Damage-control resuscitation in obstetrics - Repositorio ...
15
Full Terms & Conditions of access and use can be found at https://www.tandfonline.com/action/journalInformation?journalCode=ijmf20 The Journal of Maternal-Fetal & Neonatal Medicine ISSN: 1476-7058 (Print) 1476-4954 (Online) Journal homepage: https://www.tandfonline.com/loi/ijmf20 Damage-control resuscitation in obstetrics Javier A. Carvajal, Isabella Ramos, Juan P. Kusanovic & María F. Escobar To cite this article: Javier A. Carvajal, Isabella Ramos, Juan P. Kusanovic & María F. Escobar (2020): Damage-control resuscitation in obstetrics, The Journal of Maternal-Fetal & Neonatal Medicine, DOI: 10.1080/14767058.2020.1730800 To link to this article: https://doi.org/10.1080/14767058.2020.1730800 Published online: 26 Feb 2020. Submit your article to this journal Article views: 28 View related articles View Crossmark data
-
Upload
khangminh22 -
Category
Documents
-
view
5 -
download
0
Transcript of Damage-control resuscitation in obstetrics - Repositorio ...

Full Terms & Conditions of access and use can be found athttps://www.tandfonline.com/action/journalInformation?journalCode=ijmf20
The Journal of Maternal-Fetal & Neonatal Medicine
ISSN: 1476-7058 (Print) 1476-4954 (Online) Journal homepage: https://www.tandfonline.com/loi/ijmf20
Damage-control resuscitation in obstetrics
Javier A. Carvajal, Isabella Ramos, Juan P. Kusanovic & María F. Escobar
To cite this article: Javier A. Carvajal, Isabella Ramos, Juan P. Kusanovic & María F. Escobar(2020): Damage-control resuscitation in obstetrics, The Journal of Maternal-Fetal & NeonatalMedicine, DOI: 10.1080/14767058.2020.1730800
To link to this article: https://doi.org/10.1080/14767058.2020.1730800
Published online: 26 Feb 2020.
Submit your article to this journal
Article views: 28
View related articles
View Crossmark data

REVIEW ARTICLE
Damage-control resuscitation in obstetrics
Javier A. Carvajala, Isabella Ramosb, Juan P. Kusanovicc,d and Mar�ıa F. Escobara
aHigh Complexity Obstetric Unit, Department of Obstetrics and Gynecology, Fundaci�on Valle del Lili, Cali, Colombia; bFaculty ofHealth Sciences, ICESI University, Cali, Colombia; cCenter for Research and Innovation in Maternal-Fetal Medicine (CIMAF),Department of Obstetrics and Gynecology, Hospital S�otero del R�ıo, Santiago, Chile; dDivision of Obstetrics and Gynecology, School ofMedicine, Pontificia Universidad Cat�olica de Chile, Santiago, Chile
ABSTRACTSevere obstetric hemorrhage is a catastrophic event and represents the main cause of maternalmorbidity and mortality worldwide. The elevated mortality rate due to hemorrhage is associatedwith metabolic complications and organ hypoperfusion that may trigger a state of irreversiblecoagulopathy. Thus, the use of conventional measures to control bleeding frequently generatesa vicious cycle in which the patient continues bleeding (prolonging surgical times). Damage-control surgery has proven to be feasible and effective in the context of obstetric hemorrhage.It combines surgical and resuscitative measures that generate successful results in the control ofrefractory bleeding, ultimately decreasing mortality in patients being in critical condition.
ARTICLE HISTORYReceived 29 September 2019Revised 19 January 2020Accepted 13 February 2020
KEYWORDSCritical care; hypovolemicshock; maternal mortality;obstetric hemorrhage;postpartum hemor-rhage; pregnancy
Introduction
Obstetric hemorrhage is a catastrophic event and rep-resents the main cause of maternal morbidity andmortality worldwide [1]. When the blood loss volumeexceeds 40% of total blood volume, global hypoxiaand multiple organ dysfunction develop, with meta-bolic damage because of hypothermia, coagulopathy,and metabolic acidosis [2]. Hemorrhagic shock is themost common form of shock in the obstetric practice[3] and although the term “severe postpartum hemor-rhage (PPH)” is widely used in medical literature, thereare inconsistencies regarding its definition. This hasresulted in a lack of consensus on what constitutesthis condition. Severe PPH has been defined as bleed-ing �1500ml [4], considering only the blood loss, butnot the metabolic decompensation state. Anotherterm frequently used is massive hemorrhage, whichcan be defined as (i) blood loss exceeding circulatingblood volume within a 24-h period, (ii) blood loss of50% of circulating blood volume within a 3-h period,(iii) continuous blood loss exceeding 150ml/min, orblood loss that requires red blood cells (RBCs), plasma,and platelet transfusion [4].
The objective of the initial phase of resuscitation isto aggressively optimize hemodynamic parameters byobtaining venous accesses to ensure resuscitation andblood products replacement that, in addition to the
subsequent surgical management, will be the first stepfor the correction of systemic acidosis, hypothermia,and coagulopathy [2]. However, if medical and surgicaltherapeutic measures fail, the obstetrician encountersa dilemma of whether to attempt a primary definitivecorrection of the hemorrhage, or to perform alterna-tive maneuvers in order to provide enough time toachieve patient survival by deferring her for a seconddefinitive intervention in the following days [5,6]. Thelatter is the basis for damage-control surgery (DCS),concept derived from general surgery in whichseverely polytraumatized patients underwent surgeryto control profuse bleeding [7].
Although maternal mortality due to hemorrhagehas been reduced in developed countries, still somecommon errors in the approach to those cases havebeen identified [8]. Therefore, the pathophysiologicalconditions of patients with severe obstetric hemor-rhage (including PPH), proper patient selection, indica-tions for the approach, and an in-depth description ofthe damage-control resuscitation (DCR) concept willbe presented in the following review.
Physiology of organ dysfunction duringsevere hemorrhage
Mortality due to hemorrhage is derived from meta-bolic complications and a general state of
CONTACT Javier Andr�es Carvajal [email protected] High Complexity Obstetric Unit, Department of Obstetrics and Gynecology,Fundaci�on Valle del Lili, Carrera 98 No. 18–49, Fundaci�on Valle del Lili, Cali, Colombia� 2020 Informa UK Limited, trading as Taylor & Francis Group
THE JOURNAL OF MATERNAL-FETAL & NEONATAL MEDICINEhttps://doi.org/10.1080/14767058.2020.1730800

hypoperfusion, which can trigger an irreversible coa-gulopathy, prolongation of the hemorrhage and ultim-ately, multiple organ dysfunction and death [9]. DCSattempts to reverse organ dysfunction avoiding thetrauma triad of death (hypothermia, acidosis, and coa-gulopathy), enabling a complete control of the hemor-rhage. In situations of severe hemorrhage, the use ofconventional measures to control bleeding is oftenineffective and create a vicious cycle, wherein thepatient continues to bleed. Prolonged surgical times,together with administration of intravenous cold flu-ids, worsen the hypothermia and abnormal coagula-tion states.
Hypothermia
Hypothermia in a severely injured patient with mas-sive hemorrhage is associated with increased mortalityand is likely caused by a combination of factors. Inaddition to the decreased metabolic activity in shock,hypothermia is exacerbated in the hospital by expos-ure and administration of cold intravenous fluids dur-ing resuscitation [10]. A series of simulations haveshown that the exposed peritoneum is the dominantfactor contributing to heat loss and bleeding rate [11].Elevation of the operating room temperature andrapid abdominal closure are effective interventionsavailable to the surgeon to modify the heat loss curve.It is important to know that during a “damage con-trol” laparotomy for exsanguinating hemorrhage, thewindow of opportunity for salvage before the onset ofan irreversible physiologic insult for hypothermia andcoagulopathy is no longer than 60–90min [11].
One of the most severe consequences of hypother-mia is coagulopathy. The effect of hypothermia on thecoagulation cascade has been proposed to result frominhibition of enzyme activity and platelet function. Theinhibition of the enzyme activity has been estimatedby the effect of cold on the prothrombin time (PT)and activated partial thromboplastin time (PTT) [10].Prolonged PT has been found in hypothermic patients,experimental animals, and in plasma samples cooledin vitro [12]. Changes in platelet function under coldconditions are less consistent, but shear-induced plate-let activation is markedly depressed at temperaturesbelow 34 �C. Sheer-induced platelet aggregation isdecreased in a swine model of hypothermia, causing a57% increment in splenic bleeding time of this animalmodel, as well as a reduction of 17% in fibrinogenconcentration (when combined with metabolic acid-osis), delaying the onset of thrombin generation [13].Effective platelet count is also decreased by
hypothermia-related sequestration of platelets in theliver and the spleen [10]. Furthermore, enzyme kineticsis slowed with hypothermia. Johnston et al. found thatat 35 �C, without dilution, there was a decrease in thefunction of several coagulation factors, such as factorsXI and XII that are active only at 65% of the normalfunction, and at 33 �C, their activities dropped to 17and 32% of the normal function, respectively [14].
Hypothermia is usually caused by a reduction incellular heat generation secondary to severe tissuehypoperfusion. Frequently, it is compounded and exa-cerbated by the intraoperative heat loss, inadequatecontrol measures such as no provision of thermalblankets, cold operating rooms, fluid resuscitation withcold crystalloids and, maybe the most important, anopen abdominal cavity exposure during prolongedsurgical periods. Patients with hypovolemic shock andbody temperature below 34 �C for periods longer than4 h are associated with a statistically significantincreased mortality. Indeed, mortality rates rise up to100% when the body temperature is below 32 �C [13].Additionally, it increases the risk for cardiac arrhyth-mias, with a general decrease in cardiac output andan alteration in the hemoglobin–oxygen dissociationcurve, resulting in an increased global oxygen debt.
Metabolic acidosis
Lactate comes from pyruvate, and the latter is pro-duced in the glycolysis cascade [15]. When concentra-tion of pyruvate exceeds its utilization by themitochondria (mitochondrial aerobic oxidation via theKrebs cycle), the production of lactate increases[15,16]. Prolonged hypoperfusion causes hypoxia,which leads cellular metabolism to enter an anaerobicstate, blocking normal functioning of the mitochon-drial cellular system [15,16]. The inhibition in ATP syn-thesis and NADH reoxidation causes a pyruvateaccumulation that, with alterations in the redox poten-tial; increases the production of lactate. This allowsthe generation of some NADþ that in anaerobic gly-colysis will originate two ATP molecules [15]. Besides,the adrenergic discharge and stress in shock patientsleads to an accelerated glycolysis that continues pro-moting lactate formation. On the other hand, someshock patients have acute liver or renal dysfunctionswhich worsen the metabolic state, because of thedecreased lactate clearance [16].
Increased blood lactate concentrations in shock,produces a drop in intracellular and extracellular pH,that consequently, leads to hemodynamic failure [16].Although “severe lactic acidosis” definition remains
2 J. A. CARVAJAL ET AL.

unclear, ICU physicians tend to consider that a pH<7.2 has harmful effects on the hemodynamic state ofthe patients; indeed, acidification causes dysfunctionof coagulation system enzymes and the inactivation ofclotting factors [13]. In addition, studies have shownthe association between severe lactic acidosis andhigher mortality rates (approximately 50%), with nosurvival reported in cases which pH <7.0 [16].
Experimental studies have demonstrated thatsevere metabolic acidosis worsens cardiovascular func-tion through an increase in the amplitude of the sys-tolic calcium transient and hence, the contractionpathway altering calcium binding to troponin C [16].Another studied mechanism consists of the BNIP3gene expression under hypoxic conditions. BNIP3 isone of the members of the Bcl-2 proapoptotic proteinfamily and promotes cardiomyocyte death. It translo-cates to mitochondrial membrane and causes therelease of another proapoptotic factors that producenuclear translocation of DNase and finally, apop-tosis [16].
Notwithstanding there is a lot of experimental stud-ies, the prior effects and mechanisms have not fullydemonstrated in humans. Lactic acidosis is one of theprincipal causes of metabolic acidosis in shock states,although others have also been reported [16].
Coagulopathy
While the mortality of trauma patients requiring mas-sive transfusion exceeds 50%, at least 10% of thosedeaths are potentially preventable; many of thesedeaths occur within the first few hours of definitivecare, with coagulopathy playing a crucial role. Indeed,coagulopathy is one of the most preventable causesof death in trauma and has been implicated as thecause of almost half of hemorrhagic deaths in traumapatients, being present at the time of admission tothe emergency department in up to 25–35% of cases.Understanding the pathophysiology of trauma-inducedcoagulopathy is key, especially with respect to the crit-ical issue of establishing therapeutic strategies for themanagement of patients. Reanimation based in crys-talloids will lead to dilution of clotting factors, devel-oping a dilutional coagulopathy. This mechanism hasbeen studied and described in trauma, and isaccepted that PPH may share some of these mecha-nisms [17]. Although no consensus has been reachedregarding a definition of acute traumatic coagulopathy(ATC), there are different approaches to the classifica-tion and naming of trauma-associated coagulationimpairment [18]. Trauma-induced coagulopathy (TIC) is
a multifactorial, global failure of the coagulation sys-tem to sustain adequate hemostasis after majortrauma, with acute coagulation alterations secondaryto an early endogenous process. This acute traumaticcoagulopathy (ATC) is driven by the combination oftissue trauma and systemic hypoperfusion, and charac-terized by global anticoagulation and hyperfibrinoly-sis [19].
It has been argued that activated protein C plays acentral role in the mechanism of ATC. In initial obser-vations in trauma patients with systemic hypoperfu-sion, defined by an elevated base deficit, a correlationwas found between ATC and increased concentrationsof activated protein C, reduced concentrations of pro-tein C, and elevated soluble thrombomodulin [19]. Theactivation of the thrombomodulin-protein C systemhas been suggested as an important pathway media-ting ATC, characterized as hyperfibrinolysis and ahypocoagulable state; this proposed mechanism is dif-ferent from clotting factor consumption or dysfunc-tion. Sustained tissue hypoperfusion is associated withelevated concentrations of soluble thrombomodulinsecondary to endothelial damage, which can increasethe availability of thrombomodulin to bound thrombin[17]. The result is the formation of a complex withthrombomodulin, and the role of thrombin can bediverted from procoagulant to anticoagulant by excessactivation of protein C. These mechanisms may leadto the hyperfibrinolytic state in patients with ATC,which is reflected in increased tissue plasminogenactivator (t-PA), decreased plasminogen activatorinhibitor-1 (PAI-1), and increased D-dimer concentra-tions. This hypothetical condition has been named“acute coagulopathy of trauma-shock” [20].
Most coagulation assays (PT, PTT, and INR) fre-quently underestimate an state of coagulopathy in itsinitial stages; therefore, clinical judgment and a judi-cious intraoperative analysis based on viscoelasticcoagulation tests as ROTEM (RotationalThromboelastometry) and TEG (thromboelastography),and risk factors for bleeding and coagulopathy ofeach patient are crucial factors for survival in thesecases [21].
Damage-control resuscitation
Resuscitation in a patient with hemorrhage has under-gone significant changes in the last few decades, lead-ing to the adoption of the novel concept of DCR orhemostatic resuscitation, moving the managementfrom a definitive surgical approach to DCS. Thismethod is used in patients with severe trauma and
THE JOURNAL OF MATERNAL-FETAL & NEONATAL MEDICINE 3

massive hemorrhage, including women with severeobstetric hemorrhage related to shock and coagulop-athy. DCR describes a systematic approach to minim-ize hemorrhage, prevent the deadly triad andmaximize the oxygenation of tissues. The key princi-ples of DCR are hypotensive and hemostatic resuscita-tion with limitation of crystalloid administration, theuse of massive transfusion protocols, bleeding control[including DCS and damage-control interventionalradiology (DCIR)], and physiological and biochemicalstabilization in the ICU [10,22].
Recently, DCR has been strengthened by thelaboratory and pharmacological agents to improve thecare of the patient with hemorrhage, such as throm-boelastography as a detailed measure of the coagula-tion cascade, and the early use of tranexamic acid(TXA; an antifibrinolytic), as a strategy for hemostaticresuscitation [10].
Initial reanimation
Among the initial strategies for reanimation, theadministration of crystalloids in boluses of 500ml isrecommended, looking for an improvement in signsand symptoms of shock resulting from blood loss. Inhemorrhage state and according to the degree ofshock, women could show diaphoresis, increasedcapillary refilling, cool extremities, tachycardia, tachyp-nea, hypotension and alterations in state of conscious-ness (agitation, confusion, or somnolence) [23]. It isimportant to recognize that symptoms like tachycardiaand hypotension do not present until blood loss issubstantial [24]. The shock index (SI) is the relationbetween heart rate/systolic blood pressure that can bedone at the time of diagnosis of PPH, at 15 and30min and 24 h after the event to establish thedegree of hemodynamic instability. Although the SIcut off points for action and to predict outcomesremains unclear and are not well established, andsome limitations have been described in relation withits use, is an utility tool in clinical practice. Valuesabove 0.9 have been considered abnormal. This indexis directly related to the need for massive blood prod-ucts transfusion and the development of coagulopathyin massive PPH [25,26], since SI values >1.7 have anodds ratio of 4.24 (95% CI 1.25–14.36) for blood trans-fusion [27]. On the other hand, Kohn et al. recentlydescribed delta-SI (difference between peak SI and SIat the last antenatal visit or at facility presentation) asa novel tool, which is the strongest predictor for PPH,transfusion and need for surgical intervention,
although the peak SI is also, by itself, a strong pre-dictor [28].
Moreover, the use of Non-Pneumatic Anti-ShockGarment (NASG) is one of the strategies that have pro-ven effectiveness in the reanimation of patients withshock for PPH. Although the NASG by itself is not atherapeutic measure in patients with PPH, it is acornerstone in the initial workup and resuscitationsince it promotes the stabilization of patients byreducing bleeding and increasing perfusion to theircore organs. Its main goal is to increase survival timein women with hypovolemic shock, extending theavailable timeframe to perform definite surgical inter-ventions [29]. Additionally, it has shown that it favorsthe improvement of clinical shock parameters, such asSI and lactate clearance, and decreases the require-ment for blood transfusions and intravenous fluids[30]. Also, the NASG allows performing surgical proce-dures, such as DCS, without the need to removeit [31].
Bleeding control
Effective DCR in PPH begins with the management ofbleeding and its etiology. A range of interventions areused in obstetrics to control the bleeding, whichinclude external aortic compression (as a temporarymeasure), intrauterine balloon tamponade (Bakri’s orcondom balloons), compressive hemostatic sutures,and resuscitative endovascular balloon occlusion ofthe aorta (REBOA) used in cases of severe pelvictrauma and placenta accreta protocols [22].
Recently, the use of endovascular balloons for vas-cular occlusion has become an important option forthe management of massive PPH, especially in compli-cated cases such as patients with abnormally adherentand invasive placenta [32]. The REBOA is a novelendovascular intervention characterized by the inser-tion of an aortic balloon in order to have a proximalcontrol of the hemorrhage. Ordo~nez et al. reportedtheir experience using REBOA in 12 patients thatunderwent cesarean section due to an abnormallyadherent and invasive placenta [32]. The balloon wasinflated after delivery of the fetus and umbilical cordclamping for all cases. The median time of aorticocclusion was 22min (IQR 20–40min), and there wereno complications secondary to the use of REBOA.Moreover, a systematic review and meta-analysis offour studies including 441 patients demonstrated thatthe use of REBOA as prophylaxis for the prevention ofmajor hemorrhage was associated with a loweramount of intraoperative hemorrhage and lower
4 J. A. CARVAJAL ET AL.

requirements of blood products transfusions com-pared to patients without REBOA [32]. These findingsdemonstrate the feasibility of REBOA as a prophylacticintervention to improve the clinical outcomes ofwomen at risk for severe PPH [32]. Recently, Morrisonet al. conducted a systematic review including 41studies about the use of REBOA for the managementof resuscitation or bleeding control in patients withhemorrhagic shock. Among those studies, five wereconducted in obstetric populations, and two of themwere case-series of patients with massive bleedingdue to uterine atony, placental remnants and vaginaltrauma that required aggressive hemostatic resuscita-tion, bleeding control using REBOA and total abdom-inal hysterectomy, with no cases of maternalmortality [33].
Because of the solid body of evidence, the use ofREBOA should be considered as a useful and efficientstrategy for bleeding control in cases of massivebleeding, since it is associated with less blood lossand lower need for transfusion of blood productswhile definitive surgical interventions are conducted,being part of the DCR spectrum [32,33].
Novel hypotensive resuscitation
The aim of hypotensive resuscitation is to achieve alower blood pressure until definitive hemostasis is per-formed in order to promote adequate tissue perfusionand hemostasis, avoiding further worsening of thecoagulopathy. This approach is based on the conceptthat small crystalloid volumes are less likely to createdilutional coagulopathy, and lower blood pressure isless likely to break or fragment the alreadyformed clots.
However, when given large fluid volumes, this mayinitiate dilution of clotting factors resulting in impair-ment of coagulation and coagulopathy [34]. Gillisenet al. performed a cohort study with the aim ofdescribing the association between administration ofdifferent volumes of fluids and concentrationsof coagulation parameters in women with PPH. In thiscohort, women with the lowest fluid administrationshowed fewer signs of shock and less administrationof blood products. Also, fibrinogen, hemoglobin, hem-atocrit, and platelets concentrations decreased overincreasing fluid administration while PT and aPTT werelonger [34]. On the other hand, Henriquez et al. usedthe same cohort of patients (TeMpOH-1) to demon-strate that resuscitation with >4-L fluids was associ-ated with subsequent bleeding and more adversematernal outcomes [35].
Sondeen et al. used a porcine aortic lesion modelto quantify the upper limit of patient blood pressureafter which fluid resuscitation becomes detrimentaldue to fragmentation of the clot. The authors deter-mined an average mean arterial pressure (MAP) of64mmHg and a systolic blood pressure (SBP) of94mmHg after which further increases in BP resultedin new hemorrhages regardless of the size of the aor-tic structural injury [36]. Other noncontrolled hemor-rhagic shock animal models have demonstrated apositive benefit in survival with mean arterial pres-sures (MAP) between 55 and 60mmHg during activebleeding. According to current evidence, hypoperfu-sion can be tolerated for short periods of time andmay decrease the volume of global hemor-rhage [10,22].
The endothelial glycocalyx (EG) has recently beenrecognized as a complex of proteoglycans, glycosami-noglycans, and plasmatic proteins that are essential inmaintaining the osmotic equilibrium and overall integ-rity of the endothelium. During hemorrhagic shock,the EG becomes thinner and the administration ofcrystalloids exacerbates this state, leading further fluidextravasation and overall volume depletion, worseningbleeding [17,22].
An excessive administration of crystalloids can alsolead to cardiac dysfunction. The Frank–Starling curvedemonstrates that an increase in cardiac volumeresults in a corresponding increase in cardiac output(through increased stroke volume) up to a certainthreshold after which additional volume expansionresults in decreased cardiac output. This decrease issecondary probably due to the deleterious effects ofintracellular edema, which causes a dysfunction ofintracellular metabolic processes and an improper cel-lular respiratory system while worsening the proin-flammatory state of the hemorrhagic shock [22].
Massive transfusion protocols and hemostaticresuscitation
Massive transfusion means transfusion requirements of�4 PRBC units (some articles considered the need for�10 PRBC within 24 h), replacement of total blood vol-ume within 24 h, or replacement of 50% of blood vol-ume within 3 h [37–39]. Massive transfusion protocolsinvolve the early utilization of blood products alongwith proportionate administration of PLT:FFP:PRBC,limiting the resuscitation based in large amounts ofcrystalloids. Therefore, it has been argued that withthis approach the clotting factors dilution and thirdspacing formation is minimized [17,40].
THE JOURNAL OF MATERNAL-FETAL & NEONATAL MEDICINE 5

It is widely accepted that a high PLT:FFP:PRBC ratioconfers an advantage in patient survival. No significantdifferences between 1:1:1 or 1:1:2 ratios have beendemonstrated in terms of patient mortality in 24 h and30 days of follow-up. Nonetheless, the PROPPR studydemonstrated that a greater proportion of patients inthe 1:1:1 group achieved hemostasis and suffered lessdeaths due to exsanguination at 24 h [36]. Furtheranalysis of the PROMTT study performed by Del Juncoet al. revealed that early administration of plasma(within the first 3 h and within the first 3–6 units aftertransfused blood components) was associated with adecrease in mortality at 24 h and 30 days (OR¼ 0.47,p¼ .009; OR¼ 0.44, p¼ .002, respectively) [41].
Fibrinogen is the first clotting factor to decrease itsconcentrations, and values of <200mg/dL are consid-ered an indication for component replacement [42,43].According to Pacheco et al., one unit of platelets willincrease the platelet count by 5000–10,000/mm3, andone unit of FFP contains all clotting factors and 2 g offibrinogen for each 1000ml; thus, a unit of FFP(200–250ml) increases serum fibrinogen by 10mg/dL [17].
Antifibrinolytic agents
The CRASH-2 trial provided evidence that an earlyadministration of TXA reduces mortality secondary tobleeding in patients with trauma by approximatelyone-third. The current guidelines suggest a loadingdose of 1 g for 10min, and then an additional 1 g isinfused for 8 h. TXA should be administered as soonas possible after the injury and within the first3 h [44].
In the scenario of obstetric hemorrhage, the fibrino-lytic activity in the immediate postpartum has led toan increased interest in TXA use [45]. The WOMANtrial studied the effect of early administration of TXAon maternal mortality after hysterectomy and othersurgical morbidities in patients with PPH. In thisrandomized, double blind, placebo-controlled trial,patients of 16 years of age and older with a clinicaldiagnosis of postpartum hemorrhage after vaginaldelivery or cesarean section in 193 hospitals through-out 21 different countries were included. A total of20,060 women were included and were randomlyassigned to receive 1 g of intravenous TXA or placebo,in addition to standard care for postpartum hemor-rhage. If bleeding continued after 30min, or stoppedand resumed within 24 h of the first dose, a seconddose of 1 g was administered (either TXA or placebo).Death due to hemorrhage was significantly reduced
among women who received TXA (RR 0.81, 95% CI0.65–1.00; p¼ .045), especially in women who receivedthe treatment within 3 h after delivery (RR 0.69, 95%CI 0.52–0.91; p¼ .008), and additionally, thrombo-embolic events did not increase in patients receivingTXA [46]. Nowadays, the use of an antifibrinolyticagent such as TXA seems to be safe, effective, inex-pensive and crucial in PPH management [45], becauseof the high chance of developing an acute coagulop-athy secondary to a massive bleeding and trauma dueto excessive fibrinolysis.
There is limited evidence about the use of fibrino-gen concentrates in PPH; however, its use may reducetransfusion of blood products [42]. On the other hand,the use of prothrombin complex concentrates (con-centrates of vitamin K-dependent clotting factors) isnot recommended in the routine setting of PPHbecause of the lack of evidence to support it [42].
Point of care test (POCT)
POCT of viscoelastic coagulation such as ROTEM(Rotational Thromboelastometry) and TEG (thromboe-lastography) perform fast viscoelastic hemostatic anal-yses that provide a graphical evaluation of the kineticsof all stages of clot formation (initiation, propagation,strength, and dissolution) in whole blood, analyzingthe enzyme kinetics of the entire coagulation processand facilitating targeted therapeutic interventions.Such tests allow for individualized treatment strategiesand can reduce the requirement of blood products tobe transfused [22].
Management of massive transfusion rests on sim-ple, reliable and rapid diagnostic coagulation tests.Monitoring dynamic changes of hemostasis with TEGor ROTEM may enable: (i) distinction between a surgi-cal cause of bleeding or coagulopathy; (ii) diagnosis ofthe specific type of coagulopathic impairment; and (iii)guidance in the choice of hemostatic treatment. Thismay reduce the use of blood products and bleeding,the need for reoperations, and the rate of complica-tions associated with hypovolemic shock [47].
The use of protocols for massive transfusion is con-sidered a useful tool for the emergency team, since ithelps standardizing the management of these patientsand improves the response to a massive hemorrhage.In a systematic review, Wikkelsø et al. evaluated thehemostatic management of an algorithm using TEG orROTEM among patients with a severe hemorrhage,and compared this management with other algorithmsbased on clinical judgement, usual treatment or stand-ard laboratory tests. The primary outcome was overall
6 J. A. CARVAJAL ET AL.

mortality, and the secondary outcomes were bleedingevents, blood loss, proportion of patients in need oftransfusion and amount of blood products transfused,complications probably related to underlying condi-tions, incidence of surgical intervention and reopera-tion due to bleeding, and complications probablyrelated to transfusion, among others. The authorsincluded 17 trials (1493 participants), most of theminvolving cardiac surgery. Thromboelastography orrotational thromboelastometry seemed to reduceoverall mortality compared to usual treatment basedin laboratory test (3.9 versus 7.4%, RR (95% CI) 0.52(0.28–0.95); I2¼ 0%, 8 trials, 717 participants).However, the quality of evidence is graded as low dueto the high risk of bias, heterogeneity, imprecision andlow event rate. TEG or ROTEM significantly reducedthe proportion of patients transfused with red bloodcells (RR (95% CI) 0.86 (0.79–0.94); I2¼ 0%, 10 trials,832 participants), fresh frozen plasma (RR (95% CI)0.57 (0.33–0.96); I2¼ 86%, 10 trials, 832 participants)and platelets (RR (95% CI) 0.73 (0.60–0.88); I2¼ 0%, 10studies, 832 participants) [47].
On the other hand, it has been suggested thatreanimation with blood products should be individual-ized and adjusted according to the results of the pointof care viscoelastic testing (PCVT). Snegovskikh et al.conducted a retrospective cohort study comparingtwo groups of patients with severe postpartum hem-orrhage: (i) those with blood transfusion guided byPCVT, and (ii) those managed using a standardizedmassive hemorrhage transfusion protocol, eitherbecause PCVT was not yet available, or because noPCVT credentialed providers were on site [48]. Therewas no statistically significant difference between thePCVT and non-PCVT groups regarding the amount ofcrystalloids, colloids, albumin, and cryoprecipitateadministered. However, patients in the PCVT groupreceived significantly fewer transfusions of PRBCs(p< .0001), FFP (p< .0001), and platelets (p< .0001).Estimated blood loss was also significantly lower inthe PCVT group (median [IQR] 2000ml [1600–2500]versus 3000ml [2000–4000], p< .001). Similarly, theincidence of puerperal hysterectomy (25% [7/28] ver-sus 54% [31/58], p¼ .013) and postoperative ICUadmission (4% [1/28] versus 43% [25/58], p< .001)were significantly lower in the PCVT group [48].
The evidence provided above shows that the use ofTEG and ROTEM as bedside tests may improve theclinical outcomes and reduce the cost by consideringclinically efficient decisions for the management ofblood and blood products transfusions in patientswith severe postpartum hemorrhage.
Damage-control surgery (DCS)
DCS is the term used to describe a series of surgicalprocedures performed in stages during a period ofpatient hemodynamic instability. These procedureshave applicability in traumatic and nontraumatic scen-arios in General Surgery, Orthopedics, as well asGynecology and Obstetrics. DCS consists of performinglimited surgical interventions to swiftly counteract life-threatening conditions, with the definitive surgicalprocedure deferred until a period of stabilization hasbeen achieved in the Intensive Care Unit (ICU). DCS isusually reserved for the severely injured patient thatmay not survive the surgical efforts to achieve primaryrepair in the operating room. Frequently, the hemor-rhage in these patients may not be able to be con-trolled surgically, mainly due to a combination ofhypothermia, acidosis, coagulopathy and hypocalce-mia [49].
The most common indications for DCS in the set-ting of hemorrhage include the following: difficult sur-gical access to the bleeding site, venous bleeding notsuitable for mechanical control, need of blood prod-ucts and intravenous fluids in nonarterial bleedingscenarios, hemodynamic instability despite use of vas-opressors, and coagulopathy. This is explained inTables 1 and 2. Other indications are exsanguinationand impossibility of abdominal closure by regularmethods [49].
Typically, these patients present with diffuse bleed-ing in the absence of clot formation despite maximumsurgical efforts. Like DCS in other surgical specialties,packing is the cornerstone in the damage control ofobstetric patients [49].
Decision of DCS: a critical point
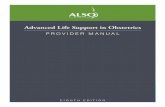
The decision to perform a DCS must be taken as earlyas possible; time is a factor that plays against survival[50]. Several patient markers, both physiological andmetabolic, have been proposed to identify patientsthat could benefit from DCS (Tables 1 and 2). Theseindicators are explained in Figure 1, and along withsound clinical judgment, are the prime determinantswhether the patient is eligible for DCS.
Table 1. Indicators for damage-control surgery (prior toentering the operating room).Systolic blood pressure <70mmHgBody temperature <34 �CMaternal blood pH <7.1
Adapted from: Pacheco et al. [49].
THE JOURNAL OF MATERNAL-FETAL & NEONATAL MEDICINE 7

Damage-control surgery technique
After identifying candidate patients, a sequentialapproach has been documented that can serve as ageneral guideline for DCS:
1. initial laparotomy: fast control of bleeding and/orcontamination, including hysterectomy
2. resuscitation in intensive care or HighDependency Unit
3. definitive surgery4. definitive closure
Initial laparotomy
The initial surgical period, where obstetric patients canpresent in different scenarios, is an important factor totake into account. This period can be regarded as themoment where the hemorrhage was generated (e.g.C-section with severe hemorrhage), an intermediatepoint of bleeding control after a B-Lynch procedure,or after a postpartum hysterectomy in which there ispersistent bleeding. Hence, due to the possible varia-tions in the initial surgical period, it is recommendedthat the obstetrician must be in constant communica-tion with the surgical team in order to assess the con-dition of the patient to determine if she is a candidate
Table 2. Intraoperative indications for damage-control sur-gery secondary to hemorrhage.Venous bleeding not suitable for surgical controlPersistent bleeding despite several transfusions of blood products (>10
units of PRBC)Massive transfusion � 6 units of Red Blood Cells (during the first 4 h)Increasing and continuous need for fluids due to an active
nonarterial bleedingHemodynamic instability, requiring persistent vasopressor support or that
results in the development of ventricular arrhythmiasCoagulopathy resulting from a combination of hypothermia (temperature
<35 �C), acidosis (pH <7.3) and loss of coagulation factorsDuration of surgery >90min
Adapted from: Pacheco et al. [49].
MASSIVE OBSTETRIC HEMORRHAGE
ACTIVATE CODE RED IDENTIFY GRADE OF SHOCK
IDENTIFY ORIGIN – 4 T
CLINICAL COAGULOPATHY HYPOTHERMIA <35º C
ACIDOSIS
TONE TISSUE TRAUMA THROMBIN
LACTIC ACID >2 EB -6
ANESTHESIOLOGY ICU
GENERAL SURGERY BLOOD BANK ACTIVATION
ACTIVATE TEAM FOR PACKING
LIQUID RESTRICTION AND
RESUSCITATION WITH LOW VOLUMES
HYPOTENSIVE RESUSCITATION INTENSIVE CARE
UNIT
ABDOMINAL PACKAGING
HEMOSTATIC RESUSCITATION
Figure 1. Algorithm of management.
8 J. A. CARVAJAL ET AL.

for DCS. A constant report and interpretation of arter-ial blood gas values, patient body temperature, surgi-cal time and number of blood units transfused is ofparamount importance.
The objective of this initial approach is to achieverapid control of bleeding. It is recommended that atthis stage the obstetrician performs an abdominal hys-terectomy. The type of hysterectomy to be performedhas to be chosen depending on the preference andexpertise of the operator, the clinical condition of thepatient, and considering other factors like age, causeof hemorrhage, hemodynamic stability and pelvicanatomy [51]. A few studies [51–53] have demon-strated that there is no statistical differences betweenthe two techniques in terms of complications, bloodtransfusions, and ICU admission; nevertheless, fasterbleeding control and shorter surgical times corre-sponds to subtotal hysterectomy (STH), which are thereasons why it is preferred over total hysterectomy(TH) [51,53]. If the origin of the hemorrhage is fromthe lower uterine segment, cervix or vaginal fornices,then a STH may not be effective controlling bleedingsince the arterial circulation of the cervix has a highblood flow rate and could cause bleeding persistence.In those cases, a TH should be performed [51,52].
Surgical time is a determining factor in patient sur-vival, and is recommended to be less than 90min,since longer operating times should be considered apredictor of adverse outcomes, because of the onsetof an irreversible physiologic insult demonstrated incomputer simulation models [11,54]. Hemorrhage con-trol of the pelvic cavity is frequently carried outthrough the means of packing [55], which can beachieved with either separated smaller compresses ora large single compress. Based on our reported experi-ence on two case series with 28 and 108 criticalpatients with obstetric hemorrhage, we recommendthat pelvic packing should be done with at least 7–10compresses [2,56]. In these case series, the mean num-ber of applied compresses was 14, with a range from8 to 22. Importantly, 73% of the patients were inter-vened with DCS within the first hour of the diagnosisof massive hemorrhage, and 88% had a total abdom-inal hysterectomy at the time of DCS.
In DCS, abdominal closure is temporary. The idealmethod should be easy to perform and remove. Themethod chosen should be able to adequately protectthe abdominal content from evisceration, prevent thedevelopment of fistulas and the lateral retraction ofthe fascia, since the latter can result in an inability tocomplete a final closure of the abdominal wall [49].Compresses should be complemented with a
temporary abdominal wall closure using a negativepressure system like Vacuum-Pack or partial closurewith a Viaflex bag (Bogota Bag) without the need fornegative pressure [2,56].
The most widespread open abdomen with negativepressure technique was described by Barker et al., inwhich after performing pelvic packing, the intestinesare protected with a cover of fenestrated polyethyl-ene, over which a layer of compresses is placed at themidline and two silicone drains are placed, beingexposed outwards to the skin by additional incisions[57]. New layers of compresses are placed over thedrains and are sealed with a cover of adherent polyes-ter. When the Vacuum Pack has been assembled, thedrains are connected to a source of negative pressurewith a reservoir of 100–125mmHg. If commercialVACVR systems are available, an intestinal coveringmust be made with polyurethane over which the flex-ible polyurethane foam included in the system mustbe applied. It is not necessary to perform additionaldrainage incisions. Subsequently, the foam is coatedwith adherent polyester and an orifice is made on theplastic coating where the negative pressure commer-cial drainage system is connected.
Evidence regarding the addition of local hemostaticagents, whether applied directly on the tissue orimmersed in sterile compresses, is limited. In some ser-ies, the addition of these agents like thrombin sprayor fibrin glue has proven to be a useful coadjuvantwhen packing with compresses is applied to limit con-tinuous bleeding [49].
Currently, there is neither consensus nor sufficientevidence regarding the use of prophylactic antibioticsin patients undergoing DCS with abdominal packing.Several surgical guidelines recommend the administra-tion of a single preoperative dose of broad-spectrumantibiotics that, in theory, should provide sufficientcoverage for aerobic and anaerobic microorganisms.Furthermore, these guidelines suggest that preopera-tive antibiotic prophylaxis should be extended to 24 hpost injury in patients who have suffered hollow vis-cous injuries [58,59]. Nevertheless, the former is notapplicable in the context of obstetric patients (as nohollow viscous injury occurs); consequently, it couldbe inferred that antibiotic use is not required. Otherexperts recommend prophylactic doses of broad-spectrum antibiotics every 6–8 h until the abdominalpacking is removed. However, further studies areneeded to provide evidence-based recommendationsin the obstetric population [49].
Interestingly, DCS can also be performed vaginallyin cases of associated vaginal tears and combined
THE JOURNAL OF MATERNAL-FETAL & NEONATAL MEDICINE 9

with other surgical techniques for effective bleedingcontrol. In our series, 8% of the patients required vagi-nal packing and 4% associated vascular ligatures.
Resuscitation – intensive care, highdependency unit
During this stage, the patient must be transferred tothe Intensive Care Unit where coagulation disordersand metabolic abnormalities should be corrected [22].These patients require a significant investment of hos-pital resources as demonstrated in our series of 108cases: 100% required massive transfusion protocolswith an average of 5 units of RBC, 6 units of plasma,4.5 units of platelets and 10 units of cryoprecipitate. Inaddition, 34% received vasoactives, 14% tranexamicacid, 8% specific coagulation factors, 5% topicalthrombin, and 2% renal replacement therapy [2].
The obstetrician must keep strict clinical vigilanceand perform care alongside the intensive care special-ist since complications could arise at any time.Significant problems that must be recognized in orderto take prompt actions during this period arethe following:
Abdominal compartment syndrome (ACS)Due to the mechanical effect of packing and progres-sive edema of the abdominal tissues during theresuscitation process, there is an increase of the intra-abdominal pressure (IAP), which is a common compli-cation after pelvic packing. This increase in the IAPmay result in Abdominal Compartment Syndrome(ACS), a common complication that is associated todecreased venous return of the inferior vena cava,producing a subsequent decrease in cardiac outputand renal perfusion (evidenced by oliguria or anuria),as well as abnormalities in mechanical ventila-tion [60,61].
Pregnancy is a state of chronically elevated intra-abdominal pressure. The median intra-abdominal pres-sure during the last stage of pregnancy is reported torange between 15 and 29mmHg. It decreases to amedian pressure of 16mmHg at 24 h after delivery.Hence, during pregnancy or the postpartum period,patients will have a higher intra-abdominal baselinepressure and should not be treated based on an iso-lated measurement of IAP in the absence of clinicalfindings consistent with ACS, such as hypotension, oli-guria that does not respond to fluid therapy, abdom-inal distension, and high airway pressures seen onmechanical ventilation [49]. All patients under post-packing management should receive continuous
measurement of IAP; values greater than 16mmHgcan be associated with hemodynamic repercussionand can indicate the need for early surgical interven-tion [62].
Once a diagnosis of ACS is confirmed, definitivetreatment involves opening the abdominal cavity (ifclosed) to allow decompression. In the scenario ofDCS with open fascia, if the opening is too small, anextension of the incision may decrease the IAP. Onthe other hand, if the packing of the cavity is tootight, repacking should be considered using a lowernumber of compresses and applying less pressurewhen placing them. Certain medical interventions candecrease IAP, such as the use of nasogastric tubes,rectal tubes, gastrointestinal prokinetic agents, diu-retics, and the use of muscle relaxants. However, theseinterventions should not replace surgical managementwhen indicated [56].
Persistent bleeding of abdominal cavityIt is very important to accurately quantify the produc-tion of fluid of the abdominal cavity; the most recom-mended device to measure it after partial abdominalclosure is the use of Vacuum Pack, which allows moreprecise quantification of bleeding during the postoper-ative period. It is considered that production higherthan 400 cc/hrs, in a patient in whom all the coagula-tion disorders have been corrected, is an early indica-tor for laparotomy.
Definitive surgery
After stabilization of the physiological variables of thepatient, it is considered safe to review the abdominalcavity. Ideally, this should be performed 48–72 h afterthe first surgical procedure. The plan and the surgicalteam should be determined based on the findings ofthe first intervention, since at this time issues thatwere partially solved should be corrected, such as thecase of ureteral ligation, bladder injury or bowel per-foration. Depending on intraoperative findings, thismay be the final surgery or the moment to definewhether the patient will need additional interventionsfor definite control. If further interventions are needed,it is recommended to continue with techniques oftemporary closure of the abdominal cavity [60]. In ourlargest case series, the mean reintervention time was48 h, with a standard deviation of 42–72 h, and in 65%of the patients total control of bleeding was achievedin the first DCS [2].
10 J. A. CARVAJAL ET AL.

Definitive closure of abdominal wall and cavity
The final stage is the definitive closure of the abdom-inal wall, which is performed after all surgeries havebeen successfully completed and all additional dam-age has been repaired. It is important to take intoaccount that the number of reinterventions is directlyrelated to a higher percentage of infectious complica-tions, wound dehiscence and abdominal wall closureproblems [62].
Complications derived from damagecontrol surgery
The majority of complications derived from DCS aredependent on when the closure of the abdominalfascia occurs. The most frequent complications areinfections and intra-abdominal collections. It is recom-mended to initiate broad-spectrum antibiotic treat-ment early, targeting the polybacterial flora present inthe female genital tract. Complications derived frominjured organs during the initial laparotomy such asurinomas, intestinal perforations, and fistulas mayrequire an interdisciplinary approach [61]. In ourcohort, the main complications included infection ofthe surgical wound in 28% of the cases, presence ofintra-abdominal collections in 20%, and evisceration in10% of the patients [2].
Final objectives in resuscitation and damagecontrol surgery
Perhaps the greatest challenge when applying DCR isto determine when to stop this therapeutic modality.Clearly, it should be sustained as long as there aresigns of bleeding and coagulopathy. A continuousassessment of the hemodynamic and physiologicalstatus of the patient is required. There is consensusthat pursuing not only one but several resuscitationparameters are essential until tissue hypoxia has beenresolved. These parameters include the following:
� pH� base deficit� lactate� hematocrit� coagulation: ideally evaluated with conventional
laboratory tests and POCT (ROTEM/TEG)
In patients with a clinical trend toward improve-ment, the decision to perform definitive surgery isappropriate. On the other hand, in those patients withcompromised micro- and macrohemodynamics, a
minimal surgical intervention that provides stabilityshould be considered until the pathophysiologicalconditions of the patient are more favorable [18].
Extension of the concept of damage control
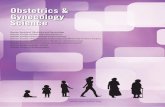
Hemostatic resuscitation should begin as soon as thepatient arrives, allowing for improvement of periopera-tive physiological conditions without delaying surgicalprocedures. The adoption of this integrated approachcombines surgical and resuscitative measures whichresults in an overall increased survival of patients withPPH. This approach should be applied during the ini-tial management of the injured patient by ambulancepersonnel, performing hemorrhage control and hemo-static resuscitation as soon as possible; this extensionof DCR to the first response team is termed remoteDCR (RDCR) [63], and is explained in Figure 2. Thisextension of damage control is also valid in the set-ting of critical obstetrics. The resuscitation of patientswith life-threatening obstetric hemorrhages shouldbegin at the site of the obstetric event (even if it is alevel I of attention), applying strategies of the obstet-ric red code and performing interventions for bleedingcontrol. DC should be given continuously during thetransfer of the patient to the highest possible com-plexity care center for comprehensive and interdiscip-linary care, with a medicalized ambulance and trainedpersonnel to ensure clinical monitoring and properresuscitation maneuvers. DCR incorporates the con-cept of damage control radiology (DCRad) for diagnos-tic and therapeutic aspects. Diagnostic DCRad(dDCRad) employs multidetector computed tomog-raphy (MDCT) to rapidly find life-threatening injuriesand sources of bleeding, facilitating decision-makingfor other treatment options.
The notion that critical patients should be withheldtransfer to the imaging service has been challengedby evidence that demonstrates that this subset ofpatients receive the highest benefit of diagnosticimaging procedures. Experienced radiologists canquickly discern and deliver a primary report to exped-ite team decision making, including transfer of thepatient to the operating room, angiography room orICU [22]. The therapeutic DCRad (tDCRad) is based onhaving a rapidly available service (typically <60min).However, this is not yet possible in the main obstetriccare centers in many countries. Minimally invasivetechniques such as balloon arterial occlusion, occlusiveembolization and vascular stents are feasible in thecontext of tDCRad and have become important toolsin treating obstetric complications, including pelvic
THE JOURNAL OF MATERNAL-FETAL & NEONATAL MEDICINE 11

arterial hemorrhage with a difficult surgical approachand vaginal and perineal trauma [22].
Impact on maternal mortality for majorobstetric hemorrhage
DCS has proven to be applicable in the context ofobstetric hemorrhage, with successful results in thecontrol of refractory obstetric hemorrhage and anoverall decreased mortality of patients in severely crit-ical conditions. This is especially true in those patientsin whom the use of conventional measurements isassociated with a high probability of failure. In a studypublished by Escobar et al. [2], currently the largestregistry of DCS in obstetrics, an adequate control ofhemostasis was achieved in 60% of the cases in thefirst surgical intervention, with subsequent control ofhemorrhage in 98% of the cases. The study alsoshowed a reduction in the expected mortality (ApacheII score average of 14) from 40 to 7%. We considerthat this strategy should be implemented in the man-agement algorithms of major obstetric hemorrhage. Itis paramount for obstetrician and gynecologists tofamiliarize themselves in depth with this approach,the technique, and indications. We emphasize thatproper training in the concept of DCS must be wide-spread, because it is an available technique to managesevere PPH in obstetric patients with severe and life-threatening conditions.
Disclosure statement
No potential conflict of interest was reported bythe author(s).
References
[1] American College of Obstetricians & Gynecologists.ACOG Practice Bulletin: Clinical ManagementGuidelines for Obstetrician-Gynecologists Number 76,October 2006: postpartum hemorrhage. ObstetGynecol. 2006;108(4):1039–1047.
[2] Ord�o~nez CA, Garcia AF, Nieto AJ, et al. Damage con-trol surgery for the management of major obstetrichemorrhage: experience from the Fundaci�on Valle DelLili, Cali, Colombia. Panam J Trauma Crit Care EmergSurg. 2017;6(1):1–7.
[3] Pacheco LD, Saade GR, Gei AF, et al. Cutting-edgeadvances in the medical management of obstetricalhemorrhage. Am J Obstet Gynecol. 2011;205(6):526–532.
[4] Hellstern P, Haubelt H. Indications for plasma in mas-sive transfusion. Thromb Res. 2002;107(Suppl 1):S19–S22.
[5] Braslow B. Damage control in abdominal trauma.Contemp Surg. 2006;62:65–74.
[6] Ghourab S, Al-Nuaim L, Al-Jabari A, et al. Abdomino-pelvic packing to control severe haemorrhage follow-ing caesarean hysterectomy. J Obstet Gynaecol. 1999;19(2):155–158.
[7] Ordo~nez C, Pino L, Badiel M, et al. The 1-2-3 approachto abdominal packing. World J Surg. 2012;36(12):2761–2766.
[8] Clark SL. Strategies for reducing maternal mortality.Semin Perinatol. 2012;36(1):42–47.
[9] Clark SL, Hankins GD. Preventing maternal death: 10clinical diamonds. Obstet Gynecol. 2012;119(2, Part 1):360–364.
[10] Bogert JN, Harvin JA, Cotton BA. Damage controlresuscitation. J Intensive Care Med. 2016;31(3):177–186.
[11] Hirshberg A, Sheffer N, Barnea O. Computer simula-tion of hypothermia during “damage control” laparot-omy. World J Surg. 1999;23(9):960–965.
Figure 2. Evolution and extension of the concept of damage-control.
12 J. A. CARVAJAL ET AL.

[12] Reed RL, 2nd, Bracey AW, Jr, Hudson JD, et al.Hypothermia and blood coagulation: dissociationbetween enzyme activity and clotting factor levels.Circ Shock. 1990;32(2):141–152.
[13] Martini WZ, Pusateri AE, Uscilowicz JM, et al.Independent contributions of hypothermia and acid-osis to coagulopathy in swine. J Trauma. 2005;58(5):1002–1010.
[14] Ho AM, Karmakar MK, Dion PW. Are we givingenough coagulation factors during major traumaresuscitation? Am J Surg. 2005;190(3):479–484.
[15] Levy B. Lactate and shock state: the metabolic view.Curr Opin Crit Care. 2006;12(4):315–321.
[16] Kimmoun A, Novy E, Auchet T, et al. Hemodynamicconsequences of severe lactic acidosis in shock states:from bench to bedside. Crit Care. 2015;19(1):175.
[17] Pacheco LD, Saade GR, Costantine MM, et al. Anupdate on the use of massive transfusion protocols inobstetrics. Am J Obstet Gynecol. 2016;214(3):340–344.
[18] Kushimoto S, Kudo D, Kawazoe Y. Acute traumaticcoagulopathy and trauma induced coagulopathy: anoverview. J Intensive Care. 2017;5(1):1–7.
[19] Davenport R. Pathogenesis of acute traumatic coagul-opathy. Transfusion. 2013;53(Suppl 1):23S–27S.
[20] Brohi K, Cohen MJ, Ganter MT, et al. Acute traumaticcoagulopathy: initiated by hypoperfusion: modulatedthrough the protein C pathway? Ann Surg. 2007;245(5):812–818.
[21] Brohi K. Diagnosis and management of coagulopathyafter major trauma. Br J Surg. 2009;96(9):963–964.
[22] West N, Dawes R. Trauma resuscitation and the dam-age control approach. Surgery (Oxford). 2018;36(8):409–416.
[23] Leduc D, Senikas V, Lalonde AB, et al. Active manage-ment of the third stage of labour: prevention andtreatment of postpartum hemorrhage. J ObstetGynaecol Can. 2009;31(10):980–993.
[24] Committee on Practice Bulletins – Obstetrics. PracticeBulletin No. 183: Postpartum hemorrhage. ObstetGynecol. 2017;130(4):e168–e186.
[25] Sohn CH, Kim WY, Kim SR, et al. An increase in initialshock index is associated with the requirement formassive transfusion in emergency departmentpatients with primary postpartum hemorrhage. Shock.2013;40(2):101–105.
[26] Pacagnella RC, Souza JP, Durocher J, et al. A system-atic review of the relationship between blood lossand clinical signs. PLoS One. 2013;8(3):e57594.
[27] Nathan HL, Seed PT, Hezelgrave NL, et al. Shock indexthresholds to predict adverse outcomes in maternalhemorrhage and sepsis: a prospective cohort study.Acta Obstet Gynecol Scand. 2019;98(9):1178–1186.
[28] Kohn JR, Dildy GA, Eppes CS. Shock index and delta-shock index are superior to existing maternal earlywarning criteria to identify postpartum hemorrhageand need for intervention. J Matern Fetal NeonatalMed. 2019;32(8):1238–1244.
[29] FIGO Safe Motherhood and Newborn HealthCommittee, International Federation of Gynecologyand Obstetrics. Non-pneumatic anti-shock garment tostabilize women with hypovolemic shock secondary
to obstetric hemorrhage. Int J Gynecol Obstet. 2015;128(3):194–195.
[30] Watson HL, Downe S. Discrimination against child-bearing Romani women in maternity care in Europe:a mixed-methods systematic review. Reprod Health.2017;14(1):1.
[31] Miller S, Martin HB, Morris JL. Anti-shock garment inpostpartum haemorrhage. Best Pract Res Clin ObstetGynaecol. 2008; 22(6):1057–1074.
[32] Ordo~nez CA, Manzano-Nunez R, Parra MW, et al.Prophylactic use of resuscitative endovascular balloonocclusion of the aorta in women with abnormal pla-centation: a systematic review, meta-analysis, andcase series. J Trauma Acute Care Surg. 2018;84(5):809–818.
[33] Morrison JJ, Galgon RE, Jansen JO, et al. A systematicreview of the use of resuscitative endovascular bal-loon occlusion of the aorta in the management ofhemorrhagic shock. J Trauma Acute Care Surg. 2016;80(2):324–334.
[34] Gillissen A, van den Akker T, Caram-Deelder C, et al.Association between fluid management and dilutionalcoagulopathy in severe postpartum haemorrhage: anationwide retrospective cohort study. BMC PregChildbirth. 2018;18(1):398.
[35] Henriquez D, Bloemenkamp KWM, Loeff RM, et al.Fluid resuscitation during persistent postpartumhaemorrhage and maternal outcome: A nationwidecohort study. Eur J Obstet Gynecol Reprod Biol. 2019;235:49–56.
[36] Holcomb JB, Tilley BC, Baraniuk S, et al. Transfusion ofplasma, platelets, and red blood cells in a 1:1:1 vs a1:1:2 ratio and mortality in patients with severetrauma: the PROPPR randomized clinical trial. JAMA.2015;313(5):471–482.
[37] Nyfløt LT, Stray-Pedersen B, Fors�en L, et al. Durationof labor and the risk of severe postpartum hemor-rhage: a case-control study. PLoS One. 2017;12(4):e0175306.
[38] Seligman K, Ramachandran B, Hegde P, et al.Obstetric interventions and maternal morbidityamong women who experience severe postpartumhemorrhage during cesarean delivery. Int J ObstetAnesth. 2017;31:27–36.
[39] Edwards HM. Aetiology and treatment of severe post-partum haemorrhage. Dan Med J. 2018;65(3):1–20.
[40] Pacheco LD, Saade GR, Costantine MM, et al. The roleof massive transfusion protocols in obstetrics. Am JPerinatol. 2013;30(1):1–4.
[41] Holcomb JB, del Junco DJ, Fox EE, et al. The prospect-ive, observational, multicenter, major trauma transfu-sion (PROMMTT) study: comparative effectiveness of atime-varying treatment with competing risks. JAMASurg. 2013;148(2):127–136.
[42] Pacheco LD, Saade GR, Hankins G. Medical manage-ment of postpartum hemorrhage: an update. SeminPerinatol. 2019;43(1):22–26.
[43] Clark SL. Obstetric hemorrhage. Semin Perinatol.2016;40(2):109–111.
[44] Roberts I, Shakur H, Coats T, et al. The CRASH-2 trial:a randomised controlled trial and economic evalu-ation of the effects of tranexamic acid on death,
THE JOURNAL OF MATERNAL-FETAL & NEONATAL MEDICINE 13

vascular occlusive events and transfusion requirementin bleeding trauma patients. Health Technol Assess.2013;17(10):1–79.
[45] Pacheco LD, Hankins GDV, Saad AF, et al. Tranexamicacid for the management of obstetric hemorrhage.Obstet Gynecol. 2017;130(4):765–769.
[46] Shakur H, Elbourne D, G€ulmezoglu M, et al. TheWOMAN Trial. (World Maternal antifibrinolytic Trial):tranexamic acid for the treatment of postpartumhaemorrhage: an international randomised, doubleblind placebo controlled trial. Trials. 2010;11(1):1–14.
[47] Wikkelsø A, Wetterslev J, Møller AM, et al.Thromboelastography (TEG) or rotational thromboe-lastometry (ROTEM) to monitor haemostatic treatmentin bleeding patients: a systematic review with meta-analysis and trial sequential analysis. Anaesthesia.2017;72(4):519–531.
[48] Snegovskikh D, Souza D, Walton Z, et al. Point-of-careviscoelastic testing improves the outcome of preg-nancies complicated by severe postpartum hemor-rhage. J Clin Anesth. 2018;44:50–56.
[49] Pacheco LD, Lozada MJ, Saade GR, et al. Damage-con-trol surgery for obstetric hemorrhage. Obstet Gynecol.2018;132(2):423–427.
[50] Duchesne JC, Islam TM, Stuke L, et al. Hemostaticresuscitation during surgery improves survival inpatients with traumatic-induced coagulopathy. JTrauma. 2009;67(1):33–37. discussion 37–39.
[51] Gungor T, Simsek A, Ozdemir AO, et al. Surgical treat-ment of intractable postpartum hemorrhage andchanging trends in modern obstetric perspective.Arch Gynecol Obstet. 2009;280(3):351–355.
[52] Mukherjee S, Arulkumaran S. Post-partum haemor-rhage. Obstet Gynaecol Reprod Med. 2009;19(5):121–126.
[53] Zhang Y, Yan J, Han Q, et al. Emergency obstetrichysterectomy for life-threatening postpartum hemor-rhage: a 12-year review. Medicine (Baltimore). 2017;96(45):e8443.
[54] Waibel BH, Rotondo MF. Damage control in traumaand abdominal sepsis. Crit Care Med. 2010;38(9Suppl):S421–S430.
[55] Dildy GA, Scott JR, Saffer CS, et al. An effective pres-sure pack for severe pelvic hemorrhage. ObstetGynecol. 2006;108(5):1222–1226.
[56] Escobar MF, Garc�ıa AF, Fonseca J, et al. Cirug�ıa decontrol de da~nos: un concepto aplicable enginecolog�ıa y obstetricia. Colomb Med. 2005;36:110–114.
[57] Barker DE, Kaufman HJ, Smith LA, et al. Vacuum packtechnique of temporary abdominal closure: a 7-yearexperience with 112 patients. J Trauma. 2000;48(2):201–206. discussion 206–207.
[58] Goldberg SR, Anand RJ, Como JJ, et al. Prophylacticantibiotic use in penetrating abdominal trauma: anEastern Association for the Surgery of Trauma prac-tice management guideline. J Trauma Acute CareSurg. 2012;73(5 Suppl 4):S321–S325.
[59] Godat L, Kobayashi L, Costantini T, et al. Abdominaldamage control surgery and reconstruction: worldsociety of emergency surgery position paper. World JEmerg Surg. 2013;8(1):53.
[60] Griggs C, Butler K. Damage control and the openabdomen: challenges for the nonsurgical intensivist. JIntensive Care Med. 2016;31(9):567–576.
[61] Burlew CC. The open abdomen: practical implicationsfor the practicing surgeon. Am J Surg. 2012;204(6):826–835.
[62] Kirkpatrick AW, Roberts DJ, De Waele J, et al. Intra-abdominal hypertension and the abdominal compart-ment syndrome: updated consensus definitions andclinical practice guidelines from the World Society ofthe Abdominal Compartment Syndrome. IntensiveCare Med. 2013;39(7):1190–1206.
[63] Malgras B, Prunet B, Lesaffre X, et al. Damage control:concept and implementation. J Visc Surg. 2017;154(Suppl 1):S19–S29.
14 J. A. CARVAJAL ET AL.