RBGO - Gynecology & Obstetrics - Febrasgo
64
RBGO Gynecology & Obstetrics ISSN 0100-7203 eISSN 1806-9339 Revista Brasileira de Ginecologia e Obstetrícia Number 12 • Volume 41 • Pages 679–726 • December 2019
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of RBGO - Gynecology & Obstetrics - Febrasgo

RBGO Gynecology & Obstetrics
ISSN 0100-7203eISSN 1806-9339
Revista Brasileira de Ginecologia e Obstetrícia Number 12 • Volume 41 • Pages 679–726 • December 2019

RBGO Gynecology and ObstetricsRevista Brasileira de Ginecologia e Obstetrícia
ISSN 0100-7203
Editor in Chief
Marcos Felipe Silva de Sá Universidade de São Paulo, Ribeirão Preto, SP, Brazil
Former Editors
Jean Claude NahoumRio de Janeiro, RJ (1979–1989)
Clarice do Amaral FerreiraRio de Janeiro, RJ (1989–1994)
Sérgio Pereira da CunhaRibeirão Preto, SP (1994–1997)
Jurandyr Moreira de AndradeRibeirão Preto, SP, Brazil (1997–2015)
Associated Editors
Agnaldo Lopes da Silva FilhoUniversidade Federal de Minas Gerais,Belo Horizonte, MG, Brazil
Alessandra Cristina MarcolinUniversidade de São Paulo,Ribeirão Preto, SP, Brazil
Ana Katherine da Silveira GonçalvesUniversidade Federal do Rio Grande doNorte, Natal, RN, Brazil
Andréa da Rocha TristãoUniversidade Estadual Paulista“Júlio de Mesquite Filho”, Botucatu, SP, Brazil
Antonio Rodrigues Braga NetoUniversidade Federal do Rio de Janeiro, Rio de Janeiro, RJ, Brazil
Corintio Mariani NetoUniversidade Cidade de São Paulo, São Paulo, SP, Brazil
Daniel Guimarães TiezziUniversidade de São Paulo,Ribeirão Preto, SP, Brazil
Diama Bhadra Andrade Peixoto do ValeUniversidade Estadual de Campinas, Campinas, SP, Brazil
Eddie Fernando Candido MurtaUniversidade Federal do Triângulo Mineiro, Uberaba, MG, Brazil
Edward Araujo JúniorUniversidade Federal de São Paulo,São Paulo, SP, Brazil
Eliana Aguiar Petri NahasUniversidade Estadual Paulista“Júlio de Mesquita Filho”, Botucatu, SP, Brazil
Fabrício da Silva CostaMonash University, Melbourne, Victoria, Australia
Fernanda Garanhani de Castro SuritaUniversidade Estadual de Campinas, Campinas, SP, Brazil
Fernando Marcos dos ReisUniversidade Federal de Minas Gerais,Belo Horizonte, MG, Brazil
Gerson Botacini das DoresGustavo Salata Romão
Universidade de Ribeirão Preto, Ribeirão Preto, SP, Brazil
Helena von Eye CorletaUniversidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil
Ilza Maria Urbano MonteiroUniversidade Estadual de Campinas, Campinas, SP, Brazil
José Geraldo Lopes RamosUniversidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil
José Guilherme CecattiUniversidade de São Paulo, Campinas, SP, Brazil
José Maria Soares JúniorUniversidade de São Paulo, São Paulo, SP, Brazil
Julio Cesar Rosa e SilvaUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Lucia Alves da Silva LaraUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Lucia Helena Simões da Costa PaivaUniversidade Estadual de Campinas, Campinas, SP, Brazil
Luiz Carlos ZeferinoUniversidade Estadual de Campinas,Campinas, SP, Brazil
Luiz Gustavo Oliveira BritoUniversidade de São Paulo,Campinas, SP, Brazil
Maria Celeste Osório WenderUniversidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil
Maria Laura Costa do NascimentoUniversidade Estadual de Campinas, Campinas, SP, Brazil
Mila de Moura Behar Pontremoli Salcedo Universidade Federal de Ciências da Saúde de Porto Alegre, Porto Alegre, RS, Brazil
Omero Benedicto Poli NetoUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Patrícia El BeituneUniversidade Federal de Ciências da Saúde de Porto Alegre, RS, Brazil
Paula Andrea de Albuquerque Salles NavarroUniversidade de São Paulo,Ribeirão Preto, SP, Brazil
Ricardo Carvalho CavalliUniversidade de São Paulo,Ribeirão Preto, SP, Brazil
Rosana Maria dos ReisUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Rosiane MattarUniversidade Federal de São Paulo, São Paulo, SP, Brazil
Rodrigo de Aquino CastroUniversidade Federal de São Paulo,São Paulo, SP, Brazil
Silvana Maria QuintanaUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Sophie Françoise Mauricette DerchainUniversidade Estadual de Campinas,Campinas, SP, Brazil
Editorial Board
Alex Sandro Rolland de SouzaInstituto de Medicina Integral Prof. Fernando Figueira, Recife, PE, Brazil
Ana Carolina Japur de Sá Rosa e SilvaUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Aurélio Antônio Ribeiro da CostaUniversidade de Pernambuco, Recife, PE, Brazil
Belmiro Gonçalves PereiraUniversidade Estadual de Campinas, Campinas, SP, Brazil
Carlos Augusto Alencar JuniorUniversidade Federal do Ceará, Fortaleza, CE, Brazil
Carlos GrandiUniversidad de Buenos Aires, Buenos Aires, Argentina

Cesar Cabello dos SantosUniversidade Estadual de Campinas, Campinas, SP, Brazil
Délio Marques CondeHospital Materno Infantil de Goiânia, Goiânia, GO, Brazil
Dick OepkesUniversity of Leiden, Leiden, The Netherlands
Dino Roberto Soares de LorenziUniversidade de Caxias do Sul, Caxias do Sul, RS, Brazil
Diogo de Matos Graça Ayres de CamposUniversidade do Porto, Porto, Portugal
Eduardo Pandolfi PassosUniversidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil
Edmund Chada BaracatUniversidade de São Paulo, São Paulo, SP, Brazil
Eliana Martorano AmaralUniversidade Estadual de Campinas, Campinas, SP, Brazil
Francisco Edson Lucena FeitosaUniversidade Federal do Ceará, Fortaleza, CE, Brazil
George CondousNepean Hospital in West Sydney, Sidney, Australia
Giuseppe RizzoUniversità degli Studi di Roma“Tor Vergata”, Roma, Italy
Gutemberg Leão de Almeida FilhoUniversidade Federal do Rio de Janeiro,Rio de Janeiro, RJ, Brazil
Iracema de Mattos Paranhos CalderonUniversidade Estadual Paulista“Júlio de Mesquita Filho”, Botucatu, SP, Brazil
João Luiz Pinto e SilvaUniversidade Estadual de Campinas, Campinas, SP, Brazil
João Paulo Dias de SouzaUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
João Sabino Lahorgue da Cunha FilhoUniversidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil
José Carlos PeraçoliUniversidade Estadual Paulista “Júlio de Mesquita Filho”, Botucatu, SP, Brazil
José Juvenal LinharesUniversidade Federal do Ceará, Campus de Sobral, Fortaleza, CE, Brazil
Joshua VogelDepartment of Reproductive Health and Research, World Health Organization, Geneva, Switzerland
Juvenal Soares Dias-da-CostaUniversidade Federal de Pelotas, Pelotas, RS, Brazil
Laudelino Marques LopesUniversity of Western Ontario, London, Ontario, Canada
Luciano Marcondes Machado NardozzaUniversidade Federal de São Paulo, São Paulo, SP, Brazil
Luis Otávio Zanatta SarianUniversidade Estadual de Campinas, Campinas, SP, Brazil
Luiz Claudio Santos ThulerInstituto Nacional do Câncer, Rio de Janeiro, RJ, Brazil
Luiz Henrique GebrimUniversidade Federal de São Paulo, São Paulo, SP, Brazil
Manoel J. B. Castello Girão, Universidade Federal de São Paulo, São Paulo, SP, Brazil
Marcelo ZugaibUniversidade de São Paulo, São Paulo, SP, Brazil
Marcos Desidério RicciUniversidade de São Paulo, São Paulo, SP, Brazil
Maria de Lourdes BrizotUniversidade de São Paulo, São Paulo, SP, Brazil
Marilza Vieira Cunha RudgeUniversidade Estadual Paulista “Júlio de Mesquita Filho”, Botucatu, SP, Brazil
Newton Sergio de CarvalhoUniversidade Federal do Paraná, Curitiba, PR, Brazil
Nuno Henrique Malhoa Migueis ClodeFaculdade de Medicina de Lisboa, Lisboa, Portugal
Olímpio Barbosa Moraes FilhoUniversidade de Pernambuco, Recife, PE, Brazil
Paulo Roberto Nassar de CarvalhoInstituto Fernandes Figueira-Fiocruz, Rio de Janeiro, RJ, Brazil
Renato Augusto Moreira de SáUniversidade Federal Fluminense, Niterói, RJ, Brazil
Rintaro MoriNational Center for Child Health and Development, Tokyo, Japan
Roberto Eduardo BittarUniversidade de São Paulo, São Paulo, SP, Brazil
Rosane Ribeiro Figueiredo AlvesUniversidade Federal de Goiás, Goiânia, GO, Brazil
Roseli Mieko Yamamoto NomuraUniversidade Federal de São Paulo, São Paulo, SP, Brazil
Rossana Pulcinelli Vieira FranciscoUniversidade de São Paulo, São Paulo, SP, Brazil
Ruff o de Freitas JuniorUniversidade Federal de Goiás, Goiânia, GO, Brazil
Sabas Carlos VieiraUniversidade Federal do Piauí, Teresina, PI, Brazil
Sebastião Freitas de MedeirosUniversidade Federal do Mato Grosso, Cuiabá, MT, Brazil
Selmo GeberUniversidade Federal de Minas Gerais, Belo Horizonte, MG, Brazil
Silvia DaherUniversidade Federal de São Paulo, São Paulo, SP, Brazil
Shaun Patrick BrenneckeUniversity of Melbourne Parkville, Victoria, Australia
Técia Maria de Oliveira MaranhãoUniversidade Federal do Rio Grande do Norte, Natal, RN, Brazil
Toshiyuki HataUniversity Graduate School of Medicine, Kagawa, Japan
Wellington de Paula MartinsUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Editorial Offi ce
Bruno Henrique Sena Ferreira
Editorial Production
Thieme Medical Publishers
Federação Brasileira das Associações de Ginecologia e ObstetríciaBrazilian Federation of Gynecology and Obstetrics Associations
ISSN 0100-7203
Society Board (2018)
PresidentCésar Eduardo Fernandes (SP)
Administrative / Financial Director Corintio Mariani Neto (SP)
Scientifi c Director Marcos Felipe Silva de Sá (SP)
Professional Status DefenceJuvenal Barreto Borriello de Andrade (SP)
Vice-president of North RegionHilka Flávia Barra do E. Santo (AM)
Vice-president of Northeast Region Flavio Lucio Pontes Ibiapina (CE)
Vice-president of Middle West Region Alex Bortotto Garcia (SP)
Vice-president of Southeast Region Agnaldo Lopes da Silva Filho (MG)
Vice-president of South Region Maria Celeste Osório Wender (RS)
Presidency and Executive Staff
Avenida das Américas, 8445 – sala 711Barra da Tijuca – Rio de Janeiro – RJ CEP: 22793-081 BrazilPhone.: (+55 21) 2487-6336 Fax: (+55 21) 2429-5133www.febrasgo.org.brpresidencia@[email protected]
RBGO Editorial Offi ce
editorial.offi [email protected]


A diverse group of award-winning Editors complement our journals in a vast variety of specialties.
http://www.thieme.com/journals
Journal Specialties
Anatomy
Cardiac Care
Chemistry
Complementary Medicine
Critical Care
Dentistry
Endocrinology
Gastroenterology
Informatics
Natural Product Research
Neurology
Neurosurgery
Nutrition
Ophthalmology
Orthopaedics
Otolaryngology
Pediatrics
Pharmacology
Plastic Surgery
Radiology
Reproductive Medicine
Respiratory
Speech-Language-Hearing
Sports Science
Surgery
Vascular Medicine
Veterinary Medicine
Read and submit http://open.thieme.com thieme.com /journals
ORDERTODAY

www.thieme-connect.com
Thieme E-Journals
For more information and a trial access, please contact:
Thieme Institutional [email protected].: + 49 711 8931 407
The Quality Choice in Medicine and Science

RBGO Gynecology and ObstetricsRevista Brasileira de Ginecologia e Obstetrícia
Volume 41, Number 12/2019
online www.thieme-connect.com/products
Editorial
679 Androgen Abuse among Recreational AthletesMaíta Poli de Araujo
Original Articles
High Risk Pregnancy
682 Risks of Maternal Obesity in Pregnancy: A Case-control Study in a Portuguese Obstetrical PopulationPatrícia Alves, Maria Filipa Malheiro, João Cavaco Gomes, Tiago Ferraz, and Nuno Montenegro
688 Perinatal Outcomes of Fetuses with Early Growth Restriction, Late Growth Restriction, Small for Gestational Age, and Adequate for Gestational AgeQuênya Antunes Silveira Inácio, Edward Araujo Júnior, Luciano Marcondes Machado Nardozza,Caetano Galvão Petrini, Victor Paranaíba Campos, and Alberto Borges Peixoto
697 Factors Associated with the Need for Insulin as a Complementary Treatment to Metformin in Gestational Diabetes MellitusMatheus Leite Ramos de Souza, Rodrigo Ribeiro e Silva, Thiago Ribeiro e Silva, Larissa Cano de Oliveira, Guilherme Dienstmann, Iramar Baptistella do Nascimento, and Jean Carl Silva
Basic and Translational Science/Mastology
703 Eff ect of Testosterone on Proliferation Markers and Apoptosis in Breasts of Ovariectomized RatsJussara Celi Conceição Oliveira, Marcelo Luis Steiner, Thérèse Rachell Theodoro, Ana Maria Amaral Antonio Mader, Giuliana Petri, Luiz Carlos Abreu, Maria Aparecida da Silva Pinhal, César Eduardo Fernandes, and Luciano Melo Pompei
Mastology/Menopause
710 Association of Menopausal Status, Expression of Progesterone Receptor and Ki67 to the Clinical Response to Neoadjuvant Chemotherapy in Luminal Breast CancerLeonardo Roberto da Silva, Renato Flora Vargas, Júlia Yoriko Shinzato, Sophie Françoise Mauricette Derchain,Susana Ramalho, and Luiz Carlos Zeferino
Teaching and Training/Gynecological Endoscopy
718 The Impact of Systematic Laparoscopic Skills and Suture Training on Laparoscopic Hysterectomy Outcomes in a Brazilian Teaching HospitalAnna Luiza Lobão Gonçalves, Helizabet Abdala Ayroza-Ribeiro, Raquel Ferreira Lima,Aline Estefane Eras Yonamine, Fabio Ohara, and Paulo Augusto Galvão Ayroza-Ribeiro
Thieme Revinter Publicações Ltda

Some of the product names, patents, and registered designs referred to in this publication are in fact registered trade marks or proprietary names even though specifi c reference to this fact is not always made in the text. Therefore, the appearance of a name without designation as proprietary is not to be construed as a representation by the Publisher that it is in the public domain.
All rights, including the rights of publication, distribution, and sales, as well as the right to translation, are reserved. No part of this work covered by the copyrights hereon may be reproduced or copied in any form or by any means—graphic, electronic, or mechanical, including photocopying, recording, taping, or information and retrieval systems—without written permission of the Publisher.
Important Note: Medical knowledge is ever-changing. As new research and clinical experience broaden our knowledge, changes in treatment and drug therapy may be required. The authors and editors of the material here-in have consulted sources believed to be reliable in their efforts to provide information that is complete and in accord with the standards accepted at the time of publication. However, in view of the possibility of human er-ror by the authors, editors, or publisher of the work herein, or changes in
medical knowledge, neither the authors, editors, or publisher, nor any other party who has been involved in the preparation of this work, warrants that the information contained here in is in every respect accurate or complete, and they are not responsible for any errors or omissions or for the results obtained from use of such information. Because of rapid advances in the medical sciences, independent verification of diagnoses and drug dosages should be made. Readers are encouraged to confirm the information con-tained herein with other sources. For example, readers are advised to check the product information sheet included in the package of each drug they plan to administer to be certain that the information contained in this publi-cation is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. This recommendation is of particular importance in connection with new or infrequently used drugs.
Although all advertising material is expected to conform to ethical (medical) standards, inclusion in this journal does not constitute a guar-antee or endorsement of the quality or value of such product or of claims made by its manufacturer.
Copyright © 2019 by Thieme Revinter Publicações Ltda Inc. RBGO Gynecology and Obstetrics/Revista Brasileiro de Ginecologia e Obstetrícia is published monthly by Thieme-Revinter Publicações Ltda., Rua do Matoso, 170, Rio de Janeiro 20270-135, Brazil.
Editorial comments should be sent to [email protected]. Articles may be submitted to this journal on an open-access basis. For further informa-tion, please send an e-mail to [email protected]. The content of this journal is available online at www.thieme-connect.com/products. Visit our Web site at www.thieme.com and the direct link to this journal at www.rbgo.com.br.
Revista Brasileiro de Ginecologia e Obstetrícia is an official publication of the Federação Brasileira das Associações de Ginecologia e Obstetrícia (Brazilian Federation of Association of Gynecology and Obstetrics, Febrasgo), It is listed in Isi - Web of Science, Web of Knowledge (Emerging), MEDLINE /PubMed, Index Medicus, Scopus (Sci Verse), SCImago, SciELO (Scientific Electronic Library Online), LILACS (Literatura Latino-Americana e do Caribe em Ciências da Saúde, Index Medicus Latino Americano), and Portal de Periódicos Capes (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior). Thieme Medical Publishers is a member of the CrossRef initiative.
ISSN 0100-7203
Complementary material is available online at www.rbgo.org.br.

Editorial
Androgen Abuse among Recreational AthletesMaíta Poli de Araujo1
1Department of Gynecology, Escola Paulista de Medicina,Universidade Federal de São Paulo, São Paulo, SP, Brazil
Rev Bras Ginecol Obstet 2019;41:679–681.
Amateur sports are the most popular form of physicalactivity in the world. While the media places its attentionon professional sports leagues or the Olympic Games, forevery professional athlete of a certain sport there are thou-sands of people who play the same sport to meet theirpersonal needs and fitness requirements.1
In women, regular and adequate levels of physical activityimprove themuscular and cardiorespiratory systems, reducethe risk of hypertension, coronary heart disease, stroke,diabetes, breast cancer and depression, and are essential toweight control.
However, in order to look thinner and athletic in a shortamount of time, the use of performance enhancing substan-ces has increased significantly. Among these substances,androgens are very attractive.
Androgen abuse epidemiology is higher in recreationalsportspeople living inEurope,NorthAmerica (theUnitedStates),Oceania (Australia and New Zealand), and South America(Brazil), and lower in Africa and Asia. A recent meta-analysisestimated that the lifetimeprevalenceofperformancesubstanceabuse worldwide is of 18.4% among recreational athletes.2
Androgens are hormones that have anabolic properties,with a direct effect on muscle hypertrophy, increased me-tabolism, and lipolysis. Testosterone is a 19-carbon steroid,and is the most potent endogenous androgen. Anabolicandrogenic steroids (AASs) are synthetic compounds thatresemble the natural hormone testosterone.3
Some athletes use AASs continuously, but others try tominimize their possible adverse effects through differentpatterns of use, as in the following:4
• Cycling: Users take AASs in cycles of 6 to 12 weeksfollowed by 4 weeks to several months off.
• Stacking: Users combine several different types of ste-roids or incorporate other supplements to maximize theeffectiveness of the steroids.
• Pyramiding: Users gradually increase the dose to a peak,and then reduce the amount.
Androgens and AASs can be taken orally (methandienone,stanozolol, and oxandrolone, for example), as pelletsimplanted under the skin (pharmaceutical compounding),by injection (nandrolone decanoate and testosterone cypio-nate, for example), or through the skin as a cream or gel(testosterone). In sports, endogenous AASs, theirmetabolitesand their isomers, when administered exogenously, areprohibited inmales and females.5 Testosteronemay promoteathletic performance not only through its long-term anabolicactions, but also by acting on specific substrates in the brainto increase aggression and motivation for competition.
Illicit steroidsmay be sold at gyms, sporting competitions,and via mail order, and buyers may be at risk of receivingadulterated or contaminated products. Anabolic androgenicsteroids are also often illegally sourced from pharmacies orsynthesized in clandestine laboratories.6
The amateur athletes who most often use anabolicsteroids are runners, followed by bodybuilders, cyclists,and weightlifters. The use commonly begins around age 20,and a typical user has at least 1 year of experience training.Most of them are aware of the risks, but believe that theside effects are temporary.6 An extensive range of seriousside effects is associated with abuse of anabolic steroids(►Fig. 1).7
The most frequently reported adverse effects amongfemale athletes include menstrual irregularities, clitoro-megaly, libido changes, uterine atrophy, hirsutism, alope-cia, and deepening of the voice. Adverse effects on thefemale reproductive systemmay occur due to depression ofgonadotropin release either by direct action on the pitui-tary gland or by suppression of the hypothalamic GnRHrelease.8
These adverse effectsmay initiate after months (menstru-al disorders, acne, and alopecia, for example), and they can bereversible (alopecia and amenorrhea, for example) or irre-versible (voice and clitoris changes, for example).
Several factors, such as the type of sport, exerciseintensity, energy balance, fat composition, irregular eating
Address for correspondenceMaíta Poli de Araujo, MD, PhD,Departamento de Ginecologia,Escola Paulista de Medicina,Universidade Federal de SãoPaulo, Rua Botucatu 740, VilaClementino, São Paulo, SP,04023-061, Brazil(e-mail: [email protected]).
DOI https://doi.org/10.1055/s-0039-3401007.ISSN 0100-7203.
Copyright © 2019 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Editorial 679

behavior, and emotional stress may contribute to a state ofhypogonadotropic hypogonadism in female athletes, evenwithout AAS abuse. However, health professionals andamateur athletes should know that prolonged periods ofhypogonadism may lead to severe adverse health conse-quences, such as effects on mood and memory, lipid abnor-malities, low bone mineral density, atherosclerosis, andincreased cardiovascular risk.9
Animal model studies have shown that some androgens(mainly those injectable) affect the sexual cycle and promotehistological alterations in the ovaries and uterus. Destructionof follicular units and an absence of corpus luteum in theovaries and vacuolated epithelium and endometrial stromafibrosis of the uterus have been observed. Although there areno controlled studies in humans, these findings are impor-tant to guide amateur athletes using anabolic steroids abouttheir reproductive future.10
Certainly, each athlete will always be responsible for theirbody and the decision to use illicit steroids. The same goes forhow people will use social media and other technologies.However, the use of AASs seems to involve other characters,such as doctors, digital influencers, bloggers, nutritionists,coaches, and backroom laboratories, and that makes it a socialand public health problem.
In conclusion, androgen abuse by recreational athletes isan emerging issue that may need special attention on the
part of gynecologists to manage the collateral effects andpreserve fertility.
References1 Henning AD, Dimeo P. The new front in the war on doping:
Amateur athletes. Int J Drug Policy 2018;51:128–136. Doi:10.1016/j.drugpo.2017.05.036
2 Sagoe D, Pallesen S. Androgen abuse epidemiology. Curr OpinEndocrinol Diabetes Obes 2018;25(03):185–194. Doi: 10.1097/MED.0000000000000403
3 Hoffman JR, Ratamess NA. Medical issues associated with anabol-ic steroid use: are they exaggerated? J Sports Sci Med 2006;5(02):182–193
4 Locquet M, Beaudart C, Larbuisson R, et al. Self-administration ofmedicines and dietary supplements among female amateur run-ners: a cross-sectional analysis. Adv Ther 2017;33(12):2257-–2268. Doi: 10.1007/s12325-016-0426-2
5 De Rose EH, Aquino Neto FR, Moreau RLM, Castro RRT. Anti-doping control in Brazil: results from the year of 2003 andprevention activities. Rev Bras Med Esporte 2004;10:289–293.Doi: 10.1590/S1517-86922004000400006
6 Lazuras L, Barkoukis V, Loukovitis A, et al. “I want it all, and I wantit now”: Lifetime prevalence and reasons for using and abstainingfrom controlled Performance and Appearance Enhancing Sub-stances (PAES) among young exercisers and amateur athletes infive European Countries. Front Psychol 2017;8:717. Doi: 10.3389/fpsyg.2017.00717
7 Nieschlag E, Vorona E. Doping with anabolic androgenic steroids(AAS): Adverse effects on non-reproductive organs and functions.
Fig. 1 Side effects associated with anabolic steroid abuse in female athletes.
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Editorial680

Rev Endocr Metab Disord 2015;16(03):199–211. Doi: 10.1007/s11154-015-9320-5
8 Christou MA, Christou PA, Markozannes G, Tsatsoulis A, Mastor-akos G, Tigas S. Effects of anabolic androgenic steroids on thereproductive system of athletes and recreational users: a system-atic review and meta-analysis. Sports Med 2017;47(09):1869-–1883. Doi: 10.1007/s40279-017-0709-z
9 Nieschlag E, Vorona E. MECHANISMS IN ENDOCRINOLOGY: Med-ical consequences of doping with anabolic androgenic steroids:
effects on reproductive functions. Eur J Endocrinol 2015;173(02):R47–R58. Doi: 10.1530/EJE-15-0080
10 Mobini Far HR, Agren G, Lindqvist AS, Marmendal M, Fahlke C,Thiblin I. Administration of the anabolic androgenic steroidnandrolone decanoate to female rats causes alterations in themorphology of their uterus and a reduction in reproductivecapacity. Eur J Obstet Gynecol Reprod Biol 2007;131(02):189–197. Doi: 10.1016/j.ejogrb.2006.07.037
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Editorial 681

Risks of Maternal Obesity in Pregnancy: A Case-controlStudy in a Portuguese Obstetrical Population
Riscos da obesidade materna na gravidez: um estudocaso-controle em uma oopulação obstétrica portuguesaPatrícia Alves1,2 Maria Filipa Malheiro1 João Cavaco Gomes1 Tiago Ferraz1,3,4
Nuno Montenegro1,3,5
1Department of Obstetrics and Gynecology, Centro HospitalarSão João, Porto, Portugal
2Department of Gynecology and Obstetrics, Centro Hospitalar deTrás-os-Montes and Alto Douro, Vila Real, Porto, Portugal
3Medicine Faculty, Universidade do Porto, Porto, Portugal4 I3S Innovation in Health and Investigation Institute, Universidade doPorto, Porto, Portugal
5Epidemology Research Unit, Institute of Public Health, Universidadedo Porto, Porto, Portugal
Rev Bras Ginecol Obstet 2019;41:682–687.
Address for correspondence Patrícia Alves, MD, Department ofObstetrics and Gynecology, Centro Hospitalar de Tr�as-os-Montes eAlto Douro, Avenida da Noruega, Lordelo, 5000-508, Vila Real, Porto,Portugal (e-mail: [email protected]).
Keywords
► cesarean section► diabetes gestational► fetal macrosomia► obesity► high-risk pregnancy
Abstract Objective The present study aims to understand to what extent obesity is related toadversematernal, obstetrical, andneonatal outcomes inaPortugueseobstetrical population.Methods A retrospective case-control study was conducted at the Department ofObstetrics of a differentiated perinatal care facility. The study compared 1,183 obesepregnant womenwith5,399normalor underweightpregnant women for theoccurrenceofgestational diabetes, hypertensive pregnancy disorders, and preterm birth. Mode ofdelivery, birthweight, andneonatal intensive careunit (ICU) admissionswerealsoevaluated.Mean blood glucose values were evaluated and compared between groups, in the firstand second trimesters of pregnancy. Only singleton pregnancies were considered.Results The prevalence of obesity was 13.6%. Obese pregnant women were significantlymore likely to have cesarean sections (adjusted odds ratio [aOR] 2.0, p< 0.001), gestationaldiabetes (aOR 2.14, p< 0.001), hypertensive pregnancy disorders (aOR 3.43, p< 0.001),and large-for-gestational age or macrosomic infants (aOR 2.13, p< 0.001), and less likely tohave small-for-gestational age newborns (aOR 0.51, p< 0.009). No significant differenceswere found in termsof pretermbirths, fetal/neonatal deaths, lowbirthweight newborns, andneonatal ICU admissions among cases and controls. Maternal obesity was significantlyassociated with higher mean blood glucose levels, in the first and second trimesters ofpregnancy.Conclusion Obesity is associated with increased risks of adverse pregnancy andneonatal outcomes. These risks seem to increase progressively with increasing bodymass index (BMI) class. Female obesity should be considered amajor public health issueand has consequences on maternal-fetal health.
receivedJuly 3, 2019acceptedOctober 9, 2019
DOI https://doi.org/10.1055/s-0039-3400455.ISSN 0100-7203.
Copyright © 2019 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Original ArticleTHIEME
682

Introduction
The World Health Organization (WHO) considers obesity aworldwide epidemic and one of the greatest public healthchallenges of the 21st century. According to the WHO, in2016, across Europe, 24.5% of women aged � 18 years oldwere obese.1 In the same year, in Portugal, the prevalencewas 21.2% and represented a 3-fold rise since 1975 (6.8%).2,3
The etiology of obesity is multifactorial and complex.Obesity is related to genetic predisposition, physiologicalchanges to the endocrine system of the body, potentialgenetic contributions over generations, cultural beliefs,and socioeconomic issues.4
Obesityhasamajor impactonbothmorbidityandmortality.Obesity is a risk factor for type 2 diabetes mellitus (DM),hypertension, dyslipidemia, and coronary heart disease. Also,obesity decreases quality of life because of associated mooddisorders, such as anxiety and depression, and aggravatedosteoarticular complaints.4,5
In pregnancy, obesity is a risk factor for adverse maternal,obstetrical, and fetal/neonatal outcomes, contributing toprolonged hospitalization periods, both for the mother andthe baby.4,6 Obesity increases risks of venous thromboem-
bolism, gestational diabetes, preeclampsia, dysfunctionallabor, cesarean delivery, postpartum hemorrhage, woundinfection, miscarriage, fetal/neonatal death, and abnormalfetal growth, either macrosomia or growth restriction.7,8
Moreover, children of obese parents have a two to threetimes higher risk of becoming obese adults. It seems that thein utero environment plays a causative role in this viciouscycle.4
Obesity in pregnancy is defined as a body mass index(BMI) equal to or greater than 30 Kg/m2 at the first prenatalvisit. It is further subclassified in: class I (30.0–34.9 Kg/m2),class II (35.0–39.9 Kg/m2), and class III (� 40 Kg/m2).8
The aim of the present study was to understand to whatextent obesity is related to adversematernal, obstetrical, andneonatal outcomes in a Portuguese obstetrical population.
Methods
Study DesignThis retrospective case-control study was conducted using4 years of data of women who gave birth at the Departmentof Obstetrics of a differentiated perinatal care UniversityHospital, between January 2013 and December 2016. Only
Resumo Objetivo O presente estudo pretende avaliar em que medida a obesidade influenciaos desfechos maternos, obstétricos e neonatais em uma população obstétricaportuguesa.Métodos Um estudo caso-controle retrospectivo foi realizado no departamento deobstetrícia de um centro perinatal diferenciado. O estudo comparou 1.183 grávidasobesas com 5.399 grávidas normoponderais ou com baixo peso para a ocorrência dediabetes gestacional, doenças hipertensivas da gravidez e parto pré-termo. Via departo, peso ao nascimento e admissão na unidade de cuidados neonatais tambémforam avaliados. Os valores glicêmicos médios foram avaliados e comparados entre osdois grupos, no primeiro e segundo trimestres de gravidez. Apenas as gravidezesunifetais foram avaliadas.Resultados A prevalência da obesidade foi de 13.6%. As grávidas obesas tiveram riscosignificativamente superior a ter uma cesariana (odds ratio ajustado [Ora] 2.0,p< 0.001), diabetes gestacional (ORa 2.14, p< 0.001), doenças hipertensivas dagravidez (ORa 3.43, p< 0.001), recém-nascidos grandes para a idade gestacional oumacrossômicos (ORa 2.13, p< 0.001) e menor probabilidade de ter recém-nascidospequenos para a idade gestacional (ORa 0.51, p< 0.009). Não houve diferençaestatisticamente significativa quanto aos partos pré-termo, mortes fetais/neonatais,baixo peso ao nascer e admissão à unidade de cuidados intensivos neonatais. O oddsratio foi ajustado para a idade, número de gestações, paridade, ganho ponderal,doenças hipertensivas da gravidez e diabetes gestacional. A obesidade materna estevesignificativamente associada a valores glicêmicos médios superiores, no primeiro esegundo trimestres de gravidez.Conclusão A obesidade está associada a maior risco de desfechos adversos nagravidez e neonatais. Este risco parece aumentar progressivamente com o aumentodo índice de massa corporal (IMC). A obesidade feminina deve ser considerada umimportante problema de saúde pública e que tem repercussões na saúde materno-fetal.
Descritores
► cesariana► diabetes
gestacional► macrossomia fetal► obesidade► gravidez de alto
risco
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Risks of Maternal Obesity in Pregnancy Alves et al. 683

singleton pregnancies were considered. Ethics approval wasobtained from the Ethics Committee of our hospital.
Atotalof9,371participantswereselected. InformationaboutBMI at the first prenatal visit was lacking from 659 medicalrecords and these pregnant women were promptly excluded.Theremaining8,712pregnantwomenwerecategorizedaccord-ing to WHO BMI categories, based on the registered weight atthe first prenatal visit.8 Overweight women (n¼ 2,130) werefurther excluded to get a more accurate comparison, becauseoverweight pregnant women are predisposed to obesity.Thefinal analysis included6,582singletonpregnancies:Agroupof 1,183 obese pregnant women (cases) were compared with agroup of 5,399 normal or underweight pregnant women (con-trols) for maternal, obstetrical, and neonatal outcomes.
Data CollectionMaternal, obstetrical, and perinatal data from singletonpregnant women who gave birth in the maternity facility,irrespective of type of pregnancy follow-up, were collectedfrom Obscare (Virtual Care, System for life, Porto, Portugal),an institutional medical record software for obstetriciansand pediatricians.
Variables DescriptionInformationwas collected onwomen’s age, parity, weight (atthe first and last prenatal visits), and BMI (Kg/m2) at the firstprenatal visit. The weight gain was calculated from thedifference inweight between the last and first prenatal visitsand used as a continuous variable.
Gestational diabetes was diagnosed according to the Inter-national Association of the Diabetes and Pregnancy StudyGroups criteria (IADPSGC).9Hypertensive pregnancy disorders(gestational hypertension and preeclampsia) were consideredwhenmaternalbloodpressurewas�140mmHg(systolic)or�90mm Hg (diastolic) on two occasions, at least 4 hours apart,after 20 weeks of gestation, in a woman with a previouslynormal bloodpressure.10Other variables studiedwere deliverymode, fetal demise, gestational age at birth, birth weight,Apgar score, neonatal intensive care unit admission, and neo-natal death. Preterm birth was classified as extreme preterm(24–28 weeks), very preterm (29–32 weeks), and moderate/late preterm (32–36 weeks). After this categorization of pre-term birth, it has also been grouped to be estimated as adichotomous variable – preterm and term births. An updatedand validated Portuguese birthweight chart was used to obtainbirthweight percentiles.11 Newborns were classified as smallfor gestational age (SGA)whenbirthweightwas< 10th percen-tile for the gestational age, and as large for gestational age (LGA)when the birth weight was� 90th percentile. Low birthweightwas considered when infants weighed � 2,500 g, and macro-somia when they weighed � 4,000 g. Gestational diabetes,hypertensivepregnancydisorders, deliverymode, fetal demise,neonatal intensive care unit admission, and neonatal deathwere evaluated as dichotomous variables.
Blood glucose values, in the first (fasting) and second(fasting, 1 and 2 hours after 75 g glucose load) trimesters ofpregnancy were evaluated and compared between groups, ascontinuous variables.
Statistical AnalysisDescriptive statistics were performed for demographic, clin-ical, and laboratory data. Mean and standard deviation (SD)were calculated for normally distributed variables. For groupcomparisons, parametric (t test student and analysis ofvariance [ANOVA]), and nonparametric tests (Mann-Whitneytest) were used, as appropriate, for continuous variables, andthe Pearson Chi2 test for categorical variables.
Logistic or linear regression analysis, as appropriate, forunivariate andmultivariatemodels were used for each of theoutcomes. Odds ratio (OR) was adjusted for age, number ofgestations, parity, weight gain, hypertensive pregnancy dis-orders, and gestational diabetes. All of the results wereconsidered significant if the p-value was< 0.05. Statisticalanalyses were performed using Stata version 12.1 (StataCorp, College Station, TX, USA).
Results
The prevalence of obesity in the obstetrical populationstudied, as registered in the first prenatal visit, was 13.6%,and the mean BMI was 24.7 Kg/m2 (►Table 1).
►Table 2 summarizes maternal characteristics. The obesegroup of women was significantly older, more frequentlymultiparous, and gained less weight during pregnancy thannormal or underweight women.
Obese women had a significantly higher prevalence ofgestational diabetes (17.6% versus 5.5%, adjusted odds ratio[aOR] 2.14; 95% confidence interval [CI]: 1.53–3.00) andhypertensive pregnancy disorders (9.0% versus. 2.6%, aOR3.43; 95%CI: 2.33–5.12). Concerning the mode of delivery,the cesarean section rate was significantly more frequent inthe obesity group compared with the control group (35.3%versus 24.4%). After adjusting for confounders, obese pregnantwomen had twice the odds of delivering by cesarean (aOR 2.0;95%CI: 1.64–2.47) compared with normal or underweightwomen. The difference was even more significant amongprimigravidae (aOR 2.27; 95%CI: 1.65–3.11). No differenceswere found in preterm birth rates between the 2 groups (8.3%versus 7.1%, obesity and control groups respectively, p¼ 0.17).The mean birth weight was significantly higher in the obesegroup (3,226� 531 g) compared with the control group(3,132� 506 g). Large for gestational age and macrosomic
Table 1 Distribution of pregnant women by body mass indexcategory
BMI category (Kg/m2) Number (prevalence %)
Underweight (< 18.5) 325 (3.7)
Normal weight (18.5–24.9) 5074 (58.2)
Overweight (25.0–29.9) 2130 (24.5)
Obesity 1183 (13.6)
Obesity class I (30.0–34.9) 819 (9.4)
Obesity class II (35.0–39.9) 268 (3.1)
Obesity class III (�40) 96 (1.1)
Abbreviation: BMI, body mass index.
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Risks of Maternal Obesity in Pregnancy Alves et al.684

newborns were significantly more prevalent among obesewomen (12.8% versus 6.9%, aOR 2.13; 95%CI: 1.54–2.96; and6.4% versus 3.2%, aOR 2.94, 95%CI: 1.95–4.45, respectively),even when adjusted for age, parity, weight gain, gestationaldiabetes, and hypertension. Considering the morbidly obesepregnant women (BMI � 40 Kg/m2), the risk of having amacrosomic newborn was> 9 times higher than that of anormal or underweight pregnant woman (aOR 9.5; 95%CI:3.7–24.6) (►Table 3). In contrast, obese pregnant women hadsignificantly fewer SGA newborns (9.7% versus. 12.1%,p¼ 0.009), but no statistical significant difference wasobserved for the low birthweight variable.
According to a local institutional policy, immediate post-partum umbilical cord blood gas analysis is performed onlyin cases of suspected fetal hypoxia/acidosis. In a total of 4,388tests, fetal acidemia (pH< 7.2 in umbilical artery) was morefrequently found in the obese group of women (8.9% versus6.7%, p¼ 0.008), but no differences were found among thegroups for severe acidemia (pH< 7.05 in the umbilicalartery). Apgar score< 7 at 5minutes was identical in bothgroups (1.2%, p¼ 0.95), and even though more newbornsfrom obese women were admitted to the neonatal intensivecare unit (ICU), the differencewas not statistically significant(6.8 versus 5.6%, p¼ 0.23).
Fetal and neonatal death rates were not significantlydifferent between obese pregnant women (n¼ 4, 0.3%) com-pared with the normal or underweight pregnant woman(n¼ 32, 0.6%).
►Table 3 presents maternal, obstetrical, and neonataloutcomes according to obesity class. The risk of gestationaldiabetes, hypertensive pregnancy disorders, cesarean deliv-ery, LGA, and macrosomic infants increased with increasingBMI class. In contrast, the odds of low birth weight and SGAinfants decreased with increasing BMI class.
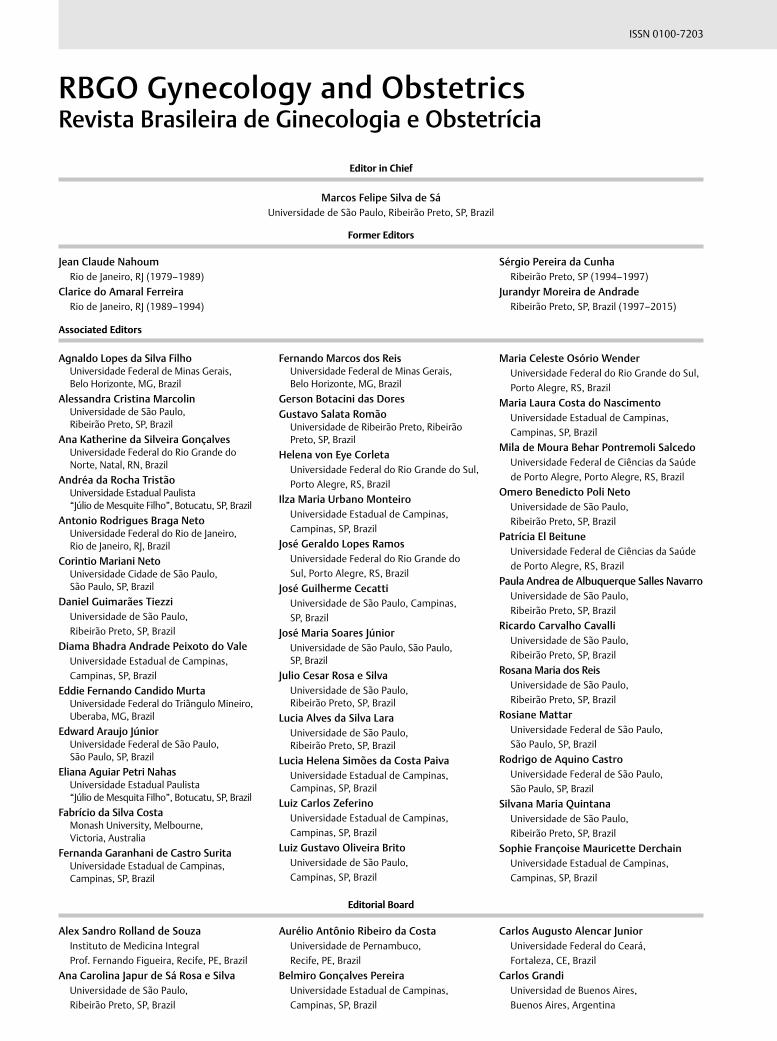
Blood glucose levels were significantly higher for obesepregnant women compared with normal or underweightwomen (p< 0.001) (►Table 4). Also, mean blood glucose
Table 2 Maternal characteristics
Obesity group (n¼ 1,183) Control group (n¼ 5,399) OR p-value
Age (years old) (mean, SD) 31.5 (5.5) 30.7 (5.6) – < 0.001
Age> 35 years old (%) 32 26 1.37 (1.2–1.57) < 0.001
Number of gestations (n‡) 2.1 1.8 – < 0.001
Nulliparous (%) 35 47.5 0.59 < 0.001
BMI (kg/m2) (mean, SD) 34.1 (3.9) 21.7 (4.9) – < 0.001
Weight gain (kg) (mean, SD) 10.5 (6.8) 14.3 (4.9) – < 0.001
Abbreviations: BMI: body mass index; kg: kilograms; n: number; OR: odds ratio; SD: standard deviation.
Table 3 Risks of maternal, obstetrical and neonatal outcomes according to obesity class
Control Obesity class I Obesity class II Obesity class III
aOR aOR (95%CI) aOR (95%CI) aOR (95%CI)
Gestational diabetes Ref 1.98 (1.35–2.9) 2.42 (1.37–4.26) 2.1 (0.92–4.80)
Hypertensive pregnancy disorders Ref 3.52 (2.27–5.45) 2.54 (1.10–5.85) 6.38 (2.49–16.35)
Cesarean section Ref 1.78 (1.41–2.25) 2.61 (1.77–3.85) 3.19 (1.79–5.71)
SGA Ref 0.59 (0.41–0.84) 0.62 (0.35–1.10) 0.1 (0.02–0.50)
Low-birthweight infant Ref 0.71 (0.49–1.03) 0.45 (0.24–0.85) 0.08 (0.20–0.38)
LGA Ref 1.69 (1.17–2.44) 3.93 (2.36–6.60) 7.0 (3.42–14.30)
Macrosomia Ref 2.25 (1.35–3.74) 5.02 (2.47–10.20) 9.53 (3.70–24.60)
Abbreviations: aOR, adjusted odds ratio; LGA, Large for gestational age; Ref, reference value; SGA, Small for gestational age.All variables are adjusted for age, number of gestations, parity, weight gain, hypertensive pregnancy disorders, gestational diabetes.
Table 4 Blood glucose levels (mg/dL)
Obesitygroup(mean, SD§)
Controlgroup(mean, SD)
p-value
1st trimesterfasting
83.5 (9.0) 79.3 (7.2) < 0.001
2nd trimesterfasting
77.8 (9.4) 73.8 (17.4) < 0.001
2nd trimester1-hourafter OGTT¶
127.6 (31.3) 113.9 (29.3) < 0.001
2nd trimester2 hoursafter OGTT¶
109 (26.6) 98.6 (24.9) < 0.001
Abbreviation: SD, standard deviation.¶OGTT (oral tolerance glucose test), 75 gr glucose load (fasting, 1 and2 hours after), at 24–28 weeks.
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Risks of Maternal Obesity in Pregnancy Alves et al. 685
levels were found to progressively increase with increasingclass of obesity (►Table 5).
Discussion
Our study reported a 13.6% prevalence ofmaternal obesity ina Portuguese population of 6,582 singleton pregnancies. Sofar, this information concerning specifically a Portugueseobstetrical population was unavailable.
Obese pregnant women included in the analysis weresignificantly older and more frequently multiparous thannormal or underweight women, reflecting a progressivetendency for weight gain with increasing age and parity.12
Excessive weight gain during pregnancy is a hallmark ofpoor metabolic control and favors adverse pregnancy out-comes.7,8 The 2013 American College of Obstetricians andGynecologists (ACOG)13 recommendations for weight gainduring pregnancy for obese women was between 5 and9.1 Kg. In our study, the average weight gain during preg-nancy in obese women exceeded the maximum allowed(10.5 Kg). This finding should alert Portuguese physiciansinvolved in women’s and antenatal medical care to specifi-cally address prevention and management of obesity,through nutritional changes, physical conditioning, and pro-motion of healthy lifestyle changes.
The results from the present study support the fact thatmaternal obesity is a major risk factor for adverse pregnancyand perinatal outcomes.
We demonstrated that gestational diabetes is twice aslikely for obese pregnant women, which is somewhat lowerthan the odds reported in the literature (OR 3.6–7.5).7,14 Wealso demonstrated increases in mean blood glucose levels,during the first and second trimesters of pregnancy, withincreasing BMI class. The HAPO study explained this meta-bolic change through increases in insulin resistance withhigher BMI values and suggested that gestational diabetesand obesity seem to share common metabolic features,such as increased insulin resistance, hyperglycemia, andhyperinsulinemia.15
Hypertensive pregnancy complications were also morelikely to occur in obese pregnant women and, specifically, inthe morbidly obese pregnant women (BMI> 40 Kg/m2) (aOR6.38; 95%CI: 2.49–16.35) (►Table 3). Analogously, anAustralian study demonstrated that obese pregnant women
had 3 times the odds of having a hypertensive disorderduring pregnancy, and the risk was even higher among themorbidly obese (OR 4.87; 95% CI: 3.27–7.24).12
In our study, maternal obesity was an independent riskfactor for deliveringmacrosomic and LGA infants. In contrast,maternal obesity reduced the risk of SGA or low birthweightnewborns.16
Cesarean delivery rates have been increasing over the past30 years in both developed and developing countries. InPortugal, by the year 2011, cesarean sections accounted for35% of total deliveries.17 These high rates led to the creation,in 2013, of a National Committee for Safe Motherhood andNewbornHealth to try to counteract this tendency toward anunnatural way of birth.18 In accordance with the publishedliterature, our study demonstrated a negative influence ofmaternal obesity on delivery mode, favoring cesarean sec-tion (►Table 3).7,19,20 Obese pregnant women were twotimes more likely to have cesarean sections compared withnormal or underweight women, and the odds were threetimes higher for the morbidly obese. This difference per-sisted even when considering only primigravidae, whichexcluded the effect caused by obstetric history, such ascesarean section. So, the increase inmaternal obesity furthercontributes to the present difficulty in achieving the 2015WHO’s goal for a cesarean section rate of 10 to 15%.17
In the literature, there is controversy regarding the asso-ciation between maternal obesity and preterm birth.7,12,16
Our study found similar rates of preterm birth for both obeseand normal or underweight women.
Our study did not demonstrate increased rates of fetal orneonatal death in the obese group of women, which isdifferent from what is already published.7,8,16 This resultmay be explained by the number of obese women, whichmay have been insufficient to evaluate infrequent adverseobstetrical and neonatal events such as fetal or neonataldeath.
The present study has further limitations. First, the presentfindings were derived from a single maternity hospital inPortugal, so that, despite the large sample, limited generaliza-tion is possible. Also, the study is a retrospective comparativeanalysis of maternal, obstetrical, and neonatal data, and somedata could not be collected. For example, in an unknownpercentage of medical records, maternal weight, as registeredin the first prenatal visit, may not have been objectively
Table 5 Blood glucose levels (mg/dL) according to obesity class
Control(χ� SD‡)
Obesity class I(χ� SD)
Obesity class II(χ� SD‡)
Obesity class III(χ� SD)
p-value(ANOVA)
1st trimester fasting 79.3 (7.2) 82.5 (8.6) 85.5 (10.1) 86.1 (8.5) < 0.001
2nd trimester fasting 73.8 (17.4) 77.5 (9.8) 77.9 (8.1) 80.0 (7.5) < 0.001
2nd trimester 1-hour after OGTT† 113.9 (29.3) 127 (32.2) 128.1 (28.5) 132.2 (28.7) < 0.001
2nd trimester 2 hours after OGTT† 98.6 (24.9) 108.8 (29.9) 109.8 (27.3) 109.1 (22.1) < 0.001
Abbreviations: ANOVA, .Analysis of variances model; SD, standard deviation.†OGTT (oral tolerance glucose test), 75 gr glucose load (fasting, 1 and 2 hours after), at 24–28 weeks.‡χ: mean.
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Risks of Maternal Obesity in Pregnancy Alves et al.686

measured, leading to self-reported errors concerning thisimportant variable.16
This is thefirst Portuguese study that specifically addressedmaternal, obstetrical, and neonatal outcomes in a populationof singleton obese pregnant women and compared themwiththose of normal or underweight pregnant women.
Conclusion
In accordance with the published literature, the present retro-spective case-control study was able to demonstrate thatobesity is associatedwith increased odds of adverse pregnancyand neonatal outcomes, such as gestational diabetes, hyper-tensive pregnancy disorders, cesarean section, macrosomia,and LGA newborns. Moreover, the occurrence of adverse out-comes increased progressively with increasing BMI class. Toconclude, the results of our study reinforce the fact that it isimperative to consider female obesity as a major public healthissue and to take measures to prevent and treat this condition,specifically among woman of childbearing age.
ContributionsAll of the the authors contributed to the conception of thework and data collection. The analysis and interpretationof data was done by Alves P., Ferraz T., Malheiro M. F. andGomes J. C.. The initial writing of the article was made byAlves P., Ferraz T. and Malheiro M. F. and was reviewed byProfessor Montenegro N. and Gomes J. C.. All of theauthors approved the final version of the article.
Conflicts of InterestsThe authors have no conflicts of interests to declare.
References1 World Health Organization. Global Health Observatory Data Repos-
itory. Prevalence ofObesity AmongAdults, BMI� 30, Age-Standard-ized Estimates by WHO Region: Europe: 2016. Geneva: WorldHealth Organization; 2017http://apps.who.int/gho/data/view.main.REGION2480A?lang¼en. Accessed February 19, 2019.
2 World Health Organization. Global Health Observatory Data Re-pository. Prevalence of Obesity Among Adults, BMI� 30, Age-StandardizedEstimates by Country: Portugal: 2016. Geneva:WorldHealth Organization; 2017http://apps.who.int/gho/data/view.main.CTRY2450A?lang¼en. Accessed May 12, 2018.
3 Sardinha LB, Santos DA, Silva AM, et al. Prevalence of overweight,obesity, and abdominal obesity in a representative sample ofPortuguese adults. PLoS One 2012;7(10):e47883. Doi: 10.1371/journal.pone.0047883
4 Mitchell S, Shaw D. The worldwide epidemic of female obesity.Best Pract Res Clin Obstet Gynaecol 2015;29(03):289–299. Doi:10.1016/j.bpobgyn.2014.10.002
5 Branca F, Nikogosian H, Lobstein T. The Challenge of Obesity in theWHO European Region and the Strategies for Response: Summa-ry. Copenhagem: World Health Organization; 2007
6 Mamun AA, Callaway LK, O’Callaghan MJ, et al. Associations ofmaternal pre-pregnancy obesity and excess pregnancy weightgains with adverse pregnancy outcomes and length of hospitalstay. BMC Pregnancy Childbirth 2011;11:62. Doi: 10.1186/1471-2393-11-62
7 Lim CC, Mahmood T. Obesity in pregnancy. Best Pract Res Clin ObstetGynaecol2015;29(03):309–319.Doi:10.1016/j.bpobgyn.2014.10.008
8 The American College of Obstetricians and Gynecologists. ACOGPractice Bulltein No 156: obesity in pregnancy. Obstet Gynecol2015;126(06):e112–e126. Doi: 10.1097/AOG.0000000000001211
9 Metzger BE, Gabbe SG, Persson B, et al; International Associationof Diabetes and Pregnancy Study Groups Consensus Panel. Inter-national association of diabetes and pregnancy study groupsrecommendations on the diagnosis and classification of hyper-glycemia in pregnancy. Diabetes Care 2010;33(03):676–682. Doi:10.2337/dc09-1848
10 American College of Obstetricians and Gynecologists. Task Forceon Hypertension in Pregnancy. Classification of hypertensivedisorders. In: American College of Obstetricians and Gynecolo-gists. Task Force on Hypertension in Pregnancy. Hypertension inPregnancy. Washington, DC: ACOG; 2013:13–15
11 Sousa-Santos RF,Miguelote RF, Cruz-Correia RJ, Santos CC, BernardesJF. Development of a birthweight standard and comparison withcurrentlyusedstandards.What is a10thcentile?Eur JObstetGynecolReprod Biol 2016;206:184–193. Doi: 10.1016/j.ejogrb.2016.09.028
12 Callaway LK, Prins JB, Chang AM, McIntyre HD. The prevalenceand impact of overweight and obesity in an Australian obstetricpopulation. Med J Aust 2006;184(02):56–59. Doi: 10.5694/j.1326-5377.2006.tb00115.x
13 AmericanCollege of Obstetricians andGynecologists. ACOGCommit-tee opinion no. 548: weight gain during pregnancy. Obstet Gynecol2013;121(01):210–212.Doi: 10.1097/01.AOG.0000425668.87506.4c
14 Ovesen P, Rasmussen S, Kesmodel U. Effect of prepregnancy mater-nal overweight and obesity on pregnancy outcome. Obstet Gynecol2011;118(2 Pt 1):305–312. Doi: 10.1097/AOG.0b013e3182245d49
15 Catalano PM, McIntyre HD, Cruickshank JK, et al; HAPO StudyCooperative Research Group. The hyperglycemia and adversepregnancy outcome study: associations of GDM and obesitywith pregnancy outcomes. Diabetes Care 2012;35(04):780–786.Doi: 10.2337/dc11-1790
16 Baeten JM, Bukusi EA, Lambe M. Pregnancy complications andoutcomes among overweight and obese nulliparous women. Am JPublic Health 2001;91(03):436–440. Doi: 10.2105/ajph.91.3.436
17 World Health Organization. Human Reproduction Programme.WHO Statement on Cesarean Section Rates. Geneva: WHO; 2015
18 OECD. Caesarean sections. In: OECD. Health at a Glance 2013:OECD Indicators. Paris: OECD; 2013:98–99
19 Kominiarek MA, Vanveldhuisen P, Hibbard J, et al; Consortium onSafe Labor. The maternal body mass index: a strong associationwith delivery route. Am J Obstet Gynecol 2010;203(03):264.e1–264.e7
20 Al-Kubaisy W, Al-Rubaey M, Al-Naggar RA, Karim B, Mohd NoorNA. Maternal obesity and its relation with the cesarean section: ahospital based cross sectional study in Iraq. BMC PregnancyChildbirth 2014;14:235. Doi: 10.1186/1471-2393-14-235
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Risks of Maternal Obesity in Pregnancy Alves et al. 687

Perinatal Outcomes of Fetuses with Early GrowthRestriction, Late Growth Restriction, Small forGestational Age, and Adequate for Gestational Age
Resultados perinatais de fetos com restrição de crescimentoprecoce, restrição de crescimento tardia, pequenos para a idadegestacional e adequados para a idade gestacionalQuênya Antunes Silveira Inácio1 Edward Araujo Júnior2,3 Luciano Marcondes Machado Nardozza2
Caetano Galvão Petrini1,4 Victor Paranaíba Campos5,6 Alberto Borges Peixoto1,4
1Universidade de Uberaba, Uberaba, MG, Brazil2Escola Paulista de Medicina,Universidade Federal de São Paulo, SãoPaulo, SP, Brazil
3Universidade Municipal de São Caetano do Sul, São Paulo, SP, Brazil4Universidade Federal do Triângulo Mineiro, Uberaba, MG, Brazil5 Faculdade de Tecnologia em Saúde, Ribeirão Preto, SP, Brazil6Universidade Barão de Mauá, Ribeirão Preto, SP, Brazil
Rev Bras Ginecol Obstet 2019;41:688–696.
Address for correspondence Edward Araujo Júnior, PhD, RuaBotucatu, 720, 04023-062, Vila Clementino, São Paulo, SP, Brazil(e-mail: [email protected]).
Keywords
► fetal growthrestriction
► small for gestationalage
► adverse perinataloutcomes
Abstract Objective To evaluate the association between early-onset fetal growth restriction(FGR), late-onset FGR, small for gestational age (SGA) and adequate for gestational age(AGA) fetuses and adverse perinatal outcomes.Methods This was a retrospective longitudinal study in which 4 groups wereevaluated: 1 — early-onset FGR (before 32 weeks) (n¼20), 2 — late-onset FGR (at orafter 32 weeks) (n¼113), 3— SGA (n¼59), 4— AGA (n¼ 476). The Kaplan-Meier curvewas used to compare the time from the diagnosis of FGR to birth. Logistic regressionwas used to determine the best predictors of adverse perinatal outcomes in fetuseswith FGR and SGA.Results A longer timebetween thediagnosis andbirthwasobserved forAGAthan for lateFGR fetuses (p< 0.001). The model including the type of FGR and the gestational age atbirth was significant in predicting the risk of hospitalization in the neonatal intensive careunit (ICU) (p<0.001). The model including only the type of FGR predicted the risk ofneeding neonatal resuscitation (p<0.001), of respiratory distress (p<0.001), and of birthat<32, 34, and 37 weeks of gestation, respectively (p<0.001).Conclusion Fetal growth restriction and SGA were associated with adverse perinataloutcomes. The type of FGR at the moment of diagnosis was an independent variable topredict respiratory distress and the need for neonatal resuscitation. The modelincluding both the type of FGR and the gestational age at birth predicted the risk ofneeding neonatal ICU hospitalization.
receivedMarch 15, 2019acceptedAugust 19, 2019
DOI https://doi.org/10.1055/s-0039-1697987.ISSN 0100-7203.
Copyright © 2019 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Original ArticleTHIEME
688

Introduction
Fetal growth restriction (FGR) is influenced by several factorsand occurs in� 7 to 15% of all gestations.1–4Within the samecountry, it can vary according to cultural and socioeconomiccharacteristics. The most widely adopted definition of FGR isan estimated fetal weight (EFW) below the 10th percentile forthe gestational age.1,2 However, some fetuses considered ashaving FGR do not present pathological growth features andare merely considered as small for gestational age (SGA).1–3
Small for gestational age differs from FGR, because it includesthe majority of constitutionally small, but healthy fetuseswith lower risk of adverse perinatal outcome.4
Themost common cause of FGR is a deficit in the transportof nutrients and oxygen to the fetus through the placenta, butseveral other maternal factors, such as poor socioeconomicand cultural condition, malnutrition, and chronic vasculardisease, as well as fetal factors, such as genetic syndromesand infections, can be involved in this growth impairment.1–3
Perinatal morbidity and mortality are greater in fetuseswith FGR than in normal fetuses, due to more frequenthypoxemia, meconium aspiration, and hypoglycemia.1–3
Furthermore, FGR is associated with a higher incidence ofcardiovascular diseases and diabetes mellitus in childhoodand adult life.5,6However, SGA fetuses are also susceptible toadverse perinatal outcomes.7,8
Themain objective of the present studywas to evaluate theadverse perinatal outcomes in early FGR, late FGR, SGA, andadequate for gestational age (AGA) fetuses. The secondaryobjectives were assessing the time between the diagnosisand the moment of delivery and the main predictors of
perinatal adverse outcomes in fetuses with early FGR, lateFGR, SGA and AGA.
Methods
This was a retrospective cohort that evaluated 476 selectedpregnant women with singleton fetuses exhibiting adequategrowth, and291womenwithsingleton fetusesdiagnosedwithfetal growth impairment. The present study was conducted atthe Fetal Medicine Unit of the Mário Palmério Hospital Uni-versitário (MPHU, in the Portuguese acronym) of the Univer-sidade de Uberaba (UNIUBE, in the Portuguese acronym),Uberaba, state of Minas Gerais, Brazil, from August 28, 2013toNovember 29, 2016. The cases included in the present studywere selected from the Astraia database (Astraia SoftwareGmbH,Munich,Germany). Thepresent studywas approvedbythe UNIUBE Committee of Ethics in Research (CAAE:99278918.0.0000.5145).
The inclusion criterion was singleton pregnancies with agestational age between 24 and 41weeks, calculated from thedate of the lastmenstrual period and confirmed by ultrasoundup to 13 weeks and 6 days, who had at least 2 ultrasoundexaminations between 24 and 41 weeks. Fetuses presentingstructural abnormalities or chromosomal diseases diagnosedby ultrasound and confirmed in the postnatal period wereexcluded, as were births that occurred outside the MPHU andcases whose postnatal data were absent in the database.
Ultrasound examinations were performed by only twoexaminers (Peixoto A. B. and Petrini C. G.) accredited by theFetal Medicine Foundation (FMF) and with 8 years of experi-ence in obstetric ultrasonography. All of the examinations
Resumo Objetivo Avaliar o efeito da restrição de crescimento fetal (RCF) precoce, RCF tardio,fetos pequenos constitucionais para idade gestacional (PIG) e fetos adequados paraidade gestacional (AIG) sobre resultados adversos perinatais.Métodos Estudo longitudinal e retrospectivo, no qual foram avaliados quatro grupos:1— RCF precoce (< 32 semanas) (n¼20), 2— RCF tardio (� 32 semanas) (n¼113), 3 —PIG (n¼59), 4 — AIG (n¼476). A curva de Kaplan-Meier foi utilizada para comparar otempo entre o diagnóstico da RCF e o parto. Regressão logística foi utilizada paradeterminação dos melhores previsores de resultados perinatais adversos entre os fetoscom RCF e PIG.Resultados Os fetos AIGs apresentaram maior tempo entre o diagnóstico e parto,enquanto fetos RCF tardio apresentaram menor tempo (p< 0,001). O modelo con-tendo tanto os tipos de RCF quanto a idade gestacional no momento do parto foisignificativo em predizer o risco de internação na unidade de terapia intensiva (UTI)neonatal (p< 0,001). O modelo incluindo apenas o tipo de FGR prediz o risco deressuscitação neonatal (p<0,001), de desconforto respiratório (p<0,001) e denascimento<32, 34 e 37 semanas de gestação, respectivamente (p< 0,001).Conclusão Os desvios do crescimento, RCF e PIG, foram associados a resultadosperinatais adversos. O tipo de RCF no momento do diagnóstico foi variável indepen-dente para predizer necessidade de reanimação neonatal e desconforto respiratório. Omodelo que incluiu o tipo de FGR e idade gestacional no nascimento prediz o risco denecessitar de internação em UTI neonatal.
Palavras-chave
► restrição docrescimento fetal
► pequeno para aidade gestacional
► resultados perinataisadversos
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Perinatal Outcomes of Fetuses with Early Growth Restriction, Late Growth Restriction Inácio et al. 689

were transabdominal and used a Voluson E6 ultrasoundsystem (General Electric Healthcare, Zipf, Austria). The ultra-sound examinations followed the protocol of the institutionfor the evaluation of fetal growth andwellbeing. The followingfetal biometric parameters were evaluated: biparietal diame-ter (BPD), head circumference (HC), abdominal circumference(AC), and femurdiaphysis length (FDL), according to the guide-lines proposed by the International Society of Ultrasound inObstetrics and Gynecology (ISUOG).9 The estimated fetalweight (EFW) was calculated using the Hadlock formula10:
log10 [birthweight]¼1.4787þ0.001837�BPD2þ0.0458�ACþ0.158� FDL�0.003343�AC� FDL
In addition to the biometric parameters, the following werealso evaluated: largest vertical pocket of amnioticfluid (LVP),11
mean uterine artery pulsatility index (PI UtA),12 umbilicalartery pulsatility index (PI UA),13 middle cerebral artery pul-satility index (PI MCA),14 middle cerebral artery peak systolicvelocity (PSV MCA),15 and cerebroplacental ratio (CPR)¼ PIMCA / PI UA.16
The patients were divided into 4 groups: 1 — early-onsetFGR, 2— late-onset FGR, 3— SGA, 4— fetuses with appropriatefor gestational age (AGA) growth (controls). Appropriate forgestational agewas defined if the estimated fetalweight (EFW)was between the 10th and 95th percentile according to therespective gestational age, following normal values of PI UA, PIMCA andmean PI UtA. Fetuses were considered to have early-onset FGR when the gestational age was<32 weeks and thefollowing criteria were present: EFW or AC below the 3rd
percentile for the gestational age or absent end-diastolic flowin UA; EFWor AC below the 10th percentile for the gestationalage, associated with a mean PI UtA or PI UA above the 95thpercentile for the gestational age. Fetuses were considered tohave late-onset FGR when the gestational age was>32 weeksand the following criteria were present: EFW or AC below the3rd percentile for the gestational age; EFWor AC below the 10th
percentile for the gestational age, associatedwith amean PI UAabove the 95th percentile for the gestational age, CPR below the5th percentile for the gestational age, or AC/EFW ratio crossingpercentiles>2 quartiles on growth percentiles.17 Fetuseswereconsidered SGA when EFW was between the 3rd and the 10th
percentile and the criteria for early- and late-onset FGR diag-nosis were not met.
According to our local protocol, 3 ultrasound examina-tions are recommended, as follows: 11–13 weeks (1st tri-mester screening for aneuploidies, pre-eclampsia and FGR),20–24 weeks (anomaly scan), 32–34 weeks (growth scan).However, ultrasound examination can be performed at anytime in the presence of obstetrical indication. The ultrasono-graphic follow-up for SGA and FGR fetuses are individualizedaccording to maternal-fetal conditions. All of the includedcases were followed longitudinally with at least two ultra-sound examinations during pregnancy, but for analyses, onlythe parameters measured at the 1st ultrasound examinationwere used when the FGR diagnosis was made. In the cases ofSGA fetuses, in which there was later development of FGR,the parameters of the 1st ultrasound examination with a
diagnosis of FGR were used. In cases of AGA fetuses, the 1st
ultrasound examination between 24 and 41 weeks wasconsidered for analyses.
The following parameterswere considered adverse perinataloutcomes: fetal death, Apgar score<7 at 5minutes, hospitali-zation in a neonatal intensive care unit (ICU), need for neonatalresuscitation, neonatal death within the first 48hours, birth-weight [BW] below the 10th percentile,18 hypothermia, hypo-glycemia, hypomagnesemia, polycythemia, thrombocytopenia,respiratory distress, and periventricular hemorrhage.
The data were analyzed using IBM SPSS Statistics for Win-dows,Version20.0 software (IBMCorp., Armonk,NY,USA). Thequantitative variables underwent the Kolmogorov-Smirnovtest for normality and were presented as means and standarddeviations (SDs). The categorical variables were described asabsolute and percentage frequencies and were represented intables and graphs. The differences between the categoricalvariables and their proportions were analyzed using the chi-squared test. The effect of FGR on continuous variables wasanalyzed with the Kruskal-Wallis test. The time elapsed fromthe diagnosis of FGR until birth was compared using survivalanalysis through Kaplan-Meier curves. Stepwise logisticregressionwasused todeterminethebestpredictorsofadverseperinatal outcomes in fetuses with some kind of growthimpairment in the prenatal period. The odds ratio (OR) forthe developmentof adverseperinatal outcomeswith statisticaldifference between the groups was determined by logisticregression. A receiver operating characteristics (ROC) curvewas used to determine the best mean PI UtA value to detectfetuses with weight below the 10th percentile during theprenatal period. The significance level for all tests was p<0.05.
Results
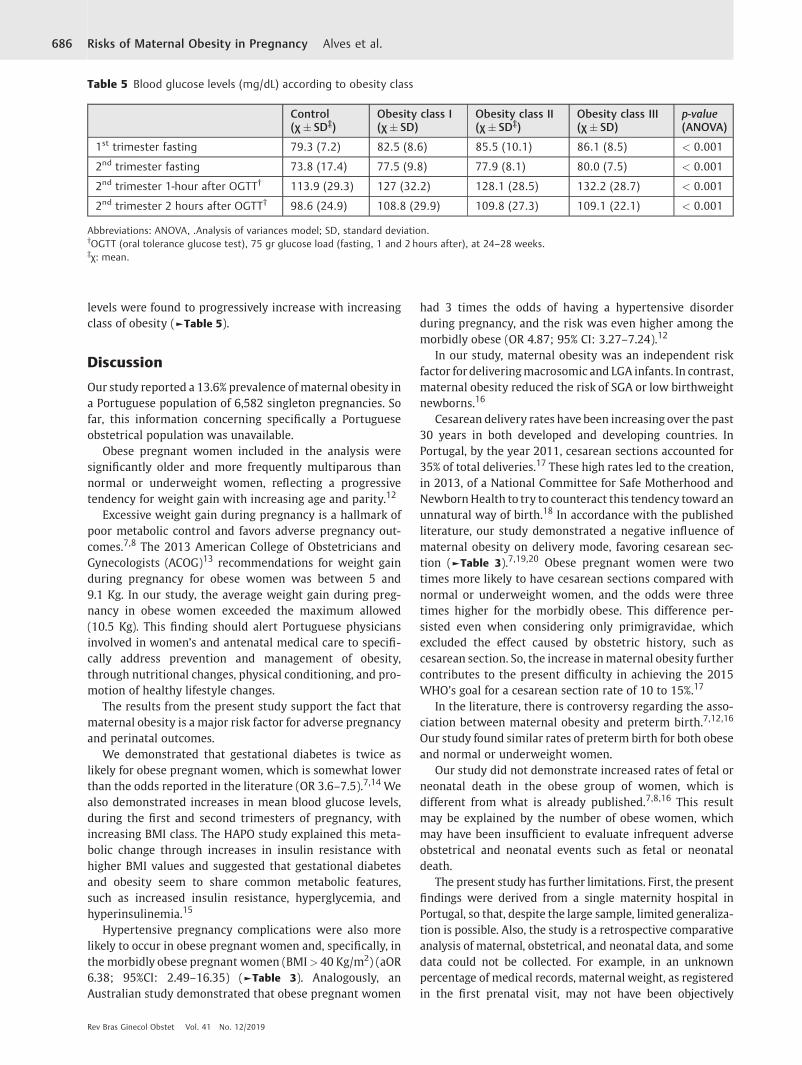
A total of 767 obstetric ultrasound examinations were evalu-ated, with gestational ages ranging from24weeks to 41weeksand 4 days. Of this total, 291 examinations (37.94%) had anEFW below the 10th percentile for their gestational age, and476 (62.05%) had an EFW between the 10th and the 95th
percentile. A total of 99 cases were excluded, of which 89 forlacking follow-up, and 10 for infection during pregnancy. Ofthe 192 remaining cases below the 10th percentile for thegestational age, 67 were SGA. As gestation progressed, 8 SGAfetuses (11.9%) were classified as having late FGR. The finalstatistical analysis considered 59 SGA fetuses (30.73%), 113fetuses with late-onset FGR (58.85%), and 20 fetuses withearly-onset FGR (10.42%) (►Fig. 1).
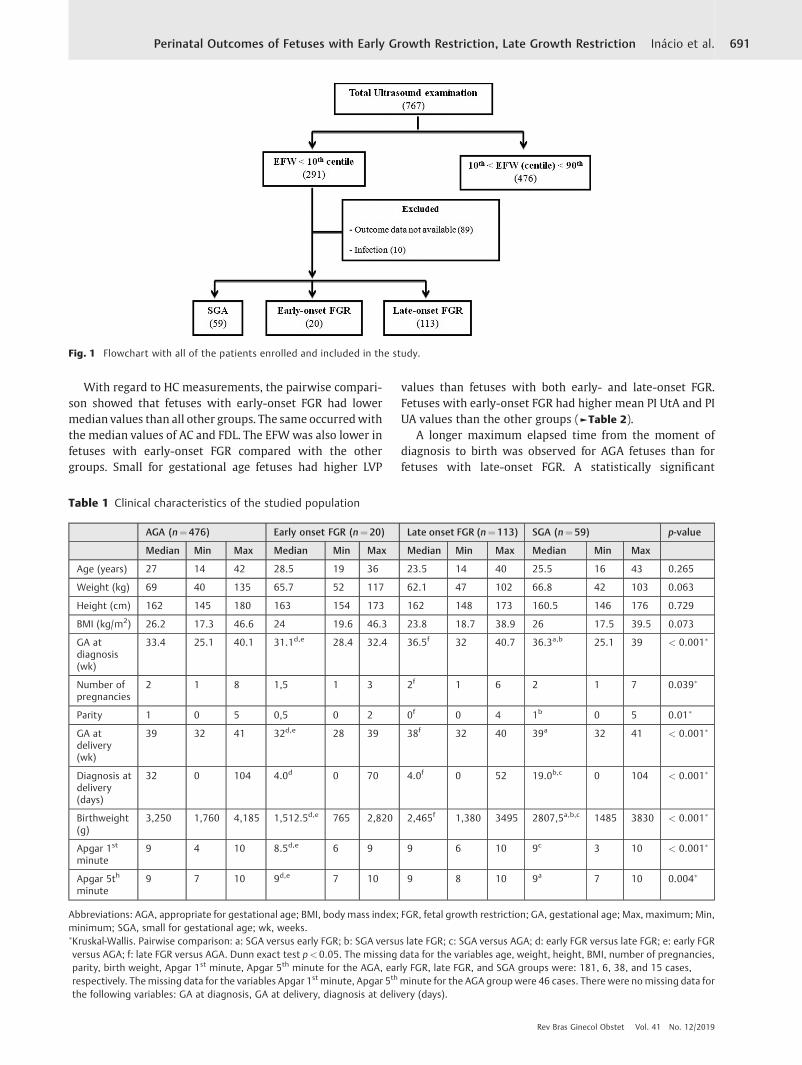
No statistically significant difference in age, weight,height, or body mass index (BMI) was found between thegroups with growth impairment at the moment of diagnosis,even though the gestational age at the moment of diagnosiswas considerably lower (31.1 weeks) in patients of the early-onset FGR group than in those with late-onset FGR (36.5weeks) and than in SGA fetuses (36.3 weeks). However,differences in the number of gestations, parity, gestationalage at delivery, time between the diagnosis and delivery, BW,Apgar scores at the 1st and 5th minutes were found to bestatistically significant (►Table 1).
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Perinatal Outcomes of Fetuses with Early Growth Restriction, Late Growth Restriction Inácio et al.690
With regard to HC measurements, the pairwise compari-son showed that fetuses with early-onset FGR had lowermedian values than all other groups. The same occurredwiththe median values of AC and FDL. The EFWwas also lower infetuses with early-onset FGR compared with the othergroups. Small for gestational age fetuses had higher LVP
values than fetuses with both early- and late-onset FGR.Fetuses with early-onset FGR had higher mean PI UtA and PIUA values than the other groups (►Table 2).
A longer maximum elapsed time from the moment ofdiagnosis to birth was observed for AGA fetuses than forfetuses with late-onset FGR. A statistically significant
Fig. 1 Flowchart with all of the patients enrolled and included in the study.
Table 1 Clinical characteristics of the studied population
AGA (n¼476) Early onset FGR (n¼20) Late onset FGR (n¼113) SGA (n¼59) p-value
Median Min Max Median Min Max Median Min Max Median Min Max
Age (years) 27 14 42 28.5 19 36 23.5 14 40 25.5 16 43 0.265
Weight (kg) 69 40 135 65.7 52 117 62.1 47 102 66.8 42 103 0.063
Height (cm) 162 145 180 163 154 173 162 148 173 160.5 146 176 0.729
BMI (kg/m2) 26.2 17.3 46.6 24 19.6 46.3 23.8 18.7 38.9 26 17.5 39.5 0.073
GA atdiagnosis(wk)
33.4 25.1 40.1 31.1d,e 28.4 32.4 36.5f 32 40.7 36.3a,b 25.1 39 < 0.001�
Number ofpregnancies
2 1 8 1,5 1 3 2f 1 6 2 1 7 0.039�
Parity 1 0 5 0,5 0 2 0f 0 4 1b 0 5 0.01�
GA atdelivery(wk)
39 32 41 32d,e 28 39 38f 32 40 39a 32 41 < 0.001�
Diagnosis atdelivery(days)
32 0 104 4.0d 0 70 4.0f 0 52 19.0b,c 0 104 < 0.001�
Birthweight(g)
3,250 1,760 4,185 1,512.5d,e 765 2,820 2,465f 1,380 3495 2807,5a,b,c 1485 3830 < 0.001�
Apgar 1st
minute9 4 10 8.5d,e 6 9 9 6 10 9c 3 10 < 0.001�
Apgar 5th
minute9 7 10 9d,e 7 10 9 8 10 9a 7 10 0.004�
Abbreviations: AGA, appropriate for gestational age; BMI, body mass index; FGR, fetal growth restriction; GA, gestational age; Max, maximum; Min,minimum; SGA, small for gestational age; wk, weeks.�Kruskal-Wallis. Pairwise comparison: a: SGA versus early FGR; b: SGA versus late FGR; c: SGA versus AGA; d: early FGR versus late FGR; e: early FGRversus AGA; f: late FGR versus AGA. Dunn exact test p< 0.05. The missing data for the variables age, weight, height, BMI, number of pregnancies,parity, birth weight, Apgar 1st minute, Apgar 5th minute for the AGA, early FGR, late FGR, and SGA groups were: 181, 6, 38, and 15 cases,respectively. The missing data for the variables Apgar 1st minute, Apgar 5th minute for the AGA group were 46 cases. There were nomissing data forthe following variables: GA at diagnosis, GA at delivery, diagnosis at delivery (days).
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Perinatal Outcomes of Fetuses with Early Growth Restriction, Late Growth Restriction Inácio et al. 691
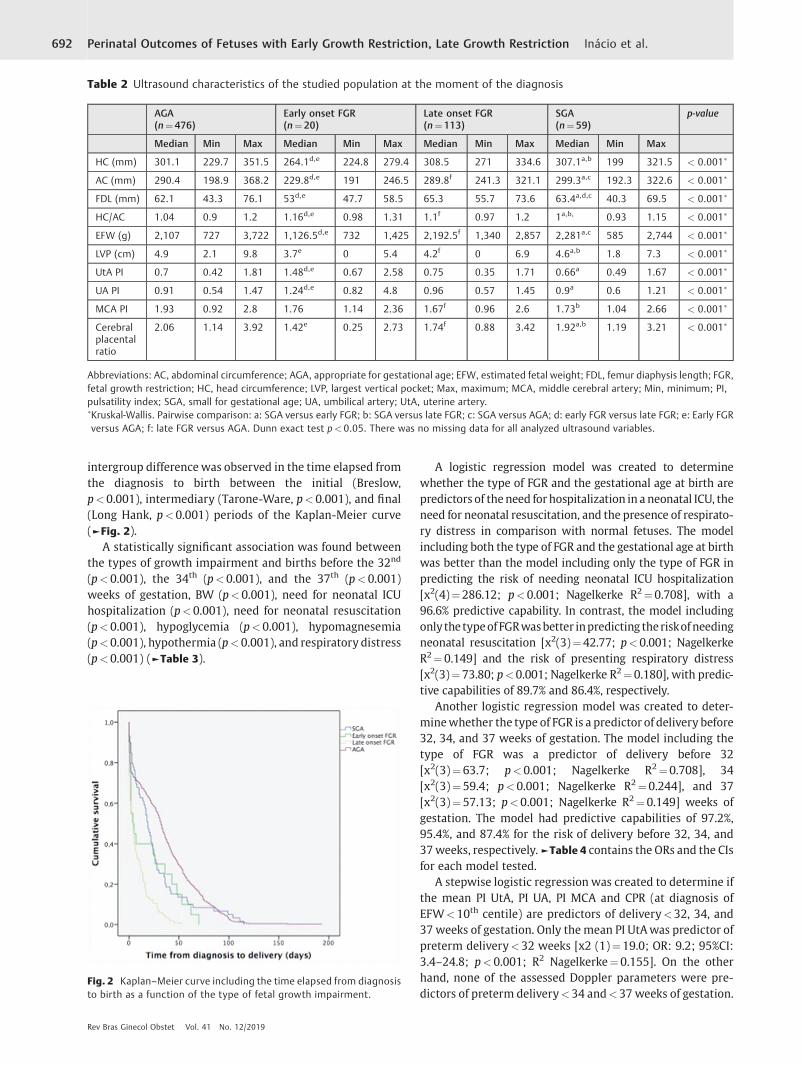
intergroup differencewas observed in the time elapsed fromthe diagnosis to birth between the initial (Breslow,p<0.001), intermediary (Tarone-Ware, p<0.001), and final(Long Hank, p<0.001) periods of the Kaplan-Meier curve(►Fig. 2).
A statistically significant association was found betweenthe types of growth impairment and births before the 32nd
(p<0.001), the 34th (p<0.001), and the 37th (p<0.001)weeks of gestation, BW (p<0.001), need for neonatal ICUhospitalization (p<0.001), need for neonatal resuscitation(p<0.001), hypoglycemia (p<0.001), hypomagnesemia(p<0.001), hypothermia (p<0.001), and respiratory distress(p<0.001) (►Table 3).
A logistic regression model was created to determinewhether the type of FGR and the gestational age at birth arepredictors of theneed forhospitalization in a neonatal ICU, theneed for neonatal resuscitation, and the presence of respirato-ry distress in comparison with normal fetuses. The modelincluding both the type of FGR and the gestational age at birthwas better than the model including only the type of FGR inpredicting the risk of needing neonatal ICU hospitalization[x2(4)¼286.12; p<0.001; Nagelkerke R2¼0.708], with a96.6% predictive capability. In contrast, the model includingonly the typeofFGRwasbetter inpredicting theriskofneedingneonatal resuscitation [x2(3)¼42.77; p<0.001; NagelkerkeR2¼0.149] and the risk of presenting respiratory distress[x2(3)¼73.80; p<0.001; Nagelkerke R2¼0.180], with predic-tive capabilities of 89.7% and 86.4%, respectively.
Another logistic regression model was created to deter-minewhether the type of FGR is a predictor of delivery before32, 34, and 37 weeks of gestation. The model including thetype of FGR was a predictor of delivery before 32[x2(3)¼63.7; p<0.001; Nagelkerke R2¼0.708], 34[x2(3)¼59.4; p<0.001; Nagelkerke R2¼0.244], and 37[x2(3)¼57.13; p<0.001; Nagelkerke R2¼0.149] weeks ofgestation. The model had predictive capabilities of 97.2%,95.4%, and 87.4% for the risk of delivery before 32, 34, and37weeks, respectively.►Table 4 contains the ORs and the CIsfor each model tested.
A stepwise logistic regression was created to determine ifthe mean PI UtA, PI UA, PI MCA and CPR (at diagnosis ofEFW<10th centile) are predictors of delivery<32, 34, and37 weeks of gestation. Only themean PI UtAwas predictor ofpreterm delivery<32 weeks [x2 (1)¼19.0; OR: 9.2; 95%CI:3.4–24.8; p<0.001; R2 Nagelkerke¼0.155]. On the otherhand, none of the assessed Doppler parameters were pre-dictors of preterm delivery<34 and<37 weeks of gestation.
Fig. 2 Kaplan–Meier curve including the time elapsed from diagnosisto birth as a function of the type of fetal growth impairment.
Table 2 Ultrasound characteristics of the studied population at the moment of the diagnosis
AGA(n¼476)
Early onset FGR(n¼20)
Late onset FGR(n¼113)
SGA(n¼59)
p-value
Median Min Max Median Min Max Median Min Max Median Min Max
HC (mm) 301.1 229.7 351.5 264.1d,e 224.8 279.4 308.5 271 334.6 307.1a,b 199 321.5 < 0.001�
AC (mm) 290.4 198.9 368.2 229.8d,e 191 246.5 289.8f 241.3 321.1 299.3a,c 192.3 322.6 < 0.001�
FDL (mm) 62.1 43.3 76.1 53d,e 47.7 58.5 65.3 55.7 73.6 63.4a,d,c 40.3 69.5 < 0.001�
HC/AC 1.04 0.9 1.2 1.16d,e 0.98 1.31 1.1f 0.97 1.2 1a,b, 0.93 1.15 < 0.001�
EFW (g) 2,107 727 3,722 1,126.5d,e 732 1,425 2,192.5f 1,340 2,857 2,281a,c 585 2,744 < 0.001�
LVP (cm) 4.9 2.1 9.8 3.7e 0 5.4 4.2f 0 6.9 4.6a,b 1.8 7.3 < 0.001�
UtA PI 0.7 0.42 1.81 1.48d,e 0.67 2.58 0.75 0.35 1.71 0.66a 0.49 1.67 < 0.001�
UA PI 0.91 0.54 1.47 1.24d,e 0.82 4.8 0.96 0.57 1.45 0.9a 0.6 1.21 < 0.001�
MCA PI 1.93 0.92 2.8 1.76 1.14 2.36 1.67f 0.96 2.6 1.73b 1.04 2.66 < 0.001�
Cerebralplacentalratio
2.06 1.14 3.92 1.42e 0.25 2.73 1.74f 0.88 3.42 1.92a,b 1.19 3.21 < 0.001�
Abbreviations: AC, abdominal circumference; AGA, appropriate for gestational age; EFW, estimated fetal weight; FDL, femur diaphysis length; FGR,fetal growth restriction; HC, head circumference; LVP, largest vertical pocket; Max, maximum; MCA, middle cerebral artery; Min, minimum; PI,pulsatility index; SGA, small for gestational age; UA, umbilical artery; UtA, uterine artery.�Kruskal-Wallis. Pairwise comparison: a: SGA versus early FGR; b: SGA versus late FGR; c: SGA versus AGA; d: early FGR versus late FGR; e: Early FGRversus AGA; f: late FGR versus AGA. Dunn exact test p< 0.05. There was no missing data for all analyzed ultrasound variables.
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Perinatal Outcomes of Fetuses with Early Growth Restriction, Late Growth Restriction Inácio et al.692

Table 3 Adverse perinatal outcomes in fetuses that were appropriate for gestational age and fetuses with intrauterine growthimpairment
AGA Early onset FGR Late onset FGR SGA p-value
n n % n n % n n % n n %
Delivery<28 wk
Yes 1 476 0.2 2 20 10.0 0 113 0.0 0 59 0.0 †
No 475 476 99.8 18 20 90.0 113 113 100.0 59 59 100.0
Delivery<32 wk
Yes 6 476 1.3 12 20 60.0 3 113 2.7 2 59 3.4 < 0.001�
No 470 476 98.7 8 20 40.0 110 113 97.3 57 59 96.6
Delivery<34 wk
Yes 13 476 2.7 13 20 65.0 8 113 7.1 3 59 5.1 < 0.001�
No 463 476 97.3 7 20 35.0 105 113 92.9 56 59 94.9
Delivery<37 wk
Yes 39 476 8.2 14 20 70.0 27 113 23.9 12 59 20.3 < 0.001�
No 437 476 91.8 6 20 30.0 86 113 76.1 47 59 79.7
Birthweight
AGA 426 472 90.3 5 20 25.0 44 113 38.9 39 59 66.1 < 0.001�
SGA 29 472 6.1 15 20 75.0 69 113 61.1 20 59 33.9
BGA 17 472 3.6 0 20 0.0 0 113 0.0 0 59 0.0
Apgar<7 at 5th minute
Yes 0 430 0.0 0 20 0.0 0 113 0.0 0 59 0.0 †
No 430 430 100.0 20 20 100.0 113 113 100.0 59 59 100.0
Neonatal ICU
Yes 20 476 4.2 17 20 85.0 28 113 24.8 6 59 10.2 < 0.001�
No 456 476 95.8 3 20 15.0 85 113 75.2 53 59 89.8
Fetal demise
Yes 0 476 0.0 0 20 0.0 0 113 0.0 0 59 0.0 †
No 476 476 100.0 20 20 100.0 113 113 100.0 59 59 100.0
Neonatal demise
Yes 0 476 0.0 1 20 5.0 1 113 0.9 0 59 0.0 †
No 476 476 100.0 19 20 95.0 112 113 99.1 59 59 100.0
Neonatal resuscitation
Yes 35 476 7.4 14 20 70.0 22 113 19.5 6 59 10.2 < 0.001�
No 441 476 92.6 6 20 30.0 91 113 80.5 53 59 89.8
Hypoglycemia
Yes 45 393 11.5 14 20 70.0 45 113 39.8 16 59 27.1 < 0.001�
No 348 393 88.5 6 20 30.0 68 113 60.2 43 59 72.9
Hypomagnesaemia
Yes 5 19 26.3 10 20 50.0 9 113 8.0 3 59 5.1 < 0.001�
No 14 19 73.7 10 20 50.0 104 113 92.0 56 59 94.9
Hypothermia
Yes 11 474 2.3 13 20 65.0 20 113 17.7 6 59 10.2 < 0.001�
No 463 474 97.7 7 20 35.0 93 113 82.3 53 59 89.8
Respiratory distress
Yes 45 475 9.5 17 20 85.0 31 113 27.4 12 59 20.3 < 0.001�
No 430 475 90.5 3 20 15.0 82 113 72.6 47 59 79.7
Abbreviations: AGA, appropriate for gestational age; FGR, fetal growth restriction; ICU, intensive care unit; SGA, small for gestational age; wk, weeks.�Chi-squared. † It was not possible to perform statistical tests on variables with< 3 patients in any category of answer.
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Perinatal Outcomes of Fetuses with Early Growth Restriction, Late Growth Restriction Inácio et al. 693

A ROC curve was plotted to determine the best sensitivityand the best mean PI UtA cutoff value to predict deliverybefore 32 weeks (►Fig. 3). Mean PI UtA values of 1.23 and1.15 were respectively able to correctly identify 57.1% and65.3% of the fetuses born before 32 weeks of gestation, withrespective false-positive rates of 10% and 15%.
Discussion
Fetal growth restriction affects� 10% of pregnancies, and it isone of the leading contributors to perinatal morbidity andmortality. Its severity greatly influences the risk of adverseperinatal outcomes.19,20
Fetal growth restriction occurs when the fetus does notreach its genetic potential for growth and development asconsequence of compromise in placental function.1Althoughthis definition seems simple, at the moment, there is no goldstandard for the diagnosis of FGR.4
In 2016, specialists established a consensus to define,classify, and diagnose FGR using the Delphi procedure.17
This consensus was a very important attempt to standardizethe diagnosis of FGR, but there is lack of studies to validatethese criteria as good predictors of adverse perinatal out-comes. Our study used it for the diagnosis of FGR, whichclassified fetuses with EFW below the 10th percentile in 3groups: SGA, early-onset FGR, and late-onset FGR.17
The present study aimed to compare perinatal outcomes ofSGA, early-onset FGR, and late-onset FGRwithAGAfetuses.Weobserved that fetuses classified as early-onset FGR had thehighest risk for adverse perinatal outcomes (need for hospital-ization in neonatal ICU, need for neonatal resuscitation, andpresence of respiratory distress) compared with AGA fetuses(OR¼77.1, 95%CI:11.27–527.75; OR¼29.4; 95%CI:10.64–81.2; OR¼54.14, 95%CI: 15.30–191.90, respectively).
The fetuses classified as late-onset FGR also had significant-ly adverse perinatal outcomes compared with AGA fetuses(OR¼7.2, 95%CI:2.8–18.01; OR¼3.0, 95%CI:1.7–5.4; OR¼3.6,95%CI:2.15–6.04 of need for hospitalization in neonatal ICU,need for neonatal resuscitation, and presence of respiratorydistress, respectively). However, fetuses classified with SGAdid not show increased risk of need for hospitalization inneonatal ICU or need for neonatal resuscitation (p¼0.23 andp¼0.44, respectively), but showed increased risk of respirato-ry distress comparedwithAGA fetuses (OR¼2.4; 95%CI: 1.20–4.93).
We also found that other adverse perinatal outcomes hada significant correlation between intrauterine growth im-pairment and AGA groups, like hypothermia (early-onsetFGR¼65%, late-onset FGR¼17.7%, SGA¼10.2%, and AGA¼2.3%, p<0,001) and hypoglycemia (early-onset FGR¼70%,
Table 4 Risk of adverse events in the neonatal periodaccording to the type of growth impairment and gestationalage at birth in comparison with fetuses with adequate growth
OR 95%CI p-value
Delivery< 32 wk
SGA 2.7 0.54–13.9 0.222
Early FGR 117.5 35.2–391.5 < 0.001�
Late FGR 2.13 0.52–8.7 0.288
Delivery< 34 wk
SGA 1.9 0.52–6.9 0.325
Early FGR 66.1 22.6–193.1 < 0.001�
Late FGR 2.7 1.09–6.7 0.031�
Delivery< 37 wk
SGA 2.9 1.4–5.8 0.004�
Early FGR 26.1 9.5–71.8 < 0.001�
Late FGR 3.5 2.0–6.0 < 0.001�
Neonatal ICU
SGA 2.3 0.59–8.69 0.23
Early FGR 77.1 11.27–527.75 < 0.001�
Late FGR 7.2 2.83–18.01 < 0.001�
Neonatal resuscitation
SGA 1.4 0.573–3.55 0.445
Early FGR 29.4 10.64–81.2 < 0.001�
Late FGR 3 1.7–5.4 < 0.001�
Respiratory distress
SGA 2.4 1.20–4.93 0.013 �
Early FGR 54.14 15.30–191.90 < 0.001�
Late FGR 3.6 2.15–6.04 < 0.001�
Abbreviations: CI, confidence interval; FGR, fetal growth restriction;ICU, intensive care unit; OR, odds ratio; SGA, small for gestational age.�Binary logistic regression.
Fig. 3 Receiver operating characteristics (ROC) curve to determinethe best value for the mean uterine artery pulsatility index (PI UtA) topredict delivery before 32 weeks of gestation in small-for-gestational-age (SGA) fetuses and fetuses with fetal growth restriction (FGR).�Area under the curve: 0.881; p< 0.001; 95%CI: 0.796–0.966.
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Perinatal Outcomes of Fetuses with Early Growth Restriction, Late Growth Restriction Inácio et al.694

late-onset FGR¼39.8%, SGA¼27.1%, and AGA¼11.5%,p<0.001).
Our findings are consistent with previous studies thatcorrelated FGR with adverse perinatal outcomes,7,19–23 butthe classification of FGR in studies used different criteria. Ourstudy was the first one that used the criteria established bythe Delphi procedure.
Regarding fetal death, neonatal death within the first48 hours andApgar score<7 at 5minutes, it was not possibleto perform statistical tests due to the small number of casesof the variables observed in all of the groups
An important factor considered to be an independentdeterminant of adverse perinatal outcomes is EFW at themoment of diagnosis.21 The lower the EFW, the higher theriskofmortality, as attestedbya studyof 355pregnantwomenwho were diagnosed with FGR in the 2nd trimester of preg-nancy. In that study, the stillbirth ratewas significantly higherin patients with EFW below the 5th percentile than that inthose with EFW between the 5th and the 10th percentile.19
Figueras et al24 consider that among fetuses with EFW belowthe 10th percentile, those below the 3rd percentile present amuch higher risk of adverse perinatal outcomes, regardless ofthe uterine artery Doppler indexes and CPR. In the presentstudy, it was possible to observe that fetuses with early-onsetFGR had a lower EFW than all other analyzed groups(p<0.001). In addition, the early-onset FGR group had 75%of the fetuses with low birthweight, the late-onset FGR grouphad 61.1%, and the SGA group had 33.9%, while the AGA grouphadonly6.1%. In the studyof Fernandez-Rodriguezetal,25onlythe cases of prenatal FGR that confirmed birth weight belowthe 3rd percentile by postnatal weight chart had increased riskof adverse perinatal outcomes.
Women with fetuses classified as early-onset FGR weremore likely to delivery in earlier gestational ages (median: 32weeks) compared with other groups: late-onset FGR (38weeks), SGA (39 weeks) and AGA (39 weeks), p<0.001.However, both groups of FGR (early- and late-onset) showedincreased risk for preterm delivery<34 weeks of gestation(OR¼66.1, 95%CI: 22.6–193.1; OR¼2.7, 95%CI¼1.09–6.7,respectively). The Doppler parameter that had the bestpredictive value for delivery<32 weeks was UtA Doppler,with sensitivity of 57.1% for false positive rate of 10% for a PIvalue of 1.23 (p<0.001). The prematurity in these cases ismainly due to elective deliveries, as observed in the study byTemming et al,19 in which FGR in the early second trimesterwas associated with increased risk of elective deliveries<37and<28 weeks compared with AGA fetuses.
Figueras et al24 consider that the only measurement thatprovides diagnostic and prognostic information for the man-agement of fetuses with FGR is the umbilical artery Dopplerexamination, either alone or in combination with CPR. Theyalso state that early-onset FGR is highly correlated to severeplacental insufficiency and chronic fetal hypoxia, whichexplains the high proportion of cases with abnormal umbili-cal-artery Doppler. In contrast, in cases of late-onset FGR,thedegreeofplacental involvement ismild,whichexplains thenormal umbilical-artery Doppler examination in nearly all ofthe cases.24 In our study, we observed the highest median
valuesofmeanPIUtA in theearly-onset FGRgroup (1.24versus0.96, 0.90, and 0.91 for early-onset FGR, late-onset FGR, SGA,andAGA, respectively, p<0.001), confirming that this group iscorrelatedwith severe placental impairment. Themedian PI ofMCA was also significantly lower for the group of late-onsetFGR in relation to the SGA and AGA groups (p<0.001), whichreflects the importance of this parameter for the diagnosis oflate-onset FGR in the differentiation of SGA fetuses, sinceMCADoppler has important value for the prediction of adverseoutcome among late-onset FGR, whereas UA Doppler is com-monly normal in these fetuses.26,27
As for the time elapsed (in days) from the diagnosis ofgrowth impairment to birth, a statistically significant corre-lationwas observed between fetuseswith late-onset FGR andSGA fetuses, with fetuses with late-onset FGR having lowermedian values. This is probably due to the fact that late-onsetFGR is diagnosed at later gestational ages; therefore, there isless time to interrupt the pregnancy. Moreover, fetuses withlate-onset FGR have fewer hemodynamic mechanisms ofadaptation to the intrauterine environment compared withfetuses with early-onset FGR, which would explain theshorter interval between the diagnosis and the interruptionof pregnancy.28 Small for gestational age fetuses can becompared with AGA fetuses, and it can take longer untilthe pregnancy is interrupted. According to Figueras et al,24
gestations of SGA fetuses, after infectious and genetic causesare excluded, may progress up to the 40th week. In gestationsof fetuses with late-onset FGR, the moment of interruptionvaries according to the stage of growth restriction of thefetus, which is determined by the changes observed onultrasound and Doppler, but interruption of the pregnancyis indicated already at 37 weeks.24
The limitations of the present study were the exclusion of30% of the cases due to the unavailability of outcome, and theretrospective nature of the study. The strengths were theinclusion of fetuseswhichwere classified as FGR according toa recent consensus definition in a single center.17
Conclusion
In summary, we have observed that the criteria establishedfor FGR by the Delphi procedure were good predictors foradverse perinatal outcomes. Additionally, the type of FGR isan independent predictor of neonatal resuscitation andrespiratory distress, and when adjusted for gestational age,it becomes also a predictor of the need for neonatal ICUhospitalization, although fetuses classified as SGA are morelikely to be constitutionally small and not present placentalpathology. These fetuses presented more risk of respiratorydistress compared with AGA fetuses. In addition, in ourcasuistic, 11.8% of the fetuses previously classified as SGAwere reclassified as late-onset FGR in their follow-up. Thus,even fetuses classified as SGA need attention to fetal wellbe-ing and proper follow-up.
ContributorsAll of the authors contributed with the project and datainterpretation, the writing of the article, the critical
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Perinatal Outcomes of Fetuses with Early Growth Restriction, Late Growth Restriction Inácio et al. 695

review of the intellectual content, and with the finalapproval of the version to be published.
Conflicts of InterestsThe authors have no conflicts of interests to declare.
References1 Frøen JF, Gardosi JO, Thurmann A, Francis A, Stray-Pedersen B.
Restricted fetal growth in sudden intrauterine unexplained death.Acta Obstet Gynecol Scand 2004;83(09):801–807. Doi: 10.1111/j.0001-6349.2004.00602.x
2 Manning FA. Intrauterine growth retardation. In:Manning FA, ed.Fetal Medicine: Principle and Practice. Norwalk, CT: Appleton &Lange; 1995:317
3 ACOG Practice Bulletin No. 204: fetal growth restriction. ObstetGynecol 2019;133(02):e97–e109. Doi: 10.1097/AOG.0000000000003070
4 Nardozza LM, Caetano AC, Zamarian AC, et al. Fetal growthrestriction: current knowledge. Arch Gynecol Obstet 2017;295(05):1061–1077. Doi: 10.1007/s00404-017-4341-9
5 Mäkikallio K, Shah J, Slorach C, et al. Fetal growth restriction andcardiovascular outcome in early human infancy: a prospectivelongitudinal study. Heart Vessels 2016;31(09):1504–1513. Doi:10.1007/s00380-015-0742-5
6 Szostak-Węgierek D, Szamotulska K. Fetal development and riskof cardiovascular diseases and diabetes type 2 in adult life. MedWieku Rozwoj 2011;15(03):203–215
7 Karlsen HO, Johnsen SL, Rasmussen S, Kiserud T. Prediction ofadverse perinatal outcome of small-for-gestational-age pregnan-cy using size centiles and conditional growth centiles. UltrasoundObstet Gynecol 2016;48(02):217–223. Doi: 10.1002/uog.15835
8 Caradeux J, Eixarch E, Mazarico E, Basuki TR, Gratacos E, FiguerasF. Longitudinal growth assessment for prediction of adverseperinatal outcome in fetuses suspected to be small-for-gestation-al age. Ultrasound Obstet Gynecol 2018;52(03):325–331. Doi: 10.1002/uog.18824
9 Salomon LJ, Alfirevic Z, Berghella V, et al; ISUOG Clinical Stand-ards Committee. Practice guidelines for performance of theroutine mid-trimester fetal ultrasound scan. Ultrasound ObstetGynecol 2011;37(01):116–126. Doi: 10.1002/uog.8831
10 Hadlock FP, Harrist RB, Carpenter RJ, Deter RL, Park SK. Sono-graphic estimation of fetal weight. The value of femur length inaddition to head and abdomen measurements. Radiology 1984;150(02):535–540. Doi: 10.1148/radiology.150.2.6691115
11 Gramellini D, Chiaie D, Piantelli G, Sansebastiano L, Fieni S, VadoraE. Sonographic assessment of amniotic fluid volume between 11and 24 weeks of gestation: construction of reference intervalsrelated to gestational age. Ultrasound Obstet Gynecol 2001;17(05):410–415. Doi: 10.1046/j.1469-0705.2001.00264.x
12 Gómez O, Figueras F, Fernández S, et al. Reference ranges foruterine arterymean pulsatility index at 11-41weeks of gestation.Ultrasound Obstet Gynecol 2008;32(02):128–132. Doi: 10.1002/uog.5315
13 Acharya G, Wilsgaard T, Berntsen GK, Maltau JM, Kiserud T.Reference ranges for serial measurements of blood velocity andpulsatility index at the intra-abdominal portion, and fetal andplacental ends of the umbilical artery. Ultrasound Obstet Gynecol2005;26(02):162–169. Doi: 10.1002/uog.1902
14 Parra-Cordero M, Lees C, Missfelder-Lobos H, Seed P, Harris C.Fetal arterial and venous Doppler pulsatility index and timeaveraged velocity ranges. Prenat Diagn 2007;27(13):1251–1257.Doi: 10.1002/pd.1868
15 Mari G, Deter RL, Carpenter RL, et al; Collaborative Group forDoppler Assessment of the Blood Velocity in Anemic Fetuses.Noninvasive diagnosis by Doppler ultrasonography of fetal ane-mia due to maternal red-cell alloimmunization. N Engl J Med2000;342(01):9–14. Doi: 10.1056/NEJM200001063420102
16 Baschat AA, Gembruch U. The cerebroplacental Doppler ratiorevisited. Ultrasound Obstet Gynecol 2003;21(02):124–127. Doi:10.1002/uog.20
17 Gordijn SJ, Beune IM, Thilaganathan B, et al. Consensus definitionof fetal growth restriction: a Delphi procedure. Ultrasound ObstetGynecol 2016;48(03):333–339. Doi: 10.1002/uog.15884
18 Alexander GR, Himes JH, Kaufman RB, Mor J, Kogan M. A UnitedStates national reference for fetal growth. Obstet Gynecol 1996;87(02):163–168. Doi: 10.1016/0029-7844(95)00386-X
19 Temming LA, Dicke JM, Stout MJ, et al. Early second-trimester fetalgrowth restriction and adverse perinatal outcomes. Obstet Gynecol2017;130(04):865–869. Doi: 10.1097/AOG.0000000000002209
20 Unterscheider J, O’Donoghue K, Daly S, et al. Fetal growth restric-tion and the risk of perinatal mortality-case studies from themulticentre PORTO study. BMCPregnancy Childbirth 2014;14:63.Doi: 10.1186/1471-2393-14-63
21 Lees C, Marlow N, Arabin B, et al; TRUFFLE Group. Perinatalmorbidity and mortality in early-onset fetal growth restriction:cohort outcomes of the trial of randomized umbilical and fetalflow in Europe (TRUFFLE). Ultrasound Obstet Gynecol 2013;42(04):400–408. Doi: 10.1002/uog.13190
22 Kabiri D, Romero R, Gudicha DW, et al. Prediction of adverseperinatal outcomes by fetal biometry: a comparison of custom-ized and population-based standards. Ultrasound Obstet Gynecol2019;•••;. Doi: 10.1002/uog.20299
23 Figueras F, Savchev S, Triunfo S, Crovetto F, Gratacos E. Anintegrated model with classification criteria to predict small-for-gestational-age fetuses at risk of adverse perinatal outcome.Ultrasound Obstet Gynecol 2015;45(03):279–285. Doi: 10.1002/uog.14714
24 Figueras F, Gratacós E. Update on the diagnosis and classificationof fetal growth restriction and proposal of a stage-based manage-ment protocol. Fetal DiagnTher 2014;36(02):86–98. Doi: 10.1159/000357592
25 Fernandez-Rodriguez B, de Alba C, Villalain C, Pallás CR, Galindo A,Herraiz I. Obstetric and pediatric growth charts for the detection offetal growth restriction and neonatal adverse outcomes in pretermnewborns before 34 weeks of gestation. JMatern Fetal NeonatalMed 2019;•••:1–8. Doi: 10.1080/14767058.2019.1626368
26 Eixarch E,Meler E, Iraola A, et al. Neurodevelopmental outcome in2-year-old infants who were small-for-gestational age termfetuses with cerebral blood flow redistribution. UltrasoundObstet Gynecol 2008;32(07):894–899. Doi: 10.1002/uog.6249
27 Hershkovitz R, Kingdom JC, Geary M, Rodeck CH. Fetal cerebralblood flow redistribution in late gestation: identification ofcompromise in small fetuses with normal umbilical artery Dopp-ler. Ultrasound Obstet Gynecol 2000;15(03):209–212. Doi:10.1046/j.1469-0705.2000.00079.x
28 Marsál K. Obstetric management of intrauterine growth restric-tion. Best Pract Res Clin Obstet Gynaecol 2009;23(06):857–870.Doi: 10.1016/j.bpobgyn.2009.08.011
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Perinatal Outcomes of Fetuses with Early Growth Restriction, Late Growth Restriction Inácio et al.696
Factors Associated with the Need for Insulin as aComplementary Treatment to Metformin inGestational Diabetes Mellitus
Fatores associados à necessidade de insulina comotratamento complementar à metformina na diabetesmellitus gestacionalMatheus Leite Ramos de Souza1 Rodrigo Ribeiro e Silva1 Thiago Ribeiro e Silva2
Larissa Cano de Oliveira1 Guilherme Dienstmann1 Iramar Baptistella do Nascimento1 Jean Carl Silva1
1Department of Medicine, Universidade da Região de Joinville,Joinville, SC, Brazil
2Department of Medicine, Universidade Positivo, Curitiba, PR, Brazil
Rev Bras Ginecol Obstet 2019;41:697–702.
Address for correspondence Matheus Leite Ramos de Souza,Universidade da Região de Joinville, Rua Ministro Calógeras 439,89202-207, Centro, Joinville, SC, Brazil(e-mail: [email protected]).
Keywords
► gestational diabetes► metformin► insulin► combined treatment
Abstract Objective To evaluate the factors associated with the need for insulin as a comple-mentary treatment to metformin in pregnant women with gestational diabetesmellitus (GDM).Methods A case-control study was performed from April 2011 to February 2016 withpregnant women with GDM who needed complementary treatments besides diet andphysical exercise. Those treated with metformin were compared with those who, inaddition to metformin, also needed the combination with insulin. Maternal character-istics and glycemic control were evaluated. Multinomial logistic regression modelswere developed to evaluate the influence of different therapies on neonatal outcomes.Results A total of 475 pregnant women who needed pharmacological therapy wereevaluated. Of these, 366 (77.05%) were submitted to single therapy with metformin,and 109 (22.94%) needed insulin as a complementary treatment. In the analysis of theodds ratio (OR), fasting glucose (FG)<90mg/dL reduced the odds of needing thecombination (OR: 0.438 [0.235–0.815]; p¼0.009], as well as primiparity (OR: 0.280[0.111–0.704]; p¼0.007]. In obese pregnant women, an increased chance of needingthe combination was observed (OR: 2,072 [1,063–4,039]; p¼0,032).Conclusion Obesity resulted in an increased chance of the mother needing insulin asa complementary treatment to metformin, while FG<90mg/dL and primiparity wereprotective factors.
Resumo Objetivo Avaliar os fatores associados à necessidade de insulina como tratamentocomplementar à metformina em gestantes com diabetes mellitus gestacional (DMG).Métodos Um estudo caso-controle foi realizado de abril de 2011 a fevereiro de 2016com gestantes portadoras de DMG que necessitaram de tratamentos complementares
receivedJune 7, 2019acceptedSeptember 9, 2019
DOI https://doi.org/10.1055/s-0039-1700796.ISSN 0100-7203.
Copyright © 2019 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Original Article 697

Introduction
Gestational diabetesmellitus (GDM) is ametabolic alterationwith prevalence between 3% and 25%, depending on theethnic group and the diagnostic criteria used.1,2 In the lastdecades, there has been a progressive increase in the numberof pregnant women diagnosed with diabetes as a result ofpopulation growth, increased maternal age, lack of physicalactivity, and an increased prevalence of obesity.3
Thematernal hyperglycemia that is a characteristic of GDMhas a negative impact on the progression of pregnancy.4,5
Therefore, GDM is an independent risk factor for obstetriccomplications, such as: preterm delivery; preeclampsia; largefor gestational age (LGA) newborns and macrossomics; birthtraumas, such as dystocia; increased need for cesarean sec-tions; and neonatal hypoglycaemia.6,7
The initial treatment recommended is lifestyle changes,such as diet and physical activity.8,9When suchmeasures arenot sufficient to reach adequate glucose levels, pharmaco-logical therapy is required, with metformin or insulin.10 It isbelieved that � 15% to 60% of patients require pharmacolog-ical treatment in combinationwith diet and physical activityto achieve control of the condition.11
Metformin is an oral anti-hyperglycemic drug derived frombiguanide that has itsmain site of action in the liver. The threemain mechanisms of action are: reduction of hepatic gluco-neogenesis, reduction of glucose absorption by the gastroin-testinal tract, and improvement in the use of peripheralglucose by increasing cellular sensitivity to insulin.12 It wasinitially developed for use in type-2 diabetes mellitus (DM2)and, because it crosses theplacental barrier, its administrationin cases of GDM was delayed. It had its safety proven inpregnancy as it was used for fertility treatments in patientswith polycystic ovary syndrome; these patients kept using themedication throughout pregnancy.13,14 Thus, because it is asafe drug,more cost-effective and easier to use comparedwith
insulin, it is indicated in cases of GDM because it is metaboli-cally similar to DM2.15
However, evenwithmetformin being as effective as insulinin glycemic control, in some patient profiles it is significantlyassociated with a low response to the monotherapy and,therefore, needs to be supplemented with insulin.16
Given this context, the objective of the present study wasto evaluate maternal and glycemic control factors that influ-ence the chance of pregnant women with GDM needinginsulin as a complementary treatment to metformin.
Methods
A case-control study was conducted. The sample was com-posed of pregnant womenwith GDM, and those who neededonly treatment with metformin were compared with preg-nant women treated with metformin who needed to beassociated with insulin.
Sample size was defined for convenience, covering all preg-nant womenwho met the inclusion criteria. The womenwerecared for in the period fromApril 2011 to February 2016 at theHigh-Risk Care Service of Maternidade Darcy Vargas (MDV), inthe city of Joinville, state of Santa Catarina, Brazil. All of thepatients had their deliveries performed at the same service.
The inclusion criteria were: pregnant women older than18 years of age, with a diagnosis of GDM, need for pharma-cological therapy complementary to diet and physical exer-cise, and complete data in the electronic patient record (EPR).The exclusion criterion was participants with incompletedata in the EPR. However, there was no need for exclusionsthroughout the study.
The project was approved under CPAE number82477318.1.0000.5363 by the Research Ethics Committee(REC) of Hospital Regional Hans Dieter Schmidt , in the city ofJoinville. We also followed item 32 of the Declaration ofHelsinki, which states that in cases in which consent is
além de dieta e exercícios físicos. Aquelas tratadas commetformina foram comparadascom aquelas que, além da metformina, também precisaram de combinação cominsulina. Foram avaliadas as características maternas e de controle glicêmico. Modelosde regressão logística multinomial foram construídos para avaliar a influência dasdiferentes terapias nos desfechos neonatais.Resultados Foram avaliadas 475 gestantes que necessitaram de terapia farmacoló-gica. Destas, 366 (77,05%) utilizaram terapia única com metformina, e 109 (22,95%)necessitaram de insulina como tratamento complementar. Na análise da razão depossibilidades (RP), a glicemia de jejum (GJ)< 90mg/dL reduziu as chances denecessidade da combinação (RP: 0,438 [0,235–0,815]; p¼0,009), bem como aprimiparidade (RP: 0,280 [0,111–0,704]; p¼0,007). Em gestantes obesas, foi obser-vada uma chance maior de necessidade da combinação (RP: 2.072 [1.063–4.039];p¼0,032).Conclusão A obesidade resultou em um aumento na chance de a mãe precisar deinsulina como tratamento complementar à metformina, enquanto a GJ<90mg/dL e aprimiparidade foram fatores de proteção.
Palavras-chave
► diabetesgestacional
► metformina► insulina► tratamento
combinado
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Factors Associated with the Need for Insulin as a Complementary Treatment Souza et al.698
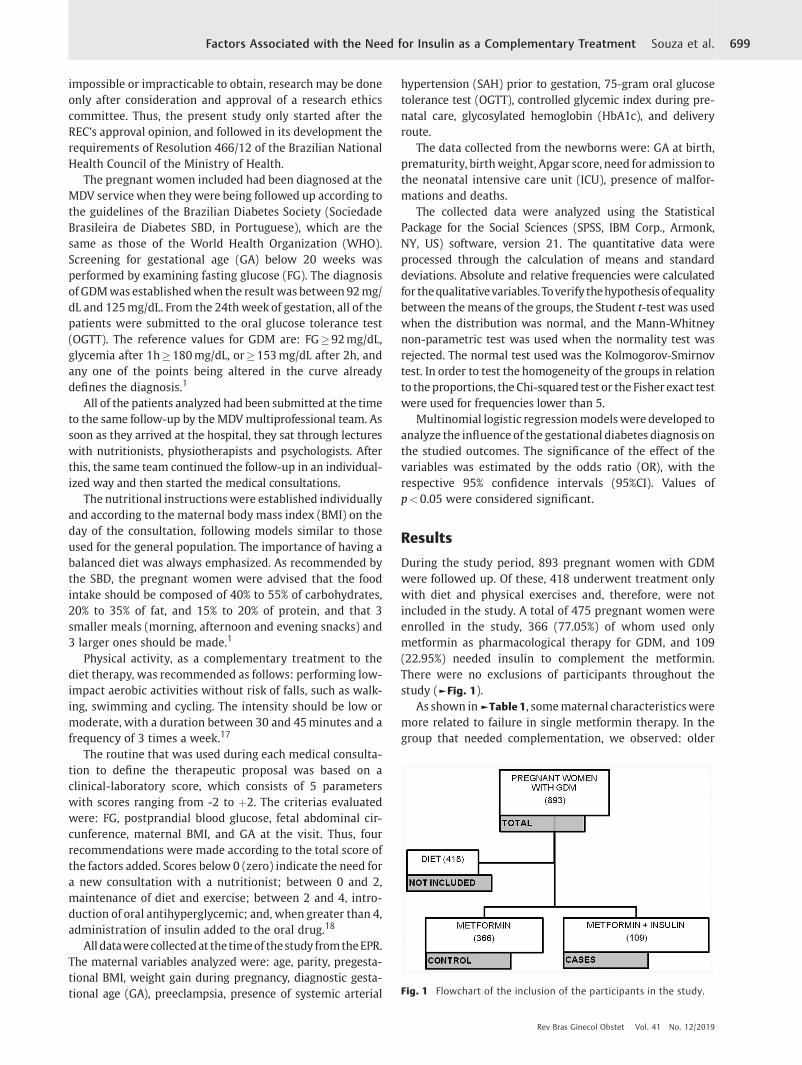
impossible or impracticable to obtain, research may be doneonly after consideration and approval of a research ethicscommittee. Thus, the present study only started after theREC’s approval opinion, and followed in its development therequirements of Resolution 466/12 of the Brazilian NationalHealth Council of the Ministry of Health.
The pregnant women included had been diagnosed at theMDV service when they were being followed up according tothe guidelines of the Brazilian Diabetes Society (SociedadeBrasileira de Diabetes SBD, in Portuguese), which are thesame as those of the World Health Organization (WHO).Screening for gestational age (GA) below 20 weeks wasperformed by examining fasting glucose (FG). The diagnosisof GDMwas establishedwhen the result was between 92mg/dL and 125mg/dL. From the 24th week of gestation, all of thepatients were submitted to the oral glucose tolerance test(OGTT). The reference values for GDM are: FG�92mg/dL,glycemia after 1h�180mg/dL, or�153mg/dL after 2h, andany one of the points being altered in the curve alreadydefines the diagnosis.1
All of the patients analyzed had been submitted at the timeto the same follow-up by theMDVmultiprofessional team. Assoon as they arrived at the hospital, they sat through lectureswith nutritionists, physiotherapists and psychologists. Afterthis, the same team continued the follow-up in an individual-ized way and then started the medical consultations.
The nutritional instructionswere established individuallyand according to the maternal body mass index (BMI) on theday of the consultation, following models similar to thoseused for the general population. The importance of having abalanced diet was always emphasized. As recommended bythe SBD, the pregnant women were advised that the foodintake should be composed of 40% to 55% of carbohydrates,20% to 35% of fat, and 15% to 20% of protein, and that 3smaller meals (morning, afternoon and evening snacks) and3 larger ones should be made.1
Physical activity, as a complementary treatment to thediet therapy, was recommended as follows: performing low-impact aerobic activities without risk of falls, such as walk-ing, swimming and cycling. The intensity should be low ormoderate, with a duration between 30 and 45minutes and afrequency of 3 times a week.17
The routine that was used during each medical consulta-tion to define the therapeutic proposal was based on aclinical-laboratory score, which consists of 5 parameterswith scores ranging from -2 to þ2. The criterias evaluatedwere: FG, postprandial blood glucose, fetal abdominal cir-cunference, maternal BMI, and GA at the visit. Thus, fourrecommendations were made according to the total score ofthe factors added. Scores below 0 (zero) indicate the need fora new consultation with a nutritionist; between 0 and 2,maintenance of diet and exercise; between 2 and 4, intro-duction of oral antihyperglycemic; and, when greater than 4,administration of insulin added to the oral drug.18
All datawerecollectedat thetimeof thestudy fromtheEPR.The maternal variables analyzed were: age, parity, pregesta-tional BMI, weight gain during pregnancy, diagnostic gesta-tional age (GA), preeclampsia, presence of systemic arterial
hypertension (SAH) prior to gestation, 75-gram oral glucosetolerance test (OGTT), controlled glycemic index during pre-natal care, glycosylated hemoglobin (HbA1c), and deliveryroute.
The data collected from the newborns were: GA at birth,prematurity, birthweight, Apgar score, need for admission tothe neonatal intensive care unit (ICU), presence of malfor-mations and deaths.
The collected data were analyzed using the StatisticalPackage for the Social Sciences (SPSS, IBM Corp., Armonk,NY, US) software, version 21. The quantitative data wereprocessed through the calculation of means and standarddeviations. Absolute and relative frequencies were calculatedfor thequalitativevariables.Toverify thehypothesisofequalitybetween themeans of the groups, the Student t-test was usedwhen the distribution was normal, and the Mann-Whitneynon-parametric test was used when the normality test wasrejected. The normal test used was the Kolmogorov-Smirnovtest. In order to test the homogeneity of the groups in relationto theproportions, the Chi-squared test or the Fisher exact testwere used for frequencies lower than 5.
Multinomial logistic regressionmodelswere developed toanalyze the influence of the gestational diabetes diagnosis onthe studied outcomes. The significance of the effect of thevariables was estimated by the odds ratio (OR), with therespective 95% confidence intervals (95%CI). Values ofp<0.05 were considered significant.
Results
During the study period, 893 pregnant women with GDMwere followed up. Of these, 418 underwent treatment onlywith diet and physical exercises and, therefore, were notincluded in the study. A total of 475 pregnant women wereenrolled in the study, 366 (77.05%) of whom used onlymetformin as pharmacological therapy for GDM, and 109(22.95%) needed insulin to complement the metformin.There were no exclusions of participants throughout thestudy (►Fig. 1).
As shown in►Table 1, somematernal characteristicsweremore related to failure in single metformin therapy. In thegroup that needed complementation, we observed: older
Fig. 1 Flowchart of the inclusion of the participants in the study.
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Factors Associated with the Need for Insulin as a Complementary Treatment Souza et al. 699

maternal age, greater number of previous pregnancies,greater weight gain, and earlier diagnosis. We also observedthat pregnant women with a higher BMI had a greater needfor the metformin and insulin combination, especially obesewomen, who represented 55.04% of the combination group.
We identified that the pregnant womenwith higher valuesof FG in the OGTT belonged to the group that represented thefailure of the metformin monotherapy. Likewise, fasting andpostprandial glycemic control data were higher in the groupthat required the combination. Furthermore, the third-trimes-ter HbA1c had a higher percentage in this same group(►Table 2).
►Table 3 shows that there was a significant differenceregarding birth weight between the newborns of the groups,which results in thefindingof a higher percentage of large forgestational age newborns (LGA NB) composing the combi-nation group, and a greater number of adequate for gesta-tional age newborns (AGA NB) in the metformin group.
Finally,►Table 4 shows that primiparityand FG<90mg/dLreduce the chance of failure of the single therapywithmetfor-min, and, therefore, they represent protective factors. On theother hand, obesity was found to cause an increase in thechance of need for insulin supplementation. The other factorsanalyzed did not show a significant influence.
Discussion
The present study aimed to define thematernal and glycemiccontrol factors that would be predictors of the need to useinsulin as a complementary treatment to metformin amongpregnant women with GDM. It was possible, therefore, toestablish an OR for the main outcomes. Primiparity andFG<90mg/dLwere deemed protective factors, andmaternalobesity, a factor of increased chance.
In the composition of the groups, a 22.95% failure rate ofthe metformin monotherapy was found, which is similar tothe results found in other studies.11,16 Silva et al,11 forexample, in a clinical trial comparing different hypoglycemic
Table 1 Maternal characteristics
Metformin(n¼366)
Combination(n¼109)
p-value
Age 31.48 (6.88) 34.40 (6.33) 0.020c
Previouspregnancies
3.00 (2.08) 3.50 (1.73) 0.008c
BMI 29.48 (5.96) 32.13 (6.99) 0.009c
BMI class
Low weight 28 (7.65%) 1 (0.91%) 0.006b
Adequate 78 (21.31%) 17 (15.59%) 0.190a
Overweight 116 (31.69%) 29 (26.60%) 0.311a
Obese 139 (37.97%) 60 (55.04%) 0.002a
Weight gain 1.31 (3.16) 3.48 (3.72) 0.009c
GA atdiagnosis
28.76 (5.83) 25.95 (5.76) < 0.001c
SHGS 21 (5.73%) 9 (8.25%) 0.346a
Previous SAH 55 (15.02%) 17 (15.59%) 0.864a
Abbreviations: BMI, body mass index; GA, gestational age; SHGS,specific hypertensive gestation syndrome; SAH, systemic arterialhypertension.Notes: aChi-squared test; bFisher exact test; cMann-Whitney test. Meanand standard deviation, absolute numbers and percentages.
Table 2 Characteristics related to diabetes
Metformin(n¼366)
Combination(n¼109)
p-value
OGTT
Fasting 92.77 (11.90) 98.30 (7.42) < 0.001c
1 hour 172.16 (33.90) 178.50 (32.58) 0.769c
2 hours 147.33 (36.58) 151.35 (30.67) 0.403c
Glycemiccontrol
Fasting 88.90 (9.81) 98.29 (10.58) <0.001c
Postprandial 120.28 (14.16) 124.03 (15.97) <0.001c
HBA1C 5.35 (0.34) 5.60 (0.38) 0.018c
Abbreviations: HBA1C, A1c glycated hemoglobin; OGTT, oral glucosetolerance test.Notes: cMann-Whitney test. Mean and standard deviation, absolutenumbers and percentages.
Table 3 Newborn characteristics
Metformin(n¼366)
Combination(n¼109)
p-value
GA at birth 38.67 (1.36) 38.55 (1.57) 0.228c
Premature 17 (4.64%) 4 (3.66%) 0.664b
Delivery route
Normal 174 (47.54%) 41 (37.61%) 0.068a
Caesarean 192 (52.46%) 68 (62.38%) 0.068a
Weight 3334.18(357.52)
3461.25(448.55)
0.001c
Weight Classification
SGA 9 (2.45%) 1 (0.91%) 0.467b
AGA 292 (79.78%) 75 (68.80%) 0.016a
LGA 65 (17.75%) 33 (30.29%) 0.005a
Apgar
1 minute 8.03 (1.20) 7.75 (1.37) 0.227c
1 minute low 28 (7.65%) 7 (6.42%) 0.806a
5 minutes 9.01 (0.69) 8.75 (0.78) 0.477c
5 minutes low 2 (0.54%) 2 (1.83%) 0.196b
Need for ICU 15 (4.09%) 15 (13.76%) < 0.001a
Malformation 13 (3.55%) 2 (1.83%) 0.537b
Death 2 (0.54%) 0 1.000b
Abbreviations: AGA, adequate for gestational age; GA, gestational age;ICU, intensive care unit; LGA, large for gestational age; SGA, small forgestational age.Notes: aChi-squared test; bFisher exact test; cMann-Whitney test. Meanand standard deviation, absolute numbers and percentages.
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Factors Associated with the Need for Insulin as a Complementary Treatment Souza et al.700

agents, observed a 21.2% rate of need for insulin supplemen-tation in the group that used metformin. Ashoush et al16
observed a rate of 23.4%.Although McGrath et al19 did not describe any differences,
weobserved in their article that thematernal agewasdifferentbetween the groups, and higher in those who needed theassociation (p¼0.02), as observed byother authors.20,21How-ever, maternal age>30 years did not increase the chance ofmetformin failure (OR: 0.879 [95%CI¼0.508–1.521];p¼0.645), a result that was contrary to expectations. Thestudy byGante et al.22 for example, showed age as a significantrisk factor (OR: 1.08 [95%CI¼1.03–1.13]; p¼0.003); Khinet al23 also observed this phenomenon. Neither of the studies,however, hypothesized this result.
Differently from maternal age, a significant associationwas found between the number of previous pregnancies andmetformin failure. There was a difference between thegroups (p¼0.008), and the effect measure analysis showedthat women in the first gestation (primiparous women) areless likely to require supplementation with insulin. Ashoushet al16 did not find the same significant relationship; how-ever, their samplewas smaller than that of the present study.
Moreover, the group that required insulin supplementa-tion had earlier diagnoses (p<0.001), in the sameway as thepopulations of other studies.19,22 Therefore, it would beexpected that those women who developed GDM earlier inpregnancywere thosewith higher risk factors and, therefore,the diagnostic GA was a predictor of metformin failure.However, no increase in oddswas found in patients requiringpharmacotherapy with GA<28 weeks (OR: 1.331 [95%CI¼0.654–2.709]; p¼0.430). In disagreement with the studyby Khin et al,23 which was published recently, we report anOR of 1.12 (95%CI¼1.1–1.2).
Maternal pregestational BMI is a factor that a large part ofthe studies described as impacting the effectiveness of thesingle therapywithmetformin. In the present study, a higherBMI was observed in the group that required insulin therapy,which had more pregnant women classified as obese thanthe other group. Therefore, an increased chance wasobtained (OR: 2.072 [95%CI¼1.063–4.039]; p¼0.032) forthe occurrence of such an event. According to twostudies22,24 that also obtained similar results (OR: 1.06[95%CI¼1.02–1.10] and OR: 4.10 [95%CI¼1.46–11.51]),this is explained due to the fact that higher BMIs and obesity
increase insulin resistance and decrease the sensitivity of theoral hypoglycemic.22,24 Sales et al,25 proving the failure ofthe drug in this context, when evaluating its impact on theoutcomes (reduction of BMI and prevention of GDM in obesepregnant women), observed that metformin was noteffective.
Finally, FG, when<90mg/dL in the OGTT, is a protectivefactor for the need for insulin supplementation (►Table 4).Therefore, pregnant women with these levels of FG have agood chance of responding to metformin monotherapy.Ashoush et al,16 Tertti et al21 and Gante et al22 also detectedthis characteristic. Similarly, Silva et al15 found a lowerfasting blood glucose value related to the success of metfor-min in their study. Finally, still corroborating this finding, astudy19 that also had the objective of evaluating the pre-dictors of insulin supplementation, even though it did notfind significance, stated that the predominant factor for sucha need would be high FG.19
The present study had some limitations, such as thecase-control design, which does not offer the highest levelof evidence possible. Another bias present is informationdue to the fact that retrospective data present in the EPRwere collected. The strengths of the study are: the largesample size and the diagnosis and follow-up of all patientsin a single hospital. Therefore, we can state that the presentstudy contributed to the improvement of the scientificknowledge regarding the identification of subgroups ofpatients who need more attention because they have agreater chance of needing a combination of insulin andmetformin as treatment.
Conclusion
In conclusion, despite the differences found among the pop-ulations, only obesity resulted in an increased chance that thepregnant woman needed insulin as a complementary treat-ment to metformin, while FG<90mg/dL and primiparitywere protective factors.
ContributionsSouza MLR contributed to collection, recording of dataand writing of the manuscript. Silva RR, Silva TR, andOliveira LC contributed to the data collection, the record-ing of data and the discussion about the implications of
Table 4 Multinomial analysis of the factors associated with the need for complementary therapy to the insulin therapy
MTF/MTFþ insulin ORa 95%CI p-value
Age>30 years 164/197 0.879 0.508–1.521 0.645
Primiparity 285/76 0.280 0.111–0.704 0.007
GA diagnosis before the 28th week 213/148 1.331 0.654–2.708 0.430
Low weight 338/23 0.300 0.038–2.396 0.256
Obese 208/153 2.072 1.063–4.039 0.032
FG< 90 mg/dL 225/136 0.438 0.235–0.815 0.009
Abbreviations: 95%CI, 95% confidence interval; FG, fasting glucose; GA, gestational age; MTF, metformin; OR, odds ratio.aGross odds ratio.
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Factors Associated with the Need for Insulin as a Complementary Treatment Souza et al. 701

this work. Dienstmann G and Nascimento IB contributedto the design of the study, the planning, the data collectionand the interpretation of data. Silva JC contributed to thedesign of the study, the planning, the coordination, thewriting, and data interpretation and analysis.
FundingThe present research did not receive any specific grant orfunding from agencies in the public, private, or not-for-profit sectors.
Conflict of InterestsThe authors have none to disclose.
References1 Oliveira JEP, Montenegro RM Junior, Vencio S. orgs. Diretrizes da
Sociedade Brasileira de Diabetes 2017–2018. São Paulo, SP:Clannad; 2017
2 National Collaborating Centre forWomen’s and Children’s Health.Diabetes in Pregnancy: Management of Diabetes and its Compli-cations from Preconception to the Postnatal Period. London:National Institute for Health and Care Excellence; 2015
3 Organização Pan-Americana da Saúde, Ministério da Saúde,Federação Brasileira das Associações de Ginecologia e Obstetrí-cia, Sociedade Brasileira de Diabetes. Rastreamento e Diagnós-tico de Diabetes Mellitus Gestacional no Brasil. Brasília, DF:OPAS; 2017
4 Gray SG, McGuire TM, Cohen N, Little PJ. The emerging role ofmetformin in gestational diabetes mellitus. Diabetes Obes Metab2017;19(06):765–772. Doi: 10.1111/dom.12893
5 Singh A, Dwivedi S. Study of adverse drug reactions in patientswith diabetes attending a tertiary care hospital in New Delhi,India. Indian J Med Res 2017;145(02):247–249. Doi: 10.4103/ijmr.IJMR_109_16
6 Ma RCW, Tutino GE, Lillycrop KA, HansonMA, TamWH. Maternaldiabetes, gestational diabetes and the role of epigenetics intheir long term effects on offspring. Prog Biophys Mol Biol2015;118(1-2):55–68. Doi: 10.1016/j.pbiomolbio.2015.02.010
7 Teh WT, Teede HJ, Paul E, Harrison CL, Wallace EM, Allan C. Riskfactors for gestational diabetes mellitus: implications for theapplication of screening guidelines. Aust N Z J Obstet Gynaecol2011;51(01):26–30. Doi: 10.1111/j.1479-828X.2011.01292.x
8 Brown J, Alwan NA, West J, et al. Lifestyle interventions forthe treatment of women with gestational diabetes. CochraneDatabase Syst Rev 2017;5:CD011970. Doi: 10.1002/14651858.CD011970.pub2
9 American Diabetes Association. Lifestyle management: standardsofmedical care in diabetes-2018. Diabetes Care 2018;41(Suppl 1):S38–S50. Doi: 10.2337/dc18-S004
10 Kalra B, Gupta Y, Singla R, Kalra S. Use of oral anti-diabetic agentsin pregnancy: a pragmatic approach. N Am J Med Sci 2015;7(01):6–12. Doi: 10.4103/1947-2714.150081
11 Silva JC, Fachin DRRN, Coral ML, Bertini AM. Perinatal impact ofthe use of metformin and glyburide for the treatment of gesta-tional diabetes mellitus. J Perinat Med 2012;40(03):225–228.Doi: 10.1515/jpm-2011-0175
12 Sinai Talaulikar V, Tang T, Yasmin E. Role ofmetformin inwomen’shealth: review of its current place in clinical practice and emerg-ing indications for future. Obstet Gynecol Surv 2016;71(05):307–317. Doi: 10.1097/OGX.0000000000000312
13 Haas J, Bentov Y. Should metformin be included in fertilitytreatment of PCOS patients? Med Hypotheses 2017;100:54–58.Doi: 10.1016/j.mehy.2017.01.012
14 Tan X, Li S, Chang Y, et al. Effect of metformin treatment duringpregnancy on women with PCOS: a systematic review and meta-analysis. Clin Invest Med 2016;39(04):E120–E131
15 Silva JC, Souza BV, SilvaMR. Preditores de sucesso dametformina notratamento do diabetes mellitus gestacional. Rev Bras Saúde MaterInfant 2013;13:129–135.Doi: 10.1590/S1519-38292013000200006
16 Ashoush S, El-Said M, Fathi H, Abdelnaby M. Identification ofmetformin poor responders, requiring supplemental insulin,during randomization of metformin versus insulin for the controlof gestational diabetes mellitus. J Obstet Gynaecol Res 2016;42(06):640–647. Doi: 10.1111/jog.12950
17 Padayachee C, Coombes JS. Exercise guidelines for gestationaldiabetes mellitus. World J Diabetes 2015;6(08):1033–1044. Doi:10.4239/wjd.v6.i8.1033
18 do Valle JB, Silva JC, Oliveira DS, Martins L, Lewandowski A, HorstW. Use of a clinical-laboratory score to guide treatment ofgestational diabetes. Int J Gynaecol Obstet 2018;140(01):47–52.Doi: 10.1002/ijgo.12326
19 McGrath RT, Glastras SJ, Hocking S, Fulcher GR. Use of metforminearlier in pregnancy predicts supplemental insulin therapy inwomen with gestational diabetes. Diabetes Res Clin Pract 2016;116:96–99. Doi: 10.1016/j.diabres.2016.04.051
20 PellonperäO,RönnemaaT,EkbladU,VahlbergT,TerttiK.Theeffectsofmetformin treatment of gestational diabetes onmaternalweight andglucose tolerance postpartum–a prospective follow-up study. ActaObstet Gynecol Scand 2016;95(01):79–87. Doi: 10.1111/aogs.12788
21 Tertti K, Ekblad U, Vahlberg T, Rönnemaa T. Comparison ofmetformin and insulin in the treatment of gestational diabetes:a retrospective, case-control study. Rev Diabet Stud 2008;5(02):95–101. Doi: 10.1900/RDS.2008.5.95
22 Gante I, Melo L, Dores J, Ruas L, Almeida MDC. Metformin ingestational diabetes mellitus: predictors of poor response. Eur JEndocrinol 2018;178(01):129–135. Doi: 10.1530/EJE-17-0486
23 Khin MO, Gates S, Saravanan P. Predictors of metformin failure ingestational diabetes mellitus (GDM). DiabetesMetab Syndr 2018;12(03):405–410. Doi: 10.1016/j.dsx.2018.01.003
24 Ali A, Shastry S, Nithiyananthan R, Ali A, Ganapathy R. Gestationaldiabetes-Predictors of response to treatment and obstetric out-come. Eur J Obstet Gynecol Reprod Biol 2018;220:57–60. Doi:10.1016/j.ejogrb.2017.11.014
25 Sales WB, Nascimento IBD, Dienstmann G, Souza MLR, Silva GDD,Silva JC. Effectiveness ofmetformin in the prevention of gestationaldiabetes mellitus in obese pregnant women. Rev Bras GinecolObstet 2018;40(04):180–187. Doi: 10.1055/s-0038-1642632
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Factors Associated with the Need for Insulin as a Complementary Treatment Souza et al.702

Effect of Testosterone on Proliferation Markersand Apoptosis in Breasts of Ovariectomized Rats
Efeito da testosterona em marcadores de proliferação eapoptose em mamas de ratas ovariectomizadasJussara Celi Conceição Oliveira1 Marcelo Luis Steiner2 Thérèse Rachell Theodoro3
AnaMaria Amaral Antonio Mader4 Giuliana Petri5 Luiz Carlos Abreu6 Maria Aparecida da Silva Pinhal3
César Eduardo Fernandes2 Luciano Melo Pompei2
1Faculdade de Medicina do ABC, Fundação do ABC, Santo André, SãoPaulo, Brazil
2Department of Gynecology and Obstetrics, Faculdade de Medicinado ABC, Santo André, SP, Brazil
3Department of Biochemistry, Faculdade de Medicina do ABC, SantoAndré, SP, Brazil
4Department of Pathology, Faculdade de Medicina do ABC, SantoAndré, SP, Brazil
5Biottery Coordination, Faculdade de Medicina do ABC, Santo André,SP, Brazil
6Outline and Scientific Writing Laboratory, Faculdade de Medicina doABC, Santo André, SP, Brazil
Rev Bras Ginecol Obstet 2019;41:703–709.
Address for correspondence Luciano Melo Pompei, PhD, Faculdadede Medicina do ABC, Fundação do ABC, Rua Procópio Ribeiro dosSantos 84, 04664-130, São Paulo, SP, Brazil(e-mail: [email protected]).
Keywords
► testosterone► proliferation► apoptosis► breast► ovariectomy
Abstract Objective To investigate the action of testosterone (T), isolated or associated withestradiol benzoate (EB), on the proliferation markers and apoptosis of breasts ofovariectomized rats.Methods A total of 48 castrated female Wistar rats were divided into 6 groups, andeach of them were submitted to one of the following treatments for 5 weeks: 1)control; 2) EB 50 mcg/day þ T 50 mcg/day; 3) T 50mcg/day; 4) EB 50 mcgþ T 300mcg/day; 5) T 300 mcg/day; and 6) EB 50 mcg/day. After the treatment, themammary tissue was submitted to a histological analysis and immunoexpressionevaluation of proliferation markers (proliferating cell nuclear antigen, PCNA) andapoptosis (caspase-3).Results There was a statistically significant difference among the groups regardingmicrocalcifications and secretory activity, with higher prevalence in the groups treatedwith EB. There was no difference among the groups regarding atrophy, but a higherprevalence of atrophy was found in the groups that received T versus those thatreceived EBþ T. There was a difference among the groups regarding the PCNA(p¼ 0.028), with higher expression in the group submitted to EBþ T 300 mcg/day.Regarding caspase-3, there was no difference among the groups; however, in the groupsubmitted to EBþ T 300 mcg/day, the expression was higher than in the isolated Tgroup.
receivedAugust 12, 2019acceptedOctober 2, 2019
DOI https://doi.org/10.1055/s-0039-3399552.ISSN 0100-7203.
Copyright © 2019 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Original Article 703

Introduction
Testosterone (T) has been used by postmenopausal women,with a positive effect on desire and sexual function.1 Throughcohort studies in worldwide populations, researchers havereported a small but significant association between T,androstenedione, dehydroepiandrosterone (DHEA) anddehydroepiandrosterone Sulfate (DHEAS), and breast cancerin postmenopausal women.2–4 Most of the studies using Tlast from 1 month to 2 years, hence the information thatassures its long-term use is unknown, which is a concern formedical professionals as well as for climacteric womenregarding the risk and its impact on breast tissue.5,6 Thus,considering the increasing use of T treatments by meno-pausal women, the lack of in vivo controlled studies using Tfor hormone replacement, and the need for further investi-gation of its biological impact on the breast tissue, it isrelevant to study such aspects in an animal model and theeffect of this therapy on the breast. The objective of thepresent study was to investigate the action of T, isolated orassociated with estradiol benzoate (EB), on proliferationmarkers and apoptosis ofmammary tissue in ovariectomizedrats.
Methods
We randomly selected 48 castrated female Wistar rats at250days of age. All of themunderwent bilateral oophorectomyunder anesthesiawithketamineandxylazine intraperitoneally.A longitudinal ventral approachwas used for the identification
and ligation of the ovarian pedicles and subsequent removal ofthe gonads. Three weeks later, microscopic examinations ofvaginal smears of all rats were performed to confirm hypoes-trogenism. Next, the animals were randomly divided into 6groups of 8 each; the groups received the corresponding dailyhormonal dose in a volume of 0.1ml by subcutaneous injec-tions in the dorsal region of each animal, during 5 consecutiveweeks. The daily treatments were as follows: group 1: control,sesame oil 0.1ml/day (n¼ 8); group 2: EB 50 mcgþ T 50mcg/day (n¼ 8); group 3: T 50 mcg/day (n¼ 8); group 4: EB50 mcgþ T 300 mcg/day (n¼ 8); group 5: T 300 mcg/day(n¼ 8); group 6: EB 50 mcg/day (n¼ 8). The animals werekept in a quiet environmentwith a constant temperature of 23°C, lighting periods of 12 hours per day, in addition towater andfeed ad libitum. Fiveweeks later, after the end of the treatment,the rats were anesthetized with ketamine 80mg/kg, andsacrificed by thiopental overdose. The second right mammarygland of each animal was resected and fixed in 10% bufferedformalinandsubsequentlyprepared forhistological and immu-nohistochemical evaluation.
Semiquantitative Histological AnalysisThe mammary glands obtained were embedded in paraffin,cut into to 3 μm sections, stained with hematoxylin-eosin(HE), and analyzed under high magnification microscopy(400x). A histological analysis with HE staining wasperformed, using a semiquantitative method (zero asabsent, þ as mild, þþ as moderate, and þþþ as intense),and the samples were observed using a Nikon (Minato,Tokyo, Japan) double-head microscope. This procedure was
Conclusion Isolated T did not have a proliferative effect on the mammary tissue,contrary to EB. Testosterone in combination with EB may or may not decrease theproliferation, depending on the dose of T.
Resumo Objetivo Investigar a ação da testosterona (T) isolada ou associada ao benzoato deestradiol (EB) na proliferação e apoptose de mamas de ratas ovariectomizadas.Métodos Um total de 48 ratas Wistar castradas foram divididas em 6 grupos, e cadaum foi submetido a um dos seguintes tratamentos durante 5 semanas: 1) controle; 2)BE 50mcg/diaþ T 50mcg/dia; 3) T 50mcg/dia; 4) BE 50mcgþ T 300mcg/dia; e) T 300mcg/dia; e f) BE 50 mcg/dia. Após o tratamento, o tecido mamário foi submetido aanálise histológica e avaliação de imunoexpressão de marcadores de proliferação(antígeno nuclear de células proliferantes, PCNA) e apoptose (caspase-3).Resultados Houve diferença estatisticamente significante entre os grupos com relaçãoàs microcalcificações e à atividade secretora, com maior prevalência nos grupos tratadoscom BE. Não houve diferença entre os grupos quanto à atrofia, mas houve maiorprevalência de atrofia nos grupos que receberam T versus os que receberam BEþ T. Houvediferença entre os grupos quanto ao ANCP (p¼ 0,028), com maior expressão no grupoBEþ T 300 mcg/dia. Com relação à caspase-3, não houve diferença entre os grupos, mas,no grupo BEþ T 300 mcg/dia, a expressão foi maior do que no grupo de T isolada.Conclusão A T isolada não apresentou efeito proliferativo do tecido mamário,contrariamente ao EB. A T em associação ao EB pode diminuir ou não a proliferação,a depender da dose de T.
Palavras-chave
► testosterona► proliferação► apoptose► mama► ovariectomia
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Effect of Testosterone on Proliferation Markers and Apoptosis Oliveira et al.704

performed by the pathologist (A.M.M.) and by the mainresearcher (J.C.C.O.), and both of them reached a consensusabout the presence or absence of atrophy, microcalcificationin the glandular lumen, and degree of glandular secretoryactivity. The quantification of secretory activitywas reportedas follows:
• þ: minimal secretion in the form of cytoplasmic vacuo-lization without accumulation or dilation of light.
• þþ: secretion in the cytoplasm and light, with minimalarchitectural distortion of the mammary lobes.
• þþþ : exuberant secretion.• 0: absent secretory activity.
Histological Analysis: HistomorphometryThe histomorphometric quantitative analysis was performedunder HE staining by the pathologist (A.M.M.), using a Zeiss(Berlin, Germany) trinocularmicroscopewith theAxiovision 4(Zeiss) image analysis software, under mediummagnification(100x). The images obtainedwere captured byadigital cameraand transferred to a computer with an image scanner. Aftercalibration to measure in mm2, the entire mammary gland(glandular tissue, fibroadipous stroma and striated muscletissue) was delineated with the computer mouse, obtainingthe total area. Then, only the glandular acini were delineated,adding their area, also expressed in mm2. Subsequently, theratio between the glandular area and the total breast areawascalculated.
ImmunohistochemistryImmunohistochemistry (IHC) was performed to analyze pro-liferating cell nuclear antigen (PCNA) and apoptosis (caspase-3)in 3-μmthick histological sections. All sampleswere submittedto IHC reaction using the following primary antibodies: PCNA(PC10) 1:1,000 (Cell Signaling Technology, Danvers, MA, US)and caspase-3 1:350 (BioVision, Milpitas, CA, US). The IHCreaction was developed using the peroxidase kit LSAB-peroxi-dase (DakoCytomation, Copenhagen, Denmark), according tothe manufacturer’s protocol. Then, they were processed withchromogen (3–3’-diaminobenzidine (DAB) 100mg (Sigma-Aldrich, St. Louis, MI, US) in 70ml of phosphate-buffered saline(PBS)þ 3ml hydrogenperoxide, andHarris hematoxylin coun-terstain (Sigma-Aldrich). Theslideswereanalyzedwith aNikonEclipse TS100 light microscope, under the same light intensityand the sameheight as the condenser, to identify the areas thatbest represent the immunostaining of the analyzed molecules(hot spot). The areas that best represented the immunostainingwere selected by an experienced pathologist, whowas blindedto the treatment groups, and analyzed under 400x magnifica-tion . Photomicrographs of consecutivemismatchedfieldswitha resolution of 640� 480 pixels were obtained using a NikonCoolpix 4300 digital camera with the same settings for allblades. In each case, the quantification of the immunostainingwas performed by digital computer analysis, and the valueswere expressed by the expression index (IE). The imagesobtainedwere analyzed using the ImageLab (Softium Informá-tica, SãoPaulo, SP, Brazil) imageprocessingandanalysis system,adjusted to the micrometer (μm) scale.
Statistical Method
The datawere organized into Microsoft Excel 2007 (MicrosoftCorp., Redmond, WA, US) spreadsheets. The qualitative vari-ableswere presented as absolute and relative frequencies, andcomparisons between the groups were performed using theChi-squared test.
The numerical datawere presented asmeans and standarddeviations, and their normal distribution was analyzed usingthe Shapiro-Wilk test. As this distributionwas not confirmed,the groupswere comparedusing theKruskal-Wallis test,whilecomparisons between pairs of groups were made using theMann-Whitney U-test. The statistical package XLStat (Addin-soft, NewYork,NY, US), version 17.01, for Excelwasused for allanalyzes. The level of statistical significance was set at 5%(p< 0.05).
Ethical AspectsAll of the study procedures were approved by the AnimalResearch Ethics Committee of the Faculdade de Medicina doABC under number 01/2016.
Results
During the study therewas no loss of animals. After dissectionand preparation of the slides, 7 samples had no glandulartissue, so 41 samples with mammary glandular tissue on theslides were included in the analysis.
►Table 1 shows the analysis of semiquantitative atrophyparameters, but no statistically significant difference wasfound among the groups. However, there is a tendency forlower occurrence of atrophy in groups receiving EB and Tversus those receiving T alone. Therefore, we decided togroup all of the cases that received EB associated with T, aswell as those that received T alone, and to perform acomparative analysis of these larger groups, noting a higherprevalence of atrophy in the group treated with isolated T ,with statistical significance (p¼ 0.015) (►Table 2). As formicrocalcifications (►Table 1), there was a statistically sig-nificant difference among the groups (p¼ 0.024), with ahigher occurrence in groups receiving EB. Similarly, wegrouped the results of the EBþ T groups, comparing themwith the groups that received only T (►Table 2) , and a higherprevalence of microcalcification in the groups that receivedEB (p¼ 0.022) was observed.
The secretory activity was also different among thegroups (p¼ 0.008), being higher in the groups that receivedisolated EB or EBþ T comparedwith the groups that receivedonly T. In ►Table 2, in the analysis performed with twogroups containing all of the cases who received Eþ T and allof the cases that received isolated T, a higher occurrence ofsecretionwas confirmed in the groups that received EB, withstatistical significance (p¼ 0.019).►Fig. 1 shows the result ofthe glandular tissue area. Although the glandular areaseemed larger in the groups receiving EB than in thosereceiving only T or the controls, no statistical significancewas found in the overall analysis among groups. In relation tothe breast area, no significance was found either.
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Effect of Testosterone on Proliferation Markers and Apoptosis Oliveira et al. 705

The graph in►Fig. 2 represents the area ratio of mamma-ry acini to the total area of breast, with larger values beingobserved in the groups treatedwith EB comparedwith thosetreated only with T or the controls, but the overall analysisshowed no statistical significance. However, when we com-pared the cases that received isolated Twith the isolated EBgroup, the difference was statistically significant (p¼ 0.047).
The PCNA quantification, shown in ►Fig. 3, presents astatistically significant difference among groups (p¼ 0.028).
The analysis of pairs of groups evidenced a significantdifference between the EB 50 mcgþ T 300 mcg group andthe controls (p¼ 0.001), between the EB 50mcgþ T 300mcgand EB 50 mcgþ T 50 mcg (p¼ 0.015) groups, and betweenthe EB 50mcgþ T 300mcg and T 300mcg (p¼ 0.027) groups.
►Fig. 4 graphically quantifies the immunohistochemistryof caspase-3. No statistically significant differencewas foundamong the groups (p¼ 0.236); however, in the analysis ofpairs of groups, a statistically significant difference wasobserved for the T 300mcg group comparedwith the control
Table 1 Results of the semiquantitative parameters by therapy (values expressed in absolute numbers and percentages inparentheses)
Semiquantitativeparameters
Placebon¼ 8
Estradiolbenzoate50 mcgn¼ 7
Estradiol benzoate50 mcg þtestosterone50 mcgn¼ 6
Testosterone50 mcgn¼ 5
Estradiol benzoate50 mcg þtestosterone300 mcgn¼ 8
Testosterone300 mcgn¼ 7
Atrophya
No 2 (25%) 3 (50%) 0 (0%) 4 (50%) 0 (0%) 2 (28.57%)
Yes 6 (75%) 3 (50%) 5(100%) 4(50%) 7 (100%) 5 (71.42%)
Microcalcificationb
Absent 7 (87.5%) 4 (66.6%) 4 (80%) 3 (37.5%) 7 (100%) 2 (28.5%)
Present 1 (12.5%) 2 (33.3%) 1 (20%) 5 (62.5%) 0 (0%) 5 (71.4%)
Secretory activityc
Absent 3 (37.5%) 1 (16.6%) 1 (20%) 1 (12.5%) 6 (85.7%) 0(0%)
Present 5 (62.5%) 5 (83.3%) 4 (80%) 7 (87.5%) 1 (14.2%) 7(100%)
Absent 3 (37.5%) 1 (16.6%) 1(20%) 1 (12.5%) 6 (85.7%) 0(0%)
þ 2 (25%) 3 (50%) 4 (80%) 2 (25%) 0 (0%) 2 (28.5%)
þþ 2 (25%) 2 (33.3%) 0 (0%) 3 (37.5%) 1 (14.2%) 3 (42.8%)
þþþ 1 (12.5%) 0 (0%) 0 (0%) 2 (25%) 0 (0%) 2 (28.5%)
Notes: ap¼ 0.143; bp¼ 0.024; cp¼ 0.008. þ: mild secretion; þþ: moderate secretion; þþþ : intense secretion.
Table 2 Results of the semiquantitative parameters (valuesexpressed in absolute numbers and percentages in parentheses)in the groups that received estradiol benzoate plus testosteroneand isolated testosterone
SemiquantitativeParameters Estradiol benzoateþ
testosteroneTestosterone
Atrophya
No 7 (50%) 0 (0%)
Yes 7 (50%) 12 (100%)
Microcalcificationb
Absent 7 (50%) 11 (91.7%)
Present 7 (50%) 1 (8.3%)
Secretory activityc
Absent 2 (14.3%) 7 (58.3%)
Present 12 (85.7%) 5 (41.7%)
Notes: ap¼ 0.015, bp¼ 0.022; cp¼ 0.019.
Fig. 1 Graphical representation of the mammary gland area in thecollected tissue per groups.
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Effect of Testosterone on Proliferation Markers and Apoptosis Oliveira et al.706

group (p¼ 0.037), and between the T 300 mcg comparedwith the Eþ T 300 mcg group (p¼ 0.025).
Discussion
Loss of sexual desire, musculoskeletal health impairment, anddecreased cognitive performance are some of the characteris-tic symptoms of the climacteric. The exogenous use of T hasbeen indicated for such complaints, especially for the decreasein sexual desire, but it generates concern among theusers. Few
studies have been published on the action and effects of Tsupplementation in women, as well as studies that clarify thecontribution of T to the risk of developing cardiovascular,musculoskeletal and cognitive disorders and cancer.7
The variety of hormone-related information, specifically Tin breast tissue, combined with the divergence of outcomesfrom studies on the risk of breast cancer and hormonereplacement therapy users8,9 was sufficient reason to devel-op this research; however, the difficulties in studying thehuman breast made us opt for the analysis of the response ofmammary tissue to the hormones tested in an experimentalmodel with rats.
The studies by Russo et al10 and Russo and Russo11
contributed with mammary tissue studies with rats andconsidered an adequate and representative model of humanbreast, which supported the decision to choose the murinemodel in the present study.
The present study did not find a statistically significantdifference among the groups for the semiquantitativeparameters of atrophy, but when comparing the isolated Tgroups to the EBþ T groups, there was a lower occurrence ofatrophy in the groups treatedwith EB. Thus, we can concludethat, in the absence of estrogen, themammary lobes atrophy,leading to a decrease in the proliferation of the epithelium,with a decrease in the number of lobes in the breast tissue, asshown by Clarke,12 who stated that estrogen is responsiblefor mitogenesis in the breast during menstruation, even inthe presence of T. The novelty is that isolated T in our studydid not lead to proliferation; on the contrary the rates ofatrophy were higher in the groups treated with isolated T.
The results found in this study are compatiblewith those ofthe study by Grynberg et al,13 who state that this increase inatrophy of the glandular tissue and fibrosis of the stromaltissues is caused in the postmenopausal period, because of the
Fig. 2 Graphical representation of the ratio between gland area andmammary area per groups.
Fig. 3 Graphical representation of quantification by immunohis-tochemistry of PCNA per groups.
Fig. 4 Graphical representation of the quantification by immuno-histochemistry of caspase-3 per groups.
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Effect of Testosterone on Proliferation Markers and Apoptosis Oliveira et al. 707

absence of estrogenic hormonal stimulation in the mammarytissue.
Regarding secretory activity, a statistically significantdifference was found in the overall analysis and the analysisamong groups, with higher secretory activity in the groupstreated with EBþ T. This shows that isolated T exerted littlestimulus in the proliferative activity of breast tissue, astimulus that was evidenced whenever EB was added.
Our study showed a statistically significant differenceamong treatment groups in the proliferative activity mea-sured by PCNA, especially the comparison of groups treatedwith higher doses of T combined with EB compared with thegroups treated with lower doses of T combined with EB,isolated T, or the controls.
Through graphic analysis and based on multiple compar-isons, a clear difference in the effect of T/EB on the epithelialproliferation expressed by PCNA is evident. In contrast, alower rate of proliferation was observed with T alone.
Our study converges with the results of the study bySomboonporn and Davis,14 which describes that androgensact in a direct protective way on cell proliferation bycontrolling the mitogenic effect of estrogen on breast tissue.In addition, one of the few human studies evaluating theeffect of T on breast-cell proliferation, conducted by Hoflinget al,15 found that postmenopausal women who receivedT (300 mcg/day) associated with hormone-replacementtherapy (2mg of estradiol and 1mg of norethisteroneacetate) showed no increase in cell proliferation; on theother hand, there was a more than five-time increase in cellproliferation in women receiving estrogen therapy associ-ated to progestogen.
This finding suggests that although the histological studyhas not shown proliferative mammary T activity, there maybe a dose-dependent effect when T is associated with EB.
The analysis of caspase-3 showed a higher apoptosis in thegroup that received EBþ T in high doses compared with thegroup that received the same dose of T, but without EB. Thisis evidence that the increased proliferationwith higher dosesof T associated with EB led to increased cell apoptosis.
The present study reinforces the findings of the study byZhou et al,16 who investigated ovariectomized rhesus maca-ques regarding the sexual steroid effects onmammary epithe-lial proliferation, with isolated estradiol increasing breastepithelial proliferation by � 50%, and T reducing the inducedestradiol proliferation by 40%, suggesting that it is a positiveandrogen replacement therapy in menopausal women.
Although not always statistically significant, our studyshows a lower proliferation in the presence of T in thegraphic analysis, but we observed a dose-dependent effectof T, which may mean that, in larger doses, T may notsuppress the proliferation induced by estrogen.
Some limitations of our study can be mentioned, such asthe fact that we have evaluated proliferation and apoptosiswith only one marker for each one, PCNA and caspase-3respectively, although these have shown results and havealready been used in previous studies such as the one byPompei et al.17 Another limiting factor was our relativelysmall number of animals in the different groups. A larger
sample would probably show statistical significance inother parameters that in the graphic analysis seem to bedifferent among groups. As a strong point, the double-blinded design was highlighted, in which the researchersand the pathologist who analyzed the slides were not awareof the treatment in each group, eliminating a source of bias.In addition, comparing different doses of T in combinationor not with estrogen helps to understand the possible dose-dependent effect and to support new studies addressingthese issues.
Conclusion
Isolated T did not have a proliferative effect on mammarytissue, contrary to EB. The combination of T andEBmayormaynot decrease the proliferation, depending on the dose of T.
Conflict to InterestsThe authors have none to disclose.
References1 Davis SR, Moreau M, Kroll R, et al; APHRODITE Study Team.
Testosterone for low libido in postmenopausal women not takingestrogen. N Engl J Med 2008;359(19):2005–2017. Doi: 10.1056/NEJMoa0707302
2 Key T, Appleby P, Barnes I, Reeves G; Endogenous Hormones andBreast Cancer Collaborative Group. Endogenous sex hormonesand breast cancer in postmenopausal women: reanalysis of nineprospective studies. J Natl Cancer Inst 2002;94(08):606–616. Doi:10.1093/jnci/94.8.606
3 Manjer J, Johansson R, Berglund G, et al. Postmenopausal breastcancer risk in relation to sex steroid hormones, prolactin andSHBG (Sweden). Cancer Causes Control 2003;14(07):599–607.Doi: 10.1023/A:1025671317220
4 Baglietto L, Severi G, EnglishDR, et al. Circulating steroid hormonelevels and risk of breast cancer for postmenopausal women.Cancer Epidemiol Biomarkers Prev 2010;19(02):492–502. Doi:10.1158/1055-9965.EPI-09-0532
5 Basaria S, Dobs AS. Safety and adverse effects of androgens: howto counsel patients. Mayo Clin Proc 2004;79(4, Suppl):S25–S32.Doi: 10.1016/S0025-6196(19)30669-X
6 Shufelt CL, Braunstein GD. Safety of testosterone use in women.Maturitas 2009;63(01):63–66.Doi: 10.1016/j.maturitas.2009.01.012
7 Davis SR, Wahlin-Jacobsen S. Testosterone in women–the clinicalsignificance. Lancet Diabetes Endocrinol 2015;3(12):980–992.Doi: 10.1016/S2213-8587(15)00284-3
8 Kaaks R, Rinaldi S, Key TJ, et al. Postmenopausal serum androgens,oestrogens and breast cancer risk: the European prospectiveinvestigation into cancer and nutrition. Endocr Relat Cancer2005;12(04):1071–1082. Doi: 10.1677/erc.1.01038
9 YasuiT,MatsuiS,TaniA,KunimiK,YamamotoS, IraharaM.Androgenin postmenopausal women. J Med Invest 2012;59(1-2):12–27. Doi:10.2152/jmi.59.12
10 Russo J,GustersonBA,RogersAE,Russo IH,WellingsSR,VanZwietenMJ. Comparative study of human and rat mammary tumorigenesis.In: Rubin E, Damjanov I, eds. Pathology reviews • 1990. New York,NY: Springer Scienceþ Business Media; 1990:217–251
11 Russo J, Russo IH. Experimentally induced mammary tumors inrats. Breast Cancer Res Treat 1996;39(01):7–20. Doi: 10.1007/bf01806074
12 Clarke RB. Steroid receptors and proliferation in the humanbreast. Steroids 2003;68(10-13):789–794. Doi: 10.1016/s0039-128x(03)00122-3
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Effect of Testosterone on Proliferation Markers and Apoptosis Oliveira et al.708

13 Grynberg M, Fanchin R, Dubost G, et al. Histology of genital tractand breast tissue after long-term testosterone administration in afemale-to-male transsexual population. Reprod Biomed Online2010;20(04):553–558. Doi: 10.1016/j.rbmo.2009.12.021
14 Somboonporn W, Davis SR; National Health and Medical ResearchCouncil. Testosterone effects on the breast: implications for testos-terone therapy for women. Endocr Rev 2004;25(03):374–388. Doi:10.1210/er.2003-0016
15 Hofling M, Hirschberg AL, Skoog L, Tani E, Hägerström T, vonSchoultz B. Testosterone inhibits estrogen/progestogen-induced
breast cell proliferation in postmenopausal women. Menopause2007;14(02):183–190. Doi: 10.1097/01.gme.0000232033.92411.51
16 Zhou J, Ng S, Adesanya-Famuiya O, Anderson K, Bondy CA.Testosterone inhibits estrogen-inducedmammary epithelial pro-liferation and suppresses estrogen receptor expression. FASEB J2000;14(12):1725–1730. Doi: 10.1096/fj.99-0863com
17 Pompei LM, Cunha EP, Steiner ML, et al. Effects of estradiol,progestogens, and of tibolone on breast proliferation and apo-ptosis. Climacteric 2015;18(04):518–522. Doi: 10.3109/13697137.2015.1020482
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Effect of Testosterone on Proliferation Markers and Apoptosis Oliveira et al. 709
Association of Menopausal Status, Expression ofProgesterone Receptor and Ki67 to the Clinical Responseto Neoadjuvant Chemotherapy in Luminal Breast Cancer
Associação de status menopausal, expressão de receptor deprogesterona e de Ki67 à resposta clínica à quimioterapianeoadjuvante no câncer luminal de mamaLeonardo Roberto da Silva1 Renato Flora Vargas1 Júlia Yoriko Shinzato1
Sophie Françoise Mauricette Derchain1 Susana Ramalho1 Luiz Carlos Zeferino1
1Universidade Estadual de Campinas, Campinas, SP, Brazil
Rev Bras Ginecol Obstet 2019;41:710–717.
Address for correspondence Luiz Carlos Zeferino, MD, PhD,Universidade Estadual de Campinas, Rua Alexander Fleming 101,13083-881, Cidade Universitária “Zeferino Vaz”, Campinas, SP, Brazil(e-mail: [email protected]).
Keywords
► antineoplastic agents► breast neoplasms► segmental
mastectomy► neoadjuvant therapy► estrogen receptors
Abstract Objective To identify the biomarkers of response to neoadjuvant chemotherapy inearly luminal breast cancer.Methods A cross-sectional study that included all patients with early or locally-advanced luminal breast cancer submitted to neoadjuvant chemotherapy between2013 and 2014. Demographic, clinic and pathologic data were retrieved from patientrecords. The expressions of the estrogen receptor (ER), the progesterone receptor (PR),and Ki67 were analyzed by immunohistochemistry (IHC). The status of the humanepidermal growth factor receptor 2 (HER2) was evaluated by IHC and fluorescent in situhybridization (FISH). Independent predictors of clinic and pathologic response wereevaluated by stepwise logistic regression models and receiver operating characteristic(ROC) curve analysis.Results Out of 298 patients identified, 115 were included in the analysis. Clinicalcomplete response (cCR) was observed in 43.4% of the patients (49/113), andpathologic complete response (pCR) was observed in 7.1% (8/115) of the patients.The independent predictors of cCR were premenopausal status (p< 0.001), low PRexpression (� 50% versus> 50%; p¼ 0.048), and Ki67 expression� 14% (versus< 14%;p¼ 0.01). Patients with cCR were more commonly submitted to breast conservingsurgery (34.7% versus 7.8%; p< 0.001). Increasing cut-off points for Ki67 expressionwere associated with an increase in specificity and a decrease in sensitivity to identifypatients with cCR.Conclusion Premenopausal status, lower PR expression and higher Ki67 expressionwere associated with a higher rate of cCR to neoadjuvant chemotherapy in luminalbreast cancer.
receivedJuly 15, 2019acceptedOctober 9, 2019
DOI https://doi.org/10.1055/s-0039-3400457.ISSN 0100-7203.
Copyright © 2019 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Original ArticleTHIEME
710

Introduction
Breast cancer is a heterogeneous group of diseases thatdiffer in terms of behavior, prognosis and response totreatment.1,2 Traditional prognostic and predictivemarkers, such as tumor size, lymph-node involvement,vascular invasion, and expression of estrogen receptor(ER), progesterone receptor (PR), and human epidermalgrowth factor receptor 2 (HER2) are used to select thetreatment. However, these factors have limited power todefine the prognosis and individualize treatment.3,4
Neoadjuvant treatment for breast cancer has become animportant strategy to downstage inoperable tumors, eval-uate tumor biology, and identify potential biomarkers in arelatively short period of time.5 Pathologic completeresponse (pCR) after neoadjuvant chemotherapy (NAC) isconsidered a surrogate endpoint for long-term outcomes.6,7
However, pCR is rarely seen in hormone-receptor-positive(luminal) breast cancer, and its prognostic impact is notclear.8,9 Still, a subgroup of luminal tumors is chemo-sensitive.10,11 There is a need to identify predictive factorsthat could help select patients with luminal breast cancerwho would benefit from NAC.
The aim of the present study was to evaluate the associa-tion between patient characteristics, expression of ER, PR,HER2 and Ki67, and the clinicopathological response to NACin patients with luminal breast cancer.
Methods
The present was a cross-sectional study conducted at Hospi-tal da Mulher Professor José Aristodemo Pinotti, Centro deAtenção Integral à Saúde da Mulher (CAISM), UniversidadeEstadual de Campinas (UNICAMP), Brazil. The study wasapproved by the Research Ethics Committee of the Schoolof Medical Sciences at UNICAMP (CEP 1246/2009). Wereviewed the medical records of 298 patients submitted toNAC between January 2013 and December 2014, and 115patients were included (►Fig. 1). The inclusion criteria werediagnosis of invasive hormone-receptor-positive breastcarcinoma, clinical stages I-III, and use of at least one cycleof NAC followed by surgery.
The tumors were histologically classified according to theWorld Health Organization criteria, the histological gradewasdetermined according to the modified Bloom–Richardsonsystem, and the tumors were grouped as low-to-moderategrade (grades I-II) and high grade (grade III).12,13 We definedpCR as the absence of invasive disease on the breast andaxilla.14 Immunohistochemistry was used to evaluate theexpression of the ER (clone 1D5, 1:1 000, Dako, Carpinteria,CA, US), PR (clone PR 636, 1:800, Dako), HER2 (Clone PN2A,1:1100, Dako), and Ki67 (clone MIB1, 1:500, Dako) proteinusing standard protocols. The ER and PR staining were classi-fied as positive if at least 1% of the nuclei stained.15 Theexpression of Ki67 was reported as an average expression
Resumo Objetivo Identificar biomarcadores de resposta à quimioterapia neoadjuvante emcâncer luminal de mama.Métodos Estudo transversal em que foram incluídas todas as pacientes com câncerluminal de mama em estádio inicial ou localmente avançado que foram submetidas aquimioterapia neoadjuvante nos anos de 2013 e 2014. Dados demográficos, clínicos epatológicos foram obtidos de prontuários médicos. As expressões de receptor deestrogênio (RE), de receptor de progesterona (RP), e de Ki67 foram avaliadas porimuno-histoquímica (IHQ). A expressão do receptor tipo 2 do fator de crescimentoepidérmico humano (human epidermal growth factor receptor 2, HER2) foi avaliada porIHQ e hibridização in situ por imunofluorescência (HISI). Análises de regressão logísticae de curva de característica de operação do receptor (COR) foram usadas parainvestigar fatores preditivos independentes de resposta clínica e patológica.Resultados De 298 pacientes identificadas, 115 foram incluídas na análise. Respostaclínica completa (RCc) foi observada em 43.4% das pacientes (49/113), e respostapatológica completa (RPc), em 7.1% (8/115). Os fatores preditivos independentes deRCc foram status menopausal (p< 0.001), baixa expressão de RP (� 50% versus> 50%;p¼ 0.048), e expressão de Ki67 � 14% (versus< 14%; p¼ 0.01). Pacientes com RCcapresentaram maior probabilidade de serem submetidas a cirurgia conservadora damama (34.7% versus 7.8%; p< 0.001). Aumento no ponto de corte para expressão deKi67 foi associado a aumento da especificidade e redução da sensibilidade naidentificação de pacientes com RCc.Conclusão Status premenopausal, baixa expressão de RP e maior expressão de Ki67estiveram associados a maior taxa de RCc à quimioterapia neoadjuvante no câncerluminal de mama.
Palavras-chave
► agentesantineoplásicos
► neoplasias da mama► mastectomia
segmentar► terapia neoadjuvante► receptores
estrogênicos
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Association of Menopausal Status, Progesterone Receptor and Ki67 to Clinical Response Silva et al. 711
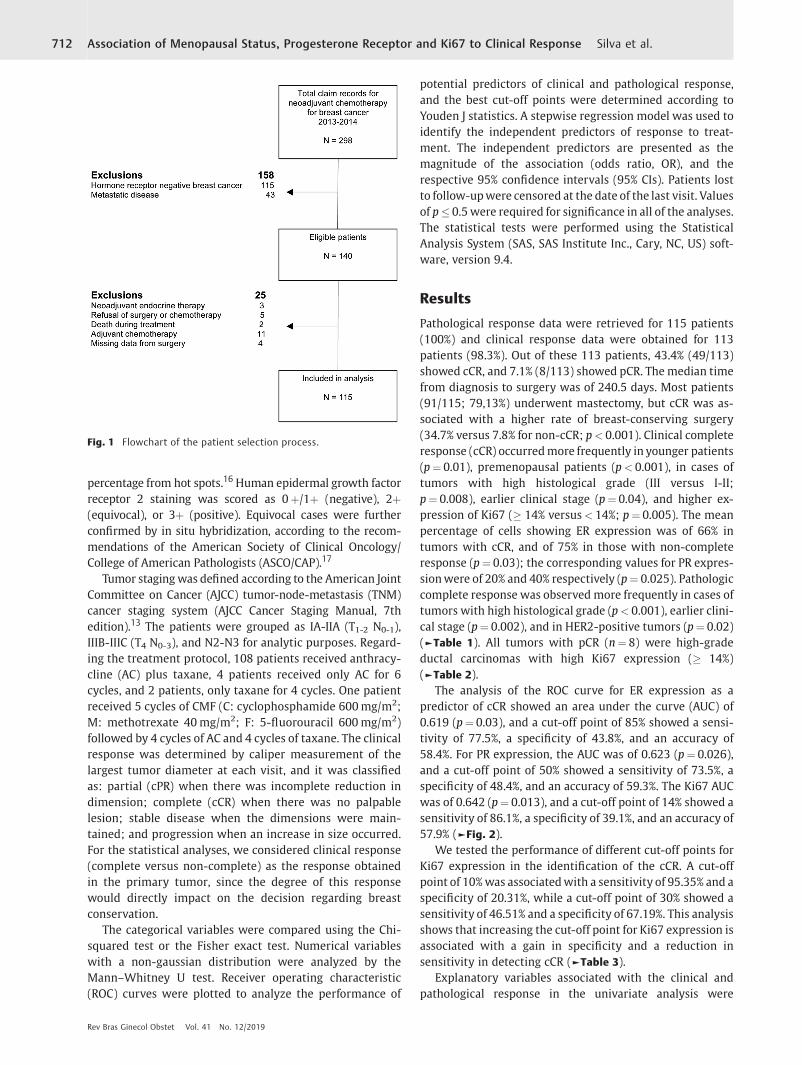
percentage from hot spots.16Human epidermal growth factorreceptor 2 staining was scored as 0þ/1þ (negative), 2þ(equivocal), or 3þ (positive). Equivocal cases were furtherconfirmed by in situ hybridization, according to the recom-mendations of the American Society of Clinical Oncology/College of American Pathologists (ASCO/CAP).17
Tumor staging was defined according to the American JointCommittee on Cancer (AJCC) tumor-node-metastasis (TNM)cancer staging system (AJCC Cancer Staging Manual, 7thedition).13 The patients were grouped as IA-IIA (T1-2 N0-1),IIIB-IIIC (T4 N0-3), and N2-N3 for analytic purposes. Regard-ing the treatment protocol, 108 patients received anthracy-cline (AC) plus taxane, 4 patients received only AC for 6cycles, and 2 patients, only taxane for 4 cycles. One patientreceived 5 cycles of CMF (C: cyclophosphamide 600mg/m2;M: methotrexate 40mg/m2; F: 5-fluorouracil 600mg/m2)followed by 4 cycles of AC and 4 cycles of taxane. The clinicalresponse was determined by caliper measurement of thelargest tumor diameter at each visit, and it was classifiedas: partial (cPR) when there was incomplete reduction indimension; complete (cCR) when there was no palpablelesion; stable disease when the dimensions were main-tained; and progression when an increase in size occurred.For the statistical analyses, we considered clinical response(complete versus non-complete) as the response obtainedin the primary tumor, since the degree of this responsewould directly impact on the decision regarding breastconservation.
The categorical variables were compared using the Chi-squared test or the Fisher exact test. Numerical variableswith a non-gaussian distribution were analyzed by theMann–Whitney U test. Receiver operating characteristic(ROC) curves were plotted to analyze the performance of
potential predictors of clinical and pathological response,and the best cut-off points were determined according toYouden J statistics. A stepwise regression model was used toidentify the independent predictors of response to treat-ment. The independent predictors are presented as themagnitude of the association (odds ratio, OR), and therespective 95% confidence intervals (95% CIs). Patients lostto follow-upwere censored at the date of the last visit. Valuesof p� 0.5were required for significance in all of the analyses.The statistical tests were performed using the StatisticalAnalysis System (SAS, SAS Institute Inc., Cary, NC, US) soft-ware, version 9.4.
Results
Pathological response data were retrieved for 115 patients(100%) and clinical response data were obtained for 113patients (98.3%). Out of these 113 patients, 43.4% (49/113)showed cCR, and 7.1% (8/113) showed pCR. The median timefrom diagnosis to surgery was of 240.5 days. Most patients(91/115; 79,13%) underwent mastectomy, but cCR was as-sociated with a higher rate of breast-conserving surgery(34.7% versus 7.8% for non-cCR; p< 0.001). Clinical completeresponse (cCR) occurredmore frequently in younger patients(p¼ 0.01), premenopausal patients (p< 0.001), in cases oftumors with high histological grade (III versus I-II;p¼ 0.008), earlier clinical stage (p¼ 0.04), and higher ex-pression of Ki67 (� 14% versus< 14%; p¼ 0.005). The meanpercentage of cells showing ER expression was of 66% intumors with cCR, and of 75% in those with non-completeresponse (p¼ 0.03); the corresponding values for PR expres-sionwere of 20% and 40% respectively (p¼ 0.025). Pathologiccomplete response was observed more frequently in cases oftumors with high histological grade (p< 0.001), earlier clini-cal stage (p¼ 0.002), and in HER2-positive tumors (p¼ 0.02)(►Table 1). All tumors with pCR (n¼ 8) were high-gradeductal carcinomas with high Ki67 expression (� 14%)(►Table 2).
The analysis of the ROC curve for ER expression as apredictor of cCR showed an area under the curve (AUC) of0.619 (p¼ 0.03), and a cut-off point of 85% showed a sensi-tivity of 77.5%, a specificity of 43.8%, and an accuracy of58.4%. For PR expression, the AUC was of 0.623 (p¼ 0.026),and a cut-off point of 50% showed a sensitivity of 73.5%, aspecificity of 48.4%, and an accuracy of 59.3%. The Ki67 AUCwas of 0.642 (p¼ 0.013), and a cut-off point of 14% showed asensitivity of 86.1%, a specificity of 39.1%, and an accuracy of57.9% (►Fig. 2).
We tested the performance of different cut-off points forKi67 expression in the identification of the cCR. A cut-offpoint of 10%was associatedwith a sensitivity of 95.35% and aspecificity of 20.31%, while a cut-off point of 30% showed asensitivity of 46.51% and a specificity of 67.19%. This analysisshows that increasing the cut-off point for Ki67 expression isassociated with a gain in specificity and a reduction insensitivity in detecting cCR (►Table 3).
Explanatory variables associated with the clinical andpathological response in the univariate analysis were
Fig. 1 Flowchart of the patient selection process.
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Association of Menopausal Status, Progesterone Receptor and Ki67 to Clinical Response Silva et al.712
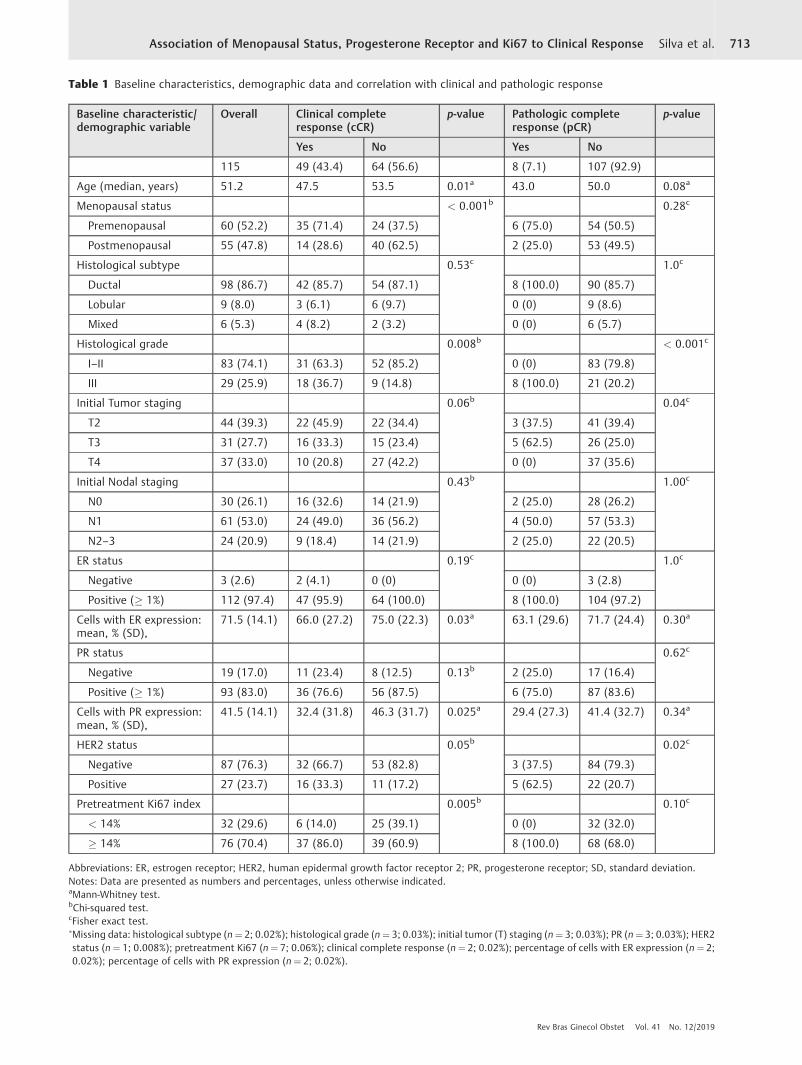
Table 1 Baseline characteristics, demographic data and correlation with clinical and pathologic response
Baseline characteristic/demographic variable
Overall Clinical completeresponse (cCR)
p-value Pathologic completeresponse (pCR)
p-value
Yes No Yes No
115 49 (43.4) 64 (56.6) 8 (7.1) 107 (92.9)
Age (median, years) 51.2 47.5 53.5 0.01a 43.0 50.0 0.08a
Menopausal status < 0.001b 0.28c
Premenopausal 60 (52.2) 35 (71.4) 24 (37.5) 6 (75.0) 54 (50.5)
Postmenopausal 55 (47.8) 14 (28.6) 40 (62.5) 2 (25.0) 53 (49.5)
Histological subtype 0.53c 1.0c
Ductal 98 (86.7) 42 (85.7) 54 (87.1) 8 (100.0) 90 (85.7)
Lobular 9 (8.0) 3 (6.1) 6 (9.7) 0 (0) 9 (8.6)
Mixed 6 (5.3) 4 (8.2) 2 (3.2) 0 (0) 6 (5.7)
Histological grade 0.008b < 0.001c
I–II 83 (74.1) 31 (63.3) 52 (85.2) 0 (0) 83 (79.8)
III 29 (25.9) 18 (36.7) 9 (14.8) 8 (100.0) 21 (20.2)
Initial Tumor staging 0.06b 0.04c
T2 44 (39.3) 22 (45.9) 22 (34.4) 3 (37.5) 41 (39.4)
T3 31 (27.7) 16 (33.3) 15 (23.4) 5 (62.5) 26 (25.0)
T4 37 (33.0) 10 (20.8) 27 (42.2) 0 (0) 37 (35.6)
Initial Nodal staging 0.43b 1.00c
N0 30 (26.1) 16 (32.6) 14 (21.9) 2 (25.0) 28 (26.2)
N1 61 (53.0) 24 (49.0) 36 (56.2) 4 (50.0) 57 (53.3)
N2–3 24 (20.9) 9 (18.4) 14 (21.9) 2 (25.0) 22 (20.5)
ER status 0.19c 1.0c
Negative 3 (2.6) 2 (4.1) 0 (0) 0 (0) 3 (2.8)
Positive (� 1%) 112 (97.4) 47 (95.9) 64 (100.0) 8 (100.0) 104 (97.2)
Cells with ER expression:mean, % (SD),
71.5 (14.1) 66.0 (27.2) 75.0 (22.3) 0.03a 63.1 (29.6) 71.7 (24.4) 0.30a
PR status 0.62c
Negative 19 (17.0) 11 (23.4) 8 (12.5) 0.13b 2 (25.0) 17 (16.4)
Positive (� 1%) 93 (83.0) 36 (76.6) 56 (87.5) 6 (75.0) 87 (83.6)
Cells with PR expression:mean, % (SD),
41.5 (14.1) 32.4 (31.8) 46.3 (31.7) 0.025a 29.4 (27.3) 41.4 (32.7) 0.34a
HER2 status 0.05b 0.02c
Negative 87 (76.3) 32 (66.7) 53 (82.8) 3 (37.5) 84 (79.3)
Positive 27 (23.7) 16 (33.3) 11 (17.2) 5 (62.5) 22 (20.7)
Pretreatment Ki67 index 0.005b 0.10c
< 14% 32 (29.6) 6 (14.0) 25 (39.1) 0 (0) 32 (32.0)
� 14% 76 (70.4) 37 (86.0) 39 (60.9) 8 (100.0) 68 (68.0)
Abbreviations: ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; PR, progesterone receptor; SD, standard deviation.Notes: Data are presented as numbers and percentages, unless otherwise indicated.aMann-Whitney test.bChi-squared test.cFisher exact test.�Missing data: histological subtype (n¼ 2; 0.02%); histological grade (n¼ 3; 0.03%); initial tumor (T) staging (n¼ 3; 0.03%); PR (n¼ 3; 0.03%); HER2status (n¼ 1; 0.008%); pretreatment Ki67 (n¼ 7; 0.06%); clinical complete response (n¼ 2; 0.02%); percentage of cells with ER expression (n¼ 2;0.02%); percentage of cells with PR expression (n¼ 2; 0.02%).
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Association of Menopausal Status, Progesterone Receptor and Ki67 to Clinical Response Silva et al. 713

subsequently tested on a multivariate stepwise regressionmodel. For ER, PR and Ki67 expression, optimal cut-off pointsdetermined at the ROC curve analysis were used. The multi-variate regression model did not identify independent pre-dictors of pCR, including histological grade, clinical staging,and HER2 expression. Premenopausal patients (OR: 4.71;95%CI: 1.9–11.7; p< 0.001), low expression of PR (� 50%versus> 50%; OR: 2.58; 95%CI: 1.01–6.62; p¼ 0.048), andhigher expression of Ki67 (� 14% versus< 14%; OR: 3.92; 95%CI: 1.33–11.53; p¼ 0.01) were identified as independentpredictors of cCR (►Table 4).
In a subgroup analysis including only luminal HER2-negative tumors (n¼ 88), 33 (37.5%) patients presentedcCR, which was associated with premenopausal status(p< 0.001) and higher pre-treatment Ki67 expression(� 14% versus< 14%; p¼ 0.0123). On the multivariate step-wise regressionmodel, premenopausal status (OR: 1.90; 95%CI: 0.81–2.98; p< 0.001) and higher pre-treatment Ki67expression (� 14% versus< 14%; OR: 1.60; 95%CI:0.32–2.88; p¼ 0.014) were independent predictors of cCR(data not shown). Regarding the luminal HER2-negativetumors, there were 3 (3.4%) cases with pCR that were
Table 2 Baseline characteristics and demographic data of patients with pCR
Patient Age Menopausalstatus
Tumorstaging
Nodalstaging
Histologicalsubtype
Histologicalgrade
HER2 PretreatmentKi67
Treatment
1 48 pre T3 N1 ductal III negative 80 AC-T
2 50 pre T2 N2 ductal III positive 70 AC-T
3 56 post T2 N0 ductal III negative 70 AC-T
4 49 post T3 N2 ductal III positive 30 AC-T
5 40 pre T3 N1 ductal III positive 20 AC-T
6 43 pre T3 N1 ductal III positive 15 AC-T
7 40 pre T3 N1 ductal III positive 20 AC-T
8 32 pre T2 N0 ductal III negative 15 AC-T
Abbreviations: AC, doxorubicin plus cyclophosphamide; ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; pCR, pathologiccomplete response; PR, progesterone receptor; T, paclitaxel or docetaxel.
Fig. 2 Receiver operating characteristic (ROC) curve analysis of estrogen receptor (ER), progesterone receptor (PR), and Ki67 expression aspredictors of clinical complete response (cCR). (A) ER expression. The calculated area under the curve (AUC) was of 0.619 (95% confidenceinterval [95%CI]: 0.516–0.722; p¼ 0.03); a cut-off point of 85% had a sensitivity of 77.5% and a specificity of 43.8% to identify patients who arelikely to develop cCR. (B) PR expression. The AUC was of 0.623 (95%CI: 0.518–0.728; p¼ 0.026); a cut-off point of 50% had a sensitivity of 73.5%and a specificity of 48.4%. (C) Ki67 expression. The AUC was of 0.642 (95%CI: 0.536–0.747; p¼ 0.013); a cut-off point of 14% had a sensitivity of86.1% and a specificity of 39.1%.
Table 3 Performanceofdifferent cut-off pointsofKi67expressionto determine the cCR according to the ROC curve analysis
Ki67 cutoff Sensitivity Specificity PPV NPV
� 10% versus< 10% 95.35 20.31 44.57 86.67
� 14% versus< 14% 86.10 39.10 48.68 80.65
� 20% versus< 20% 76.74 43.75 47.83 73.68
� 30% versus< 30% 46.51 67.19 48.78 65.15
Abbreviations: CCR, clinical complete response; NPV, negative predic-tive value; PPV, positive predictive value; ROC, receiver operatingcharacteristic.Note: Data are presented as percentages.
Table 4 Stepwise regression model results for independentpredictors of cCR
Explanatory variable Odds ratio (95% CI) p-value
Menopausal status:pre versus post
4.71 (1.9–11.7) < 0.001
Mean PR expression:� 50% versus> 50%
2.58 (1.01–6.62) 0.048
Ki67 expression:� 14% versus< 14%
3.92 (1.33–11.53) 0.01
Abbreviations: 95%CI, 95% confidence interval; CCR, clinical completeresponse; PR, progesterone receptor.
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Association of Menopausal Status, Progesterone Receptor and Ki67 to Clinical Response Silva et al.714

characterized by high histological grade (III versus I-II;p¼ 0.008) (data not shown).
Discussion
In our study,we investigated the association between clinicaland pathological parameters to predict cCR and pCR to NACin luminal breast cancer. In the univariate analysis, youngerage, premenopausal status, high histological grade andhigher expression of Ki67 were associated with cCR. Patho-logic complete responsewas observed in less than 10% of thepatients, and all of their tumors were of ductal histology,with high histological grade and higher Ki67 expression.Premenopausal status and higher expression of Ki67 wereindependent predictors of cCR in luminal breast cancerirrespective of HER2 expression. Low expression of PR wasan independent predictor of cCR only in luminal HER2-positive tumors. Our ROC curve analysis for ER, PR andKi67 expression showed amoderate performance to identifytumors with cCR. Increasing cut-off points for Ki67 expres-sion were associated with an increase in specificity anddecrease in sensitivity to identify the cCR.
In our cohort of patients, objective clinical response wasobserved in 88.6% of tumors, with a cCR rate of 43.4% on thebreast. These response rates are somewhat higher thanwhathas been previously described.18 However, these differencesmay be explained by two main factors: firstly, in the presentstudy,we classified the clinical response based exclusively onthe clinical examination. Moreover, evidence shows thatthere is a poor correlation between the response evaluatedby physical examination and imaging methods, and this mayreflect the dynamics of tumor response to treatment.19,20
Secondly, in the present study, 94% of the patients weretreatedwith an anthracycline and a taxane, opposed to 74.9%in the American College of Surgeons Oncology Group (ACO-SOG) Z1071 trial. Indeed, improvement in response ratesobtained by the addition of a taxane to an anthracycline inthe neoadjuvant setting is well documented.21,22
Our results showedthat premenopausalpatientsweremorelikely to achieve cCR. In several studies, young age at diagnosiswas identified as an independent predictor of recurrence andmortality in breast cancer patients.23,24 The poorer prognosisof these patients may be related to their higher likelihood ofdevelopingmoreaggressive tumors. In theProspective StudyofOutcomes in SporadicVersusHereditary Breast Cancer (POSH),2.956 young patients (aged 40 years or younger) with a breastcancer diagnosis were recruited, and the study showed that50.2% of the patients had a node-positive disease, 58.9% hadhigh grade tumors, and 33.7%were ER-negative, factors associ-ated with a higher response to chemotherapy.25 Similar find-ings were reported by other authors, along with high rates oflymphovascular invasion and lymphocytic infiltration.23,26
Tumorswithin the samemolecular subtypeareheterogeneous,and, although the reasons for these differences are not clear,recent evidence suggests that tumors inyounger patients showhigher expression of genes related tomammary stem cells andderegulation of mitogen-activated protein kinase (MAPK) andphosphoinositide 3-kinase (PI3K) pathways, which can con-
tribute to endocrine therapy resistance and chemosensitivityin ER-positive tumors.27–29 Tumors with lower PR expressionhad a higher probability of achieving cCR. In fact, it has beenshown that PR expression in ER-positive tumors is associatedwith less aggressive phenotypes, and that tumors with lowerPR expressionmay be less dependent on ER pathway signalingand show upregulation of the PI3K pathway.30–34
Ki67 expression was also an independent predictor of cCR,and higher expression levels are associated with a higherlikelihood of acieving cCR. Xu et al35 evaluated 129 breastcancer patients submitted to NAC, and showed that tumorswith Ki67 expression> 10% had better clinical response. Theuse of Ki67 as a predictive and prognosticmarker is amatter ofdebate due to poor reproducibility.16 To date, different Ki67expression cut-off points have been suggested to identifytumorswith ahigherprobabilityof response to chemotherapy.As we have shown, the accuracy of different cut-off points isquite variable. Finding a unique cut-off point is unlikely, andthis evaluation should consider the clinical scenario.36 OurROC curve analysis showed that the expressions of Ki67, ERand PRhave amodest ability to identify patientswith cCR. But,despite the relatively poor predictive performance, the curvesareplottedabove the line ofnodiscrimination,which implies abetter classification than random results.
In the present study, the pCR ratewas comparablewith datapublishedbyotherauthors,7,11,37 reflecting the relative chemo-resistance of ER-positive tumors. However, the pCR does notappear to have a prognostic impact on luminal breast cancerpatients, especially among low-grade and HER2-negativetumors.6,37 Although we could not identify independent pre-dictors of pCR, all tumors with pCR were ductal, had highhistological grade, Ki67 expression> 14%, and most wereHER2-positive. Histological grade and Ki67 reflect tumor pro-liferation, and tumors with high proliferative activity are moresensitive to chemotherapy.38 Rates of pCR are particularly highamong tumors that are HER2-positive, even in the absence ofanti-HER agents.6,7,37,39
The limitations of the present study include its retrospec-tive nature, which exerted an impact on our ability toretrieve some data. We studied a small sample of patients,but other authors11,35 reported on similar sample sizes. Thesmall number of patients with pCR may have limited theidentification of independent predictors for this outcome.One strength of our study is that the majority of our patientsunderwent a modern and standardized chemotherapy regi-men using the most advanced cytotoxic agents available inneoadjuvant settings, especially in the context of limitedaccess to anti-HER2 agents.
Conclusion
In conclusion, patients with hormone-receptor-positivetumors show high rates of clinical response to NAC, andachieving cCR is associated with a higher probability ofbreast-conserving surgery. Premenopausal status, lowerexpression of PR and higher expression of Ki67 were associ-ated with a higher likelihood of achieving cCR, and may beused to select patients with hormone-receptor-positive
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Association of Menopausal Status, Progesterone Receptor and Ki67 to Clinical Response Silva et al. 715

tumors who might benefit more from the NAC. This strategyhas the potential of effectively reducing overtreatment andcosts. Additional studies are necessary to better understandthe underlying mechanisms of these associations.
Contributions1. Substantial contributions to the conception or design of
thework; or the acquisition, analysis, or interpretation ofdata for thework: LeonardoRobertodaSilva,RenatoFloraVargas, JúliaYorikoShinzato, SophieFrançoiseMauricetteDerchain, Susana Ramalho, Luiz Carlos Zeferino.
2. Draft of the work or critical revision critically regardingimportant intellectual content: Leonardo Roberto daSilva, Renato Flora Vargas, Júlia Yoriko Shinzato, SophieFrançoise Mauricette Derchain, Susana Ramalho, LuizCarlos Zeferino.
3. Final approval of the version to be published: LeonardoRoberto da Silva, Renato Flora Vargas, Júlia YorikoShinzato, Sophie Françoise Mauricette Derchain, Sus-ana Ramalho, Luiz Carlos Zeferino.
Conflict of InterestsThe authors have none to declare.
AcknowledgmentsEditorial services were provided by the Edanz Group,Fukuoka, Japan.
References1 Perou CM, Sørlie T, Eisen MB, et al. Molecular portraits of human
breast tumours. Nature 2000;406(6797):747–752. Doi:10.1038/35021093
2 Sørlie T, Perou CM, Tibshirani R, et al. Gene expression patterns ofbreast carcinomas distinguish tumor subclasseswith clinical impli-cations. Proc Natl Acad Sci U S A 2001;98(19):10869–10874. Doi:10.1073/pnas.191367098
3 Weigelt B, Reis-Filho JS. Molecular profiling currently offers nomore than tumour morphology and basic immunohistochemis-try. Breast Cancer Res 2010;12(Suppl 4):S5. Doi: 10.1186/bcr2734
4 Banin Hirata BK, Oda JM, Losi Guembarovski R, Ariza CB, deOliveira CE, Watanabe MA. Molecular markers for breast cancer:prediction on tumor behavior. Dis Markers 2014;2014:513158.Doi: 10.1155/2014/513158
5 Carey LA,Winer EP. Defining success in neoadjuvant breast cancertrials. Lancet 2014;384(9938):115–116. Doi: 10.1016/S0140-6736(14)60034-9
6 von Minckwitz G, Untch M, Blohmer JU, et al. Definition andimpact of pathologic complete response on prognosis afterneoadjuvant chemotherapy in various intrinsic breast cancersubtypes. J Clin Oncol 2012;30(15):1796–1804. Doi: 10.1200/JCO.2011.38.8595
7 Fasching PA, Heusinger K, Haeberle L, et al. Ki67, chemotherapyresponse, and prognosis in breast cancer patients receiving neo-adjuvant treatment. BMCCancer 2011;11:486. Doi: 10.1186/1471-2407-11-486
8 ColleoniM,VialeG, ZahriehD, et al. Chemotherapy ismore effectivein patients with breast cancer not expressing steroid hormonereceptors: a study of preoperative treatment. Clin Cancer Res 2004;10(19):6622–6628. Doi: 10.1158/1078-0432.CCR-04-0380
9 Yerushalmi R,Woods R, Ravdin PM, HayesMM, Gelmon KA. Ki67 inbreast cancer: prognostic and predictive potential. Lancet Oncol2010;11(02):174–183. Doi: 10.1016/S1470-2045(09)70262-1
10 Sueta A, Yamamoto Y, Hayashi M, et al. Clinical significance ofpretherapeutic Ki67 as a predictive parameter for response toneoadjuvant chemotherapy in breast cancer: is it equally usefulacross tumor subtypes? Surgery 2014;155(05):927–935. Doi:10.1016/j.surg.2014.01.009
11 Horimoto Y, Arakawa A, Tanabe M, et al. Ki67 expression and theeffect of neo-adjuvant chemotherapy on luminal HER2-negativebreast cancer. BMC Cancer 2014;14:550. Doi: 10.1186/1471-2407-14-550
12 Tavassoeli FA, Devilee P. Pathology and Genetics of Tumors of theBreast and Female Genital Organs. 3rd ed. Lyon: IARC; 2003
13 Singletary SE, Allred C, Ashley P, et al. Revision of the AmericanJoint Committee on Cancer staging system for breast cancer. J ClinOncol 2002;20(17):3628–3636. Doi: 10.1200/JCO.2002.02.026
14 Mazouni C, Peintinger F, Wan-Kau S, et al. Residual ductalcarcinoma in situ in patients with complete eradication of inva-sive breast cancer after neoadjuvant chemotherapy does notadversely affect patient outcome. J Clin Oncol 2007;25(19):2650–2655. Doi: 10.1200/JCO.2006.08.2271
15 Hammond MEH, Hayes DF, Dowsett M, et al. American Society ofClinical Oncology/College Of American Pathologists guidelinerecommendations for immunohistochemical testing of estrogenand progesterone receptors in breast cancer. J Clin Oncol 2010;28(16):2784–2795. Doi: 10.1200/JCO.2009.25.6529
16 DowsettM,NielsenTO, A’Hern R, et al; International Ki-67 in BreastCancer Working Group. Assessment of Ki67 in breast cancer:recommendations from the International Ki67 in Breast Cancerworking group. J Natl Cancer Inst 2011;103(22):1656–1664. Doi:10.1093/jnci/djr393
17 Wolff AC, Hammond MEH, Hicks DG, et al; American Society ofClinical Oncology; College of American Pathologists. Recommen-dations for human epidermal growth factor receptor 2 testing inbreast cancer: American Society of Clinical Oncology/College ofAmerican Pathologists clinical practice guideline update. J ClinOncol 2013;31(31):3997–4013. Doi: 10.1200/JCO.2013.50.9984
18 Boughey JC, McCall LM, Ballman KV, et al. Tumor biology corre-lates with rates of breast-conserving surgery and pathologiccomplete response after neoadjuvant chemotherapy for breastcancer: findings from the ACOSOG Z1071 (Alliance) ProspectiveMulticenter Clinical Trial. Ann Surg 2014;260(04):608–614, dis-cussion 614–616. Doi: 10.1097/SLA.0000000000000924
19 Fiorentino C, Berruti A, Bottini A, et al. Accuracy ofmammographyand echography versus clinical palpation in the assessment ofresponse to primary chemotherapy in breast cancer patients withoperable disease. Breast Cancer Res Treat 2001;69(02):143–151
20 Shin HJ, Kim HH, Ahn JH, et al. Comparison of mammography,sonography, MRI and clinical examination in patients with locallyadvanced or inflammatory breast cancer who underwent neo-adjuvant chemotherapy. Br J Radiol 2011;84(1003):612–620. Doi:10.1259/bjr/74430952
21 Rastogi P, Anderson SJ, Bear HD, et al. Preoperative chemotherapy:updates of national surgical adjuvant breast and bowel projectprotocols B-18 and B-27. J Clin Oncol 2008;26(05):778–785. Doi:10.1200/JCO.2007.15.0235
22 Evans TRJ, Yellowlees A, Foster E, et al. Phase III randomized trialof doxorubicin and docetaxel versus doxorubicin and cyclophos-phamide as primary medical therapy in women with breastcancer: an anglo-celtic cooperative oncology group study. J ClinOncol 2005;23(13):2988–2995. Doi: 10.1200/JCO.2005.06.156
23 Gnerlich JL, Deshpande AD, Jeffe DB, Sweet A, White N, Mar-genthaler JA. Elevated breast cancer mortality in women youngerthan age 40 years compared with older women is attributed topoorer survival in early-stage disease. J Am Coll Surg 2009;208(03):341–347. Doi: 10.1016/j.jamcollsurg.2008.12.001
24 Fredholm H, Eaker S, Frisell J, Holmberg L, Fredriksson I, LindmanH. Breast cancer in young women: poor survival despite intensivetreatment. PLoS One 2009;4(11):e7695. Doi: 10.1371/journal.pone.0007695
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Association of Menopausal Status, Progesterone Receptor and Ki67 to Clinical Response Silva et al.716

25 Copson E, Eccles B, Maishman T, et al; POSH Study Steering Group.Prospective observational study of breast cancer treatment out-comes forUKwomenaged18-40yearsatdiagnosis: thePOSHstudy.J Natl Cancer Inst 2013;105(13):978–988. Doi: 10.1093/jnci/djt134
26 Collins LC, Marotti JD, Gelber S, et al. Pathologic features andmolecular phenotype by patient age in a large cohort of youngwomenwith breast cancer. Breast Cancer Res Treat 2012;131(03):1061–1066. Doi: 10.1007/s10549-011-1872-9
27 Azim HA Jr, Michiels S, Bedard PL, et al. Elucidating prognosis andbiology of breast cancer arising in young women using geneexpression profiling. Clin Cancer Res 2012;18(05):1341–1351.Doi: 10.1158/1078-0432.CCR-11-2599
28 Li X, Zhang R, Liu Z, Li S, Xu H. The genetic variants in thePTEN/PI3K/AKT pathway predict susceptibility and CE(A)F chemo-therapy response to breast cancer and clinical outcomes. Oncotar-get 2017;8(12):20252–20265. Doi: 10.18632/oncotarget.15690
29 Deng L, Chen J, Zhong XR, et al. Correlation between activation ofPI3K/AKT/mTOR pathway and prognosis of breast cancer in Chinesewomen. PLoS One 2015;10(03):e0120511. Doi: 10.1371/journal.pone.0120511
30 Ravdin PM, Green S, Dorr TM, et al. Prognostic significance ofprogesterone receptor levels in estrogen receptor-positivepatients with metastatic breast cancer treated with tamoxifen:results of a prospective Southwest Oncology Group study. J ClinOncol 1992;10(08):1284–1291. Doi: 10.1200/JCO.1992.10.8.1284
31 Bardou VJ, Arpino G, Elledge RM, Osborne CK, Clark GM. Proges-terone receptor status significantly improves outcome predictionover estrogen receptor status alone for adjuvant endocrine ther-apy in two large breast cancer databases. J Clin Oncol 2003;21(10):1973–1979. Doi: 10.1200/JCO.2003.09.099
32 Yamamoto Y, Yamamoto-Ibusuki M, Iwase H. Menopausal statusshouldbetaken into consideration forpatientswith luminal abreast
cancer in terms of the effect of differential biology on prognosis.J Clin Oncol 2013;31(19):2516. Doi: 10.1200/JCO.2013.49.4062
33 Creighton CJ, Kent Osborne C, van de Vijver MJ, et al. Molecularprofiles of progesterone receptor loss in human breast tumors.Breast Cancer Res Treat 2009;114(02):287–299. Doi: 10.1007/s10549-008-0017-2
34 Tokunaga E, Kataoka A, Kimura Y, et al. The association betweenAkt activation and resistance to hormone therapy in metastaticbreast cancer. Eur J Cancer 2006;42(05):629–635. Doi: 10.1016/j.ejca.2005.11.025
35 XuL, LiuYH,Ye JM,et al. [RelationshipbetweenKi67expressionandtumor response to neoadjuvant chemotherapywith anthracyclinesplus taxanes in breast cancer]. Zhonghua Wai Ke Za Zhi 2010;48(06):450–453. Doi: 10.3760/cma.j.issn.0529-5815.2010.06.015
36 Esposito A, Criscitiello C, Curigliano G. Highlights from the 14thSt Gallen International Breast Cancer Conference 2015 inVienna: dealing with classification, prognostication, and pre-diction refinement to personalize the treatment of patientswith early breast cancer. Ecancer 2015;9:518. Doi: 10.3332/ecancer.2015.518
37 Cortazar P, Zhang L, Untch M, et al. Pathological complete re-sponse and long-term clinical benefit in breast cancer: theCTNeoBC pooled analysis. Lancet 2014;384(9938):164–172.Doi: 10.1016/S0140-6736(13)62422-8
38 Alba E, Lluch A, Ribelles N, et al. High proliferation predictspathological complete response to neoadjuvant chemotherapyin early breast cancer. Oncologist 2016;21(02):150–155. Doi:10.1634/theoncologist.2015-0312
39 Carey LA, Dees EC, Sawyer L, et al. The triple negative paradox:primary tumor chemosensitivity of breast cancer subtypes. ClinCancer Res 2007;13(08):2329–2334. Doi: 10.1158/1078-0432.CCR-06-1109
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
Association of Menopausal Status, Progesterone Receptor and Ki67 to Clinical Response Silva et al. 717
The Impact of Systematic Laparoscopic Skills andSuture Training on Laparoscopic HysterectomyOutcomes in a Brazilian Teaching Hospital
O impacto do treinamento laparoscópico sistematizadode habilidades e sutura nos resultados da histerectomialaparoscópica em hospital universitário brasileiroAnna Luiza Lobão Gonçalves1 Helizabet Abdala Ayroza-Ribeiro1 Raquel Ferreira Lima1
Aline Estefane Eras Yonamine1 Fabio Ohara1 Paulo Augusto Galvão Ayroza-Ribeiro1
1Gynecological Endoscopy and Endometriosis Sector, Department ofObstetrics and Gynecology, Faculdade de Ciências Médicas, SantaCasa de São Paulo, São Paulo, SP, Brazil
Rev Bras Ginecol Obstet 2019;41:718–725.
Address for correspondence Anna Luiza Lobão Gonçalves, Master,Rua Cesário Motta Junior 61, 01221-020, São Paulo, SP, Brazil(e-mail: [email protected]).
Keywords
► hysterectomy► laparoscopic surgery► education► suture training
Abstract Objective To evaluate the impact of systematic laparoscopic skills and suture training(SLSST) on the total laparoscopic hysterectomy intra- and postoperative outcomes in aBrazilian teaching hospital.Methods A cross-sectional observational study in which 244 charts of total laparo-scopic hysterectomy (TLH) patients operated from 2008 to 2014 were reviewed.Patient-specific (age, parity, previous cesarean sections, abdominal surgeries andendometriosis) and surgery-related variables (hospital stay, operative time, uterinevolume and operative complications) were analyzed in three different time-framegroups: 2008-09 (I-1) – TLHs performed by senior attending physicians; 2010-11 (I-2) –TLHs performed by residents before the implementation of the SLSST program; and2012-14 (I-3) – TLHs performed by residents after the implementation of the SLSSTprogram.Results A total of 244 TLH patients (mean age: 45.93 years) were included: 24 (I-1), 55(I-2), and 165 (I-3). The main indication for TLH was uterine myoma (66.4%). Group I-3presented a decrease in surgical time compared to group I-2 (p¼0.010). Hospital staylonger than 2 days decreased in group I-3 compared to group I-2 (p¼0.010). Althoughwe observed decreased uterine volume (154.2 cm3) in group I-2 compared to group I-1(217.8 cm3) (p¼ 0.030), logistic regression did not find any association betweenuterine volume and surgical time (p¼ 0.103).Conclusion The total operative time for laparoscopic hysterectomy was significantlyshorter in the group of patients (I-3) operated after the systematic laparoscopic skillsand suture training was introduced in our hospital.
receivedMay 15, 2019acceptedSeptember 16, 2019
DOI https://doi.org/10.1055/s-0039-1700587.ISSN 0100-7203.
Copyright © 2019 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Original ArticleTHIEME
718

Introduction
Laparoscopy-assisted hysterectomy has evolved as an alterna-tive to conventional opensurgerysince theendof the twentiethcentury.1 It uses cameras and specific instruments to removethe uterus, the fallopian tubes, and/or the ovaries through aminimally-invasive trans-vaginal access.2,3 The procedure iscalled total laparoscopic hysterectomy (TLH) when hemostaticclampingof the uterine vessels, resectionof theuterosacral andcardinal ligaments, and colporrhaphy are all performedthrough a minimally-invasive video-assisted approach.3 Thebenefits of TLHare diminished postoperative pain, lower use ofopioid analgesics, shorter hospital stay, early rehabilitation andreturn to work, minimal blood loss, enhanced visualization ofintra-abdominal structures, which minimizes the risk of iatro-genic lesion to bladder and ureters, and lower rate of short- andlong-term complications.4–6 Additonally, the intrafascial dis-section technique preserves the vaginal apex support struc-tures, maintaining vaginal length.6–9
However, TLH is not widespread in many coun-tries.5,7,10–12 Data from the Brazilian Unified HealthcareSystem reveals only 2,947 laparoscopic procedures out of932,382 hysterectomies performed from 2008 to 2017.13
Developed countries like the United States and Englandestimate that 20% to 30% of hysterectomies are laparosco-pic-assisted.10,14 The major struggle regarding laparoscopicsurgery expansion has been to train new surgeons. The longlearning curve to achieve proficiency in two-dimensionscreen vision, camera navigation, hand-eye coordination,and psychomotor skills to handle laparoscopic tools with
dexterity conflict with a limited number of procedures andprofessionals in teaching hospitals with scarce resour-ces.7,12,15,16 On the other hand, increased demand for lapa-roscopic procedures in private health systems pressurejunior surgeons to take up complex cases they may not beproficient to deal with, resulting in lower surgical perform-ances and increased morbidity and mortality.15,17
Laparoscopic psychomotor skills must be preliminarilyacquired by practicing on specific validated training modelsoutside the operating room.15–17 Similar to a video game,training platforms enable the repetitive practice of standardlaparoscopic tasks. They also evaluate performance objec-tively, and provide feedback to the trainees.18 Simulatorswere proven to shorten surgical time and improve perioper-ative morbidity in TLH procedures,19 and they potentiallyreduce the learning curve compared to traditional surgicalteaching methods.20 Current surgical practice regulationsdemand a controlled, standardized and validated trainingprogram for new laparoscopic surgeons, such as the “Win-ners” program in Europe and the American College ofObstetricians and Gynecologists (ACOG) Fundamentals ofLaparoscopic Surgery (FLS) program, in the US.15 In an effortto validate an implemented standardized laparoscopic train-ing in Brazil, the present study evaluated the impact of thesystematic laparoscopic skill and suture training (SLSST) onthe outcomes of TLH performed in a teaching hospital (SantaCasa de Misericórdia de São Paulo, in the city of São Paulo,Brazil) from 2008 to 2014. We hypothesized that the SLSSTwould have a positive impact on the intra- and postoperativeoutcomes of TLH.
Resumo Objetivo Avaliar o impacto do treinamento laparoscópico sistematizado de habili-dades e sutura (TLSHS) nos resultados intra e pós-operatórios da histerectomialaparoscópica em um hospital universitário brasileiro.Métodos Estudo observacional transversal de revisão de 244 prontuários de pacien-tes submetidas a histerectomia total laparoscópica (HTL) operadas entre 2008 e 2014.Os fatores específicos das pacientes (idade, paridade, cesariana prévia, cirurgiasabdominais, e endometriose) e as variáveis relacionadas à cirurgia (tempo de hospi-talização, tempo de cirurgia, volume uterino e complicações operatórias) foramanalisados em três grupos temporais: 2008-09 (I-1) – HTLs realizadas por médicosexperientes; 2010-11 (I-2) – HTLs realizadas por residentes sem TLSHS; 2012-2014 (I-3)– HTLs realizadas por residentes após a implementação do TLSHS.Resultados Um total de 244 pacientes submetidas a HTLs foram incluídas (média deidade de 45,93 anos): 24 operadas no período I1, 55 no I2, e 165 no I3. A principalindicação para HTL foi mioma uterino (66,4%). O grupo I-3 apresentou diminuição notempo cirúrgico quando comparado ao grupo I-2 (p¼ 0,010). Hospitalização superior a2 dias diminuiu no grupo I-3 comparado ao grupo I-2 (p¼0,010). Apesar de observar-mos diminuição no volume uterino dos pacientes do grupo I-2 (154,2 cm3) emcomparação com os do grupo I-1 (217,8 cm3) (p¼0,030), a regressão logística nãorevelou associação entre volume uterino e tempo cirúrgico (p¼0,103).Conclusão O tempo cirúrgico na HTL foi significativamente menor no grupo depacientes submetidas à cirurgia após a implantação do TLSHS em nosso hospital.
Palavras-chave
► histerectomia► cirurgia laparoscópia► educação► treinamento de
sutura
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
The Impact of Systematic Laparoscopic Skills and Suture Training Gonçalves et al. 719

Methods
The present research was approved by the Ethics in HumanResearch Committee and Institutional Review Board ofSanta Casa de Misericórdia de São Paulo (under number:14945313.8.0000.5479)
We conducted a cross-sectional observational study inwhich 610 charts of patients submitted to hysterectomy atSanta Casa de Misericórdia de Sãoo Paulo from 2008 to 2014were reviewed. All TLHs were included in the study, corre-sponding to40% (244)of theprocedures. Theexclusioncriteriawere: subtotal or partial hysterectomy; hysterectomies asso-ciated with open rectosigmoidectomy and/or partial cystec-tomy due to endometriosis; and malignant diseases requiringtotal hysterectomy with open retroperitonial exploration.
Patient-specific (age, parity, previous cesarean sections,abdominal surgeries and endometriosis) and surgery-related(hospital stay, operative time, rate of conversion to openprocedure, uterine volume, intra- and postoperative compli-cations) variables were analyzed.
The postoperative complications were divided accordingto the Clavien-Dindo (C-D) classification (►Table 1), whichwas created in 1992 (by Clavien PA, Dindo D and DemartinesN at University Hospital of Zurich, Zurich, Switzerland) iswidely used, and is based on the type of therapy needed tocorrect the complication.21
In our institution, we receive every year 4 first-year resi-dents (PGY-4 OB/GYN) of the Gynecologic Endoscopy andEndometriosis Fellowship Program, and 2 second-year resi-dents (PGY-5 OB/GYN) of the Gynecologic Endoscopy andEndometriosis Fellowship Program. The surgeries were divid-ed into three different time-frame groups reflecting distinctbenchmarks of the SLSST curriculum implemented for theGynecology Endoscopy and Endometriosis Fellowship Pro-gram: 2008-09 (I-1) – TLH performed by senior attendingphysicians withmore than 5 years of experience in laparosco-pic surgery; 2010-11 (I-2) – TLH performed by the new first-year residents (PGY-4 OB/GYN) before the implementation of
the SLSST, supervised by senior physicians; and 2012-14 (I-3)–TLH performed by the new first-year residents (PGY-4 OB/GYN) after the implementation of the SLSST. The surgeriesperformed during the first 14 weeks of the SLSST (dominanthand training period) were excluded from this group. Thesurgerieswere assisted and supervisedbya second-year (PGY-5 OB/GYN) resident who was also submitted to the sametraining program, but at the end of the previous year.
An average of 7 TLHs per PGY-4/year was observed in theI-2 group, and an average of 14 TLHs per PGY-4/year wasobserved in the I-3 group.
Standard Total Laparoscopic HysterectomyThe intrafascial technique has been standardized to all TLHsperformed by the Gynecologic Endoscopy and EndometriosisGroup of Santa Casa deMisericórdia de São Paulo since 2008.The same standard steps are performed in the same order forevery TLH.
1. Position on the gynecological table with the legs on thegaiters, the buttocks 5 cm above the table, and arms onjambs along the body, asepsis/antisepsis, followed by latebladder catheterization using a no. 14 Foley catheter,hysterometry and uterine manipulator placement.
2. Intra-umbilical incision (longitudinal or arch-shaped),abdominal puncture using a Veress needle followed bysafetymaneuvers (dual recoil test, saline infusion-suctiontest, and pendant drop test), peritoneum distention withCO2 (6mmHg to 20 mmHg), assessment of abdominaldistension symmetry, and loss of liver solidness to per-cussion sign.
3. Introduction of the intra-umbilical trocar and cavityinventory to assess puncture accidents and adherences.Low pneumoperitoneum pressure to 14 mmHg, Trende-lemburg position, and establishment of accessory portalsusing 5-mm trocars (►Figure 1).
4. Left round ligament styptic section, dissection of theanterior peritoneum from the broad ligament to the
Table 1 Clavien-Dindo classification
Grades Definition
Grade I Any deviation from the normal postoperative course without the need for pharmacological treatment or surgical,endoscopic and radiological interventions.The allowed therapeutic regimens are: drugs as antiemetics, antipyretics, analgesics, diuretics and electrolytes andphysiotherapy. This grade also includes wound infections opened at the bedside.
Grade II Requiring pharmacological treatment with drugs other than those allowed for grade I complications. Bloodtransfusions and total parenteral nutrition are also included.
Grade III Requiring surgical, endoscopic or radiological interventions.
IIIa Intervention not under general anesthesia..
IIIb Intervention under general anesthesia
Grade IV Life-threatening complications (including central nervous system complications)� requiring management atintermediate care or intensive care unit.
IVa Single-organ dysfunction (including dialysis).
IVb Multiple-organ dysfunction.
Grade V Death of a patient.
Note: �Brain hemorrhage, ischemic stroke, subarachnoid bleeding, but excluding transient ischemic attacks.
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
The Impact of Systematic Laparoscopic Skills and Suture Training Gonçalves et al.720

bladder reflex, and establishment of an avascular planeleft uterus-ovarian ligament styptic section, followed byleft salpingectomy. If left oophorectomy is required, iden-tify the left ureter and perform the styptic section of theinfundibulum (►Figure 2).
5. Dissect the posterior peritoneum from the broad ligamentof the uterus to the sacrouterine ligament and perform thestyptic section of the left uterine vessels (►Figure 3A).
6. The same sequence (4 and 5) is then repeated on the rightside.
7. Bladder retracted inferiorly (►Figure 3B), colpotomyusing amonopolar cautery (►Figure 3C), and transvaginalremoval of the uterus employing a vaginal liner.
8. Place a vaginal tampon to hold the pneumoperitoneum,followed by trans-peritoneal colporrhaphy using no. 0Vicryl (polyglactin 910 manufactured by Ethicon Inc., asubsidiary of Johson and Johnson) with x-shaped stitchesat the angles of the vagina and continuous stitches in thecenter (►Figure 3D).
9. Review the hemostasis, remove the vaginal tampon, per-form the suction of the pneumoperitoneum, return tohorizontal decubitus, and perform the intra-umbilicalaponeurosis suture and trocar incision closure.
Systematic laparoscopic skills and suture training(SLSST)The training was implemented to the curriculum of theGynecologic Endoscopy and Endometriosis FellowshipProgram in 2012. Based on the Romeo Gladiator Rule sev-en-week activities22 (►Table 2), the SLSST consisted of a 21-week (4 hours per week) hands-on training at the experi-mental laboratory. Each week, the residents had to practicethe scheduled exercise for a minimum of 4 hours. The coreexercises were performed with the dominant hand onthe lateral trocar for the initial 7 weeks of the program,followed by the dominant hand on the central trocar fromthe 8th to the 14thweeks, and the non-dominant hand on thelateral trocar from the 15th to the 21st weeks.
Statistical AnalysisAll data were recorded in Excel (Microsoft Corp., Redmond,WA, US), version 14.5.7, spreadsheets, and the statisticalanalyses were performed using in the Statistical Package forthe Social Sciences (SPSS, IBM Corp., Armonk, NY, US)software, version 22. The calculation of the sample sizewas estimated based on a pilot group of 10 patients obtainedfrom the first period of time (I-1). Using a standard deviationof 50minutes and an estimated difference of 30minutes, asample of 34 patients was suggested to obtain a study powerof 80% with a significance of 5%. The Kolmogorov-Smirnovtest was performed for each independent variable to deter-mine normal distribution. The Chi-squared test was used tocompare parametric variables. The Student t-test was used tocompare parametric continuous variables, and logisticregression was performed to determine the associationbetween the variables. Data are shown as mean� standard
Fig. 1 Locations of the portals.
Fig. 2 (A) Hemostatic section of the left round ligament; (B) dissection of the left broad ligament of the uterus; (C) left avascular window; (D)hemostatic section of the left uterus-ovarian ligament.
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
The Impact of Systematic Laparoscopic Skills and Suture Training Gonçalves et al. 721
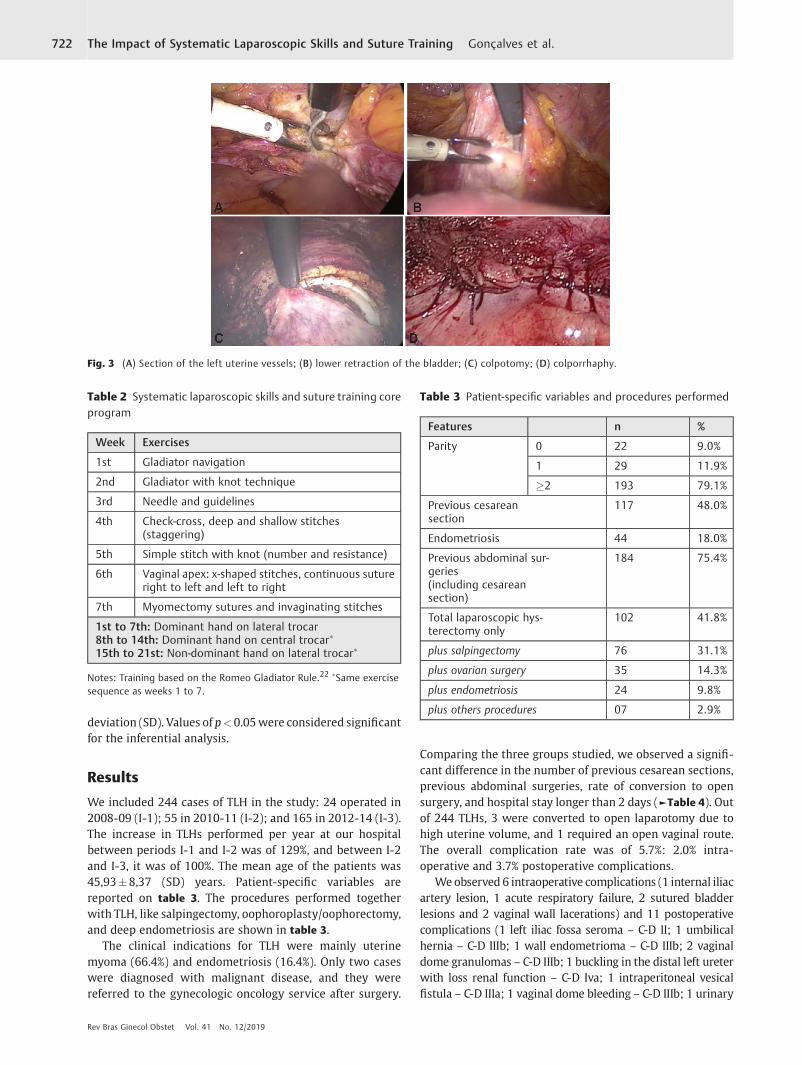
deviation (SD). Values of p<0.05were considered significantfor the inferential analysis.
Results
We included 244 cases of TLH in the study: 24 operated in2008-09 (I-1); 55 in 2010-11 (I-2); and 165 in 2012-14 (I-3).The increase in TLHs performed per year at our hospitalbetween periods I-1 and I-2 was of 129%, and between I-2and I-3, it was of 100%. The mean age of the patients was45,93�8,37 (SD) years. Patient-specific variables arereported on table 3. The procedures performed togetherwith TLH, like salpingectomy, oophoroplasty/oophorectomy,and deep endometriosis are shown in table 3.
The clinical indications for TLH were mainly uterinemyoma (66.4%) and endometriosis (16.4%). Only two caseswere diagnosed with malignant disease, and they werereferred to the gynecologic oncology service after surgery.
Comparing the three groups studied, we observed a signifi-cant difference in the number of previous cesarean sections,previous abdominal surgeries, rate of conversion to opensurgery, and hospital stay longer than 2 days (►Table 4). Outof 244 TLHs, 3 were converted to open laparotomy due tohigh uterine volume, and 1 required an open vaginal route.The overall complication rate was of 5.7%: 2.0% intra-operative and 3.7% postoperative complications.
We observed 6 intraoperative complications (1 internal iliacartery lesion, 1 acute respiratory failure, 2 sutured bladderlesions and 2 vaginal wall lacerations) and 11 postoperativecomplications (1 left iliac fossa seroma – C-D II; 1 umbilicalhernia – C-D IIIb; 1 wall endometrioma – C-D IIIb; 2 vaginaldome granulomas – C-D IIIb; 1 buckling in the distal left ureterwith loss renal function – C-D Iva; 1 intraperitoneal vesicalfistula – C-D IIIa; 1 vaginal dome bleeding – C-D IIIb; 1 urinary
Fig. 3 (A) Section of the left uterine vessels; (B) lower retraction of the bladder; (C) colpotomy; (D) colporrhaphy.
Table 2 Systematic laparoscopic skills and suture training coreprogram
Week Exercises
1st Gladiator navigation
2nd Gladiator with knot technique
3rd Needle and guidelines
4th Check-cross, deep and shallow stitches(staggering)
5th Simple stitch with knot (number and resistance)
6th Vaginal apex: x-shaped stitches, continuous sutureright to left and left to right
7th Myomectomy sutures and invaginating stitches
1st to 7th: Dominant hand on lateral trocar8th to 14th: Dominant hand on central trocar�
15th to 21st: Non-dominant hand on lateral trocar�
Notes: Training based on the Romeo Gladiator Rule.22 �Same exercisesequence as weeks 1 to 7.
Table 3 Patient-specific variables and procedures performed
Features n %
Parity 0 22 9.0%
1 29 11.9%
�2 193 79.1%
Previous cesareansection
117 48.0%
Endometriosis 44 18.0%
Previous abdominal sur-geries(including cesareansection)
184 75.4%
Total laparoscopic hys-terectomy only
102 41.8%
plus salpingectomy 76 31.1%
plus ovarian surgery 35 14.3%
plus endometriosis 24 9.8%
plus others procedures 07 2.9%
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
The Impact of Systematic Laparoscopic Skills and Suture Training Gonçalves et al.722
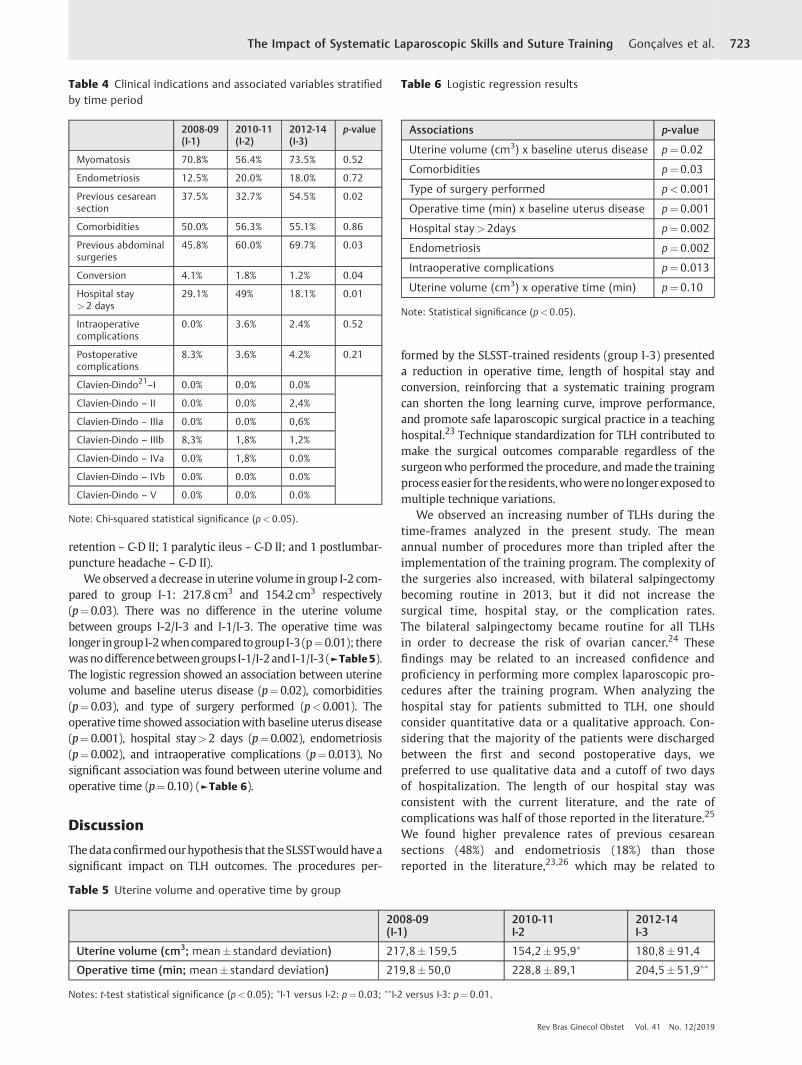
retention – C-D II; 1 paralytic ileus – C-D II; and 1 postlumbar-puncture headache – C-D II).
We observed a decrease in uterine volume in group I-2 com-pared to group I-1: 217.8 cm3 and 154.2 cm3 respectively(p¼0.03). There was no difference in the uterine volumebetween groups I-2/I-3 and I-1/I-3. The operative time waslonger ingroupI-2whencomparedtogroupI-3(p¼0.01); therewasnodifferencebetweengroups I-1/I-2andI-1/I-3 (►Table 5).The logistic regression showed an association between uterinevolume and baseline uterus disease (p¼0.02), comorbidities(p¼0.03), and type of surgery performed (p<0.001). Theoperative time showed associationwith baseline uterus disease(p¼0.001), hospital stay>2 days (p¼0.002), endometriosis(p¼0.002), and intraoperative complications (p¼0.013). Nosignificant association was found between uterine volume andoperative time (p¼0.10) (►Table 6).
Discussion
Thedataconfirmedourhypothesis that theSLSSTwouldhaveasignificant impact on TLH outcomes. The procedures per-
formed by the SLSST-trained residents (group I-3) presenteda reduction in operative time, length of hospital stay andconversion, reinforcing that a systematic training programcan shorten the long learning curve, improve performance,and promote safe laparoscopic surgical practice in a teachinghospital.23 Technique standardization for TLH contributed tomake the surgical outcomes comparable regardless of thesurgeonwho performed the procedure, andmade the trainingprocess easier for theresidents,whowereno longerexposed tomultiple technique variations.
We observed an increasing number of TLHs during thetime-frames analyzed in the present study. The meanannual number of procedures more than tripled after theimplementation of the training program. The complexity ofthe surgeries also increased, with bilateral salpingectomybecoming routine in 2013, but it did not increase thesurgical time, hospital stay, or the complication rates.The bilateral salpingectomy became routine for all TLHsin order to decrease the risk of ovarian cancer.24 Thesefindings may be related to an increased confidence andproficiency in performing more complex laparoscopic pro-cedures after the training program. When analyzing thehospital stay for patients submitted to TLH, one shouldconsider quantitative data or a qualitative approach. Con-sidering that the majority of the patients were dischargedbetween the first and second postoperative days, wepreferred to use qualitative data and a cutoff of two daysof hospitalization. The length of our hospital stay wasconsistent with the current literature, and the rate ofcomplications was half of those reported in the literature.25
We found higher prevalence rates of previous cesareansections (48%) and endometriosis (18%) than thosereported in the literature,23,26 which may be related to
Table 4 Clinical indications and associated variables stratifiedby time period
2008-09(I-1)
2010-11(I-2)
2012-14(I-3)
p-value
Myomatosis 70.8% 56.4% 73.5% 0.52
Endometriosis 12.5% 20.0% 18.0% 0.72
Previous cesareansection
37.5% 32.7% 54.5% 0.02
Comorbidities 50.0% 56.3% 55.1% 0.86
Previous abdominalsurgeries
45.8% 60.0% 69.7% 0.03
Conversion 4.1% 1.8% 1.2% 0.04
Hospital stay> 2 days
29.1% 49% 18.1% 0.01
Intraoperativecomplications
0.0% 3.6% 2.4% 0.52
Postoperativecomplications
8.3% 3.6% 4.2% 0.21
Clavien-Dindo21–I 0.0% 0.0% 0.0%
Clavien-Dindo – II 0.0% 0.0% 2,4%
Clavien-Dindo – IIIa 0.0% 0.0% 0,6%
Clavien-Dindo – IIIb 8,3% 1,8% 1,2%
Clavien-Dindo – IVa 0.0% 1,8% 0.0%
Clavien-Dindo – IVb 0.0% 0.0% 0.0%
Clavien-Dindo – V 0.0% 0.0% 0.0%
Note: Chi-squared statistical significance (p< 0.05).
Table 5 Uterine volume and operative time by group
2008-09(I-1)
2010-11I-2
2012-14I-3
Uterine volume (cm3; mean� standard deviation) 217,8�159,5 154,2� 95,9� 180,8�91,4
Operative time (min; mean� standard deviation) 219,8�50,0 228,8� 89,1 204,5�51,9��
Notes: t-test statistical significance (p< 0.05); �I-1 versus I-2: p¼ 0.03; ��I-2 versus I-3: p¼ 0.01.
Table 6 Logistic regression results
Associations p-value
Uterine volume (cm3) x baseline uterus disease p¼ 0.02
Comorbidities p¼ 0.03
Type of surgery performed p< 0.001
Operative time (min) x baseline uterus disease p¼ 0.001
Hospital stay>2days p¼ 0.002
Endometriosis p¼ 0.002
Intraoperative complications p¼ 0.013
Uterine volume (cm3) x operative time (min) p¼ 0.10
Note: Statistical significance (p< 0.05).
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
The Impact of Systematic Laparoscopic Skills and Suture Training Gonçalves et al. 723

the extraordinary number of cesarean sections performedin Brazil,25 and to the fact that our hospital is a center ofexcellence for endometriosis care.
The present study did not find an association betweenuterine volume and operative time, neither between uterinevolume and rate of complications. Our trained residentswereable to significantly reduce TLH operative time in about25minutes, despite the fact that they resected a highervolume of uteri than the non-trained residents, suggestingthat adequate training provided time-efficient abilities toyoung surgeons.
The traditional apprentice-tutor model is no longer validto develop all skills necessary in gynecological surgery; thecomplexity of modern surgery has increased the demandsand challenges to surgical education and the quality con-trol.27 Simulators motivate residents through the journeyof proficiency in laparoscopy.28 The positive impact thatsimulator-acquired skills have on real surgeries was pub-lished in a recent systematic review.19 A positive relation-ship between systematic training in simulators andreduced operative time and complications were alsoreported in cases of bariatric and urologic laparoscopicsurgery.29,30 In a Turkish study, Asoglu et al31 concludedthat a simulator lab improves the outcomes of hysterecto-my performed at a teaching institution, and may play anadjunct role in developing the resident’s surgical skills; theresults found by them are in line with the findings of ourstudy.
In the present study, repetitive practice in simulatorsenabled the fellows to improve their psychomotor skillswithout the fear of making mistakes that could had beenfatal in an actual surgery. The mistakes were analyzed bytutors who provided feedback and guided the residents toovercome obstacles. Tutorship in a stress-free environmenttranslated into faster, safer and efficient surgical perfor-mance even for more experienced attending physicians.32
Many countries have established systematic training onsimulators as requirements for laparoscopic surgeons.33
The present study was the initial step to validate a laparo-scopic training program in Brazil. Our model may stimulateother academic hospitals to expand their proficiency lapa-roscopic skills, serving a bridge to a safe and effective fullpractice of in vivo laparoscopy.
Our study had several limitations. The cross-sectionaldesign did not enable us to establish a temporal relationshipbetween the training and surgical outcomes, or to deter-mine if the experience of the surgeon measured by thenumber of TLHs previously performed had any influenceover the surgical outcomes. Moreover, the substantial dif-ference in the number of TLHs among the groups, and thevariable skill levels of the senior attending physicianswhose surgeries were included in group I-1 may be possiblebiases. Further prospective studies may define the numberof previous TLHs necessary to reduce complications. On theother hand, the present study was, to our knowledge, thisfirst clinical study to apply and evaluate the interference ofthe Romeo Gladiator training method on the outcomes of asurgical procedure.
Conclusion
The operative time for TLH was significantly shorter in thegroup of patients operated after the SLSSTwas introduced inour hospital.
ContributorsAll authors contributed with the project and the interpre-tation of data, thewriting of the article, the critical reviewof the intellectual content, and with the final approval ofthe version to be published.
Conflict of InterestsThe authors have none to disclose.
References1 Arbogast JD, Welch RA, Riza ED, Ricaurte EL, Pieper DR. Laparo-
scopically assisted vaginal hysterectomy appears to be an alter-native to total abdominal hysterectomy. J Laparoendosc Surg1994;4(03):185–190
2 Reich H. New techniques in advanced laparoscopic surgery.Baillieres Clin Obstet Gynaecol 1989;3(03):655–681
3 Ng CC, Chern BS. Total laparoscopic hysterectomy: a 5-yearexperience. Arch Gynecol Obstet 2007;276(06):613–618. Doi:10.1007/s00404-007-0385-6
4 Chapron C, Laforest L, Ansquer Y, et al. Hysterectomy techniquesused for benignpathologies: results of a Frenchmulticentre study.Hum Reprod 1999;14(10):2464–2470. Doi: 10.1093/humrep/14.10.2464
5 Chapron CM, Dubuisson JB, Ansquer Y. Is total laparoscopichysterectomy a safe surgical procedure? Hum Reprod 1996;11(11):2422–2424. Doi: 10.1093/oxfordjournals.humrep.a019128
6 Hohl MK, Hauser N. Safe total intrafascial laparoscopic (TAIL)hysterectomy: a prospective cohort study. Gynecol Surg 2010;7(03):231–239. Doi: 10.1007/s10397-010-0569-0
7 Chapron C, Dubuisson JB. Ureteral injuries after laparoscopic hys-terectomy. HumReprod 2000;15(03):733–734. Doi: 10.1093/hum-rep/15.3.733
8 Shwayder JM. The learning curve for laparoscopically assistedvaginal hysterectomy/laparoscopic hysterectomy. J Am AssocGynecol Laparosc 1994;1(4, Part 2):S33
9 Cavalli N, Sória HL, Galletto D, Sória-Vieira S, Bandeira CP,Fagundes DJ. Histerectomia vaginal assistida por videolaparosco-pia associada à técnica intrafascial (HVALi) em 579 operações. RevBras Videocir 2003;1:128–134
10 Einarsson JI,MattesonKA, Schulkin J, ChavanNR, Sangi-HaghpeykarH. Minimally invasive hysterectomies-a survey on attitudes andbarriers among practicing gynecologists. JMinim Invasive Gynecol2010;17(02):167–175. Doi: 10.1016/j.jmig.2009.12.017
11 Cosson M, Lambaudie E, Boukerrou M, Querleu D, Crépin G.Vaginal, laparoscopic, or abdominal hysterectomies for benigndisorders: immediate and early postoperative complications. EurJ Obstet Gynecol Reprod Biol 2001;98(02):231–236
12 Sória HLZ, Fagundes DJ, Sória-Vieira S, Cavalli N, Santos CRC.[Hysterectomy and benign gynecological diseases: what has beenperformed inMedical Residency in Brazil?] Rev Bras Ginecol Obstet2007;29:67–73. Doi: 10.1590/S0100-72032007000200002
13 Ministério da Saúde. Procedimentos Hospitalares do SUS – PorLocal de Internação - Brasil.2017http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sih/cnv/qiuf.def. Accessed April 29, 2017.
14 Sculpher M, Manca A, Abbott J, Fountain J, Mason S, Garry R. Costeffectiveness analysis of laparoscopic hysterectomy comparedwith standard hysterectomy: results from a randomised trial.BMJ 2004;328(7432):134. Doi: 10.1136/bmj.37942.601331.EE
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
The Impact of Systematic Laparoscopic Skills and Suture Training Gonçalves et al.724

15 Campo R, Molinas CR, DeWilde RL, et al. Are you good enough foryour patients? The European certification model in laparoscopicsurgery. Facts Views Vis ObGyn 2012;4(02):95–101
16 Takeda J, Kikuchi I, Kono A, Ozaki R, Kumakiri J, Takeda S. Efficacyof short-term training for acquisition of basic laparoscopic skills.Gynecol Minim Invasive Ther 2016;5:112–115. Doi: 10.1016/j.gmit.2015.06.001
17 Ahlberg G, Enochsson L, Gallagher AG, et al. Proficiency-basedvirtual reality training significantly reduces the error rate forresidents during their first 10 laparoscopic cholecystectomies. AmJ Surg 2007;193(06):797–804. Doi: 10.1016/j.amjsurg.2006.06.050
18 Sroka G, Feldman LS, Vassiliou MC, Kaneva PA, Fayez R, Fried GM.Fundamentals of laparoscopic surgery simulator training toproficiency improves laparoscopic performance in the operatingroom-a randomized controlled trial. Am J Surg 2010;199(01):115–120. Doi: 10.1016/j.amjsurg.2009.07.035
19 Clark NV, Gujral HS, Wright KN. Impact of a fellowship-trainedminimally invasive gynecologic surgeon on patient outcomes.JSLS 2017;21(03):e2017.00037. Doi: 10.4293/JSLS.2017.00037
20 Seymour NE, Gallagher AG, Roman SA, et al. Virtual reality trainingimproves operating room performance: results of a randomized,double-blinded study. AnnSurg2002;236(04):458–463, discussion463–464. Doi: 10.1097/00000658-200210000-00008
21 Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindoclassification of surgical complications: five-year experience. AnnSurg 2009;250(02):187–196. Doi: 10.1097/SLA.0b013e3181b13ca2
22 Liceaga A, Fernandes LF, Romeo A, Gagstatter F. Romeo’s gladiatorrule: knots, stitches and knot typing techniques: a tutorial basedon a few simple rules; new concepts to teach suturing techniquesin laparoscopic surgery. 2nd ed. Schramberg: Endo Press; 2015.
23 Nácul MP, Cavazzola LT, de Melo MC. Current status of residencytraining in laparoscopicsurgery inBrazil: acritical review.ArqBrasCirDig 2015;28(01):81–85. Doi: 10.1590/S0102-67202015000100020
24 Dilley SE, Straughn JM Jr, Leath CA III. The evolution of andevidence for opportunistic salpingectomy. Obstet Gynecol 2017;130(04):814–824. Doi: 10.1097/AOG.0000000000002243
25 Viganò P, Parazzini F, Somigliana E, Vercellini P. Endometriosis:epidemiology and aetiological factors. Best Pract Res Clin ObstetGynaecol2004;18(02):177–200.Doi:10.1016/j.bpobgyn.2004.01.007
26 Nakamura-Pereira M, Esteves-Pereira AP, Gama SGN, Leal M.Elective repeat cesarean delivery in women eligible for trial oflabor in Brazil. Int J Gynaecol Obstet 2018;143(03):351–359. Doi:10.1002/ijgo.12660
27 Ferreira H, van Belle Y, Tanos V, et al. Simulation and training ofgynaecological skills. Facts Views Vis ObGyn 2018;10(01):21–27
28 Munz Y, Almoudaris AM,MoorthyK, Dosis A, Liddle AD, Darzi AW.Curriculum-based solo virtual reality training for laparoscopicintracorporeal knot tying: objective assessment of the transfer ofskill from virtual reality to reality. Am J Surg 2007;193(06):774–783. Doi: 10.1016/j.amjsurg.2007.01.022
29 Thuler FR, de Freitas WR Jr, Ilias EJ, Kassab P, Malheiros CA.Laparoscopic bariatric surgery training program model: gastricbypass. BMC Surg 2014;14:101. Doi: 10.1186/1471-2482-14-101
30 Mucksavage P, Lee J, Kerbl DC, Clayman RV, McDougall EM.Preoperative warming up exercises improve laparoscopic opera-tive times in an experienced laparoscopic surgeon. J Endourol2012;26(07):765–768. Doi: 10.1089/end.2011.0134
31 AsoğluMR,AchjianT,AkbilgiçO, BorahayMA,KılıçGS. The impactof asimulation-basedtraining labonoutcomesofhysterectomy. J TurkGerGynecol Assoc 2016;17(02):60–64. Doi: 10.5152/jtgga.2016.16053
32 Korndorffer JR Jr, Stefanidis D, Scott DJ. Laparoscopic skills laborato-ries: current assessment and a call for resident training standards.AmJSurg2006;191(01):17–22.Doi:10.1016/j.amjsurg.2005.05.048
33 NickelF,KowalewskiKF,Müller-StichBP. [Riskawarenessandtrainingfor prevention of complications in minimally invasive surgery].Chirurg 2015;86(12):1121–1127. Doi: 10.1007/s00104-015-0097-6
Rev Bras Ginecol Obstet Vol. 41 No. 12/2019
The Impact of Systematic Laparoscopic Skills and Suture Training Gonçalves et al. 725
@thiemepublishers @ThiemeNY @thieme-group @thieme.ny
Connect with us on social media
GET 15% OFF YOUR NEXT BOOK ORDER!Visit thieme.com/news or scan here to sign up!
Sign up for emails from Thieme!
MORE SALES MORE BOOKS MORE EVENTS
MORE, FULL STOP.

Instructions to AuthorsScope and policyAll content of the journal, except where otherwise noted, is licensed under a Creative Commons License.
The material submitted for analysis cannot be simultaneously submitted for publication in other journals or previously published. In the selection of man-uscripts for publication, are evaluated the originality, relevance of the theme, quality of the methodology used, and adequacy to the editorial standards adopted by the journal. The published material becomes intellectual prop-erty of the Brazilian Journal of Gynecology and Obstetrics and Febrasgo.
Manuscripts evaluation
The manuscripts submitted to the journal are received by the Editorial Offi ce that checks the mandatory documentation and examines if the edi-torial norms contained in the Instructions to Authors have been fulfi lled. If the process is in compliance, the manuscript is sent to the Editor-in-Chief, who will make a merit evaluation of the material. If the Editor-in-Chief concludes the work is in favorable scientifi c and technical conditions, the manuscript is forwarded to the Associate Editors, who will designate re-viewers (double mind process) to evaluate it. Then, the reviewers’ opin-ions and editor’s instructions are sent to authors to inform them about changes to be made. Then, the authors resubmit the text with the sug-gested changes within the requested deadline. When resubmitting the manuscript, the requested corrections should be highlighted in yellow. In cases of disagreement with the suggestions, observations should be included in the comments balloons. Be assertive and punctual with the inquiry, and support the hypothesis with references.
IMPORTANT! Authors must comply with the deadlines, since non-attend-ance will result in delay of manuscript publication or even archiving of the process. At any point in the process of analysis and editing of the text, the authors may request the process suspension and withdrawal of the manuscript, except when it is accepted for publication. The concepts and statements contained in the articles are of the authors’ responsibility.
Preparing a manuscript for submission
Mandatory submission documents
When submitting a manuscript to RBGO, attach the documents listed below on the ScholarOne submission platform. Note that not attach-ing the documents will result in cancellation of the submitted process. Mandatory documentation for online submission:
• Authorization of copyright transfer signed by all authors (scanned and attached as supplementary document) Model;
• In accordance with chapter XII.2 of Res. CNS 466/2012, in Brazil, research involving human subjects needs to inform the registration number referring to the Certifi cate of Ethical Assessment (CAAE) or the approval number of the research (CEP/CONEP) in the Ethics Committee. International manuscripts must present local ethical documentation to proceed with the submission process;
• Cover Letter: written to justify the publication. The authors should be identifi ed, together with the title of the team that intends to pub-lish, origin institution of the authors and intention of publication;
• Title page;
• Manuscript.
Title Page
• Title of the manuscript in English with a maximum of 18 words;
• Authors’ full name without abbreviations (maximum six);
• Corresponding author (full name, professional mailing address and contact email);
• Institutional affi liation of each author. Example: Faculty of Medicine, University of São Paulo, Ribeirão Preto, SP, Brazil;
• Confl icts of interest: authors should report any potential confl icts of interest whether political, economic, of resources for research execution or intellectual property;
• Acknowledgements: restricted to people and institutions that contrib-uted to research development in a relevant way. Any fi nancial support provided by development agencies or private companies should be men-tioned in the section Acknowledgments. For Brazilian authors, RBGO re-quests the citation of CNPq, Capes, FAPESP and other fi nancing agencies, together with the number of research process or granted scholarships.
• Contributions: according to the criteria for scientifi c authorship of the International Committee of Medical Journal Editors (ICMJE), authorship credit must be based on three conditions met in full: 1. Substantial contributions to conception and design, data collection or analysis, and interpretation of data; 2. Writing of the article or critical review of the in-tellectual content; and 3. Final approval of the version to be published.
ManuscriptInstructions to Authors
The Brazilian Journal of Gynecology and Obstetrics publishes the follow-ing categories of manuscripts:
Original Articles, complete prospective, experimental or retrospec-tive studies. Manuscripts containing original clinical or experimental research results have priority for publication.
Case Reports, of great interest and well documented from the clinical and laboratorial point of view. In the letter of referral, authors should in-dicate new or unexpected aspects in relation to already published cases. The text of Introduction and Discussion sections should be based on an updated bibliographic review.
Review Articles, including comprehensive reviews, meta-analysis or systematic reviews. Spontaneous contributions are accepted. The meth-ods and procedures adopted for obtaining the text should be described, and based on recent references, including the current year. As this sub-ject is still subject to controversy, the review should discuss the trends and lines of research under way. In addition to the text of the review, there should be an abstract and conclusions. See the ‘Instructions to Authors’ section for information on the text body and title page;
Letters to the Editor, dealing with editorial matters or not, but presenting relevant information to readers. Letters can be summarized by the editor, but maintaining the main points. In case of criticism to published works, the letter is sent to the authors so their reply can be published simultaneously;
Editorial, only at the publisher’s invitation.
Title
When writing a scientifi c article, the researcher should focus on the manuscript title, which is the business card of any publication. It should be elaborated very carefully, and preferably written only after the article fi nalization. A good title adequately describes the manuscript content. Generally it is not a phrase, because it does not contain the subject, only verbs and arranged objects. Titles rarely contain abbreviations, chemical formulas, adjectives, names of cities, among others. The title of manu-scripts submitted to RBGO must contain a maximum of 18 words.
Abstract
The abstract should provide the context or basis for the study, establish the objectives, basic procedures, main outcomes and key fi ndings. It should emphasize new and important aspects of the study or observa-tions. Since the abstract is the only substantive part of the article in-dexed in many electronic databases, authors should ensure it refl ects the article content in an accurate and highlighted manner. Do not use abbreviations, symbols and references in the abstract. In case of original articles from clinical trials, authors must inform the registration number at the end of the text.

Informational abstract of structured type of original articles
Abstracts of original articles submitted to RBGO must be structured in four sections and contain a maximum of 250 words:
Objective: What was done; the question posed by the investigator.
Methods: How it was done; the method, including the material used to achieve the objective.
Results: What was found, the main fi ndings and, if necessary, the sec-ondary fi ndings.
Conclusion: The conclusions; the answer to the question asked.
Informational abstract of structured type of systematic review articles
Among the included items are the review objective to the question asked, data source, procedures for selecting the studies and data collec-tion, the results and conclusions. The abstracts of systematic review ar-ticles submitted to RBGO must be structured in six sections and contain a maximum of 250 words:
Objective: Declare the main purpose of the article.
Data sources: Describe the data sources examined, including the date, indexing terms, and limitations.
Selection of studies: Specify the number of studies reviewed and the criteria used in their selection.
Data collection: Summarize the conduct used for data extraction and how it was used.
Data synthesis: State the main results of the review and the methods used to obtain them.
Conclusions: Indicate the main conclusions and their clinical usefulness.
Informational abstract of unstructured type of review articles, except systematic reviews and case studies
It shall contain the substance of the article, covering the purpose, method, results and conclusions or recommendations. It exposes enough details so readers can decide on the convenience of reading the full text (Limit of words: 150).
Keywords
The keywords of a scientifi c paper indicate the thematic content of the text they represent. The main objectives of the aforementioned terms are the thematic content identifi cation, indexing of the work in databases, and rapid location and retrieval of contents. The keyword systems used by RBGO are DeCS (Health Sciences Descriptors - Lilacs Indexer) and MeSH (Medical Subject Headings - MEDLINE-PubMed Indexer). Please choose fi ve descriptors that represent your work on these platforms.
Manuscript body (Manuscripts submitted to RBGO must have a maximum of 4000 words. Note that tables, charts and fi gures in the Results section and References are not counted).
Introduction
The Introduction section of a scientific article has the purpose of in-forming what was researched and the reason for the investigation. This part of the article prepares the reader to understand the investigation and justification of its realization. The content informed in this sec-tion should provide context or basis for the study (i.e. the nature of the problem and its importance); state the specific purpose, research objective, or hypothesis tested in the study or observation. The study objective usually has a more precise focus when formulated as a ques-tion. Both the primary and secondary objectives should be clear, and any analyzes in a pre-specified subgroup should be described; provide strictly relevant references only and do not include data or conclusions of the work being reported.
MethodsAccording to the Houaiss dictionary, Methods “is an organized, logical and systematic process of research”. The method comprises the ma-terial and procedures adopted in the research in order to respond to the central research question. Structure the Methods section of RBGO starting with the study design; research scenario (place and period in
which it was performed); sample of participants; data collection; in-tervention to be evaluated (if any) and the alternative intervention; statistical methods used and the ethical aspects of the study. When thinking about the writing of the study design, refl ect if it is appropri-ate to achieve the research objective, if the data analysis refl ects the design, and if what was expected with use of the design was achieved to research the theme. Following, the guidelines used in clinical or epi-demiological research that should be included in the section Methods of manuscripts sent to RBGO:
Types of study (adapted from Pereira, 2014*):
Case Report (Case study): In-depth investigation of a situation in which one or a few people are included (usually up to ten);
Case series: A set of patients (for example, more than ten people) with the same diagnosis or undergoing the same intervention. In general, these are consecutive series of patients seen in a hospital or other health institu-tion for a certain period. There is no internal control group formed simul-taneously. The comparison is made with external controls. The name of external or historical control is given to the group used to compare the results, but that was not constituted at the same time within the study: for example, the case series is compared with patients from previous years.
Transversal (or Cross-sectional) study: Investigation to determine prevalence; examine the relationship between events (exposure, dis-ease, and other variables of interest) at any given time. Cause and eff ect data are collected simultaneously: for example, the case series is com-pared with patients from previous years.
Case-control study: Particular form of etiological investigation of ret-rospective approach in which the search of causes starts from the ef-fects. Groups of individuals, respectively with and without a particular health problem are compared in relation to past exposures in order to test the hypothesis that exposure to certain risk factors is the contrib-uting cause of the disease. For example, individuals affl icted with low back pain are compared with an equal number of individuals (control group) of the same sex and age, but without low back pain.
Cohort study: Particular form of investigation of etiological factors in which the search of eff ects starts from the cause; therefore, the oppo-site of case-control studies. A group of people is identifi ed, and perti-nent information on the exposure of interest is collected, so the group can be monitored over time, checking those who do not develop the disease in focus, and if the prior exposure is related to occurrence of disease. For example, smokers are compared to nonsmoker controls; the incidence of bladder cancer is determined for each group.
Randomized study: This has the connotation of an experimental study to evaluate an intervention hence the synonym of intervention study. Can be performed in a clinical setting; sometimes referred to simply as clini-cal trial or clinical study. It is also conducted at the community level. In clinical trials, participants are randomly assigned to form groups called study (experimental) and control (or testimony), whether submitted or not to an intervention (for example, a drug or vaccine). Participants are monitored to verify the occurrence of outcome of interest. This way, the relationship between intervention and eff ect is examined under controlled observation conditions, usually with double-blind evaluation. In the case of a randomized study, inform the number of the Brazilian Registry of Clinical Trials (REBEC) and/or the number of the International Clinical Trials Registration Platform (ICTRP/OMS) on the title page.
Ecological study: Research performed with statistics: the unit of observa-tion and analysis is not constituted of individuals, but of groups of individuals hence the synonyms: study of groups, aggregates, clusters, statistics or com-munity. For example, research on the variation of mortality coeffi cients for diseases of the vascular system and per capita consumption of wine among European countries.
Systematic Review and Meta-analysis: Type of review in which there is a clearly formulated question, explicit methods are used to critically iden-tify, select and evaluate relevant research, and also to collect and analyze data from the studies included in the review. There is use of strategies to

limit bias in the localization, selection, critical evaluation and synthesis of relevant studies on a given topic. Meta-analysis may or may not be part of the systematic review. Meta-analysis is the review of two or more stud-ies to obtain a global, quantitative estimate of the question or hypothesis investigated; and employs statistical methods to combine the results of the studies used in the review.
Source: *Pereira MG. Artigos Científi cos – Como redigir, publicar e avaliar. Rio de Janeiro: Guanabara-Koogan; 2014.
Script for statistical review of original scientifi c papers
Study objective: Is the study objective suffi ciently described, including pre-established hypotheses?
Design: Is the design appropriate to achieve the proposed objective?
Characteristics of the sample: Is there a satisfactory report on the selection of people for inclusion in the study? Has a satisfactory rate of responses (valid cases) been achieved? If participants were followed up, was it long and complete enough? If there was a pairing (eg. of cas-es and controls), is it appropriate? How did you deal with missing data?
Data Collection (measurement of results): Were the measurement methods detailed for each variable of interest? Is there a description of comparability of the measurement methods used in the groups? Was there consideration of the validity and reproducibility of the methods used?
Sample size: Has adequate information on sample size calculation been provided? Is the logic used to determine the study size described, includ-ing practical and statistical considerations?
Statistical Methods: Was the statistical test used for each comparison informed? Indicate if the assumptions for use of the test were followed. Was there information about the methods used for any other analysis? For example, subgroup analysis and sensitivity analysis. Are the main results accompanied by accuracy of the estimate? Inform the p value and confi dence interval. Was the alpha level informed? Indicate the al-pha level below which the results are statistically signifi cant. Was the beta error informed? Or indicate the statistical power of the sample. Has the adjustment been made to the main confounding factors? Were the reasons that explained the inclusion of some and the exclusion of oth-ers described? Is the diff erence found statistically signifi cant? Make sure there are suffi cient analyzes to show the statistically signifi cant diff er-ence is not due to any bias (eg. lack of comparability between groups or distortion in data collection). If the diff erence found is signifi cant, is it also relevant? Specify the clinically important minimal diff erence. Make clear the distinction between statistically relevant diff erence and relevant clinical diff erence. Is it a one- or two-tailed test? Provide this information if appropriate. What statistical program is used? Inform the reference where to fi nd it, and the version used.
Abstract: Does the abstract contain the proper article synthesis?
Recommendation on the article: Is the article in acceptable statistical stand-ard for publication? If not, can the article be accepted after proper review?
Source: *Pereira MG. Artigos Científi cos – Como redigir, publicar e avaliar. Rio de Janeiro: Guanabara-Koogan; 2014.
IMPORTANT!
RBGO joined the initiative of the International Committee of Medical Journal Editors (ICMJE) and the EQUATOR Network, which are aimed to improve the presentation of research results. Check the following international guides:
Randomized clinical trial: http://www.consort-statement.org/downloads/consort-statement
Systematic reviews and meta-analysis: http://www.scielo.br/pdf/ress/v24n2/2237-9622-ress-24-02-00335.pdf
Observational studies in epidemiology: strobe-statement.org/fi lead-min/Strobe/uploads/checklists/STROBE_checklist_v4_combined.pdf
Qualitative studies: http://intqhc.oxfordjournals.org/content/19/6/349.long
Results
The purpose of the Results section is to show the study fi ndings. It is the original data obtained and synthesized by the author with the aim to answer the question that motivated the investigation. For the writing of the section,
present the results in logical sequence in the text, tables and illustrations, fi rst mentioning the most important fi ndings. Do not repeat all information of the tables or illustrations in the text. Emphasize or summarize only important ob-servations. Additional or supplementary materials and technical details may be placed in an appendix where they will be accessible without interrupting the fl ow of the text. Alternatively, this information may be published only in the electronic version of the Journal. When data are summarized in the results section, provide numerical results not only in derived values (eg. percentages),but also in absolute values from which the derivatives were calculated, and specify the statistical methods used for their analysis. Use only the tables and fi gures necessary to explain the argument of the work and evaluate its foun-dation. When scientifi cally appropriate, include data analysis with variables such as age and sex. Do not exceed the maximum limit of fi ve tables, fi ve charts or fi ve fi gures. Tables, charts and/or fi gures should be included in the body of the manuscript and do not count the requested limit of 4000 words.
ATTENTION!
In Case Studies, the Methods and Results sections should be replaced by the term Case Description.
Discussion
In the Discussion section, emphasize the new and important aspects of the study and the conclusions derived therefrom. Do not repeat details of data or other information presented in the introduction or results sections. For experimental studies, it is useful to begin the discussion by briefly summarizing the main findings, comparing and contrasting the results with other relevant studies, stating the limita-tions of the study, and exploring the implications of the findings for future research and clinical practice. Avoid claiming precedence and referring to incomplete studies. Do not discuss data not directly related to the results of the presented study. Propose new hypotheses when justifiable, but qualify them clearly as such. In the last paragraph of the Discussion section, cite which information of your work contributes relatively to advancement of knowledge.
Conclusion
The Conclusion section has the function of relating the conclusions to the objectives of the study, but authors should avoid unfounded statements and conclusions not adequately supported by data. In particular, authors should avoid making statements about economic benefi ts and costs unless their original includes economic analysis and appropriate data.
References
A study is based on the results of other research that preceded it. Once published, it becomes support for future work on the subject. In the report of their research, authors state the references of prior works consulted that they deem pertinent to inform readers, hence the im-portance of choosing good References. Properly chosen references lend credibility to the report. They are a source for convincing readers of the validity of facts and arguments presented.
Attention! For manuscripts submitted to RBGO, authors should num-ber the references in order of entry into the manuscript and use those numbers for text citations. Avoid excessive references by selecting the most relevant for each statement and giving preference to the most recent work. Do not use hard-to-reach quotations, such as abstracts of papers presented at congresses, theses or restricted publications (non-indexed). Seek to cite the primary and conventional references (ar-ticles in scientifi c journals and textbooks). Do not use references such as ‘unpublished observations’ and ‘personal communication’. Authors’ publications (self-citation) should be used only if there is a clear need and relationship with the topic. In this case, include in bibliographical references only original works published in regular journals (do not cite chapters or revisions). The number of references should be 35, in ex-ception review articles. Authors are responsible for the accuracy of data contained in the references.
Please check the American Medical Association (AMA) Citation Style to format your references.

*The Instructions to Authors of this journal were elaborated based in the literary work Artigos Científi cos: Como redigir, publicar e avaliar de Maurício Gomes Pereira, Editora Guanabara Koogan, 2014.
Submission of papers
The articles must, necessarily, be submitted electronically, accord-ing to the instructions posted on the site: http://mc04.manuscript-central.com/rbgo-scieloThere is no fee for submission and review articles.
Revista Brasileira de Ginecologia e ObstetríciaAddress: Brigadeiro Luiz Antonio Avenue, 3421, 01401-001, 903 room, Jardim Paulista, São Paulo, SP, Brazil. Phone: + 55 11 5573.4919 E-mail: editorial.offi [email protected] Home Page: https://www.thieme.com/rbgo

https://publons.com/in/thieme/
How does Publons speed up science?••
•
promotion and funding applications
Publons is a completely free service for academics.
Show your true contributions to scienceTrack and verify your peer review
Thieme Medical Publishers Publons

Anuncio_Ela_20.2x26.06cm.indd 1 8/14/17 4:45 PM