Comparison of Manual and Automated Determination of Hippocampal Volumes in MCI and Early AD

Verbal Fluency Performance in Amnestic MCI and Older Adultswith Cognitive Complaints
Katherine E. Nutter-Uphama,b, Andrew J. Saykina,c,*, Laura A. Rabina,b, Robert M. Rotha,Heather A. Wisharta, Nadia Parea, and Laura A. FlashmanaaNeuropsychology Program, Department of Psychiatry, Dartmouth Medical School/DHMC,Lebanon, NH, USAbDepartment of Psychology, Brooklyn College, City University of New York, Brooklyn, NY, USAcCenter for Neuro-imaging Department of Radiology, Indiana University School of Medicine,Indianapolis, IN, USA
AbstractVerbal fluency tests are employed regularly during neuropsychological assessments of older adults,and deficits are a common finding in patients with Alzheimer’s disease (AD). Little extant research,however, has investigated verbal fluency ability and subtypes in preclinical stages ofneurodegenerative disease. We examined verbal fluency performance in 107 older adults withamnestic mild cognitive impairment (MCI, n = 37), cognitive complaints (CC, n = 37) despite intactneuropsychological functioning, and demographically-matched healthy controls (HC, n = 33).Participants completed fluency tasks with letter, semantic category, and semantic switchingconstraints. Both phonemic and semantic fluency were statistically (but not clinically) reduced inamnestic MCI relative to cognitively intact older adults, indicating subtle changes in both the qualityof the semantic store and retrieval slowing. Investigation of the underlying constructs of verbalfluency yielded two factors: Switching (including switching and shifting tasks) and Production(including letter, category, and action naming tasks), and both factors discriminated MCI from HCalbeit to different degrees. Correlational findings further suggested that all fluency tasks involvedexecutive control to some degree, while those with an added executive component (i.e., switchingand shifting) were less dependent on semantic knowledge. Overall, our findings highlight theimportance of including multiple verbal fluency tests in assessment batteries targeting preclinicaldementia populations and suggest that individual fluency tasks may tap specific cognitive processes.
KeywordsMild cognitive Impairment; Verbal Fluency; Assessment; Cognition
© 2008 National Academy of Neuropsychology. Published by Elsevier Ltd. All rights reserved.*Corresponding author at: Center for Neuroimaging, Department of Radiology, Indiana University School of Medicine, Indianapolis,IN, 46202, United States. E-mail Address: [email protected]. Phone: 317-278-6947.This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing thisearly version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it ispublished in its final citable form. Please note that during the production process errors may be discovered which could affect the content,and all legal disclaimers that apply to the journal pertain.
NIH Public AccessAuthor ManuscriptArch Clin Neuropsychol. Author manuscript; available in PMC 2009 September 14.
Published in final edited form as:Arch Clin Neuropsychol. 2008 May ; 23(3): 229–241. doi:10.1016/j.acn.2008.01.005.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

1. IntroductionAmnestic mild cognitive impairment (MCI) is characterized by memory complaints anddeficits in the absence of dementia, global cognitive decline, or significant problems withactivities of daily living (ADLs) (Petersen et al., 1999). Numerous epidemiological studieshave documented an accelerated rate of progression to Alzheimer’s disease (AD) in MCIpatients (Tierney, Yao, Kiss & McDowell, 2005), with annual conversion rates from about 10to 15 percent per year, contrasted with the rate of 1 to 2 percent reported for healthy elderly.Over a six year period, approximately 80 percent of those diagnosed with MCI will convert toAD (Petersen et al., 1999; 2001a). Because the symptomatic treatments available for MCI (e.g.,acetylcholinesterase inhibitors) exert the greatest utility if implemented early in the diseasecourse (Gauthier, Feldman, Hecker, 2002; Farlow & Evans, 1998), clinicians and researchersare increasingly examining the neuropsychological profiles of MCI patients to identifycognitive decline at its first sign. Traditionally, emphasis has been placed on episodic memorydeficits, but recent research indicates that some MCI patients show subtle, non-amnesticcognitive difficulties. Changes in aspects of executive function, such as verbal fluency, havebeen observed in people years before the clinical diagnosis of AD (Backman, Jones, Berger,& Laukka, 2005). Verbal fluency performance has often been included in predictive conversionmodels, and older adults who eventually develop AD may show baseline decline in verbalfluency 3 to 5 years before diagnosis (Artero, Tierney, Touchab, & Ritchie, 2003; Saxton, etal., 2004). Consistent with subtle executive dysfunction, neuroimaging studies of MCI haveshown reduced gray matter density in frontal lobe subregions (Saykin, et al., 2006) anddifferential activation of frontal lobe systems during executive function tasks (Rosano, et al.,2005; Saykin, 2004). Investigation of verbal fluency in preclinical AD is therefore of diagnosticand predictive importance.
Verbal fluency is typically defined as the ability to produce words under specific constraints,and within a fixed time interval (Lezak, Howieson, Loring, Hannay, & Fischer, 2004). Severalforms of verbal fluency are regularly utilized in clinical neuropsychological or experimentalassessments. Category fluency, which requires the ability to rapidly name words that aremembers of a specific category, is known to put strong demands on the hierarchical structureof semantic knowledge (Butters, Granholm, Salmon, Grant, & Wolf, 1987). Letter fluency,which requires the ability to name words that begin with a specific letter, is thought to rely lesson semantic knowledge stores and more on “frontal control” regions (Bryan, Luszcz, Crawford,1997; Delis & Kaplan, 2001). In comparison to healthy elderly, AD patients tend to showsignificant deficits in verbal fluency (Butters, et al., 1987; Hart, 1988; Hodges, Salmon, &Butters, 1991; Rosen, 1980; for review see Nebes, 1989), with greater impairment on semanticrelative to letter fluency tasks (Chan, Butters, Salmon, McGuire, 1993; Martin & Fedoi,1983). Investigation of the discriminative value of fluency subtypes in AD has revealed thatsemantic fluency (100% sensitivity, 90.9–92.5 % specificity) is superior to letter fluency(81.8% sensitivity, 83–84.1% specificity) in predicting group membership (Monsch, et al.,1994).
Several explanations have been proposed to account for the discrepancy between performanceon tests of semantic and letter fluency in AD. One model posits that AD patients suffer fromimpaired retrieval from an otherwise intact semantic memory store (Nebes & Brady, 1988;Nebes, Brady, 1989; Nebes, Martin, & Horn, 1984). In this conceptualization, associationsbetween attributes of a given semantic store (e.g., elephant attributes might include, heavy,big, wild) are intact, and deficits are entirely due to slowed retrieval. This is considered to bea non-linguistic or executive control deficit (Henry, Crawford, & Phillips, 2004). A secondmodel attributes impaired semantic verbal fluency to a loss (Hodges, Salmon, Butters, 1992;Monsch, et al., 1992; Salmon, Butters, & Chan, 1999) or disorganization (Grober, Buschke,
Nutter-Upham et al. Page 2
Arch Clin Neuropsychol. Author manuscript; available in PMC 2009 September 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Kawas, & Fuld, 1985) in the actual structure or content of semantic knowledge. Loss of storedrepresentations or attributes is thought to slow word production.
Empirical investigations of the proposed models have been conducted by comparing patients’performance on various verbal fluency tasks. When AD patients were asked to rapidly namesupermarket items on the Mattis Dementia Rating Scale (DRS-2; Jurica, Leitten, & Mattis,2001) they produced many super-ordinate responses but few exemplars (Martin & Fedoi,1983). For example, participants were able to name categories (i.e. meat) but unable to givespecific exemplars of that category (i.e. lamb, beef). Inability to access exemplars wasconsidered to be evidence for the disruption of semantic memory stores. Participants in thisstudy can access the memory store but all the information believed to be contained in the storeis not present. Henry and Crawford (2004) examined focal lesion cohorts and found thatseverity of frontal lobe injuries was associated with both letter (r = .52) and semantic (r = .54)fluency, while severity of temporal lobe lesions showed a differential association with letter(r = .44) and semantic (r = .61) fluency. These findings point to the use of frontal regions inboth tasks, but highlight the contribution of temporal lobe regions for semantic fluency.Research also has shown that AD patients experience a loss of semantic knowledge moregenerally (Norton, Bondi, Salmon, & Goodglass, 1997), and they tend to produce moresemantic-related errors on confrontation naming tasks compared with healthy elderly (Bayles& Tomoeda, 1983).
AD also has been shown to be associated with a distortion in the organization of semanticmemory. For example, using cognitive maps Chan, Butters, Salmon, & McGuire (1993)observed that AD patients used attributes less consistently and categorized more often onconcrete criteria as compared to normal healthy elderly. Furthermore, functional magneticresonance imaging (fMRI) and positron emission tomography (PET) studies have revealedanomalous activity in patients with early AD during semantic and episodic memory processingincluding spatially extended areas of activation (Becker et al., 1996; Becker, Lopez, & Butters,1996; Saykin, 1999). The implication of this finding is that participants with Alzheimer’sdisease allocate more brain tissue to complete a semantic task as compared with older adultcontrols. Although much of the available research appears to support the idea that increaseddifficulty in semantic relative to letter fluency is related to a genuine loss of semanticknowledge rather than a deficit in retrieval from an intact semantic store, it is unclear if this isthe case in early preclinical stages.
Researchers have yet to systematically investigate performance on verbal fluency subtypes inolder adults with mild cognitive impairment (MCI). Standish, Molloy, Cunje and Lewis(2007) found that a subtest of verbal fluency (type not specified, within a 135-item cognitivescreening test) was best able to discriminate between healthy older adults and those with MCIafter controlling for age and education. Saxton and colleagues (2004) included verbal fluencytasks in research on neuropsychological performance approximately 1.5 to 5 years prior to theonset of AD. Results indicated that decline in category (semantic) fluency was one of thepredictors of subsequent conversion to AD in older adults. Another study investigated practiceeffects on category fluency over a one week interval, and found that amnestic MCI and ADparticipants did not benefit from repeated exposure to the task while healthy elders did benefit(Cooper, Lacritz, Weiner, Rosenberg, & Cullum, 2004) suggesting a decline in categoryfluency performance for these populations. Recent work by Murphy, Rich, and Troyer(2006) found that amnestic MCI participants produced significantly fewer words on category(semantic), but not phonemic fluency when compared to healthy controls, though overallperformance on both tasks fell within normal limits clinically. The researchers concluded thatMCI patients experienced difficulties making semantic associations between exemplars ofsubcategories rather than difficulties searching through lexical representations, suggestingdegeneration of brain areas beyond that of the hippocampus (i.e., inclusion of cortical areas
Nutter-Upham et al. Page 3
Arch Clin Neuropsychol. Author manuscript; available in PMC 2009 September 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

supporting semantic memory) at this early disease stage. Overall, extant research suggests apossible decline in verbal fluency for individuals with amnestic MCI, particularly apparent onsemantic fluency subtests.
The goal of the current study was to systematically investigate performance on various subtypesof verbal fluency in nondepressed older adults with amnestic MCI, older adults with significantcognitive complaints (CC) despite neuropsychological test performance within normal limits,and healthy matched controls (HC). We evaluated the differential ability of the various fluencymeasures to detect differences among our participant groups. The CC group is of special interestin light of recent research suggesting that these individuals show brain changes intermediatebetween those seen in MCI and healthy older adults without complaints, and may represent a“pre-MCI” stage (Saykin et al., 2006). Another goal was to explore the underlying constructsof fluency measures to clarify the relative contributions of executive functioning and semanticknowledge on performance. While marked fluency deficits are not typically expected inpreclinical dementia, we hypothesized the presence of subtle difficulties that could relate toorganization of the attributes of semantic stores or other aspects of executive function. Inaddition to commonly used tests of semantic and letter fluency, we included other subtypesthat have yet to be investigated with regard to the contributions of semantic knowledge versusexecutive control features. These include switching tasks, which require participants toalternate between semantic categories (and more explicitly involve executive functions) andaction/verb naming tasks, also believed to be mediated by frontal regions (Baxter & Warrington1985; Cappa, Sandrini, Rossini, Sosta, & Miniussi, 2002; Miozzo, Soardi, Cappa, 1994; Piatt,Fields, Paolo, & Troster, 2004).
2. Methods2.1 Recruitment
Participants included 37 older non-depressed adults diagnosed with amnestic MCI, and 33demographically-matched healthy older adult controls (HC). We also included a third groupof 37 non-depressed older adults who presented with significant cognitive complaints (CC)but who performed within normal limits on neuropsychological testing. Participants wereenrolled consecutively in a longitudinal study of preclinical and early dementia, throughcomprehensive screening including a standardized phone interview (Rabin et al., 2007) andreview of medical records. Participants were recruited from flyers, newspaper ads, publiclectures, and referrals from Dartmouth Hitchcock Medical Center clinics. Enrollment criteriaincluded: at least 60 years of age, right-handed, fluent in English and a minimum of 12 yearsof formal education. Participants were excluded for any medical, psychiatric, or neurologicalconditions (other than MCI) that could affect brain structure or cognition. History of headtrauma with loss of consciousness for more than five minutes and current or past substanceabuse also served as exclusionary criteria. Participants provided written informed consentaccording to procedures approved by the Institutional Committee for the Protection of HumanSubjects.
2.2 Neuropsychological Assessment and Group ClassificationParticipants underwent comprehensive neuropsychological evaluation including measures ofmemory, attention, executive function, processing speed, language, general intellectual abilityand standard dementia screens. Tests included: Verbal Fluency subtests of the Delis-KaplanExecutive Function System (D-KEFS, Delis & Kaplan, 2001); action naming Test (Piatt,Fields, Paolo, & Troster, 1999); DRS-2; Mini Mental State Examination (MMSE, Folstein,Folstein, & Metlugh, 1975); California Verbal Learning Test, Second Edition (CVLT-II, Delis,Kramer, Kaplan & Ober, 2000), Boston Naming test (BNT, Goodglass, Kaplan & Barresi,2001); D-KEFS Trail Making Test; Wechsler Adult Intelligence Scale, Third Edition (WAIS-
Nutter-Upham et al. Page 4
Arch Clin Neuropsychol. Author manuscript; available in PMC 2009 September 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
III, Digit Symbol, Digit Span, Block Design, Vocabulary, and Information subtests, Wechsler,1997); Wechsler Memory Scale, Third Edition (WMS-III, Logical Memory and VisualReproduction subtests, Wechsler, 1997); and Wisconsin Card Sorting Test (WSCT short form;Heaton, Chelune, Talley, Kay, & Curtiss, 1993). Estimates of baseline intellectual functioningincluded the American National Adult Reading Test (ANART; Grober, Buschke, Kawas &Fuld, 1989) and the Barona Index (Barona, Reynolds, & Chastian, 1984). Level of cognitivecomplaint was assessed using self- and informant- report questionnaires including: Memoryand Aging Telephone Screen (Rabin et al., 2007); Memory Self-Rating Questionnaire (Squire,Wetzel, & Slater, 1979), Neurobehavioral Function/Activities of Daily Living Scale (NBF-ADL self- and informant-versions; Saykin et al., 1991), Memory Assessment Questionnaire(Pfeffer, Kurosaki, Harrah, Chance, Filos, 1982; Santulli et al., 2005), Informant Questionnaireon Cognitive Decline in the Elderly (self- and informant-versions; Jorm, 1989), and cognitiveitems from the Geriatric Depression Scale (GDS; Yesavage et al., 1983). A CognitiveComplaint Index ranging from 0 – 100 was calculated based on the total number of items thatcould be endorsed across all subjective measures (for details see Saykin et al., 2006). A Board-certified geropsychiatrist conducted a semi-structured interview to rule out depression or otherpsychiatric disorders. Blood samples were obtained to determine Apolipoprotein E (ApoE)genotype, and participants underwent structural brain MRIs, which were reviewed by a Board-certified neuroradiologist to rule out incidental pathology.
All data were derived from participants’ baseline evaluation in our longitudinal study, with theexception of four participants who received earlier versions of the fluency tasks; for theseindividuals, we used data from the second study visit (approximately one year followingbaseline). The group membership of the five participants whose second study visit data wereutilized was as follows: 2 HCs, 2CCs, and 1 MCI. A
Group classifications were made following careful review of neuropsychological assessmentresults, self- and informant-report data, and geropsychiatric evaluation. Group classificationwas determined by a consensus panel review using Petersen workgroup criteria for amnesticMCI (Petersen et al., 2001b). Participants diagnosed as MCI had: 1) preserved general cognitivefunctioning (as measured by cutoff scores on the DRS-2 and MMSE); 2) generally normalactivities of daily living (as reported on self- and informant versions of the NBF-ADL scale);3) no dementia; 4) significant memory complaints (endorsed at least 20% of possiblecomplaints across all inventories or complaints deemed significant by clinical consensus); and5) impaired memory (memory scores 1.5 S.D. below the mean established for age- andeducation-matched controls). Participants classified as CC had: 1) preserved general cognitivefunctioning; 2) generally normal activities of daily living; 3) no dementia; 4) significantmemory complaints; and 5) intact memory ability. Participants classified as HC had: 1)preserved general cognitive functioning; 2) generally normal activities of daily living; 3) nodementia; 4) no significant cognitive complaints; and 5) intact memory ability. The Petersonworkgroup criteria for MCI dictate that participants have preserved general cognition andisolated memory problems; notable executive or language impairment (including verbalfluency) was grounds for exclusion.
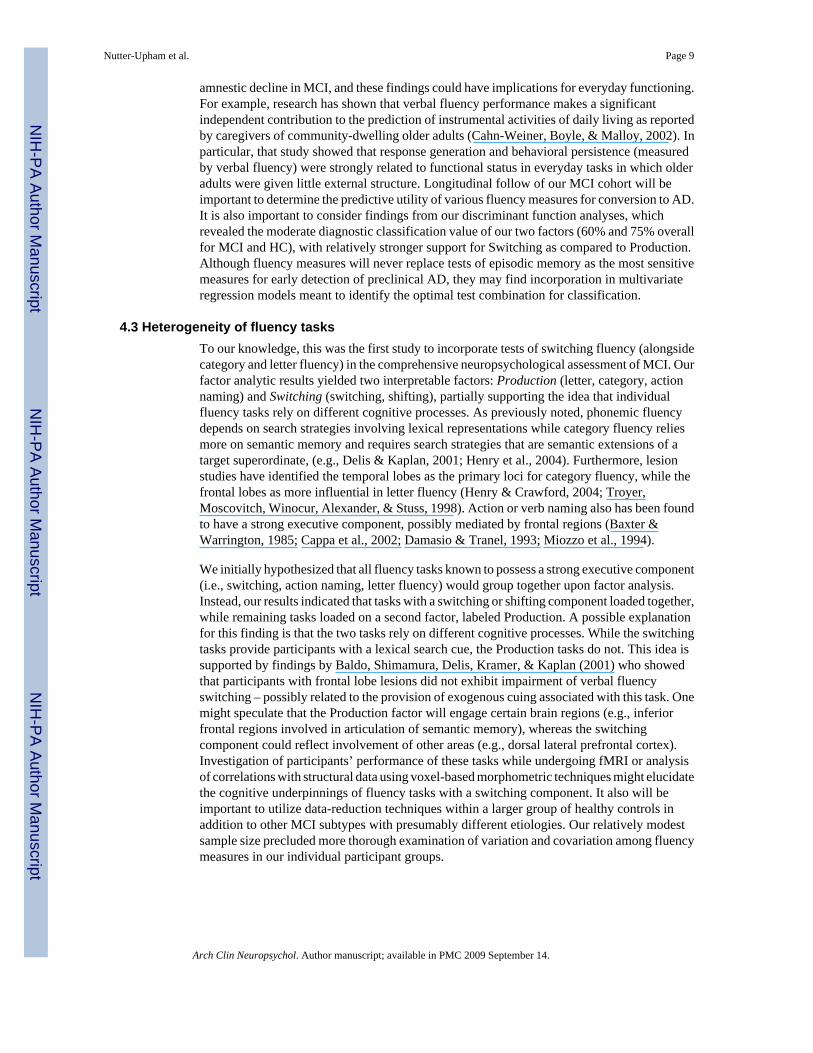
Select demographic and neuropsychological test variables are presented in Table 1. Theaverage age of participants was 72.3 (S.D. = 6.0) years and the average level of education was16.7 (S.D. = 2.8) years. All other key demographic variables were shown to be insignificant.Though no participant was clinically depressed or scored in the depressed range on the adjustedGDS (excludes the four cognitive items), CC and MCI participants tended to endorse severalmore items than HC. As expected based on study classification criteria, scores on the DRS-2and MMSE were reduced in MCI relative to the other groups, though MCI participants scoredabove the cutoff for dementia. MCI participants also showed significant deficits on tests ofmemory (e.g., DRS-2, CVLT-II, WMS-III) relative to HC. Based on study classification
Nutter-Upham et al. Page 5
Arch Clin Neuropsychol. Author manuscript; available in PMC 2009 September 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

criteria, the Cognitive Complaint Index was significantly elevated in both MCI and CC relativeto HC.
2.3 Fluency TasksAll participants were administered five verbal fluency tasks as part of a larger test battery, eachwith a 60 second time limit. Responses were given orally and recorded by hand by highlytrained technicians or postdoctoral fellows. Three of the fluency tasks were D-KEFS subtests,and required participants to rapidly generate words that: 1) begin with a certain letter (letterfluency), 2) belong to a specific category (semantic fluency), or 3) alternate between twodifferent semantic categories (switching fluency). Participants also completed 4) action namingfluency, which required them to name things “that people do” (i.e., verbs). The final task: 5)supermarket naming fluency, was a subtest of the DRS-2, and required participants to nameitems they could “find or buy in a supermarket.” All fluency scores were derived by summingcorrect utterances and excluded repetitions. For the DRS-2 supermarket naming test, themaximum number of points awarded was 20 (as per the standardized instruction manual). Forthe D-KEFS subtests, participants were randomly administered either the standard or alternatetest form to reduce practice effects engendered by multiple administrations of the same items.Alternate test forms were not available for the action naming or supermarket item fluency tasks.Form equivalency has been demonstrated by previous research (Delis & Kaplan, 2001; Cunje,Molloy, & Standish, 2007), and our analysis yielded insignificant results: χ2 (2, N = 107) = .708, p > .05. Therefore the different versions of the fluency scores were collapsed into fourvariables for all participants: “letter,” “category,” “switching,” and “shifting.” Letter fluencyscores were a combination of the three individual letter trials (FAS or BHR), category scoreswere a composite of the two individual trials (animals and boys or clothing and girls), andswitching scores comprised a single trial with two categories (fruits and furniture orinstruments and vegetables). Number of correct shifts between semantic categories also wasanalyzed. In all six fluency variables were included: letter, category, switching, shifting, actionnaming, and supermarket naming.
2.4 Statistical ProceduresSkew and kurtosis statistics were calculated for each fluency measure to explore the shape ofthe distributions. Supermarket naming was highly negatively skewed (statistic = −3.19, 11standard error = .23), while all other fluency measures where normally distributed. One-waymultivariate analysis of variance (MANOVA) was conducted to evaluate whether the groups(MCI, CC, HC) showed an overall difference on the fluency measures, as well as to providecontrol over Type I error. MANOVA was followed by analyses of variance (ANOVAs) andTukey’s HSD post-hoc tests to identify the loci of group differences for each measure.Significance level was set at p < .05 for the MANOVA and for the ANOVA and post-hoc tests.Eta-squared was employed as the measure of effect size. In order to evaluate the underlyingconstructs of multiple verbal fluency measures, a factor analysis with varimax rotation wasused. Number of factors extracted was determined using a minimum eigenvalue of onecriterion. In order to investigate the classification value of our factors, we conducteddiscriminant analyses using the MCI and HC participants. We also examined correlationsamong fluency scores and their relation with select neuropsychological variables (usingPearson correlation coefficients).
3. Results3.1 Group Differences
Descriptive statistics for the fluency measures are presented in Table 2. The overall multivariatetest (Wilk’s Lambda) was significant [F(2,104) = 4.16, p < .001], and follow-up ANOVAsindicated that the groups differed with respect to letter [F(2, 104) = 5.20, p < .01, η2 = .091,
Nutter-Upham et al. Page 6
Arch Clin Neuropsychol. Author manuscript; available in PMC 2009 September 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

power = .82] category [F(2, 104) = 7.77, p < .001, η2 = .130, power = .95], switching [F(2,104) = 16.90, p < .001, η2 = .245 power = 1.00], shifting fluency [F(2, 104) = 14.56, p < .001,η2 = .219, power = 1.00], and action naming [F(2,104) = 4.24, p = .017, η2 = .075, power = .73]. We repeated the MANOVA and subsequent ANOVAs excluding the five participants,whose second study visit data were utilized, with no change in the pattern of results.
Due to the high degree of skewness in the supermarket naming, a Kruskal-Wallis test wasperformed, but results did not reach the .01 cutoff value: χ2 (2, N=107) = 7.521, p < .05. Posthoc analyses to the univariate ANOVAs using the Tukey HSD correction revealed that MCIparticipants scored significantly lower than CC and HC on letter, category, switching, shifting,and action naming tasks. We repeated the multivariate analyses with adjusted GDS score as acovariate, with the same overall pattern of findings. Results indicated that depressive symptoms(i.e. adjusted GDS score) did not account for a significant amount of the variance betweengroups (3 percent of the variance; p > .05).
3.2 Factor Analysis of Fluency TasksFactor analysis was employed to investigate the heterogeneity of fluency tasks with a cutoffeigenvalue of one. Table 3 provides the factor loadings for the cognitive measures. Twosignificant factors emerged, which we termed Switching and Production. Switching accountedfor 56.1% of the variance while the Production factor accounted for 22.8%. In all, 78% of thevariance in fluency performance was explained by these two factors. Switching includedswitching and shifting fluency tasks. Production had loadings from letter, category, and actionnaming tasks. It is worth noting that the effect sizes for the individual tasks were adequate forthe Switching component tasks and poor for the Production component tasks (Table 2).
To investigate the ability of these two factors to discriminate groups, a group-by-factor analysiswas conducted. Factor scores were calculated by taking participants’ Z-scores for each of thefive fluency tasks, multiplied by the amount of variance accounted for on the given factor, andsumming the product of these variables. The resulting values were Z-scores on each factor,accounting for the variance described by each individual test; both factors scores were normallydistributed (Production factor skewness statistic = −0.099; Switching factor skewness statistic= 0.056).
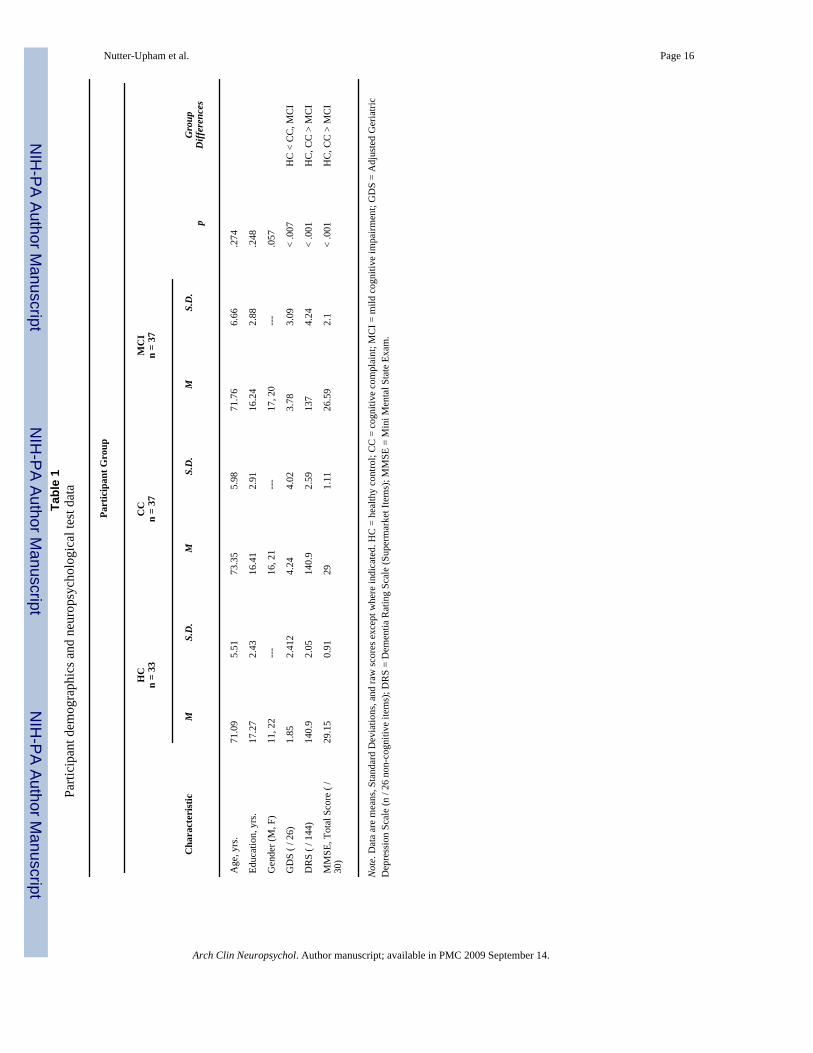
Notably, Z-scores were calculated using the entire sample (instead of HC exclusively), ensuringa conservative approach. Results revealed a significant difference for both the Switching [F(2,104) = 12.47 p < .001, η2 = .197] and Production [F(2,104) = 4.56, p = .013, η2 = .081]factors (see Figure 1). Post hoc analysis using Tukey’s HSD correction revealed that MCIparticipants were significantly lower than CC, and HC on the Switching factor, and that MCIparticipants were significantly lower than HC on the production factor.
Two discriminant function analyses were conducted to determine which factor best predictedmembership as an MCI or HC. For the Switching factor, the discriminant analysis yielded asignificant Wilk’s lambda Λ = .78, χ2 (1, N = 70) = 16.66, p < .01, and correctly classified 24of 33 HC and 25 of 37 MCIs. Overall, the Switching factor correctly classified 75% of theparticipants. The discriminant analysis for the Production factor also yielded a significantWilk’s lambda Λ = .88, χ2 (1, N = 70) = 8.36, p < .01, and correctly classified 20 of the 33 HCand 22 of 37 MCIs. Overall, the Production factor correctly classified 60% of the participants.
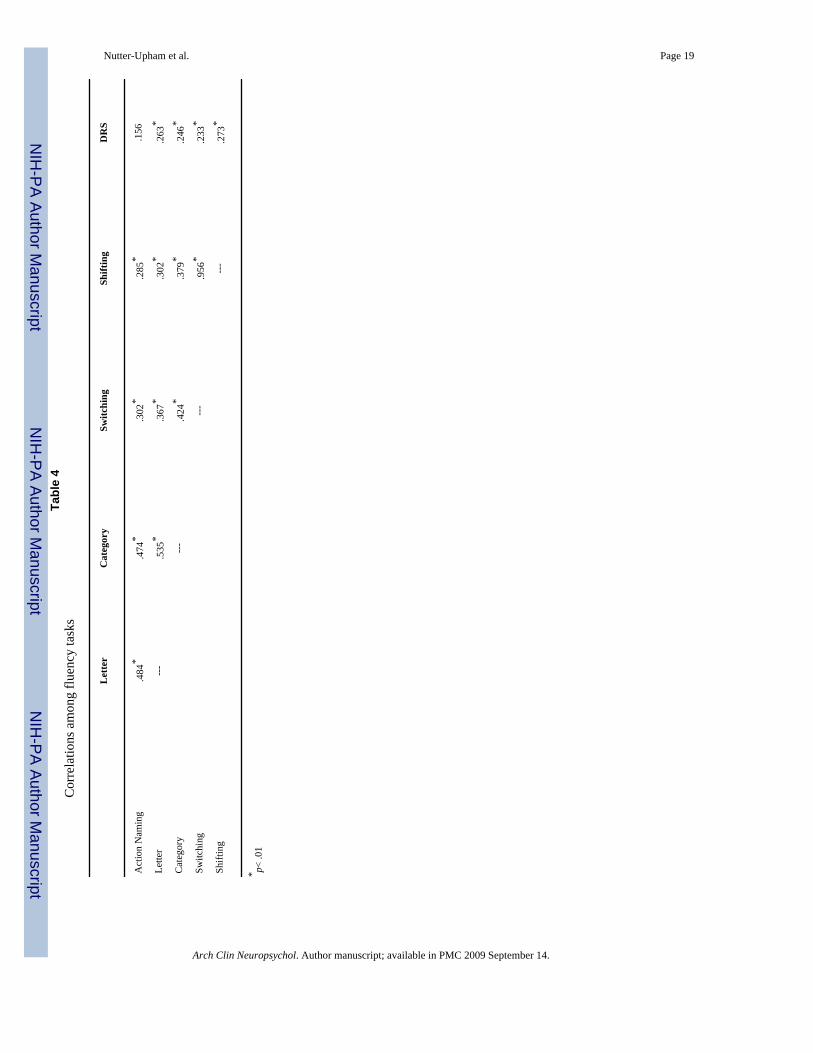
3.3 Neuropsychological CorrelatesA final set of analyses examined relations among fluency tasks and between fluency tasks andselect neuropsychological variables. Pearson correlation coefficients (p < .01 level) revealedstatistically significant relations among all six fluency measures (range = .23 to .96; Table 4),
Nutter-Upham et al. Page 7
Arch Clin Neuropsychol. Author manuscript; available in PMC 2009 September 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

with the exception of supermarket naming and action naming. Statistically significant,moderate correlations were observed between fluency measures and variousneuropsychological test scores (Table 5). Of particular interest are relations between fluencymeasures and tests known to represent verbal knowledge (WAIS-III Vocabulary, Information,and the BNT) or executive function (WCST, WAIS-III Digit Symbol, and D-KEFS TrailMaking Test, Switching condition). WAIS-III Vocabulary, WAIS-III Information, and theBNT were correlated with action naming (r =.55, .46, .31 respectively) and letter fluency (r= .51, .36, .31). WAIS-III Vocabulary and the BNT were correlated with category fluency (r= .33, .27, respectively), though WAIS-III Information was not. Switching and shifting taskswere not significantly correlated with WAIS-III Vocabulary, WAIS-III Information, or theBNT (all r values ≤ .24). The WCST (total categories and number of perseverative errors) didnot correlate with any fluency measure, but WAIS-III Digit Symbol correlated with actionnaming (r =.44), letter (r = .37), category (r =.40), switching (r = .40), and shifting (r = .39)scores.
4. Discussion4.1 Overview
Amnestic MCI is conceptualized as memory complaints and episodic memory impairment inthe absence of dementia or global cognitive decline. Recent research has indicated that subtledecline in other areas of cognition, such as executive functioning, may coexist with episodicmemory deficits. Researchers have included verbal fluency in predictive models for conversionto AD, raising the question of when verbal fluency becomes compromised in the course ofdisease. Results of the current study revealed an overall decline in verbal fluency performancein patients diagnosed with amnestic MCI relative to demographically matched healthy controls.Additionally, factor analytic results suggested that individual fluency tasks may tap specificcognitive processes, and correlational findings implied that all fluency tasks involved executivecontrol to some degree, while those with an added executive component (i.e., switching andshifting) were less dependent on semantic knowledge.
4.2 Group differencesExamination of group differences revealed that MCI participants scored lower on most fluencytasks (i.e., letter, category, switching, shifting) tasks as compared to HC. In contrast to recentfindings by Murphy, Rich, and Troyer (2006), which showed reduced semantic fluency andintact phonemic fluency, our MCI group showed reduced fluency (relative to healthy controls)on both phonemic and semantic tasks. Future research should further explore the degree towhich various fluency subtypes are selectively compromised in MCI and the relation betweenthis compromise and the underlying cognitive demands of the tasks in question. Anotherimportant study finding was that mean scores across all fluency tasks followed the pattern ofHC > CC > MCI. As with previous findings from our laboratory (Saykin et al., 2006), CCsshowed normal performance despite significant complaints about aspects of cognition. Theseindividuals are known to manifest subtle structural and functional brain changes (Saykin et al.,2004; 2006), and may be a prodrome of MCI1. It therefore will be important to follow this at-risk cohort longitudinally to determine when, and under what conditions, fluency deficits arise.
Although statistically significant group differences were obtained across fluency measures,mean MCI scores generally fell within the low average range clinically (i.e., approx 1 S.D.below of the mean of HC)2. Verbal fluency measures thus appear to be sensitive to subtle, non-
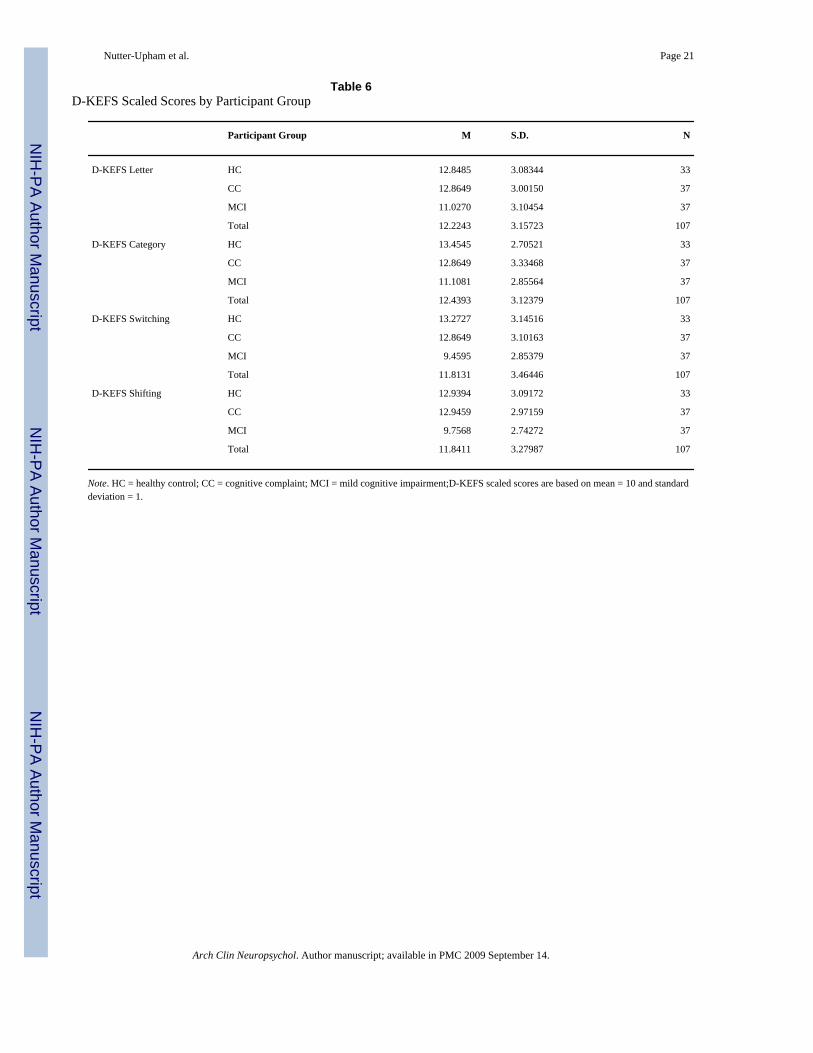
1Refer to Saykin et al. (2006) for further details regarding this cohort [overlap > 86% with participants in the current study]).2This analysis also was preformed using the D-KEFS scaled scores and the same pattern of findings emerged. Scaled score means andstandard deviations for the three groups are reported in Table 6.
Nutter-Upham et al. Page 8
Arch Clin Neuropsychol. Author manuscript; available in PMC 2009 September 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
amnestic decline in MCI, and these findings could have implications for everyday functioning.For example, research has shown that verbal fluency performance makes a significantindependent contribution to the prediction of instrumental activities of daily living as reportedby caregivers of community-dwelling older adults (Cahn-Weiner, Boyle, & Malloy, 2002). Inparticular, that study showed that response generation and behavioral persistence (measuredby verbal fluency) were strongly related to functional status in everyday tasks in which olderadults were given little external structure. Longitudinal follow of our MCI cohort will beimportant to determine the predictive utility of various fluency measures for conversion to AD.It is also important to consider findings from our discriminant function analyses, whichrevealed the moderate diagnostic classification value of our two factors (60% and 75% overallfor MCI and HC), with relatively stronger support for Switching as compared to Production.Although fluency measures will never replace tests of episodic memory as the most sensitivemeasures for early detection of preclinical AD, they may find incorporation in multivariateregression models meant to identify the optimal test combination for classification.
4.3 Heterogeneity of fluency tasksTo our knowledge, this was the first study to incorporate tests of switching fluency (alongsidecategory and letter fluency) in the comprehensive neuropsychological assessment of MCI. Ourfactor analytic results yielded two interpretable factors: Production (letter, category, actionnaming) and Switching (switching, shifting), partially supporting the idea that individualfluency tasks rely on different cognitive processes. As previously noted, phonemic fluencydepends on search strategies involving lexical representations while category fluency reliesmore on semantic memory and requires search strategies that are semantic extensions of atarget superordinate, (e.g., Delis & Kaplan, 2001; Henry et al., 2004). Furthermore, lesionstudies have identified the temporal lobes as the primary loci for category fluency, while thefrontal lobes as more influential in letter fluency (Henry & Crawford, 2004; Troyer,Moscovitch, Winocur, Alexander, & Stuss, 1998). Action or verb naming also has been foundto have a strong executive component, possibly mediated by frontal regions (Baxter &Warrington, 1985; Cappa et al., 2002; Damasio & Tranel, 1993; Miozzo et al., 1994).
We initially hypothesized that all fluency tasks known to possess a strong executive component(i.e., switching, action naming, letter fluency) would group together upon factor analysis.Instead, our results indicated that tasks with a switching or shifting component loaded together,while remaining tasks loaded on a second factor, labeled Production. A possible explanationfor this finding is that the two tasks rely on different cognitive processes. While the switchingtasks provide participants with a lexical search cue, the Production tasks do not. This idea issupported by findings by Baldo, Shimamura, Delis, Kramer, & Kaplan (2001) who showedthat participants with frontal lobe lesions did not exhibit impairment of verbal fluencyswitching – possibly related to the provision of exogenous cuing associated with this task. Onemight speculate that the Production factor will engage certain brain regions (e.g., inferiorfrontal regions involved in articulation of semantic memory), whereas the switchingcomponent could reflect involvement of other areas (e.g., dorsal lateral prefrontal cortex).Investigation of participants’ performance of these tasks while undergoing fMRI or analysisof correlations with structural data using voxel-based morphometric techniques might elucidatethe cognitive underpinnings of fluency tasks with a switching component. It also will beimportant to utilize data-reduction techniques within a larger group of healthy controls inaddition to other MCI subtypes with presumably different etiologies. Our relatively modestsample size precluded more thorough examination of variation and covariation among fluencymeasures in our individual participant groups.
Nutter-Upham et al. Page 9
Arch Clin Neuropsychol. Author manuscript; available in PMC 2009 September 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

4.4 Theoretical Implications and Directions for Future ResearchFluency tasks rely on numerous cognitive processes to a greater or lesser degree includingaccessing semantic memory stores and engaging various executive processes includinginitiation, monitoring, organization, rule implementation, and set shifting. Several models havebeen proposed to explain verbal fluency deficits in AD, and difficulties usually are ascribed toa differential loss or disorganization of semantic knowledge (Grober et al., 1985; Hodges etal., 1992; Monsch et al., 1992; Salmon et al., 1999), although some studies have highlightedimpaired retrieval (Nebes & Brady 1988; Nebes, 1989; Nebes et al., 1984). Most studies ofAD that include both semantic and phonemic fluency tasks find a significantly larger semanticdeficit thought to reflect the greater demands upon the integrity of the semantic network butthe two measures are considered equivalent in sensitivity to executive control processes suchas effortful retrieval (Henry et al., 2004). In our study, both phonemic and semantic fluencywere reduced in MCI relative to cognitively intact older adults, suggesting subtle changes inboth the quality of the semantic store and retrieval slowing. Further, switching (η2 = .245) andshifting (η2 = .219) fluencies showed the largest effect sizes, identifying them as most reliablydiscerning group membership, followed by category (η2 = .130), letter fluency (η2 = .091) andthen action (η2 = .245) (i.e., verb) generation and supermarket naming did not show groupdifferences and appear to be less valuable clinically.
The present results suggest that tasks imposing substantial demands on both semantic storesand effortful retrieval will show greater effects due to the additive features of semanticknowledge degeneration and retrieval impairment. Correlational data further revealed that allfluency tasks correlated with WAIS-III Digit Symbol, a psychomotor processing speed taskwith known executive components. In addition, while category fluency correlated with testsknown to assess semantic knowledge (i.e., WAIS-III Vocabulary and Information), switchingfluency did not. Thus, although executive difficulties are known to be increasingly prominentin later neurodegenerative disease stages, the present results imply that the relativecontributions of subtle executive versus semantic memory storage difficulties are largelyequivalent at this early stage of disease. This finding may have implications for currentconceptualizations of MCI (Winblad et al., 2004). Further investigation of the D-KEFSswitching task is warranted to clarify the relative contributions of both semantic and executiveprocesses to task performance.
4.5 Study Limitations and ConclusionsAn important study limitation was the homogeneity of the participants with regard to baselineintellect, level of education, and ethnicity. Although reflective of the region of northern NewEngland from which the sample was drawn, these factors limit the generalizability of ourfindings, and we are actively recruiting a more demographically diverse cohort. Anotherlimitation was the cross-sectional nature of our data, which prevented us from investigatingthe longitudinal course of verbal fluency performance and predictive value of fluency tasks.We are following-up with study participants and plan to investigate temporal changes in verbalfluency. Although adequate for the current set of analyses, a larger sample size would bedesirable in addition to a more heterogeneous cohort of MCI participants (e.g., multiple-domain, single nonmemory domain) to enable further exploration of verbal fluencyperformance patterns and underlying cognitive processes tapped by specific tasks. Due tosample size constraints, we utilized data from the same group of participants for both the factoranalysis and discriminant function analysis. Ideally, we would have used a validation samplein which factors derived from the first sample were used to assign classifications to an unrelatedsample, and this represents a future direction for us.
Overall, study findings indicated that various subtypes of verbal fluency become statisticallybut not clinically compromised in the preclinical dementia stage of amnestic MCI. Factor
Nutter-Upham et al. Page 10
Arch Clin Neuropsychol. Author manuscript; available in PMC 2009 September 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

analytic and correlational results further indicated involvement of both semantic stores andeffortfull retrieval in verbal fluency processes. The D-KEFS switching task most stronglydiscriminated group membership, and loaded on its own factor, suggesting that it measuressomewhat different cognitive processes than other fluency tasks. These findings underscorethe importance of including multiple verbal fluency tests (and other non-memory tasks) inassessment batteries targeting preclinical dementia populations. We also are examiningrelations of verbal fluency with structural neuroimaging data to investigate the neural basis fordeclining fluency abilities.
AcknowledgementsThis research was supported by funding from the NIA (R01 AG19771), Alzheimer’s Association, National ScienceFoundation, and Ira De Camp Foundation. Portions of this article were presented at the 25th Annual Conference ofthe National Academy of Neuropsychology in Tampa, FL, USA.
We thank Margaret Nordstrom and Dr. Robert Santulli for their assistance with this project.
REFERENCESArtero A, Tierney MC, Touchab J, Ritchie K. Prediction of transition form cognitive impairment to senile
dementia: A prospective longitudual study. ACTA Psychiatrica Scandinavica 2003;107:390–393.[PubMed: 12752036]
Backman L, Jones S, Berger AK, Laukka EJ. Cognitive Impairment in Preclinical Alzheimer’s Disease:A Meta-Analysis. Neuropsychology 2005;19:520–531. [PubMed: 16060827]
Baldo JV, Shimamura AP, Delis DC, Kramer J, Kaplan E. Verbal and design fluency in patients withfrontal love lesions. Journal of the International Neuropsychological Society 2001;7:586–596.[PubMed: 11459110]
Barona A, Reynolds C, Chastian R. A demographically based index of pre-morbid intelligence for thewais-r. Journal of Consulting Clinical Psychology 1984;52:885–887.
Baxter DM, Warrington EK. Category-specific phonological dysgraphia. Neuropsychologia1985;23:653–666. [PubMed: 4058709]
Bayles KA, Tomoeda CK. Controntation naming impairment in demantia. Brain and Language1983;19:98–114. [PubMed: 6222782]
Becker JT, Mintun MA, Aleva K, Wiseman MB, Nichols T, DeKosky ST. Compensatory reallocationof brain resources supporting verbal episodic memory in Alzheimer’s disease. Neurology1996;46:692–700. [PubMed: 8618669]
Becker, JT.; Lopez, OL.; Butters, MA. Episodic memory: Differential patterns of breakdown. In: Morris,RG., editor. The cognitive neuropsychology of Alzheimer-type dementia. New York: OxfordUniversity Press; 1996. p. 70-88.
Bryan J, Luszcz MA, Crawford JR. Verbal Knowledge and speed of information processing as mediatorsof age differences in verbal fluency performance among older adults. Psychology and Aging1997;12:471–478.
Butters N, Granholm E, Salmon DP, Grant I, Wolf J. Episodic and semantic memory: A comparison ofamnesic and demented patients. Journal of Clinical and Experimental Neuropsychology 1987;9:479–497. [PubMed: 2959682]
Cahn-Weiner DA, Boyle PA, Malloy PF. Tests of executive function predict instrumental activities ofdaily living in community-dwelling older individuals. Applied Neuropsychology 2002;9:187–191.[PubMed: 12584085]
Cappa SF, Sandrini M, Rossini PM, Sosta K, Miniussi C. The role of the left frontal lobe in sction naming.Neurology 2002;59:720–723. [PubMed: 12221163]
Chan AS, Butters N, Salmon DP, McGuire KA. Dimensionality and Clustering in the Semantic Networkof Patients With Alzheimer’s Disease. Psychology of Aging 1993;3:411–419.
Cooper DB, Lacritz LH, Weiner MF, Rosenberg RN, Cullum CM. Category Fluency in Mild CognitiveImpairment Reduced effect of Practice in Test-Retest Conditions. Alzheimers Disease and AssociatedDisorders 2004;18:120–122.
Nutter-Upham et al. Page 11
Arch Clin Neuropsychol. Author manuscript; available in PMC 2009 September 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Cunje A, Molloy DW, Standish TI, Lewis DL. Alternate forms of logical memory and verbal fluencytasks for repeated testing in early cognitive changes. International Psychogeriatric 2007;19:65–75.
Damasio A, Tranel D. Nouns and verbs are retrieved with differently distributed neural systems.Proclamations of the National Academy of Science 1993;90:4957–4960.
Delis, DC.; Kramer, JH.; Kaplan, E.; Ober, BA. The California Verbal Learning Test-Second Edition:Adult version manual. San Antonio, TX: Psychological Corporation; 2000.
Delis, D.; Kaplan, E. Delis-Kaplan Executive Function Battery. San Antonio, TX: PsychologicalCorporation; 2001.
Farlow MR, Evans RM. Pharmacologic treatment of cognition in Alzheimerȁ9s dementia. Neurology1998;51:36–44.
Folstein MF, Folstein SE, McHugh PR. Mini-mental state. Mini-Mental State: A practical method forgrading the cognitive state of patients for the clinician. Journal of Psychiatric Research 1975;12:189–198. [PubMed: 1202204]
Gauthier S, Feldman H, Hecker J. Efficacy of donepezil on behavioral symptoms in patients withmoderate to severe Alzheimer's disease. International Psychogeriatrics 2002;14:389–404. [PubMed:12670060]
Goodglass, H.; Kaplan, E.; Barresi, B. Boston Diagnostic Aphasia Examination-Third Edition.Philadelphia: Lippincott Williams & Wilkins; 2001.
Grober E, Sliwinski M, Schwartz M, Saffran E. The American Version of the NARTfor predictingpremorbid intelligence. 1989Unpublished Manuscript
Grober E, Buschke H, Kawas C, Fuld P. Impaired ranking of semantic attributes in dementia. Brain andLanguage 1985;26:276–286. [PubMed: 4084766]
Hart S. Language and dementia: A review. Psychological Medicine 1988;18:99–112. [PubMed: 3283810]Heaton, RK.; Chelune, GJ.; Talley, JL.; Kay, GG.; Curtiss, G. Wisconsin Card Sorting Test manual:
Revised and expanded. Lutz, FL: Psychological Assessment Resources; 1993.Henry JD, Crawford JR, Phillips LH. Verbal fluency performance in dementia of Alzheimer's type: a
meta-analysis. Neuropsychologia 2004;42:1212–1222. [PubMed: 15178173]Henry JD, Crawford JR. A Meta-Analytic Review of Verbal Fluency Performance Following Focal
Cortical Lesions. Neuropsychology 2004;18:284–295. [PubMed: 15099151]Hodges JR, Salmon DP, Butters N. The nature of the naming deficit in Alzheimer’s and Huntington’s
disease. Brain 1991;114:1547–1558. [PubMed: 1832072]Hodges JR, Salmon DP, Butters N. Semantic Memory impairment of Alzheimer's disease: Failure of
access or degraded knowledge? Neuropsychologia 1992;30:301–314. [PubMed: 1603295]Jorm AF, Scott R, Jacomb PA. Assessment of cognitive decline in dementia and by informant
questionnaire. International Journal of Geriatric Psychiatry 1989;4:35–39.Jurica, P.; Leitten, C.; Mattis, S. Dementia Rating Scale-2. Lutz, FL: Psychological Assessment
Resources; 2001.Lezak, MD.; Howieson, DB.; Loring, DW.; Hannay, HJ.; Fischer, JS. Neuropsychological Assessment.
Vol. 4th ed. New York: Oxford University Press; 2004.Martin A, Fedio P. Word production and comprehension in Alzheimer’s disease: Breakdown of semantic
knowledge. Brain and Language 1983;19:124–141. [PubMed: 6860932]Miozzo A, Soardi M, Cappa SF. Pure Anomia with spared action naming due to a left temporal lesion.
Neuropsychologia 1994;32:1101–1109. [PubMed: 7991077]Monsch AU, Bondi MW, Butters N, Salmon DP, Katzman R, Thal LJ. Comparisons of verbal fluency
tasks in the detection of dementia of the Alzheimer’s type. Archives of Neurology 1992;49:1253–1258. [PubMed: 1449404]
Murphy KJ, Rich JB, Troyer AK. Verbal fluency patterns in amnestic mild cognitive impairment arecharacteristic of Alzheimer’s type dementia. Journal of the International Neuropsychological Society2006;12:570–574. [PubMed: 16981610]
Nebes RD, Martin DC, Horn LC. Sparing of semantic memory in Alzheimer’s disease. Journal ofAbnormal Psychology 1984;93:321–330. [PubMed: 6470317]
Nebes RD, Brady DB. Integrity of semantic fields in Alzheimer’s disease. Cortex 1988;24:291–299.[PubMed: 3416611]
Nutter-Upham et al. Page 12
Arch Clin Neuropsychol. Author manuscript; available in PMC 2009 September 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Nebes RD. Semantic memory in Alzheimer’s Disease. Psychological Bulletin 1989;106:377–394.Norton LE, Bondi MW, Salmon DP, Goodglass H. Deterioration of Generic Knowledge in Patient with
Alzheimer’s disease: Evidence from the Number Information Test. Journal of Clinical andExperimental Neuropsychology 1997;19:857–866. [PubMed: 9524880]
Petersen RC, Doody R, Kurz A, Mohs RC, Morris JC, Rabins PV, et al. Current concepts in mild cognitiveimpairment. Archives of Neurology 2001a;58:1985–1992. [PubMed: 11735772]
Petersen RC, Smith GE, Waring SC, Ivnik RJ, Tangalos EG, Kokmen E. Mild cognitive impairment:Clinical characterization and outcome. Archives of Neurology 1999;56:303–308. [PubMed:10190820]
Petersen RC, Stevens JC, Ganguli M, Tangalos EG, Cummings JL, DeKosky ST. Practice parameter:Early detection of dementia: Mild cognitive impairment (an evidence-based review): Report of theQuality Standards Subcommittee of the American Academy of Neurology. Neurology 2001b;56:1133–1142. [PubMed: 11342677]
Pfeffer RI, Kurosaki TT, Harrah CH, Chance JM, Filos S. Measurement of functional activities in olderadults in the community. Journal of Gerontology 1982;37:323–329. [PubMed: 7069156]
Piatt AL, Fields JA, Paolo AM, Troster AI. Action (verb naming) fluency as an executive functionmeasure: Convergent and divergent evidence of validity. Neuropsychologia 1999;37:1499–1503.[PubMed: 10617270]
Piatt AL, Fields JA, Paolo AM, Troster AI. Action verbal fluency normative data for the elderly. Brainand Language 2004;89:580–583. [PubMed: 15120548]
Rabin LA, Saykin AJ, Wishart HA, Nutter-Upham KE, Flashman LA, Pare N, Santulli RB. The Memoryand Aging Telephone Screen (MATS): Development and preliminary validation. Alzheimer’s &Dementia 2007;3:109–121.
Rosano C, Aizenstein HJ, Cochran JL, Saxton JA, De Kosky ST, Newman AB, et al. Event-relatedfunctional magnetic resonance imaging investigation of executive control in very old individualswith mild cognitive impairment. Biological Psychiatry 2005;57:761–767. [PubMed: 15820233]
Rosen W. Verbal Fluency in aging and dementia. Journal of Clinical Neuropsychology 1980;2:135–146.Salmon DP, Butters N, Chan AS. The deterioration of Semantic Memory in Alzheimer’s Disease.
Canadian Journal of Experimental Psychology 1999;53:108–116. [PubMed: 10389493]Santulli, RB.; Saykin, AJ.; Rabin, LA.; Wishart, HA.; Flashman, LA.; Pare, N. Differential sensitivity
of cognitive complaints associated with amnestic MCI: Analysis of patient and informant reports;June, 2005; Presented at the Alzheimer’s Association International Conference on Prevention ofDementia; Washington, D.C. 2005.
Saxton J, Lopez OL, Ratcliff G, Dulberg C, Fried LP, Carlson MC, et al. Preclinical Alzheimer disease:Neuropsychological test performance 1.5 to 8 years prior to onset. Neurology 2004;63:2341–2347.[PubMed: 15623697]
Saykin AJ, Flashman LA, Frutiger SA, Johnson SC, Mamourian AC, Moritz CH, O’Jile JR, Tiordan HJ,Santulli RB, Smith CA, Weaver JB. Neuroanatomic substrates of semantic memory impairment inAlzheimer’s disease: pattern of functional MRI activation. Journal of InternationalNeuropsychological Society 1999;5:377–392.
Saykin AJ, Janssen R, Sprehn G, Spira T, Kaplan J, O'Connor B. Longitudinal evaluation ofneuropsychological function in homosexual men with hiv-1 infection; 18 month follow-up. Journalof Neuropsychiatry and Clinical Neuroscience 1991;3:286–298.
Saykin AJ, Wishart HA, Rabin LA, Flashman LA, Mamourian AC, Santulli RB. Cholinergicenhancement of frontal lobe activity in mild cognitive impairment. Brain 2004;127:1574–1583.[PubMed: 15140813]
Saykin AJ, Wishart HA, Rabin LA, Santulli RB, Flashman LA, West JD, McHugh TL, Mamourian AC.Older adults with cognitive complaints show brain atrophy similar to that of amnestic MCI.Neurology 2006;67:834–842. [PubMed: 16966547]
Squire LR, Wetzel CD, Slater PC. Memory complaints after electroconvulsive therapy: Assessment witha new self-rating instrument. Biological Psychiatry 1979;14:791–801. [PubMed: 497304]
Standish IM, Molloy DW, Cunje A, Lewis DL. Do the ABCS 135 short cognitive screen and its subtestsdiscriminate between normal cognition, mild cognitive impairment and dementia? InternationalJournal of Geriatric Psychiatry 2007;22:189–194. [PubMed: 16977680]
Nutter-Upham et al. Page 13
Arch Clin Neuropsychol. Author manuscript; available in PMC 2009 September 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Troyer AL, Moscovitch M, Winocur G, Alexander MP, Stuss D. Clustering and switching on verbalfluency; The effects of focal frontal- and temporal-lobe lesions. Neuropsychologia 1998;36:449–504.
Tierney MC, Yao C, Kiss A, McDowell I. Neuropsychological test accurately predict incident Alzheimerdisease after 5 and 10 years. Neurology 2005;64:1853–1859. [PubMed: 15955933]
Winblad B, Palmer K, Kivipelto M, Jelic V, Fratiglioni L, Wahlund LO, et al. Mild cognitive impairment– beyond controversies, towards a consensus: report of the International Working Group on MildCognitive Impairment. Journal of Internal Medicine 2004;256:240–246. [PubMed: 15324367]
Wechsler, D. Wechsler Adult Intelligence Scale-Third Edition. San Antonio, TX: The PsychologicalCorp; 1997.
Yesavage JA, Brink TL, Rose TL, Lum W, Huang V, Adey M, Leirer VO. Development and validationof geriatric depression screening scale: A preliminary report. Journal of Psychiatric Research1983;17:37–49. [PubMed: 7183759]
Nutter-Upham et al. Page 14
Arch Clin Neuropsychol. Author manuscript; available in PMC 2009 September 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 1. Median and Standard Error for Factors by Group
Nutter-Upham et al. Page 15
Arch Clin Neuropsychol. Author manuscript; available in PMC 2009 September 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Nutter-Upham et al. Page 16Ta
ble
1Pa
rtici
pant
dem
ogra
phic
s and
neu
rops
ycho
logi
cal t
est d
ata
Part
icip
ant G
roup
HC
n =
33C
Cn
= 37
MC
In
= 37
Cha
ract
eris
ticM
S.D
.M
S.D
.M
S.D
.p
Gro
upD
iffer
ence
s
Age
, yrs
.71
.09
5.51
73.3
55.
9871
.76
6.66
.274
Educ
atio
n, y
rs.
17.2
72.
4316
.41
2.91
16.2
42.
88.2
48
Gen
der (
M, F
)11
, 22
---
16, 2
1--
-17
, 20
---
.057
GD
S ( /
26)
1.85
2.41
24.
244.
023.
783.
09<
.007
HC
< C
C, M
CI
DR
S ( /
144
)14
0.9
2.05
140.
92.
5913
74.
24<
.001
HC
, CC
> M
CI
MM
SE, T
otal
Sco
re (
/30
)29
.15
0.91
291.
1126
.59
2.1
< .0
01H
C, C
C >
MC
I
Not
e. D
ata
are
mea
ns, S
tand
ard
Dev
iatio
ns, a
nd ra
w sc
ores
exc
ept w
here
indi
cate
d. H
C =
hea
lthy
cont
rol;
CC
= c
ogni
tive
com
plai
nt; M
CI =
mild
cog
nitiv
e im
pairm
ent;
GD
S =
Adj
uste
d G
eria
tric
Dep
ress
ion
Scal
e (n
/ 26
non
-cog
nitiv
e ite
ms)
; DR
S =
Dem
entia
Rat
ing
Scal
e (S
uper
mar
ket I
tem
s); M
MSE
= M
ini M
enta
l Sta
te E
xam
.
Arch Clin Neuropsychol. Author manuscript; available in PMC 2009 September 14.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Nutter-Upham et al. Page 17Ta
ble
2V
erba
l flu
ency
scor
es b
y di
agno
stic
gro
up
Part
icip
ant G
roup
HC
n =
33C
Cn
= 37
MC
In
= 37
Flue
ncy
Tas
kM
S.D
.M
S.D
.M
S.D
.p
η2G
roup
Diff
eren
ces
Lette
r44
.52
10.4
744
.14
10.0
437
.49
10.7
5<
.01
.091
HC
, CC
> M
CI
Cat
egor
y42
.12
6.81
41.0
39.
2235
.38
6.97
< .0
01.1
30H
C, C
C >
MC
I
Switc
hing
14.8
52.
6214
.49
2.86
11.5
42.
44<
.001
.245
HC
, CC
> M
CI
Shift
ing
13.8
23.
0613
.76
3.02
10.5
42.
8<
.001
.219
HC
, CC
> M
CI
DR
S19
.94
.348
19.6
5.9
1919
.30
1.43
nsb
---
---a
Act
ion
Nam
ing
20.9
74.
2519
.05
4.59
17.8
44.
67ns
.075
---a
Not
e. H
C =
hea
lthy
cont
rol;
CC
= c
ogni
tive
com
plai
nt; M
CI =
mild
cog
nitiv
e im
pairm
ent;
p va
lues
and
η2
valu
es w
ere
obta
ined
from
AN
OV
A re
sults
; gro
up d
iffer
ence
s wer
e ob
tain
ed fr
om T
ukey
’sH
SD p
ost h
oc a
naly
ses.
a AN
OV
A d
id n
ot re
ach
stat
istic
al si
gnifi
canc
e, a
nd p
ost h
oc a
naly
ses w
ere
not p
refo
rmed
b p va
lue
atta
ined
from
Kru
skal
-Wal
lis te
st (n
o ef
fect
size
ava
ilabl
e).
Arch Clin Neuropsychol. Author manuscript; available in PMC 2009 September 14.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Nutter-Upham et al. Page 18
Table 3Factor Loadings: Switching and Production
Factors
Fluency Tasks Switching Production
Letter .174 .804
Category .280 .803
Action Naming .095 .764
Switching .960 .236
Shifting .971 .180
Arch Clin Neuropsychol. Author manuscript; available in PMC 2009 September 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Nutter-Upham et al. Page 19Ta
ble
4C
orre
latio
ns a
mon
g flu
ency
task
s
Let
ter
Cat
egor
ySw
itchi
ngSh
iftin
gD
RS
Act
ion
Nam
ing
.484
*.4
74*
.302
*.2
85*
.156
Lette
r--
-.5
35*
.367
*.3
02*
.263
*
Cat
egor
y--
-.4
24*
.379
*.2
46*
Switc
hing
---
.956
*.2
33*
Shift
ing
---
.273
*
* p< .0
1
Arch Clin Neuropsychol. Author manuscript; available in PMC 2009 September 14.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Nutter-Upham et al. Page 20Ta
ble
5Fl
uenc
y ta
sk c
orre
latio
ns w
ith n
euro
psyc
holo
gica
l tas
ks
Let
ter
Cat
egor
ySw
itchi
ngSh
iftin
gA
ctio
n N
amin
g
WA
IS-I
II V
ocab
ular
y.5
2**.3
3**.2
2*.1
9.5
4**
WA
IS-I
II D
igit
Sym
bol
.40**
.40**
.41**
.40**
.45**
WA
IS-I
II In
form
atio
n.3
8**.2
4*.1
7.1
5.4
5**
DK
EFS,
Tra
il M
akin
g−.
28**
−.30
**−.
32**
−.28
**−.
29**
Bos
ton
Nam
ing
Test
.33**
.27**
.25*
.21*
.30**
* p< .0
5
**p<
.01
Arch Clin Neuropsychol. Author manuscript; available in PMC 2009 September 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Nutter-Upham et al. Page 21
Table 6D-KEFS Scaled Scores by Participant Group
Participant Group M S.D. N
D-KEFS Letter HC 12.8485 3.08344 33
CC 12.8649 3.00150 37
MCI 11.0270 3.10454 37
Total 12.2243 3.15723 107
D-KEFS Category HC 13.4545 2.70521 33
CC 12.8649 3.33468 37
MCI 11.1081 2.85564 37
Total 12.4393 3.12379 107
D-KEFS Switching HC 13.2727 3.14516 33
CC 12.8649 3.10163 37
MCI 9.4595 2.85379 37
Total 11.8131 3.46446 107
D-KEFS Shifting HC 12.9394 3.09172 33
CC 12.9459 2.97159 37
MCI 9.7568 2.74272 37
Total 11.8411 3.27987 107
Note. HC = healthy control; CC = cognitive complaint; MCI = mild cognitive impairment;D-KEFS scaled scores are based on mean = 10 and standarddeviation = 1.
Arch Clin Neuropsychol. Author manuscript; available in PMC 2009 September 14.
Copyright © 2022 FDOKUMEN