Use of the Learning Curve–Cumulative Summation test for quantitative and individualized assessment...
9
EDUCATION Use of the Learning Curve–Cumulative Summation test for quantitative and individualized assessment of competency of a surgical procedure in obstetrics and gynecology: fetoscopic laser ablation as a model Ramesha Papanna, MD, MPH; David J. Biau, MD, PhD; Lovepreet K. Mann, MBBS; Anthony Johnson, DO; Kenneth J. Moise Jr, MD OBJECTIVE: We sought to determine the learning curve (LC) for feto- scopic laser photocoagulation (FLP) as a model for the evaluation of training in surgical procedures. STUDY DESIGN: A retrospective review of consecutive case series of FLP from 2 centers with 3 operators (operator I [O-I], observer trained; operator II [O-II], hands-on trained; and operator III [O-III], clinical fellow) was performed and the LC-cumulative summation (CUSUM) test was plotted. RESULTS: The acceptable and unacceptable success rates for at least 1 fetus survival after FLP were set at 82% and 70%, respectively, from a systematic review. A total of 171 consecutive cases were performed by the 3 operators (O-I, 91; O-II, 49; and O-III, 31). From LC-CUSUM test O-I needed 60 procedures, O-II needed 20 procedures, and O-III needed 20 procedures to reach an acceptable performance rate for at least 1 survivor. CONCLUSION: The LC-CUSUM test can be used to accurately assess the LC in a surgical procedure in obstetrics and gynecology. Hands-on trained operators exhibit a shorter LC. Key words: formal training, laser photocoagulation, learning curve- cumulative summation, twin-twin transfusion syndrome Cite this article as: Papanna R, Biau DJ, Mann LK, et al. Use of the Learning Curve–Cumulative Summation test for quantitative and individualized assessment of competency of a surgical procedure in obstetrics and gynecology: fetoscopic laser ablation as a model. Am J Obstet Gynecol 2010;204:x.ex-x.ex. P roficiency for most surgical proce- dures is determined by 1 of 2 meth- ods. A predetermined number of cases is prescribed–a technique that fails to take into account that all individuals may not achieve proficiency with a fixed sample size. 1 Alternatively, observation by a tu- tor is used to determine when compe- tency has been reached–a method with considerable subjective bias. 2 Until re- cently, there has been very little interest in applying statistical methods to deter- mine when a trainee becomes proficient at a particular surgical procedure. Biau et al 3 reviewed the surgical literature from 1991 through 2006 and noted 22 papers that used the cumulative summation (CUSUM) test to determine the learning curve (LC). CUSUM was first intro- duced into industry to assess the mainte- nance of proficiency once a process was “in control.” 4 As an operator begins a new procedure, by definition, the pro- cess is “out of control” until a level of steady proficiency is attained. In 2008, Biau et al 5 introduced a modification of the CUSUM method called LC-CUSUM that was specifically designed to deter- mine when a level of proficiency has been attained. This new method objectively determines the LC for a procedure as to when the trainee has reached a pre- defined level of performance. 6 The importance of establishing a LC is to reduce risks to patients of incom- pletely trained providers performing complex procedures. Additionally, eval- uation of a LC can limit wastage of the available resources needed to train those who are already proficient. Thus both patient safety and cost containment are benefits that are realized. LC-CUSUM has been reported in studies for deter- mining the LC for endoscopic retrograde cholangiopancreatographies. 5 Studies using this method in obstetrics and gy- necology have been limited to embryo transfer for in vitro fertilization, 6 vitrifi- cation of the embryo, 7 and more recently From the Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, Baylor College of Medicine and Texas Children’s Fetal Center, Houston, TX (Drs Papanna, Mann, Johnson, and Moise), and the Département de Biostatistique et Informatique Médicale, APHP–Hôpital Saint-Louis, Université Paris VII and INSERM UMR-S 717, Paris, France (Dr Biau). Presented as an oral presentation at the 20th World Congress 2010 of the International Society of Ultrasound in Obstetrics and Gynecology at Prague, Czech Republic, Oct. 11, 2010. Received May 14, 2010; revised Oct. 8, 2010; accepted Oct. 13, 2010. Reprints: Ramesha Papanna, MD, MPH, Baylor College of Medicine, Obstetrics and Gynecology, 6620 Main St., Room 1100, Houston, TX 77030. [email protected]. 0002-9378/free • © 2010 Mosby, Inc. All rights reserved. • doi: 10.1016/j.ajog.2010.10.910 For Editors’ Commentary, see Table of Contents Research www. AJOG.org MONTH 2010 American Journal of Obstetrics & Gynecology 1.e1
Transcript of Use of the Learning Curve–Cumulative Summation test for quantitative and individualized assessment...

E
UqofRA
Ost
SFowp
R1
Cc
Popiasttcci
FBMMF
PU
R
R6
0
Research www.AJOG.org
DUCATION
se of the Learning Curve–Cumulative Summation test foruantitative and individualized assessment of competencyf a surgical procedure in obstetrics and gynecology:etoscopic laser ablation as a modelamesha Papanna, MD, MPH; David J. Biau, MD, PhD; Lovepreet K. Mann, MBBS;nthony Johnson, DO; Kenneth J. Moise Jr, MD
stOnl
Ctt
K
BJECTIVE: We sought to determine the learning curve (LC) for feto-copic laser photocoagulation (FLP) as a model for the evaluation ofraining in surgical procedures.
TUDY DESIGN: A retrospective review of consecutive case series ofLP from 2 centers with 3 operators (operator I [O-I], observer trained;perator II [O-II], hands-on trained; and operator III [O-III], clinical fellow)as performed and the LC-cumulative summation (CUSUM) test waslotted.
ESULTS: The acceptable and unacceptable success rates for at least
ompetency of a surgical procedure in obstetrics and gynecology: fetoscopic laser a
maa1t(cdn“
ystematic review. A total of 171 consecutive cases were performed byhe 3 operators (O-I, 91; O-II, 49; and O-III, 31). From LC-CUSUM test-I needed 60 procedures, O-II needed 20 procedures, and O-IIIeeded 20 procedures to reach an acceptable performance rate for at
east 1 survivor.
ONCLUSION: The LC-CUSUM test can be used to accurately assesshe LC in a surgical procedure in obstetrics and gynecology. Hands-onrained operators exhibit a shorter LC.
ey words: formal training, laser photocoagulation, learning curve-
fetus survival after FLP were set at 82% and 70%, respectively, from a cumulative summation, twin-twin transfusion syndromeite this article as: Papanna R, Biau DJ, Mann LK, et al. Use of the Learning Curve–Cumulative Summation test for quantitative and individualized assessment of
blation as a model. Am J Obstet Gynecol 2010;204:x.ex-x.ex.ncsBttmadwd
tpcuawpbhmcunt
roficiency for most surgical proce-dures is determined by 1 of 2 meth-
ds. A predetermined number of cases isrescribed–a technique that fails to take
nto account that all individuals may notchieve proficiency with a fixed sampleize.1 Alternatively, observation by a tu-or is used to determine when compe-ency has been reached–a method withonsiderable subjective bias.2 Until re-ently, there has been very little interestn applying statistical methods to deter-
rom the Division of Maternal-Fetal Medicinaylor College of Medicine and Texas Childreann, Johnson, and Moise), and the Départeédicale, APHP–Hôpital Saint-Louis, Univer
rance (Dr Biau).
resented as an oral presentation at the 20th Wltrasound in Obstetrics and Gynecology at Pra
eceived May 14, 2010; revised Oct. 8, 2010; a
eprints: Ramesha Papanna, MD, MPH, Baylor620 Main St., Room 1100, Houston, TX 77030
002-9378/free • © 2010 Mosby, Inc. All rights
For Editors’ Commentary, see Table
ine when a trainee becomes proficientt a particular surgical procedure. Biau etl3 reviewed the surgical literature from991 through 2006 and noted 22 papershat used the cumulative summationCUSUM) test to determine the learningurve (LC). CUSUM was first intro-uced into industry to assess the mainte-ance of proficiency once a process wasin control.”4 As an operator begins a
epartment of Obstetrics and Gynecology,Fetal Center, Houston, TX (Drs Papanna,t de Biostatistique et InformatiqueParis VII and INSERM UMR-S 717, Paris,
Congress 2010 of the International Society of, Czech Republic, Oct. 11, 2010.
pted Oct. 13, 2010.
llege of Medicine, Obstetrics and Gynecology,[email protected].
erved. • doi: 10.1016/j.ajog.2010.10.910
ontents
cMONTH 2010 Ame
ew procedure, by definition, the pro-ess is “out of control” until a level ofteady proficiency is attained. In 2008,iau et al5 introduced a modification of
he CUSUM method called LC-CUSUMhat was specifically designed to deter-
ine when a level of proficiency has beenttained. This new method objectivelyetermines the LC for a procedure as tohen the trainee has reached a pre-efined level of performance.6
The importance of establishing a LC iso reduce risks to patients of incom-letely trained providers performingomplex procedures. Additionally, eval-ation of a LC can limit wastage of thevailable resources needed to train thoseho are already proficient. Thus bothatient safety and cost containment areenefits that are realized. LC-CUSUMas been reported in studies for deter-ining the LC for endoscopic retrograde
holangiopancreatographies.5 Studiessing this method in obstetrics and gy-ecology have been limited to embryo
ransfer for in vitro fertilization,6 vitrifi-
e, Dn’smensité
orldgue
cce
Co. rp
res
of C
ation of the embryo,7 and more recentlyrican Journal of Obstetrics & Gynecology 1.e1

btoicncCtttittr
trtfdTmc
MTapaoAfc2sHAtsvtpcp
Omwtnsfiat
gwwttTncvttpgaTecOmaeeOudpafcaceAccfpvfiptc1frpmtpaab
a
sCwgwActvvcLgnopsS
tpLhamssstdhp
pstgdciscdCbttsrifipma
Research Education www.AJOG.org
1
ecoming proficient at certain diagnos-ic ultrasound procedures.8 The processf LC-CUSUM analysis has broader
mplications for training in surgical spe-ialties, specifically in obstetrics and gy-ecology. Recently there has been in-reased emphasis by the Accreditationouncil for Graduate Medical Educa-
ion to assess the competency of arainee, both qualitatively and quantita-ively. Use of LC-CUSUM would helpmprove the efficiency in determininghe training necessary to achieve compe-ency for selected surgical procedures foresidents and fellows.
The purpose of the present study waso determine the LC of fetoscopic-di-ected laser therapy in the treatment ofwin-twin transfusion syndrome (TTTS)or 3 fetal interventionists who had un-ergone different methods of training.he CUSUM test was then employed toonitor the ongoing performance once
ompetence had been reached.
ATERIALS AND METHODSo establish acceptable and unaccept-ble success rates for fetoscopic laserhotocoagulation (FLP), we performedsystematic review of published articlesf consecutive case series (Appendix 1).
retrospective study was conductedrom the review of our online database ofases that underwent FLP from June005 through September 2006 at Univer-ity of North Carolina (UNC) at Chapelill and from November 2006 throughugust 2009 at the Texas Children’s Fe-
al Center (TCFC) in Houston, TX. Thetudy was approved by institutional re-iew boards of both institutions. Fetaleam members prospectively collectedatient outcome data by direct patientontact and by contact with the referringhysician.There were 3 operators in the group.perator I (O-I) was a board-certifiedaternal-fetal medicine specialist whoas in active clinical and academic prac-
ice for �25 years with an equivalentumber of years of experience in ultra-ound-guided procedures. O-I was therst to learn the procedure in the groupfter an observation period in laser cen-
ers in Paris, France, and Leuven, Bel- p.e2 American Journal of Obstetrics & Gynecology
ium, for 1 month. Twelve live casesere observed between the 2 units, alongith multiple hours of reviewing video-
apes from previous cases. In addition,his operator visited a laser center inampa, FL, for a 2-day course on diag-osis and management of TTTS. Theourse included a series of lectures andideotape presentations on selective fe-oscopic laser photocoagulation in thereatment of TTTS. O-I performed allrocedures at UNC as the primary sur-eon after an institutional review boardpproved performing the procedure.he patients were counseled about thexperience of the surgeon during theonsenting process for the procedure.perator II (O-II) was a maternal-fetaledicine specialist in active clinical and
cademic practice for �25 years with anquivalent number of years of experi-nce in ultrasound-guided procedures.-II assisted O-I for FLP by providingltrasound guidance during the proce-ure for the first 30 cases. O-II startederforming the laser procedure at TCFCs the primary surgeon, initially per-orming only cases with a posterior pla-enta and then advancing to cases withn anterior placenta. O-I assisted in allases during O-II’s learning phase. Op-rator III (O-III) was a graduate from anmerican Board of Obstetrics and Gyne-ology–approved obstetrics and gyne-ology residency program and had per-ormed �300 laparoscopic gynecologicrocedures. O-III joined the fetal inter-ention team in July 2008 as a clinicalellow and observed 10 cases and assistedn the next 15 cases, before starting toerform FLP as the primary surgeon. Inhe beginning, O-III performed FLP onases with posterior placentation (n �5) and gradually transitioned to per-orm the procedure on cases with ante-ior placentation. O-I or O-II partici-ated in all of O-III’s cases and in theajority of cases both were present in
he operating suite when the fellow waserforming the procedure. The detailsnd the evaluation of the TTTS patientsnd the procedure at our center haveeen previously described.9,10
The data for maternal demographicsnd for preoperative, intraoperative, and
ostoperative variables were extracted to (MONTH 2010
oftware (SPSS version 11.0; SPSS Inc,hicago, IL). Comparison of parametersas performed using the �2 test for cate-orical variables and Fisher’s exact testhen an expected frequency was �5.nalysis of variance was performed forontinuous variables. Kruskal-Wallisest was used to compare nonparametricariables among the 3 operators. A Palue � .05 was considered as signifi-ant. The data needed for calculatingC-CUSUM and CUSUM included sur-eon’s identity, consecutive case seriesumber for each surgeon, and numberf surviving fetuses to birth for eachregnancy. These data were extracted tooftware (R-Software; R Foundation fortatistical Computing, Vienna, Austria).The LC-CUSUM was developed to de-
ermine when a trainee has reached aredefined level of performance.11 TheC-CUSUM sequentially tests the nullypothesis “performance is unaccept-ble” against the alternative “perfor-ance is acceptable.” It computes a
core from the successive outcomes, withuccesses yielding an increase in thecore and failures yielding a decrease inhe score. Once the score reaches a pre-efined limit (h), the test rejects the nullypothesis in favor of the alternative anderformance is deemed acceptable.Graphically the LC-CUSUM score is
lotted on the y-axis against the succes-ive procedures on the x-axis. As long ashe score remains in the continuation re-ion, namely between the x-axis and theecision limit h, performance cannot beonsidered as acceptable and monitor-ng continues. With accumulation ofuccesses the score increases until itrosses the limit h where proficiency iseclared. A particular feature of the LC-USUM is that it incorporates a holdingarrier at 0 that cannot be crossed andhe score St thus remains at 0 if therainee accumulates numerous succes-ive failures. In this way, the LC-CUSUMemains responsive at all times and if, fornstance, poor performance resultedrom poor technique, with improvementn skills the trainee will not have to com-ensate unnecessarily for all the accu-ulated failures and may be able to show
cceptable performance in due course
Appendix 1). For the LC-CUSUM for at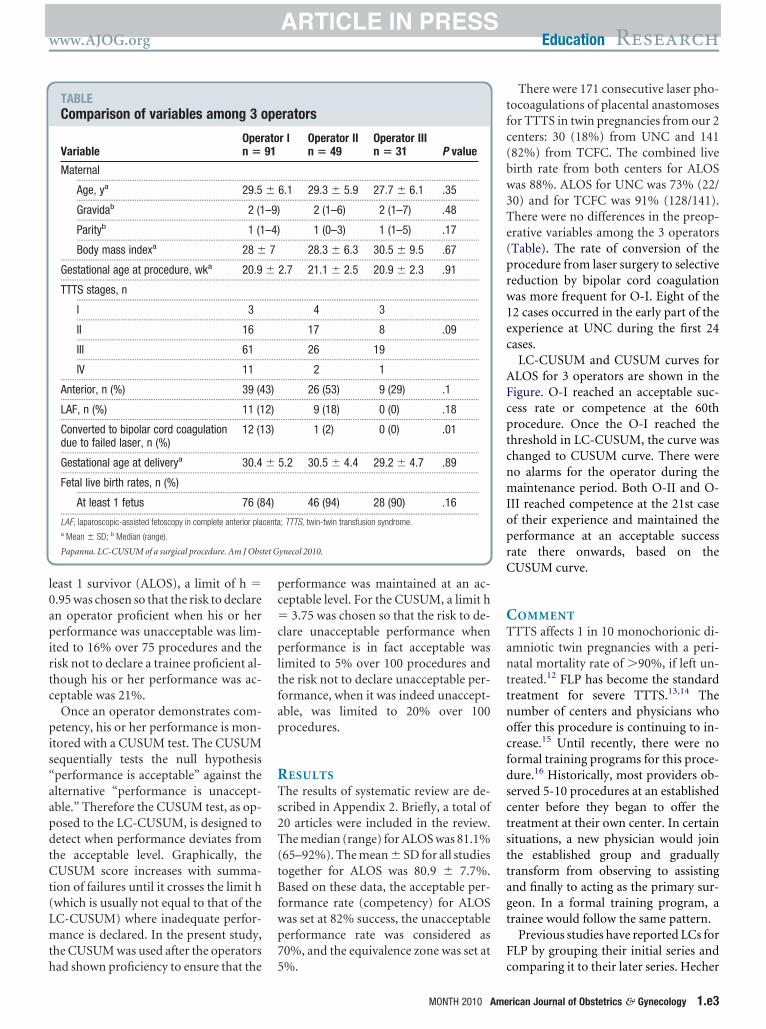
l0apirtc
pis“aapdtCt(Lmth
pc�cpltfap
RTs2T(tBfwp7
tfc(bw3Te(prw1ec
AFcptcnmIoprC
CTanttnocfdsctsttagt
F
et G
www.AJOG.org Education Research
east 1 survivor (ALOS), a limit of h �.95 was chosen so that the risk to declaren operator proficient when his or hererformance was unacceptable was lim-
ted to 16% over 75 procedures and theisk not to declare a trainee proficient al-hough his or her performance was ac-eptable was 21%.
Once an operator demonstrates com-etency, his or her performance is mon-
tored with a CUSUM test. The CUSUMequentially tests the null hypothesisperformance is acceptable” against thelternative “performance is unaccept-ble.” Therefore the CUSUM test, as op-osed to the LC-CUSUM, is designed toetect when performance deviates fromhe acceptable level. Graphically, theUSUM score increases with summa-
ion of failures until it crosses the limit hwhich is usually not equal to that of theC-CUSUM) where inadequate perfor-ance is declared. In the present study,
he CUSUM was used after the operators
TABLEComparison of variables among 3 o
VariableOpern �
Maternal..........................................................................................................
Age, ya 29.5..........................................................................................................
Gravidab 2 (1..........................................................................................................
Parityb 1 (1..........................................................................................................
Body mass indexa 28 �...................................................................................................................
Gestational age at procedure, wka 20.9...................................................................................................................
TTTS stages, n..........................................................................................................
I 3..........................................................................................................
II 16..........................................................................................................
III 61..........................................................................................................
IV 11...................................................................................................................
Anterior, n (%) 39 (4...................................................................................................................
LAF, n (%) 11 (1...................................................................................................................
Converted to bipolar cord coagulationdue to failed laser, n (%)
12 (1
...................................................................................................................
Gestational age at deliverya 30.4...................................................................................................................
Fetal live birth rates, n (%)..........................................................................................................
At least 1 fetus 76 (8...................................................................................................................
LAF, laparoscopic-assisted fetoscopy in complete anterior plaa Mean � SD; b Median (range).
Papanna. LC-CUSUM of a surgical procedure. Am J Obst
ad shown proficiency to ensure that the 5
erformance was maintained at an ac-eptable level. For the CUSUM, a limit h
3.75 was chosen so that the risk to de-lare unacceptable performance whenerformance is in fact acceptable was
imited to 5% over 100 procedures andhe risk not to declare unacceptable per-ormance, when it was indeed unaccept-ble, was limited to 20% over 100rocedures.
ESULTShe results of systematic review are de-
cribed in Appendix 2. Briefly, a total of0 articles were included in the review.he median (range) for ALOS was 81.1%
65–92%). The mean � SD for all studiesogether for ALOS was 80.9 � 7.7%.ased on these data, the acceptable per-
ormance rate (competency) for ALOSas set at 82% success, the unacceptableerformance rate was considered as0%, and the equivalence zone was set at
rators
r I Operator IIn � 49
Operator IIIn � 31 P value
..................................................................................................................
6.1 29.3 � 5.9 27.7 � 6.1 .35..................................................................................................................
2 (1–6) 2 (1–7) .48..................................................................................................................
1 (0–3) 1 (1–5) .17..................................................................................................................
28.3 � 6.3 30.5 � 9.5 .67..................................................................................................................
2.7 21.1 � 2.5 20.9 � 2.3 .91..................................................................................................................
..................................................................................................................
4 3..................................................................................................................
17 8 .09..................................................................................................................
26 19..................................................................................................................
2 1..................................................................................................................
26 (53) 9 (29) .1..................................................................................................................
9 (18) 0 (0) .18..................................................................................................................
1 (2) 0 (0) .01
..................................................................................................................
5.2 30.5 � 4.4 29.2 � 4.7 .89..................................................................................................................
..................................................................................................................
46 (94) 28 (90) .16..................................................................................................................
; TTTS, twin-twin transfusion syndrome.
ynecol 2010.
%. c
MONTH 2010 Ame
There were 171 consecutive laser pho-ocoagulations of placental anastomosesor TTTS in twin pregnancies from our 2enters: 30 (18%) from UNC and 14182%) from TCFC. The combined liveirth rate from both centers for ALOSas 88%. ALOS for UNC was 73% (22/0) and for TCFC was 91% (128/141).here were no differences in the preop-rative variables among the 3 operatorsTable). The rate of conversion of therocedure from laser surgery to selectiveeduction by bipolar cord coagulationas more frequent for O-I. Eight of the2 cases occurred in the early part of thexperience at UNC during the first 24ases.
LC-CUSUM and CUSUM curves forLOS for 3 operators are shown in theigure. O-I reached an acceptable suc-ess rate or competence at the 60throcedure. Once the O-I reached thehreshold in LC-CUSUM, the curve washanged to CUSUM curve. There wereo alarms for the operator during theaintenance period. Both O-II and O-
II reached competence at the 21st casef their experience and maintained theerformance at an acceptable successate there onwards, based on theUSUM curve.
OMMENTTTS affects 1 in 10 monochorionic di-mniotic twin pregnancies with a peri-atal mortality rate of �90%, if left un-
reated.12 FLP has become the standardreatment for severe TTTS.13,14 Theumber of centers and physicians whoffer this procedure is continuing to in-rease.15 Until recently, there were noormal training programs for this proce-ure.16 Historically, most providers ob-erved 5-10 procedures at an establishedenter before they began to offer thereatment at their own center. In certainituations, a new physician would joinhe established group and graduallyransform from observing to assistingnd finally to acting as the primary sur-eon. In a formal training program, arainee would follow the same pattern.
Previous studies have reported LCs forLP by grouping their initial series and
pe
ato91
.........
�.........
–9).........
–4).........
7.........
�.........
.........
.........
.........
.........
.........
3).........
2).........
3)
.........
�.........
.........
4).........
centa
omparing it to their later series. Hecher
rican Journal of Obstetrics & Gynecology 1.e3

ettFetiHtnnFtseoCwifott
ossofipmuvuctofapmo
pst
pfotcwutwcrscsssbjooas
L
P
Research Education www.AJOG.org
1
t al17 reported improved outcomes inheir later series from their center, whichhey attributed to different methods ofLP. De Lia et al18 grouped their initialxperience of 50 cases and comparedhem to their later 73 cases showing anmprovement in fetal rates of survival.
owever, these studies do not describehe operator-specific outcomes or theumber of cases that an operator wouldeed to reach competency to performLP. In our study, we first determinedhe acceptable and unacceptable rates ofuccess from a thorough review of thexisting literature. Using these thresh-lds, a LC was plotted using the LC-USUM test for FLP for each operator,hich varied based on method of train-
ng. We then employed a CUSUM testor continuous monitoring of outcomence the operator had reached compe-ence. Our findings suggest that opera-
FIGURELearning Curve-Cumulative Summa
C-CUSUM, learning curve-cumulative summation.
apanna. LC-CUSUM of a surgical procedure. Am J Obstet G
ors who were trained by an experienced T
.e4 American Journal of Obstetrics & Gynecology
perator (O-II and O-III) exhibited ahorter LC to reach an acceptable rate ofuccess compared to an operator trainednly through observation (O-I). The re-nement of surgical issues such as ap-ropriate case selection, choice of opti-al entry site for the fetoscopic trocar,
se of rapid infusion of fluids to improveisualization, and use of uterine manip-lation to optimize visualization of pla-ental anastomoses are only achievedhrough extensive experience with previ-us cases. In addition, transitioningrom easier procedures such as cases withposterior placentation to more difficultrocedures with anterior placentationay have contributed to the shorter LC
f O-II and O-III.One might initially propose that com-
lete obliteration of all anastomotic ves-els should be the outcome used to assesshe proficiency of laser ablation for
n test in assessment of competency
col 2010.
TTS. Such an outcome would require s
MONTH 2010
lacental injection studies to be per-ormed after birth. However, the demisef one or both twin fetuses after laserherapy will affect the placental angioar-hitecture so that injection studiesould not be possible. Moreover, resid-al anastomoses have been noted in up
o 33% of placentas after laser surgeryithout an affect on fetal outcome in
ases of dual fetal survival.19 Successates of FLP for TTTS have been de-cribed in literature by different out-ome measures including at least 1 fetusurvival, 2 fetal survivals, and overall ob-erved-to-expected fetal and neonatalurvivals.14,20 No single measure haseen proposed as the best parameter to
udge the outcome of laser therapy. Inur study, we chose survival to live birthf at least 1 fetus as the primary outcomes we believe that this parameter repre-ents the most direct outcome of laser
tio
yne
urgery. Conditions such as dispropor-

tsptictlacltdatftp
oi2(ctCcsispcp[aWHapmfatvfootspacmtfic
roecfotoslt
agcengmiptectuwuapwg
R1csS2Sap13NaC4a25RaC6sLf
7LmC8Zibt29Jotd31Ofss1icS1Tpgabn1tps1Wst21AsO1BiG1Hpss21iwi21KRsf
www.AJOG.org Education Research
ionate placental share or a premoribundtate of 1 of the fetuses are often presentrior to laser therapy and contribute tohe survival of the individual twin fetusn cases of TTTS. Therefore the profi-iency of performing laser therapy is bet-er determined through the survival of ateast 1 fetus to take these variables intoccount. In addition, fetal survival washosen over neonatal survival since theatter is related to many different factorshat may not be impacted by the proce-ure, per se. An example is gestationalge at birth, which is influenced by mul-iple factors such as maternal indicationor delivery, preterm labor, and thehreshold for delivery by the referringhysician based on fetal well-being.There are at least 2 major limitations to
ur study. Early in the series, the predom-nant fetoscope that was used by O-I was a-mm semirigid fiberoptic 0-degree deviceStorz, Vianen, The Netherlands). Foromplete anterior placentation a fiberop-ic bronchoscope (Olympus America Inc,enter Valley, PA) was used without suc-
ess for a single case that was converted to aelective reduction due to the poor visual-zation. On arrival to TCFC, new rod lenscopes with better visualization and im-roved ability to access the anterior pla-enta were routinely employed in laserrocedures (2.2-mm 30-degree scopeKarl Storz GmbH, Tuttlingen, Germany]nd 3.0-mm 0-degree scope [Richard
olfe Medical Instruments Corp, Vernonills, IL]). The use of these scopes by O-II
nd O-III was of clear benefit due to im-roved visualization of placental anasto-oses for these operators. The findings
rom this study are important as they couldssist in establishing guidelines for traininghe future generation of fetoscopic inter-entionists as well as establishing methodsor the self-monitoring of the performancef individual operators or centers on anngoing basis. Based on our findings, aypical new trainee might observe and as-ist in 15-20 cases and then perform ap-roximately an additional 20 cases of FLPs a primary surgeon before achievingompetency. Assessment of data fromultiple centers would help in establishing
he range of cases needed for attaining pro-ciency in FLP. Finally, we were unable to
ompare statistical differences in the cur- 2ent study between the LCs of the 2 meth-ds of training since there were only 3 op-rators. Access to outcomes from severalenters and different operators may allowor a further analysis of learning method-logies. Establishment of proficiency in fe-al intervention procedures followed byngoing monitoring of outcomes wouldeem plausible and prudent for the estab-ishment of centers of excellence in fetalherapy as well.
Our study demonstrates a systematicpproach to determine the LC for a sur-ical procedure in obstetrics and gyne-ology. This methodology can be used tostimate the LCs for other surgical oronsurgical procedures in training pro-rams to safely prove competency and toonitor outcomes once the competency
s reached. While determining the LCrovides an approximate estimation ofhe number of procedures required toducate a trainee, this methodologyould also be used to evaluate otherraining methods such as computer sim-lations and animal surgeries. Thisould assist in directing resources to ed-cate those who need additional trainingnd to declare competency at the appro-riate time interval for those traineesho achieve the prescribed outcome tar-et early. f
EFERENCES. Dagash H, Chowdhury M, Pierro A. Whenan I be proficient in laparoscopic surgery? Aystematic review of the evidence. J Pediatrurg 2003;38:720-4.. Sloan DA, Donnelly MB, Schwartz RW,trodel WE. The objective structured clinical ex-mination: the new gold standard for evaluatingostgraduate clinical performance. Ann Surg995;222:735-42.. Biau DJ, Resche-Rigon M, Godiris-Petit G,izard RS, Porcher R. Quality control of surgicalnd interventional procedures: a review of theUSUM. Qual Saf Health Care 2007;16:203-7.. Wohl H. The CUSUM plot: its utility in thenalysis of clinical data. N Engl J Med 1977;96:1044-5.. Biau DJ, Williams SM, Schlup MM, NizardS, Porcher R. Quantitative and individualizedssessment of the learning curve using LC-USUM. Br J Surg 2008;95:925-9.. Dessolle L, Freour T, Barriere P, et al. Howoon can I be proficient in embryo transfer?essons from the cumulative summation testor learning curve (LC-CUSUM). Hum Reprod
010;25:380-6. cMONTH 2010 Ame
. Dessolle L, Biau DJ, de Larouziere V, et al.earning curve of vitrification assessed by cu-ulative summation test for learning curve (LC-USUM). Fertil Steril 2009;92:943-5.. Balsyte D, Schaffer L, Burkhardt T, Wisser J,immermann R, Kurmanavicius J. Continuous
ndependent quality control for fetal ultrasoundiometry provided by the cumulative summa-ion technique. Ultrasound Obstet Gynecol010;35:449-55.. Papanna R, Molina S, Moise KY, Moise KJ Jr,ohnson A. Chorioamnion plugging and the riskf preterm premature rupture of membranes af-er laser surgery in twin-twin transfusion syn-rome. Ultrasound Obstet Gynecol 2010;35:37-43.0. Papanna R, Johnson A, Ivey RT, OlutoyeO, Cass D, Moise KJ. Laparoscopy-assisted
etoscopy for laser surgery in twin-twin transfu-ion syndrome with anterior placentation. Ultra-ound Obstet Gynecol 2010;35:65-70.1. Biau DJ, Porcher R. A method for monitor-
ng a process from an out of control to an inontrol state: application to the learning curve.tat Med 2010;29:1900-9.2. Yamamoto M, El Murr L, Robyr R, Leleu F,akahashi Y, Ville Y. Incidence and impact oferioperative complications in 175 fetoscopy-uided laser coagulations of chorionic platenastomoses in fetofetal transfusion syndromeefore 26 weeks of gestation. Am J Obstet Gy-ecol 2005;193:1110-6.3. De Lia JE, Cruikshank DP, Keye WR Jr. Fe-oscopic neodymium:YAG laser occlusion oflacental vessels in severe twin-twin transfusionyndrome. Obstet Gynecol 1990;75:1046-53.4. Senat MV, Deprest J, Boulvain M, Paupe A,iner N, Ville Y. Endoscopic laser surgery ver-
us serial amnioreduction for severe twin-to-win transfusion syndrome. N Engl J Med004;351:136-44.5. Molina S, Papanna R, Moise KJ Jr, Johnson. Management of stage I twin twin transfusionyndrome: an international survey. Ultrasoundbstet Gynecol 2010;36:42-7.6. Moise KJ Jr, Johnson A, Carpenter RJ,aschat AA, Platt LD. Fetal intervention: provid-
ng reasonable access to quality care. Obstetynecol 2009;113:408-10.7. Hecher K, Diehl W, Zikulnig L, Vetter M,ackeloer BJ. Endoscopic laser coagulation oflacental anastomoses in 200 pregnancies withevere mid-trimester twin-to-twin transfusionyndrome. Eur J Obstet Gynecol Reprod Biol000;92:135-9.8. De Lia JE, Kuhlmann RS, Lopez KP. Treat-
ng previable twin-twin transfusion syndromeith fetoscopic laser surgery: outcomes follow-
ng the learning curve. J Perinat Med 1999;7:61-7.9. Lopriore E, Middeldorp JM, Oepkes D,lumper FJ, Walther FJ, Vandenbussche FP.esidual anastomoses after fetoscopic laserurgery in twin-to-twin transfusion syndrome:requency, associated risks and outcome. Pla-
enta 2007;28:204-8.rican Journal of Obstetrics & Gynecology 1.e5

2ItS
ALTtfipaiteneat�tm
ro
2
wnactscbc
a
w
wueca
fird1itSwt
Research Education www.AJOG.org
1
0. Roberts D, Neilson JP, Kilby M, Gates S.nterventions for the treatment of twin-twinransfusion syndrome. Cochrane Databaseyst Rev 2008;1:CD002073.
PPENDIX: 1C-CUSUMhe LC-CUSUM test is designed to de-
ermine when a trainee has reached pro-ciency. We consider that the null hy-othesis is H0: “performance is notdequate” and the alternative hypothesiss H1: “performance is adequate.” Inerms of measurements, the null hypoth-sis corresponds to a performance that isot centered on a target, namely the ad-quate performance �0, but deviates onverage at least by �. This can be rewrit-en in mathematical terms as H0: � – �0
�. The alternative hypothesis is thathe performance does not deviate by
ore than �, the equivalence limit, thus
SUPPLEMENTARY TABLE 1Probability of an alarm at different
h p15 p18 p23
0.5 99.97% 99.39% 96.0...................................................................................................................
0.55 99.66% 98.53% 91.8...................................................................................................................
0.6 99.07% 96.59% 86.0...................................................................................................................
0.65 98.54% 95.23% 79.9...................................................................................................................
0.7 98.12% 93.23% 74.5...................................................................................................................
0.75 97.81% 91.72% 71.7...................................................................................................................
0.8 95.84% 88.17% 64.0...................................................................................................................
0.85 94.80% 84.59% 58.2...................................................................................................................
0.9 92.83% 81.34% 52.7...................................................................................................................
0.95 91.67% 78.82% 48.4...................................................................................................................
1 90.36% 75.20% 44.3...................................................................................................................
1.05 87.58% 70.49% 39.0...................................................................................................................
1.1 85.09% 67.67% 33.5...................................................................................................................
1.15 83.56% 63.81% 30.0...................................................................................................................
1.2 80.99% 60.28% 28.4...................................................................................................................
1.25 78.13% 56.79% 24.3...................................................................................................................
1.3 75.16% 54.25% 21.0...................................................................................................................
1.35 72.22% 50.07% 18.5...................................................................................................................
1.4 70.12% 46.56% 16.4...................................................................................................................
1.45 68.33% 43.58% 15.0...................................................................................................................
1.5 64.73% 41.25% 13.0...................................................................................................................
For each h value and at every performance levels, 10,000 sim
Papanna. LC-CUSUM of a surgical procedure. Am J Obstet G
.e6 American Journal of Obstetrics & Gynecology
egarded as an acceptable deviation fromptimal performance, H1: � – �0 � �The null hypothesis H0 is the union of1-sided hypotheses:H01: � – �0 � � and H02: � – �0 � –�.Since we are interested in testing
hether the failure rate of a trainee doesot deviate by more than an acceptablemount above adequate performance, theorresponding hypothesis H01 only isested. A CUSUM test statistic is then con-tructed in a traditional way, and we con-lude that an acceptable performance haseen reached when the test statistic hasrossed a predetermined limit (h).
Detailed application of the data:The LC-CUSUM and CUSUM scores
re written as:
St � max (0, St – 1 � Wt),
ith,
p27 p30 p33
88.63% 80.85% 69.76%..................................................................................................................
80.93% 68.56% 55.37%..................................................................................................................
70.20% 56.30% 42.35%..................................................................................................................
60.19% 46.00% 32.98%..................................................................................................................
53.12% 38.79% 25.38%..................................................................................................................
50.32% 35.94% 24.52%..................................................................................................................
41.56% 28.35% 17.60%..................................................................................................................
34.72% 22.13% 13.28%..................................................................................................................
30.11% 17.73% 9.29%..................................................................................................................
26.85% 15.93% 7.93%..................................................................................................................
23.05% 12.68% 6.75%..................................................................................................................
19.18% 9.89% 4.60%..................................................................................................................
16.08% 7.75% 3.78%..................................................................................................................
13.08% 5.91% 2.63%..................................................................................................................
11.02% 5.61% 2.25%..................................................................................................................
9.56% 4.41% 1.86%..................................................................................................................
7.94% 2.96% 1.52%..................................................................................................................
6.65% 2.55% 1.01%..................................................................................................................
5.55% 1.92% 0.67%..................................................................................................................
4.45% 1.96% 0.82%..................................................................................................................
4.17% 1.47% 0.38%..................................................................................................................
ons are performed.
ynecol 2010.
MONTH 2010
Wt � log{[(P1Xt(1–P1)1–Xt]/[P0Xt(1–P0)1–Xt]}
here P1 and P0 are the failure ratesnder the alternative and null hypoth-ses, respectively, and Xt is the out-ome with failures as 1 and successess 0.In the present study, adequate per-
ormance was set at 18% failure rate,nadequate performance at 30% failureate, and � at 5%. Error rates for h wereetermined based on simulations of0,000 samples under the adequate andnadequate performance levels, respec-ively, for the CUSUM and LC-CU-UM. First levels of h from 0.5-9.5ere tested by increments of 1. Then
he simulations were narrowed for lev-
SUPPLEMENTARY TABLE 2Computation ofLC-CUSUM/CUSUM
Observation OutcomeLC-CUSUMscore
CUSUMscore
0 � 0 �...........................................................................................................
1 0 0.0629 �...........................................................................................................
2 0 0.1258 �...........................................................................................................
3 0 0.1887 �...........................................................................................................
4 0 0.2517 �...........................................................................................................
5 1 0.0065 �...........................................................................................................
6 0 0.0694 �...........................................................................................................
7 0 0.1324 �...........................................................................................................
8 0 0.1953 �...........................................................................................................
. . . . . . . . . . . .
...........................................................................................................
19 0 0.8873 �...........................................................................................................
20 0 0.9502 0...........................................................................................................
21 0 � 0...........................................................................................................
22 0 � 0...........................................................................................................
23 0 � 0...........................................................................................................
24 0 � 0...........................................................................................................
25 0 � 0...........................................................................................................
26 0 � 0...........................................................................................................
27 1 � 0.511...........................................................................................................
28 0 � 0.353...........................................................................................................
29 0 � 0.194...........................................................................................................
. . . . . . . . . . . .
...........................................................................................................
CUSUM, cumulative summation; LC, learning curve.
Papanna. LC-CUSUM of a surgical procedure. Am J
h
2%.........
9%.........
4%.........
2%.........
1%.........
2%.........
5%.........
3%.........
3%.........
7%.........
4%.........
2%.........
5%.........
8%.........
8%.........
2%.........
5%.........
5%.........
6%.........
3%.........
2%.........
ulati
Obstet Gynecol 2010.

eLC1Lapp91mp2mLpC0C
ASMTaatttdttRwrvada
raswfmtlcscatvdlnrD
www.AJOG.org Education Research
ls of h ranging from 0.5–1.5 for theC-CUSUM and from 3-4.5 for theUSUM, by increments of 0.05. Tableshows the final simulations for the
C-CUSUM. The probability of anlarm is displayed for various levels oferformance. For a limit h at 0.95, therobability of an alarm is, respectively,1.67%, 78.82%, 48.47%, 26.85%,5.93%, and 7.93% for levels of perfor-ance at 15%, 18% (adequate level of
erformance), 23% (equivalence),7%, 30% (inadequate level of perfor-ance), and 33%. Table 2 shows the
C-CUSUM and CUSUM scores com-uted for O-II. When the LC-USUM score reaches the limit h �.95, proficiency is declared and theUSUM score is started.
SUPPLEMENTARY TABLE 3Results from systematic review
Serialno. Article, y St
1 De Lia et al, 19951 Oc...................................................................................................................
2 Ville et al, 199520 19...................................................................................................................
3 De Lia et al, 19992 Ap...................................................................................................................
4 Hecher et al, 19993 Ja...................................................................................................................
5 Hecher et al, 200011 Ju...................................................................................................................
6 Zikulnig et al, 19994 Ja...................................................................................................................
7 Quintero et al, 20005 Ma...................................................................................................................
8 Martinez et al, 20036 Oc...................................................................................................................
9 Senat et al, 20047 Ja...................................................................................................................
10 Yamamoto et al, 200518 No...................................................................................................................
11 Huber et al, 20069 Se...................................................................................................................
12 Middeldorp et al, 200717 Au...................................................................................................................
13 Crombleholme et al, 200715 5 y...................................................................................................................
14 Sepulveda et al, 200716 Se...................................................................................................................
15 Muratore et al, 200919 5 y...................................................................................................................
16 Habli et al, 20098 Se...................................................................................................................
17 Nakata et al, 200914 Ju...................................................................................................................
18 Cincotta et al, 200913 Ma...................................................................................................................
19 Chmait et al, 201010 Ma...................................................................................................................
20 Crisan et al, 201012 Ap...................................................................................................................
21 Current study Oc...................................................................................................................
To...................................................................................................................
ALOS, at least 1 survivor; CI, confidence interval; TFS, 2 fetal
Papanna. LC-CUSUM of a surgical procedure. Am J Obstet G
PPENDIX 2ystematic reviewethod
o establish acceptable and unaccept-ble success rates for FLP, we performedsystematic review to obtain relevant ar-
icles. PubMed was searched from 1980hrough January 2010 using the keyerms “twin-twin transfusion syn-rome” OR “TTTS” AND “laser abla-ion” OR “laser photocoagulation” to re-rieve articles related to FLP for TTTS.elevant bibliographies in these articlesere further searched to find additional
eferences. Selected studies were re-iewed by 2 independent reviewers (R.P.nd L.K.M.) for the inclusion and theata were extracted. If there was a dis-greement among the reviewers, a third
periodn (onlytwins) ALO
988 through Aug. 1994 26 17.........................................................................................................................
through 1994 45 32.........................................................................................................................
995 through March 1998 67 55.........................................................................................................................
995 through May 1997 73 58.........................................................................................................................
997 through Sept. 1999 127 103.........................................................................................................................
995 through March 1998 121 98.........................................................................................................................
994 through Dec. 1999 89 70.........................................................................................................................
997 through Feb. 2001 110 97.........................................................................................................................
999 through March 2002 72 55.........................................................................................................................
999 through April 2004 175 128.........................................................................................................................
1999 through Nov. 2003 200 167.........................................................................................................................
000 through Nov. 2004 100 81.........................................................................................................................
20 13.........................................................................................................................
2003 through Dec. 2006 33 27.........................................................................................................................
163 124.........................................................................................................................
2005 through Feb. 2008 149 131.........................................................................................................................
002 through May 2006 52 47.........................................................................................................................
2002 through June 2007 100 85.........................................................................................................................
2006 through March 2008 99 90.........................................................................................................................
001 through Sept. 2005 314 289.........................................................................................................................
006 through May 2009 171 150.........................................................................................................................
2306 1917.........................................................................................................................
vals.
ynecol 2010.
MONTH 2010 Ame
eviewer (K.J.M.) was consulted. Onlyrticles that reported consecutive caseeries or randomized controlled trialsere included. In cases where reports
rom the same center included �6onths of an overlapping study period,
he study with a larger sample size or theonger duration was included. We ex-luded studies that reported a selectiveubgroup of patients, those with a dupli-ation of the previously reported studies,nd those with a sample size of �20 pa-ients. The rates for ALOS and 2 fetal sur-ivals were calculated from the givenata excluding triplet pregnancies. If the
ive birth rates were not given, the neo-atal survival rate or 6-month survivalates were chosen as surrogate endpoint.ata from selected studies were ex-
TFS
5) 8 (31)..................................................................................................................
1) 16 (36)..................................................................................................................
2) 38 (57)..................................................................................................................
9) 30 (42)..................................................................................................................
1) 69 (54)..................................................................................................................
1) 58 (48)..................................................................................................................
9) 35 (39.3)..................................................................................................................
8.2) 54 (49.1)..................................................................................................................
6) 26 (36)..................................................................................................................
3) 61 (35)..................................................................................................................
3.5) 119 (59.5)..................................................................................................................
1) 58 (58)..................................................................................................................
5) 4 (20)..................................................................................................................
1.3) 16 (48.5)..................................................................................................................
6) 81 (50)..................................................................................................................
8) 98 (66)..................................................................................................................
0) 25 (48)..................................................................................................................
5) 66 (66)..................................................................................................................
0.9) 71 (71.7)..................................................................................................................
2) 211 (67)..................................................................................................................
8) 99 (58)..................................................................................................................
3%; CI 82-85%) 1243 (54%; CI 52-56%)..................................................................................................................
udy S
t. 1 (6......... .........
92 (7......... .........
ril 1 (8......... .........
n. 1 (7......... .........
ne 1 (8......... .........
n. 1 (8......... .........
y 1 (7......... .........
t. 1 (8......... .........
n. 1 (7......... .........
v. 1 (7......... .........
pt. (8......... .........
g. 2 (8......... .........
(6......... .........
pt. (8......... .........
(7......... .........
pt. (8......... .........
ly 2 (9......... .........
rch (8......... .........
rch (9......... .........
ril 2 (9......... .........
t. 2 (8......... .........
tal (8......... .........
survi
rican Journal of Obstetrics & Gynecology 1.e7

tSviovrcSs
RAra(iHttwystltretticgtrt
R1sts12pft63Msvs4Htdn
5MltO6Jsds27Wst28odas9Bts21KlsM1Hpss21Apt21Bits1ictt31paptG1vifa21
wi11Tpgabn1asJ2lgN2Tpts22Oss2Efvan2as12PliM2Gtst2Lwmt22dnt2lpcts3J
Research Education www.AJOG.org
1
racted to software (SPSS version 11.0;PSS Inc, Chicago, IL). The medianalue for survival from the selected stud-es was considered as an acceptable ratef performance rate and the minimumalue was considered the unacceptableate of performance. These rates wereompared to the cumulative mean andD obtained from combining all of theelected studies.
esultfter an online search, 319 articles were
etrieved and 291 articles were excludedfter reviewing the title (244), abstract36), and manuscript (39). This resultedn 28 articles that met selection criteria.
and-searching of the bibliographies ofhese articles yielded an additional 7 ar-icles. Thus, a total of 35 articles under-ent a detailed review. In the final anal-
sis, we included only 20 of thesetudies.1-20 We excluded 15 studies forhe following reasons: duplication of ear-ier studies,12 sample size of �20 pa-ients,21,22 not a consecutive case se-ies,23 part of the current study,24-30
xcluded patients after laser therapy dueo residual placental anastomoses,31 pa-ients only with stage II disease,32 miss-ng information,33 lack of fetal out-omes,34,35 and a report of only a selectroup of patients with anterior placenta-ion.36 The results from the systematiceview are described in the Supplemen-ary Table.
EFERENCES. De Lia JE, Kuhlmann RS, Harstad TW, Cruik-hank DP. Fetoscopic laser ablation of placen-al vessels in severe previable twin-twin transfu-ion syndrome. Am J Obstet Gynecol 1995;72:1202-11; discussion 1208-11.. De Lia JE, Kuhlmann RS, Lopez KP. Treatingreviable twin-twin transfusion syndrome with
etoscopic laser surgery: outcomes followinghe learning curve. J Perinat Med 1999;27:1-7.. Hecher K, Plath H, Bregenzer T, Hansmann, Hackeloer BJ. Endoscopic laser surgery ver-
us serial amniocenteses in the treatment of se-ere twin-twin transfusion syndrome. Am J Ob-tet Gynecol 1999;180:717-24.. Zikulnig L, Hecher K, Bregenzer T, Baz E,ackeloer BJ. Prognostic factors in severe
win-twin transfusion syndrome treated by en-oscopic laser surgery. Ultrasound Obstet Gy-
ecol 1999;14:380-7. a.e8 American Journal of Obstetrics & Gynecology
. Quintero RA, Comas C, Bornick PW, AllenH, Kruger M. Selective versus non-selective
aser photocoagulation of placental vessels inwin-to-twin transfusion syndrome. Ultrasoundbstet Gynecol 2000;16:230-6.. Martinez JM, Bermudez C, Becerra C, Lopez, Morales WJ, Quintero RA. The role of Dopplertudies in predicting individual intrauterine fetalemise after laser therapy for twin-twin transfu-ion syndrome. Ultrasound Obstet Gynecol003;22:246-51.. Senat MV, Deprest J, Boulvain M, Paupe A,iner N, Ville Y. Endoscopic laser surgery ver-
us serial amnioreduction for severe twin-to-win transfusion syndrome. N Engl J Med004;351:136-44.. Habli M, Bombrys A, Lewis D, et al. Incidencef complications in twin-twin transfusion syn-rome after selective fetoscopic laser photoco-gulation: a single-center experience. Am J Ob-tet Gynecol 2009;201:417.e1-7.. Huber A, Diehl W, Bregenzer T, HackeloerJ, Hecher K. Stage-related outcome in twin-
win transfusion syndrome treated by feto-copic laser coagulation. Obstet Gynecol006;108:333-7.0. Chmait RH, Khan A, Benirschke K, Miller D,orst LM, Goodwin TM. Perinatal survival fol-
owing preferential sequential selective laserurgery for twin-twin transfusion syndrome. Jatern Fetal Neonatal Med 2010;23:10-6.1. Hecher K, Diehl W, Zikulnig L, Vetter M,ackeloer BJ. Endoscopic laser coagulation oflacental anastomoses in 200 pregnancies withevere mid-trimester twin-to-twin transfusionyndrome. Eur J Obstet Gynecol Reprod Biol000;92:135-9.2. Crisan LS, Kontopoulos EV, Quintero RA.ppraisal of the selectivity index in a cohort ofatients treated with laser surgery for twin-twinransfusion syndrome. Am J Obstet Gynecol010;202:157.e1-5.3. Cincotta RB, Gray PH, Gardener G, Soong, Chan FY. Selective fetoscopic laser ablation
n 100 consecutive pregnancies with severewin-twin transfusion syndrome. Aust N Z J Ob-tet Gynaecol 2009;49:22-7.4. Nakata M, Murakoshi T, Sago H, et al. Mod-
fied sequential laser photocoagulation of pla-ental communicating vessels for twin-twinransfusion syndrome to prevent fetal demise ofhe donor twin. J Obstet Gynaecol Res 2009;5:640-7.5. Crombleholme TM, Shera D, Lee H, et al. Arospective, randomized, multicenter trial ofmnioreduction vs selective fetoscopic laserhotocoagulation for the treatment of severewin-twin transfusion syndrome. Am J Obstetynecol 2007;197:396.e1-9.6. Sepulveda W, Wong AE, Dezerega V, De-oto JC, Alcalde JL. Endoscopic laser surgeryn severe second-trimester twin-twin trans-usion syndrome: a three-year experience from
Latin American center. Prenat Diagn 2007;7:1033-8.7. Middeldorp JM, Sueters M, Lopriore E, et
l. Fetoscopic laser surgery in 100 pregnancies cMONTH 2010
ith severe twin-to-twin transfusion syndromen the Netherlands. Fetal Diagn Ther 2007;22:90-4.8. Yamamoto M, El Murr L, Robyr R, Leleu F,akahashi Y, Ville Y. Incidence and impact oferioperative complications in 175 fetoscopy-uided laser coagulations of chorionic platenastomoses in fetofetal transfusion syndromeefore 26 weeks of gestation. Am J Obstet Gy-ecol 2005;193:1110-6.9. Muratore CS, Carr SR, Lewi L, et al. Survivalfter laser surgery for twin-to-twin transfusionyndrome: when are they out of the woods?Pediatr Surg 2009;44:66-9; discussion 70.0. Ville Y, Hyett J, Hecher K, Nicolaides K. Pre-
iminary experience with endoscopic laser sur-ery for severe twin-twin transfusion syndrome.Engl J Med 1995;332:224-7.
1. Thilaganathan B, Gloeb DJ, Sairam S,ekay A. Sono-endoscopic delineation of thelacental vascular equator prior to selective fe-oscopic laser ablation in twin-to-twin transfu-ion syndrome. Ultrasound Obstet Gynecol000;16:226-9.2. Pedreira DA, Acacio GL, Drummond CL,liveira Rde C, Deustch AD, Taborda WG. La-er for the treatment of twin to twin transfusionyndrome. Acta Cir Bras 2005;20:478-81.3. Gratacos E, Van Schoubroeck D, Carreras, et al. Transient hydropic signs in the donor
etus after fetoscopic laser coagulation in se-ere twin-twin transfusion syndrome: incidencend clinical relevance. Ultrasound Obstet Gy-ecol 2002;19:449-53.4. Quintero RA, Dickinson JE, Morales WJ, etl. Stage-based treatment of twin-twin transfu-ion syndrome. Am J Obstet Gynecol 2003;88:1333-40.5. Quintero RA, Ishii K, Chmait RH, BornickW, Allen MH, Kontopoulos EV. Sequential se-
ective laser photocoagulation of communicat-ng vessels in twin-twin transfusion syndrome. J
atern Fetal Neonatal Med 2007;20:763-8.6. Chavira ER, Khan A, Korst LM, Miller D,oodwin TM, Chmait RH. Are patients with
win-twin transfusion syndrome and a veryhort cervix candidates for laser surgery? J Ul-rasound Med 2009;28:633-9.7. Huber A, Baschat AA, Bregenzer T, et al.aser coagulation of placental anastomosesith a 30 degrees fetoscope in severe mid-tri-ester twin-twin transfusion syndrome with an-
erior placenta. Ultrasound Obstet Gynecol008;31:412-6.8. Chmait RH, Rossi AC, Quintero RA. Para-oxical scalloped placenta with polyhydram-ios in twin-twin transfusion syndrome. J Ma-ern Fetal Neonatal Med 2007;20:29-32.9. Robyr R, Lewi L, Salomon LJ, et al. Preva-
ence and management of late fetal com-lications following successful selective laseroagulation of chorionic plate anastomoses inwin-to-twin transfusion syndrome. Am J Ob-tet Gynecol 2006;194:796-803.0. Quintero RA, Bornick PW, Allen MH,ohson PK. Selective laser photocoagulation of
ommunicating vessels in severe twin-twin
tp3KRsfc3Ftse
3dctp23tcs23
Ltf23tptwcn
www.AJOG.org Education Research
ransfusion syndrome in women with an anteriorlacenta. Obstet Gynecol 2001;97:477-81.1. Lopriore E, Middeldorp JM, Oepkes D,lumper FJ, Walther FJ, Vandenbussche FP.esidual anastomoses after fetoscopic laserurgery in twin-to-twin transfusion syndrome:requency, associated risks and outcome. Pla-enta 2007;28:204-8.2. Ierullo AM, Papageorghiou AT, Bhide A,ratelli N, Thilaganathan B. Severe twin-twinransfusion syndrome: outcome after feto-copic laser ablation of the placental vascular
quator. BJOG 2007;114:689-93. O3. Stirnemann JJ, Nasr B, Quarello E, et al. Aefinition of selectivity in laser coagulation ofhorionic plate anastomoses in twin-to-twinransfusion syndrome and its relationship toerinatal outcome. Am J Obstet Gynecol008;198:62.e1-6.4. Rossi AC, Kaufman MA, Bornick PW, Quin-ero RA. General vs local anesthesia for the per-utaneous laser treatment of twin-twin transfu-ion syndrome. Am J Obstet Gynecol008;199:137.e1-7.5. Lopriore E, Middeldorp JM, Sueters M,
epkes D, Vandenbussche FP, Walther FJ.MONTH 2010 Ame
ong-term neurodevelopmental outcome inwin-to-twin transfusion syndrome treated withetoscopic laser surgery. Am J Obstet Gynecol007;196:231.e1-4.6. Quintero RA, Chmait RH, Bornick PW, Kon-opoulos EV. Trocar-assisted selective laserhotocoagulation of communicating vessels: aechnique for the laser treatment of patientsith twin-twin transfusion syndrome with inac-essible anterior placentas. J Matern Fetal Neo-atal Med 2010;23:330-4.
rican Journal of Obstetrics & Gynecology 1.e9