Obstetrics and gynecology.pdf - Crimea State Medical ...
704
1 A. N. Rybalka, V. A. Zabolotnov, I. K. Kamilova, A. N. Sulima, S. S. Anikin, V. V. Litvinov, I. M. Shlapak, S. E. Regushevsky, D. A. Beglitce, Z. S. Rumyanceva, I. A. Khomulenko, N. S. Demidova, O. P. Miklin, G. N. Bagrova OBSTETRICS AND GYNECOLOGY Textbook in 2 volumes Edited by Professor A. N. Rybalka Volume 2 GYNECOLOGY Simferopol 2018
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Obstetrics and gynecology.pdf - Crimea State Medical ...

1
A. N. Rybalka, V. A. Zabolotnov, I. K. Kamilova,
A. N. Sulima, S. S. Anikin, V. V. Litvinov, I. M. Shlapak,
S. E. Regushevsky, D. A. Beglitce, Z. S. Rumyanceva,
I. A. Khomulenko, N. S. Demidova, O. P. Miklin, G. N. Bagrova
OBSTETRICS AND
GYNECOLOGY
Textbook
in 2 volumes
Edited by Professor A. N. Rybalka
Volume 2
GYNECOLOGY
Simferopol
2018

2

3
N. Rybalka, V. A. Zabolotnov, I. K. Kamilova, A. N. Sulima,
S. S. Anikin, V. V. Litvinov, I. M. Shlapak,
S. E. Regushevsky, D. A. Beglitce, Z. S. Rumyanceva, I. A. Khomulenko,
N. S. Demidova, O. P. Miklin, G. N. Bagrova
OBSTETRICS AND
GYNECOLOGY
Textbook
in 2 volumes
Edited by Professor A. N. Rybalka
Simferopol
2018

4
УДК 618.2/7
ББК
R 98
Rybalka A. N., Zabolotnov V. A., Kamilova I. K. at al.
R 98 Obstetrics and gynecology. Textbook - in 2 vol. Vol. 2 Gynecology. –
Simferopol, 2018. – 704 p., 134 pic., 20 +ав.
ISBN 978-966-2913-33-0
Annotation
The manual on obstetrics and gynecology is designated for English-speaking
students of the 5-6 courses of medical higher schools. Short lectures on the main
topics of obstetrics and gynecology are presented in the manual. The book acquaints
the reader with up-todate notions in etiology, pathogenesis, diagnosis and treatment
of gynecological diseases. The book is intended as a handbook on obstetrics and
gynecology for the English-speaking students.
© A. N. Rybalka, V. A. Zabolotnov, I. K. Kamilova, A. N. Sulima,
S. S. Anikin, V. V. Litvinov, I. M. Shlapak, S. E. Regushevsky,
D. A. Beglitce, Z. S. Rumyanceva, I. A. Khomulenko, N. S. Demidova,
O. P. Miklin, G. N. Bagrova, 2018

5
Volume 2
GYNECOLOGY
Recommended by the Scientific Council of the Midical Academy named after
S. I. Georfievsky V. I. Vernadsky Crimean Federal University as “Obstetrics and
gynecology” textbook in 2 volumes in English for students, internus and doctors of
higher medical schools, who study the academic discipline in English 27. 12. 2016
(Protocol №14)

6
Authors:
A. N. Rybalka – DM, Professor, Academician, Head of the Department of
Obstetrics, Gynecology and Perinatology.
V. A. Zabolotnov – DM, Professor, Head of the Department of Obstetrics and
Gynecology.
I. K. Kamilova – PhD, Associate Professor of the Department of Obstetrics
and Gynecology.
A. N. Sulima – DM, Professor of the Department of Obstetrics, Gynecology
and Perinatology.
S. S. Anikin – PhD, Associate Professor of the Department of Obstetrics,
Gynecology and Perinatology.
V. V. Litvinov – PhD, Chief Physician of the Human Reproduction Clinic
“Altra Vita” (LLC “ECO Center”), Moscow.
I. M. Shlapak – DM, Professor of the Department of Obstetrics, Gynecology
and Perinatology, Chief Physician of the Crimean Republican
Clinical Perinatal Center.
S. E. Regushevsky – PhD, Associate Professor of the Department of Obstetrics,
Gynecology and Perinatology, Chief Obstetrician and
Gynecologist of the Ministry of Health of the Crimea, Deputy
Chief Republican of Crimean Republication Clinical Perinatal
Center.
D. A. Beglitce – PhD, Associate Professor of the Department of Obstetrics,
Gynecology and Perinatology, Chief Physician of Clinical
Maternity №1.
Z. S. Rumyanceva – PhD, Associate Professor of the Department of Obstetrics
and Gynecology №1.
I. A. Khomulenko – PhD, Associate Professor of the Department of Obstetrics,
Gynecology and Perinatology.
N. S. Demidova – PhD, Associate Professor of the Department of Obstetrics,
Gynecology and Perinatology.
O. P. Miklin – PhD, Associate Professor of the Department of Obstetrics
and Gynecology №1.
G. N. Bagrova – PhD, Associate Professor of the Department of Obstetrics,
Gynecology and Perinatology.

7
CONVENTS
INTRODUCTION. ....................................................................................................... 7
Gynecology as a science. Historical Perspective. Deontological ethic in
gynecological practice .............................................................................................. 7
CHAPTER 1. Anatomical and Physiological changes in women in different
periods of the life. Puberty ......................................................................................... 11
Puberty stages in girls. ............................................................................................. 15
Menstruation ............................................................................................................. 19
Menopause. ............................................................................................................... 20
CHAPTER 2. Examination of Gynecological Patients ............................................... 23
Clinical breast examination. ..................................................................................... 31
Inspection of external genitalia. ............................................................................... 47
Vaginal smears ......................................................................................................... 56
Tests for evaluation of vaginal ecology ............................................................ 56
Tests for evaluation of endocrine status ............................................................ 61
Tests for evaluation of abnormal (precancerous and cancerous) conditions .... 70
Invasive methods of examination sounding of the
uterus ...................................................................................................................... 172
Histological investigations. Cervical biopsy. ......................................................... 174
CHAPTER 3. Congenital anomalies and displacements of the female genitalia .... 186
CHAPTER 4. Inflammaory diseases of the
female genitalia ......................................................................................................... 203
Sexually transmitted pelvic inflammatory diseases. .............................................. 236
CHAPTER 5. Neurohumoral control of the
menstrual cycle .......................................................................................................... 253
CHAPTER 6. Menstrual disorders ............................................................................ 270
CHAPTER 7. Neuroendocrinal syndromes in
gynecology ............................................................................................................... 299

8
CHAPTER 8. The infertile couple ............................................................................ 322
CHAPTER 9. Contraception ..................................................................................... 332
CHAPTER 10. Typical operations in gynecology .................................................... 354
CHAPTER 11. Acute abdomen in gynecologic practice .......................................... 435
CHAPTER 12. Injuries of the female genital tract.................................................... 452
CHAPTER 13. Myoma of the uterus. Endometriosis. Sarcoma of the uterus .......... 470
CHAPTER 14. Breast diseases .................................................................................. 500
CHAPTER 15. Premalignant diseases of the vulva and vagina. Cancer and
sarcoma of the vulva and vagina .............................................................................. 519
CHAPTER 16. Background processen and premalignant lesions of cervix.
Cervical cancer ......................................................................................................... 545
CHAPTER 17. Premalignant diseases of the endometrium. Cancer of the uterus.
Sarcoma of the uterus ................................................................................................ 573
CHAPTER 18. Cysts of the ovary. Ovarian tumors ................................................. 589
CHAPTER 19. Cancer of the fallopian tubes ........................................................... 605
CHAPTER 20. Trophoblastic diseases .................................................................... 609
CHAPTER 21. Gynecological diseases in childhood and adolescence .................... 617
CHAPTER 22. Female dispensary – prophylactic medical examination of
gynecological patients .............................................................................................. 635
CHAPTER 23. Hygienic regimen in female ............................................................. 640
CHAPTER 24. Urinary tract diseases in female ....................................................... 647
CHAPTER 25. Appendices ....................................................................................... 681
Appendix 1. Tests 1. ............................................................................................... 681

9
PART II. GYNAECOLOGY
INTRODUCTION
Gynecology as a science. Historical Perspective
Gynaecology (British) or gynecology (North American) literally means
'the science of women', - “the science of womankind” (Oxford Dictionary);“the
medical specialty concerned with diseases of the female genital tract as well as
endocrinology and reproductive physiology of the female”(Stedman
Dictionary). Almost all modern gynecologists are also obstetricians.
Gynecology is a typically consultant specialty. In most countries, women must
see a general practitioner first. If their condition requires knowledge or
equipment unavailable to the general practitioner, they are referred to a
gynecologist. However, in many countries law and many health insurance
plans allow gynecologists to provide primary care and some women select
that option.
Clinical history and examination generally accepted in medicine are the
main tools of diagnosis in gynecological practice. Gynecological examination
is a special one as it is quite intimate and it involves special equipment.
Various taboos associated with the study of female genitalia, for a long time
hampered the development of the science of gynecology. This drawing of 1822
by Jacques-Pierre Maigreira (Fig.1) shows a "compromise" procedure in
which the doctor kneels in front of a woman, but cannot see her genitals.
Modern gynecology no longer uses this position
Historical Perspective (see also Volume I). Down to the sixteenth
century gynecology was almost exclusively in the hands of midwives, who
were trained for it as for a trade. Only in rare cases was a surgeon called in.
Almost all the achievements of ancient times seemed to be forgotten, and only
10
after anatomical studies had been resumed and surgery had made some
progress those things began to improve.
The most important accounts of the condition of ancient gynecology are
found in famous Indian Ayurvedic books, which mean “the Science of Life”, in
the Hippocratic writings, one of the books named “About female diseases”. In
ayurvedic books there is some information about displacements of uterus,
condylomas of vulva, amenorrhea. Important information about
inflammatory processes of the uterus and vagina (diagnosis and treatment of
endometritis and vaginitis) are found in the Hippocratic writings, as well as
material about swellings of the female genitalia, some types of surgical
treatment of uterus tumors (removing of the tumor with tongs, knife and red-
hot iron).
The first scientific background of gynecological science appeared in the
16th century, in writings of Kuper, Vesalius, Bartoline, Fallopio and others.
(Fig. 2). The detailed description of female anatomy was done at this period of
time. Mercado, the professor of the university in Toledo (Spain) wrote one of
the oldest books on gynecology in the 16th century. Much was done to enlarge
and enrich the study of this branch of medicine by the works of Jacques
Guillemeau (1560 to about 1609), Scipione Mereurio (1595), Ambroise Paré
(1517–1590), Renie Graaf (1641–1673).
Fig. 1. A compromise" procedure of gynecological examination.

11
Fig.2. A - Gabriello Fallopio, 1523–1562; B - Ambroise Paré, 1517– 1590.
The gynecology was a part of surgery, it wasn’t an independent science
over a long period of time. Historically, gynecology has been one of the few
medical practices dominated by female practitioners. From Agnodice in
ancient Greece to the 18th century in Europe, the care of mothers and delivery
of infants has been regarded, both by the patients and by the specialists of
medical profession, as a profession carried out by women.
In the 18th century, a gap between surgeons and midwives arose as
medical men began to assert that their modern scientific processes were
better for mothers and infants than the midwives. A number of excellent full-
length studies of these historical changes have been written. The powerful
progress of natural science, medicine, physiology and anatomy became the
basis for development of gynecology in many countries of the world. In the
40th of the 18th century special gynecological clinics were opened in some
countries of Europe (Russia, England, France, and Germany). Up to this time
gynecology had been only a part of obstetrics and surgery. Since this time
gynecology has become the independent science studying female reproductive
system, its physiology and pathology. French scientist J. Astruc was a pioneer
of study of the septic endometritis, he detailed clinical features and supposed

12
the pyaemia to be a reason of fever, sweats, emaciation, weight loss.
F. Osiander (1759–1822) proposed to perform the amputation of the uterus
cervix in case of cancer and invented a novel device – special forceps for this
operation. The introduction of scientific gynecology in different countries was
important at that time. The science of gynecology has long inhibited the
shame associated with the examination of female genitalia. This 1822 drawing
by Jacques-Pierre Maygnier shows a "compromise" procedure, in which the
physician is kneeling before the woman but cannot see her genitalia. Modern
gynecology has overcome these inhibitions. J. Simpson, J.-L. Baudelocque,
K. Schroeder, V. A. Krasovsky, J. Pean, A. Hegar, I. Semmelveis, D. Lister,
V. Stroganov, A. Neisser, V. Snegirev, A. Gubarev, D. Ott are famous due to
their important contribution to the science.
Fig. 3. Professor V. F. Snegirev, 1847-1916
Deontological ethics in gynecological practice
The study of ethics has been defined as the way of understanding and
examining the moral life, and as the study of conduct and moral judgment
standards. Thus, the study of ethics is the study of morality, careful and
systematic reflection and analysis of moral decisions and behaviour. Since
ethics deals with all aspects of human behaviour and decision-making, it is a

13
very large complex field of study with many branches. Medical ethics
(deontological ethics) is the branch of ethics that deals with moral issues in
medical practice. The Hippocratic oath is referred to the one of the oldest
codes of medical ethics. It was Hippocrat who suggested the most important
ethical principle “do no harm” (“non nocere”) in this code.
In recent times medical ethics has been greatly influenced by the
development in human rights. It is closely related to law. But ethics and law
are not identical. As for the laws, they differ from one country to another
while ethics is applicable across national boundaries. At the same time,
medical ethics vary from one country to another depending on the
development in medical science and technology, social values, cultural wealth
and moral traditions. Although these differences may seem significant, the
similarities are far greater. Physicians throughout the world have much in
common. The fundamental values of medical ethics such as compassion,
competence, autonomy, beneficence, do no harm, confidentiality, honesty,
respect for a patient and respect for the law are common for all physicians all
over the world.
Physicians caring for patients should follow these fundamental ethical
principles.
Autonomy.
Physician’s autonomy, or self-determination is the core value of
medicine. Any physician traditionally enjoyed a high degree of clinical
autonomy in deciding how to treat a patient. On the other hand, physicians in
general (the medical profession) have been free to determine the standards of
medical education and medical practice. Both of these ways of exercising
physician autonomy have been moderated in many countries by the
government and other authorities imposing controls on physicians.
At the same time, there has been a widespread acceptance of patient
autonomy, which means, the patients should be the ultimate decision-makers
in matters that affect them. Physicians must respect a patient's right to make

14
decisions regarding medical care. Competent, informed patients have the
right to choose treatment options and refuse any unwanted medical
interventions.
Decisions for Competent Patients
One of the most important ethical principles of ethical delivery of care is
informed decision making. Informed, competent patients have the power to
choose consent to, or refuse medically feasible options for care, even when the
result will be disability or death.
Decision-Making for Incompetent Patients
Patients may be incompetent to make decisions for themselves.
Examples include young children, individuals affected by certain neurological
or psychiatric conditions, and those, who are temporary unconscious or
comatose. The World Medical Association Declaration on the Rights of the
patients states the physician’s duty in this matter as follows:
If the patient is unconscious or otherwise unable to express the will,
informed consent must be obtained from a legally entitled representative
where legally relevant. If a legally entitled representative is not available, but
a medical intervention is urgently needed, consent of the patient may be
presumed, unless it is obvious and beyond any doubt on the basis of the
patient’s previous firm expression or conviction that she/he would refuse
consent to the intervention in that situation.
Refusal of Therapy
Most patients accept treatment recommended by their physician.
However, some patients may refuse treatment that the physician believes to
be highly beneficial (e. g., amputation of a myomatous uterus). In such
circumstances it is appropriate for the physician to try to persuade the patient
to accept beneficial treatment, although the physician should refrain from
badgering the patient or misrepresenting the facts. The physician should
check that the patient is fully informed of the consequences of the decision
and has the capacity to make informed decisions. In the end, the physician

15
must respect a competent, informed patient's right to make decisions about
medical care, even if the physician believes the decision is unwise.
Compassion, defined as understanding and concern for another
person’s distress, is essential for the practice in medicine, especially in
gynaecology. In order to deal with the patient’s problems, the physician must
identify the symptoms that patient is experiencing and their underlying
causes and must want to help the patient achieve relief. Patients respond
better to treatment if they perceive that physician appreciates their concerns
and is treating them rather than just their illness.
Competence is defined as the totality of scientific knowledge and
practical skills of a physician. The lack of competence can result in death or
serious morbidity for patients.
Beneficence.
Fundamental in the doctor-patient relationship is the principle of
beneficence. It is the core ethical principle of the Hippocratic writings:
“Declare the past, diagnose the present, foretell the future; practice in such a
way. As for disease, make a habit of two things, help or at least “do no harm”.
Physicians must do their best acting in the interests of their patients. Patients
are vulnerable because of illness and lack of medical expertise. Therefore,
they rely on physicians. Physicians must put the interests of their patients
above their own interests or those of the third parties, such as insurers or
managed care organizations. If patients lack decision-making capacity, they
need to be protected from making decisions that are contrary to their
interests.
Do no harm.
The related principle directs physicians to “do no harm” to patients.
Physicians must refrain from providing ineffective treatment or acting with
malice towards patients. This principle, however, offers little useful guidance
to physicians, as many beneficial therapies also have serious risks. The
pertinent ethical issue is whether the benefits outweigh the burdens.

16
Confidentiality.
Physicians must maintain the confidentiality of medical information.
Confidentiality respects patient autonomy and encourages patients to seek
care and be candid. A physician will preserve absolute confidentiality on all he
knows about his patient even after the patient has died. The World Medical
Association Declaration on the Rights of the Patient summarized the patient‘s
right to confidentiality as follows:
All identifiable information about a patient’s health status, medical
condition, diagnosis, prognosis and treatment and all other information of a
personal kind, must be kept confidential, even after death.
Confidential information can only be disclosed if the patient gives consent or
if expressly provided for in the law. Information can be disclosed to other
healthcare providers only on a strictly “need to know” basis unless the patient
has given explicit consent.
All identifiable patient data must be protected. The protection of the
data must be appropriate to the manner of its storage. Human substances
from which identifiable data can be derived must be likewise protected.
Many of the most prominent issues in medical ethics relate to special
gynaecological conditions, such as contraception, assisted reproduction,
prenatal genetic screening, abortion, severely compromised neonates, etc.
Any information of these conditions is confidential.
The world medical association declaration of Geneva
At the time of being admitted as a member of the medical profession:
I solemnly pledge myself to consecrate my life to the service of humanity;
I will give to my teachers the respect and gratitude, which is their due;
I will practise my profession with conscience and dignity; The health of my
patient will be my first consideration;
I will respect the secrets, which are confided in me, even after the patient has
died;

17
I will maintain by all the means in my power, the honour and the noble
traditions of the medical profession;
My colleagues will be my sisters and brothers;
I will not permit considerations of age, disease or disability, creed, ethnic
origin, gender, nationality, political affiliation, race, sexual orientation, or
social standing to intervene between my duty and my patient;
I will maintain the utmost respect for human life from its beginning even
under threat and I will not use my medical knowledge contrary to the laws of
humanity;
I make these promises solemnly, freely and upon my honour.

18
Chapter 1. ANATOMICAL AND PHYSIOLOGICAL
CHANGES IN WOMEN IN DIFFERENT PERIODS OF
LIFE
PUBERTY
Puberty is an exciting but perplexing stage of life that both girls and
boys go through. In girls, it is a time of physical transition between childhood
and womanhood. Rapid physical change goes hand in hand with
psychological change.
One of the changes is the first menstrual period, which occurs at this
time. The changes of puberty are usually complete by the age of eighteen, by
that time the girl is a full-grown woman.
A girl-child starts becoming a woman at the age from 9 to 14, when the
pituitary gland and the hypothalamus in her brain send a signal to her
ovaries. This signal instructs the ovaries to increase production of the female
sex hormones. It is due to this increased hormonal production that causes the
changes of puberty for the period from two to six years. Some girls experience
puberty early others experience it late. Usually they enter puberty about the
same age as their mother or any of their father’s close female relatives.
Outward Changes of Puberty
Physical change is to be expected mostly during puberty. Secondary
sexual characteristics and other changes that develop or occur at this stage
include:
Development of breasts (thelarche);
Growth of pubic hair (pubarche);
Changes in body shape;
Increased height (accelerated growth);
Increased weight;
Growth of external genitalia;
19
Increased sweating;
Pimples;
Vaginal discharge;
The first menstrual period (menarche).
Development of breasts: The area around the nipples grows first,
followed by the actual breasts. Breast development continues approximately
until the age of 18. The growing girl often worries because one breast develops
faster than the other. She needs to be reassured that this happens to many
other girls and the pace of development will soon even out her figure.
Growth of pubic hair: Hair begins to grow in new places during puberty.
Pubic hair begins to grow in a triangular patch in the pubic area, lightly at
first. This is followed by hair growth under the arms. Hair on the legs and
sometimes hair on the arms begins to darken. Some girls are worried by
excessive hair on their limbs and upper lip and may request cosmetic
attention.
Changes in body shape: The hips and thighs widen and the pelvis
expands. The shape of the girl’s body becomes more curvaceous, she prepares
to carry a baby during future pregnancies.
Increased height: Girls enter puberty earlier than boys, and thus enter
their 'growth spurt' before boys. The growth spurt is one of the first signs of
puberty. A girl may grow as much as four inches taller in a single year. After
this, growth slows down considerably. Most girls completely stop growing
about one to three years after the first period, while some gain an inch or so
up to the age of 21. A girl’s feet grow at a fast pace, reaching their full adult
size much before the rest of the body.
Increased weight: A girl tends to be hungrier and have a better appetite
during puberty than she had earlier. Her body needs more calories as it is
growing very quickly. There is an increase in weight as well.

20
Growth of external genitalia: The genitals, which are not conspicuous in
a child, grow and become more evident during puberty. The female external
genitals include the vulva, labia and clitoris.
Increased sweating: Girls now tend to perspire more than they did as
children. Body odor also develops, sometimes necessitating the use of a
deodorant or anti-per- spirant. Daily bathing and frequent change of clothes,
particularly in hot weather, helps to reduce the unpleasant effects of excessive
sweating.
Pimples: One of the difficult changes a young girl may have to endure is
the crop of pimples on her face. Puberty causes her skin to break out because
the oil glands are now more active. The best way of dealing with pimples is to
keep the area clean and to prevent the pores from clogging. This is
particularly important in cities with their high levels of pollution.
Vaginal discharge: Six months to a year before the first period, a girl
usually notices a clear, white vaginal discharge. This is normal, and might
turn yellow on contact with underwear. It is important to change underwear
regularly.
The first period: Shortly after the breasts and pubic hair begin to grow,
the first period occurs (menarche). Girls must be forewarned about menstrual
bleeding, as the first period can otherwise come as a frightening shock. They
need to be taught to use sanitary towels and proper hygiene. Sanitary towels
should be changed at least three to four times a day. This is also the right time
to explain the menstrual cycle to a young girl. Menstrual irregularities in
puberty include a number of conditions, some of which require medical
attention.
Invisible Changes of Puberty
Growth of internal sex organs: The uterus and vagina, which are the
female sex organs within the body, grow during puberty. The uterus increases
in size and sheds its lining in a monthly discharge called the menstrual
period. The vagina grows longer and its walls stretch and become more

21
elastic. Girls going through puberty should be taught about work and
anatomy of the female reproductive system.
Puberty does not begin at the same age for every girl. It can occur
normally at any time in the age from 9 to 14. However, a doctor should be
consulted under certain circumstances, to make sure there is nothing wrong:
- Puberty begins before the age of 9. This is called precocious puberty;
- Pubic hair and breasts (secondary sexual characteristics) have not
begun to appear by the age of 13. This is referred to as delayed puberty;
- The first period has not occurred by the age of 16 (primary
amenorrhea), or the menstruation has stopped for a period of six
months or more (secondary amenorrhea).
Puberty has been divided into five Sexual Maturity Rating (SMR) stages
by two doctors, W. Marshall and J. M. Tanner. These ratings are often
referred to as Tanner Stages one through five. Staging is based on pubic
hair growth, on genital development, and female breast development. Staging
helps determine whether development is normal for a given age. Both sexes
also grow armpit hair and develop pimples. Males develop muscle mass, a
deeper voice, and facial hair. Females redistribute body fat. Along with the
maturing of the sex organs, there is a pronounced growth spurt averaging 8–
10 centimeters and culminating in full adult stature.
Puberty stages in girls
Stage 1. Age Range: Usually 8-11
In Stage 1 there are no outside signs of development, but a girl's ovaries
are enlarging and hormone production is beginning.
Stage 2. Age Range: Usually 8-14. Average: 11-12
The first sign is typically the beginning of breast growth, including
"breast buds." A girl may also grow considerable height and weight. The first
signs of pubic hair start out fine and straight, rather than curly. (Fig. 4)
Stage 3. Age Range: Usually 9-15. Average: 12-13

22
Breast growth continues, and pubic hair coarsens and becomes darker,
but there still isn't a lot of it. The body is still growing, and vagina is enlarging
and may begin to produce a clear or whitish discharge, which is a normal self-
cleansing process. (Fig.5). Some girls get their first menstrual periods late in
this stage.
Fig. 4. Illustration of the Tanner scale for females:

23
I - no glandular tissue: areola follows
the skin contours of the chest
(prepubertal)
no pubic hair at all
(prepubertal)
II - breast bud forms, with small area
of surrounding glandular tissue; areola
begins to widen
small amount of long,
downy hair with slight
pigmentation on the labia
majora
III - breast begins to become more
elevated, and extends beyond the
borders of the areola, which continues
to widen but remains in contour with
surrounding breast
hair becomes more coarse
and curly, and begins to
extend laterally
IV - increased breast size and
elevation; areola and papilla form a
secondary mound projecting from the
contour of the surrounding breast
adult–like hair quality,
extending across pubis but
sparing medial thighs
V - breast reaches final adult size;
areola returns to contour of the
surrounding breast, with a projecting
central papilla.
Stage 4. Age Range: Usually 10-16. Average: 13-14
Pubic hair growth takes on the triangular shape of adulthood, but
doesn't quite cover the entire area. Underarm hair is likely to appear in this
stage, as is menarche. Ovulation (release of egg cells) begins in some girls, but
typically not in a regular monthly routine until Stage 5.
Stage 5. Age Range: Usually 12-19. Average: 15
This is the final stage of development, when a girl is physically an adult.
Breast and pubic hair growth is complete, and full height (stature) is usually
attained by this age range. Menstrual periods are well established, but within

24
the first 1,5-2 years after menarche most menstrual cycles are anovulatory. An
ovulatory menstrual cycle is formed in 1-2 years after menarche and ovulation
occurs monthly. Irregular menstrual patterns are also common within 24
months of menarche.
Fig. 5. The pre-pubertal uterus compare with the adults
To evaluate the rating of sexual maturity special table is used now-a-
days (Table 1)

25
Table 1
Female Sexual Maturity Rating (SMR)
Stage 1 2 3 4 5
Age range 8 -10 yrs 10.5-12.9
yrs
11.3 – 13.5
yrs
11.8 – 14.0
yrs
13.3 –
15.5 yrs
Breast External
development
is not yet
visible.
Breast and
papilla
elevated as
small
mound, or
breast
bud,
areolar
diameter
increased
Breast and
areola
enlarged,
no
contour
separation
Areola and
papilla form
secondary
mound
projecting
from the
contour of
the
surrounding
breast
Adult
size and
contour.
Areola
returns
to part of
general
breast
contour,
nipple
projects
Pubic
Hair
- // - Hair is
sparse,
lightly
pigmented
and
straight,
located on
medial
border of
labia
majora
Hair is
darker,
more
coarse and
beginning
to curl,
increased
in amount
and begins
to extend
laterally
Hair is
coarse and
curly as in
the adult,
hair extends
across the
pubis but
spares the
medial
thighs
Adult
hair –
coarse
and
curly,
spreads
to medial
surface
of thighs
Menarche
(10.8 –
14.5 yrs)
- 10% 30% 90% 100%
Acne Mean age
of onset –
13.2 years

26
MENSTRUATION
The menstrual cycle is the scientific term for the physiological changes that
can occur in fertile women for the purposes of sexual reproduction and
fertilization. The menstrual cycle means a monthly cycle of changes in the
hypothalamus, pituitary gland, in the ovaries and endometrium, aimed at
maturing the eggs for fertilization and preparing the endometrium for the
implantation of a fertilized egg. The menstrual cycle is also described based
on its length (number of days between onset of menstrual bleeding in one
cycle and the onset of bleeding of the next cycle). If fertilization will not
happen, the cycle would completed with menstruation (aka periods,
menstrual flow, etc). Menstruation is the periodic bleeding from the vagina.
Menstruations begin during puberty, in the age from 9 to 14 and ends at
menopause (usually in the age from 45 to 50). For a regular menstrual cycle,
the median age of menarche is 12.77 years. The median duration of a
menstrual cycle is 28 days with most cycle lengths between 25 to 30 days.
Patients, who experience menstrual cycles that occur at intervals less than 21
days are termed polymenorrheic, while patients who experience prolonged
menstrual cycles greater than 35 days, are termed oligomenorrheic. The
typical volume of blood lost during menstruation is approximately 30 mL.
Any amount greater than 70-80 mL is considered abnormal. The duration of
the period (menses) varies in women. Normally, it should last from 3 to 5
days. A woman typically will have about 500 menstrual cycles in her lifetime.
Since it is a cycle, there is no beginning or end, and the changes that
occur are generally gradual. It is convenient, however, to call the first day of
menstruation "day one" of the cycle, because the flow of menstrual blood is
the most apparent of the changes that occur. It is also convenient to divide the
cycle into phases based on changes that occur in the ovary and in the
endometrium.

27
However, a normal cycle can range from 18 to 40 days. And the first day
of the menstrual cycle, when the bleeding begins, is the first day of the period.
MENOPAUSE
Menopause is the cessation of menstruation, in women over the age of
45, for at least 6 to 12 months. Menopause is accompanied with some physical
and psychological changes. It occurs over a few years. Ovarian failure also
takes place during this time. Needless to say, once a woman stops
experiencing the menstrual cycle, her child-bearing years are over.
Today, women’s health and longevity have improved significantly. Even
as recently as a century ago, a large percentage of women did not live up to
menopause. Improved nutrition and medical care have contributed to the
longer life of women. Nowadays, women are encouraged to live in good health
and happiness after their fertile years are over. Menopause might mean the
end of fertility but there is no valid reason why a woman should not be well
and comfortable in the years or decades ahead.
Menopause is a physiological change in the Hypothalamic-Pituitary-
Ovarian Axis (HPOA) according to the age of the woman. In order to
understand the context in which the physiological changes of the menopausal
transition are happening, it is necessary to consider the definitions and stages
associated with reproductive aging. The premenopause is typically defined as
the phase of a woman’s life from the menarche (onset of menstruation) until
the beginning of the perimenopausal stage. The perimenopause comprises
the time from a woman’s mature reproductive state at the point when she
begins to experience variability in the length of her cycle or characteristic
symptoms of the menopausal transition, to the year following her final
menstrual period (FMP). It is only following this 12-month period of
amenorrhea that a diagnosis of menopause can be made. The terms

28
“menopause” and “postmenopause” are often used interchangeably to
describe the phase of a woman’s life from this point
The age of menopause varies. In India, which has a warm climate,
women reach menopause in the age of 45 to 50. In colder climates, women
experience menopause a few years later. In the USA, for instance, the average
age of menopause is 50 to 52 years. In Russian Federation the average age of
menopause is 45–55 years. Apart from climate, the age of menopause also
depends on hereditary factors.
Psychological Features of Menopause
The frequency of the menstruation reduces gradually as a woman
approaches perimenopause. In rare cases menstruation ceases abruptly. Some
women get their periods at frequent intervals with scanty or prolonged flow.
This is because of limited follicle maturation as the remaining follicles in the
ovaries become less sensitive to gonadotropin stimulation.
There are some common psychological features of menopause. These
include increased moodiness, irritability and greater anxiety and fearfulness.
Some women undergo depression and experience insomnia (inability to
sleep). Others report a decreased libido. The vagina becomes narrow closer to
menopause. The uterus also decreases in size and the endometrial tissue
becomes sparse. The vaginal part of the cervix becomes smaller as the muscle
atrophies. The pelvic tissues and ligaments that support the vagina and uterus
lose their tone and become weaker. This predisposes to prolapse of the uterus.
If there are fibroids in the uterus, they become smaller, but do not disappear.
The fat in the breasts gradually reduces. Nipples become smaller. In general,
the breasts become softer, less full and lose the form they had in the child-
bearing years.
All these psychological symptoms form part of the menopausal
syndrome, which follows reduced estrogen in the body. Menopause, like
puberty, is another time when women require a lot of reassurance.
Menopausal women also have to cope with a changing self-image. Emotional

29
disturbances and insecurity only worsen the uncomfortable symptoms of
menopause (see also chapter “Neuro-endocrinal syndromes in gynecology”).
Self test
1. The changes of puberty are complete in the age of
A. 16-18
B. 13-14
C. 9-14
D. 20
2. The first period is named
A. menarche
B. menopause
C. menstruation
3. Girls usually notice vaginal discharge
A. six months to a year before the first period
B. one month before the menarche
C. after the appearing of the first period
4. The average blood loss in periods is
A. 35 ml
B. 20-25 ml
C. 50 ml
D. 0. 5 % of body weight
5. The first day of the menstrual cycle is
A. the first day of the period
B. the first day after the finishing of blood loss
C. the first day of increased basal temperature
6. What hormone is responsible for the release of the egg
(ovulation)?
A. the follicle stimulating hormone

30
B. the luteinizing hormone
C. the somatotropic hormone
D. the adrenocorticotropic hormone
7. The age of menopause is
A. over the age of 45
B. over the age of 65
C. over the age of 35
8. The uterus in menopause
A. decreases in size
B. increases in size
C. is without changes
9. Precociuos puberty means
A. puberty before the age of 9
B. puberty before the age of 14
C. puberty before the age of 18

31
Chapter 2. EXAMINATION OF GYNECOLOGIC
PATIENTS
Examination of gynecologic patients includes history taking, physical
examination, and examination with the help of additional techniques.
This is the scheme of questioning:
1. Biographical details;
2. Chief complaints;
3. Anamnesis or medical history;
4. Physical examination: a) general examination, b) special gynecologic
examination;
5. Additional methods of examination.
BIOGRAPHICAL DETAILS
First is the identification of a patient: name and surname, age of the
patient, home address, occupation, family status, sex, education, nationality,
and so on.
CHIEF COMPLAINTS
The most typical and frequent complaints of gynecologic patients
include pains, leucorrhoea, bleeding and menstrual disorders, infertility and
dysfunction of the adjacent organs. Pain is the most frequent complaint
associated with gynecologic diseases. It may be caused by spastic uterine
contractions, and contractions of the uterine tubes, compression of nerve
endings and plexuses of tumors and infiltrates of the inflammations. In all
cases the nature, intensity, localization, irradiation of pain must be
established. In cases of abnormal bleeding, its relation to the periods
(premenstrual, intermenstrual or postmenopausal), or to coital experience

32
must be defined. Its frequency and duration, and information about
amenorrhea, if any, the type of contraceptive used (whether hormonal or
intrauterine device), the quantum of flow and whether it is associated with
clots and pain, are important.
The periods may be profuse or prolonged (menorrhagia), or frequent
(polimenorrhea), or irregular with bleeding between the periods
(metrorrhagia).
Leucorrhoea or abnormal vaginal discharge: the quantum (profuse or
scanty), color (white, yellowish, blood-stained, brownish), nature (curdy or
frothy or mucoid), odor (offensive, urinary or ammoniac), its relation to the
menstrual cycle (intermenstrual or premenstrual) and associated symptoms
such as pruritus and burning micturition should be ascertained. An ulcerated
lesion in the genital tract (cancer, polyp) will result in an irregular blood-
stained discharge. If the growth is infected and covered over with slough, the
discharge is likely to be offensive. In rectovaginal fistula the discharge may be
fecal.
MEDICAL HISTORY (ANAMNESIS)
It is important to obtain the detailed history before a gynecological
examination. Incomplete history may lead to a wrong diagnosis.
HISTORY OF LIFE.
At the beginning one should question the history (anamnesis) of life,
including development in childhood, living conditions. For example, the
nature of nutrition, whether sufficient and adequate, which is of importance,
especially during puberty. Insufficient, excessive or inadequate nutrition may
lead to an incorrect genital system formation, as well as to menstrual
reproductive disorders. One should inquire about the woman’s living
conditions and the way in which her household and rest are organized.

33
Excessive physical work at home may trigger off a number of diseases.
Heavy lifting soon after the delivery and hard work in advanced age may
result in genital prolapse. The patient’s working conditions and occupational
hazards (dusty working environment, chemicals, vibration, noise and others)
may affect the course of some diseases.
HEREDITY.
In the course of questioning the examiner should determine whether
any relatives of the patient have suffered or suffer from mental and endocrine
diseases, alcoholism, cancer, blood and metabolic diseases. A family history of
tuberculosis, diabetes or pelvic malignancy should alert the gynecologist to
any early evidence of these conditions in the patient during the check-up.
HISTORY OF PREVIOUS DISEASES.
The history of systemic diseases should be taken in the chronological
order.
Chronic tonsillitis, epidemic parotitis and measles occurring during
puberty may have an influence on the establishment of menstrual function
and be responsible for underdevelopment of the female genital organs.
Information about any major previous illness such as tuberculosis,
appendicitis or surgery involving the abdominal or pelvic viscera should be
recorded in detail. The indication, findings at surgery, details of the procedure
and pathology report on the tissue (resected organ) would be useful. Previous
surgery especially on the abdominal organs may be responsible for
inflammation of the uterus adnexa , adhesions and ectopic pregnancy. It is
important to find out whether the patient has been taking any drugs, such as
cortisone, hypotensors, antituberculous agents or sex steroids recently.
Of particular significance is a history of blood transfusions. To obtain
the necessary information, one should inquire if the patient has ever been

34
subjected to blood transfusion, what necessitated the transfusion, and
whether it was followed by any abnormal response.
Allergy History should also be taken; it should be ascertained whether
the patient has ever had allergic reactions to any foods or drugs. This
information is essential at prescribing any medical therapy which should be
done with taking into consideration the patient’s drug tolerance.
MENSTRUAL HISTORY.
The following factors are of particular importance:
- age of menarche, regularity and length of cycle;
- date of last normal period;
- premenstrual symptoms, for example, mastalgia, tension,
headache, weight gain;
- duration of flow;
- whether menstruation is associated with pain, and facts relating
to it, for example, the site of pain, time of onset and subsidence,
accompanying nausea or vomiting;
- amount of flow, judged by the number of pads or tampons used
per day.
If the person is menopausal, the age of menopause and associated
menopausal symptoms, if any, should be ascertained.
MARITAL HISTORY. This would include facts relating to the age of
marriage, duration of the marriage, frequency of coitus and whether it is
associated with dyspareunia or not, the type of contraceptive used, its
duration and side effects, if any. Information about patient’s husband must
include: his age, occupation, blood group, Rhesus factor, his health condition
and pernicious habits (alcohol, smoking, drugs).

35
SECRETORY FUNCTION.
The patient should be questioned about the presence of leucorrhoea, its
nature (color, odor, consistence, amount), periodicity of its appearance.
GYNECOLOGIC DISEASES.
If the present disease is not the first gynecologic complaint, the patient
should be questioned about the course of the previous disease as well as the
nature and outcome of the treatment.
OBSTETRIC HISTORY.
The obstetric history should include the following information:
a) the number of pregnancies: normal or complicated by (reason);
the end of each (delivery or abortion);
b) deliveries: premature or full term (and date);
c) nature of delivery: spontaneous , instrumental, cesarean
section;complications, if any;
d) the condition of the baby at birth: live birth, fetal or neonatal
death;
e) weight of the baby at birth;
f) postpartum complications;
g) duration of breast feeding;
h) resumption of menses after the delivery;
i) the number of abortions, the date of every abortion, the period
of gestation at each termination, whether abortion was
spontaneous or induced (what method of induction) and
postabortal complications, if any;
j) the date of the last pregnancy and delivery or abortion.
For the description of the obstetric anamnesis the unified systems are
used in the most different countries. And they are understandable to any
practitioner. 3 systems used to designate OB history in females.

36
TPAL terminology is a system used to describe obstetrical history.
T — term births
P — preterm births (prior to 37 weeks gestation)
A — abortions
L — living children
TPAL numbers should be separated by hyphens.
Example: A pregnant woman who carried one pregnancy to term with
a surviving infant; carried one pregnancy to 35 weeks with surviving infant;
carried one pregnancy to 11 weeks as an spontaneous miscarriage; and has
two living children would have a TPAL annotation of T1, P1, A1, L2. This could
also be written as 1-1-1-2.
GPA Terminology
GPA is the abbreviation for gravida, para, abortus.
G - gravida (number of pregnancies)
3 types of “gravid” condition are distinguished:
- Nulligravida = 0 pregnancies.
- Primigravida = 1 pregnancy.
- Multigravida = 2+ pregnancies.
P - para (number of births, live or stillborn)
3 types of "para" conditions are distinguished:
- Nullipara = 0 births.
- Primipara = 1 birth.
- Multipara = 1+ births.
A or Ab - abortus (abortions). Number of terminated pregnancies,
including:
- Spontontaneous and missed abortions.
- Ectopic pregnancy.
- Elective abortion.
If using GPA to report pregnancy history, the G P and A should be
separated by (commas/dashes). Accompanied by Arabic numbers, G, P, and A

37
(or Ab) describe the patient’s obstetric history. Roman numerals are not used.
Alternatively, spell out the terms in lower case.
For example, when recording the history of a woman who has had two
pregnancies (both of which resulted in live births), it would be noted as G2P2.
The obstetric history of a woman who has had four pregnancies, one of which
was a miscarriage before 20 weeks, would be noted as G4P3A1.
That of a woman who has had one pregnancy of twins with successful
outcomes would be noted as G1P1. When one or more of the numbers is 0, the
preferred form is to write out the terms: gravida 2, para 0, abortus 2.
GTPAL system
Very often, GPA terminology is combined with TPAL terminology aka
GTPAL system (or TPALM when GTPAL is followed by number of multiple
pregnancies). In this case, G separated by comma, TPAL by hyphens: e.g. G,T-
P-A-L.
For example, gravidity and parity of a woman who has given birth at
term once and has had one miscarriage at 12 weeks would be recorded as G2
T1 P0 A1 L1. This notation is not standardized and can lead to
misinterpretations.

38
PHYSICAL EXAMINATION
GENERAL EXAMINATION
This should include, assessment of height, weight, nutrition status, skin
condition (color, turgor, cicatrices, scratches, ulcers, hemorrhages). Tongue,
its status: color, fur. Blood pressure and pulse rates, and temperature must be
recorded. Attention should be paid to the patient’s condition (mild, moderate,
severe). Сonstitution should be ascertained (asthenic, normosthenic,
hypersthenic). Infantile, intersexual types of constitution are also found in
gynecologic patients.
The chest examination should include the heart, lungs and breast. The
breasts are examined (inspection, palpation) for any abnormality: skin
retractions, masses (mobile, fixed), erythema, axillary or supraclavicular node
enlargement (see below).
Examination of the respiratory, cardio-vascular, gastro-intestinal and
urinary systems involves inspection, percussion, palpation and auscultation.
Detection of systemic diseases helps to specify the etiology of the gynecologic
diseases. Thus, in the presence of pulmonary or any other tuberculosis,
adnexal tuberculosis may be suspected.
Examination of abdominal organs not infrequently helps to reveal a
gynecologic disease. Abdominal examination is done with the patient in a
dorsal recumbent position with the knees slightly flexed as it promotes the
abdominal relaxation. The inspection reveals whether the abdomen moves
freely on respiration, it also indicates enlargement or prominence, scars from
previous surgery and skin changes which have followed earlier pregnancies.
Superficial palpation of the abdomen helps to ascertain the muscular
tension of the abdominal wall, diffuse or local tenderness or pain. Deep
palpation allows to determine the presence of tumors and infiltrates, their

39
localization, size, consistence, mobility and tenderness in palpation. The
surface of the tumor may be smooth or tuberous.
Abdominal percussion helps to identify the presence of meteorism (high
thympanitis) and fluid in the abdominal cavity.
SPECIAL GYNECOLOGIC EXAMINATION.
It involves a complex of methods for the examining of the genital system
in women. The basic methods include:
clinical breast examination;
inspection of external genitalia;
speculum examination;
vaginal examination: manual and/or bimanual
(vaginoabdominal).
Clinical breast examination
The reproductive system is typically described as including the organs
needed for sex and reproduction. Mammary glands are part of the
reproductive system, a hormone dependent organ, a target for the action of
sex hormones and other hormones of the endocrine system. Breasts do feed
infants once they're born. Breasts are influenced by hormonal changes during
the development of the reproductive system and during and after pregnancy.
(Fig.6)
Prolactin - produced by: anterior pituitary. The target organ: breasts
(female) . Action (females): stimulates secretion of milk (lactogenesis);
estrogen and progesterone from placenta have an inhibiting effect on milk
production until after placenta is expelled at birth; suckling of newborn
stimulates prolactin secretion to maintain milk production.
Oxitocin - produced by: posterior pituitary. The target Organs: uterus and
breasts (female). Action females: uterus: stimulates contractions during birth
and stimulates postpartum contractions to compress uterine vessels and

40
control bleeding. Stimulates let-down, or milk-ejection reflex, during
breastfeeding.
Estrogens - produced by ovaries under the influence of FSH and LH during
menstrual cycle. They are responsible for:
- development of breasts
- development of the uterus and vagina
- broadening of the pelvis
- growth of pubic and axillary hair
- increase in adipose (fat) tissue
Fig.6. Female reproductive system.
Since the mammary glands are part of the reproductive system, examination
and palpation of mammary glands by gynecologist is necessary, as are other
methods of special gynecological examination. Breast examination by a
specialist in medical treatment (clinical breast exam) is an important part of
routine physical examinations.
The clinical breast examination (CBE) is a widely used practice as a screening
tool for early detection and prevention of breast cancer; it has become a

41
standard part of the annual preventive well-woman examination. A
significant number of cancers would have been missed if CBE had not been
performed. Currently, there are many recommendations regarding use and
frequency of the clinical breast exam among various organizations, but no
consensus.
The most commonly used recommendations of the American Cancer Society
(2015):
Women 20-39 should have a physical examination of the breast (CBE) at
least every three years, performed by health care professional such as a
physician, physician assistant, nurse or nurse practitioner. Women 20-
39 should also perform monthly breast self-exam (BSE).
Women 40 and older should have CBE every year, performed by a health
care professional, such as a physician, physician assistant, nurse or nurse
practitioner. CBE can often be performed in the same visit as a
mammogram. Monthly BSE should also be performed.
Women 40 years of age should receive a screening mammogram every
year. The National Cancer Institute recommends mammography every
one to two years for women between 40-50 years of age. Beginning at age
50, screening mammography should be performed every year.
The goal of the breast examination is to determine if the breasts are
normal or abnormal. If abnormal, any or all of the following may be
indicated: surgical consultation, reexamination at a different time of the
menstrual cycle, mammograms, and possibly ultrasound.
It may be recommended to perform clinical breast exam during any visit
to gynecologist, regardless of the cause and frequency of visits, for prevention
and early diagnosis of breast cancer for those, who have strong family history
of breast cancer. Finding a breast cancer tumor when it is smaller improves
the chances of saving a breast by avoiding a mastectomy, and may reduce the
need for chemotherapy.

42
CBE procedure
I. Preparation
For a proper breast examination :
1. Patient should be undressed down to the waist.
2. A mobile bright light with an assistant is necessary to focus the
light from one area to another as the examination is being conducted.
II. Introduction (WIIPPPE)
For a breast examination the introduction is vital. The patient must feel
at ease with you and know why you are carrying out each step.
Wash your hands (and try to ensure your hands are warm)
Introduce yourself (name and position)
Identity of patient (confirm name and date of birth)
Permission (consent and explain examination: “I’m going to
examine your breasts now. This will involve inspecting and pressing them
quite firmly. Is that OK?”)
o Note that any intimate examination (including the breast exam)
should be done with a chaperone present, particularly if the
doctor is male
Pain?
o Inform the patient they should let you know if you cause them any
discomfort
Position
o Initially sitting on the edge of the couch for inspection. Then lying
flat (with one arm above head) to palpate
Privacy
o Provide a cover such as a blanket or a hospital gown (with the
opening at the front) and ensure the curtain or door is firmly
closed
Exposure

43
o You need to be able to compare both breasts visually and then
palpate both breasts in turn. Most women will not have any issue
with such exposure provided you are relaxed and explain fully.
III. Inspection
Begin by asking the patient to point to the area of concern, and always
explain what you are doing to avoid any embarrassment
Asymmetry
o Look for any asymmetry in the size of the breasts and in the breast
contour
o The size and shape of the breasts in healthy women varies
and having one breast larger than the other is common (Fig.8)
Skin change
o Look for lumps and associated skin changes including signs
of inflammation, ulceration and skin retraction which may be
caused by an underlying cancer (Fig.9).
o Dimpling known as “orange peel” (“peau d’orange ”) may be
visible. This arises due to obstruction of lymphatics (which can be
caused by tumour cells, infection, or treatment with radiotherapy)
resulting in skin oedema with multiple small indentations caused
by the hair follicles of the breast (Fig.10)
o Colour changes which may be a sign of imminent ulceration
Scars
o Indicating previous surgery
Nipple skin change
o Scaling and flaking around the nipples is commonly due to
primary dermatitis and will often be present elsewhere on the
body
o Unilateral eczematous skin changes on the nipple may
indicate Paget’s disease which is caused by carcinoma cells
migrating along ducts to the nipple

44
Nipple inversion, deviation and colour
o Benign nipple inversion is bilateral and slit-like and is typical of
duct ectasia
o Nipple retraction due to malignant disease is asymmetrical and
distorting and can pull the nipple away from its central position
leading to nipple deviation
o If an inverted nipple is seen, it is important to ask the patient if it
is normal for her or she can evert it
o Unless it is longstanding, formal investigation is essential to rule
out the possibility of carcinoma
o The ability to evert a newly inverted nipple is suggestive of benign
breast disease
Fig.8. Enlargement and asymmetry of breasts
Fig.9. Retraction (dimpling) of the skin noticeable
when raising the ipsilateral arm

45
Fig.10. Breast edema giving the skin an “orange peel” (peau d’orange)
appearance
Evaluation of masses
Some movements can be used to accentuate any subtle masses. The
examiner should demonstrate these movements and ask the patient to copy.
Watch the breast closely as the patient moves.
o Ask the patient to raise her arms above their head so that skin
tethering becomes more apparent
o Ask patient to press her hands against her hips in order to tense
her pectoral muscles to accentuate chest wall tethering.
o Ask patient to make some other maneuvers to observe breasts.
(Fig.11.)
Fig.11. A - Patient standing with arms down. B - Patient standing with arms
elevated. C – Pushing on hips to tense pectoral muscles. D - Patient standing
with palms pressed together in front of the forehead, contracting the pectoral
muscles.

46
Observing the breasts while the patient sits up may increase your ability
to detect asymmetry or other surface abnormalities, particularly if the person
has large breasts. (Fig.12).
Fig.12. The patient sits, bending forward so breast hangs free
IV. Palpation
There are 3 specific components of the clinical breast palpation that
influence the accuracy of the examination. These are the amount of time
spent on the examination, the search pattern utilized, and the finger
technique in palpation.
Time spent on clinical breast examination is one of the best predictors
of sensitivity. Spending 2 minutes on the breast examination improves
sensitivity.
The second critical aspect of the clinical breast examination technique is
the search pattern used to identify abnormalities. Use a systematic search
pattern that ensures that all areas of the breast tissue are clearly examined.
This will increase the effectiveness of clinical breast research. In this case,
keep in mind that about 50% of the breast tissue is located in the upper outer
quadrant of the gland, about 20% are located under the nipple and areola
nipple. (Fig.12.)

47
Fig. 13. Distribution of breast tissue across chest wall. Most breast
tissue is seen in upper outer quadrant.
In systematic search pattern (with the patient supine during the
examination, and her hands above her head), the area for examination should
extend from the clavicle, medially to the midsternum, laterally to the
midaxillary line, and to the inferior portion of the breast. In addition, the
examination should include the axillary tail of breast tissue and the axilla to
search for palpable lymphadenopathy.
The third critical aspect of the clinical breast examination is the finger
technique (see below).
Ask the patient to lie on the couch to palpate the breasts. Have the
patient remove their arms from the sleeves of the gown - though keep both
breasts covered by laying the garment on top of their chest. Alternatively, the
patient may put on the gown so that it opens in the front, which may make
exposing one breast at a time a bit easier.
Patient should be lying flat on the table - It may help to have them place
hand on side to be examined behind their head, allowing easier access to
breast and axilla.
Uncover only the breast that you are going to examine.

48
For the lateral examination of the breast, the patient places the
ipsilateral arm on the forehead. For medial examination, the patient's elbow
should be aligned with the shoulder. (Fig.14, 15).
Fig.14. Position of patient and direction of palpation for the CBE. The top
figure shows the lateral portion of the breast, and the bottom picture shows
the medial portion of the breast. Arrows indicate the vertical strip pattern of
examination.
Figure 15. Position of patient for the CBE.

49
With patient in supine position, observe again the breast, looking for
evidence of skin or nipple dimpling/retraction, discoloration, obvious masses
or asymmetry.(Fig. 16)
Fig.16. Clinical breast exam findings
Boundaries of the breast for palpation
Consider the main area of breast tissue as a rectangle bordered by
the clavicle superiorly, the bra-strap line inferiorly, the midsternum medially
and the midaxillary line laterally. The tail of the breast extends beyond the
midaxillary line into the axilla and must also be examined carefully.
Methods for systematic palpation of the breast (the search patterns)
Wedge or radial spoke pattern (1)
o Imagine that the breast is broken into a series of wedge-type slices, with
the nipple at the center.
o Start at the nipple, working outwards toward the periphery of the slice
that you're examining. Move your hands a few centimeters along each
time.
o When you are clearly no longer over the breast, move to the next slice
o There is a "tail" of breast tissue that extends from the lateral aspect of
the structure towards the axilla. Make sure that you palpate this
region as well.

50
Vertical strip pattern (2)
o To use this technique, start in the mid-axillary line at the bra-strap line,
and palpate by moving your fingers in a vertical strip upwards until you
reach the apex of the axilla.
o Then move your gingers medially and palpate downwards in a vertical
strip to the bra-strap line, moving your fingers medially again and
palpate up to clavicle.
o Continue palpating in a linear pattern until the sternum is reached and
all breast tissue has been palpated.
o Make sure that you palpate the “tail” of the breast as described above.
Circular pattern (3)
o Start at the nipple.
o Work along in circular fashion, moving in a spiral towards the
periphery.
o Make sure that you palpate the "tail" of the breast as described in
above.(Fig. 17)
Fig.17. Breast palpation techniques
There is conflicting evidence for the effectiveness of each method. The
most important point as a clinician is that you are confident in your palpation
that you have examined all the important areas. As such, use the method you
are most confident with.

51
Finger techniques
Three-finger technique
Palpate the breast using the pads of the middle 3 fingers of one hand (Fig.18)
Fig.18. Three –fingers for palpation of breast
Two hands can be used in women with larger breasts in order to fix the area
you wish to palpate
If a lump is found, use two hands to assess its characteristics:
o Side
o Site
o Size (measured in mm)
o Consistency (Soft; firm; hard)
o Margins (discrete vs diffuse)
o Surface (smooth vs irregular)
o Mobility
o Skin fixation or tethering
A tethered lesion is suggestive of locally advanced cancer and occurs
when the fibrous ligaments that separate the lobules of breast tissue are
shortened
These ligaments are anchored to the skin so that shortening them
puckers the skin and pulls it inwards although the lesion is mobile and can be
moved independently of the skin.

52
A fixed lesion has spread into the skin itself so that the mass cannot be
moved independently of the skin and implies more advanced local disease.
Documentation
Any abnormality found on examination must be documented, and
include the size of the mass in centimeters, its location (often described by
hours on a clock-face) and characteristics (soft, firm, hard, tender, mobile or
fixed). If a mass or other abnormality is identified, it's location can be
described as being in one of 4 quadrants (left upper, left lower, right upper,
right lower) of the breast. Alternatively, it can be described relative to it's
position, imagining a clock face were superimposed on the breast.(Fig. 19.).
Fig. 19. Description of the location of pathological formation.
In patients with large or pendulous breasts it may be necessary to use
maneuvers to flatten the breast tissue against the chest wall to optimize the
examinationю To flatten the lateral part of the breast, ask the patient roll onto
her contralateral hip, with her shoulders in a supine position, and place her
ipsilateral forearm on her forehead. To flatten the medial part, ask the patient
to lie flat on her back and move her elbow up until it is level with her
shoulder. (Fig.15)

53
Nipple discharge
Nipple discharge is a common symptom and may be clear, cloudy, or
blood-stained. It is most often due to duct ectasia, but can also be the result of
lactation, a duct papilloma, or carcinoma. If the patient is complaining of
discharge, ask them to try to express some discharge if they are comfortable
to. On no condition try to express it yourself unless the patient is totally agree
do so! Try to evaluate, is discharge originating from a single duct or multiple
ducts? Note its color.
Palpation for axillary and supraclavicular lymphadenopathy
Following direct palpation of the breast, the axillary region should be
palpated. This is because the axillary lymph nodes are usually the first site of
spread in the setting of breast cancer. While this is of greatest importance
when you identify a concerning mass in the breast itself, include the axilla in
all of breast exams. To examine, proceed as follows:
o It may help to have the patient lower their arm so it is next to their side,
as when the hand is behind their head, the axillary skin is taught and
perhaps more difficult to palpate thru.
o Gently move the arm 20-30 cm away from the patient's body, so that
you can gain access to the axillary region.
o Direct the finger tips of the examining hand (it's a bit easier to use your
L hand when examining the R breast, and vice versa) toward the top of
the axilla.
o Then push the palmar aspect of the hand towards the chest wall. You
are trying to identify any abnormal nodules/lumps that could represent
axillary adenopathy. In addition, you may be able to trap the nodes
between your hand and the chest wall, which can then be better
characterized.
o Most women will not have palpable axillary lymph nodes. If you do feel
discrete masses, make note of: firmness, quantity and degree of

54
mobility. In general, malignancy is associated with: firmness, increased
quantity, adherence to each other and/or the chest wall.
o Recognize that adenopathy may not be due to breast disease. For
example, infections of the hand can cause acute, painful axillary
adenopathy. Similarly, systemic diseases (e.g. lymphoma, sarcoidosis)
may also cause lymph node enlargement. Thus, as with all other aspects
of the exam, history and findings in other regions are of great
importance.(Fig.20)
Fig.20.Axillary lymph node examination
Finally, examine the supraclavicular fossa.
Examine from in front of the patient, place your fingers in the supraclavicular
fossae and move them in small circles to try and identify any enlarged lymph
nodes as illustrated in fig. 21.
Fig.21. Palpation of the supraclavicular areas with the patient sitting.
55
Completing the examination
o Thank the patient, help them back into comfortable posture and wash
your hands
o Give the patient some privacy to re-dress.
o In an exam situation you should finish by addressing the examiner,
stethoscope behind your back, not looking back at the patient and
presenting your findings slowly and concisely. In clinical practice the
patient should be given privacy to redress before discussing the findings
of the examination with them.
All patients with signs of breast cancer, and those presenting with
breast symptoms in whom cancer cannot be excluded by examination, must
be formally assessed with ‘triple assessment’
The three elements are:
o Clinical examination
o Imaging (ultrasound or mammography)
o Pathological analysis (core biopsy or fine needle aspirate)
Ultrasound is usually the imaging modality of choice in women under
35 years of age, whereas mammography is preferred for women over 35 years.
If there is any abnormality detected in the examination, or imaging, then
biopsies are taken. This can be in the form of Fine Needle Aspiration Cytology
(FNAC) or a core (Tru-Cut) biopsy. If neither of these provide a reliable
answer then an open surgical biopsy may be required.
Inspection of external genitalia
The first step is to establish whether the vulva is healthy. Routine
evaluation of the vulvar area includes basic developmental assessment,
symmetry, hair quality and growth distribution, skin abnormalities, swelling,
ulcerations, growths such as external genital warts (EGW) or tumors, rashes,
lacerations, piercings, bruising, and discharge. Evaluation of signs of

56
inflammation, leukoplakia, if any, perineal relaxation, presence of tears, scars
due to previous deliveries should be made. The patient is asked to strain to
see whether there is a cystocele of the uterus. Discharge of any kind from the
urethral meatus (bloody or purulent), the vaginal or hymenal orifices and the
opening of ducts of Bartholin must be noted. (Fig.22). Sexual maturity rating
should be made according to the stage of pubertal age (Tanner scale).
Speculum examination
It should be done prior to manual examination. This is carried out
mainly to view the cervix and the vagina and to determine whether they are
healthy or not. The walls of the vagina are inspected for discharge,
estrogenization (presence or absence of atrophy), erythema, and lesions. The
cervix should be examined for contour, amount of erosion, shape of the os
(patulous, scarred, parous, nonparous), discharge, lacerations, polyps,
neoplasias, and lesions (eg, warts). It is necessary also to evaluate the color of
the vaginal and cervical mucosal coat, for example, in a pregnant woman, the
cervix may appear to have a purple tone (cyanotic).
Speculum examination (CE) is also necessary for the obtaining of
smears for cytology and biopsy of the cervix.
There are several different types of vaginal specula: Sims’s, Cuscos’s,
Otto’s, Fergusson’s and Graves’ are well known and each is available in three
sizes. (Fig 23, 24, 25) For this examination most clinicians prefer Sims’s

57
specula (or spoon-shaped specula). Most often, disposable specula are
currently used. Metallic specula are sterilized according to the rules of
metallic instrument preparation. When introducing the blade of Sims’s
speculum, the labia are gently separated and the speculum is inserted
obliquely and carefully passed along the posterior vaginal wall up to the
posterior fornix of the vagina, pressing the single blade against the posterior
vaginal wall will bring the cervix and the anterior vaginal wall into the view.
(Fig. 26).
Cuscos’s speculum (bivalve speculum) is inserted with the blades closed,
and after the blades have met the cervix or vaginal vault, they are opened to
retract the anterior and posterior vaginal walls thus exposing the cervix fully
for examination. The blades can be fixed in position by tightening a screw.
Since it is a self-retaining speculum, the physician is then free to do any tests:
to collect smears, to obtain material for culture with a platinum loop, to do a
biopsy of the cervix, etc.

58
Fig. 24. Sim’s speculum
After exposing the cervix it is inspected for the shape, cicatrices, ulcers,
polyps, fistulas. A conical-shaped cervix with a point-like os is a characteristic
of nulliparous woman. Cicatricial deformation points to intrapartum
ruptures. Hypertrophy of the cervix may indicate its chronic inflammation. A
slit-like form of the external os is seen in parous women.

59
As the speculum is being withdrawn gradually, the vaginal walls are
examined carefully. Instead of the pink thick mucosa, one may find it bluish
in pregnancy, congested or covered with discharge in vaginitis, or ulcerated
due to pathological lesions.
Vaginal examination
It is divided into manual, bimanual vaginal (vagino-abdominal), and
rectovaginal examination (rectal).
Manual examination
The labia are gently separated and one or two lubricated fingers (index
and middle finger) of the gloved right hand are carefully introduced into the
vagina. During examination one should palpate the area of glands of
Bartholin and the urethra, and determine the state of pelvic floor muscles.
The next step is the palpation of the cervix. The cervix is felt as the
fingers are passed into the vaginal vault. The length, consistency, mobility,
tenderness, opening of the cervical canal should be determined by palpation
of the cervix. If the uterus is anteverted, the anterior lip is the first to be felt,
and if it is retroverted, the posterior lip is palpated first. In nulliparous
women the cervix is conical and the external os is circular. But in multiparous
women it may be enlarged or hypertrophied and external os is often slit

60
transversely. The cervix lightly outlined with the fingers to identify the size,
position, consistency, texture and dilation of the orifice. It is normally smooth
and firm. In pregnant women the cervix is soft. Its surface around the
external orifice may feel velvety in cases of erosion. In cases of pelvic
inflammation and fallopian gestation there is tenderness when the cervix is
moved. The patient is then asked to strain to see whether there is any descent
of the uterus.
Bimanual examination
In bimanual examination (examination with both hands) the internal
(dominant) hand is introduced into the vagina and is placed over the anterior
surface of the cervix. The non-dominant hand outside is placed over the
patient’s lower abdomen and firm pressure is applied to displace the lower
abdomen and pelvic organs towards the fingers in the vagina to meet the
uterus. The patient is requested to breath through the mouth to avoid
marking the abdominal wall tense. Then two internal fingers, which are
placed in the anterior vaginal fornix against the anterior
lip of the cervix press the uterus upwards while the external hand placed
over the lower abdomen pushes it downwards. The uterine outline between
the two hands can be clearly noted. (Fig. 27).
Fig. 27.Bimanual exam

61
If the uterus is retroverted, the internal fingers are inserted into the
posterior fornix to push up the uterus and thus feel it more easily bimanually.
When the uterus is felt, one can determine its:
• position,
• size,
• shape,
• consistency,
• contour,
• surface characteristics (smooth vs nodular)
• tenderness
• mobility.
Normally it is in the midline in the upper half of the pelvis with the
external os in the same plane as the ischial spine. The uterine fundus is
directed forwards and is said to be anteverted. It is normally pear-shaped,
firm and smooth. Normal or abnormal size can be made out only with some
experience as in the relationship of the size of the cervix to that of the corpus.
For palpation of the adnexa the fingers in the vagina are placed in the
lateral fornix and the external hand is pressed down over the vaginal fingers
in the attempt to outline the uterine adnexa. Normally, the healthy tubes are
not palpable but the ovaries may be felt when prolapsed, cystic or enlarged. In
acute pelvic inflammatory diseases (PID) the fornices may be tender and in
chronic cases a thickened tube or a fixed, tender, retort-shaped pyosalpinx
may be felt on one or both sides of the uterus. The pouch of Douglas may be
felt through the posterior fornix, one may find the body of the uterus when it
is retroverted, an adnexal inflammatory swelling, pelvic hematocele, pelvic
abscess, the lower pole of an ovarian tumor. If the rectum is overfilled, one
may feel the fecal masses and lack of experience may lead to a wrong
diagnosis.

62
Bimanual recto-vaginal examination
The rectovaginal exam is a diagnostic tool that helps gynecologist to
more fully examine the internal pelvic anatomy and check the vaginal and
rectal areas for abnormalities. The recto-vaginal exam is not a particularly
accurate screening exam and is usually reserved for women who either have
rectal or pelvic pain or are experiencing symptoms related to the
genitourinary tract (such as pain, urinary urgency, abnormal bleeding). It is
used to determine whether the tumor or other formation is originated from
genital organs or from the rectum. As for procedure, the index finger is
inserted into the vagina, and at the same time, the middle finger is inserted
into the rectum. (Fig. 28).
By putting one finger inside the vagina and another into the rectum, a
provider can:
• evaluate the back side of the uterus and the wall between the vagina and
rectum;
• check on the tone and alignment of the pelvic organs: ovaries, Fallopian
tubes, and ligaments of the uterus;
• determine if the uterus is retroverted (tilted);
• more thoroughly investigate complaints of pelvic or rectal pain;
• feel for rectal growths, check for blood in the stool, and look for other
early signs of colon cancer, especially in women over the age of 40.

63
Fig.28. Bimanual recto-vaginal examination
Bimanual recto-abdominal examination
It is not an obligatory part of routine gynecologic examination of a
patient. It is reserved for those who are virgin, for patient in pubertal age, for
patient who cannot tolerate a vaginal exam, also for cases, when vaginal exam
is impossible. (Fig.29). Hematocolpos, congenital abnormalities of internal
genitals are also indications for recto-abdominal palpation
Fig.29. Bimanual recto-abdominal examination

64
Vaginal smears
I.Tests for evaluation of vaginal ecology
Investigation of vaginal smears is used to assess the vaginal ecology, for
the diagnosis of the inflammatory diseases and the identification of the types
of infectious agents. Routine investigations of vaginal smear include:
• pH test;
• vaginal microscopy;
• vaginal discharge culture and sensitivity.
The pH of the vaginal secretions. The vaginal microbiota of
healthy women consists typically of a diversity of anaerobic and aerobic
microorganisms. Lactobacilli are the most prevalent and often numerically
dominant microorganisms and are relevant as a barrier to infection. The
capacity of lactobacilli to adhere and compete for adhesion sites in the vaginal
epithelium and the capacity to produce antimicrobial compounds (hydrogen
peroxide, lactic acid, bacteriocin-like substances), are important in the
impairment of colonization by pathogens. The dominance of lactobacilli
results in a normal pH of the vaginal fluid. The dominance of lactobacillus
leads to a normal pH of the vaginal environment, whereas a decrease in their
number leads to a change of the pH of vaginal secret and is the basis for the
vaginal population to be filled with pathogenic microorganisms,and
development of infectious and inflammatory processes. Vaginal secretions
should be collected from the lateral vaginal walls using a swab or small loop
and pH should be elucidated using litmus paper.(Fig. 30). The normal pH is 4-
4.5.(Fig31) .

65
Fig.30. Litmus paper strips for evaluation of pH of smears
Fig.31. The pH scale.
Whiff test. Additionally, whiff test is widly useful now-a-days. Several drops of
a potassium hydroxide (KOH) solution are added to a sample of the vaginal
discharge. A strong fishy odor from the mix means bacterial vaginosis (vaginal
dysbiosis) is present. The odor results from the liberation of amines and
organic acids produced from the alkalization of anaerobic bacteria. A positive
whiff test is suggestive of bacterial vaginosis.
Vaginal microscopy. Microscopy involves use of the:
• wet mount(wet smear, wet prep, vaginal smear, vaginalysis, or
hanging drop),
• KOH slide,
• Gram staining smears.
Vaginal microscopy is an important laboratory tool for evaluation of the
vaginal health. It include: microscopy for white blood cells (WBC),
bacterioscopy for determination of vaginal flora.

66
Wet mount observes living vaginal organisms in order to study the
ecology of the lower genital tract in women. It acts as an accessory tool to the
patient history, inspection of the vulvar and vaginal mucosa, and pH
determination in order to arrive at a presumptive etiologic diagnosis. A smear
should not be obtained after vaginal examination and therapeutic procedures
involving the intravaginal administration of drugs. Thus, it is done whit the
specula examination, before manual palpation and other procedures. A
specimen of the vaginal discharge should be collected from the wall of the
vagina using a cotton swab or sterile platinum loop. It is then placed on a
glass slide, mixed with a drop of saline and immediately examined under a
microscope. Alternatively, the vaginal discharge can be put into a 2-mL test
tube containing saline solution and then placed on a slide. The slide is
examined microscopically using low power (10×) and high dry power (400×).
This test can be carried out by any doctor. The microscopic appearance of the
discharge, in addition to a test of vaginal acidity (pH) will distinguish one type
of vaginitis from another. Microscopic examination of a wet-mount
preparation can also detect “clue cells,” which are vaginal epithelial cells that
are coated with the coccobacilli. When a skilled examiner performs the search
for clue cells, examination of wet-mount preparations can have a sensitivity of
60 percent and a specificity of up to 98 percent for the detection of bacterial
dysbiosis. The examination may also detect fungal hyphae, increased
numbers of polymorphonuclear cells (seen in trichomoniasis) or round
parabasal cells (seen in atrophic vaginitis).
The presence or absence of a large number of leukocytes (WBC) should be
noted. A few may be normal, but more than 10 per high-power field is abnormal
(Fig.32).

67
Fig.32. Normal flora.
Depending on the nature of smears, four degrees of vaginal colonization
are recognized:
• grade I colonization: it is characterized by the presence of squamous
epithelium and vaginal bacilli (normal flora); the reaction is acid;
• grade II colonization: in this case the number of vaginal bacilli is
smaller than in grade 1 colonization; epithelial cells, individual cocci
and leucocytes are observed; the reaction is acid ( grade I and grade II
colonization are considered normal);
• grade III colonization: there are few vaginal bacilli with other types of
bacteria being predominant; leucocytes are present in large numbers;
the reaction is weakly alkaline;
• grade IY colonization: there are no vaginal bacilli, but there are many
pathogenic microbes, including even gonococci and trichomonads; large
number of white blood cells are present; the reaction is alkaline (grade
III and grade IV colonization suggests abnormality).
KOH slide is another component of wet mount. An additional swab
should be taken and some discharge placed on a slide and mixed with a drop of
10% solution of potassium hydroxide (KOH) and covered with a cover slip. The
slide may be warmed briefly (heating promotes cell lysis) and should be
looked at promptly. The KOH kills bacteria and cells from the vagina, leaving

68
only yeast for a yeast infection. The slide should then be examined carefully for
the presence of budding yeast or hyphae. This is useful for detecting candidal
hyphae, mycelial tangles and spores. The test is positive in 50 to 70 percent of
women with candidal infection. During preparation of the KOH slide, a whiff
test can be performed. The whiff test is positive if a “fishy” or amine odor is
detected when KOH is added to the vaginal discharge.
Gram staining smears. The Gram stain involves applying a sample
from an infected area or a sample of bacteria grown in culture onto a glass
slide. The slide is then treated with a special stain and examined under a
microscope by a trained laboratorian. This method is used to distinguish and
classify bacterial species into two large groups (gram-positive and gram-
negative). Gram positive bacteria stain violet. Alternatively, Gram negative
bacteria stain red. The color and shape of the bacteria help classify which
general types of bacteria are present.
Vaginal discharge culture and sensitivity. It is bacteriological
investigation of vaginal discharge to evaluate culture and sensitivity to
antibiotics. It is aka high vaginal swab (HVS). It helps to evaluate culture for
yeasts; culture for bacterial pathogens, if indicated by microscopy or clinical
information. Bacteriological study helps to reveal sexually transmitted
diseases (STD). The material for bacteriological study is taken from the
urethra, cervical canal, and the upper third of the vagina (from posterior
fornix of the vagina). The discharge is transferred with a sterile applicator to a
dry sterile test tube or special container (Fig. 33.) and sent immediately to
the laboratory or is inoculated on to a sterile agar. Cultures should never
substitute for a careful history, physical examination, and microscopic
examination of the wet prep. Depending on the results of a vaginal culture
without microscopic examination of the secretions will result in frequent
errors in treatment. Nevertheless, cervical cultures may be especially helpful
in some cases.

69
Fig.33. Container for HVS.
II. Tests for evaluation of endocrine status
Endocrine status is assessed by such a functional diagnosis parameters
as the cytologic pattern of a vaginal smear, the “pupil” symptom, “fern”
symptom (arborization of cervical mucus), a viscosity and stretch ability of
cervical mucus, and rectal (basal) temperature, as well as by findings of
endometrial biopsy, hormonal levels in the blood plasma and urine and by
hormone assays.
Cytologic pattern of a vaginal smear. To study the cytologic
pattern of vaginal smears, the discharge from one of the lateral fornices is
spread in a thin layer on a glass slide, air-dried, fixed in an alcohol-ether
mixture, and then stained with hematoxylin-eosin. The effect of estrogens on
the stratified squamous epithelium is expressed in epithelial cornification,
degree of which is directly correlated with estrogen concentrations. The
predominance in a smear of cornified cells testifies to a high content of
estrogen (hyperestrogenism). When estrogen levels are moderate, the so-
called intermediate cells are sloughed from the vaginal wall. In patients with
low concentrations of estrogens (hypoestrogenism associated with ovarian
hypofunction or menopause) basal cells from deeper layers are shed and
prevail in a smear. (Fig 34)

70
Fig. 34.Types of epithelial cells of vagina.
Depending on the ratio between the types of epithelial cells, four types
of vaginal smears are distinguished:
type I: a smear consists of basal cells (small round or oval in shape with a
relatively large nucleus) and leucocytes. This type is typical of very
pronounced estrogen deficiency. It is observed in postmenopausal women
and in young women with ovarian hypofunction and amenorrhea;
type II: a smear contains basal and intermediate cells, with the
predominance of basal cells and leucocytes. It occurs in considerable estrogen
deficiency (ovarian hypofunction, post menopause);
type III: intermediate cells are the most predominant in a smear. It is a
characteristic of moderate estrogen deficiency;
type IV: a smear is composed of cornified cells. It is observed in sufficient
estrogen saturation. (Fig. 35 a,b,c,d)
Types III and IV are noted in normal menstrual cycle (depending on the
phase of the cycle).

71
Fig.35. Types of vaginal cytology depending on the types of epithelial
cells: a – type I; b - type II;
c – type III; d – type IV.
The cytologic pattern may also be quantitated, which involves the
determination of the percentage ratio of surface cells with pyknotic nuclei to
the total number of surface cells (caryopyknotic index, ripening index).
The Karyopyknotic Index (KPI). The karyopyknotic index expresses the
percentile relationship of superficial squamous cells with pyknotic nuclei to
all mature squamous cells (with vesiculae nuclei). Usually, 200 to 400
consecutive cells in three or four different fields on the smear are evaluated.
The smear is taken from the lateral fornix of the vagina as cells here respond

72
to cyclical changes in hormone that occurs in the menstrual cycle. The KPI
correlated significantly with the plasma estradiol. The peak of KI usually
coincides with the time of ovulation.
Examples: KPI > 25% - in proliferative phase of endometrial cycle
KPI < 3-5% -very low, corre3spond to secretory phase
KPI : 50-85% - typical for day of ovulation
KPI > 10% in pregnancy – progesterone deficiency
The Eosinophilic Index (EI). The eosinophilic index expresses the
percentile relationship of mature squamous cells with eosinophilic cytoplasm
to all mature squamous cells, regardless of the status of the nucleus. In a
normal menstruating woman, the peak of EI coincides with the peak of KI
and may reach 50% to 75% at the time of ovulation.
The Maturation Index (MI) expresses the maturation of the squamous
epithelium as a percentile relationship of parabasal cells to intermediate cells
to superficial cells. MI is determined by the count of 100-200 cells in 5-8- eye
shots (field of vision), and expressed in per cents. MI is designated as a
formula, where the amount of basal cells is written down on the left, in the
middle – intermediate, on the right – cornified cells. 0 designates the absence
of some types of cells.
In a normal menstruating woman at the time of ovulation, an MI of
0:35:65 would indicate that the smear contained no parabasal cells, 35% of
intermediate cells, and 65% of superficial cells.
MI Examples.
MI = 100/0/0: there are only basal cells in the smear, no intermediate
and cornified, means significant atrophy.
MI=70/30/0: there is 70% of basal and 30% of intermediate cells in the
smear, no cornified, means moderate atrophy.
MI= 0/80/20: no basal cells in the smear, there is predominance of
intermediate cells (80%), and about 20% of cornified cells, means moderate
proliferation.

73
MI=0/20/80: no basal cells, there is about 20% of intermediate and
80% of cornified cells in the smear, means significant proliferation.
MI shows the functional activity of ovaries, it helps to determine the
changes of ovarian function depending on hormonal therapy.
Cervical mucus reveals a number of rheologically related properties
including viscosity, stretchability, flow elasticity or retraction, plasticity and
tack. Rheology is the study of the flow and deformation of matter. In the case
of the cervical mucus, however, this term is extended to include various
biophysical properties and also some viscoelastic characteristics of molecular
physics.
“Pupil” symptom. The “pupil” symptom consists in the following. In
the follicular phase the cervical glands produce a mucous secretion, the
largest amount of which is accumulated by the mid-cycle. The external os of
the cervix is dilated by this secretion as a result and resembles a pupil, which
can be seen during speculum examination. This symptom is observed from
day 10 to day 17 of the cycle, being most pronounced on day 14-15. In women
with estrogen deficiency this symptom is either weak or absent, whereas in
patients with excessive estrogen production it may persist for longer time.
The less degree of dilatation of external os due to accumulation of mucus is
designated as +, moderate ++, maximal (0. 25-0. 3 cm) +++.
Crystallization of cervical mucus (syn.: “fern” symptom,
arborization symptom). Of all the properties of mucus “crystallization”, i. e.
arborization or fern phenomenon, is undoubtedly one of the most sensitive to
changes in the level of sex hormones. Thus “ferning” is widely used for the
detection of ovulation and for assessing corpus luteum function, in the early
diagnosis of pregnancy and even of a threatened abortion, and in monitoring
the induction of ovulation. The arborization is not specific to cervical mucus;
it can be seen in other mucous secretions and in most body fluids as well. It
occurs in all solutions containing proteins or other organic compounds and
electrolytes, particularly sodium chloride. Although not specific in other body

74
fluids, arborization in cervical mucus is distinctly dependent upon the action
of estrogen and bears a close relationship to the two rheological properties
described above, viscosity and spinnbarkeit. The extent of crystallization of
the mucus bears a direct relationship to sperm receptivity.
The fern pattern appears during the early proliferative phase, usually at
about the 5th or 6th day of the 28-day cycle increasing proportionally with the
degree of estrogenic activity. It reaches a maximum at ovulation and 24-72
hours later it begins to be replaced by a cellular pattern characteristic of
progestational activity. The fern pattern usually disappears completely by the
22nd day of the cycle. Pregnancy and the administration of progesterone both
produce the same qualitative picture as seen in the luteal phase of the normal
cycle. Maximal arborization is likely to be found at the time of maximal
spinnbarkeit and will usually precede the shift in basal body temperature by
24-48 hours. The peaks of arborization and spinnbarkeit also coincide with
maximal receptivity to sperm and greater sperm penetrability.
The test, easily performed in the office or clinic, is carried out as follows:
after the cervix is exposed and gently swabbed clean, a sample of endocervical
mucus is obtained with a dry sterile plastic cannula or glass pipet and is
spread on a clean glass slide. If the secretion is spread too thinly or if blood is
present, arborization does not occur, even when adequate estrogen levels
exist. The slide is air-dried for at least 10 to 20 minutes (drying must be
absolutely complete) and then is read under both low- and high-power
magnification on the microscope. If true arborization with crystallization is
present, it is indicative of a predominant estrogen effect, and the test is
positive If a cellular pattern without crystallization and arborization is seen,
the test is negative and indicates either little or no estrogen effect or, more
commonly, suppression of estrogen activity by progesterone. As an indirect
quantification of the extent and intensity of estrogen effect, the cervical
ferning can be graded according to the branching of the ferning pattern upon
crystallization: grade 1 for primary branching, grade 2 for secondary
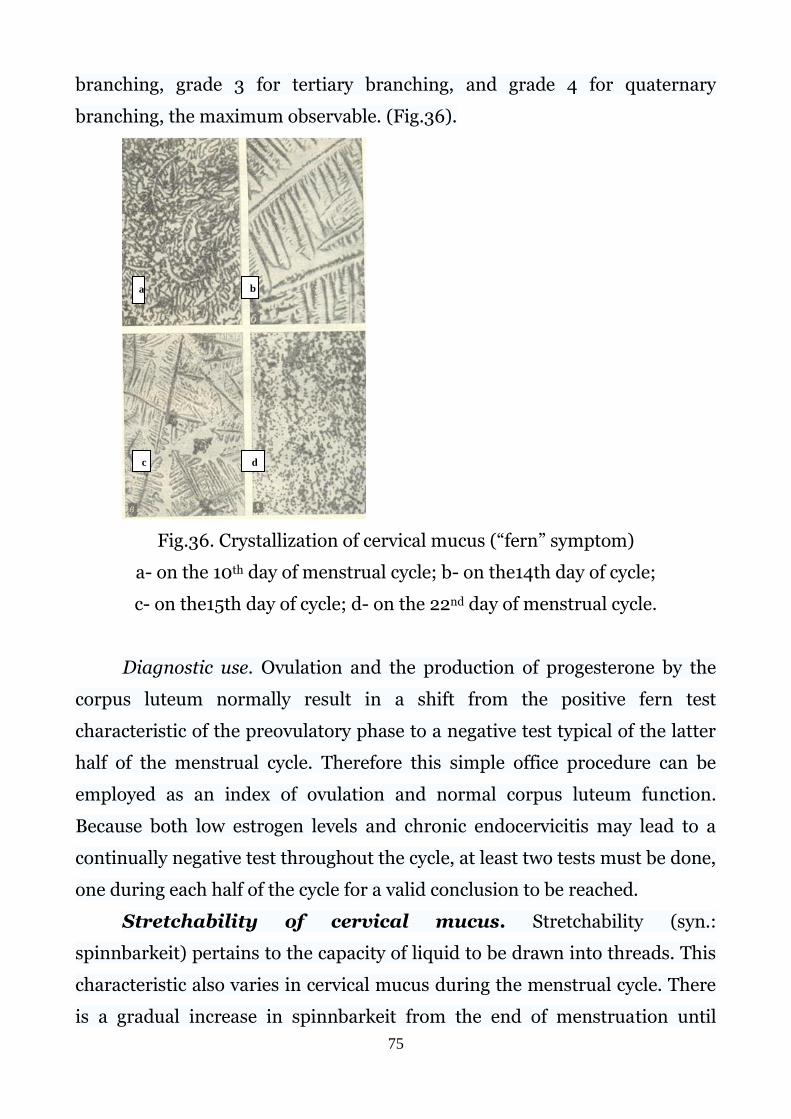
75
branching, grade 3 for tertiary branching, and grade 4 for quaternary
branching, the maximum observable. (Fig.36).
Fig.36. Crystallization of cervical mucus (“fern” symptom)
a- on the 10th day of menstrual cycle; b- on the14th day of cycle;
c- on the15th day of cycle; d- on the 22nd day of menstrual cycle.
Diagnostic use. Ovulation and the production of progesterone by the
corpus luteum normally result in a shift from the positive fern test
characteristic of the preovulatory phase to a negative test typical of the latter
half of the menstrual cycle. Therefore this simple office procedure can be
employed as an index of ovulation and normal corpus luteum function.
Because both low estrogen levels and chronic endocervicitis may lead to a
continually negative test throughout the cycle, at least two tests must be done,
one during each half of the cycle for a valid conclusion to be reached.
Stretchability of cervical mucus. Stretchability (syn.:
spinnbarkeit) pertains to the capacity of liquid to be drawn into threads. This
characteristic also varies in cervical mucus during the menstrual cycle. There
is a gradual increase in spinnbarkeit from the end of menstruation until
a b
c d
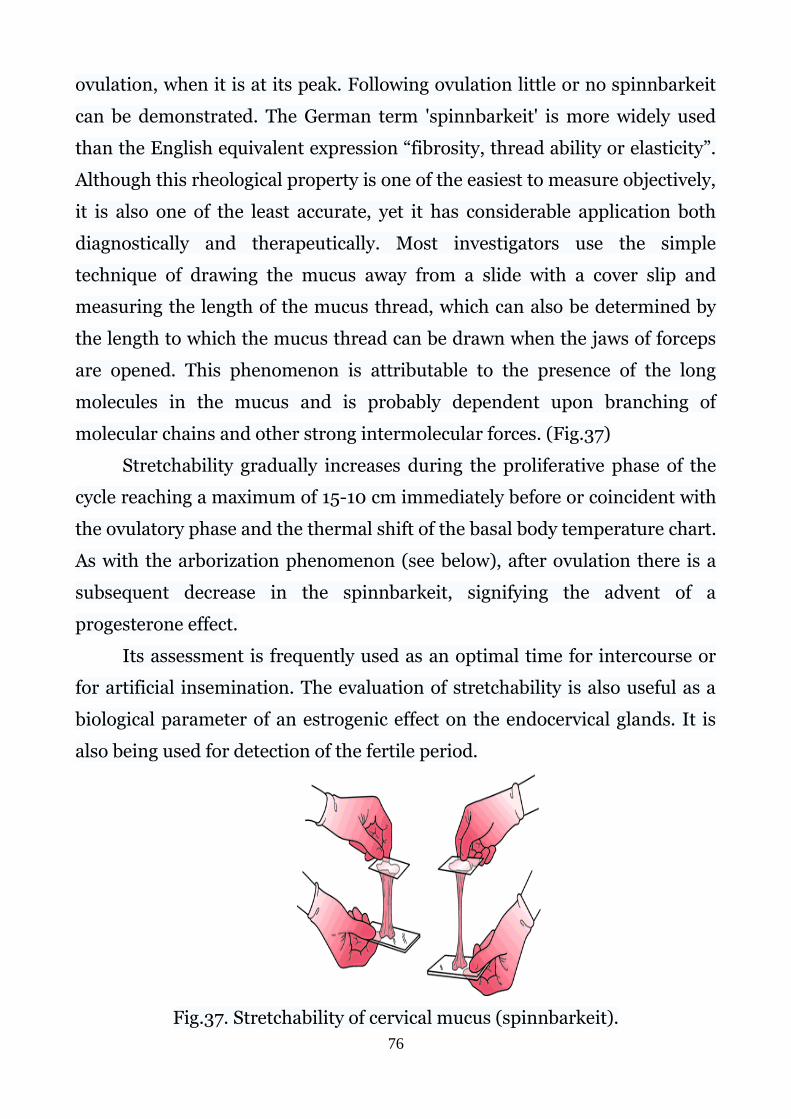
76
ovulation, when it is at its peak. Following ovulation little or no spinnbarkeit
can be demonstrated. The German term 'spinnbarkeit' is more widely used
than the English equivalent expression “fibrosity, thread ability or elasticity”.
Although this rheological property is one of the easiest to measure objectively,
it is also one of the least accurate, yet it has considerable application both
diagnostically and therapeutically. Most investigators use the simple
technique of drawing the mucus away from a slide with a cover slip and
measuring the length of the mucus thread, which can also be determined by
the length to which the mucus thread can be drawn when the jaws of forceps
are opened. This phenomenon is attributable to the presence of the long
molecules in the mucus and is probably dependent upon branching of
molecular chains and other strong intermolecular forces. (Fig.37)
Stretchability gradually increases during the proliferative phase of the
cycle reaching a maximum of 15-10 cm immediately before or coincident with
the ovulatory phase and the thermal shift of the basal body temperature chart.
As with the arborization phenomenon (see below), after ovulation there is a
subsequent decrease in the spinnbarkeit, signifying the advent of a
progesterone effect.
Its assessment is frequently used as an optimal time for intercourse or
for artificial insemination. The evaluation of stretchability is also useful as a
biological parameter of an estrogenic effect on the endocervical glands. It is
also being used for detection of the fertile period.
Fig.37. Stretchability of cervical mucus (spinnbarkeit).

77
Basal body (rectal) temperature (BBT). The basal body (rectal)
temperature is measured in the morning before getting up. In the normal
cycle the rectal temperature fluctuates throughout the cycle: in the follicular
phase the basal body temperature is 36. 2 - 36. 7°C, in the luteal phase it
increases by 0. 4-0. 5°C, declining again with the onset of menstruation. (Fig.
38).
Fig.38. Basal body temperature chart.
The basal body temperature fluctuations depend on the
estrogen/progesterone ratio. Normally, the biphasic chart indicates the
ovulation (ovulatory or biphasic menstrual cycle). In the absence of ovulation
the temperature chart will be monotonous, monophasic (anovulatory
menstrual cycle).
The presence of the ovulatory and luteal phases is confirmed by a
histological examination of the endometrium, namely its secretory
transformation. The curettage of the uterine cavity (scrapping of the
endometrium) should be performed in the second half of the menstrual cycle.
The absence or insufficiency of the secretory transformation of endometrium
suggests luteal dysfunction.

78
The endocrine status of the patient is also evaluated by hormonal
concentrations in the blood serum and urine. To specify the level of the
impairment (hypothalamus, pituitary gland, ovaries, adrenal cortex) and the
cause of endocrine lesion, various functional tests may be employed
(progesterone, releasing hormones, LH, FSH, HCG, ACTH, synthetic
progestins, glucocorticoids etc).
III. Tests for evaluation of abnormal
(precancerous and cancerous) conditions
Cytological examination (the Papanicolaou test). The
Papanicolaou test, also known as the Pap test or the Pap smear, was
developed in the 1940s by Georgios Papanikolaou. It is a cytology-based
screening, the main purpose of screening with the Pap test is to detect
abnormal cells that may develop into cancer if left untreated. The Pap test can
also find noncancerous conditions, such as infections and inflammation. It
can also find cancer cells. In regularly screened populations, however, the Pap
test identifies most abnormal cells before they become cancer. A Pap smear is
a microscopic examination of cells taken from the uterine cervix. A Pap smear
can detect certain viral infections such as human papillomavirus (HPV),
which is known to cause cervical cancer. Early treatment
of precancerous changes detected on the Pap smear can stop
cervical cancer before it fully develops. A woman may have cervical cancer
and not know it because she may not have any symptoms.
The test itself involves collection of a sample of cells from a woman's cervix
during a routine pelvic exam. Exfoliating cells from the transformation zone
of the cervix are taken for microscopic examination to reveal the presence of
malignant or precancerous lesions. The transformation zone is an area of
actively maturing epithelium, between two kinds of cells of the cervix:
79
rectangular columnar cells and flat, scale-like squamous cells. Columnar cells
are constantly changing into squamous cells in an area of the cervix called the
transformation (transitional) zone. And it is the most common place on the
cervix for abnormal cells to develop. These abnormal cells can be detected on
a Pap smear. The location of the transformation zone varies among women.
In teenage girls, the transformation zone is on the immature cervix's outer
surface (vaginal portion of the cervix) and is more susceptible to infection
than in adult women. In older women, the transformation zone may be higher
in the cervical canal.
There are two techniques of taking and making Pap-test: Pap-smear and
Liquid-Based Pap-Test (E-Prep)
Pap-smear technique: the cells, taken form transformation zone, are
placed directly on a glass slide and stained with a substance known as
Papanicolau stain. The stained cells are then examined under a microscope to
look for pre-malignant (before-cancer) or malignant (cancer) changes.
Liquid-Based Pap-Test - sample cells are placed into a vial of liquid
preservative that is then used in the cytology lab to produce a slide for
microscopic evaluation of the cells. (Fig.39)
In both cases a “broom” device or a brush/spatula combination is used to
collect the cells. To obtain the specimen, a cervical broom or cervical spatula
is applied to the surface of the cervix and turned in a single direction to
achieve an adequate sample for cytology, making sure to rotate it at least 360
º for the spatula and 5 rotations for the broom. If the spatula is used, a
cytobrush is additionally needed and must be inserted into the cervix so that
the outermost bristles are still visible at the external os. The brush is then
rotated one half turn in a single direction to achieve an adequate cytology
sample (see image below).

80
Fig.39. Pap-testing: 1- taking cells for examination; 2- placing of smear
on glass for further staining and examination; 3-placing of smear into
container with special liquid for
Liquid-based pap-test
To get adequate results, special preparation of the patient for testing is
necessary, which includes:
• avoidance of day of menstruation for Pap-testing;
• avoidance of vaginal intercourse, douching, use of tampons, use of
medicinal vaginal cream or contraceptive cream for 24-48 hrs prior to
cervical screening.
• ideally, pre-existing cervicitis should be treated prior to cervical
screening.
The smears show normal or abnormal cells. The abnormal cells are
identified by their big nuclei, chromatin network and nuclear-cell ratio. All
women over 25 years of age should be annually screened.
Depending on the type of cells seen (Fig.40), the Pap smears are
classified by Bethesda system:
• Squamous cell abnormalities (SIL)
• Atypical squamous cells of undetermined significance (ASC-US)
• Atypical squamous cells – cannot exclude HSIL (ASC-H)
• Low-grade squamous intraepithelial lesion (LGSIL or LSIL)
• High-grade squamous intraepithelial lesion (HGSIL or HSIL)

81
• Squamous cell carcinoma
• Glandular epithelial cell abnormalities
• Atypical glandular cells (AGC), specify endocervical, endometrial, or not
otherwise specified (NOS)
• Atypical endocervical cells, favor neoplastic, specify endocervical or
NOS
• Endocervical adenocarcinoma in situ (AIS)
• Adenocarcinoma
• Other
Endocervical and endometrial abnormalities can also be detected, as can a
number of infectious processes, including yeast, herpes simplex
virus and trichomoniasis. However it is not very sensitive at detecting these
infections, so absence of detection on a Pap does not mean absence of the
infection.
The past decade has witnessed several changes in the realm of cervical cancer
screening, prevention, and management. These include the increased use of liquid-
based preparations.
In 2014, the Bethesda system received some changes:
• reporting of benign-appearing endometrial cells is now recommended for
women aged 45 years;
• terms such as “LSIL, cannot exclude HSIL” or “LSIL-H” have been proposed;
• an interpretation of atypical squamous cells (ASC) cannot rule out HSIL (ASC-
H) may be made in addition to an LSIL interpretation. This would indicate that
definite LSIL is present as well as some cells that suggest the possibility of
HSIL. In general, follow-up guidelines for these interpretations are for
colposcopy and biopsy; however, in patients (such as young women) who have
samples for which the guidelines differ between LSIL.
• and ASC-H, the addition of the ASC-H interpretation should lead to
colposcopic evaluation.

82
Fig.40. Changing of cervical cells over time and becoming abnormal. LSIL
and HSIL are two types of abnormal changes to cervical squamous cells.
However, in case of negative results, smears need to be repeated every
1-3 years.
When abnormal cells are detected on the Pap-test, further diagnostic
procedures are indicated. These tests include: colposcopy, cervical
biopsy, colposcopic biopsy, endocervical curettage, cone biopsy, LEEP (Loop
Electro-Surgical Excision Procedure). Subsequent cervical cancer may be
prevented through the diagnosis and treatment of these cervical cancer
precursors.

83
Additional methods of examination
Endoscopic methods
Endoscopy is the examination of body cavities using an optical device
equipped with an illuminating device. At present, the method has ceased to be
of a purely diagnostic nature; various endoscopic operations have already
been developed and put into practice. In gynecology, endoscopy is used to
examine the cervix (colposcopy), the uterine cavity (hysteroscopy), and the
pelvic organs (laparoscopy), as well as for operations on them.
Colposcopy - examination of the vagina and vaginal part of the cervix
using a binocular or monocular loupe equipped with a lighting device (an
increase in the study area is 30 times or more).
Hysteroscopy - examination of the inner surface of the uterus in
order to detect pathological changes in the endometrium;
Laparoscopy (peritoneoscopy) - is examination of abdominal
cavity with the help of an optical instrument inserted into the abdominal
cavity; as well as a method of minimally invasive surgery.
Culdoscopy - is the examination of the pelvic organs with the help of
an optical instrument inserted into the abdominal cavity through the
posterior vaginal fornix (aka cul-de-sac, rectouterine pouch, the pouch of
Douglas).
Colposcopy
A colposcopy is an examination of the vagina and cervix using a lighted
magnifying instrument called a colposcope (special microscope), to examine
cervical and vaginal tissues in real time (in vivo). The colposcope (Fig. 41)
magnifies the image many times, thus allows the health care provider to see
the tissues on the cervix and vaginal walls more clearly and determine
anomalies. (Fig.42). A colposcope is placed in the vagina and used to

84
microscopic examination of the area of the cervix where an abnormality is
suspected.
Fig.41. Colposcope.
Fig.42. Colposcopy
Comparatively with Pap-test, which is a screening method, colposcopy
is the diagnostic test to evaluate patients with an abnormal cervical
cytological smear or abnormal-appearing cervix. The most common

85
indication of referral for colposcopy is positive screening tests (e.g., positive
cytology, positive on visual inspection etc.).
The simple colposcopy and extended colposcopy are used in clinical
practice.
The key ingredients of colposcopic examination are the observation of
features of the cervical epithelium after application of normal saline, 3-5%
dilute acetic acid, and Lugol’s iodine solution in successive steps.
The simple colposcopy is the examination of the cervix after removal of
the discharge from its surface without the use of medications. It is the first
phase of the survey, which is performed at the beginning of the study, and
allows identifying anomalies of cells, their location and the degree of change,
if any. (Fig.43). When a white area is observed on the cervix prior to the
application of acetic acid, it is called leukoplakia. (Fig.44).These areas
represent hyperkeratosis and can be associated with infection by HPV,
chronic trauma or scarring. It is generally recommended that biopsy of at
least one representative area of leukoplakia be performed during a
colposcopic examination.
Extended colposcopy is the examination of the cervix after application
of 3% acetic acid solution or 2% Lugol solution (Schiller's test), hematoxylin,
adrenaline on its vaginal part.
Acetic acid is applied to the cervix using a cotton wool ball or with a
spray. The action is manifested 30-60 sec after the application of the solution
and lasts 4 minutes. 3-5% solution of acetic acid causes a short-term swelling
of the epithelium, swelling of the cells of the Malpighian layer of cervical
epithelium, a reduction in the subepithelial vessels and a decrease in blood
supply. Abnormal areas, such as cervical intraepithelial neoplasia (CIN), will
tend to turn white (acetowhite). (Fig.45, Fig. 46). The characteristics of
acetowhite changes, if any, on the cervix following the application of dilute
acetic acid are useful in colposcopic interpretation and in directing biopsies.

86
The colposcopic diagnosis of cervical neoplasia depends on the
recognition of four main features: intensity (colour tone) of acetowhitening,
margins and surface contour of acetowhite areas, vascular features and colour
changes after iodine application. The occurrence of abnormal features in a
localised area in the transformation zone increases the probability of
diagnosis of a neoplastic lesion. Low-grade CIN is often seen as thin, smooth
acetowhite lesions with well-demarcated, but irregular, feathery or digitating
or angular margins. High-grade CIN are associated with thick, dense, dull,
opaque or greyish-white acetowhite areas with well-demarcated, regular
margins. Abnormal vascular features such as punctation and mosaics are
significant if these are seen confined to acetowhite areas. Other
abnormalities, such as cervical condyloma, endometriosis are also identified
in colposcopy (Fig.47 – Fig.53).
The Schiller’ test is based on the ability of normal epithelium to change
the coloration under the influence of iodine on dark brown, depending on the
content of glycogen epithelium in cells. (Fig.54). Areas containing glycogen
turn brown or black; areas lacking glycogen remain colourless or pale or turn
mustard or saffron yellow. Normally, uniform brown coloration is noted.
Yodnegative sites indicate a sharp decrease in glycogen in the cells of the
integumentary epithelium of the cervix. CIN lesions do not contain glycogen
and thus do not stain with iodine and remain mustard or saffron yellow areas.
To identify cell changes iodine cannot be used alone because immature
epithelium does not turn brown. Inflammation creates a lighter yellow-
stained area. Columnar epithelium is usually being stained with orange spots
by iodine. Iodine is not relevant in women with low estrogen levels in vaginal
epithelium, as in breastfeeding or after menopause, when the epithelium
contains little or no glycogen.

87
Fig.43. Normal cervix as seen through a colposcope without the application of
vinegar. The red color around the os is produced by columnar cells and the
lighter pink on the remainder of the cervix result from normal squamous
cells. The presence of visible columnar cells outside the internal os is called
ectropion and is a normal finding in young women and women on estrogen-
containing contraception. The junction between the two cell types and colors
is the squamocolumnar junction.
Fig.44. Leukoplakia (hyperkeratosis) – a.

88
Fig.45. A colposcopic picture of a woman with low-grade squamous
intraepithelial lesion cytology.
Fig 46. Acetowhiate areas on the cervical surface

89
Fig.47.Cervix with circumorificial, mild to dense acetowhite lesion with fine
mosaic (arrow)
Fig.48. Dense, well defined acetowhite area with regular margins and coarse
mosaic

90
Fig.49. Punctation (1) within a field of intraepithelial neoplasia. This
widespread and variable field of punctuated vessels indicates the presence of
various degrees of high- and low-grade cervical intraepithelial neoplasia
(CIN). Capillaries toward the center of the field are more spaced, indicating a
higher degree of CIN than in the capillaries at the periphery, which are more
closely spaced and indicate a lesser degree of abnormality.
Fig.50. Cervical cancer (indicated by the yellow arrows) is seen on both the
anterior and posterior lips of the cervix. The epithelial surface is elevated,
friable and yellowish in color. Atypical blood vessels are noted, the hallmark
of invasive cervical cancer.

91
Fig. 51. Cervical condyloma (indicated by the arrow) detected during
colposcopy. The long villous-like projections are a common morphologic
appearance of HPV-induced lesions.
Fig.52. Cancer precursor (indicated by the arrow)seen by colposcopy. The
opaque white epithelium and coarsely dilated mosaic blood vessels are
diagnostic of CIN 3(photo courtesy of Daron Ferris, MD).

92
Fig 53. Cervical endometriosis
Fig.54. The Shiller’ test: unpainted areas indicate pathology, are take material
for biopsy. Schiller’s test does not allow to answer the question about what
process was going on.
Chromocolposcopy is another aspect of colposcopy method. It is the use
of special filters for during colposcopy examination. The filters help the
physician examine tiny blood vessels (capillaries) in the area of the
squamocolumnar junction (SCJ). Blue or green filtered light can cause
abnormal capillaries to become more obvious, usually inside an acetowhite

93
area. Normal capillaries are slender and spaced out evenly. In contrast,
abnormal capillaries can appear as red spots (thickened capillaries seen on
end) or can produce a pattern resembling hexagonal floor tiles. The worse the
cervical disease, the thicker and more widely spaced out are the capillaries.
The abnormal capillary pattern ranges from mild, as with pre-cancer
(dysplasia), to severe, as with established cancer.
Colpomicroscopy (microscopic colposcopy) - colposcopy under high
magnification (160-280 times) with the help of a contact lens and with
preliminary staining of the study area. The peculiarities of the structure of
nuclei and cytoplasm of cells of surface layers of epithelium may be examined
with microscopic colposcopy.
Biopsy should be directed whenever in doubt. Using a special scoring
system and terminology, colposcopic index may guide colposcopic
interpretation and diagnosis.
The latest version of the international terminology, which is used in this
book, was formulated by the International Federation for Cervical Pathology
and Colposcopy (IFCPC) with the International Society for the Study of
Vulvar Disease (ISSVD) in Rio de Janeiro, Brazil, in 2011. (Table 2).
Table 2.
2011 IFCPC Colposcopic terminology
2011 IFCPC Colposcopic terminology
General assessment • Adequate/inadequate PGA (for example bleeding, scars,inflammation)
• Squamocolumnar junction visibility: Completely visible, partially visible, not visible
• Transformation zone(TZ) types 1,2,3
Normal colposcopic findings
Original squamous epithelium:
• Mature
• Atrophic

94
Cylindrical epithelium
• Ectopy
Metaplastic squamous epithelium
• Nabothian cysts
• Crypt (gland) openings
• Deciduosis in pregnancy
Abnormal colposkopic findings
General principles
Location of the lesion: Inside or outside the T-zone. Location of the lesion by clock position
Size of the lesion:Number of cervical quadrants the lesion covers. Size of the lesion in percentage of cervix.
Grade 1 (Minor)
Thin aceto-white epithelium, irregular, geographic border
Fine mosaic, fine punctuation
Grade 2 (Major)
Dense aceto-white epithelium, rapid apperance of acetowhitening, Cuffed crypt (gland) openings
Coarse mosaic, coarse punctuation, sharp border, inner border sign, ridge sign?
Non specific
Leukoplacia, erosion, iodine/Lugol´s staining (brown/yellow)
Suspicious for invasion
Atypical vessel. Additional signs: Fragile vessles, irregular surface, exophytic lesion, necrosis, ulceration (necrotic tumor)
Miscellaneous finding
Congenital transformation zone, condyloma, polyp, (ectocervical/endocervical), inflammation
Stenosis, congenital anomaly, post treatment consequence, endometriosis
Strander/Swede colposcopic score
• Five variables equivalent to 1-5 above has a value of 0,1 or 2
• At full deflection, the maximum is 10 point
• 1-4 points speak against CIN2+, while 8-10 points indicates for
CIN2+ (CIN3, cancer in situ)

95
Strander/Swede colposcopic score (Table 3) is a newer and international
approved scoring system, easy to use and helpful to systematize colposcopic
findings and knowing where to take biopsies.
Table 3
Strander/Swede colposcopic score
Score 0 1 2
Uptake of
asetic acid
None or
transparent
Shady, milky (not
transparent not
opaque)
Stearin-like (distinct, opaque
white)
Margins Diffuse Sharp, but
irregular, jagged,
“geographic”
satelittes
Sharp end even, difference in
surface level
Vessels Fine,
regular
Absent Coarse or atypical vessels
Size < 5mm 5-15 mm or 2
quadrants
> 15 mm or spanning, 3-4
quadrants or endocervically
undefined
Iodine
absorbtion
Brown Faintly or patchy
yellow
Distinct yellow
Factors affecting the outcome of colposcopy:
qualification of a doctor conducting colposcopy
bleeding
severe inflammation
marked atrophy of an ectocervix
Colposcopy harms include pain, cost, psychological impact, and possible
impact of subsequent cervical procedures on obstetrical outcomes.

96
Contraindications. No absolute contraindications to the performance of
a colposcopic examination exist, although special precautions may be
required in special circumstances, such as a pregnant patient who harbors a
placenta previa. The patient's ability to tolerate a standard speculum
examination is the only true limiting factor. Pregnancy by itself is not a
contraindication. Active cervicitis and vulvovaginitis should be treated before
undertaking the examination, because inflamed tissues can alter the ability to
obtain an accurate assessment, and it can make the discomfort of the
examination markedly worse.
When any lesion is identified, at least 2 biopsy specimens should be
taken to improve the accuracy of colposcopy. A biopsy should be performed
on specimens taken of the most severe area found on colposcopic examination
to confirm or rule out malignant lesions.
Hysteroscopy
Hysteroscopy is forms of minimally invasive surgeries, which allows
visualizing the internal surface of the uterus with the cervical canal to exam or
treat it. The equipment is a tiny telescope (hysteroscope), which is inserted
through the cervix into the uterus. The hysteroscope allows the surgeon to
visualize the inside of the uterine cavity on a video monitor. The inside of the
cervical canal, openings of the Fallopian tubes are visualized too.
Hysteroscopy is one of the most informative and effective methods of
diagnosis and treatment in modern practice. It helps to determine
intrauterine pathology, to make topical diagnostics and perform some
surgical intervention. Hysteroscopy has allowed not only to increase the
efficiency of diagnosis and treatment of a number of intrauterine and
endocervical problems, but also to significantly reduce surgical aggression in
modern practices. Since hysteroscopy examines the endometrium only, it is
not appropriate for examination or diagnosis of problems or conditions that
occur within the muscular layer or serous coat of the uterus. It also does not

97
allow for direct examination of the Fallopian tubes, because of makes
visualization of the openings to the Fallopian tubes, but not tubes in whole.
The procedure can be performed as an aid in the diagnosis of problems
with the uterus, or it may be combined with simple surgical techniques for
treatment purposes. Thus, diagnostic and operative hysteroscopy are
distinguished.
Diagnostic hysteroscopy - is a procedure performed to evaluate the
endometrial cavity. Two systems of diagnostic hysteroscopy exist: panoramic
(also known as direct optical) and contact (also known as contact
microhysteroscopy). The most often used a panoramic technique. In this case
the uterine cavity is distended by a medium (which could either be fluid or
carbon dioxide), to achieve adequate visualisation of the uterine cavity.
Carbon dioxide is mostly used for diagnostic hysteroscopy, because the
bleeding that appears during operative hysteroscopy obscures visibility.
Carbon dioxide is a safe distension media when used at pressures below the
mean arterial pressure (MAP) of approximately 100 mmHg and flow rates
less than 100 mL per min. The advantages of CO2 include high solubility in
blood, high image clarity, and ubiquity in all operating rooms equipped for
laparoscopy. Its use for hysteroscopy is limited to diagnostic cases and has
significant disadvantages: the combination of intrauterine blood and
CO2 creates bubbles that can dramatically reduce the viewable area and limit
the diagnostic survey. 0.9% sodium chloride solution and lactated Ringer
solution are isotonic, conductive, low-viscosity fluids that are used for
diagnostic hysteroscopy and operative procedures. 0.9% sodium chloride
solution and lactated Ringer's solution are isotonic, conductive, low-viscous
liquids, which are used for diagnostic hysteroscopy and for limited
operational procedures. 5% mannitol, 3% sorbitol and 1.5% glycine are
hypotonic, non-conductive liquid with low viscosity, they improve
visualization in bleeding. They can be used in both diagnostic and operative
hysteroscopy.

98
Contact hysteroscopy is a related procedure in which no distending
media is used and the hysteroscope is passed directly into the uterus and put
in gentle contact with the endometrial lining to obtain maximum
magnification. Only tissue that is in direct contact with the distal tip can be
inspected and evaluated.
Indications for diagnostic hysteroscopy:
abnormal premenopausal or postmenopausal uterine bleeding
confirmation of abnormal test findings (thickened endometrial lining
on sonography)
evaluation of the effectiveness of a hormone therapy
control of the uterine cavity after previous operations on the uterus
suspected Müllerian anomalies
suspected submucosal leiomyoma
suspected adenomyosis
suspected intrauterine synechiae
suspected the remnants of a fertilized ovum in the uterus after
miscarriage/abortion
suspected foreign body in the uterine cavity (IUD/fragments of IUD,
etc)
endometrial polyps
suspected perforation of a uterine wall.
Contraindications for diagnostic hysteroscopy:
Few contraindications to hysteroscopy exist. Severe medical
comorbidities may be a contraindication and should be assessed for each
individual’s needs and tolerances. Contraindications to hysteroscopy include
the following:
viable intrauterine pregnancy
female genital tract cancer, including cervical or uterine cancer
active pelvic infection

99
inexperienced surgeon
Treatment of pelvic infections is mandatory prior to hysteroscopy and
can decrease the chance of propagating gynecologic infections that can lead to
pelvic pain, tubal factor infertility, and even death.
Preoperative preparation includes:
general clinical examination, including gynecological exam and imagine
studies, is made with spеcial attention to inflammation, anemia, the
circulation and the lungs.
CBC
urinalysis
HVS should be taken for microscopy for white blood cells, epithelial
cells, yeasts, bacterial vaginosis and Trichomonas vaginalis, and
bacteriology culture for bacterial pathogens and sensitivity to antibiotic
agents. electrocardiography
chest x-ray
blood sugar level
other tests by indications
the rectum and the bladder should be empty before operation.
Diagnostic hysteroscopy should be performed in the proliferative phase
of the menstrual cycle after cessation of menstrual flow. The procedure is
typically performed at day 5-7 of menstrual cycle. Examinations during the
secretory phase should be avoided to allow for optimal views of the cavity
since secretory endometrium can mimic intrauterine pathology. However,
there are exceptions when it is necessary to assess the state of the
endometrium in the secretory phase of the cycle. In such cases, the procedure
is performed 3-5 days before menstruation. In patients with perimenopause,
in postmenopausal patients, as well as in emergency cases, with bleeding, the
time of hysteroscopy does not matter. Some patients with anovulatory cycles
sometimes need in pharmacological preparation of endometrium for

100
Hysteroscopy. In such cases pharmacologic thinning of the endometrium can
be done with a course of progestins, oral contraceptives, danazol, or GnRH
agonists. However, endometrial preparation is more typically performed prior
to operative hysteroscopy.
Fig. 55. A diagnostic hysteroscopy
Technique. The procedure may be done in specially equipped out-patient
office or in the hospital, under the local or general anesthesia. A patient
should be placed in the dorsal lithotomy position. A 10% povidone-iodine
vaginal and perineum preparation is preferred for hysteroscopic procedures.
After a bimanual examination, sim’s specula are used to bring the cervix into
view. The cervix should be cleaned with an antiseptic solution (10% povidone-
iodine or 4% chlorhexidine gluconate solution). A single-toothed tenaculum is
then applied to the anterior lip of the cervix. A small amount of local
anesthetic can be used prior to applying the tenaculum. If necessary,
administer the paracervical block with the cervix under gentle traction. In
order to achieve an adequate paracervical block for the nonpregnant female,
10-20 ml of anesthetic should be injected 10 mm deep at the 4 o'clock and 8
o’clock position in the cervicovaginal junction with a 25-gauge spinal needle.
The cervical canal should be dilated before insertion of hysteroscope into the
cervix. Special dilators usually used or patient may be given medication
(misoprostol, a synthetic prostaglandin e1 analogue) that is inserted into the

101
cervix for cervical ripening to improve the likelihood of successful cervical
dilation and decrease intraoperative pain with few adverse events. Then
equipment for distention media is activated and the flow of the medium can
be started. The hysteroscope is introduced to the external cervical os and
advanced into the endocervical canal. The flow of media should function to
"wedge" a path to uterine entry. The walls of the cervical canal, the uterine
internal surface, walls should be examined accurately during the
procedure.(fig.55, fig.56.). If hysteroscopy is being performed to evaluate
endometrial polyps or other intrauterine pathology, tissue samples can be
obtained with hysteroscopic forceps.
Fig.56. Hysteroscopic picture of a normal uterine cavity
Operative hysteroscopy is a minimally invasive gynecological operation in
which an endoscopic optical lens is inserted through the cervix into the
endometrial cavity to direct treatment of various types of intrauterine
pathology. Operative hysteroscopy is can be combined with diagnostic one,
where after accurate examination of the uterine cavity and determination of
pathology, the surgical treatment may be done. This procedure is performed
in the operating room under IV sedation administered by an anesthesiologist

102
(IV infusion of Tramadol, opioid pain medication).Transcervical instillation of
5 mL of 2% mepivacaine lowers pain scores and decreases the rate of
vasovagal reactions for women undergoing diagnostic hysteroscopy followed
by endometrial biopsy. Regional anesthesia (paracervical block), is also used.
General anesthesia may be indicated for more extensive procedures or for
patients who have lower pain tolerance and/or anxiety. General endotracheal
anesthesia is required for more complex or lengthy procedures or when
concurrent laparoscopy is expected. Thus, operative hysteroscopy may be
done under local, regional, or general anesthesia.
Operative hysterectomy is done to:
Take a tissue sample (biopsy)
Remove polyps or fibroid tumors
Prevent bleeding by destroying tissue using electric current, freezing,
heat, or chemicals
During operative hysteroscopy, equipment similar to the diagnostic
procedure (for example, a hysteroscope, light source, stretching means,
camera and gynecological instruments) is used, as well as special equipment,
need for surgical intervention with hysteroscopy. Equipment unique to
operative hysteroscopy includes:
an operative bridge that contains ports for hysteroscopic
instruments (ie, shears, graspers, and biopsy forceps),
the input and output channels that allow for continuous laminar
flow and irrigation,
the automated system that provides real-time fluid deficit
calculations and can control the pressure at which distension
medium is instilled,
the hysteroscopic morcellators
etc.
High-viscosity fluids are more preferred in operative hysteroscopy to limit
image distortion due to intrauterine bleeding. Currently, the only high-

103
viscosity fluid option is Dextran 70. Dextran 70 is void of electrolytes and is
therefore nonconductive. Intraoperative fluid management is an important
aspect of hysteroscopy. Infusion pressure can be generated by elevating the
fluid bag or by using an automated pressure infuser or blood pressure cuff.
Pressure devices may increase fluid absorption and should be kept less than
the patients MAP, especially during prolonged cases. In cases in which
visualization is not optimal, the intrauterine distending pressure may be
increased 5-10 mmHg above the mean arterial pressure for short periods of
time.
Indications for operative hysteroscopy:
abnormal uterine bleeding (AUB) or heavy menstrual bleeding
(transcervical resection of endometrium is made to prevent
bleedings).Fig.57.
submucous leiomyoma (hysteroscopic removal of submucosal fibroids if
they are less than 3 cm. in diameter); Fig. 58.
uterine polyps (polips can cause AUB, infertility, also are dangerous due
to risk for malignant transformation); Fig. 59.
uterine septum (it is noted to be a major etiology of recurrent pregnancy
loss (RPL) and resection significantly improves live birth rates); Fig.60.
intrauterine adhesions (aka Asherman syndrome, which can lead to
AUB, infertility, or RPL, and hysteroscopic resection is the standard
treatment of symptomatic intrauterine adhesions);Fig.61, Fig. 62.
tubal infertility (hysteroscopic proximal tube cannulation can be
performed to open blocked tubes with operative hysteroscopy);Fig.63.
foreign bodies in the uterus (removal of a retained intrauterine
contraceptive device, or parts of device, as well as other foreign
bodies);Fig.64.
sterilization (it is hysteroscopic alternatives to laparoscopic or mini-
laparotomy sterilization techniques).

104
Operative hysteroscopy can be performed in all of these situations with
minimal or no anesthesia and minimal surgical risk.
Contraindications:
pregnancy,
cervicitis,
active pelvic infection,
known cervical or endometrial cancer,
surgeon inexperience.
Comorbidities that may be exacerbated by intravascular volume expansion
are a relative contraindication
Technique. Operative hysteroscopy is best performed in the proliferative
phase of the menstrual cycle after menstrual flow has stopped when the
endometrium is thin. The initial steps of procedure are similar to those for
diagnostic hysteroscopy. A paracervical or intracervical block may be used
additional anesthesia. The cervix is then progressively dilated to the required
diameter (depending on the operative hysteroscope being used) with the
surgeon’s preference of cervical dilators (ie, Hegar, Hank, or Pratt).
Then the flow of distension medium is started and flushed through the
hysteroscope. The scope is then introduced to the external cervical os and
advanced into the dilated cervical canal. As the hysteroscope is slowly
advanced into the uterine cavity, continuous gentle counter-traction is
applied with the tenaculum. Once the distal tip of the hysteroscope appears in
the uterine cavity, the distension medium is allowed to expand the
intrauterine space. Uterine cavity should be accurately described, any
pathology should be noted at this time. Pathology may be treated as described
above.

105

106

107
Hysteroscopy complications. The most common complication that has been
reported is accidental perforation of the uterus. Uterine perforations occur
most frequently during adhesiolysis, but can also occur during insertion of the
hysteroscope. Perforations are generally diagnosed by direct visualization, but
should also be suspected in cases of unexplained rapid increase in the fluid
deficit, uncontrolled hemorrhage, and hemodynamic instability. Observation

108
in intensive care unit should consist of monitoring vital signs, urine output,
and, in some cases, hematocrit. Perforations through the posterior or lateral
uterus or by sharp or electrocautery instruments should prompt laparoscopy
because of the potential for injury to the pelvic viscera or vasculature. A
cystoscopy should be performed to evaluate for bladder injury if an anterior
perforation is noted.
Fluid overload and electrolyte imbalance may happen as a result of
prolonged duration of a hysteroscopy, myomectomy, uterine septum
resection, extensive lysis of adhesions. Electrolyte free distension media can
cause rapid and profound hyponatremia if absorbed in large quantities. For
this reason, fluid deficits should be carefully managed, and intrauterine
pressures should be kept below the mean arterial pressure. Once the fluid
deficit reaches 750 mL, the surgeon should plan for completion of the
procedure. The operation is terminated when deficits reach 1500 mL for
nonelectrolyte fluids and 2500 mL for isotonic fluids.
Bleeding may arise during or after hysteroscopy. The surgeon should first
ensure that the noted bleeding is not a result of uterine perforation. Mild
bleeding is typically self-limited and generally does not require intervention.
If bleeding occurs, electrocautery may be used to coagulate small vessels. If
these conservative approaches fail to control heavy bleeding or if there is
bleeding from larger vessels, an intrauterine balloon can be inserted into the
cavity and inflated to tamponade the hemorrhage.
Other possible (but rare) complications include infection, medical
complications resulting from reactions to drugs or anesthetic agents,
gas embolism from the gas that is injected to distend the uterine cavity during
the procedure.
Laparoscopy
Laparoscopy is a method of investigation, by which organs of pelvic and
abdominal cavities are examined by an optical instrument inserted into the

109
abdominal cavity through an opening in the anterior abdominal wall.
Synonyms are: endoscopy, pelviscopy, peritoneoscopy, ventroscopy, aka
keyhole surgery). The term originated the mid 19th century term from Greek
“lapara” (flank), plus - scopy. With the help of laparoscopy, a number of
gynecological surgeries can be performed: sterilization (tubal coagulation,
tantalum brace or seam imposition), dissection and coagulation of adhesions
in the small pelvis, coagulation of the endometrioid nodes, puncture of the
retention formations of the ovaries, coagulation of ovarian tissue in patients
with ovarian apoplexy.
The advantages of the method are that it is a minimally invasive type of
surgical intervention that allows manipulation through several small (5-10
mm) incisions. With its help, almost without blood loss, doctors perform
surgical treatment of diseases of the pelvic organs, in particular the uterus,
fallopian tubes and ovaries. Laparoscopy provides a much better overview of
the abdominal organs in comparison with traditional surgical methods
(laparotomy) due to the optical enlargement of the organs under
examination; allow visualizing all the floors of the abdominal cavity and
retroperitoneal space and performing surgical treatment if necessary.
(Fig.65). Other benefit of laparoscopy is that simultaneously with direct
viewing of the organs of abdominal cavity it enables the surgeon to take a
small sample of tissue for histological study (biopsy), if necessary. It
increases the accuracy of the diagnostic procedure many times over. Also
makes possible to perform needed surgical operation after immediate
histological examination of samples of tissue, making more invasive surgery
(laparotomy) unnecessary. So, with the help of small incision the diagnostic
inspection of abdominal cavity, biopsy, and surgical treatment, based on
histological study, may be performed. And the total duration of this procedure
is usually calculated in minutes. Other advantages of minimally invasive
laparoscopic procedures are also:
much smaller scars

110
decreased blood loss
less post-operative discomfort since the incisions are much smaller
shorter hospital stays
quicker recovery times and earlier return to full activities
there may be less internal scarring when the procedures are performed
in a minimally invasive fashion compared to standard open surgery.
Fig.65. The technique of laparoscopic surgery: carbon dioxide gas inflates the
abdominal cavity to help with procedure; telescope and instruments allow the
surgeon to examine the abdomen.
As laparoscopy may be done to diagnose a pathological condition or to
perform certain surgical procedures, diagnostic (exploratory) and operative
laparoscopic procedures are distinguished. Diagnostic laparoscopy is applied
to find the cause of the symptoms such as pelvic pain, infertility problems or
other gynecological conditions that cannot be confirmed with clinical
examination or an ultrasound scan. Operative laparoscopy is used to treat a
disease that has already been diagnosed. As mentioned above, if an
abnormal condition is detected during the diagnostic procedure, operative
laparoscopy or hysteroscopy can often be performed to correct it at the same
time, avoiding the need for second surgery.

111
Today, laparoscopy is one of the most widely used methods of diagnosis
and treatment, which is widely used practically all over the world. Due to its
characteristics laparoscopy has evolved from a limited gynecologic surgical
procedure used only for diagnosis and tubal ligations to a major surgical tool
used for a multitude of gynecologic and nongynecologic indications.
Laparoscopy is performed according to planned or emergency
indications
Indications for planned laparoscopy:
tubal and peritoneal infertility,
ovarian tumors,
leiomyoma,
genital endometriosis,
Mullerian anomalies,
sterilization,
lower abdominal pains of unclear etiology.
Indications for emergency laparoscopy:
ectopic pregnancy,
ovarian apoplexy,
rupture of ovarian cyst or tumor-like formation,
pelvic inflammatory diseases,
torsion of the pedicle of an ovarian tumor or a subserous
myomatous node,
differential diagnosis of acute gynecological and surgical
pathology.
Absolute and relative contraindications for laparoscopy are
diatinquished.
Absolute contraindications:
hemorrhage shock
uncorrected coagulopathy

112
diseases in which a patient cannot be located in the Trendelenburg
position (brain trauma, cerebral vascular disease
acute and chronic renal-hepatic insufficiency
Acute intestinal obstruction associated with a massive (>4 cm)
bowel dilatation, which may obscure the laparoscopic view and
increase the likelihood of bowel injury
Trauma with hemodynamic instability or a clear indication of
bowel injuries, such as presence of bile or evisceration
Relative contraindications
multivalent allergy;
presence of anterior abdominal wall infection (cellulitis or soft-
tissue infection),
ICU patients who are too ill to tolerate pneumoperitoneum or
general anesthesia;
recent laparotomy (within 4-6 weeks) or extensive adhesions
secondary to previous abdominal surgery
aortoiliac aneurysmal disease (may be associated with
increased risk of vascular rupture)
pregnancy (may be associated with injury to gravid uterus or
fetal distress)
cardiopulmonary compromise
morbid obesity
Preparation for laparoscopy. The preparation for surgery starts before
the patient even arrives in the preoperative area, and includes a discussion of
informed consent and home bowel preparation. Many patients with comorbid
medical conditions undergo a review of their treatment strategy with their
primary care physicians. Although commonly termed “medical clearance,”
this process really provides an opportunity to optimize the patient’s medical
management prior to scheduled surgery. The implementation of a method to

113
prevent venous thromboembolism begins based on the procedure and the
patient’s risk factors. Preoperative antibiotic prophylaxis typically commences
before arrival in the surgical theater, with the goal of having therapeutic levels
of the medication in the skin prior to incision. Proper skin preparation and
sterile draping of the patient is also necessary to decrease infectious mortality,
as has been done for almost a century. Obtaining a detailed list of current
medications is essential in a preoperative assessment. It is important to pay
attention to any supplements or herbal medications, because these may affect
coagulation and wound healing. Medications that affect blood clotting, such
as ibuprofen, ginko biloba, clopidogrel, and others, should be discontinued 7
days to 10 days before surgery. Angiotensin-converting enzyme inhibitors and
angiotensin II antagonists should be discontinued at least 10 hours before
general anesthesia is administered to reduce intraoperative hypotension.
Although it is advisable to stop aspirin prior to surgery, a daily low-dose pill
may be considered safe to continue into the perioperative period for patients
with a strong cardiovascular history; the risks and benefits of anticoagulation
should be balanced with the potential for increased blood loss. Elastic
compression stockings applied to legs can improve venous return but may not
be sufficient. For patients with moderate to high risk of developing deep
venous thrombosis (morbid obesity, operative duration >30 min, history of
previous deep venous thrombosis [DVT] or pulmonary embolism [PE],
certain cancers with increased association of DVT) should receive prophylaxis
with fractionated or unfractionated heparin.
CBC, urinalysis, biochemical tests, such as liver function tests or
electrolytes, blood clotting test, pregnancy test, as well as determination of
the blood group and Rh factor are made as before any surgical intervention.
Electrocardiogram, chest radiograph, other imaging studies may be used if
indicated.
Anesthesia. Laparoscopic surgical procedures are most commonly
performed with general anesthesia and skeletal muscle relaxation. However,

114
in rare circumstances, such as in trauma and intensive care unit (ICU)
patients, local anesthesia with intravenous (IV) sedation has been successfully
used.
The laparoscopic procedure. The majority of abdominal laparoscopic
procedures are performed with patients in the supine position, whereas the
lithotomy position is favored for pelvic pathologies (rectal cancer, gynecologic
malignancies, and pelvic conditions). (Fig.66). Then abdomen is cleansed and
draped for the procedure.
The operation begins usually with an intra- or infraumbilical incision
from where the Veress needle is inserted creating the pneumoperitoneum
(Fig.67). The abdominal wall is elevated by manually grasping the skin and
subcutaneous tissue to maximize the distance between the umbilicus and the
retroperitoneal vessels. The Veress needle is placed through the umbilicus
into the peritoneal cavity, avoiding of both the retroperitoneal vessels and the
intestinal tract(Fig.68). A gas, such as carbon dioxide or nitrous oxide or air is
then allowed to flow into the abdomen just below the belly button. This gas
creates a space inside by pushing the abdominal wall and the bowel away
from the organs in the pelvic area and makes it easier to see the reproductive
organs clearly.
The main (10mm) trocar is inserted through the same incision, after
removing the Veress neddle, and the laparoscope is positioned through it.
Types of trocars and placement methods are widely variable. Usually two to
three extra trocars (5mm usually or 10mm) are placed for most operative
gynaecologic laparoscopic surgeries, two lateral and in some cases one
suprapubic (Fig. 69.). The suprapubic port should be placed 3 to 4 cm above
the symphysis pubis to avoid bladder injury. A small trocars are placed
through another incision in order to move the pelvic organs into clear view. A
diagnostic laparoscopy is incomplete without a "second puncture" because,
without this second probe, it is not possible to visualize all the structures
completely.

115
During the laparoscopy the entire pelvis is carefully scanned and the
organs inspected systematically - the uterus; the ovaries; and the lining of the
abdomen, called the peritoneum. In addition to looking for diseases affecting
these structures, the doctor also looks for adhesions (bands of scar tissue),
endometriosis and tubercles. In case abnormalities are found, the doctor can
either try to correct them (operative laparoscopy), or take out bits of tissue for
histologic examination (biopsy) with a biopsy forceps. When the surgery is
complete, the gas is removed and one or two stitches inserted to close the
incisions. Videolaparoscopy, in which a video camera is connected to the
laparoscope, so that what the surgeon sees, can be displayed on a TV monitor
very often used today. This kind of laparoscopy can be very useful for
documentation and record-keeping.
Fig.66. Position of the patient
Fig.67.Diagram of a Veress needle.

116
Fig.68. Veress needle insertion
Fig. 69. Position of trocars in gynecologic laparoscopy.
Complications. In addition to the traditional risks of surgery such as
infection and generalized bleeding, laparoscopy is a technique that presents
its own unique complications.
1. Gas embolism. Embolization usually is caused by inadvertent placement
of the Veress needle in a major vessel prior to insufflation of the
abdominal cavity with carbon dioxide. Usually the carbon dioxide is
quickly absorbed from the artery, and no serious results have been

117
reported secondary to arterial embolization. In these cases, arterial
bleeding would be the major complication. On the other hand,
embolization of carbon dioxide into the venous system may be fatal due
to complete occlusion of the pulmonary artery by a large carbon dioxide
embolism. To avoid this complication, the operator must verify
intraperitoneal placement of the Veress needle prior to insufflation.
Treatment includes immediately stopping insufflation, removing the
needle, placing the patient in the left lateral decubitus position,
administering 100% oxygen, and giving cardiac support.
2. Retroperitoneal major vessel injury. Laceration of major abdominal
blood vessels is one of the least common but most life-threatening
complications in laparoscopy. When placing the Veress needle, the
patient must be in the horizontal position (not Trendelenburg), and the
angle of entry varies depending on patient weight. Open laparoscopy
remains an alternative for avoiding retroperitoneal injury. Immediate
recognition of the injury is paramount to patient survival. If blood flows
from the open Veress needle or if the patient's vital signs rapidly
decompensate after Veress or trocar insertion, prompt action must be
taken: to place a central line and order blood products, make a midline
incision for good exposure and suturing.
3. Abdominal wall vessel injury. The first step to avoiding injury is
knowing the positions of these vessels. When an injury occurs, the
operator must be prepared to control the bleeding promptly. An attempt
can be made to coagulate the vessel with electrocautery. If this approach
does not result in homeostasis, transabdominal sutures have been
advocate.
4. Intestinal or urologic injury. If injury is recognized at the time of
surgery, immediate action must be taken to repair the damage.

118
Imaging studies in gynecology
An x-ray (radiograph) is a noninvasive medical test that helps
physicians diagnose and treat medical conditions. Images with X-rays include
the effect of a small dose of ionizing radiation on a specific part of the body to
create images of its internal structure. X-ray wavelengths are shorter than
those of UV rays and typically longer than those of gamma rays. X-ray is one
of the oldest forms of medical imaging. With the development of ultrasound
and endoscopic methods, X-ray diagnostics began to be used much less
frequently. In modern gynecology, X-ray methods of investigation are most
relevant in oncogynecology, urogynecology, and also in a number of cases of
differential diagnosis of gynecological and surgical diseases.
Since the body is made up of various substances with differing densities,
X-rays can be used to reveal the internal structure of the body on film by
highlighting these differences using attenuation, or the absorption of X-ray
photons by the denser substances (like calcium-rich bones). Medical
radiography includes a range of modalities producing many different types of
image.
For detection of the reproductive system diseases, following methods
are used in gynecological practice:
hysterosalpingography (metrosalpingography – MSH);
contrasting peritoneography;
vaginography;
mammography;
arteriography, phlebography, lymphography of the pelvis and
retroperitoneal space.
Pneumopyelviography
Pneumopyelviography (gynecography, pneumogynecography, X-ray
and neovigraphy, etc.) is the second most frequently used radiographic
method in gynecology. As a contrast medium, nitrous oxide, carbon dioxide

119
and oxygen can now be used. The first two gases can only be used in a
specialized X-ray room. Their advantage is a rapid (within 30 - 120 min)
resorption in the cavity. In the absence of such a cabinet, it is more
appropriate to use oxygen, which is delayed in the abdominal cavity for 24
hours or more. The advantage of oxygen insufflation is the possibility of long-
term X-ray examination, its bactericidal and analgesic properties. Before the
procedure, 750-1500 ml of gas are administered depending on the length of
the body and the completeness of the woman at 100-200 ml per 1 min under a
pressure of no more than 40 mm Hg. Indications for pneumopyleviography
are obtaining information about the external contours of the internal genitalia
in girls and non-sexually active women, the necessary information for vaginal
examination in the presence of pronounced cicatricial or atrophic changes in
the vagina, adhesions in the small pelvis, etc .; anomalies and malformations
of internal genitalia; ovarian tumors; pseudohermophroditism and primary
amenorrhea; differential diagnosis of tumors of the uterus and appendages,
as well as genital and extragenital neoplasms. A variation of this method of
research is contrasting peritoneography, which is used to diagnose effusion
and adhesions in the abdominal cavity.
Vaginography
Vaginography is performed using a two-channel catheter (Foley type).
The expanded part of it is inserted into the vagina, and the balloon is filled
with an indifferent fluid or gas (air) in an amount of 100-150 ml, as a result of
which the entrance to the vagina is blocked. The main catheter is injected
with 150-250 ml of contrast medium (20-30% for diagnosis of vesicovaginal
fistulas and 40-50% for ureteral-vaginal). If possible, radiography should
preferably be carried out using X-ray television equipment or an ordinary X-
ray image table.

120
Hysterosalpingography
Hysterosalpingography ((HSG), is an x-ray examination of
a uterus and fallopian tubes that uses a special form of x-ray called
fluoroscopy and a contrast material.
An x-ray (radiograph) is a noninvasive medical test that helps
physicians diagnose and treat medical conditions. Imaging with x-rays
involves exposing a part of the body to a small dose of ionizing radiation to
produce pictures of the inside of the body. X-rays are the oldest and most
frequently used form of medical imaging. Fluoroscopy is a special x-ray
technique that makes it possible to see internal organs in motion. During a
hysterosalpingogram, the uterus and fallopian tubes are filled with a water-
soluble contrast material and the radiologist is able to use fluoroscopy to view
and assess their anatomy and function. HSG is a real-time form of x-ray
examination
Indications for HSG include detection of:
tubal patency
uterine polyps,
submucosal leiomyomas,
uterine synechiae,
Müllerian anomalies,
hydrosalpinges,
salpingitis isthmica nodosum (SIN),
peritubal adhesions.
Contraindications are:
pregnancy
known contrast allergy
active pelvic infection
recent uterine or tubal surgery

121
To minimize the possibility that the patient may be pregnant, a β- hCG
is warranted prior to commencing.
Technique. The procedure should be performed during the proliferative
phase of the patient’s menstrual cycle (days 6-12), when the endometrium is
thinnest. This improves visualisation of the uterine cavity, and also helps to
prevent false-positive intrauterine filling defects and proximal tubal occlusion
due to endometrial thickening. After an antiseptic cleaning of the external
genital area, a vaginal speculum is inserted with the patient in the lithotomy
position; the cervix is cleaned with an aseptic solution. Catheterisation of the
cervix is then performed; the type of device used depends on local practice
preferences: e.g. Foley catheter with balloon inflation, or any one of a range of
available HSG catheters or metal cannulas. Whatever the device, it should be
primed with contrast prior to commencing to avoid the introduction of gas
bubbles which may provide a false positive appearance of a filling defect.
Water soluble iodinated contrast is subsequently injected slowly under
fluoroscopic guidance. Some radiologists use iodinated oil (Lipiodol) as
contrast when the indication is for lack of fertility. Patient feels discomfort
during the procedure, it is related to cervical manipulation, uterine cavity
distention with the instillation of the contrast media, and peritoneal irritation
from dye that has spilled into the pelvis. Endocervical and exocervical topical
application of lidocaine-prilocaine cream 10 minutes before performing
hysterosalpingography helps to reduce pain during cervical manipulation
with tenaculum and cannula and during cervical traction. To decrease uterine
spasm, the media should be warmed to body temperature and injected slowly.
A typical fluoroscopic examination includes preliminary frontal view of the
pelvis, as well as subsequent spot images that demonstrate uterine
endometrial contour, filled fallopian tubes and bilateral intraperitoneal spill
of contrast, to establish tubal patency. For this aim the scout radiograph is
taken prior to the instillation of contrast. Then a series of at least 4 more
images should be captured as the contrast spreads through the genital tract.

122
The first image after the scout film documents initial cavity fill and is best for
visualizing small filling defects. The subsequent image should be obtained
when the cavity is fully distended to assess uterine shape. The third and
fourth images after the scout are obtained as the fallopian tubes are filling and
after dye has spilled into the pelvis, respectively.(Fig. 70). Additional images
may be required to better document any pathology that is seen.
Complications from HSG are rare. The most common adverse event
are:
abdominal cramping;
vaginal spotting;
venous extravasation;
contrast reaction (vasovagal reaction with bradycardia and hypotension,
potentially resulting in syncope);
pelvic infection
Hysterosalpingogram results interpretation. Conditions which may be
detected with HSG include:
uterine congenital anomalies (Fig.71);
submucosal uterine fibroids (Fig.72);
uterine malignancy;
adenomyosis;
intrauterine adhesions (Fig.73);
uterine (endometrial) polyps (Fig.74);
obliteration of fallopian tubes (Fig.75, Fig. 76);
tubal polyps;
tubal malignancy;
hydrosalpinx (Fig. 77);
salpingitis isthmica nodosa;
tubal spasm;
salpingectomy.

123
Fig.70. Normal HSG
Fig. 72. Uterine fibroid: the radiograph shows a well-defined
filling defect (arrow) in the fundus.

124
Fig.73. Uterine adhesions: intrauterine adhesions
(scar tissue) inside the uterus are seen as irregular
dark shadows (white arrows) within the triangular shaped uterine cavity
Fig. 74. Endometrial polyp
Fig. 75. Tubes are closed off at their ends (liquid,
injected into the uterus, accumulated at their ends)

125
Fig.76. Proximal tubal occlusion (liquid, injected into the uterus,
cannot enter the fallopian tubes)
Fig. 77. Hydrosalpinx: the radiograph shows dilatation of the ampulla
portion of the right fallopian tube (arrow). The left tube is normal in caliber
Phlebography, arteriography and lymphography are used in
oncogynecologic practice to determine the localization and nature of the
primary process, the extent of its spread. Lymphography can be repeated and
repeated to study the dynamics of the process at various intervals after
treatment. In gynecological practice, these methods are used extremely rarely.

126
X-ray studies of the chest, gastrointestinal tract and genitourinary
system are conducted by appropriate specialists, if necessary with the
participation of an obstetrician-gynecologist.
Mammography
A mammogram is an x-ray picture of the breast. An x-ray (radiograph) is a
noninvasive medical test that helps physicians diagnose and treat medical
conditions. Imaging with x-rays involves exposing a part of the body to a
small dose of ionizing radiation to produce pictures of the inside of the body.
X-rays are the oldest and most frequently used form of medical
imaging.(Fig.78)
Fig.78. Mammography
Mammography is specialized medical imaging that uses a low-dose x-
ray system to see inside the breasts. A mammography exam, called a
mammogram, aids in the early detection and diagnosis of breast diseases in
women.
There are 3 recent advances in mammography, widely used in current
clinical practice, they are:
digital mammography,
computer-aided detection
breast tomosynthesis.

127
Digital mammography, also called full-field digital mammography
(FFDM), is a mammography system in which the x-ray film is replaced by
electronics that convert x-rays into mammographic pictures of the breast.
These systems are similar to those found in digital cameras and their
efficiency enables better pictures with a lower radiation dose. These images of
the breast are transferred to a computer for review by the radiologist and for
long term storage. Conventional mammography stores the image directly on
film. (Fig.79). Digital mammography is an electronic image stored as a
computer file. The digital image can be enhanced, magnified and or
manipulated for further evaluation much more easily than the film
counterpart.
Computer-aided detection (CAD) systems search digitized
mammographic images for abnormal areas of density, mass,
or calcification that may indicate the presence of cancer. The CAD system
highlights these areas on the images, alerting the radiologist to carefully
assess this area.
Breast tomosynthesis, also called three-dimensional (3-D)
mammography and digital breast tomosynthesis (DBT), is an advanced form
of breast imaging where multiple images of the breast from different angles
are captured and reconstructed ("synthesized") into a three-dimensional
image set. In this way, 3-D breast imaging is similar to computed tomography
(CT) imaging in which a series of thin "slices" are assembled together to
create a 3-D reconstruction of the body. Although the radiation dose for some
breast tomosynthesis systems is slightly higher than the dosage used in
standard mammography, it remains within the safe levels for radiation from
mammograms.
A mammogram allows the doctor to have a closer look for changes in
breast tissue that cannot be felt during a breast exam. Women ages 50 to 74
years should get a mammogram every 2 years. Women younger than age 50

128
should talk to a doctor about when to start and how often to have a
mammogram.
Different types of mammograms are distinguished:
Screening mammograms are done for women who have no
symptoms of breast cancer. Usually it includes two x-rays of each
breast. Screening mammograms can detect lumps or tumors that are
not felt in palpation. They can also find microcalcification or tiny
calcium deposits in the chest, which sometimes means that breast
cancer is present. Current recommendations in most countries
recommend screening mammography for women starting at age 40.
Regular mammograms (once a year or once every two years) lead to
early detection of breast cancer, when they are the most curable and
contribute to breast preservation.
Diagnostic mammography is used to evaluate a patient with
abnormal clinical findings—such as a breast lump or nipple discharge—
that have been found by the woman or practitioner. Diagnostic
mammography may also be done after an abnormal screening
mammogram in order to evaluate the area of concern on the screening
exam. This type of mammogram also can be used to find out more
about breast changes found on a screening mammogram, or to view
breast tissue that is hard to see on a screening mammogram. A
diagnostic mammogram takes longer than a screening mammogram
because it involves more x-rays in order to obtain views of the breast
from several angles. The technician can magnify a problem area to make
a more detailed picture, which helps the doctor make a correct
diagnosis.(Fig.80, 81,82, 83)

129
A. B.
Fig. 79. A – Digital mammogram. B – Conventional mammograpgy (film)
Fig. 80. Normal mammogram.

130
Fig.81. Fibroadenoma
Fig.82.Bilateral cysts associated to duct ectasia, no prior history of
breast disorders
Fig.83. Breast cancer

131
It is proved that screening with breast mammography results in improved
breast cancer detection rates. Finding breast cancer as early as possible before
it has grown or spread greatly improves a woman’s chance for a successful
treatment.
Computer tomography
Computer tomography is based on the change (weakening) of the
intensity of X-ray radiation when passing through tissues of various densities.
Computed tomography or CT scan uses a high amount of ionizing
radiation (in the form of X-rays) in conjunction with a computer to create
images of both soft and hard tissues. These images look as though the patient
was sliced like bread (thus, "tomography"- "tomo" means "slice"). The exams
are generally short, most lasting only as long as a breath-hold. Contrast
agents are often used, depending on the tissues needing to be seen. Computed
tomography (CT) has become essential in the diagnostic evaluation of the
female pelvic. CT allows accurate delineation of neoplastic and inflammatory
processes and provides an effective means of guiding percutaneous needle
biopsy of masses and aspiration/drainage of fluid collections.
The most popular is spiral CT that not only acquires sliced images, but
also obtains volume images. CT scanners are now widely available in most
hospital settings and in many outpatient facilities as well. Images are now
acquired with the use of multidetector machines that complete their
acquisitions within seconds, and they can be displayed in multiple planes via
reconstruction of data and images. The spatial resolution is excellent and
different circulatory phases can be obtained allowing better interpretation of
images. CT helps to differentiate blood vessels, lymph nodes, and the
presence of tumors. When using contrast, the method helps identify ureters
and the bladder due to the turbidity of these tissues. Oral and rectal contrast
opacifies the bowel and aids in differentiating these anatomic markers from

132
gynecologic structures. A large field of view is presented and total body CT
scanning can be accomplished quickly and easily.
Conventional CT scanners are equipped with a tube that produces a
narrow x-ray beam that passes through the patient and is picked up by a row
of detectors on the other side. The tube and detectors are positioned on the
opposite sides of a ring and rotate around the patient. The tube rotates in a
single direction indefinitely (spiral or helical CT). While the tube is rotating,
the table supporting the patient also moves continuously so that a volume of
tissue rather than an individual slice is scanned. The data are then
reformatted automatically to display the images as axial slices. Thus, the scan
time is much shorter. This spiral CT is not even as fast as the newer multislice
scanners, which acquire images 2 to 3 times faster than a single slice scanner.
The multislice CT may be considered a "turbo-charged" spiral CT. Whereas
conventional and spiral CT use a single row of detectors to pick up the x-ray
beam after it has passed through the patient, the multislice CT has up to 16
active rows of detectors.(Fig. 84)
Fig. 84 CT scan
The disadvantages include radiation exposure and the risks of IV
contrast action. The use of ionizing radiation should always be very deliberate

133
and applied in absolute indications, when alternative methods (MRI or
ultrasound) can not be applied or are insufficient.
Positron emission tomography as a functional method, combined with
CT as a morphological method (PET/CT), is an optimum method in
diagnostics and the therapeutic management of relapses of gynecological
tumors, as it makes it possible to find a viable tumor tissue, and – unlike PET
by itself – to exactly specify its localization. It may also be beneficial in finding
the primary source of the disease for disseminated tumors or where duplicity
of the tumor is detected. PET/CT is also used in clinical staging and restaging
of gynecological tumors, particular where the conclusions of the other
imaging techniques are ambiguous.
CT scan can visualize abnormal masses but definitive pathologic
diagnosis is established only with surgical biopsy. CT scan is more expensive
than ultrasound.
Indications for CT in gynecology:
to detect pituitary tumor;
to detect ovarian tumor;
to determine the cancer of genital tract;
to detect the staging of cancer cervix;
to determine myometrial involvement in endometrial cancer;
to detect para-aortic nodes and obtain needle biopsy to determine
retroperitoneal spread of cancer;
to determine the spread of ovarian cancer;
to detect intraabdominal abscess and hematoma;
to diagnose pelvic vein thrombophlebitis;
to evaluate peritoneal adhesions;
to make pelvimetry by 3d CT of non-pregnant women(Fig. 85, Fig. 86).
Summary of optimum use of imaging methods presented in gynecology
presented in Table 4.

134
Table 4
Summary of optimum use of imaging methods in
gynecology:
Ultrasonography
(TVUS, TRUS,
TAS)
Magnetic
resonance
image (MRI)
Computer
tomography
(CT)
Positron emission
tiomography/Computer
tomography (PET/CT)
Assessment of
early and
advanced stages
of the disease,
lymph glands,
presence of
metastases.
Navigation in
biopsy
procedures.
Assessment of
early stages of
the disease for
tumors of the
cervix and
uterus, local
spreading of
tumors into
surrounding
organs and
closest lymph
nodes,
detection of
metastatic
lesions.
Diagnostic of
unclear adnexal
lesions.
Endometriosis.
Planning of
radiotherapy.
Diagnostics of
relapse.
Assessment of
advanced
disease,
affected lymph
nodes,
metastases.
Planning of
radiotherapy.
Monitoring
response to
therapy.
Diagnostics of
relapse.
Navigation in
biopsy
procedures and
radiofrequency
ablation (RFA).
Determining relapse.
Staging of
gynecological tumors,
especially detection of
infiltrated nodes and
other metastases.
Complementary
method in the event of
ambiguous conclusions
of other imaging
techniques
(distinguishing
between benignant and
malignant lesions).
Assessment of response
to therapy. Detection of
occult primary tumor
where metastases are
known.

135
(TVUS – transvaginal ultrasound examination, TRUS – transrectal
ultrasound examination, TAS – transabdominal ultrasound examination)
Fig.85. A contrast enhanced CT scan showing a mass growing in the left
ovary (white arrow).
Fig. 86. Axial CT scan of the pelvis in a patient with stage IIIB cervical
carcinoma shows a cervical mass (c) with right pelvic sidewall invasion
(arrow)

136
When carrying out X-ray studies in gynecological practice, several well-
known basic rules should be followed.
Any X-ray examination is accompanied by irradiation of the body,
including gonads, which is a drawback of these methods. Taking into account
the harmful effect of ionizing radiation on the generative function of a
woman, one should strive to reduce the dose of irradiation with this or that
method. This is achieved by carrying out research at a high technical level
using modern equipment that allows it to be carried out with the maximum
hard radiation and ensuring optimum safety. Highly sensitive films should be
used to reduce exposure, large-frame fluorography and electron-optical
amplifiers.
The main rule - to X-ray studies should be resorted to strict clinical
indications and, if necessary, in cases when other harmless methods
(ultrasonic, endoscopic, hormonal, functional diagnostics tests, etc.) cannot
be used.
Ultrasound examination
An ultrasound scan (US), aka sonography, is a diagnostic technique which
uses high-frequency sound waves to create an image of the internal organs.
During an ultrasound exam, a transducer sends sound waves through the
body. The sound waves come into contact with tissues, body fluids, and bones.
The waves then bounce back, like echoes. The transducer receives these
echoes, which are turned into images. The images can be viewed as pictures
on a video screen. The term "ultrasound" refers to sound waves of a frequency
greater than that which the human ear can appreciate, namely frequencies
greater than 20,000 cycles per second or Hertz (Hz). To obtain images of the
pregnant or nonpregnant pelvis, frequencies of 2 to 10 million Hertz (2 to 10
megahertz [MHz]) are typically required. Real-time imaging is the most
common sonographic technique used in obstetrics and gynecology. Multiple
individual B-mode gray-scale images are obtained and rapidly displayed in

137
succession, thereby creating a video of the area of interest over time that can
be used to evaluate its structure and some aspects of its function. Real-time
ultrasound is especially useful for imaging mobile subjects, such as the fetus
or heart, and for quickly viewing an organ from different orientations. For
optimum ultrasonographic visualization, certain mechanical, physical, and
ultrasonographic principles must be understood. The quality of an image
ultimately depends on the degree of resolution. In general, the closer the
transducer tip is to the imaging target, the greater the resolution and,
therefore, the clearer the image.
Basic physics and principle of ultrasound examination. Basic Theory:
Sound waves are simply organized mechanical vibrations traveling through a
medium, which may be a solid, a liquid, or a gas. These waves will travel
through a given medium at a specific speed or velocity, in a predictable
direction, and when they encounter a boundary with a different medium they
will be reflected or transmitted according to simple rules. This is the principle
of physics that underlies ultrasonic examination of internal organs. All sound
waves oscillate at a specific frequency, or number of vibrations or cycles per
second, which we experience as pitch in the familiar range of audible sound.
Human hearing extends to a maximum frequency of about 20,000 cycles per
second (20 KHz), while Ultrasound is the term used to describe sound of
frequencies above 20 000 Hertz (Hz), beyond the range of human hearing.
Frequencies of 1–30 megahertz (MHz) are typical for diagnostic ultrasound.
At frequencies in the megahertz range, sound energy does not travel
efficiently through air or other gasses, but it travels freely through all liquids
and biological tissues. The velocity of sound depends on the density and
compressibility of the medium. The construction of images with ultrasound is
based on the measurement of distances, which relies on this almost constant
propagation velocity. The wavelength of ultrasound influences the resolution
of the images that can be obtained; the higher the frequency, the shorter the
wavelength and the better the resolution. Energy is lost as the wave

138
overcomes the natural resistance of the particles in the medium to
displacement, i.e. the viscosity of the medium. The higher the difference of
the acoustic reflection of ultrasound energy between two media, the more
significant is the reflection of the ultrasound. That is why we use coupling gel
between the ultrasound transducer and the skin. By using the gel, we decrease
the impedance and allow the ultrasound to penetrate into the tissue. Thus,
absorption increases with the viscosity of the medium and contributes to the
attenuation of the ultrasound beam. Absorption increases with the frequency
of the ultrasound. Echo is the usual term for the reflected or back-scattered
parts of the emitted ultrasound pulses that reach the transducer. For each
echo, the intensity and time delay are measured at the transducer and
electronically processed to allow calculation of the distance travelled. The
displayed results form the basis of diagnostic ultrasound images. The origin of
echoes reflected from broad boundaries, such as the surface of organs or the
walls of large vessels, is easily identified.
The piezoelectric effect is a basis for ultrasound scanning. Piezoelectric
crystals or materials are able to convert mechanical pressure into electrical
voltage on their surface). Conversely, voltage applied to the opposite sides of a
piezoelectric material causes an alteration in its thickness (the indirect or
reciprocal piezoelectric effect). If the applied electric voltage is alternating, it
induces oscillations which are transmitted as ultrasound waves into the
surrounding medium. The piezoelectric crystal, therefore, serves as a
transducer, which converts electrical energy into mechanical energy and vice
versa. Ultrasound transducers are usually made of thin discs of an artificial
ceramic material such as lead zirconate titanate. The thickness (usually 0.1–1
mm) determines the ultrasound frequency. The basic design of a plain
transducer is shown in Fig. 87. Sound is a vibration transmitted through a
solid, liquid or gas as mechanical pressure waves that carry kinetic energy.

139
Fig. 87. Basic design of a single-element transducer.
Thus, the ultrasound probe has piezoelectric crystals in it, which convert
the electric current into sound waves. These sound waves pass through the
woman's abdomen as the clinician moves the transabdominal transducers
over the mother’s abdomen after application of water soluble gel, which acts
as a coupling agent. As these sound waves pass through the internal
structures and hit various body’s structures, they get reflected back which can
be used to identify distance between body parts and their size and shape.
When the sound waves hit a high density structure like bone, they are
reflected back in form of high velocity waves, giving a white appearance on
the screen. However, when these sound waves hit a less dense structure,
reflected waves are of a lower velocity. These waves give a gray or black
appearance on the screen. These reflected waves are picked up by the
piezoelectric crystals inside the transducer and get converted into electric
signals which are then displayed on the screen. (Fig. 88). The term
echogenicity of the tissue refers to the ability to reflect or transmit US waves
in the context of surrounding tissues. Whenever there is an interface of
structures with different echogenicities, a visible difference in contrast will be
apparent on the screen. Based on echogenicity, a structure can be
characterized as hyperechoic (white on the screen, high density structure like

140
bone), hypoechoic (gray on the screen) and anechoic (black on the screen, less
dense structure like a fluid).
Fig. 88.The pelvic ultrasound exam, suprapubic view
Ultrasound techniques. The various ultrasound techniques are used
today: A-mode, B-scan, two-dimensional, M-mode or TM-mode, Three- and
four-dimensional techniques, Doppler ultrasound, Sonohysterography, etc.
There are three types of pelvic ultrasound: transabdominal,
transvaginal, and transrectal . Transabdominal (Fig. 89) and transvaginal
ultrasound (Fig.90) are mostly used in gynecological practice. A woman may
have both transabdominal and transvaginal ultrasounds to look at the whole
pelvic area. Transrectal is used for men and in sometimes in oncogynecology.
Transabdominal ultrasound (TAUS) involves scanning through the
lower abdomen. TAUS usually provides an overview of the pelvis rather than
detailed images. The transabdominal assessment is particularly helpful for
the examination of large pelvic masses extending into the abdomen, which are
not always well viewed with transvaginal ultrasound. A small amount of
ultrasound gel is put on the skin of the lower abdomen, with the ultrasound
probe then scanning through this gel.

141
Fig. 89. Transabdominal ultrasound, the standard midline sagittal view
Transvaginal ultrasound (TVUS) is an internal ultrasound. It involves
scanning with the ultrasound probe lying in the vagina. Transvaginal
ultrasound usually produces better and clearer images of the female pelvic
organs, because the ultrasound probe lies closer to these structures. The
transvaginal ultrasound probe is thin, about 2cm diameter. The probe is
covered with a disposable protective sheath. A small amount of ultrasound gel
is placed on the end of this probe. The probe is then gently inserted a short
distance into the vagina. All transvaginal examination is made according to
the rules of cleaning and sterilization according to recommended protocols.
Fig. 90. The standard transvaginal sagittal view: it produces a
longitudinal image of the uterus similar to the transabdominal sagittal view,
but rotated 90 degrees counterclockwise

142
Indications for pelvic ultrasound in gynecological practice include:
pelvic pain,
dysmenorrhea (painful menses),
amenorrhea (absence of menses),
menorrhagia (excessive menstrual bleeding),
menometrorrhagia (excessive irregular uterine bleeding),
follow-up a previously detected abnormality,
evaluation, monitoring and treatment of infertility patients,
delayed menses, precocious puberty, vaginal bleeding in a prepubertal
child,
postmenopausal bleeding,
abnormal or technically limited manual pelvic examination,
signs or symptoms of pelvic infection,
evaluation of congenital uterine anomalies,
excessive bleeding, pain, or signs of infection after pelvic surgery,
delivery, or abortion,
localization of an intrauterine contraceptive device,
screening for malignancy in patient at increased risk,
urinary incontinence or pelvic organ prolapse,
guidance for interventional or surgical procedures,
etc.
The anatomical structures which the sonographer should be able to
examine correctly are:
The anatomical structures which the sonographer should be able to
examine correctly are:
uterus (Fig. 91) :
o position,
o size,
o shape

143
o ultrasound characteristics of endometrium and myometrium (Fig.
92);
ovaries (Fig .93):
o position,
o size,
o shape ultrasound characteristics
o number,
o size and internal echo pattern of follicles (Fig.94,Fig.95);
cervix (Fig.96)
o length,
o the angle between the cervix and uterus body;
fallopian tubes where visible (Fig.97, Fig.98)
broad ligaments
pelvic muscles
pelvic blood vessels
vagina (Fig. 99)
A transvaginal ultrasound is usually performed to view
the endometrium, myometrium and the ovaries.
Fig. 91. Transvaginal scan of a uterus (U) in the proliferative phase. E –
endometrium; C-cervix.

144
Fig. 92. Normal appearances of cyclical endometrium. (A) Menstrual
phase showing the endometrium as a thin line; (B) follicular/proliferative
phase showing a trilaminar appearance of the endometrium; (C)
periovulatory phase showing the echogenicity of the basal layer of
endometrium has extended to the midline echo; (D) luteal/secretory phase
showing thickened uniform echogenicity.

145
Fig. 93 Ultrasound image of a normal ovary with dominant follicles
Fig. 94. Longitudinal image of ovary displaying enlarged ovary with
multiple large peripheral follicles and free fluid: ovarian hyperstimulation
syndrome

146
Fig. 95. Polycystic ovary syndrome US picture
Fig. 96. TVUS of a normal cervix, showing the most commonly used
method of cervical length measurement (double-headed arrow)

147
Fig. 97. Pyosalpinx on US: patient with lower abdominal pain and
increased inflammatory markers
Fig. 98. Eight-week-old embryo in the right fallopian tube
Fig. 99. Normal appearance of the vaginal cuff in US.

148
Technique. The ultrasound examination is usually initiated
transabdominally. The bladder does not have to be full; however, if the pelvis
cannot be seen well, it may be necessary to have the patient fill her bladder to
a comfortable capacity. This may be especially important for those women
who are unable to tolerate placement of a transvaginal ultrasound probe.
Often in these cases, the entire examination can be performed
transabdominally. If a specific question remains unanswered, or if an
abnormality is suspected, other approaches, such as a transrectal examination
or even a transperineal examination, may be considered. Transabdominal
scanning is important for evaluating the upper pelvis and abdomen, such as
with large fibroids, ovarian neoplasms that extend into the upper abdomen,
or ovaries lying high in the pelvis. Images only obtained by transvaginal
scanning may not be adequate, or may miss pathology, as distance between
the area under investigation and the vagina increases.
After evaluation of the pelvis transabdominally, the patient is asked to
void because transvaginal sonography is best performed with an empty
bladder. Guiding the probe toward the area of interest, such as an ovary, and
watching how this area moves in relation to the other pelvic organs is helpful
for evaluation of complicated or unclear pelvic anatomy, especially in the
setting of abnormalities. As an example, a pelvic mass (pedunculated fibroid
or solid ovarian mass) may lie between the uterus and normal appearing
ovarian tissue. On a still image, the uterus, mass, and normal ovary may
appear contiguous. With movement of the probe, the specific origin of the
mass can usually be determined.
Visualization of pelvic structures with the transvaginal probe is limited
by the relative positions of the pelvic organs and the presence of any pelvic
masses. The resolution of high-frequency vaginal probes is good up to a depth
of 6 to 8 cm. TVUS can be performed concurrently with an abdominal
examination to better define normal and abnormal anatomy. As an example,

149
by applying pressure abdominally, the uterus with any associated fibroids,
and even the intestines, can be moved away from the ovaries, allowing better
visualization. Uterine measurements are most accurately obtained by TVUS.
The average transverse width of the endometrial cavity (ie, inside dimension
of the uterus) is 2.7 cm among nulliparas, 3.0 cm among primiparas, and 3.2
cm among multiparas.
The typical measurement of endometrial thickness includes both the
anterior and posterior endometrial walls. If fluid is present within the
endometrial cavity, the anterior and posterior endometrial echoes can be
measured independently and summed. Immediately after menses, the
endometrium is 1 to 4 mm thick; as the estrogen concentration rises, the
thickness increases to 7 to 10 mm. After ovulation, echogenicity increases
starting in the basal area; by the luteal phase, the entire endometrium is
hyperechogenic with a thickness of 8 to 16 mm. In postmenopausal women, a
thick endometrial lining (defined as >4 mm) can be a marker of endometrial
hyperplasia or malignancy.
Multiple 2 to 5 mm follicles may be seen in the ovaries. A leading follicle
of about 10 mm can be identified at the 9th or 10th cycle day; it grows rapidly
and is 20 to 24 mm in diameter just before ovulation. After ovulation, the
corpus luteum develops and may have a slightly heterogeneous consistency.
The wall typically appears to be thick with low-level internal echoes and
circumferential blood flow. The diameter of a normal follicle or corpus luteum
does not usually exceed 30 mm. A corpus luteum cyst appears as a
homogeneous hypoechogenic thin-walled structure.
Any abnormality noted should be described, as appropriate: size, shape,
location, echogenicity, echo pattern (cystic, solid, complex, septations), and a
differential diagnosis of the most likely causes of the abnormality should be
provided. Additional studies, such as Doppler velocimetry or saline infusion
sonohysterography, may be useful in defining suspected lesions, or three-

150
dimensional sonography, which may be helpful for evaluating the uterine
shape in those patients with infertility.
Doppler effect. The Doppler effect was originally postulated by the
Austrian scientist Christian Doppler in relation to the colors of double stars.
The effect is responsible for changes in the frequency of waves emitted by
moving objects as detected by a stationary observer: the perceived frequency
is higher if the object is moving towards the observer, and lower if it is moving
away. The difference in frequency (Δf) is called the Doppler frequency shift,
Doppler shift or Doppler frequency. The Doppler frequency increases with the
speed of the moving object. With Doppler sonography, one can evaluate
changes in waveform (sound, radar, light), determine the speed and direction
of the object (blood flow).
In medicine, Doppler effects are used mainly to analyze blood flow, to
calculate blood velocity, because the velocity of the ultrasound is known and
the angle of the vessels to the beam direction can be measured, allowing angle
correction. Doppler ultrasound images (Fig.100) can help the physician to see
and evaluate:
blockages to blood flow (such as clots)
narrowing of vessels
tumors and congenital vascular malformations (Fig.101)
character of blood flow to various organs (Fig. 102)
increased vasculature of genital organs, which is sometimes seen in
hyperplasia, tumors, in infections, etc.(Fig. 104)
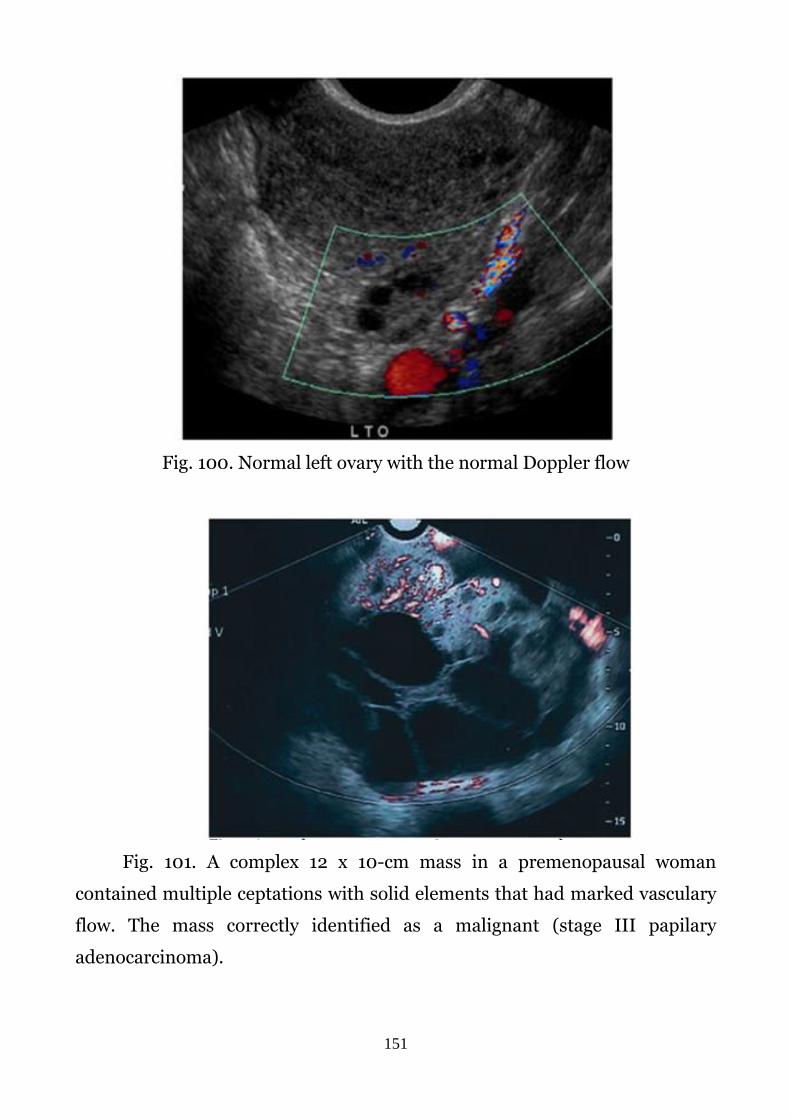
151
Fig. 100. Normal left ovary with the normal Doppler flow
Fig. 101. A complex 12 x 10-cm mass in a premenopausal woman
contained multiple ceptations with solid elements that had marked vasculary
flow. The mass correctly identified as a malignant (stage III papilary
adenocarcinoma).

152
Fig. 102. Color Doppler image of the ovarian flow in the luteal phase
of the menstrual cycle
Fig. 103.Myometrial vascularization. (A) - Greyscale ultrasound showing
secretory phase of endometrium (arrows) in a woman with heavy periods.
(B) Color Doppler in the same patient reveals increased myometrial
vascularity.
Sonohysterography allows for a more in-depth investigation of
the uterine cavity. It is a specialized procedure where sterile saline is installed
into the uterine cavity, and an ultrasound is performed at the same time. The
procedure helps to delineate intrauterine pathology such as polyps, fibroids
and uterine malformations.

153
Three-dimensional (3-D) ultrasound (3D US) is a fast-evolving imaging
technique that holds a great potential for use in gynecology. 3D US is more
sensitive and specific than two-dimensional ultrasound (2D US) in defining
and mapping uterine lesions, such as fibroids, adenomyosis, and intrauterine
synechia. In cases of suspected malignancy, 3D US is mainly used in the
initial evaluation of patients. 3D US permits evaluation of the uterus and
ovaries in planes that cannot be imaged directly.
These exams are typically performed to detect:
uterine anomalies (Fig.104)
uterine scars
endometrial polyps, fibroids(Fig.105)
cancer, especially in patients with abnormal uterine bleeding

154
3D/4D ultrasound allows visualization of dimensional surface
structures such as a baby’s face. The 4D simply shows a 3D image in motion.
Interventional ultrasound - is defined as any diagnostic or therapeutic
procedure performed under ultrasound guidance for any tissue or organ that
is visualized by ultrasound. Diagnostic procedures: ultrasound-guided
aspiration of fluid or cystic fluid for biochemical or cytological and culture
examinations as well as for cytological or tissue sampling with fine-needle.
(Fig.106, Fig.107, Fig. 108)
Fig.106.Interventional ultrasound
Fig. 107. Cyst aspiration under ultrasound guidance

155
Fig.108. Core biopsy under ultrasound guidance
Magnetic resonance imaging
Magnetic resonance imaging (MRI) is an imaging modality that has been
developed and used since the mid-1970s. It is a test that uses a magnetic field
and pulses of radio wave energy to make pictures of organs and structures
inside the body. The imaging components include a large static magnetic field
and an electromagnetic field produced by radio frequency (RF) waves.
Although once termed nuclear magnetic resonance imaging, MRI uses no
ionizing radiation. The nucleus being studied in this form of imaging is the
naturally occurring hydrogen nucleus, a proton, which is ubiquitous in the
body by virtue of its presence in water. MRI has several advantages over
computed tomography (CT) and ultrasonography. One important feature is
its noninvasiveness.
MRI also gives possibility to obtain a simultaneous display of a large
portion of the body without repositioning the patient. Transverse, sagittal,
coronal, not comparable views may be obtained in a short time. Compared
with MRI, ultrasonographic examination allows more tissue planes to be
observed in real time. But, the window of view is actually relatively small, and
a simultaneous display of a large portion of the body is not possible. This is
another advantage of MRI, widely used in clinical practice.

156
A third advantage of MRI is its excellent tissue-differentiating
capabilities. MRI acquisitions may further alter and differ contrast. These
signals are not influenced by the amount of bladder filling, the size of a
patient, or the amount of gas in the surrounding bowel, but these factors have
an important role in the quality of an ultrasonographic image. With MRI,
excellent tissue differentiation is possible without the use of contrast agents.
Besides, newly developed contrast agents may further augment tissue
contrast and are much safer than the iodinated equivalents used in CT. In
many cases, MRI gives different information about structures in the body
than can be seen with an ultrasound, X-ray, or computed tomography (CT)
scan. MRI shows problems that cannot be seen with other imaging method.
For an MRI test, the area of the body being studied is placed inside a
special machine that contains a strong magnet. Pictures from an MRI scan are
digital images that can be saved and stored on a computer for more study.
The images also can be reviewed remotely, such as in a clinic or an operating
room. Additionally, contrast material may be used during the MRI scan to
show certain structures more clearly. The use of MRI is rapidly expanding in
gynecological oncology, gynecologic surgery. Pelvic MRI has excellent soft
tissue contrast and multiplanar imaging ability to demonstrate either normal
or pathological processes.
MRI is extremely sensitive to blood flow. As with Doppler
ultrasonography, flow direction and speed may be determined. Both arterial
and venous abnormalities can be assessed by MRI. Additionally, biochemical
states of blood can be characterized by MRI because characteristic signals are
derived from oxyhemoglobin, deoxyhemoglobin, methemoglobin, and
hemosiderin in red blood cells in different stages of hematoma formation.
Together, these two capabilities for studying blood allow sensitive MRI
diagnosis of thrombotic diseases.

157
In gynecological oncology the rapidly evolving role of MRI includes not
only diagnosis but also disease staging, planning of therapy and monitoring
response to treatment.
Basic physics and principle of MRI. Certain atomic nuclei in molecules
possess nuclear angular momentum, or spin. These spinning charged
particles create a magnetic field or moment. Hydrogen nucleus, the proton, is
currently the only nucleus extensively used for MRI because of its relative
abundance in the human body. In the absence of an external magnetic field,
hydrogen nuclei are randomly oriented within a tissue. When a uniform
external magnetic field is applied to these nuclei, the nuclei tend to align in
the direction of the applied field because this is the lowest energy state. The
aligned nuclei will spin at a frequency that is determined by the strength of
the magnetic field being sensed by the nuclei—that is, the larger the external
magnetic field, the higher the frequency of spinning. The magnetic moments
of multiple similarly aligned nuclei produce a net magnetic moment that is
used to produce the MRI signal. After electromagnetic excitation, nuclei
absorb energy and a higher percentage of the nuclear population exists at a
higher energy state. By transferring this energy from the excited nuclei to
surrounding molecules, the nuclei return to a lower energy state, realigning
with the main magnetic field. The efficiency with which energy is transferred
depends on the molecular structure of the surrounding tissues (i.e.,
transferring of energy in fat would differ from transferring if energy in
muscle). The spinning of the proton induces a voltage which is then translated
into a signal that results in a magnetic resonance image. Computer, getting
information about different energy, builds the corresponding images of
different regions. It is the ability of the MRI to evaluate the variations in the
net magnetization of the nuclei in different tissues, allowing for excellent
tissue contrast, that is, a unique feature of MRI.
MRI scans are usually performed in the sagittal (longitudinal) and axial
(transverse) planes. Scanning in the sagittal plane is called a T1 image, and

158
scanning in the axial plane is a T2 image. MRI scanning may also be done in
coronal plane.
Indications
Indications for MRI of the pelvis organs in women include, but are not
limited to:
detection and staging of gynecologic malignancies, including those
originating in the vulva, cervix, uterus, ovaries, and fallopian tubes;
evaluation of pelvic pain or mass, including detection of adenomyosis,
ovarian cysts, torsion, tubo-ovarian abscess and benign solid masses,
obstructed fallopian tubes, endometriomas, and fibroids;
identification of a congenital anomaly of the female pelvic organs;
determination of number, location, and type (solid or hemorrhagic) of
fibroids prior to myomectomy, hysterectomy, or uterine artery
embolization;
assessment of pelvic floor defects associated with urinary or fecal
incontinence;
assessment for recurrence of tumors of the bowel, bladder, or
gynecological organs following a surgical resection or exenteration;
evaluation of complications following pelvic surgery, including abscess,
urinoma, lymphocele, radiation enteritis, and fistula formation;
determination of arterial and venous anatomy and patency;
identification and staging of soft tissue origin sarcomas;
identification of the source of lower abdominal pain in pregnant
women, including appendicitis and ovarian and uterine masses;
assessment of fetal and placental abnormalities;
injury or trauma in the pelvic area;
abnormal X-ray results;
unexplained difficulties urinating or defecating;
infertility;

159
irregular vaginal bleeding
Contraindications
Contraindications for pelvic MRI are:
any electrically, magnetically or mechanically activated implant (e.g.
cardiac pacemaker, insulin pomp biostimulator, neurostimulator,
cochlear implant…);
intracranial aneurism clips (unless made of titanium);
pregnancy (risk vs benefit ratio to be assessed);
ferromagnetic surgical clips or staples;
metallic foreign body inside;
metal shrapnel or bullet.
Patient preparation
A satisfactory written consent form must be taken from the patient
before entering the scanner room
Ask the patient to remove all metal object including keys, coins, wallet,
any cards with magnetic strip, jewellery, hearing aid and hairpins
Ask the patient to undress and change into a hospital gown
Contrast injection risk and benefits must be explained to the patient
before the scan
Gadolinium should only be given to the patient if glomerular filtration
rate (GFR) is>30
An intravenous line must be placed with extension tubing extending out
of magnetic bore
Claustrophobic patients may be accompanied into the scanner room e.g.
by staff member or relative with proper safety screening
Offer earplug or headphones possibly with music for extra comfort
Explain the procedure to the patient and answer questions
Note down the weight of the patient

160
Fasting for six hours prior to the examination diminishes bowel
peristalsis. At some institutions glucagon is given to decrease bowel motion. It
is also useful to empty the urinary bladder to eliminate deformation by an
enlarged bladder.
MRI machines are intended for certain areas of the body. They can be
closed or open type. Closed MRI’s have been around the longest and make
use of a capsule-like space to take high quality images.(Fig.109) Closed
machine are also known as 3 Tesla MRI. A MRI is measured in Tesla units,
which indicates the power of the electromagnet within the system. Some tests
may require a stronger signal to tell if there are issues occurring internally. A
closed MRI systems power varies from .35 to 1.5 Tesla, which offers a high
level of power.
Fig. 109. Closed MRI – Siemens MAGNETOM Trio 3.0T
As the name indicates an open MRI is an open system that doesn’t use
the tube like design. Instead of an enclosed capsule, the open MRI uses a
magnet top and bottom and is open on all four sides. An Open MRI offers .2
to .3 Tesla that scan between two large metal discs; it doesn’t enclose entire
body of the patient. Open machines are used to exclude an attack of
claustrophobia, while the patient lies in a tubular body with a width of 60 cm.
These decrease the risk of claustrophobia and panic attacks and allow patients
of all shapes and sizes to be able to make use of an MRI to accurately diagnose

161
their problems. In some cases, it is the only alternative for patients. However,
because of the shape of the open MRI, it is unable to take images of certain
areas of the body and the images it does take are of lesser quality as the
strength of the open machines is less than that of a closed or wide bore MRI.
For this reason, an open MRI is not always an option. Certain scans must be
taken with a closed machine. (Fig.110).
Fig. 110. Open MRI – Siemens MAGNETOM C 0.35T
Thus, choosing the right system depends on patients quality-of-care
preferences, as explained below, and medical indications:
closed MRI systems are more powerful, but they don’t address patient
comfort and claustrophobia concerns.
low field open MRI systems are less powerful, but they do address
patient comfort and claustrophobia concerns.
Technique. MRI examinations may be performed on outpatients or
inpatients. The examination is preferably carried out from 6 to 14 day cycle.
For an MRI test, the patient is placed in a horizontal position on a movable
table in a special chamber of the imager that integrates several magnetic coils
of the apparatus. Through the latest and scans the required area. Patient on a
movable table will enter into the magnet of the MRI unit and the radiologist

162
and technologist will perform the examination while working at a computer
outside of the room. Images will be obtained while patient contracting or
squeezing the pelvic muscles and while the pelvic muscles are relaxed. Patient
may also be asked to bear down or forcibly exhale while keeping your mouth
and nose closed. The entire exam is usually completed within 15 -30 minutes.
Pictures from an MRI scan are digital images that can be saved and stored on
a computer for more study. The images also can be reviewed remotely, such
as in a clinic or an operating room. In some cases, contrast material may be
used during the MRI scan to show certain structures more clearly. Some
patients are assigned an MRI of the pelvis with contrast. The study represents
the intravenous administration of a special extracellular low molecular weight
substances based on the chemical element gadolinium — OmniScan,
Magnevist. These drugs have strong paramagnetic properties, absorption and
emission of electromagnetic waves in the radio frequency range. They rarely
cause allergic reactions and do not lead to anaphylaxis, in contrast to the
iodine radiopaque drugs. After the introduction into the blood under the
influence of the electromagnetic field contrast solution that accumulates and
is distributed in the tissues of the area to which this field is directed, which
gives the opportunity to obtain much more information.
Complications
Complications of MRI scans are very rare. The most frequents risks are:
The strong, static magnetic field will attract magnetic objects (from
small items such as keys and cell phones, to large, heavy items such as
oxygen tanks and floor buffers) and may cause damage to the scanner or
injury to the patient or medical professionals. Careful screening of
people and objects entering the MR environment is critical to ensure
nothing enters the magnet area that may become a projectile.
The magnetic fields that change with time create loud knocking noises
which may harm hearing if adequate ear protection is not used. They

163
may also cause peripheral muscle or nerve stimulation that may feel like
a twitching sensation.
The radiofrequency energy used during the MRI scan could lead to
heating of the body. The potential for heating is greater during long
MRI examinations.
The use of gadolinium-based contrast agents (GBCAs) risk of allergic
reactions to the contrast agent.
Some patients may experience claustrophobia. Imaging in an open MRI
scanner may be an option for some patients, practitioner should be able
to prescribe medication to make the experience easier for patient.
To produce good quality images, patients must generally remain very
still throughout the entire MRI procedure. Infants, small children, and
other patients who are unable to lay still may need to be sedated or
anesthetized for the procedure. Sedation and anesthesia carry risks not
specific to the MRI procedure, such as slowed or difficult breathing, and
low blood pressure.
The MR environment presents unique safety hazards for patients with
implants, external devices and accessory medical devices. Examples of
implanted devices include artificial joints, stents, cochlear implants,
and pacemakers. An external device is a device that may touch the
patient like an external insulin pump, a leg brace, or a wound dressing.
An accessory device is a non-implanted medical device (such as a
ventilator, patient monitor) that is used to monitor or support the
patient. The strong, static magnetic field of the MRI scanner will pull on
magnetic materials and may cause unwanted movement of the medical
device; heating of devise may lead to burns, may cause electrically active
medical devices to malfunction and failure of the device function.
The presence of the medical device will degrade the quality of the MR
image, which may lead to an inaccurate clinical diagnosis, resulting in
inappropriate medical treatment.

164
Therefore patients with implanted medical devices should not receive
an MRI exam unless the implanted medical device has been positively
identified as MR Safe or MR Conditional. An MR Safe device is
nonmagnetic, contains no metal, does not conduct electricity and poses
no known hazards in all MR environments. An MR Conditional device
may be used safely only within an MR environment that matches its
conditions of safe use. Any device with an unknown MRI safety status
should be assumed to be MR Unsafe.
Thus, the majority of complications include: heating and/or burns
(thermal injuries), injuries from projectile events (objects being drawn toward
the MRI scanner), crushed and pinched fingers from the patient table, patient
falls, and hearing loss or a ringing in the ear (tinnitus). The correct technique
allows avoiding these complications
Interpretation of a pelvic - MRI results
Leiomyoma - a common gynecologic pathology. Leiomyomas tend to
be of low signal intensity regardless of the pulse sequence used. They are
usually surrounded by a smooth capsule of low signal intensity. When
compared with ultrasonography or hysterosalpingography, MRI is more
accurate in detecting the presence, size, number, and location of leiomyomas.
In patients with menorrhagia or infertility secondary to submucosal
leiomyomas, MRI may be useful in optimizing patient management. In
patients undergoing myomectomies to restore fertility, MRI before the
procedure may help in planning the extent of surgery (Fig. 111).

165
Fig. 111. A. Leiomyoma. The sagittal (T1) image of a woman with a pelvic
mass. On both clinical examination and US, distinction between an ovarian
and uterine mass could not be made. B. Axial image (T2) shows the
leiomyoma ( m) to have decreased signal intensity when compared with the
uterus ( u ).
Adenomyosis is a relatively common disease, occurring in about 15-25%
of women in the premenopausal period. This leads to progressive severe and
longer menstrual periods and is often associated with severe dysmenorrhea.
The diagnosis is usually done after a hysterectomy of pathological specimens.
MRI is used to evaluate this disease. When visualizing the uterus with
adenomyosis increases and has smooth external configurations. Diffuse
adenomyosis distorts the normal zonal anatomy of the uterus, causing
enlargement of the junctional zone. Old hemorrhagic regions a few
millimeters in diameter are often considered as high-intensity spots both on
T1 and T2-weighted images. Unlike leiomyomas that have well-defined edges,
adenomyosis has irregular and fuzzy edges due to its more invasive nature.
Since adenomyosis is often treated with a hysterectomy, but myomectomy

166
may be sufficient for some leiomyomas, such visualization can be a very
useful clinical tool for preoperative evaluation and surgical planning.(Fig. 112,
Fig 113).
Fig.112. Sagittal MRI of the uterus of the patient with focal uterine
adenomyosis showing focal thickening of the junctional zone along the
posterior wall (arrow), heterogeneity of the myometrium and small cervical
cysts.
Fig. 113. A. Adenomyosis. Sagittal T2-weighted image of adenomyosis (a)
seen as an irregular, hypointense, enlarged junctional zone with indistinct
margins infiltrating into the myometrium (arrowheads ). B. Transverse
T2-weighted image of the same patient showing adenomyosis (a).

167
Endometrium. MRI is particularly useful for assessing the
endometrium, which can easily be identified and distinguished from the
myometrium. The endometrial tissue is approximately isointense with
myometrium onT1-weighted images but appears higher in signal intensity
relative to myometrium on T2-weighted images. The thickness of the
endometrium in a normal menstruating female varies depending on the phase
of the menstrual cycle, being thinner in the follicular phase and thicker in the
secretory phase. Among patients who use oral contraceptives, the endometrial
width is significantly smaller in both the follicular and secretory phases.
Additionally, the junctional zone is also smaller in both phases of the
menstrual cycle. Myometrial thickness tends to remain the same regardless of
the phase of the menstrual cycle and the use of oral contraceptives. Such
differentiation allows better assessment of the endometrium and may be
particularly useful when Asherman's syndrome is suspected. The normal
endometrial width varies between individuals, ranging from 1 to 8 mm,
whereas the myometrial width varies from 1.5 to 2.5 cm. During the normal
follicular phase, endometrial width can grow from 1 to 3 mm. MRI is able to
define depth of myometrial invasion, tumor site, and cervical involvement in
patients with endometrial cancer. Invasion of the myometrium is
demonstrated by distortion of the junctional zone (Fig. 114). In patients with
deep myometrial invasion, this low-intensity band is absent. MRI allows
preoperative evaluation of the degree of invasion before a postoperative
pathology assessment. Although MRI cannot diagnose endometrial cancer in
situ (confined to endometrium), it is 92% accurate in the overall staging of
endometrial carcinoma.

168
Fig.114. A. Endometrial carcinoma. Slightly T2-weighted sagittal image in a
patient with endometrial carcinoma (e). Normal zonal anatomy has been
disrupted. The central region of high signal intensity represents endometrial
carcinoma that has invaded through the junctional zone and extends deeply
into the myometrium. Only a small rim of normal myometrium remains
(arrow). B. A more T2-weighted image than in A, showing similar findings.
Ovary. Several types of ovarian lesions are particularly well evaluated
by MRI; these include hemorrhagic cysts, endometrial cysts, benign
teratomas, and simple follicular cysts. (Fig.114). MRI can readily identify
hemorrhage because of relaxation differences (difference of transferring of
energy) between methemoglobin, fresh hemoglobin, and hemosiderin.
However, depending on the biochemical state and age of the blood, the signal
may be bright or dark on either T1- or T2-weighted images. Endometrial cysts
tend to have more adhesions on the external surface and may lack a distinct
margin from the uterine body.They may also demonstrate multiple
loculations within the cyst. These loculations tend to have high-intensity
signals on T1- and T2-weighted images, in contrast to water, which has high
signal intensity on T2- and low signal intensity on T1-weighted images. In the
fibrous tissue surrounding the cyst, a low-intensity area is occasionally
identified surrounding areas of acute and chronic bleeding and is thought to

169
represent the presence of hemosiderin-laden macrophages at the hematoma
margin. One other feature that is characteristic of endometrial cysts is
shading within loculi. It is thought to be due to the presence of
deoxyhemoglobin in unlysed red blood cells or a higher concentration of
paramagnetic (signal-enhancing) methemoglobin within those regions. The
presence of any or all of these features should strongly suggest an endometrial
cyst (Fig. 116). Because of the large fat content within these tumors, ovarian
cystic teratomas produce signal intensities very similar to that of adjacent fat
on both T1- and T2-weighted images (Fig. 117).
F
Fig.115.A. Hemorrhagic cyst. Longitudinal view of the pelvis on US showing a
large fluid-filled mass in the pelvis. B. Sagittal T1-weighted image showing a
mass with high signal intensity superior to the bladder (c). C. T2-weighted
sagittal image showing the cyst to have persistently high signal intensity.
Findings are consistent with a hemorrhagic cyst subsequently confirmed at
surgery.

170
Fig. 116. Endometrioma. Transverse T1-weighted image showing a left
adnexal mass with areas of both increased and decreased signal
(arrow). B. T2-weighted image showing change in signal intensities within
the cyst consistent with different stages of blood. Findings are consistent with
the final diagnosis of an endometrioma.
Fig. 117. A. Dermoid. T1-weighted transverse image showing a left adnexal
cyst of high signal intensity (arrow). B. With increased T2 weighting, the cyst
shows persistently high signal intensity. Findings are consistent with the
diagnosis of a dermoid.
Solid ovarian benign and malignant tumors tend to have variable T1 and
T2 values and tend to have lower signal intensities overall. Improving the
image with gadolinium gives higher accuracy. The size of the lesion, the
presence of solid components and septations, the presence of a thickened cyst
wall and extravariant interference are determined.(Fig.118).

171
Fig.118. A. Simple ovarian cyst. T1-weighted image showing a right adnexal
soft-tissue density of low signal intensity (arrow). B. With increased T2
weighting, the abnormality shows high signal intensity. The thin wall and the
appearance on both T1- and T2-weighted images are consistent with the final
diagnosis of a simple ovarian cyst.
Fallopian tubes. A fallopian tube MRI scan is done to check for certain
cancers or other illness. Primary fallopian tube carcinoma (PFTC) is an
extremely rare malignancy that arises from the fallopian tube. Typical
symptoms, together with the presence of some of the most characteristic MRI
signs, such as a “sausage-shaped” pelvic mass, hydrosalpinx, and hydrometra,
may signal the presence of primary fallopian cancer, and allow the radiologist
to report it as a differential diagnosis.(Fig.119).
Fig.119. Serous PFTC in a 63-year-old female, presenting with pelvic pain. c -
Coronal MRI, with the “sausage”-shaped mass (asterisk) folded upon itself, as
depicted by the portions of wall visible inside the mass (red arrow), which
approximates the “spoke-wheel” sign, usually better depicted when the mass
is predominantly cystic. Once again, the “synechiae” sign can be observed
(red arrowhead).
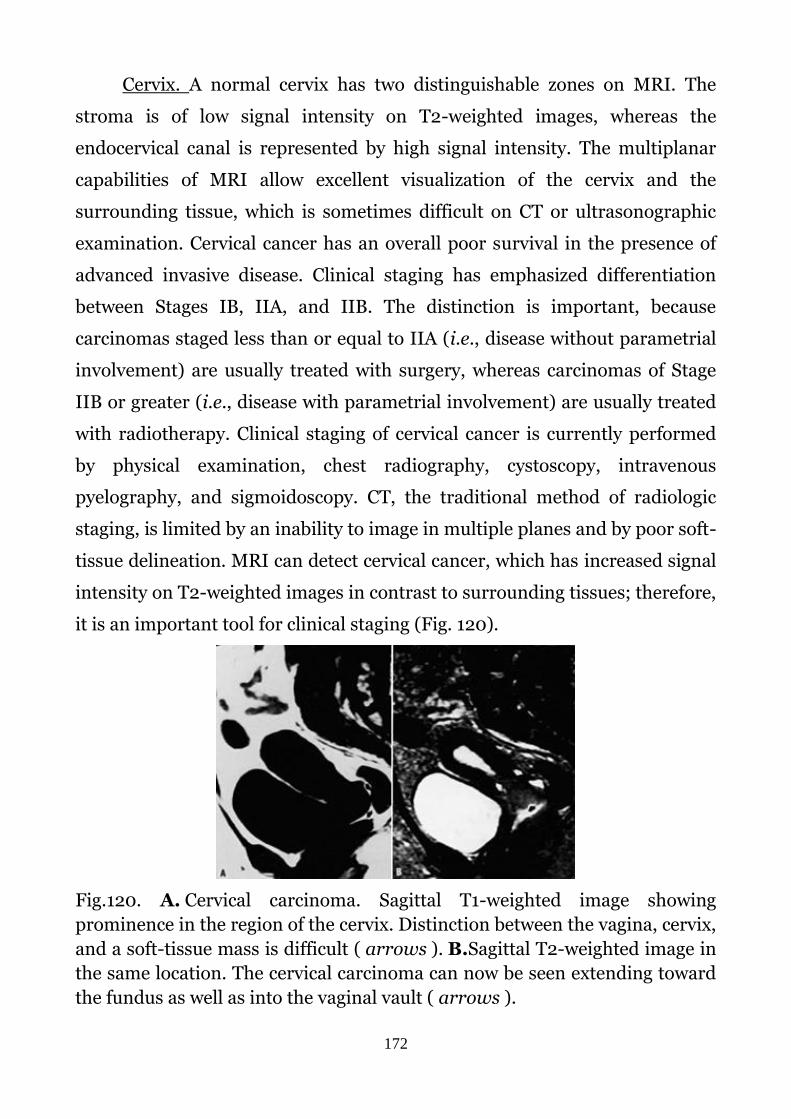
172
Cervix. A normal cervix has two distinguishable zones on MRI. The
stroma is of low signal intensity on T2-weighted images, whereas the
endocervical canal is represented by high signal intensity. The multiplanar
capabilities of MRI allow excellent visualization of the cervix and the
surrounding tissue, which is sometimes difficult on CT or ultrasonographic
examination. Cervical cancer has an overall poor survival in the presence of
advanced invasive disease. Clinical staging has emphasized differentiation
between Stages IB, IIA, and IIB. The distinction is important, because
carcinomas staged less than or equal to IIA (i.e., disease without parametrial
involvement) are usually treated with surgery, whereas carcinomas of Stage
IIB or greater (i.e., disease with parametrial involvement) are usually treated
with radiotherapy. Clinical staging of cervical cancer is currently performed
by physical examination, chest radiography, cystoscopy, intravenous
pyelography, and sigmoidoscopy. CT, the traditional method of radiologic
staging, is limited by an inability to image in multiple planes and by poor soft-
tissue delineation. MRI can detect cervical cancer, which has increased signal
intensity on T2-weighted images in contrast to surrounding tissues; therefore,
it is an important tool for clinical staging (Fig. 120).
Fig.120. A. Cervical carcinoma. Sagittal T1-weighted image showing
prominence in the region of the cervix. Distinction between the vagina, cervix,
and a soft-tissue mass is difficult ( arrows ). B.Sagittal T2-weighted image in
the same location. The cervical carcinoma can now be seen extending toward
the fundus as well as into the vaginal vault ( arrows ).

173
Breast. For a breast MRI, the woman usually lies face down, with her
breasts positioned through openings in the table. In order to check breast
positioning, the technologist watches the MRI through a window while
monitoring for any potential movement.
A breast MRI usually requires the use of contrast that is injected into a vein in
the arm before or during the procedure. For premenopausal women, the best
timing for breast MRI is day 7-15 of the menstrual cycle. There is no
recommended timing for breast MRI for women after menopause. The dye
may help create clearer images that outline abnormalities more easily.
(Fig.121).
Fig.121. Breast MRI
MRI can locate some small breast lesions sometimes missed by
mammography. It can also help detect breast cancer in women with breast
implants and in younger women who tend to have dense breast tissue.
Mammography may not be as effective in these cases. Since MRIs do not use
radiation, they may be used to screen women younger than 40 and to increase
the number of screenings per year for women at high risk for breast cancer.
Some common uses for breast MRI include:
Further evaluation of abnormalities detected by mammography

174
Finding early breast cancers not detected by other tests, especially in
women at high risk and women with dense breast tissue
Examination for cancer in women who have implants or scar tissue that
might produce an inaccurate result from a mammogram. This test can
also be helpful for women with lumpectomy scars to check for any
changes.
Detecting small abnormalities not seen with mammography or
ultrasound (for example, MRI has been useful for women who have
breast cancer cells present in an underarm lymph node, but do not have
a lump that can be felt or can be viewed on diagnostic studies)
Assess for leakage from a silicone gel implant
Evaluate the size and precise location of breast cancer lesions, including
the possibility that more than one area of the breast may be involved
(this is helpful for cancers that spread and involve more than one area)
Determining whether lumpectomy or mastectomy would be more
effective
Detecting changes in the other breast that has not been newly diagnosed
with breast cancer (There is an approximately 10 percent chance that
women with breast cancer will develop cancer in the opposite breast. A
recent study indicates that breast MRI can detect cancer in the opposite
breast that may be missed at the time of the first breast cancer
diagnosis.)
Detection of the spread of breast cancer into the chest wall, which may
change treatment options
One should describe morphology of a mass: round, oval lobulated or
irregular shape of a mass in a breast tissue. Margins can be described as
smooth, irregular, or speculated. Spiculated margins are frequently a
feature of malignant breast lesions and radial scars. If a mass has
spiculated margins, it has an 80% chance of being malignant. The pre-
contrast T1 sequence can show the presence of fat in a lesion. Breast

175
lesions containing fat are benign unless they are rapidly growing. Rapidly
growing lesions should be biopsied.(Fig.122, Fig.123). Very small and deep
lesions, found on breast MRI, also require an MRI guided biopsy.
Fig.122. Fibroadenoma (left) and a colloid carcinoma (right
Fig. 123. The image on the far left shows an irregularly shaped mass
with irregular margins, this was an invasive ductal carcinoma. The image
on the right shows a similarly irregularly shaped and irregularly
emarginated lesion, this time an adenoid cystic carcinoma.
Mammography
A mammogram is an x-ray picture of the breast. An x-ray (radiograph) is a
noninvasive medical test that helps physicians diagnose and treat medical
conditions. Imaging with x-rays involves exposing a part of the body to a
small dose of ionizing radiation to produce pictures of the inside of the body.

176
X-rays are the oldest and most frequently used form of medical imaging.
(Fig.124)
Fig.124. Mammography
Mammography is specialized medical imaging that uses a low-dose x-
ray system to see inside the breasts. A mammography exam, called a
mammogram, aids in the early detection and diagnosis of breast diseases in
women.
There are 3 recent advances in mammography, widely used in current
clinical practice, they are:
digital mammography,
computer-aided detection
breast tomosynthesis.
Digital mammography, also called full-field digital mammography
(FFDM), is a mammography system in which the x-ray film is replaced by
electronics that convert x-rays into mammographic pictures of the breast.
These systems are similar to those found in digital cameras and their
efficiency enables better pictures with a lower radiation dose. These images of
the breast are transferred to a computer for review by the radiologist and for
long term storage. stores the image directly on film. (Fig.125). Digital
mammography is an electronic image stored as a computer file. The digital

177
image can be enhanced, magnified and or manipulated for further evaluation
much more easily than the film counterpart.
Computer-aided detection (CAD) systems search digitized
mammographic images for abnormal areas of density, mass,
or calcification that may indicate the presence of cancer. The CAD system
highlights these areas on the images, alerting the radiologist to carefully
assess this area.
Breast tomosynthesis, also called three-dimensional (3-D)
mammography and digital breast tomosynthesis (DBT), is an advanced form
of breast imaging where multiple images of the breast from different angles
are captured and reconstructed ("synthesized") into a three-dimensional
image set. In this way, 3-D breast imaging is similar to computed tomography
(CT) imaging in which a series of thin "slices" are assembled together to
create a 3-D reconstruction of the body. Although the radiation dose for some
breast tomosynthesis systems is slightly higher than the dosage used in
standard mammography, it remains within the safe levels for radiation from
mammograms.
A mammogram allows the doctor to have a closer look for changes in
breast tissue that cannot be felt during a breast exam. Women ages 50 to 74
years should get a mammogram every 2 years. Women younger than age 50
should talk to a doctor about when to start and how often to have a
mammogram.
Different types of mammograms are distinguished:
Screening mammograms are done for women who have no
symptoms of breast cancer. Usually it includes two x-rays of each
breast. Screening mammograms can detect lumps or tumors that are
not felt in palpation. They can also find microcalcification or tiny
calcium deposits in the chest, which sometimes means that breast
cancer is present. Current recommendations in most countries

178
recommend screening mammography for women starting at age 40.
Regular mammograms (once a year or once every two years) lead to
early detection of breast cancer, when they are the most curable and
contribute to breast preservation.
Diagnostic mammography is used to evaluate a patient with
abnormal clinical findings—such as a breast lump or nipple discharge—
that have been found by the woman or practitioner. Diagnostic
mammography may also be done after an abnormal screening
mammogram in order to evaluate the area of concern on the screening
exam. This type of mammogram also can be used to find out more
about breast changes found on a screening mammogram, or to view
breast tissue that is hard to see on a screening mammogram. A
diagnostic mammogram takes longer than a screening mammogram
because it involves more x-rays in order to obtain views of the breast
from several angles. The technician can magnify a problem area to make
a more detailed picture, which helps the doctor make a correct
diagnosis. (Fig.126, 127,128. 129)
A. B.
Fig. 125. A – Digital mammogram. B – Conventional mammograpgy (film)

179
Fig. 126. Normal mammogram.
Fig.127. Fibroadenoma
Fig.128.Bilateral cysts associated to duct ectasia, no prior history of
breast disorders

180
Fig.129. Breast cancer
It is proved that screening with breast mammography results in improved
breast cancer detection rates. Finding breast cancer as early as possible before
it has grown or spread greatly improves a woman’s chance for a successful
treatment.
Invasive methods of examination
Sounding of the uterus
Sounding of the uterus (uterine probing). It is employed to measure the
length and determine the shape of the uterine cavity, relief of the walls and
the length and patency of the cervical canal. A metallic uterine sound is used
for this purpose. (Fig. 130). Uterine sounding is contraindicated in patients
with purulent vaginal discharge (grade III and IV colonization), signs of acute
or subacute uterine and adnexal inflammation, and pregnancy. After exposing
the cervix it is cleaned with an antiseptic. A uterine sound is passed through
the cervix to check the direction and length of the uterus.

181
(A) B. C.
Fig. 130. Utyerine probing: A - Uterine probe; B - Uterine probing; C –
Measuring of the uterine depth
Culdocentesis
Culdocentesis is the transvaginal puncture of posterior vaginal fornix and
aspiration of peritoneal fluid from the Douglas pouch (aka as cul-de-suc).
Indications:
suspected interrupted ectopic pregnancy or other causes producing
haemoperitoneum,
suspected pelvic abscess.
Technique. The procedure is done under sedation. The patient is put in
lithotomy position. Vagina is purified by betadine or another drug to comply
with asepsis rules. Using the vaginal speculum, the posterior vaginal fornix is
exposed. A needle (18 gauge), equipped with a syringe, is inserted at a point 1
cm below the cervicovaginal junction in the posterior fornix. After inserting
the needle to a depth of about 2 cm, the content of a Douglas pouch is sucked
(Fig. 131). If unclotted blood is obtained, the diagnosis of intraperitoneal
bleeding is established. If purulent content is obtained, the diagnosis of pelvic
inflammatory diseases is established. In case of rupture of a follicular cyst, the

182
follicular fluid would be obtained. The diagnosis is confirmed with the help of
microscopic and biochemical exam of obtained fluid.
Fig. 131. Culdocentesis: check for abnormal fluid in the abdominal cavity
behind the uterus corpus.
Histological investigations
Cervical biopsy
Cervical biopsy: A cervical biopsy is the removal of tissue from the
cervix, the lower third of the uterus to be analyzed for cellular abnormalities,
precancerous conditions, or cervical cancer. In a biopsy, the healthcare
provider removes a small amount of tissue for examination under a
microscope to look for precancerous cells or cancer cells. Most women have
the biopsy outpatient office, and no anesthesia is needed. A cervical biopsy is
performed to evaluate abnormal cervical tissue found during a Pap test or
colposcopy.
Colposcopic biopsy: A biopsy can be done during a colposcopyWhen an
extended colposcopy is performed after applying 3% acetic acid solution or
2% Lugol solution, the health care provider removes a tiny part of the

183
acetochite or dark brown tissue from the cervical surface at the border
between the normal and colored (abnormal) part with special tweezers. The
deleted site is then subjected to a histological examination.
Types of cervical biopsy:
Punch biopsy: A surgical procedure to remove a small piece of tissue
from the cervix. One or more punch biopsies may be performed on
different areas of the cervix. This procedure uses a circular blade, like a
paper hole puncher, to remove a tissue sample. One or more punch
biopsies may be done on different areas of the cervix.(Fig. 132).
Cone biopsy or Conization: A surgical procedure that uses a laser or
scalpel to remove a large cone-shaped piece of tissue from the
cervix. This procedure uses a laser or scalpel to remove a large cone-
shaped piece of tissue from the cervix.(Fig. 132). A loop electrosurgical
excision procedure (LEEP) is advanced modification of a knife (cone)
biopsy, it uses an electrical current passed through a thin wire hook.
The hook removes tissue for examination in the laboratory. A LEEP may
also be used to remove a precancer or an early-stage cancer.(Fig. 133)
Endocervical curettage (ECC). This procedure uses a narrow
instrument called a curette to scrape the lining of the endocervical
canal. This is an area that can’t be seen from the outside of the cervix.
During the procedure the mucous membrane of the cervical canal is
scraped using a spoon-shaped instrument (a curette). The procedure
may be done both in out-patient office and in-patient department. May
be done without anesthesia. Can be done without anesthesia. After the
procedure, there may be some cramping and bleeding. A scrap of the
cervical mucosa is subjected to a histological examination to determine
the presence of abnormal cells.

184
Fig. 132. Types of cervical biopsies.
Fig. 133. A loop electrosurgical excision procedure (LEEP)

185
Endometrial biopsy
The endometrial biopsy is a medical procedure that involves taking a
tissue sample of the lining of the uterus. The tissue subsequently undergoes
histologic evaluation which aids the physician in forming a diagnosis
Indications for endometrial biopsy include:
abnormal uterine bleeding: postmenopausal bleeding,
malignancy/hyperplasia, ovulation/anovulation;
evaluation of patient with one year of presumed menopausal
amenorrhea;.
assessment of enlarged uterus (both US and HCG do not detect
pregnancy);
evaluation of infertility;
abnormal Pap smear with atypical cells;
Follow-up of previously diagnosed endometrial hyperplasia
cancer screening (e.g., hereditary nonpolyposis colorectal cancer)
inappropriately thick endometrial stripe found on US;
detection of precancerous hyperplasia and atypia;
etc…
Contraindications for endometrial biopsy include:
pregnancy;
acute pelvic inflammatory disease;
clotting disorders (coagulopathy);
acute cervical or vaginal infections;
cervical cancer;
conditions possibly prohibiting endometrial biopsy;
morbid obesity;
severe pelvic relaxation with uterine prolapse;
severe cervical stenosis.

186
Endometrial biopsy is a blind procedure and should be considered part
of the evaluation that could include imaging studies, such as hysteroscopy or
transvaginal ultrasonography.
Types of endometrial biopsy:
diagnostic dilatation and curettage (D&C) of the cervical and uterine
mucosal membranes,
suction biopsy of endometrium (non-invasive diagnostic procedure)
Diagnostic dilatation and curettage (D&C) of the cervical and uterine
mucosa membranes (separate D&C of the cervical and uterine mucosa). This
is necessary to diagnose ovulation in case of sterility or to determine the type
of endometrium in dysfunctional bleeding.
Technique.
1. The patient is placed in the lithotomy position and bimanual
examination is performed (with nonsterile gloves) to determine the
uterine size and position, and whether marked uterocervical angulation
exists. Then the speculum should be inserted in to the vagina . Once the
cervix is centered in the speculum, the cervix can be anesthetized by
spraying 20 percent benzocaine spray for 5 seconds and then cleansing
it with povidone-iodine solution.
2. The tenaculum is placed on the anterior lip of the cervix, grabbing
enough tissue that the cervix will not lacerate when traction is applied.
The cervix is gently probed with the uterine sound.
3. If the uterine sound will not pass through the internal os, consider
placement of small Pratt uterine dilators. The smallest size is inserted,
followed by insertion of successively larger dilators until the sound
passes easily to the fundus. The distance from the fundus to the external
cervical os can be measured by the gradations on the uterine sound and
generally will be 6 to 8 cm. (Fig. 134)
4. The biopsy curette will be inserted into the uterine fundus and with a
scraping and rotating motion some tissue will be removed. The removed

187
tissue will be placed in formalin or equivalent for preservation. The
tissue will be sent to a laboratory, where it will be processed and tested.
It will then be read microscopically by a pathologist who will provide a
histologic diagnosis.
5. The uterine cavity should be treated with an antiseptic solution for the
prevention of inflammation. If necessary, the contractile agent should
be used to minimize bleeding.
Fig. 134. Dilatation and curettage of the cervical and uterus mucosa
membrane
Suction biopsy of endometrium is an office procedure that serves as a
helpful tool in diagnosing various uterine abnormalities. The technique is
fairly easy to learn and may be performed without assistance. The biopsy is
obtained through the use of an endometrial suction catheter that is inserted
through the cervix into the uterine cavity. Twirling the catheter while moving
it in and out of the uterine cavity enhances uptake of uterine tissue, which is
aspirated into the catheter and removed. Postoperative infection is rare but
may be further prevented through the use of prophylactic antibiotic therapy.
Intraoperative and postoperative cramping are frequent side effects.
Endometrial biopsy is a safe and accepted method for the evaluation of
abnormal or postmenopausal bleeding. The procedure is often performed to
exclude the presence of endometrial cancer or its precursors (Tables 1 and 2).

188
Office endometrial suction catheters are easy to use, and several have been
reported to have diagnostic accuracy that is equal or superior to the dilatation
and curettage (D&C) procedure. Suction is generated by withdrawing an
internal piston from within the catheter, and the tissue sample is obtained by
twirling the catheter while moving it up and down within the uterine cavity.
Technique.
1. The patient is placed in the lithotomy position and bimanual
examination is performed (with nonsterile gloves) to determine the uterine
size and position, and whether marked uterocervical angulation exists. Then
the speculum should be inserted in to the vagina . Once the cervix is centered
in the speculum, the cervix can be anesthetized by spraying 20 percent
benzocaine spray for 5 seconds and then cleansing it with povidone-iodine
solution.
2. The tenaculum is placed on the anterior lip of the cervix, grabbing
enough tissue that the cervix will not lacerate when traction is applied.The
cervix is gently probed with the uterine sound.
3. The endometrial biopsy catheter tip is inserted into the cervix,
avoiding contamination from the nearby tissues. The catheter tip is then
inserted into the uterine fundus or until resistance is felt. Once the catheter is
in the uterine cavity, the internal piston on the catheter is fully withdrawn,
creating suction at the catheter tip. The catheter tip is moved with an in-and-
out motion, but the tip does not exit the endometrial cavity through the
cervix, which maintains the vacuum effect. Use a 360-degree twisting motion
to move the catheter between the uterine fundus and the internal cervical os
(Fig. 134). Make at least four up and down excursions to ensure that adequate
tissue is in the catheter.
5. Once the catheter fills with tissue, it is withdrawn, and the sample
is placed in the formalin container. To remove the sample from the
endometrial catheter, the piston can be gently reinserted, forcing the tissue
out of the catheter tip. Some physicians prefer to make a second pass into the
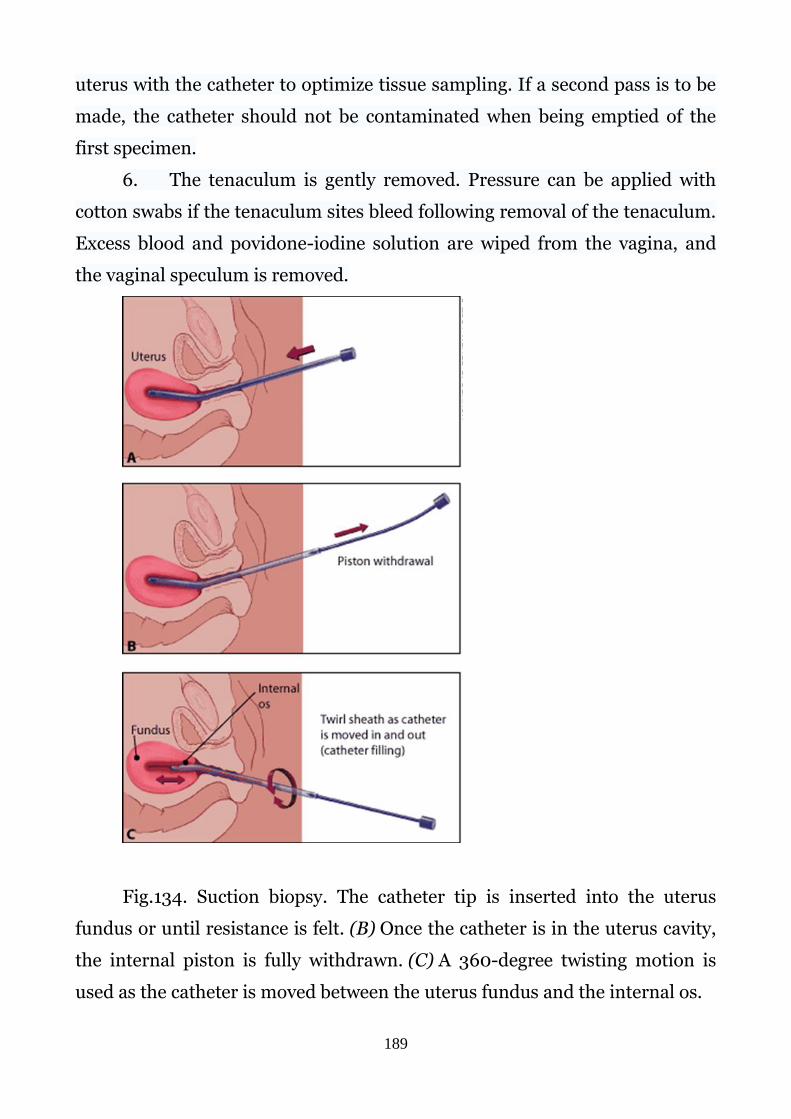
189
uterus with the catheter to optimize tissue sampling. If a second pass is to be
made, the catheter should not be contaminated when being emptied of the
first specimen.
6. The tenaculum is gently removed. Pressure can be applied with
cotton swabs if the tenaculum sites bleed following removal of the tenaculum.
Excess blood and povidone-iodine solution are wiped from the vagina, and
the vaginal speculum is removed.
Fig.134. Suction biopsy. The catheter tip is inserted into the uterus
fundus or until resistance is felt. (B) Once the catheter is in the uterus cavity,
the internal piston is fully withdrawn. (C) A 360-degree twisting motion is
used as the catheter is moved between the uterus fundus and the internal os.

190
Pipelle biopsy. It is an advanced type of aspiration biopsy of
endometrium.
In the course of this procedure, a flexible small tube is introduced, the
diameter of which is about 3 mm. The inner part of the tube is equipped with
a piston as on a syringe. When the tube is inserted into the uterine cavity a
small number of endometrial cells is taken. According to the patients' reviews
such manipulation does not cause painful sensations. Features of the
procedure When a pin is inserted into the uterus, the doctor pulls the piston
in the tubule by half. This creates a negative pressure with simultaneous
absorption of endometrial tissue. The procedure lasts only 30 seconds, which
makes it easier to conduct.(Fig. 135). Also, the patient cannot be afraid of
infections, because the pipe is a one-time tool. If suspicions of carcinoma
occur, the analysis can be carried out at any time. In other cases, precision is
needed for what the pipette of the endometrial biopsy shows:
with bleeding: an analysis on the first day of the onset of bleeding;
with global bleeding: analysis for 5-10 days themselves monthly;
infertility: analysis at the beginning of the menstrual period or the day
before the onset;
no pregnancy in the absence of menstruation: biopsy once a week;
establishing the exact day of the cycle itself: between 18 and 24 in the
afternoon.

191
Fig.135. Pipelle biopsy
Other diagnostic procedures.
Hydrotubation.
To assess the patency and functional capacity of the uterine tubes
(oviducts, fallopian tubes) air (perturbation) or fluid (hydrotubation) may be
administered into the tubes.
To perform perturbation or hydrotubation special devices are imployed,
which consists of a tip connected through a system of tubes with an air
balloon (or a device for fluid administration) and a pressure gauge.
Both procedures are performed under aseptic and antiseptic conditions.
Both show permeability of tubes and may be used for diagnosis of
infertility (evaluation of tubal factor).

192
Self test
1. Which of the following is not a special gynecological
examination?
A. speculum examination
B. vaginal examination
C. rectal or rectovaginal examination
D. palpation of lower abdomen
2. Which examination is the best to reveal the cause of infection?
A. microscopic examination of vaginal smears
B. bacteriological examination of smears
C. examination of the clinical signs of infection
D. patient complaints
3. Cusco’s specula are
A. bivalved specula
B. spoon-shaped specula
C. tubular specula
D. univalve specula
4. Cytological examination is used for
A. early detection of uterine and oviduct cancer
B. determination of causative agents of inflammation in female
genitalia
C. determination of organic disorders of female genital organs
D. determination of congenital abnormalities of female genitalia
5. Diagnostic dilatation and curettage of the cervical and uterine
mucous membranes should be used to diagnose
A. the histological abnormalities of the mucosa
B. the placement of the uterus in abdominal cavity
C. congenital abnormalities of internal genital organs
D. the pregnancy

193
6. The basal body temperature is measured
A. in the morning before getting up
B. in the evening before sleeping
C. in the daytime before eating
D. three times a day before eating
7. The Schiller’s test is negative if
A. the entire cervix and vagina take up the stain
B. the certain areas or islands remain unstained
C. the entire cervix and vagina remain unstained
D. the uterine mucosa remain unstained
8. The positive Schiller’s test means
A. the abnormal areas may be the seat of carcinoma-in-situ or
dysplasia
B. the abnormal areas have the inflammation
C. the abnormal areas have scars
D. the abnormal area is congenitally malformed
9. Histologic examination involve all enumerated below, except of
A. uterine probing
B. diagnostic dilation and curettage of the uterus cavity
C. suction biopsy
D. cone biopsy
10. Type III of vaginal cytology means
A. pronounced estrogen deficiency
B. moderate estrogen deficiency
C. sufficient estrogen saturation
D. absence of estrogenic hormones
D. absence of estrogenic hormones

194
Chapter 3. CONGENITAL ANOMALIES AND
DISPLACEMENTS OF THE FEMALE GENITALIA
Congenital anomalies of female genital organs
Congenital anomalies of female genital organs occur in 1,0–2,7 % of
gynecologic patients. They associate with various disturbances of
reproductive system (disturbances of menstrual function, sterility,
spontaneous abortions, premature delivery). More frequently they may be
due to failure of fusion of Mullerian ducts. The Müllerian ducts are the
primordial anlage of the female reproductive tract. They differentiate to form
the fallopian tubes, uterus, the uterine cervix, and the superior aspect of the
vagina. A wide variety of malformations can occur when this system is
disrupted. The most important kinds of such anomalies are: atresia, aplasia
and hypoplasia of organs. Most Müllerian duct anomalies (MDAs) are
associated with functioning ovaries and age-appropriate external genitalia.
These abnormalities are often recognized after the onset of puberty. In the
prepubertal period, normal external genitalia and age-appropriate
developmental milestones often mask abnormalities of the internal
reproductive organs. After the onset of puberty, young women often present
to the gynecologist with menstrual disorders. Late presentations include
infertility and obstetric complications.
Atresia of the Hymen
It is the most common form of genital atresia. Imperforate hymen may
be diagnosed with prenatal ultrasound documentation of bladder outlet
obstruction due to hydrocolpos or mucocolpos. However, in spite of the
recommendations for inspection of the external genitalia during the neonatal
and early childhood period, variations in hymenal anatomy commonly escape
diagnosis until the time of menarche. An imperforated hymen usually escapes

195
attention until puberty, when menstruation fails to appear, or is absent, and
the patient has periodic attacks of lower abdominal pain. With recurrent
menstrual cycles the blood collects in the vagina behind the hymenal
membrane and forms a hematocolpos. (Fig. 136) In a few progressive cases,
besides the hematocolpos the uterus (hematometra) or even the tubes
(hematosalpinx) may be involved.
A. B.
Fig. 136. A - imperforated hymen. B – Haematocolpos
Symptoms and diagnosis in infancy and childchood. Bulging, yellow-
gray mass at or beyond the introitus, the presence of an abdominal mass in
association with urinary obstruction may be find in carefull examinationof a
child. Before puberty careful examination with pressure applied to the
fourchette may reveal microperforations, sometimes with an anteriorly
displaced opening just beneath the urethra. Sometimes, a cribriform
(fenestrated), septate, or navicular configuration may take place in patient,
and this can be associated with retention of vaginal secretions (up ti
hematocolpos) and development of a mixed bacterial vulvovaginitis.
Symptoms and diagnosis in adolescence. Usually, shortly after the
breasts and pubic hair begin to grow, the first period occurs (menarche). In
patients with imperforated hymen with the onset of menarche (which may be

196
suspected due to breast development and appearance of other signs of
puberty) menstruations are absent. Failure to menstruate beyond 6 months
from the telarche and pubacrhe, is statistically uncommon, and should be
investigated to determine a cause. Imperforate hymen is one uncommon, but
important, anatomic cause of primary amenorrhea. Thus the typical
presenting complaint is primary amenorrhea. If the unperforated hymen has
not been diagnosed before, after a few months of amenorrhea, there are
complaints of frequent urination and painful bloating, first cyclically for a
month, then the symptoms become more pronounced and permanent. The
most common scenario is that in which a young woman presents with
increasingly severe intermittent abdominal and pelvic pain due to a large
hematocolpos and hematometra. Examination shows excessive stretching of
the vagina, protrusion of the lower sections of the anterior abdominal wall,up
to appearance of abdominal mass, the uterus is elevated upwards. (Fig. 137).
When examining the vulva, a bluish, sometimes convex, hymenal membrane
is found. TAUS shows collection of fluid (the menstrual blood) in the uterine
cavity (hematometra), in vagina (hematocolpos).
Treatment. The use of nonsteroidal anti-inflammatory drugs can
provide pain relief; narcotic analgesics may be required. Surgical repair after
the onset of puberty but before menarche is optimal. Hymenotomy - a
surgical technique, used to correct such a defect. In asymptomatic patients,
waiting until puberty is generally recommended before deciding whether such
a technique is necessary. The hymenal changes that result from
estrogenization (increased elasticity and fimbriation) may reveal the hymen
to be open and obviate the need for surgery with the onset of pubertal period.
With estrogen stimulation, the hymen could be described as having the
appearance of an annular "scrunchie" (ie, a fabric-covered elastic hair tie). In
addition, surgical procedures to the vagina and hymen during childhood,
when endogenous estrogen levels are low, may result in scarring and the need
for subsequent surgical revision. Thus, surgery during this time should

197
generally be avoided if possible. If the hymen is suspected to be imperforate
during childhood, re-examination should be performed after the onset of
estrogen production, as signaled by breast development. If required, surgery
can be performed at this time when healing is optimal and prior to the
accumulation of a hematocolpos.
Fig. 137. Abdominal mass with imperforated humen
The technique of hymenotomy. The objective of a hymenotomy
procedure is to open the hymenal membrane in such a way as to leave a
normally patent vaginal orifice that does not scar. Infiltration of the
membrane prior to the incision with a long-acting local anesthetic (eg, 0.25%
bupivacaine) provides preemptive analgesia. If a large hematocolpos is
present, it typically is under pressure, and the surgeon should be prepared to
dodge the pressure-driven stream of thickened old blood (typically the
consistency and color of chocolate syrup) and to evacuate the hematocolpos
and hematometra using one or more suction cannulae. The revision of the
initial incision in the hymenal membrane must await the evacuation of the
hematocolpos. The hymenal orifice is enlarged using a circular incision
following the lines of the normal annular hymenal configuration.
Alternatively, a cruciate incision along the diagonal diameters of the hymen,

198
rather than anterior to posterior, avoids extension injury to the urethra and
can be enlarged by removal of excess hymenal tissue. In either approach,
hemostasis is required using interrupted stitches with fine absorbable suture
(eg, 4-0 polyglycolic acid suture). The technique of making a small central
incision with the placement of a Foley catheter, which is then left in place for
2 weeks, accompanied by the application of estrogen cream may also be used
as less invasive. This technique may require a repeat surgical procedure in a
small number of cases. The application of 2% lidocaine jelly to the vaginal
introitus is suggested to provide postoperative analgesia.
Atresia of the Vagina
Atresia of the vagina is congenital anomalies of the female genitourinary tract
and may occur as an isolated developmental defect (extremely rare) or as part
of a complex of anomalies (more common). Vagina may be absent, in whole
or in part, (in upper, middle and lower part and have any length) with absent
or rudimentary non-functional uterus and tubes. In these cases the ovaries
are present and function normally. Rarely the uterus and tubes may be
normal and give rise to a hematometra. If vagina is absent in whole it is called
aplsia of vagina.
More frequently, vaginal atresia associated with complex of anomalies, such
as:
Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome, also referred to
as Mayer-Rokitansky syndrome, or Rokitansky-Küster-Hauser
syndrome, or, simply, Rokitansky syndrome
Bardet-Biedl syndrome
Kaufman-McKusick syndrome
Fraser syndrome
Winters syndromeSym

199
Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome consists of
vaginal aplasia with other müllerian (ie, paramesonephric) duct
abnormalities. This condition causes the vagina and uterus to be
underdeveloped or absent, although external genitalia are normal. Affected
women usually do not have menstrual periods due to the absent uterus.
Often, the first noticeable sign of MRKH syndrome is that menstruation does
not begin by age 16 (primary amenorrhea). Women with MRKH syndrome
have a female chromosome pattern (46,XX) and normally functioning
ovaries. They also have normal breast and pubic hair development. Although
women with this condition are usually unable to carry a pregnancy, they may
be able to have children through assisted reproduction.
McKusick-Kaufman syndrome is an autosomal recessive disorder, in
this case vaginal atresia is associated with hydrometrocolpos, postaxial
polydactyly, imperforate anus, and congenital heart defects; the patient has
secondary sexual characteristics
Bardet-Biedl syndrome is a genetically heterogeneous group of autosomal
recessive disorders; vaginal atresia in Bardet-Biedl syndrome is associated
with retinal dystrophy or retinitis pigmentosa (appears at age 10-20 years),
postaxial polydactyly, obesity, nephropathy, and mental disturbances.
Fraser syndrome consists of vaginal atresia associated with eye
anomalies.
Winter's syndrome is an ear anomaly in combination with vaginal
atresia.
Symptoms. Symptoms in adolescents may include abdominal pain,
difficulty voiding, and backache, the most of them are associated with
primary amenorrhea. Adults have complaints of sexual intercourse and
infertility. The diagnosis can also be determined before puberty as an
unexpected result in an ultrasound study that was caused by other complaints
or indications. If any of these symptoms are present, an evaluation for vaginal

200
obstruction should be performed, in addition to assessment of the whole
reproductive system and renal system.
Diagnosis. Ultrasound examination, sounding of the vagina, and rectal
examination can help to determine the length of atresia. One can palpate an
elastic formation in front of the rectum during the rectal examination. In
cases with hematometra and hematosalpinx, there are some elastic
formations in small pelvis. In all cases complex anomalies should be
excluded.
Standard evaluation of primary amenorrhea includes an evaluation of
levels of luteinizing hormone (LH), follicle-stimulating hormone (FSH),
prolactin, estradiol, and progesterone. A study of the total testosterone level is
a way to differentiate between Mayer-Rokitansky-Küster-Hauser (MRKH)
syndrome and androgen insensitivity. If the level is in the reference range for
males, high for females, it is consistent with androgen insensitivity.
Karyotyping should also be performed.
Assessment of kidney function is reasonable because of the association
of congenital anomalies of the genitals with anomalies of the urinary system.
Ultrasonography is the cornerstone of imaging in patients with
suspected vaginal atresia. Abdominal, pelvic and transperineal sonograms
represent the ovaries, uterus and proximal vagina. They allow an anatomical
evaluation of the urinary tract to identify abnormalities. MRI, three-
dimensional US may also be used in diagnosis and planning of the further
follow-up of the patient. Laparoscopy may be necessary to evaluate the uterus
and adnexal structures if they are not clearly identified on ultrasonography or
MRI.
Treatment. Treatment options for vaginal agenesis include creation of a
neovagina. If a functioning uterus is diagnosed early, reconstructive vaginal
surgery can give a good effect. In all cases of congenital atresia, surgery for
artificial vagina should be delayed till sexual activity. It is impossible to have
pregnancy if the uterus is poorly developed and vagina is absent.

201
Anomalies of the Uterus
Anomalies of the uterus may be due to congenital defects with a failure
of the fusion of Mullerian ducts giving rise to uterus unicornis or absence of
urogenital system on the opposite side. Failure of the fusion in whole gives
rise to uterus didelfus (double uterus): two uteri, two cervices and two
vaginae. Other kinds of malformations: uterus unicornis with normal vagina;
uterus bicornis with two cervices and one normal vagina; uterus unicornis
with hypoplastic (or rudimentary) opposite horn and normal vagina; partition
of the uterus and vagina – uterus septus or uterus subseptus, when the
partition is only partial may rarely be.
In whole, uterine anomalies are categorized as follows (Fig. 138):
I. Hypoplasia/Agenesis
II. Unicornuate uterus – a banana shaped uterus with a single horn and
sometimes a rudimentary second horn. Bicornuate uterus is characterized by
a heart shape.
III. Uterus didelphys – a double uterus that may also be associated with a
double cervix and/or vagina.
IV. Uterus bicornuate - A uterus which has 2 horns
V. Septate uterus – a wall or septum partially or fully divides the uterus into
two cavities.
VI. Arcuate uterus - A uterus that has an arc

202
Fig. 138.Uterine anomalies.
Symptoms depend on menstrual drainage, fertility and character of
pregnancy. In most cases of duplication or fusion defect no symptoms are
present and diagnosis may be accidental in the course of a bimanual
examination or during a cesarean section or laparotomy. These women are
fertile and have delivery at term.In many cases uterine anomaly may remain
undetected until menstruation begins or pregnancy is attempted. If a uterine
anomaly such as bicornuate uterus results in a rudimentary uterine horn with
no outlet, menstrual outflow will be obstructed. This can result in pain and/or
a mass similar to endometriosis that gets worse during periods. If untreated,
blood collects in the uterus and may become infected. A uterine anomaly may
also be associated with dyspareunia and reproductive problems. These
include: infertility, ectopic pregnancy, recurrent miscarriage, premature
delivery, intrauterine fetal growth restriction, abnormal fetal presentation –
breech and transverse lies. Some patients, however, complain of

203
dismenorrhea, menorrhagia, sterility, etc. Thus, the incidence of reproductive
complications depends on the particular type of anomaly.
Diagnosis: bimanual examination, ultrasound examination,
hysterosalpingography, laparoscopy, hysteroscopy, MRI.
Treatment. Many cases of such anomalies call for surgical corrections.
Metroplasty is most often used to reshape the uterus. However, surgery is not
indicated in every case and it can not be performed on a unicornuate uterus,
as there is no way to surgically enlarge a uterus. Cervical cerclage may be
performed in some cases to prevent the cervix from dilating prematurely and
to increase the fetal survival rate.
Acquired anomalies of female genital organs
Displacement of the Uterus
The normal disposition of the uterus is in the center of the small pelvis,
at the same distance from symphysis, sacrum and lateral walls of the pelvis.
The fundus of the uterus is tilted forward and the cervix is backward, so that
the corpus lies almost horizontally, when a woman stands erect. There is an
obtuse angle between the corpus and the cervix of the uterus, and this angle is
opened forward (disposition anteversion and anteflexion).
Classification of the uterus, displacement:
1. Displacements of the uterus along the vertical plane (upwards and
downwards). They include: elevation of the uterus, descent of the uterus
(womb), prolapse of the uterus (complete and incomplete).
2. Displacement of the uterus along the horizontal plane.
3. Displacement of the uterus around the longitudinal axis (rotation and
torsion of the uterus).

204
Displacement of the Uterus along the Vertical Plane.
Elevation of the Uterus.
The uterus is elevated upward, the fundus of the uterus is situated
higher than the plane of the pelvic inlet. The external os of the cervix is
situated higher than the spinal plane. This displacement may occur due to
overfilling of the bladder and rectum and it is a kind of norm. Pathological
elevation of the uterus may occur as a result of hematocolpos due to vaginal
or hymenal atresia, sometimes due to voluminous tumor of the vagina and
rectum, exudate and hemorrhage in Douglas, pouch, adhesion (or union) of
the uterus with abdominal wall, etc.
Descent of the Uterus.
The uterus is situated lower than normally, the external os of the cervix
is lower than the spinal plane, but not protruding even when it is
strengthened. Descent of the uterus can occur only if the cardinal and
uterosacral ligaments are stretched, the perineal body does not support the
uterus. The vagina usually descends first, but in a few cases the uterus
descends first and the vaginal walls follow it. Degrees of descent are: 1)
descent of the cervix to the vaginal orifice; 2) cervix protrusion, 3) uterus is
outside the vulva with complete vaginal inversion.
Prolapse of the Uterus.
It may be complete and incomplete. Incomplete prolapse: cervix is
protruding; the corpus of the uterus is behind the introitus of vagina.
Complete uterine prolapse: uterus is outside the vulva with complete vaginal
inversion. (Fig. 139)

205
Fig. 139. Complete prolapse of the uterus.
The prolapsed mass contains bladder, uterus, adnexae, peritoneal
pouches, gut, rectal wall. Anterior vaginal wall together with bladder descent
(cystocele) and posterior vaginal wall together with rectum descent
(rectocele) occur with uterine descent, but can occur alone.
Etiology. Prolapse (and descent) of the uterus is the result of weakening
of the pelvic supports. In 99 % of cases the patients are parous. During
pregnancy the structures are hyperemic and softened, and during labor the
fascia and muscles of perineum may be stretched or torn. If pregnancies are
repeated at short intervals the supports will have little chance to recover.
After the menopause the pelvic structure atrophies, and prolapse frequently
appears. Sometimes prolapse and descent of the uterus (and vagina) may
occur as a result of atrophy due to infantilism, congenital hypoplasia of
perineal muscles, failure of pelvic innervation, general asthenia, etc.
Symptoms. There is a sensation of perineal discomfort. Urinary
symptoms include frequency, incontinence or retention of urine. One of the
frequent complaints is feeling of foreign body in vagina, and between the legs.

206
Discharge may occur from the exposed cervix. The prolapsed mass usually
becomes ulcerated, infected. The chronic ulcer is developed around the
cervical os.
Treatment. Operating treatment is recommended whenever possible.
Palliative: pessary treatment may be recommended to patients, who are too
old for operation, or for young women, who hope for further pregnancies, and
in early pregnancy. Pregnancy in patients with descent and incomplete
prolapse is possible, it is often complicated due to failure of blood supply of
the uterus, fetus and in most cases caesarian section is considered.
Displacement of the Uterus along the Horizontal
Plane.
1. Position. It is a displacement of the uterus in whole.
Anteposition is a displacement of the uterus forwards. It may be as a physical
sign when the rectum is overfull. At the same time, it may be a pathological
sign due to tumors in Douglas’ pouch.
Retroposition is a displacement of the uterus backwards. It may be due to
overfilling of the bladder, tumors and cysts.
Lateroposition (dextroposition and sinistroposition) – lateral displacements
of the uterus. It is very often due to inflammatory processes in parametric fat.
2. Pathological version. Corpus of the uterus displaces to one side, but
the cervix – to the other (opposite) side. There are:
Anteversion – corpus of the uterus is displaced forwards, and the cervix –
backwards.
Retroversion – corpus of the uterus is displaced backwards, and the cervix –
forwards.
Dextroversion – corpus is displaced to the right, and the cervix – to the left.
Sinistroversion – corpus of the uterus is displaced to the left, and the cervix –
to the right.

207
Pathological versions of the uterus most often may be due to inflammatory
diseases in peritoneum, ligaments and fat.
3. Flexion of the uterus. There is an obtuse angle between the corpus
and cervix of the uterus, and it is a normal sign. This angle is opened
forwards. Pathological changes are:
Hyperanteflexion of the uterus. This is the flexion forwards, and there is an
acute angle between the corpus and cervix of the uterus. Most often it may be
due to congenital anomalies, inflammations. Symptoms: painful menses,
sterility, pain in the sacrum and lower abdomen.
Retroflexion. This is the flexion of the uterus backwards, and the acute angle
between the corpus and cervix of the uterus is opened backwards.
Symptoms. Painful menses, sterility, pains in the sacrum, constipation.
(Fig. 140)
Treatment. Sports, vitamins, symptomatic treatment, gynecological
massage (Fig. 141) There are some operations, which can help to correct
displacements of the uterus, such as ventrofixation, and one can do it if it is
necessary.

208
Fig. 140. Displacements of the uterus: A- Anteversion of the uterus; B –
Anteflexion;
C - Retroversion; D- Retroflexion.
Fig. 141. Gynecologic massage: manipulations on retroverted uterus

209
Displacement of the uterus along its longitudinal axis
1. Rotation of the whole uterus (the corpus and the cervix). This may be to
any side (right or left);
2. Torsion of the uterus. This is the turning of the corpus to the right or left,
when the cervix is fixed (immobile).
Symptoms: painful menses, sterility, pains in the sacrum, constipation.
Treatment is the same.
Self test
1. The normal disposition of the uterus is
A. in the center of the small pelvis, at the same distance from symphysis,
sacrum and lateral walls of the pelvis
B. near the symphysis pubis
C. near the rectum
D upper then the pelvic inlet
2. Anteposition is a
A. displacement of the uterus forwards
B. displacement of the uterus backwards
C. displacement of the uterus downwards
D. displacement of the uterus upwards
3. Displacement of the uterus may be
A. only congenital
B. due to another reasons
C. without any reason
D. due to mental disorder
4. Anomalies of the uterus may lead to
A. disturbances of menstrual cycle
B. сomplications during pregnancy and labor
C. malignant tumors
D. benign tumors

210
5. Pathological version means
A. displacement of the uterus along the horizontal plane
B. displacement of the uterus along the vertical axis
C. uterine eversion
D. uterine inversion
6. Rotation of the uterus means
A. displacement around its longitudinal axis
B. displacement around its horizontal plane
C. twist downwards
D. twist upwards
7. The elevation of the uterus may be only in pathological
condition.
A. yes
B. no
C. absolutely impossible
D only regular position of the uterus is possible
8. The treatment of prolapse of the uterus should be
A. surgical
B. conservative (pessaries)
C. both surgical and conservative
D. not treated at all
9. Retroposition is a
A. displacement of the uterus forwards
B. displacement of the uterus backwards
C. displacement of the uterus downwards
D. displacement of the uterus upwards
10. Which is the most common complaint in case of vaginal
atresia?
A. purulent discharge from vagina
B. periodic pains in the lower abdomen and absence of menstruation
C. absence of any discharge from vagina
D. absence of vagina

211
Chapter 4. INFLAMMATORY DISEASES OF THE
FEMALE GENITALIA
Inflammatory diseases of the female genitalia occur in 60-65 per sent of
all gynecologic patients. The most frequent causes of inflammatory diseases of
the female genitalia are infection pathogens, as well as thermal, chemical,
mechanical factors.
Classification
All gynecological disorders, accompanied by inflammatory processes in
the reproductive system, are usually differentiated depending on:
the clinical course of the pathological process,
the pathogen,
the localization of the inflammatory process.
So, depending on the clinical course of the pathological process
following forms of inflammatory disease are distinguished:
acute (disease develops rapidly, duration is 2-3 weeks);
subacute (symptoms for these disorders are observed within 6
weeks);
chronic (signs of the disease may experience more than one and a
half months, disease develops slowly, is continual or recurrent).
latent/silent: the pathogen remains inactive for a long period of
time before beoming active.
Depending on the origin, specific and nonspecific diseases are
distinguished in RF.
Specific inflammatory diseases affecting the female genital organs
usually include chlamydia, TB disease, gonorrhea, trichomoniasis, herpes
infection, and others. The term “sexually transmitted diseases” (STD) is
currently used for most of these diseases.

212
Among nonspecific inflammatory diseases affecting the female sexual
organs are most often those caused by effects on the reproductive system of
staphylococci, streptococci, E. coli, Pseudomonas aeruginosa and Proteus.
Depending on the localization of inflammatory lesions, diseases of the
lower reproductive organs (vulvitis, colitis, bartholinitis, endocervicitis) and
upper (endometritis, metendomitis, parametritis, salpingo-oophoritis) are
distinguished. The term: "Diseases, characterized by abnormal
vaginal discharge» is currently used for inflammation of the lower
genitalia. The term: "Pelvic inflammatory disease (PID)” is currently
used for inflammation of the upper genital organs.
Epidemiology. The rate of inflammatory diseases is over 60% of all
gynecologic diseases and about 30% patients of female hospitals have the
inflammatory processes of genital organs. The number of inflammatory
diseases has increased due to increased sexual activity at a young age, liberal
sexual orientation, prostitution. Those who are most at risk are young
unmarried women with several sexual partners. First of all, inflammatory
diseases affect the fertility of a person due to infections of the female upper
reproductive tract and their continuation. Women with a stable viral infection
are particularly at risk for developing cervical dysplasia and fetal death.
Pathogenesis. Inflammatory diseases of female genital tract are
considered as a result of a complex interaction between the infected organism
and the causative microorganism. It is established that the occurrence and
progression of the inflammatory process in the reproductive system of a
woman depends on its systemic resistance, which is determined by such
factors as age, general condition and the presence of other diseases (anemia,
vitamin deficiency, etc.).
Anatomically, the female genital tract consists of cavities (fallopian
tubes, uterine cavity, endocervix, vagina) that communicate with the vulvar
cleft. This structure allows for the exteriorization of the menstrual flow and
the delivery of the fetus during childbirth; on the other hand, it allows sexual

213
intercourse, and the penetration of pathogenic microorganisms to the
overlying cavities. The vaginal microflora is one of the most important
mechanisms for protecting the reproductive system of a woman, maintaining
a normal environment in the vagina and preventing the spread of
microorganisms into the vagina.
The female genital tract, especially the vaginal secretions, contain from
108 to 109 bacteria per gram of fluid examined. Bacterial flora of the vagina
makes up the normal part of female physiology from the life of the fetus to
death. Flora changes typically throughout the entire life cycle of a woman. At
birth, the vagina is sterile. A few days later, when estrogen from the mother
leads to an increase in the glycogen content in the epithelial cells of the vagina,
the colonization of lactobacilli from the mother occurs. With estrogen levels
slowly diminishing, glycogen disappears. But due to breast-feeding,
colonization of a new-born organism with appropriate flora happens. Human
milk not only contains bacteria, but is also the predominant source for creating
a "healthy microbiome" in a newborn. Thus, breastfeeding is the reason for the
colonization of a healthy newborn with normal flora (hydrogen peroxide-
producing lactobacilli. At the time of menarche, the rise in estrogen increases
glycogen deposition in the vaginal epithelial cells, which is a prerequisite for
the development of the adult vaginal microflora. In adult women more than 50
different species of bacteria live in a woman’s vagina, with lactobacilli being the
predominant microorganism found in healthy women. Lactobacilli produce
lactic acid from glucose keeping the vagina at an acidic pH (3,8-4,2). Lactic
acid is a major antimicrobial factor produced by lactobacilli. Cells of vaginal
epithelium contain glycogen, which serves as a substrate for Lactobacilli, which
then metabolized to glucose. Lactobacilli from a healthy vaginal ecosystem
produce H2O2. Production of hydrogen peroxide (H2O2) is a mechanism of
inhibiting growth of microorganisms via direct interaction or via human
myeloperoxidase. Hydrogen peroxide-producing lactobacilli have been shown

214
to inactivate HIV-1, herpes simplex virus type 2 (HSV-2), Trichomonas
vaginalis, G. vaginalis, P. bivia and E. coli.
In turn, the level of glycogen is dependent on the level of estrogens in
female organism. The hydrogen peroxide-producing flora is predominant until
menopause, when it is replaced with a flora similar to the flora found prior to
the menarche, unless hormonal replacement therapy is started.
But not only Lactobacillus acidophilus provide the self-cleaning of the
vagina. The normal vaginal ecosystem of reproductive age women contains 7
kinds of Lactobacillus: L acidophilus (42,8%), L. Paracasei, L. Fermentum, L.
Plantarum (10-18,6%)), L.cateforme, L.corineformis, L. Brevis (2,5-5,7%), H202
producing Lactobacillus may play an important role in acting as a natural
microbicide within the vaginal ecosystem. Normal vaginal microflora
contains: Lactobacillus (70-90%), Staphylococcus epidermalis (30-60%>),
diphteroids (30-60%>), Hemolytic Streptococci (10-20%), nonhaemolytic
streptococci (5-30%>), Escherichia coli (20-25%), Bacte-roides (5-15%),
Peptococcus (10-60%), Peptostreptococcus (10-40%), Clostridium (5-15%).
Presence of pathogenic flora without inflammation isn't a sign of patho-
logic processes.
Many endogenous and exogenous factors can change the balance of the vaginal
ecosystem. Some vaginal microorganisms can cause inflammation in certain
conditions. Both vaginal and cervical epithelial cells have the ability to convert
glycogen into glucose, which is further metabolized to lactic acid. Vaginal acidity
depends on adequate estrogen levels, as well as on the presence of bacteria
producing lactic acid, such as Lactobacilli. The concentrations of lactobacilli are
likely to be important determinants of vaginal pH. An increased concentration of
bacteria producing lactic acid in the vaginal fluid can lead to a decrease in pH,
which determines a decrease in susceptibility to infection. Estrogens have a
direct effect on the number of organisms and the composition of the bacterial
flora. The surface of the mucous membrane provides protection from penetrating
pathogens. Mucous can act to eliminate a variety of pathogens or antigens.

215
Mucous also serves to attach immunoglobulin A, lysozyme, lactoferrin and other
biologically active substances. The mucous membrane of the female genital tract
is under hormonal control. Any abnormality with a low level of estrogen and a
decrease in the level of estrogen with age can damage the protective mechanisms
of the female reproductive tract. Using contraceptives, excessive use of the
shower can affect the vaginal ecosystem by changing the vaginal pH, changing
the vaginal fluid by direct dilution. Imbalances of the vaginal flora caused by a
reduction in the proportion of Lactobacilli can lead to failure of a vaginal
microbiome, to overgrowth pathogens, up to development of inflammatory
process.
DISEASES, CHARACTERIZED BY ABNORMAL
VAGINAL DISCHARGE
Normal physiological discharge changes with the menstrual cycle. It is
thick and sticky for most of the cycle, but becomes clearer, wetter, and
stretchy for a short period around the time of ovulation. These changes do not
occur in women using oral contraceptives. Abnormal vaginal discharge is
characterized by a change of color, consistency, volume, or odor, and may be
associated with symptoms such as itch, soreness, dysuria, pelvic pain, or
intermenstrual or post-coital bleeding.
A number of different infections can cause a change in the amount,
consistency, color, or odor of vaginal discharge. These include:
Bacterial vaginosis
Trichomoniasis (trich)
Gonorrhea
Chlamydia
Yeast infection (candidiasis)

216
Trichomoniasis, Gonorrhea, and Chlamydia are examples of sexually-
transmitted diseases (STDs), while bacterial vaginosis and yeast infection are
not considered to be STDs.
On the other hand, inflammatory process may develop due to
overgrowth of any pathogens, especially against the background of decreased
immune protection, trauma, etc.
Bacteriology. Diseases, characterized by abnormal vaginal discharge
include following (according to localization):
bartholinitis
vulvitis
vaginitis
vulvovaginitis
bacterial vaginosis
cervicitis
Etiology. Inflammation of genitals may happen because of lack of
hygiene, unprotected sexual intercourse, use of some drugs (antibiotic
agents), diabetes mellitus, other metabolic disorders, as well as due to
hormonal imbalance, etc.
Genital inflammations are often associated with abortions (criminal,
artificial, spontaneous), labors and diagnostic therapeutic intrauterine
manipulations. Genital infection may occur due to inflammation of other
organs of the abdominal cavity (appendicitis, sigmoiditis, etc.), which is
explained by close anatomical relationships between these organs.
Bartolinitis
Bartolinitis - is an inflammation of Bartholin’s Glands. Bartholin’s
glands are paired glands, which are located in 4 O’ clock and 8 O’ clock
positions in the labia minora, or the two inner folds of the vagina.
Etiology. Pathogens, causing the disease, are:
staphylococci and streptococci;

217
E. coli;
fungi.
gonorrhea;
trichomoniasis;
chlamydia.
Pathogenic microbes enter the duct through the urethra or through the
vagina. In some cases, the infection penetrates into the gland with blood flow.
When infection occurs, swelling of the tissue, irritation and retention of
secretion develop, leading to blockage of the excretory ducts of Bartolin's
glands. This leads to the formation of the Bartholin gland cyst. If left
untreated, the Bartolin cyst can turn into an abscess, which, as a rule, does
not break up spontaneously. On the other hand, the spread of infection is
possible. The recurrent course of bartholinitis is rather frequent.
Symptoms: extreme pain in labia when sitting and walking, fever and an
elevated pulse rate. Physical examination reveals edema and hyperemia in the
area of vestibulum of vagina. The onset of an abscess is characterized by the
appearance of an extremely painful tumor in the genital area. It can be
clinically detected as a local redness, which begins to bulge, and then
progresses to a fluctuation (abscess). (Fig. 142). Suppuration, softening and
fluctuation are typical for Bartilin's gland abscess.
Diagnosis is based on clinical findings and the patient’s history.
Treatment: bed rest; local hypothermia (cold applications); administration of
antibiotics and sulfanilamides. Antibiotics should be administered under the
results of bacteriological examination of a secret:
Ceftriaxone (Rocephin)
Ciprofloxacin (Cipro)
Doxycycline (Bio-Tab, Doryx, Vibramycin)
Example: oral cephalexin therapy (500mg) every six hours for 7 days;
doxycycline 100 mg PO q12hr for 7 days.

218
Fig. 142. A – Bartolinitis. B – abscess of a Bartolin’s gland
Operative treatment is administered in cases of suppuration and
abscess forming. The excision of an abscess, its drainage should be
performed. After the opening of abscess the instillations of a 5% iodine
solution may be used every two days.(Fig. 143). Antibiotic treatment should
be continued within 7 days after surgical intervention.

219
Fig. 143. Surgical treatment of Bartolin’s gland abscess
Vuivitis
Vulvitis is inflammation of the female external genitalia – vulva that
include the labia majora, labia minora, clitoris, and introitus. Vulvites are
usually combined with vaginitis, and are called vulvovaginitis in such a case.
Causes of vulvitis: 1). general diseases (such as diabetes); 2). infection
pathogens; 3). mechanical, chemical and thermal factors, 4). allergy to some
substances. Vulvitis commonly occurs in girls and old women. In postpubertal
women it may be associated with ovarian hypofunction and avitaminoses.
Vulvitis is differentiated into primary (isolated vulval inflammation) and
secondary (attending inflammations of the internal female genitalia).
Symptoms: burning tenderness, extreme and constant itching in the
paravulval area, especially after walking, vaginal discharge, micturition. On
examination: edema, hyperemia and swelling of the external genitalia, ulcers
with a purulent coat.

220
Diagnosis is based on: patient’ complaints, clinical findings, CBC,
urinalysis, microscopic and bacteriological examination of discharge.
Treatment. It is depend on underlying disease, if any, and results of
laboratory investigations. In general, treatment of genitalia with 5 % solution
of potassium permanganate, chamomile tea, 3% solution of boric acid several
times a day; “sitting” bath with the described solutions are also effective.
After washing the skin of the vulva may be powdered with talcum and
powder, containing antibiotic agent. Medication is dependent on the origin of
inflammation: allergy, pathogens, etc. Anti-fungal creams and low-dose
hydrocortisone creams help reduce the inflammation. "Bed rest" regimen
may be administered in severe cases simultaneously with medication
Vaginitis and vulvovaginitis
Vaginitis (inflammation of the vagina) is the most common gynecologic
condition encountered in the outpatient office. It is an inflammation of a
vaginal cavity. Vaginitis may be accompanied with vulvitis (vulvovaginitis)
and cervicitis (inflammation of the uterus’ cervix.
Etiology. Approximately 90% of all cases of vaginitis are thought to be
attributable to 3 causes: bacterial vaginosis, vaginal candidiasis (or
vulvovaginal candidiasis [VVC]), and Trichomonas vaginalis infection
(trichomoniasis).
Symptoms. A major symptom common to all these forms is a pathological
vaginal discharge. The character of discharge so typical for the flora that
caused the inflammation that the primary diagnosis is sometimes
formulated based on the type of discharge from vagina. Discharge in
vaginitis may be purulent, mucous, bloody, curd-like; yellow-green,
white; thin, thick, plentiful, malodorous, etc. Discharge due to vaginitis is
accompanied by pruritus, erythema, and sometimes burning, pain, or mild
bleeding. Pruritus may interfere with sleep. Dysuria or dyspareunia may
also occur.

221
In atrophic vaginitis, discharge is scant, dyspareunia is common, and
vaginal tissue appears thin and dry. Symptoms vary among particular
types of causative agent.
The diagnosis based on the presence of symptoms of abnormal
discharge, vulvovaginal discomfort, or both; and results of clinical and
laboratory examination:
specula (and bimanual) exam;
serum human chorionic gonadotropin (hCG).
saginal pH,
microscopy of smears,
KOH wet mounts,
Whiff test;
bacteriological investigation of vaginal smears.
Bacterial vaginosis
BV is a polymicrobial clinical syndrome resulting from replacement of
the normal hydrogen peroxide-producing Lactobacillus sp. in the vagina with
high concentrations of anaerobic bacteria (e.g., Prevotella sp.
and Mobiluncus sp.), G. vaginalis, Ureaplasma, Mycoplasma, and numerous
fastidious or uncultivated anaerobes. BV is the most prevalent cause of
vaginal discharge or malodor. It is not a true bacterial infection but rather an
imbalance of the bacteria that are normally present in the vagina. Bacterial
vaginosis, also known as vaginal dysbiosis.
Risk factors that may predispose patients to BV include the following:
Recent antibiotic use
Decreased estrogen production
Wearing an intrauterine device (IUD)
Douching
Sexual activity that could lead to transmission (eg, having a new sexual
partner or a recent increase in the number of sexual partners)

222
Symptoms. Typical sign and symptoms of BV include following:
vaginal odor (fishy odor is the most common, and often initial,
symptom of BV); often after sexual intercourse and during
menstruation;
increased vaginal discharge;
itching and irritation
dysuria or dyspareunia (rare).
Physical findings in BV may include the following:
gray, thin, and homogeneous vaginal discharge, which adheres to the
vaginal mucosa;
increased light reflex of the vaginal walls, but typically with little or no
evidence of inflammation;
normal-appearing labia, introitus, cervix, and cervical discharge;
in some case, evidence of cervicitis.
Characteristics of vaginal discharge:
thin,
white or gray
cloudy
malodorous (with a fishy odor, which may become stronger after sexual
intercourse or during menstrual periods)
Diagnosis is made by:
Physical examination
o observation made with the naked eye and nose
o undergoing a pelvic examination
Laboratory tests:
o pH of vaginal secretions
o Whiff test (clue cells)
o KOH slide ((fisher odor)
o Gram staining smears.
o High vaginal swab (vaginal discharge culture and sensitivity)

223
A sample of the vaginal discharge is obtained and viewed under the
microscope, either stained or in special lighting, to determine: absence
of Lactobacilli, presence of 'clue cells', presence of Gardnerella bacteria,
Mobiluncus. Demonstration of clue cells on a saline smear is the most specific
criterion for diagnosing BV. Clue cells are vaginal epithelial cells that have
bacteria adherent to their surfaces. The edges of the squamous epithelial cells,
which normally have a sharply defined cell border, become studded with
bacteria. The epithelial cells appear to be peppered with coccobacilli.
BV can be diagnosed by the use of clinical criteria (i.e., Amsel's
Diagnostic Criteria) or Gram stain (considered the gold standard laboratory
method for diagnosing BV). If a Gram stain is not available, clinical criteria
can be used and require three of the following symptoms or signs ( aka
Amsel's Diagnostic Criteria for Bacterial Vaginosis):
Homogeneous, thin, white discharge that smoothly coats the vaginal
walls
Presence of clue cells on microscopic examination
pH of vaginal fluid >4.5
Clue cells
Amine (fishy) odor when potassium hydroxide solution is added to
vaginal secretions (commonly called the "whiff test")
Treatment. Antibiotics are the mainstay of therapy for bacterial
vaginosis (BV), but asymptomatic women with Gardnerella
vaginalis colonization do not need treatment.
Recommended Regimens:
o Metronidazole 400 mg BD (twice a day) orally within 5 - 7 days;
o Metronidazole 0.75% vaginal gel (5g applicator-full at night) or
Clindamycin 2% cream (5g applicator-full at night) – 5-7 nights
After anthibacterial therapy, it is necessary to restore the normal
vaginal microflora. For this purpose, the Lactoginal vaginal capsules are
prescribed: 1 capsule per day (14 days) or 1 capsule twice a day (7 days).

224
Trichomonas vaginitis
Trichomonas vaginitis is a sexually transmitted infection (STI), caused
by one-celled parasite called Trichomonas vaginalis.
Risk factors that may predispose patients to Trichomonas vaginitis
include the following:
o multiple sexual partners;
o having unprotected sexual intercourse
o a history of other sexually transmitted infections;
o a previous episode of trichomoniasis;
Symptoms. Many women with trichomoniasis have no symptoms, at
least not at first. Most of the symptoms described below are not specific for
trichomoniasis and can occur in other vaginal or cervical infections. Typical
sign and symptoms of Trichomonas vaginitis include following:
A profuse and often foul-smelling vaginal discharge
Genital redness, burning and itching
Pain with urination or sexual intercourse
Lower-abdominal tenderness
Physical findings in Trichomonas vaginitis may include the following:
o Profuse vaginal discharge, thin and frothy;
o Edema and erythema of vaginal mucosa (colpitis macularis)
o Cervicitis: a diffuse or patchy macular erythematous lesion of the cervix
o (strawberry cervix)
o Offensive vaginal odor
Characteristics of vaginal discharge:
The discharge profuse, classically thin and frothy,
The discharge is often yellow, may be green, gray,
Edema and erythema
Vaginal pH is often elevated (>4.5). which may be white, gray, yellow or
green

225
Complications of Trichomonas vaginalis infection (TVI) include:
In women, vaginitis is the most common manifestation of infection.
Other complications include infection of the adnexa, endometrium, and
Bartholin glands. Pelvic inflammatory disease and tubo-ovarian abscess
may also occur.
Research has shown that infection with Trichimonac vaginalis
increases the risk of HIV transmission in both men and women.
TVI also increases the susceptibility to other viruses, including herpes
and human papillomavirus (HPV).
TVI also increases the risk of cervical intraepithelial neoplasia.
In pregnant women, TVI has been associated with an increased risk of
miscarriage, low birth weight, preterm delivery, and intrauterine
infection.
Diagnosis is made by:
Physical examination
o evaluation of previous history
o visual inspection
o undergoing a pelvic examination
Laboratory tests:
o pH of vaginal secretions
o Whiff test
o KOH slide,
o Gram staining smears (shows parasite Trichomonal vaginalis).
o High vaginal swab (vaginal discharge culture and sensitivity)
o Vaginal or endocervical swab for Chlamydia
Criteria for diagnosis of Ttichomonas vaginitis:
o Identification of causative organism by microscopy (occasionally by
culture)
Treatment. Treatment should be instituted immediately and, whenever
possible, in conjunction with all sexual partners. Patients undergoing

226
pharmacotherapy should be advised to avoid alcohol consumption during the
course of treatment and for an appropriate amount of time after the
completion of their medication.
Recommended Regimens:
o Metronidazole (Flagyl, Protostat, Metronid, Novonidazolo) orally 500
mg twice daily for 7 days.
o When standard treatment regimens fail, a regimen of 2 g of oral
metronidazole or tinidazole for 5 days may be considered.
o Inpatient intravenous (IV) therapy may be indicated when resistance is
present.
After anthibacterial therapy, it is necessary to restore the normal
vaginal microflora. For this purpose, the Lactoginal vaginal capsules are
prescribed: 1 capsule per day (14 days) or 1 capsule twice a day (7 days).
Vulvovaginal candidiasis (VVC)
Vulvovaginal candidiasis develops due to an overgrowth of yeasts within
the vagina, most often C albicans. About 20% of non-pregnant women aged
15–55 have C albicans in the vagina without any symptoms. The disease
spectrum ranges from “innocent bystander,” where visible symptoms are
absent, to complicated disease where VVC is severe, persistent, or recurrent.
Risk factors. Vulvovaginal candidiasis is most commonly observed in
women the reproductive age group. It is quite uncommon in prepubertal and
post menopausal females. The higher risk to get VVC may be associated with
the following factors:
o Pregnancy
o Higher dose combined oral contraceptive pill
o Oestrogen-based hormone replacement therapy after the
menopause, including vaginal oestrogen cream
o A course of broad spectrum antibiotics such as tetracycline or
amoxicillin

227
o Diabetes mellitus
o Obesity
o Iron deficiency anemia
o Immunodeficiency eg, HIV infection
o An underlying skin condition, such as vulval psoriasis, lichen
planus or lichen sclerosus
o Other illness.
Symptoms of VVC include:
o Itching, soreness and/or burning discomfort in the vagina and vulva
o Stinging when passing urine (dysuria)
o Heavy white curd or cottage cheese-like vaginal discharge
o Pain during sexual intercourse
o Flares just before and during menstruation are typical
o Non-offensive odor
Physical findings in VVC may include the following:
o pH of vaginal secretions is < 4.5
o Vulval edema, erythema, fissures and excoriations
o Thrush patches - Usually found loosely adherent to the vulva
o Thick, white, curdlike vaginal discharge
o Bright red rash affecting inner and outer parts of the vulva,
sometimes spreading widely in the groin to include pubic areas,
groin and thighs.
Characteristics of vaginal discharge:
o Сopious
o Thick,
o White,
o Cottage cheese-like discharge adhered to vaginal wall, with fissures,
ulcers under these patches
Complications of VVC include:
o Recurrent VVC (>4 episodes within 1 year)
228
o Chronic, persistent VVC
o Atrophic vaginitis
o Lichen simplex (localized area of chronic,
lichenified eczema/dermatitis, neurodermatitis).
o Depression and sexual problems
o Candidemia, invasive candidiasis (the yeast infection affects other
parts of the body including the blood, brain, and heart).
Diagnosis is made by:
Physical examination
o evaluation of anamnestic data and visual inspection
o pelvic examination
Laboratory tests:
o pH of vaginal secretions
o a wet mount with KOH
o Whiff test
o Gram staining smears (budding yeasts, hyphae, or pseudohyphae)
o High vaginal swab (vaginal discharge culture and sensitivity) may not
need unless recurrent
Criteria for diagnosis of VVC:
o Identification of causative organism by microscopy (occasionally by
culture)
Treatment.
Recommended Regimens:
Topical use:
o Clotrimazole 1% cream 5 g intravaginally (one applicator-full)
daily for 7-14 days
o Miconazole 2% cream 5 g (one applicator-full) daily for 7 days
o Butoconazole 2% cream 5 g intravaginally in a single application
Oral agents:
Fluconazole 150 mg orally in a single dose

229
Fluconazole 100 mg oral once weekly for 3-6 months (for recurrent
VVC)
Itraconazole 400 mg orally once monthly before menses for 3-6 months
(for recurrent VVC)
After anthibacterial therapy, it is necessary to restore the normal
vaginal microflora. For this purpose, the Lactoginal vaginal capsules are
prescribed: 1 capsule per day (14 days) or 1 capsule twice a day (7
days).Treatment of underlying disease/condition.
PELVIC INFLAMMATORY DISEASE
Pelvic inflammatory disease (PID) comprises a spectrum of infectious
and inflammatory diseases of the upper genital tract of women. PID can
involve infection of the endometrium (endometritis), the oviducts
(salpingitis), the ovaries (oophoritis), the uterine wall (myometritis), or
portions of the parietal peritoneum (peritonitis), including perihepatic
structures (Fitz-Hugh−Curtis syndrome).
Etiology (or bacteriology). PID is usually the result of a sexually transmitted
disease (STD) and less often results from iatrogenic causes after
instrumentation of the female reproductive tract. Chlamydia trachomatis is
the predominant sexually transmitted organism associated with PID. Other
organisms implicated in the pathogenesis of PID include Neisseria
gonorrhoeae, Gardnerella vaginalis, Haemophilus influenzae, and
anaerobes such as Peptococcus and Bacteroides species. Other causative
agents of PID are: staphylococci, streptococci, viruses, Escherichia coli,
peptostreptococci, etc. Currently, the most of PIDs are developed against the
background of microbe associations (combinations of several types of
pathogens).

230
Pathogenesis. PID is initiated by infection that ascends from the vagina and
cervix into the upper genital tract. PID should be considered as a result of a
complex interaction between the infected organism and the causative
microorganism. Hence, emergence and progression of the inflammatory
process in the reproductive system of a woman depends on her systemic
resistance which is determined by such things as age, the general state and
the presence of other diseases (anemia, avitaminosis, etc.).
Classification of PID by the clinical course:
• Acute PID
o Acute PID refers to the acute symptoms accompanying ascending
infection from the cervix to the endometrium, tubes, ovaries, and pelvic
peritoneum.
• Chronic PID
o Chronic PID refers to chronic pelvic pain, often periodic in
exacerbation, that can follow an acute episode of PID, a sequela to an
inflammatory response to an acute infection in the pelvis. Chronic
pelvic infection can also be caused by the more rare pelvic infection with
tuberculosis (TB) and actinomycosis.
• Silent PID
• Silent PID refers to asymptomatic or mildly symptomatic pelvic
infection, which is usually diagnosed when the sequela of tubal damage
is found at a later date.
PID can occur at any age in women who are sexually active. It is most
common among young women. Those younger than age 25 years are more
likely to develop PID. Women with the following risk factors also are more
likely to have PID:
Infection with an sexually transmitted infection, most often
gonorrhea or chlamydia
Multiple sex partners (the more partners, the greater the risk)
A sex partner who has sex with others

231
Past PID
Other sources if infection in the organism, because it may spread by
blood and lymph vessels.
The inciting event, leading to PID include:
• Menstrual periods.
o Degenerating endometrium is a good culture medium and retrograde
menstruation encourages ascending infection. In addition, cervical
mucus changes during menses allow ascending infection. Two-thirds of
acute PID cases begin just after menses.
• Sexual intercourse.
o Bacteria-laden fluids may be pushed into the uterus, and uterine
contractions may assist their ascent.
• Iatrogenic events
o Elective abortion
o Dilation and curettage or endometrial biopsy
o IUD insertion or use
o Hysterosalpingography
o Chromopertubation at laparoscopy
Characteristic signs of the inflammation are: damage to tissues,
impaired blood circulation, transudation of fluid, migration of leucocytes and
lymphocytes into tissues, and impaired tissue metabolism.
Clinical features, common for PID are: lower abdominal pain, usually
bilateral, combined with either adnexal tenderness or cervical excitation on
vaginal examination. The initial diagnosis of PID is based on the presence of
these features.
Other clinical features can support a diagnosis of PID but are not
essential before starting empirical therapy:
• intermenstrual or post coital bleeding – resulting from endometritis
and cervicitis

232
• deep dyspareunia
• abnormal vaginal discharge – indicating lower genital tract infection
• fever – non-specific and usually only present in moderate to severe PID
• nausea/vomiting – may occur in severe PID but is more commonly
associated with appendicitis.
Diagnosis. The diagnosis is based on clinical finding. It is very
important to establish whether the inflammatory process is primary or
secondary. It is necessary to do a microscopic examination to establish
etiology of this process (to differentiate pathogens of this process).
Clinical criteria for diagnosis of PID:
Minimum criteria for diagnosis
o Lower abdominal tenderness
o Uterine or adnexal tenderness
o Cervical motion tenderness: lateral motion of the cervix on
examination causes pain by putting tension on the adnexa.
• Additional criteria. For women with severe signs, these additional
criteria are used to increase the specificity of the diagnosis:
o Body temperature higher than 38.3В°C
o Abnormal cervical or vaginal discharge. Mucopurulent
cervical discharge with white blood cells (WBCs) seen on
wet mount is almost always seen in women with PID. If this
finding is not present, other diagnoses should be seriously
entertained.
o Elevated erythrocyte sedimentation rate (ESR)
o Elevated C-reactive protein
o Positive test for gonorrhea or chlamydia
o Tubo-ovarian abscess seen on ultrasound
o Evidence of endometritis on endometrial biopsy
o Laparoscopic evidence of PID

233
Differential diagnosis of PID(Table 5) should include:
• Ectopic pregnancy
• Ruptured ovarian cyst
• Appendicitis
• Endometriosis
• Inflammatory bowel disease
• Degenerating fibroids
• Spontaneous abortion
• Diverticulitis
Table 5.
Differential diagnosis of PID
Differential diagnosis Significant features
Ectopic pregnancy Menstrual history, initially unilateral
pain
Ovarian accident Initially unilateral pain, often mid-
cycle
Appendicitis Gastrointestinal symptoms, right
sided pain
Irritable bowel syndrome Central or left sided pain, no cervical
exitation
Inflammatory bowel disease Colicky central or left sided pain,
bowel symptoms
Urinary tract infection Urinary symptoms, loin pains,
Bowel torsion Central pain
Psychosomatic pain Usually inconsistent symptoms

234
Recommended diagnostic techniques are:
• Cervical Gram stain. If Gram-negative intracellular diplococci are
present, gonorrhea is the presumed diagnosis. However, Gram stain
alone misses one-half of the gonorrhea cases. Chlamydia is not
diagnosed on Gram stain.
• Blood studies
o Leukocytosis is not a reliable indicator of acute PID. Less
than 50% of women with acute PID have a WBC count
greater than 10,000 cells/mL. Also, it is nonspecific; other
infectious causes of symptoms are associated with an
elevated WBC count.
o An increased ESR is a nonspecific finding, but the ESR is
elevated in approximately 75% of women with
laparoscopically confirmed PID.
• Serum human chorionic gonadotropin (hCG). A sensitive pregnancy test
is important in the differential diagnosis of pelvic pain to rule out the
possibility of ectopic pregnancy.
• Ultrasound. This technique may help define adnexal masses and
intrauterine or ectopic pregnancies, especially when a patient has a
tender abdomen that does not permit an adequate pelvic examination.
This is important for detecting the presence of tubo-ovarian abscesses
since antibiotic therapy protocols may be different from PID without
tubo-ovarian abscesses. Response to therapy can be measured
objectively as pelvic masses and induration regress. Transvaginal
ultrasound of the pelvis mostly useful.
• Culdocentesis. If purulent fluid is obtained, a culture may assist in
antibiotic selection. However, infections may be secondary to another
primary process. In addition, the pain associated with this test limits its
use.

235
• Laparoscopy. If the disease process is unclear, this technique is the
ultimate way to establish the diagnosis.
• Follow-up. After initiation of appropriate treatment, clinical
improvement should be observed in 48 to 72 hours. If no improvement
occurs, alternative diagnoses should be considered.
• Testing for HIV and assurance of current Pap smear screening should
be offered to all women diagnosed with PID. Additionally, testing for
syphilis and hepatitis B should be considered.
PID has three principal complications, as follows:
Chronic pelvic pain
Infertility
Ectopic pregnancy
Management of PID. Common principles of management of patients
with acute PID include:
• Treatment should always include sexual partners.
• The physician must decide between outpatient management of the
woman, with close follow-up in 48 to 72 hours, or hospitalization.
• Hospitalization of PID patients and intravenous antibiotic therapy is
indicated in the following scenarios:
o Until other serious diagnoses are excluded, including appendicitis and
ectopic pregnancy
o If the patient is an adolescent
o If a pelvic abscess is suspected on examination or ultrasound
o Severe systemic/peritoneal symptoms including high fever, or signs of
peritonitis
o Inability to tolerate oral outpatient treatment because of vomiting
o If the patient is pregnant
o If the patient is unable or unlikely to comply with outpatient therapy
and/or 48-to 72-hour follow-up
o If HIV infection is present

236
o If the patient has not responded to outpatient management at 48-to 72-
hour follow-up
Recommended regimens for out-patient treatment of patient with PID:
• Regimen A
Ofloxacin (Floxin) 400 mg orally two times a day for 14 days or
Levofloxacin 500 mg orally once daily for 14 days with or without
Metronidazole (Flagyl) 500 mg orally two times a day for 14 days
• Regimen B
Ceftriaxone (Rocephin) 250 mg intramuscularly once or Cefoxitin
(Mefoxin) 2 g intramuscularly plus probenecid 1 g orally in a single dose
concurrently once or
Other parenteral third-generation cephalosporin (e.g., ceftizoxime [Cefizox]
or cefotaxime [Claforan])plus Doxycycline (Vibramycin, Doryx) 100 mg orally
two times a day for 14 days with or without Metronidazole (Flagyl) 500 mg
orally two times a day for 14 days.
• Regimen C
Moxifloxacin 400 mg QD
Recommended regimens for in-patient treatment of patient with PID:
• Regimen A
Cefotetan (Cefotan) 2 g IV every 12 hours hours plus Doxycycline
(Vibramycin) 100 mg orally or intravenously every 12 hours
• Regimen B
Clindamycin (Cleocin) 900 mg intravenously every 8 hours plus
Gentamicin (Garamycin) loading dose intravenously or intramuscularly
(2 mg/kg of body weight), followed by a maintenance dose (1.5 mg/kg)
every 8 hours.
• Alternative parenteral regimens
Ofloxacin (Floxin) 400 mg intravenously every 12 hoursorLevofloxacin
500 mg intravenously once daily with or without Metronidazole
(Flagyl) 500 mg intravenously every 8 hours or Ampicillin/sulbactam

237
(Unasyn) 3 g intravenously every 6 hours plus doxycycline (Vibramycin,
Doryx) 100 mg intravenously or orally every 12 hours.
• Regimen C
• Ofloxacin 400 mg BD IV+ IV Metronidazole 500 mg TID followed by
oral Ofloxacin 400 mg BD =otral metronidazole 400 mg BD
• Regimen D
• IV Ciprofloxacin 400 mg +oral Doxycycline 100 mg BD + IV
Metronidazole 500 mg TID followed by oral Doxycycline 100 mg+
Metronidazole 400 mg BD
These regimens are to be used until at least 24 hours after the patient
demonstrates substantial clinical improvement. They may then be changed to
doxycycline (Vibramycin) 100 mg orally two times a day for a total of 14 days
of treatment. If tubo-ovarian abscess is present, many health care providers
use clindamycin (Cleocin) 900 mg orally three times a day or metronidazole
500 mg twice a day for continued therapy with doxycycline.
Hospitalization of PID patients and intravenous antibiotic therapy is
indicated in the following scenarios:
• Until other serious diagnoses are excluded, including appendicitis and
ectopic pregnancy
• If the patient is an adolescent
• If a pelvic abscess is suspected on examination or ultrasound
• Severe systemic/peritoneal symptoms including high fever, or signs of
peritonitis
• Inability to tolerate oral outpatient treatment because of vomiting
• If the patient is pregnant
• If the patient is unable or unlikely to comply with outpatient therapy
and/or 48-to 72-hour follow-up
• If HIV infection is present

238
• If the patient has not responded to outpatient management at 48-to 72-
hour follow-up
Surgery isn't usually done to treat PID unless it is needed to:
• Drain or remove a pocket of pus, such as a tubo-ovarian abscess.
• Cut scar tissue that is causing pain. This hasn't been shown to relieve
pain when the scarring is severe.
• Surgery-usually laparoscopy- is sometimes used when a diagnosis is still
unclear after other tests are done or when antibiotic treatment is not
working.
Endometritis
Endometritis is an inflammation of the mucosa membrane of the
uterine body. Rarely it may be isolated, most often the muscular layer of the
uterus is also involved in the process (metroendometritis).
Clinical picture: The acute stage of endometritis (metroendometritis) is
characterized by pain in the lower abdomen, which irradiates to the loin and
thighs, malaise, fever and profuse purulent discharge. Chronic endometritis
is a rare condition because of the frequency with which the endometrium is
shed. In the chronic stage these symptoms are less pronounced, there are no
specific signs or symptoms. Patient may complain of disturbances of
menstrual cycle, infertility. Acyclic sanguineous discharge may be observed
too. Sometimes patients at gynecological examination are found to have an
enlarged mobile “flabby” uterus, often retroverted and sometimes associated
with general pelvic inflammation or inflammation in anamnesis. Menstrual
irregularities and congestive discomfort or pain are complained of and the
cause is not known.
Diagnosis. It is based on the history (connection of the disease with
parturition, abortion, diagnostic curettage of the uterine cavity,
hydrotubation and other diagnostic manipulations). Objective findings in case

239
of acute endometritis include general signs of the inflammatory process
(fever, tachycardia, tenderness upon abdominal palpation, purulent vaginal
discharge, enlargement and tenderness of the uterus). Laboratory studies
help to detect leucocytosis and increased erythrocytes sedimentation rate
(ESR).
Data on the history of acute endometritis help to make the diagnosis in
the chronic stage of endometritis. The diagnosis of chronic endometritis is
histological, but the microscopic appearances are of infiltration mainly by
plasma cells and lymphocytes.
Treatment. Bed rest. Cold applications to the lower abdomen.
Antibiotics (see above), non-steroid anti-inflammatory drugs (NSAIDs),
desensitizing and vitamin drugs.
Salpingitis and Salpingo–Oophoritis (adnexitis)
Salpingitis means inflammation of Fallopian tube. It may be unilateral
and bilateral (Fig. 144). Salpingo-oophoritis means inflammation of uterine
tube and the associated ovary. Non-specific infection (staphylococci,
streptococci, Escherichia coli, associations of microbes), as well as (gonococci,
mycobacteria tuberculosis) can be the causative agents of this inflammation.
Salpingo-oophoritis ascends from the uterus and descends from peritoneum.
It may also have lymphogenous (from the rectum, sigmoid colon) and
haematogenous (from remote foci of infection in the body) routes. Edema and
damage of tissues lead to obstruction of the lumen in the tube with the
accumulation of exudate and formation of sactosalpinx (bag-like tumor in the
tube) and pyosalpinx in the presence of pus. Isolated inflammation of
fallopian tube is a rare finding since it also involves the ovary, which becomes
edematous and hyperemic. Abscess of the ovary (pyo-ovarium) emerges with
the development of marked purulent inflammation in the ovary. Purulent
process in the uterine tube and ovary leads to destruction and the formation
of a tuboovarian abscess.

240
Fig, 144. PID – salpingitis: A – drawing , B – photo
Clinical picture. Typical symptoms are pain, whites, menstrual cycle
disorders (bleeding) and infertility. Adnexitis is commonly accompanied by
gnawing pain, which may gradually intensify. In rupture of the pyosalpinx the
pain becomes violent, knife-like. Pain is localized in the iliac area and
irradiates to the sacrum. General clinical symptoms include fever (from
subfebrile to high), chill, indisposition, headache, dry mouth, nausea and
vomiting, tachycardia, dry tongue, abdominal flatulence and its tenderness to
palpation.

241
Painful tenesmus, compressed rectum and bladder are common in the
case of imminent rupture of pus into the gut. The chronic stage of the disease
is characterized by constant, dull pain intensifying during menstruation,
physical overstrain, gynecologic examination, sexual intercourse. Another
symptom is leucorrhea; it may be mucous, serous or purulent. When
pyosalpinx drains into the uterus, a large amount of purulent discharge can be
suddenly evacuated from the vagina. Patients complain of itching and
irritation of external genitalia, which occur due to secondary vulvitis.
Menstrual cycle disorders can be manifested both by cyclic and acyclic
bleedings. Menstruations are scant but last longer. Infertility occurs when
inflammation is transformed into a chronic stage and is associated with
occlusion of fallopian tubes due to adhesion of their mucosa or the
peritoneum. Hormonal dysfunction of the ovaries, which may also develop as
a result of inflammation, leads to sterility as well.
Diagnosis is based on history (abortions, diagnostic intrauterine
manipulations, chronic diseases such as tonsillitis, recent appendectomy,
overcooling) and typical development of a disease. Objective findings: fever,
tachycardia, dry coated tongue, abdominal flatulence, abdominal muscles,
which are tender and tense on palpation, and positive (Shchetkin-Blumberg
symptom). Dullness in sloping places, which is related to exudation, can be
elicited by percussion. Large tuboovarian abscess can be diagnosed on
abdomen palpation. Gynecologic examination discloses purulent discharge
from the cervical canal, displacement of the cervix, and tenderness of the
uterus. Thickened, soft and tender adnexa are palpated laterally to the uterus,
while a tuboovarian abscess is palpated as a tumor-like formation.
Flattening or overhanging of the posterior and lateral fornices is observed in
the presence of exudate in the abdominal cavity.
Treatment. Conservative treatment should include antibacterial therapy
(see above), hypothermy (ice bags applied to the lower abdomen and
hypothermy of the vagina), desensitizing agents, desintoxication (infusion)

242
therapy, vitamins, resolution therapy (biostimulator, enzymes) and
physiotherapy (diadynamic currents, ultrasound, inductotermy) in subacute
and chronic stages. The indications for surgical treatment of salpingitis,
salpingo-ophoritis may arise in the acute stage of the diseases:
o rupture of abscess, (or pyosalpinx, pyovarium) or suspicion on
rupture
o pelvioperitonitis resisting conservative treatment,
o tuboovarian abscess
o diffuse peritonitis,
o ineffectiveness of laparoscopic drainage during 24-48 hours
o etc
Parametritis
It is isolated inflammation of the parauterine cellular tissue. Anterior,
posterior and lateral parametritis are distinguished.
Etiologically parametritis is caused by pathogenic microorganisms
(streptococci, staphylococci, Escherichia coli, anaerobes).
Clinical picture. Usual symptoms include malaise, shivering, fever, low
abdominal pain. Micturition and defecation are painful and difficult. The
formation of an abscess in the parametrical infiltrate is associated with abrupt
increase of temperature, shivering, intensification of pain and its irradiation
to the sacrum and hip. Rupture of the abscess is evidenced by profuse effusion
of pus from the gut or its passage with the urine (if the abscess is ruptured
into the bladder). Parametritis has a long course. The process may
occasionally subside, just to resume again with a new force later. Parametritis
may cause scarring of the cellular tissue, which may alter the position of the
uterus and adnexa.
Diagnosis. The objective findings include symptoms of intoxication
attending the inflammatory process: high pyrexia, tachicardia, dry coated
tongue, change of blood formula. Abdominal palpation reveals a dense,

243
immobile, tender infiltrate communicating with the internal surface of the
iliac bone (most often from the side). Percussion elicits dullness in the
infiltrate area. Vaginal examination demonstrates uterine displacements (to
the healthy side), laterally to the uterus there is an infiltrate, which either
smoothes out or protrudes the lateral fornix of the vagina.
Treatment. In the stage of edema and infiltration the treatment includes
bed regimen, cold applications to the lower abdomen, and vaginal
hypothermia. Antibacterial (see above), NSAIDs, desensitizing,
desintoxication (infusion) and sedative therapy are administered as a rule.
Symptomatic therapy consists of administration of analgesic (suppositories
with belladonna, analgin).
At the stage when an abscess is formed in the area of the parametrical
infiltrate it is recommended to empty it through the posterior fornix (by
puncturing and drawing).
Pelvic Peritonitis
Pelvioperitonitis is an inflammation of the pelvic peritoneum
developing as a complication of inflammatory process in the pelvic organs
(salpingo-ophoritis, pyo-ovarium, torsion of the ovarian cyst pedicle, necrosis
of a myomatous node).
Clinical picture. Acute and chronic pelvioperitonitis are recognized.
Clinical symptoms include sharp abdominal pain, particularly in the lower
abdomen, high pyrexia, tachycardia, nausea, vomiting, abdominal distension,
flatulence and constipation. Abdominal examination reveals that the
abdominal wall does not participate in respiratory movements. Other findings
include tension of the abdominal wall, tenderness, positive Shchetkin-
Blumberg symptom. All these symptoms are more pronounced in the lower
abdomen. Bimanual examination discloses overhanging of the posterior
fornix, its tenderness upon palpation, and tenderness with cervical

244
displacement. The uterus and adnexa cannot usually be palpated since
examination is very painful and the anterior abdominal wall is tense.
Diagnosis is based on clinical findings, bimanual disclosing and
laboratory evaluations.
Treatment. The treatment should be combined and include:
1) antibiotic therapy;
2) NSAIDs
3) sedative and soporific drugs;
4) infusion therapy is recommended to control intoxication and impaired
metabolism;
5) If there is a danger that the process may spread to the peritoneum of the
upper abdominal cavity surgical intervention is indicated.
SEXUALLY TRANSMITTED PELVIC INFLAMMATORY
DISEASES
Gonorrhea
Etiology. Gonorrhea refers to the infection caused by Neisseria
gonorrhoeae (gonococcus). It is an intracellular, Gram-negative diplococcus.
Gonococcal PID is seen most often in younger women. The bacterium infects
the mucous membranes of the reproductive tract as well as those of the
mouth, throat, eyes, and anus. When symptoms are present, they may include
burning with urination, and vaginal discharge and pelvic pain in women.
Untreated gonorrhea can lead to pelvic inflammatory disease (PID),
infertility, and, rarely, disseminated gonococcal infection (DGI), a life
threatening infection of the blood. The incubation period of gonorrhea is 2 – 7
days, rarely 10 –15 days. Gonococci usually propagate in place with cylindrical
epithelium: in the cervix, uterine tubes, rectum, and urethra. Yet, the
gonococci may also infect the vaginal wall (in puerperants, girls).

245
Traditionally, Classification of gonorrhea is based on the duration of the
process and the clinical course of the disease.
Fresh (with duration of the disease up to two months) and chronic
forms of gonorrhea are distinguished.
Fresh gonorrhea is divided into acute, subacute and torpid. In fresh
torpid gonorrhea (G) the clinical manifestations are either insignificant or
absent. Examination of smears obtained in patients with fresh G usually
reveals gonococci. In fresh subacute gonorrhea the duration of process is
about 2 weeks, and clinical symptoms consist of subfebrile condition and
non-marked (non-pronounced ) signs.
Chronic gonorrhea. When the disease with torpid course has continued
for over two months or when its onset is unknown. Gonorrhea is often
combined with trichomoniasis, and staphylococcal and colibacillary infection.
With regard to the localization of the process gonorrhea of the lower
urogenital tract and gonorrhea of the upper genital tract are recognized. The
first form includes gonorrhea of the urethra, para-urethral ducts, Bartholin’s
glands and cervix. The second form includes gonorrhea of the uterine body,
oviducts, ovaries, peritoneum. The clinical courses of these two forms are
different.
The ICD10 coding system does not distinguish between acute and
chronic gonorrhea (table 6).

246
Table 6
ICD 10 codes of gonorrhea in women
Condition ICD-10-CM Codes
Gonorrhea
acute
A 54 (gonococcal infection)
-A 54.0 Gonococcal infection of lower genitourinary
tract without periurethral or accessory gland abscess
-A54.00 (gonococcal infection of lower genitourinary
tract, unspecified)
- A54.01 (gonococcal cystitis and urethritis,
unspecified)
- A54.02 (gonococcal vulvovaginitis, unspecified)
- A54.03 (gonococcal cervicitis, unspecified)
- A54.09 (other gonococcal infection of lower
genitourinary tract)
- A54.1 (gonococcal infection of lower genitourinary
tract with periurethral or accessory gland abscess)
- A54.2 (gonococcal pelviperitonitis and other
gonococcal genitourinary infection)
Gonorrhea of the Lower Urogenital System in Women.
Gonorrheal urethritis
The characteristic symptoms are unremarkable, may be mild pain and
burning during micturition (in patients with fresh acute form). Inspection of
the external orifice of the urethra discloses hyperemia and edema of the
mucous membrane, and the appearance of purulent exudate from the urethra.
Urethral palpation through the anterior vaginal wall is painful. Symptoms of
chronic urethritis are rather insignificant; micturition may be frequent.

247
Gonorrheal endocervicitis
Gonorrheal endocervicitis is observed in 82 – 90 % of patients with
fresh gonorrhea. The acute stage is characterized by dull low abdominal pain
and mucous or purulent discharge from the vagina. Examination of the cervix
discloses infiltrates, hyperemia, and exudation of mucous and purulent
discharge from the cervical canal. In the chronic form of gonorrheal
endocervicitis one can see insignificant pyo-mucous discharge from the
vagina and occasionally dull low abdominal pain. Menstrual disorders and
infertility (primary or secondary) are also diagnostically important.
Gonorrheal Bartholinitis, vulvitis and proctitis have similar symptoms.
Gonorrhea of the Upper Genital Tract in Women.
Gonorrheal endometritis
Having found the way into the uterine cavity, gonococci spread in its
mucous membrane, then the epithelial desquamation takes place in
individual sites, and gonococci penetrate into the subepithelial layer, where
leukocyte infiltration occurs. If infection with gonorrhea happens during
menstruation, gonococci get directly into the basal layer of the mucous
membrane.
Clinical picture. Acute gonorrheal endometritis is characterized by
fever, malaise, sharp low abdominal pain, and purulent discharge from the
uterus. The menstrual cycle is disrupted (menstrual delay, acycling bleeding).
General symptoms of intoxication are observed (dry tongue, tachycardia).
Gynecologic examination reveals an enlarged, soft and tender uterus, as well
as pyo-mucous and sanguineous purulent discharge.
Diagnosis is based on clinical findings and confirmed by laboratory
tests.

248
Gonorrheal salpingo-oophoritis
Gonorrheal infection first localized in the uterine cavity usually spreads
to the tubal mucosa by the canalicular pathway and then spreads to the ovary
and peritoneum.
Clinical picture. Gonorrheal salpingo-oophoritis has very pronounced
manifestation in the acute stage: acute pain through the abdomen, nausea
and vomiting, abdominal distension, constipation, fever and chill.
Intoxication symptom, namely dry tongue, tachycardia, headache, etc, are
also present. The abdomen is very tender upon palpation and percussion, and
tense in its lower portions; the Shchetkin-Blumberg symptom is very
pronounced. Percussion reveals tympany. Chronic form of gonorrheal
salpingo-oophoritis has the following symptoms: malaise, dull pain in the low
abdomen, periodically menstrual disorders (dysmenorrhoea,
menometrorrhagia), infertility and bladder and intestinal dysfunctions.
Patient’s working capacity is decreased.
Gonorrheal Pelvioperitonitis
The gonococci reach the abdominal cavity through its fimbrial end. As a
result, an exudative-inflammatory process develops in the peritoneum.
Clinical picture. Meteorism, constipation, difficult micturition, high
fever and chill are the main symptoms. Objective findings include
tachycardia, dry tongue, distended abdomen (which is tense and very tender
on palpation and percussion), and a positive Shchetkin-Blumberg symptom.
Gynecological examination may elucidate urethritis and endocervicitis, and
overhanging of the vaginal fornices.
Complication of gonococcal infection
Complication in women include:
PID development (because of the possibility of ascending infection)
Tubal scarring and infertility

249
Perihepatitis secondary to gonorrhea
Ectopic pregnancy with increased fetal and maternal mortality rates.
Diagnosis of gonococcal infection
Diagnosis is based on history, clinical findings and confirmed by
laboratory tests.
Laboratory Criteria for Diagnosis
Observation of gram-negative intracellular diplococci in a urethral
smear obtained from a male or an endocervical smear obtained from a
female, or
Isolation of typical gram-negative, oxidase-positive diplococci by
culture (presumptive Neisseria gonorrhoeae) from a clinical specimen, or
Demonstration of N. gonorrhoeae in a clinical specimen by detection of
antigen or nucleic acid NAAT). Culture and NAAT are available for the
detection of genitourinary infection with N. gonorrhoeae ; culture requires
endocervical swab specimens in females. A nucleic acid test (NAT) or
nucleic acid amplification test (NAAT) is a molecular technique used to
detect a particular pathogen (virus or bacterium) in a specimen of blood or
other tissue or body fluid. It does so by detecting and amplifying the RNA
or DNA of the pathogen, that is, making extra copies of its nucleic acids.
The term includes any test that directly detects the genetic material of the
infecting organism or virus, such as polymerase chain reaction, ligase
chain reaction, and others.
The most important methods of the laboratory diagnosis of gonorrhea
are bacterioscopic, cultural and serological. Specific microbiologic diagnosis
of infection with N. gonorrhoeae should be performed in all persons at risk for
or suspected to have gonorrhea. A specific diagnosis can potentially reduce
complications, reinfections, and transmission. Any patients with insignificant,
chronic forms of PID should be suggested with gonorrhea. The examination
and evaluation of the diagnosis of such cases, and chronic and fresh torpid

250
forms, may be performed after provocation, which increases the significance
of specific signs and helps to confirm diagnosisin latent, chronic, and mixed
forms of infection.
Methods of provocation. Provocation of gonorrhea is an artificial
exacerbation of the inflammatory process, which helps to diagnose and treat
the disease successfully.
Physiological provocation means the obtaining of smears for
bacterioscopy during menstruation.
Biological provocation consists in a single intramuscular administration
of gonovaccine (500 million microbic bodies).
Thermal provocation makes use of inductothermy with a vaginal
electrode.
Chemical provocation involves treatment of the urethral and rectal
mucosa with
1% solution of silver nitrate and the cervical canal with 5% solution of
silver nitrate
or Lugol’s solution in glycerol.
Combined provocation. Smears are taken 24, 48 and 72 hours after the
above mentioned procedures.
Treatment of gonorrhea
Gonorrhea therapy should be combined and include both systemic
effect and local influence on inflammation foci. A patient with an acute stage
of fresh gonorrhea, as well as a patient with exacerbation of chronic
gonorrhea, should be hospitalized. General treatment is: bed rest, special diet
(alcoholic beverages and spicy food should be excluded), antibacterial
therapy, methods aimed at increasing of immune resources, symptomatic
treatment.

251
Recommended Regimen of antibacterial treatment:
o Ceftriaxone 250 mg IM in a single dose
PLUS
o Azithromycin 1g orally in a single dose
Alternative Regimens, if ceftriaxone is not available:
o Cefixime 400 mg orally in a single dose
PLUS
o Azithromycin 1 g orally in a single dose
Gonovaccine is used after ineffective treatment with antibiotics and
relapses in the latent fresh torpid and chronic form of the disease (200-300
million from microbial bodies, 2-3 days later intramuscularly). During
pregnancy, immunotherapy and antibiotics with a negative effect on the fetus
are not applied.
For topical treatment of external genitalia, 0.002% solution of
Chlorhexidine, Rekutan, Baliz-2 is prescribed. Local treatment for chronic
gonorrhea is performed after the disappearance of signs of acute
inflammation. In the chronic and subacute stages of the inflammatory
process, physiotherapeutic methods of treatment are used: laser radiation,
paraffin therapy, mud therapy, diathermy, inductothermy.
Syphilis
Syphilis is a chronic systemic disease caused by Treponema pallidum
that has a multitude of clinical manifestations. The disease is contagious
during the primary and secondary stages and through the first year of the
latent stage. The organism can penetrate skin or mucous membranes, and the
incubation period is 10–90 days.
Primary syphilis. Signs and symptoms include a hard, painless chancre
that is usually solitary and that may appear on the vulva, vagina, or cervix.

252
Commonly, lesions occur on the cervix or in the vagina and go unrecognized.
Extragenital lesions may occur. Nontender inguinal lymphadenopathy
frequently is present. Even without treatment, the primary chancre resolves
within 2–6 weeks.
Secondary syphilis is a systemic disease that occurs 6 weeks to 6 months
after the primary infection through hematogenous spread of the organism.
Patients in this stage present with skin and mucous membrane lesions. Signs
and symptoms are generalized maculopapular rash involving the palms and
soles, mucous patches, condyloma latum (large, raised gray-white lesions),
and generalized lymphadenopathy. These symptoms spontaneously clear in
2–6 weeks.
Latent-stage syphilis follows untreated secondary stage disease and can
last 2–20 years. Signs and symptoms of the early latent phase (less than 1
year) include exacerbations of secondary syphilis in which the mucocutaneous
lesions are infectious. The late latent phase (longer than 1 year) is not
infectious by sexual transmission, but the spirochete may infect the fetus
transplacentally.
Tertiary syphilis develops in up to one-third of untreated or inadequately
treated patients. Signs and symptoms include involvement of the
cardiovascular system (e. g., endarteritis, aortic aneurysms, and aortic
insufficiency) and involvement of the CNS and musculoskeletal system, which
results in varied disorders. Gummata of skin and bones occur in late tertiary
syphilis. The CNS manifestations may include generalized paresis, tabes
dorsalis, changes in mental status, optic atrophy, and Argyll Robertson pupil,
which is pathognomonic of tertiary syphilis. Neurosyphilis must be ruled out
in those with more than 1 year's duration of disease. Cerebrospinal fluid
should be tested for fluorescent treponemal antibody absorption reactivity.
Diagnosis is made definitively by Wassermann test, dark-field
examinations and direct fluorescent antibody tests of lesion exudate or tissue.
After screening with nonspecific serologic tests and rapid plasma reagin
253
(RPR) tests, clinicians can then use specific tests to confirm the diagnosis.
The specific serologic tests are FTA-ABS and microhemagglutination assay for
antibody to T. pallidum. False-positive results may be seen in 1% of the
nonspecific serologic tests. Biologic false-positive results, usually of low titers,
may be caused by pregnancy, autoimmune disorders, chronic active hepatitis,
intravenous drug use, febrile illness, and immunization. Serologic tests
become positive 4–6 weeks after exposure, usually 1–2 weeks after
appearance of the primary chancres.
Treatment. T. pallidum is sensitive to many antibiotics, but reactions
are common and care is required in treatment. Most patients receiving
effective treatment for early syphilis with any antibiotics will display some
degree of reactions – rigors, sweating, headache, for about 24 hours. It can be
modified by giving prednisolon 5mg 6-hourly. Erythromycin 2,0 g per day in
the course of 15 days. Doxycycline, azithromycin may be used too.
Molluscum Contagiosum
Molluscum contagiosum is a benign infection of the skin by poxvirus and is
spread by sexual or nonsexual contact and autoinoculation. The incubation
period ranges from several weeks to months.
Clinical picture. Signs and symptoms include the appearance of dome-
shaped papules with central umbilication ranging from 1 to 5 mm in diameter.
Multiple lesions may arise but generally fewer than 20. The lesions are
usually asymptomatic but occasionally are pruritic. They are usually self-
limited and may last for 6–9 months.
Diagnosis is made by gross inspection or microscopic examination of
white, waxy material expressed from a nodule.
Treatment consists of evacuation of the white material, excision of the
nodule with a dermal curette, and treatment of the base with ferric subsulfate
(Monsel's solution) or 85% trichloroacetic acid. Cryotherapy with liquid

254
nitrogen can also be used. Sexual partners should be examined and treated as
well.
Genital Herpes
Genital herpes is a recurrent, sexually transmitted infection by the
herpes simplex virus (HSV) (80% of cases are due to type II) that results in
genital ulcers. Infection with genital herpes has reached epidemic
proportions, with an incidence in the United States of 500,000 to 2 million
cases per year. The prevalence is 10 million to 30 million cases per year. The
incubation period is 3–7 days.
Clinical picture. Primary infection may result in systemic as well as local
manifestations. The patient may experience a virus-like syndrome with
malaise and fever, then paresthesias of the vulva that are followed by vesicle
formation. These are often multiple, resulting in shallow, painful ulcers that
may coalesce. Multiple crops of vesicles and ulcers can occur in a 2–6 week
period. The symptoms last for approximately 14 days, peaking at
approximately day 7. The outbreak is self-limited, and lesions heal without
scar formation. Viral shedding can continue for 2–3 weeks after the
appearance of lesions. Cervical lesions are common in true primary
infections.
Recurrent herpetic outbreaks are usually shorter in duration (averaging
7 days), with less severe symptoms. They are often preceded by a prodrome of
itching or burning in the affected area. Systemic symptoms are usually absent.
Fifty percent of infected women experience their first recurrence within 6
months and have an average of 4 recurrences in the first year. Thereafter, the
rate of recurrence is quite variable. Latent herpes virus resides in the dorsal
root ganglia of S2, S3, and S4. Its reactivation can be triggered by an
immunocompromised state such as pregnancy.

255
Complications include herpes encephalitis (rare) and infection of the urinary
tract, which results in retention or severe pain or both.
Diagnosis is usually by inspection alone; however, if a definitive
diagnosis is needed, a viral culture can be obtained. The vesicle should be
opened, then vigorously swabbed. Sensitivity of a viral culture is
approximately 90%. Immunologic or cytologic tests are not as sensitive.
Polymerase chain reaction (PCR) has potential use as a rapid and sensitive
diagnostic technique but needs further testing.
Treatment. Aciklovir 200 mg orally 4-5 times a day 1 -10 weeks course
is administered. Viferon 150,000 – 500,000 units of interferon in vaginal
suppositories may be used 2 times a day during 5-7 days.
Goals of treatment are to shorten the clinical course, decrease transmission,
and prevent complications and recurrence. The virus cannot be completely
eradicated. An effective HSV vaccine is not yet available.
Counseling. Patients should be advised to remain abstinent from the
onset of prodromal symptoms until complete reepithelialization of lesions.
HSV infection may facilitate human immunodeficiency virus (HIV) infection.
There is no probable association with the development of squamous
intraepithelial lesions.
Chlamydia infection in women
Chlamydial Infection of the genitourinary tract is the most common
sexually transmitted disease (STD) in females. It is caused by chlamydial
strains D-K (which means chlamydial strain D, chlamydial strain E, etc., until
chlamydial strain K. The causative agent of chlamydial infection is a gram
negative bacteria Chlamydia trachomatis. Chlamydia - very interesting from a
scientific point of view, microorganisms. Despite the fact that they belong to
the kingdom of bacteria, nevertheless, chlamydia has certain traits that bring
them closer to viruses. This applies, above all, to their ability to infect cells of
the body and multiply directly in them. Bacteria are not able to produce some

256
enzymes necessary for their life, and therefore can live only in foreign cells.
Thus, chlamydia are intracellular parasites. Chlamydial transmission usually
is caused by sexual contact through oral, anal, or vaginal intercourse.
Neonatal infection (eg, conjunctivitis or pneumonia) may occur secondary to
passage through the birth canal of an infected mother.
Risk factors that may predispose patients to Chlamydial infection (ChI)
include the following:
Multiple sexual partners or a new sexual partner
Age 15-24 years (especially < 19 years)
Poor socioeconomic conditions (eg, homelessness)
Commercial sex workers
Non-use of barrier contraceptives
History of previous sexually transmitted disease: Chlamydial Infection
is often accompanied by other STDs
This infection is easily spread because it often causes no symptoms and
may be unknowingly passed to sexual partners. In fact, about 75% of infections
in women are without symptoms. Chlamydia infects columnar epithelial cells,
which places the adolescent female at particular risk because of the presence
of the squamocolumnar junction on the ectocervix until early
adulthood. Infection with chlamydial organisms invokes a humoral cell
response, resulting in secretory immunoglobulin A (IgA) and circulatory
immunoglobulin M (IgM) and immunoglobulin G (IgG) antibodies and a
cellular immune response.
Symptoms. Early-stage Chlamydia trachomatis infections often cause
few or no signs and symptoms. When signs or symptoms occur, they usually
start one to two weeks after exposure to chlamydia. Even when signs and
symptoms occur, they're often mild and passing, making them easy to
overlook. Chlamydia trachomatis can also infect the rectum. While these
infections often cause no signs or symptoms, patient may experience rectal

257
pain, discharge or bleeding. It's also possible to acquire chlamydial eye
infections (conjunctivitis) through contact with infected secretions.
Signs and symptoms of chlamydia trachomatis infection may include:
Painful urination (dysuria)
Lower abdominal pain
Mucopurulent cervical or vaginal discharge
Urethral discharge( thin and mucoid)
Mucopurulent rectal discharge
Painful sexual intercourse in women
Intermenstrual bleeding and bleeding after intercourse
In gynecological examination one can find cervical friability ( easy
bleeding on manilulation), cervical motion tenderness, adnexal fullness or
tenderness, associated with progression to pelvic inflammatory disease,
lower abdominal tender to palpation,upper right quadrant abdominal
tenderness (Fitz-Hugh-Curtis syndrome).
Complications. The complications associated with Chlamydial Infection
in Females could include:
Pelvic inflammatory disease, which is an infection of the uterus, ovaries,
and fallopian tubes
Sepsis: A severe infection that spreads via the blood stream
Fitz-Hugh Curtis disease: Perihepatitis, inflammation of membrane
around the liver
Tubo-Ovarian abscess: Abscess formation in the ovaries and fallopian
tubes
Infected pregnant women can transmit the infection to the child during
delivery, causing chlamydial pneumonia and chlamydial conjunctivitis
in the newborn
Ectopic pregnancies due to scarring of fallopian tubes
Infertility (either relative or absolute).

258
Reactive arthritis. People who have chlamydia trachomatis are at higher
risk of developing reactive arthritis, also known as Reiter's syndrome.
Diagnosis. Nucleic acid amplification tests (NAATs) are the most
sensitive tests for detecting chlamydia and gonococcal infections. NAATs can
be performed on endocervical, urethral, vaginal, pharyngeal, rectal, or urine
samples (first-void is preferred).The accuracy of NAATs on urine samples has
been found to be nearly identical to that of samples obtained directly from the
cervix or urethra. On wet mount, a finding of leukorrhea (more than 10 white
blood cells per high-power field on microscopic examination of vaginal fluid)
has been associated with chlamydial and gonococcal infections of the cervix.
Oropharyngeal and rectal swabs may also be used.
Treatment of Chlamydia infection. Antibacterial treatment is effective
in 95% of patient with uncomplicated Chlamydial infection. Uncomplicated
genitourinary chlamydia infection should be treated with azithromycin
(Zithromax; 1 g, single dose) or doxycycline (100 mg twice daily for 7days).
Alternatives regimens are:
Erythromycin, 500 mg four times daily for 7 days
or
Erythromycin ethylsuccinate, 800 mg four times daily for 7 days
or
Levofloxacin (Levaquin), 500 mg once daily for 7 days
or
Ofloxacin (Floxin), 300 mg twice daily (or 600 mg once daily) for 7
days
Partners should be notified of infection and treated appropriately.

259
Self test
1. Which of the following is not a characteristic of acute
endometritis ?
A. increasing of temperature
D. enlargement of the uterus
C. softening of the uterus
D. induration of the uterus
2. Acute bartolinitis:temperature is 38. 2, infected area is
hyperemic,painful, and fluctuated. What is the likely
treatment?
A. antibiotics
B. antibiotics+ sulfanilamides
C. surgical incision, dreinage, antibiotics
D bed-rest, cold application, and waiting for spontaneous resorption
3. Which of the following is more frequent causative agent of acute
endometritis?
A. trichomonas
B. streptococcus
C. staphylococcus
D. mixed infection
4. Which of the following is not a characteristic of acute
endometritis?
A. pain in lower abdomen
B. high temperature
C. enlargement of the uterus
D. normal general condition
5. Which of the following is not an indication for the surgical
treatment?
A. diffuse peritonitis
B. peritubal abscess

260
C. gonorrheal pelvioperitonitis
D. acute bartolinitis
6. In fresh subacute gonorrhea the duration of process is
A. about 2 weeks
B. about 2 months
C. about 2 days
D. about 2 hours
7. The treatment of gonorrheal pelvioperitonitis should be
A. surgical
B. conservative
C. short-distance radiation therapy
D. treatment is not necessary at all
8. Diagnosis of vulvovaginal candidiasis is made by
A. specula examination, microscopic examination of smears
B. questioning of the patient
C. surgical intervention
D. questioning of patient’s family
9. What drugs should be used for treatment of candida infection?
A. antibiotic drugs
B. hormonal drugs
C. antifungal drugs
D. antipruritic drugs
10. What should be used for treatment of trichomonas vaginitis?
A penicillin
B. fluconazole
C. metronidazole
D. aciklovir

261
Chapter 5. NEYROHUMORAL CONTROL OF THE
MENSTRUAL CYCLE
Each menstrual cycle is a complex interaction between the
hypothalamus, pituitary, ovaries and endometrium, which are integrated into
an functional system called the hypothalamus-pituitary-ovarian axis. The
menstrual cycle is controlled by this axis, which acts as a system with negative
feedback in addition to its burst gonadotropin mean cycle, resulting peptide
gonadotropins stimulate the production of steroid hormone in the ovaries,
which in turn inhibits the secretion of gonadotropin, thus allowing carry out
cycles.
The biological clock, which is responsible for the rhythmicity of the
cycles, consists in the pulsatile release of an hypothalamic decapeptides: the
Gonadotropin Releasing Hormones (GnRH). The hypothalamus secretes
follicle-stimulating hormone releasing hormone (FSH-RH) and luteinizing
hormone releasing hormone (LH-RH). These decapeptides act on the
pituitary gland in a pulsatile manner, which leads to the secretion of the
gonadotropins: follicle-stimulating hormone (FSH) and luteinizing hormone
(LH). It is the frequency and amplitude of these pulses, which determine the
quantity of each hormone ultimately secreted. The pulsatile secretion of
GnRH depends on external events (psychological factors, the nyctohemeral
rhythm) which reach the hypothalamus from the cortex through the limbic
system, but depends also on the feed-back effect that the ovarian steroids
exert on the hypothalamus and the pituitary.
FSH allows recruitment and growth of the ovarian follicles as well as the
selection of the dominant follicle whereas LH induces follicular rupture and
sustains the corpus luteum.

262
Ovaries during the menstrual cycle
Ovarian follicles are composed of an outer layer of thecal cells and an
inner layer of granulosa cells, which engulf the oocyte and host an antrum
(fig.145)
At the start of the menstrual cycle, the ovary contains several antral
follicles. These follicles consist of an oocyte, which is separated from a fluid-
filled sac called the antrum, both of which are surrounded by a layer of
granulosa cells (cumulus cells and mural cells respectively). These cells are
surrounded by a basal membrane, around which lies another layer of theca
cells. The thecal cells have LH receptors, and produce androgens
(testosterone and androstenedione) in response to LH. The androgens cross
the basement membrane to reach the granulosa cells where aromatase
transforms them into estrogens (estradiol and estrone respectively).
Conversely, granulosa cells have FSH receptors; androgens are absorbed by
these cells and metabolized to estradiol (E2). Granulosa cells also produce the
peptide hormone inhibin, which includes two isoforms, A and B. Aromatase is
an FSH dependent enzyme and the FSH receptors are located on the
granulosa cells. FSH stimulates maturation of primary oocyte in an immature
follicle.
During the first week after menses (in a 28 days cycle), FSH continues
to increase, the follicles grow intensely and FSH increases the expression of
its own receptor and of the LH receptor on the granulosa cells. During this
period, the follicles produce relatively small amounts of estradiol and the
circulating concentration of this steroid is relatively constant (fig.146).
During the second week, the follicles continue to grow and since they
have increased their FSH receptors on the granulosa cells their aromatase
actively transforms the thecal androgens into estrogens and the circulating
estradiol levels increase. This increase induces a negative feed-back on FSH
which decreases slightly in the blood. 10-15 primordial follicles start
maturing, but only one matures to fully dominant (Graffian) follicle. The

263
follicle, which has the highest number of FSH receptors, the maximal
aromatase activity and thus produces the highest concentration of estradiol is
named the dominant follicle (Graffian) and will be selected for ovulation, the
others gradually degenerate during a process called atresia (degeneration).
Fig. 145. The ovarian follicle: structure and hormones (Geneva Foundation for
Medical Education and Research, Training Courses, Edited by Aldo
Campana, September 27, 2017)

264
With its development, the dominant follicle secretes increasing levels of
estradiol (E2); this acts on the endometrium to stimulate proliferation. At the
pituitary gland, rising levels of E2 and inhibin B act to reduce FSH secretion
through a negative feedback mechanism. This phase of the cycle (from day 1
to 13) is called follicular phase. The follicular phase of the ovarian cycle
corresponds to uterine phase, which is called proliferative phase
(proliferation of the functional layer of the endometrium cycle is taking place
here). Under the influence of E2 marked cellular proliferation of the epithelial
lining, the endometrial glands and the connective tissue of the stroma of
endometrium.

265
Fig. 146. FSH and LH changes in menstrual cycle (Geneva
Foundation for Medical Education and Research, Training Courses, Edited by
Aldo Campana, September 27, 2017)

266
During the early and mid-follicular phases, E2 exerts negative feedback
on LH secretion, which ensures basal levels during this period. When ovum
has nearly matured, estrogen levels reaches a threshold above which they
stimulate production of LH, LH Surge (Positive feedback). In the late
follicular phase (i.e about 36 hours prior to ovulation), E2 reaches levels in
the circulation which switch this negative feedback effect to a positive
feedback effect. This leads to a surge in LH (which is accompanied by a
smaller surge in FSH) over a 24-hour period in the 24 hours prior to
ovulation. This LH surge leads to rupture of the dominant follicular wall and
release of the oocyte. Follicular rupture is called ovulation, which occurs
about 36h after the LH peak. It is because granulosa cells have acquired LH
receptors (effect of FSH) and are now responsive to LH. This peptide induces
the secretion of enzymes, which digest the follicular wall. The initial rise of
LH (at the beginning of the peak) is sufficient to allow the granulosa cells to
secrete small amounts of progesterone, which participate in the mechanism of
induction of the LH peak.
The released egg cell is swept into the fallopian tube by the cilia of the
fimbriae. Fimbriae are finger like projections located at the end of the
fallopian tube close to the ovaries and cilia are slender hair like projections on
each fimbria. Ovulation takes place at midpoint of menstrual cycle, thus at
28-days cycle ovulation happens at day 14th.
Once the oocyte has been expelled from the ruptured follicle, LH
induces the secretion of progesterone from the remaining granulosa cells that
organize themselves in a new gland called the corpus luteum (a process
known as luteinisation).
On the 15th day of menstrual cycle, the luteal phase begins. It lasts
until day 28 of the cycle. The following events occur during this phase:
the egg cell released during the ovulation phase stays in the fallopian
tube for 24 hours;

267
if a sperm cell does not impregnate the egg cell within that time, the egg
cell disintegrates.
Luteal phase corresponds to secretory phase of endometrial cycle.
Luteal phase is characterized with fixed duration – 14 days.
Following ovulation, there is an abrupt fall in E2 production from the
ruptured follicle. The follicle undergoes a series of changes, which convert it
into an endocrine structure called the corpus luteum (“yellow body” or
“corpus luteum”). This produces E2 and progesterone, which act on the
endometrium to promote implantation. Progesterone hormone (17α-
hydroxyprogesterone):
• it is a steroidal hormone, produced by the mature ovarian follicle;
• it is the predominant hormone is the secretory phase.
17α-hydroxyprogesterone:
stimulates the glandular cells to secrete glycogen, mucus and
other substances (thus the naming is secretory phase, or secretory
change of endometrium);
the glands become torturous and the lumens are dilated and filled
with these substances;
the stroma becomes edematous;
the spiral arteries extend into the superficial layer of the
endometrium and become convoluted.
Progesterone and estradiol increase and reach a plateau around day 22.
This induces a negative feed-back on LH and FSH which decrease in the
circulation. If implantation does not occur, Human Chorionic Gonadotropin
(hCG) is not present, the corpus luteum is not sustained any longer and
estradiol and progesterone decline. The normal life span of the corpus luteum
is 10 days then it regresses and is replaced by an avascular scar called corpus
albicans. If pregnancy doesn’t occur by day 23, the corpus luteum regresses,
secretion of progesterone and estradiol declies, and the endometrium
undergoes involution. This decline induces an increase in FSH, which will

268
recruit the follicles for the next cycle. If pregnancy does happen, the embryo
(the fertilized egg) releases human chorionic gonadotropin (HCG). HCG
maintains the corpus luteum instead of it degenerating. The corpus luteum
goes on secreting estrogen and progesterone. The lining of the uterus is thus
maintained and the period does not occur. The lining of the uterus provides
the right environment for the embryo to implant and develop into a baby.
The endometrium during the menstrual cycle
The endometrium is composed of the basal (stratum basalis) and
functional (stratum functionalis) layers. The basal layer is deep and
adjacent to the myometrium, while the functional layer comprises the
superficial two-thirds of the endometrium. The functional layer is divided
into stratum compactum and stratum spongiosum. The stratum compactum
is a superficial thin layer with gland necks and dense stroma, while the
stratum spongiosum is the deeper part of functional composed of glands
and loosely arranged stroma. Only the functional layer of endometrium
is shed with each cycle. The basal layer contains the progenitor cells that
regenerate the functional layer in each cycle. Endometrial tissue responds to
sex steroid hormones produced in the follicular and luteal phases of the
ovarian cycle.
Endometrial Vascular Supply
Arcuate arteries arise from the uterine arteries in the myometrium. The
arcuate arteries divide just inside the border of the endometrium and give rise
to numerous straight arterioles that supply the lower third of the
endometrium. These vessels continue as the spiral arteriole and supply the
functional two-thirds of the endometrium. Endometrial blood vessels have
abundant smooth muscle cells and just beneath the surface of the
endometrium, the capillaries are fenestrated. The venules from the area
drain into the uterine vein. A sketch of the endometrial vascular system can
be seen in Fig. 147.

269
Fig.147. Schematic presentation of the endometrial vascular system. The
endometrium is comprised of the stratum basalis (s. basilis) and stratum
functionalis (s. functionalis). Uterine arteries branch within the
myometrium to yield the arcuate and radial arteries. The radial artery
branches within the s. basilis to yield numerous straight and spiral arterioles
in the lower third of the endometrium. Spiral arterioles provide the vascular
blood supply to the s. functionalis through a vast network of fenestrated
capillaries.
In relation to the endometrial change, the menstrual cycle is divided
into proliferative and secretory phases, and cytoarchitectural and molecular
differences between the phases reflect endometrial responses to cyclic
changes in ovarian hormone.
Menstrual phase (from day 1 to 5 of 28th days cycle)
The functional layer (upper 2/3) of the endometrium is shed during
each menstrual cycle. Shedding of the endometrium presents menstrual
bleeding (syn.: menstruation, period). Endometrial bleeding occurs because
the progesterone levels have fallen below those required to maintain a

270
secretory endometrium. Because of the minimally lower level of
progesterone, the arteries supplying blood to the functional layer, constrict, so
that cells in that layer become ischaemic and die. A woman’s menstruation
consists of dark-colored blood from the endometrial lining of the uterus
mixed with the mucous secretion of the cervical canal and the secretion of the
vagina. Menstrual blood does not normally clot, as it is low in fibrinogen, does
not contain prothrombin, and is rich in calcium. The mean amount of total
blood loss during menstruation is 30 – 70 ml. Simultaneously with shedding
of the functional layer of endometrium, the process of regeneration starts
because of the influence of FSH and E2.
Proliferative Phase (from day 1 to 13, corresponds to follicular phase in
ovaries)
By the end of menstruation, the endometrial lining is about 2 mm thick
and is composed of epithelial cells that arise from the glands in the basal layer
and migrate to the denuded surface of the endometrium. Of note, the thin
epithelialized basal layer seen in early menstrual cycle is similar to the
endometrial cytoarchitecture observed in postmenopausal women and in
women with hypothalamic amenorrhea. Estradiol, produced by the ovaries on
approximately day 4 or 5 of the 28th day cycle, induces growth and
proliferation of the endometrium. The epithelial and stromal cells undergo
mitoses and multiply, thus causing the glands to increase in length, while the
stromal cells grow and expand the extracellular matrix. There is rapid
growth of the endometrium from cycle D4 or 5. Endometrial thickness
begins from a nadir of approximately 4.5 mm on cycle D4 and increases
linearly to a plateau of approximately 10 mm on cycle D9 or 10. The cessation
of endometrial growth occurs before estradiol levels reach their peak and
prior to the onset of secretory phase progesterone production.

271
Secretory Phase (from day 15 to 28, corresponds to ovarian luteal phase)
Secretion of progesterone after ovulation causes complete cessation of
endometrial epithelial proliferation. Progesterone exposure induces sub-
nuclear glycogen-rich vacuoles to appear on approximately day 16 (D16) of
the cycle and inhibits epithelial cell mitosis by D17. The vacuoles become
supranuclear on D18 and secretions are found in the gland lumen by D19–20.
Peak secretory activity is seen by D20–21. These changes are essential for
conception and the generation of an endometrial surface receptive to
blastocyst attachment (implantation). Progesterone provokes profound
stromal fibroblast changes characterized by cellular enlargement, as well as
laminin and type 4 collagen accumulations. In the luteal phase, type 4
collagen and laminin are present in the extracellular space of the
endometrial stroma and the basement membrane of glands and blood vessel
walls. The endometrium also makes large quantities of prolactin and the
insulin-like growth factor (IGF) binding proteins (IGFBP-1). The IGFBP-1
have several functions, including transporting the IGFs in the circulation,
mediating IGF transport out of the vascular compartment, localizing the IGFs
to specific cell types, and modulating both IGF binding to receptors and
growth-promoting actions. These changes in response to progesterone result
in dramatic alterations in both the extracellular matrix and secretory products
of the endometrium. Stromal edema is apparent by D20–23 and in the
few days immediately preceding menstruation, the stroma becomes
infiltrated by natural killer cells, macrophages, and T cells.
Summary:
The early follicular phase starts on the first day of the cycle and ends
when estradiol begins to increase (D1–D5). It is characterised by
increasing LH and FSH and constant low levels of estradiol. Shed of the
functional layer of endometrium takes place in the uterus, presenting
menstrual bleeding (menstrual phase and regeneration in uterus).

272
The late follicular phase starts with the increase in estradiol and ends at
its preovulatory peak. It is characterised by increasing estradiol and
decreasing FSH and LH levels (D6-D13).
Ovulation phase – rupture of follicular membrane and release of a
matured ovum from the ovary (D-14).
The early luteal phase starts on the day of ovulation (the day after the
LH peak) and ends when progesterone has reached its plateau. It is
characterized by increasing progesterone and decreasing LH and FSH
levels.
The mid luteal phase corresponds to plateauing progesterone levels. It is
characterized by constant elevated progesterone and constant low levels
of LH and FSH.
The late luteal phase starts when progesterone decreases and ends on
the day preceding the next menses. It is characterized by decreasing
progesterone and increasing LH and FSH levels. The luteal phase of
menstrual cycle corresponds to endometrial secretary phase).
THE NORMAL VALUES OF HORMONES DURING THE
MENSTRUAL CYCLE
Concentrations of pituitary gonadotropins and ovarian steroids stratified by
functional phases are presented in tables I to VI. The functional periods of the
cycle as defined above are compared to the days of the cycle either calculated
from the day of the LH peak or estimated for a 28 and a 35 days cycle. The
distribution of the observed values is given by the concentration of each
hormone at the 2.5th, 50th (median) and 97.5th percentile. By definition,
95% of the normal population is between the 2.5th and the 97.5th percentiles
of the distridution.

273
Table 7
FSH values in IU/l during the functional periods of the cycle
Period Days
28 days Cycle
Days
35 days
Cycle
Mean
Early Follicular 1-9 1-15 5.59
Late Follicular 10-14 16-20 4.09
Ealy Luteal 15-17 21-23 5.20
Mid Luteal 18-23 24-29 2.71
Late Luteal 24-29 30-35 2.48
Table 8.
LH values in IU/l during the functional periods of the cycle
Period Days
28 days Cycle
Days
35 days
Cycle
Mean
Early Follicular 1-9 1-15 3.40
Late Follicular 10-14 16-20 5.65
Ealy Luteal 15-17 21-23 7.00
Mid Luteal 18-23 24-29 3.64
Late Luteal 24-29 30-35 2.77

274
Table 9.
Estradiol values in pg/ml during the functional periods of the
cycle
Period Days
28 days
Cycle
Days
35 days Cycle
Mean
Early Follicular 1-9 1-15 57.6
Late Follicular 10-14 16-20 196.3
Ealy Luteal 15-17 21-23 129.0
Mid Luteal 18-23 24-29 203.5
Late Luteal 24-29 30-35 132.8
Table 10.
Estradiol values in pmol/l during the functional periods of the
cycle
Period Days
28 days
Cycle
Days
35 days Cycle
Mean
Early Follicular 1-9 1-15 211.4
Late Follicular 10-14 16-20 720.4
Ealy Luteal 15-17 21-23 473.4
Mid Luteal 18-23 24-29 746.9
Late Luteal 24-29 30-35 487.4
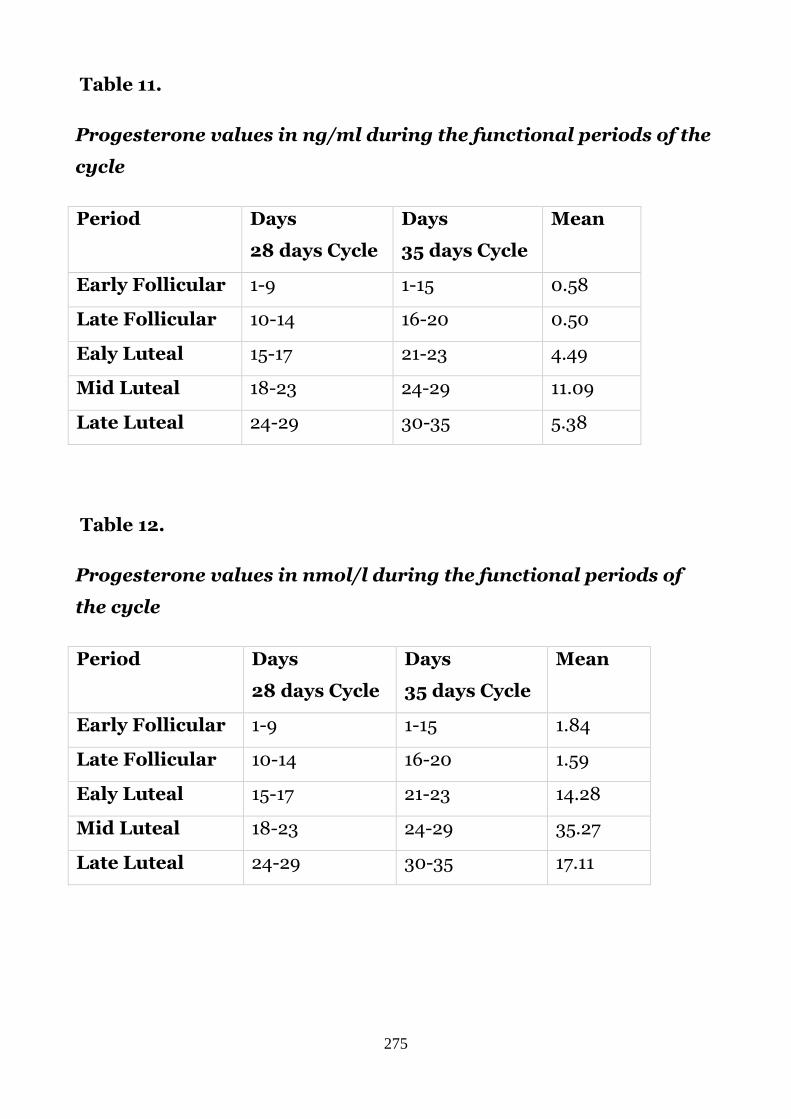
275
Table 11.
Progesterone values in ng/ml during the functional periods of the
cycle
Period Days
28 days Cycle
Days
35 days Cycle
Mean
Early Follicular 1-9 1-15 0.58
Late Follicular 10-14 16-20 0.50
Ealy Luteal 15-17 21-23 4.49
Mid Luteal 18-23 24-29 11.09
Late Luteal 24-29 30-35 5.38
Table 12.
Progesterone values in nmol/l during the functional periods of
the cycle
Period Days
28 days Cycle
Days
35 days Cycle
Mean
Early Follicular 1-9 1-15 1.84
Late Follicular 10-14 16-20 1.59
Ealy Luteal 15-17 21-23 14.28
Mid Luteal 18-23 24-29 35.27
Late Luteal 24-29 30-35 17.11

276
Self test
1. Follicle-stimulating hormone (FSH) stimulates
A. growth and maturation of follicle in the ovaries
B. beginning of menstrual bleeding
C. formation of corpus luteum
D. secretory changes of endometrium
2. The number of primordial follicles is about
A. 35,000-40,000
B. 400,000-500,000
C. 350-450
D. 35 -45
3. The estrogens
A. increase the muscular tone of the uterus
B. decrease the muscular tone of the uterus
C. have no influence on the muscular tone of the uterus
D. increase the depth of muscular layer of the uterus
4. The duration of secretory phase of menstrual cycle is
A. 14-15 days
B. 10-11 days
C. 24-25 days
D. 3-5 days
5. The duration of the desquamation phase is
A. 3-5 days
B. 14-15 days
C. 10-12 days
D. 24-25 days
6. All of the following are stages of the uterine cycle, except of
A. desquamation
B. regeneration

277
C. proliferation
D. ovulation
7. Rhythmic changes in the ovaries are divided into
A. three phases
B. two phases
C. four phases
D. five phases
8. What is the ovulation?
A. follicle ripening
B. rupture of the mature follicle
C. formation of the corpus luteum
D. rupture of the yellow body
9. The menstrual bleeding is caused by desquamation
A. of the functional layer of endometrium
B. of the basal layer of endometrium
C. of the intermediate layer of endometrium
D. of the endometrium in whole
10. The corpus luteum is formed during
A. each menstrual cycle
B. menarche
C. every other menstrual cycle
D. the issue of fertilization

278
Chapter 6. MENSTRUAL DISORDERS
Definitions and classifications
Menstrual disorder is a physical or emotional problem that interferes with a
normal menstrual cycle, causing various cycle disorders.
Violations of menstrual bleeding are manifested in a wide range. The
key characteristics of the menstrual cycle are the regularity, frequency,
intensity (severity) of bleeding, and the duration of menstrual bleeding.
Violations of the menstrual cycle are expressed in changes in each of these
indicators.
Postulation norms for menstrual bleeding are:
Frequency of menses within a 24 to 38 day window
Regularity (cycle-to-cycle variation) within ± 2 to 20 days
Duration of flow from 4 to 8 days
Volume of blood loss from 5 to 80 ml
Symptoms outside this normal range, or different from normal for the
individual, can become problematic and deserve a trial.
In general, three main groups of menstrual disorders are distinquished:
Classification of menstrual disorders:
Painful cramps (dysmenorrhea) during menstruation.
Heavy menstrual bleeding includes prolonged menstrual periods or
excessive bleeding.
Absence of menstruation (amenorrhea).
Light or infrequent menstruation refers to menstrual flow that occurs
one or two episodes in a 90-day period (menstruation that occur more
than 35 days apart).
In October 2009 the FIGO (International Federation of Gynecology and
Obstetrics) World Congress of Gynecology and Obstetrics in Cape Town
reviewed a series of recommendations, which are used today. According to

279
recommendations of FIGO world congress of gynecology and obstetrics
(October 2009) number of previously used terminology should be discarded:
because of their controversial, confusing, and poorly defined usage (Table 13).
Table 13
Discarded gynecological terminology
Menstrual terminologies that should be discarded
Menorrhagia (all usages, including ‘‘essential menorrhagia,’’ ‘‘idiopathic
menorrhagia,’’ ‘‘primary menorrhagia,’’ ‘‘functional menorrhagia,’’
‘‘ovulatory or anovulatory menorrhagia’’)
Metrorrhagia
Hypermenorrhea
Hypomenorrhea
Menometrorrhagia
Polymenorrhea
Polymenorrhagia
Epimenorrhea
Epimenorrhagia
Metropathica hemorrhagica
Uterine hemorrhage
Dysfunctional uterine bleeding
Functional uterine bleeding
The new terminology according abnormal uterine (menstrual) bleeding
and new classification (The PALM-COEIN Classification System) were
accepted.
Disturbances of regularity
o Irregular menstrual bleeding (IrregMB): bleeding of >20 days in
individual cycle lengths over a period of one year.

280
o Absent menstrual bleeding (amenorrhea): no bleeding in a 90-day
period.
Disturbances in frequency
o Infrequent menstrual bleeding: one or two episodes in a 90-day period.
o Frequent menstrual bleeding: more than four episodes in a 90-day
period.
Disturbances of heaviness of flow
o Heavy menstrual bleeding (HMB): excessive menstrual blood loss that
interferes with the woman’s physical, emotional, social, and material
quality of life and can occur alone or in combination with other
symptoms.
o Heavy and prolonged menstrual bleeding (HPMB): Less common than
HMB. It is important to make a distinction from HMB given they may
have different etiologies and respond to different therapies.
o Light menstrual bleeding: based on patient complaint, rarely related to
pathology.
Disturbance of the duration of flow
o Prolonged menstrual bleeding: menstrual periods exceeding 8 days in
duration on a regular basis.
o Shortened menstrual bleeding: uncommon, defined as bleeding of no
longer than 2 days.
*Irregular nonmenstrual bleeding
o Irregular episodes of bleeding, often light and short, occurring between
normal menstrual periods. Mostly associated with benign or malignant
structural lesions. May occur during or following sexual intercourse.
**Bleeding outside reproductive age
o Postmenopausal bleeding (PMB): Bleeding occurring >1 year after the
acknowledged menopause.
o Precocious menstruation: usually associated with other signs of
precocious puberty, occurring before 9 years of age.

281
* Irregular nonmenstrual bleeding and ** Bleeding outside reproductive age
are not violations of the actual menstrual cycle, refer to abnormal uterine
bleeding in general.
Additionally, following terms are used today
Acute AUB
An episode of bleeding in a woman of reproductive age, who is not
pregnant, of sufficient quantity to require immediate intervention to prevent
further blood loss
Chronic AUB
Bleeding from the uterine corpus that is abnormal in duration, volume,
and/or frequency and has been present for the majority of the last 6 months.
Patterns of Bleeding
The “shape” of the volume of the bleeding pattern over the days of one
menstrual period. It is usually recognized that about 90% of the total
menstrual flow is lost within the first 3 days of the cycle, with day 1 or 2 the
heaviest. In women with AUB this pattern is variable.
The following definitions are proposed for use in practice
Bleeding:
o Any bloody vaginal discharge that requires the use of protection such as
pads or tampons
Spotting:
o Any bloody vaginal discharge that is not large enough to require
sanitary protection
Bleeding/spotting episode:
o One or more consecutive days on which bleeding or spotting has been
entered on the diary card
Bleeding/spotting-free interval:

282
o One or more consecutive days on which no bleeding or spotting has
been entered on the diary card
Bleeding/spotting segment:
o One bleeding/spotting episode and the immediately following
bleeding/spotting-free interval
Reference period:
o The number of consecutive days on which the analysis is based (usually
taken as 90 days for women using long-acting hormonal systems and 28
or 30 days for women using once-a-month systems, including combined
oral contraception)
Different types of analysis that can be undertaken on bleeding patterns
within a reference period:
o Number of bleeding/spotting (B/S) days
o Number of bleeding/spotting episodes
o Mean, range of lengths of bleeding/spotting episodes (or medians and
centiles for box-whisker plot analysis)
o Mean, range (medians and centiles) of lengths of bleeding/spotting-free
intervals Number of spotting days and spotting-only episodes
No bleeding:
o no days of bleeding/spotting entered throughout the reference period
Prolonged bleeding:
o 10 days in one episode
Frequent bleeding:
o >4 episodes in one 90-day reference period
Infrequent bleeding:
o 17 days within one 90-day reference period
o
The etiology of menstrual disorders includes nervous and mental
diseases, malnutrition, some occupational hazards, systemic and gynecologic

283
inflammatory diseases, illness of the hemopoiesis, cardiovascular and other
systems, gynecologic operations, puberty disorders, and age-specific
reconstruction of the functional state in hypothalamic - pituitary - ovarian
axis in the menopause.
Causes of irregular periods (generally light) include:
Perimenopause (generally in the late 40s and early 50s)
Primary ovarian insufficiency (POI)
Eating disorders (anorexia nervosa or bulimia)
Excessive exercise
Thyroid dysfunction (too much or too little thyroid hormone)
Elevated levels of the hormone prolactin, which is made by the pituitary
gland to help the body produce milk
Uncontrolled diabetes
Cushing's syndrome (elevated levels of the hormone cortisol, used in the
body's response to stress)
Late-onset congenital adrenal hyperplasia (problem with the adrenal
gland)
Hormonal birth control (birth control pills, injections, or implants)
Hormone-containing intrauterine devices (IUDs)
Scarring within the uterine cavity (Asherman's syndrome)
Medications, such as those to treat epilepsy or mental health problems
Common causes of heavy or prolonged menstrual bleeding include:2,7
Adolescence (during which cycles may not be associated with ovulation)
Polycystic ovary syndrome (PCOS) (bleeding irregular but heavy)
Uterine fibroids (benign growths of uterine muscle)
Endometrial polyps (benign overgrowth of the lining of the uterus)
Adenomyosis (the presence of uterine lining in the wall of the uterus)
Nonhormonal IUDs
Bleeding disorders, such as leukemia, platelet disorders, clotting factor
deficiencies, or (less common) von Willebrand disease

284
Pregnancy complications (miscarriage)
Common causes of dysmenorrhea (menstrual pain) include:
Endometriosis (uterine lining grows outside the uterus)
Uterine abnormalities (fibroids or adenomyosis)
IUDs
Pelvic scarring due to sexually transmitted infections, such as chlamydia
or gonorrhea
Heavy menstrual flow
Dysmenorrhea
Dysmenorrhea is the occurrance of painful cramps during menstruation
(painful abdominal cramps). More than half of all girls and women suffer
from dysmenorrhea (cramps), a dull or throbbing pain that usually centers in
the lower mid-abdomen, radiating toward the lower back or thighs.
Menstruating women of any age can experience cramps.
While the pain may be only mild for some women, others experience
severe discomfort that can significantly interfere with everyday activities for
several days each month.
Pain can develop before the onset of menstruation and continue
throughout the period of menstrual flow. Sometimes, pain is severe and
attended by nausea, vomiting and other disturbances, which reduce the
patient’s working capacity. In many cases dysmenorrhea is just a
manifestation of systemic diseases. It may be attributed to retroflexion or
anteflexion of the uterus, cicatricial changes and narrowing of the cervical
canal, infantilism, and disturbances of central nervous system, nervous
stresses.
Primary and secondary forms of dysmenorrhea are distinguished. The
1st form does not appear to be linked to any organic disease and is congenital.
It develops in women with previously normal menstruations. Primary

285
dysmenorrhea is caused by menstruation itself. It is considered when a girl
does not begin to menstruate by the age of 16.
Secondary dysmenorrhea is triggered by another condition, such as
endometriosis or uterine fibroids. It occurs when periods that were previously
regular stop for at least 3 months.
Etiological factors of primary dysmenorrhea include:
o Elevated prostaglandin levels in the endometrial fluid
o The posterior pituitary hormone vasopressin may be involved in
myometrium hypersensitivity, reduced uterine blood flow, and pain in
primary dysmenorrhea
o Primary dysmenorrhea has also been attributed to behavioral and
psychological factors
Clinical features of primary dysmenorrhea:
o Onset shortly after menarche
o Usual duration of 48-72 hours (often starting several hours before
or just after the menstrual flow)
o Cramping or labor-like pain
o Often unremarkable pelvic examination findings (VE or rectal
exam)
Diagnosis of primary dysmenorrhea:
o Primary dysmenorrhea usually appears within a year after menarche
o The pain begins with the onset of menstruation (or just shortly before)
and persists throughout the first 1-2 days.
o The pain is described as spasmodic and superimposed over a
background of constant lower abdominal pain, which radiates to the
back or anterior and/or medial thigh
o Associated general symptoms, such as malaise, fatigue, nausea and
vomiting, diarrhea, lower backache, and headache may be present with
primary dysmenorrhea

286
o Dizziness, nervousness, and even collapse are also associated with
dysmenorrhea
Treatment of primary dysmenorrhea is directed at providing relief
from the cramping pelvic pain and associated symptoms that typically
accompany the onset of menstrual flow. To date, pharmacotherapy has been
the most reliable and effective treatment for relieving dysmenorrhea.
Nonsteroidal anti-inflammatory drugs (NSAIDs), which prevent the
formation and release of prostaglandins, and combination oral contraceptives
(OCs) are the most commonly used therapeutic modalities for the
management of primary dysmenorrhea.
The NSAIDs for treatment of primary dysmenorrhea include:
o Ibuprofen - 400 mg PO q4-6h; not to exceed 3.2 g/d
o Naproxen - 500 mg PO followed by 250 mg PO q6-8h or 500 mg q12h;
not to exceed 1.25 g/d
o Ketoprofen - 25-50 mg PO q6-8hr as necessary; not exceed 250
mg/day;
If an NSAID is not available, opioid analgesics, such as
acetaminophen (Tylenol,Vicodin) may help ease severe pain.
Other option is hormonal treatment: combined oral contraceptive pills
(COCPs), the levonorgestrel intrauterine device, and depot
medroxyprogesterone acetate provide effective pain relief and are associated
with a reduced menstrual flow. COCPs suppress the hypothalamic-pituitary-
ovarian axis and thereby inhibit ovulation and prevent prostaglandin
production in the late luteal phase. This generally significantly reduces the
amount of menstrual flow and effectively alleviates primary dysmenorrhea in
most patients. Ethinyl estradiol and norgestimate (Ortho Tri-Cyclen,
MonoNessa, Previfem, TriNessa): 1 tab/d PO for 21 d followed by 7 d off
medication (or taking inactive tab); begin new course on day 8 after taking
last active tablet. (Fig. 149).

287
Fig. 149. Ortho-Cyclen (norgestimate and ethinyl estradiol) 28 tablets
0.25 mg / 0.035 mg
Medroxyprogesterone acetate (DepoProvera) - inhibits secretion of
gonadotropins, thereby inhibiting ovulation and decreasing the thickness of
the endometrium. Usually administered as: 150 mcg IM once every 3 months.
Levonorgestrel-releasing intrauterine device (Mirena) - inhibits
secretion of gonadotropins, thereby inhibiting ovulation and decreasing the
thickness of the endometrium. Should be removed after 5 years.
Heat applied to the painful area may bring relief, and a warm bath twice
a day also may help. Simply changing the position of the body can help ease
cramps. The simplest technique is assuming the fetal position, with knees
pulled up to the chest while hugging a heating pad or pillow to the
abdomen. Dietary recommendations to ease cramps include increasing fiber,
calcium, and complex carbohydrates, cutting fat, red meat, dairy products,
caffeine, salt, and sugar. Smoking also has been found to worsen cramps.
Some research suggests that vitamin B supplements, primarily vitamin B6 in
a complex, magnesium, and fish oil supplements (omega-3 fatty acids) also
may help relieve cramps.

288
Secondary dysmenorrhea may be related to inflammatory processes,
endometriosis, and genital tumors.
Treatment. The aim of the secondary dysmenorrhea treatment is
elimination of the underlying cause (antiinflammatory, surgical, and
hormonal). When dysmenorrhea is coupled with infantilism, the treatment
should include invigorating, thermal and hormone therapy.
Symptomatic therapy should be directed at elimination of pain (analgin,
baralgin, papaverine, sedative means and microenemas with a warm
chamomile decoction).
Heavy menstrual bleeding
Heavy menstrual bleeding, heavy and prolonged menstrual periods are
menstrual bleeding due to ovulatory dysfunction (AUB-O) (PALM-COEIN
classification). Abnormal uterine bleeding (formerly, dysfunctional uterine
bleeding [DUB]) is irregular uterine bleeding that occurs in the absence of
recognizable pelvic pathology, general medical disease, or pregnancy. It
reflects a disruption in the normal cyclic pattern of ovulatory hormonal
stimulation to the endometrial lining.
ANOVULATORY MENSTRUAL BLEEDING
Anovulatory uterine bleeding is associated with anovulation caused by
impaired or unestablished functional relationships in the hypothalamic –
pituitary – ovarian axis.
There are various causes for the development of anovulatory uterine
bleedings: impaired secretion of hormones as a result of diseases and psychic
traumas, hypovitaminoses, intoxications, impaired function of the thyroid,
adrenals, and other endocrine glands.
The disease can develop in juvenile and reproductive age and in the
premenopausal period. When occurring in puberty (before 17-18 years of age),
anovulatory bleedings are referred to as juvenile. Occurring in reproductive

289
age (18-40 years of age), they are referred to as reproductive age bleedings,
and in menopausal period (after 40-45 years) - as menopausal bleedings. In
reproductive age this condition is commonly consequent upon the genital
inflammation.
In the pubertal period anovulatory uterine bleedings usually occur due
to unestablished interrelations in the hypothalamus – pituitary – ovaries -
uterus system.
In the premenopausal women the age-related changes take place in the
hypothalamic centers, which regulate the secretion of gonadotropic hormones
by the pituitary gland; there are alterations in the cyclic character of secretion
of these hormones and the corresponding ovarian hormones. Primary
changes in the ovaries and uterus can also provoke the disturbances of the
neurohormonal interrelationships.
Anovulatory bleedings are induced by the absence of ovulation and
luteal phase of the cycle. Anovulatory cycles are normal during puberty,
lactation and menopause. According to the age of patient anovulatory
menstrual bleedings are classified as juvenile (at pubertal, at adolescent
patients), bleeding of reproductive age patient, and premenopausal bleeding
(in premenopausal patients).
Anovulatory uterine bleeding develops in patients with persistence of
ovarian follicle or atresia of a few follicles. Persistent follicle prolongs to grow
within several weeks without ovulation, and releases a large number of
estrogens. When ovulation does not occur, no progesterone is produced to
stabilize the endometrium; thus, proliferative endometrium
persists, endometrium become thick. As a result, these patients have
constant, noncycling estrogen levels that stimulate endometrial growth.
Proliferation without periodic shedding causes the endometrium to outgrow
its blood supply. The tissue breaks down and sloughs from the uterus.
Subsequent healing of the endometrium is irregular and dyssynchronous.

290
Atresia of some small (unripe) follicles is associated with a low level of
FSH and with hypoestrogenism and the absence of ovulation. Low levels of
estrogen (hypoestrogenism) in such patients continue for a very long time -
more than 3 months. Because of this, the result in patients with follicular
atresia is almost the same: marked proliferation of the endometrium without
periodic shedding causes the endometrium to outgrow its blood supply. The
tissue breaks down and sloughs from the uterus. Subsequent healing of the
endometrium is irregular and dyssynchronous.
Both persistence and atresia are characterized by continuous,
monotonous secretion of estrogens. The persistence of a follicle is
characterized by continuous, monotonous high secretion of estrogens,
whereas atresia is characterized by continuous, monotonous low secretion of
estrogens. Ovulation does not occur and the corpus luteum fails to form, there
is no secretion of progesterone. Excessive proliferation of the endometrium
occurs as a result of prolonged exposure to estrogens in both processes.
Circulation in the endometrium is impaired, the capillary permeability is
decreased, and the sites of dystrophy and necrosis are manifested. In the end
persistent and atretic follicles undergo involution. The necrotic mucosa is
rejected slowly, which causes prolonged bleeding. Anovulatory uterine
bleedings are not attended with pain.
Clinical picture. Anovulatory bleedings normally occur at different
periods of amenorrhea: in 4-8 weeks in case of persistent follicle and 3-4
months in atretic one. Bleedings are more abundant in persistent follicles,
being occasionally profuse. It may lead to anemia and decrease the patient’s
working capacity. Patients complain of general fatigue, headache, poor
appetite and sleep, and so on. There may be pale skin, tachycardia, and
reduced blood pressure.
Secondary blood coagulation disorders, which can develop in the process of
bleeding, disappear when the menstrual cycle is normalized.

291
Diagnosis is based on general and gynecologic examination. At general
examination one should pay attention to the typical signs: bleedings that
follow the supression of menses, monophase basal body temperature, high or
low karyopycnotic index. These symptoms are less manifested in the presence
of atretic follicles.
Histological study of the endometrial scrape (preferably on the first
days of bleedings) reveals different types of hyperplasia, which may be
coupled with endometritis.
Anovulatory uterine bleedings should be differentiated from many
disease forms that are attended with bleedings (spontaneous abortions,
interrupted fallopian pregnancy, tumors of the uterus, hormone- producing
tumors of the ovaries, etc.).
Management. The major principles of treatment are: the arresting of
bleeding, prevention of its recurrence and regulation of ovarian function.
Stages of treatment depend on the patient’s age and her general condition.
Sometimes uterine bleedings can be so abundant that emergency care is
required, and the physician should take energetic steps to arrest the bleeding.
The doctor’s tactics largely depends on the patient’s age:
o at juvenile age (puberty) medical treatment is appropriative, while
surgical (D&C) used as a last resort, or in severe case (Hb< 90g/L;
o at reproductive and premenopausal agers D&C with histology –
mandatory ( to exlude malignancy).
Juvenile bleedings are usually treated by conservative methods. In all
patients with heavy menstrual bleeding (HMB), iron deficiency should be
assessed and treated. The target dose is in the range of 150 mg/day to 200
mg/day of elemental iron in 1 to 3 divided doses/day. To aid in absorption,
iron supplements should be taken on an empty stomach with a glass of orange
juice. The duration of replacement should extend at least 3 months beyond
normalization of hemoglobin to allow for replenishment of iron stores.

292
Because the underlying problem is bleeding from a hyperproliferative
endometrium that has outgrown its estrogen supply, the primary therapeutic
goal is reestablishment of estrogen supply in the form of high-dose oral or
parenteral estrogen. Estrogen provides hemostasis and progesterone
stabilizes the endometrium. The easiest way to administer these hormones is
by use of combined oral contraceptive pills (COCPs). Monophasic pills
containing at least 30—35 µg of ethinyl estradiol should be used initially and
can be given once daily in the adolescent who is not actively bleeding. Those
who bleed quickly (changing pads or swabs every few hours) may require 4
times a day until the bleeding stops (usually within 2-3 days). Then one tablet
three times a day for 3 days, then one tablet twice a day for 2 days, then one
tablet once a day for 21 days, then 7 days without taking the tablets. with
these 7 days a new menstruation will begin, and from the 1st day of the new
flow a new set of the same COCP tablets should begin with the usual scheme:
1 tablet once a day on the mouth during sleep for 21 days. Consumption of
COCP should be administered within 3-6 months.
In cases of ineffective conservative treatment, when there is a threat to
the life of the patient, the surgical curettage should be used for arresting of
bleeding.
Treatment of bleedings in the child-bearing age and, particularly, the
premenopausal bleedings should be started with curettage of the uterine
mucosa for arresting of bleeding and histological examination of the
endometrial scrape, which is followed by the arrest of bleeding. The day,
when D&C was done would register as the 1st day of the cycle and COCP
should be administered by scheme 1 tablet per mouth once a day at bed time
within 21 days, etc. The COCP should be administered for 6 months. The
histological study of the obtained sample helps to confirm the diagnosis.
As to conservative treatment, hormonal drugs are prescribed to arrest
bleeding (hormonal haemostasis) and for the regulation of the menstrual
cycle. The estrogen hemostasis consists in administration of estrogens, which

293
cause regeneration of the endometrium. With this aim, COCP 3 tbl /daily
until arrest of bleeding followed with 1 tbl/day within 21 days. Then – by
schedule 21 days, 3-6 months.
In case of acute, profuse bleeding, 3 steps of treatment are offered.
1. To stop bleeding: Premarin IV 25 mg every 4 hours until bleeding stops.
2. Exogenous progesterone to create secretory changes in the
endometrium and prepare for shading off: Medroxyprogesterone
acetate 10 mg of orally once a day for 10 days, followed by withdrawal
bleeding 3-5 days after completion of the drug.
3. COCP on schedule, 3-6 months.
The progesterone haemostasis is based on the ability of gestagens to
induce secretory changes in endometrium and desquamation of the
endometrium due to sudden stopping of treatment with progesterone
(“medicamentous curettage“). Progesterone is injected intramuscularly, 10-15
mg for 5-6 days. At the onset of treatment with progesterone, the bleeding
normally intensifies after which it gradually lessens and stops. When bleeding
has been arrested, cyclic hormone therapy is administered for 2 or 3 cycles.
Coagulants, hemostatic agents, stimulants of uterine- contractility
(Ergot-dugs) should be used as additional drugs. In all patients with heavy
menstrual bleeding iron deficiency should be assessed and treated. The target
dose is in the range of 150 mg/day to 200 mg/day of elemental iron in 1 to 3
divided doses/day.
In premenopausal and menopausal women the treatment begins with
diagnostic curettage obligatorily. If bleeding is combined with a subacute or
acute inflammatory process, the diagnoctic curettage is carried out only after
anti-inflammatory therapy. Hormone therapy is initiated after the histological
analysis of the endometrial sample. The therapy is directed at regulating the
menstrual function (in women under 48-50 years) or its suppression (in
women over 48-50 years). The drugs used are progesterones, synthetic
progestins,and androgens. Symptomatic treatment with contractile,

294
hemostatic, hemostimulating and sedative agents and vitamin therapy are
conducted simultaneously.
In ovulatory dysfunctional uterine bleeding, bleeding occurs cyclically,
and menorrhagia is thought to originate from defects in the control
mechanisms of menstruation. It is thought that, in women with ovulatory
dysfunctional uterine bleeding, there is an increased rate of blood loss
resulting from vasodilatation of the vessels supplying the endometrium due to
decreased vascular tone, and prostaglandins have been strongly implicated.
Therefore, these women lose blood at rates about 3 times faster than women
with normal menses.
OVULATORY MENSTRUAL BLEEDING
In ovulatory uterine bleeding is a bleeding, which occurs cyclically, and
it is thought to originate from defects in the control mechanisms of
menstruation. They are bleedings at three-phase menstrual cycle, (follicular
phase, ovulation and luteal phase), thus named ovulatory bleedings. 3 types of
ovulatory bleedings are distinguished:
shortened follicular phase, resulting in frequent
menstruations (proiomenorrhea);
shortened lutein phase (hypoluteinism);
prolonged lutein phase (hyperluteinism).
Uterine bleedings depending on shortened follicular phase of menstrual
cycle are often in puberty, in patients with inflammations of the uterus and
adnexas.
Clinical picture: the duration of follicular phase is 7-8 days, thus the
duration of menstrual cycle becomes shortened by 14-20 days, while the
duration and volume of menstrual blood loss sometimes increases
(hyperpolymenorrhea); the basal temperature is increased earlier than the10-
th day of cycle and the endometrial secretory phase is present.

295
Treatment: uterotonics, cyclic hormonal treatment, or assigning of
small doses of estrogens for 2-4-6 days of cycle.
Uterine bleedings depend on shortening of luteal phase of menstrual
cycle. They occur due to anticipatory involution of a corpus luteum, the
secretory transformation of the endometrium is incomplete. The detaching of
a functional layer of endometrium forming the uterine wall is not
synchronous, so the duration and volume of the flow may be increased
(polymenorrhea, hypermenorrhea).
Treatment: progesterone 1 ml of 1% solution (10 mg) intramuscularly
should be given during 8 days before menstrual flow. Or
Medroxyprogesterone acetate 10 mg should be given orally once daily for 10
days, it would lead to withdrawal bleeding 3-5 days after completion of the
course. Cyclic hormonal treatment may be used too. Vitamin E (50-60
mg/daily) and vitamin C (500 mg/daily) should be given.
Uterine bleedings depend on prolonged luteal phase of menstrual cycle.
They happen due to persistence of yellow body (corpus luteum) because of
prolonged secretion of LH and LTH.
Clinical picture: prolonged luteal phase of menstrual cycle (for 20-25
days), high level of progesteron, prolonged secretory phase of endometrium,
delayed menstrual flow, the duration of menstrual bleeding is about 1-1,5
months (polymenorrhea).
Treatment should be started with curettage of the uterine mucosa for
arresting of bleeding and histological examination of the endometrial scrape.
The n COCP should be administered: 1 tablet once a day within 21 days, from
the 22 day –arrest of intake of tablets, followed by withdrawal bleeding. The
new set of tablets should be started with the 1st day of a next flow.

296
Amenorrhea
Amenorrhea is an absent of menstrual bleeding in a 90-day period.
Amenorrhea may be physiological and pathological.
Amenorrhea is physiological before puberty, during pregnancy and
lactation, and after the menopause.
Pathological amenorrhea is termed primary when the patient has never
menstruated, or secondary when the periods are absent for more than 90
days.
Pathological amenorrhoea may be false (cryptomenorrhoea), when the
flow does not escape because of some obstruction, while the cyclic changes in
hypothalamus, pituitary gland, ovaries and uterus are normal; or true, when
the cyclic changes in female organism are absent. Pathological amenorrhea
may also be primary or secondary. Secondary amenorrhea is more common
than primary amenorrhea. The most common etiology is dysfunction of the
hypothalamic-pituitary-ovarian (HPO) axis.
Etiology of pathological amenorrhea includes:
nervous and mental diseases,
malnutrition,
some occupational hazards,
systemic and gynecologic inflammatory diseases,
illness of the haemopoiesis,
cardiovascular and other systems,
gynecologic operations,
puberty disorders, and age-specific reconstruction of the functional
state in hypothalamic - pituitary - ovarian axis in the menopause.
Classification of pathological amenorrhea
Pathological amenorrhea classified depending on the localization of
failure.

297
Central, or hypothalamic amenorrhea, sometimes named
stress amenorrhea
Anorexia nervosa
This is a condition, which may be considered as psychological. It occurs
in women in whom the desire to slim becomes obsessional. Fasting affects
hypothalamic function in some way not understood and amenorrhea results.
It is sometimes seen in ballet dancers, models, etc.
Weight loss (acute), malnutrition (chronic). Some acute infectious
diseases (sepsis, typhus), diabetes mellitus, pulmonary tuberculosis, other
severe diseases, chronic poisoning (mercuric, plumbic, phosphoric),
narcomania, alcocholism etc. usually result in amenorrhea due to depression
of hypothalamus and hypophysis.
Psychogenic amenorrhea
It’s occurring in patients with severe stress, for example, during war.
The nervous impulses in a hypothalamus are transformed in humoral
resulting in increased secretion of adrenocorticotropic hormone (ACTH),
depression of LH, FSH, and LTH secretion, low level of estrogen in ovaries
and absence of menses. Adipogenital dystrophy is characterized by dwarfing,
adiposity and genital infantilism, and is usually caused by a
craniopharyngioma that involves the pituitary gland and hypothalamus. The
treatment is surgical.
Pseudopregnancy
This is a curious isterical condition in which the patient either yearns
for or fears a pregnancy. Besides missing periods, she develops symptoms
such as nausea and vomiting, breast discomfort and tightness of her clothes
due to abdominal swelling.
“Amenorrhea and galactorrhea”
“Amenorrhea and galactorrhea” also known as Chiari-Frommel
syndrome. It is characterised with amenorrhea, prolonged galactorrhea, and

298
moderate adiposity, significant uterine and ovarian atrophy. It may be
functional due to excessive sedative therapy, it may occur in patients with
pseudopregnancy, in postpartum period. Small pituitary adenoma may
secrete prolactin and cause amenorrhea with galactorrhea. It also may be due
to primary hypothyroidism.
Pituitary amenorrhea due to pituitary disorders
There is a failure of production of gonadotropic hormones. Amenorrhea
is one of the aspects of general disorders and the gynecologist is seldom
responsible for treatment.
Pituitary infantilism (Levi-Loraine syndrome)
The adult resembles a child. No effective treatment is known. It happens
due to insufficiency of gonadotropic and somatotropic hormones, and may be
congenital and acquired, because of severe diseases, tumors of pituitary gland
etc.
Pituitary cachexia (Simmond’s disease)
This is usually due to ischemic necrosis of the pituitary glands
(hypophysis) due to thrombosis of pituitary vessels after postpartumsepsis,
tumors of pituitary gland, tuberculosis, syphilis. The main symptoms are:
weakness, anorexia, significant atrophy of muscles. Treatment with cortisone,
thyroxin and anabolic steroids may cause some improvement.
Amenorrhea and pituitary tumors
It happens due to poor secretion of gonadotropic hormons. In
acromegaly the eosinophillic adenoma of the pituitary gland may destroy the
gonadotropic cells, and the same may happen with other pituitary tumors. In
patients with basophillic adenoma Cushing syndrome develops. This is an
excess production of ACTH and depression of gonadotropic function. Clinical
signs are amenorrhea, obesity, hirsutism, hypertension, and hyperglycemia.

299
Postpartum unsufficiency of a hypothalamus and pituitary gland
(Sheehan's syndrome)
It is characterized with amenorrhea, hypotrophy of genital organs, and
loss of pubic hair, hypothyrosis, and depression of the adrenal cortex. The
principal causes are: excessive bleeding after delivery of the fetus, postpartum
sepsis, shock resulting in prolonged and significant failure of blood perfusion
in the area of hypothalamus and hypophysis.
Ovarian disorders
Failure of ovarian development occurs in cases of gonadal dysgenesis.
Stein–Leventhal syndrome is a disorder of unknown cause. After
some years of normal menstruation amenorrhoea occurs with hirsuties,
infertility. Both ovaries are enlarged due to cortical hyperplasia, which is a
characteristic of the disease, and they contain multiple small follicular cysts.
There are now corpora lutea. There is a block in the normal conversion of
progesterone to estrogen so that an intermediate androgen substance
androstenedione appears in excess. The urinary excretion of estrogens is
normal or low, while that of pregnanetriol (a metabolic product of certain
androgens) is raised.
Arrhenoblastoma is a very rare cause of amenorrhea.
Ovarian infections or new growths are processes destroying all ovarian
tissue.
Uterine disorders
Uterus may be congenitally defective.
Endometrium atrophies after irradiation with X-ray or radium, and
hysterectomy.
Other endocrine disorders
Amenorrhea occurs:
o in severe cases of hyperthyreoidism, myxoedema and cretinism;
o in some cases of diabetes;

300
o in Addison’s disease;
o with adrenocortical tumors or hyperplasia.
Oral contraception
A delayed first period is common after stopping oral contraception. More
prolonged amenorrhea sometimes occurs.
Diagnosis is based on general and special gynecologic examination,
ultrasonic, X-ray and hormonal tests.
Delayed menses should be evaluated if a girl has no signs of puberty by
age of 13, if menarche has not occurred by age of 16, or if 5 and more than 5
years have passed without menarche since the onset of puberty. Women of
reproductive age who have had menses should be evaluated if they are
amenorrheic for 3 and more than 3 months. First of all pregnancy should first
be ruled out.
History and physical examination can often determine the cause of
amenorrhea. Patients should be asked about abnormal growth and
development, family history of genetic anomalies, dietary and exercise habits,
lifestyle and environmental stresses. Noting hormonal alterations of the
pubertal process and of secondary sexual characteristics is central to the
diagnosis. Signs of virilization (masculinization) due to increased androgen
secretion (hyperandrogenism), especially hirsutism (an increase in hair
stimulated by andrigens), may occur. Other signs of hyperandrogenism
include temporal balding, voice deepening, increased muscle mass,
clitoromegaly, increased libido, and a decrease in feminine secondary sexual
characteristics (defeminisation), such as decreased breast size, and vaginal
atrophy. Galactorrhea may occur. The breast should be inspected accurately
for development and other signs (nonpuerperal secretion of milk, tumor etc).
Internal abnormalities may obstruct menstrual blood flow, causing
hematocolpos, hematometra. Visual inspection of vaginal and cervical mucus
is important because they are sensitive to estrogen. Special tests of functional

301
diagnosis (basal, or rectal, temperature, karyopyknotic index, “pupil” test, the
test of extensibility of the cervical mucus) are more appropriate. Usually they
help to determine the phase of menstrual cycle, and approximate level of
estrogen in the organism
Tests of hormonal diagnosis are more appropriate.
A progesterone test can help to differentiate ovarian and uterine forms of
amenorrhea. Medroxyprogesterone acetate 5 to10mg/day orally for 5 days or
progesterone 1 ml of 1% solution (10 mg) intramuscularly is given. Bleeding
confirms the presence of normal endometrium and of sufficient estrogen to
stimulate growth, and it helps to establish the diagnosis of anovulation or
incompetence of the corpus luteum. Absence of bleeding confirms anatomic
abnormality of endometrium (uterine emenorrhea), or absence of estrogen
priming of the endometrium. Thus estrogen – progesterine test should be
performed. Giving orally active estrogen (microfollin 0. 1 mg/day orally for 21
days, plus medroxyprogesterone acetate 5 to 10mg/day orally for the last 5 of
those days produces bleeding if there is no uterine amenorrhea.
Tests with hypothalamic releasing factors, with synthetic progestines,
chorionic gonadotropin, ACTH, and others are useful too. Basal serum level of
FSH, prolactin, thyroid stimulating hormone (TSH) should be measured in all
women with amenorrhea to confirm the clinical impression. X-ray of sella
turcica is indicated for women with hyperprolactinemia and for women with
low gonadotropin levels. It usually helps to ascertain the size of the area,
which is necessary in cases with tumor etc. Hystological examination of
endometrial specimen, obtained with curettage of the uterine cavity, is useful
too. Ultrasonography and computed tomography can usually localize an
androgen-producting neoplasm, and any other types of neoplasm.
By steps, testing of secondary (pathological amenorrhea) includes:
o A pregnancy test (measurement of serum or urinary human chorionic
gonadotropin) is recommended as a first step in evaluation of a
secondary amenorrhea.

302
o A CBC, urinalysis, and serum chemistries should be evaluated to help
rule out systemic disease.
o Serum prolactin, FSH, estradiol, and thyrotropin levels should also be
measured routinely in the initial evaluation of amenorrhea once
pregnancy has been excluded.
o Pelvic US may identify congenital abnormalities of the uterus, cervix,
and vagina, or absence of these organs.
o Magnetic resonance imaging can detect hypothalamic/pituitary lesions.
o Hysterosalpingography and hysteroscopy are indicated in cases of
possible Asherman syndrome.
The scheme of investigating to evaluate origin of secondary amenorrhea
presented in Fig.148.
Management. The need for treatment depends on:
o Underlying causes
o Need for regular periods
o Trying to conceive
Treatment depends on the level of damage ( Table 14).
If amenorrhea is of a hypothalamic nature the recommended treatment
includes sedative therapy, physiotherapy (endonasal electrophoresis with 2
per cent solution of vitamin B1, 0. 25 per cent solution of dyphenhydramine
hydrochloride).
In hyperprolactinemic amenorrhea drugs suppressing prolactin
secretion (bromocriptine 2. 5 mg thrice a day) are employed.
The treatment of ovarian amenorrhea (gonadal dysgenesis) is conducted
to facilitate the development of secondary characters and to normalize
processes in the hypothalamic – pituitary – ovarian – uterine axis
(substituting hormonal therapy).
Administration includes adequate nutrition, vitamin therapy, exercise
therapy, and a special diet intended to decrease the body weight in cases with
obesity. The peritoneal – sacral diathermia improving the blood inflow to the

303
genital organs is also used. Hormonal therapy of the cyclic hormones
(estrogens followed by progesterone) is administered.
Fig. 148. Investigating secondary amenorrhea

304
Table 14
Treatment of amenorrhea
Underlying causes Management
Pituitary tumor Promocryptine/ Surgery
Androgen producing ovarian tumor Surgery
Testicular feminization Gonad removal+ Hormone replacing
therapy
Turner’s syndrome Hormone replacing therapy
Atresia of a hymen Surgical incision
Thyroid disease Appropriate medical treatment
PCOS Appropriate medical treatment
Asherman syndrome Surgical incision of adhesions + IUD
insertion
Self test
1. Amenorrhea and galactorrhea is
A. Sheehan’s syndrome
B. Chiari-Frommel syndrome
C. meno-metrorrhagia
D. uteropathy
2. Heavy menstrual bleeding is
A. a long menstruation
B. a rare menstruation
C. a frequent menstruation
D. a short menstruation
3. Juvenile bleedings should be arrested
A. by conservative methods
B. by curettage of the uterine cavity
C. by physiotherapeutic methods

305
D. by manual technique
4. In premenopausal and menopausal women the treatment begins with
A. curettage of the uterine cavity and cytological examination of uterine mucosa
B. hormonal hemostasis
C. contractile agents
D. sedative drugs, cold application, bed rest, contractile agents
5. Cyclic uterine bleeding means
A. anovulatory bleeding
B. ovulatory bleeding
C. menopausal bleedings
D. bleeding due to genital inflammation
6. The principal causes of Sheehan's syndrome are all of the following, except of
A. excessive bleeding after delivery of the fetus
B. postpartum sepsis
C. significant failure of blood perfusion in area of hypotalamus and hypophysis
D. tumor of pituitary gland
7. Which of the following drugs can help to differentiate ovarian and uterine
forms of amenorrhea?
A. progesterone
B. estrogen
C. epinephrine
D. testosterone
8. The cause of uterine bleeding depending on prolonged luteal phase of
menstrual cycle is
A. the persistence of yellow body
B. the shortening of luteal phase
C. inflammations of the uterus and adnexa
D. infantilism
9. The treatment of juvenile bleeding should be started with
A. curettage of the uterine cavity

306
B. hormonal hemostasis
C. blood transfusion
D. sedative drugs, cold application, bed rest, anti-inflammatory treatment
10. In premenopausal women the treatment begins with
A. curettage of the uterine cavity
B. hormonal hemostasis
C. blood transfusion
D. sedative drugs, cold application, bed rest

307
Chapter 7. NEUROENDOCRINAL SYNDROMES IN
GYNAECOLOGY
Premenstrual syndrome
Premenstrual syndrome (PMS) is defined as the cyclic psychological and
somatic changes that occur for 10 to 14 days during the luteal phase of the
ovulatory cycle. All the changes disappear dramatically within 2 days
following the onset of menstrual flow or the onset of the following cycle in the
case of hysterectomy, and the patients are free of symptoms for at least 2
weeks afterward. Pathological changes include irritability, tension, anxiety,
mood swings, emotional lability, restlessness, decreased concentration,
depression, aggression, and lethargy, poor coordination, craving for sweet or
salty food, crying easily, and increased or decreased sexual desire. Somatic
changes include generalized swelling; breast tenderness; abdominal bloating;
face swelling, hands, and feet; weight gain; change in bowel habits; headache;
dizziness; hot flushes; and acne.
For many years, both physicians and patients were ignorant of this
syndrome; however, recent reports have drawn great interest from patients,
media persons, and health care professionals. The social and economic
concerns are further enhanced by the high prevalence of premenstrual
symptom and the increased number and role of women in the work force.
There is now a definite demand for professional attention to the condition.
ETIOLOGY
Numerous hypotheses regarding etiology have been proposed in the
past 50 years. Although many investigators believe that PMS, like all physical
diseases, arises from disordered physiology, others attempt to explain
premenstrual symptoms on a psychogenic basis, and the pathophysiology
remains elusive. Central nervous system (CNS), hormone dysregulation has
been linked to PMS by the similarity of symptoms or by association with other
emotional syndromes. These hormones include small peptides with opiate

308
receptor activity (endogenous opioid peptides) such as serotonin,
norepinephrine, dopamine, α-melanocyte-stimulating hormone, melatonin,
and acetylcholine. Other theories include hypothalamic-pituitary-adrenal
dysregulation, progesterone deficiency or withdrawal, fluid retention,
hyperprolactinemia, abnormal prostaglandin metabolism, hypoglycemia, and
thyroid dysfunction. However, no definite etiology has been identified, and
PMS is still considered as a multifactorial psychosocial-neuroendocrinologic
disorder.
DIAGNOSIS
The most important factor at the first visit is to devote considerable
time listening to the patient relating her history. One should assess the
patient's psychiatric history and explore her relationship with her family
members and co-workers, if any. External stress associated with these
relationships can make the premenstrual symptoms worse. Premenstrual
changes may be confused with other gynecologic or psychiatric problems. The
evaluation should include not only a detailed history, but the formulation of a
differential diagnosis of each complaint and a thorough physical and
psychological examination, with laboratory and radiological tests, if indicated,
and referral to other specialists when appropriate. It has been shown that
PMS is associated with the number of deliveries, postpartum depression, past
birth control pill use, alcohol and drug use, and history of PMS in first-degree
relatives. It is also important to differentiate PMS from psychiatric disorders
with premenstrual aggravation.
It is critical, in establishing the diagnosis of PMS, that symptoms occur
specifically during the luteal phase of the cycle and that there is a symptom-
free period of at least 1 week following the cessation of menstruation.
Symptoms continuing after the fifth day of the menstrual cycle are not
generally considered as PMS. There are still no uniformly accepted objective
criteria for the diagnosis of PMS, and we have to depend on the patient's
subjective report. Prospective recording of symptoms for at least 1 to 2

309
months using a daily diary, specific mood assessment charts, or specific visual
linear analogue scales is much more predictive of premenstrual changes than
are retrospective reports, which tend to misdiagnose PMS. Keeping careful
records is also helpful in increasing the patient's awareness of the problems.
Laboratory Evaluation
Thyroid dysfunction, hyperandrogenism, diabetes mellitus,
hypoglycemia, and hyperprolactinemia can cause somatic and affective
symptoms that are occasionally mistaken for PMS. Therefore, thyroid work-
up and measurement of serum afternoon cortisol, testosterone, glucose, and
prolactin levels may be performed to rule out the underlying medical
problems. However, the routine use of peripheral hormonal tests for patients
with premenstrual complaints is not only costly but also not indicated at this
time. This conclusion is based on the findings that no differences in hormone
concentrations were observed in the serum levels or patterns of secretion of
progesterone, estradiol, follicle-stimulating hormone, luteinizing hormone,
sex hormone-binding globulin, dehydroepiandrosterone sulfate,
dihydrotestosterone, prolactin, cortisol, growth hormone, or aldosterone
during the follicular and luteal phases between patients with PMS and healthy
women.
MANAGEMENT
Treatment of PMS requires a multidisciplinary team that integrates the
efforts of a gynecologist, an endocrinologist, a psychiatrist or psychologist, a
social worker, and a nutritionist.
Patient Education
The patient should be reassured that this is a problem common to many
women and that "she is not going crazy. " The physician must attempt to
familiarize the patient with the nature of the syndrome. With this knowledge
and awareness, the patient may recognize the changes in herself and find a
way to cope. The articulate patient can be encouraged to write a diary of her
moods, feelings, activities, and functions during this premenstrual period.

310
The diary can serve as another mode of ventilation and describe the pattern of
the patient's premenstrual tension as well. She can then become more
conscious of the changes that seem to occur in that week. Particularly
important is the physician's sensitivity in helping the patient repair her
emotional environment. The patient should be encouraged to join a local PMS
support group, if one is available.
Diet and Exercise
The PMS Prevention Diet emphasizes whole fresh foods. Eating regular
frequent small meals; decreasing the intake of salts, fats, sugar, and caffeine;
and increasing exercise are helpful. Foods that are high in refined sugars and
fats and that are highly processed are to be avoided. Intake of foods made
from whole grains, legumes, seeds, nuts, vegetables, fruits, and vegetable oils
should be encouraged.
Previous studies revealed that women who participated in sports
experienced less premenstrual anxiety than nonathletic women. How exercise
helps PMS is not clear, but exercise was noted to increase beta-endorphin
levels, which may explain the sense of well-being reported by some patients.
If beta-endorphin withdrawal contributes to PMS, it might be corrected, at
least partially, by exercise.
Pharmacologic Therapy
If no improvement is reported within 1 to 2 months using the approach of
education, diet, and exercise, pharmacologic therapy is added.
Treatment of Specific Symptoms
250 mg of prostaglandin synthetase inhibitor mefenamic acid (Ponstel),
administered daily during the luteal phase, significantly improved many
symptoms, particularly fatigue, headache, general aches and pains, and mood
swings. Nonsteroidal anti-inflammatory agents such as acetylsalicylic acid
(aspirin) or acetaminophen (Tylenol) with or without codeine are also used to
relieve headaches, muscle, and joint pain.

311
Sumatriptan (Imitrex), a 5-hydroxytryptamine receptor agonist, has
been shown to be effective and well tolerated by patients for menstruation-
associated migraine as it is for nonmenstrual migraine. Women were treated
for a menstruation-associated migraine (1 day before and 4 days after the
onset of menstrual flow) with 6 mg of sumatriptan in a 0. 5-mL subcutaneous
injection. A second injection was available to those who did not have
significant improvement of headache 1 hour after the first injection. At 1 hour,
80% of the sumatriptan-treated patients had significant headache relief,
compared with 19% of the placebo group.
Anxiolitic alprozalam by 0.25–0.5 mg/day during 2-3 months is usually
administered too.
Other associated symptoms, such as nausea and photophobia were also
improved. The most common adverse side effects were injection-site
reactions, dizziness, tingling, nausea and vomiting, warm sensation, and chest
tightness. Most adverse side effects lasted less than 1 hour. Clinical trials
using other forms of the medication, such as rectal suppositories and oral
pills, are currently under way.
Studies have shown significant improvement in reduction in weight and
psychological symptoms using spironolactone (Aldactone, Veroshpiron), a
potassium-sparing diuretic. If the patient gains weight, experiences bloat-
edness and edema premenstrually, and weight loss occurs dramatically after
the onset of menstruation, spironolactone, 25 mg four times a day, or 100 mg
once daily during the luteal phase, is recommended.
The dopaminergic agonist bromocriptine (Parlodel, Bromocriptin), 2. 5
- 5 mg at night daily from days 10 to 26 of the cycle, was noted to produce a
significant reduction in breast tenderness and swelling but was ineffective in
controlling other symptoms of PMS. The dose should be administered
individually: from 1. 25 to 5 mg/day depending on the level of prolactin in
blood.

312
Danazol (Danocrine), 200 mg once or twice daily, could effectively suppress
breast and other generalized symptoms.
Treatment of Generalized Symptoms
Naltrexone (Trexan). The beta-endorphin withdrawal and deficiency of
hypothesis suggests treatment of PMS with exogenous beta-endorphin, but it
is not practical because of addiction and the route of administration
(intramuscular or intravenous). An opiate antagonist, given before the
periovulatory beta-endorphin peak and withdrawal, might offer a rational
treatment for PMS by keeping a rather constant level of beta-endorphin.
Naltrexone is an oral pure narcotic antagonist that has been used in the
treatment of withdrawal symptoms for patients with heroin addiction. Unlike
drugs that have mixed agonist and antagonist effects, it does not cause
addiction or withdrawal.
Progesterone by vaginal suppository, or by injection (5 to 10 mg
intramuscularly) for 10 to 12 days premenstrually may be effective in some
cases. Progesterone has been noted to increase beta-endorphin levels in
blood. It is possible that the beneficial effect of progesterone is mediated by
beta-endorphin; however, such data on human subjects are still lacking.
Gonadotropin-releasing hormone agonists with low-dose estrogen-
progestin therapy to eliminate cyclic changes may also be used.
Recent studies suggest that naltrexone alleviates PMS symptoms and may be
an effective treatment for this syndrome. The acceptability of this medication
in the study was good, with only low incidence of nausea, decreased appetite,
dizziness, and fainting, which may be minimized by further dividing or
decreasing of the dosage. Previously, we demonstrated a decrease of plasma
beta-endorphin at periovular period and near menses in PMS patients, and
proposed that the premenstrual decrease of beta-endorphin may be
responsible for the PMS symptoms. It is possible that naltrexone inhibited

313
beta-endorphin withdrawal prevented the decrease of beta-endorphin levels,
and thus, reduced the severity of symptoms significantly.
Vitamins and Minerals
It has been suggested that deficiencies of vitamins and minerals are
related to PMS. However, recent studies did not demonstrate serum vitamin
A, B6, or E or magnesium deficiency in PMS patients compared with the
controls in peripheral blood obtained at 2- or 3-day intervals throughout
three menstrual cycles. However, serum zinc deficiency and copper excess
were found during the luteal phase in PMS patients. Because copper competes
with zinc for intestinal absorption and I serum protein binding sites, the
elevated copper in premenstrual patients reduced the availability of zinc
further. PMS patients were also found to have lower serum calcium levels in
the peripheral blood than controls. Whether these peripheral concentrations
reflect central changes requires further studies.
Although deficiencies of vitamins and minerals in patients with PMS could
not be demonstrated, a number of these supplements have appeared widely
on the market over the past few years. It was reported that a tablet of vitamin
B6 and other essential micronutrients reduced the severity of many PMS
symptoms at daily doses of 2 to 12 tablets that contained 100 to 600 mg of
vitamin Be. In contrast, another study showed that 150 mg of vitamin B6
could improve only those premenstrual symptoms related to automatic
reactions and behavioral changes but not physical or affective symptoms. The
efficacy of vitamin E in the treatment of PMS was studied in a double-blind,
placebo-controlled trial. A significant improvement in certain affective and
physical symptoms was noted in subjects treated with daily 400 IU of vitamin
E.
The effects of vitamins and minerals in these studies could be due to a
pharmacological response rather than correction of a deficiency state. The
roles of these supplements in beta-endorphin and other central
neurohormone activities need to be clarified. Until these issues are addressed,

314
the supplementation of vitamins and minerals can be considered only as
empirical therapy for PMS.
Serotonin Uptake Inhibitor. Enhancement of serotonin synthesis and
neurotransmission by administration of tryptophan or serotonin-specific
drugs has been used to treat some types of depressive illness. Administration
of large doses of pyridoxine (vitamin B6), a cofactor in serotonin synthesis,
has been observed to alleviate depression, anxiety, irritability, and a number
of other PMS symptoms.
Psychotropic Agents. Several psychotropic agents (tranquilizers) have
been used in the treatment of PMS, such as diazepam (Valium), buspirone
hydrocholoride (BuSpar). Trioxazine
0. 3 g per day may be used for irritability. Because of the required long-term
therapy for PMS patients, these agents may produce undesirable side effects
over time. It is recommended that these agents be given only to patients with
severe symptoms as a short-term adjuvant to other therapies.
Antidepressants: tianeptin 12. 5 mg/day 1-2 times a day for 2-3 months or
sertralin 50-100 mg/day.
Medical oophorectomy
In a cross-over study, it was demonstrated that elimination of ovarian
cyclicity through down-regulation of pituitary gonadotropin secretion with a
daily subcutaneous injection of gonadotropin-releasing hormone agonist
resulted in marked attenuation of premenstrual symptoms. The therapy was
rapidly reversible with no influence on subsequent cycles. Medical
oophorectomy is supposed to prevent the fluctuation and deficiency of beta-
endorphin levels by causing temporary cessation of cyclic ovarian activity.
Studies using monthly leuprolide acetate (Lupron Depot), daily nafarelin
acetate (Synarel), and other gonadotropin-releasing hormone agonists
showed similar results. Danazol (Dan-ocrine), at a dosage of 600 to 800 mg
daily, can also achieve reversible medical oophorectomy. One study showed

315
PMS symptoms were improved with danazol, 200 mg daily for 90 days,
during the anovulatory cycles but not during the ovulatory cycles.
The safety and side effects of long-term medical oophorectomy remain to be
determined. Studies using "add-back" synthetic sex steroid therapy to prevent
bone loss in patients given gonadotropin-releasing hormone agonists are
currently under investigation. The use of gonadotropin-releasing hormone
antagonists, which can achieve medical oophorectomy in a much more rapid
fashion with rapid reversal, is anticipated in the near future, assuming its side
effects, such as effects caused by histamine release, and can be minimized.
Climacteric syndrome (syn.: menopausal syndrome)
The mean age of menopause is about 51 years, with a normal
distribution curve and 95% confidence limits between ages 45 and 55. The
average life expectancy for a woman in the Ukraine is about 75 years, and
about one-third of a woman's life will be spent after menopause. This time of
life should be considered an estrogen-deficiency state, and improvement in
both the quality and the quantity of life can be obtained with the use of
estrogen replacement during the postmenopausal years.
Clinical picture
The climacteric syndrome is a complex of abnormal symptoms, which
occur in menopausal period. The clinical picture is characterized by
vegetovascular, endocrine and neuropsychic disorders. The main causes of
menopausal syndrome are the age-related changes in the hypothalamic
centers: decreased level of FSH, LH, reduced level of circulating estrogens
and progesterone. The androgen androstenedione is reduced by half, but
testosterone decreased only slightly.
Genitourinary effects
Atrophy of the genitourinary tract can produce symptoms of atrophic
vaginitis, with itching, burning, dyspareunia (painful coitus), and possible
316
vaginal bleeding. Local estrogen therapy rapidly relieves these symptoms, but
because vaginal administration of estrogen results in irregular systemic
absorption, estrogen is best administered systemically for long-term
prevention of vaginal atrophy as well as osteoporosis. Estrogen deficiency
may also cause uterine prolapse because the supporting ligaments lose their
tonicity. In addition, cystocele and rectocele may develop as a result of
estrogen deficiency. These changes can be prevented or alleviated by
administering estrogen. The trigone of the bladder and the urethra are
embryologically derived from estrogen-dependent tissue, and
postmenopausal estrogen deficiency causes atrophy of these structures,
producing symptoms of urinary urgency, incontinence, dysuria, and urinary
frequency. Because of atrophy of collagen in the periurethral fascia, urinary
stress incontinence can also occur. If these symptoms develop after
menopause, estrogen replacement alleviates the problem in a high percentage
of women.
Central nervous system changes
The pathognomonic symptom of the menopause is the hot flush or
flash, which is caused by a decrease in circulating estrogen levels. The best
treatment for the hot flush is estrogen, which has been shown to alleviate
symptoms better than placebo. It is best to administer estrogen at bedtime to
prevent the hot flushes that can interfere with sleep. The usual initial dosage
is 0. 625 mg of conjugated estrogen (Premarin), or 1 mg of estradiol, although
higher doses may be necessary, especially when the ovaries are removed in a
premenopausal individual. For women with contraindications to estrogen
therapy (for example, cancer of the breast or endometrium), other
medications that are effective in treating hot flushes include oral
medroxyprogesterone acetate (Provera) in a dosage of 10 mg per day. Hot
flushes can also be relieved by a single injection of Depo-Provera, 150 mg
given once every 3 months. In addition, clonidine (Catapres) in a dosage of
150 µg per day can also reduce the incidence of hot flushes.

317
Symptoms such as anxiety, depression, irritability, and fatigue increase
after the menopause, and it has been shown that estrogen replacement
significantly relieves these symptoms even in women who do not have hot
flushes that interfere with sleep. In addition to decreasing the incidence of
depression, recent studies show that estrogen users are less likely to develop
Alzheimer's disease. Because urinary incontinence and dementia are the two
major reasons why women are admitted to chronic care facilities, estrogen
replacement can enable them to stay in a self-care environment.
Studies have shown that postmenopausal estrogen users have a
significantly thicker skin and a greater amount of collagen in the dermis than
do postmenopausal women who do not use estrogen. Thus, systemic estrogen
use can retard the wrinkling and thinning of the skin that occurs
postmenopausally.
Osteoporosis
Postmenopausal osteoporosis affects about 25% of women but is
uncommon in black persons and in obese women. In thin white and Asian
women, about 1% to 1. 5% of bone mass is lost each year after the menopause.
Bone loss is more rapid in trabecular bone, which is found mainly in the
thoracic spine, than in cortical bone, which is present in the axial skeleton.
Beginning about age 60, fractures occur in the vertebral spine as well as the
distal portion of the radius, which is also composed of trabecular bone. The
incidence of fractures of the neck of the femur, which is made up mainly of
cortical bone, usually start to increase at about age 70 and increase at a
logarithmic rate thereafter. Estrogen therapy reduces the bone loss associated
with postmenopausal osteoporosis and thus reduces the fracture rate in
women, prolonging their productive life span as well as providing great
savings in health care costs. Supplemental calcium therapy and weight-
bearing exercise are ancillary measures that, by themselves will retard but not
prevent postmenopausal bone loss. The following factors are known to
increase the risk of osteoporosis: (1) reduced weight for height; (2) early

318
spontaneous menopause or early surgical menopause; (3) family history of
osteoporosis, (4) a diet low in calcium intake, high in caffeine intake, or high
in alcohol intake; (5) cigarette smoking; and (6) sedentary lifestyle. Routine
screening by densitometry or computed tomography scanning is not cost
effective and is not recommended to determine whether osteoporosis is
developing postmenopausally.
Osteoporosis is associated with an increased rate of bone resorption,
and the administration of estrogen will return the resorption rate to normal.
Numerous prospective and retrospective epidemiologic studies have shown
that estrogen therapy reduces the amount of postmenopausal bone loss:
When estrogen is discontinued, the rate of bone loss rapidly increases to the
same rate as that occurring immediately postmenopausally. Therefore,
estrogen replacement therapy should be maintained as long as a woman is
ambulatory. The minimum dosage of estrogen needed to prevent osteoporosis
is 0. 625 mg of conjugated equine estrogen (Premarin), 0. 625 mg of
piperazine estrone sulfate (Ogen), or 0. 5 mg of micronized estradiol
(Estrace). It is recommended that in addition to estrogen, about 700 mg of
calcium should be ingested daily, and weight-bearing exercise such as walking
should be encouraged. Supplemental use of vitamin D is of no benefit. There
is no need for additional calcium supplementation beyond the 700 mg of daily
dietary calcium in women receiving adequate estrogen replacement.
Cardiovascular effects
Because estrogen replacement regimens have a minimal effect on liver
globulins, postmenopausal estrogen users do not have an increase in mean
blood pressure compared with women not ingesting estrogen. It is safe to
provide estrogen replacement for postmenopausal women with or without
pre-existing hypertension. Because natural estrogens do not produce a
hypercoagulable state, available data indicate that postmenopausal women
with or without a past history of thrombophlebitis do not have an increased
incidence of thrombophlebitis with estrogen replacement therapy. Use of

319
estrogen replacement has been shown in numerous retrospective as well as
prospective epidemiologic studies to reduce the risk of myocardial infarction
by about 50%. Estrogen replacement also reduces the risk of stroke by about
50%. Oral estrogen increases levels of the cardioproductive high-density
lipoprotein cholesterol as well as directly increasing coronary artery blood
flow. The substantial reduction of rate of myocardial infarction, which is the
major cause of mortality in women, is a major beneficial effect of estrogen.
Age-adjusted data from several studies indicate that the mortality rate from
all causes is significantly lower in estrogen users than in nonusers.
Neoplastic effects
Six meta-analyses, each combining the data of several epidemiologic
studies, have shown there is no significantly increased risk of breast cancer in
women using estrogen replacement therapy compared with nonusers. Only a
few of any epidemiologic studies investigating the relation of estrogen use and
breast cancer have shown an increased risk of breast cancer in some subsets
of postmenopausal estrogen users, specifically long-term users of high doses
of estradiol but not conjugated equine estrogen. Several studies show no
effect of conjugated equine estrogen on this cancer. Because estrogen can
stimulate the growth of a nonpalpable breast cancer, it is advisable that all
women have mammograms performed before the initiation of estrogen
therapy. If no tumor is found, patients can be told that oral estrogen use will
not increase the risk of developing breast cancer. There is a significantly
increased risk of developing endometrial cancer in postmenopausal women
who are ingesting estrogen without progestins. This risk increases with
increased duration of estrogen use as well as with increased dosage. The
endometrial cancer that develops in estrogen users is usually well
differentiated and is usually cured by performing a simple hysterectomy. The
increased risk of developing this endometrial carcinoma in women receiving
estrogen replacement can be eliminated by also administering progestins. The
duration of progestin therapy is more important than the dosage, and it is

320
now recommended that the progestin be administered for at least 12 days per
month. The addition of progestin to the estrogen therapy acts synergistically
to cause a slight increase in bone density. However, progestins reverse some
of the beneficial effects of estrogen on serum lipids and, thus, should not be
given to women who do not have uterus. Several epidemiologic studies
investigating the use of progestins with estrogen and the risk of breast cancer
have yielded conflicting results. Therefore, a beneficial effect of progestin on
breast cancer risk has not been substantiated.
Treatment regimens
The treatment consists of replacing hormonal therapy. The treatment
regimen is mostly the sequential regimen of 0. 625 mg of conjugated
estrogen or 1 mg of estradiol orally for the first 25 days each month.
Beginning on day 12 to 15 of estrogen treatment, 5 to 10 mg of
medroxyprogesterone acetate is added daily for 10 to 13 days. With this
regimen, more than half of the women have regular withdrawal bleeding, an
annoying problem that decreases patient compliance to continued use. It is
not necessary to have withdrawal bleeding to slough the endometrium, to
reduce the risk of endometrial cancer. A continuous regimen in which the
estrogen is given daily together with a small dose of oral progestin, such as 2.
5 or 5 mg of medroxyprogesterone acetate, reduces the chance of developing
uterine bleeding as well as avoiding a week off treatment, in which symptoms
may appear.
Climonorm (two types of tablets: estradiol and estradiol + levonorgectrel),
climen (estradiol and estradiol + ciproteron), climodien (estradiol and
dienogest), climara (plaster), divigel (gel) as combined replacing hormonal
therapy may be administered.
Most women do not bleed on this regimen, and the endometrium usually
remains atrophic.

321
Post-castration Syndrome
This is a combination of neuropsychic, vegetovascular, and endocrine
disorders. It develops after surgical operations in which the ovaries are
removed. The clinical signs are similar to those at menopausal syndrome:
irritability, fatigability, afflux of fever, tachycardia, violation (disturbance) of
dream, memory etc.
Treatment
It should be combined and include therapeutic gymnastics,
balneotherapy, sedative therapy, physiotherapy, and replacement hormonal
therapy (or additional hormonal therapy). Oral contraceptives are useful as
replacement combined hormonal therapy.
Mono-phase: marvelon, janin, logest, miniziston, microginon -1 tablet once a
day during 21 day is starting from the 1 day of menstrual cycle, then 7 days-
interval (without tablets).
Two-phase: anteovin, and three-phase: trimercy, triregol, tricvilar – 1 tablet a
day from the 1 day of menstrual cycle, then 7 days-interval.
The Stein-Levental Syndrome also known as polycystic ovarian disease is an
important cause of secondary amenorrhea in young women. Main complaints
are amenorrhea with hirsutism and infertility.
These patients are infantile, often obese, hirsute and frequently have
hyperplasia of the breast. On vaginal examination, either ovaries are enlarged
to two or three times their normal size and, laparotomy shows a firm, rubbery
consistence. Estrogen and 17-ketosteroid excretion levels are normal and the
latter point differentiates the Stein-Levental from the adreno-genital
syndrome. Luteinising hormone (LH) level is raised. LH/FSH ratio is raised.
At operation, multiple cysts are found on the surface of the ovaries and, on
histological examination, a thick layer of theca cells surrounds the cysts. No
corpus luteum is present. The endometrium is estrogenic and there is no
secretors change. It is suggested that the hyperthecosis is androgen-
producing and is responsible for hirsutism. Ultrasound reveals multiple small

322
cysts on the surface of the both ovaries, and laparoscopy is not always needed
to confirm the diagnosis.
Treatment
Bilateral wedge resection of the ovaries, at one time very popular, is now
not recommended because of postoperative ovarian adhesion formation.
Laparoscopic multiple punctures of the ovaries with monopolar cautery or
laser is recommended in women who do not respond favorably to medical
treatment.
Clomiphene is the drug of choice in infertile patients suffering from
polycystic ovaries. It is of utmost importance, however, that patients should
be properly and adequately investigated before commencing treatment with
clomiphene, the dosage of which is 50-100 mg daily for five days each month,
for six months. Those not responding to drug therapy should have
cauterization or laser ablation of the cysts laparoscopically, preferably under
videopelviscopy. Menses are restored and 60% conceive.
Adreno-genital syndrome (adrenal virilism, AGS)
This is due to hyperplasia of the adrenal cortex and there are two types:
congenital and post-natal.
CONGENITAL OR INTRAUTERINE ADRENO-GENITAL
SYNDROME
It is a syndrome in which the primary defect is a block in the conversion
of 17-hydroxy progesterone into hydrocortisone due to enzyme failure. The
normal adrenal cortex produces three C21 compounds: hydrocortisone,
corticosterone and aldosterone, and in addition, certain androgens - C19
compounds. The production of 17-hydroxy-progesterone, which is mildly
androgenic in action, is controlled by ACTH, and this in turn is controlled by

323
the reciprocal action of hydrocortisone. If therefore the hydrocortisone -
ACTH interaction is upset by a deficiency of hydrocortisone, the pituitary
produces an excess of ACTH, which in turn leads to adrenal cortical
hyperplasia and excess output of androgens, notably 17-hydroxy-
progesterone. The main androgenic activity of 17-hydroxyprogesterone is due
to its conversion into Д4 androstenedione and hence to other orthodox
androges. These androgens are responsible for phallus of the female
pseudohermaphrodite showing hypertrophy, the masculine appearance of the
glans, and the persistence of fusion of the labia majora to resemble a scrotum.
The miniature vagina opens into the urogenital sinus and the external
appearance is that of a male with hypospadias.
The diagnostic feature is the very high value of 17-ketosteroids excreted.
As expected the chromosomal pattern in these girls is invariably XX.
Clinical features. The chromosomal and gonadal sex is female and the
accessory sex organs of Mullerian origin are also feminine. The external
genitalia, however, resemble the male. The body conformity is largely male
with good muscular development and broad shoulders. The voice is deep and
the thyroid cartilage is prominent. Hirsutism is present to a remarkable
degree, with a male distribution of hair. The psycological sex is often, but not
invariably, male.
The external genitalia show hypertrophy of the clitoris and fusion of the
labia majora due to failure of the cloacal membrane to divide. The vagina is
often absent if the cause is congenital. The breasts are under-developed.
Treatment of this condition consists in the administration of cortisone or
hydrocortisone or the newer synthetic corticosteroids such as prednisone or
prednisolone (2. 5 mg twice daily is an adequate maintainance dose in the
adult and will restore the output of 17-ketosteroids to normal). The continued
use of these drugs carries certain dangers of adrenal deficiency due to
suppression of ACTH and this especially operates at times of stress such as
when a patient needs an anaesthetic, at which time cortisone coverage should

324
be given during the period of stress (i. e. one day before, on the day of
operation and for three days afterwards).
The vulval abnormality is simply corrected by a small plastic operation and as
a rule it is wise to amputate the hypertrophied clitoris between 5 and 10 years
of age.
Certain cases of virilization of the fetus in-utero have been reported following
the use of progesterone in the pregnant mother. The synthetic progestogens
ethisterone and nor-ethisterone are comparatively more androgenic. In fact
all progestogens if given in sufficient dosage are suspect with the exception of
17-hydroxyprogesterone caproate, so that if progestogen is to be used at all on
the pregnant woman, this is the drug of choice.
The effect on the fetus depends largely on the duration of the pregnancy at the
time of administration and the dosage employed. If progestogens are given
before the 12th - 14th weeks of gestation, the neonatal picture may be similar
to that of the intrauterine adreno-genital syndrome, i. e. enlarged phallus and
imperforate perineal membrane.
POST-NATAL ADRENO-GENITAL SYNDROME
This can be due to excessive output of ACTH from a basophil adenoma
of the anterior pituitary (Cushing's syndrome) which gives rise to adrenal
cortical hyperplasia. An adrenal tumour, which can be benign or malignant,
has the same effect. An adrenal tumour is not dependent on pituitary
influence.
Certain virilising tumours and conditions of the ovary such as
arrhenoblastoma, hilus cell tumour, Stein-Leventhal syndrome and hyper-
thecosis. These ovarian causes of virilism produce a clinical picture,
somewhat similar to the postnatal adreno-genital syndrome, and, are due to
excess of testosterone secreted by the ovary. In the postnatal variety of
virilism, the genital tract is normal but the clitoris enlarges, the uterus
atrophies with resulting amenorrhoea, the voice deepens, hirsutism is marked

325
and the breasts atrophy. 17 -ketosteroids excretion is raised only if the adrenal
gland is hyperplastic or neoplastic, whereas with a virilising ovarian tumour it
is unaltered. (Fig. 150)
Treatment. If the fault is an enzyme block at the level of 17-
hydroxyprogesterone, the administration of cortisone or synthetic
corticosteroids will effectively control the excess production of ACTH. The
external genitalia can be restored to a feminine pattern by plastic surgery, e.
g. the formation of an artificial vagina if the patient is engaged or married.
Cortisone therapy, if successful, may restore menstruation in a patient with
amenorrhea. It is important in such patients to correct any anatomical defects

326
of the lower genital tract in order to obviate the complication of retained
menstrual products such as haematocolpos or haematometra.
If the virilism is due to adrenal hyperplasia or tumor, surgical removal is
the method of choice. This also applies to ovarian androgenic tumors.
A regular maintenance dose of estrogen is usually effective in restoring
some of the secondary sex characteristics, e. g. breast development.
Additional intermittent progesterone therapy prevents breast and uterine
malignancy.
The most effective treatment of facial hirsutism is shaving and
cosmetics.
Icenko-Cushing Disease is due to a basophile adenoma of anterior
pituitary gland, which leads to hyperfunction of the suprarenal cortex. The
main symptoms and signs are those due to a disorder of the suprarenal gland.
(Fig. 151)
Sheehan’s Syndrome. It is the condition, which develops owing to
excessive post-partum hemorrhage, and results with vascular thrombosis
leading to extensive pituitary necrosis. In the fully developed case, all
pituitary functions are suppressed so that the syndrome consists of frigidity,
amenorrhea and loss of thyrotropic hormone. The patient is lethargic and
poikilothermic. The blood sugar is lowered. In some cases there is no loss of
weight and no wasting, though this feature is often included in the syndrome.
Auxiliary and pubic hair is lost and the uterus on bimanual examinarion is
hypoplastic. Skin pigmentation is also deficient, but the patient will often
show areas of the erythema where in attempt to keep warm she has burned
her legs in front of the fire. (Fig. 152)
Chiari-Frommel Syndrome. It is an interesting example of pituitary
dysfunction. Amenorrhea, persistent galactorhea, obesity and headache occur
after delivery. Follicle stimulating hormone (FSH) excretion is diminished
while luteinizing hormone (LH) is increased and lactogenic stimulation
causes increased prolactin secretion. The occasional finding of expansion of

327
the pituitary fossa on X-ray suggests an acidophil adenoma as possible cause
and this may later lead to narrowing of the visual field.

328
Self test
1. Premenstrual changes usually occur during
A. the luteal phase of the ovulatory cycle
B. the follicular phase
C. the ovulation
D. desquamation phase
2. Which of the following drugs may be used to relieve headaches, muscle, and
joint pain in patients with PMS?
A. tylenol
B. cortizol
C. analgin
D. promedol
3. Parlodel is usually used for treatment of
A. patients with PMS
B. patients with climacteric syndrome
C. patients with post-castration syndrome
D. Icenko – Cushing disease
4. The following factors are known to increase the risk of osteoporosis, except of
A. reduced weight for height
B. early spontaneous menopause or early surgical menopause
C. a diet low in calcium intake, high in caffeine intake
D. increased body weight
5. What drugs cannot be used for replacing of hormonal therapy in patients with
climacteric syndrome?
A. climen
B. climodien
C. climara
D. progestogel
6. The main cause of adreno-genital syndrome is

329
A. the hyperplasia of the adrenal cortex
B. the hypoplasia of the adrenal cortex
C. congenital underdevelopment of the adrenal cortex
D. congenital underdevelopment of adnexa
7. Main complaints of the Stein-Levental syndrome are
A. amenorrhea with hirsuties and infertility
B. amenorrhea with galactorrhoea
C. uterine bleeding and infertility
D. persistent obesity and headache
8. Icenko – Cushing disease is due to a basophil adenoma of
A. anterior pituitary gland
B. adrenal gland
C. hypothalamus
D. ovary
9. All of the following are symptoms of Chiari-Frommel disease, except of
A. amenorrhea
B. persistent galactorhea
C. obesity and headache
D. anovulatory cycles
10. Congenital adreno-genital syndrome usually happens due to
A. abnormal conversion of progesterone
B. abnormal conversion of cortisol
C. abnormal conversion of epinephrine
D. abnormal conversion of estriol

330
Chapter 8. THE INFERTILE COUPLE
The couple is considered infertile if it has failed to conceive within two
years of unprotected sex life.
If a couple has never achieved pregnancy at any time the infertility is
described as primary; if infertility follows a pregnancy, whatever the outcome,
it is called secondary. Infertility is not an independent disease but a symptom
of various illnesses. Sterility may be classified as male and female infertility.
Male infertility
Male infertility occurs in about 15 per cent of sterile marriages. The
most common cause of male infertility is impaired spermatogenesis due to
inflammatory processes, injuries, damaging chemical and thermal factors,
alcoholism, and neuroendocrine disturbances. Male infertility may also link
cicatricial changes in the deferent duct and urethra. Spermatogenesis may be
depressed by many factors including excessive smoking or alcohol
consumption and overwork. Infertility may be due to azoospermia (absence of
spermatozoa), neсrospermia (dead or motionless spermatozoa), aspermia
(failure of formation or emission of sperm), oligospermia(deficiency of
spermatozoa). Qualitative changes of sperm may lead to infertility and
depend on the biochemical composition of the seminal fluid.
Diagnosis. In some cases the cause of male infertility may be
established already after the patients questioning and inspection. But the
examination of sperm is a more important method of diagnosis. Fresh sperm
is obtained by masturbation and kept in a sterile glass vessel at less than body
temperature during transit to the laboratory, which should be reached within
one or two hours.
Normally, the volume is 2. 5-5 ml, with an alkaline pH about60-80% of
sperms are motile within two hours; about 50% are motile within 4 hours. As

331
to sperm count, the normal range is 60-150 million/ml and 20 million/ml is
considered the minimum requirement for fertility. A normal specimen
contains abnormal forms, but less than 25%.
Seminal fluid contains both sperms and plasma. Biochemical investigation of
the plasma gives an index of the function of the male accessory glands.
Fructose, from the seminal vesicle, provides the spermatozoa with the energy
requirements. Phosphate, from the prostate, and glyceryl phosphoryl choline,
from the epididymis, can also be measured. If all these are normal the
deferent duct must be patent and accessory gland function is normal.
In addition a post-coital examination of the cervical mucus for the presence of
sperms may be made.
Female infertility
The causes of infertility in the female can be divided into 5 groups,
which indicate the main areas requiring investigation. The incidence of these
cases is as follows:
Hormonal factors controlling the process of ovulation – 41%.
Abnormalities involving the fallopian tube – 32%.
Uterine factors – 16%.
Cervical factors – 4-5%.
General factors – 4-5%
In some patients no abnormality can be found. The incidence of these
cases is around 5%.
Hormonal Factors
In normal circumstances the control of these factors is initiated at
hypothalamic level.
Primary hypothalamic failure is rare and only occurs as a congenital
autosomal condition. Secondary hypothalamic failure is comparatively

332
frequent. In the majority of cases it is a functional condition, the result of a
psychological upset at anorexia nervosa.
Pituitary factors are not so common and are usually limited to two
situations: 1) Hyperprolactinemia, which may be caused by an adenoma of the
pituitary gland, pregnancy or drugs which are antagonistic to dopamine. The
patient frequently complains of amenorrhea, loss of libido and occasionally
may show signs of acromegaly. 2) Pituitary damage by injury or ischemia.
Gonadotropin secretion becomes deficient but more commonly secretion of
all pituitary hormones ceases. The best known clinical example of this is
Sheehan’s syndrome caused by shock due to gross hemorrhage in pregnancy.
Ovarian factors. This group of patients often presents the greatest
difficulty in determining where the fault lies. In some the cases of anovulation
are obvious. Examples are ovarian damage by radiotherapy or chemotherapy,
congenital or genetic disorders, some ovulatory cyclic ones (incompetence of
the luteal phase). Premature menopause is another such condition.
Anovulation is responsible for around 25% of cases of infertility. The
most important ovarian abnormality is the polycystic syndrome. In
approximately 80% of cases menstruation is irregular or absent. It is difficult
to determine whether the initiation of this syndrome is due to a defect in
pituitary or ovarian function. There appears to be an excess of LH production
plus a diminished FSH secretion. The result is a lack of estrogen and an
excess of androgenic substances.
Two other conditions have been suggested as ovarian causes of
infertility. The first is the Luteinized unruptured follicle syndrome (LUF).
In this condition the cyclical changes in endocrine values are apparently
normal, the granulosa layer undergoes luteinization but the follicle fails to
rupture. Diagnosis is very difficult because of normal tests of functional
diagnosis, and normal hormonal level in blood and urine. A luteinized
unrupted follicle can be found in an ovary containing a fresh corpus luteum.

333
Another cause of infertility is luteal phase deficiency, either deficient
in length or deficient in progesterone production. It results in incomplete
secretory change of endometrium and violation of an implantation of
fertilized ovum.
Abnormalities of Fallopian Tubes
There are two prominent etiological factors producing changes in the
fallopian tubes leading to infertility. The main factor is infection. This may be
sexually transmitted. Two of the commonest organisms are chlamydia and
gonococci. In many cases, however, the infection arises as a result of
termination of pregnancy, abortion, wearing an intrauterine contraceptive
device and inflammatory condition in other abdominal organs. The damage of
the tubes may be mild, consisting of destruction of the epithelial cilia, but
more commonly the changes are gross and lead to obstruction of the tube, to
pelvic adhesions, etc.
The second factor is endometriosis. Not only endometriosis per se is
important, it is the adhesions formed during the healing of hemorrhages,
especially if these affect the ovary. One more cause is careless surgery.
Uterine Factors
The uterus performs many significant roles in reproduction.
There are several uterine lesions, which can lead to infertility.
Sometimes fibriods can cause gross destruction of the cervical canal, the
uterine cavity or tubal ostia and careful removal will relieve the infertility.
Endometriosis is another condition which certainly results in infertility and
leads to internal adhesions. Chronic endometritis is also one of the reasons of
infertility. It may be nonspecific and specific inflammation (for example,
tuberculosis, which leads to intra- uterine adhesions, or synechiae). Other
factors are congenital abnormalities of the uterus and vagina (uterus
didelphys, bicornus, septus, atresia or aplasia of vagina etc.).

334
Cervical Factors
The main problem is damage to the cervix due to childbirth or
spontaneous abortion in late terms of pregnancy, or surgery (careless
dilatation of the cervical canal during artificial abortion, diagnostic curettage
etc.). Thick mucus has been blamed for obstructing the passage of sperm.
Some women have antibodies to their husband’s sperm and positive test
can be demostrated in both plasma and cervical mucus. These cases are rare.
Genital Infantilism and hypoplasia also account for a considerable
number of infertility cases. In this event infertility is due to both anatomical
and functional peculiarities of the genital system linked to its
underdevelopment (long narrow cervical canal, decreased hormonal function,
impaired function of the oviduct etc).
General Factors
Poor general health due to social behaviour may be important. Drugs,
alcohol, smoking, caffeine and obesity will all defect fertility. Similarly,
exposure to toxic chemicals and pesticides at work will influence fertility
although this is more likely in the case of men.
Investigation and Treatment of the infertile couple
Confirmation of ovulation.
Seminal fluid analysis and postcoital test.
Tests for tubal patency.
Endometrial sampling by biopsy.
Endometrial culture to determine the infection.
Hysterography, hysteroscopy.
Laparoscopy.
Postcoital test.

335
Postcoital test.
Mucus is examined between 2 and 3. 5 hours after coitus at midcycle for
total number of sperm seen per high-powered field and percentage and
quality of motility. A satisfactory test is one in which more than 10 motile
spermatozoa are seen per high-powered field. An unsatisfactory test (no or
few spermatozoa seen; nonmotile spermatozoa or those with a “shaking”
movement) may be the result of:
azospermia (no spermatozoa in ejaculate),
poor inherent spermatozoa motility,
hostile cervical mucus (infection, antidodies, or not enough estrogen),
poor coital technique.
Treatment of infertility
The aim of the treatment is elimination of the underlying cause
(antiinflammatory, surgical, hormonal).
Treatment of hypothalamic is dependent on underlying condition
(stress, failure of blood supply, tumors etc0.
Treatment of ovarian factors
Ovulation induction. The ovulation induction agents used include
clomiphene citrate (CC), Human menopausal gonadotropin (hMG), Human
Chorionic gonadotropin (hCG), recombinant FSH, and recombinant LH.
Recommended Regimen of Clomiphene citrate (CC) (basic):
The standard dose of CC is 50 mg PO qd for 5 days, starting on the 5th
day of menstrual cycle or after progestin-induced bleeding.
The CC response is monitored using pelvic US starting on the 12th
menstrual cycle day. The follicle should develop to a diameter of 23-24
mm
If a dominant follicle develops, but there is no spontaneous LH surge,
hCG (10,000 units given intramuscularly) can be used for final follicular
maturation/ovulation, followed by timed intercourse or IUI.

336
Luteal phase defects treatment. Intramuscular or intravaginal
progesterone until the luteoplacental shift occurs at 8–10 weeks gestational
age.
Treatment of hyperprolactinemia. The aim is blocking of the release of
prolactin from pituitary gland.
Recommended Regimen:
Bromocriptine: 2.5mg on first day, increasing after 2 to 3 days to 2.5mg
twice daily for 14 days.
Treatment of tubal factors
For treatment of inflammations of Fallopian tubes special
investigations, antibacterial, anti-inflammatory treatment are indicated. If
ineffective- assisted reproductive techniques up to gestational carrier may be
used.
Tubal obstructions, adhesions, hydrosalpinx need in surgical correction:
tubal cannulation, microsurgical tubo-cornual reanastomosis. If necessary –
in vitro fertilization may be used.
Treatment of uterine factors
The treatment of uterine factors depend on underlying disease.
The treatment of uterine malformations depends on the severity of the
problem. Unicornuate uterus: patient can have norml pregnancy
Bicornuate uterus: can be associated with a history of recurrent miscarriages,
and its repair is indicated only if other etiologies for the miscarriage have
been excluded.
Arcuate uterus: In general, an arcuate uterus does not cause infertility.
Whether it should be corrected in cases of primary infertility is controversial.
Septate uterus: The hypothesis that a uterine septum can cause infertility is
controversial. Advising surgery in cases of primary infertility is difficult. The
avascular nature of the septum is theorized to interfere with implantation and
maintenance of the embryo.
Uterine malformations: not require treatment /or plastic surgery/ART

337
Uterine synechiae: are corrected using operative hysteroscopy.
Leyomyoma, adenomiosis – medication/surgery.
Treatment of cervical factors
Chronic cervicitis should be treated with anti-inflammatory and antibacterial
drugs, physiotherapy.
Treatment of cervical incompetence is surgical:
application of special sutures during pregnancy, known as cervical
cerclage
plastic surgery of the cervix before pregnancy
Assisted Reproductive Techniques
In vitro fertilization is used increasingly, e. g., for patients with tubal
disease, endometriosis, oligospermia, sperm antibodies, and unexplained
infertility. The procedure involves ovarian hyperstimulation, oocyte retrieval,
fertilization, embryo culture, and embryo transfer. Ovarian hyper-stimulation
with clomiphene citrate and HMG, HMG alone, or a GnRH agonist plus HMG
causes 1 to 20 oocytes to mature, depending on the patient's age and ovarian
reserve. After follicular growth is sufficient, hCG is given to induce final
follicular maturation. About 34 h after hCG administration, the oocytes are
retrieved by direct needle puncture of the follicle, usually transvaginally with
ultrasound guidance or less commonly with laparoscopy. The oocytes are
inseminated in vitro with washed sperm, and the embryos are cultured for
about 40h, after which three to four embryos are transferred to the uterine
cavity. Additional embryos can be frozen in liquid nitrogen for transfer in a
subsequent natural cycle. Despite the transfer of multiple embryos, the
average term-pregnancy rate is about 20 to 25% per attempt.
Gamete intrafallopian tube transfer (GIFT) may be used for women
who have normal tubal function and unexplained infertility or endometriosis.
Multiple oocytes and sperm are obtained as for in vitro fertilization but are
transferred—laparoscopically or transvaginally with ultrasound guidance—to
338
the distal fallopian tubes, where fertilization occurs. Success rates are about
25 to 35% at most infertility centers.
Other procedures include a combination of in vitro fertilization and
GIFT, zygote intrafallopian tube transfer, use of donor oocytes, and transfer
of frozen embryos to a surrogate mother. Some of these techniques raise
moral and ethical issues—eg, disposition of stored embryos (especially in
cases of death or divorce), legal parentage in surrogate motherhood, and
selective reduction of the number of implanted embryos in multiple
pregnancies.
Intracytoplasmic sperm injection is the primary method of achieving
pregnancy when other techniques have not resulted in fertilization or when
the semen analysis detects marked abnormalities. Sperm is injected into the
oocyte, bypassing sperm abnormalities that affect attachment to or
penetration of the oocyte.
Self test
1. The most serious causative factor of infertility that can be reflected in the
postcoital test is
A. azoospermia
B. congenital abnormalities of the uterus
C. tubal dysfunction
D. luteal dysfunction
2. Which of the following procedures is not appropriate for the evaluation of the
endometrial cavity?
A. laparoscopy
B. endometrial biopsy
C. hysteroscopy
D. endometrial culture
3. Which of the following does not indicate ovulation?

339
A. rise of basal temperature
B. secretory endometrium
C. occurence of menses
D. estrogen level dropping
4. Which of the following is not reflected in postcoital test?
A. blocked fallopian tubes
B. low sperm count
C. poor sperm motility
D. high sperm count
5. Which of the following does not contribute to abnormalities in the cervical
mucus?
A. colonization of the cervix with cytotoxic organisms
B. uterine retroversion
C. antisperm antibodies
D. uterine anteflexion
6. What is the indication for in vitro fertilization?
A. oviduct diseases
B. hormonal disturbances
C. vaginal atresia
D. intrauterine synechia
7. What is the indication for gamete intrafallopian tube transfer?
A. normal tubal function and unexplained infertility
B. oviduct diseases
C. hormonal disturbances
D. chronic inflammatory processes of genital organs
8. The incidence of hormonal infertility is
A. 41%
B. 32%
C. 16%
E. 4-5%

340
Chapter 9. CONTRACEPTION
Advice on family planning is an important part of gynecological
practice. Such advice is not only for benefit of the individual woman, but also
is of world-wide importance.
Methods will be described in rough order of effectiveness.
Methods can be divided into:
Sterilization
Hormonal contraception
Intrauterine devices
Mechanical methods
Chemical methods
Contraception based on time of ovulation
Coitus interruptus.
Sterilization
Sterilization, named surgical contraception. This method of
contraception is permanent and is therefore only used for those with
completed families or with medical contraindications to pregnancy. Before
sterilization of either partner it is important to obtain detailed information
about the family unit, with social and medical histories and the reasons for
preferring sterilization to contraception. It is wise to obtain the written
consent of both partners.
Female sterilization is performed:
By excision of parts of both tubes and ligature of the cut
ends, through a small abdominal incision. (Fig.153)
By diathermy coagulation of a section of each tube with the
aid of a laparoscope. Another type of sterilization is

341
occlusion of the tube by the application of clips or rings
under laparoscopic vision (Fig. 154)
Occasional failures occur with either method, usually because of
recanalization of the uterine end of the tube.
Male sterilization. Vasectomy is usually performed under local
anesthesia. Through a small scrotal incision the deferent duct is identified,
and after excising a small section both ends are doubly ligatured. (Fig. 155).

342
Hormonal contraception
Two main types of hormonal contraception are now commonly used:
oral and injections. More common type is oral contraception. Besides,
transdermal administration is useful nowadays. Though, intravaginal
administration of hormonal contraceptives is used too.
Oral contraceptives
Oral contraceptives are subdivided into combined and those containing
only progestogen (acontinuous method).
Combined oral contraceptives
Combined oral contraceptives (COCP) - is the usual method with a very
low failure rate. A pill containing synthetic estrogen plus progestogen is taken
each night for 21 days starting on the 5th day of menstrual cycle. There are
then 7 days without tablets and during this week a withdrawal bleeding
occurs. If the patient forgets to take the pill on one evening she should take
two pills the next night. If the bleeding does not occur within 7 days of taking
the last tablet the next course still begins. In the unlikely event of two

343
“periods” being missed the patient should have a pregnancy test. To ensure
maximum contraceptive efficacy, oral contraceptives should be taken as near
as possible to the same time each day (i. e., at regular 24-hour intervals). Most
oral contraceptives are commercially available in a mnemonic dispensing
package that is designed to aid the user in complying with the prescribed
dosage schedule; these containers should be used whenever possible.
Many сombined contraceptives are available. They may be mono-phase,
two-phase and three-phase. In modern practice the lowest effective dose of
estrogen is used to reduce the risk of thrombosis. The dose of progestogen
may be varied.
Mono-Phase
Those tablets contain the same dose of estrogen+ progestogen for 21 or
22 days of cycle, and then there is a 7-day interval without tablets.
For example:
Minovlar Ethinylestradiol 0. 05 mg + norethisterone acetate 1mg
Euginon 50 Ethinylestradiol 0. 05 mg + d-norgestrel 0. 5 mg.
Others: Ovidon, Marvelon, Minulet.
Two-Phase
Those sets contain two types of tablets: for the 1st phase (from the 5th to
15th day of the cycle) – only estrogen, or estrogen + the least dose of
progestogen, and for the 2nd phase (from the 16th to 25th day of the cycle) –
usual combination (scheme) of estrogen + progestogen.
For example:
Anteovin Ethinylestradiol 0. 05 mg + levonorgestrel 0. 05 mg
Ethinylestradiol 0. 05 mg + levonorgestrel 0. 125 mg

344
Three-Phase
There are different contents of estrogen and progestogen for different
days of cycle, like in normal menstrual cycle. Usually those drugs are of low
dosage.
For example:
Tri-Regol Ethinylestradil 0. 03 mg + levonorgestrel 0. 05 mg
(6 yellow tablets) for the 1st phase.
Ethinylestradiol 0. 04 mg + levonorgestrel 0. 075 mg
(5 tablets of apricot colour) for the 2nd phase.
Ethinylestradiol 0. 03 mg + levonorgestrel 0. 125 mg
(10 white tablets) for the 3rd phase.
Others: Loginon, Trisiston, Triphasil, Ortho-Tri-Cyclen, Tri-Norinyl.
Combined hormonal contraceptives may be used in injections.
For example:
Ciclofem Estradiol sipionat 0. 05 mg + medroxyprogesterone acetate 0.
25 mg . Injection once monthly.
Mesigina Estradiol valerianat 0. 05 mg + noretindron enantat 0. 50 mg.
Injection once monthly.
Four-phase
Qlaira (Natazia) is 4 progestin/estrogen dosing combinations during
each 28-day cycle and is the first "4-phasic" oral contraceptive. It also is the
first contraceptive to contain the bioidentical synthetic estrogen estradiol
valerate, rather than ethinyl estradiol. It is composition of the colored tablets
containing one or two active substances:
2 dark yellow tablets each containing 3 mg estradiol valerate
medium red tablets each containing 2 mg estradiol valerate and 2
mg dienogest
17 light yellow tablets each containing 2 mg estradiol valerate and
3 mg dienogest

345
2 dark red tablets each containing 1mg estradiol valerate Qlaira
composition of the white inactive tablets: these tablets do not
contain any active substances.
Estradiol valerate/dienogest contraceptive tablets (Qlaira or Natazia)) may be used
for the treatment of excessive, prolonged, and frequent menstrual bleeding, also may
be administered for contraception for women in premenopausal age.
Progestogen - only pills (continuous method)
Because of side effects of estrogens this method was introduced. The
pills, which only contain a progestogen, are taken daily without intermission.
Every set of drugs has 35 or 28 tablets with the same dose of levonorgestrel or
noratindron. The failure rate is higher than with combined method, but the
regime is simple for the patient. The pills, which only contain a progestogen,
are named mini-pills.
They are:
Microlut Levonorgestrel 0. 05 mg
Micronor Noratindron 0. 35 mg
Ovrette Norgestrel 0. 075 mg
A modification of this method is to inject a long-acting progestogen.
Depo-Provera. A single deep intramuscular injection of medroxyprogesterone
acetate 150 mg (Depo-Provera) is given at 3 monthly intervals.
Noristerat Noretindron-anantate 200 mg, one injection for every two
months.
In contrast to estrogen-progestin combinations, progestin-only oral
contraceptives are administered in a continuous daily dosage regimen
beginning on the first day of menstruation and continued each day of the
year. To achieve maximum effectiveness, patients should be instructed to take
the drug exactly as directed and at intervals not exceeding 24 hours. Strict
adherence to the dosage regimen is especially important during the first 6

346
months of use. The drug should be taken at the same time each day and
continued daily, without interruption, whether bleeding occurs or not.
Women should be advised to contact their physician, if prolonged bleeding
occurs during oral contraceptive use.
Progestin-only oral contraceptives are generally reserved for women
who do not tolerate estrogens or in whom estrogens are contraindicated, since
progestin-only oral contraceptives are less effective than estrogen-progestin
combinations and require a high level of patient compliance. When taken
according to the prescribed regimen, progestin-only oral contraceptives
provide almost completely effective contraception. The efficacy of oral
contraceptives mainly depends on compliance with the prescribed regimen.
Unlike estrogen-progestin combinations, progestin-only oral contraceptives
must be taken daily, without interruption, to be effective.
Levonorgestrel for subcutaneous implantation (Norplant®) has been
used for prevention of conception in women who elect to use subcutaneous
progestin implants as a method of contraception. The system consists of 6
silicone capsules containing levonorgestrel that are implanted subcutaneously
in the upper arm to provide contraception for up to 5 years.
Common rules of administration of oral contraceptives
Whenever possible, the smallest dosage of estrogen and progestin
should be used. The amount of both hormones should be considered in the
choice of an oral contraceptive preparation. It is prudent and in keeping with
good principles of therapeutics to minimize exposure to estrogen and
progestin. The combination used should be one, which contains the least
amount of estrogen and progestin that is compatible with a low failure rate
and with the individual needs of the woman. Common adverse effects are
usually most pronounced during the first oral contraceptive cycle and
generally disappear or diminish after 3 or 4 cycles; there it does not appear to

347
be any advantage in changing preparations during this period. If minor
adverse effects persist after the fourth cycle, a different combination of drugs
or a different dosage may be tried.
Most fixed combinations are available as 21- or 28-day dosage
preparations (conventional-cycle oral contraceptives). The 28-day
preparations contain 21 hormonally active tablets and 7 inert or ferrous
fumarate-containing tablets. In establishing an oral contraceptive dosage
cycle, the menstrual cycle is usually considered to be 28 days. The first day of
bleeding is counted as the first day of the cycle.
Administration of monophasic fixed-combination conventional-cycle
oral contraceptives usually begins on the first day of the menstrual cycle or on
the first Sunday after menstrual bleeding has started. A back-up method of
contraception (e. g., condoms, foam, sponge) should be employed for 7 days
following initiation of oral contraceptive therapy if the first dose of the oral
contraceptive is begun on the first Sunday after menstrual bleeding starts. A
back-up method of contraception is not needed if the first dosage cycle is
initiated on the first day of the menstrual cycle. Some clinicians suggest that
women switching from higher-dose preparations to low-dose preparations
may begin administration of the low-dose preparation on the first day of
withdrawal bleeding; however, if withdrawal bleeding does not occur after
discontinuance of the higher-dose preparation, administration of the low-
dose preparation should begin on the eighth day after taking the last
hormonally active tablet of the higher-dose preparation and the woman
should be advised to take additional contraceptive measures. Monophasic
fixed combinations are usually administered once daily for 21 consecutive
days, followed by up to 7 days without drugs; when the 28-day dosage
preparations are used, inert tablets or tablets containing ferrous fumarate are
administered during this latter 7-day period. Withdrawal bleeding usually
occurs within 2 or 3 days after the last hormonally active tablet has been
taken. Repeat dosage cycles begin on the same day of the week as the initial

348
cycle. Repeat cycles should generally begin regardless of whether
menstruation has stopped; after several cycles of fixed-combination
preparations, menstrual flow may be considerably reduced. If a repeat 21-day
cycle is started later than the eighth day after taking the last hormonally
active tablet (or later than the next day after taking the last inactive tablet
with 28-day dosage preparations), a back-up method of contraception should
be employed until the patient has taken a hormonally active tablet daily for 7
consecutive days.
When a biphasic oral contraceptive is used, each dosage cycle consists of
2 sequentially administered fixed combinations; the first sequence consists of
10 tablets containing a fixed combination of low-dose estrogen and low-dose
progestin and the second sequence consists of 11 tablets containing a fixed
combination of low-dose estrogen and higher-dose progestin. Although
biphasic oral contraceptives consist of 2 sequentially administered fixed
combinations, they are not the same as previously available "sequential" oral
contraceptives, which consisted of an estrogen alone for the first sequence.
Administration of a biphasic oral contraceptive usually begins on the first
Sunday after or on which bleeding has started. Tablets from the first sequence
are administered once daily for 10 consecutive days, followed by once-daily
administration of tablets from the second sequence for 11 consecutive days
and then a period of 7 days without drugs; when a 28-day dosage preparation
is used, inert tablets are administered during this latter 7-day period. A back-
up method of contraception (e. g., condoms, foam, sponge) should be
employed for 7 days following initiation of oral contraceptive therapy, if the
first dose of the oral contraceptive is begun on the first Sunday on or after
menstrual bleeding starts; a back-up method of contraception is not
necessary if the first dosage cycle is initiated on the first day of the menstrual
cycle. Repeat dosage cycles begin on the eighth day after taking the last
hormonally active tablet.

349
Triphasic oral contraceptives contain graduated sequences of progestin
or estrogen. With most commercially available triphasic oral contraceptives,
each dosage cycle consists of 3 sequentially administered fixed combinations
of the hormones in which the ratio of progestin to estrogen progressively
increases with each sequence. The first sequence consists of tablets containing
a fixed combination of low-dose estrogen and low-dose progestin, the second
sequence consists of tablets containing a fixed combination of low-dose and
higher-dose progestin, and the third sequence consists of tablets containing
low-dose estrogen and either an even higher-dose progestin or low-dose
progestin (i. e., Tri-Norinyl).
Triphasic oral contraceptives, in which the estrogen component
progressively increases with each sequence, also are available. The first
sequence consists of tablets containing a fixed combination of a progestin and
low-dose estrogen, the second sequence consists of tablets containing a fixed
combination of progestin and a slightly higher dosage of estrogen, and the
third sequence consists of tablets containing a progestin and an even higher
dosage of estrogen. Administration of a triphasic oral contraceptive usually
begins on the first Sunday after or on which bleeding has started or on the
first day of the menstrual cycle. Tablets from the first sequence of Ortho-
Novum® 7/7/7, Ortho-Tri-Cyclen®, or Ortho-Tri-Cyclen® are administered
once daily for 7 consecutive days, followed by once-daily administration of
tablets from the second sequence for 7 consecutive days and then once-daily
administration of tablets from the third sequence for 7 consecutive days.
Tablets from the first sequence of Tri-Norinyl® are administered once daily
for 7 consecutive days, followed by once-daily administration of tablets from
the second sequence for 9 consecutive days and then once-daily
administration of tablets from the third sequence for 5 consecutive days.
Tablets from the first sequence of Tri-Levlen® or Triphasil® are
administered once daily for 6 consecutive days, followed by once-daily
administration of tablets from the second sequence for 5 consecutive days and

350
then once-daily administration of tablets from the third sequence for 10
consecutive days. Tablets from the first sequence of Estrostep® are
administered once daily for 5 consecutive days, followed by once-daily
administration of tablets from the second sequence for 7 consecutive days and
then once-daily administration of tablets from the third sequence for 9
consecutive days. The 3 sequences are then followed by a period of 7 days
without drug; when a 28-day dosage preparation is used; inert tablets are
administered during this latter 7-day period. Repeat dosage cycles begin on
the eighth day after taking the last hormonally active tablet. If a repeat 21-day
cycle is started later than the eighth day after taking the last hormonally
active tablet (or later than the next day after taking the last inactive tablet
with 28-day dosage preparations), a back-up method of contraception should
be employed until the patient has taken a hormonally active tablet daily for 7
consecutive days.
Administration of a triphasic oral contraceptive usually begins on the
first Sunday after or on which bleeding has started or on the first day of the
menstrual cycle. Tablets from the first sequence of these preparations are
administered once daily for 7 consecutive days, followed by once-daily
administration of tablets from the second sequence for 7 consecutive days and
then once-daily administration of tablets from the third sequence for 7
consecutive days.
If oral contraceptives are first taken postpartum or later than the fifth
day of the menstrual cycle, the contraceptive effect should not be relied on
until after 7 consecutive days of drug administration, since there is a
possibility that ovulation and conception may have occurred. In all patients,
additional contraceptive measures may be advisable through the first week of
the initial regimen. In determining whether to initiate oral contraceptive
therapy in the postpartum period, the increased risk of thromboembolism
during this period must be considered since use of oral contraceptives is also

351
associated with an increased risk of thromboembolic and thrombotic
disorders.
Side effects and complications
Minor side effects mostly when starting medication
Nausea is common in the first cycle and can be reduced by taking the
pill last thing at night. It is due to estrogen. To minimize nausea, oral
contraceptives should be taken with or after the evening meal or at bedtime.
As vomiting or diarrhea may decrease absorption of oral contraceptives and
potentially result in treatment failures, a back-up method of contraception (e.
g., condoms, foam, sponge) should be used until the next clinician contact.
If it persists the patient should be examined to exclude pregnancy and a
change is made to a pill containing less estrogen.
Tenderness and slight enlargement of the breasts may occur, but they
usually cease after few cycles.
The “menstrual” loss is usually reduced. Intermenstrual spotting (break
through bleeding) may occur. If this persists it is usually controlled by
changing the progestogen or increasing the dose of progestogen.
An initial weight-gain of 0. 5 kg is common. This is usually lost after a
few cycles; changing to another pill sometimes decreases the weight gain.
Major complications
Hypertension may occur especially during the first year of use and in
patients over 30. The pressure must be recorded at each visit to the doctor or
clinic. If medication is stopped the pressure becomes normal.
The risk of venous thrombosis and embolism is increased in women
taking the combined contraceptives, but the risk must not be exaggerated.
Combined oral contraceptives are not advised for any woman with a history of
thrombosis or embolism.
352
The first period after stopping oral contraception is often late. More
persistent amenorrhea is uncommon, and usually recovers spontaneously.
If a woman has had an estrogen depended tumor (e. g., breast cancer)
pills containing estrogens are contraindicated.
Other side effects.
Cervical erosions are common.
Vaginal candidiasis may occur.
Chloasma (facial pigmentation like sometimes seen in pregnancy) has
been reported.
Migrainous headaches may occur.
Psychological effects are difficult to assess. Depression is sometimes
attributed to the pill, but seldom with much evidence.
Postcoital hormonal contraception.
Oral administration.
The “morning after pills” can be used after unprotected coitus around
the time of ovulation. They are diethylstilbestrol 25 mg, ethinyl estradiol 0. 03
mg, norgestrel 0. 3 mg. The drugs are administered in a short-course regimen
of 2 doses (consisting of 2 tablets per dose) administered 12 hours apart.
Other short-course, postcoital contraceptive regimens usually consist of 2 or 4
tablets per dose administered 12 hours apart. Women should be advised of
the importance of taking the second dose 12 hours after the initial dose, and
to schedule the first dose as conveniently as possible (but no later than 72
hours after intercourse) so that the likelihood of missing the second dose 12
hours later is minimized (e. g., if the first dose were taken at 3 p. m., the
second dose would need to be taken at 3 a. m., which might present a problem
of compliance for heavy sleepers). The high doses of steroids just after
ovulation may disrupt the endometrium enough so that implantation of the
embryo does not take place.
Because the high dosage in the combination regimens may cause severe
nausea and vomiting in a substantial proportion of women, which could limit

353
compliance with postcoital contraception, use of an antiemetic (e. g.,
meclizine, diphenhydramine, trimethobenzamide, promethazine) prior to
administration of each dose of the combination should be considered.
Administering the dose with food also has been suggested as a means of
reducing the risk of nausea and vomiting. If breakthrough vomiting does
occur within one hour after administration of a dose of the estrogen-progestin
combination despite concomitant administration of an antiemetic,
consideration should be given to repeating the dose.
Because of the short time frame of effective postcoital use (i. e., therapy
must commence within 72 hours of unprotected intercourse), clinicians
ideally should inform women of the availability of postcoital contraception
before such use is warranted, advising them to contact a clinician immediately
if the need for such contraception arises. Alternatively, women can be given
an appropriate estrogen-progestin combination in advance, with careful
instructions on how to safely and effectively use the combination for
emergency postcoital contraception; if a supply of the drugs is given to a
woman in advance, she also should be advised that postcoital contraceptives
are for emergency situations (e. g., unprotected intercourse, missed doses of
oral contraceptives (more than 2 tablets), missed parenteral contraceptive
dose [more than 2 weeks past scheduled injection], contraceptive failure) only
and should not be employed as the primary method of contraception.
Hormonal injections
Women may receive the transdermal contraceptive containing ethinyl
estradiol and norelgestromin (Ortho Evra®). The transdermal system is
applied topically to a clean and dry area of intact skin on the buttock,
abdomen, upper outer arm, or upper torso, by firmly pressing the system with
the adhesive side touching the skin. The system should be pressed firmly in
place with the palm of the hand for about 10 seconds, ensuring good contact,

354
particularly around the edges. The application site should not be oily,
damaged, or irritated. The transdermal system should not be applied to the
breasts or to areas where tight clothing may cause the system to be rubbed
off. If the system inadvertently gets detached during the period of use, and is
off for less than one day, the system may be reapplied or, if necessary, a new
system (if the system is no longer sticky) may be applied; in either case, the
application schedule employed should be continued. If the system is off for
longer than one day or for an unknown duration, a new system should be
applied immediately and a new 4-week cycle should be started; a back-up
method of contraception (e. g., condoms, spermicides, diaphragm) must be
used for the first week of the new cycle. Patients should be instructed to
handle the used transdermal system carefully (e. g., fold the system in half
with the sticky sides together) and then discard the system.
This is a very effective method, provided that the patient does not fail to
take the tablet
Intravaginal administration of contraceptives
Patients receiving the vaginal contraceptive ring containing ethinyl
estradiol and etonogestrel (NuvaRing®) should be carefully instructed in the
use of the vaginal ring. The ring should be inserted into the vagina by the
patient; the manufacturer states that the exact position of the ring inside the
vagina is not critical for its proper functioning. If the ring is accidentally
expelled, it can be rinsed with cool or lukewarm water and reinserted or, if
necessary, a new ring should be inserted as soon as possible; in either case,
the administration schedule employed should be continued. If the
contraceptive ring has been out of the vagina for longer than 3 hours, a back-
up method of contraception (e. g., condoms, spermicides) must be used until
the ring has been used continuously for 7 days.
355
Other hormonal contraception
Not long ago it was founded, that chronic GnRH agonist treatment,
which is usually used to facilitate treatment of hypogonadism, resulted in
down regulation of the pituitary processes responsible for gonadotropin
synthesis and release. Thus, buserelin, a GnRH analogue, when given daily
doses of 400 or 600 µg intranasally over 3 to 6 months, obtained a safe and
effective method of birth control that works by interfering with normal
ovulation. So, the main mechanism of action of chronic GnRH agonist
treatment seems to be pituitary desensitization of the processes responsible
for gonadotropin secretion. The reserve capacity for gonadotropin secretion is
rapidly reduced during repeated administration of GnRH agonists.
Intrauterine devices
These are made of radio-opaque elastic in various shapes that are
intended to prevent their extrusion from the uterus. They can be compressed
or straightened for insertion through a cannula, without anesthesia. They are
most easily inserted just after a period, or immediately after termination of
pregnancy or in puerperium. Most forms have a thread attached, which
projects through the cervix so that the presence of the device can be checked.
A normally situated device can usually be easily removed by traction on this
thread.
The action of the original devices was mechanical, presumably by
interference with the embedding of the ovum. Recently smaller devices have
been introduced, which carry drugs into the uterus. The commonest
medicated device has fine copper wire wound round the vertical limb. (Fig.
156). Copper ions are released and enter the endometrial cells, but there is no
significant absorbtion into the blood stream. Mechanism of action is:
disturbed implantation of the fertilized ovum, increased peristalsis of the
tubes etc. The device carries enough copper for 2 to 3 years of use.

356
Another type of medicated device releases progesterone slowly. The
endometrium becomes atrophic, but insufficient progesterone is absorbed to
affect ovarian function.
The medicated devices are more effective than the simple varieties, and
are easier to insert as they are smaller.
Although a device is less effective than an oral contraceptive, it has the
advantage that the patient has no responsibility once it is in place. They are
useful for patients who dislike oral contraceptives, or who are incapable or
untrustworthy in their use.
Side effects
The common side effects are pain, chiefly dysmenorrhea, and increasing
menstrual bleeding. A device may be expelled by uterine contractions. Both
expulsion and symptoms are most common in the first six months of use.
Pregnancy may occur if the device is partly extruded or incorrectly
placed. If this happens the device should be removed by traction on the string.
There is a risk of infection during the pregnancy.
Occasionally an intrauterine device may perforate the uterine wall. X-
ray will show the device lying outside the uterus. The device should be
removed from peritoneal cavity with the aid of a laparoscope.

357
Mechanical methods
They also may be male and female. As to female, the most common is
vaginal diaphragm (‘Dutch cap’). This is a dome-shaped rubber diaphragm
with a flexible rim that fits over the cervix, acts as a barrier to sperm. The
diaphragm is made in different sizes and the commonest size required is 50-
70 mm in diameter. The woman must be shown how to insert it so that the
cervix is covered. Spermicidal cream, (all of them are mainly Nonoxynol
based) is placed on both aspects of the diaphragm before insertion.
Spermicides should always be used with the diaphragm to improve
contraceptive effectiveness in case the diaphragm is displaced during coitus.
The diaphragm should cause no discomfort to either partner. It should be
inserted before coitus and remain in place for at least 6 hours after the last
coitus, if intercourse is repeated in that period more cream must be injected
with an applicator.
The diaphragm is less efficient than oral contraceptives or IUD unless
used strictly according to instructions, but it has no side effects
Chemical methods
Spermicidal agents are inserted into the vagina in the form of creams,
pessaries, gels or aerosols. All of these are mainly Nonoxynol based. For
example: pharmatex. One dose of spermicide must be injected before each act
of coitus. The method is not very effective. The active agents work by killing
the sperm, decreasing sperm motility, or inactivating the enzymes needed for
the sperm to penetrate the ova. Surface-active agents, for example, nonoxynol
9 and octoxynol 9 are spermicidal agents that disrupt the outer lipoprotein
surface layer of spermatozoa.

358
Contraception based on time of ovulation
Natural family planning (periodic abstinence)
This method requires abstaining from coitus during the fertile period.
Ovulation usually occurs about 14 days before onset of the next menses.
Although the human ovum can probably be fertilized for only a few hours
after ovulation, sperm can fertilize the ovum for several days after entering
the cervical canal; thus, fertilization can result from coitus that occurs up to 5
days before ovulation. So, natural family planning is not very effective.
The calendar rhythm method (‘safe period’)
The period of abstention is determined by subtracting 18 days from the
shortest period of the previous 12 cycles and 11 days from the longest. Thus, if
the woman’s cycles vary between 26 and 29 days, the couple must abstain
from coitus from day 8 through day 18 of each cycle. This method of
contraception is the least effective type of contraception.
Basal body temperature
This method is more effective, requires training and a high degree of
motivation.
The woman must take her rectal temperature every morning for the
sustained rise, which indicates ovulation. Basal temperature rises about 0. 5%
after ovulation. The couple abstains from coitus for at least 48 to 72 hours
after the rise in temperature. Such graphs of basal temperature are not now
accepted as being very precise indicators, but women with regular periods can
usually identify the peri-ovulatory time with a fair degree of accuracy.
However, even with careful training, the pregnancy rate is about 10%.

359
Symptothermal method
Symptothermal method is the most effective method for determining of
periodic abstinence, involves observing changes in cervical mucus (increased
cervical mucus secretion, the “spinnbarkeit” phenomenon, increased
extensibility of the cervical mucus) and in temperature as well as other
symptoms associated with ovulation.
Coitus interruptus
This means withdrawal of the penis just before ejaculation. It is widely
practiced and probably adequate for couples of low fertility, but some sperms
must enter the vagina, and withdrawal at the point of orgasm is unnatural.
Self test
1. Surgical contraception is indicated for
A. young women
B. women in reproductive age
C. women with medical contraindications to pregnancy
D. women in menopausal age
2. Which of the following is not mono-phase oral contraceptive?
A. minovlar
B. euginon
C. marvelon
D. anteovin
3. Loginоn is
A. the three-phase contraceptive
B. the two-phase contraceptive
C. the monophase contraceptive
D. the progesterone only pill

360
4. Intrauterine device is contraindicated for
A. patients with isthmico-cervical insufficiency
B. patients with active sexual life
C. multiparae patients
D. patients with extragenital diseases
5. Intrauterine device is most easily inserted
A. just after a period
B. in every day of period
C. just before the beginning of menstrual flow
D. in day of ovulation
6. Microlut is
A. progesterone-only pills
B. mono-phase pills
C. two-phase pills
D. three-phase pills
7. Which of the following is not a contraceptive action of the spermicides?
A. killing the sperm
B. decreasing sperm motility
C. disrupting the outer lipoprotein surface layer
D. neutralizing vaginal acidity
8. The medicated device carries enough copper for
A. 2 to 3 years of use
B. 3 to 4 years of use
C. 4 to 5 years of use
D. 5 to 6 years of use
9. Which of the following is not a physiologic change affected by oral
contraceptives?
A. suppression of the ovulation
B. a hypoestrogenic state
C. inactive endometrium

361
D. reduction of gonadotropins
10. Which of the following methods of contraception suppresses ovulation as its
primary mechanism of action?
A. medicated intrauterine device
B. postcoital norgestrel
C. barrier contraceptives
D. buserelin

362
Chapter 10. TYPICAL OPERATIONS IN
GYNECOLOGY
In the treatment of certain gynecologic affections it is necessary to
invade the peritoneal cavity. This invasion of the great peritoneal sac in the
center of the body necessarily carries with it considerable risk to the patient.
On the preantiseptic days the mortality was great- so great that operation was
but rarely resorted to. By modern antiseptic and aseptic methods; however,
the mortality has been reduced to a very small percentage. But, though the
mortality of the operation is small, we must not forget that there is mortality
due directly to the operation.
The danger varies much in different cases, depending on the particular
form of disease present and on the condition of the patient at the time of
operation- but there is some danger in every case. It is well to call particular
attention to this, because some physicians seem prone to overlook, or at least
fail to give proper weight to, the fact that occasionally a patient, with
everything apparently favorable, will die; and no one can promise any patient
absolutely that she will survive. One may say, in a favourable case, that the
risk is very slight and that in all probability the patient will go through the
operation and convalescence without trouble. But though the risk is slight, it
is nevertheless a risk, and the patient or her friends must so understand it.
The operation is carried out because of some condition, which is more
dangerous – that is, in that particular case the risk of waiting is greater than
the risk of operation.
This serious decision as to whether or not to operate at a certain time is
based on many factors, including knowledge of the disease in its various
forms and of the patients ability to stand the operation and the character of
the hospital facilities immediately available. The correctness of our judgment
in making such decision improves with study and experience, and some of the

363
informing experiences are bitter as we compare the action taken with the later
developments.
Preoperative preparation of patient, operative technique, postoperative
care is important to successful surgical treatment.
Preoperative Preparation
In order to reduce to a minimum the danger of the operation, careful
preparation is required.
The operation should be carried out in the clean, well arranged
operation room of a hospital, even though the patient has to be moved a
considerable distance to obtain the requisite hospital facilities.
The further preparations for the operation will be given under the
following subheads:
preparation of the patient;
preparation of sponges and dressings;
preparation of instruments and sutures;
preparation of operator and assistants.
Preparation of the patient
The patient, having been subjected to a careful general examination
including urine analysis, to exclude contraindications, is sent to the hospital
one or two days before operation that the proper preparation may be carried
out. Of course, there are cases of rapidly spreading pelvic inflammation, or of
intra-abdominal hemorrhage or injury, in which the abdomen must be
opened at the earliest possible moment. In such a case there is no time for
preliminary prepa-ration. Careful immediate sterilization is carried out and
the abdomen is then opened. But when the case is not an emergency one, the

364
preliminary preparation should be made. It gives the patient a decidedly
better chance of complete and uninterrupted recovery.
When the patient enters the hospital for operation, orders are left for
her as to diet, needed laboratory work, provision of rest and sleep, bowel
regulation, preliminary preparation of the operation field, and preanesthetic
sedation. The details vary with the surgeon and with the condition of the
patient.
A general examination is made with spеcial attention to inflammation,
anemia, the circulation and the lungs. The urine is tested for protein and
sugar, and a catheter specimen is often required for microscopy and
bacteriology. Vaginal smears should be taken for microscopy and
bacteriology. Cases of severe uterine bleeding often require blood transfusion.
The rectum and the bladder should be empty before operation.
Light diet is to be given up to and including noon of the day before
operation, then liquids only, but with water in abundance. After midnight,
just preceding operation, nothing is to be given by mouth but water, and the
water may be continued to within an hour of the operation.
An enema is to be given the night before, and again the next morning.
The idea is to have the intestinal tract in as nearly normal condition as
possible, with just a good clearing out of the lower bowel just before the
operation. Experience has shown that this simple method of preparation
brings the patient to the operating table in better condition and causes less
disturbance after the operation than the prolonged dieting and purging
formerly employed.
In cases of marked habitual constipation and eases in which the bowels
are not to be moved for some time after operation, such as in repair of
complete laceration into the rectum, it is well to clear out the intestines some
days before, but avoid prolonged increased peristalsis to the operation. When
there are complications that may necessitate resection of the intestine or

365
opening of the stomach, then, of course, the usual preoperative measures for
approximate sterilization of the upper intestinal tract would be indicated.
Preliminary sterilization of the field. In the preparation of the operative
field, as in the intestinal preparation, the trend of practice has been toward
simplicity. It has been found that some of the measures formerly employed
served to irritate the skin and increased rather than diminished the chance of
inflammation. This was true particularly of the strong antiseptics applied for
long periods preceding operation. Instead of the extensive soap poultice and
the prolonged antiseptic pack, the following method, with minor
modifications, is now employed generally:
The afternoon before operation the abdomen is lathered and shaved. It
is then scrubbed with soap and, after soap is removed, with sterile water, and
then the surface is washed with alcohol. The cleansed surface is covered with
a sterile towel or sterile cotton held in place with a binder.
In most of the gynecological cases, vaginal preparation also is needed,
because part of the operation is vaginal, or the vagina is to be opened into, or
conditions may be found requiring it to be opened. On this account,
preoperative vaginal preparation along with the abdominal is made routinely,
unless otherwise ordered in some exceptional case.
Medication (syn.: premedication). Sleep is important, and it is well to
have a regular order for sodium bromide or other sedative, to be given as
needed to quiet the nervous system and avoid wakefulness.
A preanesthetic sedative eliminates the anxiety of the trip to the
operating room and starting the anesthesia, and also reduces the amount of
anesthetic required. For this purpose, promedol, 1–1. 5 mL of 2% solution,
and atropine sulphate, 0. 5–1 mL of 0. 1% solution, and dimedrol, 1–2 mL of
1% solution, given about thirty-five or forty-five minutes before operation,
intramuscularly in one syringe, are used by many. The patient is then kept
quiet with the room darkened until taken to the operating room.

366
The preanesthetic sedative analgesia eliminates the preoperational
anxiety, which is so troublesome to some patients and more or less
troublesome to all. As a rule, the patient knows nothing about the trip to the
operating room and the induction of anesthesia and is surprised when she
learns that the operation is over. Also, the patients take the anesthetic more
quietly and require less for operations of the same length. Again, there is less
postoperative vomiting and distress. The dose of the drugs should of course
be adjusted to the size and condition of the patient, being somewhat less than
the above for small or weak individuals.
When spinal anesthesia is to be employed, the following preanesthetic
sedation is pre-ferred: 0.5 mL of atropine +0,5–1 mL of ephedrine
hydrochloride +1–2 mL of 1% solution of dimedrol in one syringe are given
intramuscularly one and one-half hours before the operation. The patient's
ears are stopped up with cotton, the eyes are covered, and the room is kept
quiet.
Catheterization. A convenient time and place for the catheterization is
during the preparation in the operating room immediately preceding
operation, during the vaginal preparation if made; otherwise just before the
abdominal preparation. Catheterization at that time has the added advantages
of emptying the bladder immediately before operation (instead of an hour
before, after which a troublesome amount of urine may collect in some cases)
and of avoiding disturbance of the patient while sedative sleep is being
induced.
Preparation in operating room. The final sterilization of the abdominal
field is ordinarily carried out as the patient is being anesthetized, though
exceptionally it may be advisable to complete this preparation before the
anesthesia is begun in order to save time under the anesthetic. As previously
explained, vaginal preparation also is advisable in most abdominal cases, and
this is usually completed just preceding the abdominal preparation. If the

367
patient is in good preanesthetic sleep, no additional anesthesia is needed for
the vaginal preparation, which may be immediately proceeded with.
The patient's hips are drawn to the edge of the table and the feet are
supported out of the way by stirrups. The external genitals and vicinity all
round are cleansed thoroughly with soap and warm water, using gauze or
cotton balls, rinsed with chlorhexidine gluconate, iodine or bichloride or
cyanide solution, or any other anticeptics.
Catheterization is now carried out with strict asepsis, the labia being
held away and the meatus specially cleansed. The sterile catheter should be
lubricated and care should be taken to avoid contaminating the bladder
portion with soap or irritating antiseptics.
The vagina is then cleansed with soap and warm water, rinsed with
sterile water, and then with the antiseptic solution, using small pieces of
gauze or cotton and opening the vagina with a speculum. If the opening is too
small for the speculum, a finger may be used beside the sponge forceps.
If the operation is to be complete abdominal hysterectomy, some iodine
solution is applied to the vaginal vault, and removed with alcohol. If the
hysterectomy is for a condition accompanied with infective uterine discharge,
the cervix is grasped with a tenaculum forceps and the uterine cavity is
packed with a quarter-inch gauze moistened with iodine solution.
When the vaginal preparation is finished, the abdominal field is
prepared. The abdominal surface is painted with 70% of ethyl alcohol iodine
(twice) and then with 2. 5% iodine solution in spirit over the large area.
Particular care should be taken to sterilize the depth of the umbilical
depression, to rub in the solution along the line of incision, and to extend the
sterilization down over the pubes well beyond the lower end of incision.
Iodine is a skin irritant and must be removed with alcohol. The following plan
may be used: the first step is thorough application to the depth of the
umbilicus, with discarding of the swab. Then by circular motion, enlarging
from the umbilicus, the central area is sterilized down to near the pubic area,

368
one or two swabs being used as needed. In the second step, with downward
and outward strikes application is made to the pubic area and adjacent thigh
surface changing swabs as necessary to avoid recontamination of sterilized
surfaces. Then, in the third step, with a fresh swab or two, application is made
to the outward portions of the abdominal field (Fig. 157), giving the complete
coverage indicated in Fig 158. The same plan is followed in the rapid removal
of the iodine with alcohol swabs. A final firm wipe is made from the umbilicus
down the median line and over the pubes.
Fig. 158. Showing the area to be painted with the antiseptic solution
(complete coverage)

369
The above account is to show in general the steps and details of the
sterilization process. The chemical preparations will vary with the hospital
and the surgeon, and also as new preparations are developed and attain
popularity. For preparation in the vagina, aqueous solutions are used, for
example, aqueous solution of phemerol (1:500) or of zephiran (1:1,000).
When the sterilization of the operative field has been complete, the area
is draped with the sterile coverings, the patient's hips are elevated to the
Trendelenburg position, and the small platforms for the operator and
assistants to stand on are slipped into place (Fig. 159)
Any considerable dropping of the feet and legs increases the tension of
the abdominal wall, and is to be avoided.
Fig. 159. Preparation of operative field. The patient has been elevated
into the Trendelenburg position and the continuous-strip sponge
bag has been clamped in place. The small platforms for the operator
and assistants to stand on have been pushed into position.

370
Preparation of sponges and dressings
The dressings, pads, towels, sheets, instruments trays, and basins are all
put through the steam sterilizer, and kept wrapped ready to use.
Preparation of instruments and sutures
The instruments used in abdominal operation for pelvic disease may be
grouped under three headings—regular set of instruments, regular set of
needles and sutures, and special instruments.
Regular Abdominal Set of Instruments (Fig. 160.):
14 Towel clips
12 Allis forceps (a, in Fig. 1164)
2 Knives with detachable blades (b)
1 Large curved Mayo dissecting scissors, (c)
1 Large straight Mayo dissecting scissors,
1 Curved blunt uterine scissors (d)
1 Straight blunt uterine scissors (e)
1 Curved sharp-pointed uterine scissors (/)
3 Tissue forceps with 2 to 4 teeth on each side (g)
1 Tissue forceps without teeth (h)
1 Tissue forceps, one with teeth (i) and one smooth 2 Large double-end
abdominal retractors (j)
1Large single-end wide abdominal retractor
1Deep single-end long-bladed retractor (k)
2 Flat flexible retractors, one narrow and one wide (I) 18 Curved clamps,
(m)("Small clamp") 32 Curved clamps, (n) ("Medium clamp")
4 Curved clamps, (o) ("Large clamp" or "Hysterectomy clamp")
24 Curved hemostats

371
32 Straight toothed clamps, (p), may be curved
4 Hegar needle holders, (r)
2 Double-toothed uterine tenaculum forceps, (t)
2 Single-toothed uterine tenaculum forceps (x)
2 Shorter tenaculum forceps
1 Grooved director with probe point (u)
1 Tumor forceps with six teeth (v)
1 Uterine sound
1 Small wire probe with eye
1 Trocars, medium and large, with rubber tubing
Set of needles and suture materials
Heavy pure gum rubber sheeting
Rubber drainage tubing, various sizes
Rubber gloves
Fig. Fig. 160. Regular abdominal set of instruments. Showing the
characteristic appearance of most of the instruments used in the abdominal
operation

372
The routine list will, of course, vary in different hospitals; certain things
frequently used in one hospital might be used only occasionally in another,
and hence would be got out only specially when called for.
Regular Needles and Suture Materials (Fig. 161):
6 Large full-curved cutting needles (a, Fig. 1165)
8 Medium Mayo needles (6), 6 No. 3, 1 No. 4, 1 No. 2
2 Slender curved intestinal needles (c)
2 Long straight trocar-point needles (d)
1 Tube 40-day No. 1 chromic catgut (e) 5 Tubes 20-day No. 1 catgut (/)
1Tubes plain No. 00 catgut (g)
1 meter of fine silk (size D) or linen (h)
8 Strands of heavy silkworm-gut (i)
Fig. 161. Regular set of needles and suture materials 'for abdominal section
for pelvic disease, showing the general appearance of the various articles.
The numbers required are given in the regular list in the text

373
Have readily available other kinds of catgut or other suture material the
particular operator may wish to use.
Needles.The large full-curved cutting needle is large enough to be used
without a needle holder, and hence is timesaving in suturing the various
layers of the long abdominal incision. The cutting point is necessary in
penetrating the skin with the stay sutures, though it occasionally starts a
small hematoma in the wall.
For inside work in the pelvis and lower abdomen, such as ligating
pedicles and suturing together pedicle ends or other surfaces, round-pointed
needles are used exclusively. These tissues are soft and easily penetrated by
the round-pointed noncutting needle, while any cutting edge on a needle used
in this suture may cut into a vessel and start a serious hematoma.
Suture materials.Different operators use many different types and sizes
of catgut in pelvic abdominal work. Each of the two suture materials, silk and
catgut, has special advantages in certain situations. For decades we have used
catgut for pelvic pedicle ligatures and for buried sutures in the abdominal
wall, and have never regretted such use. The senior author recalls that when
he began his abdominal surgery, silk was the ligature material, and the later
attainment of reliable catgut for ligatures and buried sutures was a great
boon, for it largely eliminated the long-lasting sinuses and the "fishing" and
other operative maneuvers to remove the nonabsorbable silk ligatures which
kept them discharging.
It is convenient and it simplifies the suture preparations to use just two
kinds of catgut (twenty-day No. 1 and plain No. 00) in routine work, with
occasionally forty-day catgut for some special condition. The terms "forty-
day" and "twenty-day" refer to the lasting period in connective tissue, but the
lasting period is very much less on peritoneal surfaces and especially on
mucous surfaces.
The plain catgut is used, in slender intestinal needles, for suturing in
conservative work on the ovaries and tubes and for suture ligation of the

374
meso-appendix and other small delicate pedicles. It is used for tying the
stump of the appendix, preceding the silk or linen inverting suture, and also
for the closing skin suture.
The twenty-day catgut is used for all the layers of the abdominal wall
except the skin.
The fine silk or lavsan or linen, as preferred, is used for the inverting
suture in appendectomy and for any emergency intestinal suturing that may
be required.
Silkworm-gut is the most satisfactory material for stay sutures in the
abdominal wall, and the thickest strands should always be chosen for use in
this situation.
Special instruments. There are a number of other instruments
occasionally used in abdominal operations for pelvic disease, because of a
special condition in the particular case or because preferred by the operator.
For example: large cyst trocar, large tumor forceps, Wertheim’s parametrial
clamps, and instruments for extra-gynecologic work.
Preparation of operator and assistants
Everything that is to come in contact with the operative field must be
sterilized. The hands and forearms of the operator and assistants must be
disinfected as far as possible, and should then be covered so that there is no
chance of direct contact of the operative field with the skin of the hands or
arms, for the skin cannot be absolutely sterilized. Again, the operator and
assistants must be so covered as to protect effectively the field of operation
from contamination by particles from the hair or beard, or by particles carried
in the breath.
The accomplishment of this thorough protection of the operative wound
has been the object of many decades of study and experimentation. The
present effective technique for the preparation of the operator, as well as all

375
the other antiseptic and aseptic preparations, was attained gradually, by
improvements added year by year, but it is all the direct outgrowth of the
epoch-making work of Pasteur and of Lister. The following are the steps in
the preparation of the operator and assistants:
The sleeves are rolled well up above the elbows and the fingernails are
trimmed short and cleaned thoroughly.
The hands and forearms are then scrubbed carefully and vigorously, for
ten to fifteen minutes, with warm water and some liquid preparation of green
soap—using a stiff brush. Pay particular attention to the irregularities about
the nails and knuckles and to the spaces between the fingers at their junction
with the hand. Where the brush causes undue irritation of the skin, gauze is
preferable for scrubbing the arms, but a brush should be used on the hands.
Then the soap is washed off with sterile water, and the hands and
forearms are scrubbed in 80 per cent alcohol with gauze.
Then they are scrubbed in bi-chloride solution (1:2,000), with gauze.
The long-sleeved sterile gown is then put on, and the cap and face mask
are applied. As the rubber gloves are put on, the gauntlet of the glove is
brought up over the lower end of the sterile sleeve to hold it in place. The arm
is thus securely covered and there is no chance for any skin surface to come in
contact with the wound. The assistants go through the same process.
The careful and prolonged scrubbing with soap is the most important
feature in any method of hand-disinfection. This fact has long been
recognized, and many operators have discarded bi-chloride and other irritant
antiseptics and depend entirely on the soap scrubbing followed by the
scrubbing in alcohol. When carried out with care and judgment, this practice
is safe and gives good results and avoids the irritation due to bi-chloride. In
some persons, however, alcohol causes more irritation than bi-chloride.
There are a lot of methods of hand-disinfection, which are much used.
The thorough scrubbing with soap and warm water is common to all of them.
The further steps differ as follows:

376
a. The "alcohol-bi-chloride" method. The various steps in this method
have just been given in detail.
b. The «pervomur (C-4 preparation)” method. The hands and forearms
are next immersed in a pervomur solution and kept there during 1 minute,
and then they are dried up with sterile gauze napkin.
c. The"cerygel"method. After the preliminary scrubbing with a soap and
brush (for 3 minutes for every hand), every hand and forearm should be
treated with cerygel gauze tampon, saturated with cerygel solution, then
thoroughly dried up with gauze napkin.
As to the choice of method of hand-disinfection, that is largely a matter
of personal preference. Any one of the above three methods, properly carried
out, will give good prac-tical hand-disinfection—i. e., from hands and arms so
prepared, infection will rarely if ever take place. The important thing is not
which method is chosen, but how thoroughly the chosen method is carried
out.
Absolute disinfection of the hands and arms is impossible by any
method, as the disinfection is necessarily confined to the superficial layers of
the epidermis. Bacteria situated in the deeper layers of the epidermis may
work to the surface during the course of the operation, hence the importance
of thorough covering of the prepared hands and arms with rubber gloves and
sterile sleeves, leaving no skin surface exposed.
Anesthesia
It may be local for minor operations (diagnostic curettage of the uterus),
for pelvic floor operations many surgeons infiltrate the tissues with local
anesthetic solutions. Peridural anesthesia, general endotracheal narcosis
should be performed for a lot of abdominal operations.

377
Abdominal operations
Technique of abdominal operation
Regular Steps.
The regular steps in technique incident to every abdominal section for
gynecologic disease are as follows:
Incision.
Exploration.
Correction of pathological conditions.
Toilet of the peritoneum.
Closure of incision.
Dressing.
1. Incision
The following types of incisions are commonly used in gynecological
practice:
vertical(median, paramedian) incisions
transverse ( by Phannenstiel, by Cherny) incisions.
Median Incision. In abdominal section for pelvic disease, the incision
employed is usually longitudinal and in the median line. All parts of the pelvis
and lower abdomen may be easily reached from such a median incision, and
in practically every case exploration of the whole region should be made.
Ordinarily the incision extends from near the umbilicus to the symphysis
pubis. If there is a large tumor, the incision must be extended upward, though
at first it is usually made the ordinary size required for exploration with the
hand. As a rule, the primary incision is about 10-12 cm long. If the abdominal
wall is very thick, it must be longer; if very thin, it may be shorter. The lower
the incision is placed, the more easily the deeper portions of the pelvic cavity
may be reached, but in extending the incision low, care must be exercised to
avoid injury to the bladder.
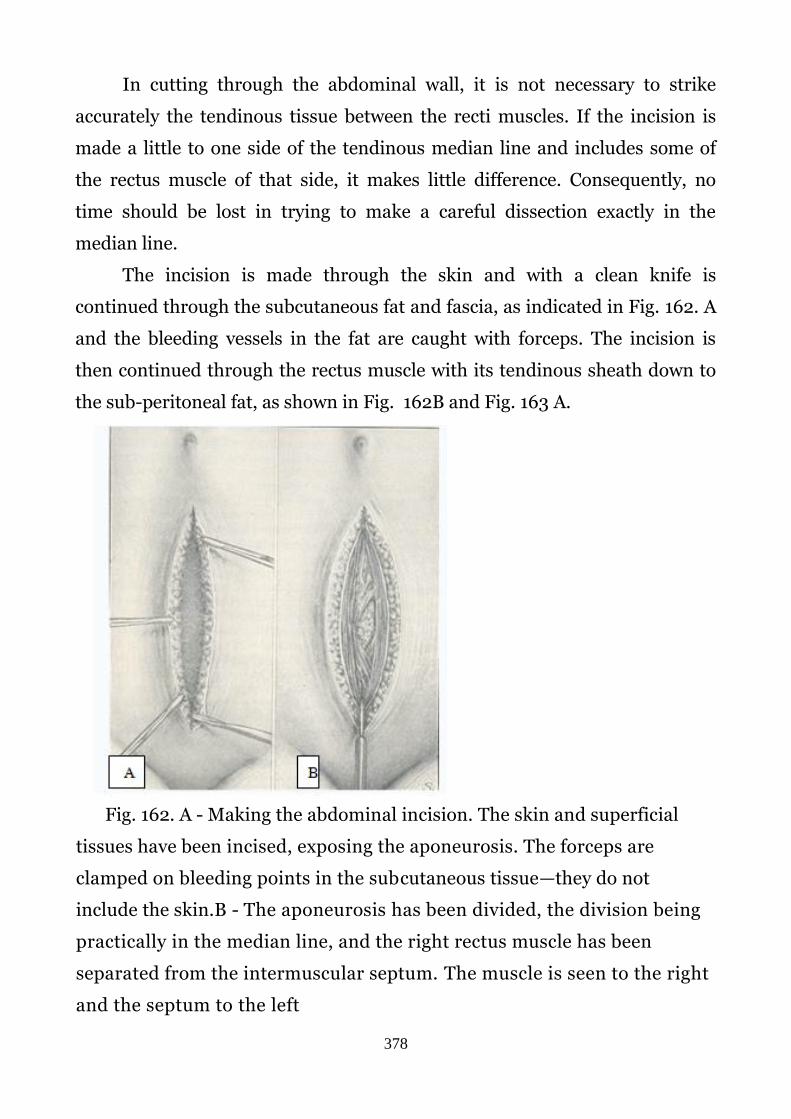
378
In cutting through the abdominal wall, it is not necessary to strike
accurately the tendinous tissue between the recti muscles. If the incision is
made a little to one side of the tendinous median line and includes some of
the rectus muscle of that side, it makes little difference. Consequently, no
time should be lost in trying to make a careful dissection exactly in the
median line.
The incision is made through the skin and with a clean knife is
continued through the subcutaneous fat and fascia, as indicated in Fig. 162. A
and the bleeding vessels in the fat are caught with forceps. The incision is
then continued through the rectus muscle with its tendinous sheath down to
the sub-peritoneal fat, as shown in Fig. 162B and Fig. 163 A.
Fig. 162. A - Making the abdominal incision. The skin and superficial
tissues have been incised, exposing the aponeurosis. The forceps are
clamped on bleeding points in the subcutaneous tissue—they do not
include the skin.B - The aponeurosis has been divided, the division being
practically in the median line, and the right rectus muscle has been
separated from the intermuscular septum. The muscle is seen to the right
and the septum to the left

379
Fig. 163. A - The few remaining muscular fibers at the bottom of the wound
are cleared away by placing the two index fingers together in the center of
the wound and then separating them to the angles, as here shown. This is
not ordinarily necessary but may be helpful if there is difficulty in
identifying the deeper tissues of the wall. B - Dividing the subperitoneal
fat.
The next step is to divide the subperitoneal fat and peritoneum. The
first small opening into the peritoneal cavity should be made in the upper
portion of the incision to avoid injury to the bladder, which may be drawn up
by an underlying tumor or inflammatory mass. The subperitoneal fat is
caught up by a dissecting forceps on each side and incised between the
forceps (Fig 163 B). A deeper portion is then caught up on each side and
divided (Fig. 164A). In this process of working through the fat, it is important
to progress directly downward toward the cavity, and not to one side. Unless
this point is watched, the dissection may extend along beside the peritoneum
and thus considerable time will be lost searching for the latter, particularly in
the cases where there is a large amount of subperitoneal fat. When the

380
peritoneum comes into view it is picked up with a forceps, to lift it from the
intestine. While thus raised, it is caught with another forceps, as shown in Fig.
164B.
Fig. 164. A — Continuing the division of the subperitoneal fat. After one
cut is made, deeper portions are picked up and divided, and thus the
process is continued until the peritoneum is reached. In dividing through
the fat, care should be taken to work directly downward toward the
peritoneum, and not laterally in the subperitoneal space.
B — Picking up the peritoneum, preparatory to incising it. It is first
caught and lifted from the intestine and then the lifted portion is caught
with another forceps.
The first forceps is then opened to release any underlying intestinal loop
that may have been held by it, and it is made to grasp the raised peritoneum
at another point (Pict. 165 A) This process is continued until it is evident the
raised peritoneum is clear of intestine. In some cases the peritoneum is so
thin that the absence of intestine or omentum may be determined by sight. In
other cases it may be determined by touch. The peritoneum is then divided
between the dissecting forceps (Pict 165 B), and the edges of the small
opening are grasped with artery forceps In cases of inflammation in the lower
abdomen, the intestinal coils may be adherent to the peritoneum, and
particular care is necessary to avoid injury to the intestine. This danger is

381
most marked in secondary operations, where the intestine may be firmly
bound by organized adhesions to the peritoneum in the vicinity of the
incision. In such a case it is advisable to extend the exposure of the
peritoneum laterally as far as necessary to find a clear area before attempting
to open it.
Fig. 165. A.— While the peritoneum is held up with the second forceps,
the first forceps are released, so that any portion of intestine caught in
them may drop away, and then the peritoneum is again caught with the
forceps. By this process, repeated if necessary, the peritoneum may be
separated from the intestine, which is sometimes inclined to adhere to it.
B.—The peritoneum incised. Notice that the opening is made at the
upper part of the abdominal wound, in order to avoid the bladder, which
may be pushed up by a tumor or pulled up by adhesions.
The next step is to enlarge the deep portion of the incision downward
and upward to the full extent of the superficial portion. A convenient way to
complete the division of the subperitoneal fat is by blunt dissection with the
scissors, as indicated in Fig. 166 A. With the heavy blunt-pointed laparotomy
scissors this division of the fat may be quickly carried to the symphysis
without danger of injuring the bladder. The peritoneum is then lifted by the

382
fingers and divided with scissors, as indicated by the dotted line in Fig. 166 B.
The divided peritoneum is then caught on each side at the lower part of the
incision and lifted out of the wound, as shown inFig. 167A. This enables the
operator to see just where the opaque bladder begins (location indicated by
dotted line in Fig. 47A, and the translucent peritoneum may be safely divided
down to it. The peritoneum at the upper angle of the wound is then divided
while the intestines are pushed away and carefully protected by the fingers
under it (Fig. 167B).
Before beginning the internal work, it is well to protect the divided
tissues of the abdominal wall by towels. The edge of a towel may be fastened
to the peritoneum of each side by hemostatic forceps, as shown in Fig. 168
A,B. Another method is to attach the edge of the towel to the opposite side of
the wound, as shown in Fig. 169A. and throw the forceps and towel over to
that side. By this maneuver the holding-forceps are covered by the towel, as
shown in Fig. 169 B. Still another method of holding the protecting towels in
place is to tuck them around the wound margins and then introduce the
retractors for holding the wound open.
Paramedian incision (syn.: rectus incision). Some operators prefer to
make the incision through the aponeurosis over the rectus muscle of one side,
usually the right. The right one is used more often as most surgeons are right-
handed. The left paramedian incision is used if the surgeon is left-handed or
the patient had several operations before. The skin incision may be made in
the median line. The skin and fat are retracted and the aponeurosis is incised
some distance from the median line, over the rectus muscle. The muscle is
then split longitudinally or retracted as preferred, and the cavity entered by
an incision immediately under the upper aponeurotic incision. The advantage
of this procedure is that it insures the interposition of a layer of muscle
between the upper and lower lines of approximation, thus giving a wide area
of union instead of the narrow one that results when the upper and lower
lines of approximation fall practically together without intervening muscle.

383
The interposition of muscle to separate the peritoneal and the aponeurotic
lines of approximation in the abdominal wall may, in the opinion of the
authors, be better attained by using the median incision and, in the closure,
dividing the intermuscular septum and approximating the two muscles in the
median line by light suturing.

384

385
Transverse incision. The transverse incision, known as the Phannenstiel
incision, is considered by some operators the preferable incision for pelvic
work. It is made by the following steps:
1. A transverse incision with a slight downward curve is made through
the skin and subdermal tissues, the middle of the incision crossing the
median line about (4 cm.) above the pubic bone (Fig. 170 A). The length of the
incision is 8 to 10 cm, and it lies largely within the region of the pubic hair.
The same incision is continued down through the aponeurosis to the
recti muscles but not through the muscles. The upper flap, consisting of skin,
fat and aponeurosis, is then raised, the fibrous septum between the muscles
being divided by scissors or knife (Fig. 170 B) as needed to permit this flap
being raised to the required extent. When completely loosened, the flap is
held out of the way by a retractor or otherwise.
The muscles are then separated in the median line and the peritoneum
divided to the required extent by a median incision (Fig. 171 A.). Retractors
are then introduced to give the necessary exposure (Fig. 171 B).

386
It is preferable to keep the incision within the area of pubic hair when
sufficient working room can be thus secured. If necessary the incision may be
extended further on one or both sides. Transverse division of the recti
muscles is permissible when required to give sufficient working room. In fact,
some operators employ this as the routine technique, making the transverse
cut through all tissues, including the muscles and the peritoneum.
The upper flap may be held out of the way by a retractor, as already
mentioned, or by traction on the aponeurosis by means of a forceps or a
suture. When all the tissues are divided transversely, the upper peritoneum
may be rolled upward and outward, or it may be sutured temporarily to the
posterior wall of the abdomen, after the intestines have been pushed up out of
the way.
When sutured across the cavity, the peritoneal flap serves to keep the
intestinal coils out of the pelvis during the subsequent steps of the operation.
The advantages of the transverse incision are: (1) the full length of the
incision is placed where most needed, viz., over the pelvis, (2) it prevents
postoperative hernia, for the suture lines do not lie immediately under each
other but cross at right angles, and (3) the scar is hardly noticeable after the
growth of the pubic hair. The disadvantages are: (1) the extensive area of
tissue traumatized increases the seriousness of infection in the wound and

387
increases the chance of oozing and hematoma, (2) proper exposure requires
persistent and strong retraction in three directions, and, (3) it is not suitable
for difficult work in the region of the umbilicus or above, which work is not
infrequently required in gynecologic cases, and the necessity for such work
may not be apparent until the abdomen is open.
Transverse incision by Cherny. It is the incision of the skin and lower
layers in transverse direction, and it is situated about 5-6 cm higher than
symphysis pubis. It may be better then Phannestiel’s incision because of its
wide opening of the abdominal cavity. But as to reparation and cosmetic view,
it is much worse.
2. Exploration
When the proper opening has been made, the hand is introduced into
the peritoneal cavity and the various pelvic organs are outlined and the
pathological conditions determined as accurately as possible. It is well to go
about the exploration in a systematic way.
The first step is to clear out the intestinal coils from the lower abdomen,
so that the pelvic organs may be seen and palpated. Having the patient in
moderate Trendelenburg posture, i. e., with the shoulders considerably lower
than the hips facilitates this step. Then with the heavy rubber sheeting,
moistened with warm saline solution, the intestines are pushed up and held
out of the field. Of course, if some of the intestinal loops are adherent in the
pelvis, the adhesions must be broken before the loops can be pushed up. In
some cases the omentum will be found adherent in the pelvis, thus covering
over and obscuring everything, even the intestinal coils. The adherent
omentum must be separated and pushed up (Fig. 172, Fig. 173). Occasionally
the margin of the omentum is so extensively or densely adherent, that it is
preferable to excise the adherent portion.

388
The omentum and intestines having been pushed out of the field, the
examination of the pelvic organs proper begins. The uterus is the central
landmark. When that organ has been recognized, the other structures, though
greatly distorted, can be identified by their relation to it. The rounded corpus
uteri can usually be easily seen and palpated and any marked abnormality

389
determined. If turned back into the hollow of the sacrum, it must be brought
forward for identification and critical palpation.
Next, the adnexa of each side are to be palpated and inspected. There
are different methods of bringing the tube and ovary up into the wound for
inspection. The most convenient method usually is to introduce the hand,
palpate the various structures, and then lift up the ovary and tube with the
fingers, as indicated in Fig. 174, first on one side, then on the other.
Another convenient method is to grasp the round ligament near the
uterus with a forceps and lift up the uterus and adnexa as shown in Fig. 175.
Care should be taken not to grasp the tube, which is more prominent than the
ligament. Still another method is to grasp the fundus uteri with a special
holding-forceps and lift the structures as shown in Fig. 176. However, this
calls for a special instrument, which unnecessarily complicates the
instrument situation.

390
Other structures to be considered in the examination are the
parametrium, bladder, ureters, glands (in carcinoma), rectum, sigmoid,
appendix, cecum, ascending colon (constricting membrane) and adjacent
ileum (bands, kinks).

391
Good exposure of the pelvic interior permits a better appreciation of the
pathological conditions and a more accurate correction of them. At the same
time it reduces the chance of injury to adjacent structures.
3. Correction of Pathological Conditions
After exploring the pelvic cavity and lower abdomen and ascertaining
the exact conditions present, the operator proceeds to deal with the lesion or
lesions according to established principles and technique, and perform the
operation properly.
The determination as to what is best to do is not always an easy matter.
In many cases the decision as to what to do and what not to do is the most
difficult feature in the whole case. On it rests the freedom of the patient from
subsequent serious disturbance and consequently, to a considerable extent,
her future happiness. Shall the damaged ovaries be removed or subjected to
conservative operation? Shall the chance of pregnancy be preserved by
leaving a portion of a tube, that may later cause trouble? Shall the myomas be
treated by myomectomy or by hysterectomy? Will the preservation of a
thickened and chronically inflamed uterus prove ultimately beneficial or
harmful to the patient? Is the malignant disease (uterine or ovarian, as the
case may be) really operable, judged according to the probability of
immediate and remote comfort to the patient? Is the patient's life and
comfort, in a case of old organized adhesions throughout the pelvis, best
protected by breaking up the adhesions in every direction or by removing the
obvious lesion with a minimum disturbance of adhesions? The list of
questions could be extended indefinitely but this is sufficient to call attention
to the serious problems encountered. The conscientious gynecologist must
bring to bear all possible knowledge of the physiology and pathology and
reparative powers of the organs involved, an understanding of the patient's
circumstances and wishes, and a judgment based upon close study, accurate

392
observation and a sympathetic consideration of the patient's comfort and
usefulness.
Most of the questions thus encountered in the exploration may be
answered promptly and positively in the individual case. A few of the
problems present features, which have not yet been fully worked out. But the
uncertain features are being eliminated gradually, as more and more reliable
information becomes available.
To prepare for leakage. An adherent inflammatory mass or cyst may
contain pus or other irritating fluid such, for example, as in an endometrial
cyst or a dermoid. In order to prevent extensive peritoneal contamination
from leakage during enucleation, special care is needed. The first thing is to
free the omentum and intestines by breaking the light adhesions, but avoid
adhesions likely to lead to leakage from the mass.
Then cover the intestines with the rubber sheeting, spreading it out so
as to give complete protection. Then spread out a towel over the rubber
sheeting to absorb any leakage as soon as it occurs in the process of
enucleating the mass, a corner of the towel to be outside and clamped to the
abdominal sheet. The amount of free fluid in the pelvis may be held to the
minimum by using the suction apparatus as soon as leakage starts. Also, when
a fluid collection is felt and leakage seems probable, it may be advisable to
evacuate the fluid with a trocar attached to the suction tube.
Appendix. Lesions of adjacent structures may be found, either
associated with a gynecologic lesion or causing symptoms attributed to a
supposed gynecologic lesion, which was not present. The gynecologist should
of course be prepared to treat such commonly encountered lesions according
to established usage as set forth by authoritative works on those subjects.
There is one question that recurs so frequently in gynecologic work that it
merits special attention here. Should the appendix be removed in every case
of abdominal section in which the patient's condition will permit? On this
point there is decided difference of opinion among operators, and there is a

393
good deal to be said on each side. Some consider it inadvisable, with the
abdomen open, to leave this structure, which may cause a second operation
and may cause the patient's death in spite of operation. Others consider it
inadvisable to open the intestinal tract in the operative field and thus run the
chance of subsequent leakage and possibly fatal peritonitis, simply to remove
a structure that is causing no trouble and may never cause trouble. The
authors have solved this problem to their own satisfaction by the adoption of
the rule that the appendix is to be removed only for a definite reason. The
accepted reasons are four in number and as a matter of fact cover most cases.
The reasons are as follows: (1) If the appendix is obviously diseased. (2) If
there have been symptoms indicating disease of the appendix. (3) If the
appendix lies in the operative field so that it is likely to be caught in the
reparative exudate. (4) If the patient requests its removal.
When the cecum and appendix are normally movable, they may be
brought sufficiently toward the median incision for convenient work. When
the structures are fixed by adhesions or congenital bands, the work must be
conducted deep in the right side, which may require strong lifting and
retraction of the right abdominal wall. Also, help may be given toward
satisfactory exposure and operating space, by keeping the patient in partial
Trendelenburg position and by pushing the small intestine to the left and
upward.
Emergency repair of injury. Injury of an adjacent structure may occur,
due to its displacement or distortion by the gynecologic lesion or involvement
in it. Such conditions, favoring injury of intestine or bladder or ureter, are
found principally with inflammatory adhesions or endometriosis, or with a
large tumor of ovary or uterus. Malignant tumors and pelvic tuberculosis are
particularly prone to involve and damage the adjacent intestinal wall or
bladder wall so that it tears on the attempt to separate adhesions.
As mentioned tinder malignant tumors of the ovary, it is well for the
gynecologist to refresh his memory in regard to the details of emergency
394
repair of intestinal and urinary tract injuries when preparing to operate in a
complicated case. The emergency treatment of bladder and urethral injuries
will be found in special textbooks.
4. Toilet of the Peritoneum
Bleeding having been completely controlled, the blood and clots are
sponged out of the pelvis and, as far as practicable, the pedicle ends are
turned under and all raw surfaces covered with peritoneum. All abdominal
sponges are then removed, the intestines are permitted to come back into the
pelvis (the patient having been lowered from the Trendelenburg posture), and
the omentum is spread out in its proper place. The objects of the toilet of the
peritoneum are to remove all injurious substances, to restore the structures to
approximately their normal relations, and to prevent serious adhesions.
The prevention of serious adhesions is a problem not yet wholly solved.
In every case of operation, more or less reparative exudate is thrown out. This
splints the injured tissues and aids in repair, somewhat on the same principle
as callus about a broken bone. If everything goes well this reparative exudate
is absorbed to a greater or lesser extent. In some cases practically all of it
disappears, while in other cases a considerable portion remains as definite,
organized adhesions. In many cases where extensive adhesions remain, no
symptoms result. In other cases postoperative adhesions cause troublesome
symptoms, the most serious of which is intestinal obstruction. So it is evident
that some adhesions cause trouble and others do not.
The preventive measures have two objects: first, the prevention of all
adhesions as far as practicable and, second, the avoidance in particular of
those special adhesions which are most likely to cause serious trouble. The
first object is obtained by a rigid asepsis to prevent all infection, by the
minimum handling and roughening of the peritoneal surfaces, by the
protection of the intestines with moist gauze pads or better still by heavy
rubber sheeting by turning in of all raw ends and edges, and by the complete

395
removal of all irritating materials from the peritoneal cavity at the close of the
operation.
In regard to the second object, it has been found that the adhesions of
the small intestine are the ones that are most likely to lead to serious trouble.
Consequently, as the toilet of the peritoneum is made, special care is taken to
keep the coils of the small intestine away from the irritated peritoneum in the
depth of the pelvis and away from the sutured peritoneum at the site of the
abdominal incision. The small intestines may be kept out of the depth of the
pelvis more or less by pushing the coils up and allowing the cecum and
sigmoid to come together across the pelvis (Fig. 177) or as near together as
possible. To prevent adhesions of the small intestine to the line of incision,
the omentum is to be spread immediately under the incision. Adhesions
between the omentum and the line of incision rarely cause trouble. In certain
cases the omentum may be used to assist in keeping the small intestines away
from irritated areas in the pelvis. The omentum, however, varies much in
length in different cases, sometimes being very short. Even when long, it
should not be tucked down forcibly into the pelvis, for omental adhesions
with tension will very probably cause troublesome symptoms.
The use of antibiotics and sulfanilamide in the peritoneal cavity in clean
cases has been much discussed pro and con—the risk of irritation and
contamination being balanced against the chance of inflammation in that case
and its prevention by the bactericide. Large series of carefully checked cases
will be needed to settle the matter.

396
5. Closure of Incision
The peritoneal edges of the wound are lifted with forceps, so as to be
clear of intestine and omentum, and then approximated by a catgut suture.
For this purpose it is well to use a running mattress suture, as shown in Fig.
1211, locked at intervals. This type of suture prevents the turning in of the raw
edge, which would favor intestinal adhesions to the wall. However, with
special care this turning in may be avoided with the ordinary running suture,
which is more convenient and rapid in application. Another item is the
tearing of the peritoneum. In cases where there is some tension and the
peritoneum is thin or friable, it may tear with each suture, and the deeper
bites taken to bring it together only cause larger tears. This difficulty is
overcome by picking up some of the muscle along with the peritoneum in the
first row of sutures. The peritoneal sutures, and, in fact, all sutures in the
abdominal wall, are ordinarily placed with large needles that can be
conveniently handled without a needle holder. In cases where the wound is
very deep, on account of a thick wall, it may be advisable to use a needle
holder here and there in the work.
After the peritoneum is sutured, the intermuscular septum is divided by
scissors, as shown in Fig. 178 B, and the two recti muscles are brought

397
together in the median line by a loosely drawn running suture. The peritoneal
and muscular suturing may be conveniently made with the same suture, by
suturing down the peritoneum, as shown in Fig. 178 A, B and up in the
muscles, as shown in Fig. 179 A,B tying the muscular portion to the upper end
of the peritoneal portion, which has been left long for that purpose.

398
The silkworm-gut stay-sutures are placed so that they lie just under the
aponeurosis and emerge on the skin surface about 1/2 cm. from the wound
margin, as shown in Fig. 179 B. Three arc usually sufficient, except in the very
long incisions, where four or five may be required. The stay-sutures prevent
undue tension on the line of union during muscular activity involving the
abdominal wall. After several days the catgut sutures become somewhat
softened and a sudden strain on the wall, such as coughing or sneezing, may
damage the union by causing separation at spots deep in the depth of the
wound or by causing the whole wound to open. This danger, the reality of
which has been established by unfortunate experiences, is minimized by the
use of stay-sutures, followed immediately on their removal by strong adhesive
strapping which is to be maintained until the end of the fourth week. In that
way adequate support supplements the approximation sutures until the union
is firm enough to stand all strains to which it is likely to be subjected.
Next the aponeurotic edges are united accurately and securely (Fig.
180). This may be accomplished by a continuous suture locked at intervals, as
shown in Pict. 61 B, or interrupted mattress sutures may be used. The suture
material is of importance. It must hold long enough to permit firm union, for
on this line of union largely depends the integrity of the scar and the
prevention of hernia. Chromic catgut is generally used. A considerable
number of operators prefer silk, lavsan or linen, and an occasional one pins
his faith to silkworm-gut or silver wire. Furthermore, there are some types of
artificial catgut (dacril), which are widely used nowadays. The nonabsorbable
sutures hold indefinitely, but if any infection takes place, sinuses are likely to
persist until the infected sutures arc removed. Such unpleasant experiences
were common in former times when silk was the universal suture material.
The ideal material is a dependable long-lasting absorbable suture. The
authors for several years have used twenty-day catgut with entire satisfaction.
The matter of suture material for the abdominal wound is considered in more
detail under preparation of instruments and sutures (Fig. 160, Fig. 161)
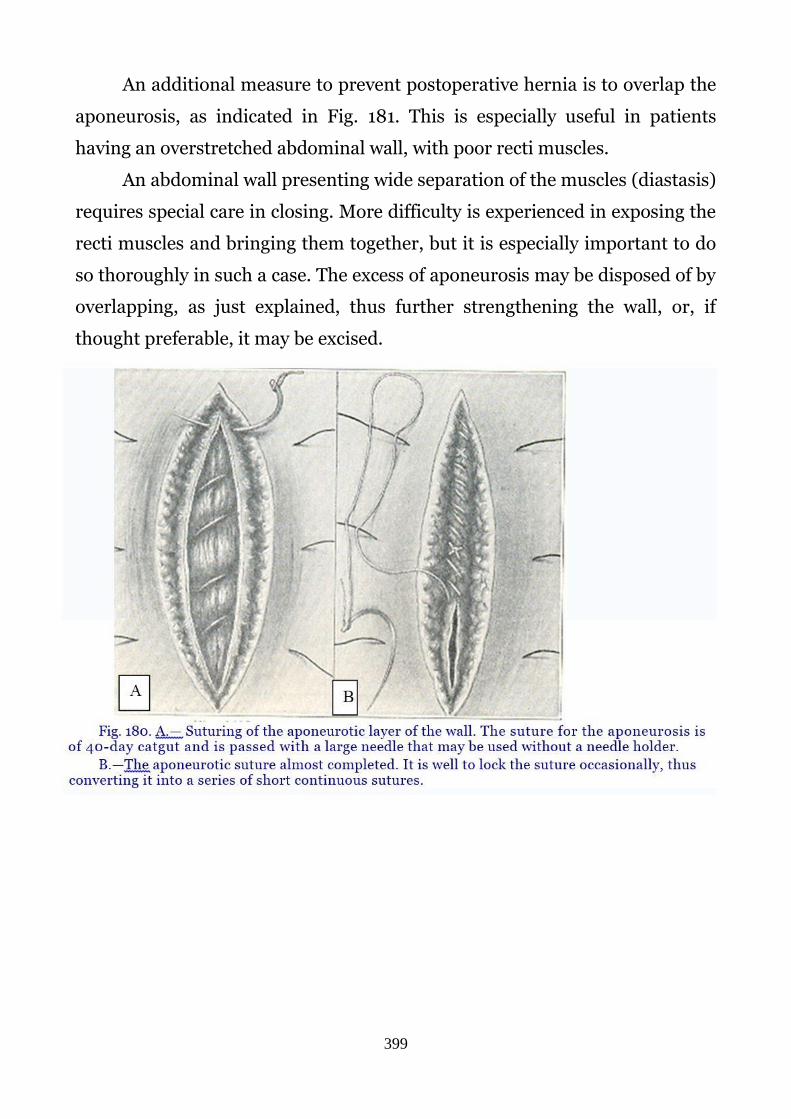
399
An additional measure to prevent postoperative hernia is to overlap the
aponeurosis, as indicated in Fig. 181. This is especially useful in patients
having an overstretched abdominal wall, with poor recti muscles.
An abdominal wall presenting wide separation of the muscles (diastasis)
requires special care in closing. More difficulty is experienced in exposing the
recti muscles and bringing them together, but it is especially important to do
so thoroughly in such a case. The excess of aponeurosis may be disposed of by
overlapping, as just explained, thus further strengthening the wall, or, if
thought preferable, it may be excised.

400
The method of skin approximation varies greatly with different
operators. The skin wound may be closed by an ordinary continuous suture of
catgut or silk or linen or by interrupted sutures of these materials. The catgut
may be placed in the form of a subcuticular suture, as explained later, or
nonabsorbable material, such as silkworm-gut or silver wire or paraffined
linen, may be used for such a suture, to be drawn out after healing. Some
operators prefer clips for closing the wound, and others depend on adhesive
plaster approximation of the skin margins.
After considerable experimentation with various methods of skin
closure, the authors have returned to the simple continuous catgut suture,
applied as shown in Fig. 182. The fine suture (No. 0) is of plain catgut and
hence is absorbed as soon as its usefulness is ended,so quickly that it does not
have to be "removed" with forceps and scissors. The outer loose unabsorbed
portion is simply brushed off. This suture is most expeditiously applied with a
slender sharp needle, large enough to be handled conveniently without a
needle holder. The needle may be straight or curved, as preferred. The

401
method of its application is shown in Fig 182 A and the completed suture in
Fig. 182 B. It can be applied rapidly, gives firm approximation, controls
oozing in the flaps, and is suitable for all conditions. Subcuticular suture is
shown in Fig. 183.
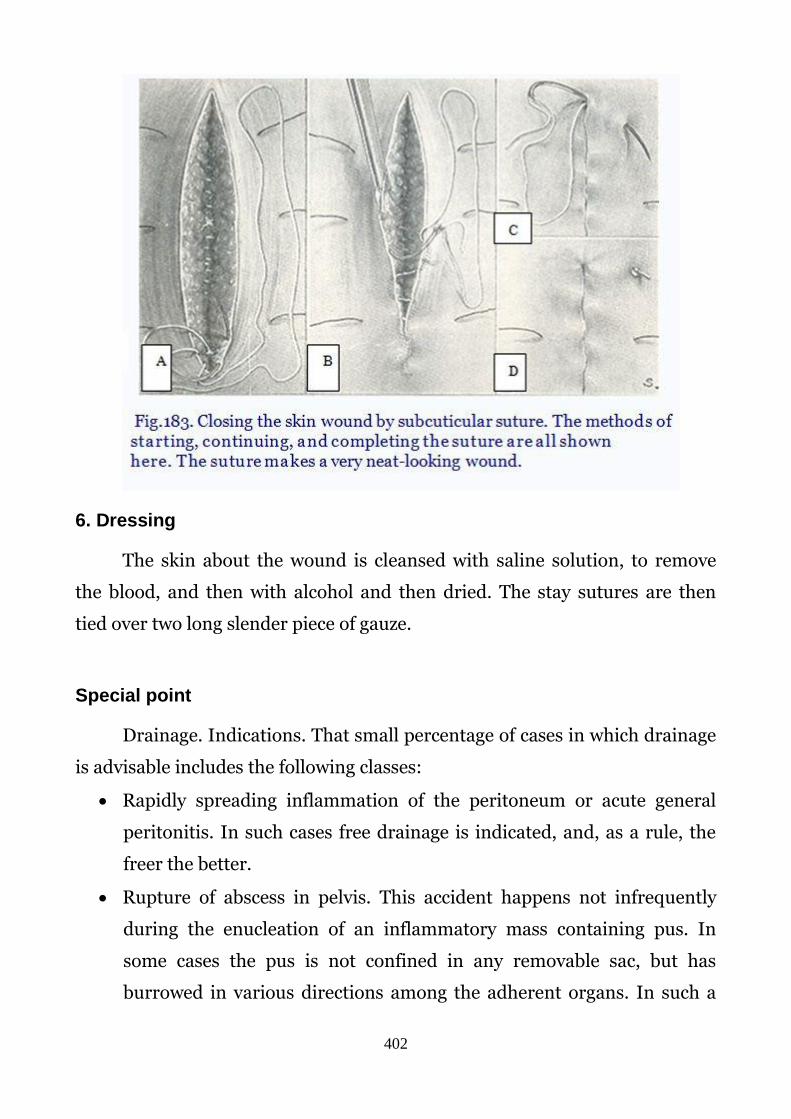
402
6. Dressing
The skin about the wound is cleansed with saline solution, to remove
the blood, and then with alcohol and then dried. The stay sutures are then
tied over two long slender piece of gauze.
Special point
Drainage. Indications. That small percentage of cases in which drainage
is advisable includes the following classes:
Rapidly spreading inflammation of the peritoneum or acute general
peritonitis. In such cases free drainage is indicated, and, as a rule, the
freer the better.
Rupture of abscess in pelvis. This accident happens not infrequently
during the enucleation of an inflammatory mass containing pus. In
some cases the pus is not confined in any removable sac, but has
burrowed in various directions among the adherent organs. In such a

403
case, as soon as the adhesions are separated the pus flows out into the
peritoneal cavity.
Persistent free oozing from surfaces left after the enucleation of an
inflammatory mass. Here the effect desired is pressure rather than
drainage, but, as the end of the gauze used for pressure must be brought
out through the abdominal wound or through the vagina, it is usually
referred to as a drain or pack. Topical thrombin preparations now take
care of oozing in most cases.
Endometrial ovarian cysts with extensive adhesions.
Methods. The method of draining depends somewhat on the extent of
the inflammation and other conditions present. If the inflammation is limited
to the true pelvis and hysterectomy has been performed, vaginal drainage is
the preferable plan. If the cervix uteri have been removed, there is already a
satisfactory opening into the vagina. If the cervix has not been removed, it
may be split posteriorly. If the inflammation is chronic and only a safety vent
is required, small red tubing may be used. If the inflammation is acute,
immediate free drainage should be provided for using good-sized rubber
tubing. Any hemostatic gauze packing beside the tubing, should be placed so
that it may be removed without disturbing the drainage tube.
If the inflammation is severe and extensive, drainage both above and
below may be advisable—the abdominal drainage being by means of a soft
rubber tube. If the uterus is preserved, it is usually preferable to drain above
only, though vaginal drainage through a special opening in the vaginal vault
may be employed if desired.
Operations on the uterus and adnexas
Amputation of the oviduct (salpingectomy)
Indications: bag-like tumor in the tube (hydrosalpinx, pyosalpinx),
double-sided severe chronic infpammational process, without effect of

404
concervative treatment, tubal pregnancy, etc. If the ovary involved into
inflammatory process it should be removed together with the tube
(adnexectomy).
Contraindication: surgical treatment is contraindicated in cases of
tuberculous disease of tubes and ovaries, because separation adhesions may
lead to development of intestinal fistula, peritonitis.
The operation may be very difficult in cases of large bag-like tumor
formations (pyosalpinx), progressive chronic inflammations due to a lot of
adhesions in abdominal cavity.
Anesthesia: general endotracheal narcosis is the most preferable in this
operation.
Stages of the operation are the following:
1. Disinfection of the skin.
2. Longitudinal or transverse incision of the anterior abdominal
wall.
3. Introduction of a dilator and shielding of the intestinal loops.
4. Gripping of the uterine tube by a hand and its elevation.
5. Placement of Kocher’s forceps on the mesosalpynx and the
uterine end of the oviduct.
6. Excision of the uterine tube, suturing and ligation of stumps.
7. Peritonization of stumps. (Fig. 67)
8. Cleaning of the abdominal cavity in case of purulent formation
(pyosalpinx, ruptured tumor-like formations), it is necessary to
perform the drainage of abdominal cavity with special sterile
polyvinyl tube, setting in one or both iliac areas.
9. The surgical nurse’s report about the accountability of all
instruments and napkins;
10. Suturing of the abdominal wound.

405
Operative treatment of ectopic pregnancy
Ectopic pregnancy is a significant health problem for women of
reproductive age and warrants an urgent well planned therapeutic strategy. It
can be a life threatening condition and is the leading cause of first trimester
mortality for women living in the developed world. The long term sequelae of
ectopic pregnancy are infertility. Critical decisions need to be taken during
the initial management of a woman with ectopic pregnancy to ensure safety
and to optimally preserve future fertility.
Ectopic pregnancies can be managed surgically either by laparotomy or
laparoscopy. Most cases should be managed laparoscopically as best practice
The traditional treatment in this stage is abdominal operation and
removal of the pregnant tube (in tubal pregnancy) as soon as the diagnosis is
fairly certain (see chapter 11). Abdominal salpingectomy (Fig. 184, Fig. 185)
as well as abdominal salpingotomy traditionally were used for surgical
treatment of non-interupted tubal pregnancy.

406
Currently ectopic pregnancies can be managed surgically either by
laparotomy or laparoscopy. Most cases should be managed laparoscopically
as best practice. The obvious benefit of laparoscopic surgery was
demonstrated convincingly in these trials – shorter operation times, less
blood loss, shorter hospital stays and lower analgesic requirements. It has
been standard teaching in the past that laparotomy should be used for women
with a haemoperitoneum. This is no longer true in the case of the experienced
laparoscopic surgeons with good operating facilities. However, in general
terms the surgical procedure that will prevent further blood loss most quickly
should be used, and in many centres laparotomy may still be the preferred
choice.
The two procedures usually performed on tubal ectopics are
salpingectomy and salpinsgotomy. In some cases with an isthmic ectopic
pregnancy, a segment of the tube can be removed which will leave sufficient
tubal length for reanastomosis at a later stage, since these cases have a poorer
outcome with conventional salpingostomy. A laparoscopic salpingostomy is
the removal of the ectopic pregnancy, by dissecting it out of the tube, leaving
the Fallopian tube in situ in an attempt to preserve fertility on that side. Fig.
186, Fig. 187.It is used for surgery of non0interrupted tubal pregnancy.

407

408
Pelvic hematocele. The typical example of pelvic hematocele is tubal
abortion. In these cases the hemorrhage has long since ceased and the
collection of blood low in the cul-de-sac is well shut off from the general
peritoneal cavity by plastic exudate and adhesions. The embryo and
membranes have probably escaped from the tube, either through a rupture in
the wall or through the end of the tube by "tubal abortion," and perhaps have
been largely absorbed. Practically all that remains is the blood in the pelvis
with the exudate and adhesions around it. This forms a tender mass low in
the culdesac back of the uterus.
In such a case the tclassic, traditional surgery was to perform urgent
laparotomy and salpingectomy, removing of blood clots and tissues of the
ovum from uterine cavity, and drainage of the uterine cavity. (Fig. 188).
Laparoscopic salpimgectomy is the benefit for managhement of such
cases today (Fig. 189).

409

410
Resection of the ovary
Indications: retention cyst of the ovary, Stein-Leventhal syndrome,
endometriosis of the ovary.
Stages of the operation are the following:
1. Disinfection of the skin.
2. Longitudinal or transverse incision of the anterior abdominal wall.
3. Introduction of a dilator and shielding of the intestinal loops.
4. Fixation of the ovary with fenestrated forceps.
5 Pathologically altered tissue of the ovary excision (with a scalpel). (Fig. 192).
6. Suturing of the ovary (with catgut).
7. Revision of the abdominal organs.
8. The nurse’s report.

411
9. Cleaning the abdominal cavity
10. Suturing of the abdominal wall (drainage should be performed in case of
endometriosis of the ovary)
11. Catheterization of the bladder
Removal of para-oophoritic cyst
Indications: para-ophoritic cyst.
Main stages of the operation are the following:
1. Disinfection of the skin.
2. Longitudinal or transverse incision of the anterior abdominal wall.
3. Introduction of a dilator and shielding of the intestinal loops.
4. Inspection of the organs of abdominal cavity and uterus especially their
topography.
5. Dissection of the anterior layer of broad ligaments (between clamp and
contraclamp).

412
6. Enucleation and removal of a cyst with the help of swab and scissors. (Fig.
193)
7. Placement of a catgut suture on the incision in the broad ligaments.
8. Nurse’s report.
9. Cleaning the abdominal cavity
10. Suturing of the abdominal wall.
11. Catheterization of the bladder
Supravaginal amputation of the uterus
There are two main types of amputation of the uterus: with or without
appendages (ovaries and tubes). The most preferable type is amputation
without adnexa. But if there is a serious damage of the ovary (or ovaries) due
to hemorrhage, inflammatory process, cysts and tumors etc, the injured ovary
(or ovaries) should be removed.

413
Indications: myoma of the uterus, endometriosis, injuries of the uterus
(perforation during artificial abortion), etc.
Main stages of the operation are the following:
1. Skin disinfection;
2. Longitudinal or transverse incision of the anterior abdominal walls;
3. Introduction of a dilator and inspection of the pelvic organs;
4. Placement of a tenaculum forcepts into the uterus and its elevation into the
wound;
5. Shielding of the intestines;
6. Application of forceps to the round ligament of the uterus, proper ligament
of the ovary, and the uterine end of the oviduct, dissection of each of those
ligaments between two forceps, and suturing of the stumps.
If it is amputation with appendages, one should apply forceps to the round
ligament, suspensory ligament, then follows dissection, ligation. Then the
tissue between forceps should be dissected;
7. Dissection of the vesicouterine fold of the peritoneum and displacement of
the bladder with a gauze swab;
8. Application of the forceps and ligation (after suturing) of vascular bundles
on both sides.
9. Dissection of the uterine corpus from the cervix; (Fig. 194).
10. Suturing of the cervical stump;
11. Peritonization;
12. Cleaning the abdominal cavity;
13. The surgical nurse’s report about the accountability of all instruments and
material;
14. Suturing of the abdominal wall;
15. Catheterization of the bladder.

414
Extirpation of the uterus (abdominal hysterectomy)
Indications: tumors of the uterus (large myoma, cancer, sarcoma),
endometriosis, unexplained repetitive uterine bleedings, ovarian tumors. This
operation is most preferable in patients after 40 years of age.
Main stages of the operation are the following:
Stages 1-3 are the same.
4. Placement of a tenaculum forcepts into the uterus and its elevation into the
wound; (Fig. 195)
5. Shielding of the intestines;
6. Application of forceps to the round ligament of the uterus, proper ligament

415
of the ovary, and the uterine end of the oviduct, dissection between two
forceps of each of those ligaments, and suturing of the stumps. (Fig. 196).
If it is extirpation with appendages, one should perform application of forceps
to the round ligament, suspensory ligament of the ovary (lig.
infundibulopeolvicum), then follows dissection, and ligation of the
formations;
7. Dissection of the vesicouterine fold of the peritoneum and displacentment
of the bladder with a gause swab. (Fig. 196);
8. Application of the forceps and ligation (after suturing) of vascular bundles
on both sides;
9. Dissection and ligation of the uterosacral ligaments;
10. Additional separation of the bladder;
11. Dissection and ligation of the uterine vessels on both sides;
12. Separation of the uterus from the vaginal fornices. The moment the vagina
is opened, the surgical nurse gives the surgeon a narrow gauze band 30 cm
long moistened with 70 per cent alcohol in the middle, which the surgeon
introduces into the vagina with the help of a long forceps; the latter is
immediately discarded after the operation. (Fig. 196);
13. Suturing of the vagina ;
14. Peritonization (Fig 197);
15. Cleaning the abdominal cavity;
16. The surgical nurse’s report about the accountability of all instruments and
material;
17. Suturing of the abdominal wall;
18. Catheterization of the bladder.

416
Conservative myomectomy
Indications: subserous myoma of the uterus.
Main stages of the operation are the following:
1. Disinfection of the skin;
2. Longitudinal or transverse incision of the anterior abdominal wall;

417
3. Introduction of a dilator and shielding of the intestinal loops;
4. Fixation of the uterus by one of the nodes with a tenaculum forceps;
5. Shielding of the abdominal cavity;
6. Dissection of the uterine wall above (may be around) the node (with
scalpel) with haemostasis using Kocher’s forceps;
7. Grasping of the exported node with a tenaculum forceps ; (Fig 198)
8. Enucleation of the node with scissors and gauze swab;
9. Ligation of bleeding vessels;.
10. Suturing of the bed of the tumor (interrupted catgut sutures in 2 layers);
11. Peritonization;
12. Cleaning the abdominal cavity;
13. The surgical nurse’s report about the accountability of all instruments and
material;
14. Suturing of the abdominal wall;
15. Catheterization of the bladder.

418
Transvaginal Operations
Preparation of operative field
The preliminary preparation of the operative field the day before has
already been mentioned. The preparation in the operating room is usually
made after the patient is anesthetized and in position for operation, though it
may be made before anesthetization if preferred. With good pre-anesthetic
sedative sleep, the preparation and often also the vaginal operation
(curettage, cervix work) can be carried out without additional anesthesia,
provided the work be conducted gently and quietly.
In arranging the patient for vaginal operation, the arms are folded over
the abdomen and each hand is caught with a gauze loop about the wrist, the
other end of the muslin strip being tied around some convenient projection
on the opposite side of the table. This method of hand tying protects the arms
from slipping over the edge of the table and also restrains the hands as
needed.
With the patient's hips drawn to the end of the table and the feet
supported out of the way by stirrups (Fig. 199.), the external genitals are
cleansed thoroughly with green soap and sterile water, using gauze or cotton
balls, then cleansed with sterile water, and then with the antiseptic solution.
419
Catheterization is then carried out with strict asepsis, the labia being
held away and the meatus specially cleansed. The sterile catheter should be
lubricated and care should be taken to avoid contaminating the bladder
portion with soap or irritating antiseptics. After the catheterization, the
vagina is cleansed with soap and water and then with the antiseptic solution.
The soap scrubbing is the most important part of surface sterilization.
As already mentioned under abdominal preparation, the other antiseptics
employed vary greatly in different institutions and at different times.
Tinctures of these and other of the newer chemicals are used for skin
disinfection, but are irritating to mucous membranes. Instead of the usual
swabbing method of application for skin sterilization, spraying has been
employed.
It is well to extend the preparation of the operative field over a wide
area. When the vaginal opening is large enough, a vaginal speculum or
retractor is introduced to facilitate the vaginal disinfection. When the opening
is too small for the speculum, a finger may be introduced alongside the gauze-
carrying forceps to spread out the vaginal folds.
When the antiseptic preparation is completed, the pad and towels are
removed, the hips are brought down well, the flat electrode is placed if there is
to be conization, and the feet are elevated in preparation for draping. In
placing the patient in position for the vaginal operation, the feet in the
stirrups should be raised high, as shown in, and then swung slightly outward
by a small twist of each support. When this is carried out correctly, the
patient's feet are slung high out of the way, giving plenty of room for the
assistants to stand immediately by the operative field where they can see what
is being done and assist to the best advantage. At the same time the feet and
legs are supported without troublesome pressure back of the knees. Of course,
for stout patients with very wide hips the usual towel padding is required
between the lower part of the leg supports and the hips. A point of importance
in arranging patients in position for operation is to watch for any stiffness of a

420
joint. Such an ankylose or painful joint is usually mentioned by the patient in
giving the history. In some cases, however, the patient does not mention this
incidental condition: hence in arranging the patient it is important to proceed
gently so that if there should be any unmentioned stiff joint, it will be noticed
and due allowance made to avoid strain.
After the patient is arranged in position, the sterile combination sheet is
applied with the steps. A waste basin is placed on the floor where it will catch
blood and soiled sponges, the operator's stool is pushed into position, the
assistants step into place, and the instrument table is pushed close to the right
side of the seated operator so that he can conveniently pick up and lay down
the few instruments ordinarily used.
Catheterization in the operating room immediately preceding operation
is advisable as part of the routine preparation. It gives an entirely empty
bladder, which tends to prevent injury in extensive pelvic operative work and
also facilitates accurate examination in those cases requiring deep palpation
under the anesthesia. Catheterization in the operating room has the
advantages that it is carried out under better antiseptic precautions and with
less trouble and loss of time than in the patient's room, and also prevents
troublesome accumulation of urine between catheterization and operation. In
the exceptional cases where catheterization is not advisable, a word in time to
the preparation-assistant will eliminate it.
Another point of importance in vaginal work is to arrange the sterile
coverings about the vaginal opening in such a way that the rectum will be kept
covered. Unless such care is exercised in the various manipulations in the
course of the operation, the rectum may become exposed sufficiently to
permit contaminating contact of sutures or instruments or the operator's
gloved fingers.

421
Operations on the cervix and vaginal walls
Cervical electroconization
Indications: cervical erosion, erosive ectropion of the cervix.
Main stages of the operation are the following:
1. Disinfection of the external genitalia and vagina with any antiseptic
solution (not alcohol);
2. Introduction of a special vaginal speculum (without electroconductive
material);
3. Fixation of the cervix with tenaculum forcepts;
4. Excision of the abnormal site with the electroconizer;
5. Treatment of the wound with 5% solution of potassium permanganate;
6. Removal of the instruments.
Conical excision of the cervix (after Sturmdorf)
Indications: glandulomuscularis hyperplasia of the cervix due to chronic
cervicitis without any effect of concervative treatment.
Main stages of the operation are the following:
1. Disinfection of the external genitalia and vagina.
2. Exposure of the cervix with the aid of a speculum.
3. Fixation of the anterior and posterior labia of the cervix with a tenaculum
forcepts ;
4. Dilatation of the cervix with Hegar's dilators (up to No. 8);
5. Circular incision of the cervical mucosa (with a scalpel);
6. Placement on the cervix of two catgut guy sutures;
7. Excision of a cone from the cervix;
8. Hemostasis;
9. Placement of two main sutures from catgut No. 6 (the nurse should give the
surgeon threads 25-30 cm long);
10. Placement of additional sutures on the cervix (catgut No. 4);

422
11. Treatment of the cervix with iodine tincture and removal of the speculum;
12. Tamponade of the vagina (liquid petrolatum, synthomycin liniment). (Fig.
200).
High amputation of the uterine cervix
Indications: elongation of the cervix, pronounced deformation of the
vaginal part of the cervix due to previous ruptures, scars, glandulomuscularis
hyperplasia of the cervix.
Main stages of the operation are the following:
1. Disinfection of the external genitalia and vagina;
2. Exposure of the cervix with the aid of a speculum;
3. Fixation of the anterior and posterior labia of the cervix with a tenaculum
forcepts;
4. Dilatation of the cervix with Hegar's dilators (up to No. 8);
5. Circular incision of the cervical mucosa (with a scalpel), reaching
submucous layer;
6. Bringing down of the cervix downwards (by tightening with forceps);

423
7. Dissection of the cervix for two parts (anterior and posterior);
8. Amputation of the anterior part of the cervix;
9. Ligation of separated cervical mucosa of anterior part with the endocervix;
10. Amputation of posterior part of the cervix;
11. Ligation of separated cervical mucosa of posterior part with the
endocervix;
12. Treatment of cervical stump with iodine tincture and removal of the
speculum;
13. Tamponade of the vagina (liquid petrolatum, synthomycin liniment).
Cervical biopsy
Indications: histological study of the cervical tissue in case of malignant
and pre-malignant diseases of the cervix.
Main stages of the operation are the following (Fig. 201):
1. Disinfection of the external genitalia and vagina;
2. Exposure of the cervix with the aid of a speculum;
3. Fixation of the cervix with a tenaculum forcepts;
4. Excision of the abnormal site of the cervix;
5. Placement of interrupted catgut sutures (catgut No. 3);
6. Treatment of the cervix with iodine tincture;
7. Marking of the material and sending it to a laboratory.

424
Plastic surgery on the anterior vaginal wall (anterior colporrhaphy)
Indications: prolapse of anterior vaginal wall.
Main stages of the operation are the following:
1. Disinfection of the external genitalia and vagina;
2. Exposure of the cervix with the aid of a speculum and its fixation with a
tenaculum forcepts (two pairs);
3. Infiltration of tissues with 0. 25 per cent solution of novocaine;
4. Dissection of the anterior vaginal wall and separation of the edges of the
vaginal flap (with a scalpel);
5. Separation of the bladder from the cervix (with scissors and a gauze swab);
6. Placement of purse-string catgut sutures (catgut No. 3-4) on the bladder
fascia;
7 Settling of the bladder into the purse-string suture with a finger ;
8. Placement of a continuous catgut suture on the vaginal wall ;
8. Excision of the excessive portion of the vaginal wall flap;
9. Catheterization of the bladder;

425
10. Treatment of the suture with iodine tincture and removal of the
instruments.
Plastic surgery on the posterior vaginal wall and the muscles of
the pelvic floor (colpoperineorrhaphy)
Indications: long-standing rupture of the perineum, prolapse of
posterior vaginal wall, prolapse of rectum.
Main stages of the operation are the following:
1. Disinfection of the external genitalia and vagina;
2. Placement of Kocher's forceps on the edges of the would-be flap;
3. Infiltration of tissues with 0. 25 per cent solution of novocaine;
4. Dissection of the vaginal wall and perineal skin;
5. Separation of a flap
6. Dissection of scars with a scissors and the fascia in the lateral corners of the
wound and exposure of the levators;
7. Placement of 2-3 interrupted sutures (catgut No. 6);
8. Placement of a continuous catgut suture on the vaginal wall;
9. Ligation of sutures on the levators;
10. Placement of buried sutures (catgut No. 3) on the superficial muscles;
11. Placement of silk sutures on the perineal skin;
12. Treatment of sutures with iodine tincture.
Manchester operation
Indications: prolapse of the uterus and vagina.
Main stages of the operation are the following:
1. Disinfection of the external genitalia and vagina;
2. Fixation of the cervix with a tenaculum forcepts;
3. Probing of the uterine cavity;
4. Infiltration of tissues with 0. 25 per cent solution of novocaine;

426
5. Incision of the anterior vaginal wall and a circular incision of the mucosa
around the vaginal portion of the cervix (with a scalpel);
6. Separation of the vaginal flap;
7. Separation of the bladder and rectum (with a scissors and a gauze swab);
8. Placement of two Kocher's forceps on the cardinal ligaments, dissection of
the ligaments and their suturing with catgut No. 4;
9. Dilatation of the cervix with Hegar's dilators (up to No. 8) and amputation
of the cervix (with a scalpel);
10. Placement of semi-purse-string sutures on the bladder fascia (catgut No.
3-4);
11. Excision of the excessive portion of the vaginal flap;
12. Fixation of the cardinal ligaments to the stump of the cervix with two
catgut sutures;
13. Placement of a continuous catgut suture on the vaginal wall;
14. Placement of sutures to form the anterior and posterior labia of the cervix
(catgut threads 25-30 cm long);
15. Catheterization of the bladder;
16. Treatment of sutures with iodine tincture (followed by
colpoperineorrhaphy as described above);
17. Placement of intravaginal tampon with petrolatum liquid or synthomycin
liniment.
Minor gynecological operations
Artificial (induced, justifiable, therapeutic) abortion
Indications: grave extragenital diseases, bad living conditions, suspicion
to congenital malformations of the fetus, hereditary diseases, etc.
Artificial abortion may be performed in term of gestation 6-12 weeks
depending on medical or social indications.
Main stages of the operation are the following:

427
1. Disinfection of the external genitalia and vagina;
2. Exposure of the cervix with the aid of a speculum;
3. Fixation of the cervix with a tenaculum forcepts;
4. Paracervical anaesthesia;
5. Probing of the uterine cavity;
6. Dilatation of the cervix with Hegar's dilators (up to No. 10-12, sometimes
to13-
14) (Fig. 202).
7. Destruction of conceptus with small curette or fenestrated forceps (Fig.
203);
8. Curettage of the mucosa of the uterine cavity;
9. Removal of the instruments and treatment of the cervix with iodine
tincture;
10. Marking of scrapings and sending the material to a laboratory.

428
Separate Curettage of the Uterine Cavity
Indications: histological study of the endometrium in case of malignant
and pre-malignant diseases of the uterus, disturbances of menstrual cycle,
etc.
Main stages of the operation are the following:
1. Disinfection of the external genitalia and vagina;
2. Exposure of the cervix with the help of a speculum and fixation of the
cervix with a tenaculum forcepts;
3. Para-cervical anesthesia;
4. Probing of the uterine cavity;
5. Dilatation of the cervical canal with Hegar's dilators;
6. Curettage of the uterine mucosa;
7. Removal of the instruments and treatment of the cervix with iodine
tincture;
8. Marking of scrapings and sending the material to a laboratory.
Puncture of the abdominal cavity through the posterior vaginal
fornix
Indications: suspicion to interrupted ectopic pregnancy, perforation of
the uterus, pelvioperitonitis or general peritonitis, to determine the character
of the exudation of tumor-like formations of appendages, etc.
Main stages of the operation are the following (Fig. 204)
1. Disinfection of the external genitalia and vagina;
2. Exposure of the cervix with the aid of a speculum;
3. Fixation of the cervix with a tenaculum forcepts ;
4. Puncture of the abdominal cavity;
5. Treatment of the cervix and the site of puncture with iodine tincture.

429
A course of the postoperative period and care for patients
When the operation is over and the patient has recovered from narcosis,
she is transferred to an intensive care unit since such patients require a
particularly thorough observation, care, and not uncommonly intensive
therapy.
The equipment of the postoperative room should meet the following
requirements: the beds should allow for the possibility to create the necessary
position (horizontal, with the elevated head or foot end), and there should be
apparatuses for observing the patient's status (tonometer, electrocardiograph,
etc.), as well as items necessary for caring for the patient and drugs.
The medical personnel working in the postoperative room should have
at their disposal a mouth opener, tongue holder, glasses or mugs, bedpans,
hot bags, ice bags, jars, colonic tubes, gastric probe, Esmarch's irrigator, and
clean bed linen. The room is equipped with a centralized supply of oxygen for
oxygen therapy.

430
A special cabinet should contain sterile systems for fluid and blood
transfusion, syringes, needles, sterile material, and sets of drugs including
cardiac means (camphor, caffeine, corglycon, strophanthin), different groups
of NSAIDS (meloxicam, acetaminophen), opioid analgesics (morphine,
promedol), haemostatic means, and drugs exerting a contractile action on the
uterus (calcium chloride, methylergometrine, syntocinon, oxytocin,
mammophysin, etc.), as well as fluids for intravenous infusion (5 per cent
glucose solution, isotonic saline) and means for providing urgent care
(adrenaline, insulin, hydrocortisone, etc.).
A nurse responsible for providing care to patients should always be
present in the room. Before the patient is brought in from the surgical theatre
it is desirable that the bed be warmed up by means of hot bags (it is
particularly important for elderly patients and persons with a heavy blood
loss). Having put the patient into the bed, place hot bags at her feet. To
prevent burns, these bags should be warm rather than very hot; they are
wrapped into a towel or placed onto the blanket. Put an oil-cloth bag with
sand on the abdomen (on the area of sutures), and then 2-3 hours later
replace it with an ice bag. An ice bag is wrapped into a cloth. It is removed for
15-20 min after 1-2 hours. An ice bag should preferably be applied for a
period of 24 hours after which it is employed only when special indications
warrant it (inflammatory process, obese abdomen, tendency to bleed). The
patient is placed on her back, without a pillow, with her head turned laterally.
These measures may prevent tongue prolapse and aspiration of the vomit.
In the postoperative period the patient needs a particularly thorough
observation, especially in the first postoperative hours when she is still
heavily sedated.
The nurse should check regularly the patient's respiration, pulse, the
state of the bandage, and vaginal discharge (following vaginal operations and
uterine extirpation). Paleness, tachycardia, weak pulse, and a drop in arterial
pressure may suggest internal bleeding and shock.

431
Tongue prolapse and aspiration are witnessed with difficult breathing
and cyanosis. If this is the case, turn the patient's head aside, support the
lower jaw, and give her oxygen.
If the patient has stopped breathing, repeated intubation is indicated to
perform artificial ventilation of the lungs. If the nurse notices any changes in
the patient's state, she should immediately report her observations to the
doctor.
A sedated patient (her consciousness not fully recovered after narcosis)
may fall off the bed, so it is advisable that she is tied to the bed with the help
of a wide cloth bandage, which is fixed above the blanket (at the level of the
hips) during the first postoperative hours.
It is important to remember about the necessity to control postoperative
pain since it interferes with deep breathing, which aggravates lung ventilation
and cardiac activity. Analgesics(particularly narcotics) should be
administered by the doctor. The method of choice is promedol administered
in combination with analgin and diphenhydramine hydrochloride (narcotics
may cause side-effects, for example, vomiting).
Vomiting during the first 1-2 postoperative days may be related to post-
narcosis intoxication. Vomiting debilitates and depresses the patient, leads to
dehydration, and may be associated with aspiration of the vomit. Therefore,
the doctor should institute disintoxication (infusion) therapy and
administration of anti-emetic means (metoclopramide, promethazine). If
vomiting persists after this period, it may indicate serious complications
(peritonitis, intestinal obstruction), which call for special intervention.
Nausea observed after the operation may be due to fasting (the patient may be
given some broth on the third day) or reaction to the administered drugs
(antibiotics, narcotics, etc.). Sometimes, the patient complains about
intensification of nausea after an injection of a definite drug (the doctor
should be informed about this).

432
The postoperative period is not uncommonly associated with metabolic
disorders (water, electrolyte, protein, carbohydrate), which may be linked
with fasting, operative trauma, and blood loss and is expressed in decreased
diuresis, nausea, vomiting, fever, weakness, bloated abdomen (intestinal
paresis), and other symptoms. These alterations are the greater, the more
extensive was the operation and the heavier was the blood loss. For 2-3 days
such patients should be given infusion therapy (blood transfusion, protein
preparations, blood substitutes, vitamins). If there are no contraindications
and vomiting, the patient should be fed, which will help to normalize
metabolism.
Nutrition and water regimen. If the patient is fully conscious and does
not suffer from vomiting, she can be given water 3-4 hours after surgery and
tea with lemon and mineral water by the end of the first day. Taking meals
fairly soon after the operation activates the function of the alimentary organs.
Following laparotomy (with the exclusion of operations on the intestine), the
patient is given sweet tea and cranberry water on the first day; raw egg, broth,
and yoghurt on the second day; liquid porridge, broth, omelette on the third
day. Beginning from the fourth day, the diet is gradually expanded.
After vaginal plastic operation the patient receives only liquid food
(broth, tea, yoghurt, fruit drink) within the first four postoperative days. On
the fifth day the patient is given a raw egg, porridge, and strained soup. The
diet is gradually expanded beginning from the 6th-7th postoperative day.
Oral hygiene. It is very important from the standpoint of stomatitis and
parotitis prevention. If the patient is unable to get up, she should be provided
with an opportunity to brush her teeth over a hand basin. In severely ill
patients the oral cavity should be treated with solution of hydrogen peroxide
or sodium tetraborate on glycerol. This is particularly important in patients
receiving antibiotics as it helps to prevent Candida-caused stomatitis.
Monitoring of intestinal function. Following planned operations
preceded by preparation, patients rarely have unassisted bowel movements.

433
So, on the 3rd day after laparotomy an enema with hypertonic (5%) solution
of sodium chloride (150-200 ml) is made.
In colitis and haemorrhoids a simple cleansing enema is recommended.
Later on, bowel movements are regulated by diet (yoghurt, prunes, dried
apricots, beets) or by prescribing plant laxative and glycerol suppositories.
Following vaginal plastic operations the intestine is emptied using of
magnesium sulphate (15 g) on the 5th-6th postoperative day, after which
bowel movements are also regulated by diet.
If the operation had to be performed urgently, without intestinal
preparation, intestinal paresis and gastric bloating may develop rather early
(by the end of the first or during the second postoperative day). Stimulation of
intestinal peristalsis is used in such cases (proserine subcutaneously, 10 per
cent solution of sodium chloride intravenously, hypertonic enema, colonic
tube).
Regulation of urinary function. Within the first 24 postoperative hours
patients are rarely capable of voluntary micturition, so, the nurse should pass
the patient's urine with a catheter at least twice daily. Occasionally, the
patient cannot urinate because she is afraid to tense her abdominal muscles
or cannot bring herself to urinate in the supine position. In such cases it is
necessary to explain to her that there is nothing to be afraid of and allow her
to sit up (if there are no contraindications). When serving a bedpan, one
should first warm it up. Sometimes, a good effect can be achieved by pouring
warm water onto the external genitalia. Patients waiting for vaginal plastic
operation should be taught how to urinate in the supine position even prior to
surgery since the normal urinary excretion may take a long time to recover
after such operations.
When urine retention is present, drug treatment may also be employed:
5-10 ml of 10-20 per cent solution of intramuscular magnesium sulphate, 1 ml
of subcutaneous pituitrin, and irrigation of the bladder with warm solution of
nitrofurazone (1:5000).

434
When multiple catheterization is necessary, it is advisable to administer
furadonin and 5-NOK. After extensive extirpation of the uterus it is expedient
to introduce a permanent catheter into the bladder for 3-4 days. Following
removal of the catheter and restoration of voluntary urination, the bladder
evacuation may not be complete in these patients since the bladder tonus may
take some time to fully recover. The degree of bladder evacuation may be
determined with palpation, percussion, or catheterization (following
micturition).
After some operations one should pay particular attention to the
amount of the excreted urine. Decreased diuresis may be associated with
shock, blood loss, traumatic surgery, and sometimes with ligation of ureters.
Postoperative anuria may be a very dangerous symptom. Having noticed a
diminution in diuresis, the nurse should immediately report to the doctor
about this development.
Postoperative regimen. It depends on the patient's age, the nature of the
underlying disease, and the scope of interference, as well as on attendant
diseases.
In recent years an active mode of the postoperative management has
been increasingly introduced into the gynaecological practice. The patient is
allowed to turn from side to side by the end of the day she was operated on,
whereas some 24 hours after the operation she may vigorously move her arms
and legs and sit up in the bed. At the same time she is recommended to do
breathing exercises to improve her respiration. Patients, on whom minor
surgery was performed, especially with a transverse incision of the abdominal
wall, may get up 24 hours after the operation. Early getting of the patient on
her feet reduces the danger of pulmonary and thrombotic complications.
Patients on an active regimen show a faster restoration of normal micturition
and improvement of intestinal peristalsis. An active mode of the
postoperative management is contraindicated in patients with pneumonia,
myocardial infarction, and heart failure. If such a mode is recommended to
435
patients suffering from obesity and anaemia and those with repeated
laparotomy, their abdomen should be tightly bandaged. An improvised
bandage from a clean towel may be used for this purpose. The patient herself
may sew such a bandage before the operation.
Following plastic surgery on the perineum, patients are permitted to get
up on the 8th day. In elderly patients the period of confinement to bed is
somewhat longer. Sitting is allowed after three weeks.
Management of sutures. Following laparotomy, the responsible
personnel should regularly check the bandage. If the dressing is not soaked
through or detached, it is replaced on the 3rd postoperative day. Then,
inspect the area of sutures for possible hyperemia or infiltrates, treat them
with iodine tincture, and place a dry bandage. Sutures are usually removed on
the 8th day, yet, in obese patients and following repeated laparotomies they
are removed on the 9th-10th day. Treat the perineal sutures daily with 5 per
cent solution of potassium permanganate and try to avoid wetting the area of
sutures when washing the patient's genitalia. Remove the sutures on the 5th-
6th day and continue to treat the scar with potassium permanganate solution
every day until it is completely healed.
Particularly important in the postoperative period is monitoring the
status of the cardiovascular system. Surgery, narcosis, and loss of blood and
fluid may lead to heart failure, especially within the first postoperative hours.
It is necessary, therefore, to carefully monitor the pulse (frequency, rhythm,
filling) and arterial pressure (electrocardiography when indicated). A fall in
blood pressure may be due to insufficient replacement of blood loss, pain-
associated shock, heart failure, and internal hemorrhage.
Respiratory alterations may be related to intubation, toxic action of
narcotics, and pneumonia. Following intubation, patient’s present hoarseness
and pain in the throat, which disappear spontaneously within 24 hours.
Usually the patient is brought from the surgical theatre only after normal
respiration has become established. Yet, respiration may fail again as an

436
after-effect of narcotics, due to aspiration, etc. It is necessary therefore to
watch the colour of the lips and nails. The development of cyanosis witnesses
oxygen deficiency. In such cases it is necessary to give oxygen urgently to the
patient and inform the responsible physician about these symptoms.
By the end of the first day following inhalation narcosis cups are put on
the patient's chest to improve her respiration and blood circulation, on the
second day circular mustard plasters are put. Prescription of breathing
exercise and expectorants as well as alleviation of postoperative pain, improve
gas exchange and blood circulation.
After minor gynecological operations (artificial abortion, diagnostic
dilatation and curettage, cervical biopsy, and puncture of the abdominal
cavity through the posterior fornix) the patient is wheeled to the ward. Proper
care involves observation of the patient's general status (pulse, arterial
pressure, color of the skin and visible mucosa) and vaginal discharge. An ice
bag is placed on the patient's low abdomen for a period of 1-2 hours. The
nurse should immediately inform the responsible physician about the
development of bleeding or any changes in the patient's status.
Complications in the postoperative period
Early detection of postoperative complications is possible only if the
patient is very closely observed. Having noticed any deviations in the patient's
status, the nurse on duty should immediately report them to the physician so
that the appropriate treatment could be instituted without delay.
Complications on the part of the operative wound include bleeding and
hematomas, infiltrates, purulent foci, and suture failure. Bleeding and
hematomas develop during the first hours after intervention and are
manifested in soaking of the dressing and change in the patient's condition
(paleness of the skin and visible mucosa, dyspnea, syncopal status,
tachycardia, and a drop in the arterial pressure). In internal hemorrhage

437
repeated laparotomy should be performed to ligate the bleeding vessels.
When the site of bleeding is in the area of sutures on the anterior abdominal
wall, it is occasionally enough to apply cold (an ice bag) or some weight (a
sand bag) onto the area of sutures in combination with hemostatic agents. If
bleeding is from the vaginal stump left after uterine extirpation, tight
tamponade of the vagina is employed. In plastic operations on the cervix it
may sometimes be necessary to place sutures on the bleeding vessels. After
bleeding has been arrested, it is necessary to replace the blood loss
(transfusion of blood and blood substitutes).
First aid in postoperative bleeding consists in application of an ice bag
on the area of sutures and abdomen and a sand bag on the area of sutures. A
nurse may also give the patient oxygen to breathe, hemostatic means and
should promptly call the physician.
Infiltrates, suppuration, and suture failure are most often related to
infection of tissues following surgery for purulent inflammatory diseases or
traumatic operations in weak and anemic patients. Patients usually present
pain, fever. The area of sutures is hyperemic and edematous. Painful
indurations are palpated, and pus may seep through the sutures. If the latter
is the case, the sutures at the area of the most severe inflammation should be
removed to ensure a better outflow of pus. Following purification of the
wound, it heals by the second intention. Simultaneously, antibacterial therapy
is conducted. Suture failure can vary in its degree from failure of sutures
placed through the skin edges to eventration. This complication is observed in
weak, emaciated or obese, and elderly patients. Signs of incipient eventration
are nausea, vomiting, and sudden profuse suffusion of the dressing with
serous fluid. Removal of the dressing reveals complete suture failure in all
layers of the abdominal wall. If the skin sutures are still intact, they hold the
intestinal loops that are readily palpated directly under the skin. Eventration
is eliminated by repeated placement of silk sutures onto the wound through

438
all layers and by antibacterial and invigorating treatment. Such sutures are
removed in 2-3 weeks.
Inflammatory complications may develop not only in the abdominal
wall but also in the pelvic organs. Their usual manifestations are pain, the
presence of dense painful infiltrates, high pyrexia, and algor.
First aid in suppurative processes consists in application of an ice bag
onto the area of sutures. When eventration is suspected, the patient is not
allowed to stand or sit up. A nurse should immediately inform the physician
about her suspicions.
Appropriate preventive measures include observation of aseptic rules,
careful treatment of tissues, good hemostasis during surgery, and
prophylactic antibacterial therapy after the operation.
Cardiovascular complications may manifest themselves in the form of
shock and collapse.
Shock and collapse develop after prolonged traumatic operations
associated with heavy blood loss and are expressed in mental inhibition,
apathy (with the consciousness preserved), small rapid pulse, paleness, cold
perspiration, fall in arterial pressure, oliguria, and shortness of breath.
Having noticed such symptoms, a nurse should immediately call the
physician.
First aid consists in immediate intravenous infusion of blood
substitutes, administration of cardiac means (20 per cent camphor oil,
caffeine), and oxygen inhalation. A key method of controlling shock is blood
transfusion, as well as administration of noradrenaline, hydrocortisone,
prednisolone, and analgesics (prescribed by the physician).
Thrombophlebitis of both superficial and deep veins of the lower
extremities is not an infrequent complication of gynecological operations. In
such cases the patient complains of pain in the limb, which becomes
edematous and larger in size. Signs of hyperemia and induration appear along

439
the course of the superficial veins (phlebitis may develop on the hand
following a vein-puncture made during the operation).
To manage this condition, the patient is confined to bed, her leg is
elevated, ice bags are applied to painful sites, and anticoagulants are
administered. Thrombophlebitis may cause pulmonary thromboembolism.
When small branches of the pulmonary artery are occluded, the patient
develops dyspnea, retrosternal pain, cyanosis, and tachycardia. Massive
embolism and embolism of the main trunk of the pulmonary artery may cause
instant death. Prophylaxis of this dire complication consists in thorough
preparation of the patient for the operation, tight bandage of the lower
extremities, an active management of the postoperative period, and
administration of anticoagulants (heparin, phenylin, acetylsalicylic acid, etc.).
Pneumonia is the most frequent respiratory complication. Elderly and
obese patients are at a particular risk of developing pneumonia. Congestive
manifestations linked to hypodynamia and poor lung ventilation serves as a
contributing factor. Measures intended to prevent pneumonia include
analgesics, active regimen (getting up in the early postoperative period and
breathing exercise), application of circular cups and mustard plasters, and
cardiac means. Pneumonia is treated with antibacterial drugs.
Gastro-intestinal complications are expressed in gastro-intestinal atony.
It may be attended by acute dilatation of the stomach, intestinal paresis, and
ileus.
In acute dilatation of the stomach, it is markedly distended with gastric
contents accumulating in it. The patient presents uncontrollable vomiting and
foul belching, which is accompanied by tachycardia and dehydration (dry
tongue). In such cases it is indicated that the stomach be irrigated with the aid
of a thin probe which is introduced through the nose (the probe is profusely
treated with petrolatum). Using Janet's syringe, introduce alkaline solution
into the stomach and actively aspirate its contents. Continue irrigation until
pure water is aspirated and leave the probe in the stomach for 10-12 hours.

440
Allow the patient to drink and periodically irrigate the stomach with small
amounts of fluid.
Intestinal paresis is manifested by abdominal flatulence, diffuse pain
throughout the abdomen, tachycardia, the absence of peristalsis, nausea and
vomiting, and stool and gas retention. If the above symptoms are very severe,
it is justified to speak about dynamic intestinal obstruction (ileus). Ileus may
also be due to a mechanical obstruction (adhesions, flexions, invagination).
This is associated with sharp paroxysmal pain attended by nausea and
vomiting. The abdomen becomes asymmetrical secondary to flatulence of
intestinal loops above the place of obstruction.
The diagnosis of ileus may be specified by X-Ray examination. It shows
intestinal loops distended with gas and horizontal levels of fluid.
Furthermore, you may give the patient half a glass of barium suspension and
examine its passage in 10-12 hours.
Paresis and dynamic ileus may be eliminated conservatively via
intestinal stimulation (injections of atropine and proserine, intravenous
administration of hypertonic saline, hypertonic enema, siphon enema,
paranephric novocaine blockade, and diadynamic currents on the area of the
solar plexus).
Mechanical obstruction not uncommonly requires surgical intervention.
Prolonged paresis and ileus may lead to the development of peritonitis.
Postoperative parotitis is a consequence of inadequate oral hygiene. The
patient presents pain at an angle of the lower jaw that irradiates to the ear,
swelling in this area, and fever. The treatment includes antibiotics, warming
compresses, and analgesics.
Anaesthesia-associated paralyses develop as a result of malposition of
the arms during the operation (putting them behind the head, compression
with the end of the operating table), which may injure peripheral nerves.

441
Self test
1. What is better for the patient before the operation?
A. - an enema the night before, and again the next morning
B. - the prolonged dieting and purging formerly employed
C. - absence of special diet and regimen before the operation
2. The afternoon before operation the abdomen
A. - is lathered and shaved without washing
B. - is lathered and shaved, then washed with soap and sterile water
C. - should be treated with iodine solution and alcohol
D. - should be treated with dimexid solution
3. Choose correct scheme of premedication before the operation.
A. - promedol 1,5 mL + atropine 1 mL, + dimedrol 2 mL
B. - analgin 1 mL+ dimedrol 1 mL + atropopin 1 mL
C. - promedol 0. 5 mL + atropine 2 mL + dimedrol 5 mL
4. The twenty-day catgut is used for
A. - all the layers of the abdominal wall except the skin
B. - suturing of the abdominal skin
5. The silk is used for
A. - any emergency intestinal suturing
B. - for suturing in conservative work on the ovaries and tubes and for suture
ligation of the mesoappendix
6. The hands and forearms are scrubbed
A. - in 80 per cent alcohol with gauze
B. - in 70 per cent alcohol with gauze
C. - in 96 per cent alcohol with gauze
7. The most preferable type of abdominal incision in modern medicine is
A. - Phannestiel incision
B. - Cherny incision
C. - rectus incision

442
D. - median incision
8. The choice of abdominal incision depends on
A. - patients condition and type of the operation
B. - the request of the operator
9. Indications for salpingectomy are as follows except
A. - hydrosalpinx, pyosalpinx
B. - severe chronic inflammation process
C. - tubal pregnancy
D. - subserous myoma of the uterus
10. What kind of operation is it in case of retention cyst of the ovary?
A. - resection of the ovary
B. - removing of the ovary with the tube
C. - extirpation of the uterus with adnexa
443
Chapter 11. ACUTE ABDOMEN IN GYNECOLOGIC
PRACTICE
Acute abdomen means such a state, which may lead to severe
complications and even death. Acute abdomen in gynecologic practice may be
due to:
internal (intraperitoneal) bleeding, caused by interrupted ectopic
pregnancy, injuries of pelvic organs, etc;
Failure of blood supply of abdominal organs (torsion of the pedicle of an
ovarian tumor or a subserous myomatous node);
acute inflammation in abdominal cavity including the peritoneum.
In all these cases rapid and correct diagnosis and therapeutic measures
save the patient’s life.
Ectopic pregnancy
Normally, the fertilized egg moves along the tube to enter the uterus
and to implant in its mucosa. But the conditions for the movement of the egg
may be disturbed and the fertilized ovum may implant elsewhere to cause
extrauterine or ectopic pregnancy.
Ectopic pregnancy includes those implanting in the uterine cervix
(cervical pregnancy), tubes (tubal pregnancy), the ovary (ovarian pregnancy),
or the abdomen (abdominal pregnancy). Abdominal pregnancy may be
primary (fertilized ovum is implanted in the abdomen from the very
beginning), and secondary (at the beginning the ovum was fertilized in the
tube, and after tubal abortion it begins to be fertilized in the abdomen). (Fig.
102)
Definition. Ectopic pregnancy is an implantation of the fertilized ovum
outside the uterus. The trophoblast can successfully be implanted in any

444
tissue with an adequate blood supply. But the most common site for an
ectopic pregnancy is the fallopian tube (98 %), but other sites are the ovary,
cervix and abdominal cavity.
Incidence. The frequency of ectopic pregnancy is about 1 in 200
pregnancies.
Classification. Ectopic pregnancy is classified according to: the location
(tubal, ovarian, abdominal, pregnancy in the cervix and others); the clinical
stage (ongoing or non-interrupted, and interrupted); the type of termination
(tubal abortion, rupture of the tube).
Etiology of ectopic pregnancy
Risk factors for ectopic pregnancy include:
Fallopian tube damage
o Previous tubal surgery (including female sterilisation) and pelvic
surgery including Caesarean section and ovarian cystectomy

445
o Previous abdominal surgery including appendicectomy and bowel
surgery
o Confirmed genital infection and pelvic inflammatory disease, commonly
caused by chlamydial infection
Infertility
o Documented tubal disease
o Assisted reproductive technology
o Endometriosis
o Unexplained infertility
Contraceptive failure
o Progestogen-only contraception
o Intrauterine contraceptive device
Cigarette smoking – including past exposure.
Age >35 years
Previous ectopic pregnancy
Previous spontaneous abortion or induced abortion
Ectopic pregnancy is more common in women attending infertility
clinics even in the absence of tubal disease. In addition, the use of ART
increases the rate of ectopic pregnancies. In vitro fertilisation (IVF) is
associated with an ectopic pregnancy risk of 2–5% and it may be higher than
this where there is tubal disease. Indeed the first IVF pregnancy, before the
first IVF live birth, was a tubal ectopic pregnancy.
Tubal Pregnancy
Clinical presentation of tubal pregnancy depends on clinical form:
interrupted or non-interrupted (ongoing).
Non-interrupted (ongoing) tubal pregnancy can terminate by the type
of tubal abortion and by the type of rupture of the uterine tube. Patient with
ongoing tubal gestation have all the changes of early physiological gestation.

446
The ovum implants in the endosalpinx and begins to grow into the muscular
wall. The growing ovum distends the attenuated and loosened walls of the
tube, which become a spindle-like. The patient displays presumption and
probably signs of gestation (change of appetite, nausea, excessive salivation,
menstrual delay, breast engorgement).
The diagnosis is difficult, diagnostic tests for ectopic pregnancy include:
o a urine pregnancy test;
o ultrasonography;
o beta-hCG measurement;
o occasionally, diagnostic curettage
While collecting the history, one can identify factors of risk for the
development of ectopic pregnancy. Physical examination reveals breast
engorgement. Gynecological examination can find cyanosis of the vaginal
walls and cervix, softening of the cervical isthmus, uterine engorgement and
disparity between the size of the uterine body and gestational age. Tumor-like
ovoid formation may be laterally and behind the uterus. The fornices are free,
cervical displacements are not painful. In patients with complicated
gynecological anamnesis, presence of risk factors, transvaginal ultrasound is
useful to assess whether a pregnancy is in the uterine cavity. The presence or
absence of an intrauterine sac is the key diagnostic marker for ectopic
pregnancy. US should be done in accordance with β-hCG level in blood
serum. In 1985, the concept of a "discriminating level of β-hCG" was
introduced to isolate the concentration of β-hCG in serum when pregnancy
should be visible in ultrasound scanning.
For TVUS, the discriminatory level of β-hCG (also known as the
discrimination zone) is 1500 IU / L. The yolk sac, if present in the uterine
cavity, should be identified in TVUS if the hCG level is 1500IU / L or more.
The absence of the yolk sac in the uterine cavity, despite the fact that a
discriminatory level of 1500 IU / L or more in TVUS basically means an
ectopic pregnancy.

447
For TAUS, the discrimination zone of hCG is 6500IU / L and more.
Thus, in the transabdominal ultrasound study, the absence of an intrauterine
gestational sac at a β-hCG concentration of more than 6500 IU / L confirms
an ectopic pregnancy. β-hCG levels may assist in interpreting ultrasound
findings. In a uterine ongoing pregnancy, the minimal rate of increase in β-
hCG is 66% in 2 days, peaking at a level greater than 100,000 mIU per mL
(100,000 IU per L). In ongoing ectopic pregnancy the level of β-hCG will also
increase, but without doubling every two days. A rapid decline in β-hCG
concentrations over 2 days, commonly by 21–35% or more, is indicative of a
spontaneous abortion or a resolving ectopic pregnancy. In cases where an
ectopic pregnancy is suspected and ultrasound is inconclusive, a diagnostic
laparoscopy may be required.
An alternative to diagnostic laparoscopy may involve a repeat
ultrasound examination, particularly when β-hCG concentrations are close to
1500 IU/l. Other strategies include alternative diagnostic tests, such as serum
progesterone or an endometrial biopsy, or empirical medical treatment as the
patient may well have an ectopic pregnancy. If β-hCG concentrations are
falling but an ectopic has not been excluded, consideration should be given to
performing serial β-hCG measurements until levels become undetectable, as
rupture can still occur. In selected cases of Pregnancy of Unknown location,
an endometrial biopsy may be taken and analyzed for the presence or absence
of chorionic villi. Their absence in the presence of a static β-hCG is suggestive
of an ectopic pregnancy.
Management of ongoing (non-interrupted) tubal pregnancy
Ectopic pregnancy may be managed surgically, medically or expectantly.
Around 70% of ectopic pregnancies with β-hCG level , 1000 mIU\mL resolve
spontaneously. It is important to remember the risks of ruptured ectopic
pregnancy. The best indicator of spontaneous resolution is β-hCG levels that
are falling by 15-25% every 48hours. If spontaneous resolution is suspected,

448
the patient will be monitored with 48hourly bloods looking for a continuous
decline in β-hCG of at least 15% each two days. If this rate stops declining or
β-hCG levels start to rise then medical or surgical treatment should be
considered.
Medical management of ectopic pregnancy. Medical treatment is
useful for patients with an unruptured tubal ectopic pregnancy who are
haemodynamically stable and have minimal symptoms. Methotrexate is a
folic acid antagonist that targets rapidly dividing cells and arrests mitosis. In
ectopic pregnancy, the drug prevents the proliferation of cytotrophoblast
cells, reducing cell viability and β-hCG secretion and thus progesterone
support for the pregnancy. This facilitates the resolution of the ectopic
pregnancy and tissue remodelling. Methotrexate is most successfully used
when the patient is asymptomatic and the beta HCG levels are lower than
3000 IU/L. The woman should be counselled that there is a failure rate
associated with medical therapy and tubal rupture may still occur in 7% of
cases.
Single dose treatment of IM methotrexate using 50mg/m 2 (most
patients require 75 – 90 mg) is effective in most cases. Β-HCG levels can be
performed on day 4 and 7 after methotrexate therapy and a minimum of 15%
drop in beta HCG would be considered acceptable between day 4 and 7.
Approximately 10% of women will require surgical intervention, although
most of these are for slowly falling β-hCG levels rather than for acute tubal
rupture. The Beta HCG levels should decrease by approximately 50% every 48
hours after the salpingotomy procedure.
Another option for the treatment of ectopic gestation is the multi-dose
protocol and direct injection of methotrexate into the ectopic pregnancy. The
multi-dose regimen consists of methotrexate treatment on Days 1, 3, 5 and 7
to a maximum of four doses and leucovorine ‘rescue-therapy’ at a dose of 0.1
mg/kg on alternate Days 2, 4, 6 and 8. This treatment may be more
appropriate for patients who present with a larger adnexal masses and greater

449
initial β-hCG levels (>5000 IU/l). Direct injection of methotrexate into the
ectopic sac, either laparoscopically or with ultrasound guidance, limits
systemic toxicity or maintains a higher therapeutic level. However, local
injection has no significant advantage in most patients and is accompanied by
a risk of provoking tubal rupture.
Contraindications to the use of methotrexate include:
o the size of embryo is .3 cm
o fetal cardiac activity, β-HCG greater than 15 000 IU/l,
o free fluid in the cul – de - sac,
o documented hypersensitivity to methotrexate,
o breastfeeding,
o immunodeficiency,
o alcoholic or other liver disease,
o anaemia, leucocytopenia, thrombocytopenia,
o active pulmonary disease,
o peptic ulcer disease,
o renal or hepatic dysfunction
Interrupted tubal pregnancy
Tubal abortion (Fig. 206): the ovum is partially or completely
separated from the wall of the fallopian tube and begins to be expelled
through its ampullar end into the abdominal cavity. It is associated with pain,
which has recurrent or continual and increased character. Pain is localized in
one of the iliac areas, irradiating into the rectum, hip, sacrum, occasionally,
into the clavicular and scapular area (lat.;phrenicus symptom). Small blood
vessels may clot, bleeding stops, and pain disappears. Expulsion of the ovum
from the uterine tube may be repeated, so termination of ectopic pregnancy
by the type of tubal abortion may be prolonged. Blood effused into the cavity
of the oviduct is gradually expelled into the abdominal cavity and then finds
its way into the rectouterine pouch, where a rectouterine hematoma may form

450
(it may also be peritubal, if blood coagulates and accumulates directly around
the fallopian tube). Between attacks the patient may experience constant
gnawing pain, heaviness in the area of the lower abdomen, and the feeling of
pressure into the rectum.
Fig. 206. Tubal abortion
Diagnosis of tubal abortion is very difficult. The most prominent
symptom is anemia of a varying degree. The patient displays presumptive and
probable signs of pregnancy. Menstrual disturbances are constant. Menstrual
delay lasts from several days to 2-3 weeks with the subsequent appearance
(soon after an attack of pain) of scanty vaginal discharge of a dark-brown
color. Sometimes sanguineous discharge appears without the preceding
menstrual delay. Examination of the abdomen may reveal its bloating and the
phenomenon of the abdominal wall lagging behind respiration-associated
movements. Percussion elicits dull sounds in sloping places. Gynecological
examination reveals cyanosis of the mucosa, scanty dark-brown discharge
from the cervical canal. Cervical displacements are painful. Uterine
engorgement does not correspond to the term of the proposed pregnancy, the
uterus is softened in the isthmus area. A sausage-like formation of the doughy
consistence is palpated in the adnexal area. This formation is tender,
moderately mobile, with a vague outline. The posterior and corresponding
451
lateral fornices may be flattened or may bulge out. The severity of the clinical
picture depends on intensity of internal bleeding.
Tubal rupture. Symptoms in patients with a ruptured uterine tube
(Fig. 207) are distinguished by severe internal bleeding, shock and acute
anemia. Rupture of a fallopian tube frequently occurs when the gestational
sac is localized in the isthmic or interstitial portion of the tube. The history is
characterized by the same factors of risk of ectopic pregnancy and delay of
menstruation. The clinical picture of tubal pregnancy, which terminates by
the type of rupture, is characterized by a sudden attack of a sharp pain in the
lower abdomen or in the iliac area with irradiation into the rectum, hip,
shoulder-blade. The patients soon become adynamic and find it difficult to
answer the questions. Any signs of internal bleeding appear, for example,
severe paleness, cyanosis of the lips, and cold sweat. The pulse is frequent,
blood pressure may be low. The abdomen is drastically bloated, the patient
spares it during breathing. Percussion and palpation of the abdomen are
tender. Percussion elicits dull sounds in sloping places. Palpation elicits
pronounced tenderness of the abdomen, the Shchotkin - Blumberg symptom
is positive. Gynecological examination reveals painful cervical displacements,
the overhanging of the posterior and lateral fornices. Palpation of the
posterior fornix is very painful ("Douglas's cry"). The uterine body is usually
enlarged, softened and tender. To one side of the adnexal area one can
palpate dough-like mass with a vague outline, occasionally pulsation may be
felt. Clinical features of this disease are so characteristic that the diagnosis is
not difficult, as a rule.

452
Fig. 207. Tubal pregnancy: rupture of the tube.
However, other clinical conditions are likely as well and should be ruled
out:
o Adnexal torsion or acute appendicitis. Although these conditions are
suggested
o by unilateral pelvis, they do not produce amenorrhea, syncope, anemia,
and early shock.
o Aborting intrauterine pregnancy. In an aborting intrauterine pregnancy,
o the external bleeding is much more severe than the pain, whereas the
reverse is true with an ectopic pregnancy.
o Corpus luteum bleeding at a normal pregnancy. Corpus luteum bleeding
usually does not produce the severity of pain or shock typical of ectopic
pregnancy. In addition, uterine bleeding is usually absent. When heavy
internal bleeding is accompanied by shock, the physician has no other
option to observe the process directly but by laparoscopy or laparotomy.
Treatment of interrupted tubal pregnancy (see also chapter 10)
Tubal pregnancy is treated surgically by removing the pregnant tube.
The patient is operated on immediately after the diagnosis has been
established, even if the condition of the patient is only satisfactory, because
the hemorrhage into the abdominal cavity may recur at any moment. If the

453
clinical picture is grave, the patient is operated on urgently, with transfusion
of blood; cardiac drugs and other means to control anemia and shock are
used.
In general the ectopic pregnancy must be removed by one of the
following techniques:
- Salpingectomy. If the tube is badly damaged, the correct treatment is
removal of the affected tube. If implantation has occurred in the interstitial
portion of the tube, then it may be necessary to resect part of the uterine horn
in addition to removing the tube.
- Salpingotomy. If the ectopic pregnancy is contained within the tube, it
may be possible to conserve the tube by removing ofthe pregnancy and
reconstitution of the tube. This is particularly important when the
contralateral tube has been lost. However, there is an increased risk of
recurrent ectopic pregnancy in the damaged tube.
- Tubal compression. Occasionally when the tubal pregnancy occurs in
the fimbrial end of the tube it may be possible to squeeze out the ovum
without opening the tube, but it is essential to be certain that adequate
hemostasis is obtained.
- Laparoscopic surgery. Salpingectomy and salpingotomy can be
performed using minimal access surgery. The Beta HCG levels should
decrease by approximately 50% every 48 hours after the salpingotomy
procedure.
Some words can be added about blood reinfusion. It may be initiated
immediately after opening the abdomen (blood reinfusion is contraindicated
when much time has passed from the moment of ectopic pregnancy
termination and in hemolysis).
Cervical Pregnancy
This is a rare variant of ectopic pregnancy, which carries a considerable
risk of severe bleeding. At the beginning of this process the clinical features
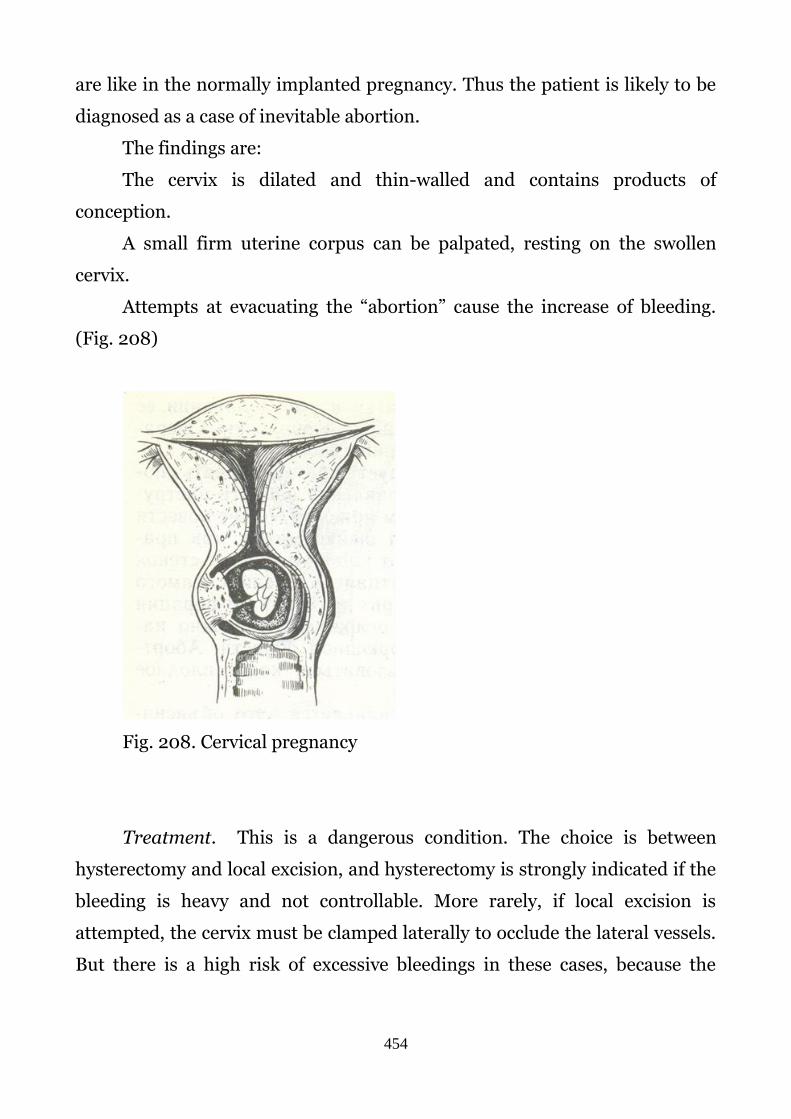
454
are like in the normally implanted pregnancy. Thus the patient is likely to be
diagnosed as a case of inevitable abortion.
The findings are:
The cervix is dilated and thin-walled and contains products of
conception.
A small firm uterine corpus can be palpated, resting on the swollen
cervix.
Attempts at evacuating the “abortion” cause the increase of bleeding.
(Fig. 208)
Fig. 208. Cervical pregnancy
Treatment. This is a dangerous condition. The choice is between
hysterectomy and local excision, and hysterectomy is strongly indicated if the
bleeding is heavy and not controllable. More rarely, if local excision is
attempted, the cervix must be clamped laterally to occlude the lateral vessels.
But there is a high risk of excessive bleedings in these cases, because the

455
altered cervical wall has no possibility of effective contractions to arrest the
bleeding.
Ovarian and abdominal pregnancies occur rarely. Implantation of the
fertilized ovum in the ovary makes up 1% of all ectopic pregnancies. The
clinical picture of the ovarian pregnancy is similar to that of the tubal
pregnancy, but the ovarian tissue is perhaps less likely to rupture than is the
muscular wall of the tube. An enlarged ovary is found at operation and if
ectopic pregnancy is suspected, the tumor should be excised. It should be
possible to preserve the ovary.
Abdominal pregnancy usually does not continue for a considerable
period of time, but still cases have been reported on full term abdominal
pregnancy. The fetus inside the membranes grows in the space between the
internal organs, the placenta being attached to the tube, the peritoneum or
the inner organs. The pregnancy is pathological and the fetus would die. The
dead fetus macerates and undergoes aseptic disintegration or mummification.
Cases have been reported in which the dead fetus was macerated and
necrotized due to the entrance of infection from the intestine.
Considerable intraabdominal bleeding may occur in connection with
separation of the placenta.
Ovarian and abdominal pregnancies are treated surgically.
Prophylaxis of extrauterine pregnancy consists in control of infantilism
(protection of children’s health), inflammatory diseases and abortions
(contraceptives, health education), which often provoke inflammatory
diseases.
The patient operated for extrauterine pregnancy requires treatment
aimed at prevention of its recurrence.
Ovarian apoplexy
Ovarian apoplexy is hemorrhage into the ovarian parenchyma due to
follicle rupture in the ovulatory period or luteal rupture attended by damage

456
to ovarian tissue and bleeding into the abdominal cavity. Most often ovarian
apoplexy occurs at the age of 16 – 30.
Etiology. The main etiological factors are inflammation of the ovary,
hormonal disturbances (increased LH secretion), injuries, overwork, etc. It
may be without any visible reason, even during the sleep.
Clinical picture. The most typical symptom is acute pain in the iliac area
spreading throughout the abdomen and irradiating to the rectum. Pain is
accompanied by dizziness, faintness, cold sweat, and nausea and vomiting.
Severity of the symptomatology is determined by the presence or
absence of intra-abdominal bleeding and its intensity (thus, two types of the
disease are distinguished: anemic and algesic). The internal bleeding is
related to skin paleness, tachycardia, and low blood pressure. The abdomen is
bloated, only weakly participating in respiration, and is painful on palpation.
Gynecological examination may elucidate overhanging of the vaginal fornices,
tenderness upon cervical displacement, the uterus of a normal size, and a
tender and enlarged ovary.
Treatment. If there are no signs of significant bleeding and the patient
feels well, conservative treatment is possible (bed rest, cold application onto
the low abdomen, hemostatic and anti-inflammatory therapy). In cases of
intra-abdominal bleeding (anemic form of apoplexy) laparotomy and ovarian
resection in the presence of hematoma or suturing of bleeding site are
performed.
The rupture of pyosalpinx, pyoovarium
An abscess of the ovary (pyo-salpinx, pyo-ovarium), or a suppurative
ovarian tumor (for example, in torsion of its pedicle), may be ruptured into
the abdominal cavity with the development of perforative peritonitis.
An abscess may rupture either spontaneously or following a physical
trauma. The main symptoms are intensification of pain, fever, increase of the
symptoms of peritoneal rebound tenderness.

457
Examination of and care for the patient in such cases should be delicate.
Rupture of the abscess with effusion of pus into abdominal cavity is
followed by acute stabbing pain throughout the abdomen, collapse (rapid
weak pulse, cold sweat, pronounced paleness and cyanosis of the lips and
nails), nausea and vomiting. The abdomen is tense and very tender when
palpated. The general state of the patient rapidly worsens, the facial features
turn sharp, and breathing becomes frequent and shallow. Other findings
include a drastically bloated abdomen due to intestinal paresis, torpid
peristalsis, and flatulence. Percussion of the abdomen elicits dull sound in
slopping places due to the formation of exudate in the abdominal cavity.
Gynecologic examination reveals overhanging of the fornices and sharp
tenderness upon displacement of the cervix. The uterus and adnexa cannot be
palpated because of marked tenderness and tension of the abdominal wall.
Diagnosis. It is based on history and clinical findings.
Treatment. The treatment is surgical. Pre-expert care consists in
ensuring that the patient is not disturbed, careful transportation to hospital,
and symptomatic therapy (cardiac and analgesic drugs), as well as
intravenous infusion of blood substitutes.
Surgery consists of laparotomy, removal of the involved organ, and irrigation
and extensive draining of the abdominal cavity.
Rupture of ovarian cyst
Rupture may be either traumatic or spontaneous. Traumatic rupture
may follow torsion of a pedicle, during bimanual examination, during labor
when the cyst is impacted in the pelvis. Spontaneous rupture is not common,
especially with malignant cysts, when the epithelial tissue outgrows the
connective tissue.
Hemorrhage may occur into these cysts, and they should not be
mistaken for endometriomata. Occasionally intra-peritoneal bleeding from a

458
ruptured cyst is sufficient to suggest an ectopic pregnancy and require
laparotomy. Thus the main clinical symptoms are the acute pain and
tenderness in lower abdomen, peritoneal symptoms, swelling in lower
abdomen due to internal bleedings.
Pseudomyxoma peritonei. This rare condition occasionally but not
inevitably follows the rupture of a mucinous cystadenoma. The epithelial cells
implant on the peritoneum and continue to secrete a gelatinous
pseudomucin; this material is not absorbed, or secretion is faster than
absorption; and the abdominal cavity is eventually filled with the jelly, while
the secreted cells spread over the parietal and visceral peritoneum. A reactive
peritonitis with adhesion is a sequel, and the patient must be operated for
removal of as much of the exudate as possible. The disease develops slowly
over several years, but will eventually cause the patient’s death from cachexia
or obstruction.
Self test
1. What percentage of women with a previous ectopic pregnancy can expect to
have another ectopic pregnancy?
A. -3%
B. -6%
C. -12%
D. -20%
E. -25%
2. What is the most accurate method of diagnosing an ectopic pregnancy?
A. -culdocentesis
B. -endometrial biopsy
C. -laparoscopy
D. -pelvic ultrasound
3. Which of the following sequele of pelvic inflammatory disease does not
enhance the possibility of ectopic pregnancy?
A. -altered cilia action
B. -distal tubal closure (hydrosalpinx)
C. -constriction of the tube

459
4. Which of the following is not a likely reason for the establishment of a tubal
pregnancy?
A. -pelvic infection
B. -peritubal adhesions
C. -tubal anastomosis
D. -assisted reproductive technology
E. -uterine myoma
5. Which of the following symptoms is more important for the development of
cervical pregnancy?
A. -dystrophy of the endometrium due to inflammations, a lot of curettage,etc
B. -acute inflammation of the uterus
C. -threatened abortion in early stage of pregnancy
D. -cervical deformarions
6. The most typical symptoms of the ovarian apoplexy are
A. acute pain in the iliac area and internal bleeding
B. delay of menstrual flow and nausea and vomiting
C. fever
7. The most effective treatment of pyoovarium is
A. - surgical treatment
B. - conservative treatment (bed-rest, antibiotics and anti-inflammatory drugs)
C. - physiotherapy
8. Are all of the following a characteristic for the rupture of the abscess with
effusion of pus into abdominal cavity ?
A. - acute stabbing pain throughout the abdomen
B. - collapse
C. - nausea and vomiting
D. - vaginal bleeding

460
Chapter 12. INJURIES OF THE FEMALE GENITAL
TRACT
Obstetric injuries
Most injuries of the female genital tract occur during childbirth. In a
normal delivery the circular fibres, which surround the external cervical os
are torn laterally on each side so that an anterior and a posterior lip of the
cervix become differentiated. As a result of stretching, the vagina becomes
more patulous, and through laceration, the hymen is subsequently
represented by irregular tags of skin, termed the carunculae myrtiformes. A
superficial laceration of the perineal skin of the first degree is common even
in uncomplicated deliveries.
In abnormal labour and when obstetrical manipulations have been
carried out, or as the result of inexpert technique, injuries of the birth canal
are frequent. Severe lacerations of the perineum are perhaps the commonest
form of birth injury. Tears of the vagina may be caused by rotation of the head
with forceps or may take the form of extension of tears either of the perineum
or the cervix. Severe lacerations of the cervix are usually caused by violent
uterine contraction at the end of the first stage of labour; others result from
the delivery of a posterior position of the occiput and some from cervical
dystocia. A vesicovaginal fistula may result from ischaemic necrosis or a
difficult forceps delivery in cases of disproportion, while a rectovaginal fistula
is the result of a complete tear of the perineum or a suture, which perforates
the rectal wall. Extensive vaginal incarceration causes fibrosis and atresia,
which may lead to dyspareunia and even apareunia.
The majority of obstetrical injuries are theoretically preventable. A case
of disproportion should be recognized antenatally and be treated in time by
caesarean section. Lacerations of the cervix and extensive tears of the
perineum, although avoidable, should be treated by immediate suturing. One

461
of the worst injuries in obstetric practice is rupture of the uterus. It occurs
mostly in delivery, when obstructed labour is not diagnosed. Uterine rupture
carries a very high maternal mortality and morbidity.
Injuries of the perineum
Lacerations are 5-6 times more frequent with primiparae than with
multiparae.
It is customary to grade lacerations of the perineum into three degrees.
In the first degree the laceration is restricted to the skin of the fourchette. In
the second degree the muscles of the perineal body are torn through, while in
the third degree the tear extends backwards through the external sphincter of
the anus into the rectum and the anal canal. A rare type of tear is the central
tear of the perineum when the head penetrates first through the posterior
vaginal wall, then through the perineal body and appears through the skin of
the perineum. It usually occurs in patients with a contracted outlet.
Perineal Lacerations. First-degree lacerations, restricted to the skin of
the fourchette, have no influence upon the integrity of the pelvic floor, but if
the lacerations are not sutured after delivery, the vaginal orifice becomes
more patulous. In practice, small lacerations of the fourchette are not sutured
unless they extend to the skin of the perineum, where they are more likely to
become infected and to cause pain.
Second-degree lacerations should always be sutured carefully
immediately after delivery. The pelvic floor is weakened unless the injury to
the muscles of the perineal body is efficiently repaired. If the decussating
tissues of the levator ani muscles are torn through, the hiatus urogenitalis
becomes patulous and prolapse of the vagina and the uterus is likely to
develop, unless these lacerations are sutured immediately after delivery.
With extensive second-degree tears, the patient should be given a local,
regional pudendal block or general anesthetic, placed in the lithotomy
462
position, and the torn muscles of the perineum identified and sutured
together with catgut. The torn edges of the vagina and the skin of the
perineum should then be sutured together with catgut. The essential part of
the after-treatment of perineal lacerations consists in keeping the perineum
clean. Frequent swabbing is therefore imperative during the puerperium. The
wound should be cleaned with an antiseptic solution such as Betadine after
micturition and defecation. Antibiotics are required.
Third-degree tears are much more important, because unless they are
efficiently repaired immediately after delivery, the patient becomes
incontinent of faeces and flatus. Amongst the predisposing causes of complete
tear of the perineum are forceps delivery in the persistent occipito-posterior
positions, and extraction of the after-coming head in breech presentation in
primiparae. Large heads and precipitate labours are also contributory factors,
but unfortunately the commonest cause is vigorous pulling in the wrong
direction during forceps delivery, especially with Kielland's forceps, so that no
opportunity is given for the head to be born by the natural mechanism of
extension. A properly performed episiotomy will very largely eliminate the
risk of a third-degree tear.
Incomplete tear of the perineum, repair should be performed as soon as
possible after the delivery. A practitioner should not undertake the repair of a
complete tear of the perineum single-handed. The operation should be
undertaken under anesthesia with the patient lying in the lithotomy position
in a good light, and with good assistance. The operation should be regarded as
a surgical emergency and there is no excuse for delay. As the facilities are not
available in the patient's home, she should be transferred to a hospital.
The immediate repair of a complete tear of the perineum is a relatively
simple procedure, since the muscles of the perineal body, though torn, can be
distinguished without much difficulty. The surrounding skin is first cleaned
and the operation area isolated with sterile towels. A sterile pack is placed in
the vagina and the limits of the laceration defined with tissue forceps. The

463
rectum and the anal canal are first repaired with fine interrupted catgut
sutures inserted with an atraumatic needle. A few sutures are then introduced
to invaginate the torn edges of the bowel wall. The muscles of the perineal
body are now sutured together, and every effort should be made to obtain
exact anatomical reposition. Particular attention must be paid to the
sphincter ani muscle, and at least two catgut sutures should be used to draw
the cut edges together. The tears in the vaginal wall and in the skin of the
perineum are now repaired with interrupted catgut sutures. Care should be
taken to avoid tying the sutures too tightly, otherwise edema of the perineum
will develop, which may lead to severe pain and cause the stitches to cut
through. If a complete tear of the perineum is treated by immediate suture,
the end result is satisfactory if correct anatomical reposition has been
attained. If primary union of the vagina and the perineal skin is not obtained
the practitioner need not despair. The wound should be kept clean and
encouraged to granulate by frequent sitz baths. The end results are often
functionally good inspite of the initial breakdown of the suture line. The
bowels should be confined for at least five days, solid foods withheld and
intestinal antiseptics given, along with stool softeners. Systemic antibiotics
are necessary.
Treatment. The treatment of complete tear of the perineum is operative.
The technical difficulties are much greater in old cases than in those operated
upon immediately after delivery. The optimum time for operation in the case
of old tears is three to six months after delivery. If the operation is attempted
earlier than this, healing by first intention is exceptional, while if the
operation is further delayed, dense scar tissue may be deposited which adds
to the operative difficulties. Preoperative preparation is of importance, and
the patient should be kept in the hospital for several days before the
operation, during this time the bowels should be emptied by aperients and
enemas and the vagina disinfected by douching and by insertion of gauze
packs soaked in flavine 1 in 1000, or betadine lotion. The bacterial flora of the

464
bowel should be controlled by phthalyl- sulphathiazole or neomycin, given in
large doses for three days before operation. The patient should be put on a
non-residual diet like milk, and fluid for two days prior to surgery. Various
techniques have been described in the operative treatment of complete tears
of the perineum, but the underlying principles are the same in all. The rectum
must be dissected from the vagina by incising the intervening scar tissue, and
by dissecting upwards in the rectovaginal septum.
Perhaps the most important step of all in the operation is to dissect the
rectum clear of scar tissue, and to mobilize it so that it can be brought down,
without tension to the anal region. The tear in the rectum and anal canal is
now repaired by excising scar tissue, freshening the cut edges and suturing
them together with fine interrupted catgut sutures mounted on an atraumatic
needle and tied within the bowel. The needles, forceps and scissors used
during this step are discarded. The wound in the bowel is now invaginated
with a layer of interrupted Lembert's sutures. Next, the deep muscles of the
perineal body and the levator ani are identified and sutured together with No.
1 catgut. It is important to ensure that the muscles are dissected clear of scar
tissue, and are mobilized. The next important step in the operation is to
suture together the torn edges of the external sphincter. These must be
carefully defined, dissected clear of scar tissue and sutured together with
three or four separate sutures. The remains of the superficial muscles of the
perineum are now sutured together with catgut and then the cut edges of the
vagina and the perineum are repaired, interrupted catgut sutures being used.
These principles are uniformly followed in the various methods described for
the treatment of a complete tear of the perineum. The modifications depend
solely upon the position of the incisions made in the vaginal walls and in the
skin of the perineum, and these, in their turn, depend not upon any particular
technique, but upon the type of complete tear, which is to be repaired.
After-treatment. The most important part of the after treatment is to
keep the wound dry. The perineum should be swabbed after micturition and

465
defecation with antiseptic solution and subsequently powdered. Betadine is
the antiseptic solution of choice these days, and it is effective. The bowels
should be confined until at least the fifth day of the operation. To achieve this,
the patient is given only intravenous fluids for the first two days and oral
fluids the next two days. On the fifth day, she receives olive oil enema. As in
all operations on the perineum, retention of urine is a common complication,
so that it may be advisable to leave a Foley's catheter for a few days in the
immediate postoperative period. Sulphathiazole or neomycin administered
preoperatively should be continued for at least a week postoperatively.
Systemic chemotherapy is necessary to prevent infection and it should be
given for a week. The end result is usually good. Another complication that
may develop is a rectovaginal fistula, which is usually the result of faulty
technique but may be due to infection.
Old-standing complete tears
Various degrees of complete perineal tears, usually resulting from
careless attempts at immediate suturing are not unusual. The rectal wall may
be torn through as high as 5 cm or more along the posterior vaginal wall, but
in most cases only the anal canal is involved. The appearance of the perineum
in the cases of old complete tear is a characteristic one. The red glistening
mucous membrane of the anal canal and rectum protrudes and fuses directly
with the vaginal wall without any of the perineal tissues intervening.
Laterally, on each side, on a level with the anus, is the depression in the skin,
which corresponds to the position of the severed edge of the torn external
sphincter. Behind the anus are the radial folds in the skin, which is corrugated
by the underlying contracted subcutaneous sphincter. The external sphincter
is only present posteriorly and the absence of the sphincteric grip is
appreciated by inserting a finger into the anus.
One of the most interesting features of the complete tear of the
perineum is that it is very rarely if ever associated with prolapse, although the

466
decussating tissues of the levator ani muscles have been torn through. The
reason is that the patient continuously draws together the two levator ani
muscles in an effort to close the bowel, so that by constant use, the tone of the
muscles becomes exceptionally good. This firmness and good development of
the levator muscles is found on clinical examination when the levator muscles
are palpated.
Symptoms. The patient complains of incontinence of faeces and flatus.
A few patients develop the tone of the levator muscles so well that they only
suffer incontinence of flatus. These women will complain of incontinence of
faeces only if they suffer an attack of diarrhea.
Rectovaginal fistula
The majority of rectovaginal fistulae result from obstetrical injuries,
usually a complete tear of the perineum, which has been imperfectly sutured
immediately after delivery. It has already been pointed out that the repair of a
complete tear of the perineum should be undertaken carefully with the
patient in the lithotomy position and under anesthesia. If, for instance, a few
sutures are placed through the lower part of the anal canal and the upper part
of the tear in the rectum is not accurately sutured, a fistulous opening may
form between the rectum and vagina. Rectovaginal fistulae may occur after
operation for old complete tears of the perineum if the wound breaks down or
if the rectum is not properly mobilized before the repair of the wound in the
rectal wall. These fistulae occur also after the operation of perineorrhaphy in
thin, elderly patients when the anterior wall of the rectum is accidentally
opened.
Other causes are tuberculosis and lymphogranuloma inguinale. In
advanced carcinoma of the cervix, when the growth has spread down the
posterior vaginal wall, a rectovaginal fistulae eventually results. Such fistulae
also occur following radiation treatment of carcinoma of the cervix or the
vagina, or following Wertheim's operation for the same condition. A fistula

467
following radiotherapy may occur three months to several years after
radiotherapy and such a fistula is surrounded by extensive stricture. A
malignant fistula is impossible to close and can only be treated by some form
of posterior pelvic exenteration or a palliative colostomy. Primary carcinoma
of the bowel can also extend forward and involve the vagina to cause
rectovaginal fistula. Congenital rectovaginal fistula is rarely seen and is the
result of mal-development of the lower part of the rectum and anal canal. In
such cases, it is customary to perform preliminary colostomy before plastic
operation.
In case of pelvic abscess when there is a collection of pus in the pouch of
Douglas, the abscess sometimes bursts into the rectum and a rectovaginal
fistula develops, particularly if the abscess is surgically opened up through the
posterior fornix. There is a form of rectovaginal fistula, which follows
infection in an anal crypt with resultant abscess formation, which bursts into
the vagina. These cases are difficult to treat surgically and good results cannot
be expected until the entire fistulous tract into the anal canal has been
excised. This necessitates division of the external sphincter, and follows the
principles laid down in the treatment of fistula-in-ano. The patient complains
of incontinence of faeces and flatus. A large fistula can easily be identified, but
a small one is very difficult to detect especially if it is surrounded by dense
fibrosis. Proctoscopy, sigmoidoscopy and injection of radio-opaque dye will
be needed to trace the fistulous tract.
Treatment. The traumatic form of rectovaginal fistula is treated by
operation. (Fig. 108) Preoperative treatment is important and the bowel
should be emptied with enema and the vagina disinfected by douches and
gauze packs soaked in antiseptic solutions such as flavine or Betadine.
Phthalyl sulphathiazole or neomycin should be given for a few days before
operation to sterilize the bowel contents.
With a small rectovaginal fistula above an intact perineal body, an
unusual event, it is sometimes feasible to excise the fistulous track and close

468
the defect successfully by a local operation. It will, however, be more
commonly found that the perineal body below the fistula is inadequate and
that the levators are not approximated. In fact, in many rectovaginal fistulae,
there is merely a thin skin bridge below the fistula and often the anal
sphincter itself is incompetent. When, in addition to these perineal defects,
the fistula is very large, the best treatment is to cut the skin bridge in the
midline and convert the fistula into a complete perineal tear. This is then
repaired exactly as described above and the results are usually satisfactory. A
high rectovaginal fistula may require a preliminary colostomy. The fistula due
to cancer of the cervix or rectum requires an exenteration operation. A fistula
following radiotherapy for cancer may be successfully closed by colpocleisis.
This operation consists of obliteration of the vaginal cavity after denuding the
entire vaginal mucosa.
Vaginal lacerations
These commonly occur following assisted instrumental vaginal
deliveries (forceps or vacuum extraction), difficult breech extractions, or
following shoulder dystocia. It is a good practice to inspect the lower genital
tract under a good light after expulsion of the placenta, identify all tears and
suture them meticulously. Sometimes a cervical tear may extend to the vault
of the vagina and cause profuse bleeding. Suturing must be done with great
care to avoid injury to the ureter. Tears extending to the base of the broad
ligament may lead to a broad ligament hematoma, which may require
recourse to a laparotomy for its evacuation.
Cervical lacerations
Minor injuries are common and need no treatment. Bilateral transverse
tears of the cervix end up as ectropions. Extensive tears involving the
sphincter of the cervix may lead to preterm deliveries or habitual painless

469
midtrimester abortions due to incompetent cervix, necessitating surgical
cerclage in future pregnancies. In women with a flat pelvis, the anterior lip of
the cervix may get caught between the fetal head and the pubic symphysis
resulting in an anterior bucket handle tear. Rarely in women with a small
gynecoid pelvis, a trial of labour may result in circumferential ischemic
necrosis of the lower part of the cervix and end up with an annular
detachment of the cervix.
Rupture of the uterus
This is almost entirely a complication of pregnancy and labour. It is
common in multiparae, usually following a neglected, obstructed delivery.
Misuse of oxytocics, or dehiscence of a previous uterine scar (cesarean
section), rarely, a haematometra or pyometra may rupture spontaneously as a
result of distension and thinning of the atrophic myometrium.
Perforation of the uterus
In the non-pregnant state, it occurs mainly during the operation of
dilatation and curettage. (Fig. 209) The perforation is more common if the
uterus is soft as in pregnancy and in malignancy. The atrophic uterus of a
menopausal woman can easily be perforated during curettage for
postmenopausal bleeding. Spontaneous perforation may also occur with
intrauterine contraceptive devices. (Fig. 210) The intrauterine coil device may
perforate the wall of the uterus, but remains within the myometrium. At times
it perforates through the entire thickness of the myometrium and either lies
freely in the peritoneal cavity or more often gets embedded in the abdominal
viscera.

470
Fig. 209. Perforation of the uterus during dilatation and curettage,
and medical termination of pregnancy
Fig. 210. Diagramm showing perforation of the uterus with Cooper T
IUD
If the uterus is empty and not malignant, laparotomy may not be
necessary. Simple observation is all that is required. In presence of pyometra
and malignancy, immediate hysterectomy is strongly advised. If the
abdominal viscera, i. e. intestine prolapes through the perforation and is seen
protruding in the vagina, immediate laparotomy becomes mandatory. The
repair of the intestinal injury or resection and end-to-end anastomosis will be

471
required depending upon the extent of the damage to the intestine. If the
uterus contains products of conception, repair of the rent will suffice. If the
perforation is a large one or if the patient has completed her family,
hysterectomy is the operation of choice. Uterine injury has been recently
reported during hysteroscopic excision of the uterine septum. Excision under
laparoscopic supervision can avoid this injury. The uterine perforation can
also occur during laser ablation of endometrium through a hysteroscope in
cases of dysfunctional uterine bleeding.
Injuries due to coitus
A slight amount of hemorrhage from the torn edges of the ruptured
hymen is normal after defloration, but the hemorrhage is sometimes very
severe, particularly when the tear has spread forwards to the region of the
vestibule. The hemorrhage can usually be controlled by the application of
gauze pressure, but suturing under anesthesia is often required and blood
transfusion may be necessary.
Bruising of the vaginal wall is not uncommon in the early days of
married life, and a urethritis may result from bruising of the urethra. Such
cases (Honeymoon pyelitis) are seen frequently and it is not uncommon for
ascending pyelonephritis to result.
Lacerations of the vagina caused by coitus are occasionally seen. Violent
coitus or rape in young girls, forceful penetration in post-menopausal women
having atrophy of the vagina, or in the presence of such malformations as an
imperforate vaginal septum, extensive and serious injuries are known to
occur. These lacerations may be of variable types. It often takes the form of a
longitudinal tear of the anterior vaginal wall. Cases have been recorded where
the posterior vaginal wall has been torn through and the peritoneal cavity
opened up and both bladder and rectum may be involved in serious coital
injuries. Similar injuries may occur in patients upon whom vaginal operations
have been previously performed, especially if coitus takes place soon after the

472
operation. All patients who have had a vaginal operation should be warned to
avoid coitus for two months. A similar injury can occur after the operation of
total hysterectomy, when coitus may disrupt the recently sewn vaginal vault.
Large or small bowel and omentum can prolapse into the vagina with
resulting shock and peritonitis. Severe hemorrhage follows injuries of this
kind. When the injuries are small, treatment consists in plugging the vagina,
provided thorough inspection has excluded the possibility of extensive or
internal injury. In more severe cases it is necessary to suture the laceration
under anesthesia. If the bowel has prolapsed, it is imperative to open the
abdomen so that a complete inspection of the gastrointestinal tract from the
jejunum to the rectum can be made. Damage to bowel or mesentery can then
be assessed and the correct treatment performed under-direct vision. It is
interesting to note that quite apart from the coitus or direct injury, a
spontaneous rupture of the vagina can occur in the upper posterior one-third.
The patients are usually elderly and the vagina is atrophic. The cause is
usually a violent bout of coughing or some severe strain associated with a
sudden rise in intra-abdominal pressure. The treatment is the same as for
coital injuries.
Direct trauma and vulval hematoma
Injuries to the vulva as the result of direct trauma are not uncommon.
Such accidents as falling astride gates and chairs are frequent, and usually
produce bruising of the labia majora. In more severe cases, large hematomas
develop in the labia majora, and the effused blood spreads widely in the lax
connective tissues. This is specially seen when the laceration involves the
region of the clitoris and the erectile tissue around the vaginal orifice. The
rupture of varicose veins of the labia majora sometimes causes comparable
hematomas of the vulva during pregnancy and the large swelling may
obstruct the delivery.

473
One of the commonest causes of the vulvo-vaginal hematoma is the
inadequate hemostasis during suturing of episiotomy or a perineal tear. The
important complications of hematoma of the vulva are hemorrhage with
subsequent anemia and local infection. A vulvae hematoma presents a painful
tender swelling, bluish black in appearance. The patient may look pale and
she may be in a condition of shock, which is out of proportion to the clinical
blood loss. A small hematoma responds well to rest in bed, sitz bath and
magnesium sulphate fomentation. Antibiotic is given to prevent infection.
With large hematoma it is sometimes necessary to incise the swelling under
anesthesia and to turn out the clot. If the hemostasis is difficult to secure,
packing with drainage is employed, but this leads to prolonged convalescence.
The deep penetrating injuries require immediate operations, suture and
repair of the injured structure. If there is a least suspicion of visceral injury or
if the pouch of Douglas has been opened, laparatomy must be performed and
perforation of the bowel or bladder sutured. A temporary colostomy may be
necessary if the rectum has been injured.
Injuries due to foreign bodies and instruments
Vaginal.
An extraordinary variety of bizarre foreign bodies have been recovered
from the vagina including safety pins, hairgrips, pencils and small jam jars.
The patient is often mentally retarded or a young child, and in both these a
persistent and a maladorous discharge should always suggest the presence of
a foreign body.
Neglected or forgotten objects employed therapeutically. The most
frequently found is the ring pessary used for prolapse. Some of these have
remained in the vagina for many years and have become encrusted with
phosphatic deposits. These neglected pessaries can cause severe ulceration of
the posterior fornix and later vaginal carcinoma. Less traumatic are forgotten
swabs and tampons, which cause a foul purulent discharge.

474
Contraceptive devices such as cervical caps and diaphragms, even a
mislaid condom when retained, can cause discharge and ulceration.
Instrumental damage caused during attempted criminal abortion.
Sound, gums, elastic bougies, hatpins, knitting needles and the like have
caused perforation of the vagina into the bladder, rectum, pouch of Douglas
and the parametrium.
Very rarely, a needle can break during suturing of an episiotomy and a
piece may remain there without causing symptoms. This is accidentally
discovered during a subsequent confinement.
Uterine.
Foreign bodies in the uterus are almost always intrauterine
contraceptive appliances such as Copper T. These are inserted in the first
place by a qualified practitioner but may be neglected or forgotten by the
patient. They cause ulceration of the endometrium and can give rise to a
serious ascending infection with inflammatory tuboovarian masses. The
foreign body may also be a cause of menorrhagia.
The other foreign body met with in the uterus has usually been
introduced in order to procure abortion. Serious intrauterine infections often
result in pelvic abscess from acute salpingooophoritis.
Perforation of the uterus may occur during dilatation and curettage, and
medical termination of pregnancy.
Perforative injuries during hysteroscopic operative procedures or
division of the uterine septum have been known. These should not be treated
lightly, the possibility of injury to hollow viscera, or vessels, must always be
borne in mind, and necessary surgical measures implemented to ensure
patient safety.
Treatment. Treatment of vaginal foreign bodies is to remove them, if
necessary under anesthesia. Simple local antiseptic douches suffice for after-
treatment. If, however, the vagina has been perforated, chemotherapy is
475
indicated and, if there are signs of peritoneal infection or bowel damage, as
with criminal abortion, laparotomy may be needed.
Uterine foreign bodies should be removed under anesthesia and, if
infection is present, a swab taken and the correct chemotherapy given.
Adnexal involvement if resistant to chemotherapy, e. g. large persistent
masses with recurrent fever and constitutional upset, call for laparotomy and
their surgical removal. In young women, it is sometimes possible to conserve
the uterus and part of one ovary. When the pelvic organs are grossly
disorganized by the pelvic inflammatory disease, total hysterectomy and
bilateral salpingo-oophorectomy is the only logical answer. Fortunately, these
severe infections from uterine foreign bodies are rare.
Chemical and other burns of the vagina
The commonest cause of these is the use of strong chemicals such as
Lysol, permanganate or corrosive sublimate. The dangerous complication of
this type of burn is that during healing, extensive vaginal adhesions and
fibrosis will obliterate the canal and prevent coitus, and even cause retention
of menstrual discharge with hematometra and pyometra. Plastic
reconstruction is the only answer to this problem.
Douches administered at a too high temperature are another cause of
burn. This is culpable error on part of the operator.
During the operation of cauterization of the cervix by the cautery or
diathermy, it is quite easy to burn the vagina directly or by conduction.
Fortunately, cryosurgery has today replaced cauterization of the cervix and
burn injuries of this nature are rare. Laser therapy for cervical lesions and
vaginal cancer in situ can also cause burns.
It must be remembered that the radium inserted into the vagina for
carcinoma of the cervix always causes radiation. During the process of
healing, the vaginal vault frequently becomes obliterated by an adhesive
vaginitis and fibrosis.
476
Treatment. Most vaginal burns, unless severe, heal with expectant
treatment. Those resulting in extensive scarring and atresia will require
plastic surgery.
Self test
1. What from the following symptoms should always suggest the presence of a
foreign body?
A. maladorous discharge
B. hemorrhage from the vagina
C. swelling in the lower abdomen
2. The dangerous complication of chemical burn is
A. - extensive adhesions of the vaginal canal
B. - vaginal tears
C. - vaginal hemorrhages
3. With second-degree tears, the torn muscles of the perineum should be sutured
with
A. - catgut
B. - silk
C. - metallic agraffe
4. Colpocleisis consists of
A. obliteration of the vaginal cavity after denuding the entire vaginal mucosa
B. temporary tamponade of the vagina
5. What may be a likely complication after operations on the perineum?
A. - retention of urine
B. - constipation
C. - diarrhea
6. What is the most dangerous complication in case of third-degree laceration of
the perineum?
A. the patient becomes incontinent of faeces and flatus

477
B. infertility
C. chronic inflammation of genital tract
7. What may be a likely complication of the cervical lacerations?
A. - isthmico-cervical insufficiency
B. - disturbances of menstrual cycle
C. - cervical erosion
D. - cervical inversion
8. Laparotomy is the only way of treatment in cases of uterine perforation.
A. yes
B. no
478
Chapter 13. MYOMA OF THE UTERUS.
ENDOMETRIOSIS. SARCOMA OF THE UTERUS
Chapter 13. MYOMA OF THE UTERUS. ENDOMETRIOSIS
LEIOMYOMA OF THE UTERUS
Leiomyomas (myomas) are the commonest of all uterine tumors.
Uterine leiomyomas are proliferative, well circumscribed,
pseudoencapsulated benign tumors composed of smooth muscle and fibrous
tissue. They are also called a fibroid, fibromyoma, myoma, fibroleiomyoma,
leiomyoma.
Incidence. Neoplasms of the uterus are almost all leiomyomas, which
may be found in nearly one woman in three over the age of 30 years. Uterine
fibroids are common, appearing in 70% of women by age 50; the 20% to 50%
that are symptomatic have considerable social and economic impact on
women’s quality of life: their health, working capacity, fertility, etc. Symptoms
of myoma are common between the age of 30 and 45. Many tumors are too
small to be palpated, and can remain asymptomatic, and are diagnosed
incidentally on clinical examination or imaging. They are present in 40% of
autopsy specimens as unexpected finding. And it is rather difficult to
determine with accuracy the true incidence of myomata. It never develops for
the first time after the menopause. They are more common in nulliparae.
Myomas are the most common indication for hysterectomy in our country.
As to its structure, it is a nonstriated muscle tumor. It develops in the
myometrium and is not encapsulated, but develops a false capsule of
compressed myometrial tissue. The cut surface is whorled, white and bulgy.
Leiomyomas may be solitary in the uterus but most frequently are multiple.
They vary in size from tiny to several cm in diameter. Some of them develop a
long pedicle and present as polyps.

479
Etiology. The cause is unknown. Cytogenetic studies suggest a role of
chromosomal abnormalities (particularly chromosome 12) in the
pathogenesis of these tumors. A limited number of genetic defects
transmitted by germ cells have been associated with familial uterine fibroid
syndromes. Most notable are germline mutations causing fumarate hydratase
deficiency, which predisposes women to the development of multiple uterine
fibroids. Recent research showed the role of stem cells, somatic genetic and
epigenetic defects, and the action of estrogen and progesterone and their
cross-talk with various signaling pathways in the development of uterine
fibroids. The inciting event responsible for the neoplastic transformation is
unknown; estrogen may be necessary for expression of this mutation. Factors
that affect growth are: estrogen, progesterone, peptide growth factors.
Evidence suggests estrogen to be a promoter of myoma growth:
o myomas are rarely found before puberty and stop growing after
menopause;
o new myomas rarely appear after menopause;
o there is often rapid growth of myomas during pregnancy.
During a woman's reproductive years, myometrial smooth-muscle cells
undergo multiple cycles of growth followed by involution under the influence
of ovarian hormones or the hormones of pregnancy. These cycles make stem
cells vulnerable to the development of mutations. It can alter key signaling
pathways such as those involving β-catenin and TGF-β, which regulate cell
proliferation, survival, and senescence and the formation of extracellular
matrix, leading to clonal expansion of the stem cells within the genetically
normal myometrium. In this context, the inherent capability of myometrial
tissue to respond to estrogen and progesterone for physiologic expansion
during the luteal phase of the ovulatory cycle or pregnancy may work to the
advantage of fibroid-tumor growth. Such growth may be mediated by high
levels of estrogen and progesterone receptors in normal myometrial cells or

480
by the differentiated population of fibroid cells that send paracrine signals to
the receptor-deficient fibroid stem cells for self-renewal.
Recent investigations implicate peptide growth factors – epidermal
growth factor, insulin-like growth factor – 1, platelet-derived growth factor –
in the regulation of leiomyoma growth. Estrogen may exert its effect through
epidermal growth factor.
Local factors, such as blood supply, adjacency to other tumors and
degenerative changes may account for variations in tumor volume and rate of
growth.
Classification. Myomas are classified according to their location within
or on the uterus into: intramural, submucous, subserous. (Fig. 211). Each
location is associated with different signs and symptoms.
Intramural myomas are the most common variety (70%), occurring
within the walls of the uterus as isolated encapsulated nodules of
varying size. As these grow, they can distort the cavity or the external
surface of the uterus. These tumors can also cause symmetric
enlargement of the uterus when they occur singly.
Submucous myoma –growing into the uterine cavity they present either
submucosal, pedunculated submucosal or pedunculated vaginal (10%)
myomatous nodes
o Submucous myomas are located beneath the endometrium. These
tumors grow into the uterine cavity, maintaining attachment to
the uterus by a pedicle. The pedunculated myomas may protrude
to or through the cervical os. These tumors are often associated
with an abnormality of the overlying endometrium, resulting in a
disturbing bleeding pattern.
Subserous myoma – these grow outwards from the uterus (20%).
Subserous myomas are located just beneath the serosal surface and
grow out towards the peritoneal cavity, causing the peritoneal surface of
the uterus to bulge. Subserous myoma can be:

481
o Subserous.
o Pedunculated subserous (abdominal). These tumors develop
a pedicle, become pedunculated, and reach a large size
within the peritoneal cavity producing pressure symptoms,
abdominal swelling. These forms may be mobile and should
be differentiated from solid adnexal lesions.
o Intraligamentous. When myomas extend into the broad
ligaments, they are known as intraligamentary myomas
o Cervical - involvement of the isthmus and cervix, fibroids at
these sites will produce their own spectrum of symptoms
and signs.
Hystopathology. Myomas consist of whorled masses of unstriped
muscle cells, but more often they consist of muscles and connective tissue.
Secondary Pathological Changes in the Fibroid Uterus
Secondary changes may occur in fibroid. These changes occur in
alteration of circulation (either arterial or venous), postmenopausal atrophy,
or infection or may be as a result of malignant transformation.

482
- Hyaline degeneration, the most common type of degeneration, is
present in almost all myomas, especially in tumors with more connective
tissue. The tumor becomes softer and the degenerated areas have a
homogenous waxy character instead of the whorl-like appearance.
Microscopically, the muscle cells become indefinite and their cytoplasm
merges with the structureless intercellular matrix.
- Cystic degeneration is the extension of hyaline degeneration with
liquefaction of some areas of the fibroid and cyst formation.
- Calcification. This more frequently occurs in the myomata of
postmenopausal women or in the subserous myoma with small pedicle. It is
practically never seen in the submucous myoma. This is associated with
circulatory impairment. In its most extreme form the fibroid is converted into
a stony mass.
- Fatty degeneration: the fatty change is associated with hyaline
degeneration and usually precedes calcification.
- Atrophy. This is noticed after menopause. The myomata become
smaller and comparatively avascular with more fibrous tissue.
- Necrosis is commonly caused by impairment of the blood supply or
severe infection. A special kind of necrosis is red, or carneous, degeneration,
which occurs most frequently in pregnancy. The lesion has a reddish hue and
is believed to be aseptic degeneration with local hemolysis.
- Infection of myoma most commonly occurs with a pedunculated
submucous leiomyoma that first becomes necrotic and then secondarily
infected.
- Sarcomatous degeneration. Malignant degeneration occurs in less
than 1% of myomas.
Associated conditions. Follicular cysts of the ovary, hyperplastic
endometrium, and endometriosis are significantly associated with myoma. All
these conditions are seen in nullipara and are due to hyperestrogenism.

483
Clinical picture. The clinical symptoms of myomata are highly variable
and are dependent on the size, site and number of tumors.
Most cases of myomata are symptomless and are found in the course of
a routine pelvic examination.
The common symptoms and signs are the following:
Menstrual disturbances:
o The most common disturbances are heavy and prolonged
menstrual bleeding with increased amount and duration of flow.
In intramural myoma abnormal uteine bleeding (AUB) may be
due to increased vascularity, hyperplastic endometrium, an
increased bleeding surface because of the larger size of the uterine
cavity and associated ovarian dysfunction. Subserous tumors do
not disturb menstruation;
o Intermenstrual bleeding or a blood-stained discharge is a feature
of submucous myoma and fibroid polyps, which have become
necrotized and infected;
o Dysmenorrhea is not uncommon symptom, which is more
characterized in submucous myomata. Submucous pedunculated
tumors produce uterine contractions causing cramp-like pain in
the lower abdomen as in spasmodic dysmenorrhae.
Abdominal swelling.
o When the myoma of uterus is larger in size than the uterus at the
12th week of gestation, it can be felt in the lower abdomen.
Pressure symptoms.
o Myoma in the fundus and the body of the uterus rarely cause
pressure symptoms.
o But a cervical myoma causes bladder irritability and frequency of
micturition. Acute retention of urine can occur premenstrual due
to the compression of the internal vesicle sphincter or the urethra
against the pubic bone.

484
o Occasionally a large broad ligament tumor may displace and press
on the urethra leading to hydroureter and a painful, tender
kidney.
o Constipation and difficult defecation can be caused by large
posterior myomas. Symptoms due to pressure on the pelvic veins
or nerves are exceptional.
Pain.
o Apart from dysmenorrhea, myomata can cause abdominal or
pelvic pain due to infection, red degeneration, torsion, due to
rapid tumor growing or sarcomatous change.
Sterility.
o About 40% of women with multiple uterine fibroids have
infertility. The presence of a submucous myoma may prevent
implantation due to poor deciduation or may give rise to an
abortion. The distortion of the uterine cavity, tubal blockage by
cornual myomata, associated salpingitis, endometriosis and
anovulation are also contributory causes of sterility.
Chronic posthemorrhagic anemia.
Diagnosis of myoma is not difficult and based on finding of abdominal,
vaginal and additional methods of examination.
Abdominal examination. Uterine may be palpated as irregular, nodular
tumors protruding against the anterior abdominal wall. Myomatous uterus
is usually firm on palpation; softness or tenderness suggests the presence
of edema, sarcoma, pregnancy, or degenerative changes.
Vaginal examination. The most common finding is uterine enlargement;
the shape of the uterus is usually asymmetric and irregular in outline. The
uterus is usually freely movable. In the case of the submucous myomas the
uterine enlargement is usually symmetric. Some subserous myomata may
be very distinct from the main body of the uterus and may move freely.

485
Additional examination:
o blood test (hemoglobin, hematocrit, erythrocytes) is obtained in the
patient with excessive vaginal bleeding to assess the degree of loss and
account of replacement,
o coagulation profile and bleeding time are ordered in a patient with
bleeding,
o endometrial biopsy or separately uterine curettage is performed in a
patient with abnormal uterine bleeding to exclude endometrial
hyperplasia, malignization.
o ultrasonography accurately assesses uterine dimension, myoma
location, interval of growth,
o evaluation of the endometrial cavity with hysteroscopy or
hysterosalpingography.
o MRI, CT scan are also used for diagnosis of leiomyoma.
Treatment. The treatment of myomata must be adapted to each patient,
and includes nonsurgical and surgical methods. Treatment decisions are
based on symptoms, fertility status, uterine size, and the rate of uterine
growth.
In general, small asymptomatic myomas do not require treatment, but
the patient should be periodically monitored. Annual examination of these
patients is mandatory and includes:
Bimanual examination every 6- 12 months to determine uterine size and
rate of growth.
o After assurance of slow growth or stable uterine size annual
follow-up may then be appropriate. Rapid growth – a change of 4
weeks in size or greater during 12 months or less of observation –
is an indication for surgical intervention.
Additional methods of examination such as:
o TAUS and TVUS,
o X-ray examination,

486
o cytological examination (Pap-testing),
o histological examination (endometrial biopsy by separate
curettage of the uterus, aspiration biopsy).
o The same about regular laboratory examination to determine Hb,
PCV, WBC, iron deficiency and so on.
Fibroids should be treated if they are associated with symptoms. Three
modalities are used to treat myomas:
o medical treatment,
o surgical treatment,
o embolization of uterine arteries
Medical treatment
Medical treatment is a temporary treatment, ideally used for patients who are
close to menopause, who are risky surgical candidates, who do not realized
their reproductive function. So, medical therapy is indicated in the following
cases:
o myoma in the late reproductive age or in premenopause;
o in case of contraindications for surgical intervention;
o before the operation to reduce uterine size and volume of
intraoperative blood loss.
Hormonal treatment of leiomyoma
o Progestogens have no stable effect on the size of leiomyoma, but
may be used in controlling the menstrual loss, especially in
anovulatory cycles, in a course of treatment of infertility, related
to leiomyoma. Progesterone is administered in the second phase
of menstrual cycle by 5 or 10 mg intramuscularly once a day for
10-12 days during 3 or 6 months; Medroxyprogesterone (Amen,
Cycrin, Provera) 10-20 mg PO qd continuously; Megestrol
(Megace) 40 mg PO qd. Use of progestins have some side effects:

487
both fibroid shrinkage and enlargement have been shown; may
induce endometrial atrophy and amenorrhea.
o Combined oral contraceptive pills (COCPs) are also used.
Norgestimate/ethinyl estradiol (Ortho-Cyclen, Ortho-Prefest,
Ortho Tri-Cycle usually administered for three months, then, if
menstrual blood loss reduced, for 6 months. COCP usually
administered by:
Schedule 1 (Sunday starter)
- Begin dose on first Sunday after onset of menstruation; start that
Sunday if menstrual period starts on Sunday
- 21-tab package: 1 tab qd for 21 d followed by 7 d off medication; new
course begins on day 8 after taking last tab
- 28-tab package: 1 tab qd without interruption
Schedule 2 (day 1 starter)
- Start dose on d 1 of menstrual cycle
Patient need in further treatment of sterility treatment and special follow up.
o Gonadotrophic-releasing hormone analogues (GnRH agonist) cause
hypoestrogenism and may be used too. They are most helpful when
given preoperatively to reduce fibroid and uterine volume. Reduction in
myoma size occurs within four months of treatment and reported range
varies from 30 to 100%. Both ischemic effect and cellular atrophy play
part in the reduction of myoma size. Some of GnRHs used are buserelin,
goserelin, 3. 75-7. 5 mg monthly for 3 -4 months. Use of GnRH agonist
therapy is not recommended for longer than 24 weeks (6 months),
because of the long-term therapy is associated with rapid bone loss
(osteoporosis), with rebound growth to pretreatment size within 6
months, often increasing bleeding and pain. For these reasons and
because of the expense of these agents, GnRH agonists are
recommended for short-term use and only in selected cases; for the
treatment of large, submucous myomata to facilitate hysteroscopic

488
resection; in the symptomatic perimenopausal patients who wish to
avoid surgery; and as presurgical treatment to decrease symptoms and
size.
o GnRH antagonists (Abarelix, Cetrorelix, Degarelix, Ganirelix) lead to
suppression of ovarian steroidogenesis production - immediate
pituitary downregulation. GnRH antagonists have the advantage of
flexibility in that they may be administered at any time during the
follicular phase of a treatment cycle. GnRH antagonists are
administered by either intramuscular injection (abarelix) or
subcutaneous injection (cetrorelix, degarelix and ganirelix). One
injection of Cetrorelix of 3 mg on day 8 or 9 of the stimulation cycle is
sufficient to prevent an LH surge.
o Antigonadotropic agents: Danazol may be administered in a dosage of
800 mg daily for six months.
o RU-486 (mifepristone), an antiprogestin, has been associated with
decrease in size of leiomyomas
o Androgens may cause the inhibition of pituitary function and atrophy of
endometrium. So, 30 mg of methyltestosterone (2 tablets three times a
day) during 20 days are administered for 3 months. Testosterone
propionate may be used in 25 mg intramuscularly in a day for 10
injections, with 10 days interval during 3 months. The treatment by
androgens may be used in the age older than 45 years.
Non-hormonal therapy is as follows:
- Ergometrine,ergonovine, which induces uterine contraction, from the
5th day of periods.
- Iodine electrophoresis daily a month with a break for menstrual flow.
- Nonsteroidal antiinflammatory drugs are also useful for treatment of
pelvic discomfort or pressure.

489
Surgical treatment
Indications for surgery are symptomatic leiomyomas:
Excessive bleeding that interferes with normal life-style or leads to
anemia.
Chronic pelvic pain.
Rapid growth (enlargement of myoma to 3-4 weeks pregnancy size in a
year of management).
Size of the uterus is more than 12 weeks pregnancy in patients less than
40 years of age and more than 14 weeks in patients older than 40 years
of age.
Uterine growth in menopause because this may represent a
malignization of fibroid.
Submucous myoma.
Pressure symptoms on surrounding organs (micturition, urinary
retention, progressive hydronephrosis, constipation, varicosity due to
compression of pelvic vessels.
Protrusion of a pedunculated submucous myoma through the cervix.
Necrosis of myomata, torsion of pedunculated myomata and so on.
Surgical treatment may be conservative and radical.
The type of surgery to be performed depends on the age of the patient, the
nature of the symptoms, and the patient’s desires regarding future fertility.
Three classes of surgical techniques are conventional:
o laparotomy,
o operative laparoscopy,
o operative hysteroscopy.
Others: Uterine fibroid embolization, laparoscopic myolysis, MRI-guided
focused ultrasound are also currently used.
Laparotomy: this technique is indicated for large myomas, for
submucous myomas larger than 3 cm in diameter, or for myomas that,
regardless of being submucous, have a portion of the myoma that

490
compromises the myometrium so that a complete resection through the
hysteroscopy is not feasible. The classic types of operations are myomectomy
and hysterectomy (see chapter 10). Myomectomy involves the removal of a
single or multiple myomata while preserving the uterus; this procedure is
usually reserved for women who desire future pregnancy and to whom
pregnancy is not contraindicated. Myomectomy can be done through
endoscopy, by laparotomy or per vagina (in cases with submucous myoma
and polyps). If the indications for surgery are present and if the patient’s
childbearing is complete, hysterectomy may be definitive treatment for
uterine myomata. Hysterectomy may be performed on the abdominal or
vaginal route. As a rule, total abdominal hysterectomy is a satisfactory and
safe operation. Large cervical or broad ligament tumors make the operation
technically difficult and there is a risk of injury of the urethra at its
displacement. In women of approximately 45 years of age both tubes and
ovaries are usually removed along with the uterus. In those who are younger,
the ovaries are preserved unless they are diseased. Vaginal hysterectomy is an
excellent operation when the uterus is not larger than 12-14 weeks pregnancy
size, especially if the patient is multiparous.
Laparoscopic myomectomy. This technique is indicated for
pedunculated and superficial intramural myomas. Also should be reserved
for myomas with a diameter less than 6 cm.(Fig. 212). In a laparoscopic
myomectomy, thin scopes are used that contain surgical and viewing
instruments. Laparoscopy requires only tiny incisions, and has a much faster
recovery time than abdominal myomectomy. Only certain fibroids can be
removed by laparoscopy. If the fibroids are large, numerous or deeply
embedded in the uterus, then an abdominal myomectomy may be necessary.

491
Laparoscopic myoma coagulation - myolysis is an alternative to
myomectomy. This procedure can be combined with endometrial ablation for
patients who have persistent uterine bleeding. Laparoscopic myomectomy is
another alternative to hysterectomy.
Robotic myomectomy. Robotic myomectomy uses a combination of
high-definition 3d magnification, robotic technology and miniature
instruments to improve a surgeon's ability to view fibroids and the
surrounding tissue, as well as enhanced ability to suture the uterus when
removing uterine fibroids and reconstructing the uterine wall. Four small
incisions are made in the abdomen to allow for slender robotic arms and tiny
surgical tools to access the uterus. Using careful techniques to continue
minimizing the bleeding, the surgeon excises the fibroid(s) from the
surrounding uterine tissue. Once the fibroid has been removed, the surgeon
uses a special device called a morcellator to cut the fibroid into smaller pieces
inside the patient's abdomen. These pieces are then removed through one of
the ports. Benefits of robotic myomectomy over abdominal myomectomy
includes less post-surgical pain, quicker recovery and return to normal

492
activities. The typical recovery involves 0-1 nights in the hospital and 4 weeks
reduced activity.
Hysteroscopic myomectomy. The removal of a submucous fibroid using
hysteroscopy should be limited to small fibroids (≤3 cm) with minimal
compromise of the myometrium. With this procedure, fibroids are removed
using an instrument called a hysteroscopic resectoscope, which is passed up
into the uterine cavity through the vagina and cervical canal. Standard
resection uses an electrosurgical wire loop to surgically remove the fibroid.
Fibroids located within the uterine wall cannot be removed with this
technique. Hysteroscopic myomectomy is an out-patient surgical procedure.
Patients go home after several hours of observation in the recovery room.
Recovery time is generally only few days. There are no scars on the skin after
the procedure. Uterine synechiae development is a potential complication
after the surgery; therefore, a postoperative HSG should be part of follow-up
care.
Uterine fibroid embolization. Uterine fibroid embolization (UFE), also
known as uterine artery embolization is performed by an interventional
radiologist, a physician who is trained to perform this and other types of
embolization and minimally invasive procedures. The procedure is performed
while the patient is conscious—but sedated and feeling no pain. It does not
require general anesthesia and usually only a hospital stay of one night.
Painkilling medications and drugs that control swelling are prescribed
following the procedure. (Fig.213). UFE consists of catheterization of the
uterine artery and the injection of micro beads of polyvinyl alcohol to
selectively occlude the circulation of the fibroid. It is not intended for patients
who desire fertility.

493
Contraindications for surgery: severe general diseases, severe inflammatory
diseases, and so on.
Endometriosis
Endometriosis is defined as abnormal growth of endometrial tissue
(glands and stroma) outside the uterus. The most frequent sites of
implantation are the pelvic viscera and the peritoneum. Endometriosis varies
in appearance from a few minimal lesions on otherwise intact pelvic organs to
massive ovarian endometriotic cysts that distort tuboovarian anatomy and
extensive adhesions often involving bowel, bladder, and ureter. It is estimated
to occur in 7% of reproductive age women and often is associated with pelvic
pain and infertility.
Pathology. The essential feature of endometriosis is the occurence of
endometrial tissue in ectopic situation. The displaced endometrial tissue is
respond to estrogen and progesterone cyclic changes, continues to act as it
normally would — it thickens, breaks down and bleeds with each menstrual
cycle. Because this displaced tissue has no way to exit the body, it becomes
trapped, leading to development of endometriotic implants, looking like

494
small, flat patches, blebs, or flecks sprinkled on the pelvic surface. The flecks
can be clear, white, brown, red, black, or blue. The color is attributed to
hemolyzed blood from ectopic endometrium that is encapsulated by
adhesions or fibrotic tissue. These peritoneal surface lesions usually range in
size from a few millimeters to 2 cm in diameter and often are surrounded by
various degrees of fibrosis that may confer a puckered appearance.
Endometriosis implants may vary considerably in appearance. Smaller fresh
lesions may be found as clusters of nodules resembling hemorrhagic vesicles,
which have been described as “raspberry” spots (Fig. 214). Other implants
may appear as clear, nonpigmented, or slightly brown vesicles, reddish
polyps, white scar tissue or plaques, petechiae, or flamelike lesions. In the
natural evolution of endometriosis, white, scarred peritoneum or the typical
pigmented lesion is considered a late-stage manifestation of endometriosis.
All types of implants may coexist within the same patient. Occasionally, foci
of endometriosis may be found at the base of adhesions formed in response to
chronic peritoneal surface irritation by the implants. Peritoneal pockets may
also be associated with endometriosis.
The severity and course of endometriosis is highly unpredictable. Some
women may have a few endometriosis implants on the surface of the pelvis,

495
the peritoneum, or pelvic organs, or they may invade the peritoneum and
grow as nodules. Endometriosis may grow on the surface of the ovary as
implants or invade the ovary and develop a blood-filled cyst called an
endometrioma, or a “chocolate cyst.” Chocolate cysts are so named because
over time the blood they contain darkens to a deep reddish-brown color.
These cysts may be as small as a pea or grow to be larger than a grapefruit.
Endometriosis may irritate surrounding tissue and produce internal scar
tissue called adhesions. These adhesions can bind the pelvic organs together,
cover them entirely, or involve nearby intestines. The adhesions may keep
fallopian tubes from picking up the egg from the ovary during ovulation.
Endometriosis also may grow into the walls of the intestine or into tissue
between the vagina and the rectum.
An “endometrioma “(the synonym of endometriosis) may be regarded
as a neoplasm, but will only survive under the influence of the ovarian
hormones. The ectopic tissue consists of both glands and stroma, in both of
which cyclical menstrual changes occur. The menstrual blood and secretion
causes secondary proliferation, and the greater part of any tumor is
adventitious tissue. Although benign, endometriosis is progressive, tends to
recur, may be locally invasive, may have widespread disseminated foci
(rare),and may exist in pelvic lymph nodes (30%).
Endometriosis occurs in the following locations (Fig. 215)
- Ovaries. Small dark endometrial “spots” appear on the surface, and the
menstrual secretion partly distends the endometrial glands and partly enters
the peritoneal cavity, where it is walled off by adhesions. A tumour mass is
formed, consisting partly of ovary, partly of adventitious fibrous tissue, and
with cystic spaces containing chocolate-coloured altered blood. The disease is
usually bilateral, and forms masses up to 10 cm in diameter.
- Uterus. Nodules (“adenomyosis”) appear in the wall, resembling
fibromiomata, except that they have no definite capsule and may show minute

496
spaces containing blood. Microscopically endometrial tissue is found, with
proliferation of adjacent muscle and fibrous tissue.
- Uterine tubes. Uncommon, except in amputation stumps.
- Rectovaginal septum. A hard fixed mass of indefinite outline appears,
and may extend backwards partially to surround the rectum. Ulceration of the
posterior fornix may occur. The rectal mucosa remains intact for a long time,
but ultimately rectal ulceration and bleeding occur. Lateral extension may
involve the ureter.
- Round ligaments, both intra- and extraperitoneal portions.
- Umbilicus.
- Lower abdominal scars, especially after hysterectomy.
- Anywhere on the pelvic peritoneum. Fibrous tissues around
endometriosis of the bowel may form a ring stricture and cause obstruction.
The peritoneal surface of the bladder may be involved.

497
Etiological theories. Endometriosis is an estrogen-dependent disease.
Three theories have been proposed to explain the histogenesis of
endometriosis:
Ectopic transplantation of endometrial tissue
Coelomic metaplasia
The induction theory
Transplantation theory. The most widely accepted hypothesis is that
endometrial cells are transported from the uterine cavity, then implant at
ectopic sites. Endometrial “spills” may be regurgitated through the tubes and
become implanted. Retrograde flow of menstrual tissue through the fallopian
tubes could cause intra-abdominal endometriosis (ovarian, peritoneal, tubal
endometriosis etc.); the lymphatic or circulatory systems could transport
endometrial cells to distant sites (for examplе, the pleural cavity). Retrograde
menstruation occurs in 70% to 90% of women, and it may be more common
in women with endometriosis than in those without the disease. The presence
of endometrial cells in the peritoneal fluid, indicating retrograde
menstruation, has been reported in 59% to 79% of women during menses or
in the early follicular phase, and these cells can be cultured in vitro. Also,
endometriosis is most often found in dependent portions of the pelvis—the
ovaries, the anterior and posterior cul-de-sac, the uterosacral ligaments, the
posterior uterus, and the posterior broad ligaments. Endometrium obtained
during menses can grow when injected beneath abdominal skin or into the
pelvic cavity of animals. Women with shorter intervals between menstruation
and longer duration of menses are more likely to have retrograde
menstruation and are at higher risk for endometriosis.
Coelomic metaplasia. Endometriosis may be due to metaplasia of the
coelomic epithelium from which the Mullerian system developed. This may
represent an abnormal response to estrogens; fibromyoma, cystic
endometrial hyperplasia, and ovarian follicular cysts are often associated with
endometriosis.

498
Induction theory. The induction theory is an extension of the coelomic
metaplasia theory. It proposes that an endogenous (undefined) biochemical
factor can induce undifferentiated peritoneal cells to develop into endometrial
tissue.
Genetic factors population studies. The risk or endometriosis is 7 times
greater if a first-degree relative has been affected by endometriosis. Because
no specific mendelian inheritance pattern has been identified, multifactorial
inheritance has been postulated. A relative risk for endometriosis of 7.2 has
been found in mothers and sisters, and a 75% (6 of 8) incidence has been
noted in homozygotic twins of patients with endometriosis.
Endometriosis also is linked to the presence of individual human
leukocyte antigens ( 28,29 and 30).
Incidence. The incidence of endometriosis for the women of
reproductive age oscillates from 7 up to 50 %.
Clinical classification of endometriosis. A number of classifications
have been developed for endometriosis. The most widely used system was
introduced by the American Society for Reproductive Medicine (ASRM) in
1979 and revised in 1985 and in 1996.(Fig. 215, Fig. 216). The ASRM system
assigns a point score for the size and location of endometriotic implants and
associated adhesions. The new ASRM endometriosis classification for
infertility includes the morphologic appearance of the implant. There is a
form published by the ASRM to assist in the management of endometriosis in
the presence of pelvic pain. Endometriosis is classified as minimal, mild,
moderate, and severe. Mild disease is characterized by superficial implants <5
cm2 in aggregate scattered on the peritoneum and ovaries. Minimal or no
adhesions are present. Moderate forms are characterized by multiple
implants, both superficial and invasive. Peritubal and periovarian adhesions
may be evident. Severe forms are characterized by multiple superficial and
deep implants, including large ovarian endometriomas. Filmy and dense
adhesions usually are present.

499
However, no staging system has been validated to correlate with the
symptoms of pain or infertility.

500
The following types of endometriosis are currently distinguished:
Peritoneal endometriosis: Peritoneal implants that consist of glandular
and stromal tissue and respond to hormonal changes associated with the
menstrual cycle showing cyclic changes similar but not identical to the normal
endometrium. These implants heal by fibrosis.
Ovarian endometriosis: benign, estrogen-dependent cyst also known as
“chocolate cyst” that contains thick, old blood that happens as a brown fluid.
This result from recurrent chronic bleeding from the endometriotic implants.
In long-standing endometriomas, the endometrioric tissue is gradually
replaced by fibrotic tissue.
Deep endometriosis: this form is characterized by proliferative
fibromuscular tissue with sparse endometrial glandular and stromal tissue,
with no surface epithelium. Deep endometriosis does not show significant
changes during the menstrual cycle. Growth of endometriotic nodules is
usually found in the uterosacral ligaments, the rectovaginal space, the upper
third of the posterior vaginal wall, the bowel, and the urinary tract.
Adenomyosis: uterine endometriosis, the growth of endometriotic
implant into - and through- the myometrial layer of the uterus. Uterine
endometriosis presented with asymmetrical enlargement of the uterus.
Disseminated endometriosis: it is the growth of endometriotic tissue in
various organs in the body including at the scar site.
Clinical picture. Small lesions may be found unexpectedly at operation,
but larger lesions cause the specific symptoms.
Pain. Pain in endometriosis presents as any of the following:
o Painful menstruation (dysmenorrhea)
o Painful intercourse (dyspareunia)
o Painful defecation (dyschezia) that may be cyclic or semi-cyclic.
o Painful micturition (dysuria)
o Lower back or abdominal discomfort
o Ovulation pain

501
o Chronic pelvic pain (non-cyclic abdominal pelvic pain of at least 6
months duration)
Atypical presentations include cyclic leg pain or sciatica (nerve
involvement), cyclic rectal bleeding or haematuria (bowel or bladder
invasion), and cyclic dyspnea secondary to catamenial pneumothorax.
These presentations are indicative of a more significant disease
involvement.
Infertility.
o Endometriosis is strongly associated strongly with infertility, mostly
due to pelvic adhesions or endometrial abnormalities. Moderate or
severe endometriosis markedly reduces fertility, because large pelvic
adhesions, when present, may prevent the release of eggs, block
sperm entry into the fallopian tube, and prevent the fallopian tube’s
ability to pick up eggs during ovulation. If pregnancy does occur,
there is often considerable improvement, at least for some time.
Abnormal uterine bleedings (heavy, prolonged menstrual bleedings),
and irregular bleeding occur from associated endometrial hyperplasia
or from uterine lesions.
Symptoms of intestinal obstruction may occur.
Chronic fatique and lack of working capacity.
The predictive value of any one symptom or set of symptoms remains
uncertain as each of these symptoms can have other causes (and a
significant proportion of affected women are asymptomatic).
Physical signs depend on the site of the disease:
“Chocolate cysts” (ovarian endometriosis) are tender, fixed bilateral
masses; simulating chronic salpingo-oophoritis, but without any history
of infection, fever or discharge.

502
Uterine lesions cause nodular or uniform enlargement, and may be
clinically indistinguishable from fibromyoma or from diffuse
hyperplasia. Three degrees of diffuse adenomyosis are known:
o the 1st is the - germination on depth of 1 cm;
o the 2nd is the germination up to the middle of endometrium,
o the 3rd is the germination up to serous coat.
Rectovaginal lesions are tender, hard, fixed, and simulate rectal
carcinoma. In contrast to carcinoma, rectal ulceration is rare and very
late.
Local lesions (e. g. in scars) may be tender at periods.
Endometriosis of bowel may be indistinguishable from carcinoma
without histological examination, except that there are often other
endometriomatous lesions.
Diagnosis. Generally, diagnosis of endometriosis is based on the
history, the symptoms and signs, physical examination and imaging
techniques.
Physical examinations should include an assessment to determine the
position, size, and mobility of the uterus. One can feel a tender nodule
behind the cervix during a combined vaginal and rectal exam, or the
uterus may be tilted back or retroverted. One or both ovaries may be
enlarged or fixed in position. Occasionally, endometriosis implants may
be visible in the vagina or the cervix. Rectovaginal examinations are
useful in determining presence of deep endometriosis.
Other than the examination of the pelvic region, inspection and
palpation of the abdomen is also advised.
Ultrasonography is the first-line investigational tool for suspected
endometriosis. It allows detection of ovarian cysts and other pelvic
disorders such as uterine fibroids. TAUS and TVUS are used for
diagnosis of endometriosis.

503
The serum level of cancer antigen 125 (CA-125) may be elevated in some
cases of endometriosis. But this is specific not only for endometriosis.
However, if the appearance of the ovarian cyst is suggestive of an origin
other than endometriosis, CA-125 and other tumor markers are
recommended.
Another serum protein, PP14, has been evaluated as a marker for
endometriosis. PP14 levels correlate with the severity of endometriosis
and decrease during suppressive medical treatment of endometriosis.
It has been traditionally believed that laparoscopy must be performed to
definitely diagnose endometriosis. Direct visualisation with
laparoscopy and histology has been regarded as the gold standard for
diagnosis. However, this view has been recently challenged as
nonsurgical diagnosis of endometriosis have proven to be highly
reliable.
In special cases, special imaging techniques such as computerized
tomography (CT ) scan, or magnetic resonance imaging (MRI) to gather
more information about patient’ pelvis may be used. These procedures
can identify cysts and help characterize the fluid within an ovarian cyst,
although an endometriotic cyst and a normal corpus luteum cyst may
have a similar appearance. These tests are useful when evaluating
women experiencing infertility and/or chronic pelvic pain.
Treatment. The treatment of endometriosis may be medical, surgical
and combined. Treatment must be individualized on the basis of age,
symptoms, desire for pregnancy, and extent of disease.
Medical treatment. Any treatment must be aimed at eliminating
pain and, if the patient desires, restoring fertility. Since ovarian hormones are
responsible for growth and activity in endometrium the immediate objective
of therapy must be to reduce their production or oppose their action.

504
A variety of steroids have been employed. At the beginning these were
mainly used to induce pseudo-pregnancy, the idea being that the ectopic
endometrium would undergo decidual change, which ultimately would be
destroyed by necrosis and healed by fibrosis. The contraceptive pills in high
dosage and provera (medroxy-progesterone acetate) were reasonably
successful in relieving pain but side effects such as weight gain, depression,
mastalgia and irregular break-through bleeding made them unacceptable to
some women. However, monophasic COCPs be used, 1 tablet daily from the
5th to 25th days of cycle, or without intermission during 6-12 months.
Provera: 20-30 mg/day orally for 6 months.
Danasol is an “impeded androgen”, i. e., a steroid hormone closely
related to testosterone, which inhibits pituitary gonadotropins, is anti-
estrogenic, anti-progestational, slightly anabolic, but has very little virilizing
activity. For the palliative treatment of endometriosis in patients with
moderate to severe disease or in patients who are infertile because of
endometriosis, the usual initial dosage of danazol is 800 mg daily given in 2
divided doses. Amenorrhea and a rapid improvement in painful symptoms
are best achieved at this dosage. Subsequent dosage may be gradually
reduced, depending on the patient's therapeutic response, to a level sufficient
to maintain amenorrhea. For the treatment of endometriosis in patients with
mild disease, the usual initial dosage is 200-400 mg daily given in 2 divided
doses. Subsequent dosage should be adjusted according to the patient's
tolerance and therapeutic response. Danazol therapy for the treatment of
endometriosis should continue uninterrupted for 3-6 months; however,
therapy may be extended to 9 months, if necessary. If symptoms recur
following discontinuance of therapy, treatment with danazol may be
reinstituted.
A daily dose of about 400 mg may abolish symptoms, and after about a
year may produce complete regression and even allow pregnancy. At that
dose level, side effects include amenorrhoea, weight gain, acne and muscle

505
cramps, none of them except amenorrhoea are invariably present. Increased
dosage may result in hot flushes and loss of libido, and mild but reversible
degrees of voice change and hirsutism.
Gestrinone. This is a derivation of 19-nortestosterone. It has slight
androgenic activity and is markedly anti-estrogenic and anti-progesterogenic.
It interacts with the pituitary steroid receptors and decreases gonadotrophic
secretion resulting in diminished follicular growth and anovulation. A bi-
weekly oral dose of 2. 5 to 5. 0 mg for 6 months induces amenorrhoea,
disappearance of pain and regression of the endometrial deposits. Side effects
include weight gain, acne, seborrhea and mild hirsutism.
Gonadotrophic-releasing hormone agonists (GnRH) are given
continuously to desensitize the pituitary receptors for the hypothalamic-
releasing hormone. GnRH suppresses the signals from the pituitary gland to
the ovaries that stimulate estrogen production, by doing this, also supress the
growth of endometriotic lesions. Leuprolide (Rx) recommended by 3.75 mg
IM monthly for up to 6 months or 11.25 mg IM every 3 months for 2 doses (6
months total).
Recommended duration of treatment is 6 months; may treat again for
additional 6 months, but with concomitant administration of norethindrone.
Surgical treatment. Small deposits on peritoneal surfaces, which are
found at laparotomy, may be coagulated with a diathermy needle. In women
over 40 more radical excision is advised, e. g. hysterectomy and removal of
both ovaries. Recto-vaginal lesions may be difficult to excise, and the
induction of the menopause by oophorectomy may be safer. Presacral
neurectomy is sometimes performed for the relief of pain. Operations for
intestinal obstruction are occasionally necessary.

506
Self test
1. Which of the following is a typical symptom associated with an abnormally
enlarged 6-8 week myomatous uterus?
A. urinary frequency
B. constipation
C. urinary retension
D. none of the above
2. Submucous myomas may be associated with all of the following signs and
symptoms except
A. abnormal bleeding
B. reproductive failure
C. anemia
D. parasitic infections
3. Abnormal uterine bleeding associated with myomata uteri is characterized by
all of the following except
A. a gradual increase in the bleeding
B. excessive bleeding during menses of normal length
C. the development of anemia
D. irregular cycles with menorrhagia
4. All of the following statements concernimng uterine myomas are true except
A. malignant degeneration occurs in less than 1% of uterine myomas
B. myomas can be found in the fallopian tubes and vagina more often
C. myomas rarely appear or grow after menopause
D. myoma and fibroid are synonyms
5. A benign tumor from a muscular tissue is a
A. leiomyoma
B. glioma
C. lipoma
D. teratoblastoma

507
6. The most frequent type of benign lesions of the uterus is
A. endometriosis
B. cervical polyp
C. trophoblastic disease
D. myoma
7. Myoma of the uterus more frequently appears
A. in the round ligament
B. in the uterine corpus
C. in the broad ligament
D. in the cervix
8. The sarcomatous degeneration of myomatous node is frequent in case of
A. subserous localization of nodes
B. intramural localization of nodes
C. submucous localization of nodes
D. any localization
9. “Chocolate cysts” are a characteristic for
A. myoma of the uterine body
B. ovarian endometriosis
C. sarcoma of the uterus
D. adenomyosis
10. What is not a characteristic for myoma of the uterine body?
A. slow growth
B. hyperpolimenorrhea
C. beginning of myoma in multiparae
D. beginning of myoma in reproductive age

508
Chapter 14. BREAST DISEASES
Evaluation of the female breast is an important part of the complete
gynecologic examination. The gynecologist performs more periodic medical
checkups of women today than does any other category of physicians. Because
they see such a large number of women for regular examinations,
gynecologists need to have a thorough knowledge of the natural history,
symptoms, and characteristic, physical findings of the various benign and
malignant breast disorders; they must also be skilled in the proper techniques
of breast examination and be able to teach self-examination to their patients.
It is essential, too, that they must be aware of the high risk category of women
especially deserving of regular surveillance. The gynecologist must be
completely familiar with the screening and diagnostic modalities available,
the proper indications for their use, and their limitations.
Although the screening and diagnosis of breast carcinoma is the
responsibility of the primary gynecologist, the patient with breast cancer
should be specifically managed by a coordinated multimodality team of
oncologists with a special interest in breast cancer. Therefore the
management of breast carcinoma is not included in this chapter, and the
interested reader is referred to a number of current texts and references for
more specifics on this subject.
Embriology.Breast development of the fetus begins at approximately 35
days of embryonic life. Embryologically, the epithelial ridge differentiates to
form lactiferous ducts and alveoli. The functional components of the breast
are complete at birth but usually lie dormant until puberty. Lactation is
occasionally noted in the neonate and is due to the influence of high levels of
maternal estrogen. As the systemic estrogen levels fall, lactation abates.
Breast development and maturation comprise one of the landmarks of
puberty. The process of breast development takes place over a three- to four-

509
year period, ultimately resulting in an adult breast in both form and function.
The process of breast development is under the influence of estrogen,
progesterone, and prolactin, ultimately resulting in the ability to lactate.
Anatomy. The functional unit of the adult breast is composed of
modified and specialized sebaceous glands. The breast parenchyma is located
underneath the superficial fascial layer of the chest wall and is composed of 15
to 20 lobes, arranged in a radial fashion, which drain to the nipple via a single
excretory duct (Fig. 218). Each lobe of the breast is composed of 30 to 40
lobules, which are the primary functional units. Each lobule is made up of 10
to 100 alveoli, which are lined by secretory cells. These are the secretory cells
that form milk under the influence of appropriate levels of prolactin. Milk is
transported from the alveoli by way of 2-mm collecting ducts to lactiferous
sinuses, which are approximately 5 to 8 mm in diameter. The lactiferous
sinuses ultimately drain through the excretory duct and into the nipple. The
ducts draining the lobules are supported by stroma composed of fibrous
tissue, fat, blood vessels, lymphatics, and nerves. Whereas the lobules occupy
the central portion of the breast, glandular tissue may extend toward the
axilla from the upper outer quadrant (tail of Spence). The periphery of the
breast is made up primarily of fat.
Fig. 218. Female breast anatomy

510
The breasts, which weigh 200 to 300 gm during the menstruating
years, are surrounded by fascial tissue and are supported by Cooper's
ligaments. These fibrous septa extend from the skin to the underlying
pectoralis fascia. With stretching caused by enlargement of the breast during
pregnancy and lactation, and with age, Cooper's ligaments become stretched,
resulting in diminished breast support.
Lymphatic drainage of the breast is especially important with regard to
the spread of breast carcinoma.
Examination and Evaluation of the Breast (see chapter 2). Routine
examination of the breast has its primary goal, the early detection and
improved survival of patients with breast carcinoma. Evaluation of the breast,
however, also allows recognition of more frequent, benign conditions and
often affords therapy to patients who presumed that they must suffer with
breast disease. Examination of the breast should therefore be part of the
routine physical examination, and breast self-examination should be taught
to every patient.
Breast examination should be carried out to maximize detection of
breast masses and associated changes in the breast, e. g., skin or nipple
retraction, subcutaneous edema, and nipple discharge. Examination in
several positions optimizes detection of abnormalities. The breast
examination is usually initiated in the sitting position; the breasts are
exposed, and the physician (or patient, viewing through a mirror) observes for
asymmetry of the breast. Special attention should be paid to possible skin or
nipple retraction or other skin changes, e. g., discoloration or edema. The
patient then raises her arms over her head, and the breasts are examined with
particular attention to the lower half of the breast. Elevating the arms pulls
upward on Cooper's ligaments and thereby accentuates skin retraction,
especially the lower half of the breast. The patient should then place her
hands on her hips and contract the pectoralis major muscle, again attempting
to accentuate skin retraction.

511
With the patient remaining in the sitting position the breast is palpated.
Examination using the whole hand as a unit and the pulps of the fingers
rather than the fingertips affords optimal capability to detect breast lesions.
The breast is palpated in an organized systematic way, with additional
attention to the supraclavicular areas, the neck, and the axillae. Any masses or
nodules palpated are noted, and attention is paid to the mobility or fixation,
size, and consistency of the mass(es). The patient is then asked to bend
forward and, with the breast dependent, is reinspected for other skin
retraction, e. g., subareolar retraction. Skin changes, especially edema of the
skin (peau d'orange), suggest an underlying cancer, although fat necrosis or
edema from obstructed lymph nodes may also cause these changes. Red,
warm skin (erythema) suggests inflammation, mastitis, or abscess, although
inflammatory carcinoma may also present erythema and pain. The nipple is
inspected with particular attention to retraction, ulceration, and discharge
(see later in this chapter for the evaluation of nipple discharge).
The patient then assumes the supine position with her arms raised over
the head. Palpation is repeated with attempts to spread out the breast tissue
so as little as possible is palpated at any one time. Again, the breast is
palpated systematically so that no areas go unexamined, with the palpation
proceeding along the tail of Spence to the axilla. Assessment on palpation
includes an evaluation of the background consistency of the breast. On
occasion, a premenstrual patient has engorged glandular tissue that is so
dense and nodular it is impossible to assess. This patient should be re-
examined several days after the menstrual period. On the other hand,
postmenopausal women should have no cyclic change in the breast (unless
they are receiving cyclic estrogen and progesterone). Examination of the
breast in the supine position includes also a search for masses or thickening.
Characteristics suggestive of benign or malignant disease are listed in table
15.

512
As the breast changes throughout a woman's lifetime, the examination
also changes. As previously noted, the menstrual woman displays increased
fullness of the breast along with engorgement of glandular epithelium, which
makes the breast more nodular and examination of the breast more difficult.
Women between 20 and 40 also tend to have an increased glandular/fat ratio
and an increased incidence of fibrocystic disease. These differences through
the menstrual cycle and throughout a patient's life should be taken into
account when the breast is evaluated.
The physician's annual breast examination is an opportune time to
teach the patient breast self-examination. Self-examination is to be
encouraged, and it is suggested that it must be performed on a monthly basis
following the menstrual period. Examination in the shower when the breast is
covered with soap increases tactile sensation by decreasing skin friction. The
patient should also be informed that repeated examinations allow her to
become familiar with her breasts, and she may therefore notice changes
sooner than her examining physician. Patient teaching information, written
material, videotapes, and models for practice examinations are widely
available.
Table 15
Findings on Breast Examination Suggesting Benign or Malignant
Conditions
Condition
Mass Nipple discharge Skin changes
Benign Soft Smooth Regular borders Not fixed
Clear or milky Bilateral
None
Malignant
Hard Irregular Fixed to skin or chest wall fascia
Bloody Unilateral
Skin or nipple retraction Peau d'orange changes of skin

513
Recognition and management of common breast disorders
Although carcinoma of the breast is the most significant breast disease
from the standpoint of the patient's overall present and future health and
well-being, patients come to the physician far more frequently because of a
variety of other benign breast disorders. Many of these disorders require
some form of evaluation and therapy for relief of symptoms; and in almost all
cases the possibility of malignancy must be excluded. This section
concentrates on the evaluation and management of such benign breast
conditions.
The therapy of breast carcinoma is constantly undergoing evolution,
and the student is referred to other current oncology textbooks for more
detailed discussions as to the appropriate surgical, medical, and
radiotherapeutic management of breast carcinoma. Because the gynecologist
most frequently sees patients with benign conditions and usually does not
manage patients once breast cancer is diagnosed, the benign conditions are
discussed in more detail in this section.
Fibrocystic changes
Fibrocystic changes of the breast are the most common benign breast
conditions encountered in the pre-menopausal woman. The older terms
fibrocystic breast disease, chronic cystic mastitis, and mammary dysplasia
have been replaced by the term fibrocystic changes. (Fig. 219) This condition
is not a true disease or pathologic condition; it is an exaggerated response of
breast tissue to fluctuating hormone levels. Therefore these changes are found
most frequently in women 20 to 50 years of age or, if estrogens are
prescribed, during menopause. The exact incidence is difficult to establish in
life, but pathologic findings suggest that at least 50 percent of autopsy breast
specimens contain fibrocystic changes. Some studies have suggested that one

514
in three premenopausal women have clinical evidence of fibrocystic changes,
and approximately 50 percent of these women have significant symptoms.
Fig. 219. Mammography: fibrocystic changes of the breast.
The etiology of fibrocystic changes is not clear. Proliferation and
hyperplasia of the lobular, ductal, and acinar epithelium is noted along with
proliferation of fibrous tissue in the breast. Because these tissues are under
the influence of estrogen and progesterone, it is hypothesized that this
condition is an exaggerated response of these tissues.
Symptoms of fibrocystic disease are usually worst during the
premenstrual days of the menstrual cycle. The patient usually experiences
cyclic bilateral breast pain with engorgement, increased density, increased
nodularity and tenderness, and occasionally a nipple discharge. Some
patients note a dominant cyst that may increase during the premenstrual
period.

515
Examination of the patient usually reveals a lumpy nodularity more
prominent in the upper outer quadrants of the breasts. The breasts may feel
rubbery with solid areas, microcysts, or macrocysts. The diagnosis is usually
based on these clinical signs and symptoms, although it may also be
established by biopsy findings. Biopsy may show adenosis and fibrosis, ductal
ectasia, apocrine metaplasia, papillomatosis, and intraductal epithelial
hyperplasia. These conditions are in general not associated with an increased
risk of breast cancer. On the other hand, findings of ductal hyperplasia with
atypia or apocrine metaplasia with atypia are associated with an
approximately fivefold risk of developing subsequent breast cancer. Another
type of diagnosis is mammography Treatment of fibrocystic breast disease
depends on the severity of symptoms. Initial therapy should include good
breast support with a firmly fitted brassiere worn both day and night. If a
dominant mass is noted on palpation or on mammography, biopsy should be
performed.
Premenstrual use of diuretics and salt restriction may be of some help in
reducing edema and breast fullness and tenderness. The complete elimination
of methylxanthines from the diet has been reported to reduce breast
symptoms in some patients, although the results of this therapy are debated
by others. If tried, caffeine (including colas, coffee, tea, and chocolates) must
be eliminated from the diet. The use of oral contraceptives and progesterone
helps some patients minimize their breast symptoms.
In patients with severe fibrocystic breast symptoms, danazol may be
tried. For the symptomatic management of fibrocystic breast disease, the
usual dosage of danazol is 100-400 mg daily given in 2 divided doses for four
to six months. Dosage should be individualized according to severity of the
disease and the patient's response to treatment. Since ovulation may not be
suppressed when danazol is administered at this dosage, an effective
nonhormonal method of contraception is recommended during therapy with
the drug. Regular menstrual patterns, irregular menstrual patterns, and

516
amenorrhea each occur in approximately one-third of patients receiving
danazol at a dosage of 100 mg daily. Irregular menstrual patterns and
amenorrhea occur more frequently when higher dosages are used.
Approximately 90 percent of patients experience a decrease in
symptomatology and decreased palpable nodularity with this regimen In most
patients, breast pain and tenderness are substantially relieved during the first
month of therapy, and eliminated in 2-3 months, but elimination of
nodularity usually requires 4-6 months of uninterrupted therapy. If
symptoms recur following discontinuance of therapy, treatment with danazol
may be reinstituted.
Unfortunately, danazol is costly, and this factor must be balanced
against the benefits the patient may experience. Alternative methods of
therapy for patients who have failed the above treatments include the use of
bromocriptine 5 mg per day or the antiestrogen tamoxifen.
Finally, in patients with severe symptoms who are unresponsive to
medical management, subcutaneous mastectomy with breast implant may be
advised. Usually, these patients are experiencing severe pain and have
undergone multiple biopsies of breast lesions. This therapy is also appropriate
in patients who have been found on biopsy to have evidence of the pre-
malignant conditions cited above.
Benign breast tumors
Fibroadenomas. Fibroadenomas are by far the most common breast
tumor and, although they may occur at any age, are most frequently seen in
women in their late teens and early twenties. They are rarely painful or
symptomatic in any way; the patient simply discovers a lump. Fibroadenomas
do not change during the menstrual cycle and are usually easily distinguished
from fibrocystic changes. Usually the mass (with an average size of 2. 5 cm) is
a firm, non-tender, rubbery-feeling, smoothly rounded, mobile, slippery
nodule most often found in the periareolar area. Its characteristic "feel" on

517
physical examination is almost diagnostic. It is most often solitary, although
occasionally (15 to 20 percent of patients) multiple lesions are present in one
or both breasts. It is sometimes difficult to distinguish fibroadenomas from
cysts. In these situations, needle aspiration is a reasonable first step of
evaluation. If the mass cannot be aspirated, surgical removal is indicated.
Because fibroadenomas persist and sometimes continue to enlarge, local
excision of these well encapsulated tumors is the treatment of choice. Most
often these procedures can be performed under local anesthesia.
Cystosarcoma phylloides. Cystosarcoma phylloides has been firmly
established as a giant, rapidly growing fibroadenoma, and approximately 25
percent of the lesions are malignant. They comprise the most common
sarcoma of the breast. The correct diagnosis is usually suggested by a rapidly
growing large, hard, lobulated mass in the breast, usually during the fifth
decade, without evidence of adjacent soft tissue or axillary involvement. Wide
local resection and sometimes mastectomy may be required because of the
large size of the benign cystosarcoma phylloides. When a microscopically
verified, truly malignant cystosarcoma phylloides is encountered, radical
mastectomy is the indicated treatment because it may be accompanied by
axillary lymph node metastases.
Intraductal papilloma. Intraductal papilloma is the second most
common benign breast tumor and the most frequent cause of bloody
discharge from the nipple. A papilloma most often arises in the lactiferous
sinus of the milk system, which is usually situated approximately at the
areolar margin. Intraductal papillomas are most often found in
perimenopausal women. The symptomatic intraductal papilloma may or may
not be large enough to be palpable, but the lobular duct system containing it
can usually be localized by the systematic periareolar point-by-point pressure
maneuver. A mammogram can also be helpful when localization is difficult.
Proper treatment is removal of the breast segment from which the
discharge has been demonstrated to arise or which contains the palpable

518
mass. Removal is important both to exclude the possibility that a much less
common intraductal papillary adenocarcinoma is responsible for the bloody
discharge and to put an end to the symptoms, which are a nuisance to the
patient.
Miscellaneous preast tumors. A variety of less common benign breast
tumors include lipomas, fibromas, sweat gland adenomas, hamartomas, and
hemangiomas. All of these lesions require local excision for definitive
diagnosis and treatment. Granular cell myoblastoma of the breast, a rare
benign tumor, is significant primarily because it sometimes presents all the
clinical signs of early breast cancer; even on cut section of the breast
specimen, it may grossly resemble a scirrhous carcinoma. As is true for solid
breast masses, biopsy and microscopic examination are essential to establish
a correct diagnosis and are usually the only way a granular cell myoblastoma
can be recognized as a benign lesion.
Postpartum mastitis is usually recognized as a localized, exquisitely
tender, edematous, erythematous region, usually of one breast. Treatment
goals are aimed at emptying the obstructed segment, which may be
accomplished by nursing, manual breast expression, or breast pumping. Ice
packs may reduce swelling, thereby allowing the duct better drainage.
Antibiotic therapy should also be employed, using a broad-spectrum
antibiotic aimed at the treatment of skin bacteria. Ampicillin and
erythromycin are the drugs most frequently selected for initial therapy.
Nonneoplastic lesions of the breast
The breast, by virtue of the fact that it is covered with skin, may develop
any of the skin changes or diseases noted elsewhere on the body. Because
these diseases are numerous, they are not discussed in this chapter, and the
student is referred to comprehensive dermatology textbooks for descriptions
and treatments of these diseases.

519
Sometimes mimic carcinoma may be caused by local breast trauma or
inflammation. They must be distinguished from malignancy, thus they are
discussed in more detail. Trauma to the breast may cause local tissue
swelling, subcutaneous bleeding, erythema, and pain. The collection of blood
in the subcutaneous tissues (hematoma) may cause additional localized
swelling, which ultimately becomes more apparent as an evolving ecchymotic
area. Treatment can usually be expectant, with spontaneous and
uncomplicated resorption usually occurring. Local application of heat and
mild analgesics may be necessary. On rare occasions, evacuation of a large
hematoma by aspiration or incision and drainage may be required.
Trauma may also cause fat necrosis, although the traumatic incident
may not be noted or remembered by the patient. The evolution of tissue
trauma with fat necrosis may ultimately lead to physical findings that closely
simulate breast cancer. As the traumatized area heals and repairs, fibrosis of
the subcutaneous tissue occurs, leading to fixation to the skin and ultimately
skin retraction. Because breast trauma is usually superficial, fibrosis and
fixation to the chest wall rarely occur. This subcutaneous scar may evolve into
dense fibrosis and a palpable mass or into a cystic cavity with calcification of
the walls. Even mammographic findings may be indistinguishable from those
of malignancy, and therefore excisional biopsy is invariably necessary to
establish the correct diagnosis.
Phlebitis of the thoracoepigastric vein (Mondor's disease) may also be
caused by local trauma or occur after cosmetic or diagnostic breast surgery.
The phlebitis of the superficial vein is progressive and painful, ultimately
resulting in a tender, fibrous cord underneath the skin. Skin retraction and
dimpling often occur, and the inexperienced clinician may mistake the
condition for some of the changes associated with breast cancer. However,
because of its superficial and linear nature, Mondor's disease must be
included in the differential diagnosis. Most often, the phlebitis resolves with

520
symptomatic therapy of heat and anti-inflammatory agents such as aspirin or
ibuprofen. Surgical intervention or anticoagulation is not necessary.
Infections in the nonpuerperal state are infrequent; and when they do
occur, the diagnosis of an inflammatory carcinoma must be considered.
Chronic subareolar abscess may occur in women in their thirties and forties.
These recurrent abscesses often drain spontaneously and ultimately may
cause areolar fistula. Obstruction of the ducts, leading to inflammation and
secondary infection, may be initially treated with heat, analgesics, and broad-
spectrum antibiotics. However, for chronic recurrent abscesses, surgical
removal of the duct and fistula tract is advised. It should be kept in mind that
inflammatory carcinoma of the breast may suggest the possibility of cellulitis
and breast abscess, and vice versa. That is, a breast abscess with surrounding
cellulitis may simulate inflammatory carcinoma, even to the cutaneous
thickening and the characteristic peau d'orange of the breast skin infiltrated
by an underlying carcinoma. Rarely, an ordinary noninflammatory type of
breast carcinoma becomes infected with or without prior ulceration of the
tumor and presents a confusing picture until biopsy clarifies the situation.
The most common causes of breast inflammation, cellulitis, and abscess
are associated with postpartum events. During the first one to three days after
delivery, breast engorgement is noted in most women, typified by swelling,
edema, and breast discomfort. A low- grade fever may be associated with this
diffuse process in both breasts. With adequate, firm breast support and ice
packs, the engorgement usually resolves within a few days. If the woman
wishes to breast-feed, it should be encouraged to reduce engorgement.
Obstruction of a duct during the postpartum period predisposes to infection
best cosmetic outcome. If a chronic infection in an old abscess cavity persists,
excision of that portion of breast may be required.

521
Breast cancer
Breast cancer is the most common invasive cancer in women, and the
second main cause of cancer death in women, after lung cancer.
Risk factors:
Personal history of breast cancer
o Women who had breast cancer in the past have a higher risk of
developing breast cancer again. The new breast cancer can
develop in the same breast as the first cancer or in the other
breast. Women who had ductal carcinoma in situ (DCIS) or
lobular carcinoma in situ (LCIS) have a higher risk of developing a
second breast cancer, but most women who had these cancers do
not develop breast cancer again.
Family history of breast and other cancers
o A family history of breast cancer means that one or more close
blood relatives have or had breast cancer. Some families have
more cases of breast cancer than would be expected by chance.
BRCA (breast cancer) gene mutations
o Some gene changes can increase the risk of developing certain
types of cancer. Inherited gene mutations are passed on from a
parent to a child. Only a small number of breast cancers (about
5%–10%) are caused by an inherited gene mutation. BRCA1
(breast cancer gene 1) and BRCA2 (breast cancer gene 2) are
normally found in the body. They are called tumor suppressor
genes because they appear to play a role in controlling the growth
of cancer cells. Mutations in the BRCA1 or BRCA2 genes can affect
them so they no longer control cancer growth. These mutations
are rare (1 in 500 people).
Certain genetic conditions

522
o Li-Fraumeni syndrome increases the risk of developing certain
types of cancer, including breast cancer, osteosarcoma, soft tissue
sarcoma and leukemia.
o Ataxia telangiectasia (AT) is caused by a mutation of the ATM
gene. This gene is responsible for repairing damaged DNA.
Certain families with a high rate of breast cancer have mutations
of this gene.
o Cowden syndrome is caused by a mutation in the PTEN gene,
which is normally a tumour suppressor gene. People with this
condition are more likely to develop breast cancer,
gastrointestinal cancers and thyroid cancer.
o Peutz-Jeghers syndrome may be related to a mutation of the
STK11 (also known as LKB1) gene. This gene appears to normally
function as a tumour suppressor gene. Peutz-Jeghers syndrome
increases the risk of developing gastrointestinal, breast, ovarian
and testicular cancers.
Other gene mutations
Ashkenazi Jewish ancestry
o BRCA1 and BRCA2 gene mutations are more common in
Ashkenazi women.
Dense breasts
Dense breasts have more connective tissue, glands and milk ducts than
fatty tissue. Breast density is an inherited trait.
Reproductive history
o Estrogen is the main hormone associated with breast cancer.
Estrogen affects the growth of breast cells. It plays an important
role in the growth of breast cancer cells as well. Early menarche,
late menopause are long estrogen’ influence; late pregnancy or no
pregnancy also lowers the total number of menstrual cycles a
woman has in her lifetime, and lead to longer estrogen exposure.

523
Exposure to ionizing radiation
Hormone replacement therapy
o Taking hormone replacement therapy (HRT) for a long time
increases the risk of breast cancer. This is especially true for HRT
that uses estrogen plus progestin (COCP).
Atypical hyperplasia
Alcohol
Being obese
Physical inactivity
High socio-economic status
Symptoms of breast cancer. Breast cancer can have a number of symptoms,
but the first noticeable symptom is usually a lump or area of thickened breast
tissue.
Other symptoms are:
a change in the size or shape of one or both breasts
discharge from nipples (which may be streaked with blood)
a lump or swelling in armpits
dimpling on the skin of breasts
a rash on or around nipple
a change in the appearance of nipple, such as becoming sunken into the
breast.
Classification. Types of cancer are usually classified based on the location and
aggressiveness of the disease.
The most common type is ductal carcinoma, which means the original
site of the disease is within the ducts (tubes) that transport milk to the nipple.
The cancer can be classified as in situ (DCIS) which means it is not invasive
and is contained inside the duct, or as an invasive breast cancer if it has
spread outside the duct.

524
Additional breast cancer types include: triple negative breast
cancer, inflammatory breast cancer, metastatic breast cancer, and other rare
forms of breast cancer.
The stages of breast cancer refer in numbers to the extent and evolution
of the breast cancer, but terms like “locally advanced” or “regionally
advanced” may also be used.
In stage 1, patients usually have invasive breast cancer, while 1A refers
to a tumor smaller than two centimeters that has spread to the lymph nodes
but not outside the breasts, and 1B to isolated cancerous patches rather than a
mass that measures 0.2 to two millimeters. Non invasive cancer, though
cancer, is concidered stage 0 (zero).
Stage 2 is when the tumor has spread to the auxiliary lymph nodes,
which can be two to five centimeters and remain localized (2A) or measure
two to five centimeters and 0.2 to two millimeters of metastasis.
Stage 3 describes a more aggressive form of invasive breast cancer and
is divided into three sub phases. Stage 4 indicates that the cancer has spread
to other organs of the body such as the lungs, the liver, distant lymph nodes,
skin, or bones.
Breast cancer screening and diagnosis. Mammographic screening is
the best available method of detecting an early breast lesion. Women with a
higher-than-average risk of developing breast cancer may be offered
screening and genetic testing for the condition.
As the risk of breast cancer increases with age, all women who are 50-70
years old are invited for breast cancer screening every three years.Women
over 70 are also entitled to screening and can arrange an appointment
through their GP or local screening unit.
The diagnosis of brteast cancer is based on anamnestic data, clinical
findings, imaging studies, biopsy with histological investigation. Breast cancer
is treated using a combination of surgery, chemotherapy and radiotherapy.

525
Surgery is usually the first type of treatment, followed by chemotherapy or
radiotherapy or, in some cases, hormone or biological treatments.
The type of surgery and the treatment are depend on the type of breast
cancer. In a small proportion of women, breast cancer is discovered after it's
spread to other parts of the body (metastasis). Secondary cancer, also called
advanced or metastatic cancer, isn't curable, so the aim of treatment is to
achieve remission (symptom relief).
Self test
1. The most important aspect of examination of the breast is
A. the use of the tips of fingers in performing the examination
B. examination in the sitting position
C. the use of a circular motion to cover all quadrants of the breast
D. the amount of time spent in performing the examination
2. A dominant mass is discovered in a 30-year-old woman. Which of the
following reflects current practice in the management of breast disease?
A. a mammogram should be performed immediately
B. aspiration should be attempted as an office procedure
C. an ultrasound should be ordered
D. the patient should be looked for an open biopsy
3. Successful management of bilateral mastalgia is associated with
A. the use of Danocrine for a 6-month trial
B. abstinence from caffeine
C. the amount of time spent with the patient
D. the use of vitamin E
4. Estrogen replacement therapy
A. is essential for all postmenopausal women to prevent osteoporosis
B. is currently used by the majority of postmenopausal women
C. is widely prescribed as a result of recent controlled randomized trials
D. has not been associated with an increased incidence of breast cancer
5. Symptoms of fibrocystic disease of the breast
A. are usually the worst during the premenstrual days of the menstrual cycle
B. disappear during the premenstrual days of the menstrual cycle
C. have no changes during the menstrual cycles

526
D. are usually the worst during the follicular phase of the menstrual cycle
6. The most freguent type of a benign tumor of the breast is
A. lipoma
B. fibroadenoma
C. adenoma
D. sarcoma
7. Fat necrosis of the breast may happen due to
A. traumatic lesions
B. inflammations
C. hormonal disbalance
D. congenital abnormalities
8. Chronic recurrent subareolar abscesses should be treated with
A. surgical removal of the duct and fistula tract
B. antibiotic therapy
C. physiotherapy
D. complex conservative treatment
9. Bloody discharge from the nipple is the common symptom of
A. intraductal papilloma
B. Mondor's disease
C. chronic subareolar abscess
D. postpartum mastitis
10. One of the most common types of breast lesion is
A. fibroadenoma of the breast
B. intraductal papilloma
C. cystosarcoma phylloides
D. fibrocystoma

527
Chapter 15. PREMALIGNANT DISEASES OF THE
VULVA AND VAGINA. CANCER AND SARCOMA OF
THE VULVA AND VAGINA
There are a lot of atrophic and hypertrophic conditions caused by a
number of stimuli. The lesions are characterized by shrinking, whitening or
reddening exclusive to the skin of the vulva. These include background
processes and true precancerous lesions. Background processes present
abnormal conditions of the skin, which may lead to the development of
precancerous conditions or cancer of the external genital organs. These
lesions do not have a uniform microscopic appearance.
Precancerous (premalignant) conditions of vulva are diseases which can
exceed into carcinomas and are called preblastomatoses.
Background diseases of the external genitalia and vulva
Background diseases include chronic dystrophic processes without
cellular displasia and cellular atypia, characterized with proliferation,
atrophic changes, without invasion. Background vulvar disease present any
chronic, dystrophic recurrent skin damages.
Background lesions of the vulva, or Nonneoplastic epithelial disorders of
vulva and mucosa, according to classification system for "Epithelial Vulvar
Disease", include:
o Lichen sclerosus
o Squamous hyperplasia
o Other dermatoses
o Mixed neoplastic and nonneoplastic disorders

528
Lichen sclerosis
The cause of this condition is not known. This condition occurs
frequently in postmenopausal women. This is a systemic atrophic dystrophy,
which occurs on the vulva and perineum. The affected areas appear whitish
and glistening with clear margins. The affected skin has a “cigarette-paper”
appearance. During the acute phase these areas may be red and purple. The
affected area on the vulva extends to the anus in a shape of Figure 8 causing
involutional adhesion of labia minora to the labia majora, thus burying the
clitoris and causing shrinkage of the introitus. (Fig.220). The leading
symptom is intense itching. If secondary infection occurs, ulceration and
contractures may follow resulting in dyspareunia and dysuria. Histologically
there is a thin inactive epithelium and loss of elastic tissue.
Fig. 220. Lichen sclerosis of the vulva.
Prognosis: areas of dysplasia or malignancy may develop in this lesion.
Other outcomes:
o Symptom improvement

529
o Disease remission
o Disease recurrence
o Disease complications
o Non-compliance with treatment
o Incidence of squamous cell carcinoma
Diagnosis is based on:
o Physical examination
o Biopsy
o Immunology (autoantibody screen, if indicated)
o Microbiology (swabs, not routinely recommended)
o Assessment of complications of lichen sclerosus, including malignancy,
scarring, sensory abnormalities (dysaesthesia), and psychosexual
problems
Histological examination (biopsy) is advisable to exclude atypical
changes. Patients under routine follow-up will need a biopsy if:
o there is a suspicion of neoplastic change, i.e. a persistent area of
hyperkeratosis, erosion or erythema, or new warty or papular
lesions;
o the disease fails to respond to adequate treatment;
o there is extragenital lichen sclerosus (LS), with features suggesting
an overlap with morphoea;
o there are pigmented areas, in order to exclude an abnormal
melanocytic proliferation;
o second-line therapy is to be used.
An autoantibody screen to look for associated autoimmune disease is
useful if there are clinical features to suggest an autoimmune disorder. In
particular, thyroid disease is common in women with LS.
Swabs are indicated in erosive disease to exclude herpes simplex
or Candida as additional complicating problems. Retesting for these

530
infections may be necessary in disease that flares or fails to respond to
treatment.
Complications:
Squamous cell carcinoma (SCC) - surgery has to be individualized
according to the tumour size and location, particularly in early invasive
disease.
Scarring
o Introital narrowing - this is rare, but, if significant and causing
dyspareunia or difficulty with micturition, surgery may need to be
considered.
o Pseudocyst of the clitoris- occasionally, clitoral hood adhesions
seal over the clitoris and keratinous debris builds up underneath
forming a painful pseudocyst. This requires a subtotal or total
circumcision).
o Stenosis of the urethral os - if this results in an impaired urinary
stream, referral for urological assessment is advisable.
Sensory abnormalities: dysaesthesia
o Vestibulodynia and Vulvodynia - These conditions may occur
after an inflammatory condition of the vulva or vestibule.
Typically, the patient remains symptomatic despite objective
clinical improvement or resolution of the skin lesions.
Neuropathic pain does not respond to topical corticosteroids, and
treatment must be directed to the eradication of the neuronal
sensitization. Initially, 5% lidocaine ointment is recommended,
with the addition of pain-modulating oral medication, such as a
tricyclic antidepressant or gabapentin, in unresponsive cases.
Psychosexual problems
o Women who have any chronic genital disorder will often lose their
interest in sexual activity, leading to problems with sexual
dysfunction.

531
Treatment. Better personal hygiene and using cotton underwear would
reduce the vulval moisture.
The recommended and accepted first-line treatment is the very potent
topical corticosteroid clobetasol propionate 0.05%. The regimen
recommended for a newly diagnosed case is clobetasol propionate 0.05%
ointment applied once daily, at night, for 4 weeks, then on alternate nights for
4 weeks, and then twice weekly for a further 4 weeks, before review. The
rationale for once-a-day application is based on pharmacodynamic studies
showing that an ultrapotent steroid only needs to be applied once a day on
extragenital skin. If symptoms recur when the frequency of application is
reduced, the patient is instructed to use the treatment more often until the
symptoms resolve. They can then try to reduce the frequency again.
Oral antihistamines and topical antipruritic agents may help to relieve
itching. A local application of estrogen cream is recommended. Estrogen may
have little effect or no direct effect on the epidermis but improves the
vascularity of the underlying dermis. Topical corticosteroid such as 1%
hydrocortisone aqueous cream has a beneficial effect on hypertrophic lesions.
In atrophic lesions, treatment with androgenic steroids is found to be more
useful, for example, 2% testosterone propionate ointment twice daily for 3 to
4 weeks. Oral retinoids or vitamin A analogues have also been used for this
condition. Topical calcineurin inhibitors, Ciclosporin, Methotrexate and other
immunosuppressive agents, may be administered.
Surgical therapy for the Lichen sclerosis of the vulva has also been
reported. Cryosurgery, photodynamic therapy, phototherapy, laser ablation,
or simple vulvectomy, though rarely, is the surgical methods followed.
Follow-up. Long-term follow-up in a secondary care specialist clinic is
appropriate for patients with genital LS associated with troublesome
symptoms, localized skin thickening, previous cancer or vulval intraepithelial
neoplasia (VIN), or pathological uncertainty about VIN. Biopsies of persistent
ulcers, erosions, hyperkeratosis and fixed erythematous areas are advised to

532
exclude intraepithelial neoplasia or invasive SCC. These patients usually have
LS with a histological pattern that has features of both LS and lichen planus
with squamous cell hyperplasia. Clinically these patients seem to have an
overlap syndrome and their disease runs a relentless course despite trials of
various therapies, and a small percentage do go on to develop one or more
SCCs.
Lichen simplex chronicus
Lichen simplex chronicus (previously known as neurodermatitis) occurs
in normal skin which becomes dry, thick, scaly, white but sometimes
pigmented, and fissured in response to the trauma of constant scratching.
Lichenification is a similar change which is superimposed on another
pathology, e.g. eczema or a contact dermatitis. These lesions are usually not
symmetrical within the vulva and usually occur in areas where they are
accessible to scratching.
Treatment consists of the use of emollients or low to moderate potency
topical corticosteroids. Sometimes sedation at night is useful to stop
nocturnal scratching.
Lichen planus
The lesions of lichen planus may be seen within mucous membrane or
on cutaneous surfaces, e.g. the inner surfaces of the wrists and lower legs.
These cutaneous lesions are usually red or purple flat topped nodules or
papules with an overlying white lacy patterned appearance (Wickham’s
striae). Involvement of the vulva is usually with areas of pruritus with white
patterned areas which are sometimes elevated and thickened (hypertrophic
lichen planus) or may appear red and raw with features of erosion; changes
within the mouth upon buccal mucosa or involving the gingival margin may
frequently be seen. The areas of change on the vulva may extend into the
vagina and subsequent desquamation will leave scarring, stenosis and
533
adhesions. Histology will show liquefactive degeneration of the basal
epidermal layer, long and pointed rete ridges, with parakeratosis and
acanthosis, and a dense dermal infiltrate of lymphocytes close to the dermal
epidermal margin. When the condition is severe treatment can be difficult,
requiring systemic steroids, azathioprine, or other immune modifying agents;
these may include cyclophosphamide, cyclosporin although the results are not
always consistent. Lesser symptoms particularly those externally on the vulva
can be managed with the application of topical corticosteroid.
Squamous hyperplasia
Squamous hyperplasia represents inadequate proliferative reaction of
vulvar epithelium on influence of plenty of irritating factors. It can develop in
any age, but more frequent than all registers in pre - and postmenopausal
periods. Microscopic signs include an acanthosis and hyperkeratinization.
Papillomatous structures usually absent, that distinguishes squamous cell
hyperplasia from acuminate condilomas.
Principles of diagnosis and management are similar to the Lichen
sclerosis.
Vulval ulceration
Vulval ulceration may be infective (syphilis chancroid, genital herpes,
HPV – vulval warts, lymphogranuloma venerum), aphthous or associated
with Behqet’s syndrome, Stevens-Johnson syndrome, dermatitis artefacta,
benign mucous membrane pemphigoid, pyoderma gangrenosum, Crohn’s
disease, and toxic epidermal necrolysis. (Fig. 221) These conditions are
uncommon. Sometimes the diagnosis can be made clinically but occasionally
biopsy will be necessary and may require immunofluorescent techniques, e.g.
benign mucous membrane pemphigoid is associated with immunoglobulin G
(IgG) deposition within the area of the basement membrane. The

534
management include treatment of underlying condition with local application
of antipruritic, moisturizing agents.
Fig. 221. Genital Ulcers: ulcers caused by genital herpes
Other dermatoses
This group of nonneoplastic epithelial disorders of vulva and mucosa
include contact dermatitis, eczema, psoriasis, which are not precancerous
conditions, but may have features of chronic, recurrent diseases with signs of
dystrophic or atrophic changes, proliferation without invasion and cellular
atypia.
The main features of recommended management is local application of
moisturizing cream or mild to moderate topical corticosteroids. Sedation at
night is useful to stop nocturnal scratching.
True precancerous lesions of vulva
The term” precancer” was chosen intentionally as it has a broad,
generic connotation that changes are present in the tissue which indicate that
a lesion, if not removed, will, with a high degree of likelihood, progress to
535
invasive carcinoma. The majority of true precancerous lesions of the vulva are
of epidermal origin. Less commonly they will arise from epidermal
appendages (e.g. hidradenoma, sebaceous adenoma), the mesoderm
(fibroma, lipoma, neurofibroma, leiomyoma, lymphangioma, haemangioma)
or from the greater or lesser vestibular glands (adenofibroma, adenoma. The
description of squamous vulvar precancerous lesions is based on the concept
of vulvar intraepithelial neoplasia (VIN) and incorporates a three grade
evaluation of the intensity of dysplastic changes (low-, intermediate- and
severe grade). There is little doubt that the intraepithelial neoplasms of the
female lower genital tract should, when they are high grade, be considered to
be precancerous. The prospective follow-up studies of such lesions have
established without a doubt that this categorization is appropriate. The use of
the term "precancer" for the low-grade lesions is problematic, however,
because it is now apparent -particularly for the uterine cervix -that some of
the epithelial changes which include the morphological features of neoplasia
may, in fact, be acute human papilloma virus (HPV) infections of the
epithelium and that the majority of such lesions will not progress to high-
grade intraepithelial neoplasia nor to invasive cancer. In the low-grade lesions
it is difficult, without HPV testing and typing, to predict the biological
behaviour of the epithelial change, but the term "precancer" has still to be
used because of the potential for such lesions to progress to high-grade
intraepithelial disease and, subsequently, to invasive cancer.
Classification of vulvar intraepithelial neoplasia
Squamous vulvar intraepithelial neoplasia (VIN):
o VIN I, mildest form
o VIN II, intermediate
o VIN III, most severe form including carcinoma in situ of the vulva
Non-squamous intraepithelial neoplasia
Extramammary Paget's disease
Tumors of melanocytes, non invasive

536
Squamous Vulvar Intraepithelial Neoplasms
Vulvar intraepithelial neoplasia (VIN) is graded as VIN 1 (mild
dysplasia), VIN 2 (moderate dysplasia), or VIN 3 (severe dysplasia or CIS) on
the basis of cellular immaturity, nuclear abnormalities, maturation
disturbance, and mitotic activity.
In VIN 1, immature cells, cellular disorganization, and mitotic activity
occur predominantly in the lower one third of the epithelium. x Dyskeratotic
cells and mitotic figures occur in the superficial layer.
In intermediate grade (VIN 2) 2/3 of the epithelial lining has dysplastic
changes. Other typical features are presence of immature cells, as well as
cellular disorganization, and mitotic activity. Additional cytopathic changes of
HPV infection, such as perinuclear halos with displacement of the nuclei by
the intracytoplasmic viral protein, thickened cell borders, binucleation, and
multinucleation, are common in the superficial layers of VIN, especially in
VIN 1 and VIN 2. These viral changes are not definitive evidence of neoplasia
but are indicative of viral exposure. Most vulvar condylomas are associated
with HPV-6 and -11, whereas HPV-16 is detected in more than 80% of VIN
cases by molecular techniques.
In VIN 3, immature cells with scanty cytoplasm and severe chromatinic
alterations occupy most of the epithelium, it is also known as vulvar
carcinoma in situ. (Fig. 222). VIN 3 can be unifocal or multifocal. Typically,
multifocal VIN 3 presents with small hyperpigmented lesions on the labia
majora. Some cases of VIN 3 are more confluent, extending to the posterior
fourchette and involving the perineal tissues. The term bowenoid papulosis
(bowenoid dysplasia) has been used to describe multifocal VIN lesions
ranging from grade 1 to 3. Clinically, patients with bowenoid papulosis
present with multiple small pigmented papules (40% of cases) that are
usually less than 5 mm in diameter. Most women with these lesions are in
their 20s, and some are pregnant. After childbirth, the lesions may regress

537
spontaneously. However, the term bowenoid papulosis is no longer
recommended by the ISSVD.
Fig. 222. VIN3 – carcinomain situ of the vulva.
Etiology. The cause of squamous neoplasia of the vulva is still unknown.
It was associated with syphilis and other granulomatous lesions, herpes
simplex viral infection, obesity, diabetes mellitus and poor hygiene. Many
authors have commented on the role that recurrent irritation appears to play,
and some have implicated previous pelvic irradiation. There is also an
association with HPV (HPV 16,18 and 31), immunosuppression , etc. VIN is
seen in patients of a wide age range, being reported in teenagers as young as
14 years and in women of 80 years of age (mean 40-45 years).
Clinical features. Most will present with pruritus, burning, and pain,
but up to 20% may be asymptomatic. Examination may reveal multicentric or
confluent areas of different size, colour including white, red and brown,
ulcerated and warty lesions, However, sometimes the lesions will only become
apparent on colposcopic examination with application of acetic acid.

538
Any part of the vulva may be involved, most commonly the perineal
skin, the periclitorial area and labia minora; approximately one-third will
have extension to involve the perianal area. requiring the anus to be examined
too.
Diagnosis. The diagnosis is always based on a careful inspection and a
targeted biopsy and histopathology, with disorderly maturation, abnormal
mitoses, basal and parabasal pleomorphism, and koilocytosis in many lesions.
Treatment. Spontaneous regression of lesions can occur in young
women and observation may well be all that is required in young or pregnant
patients unless they are symptomatic. Nevertheless, all patients need in
careful follow up.
Popular treatment modalities include:
topical chemotherapy,
carbon dioxide (CO2) laser ablation,
surgical excision.
For medical therapy, reported to be effective in at least some cases of VIN,
following are recommended:
Imiquimod cream, applied 3 times weekly for 12 to 20 weeks. This
result in red inflamed and eroded tissue often accompanied by
considerable discomfort.
5-fluorouracil (5-FU) cream, applied twice daily for several weeks. This
causes quite severe chemical dermatitis (several weeks) of the vulva
which takes some 5-6 weeks before healing starts and the results are
generally disappointing; thus, will not be tolerated by all women. It is
less effective than imiquimod cream.
Photodynamic therapy (PDT) requires specialised equipment and can
also be very painful.
The mainstay of treatment is to remove all affected tissue with a margin
of apparently unaffected tissue. This may be done by surgical incision.
Sometimes a complete vulvectomy is undertaken because of the extent of

539
disease or because of several independent areas of VIN. The carbon dioxide
laser may be used with treatment success greater than 90%. The depth of skin
and appendage removal in VIN is 1 mm in non-hairy and 2 mm in hairy skin
assigned as appropriative for successful treatment. Rarely, skin appendage
involvement to a depth of 4.6 mm may occur.
Paget’s Disease of the vulva
The vulva is one of the sites for extramammary Paget’s disease. Paget's
disease of the vulva predominantly affects postmenopausal white women, and
the presenting symptoms are usually pruritus and vulvar soreness. The lesion
has an eczematous, erythematous, or scaly appearance macroscopically with a
clearly demarcated and slightly elevated edge. The lesion usually begins on
the hair-bearing portions of the vulva. It may extend to involve the mons
pubis, thighs, and buttocks. Extension to involve the mucosa of the rectum,
vagina, or urinary tract also has been described . The more extensive lesions
are usually raised and velvety in appearance.
The clinical manifestations consist in varying degrees of pruritus,
burning and tingling of the involved vulval areas. The histologic picture shows
little or no alteration of the general pattern of maturation of the epidermis.
Superficial keratinization is present. The epidermis contains distinctive clear
cells (Paget’s cells), which are large, round or oval and have a pale cytoplasm.
The diagnosis is based on histology. Most cases of vulvar Paget's disease are
intraepithelial. Because these lesions demonstrate apocrine differentiation,
the malignant cells are believed to arise from undifferentiated basal cells,
which convert into an appendage type of cell during carcinogenesis. The
“transformed cells” spread intraepithelially throughout the squamous
epithelium and may extend into the appendages. In most patients with an
underlying invasive carcinoma of the apocrine sweat gland, Bartholin gland,
or anorectum, the malignant cells are believed to migrate through the dermal

540
ductal structures and reach the epidermis. In such cases, metastasis to the
regional lymph nodes and other sites can occur.
Management involves identification of any underlying or associated
malignant lesion, and wide excision. Prognosis is influenced by the nature
and stage of the associated neoplasm, if present. Paget’s disease will recur in
about one-third of those without associated neoplasm, due to the multicentric
distribution and difficulty in ensuring complete excision of the lesions.
Background diseases of the vagina
Vaginal background lesions are non-neoplastic processes, represent any
chronic mucosa damages, characterized with dystrophic changes without
cellular dysplasia and cellular atypia, proliferation, atrophic changes, without
invasion. Recurrent dystrophic or proliferative process is a background for
development of dysplasia, and the risk of neoplastic appearance cannot be
excluded.
Clinical picture consist in varying degrees of pruritus, burning,
discharge, dyspareunia.
The diagnosis is based on:
Evaluation of previous history (duration of chronic diseases,
irrespective for treatment, recurrence of process)
Physical examination
Microbiology (swabs, not routinely recommended)
Assessment of complications of chronic vaginitis, including scarring,
sensory abnormalities (dysaesthesia), and psychosexual problems
(dyspareunia).
Aceto-white colposcopy
Targeted biopsy with histological examination
These diseases may be presented with patches of white or red color,
often named leukoplakia or erythroplakia. A cornification of multi-layered flat

541
epithelium, thinning of superficial layers of epithelium with the phenomena
of cornification are typical findings in these cases. Erythroplakia has the
appearance of bright red spots with a brown tint, sharp-edged scopes and
brilliant surface.
Clinical picture consist in varying degrees of pruritus, burning,
discharge, dyspareunia.
Treatment consists of:
Oral antihistamines and topical antipruritic agents
Local application of estrogen cream
Topical corticosteroid
In atrophic lesions: androgenic steroids (2% testosterone propionate
ointment twice daily for 3 to 4 weeks.
Oral retinoids or vitamin A analogues have also been used for this
condition.
Surgical excision or cryolysis of pathological foci is more effective.
True precancerous lesions of the vagina
Precancerous conditions of the vagina are diseases which can exceed
into carcinomas and are called preblastomatoses. Vaginal intraepithelial
neoplasia (VAIN) may be extensions onto the vagina from the primary
cervical intraepithelial neoplasia(CIN), or they may be satellite lesions
occurring mainly in the upper vagina. Because the vagina does not have a
transformation zone with immature epithelial cells to be infected by HPV, the
mechanism of entry of HPV is by way of skin abrasions from coitus or tampon
use. As these abrasions heal with metaplastic squamous cells, the HPV may
begin its growth in a manner similar to that in the cervical transformation
zone.
VAIN can occur in just one area of the vagina, but it more often affects
several different areas at once (multifocal).
Classification of VAIN:

542
Three degrees (stages) of VAIN are distinquished: VAIN 1, 2, and 3.
In VAIN 1, a third of the thickness of the cells in the vaginal skin are
abnormal,
VAIN 2 - two-thirds of the thickness of the surface layer of the vagina is
affected.
AIN 3 - the full thickness of the surface layer of the vagina is affected. It
is also known as carcinoma in situ, or stage 0 vaginal cancer
Causes of VAIN:
HPV is a very common infection. Types 16 and 18 are most commonly
associated with VAIN.
Other factors that depress the body's immune system also need to be
present for VAIN to occur. These include Herpes simplex virus (HSV),
Cytomegalovirus, smoking, inherited immunity problems, particular
medicines (for example those taken after transplant surgery), and some
rare bone marrow and blood disorders.
Clinical features. VAIN doesn't cause any symptoms. Most women are
diagnosed with it while having medical tests for other reasons.
VAIN can’t be detected by the naked eye.
VAIN can be detected by the presence of abnormal cells in a Pap-tests
Diagnosis. Most useful method of VAIN diagnosis is a targeted biopsy
with histologic examination. Typically, the lesions are located along the
vaginal ridges, are ovoid in shape and slightly raised, and often have surface
spicules. VAIN 1 lesions usually are accompanied by a significant amount of
koilocytosis, indicating their HPV origin. As the lesions progress to VAIN 2,
they have a thicker acetowhite epithelium, a more raised external border, and
less iodine uptake. When VAIN 3 occurs, the surface may become papillary,
and the vascular patterns of punctation and mosaic may occur. The more
coarse the punctation or mosaicism, the more severe is the dysplasia.
Treatment.

543
Local ablation treats VAIN by removing or destroying the abnormal
cells in the vagina. This can be done in two ways:
o Carbon dioxide (CO2) laser treatment. A laser is directed at the
abnormal cells and destroys them. This procedure is usually
carried out under a general anesthetics.
o Diathermy treatment. This treatment is sometimes used to
remove the abnormal cells. It’s done under local anesthetics. A
thin wire uses an electric current to destroy the affected area.
Surgery may be recommended if there is any possibility of there being
undetected cancer in the vagina.
o It may also be used if VAIN comes back after previous treatment.
o Surgery may involve removing part or all of the vagina (partial or
total vaginectomy).
Other modalities are:
Radiotherapy
Chemotherapy cream (topical fluorouracil 5FU in multifocal lesions is
used)
Follow-up: colposcopy twice a year.
Cancer and sarcoma of external genitalia and vagina
Vulvar cancer
It more often occurs in elderly women and is localized in the area of
clitoris, labia majora and minora, and Bartholin’s gland. Vulvar cancer is
uncommon, the incidence varying from 0.5 to 2 per loo ooo women per year.
Histological variants of vulvar cancer.
Squamous cancers account for 90% of malignant vulvar
neoplasms and 5% of all female genital cancers. They metastasize

544
to the local lymph nodes, primarily the superficial and deep
inguinal nodes and they may be involved bilaterally. They usually
present with a nodule or ulcer and may cause pruritus or soreness
and pain. Bleeding and an offensive odor may be present with
larger lesions.
Verrucous carcinomas and basal cell carcinomas are squamous
variants and rarely if ever metastasize locoregionally and
therefore management is primarily aimed at local disease control
by whichever route affords the lowest morbidity. Verrucous
carcinomas present as slow growing wart-like lesions with a
tendency to local recurrence after excision.
Malignant melanoma of the vulva accounts for 10% of all vulvar
malignancies. The overall 5-year survival ranges between 8 and
50% and appears to be worse than for cutaneous melanomas
elsewhere. The single most important prognostic indicator in this
disease is the depth of invasion. Non-vulvar cutaneous melanoma
is usually staged according to the depth of histological
involvement. As some observers question the presence of a
papillary dermis in vulvar skin, absolute depth might be the best
compromise and invasion greater than 1.75 mm has such a high
risk of recurrence that even the use of radical surgery with
bilateral block dissection is unlikely to improve survival.
Adenocarcinomas of the vulva are exceedingly rare and are more
likely to represent metastases from another site.
Sarcomas are very uncommon and in general are biologically
similar to soft tissue sarcomas at other sites. Generally there is
poor prognosis after the appearance of regional or distant relapse.
Wide local excision appears to offer the best chance of preventing
local recurrence. Elective treatment of the regional nodes is not
indicated and there is no advantage in resecting metastatic nodes.

545
The role of adjuvant radiation and chemoradiation has not been
assessed largely because of its rarity.
Metastatic tumours are rare and account for about 8% of all vulvar
neoplasms. Cervix, endometrium and renal carcinomas have been
the most frequently documented primary sites.
Carcinoma of Bartholin’s gland is also rare and may be either
squamous, adenocarcinoma or an adenoid cystic carcinoma. They
occur more often in younger, premenopausal women and overall
have a survival of about 35% at 5 years.
Vulvar cancer is divided into infiltrative and nodular (with possible
ulceration).
Stages of lesions:
I – lesions 2 cm in size confined to the vulva or perineum;
II – tumor 2 cm in largest dimension confined to the vulva or
perineum, no nodal metastasis;
III – tumor of any size with adjacent spread to the lower urethra, the
vagina, or the anus or with unilateral regional lymph nodes metastasis;
IV – tumor invаding any of the following: upper urethra, bladder,
rectum, pelvic bone, or bilateral regional nodes. In stage IV distant metastasis
occur.
Itching, pain, leucorrhea, and sanguineous discharge occur rather
rarely. The final diagnosis is established after biopsy and histological
examination. (Fig. 223).
Treatment. The objectives of managing the primary lesions are to
remove the cancer, minimize the risk of local recurrence and preserve as
much function as possible. These objectives have initially been addressed by
modifications of the surgical approach and more latterly by considering
combined modality management, especially combinations of surgery and
radiotherapy. The site, size and relation of the lesion to important functional

546
structures will determine the most appropriate method to treat the vulvar
lesion.
Two broad categories of patient can be identified at the outset: those
who have small unifocal vulvar lesions with no clinical evidence of nodal
involvement (early disease), and those who have more advanced vulvar
disease and/or clinical evidence of nodal involvement (late disease). Radical
vulvectomy is excessive treatment for the majority of unifocal and early
cancers. Wide local excision is usually sufficient for the majority of TI and T2
tumors.
The elderly woman with extensive or multifocal disease with an
associated symptomatic maturation disorder such as lichen sclerosus might
well gain an overall benefit from radical vulvectomy with subsequent grafting.
Conversely, the young woman with a clitoral cancer might initially be
managed by radiotherapy, reserving surgery for failed local control. These
types of cases form the basis for local management of advanced vulvar
lesions. The prime objective is to maximize local control, closely followed by
consideration of further function and cosmesis in that particular woman.
Combined radiotherapy is also used. External beam megavoltage
radiotherapy is the treatment most frequently applied as an adjuvant in
women found to have two or more involved lymph nodes following groin node
dissection. The treatment field encompasses the superficial and deep inguinal
and pelvic nodes. It is in this role that radiotherapy is most frequently used in
treating vulvar cancer.

547
Vaginal cancer
Vaginal cancer is rare accounting for only 1-2% of all gynecological
malignancies. It is most often metastatic in nature. It arises as primary
squamous cancers or is the result of extension from the cervix or vulva.
Primary cancer of the vagina occurs very rarely. A wide age range (18-95
years) with the peak incidence in the sixth decade of life and a mean age of
approximately 60-65 years is typical for vaginal cancer.
The etiology is unknown, but several predisposing factors are
distinguished:
Prior lower genital tract intraepithelial neoplasia - mainly cervical
intraepithelial neoplasia (CIN) and/or cervical carcinoma.
HPV infection. This may explain the relative frequency of
multicentric lower genital tract tumors.

548
Previous gynecological malignancy. Several authors report
approximately one-quarter or as high as one third of patients as
having had a previous gynecological malignancy.
Clinical features. The symptoms depend on the stage of the tumor. The
most common presenting features are as follows:
Vaginal bleeding, accounting for more than 50% of presentations.
Vaginal discharge.
Urinary symptoms.
Abdominal mass or pain.
Asymptomatic. Approximately 10% of tumors will be
asymptomatic at the time of diagnosis. Vaginal tumors may be
easily missed at vaginal examination, particularly when a bivalve
speculum is used. Careful inspection of the vaginal walls whilst
withdrawing the speculum is necessary in order to avoid this as
otherwise the blades of the speculum may obscure a tumor on the
anterior or posterior vaginal wall.
Tumors can occur at any site in the vagina. The upper third of the
vagina is the site most frequently involved either alone or together with the
middle third in approximately two-thirds of cases. Approximately 1 in 6 will
be found to involve the entire length of the vagina. The size of tumor shows
great variation at presentation ranging from small ulcers less than 1 cm in
diameter to large pelvic masses, although the majority of tumors are 2-4 cm
in diameter. Vaginal cancer may be exophytic (looking like cauliflower) and
endophytic, with infiltration of adjacent tissues.(Fig. 224)

549
Fig. 224. Vaginal cancer.
Staging is carried out according to the FIGO classification (Table 16).
Table 16.
FIGO clinical staging of primary vaginal carcinoma
FIGO stage Definition
0 VIN 3 (carcinoma in situ)
I Invasive carcinoma limited to vaginal wall
IIA Carcinoma involves subvaginal tissue but does not extend
to parametrium
IIB Carcinoma involves parametrium but does not extend to
pelvic side wall
III Carcinoma extends to pelvic side wall
IVA Involvement of mucosa of bladder or rectum or direct
extension beyond true pelvis
IVB Spread to distant organs

550
Diagnosis. This is best performed under general anesthesia.
The site and limits of the tumor can be accurately determined and
a full thickness biopsy taken for histological analysis.
Combined rectal and vaginal examination is particularly helpful in
order to determine if there is any extension of the tumor beyond
the vagina and the extent of any spread.
Cystoscopy and sigmoidoscopy are required to exclude or confirm
the involvement of bladder or rectum.
Chest X-ray
Intravenous urogram.
More complex radiological investigations such as rectal
ultrasound scanning or MRI may be helpful in selected instances
in order to define the dimensions of the tumor.
Treatment. The majority of cases of vaginal carcinoma are treated using
pelvic radiotherapy although surgical excision is an appropriate form of
management in selected cases. Experimental chemotherapeutic regimes are
being developed both alone and in conjunction with radiotherapy for
advanced cases or recurrent disease.
Sarcomas of the vagina
Leiomyosarcomas are most frequently diagnosed with other types
reported including adenosarcoma and angiosarcoma. Sarcoma of the vagina
rarely occurs in adult women. It is more frequent in girls and is commonly
localized in the area of the clitoris, labia, and vagina. Sarcoma appears as a
limited node, growing into the underlying tissues and disintegrating with the
formation of ulcers.
Treatment. Primary therapy is surgical removal of affected organs and
subsequent radiotherapy. Adjuvant radiotherapy has been advocated for high
grade tumors or in recurrent disease. Adjuvant chemotherapy has been
utilized by some but has not been shown to confer a survival advantage in soft

551
tissue sarcomas of the extremities. The majority of women present with
discomfort and/or bleeding.
Self test
1. Which of the following is precancerous disease of external genitalia?
A. vulval fibroma
B. hidradenoma
C. vulvitis
D. leukoplakia of the vulva
2. Kraurosis of the vulva
A. usually happens in young women
B. is connected with itching
C. is not characterized with psychoemotional disturbances
D. is a hyperplasia
3. Lichen sclerosis occurs in
A. postmenopausal women
B. reproductive age
C. pubertal age
D. premenopausl age
4. Sarcoma of the vulva usually occurs in
A. postmenopausal women
B. reproductive age
C. pubertal age
D. premenopausl age
5. Vaginal cancer is most often
A. a metastatic process
B. an original process
6. Displasia of the vulva is
A. a true precancer of the vulva

552
B. a background process of the vulva
C. a true malignant growth of the vulva
D. a benign lesion of the vulva
7. In case of Paget’s disease one can find
A. a red colored, well defined maculae, which may be infiltrated and inflamed
B. dry spots of a white or yellow colour mainly over the labia majora
C. thinning and fibrosis of the vulval skin, causing stenosis of the vaginal
introitus
D. cauliflower lesion of the vulval tissue
8. The affected areas appear whitish and glistening with clear margins in
A. a Paget’s disease
B. a vulval cancer
C. a leukoplakia of the vulva
D. a lichen sclerosis
9. Fibroma of the vulva is
A. a malignant tumor
B. precancerous lesions
C. a background process
D. a benign tumor
10. The final step of the diagnosis of vulval cancer is
A. the patient’s complaints and anamnesis
B. clinical findings
C. colposcopy and colpomicroscopy
D. histological data

553
Chapter 16. «BACKGROUND» PROCESSES AND
PREMALIGNANT LESIONS OF CERVIX. CERVICAL
CANCER
«Background» processes of cervix of the uterus
The pathology of the cervix is one of the most frequent groups of female
genital diseases, accounting for 10-15% of all patients in gynecological
departments. Among them, background and precancerous diseases constitute
a group of increased risk of development cervical malignancies. Background
diseases of the vaginal part of the cervix are pathological processes that are
characterized by chronic recurrent course, hyperplasia of epithelial cells with
the formation of new glandular structures with preservation of epithelial
normoplasia, ie, the correct mitotic division of epithelial cells, their
differentiation, maturation, exfoliation are preserved. In the future, against
the background of ongoing hyperplasia, a real tumor process can occur.
Background processes present abnormal conditions of the congenital or
acquired nature, which may lead to the development of precancerous
conditions or cancer of the cervix. These diseases include cervical erosions,
pseudoerosions, chronic cervicitis, polyps, cervical ectropion, leukoplakia,
cervical warts.
Risk factors
Inflammatory processes
o necrobiosis of the multilayered squamous epithelium of the cervix
and its desquamation because of the inflammatory process
followed by the formation of erosion areas, the healing of which is
due to the overgrowth of cylindrical epithelium of the cervical
canal, which is not characteristic for the vaginal portion of the
cervix. In this zone pseudoerosion is formed. The human

554
papillomavirus (HPV) plays important role in the development of
dysplasia of the cervix.
Traumatic lesions of the cervix after childbirth or abortion
o leading to the violation of trophism and innervation of tissues
Hormonal misbalance:
o shifts in the metabolism of estrogens with the predominance of
estradiol and increase in oxygenated forms of 17-ketosteroids
Immune disorders:
o increase of cytotoxic T-lymphocytes, decrease of Langerhans cells
in the cervix, the degree of changes is proportional to the level of
immunosuppression
Sexual activity:
o early onset of sexual life and multiple sex partners
Involutional (age-related) changes of the pelvic organs
o as well as a decrease in total body resistance, the age-related
changes of metabolic and hormonal balance.
Smoking
o the risk of the disease increases with the increase in the number of
cigarettes per day and the duration of smoking
Hereditary factor
o the risk of cervical cancer in women with a history of family
history.
Methods of diagnostics
The following methods of diagnostics of background diseases are currently
used:
Evaluation of anamnestic data
gynecological examination (specular and bimanual examination)
laboratory study: CBC, Urinalysis, high vaginal swab for microscopic

555
and bacteriological examination, Pap-testing, Polymerase Chain
Reaction (PCR), Immunoenzyme Analysis to determine the type of
specific infectious agent, etc.
simple and extended colposcopy, colpomicroscopy, chromocolposcopy
with targeted biopsy, endocervical biopsy to exclude atypical changes,
as well as dysplasia
evaluation of the hormonal balance
TVUS;
optical coherence tomography.
Chronic cervicitis
Cervicitis is an inflammation of the cervix, acute and chronic forms are
distinguished. Typical symptoms are:
release of purulent or mucopurulent endocervical exudate in the
endocervical canal
sustained, easily induced endocervical bleeding, when the cotton
swab gently passes through the cervical os.
Noninfectious and infectious cervicitis are distinquished.
Noninfectious cervicitis can be caused by the following:
Local trauma - eg, cervical irritation caused by tampons, a cervical cap,
the string from an intrauterine contraceptive device, a pessary, or a
diaphragm
Radiation
Chemical irritation - eg, vaginal douches, latex exposure, or
contraceptive creams
Systemic inflammation
Malignancy
Infectious cervicitis may be caused by:
Chlamydia trachomatis, Neisseria gonorrhoeae,

556
herpes simplex virus (HSV).
Human papilloma virus (HPV)
Trichomonas vaginalis
Others
The development of the disease is determined by a combination of
several pathogenetic links. The signs of the inflammatory process are
expressed moderately and are localized mainly in endocervix. Mucous cervical
canal becomes edematous, thickened, folded. There is fullness of the vessels,
lymphohystiocytic inflammatory infiltrates are formed, epithelial cells secrete
more mucus. In exo - and endocervix, regenerative processes slow down and
dystrophic changes occur. In the lower layers of the mucosa, connective tissue
elements grow. The terminal orifices of the glands overlap with a flat
epithelium with the formation of retinal cysts. As the disease progresses,
connective tissue and cervical muscles are involved in inflammation.
The cellular and humoral immune system functions inferiorly: the
number of B- and T-lymphocytes decreases, T-dependent immune responses
are inhibited, and phagocytic activity is disrupted. As a result, the causative
agents of the infection are able to persist in both the cervical epithelium and
the cells of the immune system. In cervical mucus, the level of
immunoglobulins G and M decreases against the background of a high
content of IgA. Developed autoimmune processes with the phenomenon of
"molecular mimicry" between foreign proteins and proteins of their own
tissues.
Chronic recurrent cervicitis lead to hyperplasia, dystrophic, atrophic
changes, ulcerations, which are a prerequisite for cervical dysplasia. Acute
cervicitis does not require surgical treatment. When the inflammation
persists to a chronic stage, it is no longer confined to the mucosa but has
spread to the underlying tissue, whether on the exposed vaginal surface or
within the canal.

557
Chronic cervicitis is seen in women with laceration of the cervix, where
there is superadded infection with mixed vaginal flora. The endocervicitis
gives rise to an excessive vaginal mucoid discharge with an active
endocervical lining growing over to replace the squamous epithelium around
the external os to present as erosion.
Some of the mucous glands get blocked with pent up secretions, distend
these glands so, that they appear as whitish-yellow Nabothian cysts.
In the clinical picture of chronic cervicitis there are certain features,
which need individual attention. These features are eversion, erosion, cyst
formation, leukoplakia, whitish-yellow Nabothian cysts, and the sequelae of
laceration. To understand the appearance on examination and the deep
conditions to be dealt with, it is necessary to understand eversion, erosion,
and cyst formation.
Cervical eversion
In chronic cervicitis, the inflammatory infiltration causes marked
thickening of the mucosa and submucosal tissues. As these tissues become
more and more thickened, they push out in the direction of least resistance,
which is at the external-os. This rolling out (eversion) from inflammatory
infiltration is most marked in the cervix, which has been lacerated, but it is
found also in chronic cervicitis in nulliparas.
Cervical erosion. Pseudoerosion
The true cervical erosion and pseudoerosion are distinguished.
The essence of the process of erosion is most accurately indicated by the
very translation of this concept - "corroding" or "destruction." Erosion - is a
small inflammation or sore that has a bright red color. (Fig. 224) It is the
damaged epithelium of the mucosa, located in the area of the outer exit of the
cervix in the vagina. This erosion easily bleeds when touched. It is visible

558
from the side of the vagina on the cervix. This sore or wound on the vaginal
portion of the cervix can last for two weeks. If timely treatment is not
provided, erosion will pass into pseudo-erosion. So, pseudo-erosion is the
phase of chronic cervicitis. In this case, in the area of the entrance to the
cervical canal one can see the area on which the tissue has grown: normal
squamous epithelium cells of external surface of the cervix are replaced by
columnar cells from the cervical canal. These cells appear red and inflamed,
but they are not cancerous, and the cervix itself does not literally erode. At the
beginning of the development of pseuderosion, erosive glands can form, in
this case the gynecologist diagnoses glandular pseudo-erosion of the cervix. It
can be observed for several years.(Fig. 225).
When the inflammatory process ceases and the cells begin to be
replaced by the epithelium, pseudo-erosion becomes glandular-epidermal. If
the disease progresses, the erosive glands are blocked by secretion, and cysts
appear on the affected area. It is dangerous that they can be infected, so the
inflammatory process may increase.
Fig. 224.Cervical erosion

559
Often this pathology is congenital and does not affect normal sexual life,
pregnancy and childbirth, which makes it possible to consider it as a variation
in the development of the female reproductive system. Assessing the
condition of the surfaces and making sure that there is no risk of tissue
degeneration or the development of inflammatory processes, the gynecologist
can completely abandon the appointment of any treatment, recommending
only regular observation. At the same time, congenital erosion can cause
inconvenience even in the period of the appearance of the first menstruation,
as well as the true, resulting from the transmitted sexual infection.
If untreated, acquired pseudo-erosion can lead to a serious
inflammatory process, infertility, dysplasia, malignant tumor. In addition, it
is worth considering that erosion is constantly recurring, so woman need to
be extremely cautious. That is why it is known as background disease.
Diagnostic points
The principal diagnostic difficulty in connection with chronic cervicitis
is the question as to whether there is or not a beginning of malignant disease.
Chronic cervicitis, in its various forms and with its long-continued irritation,
is an important factor in the development of cancer in this situation. This is
readily appreciated when we consider the persistent irritation from erosion,
eversion, and cyst formation, with the resulting proliferative cell changes in
this danger area where two types of epithelium meet.
There are no symptoms in the real beginning. As far as this form of
cancer is concerned, the so-called "early" symptoms are early only in the
symptomatic sense. They are the first symptoms noticed by the patient, but
they do not represent the early stage of the pathologic process. The
microscopic change, which constitutes the beginning of tumor does not cause
bleeding or discharge. When these symptoms appear, the cancer usually has
deep prolongations.

560
Cervix cancer is usually preceded by local chronic cervicitis. There are
many things not yet known about cancer, but two known things are a). cancer
development favors in a susceptible individual chronic irritation; b). this
tendency is increased by the aging process (involution). In the cervix this
chronic irritation usually appears in the form of chronic cervicitis. Even when
marked, this causes little discomfort beyond annoying discharge, which is
easily controlled by douches. In milder cases, there may be no troublesome
discharge to call the patient's attention to this minor disturbance. In the
meantime, however, the mild inflammation penetrates into the cervical
glands and keeps up chronic irritation.
Diagnosis of pseuderosion:
Analysis of the microflora, for this is taken a smear from the urethra,
vagina and cervix to timely identify the inflammatory process.
Pap-testing
A hormone level test is performed.
Colposcopy makes it possible to completely examine the cervix under a
microscope, to reveal the structure of tissues.
Cervical biopsy with histological exam
Pseudo-erosion treatment
As a first stage of treatment, antimicrobial agents and antibiotics may be
required. In severe cases, surgical methods of treatment are used:
Diathermocoagulation is the cauterization of an electric current.
Laser surgery (carbon-dioxide laser).
Cryodestruction (cryoablation) - freezing by the action of nitrogen.
Radio wave effect.
Chemical coagulation.
Thus, a woman with pseudo-erosion should be constantly observed at
the gynecologist, only in this way serious complications can be avoided.

561
Cyst formation
The formation of small retention cysts in the cervix is due to obstruction
of the ducts of normally situated glands by inflammatory infiltration and to
the formation of glandlike cavities in areas of erosion. If there has been a
laceration of the cervix, the resulting scar tissue may obstruct ducts and this
aids in cyst formation.
These retention cysts are felt as small hard nodules, like shot of various
sizes, in the cervix, and may give rise to an erroneous diagnosis of cancer. The
cervix may be honeycombed with these small cysts, producing a condition
designated as "cystic degeneration" of the cervix. The mucus in these cysts is
usually clear and presents the characteristic tenacious, stringy consistency. In
some cases a cyst may contain pus and appear as a yellow spot.
Cervical polyps
Polyp formation in the cervix is due to chronic irritation from the
persisting inflammation and discharge. In most cases the polyp represents
simply a localized and projecting portion of the thickened mucosa (mucous

562
polyp). Occasionally, however, the polyp is a projecting portion of a
carcinoma, and as the distinguishing features can be determined with
certainty only by microscopic examination, all polyps should be sent for
laboratory examination. (Fig. 226).
Fig. 226. Cervical polyp.
These are often due to endocervical hyperplasia caused by endocervicitis
or, rarely, by oral contraceptives. These small, pea-sized mucus polyps, give
rise to a vaginal discharge, which may be mucoid and blood-stained. The
patient may also complain of postcoital bleeding.
Speculum examination shows pedunculated mucus polyps. These can be
easily twisted off, avulsed and sent for pathologic examination.
Leukoplakia
Leukoplakia is the term applied to certain small white areas occasionally
seen on the cervix. They are smooth and there may be several ones, differing
in size and shape. (Fig . 227). If the patch is wiped off, it is likely to return in a
few days. Leukoplakia, like other forms of chronic irritation in the cervix, is

563
important because of its relation to the development of carcinoma in this
location. The white color is due to abnormal proliferation of certain cells of
the epithelial layer, the types of proliferation differing somewhat in different
cases. In some cases the type of proliferation borders very closely on the
malignant one.
Leukoplakia of the cervix should be promptly removed, the same as any
other area of chronic irritation. There is likely to be associated irritation in the
form of erosion or cyst formation, and the whole affected area should be
removed by electric wire-loop conization or by conical excision with the knife.
The removed tissue is of course to be subjected to thorough microscopic
investigation. In this connection it is to be remembered that when the
specimen is removed the leukoplakic color distinction disappears. On this
account it is important, before removing such specimen, to mark the
leukoplakic area with one or two small sutures just outside the boundary—
otherwise it will be missed in the laboratory.
Fig. 227. Cervical leukoplakia, front view, macroscopic.

564
Laceration
Laceration of the cervix in labor is one source of infection and resulting
chronic cervicitis. Also, the laceration has much to do with the shape and
appearance of the chronically inflamed cervix. The splitting of the cervix by
the laceration allows much more rolling-out of the infiltrated tissues. This
eversion is a progressive process, and may go on till the laceration-notch is
obliterated and the cervix appears round like a ball.
Troublesome symptoms from cervix laceration and conditions requiring
treatment are due largely to inflammation. If there is no complicating
inflammation, the torn surfaces may fall together and unite, leaving only a
small notch, or they may heal over by granulation and scarring, leaving two
thin lips. In either case the condition causes no trouble and requires no
treatment. But if inflammation supervenes, there follows the interesting
series of progressive changes resulting in the conditions seen in chronic
cervicitis.
Precancerous lesions of cervix
Precancerous conditions imply processes in which hypertrophy,
proliferation, and various abnormalities in the vital activity of epithelial cells
occur. Precancerous conditions arise due to benign processes of ectopy and
metaplasia, which are observed in the epithelium. Ectopy develops when
cylindrical epithelial cells are formed from the reserve cells or the flat
epithelium is replaced by a cylindrical one that covers the area of the cervical
canal. Metaplasia is characterized by the transformation of reserve cells into a
tissue of flat epithelium. In general, precancerous conditions of the cervix
may be described as presence of various dysplasias. Dysplasia means the
presence of cells of an abnormal type within a tissue, which may signify a
stage preceding the development of cancer, also the abnormal growth or
development of a tissue or organ.

565
Precancerous conditions have the potential to develop into cancer. With
a precancerous condition, abnormal changes have taken place in the cells of
the cervix. Over time, some of these precancerous changes can turn into
cancer if left untreated. It may take many years (typically about 10 years or
more) for precancerous conditions to progress into an invasive cervical
cancer, but sometimes this can happen in less time.
Precancerous conditions of the cervix occur in an area called the
transformation zone. This is where one type of lining (glandular, columnar
cells of the cervical canal) is constantly being changed into another type of
lining (squamous cells of superficial layer of vaginal portion of the cervix).
The transformation zone is an area of changing cells, and it is the most
common place on the cervix for abnormal cells to develop. These abnormal
cells can be detected on a Pap smear. The location of the transformation zone
varies among women. In teenage girls, the transformation zone is on the
immature cervix's outer surface and is more susceptible to infection than in
adult women. In older women, the transformation zone may be higher in the
cervical canal.
The transformation of columnar cells into squamous cells is a normal
process, but it makes the cells more sensitive to the effect of human
papillomavirus (HPV).
Precancerous changes in the cervix are quite common. They can develop
at any age, but they occur most often in women in their 20s and 30s.
The main risk factor for precancerous changes in the cervix and cervical
cancer development is infection with the human papillomavirus (HPV).
Precancerous conditions in the cervix are described based on how
abnormal cells look under the microscope and how severe the cell changes
are. They are grouped based on the type of cell that is abnormal.
The mainstay of cervical cancer screening for the last 60+ years has
been the Papanicolaou test. The Papanicolaou test, also known as the Pap
test or the Pap smear, was developed in the 1940s by Georgios Papanikolaou.

566
It involves exfoliating cells from the transformation zone of the cervix to
enable examination of these cells microscopically for detection of cancerous
or precancerous lesions.(see Chapter 2). Precancerous conditions in the
cervix are described based on how abnormal cells look under the microscope
and how severe the cell changes are. They are grouped based on the type of
cell that is abnormal.
The current classifications of precancerous lesions of cervical squamous
epithelium is based on new findings on HPV-related carcinogenesis; the key
assumption in this context is that two early genes of HPV (E6 and E7) trigger
neoplastic transformation of the squamous epithelium. These types are
referred to as transforming HPV infections. After constant expression of E6
and E7 oncogenes the oncoproteins encoded by E6 and E7 bind to cell cycle
proteins, leading to loss of cell cycle control. Mutations gradually accumulate
and cells become genetically unstable. HPV represents a family of double-
stranded, circular DNA viruses that can infect skin or mucosal cells, including
the anogenital region and the oral cavity, and may be transmitted easily via
sexual intercourse or direct contact. More than 100 types of HPV exist, 12 of
which can involve the anogenital region and are considered "high risk" or
oncogenic in nature. These include HPV types 16, 18, 31, 33, 35, 39, 45, 51, 52,
56, 58, and 59. Of these, HPV 16 is responsible for the largest number of CIN
3 and cervical cancer cases, and HPV 16 and 18 combined are thought to be
responsible for nearly 70% of all cases of cervical cancer. Although HPV is a
necessary factor in the development of cervical dysplasia that can eventually
lead to cervical cancer, most women infected with HPV will not develop
cervical dysplasia. The presence of high-risk HPV DNA is accompanied by
cytologic abnormalities approximately one third of the time. Whether an HPV
infection will progress relates to the persistence of the infection and also
possibly to the immune response and smoking status of the woman.
Classification of precancerous lesions of the cervix. Since the Pap
smear was introduced in 1943, a number of methods have been developed to

567
classify the results. The two methods commonly used today are the CIN
Grading System and the Bethesda System.
CIN Grading System for Cervical Dysplasia uses term cervical
intraepithelial neoplasia (CIN). Cervical intraepithelial neoplasia refers to
new abnormal cell growth. Intraepithelial refers to the surface layers of the
cells. The CIN System grades the degree of cell abnormality numerically, CIN
1 is the lowest and CIN 3 is the highest.
The Bethesda System to Stage Cervical Dysplasia is a system of terminology
for reporting the results of cervical cytology. It was developed in 1988, revised
in2001 and 2014 and is now widely used in the world. It uses the
term squamous intraepithelial lesion (SIL) to describe abnormal changes in
the cells on the surface of the cervix. Squamous refers to thin, flat cells that lie
on the outer surface of the cervix. An intraepithelial lesion occurs when
normal cells on the cervical surface are replaced by a layer of abnormal cells,
and these changes are classified as high grade or low grade. Precancerous
conditions of the cervix occur in an area of transformation zone. This is where
one type of lining (glandular, columnar cells) is constantly being changed into
another type of lining (squamous cells). The transformation of columnar cells
into squamous cells is a normal process, but it makes the cells more sensitive
to the effect of human papillomavirus (HPV). And so, abnormal
(precancerous) changes may happen in both glandular, columnar cells of the
cervical canal and squamous cells of superficial layer of vaginal portion of the
cervix.
The abridged Bethesda system (2001) presented in table 17.

568
Table 17
The 2001 Bethesda system (Abridged)
Specimen adequacy
Satisfactory for evaluation (note presence/absence of endocervical/
transformation zone component)
Unsatisfactory for evaluation...(specify reason)
o Specimen rejected/not processed (specify reason)
o Specimen processed and examined, but unsatisfactory for
evaluation of epithelial abnormality because of (specify reason)
General categorization (optional)
Negative for intraepithelial lesion or malignancy
Epithelial cell abnormality
Other
Interpretation/result
Negative for Intraepithelial Lesion or Malignancy
o Organisms
-Trichomonas vaginalis
-Fungal oganisms morphologically consistent with
Candida species
-Shift in flora suggestive of bacterial vaginosis
-Bacteria morphologically consistent with Actinomyces
species
-Cellular changes consistent with herpes simplex virus
Other non-neoplastic findings (Optional to report; list not
comprehensive)
o Reactive cellular changes associated with
- inflammation (includes typical repair)

569
-radiation
- intrauterine contraceptive device
o Glandular cells status posthysterectomy
o Atrophy
Epithelial Cell Abnormalities
Squamous cells
o Atypical squamous cells (ASC)
- of undetermined significance (ASC-US)
- cannot exclude HSIL (ASC-H)
o Low grade squamous intraepithelial lesion (LSIL)
encompassing human papillomavirus/mild dysplasia/cervical
neoplasia (CIN) 1
o High grade squamous intraepithelial lesion (HSIL)
encompassing moderate and severe dysplasia, carcinoma in
situ; CIN 2 and CIN 3
o Squamous cell carcinoma
Glandular cell
o Atypical glandular cells (AGC)
- Endocervical
- Endometrial
- Glandular
o Atypical glandular cells, favor neoplastic
o Endocervical adenocarcinoma in situ (AIS)
o Adenocarcinoma: Endocervical endometrial, extrauterine, NOS
Other (List not comprehensive)
Endometrial cells in a woman ≥40 years of age
(http://www.svgo.es/sites/default/files/Bethesda%202001pdf.pdf)

570
Interpretation of the results of cytology and description of the results are
presented in Table 18, Table 19.
Table 18.
Abnormal squamous cells
Bethesda system Also includes Description
Atypical squamous cells
(ASC)
Cells do not appear
normal.
Atypical squamous cells
– undetermined
significance (ASC-US)
Cells do not appear
completely normal.
It is uncertain what the
cell changes mean.
This is considered a
mild abnormality
Atypical squamous cells
– cannot rule out high-
grade squamous
intraepithelial lesion
(ASC-H)
Cells do not appear
normal.
It is uncertain what the
cell changes mean, but
a high-grade lesion
cannot be ruled out.
This may have a higher
risk of becoming
precancerous.
Low-grade squamous
intraepithelial lesion
(LSIL)
mild dysplasia / CIN 1:
older terms
There are early changes
to the cells.
This is considered a
mild abnormality.
High-grade squamous
intraepithelial lesion
(HSIL)
moderate or severe
dysplasia/ CIN 2 or
CIN 3 (older terms)
There are marked
changes to the size and
shape of the cells, and
cells are considered
abnormal and have the
potential to develop
into cancer

571
carcinoma in situ (CIS)
Cancer cells are found
only in the surface layer
of cells lining the cervix
but have not spread
into the deeper tissues
of the cervix or
surrounding tissue
(non-invasive or pre-
invasive).
Squamous cell
carcinoma
Cancer
Table 19
Abnormal glandular cells
Bethesda system
Also includes
Description
Atypical glandular cells
(AGC)
endocervical dysplasia
atypical hyperplasia
endocervical glandular
atypia
cervical intraepithelial
glandular neoplasia
(CIGN) grade 1 or 2
Cells do not appear
normal.
This is considered a
significant abnormality.
Adenocarcinoma in situ
(AIS)
endocervical AIS
CIGN grade 3
Cancer cells are found
in the glandular tissue
of the cervix
(endocervix) but have
not spread into the
deeper tissues of the
cervix or surrounding
tissue (non-invasive or
pre-invasive).
Adenocarcinoma Cancer

572
Treatment. Conservative treatment is indicated in younger women and
in mild degree. Surgical procedures that preserve the uterus and may permit
future childbearing include cryosurgery (freezing), laser surgery, loop
electrosurgical excision procedure (LEEP) or cold-knife conization.
Cryosurgery, laser surgery, and LEEP can be performed in the out-patient
office or short procedure facility, often with local anesthesia. A cold-knife
conization is a more extensive operation that involves removal of part of the
cervix under general anesthesia. Not all patients can be adequately treated
with cryosurgery, laser surgery or LEEP. This decision depends on the extent
and appearance of the disease upon examination.
Women treated with conservative surgery require lifelong visits to their
doctor to ensure that recurrence of cervical disease can be detected in the
precancerous state or early while the cancer is still curable.
If the precancerous disease is more extensive or involves
adenocarcinoma in situ (AIS), and the woman has completed childbearing, a
total hysterectomy may be recommended. During a total hysterectomy, the
entire uterus (including the cervix) is removed. In addition, a bilateral
salpingo-oophorectomy, which is the removal of the ovaries and fallopian
tubes, may be performed. The decision to perform a bilateral salpingo-
oophorectomy depends on the woman’s age and whether the ovaries are still
functioning.
A total hysterectomy and/or a bilateral salpingo-oophorectomy are the
most extensive surgical options used for precancerous disease and require
general anesthesia and a hospital stay.
Cervical Cancer
Cervical cancer is the most commonly occuring tumour of the female
genital organs. Most commonly this disease occurs at the age of 40-49 years.
The rate of the disease is much higher in parous women. The most typical
background for the development of cervical cancer is cicatricial deformation

573
and ectropion of the cervix postpartum, as well as dysplasia of the cervix
(severe form).
Exophytic, endophytic, and mixed forms of cervical cancer are
distinguished.
In the exophytic form the tumorappears as a cauliflower and is
positioned on the cervical surface. Occasionally, it may be rather large (Fig.
228).
In the endophytic (Fig.229) form the tumour grows into the depth of the
cervix, which results in cervical enlargement. A deep crater-like ulcer forms
upon disintegration of the tumour. In terms of the histological structure
squamous cell cancer and glandular cancer of the cervix are differentiated.
The former originates from the squamous epithelium covering the vaginal
portion of the cervix, whereas the latter originates from the mucous
membrane of the cervical canal (it is encountered less frequently).

574
The process spreads via the lymphatic pathways, cellular tissue of the
true pelvis, and blood.
Classification of Cervical Cancer by the Degree of Its Propagation
Stage 0: preinvasive cervical cancer.
Stage I: only the cervix is involved (micro-invasive cervical cancer):
Stage IA micro-invasive tumor not extending more than 3 mm beyond
the basement membrane and not invading capillary or lymphatic channels;
Stage IB the growth is confined to the cervix extending more than 5 mm
beyond the basement membrane, the horizontal spread is more than 7 mm
(invasive cancer).
Stage II: the tumor extends beyond the cervix, but does not extend onto
the pelvic wall.
Stage IIA parametrial variant (infiltration of the parametrium from one
or two sides without the involvement of the pelvic wall);
Stage IIB vaginal variant (infiltration of the vagina, but not the lower
third);

575
Stage IIC uterine variant (the tumour spreads to involve the uterine
corpus)
Stage III: tumor has extended onto the pelvic wall:
Stage IIIA parametrial variant (infiltration of the parametrium from one
or two sides, which involves the walls of the small pelvis);
Stage IIIB vaginal variant (the tumor involves the lower third of the
vagina);
Stage IIIC regional metastatic variant (involvement of the regional
pelvic lymph nodes)
Stage IV:tumor has extended beyond the true pelvis or has clinically
involved the mucosa of the bladder or rectum.
Stage IVA vesicular variant (spreading of cervical cancer onto the
bladder);
Stage IVB rectal variant (spreading of cervical cancer onto the rectum);
Stage IVC metastatic variant (spread to distant organs, distant
metastases).
Most commonly cervical cancer metastasizes into the lungs, liver, bones,
kidneys, and some other organs.
There is also another classification known as the TNM staging where T
denotes a primary tumour, N - involvement of lymph nodes, and M -
metastases.
In the preinvasive stage of cervical cancer (stage 0, carcinoma in situ)
there is no growth into the underlying tissues, and altered "cancer" cells are
found only within the epithelium. The presence or absence of invasion and its
depth are established only upon histological study.
Clinical picture. Characteristic symptoms of cervical cancer are acyclic
sanguineous discharge, leucorrhea (often with threads of blood), and pain
with a further spreading of the tumour. Pre- and microinvasive cervical
cancer is characterized by dull gnawing (often nocturnal) pain in the lower
abdomen, rapid fatiguability, and irritability. Progression of the disease may

576
be associated with life-threatening bleeding. When the process spreads onto
the bladder and rectum, one observes corresponding symptomatology in the
form of persistent cystitis, constipation, etc. Compression of ureters by a
cancerous infiltrate may be linked with dysuria and hydro- and pyonephrosis.
Early detection is very important.
Diagnosis of cervical cancer. When collecting the history, one should
pay attention to the status of menstrual, secretory, and reproductive functions
and to peculiarities of the parturition, which might have associated ruptures
of the cervix and the subsequent formation of an ectropion. Not uncommonly
it can be ascertained that the patient has long been suffering from
unresponsive cervical "erosion" which developed after the delivery (as a rule,
it is an erosion-affected ectropion of the cervix).
Speculum inspection of the cervix should be performed carefully in view
of possible injury to tissues and bleeding. The revealed picture may be varied.
For example, one can see minor changes on the cervix in the form of "erosion"
or greyish easily disintegrating tumorous formations of the "cauliflower" type,
which bleed readily upon touching (exophytic form). Patients with cancer of
the cervical canal exhibit no particularly visible alterations. The mucous
membrane covering the vaginal portion of the cervix is lustrous, as if tense,
whereas the cervix itself is barrel-shaped (endophytic form). Sanguineous
discharge may appear from the cervical canal during examination. The
spreading of the cervical cancer onto the vagina is associated with effacement
of the folds and a certain whitishness of its walls.
Rectovaginal and rectoabdominal examinations help to specify the
propagation of the process onto the parametrial cellular tissue and walls of
the vagina and small pelvis. The neoplastic process is characterized by dense
infiltration, occasionally (in stage III) reaching the walls of the true pelvis and
limiting cervical mobility.

577
Schiller's test makes it possible to specify borders of abnormal sites of
the cervix that remain negative when treated with Lugol's solution. Yet, this
test is not specific for cervical cancer.
Cervical cancer may also be recognized by a characteristic colposcopic
pattern: corkscrew-like vessels are positioned on the periphery of reddish
millet-like growths with hemorrhages. In cases of crater-like ulceration one
can visualize pyonecrotic overlying formations.
Expanded colposcopy helps to elucidate the most suspicious sites for
cervical biopsy with subsequent histological examination of the obtained
tissue. Biopsy should be extensive and performed by making a wedge-like
excision of the pathologically altered site of the cervix within the healthy
tissue. In addition, curettage of the mucous membrane of the cervical canal is
performed.
Cervical cancer should be differentiated from tuberculosis, syphilis,
protruding submucosal myoma through the cervical canal, and cervical polyp.
As a rule, histological examination of the excised tissue of the tumor makes it
possible to diagnose the case.
Treatment. It depends on the stage of the disease. In stage 0 of cervical
cancer in patients under 50 years electroconization of the cervix or
amputation of its vaginal portion (Sturmdorf operation) is conducted. In
patients over 50 years of age and in those with attendant uterine myoma
extirpation of the uterus without the adnexa is indicated.
In stage I the treatment is usually combined (surgery and radiotherapy):
extended extirpation of the uterus with the adnexa (as proposed by
Wertheim) in combination with radiotherapy before and after the operation.
In stage II combined radiotherapy is employed. Multimodality
treatment is used rarely, (when the tumor has spread onto the uterus—uterine
variant).
In stage III only combined radiotherapy is usually performed.
In stage IV only symptomatic treatment is actually possible.

578
Combined radiotherapy involves alternation of external distance
radiation and intraluminal gamma-therapy. The net focal dose is 15-20 Gr.
The prognosis is favourable at the initial stages of the disease: in stage I
it is 75-85 per cent, in stage II - 60-65 per cent of five-year survival.
Urgent care is necessary for patients with cervical cancer in cases of
bleeding linked to an expanded neoplastic process. Bleeding may become
profuse and life threatening. If this is the case, a gynecological nurse or
midwife, even in the absence of a doctor, should conduct a very careful
speculum examination to exclude the presence of an injury to the vagina or
protrusion of a pedunculated submucous myoma through the cervix.
Upon the detection of a "crater-like ulcerated" cervix or growths in the
cervical area of the "cauliflower type" with bleeding vessels it is necessary to
tightly insert tampons into the vagina, with the internal end of a tampon
soaked with hydrogen peroxide or calcium chloride solution. The tampon is
left in place for 6-8 hours after which it is carefully removed. If the bleeding
continues, tamponade should be repeated. Simultaneously, acute anaemia is
treated (transfusion of blood and blood substitutes, as well as other types of
anti-anaemic therapy are carried out).
Self test
1. Which of the following may be established as background process of cervix?
A. acute cervicitis
B. chronic cervicitis
C. isthtmico-cervical incompetency
D. cervical pregnancy
2. Cervical dysplasia is characterized by
A. intensive proliferation of atypical cells
B. ectopy of columnal epithelium
C. endocervical atrophy
D. proliferation of cervical muscles

579
3. In Shiller’s test a failure zоne is
A. white in colour
B. brown
C. red
D. unaltered
4. Prior to examination with the colposcope the cervix is swabbed with
A. acetic acid
B. Lugol’s solution
C. chlor zinc iodine
D. iodine water
5. In colposcopic examination the area of suspected dysplaia is
A. white in colour
B. brown
C. red
D. unaltered
6. ”Background” diseases of cervix of the uterus are all of the following except
A. eversion
B. erosion
C. cervical polyps
D. cervical dysplasia.
7. Cervical dysplasia is
A. background process of the cervix
B. precancerous process of the cervix
C. initial stage of malignancy
D. typical malignant lesion of the cervix
8. Epidermoid cancer takes place in case of
A. ovarian cancer
B. cervical cancer
C. cancer of uterine body
D. cancer of fallopian tube

580
9. In case of cervical cancer the most frequent hystological type is
A. epidermoid cancer
B. glandular neoplasm
C. solid carcinoma
D. sarcoma
10. In case of profuse bleeding due to cervical cancer the urgent care means
A. vaginal tight tamponade with subsequent surgical intervention
B. vaginal tight tamponade
C. cryosurgery of the cervix
D. conservative hemostatic treatment

581
Chapter 17. PREMALIGNANT DISEASES OF THE
ENDOMETRIUM. CANCER OF THE UTERUS.
SARCOMA OF THE UTERUS
Precancerous diseases of the endometrium
Hyperplastic diseases of endometrium are identified as precancerous
diseases in our country. Endometrial hyperplasia is of clinical significance
because it is often a precursor lesion to adenocarcinoma of the endometrium.
It is known that both endometrial hyperplasia and adenocarcinoma are
estrogen dependent conditions; the development of malignancy is
proportionate to the duration of estrogen exposure. Estrogenic stimulation of
the endometrium, unopposed by progestins, causes proliferative glandular
epithelial changes. This finding, due to prolonged hormonal exposure, is
biologically distinct from true precancerous lesions and true neoplasia.
Making the distinction between hyperplasia and true precancerous lesions or
true neoplasia has significant clinical effect because their differing cancer
risks must be matched with an appropriate intervention to avoid
undertreatment or overtreatment.
The classification of endometrial hyperplasia has had numerous
terminologies. Terms that have been used include "adenomatous
hyperplasia," "atypical hyperplasia," and "carcinoma in situ." Some, but not
all, of these lesions represent endometrial carcinoma precursors. The
diagnosis of these proliferative lesions is poorly reproducible because it is
difficult to distinguish between non-neoplastic proliferations and neoplastic
proliferations, and it is difficult to determine endometrial invasion in a
nonhysterectomy specimen. As a result, any proliferative process of
endometrium in addition to the frequent occurrence of hyperplasia of the
endometrium in association with subsequent cancer of the uterine body is a
marked reason for intensive inspection of the patient.

582
Classification systems.
The WHO94 classification was the most commonly used system
since 1994. This system characterizes the glandular architectural pattern as
simple or complex and describes the presence or absence of nuclear atypia.
Simple hyperplasia - Increased number of glands but regular glandular
architecture
Complex hyperplasia - Crowded irregular glands
Simple hyperplasia with atypia - Simple hyperplasia with presence of
cytologic atypia (prominent nucleoli and nuclear pleomorphism)
Complex hyperplasia with atypia - Complex hyperplasia with cytologic
atypia
Endometrial intraepithelial neoplasia classification - The
endometrial intraepithelial neoplasia (EIN) classification system was
proposed by an international group of gynecologic pathologists in 2000.
The EIN system defines two classes of endometrial changes: benign and
intraepithelial neoplasia.
●Benign endometrial hyperplasia (EH, non-neoplastic)
o Changes typically observed with anovulation or other etiology of
prolonged exposure to estrogen. The morphology of EH varies from
proliferative endometrium with a few cysts (persistent proliferative
endometrium) to bulkier endometria with many dilated and
contorted glands that in other systems have been designated as
"cystic glandular hyperplasia," "mild hyperplasia," or "simple
hyperplasia."
●Endometrial intraepithelial neoplasia (EIN)
o Endometrial precancers. Epithelial crowding in EIN displaces
stroma to a point at which stromal volume is less than
approximately half of total tissue volume in nonsecretory
endometrium, and typically cells appear morphologically clonal and
distinct from the surrounding endometrium.

583
World Health Organization classification — The 2015 WHO
endometrial hyperplasia classification system has only two categories:
●Hyperplasia without atypia (non-neoplastic)
●Atypical hyperplasia (endometrial intraepithelial neoplasm)
Morphological distinguishing
Normal proliferative endometrium exhibits no crowding of glands
within the stroma (<50 percent ratio of glands to stroma). Normal secretory
endometrium may have >50 percent gland-to-stroma ratio. Although
secretory phase glands exhibit crowding, they are organized, and cells
comprising the glands are spaced and are not mitotically active.
Benign endometrial hyperplasia is characterized by a proliferation of
endometrial glands resulting in a greater gland-to-stroma ratio (>50 percent)
than observed in normal proliferative endometrium. The proliferating glands
vary in size and shape, and cells may have cytologic atypia. Mitoses are
typically present in the glandular cells.
Endometrial intraepithelial neoplasia (EIN) is defined as when the
volume of glandular crowding is greater than the stromal volume, the
presence of cytologic alterations, a lesion larger than 1 mm, and exclusion of
mimics or carcinoma.
It is sometimes difficult to distinguish a precursor lesion (EIN) from
endometrial carcinoma. Atypical hyperplasia or EIN is distinguished from
grade 1 endometrial carcinoma by findings that suggest invasion, including:
invasive pattern of glands infiltrating reactive stroma (the most definitive),
cribriform glands, or confluent growth (lack of stroma between glands).
Marked nuclear atypia, especially in the context of atrophic background
endometrium, may be present in either endometrial intraepithelial serous
neoplasm or "intraepithelial carcinoma," which is frequently associated with
invasive serous carcinoma.

584
Etiology. Endometrial hyperplasia results from continuous estrogen
stimulation that is unopposed by progesterone. This can be due to
endogenous estrogen or exogenous estrogenic sources. These diseases
develop in the presence of impaired hypothalamic-pituitary-ovarian
interrelationships and may be accompanied by abnormal uterine bleedings.
Those are:
Chronic anovulation associated with polycystic ovary syndrome
(PCOS).
Obesity, which contributes to unopposed estrogen exposure due to
chronic high levels of estradiol that result from aromatization of
androgens in adipose tissue and conversion of androstenedione to
estrone.
Endometrial hyperplasia and cancer, which are the result of
estradiol-secreting ovarian tumors, such as tumors of granulosa
cells.
Other risk factors include obesity, nulliparity, early menarche, and
late menopause.
Clinical picture. A major symptom of precancerous change of
endometrium is acyclic uterine bleeding. Bleeding may be sudden and profuse
in nature or occur as prolonged and scanty sanguineous discharge. Both
variants of uterine bleeding are linked with weakening of the patient; anemia
is frequently found. Bleeding is more frequent after menstrual delay lasting
from 6-8 weeks to several months. Cyclic bleeding occurring at the time of
expected menstruation and continuing for a long time is also possible.
Sanguineous discharge in postmenopausal women should always be
considered a sign of precancerous state or cancer of the endometrium.
Women with precancerous diseases of the endometrium are often
characterized by neuroendocrine and metabolic disorders (obesity, diabetes
mellitus, essential hypertension), prolonged menstrual disturbances,
impaired fertility, and delayed menopause (after 50-52 years of age).

585
Diagnosis of endometrial hyperplasia. Endometrial hyperplasia is a
histologic diagnosis made based upon the results of evaluation of an
endometrial biopsy, endometrial curettage sample, or hysterectomy
specimen.
Tissue sampling should be performed in women with risk factors who
present with symptoms of abnormal vaginal bleeding or discharge. This
includes:
women older than 35 years with abnormal bleeding,
women younger than 35 years with bleeding and risk factors,
women with persistent bleeding,
women with unopposed estrogen replacement, tamoxifen therapy,
and hereditary nonpolyposis colorectal cancer (HNPCC) cancer
syndrome.
women with atypical glandular cells (AGC) Pap smear or
endometrial cells in Pap smears of women older than 40 years
when out of synch with menstrual cycle.
If insufficient tissue is obtained on suction curettage, or if a patient
continues to have abnormal bleeding, a formal D&C with histilogy is
recommended.
Imaging studies are also used for diagnostics:
TVUS can visualize the endometrium and the thickness of the
endometrium can be measured
Magnetic resonance imaging and computed tomography areuseful
for obtaining preoperative data on the extent and depth of
myometrial invasion by endometrial carcinoma rather than in the
primary diagnosis of endometrial carcinoma and its precursors
Hysteroscopy can be used in any woman with abnormal uterine
bleeding in whom an intrauterine abnormality is suspected
The accurate diagnosis of hyperplasia type is vital for appropriate
treatment based on risk of cancer without over or under treatment.

586
Treatment and management. Treatment depends on degree of
hyperplasia, the patient's symptoms such as severity of bleeding, surgical
risks, and wish for future childbearing. Management depends on whether the
underlying disease is primarily hormonal (non-neoplastic endometrial
hyperplasia) or intrinsic premalignant disease (EIN).
Hyperplasia without atypia (non-neoplastic) responds well to
progestins. Changes in the hormonal environment, such as the administration
of progesterone, help control bleeding and prevent the progression of cancer,
reducing the degree of cytological atypia. The duration of progestin
administration is crucial for inhibiting endometrial mitotic activity; this is
important because control of endometrial growth is primarily related to
control of epithelial mitotic activity.
Clinical management of EIN is usually hysterectomy. There is a clinical
need for nonsurgical alternative therapies in women who wish to retain
fertility, or are poor surgical candidates. Medical hormone therapy may be
given to women whose general health is unsuitable to withstand surgery. High
dose progestin therapy can succeed in ablating some EIN lesions, but,
because of the high concurrent cancer rate and unpredictable response, must
be accompanied by careful clinical surveillance.
Recommended regimen for non-neoplastic endometrial hyperplasia:
Medroxyprogesterone acetate (MPA), 10 mg orally, or micronized
progesterone, 300 mg orally, once a day for 14 days per month for 3
months. Such cyclic regimens lead to withdrawal bleeding; a biopsy
specimen is obtained at the end of the progestin therapy at 3–4 months.
o Complete responders (reversal of endometrial hyperplasia to
progestational-type endometrium) should be maintained on cyclic
progesterone therapy or, if appropriate, combined cyclic or
continuous HRT.

587
o If a partial response is obtained, another 3-month trial with MPA,
10 mg orally four times per day, or megestrol acetate, 80 mg, for 3
months may be carried out.
o Nonresponders and patients with intractable breakthrough
bleeding may have transabdominal hysterectomy.
Recommended regimen for endometrial intraepithelial neoplasia:
Progestin therapy for premenopausal women with EIN calls for larger
doses of MPA, 100 mg orally daily; megestrol acetate, 160 mg; or 1
g/week of MPA intramuscularly for 12 weeks.
Another option of hormonal therapy for endometrial hyperplasia
with or without atypia is medicated intrauterine device (IUD) such as the
LNG- (levonorgestrel) releasing intrauterine system (Mirena®, Bayer
Healthcare Pharmaceuticals, Inc. Wayne, NJ, USA). In general, EH
responds better (90–100%) than EIN (67–88%) to intrauterine LNG. In
addition to the powerful progestational effect of Mirena on the
endometrium, adverse events (side effects) that are commonly experienced
by patients with oral progestational therapy are considerably reduced. This
is because the systemic absorption of LNG is considerably reduced
compared to oral progestational therapy. The biopsy specimen should
show progestational-type endometrium with marked stromal
decidualization. Careful follow up surveillence, including repeated biopsy
at approximately 6 month intervals until several are free of disease is
advised to ensure complete ablation. Induction of ovulation should follow
the progestational therapy.
Any progestin should be adequate for treatment of hyperplasia
without atypia or for maintenance after resolution of atypical hyperplasia.
Patient should be sampled to assess for response every 3 to 6 months for
regression to normal endometrium. If there is inadequate response in 6
months, consider increasing dose or changing progestins. Continued

588
surveillance after regression of the lesion is recommended every 6-12
months if risk factors persist. Repeat biopsy is also indicated for recurrent
abnormal bleeding or discharge. Prevention of recurrence include use of
daily or cyclic progesterone, indwelling levonorgestrel IUD, along with
weight loss for obese patients.
Surgical treatment.
Surgery (i.e., transabdominal hysterectomy) with or without bilateral
salpingo-oophorectomy is recommended for women who have persistent
benign endometrial hyperplasia but are symptomatic (abnormal uterine
bleeding) and women in the postreproductive age group with EIN.
Total hysterectomy is indicated for endometrial intraepithelial
neoplasia; it provides definitive assessment of a possible concurrent
carcinoma and effectively treats premalignant lesions. Current surgical
options include abdominal, vaginal, and minimally invasive procedures.
Surgical option may also include total hysterectomy with or without bilateral
salpingo-oophorectomy in patients with a biopsy diagnosis of endometrial
intraepithelial neoplasia. Removal of the cervix together with the uterine
corpus permits staging of any incidentally discovered cancer and reduces the
risk of leaving behind residual disease.
Cancer of the Uterus
Cancer of the uterine corpus (uterine cancer) is observed in women over
50 years of age. More commonly the disease affects nulliparous women or
women of low parity with a delayed menarche or menopause. The incidence
of uterine cancer varies considerably in women of different nationalities.
More frequently the disease develops against the background of
hyperplastic processes of the endometrium (first pathogenetic variant) and is
combined with neuro-endocrine disturbances, diabetes mellitus, obesity, and
essential hypertension. Cancer may also develop in the presence of atrophic

589
endometrium (second pathogenetic variant) in women without
neuroendocrine diseases.
Classification of Cancer of the Uterine Corpus
Stage 0: histological findings allowing to suspect malignancy of the
hyperplastic process of the endometrium.
Stage I: the tumor remains within the uterine body (Fig. 230).
Stage lA: the length of the uterine cavity does not exceed 8 cm.
Stage IB the uterine cavity is more than 8 cm.
The following histological groups are distinguished within stage I: G1 —
highly differentiated adenocarcinoma, G2 — differentiated adenocarcinoma
with zones of solid structure, G3 — undifferentiated carcinoma.
Stage II: the tumor has spread onto the corpus and cervix of the uterus
(Fig. 231).
Stage III: the tumor has spread outside the corpus but not outside the
true pelvis (Fig. 232).
Stage IV: the tumor has spread beyond the pelvis, has grown into the
bladder and rectum, or has given rise to distant metastases.
Clinical picture. The main symptom of endometrial cancer is abnormal
uterine bleeding in the reproductive or the premenopausal period, as well as
bleeding after the menopause (uterine cancer is found in every second
postmenopausal patient with uterine bleeding). Frequent findings are serous
leucorrhea with blood threads or leucorrhea of "meat slops" type, pain and
feeling of heaviness in the lower abdomen, which intensify and may be
convulsive in nature when there is accumulation of pus in the uterus
(pyometra).
Further progression of the process (stages III-IV) may be characterized
by marked symptomatology typical of impaired function of the adjacent
organs, and emaciation (cachexia).
Diagnosis. The diagnosis of uterine cancer is based on the history,
general physical and gynecological examination, as well as on additional

590
methods of examination. Gynecological examination is directed at
determining the size and mobility of the uterus, the degree of possible
infiltration of parametrial and rectovaginal cellular tissue, and adnexal
enlargement.
Mandatory components also include cytological and histological
examination. Smears for the former are prepared from the material obtained
from the posterior vaginal fornix, cervical canal, and uterine cavity (in the
latter case the material is taken with the help of aspiration biopsy and by
washing off a sample with a Braun syringe). Histological examination of the
material is conducted after separate curettage of the mucous membrane of the
cervical canal and uterine mucosa. If following an insignificant dilatation of
the cervical canal, there is a discharge of crumby masses from the uterine
cavity; only scraping should be performed since diagnostic dilatation and
curettage in this case is unwarranted in view of possible perforation of the
altered uterine wall.
Fig. 230. Cancer of the uterus. Stage I

591
Fig. 231. Cancer of the uterus, stage II Fig. 232. Cancer of the uterus,
stage III
In cases when an extended process is suspected (stages III-IV) separate
diagnostic dilatation and curettage may be substituted by radioisotope
examination.
Hysteroscopy (visual examination of the walls of the uterine cavity) has
been finding an increasingly wide application in recent years. Occasionally,
hysterosalpingography is performed for the diagnostic purpose.
Treatment given to patients with cancer of the uterine body should be
combined (surgical, X-ray, and hormonal).
The scope of surgical intervention (extirpation of the uterus along with
the adnexa, extirpation of the uterus with the adnexa plus lymphadenectomy,
expanded extirpation of the uterus with the adnexa by the type of surgery
described by Wertheim) depends on the stage of the disease as well as on the
patient's age and general status. In elderly patients with somatic diseases and
the neuroendocrine syndrome with marked obesity simple extirpation of the
uterus together with the adnexa is the most commonly employed procedure.
If there are no contraindications, the scope of surgery may be expanded since
removal of the lymph nodes of the true pelvis is also indicated in such
patients.

592
In the second stage of multimodality treatment the patient is subjected
to distance radiation in a dose of 40 Gr.
Hormonal therapy consists of prolonged (up to 3-5 years) intramuscular
administration of 12. 5 per cent solution of hydroxyprogesterone caproate.
Within the first 2 months of the therapy the daily dose of the solution is 500
mg; later on, the dose is gradually decreased to 500 mg once a week.
Quite often one employs a multimodality treatment (surgical and X-ray)
and combined radiotherapy (combination of distance irradiation and
intracavitary gamma-therapy).
The prognosis is favourable in the initial stages of the disease
comprising 91. 5 per cent of five-year survival in stage I, 85. 5 per cent in stage
II and 57. 5 per cent in stage III.
Urgent care in endometrial cancer is necessary in patients with uterine
profuse bleeding or in those with a pyometra attended by manifestations of
acute inflammation in the true pelvis and systemic intoxication.
In the case of profuse uterine bleeding which cannot be arrested by
haemostatic therapy the method of choice is urgent surgical intervention
(hysterectomy).
To diagnose pyometra, one should perform bougienage and cervical
dilatation with Hegar's dilators, with the subsequent evacuation of pus.
Bougienage is carefully performed with a thin bulbous-end probe. In the case
of complication (uterine perforation) urgent surgical intervention is needed.
Uterine bougienage should be followed by a course of antibacterial and
disintoxication therapy after which separate diagnostic dilatation and
curettage become possible.
The diagnostics and management of precancerous diseases of
endometrium and endometrial cancer are summarized in table 20.

593
Table 20.
Precancerous diseases of the endometrium m and endometrial
cancer management
Nomenclature Criteria Functional Category
Management
Benign endometrial hyperplasia (BEH)
1. Irregular glands with cysts 2. More glands than stroma 3. No cytologic change 4. Field-wide changes
Estrogen effect
Hormonal therapy
Endometrial intraepithelial neoplasia (EIN)
1. Cytologic change 2. Gland exceeds stromal area 3. Size >1 mm in single fragment 4. Exclusion of mimics 5. Exclusion of carcinoma
Precancer
Hormonal or surgical therapy
Adenocarcinoma
1. Myoinvasion 2. Solid epithelium 3. Maze-like glands 4. Cribriform architecture
Cancer
Surgical and/or radiotherapy

594
Sarcoma of the Uterine Body
Sarcoma of the uterine body is a malignant tumour developing from
connective tissue of the myometrium or from muscle fibres. (Fig. 111). Not
uncommonly it develops inside uterine myoma. The rate of the disease is the
highest at the age of 45-50. Developing interstitially the tumour is
characterized by early and rapid metastatic spread. In many cases the main
symptom of uterine sarcoma is a rapid growth of a tumour. Other
characteristic features include prolonged and profuse menstruations, with
possible acyclic (breakthrough) uterine bleeding. However, histological
examination of the endometrium may reveal no sarcoma elements since the
uterine mucosa is rarely affected.
Treatment. The treatment usually involves extirpation of the uterus
together with the adnexa and subsequent radiotherapy. In view of very
unsatisfactory results of the treatment for uterine sarcoma and a rapid
propagation or recurrence of the tumour chemotherapy has been finding an
increasingly wide application. Such drugs as methotrexate, fluorouracil,
prospidine, adriamycin, etc. are recommended for this purpose.
Early surgical intervention in cases of a rapid growth of uterine myoma
may prevent the most prevalent forms of sarcoma of the uterine corpus.
Self test
1. Which of the following is not precancerous lesion of endometrium?
A. adenomatosis
B. cystic hyperplasia
C. adenomiosis
D. proliferation of the functional layer
2. Leucorrhea is a symptom of
A. cervical cancer
B. cancer of the uterus

595
C. ovarian cancer
D. fallopian tube cancer
3. Hormonal therapy may be used in
A. cervical cancer
B. cancer of the uterine body
C. ovarian cancer
D. vaginal cancer
4 Does the treatment of uterine cancer depend on the age of patients?
A. Yes
B. No
5. Which of the following may be used for hormonal treatment of endomtrial
cancer?
A. hydroxyprogesterone caproate
B. progesterone
C. synestrol
D. legalon
6. Histologically the uterine cancer is not a
A. malignant adenoma
B. malignant acanthoma
C. adenocarcinoma (glandular neoplasm)
D. epidermoid carcinoma
7. What is the immediate cause of hyperplastic lesion of the endometrium?
A. inflammatory processes of the uterus
B. low estrogen level in the organism
C. high level of estrogens in the organism
D. just listed above
8. In patient of 30 years of age there is adenomatous hyperplasia of
endometrium. What is the treatment?
A. radiotherapy
B. chemotherapy

596
C. treatment with estrogen drugs
D. treatment with gestogen drugs
9. Surgical treatment of endometrial cancer is indicated
A. in early stages of diasease (stage I)
B. in the late stage of disease
C. In every stage of disease
D. Is not indicated at all
10. In the case of profuse uterine bleeding which cannot be arrested by
hemostatic therapy? The method of choice is
A. urgent surgical intervention (hysterectomy)
B. curettage of the uterine cavity
C. urgent radiotherapy
D. urgent chemotherapy

597
Chapter 18. CYSTS OF THE OVARY. OVARIAN
TUMORS
Cysts of the ovary
Retention cysts
Retention cysts belong to tumor-like formations of the female genital
organs. A cyst is a cavity filled with fluid and is secondary to either retention
or excessive secretion of fluid. Cysts enlarge as a result of fluid accumulation
and may be encountered in all parts of the female genital system: vulva,
vagina, cervix, ovary, and broad ligament of the uterus. Most commonly cysts
are localized in the ovary and supra-ovarian adnexa (paroophoritic cyst).
Cysts developing in the ovaries are divided into follicular cysts and lutein
cysts (Fig. 233).
Fig. 233. Retention cyst of the ovary
A follicular cyst develops from an atretic follicle, most frequently due to
an inflammatory process. A follicular cyst does not exceed 10-12 cm in
diameter; it has thin walls and its contents is transparent fluid of a straw or
orange color. The cyst is movable and softly elastic. On one of the cyst poles

598
there may be unchanged ovarian tissue spread on the capsule. The internal
surface of the cyst is even, smooth, and lustrous.
Most often the wall of a follicular cyst consists of connective tissue and
has no internal epithelium or is lined with cubical single-layer epithelium.
A lutein cyst is less frequent than a follicular one. It is also caused by an
inflammation. In macro- and microscopic terms it is similar to a follicular
cyst.
A paroophortic cyst (cyst of the paroophoron) forms as a result of
secretion retained in the lumen of the tubules of the paroophoron situated
between the ovary and oviduct in the broad uterine ligament. A paroophoritic
cyst has two capsules because of its intraligamentous position: an inherent
one and one in the form of layers of the broad uterine ligament with a
crosswise vascular pattern (feature distinguishing it from other retention
formations) (Fig. 234). A cyst may measure up to 20 cm in diameter. It has
thin walls and is slightly mobile. Alongside a cyst one can usually palpate or
visualize by laparoscopy the unaltered ovary and oviduct flattened on the cyst
surface. The internal surface of the cyst is smooth, lustrous, and covered with
cylindrical or squamous epithelium.
Theca-lutein cysts are also classified as retention cysts of the ovaries
since they can spontaneously resolve as a result of the treatment of the
underlying disease (hydatidiform mole or uterine chorionepithelioma) with
which they are associated, being its manifestation.
Fig. 234. Paraoophoritic cyst

599
Clinical picture. Retention cysts of the ovary are often asymptomatic
and only in the event of their complicated course related to torsion of the cyst
pedicle, or impaired nutrition or rupture of its capsule, clinical manifestations
of acute abdomen are encountered.
Diagnosis. The diagnosis of retention cysts is usually based on findings
of bimanual vaginal examination and is made when a formation measuring up
to 10-12 cm is palpated to the left or right side from the uterus. It is softly
elastic, mobile, and painless. Retention cysts are more frequently observed in
young age. The diagnosis of a retention cyst of the ovary in elderly women
should be made with considerable caution and only following the exclusion of
a true ovarian tumour.
Ovarian cysts should be differentiated from true ovarian tumours,
uterine myoma (subserous nodes), tubo-ovarian formations of the
inflammatory nature, and extragenital tumours.
To specify the diagnosis, one can resort to laparoscopy. In this case a
retention cyst is visualized as a thin-walled formation; one can see only an
unaltered portion of the ovary (most commonly in the area of its hilum) and
the uterine tube.
Treatment. Small retention cysts may resolve as a result of anti-
inflammatory therapy, which can be continued for no longer than 4-6 weeks.
If it is unsuccessful, surgical intervention is indicated (resection of the ovary
and even, when indicated, its removal). In the event of a paroophoritic cyst
surgery consists of its enucleation following resection of the layer of the broad
uterine ligament without removal of the ovary and fallopian tube.
Prevention of retention cysts is difficult and relies on the early and
adequate treatment of acute inflammatory processes of the internal genital
organs. In view of a possible relationship between retention cysts and
hormonal dysfunction of the ovaries, prevention of cysts should be aimed at
the study and correction of impaired hormonal relationships in the patient's
body.
600
Upon making the diagnosis of an ovarian cyst the patient should be
followed up. Modern methods of the diagnosis and treatment of retention
cysts may finally be considered as methods preventing ovarian cancer since in
every fourth patient with the diagnosis of "a retention cyst" a true ovarian
tumour is finally diagnosed.
Ovarian tumors
Ovarian neoplasms are diverse in their nature since the ovary contains
elements of all three germinal layers.
Histological classification of ovarian tumors
I. Epithelial tumors
A. Serous tumors
1. Benign:
cystadenoma and papillary cystadenoma;
superficial papilloma;
adenofibroma and cystadenofibroma
2. Borderline (of a potentially low degree of malignancy):
cystadenoma and papillary cystadenoma;
superficial papilloma;
adenofibroma and cystadenofibroma.
3. Malignant:
adenocarcinoma; papillary adenocarcinoma and papillary
cystadenocarcinoma; surface papillary carcinoma;
malignant adenofibroma and cystadenofibroma.
B. Mucinous tumors
1. Benign:
cystadenoma;
adenofibroma and cystadenofibroma

601
2. Borderline (potentially of a low degree of malignancy):
cystadenoma;
adenofibroma and cystadenofibroma
3. Malignant:
adenocarcinoma and cystadenocarcinoma;
malignant adenofibroma and cystadenofibroma
C. Endometrioid tumors
1. Benign:
adenoma and cystadenoma;
adenofibroma and cystadenofibroma.
2. Borderline (potentially of a low degree of malignancy):
adenoma and cystadenoma;
adenofibroma and cystadenofibroma
3. Malignant:
carcinoma, adenocarcinoma, adenoacanthoma, malignant
adenofibroma and cystadenofibroma;
endometrioid stromal sarcoma;
mesodermal (Muller's) mixed tumors
D. Light cell (mesonephroid) tumors:
1. Benign: adenofibroma.
2. Borderline (potentially of a low degree of malignancy).
3. Malignant: carcinoma and adenocarcinoma.
E. Brenner's tumors:
1. Benign
2. Borderline
3. Malignant
F. Mixed epithelial tumors:
1. Benign
2. Borderline
3. Malignant

602
G. Undifferentiated carcinoma.
H. Unclassified epithelial tumors.
II. Tumors of the genital cord stroma:
A. Granulosostromal cell tumors:
1. Granulosa-cell tumors (folliculomas).
2. Group of thecomas-fibromas:
thecoma;
fibroma;
unclassified.
B. Androblastomas: Sertoli and Leydig cell tumors:
1. Highly differentiated:
tubular androblastoma; Sertoli cell tumor;
tubular androblastoma with accumulation of lipids; Sertoli
cell tumor with accumulation of lipids (Lesen's lipid
folliculoma);
Sertoli and Leydig cell tumors;
Leydig cell tumor (hilum cell tumor).
1. Intermediate (transitional) differentiation
2. Poorly differentiated (sarcomatoid)
3. With heterologous elements
C. Gynandroblastoma
D. Unclassified tumours of the genital cord stroma
III. Lipid-cellular tumors.
IV. Germinal tumors:
A. Disgerminoma
B. Tumor of the endodermal sinus
C. Embryonic carcinoma
D. Polyembryoma
E. Chorionepithelioma
F. Teratomas:

603
1. Immature;
2. Mature:
solid;
cystic (dermoid cyst, dermoid cyst with malignancy).
3. Monodermal (highly specialized):
ovarian struma;
carcinoid;
ovarian struma and carcinoid;
others.
G. Mixed germinal tumors
V. Gonadoblastoma:
A. Pure (without admixture of any other forms);
B. Mixed with disgerminoma and other forms of germinal
tumors;
VI. Soft tissue tumors, non-specific for the ovaries
VII. Unclassified tumors.
VIII. Secondary (metastatic) tumors.
The most frequent type of benign ovarian tumours is epithelial tumors
(cystomas).
Serous cystadenoma (simple serous cystoma) develops from the
mesodermal epithelium, most commonly in women aged from 40 to 50 years.
Cystadenomas usually measure up to 12 cm in diameter, but larger
tumours may also be encountered. Their content is liquid and transparent.
The capsule is denser than in retention cysts and is characterized by a marked
vascular pattern. Upon palpation the tumour feels as densely elastic.
In 5-10 per cent of all cases cystadenoma becomes malignant.
Serous papillary cystadenoma (cilioepithelial papillary cystoma) opens
the list as far as the potential possibility of a tumour to become malignant is
concerned (every other papillary cystadenoma turns cancerous). Up to 70 per
cent of cancerous tumours of the ovaries are papillary cystadenomas turning

604
malignant. Most frequently this tumour occurs at the age of 50-60 years.
Most often it is bilateral, middle-sized, roundish or ovoid, densely elastic,
with smooth or tuberous surface and papillary internal growths (Fig. 235).
Fig. 235. Bilateral papillarycystoma of the ovaries.
Mucinous cystadenoma is the largest ovarian tumor, occasionally
occupying the entire abdominal cavity (tumors have been described which
weighed 50 kg and more), tuberous, multi-chamber with thick mucoid
contents, usually unilateral. Up to 5 per cent of such tumors turn malignant.
As for the degree of potential malignancy, granulosa-cell tumors
(folliculomas) come second after papillary cystadenomas and become
malignant in 25-30 per cent of all cases. Most granulosa-cell tumors are
unilateral. They may both be small and occupy the entire abdominal cavity.
Granulosa-cell tumors are most common in postmenopausal women and
possess (due to oestrogen secretion) feminizing hormonal activity.
Theca-cell ovarian tumors (thecomas) occur significantly less
commonly than granulosa-cell ones and also present a feminizing hormonally
active tumor. Structurally, it resembles the form of the ovary, is small, dense
to palpation, usually of solid structure on section, and yellow in color.
Microscopic findings include theca cells enclosed in the tumor. Thecomas are

605
more frequent in postmenopausal women. Tumors become malignant in 1-5
per cent of cases.
Ovarian fibroma actually presents as thecoma, i. e., a tumor made of
thecal cells that does not have hormonal activity. Malignancy is a rare
occurrence (1 per cent of cases). It follows the shape of the ovary, varies in
size (most often measuring up to 10-12 cm in diameter), and is very dense.
Sectional appearance is whitish in colour and fibrous in structure.
Androblastoma (arrhenoblastoma) belongs to masculinizing ovarian
tumors. It possesses androgenic activity, appears as smooth greyish-whitish
nodes, averaging 10-12 cm in diameter, and is usually unilateral. Tumor
consists of cells resembling those of the male sexual gland. Most commonly it
occurs in young age (25-35 years). Androblastomas have a benign course in
most cases. Yet, malignant forms are not infrequent.
Mature teratoma (dermoid cyst) is a neoplasm of variable consistency
(tight elastic with indurated sites) with the roundish or oval shape. It tends to
be localized anteriorly to the uterus, is unilateral, and averages 10-12 cm in
size. Section examination demonstrates fat, hair, cartilaginoid and bone
formations. A dermoid cyst occurs most commonly at the age of 20-40 years.
It accounts for 15 per cent of all ovarian tumors, with malignancy occurring in
1-1. 5 per cent of cases.
Disgerminoma is almost always malignant and usually occurs in
childhood. The tumour varies in size and is roundish or tuberous in shape.
The tumour is usually unilateral; its consistency is dense or tight elastic.
Clinical picture. Ovarian tumor may be asymptomatic. However, in
cases of large neoplasms, dysfunction of the adjacent organs (bladder and
rectum), torsion of the tumor pedicle, and impaired nutrition of the tumor
one can observe the corresponding symptomatology (low abdominal pain,
impaired micturition and defecation).
Almost all ovarian tumors possess some hormonal activity, which is not
uncommonly expressed in menstrual disorders. Tumors of the genital cord

606
stroma display the greatest hormonal activity. Thus, granulosa-cell and theca-
cell tumors can secrete elevated levels of estrogens and may cause
proliferative processes in the uterus, which leads to breakthrough (acyclic)
bleeding and to sanguineous discharge in postmenopausal women. Patients
feel a burst of vigor; "the second youth" appears to have come.
Arrhenoblastoma, having a masculinizing property, induces
amenorrhea, breast reduction, growth of hair on the face, and hoarse voice.
Ovarian fibroma is often accompanied by the development of ascitis and
hydrothorax.
The most common ovarian tumor in girls is mature teratoma. Yet, other
tumors, including malignant ones, may also be encountered. The clinical
picture of ovarian tumors in girls is distinguished by their ability to affect
sexual development. Thus, feminizing tumors are associated with precocious
puberty. On the other hand, disgerminomas are related to genital hypoplasia,
underdevelopment of secondary sex characters, and delayed menarche.
Arrhenoblastoma may also be reflected in delayed puberty.
Diagnosis. It is based on the history and general physical and
gynecological examinations. Of major significance are results of bimanual and
rectovaginal examinations. The diagnosis of an ovarian tumor is established
with consideration of the size, position, consistence, and mobility of a
formation palpated in the true pelvis laterally to the uterus.
The nature of a tumor may be determined only after laparotomy and its
removal, often only after histological examination.
Ovarian tumors should be distinguished from uterine and intestinal
tumors, retention cysts, inflammatory adnexal processes, and a dystopic
kidney. The diagnosis is specified with the help of sounding of the uterine
cavity, ultrasound scanning, laparoscopy, radiographic methods, and
examination of the gastro-intestinal tract and urinary system.
Treatment. The only available method of treatment is surgical. Only
true ovarian tumors call for mandatory surgical intervention. The scope of

607
surgery depends on the nature of the tumor. Usually, the involved ovary
should be removed. The slightest suspicion of malignancy is an indication for
urgent histological examination to determine the scope of surgery. However,
exclusions are possible. For example, if a girl or a young woman has a
dermoid cyst, one can resort to ovarian resection. In cases of a papillary
ovarian cystadenoma (a high degree of potential malignancy) supravaginal
amputation of the uterus with the adnexa and resection of the omentum are
performed.
The main guarantee of reliable prophylaxis is regular (twice a year)
examinations. At present groups of patients at risk for the development of
tumors, including ovarian ones (since any true tumour of the ovary is
potentially malignant), have been identified. Such patients include those who
have been observed at a women's consulting centre for a long time for uterine
myoma and undifferentiated tumor-like formations of the small pelvis. Early
diagnosis and treatment of true tumors present reliable ovarian cancer
prophylaxis.
Ovarian Cancer
Ovarian cancer may be primary, secondary, and metastatic. Primary
cancer occurs in 4-5 per cent of cases, this tumor from the very beginning has
malignant nature. Secondary cancer – is one of the most frequent forms of
ovarian cancer, the incidence is about 80-85% in relation to all forms of
ovarian cancer. It may delevelop in papillary cystoma of the ovary; rarely in
pseudomucinous cystoma (other name is «cancer in cystoma»).
Metastatic tumors account for 20 per cent of all malignant neoplasms of
the ovaries. Most frequent findings are a metastatic tumor of the Krukenberg
type (metastases of cancer of the gastrointestinal tract) and metastases into
the ovaries in patients with breast cancer.

608
Symptomatology and choice of the method of treatment depend on
manifestations of the underlying disease. Of the greatest clinical interest is
secondary ovarian cancer developing from previous benign true tumors.
Four stages of ovarian cancer are distinguished.
Classification. (as described by the international federation of
Gynecology and Obstetrics (FIGO).
Stage I: Growth limited to the ovaries;
Stage IA: Growth limited to one ovary, no tumour on the external
surface, and capsule intact;
Stage IB: Growth limited to both ovaries; no tumour on the external
surface, and capsule intact.
Stage IC: IA or IB but with tumor on the surface of one or both ovaries,
with capsule rupture, or with ascites or peritoneal washings containing
malignant cells;
Stage II: Involving one or both ovaries with pelvic extension.
Stage IIA: Extension and/or metastases to the uterus and/or tubes.
Stage IIB: Extension to other pelvic tissues.
Stage IIC: Stage IA or IB but with tumour on the surface of one or both
ovaries, with capsule rupture, or with ascites or peritoneal washings,
containing malignant cells.
Stage III: Involving one or both ovaries with histologically confirmed
peritoneal implants outside the pelvis and/or positive retroperitoneal or
inguinal lymph nodes.
Stage IIIA: Grossly limited to the true pelvis with negative lymph nodes,
but with histologically confirmed microscopic tumour outside pelvis.
Stage IIIB: Involving one or both ovaries with histologically confirmed
implants on abdominal peritoneal surface 2 cm in diameter and with
negative lymph nodes.
Stage IIIC: Abdominal implants 2 cm in diameter and/or positive
retroperitoneal or inguinal lymph node

609
Stage IV: involving one or both ovaries with distant metastases.
Clinical picture. In early stages the relevant symptoms are
unremarkable and only torsion of the tumor pedicle or rupture of the tumor
capsule may be associated with acute pain in the lower abdomen.
Dissemination of the process is attended by impairment of the general status
and functions of the pelvic organs. Other findings include weakness,
perspiration, loss of weight, rapid fatiguability, constant dull pain in the lower
abdomen, a feeling of abdominal bloating and abdominal enlargement due to
ascitis, dyspnea secondary to the presence of exudate in the pleural cavity,
and constipation. Acyclic uterine bleeding may occur.
Diagnosis. It is difficult in early stages of the disease because of
unremarkable symptomatology. Not uncommonly, a tumor is found during a
prophylactic examination. Ovarian cancer should be suspected if an indurate
ovarian tumor with a tuberous surface, which is somewhat mobile and is
combined with ascitis, is determined during gynecological examination.
Through the posterior fornix one can palpate dense "spikes" presenting
tumor-like masses.
In stages III-IV the disease is attended by ascitis and hydrothorax. In
the upper abdomen one can palpate a dense tuberous greater omentum, in
which metastases of the tumor are most often found. Metastatic masses may
affect virtually all portions of the abdominal cavity, including the hepatic area.
A group of risk for the development of ovarian cancer includes patients
with a prolonged recurrent inflammatory process of the uterine adnexa,
multiple uterine myoma, retention cysts, and vague tumor-like formations in
the true pelvis.
To establish the differential diagnosis, one can use such additional
methods as pelviography, laparoscopy, and ultrasound scanning. To specify
the stage of tumor dissemination, one should examine the gastrointestinal
tract (roentgenoscopy of the stomach, irrigoscopy) and the urinary tract
(excretory urography).

610
Treatment. The treatment should be combined (surgical intervention
and chemotherapy). Extirpation of the uterus and adnexa and resection of the
greater omentum are carried out. Yet, in the case of an extended process such
scope of surgical intervention is technically impossible. It is advisable to
remove major tumor-like masses in such cases.
Chemotherapy (thiotepa, cyclophosphamide, sarcolysine, fluorouracil,
etc.) is employed before and after surgery. Repeated courses of
polychemotherapy have found wide application.
Androgens are also employed in the combined treatment of ovarian
cancer.
Self test
1. Krukenberg’s tumor is
A. a primary tumor
B. a metastatic tumor
2. Which of the following is not a high risk for the development of ovarian
cancer?
A. a prolonged recurrent inflammatory process of the uterine adnexa
B. a multiple uterine myoma
C. the retention cysts
D. a chronic endocervicitis
3. The treatment of ovarian cancer should be
A. surgical
B. chemotherapeutical
C. combined (surgical intervention and chemotherapy)
D. only X-ray therapy
4. Which of the stages of ovarian cancer is characterized by dissemination of the
tumour outside the parietal pelvic peritoneum?
A. stageI

611
B. stage II
C. stage III
D. stage IY
5. The treatment of mature teratoma should be
A. surgical
B. hormonal
C. physiotherapeutical
D. radiotherapeutical
6. Granulosa-cell tumors become malignant in
A. 25-30 per cent of all cases
B. 35-40 per cent of all cases
C. 45-50 per cent of all cases
D. 55-60 per cent of all cases
7. A paroophoritic cyst forms as a result of
A. secretion retained in the lumen of the tubules of the paroophoron
B. hydrogenous transformation of the paraoophoron
C. radiotherapy
D. congenital formation
8. Arrhenoblastoma, having a masculinizing property, induces all of the
following except
A. amenorrhea
B. breast reduction
C. growth of hair on the face
D. adiposogenital dystrophy
9. The risk of malignization of ovarian fibroma is in
A. 1 per cent of cases
B. 10 per cent of cases
C. 25-30 per cent of cases
D. 0. 1-0. 5 per cent of cases

612
10. Most frequently papillary cystadenomas occur at the age of
A. 10-20 years
B. 25-35 years
C. 35-48 years
D. 50-60 years

613
Chapter 19. CANCER OF THE FALLOPIAN TUBES
Cancer of the fallopian tubes is the rarest gynecologic malignancy.
Overall, tubal cancer accounts for 0. 1 to 0,5 percent of all gynecologic
cancers.
Primary cancer of the uterine tube is rarely encountered. More
frequently it is secondary to propagation of the malignant process from the
uterus or ovary onto the oviduct.
The average age of the patients with this cancer is 50 to 60 years. Risk
factors are not well defined, however, chronic inflammatory disease, such as
salpingitis, tuberculosis is a possible etiologic factor. Patients sometimes have
a remote history of infertility.
Because of the rarity, information regarding etiology, epidemiology and
treatment is limited.
More than 95% of fallopian tube cancers are papillary serous
adenocarcinomas, arising from the epithelium of the fallopian tubes. A few
are sarcomas (Fig. 236).
The spread pattern is similar to that of ovarian cancer. Fallopian tube
cancer is spread by direct extension, by peritoneal seeding, or through the
lymphatics.
Classification depends on stages.
Staging is similar to that for ovarian cancer:
Stage 0: carcinoma in situ (limited to tubal mucosa).
Stage I: limited to the fallopian tubes
Stage IA: limited to one tube,
Stage IB: limited to both tubes,
Stage IC: stage 1А or 1В + ascites containing malignant cells
Stage II: involving one or both fallopian tubes with pelvic extension
Stage IIA: extension and/or metastasis to the uterus or ovaries,

614
Stage IIB: extension to other pelvic tissues,
Stage IIC: stage 2А or 2В + ascites containing malignant cells
Stage III: involving one or both fallopian tubes with peritoneal implants
outside the pelvis or positive retroperitoneal or inguinal lymph nodes.
Stage IV: involving one or both fallopian tubes with distant metastasis.
Fig. 236. Cancer of a Fallopian tube
Clinical picture. The signs and symptoms of fallopian tube cancer are
often vague, with the patient giving a history of lower abdominal and pelvic
pain that has been mild but chronic in nature. Most patients present with an
adnexal mass or vague abdominal or pelvic complaints such as abdominal
discomfort, bloating or pain. As the disease progresses, intraperitoneal
metastases lead to other gastrointestinal symptoms and, with progression,
abdominal distension and ascites. Some patients have vaginal bleeding, and
many report an amber-yellow discharge prior to diagnosis. Less than 1/3 of
patients present with hydrops tube profluens – a triad of pelvic pain, copious
watery discharge, and adnexal mass. Some authors have suggested that
abdominal pain relieved by the rapid release of a “tea-coloured” vaginal
discharge (hydrops tubae profluens) is pathognomonic for fallopian tube
cancer.
Diagnosis. The diagnosis is difficult. Cytological examination of an
aspirated sample from the uterine cavity or cervical canal may reveal atypical

615
cells, whereas examination of samples obtained by curettage of the
endometrium ascertains benign alterations. The diagnosis may be specified
by laparoscopy.
Treatment. The treatment is combined, including removal of the uterus
with the adnexa, omentectomy, pelvic and para-aortic lymph node dissection,
and subsequent radio- and chemotherapy.
Regular medical examination is the best type of prevention of any
genital tumours, and tubal tumours particularly.
Self test
1. Cancer of the fallopian tubes is the most rare gynecologic malignancy.
A. yes
B. no
2. The average age of the patients with the cancer of fallopian tubes is
A. 50 to 60 years
B. 20-30 years
C. 40-50 years
D. 12-16 years
3. “Tea-colored” vaginal discharge is
A. typical for tubal cancer
B. uncharacteristic for tubal cancer
C. more characteristic for vaginal cancer
D. characteristic for ovarian cancer
4. All of the following is a characteristic of tubal carcinomas except
A. adenomatous cell type
B. papillary excrescences
C. bilaterality
D. watery vaginal discharge

616
5. Which of the following is the most important prognostic factor for patients with
advanced tubal carcinoma?
A. grade of tumour
B. bulk of residual tumour left behind after initial surgery
C. stage of initial presentation
D. duration of symptoms preoperatively
6. Hystologically fallopian tube cancers usually are
A. papillary serous adenocarcinomas
B. neurosarcomas
C. fibroadenomas
D. adenomyosis
7. A malignant tumor from epithelial tissue is
A. adenoma
B. carcinoma
C. fibroadenoma
D. sarcoma
8. What is the main method of tubal malignancy diagnostics?
A. histological examination of samples obtained by curettage of the
endometrium
B. chief complaints and anamnesis data
C. US
D. laparoscopy
9. What operation is indicated in case of tubal malignancy?
A. amputation of failured tube
B. amputation of both tubes
C. extirpation of the uterus with adnexa
D. Wertheim’s operation with subsequent radio- and chemotherapy
10. Tubal cancer is
A. the rarest malignant disease
B. the most freguent malignant disease

617
Chapter 20. TROPHOBLASTIC DISEASES
Trophoblastic Disease (HydatiformMole)
Gestational trophoblastic disease is a term for a group of neoplasms,
derived from the human placenta. Trophoblastic diseases can follow a
spontaneous abortion, an actopic pregnancy, or a full-term pregnancy.
Histologically, the forms of trophoblastic disease include hydatidiform
mole (complete and partial), invasive mole (choriocarcinoma destruen),
choriocarcinoma.
Hydatiform Mole
Hydatidiform mole is a disease of the ovum, which is characterized by
excessive growth of the epithelium of chorionic villi. The villi have become
hydropic and trophoblastic elements have proliferated. Hydatidiform mole is
localized in the uterus. The placental tissue in hydatidiform mole presents a
mass of vesicles of various sizes, which are filled with fluid. Two distinct types
of hydatidiform mole have been described: partial and complete (total)
hydatidiform moles. Partial hydatidiform mole is pregnancy characterized by
replacement of a portion of the placenta by hydropic villi. With complete
moles the fetus and membranes are absent and generalized hydropic changes
are present, resulting in the characteristic gross appearance of a mass of
grape-like tissue replacing the placenta. Variable amounts of trophoblastic
proliferation are present, and fetal vessels are not identified microscopically.
Partial moles are characterized by focal hydrops of placental changes that
may not be identified and are more frequently associated with a fetus or
amniotic membranes. Hystologically, there is focal trophoblastic proliferation
and evidence of fetal vessels in placental villi.

618
Some hydatidiform moles erode the wall of the uterus, burrow into
myometrium and may even burst through the uterus into either the peritoneal
cavity or the broad ligament giving rise to internal hemorrhage. This is known
as invasive (destructive hydatidiform) mole. (Fig. 133)
Hydatidiform mole without atypia and proliferation should be
considered a benign disease while destructive hydatidiform mole presents a
malignant tumour since it destroys tissues and metastasizes into various
organs.
Hydatidiform mole may transform into choriocarcinoma.
Choriocarcinoma is an invasive, usually widely metastatic tumour
composed of malignant trophoblastic cells without hydropic villi. Incidence of
transformation of hydatidiform mole into choriocarcinoma ranges from 1 to
18 per cent.
Placental site trophoblastic tumour, consisting of intermediate
trophoblastic cells that persist after a term of pregnancy, is rare.
Clinical features.
A hydatidiform mole is more common after pregnancies in very young
(less than 17 years) or older (late 30s and 40s) patients. A hydatidiform mole
often manifests within 10-16 weeks after conception by a rapidly enlarging
uterus, which is often larger than expected for estimated gestational age.
Patients often present with vaginal hemorrhage and spontaneous
abortion of atypical hydropic vesicles. Benign ovarian cysts (theca-lutein
cysts) are caused by ovarian stimulation of human chorionic gonadotropin
(hCG) and are detected in approximately 20 percent of patients with complete
moles. Hydatidiform mole usually leads to abortions, although the mole may
be retained in the uterus.
The most frequent symptoms are:
-Vaginal bleeding. It occurs as irregular, small hemorrhage combined
with watery discharge. The hemorrhage usually starts during the 2nd month

619
of pregnancy and recurs irregularly until the time of abortion when severe
bleeding may develop.
-Symptoms of toxemia are very significant and often in patients with
hydatidiform mole. Excessive vomiting is not uncommon, blood pressure may
be raised. Feet may become edematous. Albuminuria may be found.
-Uterus is usually longer than would be expected in this term of
gestation and has a peculiar doughy consistence.
-A fetus is frequently identified in partial mole.
In complete form of hydatidiform mole there is no fetus in the uterus,
only changed chorion. There is no fetal heart sounds, fetus is not detected on
ultrasound examination, X-ray.
Diagnosis. It is based on the clinical picture, which, apart from signs
of pregnancy and occasional symptoms of gestosis, is characterized by an
extremely rapid growth of the uterus, inconsistent with the gestational age,
non-uniform uterine consistency, and ovarian enlargement. The clinical
diagnosis of molar gestation is supported also by characteristic
ultrasonography findings consisting of a “snow storm” pattern of mixed
echogenic foci, reflecting the edematous hydropic villi and intrauterine
hemorrhagе.
Thecal cysts may develop in the ovaries. Urine levels of HCG are
dramatically elevated. Reliable signs of pregnancy (foetal movements and
heartbeat) are absent in patients with complete form of hydatidiform mole.
Hydatidiform mole should be differentiated from threatened abortion,
hydramnion, multiple pregnancy, placenta abruptio, and uterine myoma.
The diagnosis can be specified by ultrasound scanning and amnioscopy.
Pregnancy tests will be positive in high dilution due to increased
output of urinary gonadotropin.
Serum HCG levels are markedly elevated in paients with hydatidiform
mole. HCG is produced by the proliferated trophoblastic tissue, and high
serum levels of the subunit of HCG aid in the diagnosis of a gestational

620
trophoblasic disease. Passage of grape-life molar suggests the diagnosis,
and histological examination confirms it.
Treatment.
In half the cases the abortion is spontaneous, but there is always a
tendency for the abortion to be accompanied by a severe uterine bleeding.
Another danger of the mole is that a malignant tumour (choriocarcinoma)
sometimes develops.
The hydatidiform mole should be removed from the uterus after the
determination of the diagnosis. Simultaneous removal (dilatation and
curettage of the uterine cavity, vacuum aspiration) of the hydatidiform
mole with the mandatory histological examination of the material obtained
is obligatory. Curettage of the uterine cavity may be done in early stages of
gestation – prior to 12 weeks of pregnancy. In terms more than 12 weeks
delivery of the hydatidiform mole should be stimulated medically. To
accelerate separation and expulsion of the mole, the woman is given
oxytocin, prostaglandine and other drugs stimulating uterine contractions.
In cases of profuse bleeding and opened cervical canal, one or two fingers
introduced into the uterine cavity should extract the mole. In cases of
profuse bleeding and the cervical canal closed for the finger, the mole
should be removed with curettage of the uterus. The curettage should be
done very accurately due to high danger of uterine perforation because of
thinning of the walls.
After the removing of the mole the special care of the patient must be
done to prevent the development of choriocarcinoma.
In the benign form of hydatidiform mole the recommended treatment
is 2-3 courses of methotrexate therapy, in destructive hydatidiform mole
three courses of polychemotherapy (methotrexate, rubomycin,
adriamycin).
With the purpose of choriocarcinoma prevention patients with a
history of hydatidiform mole are subjected to a 2-6 year follow-up. Apart

621
from ordinary clinical examination, urinary HCG levels are measured twice
weekly for two months and monthly thereafter; lung roentgenography is
performed once every three months. If the course is favourable, the HCG
titre becomes negative three weeks after removal of the hydatidiform mole.
Choriocarcinoma.
Choriocarcinoma (chorionepithelioma) (Fig. 134) is a malignant uterine
tumour developing in half of all cases from the hydatidiform mole; less
commonly it develops after deliveries and abortions. The tumour develops
from trophoblast elements. Choriocarcinoma in the form of a nodular
crimson tumour may be positioned under the mucous membrane or in the
midst of the muscular layer (interstitially), gradually growing through all
layers of the uterus; it easily disintegrates, which is often accompanied by
profuse bleeding. Choriocarcinoma in the form of friable dark blue nodes
often metastasizes into the vagina, less frequently into the ovaries and uterine
tubes.
Clinical picture.
It is characterized by acyclic prolonged, occasionally profuse uterine
bleeding (absent in intramuscular position of nodes), serous sanguineous
leucorrhea, often with a putrefactive odour, and mild low abdominal pain.
Prolonged bleeding may lead to secondary anemia, while attendant infection
may be a cause of the inflammatory process of the female genital organs.
Choriocarcinoma is characterized by early metastatic spread via blood to the
vagina, liver, brain, and, more commonly, to the lungs. In the latter case the
disease is attended by cough and blood-tinted sputum. The disease progresses
rapidly and may lead to the lethal outcome.
Diagnosis. It is based on the thorough study of the history (a history
of a hydatidiform mole, delivery, abortions). Of great significance is
determination of HCG titres in the urine and separate diagnostic dilatation
and curettage (in most cases tumour elements may be determined

622
histologically). Thecal cysts developing in choriocarcinoma in 40-50 per
cent of cases have a definite diagnostic significance since they are able to
undergo inverse development in the time course of the disease.
Treatment. The treatment may be conservative (chemotherapy) and
surgical.
Chemotherapy is based on the use of methotrexate, mercaptopurine,
and rubomycin.
Systemic measurement of HCG levels in the urine serves as a criterion
of treatment efficacy.
Surgical treatment is indicated in profuse uterine bleeding, tendency
of the tumour to grow into the surrounding tissues and threat of uterine
perforation, a large size of the tumour (the uterus is larger than the 10-week
gravid uterus), and the absence of response to chemotherapy. Extirpation
of the uterus is performed; in young women the adnexa are left intact where
it is possible.
Following conservative treatment, the patient may conceive and have
a normal delivery.
Prevention of choriocarcinoma consists in the early and correct
treatment of hydatidiform mole. Since choriocarcinoma may also develop
after normal pregnancy, to prevent the disease it is necessary to inspect
thoroughly the afterbirth (to determine its integrity) and to perform
correctly all manipulations related to pregnancy termination.
Self test
1. Which of the following is consistent with hydatidiform mole?
A. a uterus that is large for dates
B. a presence of a fetus
C. theca-lutein cysts
D. a uterus firm and irregular in shape

623
2. A 25-year-old woman presents with a molar gestation at 12 weeks from her last
menstrual period. Which of the following is the most appropriate management for
this patient?
A. removing of the hydatidiform mole and the chemotherapy
B. obtaining of a quantitative HCG titer
C. hysterotomy
D. observation of the patient and prolongation of the pregnancy
3. Which of the following factors are poor prognosis indicators for metastatic
gestational trophoblastic neoplasma?
A. a patient of 35
B. diagnosis of disease at 6 weeks postpartum
C. presence of a fetus
D. hysterectomy as treatment
4. Choriocarcinoma more often develops from the
A. hydatidiform mole
B. hysterectomy
C. pelvic inflammation
D. adenomyosis
5. Which of the folllowing is not an indication for surgical treatment of
choriocarcinoma?
A. profuse uterine bleeding
B. tendency of the tumour to grow into the surrounding tissues
C. hreat of uterine perforation
D. effective chemotherapy
6. Hydatidiform mole usually results from
A. abortion, hemorrhage
B. fetal malformations
C. postmaturity
D. cephalo-pelvic siaproportion due to a big fetus

624
7. Incidence of transformation of hydatidiform mole into choriocarcinoma ranges
A. from 1 to 18 per cent
B. from 20 to 30 per cent
C. from 40 to 50 per cent
D. more than 50 per cent
8. Choriocarcinoma is a real malignant uterine tumour.
A. yes
B. no
9. The most appropriate method of evacuation of complete hydatidiform mole is
A. a hysterectomy
B. an induction of abortion
C. a curettage of the uterine cavity
D. a suction curettage
10. Staging of trophoblastic malignancy usually utilizes all of the following except
A. quantified HCG
B. chest X-ray
C. cheast/head/abdominal CT scan
D. angiography

625
Chapter 21. GYNECOLOGICAL DISEASES IN
CHILDHOOD AND ADOLESCENCE
The development of pediatric gynecology as a separate trend of science
has considerably extended the notion of specific features of genital diseases in
girls. At present, the principles of prevention and treatment of gynecological
diseases of childhood and adolescence have been elaborated, which call for:
(1) health education of girls, their parents and teachers at kindergartens and
schools; (2) organization of regional gynecological centers for children and
adolescents; (3) establishment of specialized gynecological clinics and
consultation centers. Despite the advances made in rendering the
gynecological care to children and adolescents, situations often arise that
require emergency aid.
Tumours
Tumours in children and adolescents are a relatively rare finding. The
data on the character and clinical course of tumours are controversial and
depend on the groups of patients hospitalized. Genital tumours of girls are
reported to be potentially malignant in 50 per cent of cases.
Genital tumours of various structures can develop in childhood and
adolescence. Germinal tumours are frequently observed before puberty. Other
tumours can develop at the onset of the pubertal period, which indirectly
indicates the role of hormonal effects in their occurrence. Morphologically,
tumours typical for the young age are divided into innocent (mature
teratomas, dermoid cysts) and malignant (teratoblastomas). These
newgrowths are referred to as germinal tumours. Dysgerminomas are worth
mentioning among the tumours of the genital cord stroma.
Various pieces of information on the incidence and clinical course of
different tumours, which are often based on individual observations, provide

626
no precise idea of the problem. We consider it necessary to briefly describe
the genital tumours in children and adolescents basing primarily on our own
observations in this age group of 150 patients. According to the data obtained,
genital tumours are not an extremely rare finding in this age group: about 4
per cent of patients under 18 that were treated at the gynecological
department of our clinic had tumours and tumour-like formations of the
genitalia.
Diseases of childhood and adolescence, which are surgically treated,
differ considerably from those of adults. The majority of girls underwent
surgery for tumours and tumour-like formations revealed in the adnexa,
whereas women are most frequently operated on for tumours of the uterus,
particularly myoma.
Tumours and tumour-like formations most often develop in the adnexa.
According to our data, innocent tumours revealed in the pubertal period are
more common. It should be emphasized that due to the specific character of
hospitalization the number of girls with malignant tumours of the ovaries is
greater among patients admitted to the oncological hospitals than to the
gynecological ones. The physician should always remember about the
possibility of a malignant tumour developing in a girl.
Innocent tumours are characterized by rapid growth. Tumours and
tumour-like formations of the adnexa are not uncommonly combined with
appendicitis.
In the absence of complications (twisted tumour pedicle, suppuration)
benign tumours of the ovaries in girls follow a milder course than in adults.
Pain commonly develops only when the ovarian formation becomes large in
size. In girls, the adhesive process in the small pelvis is encountered
extremely rarely.
The ovarian cysts in infants and girls are a less common finding than in
adults. Small follicular cysts may remain undiagnosed.

627
Torsion of ovarian tumour is most often associated with a dermoid cyst
owing to the specific anatomy (long pedicle). This tumour has teratoid origin
and can be found at any age (cases have been described of twisted tumour
pedicle in girls aged 4 and 5, the tumours reaching considerable size); the
symptoms of the acute abdomen develop therewith.
Malignant newgrowths of the ovaries (teratoblasto-mas,
dysgerminomas) can also cause conditions requiring emergency care. Like in
adults, the need for emergency surgery in girls with ovarian tumours arises
when the surgical intervention has not been performed in time. The principle
that must be observed while treating the women with ovarian tumours
(immediate operation) applies in full measure to girls.
Hormone-producing tumours are a rare finding; granulosa-cell tumours
and, less commonly, thecomas develop in this age group.
Feminizing ovarian tumours in girls are usually characterized by vivid
clinical manifestations due to the large amount of estrogenic hormones
produced by the tumour. Signs of precocious puberty are witnessed by the
engorged breasts, secondary sex characters (growth of hair on the pubis,
enlarged clitoris and labia pudenda), and uterine bleedings that precede the
menstrual-like discharge.
In children and adolescents, masculinizing ovarian tumours are found
exceptionally rarely. If the symptoms of virilization are manifested, the
masculinizing tumour of the ovary can be suspected. Delayed sexual
development may be observed as a symptom of masculinizing tumour though
this happens extremely rarely. In these cases the differential diagnosis is
difficult. The patients should be followed-up at a specialized in-patient
setting.
A well-timed operation can help to prevent the development of obesity
and severe essential hypertension. Besides, early surgery for a malignant
tumour may bring favourable long-term results.

628
Tumours of the external genitalia, vagina, and uterus are rarely
observed among children and adolescents (8 per cent of all the tumours and
tumour-like formations of the adnexa). These newgrowths are malignant as a
rule (sarcoma of the vagina, cervix or corpus uteri).
When malignant tumour develops, the blood-tinted reeking vaginal
discharge, which is the leading symptom of the disease, appears. Later, pain
of various intensity concurs. Parents promptly consult the physician in the
event of blood-tinted vaginal discharge occurring in little girls. The older girls
(after the menarche has set in) do not visit the doctor for a long time as a
result of which in most cases the disease is diagnosed in the advanced stage.
The physician should bear in mind that the formation arising from the
ovary is most likely the tumour but not the cyst. A malignant newgrowth
should be suspected in cases where the tumour originates in the external
genitalia, vagina, or corpus uteri. The diagnosis of tumours and tumour-like
formations of the uterus and adnexa may present considerable difficulties,
which is to a large extent explained by the lack of information.
The diagnosis may not be established in time because the possibility of
occurrence of tumour in infants or girls is neglected. When a girl complains of
pain in the lower abdomen and her behavior changes, the pediatrician should
refer her to the gynecologist. Commonly, the tumour is easily palpated
through the peritoneal coat. The diagnosis is confirmed during the rectal
examination. In girls the uterus and adnexa are placed rather high and
descend into the true pelvis only by the end of pubertal period to occupy the
adult position.
Limited dimensions of the true pelvis do not allow the tumours to be
located in the pelvic cavity even when the ovarian formations are
comparatively small. These specific anatomical features determine the
absence of symptoms of compressed urinary bladder and rectum. When
indicated, the rectum can be examined under anesthesia. The short-term
anesthesia ensures adequate relaxation of the anterior abdominal muscles

629
and makes palpation of the internal genitalia easier. Ultrasound or X-ray
examination of the true pelvis is indicated under the conditions of
pneumoperitoneum, when the diagnosis is uncertain.
As our experience shows, ovarian tumour may be mistaken for
pregnancy, and a serious psychic trauma may be inflicted to a girl through the
physician's fault.
Before the diagnosis of pregnancy is established, it should be thoroughly
verified (gynecologist’s consultation, ultrasound study, determination of
human chorionic gonadotropine).
Tumours and tumour-like formations of the adnexa in girls have to be
differentiated primarily from appendicitis, particularly when the pedicle of
the tumour is twisted. Rectal examination helps to specify the diagnosis.
Ovarian tumour combined with appendicitis was observed in every fifth of our
patients operated on.
The dystopic kidney or its tumour, as well as overfilled urinary bladder,
can simulate a newgrowth of the ovary. To avoid diagnostic errors, it is
necessary to inspect the rectum when the urinary bladder has been emptied.
Intravenous pyelography is indicated in suspected renal pathology.
Auxiliary methods of examination, such as vagino-scopy, endoscopy,
radiography of the true pelvic organs under the condition of
pneumoperitoneum, and ultrasound study are recommended to verify the
diagnosis of genital tumours and tumour-like formations.
Surgery for genital tumours in children and adolescents should be
maximally sparing (partial resection of the ovary or enucleation of the
tumour). When the cyst is paroophoritic, only enucleation is performed. The
adnexa have to be completely removed in torsion of the tumour pedicle, when
the ovarian tissue has undergone pathological changes to the extent that calls
for its elimination.
Urgent histological study of the removed specimen is of particular
importance since the range of surgical intervention largely depends on its

630
results. In the climacteric or postmenopausal women, visual inspection of the
affected organ can be decisive with respect to the volume of surgery, whereas
in girls the need for radical surgery should be grounded on the histologically
confirmed malignancy of the newgrowth. It is necessary to refer infants and
girls to the specialized in-patient settings, where the highly skilled specialists
can perform auxiliary examinations.
Like women, girls should be subjected to emergency surgery in torsion
of the tumour pedicle, rupture and suppuration of the capsule.
Intraoperative examination of the appendix is essential, since in a large
number of girls appendectomy has to be simultaneously resorted too owing to
its chronic inflammation. Inspection of the adnexa during appendectomy is
equally important, because there were cases of the appendix removal where
the ovarian formation with the twisted pedicle remained. We had to re-
operate on such patients.
Inflammatory Diseases of the Genitalia
Conditions, which induce adnexitis in girls, fall far short of those in
women. Septic infection and gonorrhea provoke inflammatory diseases
extremely rarely. Adnexitis of tuberculous etiology may be encountered
among little girls. Severe inflammation is observed in suppuration of the
hematosalpinx originating as a result of a developmental defect of the internal
genitalia. The disease runs with the typical clinical picture of the acute
abdomen.
The diseases of the large intestine, particularly appendicitis, are the
most frequent causes of adnexitis in girls. This is explained by the close
anatomical relationships between the appendix and adnexa. Inflammation of
the appendix often involves the adnexa.
Appendectomy may be followed by adnexal inflammation a few months
later, which is probably explained by the latent inflammatory process that

631
manifests itself as a result of a provoking effect (cooling, extragenital
infection, etc.).
The clinical picture is characterized by sudden pain in the lower
abdomen attended with nausea and vomiting, frequent urination, and high
body temperature. A 'tumour' is diagnosed after the acute abdominal
symptoms disappear. The diagnosis is often late since it does not occur to
physicians to relate this condition to adnexal inflammation. The examination
demonstrates tender formations in the adnexal area. When these patients are
examined through the rectum, tenderness of the uterus is revealed on its
displacement. A tender formation of varying form and size is palpated
posterior to the uterus, mostly to the right. Its consistence is uneven, varying
from dense to tight elastic, and the surface is irregular; absence of mobility of
these tumour-like formations is characteristic.
Purulent tubo-ovarian formations of the adnexa that occasionally
adhere to the appendix are most often found during the operation. We
observed a patient in whom the gangrenous appendix, which was intimately
fused with purulent tubo-ovarian formation, was self-amputated. It should be
pointed out that surgical treatment is commonly associated with considerable
difficulties when purulent tubo-ovarian formations are combined with
inflammatory changes in the appendix.
Important practical conclusions result from the above. When
appendicitis is diagnosed in girls, the gynaecologist's consultation is a must to
find out the condition of the adnexa. To reveal inflammatory changes in time,
the adnexa should necessarily be inspected during surgery for appendicitis,
and while operating on inflammatory changes in the adnexa, the appendix
should be examined; appendectomy is performed when the abnormality is
visualized.

632
Developmental Defects of the Vagina and Uterus
The attention of many researchers has been drawn to studying the
genesis of congenital anomalies of the urogenital system. This is connected
with the fact that these defects not only make the woman suffer badly but also
cause disturbances of the reproductive function. Some authors voice the
opinion on the possible role of the environmental factors during
embryogenesis (intoxication, temperature effects, etc.).
Hereditary factors in the form of chromosomal and gene mutations can
also induce developmental defects. According to our data, the aggravated
heredity was evident in 40 per cent of women (spontaneous abortions,
idiopathic infant mortality, impaired menstrual function, childless couples,
developmental defects in the family). Parents are often over 35-40 years of
age.
Mothers of many patients have experienced stress situations associated
with war, prolonged starving, and injury. Parents of some of the patients were
alcoholics or were exposed to the occupational (chemical or radioactive)
hazards.
Congenital anomalies of the vagina and uterus are among the frequent
causes of an urgent surgical intervention. Developmental defects attended
with completely or partially delayed outflow of the menstrual blood are
clinically manifested during puberty.
The developmental defect of the vagina is characterized by completely
impaired menstrual outflow, the uterus functioning normally. In these
patients the uterus occupies normal median position; its lower pole can be
reached during the recto-abdominal examination. This abnormality manifests
itself at the menarche age and often requires emergency surgical aid.
Diagnostic errors are made in many cases: ovarian tumour, appendicitis, etc.
are diagnosed. Young girls with acute pain in the lower abdomen are
erroneously subjected to the ungrounded, occasionally repeated laparotomies.

633
The uterus is extirpated in cases where only the septum of the vagina should
be dissected.
While making the diagnosis, it is necessary to pay attention to the size of
the missing portion of the vagina, the time and intensity of pain, and also to
the dimensions of the tumour-like formation in the true pelvis. The case in
point may be atresia of the hymen, aplasia of the lower third of the vagina,
aplasia of lower two thirds of the vagina, absence of the upper third of the
vagina, and finally, complete absence of the vagina with the functioning
uterus.
The diagnosis and treatment of atresia of the hymen are most simple. In
these patients a cyanotic swelling, which is well seen on inspecting the
external genitalia, bulges out in the area of the vaginal orifice. Treatment
consists in dissecting the hymen.
It is more difficult to make the diagnosis if from one to two thirds of the
vagina are missing. The tumour-like formation, which may have the form of a
sand glass, is determined in the centre of the true pelvis during the recto-
abdominal examination. In the event of the distended cervix, the common
receptacle for the menstrual blood is formed (distended uterus, cervix, and
vagina). Surgical correction consists in the restoration of the patency of the
vaginal tube by incising the septum, lowering the edges of the distended
vagina, and suturing them in the area of the vaginal orifice.
The absence of the upper vaginal third is nearly always related to the
underdeveloped cervix. Pain develops early. The rounded formation, which is
tender to palpation, is found in the centre of the pelvis during the recto-
abdominal inspection. The uterus is emptied during surgery, but since the
cervical canal is absent this will eventually lead to the cicatrization at this site,
which interferes with the menstrual outflow. The repeated bougienage and
dissection of the cicatrices in the vaginal cupola usually prove ineffective and,
therefore, extirpation of the uterus has to be resorted to in many cases. When

634
the vagina is completely absent and the uterus is functioning, artificial vagina
is created in rare cases where the cervix is present.
If emptying of the hematometra through the cervical canal and suturing
the cervix to the vaginal cupola are managed, this operation is normally a
success. When the hematometra is emptied through an orifice artificially
created in the uterus, and this site is sutured to the vaginal cupola, the orifice
soon becomes obliterated, and the hematometra recurs.
In the event of a completely delayed menstrual outflow and the late
performance of surgery (which often happens), the hematocolpos (in the
presence of a vaginal portion), hematometra, and hematosalpinx occur. The
days of menstrual bleeding are characterized by severe pain. When infection
concurs, the contents of the uterus and fallopian tubes suppurate. The body
temperature is elevated, and the pain sharply intensifies; the peritoneal
manifestations develop. The sharply tender tumour-like formations are
palpated in the true pelvis. Emergency surgery is needed in these cases. The
diagnosis is based on the history, results of examination of the external
genitalia and rectum.
The success of surgery largely depends on what vaginal portion is
missing. In atretic hymen its cross-like dissection and emptying of the
hematocolpos are warranted. When the lower third of the vagina is absent,
the tissues are separated and incised reaching the vaginal tube after which the
edges of the vagina are sutured to the area of the vaginal orifice. When the
middle third of the vagina is absent, the tissues are incised between the lower
and upper thirds of the vagina, which is followed by suturing of their mucosa.
As a rule, such procedure is effective in this abnormality. Absence of the
upper third or the entire vagina are most unfavourable and characterized by
the absence of the vaginal fornices; the cervix is normally underdeveloped or
absent. As was noted above, surgical correction is of little effect and
technically complicated.

635
Partially impaired menstrual outflow develops in functioning of the
rudimentary closed horn of the uterus. The sharply pronounced pain, which
appears early, is typical for the clinical picture.
The diagnosis presents difficulty (we observed patients in whom acute
appendicitis or other intra-abdominal abnormality was diagnosed). Excretory
urography, which is one of the efficacious auxiliary methods of investigation,
demonstrates absence of the kidney on the side of the rudimentary horn.
Besides, the adnexa are absent in half the patients. Laparotomy with removal
of the rudimentary uterus is necessary in such cases.
The pathological condition described is very difficult to diagnose.
Persistent primary algomenorrhea, blood-tinged or purulent vaginal
discharge, and also a tumour-like formation in the true pelvis allow a
congenital anomaly to be suspected. When the condition is diagnosed,
surgical treatment presents no difficulty. The site of the rudimentary closed
vagina is dissected sufficiently widely, thereby creating conditions for the
outflow of the menstrual blood.
It should be pointed out that the diagnostic errors are common in
genital developmental defects and ungrounded surgical interventions are
often performed.
This is explained by the lack of information on the given pathology,
whereas the monthly recurring pain in the lower abdomen and the tumour-
like formation in the true pelvis in girls of the pubertal age should always
suggest congenital anomalies of the reproductive system.
Pain is typical for all types of genital developmental defects; however,
the intensity and character of pain have specific features that are determined
by the form of the anomaly. A periodically recurring and intensifying,
gnawing pain is most typical for atresia of the hymen, aplasia of the vaginal
portion, and duplex vagina and uterus with partial aplasia of one of the
vaginas. A primary colicky pain that rapidly becomes permanent and grows in
intensity is more characteristic of girls with aplasia of the entire vagina and

636
the functioning uterus and of patients with rudimentary, closed and
functioning horn of the uterus. The disease runs the most severe clinical
course in the latter cases.
Occasionally, the disease can be diagnosed only after the auxiliary
methods of investigation have been employed: ultrasound study, radiography
of the small pelvis under the conditions of pneumoperitoneum, excretory
urography, and laparoscopy.
The duplex vagina and uterus with partial aplasia of one of the vaginas
combined with the rudimentary, closed and functioning horn of the uterus
present the greatest difficulties for the diagnosis.
As it was already emphasized, excretory urography must be indicated
for all the patients in whom a congenital anomaly of the genitalia is suspected
not only because the developmental defects of the uterus and vagina are
frequently combined with anomaly of the urinary system, but also due to the
fact that absence of the kidney revealed by the excretory urography in
algomenorrhoea patients almost reliably indicates partially aplastic vagina in
case it is duplicated. Presence of the closed horn of the uterus can also be
suspected on the side of the absent kidney.
Although the condition of young girls with impaired menstrual outflow
due to a developmental genital defect not infrequently requires emergency
surgery, they should be transported to a specialized hospital to specify the
diagnosis and to undergo surgery, which presents considerable technical
difficulties.
Bleedings
Dysfunction of the ovaries, genital tumours, diseases of the blood, and
injury in childhood and adolescence can induce vaginal hemorrhage. Internal
hemorrhage is commonly associated with apoplexy of the ovary usually
encountered among girls with established menstrual function, though the
condition can also develop at an early age. The cases are reported of apoplexy

637
of the ovary with heavy blood loss in girls of 8 and 10 years of age. Juvenile
bleedings are typical for the pubertal age.
Juvenile bleeding is a dysfunctional uterine hemorrhage, which is
manifested during the period of sexual maturity. It is caused by altered
secretion of sex hormones due to disturbed neuro-endocrine regulation of the
menstrual cycle during puberty. Chronic and acute infections and somatic
diseases, hypovitaminoses, stressful situations, and unfavourable course of
the antenatal development facilitate the occurrence of juvenile bleedings
affecting the functioning of the hypothalamic-pituitary-ovarian system.
In adolescence, the immaturity of morphological structures of the
hypothalamus and other links of the system that ensure the normal menstrual
cycle can give rise to particularly severe bleedings. Hypoplasia of the uterus
increases the duration of bleeding. Bleedings are mostly anovulatory in nature
and develop against the background of atretic follicles rapidly leading to
anemia. The heavy blood loss can induce the secondary changes in the blood
coagulation and anticoagulation systems. Deviations in somatic development
(infantile body build or morphotype exceeding the norm) are often noted in
young girls suffering from juvenile bleedings.
Disturbances of the menstrual cycle are typical for patients with juvenile
bleedings: suppressed menses precede abundant bleeding. Pathological
bleeding often develops during the first menstruation.
When the diagnosis of the 'juvenile bleeding' is being made, diseases of
the blood and organic lesions of the genitalia (feminizing tumours of the
ovary, tumours of the uterus or vagina, etc.) should first of all be excluded.
When bleeding arises during the first menstruation or resembles
menorrhagia, a blood disease should be suspected; similar bleedings are
observed in the Werlgof disease, hypoproconvertinaemia, and various
thrombocytopenic conditions.
Nasal and gingival bleedings, easily occurring subcutaneous
extravasates, and the cyclic character of uterine bleedings suggests disease of

638
the blood, the study of which helps to confirm the diagnosis. The Werlgof
disease is accompanied by reduction of the thrombocyte level;
hypoproconvertinaemia is characterized by low prothrombin level (50-30 per
cent). When a blood disease is suspected, it is necessary to consult the
hematologist because these diseases, which are occasionally manifested only
during the first menstruation, should be diagnosed and treated by a specialist.
Estrogen-producing tumours of the ovary, as well as tumours of the
uterus or vagina, can induce uterine bleedings. In these cases rectal and
auxiliary examinations (ultrasound, vaginoscopy, radiography of the small
pelvic organs under conditions of pneumoperitoneum) help to confirm the
diagnosis.
Treatment of juvenile bleedings should include invigorating therapy, the
use of agents contracting the uterus and hemostatics (Ergot, Ergotal,
Ergotamine), hormone therapy, and diagnostic dilatation and curettage as an
extreme measure. Occasionally, bleeding can be spontaneously arrested
following invigorating therapy and elimination of factors that cause emotional
stress.
When bleeding is profuse, urgent measures should be taken to arrest it
for which purpose the estrogen hemostasis is employed. The point is that the
dysfunctional bleeding always occurs in response to a fall in the hormone
level, which is eliminated by the administration of estrogens (these
preparations are preferable during puberty). Proliferation of the
endometrium recurs in the mucosa of the uterine corpus, and the bleeding
stops. Elimination of the fall in the hormone-level, in its turn, normalizes the
ratio between the-follicle-stimulating hormone (FSH) and luteinizing
hormone (LH).
The estrogen hemostasis is accomplished by administering 1 ml of 0. 1
per cent of dihydrostilboestrol solution intramuscularly every 2-4 hours, or
folliculin by 10 000-20 000 MU every 2-3 hours.

639
As a rule, bleeding stops a day after the administration of hormones was
begun. The hormone therapy should not be discontinued immediately after
the arrest of bleeding, since in response to a fall of the hormone level bleeding
recurs. Administration of estrogens should be continued in gradually reduced
doses, and then followed by treatment with progesterone (1 ml of 1 per cent
solution intramuscularly for 5-6 days). The menstrual-like reaction ensues
after the progesterone has been discontinued.
Invigorating and antianemic therapy should not be neglected during the
hormonal hemostasis. These patients should be followed-up by a specialist for
a long time after the emergency aid has been rendered. There are other
schemes for the hormonal hemostasis to be carried out (with the help of
synthetic progestins). In girls, the diagnostic dilatation and curettage is
performed only for vital indications, when all the methods of therapy that
have been used prove ineffective. During the curettage the necrotized
hyperplastic mucosa of the uterus is removed which arrests the bleeding. In
the majority of patients histological study of the obtained sample reveals
hyperplastic processes in the endometrium including the development of
atypical hyperplasia and adenomatous polyps.
Patients with juvenile bleedings should be systematically followed-up
and treated by the pediatric gynecologist.
Injuries to the Genitalia. Foreign Bodies in the Vagina
Genital organs can be injured as a result of falling on acute objects, in
street traumas, etc. Traumas can be extremely severe and accompanied by
ruptures of the adjacent organs, particularly in little girls.
Injury to the genitalia is usually attended with abundant bleeding,
especially when the clitoris is damaged. Emergency care includes the arrest of
hemorrhage by ligating the bleeding vessels and restoring the intactness of
the injured tissues. The anesthesia should be given to examine the girls with a
genital trauma and to suture the ruptures. When anemia is marked,

640
transfusion of blood and its substitutes is warranted. In addition, the
antitetanus serum should be administered. The principles of treatment of
hematomas do not differ from those in adults.
Penetration of foreign bodies into the vagina is mostly observed among
girls under 8 years of age. A foreign body causes inflammatory changes in the
vaginal mucosa. The puriform discharge, sometimes mixed with blood,
appears. It is not always easy to detect the foreign body. A carefully performed
rectal examination and particularly vaginoscopy allow the diagnosis to be
verified.
When a foreign body provokes inflammatory changes in the
surrounding tissues and adhesions, it should be removed under anesthesia,
because the procedure is extremely painful. Besides, the child's restless
behaviour does not allow the foreign body to be carefully removed without
injuring the adjacent organs. In the event the foreign body is mobile the
physician manages to remove it by pushing to the vaginal orifice manipulating
by the finger introduced into the rectum.
Self test
1. Which from the following infectious processes are frequent in girls
A. septic infection
B. gonorrhea
C. adnexitis of tuberculous etiology
D. colibacillus infection
2. Prescribe the medicine, which leads to uterine contraction.
A. Folliculin
B. norephedrine
C. methylergometrine
D. partusisten

641
3. Treatment of juvenile bleeding should include all of the following except
A. antianemic therapy
B. hormonal therapy
C. heparin
D. hemostatric drugs
4. Genital tumours of girls are reported to be potentially malignant in
A. 50 per cent of cases
B. 25 per cent of cases
C. 75 per cent of cases
D. 15 per cent of cases
5. What is the most freguent type of tumour in girls?
A. hormone-producing tumours
B. germinal tumours
C. hysteromyoma
D. choriocarcinoma
6. Treatment of juvenile bleedings should be started with
A. agents contracting the uterus and hemostatics, hormone therapy
B. diagnostic dilatation and curettage
C. antianemic drugs
D. vitamins and antianemic drugs
7. Hymenal anomalies are usually associated with
A. renal anomalies
B. uterine anomalies
C. no other anomalies
D. patent ductus arteriosus
8. In children vaginitis due to poor hygiene is frequently because of
A. chlamidia
B. fungus
C. coliform bacteria
D. anaerobic bacteria

642
9. Injury to the genitalia is usually attended with
A. abundant bleeding
B. red colour of affected area
C. genital itch
D. anemia
10. The diagnosis of atresia of the hymen is based on findings of
A. cyanotic swelling, bulges out in the area of the vaginal orifice
B. encreased amount of menstrual flow
C. Decreased amount of menstrual flow
D. Retension of urine

643
Chapter 22. FEMALE DISPENSARY-
PROPHILACTIC MDICAL EXAMINATION OF
GYNECOLOGICAL PATIENTS
Female dispensary is an ambulatory clinic for women. There are two
types of female dispensary:
- The first is female dispensary only for pregnant
- The second is female dispensary only for gynecological patients.
Sometimes may be mixed dispensary both for obstetrical and
gynecological patients. The main mission of this ambulatory is prophylactic
medical examination of women. The prophylactic medical examination of
patients is an active determination of gynecological diseases of women at
early stages of processes, dynamic and complex treatment. On the other hand
it should be prophylaxis of gynecological diseases, and prophylaxis of disease
spreading.
Patients with cervicitis and endocervicitis, condilomas, cervical erosion,
endometritis, parametritis, pyosalpinx need prophylactic medical care.
Noninflammatory diseases, such as leukoplakia, kraurosis, disturbances of
menstrual cycle, infertility, neuroendocrine syndromes, benign tumours of
female genitalia, endometriosis are indications for prophylactic medical care.
The duration of dispensary prophylactic observation of those patients is
different. For example, patients with acute and subacute inflammations of
female genitalia should be observed about 3 months after special treatment in
a hospital.
Patients with precancerous diseases (kraurosis, leukoplakia, and others)
must be observed continually: patients before 40–2 times a year, patients
after 40–3 times a year, even after surgical treatment.

644
Patients with uterine myoma must be observed with special gynecologic
examination continually, once in 3 months, and even more depending on
their health.
If a patient does not come to ambulatory clinic for planned
examination, she must be invited to the ambulatory by phone, post, or nurse
may be send for inviting a patient for the examination and observing her
living conditions.
Moreover, every woman must be prophylactically observed once a year.
Prophylactic examination may be arranged at factories, plants, colleges, and
schools. During those prophylactic examinations one can pay attention to the
character of menstrual cycle, reproductive function, any pains. External
genitalia, perineum, the region of anus would be inspected. For virgins rectal
examination is used depending on indications. Other patients must undergo
speculum vaginal examination, and microscopic and bacteriological
examination of smears must be done as well. For women in premenopausal
age, and after menopause cytologic examination of smears is necessary. If any
gynecological disease is found, the patient is recommended a special care and
observation. If it is indicated, patients must be hospitalized for special
treatment.
In Ukraine there are regular medical check-ups aimed at the prevention
of malignant tumours, including cancer of the female genital organs. The key
place belongs to mass prophylactic examinations (at least twice annually) of
women aged 30 years and over. Prophylactic examinations are conducted in
women's consulting centers, industrial enterprises, and special gynecological
rooms in polyclinics. A high quality of prophylactic examinations is ensured
by mandatory use of colposcopy and cytological examination of cervical
smears. Women with gastric and breast cancer should be examined by a
gynaecologist to detect metastatic ovarian cancer at early stages.
The most important components in the prevention of cancer of the
ovaries and other female genital organs are recognition of precancerous

645
diseases, their early and appropriate treatment, and active follow-up of these
patients. With this purpose it is helpful to identify groups of risk for the
development of genital tumours and to ensure a follow-up and treatment of
such patients.
Five groups of high risk for cancer of the female genitalia are identified.
Group I: women at risk for the development of cancer of the external
genitalia (patients with vulval kraurosis and vulval and vaginal leucoplakia).
Group II: women at risk for the development of cervical cancer (patients
with ectopia, erosion-affected ectropion, recurrent polyps, leucoplakia and
dysplasia of the cervix).
Group III: women at risk for the development of uterine cancer
(patients with aggravated oncological heredity, neuroendocrine and metabolic
disturbances, ovulatory disorders, hyperplastic processes in the
endometrium, hormone-active ovarian tumours, and uterine myoma).
Group IV: women at risk for the development of ovarian cancer
(patients with aggravated oncological heredity, with a history of ovarian
surgery, ovarian cysts, chronic adnexitis, multiple uterine myoma, ovarian
dysfunction, and benign ovarian tumours).
Group V: women at risk for the development of tubal cancer (patients
with chronic recurrent adnexitis).
Health education in the form of talks and lectures plays a large role in
the prevention of genital cancer in women.
Rational management of parturition reduces the incidence of cervical
injuries and diminishes the risk of the development of cervical ectropion.
Women with an identified or suspected precancerous process or a
genital tumour should be referred to specialized hospitals for the appropriate
examination and treatment.

646
Medical examination of working capacity. In Ukraine special medical
committees assess working capacity of patients, following the appropriate
treatment and follow-up.
Self test
1. dispensary prophylactic system of gynecological patients means
A. treatment of patients in a hospital
B. treatment of patients in an ambulatory clinic
C. prophylactic and dynamic medical examination and complex
treatment of patients
in female dispensary
D. public health education
2. Patients with precancerous diseases of female genitalia must be observed
A. 2-3 times a year
B. once a year
C. about 3 months after special treatment in hospital
D. every month
3. A patient with uterine myoma must be observed
A. once in 3 months
B. once in 6 months
C. depending on her complaints
4. Patients with acute inflammations of female genitalia should be observed
A. about 3 months after special treatment in hospital
B. once a year
C. once in 6 months
D. no special after treatment observation
5. The main mission of female ambulatory clinic is
A. a prophylactic medical observation of women
B. a treatment of the out-patients
647
6. Every woman must be observed for prophylaxis once
A. a year
B. in 6 months
C. in 3 months
D. in 3 years
7. For women in premenopausal age, and after menopause cytologic examination
of smears is
A. necessary
B. is not necessary
8. If a patient does not come to ambulatory clinic for planned examination
A. gynecologist should wait for her in his office
B. gynecologist may break off dispensary prophylactic observation of
this patient
C. nurse should be send for inviting a patient for the examination and
observing her
living conditions
D. patient should be hospitalized under compulsion
9. Erosion-affected ectropion means
A. I group of risk for cervical cancer
B. II group of risk for cervical cancer
C. III group of risk for cervical cancer
D. IV group of risk for cervical cancer
10. Group IV means
A. women at risk for the development of ovarian cancer
B. women at risk for the development of tubal cancer
C. women at risk for the development of cervical cancer
D. women at risk for the development of intestinal cancer

648
Chapter 23. HYGIENIC REGIMEN IN FEMALE
Hygiene of Girls
Proper hygiene is necessary from the first day of a girl's life. Apart from
the general care for the newborn, special care of the genitalia is required. It is
recommended that the external genitalia be regularly washed with a spray of
warm water with a small amount of potassium permanganate solution or with
children's soap (a spray of water should be directed from the genital organs to
the anus) with the subsequent drying and treatment of the area of the external
genitalia, inguinal and intergluteal folds, with a wool cotton tampon soaked in
sterile vegetable oil or children's cream.
A nurse should teach the mother the rules of caring for the newborn.
Thorough observance of all hygienic rules of caring for the newborn girl will
reliably prevent the development of genital infections.
The child should have a separate bed and bathtub. Her clothes and linen
should be laundered separately.
In the neutral period of genital development girls should take hygienic
showers, wash daily the genitalia (with water and children's soap), and
change the underwear regularly. In case of irritation of the external genital
organs, chamomile and bur marigold teas are used for washing the genitalia.
Genital hygiene should be particularly thorough in girls suffering from
exudative diathesis, obesity, diabetes, and systemic infectious diseases since
they are at a high risk for developing vulvovaginitis.
In the prepubertal period girls display significant changes in the
external and internal genitalia and the appearance of secondary sex
characters. Walks in the fresh air, exercise, active physical games, and regular
and adequate meals facilitate the proper physical development. Physical loads
should correspond to the possibilities of the growing body. Hard physical
work is unacceptable at this age.

649
In the course of lectures and talks with parents and girls it is necessary
to let them know the physiological peculiarities of the pubertal period and
rules of the proper genital hygiene.
In the pubertal period girls should be explained the necessity to observe
the proper hygienic rules during menstruations (washing of the genitalia
twice-thrice per day and frequent change of sanitary pads).
Lectures and talks carried out by physicians and nurses are also
important from the viewpoint of moral upbringing of future females and
mothers. Older girls should be explained that the appearance of
menstruations does not mean that they have become sexually mature since
the process of sexual maturation is completed only at about 18 years of age.
Smoking and drinking of alcoholic beverages exert a particularly harmful
effect on the body at this age. A premature onset of sexual activity, pregnancy,
abortions, and deliveries in the period of physiological immaturity are
detrimental for a growing body.
Hygiene of Women
General Hygienic Regimen
A hygienic regimen is the correct alternation of work and leisure.
Women in the Ukraine have an opportunity to work in any branch of the
national economy they choose. But wherever they work they are always
covered by measures aimed at ensuring healthy working conditions for
women. Much attention is also paid to physical development of women and
involvement of them into exercise. Groups of health are set up on the basis of
stadiums, swimming pools, and voluntary sports societies where people swim,
jog, do aerobic exercises, etc. Students are encouraged to join sports circles or
clubs. At working places special breaks are envisaged for doing occupational
gymnastic exercises, which help to combat fatigue and improve respiration
and blood circulation.

650
Skin hygiene should be adequate (regular hygienic showers, hygienic
baths). Women are recommended to do morning exercises, to sponge down
with cold water (to improve general resistance to colds), and to take hygienic
showers in the evening. In summer time it is useful to bathe in open pools,
take air and, if not contraindicated, sun baths.
Rational diet plays an important role in the proper hygienic regimen.
Food should be diverse, while its energy value (calory intake) should
correspond to physical expenditures. Meals should be taken regularly. Apart
from the main nutrients, food should contain sufficient amount of vitamins
(vegetables and fruits). Women with a tendency to obesity are recommended
to restrict the intake of carbohydrates (sugars, flour products, sweets).
In the course of health education activities (talks and lectures) it is
necessary to convey to the audience the knowledge about the harmful effect of
smoking and drinking. The use of alcoholic beverages may greatly affect the
female body at any age. Hence, the task of health workers is to constantly and
everywhere conduct a campaign against alcohol.
A woman should take necessary measures to prevent any deviations in
her urinary and bowel habits.
Clothes should be chosen with due regard to the hygienic norms and
current weather. Cotton or wool underwear is preferable.
Hygiene During the Menstrual Period
Menstruation is a manifestation of a specific function of the female
body; it denotes the onset of sexual maturity and influences all the bodily
functions. Menstrual blood should be allowed to have a free outflow. For this
purpose absorbable sanitary pads (from cotton wool) or tampons (to be
changed several times per day) are employed.
During the menstrual flow the external genitalia should be washed with
warm water and soap several times a day. During menstruation the woman is
not allowed to take a bath, go to the bathhouse, bathe in a swimming pool or

651
any other water reservoir but should take a warm hygienic shower. Any sports
activities are forbidden during the menstruation. The woman is also
recommended to shun overcooling and poignant food and spices. The woman
should have regular bowel movements.
Intercourse is strictly forbidden during the menstruation since it may
cause infection or intensify the menstrual bleeding. Vaginal irrigation and
other therapeutic vaginal procedures are not permitted during menstruation
either.
Sexual Hygiene
The legitimate age for marriage in the Ukraine is 18 years when the
pubertal period is over and the woman becomes sexually mature. It should be
explained to the woman that the observance of sexual hygiene is essential for
her health and that sexual promiscuity poses a high risk of contracting
sexually transmitted diseases.
The first coitus is attended by hymenal rupture and the formation of
lacerations on the mucosa of the vaginal vestibule. To prevent possible
infection, it is necessary to institute a particularly thorough care for the
genital organs, including their careful washing with warm water and
abstinence from coitus for a few days.
Some deviations from normal sexual life suggest genital diseases and
may lead to neurosis and reactive depression.
One of the most common sexual disorders is frigidity. It may be
expressed as either the absence of sexual satisfaction or decreased or even
absent sexual excitability. Frigidity is more common in women and may be a
sequela of pathological states or caused by such non-physiological factors as
improper upbringing, the absence of love for the spouse, and/or conditions,
which interfere with the creation of an intimate set-up.
Diseases that may be attended by frigidity include ovarian dysfunction,
central nervous system and metabolic diseases, chronic intoxication with

652
nicotine and alcohol. Frigidity may also be associated with genital
malformations in both females and males. Of definite importance may be
poor personal hygiene, in particular genital hygiene, of one of the partners.
The decision, whether the given deviation from the norm is physiological or
pathological, is made by a sexopathologist following the examination of both
partners. The proper option for medical personnel in such cases is to
promptly refer such patients to a sexopathologist.
In the wake of the first coitus attended by sharp pain the woman may
develop vaginismus (reflex spastic contraction of muscles of the vaginal
vestibule and pelvic floor hampering intercourse). This is most often due to
functional disturbances of the nervous system, and such patients should be
referred to a neuropathologist. There is a close correlation between the
unsatisfactory sex life, sexual disorders, and neuroses. Any abnormalities of
the sexual life may finally result in neurosis. A neuropathologist and a
sexopathologist working as a team should treat sexually related neuroses.
It is impossible to establish any common denominator with regard to
the normal frequency of intercourse since the latter depends on the age,
temperament and health of both partners. The major yardstick in this respect
is how the partners feel after coitus. If it is followed by drastic fatigue,
weakness, and malaise, the partners are recommended to cut down on the
frequency of intercourses they have. Coitus is forbidden during
menstruations, in the period of treatment from sexually transmitted diseases,
during the first and last two months of pregnancy, and during four weeks
after abortion and six weeks postpartum.
Before getting married, it is advisable for both partners to consult a
doctor about her or his health status, which may help to reveal possible
asymptomatic diseases that could adversely affect their progeny. Special
genetic consultative centres deal with the questions pertaining to
transmission of hereditary diseases. People with a family history of hereditary
diseases about to get married and spouses who have already given birth to

653
children with hereditary disorders or malformations should be referred to
these genetic centres.
Self test
1. Choose the solution, which may be used for washing of external genitalia in
girls.
A. chamomile tea
B. oxygen peroxide
C. 0. 9% solution of natrium chloridum
D. tincture of iodine
2. During menstrual flow tampons should be changed
A. several times per day
B. once a day
C. owing to volume of bleeding
D. should not be changed during a day
3. During the menstrual flow the external genitalia should be washed with warm
water and soap for
A. several times a day
B. six times a day
C. two times a day
D. four times a week
4. Diseases that may be attended by poor hygiene are the following except
A. ovarian dysfunction
B. central nervous system diseases
C. inflammatory diseases
D. disturbances of a sexual function
5. The first coitus may lead to inflammations of the mucosa of the vaginal vestibule
due to
A. lacerations

654
B. changing of a hormonal status
C. alteration of a vaginal mycroflora
D. psychologic stress
6. The warm bath is
A. indicated during menstrual flow for women
B. contraindicated during menstrual flow for women
7. What is better for women during menstrual flow?
A. to have a bath for personal hygiene
B. to have a shower-bath (douche)

655
Chapter 24. URINARY TRACT DISEASES IN
FEMALE
Urinary Tract Infections in Women
Urinary tract infections (UTIs) in women are among the most common
problems encountered by the gynecologist. Twenty percent to 40% of women
will have a UTI sometimes in their lifetime. Women are 30 times more likely
than men to suffer a UTI, and of those women affected, 20% have more than
three UTIs per year. It is not surprising, then, that complaints related to the
urinary tract account for 7 million annual outpatient visits, 1 million
hospitalizations.
UTIs comprise a collection of diseases that can be classified based on
both the anatomy and the complexity of the disease. Anatomically, upper
UTIs involve the kidney, resulting in pyelonephritis. Pyelonephritis may be
chronic, subclinical, or acute, with this chapter focusing on management of
the latter. Lower UTIs involve the urethra and bladder, resulting in acute
urethritis and acute cystitis, respectively.
UTIs can be further classified as complicated or uncomplicated. A
complicated UTI is associated with a condition that increases risk for
acquiring infection, failing therapy, or suffering increased morbidity. These
associated conditions may be structural (obstruction, catheterization, renal
calculi), metabolic (diabetes, pregnancy, chronic renal failure), or functional
(impaired host [AIDS, neutropenia] or unusual pathogen).
Complicated UTIs can range in severity from simple cystitis to urosepsis
with shock; thus, it is the associated conditions, not severity of disease, that
make a UTI complicated. Some authors argue that true uncomplicated UTIs
only occur in nonpregnant, healthy adult women with no neurologic or
structural dysfunction. Eighty percent of UTIs fall into this group.

656
The urinary tract is normally an enclosed, protected, and sterile
mucosal surface. Washout of bacteria by urine flow is the primary host
defence against infection. This process is nearly continuous in the upper tract
but only intermittent in the lower. Uropathogens are generally not virulent,
but instead are highly adapted to ascend, colonize, and grow in the urinary
tract, subsequently causing cell damage and infection. The colon is the
primary reservoir for most uropathogens. Over 95% of infections result from
enteric bacteria ascending the urinary tract. Although the exact process of
ascent is unknown, enteric bacteria colonize the vagina and periurethral area,
ascend the urethra into the bladder, multiply in the urine, reflux into the
ureters, and ultimately colonize and invade the renal parenchyma. Factors
that alter urine washout, change the characteristics of the urine, or facilitate
entry of bacteria into the urinary tract increase risk for development of a UTI.
The primary risk factors in young healthy women for development of an
uncomplicated UTI are sexual intercourse and diaphragm use with
spermicide. Less than 5% of UTIs result from hematogenous spread during
septicemia. These organisms tend to be more virulent, causing severe
pyelonephritis or even microabscesses within the kidney.
The most common uropathogens responsible for development of a UTI
are enteric gram-negative bacilli of the class Enterobacteriaceae. Escherichia
coli is responsible for over 80% of UTIs in reproductive-aged females.
Staphylococcus saprophyticus causes 5% to 20% of UTIs in this group, with
other enterics such as Klebsiella, Enterobacter, Enterococcus, Proteus,
Pseudomonas, and Group B Streptococcus causing the balance of infections.
Hospitalized, catheterized, and immunosuppressed patients tending to suffer
UTIs from more virulent bacteria as well as Candida, colibacillus infections
are much less common in this group, causing less than 40% of infections.

657
Clinical Presentation
Asymptomatic Bacteriuria
Asymptomatic bacteriuria is simply the presence of bacteriuria in a
patient with no symptoms of cystitis or pyelonephritis. This condition is most
common in elderly and pregnant women. The incidence of asymptomatic
bacteriuria increases with the age to as high as 40% in women over 60. Thirty
percent of individuals become symptomatic within 1 year. Identification of
asymptomatic bacteriuria in elderly women is of questionable benefit, as no
association with excess morbidity and mortality has been demonstrated. In
contrast, it is critical that the gynecologist identify asymptomatic bacteriuria
in a pregnant woman. While only 4% to 7% of pregnant women will have
asymptomatic bacteriuria, 30% of these will subsequently develop
pyelonephritis if untreated. Asymptomatic bacteriuria has also been
implicated in stillbirth and preterm labour, but this remains controversial.
Acute Cystitis
Acute cystitis is most commonly seen in reproductive-aged women. The
most typical symptoms include dysuria, frequency, urgency, and suprapubic
or abdominal discomfort. Hematuria occurs in up to 40% of women with
acute cystitis. More general complaints may also be described, such as fatigue,
malaise, irritability, and diaphoresis, dysuria. Fever (greater than 38°C) and
severe abdominal pain are rare, and should make the emergency physician
consider upper tract disease or alternative diagnoses. Microscopic urinalysis
reveals pyuria, bacteriuria, and, frequently, hematuria.
Acute Recurrent Cystitis
Acute recurrent cystitis is defined as three or more episodes of acute
cystitis within a year. It occurs in 20% of individuals with acute cystitis,
usually as the result of separate episodic uncomplicated infections.
Individuals with recurrent cystitis should be identified for consideration of
UTI prophylaxis.

658
Acute Urethritis
Acute urethritis presents with symptoms nearly identical to those of
cystitis. There may be a coexistent cervicitis and vaginal discharge. Pyuria
without evidence of bacteriuria is common on urinalysis, with subsequent
cultures growing minimal uropathogens. Chlamydia trachomatis, Neisseria
gonorrhoeae, and the herpes simplex virus are the usual causative organisms.
Acute Pyelonephritis
Acute pyelonephritis can present with variable severity, from a mild
cystitis-like illness with flank pain to a more severe illness with fever, chills,
nausea, vomiting, sweats, and flank and/or abdominal pain. Absence of
cystitis symptoms is not uncommon. Costovertebral angle tenderness is a
common physical finding. Urinalysis reveals pyuria, bacteriuria, hematuria,
and white blood cell casts; the latter are highly specific for acute
pyelonephritis.
Urosepsis
Urosepsis is most likely to manifest in women with indwelling catheters,
immunosuppressive disorders, urinary obstruction, complicated UTIs, or
serious underlying medical problems. Elderly women from extended care
facilities are at greatest risk. Typically, such patients present with nonspecific
signs and symptoms, including fever, confusion, weakness, tachycardia,
tachypnea, and dehydration. Family members or nursing home staff may
provide valuable history, as the patient often cannot provide one herself. If
alert, the patient may complain of incontinence, abdominal pain, thirst,
dyspnea, or even cough. Fever is often present, but hypothermia is not
unusual. Examination will usually reveal dehydration or compensated shock,
but delayed presentation may result in severe hypotension and septic shock.
Symptomatic catheterized patients
Urinary catheterization is responsible for the vast majority of
nosocomial UTIs. Incidence of infection for indwelling catheters is 5% per
catheter-day. Such UTIs are, by definition, complicated, with manifestations

659
ranging from mild suprapubic pain, bladder spasms, and incontinence
around the catheter to fulminant sepsis. All symptomatic catheterized
patients should be treated with broad-spectrum antibiotic therapy.
Differential Diagnosis
The gynecologist should be aware that female patients differ from those
of other outpatient settings. Patients presenting with urinary symptoms are
more likely to have gynecologic disease (vaginitis, pelvic inflammatory
disease, and sexually transmitted disease), upper tract disease, and social
circumstances that complicate access to care and follow-up when compared
with other outpatient settings.
The differential diagnosis of acute dysuria includes the following:
acute urethritis, acute cystitis, and vaginitis. Generally, urethritis is
characterized by a more gradual onset and occurs in patients who have
concomitant vaginal symptoms. Urgency, frequency, and urinary
incontinence commonly accompany the dysuria of acute cystitis. The
bladder, when infected or inflamed, contracts spasmodically to create these
symptoms. Vaginitis is common and presents with external dysuria and
vaginal discharge. Frequency and urgency are lacking because the bladder
is not involved.
Flank pain typical of pyelonephritis is common in other diseases as
well. Patients with unilateral costovertebral angle tenderness may have
renal calculi, perinephric abscesses, renal infarcts, and neoplastic or
traumatic processes.
The gynecologist must base the differential diagnosis on the
presenting complaint, and then narrow it with additional history, physical
examination, and laboratory examination.
History
Historical information of importance includes the nature of the
dysuria (external or internal), the duration of symptoms, and
accompanying symptoms of urgency, frequency, incontinence, abnormal

660
vaginal discharge, external genital lesions, fever, back pain, hematuria, or
foul-smelling urine. A detailed sexual history, including the possibility of
pregnancy, the number of partners, and the type of birth control method
used, is also prudent. The medical history should be explored in an effort to
identify any factors that would make an otherwise uncomplicated UTI
complicated.
Physical Examination
The examination begins with an assessment of vital signs and
hydration status. Examination of the genitourinary tract includes
assessment of costovertebral angle tenderness, suprapubic mass, or
tenderness, and examination of the external genitalia and urethra. A pelvic
examination should be performed in women in whom the diagnosis is
unclear and in women whose history suggests a diagnosis of either
urethritis or vaginitis. It is important to note the presence or absence of
indwelling catheters, as they place the patient at risk for a complicated UTI.
When combined with a good history, a careful physical examination
should enable the physician to identify patients with urosepsis, acute
cystitis, and acute pyelonephritis, and should allow the physician to predict
whether the patient has a complicated or uncomplicated infection.
Urinalysis Collection
A urine specimen should be collected by the method most appropriate
for the patient's clinical status and capacity to cooperate with cleansing
guidelines. In the presence of obesity, menstrual blood, copious vaginal
discharge, or an anatomic abnormality, the preferred method for obtaining
a urine specimen is an in-and-out urethral catheterization of the bladder.
The main risk is induction of UTI, but this occurs less than 1% of the time
in a normal host. For non-menstruating, thin patients lacking vaginal
discharge, a clean-catch urinalysis can be utilized. The sample should be a
midstream specimen obtained after perineal cleansing with gauze
moistened by either saline or tap water. No benefit has been proven from

661
soap cleansers. Some experts suggest that urine from a freshly wet diaper
can be collected for accurate analysis. Regardless of the means by which the
urine is obtained, the specimen should be processed promptly after
collection, as stagnation increases colony counts.
Dipstick Chemical Tests/Urine Microscopy
The nitrite test depends on bacterial reduction of nitrate to nitrite.
The test is more likely to be positive with gram-negative bacteria. It may be
falsely negative in the presence of low-count UTIs, dilution, antimicrobial
therapy, and infections caused by non– nitrate-reducing bacteria such as S.
saprophyticus, Acinetobacter, and enterococcus. While the negative
predictive value of a nitrite test ranges from 0. 27 to 0. 70, the positive
predictive value is 0. 96. Thus, a positive nitrite test strongly suggests the
presence of bacteriuria, while a negative test does not exclude it. The
leukocyte esterase test detects the presence of neutrophil granules and
connotes pyuria greater than or equal to 8 to 10 white blood cells per high-
power field. The sensitivity for the leukocyte esterase test ranges from 0. 75
to 0. 90, while the specificity is more precisely defined as being 0. 95. False-
positive results have been reported with Trichomonas, and false-negative
results have been seen in urinalysis with dipsticks positive for glucose and
ketones.
The ease of use and availability of these tests can assist the emergency
physician in identifying UTIs. Generally, a completely negative dipstick
analysis corresponds to a negative microscopy evaluation, although 5% of
UAs with negative dipstick results are found to have abnormal urine
microscopy. Urinary microscopy has been shown to change patient
management in only 5% of patients, and, therefore, consideration must be
paid to both the turn-around time and the cost of each test. For cases in
which the diagnosis is clear, a dipstick should suffice. Full microscopic
evaluation may be of assistance in the more complicated cases and in cases
in which false-negative or false-positive results are expected.

662
Understanding the limitations of the nitrite and leukocyte esterase tests
better enables the clinician to decide when to employ microscopic analysis.
Urine Culture
Isolation and quantification of uropathogens in culture may help
differentiate the various UTIs.
The vast majority of young, otherwise healthy women with probable
UTI do not need cultures or sensitivity tests. Urine cultures should be
obtained in any woman with potential for a complicated UTI; acute
bacterial pyelonephritis; fever without focus; relapsing UTI; recently
treated, documented UTI; fever and neutropenia; indwelling bladder
catheterization; or sepsis.
Other Laboratory Studies
Patients with urosepsis, acute bacterial pyelonephritis, or complicated
UTI should have creatinine assessed, as renal dysfunction may occur with
upper tract infections. Similarly, several studies have shown little to no
discrepancy between the organism cultured from the urine and that
cultured from the blood. Because blood cultures are costly and often do not
add to the clinical evaluation, careful thought should be given as to whether
they are necessary. In the adult patient with a UTI, blood cultures are
recommended when the diagnosis is unclear, when urine culture cannot be
obtained (catheterization impossible), or when bacteremic seeding of the
kidneys is possible (endocarditis). They need not be performed for routine
pyelonephritis. Vaginal cultures can be helpful when vaginitis and
urethritis are likely, though their results are not available for initial
management decisions. A pregnancy test is indicated if pregnancy is
possible.
Imaging Studies
Radiologic imaging of the woman with uncomplicated UTI is seldom
indicated. Routine imaging of women with pyelonephritis is also not
recommended, as 75% of adults with pyelonephritis have normal anatomy.

663
Indications for emergent or urgent imaging are not clearly defined, but in
general, patients who are severely ill, patients who fail to respond to
appropriate antimicrobial therapy, and patients with recurrence within 3
days of finishing treatment may deserve radiographic evaluation in the
form of either ultrasonography or computed tomography.
Treatment
Urosepsis
Prehospital management and immediate resuscitative efforts are
necessary for women with urosepsis. Airway management and the
provision of supplemental oxygen, intravenous crystalloids, and antibiotics
are the mainstays of care. Administration of appropriate antimicrobial
agents should begin in the ED as soon as possible. Although urine and
blood cultures should ideally be obtained prior to the administration of
antibiotics, culture acquisition should not delay the administration of
appropriate therapy. Examples of suitable antibiotic choices include a
third-generation cephalosporin, imipenem–cilastatin, ticarcillin–
clavulanate, or ampicillin in combination with an aminoglycoside.
Uncomplicated Cystitis
Patients with cystitis can be treated with oral antimicrobial agents as
outpatients. Due to growing concerns about antimicrobial resistance,
increasing attention has been placed on the choice of antimicrobial therapy
and its duration. In vitro studies have found increasing resistance of
common urinary pathogens to commonly used agents. As with all
antimicrobial therapy, the choice of agent must be tailored to regional
susceptibility patterns. Despite the increasing resistance of many urinary
pathogens to trimethoprim–sulfamethoxazole (TMP/SMX), this agent
remains an extremely well tolerated and effective agent in most of the
cases. Furthermore, there are increasing data to suggest that overuse of
fluoroquinolones is leading to increasing uropathogen resistance. Overall,
TMP/SMX remains an excellent first-line agent for most cases of

664
uncomplicated UTIs. For patients with a contraindication to TMP/SMX or
those in an area where resistance is a significant concern, fluoroquinolones
or nitrofurantoin remain viable alternatives. Several experts feel that if
treating with nitrofurantoin, a 7-day regimen is more effective than a 3-day
one. Beta-lactam antibiotics cannot be advocated as first-line agents in
patients without contraindications to the aforementioned agents due to the
high incidence of resistance to these drugs. Three-day regimens of
treatment seem to confer an advantage over single-dose therapy in terms of
the incidence of symptom recurrence. This is thought to be due to the
inability of the single-dose regimens to eradicate uropathogens from the
vagina, urethra, and rectum. For patients with severe dysuria, a 1- to 2-day
course of a urinary analgesic, such as phenazopyridine 200 mg three times
per day, is also advisable.
Uncomplicated Pyelonephritis
Patients with pyelonephritis who are febrile and vomiting should be
treated with antipyretics, antiemetics, and intravenous fluids.
Antimicrobial therapy is similar to that for patients with uncomplicated
cystitis. Many authors advocate the use of single-dose parenteral therapy
followed by oral therapy for duration of 10 to 14 days. Acceptable
parenteral agents include gentamicin or third-generation cephalosporins.
Because some patients develop worsening symptoms within 24 to 36 hours
of hospital discharge, early follow-up is recommended.
Complicated Urinary Tract Infections
In general, agents used for the treatment of complicated UTIs are
similar to those used for uncomplicated infections, with the specific agent
chosen on the basis of known or presumed susceptibilities of the infecting
organism. Due to the structural abnormalities inherently associated with
complicated infections, a longer course of therapy is warranted to
effectively sterilize the urinary tract. In addition, close follow-up is
mandatory to ascertain effective cure.

665
Urinary Tract Infections Complicating Pregnancy
Antibiotics commonly used to treat UTIs are contraindicated in
pregnancy. TMP/SMX is relatively contraindicated in the first trimester
due to its inhibition of folate metabolism, and is contraindicated in the
third trimester due to its potential to cause kernicterus in the newborn.
Fluoroquinolones may damage growing cartilage and epiphyses of long
bones, their use in pregnancy is contraindicated. Other viable alternatives
for treating the parturient with cystitis include nitrofurantoin,
sulfisoxazole, and cephalexin. Due to the high incidence of complications
affecting both the mother and the fetus, pyelonephritis in pregnancy has
historically been an infection treated as an inpatient. Recent studies,
however, have shown that patients may be managed as outpatients with
close follow-up. If outpatient management is elected, 10 to 14 days'
treatment is recommended, as is consultation with the patient's
obstetrician to assure close follow-up.
Asymptomatic Bacteriuria
Treatment of asymptomatic bacteriuria is not advocated except
during pregnancy. Pregnant women with bacteriuria have a markedly
increased risk of acute pyelonephritis and the accompanying risks of
prematurity and low-birth-weight infants. Treatment is again directed at
the etiologic organism. Recommended regimens include 3-day courses of
amoxicillin, an oral cephalosporin, or nitrofurantoin.
Recurrent Cystitis
Women with more than three UTIs within 1 year may benefit from
longer term prophylactic therapy. Postcoital prophylaxis with one-half of a
TMP/SMX tablet (40/200 mg) may benefit those whose recurrences have
clearly been related to intercourse. Continuous daily prophylaxis for 6
months with TMP/SMX, nitrofurantoin, norfloxacin, cephalexin, or
trimethoprim has also been shown to decrease the morbidity of recurrent
UTIs. Unfortunately, approximately 40% to 60% of these women will

666
reestablish their pattern of frequency of infections within 6 months of
discontinuing prophylactic therapy.
Disposition
Role of the Consultant
Consultants are seldom required for uncomplicated UTI in women.
Patients with cystitis do not require follow-up unless symptoms worsen or
recur. Uncomplicated acute pyelonephritis may be referred to primary care
physicians for subsequent management. As noted, pregnant women with
pyelonephritis require close follow-up, and consultation with their
obstetricians is advised. Some women with complicated UTI may require
urologic and medical consultation.
Indications for Admission
Patients with urosepsis and serious underlying medical problems may
require critical care admission if they are hemodynamically unstable, require
mechanical ventilation, or have complicating medical conditions. Patients
with complicated pyelonephritis or uncomplicated pyelonephritis associated
with toxicity are candidates for hospital admission (serious medical
conditions, dehydration with inability to maintain a normovolemic state, and
inability to take oral medication). The young, nonparous, otherwise healthy
woman with acute, uncomplicated, and nontoxic pyelonephritis may respond
within hours of initiating appropriate therapy and may be subsequently
managed as an outpatient.
Wetness /Urinary Incontinence
Urinary incontinence, the involuntary loss of urine, is a symptom or
sign of urinary tract dysfunction; it is not a disease. The presence of even
minor degrees of urinary incontinence may be a devastating problem for
patients, preventing them from leaving home or enjoying normal activities.
The clinician must determine (a) whether it is urine that is leaking, (b) the

667
source of the urinary loss, (c) the underlying pathophysiologic mechanism,
and (d) the appropriate therapy.
I. Nonurinary Wetness
As a first step, the type of fluid actually leaking should be identified.
Nonurinary perineal wetness may easily be confused with incontinence. Urine
may be identified by measuring the creatinine level of the fluid, which will be
markedly elevated in urine. Agents that colour the urine, such as indigo
carmine or phenazopyridine, can also be used. If the perineal fluid does not
obviously stain with these agents, it is not urine. A perineal pad is helpful in
collecting the perineal fluid, and it can be weighed to quantify the leakage.
Nonurinary perineal wetness can occur from various sources.
A. Gastrointestinal tract: diarrhea, fistula, or leakage from a colostomy
or ileostomy
B. Vagina: vaginal discharge, exudate, or transudate
C. Serous or purulent drainage from perineal infection or hidradenitis
D. Perspiration
E. Subjective wetness: a complaint of wetness when no wetness is
demonstrated
II. Nonurethral Wetness
A. Fistula.
Wetness caused by fistulae may follow hysterectomy, radiation to the
pelvis, or birth trauma. The most common type of fistula is vesicovaginal. A
fistula may develop years after radiation therapy has been completed. The
patient typically will complain of constant urinary wetness. Urinary fistulae
are generally easy to diagnose on physical examination or cystoscopy. If the
fistula is not obvious but is suspected on clinical grounds, the patient may be
given a urinary coloring agent and instructed to wear a vaginal tampon and
perineal pad. In the case of a urinary fistula to the vagina, the tampon will be

668
stained but the perineal pad will not. Vesicovaginal and urethrovaginal
fistulae may be repaired by a transvaginal or transvesical approach,
depending on the location of the fistula and the experience and preference of
the surgeon. Ureterovaginal fistulae require an abdominal approach because
reimplantation of the ureter into the bladder is usually necessary.
B. Ureteral ectopia, in which the ureter congenitally inserts into a
location other than the normal bladder trigone, may cause incontinence in
female patients if the insertion is distal to the external urethral sphincter.
Although ureteral ectopia is usually associated with a duplex renal collecting
system in female patients, single ectopic ureters are encountered on rare
occasions. The ectopic orifice usually drains the upper pole of a duplex system
and may insert in the urethra, vagina, or perineum. Male patients with
ureteral ectopia are generally not incontinent because ureteral insertion will
always be proximal to the external sphincter; however, they may present with
epididymitis. Ectopic ureter is almost always discovered in childhood. The
patient or parents may note continuous urinary incontinence despite a
normal voiding pattern. In the case of a duplicated system with a poorly
functioning upper pole segment, treatment may consist of excision of the
upper pole and a varying length of its draining ureter. In the case of a single
collecting system or a duplex system with good function of the upper pole
moiety, treatment is reimplantation of the ureter into the bladder.
C. Vaginal reflux of urine during voiding may result in postvoiding
wetness. This condition may occur with vaginal stenosis or atrophy,
congenital urethral “female hypospadias,” or repositioning of the urethra
intravaginally following incontinence surgery.
III. Urethral Incontinence
Pathophysiology of continence.
Urinary continence requires that the bladder store an adequate volume
of urine at low pressure, efficient urethral sphincteric function, and integrity

669
of the neurologic control mechanisms to coordinate voiding and continence.
The bladder neck must remain closed at all times, except during voiding, and
must be able to withstand momentary increases in intraabdominal pressure.
The prostatic and membranous portions of the male urethra act as the
primary continence mechanism; the entire female urethra performs this
function. In both sexes, the urethra prevents leakage by several important
mechanisms.
1. Smooth-muscle tone is the single most important factor in
maintaining minute-to-minute continence.
2. Striated muscle fibers are found within the urethral wall and in the
periurethral area. The striated muscle constitutes the second line of defence
against incontinence. The striated muscle within the urethral wall consists of
“slow-twitch” fibers specialized to maintain constant tone. The periurethral
fibers consist of “fast-twitch” fibers that can be rapidly activated to provide
auxiliary compression, such as might be required during coughing. The
periurethral striated muscle, innervated by the pudendal nerve, is much
stronger in males than in females.
3. Coaptation of the mucosa acts as a seal and reduces the urethral
muscular tone required to prevent leakage. Female estrogens cause the
urethral mucosa to proliferate and mature. It has been suggested that this
factor may partially explain the increased incidence of stress incontinence in
postmenopausal women. Urethral scarring, such as after multiple incisions
for recurrent urethral strictures, may affect the ability of the urethra to coapt
effectively.
The classification of incontinence is traditionally based on clinical
symptoms rather than the pathophysiology.
1. Stress incontinence is defined as the involuntary loss of urine during
physical effort that is not caused by a bladder contraction. Terms such as
genuine stress incontinence and urethral incompetence are sometimes used
as synonyms. As a symptom or sign, stress incontinence does not indicate any

670
particular disease. It may be seen in both male and female patients but is
much more common in women. Most commonly, this type of incontinence
occurs in the upright position. Maneuvers that commonly elicit stress
incontinence include coughing, lifting, straining, and laughing. The amount of
urine lost is usually small, unless a bladder contraction is precipitated at the
same time. Minimal or occasional stress incontinence probably occurs in all
women at some point in their lives; however, significant stress incontinence
(defined as occurring two or more times a month) affects 5% to 10% of
women between the ages of 35 and 64. Stress incontinence is unusual in
nulliparous women and becomes more prevalent as parity increases. In
women, most instances of stress incontinence result from a defect in the
pelvic support of the bladder neck (type I stress incontinence) or both the
bladder neck and urethra (type II). In both of these types, increased
intraabdominal pressure causes hypermobility of the bladder neck or urethra.
In type III stress incontinence, there is no urethral hypermobility, but an
intrinsic urethral defect is the cause of incontinence. Type III incontinence
(sphincteric insufficiency) may be caused by trauma, denervation, multiple
surgical procedures, radiation therapy, or postmenopausal atrophy.
2. Urge incontinence is loss of urine associated with marked urinary
urgency. Other storage symptoms are typically also present, such as
frequency, urgency without incontinence, nocturia, and enuresis. By
definition, involuntary bladder contractions that are idiopathic are referred to
as detrusor instability, whereas those that occur in conjunction with a known
neurologic disease (e. g., stroke, multiple sclerosis, spinal cord injury) are
known as detrusor hyperreflexia. Typically, the patient reports the loss of
considerable amounts of urine under specific circumstances, such as during
cold weather, hand washing, or emotional upsets. In about one-third of
patients with detrusor instability, there is a history of enuresis in childhood.
In contrast to genuine stress incontinence, urge incontinence becomes
increasingly likely as the bladder fills to capacity. Coughing or other stressful

671
episodes may provoke bladder contractions (stress hyperreflexia of the
bladder), making this type of incontinence difficult to differentiate from
genuine stress incontinence.
3. Overflow incontinence is sometimes called paradoxical incontinence
because it results from chronic urinary retention. The patient leaks urine
episodically and never voids normally. Leakage may be worsened by any
increase in intraabdominal pressure. This type of incontinence may be caused
by neurogenic impairment of bladder contractility or by outflow obstruction.
4. Total incontinence refers to constant diurnal and nocturnal
incontinence without normal voiding. The symptoms may be similar to those
of overflow incontinence, but total incontinence may be differentiated from
overflow incontinence in that little or no urine is obtained on catheterization
of the bladder. This type of incontinence may be seen in neuropathic bladder
dysfunction (especially peripheral neuropathy), after obstetric or surgical
injury to the female urethra.
5. In functional incontinence, the urinary organs are normal but the
patient voids without regard to the social norms of time and place. This may
be seen in patients with organic dementia, psychiatric disease, or physical
problems of mobility or dexterity.
6. Mixed incontinence is frequently encountered in clinical practice. For
example, an elderly male diabetic may have impaired detrusor contractility
leading to increased postvoid residual as well as detrusor hyperreflexia
resulting from small cerebral lacunar infarcts.
7. Postvoid dribbling may be caused by collection of urine in the
urethral bulb or in a urethral diverticulum.
The major mechanisms of incontinence are classified below.
1. Detrusor abnormalities may cause incontinence by interfering with
the ability of the bladder to store urine.
a. Loss of compliance. A bladder that cannot maintain a low intra-
vesical pressure during filling is said to have low compliance. Once the

672
intravesical pressure exceeds that of the urethra, incontinence occurs even
without a bladder contraction. This sequence of events can be seen in cases of
myelodysplasia or other forms of neurogenic bladder dysfunction, and after
bladder operations or pelvic irradiation.
b. Overactivity. This term denotes an involuntary detrusor contraction
(pressure >15 cm H2O) that occurs during filling, either spontaneously or
with provocative maneuvers such as standing upright. As mentioned before,
when a specific neurologic cause, such as cerebrovascular disease exists, the
term detrusor hyperreflexia is used. Detrusor instability in men is most often
associated with outflow obstruction. In women, the cause of detrusor
instability is most often idiopathic. Detrusor instability can be demonstrated
in approximately one-third of all women presenting with incontinence. If
severe urgency is present, inflammatory or malignant conditions of the
bladder (such as carcinoma in situ) should be ruled out with cystoscopy and
urinary cytology.
2. Urethral sphincter incompetence may result from various causes.
a. Loss of anatomic support is by far the most common and most
important cause of urethral incompetence in female patients (see Table 11-3).
Anatomic support of the female bladder neck and urethra results from the
combined action of the pubourethral and urethropelvic ligaments and the
supportive elements of the pelvic diaphragm. Loss of pelvic support may
result from age-related loss of elasticity or multiparity. Of patients with
urethral incompetence, about 50% have an associated cystocele or
cystourethrocele and 25% have a rectocele. These manifestations of pelvic
floor prolapse should be corrected at the time of surgery for stress urinary
incontinence. With lesser degrees of pelvic floor laxity, there may be no
obvious prolapse of pelvic organs, but abdominal straining may displace the
urethra and bladder neck downward into the vagina "hypermobility of the
urethra". Why displacement of the urethra is associated with stress
673
incontinence is not clearly understood, but several hypotheses have been put
forward:
- Unequal transmission of pressure occurs as the urethra is displaced
from an intraabdominal position. During episodes of increased
intraabdominal pressure (stress), more pressure is transmitted to the bladder
than to the urethra, and urine is forced out.
- Mechanical disadvantage to the periurethral muscles results when the
urethra is excessively mobile. These muscles cannot efficiently occlude the
urethra during stress, became their anatomic relation to the urethra, which is
no longer normal.
- Slow sphincter contraction in women with stress incontinence has
been documented. In some women with stress incontinence, the ability of the
urethra to compress rapidly enough to prevent leakage during episodes of
stress is decreased. The relation of this finding to urethral hypermobility is
not understood.
b. Estrogen deficiency leading to loss of urethral mucosal coaptation has
been suggested as a factor in urethral incompetence.
c. Denervation of the urethra may occur in conjunction with peripheral
neuropathy, such as that found in diabetes mellitus.
d. Urethral scarring may result from interference with the urethral
blood supply. Multiple surgical operations or trauma may result in a urethra
that is noncompliant and unable to coapt, frequently producing total
incontinence.
Diagnosis of incontinence
Initial evaluation of the incontinent patient:
- The history is very helpful in determining the nature, duration, and
severity of incontinence.
- Physical examination in female patients should include a speculum
examination, bimanual pelvic and rectal examination, and occasionally

674
cystoscopy (particularly if prior incontinence surgery has been performed).
The presence of cystocele and rectocele on straining should be noted and
graded. In most cases, the diagnosis can be made reliably on the basis of
history, physical examination, and a few specialized tests.
1. Pad tests may be used to quantify the amount of urine lost during a
24-hour period. The wet pads are weighed and the weight of the dry pads
subtracted, leaving the weight of urine lost.
2. Postvoid residual urine should be determined after the patient has
voided. A low voided volume may reflect diminished bladder capacity. If
there is little postvoid residual urine, overflow incontinence can be ruled
out. The postvoid residual can be determined by catheterization.
Alternatively, the use of small, portable ultrasound (US) postvoid bladder
scanners can obviate the need for catheterization.
3. The Marshall-Bonney test is performed during the pelvic
examination by asking the patient to bear down or cough with a full
bladder. If incontinence is observed, the test is repeated, after the urethra is
gently elevated (but not obstructed) by two fingers, placed inside the
vagina. If incontinence is corrected by this maneuver, it indicates that a
urethropexy or colposuspension should be successful. Although many
authorities place little credence in this aspect of the Marshall-Bonney test,
the objective demonstration of stress incontinence is valuable.
4. The Q-tip test is used to diagnose urethral hypermobility. After a
sterile Q-tip is placed within the urethra, the patient is asked to cough or
bear down. The normal urethra allows little movement of the shaft of the Q-
tip during this maneuver. With urethral hypermobility, there is obvious
movement.
Urodynamic tests are designed to measure pressure or flow during
bladder filling or voiding.

675
1. Cystometrogram. The intravesical pressure is measured during
bladder filling and during contraction to assess bladder function. The most
common abnormality found is detrusor instability. Because detrusor
instability and urinary incontinence may coexist, the presence of detrusor
instability is not a contraindication to surgical therapy of incontinence;
however, the patient should be forewarned that irritative symptoms might
persist even after successful surgery. Conversely, the finding of detrusor
areflexia, especially if associated with diminished bladder sensation,
indicates the possibility of neuropathic incontinence. In patients with
detrusor areflexia, there is a high likelihood that intermittent
catheterization will be required after surgery for incontinence.
2. Long-term ambulatory monitoring of bladder pressure is
performed with solid-state transducers and portable data storage devices.
This technique monitors bladder pressure over an extended period (24 to
72 hours) and is much more sensitive than conventional cystometry in
detecting detrusor instability.
3. Abdominal leak point pressure is measured during a conventional
cystometrogram and is useful in both men and women with incontinence.
The bladder is gradually filled with contrast and monitored
fluoroscopically. After a volume of at least 200 mL is reached, the patient is
placed in a sitting or upright position and asked to perform the Valsalva
maneuver gradually. The lowest total bladder pressure at which leakage is
detected is the abdominal leak point pressure. If no leakage occurs with the
Valsalva maneuver, the patient is asked to cough several times, with
repeated fluoroscopic observation for the presence of leakage. The
abdominal leak point pressure of female patients with type I stress
incontinence typically is above 120 cm H2O; among those with type II
incontinence, it is usually between 60 and 120 cm H2O; and among those
with type III incontinence, it is usually below 60 cm H2O.

676
4. Urethral pressure profile. This test, which measures pressures
generated along the length of the urethra, is occasionally useful in the
evaluation of incontinence. Although patients with urethral incompetence
tend to have lower values than healthy persons, there is so much overlap
that static measurement of the urethral pressure profile is of little
diagnostic use. The stress urethral pressure profile is more useful; it
requires simultaneous measurement of intravesical and urethral pressure.
In women with urethral incompetence, urethral pressure falls below
bladder pressure during coughing or stress and allows leakage of urine.
This abnormality is corrected by successful surgery.
5. Uroflow measurements in patients with incontinence are used to
detect outflow obstruction. In female patients, this is an extremely rare
cause of incontinence. It is much more common in male patients and may
be the cause of detrusor instability. The uroflow pattern in detrusor
instability is one of rapid attainment of high peak flow rates, whereas
obstructed voiding is characterized by a low maximal flow rate and
prolonged duration of voiding.
6. Voiding cystourethrography is often a useful test in the diagnosis of
incontinence and may be combined with simultaneous urodynamic studies.
Voiding cystourethrography is performed by filling the bladder with
radiographic contrast and it allows voiding to occur. Fluoroscopic
visualization of the bladder and urethra may give valuable information
about vesicoureteral reflux, trabeculation of the bladder, sphincteric
function, and outflow obstruction. In the upright position, contrast should
not leak below the bladder neck. Intrinsic urethral dysfunction (caused by
neuropathy or trauma) is possible if an open bladder neck exists at rest.
With urethral incompetence, increased intraabdominal pressure will cause
the bladder base and urethra to move inferiorly and the urethra to fill with
contrast.

677
7. The pressure-flow video study is the urodynamic study combined
with simultaneous voiding cystourethrography. It is useful when it is
difficult to determine whether or not a bladder neck opening is a result of
detrusor contraction. This technique permits accurate diagnosis of detrusor
instability, detrusor-sphincter dyssynergia, and intrinsic urethral
dysfunction. It is indicated in patients with neurogenic incontinence, those
who have failed surgery, or patients with combined incontinence and
obstruction.
8. Sphincter electromyography is occasionally useful in the diagnosis
of incontinence. Proper innervation and function of the striated muscle
(external) sphincter is important for coordinated micturition.
Electromyography can therefore be used to demonstrate neuropathic
involvement of the striated perineal muscles in peripheral neuropathies
associated with diabetes mellitus, alcoholism, multiple sclerosis, and
myelodysplasia. Electromyography is often performed simultaneously with
a cystometrogram.
Endoscopy may be useful in either sex to rule out bladder
trabeculation, stones, tumour, or diverticulum. In men with
postprostatectomy incontinence, endoscopy may be used to assess the
presence of strictures or bladder neck contractures.
Pharmacologic treatment
An authoritative drug reference should be consulted before any
medications are prescribed. The following sections contain guidelines only
and describe many, but not all of the drugs used in treating incontinence.
a). Detrusor instability may be treated effectively in many instances
with anticholinergic agents or related compounds. Most of the drugs in this
class produce dry mouth, blurred vision, mild tachycardia, drowsiness, and
constipation. Dryness of the mouth is so common with most anticholinergic
agents that it can be used to monitor for adequacy of drug effect. In general,
if no effect on the bladder is noted, the dosage can be increased, until

678
significant dryness of the mouth is reported by the patient. Dryness of the
mouth tends to become less prominent after several weeks of therapy. This
class of agents is contraindicated in patients with narrow-angle glaucoma
because mydriasis may cause acute intraocular hypertension. In addition,
all the medications listed below have prominent anticholinergic effects and
should therefore be used with caution in the elderly and in all patients with
autonomic neuropathies, hepatic or renal disease, hyperthyroidism,
coronary artery disease, congestive heart failure, cardiac tachyarrhythmias,
hypertension, or hiatal hernia associated with reflux esophagitis. In
patients with detrusor instability resulting from outlet obstruction, the use
of these medications may lead to urinary retention.
1. Oxybutynin chloride is widely prescribed for detrusor overactivity.
It has anticholinergic, antispasmodic, and local anesthetic actions. The
recommended dose is 5 mg orally two to four times daily. It is available in
liquid form for children. A slow-release form (Ditropan XL) is now
available.
2. Tolterodine tartrate is a new anticholinergic agent with a
significantly lower profile of side effects. In particular, dry mouth is less
prominent, so that patient compliance is improved. It is given in doses of 2
mg twice daily.
3. Flavoxate hydrochloride is similar to dicyclomine in its
pharmacologic properties. The recommended dose is 100 to 200 mg orally
three or four times daily.
4. Imipramine hydrochloride is a tricyclic antidepressant that blocks
uptake of norepinephrine by peripheral adrenergic nerves. Clinically, it
suppresses bladder contractions and increases urethral pressure, but the
mechanisms involved are unclear. The usual adult dose is 25 to 50 mg
orally four times daily, reduced in elderly patients. Caution should be used
when treating any patient with underlying cardiac disease. The drug can be
combined with an anticholinergic agent such as oxybutynin, which permits

679
a lower dose of these agents to be effective. The side effects of imipramine
and the precautions regarding its use are similar to those for the other
drugs listed above, but when it is combined with anticholinergic agents, its
anticholinergic side effects may be additive. Other important side effects
include obstructive jaundice, abnormal liver function, skin rash, and
agranulocytosis. Central nervous system effects include parkinsonism,
sedation, irritability, and fine tremor. A baseline electrocardiogram should
be obtained in elderly patients or in those with underlying cardiac disease.
b). Urethral incompetence. Drug therapy should be considered for
patients who have intrinsic urethral incompetence without hypermobility,
those who refuse or are not well enough for surgery, and those for whom
surgical procedures have failed.
1. Pseudoephedrine hydrochloride is a sympathomimetic agent that is
available alone or as a component in cold and allergy preparations. The
usual dose is 30 to 60 mg orally up to four times daily. All
sympathomimetic agents should be used with caution in the elderly and in
patients with hypertension, diabetes mellitus, ischemic heart disease,
hyperthyroidism, increased intraocular pressure, and bladder outlet
obstruction from prostatic hyperplasia.
2. Phenylpropanolamine hydrochloride is an adrenergic agonist used
in doses of 50 mg orally three times daily. Like pseudoephedrine, this drugs
work by increasing the muscular tone at the bladder neck and in the
urethra. If detrusor instability is present, an anticholinergic agent may be
used concurrently. Phenylpropanolamine is contraindicated in patients
receiving monoamine oxidase inhibitors.
3. Estrogens have been reported to produce subjective improvement
in postmenopausal women with stress incontinence, apparently by
enhancing the mucosal quality (and therefore coaptation potential) of the
urethra. Various preparations have been used, including 0. 3- to 1. 25-mg
Premarin tablets daily, one applicator full of Premarin vaginal cream daily,

680
and 1 mg of estradiol orally three times daily. Because estrogens have been
reported to increase the risk for endometrial carcinoma and
thromboembolic events, patients should receive the lowest effective dose
and should be monitored every 3 to 6 months during therapy for vaginal
bleeding.
VI. Surgical treatment
A. Fistulae. Small vesicovaginal fistulae sometimes respond to
endoscopic fulguration of the fistula tract. Most, however, require some
type of surgical procedure. Repair may be either by the transvaginal or
transabdominal route, depending on the preference and experience of the
surgeon. Basic principles of fistula repair include (a) complete separation of
the involved organs around the area of the fistulous tract; (b) watertight
closure of each organ, preferably with nonoverlapping suture lines; (c)
interposition of another tissue, if possible, such as omentum or
peritoneum. Approximately 80% of traumatic fistulae are closed
successfully with one operation, although in patients who have had
radiation therapy, the success rate is only 50%.
B. Ureteral ectopia. Usually, the ectopic ureter is draining the upper
pole of a duplicated renal unit.
C. Sphincteric incompetence
1. Intraurethral and bladder neck injections should be considered in
female patients with a well-supported urethra and urinary incontinence.
a. Cross-linked bovine collagen elicits a minimal foreign-body
reaction and has not been associated with particle migration. It has recently
gained popularity for use as a urethral bulking agent in both male and
female patients with incontinence. It is injected through a special needle
into the submucosal space of the urethra near the bladder neck. This can be
done either transurethrally or periurethrally. The material begins to
degrade in 3 months and is completely resorbed within 1 year. The
procedure may need to be repeated but has a reasonable success rate (25%

681
to 50%) and very low morbidity in well-selected patients. In men with
incontinence after transurethral prostatic resection (post-TURP
incontinence), moderate success rates have been reported. In patients who
have had radical prostatectomy or pelvic irradiation, success rates are
significantly lower because of tissue fibrosis.
2. Retropubic suspension procedures
a. Marshall-Marchetti-Krantz procedure. The retropubic space is
developed, allowing placement of absorbable sutures adjacent to the
urethra and at the bladder neck. The sutures are tied to the periosteum of
the pubis, so that the urethra and bladder neck are elevated toward the
pubis. The operation has a success rate of about 85% and rarely causes
outflow obstruction. Its major disadvantage is that it cannot repair
coexistent cystocele or urethrocele. The major complication is osteitis pubis
(3%).
b. Burch colposuspension. Nonabsorbable sutures are placed in the
anterior wall lateral to the urethra and bladder neck and are tied to the
iliopectineal (Cooper's) ligaments. The success rate is reported to be more
than 80%. The procedure can be used to correct coexistent mild-to-
moderate cystoceles. Complications include detrusor instability, bladder
trauma, postoperative retention, and osteitis pubis.
c. Sling procedures are usually reserved for patients with type III
incontinence or in whom a previous operation has failed. The urethra is
dissected out to permit placement of various materials, such as rectus
fascia, Marlex, Mersilene, or Silastic, around it. The tension of the sling is
adjusted to allow elevation of the bladder neck. Voiding difficulties are
common, and most patients must use intermittent self-catheterization for
an average of 30 days. Success rates vary from 75% to 95%. The major
complications are operative injury to the urethra or bladder and delayed
erosion of the sling into the urethra.

682
3. Vaginal procedures
a. Anterior colporrhaphy is commonly used to repair mild stress
incontinence, especially when associated with cystocele or rectocele.
Through a vaginal incision, the bladder neck and urethra are exposed. The
pubocervical fascia is sutured in the midline to provide support for the
bladder neck. Although the success rate of anterior colporrhaphy (65%) is
not as high as that of suprapubic procedures, anterior colporrhaphy can
correct coexistent prolapse, is very well tolerated, and has a low morbidity
rate.
b. The Stamey procedure is a vaginal sling procedure performed both
vaginally and through a small suprapubic incision. A nylon bolster suture is
used bilaterally to suspend the urethra. Endoscopy is performed to make
sure no injury to the urethra or bladder has occurred. The procedure is
simple to perform and has a success rate of approximately 90%. The
complications include infection of the suture material, which requires its
removal.
c. The Raz procedure is similar to the Stamey procedure except that
the sutures are not placed near the urethra but are situated well laterally
into the anterior vaginal wall. It is thus a colposuspension from below.
Success rates are similar to those for the Stamey procedure.
d. Pubovaginal sling procedures, as stated above, are usually reserved
for patients with type III incontinence or in whom a previous operation has
failed. The urethra is dissected vaginally to permit placement of a sling,
usually a strip of rectus fascia. The sling is then brought out through a
suprapubic incision and tied loosely. Voiding difficulties are common, and
most patients must use intermittent self-catheterization for an average of
30 days but occasionally longer. Success rates are reported to be above
90%. The major complications are operative injury to the bladder, erosion
of the sling, wound infection, and prolonged retention.

683
4. Artificial urinary sphincter. This device consists of a periurethral
cuff, a pressure-regulating balloon inflated in the prevesical space, and a
control valve implanted into the labia (or scrotum if used in men) (Fig. 11-
1). When the control valve is activated (with a gentle squeeze), the
periurethral cuff pressure lowers for several minutes to allow voiding, then
automatically repressurizes. To prevent erosion into the urethra, the device
is activated 6 weeks after implantation, when healing has progressed. The
device should be used only in complicated instances of incontinence in
which the standard procedures previously described have failed. Like all
prosthetics, these devices may be complicated by mechanical failure or
infection. In male patients, the cuff can be placed around the urethra or
around the bladder neck. The control valve is then implanted into the
scrotum. Patients with good manual dexterity who are highly motivated are
candidates for this procedure. Detrusor instability or poor bladder
compliance are relative contraindications. Approximately one-third of
patients require revision of the device at some point. Nevertheless, the
overall success rate is reported to be as high as 95% (including
reoperations).
D. Diminished bladder capacity leading to incontinence may be
managed by augmenting the native bladder with a detubularized segment
of bowel. The goal of this surgery is to produce a compliant, low-pressure
reservoir without contractions that cannot be inhibited.
1. Augmentation cystoplasty may be accomplished by a variety of
techniques with an isolated segment of bowel, such as ileum, cecum,
stomach, or ileocecal segment, to improve the bladder capacity and lower
the intravesical pressure.
2. Urinary diversion. Supravesical diversion is generally applied as a
last resort in incontinent patients. The simplest method is an ileal conduit,
in which the ureters are implanted into an isolated segment of small bowel.
A cutaneous ostomy is then created, and the urine collected in a bag.

684
Continent supravesical diversions have also been designed, in which
detubularized bowel is used to fashion a urinary reservoir. The patient then
empties this “substitute bladder” several times a day by catheterizing a
small stoma brought up to the skin. Because the stoma is continent, no
external appliance is needed. Supravesical diversion is indicated when
incontinence is unmanageable by other means or when serious upper
urinary tract deterioration is caused by high intravesical pressure or
vesicoureteral reflux.
The vaginal pessary is in some ways the female counterpart of the
Cunningham clamp. Available in various sizes, a vaginal pessary is a hard,
rubber, doughnut-shaped device placed in the vagina to compress the
urethra. It is generally fitted by a gynecologist.
E. Absorbent aids are usually made of disposable material with a
waterproof backing.
1. Pads are commonly used by both women and men for mild-to-
moderate incontinence. It has been estimated that 10% to 20% of sanitary
napkins sold in the United States are purchased for incontinence rather
than menstruation. The pads can be worn under the patient's usual
underwear or under absorbent underwear.
Injuries During Operations
The injury may involve the bladder or one of the ureters. Bladder
injuries are easily repaired, and usually heal and give no further trouble. On
the other hand, ureteral injuries are difficult to repair satisfactorily and are
very likely to interfere with kidney function later.
Bladder injury.
There are certain precautions, which should be taken before doing any
operative work in the region of bladder. First, the bladder should always be
emptied by catheterization shortly before the operation. If by oversight this

685
has not been done before the patient comes to the operating room, time will
be saved in the end if the operation is delayed long enough for the patient to
be catheterized.
There are numerous dangers involved when the incision is made with
the bladder distended. First, there is a danger of opening the bladder in
incising the peritoneum. This danger is also present when the bladder is
pulled high up on the surface of the tumour. To avoid this danger the first
incision through the peritoneum is always made at the upper end of the
incision. It must be taken in enlarging the incision downward to be sure of the
location of the upper edge of the bladder, so as to avoid cutting into it.
After the peritoneum is opened, if the bladder has not previously been
emptied, it presents as a large cystic mass constantly pushing into the field,
interfering with the accuracy of the work and prolonging materially the time
of the operation.
In doing hysterectomies and removing abdominal tumours, the bladder
should be located and separated from the anterior wall of the uterus or from
the tumour early in the operation, so as to avoid cutting or clamping it.
In complete hysterectomy care should be taken to identify the bladder-
roll and the ureteral-roll on each side and to push them well out of danger.
If in spite of precautions mentioned, the bladder is injuried, it is to be
repaired. Sometimes the injury consists simply of a stripping off of a small
portion of the muscular wall. This is repaired by putting in a few sutures,
which reinforce the thin area with the thicker portion of the wall.
More serious injuries are to be observed when the bladder cavity is
opened. If the opening is small and the condition such that the remaining
separation of the bladder can be carried out without further injury, it is
advisable to close the opening as soon as made. If, on the other hand, the
bladder wall is so adherent as to be likely to be further turn, it is well to
complete the removal of the tumour and then make all bladder repair at one
time. Whether the opening is large or small, the principles of its closure are
686
the same. The first row of sutures should be of fine silk, threaded in a small
full-curved round-pointed needle. These sutures are preferably interrupted
and, taking firm hold of the bladder wall, extend close to the mucosa but not
into it. The reinforcing sutures, which bury the first row, may be of catgut and
continuous.
Ureteral injury.
Ureter ligated. – If it is discovered during the course of an operation
that a ureter has been tied, an attempt is made to loosen the ligature, which
blocks it. This can usually be done, any vessels that start bleeding are being
caught again. Exceptionally, the patient may be in such a poor condition and
the suspected ligature in such a critical position in regard to possible
hemorrhage, that it may be thought best to leave the ligature and depend on
postoperative nephrostomy and drainage of the kidney until the ligature is
absorbed and the ureter reopenes.
Ureter clamped. - The decision as to what to do is determined by the
extent of the injury. If the ureter has been severely crushed, probably to the
point of disorganization of the wall and mucosa and consequent obliteration
of the lumen, division of the ureter and uretero-ureteral anastomosis of
healthy end are advisable if the patient is in condition to stand the additional
work.
If the patient condition is poor, it is best to depend on postoperative
attempt to open the ureter by cystoscopic ureteral catheterization with resort
to nephrostomy for kidney drainage, if the ureter cannot be opened.
Ureter cut. – Uretero-ureteral anastomosis is preferable to
ureterovesical anastomosis because it preserves the function of the normal
ureterovesical junction.

687
Self test
1. The incidence of UTIs in women is about
A. 10-20 %
B. 20-40 %
C. 40-50%
D. 1-2%
2. The most common uropathogens responsible for development of a UTI are
A. enterobacteriaceae
B. escherichia coli
C. staphylococcus saprophyticus
D. klebsiella;,enterobacter
3. Acute recurrent cystitis is defined as
A. two episodes of acute cystitis within a year
B. three or more episodes of acute cystitis within a year
C. two episode of acute cystitis within 2 years
D. three episodea of acute cystiris within 2 years
4. Urine cultures should be obtained in women with all of the following conditions
except
A. potential for a complicated UTI
B. acute bacterial pyelonephritis
C. fever without focus
D. asymptomatic bacteriuria
5. Type I stress incontinence in women means
A. defect in the pelvic support of the bladder neck
B. both the bladder neck and urethra
C. internal urethral defect
D. nothing from listed above
6. Type II stress incontinence in women means
A. defect in the pelvic support of the bladder neck and urethra

688
B. defect in the pelvic support of the bladder
C. internal urethral defect
D. nothing from listed above
7. In postmenopausal women with stress incontinence estrogens may be used
A. yes
B. no
8. If the bladder is wounded during the operation , it should be closed
A. as soon as made
B. after the main operation is complete
C. in a few days after the first operation
D. in a few weeks after the first operation
9. Cateterization of bladder before abdominal operation is necessary for prevention
of its injury.
A. yes
B. no

689
Chapter 25. APPENDICES
Appendix 1. Tests
Task 1.
A 52-year - old woman suffering from obesity complains of bloody
discharges from genital tract during 4 days. Last normal menses were 2 years
ago. Histological investigation of biopsy of the endometrium has revealed
adenomatous hyperplasia. Which reasons from listed below promoted the
development of disease?
1. Hypersecretion of estrogens by ovaries
2. Excessive transformation of preandrogens from fatty tissues
3. Poor aromatization of preandrogens owing to hypothyroidism
4. The increased contents of FSH
5. Supersecretion of androgens by the cortex of adrenal glands
Task 2.
The data of a separate diagnostic curettage of the uterus made up in
connection with bleeding in a postmenopausal period reveals no pathology in
the scraping of the mucous of the cervical canal but a highly differentiated
adenocarcinoma is found at endometrium. Metastases are not found. Which
method of treatment is the most correct?
1. Surgical treatment + chemotherapy
2. Surgical treatment and radiotherapy
3. Radiotherapy
4. Surgical treatment and hormonal treatment (hormonal therapy)
5. Surgical treatment and hormonal therapy

690
Task 3.
A 27-year-old woman complains of the disorders of menstrual function
for 3 months, irregular pains in the abdomen. On bimanual examination,
there is an elastic globulous formation, painless, 7cm in diameter in the right
appendages. A fluid formation, unicameral, smooth, 4 cm in diameter in a
right ovary is observed on ultrasound.
What method of treatment is the most preferable?
1. Administration of an estrogen–gestogen complexes within 3 months with
the new survey
2. Operative treatment
3. Prophylactic medical examination on an outpatient basis
4. Anti-inflammatory therapy
5. Chemotherapy.
Task 4.
A 40-year-old patient complains of colic pains in the lower abdomen
and abundant bloody discharge from reproductive tract. Last 2 years she had
menses for 15-16 days, abundant, with clots, painful. In anamnesis there are 2
medical abortions. On bimanual examination myomatous node, protruding
into the cervix, 3 cm in diameter, is revealed. Discharges are bloody,
moderate. Choose a correct procedure to perform
1. Operation: untwisting of the nodes protruding into the cervix
2. Hormonal hemostasis
3. Vitamin therapy
4. Supravaginal amputation of the uterus without appendages
5. Hysterectomy without appendages

691
Task 5.
A 40-year-old patient complains of yellow colour discharges from the
vagina. Bimanual examination shows no pathological alteration Smear test
reports trichomonas vaginalis and mixed (compound) flora. Colposcopy
reveals two hazy fields on the front (anterior) labium of the cervix with a
negative iodine probing.
Your next possible step to do.
1. Diathermocoagulation of the uterus cervix
2. Specific treatment of trichomoniasis
3. Amputation of the cerix
4. Treatment of specific vaginitis with the subsequent biopsy
5. Cryotherapy of uterus cervix
Task 6.
A32-year-old woman consulted a gynecologist concerning abundant
long menses within 3 months. On bimanual examination the body of the
uterus is enlarged according to about 12 weeks of pregnancy, distorted,
tuberous, of dense consistence. Appendages are not palpated. Histologyical
investigation of mucosa of the body of the uterus reveals cystic and
adenomatous hyperplasia of endometrium.
Optimum medical procedure to be done
1. Surgical treatment
2. Hormonal therapy
3. Phytotherapy
4. Radiation therapy
5. Vitamin therapy

692
Task 7
A 24- year-old woman having normal menstrual function has got
irregular cycles, according to the tests of functional diagnostics anovulatory.
The content of prolactin in blood is increased. Choose the most suitable
investigation method (examination).
1. Determination of level of gonadotrophic hormones
2. Computer tomography of the head
3. Ultrasound of a pelvic cavity
4. Progesteron assay
5. Determination of the contents of testosterone-depot in blood serum
Task 8.
A 29- year -old patient has had a surgical treatment concerning the
benign serous epithelial tumor of the ovary. The postoperative period has
passed without complications. What is necessary to prescribe in the
rehabilitation period?
1. Hormonal therapy and proteolytic enzymes
2. Antibacterial therapy and adaptogens
3. Laser therapy and enzyme therapy?
4. Magnetotherapy and vitamin therapy
5. No further observation is necessary
Task 9.
A 26-year-old woman complains of sudden pains in the lower abdomen,
irradiating to the anus, nausea, giddiness, dark bloody discharge from genital
tract within one week, the delay of menses for 4 weeks. Signs of irritation of
the peritoneum are positive. On bimanual examination borders of the body of
the uterus and its appendages are not determined because of sharp pain. The

693
fornixes of the vagina on the back and right sides of the vagina are painful and
protruded. What is the most probable diagnosis?
1. Interrupted tubal pregnancy
2. Apoplexy of the ovary
3. Acute right-hand adnexitis
4. Torsion of the leg of the tumour of the ovary
5. Acute appendicitis
Task 10.
At the gynecology department there is a 32-year-old patient with the
diagnosis: "the acute bartholinitis". The body temperature is 38,2C,
leucocytes = 10,4 x109, the ESR = 24 mm / hour. In the area of big gland of
the vestibulum there is a hematoma, the sign of the fluctuation is positive,
sharp pain.
What treatment is the most correct one? (What method of treatment is
the most preferable)?
1. Antibiotics, Sulfanilamides
2. Surgical dissection, drainage of an abscess of the gland, antibiotics
3. Surgical dissection, drainage of the abscess of the gland
4. Antibiotic therapy
5. Antibiotics, detoxication and bio-stimulating drugs
Task 11.
A 33-year-old woman has got a perforation of a uterine wall in the area
of fundus during curettage of the uterus cavity concerning incomplete
infected abortion.
What is the most appropriate procedure to perform?
1. Suturing of a perforated foramen (aperture) after excision of the edges

694
(borders) of the wound
2. Suturing of a perforated aperture
3. Hysterectomy
4. Antibiotic agents, observation
5. Absolute bed rest, observation.
Task 12.
In case of bleeding appearance caused by infiltrating cancer of the
uterus cervix, it's necessary to conduct
1. A tight tamponade of vagina
2. An amputation of uterus cervix
3. Clamping of lateral parametriums
4. Laparotomy, ligation of internal iliac artery
5. Laparotomy, expanded extirpation of the uterus (Wertheim's
hysterectomy)
Task 13.
For treatment of vaginitis caused by Candida's fungus it is better to use
1. "Polyjnuks"
2. Progestogel
3. "Clotremazol"
4. Vagilac
5. The above given answers are wrong
Task 14.
These are characteristic signs of gonococcus.
1. The intracellular diplococci

695
2. The positive Gram’s-stain
3. Rounded shape
4. Tropism for the laminated flat epithelium
5. Everything enumerated above
Task 15.
In case of tuberculosis of genital organs a primary focus is located most
often in
1. Lungs
2. Bones
3. Urinary excretory system
4. Lymph nodes
5. At the peritoneum
Task 16.
All of the listed below are methods of provocation of gonorrheal process,
except
1. Intake of a spice and salted food
2. Smearing of the cervical canal with combined Lugol's iodine solution and
glycerin
3. Intramuscular injection of a sinestrol 2% solution
4. Diathermy of a lumbosacral area
5. Regional injection of a gonovaccine
Task 17.
What disorders of menstrual function are the most characteristic of the
uterus myoma?

696
1. Oligomenorrhea
2. Hyperpolymenorrhea
3. Algomenorrhea
4. Amenorrhea
5. Metrorrhagia
Task 18.
Which of the methods of examination is the most informative in the
diagnostics of tube infertility?
1. Tubal insufflation
2. Hysterosalpingography
3. Transvaginal echography
4. Laparoscopy with chromosalpingoscopy
5. Contrast pelviography
Task 19.
Making the diagnosis of cervical cancer with the detection of initial
stage is possible at
1. the expanded colposcopy
2. Histological investigation of the biopsy material
3. Cytological investigation of the smears
4. Hysterocervicoscopy
5. Ultrasound of the pelvic organs
Task 20.
The majority of benign ovarian tumors are transformed into
1. Fibroma

697
2. Serous cystadenoma
3. Mucinous cystadenoma
4. Thecoma
5. Teratoma
Task 21.
Everything enumerated below is attributed to the retention cysts of the
ovaries, except
1. Follicular cyst
2. Dermoid cyst
3. Yellow body's cyst
4. Paraovarian cyst
5. "Chocolate cyst
Task 22.
A 35 –year-old patient having the right ovarian cyst after a quick
bending felt sharp pain in abdomen on the right. At the moment of admission
to the hospital the condition is satisfactory, the pulse is 86 b/min, AP –
115/80 mm Hg, to – 37,2ºC. Abdomen is soft, painful at the right
illiohypogastric area where muscle tension is noted. A menstrual function is
normal. On vaginal examination the vagina is bulky, fornices are free and
painless. The uterus has normal size. It is dense and mobile. The left adnexa
are without any peculiarities. In the area of the right adnexa a tumor-like
mass of 12x8x8 cm is palpated, its consistency is elastic, painful. There were
noted increasing pains during examination. What kind of complication was in
that case?
1. Rupture of cyst
2. Infection of cyst

698
3. Torsion of cyst
4. Malignant degeneration
5. Bleeding into cyst
Task 23.
A 75-year-old patient complains of appearing a tumor-like mass from
vagina at small physical exertion and suppression of urine. In a recumbent
position the above-mentioned tumor can be easily set into the vagina after
which the urination renews. On examination pudental fissure gapes at the
time of exertion, the whole uterus and vagina walls with a urinary bladder and
a rectum come out, mucosa of the uterus is dry, atrophic. The patient has
severe somatic pathology an ischemic heart disease, cardiosclerosis, in
anamnesis, double myocardial infarction. Surgical treatment is offered.
Which volume of surgical intervention is the most rational for that patient?
1. Frontal and back colporrhaphy
2. Ventrosuspension
3. Vaginal hysterectomy
4. Median colporrhaphy
5. Manchester operation
Task 24.
A 26-year-old patient is 7 months after last labor (childbirth). She is
breast-feeding now and she has not had menstrual flow for all this time. But 2
weeks ago the patient complained of nausea, vomiting in the morning.
What is the probable diagnosis?
1. Gastrointestinal disorder.
2. Disturbances of menstrual cycle.
3. Early pregnancy. What likely diagnosis should be made?

699
1. Colposcopy.
2. Ultrasound examination.
Task 25.
A 16-year-old patient with developed secondary genital signs complains
of extended pains in the lower abdomen, irradiating to rectum, discomfort in
her monthly menstrual cycle for 1-2 days, absence of menstrual flows.
Somatically she is healthy. On examination non -perforated hymen of tumor-
like consistency in posterior vaginal area is felt on the tip of which the uterus
can be palpated, appendages cannot be felt.
What disease can be diagnosed?
1. Tumor of genital organs.
2. Tumor of intestine.
3. Atresia of vagina.
4. Algodismenorrhea.
5. Primary false amenorrhea, hematocolpos. What does this symptom cause?
1. Hypofunction of ovaries.
2. Congenital anomaly of hymen.
3. Chronic vulvovaginitis.
Task 26.
A 48-year-old patient has no menstrual bleeding for 2 months and after
this a severe loss of blood from the uterus started. 2 years ago menstrual cycle
was disturbed with intervals of 2-3 months between cycles. On speculum
examination there are no abnormalities except of the blood loss from the
uterus.
What disease can you think of?
1. Shreder hemorrhagic metropathy

700
2. Cancer of the uterus
3. Incomplete abortion
4. Myoma of the uterus
5. Climacteric disturbance of menstrual cycle What additional method of
investigation can be used in this case?
1. Fractional diagnostic curettage of mucosal membrane from uterine cavity,
with the following histological examination
2. Colposcopia
3. X-ray of pelvic area
Task 27.
A 25-year-old patient is infertile for 3 years. She complains of painful
and prolonged menstruations, accompanied by spasmodic pains. On
bimanual examination uterus is increased in size and looks like 8 weeks of
pregnancy; appendages cannot be palpated. Using probe and diagnostic
curettage of the uterine cavity its deformation is found. Specimen of the
curettage is normal in volume.
What is the probable diagnosis?
1. Cancer of the body of the uterus
2. Submucosal myoma of the uterus
3. Internal endometritis
4. Menorrhagia, algodismenorrhea
Task 28.
A 20-year-old woman in a few days after unexpected sexual act had a lot
of discharge from the cervix with a bad odor, pain in lower abdomen and
cutting pain while micturition.

701
On examination uterus was in normal size, adnexa were enlarged, while
palpating pain was felt.
Which pathologic condition can be thought of?
1. Acute adnexitis due to gonorrhea
2. Chronic bilateral adnexitis in the stage of attack
3. Chronic tuberculosis of appendages
Task 29.
A 57-year-old patient has reddish discharge after 10 years of
menopause. On bimanual examination blood discharge from genital tract is
found. Size of the uterus is normal. Adnexa are not found.
What pathology can it be?
1. Submucous myoma of the uterus
2. Poliposis of the uterus
3. Cancer of the corpus of the uterus
4. Internal endometriosis
Task 30.
A 32-year-old woman presents with a 4-year history of infertility. Diagnostic
evaluation reveals no abnormalities other than mild endometriosis on laparoscopy.
Treatment expecting to enhance fertility includes
1. Danazol
2. Medroxyprogesterone
3. GnRH
4. All of the above
5. None of the above

702
1 - 2
2 - 5
3 - 1
4 - 1
5 - 5
6 - 1
7 - 2
8 - 1
9 - 1
10 - 2
11 - 1
12 - 1
13 - 3
14 - 1
15 – 1
16 – 3
17 – 2
18 – 4
19 – 2
20 – 2
21 – 2
22 – 3
23 – 4
24 - 3
25 - 5, 2
26 - 5, 1
27 - 2
28 - 1
29 - 3
30 - 5

703

704
Учебное издание
Rybalka A. N., Zabolotnov V. A., Kamilova I. K. at al.
OBSTETRICS AND GYNECOLOGY
Textbook in 2 volumes
(на английском языке)
Edited by Professor A. N. Rybalka
Под редакцией профессора А. Н. Рыбалка
г. Симферополь, ул. К. Маркса, 60
Тел. (0652) 510-916, 510-89
Подписано к печати 27.04.2018 г. Печать офсетная.
Бумага офсетная 80 г/кв.м.
Формат 60х84 1/16. Физ. печ. л. 44,0 Усл. печ. л. 40,92
Тираж 500 экз. Заказ № 77.
Отпечатано в ИП Барановский А.Э.
г. Симферополь, Севастопольская, 94
295021 Российская Федерация, Республика Крым