veterinary equine education
80
American Edition | January 2014 in this issue: The official journal of the American Association of Equine Practitioners, produced in partnership with BEVA. veterinary equine education Meet 2014 AAEP President Dr. Jeff Blea Navicular bone osteomyelitis and navicular bursitis with associated fistula diagnosed with magnetic resonance fistulography in the horse Evaluation of laryngeal function under the influence of various head and neck positions during exercise in 58 performance horses Photo by AAEP member Dr. Nat White
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of veterinary equine education

American Edition | January 2014
in this issue:
The official journal of the American Association of Equine Practitioners, produced in partnership with BEVA.
veterinaryequine
education
Meet 2014 AAEP President Dr. Jeff Blea
Navicular bone osteomyelitis and navicular bursitis with associated fistula diagnosed with magnetic resonance fistulography in the horse
Evaluation of laryngeal function under the influence of various head and neck positions during exercise in 58 performance horses
Photo by AAEP member Dr. Nat White

Pssst!
The secret’s out. Horses know how good Buckeye® Nutrition is. So do horse owners. For over 100 years, we’ve been quietly producing horse feed of unsurpassed quality. We’ve perfected the art and science of equine nutrition and put into play quality assurance standards that are far from standard. We implement many programs mandated in human food manufacturing facilities. We rely on local farms for grain to make our feed the best it can be. One look at a Buckeye® Nutrition horse and it’s no secret what feed he’s on. Learn more at BuckeyeNutrition.com.
©2013 Mars Horsecare US, inc.
HEALTHY FEED. HAPPY HORSE.

c o n t e n t s
American Edition
Meet 2014 AAEP President Dr. Jeff Blea ................................................................................ III
Practitioners, others overcome adverse weather to make Nashville a top-5 convention ....... IV
Foundation grants supporting industry efforts to alleviate the plight of the unwanted horse ............................................................................................VII
Peer reviewers 2013 ...................................................................................................................1
S. WRIGHT ...............................................................................................................................2
EVE and EVJ online collection of equine endocrinology: Recent and future directions; a great start but still a long way to go C. M. MARR and T. S. MAIR ..................................................................................................4
Current best practice in clinical management of equine endocrine patients N. FRANK and R. GEOR .........................................................................................................6
Navicular bone osteomyelitis and navicular bursitis with associated fistula diagnosed with magnetic resonance fistulography in the horse E. B. GARCIA, N. RADEMACHER, C. T. MCCAULEY and L. GASCHEN ......................10
Multimodal therapy including electroacupuncture for the treatment of facial nerve paralysis in a horse C. DE FOURMESTRAUX, C. TESSIER and G. TOUZOT-JOURDE...................................18
Treatment of a femoral fracture with a titanium locking compression plate distal femur ( LCP - DF ) in a young donkey S. BUMBACHER, M. F. BRYNER, A. E. FÜRST, F. DEL CHICCA, S. K. RINGER and M. A. JACKSON .....................................................................................27
The use of magnetic resonance imaging for the diagnosis of osteomyelitis N. WERPY ...............................................................................................................................15
Electroacupuncture for nerve injury in the horse D. G. VON SCHWEINITZ .....................................................................................................24
Diaphyseal femoral fractures in young horses A. R. S. BARR ..........................................................................................................................32
Laparoscopic castration of the normal horse: Is it indicated? A. T. FISCHER JR ...................................................................................................................40
Evaluation of success rate of laparoscopic castration without orchidectomy in 32 mature horses C. DE FOURMESTRAUX, O. GEFFROY, B. SILIART, O. ALBARIC and C. TESSIER .......................................................................................................................34
Evaluation of success rate of laparoscopic castration without orchidectomy in 32 mature horses C. DE FOURMESTRAUX, O. GEFFROY, B. SILIART, O. ALBARIC and C. TESSIER .......................................................................................................................34
Abortogenic viruses in horses B. A. BAZANÓW, N. A. JACKULAK, A. B. FRACKA and Z. M. STARONIEWICZ ..........48
............................................................................................................... 47
veterinaryequine
education

Equine Veterinary Education is a refereed educational journal designed to keep the practicing veterinarian up to date with developments in equine medicine and surgery. Submitted case reports are accompanied by invited reviews of the subject (satellite articles) and clinical quizzes. Tutorial articles, both invited and submitted, provide in-depth coverage of issues in equine practice.
Equine Veterinary Education (American Edition ISSN 1525-8769) is published monthly by the American Association of Equine Practitioners, an international membership organization of equine veterinarians. Office of publication is 4075 Iron Works Parkway, Lexington, KY 40511. Periodicals Postage paid at Lexington, KY and additional mailing office. POSTMASTER: Send address changes to: Equine Veterinary Education, 4075 Iron Works Parkway, Lexington, KY 40511.
Communications regarding editorial matters should be addressed to: The Editor, Equine Veterinary Education, Mulberry House, 31 Market Street, Fordham, Ely, Cambridgeshire CB7 5LQ, UK. Telephone: 44 (0) 1638 720250, Fax: 44 (0) 1638 721868, E-mail: [email protected].
All manuscript submissions for the journal should be submitted online at http://manuscriptcentral.com/eve. Full instructions and support are available on the site and a user ID and password can be obtained on the first visit. If you require assistance, click the Get Help Now link that appears at the top right of every ScholarOne Manuscripts page.
All subscription inquiries should be addressed to: Subscriptions Department, AAEP, 4075 Iron Works Parkway, Lexington, KY 40511, Telephone: (859) 233-0147, E-mail: [email protected]. Subscription rates: AAEP annual membership dues include $40 for a subscription to Equine Veterinary Education. Other subscriptions at $151.80. Single copies $37.50.
Canadian Subscriptions: Canada Post Agreement Number 7178957. Send change address information and blocks of undeliverable copies to IBC, 7485 Bath Road, Mississauga, ON L4T 4C1, Canada.
© World copyright by Equine Veterinary Journal Ltd 2014.
The authors, editors and publishers do not accept responsibility for any loss or damage arising from actions or decisions based or relying on information contained in this publication. Responsibility for the treatment of horses under medical or surgical care and interpretation of published material lies with the veterinarian. This is an aca-demic publication and should not be used or interpreted as a source of practical advice or instruction.
The American Association of Equine Practitioners cannot accept responsibility for the quality of products or ser-vices advertised in this journal or any claim made in relation thereto. Every reasonable precaution is taken before advertisements are accepted, but such acceptance does not imply any form of recommendation or approval.
All companies wishing to advertise in Equine Veterinary Education, American edition, must be current AAEP exhibitors. AAEP retains the right, in its sole discretion, to determine the circumstances under which an exhibitor may advertise in this journal. While all advertisers must comply with applicable legal guidelines, Compounding Pharmacies are specifically directed to limit themselves to pharmacy practices as dictated by the FDA Center for Veterinarian Medicine, Compliance Policy Guideline (www.fda.gov/ora/compliance_ref/ cpg/cpgvet/cpg608-400.html). Advertising any complete or partial mimicry of drugs and dosage forms of FDA approved formulations will not be accepted. Compounding Pharmacies, or any other exhibitors/advertisers who violate this rule in any fashion, will render their advertising contract null and void.
As a private organization, the AAEP reserves the right to exclude any company from advertising in Equine Veterinary Education, American edition, for any reason. The signing and delivery of the advertising contract shall constitute an offer subject to acceptance by the AAEP. In its sole and absolute discretion, the AAEP may revoke its acceptance of the advertising contract or may terminate any contract by delivery of written notice, in which event the AAEP shall have no liability to the advertiser for damages for any other remedy.
Printed by: Cadmus Professional Communications, Lancaster Division, Lancaster, PA.
E q u i n e v e t e r i n a r y e d u c a t i o nA m e r i c a n E d i t i o n
Editor (UK) T. S. Mair, BVSc, PhD, DEIM, DESTS, DipECEIM, MRCVS
Editors (USA) N. A. White II, DVM W. D. Wilson, MRCVS
Management Group D. Foley T. S. Mair N. A. White W. D. Wilson J. L. N. Wood
Management Board A. R. S. Barr S. E. Palmer D. Foley N. A. White (US Editor) K. Garrett S. White P. Harris W. D. Wilson (US Editor) T. S. Mair (Editor) J. L. N. Wood (Chairman)
American Association of Equine Practitioners4075 Iron Works Parkway Lexington, KY 40511
FAX (859) 233-1968E-MAIL [email protected]
To access our website, go to www.aaep.org, click on Members, select LOGIN, then enter your e-mail and password or, for first-time visitors, enter your e-mail as your Username and your member number with the letter ‘a’ in front as your Password.Published monthly. Deadlines are the seventh of the preceding month.
2014 AAEP Officers
Jeff Blea, DVM, President
G. Kent Carter, DVM, President-Elect
Kathleen Anderson, DVM, Vice President
James Morehead, DVM, Treasurer
Ann Dwyer, DVM, Immediate Past President
AAEP Staff
David Foley, CAE, Executive Director [email protected]
Brad Mitchell, Director of Finance & Operations [email protected]
Sally J. Baker, APR, Director of Marketing & Public Relations
Keith Kleine, Director of Industry Relations [email protected]
Sue Stivers, Executive Assistant [email protected]
Carey Ross, Scientific Publications Coordinator [email protected]
Amity Brannock, Communications Coordinator [email protected]
Dana Kirkland, Industry Education and Development Coordinator [email protected]
Deborah Miles, CMP, Meetings Coordinator [email protected]
Elaine Young, Student Programs Coordinator [email protected]
Pam Shook, Foundation Programs Coordinator [email protected]
Cynthia Hinkle, Office Manager [email protected]
John Cooney, Publications Coordinator [email protected]
Nick Altwies, Membership Services Coordinator [email protected]
Jodie Bingham, Foundation Development Coordinator [email protected]
Julie Dunn, Meetings Assistant [email protected]
Megan Gray, Membership Assistant [email protected]
Kristin Walker, Member Relations [email protected]
All advertising inquiries should be addressed to: Dana Kirkland (859) 233-0147 [email protected]
AAEP Mission Statement: To improve the health and welfare of the horse, to further the professional development of its members, and to provide resources and leadership for the benefit of the equine industry.
Assistant Editors F. Andrews D. Archer F.T. Bain A.R.S. Barr A. Blikslager M. Bowen N. Cohen A. Dart J.-M. Denoix T. Divers P. Dixon W. Duckett B. Dunkel S. Dyson T. Fischer D. FreemanT. Greet R. Hanson P. Harris M. Hillyer M. Holmes
P. Johnson J.-P. Lavoie S. Love M.J. MartinelliI.G. Mayhew M. Mazan C.W. McIlwraith R. Moore A. Parks S. Puchalski C. Riggs H. Schott J. Schumacher S. Semevelos B. Sponseller C. Sweeney H. Tremaine S. Weese P. Wilkins Ex-officio J. Cooney

EQUINE VETERINARY EDUCATION / AE / JANUARY 2014 III
Hometown: Santa Fe, N.M.Current Residence: Sierra Madre, Calif.Current Position: Partner in Von Bluecher, Blea, Hunkin Inc., Equine Medicine and Surgery, a five-veterinarian Thoroughbred racetrack practice in Southern California. Describe how you ventured into equine veterinary medicine?My family always had riding horses and, eventually, racehorses. My grandfather would take us riding after school and on weekends. When my family moved to New Orleans in the 1970s, my father trained racehorses, and my brother and I were at the track helping him every chance we could.
As time passed, I decided to start galloping racehorses, and eventually started riding in races in the early 1980s. I enjoyed the people and the horses at the racetrack, and when my brief career as a jockey ended, a trainer that I rode for suggested that I go to vet school. I always knew that my life would involve horses, and his advice resonated deeply in me. What issues in equine veterinary medicine are top priorities for you and why? We, as equine practitioners, are losing our respected role as the voice of authority for the health and welfare of the horse, and we, as a profession, need to figure out how to regain that role in the face of escalating challenges from the lay individual.
Currently there are farriers taking radiographs and providing a diagnosis and treatment; lay dentists performing medical procedures without proper training; drug companies selling bulk product to trainers, farms and owners without a valid VCPR; and the list goes on. Government agencies are in place to protect the public from the veterinarian, yet there is no protection from the unlicensed paraprofessionals.
Another issue that is important to me is medication uniformity and integrity in horse racing. AAEP has played an integral role in improving the sport and continues to focus on what is best for the horse, its members, and the
industry. As an association, we need to keep our focus on what is best for the horse.
How has your AAEP membership influenced your career?Through the years I have been fortunate to meet and interact with many AAEP members who provided mentorship, while others became great friends and colleagues. It is an organization of talented, ethical and passionate individuals who share a common goal. Because of these relationships, I have become a better practitioner in many regards and have come to appreciate organized veterinary medicine and how to solve problems within the context of organized associations. What do you consider to be your greatest contribution to the equine veterinary profession?I’m not sure I’ve reached that pinnacle yet. I’m quite proud that many of the students who have externed with our practice left us with a better appreciation of veterinary medicine at the racetrack, a better understanding of the industry, and a respect for the racetrack practitioner.
What goals do you have for your term as AAEP president?One of my main goals is to resurrect the veterinarian’s role as the expert for the health and welfare of the horse. As a profession, we are well trained for this role; however, we are not well branded, nor are we vocal about our position.
Other goals are to continue:
of the equine practitioner
How have your experiences as a veterinarian and member of the AAEP prepared you to lead the association?I’ve learned to listen more and talk less – qualities that have served me well in practice. It’s critical to listen to the discussion to determine if, in fact, an issue exists before attempting to resolve any conflict. As a racetrack practitio-ner, my job is to solve problems and promote the success of the team; that applies to my role in AAEP as well.
Please describe your interests outside of veterinary medicine.I enjoy spending quality time with my wife and our two daughters. Our favorite place to go is Jackson Hole, Wyo., where we just truly enjoy the outdoors and its beauty. Fly-fishing in Wyoming is something that I truly enjoy, and I hope to improve my technique in the years to come.
Meet 2014 AAEP President Dr. Jeff Blea
Dr. Jeff Blea

IV EQUINE VETERINARY EDUCATION / AE / JANUARY 2014
Practitioners, others overcome adverse weather to make Nashville a top-5 convention
Nashville is known for its country music stars, but the city’s real stars Dec. 7-11 were the 6,592 equine veterinarians, students, guests and exhibitors who persevered through inclement weather and travel delays across a wide swath of the United States to make the AAEP’s 59th Annual Convention the fourth-most attended ever.
Their perseverance was rewarded with an outstanding educational program that featured 200 presentations and discussions during 34 educational sessions. Near-capacity attendance was commonplace in the meeting rooms during many of the featured sessions, and the critical area of lameness received special attention as the focus of at least one session each day.
Supplementing the leading-edge information presented during the educational program were the latest technologies, services and products for equine practice from 340 trade show exhibitors. Students, meanwhile, benefited from a significantly expanded student program that included dry labs and career development sessions with veteran practitioners.
“While the weather certainly presented some initial challenges, it didn’t diminish the enthusiasm of attendees,” said AAEP Executive Director David Foley. “I sincerely thank our program chair, Dr. Jeff Blea, and the entire Educational Programs Committee for assembling a program that received strong praise from attendees for its depth and practicality.”
AAEP Touch campaign launched
During the opening session on Dec. 8, the AAEP launched Touch: Tools to Connect to Your Clients and Their Horses. Touch is a long-term investment into the practice success of AAEP members based on extensive research with thousands of horse owners and trainers. For more information about AAEP Touch, see the article on page IX.
More than $84,000 generated for AAEP Foundation
Combined proceeds from the live auction held during the 17th Annual Foundation Celebration, the second annual sporting clay shoot tournament and from individual donations totaled more than $84,000 in support of the AAEP Foundation’s mission to improve the welfare of the horse.
Annual awards bestowed on five members
Five AAEP members were honored during the Dec. 10 President’s Luncheon for their outstanding service on behalf of the horse and the association. Congratulations to the following 2013 honorees:Distinguished Educator Award (Academic) –
Dr. Frank NickelsDistinguished Educator Award (Mentor) –
Dr. Barrie GrantDistinguished Life Member Award –
Dr. Benjamin Franklin Jr.Distinguished Service Award – Dr. Harry WernerPresident’s Award – Dr. Edward Kanara
The 2014 Officers took office during the Dec. 10 President’s Luncheon. From left: Dr. Jim Morehead, treasurer; Dr. Ann Dwyer, immediate past president; Dr. Jeff Blea, president; Dr. Kathleen Anderson, vice president; and Dr. G. Kent Carter, president-elect.
Fun and philanthropy merged at the Wildhorse Saloon during a sold-out Foundation Celebration.

EQUINE VETERINARY EDUCATION / AE / JANUARY 2014 V
Lameness spotlighted during Milne Lecture
Equine orthopaedic expert Dr. Sue Dyson equipped a standing-room only crowd of equine practitioners with the advanced knowledge necessary to diagnose and treat lameness during her Dec. 9 Frank J. Milne State-of-the-Art Lecture “Equine Lameness: Clinical Judgment Meets Advanced Diagnostic Imaging.”
Describing the diagnosis of lameness as both art and science, Dr. Dyson said longeing is superior to trotting in hand on a circle during a lameness evaluation because it is easier to assess how the horse is holding its body, which may be an adaptation to pain. When observing a horse with a rider on its back, the practitioner should be cognizant of the rider’s proficiency because a good rider can mask the appearance of lameness while a less-skilled rider can induce the appearance of lameness.
A transcript of Dr. Dyson’s presentation can be found in the 2013 AAEP Convention Proceedings book, beginning on page 92.
Osteoarthritis researcher awarded 2013 Past Presidents’ Research Fellow
Colorado State University doctoral candidate Dr. Brad Nelson received the 2013 AAEP Foundation Past Presidents’ Research Fellow for his research that seeks to detect cartilage injury in the early stages of osteoarthritis, which would enable institution of earlier treatments that have better success providing long-term comfort to the horse.
The $5,000 grant, made possible through the monetary contributions of AAEP past presidents, is awarded annually to a doctoral or residency student who has made significant progress in the field of equine health care research. Dr. Nelson was recognized during intermission of the Frank J. Milne State-of-the-Art Lecture on Dec. 9.
Researchers from Virginia Tech, Texas A&M receive 2013 EQUUS Foundation Research Fellows
Virginia Tech equine surgery resident Dr. Kendra Freeman and Texas A&M University post-doctoral research
associate Dr. Amanda-Jo Joswig received the 2013 EQUUS Foundation Research Fellows for their work to advance veterinary knowledge. Each received a $5,000 fellow during
intermission of the Milne Lecture to support their endeavors in equine research.
Dr. Freeman’s research evaluates the effect of tendon repair techniques on intrinsic tendon vasculature. Meanwhile, Dr. Joswig’s research investigates
the use of mesenchymal stem cells (MSCs) in equine corneal ulcers as well as the safety of allogeneic MSCs used subconjunctivally.
The fellows are supported in partnership by the AAEP Foundation and The EQUUS Foundation.
Kester News Hour articles available online
Equine Veterinary Journal is offering complimentary access until Feb. 3 to all of the EVJ and EVE articles discussed during the Kester News Hour on Dec. 8. The articles are available at http://bit.ly/1hYXWmm.
Kester News Hour articles may also be requested through the Texas A&M Medical Sciences Library Get It For Me service, which is a free benefit of your AAEP membership. A Get It For Me account is required and can be established at no cost. Bibliographies and instructions are available at http://guides.library.tamu.edu/aaep.
Reporting of CE credits
Convention attendees are reminded to report their continuing education credits using the CE form that was included in the packet received at registration. Attendees who have misplaced this form should contact the AAEP office at (859) 233-0147 or [email protected] to request a replacement form.
From left: AAEP Foundation Chairman Dr. Wayne McIlwraith, 2013 EQUUS Foundation Research Fellow recipient Dr. Amanda-Jo Joswig, AAEP President Dr. Ann Dwyer and EQUUS Foundation board member Dr. Rick Mitchell.
Dr. Brad Nelson, center, receives the 2013 AAEP Foundation Past Presidents’ Research Fellow from 2013 AAEP Foundation Chairman Dr. Wayne McIlwraith and 2013 AAEP President Dr. Ann Dwyer.

VI EQUINE VETERINARY EDUCATION / AE / JANUARY 2014
Nominate a distinguished researcher for the 2015 AAEP Milne Lecture
Nominations deadline is January 30
Nominations from the AAEP membership are being accepted until Jan. 30, 2014, for the 2015 Frank J. Milne State-of-the-Art Lecture.
The Milne Lecture was created in 1997 to recognize an individual with a distinguished career in research and discovery, and who has presented and published their findings in a specific area of equine health. The lecture is intended to honor the accomplishments of the presenter and bring a meaningful learning experience to the AAEP membership. The lecture is a perspective on the state-of-the-art in the presenter’s area of expertise.
The award recipient will be determined by a subcommittee of the AAEP Educational Programs Committee in February 2014 and then presented to the board of directors for approval. The selected individual will deliver their lecture and be presented with their award at the AAEP’s 2015 Annual Convention in Las Vegas, Nev.
Nominees should be an expert in their field with a track record of accomplishments and the ability to relate the topic to the audience. A detailed nomination letter is required and must include qualifications and accomplishments of the nominee.
Nomination letters for the 2015 Milne Lecture must be submitted by Jan. 30, 2014, to Carey Ross, AAEP scientific publications coordinator, at [email protected].
Dr. Sue Dyson delivers the 2013 Frank J. Milne State-of-the-Art Lecture “Equine Lameness: Clinical Judgment Meets Advanced Diagnostic Imaging.”
Thanks to the following members who volunteered time and expertise for AAEP programs during the period May-December 2013.
AAEP On Call
Dr. Larry Bramlage – Belmont Stakes on NBC from Belmont Park; Fourstardave Handicap on NBC from Saratoga Racecourse; Breeders’ Cup World Championships on NBC and NBC Sports Network from Santa Anita Park
Dr. Stephen Carr – Diana Stakes, Jim Dandy Stakes, Alabama Stakes, Sword Dancer Invitational, Bernard Baruch Handicap, Forego Stakes and Woodward Stakes on NBC Sports Network from Saratoga Racecourse
Dr. Scott Hay – Whitney Invitational Handicap on NBC from Saratoga Racecourse
Dr. Wayne McIlwraith – Breeders’ Cup World Championships on NBC and NBC Sports Network from Santa Anita Park
Dr. Scott Palmer – Preakness Stakes on NBC from Pimlico Racecourse; Hambletonian on CBS Sports Network from The Meadowlands; Adirondack Stakes and Saratoga Special Stakes on NBC Sports Network from Saratoga Racecourse; Foxwoods King’s Bishop Stakes and Travers Stakes on NBC from Saratoga Racecourse
Dr. Mary Scollay – Kentucky Derby on NBC from Churchill Downs
Ask the VetDr. Kerry Beckman – Reproduction Dr. Christina Dayton-Wall – Immunizations: Have You
Vaccinated Your Horse(s) Yet?Dr. Lydia Gray – NutritionDr. Christina Hewes – ColicDr. Rebecca Linke – Tendon and Ligament Injuries and
RehabilitationDr. Frank Reilly – Summer Eczema/Summer ItchDr. Phoebe Smith – Infectious Disease
Dentistry Short CoursesDr. Dave Bell and Dr. Roxy Bell – University of MontrealDr. Tom Daugherty and Dr. Jon Gieche – University of
GeorgiaDr. Dave Foster and Dr. Travis Boston – University of
PennsylvaniaDr. Jeff Reiswig – The Ohio State UniversityDr. Bruce Whittle – Iowa State University
Farrier Short CoursesDr. Steve O’Grady – Louisiana State University
Horsemanship Short CoursesDr. Casey Gruber and Dr. Jordan Cook – Ontario
Veterinary CollegeDr. David Hayes – Tufts UniversityDr. Joan Norton – Purdue UniversityDr. Mike Rogers – University of MissouriDr. Caroline Smith – North Carolina State University
AAEP Working For You

EQUINE VETERINARY EDUCATION / AE / JANUARY 2014 VII
Determined to raise awareness in hopes of mitigating a burgeoning and unfortunate trend, the AAEP in April 2005 initiated a dialogue among equine industry stakeholder
groups to address the plight of the unwanted horse in the United States. That dialogue – formalized as the Unwanted Horse Summit – spawned creation of the Unwanted Horse Coalition
(UHC) with a mission to reduce the number of unwanted horses and to improve their welfare through education and the efforts of organizations committed to the health, safety, and responsible care and disposition of these horses.
Placed under the auspices of the American Horse Council in June 2006, the initiative’s timing proved opportune as the issue of unwanted horses would come into sharper focus soon thereafter as a result of a combination of factors, including the economic downturn, overproduction in the breeding shed, closing of the nation’s processing facilities and high cost of euthanasia and carcass disposal.
The AAEP is a founding member – and one of 27 members in total – of the UHC and supports the coalition through annual grant funding from the AAEP Foundation, whose mission to improve the welfare of the horse meshes with that of the UHC. In fact, one of the UHC’s most visible programs, Operation Gelding, was instituted by the Foundation and continues to benefit from an annual grant specifically earmarked to the program.
Since inception of the Operation Gelding Program in 2010, support from the AAEP Foundation has helped fund the castration of 837 stallions in 28 states. Not only do the castration clinics help prevent a future generation of potentially unwanted horses, they often provide equine veterinary students with practical skills training in the procedure.
“With the support of the AAEP Foundation, the Operation Gelding Program has become an industry role model for castration grant programs and has aided in the castration of almost 1,000 stallions and helped organizations around the country host over 70 clinics in the past three years,” said UHC Director Ericka Caslin. “We are truly grateful for the continued support of the Foundation that has helped benefit so many unwanted horses and horses in need.”
Additional grant funding from the AAEP Foundation supports the UHC’s varied and ongoing efforts to fulfill its important mission.
With education as a primary focus, the UHC is an information-rich resource for horse owners and others. Its website, www.unwantedhorsecoalition.org, provides a list by
state of more than 700 facilities that accept horses as well as a directory of available resources for horse owners in need, including grant opportunities, haybanks, feedbanks, vaccination programs, castration clinics and more.
Relevant information is also disseminated through the UHC Ambassador Program, which includes approximately 150 volunteer subject matter experts
available by request to speak on the UHC’s behalf at equine events. Each ambassador is provided with a PowerPoint presentation and supplemental materials to distribute.
These materials and other brochures, flyers and documents – produced by the UHC and by its member organizations, including the AAEP – are available for free download on the UHC website or in hardcopy format. Among them is Best Practices: How Your Organization Can Help Unwanted Horses, a handbook for creation and operation of programs and activities to assist the unwanted horse based on already established and successful initiatives.
As an industry-wide response to an industry-wide issue, the UHC is making inroads into the predicament of the unwanted horse and will continue to do so with the steadfast support of the AAEP, AAEP Foundation and other concerned and committed industry organizations.
Foundation grants supporting industry efforts to alleviate the plight of the unwanted horse
Preparing for a castration at an Operation Gelding clinic held by Changing Leads Equine Rescue in Kansas City, Mo.
Unw
ante
d Ho
rse
Coal
ition

VIII EQUINE VETERINARY EDUCATION / AE / JANUARY 2014
New member and renewal donations in 2013 generate more than $21,000 for Foundation
A total of 374 AAEP members expressed their commitment to the welfare of the horse with a donation to the AAEP Foundation when renewing their annual dues or joining as a member in 2013. The AAEP Foundation thanks the following donors, who contributed $21,516 between Jan. 1 and Nov. 30, 2013.
The entirety of each gift goes directly to improve the welfare of the horse; no portion is used for administrative or fundraising costs. To donate or learn more about giving options, visit http://foundation.aaep.org.
Andrea AdamsRebecca AdkinsMaia AerniRenee Aguirre-HallJohn R. AllenderKirsten AndersonRebecca L. AndersonFrank M. AndrewsJulio S. AriasAnna M. ArimborgoJohn FG AtackLisa AtckisonChristopher Allen BaileyJames W. BaileyShannon S. BakerVincent A. BakerD. Craig BarnettRoger A. BechtelMary H. BellHendrik-Jan BergmanColleen BestMark BianchiR. Jerry BlackJames T. BlackfordTerry L. BlanchardScott BlondCeleste Boatwright
GraceJacek BobkiewiczEdward BoldtLarry A. BorgPage BouchardMarilyn Irene BoydBenjamin B. BraatJesse Scott BrandonNatalie BroomhallJesse Michael BrothersKirstin A. BubeckAnne J. BukenhoferKaren M. BulluckLinda ByerJennifer M. CardAdam N. CarrStephen CarrKathryn Allyson CarterJames P. CartnerAda CaruthersJarbas CastroCrystal ChappleCaren ChellgrenPatricia N. Chism
Katherine B. ChopeJaclyn Marie ChristakosAndrew R. ClarkDennis A. ClarkJane A. ClarkRodger ClarkChrysann CollatosCatalina Perez CompancH. Steve ConboyToby Twain ConnollyWilliam T.M. CookDane CoombsTy B. CorbiellChristine A. CornishDante CostagliolaNathalie CoteR. Reynolds CowlesRyan CoyBryant W. CraigMichal CuthbertsonPaulo Celso Da SilvaTom V. DavidEllen E. DaviesTraci Lynn DaviesEric W. DavisGeorge D. DavisShannon De ArmasInes Nicoloso De CastroRichard M. DeBowesPatricia G. Dedrick-
TerryJamie Lynn DeRoinRobert DeWardDaria Lynn DigiovanniDanielle DimonHaley A. DingfelderEnrique DominguezSharon Anne DreifusRoland C. DunavantAnn E. DwyerJanine Frances DwyerNoel DybdalAdam Charles
EichelbergerEdda C. EliassonNancy D. ElliotSteven D. EngleApril EsquivelFernando EstradaVernon Scott EvansBud Fackelman
Joanne Marie FagnouSteve G. FairbrotherDennis M. FarrellSandi FarrisLaura FaulknerJean Frances FeldmanMegan FineLeah FischerMary M. FlitnerStephanie FlowersRichard ForfaThera L. FoxBryan FraleyMichael FrederickDennis D. FrenchMichael W. GiacopuzziJocelyn D. GibsonJacqueline Danielle GilesKim Gill-FavierLyndi Liane GilliamEdward GilsleiderJudith S. GoelkelAlan A. GoldhahnRenee GolenzConstance Eileen
GormanMarta E. Granstedt-
VolkmannBarrie GrantHenry GreenwaldRichard G. GuthrieCarol A. HabigLydia Gathagan
HamiltonMary Beth HamorskiDavid HarrisKurt HarrisLaura M. HarrisKatie HayesEthan McRee HefnerNeal R. HeilmanJulie D. HendersonMartin HennFlynn Michele HenryRay A. HephnerCarlos Hernandez-
OlivaresMiles HildebrandMarcia A. HillardCorinne HillsMary Joan Hiltz
Manuel G. HimenesNicole HjelleLari Hullender HobackStephanie HobbsMichael G. HopkinsPaula Alves HorneChristina Marie HowardDavid A. HuntKate IslerBrad JackmanKaren JackmanDennis JenkinsManuel JimenezWolfgang JochleMike JohnstonCecilia JonssonFriedrich Frey JuniorAlbert KaneCrystalyn Jennifer KasaAtsushi KatoAlessandra Vittoria
KeenanAudrey A. KellemanEileen KellnerHarold M. KempHeather KerrLogan KingSteven Andrew KingRoy C. KipperKathleen T. KleinGaston KojusnerDarrel R. KramerMegan Downey KraskiKatsumi KuribaraSusy LangePeter J. LangleyJeffery L. LapointAmy McCanless LawsonBruce D. LeeAmy R. LeibeckKathleen Alecia LennonHannah Rani LeventhalRebecca B. LillardCassandra L. LodgeKate J. LombardiJohanne LongtinTroy LooperJoaquin Lopez de AldaNicholas G. LoutsionBrad D. LuckenbillJoseph Everett Lynch
Marianne MackayMargo MacphersonGail MahnkeCassandra MahoneyNicole R. MailhotJoseph MaloneJill Felix MarquezMark J. MartinelliKimberly Anne MayMark B. MayoE. Scott McAllisterMarc R. McCallJennifer McDonaldVenaye P. McGlashan-
ReeceCarol McLeodPatrick Joseph
McMahonNorifum MeguroLindsay MeharryElizabeth MetcalfGeert MeursingJacob MeursingJoseph Frank MigliacciShane MillerSylvia A. MillerJill A. MixerPercy ModomoRomy G. ModomoEddie L. MooreEvan A. MooreJames N. MooreMakensie R. MooreDean D. MorganKenton MorganRobin MundtSteven MurphyHiroshi NagataSteve NaileJimmy C. NashJoseph A. NebzydoskiGretchen NelsenC. Richard NelsonHeather E. NemanicCharlotte M. NewellRobert L. NewmanKaisa Helena NivolaKen NoguchiKaren A. NyropAlison Herr OliverWilliam Edgard Oppen

EQUINE VETERINARY EDUCATION / AE / JANUARY 2014 IX
Foundation donors, continued
Jane G. OwensBarbara T. PageRichard PankowskiDana PantanoErnest H. PattersonWilliam G. PaullSarah Kate PedersenRyan PennoDuncan PetersSarah T. PetersKimberly M. PetersonLarry A. PickeringRob PilsworthFederico Manuel PitaCandace K. PlatzThierry G. PoignonJames C. PrendergastCynthia PrestageMichael A. PrichardReal ProvencherMichael PuckettTricia Marie PughTamara L. QuaschnickMauro QuercioliDoug QuesnelSuzanne Suster QuinnAmy Rabanal
Sharanne RaidalPeter C. RakestrawMatt T. RandallRachel Morgan ReedyElizabeth ReeseMark T. ReillySarah E. ReynoldsMark RickRebecca Elaine RifkinMelinda N. RocheMaurilio RosaTerry W. RuchDennis A. RuksznisAndrea L. RussellMarvin E. RydbergJuan SamperMacarena SanzDebra SauberliBob SaundersWilliam J.A. SavilleRobert C. SchmittHarvey SchneiterElizabeth L. ScholtzJos SchreursAnne SchwartzCharles F. ScogginGregg Scoggins
David ScovilleRandal SebringNicole SeehaferHiroyuki SembaKirk A. ShinerJoseph ShrackMichael SigmanErnest Paul SilviaDebra SimeRena Rachel SingerErin Hardy SlaughterJohn C. SmithKelly SmithSuzanne J. SmithCheryl D. SofalyLouis T. SolonynkaTamara SorleyKara Lynette SpillmanMax L. SponsellerMichael T. StabbeTed Stanley StashakMeredith A. SteudleSusan M. StoverDevon W. StricklandSylvie SurprenantWilliam E. SwyersCathe Tallarico
Nicholas TallaricoJean TanguaySusan M. TanhauserD. Scott TaylorJames R. TaylorShelley May TeakleMary A. ThomasKirste TimmNathalie TokateloffMasataka TominariJosie L. Traub-DargatzKirsten Ann TraulToni L. TregoAngel Carlos Antonio
TrioniGayle W. TrotterDiane TroyerRobert TugelLeah TurnerLeslie TurnerMargaret Miller TurpinShigeto UshiyaPeter W.C.M. Van OijenMarco Van SchiePaul Rene Van WeerenTaeke Van ’t RietHenry M. Vaupel
J. Donald ViceCarol VischerWilliam C. WaferJohn WaltersJeffrey WarrenKelly Ann WasylciwAmanda Ruth WatkinsKathleen WeatherallEmily WeaverErika WeberWill Clay WernerShannon Sarah
WhatmanSusan L. WhiteJami L. WhitingCarly R. WhittalGlen Earl WilkinsonMichael D. WilliamsAmanda WilsonDavid A. WilsonJulia WilsonWilliam David WilsonA. Barry WoodJeanine A. WoodsKosei YamagiwaRyan R. ZimmermanDavid G. Zipf
AAEP Touch program helps you boost your clients’ satisfaction with your services
What if you had a blueprint for delivering the veterinary care and services your clients most desire?
During the 2013 Annual Convention, the AAEP unveiled this blueprint – a program exclusively for AAEP members that will help equine veterinarians provide better care to patients, develop long-term relationships
with clients, and deliver the services horse owners and trainers most value.
AAEP Touch: Tools to Connect to Your Clients and Their Horses was developed from market research
conducted with more than 6,100 horse owners, trainers, breeders and farm managers in the United States. An independent market research firm conducted the study in fall 2012.
The important findings from the research have been packaged into a comprehensive website of tools and resources that will help you understand your clients better than you already do.
At touch.aaep.org, you will find the Top 10 lessons for your practice; profiles of 13 different client types based on the attributes they value most in veterinary care; videos and tools to help you perform a client-focused examination; client education materials on important topics that emerged from the research; and much more.
Explore touch.aaep.org today!
X EQUINE VETERINARY EDUCATION / AE / JANUARY 2014
Being an AAEP Educational Partner is just one of the ways IDEXX Laboratories supports equine care and the practitioners who provide it.
Our extensive range of solutions includes innovative diagnostic tests, expert consulting, digital radiography and advanced patient-monitoring technologies. Each product or service is designed to help equine practitioners meet their clients’ need for faster, more accurate diagnoses.
The IDEXX EliteVisionTM Digital Imaging System, for example, instantly produces images with outstanding sharpness and clarity in the field or in-hospital. The IDEXX VetLab® integrated suite of in-house analyzers produces a comprehensive patient picture in just minutes. The suite includes the Catalyst Dx® Chemistry Analyzer, featuring the Equine 15 CLIP of 13 essential chemistries, along with 2 ratios for screening and identifying equine health concerns. Practitioners can turn to the ProCyte Dx® Hematology Analyzer for precise and comprehensive hematology results, including flags for banded neutrophils and equine fluid analysis. And for fast, critical answers in the field, there’s the SNAP® Foal IgG Test.
For routine and advanced testing, or case consultations, equine practitioners can rely on our local network of IDEXX Reference Laboratories. IDEXX provides exclusive equine advanced testing protocols, including the Comprehensive Equine Respiratory RealPCR™ Panel, which lets veterinarians submit one sample to test for 10 pathogens: equine rhinitis A and B viruses, equine herpesvirus types 1, 2, 4 and 5 and equine adenovirus, as well as Streptococcus equi subsp. equi and equine influenza virus, with the option to add a test for equine arteritis virus. They also offer the new Strangles RealPCR™ Screen, an economical way to test for the three pathogens that can cause Strangles or Strangles-like disease; and the Equine Diarrhea RealPCR™ Panel, which uses just one sample to test for 10 gastrointestinal pathogens for more focused treatment decisions.
IDEXX is committed to delivering solutions that protect the welfare of horses and support those who care for them. For the latest information on IDEXX diagnostics, go to idexx.com/equine.
AAEP Educational Partner Profile: IDEXX Laboratories
The AAEP welcomes new members and congratulates recent graduates
NEW MEMBERS:Graham J. Adams, BVSc,
NSW, AustraliaRoberto Ragni Alunni, DVM,
Dubai, United Arab EmiratesJonit G. Barsky, DVM,
Waterbury Center, VTNicola Cribb, MA, Diplomate,
Guelph, ON, CanadaDarlene Donszelmann, BSc,
DVM, Olds, AB, CanadaJarred Clayton Forrest, DVM,
Surprise, AZJames W. Marmion, BSc, BVM,
Versailles, KYKevin Martens, DVM,
Tillamook, ORJennifer Charlotte Pond,
St. Paul, MNKristin E. Richwagen, DVM,
Ravena, NYJulia Roque, DVM, Peotone, IL
RECENT GRADUATES:Travis Beasley, DVM,
Whitesboro, TXShannon Brown, DVM,
Corona, CABelinda Buchholz, DVM,
Bend, ORChad Calice, DVM, Pittston, PAMadison Taylor Cloninger,
DVM, Fort Collins, COStephanie Dam, BSc,
Dundas, ON, CanadaIan Frank Devick, DVM,
Littleton, CORebecca Jean Domenigoni,
DVM, Lockeford, CAJenna K. Donaldson, DVM,
Sherwood Park, AB, CanadaMegan Nicole Eckert, DVM,
Edmond, OKKyle Fisk, DVM, Micanopy, FL
Kristen Hampshire, DVM, Littleton, CO
Sophie Michelle Heikkila, DVM, Plympton, MA
Sandra Viviana Hernandez, DVM, Mexico City, Mexico
Jessica Jo Huwa, DVM, Prosperity, SC
Russ R. Lapierre, DVM, Mendenhall, PA
Katie Lewis, DVM, Bexley, OHVictoria Martin, DVM,
Champaign, ILJenn Megens, DVM,
Uxbridge, ON, CanadaEric Allen Metteauer, DVM,
Beaumont, TXKrystle Ocull, DVM,
Bellflower, CAAlexander William Parkes,
DVM, Edinburgh, Scotland
Lisa Rincon, DVM, Davis, CAMarcos Vinicius Dias Rosa,
DVM, Niteroi, Rio de Janeiro, Brazil
Dana Shackelton, DVM, Oakdale, CA
Susan Elizabeth Shaffer Sookram, DVM, Albuquerque, NM
Shane David Smith, DVM, Nampa, ID
Alyssa Struzyna, VMD, Rhinebeck, NY
Kelly Frances Warner, DVM, Weatherford, TX
Annie F. Williams, DVM, Bloomsbury, NJ

EQUINE VETERINARY EDUCATION / AE / JANUARY 2014 XI
The service and stewardship of the AAEP’s many dedicated volunteers is the cornerstone of the association’s ability to improve the health and welfare of the horse, further the professional development of its members and provide resources and leadership for the benefit of the equine industry. Thanks to the following members whose volunteer service on the board of directors or on a particular council or committee concluded in 2013.
Board of DirectorsDr. Benjamin EspyDr. Brad JackmanDr. John MitchellDr. Eric PetersonDr. Emma Read
Foundation Advisory CouncilDr. Kathleen AndersonDr. Jerry BlackDr. Kathy CarterDr. Tom LenzDr. Wayne McIlwraith (chair)Dr. Bill Rood
Educational Programs CommitteeDr. George MartinDr. Steve O’GradyDr. Andy ParksDr. Kim Sprayberry
Educational Programs Committee 2013 Reviewer ListDr. Rob Franklin Dr. David Frisbie Dr. Brad Jackman
Finance & Audit CommitteeDr. Jeff Blea
Leadership Development CommitteeDr. Kathleen AndersonDr. Kenton MorganDr. Mark RickDr. Hannah Wellman
Nominating CommitteeDr. Brad JackmanDr. Deb SellonDr. Nat White
Professional Conduct & Ethics CommitteeDr. Jeff BerkDr. Miles HildebrandDr. Terry SwansonDr. Kim Voller
If you desire to have a larger voice in the AAEP by sharing your time and expertise on behalf of the horse and the association, the AAEP would love to hear from you. Simply log into www.aaep.org and click “Volunteer Opportunities” on your dashboard. Select from among the many volunteer opportunities listed on the Volunteer Interest Form, complete the remainder of the form and click “Finish.”
AAEP recognizes outgoing board, council and committee members
AAEP members and others are invited to submit educational papers for consideration for presentation during the AAEP’s 60th Annual Convention, Dec. 6-10, 2014, in Salt Lake City, Utah.
Scientific papers, “how-to” papers, review papers, abstracts ≤ 250 words and The
Business of Practice papers are eligible for consideration. For
complete considerations and ethical guidelines, visit www.aaep.org.
As an aid to private practitioners, first-time authors or members seeking guidance with their submission, the AAEP offers a mentorship program in which experienced presenters are available to provide advice and direction. However, mentors are not responsible for rewriting or selecting material. To access a list of available mentors or view sample paper submissions, visit www.aaep.org.
All papers must be submitted at http://aaep2014.abstractcentral.com by March 17, 2014, 3:00 p.m. ET. Authors should visit the site in advance to set up a profile and provide paper and author information before uploading the paper when it is complete. Contact Carey Ross, scientific publications coordinator, at [email protected] with questions concerning the Annual Convention and educational paper submission.
Present an educational paper during the 2014 Annual Convention
Paper submission deadline is March 17

February 6-8, 2014
16th Annual
Resort Symposium
Gran Melia Golf Resort
Rio Grande, Puerto Rico
July 20-22, 2014
Focus on the Sport Horse
Louisville, Kentucky
September 11-13, 2014
Focus on the First Year of Life
Phoenix, Arizona
December 6-10, 2014
60th Annual Convention
Salt Lake City, Utah
AAEP Meetings and Continuing Education
XII EQUINE VETERINARY EDUCATION / AE / JANUARY 2014
For more information, contact the AAEP office at (859) 233-0147 or (800) 443-0177 or online at www.aaep.org.
Membership Benefits
AAEP group purchasing program qualifies your practice for substantial savings
As an AAEP member, you are eligible for substantial savings on supplies and services to operate your veterinary practice. The AAEP and The Veterinary Club have partnered to provide all AAEP members with access to the industry’s most robust catalog of contracts offering substantial, quantifiable savings. Discounts are available at such companies as Verizon, UPS, FedEx, Staples, OfficeMax, Office Depot and Sherwin-Williams.
Participation in the group purchasing program is free with your AAEP membership.
To participate, AAEP members must register at www.theveterinaryclub.com. For more information about this
membership benefit, contact Nick Altwies, membership services coordinator, at (859)
233-0147 or [email protected].
Request research articles through the Texas A&M Medical Sciences Library
Your AAEP membership enables you to access valuable research articles from the Texas A&M Medical Sciences Library. To request mediated database searches and have documents delivered to your practice using the library’s Get It For Me service, go to http://getitforme.library.tamu.edu/msllocal and log in.
If you are a first-time user, you must register with your e-mail address and a password. Get It For Me will encrypt your password so it remains secure. Only you will know your password. Search results and articles will be delivered to your inbox within two business days.
AAEP Rounds a convenient forum to discuss specific veterinary topics
You don’t have to work through the challenges of equine veterinary practice alone. You can get answers and advice from your fellow AAEP members by joining the interactive discussion taking place year-round in any of 15 AAEP Rounds.
Rounds are e-mail commu-nities centered on a specific topic and are an ideal way to exchange ideas and share expertise with AAEP members around the world. You can subscribe to the following Rounds:
In addition, you may also join the AAEP’s General Discussion List, which is open to a wide variety of topics of interest to AAEP members. For more information or to join a Round, log into www.aaep.org and click the “My AAEP” button.
Business EducationComplementary &
Alternative (Integrative) Medicine
DentistryEnglish Sport HorseInfectious DiseaseNew PractitionersParenting
PodiatryPublic AuctionPurchase ExamRacingReproduction/PerinatologySolo PractitionerStudentWestern Performance
Horse

SENIOR LIVING. REDEFINED.
©2013 Cargill, Incorporated. All Rights Reserved.
Exclusive Nutri-Bloom AdvantageTM increases fiber digestion up to 15% for better health and bloom.
FROM DENTAL TO DIGESTION ISSUES, NEW SAFECHOICE® SENIOR RESETS EXPECTATIONS FOR WHAT HORSE FEED CAN BE.Only SafeChoice® Senior has NutriBloom Advantage,TM which increases fiber digestion up to 15% for better health and bloom. Prebiotics and probiotics further aid in nutrient digestion and digestive health. And for horses with dental issues, SafeChoice® Senior can make a QuickMashTM in just three minutes. So you can confidently recommend it to clients with senior horses. Visit SafeChoiceFeed.com.

To be successful in today’s veterinary market you need
satisfied clients and a profitable practice.
Here’s how we can help.
Developed by:
Nutritional Supplements
EVE2013-11
Developed to enhance client satisfaction and increase yourprofitability.
For more information, call 859-873-2974 or visit KPPvet.com.
Available only through
licensed veterinarians.
Peer reviewers 2013
The following colleagues gave their time to peer review between November 2012 and October 2013, for which we arevery grateful.
Adams, StephenAinsworth, DorothyAllen, AndrewAlmeida, JulianaAndrews, FrankArcher, DebbieAudigie, FabriceBall, BarryBarakzai, SafiaBardell, DavidBarr, AlistairBarr, ElizabethBarton, AkiBathe, AndyBergman, ErikBertone, JosephBidwell, LoriBladon, BruceBlissitt, KarenBooth, ToddBowen, MarkBrearley, JacquelineBrooks, DennisCampbell, MadeleineCanisso, IgorCarmalt, JamesCaron, JohnCary, JulieChaffin, KeithCillan-Garcia, EugenioCoenen, ManfredColles, ChrisConwell, RachaelCooke, CharlesCoomer, RichardCoudry, VirginieCoumbe, KarenCox, AlistairCrabtree, JamesCramp, PhilDakin, StephanieDel Piero, FabioDenoix, Jean-MarieDivers, TomDixon, Paddydu Toit, NicoleDugdale, AlexDurham, AndyDwyer, AnnElce, YvonneEnsink, Jos
Epstein, KiraEsteller-Vico, AlejandroFielding, C. LangdonFischer, Jr., AndrewFischer, TedFiske-Jackson, AndrewFjordbakk, CathrineFraipont, AudreyFrank, NicholasFranklin, SamanthaFreeman, DavidFubini, SusanFurr, MartinGarrett, KatherineGaughan, EarlGerard, MathewGerlach, KerstinGilger, BrianGilkerson, JamesGrant, BarrieGreet, TimGrint, NicolaHackett, RichardHaga, HenningHaggett, EmilyHahn, CarolineHallowell, GayleHanson, ReidHardy, JoanneHassel, DianaHaussler, KevinHawkins, JanHead, MarcusHepburn, RichardHockenhull, JoHolbrook, ToddHolcombe, SueHoupt, KatherineHurcombe, SamuelIrby, NitaIvens, PhilipJohns, ImogenJohnson, AmyJohnson, PhilipJohnson, ShyloJones, RonKnottenbelt, DerekKnowles, EdwardLabelle, AmberLabens, Raphael
Lavoie, Jean-PierreLeBlanc, MichelleLescun, TimothyLester, GuyLindegaard, CasperLischer, ChristophLove, EmmaLove, SandyMacKay, RobertMartinelli, MarkMatthews, AndyMazan, MelissaMcCluskey, BrianMcDonnell, SueMcGorum, BruceMcIlwraith, WayneMilne, ElspethMilner, PeterMohammed, HussniMorello, SamanthaMorley, PaulMueller, P.O. EricMuir, WilliamMunroe, GrahamNieto, JorgeNolen-Walston, RoseNout, YvetteOlsen, EmilPalmer, JonathanPascoe, RobPatterson-Kane, JanetPearce, ChrisPearson, GeoffPease, AnthonyPerkins, GillianPirie, ScottPollock, PatrickProudman, ChrisPuchalski, SarahPusterla, NicolaRendle, DavidRicketts, SidneyRiggs, ChristopherRijkenhuizen, AstridRobert, CélineRoberts, VeronicaRöcken, MichaelRogers, PhilRuggles, AlanRush, Bonnie
Sandersen, CharlotteSantschi, ElizabethScholes, SandraSchott, HaroldSchramme, MichaelSchumacher, JamesSchumacher, JohnScott, DannySenior, MarkSherlock, CeriSinger, EllenSlocombe, RonSlone, DonnieSlovis, NathanSmith, KatieSmith, KenSmith, MatthewSmith, MeredithSmith, SionaghSnalune, KatieSouthwood, LouiseSponseller, BrettStewart, AllisonStick, JohnSullins, KenSuthers, JoannaSutton, DavidTamzali, YoussefTaylor, AlanTaylor, PollyTextor, JamieTimoney, JohnTimoney, PeterToth, FerencTownsend, NeilTremaine, HenryTucker, RussValentine, Bethvan Loon, ThijsVerwilghen, DenisVoute, LanceWeese, ScottWeller, RenateWhite, NathanielWilson, GaryWitte, StefanWitte, ThomasWoodford, NigelWoodie, BrettWright, Ian
1
© 2013 EVJ Ltd
EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

Highlights of recent clinically relevant papers
Sesamoidean approaches for digital flexortendon sheath synoviocentesis and injectionRichard Rocconi and Sarah Sampson from the Mississippi StateUniversity, USA, have recently published their study comparingbasilar and axial sesamoidean approaches for digital flexortendon sheath (DFTS) synoviocentesis and injection in horses.
Accurate synoviocentesis and injection of the DFTS areimportant procedures for diagnosis and treatment of injuryassociated with this structure in horses. This study aimed todefine a method for the basilar sesamoidean approach (BSA)to the DFTS and compare it with the axial sesamoideanapproach (ASA) for DFTS synoviocentesis and injection.Twelve healthy adult mares with no lower limb abnormalitieshad one forelimb and one hindlimb assigned to each DFTSapproach. All procedures were performed in standingsedated horses.
Median time for injection was significantly shorter for theBSA, compared with the ASA. The median number of times theneedle was redirected was also significantly less for the BSA.Odds of obtaining synovial fluid via the BSA were 5.7 times asgreat as for the ASA. Successful injection of contrast materialinto the DFTS did not differ significantly between methods.
The authors concluded that the BSA was a useful methodfor DFTS synoviocentesis in the fore- and hindlimbs of standingsedated horses and was superior to the ASA in most aspects.This approach to the DFTS should be considered when DFTSinjection or synovial fluid retrieval is desired, particularly inhorses with minimal DFTS effusion.
Melanoma in grey Quarter HorsesR. Teixeira and colleagues in the USA have recently reportedon coat colour genotypes and risk and severity of melanomain grey Quarter Horses (QH).
Both greying and melanoma formation in horses haverecently been linked to a duplication in the STX17 gene. Thisduplication, as well as a mutation in the ASIP gene thatincreases MC1R pathway signalling, affects melanoma riskand severity in grey horses. This study was performed todetermine if melanoma susceptibility in grey QH is lower thangrey horses from other breeds because of decreased MC1Rsignalling resulting from a high incidence of the MC1R chestnutcoat colour allele in the QH population. Blood or hair rootsamples were collected from 335 grey QH with and withoutdermal melanomas for DNA extraction and genotyping forSTX17, ASIP and MC1R genotypes. Age, sex, and externalmelanoma presence and grade were recorded.
Melanoma prevalence (16%) and grade (0.35) in this QHcohort was lower than that reported in other breeds. Agewas significantly associated with melanoma prevalenceand severity. No significant effect of MC1R genotype onmelanoma prevalence or severity was identified. An effect ofASIP genotype on melanoma risk was not detected. Low STX17homozygosity precluded evaluation of the grey allele effect.The authors concluded that melanoma prevalence andseverity is lower in this population of grey QH than has beenreported in other breeds. This could be because of theinfrequent STX17 homozygosity, a mitigating effect of theMC1R mutation on ASIP potentiation of melanoma, other
genes in the MC1R signalling pathway, or differences in breedgenetic background.
Comparison of anastomosis methods followingproximal ileal resectionThis retrospective study by S. Stewart and colleagues from theUniversity of Pennsylvania, USA, compares complications andsurvival rates with three different anastomosis methodsfollowing proximal ileal resection; namely jejunojejunostomy,jejunoileostomy and jejunocaecostomy.
Medical records for 112 horses were reviewed and, as thiswas a retrospective study, the surgical procedure was notrandomised but was based on lesion type and surgeonpreference. Short-term outcome was measured by survival todischarge and was not different between groups. Those whounderwent a jejunoileostomy were more likely to have a repeatceliotomy during the period of hospitalisation. Long-termfollow-up was measured using a Kaplan–Meier estimate ofsurvival function and found that horses who had undergone ajejunocaecostomy were more likely to have repeated episodesof colic and were less likely to survive long-term than those whohad undergone one of the alternative procedures. Survivalfollowing jejunoileostomy at one-year follow up was 100%,compared with 97% for jejunojejunostomy and 83% forjejunocaecostomy. The authors also noted that anastomosispattern may reflect outcome, with a double layer appositionalpattern performing best although numbers were too low to beof statistical significance.
The authors concluded that following proximal ilealresection jejunoileostomy may be the anastomosis techniqueof choice due to better long-term survival rates and lowerincidence of colic in the long term.
Mesenchymal stem cell administration methodsIn this study, J.M. Trela and colleagues from the University ofCalifornia, USA, used scintigraphy to compare intra-arterialinjection and distal intravenous regional limb perfusion foradministration of mesenchymal stem cells to the equine foot.
Mesenchymal stem cells have recently been administeredvia a regional limb perfusion; however, previous studies havefound that intravenous administration resulted in poor uptakeand intra-arterial injection resulted in thrombosis in some cases.This study used labelled mesenchymal stem cells andcompared intravenous and intra-arterial administration, withuptake being measured by scintigraphy. Six horses weresubjected to general anaesthesia and labelled mesenchymalstem cells were administered via a catheter placed in themedian artery of one forelimb, followed by the lateral palmardigital vein in the opposite forelimb. A tourniquet was usedonly for intravenous administration. Mesenchymal stem cellswere found to be retained in the distal limb despite not using atourniquet for intra-arterial injection. Contrary to previousstudies, there were no thrombi detected ultrasonographicallyfollowing the procedure for intra-arterial injection; however, inthe limb where the intravenous technique was used, thrombiwere detected in 4 of the 6 horses.
The authors concluded that the tourniquet and resultinghaemostasis was sufficient to create subclinical thrombi. The
2
© 2013 EVJ Ltd
EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

intra-arterial technique resulted in a more homogenousdistribution of labelled mesenchymal stem cells than theintravenous technique, and both techniques resulted in asimilar uptake when measured at 24 h post injection.
Doxorubicin chemotherapy in horsesThe aim of this study by A.P. Théon and colleagues from theUniversity of California, USA, was to determine dose-limitingtoxicosis (DLT) and maximum tolerated dose (MTD) ofdoxorubicin in tumour-bearing horses.
Seventeen horses with 34 localised or multicentricadvanced tumours were treated using a two-stagedose-ranging design involving intrapatient and interpatientdose escalation. Six treatment cycles were given at 3-weekintervals with dosages ranging from 40 to 85 mg/m2. Clinicalsigns were evaluated.
Total doses ranged from 1127 to 2900 mg in 12 horsesthat completed the assigned treatment protocols. The MTDwas 75 mg/m2. Hypersensitivity reactions and neutropeniawere dose limiting. Hypersensitivity was dose-dependentbut schedule invariant. Neutropenia was dose- andcycle-dependent but dose-escalation schedule invariant.Cardiotoxicity was not observed.
The authors concluded that the recommended dosageof doxorubicin to treat horses is 70 mg/m2 given at 3-weekintervals as single agent. Adjunctive treatment withantihistamines and nonsteroidal anti-inflammatory drugs isrecommended to control hypersensitivity.
Equine exuberant granulation tissue andhuman keloidsIn this study, C. Theoret and colleagues in Canada andthe USA compared histopathological features of afibroproliferative disorder in horses (exuberant granulationtissue) and humans (keloid).
Archival tissue samples of exuberant granulation tissue(EGT) and keloid were used for this study. After automatedhaematoxylin and eosin, histochemical (Gomori trichrome,Verhoeff-van Gieson elastin) and immunohistochemical(vimentin, α-smooth muscle actin, CD34, CD68, CD117)stainings, tissue sections were evaluated using asemi-quantitative grading scale for presence or absence ofulceration, keloidal collagen, myofibroblasts and elastic fibresas well as degree of inflammation, fibrosis, vascularity andorientation of collagen fibres.
Superficial dermis and deep dermis of both horses andhumans had increased numbers of haphazardly orientedthickened collagen fibres; however, only keloids contained‘keloidal’ collagen. Fibroblast numbers were markedlyincreased in both groups but only EGT had myofibroblasts.Minimal vascularity was observed in the deep dermis of bothgroups. The superficial dermis in EGT was characterised bysmall vessels within immature granulation tissue. Macrophagesand mast cells were infrequently found in both groups butpolymorphonuclear cells were markedly increased in EGT.
Humans and horses are the only mammals known tonaturally develop excessive granulation during woundhealing; however, similarities and differences betweenfibroblast populations and associated collagen have not beenreported. Inflammatory response may contribute to observeddifferences in the cellular populations, with EGT possessingmarkedly increased myofibroblasts, small vessels and acute
inflammatory cells compared with keloids. Further work iswarranted to develop common treatment strategies for thesefibroproliferative conditions.
Characteristics of the normal equine proximalsuspensory ligamentIn this study, N. Werpy and colleagues in the USA and Francecompared the use of standard ultrasonography, anglecontrast ultrasonography, magnetic resonance imaging (MRI)and histology for identification of the anatomic characteristicsof the normal equine suspensory ligament in the forelimb.
Horses free from forelimb lameness with no palpableabnormalities in the region of the suspensory ligament wereincluded in this study. The proximal suspensory ligaments in 20forelimbs were examined using the standard ultrasoundtechnique, angle contrast ultrasound technique and MRI,followed by histological evaluation. Total transverse(cross-sectional) area of the proximal suspensory ligament wasestimated using standard ultrasound and angle contrastultrasound techniques, MRI and histological sections for thefollowing parameters: total area of the ligament, ligamentfibres, muscle and fat. The proximal suspensory ligament lobesize and tissue distribution were compared and subjectivelygraded for asymmetry. Subjectively, angle contrast ultrasoundtechnique improved differentiation of fibres from theremaining tissue types and allowed identification of theperipheral ligament margin. There was no significantdifference in asymmetry scores between modalities. Theasymmetry scores of the right and left forelimbs weresignificantly different with both ultrasound and MRI, based onthe level of measurement. The angle contrast ultrasoundtechnique has limitations compared to MRI. However, itprovides additional diagnostic information that is not availablewith the standard ultrasound technique.
S. WRIGHTEVE Editorial Office
ReferencesRocconi, R.A. and Sampson, S.N. (2013) Comparison of basilar and axial
sesamoidean approaches for digital flexor tendon sheathsynoviocentesis and injection in horses. J. Am. Vet. Med. Assoc. 243,869-873.
Stewart, S., Southwood, L.L. and Aceto, H.W. (2013) Comparison ofshort- and long-term complication and survival followingjejunojejunostomy, jejunoileostomy and jejunocaecostomy in 112horses: 2005-2010. Equine Vet. J. Epub ahead of print10.1111/evj.12143.
Teixeira, R.B., Rendahl, A.K., Anderson, S.M., Mickelson, J.R., Sigler, D.,Buchanan, B.R., Coleman, R.J. and McCue, M.E. (2013) Coat colorgenotypes and risk and severity of melanoma in gray quarter horses.J. Vet. Intern. Med. 27, 1201-1208.
Théon, A.P., Pusterla, N., Magdesian, K.G. and Wilson, W.D. (2013) PhaseI dose escalation of doxorubicin chemotherapy in tumor-bearingequidae. J. Vet. Intern. Med. 27, 1209-1217.
Theoret, C.L., Olutoye, O.O., Parnell, L.K. and Hicks, J. (2013) Equineexuberant granulation tissue and human keloids: A comparativehistopathologic study. Vet. Surg. 42, 783-789.
Trela, J.M., Spriet, M., Padgett, K.A., Galuppo, L.D., Vaughan, B. andVidal, M.A. (2013) Scintigraphic comparison of intra-arterial injectionand distal intravenous regional limb perfusion for administration ofmesenchymal stem cells to the equine foot. Equine Vet. J. Epubahead of print 10.1111/evj.12137.
Werpy, N.M., Denoix, J.M., McIlwraith, C.W. and Frisbie, D.D. (2013)Comparison between standard ultrasonography, angle contrastultrasonography, and magnetic resonance imaging characteristicsof the normal equine proximal suspensory ligament. Vet. Radiol.Ultrasound 54, 536-547.
© 2013 EVJ Ltd
3EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

Editorial
EVE and EVJ online collection of equine endocrinology: Recentand future directions; a great start but still a long way to go
This month, Equine Veterinary Education and Equine VeterinaryJournal have combined forces to create a free onlinecollection of our recent articles on equine endocrinology. Thisinitiative has been made possible with the support of the BritishEquine Veterinary Association Trust, and we are extremelygrateful to Professor Nick Frank and Professor Philip Johnson,who have served as guest editors for this collection.
Equine endocrinology is a fast-moving field; in anintroductory editorial, Philip Johnson, writing with ProfessorSojka-Kritchevsky, reflects on the pace of progress that hasgenerated a vast number of publications in the last decade(Sojka-Kritchevsky and Johnson 2014). The online collectionencompasses a comprehensive range of topics within the fieldof endocrinology and includes authoritative review articles oninsulin dysregulation (Frank and Tadros 2014), glucocorticoidsand laminitis (Cornelisse and Robinson 2013) andparaneoplastic syndromes (Axiak and Johnson 2012).
Pituitary pars intermedia dysfunction (PPID) (McGowanet al. 2013a) and equine metabolic syndrome (Frank andTadros 2014) are both associated with insulin dysregulation andare now recognised as important and common problems inequine medicine that affect the health and well-being ofmany horses and ponies globally. Both become extremelysignificant due to their link with recurrent laminitis, which raisestheir impact in terms of both morbidity and mortality (Tadrosand Frank 2011). The exact mechanisms that link insulin,glucocorticoids, lipid metabolism and inflammation,endothelial function and the laminae remain to be clarified(Sojka-Kritchevsky and Johnson 2014), but the online collectionhighlights several studies that represent important pieces of thisjigsaw (Tóth et al. 2010; Venugopal et al. 2011; Borer-Weir et al.2013; Burns et al. 2013; Gauff et al. 2013; Dunkel et al. 2014).
Current best practice for management of equinemetabolic syndrome is outlined by Professors Nick Frank andRay Geor in this month’s issue of Equine Veterinary Education(Frank and Geor 2014). The first goal of management is toinduce weight loss, and helpful and explicit guidelines fordesigning diets for obese equids are provided. There is littledoubt that exercise together with dietary management(Hudson et al. 2012) can reduce the clinical signs and indicesof inflammation in equine metabolic syndrome (Hudson et al.2012; Menzies-Gow et al. 2013; Frank and Geor 2014); however,further studies are needed to quantify the efficacy of thesemanagement changes on long-term outcomes.
In cases that are refractory to this approach, metformin(Rendle et al. 2013) or levothyroxine (Frank and Geor 2014)may be helpful. However, questions remain regarding the mosteffective medication, if any, for management of insulindysregulation. It seems reasonable to postulate that removalor control of the underlying causes will be more rational thansimply treating the effects, and it is essential that horse-ownersunderstand that with sufficient effort on their part, equineobesity can be tackled (Owers and Chubbock 2013).
The online collection includes several studies addressingthe diagnosis of PPID, and in particular, the value of plasmaadrenocorticotropic hormone (ACTH) when interpreted with
seasonally adjusted reference ranges is discussed by severalauthors (Copas and Durham 2012; McGowan et al. 2013b;Rendle et al. 2014); this is advocated by Professors Frank andGeor as the most readily accessible test for monitoring PPIDcases in a field setting, although the thyroid-releasing hormonestimulation test is more sensitive and therefore has advantagesin confirmation of diagnosis (Frank and Geor 2014).
There are some significant problems emerging with theway that horse-owners interpret the information that can begleaned from screening horses for PPID with the plasma ACTHassay. Perusal of the extremely popular and highly influentialHorse and Hound forum in the UK (http://www.horseandhound.co.uk/forums/) on 21 October 2013 reveals some interestingstrands on this topic. In a query entitled ‘Cushings, how highcould a false positive be?’ a horse owner outlines her concernas follows:
Had vet out for routine stuff the other day and decided toget a mare tested for Cushings purely because it was freeand she is in her 20’s. She doesn’t show any outward signsof Cushings. The result came back 119. Could this be a falsepositive or a natural spike or is it too high to be false?
In reply, another forum user describes some typical clinicalsigns of PPID, but nevertheless encourages treatment in theabsence of any other clinical evidence of a problem, offeringthe following in response:
ACTH levels are naturally higher at this time of year fornormal horses but for Cushings horses the levels go quite abit higher. Some horses hardly show any signs of Cushingsand the first sign can be an attack of laminitis. . .when minewas first diagnosed she had a thick coat which didn’t [sic]shed properly and fat pads above her eyes and quarters,her level was 172. . .so your [sic] may be at the beginningof Cushings and it may be worth putting her on themedication to control it and then getting her tested againto see if it has made a difference. Unfortunately themedication is quite pricey but you may find she only needsa low dose.
Pituitary pars intermedia dysfunction is aneurodegenerative disorder, and current knowledge on itspathogenesis is discussed in detail by Professors Sojka-Kritchevsky and Johnson in their introduction to the onlinecollection published in this month’s issue of Equine VeterinaryJournal (Sojka-Kritchevsky and Johnson 2014). The odds ofdeveloping clinical signs associated with PPID increase byapproximately 20% per year in horses over 15 years of age. Theprevalence of clinical signs in a group of Australian horses was21.5% (McGowan et al. 2013a). The prevalence of clinical signsin horses younger than 15 years of age has not been reportedbut, while there is little doubt that clinical PPID can occur inyounger horses, it seems reasonable to speculate that theprevalence is lower than 20%. The studies on use of plasmaACTH assays for diagnosis of PPID suggest that the sensitivityand specificity are very satisfactory in autumn, but only around80% in other seasons. Studies on the sensitivity and specificity of
4
© 2013 EVJ Ltd
EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

plasma ACTH as a diagnostic test for PPID are hampered bythe lack of a readily available ‘best’ or ‘gold standard’ test forthe condition.
So, where does prevalence come in? Sensitivity andspecificity are indicators that relate directly to the test underscrutiny, while for calculation of positive and negativepredictive values, prevalence is included in the denominator.In the study by McGowan et al. during autumn the positivepredictive value (in other words, the proportion of positive testresults that truly are positive) was only 75%, while in spring,summer and winter the positive predictive value fell to around45% (McGowan et al. 2013b), indicating that 3 of 4 horses withpositive test results in autumn were affected, but in the otherseasons, when a ‘positive’ result was obtained, slightly morehorses did not have the disease than did. The population fromwhich those estimates were derived was restricted to horses≥15 years old. The positive and negative predictive values fallas prevalence decreases, and a test useful for diagnosis is notnecessarily appropriate for screening apparently healthypopulations for subclinical disease. Horse-owners areincreasingly aware of PPID and want to screen their horsesbecause the concept of early diagnosis and treatment isattractive. However, studies are urgently required to providethe evidence on which to base screening programmes.Overdiagnosis leads to overtreatment, and treating animalsunnecessarily creates unnecessary concern for their owners aswell as inappropriate financial investment in drug therapy. Inaddition, the risk of untoward effects of drug treatment mustalways be considered; pergolide was removed from themarket for human use in the USA in 2007 because of aperceived increase in the risk of valvular heart disease.
Pergolide has emerged as the drug of first choice fortreatment of PPID, and it has the advantage that it is licensedfor use in the horse in many regions (Frank and Geor 2014).While the early introduction of medication may avert thespectre of laminitis, clinicians should be aware that, at present,there are no randomised controlled trials comparing pergolidewith alternatives. Furthermore, there have been no long-termstudies to show that horses that are treated with low-dosepergolide before the onset of clinical signs of PPID have betteroutcomes, including a reduced incidence of developinglaminitis, than horses in which treatment is delayed until clinicalsigns become apparent. Perhaps the next decade will providethe evidence base that is needed to provide robust guidelineson this and other medications?
NoteThis article is co-published in Equine Veterinary Education andEquine Veterinary Journal.
C. M. MARR and T. S. MAIREVJ and EVE Editorial Office
ReferencesAxiak, S. and Johnson, P.J. (2012) Paraneoplastic manifestations of
cancer in horses. Equine Vet. Educ. 24, 367-376.
Borer-Weir, K.E., Menzies-Gow, N.J., Bailey, S.R., Harris, P.A. and Elliott, J.(2013) Seasonal and annual influence on insulin and cortisol resultsfrom overnight dexamethasone suppression tests in normal poniesand ponies predisposed to laminitis. Equine Vet. J. 45, 688-693.
Burns, T.A., Watts, M.R., Weber, P.S., McCutcheon, L.J., Geor, R.J. andBelknap, J.K. (2013) Distribution of insulin receptor and insulin-likegrowth factor-1 receptor in the digital laminae of mixed-breedponies: an immunohistochemical study. Equine Vet. J. 45, 326-332.
Copas, V.E.N. and Durham, A.E. (2012) Circannual variation in plasmaadrenocorticotropic hormone concentrations in the UK in normalhorses and ponies, and those with pituitary pars intermediadysfunction. Equine Vet. J. 44, 440-443.
Cornelisse, C.J. and Robinson, N.E. (2013) Glucocortioid therapy andthe risk of equine laminitis. Equine Vet. Educ. 25, 39-46.
Dunkel, B., Wilford, S.A., Parkinson, N.J., Ward, C., Smith, P., Grahame, L.,Brazil, T. and Schott, II, H.C. (2014) Severe hypertriglyceridaemia inhorses and ponies with endocrine disorders. Equine Vet. J. 46,118-122.
Frank, N. and Geor, R. (2014) Current best practice in clinicalmanagement of equine endocrine patients. Equine Vet. Educ. 26,6-9.
Frank, N. and Tadros, E.M. (2014) Insulin dysregulation. Equine Vet. J. 46,103-112.
Gauff, F., Patan-Zugaj, B. and Licka, T.F. (2013) Hyperinsulinaemiaincreases vascular resistance and endothelin-1 expression in theequine digit. Equine Vet. J. 45, 613-618.
Hudson, A.B., McGowan, C.M. and Morgan, R. (2012) The clinicalmanagement of EMS at the Philip Leverhulme equine hospital.Equine Vet. J. 44, Suppl. 42, 7-8.
McGowan, T.W., Pinchbeck, G.P. and McGowan, C.M. (2013a)Prevalence, risk factors and clinical signs predictive for equinepituitary pars intermedia dysfunction in aged horses. Equine Vet. J.45, 74-79.
McGowan, T.W., Pinchbeck, G.P. and McGowan, C.M. (2013b)Evaluation of basal plasma α-melanocyte-stimulating hormone andadrenocorticotrophic hormone concentrations for the diagnosis ofpituitary pars intermedia dysfunction from a population of agedhorses. Equine Vet. J. 45, 66-73.
Menzies-Gow, N.J., Wray, H., Bailey, S.R., Harris, P.A. and Elliott, J. (2013)The effect of exercise on plasma concentrations of inflammatorymarkers in normal and previously laminitic ponies. Equine Vet. J.Epub ahead of print; doi: 10.1111/evj/12132
Owers, R. and Chubbock, S. (2013) Fight the fat! Equine Vet. J. 45, 5.
Rendle, D.I., Litchfield, E., Heller, J. and Hughes, K.J. (2014) Investigationof rhythms of secretion and repeatability of plasmaadrenocorticotropic hormone concentrations in healthy horses andhorses with pituitary pars intermedia dysfunction. Equine Vet. J. 46,113-117.
Rendle, D.I., Rutledge, F., Hughes, K.J., Heller, J. and Durham, A.E. (2013)Effects of metformin hydrochloride on blood glucose and insulinresponses to oral dextrose in horses. Equine Vet. J. 45, 751-754.
Sojka-Kritchevsky, J.E. and Johnson, P.J. (2014) Current status and futuredirections: equine pituitary pars intermedia dysfunction and equinemetabolic syndrome. Equine Vet. J. 46, 99-102.
Tadros, E.M. and Frank, N. (2011) Endocrine disorders and laminitis.Equine Vet. Educ. 25, 152-162.
Tóth, F., Frank, N., Martin-Jiménez, T., Elliott, S.B., Geor, R.J. and Boston,R.C. (2010) Measurement of C-peptide concentrations andresponses to somatostatin, glucose infusion, and insulin resistance inhorses. Equine Vet. J. 42, 149-155.
Venugopal, C.S., Eades, S., Holmes, E.P. and Beadle, R.E. (2011) Insulinresistance in equine digital vessel rings: an in vitro model to studyvascular dysfunction in equine laminitis. Equine Vet. J. 43, 744-749.
© 2013 EVJ Ltd
5EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

Editorial
Current best practice in clinical management of equineendocrine patients
Endocrine disorders are commonly diagnosed in horses and ourknowledge of equine endocrinology has expanded in recentyears. Original research reports, case series and review articlesincluded in this virtual issue of Equine Veterinary Educationand Equine Veterinary Journal are examples of the workbeing conducted in this developing area of equine medicine.Pituitary pars intermedia dysfunction (PPID) and insulindysregulation (ID) are the most common endocrine disordersencountered in horses and have high prevalence rates.McGowan et al. (2013a) report a prevalence rate of 21.2% forPPID in horses aged ≥15 years from a cross-sectional survey ofhorse owners in Queensland, Australia and this is consistent withthe previously reported 22% prevalence rate for haircoatchanges associated with PPID in aged horses in the UnitedKingdom (Ireland et al. 2012). Insulin dysregulation also appearsto be common in horses, as a component of equine metabolicsyndrome (EMS) or accompanying PPID (Frank and Tadros2013). Hyperinsulinaemia (fed plasma insulin concentration≥30 mu/l) occurred with a prevalence of 10% in a cross-sectional study of mixed light-breed horses in Virginia, USA(Pleasant et al. 2013) and basal hyperinsulinaemia (>20 mu/l)was detected in 32% of aged (≥15 years) horses with PPIDin Queensland (McGowan et al. 2013b). There appears tobe a genetic basis to ID, with certain breeds of horse,including ponies, Morgan horses and Arabians beingoverrepresented. Other endocrine disorders of horses includehyperparathyroidism, as discussed by Axiak and Johnson (2012)in their article focused on paraneoplastic syndromes, anddiabetes mellitus (Durham et al. 2009; Dunkel et al. 2013). Incontrast, some of the common endocrinopathies of humanpatients, dogs and cats such as Addison’s disease,hyperthyroidism and hypothyroidism, are rarely seen in horses.This discussion of best practices in clinical management ofequine endocrine patients focuses on PPID and ID because oftheir high prevalence rates.
Before making management decisions, the clinician shouldfirst consider the stage of the endocrinopathy and appreciatethe dynamic nature of endocrine disorders. Pituitary parsintermedia dysfunction is a neurodegenerative condition thatprogresses over time and occurs in its advanced form in oldhorses. It is important to recognise, however, that this disorderfirst develops at a younger age and advances in diagnostictesting have allowed us to detect PPID in its earlier stages.Pituitary pars intermedia dysfunction should be considered inhorses aged >10 years that exhibit poor performance, loss ofmuscle mass and subtle haircoat changes such as retainedhairs in small areas (regional hypertrichosis). Detection of earlyPPID is important because the disorder is easily managed withpergolide treatment and it is advisable to prevent laminitis,rather than wait for this condition to develop. Both PPID and IDare associated with laminitis, and relationships among theseconditions were reviewed by Tadros and Frank (2013) anddiscussed extensively in the Equine Veterinary Journal virtualissue on laminitis (http://onlinelibrary.wiley.com/journal/10.1001/(ISSN)2042-3306/homepage/laminitis__recent_advances_and_future_directions.htm).
Insulin dysregulation can also change over time. If weconsider certain horses to be genetically predisposed to thisproblem, the degree of ID is determined by the managementof the horse and development of concurrent medicalconditions. A genetically predisposed horse that is wellmanaged can remain free of health problems whereasobesity, hyperinsulinaemia and laminitis may develop if thesame animal is overfed or exposed to feeds and forages thatelicit a marked insulinaemic response. Obesity, regionaladiposity, ID, hypertriglyceridaemia and hyperleptinaemia areall components of EMS, a collection of endocrine andmetabolic abnormalities associated with the development oflaminitis in equids. Insulin dysregulation can also beexacerbated by PPID and anecdotal evidence suggests thathorses with EMS are predisposed to PPID. This concern has ledto the recommendation that all horses with EMS that are aged>10 years be closely monitored for signs of pituitarydysfunction.
Management and monitoring of PPIDPergolide is recommended for the treatment of PPID inhorses at a dosage of 0.002 mg/kg bwt and is available asPrascend®1 in 1 mg tablets. Anorexia can be encounteredas pergolide treatment is initiated, so it is advisable to starthorses on half the dose every other day for 2 doses andthen half the dose daily for 3 days to avoid this complication.Cyproheptadine is also used for the management of PPID, butis reserved for horses with advanced PPID on higher dosages ofpergolide. In these situations cyproheptadine is administeredat a dosage of 0.25 mg/kg bwt orally every 12 h and given toanimals concurrently receiving pergolide.
Best practices for managing PPID include measurement ofplasma adrenocorticotropin hormone (ACTH) concentrations30 days after pergolide treatment is initiated at the full dose.Plasma ACTH concentrations are also measured to diagnosePPID and this is an easy test to perform because only a singleblood sample is required. The other recommended diagnostictest for PPID is the thyrotropin-releasing hormone (TRH)stimulation test and this is performed by collecting a bloodsample, injecting 1.0 mg TRH i.v. and collecting a secondblood sample 10 min later. Horses with PPID have a markedincrease in plasma ACTH concentrations in response to TRH.The TRH stimulation test appears to have greater sensitivitythan resting ACTH measurements and is thereforerecommended when clinical signs are subtle and early PPID issuspected.
Reference intervals are required when plasma ACTHconcentrations are used to diagnose and monitor PPID, andthese intervals must be appropriate for the time of year whenthe horse is tested and assay used. Copas and Durham (2012)established seasonal reference intervals for plasma ACTHconcentrations in horses and reported upper limits of29 pg/ml between November and July and 47 pg/mlbetween August and October for horses in the UK. Seasonallyadjusted reference intervals allow horses to be evaluatedin the late summer and autumn when ACTH concentrations
6
© 2013 EVJ Ltd
EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

are higher and melanotrophs within the pars intermediaare more active. Alpha melanocyte-stimulating hormoneconcentrations are also increased with PPID and are affectedby season (McGowan et al. 2013a), but this measure is notoffered by laboratories. The August to October periodwas avoided in the past, but this time of year is nowrecommended as an appropriate time to assess horses onpergolide treatment. Plasma ACTH concentrations should bemeasured biannually, in the autumn and spring, and thepergolide dosage should be adjusted to maintain plasmaACTH concentrations within reference intervals at both timesof the year.
Only the laboratory response to pergolide treatment hasbeen discussed so far and this is the recommended approachwhen managing horses with early PPID that respond well totreatment. However, horses with advanced PPID at the timeof first diagnosis often have very high plasma ACTHconcentrations, sometimes in excess of 1000 pg/ml. It may notbe possible to return plasma ACTH concentrations to normal inthese cases, so other approaches must be considered. The firstapproach is to adjust the pergolide dosage until a significantdownward shift in ACTH concentrations is detected. Forexample, a downward shift to 250 pg/ml represents asignificant improvement in a horse with a plasma ACTHconcentration of 1000 pg/ml. If the owner can afford toadminister pergolide at higher doses, the dosage should beincrementally increased to try and return plasma ACTHconcentrations to within the reference interval. In the authors’experience, pergolide can be administered to a maximumdosage of 0.01 mg/kg bwt (5 mg for a 500 kg horse) withoutadverse health effects. Although this is the preferredapproach, it is also practical to consider the finances of theowner and select a dosage that elicits a significant downwardshift in plasma ACTH concentration, even if concentrationsremain above reference interval. When discussing prognosis,clinicians can point out that only some of the ACTH producedin horses with advanced PPID is likely to be biologically active,so the laboratory values might be only loosely correlated withclinical signs. In the same example, lowering the ACTHconcentration to 250 pg/ml could therefore be associatedwith a significant improvement in clinical signs. Our secondrecommendation is therefore to monitor clinical responsesto treatment. Outcomes of pergolide treatment includeincreased alertness and activity, resolution of polyuria andpolydipsia, lower incidence of laminitis, improved immunefunction and fewer bacterial infections, mitigation ofhyperglycaemia and hyperinsulinaemia, increased musclemass, and improvements in haircoat quality, hair length andshedding. If a downward shift in ACTH concentrations isdetected and clinical signs improve, owners should beencouraged to continue long-term treatment. Some horsesshow gradual improvement in clinical signs over time, evenwhen receiving pergolide at a dosage suboptimal from alaboratory standpoint. Pituitary pars intermedia dysfunction isa manageable endocrine disorder, even in its advancedstages, and geriatric medicine is a growing field in equinepractice.
There are a number of secondary problems encounteredin horses with advanced PPID that should be kept in mind. Asmentioned above, polyuria and polydipsia are encountered inhorses with advanced PPID and result from the reduced actionof antidiuretic hormone on the kidney, as described in arecent report by Moses et al. (2013). Hypertriglyceridaemia is
also a concern when horses enter negative energy balance,as occurs with colic, dental disease or systemic illness. Dunkelet al. (2013) describe this problem in their recent retrospectivestudy of hospitalised horses and ponies. Of the 7 animalsidentified with endocrine disorders and hypertriglyceridaemia(serum triglyceride concentration >5.65 mmol/l), 3 horses and 3ponies were diagnosed with PPID and 5 had concurrent type2 diabetes mellitus. This report and the 3 horses with type 2diabetes mellitus described by Durham et al. (2009), haveraised our awareness of these problems in horses with PPID.Glucose concentrations must be closely monitored in horseswith PPID that encounter stress associated with medicalconditions or hospitalisation, and insulin therapy should beconsidered if hyperglycaemia and hypertriglycerideaemia areencountered.
Management and monitoring ofinsulin dysregulationInsulin dysregulation collectively refers to increased insulinresponses to oral sugars, hyperinsulinaemia and insulinresistance, and these problems manifest to different degrees ingenetically susceptible horses and ponies. The degree of IDdepends upon modifying factors, including obesity, diet andPPID. Adiposity and tissue insulin sensitivity are negativelycorrelated in horses (Carter et al. 2009), so the first goal ofmanaging ID in an obese horse or pony is to induce weightloss. Exercise should be increased and energy intake restrictedby removing energy-dense feeds such as grain from the dietand limiting pasture access. Obese equids should bemaintained on a diet of hay plus a ration balancer to provideessential nutrients. Amounts of hay can be calculated usingdigestible energy requirements or a simple approach can befollowed in which hay is fed in amounts equivalent to 1.5% ofcurrent bodyweight. If body fat mass does not decrease after4 weeks, the daily amount of hay should be lowered to 1.25%of bodyweight. A further reduction in hay ration to 1.0% ofbodyweight is needed in some cases. Some horses and poniesremain obese on low-energy diets even after exercise isincreased to consume energy; and this is referred to as weightloss resistance (Argo et al. 2012). Levothyroxine sodium can beadministered to accelerate weight loss in these animals, butthis approach is only practical in the USA where the drug isinexpensive.
Our understanding of the relationships between insulin andlaminitis is improving as more research is performed, includingthe 3 studies described in this virtual issue (Venugopal et al.2011; Burns et al. 2013; Gauff et al. 2013), and these findingsemphasise the need for ID to be diagnosed and managed inhorses to prevent laminitis. Two tests are recommended fordiagnosing and monitoring ID: 1) an oral sugar/glucose testand 2) measurement of fasting insulin concentrations. The firsttest evaluates insulinaemic responses to ingested sugars andthe oral sugar test (OST) or in-feed oral glucose test (OGT) canbe performed. The OST is more commonly used in the USAwhere corn syrup is readily available for purchase insupermarkets. When this test is performed, the horse is fastedfrom midnight onwards and corn syrup (0.15 ml/kg bwt) isadministered orally using dose syringes the next morning. Bloodsamples are collected at 60 and 90 min and a high insulinresponse is currently defined by an insulin concentration>60 mu/l at either time point. The OGT is also performed afterfasting and the horse is fed 0.5 kg chaff-based feed that
© 2013 EVJ Ltd
7EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

contains added dextrose powder (1 g/kg bwt) mixed withwater. A blood sample is collected 2 h later and an insulinconcentration ≥87 mu/l is a high insulin response. Fasting insulinconcentrations can also be measured to test horses for ID. Asingle blood sample is collected after a short fast and fastinghyperinsulinaemia is defined by an insulin concentration>20 mu/l. This test is easy to perform and can be used whenowners have concerns about the OST or OGT. However,breed-specific reference intervals are required to improvethe performance of this test and its sensitivity is low, whichraises concern about false negative results in mildly affectedhorses.
If it is established from OST or OGT results that insulinresponses to ingested sugars are high, a diet should beselected to minimise post prandial hyperinsulinaemia bylimiting the intake of simple sugars and starches, which arerapidly hydrolysed to glucose. Grain and sweet feeds shouldbe fed with caution and the amount of grass consumed onpasture should be limited by restricting the area for grazing orplacing a grazing muzzle on the horse to decrease feedintake. If insulin concentrations markedly increase during theOST, hay with low nonstructural carbohydrate content shouldbe selected and forage analysis is recommended. Hay can besoaked in cold water for 30 min to lower the sugar contentalthough this method does not yield a predictable decrease insugars.
Metformin hydrochloride is administered to horses with IDdespite its low oral bioavailability (Hustace et al. 2009) and astudy performed by Rendle et al. (2013) examines themechanism of action of this drug in equids. Results indicatethat metformin acts locally at the intestinal level to lower postprandial glucose and insulin concentrations. Only healthyhorses were evaluated in the study, but results support the useof metformin to limit post prandial hyperinsulinaemia in horseswith ID, and current recommendations are to administermetformin at a dosage of 30 mg/kg bwt orally every 8–12 h,with the drug administered 30–60 min before the horse isfed, if possible. The authors reserve metformin treatment forhorses and ponies with markedly increased OST insulinconcentrations, even after loss of body fat mass and dietarymanagement.
Insulin dysregulation should be monitored by measuringfasting insulin concentrations (if initially elevated) or repeatingthe OST or OGT. High plasma triglyceride and leptinconcentrations can also accompany ID and obesity, andshould decrease with appropriate management. Adiposity ismonitored through body condition scoring, measuringabdominal circumference at the umbilicus, or neck crestscoring. Pituitary pars intermedia dysfunction exacerbates IDand horses aged >10 years should be closely monitored for thedevelopment of this condition.
ConclusionsEquine endocrine disorders are increasingly recognised andhave become an integral part of wellness evaluations inhorses. Establishing best practices in the diagnosis andmanagement of the 2 common endocrine disorders, PPID andID, will lower the risk of laminitis and improve the healthof horses. Increased awareness of endocrine disorders,including rarer conditions such as diabetes mellitus andhyperparathyroidism, is expanding our knowledge in this areaof veterinary medicine.
Authors’ declaration of interestsDr Frank is a consultant on study design for BoehringerIngelheim Vetmedica, manufacturer of Prascend®.
Manufacturer’s address1Boehringer Ingelheim Vetmedica, Ingelheim, Germany.
N. FRANK†‡ and R. GEOR§
†Clinical Sciences, Tufts Cummings School of VeterinaryMedicine, North Grafton, Massachusetts, USA; ‡Division of
Medicine, School of Veterinary Medicine and Science,University of Nottingham, Leicestershire, UK; and §Large
Animal Clinical Sciences, Michigan State University,East Lansing, USA.
ReferencesArgo, C.M., Curtis, G.C., Grove-White, D., Dugdale, A.H., Barfoot, C.F.
and Harris, P.A. (2012) Weight loss resistance: a further considerationfor the nutritional management of obese Equidae. Vet. J. 194,179-188.
Axiak, S. and Johnson, P.J. (2012) Paraneoplastic manifestations ofcancer in horses. Equine Vet. Educ. 24, 367-376.
Burns, T.A., Watts, M.R., Weber, P.S., McCutcheon, L.J., Geor, R.J. andBelknap, J.K. (2013) Distribution of insulin receptor and insulin-likegrowth factor-1 receptor in the digital laminae of mixed-breedponies: an immunohistochemical study. Equine Vet. J. 45, 326-332.
Carter, R.A., McCutcheon, L.J., George, L.A., Smith, T.L., Frank, N. andGeor, R.J. (2009) Effects of diet-induced weight gain on insulinsensitivity and plasma hormone and lipid concentrations in horses.Am. J. Vet. Res. 70, 1250-1258.
Copas, V.E. and Durham, A.E. (2012) Circannual variation in plasmaadrenocorticotropic hormone concentrations in the UK in normalhorses and ponies, and those with pituitary pars intermediadysfunction. Equine Vet. J. 44, 440-443.
Dunkel, B., Wilford, S.A., Parkinson, N.J., Ward, C., Smith, P., Grahame, L.,Brazil, T. and Schott, H.C. 2nd (2013) Severe hypertriglyceridaemia inhorses and ponies with endocrine disorders. Equine Vet. J. 46,118-122.
Durham, A.E., Hughes, K.J., Cottle, H.J., Rendle, D.I. and Boston, R.C.(2009) Type 2 diabetes mellitus with pancreatic beta celldysfunction in 3 horses confirmed with minimal model analysis.Equine Vet. J. 41, 924-929.
Frank, N. and Tadros, E.M. (2013) Insulin dysregulation. Equine Vet. J. 46,103-112.
Gauff, F., Patan-Zugaj, B. and Licka, T.F. (2013) Hyperinsulinaemiaincreases vascular resistance and endothelin-1 expression in theequine digit. Equine Vet. J. 45, 613-618.
Hustace, J.L., Firshman, A.M. and Mata, J.E. (2009) Pharmacokineticsand bioavailability of metformin in horses. Am. J. Vet. Res. 70,665-668.
Ireland, J.L., Clegg, P.D., McGowan, C.M., McKane, S.A., Chandler, K.J.and Pinchbeck, G.L. (2012) Disease prevalence in geriatric horses inthe United Kingdom: veterinary clinical assessment of 200 cases.Equine Vet. J. 44, 101-106.
McGowan, T.W., Pinchbeck, G.P. and McGowan, C.M. (2013a)Evaluation of basal plasma α-melanocyte-stimulating hormone andadrenocorticotrophic hormone concentrations for the diagnosis ofpituitary pars intermedia dysfunction from a population of agedhorses. Equine Vet. J. 45, 66-73.
McGowan, T.W., Pinchbeck, G.P. and McGowan, C.M. (2013b)Prevalence, risk factors and clinical signs predictive for equinepituitary pars intermedia dysfunction in aged horses. Equine Vet. J.45, 74-79.
Moses, M.E., Johnson, P.J., Messer, N.T. and Wilson, D.A. (2013)Antidiuretic response of a horse affected with pituitary parsintermedia dysfunction to desmopressin acetate. Equine Vet. Educ.25, 111-115.
© 2013 EVJ Ltd
8 EQUINE VETERINARY EDUCATION / AE / JANUARY 2014
Continued on page 39

Thank you for supporting
the facts.Brief Summary Indications: For the intramuscular treatment of non-infectious degenerative and/or traumatic joint dysfunction and associated lameness of the carpal and hock joints in horses. There are no known contraindications to the use of intramuscular Adequan® i.m. brand Polysulfated Glycosaminoglycan in horses. Studies have not been conducted to establish safety in breeding horses. WARNING: Do not use in horses intended for human consumption. Not for use in humans. Keep this and all medications out of the reach of children. Caution: Federal law restricts this drug to use by or on the order of a licensed veterinarian. Each 5 mL contains 500 mg Polysulfated Glycosaminoglycan. SEE PRODUCT PACKAGE INSERT FOR FULL PRESCRIBING INFORMATION. Adequan® is a registered trademark of Luitpold Pharmaceuticals, Inc. ©LUITPOLD PHARMACEUTICALS, INC., Animal Health Division, Shirley, NY 11967. AHD 1528, lss. 2/12 D-LPI12001aR-AAEP
There is NO GENERICADEQUAN® i.m.(polysulfated(polysulfated glycosaminoglycan)glycosaminoglycan)ycan
Get the facts at nogenericadequan.com

Case Report
Navicular bone osteomyelitis and navicular bursitis with associatedfistula diagnosed with magnetic resonance fistulographyin the horseE. B. Garcia, N. Rademacher*, C. T. McCauley† and L. GaschenDepartment of Veterinary Clinical Sciences, Section of Diagnostic Imaging; and †Equine Health Studies Program,School of Veterinary Medicine, Louisiana State University, Louisiana, USA.*Corresponding author email: [email protected]
Keywords: horse; draining tract; navicular bursa; osteomyelitis; deep digital flexor tendon; tendonitis
SummaryA 7-year-old Quarter Horse gelding was referred for magneticresonance (MR) imaging due to chronic left hindlimb lamenesslocalised to the foot. On presentation, a previouslyundiagnosed draining tract was identified at the plantaraspect of the pastern. Radiographs revealed severe osteolysisof the navicular bone. Positive contrast MR fistulography wasperformed using a gadolinium based contrast agent followingconventional MR imaging of the left hind foot. Fistulographyallowed characterisation of a fistulous tract, which was closelyassociated with the deep digital flexor tendon, navicular bursaand osteomyelitis of the navicular bone.
History and clinical findingsA 7-year-old Quarter Horse gelding was referred for magneticresonance imaging (MRI) of the left hind foot for theinvestigation of intermittent lameness of 3 months’ duration.Recurrent subsolar and coronary band abscesses werediagnosed by the referring veterinarian. Treatment prior toreferral included debridement of devitalised tissue fromboth the sole and coronary band, oral administration ofnonsteroidal anti-inflammatory medication, oral administrationof antibiotics, and administration of antibiotics by regional limbperfusion.
At presentation, the horse was grade 4–5 out of 5 lameusing the AAEP lameness scale on the left hindlimb (Anon1999). A draining tract not previously reported by the referringveterinarian was identified at the plantar aspect of thepastern. A low 4-point nerve block and a dorsal ring blockperformed proximal to the metatarsophalangeal joint resultedin marked decrease in the degree of lameness.
Imaging
RadiographyRadiography of the left hind foot revealed severe navicularbone osteolysis of the distal half of the flexor cortex extendinginto the medullary cavity (Fig 1). Moderate concentric softtissue swelling was evident from the metatarsophalangeal jointto the level of the coronary band. The findings were mostconsistent with infectious osteomyelitis.
Magnetic resonance imagingThe horse was placed under general anaesthesia using astandard anaesthetic protocol. Magnetic resonance imagingwas performed using a 1.5 T magnet (Echelon)1 with the horse
in left lateral recumbency. Sagittal proton density (PD) at 3 mmslice thickness, T2-weighted fast spin echo (T2W FSE) at4 mm slice thickness, fast inversion recovery (FIR) at 4 mmslice thickness, transverse PD and T2W FSE both at 3 mm slicethickness, and a dorsal PD sequence at 3 mm slice thicknesssequences were acquired from the tip of the foot to themidpoint of the proximal phalanx. A transverse 3D T2*sequence was acquired and reconstructed in 1 mm thickslices in the sagittal plane.
The distal aspect of the navicular bone flexor cortexshowed a large ill-defined zone of hyperintensity on PD,T2* and FIR sequences (Fig 2). Multifocal, 1–2 mm diameter
Fig 1: Lateromedial radiograph of foot of left pelvic limb. The distalaspect of the flexor cortex is lytic and irregularly bordered withextension of lysis into the adjacent medullary region. The distalinterphalangeal joint is dorsally subluxated. The horse was unableto bear full weight on the left pelvic limb during acquisition of thisimage.
10
© 2013 EVJ Ltd
EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

hypointense structures were present within the region of theabnormal hyperintense signal at the distal and lateral flexorsurface of the navicular bone. The distal sesamoidean imparligament was subjectively thickened and surrounded by aregion of PD, T2W and FIR mixed signal intensity, which wasprimarily hyperintense. The dorsal aspect of the deep digitalflexor tendon (DDFT) at the level of the navicular bone wassubjectively thin, most severe in the medial lobe. A T2W, PDand T2* hyperintense signal was evident at the dorsal border ofthe DDFT, more severe in the medial lobe compared to thelateral lobe (Fig 3). Proton density and T2* hyperintensity of theDDFT was more extensive compared with T2W sequences andextended full thickness through the medial lobe of the tendonand partial thickness through the lateral lobe. The navicularbursa was poorly visualised on all sequences.
Within the plantar aspect of the pastern, the soft tissuesdorsal to the digital cushion showed a faint PD isointense andwell defined T2W and FIR hyperintense tract on sagittalimages. However, the course of this tract was faintly visible asit approached the DDFT and the dorsal extent of the tractcould not be delineated on either sagittal or transverse PD andT2 weighted sequences. Diagnoses of navicular bone necrosis,navicular bursitis, impar ligament desmitis and distal borderfragmentation, focal deep digital flexor tendonitis and afistula of the left hind foot were made. To determine ifcommunication existed between the fistulous tract andcomponents of the podotrochlear apparatus, fistulographywas performed.
Immediately following initial image acquisition, the surfacecoil was removed and the left hind pastern region wasaseptically prepared. A sterile stainless steel probewas placed temporarily into the fistulous tract so that 6 ml of1% Gd-DPTA (Magnevist)2 could be introduced. Sagittal T1W
FIR 3D T2*
Fig 2: Mid-sagittal FIR and 3D GRE T2* images of the left hind foot. The FIR image was acquired with 4 mm slice thickness and theGRE reconstructed with 1 mm thickness. The distal sesamoidean impar ligament is severely thickened and has increased signal intensityon both sequences (arrowhead). The hypointense signal from the flexor cortical bone is absent (*) and there is increased FIRsignal intensity within the navicular bone medullary cavity. The DDFT is thinned with irregular borders (long arrow). A faint FIR hyperintensetract is visible within the plantar soft tissues, proximal to the digital cushion and progresses towards the podotrochlear apparatus (shortarrows).
3D T2*
Fig 3: Transverse 3D GRE T2* image at the level of the mid middlephalanx, just proximal to the proximal recess of the navicularbursa. Medial is to the left. There are biaxial dorsal borderhyperintensities of the DDFT (arrows), which were also observed infurther distal images (not shown), extending to the level of proximalaspect of the distal phalanx. Additionally, the dorsal border ofthe DDFT is irregular and poorly delineated. Further proximal to thisimage, the signal intensity of the DDFT was hypointense andsymmetrical.
© 2013 EVJ Ltd
11EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

FSE 4 mm thick and dorsal and transverse 3 mm thick imageswere acquired. Hyperintense contrast agent confirmed thelocation of the fistulous tract from the plantar aspect of thepastern, which coursed through the mid-sagittal digitalcushion, and diverted laterally around the DDFT to end at thelateral aspect of the proximal navicular bursa recess (Fig 4).Following fistulography a diagnosis of navicular bone necrosis,and navicular bursitis due to a fistulous tract at the pastern wasconfirmed.
Surgery and outcomeFollowing MRI, navicular bursoscopy was unsuccessfullyattempted due to loss of structural integrity of the bursa (Wrightet al. 1999). For this reason an alternative approach throughthe sole of the frog was used to access the podotrochlearapparatus (Fürst and Lischer 2006). Goals of surgery weredebridement of the navicular bone and therapeutic lavage ofthe navicular bursa. Surgical findings included soft andnecrotic bone at the flexor surface of the navicular bone,which extended into the medullary cavity. The navicular bursawas unidentifiable surgically. Following surgery, the horse failedto show improvement despite aggressive systemic andregional antibiotic therapy, aggressive multi-modal painmanagement, anti-inflammatory therapy and supportive careto prevent support limb laminitis. During a second surgery,deep digital flexor tenotomy was performed in an attempt tomanage pain by minimising pressure applied to the navicularbone by the DDFT (Hunt et al. 1991).
Due to failure to respond to therapy, the owner declinedfurther treatment and the horse was discharged foreuthanasia by the referring veterinarian. No necropsy wasperformed. The case described in this study was treated
according to current veterinary ethical and professionalguidelines as described by Anon (2012).
DiscussionMagnetic resonance fistulography allowed the causeof lysis of the navicular bone, focal DDFT lesions anddestruction of the navicular bursa to be linked to a fistuloustract. In this study, a gadolinium based paramagnetic contrastagent was used that has the effect of decreasing T1 relaxationtime which results in increased signal produced during a T1weighted sequence (McRobbie 2007). One report of equineMRI fistulography is available and only describes the use ofiodinated contrast that remained present followingradiographic fistulography (Kinns and Mair 2005). Anotherstudy reported the use of 3D GRE T1 weighted imaging todiagnose experimentally created thoracic duct fistulae in pigsfollowing administration of gadolinium contrast agent into thehindlimb interstitium (Staatz et al. 2003). We found a similarimproved ability to identify the fistula following contrastadministration in our study using a 3D T1W GRE sequence.Magnetic resonance fistulography has been described morecommonly in man for perianal and anovaginal fistulae (Sabiret al. 2000; Ergen et al. 2007; Waniczek et al. 2011). Postcontrast T2W GRE, and to a lesser extent precontrast STIRsequences, provided the greatest ability to identify perianalfistulous tracts using gadolinium enhanced fistulography withMRI (Sabir et al. 2000). Post contrast T1W sequences were lesseffective at highlighting fistulous tracts due to the inability todistinguish hyperintense Gd-DTPA from hyperintense perinealfat (Sabir et al. 2000). This differed from our findings where T1Wimages following administration of Gd-DTPA allowed forexcellent contrast with the relatively hypointense digital
T1 T1
Fig 4: Post fistulography sagittal and transverse T1W images. The fistulous tract (arrows) is observed clearly traversing the plantar soft tissues,tracking to the level of the DDFT, redirecting laterally and then dorsally to the level of the proximal border of the navicular bone andnavicular bursa. Multifocal foci of signal void are located within the centre of the fistulous tract, probably representing air that wasintroduced iatrogenically during contrast administration. The full extent of the fistulous tract was not evident on precontrast images.
© 2013 EVJ Ltd
12 EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

cushion and surrounding plantar soft tissue structures. Thisdifference from human perianal MRI fistulography can beexplained by a difference in regional tissue composition, withthe digital cushion containing collagenous and elastic fibreswith minimal fat and cartilage (Dyce et al. 2010).
Even though it was unable to be confirmed in this case,penetrating solar trauma is reported as a cause for septicnavicular bursitis in mature horses (Honnas 1992). Injuries frompenetrating foreign objects in the foot often result in ahypointense tract with MRI that persists for weeks following theinitial injury, which would not be possible to diagnose withradiography unless osseous changes develop (Kinns and Mair2005). T1W and T2W hypointensity of tracts is explained inacute stages as a signal void due to air, and in chronic stagesas a result of mineralisation or haemosiderin (Kinns and Mair2005; Murray et al. 2006). Similar findings at the distal flexorsurface of the navicular bone were present in the currentcase. Penetrating foot trauma is less common than other typesof foot injury in the horse and was identified in 5 of 347 horsesexamined for foot pain using MRI that also exhibitedhypointensity in the palmar soft tissues (Dyson and Murray2007). Penetrating foot trauma is often identified inconjunction with injury to other soft tissue structures such as theDDFT, navicular bursa, distal sesamoidean ligament or distalphalanx (Dyson et al. 2005; Kinns and Mair 2005; Dyson andMurray 2007). Magnetic resonance imaging has been shownto be an excellent modality for diagnosing penetrating footinjury in the horse (Boado et al. 2005; Kinns and Mair 2005).
Radiographic fistulography is the traditional method fordefining fistulous tracts in the equine digit or other anatomysecondary to penetrating trauma and to improveidentification of foreign bodies (Barber 1983). Its usage hasbeen described and shown to aid in determination ofsoft tissue involvement, communication with synovial structuresand communication with bone in horses (Lamb 1991).Computed tomographic fistulography has also beendescribed in veterinary and human literature anddemonstrates improved identification of fistulous tracts, foreignbodies and diagnosis of osteomyelitis compared toradiography (Vasil’ev et al. 2003; Johnson-Neitman et al.2006). Magnetic resonance imaging was indicated based onthe history of chronic foot pain and the need for evaluation ofthe soft tissue structures in the foot for determination ofprognosis and potential surgical approach (Dyson et al. 2005).During initial acquisition, the course of the draining tract couldnot be determined with standard MRI sequences. Therefore,it was decided to add a fistulography to gain more informationfor prognosis and surgical approach. Superimposition andpoor soft tissue resolution of a radiographic contrastfistulography compared to MRI would have limited the abilityto determine the course of the draining tract and itsrelationship with soft tissue structures within the foot and wouldhave prolonged anaesthesia time.
Magnetic resonance bursography may have providedfurther evidence of communication with the fistuloustract and the navicular bursa or information regardingthe integrity of the bursa. Since the time of the initialexamination of the horse in this report, 2 reports describingcontrast navicular bursography in the horse have beenpublished. One cadaver study reports that administration ofsaline into the navicular bursa allowed for separationof the dorsal border of the DDFT and the palmar border of thenavicular bone, which improved evaluation of navicular
fibrocartilage (Schramme et al. 2009). Another study describesimproved identification of adhesions between the navicularbursa and DDFT using MRI following bursal distension withiodinated contrast agent (Maher et al. 2011). Hadbursography been used in the case described here, the fullestextent of navicular bursal involvement may have beenappreciated. We attempted navicular bursoscopy in ourpatient but were unable to enter the bursa or visualise anynormal bursal tissue. This is probably due to the destruction ofthe navicular bursa by a suspected septic process and mayhave prevented our ability to perform MRI bursography had itbeen attempted.
This report describes the use of gadolinium contrast agentto improve the identification of a fistulous tract inthe foot of a horse. Portions of the fistulous tract could beidentified prior to fistulography, especially with T2W FSEsequences, but the location and full extent were only evidentin T1W post contrast images and confirmed the extremelyclose association with the navicular bone, DDFT and navicularbursa lesions. Magnetic resonance fistulography was ideal forthe simultaneous description of the soft tissue pathology anddefinition of the fistulous tract with the use of one imagingmodality.
Authors’ declaration of interestsNo conflicts of interest have been declared.
Manufacturers’ addresses1Hitachi Medical Systems America, Twinsburg, Ohio, USA.2Bayer Health Care Pharmaceuticals Inc., Wayne, New Jersey, USA.
ReferencesAnon (1999) Guide to Veterinary Services at Horseshows, American
Association of Equine Practitioners, Lexington.
Anon (2012) A.A.E.P. Directory, American Association of EquinePractitioners, Lexington.
Barber, S.M. (1983) An unusual location of foreign body in the horse.Can. Vet. J. 24, 63-66.
Boado, A., Kristoffersen, M., Dyson, S. and Murray, R. (2005) Use ofnuclear scintigraphy and magnetic resonance imaging to diagnosechronic penetrating wounds in the equine foot. Equine Vet. Educ.17, 62-68.
Dyce, K.M., Sack, W.O. and Wensing, C.J.G. (2010) The forelimb of thehorse. In: Textbook of Veterinary Anatomy, 4th edn., Eds: K.M. Dyce,W.O. Sack and C.J. Wensing, Saunders Elsevier, St Louis. pp 586-623.
Dyson, S. and Murray, R. (2007) Magnetic resonance imaging of theequine foot. Clin. Tech. Equine Pract. 6, 46-61.
Dyson, S.J., Murray, R. and Schramme, M.C. (2005) Lamenessassociated with foot pain: results of magnetic resonance imagingin 199 horses (January 2001-December 2003) and response totreatment. Equine Vet. J. 37, 113-121.
Ergen, F.B., Arslan, E.B., Kerimoglu, U. and Akata, D. (2007) Magneticresonance fistulography for the demonstration of anovaginal fistula:an alternative imaging technique? J. Comput. Assist. Tomogr. 31,243-246.
Fürst, A.E. and Lischer, C.J. (2006) Foot. In: Equine Surgery, Eds: J.A. Auerand J.A. Stick, Saunders Elsevier, St Louis. pp 1184-1216.
Honnas, C.M. (1992) The surgical treatment of septic navicular bursitis.Equine Vet. Educ. 4, 183-188.
Hunt, R.J., Allen, D., Baxter, G.M., Jackman, B.R. and Parks, A.H. (1991)Mid-metacarpal deep digital flexor tenotomy in the managementof refractory laminitis in horses. Vet. Surg. 20, 15-20.
Johnson-Neitman, J.L., Bahr, R.J. and Broaddus, K.D. (2006) Fistulaformation secondary to a nylon cable band in a dog. Vet. Radiol.Ultrasound 47, 355-357.
© 2013 EVJ Ltd
13EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

Kinns, J. and Mair, T.S. (2005) Use of magnetic resonance imaging toassess soft tissue damage in the foot following penetrating injury in 3horses. Equine Vet. Educ. 17, 69-73.
Lamb, C.R. (1991) Contrast radiography of equine joints, tendonsheaths, and draining tracts. Vet. Clin. North Am. Equine Pract. 7,241-257.
Maher, M.C., Werpy, N.M., Goodrich, L.R. and McIlwraith, C.W. (2011)Positive contrast magnetic resonance bursography for assessmentof the navicular bursa and surrounding soft tissues. Vet. Radiol.Ultrasound 52, 385-393.
McRobbie, D.W. (2007) MRI from Picture to Proton, Cambridge UniversityPress, Cambridge.
Murray, R.C., Schramme, M.C., Dyson, S.J., Branch, M.V. and Blunden,T.S. (2006) Magnetic resonance imaging characteristics of the footin horses with palmar foot pain and control horses. Vet. Radiol.Ultrasound 47, 1-16.
Sabir, N., Sungurtekin, U., Erdem, E. and Nessar, M. (2000) Magneticresonance imaging with rectal Gd-DTPA: New tool for the diagnosisof perianal fistula. Int. J. Colorectal Dis. 15, 317-322.
Schramme, M., Kerekes, Z., Hunter, S., Nagy, K. and Pease, A. (2009)Improved identification of the palmar fibrocartilage of the navicularbone with saline magnetic resonance bursography. Vet. Radiol.Ultrasound 50, 606-614.
Staatz, G., Spuntrup, E., Bucker, A., Vazquez-Jimenez, J., Liakopoulos,O.J., Pfluger, D., Grosskortenhaus, S., Misselwitz, B. and Gunther, R.W.(2003) Interstitial T1-weighted MR lymph fistulography withGadomer-17 in an experimental animal model. Rofo 175, 275-281.
Vasil’ev, A., Bulanova, T.V. and Onishchenko, M.P. (2003) Spiralcomputed tomography in the diagnosis of limb osteomyelitis. Vestn.Rentgenol. Radiol. 6, 44-49.
Waniczek, D., Adamczyk, T., Arendt, J., Kluczewska, E. andKozinska-Marek, E. (2011) Usefulness assessment of preoperative MRIfistulography in patients with perianal fistulas. Pol. J. Radiol. 76, 40-44.
Wright, I.M., Phillips, T.J. and Walmsley, J.P. (1999) Endoscopy ofthe navicular bursa: a new technique for the treatment ofcontaminated and septic bursae. Equine Vet. J. 31, 5-11.
© 2013 EVJ Ltd
14 EQUINE VETERINARY EDUCATION / AE / JANUARY 2014
EQUIOXX® (firocoxib) Oral Paste for HorsesNon-steroidal anti-inflammatory drug for oral use in horses only.CAUTION: Federal law restricts this drug to use by or on the order of a licensed veterinarian.Indications: EQUIOXX® Oral Paste is administered for up to 14 days for the control of pain and inflammation associated with osteoarthritis in horses.Contraindications: Horses with hypersensitivity to firocoxib or other NSAIDs should not receive EQUIOXX® Oral Paste.Warnings: For oral use in horses only. Do not use in horses intended for human consumption.Human Warnings: Not for use in humans. Keep this and all medications out of the reach of children. Consult a physician in case of accidental ingestion by humans.Animal Safety: Client should be advised to observe for signs of potential drug toxicity and be given a Client Information Sheet with each prescription.For technical assistance or to report suspected adverse events, call 1-877-217-3543.Precautions: Horses should undergo a thorough history and physical examina-tion before initiation of NSAID therapy. Appropriate laboratory tests should be conducted to establish hematological and serum biochemical baseline data before and periodically during administration of any NSAID. Clients should be advised to observe for signs of potential drug toxicity and be given a Client Information Sheet with each prescription. See Information for Owner or Person Treating Horse section of this package insert.Treatment with EQUIOXX® should be terminated if signs such as inappetence, colic, abnormal feces, or lethargy are observed.As a class, cyclooxygenase inhibitory NSAIDs may be associated with renal and gastrointestinal toxicity. Sensitivity to drug-associated adverse events varies with the individual patient. Patients at greatest risk for adverse events are those that are dehydrated, on diuretic therapy, or those with existing renal, cardiovascular, and/or hepatic dysfunction. Concurrent administration of potentially nephrotoxic drugs should be carefully approached or avoided. NSAIDs
may inhibit the prostaglandins that maintain normal homeostatic function. Such anti-prostaglandin effects may result in clinically significant disease in patients with underlying or pre-existing disease that has not been previously diagnosed. Since many NSAIDs possess the potential to produce gastrointestinal ulcerations, concomitant use with other anti-inflammatory drugs, such as NSAIDs or corticosteroids, should be avoided or closely monitored. The concomitant use of protein bound drugs with EQUIOXX® Oral Paste has not been studied in horses. The influence of concomitant drugs that may inhibit the metabolism of EQUIOXX® Oral Paste has not been evaluated. Drug compatibility should be monitored in patients requiring adjunctive therapy.The safe use of EQUIOXX® Oral Paste in horses less than one year in age, horses used for breeding, or in pregnant or lactating mares has not been evaluated.Consider appropriate washout times when switching from one NSAID to another NSAID or corticosteroid.Adverse Reactions: In controlled field studies, 127 horses (ages 3 to 37 years) were evaluated for safety when given EQUIOXX® Oral Paste at a dose of 0.045 mg/lb (0.1 mg/kg) orally once daily for up to 14 days. The following adverse reactions were observed. Horses may have experienced more than one of the observed adverse reactions during the study.EQUIOXX® (firocoxib) Oral Paste was safely used concomitantly with other therapies, including vaccines, anthelmintics, and antibiotics, during the field studies.Information for Owner or Person Treating Horse: You should give the Client Information Sheet to the person treating the horse and advise them of the potential for adverse reactions and the clinical signs associated with NSAID intolerance. Adverse reactions may include erosions and ulcers of the gums,
tongue, lips and face, weight loss, colic, diarrhea, or icterus. Serious adverse reactions associated with this drug class can occur without warning and, in rare situations, result in death. Clients should be advised to discontinue NSAID therapy and contact their veterinarian immediately if any of these signs of intolerance are observed. The majority of patients with drug-related adverse reactions recover when the signs are recognized, drug administration is stopped, and veterinary care is initiated.Effectiveness: Two hundred fifty-three client-owned horses of various breeds, ranging in age from 2 to 37 years and weighing from 595 to 1638 lbs, were randomly administered EQUIOXX or an active control drug in multi-center field studies. Two hundred forty horses were evaluated for effectiveness and 252 horses were evaluated for safety. Horses were assessed for lameness, pain on manipulation, range of motion, joint swelling, and overall clinical improvement in a non-inferiority evaluation of EQUIOXX compared to an active control. At study’s end, 84.4% of horses treated with EQUIOXX were judged improved on veterinarians’ clinical assessment, and 73.8% were also rated improved by owners. Horses treated with EQUIOXX showed improvement in veterinarian-assessed lameness, pain on manipulation, range of motion, and joint swelling that was comparable to the active control.Storage Information: Store below 86°F (30°C). Brief excursions up to 104°F (40°C) are permitted.How Supplied: EQUIOXX is available in packs of 20, 72 and 216 individually-boxed syringes. Each syringe contains 6.93 grams of EQUIOXX® paste, sufficient to treat a 1250 lb. horse.Marketed by: Merial LLC, Duluth, GA 30096-4640Made in BrazilFor technical assistance or to report suspected adverse reactions, call 1-877-217-3543.NADA 141-253, Approved by FDA©2010 Merial. All Rights Reserved.U.S. Pat. No.: 5981576, 6020343
®EQUIOXX is a registered trademark of Merial.
Adverse Reactions Seen In U.S. Field Studies
AdverseReactions EQUIOXX n=127 Active Control
n=125
Abdominal pain 0 1
Diarrhea 2 0
Excitation 1 0
Lethargy 0 1
Loose stool 1 0
Polydipsia 0 1
Urticaria 0 1

®EQUIOXX is a registered trademark of Merial. ©2013 Merial Limited, Duluth, GA. All rights reserved. EQUIEQX1301-F (07/13)
*Joint pain and inflammation associated with equine osteoarthritis, also called degenerative joint disease.1 Shlueter AE, Orth MW. Equine osteoarthritis: a brief review of the disease and its causes. Equine Comp Exerc Physiol. 2004;1(4):221-231. 2 EQUIOXX product labels.3 American Quarter Horse Association. Show rules and regulations. Official Handbook of Rules and Regulations. 2012:130. Available at: http://www.aqha.com/About/Content-Pages/About-the-Association/AQHA-Handbook.aspx. Accessed January 1, 2012. 4 United States Equestrian Federation. Rule Book; Chapter 4: Drugs and Medications. 2011(4):GR401-GR408. Available at: http://www.usef.org/_Iframes/RuleBook/2012Chapters.aspx. Accessed January 1, 2012.
Equine osteoarthritis can cut your clients’ horses’ careers short.1 EQUIOXX® (firocoxib) Oral Paste is proven to control the joint pain and inflammation associated with equine osteoarthritis with one daily dose.*2
And EQUIOXX Oral Paste is allowed by both the AQHA and USEF for use for up to 14 consecutive days – versus just five with other NSAIDs.3,4
YOUR CLIENTS’ HORSES CAN DO MORE FOR LESS WITH NEW LOWER PRICING. Talk to your Merial Representative or visit equioxx.com to learn more.
IMPORTANT SAFETY INFORMATION: As with any prescription medication, prior to use, a veterinarian should perform a physical examination and review the horse’s medical history. A veterinarian should advise horse owners to observe for signs of potential drug toxicity. As a class, nonsteroidal anti-inflammatory drugs may be associated with gastrointestinal, hepatic and renal toxicity. Use with other NSAIDs, corticosteroids or nephrotoxic medication should be avoided. EQUIOXX has not been tested in horses less than 1 year of age or in breeding horses, or pregnant or lactating mares. For additional information, please refer to the prescribing information or visit www.equioxx.com.

Take A Stand Against Anesthetic RiskNew Standing MRI technology offers
clearer images with less risk.
Standing equine MRI machines are becoming the new norm in helping equine
veterinarians diagnose lameness problems. Hallmarq Veterinary Imaging’s standing MRI
machine allows horses to stand for scans of the foot and lower leg. The horse is
simply walked into the machine instead of undergoing general anesthesia, which can
lead to problems including death in some healthy horses. The new motion correction
technology offers quality diagnostic images
while providing a safe and comfortable
experience for the horse.
To find out more about Hallmarq’s standing equine MRI machines visit www.hallmarq.net or call (978) 266 1219.
Photo courtesy of Rossdale and Partners, Newmarket UK. © Hallmarq Veterinary Imaging Ltd (2013)

Clinical Commentary
The use of magnetic resonance imaging for the diagnosisof osteomyelitisN. WerpyDiagnostic Imaging Department, University of Florida, Gainesville, Florida, USA.Corresponding author email: [email protected]
The case presented in this issue by Garcia et al. (2014)demonstrates the use of magnetic resonance imaging (MRI)positive contrast fistulography in a horse with a penetratingfoot wound and associated osseous and soft tissue injury.Based on the history, and clinical and imaging examinations,infectious osteomyelitis was strongly suspected. Radiographsdemonstrated evidence of osteolysis of the navicular bone,but further imaging was needed to confirm this finding andevaluate the soft tissues (Urraca Del Junco et al. 2012). The softtissue detail and exquisite fluid sensitivity make MRI themodality of choice when evaluating a penetrating woundand particularly when extension to the osseous column issuspected (Fig 1). No other modality has the ability to definethe extent or involvement of associated structures with thesame accuracy.
Differentiating septic conditions such as osteomyelitis fromregional inflammation or trauma is difficult to impossiblewithout the identification of bone lysis regardless of theimaging modality. The clinical history and examination iscritical for accurate interpretation of the imaging findings.However, there can be significant overlap between horsespresenting with infection vs. inflammation. These casesare challenging, and often require additional diagnosticimaging to aid in the differentiation between infection andinflammation. This can be most difficult when attemptingto differentiate joint sepsis with periarticular/subchondralosteomyelitis from a joint flare with osseous inflammation. This isbecause the same overlap in these cases that can occur withthe clinical presentation can also occur with imaging findings.
One of the earliest pathological changes in thedevelopment of osteomyelitis is osseous fluid accumulationand MRI is the only imaging modality that can be used for itsidentification (Yang et al. 2006; Jaramillo 2011; Guillerman2013). The earliest pathological changes in osteomyelitis canbe identified using skeletal nuclear scintigraphy. However, thismodality is dependent on the presence of actual boneturnover and not specifically the presence of osseous fluid. Forthis reason, nuclear scintigraphy is sensitive for early bone injurybut not specific for osteomyelitis (Boado et al. 2005; Jaramillo2011; Urraca Del Junco et al. 2012). Fat suppressed and fluidsensitive MRI sequences, such as the STIR sequence, are mostfrequently used to identify fluid in bone. While normal bone isrelatively homogenous dark grey to black on images acquiredusing the STIR sequence, fluid in bone is detected as regions ofincreased signal intensity and the affected area appears greyto white. The degree of hyperintensity (dark grey, light grey orwhite) is based on the severity of the fluid accumulation andthe fluid composition. Pure fluid will appear a different shadeof grey to fluid with cells and/or protein, depending on the MRIsequence. Although fat suppressed sequences are most
commonly used for the identification of osseous fluid and aregenerally most sensitive, other MRI sequences can also beutilised. All MRI sequences should be compared as thedifferent sequences provide different pieces of information(Werpy and Barrett 2012).
The diagnostic imaging challenge in these cases is that thesignal patterns for these conditions, joint sepsis vs. joint flare,are not specific, and at different stages and severities therecan be marked similarities in the appearance of the MRIimages (Kuemmerle et al. 2006). The interpretation of theimages must utilise all of the available signs including theassociated or adjacent synovial and soft tissue structures. Jointcapsule inflammation and synovitis, as well as soft tissueswelling are important indicators, as they are often moreprominent with sepsis (Yang et al. 2006; Jaramillo 2011;Guillerman 2013).
Although the imaging modality of MRI is uniquely sensitiveto the identification of osseous fluid, the fluid can also bea nonspecific finding (Fig 2). Fluid is seen in cases withosteomyelitis, osteonecrosis, resorption, trauma, inflammation,limb overuse and altered biomechanics (Schweitzer andWhite 1996; Grampp et al. 1998). It is important to understand
Fig 1: A penetrating wound is present, evidenced by a tractcontaining haemorrhage (arrow). The tract extends from the solethrough the digital cushion into the proximal recess of the navicularbursa (asterisk). Magnetic resonance imaging provides anexcellent method for determining the extent of abnormalitiesresulting from a penetrating wound.
15
© 2013 EVJ Ltd
EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

that osseous fluid from osteomyelitis can appear as the sameshade of grey as fluid from inflammation or trauma. The shadeof grey in the region of fluid, which is determined by theseverity and the composition of the fluid, is an important factor
in ranking the differential diagnoses for these cases inconjunction with the clinical presentation. In order todifferentiate the aetiology of the fluid accumulation better, i.v.administration of gadolinium can be considered (Morrisonet al. 1993). The synovial membrane is expected to havemarked contrast enhancement in sepsis. However, this canalso be difficult to differentiate from severe inflammation andenhancement is considered a nonspecific finding (Ledermannet al. 2002; Averill et al. 2009).
Lysis is the most definitive diagnostic imaging abnormalitythat can lead to a confident diagnosis of osteomyelitis (Pinedaet al. 2006). In the earliest stages of osteomyelitis, lysis may notbe initially visible, and then becomes visible on subsequentstudies. The cross sectional nature of MRI makes it very sensitiveto the progression of bone lysis that can occasionally occurvery rapidly, resulting in significant lysis in 1–2 weeks that wasnot present on the initial study. The use of standing, sedatedMRI is particularly useful in this situation for frequent recheckexaminations when attempting to monitor treatment anddisease progression. In certain cases, it will not be possible todiagnose osteomyelitis using only one MR examination and asecond may be necessary to evaluate the affected structures(Werpy 2012).
In the case of a penetrating wound, bone loss as a result ofosteomyelitis is a great concern. However, it is important tonote that bone loss can occur without infection. Trauma to thebone by the penetrating object can result in osteonecrosis orresorption. In these cases the MRI images and radiographsshould be evaluated together as the fine bone detail can bebetter assessed on radiographs when it is in a visible location.Regardless of these assessments, when in doubt these casesshould be treated like sepsis with osteomyelitis until provenotherwise (Jann and Pasquini 2005; Murray 2012). Typically,even in the absence of infection, there is initially significantinflammation in the bone recognised on MR images by thepresence of fluid. Trauma and/or joint flares can result inenough inflammation to see abnormalities develop in thearticular cartilage and the periarticular margins. The lack ofinfection in cases with severe inflammation does not decreasein importance of this relative to the long-term health of thejoint.
The case presented in this issue by Garcia et al. (2014)demonstrates the use of positive contrast fistulography in ahorse with a suspected penetrating wound. Clear signs ofosteomyelitis were present in this case. However, it is importantto remember that the distinction between infection andinflammation can be difficult even with MRI and may requiremore than one imaging study.
Author’s declaration of interestsNo conflicts of interest have been declared.
ReferencesAverill, L.W., Hernandez, A., Gonzalez, L., Peña, A.H. and Jaramillo, D.
(2009) Diagnosis of osteomyelitis in children: utility of fat-suppressedcontrast-enhanced MRI. AJR Am. J. Roentgenol. 192, 1232-1238.
Boado, A., Kristoffersen, M., Dyson, S. and Murray, R. (2005) Use ofnuclear scintigraphy and magnetic resonance imaging to diagnosechronic penetrating wounds in the equine foot. Equine Vet. Educ.17, 62-68.
Garcia, E.B., Rademacher, N., McCauley, C.T. and Gaschen, L. (2014)Navicular bone osteomyelitis and navicular bursitis with associatedfistula diagnosed with magnetic resonance fistulography in thehorse. Equine Vet. Educ. 26, 10-14.
Case 1
Case 2
Fig 2: STIR sagittal images from 2 different cases. Case 1 becameseverely lame 4 days after treatment of the navicular bursa. Fluid ispresent in the navicular bone and distal phalanx. Synovial fluidanalysis from the navicular bursa was not definitive for infection.Case 2 has a penetrating wound (white arrow) with lysis of thenavicular bone (arrowhead), severe deep digital flexor tendoninjury and osseous fluid affecting the navicular bone and distalphalanx. The osseous fluid appears similar in these 2 cases in bothits location and intensity. However, the cause of the fluid may bequite different. In Case 2, osteomyelitis is the most likely cause ofthe fluid. However, in Case 1 there is not clear distinction betweeninflammation or infection, and both remain possible.
© 2013 EVJ Ltd
16 EQUINE VETERINARY EDUCATION / AE / JANUARY 2014
Continued on page 31

Since hay is the first consideration when it comes to nutrition, skimping on quality could keep your horse from doing his best for you.
Do your best for your horse.Feed Standlee Premium Western Forage™. All natural. Always available.
CHECK OUT OUR COMPLETE PRODUCT LINE OR FIND A STORE NEAR YOU AT
WWW.STANDLEEFORAGE.COM

Case Report
Multimodal therapy including electroacupuncture for the treatmentof facial nerve paralysis in a horseC. de Fourmestraux*, C. Tessier and G. Touzot-JourdeSurgery Department, Equine Clinic, ONIRIS, Nantes-Atlantique, National College of Veterinary Medicine, FoodScience and Engineering, Nantes, France.*Corresponding author email: [email protected]
Keywords: horse; anaesthesia; facial nerve paralysis; electrostimulation
SummaryThis Case Report describes a 5-year-old Standardbred geldingthat was referred to the Equine Hospital of ONIRIS VeterinarySchool of Nantes, France for a surgical procedure undergeneral anaesthesia. Anaesthesia was induced andmaintained intravenously and the horse was placed in leftlateral recumbency with a padded halter. On post operativeDay 1, a post anaesthetic distal facial nerve branch paresiswas diagnosed based on clinical signs. The horse wasdischarged on post operative Day 2 with medical treatmentbased on anti-inflammatory drug administration locally andsystemically. The horse was re-examined 2 weeks after thesurgery; the left partial facial paralysis was still present andassociated with amyotrophy of the muscles supplied by thebuccal branches of the facial nerve. In accordance with theowner, the horse was hospitalised to start an electrostimulationtreatment. The horse was treated every day for the first 4 days,then every 2 or 3 days during the following 3 weeks, for a totalof 11 sessions. At the end of the second week of treatment,the horse was able to normally prehend the food andatrophy seemed reduced. The horse was discharged fromhospitalisation at the end of the third week of treatment withspecific recommendations. One month after discharge fromthe hospital just a slight asymmetry could be noticed at rest. Sixmonths later, the training season began and the horse wasable to perform. Facial paralysis due to nerve compression is awell-known complication of anaesthesia. Gradual recovery offunction over the weeks of treatment suggests thatelectroacupuncture may promote recovery and may hastentime of recovery.
IntroductionFacial nerve paralysis has been identified in several domesticspecies (DeLahunta and Glass 2009). The most common causein horses is a facial nerve traumatic injury, which can be aconsequence of direct trauma to the nerve or a result of localinflammatory changes involving the nerve (Sumano et al.1997; Rose and Hodgson 2000). It may improve over days,weeks or months without treatment, but can also persist formonths to years and lead to inability to perform (Jeong et al.2001; Smith and George 2009). In man, there is some evidenceto support acupuncture as a treatment for facial paralysis(Dong and Xie 2002; Mayor 2007). Electroacupuncture hasbeen regarded as a therapeutic option for various muscularand neurological conditions and may also be able to facilitatethe treatment of facial paralysis in horses (Sumano et al. 1997;Fleming 2001; Kim and Xie 2009). Electroacupuncture elevatesneurotrophic factors such as neurotrophine 3 (NT-3) and level
of cyclic adenosine monophosphate in injured spinal cordtissue (Ding et al. 2009). Neurotrophine 3 plays an importantrole in nervous system development, neuronal survival anddifferentiation, and neural repair. Elevated NT-3 expression canimprove the microenvironment of injured spinal cord (Yanet al. 2011). In addition, a previous study reported thatelectroacupuncture treatment can prevent the formation of aglial scar after spinal cord injury (Yang et al. 2005). Moreinterestingly, regarding functional peripheral nerveregeneration it has been shown that electroacupunctureexerts a positive influence on motor recovery and reducedpain related behaviour in mice after sciatic nerve crush injury(Hoang et al. 2012). This clinical case reports the use ofelectrostimulation in the treatment of traumatic partial facialnerve palsy following a surgery under general anaesthesia in ahorse.
Case historyA 5-year-old Standardbred gelding was referred for surgicalrelease of an epiglottic fold entrapment to the Equine Hospitalof ONIRIS Veterinary School of Nantes, France. The surgery wasperformed under general anaesthesia with the horse placedin left lateral recumbency in a padded recovery box.Anaesthesia was induced intravenously with diazepam(Valium)1 at 0.05 mg/kg bwt and ketamine (Imalgene)2
at 2.2 mg/kg bwt after a romifidine premedication (Sedivet)3,at 0.08 mg/kg bwt and maintained by administration ofa triple drip (guaifenesin 5%, ketamine 1 g/l, romifidine0.05 g/l). The surgical site was accessed by the oral cavity andthe procedure was performed under endoscopic guidance.No intraoperative complications were encountered. Theprocedure lasted 18 min and the total recumbency durationlasted 60 min. During the procedure, a padded halter waskept on the horse in order to mobilise the head easily and wasleft during recovery.
Clinical findings and diagnosisOn post operative Day 1, the horse presented a markedmuzzle deviation towards the right side, the left nostril wascollapsed and sagging inwards during inspiration. The lower lipon the left side hung loosely from its attachment and the horsehad difficulty prehending food. The left eyelid and the left eardid not show any weakness. Additionally, swelling was presenton the left lateral aspect of the masseter at the level of thefacial nerve buccal branches. A traumatic distal facial nervebranch paresis was diagnosed based on clinical signs (Fig 1).The initial treatment was comprised of a single i.v.administration of dexamethasone (Dexadreson)4 at 0.1 mg/kg
18
© 2013 EVJ Ltd
EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

bwt and local application twice a day of a topical gelcontaining dimethyl sulfoxide and prednisolone. The horsewas discharged on post operative Day 2. The owner wasinstructed to administer a 5-day course of phenylbutazone(Equipalazone)4 at 2.2 mg/kg bwt per os s.i.d., to rest the horse
for 2 weeks (1 week of box rest and 1 week in the paddock),and to return for follow-up.
The horse was re-examined 2 weeks after the surgery for apost operative evaluation of the upper airway and the facialparalysis. The left partial facial paralysis was still present and a
a) b)
Fig 1a) and b): The horse with distal facial nerve palsy associated with a marked muzzle deviation towards the right side and the lower lipon the left side hung loosely.
Facial nerve
13
4
6
7
2
5
Dorsal buccalbranchVentral buccalbranch
Zygomaticus
Levatornasolabialis
Levatorlabiisuperioris
Orbicularisoris
Depressor labiiinferioris
BuccinatorCaninus
Fig 2: Superficial structures of the head; the course of the facial nerve and muscles supplied by its buccal branches.
© 2013 EVJ Ltd
19EQUINE VETERINARY EDUCATION / AE / JANUARY 2014
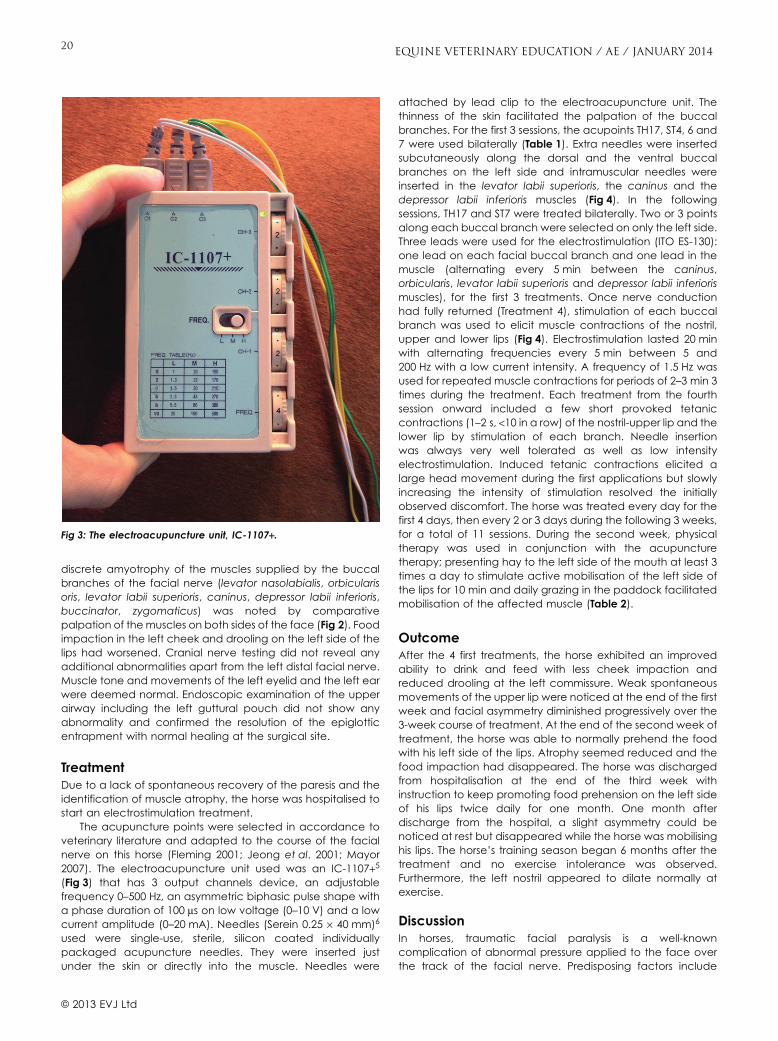
discrete amyotrophy of the muscles supplied by the buccalbranches of the facial nerve (levator nasolabialis, orbicularisoris, levator labii superioris, caninus, depressor labii inferioris,buccinator, zygomaticus) was noted by comparativepalpation of the muscles on both sides of the face (Fig 2). Foodimpaction in the left cheek and drooling on the left side of thelips had worsened. Cranial nerve testing did not reveal anyadditional abnormalities apart from the left distal facial nerve.Muscle tone and movements of the left eyelid and the left earwere deemed normal. Endoscopic examination of the upperairway including the left guttural pouch did not show anyabnormality and confirmed the resolution of the epiglotticentrapment with normal healing at the surgical site.
TreatmentDue to a lack of spontaneous recovery of the paresis and theidentification of muscle atrophy, the horse was hospitalised tostart an electrostimulation treatment.
The acupuncture points were selected in accordance toveterinary literature and adapted to the course of the facialnerve on this horse (Fleming 2001; Jeong et al. 2001; Mayor2007). The electroacupuncture unit used was an IC-1107+5
(Fig 3) that has 3 output channels device, an adjustablefrequency 0–500 Hz, an asymmetric biphasic pulse shape witha phase duration of 100 ms on low voltage (0–10 V) and a lowcurrent amplitude (0–20 mA). Needles (Serein 0.25 ¥ 40 mm)6
used were single-use, sterile, silicon coated individuallypackaged acupuncture needles. They were inserted justunder the skin or directly into the muscle. Needles were
attached by lead clip to the electroacupuncture unit. Thethinness of the skin facilitated the palpation of the buccalbranches. For the first 3 sessions, the acupoints TH17, ST4, 6 and7 were used bilaterally (Table 1). Extra needles were insertedsubcutaneously along the dorsal and the ventral buccalbranches on the left side and intramuscular needles wereinserted in the levator labii superioris, the caninus and thedepressor labii inferioris muscles (Fig 4). In the followingsessions, TH17 and ST7 were treated bilaterally. Two or 3 pointsalong each buccal branch were selected on only the left side.Three leads were used for the electrostimulation (ITO ES-130):one lead on each facial buccal branch and one lead in themuscle (alternating every 5 min between the caninus,orbicularis, levator labii superioris and depressor labii inferiorismuscles), for the first 3 treatments. Once nerve conductionhad fully returned (Treatment 4), stimulation of each buccalbranch was used to elicit muscle contractions of the nostril,upper and lower lips (Fig 4). Electrostimulation lasted 20 minwith alternating frequencies every 5 min between 5 and200 Hz with a low current intensity. A frequency of 1.5 Hz wasused for repeated muscle contractions for periods of 2–3 min 3times during the treatment. Each treatment from the fourthsession onward included a few short provoked tetaniccontractions (1–2 s, <10 in a row) of the nostril-upper lip and thelower lip by stimulation of each branch. Needle insertionwas always very well tolerated as well as low intensityelectrostimulation. Induced tetanic contractions elicited alarge head movement during the first applications but slowlyincreasing the intensity of stimulation resolved the initiallyobserved discomfort. The horse was treated every day for thefirst 4 days, then every 2 or 3 days during the following 3 weeks,for a total of 11 sessions. During the second week, physicaltherapy was used in conjunction with the acupuncturetherapy; presenting hay to the left side of the mouth at least 3times a day to stimulate active mobilisation of the left side ofthe lips for 10 min and daily grazing in the paddock facilitatedmobilisation of the affected muscle (Table 2).
OutcomeAfter the 4 first treatments, the horse exhibited an improvedability to drink and feed with less cheek impaction andreduced drooling at the left commissure. Weak spontaneousmovements of the upper lip were noticed at the end of the firstweek and facial asymmetry diminished progressively over the3-week course of treatment. At the end of the second week oftreatment, the horse was able to normally prehend the foodwith his left side of the lips. Atrophy seemed reduced and thefood impaction had disappeared. The horse was dischargedfrom hospitalisation at the end of the third week withinstruction to keep promoting food prehension on the left sideof his lips twice daily for one month. One month afterdischarge from the hospital, a slight asymmetry could benoticed at rest but disappeared while the horse was mobilisinghis lips. The horse’s training season began 6 months after thetreatment and no exercise intolerance was observed.Furthermore, the left nostril appeared to dilate normally atexercise.
DiscussionIn horses, traumatic facial paralysis is a well-knowncomplication of abnormal pressure applied to the face overthe track of the facial nerve. Predisposing factors include
Fig 3: The electroacupuncture unit, IC-1107+.
© 2013 EVJ Ltd
20 EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

anatomic features in the horse, such as the nerve passingover prominent facial bony structures (rim of the ramusmandibulae, supraorbital ridge) and nerve location in thinsubcutaneous tissue as well as prolonged periods of completelateral recumbency on hard surfaces or wearing a halter withlarge buckles and thick leather or fabric (DeLahunta and Glass2009; Smith and George 2009). Despite padding precautionsand a short duration of recumbency, facial paralysis
developed in this horse and was probably a result of keepinga large, thick and insufficiently padded halter on the head.
The World Health Organisation has included Bell’s palsy inits list of diseases for which acupuncture therapy is indicatedand a wide variety of human facial paralyses are commonlytreated by acupuncture and electroacupuncture (Dong andXie 2002; Mayor 2007). Point selection based on traditionalacupoints has been shown to be more effective when it isadapted to the anatomical distribution of the facial nervebranches and anatomical location of muscles targeted forstimulation (Fleming 2001; Jeong et al. 2001; Mayor 2007). Inthe treatment of various problems including paralysis,electroacupuncture, as compared to simple needling, hasbeen shown to allow for more rapid, more intense and longerlasting results (Mayor 2007). While experimental data havesupported the benefit of electrical nerve stimulation for axonalregeneration following nerve trauma (Shi et al. 2000), directstimulation of denervated muscles has been a subject ofcontroversy. Excessive stimulation and movement of muscleswith reduced circulation is thought to increase fibrosis anddelay nerve regrowth and reconnection to muscles (Mayor2007). However, electrical stimulation by its beneficial effectson microcirculation and inflammation can improve tissuenourishment and healing as well as delay atrophy and fibrosis.Selection of electrical parameters based on intrinsic firingcharacteristics of motor units themselves like in trophicelectrical stimulation (low frequencies and amplitudes)appears to be less fatiguing and more able to maintain muscletone by altering metabolism rather than muscle fibre training(Mayor 2007). Low frequency and low intensity stimulation forshort periods of time were therefore initially used to obtainweak contractions of atrophied muscle in this horse. Oncenerve conduction had been regained, alternating high andlow frequency stimulation at low amplitude was used as it hasbeen shown to be more efficacious than a continuousstimulation at a set frequency (Mayor 2007). This constitutes adifference with the stimulation mode used by Sumano in his 12clinical cases.
When the injury is mild, clinical signs often disappear in afew days/weeks and it is thought that no nerve degenerationoccurs, only interruption of nerve conduction (neuropraxia).The myelin sheath is temporarily damaged causing a focaldemyelination and a partial denervation of the muscles, whichcan still be excited by stimulation of the motor nerve (Mayor2007). If the lesion is more severe (neurotmesis), a completedenervation leads to muscle degeneration and fibrosis startingwithin 1–2 weeks of the nerve injury and is completed in about3 years. In this sort of clinical case, the muscle fibres need to bedirectly stimulated to contract. The severity of the lesion wasnot clearly established; however, absence of spontaneous
TABLE 1: Description of acupuncture points used
Point, Chinese name Meridian Location area
ST4, Di Cang Stomach meridian Caudal to the corner of the mouth, at the ‘V’ junction of the levator nasolabialism. and zygomaticus m., on the outer margin of the orbicularis muscle.
ST6, Jiache Stomach meridian In the centre of the masseter muscle belly, just dorsal to the ventrolateral aspectof the jaw. Located in a depression when the jaw is opened (where the ringhalter is).
ST7, Xia Guan Stomach meridian At the temporo-mandibular joint, ventral to the zygomatic arch, caudodorsal tothe lateral canthus, in the masseter m.
TH17, Yi Feng Triple heater Posterior to the ear in depression between the mandible and mastoid process.
TH17
ST6
ST7
ST4
Fig 4: Electroacupuncture treatment of a horse with left distal facialparalysis and localisation of the acupuncture points used in thetreatment.
© 2013 EVJ Ltd
21EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

recovery and muscle atrophy seems to be in favour ofneurotmesis. Rapid recovery of nerve conduction as identifiedby muscle contraction elicited by stimulation of the nerve onthe third treatment probably indicates a less severe lesion thaninitially assessed. Electroacupuncture treatment is believed tohave been beneficial in this case as observed by the recoveryand improvement of clinical signs over time. No improvementwas seen during the first 2 weeks with the initial medicaltreatment and facial muscle atrophy had begun. Gradualrecovery of function over the 3-week electroacupuncturecourse suggests that it is a favourable treatment. Sumano et al.(1997) reported successful outcomes with a similar treatmentcourse: first stimulation within the 10 days (2 weeks for this case)following paralysis onset with a mean of 13 (7–17) treatmentsdone every other day over a course of 3–4 weeks (11 sessionsover 3 weeks for the present case). Progressive improvementswere seen over the course of the treatment and very visibleafter the first or second treatment as in the presentcase. Although the factors involved in the decision oftreatment termination are not clearly stated, ownersatisfaction seemed to have played an important role.Follow-up at 6 months showed no recurrence of clinical signs inboth case reports. Rehabilitation exercises were added to theelectroacupuncture for the present case during the secondweek of treatment and likely also played a role in recovery.Human and experimental data show that there areadvantages in combining electrotherapy and physiotherapy(Angelov et al. 2007; Mayor 2007).
ConclusionsDistal facial paralysis in the horse as described in the presentcase affects food prehension ability and nostril dilation. It canresult in dysphagia and inability to perform. Spontaneousrecovery can be long and incomplete, jeopardisingan athletic career. The use of electrotherapy seemsadvantageous in promoting recovery and may hasten time ofrecovery. However, as the amount of nerve injury was notassessed before treatment and a multimodal therapeuticapproach was used, it is not possible to determine which part
of the treatment was the most efficacious, although thetreatment success was assumed to be due to the combinedtherapy (electroacupuncture and physical therapy) afterinitial medical treatment failed. Finally, it is important to keep inmind that facial paralysis might occur even after a short lateralrecumbency and halters should be always removed whenpossible. Discussion about appropriate positioning andpadding to avoid nerve lesion is the primary way to avoidfacial paralysis in horses undergoing general anaesthesia.
Authors’ declaration of interestsNo conflicts of interest have been declared.
Manufacturers’ addresses1Roche, Boulogne-Billancourt, France.2Merial, Lyon, France.3Boehringer Ingelheim, Paris, France.4MSD, Courbevoie, France.5ITO, Tokyo, Japan.6Seirin Corporation, Shizuoka, Japan.
ReferencesAngelov, D.N., Ceynowa, M., Guntinas-Lichius, O., Streppel, M.,
Grosheva, M., Kiryakova, S.I., Skouras, E., Maegele, M., Irintchev, A.,Neiss, W.F., Sinis, N., Alvanou, A. and Dunlop, S. (2007) Mechanicalstimulation of paralyzed vibrissal muscles following facial nerve injuryin adult rat promotes full recovery of whisking. Neurobiol. Dis. 26,229-242.
Delahunta, A. and Glass, E. (2009) Lower motor neuron: general somaticefferent, cranial nerve. In: Veterinary Neuroanatomy and ClinicalNeurology, Eds: A. Delahunta, E. Glass and M. Kent, W.B. Saunders,St Louis. pp 134-167.
Ding, Y., Yan, Q., Ruan, J.W., Zhang, Y.Q., Li, W.J., Zhang, Y.J., Li, Y., Dong,H. and Zeng, Y.S. (2009) Electro-acupuncture promotes survival,differentiation of the bone marrow mesenchymal stem cells as wellas functional recovery in the spinal cord-transected rats. BMCNeurosci. 10, 1-13.
Dong, H.G. and Xie, Z.F. (2002) Acupuncture: review and analysis ofreports on controlled clinical trials. World Health Organisation,Geneva.
TABLE 2: Therapeutic table
Type oftreatment
Day aftersurgery Detailed description
Medical D1D1–D5
Dexamethasone (Dexadreson, i.v.)4 at 0.1 mg/kg bwt, s.i.d.Topical gel (dimethyl sulfoxide, prednisolone), b.i.d.Phenylbutazone (Equipalazone)4 2.2 mg/kg bwt per os, s.i.d.
AcupunctureFirst week
D16, D17, D18 Acupoints Extra needles Leads Mode and frequencyBilaterally Left side Left side Treatment duration: 20 minTH17, ST4, ST6, ST7 Subcutaneously
Along the dorsal and theventral buccal branches
Intramuscular needles(Levator labii superioris,
caninus, depressor labiiinferioris)
One lead on needles placedalong left dorsal branch
One lead on needles placedalong left ventral branch
One lead on intramuscularneedles (levator labiisuperioris, caninus)
Alternating every 5 min(5–200 Hz)
Second andthird week
D19, D21, D23, D25,D28, D31, D34, D37
TH17 and ST7 Along the dorsal and theventral buccal brancheswith the proximal needlejust caudally to the origin ofthe branches and the distalneedle proximal to therostral border of themasseter
One lead on needles placedalong left dorsal branch
One lead on needles placedalong left ventral branch
Alternating every 5 min(5–200 Hz)Low current intensity1.5 Hz for repeated muscle
contractions for periods of2–3 min, 3 times during thetreatment
Physicaltherapy
D23 to the end Hay presentation by hand of the left side to stimulate mobilisation of the affected muscles for 10 min, t.i.d. andall day grazing.
© 2013 EVJ Ltd
22 EQUINE VETERINARY EDUCATION / AE / JANUARY 2014
Continued on page 40

Find the solution to your horse’s needs – discover your Platinum! To find the right Platinum Performance® solution, and to learn about the science behind the supplements call 1-800-553-2400, visit PlatinumPerformance.com or speak with your equine veterinarian.© 2013 PLATINUM PERFORMANCE, INC.
www.PlatinumPerformance.com
Ashlee BondInternational Grand Prix Show JumperPlatinum Performance® Client since 1996
Ashlee Bond is a sponsored endorsee and actual client.
Platinum Gastric Support®Plat
• Joint Health• Hoof Health• Skin & Coat Health
• Performance & Recovery• Digestive health• Bone & Tendon Health
• Helps maintain healthy gastric acid levels• Supports a healthy appetite and digestion
Available in 3 Flavors:
OriginalApple
Natural Cherry
Cinnamon Spice
Platinum Performance® CJ Supports
I've been so fortunate to be able to ride great horses like Cadet and Wistful. Agro Star is another one with a bright future, and I'm excited to see him now spread his wings at the Grand Prix level. As an equestrian athlete, it is such an honor to represent the USA. Before every show, I make every effort to prepare each of my horses to be their best. A lot of things have come and gone in our program. But when something works, you stick with it. Platinum Performance has been in our barn since 1996. You can see it in the horses fitness and performance. We literally wouldn't be without it.
This is my horse™
to ride great horses like Cadet andWistful. Agro Star is another onewith a bright future, and I'm excitedto see him now spread his wings atthe Grand Prix level. As an equestrianathlete, it is such an honor torepresent the USA. Before everyshow, I make every effort to prepareeach of my horses
y to be their best.
A lot of thingsyy
have come and gonein our program. But when somethingworks, you stick with it. PlatinumPerformmaance
yhas been in our barn
since 19996. You can see it in thehorses fitness and performance. Wel ll ld '
I've been so fortunate to be ableb f t t t b bl
literally wouldn't be without it.
I've been so fortunate to be able to ride great horses like Cadet and Wistful. Agro Star is another one with a bright future, and I'm excited to see him now spread his wings at the Grand Prix level. As an equestrian athlete, it is such an honor to represent the USA. Before every show, I make every effort to prepare each of my horses to be their best. A lot of things have come and gone in our program. But when something works, you stick with it. Platinum Performance has been in our barn since 1996. You can see it in the horses fitness and performance. We literally wouldn't be without it.
AshAshAshAshshshshhhhhleeleeleeleeleeleeleelee BoBoBoBoBoBoBoBondndddndndndnnnnIIInInnnnttttteeerernrnnrn tiatiationanaaonalll GrGrGrGrGrG andndddandandandaall PPPrPrPriixixixdddddd ShShShShShowowowowowoxxx JuJuJuJuJumpempempempemp rrwwwwwPPPlPlaPlalalaaaaatintininntitt umumumum PePePePerfrforfof rmrmrmamamancee®® CClient®® sinceet 1999911 9699
Ashlee Bond is a sponsored endorsee and actual client.
Ashlee BondInternational Grand Prix Show JumperPlatinum Performance® Client since 1996
Ashlee Bond is a sponsored endorsee and actual client.
Agro Star Agro StarGrand Prix Show Jumping Horse

Clinical Commentary
Electroacupuncture for nerve injury in the horseD. G. von SchweinitzOrchard Paddocks, Iron Lane, Surrey, Bramley, Guildford, UK.Corresponding author email: [email protected]
Keywords: horse; electroacupuncture; acupuncture; nerve injury; transcutaneous electrical nerve stimulation; electricalstimulation; nerve regeneration
The case report from de Fourmestraux et al. (2014) describesthe use of electroacupuncture (EA) in the treatment of a facialnerve paralysis occurring as a post anaesthetic complicationin a horse. It was applied in addition to conventional treatmentin an effort to maximise the chances of recovery of nervefunction. Nerve trauma with varying degrees of nerve deficitand associated pain are not uncommon in the horse. Thereare many indications and opportunities for EA to improve theoutcome of injuries involving nerve damage, and there is goodevidence from clinical and experimental trials in other speciesin the use of EA for these cases.
A recent review of the EA literature through PubMed givesan account of the breadth of research in this area from 1975 to2012 (Mayor 2013). This found 548 clinical studies of EA in manand 1607 predominantly experimental animal studies. Thesewere mainly pain studies investigating endogenous opioidmechanisms. More recently, nonpain studies dominate. Thefindings support the upregulation of β-endorphins occurring inthe brain from low frequency EA (1–7 Hz) and the upregulationof dynorphin in the spinal cord occurring from high frequencyEA (15–100 Hz). Electroacupuncture delivers a stronger dose ofacupuncture, more effectively upregulates the endogenousopioid mechanisms, and is more easily standardised forresearch purposes than manual acupuncture.
Peripheral nerve injuries result in partial or total loss of motor,sensory, and autonomic functions in the denervated area dueto the interruption of axons, degeneration of distal nerve fibres,and eventual death of axotomised neurons (Allodi et al. 2012).Deficits can be compensated by regenerating injured axonsor by collateral branching of undamaged axons, andremodelling of nervous system circuitry related to the lostfunctions. Plasticity of central connections may compensatefunctionally for the lack of adequate target reinnervation;however, plasticity has limited effects on disturbed sensorylocalisation or fine motor control after injuries, and may evenresult in maladaptive changes, such as neuropathic pain andhyper-reflexia (Navarro 2009). The lack of specificity of nerveregeneration, in terms of motor and sensory axon regrowth,pathfinding and target reinnervation, is one of the mainshortcomings for recovery.
Peripheral nerve regeneration has been extensivelystudied in function and gene expression using a sciaticnerve crush model in mice and rats (Vogelaar et al. 2004).Recovery of sensory and some motor function occurred inapproximately 3 weeks; however, with the return of sensoryfunction, a state of mechanical allodynia (painful experiencegenerated by non-noxious stimuli) develops and is slow toretreat. This is a component of neuropathic pain known to existin man and studied in laboratory animals, but only relativelyrecently considered as a source of chronic pain in horses (Graf
von Schweinitz 1999; Macgregor and Graf von Schweinitz2006; Jones et al. 2007; Driessen et al. 2010; Muir 2010).Considering the risks of neuropathic pain from peripheral nerveinjury it is interesting to note the ongoing efforts to treatidiopathic headshaking in the horse by compression of theinfraorbital nerve, which has a reported initial success rate of63%, post operative nose rubbing rate of 63%, and symptomrecurrence rate of 26% (Roberts et al. 2013).
Different therapies have evolved to improve recoveryfrom nerve injury including exercise, and electrical stimulation,but the functional outcome of nerve repair can still bedisappointing due to muscle atrophy, scar tissue, neuroma,disturbed sensory evolution, and poor motor control. Averageaxonal regeneration rate in mammals is 1–3 mm/day (Gordonet al. 2009) and the length of nerve damage in the horsemay easily be several centimetres leading to a lengthyregeneration time with increased risks of unsatisfactoryregeneration.
Electrical stimulation has shown positive results onperipheral nerve regeneration effects in laboratory animals,mostly using EA with implanted electrodes with differentelectrical parameters: weak constant direct current andpulsed alternating current (Pomeranz et al. 1984; McDevittet al. 1987; Beveridge and Politis 1988; Pomeranz andCampbell 1993; Chen et al. 2001; Inoue et al. 2003; Mendonçaet al. 2003). One of the emerging links of EA being investigatedis with the modulation of nerve growth factor in nerve repair(Manni et al. 2011).
In a study of rats with transected median nerves one groupreceived plain acupuncture for 15 min every 2 days from oneweek after injury using points (PC 3 and 7) near the proximaland distal nerve stumps; another group received EA (1 mA at2 Hz) to produce a visual muscle contraction; a third groupwere untreated controls (Ho et al. 2013). Both treatmentgroups had better morphological, electrophysiological andfunctional outcomes than the control group.
Not all electrical stimulation forms are helpful. Somestudies of electrical stimulation have also had negativeoutcomes illustrating that the intensity and frequency of theelectrical field plays an important role (Aydin et al. 2006). Aninvestigation of transcutaneous electrical stimulation with low(4 Hz) and high (100 Hz) frequency transcutaneous electricalnerve stimulation (TENS) was undertaken as this technique isfrequently employed to control neuropathic pain (Baptistaet al. 2008). Using mice with a sciatic crush lesion treated30 min daily, TENS 5 days/week for 5 weeks led to a delayedregeneration with negative morphological changes of nervetissue compared to an untreated control group, especially inthe high frequency TENS group. The timing of the applicationof EA after nerve injury also appears to be an important factor
24
© 2013 EVJ Ltd
EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

(Yeh et al. 2010). In rats subjected to sciatic nerve section,those treated 8 days or 15 days later with low frequency (2 Hzat 1 mA) EA for 15 min every other day for 2 weeks hadsignificantly improved nerve regeneration, which was not thecase in the group treated from the first day.
Similarly, exercise has been shown to be a positive ornegative factor in nerve regeneration investigationsdependent on the exercise intensity and stress caused to theanimal (van Meeteren et al. 1998). Recently, low energyextracorporeal shock wave treatment has been shown toaccelerate the recovery of muscle sensitivity and function bypromoting regeneration after nerve compression injury in rats(Hausner et al. 2012; Mense and Hoheisel 2013). This stillrequires work to determine the appropriate dose andfrequency of treatment before it can be confidently used inthe horse.
In the case report from de Fourmestraux et al. (2013), carewas taken to select appropriate points and electricalstimulation properties based on the research, and to includean exercise tailored to the condition to optimise the chancesfor recovery. The significance being that it is possible to treatinappropriately, cause additional harm, and bring about anegative outcome from the use of EA. Similar case reports arelacking in the literature and hopefully this report will encouragesimilar ones.
A case report of acupuncture in a dog with idiopathicfacial nerve paralysis makes an interesting comparison (Jeonget al. 2001). A terrier with a 35 day acute onset of unilateralfacial nerve paralysis and no improvement on dailyprednisolone at 1 mg/kg bwt was treated with dry needleacupuncture. Points on the face (LI 20, ST 2, ST 7, SI 18, TH 17and GB 3) were needled only on the contralateral side, and adistal forelimb and a hindlimb point was treated bilaterally (LI 4and GB 34 respectively) for 20 min every other day for the firstweek, then weekly for the next 3 weeks. Lip drooping anddrooling were abolished after the first treatment, with progressto complete facial symmetry achieved by the last treatment.In this case there was no local stimulation on the affected sideindicating central neural reflexes and mechanisms wereresponsible for the improvements. Studies of neuropathicmechanisms from nerve injury demonstrate a unilateral injuryoften progresses to bilateral neuropathic changes (Beheraet al. 2013); interestingly, acupuncture treatment on thecontralateral side has been shown to treat the opposite side(Kim et al. 2010).
The use of EA in nerve regeneration in man has beenreported, e.g. in carpal tunnel syndrome with severe axondegeneration and release surgery (Gordon et al. 2008). Trainsof 20 Hz electrical stimulation for one hour to 2 weeksaccelerated axon outgrowth across the suture site inassociation with elevated neuronal neurotrophic factor andreceptors and promoted the full reinnervation of thenarmuscles in contrast to a nonsignificant increase in motor unitnumbers in the control group.
Some critics may take issue with this example as notrepresenting acupuncture because of a lack of adherence tothe traditional Chinese medicine language of yin and yang,and the flow of Qi, and one may then consider this anexample of western medical acupuncture. Acupuncture hashistorically evolved and traditional Chinese medicine isarguably grossly misrepresented by translation errors of theancient Chinese texts and the politics of the practice from laypractitioners (Birch and Felt 1999; Kendall 2002; Unschuld 2003;
Schnorrenberger 2011). The advances in neuroscience havebrought an increasing amount of evidence for the usefulnessand relatively low risks in a competent application ofacupuncture including the more modern forms of EA and laseracupuncture. More evidence in the form of controlled trialsand clinical trials are required, but this can equally be appliedto most of veterinary medicine.
Author’s declaration of interestsNo conflicts of interest have been declared.
ReferencesAllodi, I., Udina, E. and Navarro, X. (2012) Specificity of peripheral nerve
regeneration: interactions at the axon level. Prog. Neurobiol. 98,16-37.
Aydin, M.A., Comlekci, S., Ozguner, M., Cesur, G., Nasir, S. and Aydin,Z.D. (2006) The influence of continuous exposure to 50 Hz electricfield on nerve regeneration in a rat peroneal nerve crush injurymodel. Bioelectromagnetics 27, 401-413.
Baptista, A.F., Gomes, J.R.S., Oliveira, J.T., Santos, S.M., Vannier-Santos,M.A. and Martinez, A.M. (2008) High- and low-frequencytranscutaneous electrical nerve stimulation delay sciatic nerveregeneration after crush lesion in the mouse. J. Peripher. Nerv. Syst.13, 71-80.
Behera, D., Behera, S., Jacobs, K.E. and Biswal, S. (2013) Bilateralperipheral neural activity observed in vivo following unilateral nerveinjury. Am. J. Nucl. Med. Mol. Imaging 3, 282-290.
Beveridge, J. and Politis, M. (1988) Use of exogenous electric current inthe treatment of delayed lesions in peripheral nerves. Plast.Reconstr. Surg. 82, 573-579.
Birch, S.J. and Felt, R.L. (1999) Understanding Acupuncture, ChurchillLivingstone, Edinburgh.
Chen, Y., Hu, C., Hsieh, C.L., Lin, J.G., Tsai, C.C., Chen, T.H. and Yao, C.H.(2001) Effects of percutaneous electrical stimulation on peripheralnerve regeneration using silicone rubber chambers. J. Biomed.Mater. Res. 57, 541-549.
Driessen, B., Bauquier, S.H. and Zarucco, L. (2010) Neuropathic painmanagement in chronic laminitis. Vet. Clin. North Am.: Equine Pract.26, 315-337.
de Fourmestraux, C., Tessier, C. and Touzot-Jourde, G. (2014) Multimodaltherapy including electroacupuncture for the treatment of facialnerve paralysis in a horse. Equine Vet. Educ. 26, 18-23.
Gordon, T., Brushart, T.M. and Chan, K.M. (2008) Augmenting nerveregeneration with electrical stimulation. Neurol. Res. 30, 1012-1022.
Gordon, T., Chan, K.M., Sulaiman, O.A., Udina, E., Amirjani, N. andBrushart, T.M. (2009) Accelerating axon growth to overcomelimitations in functional recovery after peripheral nerve injury.Neurosurgery 65, A132-A144.
Graf von Schweinitz, D. (1999) Thermographic diagnostics in equineback pain. Vet. Clin. North Am.: Equine Pract. 15, 161-177.
Hausner, T., Pajer, K., Halt, G., Hopf, R., Schmidhammer, R., Redl, H. andNógrádi, A. (2012) Improved rate of peripheral nerve regenerationinduced by extracorporeal shock wave treatment in the rat. Exp.Neurol. 236, 363-370.
Ho, C.Y., Yao, C.H., Chen, W.C., Shen, W.C. and Bau, D.T. (2013)Electroacupuncture and acupuncture promote the rat’s transectedmedian nerve regeneration. Evid. Based Complement. Alternat.Med. 2013: 514610.
Inoue, M., Hojo, T., Yano, T. and Katisumi, Y. (2003) The effects ofelectroacupuncture on peripheral nerve regeneration in rats.Acupunct. Med. 21, 9-17.
Jeong, S.M., Kim, H.-Y., Lee, C.H., Kweon, O.K. and Nam, T.C. (2001) Useof acupuncture for the treatment of idiopathic facial nerve paralysisin a dog. Vet. Rec. 148, 632-633.
Jones, E., Vinuela-Fernandez, I., Eager, R.A., Delaney, A., Anderson, H.,Patel, A., Robertson, D.C., Allchorne, A., Sirinathsinghji, E.C., Milne,E.M., MacIntyre, N., Shaw, D.J., Waran, N.K., Mayhew, J. andFleetwood-Walker, S.M. (2007) Neuropathic changes in equinelaminitis pain. Pain 132, 321-331.
© 2013 EVJ Ltd
25EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

Kendall, D.E. (2002) Dao of Chinese Medicine: Understanding AnAncient Healing Art, Oxford University Press, New York. 0-19-592104-6.
Kim, M.K., Choi, T.Y., Lee, M.S., Lee, H. and Han, C.H. (2010) Contralateralacupuncture versus ipsilateral acupuncture in the rehabilitation ofpost-stroke hemiplegic patients: a systematic review. BMCComplement. Altern. Med. 10, 41.
Macgregor, J. and Graf von Schweinitz, D. (2006) Needleelectromyographic activity of myofascial trigger points and controlsites in equine cleidobrachialis muscle–an observational study.Acupunct. Med. 24, 61-70.
Manni, L., Rocco, M.L., Barbaro Paparo, S. and Guaragna, M. (2011)Electroacupuncture and nerve growth factor: potential clinicalapplications. Arch. Ital. Biol. 194, 247-255.
Mayor, D. (2013) An exploratory review of the electroacupunctureliterature: clinical applications and endorphin mechanisms.Acupunc. Med. doi: 10.1136/acupmed-2013-010324. [Epub aheadof print].
McDevitt, L., Fortner, P. and Pomeranz, B. (1987) Application of weakelectric field to the hindpaw enhances sciatic motor nerveregeneration in the adult rat. Brain Res. 416, 308-314.
Mendonça, C., Barbieri, C. and Mazzer, N. (2003) Directly applied lowintensity direct current enhances peripheral nerve regeneration inrats. J. Neurosci. Methods 129, 183-190.
Mense, S. and Hoheisel, U. (2013) Shock wave treatment improves nerveregeneration in the rat. Muscle Nerve 47, 702-710.
Muir, W.M. (2010) Pain: mechanisms and management in horses. Vet.Clin. North Am.: Equine Pract. 26, 467-480.
Navarro, X. (2009) Neural plasticity after nerve injury and regeneration.Int. Rev. Neurobiol. 87, 483-505.
Pomeranz, B. and Campbell, J. (1993) Weak electric currentaccelerates motoneuron regeneration in the sciatic nerve often-month-old rats. Brain Res. 603, 271-278.
Pomeranz, B., Mullen, M. and Markus, H. (1984) Effect of appliedelectrical fields on sprouting of intact saphenous nerve in adult rat.Brain Res. 303, 331-336.
Roberts, V.L., Perkins, J.D., Skärlina, E., Gorvy, D.A., Tremaine, W.H.,Williams, A., McKane, S.A., White, I. and Knottenbelt, D.C. (2013)Caudal anaesthesia of the infraorbital nerve for diagnosis ofidiopathic headshaking and caudal compression of the infraorbitalnerve for its treatment, in 58 horses. Equine Vet. J. 45, 107-110.
Schnorrenberger, C.C. (2011) Epistemological evaluation of Chinesemedicine and acupuncture. J. Chin. Med. 22, 1-17.
Unschuld, P.U. (2003) Huang Di Nei Jing Su Wen. Nature, Knowledge,Imagery in An Ancient Chinese Medical Text, University of CaliforniaPress, Berkeley.
van Meeteren, N.L., Brakkee, J.H., Helders, P.J. and Gispen, W.H. (1998)The effect of exercise training on functional recovery after sciaticnerve crush in the rat. J. Peripher. Nerv. Syst. 3, 277-282.
Vogelaar, C.F., Vrinten, D.H., Hoekman, M.F., Brakkee, J.H., Burbach, J.P.and Hamers, F.P. (2004) Sciatic nerve regeneration in mice and rats:recovery of sensory innervation is followed by a slowly retreatingneuropathic pain-like syndrome. Brain Res. 1027, 67-72.
Yeh, C.C., Lin, Y.C., Tsai, F.J., Huang, C.Y., Yao, C.H. and Chen, Y.S. (2010)Timing of applying electrical stimulation is an important factordeciding the success rate and maturity of regenerating rat sciaticnerves. Neurorehabil. Neural Repair 24, 730-735.
© 2013 EVJ Ltd
26 EQUINE VETERINARY EDUCATION / AE / JANUARY 2014
For subcutaneous injection in the posterior aspect of the ear where it attaches to the head (base of the ear) in lactating dairy cattle. For subcutaneous injection in the middle third of the posterior aspect of the ear or in the posterior aspect of the ear where it attaches to the head (base of the ear) in beef and non-lactating dairy cattle. Not for use in calves to be processed for veal.
CAUTIONFederal (USA) law restricts this drug to use by or on the order of a licensed veterinarian.
INDICATIONSEXCEDE Sterile Suspension is indicated for treatment of bovine respiratory disease (BRD, shipping fever, pneumonia) associated with Mannheimia haemolytica, Pasteurella multocida, and Histophilus somni in beef, non-lactating dairy, and lactating dairy cattle.
EXCEDE Sterile Suspension is also indicated for the control of respiratory disease in beef and non-lactating dairy cattle which are at high risk of developing BRD associated with M. haemolytica, P. multocida, and H. somni.
EXCEDE Sterile Suspension is also indicated for the treatment of bovine foot rot (interdigital necrobacillosis) associated with Fusobacterium necrophorum and Porphyromonas levii in beef, non-lactating dairy, and lactating dairy cattle.
EXCEDE Sterile Suspension is also indicated for treatment of acute metritis (0-10 days postpartum) associated with bacterial organisms susceptible to ceftiofur in lactating dairy cattle.
CONTRAINDICATIONSAs with all drugs, the use of EXCEDE Sterile Suspension is contraindicated in animals pre viously found to be hypersensitive to the drug.
WARNINGSFOR USE IN ANIMALS ONLY. NOT FOR HUMAN USE.KEEP OUT OF REACH OF CHILDREN.
Penicillins and cephalosporins can cause allergic reactions in sensitized individuals.
Topical exposures to such antimicrobials, including ceftiofur, may elicit mild to severe allergic reactions in some individuals. Repeated or prolonged exposure may lead to sensitization. Avoid direct contact of the product with the skin, eyes, mouth and clothing. Sensitization of the skin may be avoided by wearing protective gloves.
Persons with a known hypersensitivity to penicillin or cephalosporins should avoid exposure to this product.
In case of accidental eye exposure, flush with water for 15 minutes. In case of accidental skin exposure, wash with soap and water. Remove contaminated clothing. If allergic reaction occurs (e.g., skin rash, hives, difficult breathing), seek medical attention.
The material safety data sheet contains more detailed occupational safety information. To obtain a material safety data sheet please call 1-800-733-5500. To report any adverse event please call 1-800-366-5288.
Intra-arterial injection may occur during administration of EXCEDE Sterile Suspension via middle third of the ear injection or base of the ear injection directed toward the opposite eye. Intra-arterial injection of EXCEDE Sterile Suspension is likely to result in sudden death of the animal.
RESIDUE WARNINGS
a 13-day pre-slaughter withdrawal period is required after the last treatment.
no milk discard period is required for this product.
BW or administration by unap proved routes (subcutaneous injection in the neck or intramuscular injection) may cause violative residues.
in pre-ruminating calves.
PRECAUTIONSFollowing subcutaneous injection in the middle third of the posterior aspect of the ear, thickening and swelling (characterized by aseptic cellular infiltrate) of the ear may occur. As with other parenteral injections, localized post-injection bacterial infections may result in abscess formation. Attention to hygienic procedures can minimize their occurrence.
Following injection at the posterior aspect of the ear where it attaches to the head (base of the ear), areas of discoloration and signs of inflammation may persist at least 13 days post administration resulting in trim loss of edible tissue at slaughter. Injection of volumes greater than 20 mL, in the middle third of the ear, may result in open draining lesions in a small percentage of cattle.
The effects of ceftiofur on bovine reproductive performance, pregnancy, and lactation have not been determined.
ADVERSE EFFECTSIntra-arterial injection may occur during administration of EXCEDE Sterile Suspension via middle third of the ear injection or base of the ear injection directed toward the opposite eye. Intra-arterial injection of EXCEDE Sterile Suspension is likely to result in sudden death of the animal. During the conduct of clinical studies, there was a low incidence of acute death (see ANIMAL SAFETY) confirmed to be the result of inadvertent intra-arterial injection. No other adverse systemic effects were noted for either the antibiotic or formulation during any of the clinical and target animal safety studies.
STORAGE CONDITIONSStore at controlled room temperature 20° to 25°C (68° to 77°F). Shake well before using. Contents should be used within 12 weeks after the first dose is removed.
HOW SUPPLIEDEXCEDE Sterile Suspension is available in the following package sizes:100 mL vial250 mL vial
NADA #141-209, Approved by FDAwww.EXCEDE.com or call 1-866-387-2287
Revised December 2011 EXD12041
Distributed byPharmacia & Upjohn CompanyDivision of Pfizer Inc, NY, NY 10017

Important Safety Information: The use of EXCEDE is contraindicated in animals with known allergy to ceftiofur or to the β-lactam group (penicillins and cephalosporins) of antimicrobials. Do not use EXCEDE in horses intended for human consumption. The administration of antimicrobials in horses under conditions of stress may be associated with diarrhea, which may require appropriate veterinary therapy. Though safe in cattle when properly administered, inadvertent intra-arterial injection is possible and fatal. EXCEDE has a pre-slaughter withdrawal time of 13 days in cattle. Do not use in calves to be processed for veal. For complete details, refer to the full prescribing information, or visit excede.com.
Treat him right the fi rst time with EXCEDE® — the only 2-treatment solution.Just because the symptoms have gone, it doesn’t mean the infection has. Fortunately, EXCEDE® (ceftiofur crystalline free acid) Sterile Suspension off ers an eff ective, less complicated approach. No more 10-dose treatments. No more hoping you didn’t miss a day. And no more fi ghting to administer for 10 straight days. Talk to your veterinarian, and discover the only FDA-approved 2-treatment solution. excede.com/equine
Join our community
/eqstable
EQStable™ available inthe Apple® App Store®
All trademarks are the property of Zoetis Inc., its affi liates and/or its licensors. All other trademarks are the propertyof their respective owners. ©2013 Zoetis Inc. All rights reserved. EQB13087
ARE NEVERTHIS EASY TO SPOT
RESPIRATORY INFECTIONSHALF-TREATED

Wellness visitshave been upgraded from “suggested” to
REQUIRED
You know that taking the best care of your clients’ horses requires regular wellness visits and preventive care. We know that, too. That’s why we require all horses enrolled in our ColiCare colic surgery reimbursement program stay up to date on annual exams, vaccinations and a deworming program�—�all through their veterinarian.
We also require that horses in the ColiCare program receive year-round, daily administration of SmartDigest® Ultra, our comprehensive GI health formula. We’re so confident in the combination of regular veterinary care and SmartDigest Ultra that every horse enrolled in ColiCare is eligible for up to $7500 of colic surgery reimbursement.
That’s how ColiCare gives you healthy patients and a healthy practice.
Learn more about the ColiCare program today at SmartPak.com/ColiCareDVM or call 1-888-472-5229
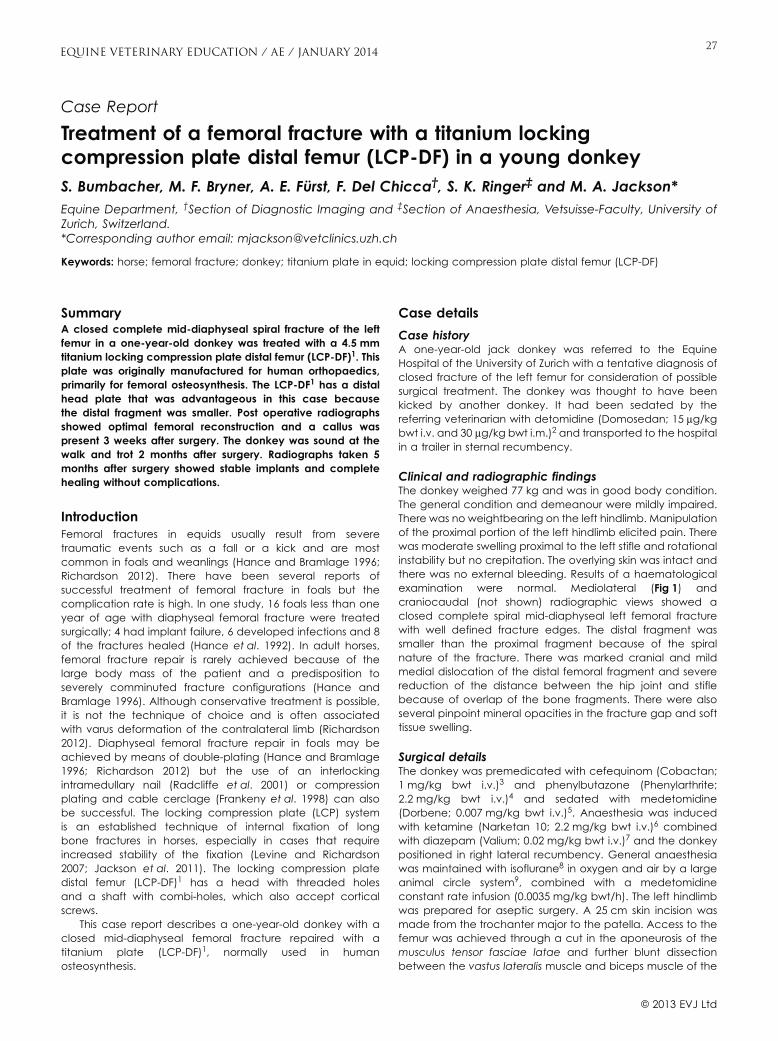
Case Report
Treatment of a femoral fracture with a titanium lockingcompression plate distal femur (LCP-DF) in a young donkeyS. Bumbacher, M. F. Bryner, A. E. Fürst, F. Del Chicca†, S. K. Ringer‡ and M. A. Jackson*Equine Department, †Section of Diagnostic Imaging and ‡Section of Anaesthesia, Vetsuisse-Faculty, University ofZurich, Switzerland.*Corresponding author email: [email protected]
Keywords: horse; femoral fracture; donkey; titanium plate in equid; locking compression plate distal femur (LCP-DF)
SummaryA closed complete mid-diaphyseal spiral fracture of the leftfemur in a one-year-old donkey was treated with a 4.5 mmtitanium locking compression plate distal femur (LCP-DF)1. Thisplate was originally manufactured for human orthopaedics,primarily for femoral osteosynthesis. The LCP-DF1 has a distalhead plate that was advantageous in this case becausethe distal fragment was smaller. Post operative radiographsshowed optimal femoral reconstruction and a callus waspresent 3 weeks after surgery. The donkey was sound at thewalk and trot 2 months after surgery. Radiographs taken 5months after surgery showed stable implants and completehealing without complications.
IntroductionFemoral fractures in equids usually result from severetraumatic events such as a fall or a kick and are mostcommon in foals and weanlings (Hance and Bramlage 1996;Richardson 2012). There have been several reports ofsuccessful treatment of femoral fracture in foals but thecomplication rate is high. In one study, 16 foals less than oneyear of age with diaphyseal femoral fracture were treatedsurgically; 4 had implant failure, 6 developed infections and 8of the fractures healed (Hance et al. 1992). In adult horses,femoral fracture repair is rarely achieved because of thelarge body mass of the patient and a predisposition toseverely comminuted fracture configurations (Hance andBramlage 1996). Although conservative treatment is possible,it is not the technique of choice and is often associatedwith varus deformation of the contralateral limb (Richardson2012). Diaphyseal femoral fracture repair in foals may beachieved by means of double-plating (Hance and Bramlage1996; Richardson 2012) but the use of an interlockingintramedullary nail (Radcliffe et al. 2001) or compressionplating and cable cerclage (Frankeny et al. 1998) can alsobe successful. The locking compression plate (LCP) systemis an established technique of internal fixation of longbone fractures in horses, especially in cases that requireincreased stability of the fixation (Levine and Richardson2007; Jackson et al. 2011). The locking compression platedistal femur (LCP-DF)1 has a head with threaded holesand a shaft with combi-holes, which also accept corticalscrews.
This case report describes a one-year-old donkey with aclosed mid-diaphyseal femoral fracture repaired with atitanium plate (LCP-DF)1, normally used in humanosteosynthesis.
Case details
Case historyA one-year-old jack donkey was referred to the EquineHospital of the University of Zurich with a tentative diagnosis ofclosed fracture of the left femur for consideration of possiblesurgical treatment. The donkey was thought to have beenkicked by another donkey. It had been sedated by thereferring veterinarian with detomidine (Domosedan; 15 mg/kgbwt i.v. and 30 mg/kg bwt i.m.)2 and transported to the hospitalin a trailer in sternal recumbency.
Clinical and radiographic findingsThe donkey weighed 77 kg and was in good body condition.The general condition and demeanour were mildly impaired.There was no weightbearing on the left hindlimb. Manipulationof the proximal portion of the left hindlimb elicited pain. Therewas moderate swelling proximal to the left stifle and rotationalinstability but no crepitation. The overlying skin was intact andthere was no external bleeding. Results of a haematologicalexamination were normal. Mediolateral (Fig 1) andcraniocaudal (not shown) radiographic views showed aclosed complete spiral mid-diaphyseal left femoral fracturewith well defined fracture edges. The distal fragment wassmaller than the proximal fragment because of the spiralnature of the fracture. There was marked cranial and mildmedial dislocation of the distal femoral fragment and severereduction of the distance between the hip joint and stiflebecause of overlap of the bone fragments. There were alsoseveral pinpoint mineral opacities in the fracture gap and softtissue swelling.
Surgical detailsThe donkey was premedicated with cefequinom (Cobactan;1 mg/kg bwt i.v.)3 and phenylbutazone (Phenylarthrite;2.2 mg/kg bwt i.v.)4 and sedated with medetomidine(Dorbene; 0.007 mg/kg bwt i.v.)5. Anaesthesia was inducedwith ketamine (Narketan 10; 2.2 mg/kg bwt i.v.)6 combinedwith diazepam (Valium; 0.02 mg/kg bwt i.v.)7 and the donkeypositioned in right lateral recumbency. General anaesthesiawas maintained with isoflurane8 in oxygen and air by a largeanimal circle system9, combined with a medetomidineconstant rate infusion (0.0035 mg/kg bwt/h). The left hindlimbwas prepared for aseptic surgery. A 25 cm skin incision wasmade from the trochanter major to the patella. Access to thefemur was achieved through a cut in the aponeurosis of themusculus tensor fasciae latae and further blunt dissectionbetween the vastus lateralis muscle and biceps muscle of the
27
© 2013 EVJ Ltd
EQUINE VETERINARY EDUCATION / AE / JANUARY 2014
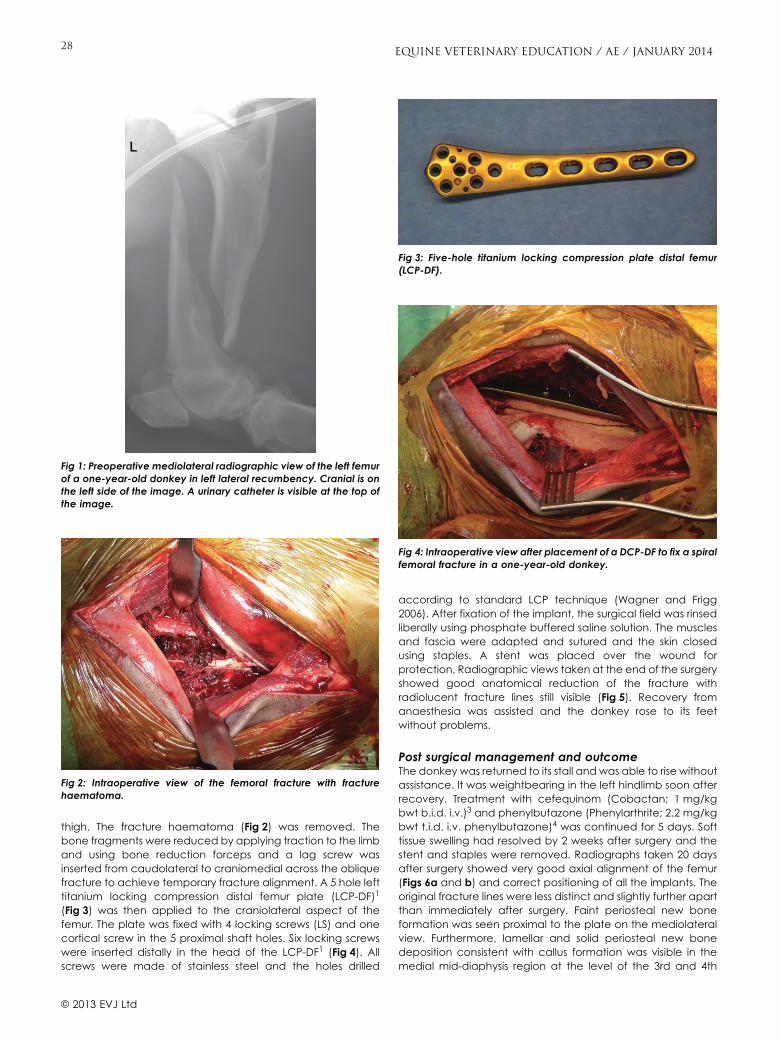
thigh. The fracture haematoma (Fig 2) was removed. Thebone fragments were reduced by applying traction to the limband using bone reduction forceps and a lag screw wasinserted from caudolateral to craniomedial across the obliquefracture to achieve temporary fracture alignment. A 5 hole lefttitanium locking compression distal femur plate (LCP-DF)1
(Fig 3) was then applied to the craniolateral aspect of thefemur. The plate was fixed with 4 locking screws (LS) and onecortical screw in the 5 proximal shaft holes. Six locking screwswere inserted distally in the head of the LCP-DF1 (Fig 4). Allscrews were made of stainless steel and the holes drilled
according to standard LCP technique (Wagner and Frigg2006). After fixation of the implant, the surgical field was rinsedliberally using phosphate buffered saline solution. The musclesand fascia were adapted and sutured and the skin closedusing staples. A stent was placed over the wound forprotection. Radiographic views taken at the end of the surgeryshowed good anatomical reduction of the fracture withradiolucent fracture lines still visible (Fig 5). Recovery fromanaesthesia was assisted and the donkey rose to its feetwithout problems.
Post surgical management and outcomeThe donkey was returned to its stall and was able to rise withoutassistance. It was weightbearing in the left hindlimb soon afterrecovery. Treatment with cefequinom (Cobactan; 1 mg/kgbwt b.i.d. i.v.)3 and phenylbutazone (Phenylarthrite; 2.2 mg/kgbwt t.i.d. i.v. phenylbutazone)4 was continued for 5 days. Softtissue swelling had resolved by 2 weeks after surgery and thestent and staples were removed. Radiographs taken 20 daysafter surgery showed very good axial alignment of the femur(Figs 6a and b) and correct positioning of all the implants. Theoriginal fracture lines were less distinct and slightly further apartthan immediately after surgery. Faint periosteal new boneformation was seen proximal to the plate on the mediolateralview. Furthermore, lamellar and solid periosteal new bonedeposition consistent with callus formation was visible in themedial mid-diaphysis region at the level of the 3rd and 4th
Fig 1: Preoperative mediolateral radiographic view of the left femurof a one-year-old donkey in left lateral recumbency. Cranial is onthe left side of the image. A urinary catheter is visible at the top ofthe image.
Fig 2: Intraoperative view of the femoral fracture with fracturehaematoma.
Fig 3: Five-hole titanium locking compression plate distal femur(LCP-DF).
Fig 4: Intraoperative view after placement of a DCP-DF to fix a spiralfemoral fracture in a one-year-old donkey.
© 2013 EVJ Ltd
28 EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

screws (from proximal). The donkey was sound and wasdischarged 21 days post operatively. Five months after surgerythe donkey was re-evaluated. It had been pastured in theAlps, was sound at the walk and trot and in good bodycondition. Radiographic views of the left femur taken with aportable x-ray machine confirmed complete healing of thefracture. The radiolucent fracture lines seen on radiographs 20days after surgery were no longer visible (Fig 7).
DiscussionAn excellent outcome was achieved with a single distalfemoral locking compression plate (LCP-DF)1 in a one-year-olddonkey with closed complete mid-diaphyseal spiral femoralfracture. The main complication of femoral osteosynthesis isseroma formation (Hance and Bramlage 1996; Bramlage andFackelmann 2000; Richardson 2012), which can result from thefracture itself or from post fracture soft tissue trauma (Hanceand Bramlage 1996). Post operative infection and implantfailure are often related to seroma formation (Hance et al.1992). Factors that led to a favourable outcome withoutcomplications in our patient were the calm temperament andlow bodyweight (77 kg). It is well known that femoral fractureosteosynthesis in foals, ponies and small donkeys has a muchbetter prognosis than in heavier equine patients (Frankenyet al. 1998; Bramlage and Fackelmann 2000; Radcliffe et al.2001; Byron et al. 2002). For this reason, surgical treatment offemoral fractures is rarely attempted in the latter and affectedhorses are often subjected to euthanasia (Hance et al. 1992).
A lower bodyweight is not the only reason why foals and otheryoung horses with femoral fracture are better surgicalcandidates (Hance et al. 1992; Bramlage and Fackelmann2000; Radcliffe et al. 2001); young horses with femoral fracturetypically have a large spiral component caused by torsionalforce (Hance et al. 1992; Frankeny et al. 1998; Bramlage andFackelmann 2000), which makes the fracture easier to stabilisethan a comminuted fracture, which typically occurs in adulthorses. Young and growing animals also have a higher rate ofbone repair and form a stronger callus than older patients(Mehta 2010).
Double-plating with one plate positioned cranially and theother laterally on the femur is an established surgical treatmentfor femoral fracture (Radcliffe et al. 2001). The double-platingconstruct neutralises bending (Hance et al. 1992; Bramlageand Fackelmann 2000) as well as rotational forces. Comparedwith other methods, this construct provides greater strengthand stiffness (Radcliffe et al. 2001). Because of the fractureconfiguration with a long spiral component through themiddle of the bone, double-plating was not feasible in ourpatient, mainly because the screws of the lateral plate wouldhave been positioned parallel to the plane of the fracture. Forthis reason, it was necessary to achieve stabilisation with asingle plate placed craniolaterally on the femur. Alternatively,a plate combined with cerclage wire (Frankeny et al. 1998),intramedullary interlocking nail (IIN) fixation or IIN fixationcombined with a dynamic compression plate (Radcliffe et al.2001) could have been used in our patient. However, because
Fig 5: Post operative mediolateral radiographic view of the leftfemur of a one-year-old donkey in left lateral recumbency. Cranialis on the left side of the left of the image. The LCP-DF has beenplaced craniolaterally on the femur and good fracture reduction isapparent. A urinary catheter is visible at the top of the image.
Fig 6: a) Craniocaudal radiographic view of the left femur of aone-year-old donkey in left lateral recumbency 3 weeks afterosteosynthesis with an LCP-DF. There is a smooth and solidperiosteal callus (arrow) on the medial aspect of the femur atmid-diaphysis. b) Mediolateral radiographic view of the left femurof a one-year-old donkey in left lateral recumbency 3 weeks afterosteosynthesis with an LCP-DF. There is periosteal new boneproliferation proximal to the plate (arrow).
© 2013 EVJ Ltd
29EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

the distal fragment was relatively short and the LCP-DF1
allowed fixation with several screws distally, we consideredosteosynthesis with this plate more adequate. It provided amore stable fixation compared with a conventional LCP thatwould allow only one or 2 screws in the distal fragment(Kirker-Head and Fackelmann 1989) and the combination ofthe titanium plate and stainless steel screws was notassociated with implant instability attributable to galvaniccorrosion (Disegi 2009). The strength of LCP-DF1 was previouslydemonstrated in a biomechanical study that showed that itsaxial stiffness was greater than that of a dynamic condylarscrew (DCS) plate (Kim et al. 2011). The main advantage of theLCP-DF1 is that short terminal fragments are more easilyfixed because up to 7 screws can be inserted, similar to thestainless steel cobra head plate (Kirker-Head and Fackelmann1989). The LCP-DF1 was originally designed for distal shaft,supracondylar, intra-articular and periprosthetic fractures inman. The LCP-DF1 is available in a right and left version toadapt to the lateral condyles of the human femur. To ourknowledge, this is the first time that this plate has been used inequine surgery and it was shown to be very beneficial.
A recent in vitro study compared the use of titanium andstainless steel in fracture fixation (Hayes and Richards 2010).Titanium is used in plates because it provides stiffness,biocompatibility, ductility and strength, prerequisites forappropriate fracture fixation. The LCP-DF1 is made of varioustitanium alloys which have higher tensile strength capabilityand lower ductility than pure titanium (Disegi 2012). The
material most often used for internal fixation in equineosteosynthesis is stainless steel. Stainless steel is also a very stiffand strong metal with high yield strength and can thereforeundergo more countering and bending cycles before failureoccurs compared with titanium. The titanium LCP-DF1 isanatomically precontoured and therefore is not meant toundergo bending by the surgeon before placement. However,this plate has been developed for human orthopaedic surgeryand some degree of bending may be unavoidable if it is usedin other species. Titanium alloy is more flexible and has higherfatigue resistance than stainless steel and therefore is capableof adapting to deformations of the bone more closely.Another difference between these 2 metals relates to theirinteraction with bone. There is always a gap between boneand stainless steel filled with fibroid tissue, but not betweenbone and titanium, and therefore titanium alloy should, atleast theoretically, better integrate with bone than stainlesssteel. The surface of a titanium alloy plate is rougher then thatof a stainless steel plate because stainless steel iselectropolished. These characteristics of titanium enhanceosseointegration providing superior implant stability.Interestingly, however, clinical evaluations of human surgicalpatients failed to show distinct differences in healing betweenstainless steel and titanium implants (Hayes and Richards2010). The use of titanium alloy implants is not commonplace inequine osteosynthesis, but because implants in this speciesmay be subjected to very large cyclic loads, titanium maynevertheless hold promise for this indication. Because thefracture healed without complications and the plateappeared well integrated in the bone, implant removal wasdeemed unnecessary in our patient.
ConclusionA titanium LCP-DF1 was used successfully for the surgical repairof a mid-diaphyseal femoral fracture in a young donkey. Wefeel that this plate provides a promising option for femur repairin small equids and possibly for other selected fractures in adulthorses. The plate head with 7 threaded holes makes it usefulfor fractures with small terminal fragments or fractureconfigurations that are not amenable to fixation with 2 LCPs.Furthermore, titanium alloys have several properties thatsupport fracture healing and possibly reduce the risk ofinfection.
Authors’ declaration of interestsNo conflicts of interest have been declared.
AcknowledgementsThe authors wish to thank Dr Stefano D’Albena for referral ofthe donkey and for follow-up examination.
Manufacturers’ addresses1Synthes, Oberdorf, Switzerland.2Provet AG, Lyssach, Switzerland.3Veterinaria AG, Pfäffikon SZ, Switzerland.4Vétoquinol SA, Lure, France.5Dr E. Graeub AG, Bern, Switzerland.6Vetoquinol AG, Ittigen, Switzerland.7Roche Pharma AG, Reinach, Switzerland.8Abbott AG, Baar, Switzerland.9Vetronic Services Ltd, Devon, UK.
Fig 7: Mediolateral radiographic view of the left femur of the patientin left lateral recumbency 5 months after osteosynthesis with anLCP-DF. The fracture lines are no longer visible.
© 2013 EVJ Ltd
30 EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

ReferencesBramlage, L.R. and Fackelmann, G.E. (2000) Femur. In: AO Principles
of Equine Osteosynthesis, Eds: L.R. Bramlage, J.A. Auer, G.E.Fackelmann and D.M. Nunamaker, Thieme, Stuttgart. pp 197-207.
Byron, C.R., Stick, J.A., Brown, J.A. and Lugo, J. (2002) Use of a condylarscrew plate for repair of a Salter-Harris type-III fracture of the femurin a 2-year- old horse. J. Am. Vet. Med. Assoc. 221, 1292-1295.
Disegi, J.A. (2009) Implant Materials, 3th edn., Synthes Inc, West Chester.
Disegi, J.A. (2012) Metallic instruments and implants. In: Equine Surgery,4th edn., Eds: J.P. Auer and J.A. Stick, Saunders Elsevier,Philadelphia. pp 1040-1047.
Frankeny, R.L., Wilson, D.A., Crson, W.L. and Keegan, K.G. (1998) An invitro biomechanical investigation of compression plating with cablecerclage for repair of oblique osteotomies in foal femurs. Vet.Comp. Orthop. Traumatol. 11, 28-33.
Hance, S.R. and Bramlage, L.R. (1996) Fractures of the femur andpatella. In: Equine Fracture Repair, Ed: A.J. Nixon, W.B. Saunders,Philadelphia. pp 284-293.
Hance, S.R., Bramlage, L.R., Schneider, R.K. and Embertson, R.M. (1992)Retrospective study of 38 cases of femur fractures in horses less thanone year of age. Equine Vet. J. 24, 357-363.
Hayes, J.S. and Richards, R.G. (2010) The use of titanium and stainlesssteel in fracture fixation. Expert Rev. Med. Devices 7, 843-853.
Jackson, M.A., Kummer, M., Auer, J.A., Hagen, R. and Fürst, A. (2011) Thetreatment of type 2 and 4 olecranon fractures with locking
compression plates (LCP) in horses: a prospective study (2002-2008).Vet. Comp. Orthop. Traumatol. 24, 57-61.
Kim, J.W., Oh, C.W., Byun, Y.S., Oh, J.K., Kim, H.J., Min, W.K., Park, S.K. andPark, B.C. (2011) A biomechanical analysis of locking plate fixationwith minimally invasive plate osteosynthesis in a subtrochantericfracture model. J. Trauma 70, E19-E23.
Kirker-Head, C.A. and Fackelmann, G.E. (1989) Use of the cobra headbone plate for distal long bone fractures in large animals. Vet. Surg.18, 227-234.
Levine, D.G. and Richardson, D.W. (2007) Clinical use of the lockingcompression plate (LCP) in horses: a retrospective study of 31 cases(2004-2006). Equine Vet. J. 39, 401-406.
Mehta, M. (2010) Callus competence in bone healing of aged rats In:Fracture Callus Competence: Factors influencing the risk ofsecondary bone healing. Julius Wolf Institute Berlin, pp 31-52.
Radcliffe, R.M., Lopez, M.J.L., Turner, T.A., Watkins, J.P., Radcliffe, C.H.and Markel, M.D. (2001) An in vitro biomechanical comparison ofinterlocking nail constructs and double plating for fixation ofdiaphyseal femur fractures in immature horses. Vet. Surg. 30,179-190.
Richardson, D.W. (2012) Femur and pelvis. In: Equine Surgery, 4th edn.,Eds: J.P. Auer and J.A. Stick, Saunders Elsevier, Philadelphia.pp 1442-1449.
Wagner, M. and Frigg, R. (2006) Techniques and procedures in LISS andLCP. In: AO Manual of Fracture Management, Internal Fixators, 1stedn., Eds: M. Wagner and R. Frigg, Thieme, Stuttgart. pp 125-161.
© 2013 EVJ Ltd
31EQUINE VETERINARY EDUCATION / AE / JANUARY 2014
Grampp, S., Henk, C.B. and Mostbeck, G.H. (1998) Overuse edema inthe bone marrow of the hand: demonstration with MRI. J. Comput.Assist. Tomogr. 22, 25-27.
Guillerman, R.P. (2013) Osteomyelitis and beyond. Pediatr. Radiol. 43,Suppl. 1, S193-S203.
Jann, H. and Pasquini, C. (2005) Wounds of the distal limb complicatedby involvement of deep structures. Vet. Clin. North Am.: EquinePract. 21, 145-165.
Jaramillo, D. (2011) Infection: musculoskeletal. Pediatr. Radiol. 41, Suppl.1, S127-S134.
Kuemmerle, J.M., Uhlig, H. and Kofler, J. (2006) Severe acuteinflammatory reaction (SAIR) of the fetlock joint after intraarticularhyaluronate injection in a horse. Vet. Comp. Orthop. Traumatol. 19,236-238.
Ledermann, H.P., Schweitzer, M.E. and Morrison, W.B. (2002)Nonenhancing tissue on MR imaging of pedal infection:characterization of necrotic tissue and associated limitations fordiagnosis of osteomyelitis and abscess. AJR Am. J. Roentgenol. 178,215-222.
Morrison, W.B., Schweitzer, M.E., Bock, G.W., Mitchell, D.G., Hume, E.L.,Pathria, M.N. and Resnick, D. (1993) Diagnosis of osteomyelitis: utility
of fat-suppressed contrast-enhanced MR imaging. Radiology 189,251-257.
Murray, S. (2012) How to manage penetrating injuries of synovialstructures in the field. Proc. Am. Ass. Equine Practnrs. 58, 221-227.
Pineda, C., Vargas, A. and Rodríguez, A.V. (2006) Imaging ofOsteomyelitis: current concepts. Infect. Dis. Clin. North Am. 20,789-825.
Schweitzer, M.E. and White, L.M. (1996) Does altered biomechanicscause marrow edema. Radiology 198, 851-853.
Urraca Del Junco, C.I., Mair, T.S., Powell, S.E., Milner, P.I., Font, A.F.,Schwarz, T. and Weaver, M.P. (2012) Magnetic resonance imagingfindings of equine solar penetration wounds. Vet. Radiol. Ultrasound53, 71-75.
Werpy, N.M. (2012) Recheck magnetic resonance imagingexaminations for evaluation of musculoskeletal injury. Vet. Clin.North Am.: Equine Pract. 28, 659-680.
Werpy, N.M. and Barrett, M.F. (2012) Advances in Equine Imaging. Vet.Clin. North Am.: Equine Pract. 28, xiii-xxiv.
Yang, W.J., Im, S.A., Lim, G.-Y., Chun, H.J., Jung, N.Y., Sung, M.S. andChoi, B.G. (2006) MR imaging of transient synovitis: differentiationfrom septic arthritis. Pediatr. Radiol. 36, 1154-1158.
Continue page 16d from

Clinical Commentary
Diaphyseal femoral fractures in young horsesA. R. S. BarrSchool of Clinical Veterinary Science, University of Bristol, UK.Corresponding author email: [email protected]
The case report by Bumbacher et al. (2014) describes themanagement of a closed, complete, spiral, mid-diaphysealfracture of the femur in a yearling donkey weighing 77 kg.Internal fixation was achieved via a lateral surgical approachusing a titanium locking compression plate distal femur(LCP-DF) applied craniolaterally along with a single lag screw.The fracture healed satisfactorily and at 5 months post surgerythe donkey was sound at the walk and trot.
Femoral fractures are said to be more common in younghorses (Richardson 2012) although as smaller, younger horsestend to be the only ones where surgical repair may becontemplated there is probably significant selection prior toreferral to surgical facilities. The high energy required tofracture the femur in an adult horse often results in severelycomminuted fractures that are rarely amenable to treatmentand usually warrant humane destruction.
Femoral fracture configurations in horses include:
Occasional stress fractures of the proximal cranial femoralcortex are also said to occur (Hawkins 2003).
Diaphyseal fractures in young horses are usually aconsequence of a fall or external blow. Clinical signs usuallycomprise acute severe lameness, swelling (and sometimesshortening) of the thigh region, pain on manipulation,rotational instability and, in some cases, crepitation onmanipulation of the limb (although the latter was not a featurein the case reported here emphasising that fragmentseparation by haemorrhage, inflammatory swelling andinterposing muscle can be sufficient to minimise this sign).Radiographic examination is best performed under generalanaesthesia or deep sedation that will allow the animal to beplaced in lateral recumbency for mediolateral views and indorsal recumbency for craniocaudal views of the entire femur.
to optimally image both proximal and distal femur.Displacement of proximal or distal physeal fractures may beminimal and good quality images will be required to diagnosethe injury in such cases.
Diaphyseal femoral fractures are generally spiral or longoblique in configuration and usually closed because of theextensive surrounding musculature (Fig 1). There may besignificant overriding of fragments due to muscle contracture.Spiral fractures may be a consequence of torsional loadingwhich results in shear stresses distributed over the entire bone.Bone strength and stiffness in torsion is dependent oncross-sectional area and the distribution of bone around theneutral axis which together determine the polar moment of
shape may concentrate stresses at certain points in the bone(stress risers). Experimentally, the weakening effect of stressrisers is particularly prominent under torsional loading(Edgerton et althe absence of bone defects in the caudal cortex followingreduction and fixation is felt to be important to prognosisclinically (Bramlage and Fackelman 2000).
Other than trochanteric fractures which can often bemanaged successfully conservatively, femoral fractures inhorses remain a major management challenge to equineorthopaedic surgeons. Conservative management is probablyonly likely to be successful for trochanteric fractures and stableminimally displaced distal physeal fractures and shouldcomprise 3 months box rest in the first instance (Hance and
diaphyseal fracture usually end up with shortening androtational deformity of the femur together with marked varusangular limb deformity of the contralateral limb due toexcessive weightbearing during healing.
Open reduction and internal fixation is thus generally theonly realistic option for management of major completefemoral diaphyseal fractures if there is to be any hope of areasonable functional outcome. The surgical approach, as inthe case reported here, is a lateral one. The incision runs fromslightly caudal to the greater trochanter to the lateralepicondyle of the femur along the cranial border of the bicepsfemoris muscle. The deep fascia is incised in the intermuscularseptum between the superficial gluteal muscle and bicepsfemoral muscle proximally and the tensor fasciae latae andbiceps femoris distally. The attachment of the superficialgluteal to the third trochanter may be incised and reflectedcranially and the insertion of the biceps femoris muscle on thelateral patellar ligament can be partially incised to provideincreased exposure in more distal fractures. The lateral aspectof the femur is then exposed by retracting the biceps femorismuscle caudally and vastus lateralis
Separated fragments should be re-attached to the mainproximal or distal fragments with lag screws trying to avoid thescrew heads being in positions that will compromisesubsequent placement of plates or using 3.5 mm screws anddeeply countersinking the heads to avoid them interfering.Reduction of the main fracture fragments can provechallenging particularly when, as is often the case, thereduced configuration is not inherently stable. Significanttraction may be required on the lower limb and anchoring thetail and body of the animal to the table in anticipation of thisis worthwhile. Large bone-holding forceps to manipulate andsecure fragments during reduction are helpful and oncereduced one or more lag screws should be placed to securealignment during plate application.
32
© 2013 EVJ Ltd
EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

Optimal implant choice has progressed over the last 40years since the first descriptions of internal fixation of equinefemoral fractures. Denny (1978) reported the attemptedsurgical management of 5 cases of femoral diaphysealfractures in neonatal foals. Two were treated with stackedintrameduallary pins, 2 with Venables plates and one with anASIF broad dynamic compression plate. In all cases, fixationfailed within 10 days of surgery and the foals had to behumanely destroyed. Since that time implants used haveincluded broad dynamic compression plates, cobra headplates, angle blade plates and dynamic condylar screwplates. Richardson (2012) recommended double plating using4.5 mm locking compression plates with 5.5 mm cortex screwsand 5 mm locking head screws. As long a plate as possible ispositioned laterally and then a shorter one placed craniallywith interdigitating screws. An interlocking intramedullary nailmay be an alternative for simple fractures not requiringadditional lag screws. Bramlage and Fackelman (2000) andRichardson (2012) emphasise the importance of closedsuction drainage to minimise serum accumulation for the first3–4 days post operatively. Seroma formation can predisposeto wound dehiscence and infection which are common postoperative complications (Richardson 2012). Approximately50% of foals with diaphyseal fractures, repaired by internalfixation with double plating, will have satisfactory healing.Bramlage and Fackelman (2000) state that the majority offoals with successful outcomes are less than 3 months of agewhen presented with their fractures.
In the case reported here a single plate was deployedcraniolaterally because the surgeons were concerned aboutthe potential for screws to end up parallel to the plane of the
fracture if a double plating technique were deployed. Theexpanded distal end of the LCP-DF also allows for up to 7screws to be placed in the distal fragment which providesadditional stability in the repair of fractures that extend closeto the distal physis. Figure 6 in the paper by Bumbacher et al.(2014) suggests the fracture in this case healed with limitedradiographically visible bony callus which implies goodfracture stability during healing and is in contrast to the largecalluses previously observed in other cases (Bramlage andFackelman 2000; Richardson 2012). Surgical removal ofimplants is rarely required unless there are problems withinfection or growth compromise by implants which cross thedistal physis. Bumbacher et al. (2014) discuss the potentialmechanical advantages of titanium alloys and theirenhanced capacity for integration with bone. There is alsosome evidence in man that titanium implants may also reducethe risk of delayed infection compared to stainless steelimplants (Glotzbecker et al. 2013).
Successful surgical treatment of femoral diaphysealfractures in young horses probably hinges particularly oncareful case selection in the first place, focusing on the sizeand temperament of the patient and configuration of thefracture together with the availability of the requisite facilities,equipment and experienced surgical staff. Balancing theconfidence and optimism to attempt the possible with theneed to recognise and heed the warning signs of likely failureremain crucial as ever to the surgical art. The successfuldeployment of new implants such as the titanium lockingcompression plate distal femur (LCP-DF) described byBumbacher et al. (2014) shows that progress continues to bemade to make such repairs more likely to succeed.
Author’s declaration of interestsNo conflicts of interest have been declared.
ReferencesBramlage, L.R. and Fackelman, G.E. (2000) Femur. In: AO Principles of
Equine Osteosynthesis, Eds: G.E. Fackelman, J.A. Auer and D.M.Nunamaker, Thieme, Stuttgart. pp 197-207.
Bumbacher, S., Bryner, M.F., Furst, A.E., Del Chicca, F., Ringer, S.K. andJackson, M.A. (2014) Treatment of a femoral fracture with a titaniumlocking compression plate distal femur (LCP-DF) in a young donkey.Equine Vet. Educ. 26, 27-31.
Denny, H.R. (1978) The surgical treatment of equine fractures. Vet. Rec.102, 273-277.
Edgerton, B.C., An, K.N. and Morrey, B.F. (1990) Torsional strengthreduction due to cortical defects in bone. J. Orthop. Res. 8, 851-855.
Glotzbecker, M.P., Riedel, M.D., Vitale, M.G., Matsumoto, H., Roye, D.P.,Erickson, M., Flynn, J.M. and Saiman, L. (2013) What’s the evidence?Systematic literature review of risk factors and preventive strategiesfor surgical site infection following pediatric spine surgery. J. Pediatr.Orthop. 33, 479-487.
Hance, S.R. and Bramlage, L.R. (1996) Fractures of the femur andpatella. In: Equine Fracture Repair, Ed: A.J. Nixon, W.B. Saunders,Philadelphia. pp 284-293.
Hawkins, D.L. (2003) The thigh. In: Diagnosis and Management ofLameness in the Horse, Eds: M.W. Ross and S.J. Dyson, SaundersElsevier, Philadelphia. pp 471-474.
Markel, M.D. (1996) Fracture biomechanics. In: Equine Fracture Repair,Ed: A.J. Nixon, Saunders, Philadelphia. pp 10-18.
Milne, D.W. and Turner, A.S. (1979) Approaches to the femur. In: An Atlasof Surgical Approaches to the Bones of the Horse, Eds: D.W. Milneand A.S. Turner, W.B. Saunders, Philadelphia. pp 154-159.
Richardson, D.W. (2012) Femur and pelvis. In: Equine Surgery, 4th edn.,Eds: J.A. Auer and J.A. Stick, Saunders Elsevier, Philadelphia.pp 1442-1449.
Fig 1: Oblique diaphyseal femoral fracture in 2-month-oldThoroughbred cross foal.
© 2013 EVJ Ltd
33EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

Original Article
Evaluation of success rate of laparoscopic castration withoutorchidectomy in 32 mature horsesC. de Fourmestraux*, O. Geffroy, B. Siliart†, O. Albaric‡ and C. TessierDepartments of Surgery, Equine Clinic, †Nutrition and Endocrinology and ‡Pathology, ONIRIS, National College ofVeterinary Medicine, Food Science and Engineering, Atlanpôle-La Chantrerie, Nantes Cedex, France.*Corresponding author email: [email protected]
Keywords: horse; laparoscopy; castration; scrotal testes; endocrine tests; behaviour
SummaryThe surgical success of laparoscopic castration withoutorchidectomy results from avascular necrosis of the testes.However, failures and subsequent production of testosteroneand stallion-like behaviour have been previously identified.Laparoscopic castration without removal of the testes wasperformed in 32 horses with 2 normal descended scrotaltestes between July 2006 and October 2012. The objectives ofour study were to evaluate the success rate of laparoscopiccastration without orchidectomy on descended testes in ourpopulation and assess complications and recovery time.Endocrine tests were performed after surgery and owners alsoasked to report on their horse’s behaviour and ability toresume exercise. Castration was deemed successful ifendocrine test results were in accordance with geldingvalues. Failed horses were castrated using a conventionaltechnique and histology performed when possible. Basaltestosterone levels decreased below 3 nmol/l after surgeryin 30/32 cases. However, in 2 horses, stallion behaviourpersisted and histological evaluation after inguinal castrationshowed residual viable tissue. Two horses maintained hightestosterone levels after surgery associated with stallion-likebehaviour. Based on these results, 12.5% of horses (4/32horses) failed to be considered a gelding based on eitherendocrine tests and/or histology. All horses, with oneexception, were able to resume exercise less than aweek after the procedure. Laparoscopic castration withoutorchidectomy appears to be a safe procedure. Whenassessing the success of laparoscopic castration, our totalfailure rate was 12.5% (4/32 horses) which is significantlyhigher than previously reported.
IntroductionLaparoscopic castration in standing horses eliminates therequirement for general anaesthesia and its associated risks.This technique also allows visual confirmation that adequatehaemostasis of the mesorchium occurs and may offer theadvantage of a more rapid return to function (Hendricksonand Wilson 1997; Hanrath and Rodgerson 2002; Hendrickson2006). Laparoscopic cryptorchidectomy using electrosurgicalcoagulation and transection is a safe, technically easyand efficient approach for ensuring haemostasis of themesorchium in horses (Fischer and Vachon 1998; Hanrath andRodgerson 2002). Laparoscopic intra-abdominal ligation/transection of the spermatic cord without orchidectomy hasbeen previously described as one method to castrate horses(Rijkenhuizen and Grinwis 1999). Earlier studies performed indonkeys, ponies and horses with normally descended testes
have shown that intra-abdominal ligation of the spermaticcord resulted in avascular necrosis of the testes and adecrease in basal testosterone (Wilson et al. 1996; Rijkenhuizenand Grinwis 1999; Walmsley 1999; Pepe et al. 2005). Onereported case of revascularisation of a testis left in the inguinalcanal following transection of the mesorchium and ductusdeferens suggested that more research was necessary(Bergeron et al. 1998). Surgical success results from avascularnecrosis of the testes. However, surgical failures and thesubsequent production of testosterone and stallion-likebehaviour have been identified (Rijkenhuizen and Grinwis1999). Recently, a study reported that even with adequatetechnique, procedural failure occurred in 7% of horseswith descended testes. Initial failures were attributed toinsufficient ligation of the spermatic cord, but a smallnumber of operations also failed despite completetransection of the entire spermatic cord (Voermans et al.2006). Revascularisation of the testes castrated usinglaparoscopy was attributed to a tributary from the externalpudendal artery. Therefore, laparoscopic castration withoutorchidectomy was not recommended as a reliable method forcastration in normal stallions (Voermans et al. 2006).Laparoscopic castration leaving the testicles in situ is a lessinvasive alternative to more conventional castrationtechniques, but may result in residual active testicular tissueand persistent stallion behaviour. Endocrine tests such astestosterone basal concentration and the human chorionicgonadotropin (hCG) response test can be used to identifyhorses that have been castrated but potentially have viabletesticular tissue remaining. Testosterone concentration hasbeen utilised as a reliable method of identifying viabletesticular tissue in horses (Wilson et al. 1996; Bergeron et al.1998). Total testosterone concentration in serum can bemeasured quantitatively with a modified testosteroneradioimmunoassay (Spectria)1 and has been shown todeliver clinically useful information in man (Norjavaara andAnkarberg-Lindgren 2011). If the baseline testosteroneconcentration is higher than expected in a gelding, it isthought to be an indicator of the presence of viable testiculartissue (Bergeron et al. 1998). Intravenous injection of8000–12,000 iu of hCG to horses possessing testicular tissuestimulate a rise in testosterone concentration. There should beno increase above basal testosterone concentrations in horseswith no viable testicular tissue (Cox et al. 1973; Searle et al.1999). Our study objectives were to evaluate the success rateof laparoscopic castration without orchidectomy throughendocrine tests and behaviour evaluation on our populationof horses. Complications and recovery time were alsoevaluated.
34
© 2013 EVJ Ltd
EQUINE VETERINARY EDUCATION / AE / JANUARY 2014
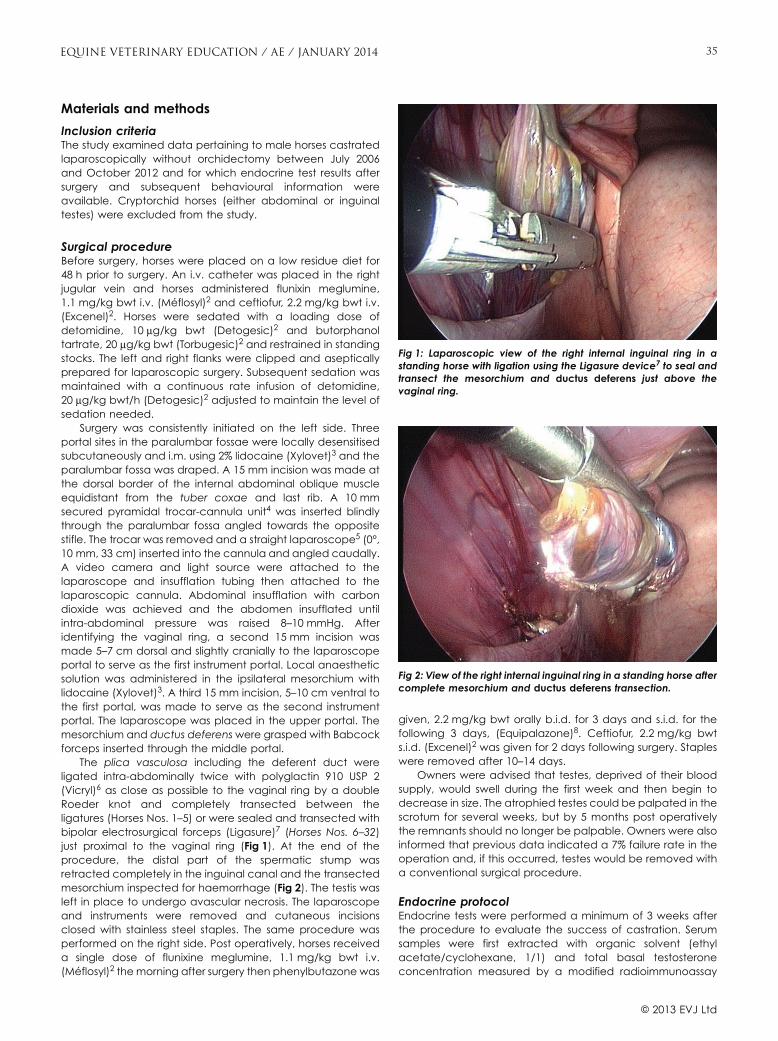
Materials and methods
Inclusion criteriaThe study examined data pertaining to male horses castratedlaparoscopically without orchidectomy between July 2006and October 2012 and for which endocrine test results aftersurgery and subsequent behavioural information wereavailable. Cryptorchid horses (either abdominal or inguinaltestes) were excluded from the study.
Surgical procedureBefore surgery, horses were placed on a low residue diet for48 h prior to surgery. An i.v. catheter was placed in the rightjugular vein and horses administered flunixin meglumine,1.1 mg/kg bwt i.v. (Méflosyl)2 and ceftiofur, 2.2 mg/kg bwt i.v.(Excenel)2. Horses were sedated with a loading dose ofdetomidine, 10 μg/kg bwt (Detogesic)2 and butorphanoltartrate, 20 μg/kg bwt (Torbugesic)2 and restrained in standingstocks. The left and right flanks were clipped and asepticallyprepared for laparoscopic surgery. Subsequent sedation wasmaintained with a continuous rate infusion of detomidine,20 μg/kg bwt/h (Detogesic)2 adjusted to maintain the level ofsedation needed.
Surgery was consistently initiated on the left side. Threeportal sites in the paralumbar fossae were locally desensitisedsubcutaneously and i.m. using 2% lidocaine (Xylovet)3 and theparalumbar fossa was draped. A 15 mm incision was made atthe dorsal border of the internal abdominal oblique muscleequidistant from the tuber coxae and last rib. A 10 mmsecured pyramidal trocar-cannula unit4 was inserted blindlythrough the paralumbar fossa angled towards the oppositestifle. The trocar was removed and a straight laparoscope5 (0°,10 mm, 33 cm) inserted into the cannula and angled caudally.A video camera and light source were attached to thelaparoscope and insufflation tubing then attached to thelaparoscopic cannula. Abdominal insufflation with carbondioxide was achieved and the abdomen insufflated untilintra-abdominal pressure was raised 8–10 mmHg. Afteridentifying the vaginal ring, a second 15 mm incision wasmade 5–7 cm dorsal and slightly cranially to the laparoscopeportal to serve as the first instrument portal. Local anaestheticsolution was administered in the ipsilateral mesorchium withlidocaine (Xylovet)3. A third 15 mm incision, 5–10 cm ventral tothe first portal, was made to serve as the second instrumentportal. The laparoscope was placed in the upper portal. Themesorchium and ductus deferens were grasped with Babcockforceps inserted through the middle portal.
The plica vasculosa including the deferent duct wereligated intra-abdominally twice with polyglactin 910 USP 2(Vicryl)6 as close as possible to the vaginal ring by a doubleRoeder knot and completely transected between theligatures (Horses Nos. 1–5) or were sealed and transected withbipolar electrosurgical forceps (Ligasure)7 (Horses Nos. 6–32)just proximal to the vaginal ring (Fig 1). At the end of theprocedure, the distal part of the spermatic stump wasretracted completely in the inguinal canal and the transectedmesorchium inspected for haemorrhage (Fig 2). The testis wasleft in place to undergo avascular necrosis. The laparoscopeand instruments were removed and cutaneous incisionsclosed with stainless steel staples. The same procedure wasperformed on the right side. Post operatively, horses receiveda single dose of flunixine meglumine, 1.1 mg/kg bwt i.v.(Méflosyl)2 the morning after surgery then phenylbutazone was
given, 2.2 mg/kg bwt orally b.i.d. for 3 days and s.i.d. for thefollowing 3 days, (Equipalazone)8. Ceftiofur, 2.2 mg/kg bwts.i.d. (Excenel)2 was given for 2 days following surgery. Stapleswere removed after 10–14 days.
Owners were advised that testes, deprived of their bloodsupply, would swell during the first week and then begin todecrease in size. The atrophied testes could be palpated in thescrotum for several weeks, but by 5 months post operativelythe remnants should no longer be palpable. Owners were alsoinformed that previous data indicated a 7% failure rate in theoperation and, if this occurred, testes would be removed witha conventional surgical procedure.
Endocrine protocolEndocrine tests were performed a minimum of 3 weeks afterthe procedure to evaluate the success of castration. Serumsamples were first extracted with organic solvent (ethylacetate/cyclohexane, 1/1) and total basal testosteroneconcentration measured by a modified radioimmunoassay
Fig 1: Laparoscopic view of the right internal inguinal ring in astanding horse with ligation using the Ligasure device7 to seal andtransect the mesorchium and ductus deferens just above thevaginal ring.
Fig 2: View of the right internal inguinal ring in a standing horse aftercomplete mesorchium and ductus deferens transection.
© 2013 EVJ Ltd
35EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

based on the competitive radioimmunoassay principle(Spectria Testosterone Radioimmunoassay Kit)1. The analyticaldetection limit is better than 0.1 nmol/l and the functionaldetection limit is approximately 0.3 nmol/l with a 10%coefficient of variation. If the test was performed less than 4weeks after castration, basal testosterone concentration onlywas measured. If endocrine tests were performed more than 4weeks after surgery, a hCG stimulation test was performed byinjecting 30 iu/kg bwt i.v. of hCG (Chorulon)9 with a maximumof 15,000 iu/horse. According to our laboratory (LDHVet)representative reference limits, horses were classified as‘gelding-like’ if the basal testosterone concentration was lessthan 3 nmol/l and/or when there was no rise in testosteroneconcentration after the stimulation test. Owners werecontacted by telephone at least 3 weeks after surgery todetermine the horse’s behaviour and ability to resume exercisefollowing the procedure. Horses with persistent stallionbehaviour (vocalising, excitement, attempts to mount otherhorses, etc), failure to decrease their testosterone levels below3 nmol/l and/or with a positive hCG stimulation test severalweeks after surgery were readmitted for castration using aninguinal closed castration. Histopathology was performed onthe excised testes when possible. Testes were fixed in a 10%neutral buffered formalin solution for 48 h and tissue sectionsstained with haematoxylin-eosin saffron and examinedmicroscopically.
ResultsThe study included 32 mature horses aged 2–10 years (mean 6years). All testes were descended in the scrotum and deemednormal in size, shape and position. The population included 28Selle Français stallions, one KWPN, one Oldenburg, one Barbe,one Holsteiner and one stallion of unknown origin. All horseswere in training at the time of surgery. Physical examination,haematology and biochemistry results showed noabnormalities prior to surgery.
OutcomeBasal testosterone levels were measured in 17/32 horses,between 3 and 4 weeks after castration. In the remaininghorses (15/32), tests measuring testosterone levels before andafter hCG stimulation were performed. Detailed results of theendocrine tests are available in Table 1. Basal testosteronelevels were below 3 nmol/l after surgery in 30/32 cases. In 2/32horses (6,25%), high testosterone levels (>3 nmol/l) weremeasured. Horse No. 8 had high testosterone levels andpersistent stallion behaviour. Horse No. 18 had 2 separatetestosterone level assays. The first assay was performedbetween 3 and 4 weeks after surgery and showed a lowtestosterone level (2.3 nmol/l) according to our laboratoryreference limits. However, the horse continued to displaystallion behaviour, and another assay was performed 6 monthslater, which showed a high testosterone level (6 nmol/l). Those2 horses were considered to have had ‘failed’ castrations. Inhorses that showed a decreased basal testosterone level(<3 nmol/l), stallion-like behaviour was still present in 2 horses.Horse No. 6 had a basal testosterone measurement of2 nmol/l, stallion behaviour was persistent and the ownersopted to have an inguinal closed castration performed. HorseNo. 7 had 2 basal testosterone assays showing low values:0 nmol/l between 3 and 4 weeks after surgery and 0.6 nmol/l8 months after surgery. An hCG stimulation test was also done
one year after laparoscopic castration and was positive. In thishorse, persistent stallion behaviour also motivated the ownersto request a closed inguinal castration.
Those 4 horses were subsequently castrated with astandard castration technique and histopathologicalexamination of the testicles was performed on only 3 horses(Nos. 6, 7 and 8). On gross examination, all epididymesappeared normal and all testes were markedly reduced insize, resulting in relative prominence of the epididymes. Oncross-section, testes were dull and yellowish green. Asobserved in a previous study, testes were largely necrotic andnormal testicular parenchyma was present in the most caudalpart of the testis, adjacent to the proper ligament (Fig 3). Inthose 4 horses, testes partially viable were larger and easy topalpate and partially visible in the scrotum. The castrationeliminated the stallion-like behaviour in all of the 4 horses.
No intra-operative complications occurred. Short-termcomplication occurred in one horse that presented asignificant important scrotal oedema associated with lamenessuntil 2 weeks after surgery, which resolved with medicaltreatment consisting of frequent lungeing, nonsteroidalanti-inflammatory drugs and diuretic administration. All horses,with the exception of this one, were able to go back to work lessthan a week after the procedure.
Histological evaluationHistological results were available for 3/4 horses (6 testes). In 2horses (Nos. 6 and 8), one testis was completely necrotic andone testis was only partially necrotic with persistence of viabletesticular tissue. In the third horse (No. 7), both testes werepartially necrotic. In all cases, the epididymis was spared.Testicular degeneration and necrosis were characterisedby the presence of ischaemic necrosis of seminiferoustubules, infiltration by pigmented macrophages, peripheralproliferative fibrosis and calcification (Figs 4a and b). Viabletissue was assessed by the presence of preserved tubulesassociated with the germinal cells (Figs 5a and b).
DiscussionCompared to conventional castration methods, thelaparoscopic castration technique shows minimal intra- andpost operative complications (Fischer and Vachon 1992, 1998;Davis 1997; Walmsley 1999; Pepe et al. 2005). The technique ofleaving the testis in situ to undergo avascular necrosisdecreases the potential for excess oedema, haemorrhage,infection, lameness and evisceration, when compared withother methods (Moll et al. 1995; Wilson et al. 1996; Bergeronet al. 1998). Swelling and signs of pain observed afterlaparoscopic surgery are less severe than those seen afterroutine castration and are an expected response to thenecrotic testicular tissue (Wilson et al. 1996). Therefore, thistechnique can be used on horses that need to be stall-restedfor various conditions including severe orthopaedic lesions andhorses not able to cope with general anaesthesia and/orrecovery. No life-threatening complications have beendescribed with this minimally invasive technique. Theconvalescence time is also considerably reduced comparedwith other conventional techniques (Rijkenhuizen and Grinwis1999; Walmsley 1999; Pepe et al. 2005; Voermans et al. 2006). Inour population, all horses but one castrated in this fashion wereable to go back to work in less than a week, which is aneconomical consideration for horses in training. It is important
© 2013 EVJ Ltd
36 EQUINE VETERINARY EDUCATION / AE / JANUARY 2014
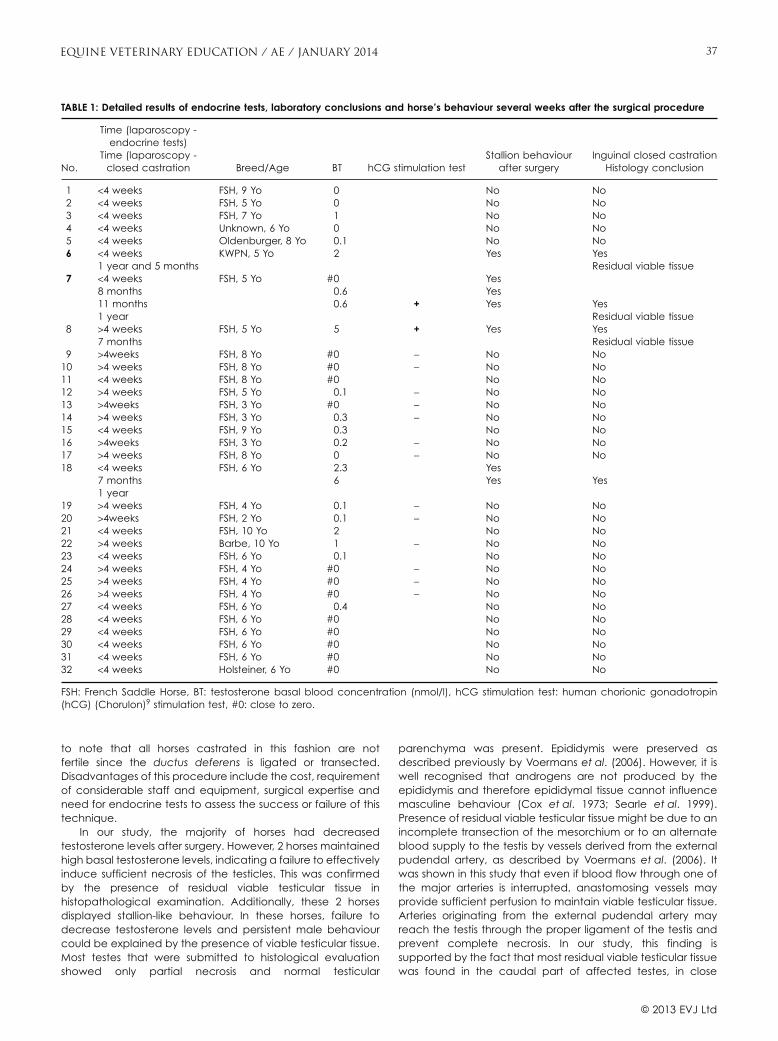
to note that all horses castrated in this fashion are notfertile since the ductus deferens is ligated or transected.Disadvantages of this procedure include the cost, requirementof considerable staff and equipment, surgical expertise andneed for endocrine tests to assess the success or failure of thistechnique.
In our study, the majority of horses had decreasedtestosterone levels after surgery. However, 2 horses maintainedhigh basal testosterone levels, indicating a failure to effectivelyinduce sufficient necrosis of the testicles. This was confirmedby the presence of residual viable testicular tissue inhistopathological examination. Additionally, these 2 horsesdisplayed stallion-like behaviour. In these horses, failure todecrease testosterone levels and persistent male behaviourcould be explained by the presence of viable testicular tissue.Most testes that were submitted to histological evaluationshowed only partial necrosis and normal testicular
parenchyma was present. Epididymis were preserved asdescribed previously by Voermans et al. (2006). However, it iswell recognised that androgens are not produced by theepididymis and therefore epididymal tissue cannot influencemasculine behaviour (Cox et al. 1973; Searle et al. 1999).Presence of residual viable testicular tissue might be due to anincomplete transection of the mesorchium or to an alternateblood supply to the testis by vessels derived from the externalpudendal artery, as described by Voermans et al. (2006). Itwas shown in this study that even if blood flow through one ofthe major arteries is interrupted, anastomosing vessels mayprovide sufficient perfusion to maintain viable testicular tissue.Arteries originating from the external pudendal artery mayreach the testis through the proper ligament of the testis andprevent complete necrosis. In our study, this finding issupported by the fact that most residual viable testicular tissuewas found in the caudal part of affected testes, in close
TABLE 1: Detailed results of endocrine tests, laboratory conclusions and horse’s behaviour several weeks after the surgical procedure
No.
Time (laparoscopy -endocrine tests)
Time (laparoscopy -closed castration Breed/Age BT hCG stimulation test
Stallion behaviourafter surgery
Inguinal closed castrationHistology conclusion
1 <4 weeks FSH, 9 Yo 0 No No2 <4 weeks FSH, 5 Yo 0 No No3 <4 weeks FSH, 7 Yo 1 No No4 <4 weeks Unknown, 6 Yo 0 No No5 <4 weeks Oldenburger, 8 Yo 0.1 No No6 <4 weeks KWPN, 5 Yo 2 Yes Yes
1 year and 5 months Residual viable tissue7 <4 weeks FSH, 5 Yo #0 Yes
8 months 0.6 Yes11 months 0.6 + Yes Yes1 year Residual viable tissue
8 >4 weeks FSH, 5 Yo 5 + Yes Yes7 months Residual viable tissue
9 >4weeks FSH, 8 Yo #0 − No No10 >4 weeks FSH, 8 Yo #0 − No No11 <4 weeks FSH, 8 Yo #0 No No12 >4 weeks FSH, 5 Yo 0.1 − No No13 >4weeks FSH, 3 Yo #0 − No No14 >4 weeks FSH, 3 Yo 0.3 − No No15 <4 weeks FSH, 9 Yo 0.3 No No16 >4weeks FSH, 3 Yo 0.2 − No No17 >4 weeks FSH, 8 Yo 0 − No No18 <4 weeks FSH, 6 Yo 2.3 Yes
7 months 6 Yes Yes1 year
19 >4 weeks FSH, 4 Yo 0.1 − No No20 >4weeks FSH, 2 Yo 0.1 − No No21 <4 weeks FSH, 10 Yo 2 No No22 >4 weeks Barbe, 10 Yo 1 − No No23 <4 weeks FSH, 6 Yo 0.1 No No24 >4 weeks FSH, 4 Yo #0 − No No25 >4 weeks FSH, 4 Yo #0 − No No26 >4 weeks FSH, 4 Yo #0 − No No27 <4 weeks FSH, 6 Yo 0.4 No No28 <4 weeks FSH, 6 Yo #0 No No29 <4 weeks FSH, 6 Yo #0 No No30 <4 weeks FSH, 6 Yo #0 No No31 <4 weeks FSH, 6 Yo #0 No No32 <4 weeks Holsteiner, 6 Yo #0 No No
FSH: French Saddle Horse, BT: testosterone basal blood concentration (nmol/l), hCG stimulation test: human chorionic gonadotropin(hCG) (Chorulon)9 stimulation test, #0: close to zero.
© 2013 EVJ Ltd
37EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

proximity to the proper ligament of the testis. A laparoscopiccastration failure rate of 7% was attributed to this phenomenon(Voermans et al. 2006).
Interestingly, in our study, 2 horses had a low basaltestosterone level according to LDHvet laboratory referencelimits but continued to display stallion behaviour several weeksto months after surgery. This behaviour resulted in the ownersopting for a standard castration to be performed. In these 2horses, histopathology also showed the presence of residualviable testicular tissue. We hypothesised that in these 2 cases,low testosterone levels might be due to a very small amountof viable testicular tissue. Subjectively, on histologicalexamination, we found that a horse with a high testosteroneconcentration post castration (Horse No. 8) seemed to have alarger amount of viable tissue compared to horses with a lowlevel of testosterone (Horse No. 7), in which a very small part ofviable tissue was observed histologically. It is likely that theamount of residual viable testicular tissue influences themeasured testosterone levels. Unfortunately, we were not ableto effectively calculate the proportion of viable tissue in ‘failedhorses’ testicles.
Those 2 horses were in the upper limit of our cut-off mark. Itis likely that with a lower cut-off value, we would haveconsidered these horses as ‘failed’ based solely on hormonalassays. As there is a ‘grey area’ with overlapping values inbasal testosterone levels between geldings and stallions,erroneous conclusion might be made. We took LDHVetlaboratory’s standards when evaluating results of hormonalassays to classify horses and it seems our cut-off value is high.However, it is important to consider the fact that we measuredtotal testosterone concentration after extraction, which mightbe a reason why our basal testosterone levels in geldings arehigher than those previously published. According toVoermans et al. (2006), cut-off value to confirm a castration is<0.09 nmol/l and according to Arighi and Bosu (1989),
concentration of ≤0.83 nmol/l is diagnostic of absence oftesticular tissue.
Examining our results and due to the fact that Horse No. 7with a repeated basal testosterone level of 0.6 nmol presentedviable testicular on histological examination, horses between0.5 and 3 nmol/l should be stimulated to assess success ofcastration. Measurement of serum testosterone alone is notsufficient to assess the gonadal function and must be backedup with other clinically relevant data, repeat endocrine test inthe following months, including spring months or hCGstimulation test. Even if behaviour does not always corroboratewith the presence of viable testicular tissue, it should beevaluated as this may be a predictor of castration failure.When assessing success of laparoscopic castration, our totalfailure rate was 12.5% (4/32 horses) which is significantly higherthan previously reported. The number of cases included in ourstudy is smaller than in the results presented by Voermans et al.(2006) and additional cases are needed to validate ourfindings. We conclude that this study confirms thatlaparoscopic castration without orchidectomy cannot berecommended for castration of normal stallions and has to be
Fig 3: Macroscopic aspect of a partially necrotic testis with apreserved caudal part and a spared epididymis.
a)
b)
Fig 4: a) Diffuse coagulative necrosis of seminiferous tubules (blackarrows) with mineralisation and degenerative interstitial cells (*)(acute lesion). (Horse No. 6). b) Vestigial seminiferous tubules(black arrows) surrounded by macrophages (+) in a dense fibroustissue (chronic lesion). (Horse No. 7).
© 2013 EVJ Ltd
38 EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

applied only in specific cases and be used only with a clearunderstanding by the owners of the failure rate. A larger futurestudy is required in order to efficiently identify factorspredisposing to surgical failure.
Authors’ declaration of interestsNo conflicts of interest have been declared.
Manufacturers’ addresses1Orion Diagnostica, Espoo, Finland.2Pfizer, Paris, France.
3CEVA, Libourne, France.4Optomed, Les Ulis, France.5Storz, Tuttlingen, Germany.6Ethicon, Johnson & Johnson, Issy les Moulineaux, France.7Covidien, Mansfield, Massachusetts, USA.8Dechra, Stock-on-Trent, Staffordshire, UK.9MSD Santé Animale (Intervet), Beaucouze, France.
ReferencesArighi, M. and Bosu, W.T.K. (1989) Comparison of hormonal methods for
diagnosis of cryptorchidism in horses. J. Equine Vet. Sci. 9, 20-26.
Bergeron, J.A., Hendrickson, D.A. and McCue, P.M. (1998) Viability of aninguinal testis after laparoscopic cauterization and transection of itsblood supply. J. Am. Vet. Med. Ass. 213, 1303-1304.
Cox, J.E., Williams, J.H., Rowe, P.H. and Smith, J.A. (1973) Testosterone innormal, cryptorchid and castrated male horses. Equine Vet. J. 5,85-90.
Davis, E.W. (1997) Laparoscopic cryptorchidectomy in standing horses.Vet. Surg. 26, 326-331.
Fischer, A.T. and Vachon, A.M. (1998) Laparoscopic intra-abdominalligation and removal of cryptorchid testes in horses. Equine Vet. J.30, 105-108.
Fischer, A.T. Jr and Vachon, A.M. (1992) Laparoscopiccryptorchidectomy in horses. J. Am. Vet. Med. Ass. 201, 1705-1708.
Hanrath, M. and Rodgerson, D.H. (2002) Laparoscopiccryptorchidectomy using electrosurgical instrumentation in standinghorses. Vet. Surg. 31, 117-124.
Hendrickson, D.A. (2006) Laparoscopic cryptorchidectomy andovariectomy in horses. Vet. Clin. N. Am.: Equine Pract. 22, 777-798.
Hendrickson, D.A. and Wilson, D.G. (1997) Laparoscopic cryptorchidcastration in standing horses. Vet. Surg. 26, 335-339.
Moll, H.D., Pelzer, K.D., Pleasant, R.S., Modransky, P.D. and May, K.A.(1995) A survey of equine castration complications. Equine Vet. Sci.12, 522-526.
Norjavaara, E. and Ankarberg-Lindgren, C. (2011) Modified spectriatestosterone RIA detects the same testosterone levels in prepubertaland pubertal children as liquid chromatography-tandem massspectrometry. Endocr. Rev. 32, 3-710.
Pepe, M., Gialletti, R., Moriconi, F., Puccetti, M., Nannarone, S. andSinger, E.R. (2005) Laparoscopic sterilization of Sardinia donkeysusing an endoscopic stapler. Vet. Surg. 34, 260-264.
Rijkenhuizen, A.B.M. and Grinwis, G.C.M. (1999) Castration of thestallion: preferably in the standing horse by laparoscopictechniques? Pferdeheilkunde 16, 425-429.
Searle, D., Dart, A.J., Dart, C.M. and Hodgson, D.R. (1999) Equinecastration: review of anatomy, approaches, techniques andcomplications in normal, cryptorchid and monorchid horses. Aust.Vet. J. 77, 428-434.
Voermans, M., Rijkenhuizen, A.B.M. and van der Velden, M.A. (2006) Thecomplex blood supply to the equine testis is a cause of failure inlaparoscopic castration. Equine Vet. J. 38, 35-39.
Walmsley, J.P. (1999) The Sir Frederick Hobday memorial lecture. Reviewof equine laparoscopy and an analysis of 158 laparoscopies in thehorse. Equine Vet. J. 31, 456-464.
Wilson, D.G., Hendrickson, D.A., Cooley, A.J. and Degrave-Madigan, E.(1996) Laparoscopic methods for castration of equids. J. Am. Vet.Med. Ass. 209, 112-114.
a)
b)
Fig 5: a) Incomplete necrosis of testis with extensive chronic fibrouslesion with vestigial seminiferous tubules (thin black arrows) andpreserved seminiferous tubules (large black arrows). (Horse No. 8).b) Complete preservation of testicular tissue with seminiferoustubules (black arrows), intact Leydig cells (L) and spermatozoids(#). (Horse No. 8).
© 2013 EVJ Ltd
39EQUINE VETERINARY EDUCATION / AE / JANUARY 2014
Pleasant, R.S., Suagee, J.K., Thatcher, C.D., Elvinger, F. and Geor, R.J.(2013) Adiposity, plasma insulin, leptin, lipids, and oxidative stress inmature light breed horses. J. Vet. Intern. Med. 27, 576-582.
Rendle, D.I., Rutledge, F., Hughes, K.J., Heller, J. and Durham, A.E. (2013)Effects of metformin hydrochloride on blood glucose and insulinresponses to oral dextrose in horses. Equine Vet. J. 45, 751-754.
Tadros, E.M. and Frank, N. (2013) Endocrine disorders and laminitis.Equine Vet. Educ. 25, 152-162.
Venugopal, C.S., Eades, S., Holmes, E.P. and Beadle, R.E. (2011) Insulinresistance in equine digital vessel rings: an in vitro model to studyvascular dysfunction in equine laminitis. Equine Vet. J. 43, 744-749.
Continue page 8d from

Clinical Commentary
Laparoscopic castration of the normal horse: Is it indicated?A. T. Fischer JrChino Valley Equine Hospital, Chino Hills, California, USA.Corresponding author email: [email protected]
The article by de Fourmestraux et al. (2014) presents a nicelyconstructed clinical study in which the authors evaluated thetechnique of laparoscopic sectioning of the mesorchium andvas deferens in standing horses, leaving the testicle to undergoischaemic necrosis in situ. Testosterone levels were thenobtained at least 3 weeks post surgically and correlated withbehavioural outcomes. Four of the 32 horses retainedstallion-like behaviour and were considered failed castrations.These subsequently underwent open castration. Two of the 4horses had an elevated testosterone at the first sampling. Ofthe remaining 2 horses, one had a testosterone level near thelevel considered consistent with being a stallion and the othera normal resting testosterone level positive on HCG stimulationtesting. This study has confirmed that the blood supply to thetesticle may be preserved via the external pudendal arterywhen only the mesorchium is transected, as shown byVoermans et al. (2006). On reading the study by Voermans etal. (2006), where there was a 7% failure rate for castration, myconclusion was that this is not a suitable technique forcastration except in very specific circumstances and thepresent study with a 12% failure rate confirms this. As theauthors suggest in the present study, this procedure might beindicated in horses where general anaesthesia is consideredunsafe, such as horses convalescing from orthopaedic injuries.Other indications for this procedure are if the horse to becastrated has an increased risk of a life threateningcomplication vs. other horses. The authors suggest that thisprocedure has a shorter convalescence time than openprocedures but this has not been my experience as normaland cryptorchid castrations are returned to full training in thesame amount of time (one week) that the authors suggest.One of the downsides of leaving the testicles in situ occurs ifthe horses are exported to the United States prior to thetesticles fully atrophying. Veterinary inspectors observe testiclesin a supposedly castrated animal and the horse must eitherundergo an expensive contagious equine metritis (CEM)
quarantine or undergo surgery for removal of the testicles priorto being released from quarantine into the US. When thisoccurs, the client has definitely not saved money by paying for2 procedures or having the horse undergo a protractedquarantine. The horse also undergoes a second surgery with itsassociated risks. Whilst articles have previously been written onovariectomy without removal of the ovary (Shoemaker et al.2004) and castration without removal of the testicle, my beliefis that removal of the testicle or ovary is indicated as a goodsurgical technique. Allowing tissue to undergo ischaemicnecrosis within the abdomen puts the horse at risk ofadhesions. I would be interested in a study that followed thelevels of inflammatory mediators in horses undergoingcastration with or without removal of the testicle.
While a staunch advocate for developing laparoscopicprocedures for horses, this technique does not address theanatomic fact that some horses’ testicles have a blood supplyvia the external pudendal artery which allows them tomaintain their stallion-like behaviour resulting in a failedsurgery. This anatomic limitation precludes the use of thisprocedure except in very specific instances.
Author’s declaration of interestsNo competing interests have been declared.
Referencesde Fourmestraux, C., Geffroy, O., Siliart, B., Albaric, O. and Tessier, C.
(2013) Evaluation of success rate of laparoscopic castration withoutorchidectomy in 32 mature horses. Equine Vet. Educ. 26, 34-39.
Shoemaker, R.W., Read, E.K., Duke, T. and Wilson, D.G. (2004) In situcoagulation and transection of the ovarian pedicle: an alternativeto laparoscopic ovariectomy in juvenile horses. Can. J. Vet. Res. 68,27-32.
Voermans, M., Rijkenhuizen, A.B.M. and van der Velden, M.A. (2006) Thecomplex blood supply to the equine testis is a cause of failure inlaparoscopic castration. Equine Vet. J. 38, 35-39.
40
© 2013 EVJ Ltd
EQUINE VETERINARY EDUCATION / AE / JANUARY 2014
Fleming, P. (2001) Acupuncture for musculoskeletal and neurologicconditions in the horse. In: Veterinary Acupuncture: Ancient Art toModern Medicine, Ed: A.M. Schoen, Mosby, St Louis. pp 443-465.
Hoang, N.S., Sar, C., Valmier, J., Sieso, V. and Scamps, F. (2012)Electro-acupuncture on functional peripheral nerve regeneration inmice: a behavioural study. BMC Complement. Altern. Med. 12, 1-9.
Jeong, S.M., Kim, H.-Y., Lee, C.-H., Kweon, O.K. and Tam, T.C. (2001) Useof acupuncture for the treatment of idiopathic facial nerve paralysisin a dog. Vet. Rec. 148, 632-633.
Kim, M.S. and Xie, H. (2009) Use of electroacupuncture to treatlaryngeal hemiplegia in horses. Vet. Rec. 165, 602-603.
Mayor, D.F. (2007) Electroacupuncture: an introduction and its use forperipheral facial paralysis. J. Chin. Med. 84, 1-19.
Rose, R.J. and Hodgson, D.R. (2000) Neurology. In: Manual of EquinePractice, 2nd edn., W.B. Saunders Company, An Imprint of Elsevier,Philadelphia. pp 503-576.
Shi, X., Yu, G. and He, D. (2000) An experimental study on physiotherapyfor traumatic facial nerve injury. Zhonghua Kou Qiang Yi Xue Za Zhi35, 450-452.
Smith, M.O. and George, L.W. (2009) Diseases of the nervous system.In: Large Animal Internal Medicine, 4th edn., Ed: B.P. Smith, Mosby,St Louis. pp 972-1111.
Sumano, H., Mateos, G. and Hoyos, L. (1997) The use ofelectroacupuncture for the management of unilateral traumaticfacial paralysis in the horse: preliminary report. Am. J. Acupunct. 25,169-174.
Yan, Q., Ruan, J.W., Ding, Y., Li, W.J., Li, Y. and Zeng, Y.S. (2011)Electro-acupuncture promotes differentiation of mesenchymalstem cells, regeneration of nerve fibers and partial functionalrecovery after spinal cord injury. Exp. Toxicol. Pathol. 63, 151-156.
Yang, C., Li, B., Liu, T.S., Zhao, D.M. and Hu, F.A. (2005) Effect ofelectroacupuncture on proliferation of astrocytes after spinal cordinjury. Zhongguo Zhen Jiu 25, 569-572.
Continue page 22d from

Original Article
Evaluation of laryngeal function under the influence of varioushead and neck positions during exercise in 58 performance horsesL. Go1*†, A. K. Barton1†‡ and B. Ohnesorge†
†Clinic for Horses, University of Veterinary Medicine Hannover, Hannover, Germany and ‡Equine Clinic, Departmentof Veterinary Medicine of Freie Universität Berlin, Berlin, Germany.*Corresponding author email: [email protected]
Keywords: horse; recurrent laryngeal neuropathy; equine larynx; head and neck position
SummaryThe objective of this study was to examine laryngeal functionat rest and during ridden exercise and to further analyse theimpact of different head and neck positions on the laryngealfunction in ridden sport horses. Fifty-eight Warmblood horseswere examined endoscopically during ridden exercise as wellas during quiet breathing at rest before and after sedation. Fourdifferent head-neck positions (unrestrained, reference,elevation and hyperflexion) were assessed during the exercisetest. Laryngeal function was graded at rest and for everycombination of gait and head and neck position duringexercise. There was a significant correlation between thegrade of laryngeal function during exercise and at rest bothbefore (correlation coefficient = 0.794) and after (correlationcoefficient = 0.741) sedation (P<0.01). No significantassociation was found between the grade of laryngealfunction during exercise and the different head and neckpositions.
IntroductionRespiratory dysfunction is a frequent cause of poorperformance in athletic horses. Recurrent laryngealneuropathy (RLN) is one of the most common forms ofdynamic upper respiratory tract obstructions in bothperformance horses and racehorses (Davidson and Martin2003; Franklin et al. 2006; Barakzai 2007; Desmaizieres et al.2009). Laryngeal function at rest usually gives an indication oflaryngeal function during exercise (Hammer et al. 1998; Martinet al. 2000; Lane et al. 2006a). Barakzai and Dixon (2011) wereable to show a significant correlation between restinglaryngeal function score using the Havemeyer grading system(Dixon et al. 2003) and exercising grades of laryngeal functionin horses undergoing high-speed treadmill endoscopy.However, a number of studies have documented thatendoscopy during exercise is required for a definite diagnosisof dynamic upper respiratory tract obstructions (Kannegieterand Dore 1995; Martin et al. 2000; Tan et al. 2005; Lane et al.2006a). High-speed treadmill endoscopy has become themost accepted method of investigating dynamic obstructionsof the upper respiratory tract, especially in racing horses. Insport horses, factors other than strenuous workload are moreimportant for diagnostic purposes. These factors includedifferent head-neck positions whose influences are easier toinvestigate during ridden exercise than on a high-speedtreadmill (Barakzai and Cheetham 2012). It has been
suggested that head-neck flexion affects upper airway flowmechanics during exercise. In a study by Petsche et al. (1995),an increased respiratory resistance was found during headflexion compared to a neutral head position. Several theoriesand models trying to explain this phenomenon have beenestablished. Gerring (1985) proposed that head position mayinfluence the airflow in the airway, because the airflow nolonger follows a straight line but has to make its way through adecreasing kink angle (between nasal airway and trachea)with increasing head flexion. Other authors assume that thechanges in shape and size of the upper airway are dependenton alteration of the head position (Cook 1965; Petsche et al.1995). This theory has been supported by studies illustratingthat head-neck flexion causes a reduction in the dorsoventraldiameter of the nasopharynx on lateral radiographs in horsesat rest (Linford et al. 1983; Cehak et al. 2010; Go et al.unpublished data). Therefore, head-neck flexion is suspectedto induce or deteriorate disorders of the upper respiratory tract(Allen et al. 2011; van Erck-Westergren 2011).
The purpose of the present study was to investigate therelationship between laryngeal function at rest and duringexercise in Warmblood sport horses and to examine theinfluence of different head-neck positions on laryngealfunction during exercise.
Materials and methodsFifty-eight German Warmblood horses (39 geldings, 16 maresand 3 stallions) aged 3–20 years free of cardiovascular ormusculoskeletal disease were included in the study. Thirty-six ofthese horses, owned by clients, were presented at theuniversity for evaluation of an abnormal respiratory noiseand/or poor performance (respiratory noise = 27, poorperformance = 3, both = 6); 9 horses were owned by theuniversity and 13 horses were owned by the Hanoverianmounted police unit. The horses’ usual working disciplinesincluded dressage (n = 16), showjumping (n = 20) and pleasureriding (n = 22). All horses were subjected to a physicalexamination, and an endoscopic examination was performedat rest and during ridden exercise.
Endoscopic examination at restEndoscopic examinations (Olympus Evis Exera II)1 were carriedout at rest before and after sedation. Horses were sedatedwith detomidine hydrochloride i.v. (0.115–0.03 mg/kg bwt,Cepesedan RP)2 and butorphanol tartrate i.v. (0.1 mg/kg bwt,Alvegesic PH)2. Laryngeal arytenoid cartilage movement wasrecorded during respiration at rest, during nasal occlusion andafter swallowing. Arytenoid function before and after sedation1These authors contributed equally to this work.
41
© 2013 EVJ Ltd
EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

was graded independently by 3 observers based on theinternationally used Havemeyer grading system for laryngealfunction, first published by Dixon et al. (2003). For furtheranalysis, median values of the laryngeal grades assigned bythe 3 observers were used.
Endoscopic examination during exerciseFor the endoscopic examination during exercise, theendoscope was inserted following a warm-up period. After thehorses had become accustomed to the Dynamic RespiratoryScope3 they were subjected to a standardised exercise test.Abnormal respiratory sounds occurring during the examinationwere documented. The exercise test included performance attrot and canter in 4 different head-neck positions (reference,elevation, hyperflexion and unrestrained) as shown in Fig 1.
The reference position was defined as the position in whichthe riders presented their horses as they would train them athome during the warm-up phase. Ideally, a posture with a lowneck and the ridge of the nose slightly in front of the verticalplane should have been achieved, independent of thehorses’ usual working disciplines. For the head-neck positionelevation, the riders were asked to present their horses with thepoll being the highest point and the ridge of the nose slightly infront of the vertical plane. In the head-neck position termedhyperflexion the horses should be adjusted as low andoverbent as they would perform willingly without resistanceagainst the rider. To achieve the unrestrained head-neckposition the riders were to loosen the reins until there was nolonger a connection between the rider’s hand and the bit. Allhorses were examined according to the following scheme: trotreference, trot elevation, trot hyperflexion, canter reference,canter elevation, canter hyperflexion and trot unrestrained.The exercise test took 20–25 min, with each combination ofgait and head-neck position lasting about 3 min. For everycombination of gait and head-neck position, endoscopy anda lateral video of horse and rider were digitally recorded along2 long sides of the indoor arena, which was 40 m long. Thetimelines of the 2 videos were synchronised and the lateralvideo of the horse and rider was used to determine the pointin time from which a combination of gait and head-neckposition started. By means of the lateral video, head-neck
position was checked by one author (L.G.) for correctexecution and was rated correct, if it could be classified intoone of the positions (reference, elevation, hyperflexion andunrestrained) defined as described above. If the requiredhead-neck position was not performed in an adequate way orwas inconsistent during the sequence, the data from this horsefor this position were excluded from further analysis.
The endoscopic videos were evaluated in real time and, ifrequired, in slow motion. Laryngeal function was graded forevery combination of gait and head-neck position into one of7 categories. For this purpose, the scoring system fromRakestraw et al. (1991) was modified (Table 1) to allow a moreprecise classification.
Data analysisAs the laryngeal function scores at rest and during riddenexercise cannot be treated as interval scaled and, in addition,data could not be transformed into normal distribution,the nonparametric tests of SPSS statistic version 204 wereapplied. The endoscopic grades of laryngeal function atrest were tested for interobserver agreement using Cronbach’sα as intraclass correlation coefficient. The Spearman-Rho coefficient was used to check for possible correlationbetween the laryngeal function score during exercise andthe score at rest with and without sedation respectively. TheWilcoxon test for paired samples was used to check fordifferences in the distribution of laryngeal function scoresduring ridden exercise between the different gaits andhead-neck positions. The Kruskal-Wallis test was used to assessdifferences in laryngeal function score during exercisebetween the 3 working disciplines (dressage, showjumpingand pleasure riding), and between horses with and without anabnormal respiratory noise, respectively. Significance was setat P<0.05.
Horses were divided into 3 groups (A, B, C) depending ontheir laryngeal function score in the reference position at trotto show the distribution of laryngeal function score in the othergait and head-neck positions for each of these groups.
ResultsThere was substantial agreement between the endoscopicscores at rest given by the 3 observers (α = 0.958 beforesedation and α = 0.936 after sedation). Two horses wereexamined at rest only without sedation. Fifty-four of theremaining 56 cases (96.4%) were rated the same (n = 28) orassigned a lower score (n = 25) without sedation than withsedation. The median values of the laryngeal function scoreswithout and with sedation at rest were significantly different(P<0.05). The distributions of the grades for laryngeal functionat rest before and after sedation as well as during exercise forall horses are shown in Table 2.
The Spearman-Rho correlation coefficient betweenevaluation of laryngeal function without sedation at rest andevaluation of laryngeal function during exercise was 0.794(P<0.01); that between rating of laryngeal function withsedation at rest and rating of laryngeal function duringexercise was 0.741 (P<0.01).
For the total of 58 horses, the distributions of laryngealfunction scores during exercise were not significantly differentbetween the investigated head-neck positions within thesame gait. However, the distributions of grades between trotand canter were significantly different (P<0.05), independentof head-neck positions.
Head-neck positions
Elevation
UnrestrainedHyperflexion
Reference
Fig 1: Photographs of a standing horse, illustrating the 4 differenthead and neck positions used in this study.
© 2013 EVJ Ltd
42 EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

Tables 3–5 show the distribution of laryngeal function scorein relation to the different head-neck positions and gaits for 3groups of horses, divided up in accordance to their laryngealfunction score in the reference position at trot.
There was no significant difference in laryngeal functionscores during exercise between the working disciplinesdressage and showjumping. Compared to these 2 groupsthe group of pleasure riding showed a significantly higherscore.
Thirty-four out of 58 horses (58.6%) had an abnormalrespiratory noise during the exercise test. These horses weresignificantly (P<0.05) more often diagnosed with a left-sidedlaryngeal dysfunction during exercise than horses without anabnormal respiratory noise.
During the exercise test, 7 combinations of head and neckpositions and gaits have been requested. Forty-seven out of 58horses (81%) fulfilled all demanded requirements correctly. The
remaining 11 horses (19%) failed at least in one of the 7combinations (7/11 in one combination and 4/11 in more thanone). Overall, 15 combinations (15/406; 3.7%) were rated asnot correctly performed. The combination canter-elevationwas found to be incorrectly implemented in 8 cases (53%),canter-hyperflexion in 3 cases (20%), trot-elevation in 2 cases(13.3%) and one case (6.6%) each in the combinationtrot-hyperflexion and trot-unrestrained respectively.
Apart from laryngeal dysfunctions, the following upperairway obstructions occurred during the exercise test: axialdeviation of the aryepiglottic fold (n = 1), dorsal displacementof the soft palate (n = 5) and pharyngeal collapse (n = 5). Eighthorses (14%) were diagnosed with more than one upperairway abnormality. Due to the few cases, a statement aboutthe relationship between head-neck position and theoccurrence of these upper airway obstructions could not bedrawn.
TABLE 1: Modified scoring system of laryngeal function from Rakestraw et al. (1991). Grades B and C were divided into sub-grades
Grade Description
A Full abduction of the arytenoid cartilage during inspirationB 1 Transient partial abduction of the affected arytenoid cartilage and/or flutter of the vocal fold
2 Partial abduction of the affected arytenoid cartilage much of the time but in steady position, flutter of thevocal cord
3 Partial abduction of the affected arytenoid cartilage much of the time but in steady position, transientcollapse of the vocal cord and/or laryngeal ventricle
C 1 Complete immobility of the affected arytenoid cartilage but in steady position2 Immobility and collapse of the affected arytenoid cartilage less than to the midline of the rima glottidis during
inspiration3 Immobility and collapse of the affected arytenoid cartilage into the contralateral half of the rima glottidis
during inspiration
TABLE 2: Number of horses and their corresponding laryngeal function score during exercise dependent on the grade of laryngeal functionat rest before sedation (written in normal style) and after sedation (written in italic style and in brackets)
Laryngealfunction at rest
Laryngeal function during exercise
A B1 B2 B3 C1 C2 C3
I 9 (2) 4 3 16 (2)IIA 2 (7) 10 (11) 10 (7) 22 (25)IIB (1) 1 (4) 7 (8) 1 (1) 9 (14)IIIA (3) (1) 1 1 (4)IIIB 2 (2) (1) 2 (3)IIIC 1 (1) 1 (1) 2 (2)IV 4 (4) 2 (2) 6 (6)
11 (10) 15 (15) 20 (18) 1 (2) 7 (7) 4 (4) 58 (56)
TABLE 3: Laryngeal function score in relation to the different head-neck positions and gaits for all horses diagnosed grade A (n = 25) inreference position at trot. Note that the number of horses is not equal for every combination of contact position and gait, due to the factthat data from some horses were excluded if the contact position was not performed correctly
Gait and head-neck position
Laryngeal function during exercise
A B1 B2 B3 C1 C2 C3
Trot reference 25 - - - - - -Trot unrestrained 23 2 - - - - -Trot elevation 22 1 - - - - -Trot hyperflexion 11 1 - - - - -Canter reference 15 7 3 - - - -Canter elevation 1 10 1 - - - -Canter hyperflexion 13 7 3 - - - -
© 2013 EVJ Ltd
43EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

DiscussionNo significant correlation between head-neck flexion andpresence or degree of laryngeal dysfunction in Warmbloodperformance horses could be confirmed in the current study.This contradicts the results of a previous study by vanErck-Westergren (2011), in which a causal relationshipbetween rider intervention (including head and neck flexion)and laryngeal function was found. It should be noted that inthe study by van Erck-Westergren (2011), the degree of pollflexion was not standardised and is only described as anincreased head and neck flexion in comparison to free headcarriage. In the present study, only head-neck positions inwhich the horses performed willingly without resistance to therider were investigated. Therefore, the possibility that anenforced overbending – as presently discussed in theequestrian community – may influence laryngeal functioncould not be ruled out. Furthermore, in the study by vanErck-Westergren (2011) the horses were first ridden with theirheads free and afterwards with increased head and neckflexion, whereas in the present study the free head positionwas investigated at the end of the exercise test. Therefore, theintensity and duration of the exercise test and the resultingfatigue are aspects that should be taken into accountregarding the different results of the 2 studies.
The hypothesis that alterations in head-neck position mayinfluence morphology and function of the upper airway isbased on the assumption that increasing flexion of the headand neck leads to a decreasing diameter of the upper airway(Cook 1965; Petsche et al. 1995). As a consequence, theresistance to airflow increases and hence the absolute valueof the intraluminal negative pressure during inhalation,especially in exercising horses, increases. The extent to which achange in diameter influences airflow and pressure conditions
inside the upper airway is still not completely clarified. Sincethe equine upper airway is not a circular tube of uniformdiameter and airflow within it is turbulent, Rakesh et al. (2008a)came up with a new approach, showing that the radius of asection of the upper airway affects the impedance to thepower of 0.85. However, this equation applies only for achange in radius in a section of the upper airway and shouldnot be applied to the entire upper respiratory tract.
Previous research has already demonstrated thathead-neck positions affect the pharyngeal diametermeasured in sedated horses at rest (Linford et al. 1983; Cehaket al. 2010), and in a recent study we could confirm thathead-neck position also affects the pharyngeal diameter ofhorses during exercise (Go et al. unpublished data).
Furthermore, increased head-neck flexion is suspected toincrease the risk of the likelihood of pharyngeal wall collapse(Smith et al. 1994; Barton et al. 2009) and promotes thedevelopment of palatal instability (Boyle et al. 2006).
Head-neck flexion is even considered to be responsible forinducing bilateral arytenoid cartilage and vocal fold collapse,which has been reported in Norwegian Coldblooded Trotters(Strand et al. 2004; Fjordbakk et al. 2008) and in a case reportabout an Icelandic Horse (Hanche-Olsen 2010).
Recent investigations about the influence of head-neckflexion on the area of the laryngeal opening have shown thatthis area is significantly smaller in hyperflexion in comparison tothe normal contact position in ridden sport horses (Gehlenet al. 2011). It should be noted that in the cited study it was nottaken into account that a modification of head-neck positionmay result in a change of distance between the endoscopeand the larynx as well as in the viewing angle and hence couldaffect the measured laryngeal opening. In the present study,the association between the alteration of head-neck position
TABLE 4: Laryngeal function score in relation to the different head-neck positions and gaits for all horses diagnosed grade B (n = 23) inreference position at trot
Gait and head-neck position
Laryngeal function during exercise
A B1 B2 B3 C1 C2 C3
Trot reference - 15 7 1 - - -Trot unrestrained 3 12 4 2 1 - -Trot elevation 1 15 6 1 - - -Trot hyperflexion 2 12 8 - 1 - -Canter reference 2 6 13 1 1 - -Canter elevation 1 9 10 1 - 1 -Canter hyperflexion 1 10 9 1 - 1 -
TABLE 5: Laryngeal function score in relation to the different head-neck positions and gaits for all horses diagnosed grade C (n = 10) inreference position at trot
Gait and head-neck position
Laryngeal function during exercise
A B1 B2 B3 C1 C2 C3
Trot reference - - - - 6 4 -Trot unrestrained - - 1 - 3 6 -Trot elevation - - 2 - 4 3 1Trot hyperflexion - - 1 - 2 6 1Canter reference - - - - - 7 3Canter elevation - - - - - 4 2Canter hyperflexion - - 1 - 1 5 3
© 2013 EVJ Ltd
44 EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

and laryngeal function was analysed. Since the utilisedgrading system is essentially based on laryngeal movement itcan be assumed that the angle at which the assessedstructures are viewed and the distance between theendoscope and the larynx has no influence on the grading oflaryngeal function.
In the present study, a significant difference between thelaryngeal function score in the 2 investigated gaits could bedemonstrated. This could be explained by the generallyaccepted fact that with increasing physical workload, thebreathing and airflow pattern changes as well.
It has been postulated by some authors that rider’sintervention has a significant effect on the morphology andstability of the upper airway, with head-neck flexion being themain contributing factor causing dynamic collapse of theupper airway or leading to deterioration of existingpathologies (Davidson et al. 2002; Franklin et al. 2006; Allenet al. 2011; van Erck-Westergren 2011). In terms of laryngealfunction, this could not be confirmed by the present study.
A conceivable explanation could be that the head-neckposition has a bigger impact on pharyngeal than on laryngealstability. This hypothesis is based on the fact that the larynx, incontrast to the pharynx, is supported by cartilaginousstructures. In addition, the cross-section area of the fullyabducted larynx is 7% greater than that of the trachea and amaximal abduction of the arytenoid cartilages may not benecessary for sufficient ventilation (Rakesh et al. 2008b).Furthermore, it is possible that the soft tissue boundaries of thepharynx are stretched longitudinally during atlanto-occipitalextension, whereas these tissues are less stretched in a moreflexed head-neck position (Cook 1965; Strand et al. 2009). As aresult, the pharyngeal walls bulge inwards, partly due to thereduced stretching, but also as a consequence of theanatomical characteristics of the head. Since the deepmuscles of mastication (M. pterygoideus medialis andM. pterygoideus lateralis) and the superficial muscle of theintermandibular space (M. digastricus) are laterally limited bythe mandible, these structures can only evade medially if theyare less stretched or even compressed during increasedhead-neck flexion. As shown by McCluskie et al. (2008), headposition significantly affects the position of the larynx in such away that flexed head position results in rostral advancement ofthe larynx. This indicates that the structures of the upperrespiratory tract are laterally restricted and are compressed inthe longitudinal axis (concerning the sagittal plane) duringhead-neck flexion.
It is well known that, apart from racehorses, performancehorses are never required to reach the point of maximalventilation coupled with complete physical exhaustion (Morris1991). The results of the present study demonstrate that themost critical factor for diagnosing a laryngeal malfunction insport horses is replicating their usually required level of work. Asmost of the presented horses had a history of an abnormalrespiratory noise during their routine type of work, theprevalence of laryngeal dysfunction (81%) in the present studywas very high despite the fact that the horses were notexercised to the point of fatigue. Previous studies, which alsoinvestigated horses with abnormal respiratory noise and/orpoor performance, reported a prevalence of 11–38%(Kannegieter and Dore 1995; Martin et al. 2000; Tan et al. 2005;Franklin et al. 2006; Lane et al. 2006b; Barakzai and Dixon2011). The difference could be explained by the choice ofsubjects. In the present study, only Warmblood horses have
been included whereas in the other studies mainly racehorses(Thoroughbreds and/or Standardbreds) have been examined.On closer inspection of the studies it becomes apparent thatthe prevalence increases along with the amount of includedWarmblood horses. This confirms the hypothesis that laryngealdysfunction is the most frequent dynamic upper airwayobstruction in Warmblood horses (Davidson and Martin 2003;Davidson et al. 2011).
In this study, the group of pleasure riding horses showed asignificantly lower laryngeal function score than the other 2groups (dressage and showjumping). It is possible that thesedifferences result from the composition of the aforementionedgroups. Since the group of pleasure horses consisted in themajority of horses not referred as patients (horses owned bythe university or the police unit), a biased distribution could besuspected.
Failure of complete abduction of the left arytenoidcartilage at rest is a reliable indicator for dynamic arytenoidcollapse during exercise and has been shown by severalresearchers (Hammer et al. 1998; Martin et al. 2000; Bartonet al. 2011). The majority of horses which are able to attain andmaintain full arytenoid abduction at rest will be classified asgrade A during exercise (Morris and Seeherman 1990; Morris1991; Rakestraw et al. 1991). However, in all reports there aresome horses with apparently normal laryngeal function at restthat progress to complete laryngeal collapse during exercise(Morris 1991; Kannegieter and Dore 1995; van Erck-Westergren2011). In the literature, predictions of laryngeal function duringexercise of horses with grade III at rest have been veryunreliable. Some authors (Hammer et al. 1998; Martin et al.2000) discovered that up to 80% of racehorses showing agrade III left laryngeal hemiplegia at rest will have a significantdynamic collapse of the arytenoid during strenuous exercise.Controversially, another author (Rakestraw et al. 1991)published that 80% of the horses with resting grade III were ableto maintain full abduction during exercise. Meanwhile, allhorses with grade IV left laryngeal hemiplegia at rest wereclassified as grade C during exercise (Morris and Seeherman1990; Kannegieter and Dore 1995; van Erck-Westergren 2011).
In accordance with previous studies (Morris andSeeherman 1990; Hammer et al. 1998; Lane et al. 2006a;Barton et al. 2011; Davidson et al. 2011), we found a significantcorrelation between resting laryngeal function grade and thegrade of laryngeal function during exercise. All horsesclassified as grade IV at rest were diagnosed with a grade Claryngeal dysfunction during exercise. Horses with grade IIIB upto grade IIIC laryngeal function at rest were also rated gradeC during exercise. All horses that showed laryngeal functionbetween grade I and grade IIIA at rest were classified grade Aor B during exercise.
The endoscopic examinations at rest were carried out withand without sedation. The ability to abduct fully is alwaysdetermined by comparison between the left and the rightarytenoid cartilage and it can be assumed that both sideswould be affected equally by sedation. It has been suggestedthat sedation may help to clarify endoscopic findings at rest toidentify early stages of recurrent laryngeal neuropathy (Cook1989; Ohnesorge et al. 1993; Lindegaard et al. 2007; Löbert2009). As in these studies sedation increased the severity oflaryngeal dysfunction, it has been hypothesised that musclerelaxation induced by the sedatives imitates muscular fatigueinduced by exercise. In accordance with previous studies(Ducharme et al. 1991; Lindegaard et al. 2007; Löbert 2009) we
© 2013 EVJ Ltd
45EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

could reproduce an exacerbation of laryngeal functiongrades with sedation in comparison to the grades withoutsedation. However, as the present study shows, sedation didnot increase the predictive value of resting endoscopy incomparison to the examination during ridden exercise.Consequently, the examiner has free choice of whether or notto use sedation during the endoscopy at rest for the diagnosisof dynamic RLN.
Because dynamic RLN could not be predicted withcomplete certainty by resting endoscopy, evaluation duringexercise should be performed in any case of doubt beforerecommendations for treatment of equine athletes are made.The results of the current study indicate that, concerning theevaluation of laryngeal function, flexion of head and neckduring the exercise examination is not required, since it doesnot influence laryngeal function.
Authors’ declaration of interestsNo conflicts of interest have been declared.
Manufacturers’ addresses1Olympus Corporation, Tokyo, Japan.2CP-Pharma Handelsgesellschaft mbH, Burgdorf, Germany.3Optomed, Les Ulis, France.4IBM Corporation, Armonk, New York, USA.
ReferencesAllen, K.J., Terron-Canedo, N., Hillyer, M.H. and Franklin, S.H. (2011)
Equitation and exercise factors affecting dynamic upper respiratorytract function: a review illustrated by case reports. Equine Vet. Educ.23, 361-368.
Barakzai, S.Z. (2007) Treadmill endoscopy. In: Equine RespiratoryMedicine and Surgery, Ed: B.C. McGorum, Saunders/Elsevier,Edinburgh. pp 235-245.
Barakzai, S.Z. and Cheetham, J. (2012) Endoscopic examination ofexercising horses: effects on diagnosis and treatment of upperrespiratory tract disorders. Equine Vet. J. 44, 501-503.
Barakzai, S.Z. and Dixon, P.M. (2011) Correlation of resting and exercisingendoscopic findings for horses with dynamic laryngeal collapse andpalatal dysfunction. Equine Vet. J. 43, 18-23.
Barton, A.-K., Cehak, A. and Ohnesorge, B. (2009) Transendoscopiclaser surgery of a transient pharyngeal collapse in flexed position ofthe head in 7 horses. In: 4th World Equine Airways Symposium, Berne.p 205.
Barton, A.-K., Löbert, H.B. and Ohnesorge, B. (2011) Zum Einfluss desSedativums Detomidin auf Diagnostik und Beurteilung derKehlkopfmotorik in der Ruheendoskopie beim Warmblutpferd.Pferdeheilkd 27, 674-680.
Boyle, A.G., Martin, B.B., Davidson, E.J., Durando, M.M. and Birks, E.K.(2006) Dynamic pharyngeal collapse in racehorses. Equine Vet. J.,Suppl. 38, 546-550.
Cehak, A., Rohn, K., Barton, A.-K., Stadler, P. and Ohnesorge, B. (2010)Effect of head and neck position on pharyngeal diameter in horses.Vet. Radiol. Ultrasound 51, 491-497.
Cook, W.R. (1965) The diagnosis of respiratory unsoundness in the horse.Vet. Rec. 77, 516-527.
Cook, W.R. (1989) Recent observations on recurrent laryngealneuropathy in the horse: applications to practice. Proc. Am. Ass.Equine Practnrs. 35, 427-478.
Davidson, E.J. and Martin, B.B. (2003) Diagnosis of upper respiratorytract diseases in the performance horse. Vet. Clin. North Am.: EquinePract. 19, 51-62.
Davidson, E.J., Martin, B.B., Boston, R.C. and Parente, E.J. (2011)Exercising upper respiratory videoendoscopic evaluation of 100nonracing performance horses with abnormal respiratory noiseand/or poor performance. Equine Vet. J. 43, 3-8.
Davidson, E.J., Martin, B.B., Parente, E.J. and Birks, E.K. (2002) Dynamicevaluation of sport horses with poor performance: 80 cases(1992-2000). In: The Elite Dressage and 3-day-event horse.Conference on Equine Sports, Medicine and Science, Essen.pp 133-136.
Desmaizieres, L.M., Serraud, N., Plainfosse, B., Michel, A. and Tamzali, Y.(2009) Dynamic respiratory endoscopy without treadmill in 68performance Standardbred, Thoroughbred and saddle horsesunder natural training conditions. Equine Vet. J. 41, 347-352.
Dixon, P.M., Robinson, N.E. and Wade, J.F. (2003) Workshop summary. In:Equine Recurrent Laryngeal Neuropathy, Stratford-upon-Avon.pp 93-97.
Ducharme, N.G., Hackett, R.P., Fubini, S.L. and Erb, H.N. (1991) Thereliability of endoscopic examination in assessment of arytenoidcartilage movement in horses Part II. Influence of side ofexamination, reexamination, and sedation. Vet. Surg. 20, 180-184.
Fjordbakk, C.T., Strand, E. and Hanche-Olsen, S. (2008) Surgical andconservative management of bilateral dynamic laryngeal collapseassociated with poll flexion in harness race horses. Vet. Surg. 37,501-507.
Franklin, S.H., Naylor, J.R.J. and Lane, J.G. (2006) Videoendoscopicevaluation of the upper respiratory tract in 93 sport horses duringexercise testing on a high-speed treadmill. Equine Vet. J. Suppl. 38,540-545.
Gehlen, H., Zebisch, A., May, A., Oel, C. and Reese, S. (2011)Hyperflexion von Kopf und Hals: Auswirkungen auf die oberenAtemwege, Blut-Cortisol, Rittigkeit und Verhalten. In: XIX. Tagungüber Pferdekrankheiten im Rahmen der Equitana, Essen. 93-96.
Gerring, E.L. (1985) Differential diagnosis of equine respiratory noises.In Pract. 7, 109-117.
Hammer, E.J., Tulleners, E.P., Parente, E.J. and Martin, B.B. (1998)Videoendoscopic assessment of dynamic laryngeal function duringexercise in horses with grade-III left laryngeal hemiparesis at rest: 26cases (1992-1995). J. Am. Vet. Med. Ass. 212, 399-403.
Hanche-Olsen, S. (2010) Bilateral dynamic laryngeal collapseassociated with collection in high poll flexion in a gaited Icelandichorse. Pferdeheilkd 26, 810-813.
Kannegieter, N.J. and Dore, M.L. (1995) Endoscopy of the upperrespiratory tract during treadmill exercise: a clinical study of 100horses. Aust. Vet. J. 72, 101-107.
Lane, J.G., Bladon, B., Little, D.R.M., Naylor, J.R.J. and Franklin, S.H.(2006a) Dynamic obstructions of the equine upper respiratory tract.Part 2: comparison of endoscopic findings at rest and duringhigh-speed treadmill exercise of 600 Thoroughbred racehorses.Equine Vet. J. 38, 401-407.
Lane, J.G., Bladon, B., Little, D.R.M., Naylor, J.R.J. and Franklin, S.H.(2006b) Dynamic obstructions of the equine upper respiratory tract.Part 1: observations during high-speed treadmill endoscopy of 600Thoroughbred racehorses. Equine Vet. J. 38, 393-399.
Lindegaard, C., Husted, L., Ullum, H. and Fjeldborg, J. (2007) Sedationwith detomidine and acepromazine influences the endoscopicevaluation of laryngeal function in horses. Equine Vet. J. 39, 553-556.
Linford, R.L., O’Brien, T.R., Wheat, J.D. and Meagher, D.M. (1983)Radiographic assessment of epiglottic length and pharyngeal andlaryngeal diameters in the Thoroughbred. Am. J. Vet. Res. 44,1660-1666.
Löbert, H.B. (2009) Zum Einfluss Des Sedativums Detomidin Und EinerLangzeitlaufbandbelastung Auf Die Endoskopisch EvaluierbareFunktion Der Oberen Atemwege Beim Pferd, tierärztl. Hochschule,Diss., Hannover.
Martin, B.B., Reef, V.B., Parente, E.J. and Sage, A.D. (2000) Causes ofpoor performance of horses during training, racing, or showing: 348cases (1992-1996). J. Am. Vet. Med. Ass. 216, 554-558.
McCluskie, L.K., Franklin, S.H., Lane, J.G., Tremaine, W.H. and Allen, K.J.(2008) Effect of head position on radiographic assessment oflaryngeal tie-forward procedure in horses. Vet. Surg. 37, 608-612.
Morris, E.A. (1991) Dynamic evaluation of the equine upper respiratorytract. Vet. Clin. North Am.: Equine Pract. 7, 403-416.
Morris, E.A. and Seeherman, H.J. (1990) Evaluation of upper respiratorytract function during strenuous exercise in racehorses. J. Am. Vet.Med. Ass. 196, 431-438.
© 2013 EVJ Ltd
46 EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

Ohnesorge, B., Deegen, E., Miesner, K. and Geldermann, H. (1993)Hemiplegia laryngis bei Warmblutpferden – eine Untersuchung anHengsten, Stuten und deren Nachkommen. J. Vet. Med. A 40,134-154.
Petsche, V.M., Derksen, F.J., Berney, C. and Robinson, N.E. (1995) Effectof head position on upper airway function in exercising horses.Equine Vet. J. 27, Suppl. 18, 18-22.
Rakesh, V., Ducharme, N.G., Cheetham, J., Datta, A.K. and Pease, A.P.(2008a) Implications of different degrees of arytenoid cartilageabduction on equine upper airway characteristics. Equine Vet. J. 40,629-635.
Rakesh, V., Ducharme, N.G., Datta, A.K., Cheetham, J. and Pease, A.P.(2008b) Development of equine upper airway fluid mechanicsmodel for Thoroughbred racehorses. Equine Vet. J. 40, 272-279.
Rakestraw, P.C., Hackett, R.P., Ducharme, N.G., Nielan, G.J. and Erb,H.N. (1991) Arytenoid cartilage movement in resting and exercisinghorses. Vet. Surg. 20, 122-127.
Smith, C.M., Taylor, R.J. and Dixon, P.M. (1994) Unilateral ventraldisplacement of the roof of the nasopharynx as a cause of stridor ina pony. Vet. Rec. 134, 140-141.
Strand, E., Fjordbakk, C.T., Holcombe, S.J., Risberg, A. and Chalmers, H.J.(2009) Effect of poll flexion and dynamic laryngeal collapse ontracheal pressure in Norwegian Coldblooded Trotter racehorses.Equine Vet. J. 41, 59-64.
Strand, E., Hanche-Olsen, S., Grønvold, A.M.R. and Mellum, C.N. (2004)Dynamic bilateral arytenoid and vocal fold collapse associatedwith head flexion in 5 Norwegian Coldblooded Trotter racehorses.Equine Vet. Educ. 16, 242-250.
Tan, R.H.H., Dowling, B.A. and Dart, A.J. (2005) High-speed treadmillvideoendoscopic examination of the upper respiratory tract in thehorse: the results of 291 clinical cases. Vet. J. 170, 243-248.
Van Erck-Westergren, E. (2011) Dynamic respiratory videoendoscopy inridden sport horses: effect of head flexion, riding and airwayinflammation in 129 cases. Equine Vet. J. 43, 18-24.
© 2013 EVJ Ltd
47EQUINE VETERINARY EDUCATION / AE / JANUARY 2014
Advertisers’ Index
AAEP CE …………………………...Cover 3 Merial ……………………………….14A Buckeye Nutrition …………………..Cover 2 Nutrena ……………………………...XIII GlobalVetLink ………………………47 Platinum Performance ………………23 Hallmarq …………………………….14B PulseVet Technologies ……………...Cover 4 Henry Schein Animal Health ……….56B SmartPak …………………………….26B Kentucky Performance Products ……XIV Standlee Hay Company ……………...17 Luitpold Animal Health …………….9 Zoetis ………………………………...26A
Equine Digital Best PracticesJoin GlobalVetLINK on Feb 5th, 2014
for a CE Webinar featuring three widely successful equine veterinarian
proffesionals who will share some of their tools of the trade by going digital.
515-817-5701 | [email protected] | GlobalVetLINK.com
Learn Morewww.globalvetlink.com/best-practices-webinar
CE Credit Pending
ADEVE14-1

Review Article
Abortogenic viruses in horsesB. A. Bazanów*, N. A. Jackulak, A. B. Fracka and Z. M. StaroniewiczDepartment of Microbiology, Faculty of Veterinary Medicine, Wrocław University of Environmental and LifeSciences, Poland.*Corresponding author email: [email protected]
Keywords: horse; EAV; EHV-1; EHV-4; abortion; latency
SummaryViral causes of abortion include equine viral arteritis (EVA) andinfection with equine herpesviruses-1 and -4 (EHV-1 andEHV-4). Transmission of equine arteritis virus (EAV) occursthrough respiratory, venereal or transplacental routes.Horizontal respiratory transmission of EAV results from exposureto infective nasopharyngeal secretions from acutely infectedhorses. For this transmission to occur, direct and close contactbetween horses is necessary. Venereal infection is an efficientmethod of transmission, with seroconversion of 85 to 100%of seronegative mares bred to virus shedding stallions.Asymptomatic carrier stallions are the essential naturalreservoir of equine arteritis virus. Equine herpesviruses-1 and -4infect a susceptible host, replicate and establish a lifelonglatent infection without any associated clinical signs.Reactivation of latent infections can result from factors such asstress and intercurrent disease. The control of these diseases isby implementation of appropriate management and hygienemeasures, supplemented by vaccination and, in the case ofEVA, by the identification of persistently infected stallions,which can be removed from breeding or continue to be bredto if managed under controlled conditions to prevent the risk ofan outbreak of the disease.
IntroductionAbortion in horses may result from a variety of causes.Infectious agents, such as bacteria, viruses or fungi, may infectthe fetus or its membranes resulting in fetal death andabortion. Other noninfectious factors connected with themare, fetus or external agents may also cause loss of theembryo or fetus. These factors include twinning, congenitaldefects, progesterone or nutritional deficiencies, ergotalkaloid toxicity, umbilical cord torsion and exposure to Easterntent caterpillars. The significant viral causes of abortion includethe following diseases: equine viral arteritis (EVA) and equineherpesvirus-related diseases, which may be due to infectionwith either of 2 closely related herpesviruses: equineherpesvirus-1 (EHV-1) or less frequently, -4 (EHV-4).
Equine viral arteritisEquine viral arteritis is a highly contagious viral infection thatcan cause a high rate of abortion among susceptiblepregnant mares. The disease is caused by equine arteritis virus(EAV). This virus is present in horse populations in manycountries. A significant percentage of stallions may becomecarriers of the virus. Equine arteritis virus was first isolatedfrom the lung of an aborted fetus in 1953 following an outbreakof respiratory disease and abortion on a Standardbredbreeding farm near Bucyrus (Ohio, USA) (Doll et al. 1957a,b).
After the isolation of the causative agent and description ofcharacteristic vascular lesions, the virus was called equinearteritis virus (Jones et al. 1957).
AetiologyEquine arteritis virus is a member of the Arteriviridae family (VanRegenmortel et al. 2000). Virions are 60 nm in diameter with anisometric nucleocapsid of about 35 nm in diameter,surrounded by a lipid envelope which possess 12–15 nmring-like surface structures. They contain a single molecule oflinear, positive-sense RNA (De Vries et al. 1996; Snijder andMeulenberg 1998; Ziebuhr et al. 2000). Equine arteritis virus isreadily inactivated by lipid solvents and by commondisinfectants and detergents. Under laboratory conditions, EAV(Bucyrus strain) can retain infectivity in a tissue culture mediumfor >75 days at 4°C, for 2–3 days at 37°C and for 20–30 min at56°C (Konishi et al. 1975).
EpidemiologySerological surveys have shown that EAV occurs in Europe,North and South America, Africa, Asia and Australia (Timoneyand McCollum 1993a). The seroprevalence of EAV infectionvaries between countries and also among horses of differentbreed and age (Timoney and McCollum 1988; Golnik andSordyl 2004).
Differences in the seroprevalence between different horsebreeds may indicate the importance of the host genotype forsusceptibility to infection. Relatively high seroprevalence insome horse breeds may be connected with specificmanagement practices which increase the risk of exposure tothe virus (Crabb and Studdert 1996).
In spite of its worldwide circulation, EAV causesdisease outbreaks only from time to time (Timoney andMcCollum 1993b). The conspicuous difference between theubiquitousness of the virus and recorded outbreaks of thedisease may indicate a lack of knowledge on the part ofowners and veterinarians about EVA, limitations in accessiblediagnostics, confusion with another equine disease andsubclinical infection with EAV. The increasing number ofconfirmed outbreaks of EVA in the 1990s can be relatedto increased international horse transport and use ofartificial insemination in the equine industry (Crabb andStuddert 1996).
PathogenesisThe pathogenesis of EVA is still not entirely clear. Many of theclinical manifestations of EVA result from vascular injury(Balasuriya and MacLachlan 2007). After infection,multiplication of virus is known to take place in alveolarmacrophages and sites in the upper respiratory tract. The virus
48
© 2013 EVJ Ltd
EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

migrates to the bronchial lymph nodes where furtherreplication takes place and the virus is disseminatedthroughout the body via the blood stream. The following tissuesites are secondary locations of virus replication: the epitheliaof adrenals, kidneys, seminiferous tubules, liver and the thyroid,and the mesothelium and cells of the tunica media (Breeseand McCollum 1973; Timoney and McCollum 1993b).Localisation of EAV may involve the endothelium and medialmyocytes (Del Piero et al. 1997). Damage of endothelial cellscould lead to anoxia and thrombosis (Estes and Cheville 1970).Equine arteritis virus is not detected beyond 28 days afterinfection other than from semen of carrier stallions (Timoneyet al. 1986b; Neu et al. 1988).
The pathogenesis of EAV abortion is not fully known andsome different, but not mutually exclusive mechanisms, havebeen proposed to explain EAV. One of the oldest theoriesproposed is that abortion is the result of a lethal fetal infectionnot connected with the dam because it usually coincides withearly maternal convalescence (Doll et al. 1957b). Otherauthors suggest that abortion results from damaged uterineand placental blood supply because of systemic vascularnecrosis in the mare (Jones et al. 1957). According to anothertheory, abortion is the result of a fetal infection which leads todeath rather than myometritis or a placental damage thatimpairs progesterone synthesis, leading to fetal expulsion(Coignoul and Cheville 1984). MacLachlan et al. (1996)contend that fetal stress and subsequent activation of thefetal hypothalamic-pituitary axis, as a consequence of viralinfection of the developing fetus, might contribute to thepathogenesis of EVA-induced abortion.
TransmissionTransmission of EAV occurs through respiratory, venereal ortransplacental routes.
Horizontal respiratory transmission of EAV is the result ofexposure to infective nasopharyngeal secretions from acutelyinfected horses. These secretions can be highly infectious, withtitres of EAV for some 7–14 days during the acute phase ofinfection (McCollum et al. 1971). For this transmission to occur,direct and close contact between horses is necessary(Timoney and McCollum 1988). Blood, lacrimal fluid, urine,faeces, vaginal secretions and aborted fetus, placenta andamniotic fluid may also contribute to horizontal virus spread(Fukunaga et al. 1981; Cole et al. 1986). Horizontal infectionposes a threat to pregnant mares, which can result in abortion(de Vries et al. 1996). The other important route of naturaltransmission of the virus is venereal transmission of EAV throughthe use of semen from an EAV carrier stallion. Most acutely andall persistently infected stallions shed virus in semen and maybe a source of infection through breeding or indirect contactwith stallion masturbates (Neu et al. 1988; Bürki et al. 1992).Venereal infection is an efficient means of transmission withseroconversion of 85–100% of seronegative mares bred toshedding stallions (Timoney et al. 1986a). Mares can also beinfected by artificial insemination with infective semen(Balasuriya et al. 1998). However, venereal transmission fromacutely infected mares to stallions has not been proven (DeVries et al. 1996). Transplacental transmission of the virus inmares infected in late gestation may result in a foal withcongenitally acquired EAV infection. These foals may developa rapidly progressive, fulminating interstitial pneumonia andfibronecrotic enteritis; however, the virus is not teratogenic
(Timoney and McCollum 1993b). Transmission earlier ingestation can result in abortion (Golnik et al. 1981; Del Pieroet al. 1997).
Asymptomatic carrier stallions are the principal naturalreservoir of EAV. Persistently infected stallions can be dividedinto 3 categories on the basis of the duration of thevirus shedding (Timoney et al. 1987). The short-term orconvalescent carriers shed the virus in semen for 2–5 weeks, anintermediate carrier state lasts for 3–8 months and long-term orchronic carriers contain the virus in their sperm for years andperhaps even for life (Timoney and McCollum 1993b) Somepersistently infected horses cease to shed virus after periodsbetween 18 months and 10 years with no apparent reversionlater to a shedding state (Timoney and McCollum 1993b). Themechanism of persistence of EAV in the male reproductivetract is unknown, but it appears to be testosterone-dependent(Little et al. 1992). Persistently infected stallions castrated andtreated with testosterone continued to shed the virus in semenas opposed to untreated animals (Little et al. 1992). The virushas not been isolated from the reproductive tract of mareslater than one month after infection or from convalescentmares (McCollum and Timoney 1984).
Clinical featuresMost natural infections are asymptomatic (McCollum andBryans 1973) or pyrexia of up to 41°C occurs. In addition, anycombination of the following clinical signs can be observed:anorexia, depression, conjunctivitis and respiratory signs withrhinitis, rhinorrhoea, nasal and ocular discharge, epiphoraand oedema of the palpebra, abdomen, prepuce andscrotum or mammary glands. Sometimes urticarial rash andstiffness of gait are present. Less frequently, ataxia, mucosalpapular eruptions, shoulder oedema and submaxillarylymphadenopathy have been observed (Del Piero 2000). Innatural cases of EVA, the clinical signs can vary significantlyamong individual horses and between outbreaks and dependon factors such as the age and physical condition of the horse,route of infection, challenge dose, environmental conditionsand strain of virus (Slater 2007). In adult horses the course ofdisease is rarely fatal. Pregnant mares which have hadcontact with infective respiratory tract secretions from acutelyinfected horses can frequently abort. Abortion rates varybetween <10% and >50% (Timoney and McCollum 1993b)and generally occurs 10–33 days after EAV infection. It isconnected with the late febrile or early convalescent phasebut it can occur even if no clinical signs are observed (Bryanset al. 1957). Frequently, but not invariably, aborted fetusesare partially autolysed and do not show any gross andmicroscopic lesions (De Vries et al. 1996), whereasEHV-infected fetuses are expelled fresh and frequently havecharacteristic gross lesions (Holyoak et al. 2008).
EHV-1 and EHV-4 infectionBefore 1981, EHV-4 and EHV-1 were known as the samevirus, namely ‘EHV-1’, for which the synonyms ‘equinerhinopneumonitis virus’ and ‘equine abortion virus’ wereuniversally used. It was supposed that ‘EHV-1’ causedrespiratory disease (equine rhinopneumonitis), establishedlatent infection and subsequently caused abortion, as anunpredictable sequel following reactivation of latency inpregnant mares. It was assumed likewise in the case ofoccurrence of EHV-1 neurological disease (Crabb andStuddert 1996).
© 2013 EVJ Ltd
49EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

The result of restriction endonuclease DNA fingerprints(Sabine et al. 1981; Studdert et al. 1981; Turtinen et al. 1981)revealed that what had been designated ‘EHV-1’ reallycomprised 2 different viruses. In 1988, The Herpesvirus StudyGroup of the International Committee on Taxonomy of Viruses(ICTV) accepted the proposal for the viruses to be designatedEHV-1 and -4 (Turtinen et al. 1981).
AetiologyEHV-1 and -4 are related members of the Alphaherpesviridaefamily and responsible for abortion and neurological disease(Campbell and Studdert 1983; Allen and Bryans 1986; Crabbet al. 1995). Virions are about 150 nm in a diameter withcomplex and characteristic structures and include bothsymmetric and nonsymmetric components (Homa and Brown1997). The spherical virions comprise a core, capsid, tegumen,and lipoprotein envelope. The core consists of the viralgenome, a single, linear, double stranded (ds) DNA molecule(Van Regenmortel et al. 2000). EHV-1 and -4 are closely relatedbut are genetically, antigenically and pathogeniticallydifferent from EHV-2, -3 and -5 (Allen et al. 1977; Staczek et al.1983; Crabb and Studdert 1993).
Both EHV-1 and -4 are environmentally labile and quicklydestroyed by lipid solvents, heat, detergents and disinfectants(Doll et al. 1959a). Environmental persistence of EHV isrelatively short, estimated to be below 7 days in mostconditions with a maximum survival of 35 days (Doll et al.1959b).
EpidemiologyThe main reservoir of EHV is the latently infected horse. Equineherpesvirus-1 most often causes abortion in mares, whileEHV-4 is usually associated with respiratory disease in younghorses. Although both viruses have the potential to causerespiratory disease, abortion and equine herpesvirusmyeloencephalopathy (EHM), cases of EHV-4 related abortionand neurological disease are rare (Slater 2007).
Epidemiological research indicates that primary infection isacquired within the first few weeks or months of life, usuallybefore or just after weaning, from adult mares that exhibit noclinical signs of disease and shed virus (Gilkerson et al. 1999).
The life styles of EHV-1 and -4 are represented by 1) earlyand widespread infection of young horses, 2) a highprevalence of latently infected carrier horses and 3)transmission of virus from latently infected adults to newgenerations of equines (Slater 2007).
PathogenesisThe upper respiratory tract is the natural gateway of entry forEHV-1 and -4 and the respiratory mucosal epithelium is themain target for infection (Allen and Bryans 1986; Gibson et al.1992; Allen et al. 2004). Close physical contact with a horse,that shed virus or inhalation of infectious aerosol maycontribute to respiratory infection. The efficacy of respiratorytransmission and active spread of herpesvirus infections is lessthan that observed with equine influenza virus (Allen 2002b).
Primary EHV-1 replication occurs in epithelial cells of theupper respiratory tract and local lymph nodes resulting in aleucocyte-associated viraemia, which can persist for at least14 days (Patel et al. 1982; Kydd et al. 1994; Lunn et al. 2009).This leucocyte-associated viraemia in an acute infection hasbeen shown to be a precondition for abortion by initiating
replication of EHV-1 in endothelial cells of blood vessels in thepregnant uterus. It is likely that this mechanism also occurs inabortions which occur long after an acute primary infectioncaused by reactivated virus from latently infected leucocytes(Patel et al. 1982; Smith et al. 1993). Detection of EHV-1 in anaborted fetus is sometimes more difficult in cases where thereis widespread infection of endometrial blood vessels resultingin a severe vasculitis and multifocal thrombosis than in cases ofless extensive uterine vascular pathology. In the latter situation,the virus can transfer across the uteroplacental barrier and it ispossible to detect it in the aborted fetus. If transplacentalEHV-1 infection occurs near term, the foals can be born alive,but usually die a few days later from a fulminent interstitialpneumonia (Smith et al. 1992, 1993).
Uterine endothelial cells are more susceptible to infectionwith EHV-1 in late pregnancy compared with early pregnancy,so mares abort usually at 6–11 months of gestation (Bryans1978; Slater 2007). This is related to the level of hormonessuch as serotonin, thromboxanes, prostaglandins and serumgonadotropin in the pregnant mare (Robinson and Maxie1993). Hormonal stability of the placenta in response tovascular injury in early gestation can be reason of resistanceof the pregnant mare to EHV-1 abortion during this time(Edington et al. 1991). Some investigations showed thatplasma fibrinogen, factor VIII:C and Von Willebrand factoractivity gradually increase from mid-gestation to delivery innormal mares and this may contribute to thrombosis invirus-infected endometrial endothelium and enhance the riskof abortion in the final third of pregnancy (Gentry et al. 1992).
In cases of abortion which occur up to 6 months, thefetuses are usually autolysed. Tissue from aborted fetusesshows a range of macroscopic and microscopic lesions. In lateabortions (after 7 months) lesions are visible in about 25% of thecases (Doll and Bryans 1962).
In comparison to EHV-1, EHV-4 has a much lowerendotheliotropism. Most EHV-4 strains do not give rise to acell-associated viraemia and consequently, rarely causeabortion or neurological disease (Patel et al. 1982). However,some isolates of EHV-4 have the capacity to cause acell-associated viraemia and can replicate in uterine and/orfetal endothelial cells and cause abortion (Whitwell et al.1994).
Usually EHV-4 infections are cleared from the respiratorytract after 7–20 days post primary infection and within 2–7 daysof subsequent infections (Allen et al. 2004). The actualpathogenesis of EHV-4 infection has not been fullydetermined. It is similar to EHV-1 because the early mucosalphase is connected with infection of the respiratory tract andits associated lymphoid system. Finally, viral DNA can persist inthe trigeminal ganglia, certain subpopulations of circulatinglymphocytes and reticuloendothelial cells associated with therespiratory tract, following recovery from infection (Welchet al. 1992; Borchers et al. 1997).
LatencyEquine herpesviruses-1 and -4 are capable of staying dormantin a carrier horse for a long time, probably for life, without anyassociated clinical signs. On large equine breedingestablishments, EHV-1 infection occurs in the first weeks ormonths of life and current vaccines and control practicescannot prevent this occurring (Gilkerson et al. 1999). Latencyin infected horses is established in lymph nodes associatedwith the respiratory tract, CD8+ T lymphocytes and in neurons
© 2013 EVJ Ltd
50 EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

within the trigeminal ganglia (Pusterla et al. 2010). Viral DNAcan also be detected in other locations, but it is unknownwhether the virus is capable of undergoing reactivation fromthese sites (Nordengrahn et al. 2002). Influence of factors suchas stress, transport, co-mingling of horses and intercurrentdisease, can lead to reactivation of latent infection (Edingtonet al. 1985). Reactivation of EHV-1 may result in mild respiratorydisease (Kydd et al. 1994) and if it occurs in mares which havenot previously aborted an EHV-1 infected fetus, they mayabort (Campbell and Studdert 1983). It may take place weeksor months post infection, after the period of thecell-associated viraemia that follows virus reactivation fromthe trigeminal ganglia or lymphatic tissue within the respiratorytract (Allen et al. 1998). Reactivation of latent EHV-4 will usuallycause recurrent disease in the host accompanied by virusshedding from the nasopharynx in the absence of clinical signs(Allen et al. 2004).
A recent study conducted in the USA among a healthyhorse population, demonstrated that subclinical shedding ofEHV-1 is rare and when it does occur it is at a very low level thatmight not pose an infectious disease threat to other horses(Pusterla et al. 2008). These observations contrast with theparadigm of common subclinical transmission of EHV-1, atleast in the absence of neonatal and juvenile horsepopulations and imply that a spread of EHV-1 among adulthorses is typically accompanied by clinical disease (Lunn et al.2009). However, the Australian studies report a silent cycle ofEHV-1 transmission and do suggest that mares are the sourceof this virus, in the absence of outbreaks of disease (Gilkersonet al. 1999).
TransmissionEquine herpesviruses-1 and -4 can spread via the respiratoryroute, through contact with an infected animal or abortedfetus, via contaminated equipment or via handler’s clothingand hands (Kydd et al. 1994) The most common transmissionroute is via the respiratory tract by aerosolised respiratorysecretions. Infection can also occur by inhalation of dropletsfrom surfaces or by ingestion. All horses with clinical diseaseand horses in which reactivation of latency has taken placeare considered to be infectious by the respiratory route, evenvirus-shedding adult horses may exhibit no clinical signs.Aborted foals, placental fluids and fetal membranes containlarge quantities of virus and are especially hazardous (Slater2007). EHV-1 can also infect conjunctival epithelium, probablythrough aerosol contact (Kydd et al. 1994). In experimentalintranasally infected pony foals and pony stallions, EHV-1 wasfound in the epididymis and testis. Semen of these horses canbe source of the virus even after the cessation of viraemia(17–25 days after infection) (Tearle et al. 1996).
Clinical features
AbortionIt has been reported that pregnant mares abort suddenly,without any evidence of previous respiratory tract infection,14–120 days after exposure (Doll and Bryans 1962; Smith et al.1992). Abortion caused by EHV-1 may be sporadic or result inmultiple abortions (‘abortion storms’). Abortion rates in suchsituations can reach up to 75% (Doll and Bryans 1963; Mumfordet al. 1987; Smith et al. 1996).
Abortion may occur when the mare is still standing or soonafter lying down. The fetus is often still enveloped in its amniotic
membrane and is usually expelled together with the placenta(Allen et al. 2004). Sometimes, fetuses are born alive, but sufferfrom respiratory distress. Progression of the disease is rapid andcan be accompanied by other signs such as pyrexia,leucopenia, hypoxia, lethargy and diarrhoea. Affected foalsfail to nurse, exhibit severe respiratory distress and eventuallydie within 10–14 days (Allen et al. 2004; Slater 2007). Thereproductive potential of a mare that has aborted is notadversely affected. The majority of mares can becomepregnant a short time after aborting and foal normally in thefollowing year. Accordingly, EHV-1 infection rarely is a cause ofabortion in successive years. Infrequently, however, mares canbecome reinfected and abort again (Bryans 1969; Allen et al.2004). Occasionally, EHV-4 is a cause of abortion. Clinical signsof such abortions are similar to those of EHV-1 abortion, butabortion storms caused by EHV-4 have not been recorded(Allen et al. 2004).
EHV-1 is generally cleared from the respiratory tract within3 weeks of primary infection and 1–2 weeks followingsubsequent infections (Gibson et al. 1992). The duration ofnasal shedding of EHV-4 is usually more transient than for EHV-1(Slater 2007).
Respiratory diseaseEquine herpesvirus-1, in comparison to EHV-4, is not socommonly found to be the cause of clinically apparentrespiratory disease (Wood et al. 2005). Both viruses generallycause disease limited to the upper respiratory tract, but inimmunocompromised, neonatal and other naïve younganimals, these viruses can also cause severe lower respiratorytract infection which can lead to secondary bacterialbronchopneumonia. These foals develop progressive disease,with depression, tachypnoea, dyspnoea and pyrexia (Slater2007). In previously infected horses, respiratory signs may bemild and duration of illness may be short-lived (Kydd et al.1994). In older horses, clinical signs may be entirely absent. Thisapplies especially to pregnant mares and mature horses thatdevelop neurological disease which may not show anyrespiratory signs before abortion or onset of neurologicaldysfunction (Goehring et al. 2005). Similarly, reactivation oflatent EHV-1 or -4 usually results in asymptomatic virus sheddingand viraemia of limited duration (Slater 2007).
Neurological diseaseEquine herpesvirus myeloencephalopathy (EHM) is becomingmore frequent and can be a devastating disease (Kohn andFenner 1987). Equine herpesvirus myeloencephalopathy is notrestricted by pregnancy, age, or gender and can occur in allcategories of horses (Greenwood and Simson 1980). It isassumed that transmission is via the respiratory route althoughendogenous reactivating virus may also be a source ofinfection. Neurological signs usually occur during, or towardsthe end of, the viraemic phase of infection, similar to thepathogenesis of abortion. Neurological signs are highlyvariable in range and severity and depend on the extent andlocation of the neurological lesions in the spinal cord and kindof lesion (Goehring et al. 2005; Slater 2007).
Diagnosis of EAV, EHV-1 and EHV-4
Equine arteritis virusAntibodies to EAV can be detected by a virus neutralisationtest (VNT), complement fixation test (CF) or enzyme-linked
© 2013 EVJ Ltd
51EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

immunosorbent assay (ELISA) within a week after infection(Fukunaga and McCollum 1977). Neutralising antibodiesgenerally persist for years and it is believed immunity againstthe disease is long-lasting, if not lifelong (Gerber et al. 1978). Aneutralisation antibody dilution titre of 1:4 or greater isregarded as positive. For virus isolation, the rabbit kidney(RK-13) line is routinely used. Virus is very frequently isolated onfirst or second passage in cell culture (Timoney 2012);development of cytopathic effect (CPE) in inoculated cells isindicative of the presence of the virus.
Immunofluorescence, immunoperoxidase staining orneutralisation tests are needed to confirm the identity of a viralisolate. For detection of nucleic acid, reverse transcriptase-polymerase chain reaction (RT-PCR), nested RT-PCR (RT-nPCR)and real-time RT-PCR assays have been developed (Balasuriyaand MacLachlan 2007).
Equine herpesvirus-1 and -4The diagnosis of EHV-1 or -4 infection can be by PCR, virusisolation or by fluorescent antibody testing. Specimens for virusisolation are usually placenta, lung, spleen, liver and kidney ofan aborted fetus which, after preparation of a tissuesuspension, are inoculated onto equine or rabbit monolayercell cultures. If the virus is present, CPE is visible within 24–48 hpost injection at which time infected cells are harvested andPCR on electron microscopy (EM) used to identify the virus asa herpesvirus. To determine the identity of the virus either PCR(Kirisawa et al. 1993), ELISA (Yeargan et al. 1985) or DNAfingerprint (Studdert 1983) can be used.
Serological testing, which demonstrates a 4-fold or higherincrease in serum antibody titre by VNT or CF test, on acuteand convalescent samples collected 7–21 days apart,provides presumptive evidence of EHV infection (Kydd et al.2006). The drawback of serological tests such as VN, CF is thefact that they do not distinguish between antibodies to EHV-1or EHV-4; however, commercially available ELISA kits forexample Svanovir EHV-1/EHV-4-Ab ELISA1 are able todifferentiate antibodies to EHV-1 from those due to EHV-4(Crabb and Studdert 1993; Crabb et al. 1995; Hartley et al.2005; Gür and Yapici 2008).
Prevention and control of EAV and EHV-1and EHV-4
Equine viral arteritisCarrier stallions have a significant role in the maintenance andspread of EAV infection in breeding populations. Outbreaks ofEAV can be prevented through identification of persistentlyinfected stallions and implementation of managementpractices to avert the introduction of EAV-infected horses.Stallions should be tested to determine their serological statusfor antibodies to EAV. If stallions are found serologically positivethey should be tested for presence of the shedding state byvirus isolation in tissue culture, RT-PCR or by test breeding toat least 2 seronegative mares. The mares are tested forthe presence of anti-EAV antibodies 14 and 28 days afterbreeding. Stallions that are confirmed carriers and shedders ofvirus in semen are castrated in some countries, in others theyare kept physically isolated and bred only to naturallyimmunised or vaccinated mares. After being bred to ashedding stallion for the first time, the mare should be isolatedfor 3 weeks from any horses seronegative for antibodies to the
virus. It is important to keep carrier stallions isolated because itavoids the risk of contamination of equipment and premiseswith the virus.
If an outbreak of EVA is suspected on a farm, theappropriate veterinary authorities should be notified andaffected and in contact horses isolated. Restrictions ofmovement of horses on and off the affected premises,vaccination of at risk horses and ceasing breeding activity toprevent further spread of the virus should be implemented.Diagnosis of EAV should be confirmed by laboratory testing assoon as possible. Stalls and equipment on the affectedpremises should be thoroughly sanitised with an appropriatedisinfectant. Equine arteritis virus is susceptible to chlorinephenolic compounds, iodine and quaternary ammoniumcompounds. Quarantine is lifted when clinical signs of diseaseor serological evidence of infection have not been observedfor at least 3 weeks (Slater 2007).
The goals of vaccination against EAV are protection ofstallions and 6–12 month old colts against infection and thepossibility of subsequent development of the carrier state,immunisation of seronegative mares before being bredwith EAV-infective semen and reduction of outbreaks innonbreeding populations (Anon. 2012, http://www.aaep.org/eva.html). A modified live-virus attenuated vaccine againstEAV (Arvac)2 is available on the market in the USA andCanada. It has also been used in New Zealand, subjectto ministerial controls, as a part of the EVA eradicationprogramme in that country. The second type of vaccine whichis a killed or inactivated vaccine (Equip Artervac, formerlyArtervac)2 is licensed for commercial use in certain Europeancountries, including Denmark, France, Germany, Hungary,Ireland, Sweden and the UK. It is recommended to vaccinatehorses at 3 or more weeks before breeding (Timoney 2012).
The vaccination of pregnant mares is not encouraged,particularly during the last 2 months of gestation, unless theyare at risk of a natural exposure (Doll et al. 1968). In somecountries, vaccination against EVA is banned because theavailable vaccines do not distinguish between vaccinatedanimals and horses seropositive through natural exposure toinfection.
Equine herpesvirus-associated abortionFor prevention and control of EHV-1 disease, the followingpractices have been described: prevention of disease entryonto premises; stress reduction; limiting the spread of EHVinfection on a premises and adjacent horse areas andvaccination (Slater 2007). The greatest danger of exogenousinfection is introduction of new horses into established groups.The addition of new animals to the herd should be, if possible,avoided or preceded by a 21 day period of isolation (Allen2002a).
For maximum protection, group size should be as small asthe physical facilities allow and different age groups shouldnot be mixed. Pregnant mares should be kept separate fromall other horses on the premises and should be subdivided intosmall groups to reduce the risk of outbreaks. Mares in thelast third of pregnancy, when the risk of EHV-1 abortion is thehighest, should be considered most at risk. In case ofsuspected EHV-1 infection, the horse should be isolated andappropriate clinical samples should be collected andimmediately transported to a diagnostic laboratory underchilled (but not frozen) conditions (Allen 2002a; Slater 2007). Alldischarges from the infected horse should be removed and
© 2013 EVJ Ltd
52 EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

the area cleaned and disinfected using an appropriatechemical disinfectant. The underlying goal of outbreak controlprocedures is limiting further spread of disease to adjacentpremises and this requires efficient communication amongpremises’ owners, veterinarians and other parties working withthe affected premises (Allen 2002a; Slater 2007).
To minimise the risk of infection in established herds, newarrivals should ideally have been vaccinated before arrivaland should be kept in isolation from other horses until sufficienttime (3–4 weeks) has elapsed for disease to become apparent(Slater 2007).
The goal of vaccination against EHV-1 and -4 is to protecthorses against respiratory disease and prevent abortion.Although there is limited evidence from the literature of somecross protection between EHV-1 and -4, it is generallyaccepted that in order to enhance the immune responses toEHV, current vaccines should contain both EHV viruses (Minkeet al. 2004). The first vaccines against EHV-1 containedinactivated EHV-1 prepared from the tissues of infectedhamsters and were used as a part of a ‘planned infection’control programme for immunising mares against abortion inKentucky many years ago (Doll et al. 1959a). The nextinactivated vaccines were prepared with different adjuvants(Thompson et al. 1979). They gave only partial clinical andvirological protection against respiratory infection with EHV-1and -4 and did not prevent cell-associated viraemia. Despitehigh VN antibody titres, mares have aborted an infected fetusafter inoculation early in gestation with live virus and thenreinoculation 4–6 months later (Doll et al. 1955; Doll and Bryans1963). There are now a variety of live (Rhinomune [Rhino-Flu])2
and inactivated (Duvaxyn EHV-1/-4 [Equi Vac EHV-1/-4]3;Equiffa4; Prestige [Resequin])5 Some contain only EHV andsome combine EHV with other equine disease agents.Immunity after vaccination against reinfection is not longlasting and it is therefore recommended that mares arevaccinated late in gestation in an effort to prevent abortion. Inthe case of an inactivated whole EHV-1/-4 vaccineadjuvanted with carbomer, a 6 month protection period hasbeen previously reported (Minke et al. 2004; Van de Walleet al. 2010).
ConclusionsAbortogenic viruses are the one of most important causes ofabortion in horses. Equine arteritis virus and EHV-1 and -4 canbe responsible for significant economic loses. The control ofthese diseases is through an implementation of appropriatemanagement and hygiene measures and vaccination, thelatter provides relative but not absolute protection againstequine herpesvirus-associated abortion.
According to research conducted in central Kentuckyduring 1988 and 1989 foaling seasons, after the introduction ofwidespread vaccination against EHV-1, the number of fetaland neonatal foal losses decreased significantly (Hong et al.1993). This is a source of encouragement for breedersto implement systematic vaccination, even thoughvaccination is not wholly efficient; most vaccines do notprevent infection but only reduce the clinical outcome ofinfection. Optimal protection is obtained when regularvaccination is implemented for some years. In the case of EVA,outbreaks can be prevented by systematic testing of horses todetermine their serological status for EAV antibodies. Semen ofseropositive stallions should be investigated virologically todetect virus shedding. Stallions confirmed virus carriers can be
removed from breeding or kept in isolation until their semen nolonger tests positive for virus. To reduce the prevalence of EAVinfection in horse populations, carrier stallions, which shed thevirus constantly in their semen, should be castrated or usedunder strictly controlled breeding conditions.
Authors’ declaration of interestsNo conflicts of interest have been declared.
Manufacturers’ addresses1Svanova Biotech AB, Uppsala, Sweden.2Pfizer, Zoetis now, New York City, USA.3Fort Dodge, Zoetis now, New York City, USA.4Merial, A Sanofi Company headquarter in the North America: Duluth,Georgia, USA; Quebec, Canada, in Europe: Lyon, France;Hallbergmoos, Germany; Milano, Italy; Velserbroek, Netherlands;Barcelona, Spain; Essex, UK and Ireland; Wien, Austria; Diegem, Belgium;Helsinki, Finland; Oslo, Norway, Malmö, Sweden; Rio de Mouro, Portugal.5Intervet, (since 29 June 2011) Merck Animal Health in USA andCanada, New York City, United States and MSD Animal Health in othercountry Boxmeer, the Netherlands.
ReferencesAllen, G.P. (2002a) Epidemic disease caused by equine herpesvirus-1:
recommendations for prevention and control. Equine Vet. Educ. 14,136-142.
Allen, G.P. (2002b) Respiratory infections by equine herpesvirus types 1and 4. In: Equine Respiratory Diseases, Ed: P. Lekeux, InternationalVeterinary Information Service, Ithaca, New York. pp 1-14.http://www.ivis.org
Allen, G.P. and Bryans, J.T. (1986) Molecular epizootiology,pathogenesis, and prophylaxis of equine herpesvirus-1 infections.Prog. Vet. Microbiol. Immunol. 2, 78-144.
Allen, G.P., Kydd, J.H., Slater, J.D. and Smith, K.C. (1998) Advances inunderstanding of the pathogenesis, epidemiology andimmunological control of equine herpesvirus abortion. In: EquineInfectious Diseases, Vol. VIII, Eds: U. Wernery, J.F. Wade, J.A. Mumfordand O.R. Kaaden, R&W Publications Ltd, Newmarket.p 129.
Allen, G.P., Kydd, J.H., Slater, J.D. and Smith, K.C. (2004) Equidherpesvirus-1 (EHV-1) and -4 (EHV-4) infections. In: InfectiousDiseases of Livestock, Eds: J.A.W. Coetzer and R.C. Tustin, OxfordPress, Cape Town. pp 829-859. Chapter 76.
Allen, G.P., O’ Callaghan, D.J. and Randall, C.C. (1977) Geneticrelatedness of equine herpesvirus types 1 and 3. J. Virol. 24, 761-767.
Anon. (2012) Codes of practice extract for contagious equine metritis(CEM), Klebsiella pneumonia and Pseudomonas aeruginosa.Horserace Betting Levy Board Parnell House 25 Wilton Road London.http://www.aaep.org/eva.html
Balasuriya, U.B., Evermann, J.F. and Hedges, J.F. (1998) Serologic andmolecular characterization of an abortogenic strain of equinearteritis virus isolated from infective frozen semen and an abortedequine fetus. J. Am. Vet. Med. Ass. 213, 1586-1589.
Balasuriya, U.B. and MacLachlan, N.J. (2007) Equine viral arteritis. In:Equine Infectious Diseases, Vol. 14, Eds: D.C. Sellon and M.T. Long,Saunders Elsevier, St Louis. pp 153-164.
Borchers, K., Wolfinger, U., Lawrenz, B., Schellenbach, A. and Ludwig, H.(1997) Equine herpesvirus 4 DNA in trigeminal ganglia of naturallyinfected horses detected by direct in situ PCR. J. Gen. Virol. 78,1109-1114.
Breese, S.S., Jr and McCollum, W.H. (1973) Electron-microscopic studiesof tissues of horses infected by equine arteritis virus. In: Proceedingsof the 3rd International Conference on Equine Infectious Disease,Eds: J.T. Bryans and H. Gerber, S. Karger, Paris. pp 273-281.
Bryans, J.T. (1969) On immunity to disease caused by equineherpesvirus-1. J. Am. Vet. Med. Ass. 155, 294-300.
© 2013 EVJ Ltd
53EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

Bryans, J.T. (1978) Immunization of pregnant mares with an inactivatedequine herpesvirus 1 vaccine. In: Equine Infectious Diseases, 4thInternational Conference of Equine Infectious Diseases, Lyon, Eds:J.T. Bryans and H. Gerber, Vet. Publ. Inc., Princeton, New Jersey. pp83-92.
Bryans, J.T., Doll, E.R., Crowe, M.E.W. and McCollum, W.H. (1957) Theblood picture and thermal reaction in experimental viral arteritis ofhorses. Cornell Vet. 47, 42-52.
Bürki, F., Hofer, A. and Nowotny, N. (1992) Objective data plead tosuspend import-bans for seroreactors against equine arteritis virusexcept for breeder stallions. J. Appl. Anim. Res. 1, 31-42.
Campbell, T.M. and Studdert, M.J. (1983) Equine herpesvirus type 1(EHV-1). Vet. Bull. 53, 135-146.
Coignoul, F.L. and Cheville, N.F. (1984) Pathology of maternal genitaltract, placenta, and fetus in equine viral arteritis. Vet. Pathol. 21,333-340.
Cole, J.R., Hall, R.F., Gosser, H.S., Hendricks, J.B., Pursell, A.R., Senne, D.A.,Pearson, J.A. and Gipson, C.A. (1986) Transmissibility andabortogenic effect of equine viral arteritis in mares. J. Am. Vet. Med.Ass. 189, 769-771.
Crabb, B.S. and Studdert, M.J. (1993) Epitopes of glycoprotein G ofequine herpesviruses 4 and 1 located near the C termini elicittype-specific antibody responses in the natural host. J. Virol. 67,6332-6338.
Crabb, B.S. and Studdert, M.J. (1996) Equine rhinopneumonitis (equineherpesvirus 4) and equine abortion (equine herpesvirus 1). In: VirusInfections of Equines, Ed: M.J. Studdert, Elsevier, Amsterdam.pp 11-37.
Crabb, B.S., Drummer, H.E., Reubel, G.H., McPherson, C.M., Browning,G.F. and Studdert, M.J. (1995) A type specific, serological test todistinguish antibodies to equine herpesviruses 4 and 1. Arch. Virol.140, 245-258.
De Vries, A.A.F., Rottier, P.J.M., Glaser, A.L. and Horzinek, M.C. (1996)Equine viral arteritis. In: Virus Infections of Equines, Vol. 15, Ed:M.J. Studdert, Elsevier, Amsterdam. pp 171-200.
Del Piero, F. (2000) Equine viral arteritis. Vet. Pathol. 37, 287-296.
Del Piero, F., Wilkins, P.A. and Lopez, J.W. (1997) Equine viral arteritis innewborn foals: clinical, pathological, serological, microbiologicaland immunohistochemical observations. Equine Vet. J. 29, 178-185.
Doll, E.R. and Bryans, J.T. (1962) Incubation periods for abortion inequine viral rhinopneumonitis. J. Am. Vet. Med. Ass. 141, 351-354.
Doll, E.R. and Bryans, J.T. (1963) A planned infection program forimmunizing mares against viral rhinopneumonitis. Cornell Vet. 53,249-262.
Doll, E.R., Bryans, J.T. and McCollum, W.H. (1957a) Isolation of a filterableagent causing arteritis of horses and abortion by mares; itsdifferentiation from the equine abortion (influenza) virus. Cornell Vet.47, 3-41.
Doll, E.R., Knappenberger, R.E. and Bryans, J.T. (1957b) An outbreak ofabortion caused by the equine arteritisvirus. Cornell Vet. 47, 69-75.
Doll, E.R., Bryans, J.T. and McCollum, W.H. (1959a) A procedure forevaluating the antigenicity of killed virus vaccines for equinerhinopneumonitis. Cornell Vet. 49, 212-220.
Doll, E.R., McCollum, W.H., Bryans, J.T. and Crowe, M.W. (1959b) Effect ofphysical and chemical environment on the viability of equinerhinopneumonitis virus propagated in hamsters. Cornell Vet. 49,75-81.
Doll, E.R., Crowe, M.E.W., Bryans, J.T. and McCollum, W.H. (1955)Infection immunity in equine abortion. Cornell Vet. 45, 387-410.
Doll, E.R., Bryans, J.T., Willson, J.C. and McCollum, W.H. (1968)Immunization against equine viral arteritis using modified live viruspropagated in cell cultures of rabbit kidney. Cornell Vet. 58, 497-524.
Edington, N., Bridges, C.G. and Huckle, A. (1985) Experimentalreactivation of equid herpesvirus 1 (EHV 1) following theadministration of corticosteroids. Equine Vet. J. 17, 369-372.
Edington, N., Smyth, B. and Griffiths, L. (1991) The role of endothelial cellinfection in the endometrium, placenta and foetus of equidherpesvirus 1 (EHV-1) abortions. J. Comp. Pathol. 104, 379-387.
Estes, P.C. and Cheville, N.F. (1970) The ultrastructure of vascular lesionsin equine viral arteritis. Am. J. Pathol. 58, 235-252.
Fukunaga, Y., Imagawa, H., Tabuchi, E. and Akiyama, Y. (1981) Clinicaland virological findings on experimental equine viral arteritis inhorses. Bull. Equine Res. Inst. 18, 110-118.
Fukunaga, Y. and McCollum, W.H. (1977) Complement fixationreactions in equine viral arteritis. Am. J. Vet. Res. 38, 2043-2046.
Gentry, P.A., Feldman, B.F., O’Neill, S.L., Madigan, J.E. and Zinkl, J.G.(1992) Evaluation of the haemostatic profile in the pre- and postparturient mare, with particular focus on the perinatal period.Equine Vet. J. 24, 33-36.
Gerber, H., Steck, F., Hofer, B., Walther, L. and Friedli, U. (1978)Serological investigations on equine viral arteritis. In: Proceedings ofthe 4th International Conference on Equine Infectious Diseases,Lyon, Eds: J.T. Bryans and H. Gerber, Veterinary Publications, Inc.,Princeton, New Jersey. pp 461-465.
Gibson, J.S., Slater, J.D., Awan, A.R. and Field, H.J. (1992) Pathogenesisof equine herpesvirus-1 in specific pathogen- free foals: primary andsecondary infections and reactivation. Arch. Virol. 123, 351-366.
Gilkerson, J.R., Whalley, J.M. and Drummer, H.E. (1999) Epidemiologicalstudies of equine herpesvirus 1 (EHV-1) in thoroughbred foals: areview of studies conducted in the Hunter Valley of New South Walesbetween 1995 and 1997. Vet. Microbiol. 68, 15-25.
Goehring, L.S., van Maanen, C. and Sloet van Oldruitenborgh-Oosterbaan, M.M. (2005) Neurological syndromes among horses inThe Netherlands: a 5 year retrospective survey (1999–2004). Vet. Q.27, 11-20.
Golnik, W., Michalska, Z. and Michalak, T. (1981) Natural viral arteritis infoals. Schweiz. Arch. Tierheilkd 123, 523-533.
Golnik, W. and Sordyl, B. (2004) Odsetek zakazen naturalnych wirusemzapalenia tetnic koni u ogierów róznych ras. Medycyna Wet. 60,849-852.
Greenwood, R.E. and Simson, A.R. (1980) Clinical report of a paralyticsyndrome affecting stallions, mares and foals on a thoroughbredstudfarm. Equine Vet. J. 12, 113-117.
Gür, S. and Yapici, O. (2008) Equine herpesvirus type 1 and 4 inindividually reared horses in Centraland Western Turkey. Acta Vet.Brno 77, 609-613.
Hartley, C.A., Wilks, C.R., Studdert, M.J. and Gilkerson, J.R. (2005)Comparison of antibody detection assays for the diagnosis ofequine herpesvirus 1 and 4 infections in horses. Am. J. Vet. Res. 66,921-928.
Holyoak, G.R., Balasauriya, U.B.R., Broaddus, C.C. and Timoney, P.J.(2008) Equine viral arteritis. Current status and prevention.Theriogenol. 70, 403-414.
Homa, F.L. and Brown, J.C. (1997) Capsid assembly and DNApackaging in herpes simplex virus. Rev. Med. Virol. 7, 197-222.
Hong, C.B., Donahue, J.M., Giles, R.C., Petrites-Murphy, M.B., Poonacha,K.B., Roberts, A.W., Smith, B.J., Tramontin, R.R., Tuttle, P.A. andSwerczek, T.W. (1993) Equine abortion and stillbirths in centralKentucky during 1988 and 1989 foaling seasons. J. Vet. Diagn. Invest.5, 560-566.
Jones, T.C., Doll, E.R. and Bryans, J.T. (1957) The lesions of equine viralarteritis. Cornell Vet. 47, 52-68.
Kirisawa, R., Endo, A., Iwai, H. and Kawakami, Y. (1993) Detection andidentification of equine herpesvirus -1 and -4 by polymerase chainreaction. Vet. Microbiol. 36, 57-67.
Kohn, C.W. and Fenner, W.R. (1987) Equine herpesmyeloencephalopathy. Vet. Clin. N. Am.: Equine Pract. 3, 405-419.
Konishi, S., Akashi, H., Sentsui, A. and Ogata, M. (1975) Studies on equineviral arteritis. Characterisation of the virus and trial survey onantibody with Vero cell culture. Jpn. J. Vet. Sci. 37, 259-267.
Kydd, J.H., Townsend, H.G. and Hannant, D. (2006) The equine immuneresponse to equine herpesvirus-1: the virus and its vaccines. Vet.Immunol. Immunopathol. 111, 15-30.
Kydd, J.H., Smith, K.C., Hannant, D., Livesay, G.J. and Mumford, J.A.(1994) Distribution of equid herpesvirus-1 (EHV-1) in respiratory tractassociated lymphoid tissue: implications for cellular immunity.Equine Vet. J. 26, 466-473.
Little, T.V., Holyoak, G.R., McCollum, W.H. and Timoney, P.J. (1992)Output of equine arteritis virus from persistently infected stallions istestosterone-dependent. In: Proceedings of the 6th InternationalConference on Equine Infectious Disease, Cambridge, 1991, Eds:W. Plowright, P.D. Rossdale and J.F. Wade, R&W Publications Ltd.,Newmarket. p 225.
© 2013 EVJ Ltd
54 EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

Lunn, D.P., Davis-Poynter, N., Flaminio, M.J.B.F., Horohov, D.W.,Osterrieder, K., Pusterla, N. and Townsend, H.G.G. (2009) Equineherpesvirus-1 consensus statement. J. Vet. Intern. Med. 23, 450-461.
MacLachlan, N.J., Balasuriya, U.B.R., Rossitto, P.V., Hullinger, P.A., Patton,J.F. and Wilson, W.D. (1996) Fatal experimental equine arteritisinfection of a pregnant mare: immunohistochemical staining of viralantigens. J. Vet. Diagn. Invest. 8, 367-374.
McCollum, W.H. and Bryans, J.T. (1973) Serological identification ofinfection by equine arteritis virus in horses of several countries. In:Proceedings of the 3rd International Conference on EquineInfectious Disease, Paris, 1972, Eds: J.T. Bryans and H. Gerber, S.Karger, Basel. pp 256-263.
McCollum, W.H. and Timoney, P.J. (1984) The pathogenic qualities ofthe 1984 strain of equine arteritis virus. In: Proceedings of theGrayson Foundation International Conference of ThoroughbredBreeders Organizations, Dromoland Castle, Ireland, 1984, pp. 34-84.
McCollum, W.H., Prickett, M.E. and Bryans, J.T. (1971) Temporaldistribution of equine arteritis virus in respiratory mucosa, tissues andbody fluids of horses infected by inhalation. Res. Vet. Sci. 12, 459-464.
Minke, J.M., Audonnet, J.C. and Fischer, L. (2004) Equine viral vaccines:the past, present and future. Vet. Res. 35, 425-443.
Mumford, J.A., Rossdale, P.D., Jessett, D.M., Gann, S.J., Ousey, J. andCook, R.F. (1987) Serological and virological investigations of anequid herpesvirus 1 (EHV-1) abortion storm on a stud farm in 1985.J. Reprod. Fertil. Suppl. 35, 509-518.
Neu, S.M., Timoney, P.J. and McCollum, W.H. (1988) Persistent infectionof the reproductive tract in stallions experimentally infected withequine arteritis virus. In: Proceedings of the 5th InternationalConference on Equine Infectious Diseases, Lexington, 1987, Ed:D.G. Powell, The University Press of Kentucky, Lexington. pp 149-154.
Nordengrahn, A., Merza, M. and Ros, C. (2002) Prevalence of equineherpesvirus types 2 and 5 in horse populations by using type-specificPCR assays. Vet. Res. 33, 251-259.
Patel, J.R., Edington, N. and Mumorfd, J.A. (1982) Variation in cellulartropism between isolates of equine herpesvirus 1 in foals. Arch. Virol.74, 41-51.
Pusterla, N., Mapes, S. and Wilson, W.D. (2008) Use of viral loads in bloodand nasopharyngeal secretions for the diagnosis of EHV-1 infectionin field cases. Vet. Rec. 162, 728-729.
Pusterla, N., Mapes, S. and Wilson, W.D. (2010) Prevalence of equineherpesvirus type 1 in trigeminal ganglia and submandibularlymphnodes of equids examined postmortem. Vet. Rec. 164,376-378.
Robinson, W.F. and Maxie, M.G. (1993) The cardiovascular system.In: Pathology of Domestic Animals, 4th edn., Vol. 3, Eds: K.V.F. Jubb,P.C. Kennedy and N. Palmer, Academic Press, San Diego, California.pp 1-100.
Sabine, M., Robertson, G.R. and Whalley, J.M. (1981) Differentiation ofsub-types of equine herpesvirus 1 by restriction endonucleaseanalysis. Aust. Vet. J. 57, 148-149.
Slater, J. (2007) Equine herpesviruses. In: Equine Infectious Diseases, Vol.13, Eds: D.C. Sellon and M.T. Long, Saunders Elsevier, St Louis. pp134-153.
Smith, K.C., Mumford, J.A. and Lakhani, K. (1996) A comparison of equidherpesvirus 1 (EHV-1) vascular lesions in the early versus latepregnant equine uterus. J. Comp. Pathol. 114, 231-247.
Smith, K.C., Whitwell, K.E., Binns, M.M., Dolby, C.A., Hannant, D. andMumford, J.A. (1992) Abortion of virologically negative fetusesfollowing experimental challenge of pregnant pony mares withequid herpesvirus-1. Equine Vet. J. 24, 246-259.
Smith, K.C., Whitwell, K.E., Mumford, J.A., Gower, S.M., Hannat, J.P. andTaerle, J.P. (1993) An immunological study of the uterus of maresfollowing experimental infection by equid herpesvirus 1. Equine Vet.J. 25, 36-40.
Snijder, E.J. and Meulenberg, J.J. (1998) The molecular biology ofarteriviruses. J. Gen. Virol. 79, 961-979.
Staczek, J., Atherton, S.S. and O’Callaghan, D.J. (1983) Geneticrelatedness of the genomes of equine herpesvirus types 1, 2, and 3.J. Virol. 45, 855-858.
Studdert, M.J. (1983) Restriction endonuclease DNA fingerprinting ofrespiratory, foetal and perinatal foal isolates of equine herpesvirustype 1. Arch. Virol. 77, 249-258.
Studdert, M.J., Simpson, T. and Roizman, B. (1981) Differentiation ofrespiratory and abortogenic isolates of equine herpesvirus 1 byrestriction endonucleases. Science 214, 562-564.
Tearle, J.P., Smith, K.C., Boyle, M.S., Binns, M.M., Livesay, G.L. andMumford, J.A. (1996) Replication of equid herpesvirus-1 (EHV-1) inthe testes and epididymis of ponies and venereal shedding ofinfectious virus. J. Comp. Pathol. 115, 385-397.
Thompson, G.R., Mumford, J.A. and Smith, I.M. (1979) Experimentalimmunization against respiratory disease due to equine herpesvirus1 infection (rhinopneumonitis) using formalin-inactivated virus withvarious adjuvants. Vet. Microbiol. 4, 209-222.
Timoney, P.J. (2012) Equine viral arteritis. In: O.I.E Manual of DiagnosticTests and Vaccines for Terrestrial Animals (Mammals, Birds and Bees),7th edn., Ed: B. O’Neill, Office International Des Epizooties, Paris.pp 904-918.
Timoney, P.J. and McCollum, W.H. (1988) Equine viral arteritis:epidemiology and control. J. Equine Vet. Sci. 8, 54-59.
Timoney, P.J. and McCollum, W.H. (1993a) Equine viral arteritis inperspective in relation to international trade. J. Equine Vet. Sci. 13,50-52.
Timoney, P.J. and McCollum, W.H. (1993b) Equine arteritis virus. Vet. Clin.N. Am.: Equine Pract. 9, 295-309.
Timoney, P.J., McCollum, W.H. and Roberts, A.W. (1986a) Detection ofthe carrier state in stallions persistently infected with equine arteritisvirus. Proc. Am. Ass. Equine Practnrs. 32, 57-65.
Timoney, P.J., McCollum, W.H., Roberts, A.W. and Murphy, T.W. (1986b)Demonstration of the carrier state in naturally acquired equinearteritis virus infection in the stallion. Res. Vet. Sci. 41, 279-280.
Timoney, P.J., McCollum, W.H., Murphy, T.W., Roberts, A.W., Willard, J.G.and Carswell, G.D. (1987) The carrier state in equine arteritis virusinfection in the stallion with specific emphasis on the venereal modeof virus transmission. J. Reprod. Fertil. Suppl. 35, 95-102.
Turtinen, L.W., Allen, G.P., Darlington, R.W. and Bryans, J.T. (1981)Serologic and molecular comparisons of several equine herpesvirustype 1 infections. Am. J. Vet. Res. 42, 2099-2104.
Van de Walle, G.R., May, M.A., Peters, S.T., Metzger, S.M., Rosas, C.T. andOsterrieder, N. (2010) A vectored equine herpesvirus type 1 (EHV-1)vaccine elicits protective immune responses against EHV-1 andH3N8 equine influenza virus. Vaccine 28, 1048-1055.
Van Regenmortel, M.H.V., Fauquet, C.M. and Bishop, D.H.L. (2000)Seventh report of the International Committee on Taxonomyof Viruses. In: Virus Taxonomy. Classification and Nomenclatureof Viruses, Eds: M.H.V. van Regenmortel, C.M. Fauquet, D.H.L. Bishop,E.B. Carstens, M.K. Estes, S.M. Lemon, J. Maniloff, M.A. Mayo, D.J.McGeoch, C.R. Pringle and R.B. Wickner, Academic Press, SanDiego, California. pp 851-856.
Welch, H.M., Bridges, C.G., Lyon, A.M., Griffiths, L. and Edington, N.(1992) Latent equid herpesviruses 1 and 4: detection and distinctionusing the polymerase chain reaction and co-cultivation fromlymphoid tissues. J. Gen. Virol. 73, 261-268.
Whitwell, K.E., Smith, K.C., Sinclair, R. and Mumford, J.A. (1994) Foetallesions in spontaneous EHV-4 abortions in mares. In: Equine InfectiousDiseases, Vol. VII, Eds: W. Plowright and H. Nakajima, R & WPublications, Newmarket, Suffolk. p 354.
Wood, J.L., Newton, J.R., Chanter, N. and Mumford, J.A. (2005)Association between respiratory disease and bacterial and viralinfections in British racehorses. J. Clin. Microbiol. 43, 120-126.
Yeargan, M.R., Allen, G.P. and Bryans, J.T. (1985) Rapid subtyping ofequine herpesvirus 1 with monoclonal antibodies. J. Clin. Microbiol.21, 694-697.
Ziebuhr, J., Snijder, E.J. and Gorbalenya, A.E. (2000) Virus-encodedproteinases and proteolytic processing in the Nidovirales. J. Gen.Virol. 81, 853-879.
© 2013 EVJ Ltd
55EQUINE VETERINARY EDUCATION / AE / JANUARY 2014

GENERAL
Equine Veterinary Education (EVE) is the official education journal of both the British Equine Veterinary Association (BEVA) and the American Association of Equine Practitioners (AAEP). As such, it is circulated to over 10,000 equine veterinarians around the world. It is published monthly and is a subscription based journal.
EVE is an educational journal and we aim to publish material of direct clinical relevance and interest to practising equine clinicians. The educational value of a submitted article is one of the most important criteria that we assess when deciding whether to accept it for publication. Articles do not necessarily need to contain original or novel information but we welcome submission of this material.
Currently, the journal publishes the following types of articles: Editorials, Case Reports, Clinical Commentaries, Review Articles, Original Articles, Correspondence and Book Reviews.
Papers submitted are assessed by at least two peer reviewers and, if accepted for publication, the copyright becomes the property of EVJ Ltd.
Authorship: Authors submitting a paper do so on the understanding that the manuscript has been read and approved by all authors and that all authors agree to the submission of the manuscript to the Journal. ALL named authors must have made an active contribution to the conception and design and/or analysis and interpretation of the data and/or the drafting of the paper and ALL must have critically reviewed its content and have approved the final version submitted for publication. Participation solely in the acquisition of funding or the collection of data does not justify authorship and, except in the case of complex large-scale or multi-centre research, the number of authors should normally not exceed six.
Conflict of Interest: Authors are required to disclose any possible conflict of interest. These include financial (for example patent, ownership, stock ownership, consultancies, speaker’s fee). Author’s conflict of interest (or information specifying the absence of conflicts of interest) will be published under a separate heading entitled: Authors’ declaration of interests.
Copyright Assignment
Authors submitting a paper do so on the understanding that the work and its essential
substance have not been published before and is not being considered for publication elsewhere. The submission of the manuscript by the authors means that the authors automatically agree to sign a Copyright Transfer Agreement form when the manuscript is accepted for publication. The work shall not be published elsewhere in any language without the written consent of the publisher.
If your paper is accepted, the author identified as the formal corresponding author for the paper will receive an email prompting them to login into Author Services; where via the Wiley Author Licensing Service (WALS) they will be able to complete the license agreement on behalf of all authors on the paper.
SUBMISSION OF MANUSCRIPTS
Equine Veterinary Education uses ScholarOne Manuscripts for online manuscript submission and peer review. The system has a whole host of benefits including:
All submissions to the journal must be submitted online at http://mc.manuscriptcentral.com/eve. Full instructions and support are available on the site and a user ID and password can be obtained on the first visit. If you require assistance then click the Get Help Now link which appears at the top right of every ScholarOne Manuscripts page. If you cannot submit online, please contact the Editorial Office.
Manuscript Files Accepted
Manuscripts should be uploaded as Word (.doc) or Rich Text Format (.rft) files (not write-protected) plus separate figure files. GIF, JPEG, PICT or Bitmap files are acceptable for submission, but only high-resolution TIF or EPS files are suitable for printing.
Manuscript Status
You can access ScholarOne any time to check your ‘Author Centre’ for the status of your manuscript. You will be informed by e-mail once a decision has been made.
MANUSCRIPT TYPES ACCEPTED
Editorials These are often written by the Editors or members of the Editorial Board. However, guest editorials are always welcome. They can relate to the content of the issue, providing a useful means of
AUTHOR GUIDELINES

introducing and generating interest in specific subjects. Editorials should be approximately 1000 words and may include a limited number of references.
Case Reports Case Reports are published when they are considered to be of educational value. Single or multiple cases are acceptable. They should be presented clearly, with events recorded in chronological order or under headings where appropriate: Introduction, Case history, Clinical findings, Diagnosis, Treatment, Outcome, Post mortem findings (where applicable) and Discussion.The recommended length is 2000 words, although this is dependent upon the nature of the report.
Clinical Commentaries The purpose of Clinical Commentaries is to expand on particular aspects of specific Case Reports. Clinical Commentaries provide expert opinion written by a colleague with a special interest and knowledge of the subject. Freedom of expression on any aspect of the Case Report is encouraged. The commentaries are 500–2000 words in length and may contain figures and illustrations where appropriate.
Original Articles Original Articles have a high scientific content and contain original work. They may include, for example analyses of data from case series or results of clinical research studies. Articles should be no more than 4000 words in length including references and tables and should include illustrations. A brief summary should be included at the beginning of the article.
Review Articles These articles summarise the current knowledge relating to the subject and, in some cases, discuss means of improving understanding. Individual articles can be up to 4000 words long and a full reference list should be supplied. A brief summary should be included at the beginning of the article.
Evidence-based clinical questions These should be 800–1000 words and address a clinically relevant question, evaluating it from an evidence-based viewpoint.
Correspondence The Editors welcome correspondence on any subject. If a letter relates to an article published in a previous issue, it is usual for a copy to be sent to the author(s) of that article who will be given a chance to respond.
Supplementary Information
Publication in electronic formats has created opportunities for adding details or whole sections in the electronic version only. Supplementary information can contain data sets, additional figures or tables or video clips which are published alongside the online version of the article.
AFTER ACCEPTANCE
Upon acceptance of a paper for publication, the manuscript will be forwarded to the Production Editor who is responsible for the production of the journal.
Proof Corrections
The corresponding author will receive an e-mail alert containing a link to a website. A working e-mail address must therefore be provided for the corresponding author. The proof can be downloaded as a PDF (portable document format) file from this site. Proofs must be returned to the Production Editor within three days of receipt.
EarlyView (Publication Prior to Print)
Equine Veterinary Education is covered by Wiley-Blackwell Publishing’s EarlyView service. EarlyView articles are complete full-text articles published online in advance of their publication in a printed issue.
Author Services
Online production tracking is available for your article through Wiley-Blackwell’s Author Services. Author Services enables authors to track their article - once it has been accepted - through the production process to publication online and in print.
For more substantial information on the services provided for authors, please see Wiley-Blackwell Publishing Author Services
Offprints and Extra Copies
A PDF offprint of the online published article will be provided free of charge to the corresponding author and may be distributed subject to the Publisher’s terms and conditions. Additional paper offprints may be ordered online. If you have queries about offprints please e-mail [email protected]
For full author guidelines, please visit wileyonlinelibrary.com/journal/eve

Digital solutions from the most trusted name in portable x-ray imaging
(855) HSAH-EQ1 (472-4371) www.henryscheinvet.com
Rely on Us for All Your Equine Product and Practice Needs

For more information, visit www.aaep.org.
The AAEP offers year-round opportunities
to broaden your professional circle and expand
your clinical knowledge in practice areas most
important to you. Mark your calendar now for
these 2014 educational events.
A m e r i c a n A s s o c i a t i o n o f E q u i n e P r a c t i t i o n e r s
2014 CE Meetings
grow.December 6-10
6006000666600thhthhtt annualnuaan lannuauuannnanan lluauaaaaa conventionovoc nnonventiooovvoooocc nnnnnn ee iitt ooooSalt Lake City, Utah
February 6-8
July 20-22
Louisville, Kentucky
16166661111 thhthhhhtt ANNUALNUAAN LANNUAUUAUUANNNNAANAAN LLUAUAAAAAAA RESORTORESRESORTOOOOSSRRERRE RTTRTTRRTTRRTTOORRRRRRRR SYMPOSIUMUSOS P I MYM O UUUUSSSSOOOOSSSS MMIIIIPPYMYMYYMMYYMM OOOORio Grande, Puerto Rico
Sponsored by
Sponsored by
September 11-13
Phoenix, Arizona

©2013 PulseVet Technologies Alpharetta, GA. | www.pulsevet.com
Back to work with the gold standard in
shock wave healingVersaTron® electrohydraulic, focused shock wave is UNMATCHED. A noninvasive treatment that uses high-energy sound waves to treat lameness & pain.
Not all shock wave is created equal.Don’t settle for anything less than the VersaTron.
VersaTronShockwave.com
RECEIVE $1,000 OFF
LOWEST PRICE WHEN YOU MENTION
THIS EVE AD
Customized penetration depths up to 110 mm – deeper than any other device
Tailor the treatment for:- Suspensory injuries - Tendon tears/strains- Osteoarthritis - Bone fractures- Back Pain - Navicular syndrome (foot lameness)- Wounds - Hocks and other joint injuries
Studied More, Proven Effective – more than a decade of clinical research validating efficacy
Used at more universities and clinics worldwide Treatments covered by most insurance companies
ASK FOR
THE VERSATRON
BY NAME