2014 Obstetrics and Gynecology Update: - Continuing ...
414
The Department of Obstetrics, Gynecology, and Reproductive Sciences University of California, San Francisco School of Medicine presents 2014 Obstetrics and Gynecology Update: What Does the Evidence Tell Us? October 22-24, 2014 Hilton Financial District San Francisco, California Course Chair Amy (Meg) Autry, MD of California, San Francisco University of California, San Francisco School of Medicine
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of 2014 Obstetrics and Gynecology Update: - Continuing ...

The Department of Obstetrics, Gynecology, and Reproductive Sciences
University of California, San Francisco School of Medicine presents
2014 Obstetrics and Gynecology Update:
What Does the Evidence Tell Us?
October 22-24, 2014 Hilton Financial District
San Francisco, California
Course Chair Amy (Meg) Autry, MD
of California, San Francisco
University of California, San Francisco School of Medicine

Acknowledgement of Commercial Support
This CME activity was supported in part by educational grants from the following:
Cook Medical
Ethicon Endo-Surgery

Exhibitors
Abbvie
Applied Medical
Bayer HealthCare
Boston Scientific
ETHICON
Hologic, Inc.
Mallinckrodt Pharmaceuticals
Merck & Co.
Progenity
Sanofi BioSurgery
Stemcyte
TEVA Women’s Health

University of California, San Francisco School of Medicine Presents
2014 Obstetrics and Gynecology Update: What Does The Evidence Tell Us?
EDUCATIONAL OBJECTIVES An attendee completing this course will be competent to:
Apply aneuploidy screening in practice; Summarize the radiologic diagnostic criteria for failed intrauterine pregnancy; Utilize the new hypertension and pregnancy guidelines in the management of
patients; Use screening guidelines for cervical cancer, STD treatment; Utilize the Quality Family Guidelines to counsel complex patients on
contraception; Appropriately counsel patients regarding uterine morcellation, vaginal mesh, and
mammography; Describe methods to prevent HIV transmission in discordant couples; Discuss unique aspects of care for transgendered patients.
ACCREDITATION
The University of California, San Francisco School of Medicine (UCSF) is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. UCSF designates this educational activity for a maximum of 23.00 AMA PRA Category 1 Credits™. Physicians should only claim credit commensurate with the extent of their participation in the activity. This CME activity meets the requirements under California Assembly Bill 1195, continuing education and cultural and linguistic competency. The cases used in this course are presented for teaching purposes only. Please observe patient confidentiality. This presentation may be protected under Evidence Code 1156, 1157. This Live activity, Obstetrics and Gynecology Update, with a beginning date of October 31, 2012, has been reviewed and is acceptable for up to 22.75 Prescribed credits by the American Academy of Family Physicians. Physicians should claim only the credit commensurate with the extent of their participation in the activity.

General Information Attendance Verification / CME Certificates Please remember to sign-in on the sign-in sheet on your first day. You only have to sign-in once for the course, when you first check in. After the meeting, please visit this website to complete the online course evaluation: http://www.ucsfcme.com/evaluation Upon completing the online evaluation, your CME certificate will be automatically generated and emailed to you.
Evaluation Your opinion is important to us – we do listen! We have two evaluations for this meeting. The speaker evaluation is the bright yellow hand-out you received when you checked in. Please complete this during the meeting and turn it in to the registration staff at the end of the conference. The overall conference evaluation is online at: http://www.ucsfcme.com/evaluation We request you complete this evaluation within 30 days of the conference in order to receive your CME certificate.
Security We urge caution with regard to your personal belongings and syllabus books. We are unable to replace these in the event of loss. Please do not leave any personal belongings unattended in the meeting room during lunch or breaks or overnight.
Exhibits Industry exhibits are located outside the general session room during breakfasts and coffee breaks.
Lunches Lunches are on your own. A list of nearby options is available at the conference registration desk.
Final Presentations PDF versions of the final presentations will be posted on the course slides website approximately 2-3 weeks post course. Only presentations that have been authorized by the presenter will be included. http://www.ucsfcme.com/2015/MOB15001/slides.html

Federal and State Law Regarding Linguistic Access and Services for Limited English Proficient Persons
I. Purpose. This document is intended to satisfy the requirements set forth in California Business and Professions code 2190.1. California law requires physicians to obtain training in cultural and linguistic competency as part of their continuing medical education programs. This document and the attachments are intended to provide physicians with an overview of federal and state laws regarding linguistic access and services for limited English proficient (“LEP”) persons. Other federal and state laws not reviewed below also may govern the manner in which physicians and healthcare providers render services for disabled, hearing impaired or other protected categories
II. Federal Law – Federal Civil Rights Act of 1964, Executive Order 13166,
August 11, 2000, and Department of Health and Human Services (“HHS”) Regulations and LEP Guidance.
The Federal Civil Rights Act of 1964, as amended, and HHS regulations require recipients of federal financial assistance (“Recipients”) to take reasonable steps to ensure that LEP persons have meaningful access to federally funded programs and services. Failure to provide LEP individuals with access to federally funded programs and services may constitute national origin discrimination, which may be remedied by federal agency enforcement action. Recipients may include physicians, hospitals, universities and academic medical centers who receive grants, training, equipment, surplus property and other assistance from the federal government. HHS recently issued revised guidance documents for Recipients to ensure that they understand their obligations to provide language assistance services to LEP persons. A copy of HHS’s summary document entitled “Guidance for Federal Financial Assistance Recipients Regarding Title VI and the Prohibition Against National Origin Discrimination Affecting Limited English Proficient Persons – Summary” is available at HHS’s website at: http://www.hhs.gov/ocr/lep/ . As noted above, Recipients generally must provide meaningful access to their programs and services for LEP persons. The rule, however, is a flexible one and HHS recognizes that “reasonable steps” may differ depending on the Recipient’s size and scope of services. HHS advised that Recipients, in designing an LEP program, should conduct an individualized assessment balancing four factors, including: (i) the number or proportion of LEP persons eligible to be served or likely to be encountered by the Recipient; (ii) the frequency with which LEP individuals come into contact with the Recipient’s program; (iii) the nature and importance of the program, activity or service provided by the Recipient to its beneficiaries; and (iv) the resources available to the Recipient and the costs of interpreting and translation services. Based on the Recipient’s analysis, the Recipient should then design an LEP plan based on five recommended steps, including: (i) identifying LEP individuals who may need assistance; (ii) identifying language assistance measures; (iii) training staff; (iv) providing notice to LEP persons; and (v) monitoring and updating the LEP plan. A Recipient’s LEP plan likely will include translating vital documents and providing either on-site interpreters or telephone interpreter services, or using shared interpreting services with other Recipients. Recipients may take other reasonable steps depending

on the emergent or non-emergent needs of the LEP individual, such as hiring bilingual staff who are competent in the skills required for medical translation, hiring staff interpreters, or contracting with outside public or private agencies that provide interpreter services.
HHS’s guidance provides detailed examples of the mix of services that a Recipient should consider and implement. HHS’s guidance also establishes a “safe harbor” that Recipients may elect to follow when determining whether vital documents must be translated into other languages. Compliance with the safe harbor will be strong evidence that the Recipient has satisfied its written translation obligations.
In addition to reviewing HHS guidance documents, Recipients may contact HHS’s Office for Civil Rights for technical assistance in establishing a reasonable LEP plan.
III. California Law – Dymally-Alatorre Bilingual Services Act. The California legislature enacted the California’s Dymally-Alatorre Bilingual Services Act (Govt. Code 7290 et seq.) in order to ensure that California residents would appropriately receive services from public agencies regardless of the person’s English language skills. California Government Code section 7291 recites this legislative intent as follows:
“The Legislature hereby finds and declares that the effective maintenance and development of a free and democratic society depends on the right and ability of its citizens and residents to communicate with their government and the right and ability of the government to communicate with them.
The Legislature further finds and declares that substantial numbers of persons who live, work and pay taxes in this state are unable, either because they do not speak or write English at all, or because their primary language is other than English, effectively to communicate with their government. The Legislature further finds and declares that state and local agency employees frequently are unable to communicate with persons requiring their services because of this language barrier. As a consequence, substantial numbers of persons presently are being denied rights and benefits to which they would otherwise be entitled.
It is the intention of the Legislature in enacting this chapter to provide for effective communication between all levels of government in this state and the people of this state who are precluded from utilizing public services because of language barriers.”
The Act generally requires state and local public agencies to provide interpreter and written document translation services in a manner that will ensure that LEP individuals have access to important government services. Agencies may employ bilingual staff, and translate documents into additional languages representing the clientele served by the agency. Public agencies also must conduct a needs assessment survey every two years documenting the items listed in Government Code section 7299.4, and develop an implementation plan every year that documents compliance with the Act. You may access a copy of this law at the following url: http://www.spb.ca.gov/bilingual/dymallyact.htm
Course Chair
Amy (Meg) Autry, MD Clinical Professor and Residency Director, Department of Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco
Course Faculty
Priscilla Abercrombie, RN, NP, PhD Health Sciences Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences University of California, San Francisco Yair J. Blumenfeld, MD Clinical Assistant Professor of Obstetrics and Gynecology, Stanford University, Stanford, CA Ami Burnham, LM, RN, IBCLC Licensed Midwife, Rites of Passage Midwifery and Lactation Consulting, San Francisco, CA Marcelle I. Cedars, MD Professor of Obstetrics, Gynecology and Reproductive Sciences Director, Division of Reproductive Endocrinology University of California, San Francisco Lee-may Chen, MD Professor of Obstetrics, Gynecology and Reproductive Sciences Edward C. Hill, MD Endowed Chair in Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Mindy Goldman, MD Professor of Obstetrics, Gynecology, and Reproductive Sciences Director, Women’s Cancer Care Program, UCSF Women’s Health and Carol Franc Buck Breast Care Center University of California, San Francisco
Juan M. González, MD, MS, FACOG Assistant Professor of Obstetrics, Gynecology, and Reproductive Sciences University of California, San Francisco Megan Huchko, MD, MPH Assistant Professor of Obstetrics, Gynecology, and Reproductive Sciences University of California, San Francisco Alison F. Jacoby, MD Professor of Obstetrics, Gynecology and Reproductive Sciences; Director, UCSF Comprehensive Fibroid Center University of California, San Francisco Vanessa Jacoby, MD, MAS Assistant Professor of Obstetrics, Gynecology and Reproductive Sciences University of California San Francisco Karla Kerlikowske, MD Professor, Departments of Medicine and Epidemiology/Biostatistics University of California San Francisco Jennifer Kerns, MD, MPH Assistant Professor of Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Robyn A. Lamar, MD, MPH Clinical Instructor, Department of Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Jennifer M. Lucero, MD Assistant Professor of Clinical Anesthesia University of California, San Francisco

Christopher Moriates, MD Assistant Professor of Medicine, Division of Hospital Medicine University of California, San Francisco Michelle Y. Morrill, MD Director of Urogynecology; TPMG Chief of Urogynecology, Kaiser Permanente, San Francisco, CA Mary E. Norton, MD Professor of Obstetrics, Gynecology and Reproductive Sciences, and of Pediatrics University of California, San Francisco Michael S. Policar, MD, MPH Professor of Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Medical Director, UCSF/ Family PACT Program Support and Evaluation, CA Office of Family Planning, Sacramento, CA Mark D. Rollins, MD, PhD Associate Professor Director, Obstetric & Fetal Anesthesia, Department of Anesthesia & Perioperative Care University of California, San Francisco Tami Rowen, MD, MS Clinical Instructor, Department of Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Kirsten Salmeen, MD Assistant Professor of Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco George F. Sawaya, MD Professor of Obstetrics, Gynecology and Reproductive Sciences and of Epidemiology and Biostatistics University of California, San Francisco Karen Smith-McCune, MD, PhD Professor of Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco
Lori M. Strachowski, MD Clinical Professor of Radiology and Biomedical Imaging; Adjunct Professor, Department of Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Stefanie Ueda, MD Assistant Professor of Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Erica Weiss, MD Northern California OB/GYN Lead, Transgender Health, Kaiser Permanente, San Francisco, CA Sara Whetstone, MD, MHS Clinical Instructor, Department of Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Sarah Wilson, MD, MEd Assistant Professor of Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Marya G. Zlatnik, MD, MMS Professor of Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco

Disclosures The following faculty speakers, moderators and planning committee members have disclosed NO financial interest/arrangement or affiliation with any commercial companies who have provided products or services relating to their presentation(s) or commercial support for this continuing medical education activity:
Amy (Meg) Autry, MD Priscilla Abercrombie, RN, NP, PhD Yair J. Blumenfeld, MD Ami Burnham, LM, RN, IBCLC Mindy Goldman, MD, MPH Juan M. González, MD, MS, FACOG Megan Huchko, MD, MPH Alison F. Jacoby, MD Karla Kerlikowske, MD Jennifer Kerns, MD, MPH Robyn A. Lamar, MD, MPH Jennifer M. Lucero, MD
Christopher Moriates, MD
Michelle Y. Morrill, MD Michael S. Policar, MD, MPH Mark D. Rollins, MD, PhD Tami Rowen, MD, MS Kirsten Salmeen, MD George F. Sawaya, MD Karen Smith-McCune, MD, PhD Lori M. Strachowski, MD Stefanie Ueda, MD Erica Weiss, MD Sara Whetstone, MD, MHS Sarah Wilson, MD, MEd Marya G. Zlatnik, MD, MMS
The following faculty speakers have disclosed a financial interest/arrangement or affiliation with a commercial company who has provided products or services relating to their presentation(s) or commercial support for this continuing medical education activity. All conflicts of interest have been resolved in accordance with the ACCME Standards for Commercial Support:
Marcelle I. Cedars, MD Research Support Ferring Pharmaceuticals Lee-may Chen, MD Moderated Advisory Board Genentech Meeting Vanessa Jacoby, MD Grant Support Halt Medical Mary E. Norton, MD Grant/Research Support Ariosa Diagnostics Grant/Research Support Natera This UCSF CME educational activity was planned and developed to: uphold academic standards to ensure balance, independence, objectivity, and scientific rigor; adhere to requirements to protect health information under the Health Insurance Portability and Accountability Act of 1996 (HIPAA); and, include a mechanism to inform learners when unapproved or unlabeled uses of therapeutic products or agents are discussed or referenced. This activity has been reviewed and approved by members of the UCSF CME Governing Board in accordance with UCSF CME accreditation policies. Office of CME staff, planners, reviewers, and all others in control of content have disclosed no relevant financial relationship.

UCSF Obstetrics and Gynecology Update: What Does the Evidence Tell Us?
October 22 – 24, 2014 COURSE AGENDA
Wednesday, October 22, 2014
7:00- 7:45 am Registration / Continental Breakfast 7:45- 8:00 Welcome and Opening Statements Dr. Amy (Meg) Autry 8:00- 8:35 What’s New in Aneuploidy Screening Dr. Mary E. Norton 8:35- 8:45 Q & A 8:45- 9:20 New Recommendations for Diagnosing Failed Intrauterine Dr. Lori M. Strachowski Pregnancy 9:20- 9:30 Q & A 9:30- 10:05 Tips, Tricks, and Controversies in Laparoscopic Hysterectomy Dr. Alison F. Jacoby 10:05- 10:15 Q & A 10:15- 10:30 Coffee Break 10:30- 11:05 Mesh Erosion and What to Do Dr. Michelle Y. Morrill 11:05- 11:15 Q & A 11:15- 11:50 New Treatments for Fibroids Dr. Vanessa Jacoby 11:50- 12:00 Q & A 12:00- 1:15 pm Lunch On Own 1:15- 1:50 Updates on Cervical Cancer Screening Dr. George F. Sawaya 1:50- 2:00 Q & A 2:00- 2:35 Treatment of CIN Dr. Karen Smith-McCune 2:35- 2:45 Q & A 2:45- 3:00 Coffee Break 3:00- 3:35 The 2014 CDC Quality Family Planning Services Guideline Dr. Michael S. Policar 3:35- 3:45 Q & A 3:45- 4:20 Complicated Contraception Dr. Jennifer Kerns 4:20- 4:30 Q & A 4:30- 5:05 PreP Guidelines Dr. Megan Huchko 5:05- 5:15 Q & A 5:15 pm Adjourn

UCSF Obstetrics and Gynecology Update: What Does the Evidence Tell Us?
October 22 – 24, 2014 COURSE AGENDA
Thursday, October 23, 2014 7:30- 8:00 am Continental Breakfast 8:00- 8:35 The New HTN Guidelines Dr. Yair J. Blumenfeld 8:35- 8:45 Q & A 8:45- 9:20 Diagnosis and Management of Diabetes in Pregnancy Dr. Kirsten Salmeen 9:20- 9:30 Q & A 9:30- 10:05 Chorioamnionitis: What is the Evidence for Clinical Management? Dr. Juan M. Gonzalez 10:05- 10:15 Q & A 10:15-10:30 Coffee Break 10:30- 11:05 Reducing OB Surgical Site Infections: A Successful Program Dr. Marya G. Zlatnik 11:05- 11:15 Q & A 11:15- 11:50 Evidence-Based Antenatal Testing Dr. Robyn A. Lamar 11:50- 12:00 Q & A 12:00- 1:15 pm Lunch On Own 1:15- 1:50 Induction of Labor Dr. Sarah Wilson 1:50- 2:00 Q & A 2:00- 2:35 Pain Management Options for Laboring Patients Dr. Jennifer M. Lucero 2:35- 2:45 Q & A 2:45- 3:20 CPR/ACLS: Obstetric Considerations and Current Guidelines Dr. Mark D. Rollins 3:20- 3:30 Q & A 3:30- 3:45 Coffee Break 3:45- 4:20 Overcoming Obstacles: Breastfeeding Success and Ami Burnham, LM, RN, IBCLC Baby-Friendly Hospitals 4:20- 4:30 Q & A 4:30- 5:05 Striving to Provide the Best Care at Lower Costs Dr. Christopher Moriates 5:05- 5:15 Q & A 5:15pm Adjourn

UCSF Obstetrics and Gynecology Update: What Does the Evidence Tell Us?
October 22 – 24, 2014 COURSE AGENDA
Friday, October 24, 2014 7:30- 8:00 am Continental Breakfast 8:00- 8:45 Hormone Replacement Dr. Marcelle I. Cedars 8:45- 8:55 Q & A 8:55- 9:30 Polycystic Ovary Syndrome Dr. Marcelle I. Cedars 9:30- 9:40 Q & A 9:40- 10:15 Sexual Dysfunction Dr. Tami Rowen 10:15- 10:25 Q & A 10:25- 10:40 Coffee Break 10:40- 11:15 Racial and Ethnic Disparities in Ob/Gyn Dr. Sara Whetstone 11:15- 11:25 Q & A 11:25- 12:00 pm Controversies in Breast Cancer Screening Dr. Karla Kerlikowske 12:00- 12:10 Q & A 12:10- 1:15 Lunch On Own
1:15- 1:50 Gynecologic Cancer Genetics Dr. Lee-may Chen 1:50- 2:00 Q & A 2:00- 2:35 Approach to the Adnexal Mass Dr. Stefanie Ueda 2:35- 2:45 Q & A 2:45- 3:00 Coffee Break 3:00- 3:35 Transgender Health for the Gynecologist Dr. Erica Weiss 3:35- 3:45 Q & A 3:45- 4:20 Integrative Approaches to the Management of Chronic Dr. Priscilla Abercrombie Pelvic Pain 4:20- 4:30 Q & A 4:30- 5:05 Gynecologic Care for Breast Cancer Survivors Dr. Mindy Goldman 5:05- 5:15 Q & A 5:15 pm Course Adjourns

10/22/2014
1
What’s New in Aneuploidy Screening?
Mary E Norton, MDProfessor of Obstetrics, Gynecology & Reproductive Sciences; UCSFOb Gyn Update, Oct 22, 2014
Disclosures
• Principal Investigator of ongoing clinical trial on cfDNA supported by Ariosa Diagnostics
• Unpaid clinical consultant for Natera• Research support from Natera• No personal financial involvement in any of the cfDNA companies
020406080
100120
Detection rate of prenatal screening for Down syndrome has
improved over time
Det
ectio
n R
ate
(%)
Hype cycle of new technology

10/22/2014
2
Hype cycle of new technologyOctober 2013
Hype cycle of new technology
October 2014
Cell free fetal DNA• Cell free fetal DNA (cffDNA) is made up of short segments of fetal DNA (<200 base pairs) that circulate in maternal plasma
• Although called “fetal”, the origin of these fragments is primarily placenta
Maternal DNA
Fetal DNA
Cell free DNA results from apoptosis

10/22/2014
3
Noninvasive Prenatal Testing (NIPT)
• Detection requires accurate quantification of DNA from a specific chromosome
• Somewhat different methods are utilized by different laboratories
Analysis of fetal DNA
Zhong, X, Holzgreve, W, Glob. libr. women's med 2009
Wts (%)
10099.1 (98.3 - 99.6)2.594.4 (72.7 - 100)1.2100 (63.1 - 100)3.5100 (86.3 - 100)4.1100 (88.4 - 100)1.6100 (71.5 - 100)4.9100 (90.3 - 100)11.0100 (95.6 - 100)1.2100 (63.1 - 100) 1.6100 (71.5 - 100)2.3100 (79.4 - 100)12.0100 (95.9 - 100)6.8100 (92.9 - 100)1.9100 (75.3 - 100)28.498.6 (95.9 - 99.7)5.3100 (91.0 - 100)
50 60 70 80 90100 DR % (95% CI) (%)
11.6100 (95.8 - 100)
Pooled analysis
Verweij et al., 2013 [18]Song et al., 2013 [8]
Nicolaides et al., 2013 [25]Guex et al., 2013 [30]
Zimmerman et al., 2012 [11]Sparks et al., 2012 [36]Norton et al., 2012 [81]
Nicolaides et al., 2012 [8]Lau et al., 2012 [11]
Jiang et al., 2012 [16]Bianchi et al., 2012 [89]Ashoor et al., 2012 [50]Sehnert et al., 2011 [13]
Palomaki et al., 2011 [212]Ehrich et al., 2011 [39]
Chiu et al., 2011 [86]Author DR (95% CI)
0 3 6 9 12 FPR % (95% CI) (%)
0.08 (0.03 - 0.17)
FPR (95% CI) Wts (%)
100
0.00 (0.0 - 0.7) 5.80.00 (0.0 - 0.2) 13.9
0.00 (0.0 - 1.8) 2.70.00 (0.0 - 2.5) 2.00.00 (0.0 - 2.7) 1.80.00 (0.0 - 2.8) 1.80.04 (0 - 0.2) 18.00.00 (0.0 - 0.2) 14.80.00 (0.0 - 3.7) 1.30.00 (0.0 - 0.4) 9.00.00 (0.0 - 0.9) 4.90.00 (0.0 - 1.1) 4.30.00 (0.0 - 10.3) 0.5
0.20 (0.0 - 0.6) 12.60.24 (0.0 - 1.4) 4.92.06 (0.4 - 5.9) 2.0
T21: n=733 11,475 non-T21
Trisomy 21 performance cfDNA testing: meta-analysis (Gil et al, Fetal Diagn Ther, 2014)
Wts (%)
10099.1 (98.3 - 99.6)
2.594.4 (72.7 - 100)1.2100 (63.1 - 100)3.5100 (86.3 - 100)4.1100 (88.4 - 100)1.6100 (71.5 - 100)4.9100 (90.3 - 100)11.0100 (95.6 - 100)1.2100 (63.1 - 100) 1.6100 (71.5 - 100)2.3100 (79.4 - 100)12.0100 (95.9 - 100)6.8100 (92.9 - 100)1.9100 (75.3 - 100)28.498.6 (95.9 - 99.7)5.3100 (91.0 - 100)
50 60 70 80 90100 DR % (95% CI) (%)
11.6100 (95.8 - 100)
Pooled analysis
Verweij et al., 2013 [18]Song et al., 2013 [8]
Nicolaides et al., 2013 [25]Guex et al., 2013 [30]
Zimmerman et al., 2012 [11]Sparks et al., 2012 [36]Norton et al., 2012 [81]
Nicolaides et al., 2012 [8]Lau et al., 2012 [11]
Jiang et al., 2012 [16]Bianchi et al., 2012 [89]Ashoor et al., 2012 [50]Sehnert et al., 2011 [13]
Palomaki et al., 2011 [212]Ehrich et al., 2011 [39]
Chiu et al., 2011 [86]Author DR (95% CI)
0 3 6 9 12 FPR % (95% CI) (%)
0.08 (0.03 - 0.17)
FPR (95% CI) Wts (%)
100
0.00 (0.0 - 0.7) 5.80.00 (0.0 - 0.2) 13.9
0.00 (0.0 - 1.8) 2.70.00 (0.0 - 2.5) 2.00.00 (0.0 - 2.7) 1.80.00 (0.0 - 2.8) 1.80.04 (0 - 0.2) 18.00.00 (0.0 - 0.2) 14.80.00 (0.0 - 3.7) 1.30.00 (0.0 - 0.4) 9.00.00 (0.0 - 0.9) 4.90.00 (0.0 - 1.1) 4.30.00 (0.0 - 10.3) 0.5
0.20 (0.0 - 0.6) 12.60.24 (0.0 - 1.4) 4.92.06 (0.4 - 5.9) 2.0
T21: n=733 11,475 non-T21
Trisomy 21 performance cfDNA testing: meta-analysis (Gil et al, Fetal Diagn Ther, 2014)
DR: 99.1% (98.3 - 99.6)

10/22/2014
4
Wts (%)
10099.1 (98.3 - 99.6)
2.594.4 (72.7 - 100)1.2100 (63.1 - 100)3.5100 (86.3 - 100)4.1100 (88.4 - 100)1.6100 (71.5 - 100)4.9100 (90.3 - 100)11.0100 (95.6 - 100)1.2100 (63.1 - 100) 1.6100 (71.5 - 100)2.3100 (79.4 - 100)12.0100 (95.9 - 100)6.8100 (92.9 - 100)1.9100 (75.3 - 100)28.498.6 (95.9 - 99.7)5.3100 (91.0 - 100)
50 60 70 80 90100 DR % (95% CI) (%)
11.6100 (95.8 - 100)
Pooled analysis
Verweij et al., 2013 [18]Song et al., 2013 [8]
Nicolaides et al., 2013 [25]Guex et al., 2013 [30]
Zimmerman et al., 2012 [11]Sparks et al., 2012 [36]Norton et al., 2012 [81]
Nicolaides et al., 2012 [8]Lau et al., 2012 [11]
Jiang et al., 2012 [16]Bianchi et al., 2012 [89]Ashoor et al., 2012 [50]Sehnert et al., 2011 [13]
Palomaki et al., 2011 [212]Ehrich et al., 2011 [39]
Chiu et al., 2011 [86]Author DR (95% CI)
0 3 6 9 12 FPR % (95% CI) (%)
0.08 (0.03 - 0.17)
FPR (95% CI) Wts (%)
100
0.00 (0.0 - 0.7) 5.80.00 (0.0 - 0.2) 13.9
0.00 (0.0 - 1.8) 2.70.00 (0.0 - 2.5) 2.00.00 (0.0 - 2.7) 1.80.00 (0.0 - 2.8) 1.80.04 (0 - 0.2) 18.00.00 (0.0 - 0.2) 14.80.00 (0.0 - 3.7) 1.30.00 (0.0 - 0.4) 9.00.00 (0.0 - 0.9) 4.90.00 (0.0 - 1.1) 4.30.00 (0.0 - 10.3) 0.5
0.20 (0.0 - 0.6) 12.60.24 (0.0 - 1.4) 4.92.06 (0.4 - 5.9) 2.0
T21: n=733 11,475 non-T21
Trisomy 21 performance cfDNA testing: meta-analysis (Gil et al, Fetal Diagn Ther, 2014)
DR: 99.1% (98.3 - 99.6) FPR: 0.08% (0.03 - 0.17)
Your patient has NIPT and results are positive for trisomy 21. What is the likelihood that the fetus actually has
Down syndrome?
G re a t
e r th a n
9 . . .
I t de p e
n d s o n
. . .
I a m n o
t s ur e .
58%
10%
32%1. Greater than 99%2. It depends on the patient’s age3. I am not sure.

10/22/2014
5
NIPT: Biologic ChallengesFalse positives:• Unrecognized or vanishing twin• Placental mosaicism• Low level maternal mosaicism, esp sex chromosomal• Maternal malignancyFalse negatives:• Low level of fetal DNA • Placental mosaicismFailed results: • Increased BMI• Low level of fetal DNA• Fetal aneuploidy
Does NIPT have risks?1. Some tests fail to provide a result
o These patients are at HIGH RISK of aneuploidyo Importance of “fetal fraction”
2. The PPV (chance that a positive is a TRUE POSITIVE) depends on maternal ageo This is often misunderstood
3. Not all abnormalities are detectableo Down syndrome comprises ~50% of aneuploidies
Fetal DNA Fraction Varies Fraction of Fetal DNA
Prenatal Diagnosis2012; 32(13) p 1233-41

10/22/2014
6
Fetal Fraction Ranges
0-4% 4-8% 8%+Fetal Fraction too
low to reportIntermediate fetal
fraction – decreased sensitivity
Fetal fraction adequate to achieve best performance
An aneuploid sample with a lower fetal fraction has a higher chance of resulting in a false negative result.
.
Published Trials of NIPT: failure rates
Trial Failure rate Detection False positive rate
Chiu et al (2011) 11/764 (1.4%) 86/86 3/146 Ehrich et al. (2011) 18/467 (3.8%) 39/39 1/410 Palomaki et al. (2011) 13/1696 (0.8%) 209/212 3/1471Bianchi et al. (2012) 30/532 (3.0%) 89/89 0/404Norton et al (2012) 148/3228 (4.6%) 81/81 1/2888Zimmermann et al (2012) 21/166 (12.6%) 11/11 0/145Pergament (2014) 85/1051 (8%) 58/58 905/905
All 241/6853 (4.1%) 482/485 (99.4%) 8/6224 (0.13%)
Fetal Fraction Fetal Fraction

10/22/2014
7
Fetal fraction of DNA and test failure
Up to 5% of samples do not provide a result
o Low fraction fetal DNA, failed sequencing, high variability in counts
o Some association with gestational age (<10 wks) o Low fetal fraction associated with maternal BMI
• 20% at >250 lbs• 50% at >350 lbs
� Low fetal fraction is associated with aneuploidy�Repeating test will provide a result in SOME cases
Fetal Fraction
Fetal Fraction Fetal Fraction

10/22/2014
8
NO….
Why is NIPT not diagnostic? Confined Placental Mosaicism (normal + trisomic cells) • THIS IS A PLACENTAL, AND NOT A FETAL TEST
False positive False negative
Normal
Trisomic
Other aneuploidies
Trisomy Detection Rate False Positive Rate
Trisomy 21 99% 0.1%Trisomy 18 97% 0.3%Trisomy 13 87% 0.6%Sex chromosomes
86% 0.6%
The performance of NIPT for other aneuploidies is NOT AS GOOD as for trisomy 21

10/22/2014
9
Wang et al, Genetics in Medicine, 2014
Aneuploidy No. of positives
No (%)confirmed
T21 41 38/41 (93%)T18 25 16/25 (64%)T13 16 7/16 (44%)45X 16 6/16 (38%)

10/22/2014
10
How Does Test Performance Differ with Risk? Low Risk (age 25; 1/1000) High Risk (age 38; 1/100)
N=1000
1 T21 999 not T21
1 TP, 0 FN 2 FP, 998 TN
OAPR = 1/3
N=1000
10 T21 990 not T21
10 TP, 0 FN 2 FP, 988 TN
OAPR = 10/12 or 5/6
(Assume >99% sensitivity and 99.8% specificity)
How Does Test Performance Differ with Risk? Low Risk (age 25; 1/8,000) High Risk (age 38; 1/1000)
N=10,000
1 T13 9,999 not T13
1 TP, 0 FN 100 FP, 9900 TN
OAPR = 1/100
N=10,000
10 T13 9,990 not T13
9 TP, 1 FN 100 FP, 9890 TN
OAPR = 9/100
(T13: Assume 99% sensitivity and 99% specificity)
• N=1914 women undergoing standard screening• Mean maternal age = 29.6 yrs• Primary outcome = false positive rates for T18 and T21
cfDNA vs Standard Screening
Bianchi et al, NEJM, 2014
FPR PPVcfDNA 0.3% 45.5% p<.001Standard 3.6% 4.2%
• Only 8 aneuploidy cases in the cohort (5: T21, 2: T18, and 1: T13)
• All were detected
10/22/2014
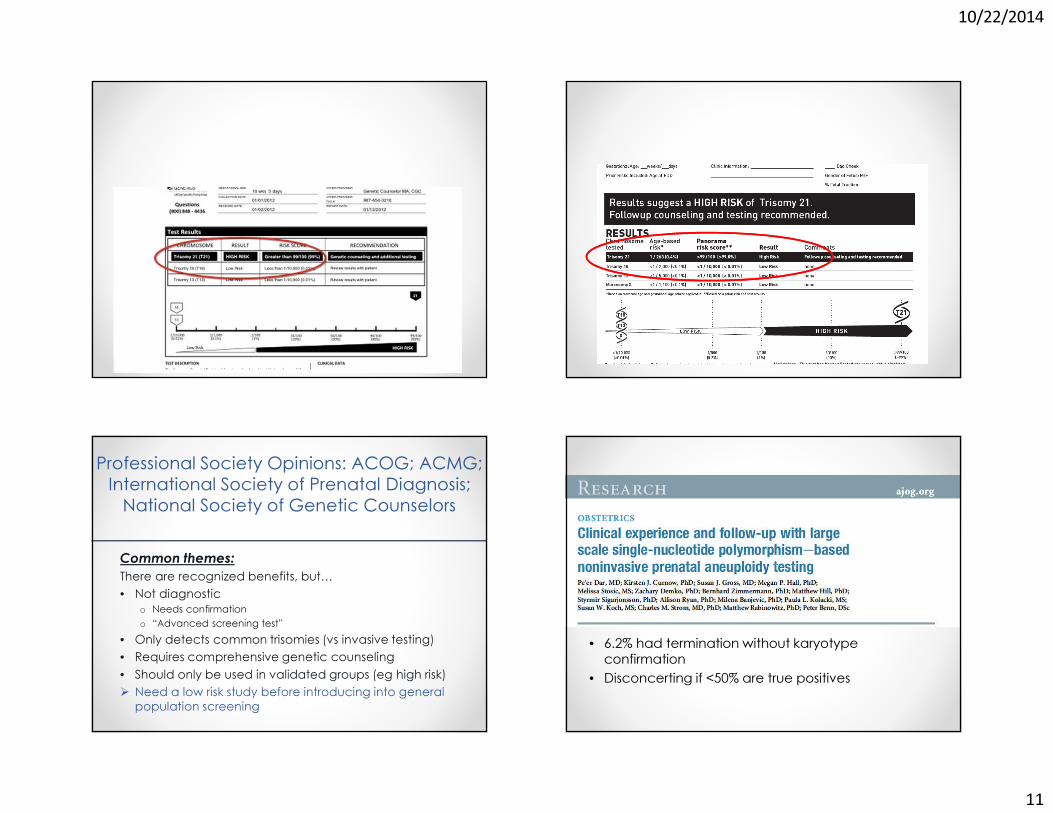
11
Professional Society Opinions: ACOG; ACMG; International Society of Prenatal Diagnosis; National Society of Genetic Counselors
Common themes:There are recognized benefits, but…• Not diagnostic
o Needs confirmationo “Advanced screening test”
• Only detects common trisomies (vs invasive testing)• Requires comprehensive genetic counseling• Should only be used in validated groups (eg high risk)� Need a low risk study before introducing into general
population screening
• 6.2% had termination without karyotype confirmation
• Disconcerting if <50% are true positives

10/22/2014
12
Consequences of false positive results
N=100,000 1% false positives
1000 abnormal results6.2% TAB w/o confirmation
62 TAB
28 TP 34FP
34 TAB of normal fetuses
NIPT
45% PPV
Consequences of false positive results
N=100,0005% false positives
5000 abnormal results0.2% loss rate
(amnio)
10 losses of normal fetuses
N=100,000 1% false positives
1000 abnormal results6.2% TAB w/o confirmation
62 TAB
28 TP 34FP
34 TAB of normal fetuses
NIPT Serum Screening
45% PPV
Where does cfDNA fit?
� Is this an outstanding screening test or an imperfect diagnostic test?� Is this best used as a secondary screening test, or as a first tier screening test?� Are we ready to abandon current screening in favor of cfDNA?
10/22/2014
13
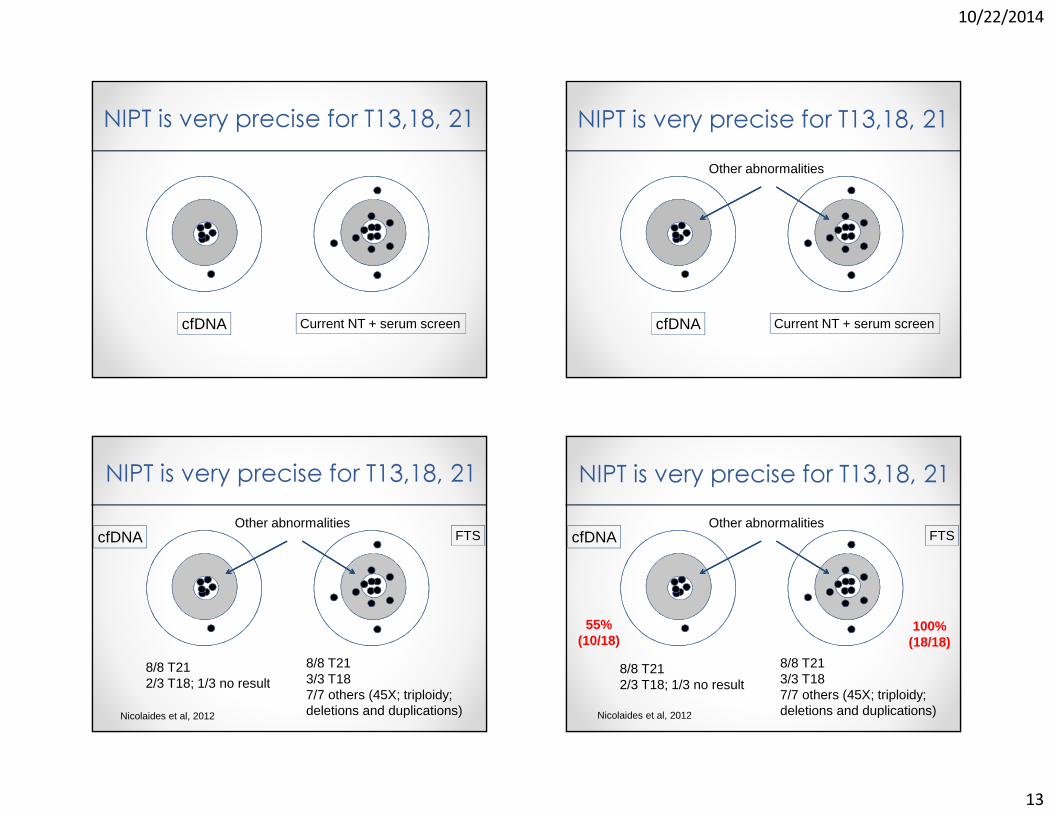
NIPT is very precise for T13,18, 21
cfDNA Current NT + serum screen cfDNA Current NT + serum screen
Other abnormalities
NIPT is very precise for T13,18, 21
NIPT is very precise for T13,18, 21
cfDNA FTSOther abnormalities
8/8 T212/3 T18; 1/3 no result
8/8 T213/3 T187/7 others (45X; triploidy; deletions and duplications)Nicolaides et al, 2012
NIPT is very precise for T13,18, 21
cfDNA FTSOther abnormalities
8/8 T212/3 T18; 1/3 no result
8/8 T213/3 T187/7 others (45X; triploidy; deletions and duplications)
55%(10/18)
100%(18/18)
Nicolaides et al, 2012

10/22/2014
14
T13, 18 and 21 are 2/3 of aneuploidies detectable by karyotype
Aneuploidies Detected by Prenatal Diagnostic Testing
Tri 21: 53.2%Sex chrom: 8.2%
Tri 13: 4.6%
Tri 18: 17.0%
Other16.9%
Norton et al, SMFM, 2014
Chromosome Abnormalities by Maternal Age
0%10%20%30%40%50%60%70%80%90%
100%
< 25 25 to 29 30 to 34 35 to 39 40 to 44 ≥ 45
Per
cent
Det
ecte
d
Age Group (Years)
NIPT Detectable
Yes
No
P<0.01
Norton et al, SMFM, 2014
NIPT Detection Rate
• ~83% of chromosomal abnormalities detected by current screening can potentially be identified by NIPT
• This varies by maternal ageo Lower detection in younger women (75-80%)o Greater detection in older women, but still only 90%

10/22/2014
15
Disorders potentially detectable by serum screening and NIPTNIPT Current Screening
• Trisomy 21• Trisomy 18• Trisomy 13• Some sex chromosomes
• Trisomy 21• Trisomy 18• Trisomy 13• Some sex chromosomes• Triploidy• Other rare aneuploidies• Congenital heart defects• Noonan syndrome• Neural tube defects• Ventral wall defects• Congenital adrenal hypoplasia• Smith Lemli Opitz syndrome• Steroid sulfatase deficiency• Adverse OB outcomes (IUGR, PreE, PTB)
NIPT: Expanded panelsLaboratories have added other trisomies and microdeletions
• Trisomies 16 and 22• Microdeletion syndromes
o 22q (diGeorge)o 5p (cri-du-chat)o 1p36o 15q (Prader Willi)o 4p (Wolf-Hirshhorn)
Genomic imbalance detected by microarray but not karyotype
Miller et al, 2010, AJHG
Microdeletion syndromesSyndrome Frequency Features22q11.2 (DiGeorge)
1/4K Varies: cardiac, palatal, immune, intellectual disability
1q36 1/5-10K Severe intellectual disability (ID), +/- obvious structural
anomaliesAngelman 1/12-20K Severe ID, seizures, speech
delayPrader-Willi 1/10-30K Obesity, ID, behavioral
problemsCri-du-chat 1/20-50K Microcephaly, ID, +/- CHDWolf-Hirshhorn
1/50K ID, seizures, +/- CL/CP

10/22/2014
16
NIPT for Rare Disorders
N=100,000
2 Wolf-Hirschhorn 99,998 not WHS
2 TP; 0 FN 800 FP; 99,198 TN
OAPR = 1/400
Population Risk = 1/50,000
(Wolf-Hirschhorn, 4p-: Assume 99% sensitivity and 99.2% specificity)
Chromosomal Microarray (CMA) for Prenatal Diagnosis
Karyotype
Resolution:>7-10 Million Base Pairs
(7-10 Mb)
Resolution:< 0.5 Million Base Pairs
(< 500 kb)
Chromosomal Microarray Diagnostic Yield in Cases with Normal
KaryotypeIndication for
TestingClinically Relevant
(N=96) U/S Anomaly
N=755 6.0%AMAN=1,966 1.7%
Positive ScreenN=729 1.7%OtherN=372 1.3%

10/22/2014
17
In patients with fetal structural abnormalities undergoing prenatal diagnosis, microarray is recommended.
New “menu” in prenatal testing
Screening test for common aneuploidies (NIPT) (1/500)
VS
Invasive diagnostic testing with CMA (1/60)
NIPT and chromosomal microarrayIF:
CMA detects an abnormality in 1.7% of cases (about 1/60)AND:
NIPT detects T13,18, 21 – about 1/500 pregnanciesTHEN:
� If NIPT is the routine screening test, it will detect only about 12% of diagnosable chromosomal abnormalities
Cost sensitivity analysis of NIPT• Calculated marginal costs of Down syndrome detection
compared to current screening
• If NIPT costs $1000, increased cost per case detected is $3.6 million more than first trimester combined screening
� Universal NIPT screening will only become cost effective if costs drop substantially
� Contingent screening of highest risk 10-20% is recommended
Cuckle et al, Prenat Diag 2013

10/22/2014
18
Down syndrome
Summary• cfDNA is a better test for Down syndrome than current screeningo MUST CONFIRM abnormal results before TAB!!o Test failure indicates an increased risk for aneuploidy
• Detects fewer disorders than traditional screening or diagnostic testing
• Patients need to be carefully counseled about the trade-offs of lower false positives but fewer disorders tested

10/22/2014
19
If only it were this simple…
Thank You!

10/22/2014
1
New Recommendations for Diagnosing Failed Intrauterine Pregnancy
Lori Strachowski, MDClinical Professor of Radiology, UCSF
Chief of Ultrasound, SFGH
Nothing to disclose.
The Article
N Engl J Med October 2013;369:1443-51
Lecture Goals• Detailed overview of update on diagnostic criteria for
nonviable pregnancy early in the first trimester– Panelists– Issue – Objective– Plan– Recommended criteria– Reasoning

10/22/2014
2
The Panelists• Society of Radiologists in Ultrasound (SRU) Multispecialty
Panel on Early First Trimester Miscarriage and Exclusion of a Viable Intrauterine Pregnancy
• 3 Specialties:– Radiologists (7)– Obstetrician-Gynecologists (5)– Emergency Medicine (3)
The Rads
• Peter M. Doubilet, M.D., Ph.D., Brigham and Women’s and Harvard Medical School*
• Carol B. Benson, M.D., Brigham and Women’s/Harvard* • Beryl R. Benacerraf, M.D., Brigham and Women’s/Harvard• Douglas L. Brown, M.D., Mayo Clinic, Rochester• Roy A. Filly, M.D., UCSF• Edward A. Lyons, M.D., Univ of Manitoba, Winnipeg, MB• Dolores H. Pretorius, M.D., UCSD
* primary authors
The OB/Gyn’s
• Tom Bourne, M.B., B.S., Ph.D., Imperial College, London*• Steven R. Goldstein, M.D., NYU School of Medicine• Ilan E. Timor-Tritsch, M.D., NYU School of Medicine• Kurt T. Barnhart, M.D., M.S.C.E., University of Pennsylvania• Misty Blanchette Porter, M.D., Dartmouth
* primary authors
The ER Docs
• Michael Blaivas, M.D., University of South Carolina*• J. Christian Fox, M.D., University of California, Irvine• John L. Kendall, M.D., Denver Health Medical Center
* primary authors

10/22/2014
3
The Issue
www.facebook.com
Pain +/- Bleeding in Early PregnancyMisuse and misinterpretation of US and β-hCG
Methotrexate inadvertently administered
Miscarriage and malformations
MALPRACTICE_ _ _ _ _ _ _ _ _ _ _
Medical Liability Action• 2009 Survey on Professional Liability conducted by ACOG
– 90.5%: ≥ 1 professional liability claim– Avg: 2.69 claims per obstetrician - gynecologist
• 62% - OB care• 38% - Gyne care
– Delayed dx of breast cancer– Inadvertent Tx of IUPs with MTX
Obstetrics and Gynecology 2010 ;116:8-15
Inadvertent Tx of IUPs with MTX• 3 diagnostic error patterns
– Perception and interpretation of findings on US
– Improper correlation of β-hCG levels and US findings
– Treatment based on a single hCG level without a definitive US diagnosis of ectopic pregnancy
Obstetrics and Gynecology 2010 ;116:8-15

10/22/2014
4
US Error Types• Perception:
– Finding seen in retrospect but initially missed• i.e. an early intrauterine GS or YS
• Interpretation:– Findings perceived but incorrectly diagnosed
• i.e. CL interpreted as EP or early GS as a pseudo-sac• Confounding factors:
– Poor quality images, noncritical image evaluation, incomplete clinical info
Obstetrics and Gynecology 2010 ;116:8-15
The Objective
First, DO NO HARM
“or the least possible”
The Plan• Set quality standards for diagnostic tests
• Standardize terminology
• Establish diagnostic criteria – Widely applicable and reproducible– Minimize risk
• Based on consequences of false positive and negative results
The Diagnostic Tests: hCG• Human chorionic gonadotropin
– Serum measured with use of WHO 3rd or 4th International Standard
– Positive serum pregnancy test is defined by > 5 mIU/ml
NOTE: low levels of hCG can occur in health non-pregnant patients.

10/22/2014
5
The Diagnostic Tests: US • Minimum quality criteria:
– TVS of uterus and adnexa– TAS for FF and mass high in the pelvis– Oversight by an appropriately trained physician– Performed by providers and interpreted by physicians, all
of whom meet at least minimum training or certification standards
– Scanning equipment permitting adequate visualization of structures early in the first trimester
The Terminology • Viable
• Nonviable
Definition: Viable (vī-ə-bəl)1: capable of living; especially: having attained such form and development as to be normally capable of surviving outside the mother's womb <a viable fetus>
www.Merriam-Webster.com
Definition: Viable (vī-ə-bəl)1: capable of living; especially: having attained such form and development as to be normally capable of surviving outside the mother's womb <a viable fetus>
www.Merriam-Webster.com

10/22/2014
6
Definition: Viable (vī-ə-bəl)1: capable of living; especially: having attained such form and development as to be normally capable of surviving outside the mother's womb <a viable fetus>
2: capable of growing or developing <viable seeds> <viable eggs>
3 a : capable of working, functioning, or developing adequately <viable alternatives> b : capable of existence and development as an independent unit <the colony is now a viable state> c (1) : having a reasonable chance of succeeding <a viablecandidate> (2) : financially sustainable <a viable enterprise>
www.Merriam-Webster.com
Definition: Viable (vī-ə-bəl)1: capable of living; especially: having attained such form and development as to be normally capable of surviving outside the mother's womb <a viable fetus>
2: capable of growing or developing <viable seeds> <viable eggs>
3 a : capable of working, functioning, or developing adequately <viable alternatives> b : capable of existence and development as an independent unit <the colony is now a viable state> c (1) : having a reasonable chance of succeeding <a viablecandidate> (2) : financially sustainable <a viable enterprise>
www.Merriam-Webster.com
The Terminology• Viable:
– A pregnancy is viable if it can potentially result in a liveborn baby.
• Nonviable: – A pregnancy is nonviable if it cannot possibly result in a
liveborn baby. • Examples: ectopic pregnancies and failed intrauterine
pregnanciesManual uterine
aspiration
The Differential
CurrentlyViable
IUPFailed/Failing
IUP
Ectopic pregnancy
Expectant management
MUA +/- MTX +/or surgery
MUA

10/22/2014
7
Currently Viable IUP The Differential
CurrentlyViable
IUPFailed/Failing
IUP
Ectopic pregnancy
Expectant management
MUA +/- MTX +/or surgery
MUA
Ectopic Pregnancy
Ov
The Differential
CurrentlyViable
IUPFailed/Failing
IUP
Ectopic pregnancy
Expectant management
MUA +/- MTX +/or surgery
MUA

10/22/2014
8
Spontaneous AB in ProgressCervix
The Differential
CurrentlyViable
IUPFailed/Failing
IUP
Ectopic pregnancy
Expectant management
MUA +/- MTX +/or surgery
MUA
What is the best diagnosis for this1st trimester pregnancy?
A. B. C. D.
20%
71%
1%7%
A. Currently viable IUPB. Failed/failing IUPC. Ectopic PregnancyD. I don’t like any of these
answers
It ain’t always that easy!

10/22/2014
9
FP + FN Consequences
CurrentlyViable
IUPFailed/Failing
IUP
Ectopic pregnancy
Expectant management
MUA +/- MTX +/or surgery
MUA
FP: Viable IUP
Short delay in dx
FN: Failure
FP + FN Consequences
CurrentlyViable
IUPFailed/Failing
IUP
Ectopic pregnancy
Expectant management
MUA +/- MTX +/or surgery
MUAShort delay in dxLikely non-life-
threatening!
FN: EP
FP + FN Consequences
CurrentlyViable
IUPFailed/Failing
IUP
Ectopic pregnancy
Expectant management
MUA +/- MTX +/or surgery
MUAShort delay in dxLikely non-life-
threatening!
FN: EP FN: Failure
FP + FN Consequences
CurrentlyViable
IUPFailed/Failing
IUP
Ectopic pregnancy
Expectant management
MUA +/- MTX +/or surgery
MUA
FP: Failure FP: EP
Short delay in dxLikely non-life-
threatening!
FN: Viable IUP FN: Viable IUP

10/22/2014
10
To “DO NO HARM”1. Criteria for non-viability require
– 100% Specificity– 100% PPV
2. Need more buckets!!!
“or as close as possible”
The Expanded Differential
CurrentlyViable
IUPFailed/Failing
IUP
Ectopic pregnancy
Expectant management
MUA +/- MTX +/or surgery
MUA
IUP of Uncertain Viability
Pregnancyof
UnknownLocation
The Expanded Differential
CurrentlyViable
IUPFailed/Failing
IUP
Ectopic pregnancy
Expectant management
MUA +/- MTX +/or surgery
MUA
IUP of Uncertain Viability
Pregnancyof
UnknownLocation
Expectant management
Expectant management
The Terminology• Intrauterine pregnancy of uncertain viability:
– Transvaginal ultrasonography shows an intrauterine gestational sac with no embryonic heartbeat and no findings of definite pregnancy failure.
• Pregnancy of unknown location:– Positive pregnancy test and no intrauterine or ectopic
pregnancy on transvaginal US.

10/22/2014
11
The Pivotal Question
Is there a chance of a viable pregnancy?
The Expanded Differential
CurrentlyViable
IUPFailed/Failing
IUP
Ectopic pregnancy
Expectant management
MUA +/- MTX +/or surgery
MUA
IUP of Uncertain Viability
Pregnancyof
UnknownLocation
Expectant management
Expectant management
Viable IUP
Failure
Short delay in dx
EP
Likely non-life threatening
Short delay in dx
Viable IUP
Failure
Likely non-life threatening
EP
The Expanded Differential
CurrentlyViable
IUPFailed/Failing
IUP
Ectopic pregnancy
Expectant management
MUA +/- MTX +/or surgery
MUA
IUP of Uncertain Viability
Pregnancyof
UnknownLocation
Expectant management
Expectant management
The Expanded Differential
Failed/Failing
IUPIUP of Uncertain Viability
Pregnancyof
UnknownLocation
Specific criteria and management algorithms

10/22/2014
12
Literature on Nonviable IUP Criteria• Serum beta level
– Largely unreliable given range of normal
• US findings– Size-based criteria
• Embryo without heart motion• GS without an embryo
– Time-based criteria• Appearance of interval findings
What is the correct order of appearance?
A. B. C. D.
12%
52%
34%
2%
A. Yolk sac – Gestational sac – Embryo – Amnion B. Yolk sac – Amnion – Embryo – Gestational SacC. Gestational sac – Yolk sac – Embryo – Amnion D. Gestational sac – Yolk sac – Amnion – Embryo
Let’s review normal.
vv
US of Early Pregnancy• In order of appearance:
– Intradecidual sign– Double decidual sac sign– Yolk sac– Embryo– Amnion
(+ heart motion)

10/22/2014
13
US of Early Pregnancy• In order of appearance:
– Intradecidual sign– Double decidual sac sign– Yolk sac– Embryo– Amnion
(+ heart motion)
“White Lines” of the EndometriumPost menses
B
Basalis (2 layers)
“White Lines” of the EndometriumEarly Proliferative Phase
Basalis (2 layers) Functionalis = Spongiosum and Compactum
B
BC S
S
“White Lines” of the Endometrium
B
B
C SS
Basalis (2 layers) Functionalis = Spongiosum and Compactum
Late Proliferative Phase
Aka: “Triple line sign”

10/22/2014
14
“White Lines” of the EndometriumSecretory Phase
Basalis (2 layers) Functionalis = Spongiosum and Compactum
“White Lines” of the Endometrium
Basalis (2 layers) Functionalis = Spongiosum and Compactum
Early Secretory Phase
“White Lines” of the Endometrium
Basalis (2 layers) Functionalis = Spongiosum and Compactum
Late Secretory Phase
“White Lines” of the Endometrium
Basalis (2 layers) Functionalis = Spongiosum and Compactum
Decidua
In Pregnancy

10/22/2014
15
“White Lines” of the Endometrium
Basalis (2 layers) Functionalis = Spongiosum and Compactum
Blastocyst
Decidua
In Pregnancy
“White Lines” of the Endometrium
Basalis (2 layers) Functionalis = Spongiosum and Compactum
In Pregnancy = DeciduaDecidua
In Pregnancy
Intradecidual Sign
Basalis (2 layers) Functionalis = Spongiosum and Compactum
In Pregnancy = DeciduaDecidua
In Pregnancy
Intradecidual Sign• ~ 3-4 weeks
• US:– ≥ 2 mm cyst– Thin echogenic rim– Eccentric to central
echogenic line – “Color flash”
• Occasionally helpful
Yeh, et.al., Radiology. 1986 Nov;161(2)

10/22/2014
16
Intradecidual Sign: Mimics• DDx:
– Intracavitary fluid– Decidual cysts
• IUP• EP
– Endometrial pathology• Polyps• Cystic hyperplasia• Malignancy
Intradecidual Sign
Grows ~ 1mm/day and becomes….
Double Decidual Sac Sign Double Decidual Sac Sign• ~ 5 weeks
• US:– Round/oval fluid
collection– 2 echogenic rims
• Inner: chorion• Outer: decidua
Bradley, Filly, et.al., Radiology.1982 Apr;143(1)

10/22/2014
17
Double Decidual Sac Sign: Mimic• Pseudo-gestational sac• DDx:
– Decidual reaction– Implantation bleed– EP (10-20%)
• US:– Fluid collection
• 1 echogenic rim• Acute ‘s, “tear -
drop” shaped
How reliable are these signs?• Intradecidual sac sign
– Specificity: 66 - 97%– Sensitivity: 48 - 92 %
• Double decidual sac sign– Specificity: 85 - 98%– Sensitivity: 64 - 95%
Absent in at least 35% of
gestational sacs
Any round/oval fluid collection = GS
“ Therefore, any round or oval fluid collection in a woman with a positive pregnancy test most likely represents an intrauterine
gestational sac and should be reported as such.”
N Engl J Med October 2013;369:1445
Mean Sac Diameter Measurement• Add dimensions of anechoic sac
(excluding echogenic rim)– Length + height + width
• Divide by 3
+ +
LONG
TRANS
Report: “If this represents a GS, the MSD measures # mm”

10/22/2014
18
Mean Sac Diameter Measurement• Add dimensions of anechoic sac
(excluding echogenic rim)– Length + height + width
• Divide by 3
+ +
LONG
TRANS
Report: “If this represents a GS, the MSD measures # mm”
Yolk Sac • ~ 5 ½ weeks
• US:– Thin round ring-like
structure– 3-5 mm
• Typically not > 6 mm
IUP MSD IUP MSD

10/22/2014
19
What do you do/say in your report/notes?
A. B. C. D.
60%
33%
7%0%
A. Too early to calculate gestational age and EDCB. Have your partner figure out interval growth when she
returns for her 18 – 20 week scanC. Measure yolk sac and add to MSDD. Use the formula MSD (mm) + 30 = GA (days) and wheel out
the EDC
IUP MSD
MSD (mm) + 30 = GA (days)i.e. 10 + 30 = 40 days (5 wks, 5 days)
Embryo • ~ 6 weeks
• US:– Flickering heart motion
adjacent to yolk sac– Grows ~ 1mm/day– Reniform, tadpole
appearance
Crown-rump length (CRL) = avg of 2-3 end-to-end measurements
Amnion• ~ 8 weeks
• US:– Very thin echogenic
membrane surrounding embryo
– Between YS and embryo – “Fuses” with chorion:
12-16 weeks
“2nd skin”
YS

10/22/2014
20
US of Early Pregnancy• In order of appearance:
– Intradecidual sign– Double decidual sac sign– Yolk sac– Embryo– Amnion
(+ heart motion)
4 criteria definitive for failure2 size based
2 time based
Discriminatory CRL• Defined as CRL size, above which, the absence of cardiac
motion is unequivocal for failure• Historically: 5 mm
– However:• Sensitivity: 50%• More recent data: 5-6 mm • Inter-observer variability: + 15%
• Most conservative scenario:Upper nl CRL (6 mm) + 15% (0.9) = 6.9 mm7.0 mm
Criteria Definitive for Failure1. CRL ≥ 7 mm without
cardiac activity – PPV for failure: 100%
“Embryonic demise”
Discriminatory MSD• Defined as MSD size, above which, the absence of an embryo
is unequivocal for failure• Historically: 16 – 18 mm
– However:• Sensitivity: 50%• More recent data = 17-21 mm• Inter-observer variability: + 19%
• Most conservative scenario:Upper nl MSD (21 mm) + 19% (4) = 25 mm

10/22/2014
21
Criteria Definitive for Failure2. MSD ≥ 25 mm and no visible
embryo– PPV for failure: 100%
“1st trimester pregnancy failure”
Time-Based Criteria for Failure• Needed as discriminatory sac or embryo sizes may never be
achieved• Based on timing of interval appearance:
– GS - 5 weeks – YS - 5 ½ weeks– Embryo with heart motion - 6 weeks
• Most conservative scenario:– Lower nl GS (4 ½ wks) - upper nl embryo (6 ½ wks) = 2 wks– Lower nl YS (5 wks) - upper nl embryo (6 ½ wks) = 1 ½ wks
+/- ½ week
11 days14 days
Criteria Definitive for Failure3. Absence of embryo with heartbeat ≥ 14 days after a scan that
showed a GS without a YS
4. Absence of embryo with heartbeat ≥ 11 days after a scan that showed a GS with a YS
8 criteria suggestive for failure

10/22/2014
22
Criteria Suggestive for Failure1. CRL <7 mm and no heartbeat
2. MSD of 16 - 24 mm and no embryo
3. Absence of embryo +HM 7–13 days after a GS without a YS
4. Absence of embryo +HM 7–10 days after a GS with a YS
“When there are findings suspicious for pregnancy failure, follow-up US at 7 to 10 days is generally appropriate.”
Do we really need to wait to call this?
Normal GS and embryo grow ~1 mm/day
Criteria Suggestive for Failure5. Empty amnion
- Amnion adjacent to YS, with no visible embryo
Criteria Suggestive for Failure5. Empty amnion
- Amnion adjacent to YS, with no visible embryo
6. Enlarged yolk sac (>7 mm)

10/22/2014
23
Criteria Suggestive for Failure5. Empty amnion
- Amnion adjacent to YS, with no visible embryo
6. Enlarged yolk sac (>7 mm)
7. Small GS in relation to size of embryo
- MSD – CRL = <5
Criteria Suggestive for Failure8. Absence of embryo ≥ 6 wk
after last menstrual period
CAUTION!!!- Would only consider if:
– Reliable historian with very regular cycles
OR– IVF patient
Pregnancy of Unknown Location• Defined as:
– Pregnant (serum beta hCG > 5 mIU/ml)– US findings:
• No intrauterine fluid collection• Normal (or near normal) adnexa
corpus luteum of pregnancy
Pregnancy of Unknown Location

10/22/2014
24
Pregnancy of Unknown Location• NOTE: Serum beta levels
– A single measurement of hCG, regardless of its value, does not reliably distinguish between EP and IUP (viable or nonviable)
– Discriminatory level of 2000 (to dx IUP) may not be high enough• Looked at likelihood ratios of different outcomes based
on range of serum beta hCG
Beta vs. Likely Outcome
Serum beta Likely outcome
< 2000 mIU/ml Viable IUP
Beta vs. Likely Outcome
Serum beta Likely outcome
< 2000 mIU/ml Viable IUP
2000 – 3000 mIU/mlNonviable IUP - 38:1
EP - 19:1 Viable IUP: 2%
Beta vs. Likely Outcome
Serum beta Likely outcome
< 2000 mIU/ml Viable IUP
2000 – 3000 mIU/mlNonviable IUP - 38:1
EP - 19:1 Viable IUP: 2%
> 3000 mIU/mlNonviable IUP - 140:1
EP - 70: 1Viable IUP: 0.5%

10/22/2014
25
Pregnancy of Unknown Location• Management recommendations:
– Beta hCG <3000 and stable:• Presumptive tx for EP with MTX or other pharmacologic
or surgical means should not be undertaken, in order to avoid the risk of interrupting a viable IUP.
– Beta hCG ≥3000 and stable:• A viable IUP is possible but unlikely. However, as the
most likely diagnosis is a nonviable IUP, it is generally appropriate to obtain at least one follow-up hCG and follow-up US before undertaking treatment for EP.
Pregnancy of Unknown Location• Management recommendations:
– Beta hCG <3000 and stable:• Presumptive tx for EP with MTX or other pharmacologic
or surgical means should not be undertaken, in order to avoid the risk of interrupting a viable IUP.
– Beta hCG ≥3000 and stable:• A viable IUP is possible but unlikely. However, as the
most likely diagnosis is a nonviable IUP, it is generally appropriate to obtain at least one follow-up hCG and follow-up US before undertaking treatment for EP.
Pregnancy of Unknown Location• NOTE:
– When US not yet performed:• No single serum beta level predicts the likelihood of EP
rupture. • When clinical findings are suspicious for EP, transvaginal
ultrasonography is indicated, even when the hCG level is low.
There isn’t a beta low enough to exclude EP.You gotta do the US!
The Basic Assumption• Pregnancy is desired.
UCSF: Meredith Warden, M.D., M.P.H. Jody Steinauer, M.D., Univ of Penn: Courtney A. Schreiber, M.D., M.P.H.

10/22/2014
26
In Conclusion• First, DO NO HARM to a potentially viable pregnancy
• Consider adding “IUP of Uncertain Viability” and “Pregnancy of Unknown Location” to your lexicon and manage expectantly
• In setting of PUL, stable pt. and desired pregnancy– Always get an US – Beta < 3000, f/u serial betas and US as indicated– Beta ≥ 3000, though viable IUP highly, may consider f/u
beta
and desired
Upper beta limit not addressed.
In Conclusion• Definitive criteria for early IUP failure:
– CRL ≥ 7 mm + no heart motion– MSD ≥ 25 mm and no embryo– No embryo ≥ 14 days after a GS without a YS – No embryo ≥ 11 days after a GS with a YS
• Suggestive for failure:– No embryonic heart motion– Empty amnion sign– YS too big, GS too small, others– Consider repeat US at 7-10 days
highly suggestive, in my opinion
sooner sometimes OK too , in my opinion
Role of beta?
Thank you for your attention.

Tips, Tricks & Controversies in Laparoscopic Hysterectomy
Alison Jacoby, MDDept of Obstetrics, Gynecology and
Reproductive Sciences
No disclosures
• Incorporate new surgical techniques into your practice
• Understand the recent controversy with Power Morcellation
• Share strategies for minimizing risk of disseminating occult malignancies
• Review incidence of sarcoma in patients presumed to have fibroids
Learning ObjectivesKeys to success

Keys to success
• Laparoscopic entry: port placement, cosmetic incisions
Keys to success
• Laparoscopic entry: port placement, cosmetic incisions
• Visualization: seeing around corners
Keys to success
• Laparoscopic entry: port placement, cosmetic incisions
• Visualization: seeing around corners
• Uterine manipulation: delineate vaginal fornices, displace ureters
Keys to success
• Laparoscopic entry: port placement, cosmetic incisions
• Visualization: seeing around corners
• Uterine manipulation: delineate vaginal fornices, displace ureters
• LSH: cervical transection made easy

Keys to success
• Laparoscopic entry: port placement, cosmetic incisions
• Visualization: seeing around corners
• Uterine manipulation: delineate vaginal fornices, displace ureters
• LSH: cervical transection made easy
• Specimen removal: the most challenging part of surgery today
Keys to success
• Laparoscopic entry: port placement, cosmetic incisions
• Visualization: seeing around corners
• Uterine manipulation: delineate vaginal fornices, displace ureters
• LSH: cervical transection made easy
• Specimen removal: the most challenging part of surgery today
Keys to success
• Laparoscopic entry: port placement, cosmetic incisions
• Visualization: seeing around corners
• Uterine manipulation: delineate vaginal fornices, displace ureters
• LSH: cervical transection made easy
• Specimen removal: the most challenging part of surgery today
Laparoscopic entry:Port Placement

Laparoscopic entry:Port Placement
Always have your scope higher than the fundus(with maximum cephalad displacement)
Laparoscopic entry: Cosmetic incisions
Umbilicus
• Incision types: Vertical and Omega
• Cosmetically appealing
• Minimize # of incisions
Omega Umbilical Incision

Omega Umbilical Incision
Visualization:Seeing around corners
Angled scopes:
• 0°, 30° & 45°
• Invaluable for seeing over and around large fibroids
Visualization:Uterine manipulation
• Places tissue on tension
• Separates ureter and uterine artery
• Delineates vaginal fornix

Tools for Cervical Amputation
• Electrosurgical loop- monopolar or bipolar
• Fast but potentially dangerous
Specimen Removal: Vaginal route
• Great option for TLH
• Less practical for a very large uterus or patient with narrow pubic arch
• Not an option for LSH
Specimen Removal: Supra-pubic mini-lap
• Addition incision
• Cosmetically less appealing
• Increased pain
Text

Specimen Removal: Intracorporeal Power Morcellation
• Introduced in 1993
• Spinning blade cuts specimen into long strips
• Passes through a 15 mm port (8- 20 mm)
• ~40,000 cases per yr in US
Specimen Removal:The Controversy
Specimen Removal:The Controversy
Power Morcellation:
Specimen Removal:The Controversy
Power Morcellation:
• November 2013- News story about dissemination of unsuspected sarcoma

Specimen Removal:The Controversy
Power Morcellation:
• November 2013- News story about dissemination of unsuspected sarcoma
• April 2014-FDA safety warning
Specimen Removal:The Controversy
Power Morcellation:
• November 2013- News story about dissemination of unsuspected sarcoma
• April 2014-FDA safety warning
• May 2014- J&J suspends sale of morcellator
Specimen Removal:The Controversy
Power Morcellation:
• November 2013- News story about dissemination of unsuspected sarcoma
• April 2014-FDA safety warning
• May 2014- J&J suspends sale of morcellator
• July 2014- FDA review panel
• FDA Warning issued 4/17/2014
• Prevalence of unsuspected uterine sarcoma in patients undergoing hysterectomy or myomectomy for presumed benign fibroids is 1 in 352, and the prevlance of unsuspected uterine leiomyosarcoma is 1 in 498.
• “If laparoscopic power morcellation is performed in women with unsuspected uterine sarcoma, there is a risk that the procedure will spread the cancerous tissue within the abdomen and pelvis, significantly worsening the patient’s likelihood of long-term survival. For this reason, and because there is no reliable method for predicting
whether a woman with fibroids may have a uterine sarcoma, the FDA discourages the use of laparoscopic power morcellation during hysterectomy for uterine fibroids.”

Can we differentiate a fibroid from a sarcoma?
• Age
• Menopausal status
• Tamoxifen
• Pelvic radiation
• HLRCC
Findings that do NOT reliably predict sarcoma
• Rapidly growing mass NOT necessarily c/w sarcoma
• Benign fibroids can double in size in 6 mo (Pedadda 2008)
• Large uterine size (>20wks) NOT associated w sarcoma (West, Fertil Steril 2006 and
Schwartz 1993)
Investigational screening protocols

Investigational screening protocols
Potential ways to differentiate sarcoma from fibroids:
Investigational screening protocols
Potential ways to differentiate sarcoma from fibroids:
•Dynamic gadopentetate dimeglumine-enhanced MRI combined with serum LDH isoenzyme analysis
Investigational screening protocols
Potential ways to differentiate sarcoma from fibroids:
•Dynamic gadopentetate dimeglumine-enhanced MRI combined with serum LDH isoenzyme analysis
•Diffusion-weighted MRI2
Investigational screening protocols
Potential ways to differentiate sarcoma from fibroids:
•Dynamic gadopentetate dimeglumine-enhanced MRI combined with serum LDH isoenzyme analysis
•Diffusion-weighted MRI2

Investigational screening protocols
Potential ways to differentiate sarcoma from fibroids:
•Dynamic gadopentetate dimeglumine-enhanced MRI combined with serum LDH isoenzyme analysis
•Diffusion-weighted MRI2
1Goto A et al, Int J Gynecol Cancer 2002;12:354
Investigational screening protocols
Potential ways to differentiate sarcoma from fibroids:
•Dynamic gadopentetate dimeglumine-enhanced MRI combined with serum LDH isoenzyme analysis
•Diffusion-weighted MRI2
1Goto A et al, Int J Gynecol Cancer 2002;12:354
2Sato K et al, Am J Obstet Gynecol 2013;210:368
Endometrial Biopsy
• EMB can sometimes detect sarcomas (Sagae
Oncology 2004 and Jin In J Gynecol Cancer 2010)
• Sensitivity of pre-operative endometrial sampling for diagnosis leiomyosarcoma: 38% (3/8) and 67% (4/6) (Leibsohn, Am J Obstet Gynecol 1990 and
Bansal, Gynecol Oncol 2008).
Prevalence of Sarcoma
• Retrospective case series
• 10 - 15 studies
• Prevalence ranged from 1 in 1000 (0.1%) to 1 in 352 (0.28)
• mostly LMS, some cases ESS • Parker 1994, Leung 2009, Leibsohn 1990, Takamizawa 1999, Leung 2012, Durand-Reville 1996, Seidman
2012, Theben 2013, Sinha 2008, Hagemann 2011, Park 2011, Kamikabeya 2010.

What is the prevalence at UCSF?
• Pre-op dx of fibroids
• 1999-2014
• # treated by hysterectomy or myomectomy- 2454
• # of unsuspected sarcomas- 8
• 3 LMS, 3 ESS, 2 AS
• Prevalence is 8/2454 = 1/306 = 0.33%
Minimizing harm/Maximizing safety
Minimizing harm/Maximizing safety
1. When possible, use alternative to uncontained power morcellation
Minimizing harm/Maximizing safety
1. When possible, use alternative to uncontained power morcellation
•mini-lap, vagina, contained morcellation

Minimizing harm/Maximizing safety
1. When possible, use alternative to uncontained power morcellation
•mini-lap, vagina, contained morcellation
•written, signed informed consent
Minimizing harm/Maximizing safety
1. When possible, use alternative to uncontained power morcellation
•mini-lap, vagina, contained morcellation
•written, signed informed consent
2. Never morcellate known or suspected cancer
Minimizing harm/Maximizing safety
1. When possible, use alternative to uncontained power morcellation
•mini-lap, vagina, contained morcellation
•written, signed informed consent
2. Never morcellate known or suspected cancer
3. PreOp evaluation for occult malignancy
Minimizing harm/Maximizing safety
1. When possible, use alternative to uncontained power morcellation
•mini-lap, vagina, contained morcellation
•written, signed informed consent
2. Never morcellate known or suspected cancer
3. PreOp evaluation for occult malignancy
•Endometrial sampling and imaging

Minimizing harm/Maximizing safety
1. When possible, use alternative to uncontained power morcellation
•mini-lap, vagina, contained morcellation
•written, signed informed consent
2. Never morcellate known or suspected cancer
3. PreOp evaluation for occult malignancy
•Endometrial sampling and imaging
•Cytologic or molecular screening of cervix
Minimizing harm/Maximizing safety
1. When possible, use alternative to uncontained power morcellation
•mini-lap, vagina, contained morcellation
•written, signed informed consent
2. Never morcellate known or suspected cancer
3. PreOp evaluation for occult malignancy
•Endometrial sampling and imaging
•Cytologic or molecular screening of cervix
•Avoid uncontained morcellation of ovaries
ACOG
• “Minimally invasive surgery, including with power morcellation, continues to be an option for some patients when performing hysterectomy and myomectomy. At the same time, it is critical to minimize the risk for patients undergoing these surgeries who may have an occult gynecologic cancer.”
AAGL
• “Power morcellation is an important tool in treating symptomatic uterine fibroids which allows 150,000 women each year to undergo minimally invasive surgery when they would otherwise require laparotomy for TAH. While research, education, and improved tissue extraction techniques can probably further enhance the safety profile of power morcellation, the elimination of power morcellation and conversion of these women to open surgery would likely increase morbidity and mortality from open surgery and cause harm to more patients. Our obligation is not only to patients with leiomyosacoma, but to all of our patients. We must not sacrifice our patients in response to a rare event. Thus, it is the AAGL’s position that we should improve but not abandon power morcellation, and that power morcellation with appropriate informed consent should remain available to all appropriately screened, low-risk women.”

Specimen Removal:Options for L/S myo & LSH
Specimen Removal:Options for L/S myo & LSH
• Colpotomy
Specimen Removal:Options for L/S myo & LSH
• Colpotomy
• Uncontained power morcellation (with informed consent)
Specimen Removal:Options for L/S myo & LSH
• Colpotomy
• Uncontained power morcellation (with informed consent)
• Contained scalpel morcellation

Specimen Removal:Options for L/S myo & LSH
• Colpotomy
• Uncontained power morcellation (with informed consent)
• Contained scalpel morcellation
• Contained power morcellation
Contained PowerMorcellaltion

• Incorporate new surgical techniques into your practice
• Understand the recent controversy with Power Morcellation
• Share strategies for minimizing risk of disseminating occult malignancies
• Review incidence of sarcoma in patients presumed to have fibroids
Learning ObjectivesKeys to success
• Laparoscopic entry: port placement, cosmetic incisions
• Visualization: seeing around corners
• Uterine manipulation: delineate vaginal fornices, displace ureters
• LSH: cervical transection made easy
• Specimen removal: the most challenging part of surgery now
Thank you
Iatrogneic complications from dissemination tissue fragments
• Peritonitis, abscess, obstruction (Lieng, J Minim Invasive Gynecol 2006)
• Case reports of iatrogenic myomas on bladder, appendix and retroperitoneally (Kho, Obstet Gynecol 2009)

• MV analysis: higher stage (OR 20.34 1.27-325.58) and morcellation (OR 3.11, 1.07-9.06) significantly associated with death at the 5-yr time point

1
Mesh Erosion and What to do
Michelle Y. Morrill, MDChief of Urogynecology, TPMG
Director of Urogynecology, Kaiser San FranciscoAssistant Professor, Volunteer Faculty Dept of Ob/Gyn, UCSF
Disclosures
None
Goals for Today
� Review the history of the use of vaginal mesh in surgery
� Discuss common and serious complications that can arise from vaginal mesh surgery
� Learn about the efficacy of various techniques for approaching vaginal mesh complications
� Mesh - Synthetic� Current standard:
Polypropylene Type 1 Mesh – Permanent, Monofilament and Macroporous

2
History
� Stress urinary incontinence (SUI) :� Variety of abdominal and vaginal surgeries
� 1997 AUA SUI Guidelines recommend retropubic suspensions or (traditional) pubovaginal slings based on 4y outcomes*Both are abdominal surgeries with noted
morbidity
� 1995 Ulmsten presents the mid-urethral sling (MUS)
History
Funk et al. Trends in the Surgical Management of St ress Urinary Incontinence. Obstet Gynecol 2012;119:845–51
History
� SUI continued…� 2014 Systematic Review of English
language RCTs with ≥12m follow-up� 127 papers on 49 unique trials
� MUS equivalent or superior to Burch and pubovaginal sling by subjective, objective and adverse event outcomes
Schimpf MO, Rahn DD, Wheeler TL, et al. Sling surgery for stress urinary incontinence in women: a systematic review and metaanalysis. Am J Obstet Gynecol 2014; Jul;211(1):71.e1-71.e27.
History
� SUI continued…� 2014 AUGS/SUFU Position Statement on
MUS
“The polypropylene mesh midurethral sling is the recognized worldwide standard of care for the surgical treatment of stress urinary incontinence. The procedure is safe, effective, and has improved the quality of life for millions of women.”

3
History
� Pelvic organ prolapse (POP)� Vaginal vs. Abdominal approach
� 1996 Benson et al. RCT avg f/u 2.5y � Abd 16% repeat surgery � Vaginal 33% repeat surgery
� 1997 Olsen et al. 30% of surgeries for POP or UI were repeats
Benson et al. Am J Obstet Gynecol, 1996; 175(6):1418-21Olsen et al. Obstet Gynecol 1997;89:501-6
History
� POP continued…
� 2001 FDA approves mesh device for prolapse� 510k – based on similarity to mesh for hernia
repair
� ~100 devices developed over the following years
Ellington DR, Richter HE. The Role of Vaginal Mesh Procedures in Pelvic Organ Prolapse Surgery in View of Complication Risk . Obstetrics and Gynecology International. Volume 2013, Article ID 356960.
Events reported in MAUDE 2005-2010
1 Erosion 528
2 Pain 472
3 Infection 253
4 Bleeding 124
5 Dyspareunia 108
6 Organ Perforation 88
7 Urinary Problems 80
8 Vaginal Scarring/Shrinkage 43
9 Neuromuscular Problems 38
10 Recurrent Prolapse 32
A. I. Brill, “The hoopla over mesh: what it means for practice,”. Obstetrics & Gynecology News, pp. 14–15, 2012.
History
� POP continued…� 2008 FDA Public Health Warning� >1000 reports in 3y of mesh device complications� Recommend specialized training� Recommend patient education

4
History
� POP continued…� 2008 FDA Public Health Warning� >1000 reports in 3y of mesh device complications
� 2011 July FDA Safety Communication� >2800 reports in 3y of mesh device complications� “Serious adverse events are NOT rare, contrary to
what was stated in the 2008 PHN”� “Transvaginally placed mesh in POP repair does
NOT conclusively improve clinical outcomes over traditional non-mesh repair.”
History
� POP continued…
� 2011 ACOG/AUGS Committee Opinion� “POP vaginal mesh repair should be reserved
for high-risk individuals in whom the benefit of mesh placement may justify the risk”� Surgeons need particular training� Further research recommendations
History
� POP continued…
� 2012 FDA mandates postmarket studies (522 studies) for transvaginal mesh devices for POP
Mesh Today
� Multi-incision MUS� Gold Standard
� Single incision MUS
� Sacrocolpopexy � Abdominal or Laparoscopic approach
� Vaginally placed mesh for POP

5
Adverse Events
1 Erosion 528
2 Pain 472
3 Infection 253
4 Bleeding 124
5 Dyspareunia 108
6 Organ Perforation 88
7 Urinary Problems 80
8 Vaginal Scarring/Shrinkage 43
9 Neuromuscular Problems 38
10 Recurrent Prolapse 32
Adverse Events
1) Mesh erosion in vaginaIntimate partner pain (His-pareunia)
2) Mesh erosion into urinary tract or bowel
3) Dyspareunia or Pelvic Pain
4) Voiding dysfunction

6
Mesh Erosion in the Vagina Presentation / Symptoms
� Symptoms : vaginal discharge, odor, vaginal pain, dyspareunia, or pain by the sexual partner
� Often asymptomatic �Wong et al. 56% incidentally found
� May present years after surgery
Wong K, et al. Adverse Events Associated With Pelvic Organ Prolapse Surgeries That Use Implants. ObstetGynecol 2013;122:1239–45
Mesh Erosion Rates
Vaginal approach prolapse surgery
� Cochrane 2013� Anterior mesh 11% erosion� Multiple compartments 18% erosion
Maher C et al. Surgical management of pelvic organ prolapse in women. Cochrane Database of Systematic Reviews 2013, Issue 4. Art. No.: CD004014.
Mesh Erosion Rates
Sacrocolpopexy
� 2.2% Mesh erosion or infection in 52 studies of >5600 patients� mean 26m f/u
� 10% Mesh erosion at 5y in RCT of open sacrocolpopexy (84% f/u)
Diwadkar et al. Complication and Reoperation Rates After Apical Vaginal Prolapse Surgical Repair A Systematic Review. Obstet Gynecol 2009;113:367–73Nygaard I, et al. Long-term Outcomes Following Abdominal Sacrocolpopexy for Pelvic Organ Prolapse JAMA. 2013;309(19):2016-2024

7
Mesh Erosion Rates
Mid-Urethral Slings
� 1.4%-2.2% (retropubic & trans-obt)
Schimpf MO, Rahn DD, Wheeler TL, et al. Sling surgery for stress urinary incontinence in women: a systematic review and metaanalysis. Am J Obstet Gynecol 2014; Jul;211(1):71.e1-71.e27.
Mesh Erosion
Risk Factors� Concomitant
hysterectomy � Vaginal Perforation� Diabetes� Smoking� Age
� Hematoma / Blood transfusion
� Trans-obt > Retropubic
Abed et al. Incidence and management of graft erosion, wound granulation, and dyspareunia following vaginal prolapse repair with graft materials: a systematic review. Int Urogynecol J (2011) 22:789–798Osborn DJ et al. Analysis of patient and technical factors associated with midurethral sling mesh exposure and perforation. Int J Urol. 2014 Jul 14. Kokanali MK, et al. Risk factors for mesh erosion after vaginal sling procedures for urinary incontinence. Eur J Obstet Gynecol Reprod Biol. 2014 Jun;177:146-50.
POP Mesh Erosion Management
Deffieux X, et al. Long-term follow-up of persistent vaginal polypropylene mesh exposure for transvaginally placed mesh procedures. Int Urogynecol J (2012) 23:1387–1390
Treatment EfficacyObservationVaginal EstrogenOffice ExcisionOR Excision
POP Mesh Erosion Management
1Wong K, et al. Adverse Events Associated With Pelvic Organ Prolapse Surgeries That Use Implants. Obstet Gynecol2013;122:1239–452Abed et al. Incidence and management of graft erosion, wound granulation, and dyspareunia following vaginal prolapse repair with graft materials: a systematic review. Int Urogynecol J (2011) 22:789–7983Crosby EC, et al. Symptom Resolution After Operative Management of Complications From Transvaginal Mesh. Obstet Gynecol2014;123:134–9
Treatment EfficacyObservation ?30% 1
Vaginal Estrogen 20% 1,2
Office Excision 43% 1
OR Excision 90-95% 1,3

8
Treatment EfficacyObservation ?30%Vaginal Estrogen 20%Office Excision 43%OR Excision 90-95%
POP Mesh Erosion Management
� OR excision may be best initial approach for symptomatic erosion
Skoczylas LC, et al. Managing mesh exposure following vaginal prolapse repair: a decision analysis comparing conservative versus surgical treatment. Int Urogynecol J 2013;24:119–25.
MUS Mesh Erosion Management
� Observation / Vaginal Estrogen� TOMUS “most” did not require surgery 1
� Vaginal mucosa flap 2
� 2/8 exposure recurrence, 8/8 persistent d/c
� Excision
1Brubaker L, et al; for the Urinary Incontinence Treatment Network. Adverse events over two years after retropubicor transobturator midurethral sling surgery: findings from the Trial of Midurethral Slings (TOMUS) study. Am J Obstet Gynecol 2011;205:498.e1-6.2Kim SY, et al. Vaginal Mucosal Flap as a Sling Preservation for the Treatment of Vaginal Exposure of Mesh. Korean J Urol 2010;51:416-419
Mesh Excision Approach
� Small / Focal� Dissect overlying epithelium off of mesh
~1cm from edge of erosion
Barber MD. Surgical Techniques for Removing Problematic Mesh. CLINICAL OBSTETRICS AND GYNECOLOGY Volume 56, Number 2, 289–302
Mesh Excision Approach
� Small / Focal� Dissect overlying epithelium off of mesh
~1cm from edge of erosion� Incise mesh and dissect from underlying tissue� Close epithelium
Barber MD. Surgical Techniques for Removing Problematic Mesh. CLINICAL OBSTETRICS AND GYNECOLOGY Volume 56, Number 2, 289–302

9
Mesh Excision Approach
� Large / Recurrent� Remove as much mesh as possible
vaginally� Know the implant� Consider epithelial augmentation with
biologic graft
Barber MD. Surgical Techniques for Removing Problematic Mesh. CLINICAL OBSTETRICS AND GYNECOLOGY Volume 56, Number 2, 289–302
Mesh Erosion or Perforation into Urinary Tract or Bowel
Mesh Erosion or Perforation into Urinary Tract or Bowel
� May happen early or late� May be asymptomatic or have subtle
symptoms� Increased risk with perforation, even if
repaired � Tip: Don’t lay mesh over a repaired -otomy
Paine M, et al. Transrectal mesh erosion remote from sacrocolpopexy: management and comment. Am J ObstetGynecol. 2010 Aug;203(2):e11-3.
Mesh in Bladder
� Consider options for approach� Vaginal � Laparoscopic / Laparotomy� Cystoscopic with Suprapubic port
� Consider possibility of ureteral involvement� Stenting / need for reimplantation
� Detailed counseling� Appropriate consults

10
Mesh in Bowel
� Consider options for approach� Rectal� Vaginal� Laparoscopic / Laparotomy
� Detailed counseling� Appropriate consults
Mesh in Urethra
� Approaches: transvaginal or transurethral� Optimize visualization� Nasal speculum� Hysteroscope� Grasp ie with Endoclose
Mesh in Urinary Tract or Bowel
Overall : Optimize Surgery
�Multi-Disciplinary Team�Wait for ideal time for patient�Very Carefully
Mesh and Pain

11
Mesh and Pain
� Dyspareunia 9%� RF = posterior colporrhaphy and mesh
erosion
� Dyspareunia rates are similar for mesh and native tissue prolapse repairs� Excision resolves pain ~50% of the time� Possible confounder: reporting /
identifying pain pre-opAbed et al. Incidence and management of graft erosion, wound granulation, and dyspareunia following vaginal prolapse repair with graft materials: a systematic review. Int Urogynecol J (2011) 22:789–798Crosby EC, et al. Symptom Resolution After Operative Management of Complications From Transvaginal Mesh. Obstet Gynecol 2014;123:134–9
Mesh and Pain
� Consider Physical Therapy � Before Pelvic Reconstructive Surgery if
patient has pain� In conjunction with surgical management
of post-operative pain
Voiding Dysfunction Voiding Dysfunction
Schimpf MO, Rahn DD, Wheeler TL, et al. Sling surgery for stress urinary incontinence in women: a systematic review and metaanalysis. Am J Obstet Gynecol 2014 Jul;211(1):71.e1-71.e27.
RetropubicMUS
Trans-obturatorMUS
Persistent voiding dysfunction
2.7% 2.4%

12
Voiding Dysfunction
� Retrospective of patients with voiding dysfunction who had Simple incision or Partial excision
� ~10% persistent retention� 50% if new incontinence procedure included
� 2% (simple) vs. 23% (partial) had repeat incontinence surgery
Agnew G, et al. Functional outcomes for surgical revision of synthetic slings performed for voiding dysfunction: a retrospective study. Eur J Obstet Gynecol Reprod Biol. Jul;163(1):113-6
Review
� Surgical mesh around the vagina provides effective and long lasting treatments� But is still a developing story…
� Mesh exposure in the vagina often does not require intervention
� Surgical excision usually is effective for mesh exposure treatment� But some women require multiple surgeries
Review
� Mesh in the bladder or bowel � Avoid placing mesh over organ repair� Multi-disciplinary approach
� Pelvic pain / dyspareunia should be queried + treated before PFD surgery
� Simple sling incision > Partial excision for Tx of post-op voiding dysfunction
Questions?

New Treatments For Fibroids
Vanessa Jacoby, MD, MASAssistant Professor
Obstetrics, Gynecology, & Reproductive SciencesUCSF
Disclosure
Principal Investigator, The ULTRA Trial Trial of laparoscopic radiofrequency ablationFunded by Halt Medical under contract with UCSF
*Investigator Initiated Research (IIR)*Study design, implementation, analysis, and publication are independent of Halt Medical
Impact of Fibroids
• 30% of premenopausal women
• #1 reason for hysterectomy (250,000/year)
• $34 billion/year to care for women with fibroids
• $17 billion for lost work and disability after surgery
Outline
• Medical Management• Antifibrinolytics• Hormonal modulations
• MR Guided Focused Ultrasound• Radiofrequency ablation
• Laparoscopic• Hysteroscopic

A 40 year old P2 presents with heavy menstrual bleeding and 2 intramural fibroids not contacting endometrium, 5cm and 4cm. Hb=11.5. Would you offer her tranexamic acid (lysteda) for heavy menstrual bleeding?
A. B.
35%
65%
A. YesB. No
Antifibrinolytic: Tranexamic Acid
• Nonhormonal• Binds to plasmin to inhibit fibrinolysis
Tranexamic Acid: RCT
Freeman et al, AJOG, 2011, pg 319. e1-7
• Placebo controlled trial (n=297)• 35% of participants had fibroids
• Excluded if number/size of fibroids required surgery based on surgeon opinion
• Starting EBL per menses 153-178cc• Tranexamic acid tid up to 5 days per menses
• 3.9g/day or 1.95g/day or placebo• Results reported for 3 cycles
Tranexamic Acid: RCT Results
Freeman et al, AJOG, 2011, pg 319. e1-7
2% decrease
26% decrease
39% decrease

Tranexamic Acid: Adverse Events and Limitations
Freeman et al, AJOG, 2011, pg 319. e1-7
• Potential risk of thromboembolism • Not observed in trials of tranexamic acid• Patients at risk have been excluded (including OCPs)• Contraindicated: hx or current thromboembolic disease
• Little known about fibroid subgroup • May be effective for women with fibroids, more
studies needed• 1300mg tid as needed day 1-5 for heavy bleeding• Patient can usually tell on day 1 if there is
improvement
Medical Management: Hormonal Manipulation
Drug Targets: Decrease hormone levelsSelectively block hormone action
Estrogen Progesterone
Progesterone Receptor Modulators
• Inhibits ovulation, decreases fibroid volume• Does not decrease serum estrogen levelsUlipristal Acetate • 2 RCTs in Europe• Participants had heavy bleeding, anemia, uterus
<16 weeks, planning surgery• 13 weeks of medication• Study underway to gain FDA approval to market in
U.S. (Watson Pharmaceuticals, NCT02147197)
Donnez et al, NEJM, 2012: 366:421-32.
Ulipristol Trials
Ulipristal vs. Placebo Ulipristal vs. Lupron
U 10mgN=94
PlaceboN=48
U 10mgN=95
LupronN=93
Amenorrhea 82% 6.3%* 89% 80%
Menstrualbleeding became normal
92% 19%* 98% 89%
Change in fibroid volume
-39% +3%* -42% -53%
Hot flashes
*p<.05 compared with U 10mg
10% 40%*
Donnez et al, NEJM, 2012: 366:421-32.

PRM Risk
• Potential for endometrial hyperplasia or cancer• Mixed results in studies with EMBs • NIH Pathology Panel classified new pattern of
endometrial changes: PRM-associated endometrial changes (PAEC)
• 10-15% of patients develop PAEC• More long-term study needed to assess natural
progression of this entity
Aromatase Inhibitors: letrozole and anastrozole
FibroidAromatase
EnzymeAndrogens Estrogen
• Blocks action of aromatase enzyme in ovaries and peripheral tissue, including fibroids
Letrozole: Decreases Fibroid Volume
Fibroid volume in cc
Parsanezhad et al, Fert Ster: Jan 2010: 93:1
46% decrease
Aromatase Inhibitors
• Side Effects• Estrogen levels in serum remain normal• No hot flashes
• Limitations• Small, uncontrolled trials, none in U.S. • Only 12 weeks of drug
• Long Term Risks• Concern for osteoporosis because studies of postmenopasual
women with breast cancer on AIs have found increased risk of fracture compared with women taking tamoxifen.
Larger, long-term, randomized trials needed to assess safety and efficacy

Other Medications
• Antiprogestin Mifepristone• Decreases fibroid size/bleeding• 10% endometrial hyperplasia/PAEC?
• Not available as needed for fibroids (5-50mg)
• GnRH antagonist Elagolix• Trial for FDA approval (recruiting, NCT01441635)
• Estrogen Receptor Modulator Raloxifene: • Preliminary studies with conflicting results, concern re: VTE
New devices to treat fibroids must be shown to be effective with comparative trials prior to FDA approval.
A. B.
61%
39%
A. TrueB. False
Fibroid Devices
• Unlike new drugs, FDA does not require comparative trials for new devices
FDA approves new device for fibroids
Insurance considers device experimental: Need RCTsDeclines coverage
RCTs conducted with support from:Industry (concern re: bias)NIH (too $$ to pay for device)
Limits ability to obtain gold standard evidence
Limits access to effective treatments
What is MRgFUS?
FDA approved 2003, very limited availability across U.S.
• Available in 9 states, 12 sites• 9/12 academic medical centers• In California:
UCSF, UCLA, UCSD, Stanford• Reimbursement is major challenge• Some sites offer treatment in research protocol

What is MRgFUS?
Diagnostic ultrasound waves•Focused ultrasound beamheats tissue to 150-1850 F
•Coagulative necrosis occurs
FDA approved 2003, very limited availability across U.S.
What is MRgFUS?
• Patient lies prone for 3-5 hours in MRI• Conscious sedation• Foley
• Hand held automatic stop button
What is MRgFUS?
A. B.
C. D.
nonperfused volume (NPV)
MRgFUS vs. UAE
UAE MRgFUS
Ioinizing radiation XHospital admission X (75%)
Return to normal activities
7-10 days 1-3 days
Potential for ovarian failure
X
Post-procedure fever/infection
X

Current Evidence on MRgFUS
• Largest study 359 women in U.S.A and abroad• Uncontrolled, all women underwent MRgFUS• Treatment volume limited due to FDA regulation• Industry sponsored
Stewart EA, Gostout B, et al, Obstet Gynecol, Aug 2007 Stewart EA, Gostout B, et al, Obstet Gynecol, Aug 2007
MRgFUS Symptom Improvement
Symptoms
No fibroids
Fibroids
MRgFUS Outcomes
Study N NPV Shrinkage Reoperation
Stewart et al 2007
(low treatment volume)
359 Variable 20% average Depends on NPV
(24% at 2 years for 45% NPV)
Gorny
2011
130 45% N/A 7.4% at 12 mo
LeBlang
2010
80 55% 31% at 6 mo N/A
Funaki
2009
91 40% at 24 mo 15% at 34 mo
Adverse Events
Outcome Percent
Abdominal pain 33%
Back or leg pain with sonications 13%
Nausea or emesis 11%
Bladder or catheter pain 14%
Abnormal vaginal discharge 11%
Skin burns 5%
Olive D, Obstet Gynecol, March 2008Parker W, Obstet Gynecol, Nov 2007

Pregnancy after MRgFUS
54 pregnancies (51 women)
Ongoing 20% (11/54)
Delivered 41% (22/54)
SAB 26% (14/54)
TAB 13% (7/54)
Antepartum hospitalization
18% (4/22)
Placenta previa 9% (2/22)
Term (14/15)
Rabinovici, et al, Fertility and Sterility, January 2010
Randomized Trials of MRgFUS• PROMISe: Pilot randomized, placebo-controlled trial
MRgFUSN=13
Sham MRgFUSN=7
RandomizedN=20
3 month change in:Fibroid Symptoms, Fibroid Size, Hematocrit
Jacoby VJ, Kohi M, Poder L, Jacoby A, Coakley F, Abstract, FUS Foundation, manuscript under consideration
Change in UFS-QOL Symptom Severity Score
p=.90 p=.20
-13
-31
Jacoby VJ, Kohi M, Poder L, Jacoby A, Coakley F, under consideration
Ongoing Randomized Trials
•Placebo-controlled trial for new MR Focused Ultrasound Device underway (Sonavelle device, Philips, NCT01504308)
•The FIRSTT Study: A Randomized Trial of MRgFUS versus UAE (NCT NCT00995878)
•NIH funded•Mayo Clinic (PI E. Stewart), UCSF, Duke•Enrollment closed August 2014

Radiofrequency Ablation The Radiofrequency Ablation Device
Generator with Foot Pedal
3mm RF Handpiece
Laparoscopic Ultrasound
• FDA approved for fibroids November 2012(Acessa)
Radiofrequency Ablation
• Fibroids identified with ultrasound
• Radiofrequency (RF) probe placed under ultrasound guidance
• Monopolar RF energy delivered to fibroids
• Tissue heats to 1000 C to cause coagulative necrosis
• Fibroid cells reabsorbed
Advantages of Acessa over Current Treatment
HospitalStay
RecoveryTime
Blood Loss Pain
Radiofrequency Ablation
0 5-9 days
32 cc Minimal
Open Hysterectomy
2-3 nights 4-6 weeks 300-500cc Moderate
Laparoscopicor Vaginal Hysterectomy
1 night 4 weeks 200cc Minimal-Moderate
Open Myomectomy
2-3 nights 4-6 weeks 250-500cc Moderate
LaparoscopicMyomectomy
0-1 2-4 weeks 200cc Minimal-Moderate

RF Ablation: Current Evidence
• Largest study, n=135 • Industry funded, FDA pivotal trial• Uncontrolled, all women treated with RF ablation• 2 year follow-up
Chudnoff et al, Green Jo, May 2013Guido et all, Health and Quality of Life Outcomes 2013, 11;139
RF Ablation: Current Evidence
UFS-QOL
Symptom SeverityScore
Quality of Life Score
3 months -52% +50%
12 months -57% +53%
24 months -59% +53%
Chudnoff et al, Green Jo, May 2013
RF Ablation: Current Evidence
Uterine Volume Fibroid Volume
3 months -15% -40%
12 months -25% -45%
Chudnoff et al, Green Jo, May 2013
RF Ablation: Current Evidence
• Adverse events: 4%
• Pregnancy (“not recommended” per FDA)• Not studied in women who desire future fertility• Insufficient data on pregnancy outcomes
Treatment Failure • <1% at 1 year, 5% at 2 years
Chudnoff et al, Green Jo, May 2013Guido et all, Health and Quality of Life Outcomes 2013, 11;139

RF Ablation: Ongoing Studies
• ULTRA• Uncontrolled nationwide study of Acessa• 3 years of follow-up to assess change in symptoms,
treatment failure, pregnancy outcomes (NCT02100904)
– Vizablate (NCT01226290): Hysteroscopic RF ablation
• TRUST (Halt Medical)
• RCT of Acessa vs. Myomectomy NCT02163525
Conclusions
• Several new medications, limited data on safety and efficacy
• Surgical treatments focused on minimally invasive approaches that leave fibroids in utero
• Long-term comparative trials are needed to confirm the durability of these treatments

Updates on Cervical Cancer Screening
George F. Sawaya, MDProfessor
Department of Obstetrics, Gynecology and Reproductive Sciences
Department of Epidemiology and BiostatisticsUniversity of California, San Francisco
Director, Cervical Dysplasia Clinic, San Francisco General Hospital
I have no financial interests in any product I will discuss today.
Objectives
• To understand the latest cervical cancer screening guidelines (updated in 2012)
• To understand areas of existing controversy
• To understand the current role of the bimanual pelvic examination in the context of less-than-annual screening
Background
• ~12,000 cervical cancer cases and 4,200 deaths per year in the US (ACS, 2010)
• ~50-60% of cases occur in never- and poorly-screened women
• ~80 million women at risk in the US• Most effective approach: screen unscreened
and poorly-screened women

SEER Cervical Cancer Rates: 2003-2007
http://seer.cancer.gov/statfacts/html/cervix.html
Effect of hysterectomy• Absolute rates and age-specific
patterns of cervical cancer incidence vary by race.
• White women: peak incidence at 65 to 69 years of age (corrected rate 83% greater than uncorrected)
• Black women: hysterectomy corrected incidence increased steadily with age up to age 65 to 69 years (corrected rate 126% greater than uncorrected)
Rostitch, Cancer, 2014
From virus to cancer
Schiffman and Wright NEJM2003;348(6):489-490
Cytology Primer
• ASC-US: atypical squamous cells of undetermined significance
• LSIL: low-grade squamous intraepithelial lesion • HSIL: high-grade squamous intraepithelial
lesion• AGC: atypical glandular cells of undetermined
significance (AGUS)

Histology Primer
Cervical intraepithelial neoplasia (CIN)Graded based on proportion of epithelium involved• CIN 1: indicates active HPV infection; treatment
discouraged since spontaneous resolution is high• CIN 2: most are treated, but about 40% resolve
over a 6-month period; treatment may be deferred in young women
• CIN 3: proximal cancer precursor
United States recommendations: the big 3
• American Cancer Society, American Society for Colposcopy and Cervical Pathology, American Society of Clinical Pathologists (ACS/ASCCP/ASCP) 2012CA Cancer J Clin2012
• American College of Obstetricians and Gynecologists (ACOG) 2012: Screening for Cervical Cancer. Number 131, November 2012
• US Preventive Services Task Force (USPSTF) 2012Cervical cancer screening. At http://www.uspreventiveservicestaskforce.org/uspstf/uspscerv.htm
Guidelines do not apply to immunocompromised women (HIV+), those with in utero DES exposure and those with prior CIN 2 or 3.
Evidence Review Evidence Based Practice Center: Evidence Report, May 2011
• Liquid-based and conventional cytology do not differ• HPV testing finds more precancerous lesions but has
unclear effects on cancer and on harms (e.g., additional colposcopies)
• HPV positivity incurs short-term adverse psychological effects
• Women with negative HPV tests and normal cytology may be at particularly low risk
http://www.uspreventiveservicestaskforce.org/uspstf11/cervcancer/cervcanceres.pdf

Age to Begin Screening
• ACS/ASCCP/ASCP (2012): begin at age 21 (“no screening” under age 21)
• ACOG (2012): same
• USPSTF (2012): begin at age 21 “regardless of sexual history”, “D” recommendation (don’t screen under age 21)
All agree: do not screen before age 21 years
Age to Begin Screening: Rationale
• Most dysplastic lesions low-grade and transient
• Long progression time of preinvasive lesions to invasive cancer
• Potential adverse effects of treatment (e.g., LEEP, cone biopsy) on pregnancy
Potential adverse effects of LEEP
Preterm delivery 70% increaseLow birth weight 82% increasePreterm premature 169% increase
ROMLancet2006 367:489-98
No randomized trials; evidence inconsistent.
Perinatal mortality 187% increaseSevere preterm delivery 178% increaseExtreme low birthweight 186% increase
BMJ 2008 Sep 18;337
Potential severe adverse effects of cone biopsy (not LEEP or cryotherapy)
Screening frequency: ages 21-29
• ACS/ASCCP/ASCP (2012): cytology every 3 years
• ACOG (2012): cytology every 3 years
• USPSTF (2012): cytology every 3 years (“A”)
All agree: no annual screening ACS/ASCCP/ASCP: “Women of any age should not be screened annually by any screening method.”
All agree: no HPV testing for primary screening USPSTF: “D” recommendation women under 30

So, should we screen virgins at age 21?
Not the intention of the USPSTF when they stated “regardless of sexual history”.
ACOG: “Speculum examinations for cervical cancer screening should begin at age 21 years, irrespective of sexual activity of the patient.”
ACOG Committee Opinion No. 534 August 2012
Screening frequency: ages 30-65
• ACS/ASCCP/ASCP (2012): screen every 3 years with cytology alone or every 5 years with cytology plus HPV testing (‘preferred’ strategy, but a ‘weak’ recommendation)
• ACOG (2012): same as ACS/ASCCP/ASCP
• USPSTF (2012): screen every 3 years with cytology alone or every 5 years with cytology plus HPV testing (but only for ‘women who want to lengthen the screening interval’)
USPSTF Conclusion: Co-testing
“Although there is evidence of harms of strategies that incorporate HPV testing in women age 30 to 65 years, the USPSTF concludes that there is adequateevidence that the longer screening interval for HPV testing with cytology reduces the magnitude of these harms by decreasing the opportunity for false-positive test results.”
ModelingFalse
positivesColposcopies CIN 2-3 Cancers Cancer deaths
Cytology q3 years, ages 21-65
350 758 80 8.5 1.55
Cytology q3 years until age 30 then co-testing q5 years
281 625 85 7.1 1.29
Per 1000 women screened over a lifetime.NB: Women with normal cytology and persistent HPV+ were returned to routine screening if colposcopy was normal.
“Modeling studies support similar benefits of co-testing every 5 years and cytology every 3 years, demonstrating small differences in expected cancer cases and cancer deaths.”

Current controversy
Should co-testing (HPV plus cytology) be preferredover cytology alone?
Commonly used HR HPV DNA tests
• Hybrid Capture 2: tests for one or more of 13 oncogenic HPV types; the low-risk probe has no clinical utility
• Cervista: tests for one or more of 14 oncogenic HPV types; type-specific testing available (16, 18)
• Cobas HPV test: tests for one or more of 14 oncogenic HPV types; type-specific testing available (16, 18)
USPSTF: Co-testing caveat
• “The percentage of U.S. women undergoing co-testing who will have a normal cytology test result and a positive HPV test result (and who will therefore require additional testing) ranges from 11% among women age 30 to 34 years to 2.6% among women age 60 to 65 years.”
USPSTF: Co-testing caveat
• “Women choosing co-testing … should be aware that positive screening results are more likely with HPV-based strategies… and that some women may require prolonged surveillance with additional frequent testing if they have persistently positive HPV results.”
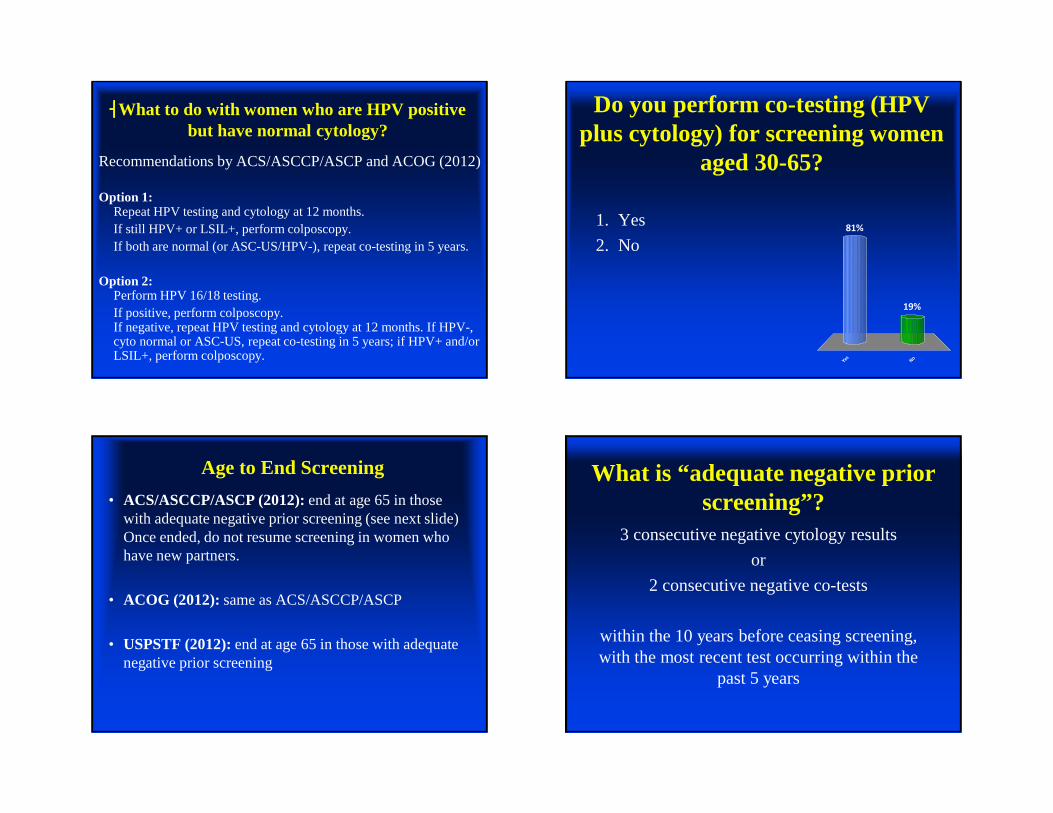
����What to do with women who are HPV positive but have normal cytology?
Recommendations by ACS/ASCCP/ASCP and ACOG (2012)
Option 1: Repeat HPV testing and cytology at 12 months. If still HPV+ or LSIL+, perform colposcopy.If both are normal (or ASC-US/HPV-), repeat co-testing in 5 years.
Option 2: Perform HPV 16/18 testing.If positive, perform colposcopy. If negative, repeat HPV testing and cytology at 12 months. If HPV-, cyto normal or ASC-US, repeat co-testing in 5 years; if HPV+ and/or LSIL+, perform colposcopy.
Do you perform co-testing (HPV plus cytology) for screening women
aged 30-65?
Y es
N o
19%
81%1. Yes
2. No
Age to End Screening
• ACS/ASCCP/ASCP (2012): end at age 65 in those with adequate negative prior screening (see next slide) Once ended, do not resume screening in women who have new partners.
• ACOG (2012):same as ACS/ASCCP/ASCP
• USPSTF (2012): end at age 65 in those with adequate negative prior screening
What is “adequate negative prior screening”?
3 consecutive negative cytology results
or
2 consecutive negative co-tests
within the 10 years before ceasing screening, with the most recent test occurring within the
past 5 years

Ending screening: regardless of age• ACOG, ACS and USPSTF: all agree that
screening following total hysterectomy with removal of the cervix for benign disease is not indicated. USPSTF: “D” recommendation
• ACOG (2003): If hysterectomy for CIN 2 or 3, may stop screening after 3 normal tests.
• ACOG (2012): Continued routine screening (cytology ever 3 years) recommended for 20 years.
USPSTF: Co-testing caveat
• “Because HPV test results may be positive among women who would otherwise be advised to end screening at age 65 years on the basis of previously normal cytology results alone, the likelihood of continued testing may increase with HPV testing.”
On the horizonCobas HPV test (14 HR types): FDA approved as a
primary screening test beginning at age 25 years
https://usdiagnostics.roche.com/en/hpv_ctng.html
What about the bimanual exam?

ACOG: bimanual pelvic examinations
• “No evidence supports the routine internal examination of the healthy, asymptomatic patient before age 21 years…” but
• “Annual pelvic examination of patients 21 years of age or older is recommended by the College.”
• Recommendation based on expert opinion
• “No evidence supports or refutes the annual pelvic examination or speculum and bimanual examination for the asymptomatic, low-risk patient.”
ACOG Committee Opinion No. 534 August 2012
Routine exams
“The decision to perform an internal pelvic examination, breast examination, or both should be made by the physician and the patient after shared communication and decision making.”
“Concerns, such as individual risk factors, patient expectations, or medical–legal concerns may influence the decision to perform an internal pelvic examination or clinical breast examination.”
ACOG Committee Opinion No. 534 August 2012
After removal of the uterus and ovaries in asymptomatic, low-risk* women
“The decision to receive an internal examination can be left to the patient…”
“Annual examination of the external genitalia should continue.”
ACOG Committee Opinion No. 534 August 2012
*no history of vulvar intraepithelial neoplasia, cervical intraepithelial neoplasia grade 2+, immunocompromise and in uteroDES exposure
“ACP recommends against perfoming screening pelvic exams in asymptomatic, nonpregnant adult women”

ACOG Response• “the College continues to firmly believe in the clinical
value of pelvic examinations, through which gynecologists can recognize issues such as incontinence and sexual dysfunction.
• While not evidence-based, the use of pelvic exams is supported by the clinical experiences of gynecologists treating their patients.
• Pelvic examinations also allow gynecologists to explain a patient’s anatomy, reassure her of normalcy, and answer her specific questions, thus establishing open communication between patient and physician.
http://www.acog.org/About-ACOG/News-Room/Statements-and-Advisories/2014/ACOG-Practice-Advisory-on-Annual-Pelvic-Examination-Recommendations
Do you perform bimanual pelvic exams in asymptomatic women?
Y es
N o
19%
81%
1. Yes
2. No
Survey: Bimanual Exams• 521 US OB/GYNs
• Nearly all perform bimanual pelvic examinations in asymptomatic women across the lifespan
• Reasons cited as “very important” included adherence to standard medical practices (45%), patient reassurance (49%), detection of ovarian cancer (47%), and identification of benign uterine (59%) and ovarian (54%) conditions.
Henderson et al AJOG2012
ACOG: focus on other important issues in women’s health
immunizations
smoking cessation
breast disease (CBE)
depression screening
violence screening
STI screening
family planning
wellness
Chelmow et al Obstet Gynecol 2012;119:695-9

Summary
• No cytology screening prior to age 21
• Annual cytology not recommended for most women
• Annual screening is recommended for high-risk women: e.g., immunocompromised (HIV+)
• Co-testing (HPV plus cytology) every 5 years may be equivalent to cytology every 3 years for women aged 30-65 years
Summary
• Women aged 30-65 who are resistant to screening every 5 years are poor candidates for co-testing (HPV plus cytology)
• Screen HPV vaccinated women same as others
• Screening with (conventional) cytology alone (without HPV testing) every 3 years is still a great option (and perhaps the least complicated)
• Be aware of limited data on benefits and harms of bimanual exams in asymptomatic women
Questions

10/22/2014
1
Treatment of Cervical Intraepithelial Neoplasia
George F. Sawaya for
Karen Smith-McCuneProfessor, Department of Obstetrics, Gynecology and
Reproductive Sciences
I have no conflicts of interest
Goals• Review literature about obstetrical outcomes
of treatments for CIN• Review morphometric considerations for
determining depth of treatment• Discuss special strategies for management of
CIN 2 and CIN 2/3 in reproductive aged women
Background• Before the advent of colposcopy, abnormal
Paps were treated by hysterectomy or conization
• With the advent of colposcopy, conservative methods were adopted: – ablative methods such as cryotherapy, laser
ablation, electrocautery or diathermy– excision with CO2 laser (laser conization)

10/22/2014
2
Background• With the introduction of the loop
electrosurgical excision procedure (LEEP, LLETZ) in the 1990’s, ablative methods mostly abandoned
• Advantages of treatment with LEEP: – provides a histological specimen– therefore can be used in a “see-and-treat” format
Choice of therapy: excision versus ablation
For ablative therapy (cryotherapy, laser ablation) the following conditions must be present:– satisfactory colposcopy– negative endocervical curettage– lesion fully visualized– no evidence of invasion– no glandular dysplasia or glandular atypia
Is ablative therapy effective?
• Cochrane review 2006
Kyrgiou et al 2006

10/22/2014
3
Choice of treatment modality• Current literature has suggested that
excisional treatment for CIN results in increased risk of preterm delivery
Obstetric sequelae of LEEP: systematic review 2003
• 5 articles included in the review• Findings: women who had LEEP had increased
risk of preterm delivery (OR 1.8, 95% CI 1.2-2.8) and low birth weight infants (OR 1.6, 95% CI 1.0-2.5)
• After matching for smoking, preterm birth remained significantly more common (OR 2.5, 95% CI 1.4-4.5)
Crane, Obstet Gynecol 2003;102:1058-62
Obstetric sequelae of cervical therapies:2006
• Systematic review and meta-analysis of the literature regarding obstetric outcomes after excisional therapy for CIN (cone, loop, laser)
• 27 studies included• Preterm birth defined as less than 37 weeks
Kyrgiou et al Lancet 2006
Obstetric sequelae of excisional therapies: meta-analysis 2006
Results:• Cold knife cone significantly associated
with preterm delivery <37 weeks – 14% versus 5%, relative risk 2.6 (95% CI
1.8-3.7)
• LEEP significantly associated with preterm delivery <37 weeks– 11% versus 7%, relative risk 1.7 (95% CI 1.2-2.3)
Kyrgiou et al Lancet 2006

10/22/2014
4
Obstetric sequelae of excisional therapies: meta-analysis 2006
- Similar adverse effects for laser conisation (relative risk for preterm delivery was 1.71 (95% CI 0.93-3.14). - laser ablation: no significantly increased risks for adverse obstetric outcomes observed
Kyrgiou et al Lancet 2006
Cochrane review
Limitations of the studies• Comparison groups mixed: some studies used
“external” controls (population based), which may not control well for confounding factors
• Some studies used “internal” controls (women who were treated before birth versus women who were treated after birth) to avoid some of the confounding
Obstetric sequelae of cervicaltreatment: meta-analysis 2011
• Excisional and ablative therapies for CIN • Separated results based on the comparison
group used in the study: external (population based)internal (birth before versus after treatment), and women with CIN treatment versus no treatment
• 30 studies- 27 were retrospectiveBruinsma and Griffin, BJOG, 2011

10/22/2014
5
Obstetric sequelae of excisional therapy for CIN: meta-analysis 2011
Results: • As seen in the other meta-analysis, excisional
treatment associated with a significantly increased risk of preterm labor:
• RR = approx 2 whether the comparison group was external or internal
• Effect of cold knife cone and laser cone (RR 3.41 and 3.58) more pronounced that LEEP (RR 1.85)
Bruinsma and Griffin, BJOG, 2011
• Ablative therapy also associated with a significantly increased risk of preterm labor: RR = 1.47 (95% CI 1.24-1.74) when the comparison group was external
• Ablative therapy not associated with a significantly increased risk of preterm labor when the comparison group was internal: RR=1.24 (95% CI 0.73-2.10)
Bruinsma and Griffin, BJOG, 2011
Control group is important
Meta-analysis 2008: perinatal mortality and other severe adverse pregnancy
outcomes associated with treatment of CIN
Cold knife cone associated with significantly increased risk of: • Preterm delivery <28 weeks (RR 5.3)• Low birth weight <2000 gm (RR 2.9)• Perinatal mortality (RR 2.87)
Arbyn et al, BMJ 2008
• LEEP associated with no increased risk of perinatal mortality (1.17, 95% CI 0.74-1.87)
• Cryotherapy and laser ablation not associated with increased risk of perinatal mortality, preterm delivery, or low birth weight
Arbyn et al, BMJ 2008
Meta-analysis 2008: perinatal mortality and other severe adverse pregnancy outcomes
associated with treatment of CIN

10/22/2014
6
Effect of size of excision • the deeper the LEEP or cone, the greater the
risk of preterm birth• For example, the risk of preterm birth
increased 6% for each mm of tissue removed (Noehr et al 2009, Obstet Gynecol)
• Height of the cone but not the volume or circumference of the cone significantly associated with the gestational age at delivery (Ortoft et al BJOG 2010)
LEEP and risk of preterm birth: U.S. data
• 241,701 singleton births at Parkland Hospital from 1992-2008– 511 had previously undergone LEEP– 842 subsequently underwent LEEP
• No differences in rates of preterm birth <34 weeks
Werner et al Obstet Gynecol 2010
Meta-analysis 2014• 19 studies that were restricted to LEEPs only • 2 categories of “unexposed” (no LEEP) women
were identified-– Those with no or unknown history of dysplasia– Those with a known history of dysplasia but no
excision
Conner et al Obstet Gynecol 2014
Meta-analysis 2014• Pooled RR of preterm labor <37 weeks for
LEEP was 1.6 (95% CI 1.3-1.9)• Pooled RR of preterm labor <34 weeks for
LEEP was 2.2 (95% CI 1.3–3.7)• Risk of perinatal mortality elevated in women
with a history of LEEP but not statistically significant (pooled RR 1.6, 95% CI 0.95–2.80).
Conner et al Obstet Gynecol 2014

10/22/2014
7
Meta-analysis 2014• There were 4 studies in which the
“unexposed” group were women with a history of dysplasia but no cervical excision
• No statistically significant difference in the risk of preterm birth when the prior LEEP group was compared to this group (pooled RR 1.08, 95% CI 0.88–1.33).
Conner et al Obstet Gynecol 2014
LEEP-to-pregnancy interval and obstetrical risks
• Multicenter retrospective cohort study 1996-2006
• 596 women had previously undergone LEEP and subsequently became pregnant
• Median time to pregnancy was 30.8 months (interquartile range 18.4-50.7)
• LEEP-to-pregnancy interval (<12 months versus ≥ 12 months) not associated with risk or preterm labor
Conner et al Obstet Gynecol 2013
LEEP-to-pregnancy interval and risk of spontaneous abortion
• LEEP-to-pregnancy interval of less that 12 months significantly associated with an increased risk of SAB (<12 weeks): 17.9% versus 4.6%, OR 5.6 (2.5-12.7)
• LEEP-to-pregnancy interval of less that 6 months showed an even stronger effect: 42.9% versus 4.3%, OR 16.8 (3.5-81.6) but the number of pregnancies in the 6 mo group was small (n=7)
Conner et al Obstet Gynecol 2013
Obstetrical outcomes after treatment for CIN: Summary of evidence
• No randomized trials• Studies limited by retrospective designs, by
the selection of control groups, and by confounding factors
• Biological mechanisms underlying the association not well understood

10/22/2014
8
Nevertheless the following results have been observed
– Excisional procedures appear to be associated with an increased risk of preterm delivery and perinatal mortality
– Shorter interval to subsequent pregnancy after LEEP (<12 months) may increase the risk of first trimester spontaneous abortion
– Data on cryotherapy and laser ablation do not show a strong association with adverse obstetrical outcomes
For treatment of CIN
What is the right depth of treatment to eradicate the disease without imparting unnecessary risk of preterm delivery in reproductive aged women?
Morphometric studies• Analysis of 319 cone specimens revealed that
an excision of 4.80 mm in depth will eradicate 99.7% of CIN3 lesions
• Depth increased with lesion severity: mean depth of CIN1 was 0.42 mm, CIN2 0.93 mm, and CIN3 1.35 mm
Abdul-Karim et al, Obstet Gynecol 1986
Morphometric studies• Analysis of 342 cone specimens revealed that
the mean depth of CIN into the cervical glands was 1.24 mm
• The deepest gland containing CIN that they found was 5.22 mm
• 99.7% of CIN lesions are located 3.80 mm from the surface
• Older women have deeper crypt involvement than younger women
Anderson and Hartley, Obstet Gynecol Survey 1979

10/22/2014
9
Effect of age on treatment outcomes• In a large retrospective study, failure rates for
each treatment modality increased with age• for treatment of CIN 3 with LEEP:
Melnikow et al, JNCI 2009
AGE FAILURE RATE21-29 8.6%30-39 9.6%40-49 12.9%>50 13.6%
Cryosurgery (Cryotherapy)• Historically was the 1st outpatient treatment
of CIN• Low cost, high patient safety• Easy to perform, well tolerated• Requires stringent patient selection guidelines• Clearance rates for CIN = 86% to 91.6%• Key predictor of success is depth of freeze
Courtesy E.J. Mayeux Courtesy E.J. Mayeux

10/22/2014
10
Cryotherapy
• Goal: create sufficient thermal injury to destroy abnormal cells
• -20 degrees Celsius necessary for cell death• For successful ablation: freeze beyond the
lesion
Cryotherapy• “Iceball” = freeze depth = lateral spread• Most tissue in this zone will necrose
Cervix
Cryoprobe
Courtesy E.J. Mayeux
Iceball

10/22/2014
11
Effect of age on treatment outcomes• In a large retrospective study, failure rates for
cryotherapy were unacceptably high for women over the age of 40:
Modality used for treatment of CIN 3
Failure rate in women aged 40-49 yr
Cone biopsy 8.5%LEEP 12.9%Laser 17.3%Cryotherapy 34.0%
Melnikow et al JNCI 2009
Laser ablation• CO2 laser common in dermatology outpatient
settings and used to be common in gynecological outpatient practices but have fallen out of fashion since the advent of the LEEP
• Modern equipment designed for easy use and storage in the outpatient setting

10/22/2014
12
LEEP• Given the results from the morphometric
studies, 99.7% of lesions are <5mm deep• Therefore it would be uncommon to need to
excise more than 7 mm of canal in women with satisfactory colposcopy
• Routine use of the “top-hat” LEEP should be avoided in women of reproductive age
CENTRAL TENETS for management of CIN in young women
• The underlying risk of cancer is very low• HPV infection and CIN lesions are common at
the onset of sexual activity• Clearance of HPV is common• Approximately 90% of CIN 1 lesions will regress• Approximately 40% of CIN 2 lesions will regress
ASCCP Guidelines for Management of CIN

10/22/2014
13
New ASCCP guidelines 2013
• In “young women” with high grade CIN, either treatment or observation is acceptable provided colposcopy is satisfactory (adequate)
• When CIN 2 is specified, observation is preferred
• When CIN 3 is specified, or colposcopy is inadequate, treatment is preferred
ASCCP.com
New ASCCP guidelines 2013
• “The term ‘young women’ indicates those who after counseling by their clinicians consider risk to future pregnancies from treating cervical abnormalities to outweigh risk for cancer during observation of those abnormalities. No specific age threshold is intended.”
Management guidelines for surveillance of CIN 2 (and CIN 2/3) in young women
• Perform colposcopy and cytology every 6 months.
• If colposcopy worsens or if HSIL persists for one year, repeat colposcopic biopsy, and if it now shows CIN 3, treatment is recommended
• IF CIN 2 persists for 24 months, treatment is recommended
Figure 17, ASCCP 2013 consensus guidelines
Case #1A 31 year old woman has an abnormal cytology result. She is referred for a diagnostic workup. Colposcopy is adequate (satisfactory), there is a visible lesion from 12-4 o’clock, and the biopsy shows CIN2. She is on oral contraceptives and has one child. She and her husband want to have another child in the next year.

10/22/2014
14
How would you treat this woman?
1 2 3 4 5
43%
8%
1%
48%
1%
1. Observation 2. LEEP3. Laser ablation4. Cryotherapy5. Cone biopsy
Case #2A 26 G1P1 year old woman has an abnormal cytology result. She is referred for a diagnostic workup. Colposcopy is adequate (satisfactory), there is a visible lesion from 12-4 o’clock, and the biopsy shows CIN3. She is on oral contraceptives and has one child. She and her husband want to have another child in the next year.
How would you treat this woman?
1 2 3 4 5
1%
65%
1%
26%
7%
1. Observation 2. LEEP3. Laser ablation4. Cryotherapy5. Cone biopsy
Questions?
1

Slide 56
1 Karen McCune, 10/23/2013

10/22/2014
15
Case #3A 26 year old G1P1 woman has an abnormal cytology result. She is referred for a diagnostic workup. Colposcopy is inadequate (unsatisfactory), there is a visible lesion from 12-4 o’clock, and the biopsy shows CIN3. She is on oral contraceptives and has one child. She and her husband want to have another child in the next year.
How would you treat this woman?
1 2 3 4 5
0% 0% 0%0%0%
1. Observation 2. LEEP3. Laser ablation4. Cryotherapy5. Cone biopsy
Countdown
10
Case #4A 48 year old woman has an abnormal cytology result. She is referred for a diagnostic workup. Colposcopy is satisfactory, there is a visible lesion from 12-4 o’clock, and the biopsy shows CIN 2/3. She has 3 children and had a tubal ligation after her last delivery.
How would you treat this woman?
1 2 3 4 5
0% 0% 0%0%0%
1. Observation 2. LEEP3. Laser ablation4. Cryotherapy5. Cone biopsy
Countdown
10

10/22/2014
16
Conner et al Obstet Gynecol 2014

The CDC 2014 Providing Quality Family Planning (QFP) Services Guidelines
Michael S. Policar, MD, MPHClinical Professor of Ob, Gyn, and Repro SciUCSF School of [email protected]
ObGyn Update: What Does the Evidence Tell Us?October 22, 2014
• There are no relevant financial relationships with any commercial interests to disclose
Purpose of the QFP• The intended audience is all providers of family planning
services, including Title X grantees• Key purposes are to
– Define which services should be offered in a family planning visit, and to describe how to do so
– Support consistent application of quality care across settings and provider types
– Translate research into practice, so the most evidence-based approaches are used
So…What’s The “Big Deal” About The QFP?• Completes, and ties together, the CDC “suite” of family
planning guidelines• Defines and prioritizes the core content of contraceptive
services• Defines the “borders” between family planning and other
preventive services• Specifies which interventions are recommended for each of
the 7 family planning service types• Emphasizes the role and content of contraceptive counseling• Refines the content of male family planning services

The “Suite” of CDC Family Planning Recommendations
MMWR 2010,59 (RR04):1-6
Focus on safety in women with a variety of medical conditions
MMWR 2013;62(5):1-60
Focus on efficacy in women and men using contraceptives
MMWR 2010; 59 (RR-12): 1
Updated Guidelines to Be Published in 2014

MMWR 2006;55(RR-14):1-17
MMWR 2006; 55 (RR06): 1-23
Filling The “Gaps”• Pregnancy testing
and counseling• Achieving pregnancy• Basic infertility• Preconception health• Preventive health
screening of women and men
• Contraceptive counseling, incl reproductive life plan
Frameworkof the QFP
Core: Family planning
Related PHS: reproductive health, but not corefamily planning
Other PHS : not reproductive health or core family planning”

How Are Core Family Planning (FP) Services Different from “Well Woman” Care?
• Core FP services focus upon – Avoiding pregnancy or becoming pregnant– Safe and effective contraceptive use– Protection of reproductive health
• Additional preventive services may be performed by– The patient’s primary care provider (PCP), or– Her family planning clinic, in the absence of a PCP
• Given limitations of time and resources, provision of core family planning services is our top priority!
Well Woman Preventive Services• Recommended, but optional, related and other
preventive health services at any given visit based upon – Individual client choice– Avoidance of duplication of services performed by
the primary care provider or elsewhere– Provider attitudes and preferences, as reflected in
site-specific policies and protocols

QFP: Other Preventive Health ServicesInterventions unrelated to core family planning
Discuss and counsel
• Healthy diet counseling• Dental health• Injury prevention• Breast cancer preventive medication• Tobacco and drug use cessation interventions• Administer vaccines: DTaP booster, influenza, rubella
Screening • Colorectal cancer screening• DM, hyperlipidemia screening (unrelated to BCM)• Skin cancer screening (high risk)• Thyroid disease (high risk)
Test• Bacteriuria screening with urinalysis• Genital herpes screening• Chlamydia screening in low risk women >26 and males of all ages• Gonorrhea screening in low risk persons• Syphilis screening in low risk persons• Bacterial vaginosis and trichominiasis screening• Hepatitis B screening• Hepatitis C screening in low risk persons• Ovarian cancer screening in low risk women• BRCA mutation testing in low risk women
QFP: Routine Interventions to Avoid…Based on USPSTF Recommendations
QFP Recommendations About Clinical Services
QFP: Contraceptive Services• Remove clinical barriers as a prerequisite to contraceptive
provision– Screening pelvic exams not routinely needed, unless
inserting IUD– Annual cervical cytology– Routine HIV screening
• In accordance with CDC’s MEC and SPR• Offer a full range of FDA-approved methods• Use an evidence-informed counseling process, which is
client-centered and includes contraceptive effectiveness

QFP: Preconception Health Services• Preconception health services should
be offered to female and male clients • Priority populations
– Trying to achieve pregnancy, including negative preg test visits
– Removal of IUC or implant to become pregnant
– Basic infertility services– Clients at high risk of unintended
pregnancy
QFP Recommendations: Counseling & Education
Five Principles of Quality Counseling
1: Establish and maintain rapport with the client
2: Assess the client’s needs3: Work interactively to
establish a plan4: Provide information that can
be understood and retained5: Confirm client understanding
Case Study• 33 year old G3P3 established patient seen for family
planning health screening visit• Using metformin for type 2 diabetes• Mutually monogamous relationship• Recent fasting lipid profile normal• LMP 3 weeks ago; using condoms for contraception• Cervical cytology test 2 years ago was negative• Screened negative for HIV in each of her 3 pregnancies

Case Study• Would like to start oral contraceptives…today if possible
– 13 cycles of monophasic dispensed• Face-to-face time: 23 minutes; 18 minutes counseling• What needs to be done in regard to…
– Counseling? – Method choice?– Screening tests?– Encounter coding?– Out-of-pocket cost sharing (e.g., co-payment)?
Reproductive Life Plan Questions • Do you hope to have any (more) children?• How many children do you hope to have?• How long do you plan to wait until you next become
pregnant?• How much space do you plan to have between your
pregnancies?• What do you plan to do until you are ready to become
pregnant?• What can I do today to help you achieve your plan?
“One Key Question”
www.onekeyquestion.org
OC/P/R POP DMPA Impl LNG-IUD
Cu-IUD
Hx gestational diabetes 1 1 1 1 1 1
Nonvascular diseasei. Noninsulin-dependent 2 2 2 2 2 1ii. Insulin-dependent 2 2 2 2 2 1
Nephropathy/retinopathy/neuropathy
3/4 2 3 2 2 1
Other vascular disease or diabetes of >20 yrs’ duration
3/4 2 3 2 2 1
US MEC 2010: Diabetes

SPR Appendix B: When To Start Using Specific Contraceptive Methods
Method When to start Back-Up ExamCu-IUC Anytime none pelvic examLNG-IUS Anytime If >7d* Pelvic examImplant Anytime If >5d* noneInjection Anytime If >7d* noneCHC Anytime If >5d* BPPOP Anytime If >5d* none
* After the first day of menstrual bleeding
SPR Appendix C: Exams And Tests Needed Before Method Initiation
Examination Needed for Blood pressure OC, patch, ringClinical breast examination NoneWeight (BMI) Hormonal methodsBimanual examination, cervical inspection IUC, cap, diaphragmGlucose, Lipids NoneLiver enzymes NoneThrombogenic mutations NoneCervical cytology (Papanicolaou smear) NoneSTD screening with laboratory tests NoneHIV screening with laboratory tests None
SPR Appendix D: Routine Follow-Up After Contraceptive Initiation
IUC Implant Injectable CHC POPReturn any time X X X X XAssess satisfaction at routine visits
X X X X X
Asses for change in health status (MEC 3,4)
X X X X X
Consider string check XConsider assessing weight change
X X X X X
Measure blood pressure X
CDC 2010: Routine STI Screening in WomenAge 18-20 21-25 26-29 30-39 40-49 50-59
CT (Both) Annually Hi riskGC (Both) Hi RiskHIV
Once, then Hi risk only
Syphilis Hi RiskVag trich Hi RiskHepatitis C- CDC 2012
Hi risk
Routine annual screening of sexually active women under 26One time screening of adults born 1945-1965

Routine Cancer Screening in Women Age 18-20 21-25 26-29 30-39 40-49 50-59
Cervix CA•Cytology•Co-testing
NoneNone
Q 3 yrsQ5 yrs
CBE•ACS
None Q 3 yrs X Annual with MG
Mammogram•ACS•USPSTF
None Hi Risk[I]
AnnualQ2y [C] Q2y [B]
Colorectalcancer None Hi Risk [A]ACOG: Am College of Ob-GynACS: American Cancer Society
CBE: Clinical breast examCDC: Centers for Disease ControlUSPSTF: US Prev Services Task Force
Preconception Care for Diabetics
• Diabetes in pregnancy is associated with higher rates of– Miscarriage– Fetal malformations: esp cardiac and neural tube defect – Pre-eclampsia, preterm labor– Macrosomia, birth injury, and perinatal mortality
• Lower risk if optimal glycemic control, before & during pregnancy– Insulin to achieve target blood glucose levels– Use metformin as an adjunct or alternative
Mahmud M, Mazza D: Preconception care of women with diabetes: a review of current guideline recommendations. BMC Women’s Health 2010 10:5
Preconception Care for Diabetics
Mahmud M, Mazza D: BMC Women’s Health 2010 10:5
Counseling• Folate 5 mg daily pre-conceptually until 12 weeks gestation• Inform about risk of miscarriage, congenital malformation and
perinatal mortality with poor metabolic control • Inform re: how DM affects pregnancy and pregnancy affects DM• Use effective contraception until target blood glucose is achieved• Encourage smoking cessation and reduction in alcohol intake• Encourage management of weight to achieve a BMI < 27Contraindications to pregnancy• HbA1C >10%• Impaired renal function (increased risk of progression to dialysis)
ADA 2014 Guidelines: Preconception CareMaintain A1c levels as close to 7.0% as possible before conceptionAll women of childbearing potential
Provide preconception counseling starting at puberty
Evaluate and treat ( if necessary) all women contemplating pregnancy
• Retinopathy• Nephropathy• Neuropathy• CVD
Evaluate and consider risk/benefit profile of medications used for DM
Contraindicated/not recommended •Statins•ACEIs (AT-converting enzyme inhibitor)•ARBs (AT receptor blocker)•Non-insulin therapy, except metformin
ADA, Diabetes Care 2014; 37 (supp 1): S14-S80

Summary of Patient Management• QFP: review reproductive life plan; discuss all methods• MEC: can use oral contraceptives with same day start• SPR: assess BP, BMI only• STD: no STI screening tests indicated• HIV: screening not necessary• Cancer screening: clinical breast exam Q 1-3 years• Preconception care:
– Discuss preconception glucose control with all diabetics• How should I code this visit???
Problem Oriented E/M Visits
HISTORY
EXAM
MEDICAL DECISION MAKING
TIME
Either:•Composite of 3 key
components (Hx + PE + MDM)
Or •TIME, when greater
than 50% of time is spent in counseling
Established Time (typical)99211 < 7 (5)99212 8-12 (10)99213 13-20 (15)99214 21-33 (25)99215 >33 (40)
New Time (typical)99201 < 15 (10)99202 16-25 (20)99203 26-37 (30)99204 38-53 (45)99205 > 53 (60)
Problem Oriented E/M: Face-to-Face Time “Midpoints”
E/M: Preventive Medicine Services
Age New patient Established12-17 yrs old 99384 9939418-39 yrs old 99385 9939540-64 yrs old 99386 9939665 yo or older 99387 99397
• Preventive medicine: “check-up” visit

Case Study: AnswerCPT code/HCPCS II code ICD9-CM
Procedure NoneSupplies NoneDrug S4993 (OCs) x 13 cycles V 25.01 (prescription of
oral contraceptives) Lab NoneE/M • 99214 (problem visit, 25 min)
or• 99395 (preventive medicine
service,18-39 yo)
1o: V 72.31 (routine GYN exam)2o: V 25.01 (prescription of oral contraceptives)
• Six CDC-developed evidence based guidelines are now available that cover most clinical circumstances that occur in family planning clients
• The QFP fill in gaps left between the guidelines and then “ties” all the guidelines cohesively
• Most family planning services will be coded based on time , not on physical assessment or lab testing
• Most women covered by commercial health insurance, Medicaid, state FP programs, and Title X will have no out-of pocket costs for contraceptives
Clinical Pearls
Go Giants!!!

10/23/2014
1
Complex contraceptionJennifer Kerns, MD, MPHAssistant Professor, UCSFObstetrics, Gynecology and Reproductive SciencesSan Francisco General HospitalOctober 2014
Disclosures• I have no relevant financial disclosures
Objectives• To review resources for assessing the safety of contraceptive methods for particular women
• To review the evidence for selected practice recommendations for women with particular medical issues
• To emphasize the need for contraception especially for medically complicated women
Contraceptive Prevalence & Maternal Deaths
Ahmed et al. Lancet. 2012

10/23/2014
2
Are you familiar with the US Medical Eligibility Criteria for Contraception?
a. b.
16%
84%
a. Yesb. No
Are you familiar with the US Selected Practice Recommendations for Contraception?
a. b.
42%
58%a. Yesb. No
Can my patient use this method?
CDC Medical Eligibility Criteria• Evidence-based guidelines for safety of methods with co-existing conditions
• Similar to WHO but US-specific www.cdc.gov/mmwr/preview/mmwrhtml/rr59e0528a1.htm
CDC Medical Eligibility Criteria (MEC)

10/23/2014
3
MEC Categories1 Can use the method No restrictions2 Can use the method Advantages generally
outweigh theoretical/proven risks
3 Should not use method unless no other method is appropriate
Theoretical/proven risks generally outweigh advantages
4 Should not use method Unacceptable health risk
Medical Condition
Birth Control Methods
MEC Category
Where do you find the US MEC?

10/23/2014
4
ACOG Resource New Textbook
Case #119 yo G0, newly sexually active, wants to start the contraceptive vaginal ring. But she is concerned about what she has read in the news about the ring causing blood clots.

10/23/2014
5
DVT Risk with the Contraceptive Vaginal Ring (CVR)• Retrospective cohort: 9,429,128 woman years• Confirmed VTE events per 10 000 woman years▫ Non-users of hormonal contraception 2.1▫ Combined Oral Contraceptives 6.2 (RR 3.2)▫ Transdermal patches 9.7 (RR 7.9) ▫ Vaginal ring 7.8 (RR 6.5)
Ring +1.6 additional cases / 10,000 women-years. Adjusted Rate Ratio 1.9 (1.3-2.7) v. COC
Lidegaard et al. BMJ 2012
DVT Risk with the Contraceptive Vaginal Ring (CVR)
• Prospective cohort - 66 489 woman years of observation• Confirmed VTE events per 10 000 woman years▫ LNG COC 7.8▫ All COC 9.2▫ Vaginal ring 8.3
Ring - no increased risk compared with any pill. HR 0.8 (0.5-1.5)
Dinger et al. Obstet Gynecol 2013
DVT Risk with the Contraceptive Vaginal Ring (CVR)• Retrospective cohort - 573, 680 women• Confirmed VTE events per 10 000 woman years▫ All COC – new users 8.2 (7-9.6)▫ Vaginal ring 11.3 (4.26-32)
Ring - no increased risk compared with the pill (after adjustment)HR 1.1 (0.6-2.2)
Sidney et al. Contraception 2013

10/23/2014
6
Case #119 yo G0, newly sexually active, wants to start the
contraceptive vaginal ring. • Conflicting level 2 evidence – may cause slight
increase risk relative to COC• Attributable risk = very, very small• Level I evidence that women use it correctly
compared with pill• May cause fewer unintended pregnancies and
therefore fewer VTE overall
VTE & Oral Progestin Type• Desogestrel and drosperinone COCs may increase risk of VTE
• BUT. . . Absolute risk remains lowNon-pregnant, no COCs: 2-4 per 10,000 ♀- yrs• Levonorgestrel COCs: 5.0 per 10,000 ♀- yrs• Desogestrel COCs: 6.5 per 10,000 ♀- yrs• Drosperinone COCs: 7.8 per 10,000 ♀- yrs
Lidegaard BMJ 2009 Heinemann Contraception 2007
Choosing a COC• Careful with very low-dose estrogen – ↑ bleeding• Monophasic fine• Levonorgestrel may cause fewer VTE• No clear benefit of drospirenone▫ PMDD: fewer sxs 6 months – equivalent at 2 yr▫ Acne: Equivalent to other pills
• 30 or 35 mcg EE + levonorgestrel• Shortened or erased placebo week if possible• Monophasic
VanViet Cochrane 2006LaGuardia Contraception, 2003Freeman Womens Health 2001van Vloten Cutis 2002
CDC MEC
All progestin-only methods are safe even if:
1) Current VTE2) No anti-coagulation3) Provoked or unprovoked VTE

10/23/2014
7
Case #238 yo G2P1T1 woman is seeking contraception.
She had pre-eclampsia during her last pregnancy but otherwise reports she is healthy.
Wt= 226 lbsHt= 5’5” (BMI = 37.6)
BP=138/89
Obesity and Contraception
Institute of Medicine. Weight gain in pregnancy: Reexamining the guidelines
Efficacy•Pharmacokinetics•Oral vs. non-oral•Risk of pregnancy
Adverse events•Risk of VTE•Risk of CV events•Metabolic effects
–Weight gain? Lipid profiles?
Obesity & Contraceptive Efficacy
1 Lopez LM Cochrane 2010 2 McNicholas Obstet Gynecol 2013 3 Edelman Contraception, 20094 Westhoff Obstet Gynecol 2005 5 Zieman Fertil Steril 2002
DMPA: no difference1
Ring: no difference1,2
Implant: lower serum level, but still inhibitory1,4
IUC: no difference
OCs: no clear difference; longer time to steady state1,2
Patch: increased failure5 if >90kg• BUT BMI more relevant measure• No effect with BMI1,2
Obesity & Contraceptive Risks• VTE risk▫ COCs & obesity are independent risk factors for VTE� Obesity doubles risk of VTE
▫ No data show synergistic, increased risk ▫ Risk is lower than pregnancy (29/10,000 ♀-yrs)
Note: no safety information on women with BMI >40

10/23/2014
8
Contraception & Weight Gain• Pill, Patch, Ring: none or age-expected change1,2,3,6
• LNG-IUS: age-expected weight gain4
• ENG implant: minimal if any effect5
• DMPA:
1. O’Connell 2001 Contraception; 2. Gallo 2004 Obstet Gynecol; 3. Berenson AJOG 20094. Ronnerdag Acta Obstet Gynecol Scand 1999 5. Darney Fertil Steril 2009 6. Beksinka Contraception 20107. Pantoja Contraception 2010 8. Bonny Contraception 2010
Pantoja 2010
•Average 5-6 kg over 3-5yrs3,6•Baseline BMI:
•Nl and overwt = �risk7•No assoc for adolescents8
•Adolescents:•More pronounced wt gain5
•Early wt gain @ 6mo (>5%) predicts future wt gain8
BMI>30
BMI 25-30
BMI<25
Metabolic Syndrome• Constellation of findings which increase risk of CHD,
stroke, & type 2 DM
• 3 or more risk factors▫ Hypertension ▫ Insulin resistance▫ Central obesity▫ High triglycerides▫ Low HDL
≥130/85FBS ≥100Waist circumference ≥35”≥150 mg/dL≤ 50mg/dL
Metabolic Syndrome & ContraceptionLIPIDS CHC: �TGL, HDL, �LDL1
For PCOS, improved LDL/HDL ratio2
DMPA: transient worsening of lipids post-injection3
ENG Implant: � Chol, LDL, HDL4,5
BLOOD PRESSURE
OCP: 5% develop reversible HTN (7mm Hg)6
INSULIN RESISTANCE
No DM:• OCs, LNG-IUS, implant: No impact7
• Ring: improved IR in PCOS8
• DMPA: no effect9 vs. small increase in FBS (3mg/dL over 2yrs)10
For obese women: DMPA increased IR v. non-obese women+ DM:• DMPA: No RCTs. Increase in FBG 103-112• OCP: No increase in insulin requirement or end-organ damage11
1. Winkler 2009 Contraception 2. Falsetti 1995 Acta Obstet Gyn Scand 3. WHO 1993 Contraception4. Merki-Feld 2008 Clin Endocrinol 5. Inal 2008 Eur J Contr Reprod HC 6. Darney & Speroff 2005 Clin Guide for Contraception7. Grimes 2009 Cochrane 8. Battaglia 2009 Fertil Steril 9. Fahmy 1991 Contraception 10. Berenson 2011 Obstet Gynecol 11. Skouby 1984 Fertil Steril
CDC MEC

10/23/2014
9
Bariatric Surgery & Contraception• Advisable to wait 1-2 years after surgery
before planning pregnancy1• Fecundity & pregnancy rates often
increase after surgery2,3
▫ Especially in adolescents(13% vs. 6%)▫ Prevent unintended pregnancy
• Recommend non-oral methods for surgeries that impair GI absorption4
▫ Decreased absorption of OCPs1. ACOG Practice Bulletin 105, 20092. Merhi 2007 Fertil Steril3. Roeherig 2007 Obes Surg4. Mehri 2007 Gynecol Obstet Invest
CDC MEC
Oral absorption
Case #2
38 yo G2P1T1 obese woman desires birth control
• Assess for other risk factors• If none, all methods are safer than pregnancy• If smoker or other risk factors – may avoid CHC• DMPA – concern for insulin resistance and weight gain• For EC – recommend ulipristal acetate or Cu-IUD
Case #3An 18yo G0 presents having had unprotected sex the night before, requesting emergency contraception. Her BMI is 34.She had been using pills, but had a hard time remembering to take them.What do you offer her?
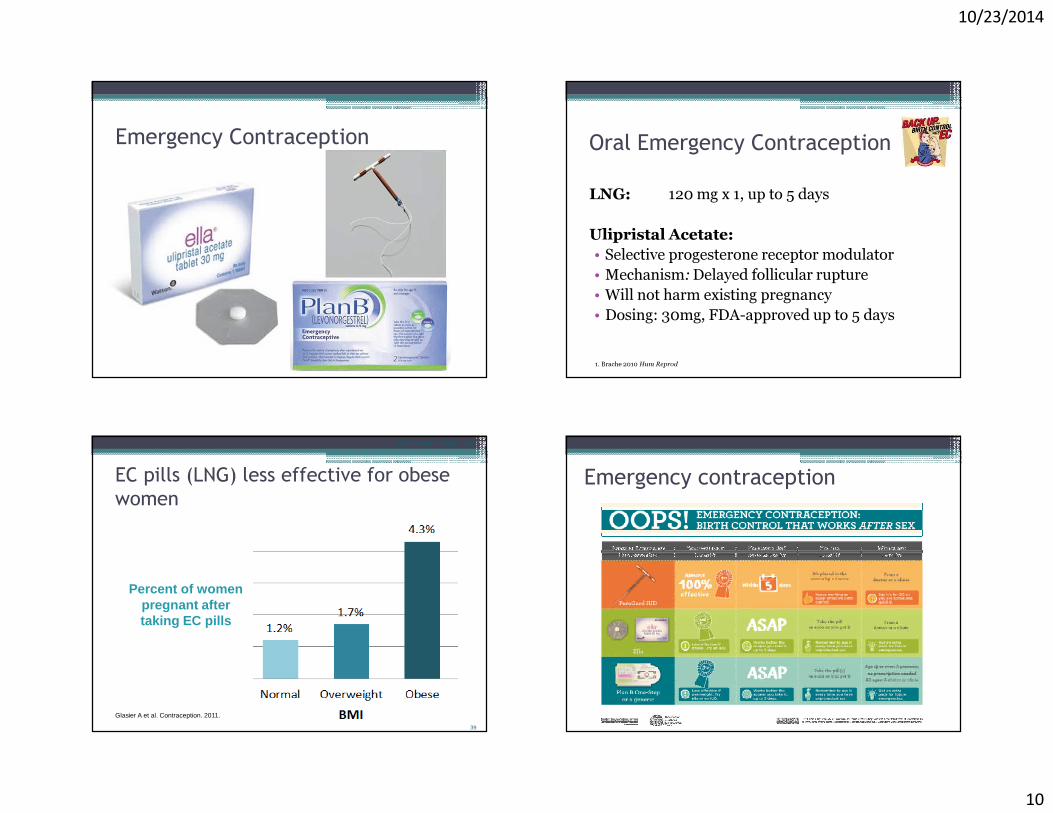
10/23/2014
10
Emergency Contraception Oral Emergency ContraceptionLNG: 120 mg x 1, up to 5 days
Ulipristal Acetate:• Selective progesterone receptor modulator• Mechanism:Delayed follicular rupture• Will not harm existing pregnancy• Dosing: 30mg, FDA-approved up to 5 days
1. Brache 2010 Hum Reprod
39
EC pills (LNG) less effective for obese women
Glasier A et al. Contraception. 2011.
Misinformation about LARC
Percent of women pregnant after taking EC pills
Emergency contraception

10/23/2014
11
Case #423 yo G0 is interested in using an IUD.History of chlamydia in college.She has had 3 male partners in the past year.Do you screen her for GC/CT?
Can women who have no children use an IUD?
Yes!
Misinformation about LARC
Veldhuis H. Eur J Gen Pract. 2004.Suhonen S et al. Contraception. 2004.Thonneau P et al. Human Reprod. 2006.ACOG Committee Opinion 539. Obstet Gynecol. 2012.
Some considerations…• Skyla (13.5mg LNG, 3yrs)• Pre-insertion pain medication• Paracervical block
43
Can women with a history of STIs use an IUD?Yes! Past infections are not a contraindication to any method of contraception.
Misinformation about LARC
ACOG Practice Bulletin. Obstet Gynecol. 2005.Skjeldestad, et al. Contraception. 1996.Centers for Disease Control. MMWR. 2010.
CDC Medical Eligibility for Initiating Contraception
ConditionLNG-IUS or Copper IUD
Sexually Transmitted Infections
Current vaginitis 2
Current chlamydia, gonorrhea, or purulent cervicitis
4
44
Can women with a history of PID use an IUD?Yes! Women with PID history can use IUDs.Active PID is a contraindication
Misinformation about LARC
ACOG Practice Bulletin. Obstet Gynecol. 2005.Skjeldestad F et al. Contraception. 1996.Centers for Disease Control. MMWR. 2010.
CDC Medical Eligibility for Initiating Contraception
ConditionLNG-IUS or Copper IUD
Pelvic inflammatory disease
Past PID, subsequent pregnancy 1
Past PID, no subsequent pregnancy
2
Current PID 4

10/23/2014
12
What we know about IUDs and PID• Unprotected sex w/ infected partners� PID• Transient increased risk at insertion
▫ 22,908 insertions: � 9.7/1000 w/in 20 days � 1.4/1000 after 20 days
• Beyond time of insertion▫ Overall decreased risk with LNG IUS ▫ No increased risk with Copper IUD
Farley Lancet 1992Walsh Lancet 1998
Routine GC/CT screening not necessary
� Retrospective cohort, n=57,728 IUD insertions� Evidence-based STI screening, tx if + test
Sufrin et al Obstet Gynecol 2013
Among all women: Risk of PID
Non-screened = ScreenedOR= 1.05 (0.78, 1.43)
Among screened women:Risk of PID
Same day = Pre-insertionOR=0.99 (0.64, 1.54)
Women appropriately selected for non-screening
Most accurate screening time is day of insertion
Who should be screened?• CDC and USPSTF guidelines for GC/CT screening at IUD insertion▫ Annually if < 26 yo and sexually active▫ Any time if risk factors (new partner, sx’s, other STI)
• Screen on same day as insertion• No cases of PID when Planned Parenthood switched to same day screening
• No benefit to prophylactic antibioticsUSPSTF Am J Prev Med 2001 CDC MMWR #59 2010 Goodman Contraception 2008Grimes Contraception 1999
Conclusions• Contraception is important for women with medical problems
• There are many methods that are appropriate for any given medical problems
• Consult the appropriate resources to help guide contraception recommendations

PrEP Guidelines for the Ob/Gyn
Dominika Seidman, MDObstetrics and Gynecology Update
October 22, 2014
I have no conflicts of interest to declare.
Outline• The need for PrEP: HIV treatment and prevention
gap
• What is the evidence?
• How do I provide PrEP?
• Special considerations: PrEP during conception, pregnancy and breastfeeding
New HIV infections in the US, 2010: most affected populations
New
HIV
Infe
ctio
ns (
Num
ber)
White Black Hispanic BlackWomen
BlackMen
WhiteWomen
HispanicWomen
BlackMale
BlackFemale
MSMHeterosexual IDUs
11,20010,600
6,700
5,300
2,700
1,300 1,200 1,100650
CDC. HIV Surveillance Report, 2010; vol 22. Published March 2012.http://www.cdc.gov/hiv/surveillance/resources/reports/2010report/pdf/2010_HIV_Surveillance_Report_vol_22.pdf.
Total EstimatedNew HIV Infectionsin 2010 (n=47,129)
~25% heterosexual sex

HIV in the US:under-diagnosed and under-treated
Num
ber
(in ‘0
00s)
Prevalence Diagnosed Treated
1,106,400-1,200,000
874,056-960,000
437,028-489,600
~80%Diagnosed
~40%Treated
Smith MK, et al. PLoS One. 2012;9:e1001260.Gardner EM, et al. Clin Infect Dis. 2011;52:793-800.Burns DN, et al. Clin Infect Dis. 2010;51:725-731.
~25% viral load<50 copies/mL
209,773-376,992
Viral Suppression
Interventions to prevent HIV transmission
• Barrier protection• STI treatment• circumcision• Blood screening• ART
– Maternal-to-child transmission– Decrease partner’s viral load– Diagnose & treat acute infection
● Barrier protection● STI treatment● Oral PEP● Oral PrEP● Topical microbicides● Circumcision● Contraception?
● Condom promotion● Individual intervention● Couples intervention● Community based intervention● Structural intervention
Decrease Sourceof HIV Infection
Decrease Host Susceptibilityto HIV Infection
Alter Risk-Taking Behavior
Modified from Mayer KH, et al. Am J Public Health. 2010;100:1867-1876.
Condoms are effective at infection prevention.
Risk of HIV transmission per unprotected act:
Hughes et al, Determinants of Per-Coital-Act HIV-1 Infectivity Among African HIV-1 Serodiscordant Couples. JID 2012: 205 (Feb. 1)Patel et al. Estimating per-act HIV transmission risk: a systematic review. AIDS (2014) volume: 28 issue: 10 page: 1509-19
Sexual Act Risk / 10,000 acts 95% CIReceptive penile-vaginal sex 8 6-11Insertive penile-vaginal sex 4 1-14Receptive anal sex 138 102-186Insertive anal sex 11 4-28
Condom use � risk 78% per-act
ARVs are effective at HIV prevention.
• HPTN 052: 96% reduction in transmission risk with immediate vs. delayed ARV
• For each log � viral load: 2.9X� risk per-act• No reported cases of heterosexual transmission
in setting of undetectable viral load
Cohen MS, Chen YQ, McCauley M, et al., HPTN 052 Study Team. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011;365(6):493–505.Hughes, 2012.Supervie et al. Heterosexual Risk of HIV Transmission Per Sexual Act Under Combined Anti-Retroviral Therapy: Systematic Review and Bayesian Modeling. Clin Infect Dis. 2014 Apr 9.

PrEP: a way for individuals to control their own infection risk.
What is PrEP?• Pre-exposure prophylaxis with antiretroviral
therapy to reduce the risk of HIV acquisition• FDA approved July, 2012 • Oral therapy given to adults at high-risk of HIV
acquisition– Tenofovir 300mg and Emtricitabine 200mg (fixed-
dose combination) once daily
Just to review…what is PEP?• PEP – post-exposure prophylaxis with
antiretroviral medications• Given AFTER occupational, sexual, IVDU
exposure, but within 72 hours• PEP after a percutaneous exposure reduces
transmission risk by 81%• CDC guidelines for occupational PEP:
emtricitabine/tenofovir AND raltegravir x 28 days
US Public Health Service Guideline. Updated US Public Health Service Guidelines for the Management of Occupational Exposures to Human Immunodeficiency Virus and Recommendations for Postexposure Prophylaxis. infection control and hospital epidemiology september 2013, vol. 34, no. 9
The evidence for PrEP:PrEP (like ART) works when taken
Study Blood Samples With TDF
Detected, %
HIV Protection Efficacy Overall,%
HIV Protection Efficacy in Subjects
with Detectable TDF
Partners PrEP[1] 81 75 90%TDF2[2] 80 62 85%iPrEx[3] 51 44 92%Thai IDU[4] 67 49FEM-PrEP[5] andVOICE[6]
< 30 No HIV protection
1. Baeten JM, et al. N Engl J Med. 2012;367:399-410. 2. Thigpen MC, et al. N Engl J Med. 2012;367:423-434. 3. Grant RM, et al. N Engl J Med. 2010;363:2587-2599. 4. Choopanya K, et al. Lancet. 2013;381: 2083-2090. 5. Van Damme L, et al. N Engl J Med. 2012;367:411-422. 6. Marrazzo J, et al. CROI 2013. Abstract 26LB.

Partners PrEP Study:Serodifferent Heterosexual Couples
Double-Blind
Phase 3, Double-Blind StudyKenya, Uganda
Serodiscordant, heterosexualcouples (n=4758)
HIV-positive partner not yeteligible for ART
Randomization1:1
Placebo (n=1584)
Tenofovir DF qd (n=1584)
Baeten J, et a. N Engl J Med. 2012;367:399-410.
Follow-Up
Up to 36 months(median 23 months; 7830 person-years)
Tenofovir/Emtricitabine qd (n=1579)
Primary Endpoints
HIV infection in HIV-negative partnerSafety
All patients received comprehensive HIV prevention services.
Partners PrEP Study: Results
0
0.01
0.02
0.03
0.04
0.05
Cum
ulat
ive
Pro
babi
lity
ofH
IV In
fect
ion
Baeten J, et a. N Engl J Med. 2012;367:399-410.
0 3 6 9 12 15 18 21 24 27 30 33 36Months
TDF/FTC(n=1568)
Placebo(n=1568)
Tenofovir DF(n=1572)
Partners PrEP Study: Results
• Both PrEP arms significantly reduced risk of HIV acquisition
– Similar results for men & women
– Safe & well tolerated
• Tenofovir levels significantly correlated with HIV protection
– Relative risk reduction of 90% associated with detectable tenofovir
• No evidence of risk compensation
• No evidence of resistance among those who became HIV infected
HIV Incidence
HIV
Inci
denc
e(p
er 1
00-p
erso
n-ye
ars)
1.99
0.65
67%Reduction(P<0.001)
0.50
75%Reduction(P<0.001)
Placebo TenofovirDF
TenofovirEmtricitabine
Baeten J, et a. N Engl J Med. 2012;367:399-410.
TDF2 Study: PrEP in Heterosexually Active Young Adults in Botswana
• Phase 2 trial in heterosexual men and women (n=1219)
– Women: 45%– Married: 94%– Completed study: 67%
• Primary results– HIV seroconversion (n=33)
• Daily oral TDF/FTC(n=9 [2 males/7 females])
• Placebo (n=24 [10 males/14 females])
Thigpen MC, et al. N Engl J Med. 2012;367:423-434.
Pro
port
ion
0 1 2 3
HIV Seroconversion (ITT)
TDF/FTC(n=610)
Placebo(n=606)
62%Reduction(P=0.03)
Years

Safety of PrEP• Serious adverse events (including renal dysfunction) are
rare and were not significantly different between PrEPand placebo arms
• PrEP is well tolerated– Nausea more common in those on PrEP than placebo– Occurred in < 10% subjects and primarily during the
first month (PrEP “start-up” symptoms)• PrEP associated with a small change (~ 1%) in bone
mineral density in men, but no increased risk of fracture over 1-2 years
CDC/US Public Health Service. Preexposure Prophylaxis for the Prevention of HIV Infection in the US: A Clinical Practice Guideline. 2014
Does PrEP cause HIV resistance?
CDC/US Public Health Service. Preexposure Prophylaxis for the Prevention of HIV Infection in the US: A Clinical Practice Guideline. 2014
Pre-exposure Prophylaxis for the Prevention of HIV Infection in the United States – 2014A Clinical Practice Guidelinehttp://www.cdc.gov/hiv/pdf/PrEPguidelines2014.pdf
May 2014
Prescribing PrEP
CDC/US Public Health Service. Preexposure Prophylaxis for the Prevention of HIV Infection in the US: A Clinical Practice Guideline. 2014
CDC: Indications for PrEP for Sexually Active Women

ACOG Committee Opinion: PrEP eligibility
• Women in sero-different relationships• Sexually active women in a high HIV-prevalence
area or social network and one of the following: – Inconsistent condom use– Recent diagnosis of sexually transmitted infection– Exchange sex– Use intravenous drugs – Incarceration– Partner(s) of unknown HIV status with any of the factors
previously listedhttp://www.acog.org/Resources-And-Publications/Committee-Opinions/Committee-on-Gynecologic-Practice/Preexposure-Prophylaxis-for-the-Prevention-of-Human-Immunodeficiency-Virus
MENTAL POLL:Do you routinely ask your patients about the HIV status or risk behaviors of their
partners?
Before initiating PrEP: take a history�Determine eligibility, ongoing risk �Take a sexual history�Determine pregnancy/breastfeeding status
and pregnancy desires�Offer contraception if not trying to
conceive!�Determine last exposure. If within 72
hours, offer PEP�Assess for signs/symptoms of acute HIV in
prior month

Before initiating PrEP: testing�Document negative HIV antibody test
immediately before starting PreP (within the week). Do NOT use an oral rapid test.
�Test for acute HIV infection if recent exposure and symptoms: 4th gen test or viral load
�Check creatinine clearance (ineligible if <60 mL/min)
�Screen for HBV (offer vaccine if susceptible) & HCV
�Screen for and treat STIs
Testing review: the ‘window period’ is closing, but not entirely.
a.k.a. ‘viral load’
a.k.a. ‘4th
gen’ test: detect IgM, IgG, p24 Ag
Detect IgM, IgG. Most rapid tests are here.
Before initiating PrEP: counseling� PrEP is part of an integrated strategy to prevent
HIV infection� Adherence = efficacy� Regular HIV testing is mandatory� Review signs/symptoms of acute HIV� PrEP is for seasons of vulnerability: continually
assess for changes in risk, opportunities for new prevention strategies (partner linkage to care!)
� Review side effects: nausea, headache
Resources for patients at the CDC website

Prescribing PrEP�Tenofovir DF/Emtricitabine (300/200 mg) 1 tablet
daily�Prescribe no more than a 90-day supply�Refill only after confirming patient remains HIV
uninfected
PrEP Patient Assistance Program
PrEP Billing: ICD-10 codes• V01.79: Contact with or Exposure to viral
HIV/AIDS virus• V01.89: Exposure to an STD
Follow-up while on PrEP
• Evaluate adherence at each visit• Pregnancy testing at each visit (?)…better to assess
pregnancy intentions and contraceptive plan!• HIV antibody test at least every 3 months• Assess risk behaviors; provide counseling &
condoms• Test for STIs every 6 months regardless of
symptoms• Check BUN/Cr 3 months after initiation, then every
6 monthsCDC/US Public Health Service. Preexposure Prophylaxis for the Prevention of HIV Infection in the US: A Clinical Practice Guideline. 2014

Discontinuing PrEP• Perform HIV test(s) to confirm HIV status
– If positive• Order CD4 count, viral load and resistance testing
• Establish linkage to care, facilitate partner notification and testing
– If negative• Establish linkage to risk-reduction support services as
indicated• Consider completion of PEP and confirmatory testing 6
& 12 weeks after last exposure• If active HBV infection
– Discuss with hepatologistCDC/US Public Health Service. Preexposure Prophylaxis for the Prevention of HIV Infection in the US: A Clinical Practice Guideline. 2014
Special considerations: PrEP for conception (PrEP-ception),
PrEP in pregnancy, & PrEP during breastfeeding
Disco Survey: HIV- in a relationship with an HIV+ & desire children
93 completed surveys•90% want children with their HIV+ male partner•25% have tried to get pregnant with their HIV+ male partner•67% had vaginal sex without condom with HIV+ partner•42% have seen a provider to discuss ways to get pregnant
Women are interested in various methods to prevent transmission• 53% PrEP• 51% Timed unprotected sex• 47% PEP• 62% sperm washing vaginal insemination• 22% IVF• 44% adoption• 9% insemination with donated sperm
Still enrolling: http://hiv.ucsf.edu/care/perinatal/pro_men.html
CDC Perinatal HIV Guidelines: March, 2014• PrEP-ception is one of many options for sero-different
couples to have a family. Counseling must include range of options: adoption, sperm donation, IUI + sperm washing, IVF, timed intercourse +/- PrEP
• PrEP offers “an additional strategy for safer conception”
• start 1 month prior and continue 1 month after exposure
• Limit condomless sex to times of peak fertility• Screen for STIs• Consider sperm preparation techniques• Maximize viral suppression prior to conception• Semen analysis for HIV-infected male partner
http://aidsinfo.nih.gov/contentfiles/lvguidelines/perinatalgl.pdf

ACOG Committee Opinion• Limited data on PrEP in pregnancy and
lactation, however emtricitabine/tenofovir is commonly used in pregnancy and has a “reassuring” safety profile
• Practice vigilance for new HIV infections in lactating women
Rationale for PrEP peri-conception, during pregnancy and breastfeeding
• Pregnancy is associated with a 2X increased risk of HIV acquisition �Contraception = HIV prevention
• Acute HIV in pregnancy associated with 8X increased risk of perinatal transmission
• Acute HIV in breastfeeding associated with 4X increased risk of neonatal transmission
Mugo et al. Increased risk of HIV-1 transmission in pregnancy: a prospective study among African HIV-1-serodiscordant couples. AIDS. 2011 Sep 24;25(15):1887-95.Humphrey et al. Mother to child transmission of HIV among Zimbabwean women who seroconverted postnatally: prospective cohort study. BMJ 2010;341:c6580Singh et al. HIV seroconversion during pregnancy and mother-to- child HIV transmission: data from the enhanced perinatal surveillance projects, United States, 2005–2010. Paper presented at: CROI 2013, Atlanta, GA.
Safety of PrEP during PrEP-ception• Partners PrEP: PrEP discontinued when
pregnancy detected, mean 5 wks GA• No difference in pregnancy incidence, birth
outcomes, and infant growth • “Signal” for PrEP associated with pregnancy loss?
– 96 of 288 pregnancies: 42.5% for FTC+TDF vs. 32.3% for placebo (difference 10.2%; 95% CI, −5.3% to 25.7%; P = .16)
• CIs for birth outcomes were wide�definitivestatements about safety of PrEP periconceptioncannot be made
Mugo et al. Pregnancy Incidence and Outcomes Among Women Receiving PrEP. JAMA Jul 2014
• Data from 1600+ pregnancies: rule out 2X increase in overall birth defects
• No impact on intrauterine growth• PHACS (US): decreased length (0.4 cm) and head
circumference (0.3 cm) at 1 year• CROI 2014 oral abstract: decreased BMD at birth• DART (Africa): no difference in growth, fractures at
2 yrs• “Pregnancy is not a contraindication to PrEP.”• Enroll patients in the ARV pregnancy registry!!!
Safety of PrEP in Pregnancy
Siberry 2012; Siberry 2014; Gibb 2012.

Safety of PrEP in lactation• Little data• Tenofovir/emtricitibine promoted for HIV
infected lactating women by the WHO in low-resource settings
• Tenofovir is secreted in breast milk, but infant levels are extremely low
• Consult to discuss risks/benefits, HIV testing while breastfeeding
CDC/US Public Health Service. Preexposure Prophylaxis for the Prevention of HIV Infection in the US: A Clinical Practice Guideline. 2014
Providing PrEP for PrEP-ception, during pregnancy and breastfeeding
• PrEP is part of a prevention package: engage partner in care, obtain consent to talk to his provider, achieve viral suppression, screen for STIs
• Women may choose to use or discontinue PrEPpericonception, during pregnancy, or postpartum for a variety of reasons – requires assessment for ongoing risk, discussion of risks/benefits in data-free zones
• Recommendations for evaluation/testing peri-conception, during pregnancy/breastfeeding are based on expert opinion – consult an experienced PrEPprovider or call the Perinatal Hotline for assistance!
Help make HIV history.Becoming a PrEP provider means you’re contributing to the end of sexual and perinatal transmission of HIV.
Resources for Providers• CDC PrEP guidelines and provider supplement
http://www.cdc.gov/hiv/pdf/guidelines/PrEPProviderSupplement2014.pdf
• CDC Perinatal HIV Guidelines:
http://aidsinfo.nih.gov/contentfiles/lvguidelines/perinatalgl.pdf
• ACOG Committee Opinion Preexposure Prophylaxis for Prevention of HIV, May 2014.
• Bay Area Perinatal HIV/AIDS Centerhttp://hiv.ucsf.edu/care/perinatal/resources.html

The Clinicians’ Consultation Center provides clinicians of all experience levels with cost-free, confidential, timely, expert responses to questions on:
•HIV/AIDS management (testing, ARVs, co-infection, care)•Occupational and non-occupational exposure management•Management of HIV in pregnant mothers and their infants•Considerations of providing PrEP as part of HIV prevention
Our mission is to improve patient health outcomes by building the capacity of healthcare providers through
expert clinical consultation and education.The CCC at UCSF/SFGH is a project of the HRSA AETC Program & the CDC.
HIV Management: 800.933.34139 am – 8 pm EST, M-F
PEPline: 888.448.49119 am – 2 am EST, every day
Perinatal HIV Hotline: 888.448.87659 am – 2 am EST, every day
PrEPline: 855.448.773711 a.m. – 6 p.m. EST, M-F
Online Consultation: nccc.ucsf.edu
Resources for Patients• Project Prepare Website: www.projectprepare.net• http://www.prepwatch.org/#women• Centers for Disease Control and Prevention:
http://www.cdc.gov/hiv/prep/• Project inform: http://www.projectinform.org/pdf/orderprepbooklets
– A new option for safer loving for women in Spanish and English• San Francisco Department of Public Health: www.prepfacts.org• PrEP watch: http://www.prepwatch.org/#guidance• Bay Area Perinatal AIDS Center: Positive Reproductive Outcomes for Men:
http://hiv.ucsf.edu/care/perinatal/pro_men.html• Positively Negative: https://positively-negative.squarespace.com
Acknowledgements• Megan Huchko• Ian McNicholl• Shannon Weber• Erika Aaron• Sarah Averbach
Additional Slides

CAPRISA 004 Study:Heterosexual Women
Double-Blind
Double-blind studySouth Africa sites(Kwa-Zulu, Natal)
Sexually active HIV-uninfectedwomen not using barrier
contraception
Screened (n=2160)
Randomization1:1
Placebo (n=444)
Tenofovir Gel (n=445)
Abdool Karim Q, et al. Science. 2010;329:1168-1174.
Administration of placebo/tenofovir DF gel•Insert 1 dose within 12 hours before sex
•Insert 1 dose ASAP, within 12 hours after sex
•No more than 2 doses within 24 hours
Similar baseline demographic characteristics, sexual history/behavior,
and contraception use
0 6 12 18 24 30
CAPRISA 004 Results:Cumulative Probability of HIV Infection
Pro
babi
lity
of In
fect
ion
0 6 12 18 24 30Month
Abdool Karim Q, et al. Science. 2010;329:1168-1174.
47% 50% 47% 40% 39%Effectiveness (%):(P=0.064) (P=0.007) (P=0.004) (P=0.013) (P=0.017)
P=0.017
TenofovirGel
PlaceboGel
CAPRISA 004 Results• Tenofovir DF gel reduced HIV
infection by an estimated 39%– Peaked at 50% after 12 months
• Protective effect of tenofovir gel use was evident irrespective of– Sexual behavior– Condom use– HSV-2 infection
– Urban/rural differences
• A trend of higher effectiveness was observed as gel adherence improved
Abdool Karim Q, et al. Science. 2010;329:1168-1174.
>80% 50%-80% <50%Adherence Level (months)
9.3%
4.2%
10.0%
8.6%54%(P=0.025)
38%(P=0.34)
6.3% 6.2%
28%(P=0.30)
HIV
Inci
denc
e R
ate
(%)
Tenofovir DF gel
Placebo
HIV Incidence
iPrEx Study: ComprehensivePackage of Prevention Services
• All subjects received HIV testing, risk-reduction counseling, condoms, and diagnosis and treatment of symptomatic STIs
• At 24-week intervals, subjects screened for – Asymptomatic urethritis, syphilis, antibodies to HSV-2, genital warts/ulcers– Treatment was provided when indicated
• Sexual partners– Offered treatment of STIs
• As needed, linkage to local prevention and treatment services• Counseled on the use of conventional methods to protect from HIV• HBV vaccination offered to susceptible subjects
Grant RM, et al. N Engl J Med. 2010;363:2587-2599.

iPrEx Study:MSM and Transgender Women
Double-Blind
Multinational studyHIV-negative men or
transgender women whohave sex with men
Peru, Ecuador, Brazil, Thailand, South Africa, US
Screened (n=4905)
Randomization1:1
Placebo (n=1248)
TDF/FTC (n=1251)
Study Outcomes•HIV seroconversion•Adverse events•Metabolic effects•HBV exacerbations•Risk behavior and STIs (including HSV)•Adherence
Similar baseline demographic characteristics
(except mean age), sexual risk factors, STIs,and HBV status
Drug resistance, HIV RNA level, immunologic respons e, and CD4 cell count assessed in people whobecome HIV positive during the study.
Grant RM, et al. N Engl J Med. 2010;363:2587-2599.
Follow-Up3324 person-years(median 1.2 years)
iPrEx Study Results:Cumulative Probability of HIV Infection
0 12 24 36 48 60 72 84 96 108 120 132Weeks
Placebo(n=1248)
TDF/FTC(n=1251)
P=0.005
Cum
ulat
ive
Pro
babi
lity
of H
IV In
fect
ion
Grant RM, et al. N Engl J Med. 2010;363:2587-2599.
Partners PrEP Study:Comprehensive Prevention Services
• Risk reduction counseling (individuals and partners)• Free condoms and condom counseling• Contraception counseling and provision
• Screening and treatment for STIs• Counseling and referral for other HIV-prevention
interventions (eg, male circumcision), per national policies
Baeten J, et a. N Engl J Med. 2012;367:399-410.
Biologic plausibility for PrEP• Maternal-child transmission: AZT acts as PrEP
& PEP• Occupational PEP: PEP reduces transmission
risk by 81% after percutaneous exposure• Animal studies of vaginal and rectal PrEP
suggested efficacy in preventing sexual transmission
CDC/US Public Health Service. Preexposure Prophylaxis for the Prevention of HIV Infection in the US: A Clinical Practice Guideline. 2014

Worldwide treatment andprevention gaps, 2011
• 35 million people living with HIV
• 2 million new infections annually
• 30-70% people don’t know their status• 15 million eligible for ART
• 8 million people on ART, 54% of those eligible
• 36% estimated coverage of ART in low and middle-income countries
Granich R, et al. Curr Opin HIV AIDS. 2013;8:41-49.
ARVs are effective at HIV prevention.• HPTN 052: 96% reduction in transmission risk
with immediate vs. delayed ARV• For each log � viral load: 2.9X� risk per-act• Risk of heterosexual transmission with HIV+
partner on ART & engaged in care > 6 months (whether or not virally suppressed!, 80% condom use) <13:100,000 acts
• No reported cases of heterosexual transmission in setting of undetectable viral load
Cohen MS, Chen YQ, McCauley M, et al., HPTN 052 Study Team. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011;365(6):493–505.Hughes, 2012.Supervie et al. Heterosexual Risk of HIV Transmission Per Sexual Act Under Combined Anti-Retroviral Therapy: Systematic Review and Bayesian Modeling. Clin Infect Dis. 2014 Apr 9.

10/23/2014
1
Updates in the Diagnosis & Management of Preeclampsia and
Hypertensive Disorders of Pregnancy ACOG and CMQCC Guidelines
Yair Blumenfeld, MDAssistant Professor
Department of Obstetrics & GynecologyStanford University School of Medicine
I have no financial disclosures to report
2014 Guidelines for the Management of Hypertension
in Pregnancyfrom ACOG and CMQCC
Maurice L. Druzin, MDProfessor and Vice-Chair
Department of Obstetrics and GynecologyDivision of Maternal Fetal MedicineStanford University Medical CenterAssociate Dean for Academic Affairs
Stanford University School of Medicine
Learning objectives� To review the most current recommendations for the diagnosis and
management of hypertensive disorders of pregnancy from ACOG and the California Preeclampsia Task Force (PTF) of CMQCC.
� To review the impact of hypertensive disorders of pregnancy on maternal and perinatal morbidity and mortality.
� To delineate the most common causes of maternal morbidity and mortality secondary to hypertensive disorders of pregnancy.
� To outline a management algorithm to optimize care for patients with hypertensive disorders of pregnancy.

10/23/2014
2
How often do you encounter preeclamspia in your practice?
5
1 2 3 4
25%
10%
30%
35%1. Almost daily2. Approximately once per week3. At least once per month4. Rarely, approximately a handful
of times per year
“Over the past year, I have seen preeclampsia mismanaged either by
the OB provider, nurse, or anesthesiologist”
61 2
48%
52%1. True2. False
“In my hospital, the entire care team (OB providers, nursing,
anesthesiology) is dedicated to managing acute severe hypertension
rapidly”
71 2
26%
74%1. True2. False
“I’ve had enough of preeclampsia talks, I’m going out to get some
coffee outside – see ya!”
81 2
90%
10%
1. True2. False

10/23/2014
3
The summary• Classification: 1) Preeclampsia (PE) • 2) Chronic hypertension (CHTN)• 3) CHTN+PE • 4) Gestational hypertension
• Management: 1) Blood pressure control!• 2) Seizure prevention• 3) Delivery - 34 weeks vs. 37 weeks• 4) Post partum surveillance
Executive Summary: Hypertension in Pregnancy
American College of Obstetricians and Gynecologists
James Martin, Jr, MD
Obstet Gynecol 2013;122:1122-31
Improving Health Care Response to Preeclampsia: A California Quality
Improvement Toolkit
Funding for the development of this toolkit was provided by: Federal Title V block grant funding from the California Department of Public Health; Maternal,
Child and Adolescent Health Division and Stanford University.11
Development of the California Toolkit ‘Improving Health Care Response to Preeclampsia’ was funded by the California Department of Public Health (CDPH), Center for Family Health, Maternal Child and Adolescent
Health (MCAH) Division, using federal Title V MCH funds.
Preeclampsia Task Force MembersMaurice Druzin, MD – StanfordElliott Main, MD – CMQCCBarbara Murphy, RN – CMQCCTom Archer, MD – UCSDOcean Berg, RN, CNS – SF General HospitalBrenda Chagolla, RNC, CNS – UC DavisHolly Champagne, RNC, CNS – Kaiser Meredith Drews – Preeclampsia FoundationRacine Edwards-Silva, MD – UCLA Olive ViewKristi Gabel, RNC CNS – RPPC SacramentoThomas Kelly, MD – UCSD
Larry Shields, MD – Dignity HealthNancy Peterson, RNC, PNNP – CMQCCChristine Morton, PhD – CMQCCSarah Kilpatrick, MD – Cedars SinaiRichard Lee, MD – Univ. of Southern CaliforniaAudrey Lyndon PhD, RNC – UC San FranciscoMark Meyer, MD – Kaiser SDValerie Cape – CMQCCEleni Tsigas – Preeclampsia FoundationLinda Walsh, PhD, CNM – UC San FranciscoMark Zakowski, MD – Cedars SinaiConnie Mitchell, MD, MPH – CDPH - MCAH
12

10/23/2014
4
The Scope of the Problem
13
Why is preeclampsia important?• The incidence of preeclampsia has increased by
25% in the United States during the past two decades.
• Preeclampsia is a leading cause of maternal and perinatal morbidity and mortality, with an estimated 50,000-60,000 preeclampsia-related deaths per year worldwide.
Ref: ACOG – HIP, 2013
Why is preeclampsia important?• For every preeclampsia-related death
that occurs in the United States, there are probably 50-100 other women who experience “near miss” significant maternal morbidity that stops short of death but still results in significant health risk and health care cost.
• What can be considered “less than optimal” care of patients with preeclampsia and other hypertensive disorders of pregnancy reportedly occurs with some frequency worldwide, contributing to maternal and perinatal injury that might have been avoidable.
Ref: ACOG – HIP, 2013
Cause of U.S. maternal mortality• CDC Review of 14 years of coded data: 1979-1992• 4024 maternal deaths• 790 (19.6%) from preeclampsia
MacKay AP, Berg CJ, Atrash HK. Obstetrics and Gynecology 2001;97:533-538
90% of CVA were from hemorrhage

10/23/2014
5
16
18
16
13
9 10
8
1011
14
9
12
78 8
1515
99
1011
10
6
666
10
9
11
111111
87
10
11
15
12
17
12
21
0
5
10
15
20
25
1970 1975 1980 1985 1990 1995 2000 2005 2010
HP Objectives – Maternal Deaths (<42days postpartum) per 100,000 Live Births
Mat
erna
l Dea
ths
per
100,
000
Live
Birt
hs
ICD-10 codes
ICD-8 codes
ICD-9 codes
Maternal mortality rate, California residents: 1970-2010
SOURCE: State of California, Department of Public Health, California Birth and Death Statistical Master Files, 1970-2010. Maternal mortality for California (deaths ≤ 42 days postpartum) was calculated using the ICD-8 cause of death classification for 1970-1978, ICD-9 classification for 1979-1998 and ICD-10 classification for 1999-2010. Healthy People Objectives: HP2000: 5.0 deaths per 100,000 live births; HP2010: 3.3
deaths, later revised to 4.3 deaths per 100,000 live births, and; HP2020: 11.4 deaths per 100,000 live births. Produced by California Department of Public Health, Center for Family Health, Maternal, Child and Adolescent Health Division, December, 2012.
California pregnancy-associated mortality review (CA-PAMR) quality improvement
review cycle1. Identification of cases
1. Identification of cases
2. Information collection, review by multidisciplinary
committee 2. Information collection,
review by multidisciplinary committee
3. Cause of Death, Contributing Factors and Quality Improvement (QI) Opportunities identified
3. Cause of Death, Contributing Factors and Quality Improvement (QI) Opportunities identified
4. Strategies to improve care and reduce
morbidity and mortality4. Strategies to improve
care and reduce morbidity and mortality
5. Evaluation and Implementation of QI strategies and
tools
5. Evaluation and Implementation of QI strategies and
toolsToolkits Developed:• Hemorrhage • Preeclampsia
CA-PAMR causes of death 2002-2004
19
Grouped Cause of Death, per CA-PAMR Committee
Pregnancy-Related Deaths N (%)
Cardiovascular disease 29 (20)
Cardiomyopathy 19 (13)
Other cardiovascular 10 (7)
Preeclampsia/eclampsia 25 (17)
Obstetric hemorrhage 16 (11)
Amniotic fluid embolism 15 (10)
DVT/ PE 15 (10)
Other 45 (31)
TOTAL 145
Pregnancy-Related Mortality Rate: 1.6 deaths /100,000 live births
400-500xSerious Morbidity: 3400/year (prolonged postpartum length of stay)
Maternal morbidity and Mortality: Preeclampsia
40-50x
Near Misses: 380/year (ICU admissions)
About 8 Preeclampsia Related Mortalities/2007 in CA
Source: 2007 All-California Rapid Cycle Maternal/Infant Database for CA Births: CMQCC

10/23/2014
6
• Cohort of pregnancy-related deaths, N=145– 25 (17%) of deaths were grouped as “Preeclampsia/Eclampsia” cause of
death
• Over half of all pregnancy-related deaths had HTN diagnoses– 50 (34%) had inpatient diagnosis of HTN– 57 (39%) had any diagnosis of HTN (inpatient, prenatal, preexisting)
Impact of hypertension in CA-PAMR cohort, 2002-2004
CA-PAMR: Chance to alter outcome grouped cause of death; 2002-2004 (N=145)
Grouped Cause of Death Chance to Alter Outcome
Strong /Good (%)
Some(%)
None(%)
Total N (%)
Obstetric hemorrhage 69 25 6 16 (11)
Deep vein thrombosis/pulmonary embolism
53 40 7 15 (10)
Sepsis/infection 50 40 10 10 (7)
Preeclampsia/eclampsia 50 50 0 25 (17)
Cardiomyopathy and other cardiovascular causes
25 61 14 28 (19)
Cerebral vascular accident 22 0 78 9 (6)
Amniotic fluid embolism 0 87 13 15 (10)
All other causes of death 46 46 8 26 (18)
Total (%) 40 48 12 145
• New best practice recommendations are greatly needed to guide clinicians in the care of women with all forms of preeclampsia and hypertension that occur during pregnancy, particularly women with acute severe hypertension and superimposed preeclampsia.
• Identification of patients with severe forms of preeclampsia continues to challenge clinicians.
Ref: ACOG – HIP, 2013
• Also needed is a system for continually updating these guidelines and integrating them into daily obstetric practice.
• Improved patient education and counseling strategies are needed to convey more effectively the dangers of preeclampsia and hypertension and the importance of early detection to women with varying degrees of health literacy.
• Research on preeclampsia and other hypertensive disorders of pregnancy in both the laboratory and clinical arenas require continued emphasis and funding.
Ref: ACOG – HIP, 2013

10/23/2014
7
Classification, Diagnosis & Management
25
Classification of hypertensivedisorders of pregnancy
• The task force chose to continue using the classification schema first introduced in 1972 by the College and modified in the 1990 and 2000 reports of the Working Group of the National High Blood Pressure Education Program, ASH and ACOG Practice Bulletins.
• Although the task force has modified some of the components of the classification, this basic, precise and practical classification was used which considers hypertension during pregnancy in only four categories.
Ref: ACOG – HIP, 2013
Classification of hypertensivedisorders of pregnancy
1) Preeclampsia-eclampsia after 20 weeks
2) Chronic hypertension (of any cause) predating pregnancy
3) Chronic hypertension with superimposed preeclampsia
4) Gestational hypertension after 20 weeks
Ref: ACOG – HIP 2013
Executive Summary: Hypertension in Pregnancy, American College of Obstetricians and Gynecologist, Obstet Gynecol 2013;122:1122-31. Copyright permission received.
Diagnostic criteria for preeclampsia

10/23/2014
8
Key clinical pearl
Forty percent of patients with new onset hypertension or
new onset proteinuria will develop classic preeclampsia.
Barton JR, Sibai BM. Prediction and prevention of recurrent preeclampsia. ObstetGynecol. 2008;112(2 PART 1): 359-372.
Key clinical pearl Patients presenting with vague symptoms of:
� headache� abdominal pain� shortness of breath� generalized swelling� complaints of “I just don’t feel right”
should be evaluated for atypical presentations of preeclampsia or “severe features”
Sibai BM, Stella CL. Diagnosis and management of atypical preeclampsia-eclampsia. Am J Obstet Gynecol. May 2009;200(5):481 e481-487.
Laboratory evaluation of preeclampsia
• Initial lab studies should include:– CBC with platelet count– AST, ALT, LDH (hemolysis)– Creatinine, Bilirubin, Uric acid, Glucose
• For women with acute abdominal pain, add:– Serum amylase, lipase and ammonia
Diagnosis of preeclampsia with severe features
Executive Summary: Hypertension in Pregnancy, American College of Obstetricians and Gynecologist, Obstet Gynecol2013;122:1122-31. Copyright permission received.
*5 grams proteinuria eliminated as a criterion

10/23/2014
9
• Acute onset, persistent (lasting 15 min or more), severe systolic (≥160 mm Hg) or severe diastolic hypertension (≥ 110 mm Hg) or both in pregnant or postpartum women with preeclampsia/eclampsia constitutes a hypertensive emergency * and it is inadvisable to wait 4 hours for treatment.
Do not wait when a patient has severe-range hypertension!
*Emergent Therapy for Acute-Onset, Severe Hypertension With Preeclampsia or Eclampsia, ACOG Committee Opinion, # 514, December 2011
The deadly triadSevere preeclampsia - HELLP syndrome - Eclampsia
Associated with an increased risk of adverse outcomes:• Placental Abruption• Renal Failure• Sub-capsular Hepatic Hematoma• Preterm Delivery• Fetal or Maternal Death• Recurrent Preeclampsia
ACOG Practice Bulletin #33, Reaffirmed 2012; ACOG Committee Opinion #514, 2012; Tuffnell D, Jankowitcz D, Lindow S, et al. BJOG 2005;112:875-880.
ACOG executive summary onhypertension in pregnancy, Nov 2013
1. The term “mild” preeclampsia is discouraged for clinical classification. The recommended terminology is: a. “preeclampsia without severe features” (mild)b. “preeclampsia with severe features” (severe)
2. Proteinuria is not a requirement to diagnose preeclampsia with new onset hypertension.
3. The total amount of proteinuria > 5g in 24 hours has been eliminated from the diagnosis of preeclampsia with severe features.
4. Early treatment of severe hypertension is mandatory at the threshold levels of 160 mm Hg systolic or 110 mm Hg diastolic.
Cause of U.S. maternal mortality• CDC Review of 14 years of coded data: 1979-1992• 4024 maternal deaths• 790 (19.6%) from preeclampsia
MacKay AP, Berg CJ, Atrash HK. Obstetrics and Gynecology 2001;97:533-538
90% of CVA were from hemorrhage

10/23/2014
10
CA-PAMR Final Cause of Death Among Preeclampsia Cases, 2002-2004 (n=25)
Final Cause of Death Number % Rate/100,000
StrokeHemorrhagicThrombotic
16142 12.5%
1.0
Hepatic (liver) Failure 4 16.0% .25Cardiac Failure 2 8.0%Hemorrhage/DIC 1 4.0%Multi-organ failure 1 4.0%ARDS 1 4.0%
37
How do women die of preeclampsia in CA?
64%87.5%
Preeclampsia mortality rates in California and UK
Cause of Death among Preeclampsia Cases
CA-PAMR (2002-04)Rate/100,000
Live Births
UK CMACE (2003-05)Rate/100,000
Live Births
Stroke 1.0 .47Pulmonary/Respiratory .06 .00
Hepatic .25 .19OVERALL 1.6 .66
38
The overall mortality rate for preeclampsia in California
is greater than 2 times that of the UK, largely due to differences in deaths
caused by stroke.
Controlling blood pressure is the optimal intervention
to prevent deaths due to stroke in women with preeclampsia.
Key clinical pearl
Over the last decade, the UK has focused QI efforts on aggressive treatment of both systolic and diastolic blood pressure and has demonstrated a reduction in deaths.
Gestational age groups of CA-PAMR deaths, 2002 to 2004
Early Preterm Birth Preeclampsia Deaths: 36% (n=9) were <34 weeks gestation
GESTATIONAL AGE GROUPS
2002-2004 CA-PAMR PREECLAMPSIA DEATHS (N=25)
CA-PAMR NON-PREECLAMPSIA
DEATHSN (%) N (%)
<24 weeks 0 (0) 2 (2%)24-31w6d 2 (8%) 13 (11%)32-36w6d 12 (48%) 29 (24%)
>37 weeks 11 (44%) 76 (63%)TOTAL 25 120

10/23/2014
11
In patients with preterm preeclampsia with severe features,
the disease can rapidly progress to significant maternal morbidity and/or mortality.
Key clinical pearl Expectant management in pregnancies with preeclampsia with severe features 24-34 weeks
With stable maternal/fetal conditions, continued pregnancy should be undertaken only at facilities with adequate
maternal and neonatal intensive care resources
Administer corticosteroids for fetal lung maturity benefit
Expectant management recommendations:
ACOG Executive Summary: Hypertension in Pregnancy. Obstet Gynecol 2013;122:1122-31
Maternal Stabilization refers to:� Seizure prophylaxis� BP control� Adequate maternal cardio-pulmonary function
� AND� Consultation with:
� NICU� MFM� Anesthesia and/or � Critical care services
Expectant management of pregnancies with preeclampsia < 34 weeks gestation
Management of suspected preeclampsia with severe features< 34 weeks gestation
Proceed to delivery for:• Recurrent severe hypertension despite therapy• Other contraindications to expectant management
Initial 24-48 hours observation• Initiate antenatal corticosteroids if not previously administered• Initiate 24 hour urine monitoring as appropriate• Ongoing assessment of maternal symptoms, BP, urine output• Daily lab evaluation (minimum) for HELLP and renal function• May observe on an antepartum ward after initial evaluation
Antenatal corticosteroid treatment completed:• Expectant management not contraindicated• Consider ongoing in-patient expectant
management
Adapted from Sibai BM. Evaluation and management of severe preeclampsia before 34 weeks’ gestation. American Journal of Obstetrics & Gynecology, September 2011, pg. 191-198.

10/23/2014
12
Expectant management of pregnancies < 34 weeks gestation(From CMQCC Preeclampsia Toolkit, 2013)
ACOG task force recommendations
• For women with gestational hypertension, less than 160/110 or preeclampsia without severe features at or beyond 37 0/7 weeks of gestation, delivery rather than continued observation is suggested.
Ref: Koopmans CM, et al. Induction of labour versus expectant monitoring for gestational hypertension or mild preeclampsia after 36 weeks gestation. (HYPITAT). Lancet 2009;374:979-88
Contributing Factor(at least one factor probably or definitely contributed)
PreeclampsiaN (%)
TOTALN (%)
OVERALL 25 (100%) 129 (89%)PATIENT FACTORS 16 (64%) 104 (72%)
Underlying significant medical conditions 8 (50%) 40 (39%)
Delay or failure to seek care 10 (63%) 27 (26%)
Lack of understanding the importance of a health event
9 (56%) 16 (15%)
HEALTHCARE PROFESSIONALS 24 (96%) 115 (79%)Delay in diagnosis 22 (92%) 62 (54%) Use of ineffective treatment 19 (79%) 48 (42%)Misdiagnosis 13 (54%) 36 (31%)
Failure to refer or seek consultation 6 (25%) 26 (23%)
HEALTHCARE FACILITY 12 (48%) 72 (50%)
Factors contributing to pregnancy-related deaths, CA-PAMR 2002-2004 Key clinical pearl
An organized tool to identify “clinical signs,” of high concern or triggers can aid clinicians to recognize and respond
in a more timely manner to avoid delays in diagnosis and treatment.

10/23/2014
13
Preeclampsia early recognition tool Eclampsia
• Eclampsia is defined as NEW ONSET grand mal seizures in a woman with preeclampsia
• Incidence is 1 in 1,000 deliveries in U.S.
• Mortality from eclampsia ranges from approximately 1% in the developed world, to as high as 15% in the developing world
Ghulmiyyah L, Sabai BM. Maternal Mortality from Preeclampsia/Eclampsia. Semin Perinatol2012;36:56-59.
Eclampsia: maternal-perinatal outcome In 254 consecutive cases over 12 years
• 83,720 deliveries, for an incidence of one in 330
• 49 patients (19%) did not have proteinuria
• 58 patients (23%) did not have hypertensionSibai BM. Eclampsia VI. Maternal-perinatal outcome in 254 consecutive cases. Am J Obstet GynecolSep 163(3):1049-1054; discussion 1054-1065 1990.
Eclampsia: Maternal-perinatal outcome in 254 consecutive cases over 12 years
• 73 (29%) occurred postpartum.
• Over half of postpartum cases, (40 cases/16%) occurred in the late postpartum period (>48 hrs)
• 18 of these 40 cases were normotensive; all 18 had symptoms of headache or visual disturbance
Sibai BM. Eclampsia VI. Maternal-perinatal outcome in 254 consecutive cases. Am J ObstetGynecol Sep 163(3):1049-1054; discussion 1054-1065 1990.

10/23/2014
14
Key clinical pearl• The critical initial step in decreasing maternal morbidity and mortality is to
administer anti-hypertensive medications within 60 minutes of documentation of persistent (retested within 15 minutes) BP ≥160 systolic, and/or >105-110 diastolic.
• Ideally, antihypertensive medications should be administered as soon as possible, and availability of a “preeclampsia box” will facilitate rapid treatment.
• In Martin et al., stroke occurred in: – 23/24 (95.8%) women with systolic BP > 160mm Hg– 24/24 (100%) had a BP ≥ 155 mm Hg– 3/24 (12.5%) women with diastolic BP > 110mm Hg– 5/28 (20.8%) women with diastolic BP > 105mm Hg
Martin JN, Thigpen BD, Moore RC, Rose CH, Cushman J, May. Stroke and Severe Preeclampsia and Eclampsia: A Paradigm Shift Focusing on Systolic Blood Pressure, Obstet Gynecol 2005;105-246.
Hypertensive medication administration:Oral versus IV
• First line therapy recommendations for acute treatment of critically elevated BP in pregnant women (160/105-110) are with either IV labetalol or hydralazine.
• In the event that acute treatment is needed in a patient without IV access oral nifedipine may be used (10 mg) and may be repeated in 30 minutes.
• Oral labetalol would be expected to be less effective in acutely lowering the BP due to its’ slower onset to peak and thus should be used only if nifedipine is not available in a patient without IV access.
ACOG Practice Bulletin #33, Reaffirmed 2012; ACOG Committee Opinion #514, 2012; Tuffnell D, Jankowitcz D, Lindow S, et al. BJOG 2005;112:875-880.
Magnesium Sulfate• Primary effect is via CNS depression• Improves blood flow to CNS via small vessel vasodilation• Blood pressure after magnesium infusion:
� 6 gm loading then 2 gm/hr.
sBPmm Hg
sBP30 min
sBP120 min
dBPmm Hg
dBP30 min
dBP120 min
Mild Group
145±10
143±13
141±14
87±10
79±9
82±9
Belfort M, Allred J, Dildy G. Magnesium sulfate decreases cerebral perfusion pressure in preeclampsia.Hypertens Pregnancy. 2008;27(4):315-27.
� Magnesium sulfate should not be considered a antihypertensive medication
Magnesium sulfate in the management of Preeclampsia
Magpie Trial Collaboration Group. Do women with pre-eclampsia, and their babies, benefit from magnesium sulfate?
• 58% reduction in seizures• 45% reduction in maternal death*• 33% reduction in placental abruption
Altman D, Carroli G, Duley L, et al. The Magpie Trial: a randomized placebo-controlled trial; Lancet 2002;359:1877–90.
*The 45% reduction in maternal death is not statistically significant but clinically important.

10/23/2014
15
Recommendations for women who should be treated with magnesium
Preeclampsia without severe
features
SeverePreeclampsia
Eclampsia
ACOG ** X XNICE X XSOGC X* X XCMQCC X* X XWHO X X X
**ACOG Executive Summary, 2013: for preeclampsia without severe features, it is suggested that magnesium sulfate not be administered universally for the prevention of eclampsia.
* Should be considered: Numbers needed to treat (NNT) = 109 for “mild”, 63 for “severe”
Key clinical pearl• Magnesium sulfate therapy for seizure prophylaxis should be
administered to any patients with:
– Preeclampsia with “severe features” i.e., subjective neurological symptoms (headache or blurry vision), abdominal pain, epigastric pain AND
– should be considered in patients with preeclampsia without severe features)
Key clinical pearl
Algorithms for acute treatment of severe hypertension and eclampsia should be readily available or preferably posted in all clinical areas that may encounter pregnant women.
Policy and Procedure: Perinatal Inpatient: IV
Labetalol/Hydralazine for Acute Hypertension
LPCH Approval: March 2014

10/23/2014
16
Labor and delivery medication box and dose guidelines for preeclampsia and eclampsia
The Post-Partum Period
62
Timing of pregnancy-related deaths CA-PAMR, 2002 to 2004
68%
8% 12%4% 4% 0% 4%
01020304050607080
0 1 2 3 4 5 6+Number of weeks between baby's birth and maternal death
Perce
nt Pr
eecla
mpsia
Dea
ths
88%
87%
Non-PreeclampsiaDeaths(n=129)
Preeclampsia Deaths(n=25)
96%
89% 63%
17
7
1 1 1
10
0
10
20
30
40
50
60
70
0 1 2 3 4 5 6+
Per
cent
Pre
gnan
cy-R
elat
ed D
eath
Number of weeks between baby’s birth and maternal d eath
ACOG task force recommendationspost partum hypertension and preeclampsia
• For women in whom GHN,PE, or superimposed PE is diagnosed, it is suggested that BP be monitored in the hospital or equivalent outpatient surveillance be performed for at least 72 hours postpartum and again 7-10 days after delivery or earlier in women with symptoms.

10/23/2014
17
Key clinical pearls• Early post-discharge follow-up recommended for all
patients diagnosed with preeclampsia/eclampsia• Preeclampsia Toolkit recommends post-discharge
follow-up:– within 3-7 days if medication was used during labor and
delivery OR postpartum– within 7-14 days if no medication was used
• Postpartum patients presenting to the ED with hypertension, preeclampsia or eclampsia should either be assessed by or admitted to an obstetrical service
Key clinical pearls• Use of preeclampsia-specific checklists, team
training and communication strategies, and continuous process improvement strategies will likely reduce hypertensive related morbidity.
• Use of patient education strategies, targeted to the educational level of the patients, is essential for increasing patient awareness of signs and symptoms of preeclampsia.
Patient education materials
This and many other patient education materials can be ordered from www.preeclampsia.org/market-place
Getting the job done in your institution • Establish tools / new recommendations• Establish champions and collaborators• Provide convincing rationale for change• Get providers to adopt the changes• Provide convincing evidence that the proposed
changes in clinical care will improve outcome
• Distribute the convincing rationale and evidence

10/23/2014
18
For More Information and to
Download the Toolkit
• Visit our website: www.cmqcc.org
• Or contact us:[email protected]
Available online at www.cmqcc.org
Thank you
70

10/23/2014
1
Diagnosis and Management of Diabetes in Pregnancy
Kirsten Salmeen, MDAssistant Professor
Department of Obstetrics, Gynecology & Reproductive Sciences
Maternal-Fetal Medicine
Disclosures
I have nothing to disclose
Type 1GDMA2
Pre-DM/Type 2
GDMA1
Overview
• Impact of Hyperglycemia• Testing• Management• Postpartum

10/23/2014
2
Glucose & Insulin
Cunningham et al. Williams Obstetrics, 23rd Edition
GLUCOSE
INSULIN
PREGNANT
NON-PREGNANT
PREGNANT
NON-PREGNANT
Normal Pregnancy: - Fasting HYPO glycemia- Postprandial HYPER glycemia- HYPER insulinemia
Normal Glucose In Pregnancy:Non Diabetics
Hernandez Diabetes Care 2011
Glucose & Insulin – Pregnancy
• Pregnancy = “Pancreatic Stress Test”
• Human placental lactogen blocks peripheral uptake and use of glucose in the mother
• Insulin sensitivity is > 50% lower
Glucose & Insulin – The Fetus
• Transfer of glucose across placenta is by facilitated diffusion via glucose transport proteins
• Glucose is the primary substrate for fetal growth
• The fetus makes its own insulin
• Hyperinsulinemia likely drives excess fetal growth

10/23/2014
3
Overview
• Impact of Hyperglycemia• Testing• Management• Postpartum
Pregnancy Outcomes in GDM
Approximate Overall % Relative Risk/Odds RatioMacrosomia 20 RR ~1.4
Pre-Eclampsia 15 RR ~1.7Cesarean Section Varies RR ~ 1.2Shoulder Dystocia 3-5 OR ~ 1.2
IUFD ~ 0.05 RR ~ 2
HAPO Study Cooperative Research Group N Engl J Med 2008Schmidt M Diabetes Care 2001Wendland E BMC Pregnancy Childbirth 2012
Hyperglycemia & Pregnancy Outcomes
Preeclampsia (%)
Macrosomia(%)
Cesarean Section (%)
50 gram, 1-hour < 100 mg/dL 3.0 12.2 17.5100 – 114 mg/dL 6.3 12.5 20.8116 – 134 mg/dL 5.6 15.4 23.0> 134 mg/dL 5.9 17.2 23.4
P-value for trend 0.01 0.001 0.001
Sermer et al AJOG 1995
Fasting Glucose Macrosomia (%)
< 72 mg/dL 9.774-76 mg/dL 14.478-82 mg/dL 14.1> 82 mg/dL 20.5
Hyperglycemia & Pregnancy Outcomes
Sermer et al AJOG 1995

10/23/2014
4
Outcome (%) Fasting < 74
Fasting 74-77
Fasting 79-81
Fasting ≥ 83
Odds Ratio 95% CI
Birth weight≥ 4000 g 23.4 27.9 28.5 31.7 1.14 1.06-1.22
Birth weight ≥ 4500 g 4.3 6.3 6.8 8.1 1.23 1.08-1.40
LGA 17.2 18.9 22.7 25.6 1.19 1.10-1.29
PIH/PreE 5.8 6.6 7.1 7.9 1.12 0.99-1.26
Shoulder Dystocia 1.4 0.8 1.7 2.2 1.21 0.92-1.62
Hyperglycemia & Pregnancy Outcomes
Jensen AJOG 2001 Jensen AJOG 2001
Outcome (%) 2 hour < 102
2 hour 102-114
2 hour 115-128
2 hour ≥ 130
Odds Ratio 95% CI
Birthweight≥ 4000 g 22.9 27.4 28.8 32.3 1.16 1.01-1.34
Birthweight> 4500 g 5.2 5.3 5.6 8.6 1.16 1.01-1.34
LGA 16.0 20.7 21.1 27.2 1.23 1.13-1.33
PIH/PreE 4.8 6.9 8.4 7.2 1.16 1.02-1.31
Shoulder Dystocia 0.4 1.2 1.8 2.9 1.78 1.32-2.40
Hyperglycemia & Pregnancy Outcomes
• Does hyperglycemia without overt diabetes during pregnancy increase risk of adverse pregnancy outcomes?
• Blinded study of ~25,000 women at 15 centers in 9 countries
• Primary outcomes: birthweight > 90%ile for GA, primary CD, neonatal hypoglycemia, cord-blood C-peptide level > 90%ile
• Primary predictor: Levels of hyperglycemia
HAPO Study Cooperative Research Group N Engl J Med 2008
HAPO Glucose Levels
Level Fast (mg/dL) 1 hr (mg/dL) 2 hr (mg/dL)1 < 75 ≤ 100 ≤ 902 75-79 106-132 91-1083 80-84 133-155 109-1254 85-89 156-171 126-1395 90-94 172-193 140-1576 95-99 194-211 158-1777 ≥ 100 ≥ 212 ≥ 178
HAPO Study Cooperative Research Group N Engl J Med 2008

10/23/2014
5
HAPO Results
HAPO Study Cooperative Research Group N Engl J Med 2008
Weight Prolonged Labor (%) Excess Bleeding (%) CD (%)3000 – 3999 g 0.9% 0.5 184000 – 4499 g 1.2 0.7 25.54500 – 4999 g 1.3 0.9 35.6
> 5000 g 1.5 1.1 50.6
Boulet SL et al. Am J Obstet Gynecol. 2003;188(5):1372-8; Acker et al. Obstet Gynecol. 1985;66:762; Nesbitt et al. Am J Obstet Gynecol. 1998;179:476; Sandmire et al. Int J Gynaecol Obstet. 1988;26:65; Overland E et al. Am J Obstet Gynecol. 2009;200(5):506
Impacts of Macrosomia – Maternal
Boulet AJOG 2003
Impacts of Macrosomia – Fetal3000 –3999 g 4,000 – 4,499 g 4,500 – 4,999 g ≥ 5,000 g
Outcome % % OR CI % OR CI % OR CI5 min
Apgar ≤ 3 0.1 0.1 1.3 1.2-1.4 0.2 2.0 1.8-2.3 0.5 5.2 4.1-6.6
Assisted ventilation ≥ 30 min
0.3 0.3 1.2 1.1-1.2 0.5 1.9 1.7-2.0 1.3 4.0 3.5-4.6
Birth injury 0.3 0.5 2 1.9-2.1 0.8 3.1 3.0-3.3 1.3 4.5 4.0-5.2
NeonatalMortality
Rate*0.7 0.6 0.87 0.8-1 0.7 1.0 0.8-1.2 1.9 2.7 1.9-3.8
* Per 1,000, < 28 days Gillman Pediatrics 2003
Cumulative hazard (risk) function for development of metabolic syndrome according to birth weight.
P = 0.56
P = 0.004
LGA
LGA
AGA
AGA
Impacts of Macrosomia -Childhood

10/23/2014
6
• Increasing blood glucose (even without overt diabetes) is associated with worsening pregnancy outcomes including macrosomia, pre-eclampsia and cesarean section in an approximately linear fashion.
Overview
• Impact of Hyperglycemia• Testing• Treatment• Postpartum
When to test?Initial Visit:
• Overweight/obese• History of gestational diabetes or glucose intolerance• Prior LGA infant• Family history of type 2 DM• Maternal age > 35• High-risk ethnic groups (non-Caucasian)• PCOS
24 – 28 Weeks:• Everyone else• High-risk patients who screened negative earlier
How are average-risk patients screened for GDM in your practice?
T wo s t
e p t e s t
. . . O n
e s te p
t e s t. . .
F as t i n
g b lo o d
. . . A
a n d C
B an d C
57%
13%7%
21%
2%
A. Two step testing (1-hour, 50 gram glucose loading test followed by fasting 3-hour, 100 gram loading test if needed) at 24-28 weeks
B. One step testing (fasting 2-hour, 75 gram loading test at 24-28 weeks
C. Fasting blood sugar and/or hemoglobin A1c in the first trimester
D. A and CE. B and C

10/23/2014
7
GDM Testing Controversy What defines disease?
HAPO Study Cooperative Research Group. N Engl J Med. 2008.
F 75-791 hr 106-1322 hr 91-108
F 90-941 hr 172-1932 hr 140-157
In your opinion, what primary cesarean section rate defines disease?
> 1 5
%
> 2 0
%
> 2 5
%
> 3 0
%
12%
24%
35%30%
A. > 15%B. > 20%C. > 25%D. > 30% More Sensitive, Less Specific
LESS women WITHOUT disease test positive
MORE women WITHOUT disease test positive
Sensitivity v Specificity
Less Sensitive, More Specific
One-Step Two-StepCarpenter Coustan National Diabetes Data GroupUniversal Screening Risk-Based Screening
Early Screening 24-28 Week ScreeningHemoglobin A1c No Hemoglobin A1c
Testing for 1 abnormal value No f/u for 1 abnormal value

10/23/2014
8
One-Step vs. Two-Step Testing
Two-StepStep 1: Non-Fasting, 50 g, 1 hr serum glucose measurement
≥ 130/140 mg/dL� Step 2Step 2: Fasting, 100 g, 3 hr glucose test
2+ abnormal values � GDM
GDM prevalence ~ 5-10%
One-StepFasting, 75 g, 1 & 2 hr serum glucose measurement
1+ abnormal value � GDM
GDM prevalence ~ 20% ControlCC
IAD-PSG
GDMby CC (%)
GDM by IADPSG (%)
Normal Glucose
Tolerance (%)*PrimaryCesarean 19.5 17.8 14.8
*Shoulder Dystocia 1.2 0.71 0.91
*PPH 1.5 1.4 1.3
Ethridge Obstet Gynecol 2014
Prenatal Outcomes and Screening Strategies
* Not statistically significant
Prenatal Outcomes and Screening Strategies
Pregnancy outcomes among 1,750 women diagnosed with GDM by Carpenter-Coustan criteria and 1,526 women diagnosed by IADPSG criteria.
GDM Rate by CC = 10.6%GDM rate by IADPSG = 35.5%
2-Step CC Criteria IADPSG CriteriaGDM
%NGT
%P:
GDM vs NGTGDM
%NGT
%P:
GDM vs NGTGest HTN 4.9 4.0 0.047 5.7 2.2 0.009Delivery 0.049 0.026
Vaginal 57.9 58.4 69.7 73.2CD 27.6 25.7 22.1 18.5Forceps 14.5 15.9 8.2 8.3
LGA 4.9 4.6 0.9 4.8 3.2 0.04Duran Diabetes Care 2014 Mayo AJOG 2014
Prenatal Outcomes and Screening Strategies
Outcome OGTT Negative (N=526)
IADPSG (N=155) CDA (N=358)
* Composite 0.9 (0.8-1.2) 1.4 (1.1 – 1.9) 1.4 (1.1-1.8)PIH/Pre-E 0.9 (0.6-1.7) 3.0 (1.7-5.6) 1.2 (0.7-2.1)CD 1.1 (0.9-1.4) 1.4 (1.01-1.2) 1.3 (1.05-1.7)LGA (> 90%ile) 1.2 (0.9-1.6) 1.8 (1.1-2.9) 1.5 (1.1-2.2)
* Composite of: hypertensive disorders, shoulder dystocia, 3rd or 4th degree laceration, LGA, NICU admission, neonatal: respiratory complication, hypoglycemia, jaundiceCDA Guidelines: 1 hr, 50 g > 140 � 2 hr, 75 g < 95/191/160
Odds of Outcome compared to 1 hr, 50 g < 140 mg/dL

10/23/2014
9
One-Step vs. Two-Step• IADPSG criteria increases rates of GDM
• IADPSG GDM is associated with pregnancy outcomes similar to CC GDM
• If treating CC GDM improves outcomes (it does), diagnosing and treating IADPSG-defined GDM seems clinically appropriate
Alternative Testing Strategies
Trujillo Diab Res Clin Prac 2014
Performance Measures Cut-off for fasting plasma glucose (mg/dL)
80 85 90 92Positive Test (%) 54.3 34.3 19.8 15.6Sensitivity (%) 96.9 92.5 88.3 86.8Specificity (%) 55.0 78.4 95.1 100
Positive Predictive Value (%) 32.0 48.3 79.8 100Negative Predictive Value (%) 98.8 97.9 97.4 97.2
Fasting plasma glucose as a predictor for GDM (by IADPSG criteria)
Alternative Testing Strategies
O’Connor Clin Chem Lab Med 2012
A1c ≥ 6.5 � DM2A1c 5.7-6.4 � Pre-DiabetesA1c < 5.7 � Normal
Non-Pregnant
1st
Trimester2nd
Trimester3rd
TrimesterHbA1c
%4.8 – 5.5
(5.2)4.3 – 5.4
(5.0)4.4 – 5.4
(4.9)4.7 – 5.7
(5.1)
Average HbA1c Values Non-Diabetic Women
4.4%
5.4%5.6%
4.7%
5.1%4.9%
Non-Preg
2nd Tri
3rd Tri
1st Tri
Jelly Beans
Lamar AJOG 1999
• Brach jelly beans, mixed assortment• 28 jellybeans = 50 g simple sugar
50 g Glucose Beverage Jelly BeansCalculated
Value 95% CI Calculated Value 95% CI
Sensitivity 80% 28-99% 40% 5-85%Specificity 82% 75-88% 85% 77-90%Positive Predictive Value 15% 4-34% 9% 1-29%Negative Predictive Value 99% 95-100% 97% 93-99%

10/23/2014
10
Overview
• Impact of Hyperglycemia• Testing• Treatment• Postpartum
• Hyperglycemia is associated with worse pregnancy outcomes.
• Does intervention help?
Treatment of GDM
• Crowther et al: – RCT of treatment for gestational diabetes – 958 women with OGT: fasting < 140 & 2 hr 140-198– 485 received dietary intervention, glucose
monitoring, and insulin therapy if indicated– 473 received routine care
Treatment of GDM
Crowther et al. N Engl J Med 2005
Intervention Group N= 490
(%)
Routine Care N= 510
(%)
Adjusted RR or Treatment Effect
Adjusted p-value
*Any serious perinatalcomplication 1 4 0.33 (0.14 – 0.75) 0.01
Admission to NICU 71 61 1.13 (1.03 – 1.23) 0.04
Macrosomia 10 21 0.47 (0.34 – 0.64) < 0.001
Neonatal hypoglycemia 7 5 1.42 (0.87 – 2.32) 0.16
Preeclampsia 12 18 0.7 (0.51 – 0.95) 0.02
Cesarean Delivery 31 32 0.97 (0.81 – 1.16) 0.73* One or more of: death, shoulder dystocia, bone fracture, nerve palsy

10/23/2014
11
Anxiety & GDM
Crowther NEJM 2005
*
***
*
**
‡ Scores for the SF-36 can range from 0 (worst) to 100 (best).
• Landon et al:– RCT of treatment of mild GDM– 958 patients with fasting glucose < 95, but 2 or
more abnormal values on 3 hour (1 hr > 180, 2 hr > 155, 3 hr > 140)
– 485 were treated (37 required insulin)– 473 had usual care (2 required insulin)
Treatment of GDM
Intervention Group N = 485
(%)
Control Group N = 473
(%)Relative Risk p-value
NICU Admission 9 11.6 0.77 (0.51 – 1.18) 0.19
Macrosomia 5.9 14.3 0.41 (0.26 – 0.66) < 0.001Neonatal
Hypoglycemia 5.3 6.8 0.77 (0.44 – 1.36) 0.32
Shoulder Dystocia 1.5 4.0 0.37 (0.14 – 0.97) 0.02
Cesarean Delivery 26.9 33.8 0.79 (0.64 – 0.99) 0.02Preeclampsia or
GHTN 8.6 13.6 0.63 (0.42 – 0.96) 0.01
Treatment of GDM
Landon et al. N Eng J Med. 2009
• Blood Sugar Monitoring (biofeedback)• Choices for Treatment:
– Dietary modification & exercise– Oral agents– Insulin therapy
Treatment of GDM

10/23/2014
12
Hawkins Obstet Gynecol 2009
Blood Sugar MonitoringWeekly (N=675) Daily (N=315) p
Vaginal Delivery 67.1% 63.2% 0.22Shoulder Dystocia 1.9% 1.6% 0.71
Birth Weight 3,690 g 3,536 g < 0.001LGA 34.4% 23.1% < 0.001
Treatment of GDM• No evidence to-date to support a
specific diet.• Carb-restriction (< 40%) seems to
improve outcomes • Usual advice: 25-30 kcal/kg/day, limit
carbs to < 40% of total calories, 20% protein, 40% fat.
Treatment of GDM – Diet
Han et al. Cochrane Database of Systematic Reviews 2013, Issue 3.Major et al. Obstet Gynecol 1998;91:600-4.
� Exercise data is lacking with regards to pregnancy outcomes
Avoiding Ketosis• Severe carb restriction can result in ketosis – resulting
from breakdown of fatty acids in absence of sufficient carbohydrates
• Ketosis may be associated with behavioral and intellectual abnormalities in offspring
• Rizzo et al: Children’s developmental scores correlated inversely with 3rd trimester beta-hydroxybutyrate levels
• Onyeije et al: Maternal ketonuria associated with increased risk of oligohydramnios, nonreactive NST, fetal heart rate decelerations
Rizzo et al. N Engl J Med 1991;325:911-6.Onyeije et al. Am J Obstet Gynecol. 2001;184(4):713-8.
In your practice, for patients who fail diet/exercise management of diabetes, what is your preferred first-line agent?
Me t f o
r m in
G ly b u
r i d e
I n su l i n
19% 22%
59%A. MetforminB. GlyburideC. Insulin

10/23/2014
13
• Glyburide (sulfonylurea) – Increases insulin release from beta cells in pancreas
• Metformin (biguanide) – Increases insulin sensitivity, decreases gluconeogenesis
Treatment of GDM – Oral Agents 400 women, GDM requiring medication, randomized to Glybruide or insulin.
Treatment of GDM – Glyburide
Langer et al. N Engl J Med 2000;343:1134-8.
Treatment of GDM – Glyburide
Langer et al. N Engl J Med 2000
Outcome Glyburide (N=201)
Insulin (N=203)
P Value
NeonatalLGA 12% 13% 0.76Birth Weight 3256 g 3194 g 0.28Hypoglycemia 9% 6% 0.25
Maternal Blood Glucose < 40 mg/dL 2% 20% 0.03Preeclampsia 6% 6% 1Cesarean Section 23% 24% NS
Langer: Secondary data analysis of RCT• Glyburide and insulin are equally efficient for treatment of
GDM in all levels of disease severity.
Langer et al. Am J Obstet Gynecol. 2005
Treatment of GDM – Glyburide
Fasting plasma glucose on oral GTT
< 95 mg/dL > 95 mg/dLInsulin Glyburide Insulin Glyburide
LGA 7.7% 8.8% 17.8% 18.4%Macrosomia 2.0% 6.3% 8.0% 9.2%Composite Outcome* 25.3% 27.5% 30.7% 29.1%
* At least one of: metabolic complications, LGA/macrosomia, neonatal ICU admission > 24 hrs, need for respiratory support.

10/23/2014
14
Glyburide should be administered 30-60 minutes before a meal
Caritis et al. Obstet Gynecol. 2013;121:1309-12.
Glyburide – Timing of AdministrationGlyburide crosses the placenta
Rochon et al: Retrospective cohort study of 235 women• Odds of Glyburide failure were 2.84 (1.01 – 7.98) times higher among
patients with glucose challenge test ≥ 200 mg/dL• Neonates born to successfully Glyburide-treated mothers were more
likely to go to the ICN as compared to women with Glyburide-failures (33% vs 10%, p = 0.037).
Jacobson et al: Retrospective study comparing outcomes between 236 Glyburide-treated patients and 268 insulin-treated patients
• Patients treated with Glyburide had higher incidence of pre-eclampsia (12% vs 6%, p = 0.02, aOR 2.32)
• Neonates more likely to receive phototherapy (9% vs 5%, p < 0.05)Schwartz et al. Abstract SMFM. Am J Obstet Gynecol 2003;S25.Rochon et al. Am J Obstet Gynecol. 2006;195:1090-4.Jacobson et al. Am J Obstet Gynecol. 2005;193:118-24.
Downsides of Glyburide
Trends in Glyburide Use
Castillo Obstet Gynecol 2014
Propo
rtion
of Pa
tients
on Gl
yburi
de
0.4
0.8
0.2
0.0
0.6
1.0Glyburide use increased from
7.4% to 64.5% from 2000 to 2011
2001 2011
Metformin• Rowan et al: RCT of 751 women to compare Metformin &
insulin in the treatment of GDM. – Primary outcome was composite of neonatal
complications– Rate of primary outcome was equal in both groups– 46% required supplemental insulin. – More women in the metformin group than in the
insulin group would choose to receive their assigned treatment again (76.6% vs 27.2%, p < 0.001).
Rowan et al. N Engl J Med. 2008;358:2003-15.Moore et al. Obstet Gynecol. 2010;115:55-9.

10/23/2014
15
Treatment of GDM - Metformin
Rowan et al. N Engl J Med. 2008;358:2003-15.
Treatment of GDM - Metformin
• Moore: RCT of 149 women comparing Metformin to Glyburide. – Generally similar outcomes– Failure rate for metformin was 2.1 x higher
than Glyburide.
Moore Obstet Gynecol 2010
Insulin
Type Onset Peak (hours) Duration (hours)Insulin Lispro/Aspart 1-15 min 1-2 hrs 4-5 hrs
NPH 1-3 hrs 5-7 hrs 13-18 hrsInsulin Glargine (Lantus) 1 hr None 24 hrs
Insulin Detemir (Levemir) 1-2 hrs None 24 hrs
Oral Agents vs. Insulin
Dhulkotia AJOG 2010
Meta-analysis of oral hypoglycemics vs insulin: No difference in birthweight
FAVORS ORAL AGENTS FAVORS INSULIN
Pooled Weighted Mean Difference 0

10/23/2014
16
Oral Agents vs Insulin
Dhulkotia AJOG 2010
Meta-analysis of oral hypoglycemics vs insulin: No difference in CS Rates
FAVORS ORAL AGENTS FAVORS INSULIN
Induction of Labor• Rosenstein: Infant mortality rates at 39 weeks are lower than
overall mortality risk of expectant management.
Rosenstein et al. Am J Obstet Gynecol. 2012;206:309.e1-7.
Overview
• Impact of Hyperglycemia• Testing• Treatment• Postpartum
Postpartum – Impact of Activity
Bao JAMA Intern Med 2014
Each 100 min/wk increase in moderate-intensity physical activity reduced the risk of DM2 by 9%.

10/23/2014
17
Postpartum – Impact of Activity
RR for Type 2 DM associated with TV watching: 0-5 hrs = 16-10 hrs = 1.28 11-20 hrs = 1.41> 20 hrs = 1.77
Bao JAMA Intern Med 2014
Effect of Life Style on Risk of DM
Ratner J Clin Endocrinol Metab 2008
Conclusions• The goal of blood sugar testing is to identify
women at increased risk for poor perinatal outcomes and provide intervention where possible
• Given the low risk of intervention and the high-potential for gain, the most sensitive testing strategy should be considered
• Testing strategy must be tailored to patients/population
Conclusions
• Dietary intervention is often adequate treatment
• Oral antihyperglycemics are an appropriate alternative to insulin
• Careful attention to diet and exercise in the postpartum period reduces the long term risk of type 2 diabetes

10/23/2014
18
Thank You!

CHORIOAMNIONITIS: WHAT IS THE EVIDENCE FOR CLINICAL MANAGEMENT?Juan M. Gonzalez, MD Assistant Professor Maternal-Fetal Medicine Department of Ob/Gyn & RSUniversity of California, San Francisco
Disclosures
• No Financial Disclosures
Definition
• Chorioamnionitis
• Amnionitis• Intramamniotic infection
Pathogenesis
• Ascending of cervicovaginal flora• Facilitated by ROM
• Tranplacental• Listeria moncytogenes
• Iatrogenic • Amnio, CVS, fetal surgery

Clin Perinatol. 2010 Jun;37(2):339-54.
EPIDEMIOLOGY
Preterm
• Intramamniotic infection with pPROM• Less than 27 weeks � 41 %• 28 to 36 weeks � 15 %
• Intraamniotic infection 1/3 of spontaneous preterm labor with intact membranes
Clin Obstet Gynecol. 1993 Dec;36(4):795-808.
Am J Obstet Gynecol. 2001 Nov;185(5):1130-6.
Term
• 2 to 4 % term deliveries
• 12 % in labor who undergo a cesarean delivery

Risk Factors
• Low parity • Prolonged labor • Prolonged rupture of membranes • Multiple vaginal examinations in labor (consequence of longer labors)
• Internal fetal monitoring • Genital tract pathogens (STI, GBS, BV)
Microbiology
• Clinical intraamniotic infection • Bacteroides species (25 %)• G. vaginalis (24 %) • GBS (12 %)• Aerobic streptococci (13 %)• E. coli (10%)• Aerobic gram-negative rods (10 %)
J Infect Dis. 1982 Jan;145(1):1-8.
Microbiology
• 35 % of patients with clinical chorioamnionitisyield Mycoplasm hominis
J Infect Dis. 1983 Apr;147(4):650-3.

Clinical Presentation
• Clinical chorioamnionitis
• Subclinical absence of clinical findings:• Most commonly presents as spontaneous preterm labor or pPROM
Clinical Chorioamnionitis
• Maternal fever (oral temp ≥ 38.0C or 100.4F) (all cases)
• At least two of the following: • wbc > 15k (70-90% of cases)• maternal tachycardia (> 100 bpm) (50-80% of cases)• fetal tachycardia (> 160 bpm) (50-80% of cases)• uterine tenderness or foul odor of the amniotic fluid (4-
25% of cases)
Clin Perinatol. 2010 Jun;37(2):339-54.
Test
Clinical parameters
Fever Temperature >100.4 F 95 – 100 sensitiveNewton ER. Clin Obstet Gynecol 1993;36:795
Maternal tachycardia > 100/min 50 – 80% sensitive
Fetal tachycardia >160/min 40 – 70% sensitive
Fundal tenderness Tenderness on palpation 4 – 25% sensitive
Vaginal discharge Foul-smelling discharge 5 – 22% sensitive
Amniocentesis
• Refractory to tocolytics
• pPROM to determine whether induction is indicated
• Discriminate between chorioamnionitis and other causes of fever and abdominal pain

Amniocentesis TEST ABNORMAL FINDING COMMENT
Maternal white blood cell count (WBC)
≥15,000 cells/mm3 with preponderance of leukocytes
Labor and/or corticosteroids also may result in elevation of WBC
Amniotic fluid glucose ≤10 to 15 mg%
Excellent correlation with positive amniotic fluid culture and clinical infection
Amniotic fluid interleukin-6 ≥7.9 ng/mL
Excellent correlation with positive amniotic fluid culture and clinical infection
Amniotic fluid leukocyte esterase ≥1+ reaction
Good correlation with positive amniotic fluid culture and clinical infection
Gabbe 6th edition 2012
TEST ABNORMAL FINDING COMMENT
Amniotic fluid gram stain
Any organism in an oil immersion field
Allows id of particularly virulent organism: GBS. However, very sensitive to inoculum effect. Cannot id pathogens such as mycoplasmas.
Amniotic fluid culture
Growth of aerobic or anaerobic microorganism
Results are not immediately available
Blood cultures
Growth of aerobic or anaerobic microorganism
+ in 5% to 10% of patients; done in seriously ill pts or at risk for bacterial endocarditis, immunocompromised, or has a poor response to initial tx
Gabbe 6th edition 2012
Test
Amniotic fluid parameters
Culture Microbial growth Diagnostic gold-standard
Gram stainBacteria or white blood cells (>6/HPF)
24% sensitive, 99% specificRomero R, et al. Am J Obstet Gynecol 1993;169(4):839–51
Glucose level <15mg/dlAffected by maternal hyperglycemia 57% sensitive, 74% specificRomero R, et al. Am J Obstet Gynecol 1993;169(4):839–51
Interleukin 6 >7.9 ng/ml 81% sensitive, 75% specificRomero R, et al. Am J Obstet Gynecol 1993;169(4):839–51
White blood cell count >30/cubic mm 57% sensitive, 78% specificRomero R, et al. Am J Obstet Gynecol 1993;169(4):839–51
Leukocyte esterase Positive (dipsticks)85–91% sensitive, 95–100% specificRiggs JW, et al. Semin Perinatol 1998;22(4):251–9Hoskins IA, et al. Am J Perinatol 1990;7(2):130–2
Clinical Management
• Maternal bacteremia:3 – 12 % of infected patients
• Cesarean delivery is required: 8 % develop a wound infection 1 % develop a pelvic abscessIncrease risk of endomyometritis and venous thrombosis
Gabbe 6th edition 2012

Clinical Management
• Three separate investigations show intrapartumtreatment is superior to treatment after delivery. • Decrease in bacteremia • Decrease pneumonia • Decrease in maternal fever and hospitalization
Sperling RS et al. Obstet Gynecol 70:861, 1987.
Gilstrap LC et al. Am J Obstet Gynecol 159:579, 1988.
Gibbs RS et al. Obstet Gynecol 72:823, 1988.
Clinical Management
• 2002 meta-analysis (N = 181) compared intrapartum versus postpartum antibiotic therapy
• Intrapartum: • Reduction in neonatal sepsis (RR 0.08; CI 0.00 - 1.44)
• Pneumonia (RR 0.15; CI 0.01 – 2.92)
Hopkins L, Cocharane Database Syst Rev 2002
Regimen
• Antibiotic should be initiated as soon as Dx is made
• Administer broad spectrum antibiotics to cover: • Beta-lactamase producing aerobes • Anaerobes
• Main goal is to target GBS and E.coli
Regimen
• Ampicillin (2 g every 6 hours) or penicillin (5 million units every 6 hours)
plus • Gentamicin (1.5 mg/kg every 8 hours or 7 mg/kg/ideal body weight every 24 hours)

Other Regimens
• Ampicillin-sulbactam• 3 grams intravenously every six hours
• Ticarcillin-clavulanate• 3.1 grams intravenously every four hours
• Cefoxitin• 2 grams intravenously every six hours
Regimen • Penicillin-allergic patients
• Substitute ampicillin for:
• Vancomycin 1 gram every 12 hours • If GBS+ and Clinda resistant/resistance unknown: Vancomycin /Gentamicin
OR
• Clindamycin 900 mg every 8 hours • If GBS-negative or Clinda-sensitive GBS: Clindamycin /Gentamicin
Regimen
Chorioamnionitis and Cesarean delivery:
• If Amp/Gent or Vanco/Gent used • add Clindamycin
or • Metronidazole
(ideally prior to skin incision) for anaerobic coverage
Duration Postpartum
• Post-partum management if vaginal delivery: • antibiotics are continued for one dose after delivery unless the
woman is diagnosed with endometritis
No difference in treatment failure or infection-related complications in RCT evaluating:
• single postpartum dose of antibiotics (Amp/Gent in study)
versus
• continuing until 24 hours afebrile postpartum
Edwards et al. Obstet Gynecol 102:957, 2003.

Duration Postpartum • Post-partum management of chorioamnionitis if Cesarean
delivery: • If Amp/Gent or Vanco/Gent used
• add Clindamycin or
• Metronidazole
Edwards’ study included vaginal delivery and cesarean.
Underpowered to compare single-dose vs. continued dose just including Cesarean.
Given the high risk of endometritis in the setting of chorioamnionitis and Cesarean, continue antibiotics until 24 hours afebrile postpartum
Edwards et al. Obstet Gynecol 102:957, 2003.
Regimen
• There is NO evidence for oral antibiotics after discontinuation of parental therapy.
Dinsmoor MJ et al. Obstet Gynecol 1991; 77:60.
Antipyretics
• Maternal fever + fetal acidosis confers a 12.5% risk of neonatal encephalopathy (OR 94, 95 % CI 29 - 307)
• Independent effect:• Fever OR 8.1, 95 % CI 3.5 - 18.6• Neonatal acidosis OR 11.5, 95 % CI 5.0 – 26.5
Impey LW et al Am J Obstet Gynecol 2008; 198:49.
Route of Delivery
• Bactericidal concentrations in fetus one-half to one hour after infusion
• Average time between diagnosis and delivery is 3 to 5 hours
• No evidence that duration of infection correlates with outcomes
Gibbs RS et al Am J Obstet Gynecol 1991; 164:1317
Gilstrap LC 3rd et al Obstet Gynecol Clin North Am 1989; 16:373

Rouse DJ et al Am J Obstet Gynecol 2004; 191:211
Rouse DJ et al Am J Obstet Gynecol 2004; 191:211
• Prolonged first or second stage of labor has been associated with an increased risk of chorioamnionitis
• Whether this relationship is causal is unclear �evolving chorioamnionitis may predispose to longer labor
• Neither chorioamnionitis nor its duration should be an indication for cesarean delivery
ACOG Number 1, March 2014

Short-Term Outcomes
• Case-control study (N = 67) microbiologically confirmed clinical chorioamnionitis at term.
• Pneumonia 4 %• Neonatal bacteremia 4 %• No difference in low Apgar scores
Yoder RP et al Am J Obstet Gynecol.145:695 1983.
Short-Term Outcomes
• Among preterm neonates those with chorioamnionitis had higher:
• Perinatal death (13 % vs 3 %, P < .05)• RDS (34 % vs 16 %, P < .01)• Infection (17 % vs 7 %, P < .05)
Garite TJ Obstet Gynecol. 59:539-545 1982.
Short-Term Outcomes
• More likely to require cesarean
• Uterine dysfunction • Inadequate uterine response to oxytocin• Abnormal labor progress
Creasy and Resink 7th Edition 2014
Long-Term Outcomes

Long-Term Outcomes Diagnosis N RR (95% CI)
PRETERM INFANTS
Cerebral Palsy
Clinical chorioamnionitis 11 1.9 (1.4-2.5)
Histologic chorioamnionitis 5 1.6 (0.9-2.7)
Cystic Periventricular Leukomalacia
Clinical chorioamnionitis 6 3.0 (2.2-4.0)
Histologic chorioamnionitis 7 2.1 (1.5-2.9)
CI, confidence interval; RR, relative risk.
Grether JK, Nelson KB JAMA278:207, 1997; Wu YW, Colford JM Jr JAMA284:1417, 2000.
Creasy and Resink 7th edition 2014.
Long-Term Outcomes
Diagnosis N RR (95% CI)
TERM INFANTS
Cerebral Palsy
Clinical chorioamnionitis 2 4.7 (1.3-16.2)
Histologic chorioamnionitis 1 8.9 (1.9-40)
CI, confidence interval; RR, relative risk.
Grether JK, Nelson KB JAMA278:207, 1997; Wu YW, Colford JM Jr JAMA284:1417, 2000.
Creasy and Resink 7th edition 2014.
Prevention
• Ineffective:• Chlorhexidine vaginal washes during labor1
• Antepartum treatment of bacterial vaginosis 2
• Broad-spectrum antibiotics in patients with preterm labor but intact membranes3
Rouse DJ et al Am J Obstet Gynecol. 176:617 1997. 1
Carey JC et al N Engl J Med. 342:534 2000. 2
Egarter C et al Obstet Gynecol. 88:303 1996. 3
Prevention
• Intrapartum prophylaxis to prevent neonatal GBS sepsis decrease chorioamnionitis
• Screening based strategy versus risk-based
Locksmith GJ et al Am J Obstet Gynecol. 180:416 1999.

Prevention
• Active management of laborLopez-Zeno JA et al N Engl J Med. 326:450 1992.
• Induction of labor after PROM at term Mozurkewich EL et al Am J Obstet Gynecol. 89:1035 1997.
• Prophylactic antibiotics in selected patients with pPROM
Mercer BM Lancet. 346:1271 1995.
Prevention
• Largest randomized study found induction with oxytocin induction in PROM • Reduced:
• the time interval between premature rupture of membranes and delivery
• chorioamnionitis• postpartum febrile morbidity• neonatal antibiotic treatments
• Without increasing cesarean deliveries or neonatal infections
ACOG PB Number 107, August 2009.Hannah ME et al N Engl J Med 1996; 334:1005–10.
Prevention • Intravaginal PGE2 for IOL with PROM appears to be safe
and effective
• Randomized study IOL with PROM at term, only 1 dose of intravaginal misoprostol was necessary for successful labor induction in 86%
• No evidence that use of either prostaglandin increases the risk of infection in women with ROM
• Insufficient evidence to guide on use of mechanical dilators in ruptured membranes.
ACOG PB Number 107, August 2009.
Ray DA, Garite TJ. Am J Obstet Gynecol 1992;166:836–43.Sanchez-Ramos L et al Obstet Gynecol 1997;89:909–12.
Prevention • Meta-analysis (N = 6,814) PROM at term compared:
• IOL with prostaglandins or oxytocin • expectant management
• In patients which underwent IOL significant reduction in the risk of:• chorioamnionitis• endometritis• number of neonates requiring admission to NICU
Dare MR et al Cochrane Database of Systematic Reviews 2006, Issue 1. Art. No.: CD005302.

Summary • Chorioamnionitis is polymicrobial
• results from migration of cervicovaginal flora through the cervical canal
• Other causes include transplacental infection • bacteremia • invasive procedures
• Maternal fever ≥100.4 F. • Clinical diagnosis is strengthened by risk factors for the disease
and excluding sources of fever • Nonspecific clinical signs: leukocytosis, maternal and fetal
tachycardia, uterine tenderness, malodorous amniotic fluid
Tita, A et al Clin Perinatol. 2010;37(2):339-354.
Summary
• Amniocentesis may be helpful in cases of diagnostic uncertainty
• Chorioamnionitis may impair myometrialcontractility �can result:• labor abnormalities• need for cesarean delivery (with higher rate of complications)
• postpartum hemorrhage
Tita, A et al Clin Perinatol. 2010;37(2):339-354.
Summary
• Broad spectrum antibiotics should be started at diagnosis to minimize maternal and fetal morbidity.• Vaginal delivery: a single dose of antibiotics after delivery
• Cesarean section: afebrile for at least 24 hours
Tita, A et al Clin Perinatol. 2010;37(2):339-354.
Summary
• In the setting of chorioamnionitis, prompt induction or augmentation of labor• cesarean delivery reserved for standard obstetrical indications
• Immediate cesarean in the setting reassuring intrapartum fetal testing, adequate progress of labor, and administration of antibiotics does not improve neonatal or maternal outcome.
• Adverse neonatal outcomes associated with chorioamnionitis
Tita, A et al Clin Perinatol. 2010;37(2):339-354.

10/23/2014 1
1
Reducing Cesarean Surgical Site Infections
Marya G. Zlatnik, MD, MMSMaternal Fetal Medicine
UCSF 2
No Disclosures
UCSF
3
Objectives�Significance of SSIs in OB�Pathogenesis of SSI� Patient factors, procedural factors
�CDC recommendations for prevention �UCSF experience� CDC recommendations� Antibiotic timing
�Other/broader strategies4
Surgical Site Infections�3rd most frequent nosocomial infxn� 15% of nosocomial infxns
� Increased hospital stay & costs� 7-10 extra hospital days� Cost >$3000 each
�C/S: Most common surgery in US� SSIs common: endometritis, wound infxn� Rate of C/S SSI at UCSF as high as 12% in past
Births: Preliminary data for 2006. National vital statistics report; Vol 56, no 7

10/23/2014 2
6
Pathogenesis of SSI• Multi-factorial event driven by � Procedure variables � Patient risk factors
• Main pathogens = pt’s own flora− from skin & vagina
• Exogenous sources of SSI pathogens (less common)− OR environment− Surgical personnel− Instruments
Dose of bacteria x VirulenceHost Resistance
7
Patient Factors Contributing to SSI � Coincident infxns� Obesity� Diabetes � Indwelling invasive
devices� Tobacco use� Severity of illness
� Loss of intact skin� Blood transfusions � Poor Nutritional
Status� Steroid Therapy� Extremes of Age
8
What can we do to prevent SSI?� National recommendations 2014� Pre-op� In OR� Post-op
�These are general recommendations, not OB specific (but most apply to OB)
9
National Recommendations: Reducing SSIs�SHEA/ISDA/AHA/TJC 2014
� Atbx prophylaxis�Appropriate timing, drug, dosing, re-dosing
� Don’t shave�Preoperative skin prep: alcohol + (CHG)� Control blood sugars perioperatively (<180mg/dl)� Normothermia�Adequate ventilation/oxygenation�Surveillance for SSI
Anderson 2014 Strategies to Prevent Surgical Site Infections in Acute Care HospitalsInfxn Contr Hosp Epi http://www.jstor.org/stable/10.1086/676022

10/23/2014 3
10
Preoperative: Hair Removal�Use clippers, not razors for hair removal
� Micro-breaks in skin barrier�Clipping immediately before associated w/
lower SSI risk than shaving or clipping night before
�Don’t remove hair unless interferes w/ operation
Seropian, 1971, othersNg J Hosp Infec 2013 http://dx.doi.org/10.1016/j.jhin.2012.09.013
A hairy tale:successful patient education strategies to reduce prehospitalhair removal by patients undergoing elective caesarean section
12
A hairy tale: education strategies to reduce prehospital hair removal by patients undergoing C/S�Fewer pts shaved (1 wk): 83% � 53% in 2011 �SSI rate decreased: 7.6% � 3.7% after patient
education interventions (P < 0.001)� Overall reduction in SSI rate primarily d/t to
reduction in superficial infections
Ng, J Hosp Infec 2013 http://dx.doi.org/10.1016/j.jhin.2012.09.013
13
Preoperative: Antiseptic Shower/Bath�Decreases skin microbial colony counts �Require pts to shower w/ antiseptic agent the
night before OR (elective cases)Cat IB
�Pre-clean skin using soap/CHG� Remove any gross contamination Cat IB�Waiting on C/S data

10/23/2014 4
14
�Skin Prep—2 elements:� Physical separation of bugs
–friction & soap� Chemical activity on bugs by antimicrobial
soln�Use fast-acting, broad spectrum antimicrobial � CHG/alcohol better than iodine� Allow to air dry
Preoperative: Skin Preparation in OR
Amer-Alshiek 2013 15
� Objectives� Remove dirt, debris & transient flora� Reduce microbial counts as much as possible� Leave antimicrobial residual on the skin
� Optimum duration unknown� 2- 5 min scrub as effective as 10 min
�Chlorhexidine gluconate (CHG)� Persistent effect, broad spectrum
Surgeon Hand/Forearm Prep
CDC/HICPAC/APIC/SHEA/IDSA hand hygiene guidelines 2002
16
Preoperative Hand Prep�Artificial Nails� Increased bacterial &
fungal colonization� Long nails increase
tears in gloves� Increased nosocomial infxns
�Nail polish & hand jewelry� SSI risk unknown
�No artificial nails or polish, nail beds free of infxn
CDC Hand Hygiene, Mayo 17
Antimicrobial Prophylaxis: Agents, Timing�1st & 2nd gen cephalosporins most common� As effective as 3rd gen for C/S
(Cochrane 1999)�Giving ≤ 2 hrs before incision reduces SSI
(0.59% vs ≥ 3.3%)�General consensus: 30-60 min before incision� Except C/S, after cord clamping CAT 1A
CDC “Guideline for Prevention of Surgical Site Infection, 1999” available online at www.cdc.gov/ncidod/hip

10/23/2014 5
18
Antibiotic Prophylaxis�Cefazolin 2g� 3g if > 80kg
�Repeat Dosing� Cochrane re: C/S prophylaxis—1 dose as good as
multiple doses� Repeat for long (>3-4 hr) cases or excess blood
loss (>1500cc)�Maintain therapeutic levels during case &, at
most, few hours after closureCat IA
Anderson 2014
19
Surgical Attire: Recommendations�Sterile gowns/gloves during case�Masks/eye protection to protect staff�Theoretically filters aerosols from staff to patient -
not proven�When sneezing or coughing w/ mask on, face sterile
field directly�Scrub clothes—Change if soiled or moist�Hair covering in OR
• Cat IB/OSHA
20
SSI Surveillance
�Surveillance of SSI w/ feedback to surgeons reduces SSI risk
�Successful surveillance program includes:� effective surveillance methods� data feedback Cat IB� Starbucks cards & emails!
� Use EHRBarwolff J Hosp Infect 2006 21
Surgical Techniques Believed to Reduce SSI Risk�Good hemostasis�Handle tissues gently �Eradicate dead space �Avoid inadvertent entry into hollow viscus�Remove devitalized tissues�Use drains & suture material appropriately�Prevent hypothermia
Cat IB

10/23/2014 6
22
Other C/S-related Methods�Avoid chorioamnionitis�Spontaneous Delivery of Placenta�5.7% vs 15.2% endometritis w/ manual
extraction @ C/S• Baksu Acta Obst Gyn Scand 2005
�? Uterine exteriorization�Quicker, less febrile morbidity
• Jakobs-Jokhan Cochrane 2004
23
C/S SSI Reduction—UC Irvine�Multi-disciplinary team:� Atbx timing, reducing op time, double gloving,
1- layer uterine closure, tincture of iodine prep, no shaving
�C/S endometritis reduced from 4.1% to 1.6%�Cost savings of $35,653 per year
W Gornick, UCI Med Ctr, Irvine CA (APIC 97)
24
Pre-Op Checklist�ACOG abstract 2014—NY �After institution: SSI 6.2%� 3%
�Electric clipper to remove hair at surgical site�Cleaning skin with chlorohexidine solution�Broad spectrum atbx prophylaxis before incision�Cefazolin 1 gm IV bolus (30-60 min before surgery) plus
azithromycin 500 mg IV (1 hour before surgery)�Removal of placenta by cord traction�Closure of deep subcutaneous layer >2cm�Skin closure with subcuticular suture
Caban 2014
SSI after C/S: Implementing 3 changes to improve the quality of patient care
Corcoran, Am J Infec Control, 2013
• Clippers to remove hair• 2% CHG instead of 0.5%• Sew skin with non-absorbable suture
(instead of absorbable)
16% SSI 5% SSI

10/23/2014 7
26
Scope & Magnitude of SSI at UCSF� 2003: 217 C/S in 6 months at UCSF
� 9% rate SSI (13 incisional, 6 endometritis)� NNIS benchmark 3%� Analysis of risk factors: only diabetes & BG >200
were significantly associated� Identified as an area for improvement in our L&D� Task force�MDs, RNs, Administrators, Hospital infection control
27
Retrain RNs in aseptic
technique
O2 Post-opPatient warming
New surgical prep
(Duraprep)
Reduce nonessential personnel in
OR
Blood Sugars
Improve scrub technique
REDUCE C/S SSIs
Reducing SSI in L&D at UCSF: Feb 2005
28
UCSF SSI before & after Protocol Changes
p= 0.68
p= 0.08
p= 0.22
29
New surgical prep
Retrain RNs in aseptic
technique
O2 PostopPatient warming
Reduce nonessential personnel in
OR
Blood Sugars
Improve scrub technique
REDUCE SURGICAL SITE
INFECTIONS
Administer atbx prior to
incision
Reducing Surgical Site Infection2006
Kaimal AJOG 2008

10/23/2014 8
30
March 2005 June 2006
Methods
Retrain RNs in aseptic technique
New surgical prep
Reduce nonessential personnel
Supplemental O2
Patient warming
Improve scrub technique
Improve BG control
Antibiotics administered prior to incision
Study completed
June 2007
Historical Controls Intervention Group 31
All Cesareans
p= 0.002
p= 0.014
p= 0.020
Kaimal SMFM 2008
32
Multivariable Regression
aOR 95% CI
Overall SSI 0.33 0.14-0.77
Endometritis 0.34 0.13-0.92
Cellulitis 0.22 0.49-0.96
Controlling for labor, parity, prior cesarean delivery, maternal age, BMI, DM
33
�Change in policy to administer prophylactic atbx prior to incision � significant decrease in C/S SSI
�Demonstrate the integration of research findings into real-life clinical practice
�Our protocol is now to ask anesthesia to routinely administer cephalosporin prior to incision (cefazolin 2-3g)
Results at UCSF

10/23/2014 9
34
� 9,010 C/S before/after change in policy: timing of cefazolin� Decreased SSI w/ preop atbx vs cord clamp� Endometritis aOR 0.6 [0.5-0.8]�Wound infxn aOR 0.7 [0.6-0.9]
� No difference in early onset neonatal infxn� Lower late onset neonatal infxn� 1.8% vs 5.7% p<0.001
� No difference in “rule-out sepsis”
Similar Results Elsewhere: Magee-Womens
Owens ObGyn 200935
ACOG Committee Opinion Sept 2010�Recommends atbx prophylaxis for all C/S�unless the patient is already receiving appropriate
atbx (eg, for chorioamnionitis)�Prophylaxis should be administered within 60
minutes of the start of the C/S
36
Extended spectrum Prophylaxis�Ureasplasma increases risk for C/S SSI�Cephalosporin doesn’t cover
�RCT at UAB: 597 pts� Cefotetan +/- doxy 100mg IV + azithro 1g po 6hrs
later vs placebo�17% vs 25% endometritis p = 0.02�1% vs 4% wound infxns p = 0/03
Andrews ObGyn 2003Tita ObGyn 2008
37
Extended spectrum Prophylaxis
� F/U in Birmingham over 14 years� In 2000, IV cefotetan or cefazolin & IV azithro at cord clamp�Decreased endometritis�Decreased wound infections Tita ObGyn 2009
Tita AJOG 2008

10/23/2014 10
38
Extended spectrum Prophylaxis
�UCSF baseline rate much lower�Hesitant to extend atbx spectrum for all C/S
pts� Concerns re atbx resistance
�Selectively extend atbx spectrum� eg, pt w/ DM/obesity� Cefazolin 3g IV preop + azithro 500mg IV after cord
clamp (mix in 250mL/give over 1 hr )
39
Some Evidence�Povidone-Iodine Vaginal Prep�Endometritis
Cochrane 2010
40
Some Evidence�Povidone-Iodine Vaginal Prep— +/-ROM
Cochrane 2010 41
Mixed Evidence�Skin Closure � Suture better than staples –Tuuli 2011� No winner—Mackeen Cochrane 2012 � Non absorbable suture better than staples,
staples better than absorbable suture—Corcoran 2013

10/23/2014 11
42
Limited Evidence�Supplemental O2—may help in GI surgery, no
benefit in C/S (and may be harmful)� Gardella 2008� Scifres 2010� Duggal 2013
43
Review: Reducing C/S SSIs�Treat chorio�Atbx prophylaxis—BEFORE INCISION
�Appropriate dosing, re-dosing� Just don’t shave it!� Preoperative skin prep: alcohol + CHG� Peri-op:
� Control blood sugars perioperatively (<180mg/dl)� Normothermia
� Think about a checklist� Surveillance for SSI
44
Conclusions�Multi-disciplinary approach �Decreasing chorioamnionitis/managing labor
may be as important as OR issues�Give pre-op prophylaxis pre-op�Consider extended spectrum atbx for high risk
pts, vag prep for ROM� Track SSIs
45
�Thank you for your attention

10/23/2014
1
Evidence-Based Antenatal Testing
Robyn Lamar, MD, MPH
Clinical Instructor, OB-GYN, UCSF
I have nothing to disclose
But I wish I’d titled my talk differently
Outline
• Brief history
• Stillbirth epidemiology
• Evidence supporting antenatal testing
• Current practice recommendations
• Areas of controversy
• Antenatal testing as a screening program
Antenatal Testing: historical perspective
• 1902: concept of antenatal care introduced by Dr. JW Ballantyne in Scotland
• Late 1960s: electronic fetal monitoring
• Late 1970s: contraction & nonstress tests
• Late 1980s: “modified BPP” widely adopted

10/23/2014
2
Goal of Testing
• ACOG (2014): “to prevent fetal death”
• NICHD Workshop (2007): “to identify fetuses at risk for intrauterine death or injury, so that these adverse outcomes can be prevented”
In essence, antenatal testing is a screening program
Implications
The goal of reducing fetal death implies:
• Some causes of stillbirth are preventable
• Some vulnerable fetuses can be identified
A few definitions
• Stillbirth: fetal death occurring at 20 weeks gestation or later
• Fetal mortality rate: stillbirths per 1000 live births + stillbirths
• Late fetal mortality rate: stillbirths at 28 weeks or greater per 1000 live births + stillbirths
• Biweekly indicates “twice a week” in this talk
Late Stillbirth rate (28wk+): 11 Developed countries

10/23/2014
3
Stillbirth rate in the US
0
2
4
6
8
10
12
14
16
1940 1950 1960 1970 1980 1990 2000 2010
>28wk
Antenatal testingintroduced
Stillbirth Rates in the US
Etiology of Antepartum Stillbirth
Antepartum Stillbirths
PlacentalHTNMaternalInfectionGeneticUmbilicalObstetricOther
From the NICHD Stillbirth Collaborative Research Network
Quick review
• Half of stillbirths happen before 28 weeks
• The etiology of some stillbirths does not lend itself to prevention, ex:– Genetic causes
– Cord accidents
– Acute infection

10/23/2014
4
What can antenatal testing detect?
Relies on the premise that a fetus with compromised oxygenation responds with a series of detectable changes
• Blood flow � brain/heart, away from kidneys � oligohydramnios
• Fetal movements decrease to conserve energy
• Vagally-mediated slowing of pulse (decels)
Commonly reported sequence
• Loss of reactivity in fetal heart rate, abnormal blood flow in umbilical artery
• Absence of fetal breathing movement
• Low amniotic fluid
• Decreased fetal movement
• Abnormal fetal tone
Types of antenatal testing
• Maternal perception of fetal movement
• Nonstress test (NST)
• Contraction stress test (CST)
• Biophysical profile (BPP)
• Modified BPP (NST + amniotic fluid assessed)
• Umbilical artery Doppler velocimetry
Formal Antenatal Testing:Performance characteristics
False negative False positive
NST 2-6.5 55-90%
CST 0.4 35-65%
BPP 0.7-0.8 40-50%
mBPP 0.8 60%
False negative: stillbirth rate within 1 week of a normal test
False positive: percent of abnormal tests where follow up testing is normal (i.e., 1-PPV)

10/23/2014
5
The tricky part
• What was the woman’s pretest probability?
• How different is her post-test probability?
• In other words, how much a normal finding on antenatal testing reduce her risk?
What is the weekly stillbirth rate at 40 weeks for all-comers in the US?
Remember, the stillbirth rate is the number of stillbirths per the total number of births (stillbirths + live births)
. 1 . 4 1 2
19%
10%
26%
46%a. 0.1
b. 0.4
c. 1
d. 2
Weekly risk of stillbirth
Gestational Age Risk of stillbirth/1000/wk37 0.2138 0.2739 0.3540 0.4241 0.6142 1.08
After antenatal testing: 0.4-0.8 (in high risk women)
Evidence that Antenatal Testing Improves Outcomes
• No appropriate randomized controlled trials
• Best data (cited by ACOG) comes from cohort studies or case series which reference either– Historic controls
– Untested (presumably lower risk) patients at the same institution

10/23/2014
6
Evidence that Antenatal Testing Improves Outcomes
• Clark et al (1989): prospective 3 year cohort study of 2628 women with high risk singleton pregnancies– Weekly or biweekly mBPP with acoustic stim
– Intervention rate: 3%
– Stillbirths: 1 (T21, declined intervention)
– Comparison: stillbirths in unmonitored women over 1 year = 10 out of 4055 births (2.5 per 1000)
Evidence that Antenatal Testing Improves Outcomes
• Nageotte et al (1994): 4 year series of all 2774 high risk women referred for antenatal testing– Biweekly mBPP with acoustic stim
– 47% of women had a positive test at some point
– Intervention rate: 9.4%
– Stillbirths: 8 (2.9 per 1000; corrected 1.8 per 1000)
– Comparison: 11 per 1000 in patient population at this hospital who delivered after 28 weeks
Evidence that Antenatal Testing Improves Outcomes
• Miller et al (1996): prospective 4 year cohort study of 15,482 high risk women – Used weekly or biweekly mBPP with acoustic stim
– Intervention rate: 15.5% (<37wk: 1.5%)
– Stillbirths: 25 (1.6 per 1000; corrected 1.3 per 1000)
– Comparison: stillbirth rate of 10.8 per 1000 among 53,027 in the untested population
Evidence that Antenatal Testing Improves Outcomes: Summary
• Stillbirth rates were low in high risk women receiving structured antenatal testing, compared to women not in testing
• Intervention rates varied from 3% to 15%
• 1 study documented about half of women required backup testing at some point
• 1 study had iatrogenic prematurity rate of 1.5%

10/23/2014
7
Concerns about Evidence for Antenatal testing
• Was antenatal testing what drove the difference in stillbirth rates between tested & untested women? Possible confounders include:– Other differences in type of care provided (what
else would have been part of high risk care?)– Differences in the patients’ access to care– Differences in patient compliance with care
• Publication Bias?
How to Test
How to test: When to initiate?
• ACOG: “Both theoretic models and large clinical studies suggest that initiating antepartum fetal testing no earlier than 32 0/7 weeks of gestation is appropriate for most at-risk patients”
• Decision hinges on– Risk of stillbirth by gestational age– Risk of neonatal death by gestational age– The false positive rate of the test
How to test:Which Test?
• No firm guidelines• By test characteristics
– All have false negative rate <1/1000 except NST– All have false positive rates ~50% or higher– Resources & personnel may be deciding factors
• Which test for backup?– Limited data suggest CST leads to more
interventions compared to BPP, but not to better outcomes

10/23/2014
8
How to test:Frequency
• ACOG: “If the maternal medical condition is stable and test results are reassuring, tests of fetal well-being (NST, BPP, modified BPP, or CST) are typically repeated at weekly intervals”
• Some reports advocate twice weekly testing for certain high risk conditions
How to test:Amniotic fluid assessment
• Use deepest vertical pocket (DVP) < 2cm:– Decreased risk of false positives
– No change in risk of false negatives
• Consider poor reproducibility– 41% of repeat assessment of oligohydramnios
showed a normal AFI 3-4 days later
• Some data suggest that maternal hydration & rest in left lateral decubitus may increase AFI
Whom to Test?
• Classic indications:– Maternal: DM, HTN, severe renal or autoimmune
disease– Pregnancy related: late/postterm, decreased fetal
movement, HTN disorders, IUGR
• But epidemiologic research shows many other consistent risk factors for stillbirth
• And half of women with stillbirth have no identifiable risk factors
Newer Indications for Testing?
ACOG:
Because antepartum fetal surveillance results have not been definitively demonstrated to improve perinatal outcome, all indications for antepartum testing must be considered somewhat relative. In general, antepartum fetal surveillance has been used in pregnancies in which the risk of antepartum fetal demise is increased.

10/23/2014
9
Newer Indications for Testing?
Executive Summary from NICHD interprets this:
The ACOG practice bulletin on antepartum fetal surveillance suggests that antepartum testing may be appropriate for any “pregnancies in which the risk of antepartum fetal demise is increased.”
NICHD Increased Risk Categories
• Advanced maternal age, or age < 20• Black women• Nulliparity• Very high parity (10+)• Assisted reproductive technology• Abnormal serum markers • Overweight & obesity• Low educational attainment
How many of your patients don’t have ANY of these risk factors?
< 15 %
1 5- 3 0
%
3 0- 5 0
% M
o r e t h
a n h a l
f . . .
83%
1%1%15%
a. <15%
b. 15-30%
c. 30-50%
d. More than half are low risk
Prevalence of Risk Factors among Californian Pregnant Women
• Age 35+ 18%• Age <20 9%• Black 5%• Nulliparity* 40%• IVF* 1.5%• Abnormal serum * 5-7%• BMI* ≥25 47%• Low education 26%
*National dataCalifornia data is from California DPH, 2010 birth data

10/23/2014
10
Newer Indications for Testing:Concerns
• High prevalence of many risk factors
• No data on the impact of antenatal testing on populations for these indications
• Would expansion of antenatal testing imply this was part of standard prenatal care, and only exceptionally low risk women could be excluded?
Stillbirth & AgeNewer Indications for Testing?
A thought experiment:Consider testing pregnant women age 35-39• Risk of stillbirth: 6.85/1000• Risk of stillbirth 28+wk: 3.35/1000
Imagine antenatal testing reduced their risk to that reported by Miller:1.6/1000
Absolute risk reduction: 3.35-1.6/1000 = 1.75 per 1000Number needed to treat = 572
A quick question on cost. . .

10/23/2014
11
How much does UCSF bill for each modified BPP?
$50 $100 $500 $1,000
1%
24%
58%
17%
a. $50
b. $100
c. $500
d. $1000
Newer Indications for Testing?A thought experiment:
Consider testing pregnant women age 35-39• Risk of stillbirth: 6.85/1000• Risk of stillbirth 28+wk: 3.35/1000
Imagine antenatal testing reduced their risk to that reported by Miller:1.6/1000
Absolute risk reduction: 3.35-1.6/1000 = 1.75 per 1000Number needed to treat = 572
Costs of tests themselves (assume ~7 tests/woman)572 * 7 * $500 = $2 million dollars spent on initial screening
tests per stillbirth avoided
Risks & unknowns to consider
• Increase in induction rate • Iatrogenic prematurity• Increase in cerebral palsy with preterm testing?• Cost of testing
– UCSF:• Bills $1395 per mBPP• Collects $435-800 per test for privately insured patients
(MediCal: $80 per test)– Doesn’t include costs of interventions that follow– Maternal time
• Maternal experience
Screening Criteria: WHO• The screening program should respond to a recognized need.• The objectives of screening should be defined at the outset. • There should be a defined target population. • There should be scientific evidence of screening program
effectiveness. • The program should integrate education, testing, & clinical services• There should be quality assurance, with mechanisms to minimize
potential risks of screening. • The program should ensure informed choice, confidentiality and
respect for autonomy. • The program should promote equity and access to screening for the
entire target population. • Program evaluation should be planned from the outset. • The overall benefits of screening should outweigh the harm.

10/23/2014
12
Screening Criteria: WHO
• There should be a defined target population. • There should be scientific evidence of screening program
effectiveness.
• There should be quality assurance, with mechanisms to minimize potential risks of screening.
• The program should ensure informed choice, confidentiality and respect for autonomy.
• Program evaluation should be planned from the outset. • The overall benefits of screening should outweigh the harm.
Summary• Currently there is a lack of data on:
– How to disentangle the unique contribution of antenatal testing in preventing stillbirth from other aspects of “high risk” prenatal care
– The potential harms & costs of screening– Who might benefit the most from screening
• Keep in mind ACOG’s admonishment:“Because antepartum fetal surveillance results have not been definitively demonstrated to improve perinatal outcome, all indications for antepartum testing must be considered somewhat relative.”
• Especially for unstudied indications for testing, counsel patients individually on the decision of if & when to initiate testing

10/23/2014
1
Induction of Labor: Update on the Evidence
Sarah B Wilson, MD MEdAssistant ProfessorDepartment of OB/GYN, UCSF
Disclosures
� I have nothing to disclose.
Induction: A Balancing Act
� Consider…– Maternal health
• Likelihood of spont labor• Risk of cesarean with IOL
– Fetal health• Risks of premature delivery• Risk of IUFD
– Maternal preferences– MD preferences? – Systems/ cost– The EVIDENCE
Background
� Labor induced in 22% of gravid women in US� Induction rate doubled from 1995 to 2006 � Medical Inductions
– IUGR, Diabetes, Preeclampsia� Elective Inductions: no medical indication
– Rate increasing even more rapidly
ACOG Practice Bulletin 107, August 2009, Reaffirmed 2013

10/23/2014
2
Objectives
� Become an agent of change against elective IOL < 39 weeks� Dive into understanding the relationship
between IOL and risk of c section� Discuss IOL timing after 41 weeks� Analyze if IOLs increase risk of autism
Elective Induction before 39 Weeks
� ACOG strongly cautions against elective IOL before 39 weeks.
� Confirmation of gestational age by– Ultrasound measurement <20 weeks
confirms 39 weeks or greater– Doppler confirmed fetal heart tones present
for 30 weeks– 36 weeks since a positive urine or serum
HCG pregnancy test
� Fetal lung maturity before 39 weeks is NOT an indication for IOL
ACOG Practice Bulletin 107, August 2009
Elective Induction before 39 Weeks
Percent Change in Distribution of Birth by Gestational Age: US between 1990-2006
Martin et al. National vital statistics report: vol 57 no 7. National Center for Health Statitstics
Elective Induction before 39 Weeks
� Early-term neonates have increased morbidity and mortality, compared to neonates ≥ 39 wks .– Clark et al: 18% of 37 wk electively delivered infants went to
the NICU.
Oshiro et al. Decreasing elective deliveries before 39 weeks in an integrated healthcare system Obstet Gynecol 2009. Adapted by Main et al. CMQCC Toolkit.

10/23/2014
3
Elective Induction before 39 Weeks
� Early-term elective deliveries have been quite common.– Retrospective study: 17,794 deliveries
• 44% of >37 week deliveries were planned, not spontaneous.
• 71% of planned deliveries were elective.
– 10% of all deliveries were elective inductions or cesareans between 37-39 wks.
Clark et al. AJOG 2009.Included all deliveries in 27 hospitals in 14 states in a 3 month period in 2007
Do you see elective early term IOLs?
Elective early-term (<39 wks) IOLs occur at my institution.
N ev e r
R ar e l y
S om e
t i me s
F r eq u e
n t l y
54%
4%5%
37%
A. NeverB. RarelyC. SometimesD. Frequently
How can we reduce early term elective IOLs?
� Clark et al AJOG 2010– 3 Strategies:
• Hard stop at the hospital level policy
• Soft stop: providers agree to not electively induce < 39 wks
• Education program about the risks– Hard stop� greatest reduction in early deliveries
� Ehrenthal et al Obstet Gynecol 2011– Hard stop with significant reduction in IOL and
NICU admissions– Tradeoff: Increased stillbirths at 37 and 38 wks
� <39 Week Toolkit CMQCC
How can we reduce early term elective IOLs?
choosingwisely.org

10/23/2014
4
What about after 39 weeks?
� Role for selective or elective IOL at full or late term
� Does this improve outcomes?
Does IOL increase the risk of c section?
Inductions increase risk of cesareans.
A gr e e
N eu t r
a l
D i sa g r
e e
58%
16%
26%
A. Agree
B. Neutral
C. Disagree
Does IOL increase the risk of c section?
� Observational studies that compare IOL vs spontaneous labor in same week show IOL has higher c section rates.
� True comparison?
Johnson DP Ostet Gynecol 2003, Caughey Evid Based Med 2014
Does IOL increase the risk of c section?
�Wood et al (2013) BJOG– Meta-analysis of 31 studies IOL vs
expectant management • Included IOL for medically indicated and elective
IOL, intact membranes• Method of IOL not the same
– IOL� moderate, but significant reduction in cesareans
– No significant differences in other maternal or neonatal outcomes

10/23/2014
5
Does IOL increase the risk of c section?
� Limitations of accepting conclusion wholeheartedly– Higher GA leads to diagnoses that
bias clinicians to c sections
Does IOL increase the risk of c section?
� Limitations of accepting conclusion wholeheartedly– Higher GA leads to diagnoses that
bias clinicians to c sections– Difference in IOL meds/ technique
depending on GA
Does IOL increase the risk of c section?
� Limitations of accepting conclusion wholeheartedly– Higher GA leads to diagnoses that
bias clinicians to c sections– Difference in IOL meds/ technique
depending on GA– What about what we know about
waiting for a favorable cervix?
Does IOL increase the risk of c section?
� Limitations of accepting conclusion wholeheartedly– Higher GA leads to diagnoses that
bias clinicians to c sections– Difference in IOL meds/ technique
depending on GA– What about what we know about
waiting for a favorable cervix?– Consider costs

10/23/2014
6
IOL Timing after 41 weeks
� ACOG: late term ≥41 wks to postterm ≥42 wks
� Fetal Neonatal Risks of Post-term: – Post-term preg have higher stillbirth rates– Post-maturity syndrome– Increased macrosomia� worse fit
� Maternal Risks– Increased severe perineal lacs, c sections, PPH,
ACOG Practice Bulletin #146, Aug 2014
IOL Timing after 41 weeks
� Hannah RCT: 41 vs Expectant Management– 3407 women at 41 wks randomly assigned to IOL or
expectant monitoring• Cesarean rate
– 21.2% IOL group vs 24.5% Monitoring group (p<0.03)– More Cesareans in monitoring group for fetal distress
• Perinatal Deaths: 2 stillbirths in monitoring group (p not significant)
Hannah et al. NEJM 1992
IOL Timing after 41 weeks
� Gulmezoglu et al (2009) Cochrane Meta-Analysis– 19 studies, 7984 women (included Hannah)– 41 week induction was associated with…
• Fewer all cause perinatal deaths RR 0.3 (95%CI 0.09-0.99)
• No significant change in cesarean rate RR 0.92 vs 0.97 for 42 wks
– Conclusion: A policy of IOL at 41 wks, is associated with fewer perinatal deaths. Women should be counseled about the relative and absolute risks of IOL at 41 wks.
� ACOG: Can consider IOL at 41-42 weeks, recommend at ≥ 42
IOL Timing after 41 weeks
� Cost Effectiveness of 41 wk IOL– Decision analytic model: 41 wk IOL vs expectant
management to 42wks, then IOL– Assumed IUFD rate in 41st wk 0.12% and C/S rate 27% in
41wk IOL– 41 wk IOL associated with…
• Incremental cost $10,945/QALY• Decreased adverse obstetric outcomes
Kaimal et al, AJOG 2011

10/23/2014
7
Do IOLs increase risk of autism?
IOLs increase the risk of autism spectrum disorders in children.
A gr e e
N ot s u
r e
D i sa g r
e e
0%
66%
34%
A. AgreeB. Not sureC. Disagree
Do IOLs increase risk of autism?
Have you been asked this question by your patients?
Y es , a
n d I h a
v . . .
Y es , a
n d I ’ m
n . ..
N o, I h
a v en ’ t
. . .
11%
73%
17%
A. Yes, and I have a planned response.
B. Yes, and I’m not sure what to say.C. No, I haven’t been asked this.
Do IOLs increase risk of autism?
� Oxytocin link with Autism Spectrum Disorder? � No causal relationship with current
evidence
ACOG Committee Opinion 597, May 2014
Do IOLs increase risk of autism?
� Guinchat et al 2012 Review– Weak nonsignificant association?
� Gregory et al 2013 JAMA Pediatr– Autism in 1.3% male, 0.4% female children – Mec, fetal distress, <34 weeks, DM, IOL,
aug and IOL+aug� increased odds

10/23/2014
8
Do IOLs increase risk of autism?
� Gregory et al 2013– Strengths
• Huge dataset ≈ 625,000 children• Multivariate log regression: control for
confounders
– Weaknesses• Increased odds but no causal effect• Missing data including some info about birth
trauma• No data re IOL method, med exposure
– Meds or act of IOL?
� Questions or comments?
� Thank you.

10/23/2014
1
Pain Management Options in Laboring
PatientsJennifer Lucero, MDAssistant ProfessorClinical Anesthesia
UCSF Dept. of Anesthesia
Objectives• Discuss the current evidence for opioids
in labor• Review the Role of Nitrous Oxide in labor• Discuss Non-Pharmacologic strategies • Review the Role of Epidural Analgesia in
labor
OPIOIDS IN LABOR

10/23/2014
2
Fentanyl Pharmacokinetics• Short acting synthetic μ-1 & μ-2 opioid
receptor agonist• Rapid onset of action in 30-60 sec• Peak analgesic effect within 2.5 min• Cumulative effect with repeated or prolonged
administration• Increased context sensitive half-life: ≈70 min • Elimination in neonates varies: 75-440 min
Remifentanil Pharmacokinetics:Ultra-Short Acting (mu-1 opioid receptor agonist)
• Rapid onset (onset = 30-60 sec; Peak = 2.5 min)
• Inactive metabolites (plasma esterases)
• Short Context-Sensitive half-life (3.5 min)
• ““““Respiratory Depression”””” half-life (2.5 min) Hinova et al. Systemic Remifentanil for Labor Analgesia. Anesthesia & Analgesia. 2009; 109(6): 1925-9. Babenco et al. The pharmacodynamic effect of a remifentanil bolus on ventilatory control. Anesthesiology 2000; 92:393-8.
Remifentanil and Pregnancy• The placenta contains nonspecific esterases• Fetal esterases nearly fully developed at birth• Within 5-10 minutes of turning off an infusion
there is virtually no residual effect.• Remifentanil can be turned off minutes before
delivery without fetal respiratory depression
Maternal-Fetal Transfer
Kan, R, et al.. Anesthesiology; 1998;88:1467-74

10/23/2014
3
Maternal-Fetal Transfer
Kan, R, et al.. Anesthesiology; 1998;88:1467-74 Douma et al. Br J Anesth 2010; 104(2): 209-15.
*
Douma et al. Br J Anesth 2010; 104(2): 209-15.
Meperidine Fentanyl RemifentanilSatisfaction 7.0 7.3 8.1*Epidural 34% 15%* 13%*Supp O2 8% 2% 12%Sat < 95% 33% 56%* 74%*Apgar 1 8.6 8.5 8.9Apgar 5 9.7 9.6 9.9
* = p<.05 vs. Demerol
RCT Remifentanil vs. Epidural
Volmanen et al. Acta Anesthesiol Scand 2008; 52: 249-55.
N=45 Total

10/23/2014
4

10/23/2014
5
• Remifentanil Group: transient maternal desaturation observed more frequently
• Fentanyl Group: larger number of neonates required resuscitation
• Pain scores were no different between the groups
NITROUS IN LABOR
Nitrous oxidePatients:11% Complete61% Considerable28% Slight or None
Midwives:7% Excellent35% Good49% Adequate9% inadequate
Rosen 1969 BMJ, Vol3:263

10/23/2014
6
• 58 publications reviewed – 2 studies good quality– 11 studies fair – 46 studies poor
• Nitrous less effective pain relief than epidural• Heterogeneous outcomes for satisfaction• No difference in neonatal outcomes• More good quality studies needed
Coping Algorithm vs. Pain Scoresin Labor
• Developed to provide an alternative pain scores
• Formalized assessment tool for laboring women
• Future Research– Validation with different cultures ethnicities– Validation from patient perspective– Generalizability at other institutions

10/23/2014
7

10/23/2014
8
NON-PHARMACOLOGIC METHODS
Listening to Mothers- 2006• Survey of women who gave birth in a hospital
in 2005• 1,573 survey participants• Ages 18-45• Only single gestations (multiple gestations
excluded)

10/23/2014
9
EPIDURAL ANALGESIA
Thorp, JA et al .The effect of continuous epidural analgesia on cesarean section for dystocia in nulliparous women.Am J Obstet Gynecol. 1989; 161(3): 670-5
Thorp, JA et al.Epidural analgesia and cesarean section for dystocia : risk factors in nulliparas.Am J perinatology1991;8 (6):402-410
Thorp, JA et al. The effect of Intrapartum Epidural Analgesia on Nulliparous Labor: Randomized, Controlled, Prospective Trial. Am J Obstet Gynecol 1993 196(4):851-858.
Historically, a Bad Reputation

10/23/2014
10
Outcome Narcotic (45) Epidural (48)Oxytocin Augmentation 26.7% 58.3%Head Malposition 4.4% 18.8%Assisted Vaginal Delivery 11.1% 18.8%Cesarean Delivery 2.2% 25.0%
Thorp, JA et al. The effect of Intrapartum Epidural Analgesia on Nulliparous Labor: Randomized, Controlled, Prospective Trial. Am J Obstet Gynecol 1993 196(4):851-858.
…when feasible, obstetric practitioners should delay the administration of epidural analgesia in nulliparous women until cervical dilatation reaches 4–5 cm and other forms of analgesia be used until that time.
Outcome Neuraxial Systemic P ValueCesarean 17.8 % 20.7% .31Instrumental 19.6% 16.0% .13Oxytocin 92.3% 94.5% .38Neuraxial Duration 440 min 330 min .001APGAR <7 (1min) 16.7% 24.0% .01APGAR <7 (5min) 1.4% 2.5% .28

10/23/2014
11
EDITORS’ CHOICE
Early versus late init iat ion of epidural analgesia inlabor: Does it increase the risk of cesarean section?A randomized trial American Journal of Obstetrics and Gynecology (2006) 194, 600–5
In the absence of a medical contraindication, maternal request is a sufficient medical indication for pain relief during labor…ACOG recognizes that many techniques are available for analgesia in laboring patients. None of the techniques appears to be associated with an increased risk of cesarean delivery.
No increased risk of Cesarean Delivery or Instrumented Vaginal Delivery with early epidural placement

10/23/2014
12
Routine Epidural analgesia may be inferior to Epidural on Request leading to more Operative Deliveries: Vaginal and Cesarean Delivery

10/23/2014
13
It’s ComplicatedLabor dysfunction causes increased pain resulting in maternal request for epidural? MaybeOREpidural causes increased second stage and operative vaginal delivery? Not Likely
Complex interplay of Labor, Labor management, and epidural analgesia
Labor epidural currently the most effective in reducing pain scores and producing most effective analgesia in labor
Conclusions• Opioids are safe for both mother and neonate• Remifentanil & Fentanyl PCA are alternative
options for women who epidural is contraindicated
• Nitrous Oxide has a role in labor analgesia
Conclusions• Pain scores should not be the only assessment
of Labor analgesia • There is a role of non-pharmacologic options
in labor• Epidurals do not increase your risk of
operative deliveries• Epidural analgesia is best at maternal request
and not as routine analgesia

10/23/2014
14

10/23/2014
1
UCSF
October 23, 2014
Mark Rollins, MD, PhDUCSF Director Obstetric Anesthesia
UCSFOB/GYN Update:What Does the
Evidence Tell Us?
Discussion of ACLS considerations in pregnancy…
• Frequency of Cardiac Mortality
• ACLS Code Modifications
• Local Anesthetic Toxicity
• Perimortem Delivery
• Checklists & Simulation
http://www.cdc.gov/reproductivehealth/maternalinfanthealth/pmss.html

10/23/2014
2
Causes of pregnancy-related death in the United States: 2006–2010
http://www.cdc.gov/reproductivehealth/maternalinfanthealth/pmss.html
Anesthesiology, June 2014
Anesthesiology, June 2014
Cardiac Arrest: 1 in 7,151 (CI 1:5,319 - 1:9,615)
Eric J. Lavonas, Farida M. Jeejeebhoy and Andrea GabrielliTerry L. Vanden Hoek, Laurie J. Morrison, Michael Shuster, Michael Donnino, Elizabeth Sinz,
Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular CarePart 12: Cardiac Arrest in Special Situations: 2010 American Heart Association

10/23/2014
3
Cardiac arrest in pregnancy• Incidence:
1:20,000 patients• Mostly: stick to
ACLS algorithms• IV above
diaphragm• Difficult airway• Left uterine
displacement• Cesarean section
• How Does This Consensus Statement Differ From Existing Guidelines?
Anesth & Analg, June 2014
Key Objectives
• Appropriate Team
• Relieve Aorto-Caval Compression
• Focus on Chest Compressions
• Do Not Delay Defibrillation
• Prepare for Emergent Delivery
• Checklists and Simulation
Call for Help“Code OB”

10/23/2014
4
Call for Help“Hey, Who’s resuscitating the baby?”
Cardiology, Anesthesia, Obstetricians & Nurses:
Can you use that pressor?
Should we stop the nitro drip?
I thought Versed was a teratogen…
The phenylephrine is causing the decels…
Isn’t supplemental oxygen bad for the baby?
Why are you tilting her to the left?
The loss of variability is just the fentanyl…Are you sure you want a stent placed? You won’t be able to place an epidural for delivery…
Where did all this fluid come from?
Slide by Elizabeth Whitlock
Aortocaval compression• The gravid uterus compresses the
IVC and aorta when supine• Hypovolemic shock
Kerr MG: Cardiovascular dynamics in pregnancy and labor. BMJ Bull 24:19, 1968.
Slide by Elizabeth Whitlock
Left uterine tilt/displacement
Slide by Elizabeth Whitlock Vanden Hoek. Circulation; 122:S829. 2010

10/23/2014
5
Left uterine tilt/displacement
Lift!
Displace!
Slide by Elizabeth Whitlock Vanden Hoek. Circulation; 122:S829. 2010
Cardiac arrest in pregnancy: CABDE• C: Circulation▫ Left uterine displacement▫ Compressions� 2 or 3 cm Higher on Sternum� 5-cm depth (Hard)� 100/min (Fast)� Rotate Compressors q 2 min� Minimize Interruptions� Capnography (> 10 mmHg)
▫ IV above the diaphragmF.M. Jeejeebhoy et al. / Resuscitation 82 (2011) 801–809
Slide by Elizabeth Whitlock
Airway and Breathing
• An example of a
“simplified algorithm”
• Call for Help
• Don’t get fixated on ETT placement

10/23/2014
6
Airway and Breathing
• 10 breaths per min.
• 500-700 ml/breath
• EtCO2 confirmation
Cardiac arrest in pregnancy: CABDE• D: Defibrillate:
• Performed on shockablerhythms ASAP
• No change in energy during pregnancy
• AED?
• Goal of < 3 min from collapse
• Removal of monitors
Slide by Elizabeth Whitlock
Cardiac arrest in pregnancy: CABDE
•D: Drugs:
• All ACLS drugs OK
• Oxytocin?
• Lipid Emulsion with Local Anesthetic Toxicity
Perioral Numbness or TinglingMetallic Taste
Tinnitus DiplopiaLightheadedness
Confusion & DrowsinessRestlessness
Sense of Impending DoomMuscular Twitching
Tonic-Clonic SeizuresUnconsciousness
Respiratory Arrest

10/23/2014
7
Tachycardia
Hypertension
Myocardial Depression
Decreased Cardiac Output
Peripheral Vasodilation
Hypotension
Conduction Block
Sinus Bradycardia
Ventricular Arrhythmias
Asystole Collapse
• Advanced Age
• Severe Cardiac Dysfunction
• Conduction Abnormalities
• Liver Disease
• Low Plasma Protein
• AcidosisNeal JM, et al. Reg Anesth Pain Med. (2012) 37:16-8
Neal JM, et al. Reg Anesth Pain Med. (2012) 37:16-8 Neal JM, et al. Reg Anesth Pain Med. (2012) 37:16-8

10/23/2014
8
Neal JM, et al. Reg Anesth Pain Med. (2012) 37:16-8
Anesth Analg. February 2013
Anesth Analg. April 2012

10/23/2014
9
BMJ. December 2003
Cardiac arrest in pregnancy: CABDE
• E: Extract (the fetus)▫ Incision at 4 minutes▫ Delivery by 5 minutes
post-arrest
Slide by Elizabeth Whitlock
No perfusing rhythm after 4 minutes?
Perimortem cesarean section Perimortem cesarean section
American Journal of Obstetrics and Gynecology (2005) 192, 1916–21

10/23/2014
10
Perimortem cesarean section
American Journal of Obstetrics and Gynecology (2005) 192, 1916–21
Perimortem cesarean section
American Journal of Obstetrics and Gynecology (2005) 192, 1916–21
Perimortem cesarean section
• Location?
• Operative Vaginal Delivery?
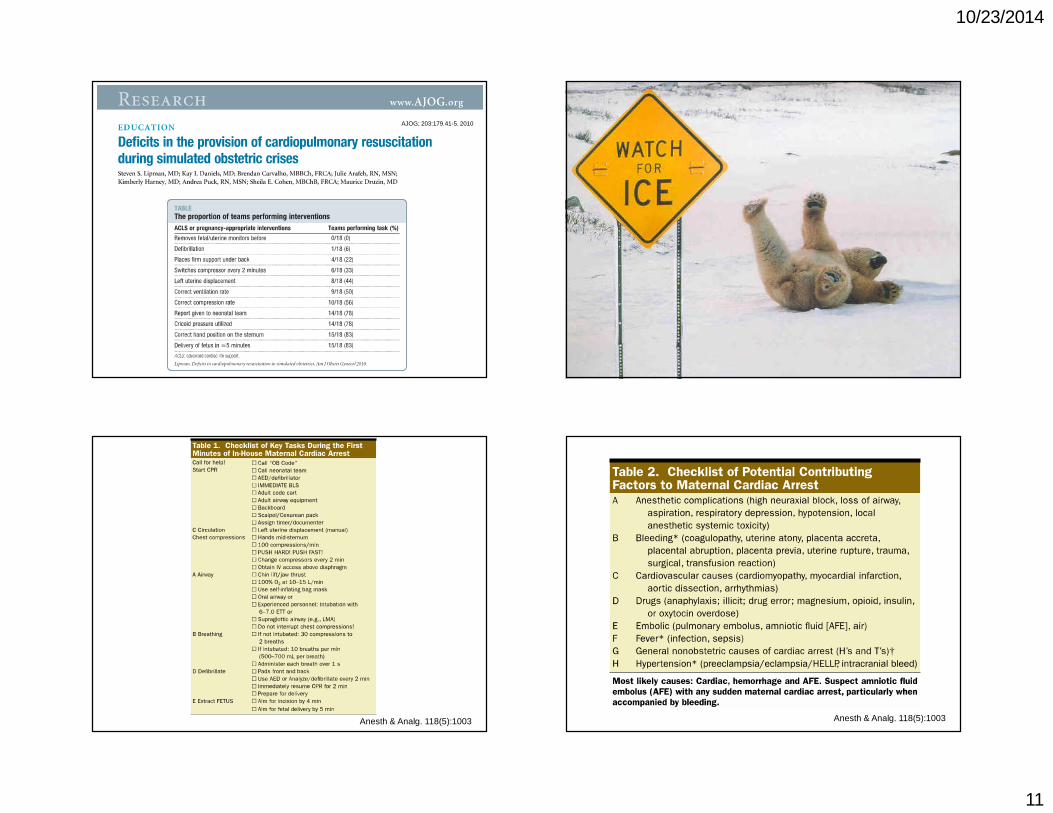
10/23/2014
11
AJOG; 203:179.41-5. 2010
Anesth & Analg. 118(5):1003 Anesth & Analg. 118(5):1003

10/23/2014
12
EMERGENCY MANUAL
COGNITIVE AIDS FOR OB PERIOPERATIVE CRITICAL EVENTS
Adapted from: Stanford Anesthesia Cognitive Aid Group’s Emergency Manual 2014, V2.0 and Gawande et al. OR Crisis Checklists NEJM 2013; 368: 246-53.
CH
EC
KLI
ST
S
Adapted from: Stanford Anesthesia Cognitive Aid Group’s Emergency Manual 2014, V2.0 and Gawande et al. OR Crisis Checklists NEJM 2013; 368: 246-53.
ACLSAsystole/PEA……………………………………………………..…....1Bradycardia – Unstable……………………………………..……..2Tachycardia – Unstable……………………………………..……..3Pulseless VF/VT……………………………………………..…………4CRITICAL EVENTS: NON-ACLSAmniotic Fluid Embolism………………………………..………..5Anaphylaxis…………………………………………………..…………6Bronchospasm…………………………………………….….……….7Difficult airway – Unanticipated………………….…………..8Fire…………………………………………………………….………..….9Post-partum Hemorrhage…………………………….…….….10Hypotension………………………………………………...………..11Hypoxia……………………………………………………..….……….12Local Anesthetic Toxicity……………………..………….……..13Malignant Hyperthermia…………………………………………14Myocardial Ischemia……………………………………………….15Tachycardia – Stable SVT………………………………….…….16Total Spinal Anesthesia………………………………….……….17Transfusion Reaction…………………………………….……….18Venous Air Embolus……………………………………………….19
Are you seeking to help clinicians deliver the best possible care during medical
emergencies?
Despite best intentions, well-trained clinicians often miss known key steps during
critical events.
This FREE perioperative Emergency Manual contains 25 critical events as well as
Crisis Resource Management key points. It has been iteratively tested with simulation
over many years.
Table of ContentsMobile DownloadPermissions & Local CustomizationAppropriate CitationDisclaimer

10/23/2014
13
Potential Drills & Simulations
Severe Fetal Bradycardia
Eclamptic Seizure
Shoulder Dystocia
Massive Hemorrhage
Failed Intubation
Anaphylaxis
Total Spinal
Magnesium Overdose
Opportunities for New Facilities
Where are the supplies located? Airway cart? Code cart?
What are the work flows?
How long does it take to transfer patient locations?
How do I call for help? A code? A crash?
How do I get emergency blood?
How do I get STAT labs? Point of care testing?
Preston P, et al. Seminars in Perinatology 2011. 35:84
• Cardiac Arrest in Pregnancy is Rare
• Appropriate Help “Code OB”
• Relieve Aorto-Caval Compression
• Focus on Compression & Defibrillation
• Use Lipid Emulsion with LAST
• Prepare Early for Emergent Delivery
• Checklists and Simulation Beneficial

10/24/2014
1
Overcoming ObstaclesBreastfeeding Success and Baby Friendly Hospitals
Ami Burnham LM, RN, IBCLC
• I have nothing to disclose
The Ten Steps to Successful Breastfeeding
• 1. Have a written breastfeeding policy that is routinely communicated to all health care staff.
• 2. Train all health care staff in skills necessary to implement this policy.
• 3. Inform all pregnant women about the benefits and management of breastfeeding.
• 4. Help mothers initiate breastfeeding within the first hour of birth.
• 5. Show mothers how to breastfeed, and how to maintain lactation even if they should be separated from their infants.

10/24/2014
2
The Ten Steps continued…• 6. Give newborn infants no food or drink other then human
milk, unless medically indicated.• 7. Practice rooming-in – that is, allow mothers and infants to
remain together – 24 hours a day.• 8. Encourage breastfeeding on demand.• 9. Give no artificial teats or pacifiers to breastfeeding infants.• 10. Foster the establishment of breastfeeding support groups
and refer mothers to them on discharge from the hospital or clinic.
• http://www.babyfriendlyusa.org/about-us/baby-friendly-hospital-initiative/the-ten-steps
Who is Baby Friendly?• Healthy People 2020 goals: 8.1% U.S. hospitals will be baby
friendly
• 2007 2.9% of hospitals were baby friendly
• 2014 8.4% (198) of U.S. Hospitals are designated baby friendly
• www.babyfriendly.org/find-facilites
Why Does it Matter?• In 2005 US facilities designated as Baby-Friendly had higher
rates of breastfeeding initiation (83.8% vs 69.5%)1
• These facilities also had higher rates of exclusive breastfeeding (78.4% vs 46.3%)1
• If 90% of Americans exclusively breastfed for 6 months: $13 billion/year in savings and 911 deaths prevented (mostly infants)2
What steps can you do?• 3. Inform all pregnant women about the benefits and
management of breastfeeding.
• 4. Help mothers initiate breastfeeding within the first hour after birth.
• 5. Show mother’s how to breastfeed and how to maintain lactation even if they should be separated from their infants.
• 10. Foster the establishment of breastfeeding support groups and refer mothers to them on discharge from the hospital or clinic.

10/24/2014
3
Step 4• “mother’s who breastfed within the first hour of birth (61%)
were significantly more likely to be exclusively breastfeeding 2-4 weeks after discharge”3
• “Lack of both 4 and 9 (pacifiers) together was related to the greatest decrease in breastfeeding duration (11.8wk decrease)”4
Steps 3,5 & 10• Educate yourselves and your colleagues in order to educate
your clients
• Targeted breastfeeding education among ObGyns, Pediatricians and Family Practice residents has been shown to significantly increase exclusive breastfeeding rates among their patients.5
• http://newborns.stanford.edu/Breastfeeding/HandExpression.html
Attitude matters• Positive association has been found between the obstetrician
and pediatricians preference for breastfeeding and exclusive breastfeeding at 1 and 3 months.6
• Prenatal care providers have extensive access to support and educate pregnant women and their families about breastfeeding.
• What can you do?
Other providers and settings• CDC found in 2011
• 57.7% of U.S. women reporting exclusive breastfeeding at 4 weeks pp7
• Homebirth midwives in the bay area: 1,916 planned home births from 2009-2014• 98.5% (1,892) reported exclusively breastfeeding
at final pp visit (5-6wks pp)8

10/24/2014
4
What are they doing?• Prenatally: Questionnaire/discussion with non-judgmental, open
ended questions re: breastfeeding plans• Ex: Are you planning on breastfeeding and if so, how long?
• Enable you to explore and educate re: the recommendations around ex breastfeeding for 6 months, with complimentary foods for at least 1 year.
• Intraprtum: primarily oral hydration • Low rates of medication use and operative delivery • Immediately postpartum: skin to skin unless medically indicated.• Standard newborn procedures done on mom’s body• Routine medications and bathing withheld until breastfeeding
established (or 2-3 hours pp. for medications)• Postpartum: extensive support in-home, referrals prn to IBCLCs,
connect all new parents with peer-to-peer support groups
Some other thoughts…Another Ten Steps for Intrapartum Care9• 1. Assess the mother’s knowledge of the benefits of
breastfeeding and risks of formula feeding to ensure informed consent for feeding choice.
• 2. Assess the mother’s knowledge of the impact analgesia and anesthesia has on labor, the infant, and the lactation process.
• 3. Assess the mother’s knowledge of, experience with, and motivation for the use of non-pharmacologic comfort measures to customize teaching and labor support to avoid or minimize pharmacologic measures.
• 4. Encourage ambulation for as long as the laboring woman is comfortable.
• 5. Discourage the recumbent position and suggest frequent position changes for mother’s confined to bed.
Another Ten Steps cont…• 6. Encourage oral hydration and nourishment, unless
contraindicated, and carefully monitor fluid intake and output.• 7. Place baby immediately on mother’s chest, and leave the
baby skin-to-skin to encourage bonding, breast-seeking and breastfeeding behaviors.
• 8. Delay routine eye prophylaxis and vitamin K injections until after the first breastfeeding is accomplished.
• 9. Delay the baby bath until after the first breastfeeding.• 10. Initiate breast pumping within the first hour if the infant is
transferred to the NICU without the opportunity for skin-to-skin contact and breastfeeding.9
Labor Pain Medications and Delayed Onset of Lactation (DOL)• DOL: onset of copious milk secretion >72 hours postpartum
• DOL: associated with shorter breastfeeding duration, in one study median breastfeeding durations 3.4 months and 11.7 months respectively
• “regardless of method of delivery, women who used pain medication reported higher rates of DOL”10

10/24/2014
5
Summary• The Ten steps are an effective tool to increase initiation and
duration of breastfeeding.
• Utilizing even some of the steps has been demonstrated to help increase breastfeeding initiation and duration.
• Small interventions during the prenatal, intrapartum and immediate postpartum periods can have big consequences when it comes to successful lactation.
Thank you!Ami Burnham LM,
RN, IBCLCammasource.com

10/24/2014
1
Striving to Provide the Best Care at Lower Costs
Christopher Moriates, MDDivision of Hospital Medicine, UCSF
October 23, 2014Email: [email protected]
Twitter: @ChrisMoriates
Disclosures
I do not have any relevant financial relationships or commercial interests to disclose

10/24/2014
2
“ Do you want to do prenatal
genetic testing?”

10/24/2014
3
Providing “Value” in Health Care
QualityCost
VALUE =
Sources of $750B of Waste and Excess in Healthcare
IOM (Institute of Medicine). 2012. Best care at lower cost: The path to continuously learning health care in America. Washington, DC: The National Academies Press.
1 Don’t schedule elective, non-medically indicated inductions of labor or Cesarean deliveries before 39 weeks 0 days gestational age.
1 Don’t schedule elective, non-medically indicated inductions of labor between 39 weeks 0 days and 41 weeks 0 days unless the cervix is deemed favorable.
1 Don’t perform routine annual cervical cytology screening (Pap tests) in women 30–65 years of age.
1 Don’t treat patients who have mild dysplasia of less than two years in duration.
1 Don’t screen for ovarian cancer in asymptomatic women at average risk.

10/24/2014
4
The only way is to get rid of
Fee-for-Service!
The problem is DEFENSIVE MEDICINE.
“Fix” malpractice or you won’t be able to
do anything!
What We Are Up Against:Video: “Overrun with Overuse, Part 2”
Teaching Value Project, Costs of Care, 2013Video clips available for FREE at www.teachingvalue.org
THEHIDDENCURRICULUM
Not paid… Fee-for-Service
Not at high risk of being sued

10/24/2014
5
“Culture Eats Strategy For Lunch”
Slide showing % of GDP goes here?
Clinicians are trained to take care of the patient in front of us
The “system”
The bedside
… not to assume responsibility for populations
Slide by Dr. Neel Shah, Costs of Care

10/24/2014
6
It Is About The Patient In Front of Us!Side-Effects May Include: Financial Ruin
• Medical bills are the leading causefor personal bankruptcy in the United States
• >75% were insured!
• More Americans than ever before are now on High-Deductible Insurance plans
Himmelstein DU, Warren E, Thorne D, Woolhandler S. MarketWatch: Illness And Injury As Contributors To Bankruptcy. Health Affairs, no.W5(63), 2005. Himmelstein DU, Thorne D, Warren E, Woolhandler S. Medical bankruptcy in the United States, 2007: results of a national study. Am J Med 2009;122(8):741–6.
Patient Affordability: Massachusetts
The Access Project, 2009
Insured non-elderly adults in MA reporting problems paying medical bills
medical debt rates unchanged
Urban Institute, MA Health Reform Survey, 2010
98% have insurance
Slide by Dr. Neel Shah, Costs of Care
An Uninsured Patient’s Perspective
Clip courtesy of This American Life from WBEZ Chicago

10/24/2014
7
Pricecheck… Costs of Care Essay Contest
Some physicians may be resigned to a reality that financial adverse effects are a known and unavoidable harm of
medical care. However, the same argument had been made previously
about central line infections, yet recent data highlight that central line infections are almost universally avoidable
through specific actions of physicians.

10/24/2014
8
“COST” interventions: Culture
OversightSystems
Training
Moriates and Shah. JAMA Internal Medicine. August, 2014
Thank YouChris Moriates, MD
Division of Hospital Medicine, [email protected]
Twitter: @ChrisMoriates

10/24/2014
1
Management of Menopause
Marcelle I. Cedars, M.D.Professor and Director
Division of Reproductive Endocrinology and InfertilityUCSF
Conflict of Interest
• Financial conflict – none
• Research conflict– Funded research:
• Ferring Pharmaceutical• Nora Therapeutics
• Off –label drug use– none
Problems in Peri-Postmenopausal Women
• Abnormal uterine bleeding
• Vasomotor symptoms
• Genital atrophy
• Decrease in skin collagen• Rapid bone loss
• Increase in coronary heart disease
• Increase in Alzheimer’s disease

10/24/2014
2
Benefits of Menopausal HT:What We Thought We Knew before WHI
• Prevents or abolishes hot flashes
• Prevents or improves genital atrophy• Prevents or slows bone loss
• Reduces risk of cardiovascular disease
• Improves cerebral blood flow
• May reduce risk of Alzheimer’s disease
• May reduce risk of colon cancer• Improves overall quality of life
Risks of Menopausal HT:What We Thought We Knew before WHI
• Breast cancer, ?RR 1.1-1.5
• Endometrial cancer, RR 4.0-11.0 (unopposed estrogen)
• Venous thromboembolism– 2 additional cases per 10,000 women– Low mortality rate of 1%
• Gall bladder disease
Publication of Clinical Trials in July, 2002
• Heart & Estrogen/Progestin Replacement Study (HERS) II– JAMA 2002;288:49-66 (July 3)
• Women’s Health Initiative (WHI)– JAMA 2002;288:321-33 (July 17)
HERS: Conclusion
• HRT should not be used to reduce the risk of further CHD events in postmenopausal women with already established CHD

10/24/2014
3
WHI HRT StudyWHI HRT StudyDisease Rates for Women on Estrogen + Progestin vs PlaceboDisease Rates for Women on Estrogen + Progestin vs Placebo
Writing Group for the Women’s Health Initiative. JAMA. 2002;288:321-333.
Numb
er of
Cases
/year
in 10,0
00 Wo
men
6050403020100
CHD Stroke Breast Cancer
PE ColorectalCancer
HipFractureEndometrilCancer
Deaths
Risks+31 Benefits- 11 Neutral
Placebo
Estrogen+Progestin+ 7
+ 8+ 8
+ 8 - 6 - 5
Number of women needing to take HT for oneextra adverse or protective event per year:
• 1100 for myocardial infarction
• 1200 for stroke• 600 for serious thromboembolism
• 1300 for invasive breast cancer
• 2000 to prevent a hip fracture
• 1700 to prevent a colon cancer
The WHI Estrogen-Alone Trial(JAMA 2004:291:1701-1712)
• Only strokes and hip fractures were significantly impactedin 10,739 postmenopausal women aged 50-79 over 6.8 years: There was an absolute excess risk of 12 additional strokes and 6 fewer hip fractures per 10,000 person-years.
• A possible reduction in breast cancer risk, inconsistent with other studies, “requires further investigation.”
• Preliminary analyses suggest lower hazard ratios (for CVD) in women aged 50 to 59 years.
Reconciling observational studies and clinical trials

10/24/2014
4
WHI vs. Observational studies
Manson JE, et al. 2006; 13:139
What’s different?
• Methodological explanations:– Confounding
• intrinsic biases of observational studies
– Incomplete capture of early clinical events• attenuation of risk
• Biological explanations– Clinical characteristics of the populations
• timing of initiation of treatment
– Characteristics of hormone therapy• type and dosage
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
22 24 27 >29
RH
for C
VD
BMI (kg/m 2)
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
WHI*
RH
for
CV
DThe Effect of Body Mass on the Risk
of CHD: Putting the WHI Results in Perspective
*Mean BMI 28.5 kg/m 2.BMI data from Willett et al, JAMA , 1995WHI data from Writing Group for the Women’s Health Initiative Investigators, JAMA , 2002
VASCULAR BIOLOGIST'S DEFINITION OFPRIMARY PREVENTION
CARDIOLOGIST'S DEFINITION OFPRIMARY PREVENTION
AdventitiaMedia
Lamina
Fatty Streak/Plaque
InternalElastic
Fibrous
Plaque
Cap
Event
Necrotic Core
Plaque
FibrousCap
MMP-9

10/24/2014
5
Metalloproteinase and Gelatinolytic Activity of Human Coronary Artery
Atherosclerotic Plaques
From Galis et al, J Clin Invest, 1994
Estrogen Effects on the Natural History of AtherosclerosisAdventitia
Media
Fatty Streak/Plaque
InternalElasticLamina
Necrotic Core
Plaque
FibrousCap
FibrousCap
Plaque Necrotic Core
Plaque
FibrousCap
MMP-9
Estrogen Effects in Atherogenesis↓LDL oxidation ⇒↓LDL atherogenicity↓LDL binding/accum ⇒↓lesion
progression↓CAMs ⇒↓monocyte adhesion/
↓macrophage accumulation↓SMC proliferation ⇒↓lesion
progression↑Endothelial function ⇒↑vasodilation
Estrogen Effects in Established Plaques↑Inflammation ⇒ ↑PQ instability
↑lesion progression↑MMP expression ⇒↑PQ instability/rupture↑Neovascularization ⇒↑PQ hemorrhage
Loss of Estrogen Benefits↓ Expression of estrogen receptors↓ Vascular responsivity
Benefits of estrogen on atherosclerosis prevention
Adverse effects ofestrogen on atherosclerosis/CHD
Patient Characteristics: Agethe “timing” hypothesis
• Grodstein et al. J Womens Health 2006– Nurse’s Health Study: evaluating time from
menopause – women near menopause reduced CV risk (RR 0.66 CI: 0.54-0.80)
• Manson et al. NEJM 2007– WHI: coronary calcium – women 50-59,
coronary calcium score lower in women on ET vs. placebo (OR 0.69 CI: 0.48-0.98)
Ovarian Aging and Somatic Aging
• Cardiovascular (CV) risk
• Osteoporosis

10/24/2014
6
Endothelial dysfunction during MT
Moreau JCEM 2012
Acceleration of CV risk
El Khoudary Menopause 2012
Ovarian aging and CV risk
Bleil Menopause 2013
Danish Osteoporosis Prevention Study (DOPS)
• 1006 women
• Randomized 45-58 years, last vaginal bleeding 3-24 months prior to enrollment and increased FSH
• Randomized, open-label, trial of estrogen (2mg daily), triphasic estradiol + norethisterone (uterus) vs. no treatment

10/24/2014
7
DOPS 2012
Schierbeck LL, BMJ 2012
DOPS 2012
• At 10 years, reduced overall mortality
• Reduced heart failure, MI
• No “apparent” increased risk cancer, VTE
Impact of MT on bone turnover
Sowers JCEM 2013
Breast CancerRisk Factors
• Starting close to menopause
• Low body weight
• High mammographic breast density
• 2 years after stopping HRT – risk equivalent to never users

10/24/2014
8
Breast CancerRisk Factors
• Was there truly a “protective” effect of estrogen in the E-only arm – WHI?
• Estrogen– Role of estrogen deprivation
• Whether natural or via anti-estrogens (tamoxifen/aromatase inhibitors)
– Estrogen as a pro-apoptotic
Breast CancerThe ‘Gap’ Hypothesis
• Starting estrogen remote from menopause decreases risk while treatment within 2 years increases breast cancer risk
• The ‘gap hypothesis’ and the ‘timing hypothesis’ are thus in conflict
Estrogen and Breast Cancer
Breast Cancer ReanalysisLancet, 1997:350:1047
Current/recent use HT: 2.3%/yearDelay in menopause: 2.8%/year
The “Menopausal Syndrome”
• Almost all signs and symptoms result from decreased circulating estrogen
• Symptoms:Hot flushes, paresthesias, cold hands and feet, headache, vertigo, irritability, anxiety, nervousness, depression, fatigue, weight gain, insomnia, night sweats, forgetfulness
• Signs:Depressed menstrual bleeding, relocation of fat deposits, decreased skin elasticity, osteoporosis in 25%, genital tract atrophy
• Some signs and symptoms may begin before menopause - and last long after

10/24/2014
9
Symptoms and the Menopausal Transition
• Hot flushes and night sweats• Stiff or painful joints• Difficulty sleeping• Poor/fair self-rated health
• Depression• Headache
Berecki-Gisolf J, et al. Menopause 2009
Trouble Sleeping by Cycle Day
Kravitz, H. M. et al. Arch Intern Med
Hot Flashes worsen Sleep
• 20 healthy premenopausal women receiving GnRHa
• 80% concordance between subjective/objective VMS (sVMS/oVMS)
• Sleep efficiency (actigraphy) worse with oVMS, quality worse with sVMS (questionnaire)
Joffe H, Menopause 2013 PMID 23481119
Adjusted OR for CES-D > 16Across Menopausal Transition
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
Pre Early Peri Late Peri Post HT Users
Bromberger, J Affect Disord 2007

10/24/2014
10
Verbal Memory
Decrement in immediate (A) and delayed (B) verbal recall
Epperson JCEM 2013
Estradiol and Depressive Disorders(Soares et al., Arch Gen Psychiatry 2001;58:529)• 50 perimenopausal women aged 40-55 with irregular
menstrual periods and FSH > 25 IU/L meeting criteria for major depressive, dysthymic, or minor depressive disorder by DSM-IV blindly randomized to transdermal estradiol (0.1 mg) or placebo for 12 wks
• Remission of depression observed in 17 of 25 (68%) on E2 and 5% on placebo
• Regardless of DSM-IV diagnosis, subjects responded similarly to E2
Headaches during the MT
Oh K, Euro Neurol 2012
Estrogen and the Brain
• Direct effects– Enhances synaptic plasticity, neurite growth,
hippocampal neurogenesis and long-term potentiation (memory)
– Protects against apoptosis and neural injury– Stimulates aceytlcholine (memory), serotonin,
noradrenalin– Decrease deposition of β-amyloid– Promotesmorphological and electrophysiological
correlates of learning and memory• Indirect effects
– Vasculature– Immune system
NIA – Frontiers proposal – Bench to BedsideEstrogen as a case-study (2009)

10/24/2014
11
Estrogen and the Brain
• Alzheimer Disease– Early and consistent symptom – loss of
episodic memory (failing to recall appointments and events)
– In the laboratory: estrogen reduces the formation of β-amyloid formation and diminishes hyperphosphorylation of tauprotein
Estrogen and the BrainAlzheimer Disease
• Observational studies suggest protection• Meta-analyses suggest risk reduction of
approximately 1/3• Contradicted by the WHIMS trial (ages 65-79)
– Risk of dementia increased two-fold with combined HRT
– Impact noted within a few years, suggesting impact primarily on the vasculature
– Past history of use associated with lowered incident risk of dementia (including Alzheimer Disease)
• Initiation in older women WITH disease is not beneficial
HRT/ET and Neuroprotection
• WHIMS (Shumaker et al., JAMA 2003;289:2651-62; Rapp et al., JAMA 2003;289:2663-72)
– increased cognitive impairment and dementia in the oldestpopulation
• Observational/animal studies– role of timing, type– improvement in certain skills (memory and verbal
fluency)– impact of smoking
Estrogen, Menopause, and the Aging Brain: How basic neuroscience can inform hormone therapy in women
• Disconnect with WHI and WHIMS– Animal and pre-clinical data supporting benefit– Timing of treatment– Administration formulations
• HT/ET at the menopausal transition and afterward could have beneficial effects on neurological symptoms
Morrison, Brinton, Schmidt, Gore: J Neuroscience: 26:10332

10/24/2014
12
Route of Estrogen Therapy
• Blood pressure – impaired endothelial function– Small impact of oral; no impact for transdermal– beneficial impact suggested with estradiol and
drospirenone
• Metabolic syndrome – menopause diabetogenic– Reduced DM and insulin resistance with estrogen– Advantage of natural progesterone/non-androgenic
progestins (drospeirenone, dydrogesterone)
Route of Estrogen Therapy
• CVD– CRP – increased with oral and not transdermal;
worsening affect with MPA– “first pass” effect on the liver (lipids)– endothelial function - improved with both
(inhibited by MPA and NET)– MMP-9 – increased by oral and not by transdermal
• Thromboembolic events– Increased risk with oral– No increase with transdermal
Route of Estrogen Therapy
• Neuroprotection– No differences available between oral and
transdermal
• Breast cancer– No differences available between oral and
transdermal– Increased risk with combined progestational
agent
Risks of Menopausal HT:What We Think We Know Now
• Breast cancer– RR 1.1-1.5 (all forms of estrogen) - 8 add’l/10,000 women– Increased with progestogen (especially continuous)– No increased risk with estrogen > 2 years post-menopause
• Endometrial cancer– R 4.0-11.0 (unopposed estrogen)– reduced by progestin
• Venous Thromboembolism (oral therapy)– 2 additional cases per 10,000– Mortality low, 1%
• Gall bladder disease• CVD
– increased risk with existing disease and remote from menopause

10/24/2014
13
Current “Truths” Regarding Menopausal HT and CVD
• The public is largely unaware that CVD is the primary cause of mortality in women.
• Women should not take estrogen to prevent CVD.
• Women with known CVD should not begin HT for treatment of heart disease.
Current “Truths” Regarding Menopausal HT and Breast cancer
• Estrogen-alone (greater than 5 years post-menopausally) lowersbreast cancer risk
• 2 years post-cessationof HRT/ET –breast cancer risk is no greater than never-users
Hormone related indicators of the risk of breast cancer
ASRM Practice Committee Report 2008
Current “Truths” Regarding Menopausal HT
• The “timing hypothesis” suggests CVD protection MAY be possible if started near the onset of menopause
• The “gap hypothesis” suggests breast cancer risk is HIGHEST when started near menopause.

10/24/2014
14
Endocrine Society 2010 Endocrine Society 2010
Assessment of Perimenopausal women
• BP• Fasting lipid profile• Fasting glucose• TSH• Assess for metabolic syndrome (decrease in insulin
sensitivity; increase in central obesity)
• Counsel re: maintenance of healthy weight• Assess sleep quality• Screen for depression• Vitamin D deficiency
• IMPORTANCE OF LIFESTYLE
Current “Truths” Regarding HRT and CVD
• A statin is the drug of choice for any woman with hypercholesterolemia
• First-line therapies for women with known CVD diseaseinclude risk-factor modification, aspirin, β-blockers, statins and angiotensin-converting enzyme inhibitors - just as in men

10/24/2014
15
Benefits of Menopausal HT:What We Think We Know Now
• Prevents or abolishes hot flashes –still the most effect treatment
• Prevents or improves genital atrophy
• Prevents or slows bone loss
• May reduce risk of Alzheimer’s disease
• May reduce risk of colon cancer• May improve overall quality of life
So Just When Is Menopausal HT Indicated Now?
• For symptomatic women
• For prevention of osteoporosis in those where other drugs may be contraindicated
• ?In women with new onset depression
• ?For those who feel better taking estrogen
Alternatives and Future Directions for Research
• Estrogen/Progestin Therapy– progestagen-IUD for uterine protection– transdermal estrogen– lower dosages– new progestational agent
• Raloxifene– no change in CRP– lowers homocysteine– increased VTE
• New SERMs– neurospecific action– bone specific action– anti-estrogenic at breast and uterus

10/24/2014
1
PCOS across the Lifespan:An Update on Treatment
Strategies
Marcelle I. Cedars, M.D.
University of California – San Francisco
Conflict of Interest
• Financial conflict – none• Research conflict
– Funded research: • Ferring Pharmaceutical• Nora Therapeutics
• Off –label drug use– none
PCOS: Overview
� Characterized by oligo-ovulation, hirsutism, polycystic ovaries� 5-10% Reproductive age females � Pathogenesis unclear:
- Androgen- Insulin- Pituitary
� Familial clustering: genetic etiology ?
Young Adult Reproductive Age Post Reproductive
PCOS across the lifespan
Diagnosis Fertility
Management of Symptoms:
Cycle Control
Hirsutism
Metabolic Alterations

10/24/2014
2
Young Adult
Making the PCOS Diagnosis
PCOS: Diagnosis
Rotterdam Criteria
Must have at least 2 out of 3:1. Oligo- or anovulation2. Clinical and/or laboratory evidence of
hyperandrogenism3. Polycystic ovaries
Exclusion of other etiologies
PCOS Diagnosis: Anovulation
Anovulation
Oligo-anovulation1. Less than 8 periods/year2. Variable bleeding pattern3. Amenorrhea rare4. Unopposed estrogen increases risk
PCOS Diagnosis: Hyperandrogenism
Clinical Evidence
• Hirsutism• Acne• Male pattern
alopecia
Lab Evidence
Total Testosterone Free Testosterone DHEA-S

10/24/2014
3
PCOS Diagnosis: Ovary
• 12 or more follicles measuring 2-9 mm in diameter
• Increased ovarian volume (>10cm 3)
Ovary Criteria:
Controversy: Follicle Number
• Specificity concerns: Follicle cut off of 12 is too low
• Relevance concerns: Follicle count does not associate with metabolic abnormalities
Rotterdam Criteria for Polycystic Ovary Syndrome (PCOS)Percentage Meeting Rotterdam Criteria, by Age
62.5
34.48
24.69
6.82
0
10
20
30
40
50
60
70
25-30 (n= 48)
31-35(n = 88)
36-40 (n = 84)
41-45 (n = 45)
Age group
AFC >12 in one ovary
Per
cent
age
Modified from Johnstone 2010
Controversy: Follicle Number
• Specificity concerns: Follicle cut off of 12 is too low
• Relevance concerns: Follicle count does not associate with metabolic abnormalities

10/24/2014
4
Metabolic Impact of Isolated PCO
Johnstone 2010
Young Adult -> Reproductive Age
•Cycle control and uterine protection
•Hirsutism
•Acne
Management: Uterine Protection
• Unopposed estrogen = risk of hyperplasia
• Options for protection:1. Cyclical Progestin 2. Combined contraceptive3. Mirena IUD
Mechanism of OCP
o Protect the uteruso Increase SHBGo Inhibit of LH
secretiono Inhibit adrenal
androgen secretion
Pituitary
liver
LH
ocp
.SHBG
ovary Testosterone
adrenal
DHEAS
uterus
Estrogen
Progestin
Estrogen

10/24/2014
5
Management: Hyperandrogenism
Acne HirsutismAndrogenic
Alopecia
Hirsutism
Mechanical Removal Pharamacologic
�Laser
�Electrolysis
�Oral Contraceptives
�Spironolactone
�Flutamide
�Finasteride
�Vaniqua
Mechanism of OCP
o Protect the uteruso Increase SHBGo Inhibit of LH
secretiono Inhibit adrenal
androgen secretion
Pituitary
liver
LH
ocp
.SHBG
ovary Testosterone
adrenal
DHEAS
uterus
Estrogen
Progestin
Summary: Hirsutism
Direct Removal
Oral Contraceptive
Second Agent: Spironolactone6 months

10/24/2014
6
Androgenetic Alopecia :
Treatment: • FDA Approved option: Rogaine • Oral contraceptive and
Spironolactone 50 mg per day
Differential Diagnosis: Importance of History/Physical - Telogen Effluvium- Alopecia Areata
Reproductive Age: Fertility
• Weight Loss and Lifestyle Change
• Clomid• Metformin• Letrozole
• Drilling• Gonadotropins
Lifestyle Changes
• Clark
et
87 women
- obese
- 79 % PCOS
6 month group program
- regular exercise
- gradual dietary changes
20 patients dropped out
•No changes in BMI
•No conceptions
67 patients completed program
•Mean change in BMI -3.7
•27% spontaneous conception
•53% conceived with assistance
•Increased self esteem
•Decreased anxiety/depression
Clark et al Human Reproduction 1995
Lifestyle Change
• 40 women with PCOS/anovulatoryinfertility
Palomba et al Human Reproduction 2008
Structured Exercise3 sessions/wkweek
HypocaloricDiet High Protein
800 kcal deficit
Patient choice….
24 weeks

10/24/2014
7
Exercise vs. Diet: Results
Exercise Diet
Age 26.8 25.8 NS
BMI 33.1 33.2 NS
Dropout 15% 35% 0.14
% Ovulatory 65% 25% 0.01
Pregnancy Rate 35% 10% 0.06
Palomba et al Human Reproduction 2008
Lifestyle
• Lifestyle interventions may increase ovulations and chance of pregnancy
• Weight reduction may reduce pregnancy complications
• Lifestyle interventions should be considered first line
Pituitary GlandFSH
LHE2
Clomid
Ovulation Induction: Mechanism
Metformin
Weight Loss
Improve insulin sensitivity
Letrozole
Clomiphene Citrate (Clomid)
• Synthetic Antiestrogen• Convenient • Inexpensive • Long-standing first choice
for ovulation induction in women with PCOS

10/24/2014
8
Imani, B. et al. J Clin Endocrinol Metab 1998;83:2361-2365
How many women will ovulate with Clomid?
Imani, B. et al. J Clin Endocrinol Metab 1999;84:1617- 1622
•160 patients
•Normogonadotropic anovulation
•Successful response to clomid
•Normal SA
•BMI >18.5
Clomid: What are the chances for conception?
Metformin for ovulation
• Biguanide Insulin Sensitizer• Category B• Not FDA approved
Reproductive Medicine Network
Legro et al. NEJM 2007; 35:551-66
• Multicenter
• Double blind
• 626 women with PCOS
ClomipheneMetformin Both
Randomized

10/24/2014
9
Results of RMN PPCOS Trial
0%
10%
20%
30%
40%
50%
60%
OVULATION Conception Livebirth Pregnancy loss
Metformin Clomid Both
P<.001
P<.001
P<.001
Legro et al. NEJM 2007; 35:551-66
Live Birth Prediction Chart
Rausch M E et al. JCEM 2009;94:3458-3466
Predictors of success:
•Low hirsutism score
•Lower BMI
•Younger age
•Shorter duration of infertility
PCOSMIC: Met/Clomid in BMI <32 and >32
0%10%20%30%40%50%
Placebo Metformin Clomid Metformin Clomid +Met
6%16%
36%29%
43%
Live Birth Rates
Johnson et al 2010 Hum. Reprod. 25 (7): 1675-1683.
BMI >32 BMI <32
• Randomized double blind trial in New Zealand• BMI >32 (n=65): placebo vs.metformin• BMI < 32 (n=106) CC vs. Met vs. CC/MET• Six month treatment period
Metformin as Pre-Treatment: Results
Morin-Papunen L et al. JCEM 2012;97:1492-1500
Pregnancy rate: Metformin 52.6%Placebo: 40.4%
Effect more pronounced
in obese women
Obese Non-Obese

10/24/2014
10
Aromatase InhibitorsClomiphene citrate vs.
Letrozole
Legro RS, NEJM 2014
Summary: Fertility
• The first line treatment for ovulation induction remains lifestyle.
• Letrozole superior to Clomiphene citrate• Metformin may add benefit as pre-treatment• Gonadotropins are second line treatment• IVF third line treatment or if over-stimulation
cannot avoided
Post-reproductivePCOS and Insulin Resistance
0102030405060708090
Lean Lean PCOS Obese Obese PCOS
Insu
lin R
esis
tanc
e(m
in -
1/nm
ol/m
l)
Adapted from Dunaif A, et al. JCEM 81: 942-947, 1996

10/24/2014
11
Insulin and the Pathophysiology of PCOS
Hyperinsulinemia
Decreased SHBG
Increased Free AndrogenClinical Hyperandrogenism
Anovulation
Insulin Resistance
Androgen production
ovary IGF RECEPTOR
HyperglycemiaDiabetes
Cardiovascular disease
Fatty Liver
Prevalence of IGT or Diabetes
0%
20%
40%
60%
80%
NGT IGT Type 2DM
Chicago n=122
Penn State n=144
Mt Sinai n=110
Rezulin Collab Group n=408
Legro, et al. JCEM 1999; 84: 165-169
Azziz et al. JCEM 2001; 86: 1626-1632
Ehrmann et al. Diabetes Care 1999; 22:141-146
Prevalence of IGT and Diabetes
0%
20%
40%
Per
cent
PCOS Lean PCOS NHANESIGT 30% 10% 1.6%T2DM 8% 0% 2.2%
PCOS versus National population
IGT Across the Lifespan
• Adolescents have impaired glucose tolerance 30% and TYPE 2 diabetes 7.4%
• Prevalence of Type 2 diabetes in perimenopausal women with history of PCOS is four fold higher compared to controls (32% vs 8%)
Palmert, MR et al JCEM 2002; 87:1017

10/24/2014
12
Metabolic Syndrome
368 Non-diabetic PCOS patients (Ages18-41)
• No Metabolic syndrome in Women with BMI <27 (n=52)
• Women with BMI > 30 had 13X chance of Metabolic syndrome0%
20%
40%
60%
80%
33%
80%66%
32%21%
5%
Ehrmann et al. J Clin Endocrinol Metab. 2006 Jan;91(1):48-53.
Meta-Analysis of BMI Matched Studies
Moran L J et al. Hum. Reprod. Update 2010;16:347-36 3
Odds Ratio (95% CI) in women with PCOS compared to BMI controls
� Impaired glucose tolerance: OR: 2.54 (1.44, 4.47)� Diabetes: OR: 4.00 (1.97, 8.10)
0%
20%
40%
60%
80%
15-20 20-25 25-30 30-35 35-40 40-45 45-50IGT or T2DM 9% 7% 42% 53% 40% 55% 44%
Per
cent
with
IGT
or
T2D
M
Impaired Glucose Metabolism by BMI
The Impact of BMI on IGT
Adapted from Legro, et al. JCEM 1999; 84: 165-169
PCOS Phenotypes
HyperandrogenismOligo or
Anovulation
Polycystic Ovaries

10/24/2014
13
137 Italian women screened with insulin glucose clamp
Insulin Resistance and PCOS Phenotype
Classic Phenotype
70%Ovulatory
15%
Normal Androgens
15%
Moghetti et al JCEM April 2013 Epub
0%
20%
40%
60%
80%
All Classic Ovulatory NormalAndrogens
Insulin Resistance
P<.001
Moghetti et al JCEM April 2013 Epub
B-coeff P
Classic -.2.13 .003
Ovulatory -1.66 .054
Normal Androgens
-.62 .451
Age .1 .016
Fat Mass -0.11 <.001
Insulin Resistance and PCOS Phenotype
Free Androgen Index and Metabolic Syndrome
Goverde A et al. Hum. Reprod. 2009;24:710-717
Natural History of Insulin Resistance in PCOS

10/24/2014
14
Progression to Type 2 Diabetes
• 67 Australian Women with PCOS followed for 6.2 years
• Mean BMI 29• 2.2% annual conversion rate
from normal glucose tolerance to impaired glucose tolerance (IGT) or Type 2 diabetes
• 8.7% annual conversion rate from IGT to DM
Norman et al. Human Reproduction 2001; 16:1995-1999
0%
10%
20%
30%
40%
50%
60%
Baseline Followup
33%40%
12%
19%
DMIGT
Progression and Population Attributable Risk
Talbottt et al. Journal of Women’s Health 2007; 16:191
• Prospective Controlled Study• 149 PCOS and 166 Controls followed for 8 years• Diagnosis of T2DM made by fasting glucose or
reported history
PCOS Controls
Age 47 49*
BMI 32 (8.8) 28 (6.1)*
Waist 95 (18.6) 85 (13/9)*
Type 2Diabetes
12.8% 3.6%**
Among 242 white women• 6.5 increase in RR when
adjusting for age• 4.0 increase in relative RR
when adjusting for BMI• 25-36% population
attributable risk based on a 6-10% prevalence of PCOS in general population
*p <.05**p.003
Progression of Insulin Resistance
Follow-up Study (2-3 years )
Legro et al JCEM 2005; 90:3236-32
0%
10%
20%
30%
40%
50%
60%
Baseline Post Baseline Post
37%45%
21%
10%
15%
0%
T2DM
IGT
• 16% conversion per year from NGT to IGT• 2% conversion/year from IGT to DM2• 2 fold increase over controls
PCOS Control
Control PCOS NGT
PCOS IGT/DM
Age 36 27 29
BMI 29 35 38
Progression of Insulin Resistance
Gambineri et al.Diabetes. 2012 : 61(9):2369-74
PCOS ItalianPopulation
39.3%
5.8%
Age Standardized Rate of Type 2 Diabetes
• Cohort of women with PCOS (n=255)
• Followed for at least 10 years (mean 16.9)
� 42 developed T2DM
� IR 1.05 per 100 person years

10/24/2014
15
Why is Screening Important?
• Identify T2DM requiring intensive treatment• Identify hyperglycemia in patient considering
pregnancy• Identify IGT or IFG that could benefit from
treatment
• Motivate!
Criteria for Defining Impaired Glucose Metabolism
WHO 2006 ADA 2007
Fasting Glucose Impaired 110 -125 mg/dlDiabetes >126 mg/dl
Impaired 100 -125 mg/dlDiabetes >126 mg/dl
2 hour Glucose Challenge
Impaired 140-199 mg/dlDiabetes >200 mg/dl
Perform in FG is normal, but suspicion is high
Impaired 140-199 mg/dlDiabetes >200 mg/dl
Screening Recommendations
Organization Who to screen Screening Test
American Association of Clinical Endocrinologists
All patients with PCOS Fasting glucose, Consider OGTT
American College of Obstetrics and Gynecology
All patients with PCOS Fasting glucose, OGTT
ADA Asymptomatic individuals under age of 45 if overweight with additional risk factors, including PCOS
Fasting glucose, OGTT in patients with IFG or if high level of concern.
ASRM and ESHRE Obese women with PCOS, consider non-obese women with additional risk factors
OGTT
Androgen excess Society All patients with PCOS OGTT
Screening: OGTT is Key
Legro R S et al. JCEM 1999;84:165-169
Patients with abnormal
OGTT with normal fasting glucose

10/24/2014
16
Screening • Population based study• OGTT administered to 105 consecutive
women with PCOS referred to an academic REI clinic
• Mean age 28, Mean BMI: 25.5• Prevalence of abnormal OGTT was 28%
�23% had IGT and �5% had diabetes
• If ADA recommendations were followed 1/7 women with PCOS would have missed dx
Baillargeon KP et al Can Med Ass J 2007 176:933
Implications of Impaired Glucose Metabolism
Impaired glucose tolerance
Tominga et al Diabetes Care 1999 22:920-926
Impaired Fasting Glucose
Funagata Diabetes StudyPatients with normal glucose, IGT and IFG
Only IGT had poor outcomes
Prevention and Treatment
Diabetes Prevention Trial
• Multi-center, 4 year study• 3234 people with impaired glucose tolerance
and mean BMI of 34• 45% of participants from higher risk minority
groups• Interventions:
�Metformin (850 mg bid) �Structured Lifestyle (goal of 7% weight loss)�No intervention
• Ended study 1 year early
Knowler et al. N Engl J Med 2002;346:393-403.

10/24/2014
17
Cumulative Incidence of Diabetes According to Study Group.
Knowler et al. N Engl J Med 2002;346:393-403.
Diabetes Prevention Trial: Results
Conversion to Diabetes:
Placebo: 29%Metformin 22%Lifestyle 14%
Risk reduction Metformin 31%Lifestyle 58%
Indian Diabetes Prevention Project
Persistent Impaired Glucose Tolerance
Mean BMI = 26Mean age= 45
Controlsn=136
Lifestylediet and exercise
advice and scores for adherence
n=133
Metformin(500mg)n=133
Metformin and
Lifestyle n=129
Ramachandran et al Diabetologia 2006 49:289-297
Indian Diabetes Prevention Project
Ramachandran et al Diabetologia 2006 49:289-297
Cumulative Incidence of diabetes 3 years :
• Controls: 55%• Lifestyle: 39%• Metformin: 41%• Both: 40%
• Risk reduction of 28%
Control s
LifestyleMetformin
Both
p=.02
Physical Activity in the Real World
Lamb et al Am J of Obste Gynecol 2011; 204:352-356
• Cross sectional study of 150 women with PCOS (Rotte rdam)
• Assessed adherence to Department of Health and Huma n Services guidelines for exercise-150 minutes of mod erate or 75 minutes of vigorous exercise per week
59%41%
PHYSICAL ACTIVITY Met DHHS Guidelines
Did not meet
DHHS Guidelines
• Active women more likely to be white (72% vs. 46%) and nulliparous (64% vs. 40%)

10/24/2014
18
Physical Activity in the Real World
Lamb et al Am J of Obste Gynecol 2011; 204:352-356
Variable Not Active Active pBody mass index kg/m2 33.7 29.9 .009
Waist circumference (cm) 98 89 0.03
Weight fluctuations (kg) 28.0 19.2 .008
Fasting glucose (mg/dL) 94.0 87.8 .04
OGTT (mg/Dl) 122.3 105.4 .07Sex hormone-binding globulin(nmol/L) 40.4 68.4 .006
Depression 5.5 3.6 .005
Recommendations for Management Consensus Recommendations for treatment of individuals with IFG, IGT or both
Population Treatment
IFG or IGT Lifestyle modification (5-10% of weight loss and moderate intensity physical activity 30 minutes per day)
Individuals with IFG and IGT and any of the following� <60 years� BMI >35� Family history� Elevated TRIG� Reduced HDL� Hypertension� AIC >6.0
Lifestyle and/or metformin
Nathan et al Diabetes Care 2007 30: 753-760
Summary: Metabolic Risk
• Insulin resistance and diabetes is common in PCOS a nd appears likely to translate into increased cardiova scular events even when controlling BMI
• Risk factors are increased BMI, family history of d iabetes, and PCOS with hyperandrogenism and increased ovarian vol ume
• Screening with OGTT is most sensitive screening met hod• Obtain fasting lipid profile as well
• Lifestyle is mainstay of treatment for IGT
• Pharmacologic intervention should be considered in select patients
UCSF Multidisciplinary Clinic for PCOS
Pre-visit
• One month off OCP’s and anti-androgen therapy
• Questionnaires• Complete Laboratory
Panel
Visit One
• Reproductive Endocrine
• Ultrasound• Dermatologist• Genetic
counselor
Visit Two
• Reproductive Endocrine
• Nutritionist• Psychologist
Clinical Care
Research Framework

10/24/2014
19
Thank You

10/24/2014
1
Tami Serene Rowen, M.D. M.S.Department of Obstetrics, Gynecology and Reproductive Sciences
University of California, San FranciscoOctober 24, 2014
• None to report
• Definitions and Epidemiology• Physiology of Female Sexual Response• Female Sexual Dysfunction
• Classification• Risk Factors• Evaluation• Treatment
• A state of physical, emotional, mental and social wellbeing in relation to sexuality
• Not merely the absence of disease, dysfunction or infirmity
• Requires the possibility of safe and pleasurable experiences
• An important and integral aspect of human development and maturation
• A human right
-WHO Tech Consultation Sex Health 2002

10/24/2014
2
• Largest study(13882 women, 29 countries)• 65% women sexually active in last year
• 38% in last week(inverse age relationship)• Agrees with US data
• 20-37% reported sex was very/extremely important to life
• 76% women felt satisfactory sex is essential to maintain a relationship
• Sexual well being significantly correlated to self perceived overall health
• Laumann et al, 2006; Nicolosi et al, 2004; Lindau 2007
Do patients want to discuss sex?• While 85% of adults want to discuss sexual functioning with their physicians…
• 71% believe their physicians doesn’t have the time• 68% don’t want to embarrass their physician• 76% thought no treatment was available for their problems
• 22% of women over 50 report discussing sex with a physician
Marwick et al, 1993; Maurice et al 1999, Lindau et al 2007
• Only 25% of primary care physicians take a sex history Jonassen et al 2002
• How do gynecologists do stack up?• Cross sectional study of 1,154 US Gynecologists
• 63% ask about sexual activity• 40% ask about sexual function• <30% ask about sexual orientation & satisfaction
Sobeicki et al 2012
• Laumann 1999: 1,749 US women age 18-59• ~43% prevalence based on 7 single item dichotomous questions
• Bancroft 2003: Interview of 987 women 20-65• 24% prevalence of self reported “distress”
• Shifren 2008: 31,581 US women >18 years• 43% reported sexual problem• 22% reported sexual distress• 12% reported both sexual problem and distress

10/24/2014
3
• Our patients would like to discuss sex• More than 10% likely have a
distressing problem• Many of us don’t ask about it
•Unsure how to ask•Uncertainty what to ask•Unfamiliar with treatment options
Masters & Johnson 1964
Male
Masters & Johnson 1964
FemaleFemale
Basson et al 2004
Numerous Incentives for Sex
Sexual Receptive-ness
Sexual Stimuli
Sexual Arousal
Responsive Desire
Rewards: Sexual
and nonsexual
Innate Sexual Desire?

10/24/2014
4
• Cross sectional study 404 women•Linear model was good fit in mixed population of women•Circular model fit better in women with “dysfunction”
• Giles & McCabe 2009
• Cross sectional study 129 nurses•2/3 subjects endorsed linear model•Sexual function scores significantly lower in women who endorsed Basson model
• Sand & Fisher 2007
Classification of Female Sexual DysfunctionDSM IV
• Persistent or recurrent, causing personal distress– Desire Disorders
• Hypoactive Sexual Desire Disorder • Sexual Aversion Disorder
– Sexual Arousal Disorder • Genital • Subjective• Mixed
– Anorgasmia– Sexual Pain Disorders
• Dyspareunia• Vaginismus• Non-coital sexual pain disorders
DSM V Updates• Must have 6 months of sx• Medical conditions, medications and other psychological dx cannot account for sx• HSDD, sex aversion and arousal disorders replaced by “Sexual desire/Arousal disorders”•• Vaginismus and dyspareunia are combined into “genito-pelvic pain/penetration disorder”• Still includes Orgasmic Disorder
• Lack of, or significantly reduced sexual interest, manifested by 3 of the following:• Absent/reduced interest in activity• Absent or reduced sexual thoughts/fantasies• No/reduced initiation of sexual activity• Absent/reduced excitement/pleasure• Absent/reduced response to cues• Absent/reduced genital sensations
• 5.3-13.6% prevalence
Shifren et al, 2008; Seagraves and Woodard, 2006

10/24/2014
5
• Genital pain associated with sexual stimulation• 8-21% among 18-59, 14% among women 40-80
• Etiology• Vulvar Vestibulitis• Endometriosis• Fibroids• Surgery• Psychosocial• Vaginal Atrophy• Inadequate lubrication
Laumann et al, 1999; Laumann et al, 2005; Walton et al, 2003
• Absence/Reduced orgasm after sufficient sexual stimulation and arousal
• Prevalence 3.4-5.8%
• Etiology• Physical• Medications• Hormonal• Psychological
Shifren et al, 2008
• Brief Index of Sexual Functioning for Women (BISF-W)• 22 items, 7 domains, relationship focusTaylor et al, 1994
• Female Sexual Function Index (FSFI)• 19 questions, 6 domains
• Desire, arousal, lubrication, orgasm, satisfaction, painRosen et al, 2000
• Female Sexual Distress Scale (FSDS, FSDS-R)• 20(12) items, all focused on self reported distressDerogatis et al, 2002
• Profile of Female Sexual Function (PFSF)• 37 items, 7 domains, validated for women w/ BSO and HSDDMcHorney et al 2004
• Physical and Emotional Health status is #1 predictor!Laumann et al, 1999; Laumann et al, 2006; Nicolosi et al, 2004; Lindau et al, 2007
• Role of age
• Other factors:• Relationship length (inverse correlation), education, mental health status, HRT and surgical menopause
Hayes, et al 2008; Dennerstein 2008
Filled circle =desireopen triangle= arousalfilled square= orgasmopen diamond=any.
Shifren et al, Obstet Gynecol 2008

10/24/2014
6
• Pregnancy• 90% still sexually active, drops dramatically third tri
• Von Sydow 2009
• Post partum• 50% rate dyspareunia
• Barret et al 2000
• NO relationship between PP FSD and C/S vs SVD• Higher rates of FSD with episiotomy and OVD
Viswanthan et al 2006; Hannah et al 2004; Klein et al 1994
• Breastfeeding associated with more dyspareunia but can stim arousal
Signorello et al 2001; Avery 2000
• Race and Ethnicity: conflicting data on sex activity among different groupsHuang et al, 2009; Avis et al, 2005
• Obesity: Higher BMI associated with more FSDBariatric Surgery significantly improves sex QOL
Kolotkin et al 2006; Sawer et al 2014
• WSW: Distress associated with partner status, OABShindel, Rowen et al 2013
• Women with Disabilities: no difference if rates of SA• However less sex ed, higher risk of traumaRowen et al, in press
• Focused history and physical• May be useful to ask patient to describe most recent sexual experience• Surveys may be of use-FSDS, domains of FSFI• Physical Exam:
• consider vulvoscopy• screen for vag infxn•PFMD
• Laboratory testing as indicated by H&PGoldstein, 2005
• SSRIs• Exception is buproprion
• Anti Psychotics• Exception is mirtazepine
• CHC• Anti-HTN• Antihistamines• ChemotherapyACOG Practice Bulletin 2011, Parrish ISWWSH 2013

10/24/2014
7
•Treat underlying disorders•Address relationship•Address psychosexual issues•Sex Education•Recalibrate expectations•Sexual Enhancement treatments: gels and devices
•Pharmacotherapy?
• Caruso 2001: 53 women with FSD•DB PC-crossover trial•Improved arousal, orgasm, frequency of sexual intercourse
•No dose response•Strong placebo effect
• Berman et al 2003: 202 menopausal women on HRT with FSD, RCT• Improved FIEI for women with FSAD•No effect on women with HSDD•No increase in “successful” sexual activity
placebosildenalfil/ HSDDsildenafil/ no HSDD
050
100
placebosildenalfil/ HSDDsildenafil/ no HSDD
% of participants
• Basson et al 2002: 781 women with FSD• stratified by estrogen status •No effects found in allcategories
• Nurnberg et al, JAMA, 2008• 98 women w/ depression on SSRI• Sildenafil 50-100 mg on demand vs. placebo• 73% improved sex fnc on sildenafil, 28% on placebo• Significant improvement in orgasmic score(0.5-0.7 above baseline on 6 point scale, CI 0.1-1.3) , p<0.01)
placebosil50sil 1000
1020304050
placebosil50sil 100
Estrogenized women% improved

10/24/2014
8
• Evidence equivocal for sildenafil use in women with arousal/hypoactive desire disorder
• Possible role of sildenafil for FSD associated with SSRI use
• Adverse Effects of sildenafil are: congestion, flushing, headache, dyspepsia, myalgias• Can’t take with nitrates(hypotension)• No significant adverse events reported in studies on
women
• Postsynaptic 5-HT1A agonist/5-HT2A antagonist (sim to buspirone)• 3 Phase III RCTs done concurrently with 24 weeks tx (7 total RCTs)• Thorp 2012 (DAISY): 1071 women with HSDD• Placebo v Flibanserin 25, 50 BID, 100 q night
• Significant increase (~2/month) in SSE • Subjective improvement of 44-47% (30% in placebo arm)
• 13.4 % discontinuation rate (vs10.1%)• No major AE
• Derogatis 2012 (VIOLET): 663 women with HSDD• Placebo v Flibanserin 50 & 100 mg • Slight but significant increase in satisfying sexual
events (SSE) from 0.8->1.4 and 1.6 (p<0.05)No major AE
• Benefits did not outweigh risks-including CNS effects• Not enough sexual benefit
• based only on SSE not on other domains of sexual health• Controversy re: how to measure improvement Kingberg and Althof, 2011
• Taken up by new company….• FDA again denied (2013)
2010:Female Viagra Hits Roadblock, FDA Denies Approval • Estrogens
• Demonstrated effect on vaginal vascularity and baseline moisture• Regular use associated with increased sex activity•May improve other health measures• Can use
• cream 3/week• Estring q 3 months• Vagifem 2-3/week
• SERMs• Ospemafine: only FDA approved tx for FSF• Tibolone: has P, E, & T activity
• Not approved in USGass et al, 2011; Kovalevsky 2005, Lobo 2003, Basson 2004, Shifren 2000, Davis 2006, Nappi 2006

10/24/2014
9
• Decreased starting age 30
Davis et al, 2005
• No single androgen level predictive of sexual response
• Male levels of T associated with improved sex health• Sig SE: hyperlipidemia, CVD, ?carnogenic
Sherwin&Gelfan 1987
SSE PFSF-Arousa
PFSF-Desire PDS AE
Braunstein 2005
447, surgically menopausal 140-450 mcg/d NR 8* ~5* NS 6%
Simon 2005 562 surgically menopausal 300mcg/d 1.1† 5† 5† -7.7† -2%
Davis 2006 77 surgically menopausal 300 mcg/d 0.5 19† 10† -19.3† -1%
Shifren 2006 238 naturally menopausal 300 mcg/d 1.6† 26%† 5.8† -9† 6%
Davis 2008b 814 menopausal, no E2‡ 150 or 300 mcg/d 1.4* ~10† ~8† ~-11† 0%
Panay 2010272 naturally
menopausal (26% on E2)
300 mcg/d 1.2† ~14† 7.6† 11.5† 9%
†= Sta�s�cally Significant (p<0.05) * = Significant differences only with 300 mcg/daily patch ‡ = women taking vaginal estrogens continued on stable dosing regimens
Study n= TreatmentDifference versus placebo in…
AE= Incidence of Adverse Events, FSFI=Female Sexual Function Index, FSDS=Female Sexual Distress Scale, NR= Not Reported, NS= Not significant, PFSF =Profile of Female Sexual Function, PDS= Personal Distress Scale, SSE=Satisfying
• Brand Name: Intrinsa• No long term safety data• More BTB, no increase hyperplasia• Breast Ca: 4 vs 0 (2 in first year, 1 in 2nd)• FDA agreed to efficacy but required more long term
safety data: rejected in 2004• Note: only 3 months safety data required for men
• Approved in Europe but no market: no longer available
Shifren ASRM 2013
• Testosterone Cream (10mg)• 1 RCT, 36 women with HSDD, surgically menopausal, on E2• sig increase in BISF-W(8.2 point, p<0.01)• no mention of adverse eventsEl-Hague et al, 2007
• Transdermal Spray (2.8-9mg)• 1 RCT, 261 pre-men women• inc in SSE 0.4-0.8• adverse events in 11-16%(acne, hirsutism)Davis et al, 2008
• Can also use T pellets, topic gels (“Axiron”)

10/24/2014
10
• Libigel: daily 1% gel application•Committed to long term safety trial
• 5 year f/u•BLOOM phase III trials
• 1172 women• no significance in ANY endpoint•Company went bankrupt•did not release safety dataShifren ASRM 2013,; Shafer 2011
• Van Kesternen et al 1997: 297 F-M Transsexuals given T for 2 mo-41 years • No difference in CAD rate compared to control Dutch women
• Braunstein 2007 : Review of TRT in women• Major AE in women appear to be hirsutism, acne, and lowering of HDL with oral T over 1-2 year time frame
• Tamimi et al 2006: 70,444 post-menopausal women in Nurses Health Study taking E, E+P, E+T, or no hormones over 24 years• Multivariate RR for breast CA was 1.77 (CI 1.22-2.56) for E+T, 1.15 (CI 1.05-1.27) for E, and 1.58 (CI 1.44-1.73) for E+P
• Ness et al 2009: 31842 women in WHI, E+T vs no HRT• Adjusted HR1.42; 95% confidence interval, 0.95-2.11 p=.67)
• End of Libigel meant end of Testosterone solo therapy for FDA approval of FSD
• Data insufficient to demonstrate sig AE, incl breast ca• Off-label use: what our societies say
• NAMS (2005): “Postmenopausal women with decreased sexual desire associated with personal distress and with no other identifiable cause may be candidates for testosterone therapy. Testosterone treatment without concomitant estrogen therapy cannot be recommended because of a lack of evidence”
• ACOG: Practice Bulletin (2012) : “Transdermal Testosterone has been shown to be effective for the short term of hypo-active sexual desire disorder, with little evidence to support long term use (longer than 6 months) Level A
• Lybrido: SL Testosterone +sildenafil+ buspirone (Emotional Brain, NY)• To be taken prior to sexual activity• Currently just completed Phase II RCT• 210 women , measuring dosage and SSE• Comparison group: placebo, sildenafil
testosterone

10/24/2014
11
• Bremalenotide• DHEA• Oxytocin• Topical Prostaglandins• Zestra• All With Essentially Conflicting to Negative data for
Effectiveness
• Female Sexual Health is complex but very important to women
• New research has opened door to physiologic factors
• Any treatment should be both medical and psychosocial
• Reliable and proven medical therapy for women with sexual problems is currently lacking• Based on both outcomes and safety concerns
Questions?

10/24/2014
1
Racial/Ethnic Disparitiesin OB/GYN
Sara Whetstone, MD, MHSClinical Instructor, UCSF OB/GYN
Disclosures� I have nothing to disclose
Objectives� To define health and healthcare disparity
� To discuss the scope of the racial health disparities in the United States
� To state 2 examples of health or healthcare disparities within OB/GYN
� To provide at least 2 reasons for health disparities
IOM: Unequal Treatment, 2002� Evidence of racial and ethnic disparities in healthcare is consistent across a range of illnesses and healthcare services.
� Racial and ethnic minorities experience a lower quality of health services and are less likely to receive even routine medical procedures than are white Americans.

10/24/2014
2
Definitions
� Health Disparities“…are preventable differences in the burden of disease, injury, violence, or opportunities to achieve optimal health that are experienced by social disadvantaged populations”1
1. CDC, 2008
Definitions
� Healthcare Disparities“…racial or ethnic differences in the quality of healthcare that are not due to access-related factors or clinical needs, preferences, and appropriateness of intervention ”1
1. IOM, Unequal Treatment, 2002.
Examples
Health Disparities Healthcare Disparities� Black women are more likely to die from ovarian cancer than white women
� Black women were less likely than white women to receive guideline-recommended care for advanced epithelial ovarian cancer (54% compared with 68%, p<0.01)1
Howell EA et al. Obstet Gynecol, 2013.
Estimating the effect of racial disparities
� In 2005, Satcher et al estimated that 83,570 excess deaths occur each year because of the difference in mortality rates between Blacks and Whites.1
Satcher D et al. Health Affairs, 2005
Leading Causes of Death in US, 20131) Heart disease: 596,5772) Cancer: 576,6913) Chronic lower respiratory diseases: 142,9434) Stroke (cerebrovascular diseases): 128,9325) Accidents (unintentional injuries): 126,4386) Alzheimer's disease: 84,9747) Diabetes: 73,8318) Influenza and Pneumonia: 53,8269) Nephritis, nephrotic syndrome, and nephrosis: 45,59110) Intentional self-harm (suicide): 39,518
6th leading cause of death

10/24/2014
3
Leading cancer deaths - 2014Women
Lung & bronchus: 72,330
Breast: 40,000
Colon & rectum: 24,040
Pancreas: 19.420
Ovary: 14.270
Men
Lung & bronchus: 86.930
Prostate: 29,480
Colon & rectum: 26,270
Pancreas: 20,170
Liver: 15,870
American Cancer Society, 2014
Black-white disparities in mortality:83,570
Broader context
Racial and ethnic disparities in health occur in the context of broader historic and contemporary social and economic inequality.
Social determinants of health
Source: Commission on Social Determinants of Health, Closing the gap in a generation: Health equity through action on the social determinants of health. Final Report on Social Determinants of Health (Geneva: World Health Organization, 2008),
Examples of health disparities within OB/GYN� Rate of maternal mortality has remained 3 to 4 times higher among black women than white women during the past 6 decades (HRSA, 2010)
� Black woman experience the highest infant mortality rate (CDC, 2011)
� Rate of preterm birth in black and Puerto Rican women is substantially higher than that for white women (CDC, 2011)
� Black women are nearly twice as likely to die of cervical cancer and uterine cancer as white women (American Cancer Society, 2014)
� Black women have a higher death rate from breast cancer than white women, despite a lower incidence rate (Whitman, 2014)
� Black women have the highest rate of unintended pregnancy of any racial or ethnic groups (Finer, 2014)

10/24/2014
4
Common interpretations for racial disparities in health� Biological differences� Economic inequality (income, level of
education, and unemployment) � Patient choice or preference
Common interpretations for racial disparities in health� Biological differences
� No biologic or genetic basis for race
� Race is a social or political category that has biological consequences because of the impact of social inequality on health
� Understanding race as social/political category “redirects attention from genetic explanations (of health disparities) to social ones.” (Dorothy Roberts, Fatal Invention, 2011)
Common interpretations for racial disparities in health� Biological differences� Economic inequality (income, level of
education, and unemployment)
� Health disparities are associated with socioeconomic differences.� However, the majority of studies show that
racial disparities remain even after adjustment for socioeconomic differences. (IOM, 2002)
Infant Mortality Rates for Mothers Age 20+, by Race/Ethnicity and Education, 2001-2003
DATA: National Center for Health Statistics, National Vital Statistics System, National Linked Birth/Infant Death Data. Health, United States, 2006, Table 20.SOURCE: Kaiser Family Foundation, Key Facts: Race, Ethnicity and Medical Care, 2007, Figure 9.
College+
Less thanHigh
School
Infant deaths per 1,000 live births
African American (Non-Hispanic)
American Indian/Alaska NativeWhite (Non-Hispanic)
Asian and Pacific IslanderHispanic
African American (Non-Hispanic)
American Indian/Alaska NativeWhite (Non-Hispanic)
Asian and Pacific IslanderHispanic
African American (Non-Hispanic)
American Indian/Alaska NativeWhite (Non-Hispanic)
Asian and Pacific IslanderHispanic
High School

10/24/2014
5
Common interpretations for racial disparities in health� Biological differences� Economic inequality (income, level of
education, and unemployment) � Patient choice or preference
� While minority patients have been found to refuse recommended treatment more often than whites, differences in refusal rates are small and have not fully accounted for racial and ethnic disparities in receipt of treatments (IOM, 2002)
Role of healthcare disparities
Healthcare disparities
Root causes of healthcare disparities• Issues related to the complexity of the
health care system and how it may be poorly adopted to and disproportionately difficult to navigate for minority patients
Health system level factors
• Issues related to health care providers, including stereotyping and the impact of race/ethnicity on clinical decision-making
Care Process Variables
• Include patient's mistrust, poor adherence to treatment, and delays in seeking care
Patient Level Variables
Diagram of patient’s experiences
Challenges navigating the health
care system
Barriers to communication
and rapport
Biases in clinical
decision-making
Lack of follow
through with
provider recs
Patient presents to health system
DISPARITIES IN HEALTH CARE
Massachusetts General Hospital, Disparities Solution Center

10/24/2014
6
A Closer LookDisparities in Maternal Mortality
Maternal Death: death of a woman while pregnant or within 42 days of termination of pregnancy
Understanding the racial disparity in maternal mortalityTucker M et al, American Journal Public Health 2007Methods:① Selected 5 complications of pregnancy: (1) pre-eclampsia, (2) eclampsia, (3) abruption, (4) placenta previa, (5) postpartum hemorrhage ② Calculated prevalence rates for Black and White women during 1988-1999③ Calculated case-fatality rates for Black and White women who died during 1988-1999
Case-fatality ratio= # of deaths attributable to that condition per 100,000 women with that condition
Pregnancy related-mortality ratio # of deaths attributable to that condition per 100,000 live births
④ Calculated the pregnancy-related mortality ratio for each condition
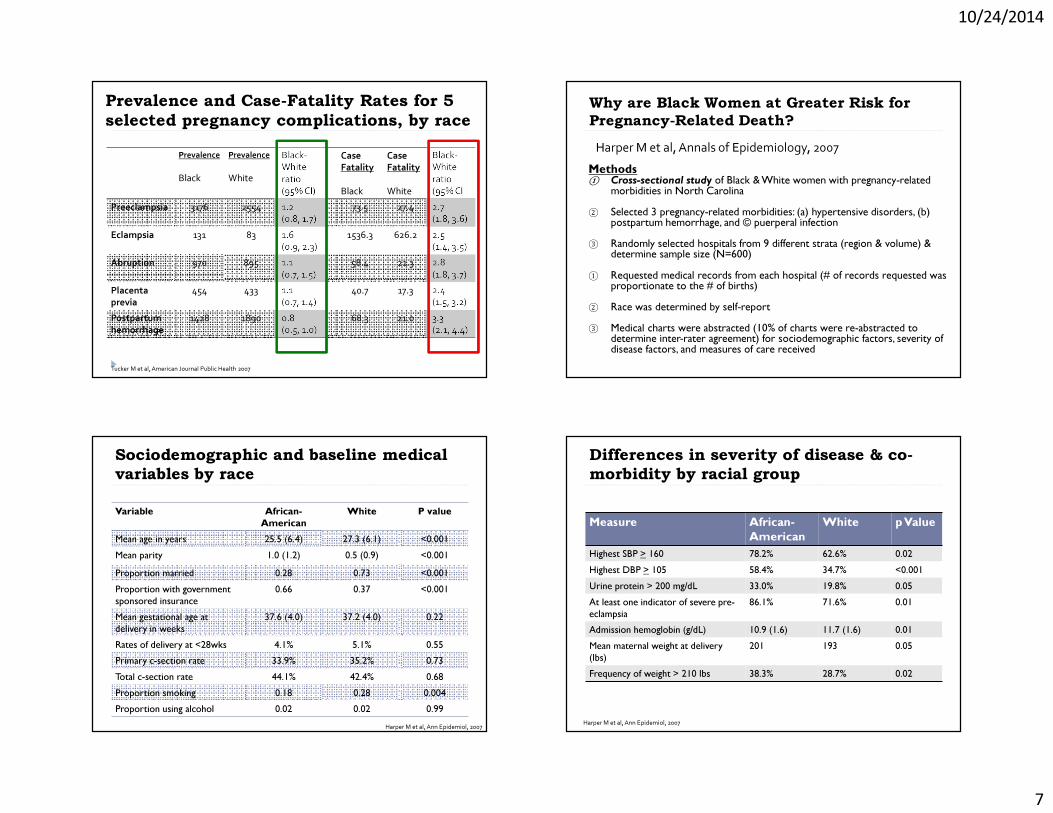
10/24/2014
7
Prevalence and Case-Fatality Rates for 5 selected pregnancy complications, by race
Tucker M et al, American Journal Public Health 2007
Prevalence
BlackPrevalence
WhiteBlack-White ratio (95% CI)
Case Fatality Black
Case FatalityWhite
Black-White ratio (95% CI
Preeclampsia 3176 2554 1.2(0.8, 1.7)
73.5 27.4 2.7(1.8, 3.6)
Eclampsia 131 83 1.6(0.9, 2.3)
1536.3 626.2 2.5(1.4, 3.5)
Abruption 970 895 1.1(0.7, 1.5)
58.4 21.3 2.8(1.8, 3.7)
Placenta previa
454 433 1.1(0.7, 1.4)
40.7 17.3 2.4(1.5, 3.2)
Postpartum hemorrhage
1428 1890 0.8(0.5, 1.0)
68.3 21.0 3.3(2.1, 4.4)
Why are Black Women at Greater Risk for Pregnancy-Related Death?
Methods① Cross-sectional study of Black & White women with pregnancy-related
morbidities in North Carolina② Selected 3 pregnancy-related morbidities: (a) hypertensive disorders, (b)
postpartum hemorrhage, and © puerperal infection③ Randomly selected hospitals from 9 different strata (region & volume) &
determine sample size (N=600)① Requested medical records from each hospital (# of records requested was
proportionate to the # of births)② Race was determined by self-report③ Medical charts were abstracted (10% of charts were re-abstracted to
determine inter-rater agreement) for sociodemographic factors, severity of disease factors, and measures of care received
Harper M et al, Annals of Epidemiology, 2007
Sociodemographic and baseline medical variables by raceVariable African-
AmericanWhite P value
Mean age in years 25.5 (6.4) 27.3 (6.1) <0.001Mean parity 1.0 (1.2) 0.5 (0.9) <0.001Proportion married 0.28 0.73 <0.001Proportion with government sponsored insurance
0.66 0.37 <0.001
Mean gestational age at delivery in weeks
37.6 (4.0) 37.2 (4.0) 0.22
Rates of delivery at <28wks 4.1% 5.1% 0.55Primary c-section rate 33.9% 35.2% 0.73Total c-section rate 44.1% 42.4% 0.68Proportion smoking 0.18 0.28 0.004Proportion using alcohol 0.02 0.02 0.99
Harper M et al, Ann Epidemiol, 2007
Differences in severity of disease & co-morbidity by racial group
Measure African-American
White pValue
Highest SBP > 160 78.2% 62.6% 0.02Highest DBP > 105 58.4% 34.7% <0.001Urine protein > 200 mg/dL 33.0% 19.8% 0.05At least one indicator of severe pre-eclampsia
86.1% 71.6% 0.01
Admission hemoglobin (g/dL) 10.9 (1.6) 11.7 (1.6) 0.01Mean maternal weight at delivery (lbs)
201 193 0.05
Frequency of weight > 210 lbs 38.3% 28.7% 0.02
Harper M et al, Ann Epidemiol, 2007

10/24/2014
8
Receipt of diagnostic & therapeutic interventions by racial group
Harper M et al, Ann Epidemiol, 2007
African-American
White p Value
COHORT WITH PREGNANCY-RELATED HYPERTENSION
Treatment for SBP > 160 and/or DBP > 105 51.80% 32.80% 0.02
Intrapartum magnesium 67.00% 50.50% 0.02
COHORT WITH HEMORRHAGE
Curettage 25.70% 27.70% 0.87Surgical procedure other than curettage 9.60% 21.20% 0.03
Hysterectomy 0 6.10% 0.03
ANTEPARTUM STEROIDS 44.50% 68.10% 0.008
Conclusions•Prevalence of selected conditions was not significantly greater among Black women•Black women had case-fatality rates that were 2 to 3 times greater than those of White women•Disease severity did vary by race•Overall there was equivalent care; however, there were examples of differences in care-process variables.
A Closer LookDisparities in Breast Cancer Mortality
Breast Cancer Incidence and Mortality, 1975-2010
SEER Cancer Statistics Review, 1975-2010, 2013

10/24/2014
9
Trends in disparities in breast cancer mortality� Hunt BR et al, Cancer Epidemiology, 2014
Methods� Calculated race-specific breast cancer mortality rates for the 50 largest US cities for 5-year intervals between 1990 and 2009
� Calculate the rate ratio (non-Hispanic black mortality rate: non-Hispanic white mortality rate) for the 50 cities for 5 years intervals
Five-Year Estimates of Breast Cancer Mortality Rates - USA (1990-2009)
Hunt BR et al, Cancer Epidemiology, 2014.
•Increase in Black:White disparity in breast cancer mortality
•Mortality rate for blacks did not change substantially; however, the mortality rate for whites declined significantly
Reasons for racial disparities in breast cancer mortality� Differential access to screening� Differential quality of screening� Differential access to treatment� Differential quality of treatment

10/24/2014
10
Reasons for racial disparities in breast cancer mortality� Differential access to screening
Cancer Screening – United States, MMWR, 2012.
Reasons for racial disparities in breast cancer mortality� Differential access to screening� Differential quality of screening� Black women are more likely to have their mammograms
performed at public facilities and less likely to be screened at academic institutions
� White women are more likely to have their mammograms performed at facilities that relied exclusively on breast imaging specialists to read mammogram and at facilities where digital mammography is available
Rauscher GH, Journal of Women’s Health, 2012.
Reasons for racial disparities in breast cancer mortality� Differential access to screening� Differential quality of screening� Differential access to treatment� Black women are less likely than White women to receive
timely follow-up after an abnormal or inconclusive screening mammogram
� Residential segregation� Black women have been found to experience treatment delays,
regardless of stage at diagnosis
Gerend MA, Cancer Epidemiology, Biomarkers & Prevention, 2008.Lund MJ et al, Breast Cancer Research and Treatment, 2008.
Reasons for racial disparities in breast cancer mortality� Differential access to screening� Differential quality of screening� Differential access to treatment� Differential quality of care� Black women are less likely than White women to receive
breast-conserving surgery� Studies have shown that Black women are less likely than white
women to receive adjuvant radiation therapy after breast-conserving surgery
Gerend MA, Cancer Epidemiology, Biomarkers & Prevention, 2008.

10/24/2014
11
IOM: Unequal Treatment� Recognize the myriad of factors that influence health disparities, including access to care and patient preferences
� “Research suggests that healthcare providers’ diagnostic and treatment decisions, as well as their feelings about patients, are influenced by patients’ race or ethnicity.” (IOM, 2002)
� Conclude that healthcare disparities can in part be attributed to discrimination by medical providers
Social determinants of health
Source: Commission on Social Determinants of Health, Closing the gap in a generation: Health equity through action on the social determinants of health. Final Report on Social Determinants of Health (Geneva: World Health Organization, 2008),
IOM Recommendations� Promote consistency and equity of care through the use of evidence based guidelines� Implement multidisciplinary teams and preventive care teams� Implement patient education programs to increase patient knowledge on how to best access care� Increase awareness of racial/ethnic disparities in health care
Summary
� Racial and ethnic disparities persist in health and occur in virtually every field of medicine
� Evidence that racial/ethnic differences in health care, including differences in diagnosis and treatment, lead to disparities in health
� Research demonstrates that health care providers play a role in perpetuating health care disparities and in turn health disparities

1
Gynecologic Cancer Genetics
UCSF Obstetrics and Gynecology Update:What Does the Evidence Tell Us?October 24, 2014
Lee-may Chen, M.D.Professor Department of Obstetrics, Gynecology, & Reproductive Sciences
October 24, 2014Gynecologic Oncology
Disclosure
• I have served as a moderator for an advisory board to Genentech
• UCSF has conducted clinical trials using bevacizumab, olaparib, veliparib, rucaparib
Gynecologic Oncology
Audience response
Have you sent a cancer genetic test for one of your patients?
3
Y es
N o
40%
60%
1. Yes2. No
Gynecologic Oncology
Audience response
What was the result?
4
P os i t i
v e N e
g a ti v e
V ar i a n
t o f u n
k n ow n
s i g ni . . .
D on ’ t
k n ow
19% 22%
13%
47%
A. PositiveB. NegativeC. Variant of unknown
significanceD. Don’t know

2
Gynecologic Oncology
Audience response
What genetic counseling did your patient receive before testing?
5
G en e t
i c co u n
s e . ..
M D P r o
v i de r
D i d n o
t g et c o
. . .
60%
8%
33%
A. Genetic counselorB. MD ProviderC. Did not get counseling
Gynecologic Oncology
Objectives
• To describe Society of Gynecologic Oncology’s initiatives towards identifying women at risk for hereditary gynecologic cancer syndromes
• To describe the complexities of direct to consumer genetic testing, and the significance of genetic counseling
• To outline management options, including screening, risk-reducing surgery, and personalized cancer care
6
Gynecologic Oncology
7
Gynecologic Oncology
8

3
Gynecologic Oncology
Next Generation Genetic Testing
BRCA1, BRCA2
MLH1, MSH2, MSH6, PMS2
9
APC, ATM, BARD1, BMPR1A, BRCA1, BRCA2, BRIP1, CDH1, CDK4, CDKN2A, CHEK2, EPCAM, FANCC, MLH1, MRE11A, MSH2, MSH6, MUTYH, NBN, NF1, PALB2, PMS2, PTEN, RAD50, RAD51C, RAD51D
Gynecologic Oncology
Universal testing?
10
Gynecologic Oncology
11
Taking a Family History
Gynecologic Oncology
12
Features of Hereditary Cancer
• Young ages at cancer diagnosis
• Multiple primary tumors in the same individual
• Bilateral cancers in paired organs (for example, bo th breasts)
• Multiple family members with cancer in two or more generations
• Types of cancer seen in known hereditary cancer predisposition syndromes

4
Gynecologic Oncology
13
Hereditary Breast-Ovarian Cancer
• Breast cancer diagnosed before age 50
• 2 or more relatives with breast cancer
• Male relative with breast cancer
• Bilateral breast cancer or multiple primaries in th e same breast
• Breast cancer and Ashkenazi, or Eastern European Jewish, ancestry
• Ovarian cancer (epithelial; non-mucinous) at any ag e Gynecologic Oncology
Patient 1
14
49yo G1P1 with BRCA1 mutation
Gynecologic Oncology
Patient 1Laparoscopic bilateral risk-reducing salpingo-oophorectomy� Right ovary with < 1cm microscopic focus of high grade papillary serous carcinoma
• Washings• Remove entire ovaries & tubes• Frozen section for suspicious
lesions only• Serial sectioning, including entire
fimbriae
Rabban et al, Am J Surg Pathol 2009Gynecologic Oncology
Patient 1Staging offered.
Patient elected expectant management.
6 years later
CA125 9� 14� 40� 28� 508 over 2 years
CT: Multiple peritoneal implants in the omentum
Exploratory laparotomy, total abdominal hysterectomy, bilateral pelvic & para-aortic lymphadenectomy, omentectomy, tumor debulking, intraperitoneal port placement� High grade serous carcinoma� Stage IIIC peritoneal carcinoma
16

5
Gynecologic Oncology
Patient 1IV/IP paclitaxel & cisplatin x 6 cycles, then observation
CA125 = 7, CT c/w complete response
3 years later
CA125 14� 36� 39� 51� 78 over 1 year
PET/CT� 1.5cm left supraclavicular lymph node, left pleural effusion, nodularity, mediastinal lymphadenopathy, no evidence of disease in abdomen & pelvis
Fine needle aspiration positive for adenocarcinoma
Options:
Veliparib clinical trial
Carboplatin, gemcitabine, +/- bevacizumab
17
Gynecologic Oncology
18
PARP Inhibition
PARP
DNA damage (SSBs)
DNA replication(accumulation of DNA DSBs)
Normal cellwith functional HR
pathway
HR-deficient tumor cell (e.g. BRCA 1/2-/-)
Cell survival Cell death
HR-mediated DNA repair
Tumor-selective cytotoxicity
PARP inhibition
Impaired HR-mediated DNA repair
Gynecologic Oncology
19
Olaparib—Phase II
Phase II trial in BRCA-deficient advanced ovarian cancer, 2 sequential cohorts, 12 sites, 6/07-3/08
n=57, 33 at 400mg BID, 24 at 100mg BIDConfirmed BRCA1 or BRCA2 mutation
Measurable disease
Good performance status (ECOG 0-2)
Response rate 400mg 100mg
BID BID
RECIST (radiology) 33% 13%
GCIG (incl CA125) 61% 17%.
Median duration of response 9.6 mo. 9.0 mo.
Audeh et al, Lancet, 2010 Gynecologic Oncology
20
Olaparib & High grade serous ovarian cancer
Four cohorts: Triple negative breast cancer, BRCA1/ 2 associated breast cancer, High grade serous ovarian cancer, BRCA1/2 associated ovarian cancer
n=23 breast cancer, 63 ovarian cancer patients, Ola parib 400mg BID
No breast cancer patients responded
41% RECIST response in BRCA1/2-positive ovarian can cer
24% RECIST response in BRCA1/2-negative ovarian can cer
Gelmon et al, Lancet Oncol 2011

6
Gynecologic Oncology
Olaparib Maintenance
N=265
Platinum sensitive ovarian cancer patients in 2nd or 3rd
remission, randomize to Olaparib 400mg BID versus placebo
Progression-free survival: 8.4 versus 4.8mo. HR 0.35, 95% CI 0.25-0.49
Overall survival (at 58% maturity): HR 0.88
For BRCA mutation carriers: 11.2 versus 4.3 mo. HR 0.18, 95% CI 0.11-0.31
21
Lederman et al, N Engl J Med 2012; Lederman et al, Lancet Oncol 2014
Gynecologic Oncology
Veliparib
GOG #280
N=52, BRCA1 or BRCA2 mutation carriers with recurrent/persistent ovarian/tubal/peritoneal cancer and measurable disease
400mg PO BID
30 platinum-resistant, 20 platinum-sensitive
Median number of cycles: 5.5, 48% with dose reduction
26% response rate (90% CI, 15-38). 1 CR, 12 PR
Median PFS: 8.1 months (90% CI, 5.5-8.8)
Toxicities: fatigue, nausea, vomiting, anemiaColeman et al, SGO 2014
Gynecologic Oncology
Rucaparib
ARIEL 2: Phase II study of rucaparib in platinum-sensitive ovarian/tubal/peritoneal cancer
Tissue biopsies pre- and post-treatment will help define subgroups of patients with homologous recombination defects
15 BRCA1/2 mutation carriers
165 BRCA1/2 negative
ARIEL 3: Phase III study of rucaparib as maintenance following platinum-based chemotherapy for patients with platinum sensitive ovarian/tubal/peritoneal cancer
23
Gynecologic Oncology
Causes of Ovarian Cancer
24
Hereditary(5%-10%)
Sporadic BRCA1 (~70%)
Other single genes (~8%)
BRCA2 (~20%)LYNCH (~2%)
Sporadic
ASCO
Familial (10%)

7
Gynecologic Oncology
Genetic Evaluation
N= 360 consecutive women with primary ovarian, tubal, peritoneal cancer
Screened for 21 germline mutations by genomic sequencing
11% BRCA1
6% BRCA2
6% Other: BARD1, BRIP1, CHEK2, MRE11A, MSH6, NBN, PALB2, RAD50, RAD51C, or TP53
31% with no family history of breast/ovarian cancer
63% less than age 60
25
Walsh et al, Proc Natl Acad Sci USA 2011Gynecologic Oncology
Genetic Evaluation
26
Walsh et al, Proc Natl Acad Sci USA 2011
Sporadic ovarian cancer
Hereditary ovarian cancer~24%
Gynecologic Oncology
Genetic Evaluation
27
Narod & Foulkes, Nature Reviews Cancer 2004Gynecologic Oncology
Genetic Evaluation
SGO Clinical Practice Statement: Genetic Testing for Ovarian Cancer
October 2014
Women diagnosed with epithelial ovarian, tubal, and peritoneal cancers should receive genetic counseling and be offered genetic testing, even in the absence of a family history.

8
Gynecologic Oncology
Genetic Evaluation
SGO Clinical Practice Statement: Next Generation Cancer Gene Panels Versus Gene by Gene Testing
March 2014
Cancer gene panels use next generation sequencing technology to assess inherited mutations in multiple genes simultaneously and are currently commercially available. Current cancer gene panels vary in size from just two genes (i.e., BRCA1 and BRCA2) to larger panels that include more than 50 genes. However, health care providers need to consider the limitations as well as the advantages of the cancer gene panels.
29
Gynecologic Oncology
Genetic Evaluation
APC, ATM, BARD1, BMPR1A, BRCA1, BRCA2, BRIP1, CDH1, CDK4, CDKN2A, CHEK2, EPCAM, FANCC, MLH1, MRE11A, MSH2, MSH6, MUTYH, NBN, NF1, PALB2, PMS2, PTEN, RAD50, RAD51C, RAD51D
Considerations:• Counseling• Costs• Variants
Gynecologic Oncology
Patient 2
49yo G0 with Stage IIIC high grade serous ovarian carcinoma.
PMHx: Benign breast lump, precancerous skin lesions
FHx: Father with colon cancer in 70s
Sister with breast cancer at age 49. BRCA1/2 neg.
Maternal grandmother with breast cancer in 70s
GeneDx Breast/Ovarian Panel�PMS2 (400C>T) mutation AND
PALB2 (172_175delTTGT) mutation
31
Gynecologic Oncology
Consequences of Panel Testing
UT Southwestern
April 2012-January 2013
N=50 next-generation sequencing panels
10% positive result
30% variant of uncertain significance or variant suspect benign
Kaiser Northern California
N=69 VUS, 30% RRSO, 11% RRM, 56% reclassified
32
Mauer et al, Genet Med 2014Garcia et al, Genet Med 2014

9
Gynecologic Oncology
Surveillance recommendations
• Breast examination and annual mammography/MRI, beginning at age 25 (or earlier based on family history)
• Pelvic examination, CA125, pelvic ultrasound every 6 months, beginning at age 30 (or earlier based on family history)
• Recommend risk-reducing salpingo-oophorectomy between ages 35-40, or on completion of childbearing
Also consider oral contraceptives for ovarian cancer risk reduction
Managing BRCA1 & BRCA2 Mutation Carriers
33
Gynecologic Oncology
Other mutations besides BRCA1&2
• BRIP1: 1.4%of ovarian cancer cases, 10-15% lifetime risk for ovarian cancer
• RAD51D: 0.6% of ovarian cancer cases, 10-15% lifetime risk for ovarian cancer
• RAD51C: 0.5% of ovarian cancer cases, 10-15% lifetime risk for ovarian cancer
• PALB2?
• BARD1?
• ATM?34
Rafnar et al, Nat Genet 2011Loveday et al, Nat Genet 2011Loveday et al, Nat Genet 2012Peltari et al, J Med Genet 2012
Gynecologic Oncology
Surveillance recommendations
• Breast examination and annual mammography/MRI, beginning at age 25 (or earlier based on family history)
• Pelvic examination, CA125, pelvic ultrasound every 6 months, beginning at age 30 (or earlier based on family history)
• Recommend risk-reducing salpingo-oophorectomy between ages 35-40, or on completion of childbearing
Also consider oral contraceptives for ovarian cancer risk reduction
Managing BRCA1 & BRCA2 Mutation Carriers
35
Gynecologic Oncology
PROSperProspective Research on Salpingo-oophorectomy
36

10
Gynecologic Oncology
Genetic Evaluation—clinical benefits
Decision making for treatment
• Better short term prognosis (Bolton et al, 2012)
• Favor platinum or Doxil chemotherapy over taxaneor topotecan (Safra et al 2014)
Opportunities for clinical trials
• PARP inhibitors (Audeh et al 2010, Lederman et al 2014)
Cancer prevention: personal, family
• Breast cancer screening by MRI (Sung & Dershaw2013)
• Risk-reducing surgery (Domchek et al, 2010)
37
Gynecologic Oncology
Ovarian Cancer Survival
38
Progress is noted over time
-Surgery
-Chemotherapy
-Targeted therapies
-Genetics
Gynecologic Oncology
Genetic Evaluation
SGO Clinical Practice Statement: Screening for Lynch Syndrome in Endometrial Cancer
March 2014
All women diagnosed with endometrial carcinoma should undergo systematic clinical screening (review of personal and family history) and/or molecular screening for Lynch syndrome, a hereditary cancer syndrome.
39
Gynecologic Oncology
Amsterdam II Criteria
• International Collaborative Group on HNPCC
• Histologically verified Lynch-associated cancer in > 3 relatives, one of whom is a first degree relative of the other two
• 2 successive generations
• At least 1 diagnosed before age 50
• Lynch-associated cancer = bowel, endometrial, ureter, renal pelvis
Vasen et al, Gastroenterology, 1999Vasen et al, Gastroenterology, 1999

11
Gynecologic Oncology
Lynch Testing through Pedigree
41
Gynecologic Oncology
Identification of Women at Risk
N=117 women from Lynch families with dual gynecologic and colorectal cancers from 5 Lynch registries
14% patients with synchronous cancers
51% with gynecologic cancer first
Median age 44, time to second cancer 11 yrs
49% with colon cancer first
Median age 40, time to second cancer 8 yrs
Lu et al, Obstet Gynecol, 2005
Gynecologic Oncology
Prevalence of Lynch
543 endometrial cancer patients underwent microsatellite instability testing
118 (21.7%) MSI positive—all underwent mutation testing
10 (1.8%) patients with deleterious germline mutation
9 of 118 MSI positive pts--MLH1, 3 MLH2, 5 MSH61 MSI stable tumor had absence of MSH6 on IHC confirmed on germline mutation
Hampel et al, Cancer Res, 2006 Gynecologic Oncology
Lynch versus HBOC Evaluation
44
Endometrial cancer
Tumor studies
Germline testing(MLH1, MSH2, MSH6, PMS2)Panel testing available
Ovarian cancer
Germline testing(BRCA1, BRCA2)

12
Gynecologic Oncology
Tumor Studies for Lynch
• Immunohistochemistry (IHC)
– Loss of staining means gene product absent
• Microsatellite instability (MSI)
– Microsatellite instability a hallmark of DNA mismatch repair
• Hypermethylation of MLH1
– Differentiates between somatic vs. germline cause of MLH1 loss
45
Gynecologic Oncology
Testing for Lynch
46
Gynecologic Oncology
Testing for Lynch
Patient 3
67yo G1P1 with Stage II grade 3 endometrial cancer
S/P LAVH/BSO/PLND/PALND�12cm FIGO grade 3 adenocarcinoma, 69% invasion, suspicious for lymphovascular space involvement, 33 lymph nodes negative, washings negative
IHC� MLH1 present, MSH2 present, MSH6 present, PMS2 absent. MSI high
Germline genetic testing� PMS2 mutation, 943C>T; arg315stop
Daughter tested negative for mutation
47
Gynecologic Oncology
Surveillance recommendations
• Colonoscopy starting at age 20-25, or 2-5 years prior to earliest colon cancer
• Option of office endometrial biopsy annually
– Dysfunctional uterine bleeding warrants evaluation
• Recommend risk-reducing hysterectomy & bilateral salpingo-oophorectomy on completion of child-bearing
• Consider endoscopy, urine analysis, CNS examination
Managing Lynch Mutation Carriers
48

13
Gynecologic Oncology
SGO Genetics Summit
• Assess the current practice of genetic testing
• Identify barriers/challenges to appropriate screening, testing and patient care
• Structure a delivery care model for future practice that is current, forward-thinking and provides optimal access to testing
49
Gynecologic Oncology
SummaryGenetics & Personalized care
Individualized cancer risk
Risk-reducing surgery, salpingectomy
Colonoscopy
Selection of systemic treatment
Platinum-based chemotherapy
Clinical trials: PARP inhibitors
Tumor testing
Who to test, how to counsel?
50
Gynecologic Oncology
AcknowledgementsBeth Crawford, MS CGC
Julie Mak, MS CGC
Amie Blanco, MS CGC
Joseph Rabban, MD MPH
Rebecca A. Brooks, MD
Stephanie M. Ueda, MD
Paul Watkins, Protocol Project Manager
Calvin Cheung, Clinical Research Coordinator
SGO Clinical Practice Committee

1
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Approach to the Adnexal Mass
Stefanie M. Ueda, M.D.
Assistant Clinical ProfessorDivision of Gynecologic Oncology
University of California, San Francisco
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
I have nothing to disclose.
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Management of Adnexal MassQuestion #1
30 y/o G1P0 female found to have adnexal fullness on routine exam. Pelvic ultrasound shows a 5 cm adnexal mass with septations and trace free fluid.
64%
3%3%
30%
1. Repeat ultrasound in 6-8 weeks2. CA-1253. OVA-14. MRI or CT
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Management of Adnexal MassQuestion #2
Patient is anxious and strongly desires surgical removal. CA-125 comes back at 67.
25%
40%
1%3%
30%
1. MRI or CT2. Referral to gynecologic oncologist3. Laparoscopic cystectomy4. Laparoscopic salpingo-oophorectomy5. Laparoscopic salpingo-oophorectomy,
washings, possible biopsies

2
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Management of Adnexal MassQuestions #3
55 y/o postmenopausal female found to have adnexal fullness on routine exam. Pelvic ultrasound shows a
4 cm adnexal mass with thin septation.
18%
3%9%
71%1. Repeat ultrasound in 6-8 weeks2. CA-1253. OVA-14. MRI or CT
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Management of Adnexal MassQuestion #4
Patient has mild hypertension and no significant family history. She is asymptomatic. CA-125 comes
back at 11.
1%12%
82%
4%
1. OVA-12. MRI or CT3. Repeat ultrasound and tumor marker
in 6-8 weeks4. Referral to gynecologic oncologist
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
The Adnexal Mass
• Characteristics of Adnexal Masses• Diagnostic Tools
– Imaging Modalities– Tumor Markers and Multivariate Assays
• Approach to Management• Referral to Gynecologic Oncologist
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Prevalence of Adnexal Mass
• 5-10% lifetime risk of requiring surgery for adnexa l mass– Asymptomatic women age 25-40 1
• 6.6% with ovarian cyst
– Asymptomatic postmenopausal women 2
• 2.5% simple cyst• 84% less than 5 cm and missed on exam
• Risk of malignancy increases with age– 6-11% in premenopausal 3
– 29-35% in postmenopausal
1Borgfeldt C et al, Ultrasound Obstet Gynecol 19992Castillo G et al, Gynecol Oncol 20043Norris HJ et al, Cancer 1972

3
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Clinical Pearls
• Presence of fever, leukocytosis, or pelvic tenderness
• Past medical history, including personal history of breast cancer
• Gastrointestinal symptoms particularly if periumbilical or left lower quadrant pain
• Hepatic, renal or cardiac disease can contribute to ascites or elevated CA-125
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Differential Diagnosis
• Physiologic or functional cysts• Ectopic pregnancy• Inflammatory Etiologies• Endometrioma• Benign or malignant neoplasms
– Serous cystadenomas most common– Mucinous cystadenomas more likely to be
multiloculated, unilocular, larger
• Metastasis to ovary
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Diagnostic Evaluation – Pooled Analysis
Diagnostic Tool Sensitivity Specificity
Bimanual exam 45% 90%
Ultrasound morphology 86-91% 68-83%
MRI 91% 87%
CT 90% 75%
PET 67% 79%
CA-125 78% 78%
1Myers ER et al, Agency Healthcare Res 2006
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Pelvic Ultrasonography• Normal ovary
– 3.5 x 2 x 1.5 cm in premenopausal– 1.5 x 0.7 x 0.5 cm postmenopausal
• 173 consecutive cases of women with pelvic mass 1
– Correct diagnosis 42%, incorrect diagnosis in 7%– 92% sensitivity and 97% specificity for
endometrioma– 90% sensitivity and 98% specificity for dermoid
1Valentin L et al, Ultrasound Obstet Gynecol 1999

4
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Normal premenopausal and postmenopausal ovary
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
DermoidEndometrioma
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Diagnosis of Ovarian Cancer by Sonography
Sonographic Findings Sensitivity Specificity
Ultrasound morphology 86-91% 68-83%
Resistive index 72% 90%
Pulsatility index 80% 73%
Presence of vessels 88% 78%
Morphology and Doppler 86% 91%
Doppler technology should be combined with morpholo gy assessment
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Pelvic Ultrasonography
• Malignancies rich in neovascularization– Lower resistive and pulsatile indices
• Gray scale with color Doppler flow better than either alone
• Likelihood of malignancy 1
– 0.3% of unilocular– 8% of multilocular– 36% of multilocular, solid– 39% of solid
1Granbery S et al, Gynecol Oncol 1989

5
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Sonographic Characteristics
• Low to medium echoes in endometrioma• Fishnet or reticular pattern in hemorrhagic cyst• Hyperechoic nodule with distal acoustic
shadowing suggestive of teratoma• Malignant mass
• Solid but not hyperechoic• Papillary• Thick septations (>2-3 mm)• Color or Doppler flow in solid component
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Multiple septations and solid elements with vascula r flow
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
CT Use in Adnexal Masses• 4.1% asymptomatic women found to have adnexal mass 1
• Mean age 56.2 years• 108 unilateral, 10 bilateral• Mean size 4.1 cm
– No ovarian cancers among those with incidental mass– 4 cases of ovarian cancer developed after negative CT at
15-44 months follow-up
• CT should not be used for screening but preferred technique in the pretreatment evaluation of ovarian cancer to define the extent of disease 2
1Pickhardt PH et al, Radiology 20102Iyer VR et al, AJR 2010
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Mucinous Borderline Tumor

6
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Pelvic MRI in Evaluating Adnexal Mass
• Retrospective cohort of 237 with indeterminate adnexal mass by ultrasound at tertiary care center– Sensitivity 95%– Specificity 94.1%– Predicted benign histologic subtype accurately in 5 6 of 57
women (98.3%)– Predicted malignancy accurately in 23 of 27 women ( 85.2%)– Offered more detailed patient counseling, surgical referral,
and conservative management of benign masses
1Haggert AF et al, Int J Gynecol Cancer 2014
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Endometrioma with hypointensity and fluid levels on T2 (left) and hyperintense blood on T1
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
PET/CT Compared to Other Modalities
• 99 patients underwent PET, ultrasound technique and T2-weighted MRI– PET depicted 7 of 12 malignant and 66 of 87 benign
tumors– False-negative PET obtained in 5 of 7 Stage I canc er
and borderline • Sensitivity 58%• Specificity 76%
– Sensitivity (83%) and specificity (84%) higher for ultrasound and for MRI (92% & 85%, respectively)
– Ultrasound remains method of choice1Fenchel S et al, Radiol 2002
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Normal premenopausal ovaries with FDG-avidity

7
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Multimodal ImagingSonographic Findings Sensitivity Specificity
Sonogram with Doppler 92% 60%
MRI 84%
PET 80%
Combination of all 3 92% 85%
• 101 patients with asymptomatic adnexal masses scheduled for laparoscopy– Preoperative ultrasound, MRI, and PET– Correct classification of 11 of 12 ovarian malignan cies– MRI & PET improved specificities but decreased sens itivities– Multimodal imaging may improve accuracy
1Grab D et al, Gynecol Oncol 2000
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
CA-125
Clinical Scenario Sensitivity Specificity PPV
Stage I 50%
Stage II 90%
Malignancy in premenopausal
50-87% 26% 73-100%
With complex or solid mass on ultrasound
85% 92%
• Elevated in >80% of advanced ovarian cancers• Higher specificity for malignancy if combined with sonography
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Human Epididymis Protein 4 (HE4)
• Disulfide family of secreted proteins that is amplified in ovarian cancer– <140-150 pmol/L for postmenopausal – <70 pmol for premenopausal
• Increased expression in serous (93%) and endometrioid subtypes (100%)• FDA approval in 2008 to monitor patients
with ovarian cancer for disease progression or recurrence
• Not elevated in endometriosis
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
HE-4 staining more common in serous and endometrioi d ovarian carcinomas, but absent in mucinous

8
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Meta-Analysis of HE-4
Clinical Scenario Sensitivity Specificity
HE-4 in Malignancy 78% 86%
CA-125 in Malignancy 80% 75%
• 45 studies of 10,671 women with ovarian tumors– Similar performance of HE-4 to CA-125– Risk of Ovarian Malignancy Algorithm (ROMA),
which includes CA-125 and HE-4, shows conflicting results of improving performance over either marker alone
1Lacerda Macedo AC et al, Int J Gynecol Cancer 2014
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
OVA-1 (Multivariate Index Assay)• 5 biomarkers
– CA-125, transthyretin, apolipoprotein A1, β2 microglobulin, transferrin
• FDA approval in 2009 to screen women with pelvic mass
• High probability of malignancy– >5.0 in premenopausal– >4.4 in postmenopausal– Assay interference if rheumatoid factor>250 IU/ml
or triglyceride >4.5 g/L
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
OVA-1 versus CA-125Clinical Scenario OVA-1
SensitivityCA-125
Sensitivity
Early stage ovarian cancer 94% 61%
Premenopausal 82% 29%
Postmenopausal 100% 78%
• 590 scheduled for surgery for ovarian mass– 27 primary care and specialty sites throughout U.S.– >50% enrolled by non-gynecologic oncologist– Females age 18 or older– High probability of malignancy
• Premenopausal >5.0• Postmenopausal >4.4 1Ueland FR et al, Obstet Gynecol 2011
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Performance in Predicting Ovarian Malignancy
Performance CA-125 (>200) Multivariate Index
Physician Assessment
Assessment +Assay
Sensitivity 69% 93% 75% 96%
Specificity 84% 43% 79% 35%
PPV 65% 42% 62% 40%
NPV 86% 93% 88% 95%
• Physician assessment + OVA-1 identified 86% of mali gnancies missed by CA-125
• 45% still referred to gynecologic oncologist despit e OVA-1 predicting 182 benign tumors
1Ueland FR et al, Obstet Gynecol 2011

9
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Probability of Malignancy with OVA-1 Score
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Risk of Malignancy Following OVA-1 & Imaging
Clinical Test Sensitivity Specificity
Ultrasound or OVA-1 98% 31%
CT 97% 22%
Ultrasound + OVA-1 68% 75%
CT + OVA-1 71% 70%
• 1110 women with adnexal mass evaluated with ovarian imaging, biomarker analysis, and surgery at 44 sites– High-risk imaging defined as complex mass with evid ence of solid
or papillary components– 24% with ovarian malignancy (45 borderline)– Only 1.6% of tumors malignant if both OVA-1 and ima ging low-risk
1Goodrich ST et al, AJOG 2014
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Fine Needle Aspiration of Cystic Mass• Limited by concerns for diagnostic accuracy & cyst
rupture– 235 ovarian cysts by FNA 1
• 56% devoid of diagnostic cells• Sensitivity ranges from 35-85%• Specificity approaches 100%
• Risk for re-formation high 2
– Randomized, controlled study of 278 women with unilocular cysts 4-7 cm
• No difference in resolution between those undergoin g cyst puncture and those observed for 6 months
1Mulvany NJ, Acta Cytol 19962Zanetta G et al, BMJ 1996
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Decisions Regarding Borderline Tumors• Greater tendency to underdiagnose borderline tumors on
frozen section (24-30%) 1
– More for mucinous than serous (33% vs. 13%)
• Upstaging not uncommon with serous borderline tumor s (12-47%) but less likely for mucinous 1
– Incomplete staging associated with a higher recurre nce rate (11.8% vs. 7.1%)
– 24.7% who underwent restaging revealed residual tum or– Stage and sub-classification of extra-ovarian disea se into
invasive and non-invasive implants together with th e presence of postoperative macroscopic residual disease most imp ortant prognostic indicators 2
1Fischerova D et al, Oncologist 20122Seldman JD et al, Human Path 2000

10
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Serous Borderline Tumors
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Surgical Management of Borderline Tumors
• Histology and fertility should be considered with c areful intraoperative exploration
– Pelvic washings– Biopsies of omentum & peritoneum– Appendectomy if mucinous
• Recurrence rate higher after cystectomy (12-58%) th an oophorectomy (0-20%)
– Recurrence in the form of invasive disease <1% for early stage disease
– Only 15% of unilateral tumors associated with extra -ovarian disease if no other suspicious peritoneal lesions or microp apillary pattern found
1Fischerova D et al, Oncologist 2012
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Bowel mesentery with several small implants
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Adnexal Masses in Pregnancy
• Expectant management– 51-70% resolve– 10% malignant– Majority borderline tumors or germ cell tumors
• Surgical intervention– Optimally early to mid-second trimester– Laparoscopy safe, particularly in those <10 cm
• Complication rate <2%– Most pushed out of pelvis

11
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
ACOG Guidelines for Referral to Gynecologic Oncolog ist
Premenopausal Postmenopausal
Elevated CA-125 (>200) Elevated CA-125 (>35)
Ascites Ascites
Abdominal or distant metastases Nodular or fixed pel vic mass
Abdominal or distant metastases
1ACOG Committee Opinion 477, Obstet Gynecol 20112Dodge JE et al, Gynecol Oncol 2012
Malignancy in Premenopausal: Sensitivity 79%, Speci ficity 70%Malignancy in Postmenopausal: Sensitivity 93%, Spec ificity 60%.
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Referral to Gynecologic Oncologist
• Predictive value of guidelines in 1035 women with pelvic mass 1
– Captures 70% of ovarian cancers– 33.8% PPV for premenopausal– 59.5% PPV for postmenopausal– 90% NPV for both groups
• Lowest sensitivity in premenopausal women with earl y stage disease
• Average delay to definitive or staging surgery ~5 weeks 2
– Delay when tumor ruptured affected survival1Im SS et al, Obstet Gynecol 20052Maiman M et al, Obstet Gynecol 1991
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Gynecologic Oncologist Involvement• Survey mailed to 3,200 physicians age <64
– Vignette described a 57-year-old symptomatic woman with a suspicious right adnexal mass with ascites
– Gynecologic oncologist referral • 39.3% of family physicians• 51.0% of general internists • 66.3% OB-GYNS• Factors associated with non-referral
– Medicaid insurance– Providers' weekly average number of patients >91– Male sex – Rural practice location – Solo practice 1Goff BA et al, Obstet Gynecol 2011
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Decision Analysis for Referral
Strategy Cost # Reoperation
CA-125 $933.9 mil 461
OVA-1 $976.9 mil 142
Refer All $939.7 mil Not applicable
• Compared CA-125 to multivariate index for referral strategy in 81,000 hypothetical patients with complex pelvic mass
• 91% of patients have appropriate staging with multi variate index approach• OVA-1 utilization resulted in more ovarian cancer p atients receiving
appropriate initial surgery, but at increased costs• Referring all patients avoids the most reoperations at reduced cost
1Kim KH et al, Gynecol Oncol 2012

12
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Conclusions
• Pelvic ultrasound remains the optimal diagnostic tool at initial evaluation
• MRI may further distinguish tumor characteristics in indeterminate masses
• OVA-1 testing may be considered, particularly in premenopausal women
• High suspicion for malignancy should lead to referral to a gynecologic oncologist
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Management of Adnexal MassQuestion #1
30 y/o G1P0 female found to have adnexal fullness on routine exam. Pelvic ultrasound shows a 5 cm adnexal mass with septations and trace free fluid.
75%
0%
25%
0%
1. Repeat ultrasound in 6-8 weeks2. CA-1253. OVA-14. MRI or CT
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Management of Adnexal MassQuestion #2
Patient is anxious and strongly desires surgical removal. CA-125 comes back at 67.
0% 0% 0%0%0%
1. MRI or CT2. Referral to gynecologic oncologist3. Laparoscopic cystectomy4. Laparoscopic salpingo-oophorectomy5. Laparoscopic salpingo-oophorectomy,
washings, possible biopsies
Countdown
10
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Management of Adnexal MassQuestions #3
55 y/o postmenopausal female found to have adnexal fullness on routine exam. Pelvic ultrasound shows a
4 cm adnexal mass with thin septation.
0% 0%0%0%
1. Repeat ultrasound in 6-8 weeks2. CA-1253. OVA-14. MRI or CT
Countdown
10

13
Approach to the Adnexal Mass UCSF Helen Diller Cancer Center
Management of Adnexal MassQuestion #4
Patient has mild hypertension and no significant family history. She is asymptomatic. CA-125 comes
back at 11.
0% 0%0%0%
1. OVA-12. MRI or CT3. Repeat ultrasound and tumor marker
in 6-8 weeks4. Referral to gynecologic oncologist
Countdown
10

10/24/2014
1
Erica Weiss, MD
Kaiser NCAL OB/GYN Lead, Transgender HealthKaiser Permanente, San Francisco
Transgender Health for the Gynecologist
I have nothing to disclose
Disclosures
OB/GYN’s: Prepare to Treat Transgender Patients
December 2011 Committee Opinion, Obstetrics and Gynecology
Objectives
� Become comfortable with language and sensitivity issues surrounding transgender patients� Review relevant data regarding trans health� Learn clinical pearls specific for the gynecologist
caring for transgender patients

10/24/2014
2
Definitions
� Sex� Gender Identity� Gender Expression� Gender Non-Conforming� Gender Dysphoria� Sexual Orientation
Challenges for the Transgender Community
� 41% have no health insurance� 42% of those with health insurance delay access to
care� 26% Unemployment� Nearly 70% report discrimination or harassment at
work� Twice as likely to live under the poverty line
Green J, et al. Increasing access to care. Center of Excellence for Transgender Health, UCSF.
Sensitivity
• Intake questionnaires• What sex were you assigned at birth?• What is your current gender identity?
• Training Staff- office and OR• Non-discrimination Policy• Sexual Health • Electronic Medical Record
National Transgender Health Summit, UCSF Center of Excellence for Transgender HealthCallahan, et al Introducing sexual orientation and gender identity into the EHR…Academic Medicine 2014

10/24/2014
3
What’s the Data?
� Endocrine Society Guidelines- 2009
� World Professional Association for Transgender Health(WPATH)- Standards of Care for the Health of Transsexual, Transgender, and Gender Nonconforming People SOC version 7
Quality of Life
“Hormonal therapy and sex reassignment: a systematic review and meta-analysis of quality of life and psychosocial outcomes” Au Murad, et al. Clin Endocrinology. 2010.
Analysis of 28 studies(observational)• 80% significant improvement in quality of life• 72% improvement in sexual function• 78% significant improvement in
psychological symptoms
Hormone Therapy
“Long-Term Evaluation of Cross-Sex Hormone Treatment in Transsexual Persons Wierckx, et
al.” J Sex Med 2011
Cross-sectional study: n=100� FTM: no osteoporosis, CV events, hormone-
related CA� MTF: 25 % osteoporosis at lumbar spine, 6%
thromboembolic event, 6% CV event after 11 years , no hormone-related tumors
Sex Reassignment Surgery
“A Sex Reassignment Thirty Years of International Follow-Up Studies SRS: A Comprehensive Review, 1961-1991”. Pfafflin,
F. and Junge, 1998 Symposium Publishing, Dusseldorf, Germany.
� Statistically significant decrease in suicide� Long term regret less than 2%
“Transsexual Surgery Follow-Up: Status in the 1990s.” Green R., and Fleming D. Annual Review of Sex Research. 1990.� 87% of MTFs & 97% of FTMs post SRS had favorable
outcomes� Technical surgical result best predicted favorable outcomes

10/24/2014
4
WPATH Standards of Care Hormone Readiness
• Persistent, well-documented gender dysphoria• Capacity to give consent for treatment• Age of a majority in a given country(if younger,
follow SOC for children and adolescents)• Well-controlled medical or mental health concerns,
if present.
Benefits of Testosterone
• Permanent changes:• Bigger clitoris• Lower voice• More body hair• More facial hair
Benefits of Testosterone
� Reversible Changes:• Coarser skin
• Increased muscle mass
• Increased strength• Amenorrhea• Increased physical energy• Increased libido
Risks of Testosterone
� Acne� Blood clots� More abdominal fat� Headaches� Elevated Blood Pressure� Infertility� Increased RBC count� Liver inflammation

10/24/2014
5
Risks of Testosterone
� Emotional changes� Vaginal dryness� Male pattern baldness� Swelling�Weight gain� Gynecologic Cancers?
Routes of Administration
� Intramuscular� Transdermal patch or gel� Subcutaneous
� Goal Estradiol levels: less than 50� Goal Testosterone levels: 320-800
Intramuscular Use
� Initial dose 50-200 mg depo-testosterone� Usual dose is 200 mg Q 2 weeks� Split dosing to 100 mg QW- helps avoid
peak and trough issues
Transdermal Preparations
� If desire slower progress� Patients who develop polycythemia� Ongoing maintenance after desired virilization� Post BSO

10/24/2014
6
GYN Cancer Risk
Published Case Reports:• Ovarian CA: 3• Vaginal Cancer: 1• Cervical Cancer: 2• Endometrial Cancer: 1
Urban R, et al. Gynecologic malignancies in female-to-male transsexuals…AJOG. 2011.
Testosterone and the Endometrium
� Assess for bleeding• Check on hormone regimen• Add progesterone� Lining
• Decreased thickness• WPath guidelines- no increased risk for
endometrial CA
AU Mueller, et al: J Clinic Endocrinology Metab 2007
Breast Cancer Risk
� 5 reported cases in the literature� Post nipple-sparing subcutaneous
mastectomy� Chest wall exams� ? mammograms
Nikolic, et al, Importance of revealing a rare case of breast cancer in a FTM after bilateral mastectomy. World J surg Oncol. Dec 2012
Bone Density“Long-term follow-up of bone mineral density and
bone metabolism in transsexuals treated with cross-sex hormones”. Auvan, et al. JSO Clin
Endocrinol. 1998.In FTM patients:
• Increased alk phos during first year• BMD did not change in first year• Significant decrease in bone density 28-63
months post BSO
Miyajima, et al A study of changes in bone metabolism in cases of gender identity disorder, J Bone Miner Metab, 2012.

10/24/2014
7
Follow-up Care
� Discuss social adjustment, libido, sexual behavior, and quality of life� Risky behaviors/STD screening� Screen for DV� Assess menses/bleeding� Review: Contraception if SA with men
Follow-up Care
� Testosterone levels
� Lipids/CBC
� Mammograms/Chest wall exams
� Pap smear screening (higher rates of unsatisfactory paps)
� Bone Density
Peitzmeier, et al, Female-to-male patients have high prevalence of unsatisfactory PAPs…, J Gen Intern Med. May 2014.
WPATH Surgical Criteria
�Letter of referral by a mental health provider with documentation of Gender Dysphoria
�Top Surgery: 1 letter, hormone therapy optional for FTM / encouraged for MTF
�SRS: 2 letters, hormone therapy, 1 year of continuous living as one’s gender identity
FTM Gender-Confirming Procedures
� Mastectomy� Hysto� Vaginectomy� Metoidioplasty� Scrotoplasty/implants� Placement of testicular prostheses� Phalloplasty

10/24/2014
8
FTM Top Surgery
� Double incision subtotal mastectomies with free areola-nipple grafts
� Keyhole or subcutaneous nipple sparing mastectomies through areola incision
� Liposuction
FTM Top Surgery-Preop
FTM Top Surgery-Postop Hysterectomy BSO
� Many FTM patients seek to align internal anatomy with external identity� To avoid gynecologic problems and cancers� Cancer screening rates may be low� Ability to decrease testosterone dose post-op� ? Increase in adenomyosis
O’Hanlan et al. Total Laparoscopic Hysterectomy for Female-to-Male Transsexuals. Obstetrics and Gynecology 2007Rachlin, et al. Hysterectomy and Oophorectomy Experiences of Female-to Male TransgenderIndividuals, Int’l Jnl Transg, 2010.

10/24/2014
9
Total Laparoscopic Hysterectomy for Female-to-Male Transsexuals
• Retrospective chart review• 593 patients(41 transsexual, 552 females)• Transsexuals
• Shorter operating time (57.5 min vs. 116 min, p<.001)
• Less blood loss (mean 27 cc vs 107 cc, p.001)• Lower uterine weight (mean 118 g vs. 167 g,
p<.001)• No significant differences in complication
rate(under-powered)• No significant differences in re-operation rates
O’Hanlan et al. Obstetrics and Gynecology 2007.
Fertility and Family Building
• Discuss fertility issues with patients considering hormones
• Discuss again pre-hysterectomy and address ovarian retention
• Assisted reproductive technologies
Wallace, et al. Fertility preservation in the transgender patient: expanding oncofertility care beyond cancer. Gynecol Endocrinol. 2014
The Next Frontier in Fertility Treatment. Sarah Elizabeth Richards. January 12, 2014.
“Over the past 15 years, activists have fought to compel insurers to cover transgender-related health care....
What’s been left out of the spotlight: having babies.”
Reproductive Desires in Transsexual Men
� Self-constructed questionnaire 50 transsexual men� 64 % involved in a relationship� 54 % desired to have children� 22 %(11) had children
8 had female partners inseminated with donor sperm3 gave birth before hormonal therapy and SRS
� 37.5% would have considered freezing germ cells if had been available
Wierckx, et al, Human Reproduction 2012

10/24/2014
10
Transmen and Pregnancy• Cross-sectional survey study of 41 trans-identified men• 25 (61%) had used testosterone• 20 (80%) resumed menstruation in 6 months after stopping• 5 (20%) conceived while still amenorrheic from T (13% unplanned)• 36 (88 %) of oocytes from participants’ own ovaries • Majority conceived within 4 months• 50% received prenatal care from an MD• 78 % delivered in a hospital• Cesarean section(25% requested)
• 36% of testosterone group, 19 % of no testosterone group• 50% breast(chest)fed
• 40% of testosterone group• 69% of no testosterone group
• Perinatal complications:• 12% hypertension, 10 % preterm labor, 10% abruption, 7 % anemia
Light et al, Transgender men who experienced pregnancy after female-to-male gender transitioning, Obstetrics and Gynecology, in press.
Transmen and Pregnancy
� “Lonely, because I was the only one”
� “Heavy time, having a baby, not passing as male, all the changes and society telling me to just be happy”
� “Began to show symptoms of postpartum depression long before anyone discussed symptoms to watch for”
Light et al, Transgender men who experienced pregnancy after female-to-male gender transitioning, Obstetrics and Gynecology, in press.
MTF Hormone Therapy
� Estrogen• Oral: 2-8 mg/day• Transdermal: 0.1-0.4 mg twice weekly• Parenteral: 5-30 mg IM every 2 week
� Spironolactone: 50-200 mg BID� Progesterone: generally not needed� Goal Testosterone level: less than 55� Goal Estradiol level: 100-200
MTF SRS Procedures
� Tracheal Shave� Labiaplasty� Vaginoplasty� Breast Augmentation� Facial Feminization� Orchiectomy

10/24/2014
11
Surgical Complications
� Vaginal stenosis� Necrosis of the vagina or labia� Fistulas from the bladder or bowel into the vagina� Stenosis of the urethra� Shortened vagina� Granulation tissue
Weiss, et al Gynecology Care for Transgender Patients, Kaiser Permanente Practice Resource, 2012
Voiding Disorders and Dyspareunia
• 7.5% prolapse greater than POP stage 2 (3.8 % required surgical intervention)
• 47% voiding difficulties• 25% urgency(17% UI)• 23% SUI • 9 % fecal urgency and 8% incomplete bowel emptying• 23% not satisfied with sexual functioning
Kuhn, et al. Vaginal prolapse, pelvic floor function, and related symptoms 16 years after sexual reassignment surgery in transsexuals, Fertility and Sterility, 2011.
The Desire to have Children and the Preservation of Fertility in Transsexual Women: A Survey
60%
40%
No Bio Children
Have Bio Children
40%
40%
20%
WantChildrenDon't WantChildrenNo Comment
De Sutter et al. Intl J Transgenderism 2002
Examinations for MTF patients� DV, HIV/STD� Visual inspection for lesions� If not having penetration, counsel on use of dilators� Breast exams and mammograms after 5-10 years of
estrogen use� Prostate screening:
• PSA not indicated in low risk patients (falsely low if androgen-deficient)
• If post SRS- best examined vaginally
Pattison, Triple negative breast cancer in a male-to-female transsexual, Internal medicine Journal 2013.Colebunders, et al, Hormonal and surgical treatment in transwomen with BRCA 1, J Sex Med 2014

10/24/2014
12
Clinical Pearls to Remember…
� Pause and Ask Ask Ask� Address dosing� Paps in FTM- tell on testosterone� Endometrial effects� Breast cancer screening� Contraception for FTM patients if sexually
active with men� Fertility preservation� Surgical complications in MTF patients
Conclusion
� Transgender people are among the last patients to be excluded from the healthcare system in the US
� Transgender people are among the last people to have universal protection from discrimination
.
Spack, N. Management of Transgenderism JAMA 2013
Resources
� Center of Excellence for Transgender Health• transhealth.ucsf.edu� World Professional Association for Transgender
Health(WPATH)• wpath.org� Trans Care Project of Vancouver, British Columbia
• vch.ca/trans health/resources/tcp.html• Kaiser documents/protocols
LET’S GO GIANTS!

10/24/2014
1
An Integrative Approach to Caring for Women with Chronic Pelvic Pain
Priscilla Abercrombie, RN, NP, PhD, AHN-BCHealth Sciences Clinical ProfessorObstetrics, Gynecology & Reproductive SciencesUCSF Chronic Pelvic Pain ClinicUCSF Osher Center for Integrative MedicineSFGH Women’s Health CenterFounder, Women’s Health & Healing
1
Disclosures� I have no disclosures� I will discuss off-label use of drugs.
2
Objectives� Define chronic pelvic pain (CPP) and
identify the most common causes of CPP.� Conduct a comprehensive holistic assessment
of the sources of pain in women with CPP. � Identify the importance of myofascial
manifestations of pain and how they are treated. � Explore the difference between treating acute
and chronic pain and how to employ a variety of different treatment modalities that treat the whole person.
3
Integrative Medicine� The practice of medicine that reaffirms the importance of the relationship between practitioner and patient, focuses on the whole person, is informed by evidence, and makes use of all appropriate therapeutic approaches, healthcare professionals and disciplines to achieve optimal health and healing.” Consortium of Academic Health Centers for Integrative Medicine � Combines mainstream medical therapies with CAM therapies for which there is some high-quality scientific evidence for safety and effectiveness. NCCAM

10/24/2014
2
Chronic Pelvic Pain Definition� “Continuous or episodic pain in the lower
abdomen or pelvis lasting ≥6 months and associated with a negative impact on quality-of-life” (Williams, et al., 2004)� Definitions vary greatly throughout the clinical
and research literature.� Can be classified as cyclic or noncyclic
� Seldom fits into those categories clinically
5
Chronic Pelvic Pain� Prevalence 12-39%� Medical Care◦ 20% of all referrals to gynecologists◦ >40% of all laparoscopies◦ 12% of all hysterectomies� Costs to Society◦ $882 million in outpatient visits alone◦ 15% time lost from work◦ 45% reduced productivity◦ Total costs estimated at > $2 billion / yr
6
Howard FM. Obstetrical and Gynecological Survey 1993;48:357-87.Mathias SD, Kuppermann M, et al. Obstetrics & Gynecology 1996;87:321-7.
Overview of CPP � Affects physical and sexual function, and emotional well-being
� Can severely impact quality of life � Multiple systems interact and contribute to the pathophysiology of CPP
� In many cases a direct cause of CPP cannot be identified
� Increased risk of a history of abuse, depression, and anxiety, which exacerbates painful symptoms
7
Case History� 35 yo with crampy lower abdominal pain x 3 years� Daily pain 3/10, worsens to 8/10 twice a week� Limits activities (including sex), enjoyment of life� Worse with her period� Pain with intercourse� Has constipation with bloating� Urinary frequency
8

10/24/2014
3
ASSESSMENT• No standard diagnostic criteria or
standard method of evaluating patients• Proceed in a holistic systematic manner
assessing for all sources of pain: physical, emotional and spiritual
9
Needs of CPP Patients� Receive legitimization of their pain from a health care professional� To be heard during the patient contact visit� To have support in numerous forms� To take personal responsibility for one’s health
Jarrell (2005), The Society of Obstetricians and Gynaecologists of Canada
Components of the CPP History� Pain history/diary: quality, location, timing with cycle, contributing or relieving factors, body map� Medical/surgical
history including Rxs� Ob/Gyn: ◦ menstrual history◦ sexual history
� GI symptoms/pain� Urinary symptoms:
IC screening� Quality of life/coping� Health habits: ◦ substance abuse◦ nutrition/exercise� Review records:◦ surgery◦ diagnostic tests
11
See International Pelvic Pain Society Website for history and PE forms:English, Spanish, French
Assess Quality of Life� Assess impact on functioning and quality of life (scale of 1 to 4) ◦ In the past month, how much has your pelvic pain kept you from doing your usual activities such as self-care, work or recreation? ◦ How much has your pelvic pain interfered with your quality of life? ◦ How much has your pelvic pain interfered with your normal or regular sexual activity? ◦ How much have the treatments you have received for your pelvic pain improved your quality of life?� How do you cope with your pain?� How does your partner, family etc. respond when you
are in pain?
12

10/24/2014
4
Emotional Health� Elicit patient’s view of illness, fears and concerns◦ Do you have any thoughts or concerns about what might be causing the pain?� Screen for current or prior physical or sexual violence, including events in childhood� Screen for depression (12-35%)◦ During the past month, have you been bothered by little interest or pleasure in doing things? ◦ During the past month, have you been bothered by feeling down or hopeless?”� Assess sexual functioning◦ Desire, frequency, satisfaction, orgasm and discomfort
13
Spiritual Health� How do you connect with your spirit?�What brings you joy?�Who are the people you choose to be close to?�What do you hope for?�Where do you find strength?�What brings you comfort when you are upset?
14
15
Patients don’t really come to us because they are in pain, they come to us because they are suffering.Ling, APS Conference 2010
16
CPP Diagnostic TestsTest RationaleUrinalysis and culture Bladder symptoms suggestive of UTIWet mount, STI screening Signs or risk factors for genital tract infectionALT and creatinine Taking multiple medications or concern for liver or
kidney diseaseTSH, CBC, FBS, Vitamin D Depressive or constitutional symptoms
Pelvic sonogram Bimanual exam limited or abnormalCT and MRI Other diagnostic studies are abnormal or inadequate
Laparoscopy Persistent symptoms, infertility, large ovarian cysts, treatment of endometriosis or adhesions
Cystoscopy Concern for IC or other bladder abnormalitiesFOBT x 3 or referral for colonoscopy
GI symptoms or concern for colon cancer

10/24/2014
5
PHYSICAL EXAM• Identify underlying pathology• Reproduce pain• Establish trust and minimize fear
17
Musculoskeletal Exam� Observe gait, posture, balance� Examine hip flexibility and symmetry� Palpate the abdomen for muscle tension, tenderness and trigger points� Perform Q-tip or cotton swab test� Examine pelvic floor muscles
Don’t confine your exam to the gyn table
18
Carnett’s Sign� Differentiates pain originating from the abdominal wall versus peritoneal cavity (Suleiman et al., 2001)� The patient raises her head and shoulders from the examination table while the provider palpates the tender area on the abdomen. � Positive Carnett’s sign: pain remains unchanged or increases when the abdominal muscles are tensed.
19
Myofascial Trigger Points
20
� Trigger points are hyperirritable palpable nodules that are taut bands of muscle fibers (Tough et al., 2007)
� When palpated the pain usually radiates to another location
� Found in abdominal wall, buttocks, hips, perineum and pelvic floor locations
� Major contributor to CPP
See also: Lavelle, E., Lavelle, W., & Smith, H. (2007). Myofascial trigger points. Anesthesiology Clinics, 25, 841-51.

10/24/2014
6
Myofascial Trigger Points
21
Levator ani
Obturator internus
Q -Tip Test
22
National Vulvodynia Association CME Course http://www.medscape.org/viewarticle/780555
Q -Tip Test� Purpose: identify and map changes in sensation including allodynia� Gently touch with a q-tip� Start at the thigh and work down to perineum bilaterally� Include clitoris and perianal areas� Proceed from labia majora to labia minora then the vestibule� Record findings
23
Examining Pelvic Floor Muscles
24

10/24/2014
7
Internal Pelvic Floor Examination� Palpate in 3 layers with a single finger� Layer one (superficial)◦ First knuckle◦ Bulbocavernosus, ischiocavernosus, superficial transverse perineal� Layer two ◦ Second knuckle◦ Urethral muscles, deep transverse perineal� Layer three (deep)◦ Third knuckle◦ Levator ani, coccygeus, piriformis, obturatorinternus
25
DIAGNOSIS
26
• Gynecologic• Gastrointestinal• Urinary tract• Musculoskeletal• Psychological
Gynecologic Causes� Endometriosis� Adenomyosis� Adhesions entrap ovaries, tether
pelvic organs� Vulvodynia, vestibulodynia� Pelvic congestion syndrome� Ovarian remnant syndrome
27
DIAGNOSIS OF VULVODYNIA
Chronic Vulvar Pain
PENo visible findings
ErythemaHyperalgesia
Allodynia
VulvodyniaGeneralized pain
Burning, stabbing, stinging, etc.
VestibulodyniaPain at vestibule only
ProvokedBurning
R/OInfectious,
inflammatory, neoplastic and
neurologic causeTreat accordingly
28

10/24/2014
8
Vulvodynia Treatments� Oral pain medications◦ TCA’s, SSNRI’s◦ Anticonvulsants◦ Opioids
� Topical Preparations◦ Anesthetics◦ Compounded formulations
◦ Hormones � Pelvic floor therapy, biofeedback
� Nerve blocks: ◦ Subcutaneous, pudendal, caudal
� Psychotherapy◦ Coping/support◦ Communication◦ CBT
� Sex therapy/education� Neurostimulation� Diet modification� Surgery:
◦ Vestibulectomy, vulvectomy
29
Gastrointestinal Conditions� Irritable bowel syndrome� Inflammatory bowel disease, diverticular disease� Hernias � Cancer (rarely)
30
Urinary Tract Conditions� Interstitial cystitis: painful bladder
syndrome� Infection: usually acute symptoms� Kidney stones: usually acute symptoms� Cancer (rarely)
Diagnosis of Interstitial Cystitis
31
� Pain related to bladder and urgency, frequency or nocturia◦ absence of objective evidence of another disease that could cause the symptoms� PUF questionnaire, IC Symptom Index� Cystoscopy and urodynamics recommended if diagnosis of IC in doubt◦ cystoscopy showing Hunner’s ulcer or glomerulations(nonspecific) on bladder wall � Potassium sensitivity test not recommended
See AUA Guidelines 2011
Treatments for IC� Patient education and self care practices: ◦ Bladder training◦ Dietary changes: acidic foods, artificial sweeteners, caffeine, alcohol
◦ Stress management/stop smoking� Oral medications: amitriptyline, cimetidine,
hydroxyzine, pentosanpolysulfate� Intravesical medications: DMSO, heparin,
lidocaine� Physical therapy/movement

10/24/2014
9
MUSCULOSKELETAL MALADAPTATIONSHypertonus and tenderness common
33
Inciting Pain Event: uterus, ovary, bowel, bladder, muscles, nerves
Secondary Muscle “Adaptations”:Lower back, buttocks, hips, pelvic floor
Initial EventResolves (naturallyor with treatment)
MYOFASCIAL PAINLOW BACK, HIP, BUTTOCK, ABDOMINAL WALL, AND PELVIC FLOOR MUSCLE DYSFUNCTION
34
Hypertonus and tenderness are common
FEAR AVOIDANCE MODEL(CATASTROPHIZING)
(Main, et al., BMJ, 2002; Alappattu & Bishop, 2011; Martin, Johnson, Wechter, Leserman, & Zolnoun, 2011). 35
Chronic pelvic pain
EMOTIONAL PAINAddress anxiety, depression and sexual pain
36

10/24/2014
10
Psychological Morbidity� Pain has impact on quality of life and functional
capacity� Women become isolated and relationships
become strained� Pre-existing psychological issues such as anxiety,
depression, and PTSD exacerbated by pain� Depression is common (22% Learman, 2011) ◦ risk for suicide x2 for patients in pain (Tang, 2006), ◦ prevalence of suicidal ideation 24% (Racine, 2014)
37
Which Patient Has More Pain?
38
Patient ADepressed
Patient BNot Depressed
Sexuality Issues� Dyspareunia is common� Can lead to sexual dysfunction and strained sexual relationships� 68% of women with CPP have sexual dysfunction◦ Hypoactive desire 54%◦ Arousal disorder 33%◦ Orgasmic disorder 22%◦ Sexual pain 74%
39(Verit, Verit, & Yeni, 2006)
TREAT CHRONIC PAIN AS A CONDITIONCentral Sensitization
40

10/24/2014
11
Pathways of Pain Perception
41
Central Sensitization
� Definition: “an amplification of neural signaling within the central nervous system that elicits pain hypersensitivity” (Woolf, 2011). � Body continues to experience pain despite healing from a precipitating injury� Pain in the setting of no known pathology� Chronic pain is a condition
42
43
Central Sensitization� CNS perpetuates pain by demonstrating exaggerated or prolonged responses to painful stimuli this is referred to as “windup” � Reduced capacity for inhibition� Occurs in many CPP disorders such as vulvodynia (Zhan, 2011), dysmenorrhea (Bajaj, 2002), and endometriosis (He, 2010)
44

10/24/2014
12
TREATMENT• Improve quality of life• Improve functional status• Decrease pain
45
Therapeutic goals� Identify and treat physical and psychological morbidity
� Assist in the development of:◦ Positive coping techniques◦ Communication strategies◦ Problem solving skills
� Set realistic treatment goals� Acknowledge and support woman� Work with PCP to provide medication management
� Convene a multidisciplinary team46
Treating Pain: Medications� Analgesics:◦ Opioids◦ NSAIDS� Topical anesthetics*� Antidepressants◦ Tricyclics*◦ SSRI’s/SNRI’s*� Anticonvulsants◦ gabapentin◦ pregabalin
� Muscle relaxants� Refer to pain management◦ nerve blocks◦ neurotoxin: OnabotulinumtoxinA*
◦ medication consult
47*Off label use
Physical Therapy for Myofascial Pain� Refer patients to physical therapists specializing in pelvic floor myofascial work (advanced training)◦ Complete assessment◦ Myofascial release◦ Biofeedback◦ Home exercise program� Abdominal breathing, rescue poses, stretching exercises
� Resource: YouTube videos in English and Spanish
48See APT Womens Health Section website for referrals

10/24/2014
13
Treatment for Trigger Points� Ultrasound energy, manual therapy� Local anesthetic injection ◦ 93% success by 5th injection in abdomen
(Kuan, 2006)◦ Lidocaine 1% x 10-15cc, bupivicaine 0.25% -
0.5% x 10-15cc
49
Treating Sexual Pain� Patient educationo Learn about your body o Explore your pleasure spotso Educate your partner
o Connect with your partner in sexual and non-sexual ways
o Prepare for sex: relax the PF muscles, use lubricants, take time for arousal
o Reinvent your sex lifeo Avoid painful activities
o Refer to sex therapist or sexologisto Use patient education materials
50Heather Howard, PhD Sexual Rehab.org
Integrative Approach� Mind/body interventions: breathing exercises, imagery, MBSR, laughter yoga, etc.
� Movement therapies: yoga, Tai Chi, Feldenkrais, etc.
� Nutrition: anti-inflammatory diet/herbs, multivitamins, B complex, fish oil, calcium/magnesium, herbal adaptogens
� Alternative providers: TCM, craniosacral, chiropractic, energy medicine, strain/counter strain, etc.
51
Clinical Pearls� Set realistic goals with your patient: improved function vs. complete remission
� Have a systematic approach to assessment� Be wary of the assumption pain is linked to pathology or obvious tissue damage
� Avoid opiates/Use medication contracts� Work as an interdisciplinary team- build a community
� Have lots of tools in your tool kit� Keep learning about innovative strategies� Use group medical visits
52

10/24/2014
14
In their own words• “I thought I was the only one in the world with this [pain]… It was so good to hear other people’s experiences and help define what I had. I thought there was something terribly wrong [with me]. I feel very reassured that its something else people have and I’ve come to terms with the fact that it might never go away. I was always hoping that some day everything would be fine if I just did the right thing. But now it’s just everything being okay is all right.”
� “To find that other people have the same experiences and the feeling that you’re not alone. Everyone was able to share so well. I always felt comfortable. It just meant a lot.”
• “My experience was positive! I feel more in control of my own life now and I feel confident that I can improve (and possibly rid my condition).”
University of California, San FranciscoCenter of Excellence in Pain Education
Interactive QuestionIn addition to obtaining an NRS/VAS pain intensity score, what additional aspects of pain should be assessed?
T i mi n g
o f p a i
n . . . B o
d y m a
p C o
n t ri b u
t i n g a . .
. Q u
a l i ty , l o
c a t. . .
A l l o f
t h e a b
o . . .
20% 20% 20%20%20%
Countdown
10
a. Timing of pain with the menstrual cycleb. Body mapc. Contributing and relieving factorsd. Quality, location and timinge. All of the above
University of California, San FranciscoCenter of Excellence in Pain Education
Answer In addition to obtaining an NRS/VAS pain intensity score, what additional aspects of pain should be assessed?a. Timing of pain with the menstrual cycleb. Body mapc. Contributing and relieving factorsd. Quality, location and timinge. All of the above• If patient is unable to give an adequate pain history then she should keep a pain diary for 3-5 days to record the information above.
University of California, San FranciscoCenter of Excellence in Pain Education
Interactive QuestionWhat is allodynia?
I n cr e a
s e d s e n
s . . .
B ur n i n
g p ai n s
. . .
P a in f r
o m a n
o . . .
33% 33%33%a. Increased sensitivity to painb. Burning pain sensationc. Pain from a non-painful
stimulus
Countdown
10

10/24/2014
15
University of California, San FranciscoCenter of Excellence in Pain Education
AnswerWhat is allodynia?a. Increased sensitivity to painb. Burning pain sensationc. Pain from a non-painful
stimulus
University of California, San FranciscoCenter of Excellence in Pain Education
Interactive QuestionWhat underlying conditions might be present in a patient with dysparuenia?
E n do m
e t r io s i s
V ul v o d
y n i a o r
. . . I n t
e r s ti t i a
l c . ..
P e lv i c
f l o or m
. . . A l l
o f t h e
a b o. . .
20% 20% 20%20%20%
Countdown
10
a. Endometriosisb. Vulvodynia or vestibulodyniac. Interstitial cystitisd. Pelvic floor muscle dysfunctione. All of the above
University of California, San FranciscoCenter of Excellence in Pain Education
AnswerWhat underlying conditions might be present in a patient with dysparuenia?
a. Endometriosisb. Vulvodynia or vestibulodyniac. Interstitial cystitisd. Pelvic floor muscle dysfunctione.All of the above
Interactive QuestionThe following statements about CPP are true, except:
60 I t is d e
f i n ed . .
. I t i
s a c o m
p l e. . .
I t af f e c
t s qu a .
. . I t i
s c om m
o n ly . . .
I t is b e
s t tr e . .
.
20% 20% 20%20%20%
Countdown
10
a. It is defined as pain in the pelvis lasting >6 months.
b. It is a complex condition that can involve many different organ systems.
c. It affects quality of life including sexual function.
d. It is commonly caused by acute pelvic inflammatory disease.
e. It is best treated using a multidisciplinary approach.

10/24/2014
16
Interactive QuestionThe following statements about CPP are true, except:a. It is defined as pain in the pelvis lasting >6 months.b. It is a complex condition that can involve many different
organ systems.c. It affects quality of life including sexual function.d. It is commonly caused by acute pelvic
inflammatory disease.e. It is best treated using a multidisciplinary approach.
61

10/24/2014
1
Gyn Care for Women with Breast CancerMindy Goldman, MD
Clinical ProfessorDept. of Ob/Gyn and Reproductive Sciences
Director, Women’s Cancer Care Program, UCSF Breast Care Center
and Women’s HealthUniversity of California, San Francisco
Case• 34 yr. G2P2 presents with a palpable breast mass –
you send her for a FNA which returns positive for carcinoma. She has no other medical history and no family history of breast cancer. She undergoes a lumpectomy for a 1.8 cm infiltrating ductal carcinoma that is ER+/PR+ and Her2Neu negative. She receives adjuvant chemotherapy with AC followed by Taxol, then radiation, and is placed on Tamoxifen. Her menses stop with chemotherapy and return 6 mos later.
Questions• 1. Is she at risk for endometrial cancer by taking
Tamoxifen?
• 2. Will Tamoxifen affect her menstrual cycles?
• 3. Would you recommend routine ultrasound surveillance?
Breast Cancer Epidemiology-• Most common invasive cancer in US women
• 232,340 new cases invasive Breast ca in US in 2013
• Median age of diagnosis is 61
• 12% diagnosed in reproductive years (ages 20-44)
• More than 25,000 cases per yr in California

10/24/2014
2
Breast Cancer Epidemiology• Lifetime risk 1 in 8 at age 85
• 2.0 million women living in US with history of Breast Cancer
• SEER data: breast cancer rates increased 1980-1990’s, declined 1999-2004, stable 2004-2011, but rates of advanced cancer increasing in young women aged 25-39
• Possible reasons for drop - less HRT, less mammography, more aggressive treatment of DCIS, use of SERM’s, fewer Medicare visits. Unclear why more advanced cancers in young women ? Environmental exposures
Breast Cancer Epidemiology• 89% women diagnosed alive at 5 yrs – 98.6% alive for
localized breast cancer
• Since 1990 breast cancer mortality has declined, and current declines 2% per year
• Risk of death from Breast Ca 1 in 35
• 40,000 deaths per year
• Second leading cause of cancer deaths after lung cancer. Leading cause of cancer deaths in US women ages 40-59
Breast Cancer Treatments• Breast surgery – either breast conserving
lumpectomy or modified mastectomy. May also include immediate or delayed reconstructive procedures
• Radiation
• Chemotherapy
• Hormonal Therapies
These treatments can all have gynecologic effects
Gynecologic Issues Related to Breast Cancer
• Chemotherapy induced menopause
• Gynecologic effects of hormonal therapies
• Treatment of menopausal symptoms– Hot flashes– Vaginal dryness/discomfort– Sexuality issues
• Gynecologic uses of hormonal therapies
• Ovarian suppression

10/24/2014
3
Breast Cancer Treatments and MenopauseMenopausal complaints often more severe
• Surgical treatments may include oophorectomy with immediate onset of menopause
• Premenopausal women with normal menstrual functioning get put into immediate menopause with chemotherapy
• Postmenopausal women taking HRT tend to abruptly stop when diagnosed with breast cancer
• Side effects of hormonal drugs like Tamoxifen may be severe
Chemotherapy Induced Menopause
• Incidence of ovarian failure dependent on chemotherapy regimen, cumulative dose and age of patient
• Most ovarian toxicity due to alkylating agents - cyclophosphamide• 33-81% after 6 cycles CMF
• Moderate ovarian toxicity with doxurubicin or cisplatin
• Less ovarian effects with 5-FU, methotrexate, and vincristine
• Less ovarian effects with taxol and taxotere, but less known regarding long term effects
Chemotherapy Induced Menopause
• Overall incidence of chemotherapy-induced amenorrhea ranges from 53% to 89%
• 50% women < 35 resume normal menses post chemotherapy
• 70 -90% women > 40 have permanent ovarian failure post chemotherapy
• Longterm cytotoxic effects - women who menstruate post chemotherapy still at increased risk for premature menopause
Can Ovarian Toxicity be Prevented?
• POEMS (Prevention of Early Menopause, phase 3 prospective trial) – presented at ASCO 5/2014
• 2004-2011, 4 year follow up
• 218 women with Stage 1-3 hormone negative breast cancer given Goserelin (GnRH agonist) with chemotherapy vs. chemotherapy alone
• primary endpoint - ovarian failure

10/24/2014
4
Can Ovarian Toxicity be Prevented?• Results: More pregnancies and more live births with goserelin
– Ovarian failure - 22% chemotherapy arm vs 8% goserelin arm (P = .04)
– Attempted pregnancy - 12 (11%) chemotherapy arm and 22 (21%) goserelin arm became pregnant (P = .03)
– Live Births - 8 patients chemotherapy arm (7%, 12 babies) and 16 patients (15%) in the goserelin arm (18 babies, P = .05)
– 4-year disease-free survival - 78% in the chemotherapy arm and 88% in the goserelin arm (P = .04).
– 4-year overall survival was 82% chemotherapy arm vs 92%, goserelinarm(P = .06)
Breast Cancer Tumors• Breast tumors are all sent for ER/PR status and to
see whether over-expression of Her2neu
• Estrogen and Progesterone positivity tells you the tumor will benefit from drugs that manipulate the hormonal environment
• 2/3 of breast cancers are hormone positive
HER-2 Tumors• The HER2 gene makes the protein HER2 receptor which
is important in controlling epithelial cell growth, cell differentiation and possibly angiogenesis
• HER2 tumors overexpress Her2-neu and are oncogene driven and a marker of more aggressive tumor
• 18-20% of breast cancers over express HER2-neu
HER-2 Tumors• Anti-angiogenic drug Trastuzumab (Herceptin) - attaches to HER2 receptors
on the surface of breast cancer cells and prevents them from receiving growth signals
• Biologic targeted therapy
• Typically used with either anthracycline-based or docetaxel and carboplatin (TCH) chemotherapy
• Studies have shown Improved 5-year disease-free survival and overall survival but more cardiotoxicity
• Recent study showing benefits of similar drug pertuzumab (Perjeta) with Herceptin and chemotherapy had improved survival for metastatic Her2-positive disease

10/24/2014
5
SF Giants TriviaIn 1883, John B. Day and Jim Mutrie, owners of the
American Association's New York Metropolitans, form a National League team called ….
T h e G i a
n t s T h
e Ne w
Y o rk G
r i z zl e y ’
s
T he N
e w Y o r
k R az o r
b a ck s
T h e G o
t h am s
55%
18%20%
7%
A. The GiantsB. The New York Grizzley’sC. The New York RazorbacksD. The Gothams
The Answer Is…..• The Gothams
• The pennant-winning Metropolitans move over to the National League franchise in 1885. On June 3, after a rousing extra-innings victory over Philadelphia, manager Jim Mutrie was so overcome with emotion that he supposedly blurted out a description of his team that immediately became the franchise's new nickname - He called them his Giants
Hormonal Treatments and Breast Cancer
• Used to reduce recurrences and overall breast cancer mortality in women with hormone receptor positive breast cancer
• Biologic goals of hormonal therapy
• Block production of estrogen• Block action of estrogen• Down-regulate the estrogen receptor
Hormonal Treatments of Breast Cancer
• SERMS: Tamoxifen (Soltamox), Raloxifene (Evista), Toremifene (Fareston)
• Estrogen Receptor Downregulators: Fulvestrant(Faslodex)
• Aromatase Inhibitors: Anastrozole (Arimidex), Letrozole (Femara), Exemestane (Aromasin)

10/24/2014
6
Hormonal Treatments of Breast Cancer - Tamoxifen
• Complex drug with estrogen and anti-estrogen properties
• Originally made as contraceptive then found to suppress mammary tumors in rats
• By 1992 shown to increase disease free interval and decrease contralateral breast ca in pre and postmenopausal women
Benefits of Tamoxifen• 5 years of tamoxifen reduces breast cancer recurrence by 40%-
50% in PMP women and 30%-50% in premenopausal women
• 5 years of tamoxifen reduces risk of a new contralateral breast cancer by about 50%
• 5 years of tamoxifen has shown improved overall survival with more than 15 years of follow up
• 5 years of tamoxifen has been found to better than 2
• Can be used as neoadjuvant therapy to shrink large, hormone-receptor-positive breast cancers prior to surgery
Tamoxifen – Longer Treatment• Earlier international trials showed differences in benefits with
longer treatment
• Adjuvant Tamoxifen, Longer vs Shorter (ATLAS) looked at >15,000 women, 5 or 10 yrs of Tam
– Reductions in recurrence, mortality, contralateral breast cancer with 10 vs 5
– More endometrial cancer, PE and Ischemic Heart Disease
Tamoxifen - Longer Treatment• Adjuvant Tamoxifen To Offer More (aTTOM) trial looked at
7000 women given 5 or 10 yrs of Tam – results 2013
– Decreased recurrence with 10 yrs, not seen until year 6– Trend toward decreased mortality after year 10– Increased endometrial cancers and endometrial cancer
death
• Standard of care changing to 10 years of adjuvant tamoxifen

10/24/2014
7
Stopping Tamoxifen for Pregnancy• Given the recommendations for longer treatment and trials
showing safety of pregnancy after breast cancer, more oncologists recommending stopping tamoxifen for pregnancy and then resuming post partum
• Typically recommended to do at least 2 years of tamoxifentherapy
• Stop for at least 2 mos (wash out) prior to attempting pregnancy
• Tamoxifen may slow milk production and should not be used when breastfeeding
Tamoxifen for Breast Cancer Prevention
• Breast Cancer Prevention Trial showed 5 years of Tamoxifen in high risk women reduced risk of hormone receptor positive breast cancer by 45%
• Approved by FDA in 1998 for breast cancer prevention
Tamoxifen – Why Don’t More Women Use for Prevention?
• Adverse side effects reported in 60% pts• 20-40% discontinue drug because of poor
tolerability and effects on QOL• Weight gain typically 7-10 lbs
Common Side Effects:Hot FlashesVaginal DischargeVaginal DrynessJoint PainHeadaches
Tamoxifen – Adverse Events• Increased rate of venous thromboembolic events, particularly
in first two years
• Additional pro-coagulant effect when tamoxifen is added to chemotherapy
• Overall 2-3 fold increased RR for DVT and PE
• If Factor V Leiden mutation 5 –fold increased risk of thromboembolism

10/24/2014
8
Tamoxifen – Adverse Events• Increased risk for arterial thromboembolism (stroke)
• Stroke risks thought to be counterbalanced by favorable effects on ischemic heart disease: – Overview of RCT of adjuvant tamoxifen showed non-significant
increased stroke deaths (3 extra per 1000 women in first 15 yrs) was exactly balanced by a non-significant reduction in cardiac deaths (3 fewer per 1000 women during the first 15 years)
• Most recommendations are to discontinue tamoxifen for few days before surgery or long travel
Tamoxifen - Biologic Effects
• Agonist and Antagonist effects
• Effects of Tamoxifen vary depending on hormonal environment
Tamoxifen and Premenopausal Women
• Induces estrogen production and ovulation - has been used for ovulation induction for IVF
• Reports of ovarian cysts in upwards of 30% women
• Menstrual irregularities- mainly oligomenorrhea or amenorrhea (but affected by prior chemotherapy)
• Growth of endometrial polyps, fibroids, endometriomas
• Not thought to increase the risk of endometrial cancer
Tamoxifen –Recommendations for Contraception
• Reports of teratogenicity in rodent studies, although series of women who have conceived on Tamoxifen and had normal pregnancy outcomes
• Non-hormonal forms of contraception recommended

10/24/2014
9
Tamoxifen and Postmenopausal Women
• Increased endometrial proliferation, cystic changes, polyp formation, adenocarcinoma and uterine sarcoma
• Frequency of cancer dependent on endometrial surveillance: TVS vs. EMB and criteria for surveillance – symptomatic vs. asymptomatic
• The reported risks of endometrial cancer in Tamoxifen users have ranged from 1.3-7.5 in RCT, and increase with longer use
• Meta-analysis of 32 RCT trials showed RR 2.7, primarily in women > 50
Tamoxifen and Endometrial Cancer• Absolute risks - about 4 cases of endometrial cancer per
1000 women taking Tamoxifen each year
• 95% of Endometrial Cancers present with Vaginal Bleeding
• Risks are thought to decrease as soon as tamoxifen is stopped
• Most women get a much greater benefit to their breast than risk to their uterus
Tamoxifen and Other Types of Endometrial Cancer
• Recent studies show more aggressive endometrial cancer subtypes in Tamoxifen users: sarcomas, papillary serous, clear cell, and mixed mullerian tumors
• Cancer registry data has shown that shorter time to development of cancer and more aggressive subtypes but no differences in endometrial cancer specific survival
• Overall felt that tamoxifen does not affect endometrial cancer survival
Endometrial Surveillance with TVS – what are the concerns?
• Increased endometrial thickness, irregular echoes, cystic changes (‘Swiss-cheese appearance”), polyps and hyperplasia
• Findings do not correlate with malignant histology
• Thickened endometrium can be atrophic. Mechanism may be stromal hypertrophy, enlargement of subendometrial glands
• No prospective data on what is normal endometrial thickness for women on tamoxifen

10/24/2014
10
What are the problems with routine surveillance?
• Absence of a defined endometrial thickness cut-off for the tamoxifen patients reduces ultrasound accuracy and increases the number of patients referred for unnecessary hysteroscopy
• Overtreatment with unnecessary surgeries
Ultrasound of Patient on Tamoxifen
Endometrial Surveillance – Other Imaging for patients on Tamoxifen
• Saline Sonogram – useful in distinguishing polyps from cystic endometrium overall improved sensitivity
• MRI useful for evaluating myometrium but less accurate in looking at intra-cavitary lesions - sensitive in evaluating endometrium but not specific enough to assess cancer vs. other pathology
• Lack of good data looking specifically at Tamoxifen
Clinical Pearls for Tamoxifen and Imaging• Get baseline sono for comparison because there are many times
that “things come up” –bloating, pain, bleeding that may require imaging
• Do not get routine surveillance
• Do not use endometrial thickness as an indicator for intervention
• Consider saline sonograms to improve PPV but no stated guidelines
• Endometrial effects are thought to stop once tamoxifen is stopped and risks back to baseline in about 5 years

10/24/2014
11
What about levonorgestrel-releasing IUD (Mirena) for women on Tamoxifen?
• Cochrane review to determine effectiveness of Mirena in preventing endometrial hyperplasia, polyps, and adenocarcinoma in pre and postmenopausal breast cancer patients taking tamoxifen
• Looked at only RCT, 2 met search criteria
• Results:– Mirena led to significant reduction in the incidence of endometrial polyps OR
0.14– Neither trial powered to detect changes in rate of endometrial hyperplasia or
adenocarcinoma or whether Mirena led to increased risk of breast ca recurrence
– More vaginal bleeding in the Mirena treatment group in the first six months only
• Chin J, et al. Cochrane Database Syst Rev. 2009 Oct 7;(4):CD007245. Review.
What about levonorgestrel-releasing IUD (Mirena) for women on Tamoxifen?
• Recent RCT 2013 in China showed similar reduction in polyps, no differences in hyperplasia or cancer and not powered to assess breast cancer recurrence
• Many oncologists feel uncomfortable based on risks of progestins to the breast
Tamoxifen and CYP Testing• Tamoxifen is converted into its active metabolites in the liver by
the CYP2D6 liver enzyme, part of the P450 detoxification pathway
• CYP2D6-mediated drug metabolism is variable. 7-10% of individuals have decreased enzyme production - Concern whether poor metabolizers may not benefit from tamoxifen and have increased risk for recurrence
• Trials have not yet shown that CYP testing is clinically useful
• Some concerns with co-administration of pure SSRI’s that are potent inhibitors of CYP - Paroxetine, Fluoxetine
Tamoxifen vs. Raloxifene for Breast Cancer Prevention – STAR Trial
• STAR trial: 5 years, one of largest breast ca prevention studies, 500 centers in US, Canada, and Puerto Rico
• Tamoxifen reduced risk of invasive breast cancer and DCIS by 50%
• Raloxifene was 75% as effective as Tamoxifen in preventing invasive breast ca and 78% as effective as Tamoxifen in preventing DCIS
• Significantly fewer endometrial cancers, thromboembolic events and cataracts
• Raloxifene - FDA approved for breast cancer prevention in PMP women in 2007

10/24/2014
12
Giants Trivia:What year did the New York Giants become the
San Francisco Giants?
1 94 8
1 95 2
1 95 8
1 96 4
0%
33%
67%
0%
A. 1948B. 1952C. 1958D. 1964
The Answer Is…..
1958
Aromatase Inhibitors• Tamoxifen competes with estrogen at receptor binding site in
the breast preventing receptor activation
• Aromatase Inhibitors prevent conversion of androstenedioneand testosterone into estrogens and decrease peripheral circulating estrogen
• Not useful in premenopausal women because blocking aromatase in the ovaries results in lower estradiol levels which reduce negative feedback and increase pituitary gonadotropin output, increasing ovarian function
Aromatase Inhibitors
• Third generation AI’s used:
• Anastrozole (Arimidex) • Letrozole (Femara)
• Exemestane(Aromasin)
Nonsteroidal - reversible
Steroidal –irreversible inhibitors

10/24/2014
13
Anastrazole, Tamoxifen, Alone or in Combination (ATAC) trial
• 9000 PMP women with early stage breast ca, treated with 5 yrsof Anastrazole vs. Tamoxifen, first interim analysis presented in 2001 with now 13 years of follow up.
• Anastrazole had improved Disease Free Survival (HR .90 at 100 mos)
• Anastrazole had improved time to recurrence (HR .81 at 100 mos)
• Anastrazole had lower incidence of contralateral breast cancer (HR .68 at 100 mos)
Anastrozole vs. Tamoxifen - Adverse Effects
• Worse with AI – only about 60% of women continue full recommended treatment
• More arthralgia, myalgia, and bone loss with AI
• Increased cardiovascular risks with AI, but no difference in MI, or MI related death
• Increase risks of fracture with AI during treatment but not seen after completion
• More colorectal and lung cancers with AI, not significant
• More vaginal dryness, dyspareunia and decreased libido with AI
Anastrozole vs. Tamoxifen - Beneficial Effects
• Better with AI:
• Fewer CVA in AI group but did not persist after treatment
• Lower thromboembolic events with AI
• Fewer endometrial, ovarian cancer and melanoma in AI - only significant for endometrial cancer
• Aromatase Inhibitors thought to prevent endometrial cancer
Aromatase Inhibitors - 2014• Many international trials have now shown efficacy of
aromatase Inhibitors in adjuvant treatment for postmenopausal women
• FDA approved Anastrazole (Arimidex) as first-line adjuvant therapy in PMP women with hormone positive breast cancer
• FDA approved Letrozole (Femara) for extended adjuvant use in women with early-stage, hormone-receptor-positive breast cancer after five years of tamoxifen
• Trial of Exemestane(Aromasin) showed 70% reduction in ER-positive invasive breast ca with exemestane compared to placebo over a 3-year period, not yet FDA approved for prevention

10/24/2014
14
Aromatase Inhibitors – Gynecologic Uses• Ovulation Induction – studies have shown pregnancy rates similar to
gonadotropins
• Ovulatory Dysfunction – PCOS. Meta-analysis of 4 published trials showed pregnancy rates similar to Clomiphene
• Treatment of Pelvic Pain and Endometriosis – aromatase is expressed at higher levels in endometriosis implants than in normal endometrium. Letrozole and Norethindrone reported to improve symptoms and histologic diagnosed endometriosis – No RCT compared to standard medical therapies
• Treatment for Fibroids – documented aromatase in myoma cells
• ACOG Technical Bulletin on Aromatase Inhibitors in Gynecologic Practice - Aug 2008
Breast Cancer – What’s New in 2014• Individualized Treatment - Advances in gene expression
technologies improves predictions of prognosis and treatment benefit
• Oncotype DX ,Mammoprint , PAM50 test - genomic tests that predict risk of cancer recurrence and likely benefit from adjuvant chemotherapy
• Recent study on the genomics of breast cancer showed four distinct genetic types of the disease
• Breast cancer treatments are becoming more individualized
Ovarian Suppression and Ablation
Ovarian Suppression and Ablation • Ovarian ablation oldest form of systemic treatment for breast ca,
first described 1896
• Methods – Surgical, Radiation-Induced, Medical with GNRH analogs (Zoladex)
• Many studies looking at ablation as adjuvant therapy
Overview of trials:
– Ovarian suppression (OS) and ovarian ablation (OA, via surgical oophorectomy) significantly decreases recurrence and improves survival in women < 50 with hormone positive tumors

10/24/2014
15
Ovarian Suppression and Ablation• OS and OA thought to be comparable to chemotherapy alone –
but data based on older regimens and not established for current anthracycline or taxane baseed regimens
• Not clear that OS/OA provides an additive benefit to chemotherapy – possibly in women under age 40 who are more likely to have return of ovarian function post chemotherapy
Ovarian Suppression and Endocrine Therapy
• Some trials suggest that ovarian suppression plus tamoxifenprovides added benefit. Many oncologists suppress ovaries for 3 yrs in high risk patients
• Current trials (TEXT, SOFT) looking at ovarian suppression to determine optimal hormonal therapy for premenopausal women with early breast cancer - recent combined data showed OS with AI had 34% lower risk of recurrence than Tamoxifen with OS, awaiting data on OS and AI vs. Tamoxifen alone
Should the Ovaries Come Out?• Although data showing ovarian suppression is
beneficial, not clear that oophorectomy should be done in all premenopausal women with hormone positive breast cancer
• ? Counterbalancing risks of subsequent heart disease with oophorectomy in early stage breast cancer, and recent reports of more osteoporosis and arthritis
Ovarian Suppression and Fertility• Recent studies showing ovarian suppression
prior to chemotherapy preserved ovarian function
• Many fertility programs focused on assisted reproductive techniques to preserve fertility –ovarian stimulation with Tamoxifen or Letrozole and embryo cryopreservation, ovarian tissue or oocyte cryopreservaton prior to chemotherapy

10/24/2014
16
More Giants TriviaWho hit the first homerun into McCovey Cove?
S a mm y
S o sa
J e ff K e
n t
B ar r y
B o nd s
W il l C
l a r k
21%
13%
46%
21%
A. Sammy SosaB. Jeff KentC. Barry BondsD. Will Clark
And the Answer Is….
• Barry Bonds
• This ball was hit over the right field wall into the Pacific Ocean against Rich Rodriguez on May 1st, 2000
Final Thoughts……
• Common questions about breast cancer
How to treat Hot Flashes in Breast Cancer Patients
• Low dose antidepressants – Venlaflaxine, Paroxetine, Fluoxetine, Citalopram, Desvenlafaxine (1/10-20th doses for depression)
• Antihypertensive Clonidine• Gabapentin (Neurontin)• Vitamin E• Soy supplements• Herbal Products: best studied Black Cohosh• Tibolone (in Europe)• Chinese Herbs• Alternative Therapies

10/24/2014
17
How to treat Vaginal Dryness in Breast Cancer Patients
• Lubricants for sexual activity
• Oils to the tissue- mineral, olive, coconut
• Vaginal Preparations of Estrogens or Testosterones -remember testosterone preparations not FDA approved and need to be compounded
• Estring (best data, limited), Vagifem
• Replens- Several studies showing improvement in vaginal itching, irritation and dyspareunia - equivalent to vaginal estrogen creams, most improvement in first 2 wks
• SERMS – Ospermifene, no data in breast cancer patients
Common Questions - Do Fertility Drugs increase the risk of Breast Cancer? - NO
• Israeli cohort showed no increased risk except for women treated with clomiphene citrate Breast Cancer Res Treat. 2006
• Large Danish cohort showed no association Cancer Epidemiol Biomarkers Prev. 2007
• Israeli cohort of IVF found women over age 40 and those who underwent > 4 cylceshad a higher risk of breast cancer Ann Surg Oncol. 2008
• Large British cohort with ovulatory disorders showed higher risk of primary breast cancer but no increased risks with fertility drugs Br J Cancer. 2009
• US cohort of 12,000 women from 1965-1988 showed no increased risk except for women using >12 cycles of Clomid Cancer Epidemiology, Biomarkers & Prevention, April 2014.
Is it safe to get pregnant after having Breast Cancer? -YES
• Large population registry studies have shown no increased risks of recurrences for women who get pregnant after prior treatment for breast cancer
• Typically recommended to wait at least 2 years from diagnosis
• Pregnancies more often in women with early stage disease so possible selection bias “healthy mother effect”
Can Women Breastfeed after Breast Cancer? - MAYBE
• Most patients report inadequate lactation in affected breast
• May have asymmetric breasts due to inadequate hypertrophy
• Breast conserving surgeries may allow for lactation
• Less likely with:
– Centrally located tumors– If prior radiation - induces fibrosis of lobules with decreased
milk production

10/24/2014
18
Is HRT after Breast Cancer safe? MAYBE
• Qualitative review of 10 prospective and 2 randomized trials in Belgium- no increased risks Human Reproduction 2007 22(2):616-622
• Retrospective study from large HMO in Washington lookingat pharmacy data showed no increased risk of recurrence or mortality J Natl Cancer Inst. 2001 May 16;93(10):754-62
• Review from Germany of four prospective randomized studies and 15 observational studies - Only the Hormonal Replacement Therapy after Breast cancer: Is iT Safe (HABITS) study showed an increased risk of recurrence Minerva Ginecol. 2007 Oct;59(5):529-41
Is HRT after Breast Cancer safe? MAYBE
• Follow up of large Stockholm trial that included lower doses of progestins did not show increased risk of recurrence at 10.8 yrs fu (originally stopped early in 2003 after HABITS published showing increased risk) Eur J Cancer. Aug 11 2012
• HT safe if DCIS only and bilateral mastectomies
• HT and breast cancer complicated: new studies using estrogen therapy to reverse acquired antihormonal resistance in the treatment of metastatic hormone positive breast cancer Clin Breast Cancer. 2008 Apr;8(2):124-33
Is breast imaging needed after bilateral mastectomies? NO
• If complete mastectomy no need for imaging
• If skin sparing, nipple sparing procedure, some centers may still recommend screening mammography
• MRI can be helpful to establish the presence of residual breast tissue after bilateral mastectomy, and routine screening not recommended if no residual breast tissue is seen
• With saline or silicone implants or autologous reconstruction procedures imaging typically not recommended
Case• 34 yr G2P2 presents with a palpable breast mass –
you send her for a FNA which returns positive for carcinoma. She has no other medical history and no family history of breast cancer. She undergoes a lumpectomy for a 1.8 cm infiltrating ductal carcinoma that is ER+/PR+ and Her2Neu negative. She receives adjuvant chemotherapy with AC followed by Taxol, then radiation, and is placed on Tamoxifen. Her menses stop with chemotherapy and return 6 mos later.

10/24/2014
19
Questions• Is she at risk for endometrial cancer by taking
Tamoxifen? • NO
• Will Tamoxifen affect her menstrual cycles? • MAYBE
• Would you recommend routine ultrasound surveillance?
• NO
Hopefully now, you will….• Know more facts about breast cancer• Understand the gyn issues related to the treatment of breast
ca• Understand when Tamoxifen and Aromatase Inhibitors are
used in breast ca treatment• Understand the gyn implications of Tamoxifen and the
Aromatase Inhibitors• Know about the role of ovarian suppression in breast cancer• Know about fertility drugs and breast cancer• Know about safety of pregnancy and hormone use after
breast cancer• Know something new about breast cancer that you didn’t
know before this talk……
Thank You• GO GIANTS!