographICC 95% CI ICC 95% CI ICC 95% CI
Tooth widths 0.96 0.93 – 0.98 0.98 0.96 – 0.99 0.85 0.73 – 0.93OBR 0.76 0.64 – 0.87 0.79 0.64 – 0.89 0.59 0.36 – 0.77ABR 0.75 0.63 – 0.86 0.84 0.72 – 0.92 0.54 0.31 – 0.74
ICC, Intra-class correlation coefficient
made with the DigiModel software, although thereare several reports of other software programmesavailable for 3-D digital study models.5,9–12
Compared to the caliper measurements, DigiModeltended to underestimate the mesio-distal widths ofthe teeth by an average of 0.08 mm, overestimate theOBR by an average of 0.18 per cent and underesti-mate the ABR by an average of 0.43 per cent. Theseover- and underestimates equated to an overall toothsize discrepancy of 0.18 mm and an anterior toothsize discrepancy of 0.24 mm, which we consider arenot clinically significant. According to Shellhart et al.,Bolton’s ratios calculated with data obtained withneedle point dividers may vary by as much as ±2.2mm, thus emphasising the relative insignificance of the discrepancies we found with the DigiModelsoftware.13
When the measurements were repeated using theDigiModel software, the replicates were strongly cor-related: the high Cronbach’s alpha scores we obtainedindicate excellent reliability. The data for repro-ducibility were also very promising. Roberts andRichmond suggested that an ICC value below 0.4constitutes 'poor' reliability, between 0.4 and 0.75 is'fair to good', and above 0.75 represents 'excellent'reliability.3 Thus, our finding of ICC scores exceed-ing 0.79 for DigiModel indicates 'excellent' reproducibility. Although the DigiModel method has the same shortcomings as other methods of producing digital models the differences are extremelysmall and are unlikely to be of clinical significance.5,9,12
The validity of tooth width measurements andBolton analyses made on the digital photographs
VALIDITY, RELIABILITY AND REPRODUCIBLITY OF TOOTH WIDTH MEASUREMENTS
Australian Orthodontic Journal Volume 25 No. 2 November 2009 101
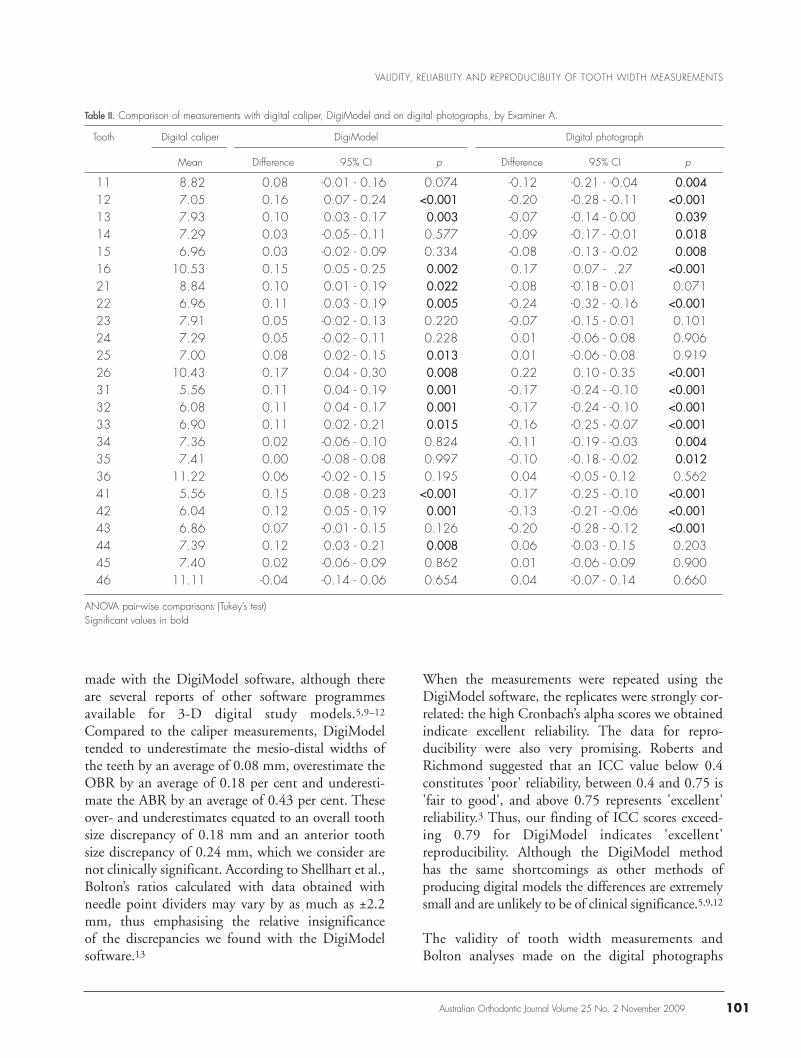
Table II. Comparison of measurements with digital caliper, DigiModel and on digital photographs, by Examiner A.
Tooth Digital caliper DigiModel Digital photograph
Mean Difference 95% CI p Difference 95% CI p
11 8.82 0.08 -0.01 - 0.16 0.074 -0.12 -0.21 - -0.04 0.00412 7.05 0.16 0.07 - 0.24 <0.001 -0.20 -0.28 - -0.11 <0.00113 7.93 0.10 0.03 - 0.17 0.003 -0.07 -0.14 - 0.00 0.03914 7.29 0.03 -0.05 - 0.11 0.577 -0.09 -0.17 - -0.01 0.01815 6.96 0.03 -0.02 - 0.09 0.334 -0.08 -0.13 - -0.02 0.00816 10.53 0.15 0.05 - 0.25 0.002 0.17 -0.07 - .27 <0.00121 8.84 0.10 0.01 - 0.19 0.022 -0.08 -0.18 - 0.01 0.07122 6.96 0.11 0.03 - 0.19 0.005 -0.24 -0.32 - -0.16 <0.00123 7.91 0.05 -0.02 - 0.13 0.220 -0.07 -0.15 - 0.01 0.10124 7.29 0.05 -0.02 - 0.11 0.228 0.01 -0.06 - 0.08 0.90625 7.00 0.08 0.02 - 0.15 0.013 0.01 -0.06 - 0.08 0.91926 10.43 0.17 0.04 - 0.30 0.008 0.22 -0.10 - 0.35 <0.00131 5.56 0.11 0.04 - 0.19 0.001 -0.17 -0.24 - -0.10 <0.00132 6.08 0.11 0.04 - 0.17 0.001 -0.17 -0.24 - -0.10 <0.00133 6.90 0.11 0.02 - 0.21 0.015 -0.16 -0.25 - -0.07 <0.00134 7.36 0.02 -0.06 - 0.10 0.824 -0.11 -0.19 - -0.03 0.00435 7.41 0.00 -0.08 - 0.08 0.997 -0.10 -0.18 - -0.02 0.01236 11.22 0.06 -0.02 - 0.15 0.195 0.04 -0.05 - 0.12 0.56241 5.56 0.15 0.08 - 0.23 <0.001 -0.17 -0.25 - -0.10 <0.00142 6.04 0.12 0.05 - 0.19 0.001 -0.13 -0.21 - -0.06 <0.00143 6.86 0.07 -0.01 - 0.15 0.126 -0.20 -0.28 - -0.12 <0.00144 7.39 0.12 0.03 - 0.21 0.008 0.06 -0.03 - 0.15 0.20345 7.40 0.02 -0.06 - 0.09 0.862 0.01 -0.06 - 0.09 0.90046 11.11 -0.04 -0.14 - 0.06 0.654 0.04 -0.07 - 0.14 0.660
ANOVA pair-wise comparisons (Tukey’s test)Significant values in bold

were also clinically acceptable. Measurements on thedigital photographs were slightly larger (Mean differ-ence: 0.07 mm) than the caliper measurements andthe OBR and ABR were overestimated by 0.59 percent and 0.82 per cent, respectively. The overestimates of the tooth widths contributed 0.44 mm to the OBR and 0.57 mm to the ABR,which are unlikely to be of clinical significance.Although the measurements and Bolton ratios made on the digital photographs had excellent reliability and good reproducibility (ICC scoresexceeding 0.54) they were slightly less reproduciblethan the same measurements made with theDigiModel software.
A variety of reasons could be responsible for the slightinaccuracies in tooth width measurements obtainedwith the two new methods. For DigiModel, the mostlikely explanation is shrinkage of the alginate impres-sions during transportation with the result that thedigital models and the crowns were slightly smaller.14
Furthermore, the occlusal anatomy and interproximalcontacts were not well-defined on all digital models,which increased the potential for measurement errors.On the digital photographs, the contact areas oftipped teeth were often difficult to identify becausethe photographs were 2-D representations of the 3-Dstudy models. This may explain the inaccurate meas-urements of the lower incisors, which were oftentipped. Despite these limitations, the errors with bothDigiModel and the digital photographs were smalland not clinically significant.
Conclusion
The validities of DigiModel and digital photographsfor tooth width measurements and Bolton analysesare clinically acceptable. The reliability of both methods is also excellent. However, DigiModel pro-
vided more accurate Bolton’s ratios and demonstratedgreater reproducibility than the digital photographs.
Corresponding author
Associate Professor Christopher T.C. HoSchool of DentistryThe University of Queensland200 Turbot StreetBrisbane Qld 4000AustraliaTel: +61 7 3365 8084Email: [email protected]
References1. Bolton WA. Disharmony in tooth size and its relation to the
analysis and treatment of malocclusion. Angle Orthod 1958;28:113–30.
2. Houston WJ. The analysis of errors in orthodontic measure-ments. Am J Orthod 1983;83:382–90.
3. Roberts CT, Richmond S. The design and analysis of relia-bility studies for the use of epidemiological and auditindices in orthodontics. Br J Orthod 1997;24:139–47.
4. McNaught AD, Wilkinson A. IUPAC Compendium ofchemical terminology, 2nd edn. Oxford: Blackwell Science,1997. URL: ‘http://www.iupac.org’. Accessed October 2007.
5. Stevens DR, Flores-Mir C, Nebbe B, Raboud DW, Heo G,Major PW. Validity, reliability, and reproducibility of plastervs digital study models: comparison of peer assessment ratingand Bolton analysis and their constituent measurements. AmJ Orthod Dentofacial Orthop 2006;129:794–803.
6. Cody PC, Smith JK. Applied statistics and the SAS pro-gramming language. Pearson Prentice-Hall: New Jersey,2006:348–9.
7. Field A. Discovering statistics using SPSS. SAGEPublications: London, 2005:667–76.
8. Hamer RM. Intracc:sas. Calculate reliabilities from intra-class correlations. URL: ‘http://www.psych.yorku.ca/lab/sas/intracc.htm’. Accessed October 2007.
9. Santoro M, Galkin S, Teredesai M, Nicolay OF, CangialosiTJ. Comparison of measurements made on digital and plastermodels. Am J Orthod Dentofacial Orthop 2003;124:101–5.
10. Tomassetti JJ, Taloumis LJ, Denny JM, Fischer JR, Jr. Acomparison of 3 computerized Bolton tooth-size analyseswith a commonly used method. Angle Orthod 2001;71:351–7.
NAIDU ET AL
Australian Orthodontic Journal Volume 25 No. 2 November 2009102
Table III. Comparison of the Bolton’s ratios using the three measurement methods, by Examiner A.
Digital caliper DigiModel Digital photograph
Mean 95% CI Mean 95% CI p Mean 95% CI p
OBR 91.66 91.30 - 92.01 91.84 91.48 - 92.19 0.75 92.25 91.89 - 92.60 0.06ABR 77.95 77.55 - 78.35 77.52 77.12 - 77.92 0.28 78.77 78.37 - 79.17 0.02
ANOVA pair-wise comparisons (Tukey’s test)Significant value in bold

11. Zilberman O, Huggare JA, Parikakis KA. Evaluation of thevalidity of tooth size and arch width measurements usingconventional and three-dimensional virtual orthodonticmodels. Angle Orthod 2003;73:301–6.
12. Quimby ML, Vig KW, Rashid RG, Firestone AR. The accu-racy and reliability of measurements made on computer-based digital models. Angle Orthod 2004;74:298–303.
13. Shellhart WC, Lange DW, Kluemper GT, Hicks EP, KaplanAL. Reliability of the Bolton tooth-size analysis whenapplied to crowded dentitions. Angle Orthod 1995;65:327–34.
14. Coleman RM, Hembree JH, Weber FN. Dimensional stabil-ity of irreversible hydrocolloid impression material. Am JOrthod 1979;75:438–46.
VALIDITY, RELIABILITY AND REPRODUCIBLITY OF TOOTH WIDTH MEASUREMENTS
Australian Orthodontic Journal Volume 25 No. 2 November 2009 103

IntroductionOrthodontic treatment relies on forces and momentsto move teeth into predetermined positions.Unfortunately, the reaction to many orthodonticforces can result in unwanted movement of theanchor teeth or ‘loss of anchorage’. As a result, ortho-dontists have developed new intra-oral sources ofanchorage that do not rely on the teeth. These newmethods use plates and/or screws inserted into thebone(s) of the facial skeleton. These devices areclaimed to provide so-called absolute anchorage: inother words, they remain stationary when subjectedto an orthodontic load.The first attempt at so-called absolute anchorage wascarried out over 60 years ago by Gainsforth and Higley,who used the anchorage provided by vitallium screwsin the ascending rami of six dogs to retract the lower
canines.1 It was almost 20 years before the anchorageprovided by screws inserted in skeletal structures wasused to treat an actual malocclusion.1,2 Since then avariety of methods has been developed to provideabsolute anchorage.3–11 The newer methods use smalltitanium-alloy screws or miniscrews that have accept-able stability under orthodontic loads.12–14
At present there is a lack of information on theimportance of miniscrew location and angulation toanchorage resistance and stability, and of the stressesin the tissues surrounding a miniscrew underload.14,15 The FEM is an effective method of investi-gating stresses in the tissues surrounding a miniscrewbecause it enables the investigator to ‘model’ a systemmade up of different tissues/structures (e.g. tooth,periodontal ligament, surrounding bone, miniscrew),assign properties to the components or elements in
Australian Orthodontic Journal Volume 25 No. 2 November 2009 © Australian Society of Orthodontists Inc. 2009104
Stresses around a miniscrew. 3-D analysis with thefinite element method (FEM)
Allahyar GeramyDepartment of Orthodontics, Tehran University of Medical Sciences (TUMS) and Dental Research Center, Tehran, Iran
Background: Miniscrews used for absolute anchorage may induce stresses in the surrounding tissues that are dependent on theirproximity to the miniscrew.Aims: To determine the stresses in the buccal walls of the sockets of lower molars adjacent to a miniscrew under load when theposition and angulation of the miniscrew are changed.Methods: Five 3-D FEM models containing the first and second lower molars, their periodontal ligaments and the surroundingspongy and cortical bone, were modelled in SolidWorks 2006 (SolidWorks, Concord, MA, USA) and transferred to theANSYS Workbench (ANSYS Inc., Southpointe, Canonsburg, PA, USA). A tensile force of 2 N, decomposed in 3-D space, was applied to a miniscrew inserted between the lower first and second molars. The von Mises (equivalent) stresses along thebuccal walls of the sockets of the first and second molars were derived following changes in miniscrew position and angulation. No direct force was applied to the molars.Results: When the miniscrew was inserted at right angles to the bone and midway between the molars the stress in the crestalarea was 0.093 MPa. This stress increased proportionally in the first molar socket as the miniscrew was moved towards thefirst molar and declined when the miniscrew was tipped towards the second molar. Stresses also decreased in the crestal areaof the second molar as the miniscrew was moved towards the first molar, but increased when it was tipped towards the secondmolar. A 30–55 per cent increase in crestal stress in the first molar socket was detected.Conclusion: Stress occurred in the tissues surrounding a miniscrew subjected to a force vector. Changes in the position or angulation of a miniscrew can affect the stress in the socket walls of adjacent teeth. (Aust Orthod J 2009; 25: 104–109)
Received for publication: January 2009Accepted: May 2009
Email: [email protected]

FEM ANALYSIS OF STRESS SURROUNDING A MINISCREW
Australian Orthodontic Journal Volume 25 No. 2 November 2009 105
the system and study the behaviour of the systemunder defined loads and conditions.16–22 The objec-tive of the present study was to investigate the hypo-thesis that a miniscrew under load induces stresses inthe surrounding tissues that vary according to theposition and angulation of the miniscrew.
Materials and methods
Five 3-D computer models of the first and secondlower molars were designed in SolidWorks 2006(SolidWorks, Concord, MA, USA) to simulate situ-ations when a force is applied to a miniscrew insertedperpendicular to the surface of the bone and midwaybetween the first and second molars, displaced bodily to one side or tipped to one side of the pointof insertion. The 3-D models contained compact andcancellous alveolar bone, the first and second lowermolars and their periodontal ligaments, and a 10 mmminiscrew inserted between the molars. The teethwere modelled according to Ash’s dental anatomy.23
The head of the miniscrew (i.e. the part protrud-ing from the bone), which plays no part in the resist-ance offered by the screw, was omitted from themodel.
In Model 1 the miniscrew was inserted perpendicularto the surface of the bone and 2.6 mm from eachmolar (Figure 1). In Model 2 the miniscrew wasinserted perpendicular to the surface of the bone, butmoved 0.5 mm mesially from the position in Model1. In Model 3 the miniscrew was inserted perpen-dicular to the surface of the bone, but moved 1.0 mmmesially from the position in Model 1. In Model 4the miniscrew was inserted with a 10-degree tilttowards the second molar with the axis of rotationthrough the point of insertion in Model 1. In Model5 the miniscrew was inserted with a 20-degree tilttowards the second molar with the axis of rotationthrough the point of insertion in Model 1.
The roots of the molars were given a periodontal ligament with a uniform thickness of 0.25 mm. The
(a) (b) (c)
Figure 1. (a) Model 1, miniscrew midway between the lower first and second molars. (b) Model 3, miniscrew 1.0 mm closer to first molar on the right. (c) Model 5, miniscrew tilted 20 degrees towards second molar on the left.
(a) (b)
Figure 2. (a) The meshed 3-D computer model. (b) The meshed 3-D computer model of the miniscrew.

GERAMY
Australian Orthodontic Journal Volume 25 No. 2 November 2009106
3-D models were designed to be as realistic as poss-ible, without using any symmetry in modelling. Eachmodel was transferred to the ANSYS WorkbenchVersion 10 (ANSYS Inc., Southpointe, Canonsburg,PA, USA). Boundary conditions restricted displace-ments of the nodes at the mesial and distal parts ofthe models. Solid bodies are free to move in 3-Dspace while under load in FEM. This rigid bodymotion was restricted by preventing definite nodesfrom moving along the 3-D space axes. The mannerof restriction was based on the anatomy of mand-ible. All nodes at the mesial and distal surfaces of the model were prevented from being displacedbucco-lingually, mesio-distally and occluso-apically.Mechanical properties were then applied and themodels were meshed (Table I, Figure 2).
A 3-D force system was then applied to the miniscrewand each molar in turn in each model, based ondecomposition of a 2.0 N force at 20 degrees to sagittal plane. The force, applied between the mini-screw and lower canine, resulted in a vertical com-
ponent of 0.685 N and a horizontal component of1.879 N. This component, in turn, decomposed to amesial vector (i.e. along the dental arch) of 1.85 Nand a medial force vector (i.e. towards the mid-sagittal plane) of 0.326 N. No direct force wasapplied to either the first or second lower molars. The3-D model was ‘sliced’ along two planes: the firstpassed through the disto-lingual line angle of themodel and the centre of the miniscrew and the secondslice through the mesio-lingual line angle of themodel and the centre of the miniscrew. The first sliceshowed the inner wall of the second molar and thesecond slice the inner wall of the first molar (Figure3). The von Mises stress, which is defined asσe=(0.5[(σ1-σ2)2+(σ2-σ3)2+(σ3-σ1)2])0.5) where σ1is the maximum principal stress; σ2 is the intermedi-ate principal stress; and σ3 is the minimum principalstress produced by the applied force system, was thenassessed along the inner walls of the tooth sockets ineach sectioned model. The forces were assessed at sixequally-spaced points between the crestal and apicalareas of each molar (Figure 4).
Results
Numeric findings of the von Mises stress at locationsindicated in Figure 4 are given in Table II. The stresscontours are shown in Figures 3, 5 and 6.
First molarIn Model 1, the miniscrew was inserted perpendicu-lar to the surface of the bone and 2.6 mm from eachmolar. The stress findings along the defined path are
Table I. Mechanical properties of the materials used in the models.
Young’s modulus Poisson’s ratio(MPa)
Tooth 20300 0.26PDL 0.667 0.49Spongy bone 13400 0.38Cortical bone 34000 0.26Titanium 96000 0.36
Figure 3. The slices defined and the von Mises stresses in the sockets of bothmolars.
Figure 4. The von Mises stresses were determined at six points along thecrestal-apical path in the buccal walls of both lower molars, only one socketis shown.

FEM ANALYSIS OF STRESS SURROUNDING A MINISCREW
Australian Orthodontic Journal Volume 25 No. 2 November 2009 107
0.093 MPa at the crestal point and 0.001 MPa at theapical point. When the miniscrew was moved 0.5 and1.0 mm towards the first molar without any changein the angulation, the stress at the crestal pointincreased to 0.101 and 0.144 MPa, respectively.Stress at the apical point increased from 0.001 MPa(0.5 mm) to 0.002 MPa (1.0 mm).
A 10-degree change in angulation of the miniscrewaway from the first molar reduced the stress at the cre-stal point to 0.074 MPa. At the apical point, the stress(0.001 MPa) was similar to the 0.001 MPa stress atthe apical point in Model 1. When the miniscrew wasinclined 20 degrees toward the second molar thestress at the crestal point was 0.061 MPa and at theapical point 0.002 MPa.
Second molar Stress at the crestal point started at 0.048 MPa andfell to 0.045 MPa and 0.031 MPa when the mini-
screw was moved mesially 0.5 mm and 1.0 mm,respectively. Stress at the apical point started andremained at 0.002 MPa.
A 10-degree tilt of the miniscrew towards the secondmolar increased the stress at the crestal point to 0.052MPa and the stress at the apical point increasedslightly to 0.002 MPa. Increasing the angulation ofthe miniscrew to 20 degrees resulted in 0.066 MPastress at the crestal point and 0.002 MPa at the apicalpoint.
Discussion
FEM analysis is seldom used to analyse the stressinduced on teeth and anchor structures by ortho-dontic forces, but it has been shown to be a cost-effective and valid method of determining the behaviour of structures under load. When a mini-screw is the anchor structure the distribution of loadsto the surrounding tissues need to be considered from
Figure 5.The von Mises stress along the crestal-apical path in the buccalwall of the lower first molar socket.
Figure 6. The von Mises stress along the crestal-apical path in the buccalwall of the lower second molar socket.
Table II. Stress findings (MPa) for different positions and angulations of the miniscrew.
Normal Normal 0.5 mm 0.5 mm 1.0 mm 1.0 mm 10 10 20 20mesial mesial mesial mesial degree degree degree degree
displace- displace- displace- displace- distal tip distal tip distal tip distal tipment ment ment ment
Tooth 6 7 6 7 6 7 6 7 6 7Crestal 1 0.093 0.048 0.101 0.045 0.144 0.031 0.074 0.052 0.061 0.066
2 0.072 0.047 0.064 0.041 0.077 0.035 0.060 0.054 0.045 0.0553 0.026 0.024 0.030 0.024 0.021 0.021 0.026 0.025 0.018 0.0274 0.011 0.010 0.012 0.010 0.009 0.009 0.011 0.012 0.008 0.0115 0.005 0.005 0.005 0.004 0.004 0.004 0.004 0.004 0.004 0.003
Apical 6 0.001 0.002 0.001 0.002 0.002 0.002 0.001 0.002 0.002 0.002
Normal, miniscrew inserted perpendicular to the bone surfaceMesial displacement, miniscrew moved towards the first molarDistal tip, miniscrew tipped towards the second molar
0.16
0.14
0.12
0.1
0.08
0.06
0.04
0.02
0
0.07
0.06
0.05
0.04
0.03
0.02
0.01
0
Cervical 2 3 4 5 Apical Cervical 2 3 4 5 Apical
Normal 60.5 mm 6
1.0 mm610 deg rot 6
20 deg rot 6
Normal 7
0.5 mm 7
1.0 mm 7
10 deg rot 7
20 deg rot 7

a stress point of view. The force on a tooth with ahealthy periodontal ligament (PDL) results in toothmovement, which is a PDL-based phenomenon, butforce on a miniscrew, which lacks a PDL, is trans-ferred directly from the miniscrew to the surroundingtissues. Relatively small variations in the placementand/or orientation of a miniscrew can increase thestress in the surrounding tissues, which may includeteeth and PDL. In the present study the main issuewas to determine if small changes in the position andangulation of a miniscrew relieved the PDL fromexternal effects or introduced new stresses on thePDL.
The present study is the first to assess stress in the tis-sues surrounding a miniscrew. It would be fair to saythat most clinicians regard a miniscrew inserted insound bone as stable anchorage, and give little con-sideration to the stress transferred from a loadedminiscrew to the surrounding tissues. The findingsshow that the stress on the PDL of the first and second lower molars changed as the miniscrew wasshifted bodily towards the first molar or tippedtoward the second molar. When the miniscrew wasmoved mesially stress increased in the tissues sur-rounding the first molar and reduced in the tissuessurrounding the second molar. The reverse occurredwhen the angulation of the miniscrew was changed.Moving the head of the miniscrew closer to the sec-ond molar increased stress in the tissues surroundingthe second molar.
If small changes in the position of a miniscrew canalter stress in the tissues surrounding a tooth, the con-sequences of the loads affecting the PDL should beconsidered. The PDL of a tooth close to a miniscrewis not completely isolated from the stresses inducedby loads on the miniscrew. The health of the tissuessurrounding a miniscrew is an important considera-tion just as the health of the PDL is important inorthodontic treatment. High loads on a miniscrewcould result in high stresses in the surrounding tis-sues, which may initiate unwanted tooth movementor, in an extreme case, unseen pathological changes.Stress in the tissues surrounding a miniscrew can becontrolled by ensuring that the miniscrew is not sub-jected to a high load, that it does not perforate thePDL and that it is inserted in thick, healthy bone. Insituations where it is necessary to insert a miniscrewclose to the PDL, a light load to the miniscrew shouldbe employed.
As we have seen, increases in stress can affect the PDLof an adjacent tooth. For example, stress in the crestalarea of the lower first molar increased up to 55 percent by moving the miniscrew 1.0 mm towards thefirst molar, and increased by 37 per cent in the secondmolar socket adjacent to the PDL by inclining theminiscrew 20 degrees towards the second molar.Changes in the location or angulation of a miniscreware followed by changes in the von Mises stresses inone location or another. Examination of the stresscurves revealed that if the position of a miniscrew isto be changed, moving a miniscrew toward a toothwill increase the stresses more uniformly than inclin-ing the miniscrew towards the tooth. The study alsoshowed the apical half of the roots of both molarswere free of the effects of the miniscrew, suggestingthat an apically-placed miniscrew with a cervicalextension/attachment would leave the critical crestalarea stress-free (Figures 5 and 6).
Conclusion
As a rule, miniscrews are reliable and safe sources ofintra-oral anchorage. The von Mises stresses in thesockets of teeth adjacent to the miniscrew are influ-enced by the proximity and angulation of the loadedminiscrew to the teeth.
Corresponding author
Dr Allahyar Geramy3rd Fl. School of Dental MedicineGhods Ave., Enghelab St.Tehran University of Medical SciencesTehranIranEmail: [email protected]
References1. Gainsforth BL, Higley LB. A study of orthodontic anchor-
age possibilities in basal bone. Am J Orthod Oral Surg 1945;31:406–17.
2. Creekmore TD, Eklund MK. The possibility of skeletalanchorage. J Clin Orthod 1983;17:266–9.
3. Douglas JB, Killiany DM. Dental implants used as ortho-dontic anchorage. J Oral Implantol 1987;13:28–38.
4. Roberts WE, Helm FR, Marshall KJ, Gongloff RK. Rigidendosseous implants for orthodontic and orthopedicanchorage. Angle Orthod 1989;59:247–56.
5. Wehrbein H, Glatzmaier J, Mundwiller U, Diedrich P. TheOrthosystem: a new implant system for orthodontic anchor-age in the palate. J Orofac Orthop 1996;57:142–53.
6. Block MS, Hoffman DR. A new device for absolute anchor-age for orthodontics. Am J Orthop Dentofacial Orthop1995;107:251–8.
GERAMY
Australian Orthodontic Journal Volume 25 No. 2 November 2009108

FEM ANALYSIS OF STRESS SURROUNDING A MINISCREW
Australian Orthodontic Journal Volume 25 No. 2 November 2009 109
7. Kanomi R. Mini-implant for orthodontic anchorage. J ClinOrthod 1997;31:763–7.
8. Costa A, Raffainl M, Melsen B. Miniscrews as orthodonticanchorage: a preliminary report. Int J Adult OrthodonOrthognath Surg 1998;13:201–9.
9. Melsen B, Petersen JK, Costa A. Zygoma ligatures: an alter-native form of maxillary anchorage. J Clin Orthod 1998;32:154–8.
10. Umemori M, Sugawara J, Mitani H, Nagasaka H, KawamuraH. Skeletal anchorage system for open-bite correction. Am JOrthod Dentofacial Orthop 1999;115:166–74.
11. De Clerck H, Geerinckx V, Siciliano S. The Zygoma anchor-age system. J Clin Orthod 2002;36:455–9.
12. Liou EJ, Pai BC, Lin JC. Do miniscrews remain stationaryunder orthodontic forces? Am J Orthod Dentofacial Orthop2004;126:42–7.
13. Wang YC, Liou EJ. Comparison of the loading behavior ofself-drilling and predrilled miniscrews throughout ortho-dontic loading. Am J Orthod Dentofacial Orthop 2008;133:38–43.
14. Brettin BT, Grosland NM, Qian F, Southard KA, Stuntz TD,Morgan TA et al. Bicortical vs monocortical orthodonticskeletal anchorage. Am J Orthop Dentofacial Orthop 2008;134:625–35.
15. Hoste S, Vercruyssen M, Quirynen M, Willems G. Risk factorsand indications of orthodontic temporary anchoragedevices: a literature review. Aust Orthod J 2008;24:140–8.
16. Zienkiewicz OC, Taylor RL. The finite element method.4thed. London: McGraw-Hill book company, 1989;1–20.
17. Geramy A, Faghihi SH. Secondary trauma from occlusion:3-D analysis using the finite element method. QuintessenceInt 2004;35:835–43.
18. Geramy A. Alveolar bone resorption and the center of resisi-tance modification: 3-D analysis by means of the finite ele-ment method. Am J Orthod Dentofacial Orthop 2000;117:399–405.
19. Geramy A. Initial stress produced in the periodontal mem-brane by orthodontic loads in the presence of varying loss ofalveolar bone: a three dimensional finite element analysis.Eur J Orthod 2002;24:21–33.
20. Geramy A. Optimization of unilateral overjet management:three-dimensional analysis by the finite element method.Angle Orthod 2002;72:585–92.
21. Geramy A, Morgano S. Finite element analysis of threedesigns of an implant-supported molar crown. J ProstheticDent 2004;92:434–40.
22. Geramy A, Ghadirian H. Comparison of methods used tocorrect a lingually tilted mandibular molar: 3-D analysisusing the finite element method. Aust Orthod J 2008;24:96–101.
23. Ash MM. Dental anatomy, physiology, and occlusion. 6thed. Philadelphia: W.B. Saunders Co., 1984;246,261.

Introduction
Separators are usually placed prior to banding tolessen the pain and discomfort of banding, preventinjury to both hard and soft tissues and ensure that a band fits the tooth.1 Separators are also used to disimpact partially erupted teeth,2,3 to create spacefor safe interproximal reduction of adjacent teeth4
and to gain space for crown restorations.5,6 To com-fortably seat a band, the space between adjacent teeth should equal the average width of the perio-dontal ligament (approximately 0.25 mm).1,7,8 Whena molar band is seated without adequate separationthe root may contact the alveolus, produce‘hyalinised’ areas in the periodontal ligament (PDL)and cause pain.9–11
Different types of separators are available, and theyvary in the amount of pain they cause during separ-ation, their effectiveness in separating teeth andmaintenance of the separation gained.1 Some separa-tors, such as brass wire separators and separatingsprings, are inclined to irritate the buccal mucosa andmake tooth cleaning more difficult than other typesof separators. Separating springs and elastomeric sep-arators are more easily placed and removed than brasswire separators, but they can loosen and fallout.1,8,12–14 Because serious periodontal problems canarise if an elastomeric separator is pushed into theinterproximal space,1,14,15 radiopaque and brightlycoloured elasto-meric separators should be used.Furthermore, elastomeric separators that remain inplace can be uncomfortable for up to a week.7,16,17
Australian Orthodontic Journal Volume 25 No. 2 November 2009 © Australian Society of Orthodontists Inc. 2009110
Perception of pain and discomfort during tooth separation
Didem Nalbantgil, Derya Germec Cakan, M. Oguz Oztoprak and Tülin ArunDepartment of Orthodontics, Faculty of Dentistry, Yeditepe University, Istanbul, Turkey
Objectives: To evaluate patients’ perceptions of pain and discomfort during tooth separation and to compare the effectivenessof brass wire and elastomeric separators.Methods: The participants were 87 adults with a mean age of 22.1 ± 1.9 years. Elastomeric and brass wire separators wereinserted mesial and distal to upper right (elastomeric separators) and upper left first molars (brass wire separators) in each subject. After seven days, the amount of tooth separation was measured with a leaf gauge, and pain perception and discomfort were evaluated with a visual analogue scale and questionnaire. Results: The elastomeric separators produced significantly more separation than the wire separators. There was a statistically significant difference in the subjects’ perceptions of pain and discomfort at rest and during chewing between the different separators (p < 0.001). In general, the brass wire separators caused the greatest pain and discomfort immediately after insertion. Pain from the wire separators subsided over seven days, whereas elastomeric separators caused the greatest pain onthe first two days after insertion. Eating was negatively influenced by the separation in 61 per cent of the subjects on the firstday. On the other hand, other daily activities were affected minimally.Conclusions: The different levels of pain and discomfort caused by these separators, together with their advantages and disadvantages, can help the clinician to choose an appropriate separator. Patients should be warned that pain due to separation may affect their chewing, social life, school work and sleeping. Analgesics and soft food are recommended following placement of separators.(Aust Orthod J 2009; 25: 110–115)
Received for publication: January 2009Accepted: May 2009
Didem Nalbantgil: [email protected] Germec Cakan: [email protected]. Oguz Oztoprak: [email protected]ülin Arun: [email protected]

PERCEPTION OF PAIN AND DISCOMFORT DURING TOOTH SEPARATION
Australian Orthodontic Journal Volume 25 No. 2 November 2009 111
Although the pain and discomfort experienced bypatients during tooth separation can vary widely, theyare the main patient complaints at the start of ortho-dontic treatment and can discourage some patientsfrom seeking treatment and others from continuingwith their treatment.7,16–25 The aims of this studywere to determine patients’ perceptions of pain anddiscomfort during tooth separation and to comparethe effectiveness of brass wire and elastomeric separators.
Materials and methods
Following ethical approval, 100 adults with an agerange of 18 to 25 years volunteered to participate inthis study. Informed consent was obtained from allsubjects. The inclusion criteria were: healthy perio-dontium, no missing or extracted upper teeth, noupper midline diastema, no orofacial pain, no inter-proximal caries or restorations, fully erupted uppersecond molars, tight mesial and distal contact areason both upper first molars. The tightness of a contactpoint was confirmed by the failure to pass a leaf gauge(Huffman Dental Products L.L.C., Springfield, OH,USA) between the upper first molars and the adjacentteeth (Figure 1).
Before placement and after removal of the separators,the Gingival and Plaque Indices and the depths of thegingival sulci around both upper first molars weremeasured. The separators used were a 0.022 inchbrass wire separator (Dynaflex, Saint Ann, MO,USA) and an elastomeric separator (Ormco,Glendora, CA, USA). The elastomeric separators
were inserted around the mesial and distal contactareas of the upper right first molars using universalseparation pliers (AEZ, Ormco, Glendora, CA, USA),and the brass wire separators were placed around themesial and distal contact areas of the upper left firstmolar and tightened using a Matthiew plier. All separators were placed by the same investigator. Thebrass wire separators were not reactivated during the observation period.
Each subject was given a worksheet containing a visual analogue scale (VAS) and a questionnaire andasked to assess their perception of pain and discom-fort at rest and during chewing before insertion of theseparators (TB), immediately after insertion of theseparators (T0), 4 hours after insertion (T04) andthen daily for 7 days. Each subject was asked torecord the level of pain for each time period andanswer questions on the impact of any pain and dis-comfort from the separators on their chewing, sociallife, school work and at night. The questionnairerequired fixed answers. The VAS was anchored at theends by the descriptors, ‘No pain’ and ‘Extreme pain’and the subjects were asked to mark the scale accord-ing to how they perceived the severity of the pain.The right and left molars were scored separately forperceived pain levels. A score was obtained by meas-uring the millimetre distance of a mark made by thesubject from the left end of the scale (i.e. the ‘Nopain’ end of the scale). On the seventh day theamount of tooth separation was measured with theleaf gauge.
The replies were evaluated with NCSS 2007 softwarefor Windows. The means and standard deviations ateach time period were calculated and ANOVA wasused to compare the measurements at each timepoint. Post-hoc Newman Keuls multiple comparisonstests were used for pair-wise comparisons, the pairedt-test was used in the assessment of pain before andafter the insertion of the separators and Student’s t-test was used to compare the separator groups.Statistical significance was set at p < 0.05.
Results
A total of 13 subjects were excluded from the study.Of these, nine subjects lost their elastomeric separ-ators, three used analgesics and one subject did notcomplete the worksheet. No brass wire separatorswere lost. The mean age of the remaining 87 subjects(32 males, 55 women) was 20.1 ± 9 years. As there
Figure 1. Measurement of the tooth separation with a leaf gauge.

were no gender differences in the amount of toothseparation after 7 days, in the subjects’ perceptions ofpain or the plaque and gingival scores, the data fromthe males and females were combined.
The elastomeric separators produced significantly (p < 0.001) more separation (0.24 ± 0.08 mm and0.29 ± 0.10 mm on the mesial and distal contactpoints, respectively) than the brass wire separators(0.16 ± 0.07 mm and 0.17 ± 0.07 mm on the mesialand distal contact points, respectively) (Table I).
There were statistically significant differences (p <0.001) in the subjects’ perceptions of pain at rest fromthe two types of separator for the whole week exceptT04 and T7. The brass wire separators produced thehighest pain and discomfort levels immediately afterthe insertion (Figure 2). The pain levels from bothseparators gradually diminished over the 7-day obser-vation period and approached baseline levels on the seventh day. Elastomeric separators were
significantly less painful than the brass wire separatorsimmediately after the placement (p < 0.001), butresulted in significantly more pain than the brass wireseparators between day 1 and day 7. The reduction inpain from both separators followed a similar patternfrom day 1.
During chewing, the brass wire separators were sig-nificantly more painful than the elastomeric separ-ators immediately after insertion (p < 0.001) (Figure3). By the fourth hour, there was no significant dif-ference between the two separators (p > 0.05), butfrom day 1 to day 7 the elastomeric separators weresignificantly more painful than the brass wire separ-ators. The elastomeric separators were most painfultwo days after insertion (p < 0.001), thereafter, the
NALBANTGIL ET AL
Australian Orthodontic Journal Volume 25 No. 2 November 2009112
VAS
VAS
Figure 2. Mean pain scores (VAS) at rest (*, p < 0.05; ***, p < 0.001). Figure 3. Mean pain scores (VAS) during chewing (***, p < 0.001).
Table I. Separation obtained with elastomeric and brass wire separators.
Amount of Brass wire Elastomericseparation (mm) separator separator p
Mesial 0.16 ± 0.07 0.24 ± 0.08 < 0.001Distal 0.17 ± 0.07 0.29 ± 0.1 < 0.001
Statistically significant differences in bold
Table II. Subjects adversely affected by tooth separation.
Chewing Social life School work Night pain(%) (%) (%) (%)
T04 59 6 1 1Day 1 61 14 10 6Day 2 60 14 7 5Day 3 51 9 6 -Day 4 40 4 2 -Day 5 30 2 1 -Day 6 9 1 1 -Day 7 1 1 - -

PERCEPTION OF PAIN AND DISCOMFORT DURING TOOTH SEPARATION
Australian Orthodontic Journal Volume 25 No. 2 November 2009 113
pain from these separators subsided, but it failed toreach the baseline level by day 7.
Approximately 5 per cent of the subjects reportedthat elastomeric separators were painful for the firsttwo nights after insertion, whereas the brass wire sep-arators were not painful at night. Table II gives thepercentage of subjects influenced by tooth separationin their daily activities. More than half of the respon-dents considered their eating habits were negativelyinfluenced by the separation from insertion to day 3.By day 7, only one per cent had changed their eatinghabits because of the separation. On day 1, schooland social activities were adversely affected by thepain associated with tooth separation in 10 and 14per cent of the subjects, respectively. There was nostatistically significant difference between the plaqueand gingival scores of the molars with brass wire separators and those with elastomeric separators.
Discussion
For many patients placement of separators marks thestart of their orthodontic treatment, which they havebeen told will be free of pain and discomfort. Thefindings of our study show that in young adults thepain from tooth separation can last up to seven days,and for the first few days the pain and discomfort willadversely affect the daily activities of approximatelyone third of them. Brass wire separators were initiallymore painful than elastomeric separators, but thepain from the elastomeric separators lasted longer andelastomeric separators were more likely to be lost thanwire separators.
The view that gender is an important predictor ofpain during tooth separation is controversial. Somestudies have reported more girls report discomfortand pain associated with orthodontic treatment thanboys,17,23 whereas other studies failed to find any cor-relation between gender and the pain associated withtooth separation.7,16 A further study reported non-linear relationships exist between the pain after inser-tion of separators and placement of initial archwiresand gender, age, psychological state and culturalbackground.18 We found there were no differencesbetween males and females in the perception of painand discomfort and the amount of tooth separation.In agreement with Hoffman,1 we found elastomericseparators consistently produced more tooth separ-ation than brass wire separators, but the differencewas small (0.10 mm) and not clinically significant.
Bondemark et al.,7 who compared the effectiveness ofelastomeric and spring separators, also found a statis-tically significant difference of only 0.10 mm andconcluded that it was not important clinically.
Davidovitch and coworkers examined the duration ofseparation and on the initial tightness of contactpoints, and reported that less space was gained whenthe contact points were tight.8 Providing they stay inplace, elastomeric separators produce more tooth sep-aration than other types of separators, and should beused in patients with tight initial contact points.1,7,13
On the other hand, elastomeric separators may causea localised periodontitis, particularly when they aredisplaced interproximally, and bacteraemia whichcontraindicate their use in patients with systemic disorders.1,14,15,22,26
Almost 10 per cent of the subjects with elastomericseparators lost their separators in the first week. Werecommend that brass wire separators are used if a patient is unable to attend for banding within aweek. Although the brass wire separators producedless tooth separation and may need to be reactivatedto ensure there is sufficient space for banding, theystayed in place and were less painful than elastomericseparators.1,8 Previous studies have reported thatorthodontic patients experience varying degrees ofpain during treatment even after a simple proceduresuch as separation.7,8,16,19–22 The pain/discomfortusually starts within 4 hours of a separator beingplaced, increases over the next 24 hours and subsidesto the pre-placement level within 7 days. Elastomericseparators were, however, an exception: they werepainful and adversely affected patients’ daily activitiesfor seven days. To avoid the discomfort experiencedwith elastomeric separators we support Davidovitch’srecommendation that elastomeric separators are usedfor short periods of time.8 Davidovitch et al.8 alsosuggested that if a separator is lost, regardless of thetype, the patient should be asked to return 3 to 4 hoursbefore his/her appointment and the separator replaced.
We used a VAS to assess the pain and impact of separator-induced discomfort on daily activities, suchas eating, social interaction and sleeping. The VAS isan established method for assessing response topain/discomfort and has several advantages over adescriptive rating scale. A subject can scale his/herresponse to a changing pattern of pain/discomfort andin this respect it is of value when assessing pain/discomfort in individuals. Comparisons of responses

by groups should be regarded with caution. Identicalscores by different individuals at the same time, oreven by the same individual at different times, do notpermit us to make assertions about the quality of theperceptions of pain/discomfort: identical scores mayhave quite different meanings. The unmarked scalewe used lacked a neutral point so a subject did notknow where the range changed from ‘mild pain’ to‘mild no pain’. Scores in the middle zone could havebeen due to uncertainty, distractions or even lack ofinterest on the part of the respondent. The majorityof subjects reported discomfort to some degree, but ithad a very small impact on their daily life. Of thedaily activities, 60 per cent of the subjects consideredtheir eating was most affected four hours after place-ment of a separator and on the first and second days.These results agree with previous studies of the dis-comfort following insertion of separators and place-ment of orthodontic appliances.7,23 We recommendthat analgesics are prescribed at the time of insertionof separators and patients advised to change their dietto soft food in the first 2 to 3 days after placement ofseparators. Good oral hygiene is important becauseseparators can cause significant bacteraemia and alocalised periodontitis.15,26 Unlike Hoffman we didnot find any difference in the accumulation of plaquearound the first molars. Therefore, the standard oforal hygiene is not a criterion for the clinician whendeciding on the type of separator to use.
Conclusions
Patients should be warned that tooth separation canbe painful and the pain/discomfort may affect theirchewing, social life, school work and sleeping.Analgesics and soft food are recommended followingplacement of separators.
The elastomeric separators were found to be morepainful than the brass wire separators.
Both types of the separator were most painful duringthe first 2 days.
There was no difference in the effectiveness of theseparators to separate upper first molars with tightinterproximal contacts.
Elastomeric separators were more likely to be lostthan brass wire separators.
The advantages and disadvantages of each separatorshould be considered when choosing an appropriateseparator.
Corresponding author
Dr Didem NalbantgilDepartment of OrthodonticsFaculty of DentistryYeditepe UniversityBagdat cad. No 238 Göztepe IstanbulTurkeyTel: +90 216 363 60 44Fax: +90 216 363 62 11Email: [email protected]
References1. Hoffman WE. A study of four types of orthodontic separator.
Am J Orthod1972;62:67–73.2. Shapira Y, Borell G, Nahlieli O, Kuftinec MM. Uprighting
mesially impacted mandibular permanent second molars.Angle Orthod 1998;68:173–8.
3. Moro N, Murakami T, Tanaka T, Ohto C. Uprighting ofimpacted lower third molars using brass ligature wire. AustOrthod J 2002;18:35–8.
4. Vlaskalic V, Boyd R, Hordt C, Miethke RR. Die kiefer-orthopädische behandlung mit dem Invisalign-system.Quintessenz Online Select Kiefer orthopädie SonderheftInvisalign 2001. Avaliable at: http://qos.quintessenz.de/ index.php?content=inhalt&layer=kfosi. Accessed January 15, 2008.
5. VanderWeele RA, Broome JC, Ramer JP. Regaining space byusing elastic orthodontic separators. Gen Dent 1998;46:454–6.
6. Keesee SM, Baty DL, Cameron SM, Lefler TB, Morris WJ.A technique for achieving prerestorative minor tooth move-ment with orthodontic separators. J Prosthet Dent 2002;88:544–7.
7. Bondemark L, Fredriksson K, Ilros S. Separation effect andperception of pain and discomfort from two types of ortho-dontic separators. World J Orthod 2004;5:172–6.
8. Davidovitch M, Papanicolaou S, Vardimon AD, Brosh T.Duration of elastomeric separation and effect on interproxi-mal contact point characteristics. Am J Orthod DentofacialOrthop 2008;133:414–22.
9. von Böhl M, Maltha JC, Von Den Hoff JW, Kuijpers-Jagtman AM. Focal hyalinization during experimental toothmovement in beagle dogs. Am J Orthod Dentofacial Orthop2004;125:615–23.
10. Sodeyama T, Maeda T, Takano Y, Hara K. Responses of peri-odontal nerve terminals to experimentally induced occlusaltrauma in rat molars: an immunohistochemical study usingPGP 9.5 antibody. J Periodontal Res 1996;31:235–48.
11. Ogawa T, Ishii N, Toda K, Soma K. Changes in responseproperties of periodontal mechanoreceptors during toothmovement in rats. J Med Dent Sci 2002;49:95–101.
12. Kottraba TM. Preventing separator loss. J Clin Orthod1977;11:60.
13. Cureton SL, Bice RW. Comparison of three types of separatorsin adult patients. J Clin Orthod 1997;31:172–7.
14. Proffit WR. Contemporary Orthodontics. (ed 4). St Louis:Mosby, 2007:412.
15. Harrington Z, Darbar U. Localised periodontitis associatedwith an ectopic orthodontic separator. Prim Dent Care2007;14:5–6.
NALBANTGIL ET AL
Australian Orthodontic Journal Volume 25 No. 2 November 2009114

PERCEPTION OF PAIN AND DISCOMFORT DURING TOOTH SEPARATION
Australian Orthodontic Journal Volume 25 No. 2 November 2009 115
16. Ngan P, Kess B, Wilson S. Perception of discomfort bypatients undergoing orthodontic treatment. Am J OrthodDentofacial Orthop 1989;96:47–53.
17. Bergius M, Berggren U, Kiliaridis S. Experience of pain during an orthodontic procedure. Eur J Oral Sci 2002;110:92–8.
18. Krishnan V. Orthodontic pain:from causes to management-a review. Eur J Orthod 2007;29:170–9.
19. Bergius M, Broberg AG, Hakeberg M, Berggren U.Prediction of prolonged pain experiences during ortho-dontic treatment. Am J Orthod Dentofacial Orthop 2008;133:339.e1–8.
20. Giannopoulou C, Dudic A, Kiliaridis S. Pain discomfort andcrevicular fluid changes induced by orthodontic elastic separators in children. J Pain 2006;7:367–76.
21. Ngan P, Wilson S, Shanfeld J, Amini H. The effect ofibuprofen on the level of discomfort in patients undergoingorthodontic treatment. Am J Orthod Dentofacial Orthop1994;106:88–95.
22. Bird SE, Williams K, Kula K. Preoperative acetaminophen vsibuprofen for control of pain after orthodontic separatorplacement. Am J Orthod Dentofacial Orthop 2007;132:504–10.
23. Scheurer P, Firestone A, Bürgin W. Perception of pain as aresult of orthodontic treatment with fixed appliances. Eur JOrthod 1996;18:349–57.
24. Oliver RG, Knapman YM. Attitudes to orthodontic treat-ment. Br J Orthod 1985;12:179–88.
25. Erdinç AM, Dinçer B. Perception of pain during ortho-dontic treatment with fixed appliances. Eur J Orthod 2004;26:79–85.
26. Lucas VS, Omar J, Vieira A, Roberts GJ. The relationshipbetween odontogenic bacteraemia and orthodontic treat-ment procedures. Eur J Orthod 2002;24: 293–301.

Introduction
The role of the orofacial musculature in determiningfacial morphology and tooth position has intrigueddental researchers for decades. Electromyographic(EMG) studies indicate that anterior temporalis,masseter and orbicularis oris muscles may play a partin the causation of malocclusion and relapse afterorthodontic therapy.1–15 Similar methods, whichhave been used to investigate the activity of the oro-facial muscles during and following use of functionalappliances, indicate that functional appliances mod-ify the neuromuscular environment of the dentitionand related bones.16 However, the EMG evidence is
by no means clear-cut: some investigators havereported reduced EMG activity in the temporalis andmasseter muscles during maximal bite, chewing andat rest in patients treated with functional appliances,while other investigators have reported increasedmuscle activity during clenching, swallowing and atrest with these appliances.9–12,17–19
It would appear that the mechanisms of neuro-muscular adaptation to functional appliance therapyare complex. Orthodontists have traditionallyappraised the soft tissue profile on lateral cephalo-metric radiographs, but the information obtainedfrom such investigations is limited as the observer has
Australian Orthodontic Journal Volume 25 No. 2 November 2009 © Australian Society of Orthodontists Inc. 2009116
Changes in soft tissue profile and electromyo-graphic activity after activator treatment
Abdulvahit Erdem,* Nihat Kilic* and Barçin Eröz†
Department of Orthodontics, Faculty of Dentistry, Atatürk University,* Erzurum and Private practice,† Rize, Turkey
Background: To date, few studies have correlated the changes in muscle activity and specific soft tissue variables in adolescents with malocclusions. Objective: To determine associations between the soft tissue profile and electromyographic activities in temporalis, masseter andorbicularis oris muscles in children with Class II division 1 malocclusions treated with activators.Methods: For this prospective study, 25 subjects with Class II division 1 malocclusions were randomly assigned to either aTreatment group (N = 15) or a Control group (N = 10). The mean skeletal ages of the subjects in the Treatment and Controlgroups were 11.3 ± 1.1 and 11.0 ± 1.3 years, respectively. The subjects in the Treatment group were treated with activatorsand the subjects in the Control group were untreated. Lateral cephalometric radiographs and EMG recordings of the anteriortemporalis and masseter muscles during clenching, chewing and swallowing and the orbicularis oris muscle during whistlingwere obtained at the start of the study and 12 months later. Changes in the soft tissue profile were correlated with changes inthe EMG activities in anterior temporalis, superficial masseter and orbicularis oris muscles.Results: The upper lip to E line distance (UL-E) decreased more in the Treatment group than the Control group (p < 0.05) andthe H angle decreased in the Treatment group, but increased in the Control group (p < 0.01). The EMG activities of temporalisand masseter muscles increased significantly in both groups. All between-group EMG differences were statistically significantwith the exception of the activities in the temporalis and masseter muscles during swallowing. In the Treatment group, a significant positive correlation (r = .57) was found between the changes in UL-E and anterior temporalis activity during swallowing, and significant negative correlations were observed between the EMG activity of masseter muscle during swallowing and changes in LL-E (r = -.54), OLp-UL (r = -.55) and OLp-LL (r = -.67). Conclusions: Activator therapy is accompanied by changes in the lips and temporalis and masseter activities during swallowing.(Aust Orthod J 2009; 25: 116–122)
Received for publication: March 2009Accepted: June 2009
Abdulvahit Erdem: [email protected] Nihat Kilic: [email protected] Barçin Eröz: [email protected]
CHANGES IN SOFT TISSUE PROFILE AND EMG ACTIVITY
Australian Orthodontic Journal Volume 25 No. 2 November 2009 117
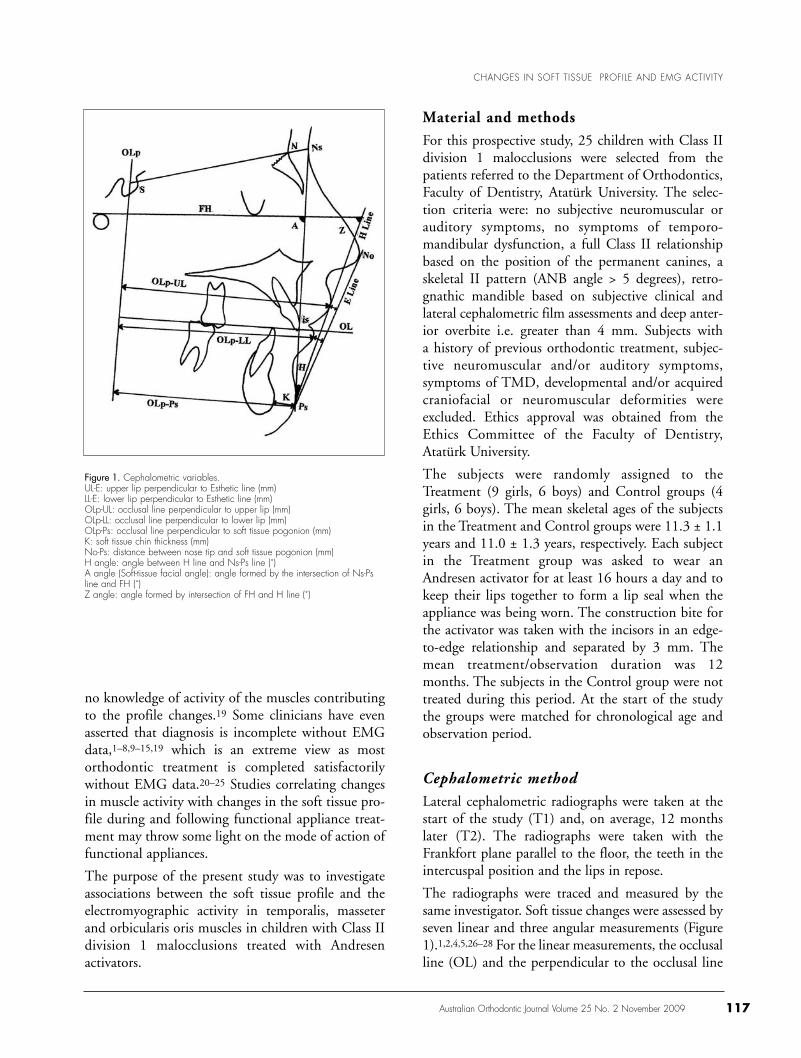
no knowledge of activity of the muscles contributingto the profile changes.19 Some clinicians have evenasserted that diagnosis is incomplete without EMGdata,1–8,9–15,19 which is an extreme view as mostorthodontic treatment is completed satisfactorilywithout EMG data.20–25 Studies correlating changesin muscle activity with changes in the soft tissue pro-file during and following functional appliance treat-ment may throw some light on the mode of action offunctional appliances.
The purpose of the present study was to investigateassociations between the soft tissue profile and theelectromyographic activity in temporalis, masseterand orbicularis oris muscles in children with Class IIdivision 1 malocclusions treated with Andresen activators.
Material and methods
For this prospective study, 25 children with Class IIdivision 1 malocclusions were selected from thepatients referred to the Department of Orthodontics,Faculty of Dentistry, Atatürk University. The selec-tion criteria were: no subjective neuromuscular orauditory symptoms, no symptoms of temporo-mandibular dysfunction, a full Class II relationshipbased on the position of the permanent canines, askeletal II pattern (ANB angle > 5 degrees), retro-gnathic mandible based on subjective clinical and lateral cephalometric film assessments and deep anter-ior overbite i.e. greater than 4 mm. Subjects with a history of previous orthodontic treatment, subjec-tive neuromuscular and/or auditory symptoms, symptoms of TMD, developmental and/or acquired craniofacial or neuromuscular deformities wereexcluded. Ethics approval was obtained from theEthics Committee of the Faculty of Dentistry,Atatürk University.
The subjects were randomly assigned to theTreatment (9 girls, 6 boys) and Control groups (4girls, 6 boys). The mean skeletal ages of the subjectsin the Treatment and Control groups were 11.3 ± 1.1years and 11.0 ± 1.3 years, respectively. Each subjectin the Treatment group was asked to wear anAndresen activator for at least 16 hours a day and tokeep their lips together to form a lip seal when theappliance was being worn. The construction bite forthe activator was taken with the incisors in an edge-to-edge relationship and separated by 3 mm. Themean treatment/observation duration was 12months. The subjects in the Control group were nottreated during this period. At the start of the studythe groups were matched for chronological age andobservation period.
Cephalometric methodLateral cephalometric radiographs were taken at thestart of the study (T1) and, on average, 12 monthslater (T2). The radiographs were taken with theFrankfort plane parallel to the floor, the teeth in theintercuspal position and the lips in repose.
The radiographs were traced and measured by thesame investigator. Soft tissue changes were assessed byseven linear and three angular measurements (Figure1).1,2,4,5,26–28 For the linear measurements, the occlusalline (OL) and the perpendicular to the occlusal line
Figure 1. Cephalometric variables.UL-E: upper lip perpendicular to Esthetic line (mm) LL-E: lower lip perpendicular to Esthetic line (mm)OLp-UL: occlusal line perpendicular to upper lip (mm)OLp-LL: occlusal line perpendicular to lower lip (mm)OLp-Ps: occlusal line perpendicular to soft tissue pogonion (mm)K: soft tissue chin thickness (mm)No-Ps: distance between nose tip and soft tissue pogonion (mm)H angle: angle between H line and Ns-Ps line (˚)A angle (Soft-tissue facial angle): angle formed by the intersection of Ns-Psline and FH (˚)Z angle: angle formed by intersection of FH and H line (˚)

(OLp) through sella (S) on the T1 radiograph wasused as a reference grid. The grid was transferred fromthe first tracing to the second tracing by super-imposing the grid on the N - S line (NSL) at S oneach subject’s T2 radiograph. The linear and angularmeasurements were made to the nearest 0.5 mm and0.5 degree, respectively. The changes during treat-ment were the T2 measurements minus the T1 measurements.
To determine the errors associated with the radio-graphic tracings and measurements, 20 radiographswere randomly selected from the Treatment andControl groups, re-traced and remeasured one monthafter the first procedure. The variables were normallydistributed, and there were no statistically significantdifferences between the first and second sets of measurements (p > 0.05).
EMG methodThe EMG activities of the left anterior temporalismuscle, the left masseter muscle and the left orbi-cularis oris muscle were recorded in the same shielded room before treatment (T1) and, on average,12 months later (T2). Before each recording session,the EMG recording procedure was explained in detail to the subjects and their parents to allay anxiety. The subjects were requested to wash theirface with soap and water and the skin over the desiredmuscles was cleaned with alcohol, dried thoroughlyand smeared with electrode jelly. Each subject was then comfortably seated with the head in natural head posture. The subjects were asked topractise habitual chewing, swallowing and whistling.Rectangular, unipolar surface electrodes were used forEMG recordings. The electrodes were taped in themain direction of the muscle fibres. The tip of the active electrode was placed on the contracted part of the muscle, while the tip of the passive electrode was placed 3 cm from the active electrode.The active regions of the anterior temporalis and masseter muscles were determined by palpation. A ground electrode was attached to the wrist of thesubject.
The EMG recordings were made with a Disa Neuro-matic 2000 electromyograph device (Dantec DISA,Scovlunde, Denmark). The sweep speed and sensitiv-ity of the device were 100 mm/sec and 1–10 mV/cm,respectively. A few trial recordings were obtained tofamiliarise each subject with the recording procedure.
EMG recordings of the anterior temporalis andsuperficial masseter muscles were obtained duringmaximal clenching, chewing and swallowing of nuts.For the latter, a readily available round hazelnut wasused. The activity in the superior orbicularis orismuscle was recorded during whistling an habitual andconstant tone. Two digital EMG recordings of each muscle were obtained at the same session and themean of the recordings of each muscle have been usedin all subsequent calculations. All recordings wereobtained by the same operator.
EMG recordings were taken before treatment/observation (T1) and approximately 12 months later(T2). The differences were calculated by subtractingthe T1 values from the T2 values. The measurementunit was in microvolts (µV), and the equipment wascalibrated manually, according to the recording sensitivity for each functional activity, range100–1000 µV. The sweep speed was set 10 msec/cm.
Statistical methodsA paired t-test was applied to determine the within-group changes in the cephalometric and electromyo-graphic variables. Student’s t-test was used to comparethe changes between the Treatment and Controlgroups. In addition, Pearson’s correlation analysis wasused to disclose associations between the changes inthe cephalometric and electromyographic variables.All statistical analyses were performed using the SPSSsoftware program (SPSS for Windows 98, version10.0, SPSS Inc, Chicago, IL, USA).
Results
There were statistically significant within-groupchanges in eight parameters in the Treatment groupand five parameters in the Control group (Table I).There were, however, only two statistically significantbetween-group T1-T2 changes: the upper lip to Edistance and the H angle. The upper lip to E distancedecreased 1.53 mm in the Treatment group, but only0.35 mm in the Control group (p < 0.05). The Hangle decreased in the Treatment group by 1.23degrees, but increased in the Control group by 1.65degrees (p < 0.01).
The activity of temporalis and masseter muscles during clenching, chewing and swallowing increasedsignificantly in both groups, particularly in theTreatment group where the EMG activity in the
Australian Orthodontic Journal Volume 25 No. 2 November 2009118
ERDEM ET AL

CHANGES IN SOFT TISSUE PROFILE AND EMG ACTIVITY
Australian Orthodontic Journal Volume 25 No. 2 November 2009 119
temporalis muscle during maximal clenchingincreased more than eight times the T1-T2 increasein the Control group (Table II). The activity in orbicularis oris during whistling increased signifi-cantly in the Treatment group, but not the Controlgroup, but the standard deviations in both groupswere large. All between-group differences were statis-tically significant with the exception of the activitiesin the temporalis and masseter muscles during swallowing.
In the Treatment group, four statistically significantcoefficients occurred between the cephalometric andelectromyographic changes (Table III). There was
significant positive correlation of .57 between thechanges in upper lip – E line distance (UL-E) andcontraction in the anterior temporalis muscle duringswallowing, and significant negative correlationsbetween the changes in the lower lip – E distance (-.54), OLp to upper lip (-.55) and OLp to lower lip (-.67) and masseter muscle activity during swallowing.
Discussion
Functional appliances are thought to modify the neu-romuscular environment of the dentition and relatedbones.16 We investigated associations between the
Table I. Comparison of the cephalometric changes (T2-T1) in the Treatment and Control groups.
Treatment group Within- Control group Within- Between-(N=15) group (N=10) group group
comparison comparison
Parameters Mean change SD t Mean change SD t t
Upper lip to E -1.53 1.61 -3.69*** -0.35 1.06 -1.05*** -2.04**Lower lip to E -1.23 1.71 -2.79*** 0.00 2.64 0.00*** -1.42**OLp-Upper lip 2.47 2.46 3.88*** 2.00 1.67 3.79*** 0.53**OLp-Lower lip 2.90 3.49 3.22*** 2.25 2.06 3.46*** 0.53**OLp-Ps 3.87 4.61 3.25*** 1.65 1.75 2.98*** 1.45**K 0.93 1.33 2.71*** 0.45 0.96 1.49*** 0.98**No-Ps 3.73 1.55 9.36*** 3.20 1.89 5.36*** 0.77**H (angle) -1.23 2.08 -2.30*** 1.65 1.76 2.96*** -3.60**A (angle) -0.17 3.87 -0.17*** 0.15 1.84 0.26*** 0.27**Z (angle) 1.37 3.72 1.51*** -0.15 2.98 -0.48*** 1.08**
* p < 0.05, **p < 0.01, ***p < 0.001
Table II. Comparison of the electromyographic differences (T2-T1) in the Treatment and Control groups.
Treatment Within- Control Within- Between-group group group group group
(N=15) comparison (N=10) comparison comparison
Muscle Parameters Mean SD t Mean SD t t
Temporal Maximal clenching 554.1 276.0 7.76*** 64.4 29.4 6.92*** 5.55***Chewing 586.0 221.0 10.28*** 130.5 56.1 7.35*** 6.34***Swallowing 71.5 57.5 4.83*** 51.6 54.6 2.99*** 0.87***
Masseter Maximal clenching 334.0 146.2 8.84*** 106.4 70.1 4.80*** 4.56***Chewing 388.4 196.2 7.66*** 85.1 74.5 3.61*** 4.64***Swallowing 69.1 65.0 4.12*** 45.4 30.0 4.78*** 1.07***
Orbicularis oris Whistling 372.0 290.0 4.97*** 111.8 203.6 1.82*** 2.46***
* p < 0.05, **p < 0.01, ***p < 0.001

changes in the soft tissue profile and changes in theactivities of anterior temporalis, masseter and orbicularis oris muscles in children with Class II division 1 malocclusions treated with Andresen acti-vators. At the start of the study, which ran for 12months, the children were randomly assigned toeither a Treatment or a Control group. The subjectsin the Treatment group were closely matched forchronological age and observation period with thesubjects in the Control group. We also took par-ticular care to standardise our cephalometric and electromyographic methods. After 12 months treat-ment relatively weak, but statistically significant,associations occurred between the lips and temporalisand masseter activity during swallowing. The signifi-cant associations were attributed to changes in the positions of the lips, possibly due to overjet reduction, and changes in muscle activity duringswallowing. In common with other studies, consider-able variation in EMG activity was encountered, butless variation occurred during swallowing than duringclenching and chewing.
The within-group cephalometric comparisonsrevealed eight significant changes (T1 to T2) in theTreatment group and five significant changes in theControl group. But when we compared the changesin the groups, only the upper lip to E distance (UL-E) and H angle were significantly different. Theupper lip was 1.5 mm less protrusive (relative to theE line) in the group treated with activators, and lessthan 0.5 mm less protrusive in the untreated group.The H angle decreased in the Treatment group byalmost 1.25 degrees, but increased in the Controlgroup by more than 1.5 degrees. The H angle is notinfluenced by growth of the nose, but it is influencedby growth and treatment-induced changes in the
upper lip and soft tissue pogonion. Others haveattributed the changes in functional appliance groupsto an appliance-induced retrusive force on maxillaand protrusive force on mandible,29–32 but our evidence does not support this conclusion. Soft tissue pogonion (OLp-Ps) increased significantly inthe Treatment group and Control groups, but thebetween-group difference was not statistically signifi-cant. It is unlikely that this measurement (OLp-Ps)was affected by growth changes in sella in the 12months of our study. The wide variation in theTreatment group is probably the reason we failed tofind a significant between-group difference for thismeasurement, and for OLp-UL and OLp-LL. Ourfindings emphasise the importance of using anato-mically stable landmarks, such as the cranial base,rather than reference lines that may be affected bygrowth.
One of the challenges in many orthodontic practicesis the successful treatment of Class II division 1 mal-occlusions. Some orthodontists routinely use func-tional appliances, either alone or in combination withsome other form of appliance, to treat these mal-occlusions. Conflicting results have been reported inthe literature regarding the EMG changes in the muscles during functional therapy. We found signifi-cant EMG changes in the temporalis and massetermuscles during maximal clenching, chewing andswallowing in both groups, and a significant EMGchange in the orbicularis oris muscle during whistlingin the Treatment group, but not in the Control group.We also found significant between-group changes inthe three muscles during clenching, chewing andwhistling, but not during swallowing. The EMG pat-terns during swallowing were not only the smallestchanges recorded, but also the least variable changes.
ERDEM ET AL
Australian Orthodontic Journal Volume 25 No. 2 November 2009120
Table III. Associations between the soft tissue and EMG changes in the activator group.
UL-E LL-E OLp-UL OLp-LL OLp-Ps K No-Ps H Angle A Angle Z Angle
Temporal Maximal clenching .295* .164* -.126 -.291** -.335 .016 -.202 .354 .043 -.206Chewing .214* .045* -.033 -.198** -.197 .145 .149 .163 -.120 -.115Swallowing .574* .088* -.332 -.069** .089 .063 .538 -.218 .030 .334
Masseter Maximal clenching .116* .090* -.282 -.117** .197 -.048 .266 .023 .172 .039Chewing .254* .125* -.164 -.306** -.122 -.324 .141 .192 -.064 -.005Swallowing -.159* -.537* -.554* -.668** -.305 .358 -.433 -.147 -.430 -.134
Orb. oris Whistling .316* .216* -.215 -.159 -.146 -.266 -.055 .156 .223 -.087
* p < 0.05, ** p < 0.01

Swallowing is an oral function with a consistent pattern of muscle activity, which does not appear tobe influenced by functional appliance treatment.
Whistling and swallowing require strong contractionsin the same circumoral musculature. Duringwhistling there was a marked increase in EMG activ-ity at the end of 12 months treatment and the differ-ence (T2 minus T1) was statistically significant. Thereduction in overjet may have contributed to thisfinding. In the Control group, however, the change inthe EMG activity in orbicularis oris was less marked,presumably because no additional effort was required(the subjects had an increased overjet on both occa-sions) and the change was not statistically significant.When we tested for between-group differences therewas a small, but statistically significant finding.
Several investigators have reported that the EMGactivities in temporalis and masseter musclesincreased in subjects treated with functional appliances,5,11,12,18 and other investigators havereported that the EMG activities in these musclesdecreased.9,10,19,33 We attribute this disagreement tothe different functional appliances and treatmentapproaches used, occlusal instability during function-al appliance treatment and to the different methodsused to record EMG patterns. For example, severalinvestigators have used hook electrodes, which areunreliable and give limited EMG data of a muscle.9,10,34
Needle electrodes also have disadvantages: theymarkedly reduce intramuscular crosstalk and arerejected by patients and clinicians because of the needfor specialised personnel to acquire data.35,36 We usedsurface electrodes because they are noninvasive, allowrecording over a large area and are reliable.34,37
A statistically significant positive correlation wasfound between the change in the upper lip to E linedistance (UL-E) and the change in anterior tempor-alis activity during swallowing. This means that theEMG activity in the temporalis muscle increased dur-ing swallowing when the upper lip to E line distanceincreased. However, measurements to the E line givean unreliable indication of change in the lips becauseof the confounding effect of nasal growth. Three statistically significant negative correlations werefound between masseter activity during swallowingand LL-E, OLp-UL, and OLp-LL. In general, thesesignificant correlations indicate that the more retru-sive the soft tissue profile, the greater the massetermuscle activity during swallowing.
Associations have been reported between the cranio-facial morphology and muscle activity duringrest,2,3,38,39 maximum intercuspation,2,3 clench-ing,2,3,8,13,14 chewing,6,39 and swallowing.3,6,8,39 Thesignificant associations we found between thechanges in EMG activity in masseter and temporalmuscles during swallowing and sagittal movements ofupper and lower lips may be due to the combinedeffects of forward growth of the face, treatment-induced changes in the lips due to overjet reductionand age-related postural changes in the lips. Althoughspecial attention was given to the EMG and cephalo-metric methods, the findings should be interpretedwith care due to the small sample sizes.
Conclusions
After 12 months treatment with Andresen activators,statistically significant associations occurred betweenthe sagittal changes in the lips and temporalis andmasseter muscles during swallowing. In general, themore retrusive the soft tissue profile, the greater the masseter muscle activity during swallowing.
Significant sagittal changes in the positions of the lipsmay have been due to the reduction in overjet.
Considerable variation in the EMG activity of tempor-alis, masseter and orbicularis muscles was encoun-tered during clenching, chewing and whistling. Lessvariation in EMG activity occurred in the temporalisand masseter muscles during swallowing.
Corresponding author
Dr Abdulvahit Erdem Atatürk Üniversitesi Dis Hekimligi FakültesiOrtodonti Anabilim Dalı 25240 ErzurumTurkeyEmail: [email protected] Tel: +90 442 2311808Fax: +90 442 2312270 - 2360945
References1. Lowe AA. Correlations between orofacial muscle activity
and craniofacial morphology in a sample of control andanterior open-bite subjects. Am J Orthod 1980;78:89–98.
2. Lowe AA, Takada K, Taylor LM. Muscle activity duringfunction and its correlation with craniofacial morphology ina sample of subjects with Class II, Division 1 malocclusions.Am J Orthod 1983;84:204–11.
3. Lowe AA, Takada K. Associations between anterior tempo-ral, masseter, and orbicularis oris muscle activity and cranio-facial morphology in children. Am J Orthod 1984;86:319–30.
CHANGES IN SOFT TISSUE PROFILE AND EMG ACTIVITY
Australian Orthodontic Journal Volume 25 No. 2 November 2009 121

4. Takada K, Lowe AA, Freund VK. Canonical correlationsbetween masticatory muscle orientation and dentoskeletalmorphology in children. Am J Orthod 1984;86:331–41.
5. Pancherz H, Aneheus-Pancherz M. Muscle activity in ClassII, Division 1 malocclusions treated by bite jumping withthe Herbst appliance: an electromyographic study. Am JOrthod 1980;78:321–9.
6. Ingervall B. Facial morphology and activity of temporal andlip muscles during swallowing and chewing. Angle Orthod1976;46:372–80.
7. Ingervall B, Helkimo E. Masticatory muscle force and facialmorphology in man. Arch Oral Biol 1978;23:203–6.
8. Miralles R, Hevia R, Contreras L, Carvajal R, Bull R, MannsA. Patterns of electromyographic activity in subjects withdifferent skeletal facial types. Angle Orthod 1991;61:227–84.
9. Ingervall B, Bitsanis E. Function of masticatory musclesduring the initial phase of activator treatment. Eur J Orthod1986;8:172–84.
10. Ingervall B, Thüer U. Temporal muscle activity during thefirst year of Class II, Division 1 malocclusion treatment withan activator. Am J Orthod Dentofacial Orthop 1991;99:361–8.
11. Miralles R, Berger B, Bull R, Manns A, Carvajal R.Influence of the activator on electromyographic activity ofmandibular elevator muscles. Am J Orthod DentofacialOrthop 1988;94:97–103.
12. Stavridi R, Ahlgren J. Muscle response to the oral-screenactivator: an EMG study of the masseter, buccinator, andmentalis muscles. Eur J Orthod 1992;14:339–49.
13. Pancherz H. Activity of the temporal and masseter musclesin Class II, Division 1 malocclusions: an electromyographicinvestigation. Am J Orthod 1980;77:679–88.
14. Tallgren A, Melsen B, Hansen MA. An electromyographicand roentgen cephalometric study of occlusal morphofunc-tional disharmony in children. Am J Orthod 1979;76:394–409.
15. Ahlgren J. Early and late electromyographic response totreatment with activators. Am J Orthod 1978;74:88–93.
16. Rakosi T. Principles of functional appliances. In: GraberTM, Rakosi T, Petrovic AG. Dentofacial orthopedics withfunctional appliances. St Louis: CV Mosby, 1997; 85–106.
17. Uner O, Darendeliler N, Bilir E. Effects of an activator onthe masseter and anterior temporal muscle activities in ClassII malocclusions. J Clin Pediatr Dent 1999;23:327–32.
18. Aggarwal P, Kharbanda OP, Mathur R, Duggal R, ParkashH. Muscle response to the twin-block appliance: an elec-tromyographic study of the masseter and anterior temporalmuscles. Am J Orthod Dentofacial Orthop 1999;116:405–14.
19. Simpson MM. An electromyographic investigation of theperioral musculature in Class II, Division 1 malocclusion.Br J Orthod 1977;4:17–22.
20. Holdaway RA. A soft-tissue cephalometric analysis and itsuse in orthodontic treatment planning. Part I. Am J Orthod1983;84:1–28.
21. Holdaway RA. A soft-tissue cephalometric analysis and itsuse in orthodontic treatment planning. Part II. Am J Orthod1984;85:279–93.
22. Bishara SE, Hession TJ, Peterson LC. Longitudinal soft-tissue profile changes: a study of three analyses. Am JOrthod 1985;88:209–23.
23. Merrifield LL. The profile line as an aid in critically evaluating facial esthetics. Am J Orthod 1966;52:804–22.
24. Subtelny JD. A longitudinal study of soft tissue facial struc-tures and their profile characteristics, defined in relation tounderlying skeletal structures. Am J Orthod 1959;45:481–507.
25. Marsan G. Effects of activator and high-pull headgear combination therapy: skeletal, dentoalveolar, and soft tissueprofile changes. Eur J Orthod 2007;29:140–8.
26. Pancherz H. The mechanism of Class II correction in Herbstappliance treatment. A cephalometric investigation. Am JOrthod 1982;82:104–13.
27. Pancherz H. Treatment of Class II malocclusions by jumpingthe bite with the Herbst appliance. A cephalometric investi-gation. Am J Orthod 1979;76:423–42.
28. Ricketts RM. Planning treatment on the basis of the facialpattern and an estimate of its growth. Angle Orthod 1957;27:14–37.
29. McNamara JA Jr, Bookstein FL, Shaughnessy TG. Skeletaland dental changes following functional regulator therapyon Class II patients. Am J Orthod 1985;88:91–110.
30. Varlik SK, Gültan A, Tümer N. Comparison of the effects ofTwin Block and activator treatment on the soft tissue pro-file. Eur J Orthod 2008;30:128–34.
31. Türkkahraman H, Sayin MO. Effects of activator and acti-vator headgear treatment: comparison with untreated ClassII subjects. Eur J Orthod 2006;28:27–34.
32. Battagel JM. The relationship between hard and soft tissuechanges following treatment of Class II, Division 1 maloc-clusions using Edgewise and Fränkel appliance techniques.Eur J Orthod 1990;12:154–65.
33. Tallgren A, Christiansen RL, Ash Jr MM, Miller RL. Effectsof a myofunctional appliance on orofacial muscle activityand structures. Angle Orthod 1998;68:249–58.
34. Burdette BH, Gale EN. Reliability of surface electromyo-graphy of the masseteric and anterior temporal areas. ArchOral Biol 1990;35:747–51.
35. Perry J, Easterday C, Antonelli D. Surface versus intra-muscular electrodes for electromyography of superficial anddeep muscles. Phys Ther 1981;61:7–15.
36. Bogey R, Cerny K, Mohammed O. Repeatability of wire andsurface electrodes in gait. Am J Phys Med Rehabil 2003;82:338–44.
37. Pease WS, Elinski MA. Surface and wire electromyographic.Recording during fatiguing exercise. Electromyogr ClinNeurophysiol 2003;43:267–71.
38. Ahlgren J, Sonesson B, Blitz M. An electromyographicanalysis of the temporalis function of normal occlusion. AmJ Orthod 1985;87:230–9.
39. Ahlgren JGA, Ingervall BF, Thilander BL. Muscle activity innormal and postnormal occlusion. Am J Orthod 1973;64:445–56.
ERDEM ET AL
Australian Orthodontic Journal Volume 25 No. 2 November 2009122

Introduction
In spite of the significant number of laboratory stud-ies published on bond strength, there is a lack of evi-dence regarding the clinical relevance of laboratoryassessments of bond strength. Orthodontic bondstrength testing can be a useful tool for the under-standing of the properties of a bonding material inthe laboratory.1
However, the actual behaviour of an orthodonticmaterial can only be determined in clinical con-ditions. In the oral cavity, complex oral flora and theirby-products are present, as well as the accumulationof plaque, and this is what distinguishes in vivo
conditions from in-vitro configurations.2 Severalparameters in the oral environment can affect bondstrength values, including saliva, chemical and physicaldegradation, erosion by food and bacterial activity.3
The development of the acid etch technique fromBuonocore4 in 1955 introduced revolutionary changesin the adhesion between tooth enamel and acrylicmaterials. Ever since, composite resins have been usedextensively as standard adhesive materials in ortho-dontic bonding. However, in vivo aging occurringduring orthodontic treatment may result in modifica-tion of the structural properties of this material andmay have effects on the longevity of its bond
© Australian Society of Orthodontists Inc. 2009 Australian Orthodontic Journal Volume 25 No. 2 November 2009 123
Effect of in vivo aging on the shear bond strengthof an orthodontic adhesive
Evangelia Chatzistavrou,* Theodore Eliades,* Spiros Zinelis,†
Athanasios E. Athanasiou* and George Eliades†
Department of Orthodontics, School of Dentistry, Aristotle University of Thessaloniki* and the Department of Biomaterials, School of Dentistry, University of Athens,† Greece
Aims: To assess the effect of intra-oral aging on the shear bond strength of a composite resin orthodontic adhesive (TransbondXT, 3M Unitek, Monrovia, CA, USA) after 6 months in the oral cavity and to compare it with control specimens not subjected tointra-oral aging.Methods: The sample consisted of patients aged 13–36 years, in need of premolar extractions for orthodontic purposes. Ten premolars were bonded with Transbond XT. After 6 months in vivo, the teeth were carefully extracted, sectioned at theamelo-cemental junction, mounted in cold cure acrylic resin cylinders and subjected to shear bond strength testing using a universal testing machine. The debonded bracket base surfaces were then studied under light microscope, photographed digitally and analysed with SigmaScan Image Measurement Software (Jandel GmbH, Erkrath, Germany) for the percentage ofcoverage of the debonded brackets with the orthodontic adhesive. The same procedure was followed for 14 premolars fromthe same patients bonded in vitro with the same adhesive.Results: No statistically significant differences were found in the shear bond strength between the two groups of composite resinadhesive systems (with and without clinical aging) or in the adhesive remnant coverage following debonding. No significantcorrelation was detected between the shear bond strength and the adhesive remnant coverage in the test specimens with andwithout aging.Conclusions: Laboratory studies of shear bond strength appear to be clinically relevant.(Aust Orthod J 2009; 25: 123–127)
Received for publication: May 2009Accepted: July 2009
Evangelia Chatzistavrou: [email protected] Eliades: [email protected] Zinelis: [email protected] E. Athanasiou: [email protected] Eliades: [email protected]

CHATZISTAVROU ET AL
Australian Orthodontic Journal Volume 25 No. 2 November 2009124
strength.2 The multifactorial nature of intra-oralaging, which includes pH fluctuation, complex cyclicloading, microbial attack and enzymatic degradation,may result in deterioration of the composite resin.Currently there is a lack of data for the in vivo behav-iour of bonding materials and the clinical relevance ofbond strength testing protocols.
The aims of this study were to evaluate the shearbond strength to enamel of a composite resin ortho-dontic adhesive after six months of intra-oral service,and to examine the potential variations in adhesiveremnant coverage with aging.
Materials and methodsSubjects and specimen preparationThe sample originated from patients attending theGraduate Orthodontic Clinic of the AristotleUniversity of Thessaloniki. The patients had a meanage of 22 years (Range: 13–36 years); 55 per centwere males and 45 per cent were females. Patientswere selected from a larger pool of participants whopresented for orthodontic treatment and wereplanned for treatment with extraction of premolars,based on the following criteria: intact buccal surfacesof premolars and absence of intervention during themonitoring period. The protocol of the study wasapproved by the Ethical Committee of the same uni-versity, and consent was obtained from all partici-pants or their guardians. No orthodontic treatmentwas initiated prior to extractions and for six monthsafter bonding.
The premolars of patients participating in the studywere cleaned and polished with a non-fluoride paste(Clean Polish, Hawe-Neos Dental, Bioggio, Switzer-land). Standard metal edgewise brackets (Mini SprintBrackets, Forestadent, Pforzheim, Germany) werebonded with composite resin (Transbond XT, 3MUnitek, Monrovia, CA, USA) following the manu-facturers’ instructions. Prior to resin bonding, theenamel was etched with 35 per cent phosphoric acidgel (Transbond XT, Etching Gel, 3M Unitek) for 30seconds. Six months later, the teeth were carefullyextracted, having the brackets intact on their buccal sur-faces, and were thoroughly rinsed with distilled water.
The control sample (Without aging) consisted of 14recently extracted premolars bonded in the labor-atory with the same composite resin adhesive mater-ial using the aforementioned metal brackets and
following the manufacturers’ instructions. Prior tobonding, the enamel was etched with 35 per centphosphoric acid gel (Transbond XT, Etching Gel, 3MUnitek) for 30 seconds.
All teeth were carefully sectioned at the amelo-cemental junction under continuous water flow. Afterthe sectioning and removal of their roots, the crownsof the bonded teeth were mounted in cold cureacrylic resin (GC Reline Chairside Hard DentureReline, GC America Inc., IL, USA) with mixing ratioof 1.8 g powder/1 ml liquid monomer, embedded inplastic cylinders of 30 mm height and external diam-eter of 16 mm. The buccal surfaces of the crownswere placed outwards, with the bonded brackets protruding from the acrylic resin.
Bond strength testThe plastic cylinders containing the embeddedcrowns were mounted on the jig of a universal testingmachine (Tensometer 10, Monsanto PLC, Wiltshire,England), connected to a computer through theMTEST II Materials Testing System, with their labial surfaces perpendicular to the horizontal plane.The jig was guided at the interface between thebracket and the buccal surface of the premolar with a loading velocity of 1 mm/min. The force at debonding (newtons) under shear loading wasrecorded. All specimens were maintained in standardroom temperature conditions (25 ºC and 30% relative humidity).
Adhesive remnant coverageThe debonded bracket base surfaces were studiedunder light microscope (Leitz, Wetzlar, Rockleigh,NJ, USA) at a magnification of x10, and photo-graphed with a digital camera (Nikon Coolpix E995,Nikon Co., Tokyo, Japan) directly connected to themicroscope. The analysis of the digital images of thedebonded surfaces of the brackets was performedusing SigmaScan and SigmaScan Pro5 (AutomatedImage Analysis Software, Jandel GmbH, Erkrath,Germany). For the assessment of the scale of meas-urement, a transparent millimetre ruler was placed ontop of the debonded bracket base and photographedwith the digital camera. The percentage coverage ofthe debonded brackets with remnants of the ortho-dontic adhesive following the shear bond strengthtesting was calculated after processing of the digitalimages with the image analysis software.

Statistical analysisDescriptive statistics (means, standard deviations,and minimum and maximum values) were calcul-ated and the data tested for normality. Independenttwo-sample t-tests were used to compare the samplemeans on shear bond strength and adhesive remnantcoverage. Further, a multivariate regression analysisbetween the two dependent variables (bond strengthand adhesive remnant coverage) and the independentvariable (aging) was carried out. The significance levelwas set at p ≤ 0.05 for all statistical analyses.
Results
Descriptive statistics on the shear bond strength ofthe composite resin and on the adhesive remnant coverage, calculated for the two groups tested (withand without aging in the oral cavity), are shown inTable I. The 6-month in vivo aged group did notshow a statistically significant difference in bondstrength compared to the control specimens. Withrespect to the adhesive remnant coverage, aging in theoral environment resulted in a slightly greater, albeitnon-significant coverage of bracket bases with adhesive (77.56%) as opposed to the non-aged group(71.31%).
Regarding the distribution of coverage with adhesiveremnants, it was demonstrated that after six monthsin vivo aging, the vast majority of specimens (9 out of10) had a coverage of >50 per cent and only 1 out of10 had 100 per cent coverage, whereas in the controlsample, 4 out of 14 had 100 per cent coverage, halfhad >50 per cent coverage and the remaining (3 outof 14) had <50 per cent coverage.
Finally, no significant correlation was demonstratedbetween the shear bond strength and the coverage ofdebonded brackets with adhesive remnant in either of
the situations tested (with and without aging, p >0.05, data not shown).
Discussion
The present study showed no effect of intra-oralaging on the shear bond strength of orthodonticadhesive to enamel. Despite the numerous in-vitrostudies, little is known regarding the true clinical conditions and since the intra-oral environment con-stitutes a complex milieu capable of affecting thephysico-mechanical properties of an adhesive mater-ial, such as the bond strength, one should be carefulwhen interpreting laboratory data.
In the orthodontic literature, there is a scarcity ofstudies examining the effect of aging on the bondstrength of composite resins5–9 apparently due to thedifficulty in simulating the in vivo effects of exposureto various intra-oral factors including masticatoryloads and mechanotherapy-related forces, and potentfactors such as saliva, acidic food and temperaturefluctuations. To overcome these obstacles, removableappliances have been used to allow dental materials to be retrieved from the oral environment and testedfor bond strength with a testing machine.6 An in vivo debonding device consisting of an elastic separator plier attached to a digital force gauge has also been tested.5,7 In the present study, the bonded premolars remained intra-orally for sixmonths, thus experiencing the in vivo environment,before being extracted and tested for shear bondstrength. Bond strength testing was similarly per-formed on non-aged specimens. The finding that 6-months of intra-oral aging did not affect the shearbond strength of composite resin adhesive is in agree-ment with a previous study,6 which examined thevariation of shear bond strength of Transbond adhesive at 4, 8 and 12 weeks post bonding.Moreover, the generalised result that bond strengthvalues for composite resin are not time-dependent, isalso supported from the work of Hajrassie and Khier7
who examined the effect of four different time frames(10 minutes, 24 hours, 1 week and 4 weeks) on bond strength. Nevertheless, it should be kept in mindthat the cohort of phenomena accompanying theintra-oral aging of the composite resin might not be reflected in the short-term bond strength performance of the adhesive.10
The results of this study provide support for the clinical relevance of laboratory bond strength testing
EFFECT OF IN VIVO AGING ON SHEAR BOND STRENGTH
Australian Orthodontic Journal Volume 25 No. 2 November 2009 125
Table I. Shear bond strength and Adhesive Remnant Coverage (ARC) ofin vivo aged and control specimens.
Shear bond strength ARCGroup Mean (N) SD Mean (%) SD
Without aging(N =14) 108.09 37.28a 71.31 21.04bWith aging(N =10) 122.64 39.23a 77.56 11.63b
Means with the same letters are not different at the 0.05 level (t - test)

CHATZISTAVROU ET AL
Australian Orthodontic Journal Volume 25 No. 2 November 2009126
for a period of six months; further research shouldvalidate the representative character of this testingprotocol for the full term of treatment.
Following debonding, the coverage of brackets withadhesive remnant demonstrated that, even thoughthe bond failure occurred mostly at the enamel-adhesive interface with 74.43 per cent of the bondingmaterial remaining on the bracket base, a small per-centage of specimens (3 out of 14 without aging) hadlarge adhesive remnants on enamel. This can beexplained by the fact that bonding to enamel is mainly achieved through micromechanical retention;the nature of retentive features may not be limited tothe formation of macro- and micro-tags, rather it mayalso include the formation of an interfacial resin-enamel interdiffusion zone within the lateral sites ofthe remaining enamel protuberances.11
In this study, adhesive remnant coverage was assessedwith the use of image measurement software(SigmaScan) as opposed to the popular AdhesiveRemnant Index (ARI).12 This particular softwareanalysis programme permits more accurate measure-ments of the quantity of adhesive remnants, even forthree-dimensional surfaces such as curved bracketbases, which are usually covered with retentive meshor grooves. Conventional ARI testing involves twomajor deficiencies: the fact that scores are derivedthrough a subjective assessment which involves visualinspection of enamel surface; and the dispropor-tional scales used. The ARI is used with four grades (0 = no adhesive remnant on enamel, 1 = less than 50per cent of adhesive on enamel, 2 = more than 50 percent of adhesive on enamel, 3 = all adhesive on enamel, along with the impression of the bracketbase) or five grades as in the modified index (5 = noadhesive remnant on enamel, 4 = less than 10 percent of adhesive on enamel, 3 = more than 10 per cent, but less than 90 per cent of adhesive onenamel, 2 = more than 90 per cent of adhesive onenamel, 1 = all adhesive on enamel, along with theimpression of the bracket base). Although many studies in the literature have utilised the ARI score,one study used the technique of map analysis ondebonded bracket bases and enamel. By using a digi-tiser attached to a computer, the adhesive is mappedaccording to three categories of thick, thin or noadhesive remaining.13 However, this method does notseem to be as accurate as the one used in the presentstudy with the analysis software.
Frequently, in the orthodontic literature, a Weibullanalysis is applied to provide the clinician with moreuseful information regarding the extrapolation of in-vitro data to clinical reality. Even though this survivalanalysis allows for fracture probability to be calculat-ed as a function of applied force or vice versa,14 thusallowing the consideration of non-parametric datawith inclusion of the smaller values of the tail of thedistribution,15–16 it is still a system based on predic-tions of bond strength values rather than on actualrecordings of in vivo bond strength values, asobtained in the present work.
Lastly, it should be noted that bond strength testingsuffers from a lack of standardisation. Factors such asstorage medium and the time prior to bonding toenamel should be taken into consideration, since theycould possibly affect the shear bond strength values.16
In the present work, the recommendations of Fox etal.15 were followed. Premolars which had beenextracted from adolescents for orthodontic purposeswere stored in distilled water for a maximum of 1–6months prior to bonding. Also, care was taken toensure the point of application and direction ofdebonding force was the same for all specimens toavoid enamel fractures or loading modes other thanthe shear (i.e. tensile or torsional), which would com-plicate the assessment of the actual shear bondstrength testing.
Conclusions
The results of this study demonstrated no significantdifferences in either the bond strengths or adhesiveremnant coverage of in vivo aged bonds after sixmonths in the oral cavity and their control counter-parts.
No correlation was demonstrated between the adhesive coverage between the two groups afterdebonding.
Corresponding author
Dr Theodore Eliades57 Agnoston Hiroon Street GR-14231 Nea IoniaGreeceEmail: [email protected]
References1. Powers JM, Kim HB, Turner DS. Orthodontic adhesives and
bond strength testing. Semin Orthod 1997;3:147–56.

2. Eliades G, Eliades T, Vavuranakis M. General aspects of biomaterials’ surface alterations following exposure to bio-logical fluids. In: Eliades G, Eliades T, Brantley WA, WattsDC, eds. Dental materials in vivo: aging and related phenomena. Chicago: Quintessence, 2003:3–23.
3. Eliades T, Bourauel C. Intra-oral aging of orthodontic mate-rials: the picture we miss and its clinical relevance. Am JOrthod Dentofac Orthop 2005;127:403–12.
4. Buonocore MG. A simple method of increasing the adhesionof acrylic filling materials to enamel surfaces. J Dent Res1955;34:849–53.
5. Pickett KL, Sadowsky PL, Jacobson A, Lacefield W.Orthodontic in vivo bond strength: Comparison with invitro results. Angle Orthod 2001;71:141–8.
6. Murray SD, Hobson RS. Comparison of in vivo and in vitroshear bond strength. Am J Orthod Dentofac Orthop 2003;123:2–9.
7. Hajrassie MK, Khier SE. In-vivo and in-vitro comparison ofbond strengths of orthodontic brackets bonded to enameland debonded at various times. Am J Orthod DentofacOrthop 2007;131:384–90.
8. Shammaa I, Ngan P, Kim H, Kao E, Gladwin M, Gunel E,Brown C. Comparison of bracket debonding force betweentwo conventional resin adhesives and a resin-reinforced glassionomer cement: An in vitro and in vivo study. AngleOrthod 1999;69:463–9.
9. Summers A, Kao E, Gilmore J, Gunel E, Ngan P.Comparison of bond strength between a conventional resinadhesive and a resin-modified glass ionomer adhesive: an invitro and in vivo study. Am J Orthod Dentofacial Orthop2004;126:200–6.
10. Eliades T. Comparing bond strengths. Am J OrthodDentofacial Orthop 2002;122:13A–15A.
11. Eliades T, Eliades G. Orthodontic Adhesive Resins. In:Brantley WA, Eliades T. Orthodontic Materials. Scientificand Clinical Aspects. Stuttgart: Thieme, 2001:201–19.
12. Årtun J, Bergland S. Clinical trials with crystal growth con-ditioning as an alternative to acid-etch enamel pretreatment.Am J Orthod 1984;85:333–40.
13. Rock WP, Abdullah MSB. Shear bond strengths produced bycomposite and compomer light cured orthodontic adhesives.J Dent 1997;25:243–9.
14. McCabe JF, Carrick TE. A statistical approach to themechanical testing of dental materials. Dent Mater 1986;2:139–42.
15. Fox NA, McCabe JF, Buckley JG. A critique of bondstrength testing in orthodontics. Br J Orthod 1994;21:33–43.
16. Eliades T, Brantley WA. The inappropriateness of conven-tional orthodontic bond strength assessment protocols. EurJ Orthod 2000;22:13–23.
EFFECT OF IN VIVO AGING ON SHEAR BOND STRENGTH
Australian Orthodontic Journal Volume 25 No. 2 November 2009 127

Introduction
Bond failure is arguably one of the most frustratingaspects of fixed appliance treatment. Failure of bonded attachments is costly in terms of clinical timeand material: it can prolong treatment and affect theoutcome. Previous clinical trials of bond failure rateshave compared bonding products and/or methods ofbonding, such as light-cured adhesive systems.1–9
Rates around 6 per cent (range 4.7 to 24.3 per cent)have been reported for first-time bond failures of anterior and premolar brackets.1–9 One studyincluded repeat failures and the rate rose to 9 percent.3 In large studies, the number of clinicians or
type of adhesive used do not appear to influence thefailure rate.1–3
Failure rates for molar tubes have received less atten-tion in the literature. Rates as low as 7 per cent havebeen reported for Speed molar tubes and rates as highas 20 per cent for conventional molar tubes whenlight-cured adhesives are used.10–12 The low profile ofSpeed molar tubes, in relation to the area of thebonding pad, and the absence of third order rotationin the tube may account for this finding. A failurerate of 34 per cent was reported when a chemically-cured adhesive was used to bond unspecified firstmolar tubes.12
Australian Orthodontic Journal Volume 25 No. 2 November 2009 © Australian Society of Orthodontists Inc. 2009128
Bond failure in clinical practice
Mark EwingSpecialist practice, Hamilton, New Zealand
Background: It has been suggested that the small bonding pads and prominent profiles of self-ligating brackets may lead tohigh failure rates when compared with conventional edgewise brackets.Aims: To compare the bond failure rates of a self-ligating bracket (Speed, Strite Industries, Cambridge, Canada) and a twinedgewise bracket (Mini-Diamond, Ormco, Orange, CA, USA) bonded with different adhesives (Sequence, Ormco, Orange,CA, USA; Transbond XT, 3M Unitek, Monrovia, CA, USA); to compare the bond failure rates of a self-ligating bracket bondedwith different adhesives (Enlight, Ormco, Orange, CA, USA; Lightbond, Reliance, Itasca, IL, USA); and to compare the bondfailure rates of molar attachments (Speed, Strite Industries, Cambridge, Canada) using different adhesives (Enlight, Ormco,Orange, CA, USA; Lightbond, Reliance, Itasca, IL, USA; Sequence, Ormco, Orange, CA, USA; Transbond XT, 3M Unitek,Monrovia, CA, USA).Methods: This retrospective study covered 17 years. Study A (1991–99): Speed and Mini-Diamond brackets were bonded inboth arches with either Sequence (Group 1) or Transbond-XT (Group 2) adhesives and the number of bond failures compared.Study B (2000–07): Speed brackets were bonded with either Lightbond (Group 3) or Enlight (Group 4) adhesives and the totalnumber of bond failures (first-time and re-failures) compared. In Study C (1991–2007) Speed upper molar mini-brackets, uppermolar tubes or ER brackets were used in the upper arch, and Speed lower buccal tubes were used in the lower arch. The fail-ure rates of the molar attachments were compared.Results: In Study A the failure rates with Sequence adhesive were: Speed 7.3 per cent, Mini-Diamond 11.9 per cent (p = 0.05). With Transbond XT adhesive the failure rates were: Speed 5.9 per cent, Mini-Diamond 6.4 per cent (p > 0.05).The teeth with the highest failure rates (central incisors and second premolars) were similar for both appliances. In Study B thefailure rates were: Group 3 (Speed/Lightbond) 4.2 per cent; Group 4 (Speed/Enlight) 6.9 per cent; Group 3 vs Group 4, p = 0.05. In Study C the failure rate of Speed upper molar mini-brackets was markedly higher than the failure rates of themolar tubes.Conclusions: The failure rates of the Speed brackets reduced over time, possibly because of improvements in the adhesives.The small bonding pads and prominent profiles of Speed brackets did not result in high failure rates.(Aust Orthod J 2009; 25: 128–135)
Received for publication: September 2008Accepted: July 2009
Mark Ewing: [email protected]

BOND FAILURE IN CLINICAL PRACTICE
Australian Orthodontic Journal Volume 25 No. 2 November 2009 129
Whether they are used on the anterior teeth ormolars, it could be argued that brackets with smallbases and prominent profiles, such as Speed self-ligat-ing brackets, are more susceptible to bond failurethan conventional attachments, which generally havelarger bases and relatively flat profiles.
The aims of this retrospective practice-based studywere threefold: to compare the bond failure rates oftwin edgewise brackets and Speed brackets over a 9-year period; to compare the failure rates for Speedbrackets bonded with two different adhesives in thesubsequent eight years; and to compare the bond fail-ure rates of Speed molar attachments using differentadhesives.
Materials and methods
Between 1991 and 2007 data were available for 1834subjects (Mean age: 13.4 years, Range: 10.1–46.9years) who had completed treatment. Of these, 179subjects had conventional edgewise twin anterior and premolar brackets bonded in both arches (Mini-Diamond, Ormco, Orange, CA, USA) and theremainder had self-ligating anterior and premolarbrackets (Speed, Strite Industries, Cambridge,Canada) bonded in both arches. Between 2000 and2007 the Speed lower second premolar brackets wereoffset gingivally and had larger bonding pads than thepremolar brackets used prior to 2000. Three types ofattachments were used on upper molars: a singleSpeed bracket with a miniature bonding pad(1991–93), a Speed upper buccal tube (1994–2002)
and a Speed ER upper first molar bracket (2002–07).On the lower first molars, Speed bondable buccaltubes were used exclusively (1991–2007). The secondmolars were excluded from this study because manywere either not bonded or were bonded late in treat-ment. All subjects had attachments bonded from firstmolar to first molar with one of four light curedadhesives: 1991–99, Sequence (Ormco, Orange, CA,USA); 1991–99, Transbond XT (3M Unitek,Monrovia, CA); 2000–06, Lightbond (Reliance,Itasca, IL, USA); 2002–07, Enlight (Ormco, Orange,CA, USA).
The following data were recorded for each subject:appliance used (i.e. type of attachment), bondingdate, adhesive used, treatment duration, originalbond failure and any subsequent bond failures.Subjects with 0.018 inch attachments, molar bandsand patients treated with appliances other than Mini-Diamond or Speed were excluded. On deep bitecases, when the upper teeth contacted the lower anter-ior and/or premolar brackets, either a removable biteplate or acrylic bite button was used to prevent theupper teeth from dislodging the lower attachment(s).The bite plates/buttons were discontinued once theposterior teeth had erupted into contact and thelower brackets were no longer liable to be dislodged.
Bonding protocolsFrom 1991 to 1999, all attachments were bonded bythe author. The teeth were cleaned with pumice andwater, etched for 30 seconds with 37 per cent
Table I. Comparison of overall bond failure rates.
Group Years used Bracket type Adhesive Subjects Treatment Bracket Debonded Overallused (N) duration (N) (N) failure rate
(Months) (Per cent)
1 1991–99 SL S 89 21.9 1680 123 7.31991–99 E S 67 24.5 1248 148 11.9
2 1991–99 SL T-XT 261 22.4 4935 291 5.91991–99 E T-XT 112 23.8 2083 134 6.4
3 2000–06 SL L 577 23.2 11304 477 4.2
4 2002–07 SL E/O 409 23.1 7981 553 6.9
Odds ratio: Group 1 (SL vs E): p = 0.05; Group 2 (SL vs E): p > 0.05Group 3 vs Group 4 (Lightbond/Speed vs Enlight/Speed): p = 0.05SL, Speed; E, Mini-DiamondE/O, Enlight/Orthosolo; L, Lightbond; S, Sequence; T-XT, Transbond-XT

EWING
Australian Orthodontic Journal Volume 25 No. 2 November 2009130
Table II. Distribution of bond failures, by bracket type.
Group 1 SequenceSpeed Bonded Failures Per cent Mini-Diamond Bonded Failures Per centTooth (N) (N) Tooth (N) (N)
11 89 9 10.1 11 67 20 29.912 89 10 11.2 12 67 7 10.413 89 3 3.4 13 67 8 11.914 74 1 1.4 14 56 3 5.415 66 11 16.7 15 48 7 14.6
21 89 13 14.6 21 67 14 20.922 89 2 2.2 22 67 8 11.923 89 3 3.4 23 67 6 9.024 73 7 9.6 24 57 6 10.525 72 7 9.7 25 49 13 26.5
31 89 11 12.4 31 67 7 10.432 89 3 3.4 32 67 1 1.533 89 2 2.2 33 67 4 6.034 83 5 6.0 34 66 7 10.635 81 7 8.6 35 51 12 23.5
41 89 7 7.9 41 67 7 10.442 89 1 1.1 42 67 1 1.543 89 3 3.4 43 67 1 1.544 84 7 8.3 44 66 3 4.545 79 11 13.9 45 51 13 25.5
Totals 1680 123 7.3 1248 148 11.9
Group 2 Transbond XTSpeed Bonded Failures Per cent Mini-Diamond Bonded Failures Per centTooth (N) (N) Tooth (N) (N)
11 261 29 11.1 11 112 14 12.512 261 25 9.6 12 112 6 5.413 261 3 1.1 13 112 5 4.514 198 4 2.0 14 80 2 1.315 221 25 11.3 15 89 11 7.9
21 261 29 11.1 21 112 18 17.022 261 18 6.9 22 112 5 2.723 261 2 0.8 23 112 4 3.624 200 8 4.0 24 79 4 5.125 220 21 9.5 25 92 12 9.8
31 261 19 7.3 31 112 3 2.732 261 10 3.8 32 112 1 0.933 261 12 4.6 33 112 2 1.834 252 6 2.4 34 105 3 2.935 230 22 9.6 35 95 22 23.2
41 261 18 6.9 41 112 3 1.842 261 5 1.9 42 112 0 0.043 261 9 3.4 43 112 3 2.744 252 7 2.8 44 105 2 1.045 230 19 8.3 45 94 14 14.9
Totals 4935 291 5.9 2083 134 6.4

BOND FAILURE IN CLINICAL PRACTICE
Australian Orthodontic Journal Volume 25 No. 2 November 2009 131
hydrophosphoric acid and dried. The sealants andadhesives were applied according to the manufact-urers' instructions and light-cured with a Demetron401 light (Kerr Corporation, Orange, CA, USA).Lost attachments were replaced with new attach-ments and were bonded using the same protocol.From 2000–2007, the same protocol was used forbonding except the teeth were cleaned by an ortho-dontic auxiliary and bonded by the author with aDemetron 501 curing light (Kerr Corporation,Orange, CA, USA). Lost attachments were sandblast-ed and rebonded by an orthodontic auxiliary. In thisperiod, first-time failures and all subsequent failureswere recorded separately.
Data managementStudy A (1991–99): Speed and Mini-Diamondbrackets were bonded in both arches with either
Sequence (Group 1) or Transbond-XT (Group 2)adhesives and all bond failures were compared.
Study B (2000–07): Speed brackets were bondedwith either Lightbond (Group 3) or Enlight (Group4) adhesive and the total number of bond failures(first-time and re-failures) recorded. The lower secondpremolar brackets were offset gingivally and had larger bonding pads than the premolar brackets usedin Study A.
Study C (1991–2007): the total failure rates of themolar attachments were compared.
As there were no detectable gender differences thedata from the boys and girls were combined. In each group the total number of bond failures wasrecorded. The percentages for each tooth and theoverall percentage failure were then calculated. Theprobability of failure at the 0.05 level of significancewas calculated with the odds ratio.
Table III. Distribution of bond failures, by adhesive.
Group 3 Group 4Lightbond/ Enlight/
Speed Bonded Failures Per cent Re-failures Per cent Speed Bonded Failures Per cent Re-failures Per cent Tooth (N) (N) (N) overall Tooth (N) (N) (N) overall
11 577 48 8.3 5 9.2 11 409 56 13.7 12 16.612 577 18 3.1 2 3.5 12 409 29 7.1 3 7.813 577 6 1.0 0 1.0 13 409 5 1.2 2 1.714 549 5 0.9 0 0.9 14 396 10 2.5 3 3.315 529 53 10.0 7 11.3 15 362 68 18.8 26 26.0
21 577 48 8.3 7 9.5 21 409 48 11.7 19 16.422 577 30 5.2 0 5.2 22 409 33 8.1 6 9.523 577 6 1.0 0 1.0 23 409 4 1.0 1 1.224 546 11 2.0 1 2.2 24 399 11 2.8 0 2.825 530 69 13.0 16 16.0 25 362 80 22.1 39 32.9
31 577 26 4.5 2 4.9 31 409 12 2.9 4 3.932 577 5 0.9 1 1.0 32 409 5 1.2 1 1.533 577 5 0.9 0 0.9 33 409 8 2.0 3 2.734 570 9 1.6 0 1.6 34 406 1 0.2 0 0.235 542 30 5.5 0 5.5 35 371 9 2.4 0 2.4
41 577 20 3.5 1 3.6 41 409 11 2.7 5 3.942 577 4 0.7 1 0.9 42 409 8 2.0 1 2.243 577 4 0.7 0 0.7 43 409 2 0.5 4 1.544 570 6 1.1 1 1.2 44 407 6 1.5 0 1.545 544 29 5.3 1 5.5 45 370 14 3.8 4 4.9
Totals 11304 432 3.8 45 4.2 7981 420 5.3 133 6.9

Results
The results are summarised in Tables I to IV.
Study A: In Group 1, the overall failure rates for Speedand Mini-Diamond brackets bonded with Sequenceadhesive were 7.3 and 11.9 per cent, respectively (TableI). There was a statistically significant differencebetween these two proportions (p = 0.05). The teethwith high failure rates were the second premolars andcentral incisors (Table II). In Group 2, the overall fail-ure rates for the Speed brackets and Mini-Diamondbrackets bonded with Transbond-XT adhesive were5.9 and 6.4 per cent, respectively (p > 0.05). Again,the teeth with the highest failure rates were the secondpremolars and central incisors (Table II, Figure 1).
Study B: The overall bond failure rates for the Speedbrackets bonded with Lightbond and Enlight adhe-sives were 4.2 and 6.9 per cent, respectively (p =0.05). The upper second premolars had the highestfailure rate with both adhesives (Table III, Figure 2).
Study C: The results are presented in chronologicalgroups corresponding to the adhesive and attachmentused (Table IV). Between 1991 and 1993 the failurerates for the Speed upper molar mini-brackets withSequence adhesive were 19.9 (tooth 16) and 28.8(tooth 26) per cent, and for the Speed lower molarbuccal tubes the failure rates were 7.8 (tooth 36) and8.3 (tooth 46) per cent. Between 1994 and 1998, thefailure rates of Speed upper and lower buccal tubes
with Transbond-XT adhesive were 8.3 per cent (tooth16), 9.5 per cent (tooth 26), 6.5 per cent (tooth 36)and 7.1 per cent (tooth 46). From 1998 to 2002, thefailure rates of Speed upper and lower buccal tubeswith Lightbond adhesive were 4.1 per cent (tooth16); 6.1 per cent (tooth 26), 1.7 per cent (tooth 36)and 4.4 per cent (tooth 46). From 2002 to 2006, thefailure rates for Speed ER upper first molar bracketsand Speed lower buccal tubes bonded withLightbond were 9.3 per cent (tooth 16), 10.5 (tooth26), 0.8 (tooth 36) and 1.2 (tooth 46). Between 2002and 2007, the combination of Enlight adhesive andSpeed ER upper first molar brackets failed in 11.7(tooth 16), 16.6 (tooth 26) per cent, and Enlightadhesive and Speed lower buccal tubes failed in 1.5(tooth 36) and 1.0 (tooth 46) per cent of the bondedmolars.
Discussion
The bond failure rates of a twin edgewise bracket(Mini-Diamond), a self-ligating bracket (Speed) anda variety of Speed molar attachments were investi-gated in this long-term, retrospective practice-basedstudy. Despite material changes during the course ofthe study it is possible to draw some conclusionsabout the bond failure rates of the brackets and buccal tubes used. The overall failure rate of Speedbrackets was less than the failure rate of Mini-Diamond brackets when Sequence adhesive was used,
EWING
Australian Orthodontic Journal Volume 25 No. 2 November 2009132
Table IV. Bond failure rates of first molar attachments, by tooth and adhesive.
Years used Attachment Adhesive Subjects Tooth 16 Tooth 26Failures Failures
(N) (N) (Per cent) (N) (Per cent)
1991–3 SL mini bracket S 159 31 19.9 45 28.81994–8 SL buccal tube T-XT 488 40 8.3 46 9.51998–2002 SL buccal tube L 521 21 4.1 32 6.1
2002–6 SL ER bracket L 257 24 9.3 27 10.52002–7 SL ER bracket E/O 409 48 11.7 68 16.6
Tooth 36 Tooth 461991–3 Buccal tube S 159 12 7.8 13 8.31994–8 Buccal tube T-XT 488 32 6.5 34 7.11998–2002 Buccal tube L 521 9 1.7 23 4.4
2002–6 Buccal tube L 257 2 0.8 3 1.22002–7 Buccal tube E/O 409 6 1.5 4 1
SL, Speed; E/O, Enlight; L, Lightbond; S, Sequence; T-TX, Transbond XT

but there was no difference between the brackets withTransbond adhesive, despite the Speed brackets having smaller bonding pads and more prominentprofiles than the Mini-Diamond brackets. The over-all failure rates for both brackets with Transbondadhesive were comparable to the first-time bond fail-ure rates reported by others using the same adhesive,and less than the rates reported by others when allbond failures were counted.1–3 Fewer Speed bracketsfailed when Lightbond adhesive was used as com-pared with Enlight adhesive, and more upper secondpremolar and upper central incisor brackets failedthan brackets bonded to other teeth. In the upperarch, fewer Speed buccal tubes failed than Speedupper molar mini-brackets or Speed ER brackets, andin the lower arch fewer buccal tubes were lost wheneither Lightbond or Enlight adhesive was used.
In a long-term practice-based study such as this, thelimitations should be mentioned. Firstly, the adhesives, the methods of application, the curinglight and the design of the Speed lower premolarbrackets were changed during the course of the study.For these reasons it was necessary to separate the datainto chronological groups. Although this procedurereduced the number of subjects in each group, thenumber of brackets bonded was still higher than
the totals reported in previous studies.1–9 Becausethere were fewer subjects (and brackets) in Groups 1and 2 the relatively high overall failure rates in thesegroups may be due to the sizes of the samples and/orthe materials and methods used. The practice of usingan orthodontic auxiliary to rebond brackets may have contributed to the high failure rate of bracketsbonded to the second premolars in Groups 3 and 4.The strengths of this study should also be mentioned:large numbers of subjects and brackets were used andevery effort was made to ensure consistent handlingof the materials by an experienced clinician. To reflectthe reality of clinical practice, all debonds wererecorded and failed brackets were either replaced withnew brackets or the original brackets were micro-etched and rebonded. It made no difference to thefailure rate what procedure was followed, whichagrees with findings in other studies.13–16
The patterns of bond failure were similar for bothtypes of bracket. More upper and lower second pre-molar and upper central incisor brackets were lostthan brackets bonded to other teeth. The failure ratesfor Speed lower anterior and lower premolar bracketsfell appreciably over time as new adhesives and gingivally offset lower premolar brackets on a largerpad were introduced.17–18 These findings suggest that
BOND FAILURE IN CLINICAL PRACTICE
Australian Orthodontic Journal Volume 25 No. 2 November 2009 133
Per
cent
age
debo
nds
Per
cent
age
debo
nds
Figure 1. Failure rates for Speed and Mini-Diamond brackets with TransbondXT adhesive.
Figure 2. Failure rates for Speed brackets bonded with either Lightbond orEnlight adhesive.

improvements in the design of the upper second pre-molar brackets, to render them less likely to fail,could reduce the bond failure rates to negligible levels. The patterns of bond failure were similar in allgroups, but the overall rate of failure of the uppercentral incisors and second premolars rose markedlyin Group 4 because of the high number of bracketsthat failed more than once. The bonding pads onfailed brackets were microetched, which should haveresulted in bond strengths similar to the bondstrengths of new brackets,13–16 but one study hasshown that replacement brackets have up to 30 percent lower shear bond strength than first-time bonded brackets.19
The similarity in the pattern of failure for both typesof appliance and for all adhesives suggests that bondfailure may be due to patient behaviour, enamel vari-ability and/or the difficulty in bonding to upper second premolars with short clinical crowns andenlarged gingivae.20–22 The higher failure rate ofupper central incisors may be correlated with activi-ties, such as participation in contact sports, eatingstone fruit and drinking from plastic drink bottles. Itis difficult to determine the precise cause(s) of bondfailure in the present study due the number of con-founding variables and lack of information on patientbehaviour.
The experience in this study indicates that improve-ments in the design of molar attachments and adhesive technology now result in acceptable failurerates for the upper and lower first molars. Failure ratesof the bonded lower molar attachments in the presentstudy were better than most of the failure rates of firstmolar bands cemented with modern glass ionomercements, and substantially less than the failure ratesof bonded upper and lower molar attachmentsreported by others.10–12,23–29 Pandis and coworkers,who also bonded Speed buccal tubes with Transbondadhesive, reported an upper first molar failure rate ofapproximately 7 per cent, which agrees with the find-ings in the present study, and a lower molar failurerate of 12 per cent which is substantially higher thanour failure rate.11
Relatively high failure rates were experienced withSpeed upper molar attachments, as compared withthe lower molar buccal tubes. In light of the high fail-ure rates with Speed upper molar mini-brackets andSequence adhesive this adhesive-bracket combinationwas discontinued. A recent in-vitro study reported
the shear bond strengths of Transbond and Light-bond were not the same for all teeth.22 The highestbond strengths were reported for the lower molarsand upper central incisors with Lightbond adhesive,which supports the findings of the present study.22 Inthe present study the failure rates of the lower buccaltubes with Enlight adhesive were similar to the failurerates with Lightbond adhesive. Higher failure ratesfor the upper first molar attachments with both adhesives lends further support to the finding thatdifferent teeth have different shear bond strengths.20–22
Conclusions
The overall failure rates of Speed anterior and pre-molar brackets were slightly better than the failurerates of the Mini-Diamond brackets, despite theSpeed brackets having smaller bonding pads andmore prominent profiles than the Mini-Diamondbrackets.
The patterns of bond failure were similar for bothtypes of bracket, which suggests that bond failure isdue to patient behaviour and/or tooth type. Failure ofbrackets bonded to the upper second premolarsremained high throughout the study.
The failure rates for Speed anterior and premolarbrackets reduced over time, possibly due to improve-ments in the adhesives used. The failure rates ofSpeed lower molar attachments were lower than thefailure rates of Speed upper first molar attachments.
Acknowledgment
I thank Lyn Hunt, Department of Statistics,University of Waikato for the statistical analysis.
Corresponding author
Dr Mark P. Ewing29 Pembroke StreetHamilton 3204New ZealandTel: +64 7 839 5870Fax: +64 7 834 1148Email: [email protected]
References1. Millett DT, Hallgren A, Cattanach D, McFadzean R,
Pattison J, Robertson M, Love J. A 5-year clinical review ofbond failure with a light cured resin adhesive. Angle Orthod1998;68:351–6.
2. Linklater RA, Gordon PH, Bond failure patterns in vivo.Am J Orthod Dentofacial Orthop 2003;123:534–9.
EWING
Australian Orthodontic Journal Volume 25 No. 2 November 2009134

BOND FAILURE IN CLINICAL PRACTICE
Australian Orthodontic Journal Volume 25 No. 2 November 2009 135
3. Adolfsson U, Larsson E, Ogaard B. Bond failure of a no-mixadhesive during orthodontic treatment. Am J OrthodDentofacial Orthop 2002;122:277–81.
4. Kinch AP, Taylor H, Warltier R, Oliver RG, Newcombe RG.A clinical trial comparing the failure rates of directly bonded brackets using etch times of 15 or 60 seconds. Am JOrthod Dentofacial Orthop 1988;94:476–83.
5. O’Brien KD, Read MJ, Sandison RJ, Roberts CT. A visiblelight-activated direct-bonding material: An in vivo compar-ative study. Am J Orthod Dentofacial Orthop 1989;95:348–51.
6. Trimpeneers LM, Dermaut LR. A clinical trial comparingthe failure rates of two orthodontic bonding systems. Am JOrthod Dentofacial Orthop 1996;110:547–50.
7. Sunna S, Rock WP. Clinical performance of orthodonticbrackets and adhesive systems: A randomized clinical trial.Brit J Orthod 1998; 25:283–7.
8. Tang ATH, Björkman L, Lindbäck KF, Andlin-Sobocki A,Ekstrand J. Retrospective study of orthodontic bondingwithout liquid resin. Am J Orthod Dentofacial Orthop2000;118:300–6.
9. Armas Galindo HR, Sadowsky PL, Vlachos C, JacobsonA,Wallace D. An in-vivo comparison between a visible light-cured bonding system and a chemically cured bonding system. Am J Orthod Dentofacial Orthop 1998;113:271–5.
10. Millett DT, Hallgren A, Fornell AC, Robertson M. Bondedmolar tubes: A retrospective evaluation of clinical perform-ance. Am J Orthod Dentofacial Orthop 1999;115:667–74.
11. Pandis N, Christensen L, Eliades T. Long-term clinical fail-ure rate of molar tubes bonded with a self-etching primer.Angle Orthod 2005;75:1000–2.
12. Banks P, Macfarlane TV. Bonded versus banded first molarattachments: a randomized controlled clinical trial. JOrthod 2007;34:128–36.
13. Mui B, Rossouw PE, Kulkarni GV. Optimization of a pro-cedure for rebonding dislodged orthodontic brackets. AngleOrthod 1999;69:276–81.
14. Grabouski JK, Staley RN, Jakobsen JR. The effect ofmicroetching on the bond strength of metal brackets whenbonded to previously bonded teeth: an in vitro study. Am JOrthod Dentofacial Orthop 1998;114:452–60.
15. Sonis AL. Air abrasion of failed bonded metal brackets: astudy of shear bond strength and surface characteristics asdetermined by scanning electron microscopy. Am J OrthodDentofacial Orthop 1996;110:96–8.
16. Sunna S, Rock WP. Effect of sandblasting on the retentionof orthodontic brackets: a controlled clinical trial. J Orthod2008;35:43–8.
17. Thind BS, Larmour CJ, Stirrups DR, Lloyd CH. An ex vivoassessment of gingivally offset lower premolar brackets. JOrthod 2004;31:34–40.
18. Thind BS, Stirrups DR, Hewage S. Bond failure of gingival-ly offset mandibular premolar brackets: A randomized con-trolled clinical trial. Am J Orthod Dentofacial Orthop 2009;135:49–53.
19. Bishara SE, Laffoon JF, Vonwald L, Warren JJ. The effect ofrepeated bonding on the shear bond strength of differentorthodontic adhesives. Am J Orthod Dentofacial Orthop2002;121:521–5.
20. Linklater RA, Gordon PH. An ex vivo study to investigatebond strengths of different tooth types. J Orthod 2001;28:59–65.
21. Hobson RS, McCabe JF, Hogg SD. Bond strength to surfaceenamel for different tooth types. Dent Mater 2001;17:184–9.
22. Öztürk B, Malkoç S, Koyutürk AE, Catalbas B, Ozer F.Influence of different tooth types on the bond strength oftwo orthodontic adhesive systems. Eur J Orthod 2008;30:407–12.
23. Fricker JP, McLachlan MD. Clinical studies of glass ionomercements. Part 1: a twelve-month clinical study comparingzinc phosphate cement to glass ionomer. Aust Orthod J1985;9:179–80.
24. Gillgrass TJ, Benington PC, Millett DT, Newell J, GilmourWH. Modified composite or conventional glass ionomer forband cementation? A comparative clinical trial. Am JOrthod Dentofacial Orthop 2001;120:49–53.
25. Mizrahi E. Glass ionomer cements in orthodontics – anupdate. Am J Orthod Dentofacial Orthop 1988;93:505–7.
26. Millett DT, McCabe JF, Bennett TG, Carter NE, GordonPH. The effect of sandblasting on the retention of firstmolar orthodontic bands cemented with glass ionomercement. Br J Orthod 1995;22:161–9.
27. Stirrups DR. A comparative clinical trial of a glass ionomerand a zinc phosphate cement for securing orthodonticbands. Br J Orthod 1991;18:15–20.
28. Millett DT, Gordon PH. The performance of first molarorthodontic bands cemented with glass ionomer cement – aretrospective analysis. Br J Orthod 1992;19:215–20.
29. Millett DT, Hallgren A, McCluskey LA, McAuley F, FornellAC, Love J et al. A clinical retrospective evaluation of twoorthodontic band cements. Angle Orthod 2001;71:470–6.
Printed with permission of the Australian Society of Orthodontists Inc. 2009

Introduction
In orthodontic treatment, sliding mechanics usingpre-adjusted brackets is a common method of trans-lating a tooth or a group of teeth. In particular, over-jet reduction or space closure with the ‘straight-wiretechnique’ is achieved by applying a force that pro-duces sliding of the archwire through the slots of thebrackets or the tubes of the posterior teeth.1 Themajor disadvantage with the use of sliding mechanicsis the friction generated between the bracket and thearchwire during orthodontic movement. The amountof friction is proportional to the force with which thetwo surfaces are pressed together and dependent onthe nature of the surfaces in contact. The forceapplied must overcome friction to achieve the desiredorthodontic movement. It has been suggested that50–60 per cent of the applied force may be lost
in overcoming frictional resistance.2 Frictional resis-tance must be kept to a minimum during slidingmechanics so that orthodontic tooth movement canbe generated through light optimal forces, sinceincreased forces in an attempt to overcome frictionalresistance during retraction of the anterior teeth mayproduce increased posterior anchorage loss.3
Elastomeric modules are widely used in orthodonticpractice for the engagement of archwires into brackets, and have gained almost universal acceptanceby the profession. Despite this popularity, there hasbeen some concern about the effect of the elasto-meric modules on frictional resistance. The frictionalbehaviour of elastomeric modules can be affected byfactors such as the method of tying, pre-stretchingand the oral environment.4,5 Low-friction elasto-meric modules have been shown to generate lower
Australian Orthodontic Journal Volume 25 No. 2 November 2009 © Australian Society of Orthodontists Inc. 2009136
Static frictional resistance with the Slide low-friction elastomeric ligature system
Steven P. Jones and Saida Ben Bihi Unit of Orthodontics, UCL Eastman Dental Institute for Oral Health Care Sciences, London, UK
Aim: This ex-vivo study compared the static frictional resistance of a low-friction ligation system against a conventional elastomeric module, and studied the effect of storage in a simulated oral environment on the static frictional resistance of bothligation systems.Methods: Eighty stainless steel brackets were tested by sliding along straight lengths of 0.018 inch round and 0.019 x 0.025inch rectangular stainless steel wires ligated with either conventional elastomerics or the Slide system (Leone, Florence, Italy).During the tests the brackets and wires were lubricated with artificial saliva. A specially constructed jig assembly was used tohold the bracket and archwire securely. The jig was clamped in an Instron universal load testing machine. Crosshead speedwas controlled via a microcomputer connected to the Instron machine. The static frictional forces at 0 degree bracket/wireangulation were measured for both systems, fresh from the pack and after storage in artificial saliva at 37 °C for 24 hours. Results: The results of this investigation demonstrated that the Slide ligatures produced significantly lower static frictional resistance than conventional elastomeric modules in the fresh condition and after 24 hours of storage in a simulated oral environment (p < 0.001). Storage for 24 hours in artificial saliva had no effect on the static frictional resistance of conventionalelastomeric modules and the Slide system (p = 0.525).Conclusions: The claim by the manufacturer that the Slide system produces lower frictional resistance than conventional elastomeric modules is upheld.(Aust Orthod J 2009; 25: 136–141)
Received for publication: May 2009Accepted: July 2009
Steven Jones: [email protected] Ben Bihi: [email protected]

FRICTION WITH THE SLIDE SYSTEM
Australian Orthodontic Journal Volume 25 No. 2 November 2009 137
forces during alignment and maxillary arch expan-sion, and shorten treatment time6–10 although theireffects on linear sliding have yet to be evaluated fully.
In this laboratory-based study, the static frictionalresistance to sliding of a low-friction ligation systemwas compared to that of conventional elastomericmodules. Frictional forces were measured in the freshstate, and after a period of storage in a simulatedintra-oral environment, to assess any deteriorationassociated with use.
Materials and methods
Stainless steel upper left central incisor brackets (MidiDiagonali, Leone, Florence, Italy) with Roth pre-scription and 0.022 x 0.028 inch slots were used.Incisor brackets were chosen because of their flat pro-file bases, which facilitated mounting for the tests.The brackets were from the same batch to ensureconsistency of manufacture.
Two different types of stainless steel archwire wereused, 0.018 inch round and 0.019 x 0.025 inch rec-tangular, both supplied as 25 cm (10 inch) straightlengths (AJ Wilcock, Whittlesea, Victoria, Australia).All wires tested were obtained from the same batch toensure consistency of manufacture. Wires were cutinto 10 cm lengths, and a new length of wire was usedfor each test.
Two different types of elastomeric modules were test-ed, conventional elastomeric modules (GlenroeTechnologies, Bradenton, USA) and low-friction lig-atures (Slide system, Leone, Florence, Italy). All mod-ules tested were obtained from the same batch toensure consistency of manufacture. A new conven-tional elastomeric module and Slide system ligaturewas used for each individual test.
An artificial saliva (Saliva Orthana, Nycomed,Birmingham, UK), which contains pig mucin, xyli-tol, and mineral salts, was used to provide lubricationfor the system.
Each group of 10 brackets was degreased in a solutionof acetone for 10 minutes and then allowed to air dryfor an equivalent amount of time. The brackets werethen transferred to a container with 5 ml of artificialsaliva and left standing for 24 hours to allow surfaceadsorption. The archwires were cut into 10 cmlengths and cleaned with alcohol immediately beforeeach test. Two groups of both conventional and Slidesystem ligatures were used. The first group was used
directly from the canes, while the second group was placed unstretched in artificial saliva and storedat a temperature of 37 °C for 24 hours in order to simulate a period in the oral environment.
The method used has been comprehensivelydescribed in a previous publication.11 Brackets weremounted in a custom-made jig assembly, with eachbracket secured in a mount by means of an adjustablevice and screw beneath the bracket base. The bracketmount was removable from the testing apparatus tofacilitate this procedure. Each bracket was mountedsuch that the bracket slot angulation was set at 0degree using a straight piece of 0.021 x 0.025 inchwire as a guide. Once the bracket had been mounted,the guide wire was removed and a sample of 10 cm oftest wire was placed passively into the bracket slot andthrough the turrets of the jig. The wire was clampedsecurely at the superior and inferior ends. The middleclamp was loosely tightened until the tensile forcehad been applied. The jig was then transferred to abench positioned heavy duty clamp, which held thejig in a vertical position. A weight of 1 kg was placedonto the most inferior clamp to put the wire sampleunder tension in order to straighten it by eliminatingany inherent curvature. The central clamp was thentightened against the jig to fix the wire in its tensioned state before the weight was removed. Theclamp system was constructed such that in the case ofthe rectangular wire, this resulted in the wire lyingpassively through the slot with no active torque dif-ferential between the wire and slot, which eliminatedany additional effect of torque on friction. A conven-tional elastomeric module or Slide system ligaturewas placed onto the bracket using a pair of mosquitoforceps. Each was placed around four tie wings of thebracket and secured the wire into the bracket slot.
A universal load testing machine with 1 kN load cell(Instron, High Wycombe, UK) was used to hold thejig in place and to produce a steady movement of thearchwire through the bracket slot. The Instronmachine was switched on and formatted automatic-ally. The assembled jig was placed into the jaw gripsof the Instron machine by first securing the inferiorarm on the jig into the machine. The Instronmachine was then calibrated and balanced once thesuperior arm of the jig was secured. The bracketmount was held in the mid-distance of the turrets, toensure that the inter-bracket distance was reproducedthroughout the test. Prior to each test, artificial saliva

was applied onto the bracket, wire and ligature usinga soft brush to ensure that the system was well-lubricated. The crosshead speed was set at 0.5 mm/minand the test was run over 1 mm. All results wererecorded on a microprocessor connected to theInstron machine. The force levels were processed bycomputer and displayed as a force/displacementgraph. The curve produced took the form of an initialpeak followed by a plateau region. The initial peakcorresponded to the force required to commence move-ment of the bracket relative to the archwire and wasrecorded as the value for the static frictional resistance.
A sample size calculation was carried out using datafrom a previous study.12,13 It was determined that inorder to detect a difference in static frictional resist-ance of 10 per cent, with a power of 90 per cent andat an α-level of 0.05, a sample size of 10 samples pergroup would be required.
Results
The data were first manually entered in MicrosoftExcel and then imported into a software statisticalpackage (SPSS 14.0 for Windows, SPSS Inc.) for statistical analysis. The data were found to be nor-mally distributed and therefore parametric tests werecarried out to investigate for statistical differencesbetween groups. A two-way analysis of variance(ANOVA) was used for inter-group examination tocompare the static friction of the conventional modules and Slide ligature system on different wires(round/rectangular) and under different conditions(fresh and 24 hours of storage in a simulated oralenvironment) and to assess interactions between factors.
Data are demonstrated in Table I with the two-wayANOVA results in Table II. The mean static fric-tional resistance produced with the Slide system waslower than that of conventional elastomeric modules(Two-way ANOVA: p < 0.001). When the ligatureswere used fresh from the canes the conventional elasto-meric modules produced a significantly higher levelof static frictional resistance for both 0.018 inchround wire (Elastomeric mean: 1.57 N, 95% CI:1.24, 1.90; Slide system mean: 0.22 N, 95% CI:0.11, 0.55; p < 0.001) and 0.019 x 0.025 inch rec-tangular archwire (Elastomeric mean: 1.17 N, 95%CI: 0.84, 1.50; Slide system mean: 0.35 N, 95% CI:0.02, 0.68; p < 0.001). When the ligatures wereimmersed in a simulated oral environment for a duration of 24 hours the conventional elastomericmodules again produced significantly higher staticfrictional resistance values for both 0.018 inch roundwire (Elastomeric mean: 1.11 N, 95% CI: 0.78, 1.45;Slide system mean: 0.34 N, 95% CI: 0.01, 0.67; p <0.001) and 0.019 x 0.025 inch rectangular archwire(Elastomeric mean: 1.16 N, 95% CI: 0.83, 1.49; Slidesystem mean: 0.39 N, 95% CI: 0.06, 0.72; p < 0.001).
Table II demonstrates that the type of ligation system(System) produces highly significant differences infrictional resistance (p < 0.001). However, the type ofwire (wire) and the storage status of the ligation system, either fresh from the canes or after a 24 hourperiod of soaking in artificial saliva (saliva) do notgive statistically significant differences (Wire: p =0.709; Saliva: p = 0.525). Table II also demonstratesthat when interactions between ligation method, wiretype and storage status were examined, there were nostatistically significant effects of interactions.
JONES AND BEN BIHI
Australian Orthodontic Journal Volume 25 No. 2 November 2009138
Table I. Static frictional resistance of elastomeric modules and the Slide system with different wires and two different conditions (Fresh, Soaked in artificialsaliva for 24 hours).
System Condition Wire Mean force SE 95% CI(N) Lower Upper
Fresh Round 1.57 0.17 1.24 1.90Elastomeric Rectangular 1.17 0.17 0.84 1.50
Soaked Round 1.11 0.17 0.78 1.45Rectangular 1.16 0.17 0.83 1.49
Fresh Round 0.22 0.17 0.11 0.55Slide system Rectangular 0.35 0.17 0.02 0.68
Soaked Round 0.34 0.17 0.01 0.67Rectangular 0.39 0.17 0.06 0.72

FRICTION WITH THE SLIDE SYSTEM
Australian Orthodontic Journal Volume 25 No. 2 November 2009 139
Discussion
This study aimed to compare the static friction of twotypes of elastomeric ligatures using different wire sizesunder different conditions (fresh from the canes, andafter 24 hours storage in a simulated oral environ-ment). The method has been used in previous studiesover many years and has been shown to produce reliable results.4,11,12,14–16
Elastomeric modules have been used widely in ortho-dontic practice since their introduction in the 1960s.Many authors have suggested that the elastomericsmay lose 50–70 per cent of their initial force in thefirst 24 hours in the oral environment.17–19 It was,therefore, considered important to study the friction-al resistance of modules after they had been stored ina simulated intra-oral environment for 24 hours, inorder to make the test more clinically relevant. In thiscomparative study, the ligatures were stored in anunstretched state, which may not be totally repre-sentative of the clinical situation wherein the ligatureis stretched around a bracket. It was considered thatto store the ligature systems in a pre-stretched modearound brackets would have complicated the experi-mental process, since setting up the jig would havemeant that the ligatures would have had to beremoved and then replaced as the wire was intro-duced, producing an additional variable. It was con-sidered that any loss of elasticity within the ligaturesystems would have resulted in a reduction in elasticrecoil after stretching onto the bracket and this wouldreflect the loss of elastic force to be expected from aligature intra-orally. To this end, both systems werestored unstretched.
The Slide ligature system is a polyurethane elasto-meric module which it is claimed, produces lowerfrictional resistance than conventional modules dur-ing sliding mechanics. In the current study, the Slidesystem showed levels of friction that were signifi-cantly lower than those produced by conventionalmodules during sliding mechanics with both 0.018inch stainless steel round and 0.019 x 0.025 inchstainless steel rectangular archwires (p < 0.001). Thestatic frictional forces exerted by the Slide systemwere minimal when compared with conventionalmodules, and these findings agree with those fromprevious research which assessed the performance ofthe low-friction system in alignment and arch expan-sion.6–10 The frictional resistance obtained in thisstudy for conventional elastomeric modules is com-parable to previously published results.4 The Slide ligation showed less static frictional resistance com-pared to conventionally placed elastomerics, elasto-merics tied in a ‘figure-of-eight’ pattern and stainlesssteel ligatures.4
Previous work has suggested that friction appears toincrease as the archwire diameter increases.20,21 In
Table II. Two-way analysis of variance (ANOVA).
Source Type IIsum of Meansquares df square F p
System 17.28 1 17.28 62.84 < 0.001Saliva 0.11 1 0.11 0.41 0.525Wire 0.04 1 0.04 0.14 0.709System * Saliva 0.51 1 0.51 1.87 0.176System * Wire 0.36 1 0.36 1.31 0.255Saliva * Wire 0.16 1 0.16 0.59 0.443System *Saliva * Wire 0.35 1 0.35 1.27 0.263
* InteractionSignificant value in bold
Figure 1. Facial (A) and longitudinal (B) views of Slide ligature in place.Reproduced with permission from Baccetti T, Franchi L. Friction produced bytypes of elastomeric ligatures in treatment mechanics with the preadjustedappliance. Angle Orthod 2006;76:211–16.24

this study the static frictional resistance of the Slidesystem and conventional modules were measuredagainst both 0.018 inch stainless steel round and0.019 x 0.025 inch stainless steel rectangular wires.The results revealed that the wire size had no statistic-ally significant effect on the static frictional resistanceof both types of modules (p = 0.709). However, itshould be noted that this study was carried out withthe bracket/archwire angulation at 0 degree. In thisstate the bracket/archwire angulation is in the passiveconfiguration, below the critical angle and only clas-sical friction is present because binding and notchingdo not occur.22 It is clear from the present results thatthe Slide system significantly reduced static frictionregardless of the wire size used. This reduction couldbe of benefit clinically. However, when consideringthe total friction generated at the bracket/archwireinterface in a clinical situation, factors other than lig-ation are also involved, including binding betweenarchwire and bracket as teeth are moved through aseries of tipping and uprighting phases. It has beenshown that the level of influence of the ligature forcediminishes as the bracket/archwire angulationincreases.23
In this study, force degradation may have been due tostress relaxation of the elastomers or the presence ofchemical factors from artificial saliva. In addition, thepresence of moisture may have resulted in weakeningof elastomeric intermolecular forces.19 The results inthis investigation demonstrated that soaking in artifi-cial saliva for 24 hours had no statistically significanteffect on static frictional force for both types of testligatures (p = 0.176). This suggests that modern elasto-merics based on polyurethane may be less prone toenvironmental effects than more traditional latexmaterials.
Conclusions
Under the conditions of this ex-vivo study, the following conclusions can be drawn:
The new Slide system appears to generate signifi-cantly less static friction at the module/archwireinterface than conventional elastomeric modules (p < 0.001).
Immersion in a simulated oral environment for 24hours did not have a statistically significant effect onthe static frictional values of the two types of ligatures(p = 0.176).
There was no statistically significant difference instatic frictional resistance for either system between around or rectangular archwire (p = 0.709).
There were no statistically significant interactionsbetween variables.
Acknowledgments
The authors would like to acknowledge the contribu-tions of Dr Graham Palmer for technical assistance,and Professor David Moles for statistical support. Weare also grateful for the support of DB OrthodonticsLtd, UK who generously donated the materials testedand Nycomed (UK) who donated the Saliva Orthana.
Corresponding author
Dr S. P. JonesOrthodontic UnitUCL Eastman Dental Institute for Oral Health Care Sciences256 Gray’s Inn RoadLondon, WC1X 8LDUnited KingdomTel: +44 (0)20 7915 1068Fax: +44 (0)20 7915 1238Email: [email protected]
References 1. Barlow M, Kula K. Factors influencing efficiency of sliding
mechanics to close extraction space: a systematic review.Orthod Craniofac Res 2008;11:65–73.
2. Drescher D, Bourauel C, Schumacher HA. Frictional forcesbetween bracket and arch wire. Am J Orthod DentofacOrthop 1989;96:397–404.
3. Omana HM, Moore RN, Bagby MD. Frictional propertiesof metal and ceramic brackets. J Clin Orthod 1992;26:425–32.
4. Edwards GD, Davies EH, Jones SP. The ex-vivo effect of lig-ation technique on the static frictional resistance of stainlesssteel brackets and archwires. Br J Orthod 1995;22:145–53.
5. Eliades T, Eliades G, Watts DC. Structural conformation ofin-vitro and in-vivo aged orthodontic elastomeric modules.Eur J Orthod 1999;21:649–58.
6. Fortini A, Lupoli M, Cacciafesta V. A new low-friction ligation system. J Clin Orthod 2005;39:464–70.
7. Franchi L, Baccetti T. Forces released during alignment witha preadjusted appliance with different types of elastomericligatures. Am J Orthod Dentofac Orthop 2006;129:687–90.
8. Franchi L, Baccetti T, Camporesi M, Lupoli M. Maxillaryarch changes during levelling and aligning with fixed appli-ances and low-friction ligatures. Am J Orthod DentofacOrthop 2006;130:88–91.
9. Camporesi M, Baccetti T, Franchi L. Forces released byesthetic preadjusted appliances with low-friction and con-ventional elastomeric ligatures. Am J Orthod DentofacOrthop 2007;131:722–5.
JONES AND BEN BIHI
Australian Orthodontic Journal Volume 25 No. 2 November 2009140

FRICTION WITH THE SLIDE SYSTEM
Australian Orthodontic Journal Volume 25 No. 2 November 2009 141
10. Baccetti T, Franchi L, Fortini A. Orthodontic treatmentwith pre-adjusted appliances and low-friction ligatures:experimental evidence and clinical observations. World JOrthod 2008;9:7–13.
11. Rajakulendran J, Jones S. Static frictional resistances ofpolycrystalline ceramic brackets with metal slot inserts. AustOrthod J 2006;22:147–52.
12. Mahmoud G. An ex-vivo laboratory study into the compar-ative frictional resistances of polymer coated and conven-tional elastomeric modules. MSc Thesis; University ofLondon. 2003
13. Altman DG. Statistics in Practice. British MedicalAssociation, London, UK. 1982
14. Keith O, Jones SP, Davies EH. The influence of bracketmaterial, ligation force and wear on frictional resistance oforthodontic brackets. Br J Orthod 1993;20:109–15.
15. Dickson J, Jones SP. Frictional characteristics of a modifiedceramic bracket. J Clin Orthod 1996;30:516–18.
16. Read-Ward GE, Jones SP, Davies EH. A comparison of self-ligating and conventional orthodontic bracket systems. Br JOrthod 1997;24:309–17.
17. Wong AK. Orthodontic elastic materials. Angle Orthod1976;46:196–205.
18. Young J, Sandrik JL. The influence of pre-loading on stressrelaxation of orthodontic elastic polymers. Angle Orthod1979;49:104–9.
19. Huget EF, Patrick KS, Nunez LJ. Observations on the elasticbehavior of a synthetic orthodontic elastomer. J Dent Res1990;69:496–501.
20. Angolkar PV, Kapila S, Duncanson MG Jr., Nanda RS.Evaluation of friction between ceramic brackets and ortho-dontic wires of four alloys. Am J Orthod Dentofac Orthop1990;98:499–506.
21. Kapila S, Angolkar PV, Duncanson, MG Jr, Nanda, RS.Evaluation of friction between edgewise stainless steel brackets and orthodontic wires of four alloys. Am J OrthodDentofacial Orthop 1990;98:117–26.
22. Kusy RP, Whitley JQ. Influence of archwire and bracketdimensions on sliding mechanics: derivations and determi-nations of the critical contact angles for binding. Eur JOrthod 1999;21:199–208.
23. Frank CA, Nikolai RJ. A comparative study of frictionalresistances between orthodontic bracket and archwire. Am JOrthod 1980;78:593–609.
24. Baccetti T, Franchi L. Friction produced by types of elastomeric ligatures in treatment mechanics with the pre-adjusted appliance. Angle Orthod 2006;76:211–16.

Introduction
Malocclusions with rotated and/or imbricated incisorsrequire long-term retention after treatment to preventrelapse.1 Although banded canine-to-canine lingualretainers were generally removed after 1 to 2 years,bonded lingual retainers can be left in place for many years and are often referred to as ‘permanent’retainers.2,3 Early bonded lingual retainers, whichcopied the design of the banded retainers, had a largediameter wire bonded to the lingual surfaces of eitherthe lower canines or premolars.4 The next develop-
ment was the use of small diameter spiral or multi-strand wires bonded to all lower anterior teeth.5,6 Itwas felt that a multistrand wire would be flexibleenough to allow physiological movement of the teethand, at the same time, retain previously rotated orimbricated teeth.7 However, the roughness of a multi-strand wire can be uncomfortable to some patientsand encourage the retention of plaque. The latter canlead to gingivitis and/or periodontal breakdown. Atleast one author felt that the flexibility of multistrandwire retainers would result in distortion of the wireduring chewing and bond failure.8
Australian Orthodontic Journal Volume 25 No. 2 November 2009 © Australian Society of Orthodontists Inc. 2009142
Gingival health and relapse tendency: a prospective study of two types of lower fixed retainers
Kazem Al-Nimri,* Rola Al Habashneh† and Mohammed Obeidat+
Departments of Orthodontics* and Preventive Dentistry,† Jordan University of Science and Technology and Private practice,+ Irbid, Jordan
Background: Different types and diameters of wire are used in bonded lingual retainers. Some clinicians bond a small diametermultistrand wire to each tooth, while other clinicians bond a large diameter wire to the lingual surfaces of the lower canines.Aim: To compare the gingival health, plaque accumulation, tooth stability and integrity of multistrand wire and round wire bonded lingual retainers.Methods: Sixty-two subjects, who had completed treatment and who required fixed retention for the lower anterior segment,were assigned to either the Round wire retainer group or the Multistrand wire retainer group. In the Round wire retainer group,a 0.036 inch round, stainless steel wire was bonded to the lingual surfaces of both lower canines. The Multistrand retainergroup had a 0.015 inch multistrand wire bonded to the lingual surfaces of all lower anterior teeth. At least 12 months afterdebonding, the subjects were recalled and the following variables were recorded: Oral Hygiene Index (OHI), Plaque Index (PI)of the lower anterior teeth, Gingival Index (GI) of the lower anterior teeth, Irregularity Index (IRI) of the lower anterior teeth, andthe number of broken retainers.Results: There were no significant differences between the PI (p = 0.165) and GI (p = 0.150) of the two groups. More plaquewas found on the distal surfaces of the lower anterior teeth in the group with multistrand wire retainers (p = 0.02). The loweranterior teeth were significantly more irregular in the group with round wire retainers compared to the group with multistrandwire retainers (p = 0.002). Although the multistrand wire retainers fractured more frequently than the round wire retainers thedifference was not statistically significant (p = 0.325).Conclusion: More plaque accumulated on the distal surfaces of the lower anterior teeth in subjects with multistrand wire retainers than in subjects with round wire retainers. Multistrand wire retainers were better at maintaining incisor alignment thansingle span, round wire retainers. (Aust Orthod J 2009; 25: 142–146)
Received for publication: April 2009Accepted: August 2009
Kazem Al-Nimri:[email protected] Al Habashneh: [email protected] Obeidat: [email protected]

GINGIVAL HEALTH AND RELAPSE TENDENCY OF LOWER FIXED RETAINERS
Australian Orthodontic Journal Volume 25 No. 2 November 2009 143
Studies of patients with bonded retainers indicatethat multistrand wire retainers are better at maintain-ing alignment of the lower incisors than single span,canine-to-canine retainers and do not promote theaccumulation of plaque.9–12 However, round wirecanine-to-canine retainers appear to be more durablethan multistrand retainers.10,12
The aims of this prospective study were to comparethe gingival health, plaque accumulation, tooth stability and integrity of lingual retainers made ofmultistrand wire bonded to all lower anterior teethwith lingual retainers made of thick, round wirebonded to the lower canines.
Materials and methods
The subjects in this prospective study were 62patients who completed orthodontic treatment at theDental Teaching Center, Jordan University of Scienceand Technology, between 2003 and 2005, and whorequired fixed retention for the lower anterior seg-ment. Alternate subjects were assigned to the Roundwire retainer group (Mean age: 20.23 ± 3.8 years) andthe Multistrand wire retainer group (Mean age: 19.97± 4.2 years). There were 22 women and 9 men inboth groups.
At the completion of treatment, the teeth in all sub-jects were thoroughly scaled and the roots planed by the same clinician. The appliances were thendebonded and impressions taken for study casts andfabrication of the retainers. The round wire retainerswere made of 0.036 inch stainless steel wire, sand-blasted at both ends, and bonded to the lingual surfaces of the lower canines only (Round wire retainer group).8 The multistrand retainers weremade of 0.015 inch multistrand wire, bonded to thelingual surfaces of all lower anterior teeth (Multi-strand wire retainer group). All retainers were bondedby the same clinician using a localising template andFiltek P60 composite resin (3M Espe, St. Paul, MN,USA). At debonding, the mean Irregularity Index for the subjects in the Multistrand retainer group was 0.38 and for the subjects in the Round wireretainer group it was 0.32 (p = 0.637). Oral hygieneinstructions were given to all participants.
At least 12 months after debonding all subjects wererecalled and the following variables were recorded:Oral Hygiene Index (OHI); Plaque Index (PI) of thelower anterior teeth; Gingival Index (GI) of the lower
anterior teeth; Irregularity Index (IRI) of the loweranterior teeth; number of breakages of the retainers.
The OHI records the amount of debris or calculus onthe buccal and lingual surfaces of the teeth in eachdental arch i.e. both buccal segments and the anter-ior segment.13 In each segment the tooth with thegreatest area covered by either debris or calculus wasused to determine the index for that particular seg-ment. The debris scores for the segments weresummed and divided by the number of segmentsrecorded. In the present study, the lower anterior segments were excluded as the amount of debris andcalculus may have been affected by the presence ofthe fixed retainer. The same method was used toobtain the Calculus Index scores. Then the debris andcalculus scores were combined to obtain the OHIscore.
To determine the PI, the buccal, lingual, mesial anddistal surfaces of the lower anterior teeth were scoredfrom 0 to 3, according to the amount of plaque oneach surface.14 The scores for each tooth weresummed and divided by 4 to give the PI for the tooth.The scores for the lower anterior teeth were averagedto give the PI score for the lower anterior segment.
To obtain the GI, the labial and lingual surfaces of thelower anterior teeth were given a score from 0 to 3;these scores were averaged to give the GI for eachtooth.15 The GI scores of the lower anterior teethwere summed and averaged to give a GI score for thelower anterior segment.
The IRI was used to measure the irregularity of thelower anterior teeth.16 Contact point displacementswere measured directly with calipers to 0.1 mm. The calipers were held parallel to the occlusal plane,and the IRI for each subject was the sum of the measurements of the five contact points.
To determine the measurement error, 10 subjects (5subjects from each group) were re-examined at least 7days after the initial examination and the measure-ment error determined using Dahlberg’s method. Theerrors varied between 0.018 for the total PI to 0.073for the GI on the lingual surfaces.
Statistical analysisMeans and standard deviations were calculated for allthe variables using SPSS (Version 11, Chicago,Illinois, USA). Statistically significant group differ-ences in PI, GI and IRI were determined using the

Student’s t-test. Chi-squared was used to examine thedifferences in the fracture rates and the IRI scores inthe two groups. Probability values less than 0.05 wereconsidered significant.
Results
The mean retention period for the group with roundwire retainers was 21.31 months, and for the groupwith multistrand wire retainers it was 19.35 months.The difference was not statistically significant ( p = 0.473).
The mean OHI, PI, GI and IRI scores and the num-ber of fractured retainers in each group are given inTable I. Only the IRI was significantly different: thelower anterior teeth in the Round wire group were significantly more irregular at recall than thelower anterior teeth in the Multistrand wire group (p = 0.002). Although more multistrand wire retainersfractured than round wire retainers, the differencewas not statistically significant. When, however, themean PI and mean GI were broken down into toothsurfaces, the distal surfaces of the lower anterior teethin the Multistrand wire group had significantly moreplaque than the distal surfaces of the anterior teeth inthe Round wire group (Table II, p = 0.020). Themean difference in the GI scores for the lingual sur-faces of the anterior teeth also approached statisticalsignificance (p = 0.053).
More subjects in the Multistrand wire group hadideal alignment of the anterior teeth compared withthe subjects in the Round wire group, and more sub-jects in the latter group had moderate crowding atrecall than the subjects in the Multistrand wire group
AL-NIMRI ET AL
Australian Orthodontic Journal Volume 25 No. 2 November 2009144
Table I. Differences between the Round wire and Multistrand wire retainer groups.
Variable Round wire group Multistrand wire groupMean (SD) Mean (SD) Mean difference p
Retention period (Months) 21.31 (8.97) 19.35 (6.67) 2.96 0.473Oral Hygiene Index 2.11 (0.98) 2.18 (0.67) 0.07 0.747Plaque Index 1.02 (0.52) 1.21 (0.48) 0.19 0.165Gingival Index 1.19 (0.44) 1.34 (0.39) 0.15 0.150Irregularity Index (mm) 3.08 (1.52) 1.92 (1.21) 1.16 0.002Fractured retainers (N) 4 9 5 0.325
Significant value in bold
Table II. Plaque Index (PI) and Gingival Index (GI) of the lower anterior segments.
Surface Round wire group Multistrand wire groupMean (SD) Mean (SD) Mean difference p
PI buccal surfaces (0.66 (0.57) 0.83 (0.66) 0.17 0.290PI lingual surfaces (0.85) 1.35 1.50 (0.45) 0.15 0.419PI mesial surfaces (1.04 (0.64) 1.30 (0.72) 0.27 0.127PI distal surfaces (0.96 (0.59) 1.33 (0.61) 0.36 0.020GI buccal surfaces (1.12 (0.60) 1.20 (0.50) 0.08 0.560GI lingual surfaces (1.25 (0.51) 1.50 (0.48) 0.25 0.053
Significant value in bold
Table III. Irregularity of the lower incisors at recall.
Irregularity Index Round wire Multistrandgroup (N) wire group (N) Total
Ideal (0-1 mm) 2 9 11Mild (2-3 mm) 15 16 31Moderate (4-6 mm) 13 6 19Severe (7-10 mm) 1 0 1
* p = 0.045, chi-squared analysis

GINGIVAL HEALTH AND RELAPSE TENDENCY OF LOWER FIXED RETAINERS
Australian Orthodontic Journal Volume 25 No. 2 November 2009 145
(Table III). The distributions were significantly different (p = 0.045)
Discussion
Bonded lingual retainers are frequently used to retainthe lower anterior teeth. These retainers are often fabricated from different types and gauges of wire and may be attached to all anterior teeth or only tothe canines. The aims of this study were to compare the gingival health, plaque accumulation, tooth alignment and fracture rate of two designs of fixedretainers after both had been in use for at least a year.The underlying intentions were to determine if bothretainers achieved what they were designed to do, i.e.retain alignment, determine if the gingival health wasacceptable at recall or if early signs of periodontalbreakdown were present. There were no statisticallysignificant differences in oral hygiene, plaque reten-tion or gingivitis. Multistrand wire retainers weremore effective at retaining alignment of the lowerincisors and were more likely to be lost than roundwire, single span retainers. There was also signifi-cantly more plaque on the distal surfaces of the anterior teeth in the group with multistrand wireretainers, which suggests that long-term studies areneeded.
Our findings that there were no differences betweenthe PI and GI scores for both types of retainer agrees
with Årtun and coworkers.7,10 They reported thatplaque was no more likely to accumulate on teethadjacent to retainers made of multistrand wire thanon the teeth adjacent to retainers made from a largediameter, round wire. However, the distribution ofthe plaque we found differs slightly from that report-ed by Årtun.7 We found there was significantly moreplaque on the distal surfaces, which suggest thatinterproximal cleaning was difficult because of theshort spans of multistrand wire.17 Årtun7 reportedthat the PI scores for teeth bonded with round wireand multistrand wire retainers were generally higherin the inter-proximal areas than on the lingual sur-faces, indicating that interproximal cleaning was dif-ficult with both types of retainer. We found the GI oflingual surfaces was higher in the Multistrand wiregroup (p = 0.053), which suggests that this surfacealso needs attention during tooth cleaning.
In agreement with Artun et al.,10 we found thatround wire retainers were less likely to maintainalignment of the anterior teeth than multistrandretainers bonded to all anterior teeth. The differencein irregularity was quite marked: fewer subjects in theRound wire group had an ideal alignment and 14subjects (45 per cent) in the Round wire group hadan unacceptable return of irregularity (IRI > 4 mm).This indicates that when the lower incisors are likelyto relapse a multistrand wire retainer should be used.
Table IV. Gingival health and relapse tendency in the present study and previous studies.
Study Observation Retainer type Number of Plaque Index Gingival Index Irregularity Index Fractureperiod subjects rate
Årtun et al.10 3 years Thick plain wire 11 0.06 0.66 1.19 9.1Thick spiral wire 13 0.10 0.49 0.36 30.8Thin spiral wire 11 0.13 0.39 0.66 27.3
Störmann and Ehmer9 2 years Thick wire 34 NA NA 80% 53.00.0195 inch 38 NA NA 0% 29.0spiral wire0.0215 inch 31 NA NA 20% 18.0spiral wire
Booth et al.11 20 years Thick plain wire 60 NA 0.58 2% 25.0>2mm
Present study 1–3 years 0.036 inch 31 1.02 1.19 3.08 13.0round wire0.015 inch 31 1.21 1.34 1.92 29.0spiral wire
NA, Not available

Because only the ends of a large diameter, round wireretainer are bonded to the canines the incisors are freeto move away from the wire.
The failure rate of retainers made of multistrand wirewas 30 per cent compared with a failure rate of 13 percent for the round wire retainers. Although this dif-ference was not statistically significant, a debondedwire may be time-consuming to repair and if a toothhas moved out of position time-consuming retreat-ment will be required.17 This finding agrees withÅrtun et al.,10 who reported failure rates of 27.3 percent for multistrand wire retainers and 9.1 per centfor round wire retainers. Our finding of a higher fail-ure rate for multistrand retainers may have occurredbecause the short spans in multistrand retainers arenot flexible enough to allow the incisors to move inde-pendently under biting loads, whereas a round wireretainer, which attached at its ends, may be flexibleenough to allow the canines to move under load.
Our failure rate for lower round wire retainers (13 per cent) is slightly higher than the 11.6 per centreported by Zachrisson4 and the 9.1 per cent reportedby Årtun et al.10 Our failure rate for the multistrandretainers (30 per cent) is also higher than the failurerates reported by Dahl and Zachrisson (20.6 percent),12 Årtun et al. (27.3 per cent)10 and by Lumb-esdun (23.2 per cent).18 Comparisons between ourresults and previous studies are summarised in TableIV.9–11 The differences in the failure rates between thevarious studies may be due to differences in the bond-ing materials and techniques used, the sizes and typesof the wires, number of teeth bonded, the observationperiod and the patients’ behaviours and habits.
Conclusions
There was no difference between the gingival condi-tions of the lower anterior teeth retained with either amultistrand wire retainer or a single round wire retainer.
More plaque accumulated on the distal surfaces of thelower anterior teeth when a multistrand wire retainerwas used as compared with a retainer made of roundwire bonded to the canines only.
Multistrand wire retainers bonded to all lower anter-ior teeth were better at maintaining tooth alignmentthan single span, canine-to-canine retainers.
Although more multistrand wire retainers failed thanround wire, single span retainers, the difference wasnot statistically significant.
Corresponding author
Dr Rola Al HabashnehDepartment of Preventive DentistryFaculty of DentistryJordan University of Science and TechnologyP.O. Box (3030)Irbid 22110JordanTel: +962 2 7278 662 Ext. 291Fax: +962 2 7278 962Email: [email protected]
References1. Nanda RS, Nanda, SK. Considerations of dentofacial growth
in long term retention and stability: is active retention needed? Am J Orthod Dentofacial Orthop 1992;101:297–303.
2. Clark JD, Kerr WJ, Davis MH. CASES clinical audit; sce-narios for evaluation and study. Br Dental J 1997;183: 108–11.
3. Durbin DD. Relapse and the need for permanent fixedretention J Clin Period 2001;35:723–7.
4. Zachrisson BU. Clinical experiences with direct-bondedorthodontic retainers. Am J Orthod 1977;71:440–8.
5. Årtun J, Zachrisson BU. Improving the handling propertiesof a composite resin for direct bonding. Am J Orthod 1982;81:269–76.
6. Zachrisson BU. The bonded lingual retainer and multiplespacing of anterior teeth. Swed Dent J Suppl 1982;15: 247–55.
7 Årtun J. Caries and periodontal reaction associated withlong term use of different types of bonded lingual retainers.Am J Orthod 1984;86:112–18.
8. Zachrisson BJ. Third generation mandibular bonded lingual3-3 retainer. J Clin Orthod 1995;29:39–48.
9. Störmann I, Ehmer U. A prospective randomized study ofdifferent retainer types. J Orofac Orthop 2002;63:42–50.
10. Årtun J, Spadafora AT, Shapiro PA. A three year follow-upstudy of various types of orthodontic canine-to-canineretainers. Eur J Orthod 1997;5:501–9.
11. Booth FA, Edelman JM, Proffit WR. Twenty-year follow-upof patients with permanently bonded mandibular canine-to-canine retainers. Am J Orthod Dentofacial Orthop 2008;133:70–6.
12. Dahl EH, Zachrisson BU. Long term experience with direct-bonded lingual retainers. J Clin Orthod 1991;25:619–30.
13. Greene JC, Vermillion JR. The simplified oral hygieneindex. J Am Dent Assoc 1964;68:7–13.
14. Silness J, Löe H. Periodontal disease in pregnancy. II.Correlation between oral hygiene and periodontal conditions. Acta Odontol Scand 1964;22:112–35.
15. Löe H, Silness J. Periodontal disease: I. Prevalence andseverity. Acta Odontol Scand 1963;21:533–51.
16. Little RM. The irregularity index: a quantitative score ofmandibular anterior alignment. Am J Orthod 1975;68:554–63.
17. Cerny R. The reliability of bonded lingual retainers. AustOrthod J 2007;23:24–9.
18. Lumsden KW, Saidler G, McColl JH. Breakage incidencewith direct bonded lingual retainers. Br J Orthod 1999;26:191–4.
AL-NIMRI ET AL
Australian Orthodontic Journal Volume 25 No. 2 November 2009146

Introduction
Orthodontic tooth movement is a unique process bywhich a tooth is made to move through bone by theapplication of an appropriate force. The force inducesbone resorption on the pressure side of the root andbone deposition on the tension side, maintaining thewidth of the periodontal ligament (PDL).1–4
Many orthodontic patients have a shortage of spaceand crowding.1 Although nonextraction treatmentapproaches have become popular, there are still a
number of patients who need treatment requiring theextraction of teeth.1 The first phase in the treatmentof many premolar extraction cases is the retraction ofthe upper canines. Using conventional methods theteeth move at a slow rate (about 1 mm per month)and it takes between 6 and 8 months to retract theupper canines and between 18 and 24 months tocomplete treatment. In some cases special extra-oraland intra-oral mechanics are required to conserveanchorage during canine retraction, particularly inso-called maximum anchorage cases. With inter-dental/
© Australian Society of Orthodontists Inc. 2009 Australian Orthodontic Journal Volume 25 No. 2 November 2009 147
Clinical investigation of periodontal ligament distraction osteogenesis for rapid orthodonticcanine retraction
Priyanka Sethi Kumar,* Ruchi Saxena,† Sameer Patil,+ Kanhoba MahabaleshwarKeluskar,± K. Nagaraj± and Sharadindu M. Kotrashetti±
Santosh Dental College and Hospital, Ghaziabad,* Vydehi Institute of Dental Sciences and Research Centre, Bangalore,†Sinhgad Dental College and Hospital, Pune,+ and The Institute of Dental Sciences, KLE University, Belgaum,± India
Aims: To investigate rapid canine distalisation by periodontal ligament distraction and to determine the effects of periodontal ligament distraction on the canine root and pulpal vitality.Methods: The sample consisted of 16 upper canines in eight patients who required first premolar extractions. The upper firstpremolars were extracted and the interseptal bone distal to each canine was thinned and undermined surgically. Custom-builtdistractors were placed and activated immediately to distract the canines into the extraction spaces. Radiographs were takenbefore canine distraction and at regular intervals thereafter. The upper canine pulps were tested with an electronic pulp testerbefore and after the distraction and the canines were examined on the post-distraction radiographs for evidence of apical andlateral root resorption. Results: The canines were retracted to proximal contact with the second premolars in 20.33 ± 1.87 days. The average amountof retraction was 5.25 mm and the canines tipped distally 15.33 degrees. Although the upper molars did not move mesially,they extruded almost 1 mm. Root resorption was minimal and there was no deterioration in pulp vitality.Conclusion: Canines can be rapidly retracted by periodontal ligament distraction without complications. However, the efficacyof the method depends upon the surgical procedure, which is technique sensitive. Resistance offered by the interseptal bone distal to the apex of the canine was thought to be the reason for the canine tipping during distraction.(Aust Orthod J 2009; 25: 147–152)
Received for publication: April 2009Accepted: August 2009
Piryanka Sethi Kumar: [email protected] Saxena: [email protected] Patil: [email protected] M. Keluskar: [email protected]. Nagaraj:[email protected] M. Kotrashetti: [email protected]

KUMAR ET AL
Australian Orthodontic Journal Volume 25 No. 2 November 2009148
periodontal ligament distraction osteogenesis theupper canines can be retracted into the first premolarextraction spaces in about three weeks with minimalloss of anchorage and little/no root resorption.5–7
Interdental/periodontal ligament distraction osteo-genesis is a major advance in orthodontics in terms ofreducing the duration of treatment and conservationof anchorage.5 However, there is little informationwith regard to the efficacy of this procedure and, as aresult, it is not used by many orthodontists. The pres-ent study was undertaken to investigate the efficacy ofrapid canine retraction by interdental/periodontal ligament distraction osteogenesis and to evaluate itseffects on the canine root and pulpal vitality. Wehypothesised that interdental/periodontal ligamentdistraction can be used as a treatment modality inpatients with high anchorage demands, and that theduration of treatment could be reduced without anycomplications.
Material and methods
The study sample consisted of eight subjects, 17 to 25years of age, who needed canine retraction, extractionof the upper first premolars due to either anteriorcrowding or dentoalveolar protrusion and had highanchorage demands. Since the treatment involvedsurgery, only subjects 16 years or older were included.All patients attended the Department of Orthodon-tics and Dentofacial Orthopedics, KLE Institute ofDental Sciences, Belgaum, for treatment. Informed
consent was obtained for all subjects and approval forthe study was granted by the ethics committee ofKLE University.
Distractor construction and surgicalmethodThe upper canines and first molars were banded anda working model obtained. The distractors used inthis study were intra-oral, custom-made tooth-bornedistracters (SK Surgical, Pune, India) cast in high-grade stainless steel and soldered to the canine andfirst molar bands (Figure 1). A custom-made key wasused to activate the distractor.
The surgical procedure5,6,8 was performed under localanaesthesia as a routine outpatient procedure (Figure2). The first premolars were extracted and the inter-septal bone distal to the canine was undermined andthinned to 1–2 mm. As the roots of the premolars areshorter than the canine roots, the premolar socketswere extended to the same depths as those of thecanines using a round carbide bur. This stage was per-formed carefully with the aid of radiographs to avoiddamaging the canine root. Two vertical grooves weremade on the mesio-lingual and mesio-buccal lineangles of the extraction socket. The verticalosteotomies were then connected with an obliqueosteotomy at the base of the socket, creating a U-shaped groove. The objective of these osteotomies wasto weaken the interseptal bone and allow the canineto move bodily. The wound was thoroughly irrigated
Figure 1. Design of the distractor. The anterior section is soldered to thecanine band, and the posterior section is soldered to the molar band. The horizontal sliding stainless steel bar and stainless steel screw join bothsections.
Figure 2. Interseptal bone removed to deepen the socket (dotted line).
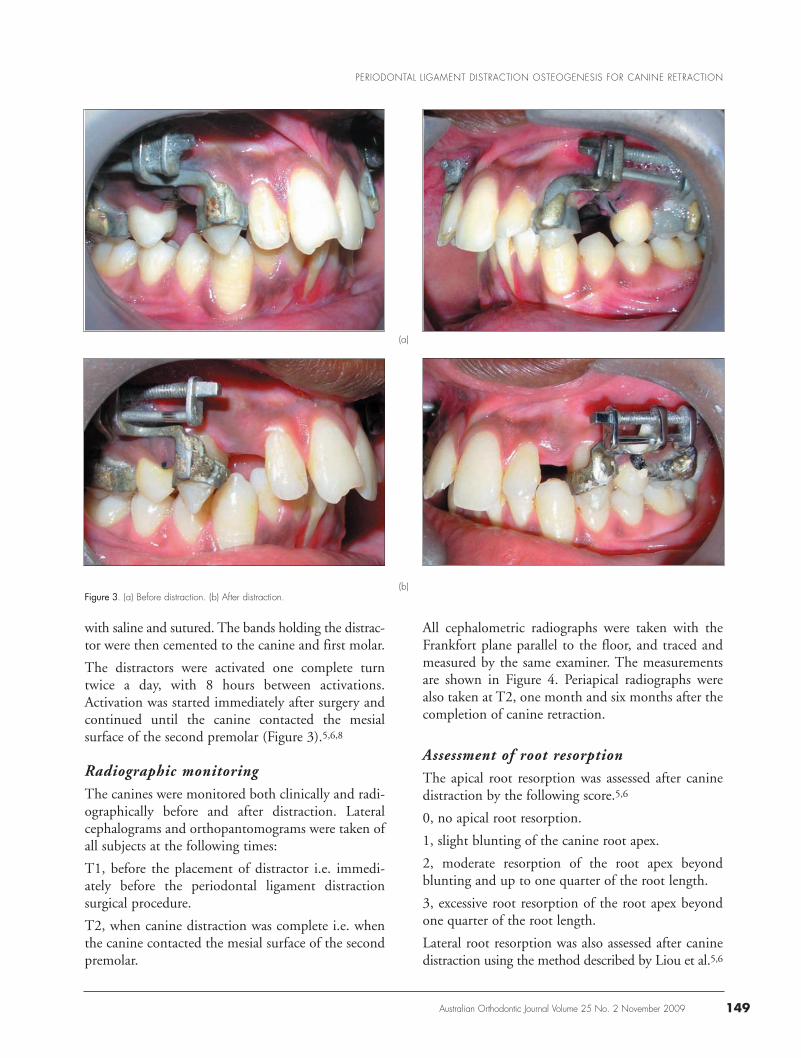
with saline and sutured. The bands holding the distrac-tor were then cemented to the canine and first molar.
The distractors were activated one complete turntwice a day, with 8 hours between activations.Activation was started immediately after surgery andcontinued until the canine contacted the mesial surface of the second premolar (Figure 3).5,6,8
Radiographic monitoringThe canines were monitored both clinically and radi-ographically before and after distraction. Lateralcephalograms and orthopantomograms were taken ofall subjects at the following times:
T1, before the placement of distractor i.e. immedi-ately before the periodontal ligament distraction surgical procedure.
T2, when canine distraction was complete i.e. whenthe canine contacted the mesial surface of the secondpremolar.
All cephalometric radiographs were taken with theFrankfort plane parallel to the floor, and traced andmeasured by the same examiner. The measurementsare shown in Figure 4. Periapical radiographs werealso taken at T2, one month and six months after thecompletion of canine retraction.
Assessment of root resorptionThe apical root resorption was assessed after caninedistraction by the following score.5,6
0, no apical root resorption.
1, slight blunting of the canine root apex.
2, moderate resorption of the root apex beyondblunting and up to one quarter of the root length.
3, excessive root resorption of the root apex beyondone quarter of the root length.
Lateral root resorption was also assessed after caninedistraction using the method described by Liou et al.5,6
PERIODONTAL LIGAMENT DISTRACTION OSTEOGENESIS FOR CANINE RETRACTION
Australian Orthodontic Journal Volume 25 No. 2 November 2009 149
(b)Figure 3. (a) Before distraction. (b) After distraction.
(a)

KUMAR ET AL
Australian Orthodontic Journal Volume 25 No. 2 November 2009150
0, smooth lateral root surface and periodontal ligament.
1, slightly irregular lateral root surface not beyondone third of the dentine width between the distal sideof the periodontal ligament and the pulp chamber.
2, moderate irregular lateral root surface beyond onethird and up to two thirds of the dentine widthbetween the distal side of the periodontal ligamentand the pulp chamber.
3, excessive irregularity of the lateral root surfacebeyond two thirds of the dentine width between thedistal side of periodontal ligament and pulp chamber.
Assessment of pulp vitalityThe vitality of each upper canine was tested with anelectronic pulp tester before distraction, immediatelyafter removal of the distractor, one month and sixmonths after the surgical procedure.5,6
Statistical methods Statistical analyses were performed using the statist-ical package for social sciences (SPSS version 13.0)
for Windows. The means and standard deviationswere calculated and the differences between thebefore and after distraction measurements comparedwith the paired t-test. Probabilities < 0.05 were considered to be significant.
Results
The mean time taken to distract the upper canineswas 20.33 ± 1.87 days (Range: 17 – 22 days). Therate of movement was 0.25 mm per day and the meantotal distance the canines were distracted was 5.25 mm.
The cephalometric findings are given in Table II. Thehorizontal distance U6M-SV increased by 0.25 mmand distance between the upper first molar and thepalatal plane (U6M-PP) increased significantly by0.66 mm. The canines were retracted (U3M-SV) onaverage 5.2 mm and extruded (U3A-PP) by 0.58mm. The inclination of the upper canines to the SNline (U3A) reduced by 15.33 degrees.
Apical and lateral root resorption was minimal andnot statistically significant for the upper canines(Table II). There were no fractured or ankylosedcanines before or after distraction.
1
2
3
6
5
4
Figure 4. Cephalometric measurements. U6M-SV, perpendicular distance from the mesial of U6 to the vertical refer-ence line (SV).U6M-PP, vertical distance between U6 and the palatal plane (PP).U3D-SV, perpendicular distance from the mesial of U3 to the vertical refer-ence line.U3D-PP, vertical distance between U3 and the palatal plane.U3A, inclination of U3 to the SN line.
Table I. Comparison of the cephalometric measurements before andafter distraction.
Measurements Before distraction After distraction p
Mean SD Mean SD
U6M-SV (mm) 41.58 3.54 41.33 4.49 0.916U6M-PP (mm) 21.41 2.22 22.08 2.34 0.011U3D-SV (mm) 56.00 5.39 50.75 5.06 0.002U3A-PP (mm) 2.75 1.69 3.33 2.20 0.063U3A (degrees) 94.50 7.66 79.16 10.7 0.002
Paired t - test, significant values in bold
Table II. Apical and lateral root resorption.
Scores for root Numner of teeth Number of teethresorption affected by apical affected by lateral
root resorption root resorption
0 5 41 11 122 0 03 0 0

Before starting the distraction procedure, the caninesand first molars were tested with an electronic pulptester and all the teeth tested positive. The same testwas repeated after removal of the distractor and againthe canines tested positive. The pulp vitality testswere not done immediately after the canines were dis-tracted as it would have given a false reading with thedistractors in situ.
Discussion
We studied the radiographic changes, pulp vitality,occurrence of root resorption and ankylosis affectingthe upper canines retracted into the first premolarextraction spaces by periodontal ligament distraction.The canines were retracted 5 mm and extruded lessthan 1 mm in 20 days with virtually no loss ofanchorage. However, they ‘uprighted’ 15 degreesindicating that some tipping occurred, possiblybecause of resistance offered by the interseptal boneadjacent to the apex of the canine and/or deformationof the distractor guide rod and screw. There was nodetectable deterioration in pulpal vitality, root resorp-tion was minimal and there were no ankylosed teeth.Using this technique it is possible to substantiallyreduce the duration of treatment and conserveanchorage, even in severe malocclusions.
When a tooth is subjected to an orthodontic forcethere is a lag period of two to three weeks beforetooth movement occurs, which has been attributed tothe formation of a hyalinised zone in the periodontalligament. The aim of periodontal ligament distrac-tion osteogenesis is to retract the upper canines in thisperiod before the first molars move mesially.2,9,10 Inthe present study the first molars, which were the solemeans of anchorage, stayed more-or-less in their initial positions although they extruded slightly.Forces acting more than three weeks can result in lossof anchorage as the canine and the anchor unit movetowards each other after the lag period.5,6 When periodontal ligament distraction is expected to takelonger than two to three weeks the second premolarsand/or second molars should be included in theanchor unit or adjuncts, such as extra-oral traction, atranspalatal arch, miniscrews or a Nance button,employed. Without some means of reinforcing theanchorage 2 to 3 mm of space can be lost during conventional orthodontic treatment.11,12
Our finding that the first molars extruded slightlyduring treatment and that the canines tipped distally
is in contrast to previous reports.5,6,8 Our distractorwas designed to facilitate translation: the screws androds passed through the centres of resistance of bothteeth. In spite of this the canines tipped distally 15degrees. Because the device was robustly constructedwe consider that extrusion was due to the root tips‘catching’ on a ledge of bone during retraction ratherthan deformation of the guide rods and screws. Thefinal osteotomy linking the two vertical cuts was dif-ficult to achieve and completeness of the cut couldnot be verified.
Faster orthodontic tooth movement and less rootresorption occur when teeth are moved in trabecularalveolar bone.5,6 After tooth extraction, healing tissuefills the extraction socket which becomes resistantand ‘solid’ in about three months. If the canine is notretracted across the first premolar socket in the firstthree weeks, the rate of tooth movement slows, thelikelihood of external root resorption increases andthe anchor unit moves forward. Initially, the inter-septal bone distal to the canine is the only obstacle todistraction and failure to reduce or weaken it willimpede movement of the canine.5,6,8 Liou andHuang6 moved the upper canines about 6 mm intothe first premolar extraction sockets within threeweeks. Despite all efforts to move the canines bodilythey reported 17 degrees of distal tipping occurred,which is similar to the 15 degrees we found.
It is generally accepted that varying amounts of rootresorption occur in patients undergoing orthodontictreatment. Although external root resorption hasbeen reported as early as one week after the applica-tion of a force, appreciable root resorption occursduring the third week of force application.2,13 Wefound little evidence of apical and/or lateral rootresorption. An association has been reported betweenroot resorption and the duration of an applied forcewhich is more critical than the magnitude of theforce.14 The amount of external root resorption is alsoless in alveolar bone with ‘loose’, bony trabeculae.5Therefore, the best way to minimise root resorptionduring periodontal ligament distraction is to com-plete canine distraction within three weeks and beginoverjet reduction before the canine sockets fill withbone.5,15
It is generally accepted that pulp vitality tests are notreliable when a tooth is being moved orthodontically.5We recorded pulp vitality with an electronic pulptester and found no change in vitality and no darken-
PERIODONTAL LIGAMENT DISTRACTION OSTEOGENESIS FOR CANINE RETRACTION
Australian Orthodontic Journal Volume 25 No. 2 November 2009 151

ing of the distracted canines. However, electronicpulp testing can be unreliable so we suggest thatfuture studies use the more reliable laser Dopplerflowmeter. Liou and coworkers reported that the pulpremained vital, even when a tooth was moved at therate of 1.2 mm/week.7 It has also been reported thatthe inferior alveolar nerve and blood vessels regen-erate a short period of time after mandibular dis-traction.16 The long-term effects of periodontal liga-ment distraction on the pulp vitality are stillunknown so future studies should closely monitorpulp vitality.7,8
Rapid canine retraction by periodontal ligament dis-traction is an attractive method because it substan-tially reduces the duration of treatment and conservesanchorage. However, it has several potential draw-backs such as root resorption, loss of tooth vitality,ankylosis, tooth discolouration and excessive tipping.Furthermore, the surgical procedure is invasive andtechnique sensitive and can be uncomfortable, thedistractor is bulky, the patient requires close monitor-ing during the distraction period and excellentpatient compliance is essential for success.
Conclusions
The results of our study led to the following con-clusions:
1. Rapid canine retraction with distraction of theperiodontal ligament reduced the time needed tocompletely retract an upper canine. The method issuitable for severe malocclusions requiring maximumanchorage control.
2. The canines undergoing distraction should beclosely monitored.
3. No signs of root resorption, loss of pulp vitality orankylosis were found during interdental/periodontalligament distraction.
4. Less bulky distractors need to be developed.
5. The long-term effects of interdental/periodontalligament distraction are unknown.
Corresponding author
Dr Priyanka Sethi Kumar Senior LecturerDepartment of Orthodontics and DentofacialOrthopedicsSantosh Dental College and Hospital1 Santosh Nagar
Ghaziabad- 201009, U.P.IndiaTel: +91 9810 723900Email: [email protected]
References1. Vig P, Weintraub JA, Brown C, Kowalski CJ. The duration
of orthodontic treatment with and without extractions: Apilot study of 5 selected practices. Am J Orthod DentofacialOrthop 1990;97:45–51.
2. Reitan K. Clinical and histological observations on toothmovement during and after orthodontic treatment. Am JOrthod Dentofacial Orthop 1967;53:721–45.
3. Davidovitch Z, Finkelson MD, Steigman S, Shanfield FL,Moutogomery PC, Korostaff E. Electric currents, boneremodeling and orthodontic tooth movement. I. The effectof electric currents on periodontal cyclic nucleotides. Am JOrthod Dentofacial Orthop 1980;77:14–32.
4. Choy K, Pae EK, Park Y, Kim K, Burstone CJ. Effect of rootand bone morphology on the stress distribution in the perio-dontal ligament. Am J Orthod Dentofacial Orthop 2000;117:98–105.
5. Liou EJ, Huang CS. Rapid canine retraction through dis-traction of the periodontal ligament. Am J OrthodDentofacial Orthop 1998;114:372–82.
6. Liou EJ, Huang CS. Rapid canine retraction using distrac-tion of the periodontal ligament. Samchukov ML, Cope JB,Cherkashin AM eds. Craniofacial distraction osteogenesis.St. Louis: Mosby, 2001;461–74.
7. Liou EJ, Figueroa AA, Polley JW. Rapid orthodontic toothmovement into newly distracted bone after mandibular dis-traction osteogenesis in a canine model. Am J OrthodDentofacial Orthop 2000;117:391–8.
8. Seher S, Osman B, Umit G, Kerim O. Rapid canine distal-ization using distraction of the periodontal ligament: A preliminary clinical validation of the original technique.Angle Orthod 2004;74:304–15.
9. Sharpe W, Reed B, Subtelny JD, Polson A. Orthodonticrelapse, apical root resorption and crestal alveolar bone levels.Am J Orthod Dentofacial Orthop 1987;91:252–8.
10. Reitan K. Tissue behavior during orthodontic tooth move-ment. Am J Orthod 1960;46:881–900.
11. Baker R, Guay A, Peterson H. Current concepts of anchor-age management. Angle Orthod 1972;42:129–38.
12. Ziegler P, Ingervall B. A clinical study of maxillary canineretraction with a retraction spring and with sliding mechanics.Am J Orthod Dentofacial Orthop 1989;95 99–106.
13. Kurol J, Owman-Moll P, Lundgren D. Time related rootresorption after application of controlled continuous ortho-dontic force. Am J Orthod Dentofacial Orthop 1996;110:303–10.
14. Brezniak N, Wasserstein A. Root resorption after orthodon-tic treatment: a literature review. Part I. Am J OrthodDentofacial Orthop 1993;103:62–6.
15. Iseri H, Kisnisci R, Tüz H, Bzizi N. Rapid canine retractionand orthodontic treatment with dentoalveolar distractionosteogenesis. Am J Orthod Dentofacial Orthop 2005;127:533–41.
16. Block M, Daire J, Stover J, Mathews M. Changes in theinferior alveolar nerve following mandibular lengthening inthe dog using distraction osteogenesis. J Oral MaxillofacSurg 1993;652–60.
KUMAR ET AL
Australian Orthodontic Journal Volume 25 No. 2 November 2009152

Introduction
The introduction of chemically-cured compositeresins for direct bonding of orthodontic brackets wasan enormous advance over banding.1–3 However, themethod had some limitations, such as the inability toprecisely control the polymerisation time of the resinand incorporation of air during mixing, whichreduced the bond strength of the resin.4 The nextmove was the introduction of ultraviolet light-sensi-tive resins. Although the setting time of these resinscould be controlled, ultraviolet radiation introduced
unacceptable health hazards.5 Resins cured with visible light between 420 and 450 nm overcame thisdisadvantage.6 Composite resins cured with visiblelight were safe to use and the polymerisation timecould be controlled.
Polymerisation of light-cured composite resins beginsin the resin adjacent to the fibre optic tip and contin-ues as a chain reaction through the resin, eventuallyreaching the resin beneath the base of the bracket,where it may take some time to reach the full bond-ing strength.7 A recommended procedure is to place
© Australian Society of Orthodontists Inc. 2009 Australian Orthodontic Journal Volume 25 No. 2 November 2009 153
Changes in shear bond strength of ceramic andstainless steel brackets with different visible lightcuring times and directions
Farzin Heravi and Shahin BayaniDepartment of Orthodontics and the Dental Research Center, School of Dentistry, Mashad, Iran
Background: Selection of the appropriate curing time and light direction may enable the appropriate shear bond strength to beobtained and avoid enamel fracture during debonding.Aims: To determine the effects of different curing times and light directions on the shear bond strengths of ceramic and stainlesssteel brackets.Method: Ninety-two recently extracted, upper premolars were randomly assigned to six groups. Either stainless steel or ceramicbrackets were bonded to the buccal surfaces of the teeth. Group 1, stainless steel brackets cured for 40 seconds from buccalsurface; Group II, stainless steel brackets cured for 40 seconds from palatal surface; Group III, stainless steel brackets cured for 80 seconds from palatal surface; Group IV, ceramic brackets cured for 40 seconds from the buccal surface; Group V, ceramicbrackets cured for 40 seconds from the palatal surface; Group VI, ceramic brackets cured for 80 seconds from the palatal surface. The shear bond strength was measured with a universal testing machine and the resin remaining after debondingscored with the Adhesive Remnant Index (ARI). The data were analysed with the one-way ANOVA, Tukey’s HSD test and theKruskal-Wallis test. Associations between the ARI and shear bond strength were determined with Pearson’s correlation coefficient. Results: Group IV (ceramic brackets cured for 40 seconds from buccal surface) had the highest shear bond strength (21.26 MPa) and Group II (metal brackets cured for 40 seconds from palatal surface) had the lowest shear bond strength(6.95 MPa).There was no significant difference in ARI scores among the groups. The association between the ARI scores andbond strength values was not statistically significant. Conclusions: Curing from the buccal surface for 40 seconds gave unacceptably high shear bond strength values for both stain-less steel and ceramic brackets. Lower shear bond strengths occurred when the light was directed from the palatal surface, buta shorter curing time is more likely to be preferred by clinicians. Future studies should investigate the possibility of reducing thecuring time for both brackets.(Aust Orthod J 2009; 25: 153–157)
Received for publication: October 2008Accepted: October 2009
Farzin Heravi: [email protected] Bayani: [email protected]

HERAVI AND BAYANI
Australian Orthodontic Journal Volume 25 No. 2 November 2009154
the curing light next to the mesial (20 seconds) anddistal edges (20 seconds) of the bracket base.8 Theresin can also be polymerised by transilluminationfrom the occlusal and/or lingual/palatal surface.4, 9–11
This method may be advantageous for bondingbrackets with high bond strengths and reduce thepossibility of enamel damage during debonding.12
The purpose of this study was to determine the effectsof different curing times and light directions on theshear bond strengths (SBS) of ceramic and stainlesssteel brackets. We were particularly interested indeveloping protocols for direct bonding of stainlesssteel and ceramic brackets to premolars that wouldprovide adequate bond strength and reduce the like-lihood of enamel damage during debonding.
Material and methods
Ninety-two recently extracted, human upper pre-molars were used for this study. Teeth with enameldefects and/or enamel cracks or treated with chemicalagents were excluded. The teeth were stored in normal saline before use. Immediately before use theteeth were cleaned and polished with non-fluoridatedpumice and rubber cups for 10 seconds, randomlyassigned to six groups, and embedded in fast settingcold-cure acrylic resin.
The buccal surfaces of the teeth were etched with 37per cent phosphoric acid for 30 seconds, rinsed thor-oughly with water and dried with moisture-free air. Athin layer of Adper Prompt LP (3M Espe, St. Paul,MN, USA) was applied to the buccal surface of eachtooth and thinned by gently blowing air on the resinfor 10 seconds. The resin was then cured with anAstralis 7 visible light unit (Ivoclar, Vivadent, Schaan,Switzerland) with the intensity of 780 mW/cm2 for20 seconds. Ultratrimm stainless steel edgewise brackets (Dentaurum, Ispringen, Germany) andFascination ceramic edgewise brackets (Dentaurum,Ispringen, Germany) were bonded to the teeth withTransbond XT (3M Unitek, Monrovia, CA, USA)and cured with the same light at 780 mW/cm2. Thefollowing curing times and light directions were used:13
Group I: Stainless steel brackets, cured for 40 secondsfrom the buccal aspect (10 seconds at the mesial, distal, occlusal and gingival edges of the bracket base).
Group II: Stainless steel brackets, cured for 40 sec-onds from palatal aspect (light tip as close as possibleto the surface of the tooth).
Group III: Stainless steel brackets, cured for 80 sec-onds from palatal aspect (light tip as close as possibleto the surface of the tooth).
Group IV: Ceramic brackets, cured for 40 secondsfrom buccal aspect (10 seconds at the mesial, distal,occlusal and gingival edges of the bracket bases).
Group V: Ceramic brackets, cured for 40 secondsfrom palatal aspect (light tip as close as possible to the surface of the tooth).
Group VI: Ceramic brackets, cured for 80 secondsfrom palatal aspect (light tip as close as possible to the surface of the tooth).
After bonding, the specimens were stored for 24 h ina dark environment in normal saline at 37 °C.14 Thespecimens were mounted in a Zwick testing machine(Zwick GmbH, Ulm, Germany) and the bracketsdebonded with shear load applied to the bracket baseby a blade at a crosshead speed of 1 mm/min (Figure1). The Adhesive Remnant Index (ARI) was used toscore the amount of resin on the tooth surface afterdebonding.15
Statistical analysisThe Kolmogorov-Smirnov test was used to determineif the data were normally distributed. The shear bond
Figure 1. Shear load applied to the bracket base by a blade at acrosshead speed of 1 mm/min.

strengths were compared with the one-way analysis ofvariance (ANOVA) and post hoc differences amongthe groups with Tukey’s honestly significant differ-ence test (HSD). The Kruskal-Wallis test was used todetermine the significance of the differences in theARI scores. Associations between the ARI and shearbond strength were determined with Pearson’s correlation coefficient. The significance level for allstatistical tests was set at p ≤ 0.05.
Results
The shear bond strengths are given in Table I. GroupIV (ceramic brackets with 40 seconds curing frombuccal aspect) had the highest mean shear bondstrength and Group II (metal brackets with 40 secondscuring from palatal aspect) had the lowest bondstrength. The mean shear bond strengths of all groupsexcept Group II exceeded 7 MPa, the shear bondstrength regarded as clinically acceptable.2
The Group I brackets differed significantly from theGroup II brackets; the Group II brackets differed sig-nificantly from the Group IV, V and VI brackets; theGroup III brackets differed significantly from theGroup IV and VI brackets; the Group IV bracketsdiffered from the Group V brackets (Table II).
The ARI scores for the groups are given in Table III.The Kruskal-Wallis test showed that there were nosignificant differences between ARI scores of thegroups. During debonding the enamel fracturedbeneath the bases of two brackets in Group I (metalbrackets with 40 seconds curing from buccal aspect)and one bracket in Group IV (ceramic brackets with40 seconds curing from buccal aspect). These caseswere assigned an ARI score of zero. There was no sig-nificant correlation between the ARI scores and thebond strength values (p = 0.55).
Discussion
In this laboratory-based study, we determined theeffects of curing time and the tooth surface exposedto the curing light on the shear bond strengths ofceramic and stainless steel brackets bonded to humanpremolars. Regardless of the method of curing, theshear bond strengths of all groups, except the GroupII steel brackets (40 seconds cure and the curing lightplaced on the palatal surface), were well above the values needed for orthodontic treatment.2 The bondstrengths of both types of bracket were higher when thecuring light was placed on the buccal surface. For thesame curing times (40 and 80 seconds) and surfaces(buccal and palatal) ceramic brackets had higher shearbond strengths than stainless steel brackets.
Our results confirm previous reports that ceramicbrackets bonded with Transbond XT adhesive and
EFFECT OF CURING TIME AND LIGHT DIRECTION ON BOND STRENGTH
Australian Orthodontic Journal Volume 25 No. 2 November 2009 155
Table I. The effect of curing time and surface illuminated on the shearbond strengths of stainless steel and ceramic brackets.
Groups N Mean SD SEM 95% CI(MPa) Lower Upper
I 15 18.59 5.92 1.53 15.31 21.87II 15 6.95 4.83 1.25 4.27 9.62III 15 12.78 3.90 1.01 10.63 14.94IV 15 21.26 7.50 1.94 17.10 25.41V 16 14.39 3.65 0.91 12.44 16.33VI 16 20.12 7.09 1.77 16.34 23.90Total 92 15.72 7.39 0.77 14.18 17.25
I = 40 seconds light curing from buccal with steel bracketsII = 40 seconds light curing from lingual with steel bracketsIII = 80 seconds light curing from lingual with steel bracketsIV = 40 seconds light curing from buccal with ceramic bracketsV = 40 seconds light curing from lingual with ceramic bracketsVI = light curing for 80 seconds from lingual with ceramic brackets
Table II. Differences in shear bond strength among the groups (Tukey'sHSD test).
Groups II III IV V VI
I .00 .07 .79 .32 .97II .06 .00 .00 .00III .00 .97 .01IV .01 .99V .06
Statistically significant differences between groups are in bold
Table III. Adhesive Remnant Index (ARI) scores.
Groups ARI Scores
0 1 2 3I 5 3 2 5II 4 2 5 4III 2 5 3 5IV 2 5 3 5V 4 5 4 3VI 1 5 9 1Total 18 25 26 23

HERAVI AND BAYANI
Australian Orthodontic Journal Volume 25 No. 2 November 2009156
cured from the buccal aspect have the highest shearbond strengths.13,16 Bishara, who used ceramic brackets and Transbond XT adhesive, reported amean shear bond strength of only 10.4 MPa when thebrackets were bonded to upper molars,17 which sug-gests that enamel quality and possibly the shape ofthe buccal surface are factors determining bondstrength. We did not measure the areas of the bracket bases, a factor which may be partially respon-sible for different shear bond strengths betweenceramic and steel brackets. Although others havereported that the area of the bracket base is not a crucial factor affecting bond strength with mesh-backed brackets,18 future studies should investigatethe influence of the base area and type of bracket onthe shear bond strength.
According to Retief, enamel fractures can occur withbond strengths as low as 13.5 MPa.19 We experiencedthree enamel fractures: two teeth in Group I (steelbrackets with a mean shear bond strength of 18.59MPa) cured for 40 seconds from buccal aspect andone tooth in Group IV (ceramic brackets with a meanshear bond strength of 21.26 MPa) also cured for 40seconds from buccal aspect. Joseph reported enamelfractures in 4 out of 12 ceramic brackets he bondedwith a chemically light-activated composite resin.11 Wefound that brackets cured for 40 seconds from thepalatal surface had a mean shear bond strength of14.39 MPa. We consider that this is a clinically accept-able shear bond strength, and that it is less likely toresult in enamel fracture during debonding than highershear bond strengths.20
An interesting finding of our study was that all adhe-sive-ceramic bracket combinations cured from thepalatal surface had higher mean shear bond strengththan steel brackets cured from the palatal surface. Wepostulate that light reflected by the underside of aceramic bracket caused further polymerisation, andless light was reflected from the retentive mesh on astainless steel bracket. Group I had the highest meanshear bond strength for stainless steel brackets (MeanSBS: 18.59 MPa). These brackets were cured for 40 seconds from the buccal aspect, but the mostappropriate mean bond strength was in Group III(Mean SBS: 12.78 MPa). The brackets in the lattergroup were cured by transillumination from thepalatal aspect for 80 seconds. However, some clini-cians may consider this is too long a curing time touse routinely.
Joseph and Rossouw11 reported a mean shear bondstrength of 17.80 MPa for metal brackets primarilycured by transillumination. Their bond strengthswere higher than our Group II and Group III bondstrengths of 6.95 MPa and 12.78 MPa, respectively.Our Group II steel bracket – adhesive combinationwas cured by transillumination for 40 seconds andthe Group III steel bracket-adhesive combination wasalso cured by transillumination, but for 80 seconds.Joseph and Rossouw11 initially cured the adhesive for20 seconds from the labial surface and followed thisup with 5 min transillumination. Moreover, theyused canine teeth rather than human premolars.
Long curing times with intense light sources can raisethe temperature of a tooth pulp. Uzel et al.21 placed aSmart-line halogen curing light, with an output of625 mW/cm2, in contact with human premolars for40 seconds and recorded an increase in the pulpaltemperature of 1.9 °C. Although we used a morepowerful light source of 780 mW/cm2 for 80 secondsfrom the palatal aspect, the longer time is inconven-ient and the increase in shear bond strength may promote enamel fractures, particularly with rigidbrackets. We recommend shorter exposures are usedto avoid the possibility of increasing the temperatureof the pulp by more than the critical value of 5–6 °C.The safety of more powerful curing lights and longcuring times should be investigated.
Conclusions
In this laboratory-based study ceramic and stainlesssteel edgewise brackets were bonded to the buccalsurfaces of upper premolars with the same light-curedadhesive and the effects of curing time and lightdirection on the shear bond strengths determined.
The highest shear bond strengths of ceramic and steelbrackets in this study were found when the adhesivewas cured for 40 seconds and the light was placed onthe buccal surface of the tooth.
For the same curing times (40 and 80 seconds) andsurfaces (buccal and palatal) ceramic brackets hadhigher shear bond strengths than stainless steel brackets.
Only the shear bond strengths of stainless steel brackets illuminated from the palatal surface for 40seconds fell below 7 MPa, the acceptable level forclinical use.
No significant differences were found in ARI scoresbetween the groups.

The enamel fractured during debonding two metaland one ceramic brackets, both cured for 40 secondsfrom the buccal surface.
There was no significant correlation between the ARIscores and the bond strength values.
Clinicians using light-cure adhesives should considerthe trade-off between a long curing time (higher shearbond strengths) and the possibility of pulp/enameldamage. We suggest the lowest possible curing time(40 seconds from buccal for ceramic and steel bracketsor 40 seconds transillumination for ceramic brackets)with conventional light-curing devices will result inclinically acceptable shear bond strengths with bothtypes of bracket.
Acknowledgment
Financial support for this study was provided by ViceChancellor for Research, Mashad Medical University.
Corresponding author
Associate Professor Farzin HeraviDepartment of Orthodontics andDental Research CenterSchool of DentistryMashad University of Medical SciencesMashad/IranTel: +98 511 8419814Fax: +98 511 8829500Email: [email protected]
References1. Johnson WT, Hembree JH, Weber FN. Shear strength of
orthodontic direct-bonding adhesion. AM J Orthod 1976;70:559–66.
2. Reynolds IR. A review of direct orthodontic bonding. Br JOrthod 1975;2:171–8.
3. Keizer S, Ten Cate JM, Arends J. Direct bonding of ortho-dontic brackets. Am J Orthod 1976;69:318–27.
4. King L, Smith RT, Wendt SL, Behrents RG. Bond strengthsof lingual orthodontic brackets bonded with light-curedcomposite resins cured by transillumination. Am J Orthod1987;91:312–5.
5. Rock WB. The use of ultra-violet radiation in dentistry. BrDent J 1974;136:455–60.
6. Douglas WH, Craig RG, Chen CJ. A new composite restora-tive based on a hydrophobic matrix. J Dent Res 1979;58:1981–6.
7. Zachrisson BU, Buyukyilmaz T. Bonding in Orthodontics.In: Graber TM, Vanarsdall RL, Vig KW. 4th ed.Orthodontics current principles and techniques. St. Louis:Mosby, 2007:594.
8. Oesterle LJ, Messersmith ML, Devine SM, Ness CF. Lightand setting times of visible-light-cured orthodontic adhesives.J Clin Orthod 1995;29:31–6.
9. Tavas A, Watts DC. Bonding of orthodontic brackets bytransillumination of a light activated composite: an in vitrostudy. Br J Orthod 1979;6:207–8.
10. Read MJF. Indirect bonding using a visible light cured adhesive. Br J Orthod 1987;14:137–41.
11. Joseph VP, Rossouw E. The shear bond strength of stainlesssteel and ceramic brackets used with chemically light-acti-vated composite resins. Am J Orthod Dentofacial Orthop1990;97:121–5.
12. Ghafari J. Problems associated with ceramic brackets suggestlimited use to selected teeth. Angle Orthod 1992;62:145–52.
13. Haydar B, Sarikaya S, Cehreli ZC. Comparison of shearbond strength of three bonding agents with metal andceramic brackets. Angle Orthod 1999;69:457–62.
14. Hocevar RA, Vincent HF. Indirect versus direct bonding:bond strength and failure location. Am J OrthodDentofacial Orthop 1988;94:367–71.
15. Artun J, Bergland S. Clinical trials with crystal growth con-ditioning as an alternative to acid etch pretreatment. Am JOrthod 1984;85:333–40.
16. Gwinnett AJ. A comparison of shear bond strength of metaland ceramic brackets. Am J Orthod Dentofacial Orthop1988;93:346–8.
17. Bishara SE, Olsen ME, VonWald L, Jakobsen JR.Comparision of the debonding characteristics of two inno-vative ceramic bracket designs. Am J Orthod DentofacialOrthop 1999;116:86–92.
18. MacColl GA, Rossouw PE, Titley KC, Yamin C. the rela-tionship between bond strength and orthodontic bracketbase surface area with conventional and microetched foil-mesh bases. Am J Orthod Dentofacial Orthop 1998;113:276–81.
19. Retief DH. Failure at the dental adhesive-etched enamelinterface. J Oral Rehabil 1974;1:265–84.
20. Bowen RL, Rodriguez MS. Tensile strength and modulus ofelasticity of tooth structure and several restorative materials.J Am Dent Assoc 1962;64:378–87.
21. Uzel A, Buyukyilmaz T, Kayaligolu M, Uzel I. Temperaturerise during orthodontic bonding with various light-curingunits: an in vitro study. Angle Orthod 2006;76:330.
EFFECT OF CURING TIME AND LIGHT DIRECTION ON BOND STRENGTH
Australian Orthodontic Journal Volume 25 No. 2 November 2009 157

Introduction
Facial symmetry is an important aspect of facialattractiveness. It is well-known that symmetrical facesare generally more attractive than asymmetricalfaces,1 although individuals with balanced and attrac-tive faces often have slight skeletal asymmetries.2Skeletal asymmetries are much less common thanother facial asymmetries, such as asymmetric facialmovements which play an important part in socialinteraction.3–5 Skeletal asymmetries are frequentlyfound in subjects with Class III malocclusion andgenerally affect the lower face, particularly themandible.6,7 Frontal facial asymmetry in ortho-gnathic surgery patients with Class III malocclusionhas been rarely investigated, in spite of the fact that
orthognathic surgery provides an opportunity to correct an underlying skeletal asymmetry.7–9
The purpose of this study was to investigate facialskeletal asymmetries in orthognathic surgery patientswith Class III malocclusions.
Materials and methods
The Class III group consisted of 29 subjects (14female, 15 male) with a mean age of 21.44 years whohad had orthognathic surgery. All subjects in thisgroup had severe dental and skeletal Class III relationships (ANB angle > -5 degrees). The Controlgroup consisted of 32 subjects (16 female, 16 male;Mean age: 19.20 years) with excellent Class I occlu-sions, no missing teeth and slight to moderate anterior
Australian Orthodontic Journal Volume 25 No. 2 November 2009 © Australian Society of Orthodontists Inc. 2009158
Facial asymmetry in subjects with Class III malocclusion
Nihat Kilic,* Songül Comert Kilic† and Gülhan Catal*
Departments of Orthodontics* and Oral and Maxillofacial Surgery,† Faculty of Dentistry, Atatürk University, Erzurum, Turkey.
Background: Facial skeletal asymmetries in Class III subjects seeking orthognathic surgery may complicate subsequent treatment.Objective: The purpose of this study was to investigate facial asymmetry in orthognathic surgery patients with Class III malocclusion.Methods: The Class III group consisted of 29 orthognathic surgery patients (14 female, 15 male; Mean age: 21.44 years)with Class III malocclusions. The Control group consisted of 32 subjects (16 female, 16 male; Mean age: 19.20 years) withexcellent Class I occlusal relationships. Facial skeletal asymmetry, based on the skeletal midline, was measured on postero-anterior radiographs. In the Class III group, the chin point deviated to the ipsilateral side. The side-to-side and between groupdifferences were compared.Results: In the Class III group, the antegonial notch – skeletal midline distance was significantly larger (p < 0.05) and menton –antegonial notch distance was significantly different (p < 0 .05). There were no statistically significant differences between theright and left side measurements in the Control group. Between-group comparisons showed that subjects in the Class III grouphad greater skeletal asymmetries in lower face. In 78 per cent of the subjects in the Class III group the chin point was dis-placed more than 2 mm to one side. Conclusions: Subjects with Class III malocclusion may have facial skeletal asymmetries, predominantly in the lower face. Frontalasymmetries should be considered during diagnosis and treatment planning. (Aust Orthod J 2009; 25: 158–162)
Received for publication: March 2009Accepted: October 2009
Nihat Kilic: [email protected]ül Comert Kilic: [email protected]ülhan Catal: [email protected]

THE FACIAL ASYMMETRY IN CLASS III MALOCCLUSION
Australian Orthodontic Journal Volume 25 No. 2 November 2009 159
crowding. Additional inclusion criteria for the sub-jects in both groups were: no developmental and/oracquired craniofacial or neuromuscular deformities;no previous orthodontic treatment; no carious lesionsor extensive restorations and healthy periodontal tis-sues. Patients with functional unilateral posteriorcrossbites, which were determined clinically, wereexcluded from the Class III group.
The pretreatment postero-anterior cephalometricradiographs of all subjects were selected from the filesin the Department of Orthodontics, Faculty ofDentistry, Atatürk University, Erzurum, Turkey. Allradiographs were taken by a single operator with theFrankfort plane parallel to the floor and with theteeth in the intercuspal position. The radiographswere taken with a Proline PM 2002 CC machine(Planmeca, Helsinki, Finland) with Kodak MXG filmand an exposure time of 1.2 seconds at 62 kV(p) and12 mA.
The postero-anterior radiographs were scanned(Epson Expression 1860 Pro, Seiko Epson Corp.,Nagono-ken, Japan) at a magnification of 100 percent and the resulting images ‘traced’ and measuredwith Quick Ceph 2000 (Quick Ceph Systems, SanDiego, CA, USA). The cephalometric measurementsused in the present study were adapted from thosedescribed by Grummons and Van de Coppello(Figure 1).10 For bilateral structures, the perpendic-ular distances from the right and left landmarks to thevertical reference line (X-Line) were measured andthe differences calculated. Mandibular (chin) devi-ation was the horizontal distance from menton to theX-Line. This deviation could be to either the right orthe left side in both groups and was given as a posi-tive value in the between-group comparisons. Theside to which the mandible (chin point) deviated relative to the X-Line will be referred as the ipsi-lateral side and the alternate side will be referred asthe contralateral side.
Statistical analysisTo determine the systematic and random errors asso-ciated with digitisation and measurement, 15 radio-graphs were randomly selected, re-digitised andremeasured two weeks later. A paired t-test wasapplied to the first and second measurements and noerrors were found.
A paired t-test was also used to determine the differ-ences between the left and right sides in the subjectsin each group. The differences in the Control groupwere obtained by subtracting the left side measure-ments from the right side measurements and in theClass III group the differences were the ipsilateral sidemeasurement minus the contralateral side measure-ment. The between-group differences and the chindeviation were compared with Student’s t-test.
All statistical analysis was performed using the SPSSsoftware package (SPSS for Windows 98, version10.0, SPSS Inc, Chicago, IL, USA).
Results
The results are given in Tables I and II. In the ClassIII group there was no statistically significant differ-ence between the jugular processes and the X-Line (p = 0.111). The antegonial notch distance was significantly greater on the ipsilateral side than on the contralateral side (p < 0.012), and the menton –antegonial notch distance was significantly smaller on
Figure 1. Cephalometric landmarks and measurements.Mandibular deviation (1): the perpendicular distance between menton (Me),the most inferior point of anterior border of mandible at the symphysis, andthe X-Line.Jugular process distances (2 and 3): the perpendicular distances betweenmaxillare (Mx), the deepest points of the lateral maxillary contours at thejunctions of right and left maxilla and zygomatic buttress, and the X-Line.Antegonial notch distances (4 and 5): the perpendicular distances betweenthe right and left antegonial notches and the X-Line.Menton - antegonial notch distances (6 and 7): the distances between ante-gonial notches (Ag) and menton (Me).Horizontal reference line (Z-Line) (8): the line connecting the right and left lat-ero-orbitale points (Lo), which are the intersections of the lateral wall of theorbit and the greater wings of the sphenoid bone (the oblique line).Vertical reference line (X-Line) (9): the perpendicular to the Z-Line passingthrough the tip of the anterior nasal spine (ANS), which represents skeletalmedian line.

the ipsilateral side than on the contralateral side (p < 0.029). There were no statistically significant dif-ferences between the right and left sides in theControl group (Table I). As there were no right – leftdifferences in the Control group, the right side minusthe left side differences were used in all subsequentcomparisons.
The between-group comparisons, including the devi-ation in the chin (mandibular deviation) are given inTable II. There were two statistically significant ClassIII group – Control group differences: the differencein the antegonial notch distance was significantlylarger in the Class III group (p = 0.004) and the dif-ference in the menton – antegonial notch distancewas also statistically significant (p = 0.011).
In the Class III group, the mandible deviated to theright side in eight subjects and to the left side in 21subjects. In other words, the chin deviated to the left
side in 72 per cent of the Class III subjects. Morethan 2 mm deviation was observed in 78 per cent ofthe subjects in this group. The mean mandibulardeviation was 3.29 mm in the Class III group and0.54 mm in the Control group.
Discussion
Facial asymmetries have been investigated by differ-ent methods including frontal facial photographs,stereophotogrammetry, three-dimensional computedtomography and postero-anterior radiographs.9,11,12
Although the beauty and harmony of the face is usually judged from the frontal or mirror view ortho-dontists rarely use postero-anterior radiographs tostudy facial asymmetry.10 Radiographs have theadvantage of disclosing the underlying skeletal formnot seen with photographic methods. The key forevaluating facial asymmetry on postero-anterior radio-graphs is the method used to determine the skeletalmidline. We found that the computer software pro-gramme we used had advantages over traditional methods of measuring radiographs. It was possible toaccurately trace the contours of bony structures, suchas the orbits, by enlarging the image and altering thecontrast when needed.13
We used the perpendicular to the line joining theright and left latero-orbitale points passing throughthe tip of the anterior nasal spine because it avoideddeviations of the nasal septum. Furthermore, thesepoints are not usually affected by severe lower faceasymmetries. Upper face asymmetries which wouldaffect construction of the Z-Line and, hence, ourmethod of determining the facial midline, are rela-tively uncommon. In a retrospective study of 1460patients, Severt and Proffit reported that upper faceasymmetry occurred in only 23 subjects (5 per cent)
KILIC ET AL
Australian Orthodontic Journal Volume 25 No. 2 November 2009160
Table I. Comparisons of the deviated side (ipsilateral) with the contralateral side in the Class III group and the right and left sides in the Control group.
Class III group Control groupIpsilateral side Contralateral side p Right side Left side p
Mean (SD) Mean (SD) Mean (SD) Mean (SD)
Jugular process distance (mm) 31.74 (2.55) 31.04 (2.24) 0.111 36.62 (3.39) 36.73 (3.44) 0.272Antegonial notch distance (mm) 46.22 (4.05) 43.84 (3.38) 0.012 49.96 (3.89) 49.95 (3.77) 0.887Menton–antogonial notch distance (mm) 54.89 (6.66) 58.52 (7.58) 0.029 57.70 (6.25) 57.72 (6.19) 0.825
Significant values in bold
Table II. Group comparisons.
Parameters Class III group Control group p
Mean Meandifference (SD) difference (SD)
Chin deviation 3.29 (2.05) 0.54 (0.39) 0.000Jugular processdistance (mm) 0.71 (2.33) -0.10 (0.53) 0.124Antegonial notchdistance (mm) 2.38 (4.77) 0.02 (0.69) 0.004Menton–antegonialnotch distance (mm) -3.63 (8.48) 0.02 (0.66) 0.011
Class III group: ipsilateral measurement minus contralateral measurementControl group: right side minus left sideSignificant values in bold

THE FACIAL ASYMMETRY IN CLASS III MALOCCLUSION
Australian Orthodontic Journal Volume 25 No. 2 November 2009 161
of the group with a dentofacial deformity.7 The analysis we used is a practical and simple method ofdetermining the locations and severity of a facialasymmetry and recently we have confirmed its validity.14
In agreement with others we found that the subjectswith severe Class III malocclusions had marked skele-tal asymmetries in the lower third of the face that arenot always visible to an observer.6,7 Severt and Proffitreported that 34 per cent of the subjects they exam-ined had clinically apparent facial asymmetry.7 In oursample, the chin deviated slightly more than 3 mm toone side, the menton to antegonial distance wasreduced on that side and the antegonial notch dis-tance was increased. Others have also reported thatsubjects with a skeletal Class III deformity frequentlyhave an asymmetrical lower face.6,15 For example,Haraguchi and coworkers found between 70 and 85per cent of their subjects had a facial asymmetry inaddition to a skeletal Class III deformity.12 Theseresults indicate that patients with severe Class III mal-occlusions frequently have skeletal facial asymmetrieswhich may influence orthognathic surgery.
Horizontal and vertical head rotations during radiog-raphy may contribute to errors in the vertical refer-ence line and reduce the effectiveness of our analysis.10 To eliminate rotations around the verticaland transverse axes, postero-anterior radiographsshould be taken with the ear rods firmly placed in theexternal auditory meati and with the head in a stan-dardised position relative to the floor. We positionedthe head with the Frankfort line parallel to the floor,but other positions can be used. The teeth should bein maximal intercuspation because this occlusal posi-tion is reproducible and readily attained by patients.16
However, some Class III patients seeking ortho-gnathic surgery may have a mandibular functionalpattern that differs from the norm.17 This may takethe form of a lateral crossbite and mandibular dis-placement which may contribute to an underlyingmandibular asymmetry.18,19 We did not attempt toeliminate or correct any functional displacement ofthe mandible on the radiographs.
Severe facial asymmetry may affect jaw function anddental and facial appearance. The latter may lead todiscrimination in social interactions.20 Althoughfunctional impairments, such as difficulty in chew-ing, discomfort and pain, are often the main reasonsfor the surgical/orthodontic treatment, poor facial
appearance can lead to feelings of inadequacy anddiscontent.21,22
Conclusion
Subjects with Class III dentofacial deformity mayhave frontal skeletal facial asymmetries, predomi-nantly in their lower third of the face. Cliniciansshould consider the possibility of these in their initialdiagnosis and treatment planning.
Corresponding author
Dr Nihat KilicAtatürk Üniversitesi Dis Hekimligi FakültesiOrtodonti Anabilim Dalı 25240 ErzurumTurkeyTel: +90 442 2311810Fax: +90 442 2312270 – 2360945Email: [email protected]
References1. Grammer K, Thornhill R. Human (Homo sapiens) facial
attractiveness and sexual selection: the role of symmetry andaverageness. J Comp Psychol 1994;108:233–42.
2. Kowner R. Perceiving and attributing hemispheric width infaces of normal adults. Percept Mot Skills 1998;87:567–72.
3. Sackeim HA, Weiman AL, Forman BD. Asymmetry of theface at rest: size, area and emotional expression. Cortex1984;20:165–78.
4. Schmidt KL, Liu Y, Cohn JF. The role of structural facialasymmetry in asymmetry of peak facial expressions.Laterality 2006;11:540–61.
5. Smith WM. Hemispheric and facial asymmetry: gender differences. Laterality 2000;5:251–8.
6. Haraguchi S, Iguchi Y, Takada K. Asymmetry of the face inorthodontic patients. Angle Orthod 2008;78:421–6.
7. Severt TR, Proffit WR. The prevalence of facial asymmetryin the dentofacial deformities population at the Universityof North Carolina. Int J Adult Orthodon Orthognath Surg1997;12:171–6.
8. Proffit WR. Contemporary Orthodontics. St Louis: MosbyYear Book, 2000;674–709.
9. Maeda M, Katsumata A, Ariji Y, Muramatsu A, Yoshida K,Goto S, Kurita K, Ariji E. 3D-CT evaluation of facial asym-metry in patients with maxillofacial deformities. Oral SurgOral Med Oral Pathol Oral Radiol Endod 2006;102:382–90.
10. Grummons DC, Kappeyne van de Coppello MA. A frontalasymmetry analysis. J Clin Orthod 1987;21:448–65.
11. Farkas LG, Cheung G. Facial asymmetry in healthy NorthAmerican Caucasians. An anthropometrical study. AngleOrthod 1981;51:70–7.
12. Koff E, Borod J, Strauss E. Development of hemiface sizeasymmetry. Cortex 1985;21:153–6.
13. Cangialosi TJ, Chung JM, Elliott DF, Meistrell ME.Reliability of computer-generated prediction tracing. AngleOrthod 1995;65:277–84.

KILIC ET AL
Australian Orthodontic Journal Volume 25 No. 2 November 2009162
14. Caglaroglu M, Kilic N, Erdem A. Effects of early unilateralfirst molar extraction on skeletal asymmetry. Am J OrthodDentofacial Orthop 2008;134:270–5.
15. Sheats RD, McGorray SP, Musmar Q, Wheeler TT, King GJ.Prevalence of orthodontic asymmetries. Semin Orthod1998;4:138–45.
16. Major PW, Johnson DE, Hesse KL, Glover KE. Landmarkidentification error in posterior anterior cephalometrics.Angle Orthod 1994;64:447–54.
17. Athanasiou AE, Melsen B, Mavreas D, Kimmel FP.Stomatognathic function of patients who seek orthognathicsurgery to correct dentofacial deformities. Int J AdultOrthodon Orthognath Surg 1989;4:239–54.
18. Bishara SE, Burkey PS, Kharouf JG. Dental and facial asymmetries: a review. Angle Orthod 1994;64:89–98.
19. Deguchi T, Garetto LP, Sato Y, Potter RH, Roberts WE.Statistical analysis of differential lissajous EMG from nor-mal occlusion and Class III malocclusion. Angle Orthod1995;65:151–60.
20. Proffit WR, White RP. Dentofacial problems: Prevalence andtreatment need. In: Proffit WR, White RP, Sarver DM,Editors. Contemporary treatment of dentofacial deformity.St. Louis: Mosby, 2003;2–28.
21. Phillips C, Bennett ME, Broder HL. Dentofacial disharmony:psychological status of patients seeking treatment con-sultation. Angle Orthod 1998;68:547–56.
22. Rivera SM, Hatch JP, Dolce C, Bays RA, Van Sickels JE,Rugh JD. Patients’ own reasons and patient-perceived rec-ommendations for orthognathic surgery. Am J OrthodDentofacial Orthop 2000;118:134–41.

Introduction
Determinations of tooth size are an important step inthe diagnostic process, particularly in management ofcomplex cases.1 Disproportions in intra- and inter-arch tooth sizes may contribute to crowding or spacing in the dental arches. Failure to compensatefor these discrepancies during treatment generallyresults in unsatisfactory alignment and occlusion ofthe teeth at the end of orthodontic treatment. Largeteeth relative to the size of the jaws are associated withcrowded dental arches and small teeth with spaceddental arches: both conditions can be localised to afew teeth or affect all teeth.2
Before we can know if a tooth is under- or oversize itis necessary to have data on tooth sizes for the rele-vant ethnic, gender and malocclusion group.3–5 Thesedata are important for orthodontic clinical diagnosisand treatment planning and may be useful in forensicdentistry6 and as records marking technologicaladvances, environmental variations and dietaryimprovements affecting tooth size.4 The accumulatedevidence indicates that tooth size reflects a com-plex interaction between a variety of genetic and environmental factors.4
The objectives of the present study were to com-pare the mesio-distal tooth sizes and dental arch
© Australian Society of Orthodontists Inc. 2009 Australian Orthodontic Journal Volume 25 No. 2 November 2009 163
Variations in tooth size and arch dimensions inMalay schoolchildren
Khalid W. Hussein, Zainul A. Rajion, Rozita Hassan and Siti Noor Fazliah Mohd. NoorSchool of Dental Sciences, Universiti Sains Malaysia, Kelantan, Malaysia
Aims: To compare the mesio-distal tooth sizes and dental arch dimensions in Malay boys and girls with Class I, Class II andClass III malocclusions.Methods: The dental casts of 150 subjects (78 boys, 72 girls), between 12 and 16 years of age, with Class I, Class II andClass III malocclusions were used. Each group consisted of 50 subjects. An electronic digital caliper was used to measure themesio-distal tooth sizes of the upper and lower permanent teeth (first molar to first molar), the intercanine and intermolar widths.The arch lengths and arch perimeters were measured with AutoCAD software (Autodesk Inc., San Rafael, CA, USA).Results: The mesio-distal dimensions of the upper lateral incisors and canines in the Class I malocclusion group were signifi-cantly smaller than the corresponding teeth in the Class III and Class II groups, respectively. The lower canines and first molarswere significantly smaller in the Class I group than the corresponding teeth in the Class II group. The lower intercanine widthwas significantly smaller in the Class II group as compared with the Class I group, and the upper intermolar width was signifi-cantly larger in Class III group as compared with the Class II group. There were no significant differences in the arch perimetersor arch lengths. The boys had significantly wider teeth than the girls, except for the left lower second premolar. The boys alsohad larger upper and lower intermolar widths and lower intercanine width than the girls. Conclusion: Small, but statistically significant, differences in tooth sizes are not necessarily accompanied by significant archwidth, arch length or arch perimeter differences. Generally, boys have wider teeth, larger lower intercanine width and upperand lower intermolar widths than girls.(Aust Orthod J 2009; 25: 163–168)
Received for publication: February 2009Accepted: October 2009
Khalid W. Hussein: [email protected] A. Rajion: [email protected] Hassan: [email protected] Noor Fazliah Mohd. Noor: [email protected]

HUSSEIN ET AL
Australian Orthodontic Journal Volume 25 No. 2 November 2009164
dimensions in Malay schoolchildren with Class I,Class II and Class III malocclusions, and to deter-mine if gender differences in tooth sizes and archdimensions are present in Malay schoolchildren.
Materials and methods
In this cross-sectional study, mesio-distal tooth sizes,intercanine and intermolar widths, arch lengths andarch perimeters were measured on the dental casts of150 Malay schoolchildren (78 boys, 72 girls) fromthe Kota Bharu District, Kelantan. The children whowere between 12 and 16 years of age had Class I (N = 50), Class II (N = 50) and Class III (N = 50)malocclusions. The mesio-distal tooth sizes, inter-canine and intermolar widths were measured on thedental casts with calipers and the upper and lowerarch perimeters and arch lengths were measured with
AutoCAD software (Autodesk Inc., San Rafael, CA,USA). The study was carried out at Universiti SainsMalaysia.
Subjects were included if all permanent teeth, exceptthe third molars, were present and there was no his-tory of previous orthodontic treatment. Subjects wereexcluded if a dental cast had an impression and/orcasting artefact affecting the crowns of the teeth, conical and/or peg-shaped incisors or hypoplastic teeth.
The following measurements were recorded: thelargest mesio-distal widths of the permanent teethexcept the second molars in each arch, the inter-canine and intermolar widths, arch length and archperimeter. The mesio-distal widths of the teeth weremeasured between the anatomical contact points andperpendicular to the long axes of the teeth on ortho-dontic models by the same examiner with an
Table I. Comparisons of the mesio-distal tooth widths (mm) in the malocclusion groups.
Arch Tooth Class I Class II Class III pMean ± SD Mean ± SD Mean ± SD
Upper 1 R 8.36 ± 0.50 8.48 ± 0.44 8.57 ± 0.64 NSL 8.36 ± 0.50 8.48 ± 0.41 8.57 ± 0.66 NS
2 R 6.68 ± 0.60 a 6.87 ± 0.47 7.03 ± 0.65 a 0.01L 6.70 ± 0.45 a 6.84 ± 0.48 6.97 ± 0.63 a 0.03
3 R 7.83 ± 0.42 a 8.06 ± 0.46 a 8.05 ± 0.51 0.05L 7.81 ± 0.45 a 8.04 ± 0.46 a 7.98 ± 0.50 0.05
4 R 7.42 ± 0.38 7.39 ± 0.39 7.52 ± 0.42 NSL 7.39 ± 0.38 7.43 ± 0.39 7.51 ± 0.43 NS
5 R 6.92 ± 0.39 7.03 ± 0.44 7.16 ± 0.48 NSL 6.49 ± 0.47 7.07 ± 0.51 6.94 ± 0.38 NS
6 R 10.21 ± 0.53 10.36 ± 0.51 10.19 ± 0.65 NSL 10.20 ± 0.53 10.40 ± 0.52 10.20 ± 0.72 NS
Lower 1 R 5.41 ± 0.36 5.45 ± 0.27 5.56 ± 0.45 NSL 5.40 ± 0.29 5.45 ± 0.27 5.34 ± 0.43 NS
2 R 6.02 ± 0.36 6.12 ± 0.32 6.10 ± 0.43 NSL 6.00 ± 0.36 6.14 ± 0.29 6.14 ± 0.41 NS
3 R 6.77 ± 0.43 a 7.00 ± 0.36 a 6.95 ± 0.52 0.02L 6.75 ± 0.43 a 7.00 ± 0.32 a 6.89 ± 0.70 0.04
4 R 7.29 ± 0.45 7.29 ± 0.44 7.31 ± 0.43 NSL 7.29 ± 0.45 7.33 ± 0.36 7.35 ± 0.46 NS
5 R 7.11 ± 0.46 7.28 ± 0.42 7.16 ± 0.48 NSL 7.17 ± 0.48 7.28 ± 0.41 7.12 ± 0.47 NS
6 R 11.16 ± 0.51 a 11.48 ± 0.61 a 11.34 ± 0.63 0.02L 11.16 ± 0.53 a 11.46 ± 0.68 a 11.40 ± 0.63 0.04
The letters indicate groups significantly different from each other (Scheffe test)Significant values in bold; NS, p > 0.05

electronic digital caliper (ProMax, Fowler Company,Newton, MA, USA) to 0.01 mm.
The intercanine widths were the horizontal distancesbetween the tips of the cusps of the upper and lowerpermanent canines, and the intermolar widths werethe horizontal distances between the right and leftcentral fossae of the upper and lower first permanentmolars.7 Arch length was the line drawn from midlinebetween the central incisors perpendicular to the tangent touching the distal surfaces of the first per-manent molars.8 Arch perimeter was a smooth curvedrawn from the distal surface of a first permanentmolar around the arch over the contact points andincisal edges to the distal surface of the contralateralfirst permanent molar.8 These measurements were
performed on images of the occlusal surfaces takenwith a Scan-jet 5550 (Hewlett-Packard Asia PacificLtd, Singapore). A piece of squared paper was included with the scanned images for the purposes of calibration and calculation of the magnification.9These images were downloaded into the AutoCAD2008 software (Autodesk Inc., San Rafael, CA, USA)and the arch lengths and arch perimeters measured towithin 0.1 mm.8
Statistical analysisTwenty pairs of dental casts were randomly selectedand remeasured one month after the initial measure-ments. There were no statistically significant differ-ences between the two sets of measurements.
TOOTH SIZES AND ARCH DIMENSIONS IN MALAY SCHOOL CHILDREN
Australian Orthodontic Journal Volume 25 No. 2 November 2009 165
Table II. Comparisons of arch length, arch width and arch perimeter in different malocclusion groups.
Arch Variable Class I Class II Class III pMean ± SD Mean ± SD Mean ± SD
Upper Intercanine 35.10 ± 1.31 34.99 ± 1.18 5.74 ± 5.78 NSIntermolar 47.87 ± 2.03 46.71 ± 2.83 a 48.42 ± 2.81 a 0.00Arch length 39.51 ± 2.09 39.48 ± 2.45 39.87 ± 2.48 NSArch perimeter 102.00 ± 4.66 103.22 ± 4.64 103.53 ± 5.09 NS
Lower Intercanine 27.03 ± 1.46 a 26.02 ± 1.08 a 27.49 ± 1.79 0.00Intermolar 41.77 ± 2.18 41.97 ± 2.98 42.28 ± 2.75 NSArch length 35.01 ± 2.05 39.48 ± 2.45 34.57 ± 2.31 NSArch perimeter 91.26 ± 4.97 91.19 ± 3.59 90.05 ± 4.81 NS
The letters indicate groups significantly different from each other (Scheffe test)Significant values in bold; NS, p > 0.05
Table III. Gender comparisons of the mesio-distal widths (mm).
Tooth Male Female p Tooth Male Female pMean ± SD Mean ± SD Mean ± SD Mean ± SD
Upper 11 8.62 ± 0.55 8.30 ± 0.47 0.00 21 8.61 ± 0.55 8.33 ± 0.48 0.0012 6.97 ± 0.55 6.75 ± 0.62 0.02 22 6.93 ± 0.51 6.74 ± 0.54 0.0313 8.15 ± 0.45 7.80 ± 0.43 0.00 23 8.14 ± 7.72 7.72 ± 0.44 0.0014 7.52 ± 0.41 7.35 ± 0.36 0.01 24 7.53 ± 0.40 7.36 ± 0.39 0.0115 7.06 ± 0.46 6.90 ± 0.43 0.03 25 7.06 ± 0.46 6.90 ± 0.43 0.0316 10.39 ± 0.48 10.11 ± 0.56 0.00 26 10.46 ± 0.48 10.06 ± 0.65 0.00
Lower 41 5.53 ± 0.38 5.41 ± 0.35 0.05 31 5.53 ± 0.37 5.39 ± 0.29 0.0142 6.18 ± 0.39 5.96 ± 0.32 0.00 32 6.18 ± 0.39 6.00 ± 0.30 0.0043 7.07 ± 0.43 6.73 ± 0.40 0.00 33 7.01 ± 0.57 6.75 ± 0.42 0.0044 7.41 ± 0.43 7.17 ± 0.41 0.00 34 7.40 ± 0.42 7.24 ± 0.42 0.0245 7.30 ± 0.44 7.06 ± 0.45 0.00 35 7.23 ± 0.47 7.14 ± 0.44 0.2046 11.46 ± 0.55 11.18 ± 0.61 0.00 36 11.5 ± 0.60 11.16 ± 0.62 0.00
Significant values in bold

HUSSEIN ET AL
Australian Orthodontic Journal Volume 25 No. 2 November 2009166
The data were analysed using SPSS version 12.0.1 forwindows (SPSS Inc., 2003). An analysis of variance(ANOVA) was used to determine whether statistic-ally significant differences existed between Class I,Class II and Class III groups and the post hoc Scheffetest was used to determine which groups were differ-ent from each other. Student’s t-test was used toinvestigate gender differences in the samples. The sig-nificance level was set at p < 0.05 for all statisticaltests.
Results
The results are given in Tables I to IV.
There were eight statistically significant mesio-distalwidth differences between the malocclusion groups:the upper lateral incisors in the Class III group weresignificantly larger than the lateral incisors in theClass I malocclusion group, both upper and lowercanines were significantly larger in the Class II groupthan the corresponding canines in the Class I group;and the lower first molars in the Class II group weresignificantly larger than the lower first molars in theClass I group (Table I).
The upper intermolar width was significantly largerin the Class III group than the Class II group and thelower intercanine width in the Class II malocclusiongroup was significantly smaller than the intercaninewidth in the Class I malocclusion group (Table II).There were no statistically significant differences inarch perimeter or arch length.
To investigate the sexual dimorphism, the malocclu-sion groups were combined. The data from 78 boys
were compared with the data from 72 girls (TableIII). The mesio-distal sizes of all upper teeth were sig-nificantly larger in the boys than in the girls. In thelower arch the mesio-distal widths of all teeth exceptthe lower left second premolar (tooth 35) were again significantly larger in the boys than in the girls.
The lower intercanine width and the upper and lowerintermolar widths were statistically significantly larger in boys than in the girls (Table IV). There wereno statistically significant gender differences in eitherthe upper and lower arch lengths or the upper andlower arch perimeters.
Discussion
The importance of tooth size discrepancies in ortho-dontic diagnosis has been widely reported in theorthodontic literature because a discrepancy mayaffect the relationship between the upper and lowerarches and the excellence of the treatment outcome.We compared the tooth sizes and arch dimensions inMalay schoolchildren with Class I, Class II and ClassIII malocclusions and in the boys and girls. We foundthat although the children in the Class III group hadlarger upper lateral incisors and tended to have largerupper teeth than the children in the Class I group,there were no statistically significant differences inarch length or arch perimeter.
The wider lower canines in the Class II group mayhave contributed to the narrower lower intercaninewidth in that group. A deep bite may inhibit devel-opment in width of the lower dentoalveolar segmentin patients with Class II malocclusions, and it could
Table IV. Gender comparisons of the dental arch dimensions (mm).
Variable Male Female t-value pMean ± SD Mean ± SD
Upper Canine 35.38 ± 3.04 35.16 ± 4.07 0.38 0.70Intermolar 48.25 ± 2.60 47.03 ± 2.60 2.87 0.01Arch perimeter 103.37 ± 5.02 102.42 ± 4.58 1.21 0.23Arch length 39.54 ± 2.37 39.70 ± 2.31 -0.42 0.67
Lower Intercanine 27.12 ± 1.63 26.55 ± 1.50 2.23 0.03Intermolar 42.54 ± 2.61 41.43 ± 2.59 2.62 0.01Arch perimeter 90.83 ± 4.18 90.83 ± 4.86 -0.00 0.10Arch length 35.08 ± 1.89 34.92 ± 2.29 0.48 0.63
Significant values in bold

be argued that the slightly larger lower canines wefound may have contributed to our finding that thelower intercanine width was reduced.10 However, thishypothesis is not supported by Sayin and Türkkah-raman11 who reported that the lower intercaninewidth was significantly larger in Class II mal-occlusions than in Class I malocclusions. Differencesin intercanine widths may be due also to the age ofthe samples and/or the severity of the maloclusions.11
Because our subjects were between 12 and 16 years ofage further changes in the arch widths were unlikelyto occur.7,8,11,12
Our finding that the upper intermolar width in theClass III group was significantly larger than that theintermolar width in the Class II malocclusion group partially agrees with Al-Khateeb and Abu Alhaija’sfinding that the upper arch is narrower in Class IImalocclusions compared with other malocclusions.3Our findings do not support Buschang et al.13 andLux et al.14 who reported that the lower arch is widerin Class I malocclusiosn than Class II malocclusion. In agreement with Poosti and Jalali,8 we found no differences in arch length or arch perimeter in themalocclusion groups.
Limited changes in arch width occur between 13 and25 years of age.15 Therefore, we assumed that the archwidths in our subjects were stable. The early perma-nent dentition provides the best time for tooth sizemeasurements because there is generally less attritionand fewer teeth have been extracted.16 It is also moreconvenient and accurate to measure the mesio-distalwidths of teeth, arch length and arch perimeter onstudy casts than intra-orally.7
The boys in our study had larger teeth than girls, withthe exception of the left lower second premolar. Thisgender difference is supported by previously published studies on the sizes of teeth in differentpopulations.3,6,17
Conclusions
Malay girls have smaller permanent teeth than Malayboys.
The lower intercanine width was significantly smallerin Malay children with Class II malocclusions thanchildren with Class I malocclusions. There were nodifferences in the upper intercanine width among thedifferent malocclusion groups.
The upper intermolar width was larger in the groupwith Class III maloccclusions as compared with thegroup with Class II malocclusions.
There were no differences in either arch length orarch perimeter among the malocclusion groups.
Corresponding author
Dr Zainul A. RajionSchool of Dental SciencesUniversiti Sains Malaysia16150 Kubang KerianKelantanMalaysia Tel: +609 766 5213Fax: +609 764 2026Email: [email protected]
References1. Santoro M, Ayoub ME, Pardi VA, Cangialosi TJ. Mesiodistal
crown dimensions and tooth size discrepancy of the per-manent dentition of Dominican Americans. Angle Orthod2000;70:303–7.
2. Bermúdez de Castro JM, Nicolas ME. Posterior dental sizereduction in hominids: the Atapuerca evidence. Am J PhysAnthropol 1995;96:335–56.
3. Al-Khateeb SN, Abu Alhaija ES. Tooth size discrepanciesand arch parameters among different malocclusions in aJordanian sample. Angle Orthod 2006;76:459–65.
4. Hattab FN, al-Khateeb S, Sultan I. Mesiodistal crown diam-eters of permanent teeth in Jordanians. Arch Oral Biol 1996;41:641–5.
5. Ho CT, Freer TJ. Clinical application of the graphical analy-sis of tooth width discrepancy. Aust Orthod J 1994;13:137–43.
6. Ling JY, Wong RW. Tooth dimensions of Southern Chinese.Homo 2007;58:67–73.
7. Hashim HA, Al-Ghamdi S. Tooth width and arch dimen-sions in normal and malocclusion samples: an odontometricstudy. J Contemp Dent Pract 2005;6:36–51.
8. Poosti M, Jalali T. Tooth size and arch dimension inuncrowded versus crowded Class I malocclusions. JContemp Dent Pract 2007;8:45–52.
9. Paredes V, Gandia JL, Cibrian R. New, fast, and accurateprocedure to calibrate a 2-dimensional digital measure-ment method. Am J Orthod Dentofacial Orthop 2005;127:518–9.
10. Walkow TM, Peck S. Dental arch width in Class II Division2 deep-bite malocclusion. Am J Orthod Dentofacial Orthop2002;122:608–13.
11. Sayin MO, Türkkahraman H. Comparison of dental archand alveolar widths of patients with Class II, division 1 mal-occlusion and subjects with Class I ideal occlusion. AngleOrthod 2004;74:356–60.
12. Banabilh SM, Rajion ZA, Samsudin R, Singh GD. Dentalarch shape and size in Malay schoolchildren with Class IImalocclusion. Aust Orthod J 2006;22:99–103.
TOOTH SIZES AND ARCH DIMENSIONS IN MALAY SCHOOL CHILDREN
Australian Orthodontic Journal Volume 25 No. 2 November 2009 167

13. Buschang PH, Stroud J, Alexander RG. Differences in den-tal arch morphology among adult females with untreatedClass I and Class II malocclusion. Eur J Orthod 1994;16:47–52.
14. Lux CJ, Conradt C, Burden D, Komposch G. Dental archwidths and mandibular-maxillary base widths in Class IImalocclusions between early mixed and permanent den-titions. Angle Orthod 2003;73:674–85.
15. Bishara SE, Jakobsen JR, Treder J, Nowak A. Arch widthchanges from 6 weeks to 45 years of age. Am J OrthodDentofacial Orthop 1997;111:401–9.
16. Puri N, Pradhan KL, Chandna A. Sehgal V. Gupta R.Biometric study of tooth size in normal, crowded, andspaced permanent dentitions. Am J Orthod DentofacialOrthop 2007;132:279 e7–14.
17. Singh SP, Goyal A. Mesiodistal crown dimensions of the per-manent dentition in North Indian children. J Indian SocPedod Prev Dent 2006;24:192–6.
HUSSEIN ET AL
Australian Orthodontic Journal Volume 25 No. 2 November 2009168

Australian Orthodontic Journal Volume 25 No. 2 November 2009 169
Guest editorial
The human dentition sustains two functions of biological significance: it has a central role in the masticatory system, and plays a complementary rolein anterior tooth display and the expression of emotion essential in social communication and socialsignalling.
In the first function the teeth within and on opposingdental arches, i.e. the occlusion, bear direct physicalloading during maturation, adulthood and aging.Thus occlusal function and occlusal stability, longviewed as discrete goals of orthodontic treatment are,in reality, each part of the ultimate objective: to ensurethe life-long function, stability and physiologicalintegrity of the dentition as an organ system.
A hundred years ago, when orthodontics was in itsinfancy in the United States, the lofty though difficultgoal of dentistry was to preserve the natural dentitionfor a lifetime. In one respect the task was less for-midable than it is today given that the average lifespan at the turn of the 20th century was approxi-mately 30 years shorter than it was at the beginning ofthe 21st century. Ushering in the modern era in dentistry, I.B. Davenport, G.V. Black, W.G.A. Bon-will, E.H. Angle, C.S. Case and many other dentistsof the late 19th century came to think that the key tothe preservation of an intact dentition is stable occlu-sion. The greatest threat to a stable occlusion at thattime was tooth loss due to caries or pyorrhoea, as peri-odontal disease was then called. Difficult though it isto imagine now, mutilated dentitions were far morecommon than intact dentitions after 20 or 30 years ofage during this period in relatively recent dental history.
Conviction that proximal contact and occlusal inter-cuspation of teeth, and stability of tooth position andocclusion are fundamental to the long-term main-tenance of the dentition led Angle to propose that the ‘science of occlusion’ serve as the basis of clinicaldentistry.1 The observation that premature loss of oneor more permanent teeth may cause adjacent andopposing teeth to migrate or drift in more or less predictable fashion prompted the conclusion that
mutilated dentitions are unstable. Yet even mutilateddentitions over time acquire stability, leading to theobvious conclusion that the dentition exists in a stateof dynamic equilibrium. Angle’s further suppositionwas that intercuspation of posterior teeth is respons-ible for tooth stability and it was hoped that the studyof the science of occlusion would illuminate the factors responsible for stability or instability.
Early orthodontists observed that positional changeeffected by orthodontic tooth movement almostalways led to some degree of instability; thus did theterm relapse become part of the orthodontic lexicon.Yet even if badly malposed, a tooth in equilibriummay attain a stable position. It is said that this observation prompted Angle to remark somewhatfacetiously, ‘There is nothing as stable as a mal-occlusion’! Another early orthodontist, it is reported,offered that he would happily treat any malocclusionas long as someone else supervised its retention.Regrettably, a broader concept of stability and relapsein clinical orthodontics has diminished in attentionover the last 50 years; today the term ‘relapse’ oftenmerely conjures post-treatment crowding of man-dibular incisors. Important though this is to practisingorthodontists it diverts attention from the crucial andvital element of stability within the whole dentition asa long-term objective of orthodontic treatment.
Angle’s assertion that intercuspation of posterior teethis the major factor in tooth stability has proved to beincorrect.2 We know now that teeth are positioned ina state of equilibrium within the enveloping soft tissues. Indeed during normal masticatory functionthe food bolus is prepared with no more than transi-tory occlusal contact during swallowing. On the otherhand, occlusal contact does occur in almost everyonein brief clenching and grinding during REM sleep,and some individuals have prolonged parafunction.
How much does occlusion really contribute to long-term health and stability of the dentition? Until fairlyrecently an unstable occlusion was thought to pro-mote the onset of periodontal disease, a misinterpreta-tion of presumed cause and effect. In fact, teeth drift
The interaction of function and stability in the dentitionJames L. Ackerman, Martin R. Kean and William R. Proffit

because of loss of periodontal attachment resultingfrom periodontal disease, not vice versa. It was con-sidered also that traumatic occlusion is a primary factor in causing periodontal disorder; it is recognisednow that occlusal trauma, if associated with a perio-dontal problem is a secondary, not primary, factor inits causation. There is also no evidence that improv-ing occlusion with orthodontic treatment enhancesperiodontal health.3,4
Another likely misinterpretation of the role of occlu-sion in oral health resulted from the potentially erroneous conclusion about the ‘high filling’ effect.Here, when a restoration creates a premature occlusalcontact, the patient invariably develops tooth painlasting days or even weeks. The conclusion drawn wasthat faulty occlusion created micro-trauma, a primaryfactor in causing pulpal hyperaemia, as well as perio-dontal lesions. But in orthodontic practice todaycomposite is often added to the occlusal surfaces ofposterior teeth temporarily to serve as temporarymini-bite planes with patients rarely complaining ofdental pain. Pulpal hyperaemia associated with a highfilling is likely the result of caries removal duringtooth preparation for restoration, with occlusal traumabeing a secondary or compounding factor in causingpain.
The same kind of misinterpretation of causality hasbeen responsible for an incorrect conclusion regard-ing the relationship between occlusion and temporo-mandibular joint disorder (TMD). It is now widelyaccepted that flawed occlusion is not a primary factorin causing TMD. In some individuals, occlusal prem-aturities may lead to the parafunctional habit ofclenching or bruxing, thereby causing secondarymuscle spasm, fasciitis or tendonitis resulting in painin the region of the joint. There is no evidence thatone specific occlusal arrangement offers an advantageover another by way of enhanced function of the den-tition (e.g. more efficient mastication) with resultantimproved oral or overall health.5 The NationalInstitute of Dental and Craniofacial Research,National Institutes of Health, cautions against treat-ing the symptoms of TMD by altering occlusion andwarns, ‘Avoid treatments that cause permanentchanges in the bite or jaw. Such treatments includecrown and bridge work to balance the bite, orthodon-tics to change the bite, grinding down teeth to bringthe bite into balance (occlusal adjustment), and repo-sitioning splints, which permanently change the bite’.6
Acknowledgment of these previous misunderstand-ings in no way alters the fundamental objectives oforthodontic treatment nor does it diminish its valuein improving quality of life and social wellbeing.What it calls into question are some of the most fer-vently held assumptions regarding the relationship ofanatomical occlusion to oral function and oral health.Although the traditional concepts of ‘functionalocclusion’ and ‘balanced occlusion’ in restorative andprosthetic dentistry have undoubted merit, in thenatural dentition these terms are not only ambiguousbut are largely misplaced. The true role of satisfac-tory proximal and occlusal contact of teeth in the natural dentition is to maintain balance within theorgan system, that is, to ensure functional stability. Inseeking occlusal stability in patients the orthodontistis faced with two considerations: first, the differentia-tion between malocclusions that are functionally stableand those that are functionally unstable. Anatomicalposterior crossbites, for example, vary in functionalstability. If, in a maxillary palatal crossbite the guid-ing cusps of the maxillary posterior teeth rest in thecentral fossae of mandibular posterior teeth, bothocclusal function and tooth position may be quitestable, and orthodontic correction not indicated. Onthe other hand, conventional clinical wisdom is thatany palatal crossbite that deflects the mandible onclosure can be considered functionally unstable andtherefore an indication for orthodontic treatment. Ina maxillary buccal crossbite (scissors bite), at leastsome of the maxillary teeth are unopposed even if thepatient shifts the mandible to one side. In AustralianAboriginals (who were renowned for their excellentocclusion and dental stability prior to the introduc-tion of modern diets), such an arrangement (so-calledW occlusion) is quite common and is compatiblewith normal masticatory function, oral health andstability. However, where a severe Class II, Class III,or deep bite malocclusion is functionally unstablebecause of the lack of coupling of anterior teeth andpotential absence of antagonists for the terminalmolars, there is a valid reason for treatment, thoughnot necessarily a compelling reason in the absence ofany concern by the patient about the psychosocialeffects of impaired facial and dental appearance.
Secondly, understanding what aspects of occlusionare important in determining stability or relapse fol-lowing orthodontic treatment. Will the establishmentof inter-occlusal contacts between opposing teeth
GUEST EDITORIAL
Australian Orthodontic Journal Volume 25 No. 2 November 2009170

stabilise their vertical position? Almost certainly, yes,because even the intermittent pressures that accom-pany swallowing and REM sleep seem adequate tocontrol vertical tooth migration so that it is no fasterthan vertical ramal growth. Will the occlusion stabilisea crossbite correction in which the maxillary arch wasgreatly expanded posteriorly, or the position of max-illary incisors proclined excessively? Almost surelynot, because light sustained force from stretched softtissues will overcome the forces of occlusion of muchshorter duration. Under the circumstances, perhapsthe most simple and practical goal of orthodontics inregard to functional stability is the establishment ofan effective occlusal platform to control eruption andvertical drift of teeth. In the anteroposterior andtransverse dimensions, teeth must be placed entirelywithin the zone of equilibrium mediated by envelop-ing soft tissues. Thus individual teeth or segments ofa dental arch in functionally unstable positions orrelationships may, as a consequence, affect oral healthadversely. This is what is implied in recognising theexistence of functional stability or instability. Makingthe distinction is an essential element of orthodonticassessment, and most important in treatment planning.
When Angle proposed that the study of occlusionbecome the backbone of dental science no one couldhave anticipated the dramatic advances that wouldoccur in the basic medical sciences and technologyover the following century, including insistence onscientific evidence for the validity of such advances.Whereas Angle was limited almost entirely tomechanical explanations for all occlusal phenomena,we now have the advantage of advances in biologicalanthropology and the molecular biology of tooth-supporting structures to help elucidate some of thestill inadequately understood aspects of clinicalorthodontics. Today, although the mechanism forpost-emergent tooth eruption is still incompletelyunderstood, we know that the intermittent forces ofocclusion cannot alone explain the relationshipbetween occlusion and stability. The soft tissue equi-librium established by the tongue and lips, and thetrans-septal fibre apparatus maintain stability of toothpositions. The flaw in Angle’s belief about the role ofcusps in chewing and stability is related to severalcritical evolutionary events.
Bonwill and Angle believed that cusps, intercuspationand the gear-like arrangement of articulated teeth
were vital to their function. Their teleological reason-ing was based on the idea that only the ‘DivineArchitect’ could possibly be responsible for such mag-nificently designed machinery. Both believed thattooth cusps and fossae serve as mini mortars and pestles for the trituration of food. Angle posited thatthe secondary function of cusps is to serve as locatorjigs for referencing the upper and lower teeth, there-by maintaining their stability. Bonwill was very con-versant with Darwin’s theory of evolution, which hadbeen proposed 25 years before, but he was entirelyunconvinced of its validity. Bonwill even published a paper in 1894 titled, ‘What has dentistry to demonstrate against the hypothesis of organic evolution?’7
During the 20th century, remarkable advances inpaleoanthropology shed light on how changes in dietand food preparation over a period of approximately2 million years led to the adaptative changes of reduc-tion in the size of jaws, teeth, mouth aperture andmouth volume in prehumans and humans. Duringthis long evolutionary period, the invention and useof stone tools for slicing through animal carcassesfacilitated the inception of man eating raw meat. Thediscovery of fire, and the invention of cooking byHomo sapiens over 250,000 years ago, markedlyreduced the essential need for the masticatory appa-ratus for fitness and survival. Perhaps most of all,changes in diet and food preparation made eating anddigestion more efficient, in turn effectively conserv-ing energy.8 It has been suggested that the relativelyrecent introduction of eating utensils that is, the knifeand fork will ultimately cause further diminution ofthe teeth and jaws of humans.9
In light of greater knowledge about the significance ofthese evolutionary events, we now recognise the serious flaws in Bonwill’s and Angle’s theories aboutthe role of cusps in chewing in modern peoples. It isalso clear from the fossil and skeletal record that bythe Stone Age, humans had almost entirely worn thecusps off their posterior teeth through attrition by thetime the permanent second molars erupted. Similarlythe cusps of the second molars were entirely wornaway by the time the third molars emerged. A similarobservation in Australian Aboriginals promptedBegg, who had been a student of Angle’s, to speculatethat the sole purpose of tooth cusps in modern manwas to serve as referencing jigs for guiding teeth intoocclusion during the development of the dentition.
Australian Orthodontic Journal Volume 25 No. 2 November 2009
GUEST EDITORIAL
171

GUEST EDITORIAL
Australian Orthodontic Journal Volume 25 No. 2 November 2009172
Begg speculated that once teeth were in occlusion,cusps no longer served a meaningful function. Heopined, ‘Generally speaking, textbook ideal occlusionhas been implicitly endowed with attributes in excessof reality’.10
Angle made a lasting contribution to dentistry by for-malising the concept that the lifetime preservation ofthe natural dentition requires establishing proximaland occlusal contacts of teeth to foster stability and equilibrium within the functioning dentition,and achieving tooth positions, promoting balance inthe relationship of the dentition to its investing softtissue and musculature. This disarmingly simple, yetultimately profound concept emphasising the criticalimportance of functional stability of the dentition,changed the future course of clinical dentistry. Toothalignment and occlusion are important in maintain-ing the long-term function and appearance of thedentition, thus optimising social wellbeing and quality of life, even if ideal interdigitation of teethdoes not prevent post-orthodontic relapse.
Perhaps Angle’s most important contribution to clin-ical orthodontics was by providing the insight thatthe goals of treatment are to maintain or establishfunctional stability of the dentition, and to achievebalance between dentition and soft tissue drape,thereby enhancing dentofacial appearance.
Addresses for correspondence
James L. Ackerman1030 Fearrington PostPittsboro, NC 27312United States of AmericaEmail: [email protected]
Martin R. Kean49 Connolly StreetGeraldine 8751New ZealandEmail: [email protected]
William R. ProffitDepartment of OrthodonticsUniversity of North Carolina School of DentistryChapel Hill, NC 27599-47450United States of AmericaEmail: [email protected]
References1. Angle EH. Classification of malocclusion. Dental Cosmos
1899;41:248–64,350–7.2. Proffit WR, Frazier-Bowers SA. Mechanism and control of
tooth eruption: overview and clinical implications. OrthodCraniofac Res 2009;12:59–66.
3. Bollen A, Cunha-Cruz J, Bakko DW, Huang GJ, Hujoel PP.The effects of orthodontic therapy on periodontal health: asystematic review of controlled evidence. J Am Dent Assoc2008;139:413–22.
4. Chung MH, Henwood RW. Inconclusive evidence of theeffects of orthodontic therapy on periodontal health. J AmDent Assoc 2009;140:575–6.
5. Luther F. TMD and occlusion Part II. Damned if we don’t?Functional occlusal problems: TMD epidemiology in awider context. Br Dent J 2007;202,E3.
6. NICDR http://www.nidcr.nih.gov/OralHealth/Topics/TMJ/LessisBest.htm
7. Bonwill WGA. What has dentistry to demonstrate againstthe hypothesis of organic evolution? Chicago, Knight,Leonard and Co. 1894;1–15.
8. Wrangham R. Catching fire, how cooking made us human.Philadelphia, Basic Books. 2009.
9. Brace CL. Occlusion to the anthropological eye. In: Thebiology of occlusal development, Moyers SymposiumMonograph Number 7. Ann Arbor, University of Michigan.1977;179–209.
10. Begg PR. Stone age man’s dentition. Am J Orthod 1954;40:298–312;373–83.

Australian Orthodontic Journal Volume 25 No. 2 November 2009 173
To unravel and pay tribute to John FrederickReading’s unique character has been an interestingproject. The writer has discovered unknown capa-bilities and perhaps the reasons for such a broadly educated, dedicated and humorous (albeit dry) mind.
Born in Sydney, he was baptised at St StephensPresbyterian Church Macquarie Street, where his parents, Fred and Daisy, (particularly his mother) wereenthusiastic parishioners. He resided in the easternsuburbs for most of his life; originally in DarlingPoint, briefly Maroubra, where he established abranch practice, and finally in Vaucluse, where heoccupied the family home.
School days were spent at The Scots College(1935–44) as he progressed from Preparatory Schoolto Senior School participating in a broad spectrum ofactivities: summer time cricket (Prep School 1st XI,Senior School 3rd XI), winter rugby (Prep School 1stXV), NCO Air Training Corps and member of schoolchoir. Encouraged by his mother in pianoforte, hebecame an accomplished pianist, and his father’s geneswere apparent in developing an analytical mind with
ability to annunciate a cryptic ‘one line response’ tomost questions.
Perhaps his father hoped his only son might join hissuccessful textile company enabling a change of namefrom F.J. Reading and Co. to F.J. Reading and Son,but, thanks to the need for an orthodontic consul-tation, he was introduced to Dr Arthur ThorntonTaylor at about 9 years of age, and this introductioninitiated his 73 years in the field of orthodontics. Hesaid he was inspired by Dr Taylor’s organising abilityand his endeavour to gain further knowledge in hisspecialty. John, while a school boy, spent holiday timein Dr Taylor’s laboratory, casting models and carryingout technical tasks. It was not surprising he enrolled inthe Dental Faculty in 1944, having successfully negotiated his leaving certificate. He described hisundergraduate training as ‘uneventful’, but he wasproud of editing The Articulator, and with his businessmanager, Bill Harvey, they introduced advertisementsfrom the trade houses, thus improving the magazine’sfinancial viability.
On graduation in 1949, John went to practise inOrange with Dr G.H. Dent, and after 18 months was
Obituary
John Frederick Reading1927 – 2009

OBITUARY
Australian Orthodontic Journal Volume 25 No. 2 November 2009174
encouraged by his friend Gordon Hutchinson totravel to England on the RMS Ormonde. England’sNational Health Scheme provided ready employmentfor Australian graduates and John practised with MrGeorge Danks, a Guy’s Hospital graduate.
John, I believe, aimed to realise the requirements setby the NSW Dental Board for a graduate to specialiseand describe himself as an orthodontist. Briefly, theBoard’s requirements were: a written undertaking torestrict practice to orthodontics, two years experiencein general practice, to have gained special skillthrough training and/or experience – ideally to havegained a higher degree.
Four 1948 Sydney graduates: Owen Makinson,Gordon Hutchinson, Geoff Harris and John Readingbecame Junior House Officers at the University ofLondon Institute of Dental Surgery; John with ascholarship (£10 sterling per week) enabling part-time work and study towards the Fellowship inDental Surgery, Royal College of Surgeons.
His experience as a graduate student in revisiting thebasic sciences (physiology, anatomy and histology)strengthened his resolve as he later pressed for a formal training course in Australia.
In 1952, with his Fellowship in Dental Surgery RCS,John was appointed a junior registrar in Orthodonticsat Eastman Dental Hospital, becoming a senior regis-trar in 1954. He was the first Australian to gain hisDiploma in Orthodontics RCS in 1954 and while atthe Eastman met, then married, June, on the 5thFebruary 1955. The newlyweds returned to Australiaenjoying their honeymoon on the Oronsay and, sub-sequently, the arrival of Graeme and Fiona set up aloving family unit.
From patient at 9 years, to orthodontic associate in1955, John rejoined ‘his orthodontist’ Dr A.T. Taylor,for two years, in which time he successfully applied tothe NSW Board for permission to describe himself asan orthodontist.
He opened his own practice at 149 Macquarie Streetin 1957 and a branch practice in his home atMaroubra, where June acted as practice manager.
Ever mindful of his qualification, first as a dentist, hebecame an active member of the Dental AlumniSociety on graduation; during his English sojourn heacted as a London correspondent for Apollonia (thealumni magazine) and for the Australian Journal ofDentistry. Always the student, he attended the
London School of Printing, Typography in 1952, nodoubt to gain basic training in this field of interest,and subsequently he applied his talents as editor ofApollonia 1958-69; he formalised the ASO Bulletinfrom which was derived the ASO Newsletter andeventually the Australian Orthodontic Journal wasborn.
He always demonstrated strict protocol in his writ-ings and his reports to referring dentists were detailedand beautifully expressed in his precise English, leaving the reader in no doubt regarding diagnosis,prognosis and treatment plan. He took responsibilityfor ongoing observation of his cases to check the stability of his result. Recognising the inevitable‘change with age’ he explained that ‘he never finisheda case’. His door was always open for future discussion if the patient was concerned.
Service to his specialty and to the ASO came first atstate level and led to Federal Council Service in allexecutive positions viz., councillor, secretary, vice-president and president. He humbly explained that his election to all positions was a progressionexpected from all members of such a small groupwhich then existed.
To enhance numbers ‘dentists with an interest inorthodontics’ were encouraged to join as Associatemembers of the Society and John, then secretary, withDr Arthur Taylor, president of the NSW branch,pushed this initiative. To accommodate the Associatemembers in branch activity, John initiated the first‘Country Clinical Day’ in 1958. This day saw aninterchange of ideas between GPs and specialistsregarding patient treatment and greatly assisted thewelfare of remote patients.
Although the ASO now has no Associate members,on 27th May 2009, the NSW branch celebrated the50th Clinical Day and the J.F. Reading prize (estab-lished in John’s honour in 1995) for the best casepresentation was again awarded. This was the firstClinical Day which recorded an apology, due to illhealth, from J.F. Reading.
The milestone in Australian orthodontic training his-tory was the establishment of the MDSc course(orthodontics) in Sydney 1964. Initially, a one yeardiploma was promoted by the Dean, Professor A.J.Arnott but fortunately J.F. Reading as NSW StatePresident and his executive, successfully lobbied for atwo year full-time training course rather than a one

Australian Orthodontic Journal Volume 25 No. 2 November 2009
OBITUARY
175
year diploma. This was the first full-time Australiancourse in orthodontics; it has since been lengthenedto three years, forming the basis of training and reg-istration to this day. With the establishment of thecourse in 1964, John served as a part-time teacher forsome 25 years and he insisted that stimulus from histeaching graduate students encouraged his extendedinterest and activity in orthodontics.
Further contributions he made to the improvementof teaching standards and training were exemplifiedby other positions he held: chairman of GraduateEducation Committee ASO; convenor and chairmanOrthodontic Registration Board, ASO; foundationmember and former secretary of the Royal College ofSurgeons Dental Society of Australia and NewZealand; inaugural member of the Australian Collegeof Dental Surgeons later FRACDS, member of theBoard of Studies in Orthodontics RACDS, lecturerNSW committee for final candidates FRACDS; inaugural member of the Australian BeggOrthodontic Society, former secretary and honorarylife member of the Society and recipient of the BeggMedallion for the best case presentation in 1986; ADANSW branch, member of the library committee,revamped Package Library, redesigned Newsletter,willing presenter to ADA meetings, country conven-tions, country group meetings and metropolitan dental group meetings; ASO Foundation forEducation and Research, former councillor, and inretirement he compiled the history of the Foundation.
John was joined in practice by Dennis Bradley in1973 and they formed a partnership in 1975 whichenjoyed 23 years happy association. Theo Baisi tookthe reins in 1995, allowing John to retire in 1996 andDennis in 1997. Recognising his huge contributionto the Society, the membership bestowed its highestaccolade, Honorary Life Membership, in 1995 at the
Melbourne Congress. Fittingly, John presented tothat meeting a collage of case presentations he hadpreviously presented to the Society through his prac-ticing life. Few have presented such a record, but thisman had few to match his clinical ability or method-ical storage or recollection of records.
You may well ask what was there outside ortho-dontics? I can report that the Marx Brothers movieswere all known to John, The Goon Show tickled hisfancy, Peter Sellers a favourite actor, and, Get Smartoften viewed on television. His popular artists included Frank Sinatra, Shirley Bassey and Nat KingCole, his favourite composer was J.S. Bach.
Service Clubs included Apex then Sydney Rotary. Hishobby, photography, with the latest available camera,he documented orthodontic meetings and travels inEurope and America and even his visits to China withthe Begg Society.
His artistic skills were well-known to his professionalcolleagues, through detailed diagrams in lecture pre-sentations, but the extent of his hobby of observingships in Sydney Harbour drawing them in everydetail, photographing them and recording theirmovements to and from Sydney was beautifully illus-trated in the display at the Royal Sydney Golf Clubon Friday the 26th June 2009 when friends and fam-ily celebrated his wonderful life.
In the sixth century BC Confucius stated: ‘If a mankeeps cherishing his old knowledge, so as continuallyto be acquiring new, he may be a teacher of others.’John Reading certainly accedes to this qualification.
To June, Graeme and Virginia, Fiona and Nicktogether with grandchildren Lucy, Georgie, Drewand Liza we express our kindest thoughts at this timeof our loss.
Jim Mackie

Australian Orthodontic Journal Volume 25 No. 2 November 2009176
Biological Mechanisms of Tooth Movement
Editors: Vinod Krishnan and Ze’evDavidovitchPublisher: Wiley (au.wiley.com)Price: AUD $240.00 / NZD $270.00ISBN: 978-1-4051-7690-3
Biological Mechanisms of Tooth Movement is a mostcomprehensive reference to the scientific backgroundof orthodontics and specifically, the biologicalresponses of the dental and paradental tissues to theapplication of mechanical loads. It is suitable for bothorthodontic students and specialist practitioners.There are 12 chapters written by 18 international con-tributors.
The book is edited by two of the authors, VinodKrishnan and Ze’ev Davidovitch, who also contributeto six of the 12 chapters. Vinod Krishnan is AssistantProfessor in the Department of Orthodontics at theRajas Dental College in Tamilnadu, India and Ze’evDavidovitch is Clinical Professor in the Departmentof Orthodontics at Case Western Reserve University,Cleveland, Ohio, USA. Both editors have publishedwidely in the orthodontic literature on the subject oforthodontic tooth movement, and this publicationincludes some of their previously published work in avery readable and logically ordered form.
The comprehensive nature of the book is perhaps bestillustrated by listing the chapter headings:
The adaptation and development of biological concepts in orthodonticsBiology of orthodontic tooth movement: an overviewThe mechanobiology of the periodontal tissuesGenetic influences on orthodontic tooth movementThe role of inflammation in defining the type andpattern of tissue response in orthodontic tooth movement
Biological aspects of bone growth and metabolismin orthodonticsMarkers of paradental tissue remodelling in the gingival crevicular fluid of orthodontic patientsEffects of systemic diseases on orthodontic toothmovementThe effect of drugs and diet on orthodontic toothmovementBiologically and clinically, what are optimal ortho-dontic forces and how are they applied in selectivecommon malocclusions?The biological background of relapse of orthodontictooth movementMechanical and biological determinants of iatro-genic injuries in orthodontics.
Chapter 1 presents a simple history of the develop-ment of orthodontics from the early application of acrude force to modern-day research of cellular, histo-chemical and molecular changes associated with toothmovement. Emphasis is placed on the need to tailor atreatment plan to the patient’s biological profile.Chapter 2 continues this theme, whilst discussing indetail the sequence of histochemical events that followthe application of force. The tissue response to variedforce applications is also discussed. Chapter 3 is writ-ten by four Israeli oral biologists and concludes thatthe periodontal ligament cells regulate the remodel-ling process, but the marginal gingival fibroblasts havea significant role to play in remodelling by releasingATP and in turn increasing calcium ion fluxes.
The author of Chapter 4 is a research professor at theCenter for Craniofacial Molecular Biology at USC.She discusses in depth, the histochemical pathwaysleading to bone resorption and deposition and the rolethat genes may have in regulating these pathways. She suggests that in the near future there may be agenetic test available to determine an individual’s susceptibility to root resorption.
Chapter 5 is written by a Japanese orthodontist whoconfirms that the tissue response to orthodontic forceis an inflammatory response – an aseptic inflamma-tion. He suggests that NSAIDs are the best treatment
Book reviews

Australian Orthodontic Journal Volume 25 No. 2 November 2009
BOOK REVIEWS
177
for orthodontic pain, but warns that protracted usewill delay tooth movement because of the anti-inflammatory effect.
Chapter 6 discusses bone growth, intramembranousand endochondral, as well as bone modelling andremodelling of the facial bones and the TMJ. There issome discussion of bone metabolism at the cellularlevel, but the chapter is worth reading if only as arefresher on bone growth. Eugene Roberts, who hasvisited Australia many times, is a co-author of thischapter.
Chapter 7 is a true academic discourse on gingivalcrevicular fluid markers in orthodontic patients,although the authors emphasise the need to directfuture studies towards an outcome with clinical sig-nificance, such as optimal forces, speed of toothmovement and a reduction in root resorption.
Chapter 8 is co-authored by the two editors. It liststhe systemic conditions that may modulate the pat-tern and velocity of tooth movement, and reminds usthat ‘the dentofacial complex affects the body, and isaffected by it’. Disorders of each system of the body,vascular, respiratory, endocrine etc. are discussed withreference to their possible effects on orthodontictreatment. Chapter 9 is also written by the editorsand discusses drugs such as bisphosphonates andNSAIDs, hormones such as thyroid and relaxin anddietary requirements such as calcium and copper aswell as Vitamins C, A, D and K.
Chapter 10 illustrates optimal tooth movement con-cepts by promoting the efficacy of using the authors’‘amalgamated technique’ or AT. It roundly condemnstreatment modalities including Begg, Tip-Edge andStraight Wire as not being compatible with minimaltooth movement and shorter treatment times andproducing damage to the teeth and paradental tissues.Several AT treated cases are used to show that ‘opti-mal orthodontics’ is a patient-orientated methodbased on recognition of individual determinants:morphological, functional and biological.
Chapter 11 discusses relapse and retention and con-cludes that relapse is probably not due to fibrous factors, as the collagen remodelling in the PDL andthe gingival fibres is very rapid. The authors stress ‘theurgent need for experimental and clinical studies toelucidate the biological basis of relapse’.
The final chapter seems superfluous to the subject ofthis book. However it is a good review of the damage
that appliances and treatment can do to the patient,intra-orally, extra-orally and psychologically.
Each of these topics has a most extensive reference listand this presents the reader with an excellent oppor-tunity to further explore a subject of particular inter-est in more detail. For example, Chapters 8 and 9,which are ordered reviews of the effect of disease,drugs and diet on tooth movement, have more than300 references. These chapters are of significant inter-est to orthodontists working with compromisedpatients.
In summary, this book is an important addition tothe orthodontic literature as it brings together someexcellent and up-to-date information on a subject whichis fundamental to everyday orthodontic practice. Thereis some repetition of information and future editionsof the book will, no doubt, produce updates andrefinements which will further enhance its status as a‘must read’. It is beautifully illustrated and indexedand should be on the shelves of every dental library.
John Armitage
Radiographic Imaging for the Dental Team.Fourth Edition
Editors: Dale Miles, Margot Van Dis,Gail Williamson and Catherine JensenPublisher: Saunders Elsevier (shop.elsevi-er.com.au)Price: AUD $101.00 ISBN: 978-1-4160-6004-8
This book is written for the dental assisting and den-tal hygiene students and their instructors. It aims tohelp the student master the art and science of oral andmaxillofacial radiology. The authors include Dale A.Miles, an Adjunct Professor at the University of TexasHealth Science Centre at San Antonio, Texas; MargotL. Van Dis and Gail F. Williamson, Professors in theDepartment of Oral Pathology, Medicine andRadiology at the Indiana University School ofDentistry and Catherine W. Jensen.
The first three chapters describe the basic techniquesof intra-oral radiographic imaging. Chapter 1 begins

BOOK REVIEWS
Australian Orthodontic Journal Volume 25 No. 2 November 2009178
by reminding the reader of the biologic cost of theradiographic examination. Guidelines are given forthe student regarding the use of lead aprons, whichare not considered mandatory if using minimal expo-sure, but essential for children and pregnant women.A step-by-step guide is provided with descriptions of elementary radiographic techniques such as theparallel and bisecting angle techniques along withanatomical considerations. Common problems arereported along with solutions and helpful hints.
The following chapter explains the processing of filmbased images, however regarding the processing ofdigital images the reader is referred to a website for anexplanation. Chapter 3 identifies common radio-graphic anatomical landmarks to aid in film arrange-ment. It contains clear and enlarged radiographicimages with excellent examples.
The student is then given a brief history of the dis-covery of X-rays by the Bavarian physicist Roentgenin 1895. An elementary lesson in quantum physicsleads to the production of X-rays. The direct andindirect effects of radiation on living organisms aredescribed, based on the latest information of theNational Council on Radiation Protection Report.Interestingly, on taking a panoramic radiograph, theradiation used is roughly equivalent to three days ofbackground radiation. However, cone beam volu-metric imaging uses 4–40 times this amount.
The remaining chapters are dedicated to the produc-tion of extra-oral radiographic images. Again, pro-cessing errors are described along with various trouble-shooting suggestions. Various specialised diagnosticradiographic techniques are listed. Tomography isdescribed, producing a slice of an image by move-ment of the source and the image receptor. Thesemovements range from linear to complex move-ments. Arthrography used pre-magnetic resonanceimaging and radio-opaque dye to view soft tissues ofthe temporomandibular joint.
Digital imaging such as computed tomography isintroduced and described as having the X-ray sourcerotating 360 degrees around the patient. The receptorreceives the remaining radiation after it passesthrough the patient. The information is digitised andmathematical formula is applied to the data. Theresulting binary computer language 0’s and 1’s arearranged in rows and columns producing an imagematrix. Each cell of the image matrix is called a pixelwhich is assigned a colour.
Magnetic resonance imaging (MRI) is also covered inthis book. The patient is placed in a large magnetwhich causes the nuclei of the atoms in the body toalign themselves in the magnetic field. A radio fre-quency is applied disturbing this alignment (particu-larly the hydrogen atoms). When the radio signal isturned off the hydrogen atoms realign themselves inthe magnetic field and energy is released. This energyis digitised via a computer. Tissues with a high watercontent are brighter than those with a low content.
Cone beam imaging is compared to conventionalcomputed tomography. Cone beam volumetric imag-ing is obtained by one 360 degree rotation, unlikeconventional CT which requires several rotations.Spatial resolution is expressed in voxels (volume elements) rather than pixels.
This book is ideal for instructors and their dentalassistants and dental hygiene students. It providessimple step-by-step instructions to assist the studentin the undertaking of the production of both intra-oral and extra-oral radiographic images. This bookboasts an ‘evolve’ learning system. This is an evolvesite where students and instructors are directedonline, with such aids as powerpoint lectures forinstructors and interactive practice exams for the student. The site also contains answers to the chapterstudy questions, which are found at the end of eachchapter. This book is well-written and could be anexcellent aid to auxiliary staff training.
Sameh Malek
Enhancement Orthodontics: Theory and Practice
Author: Marc Bernard AckermanPublisher: Wiley-Blackwell (au.wiley.com)Price: AUD $120.00 /NZD $135.00ISBN: 978-0-8138-2623-3
This book offers a practical clinical guide in the eval-uation of a patient for orthodontic care. The method-ology focuses on using a ‘patient-centred paradigm’.It extends from the clinical assessment of the mal-

Australian Orthodontic Journal Volume 25 No. 2 November 2009
BOOK REVIEWS
179
occlusion and the extra-oral features of the in-dividual’s face to also include contemporary views inthe classification of dentofacial traits and differentaspects of a patient’s smile in the decision-makingprocess.
The first two chapters define orthodontics relative tothe health and disability to the patient. The authordescribes a strategy for establishing a good communi-cation with the patient (and/or their parents) toderive to a patient-centred care that satisfies both theclinician’s desire to provide the highest level of careand service the needs of the patient.
The later chapters describe a systematic and contem-porary guide in the clinical examination of the patientand how various modern imaging tools could be usedto assist in the diagnosis of the dentofacial trait.
This concise book is simple to follow and supple-mented with clinical illustrations. One of its strengthsis the implementation of the guidelines in everydaypractice through the use of 10 case studies. This mayappeal in particular to studying orthodontists andgraduate students in prosthodontics and restorativedentistry.
Hong Chan
Mini-Implants in Orthodontics: InnovativeAnchorage Concepts
Authors/Editors: Björn Ludwig, SebastianBaumgaertel and Jay S. BowmanPublisher: Quintessence(www.quintpub.com)Price: US $185.00ISBN: 978-3-938947-47-0
There is no doubt that the increasing acceptance andusage of temporary anchorage devices or TADs (alsocalled pins, miniscrews or mini- or micro-implants)have certainly added a whole new dimension in theway we may practice clinical orthodontics today. Thisbook, Mini-implants in Orthodontics, comprises eightchapters dealing with all the issues pertaining toanchorage, the different types of TADs, their accessories, the science and biology related to their
placement and integration, indications and con-traindications in their use in clinical practice with anabundance of tables, colour illustrations and flowcharts.
Chapters 1 and 2 deal with general definitions andthe issues surrounding anchorage in orthodontics.Chapter 3 introduces the different types of screwsavailable providing details regarding design, dimen-sion and material type. With significant detail spenton the pros and cons of the different designs andtypes of screws, the clinician is left with a clear under-standing of what is available and the associated limitations. This chapter is not purely technically ori-entated as almost every aspect of TADs is well supported by a sound scientific explanation. The dif-ferent methods of insertion and instruments requiredincluding the biology behind osseointegration, heal-ing and the factors that influence the success of TADsare well described here.
All aspects of the procedures involved in the insertionprocess are thoroughly described in Chapter 4.Chapter 5 is probably the most well illustrated andinteresting chapter in the book. This chapter is fur-ther complimented by Chapter 8. These two chaptersare devoted to discussing all the clinical applicationsfor TADs used as either an indirect or direct form ofanchorage. Different solutions with use of TADs areoffered to numerous clinical problems with clearcolour clinical photographs. In this textbook, TADsare used in maxillary expansion, space closure, molaruprighting, occlusal cant, midline, CII and CIII correction, intrusion and other complex tooth move-ments. Immediately the reader is able to see the difference TADs can make in certain clinical situa-tions which otherwise would involve very complexmechanics with untoward side effects. There are cer-tainly some examples provided where more TADswere used than required, or the case may have beentreated without TADs, however one must appreciatethe fact that the authors have so-called ‘pushed theboundaries’ in order to determine what is achievablewith TADs. It is up to the reader/clinician to deter-mine whether it is practical or feasible to carry out inclinical practice. The one thing this text has the leastamount of information in is a thorough explanationor description of the vectors and biomechanicsinvolved in the use of TADs. There is, however, abasic description for the various presenting clinicalsituations.

Chapters 6 and 7 deal with the important issues ofhow to safely incorporate TADs into clinical practice.The risks associated with TAD placement and how tominimise these risks are thoroughly discussed.Further, once the need of TADs has been established,the authors discuss how to obtain adequate informedconsent and plan towards the effective placement ofthe TAD.
It is refreshing to see that the authors do not push anyparticular product and throughout the text allude tothe fact that TADs are not the panacea in ortho-dontics nor are they there to make up for poor diag-noses and treatment planning. They are easy to usetools with a myriad of applications for orthodontics,enabling orthodontists for the first time to put teethwhere they need to be put, rather than accept where they end up as a result of the limitations posedby the other appliances used today, or poor patientcompliance.
This book is as an excellent guide for the orthodon-tist thinking about getting involved with TADs, orthe orthodontist who wants to broaden and build onhis/her current knowledge base. The clear colour clin-ical photos and illustrations serve as a handy quickreference in practice. It also serves as a good teachingtext for orthodontic residents keen to develop asound foundation on TADs and their applications.
Sanjivan Kandasamy
The Herbst Appliance: Research-basedClinical Management
Editors: Hans Pancherz and Sabine RufPublisher: Quintessence(www.quintpub.com)Price: US $198.00ISBN: 978-1-85097-169-6
This book is a comprehensive review of the literaturerelating to fixed functional appliance treatment andin particular, the scientific and clinical informationfor consideration when using the Herbst appliance.
The first three chapters provide an excellent descrip-tion of the history and development of the Herbst
appliance including the limitations and possible com-plications associated with various appliance designs.Anchorage concepts of the Herbst appliance, designvariations and pitfalls of each design are clearlyexplained. The authors recommend that when considering both anchorage control and appliancedurability, the cast cobalt-chrome splint Herbst appliance is the design of choice. Of particular note is Chapter 3, which provides detailed prescrip-tions for the laboratory technician including recom-mended manufacture techniques. The accompanying photographs simplify the instructions for such manufacture.
Chapter 4 refers to the ‘reintroduction’ of the Herbstappliance by Pancherz in 1979 and how many of thenew inventions are derivates, or hybrids, of the orig-inal Herbst appliance. Chapter 5 provides an evidence base, with discussion of the adaptiveanatomical changes observed in rats and monkeysthat had been fitted with bite jumping appliances.This chapter is well researched and informative anddemonstrates histologically the TMJ changes inexperimental animal studies. This evidence can hypo-thetically be used when interpreting clinical changesobserved in Herbst appliance wearing patients. Thischapter leads into the research base on which theremainder of the text is centered.
Chapter 6 discusses the analysing methods used inthe subsequent chapters and Chapters 7 to 25 aredetailed, with numerous case studies and references tosupport the outcomes from Herbst appliance treat-ment. The evidence provided is supported by long-term studies comparing lateral head films and dentalrecords obtained before, during and up to 13 yearspost active Herbst treatment. Short-term and long-term treatment effects are examined and clinicians areencouraged to make use of the high pull headgeareffect of the Herbst appliance.
Chapter 10 focuses on the altered condylar positionwithin the fossa, the condylar remodelling and theglenoid fossa changes associated with Herbst appli-ance therapy. The adaptive TMJ changes are shownto result in advancement of the mandible and as suchthe use of the Herbst appliance is recommended forthe treatment of skeletal Class II malocclusions.Mandibular growth changes, ‘effective TMJ growth’and the effects on the skeletofacial growth pattern areexamined with good cross-referencing between chap-ters and scientific journal articles. Hypotheses are
BOOK REVIEWS
Australian Orthodontic Journal Volume 25 No. 2 November 2009180

presented from research results and consideration isgiven to somatic and skeletal maturation. Resultspublished show much of the mandibular growthobserved during Herbst treatment reverted after treatment and much of the ‘effective TMJ growth’recovers post-treatment. The Herbst appliance alsoappears to have only a short-term impact on theskeletofacial growth pattern. Despite these obser-vations, clinical studies have reported that the soft tissue and skeletal changes during treatment werebeneficial for Class II correction at that time.Evidence is provided and credence is given to estab-lishing a stable occlusion as part of treatment in orderto counteract any occlusal relapse after functionalappliance therapy. Pancherz and Ruf recommendsolid Class I interdigitation of the teeth followingHerbst therapy as being essential for long-term stability.
In Chapter 14 the authors espouse the advantages ofusing the Herbst appliance to improve the facial profile in Class II division 1 patients, but the text also mentions the unpredictability of long-term softtissue changes. Chapters 15 and 16 provide discus-sion relating to treatment effects on muscle activityand TMJ function, with evidence to indicate that theappliance does not cause TMD, but further studiesare suggested to investigate masticatory muscle activity during and post-orthodontic treatment.
As the text continues through Chapters 17 to 21 thebook elaborates on treatment specifics and providesinformation true to the title, The Herbst ApplianceResearch-based Clinical Management. It becomes clearthat the text is not an undergraduate textbook, but abook suitable for postgraduate education and a wonderful text for those orthodontists who use functional appliances. The text provides an evidencebase for dentofacial orthopaedics and, in particularpresents guidelines for the use of the Herbst appli-ance. The book outlines the indications for Herbsttreatment, with the authors recommending fixedappliance therapy after using a Herbst appliance. Thediscussion relating to indications and contrain-dications for extractions is useful. Chapter 22 con-siders the appropriate timing for Herbst treatmentand Chapter 23 offers an alternative to orthognathicsurgery by proposing the use of Herbst appliances in borderline Class II skeletal adults. Appliance failures are described together with reports of complications.
Chapter 26, Concluding Remarks, provides a neatsummary of the content of the book and if this chap-ter stirs your interest then the preceding pages shouldbe read. Overall, the book provides clear informationand guidelines that practitioners could refer to whenconsidering using a fixed bite jumping type appli-ance. The book is comprehensive, with its use of dia-grams, graphs and photographs, the quality of whichare excellent. However, the index, which is merely alist of contents, chapter by chapter, could beimproved. Although written specifically on over 30years of scientific and clinical work with a non-compliance fixed functional appliance, the bookstimulates thought on functional appliance treatmentper se and should stimulate lateral thinking for anypractitioner using functional appliances in their prac-tice. The style is easy to read and understand withnumerous case studies, but in parts becomes some-what repetitive. Nonetheless, at the end one has aclear understanding of indications, construction,management and potential complications when usingthe Herbst appliance.
Helen McLean
Current Experimental Study for Treatment ofCleft Lip and Palate
Editors: Tsuyoshi Kawai, NagatoNatsume and David S. PreciousPublisher: Quintessence(www.quintpub.com)Price: US $128.00ISBN: 4931537049
The introduction provides personal biographies foreach of the editors rather than an insight to the textand the reader needs to move to the table of contentsfor an overview of the text.
The book is printed on A4 semigloss paper and isdivided into five chapters as follows:
Basic research concerning treatment of cleft lipand/or cleft palate (CL/P)
Research concerning the mechanism of CL/Pdevelopment
Australian Orthodontic Journal Volume 25 No. 2 November 2009
BOOK REVIEWS
181

Research concerning prevention of CL/P
Clinical research for prevention of CL/P
Future perspective.
Chapter 1 contains 14 separate articles covering surgery, growth and speech. Chapter 2 contains 11separate articles covering genetics, embryogenesis andaetiological factors such as bacterial infections.Chapter 3 is a single article, which is a review ofexperimental studies on the effects of folic acid andvitamins on congenital anomalies. Chapter 4 con-tains two articles covering attempts for preventionand methods of dietary surveys. Chapter 5 is also asingle article discussing the goals of clarifying the aetiology of CL/P and to establish preventive measures for same.
There is a list of authors and investigators at thebeginning of the book, their institutional associationsand the articles they have contributed to. This reviewer suggests that the reader would find the textmore user-friendly if the individual authors were listed at the beginning of each article, rather thanhaving to search through the author list. Particularlyso, as it appears that the book is a collection of previously published papers as seen from the lack ofconsistency in style between articles and the differentreferencing protocols used from article to article.
In general, the illustrations are excellent, with clearline drawings and colour photographs, yet let downin some articles by being too small, such as on page 16.
Overall, the book covers a broad cross section of thetopic of cleft lip and palate. However for a publica-tion dated 2008 it is let down by the observation thata number of articles have not been updated in theirreferencing, e.g. Chapter 2, article 10, where the mostrecent reference is 1988. This severely limits the currency of the book as demanded by the title.
The presentation of the book is poor and suggests arush to publication as a draft without adequate proof-reading. A consistent style with a larger font wouldmake the text more readable and there are manyspelling and grammatical errors throughout the text,which are frustrating. While the grammatical errorscan be forgiven as a consequence of translation intoEnglish, spelling errors should be relatively simple topick up. The lack of proofreading is glaringly obviouseven in the naming of the editors where the inside
cover names the first editor as: Kawai Tsuyoshi, yetrecords this as Tsuyoshi Kawai in the introduction.
I was looking forward to reading this publicationfrom Quintessence, however, this was a disappointingbook and not up to my expectations from readingother publications from this publisher. It may be use-ful as a reference for the practitioner, but only of limited appeal to the postgraduate student due to thelack of up-to-date referencing and no index.
John Fricker
Orthodontics at a Glance
Author: Daljit S. Gill Publisher: Wiley-Blackwell (au.wiley.com)Price: AUD $69.95 / NZD $78.99ISBN: 978-1-4051-2788-2
This is the second title in the ‘At a Glance’ series,Periodontology being the subject of the first publica-tion. The aim of this series is to present a conciseintroduction to the field of interest in a slim volume– the current title runs to 106 pages, with numerousillustrations. As such it admirably achieves a summ-ary of orthodontics, although the brevity of the publication is also its biggest drawback. The targetreadership is stated to include dental nurses, generalpractitioners and those who wish to specialise inorthodontics – an ambitious scope and any attemptto satisfy all readers is bound to have some failings.Serious students of orthodontics will find the contentdeficient – every topic is assigned two pages, no moreor less.
For the most part the topics are divided into approx-imately one page of text and one of illustrations.While this may suffice for topics such as super-numerary teeth, it is sadly brief for topics such asdevelopment of the dentition, biology of tooth move-ment or treatment of Class III malocclusions.Disappointingly for a new publication, no mention atall is made of ceramic brackets, lingual appliances,sequential plastic aligners or of temporary anchoragedevices.
BOOK REVIEWS
Australian Orthodontic Journal Volume 25 No. 2 November 2009182

Even within the two pages assigned to each topicthere are some glaring omissions – for example in thesection on biomechanics we are told there are threebasic types of tooth movement – tipping, bodilymovement and rotation. No mention is made ofintrusion or extrusion, although there is still plenty ofroom on the page assigned. Additionally, Orthodon-tics at a Glance provides no references whatsoever, sodoes not facilitate further examination of any topicpresented.
The above notwithstanding, a thorough knowledgeof the contents of this publication would enable theaverage dental student to more than successfully passundergraduate orthodontic courses. The illustrationsare clear, well-designed and appropriate to the subjectunder discussion. The structure of the book is wellthought-out, following a logical sequence in coveringtopics from growth and development, diagnosis andtreatment planning, management of malocclusionand finally treatment techniques.
Orthodontics at a Glance is a more approachable pub-lication than more serious contenders as orthodontictexts, such as Contemporary Orthodontics by WilliamProffit and as such perhaps most useful for thosewhose requirements are for a shallow overview.
Tony Weir
Sleep Medicine for Dentists – A PracticalOverview
Editors: Giles J. Lavigne, Peter A. Cistulliand Michael T. SmithPublisher: Quintessence(www.quintpub.com)Price: US $68.00ISBN: 978-0-86715-487-0
In essence, this is the first comprehensive text on dental sleep medicine. To quote Professor ColinSullivan (a leading world authority on sleep medi-cine), ‘generations of dentists have looked in themouths of countless individuals with sleep disorderedbreathing without knowledge of the disorder – a goodknowledge of sleep apnoea should be part of the profession’s knowledge base’.
A total of 45 contributors was involved in the com-pilation of this text, many undoubtedly worldauthorities in their own areas of expertise. SleepMedicine for Dentists is divided into four primary sections, the first of which reviews the nature of sleep,sleep neurobiology and the classification of sleep disorders. Section II focuses on sleep breathing dis-orders, especially the pathophysiology of obstructivesleep apnoea (OSA), its long-term sequelae and theclinical diagnosis and treatment of OSA as it relatesto the dental profession.
Section III is devoted to sleep bruxism and movementdisorders, which highlights the difficulties of differ-ential diagnosis and treatment in this complex groupof patients. The final section (Section IV) investi-gates sleep and orofacial pain, including the effect oftemporomandibular disorders on sleep.
From a personal perspective it appears that the pur-pose of this text was to introduce the dental pro-fession to the realms of sleep medicine. Althoughwell-written, this text is not ‘an easy read’ as the titleA Practical Overview would have us believe. In manyrespects this text highlights the complexities of thenature of sleep medicine and in reality asks morequestions than it gives answers. The section review-ing obstructive sleep apnoea, although concise andinformative, should have been more expansive and included more aspects of oral appliance use anddesign, as undoubtedly this would be the area ofgreatest importance to the clinician. Likewise the section on upper airway imaging only brieflydescribes the use of cephalometrics as a diagnostictool in the treatment of OSA. Cephalometry has beenused extensively over the years to establish cranio-facial anomalies regarded as ‘risk factors’ for the onsetof OSA. An elaboration of these studies may havebeen appropriate.
Sections III and IV relating to bruxism and move-ment disorders and sleep and orofacial pain, respec-tively, were relatively expansive in relation to the section on OSA. Although bruxism is important tothe dental profession, the reality is that it can only beformally diagnosed by polysomnography, yet as clinicians we can do little about it except deal with itsaftermath. It does not, however, carry the pathogene-sis of OSA, yet a significant part of this text wasdevoted to this condition.
Section IV (Sleep and orofacial pain) was undoubt-edly the most difficult section to read. There was a
Australian Orthodontic Journal Volume 25 No. 2 November 2009
BOOK REVIEWS
183

BOOK REVIEWS
Australian Orthodontic Journal Volume 25 No. 2 November 2009184
heavy neurobiological bias to this section, which in aclinical setting was possibly of limited value. A rec-ommendation for dentists to become involved in cognitive-behavioural therapy for the treatment ofinsomnia was optimistic to say the least.
Overall, Sleep Medicine for Dentists – a PracticalOverview is a significant text and any previous com-ments are in reality of a minor nature. It is note-worthy that two of the most influential authorities in
sleep medicine today, namely Professors ColinSullivan and Alan Lowe wrote both the Introductionand Conclusion, respectively.
In conclusion, this text is not a ‘how to do it manual’for the dental profession as the title would lead us tobelieve, but a text that highlights the complexitiesand nature of sleep and its many associated disorders.
Chris Robertson

Australian Orthodontic Journal Volume 25 No. 2 November 2009 185
Tooth size discrepancy in orthodontic patientsamong different malocclusion groups
M. Strujic, S. Anic-Milosevic, S. Mestrovic and M. Slaj
The correct maxillary to mandibular tooth size ratio isimportant for the attainment of correct occlusal inter-digitation, overjet and overbite. The Bolton ratioshave also been used to assess the relationship thatexists between tooth dimensions and supporting boneas well as to predict final tooth positions. The questionwas then asked whether there was a difference in theincidence of tooth size discrepancies among differentskeletal malocclusion groups and whether genderdimorphism existed? In order to investigate the prob-lem, study models and lateral head radiographs from auniversity clinic were obtained. The inclusion criteria,requiring the presence of all permanent teeth, withoutwear or abrasion or having undergone orthodontictreatment, identified 301 casts. Occlusal classificationwas based on Angle and coincided with the skeletalclassification which was based on the ANB angle. Themesio-distal dimensions of all teeth from first molar tofirst molar were measured and recorded using digitalcalipers and a Bolton analysis performed. Measure-ment error was identified as minimal and a number ofstatistical tests were applied.Results showed a statistically significant gender differ-ence in the anterior Bolton ratio indicating that maleshad slightly larger ratios. A tendency was foundtoward mandibular tooth size excess in Angle Class IIImalocclusions and maxillary tooth size excess in ClassII malocclusions. Posterior and overall Bolton ratioswere greater in Class III malocclusions than in otherocclusal categories. The authors concluded and recommended that attention be paid to tooth size discrepancies particularly during the finishing stagesof treatment so that treatment results and stabilitywere optimised.
European Journal of Orthodontics 2009;doi:10.1093/ejo/cjp013
Cervical vertebral anomalies in orthodonticpatients: a growth based superimpositionapproach
D.D. Koletsis and D.J. Halazonetis
The use of cervical vertebral maturity indicators todetermine the growth status of orthodontic patientshas focussed attention on the spine. Vertebral anom-alies are being discovered that may be associated withcraniofacial syndromes. Vertebral fusion is a relativelycommon identifiable problem that falls into the cate-gory of congenital malformation. The present studyaimed to present a growth-based superimpositionalapproach for assessing cervical vertebral fusions and toapply this method to record the type and prevalence ina skeletally heterogeneous orthodontic population. Asecondary aim was to determine any correlationbetween cervical spine anomalies and craniofacialskeletal pattern.The sample consisted of 156 standardised lateralcephalograms of consecutive patients from a univer-sity and a private clinic. The radiographs were scannedand digitised using specific software and a com-prehensive cephalometric analysis completed. In addition, each radiograph was visually assessed by theauthors to determine the prevalence of cervical spineanomalies such as vessel canal morphology, atlas dehiscence, accessory ossicles and fusions. Kappa statistics were applied for inter-observer error. A smallpercentage of patients was identified as having secondary ossicles, vertebral canal anomalies anddehiscence particularly of the atlas.Fourteen patients were possibly identified as havingfusion of the second and third vertebrae. However,there was no agreement between observers. A growth-based superimposition revealed that no patientshowed actual vertebral fusion even though the lateralcephalometric analysis revealed a number of extremeskeletal patterns, which have previously been relatedto cervical fusion.
Recentpublications
Abstracts of recently published papers reviewed by the Assistant Editor, Craig Dreyer

RECENT PUBLICATIONS
Australian Orthodontic Journal Volume 25 No. 2 November 2009186
Although the findings of the study revealed a low per-centage of atlas anomalies, the authors concluded thatit was not possible to correlate skeletal pattern tofusion of cervical vertebrae because there was uncer-tainty over the recognition of fusion. The subjectivevisual examination of a single cephalogram may resultin false-positive findings and growth-based super-imposition has been recommended. Clinicians, how-ever, should be on the alert for anomalies.
European Journal of Orthodontics, 2009doi:10.1093/ejo/cjp049
Palatally impacted canines and the modifiedindex of orthodontic treatment need
S.T. Barlow, M.B. Moore, M. Sherriff, A.J. Ireland and J.R. Sandy
Most indices that assess the severity of a malocclusionare based on aesthetic and/or functional criteria.These, in turn, provide quantification of the need fortreatment and its outcome. Significant local problemsdo not often contribute to a treatment need indexand the authors identified maxillary impacted caninesas an orthodontic problem that can produce majortreatment complications. The authors pursued theuse of a modification of the dental health componentof the IOTN, which excluded the 5i score relating topalatally impacted canines. This was expected to scoreother features of the malocclusion and enable ananecdotal impression of the difficulty of impactedcanine management to be supported or refuted.The sample consisted of 54 pretreatment study models of patients who had undergone successful sur-gical exposure and orthodontic treatment of at leastone palatally impacted canine. The patients weretreated in two different institutions, but by the samesurgical/orthodontic team. The modified treatmentindex excluded the 5i score for the impacted canine,but graded the other features of the malocclusionusing the IOTN ruler. Statistical tests and re-examination applied Kappa statistics to analyseresults and examiner consistency.As all patients in the study had impacted canines andwould have been placed in the 5i category of treat-ment need, the removal of this category meant thatthe examiners graded many cases to a lower IOTNlevel. However, there was still a significant number of cases (41%) who possessed malocclusion traitswhich still placed the patients in the higher categoriesof treatment. However, 25 per cent of the cases hadadjusted scores that indicated little or no need for
treatment. The results therefore demonstrated that inthe absence of a palatally impacted canine, therewould be little need for treatment in a significantnumber of cases. The authors emphasised the impor-tance of early diagnosis of an impacted canine and the implementation of interceptive techniques, par-ticularly when patients would otherwise require noother orthodontic care.
European Journal of Orthodontics 2009;31: 362-366
A systematic review of the effects of bone-borne surgically assisted rapid maxillary expansion
J. Verstraaten, A.M. Kuijpers-Jagtman, M.Y. Mommaerts,S.J. Bergé, R.M. Nada and J.G.J.H. Schols
The management of transverse maxillary deficiency isdependent on the underlying aetiology and thepatient’s developmental status. Treatment optionsrange from slow maxillary expansion for mild dentalproblems, to rapid expansion for skeletal dishar-monies. Rapid expansion in adults frequently requiressurgical assistance, but still employs a tooth-borneappliance which does not eliminate side effects ofperiodontal deterioration and post-treatment collapse.In 1999, a bone-borne appliance was introduced thatdelivered the expansion force directly to the maxillarybone and was therefore expected to avoid negativeorthodontic and periodontal sequelae.The authors’ objectives were to conduct a systematicreview of the literature to determine whether bone-borne surgically-assisted rapid maxillary expansionconstituted an effective orthodontic and orthopaedictreatment option, while at the same time, eliminatingorthodontic (buccal tilting, extrusion) and perio-dontal (root resorption, tooth mobility) side effects.Seven popular medical databases were searched forrandomised controlled trials, controlled clinical trialsand case studies of patients who had undergone a sur-gically-assisted bone-borne palatal distraction. Themajority of the studies were located in PubMed orMEDLINE databases and after applying exclusioncriteria, the final number was 10. All were case stud-ies, mostly prospective but with one retrospectivestudy. No randomised controlled trials or controlledclinical trials were found. The results indicated thatthe expected advantages of bone-borne versus tooth-borne assisted maxillary expansion were minimal.There was weak evidence suggesting that there wasless buccal tipping of teeth used as anchors in the

Australian Orthodontic Journal Volume 25 No. 2 November 2009
RECENT PUBLICATIONS
187
tooth-borne appliances. The retrieved articles showedsignificant heterogeneity and wide variability of out-come, which posed serious restrictions on the inter-pretation of the literature in a quantitative systematicmanner. It was concluded that there was an acuteneed for a well-designed clinical trial to research thepossible effects of tooth-borne and bone-borne maxillary expansion.
Journal of Cranio-Maxillofacial Surgery, 2009doi:10.1016/j.jcms.2009.06.006
Long term effects of surgically assisted rapidmaxillary expansion without performingosteotomy of the pterygoid plates
R. Seeberger, W. Kater, R. Davids and O.C. Thiele
In patients whose circum-maxillary sutural activityhas reduced, a surgically-assisted rapid maxillaryexpansion procedure is a common therapy to correcta transverse maxillary deficiency. However, the pillarsof the upper facial skeleton create resistance to widen-ing and are a possible reason for post-surgical col-lapse. The study therefore evaluated the long-termstability of surgically-assisted rapid palatal expansionwithout performing osteotomy of the pterygoidplates. The study further examined the effects onnasal airway volume and was designed as a retro-spective clinical study. Thirteen non-syndromicpatients (8 female, 5 male) with a mean age of 31.2years underwent a surgically assisted RME withoutseparation of the pterygoid plates. An acoustic rhinometry measurement was performed one monthprior and an average of 63 months after the ope-ration. The measurement was achieved by the delivery of an acoustic pulse and the recording ofimpedance differences in the hollow spaces of thenasal cavity. A study model analysis to determine theexpansion across the first molars was also performed.All patients showed a significant enlargement of nasalvolume as a result of palatal transverse distraction.There was also enhanced nasal respiration reported byall. A mean distraction width increase of 8.29 ± 1.68mm was measured from the casts producing an occlu-sion that was stable after five years. The authors con-tend that long-term benefits of a stable expandedocclusal relationship and a significant improvementin nasal function are achievable without separation ofthe pterygoid plates, which provides a preferable risk-benefit ratio for the patient.
Journal of Cranio-Maxillofacial Surgery, 2009doi:10.1016/j.jcms.2009.07.003
Craniofacial growth patterns in patients withcongenitally missing permanent teeth
N. Bauer, K. Heckmann, A. Sand and J.A. Lisson
Is there a correlation between the congenital absenceof certain permanent teeth and individual cranio-facial growth patterns? This was the question posedby the authors who recognised that permanent toothagenesis was an increasing problem, influenced by theenvironment but largely of genetic origin. Past stud-ies suggested that a possible correlation existed, butno previous work had focussed on the extent to whichthe type of tooth absence correlated with a particularindividual growth pattern.A collection (101) of lateral cephalograms of patientssuffering agenesis was obtained from an orthodonticpractice. The radiographs were divided into thosepatients with missing second premolars, upper lateralincisors or other missing teeth. The lateral head radio-graphs were analysed using the Hasund method, whichinvolved digitisation and reading into a computerusing appropriate software. Additional software allowedthe on-screen identification of cephalometric pointsfrom which distance and angular measurements weremade following adjustments for magnification. Appro-priate statistics were applied. Interesting results fromthe study indicated that females were twice as affectedby agenesis compared with males and that lower secondpremolars were the most commonly missing teeth fol-lowed by upper lateral incisors. Growth patterns wereconsidered horizontal or vertical if angular measure-ments fluctuated more than 2.5° from the mean.Using this criterion, the study showed that patientswith congenitally missing lower second premolars weremore likely to have a horizontal growth pattern, butthis likelihood was not highly significant. No signifi-cant correlations were found between individual growthpatterns and the absence of specific permanent teeth inpatients with other congenitally missing teeth. Patientswith congenitally missing teeth had a smaller basalplane angle (palatal plane–mandibular plane) comparedwith controls. Those patients with agenetic premolarshad a reduced mandibular plane angle to sella-nasionline, which signified a reduction in lower anteriorfacial height. While no statistically relevant correla-tion between type and location of missing teeth wasapparent, it was expected that patients with congeni-tally missing teeth exhibited lower vertical values.
Journal of Orofacial Orthopedics 2009;70: 139-151

Alignment of impacted maxillary canines:critical analysis of eruption path and treatment time
M. Schubert and U. Baumert
Impacted maxillary canines cause a substantial clinical concern and invite a number of treatmentpossibilities. In deciding amongst the options, treat-ment duration is likely to be of high importance tothe patient and it is argued that this aspect of management is usually reliant on the experience andsubjectivity of the clinician. This retrospective studyaimed to determine to what extent parameters of vertical and anteroposterior position and the angula-tion of impacted canines influenced treatment time.Management of all reported impacted caninesinvolved surgical exposure and mechanical elevation.Fifty-seven adolescent patients were identified whofulfilled the following criteria. They were no olderthan 18 years, underwent surgical exposure and aclosed-eruption approach as a nonextraction pro-cedure. Orthopantomograms were analysed from anocclusal plane defined by the mesio-buccal cusps ofthe upper first molar and the upper central incisoredge of the same side. A vertical reference line wasdefined as a midline axis between the upper centralincisors and longitudinal axes were also drawn of theimpacted canine and the adjacent lateral incisor. Anumber of angular and distance measurements weretaken.Results indicated that the length of treatment time,defined by the time from the surgical exposure to theremoval of appliances, correlated significantly withthe canine’s position relative to the surrounding teeth.An important measurement was the distance of thedisplaced canine cusp tip to its target position on theocclusal plane between the lateral incisor and the firstpremolar. Regression analysis demonstrated that thismeasurement was sufficient to predict the activetreatment time for canine alignment. The authorspointed out that the canine tip to occlusal planemeasurement provided a practice-orientated parame-ter to predict treatment timing for impacted canines.However, it was conceded that current 2D imagingdiagnostics most likely limit the ability to predict thelength of therapy to 40 per cent.
Journal of Orofacial Orthopedics 2009;70: 200-212
Conventional wisdom and the surgical exposure of impacted teeth
A. Becker, N. Casap and S. Chaushu
It is accepted that the dental follicle plays an integralrole in the normal eruption of a tooth requiring thatbone resorption occurs in the eruptive pathway followed by fusion of the follicle with the oral epi-thelium. An unerupted tooth that has been surgicallydeprived of its dental follicle is believed to stay inplace as the enamel-to-bone interface does not stimu-late bone resorption. ‘Conventional wisdom’ has itthat the tooth will not erupt by itself nor be amenableto mechanically applied orthodontic traction exceptby a slow pressure generated, pathological resorptionof alveolar bone. The authors contend that the conventional surgicalexposure of an impacted tooth requires substantialbone and soft tissue removal in an open procedure.This is likely to result in periodontal complicationsduring treatment and thereafter. It is recommendedthat the clearance of bone around an impacted toothshould be minimal and involve a closed surgical pro-cedure. Several clinical cases were presented to sup-port their hypothesis. Patients reported they wereaffected by impacted teeth, from otherwise healthy,normal patients with and without resorption of adjacent incisor roots. In addition, patients sufferingfrom cleidocranial dysplasia and increased bone density and also patients with autogenous and syn-thetic bone grafts were assessed. A closed eruptionsurgical technique was used in which only a smallwindow was opened into the dental follicle whichtherefore preserved the maximum amount of sur-rounding bone. The cases were chosen to show therapid responses to extrusive forces and the unneces-sary need for the radical removal of bone. This articleprovides anecdotal and empirical examples to supporta viewpoint that challenges the potentially harmfulperiodontal prognosis that is likely with conventionalexposure surgery.
Orthodontics and Craniofacial Research 2009;12: 82-93
RECENT PUBLICATIONS
Australian Orthodontic Journal Volume 25 No. 2 November 2009188

Australian Orthodontic Journal Volume 25 No. 2 November 2009 189
In appreciationReviewers for the Australian Orthodontic Journal
Hussam Abdel-Kader, Cairo, EgyptNiwat Anuwongnukroh, Bangkok, ThailandPaul Armbruster, Louisiana, USADavid Armstrong, Sydney, NSWJonathan Ashworth, Adelaide, SASaeed Banabilh, Kelatan, MalaysiaAndrew Barry, Wollongong, NSWPhillip Benson, Sheffield, United KingdomJim Bokas, Burwood, VicStephen Brown, Fairy Meadow, NSWBarbara Carach, North Ringwood, VicHong Chan, Doncaster East, VicRobert Cerny, Warners Bay, NSWIsmail Ceylan, Erzurum, TurkeyLuke Chapman, Louisiana, USATony Collett, Ferntree Gully, VicRichard Coltman, Strathfield, NSWRichard Cook, Perth, WAJohn Coolican, Chatswood, NSWMark Cordato, Bathurst, NSWAmy Counts, Florida, USARhonda Coyne, Edge Hill, QAli Darendeliler, Sydney, NSWSaxton Dearing, Napier, New ZealandAnton Demling, Hannover, GermanyPeter Dysart, Dunedin, New ZealandMark Ewing, Hamilton New ZealandMarcelo Ferreira, Paraná, BrazilPadhraig Fleming, London, United KingdomJohn Fricker, Manuka, ACTJoseph Geenty, Fairy Meadow, NSWAllahyar Geramy, Tehran, IranFarzin Heravi, Mashad, IranMithran Goonewardene, Perth, WA Fiona Hall, Mount Lawley, WAPaul Hanrahan, Townsville, QJames Hawkins, Sydney, NSWAbdalla Hazza’a, Irbid, JordanChristopher Ho, Brisbane, QMichael Hyde, Canberra, ACTHideki Ioi, Fukuoka, JapanSteven Jones, London, United KingdomViral Kachiwala, Muscat, OmanVignesh Kailasam, Chennai, IndiaMark Kebsch, Mosman, NSWOm Kharbanda, New Delhi, India
Russell Kift, Maitland, NSWThomas Kluemper, Kentucky, USAEden Lau, Lower Mitcham, SAIgor Lavrin, Mebourne, VicRobert Lee, London, United KingdomGavin Lenz, Brisbane, QKerry Lester, Woollahra, NSWPeter Lewis, Gordon, NSWAtul Mehta, North Parramatta, NSWMurray Meikle, SingaporeAna Claudiá Melo, Curitiba, BrazilChristopher Miles, Clifton Hill, Vic Shunsuke Nakata, Fukuoka, JapanJames Noble, Ontario, CanadaDesmond Ong, Brisbane, QTakashi Ono, Tokyo, JapanKunihiko Otsubo, Tokyo, Japan Konstantina Papadopoulou, Bonn, GermanyYyonne Poon, Gladesville, NSWAndrew Quick, Dunedin, New ZealandSarbin Ranjitkar, Adelaide, SAMike Razza, Booragoon, WA David Roberts-Harry, Harrogate, United KingdomChristoper Robertson, Dunedin, New ZealandRichard Salmon, Adelaide, SAWayne Sampson, Adelaide, SA Ozgur Sayin, Isparta, TurkeyD.G. Singh, San Juan, USAJonathan Skilton, Melbourne, VicAisha Gomes Stumph, Porto Alegre, BrazilGuilherme Thiesen, Florianópolis, BrazilMarcus Tod, Upper Mount Gravatt, QGrant Townsend, Adelaide, SAChristine Underhill, Edgecliff, NSWTancan Uysal, Kayseri, TurkeyJan van Gastel, Leuven, BelgiumVicky Vlaskalic, Hawthorn East, VicWilliam Weekes, Gosford, NSWGeoffrey Wexler, Toorak, Vic Peter Wilkinson, Helensvale, QGuy Willems, Leuven, BelgiumAlbert Wong, East Reservoir, VicMichael Woods, Melbourne, VicNoriaki Yoshida, Nagasaki, Japan
Over the past year the following individuals have generously contributed their time, knowledge and expertise reviewing articles for the Journal. We sincerely thank them and acknowledge their considerable contributions which have improved the quality of the Journal.

Australian Orthodontic Journal Volume 25 No. 2 November 2009190
InVu bracket with adhesiveThe InVu aesthetic bracket isnow even easier to use, withthe addition of Readi-Base pre-applied adhesive for conven-ient application, according tothe manufacturer. InVu bracketscan be positioned precisely onthe teeth without drift and aretranslucent, thus providing anoptimum colour-match.
For further information contact TP OrthodonticsTel: 1800 643 055Website: www.invuortho.comEmail: [email protected]
Mystique MBThe bonding base of theMystique ceramic brackethas been completely rede-signed to further increasebond strength and improvepredictability when debond-ing, according to the manu-facturer. As can be seen inthe photo, Mystique MB now utilises a 100 per cent mechan-ical lock base whilst retaining the original performance of the polycrystalline bracket construction and aesthetics of a silica-lined slot.For further information contact GAC Australia Pty LtdTel: 1800 422 287Website: [email protected]
CephMate digitising software CephMate by tops Softwareis a new generation of tracingsoftware. A single windowinterface makes tracing and
analysis easy for the doctor and staff, according to the man-ufacturer. Key features include the ability to adjust landmarkswithout re-digitising, the new RADIAL menu and realistic, livesoft tissue morphing. CephMate works with any X-ray imagingsoftware or digital camera.For further information contact topsOrthoWebsite: topsOrtho.com
topsOrtho softwaretopsOrtho is the only nativeMac OS X orthodontic prac-tice management and imag-ing software. It provides afast, easy and reliable solu-
tion to minimise IT headaches, according to the manufacturer.It uses a single server for multi-office set-ups.For further information contact topsOrthoWebsite: topsOrtho.com
Quattro Sentalloy coil springsThe Quattro Sentalloy coil springsare specifically designed for usewith temporary anchorage devicessuch as the Quattro system. Oneend of the springs has beenenlarged to allow clearance overthe head of the TAD and the overalllength has been reduced to facili-tate TAD treatment. The Sentalloyspring provides a superelastic, nearconstant force of 50 g. For further information contact GAC Australia Pty LtdTel: 1800 422 287Website: [email protected]
3M Unitek Ortholux curing lightThis new curing light has high intensity1600mW/cm2 LED technology which, themanufacturer claims, will cure ceramicbrackets in 3 seconds and metal brackets in6 seconds. The manufacturer claims theOrtholux Luminous has the same curing timeas plasma arc curing lights, but portableand lighter. The lithium ion battery has 1.5to 2 times the storage capacity of nickelmetal hydride batteries and does not needto be discharged completely betweenrecharge cycles. For further information or to arrange ademonstration contact your 3M UnitekTerritory Manager on 1300 363 484.
New products
New products are presented as a service to our readers, and in no way imply endorsement by the Australian Orthodontic Journal.

Lotus passive self-ligating bracket system Lotus is a new self-ligatingbracket system from OrthoTechnology. It was designedby orthodontists to be comfort-able and hygienic for patients.It is a rhomboid, twin bracket
with a level slot allowing for fast and accurate placement,according to the manufacturer. It also features a uniquepatented clip which can be removed to provide improvedcontrol when finishing a case. Now available in Australiafrom Orthology Pty Ltd.Tel: 1800 678 407Website: www.orthotechnology.com/lotusEmail: [email protected]
SmartClip SL3 with next generation clip 3M Unitek’s self-ligatingappliance system now fea-tures a clip that, the manu-facturer claims, reducesengagement and disen-gagement forces. The appliance incorporates twin bracketsfor enhanced levelling and aligning and the gate-free designis claimed to improve patient hygiene, simplify archwirechanges and reduce chair time. SmartClip SL3 is fully com-patible with the Clarity SL self-ligating appliance system, andbrackets can be ordered pre-coated with adhesive.For further information contact your 3M Unitek TerritoryManager on 1300 383 484.
Australian Orthodontic Journal Volume 25 No. 2 November 2009
NEW PRODUCTS
191
Charlene White’s SOSDolphin Management has released its newest Legend Series module – Charlene White’s SOS Syste-matic Office Solutions. According to the manufacturers, it compares your practice statistics to Charlene’sbenchmarks then offers suggestions for improvement. It has conversational scripting for different employee roles and informs you if your treatment time frame is efficient or if your recall system isn’t up-to-date. Charlene White and her team at Progressive Concepts Orthodontic Consulting and Manage-ment Solutions have worked closely with Dolphin to make their expertise available to practices usingDolphin. A 60-minute DVD ‘Scheduling from the Team Approach’ and a $400 voucher for ‘Charlene’sComplete Marketing Tool Kit’ are included.
For further information contact Dolphin Imaging and Management SolutionsTel: 1300 326 354 Website: www.dolphinimaging.com

Australian Orthodontic Journal Volume 25 No.2 November 2009192
2010
February 6-97th International Orthodontic Congress and 4th Meeting of theWorld Federation of Orthodontists, Sydney, Australia.Website: www.wfosydney.com
April 14-18Annual Meeting of the International Association for Orthodontists,Hilton Clearwater Beach Resort, Florida, USA.Website: www.iaortho.com
April 30 – 4 MayAmerican Association of Orthodontists’ 110th AAO AnnualSession, Washington Convention Center, Washington DC, USA.Website: www.aaomembers.org
May 15-1611th International Symposium of the Greek Orthodontic Society,Hotel Divani-Akropolis, Athens, Greece.Website: www.grortho.grEmail: [email protected]
June 15-1986th Congress of the European Orthodontic Society, St BernardinAdriatic Resort and Convention Centre, Portoroz, Slovenia.Website: www.eos2010.siEmail: [email protected]
June 30 – July 3New Zealand Association of Orthodontists’ Biennial Conference,Hotel Grand Chancellor, Christchurch, New Zealand.Website: www.conference.co.nz
August 18-21XIII International Orthodontic Congress of the Chilean OrthodonticSociety, Centro de Eventos Casa Piedra, Santiago, Chile.Website: www.sociedadortodonciachile.orgEmail: [email protected]
September 18-21British Orthodontic Society Conference, Brighton, UnitedKingdom.Website: www.bos.org.uk
Orthodontic calendar
For a list of meetings and links to websites of national and international orthodontic societies, visit the World Federation of Orthodontics, www.wfo.orgFor inclusion in the Australian Orthodontic Journal please contact: Dr Tony Collett Tel: (+61 3) 9756 0519 Email: [email protected]

Australian Orthodontic Journal Volume 25 No. 2 November 2009 193
Author indexAckerman J, 169Al Habashneh R, 142Al-Nimri K, 142Ameri H, 19Armbruster P, 1Arun T, 110Athanasiou A, 123Azimi S, 41Bagheban A, 8, 41Bayani S, 153Ben Bihi S, 135Cakan D, 110Catal G, 158Chalakkal P, 59Chapman L, 1Chatzistavrou E, 123Cheuk G, 12Chopra S, 59Conti C, 34Coreil M, 1DiBiase A, 76Du J, 1Eliades G, 123Eliades T, 63, 123Erdem A, 116Eröz B, 116Eslamian L, 8Ewing M, 128Favoni O, 34Fereidooni F, 41Ferraris P, 34Fleming P, 76Georgiou G, 12Geramy A, 104Gracco A, 34Guarneri M, 34Hadizadeh B, 30Harkness M, 82Hassan R, 163Heravi F, 153Ho C, 97Hughes T, 48
Hussein K, 163Jahanbin A, 19Jones S, 12, 135Kachiwala V, 24Kalha A, 24Kean M, 169Keluskar K, 147Khaleghimoghaddam R, 19Kheirieh S, 8Kianoush K, 30Kilic N, 116, 158Kilic S, 158Kotrashetti S, 147Kumar P, 147Lau E, 48Machado G, 24Massudi R, 41Mazzoli A, 34Moles D, 12Nagaraj K, 147Naidu D, 97Nalbantgil D, 110Noor S, 163Nouri M, 8, 41Obeidat M, 143Ong D, 97Oztoprak M, 110Papadopoulou K, 63Patil S, 147Poosti M, 30Proffit W, 169Rad H, 30Rajion Z, 163Safavi S, 8Sampson W, 48Saxena R, 147Scott J, 97Seehra J, 76Sefidroodi A, 8 Thomas A, 59Tosi G, 34Townsend G, 48Zinelis S, 123
Subject index
2 x 4 appliance
Orthodontic treatment of localised gingival recession associated withtraumatic anterior crossbite, 76
3-D digital study models
The accuracy of a 3-D laser scannerfor crown width measurements, 41
Activator
Changes in soft tissue profile and elec-tromyographic activity after activatortreatment, 116
Adhesive
Effect of adhesive types on enameldiscolouration around orthodonticbrackets, 19
Aligner transparency
Short-term chemical and physicalchanges in Invisalign appliances, 34
Alloys
Microbiologically-influenced corrosionof orthodontic alloys: a review of pro-posed mechanisms and effects, 63
Anchor loss
Clinical investigation of periodontalligament distraction osteogenesis forrapid orthodontic canine retraction,147
Arch dimensions
Variations in tooth size and archdimensions in Malay schoolchildren,163
Arch length
Variations in tooth size and archdimensions in Malay schoolchildren,163
Arch perimeter
Variations in tooth size and archdimensions in Malay schoolchildren,163
Index to Volume 25The Australian Orthodontic Journal

Bimaxillary protrusion
Soft tissue changes associated withfirst premolar extractions in adultfemales, 24
Biofilm
Microbiologically-influenced corrosionof orthodontic alloys: a review of pro-posed mechanisms and effects, 63
Bolton analysis
Validity, reliability and reproducibilityof three methods used to measuretooth widths for Bolton analyses, 97
Bond failure rate
Bond failure in clinical practice, 128
Bond strength
Shear bond strengths of molar tubesbonded with different adhesives, 1
Bonding
Shear bond strengths of molar tubesbonded with different adhesives, 1
Book reviews
Biological Mechanisms of ToothMovement, 176Clinical Endodontics. A textbook.Third Edition, 86Current Experimental Study forTreatment of Cleft Lip and Palate, 181Dental Instruments – A Pocket Guide.Third Edition, 85Enhancement Orthodontics: Theoryand Practice, 178The Herbst Appliance: Research-based Clinical Management, 180Mini-Implants in Orthodontics:Innovative Anchorage Concepts, 179Orofacial pain. Guidelines for Assess-ment, Diagnosis and Management.Fourth Edition, 86Orthodontic Diagnostic Principles.Third Edition, 85Orthodontic Miniscrew Implants, 83Orthodontic Radiographs – Guide-lines. Third Edition 2008, 83Orthodontics at a Glance, 182Radiographic Imaging for the Dentalteam. Fourth Edition, 177Sleep Medicine for Dentists – APractical Overview, 183
The 20 Principles of the AlexanderDiscipline, 87
Brass wire separator
Perception of pain and discomfort during tooth separation, 110
Canine retraction
Clinical investigation of periodontalligament distraction osteogenesis forrapid orthodontic canine retraction,147
Case report
Orthodontic treatment of localised gin-gival recession associated with trau-matic anterior crossbite, 76
Clark twin block treatment
An evaluation of maxillary andmandibular rotational responses withthe Clark twin block appliance, 48
Class III malocclusion
Facial asymmetry in subjects withClass III malocclusion, 158
Composite resin
Effect of in vivo aging on the shearbond strength of an orthodontic adhesive, 123
Corrosion
Microbiologically-influenced corrosionof orthodontic alloys: a review of pro-posed mechanisms and effects, 63
Curing light direction
Changes in shear bond strength ofceramic and stainless steel bracketswith different visible light curing timesand directions, 153
Curing times
Changes in shear bond strength ofceramic and stainless steel bracketswith different visible light curing timesand directions, 153
Dental cast analysis
The accuracy of a 3-D laser scannerfor crown width measurements, 41
Dental health component (DHC)
Orthodontic treatment need in 14-–16year-old Tehran high school students,8
Digital analysis
Validity, reliability and reproducibilityof three methods used to measuretooth widths for Bolton analyses, 97
Digital callipers
Validity, reliability and reproducibilityof three methods used to measuretooth widths for Bolton analyses, 97
DigiModel software
Validity, reliability and reproducibilityof three methods used to measuretooth widths for Bolton analyses, 97
Discomfort
Perception of pain and discomfort during tooth separation, 110
Distraction osteogenesis
Clinical investigation of periodontalligament distraction osteogenesis forrapid orthodontic canine retraction, 147
Ectopic upper canines
Reliability of the magnification methodfor localisation of ectopic uppercanines, 59
Edgewise brackets
Bond failure in clinical practice, 128
Editorial
Some factors that may affect yourchoice of appliance, 82
Elastomeric separator
Perception of pain and discomfort during tooth separation, 110
Elastomerics
Static frictional resistance with theSlide low-friction elastomeric ligaturesystem, 136
Electromyography
Changes in soft tissue profile and elec-tromyographic activity after activatortreatment, 116
Energy dispersive X-ray micro-analysis
Short-term chemical and physicalchanges in Invisalign appliances, 34
Enzymes
Microbiologically-influenced corrosionof orthodontic alloys: a review of pro-posed mechanisms and effects, 63
INDEX
Australian Orthodontic Journal Volume 25 No. 2 November 2009194

Facial asymmetry
Facial asymmetry in subjects withClass III malocclusion, 158
Facial profile
Soft tissue changes associated withfirst premolar extractions in adultfemales, 24
Finite element method
Stresses around a miniscrew. 3-Danalysis with the finite element method(FEM), 104
First premolar extractions
Soft tissue changes associated withfirst premolar extractions in adultfemales, 24
Fluoridated apatites
Comparison of fluoridated apatiteswith pure hydroxyapatite as potentialbiomimetic alternatives to enamel for laboratory-based bond strengthstudies, 12
Fourier transform infra-redmicrospectroscopy
Short-term chemical and physicalchanges in Invisalign appliances, 34
Friction
Static frictional resistance with theSlide low-friction elastomeric ligaturesystem, 136
Functional appliance
An evaluation of maxillary andmandibular rotational responses withthe Clark twin block appliance, 48
Gas chromatography-massspectrometry
Short-term chemical and physicalchanges in Invisalign appliances, 34
Gingival index
Gingival health and relapse tendency:a prospective study of two types oflower fixed retainers, 142
Growth rotation
An evaluation of maxillary andmandibular rotational responses withthe Clark twin block appliance, 48
Guest editorial
The interaction of function and stability in the dentition, 169
Hydroxyapatite
Comparison of fluoridated apatiteswith pure hydroxyapatite as potentialbiomimetic alternatives to enamel for laboratory-based bond strengthstudies, 12
Index of orthodontic treatmentneed (IOTN)
Orthodontic treatment need in 14–16year-old Tehran high school students,8
Interdental/periodontal ligament distraction
Clinical investigation of periodontalligament distraction osteogenesis forrapid orthodontic canine retraction,147
Invisalign aligners
Short-term chemical and physicalchanges in Invisalign appliances, 34
In vitro testing
Effect of in vivo aging on the shearbond strength of an orthodontic adhesive, 123
In vivo aging
Effect of in vivo aging on the shearbond strength of an orthodontic adhesive, 123
Irregularity index
Gingival health and relapse tendency:a prospective study of two types oflower fixed retainers, 142
Laser scanning
The accuracy of a 3-D laser scannerfor crown width measurements, 41
Light cure adhesives
Changes in shear bond strength ofceramic and stainless steel bracketswith different visible light curing timesand directions, 153
Lip changes
Soft tissue changes associated withfirst premolar extractions in adultfemales, 24
Localised gingival recession
Orthodontic treatment of localised gingival recession associated withtraumatic anterior crossbite, 76
Magnification method
Reliability of the magnification methodfor localisation of ectopic uppercanines, 59
Malay schoolchildren
Variations in tooth size and archdimensions in Malay schoolchildren,163
Malocclusion
Orthodontic treatment need in 14–16year-old Tehran high school students,8
Masseter muscle
Changes in soft tissue profile and elec-tromyographic activity after activatortreatment, 116
Mesio-distal crown widths
The accuracy of a 3-D laser scannerfor crown width measurements, 41
Micro-organisms
Microbiologically-influenced corrosionof orthodontic alloys: a review of pro-posed mechanisms and effects, 63
Mini-Diamond brackets
Bond failure in clinical practice, 128
Miniscrew angulation
Stresses around a miniscrew. 3-Danalysis with the finite element method(FEM), 104
Miniscrew position
Stresses around a miniscrew. 3-Danalysis with the finite element method(FEM), 104
Molar tubes
Shear bond strengths of molar tubesbonded with different adhesives, 1
Nickel
Are more nickel ions released fromNiTi wires after sterilisation? 30
Nickel ion release
Are more nickel ions released fromNiTi wires after sterilisation? 30
Australian Orthodontic Journal Volume 25 No. 2 November 2009
INDEX
195

INDEX
Australian Orthodontic Journal Volume 25 No. 2 November 2009196
NiTi archwire
Are more nickel ions released fromNiTi wires after sterilisation? 30
Obituary
John F. Reading, 173
Orbicularis oris muscle
Changes in soft tissue profile and elec-tromyographic activity after activatortreatment, 116
Orthodontic adhesive
Effect of in vivo aging on the shearbond strength of an orthodontic adhesive, 123
Orthodontic tooth movement
Static frictional resistance with theSlide low-friction elastomeric ligaturesystem, 136
Pain perception
Perception of pain and discomfort during tooth separation, 110
Palatally placed canines
Reliability of the magnification methodfor localisation of ectopic uppercanines, 59
Panoramic radiograph
Reliability of the magnification methodfor localisation of ectopic uppercanines, 59
Parallax method
Reliability of the magnification methodfor localisation of ectopic uppercanines, 59
Plaque index
Gingival health and relapse tendency:a prospective study of two types oflower fixed retainers, 142
Postero-anterior radiographs
Facial asymmetry in subjects withClass III malocclusion, 158
Relapse
Gingival health and relapse tendency:a prospective study of two types oflower fixed retainers, 142
Reliability
The accuracy of a 3-D laser scannerfor crown width measurements, 41
Validity, reliability and reproducibilityof three methods used to measuretooth widths for Bolton analyses, 97
Reproducibility
Validity, reliability and reproducibilityof three methods used to measuretooth widths for Bolton analyses, 97
Retention
Gingival health and relapse tendency:a prospective study of two types oflower fixed retainers, 142
Retrospective study
Bond failure in clinical practice, 128
Review
Microbiologically-influenced corrosionof orthodontic alloys: a review of proposed mechanisms and effects,63
Scanning electron microscopy
Short-term chemical and physicalchanges in Invisalign appliances, 34
Self-ligating brackets
Bond failure in clinical practice, 128
Sensitivity
Reliability of the magnification methodfor localisation of ectopic uppercanines, 59
Shear bond strength
Shear bond strengths of molar tubesbonded with different adhesives, 1Comparison of fluoridated apatiteswith pure hydroxyapatite as potentialbio-mimetic alternatives to enamel forlaboratory-based bond strength studies, 12Effect of in vivo aging on the shearbond strength of an orthodontic adhesive, 123Changes in shear bond strength ofceramic and stainless steel bracketswith different visible light curing timesand directions, 153
Sliding mechanics
Static frictional resistance with theSlide low-friction elastomeric ligaturesystem, 136
Soft tissue profile
Changes in soft tissue profile and elec-tromyographic activity after activatortreatment, 116
South Indian adult females
Soft tissue changes associated withfirst premolar extractions in adultfemales, 24
Specificity
Reliability of the magnification methodfor localisation of ectopic uppercanines, 59
Spectrophotometry
Short-term chemical and physicalchanges in Invisalign appliances, 34
Speed brackets
Bond failure in clinical practice, 128
Speed molar attachments
Bond failure in clinical practice, 128
Sterilisation
Are more nickel ions released fromNiTi wires after sterilisation? 30
Tehran high school children
Orthodontic treatment need in 14–16year-old Tehran high school students,8
Temporalis muscle
Changes in soft tissue profile and elec-tromyographic activity after activatortreatment, 116
Tooth discolouration
Effect of adhesive types on enameldiscolouration around orthodonticbrackets, 19
Tooth separation
Perception of pain and discomfort during tooth separation, 110
Tooth size
Validity, reliability and reproducibilityof three methods used to measuretooth widths for Bolton analyses, 97Variations in tooth size and archdimensions in Malay schoolchildren,163

Australian Orthodontic Journal Volume 25 No. 2 November 2009
INDEX
197
Tooth widths
Validity, reliability and reproducibilityof three methods used to measuretooth widths for Bolton analyses, 97
Traumatic anterior crossbite
Orthodontic treatment of localised gin-gival recession associated with trau-matic anterior crossbite, 76
Upper removable appliance
Orthodontic treatment of localisedgingival recession associated withtraumatic anterior crossbite, 76
Validity
The accuracy of a 3-D laser scannerfor crown width measurements, 41Validity, reliability and reproducibilityof three methods used to measuretooth widths for Bolton analyses, 97
von Mises stress
Stresses around a miniscrew. 3-Danalysis with the finite element method(FEM), 104