
Update on Axxess stent in bifurcation lesion
71
Update on Axxess stent in bifurcation lesion Carlo Briguori, MD, PhD Clinica Mediterranea, Napoli
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Update on Axxess stent in bifurcation lesion

Update on Axxess stent in
bifurcation lesion
Carlo Briguori, MD, PhD Clinica Mediterranea, Napoli

Treating bifurcations lesions with conventional stents may be difficult

Carina Shift After over-sizes stent in MV
Finet’s adapation of the Murrary’s law

Stent selection for treament of bifurcation lesion
4

Side branch occlusion

Bifurca(on angle & shear stress
Moore JE et al. Catheterization Cardiovascular Interventions 2010; 76:836
Larger angle higher shear stress Δ between medial and lateral wall • Mean angle in LM bifurcation = 84±14° (47-107) Arterioscler Thromb Vasc Biol 1997;17:1356–1360
low and oscillating WSS at the lateral wall higher restenosis rate


Site of recrossing
Foin N et al. International J Cardiol 2013

Conven(onal Strategy for Bifurca(on Lesion Treatment
Legrand V. et al. Eurointervention 2007;3:44
Dedicated Devices
Device needed which could:
1. Reduce complexity • sized to the vessel proximally and distally • enable side-‐branch access
2. Improve safety • less metal • beCer apposi(on

The AXXESSTM stent
• Dedicated bifurca(on drug-‐elu(ng stent • Self-‐expanding and conical shaped Nickel –(tanium
stent • Abluminal bioabsorbable PLA/BA9 coa(ng technology • 4 sizes are currently CE-‐approved (7F):
– 3.0 and 3.5 mm in diameter – 11 and 14 mm in length
• A successful implant will span the os(a of both branching vessels, indicated by the presence of one marker in each branch vessel
The AxxessTM Stent
Dedicated bifurcation drug-eluting stent (DES)
� Nitinol self-expanding stent � Abluminal biodegradable PLA
polymer/Biolimus BA9™ coating technology
� Available sizes: • 3.0 and 3.5 mm in diameter* • 11 and 14 mm in length*
Axxess™ bifurcation DES is CE approved
* Current sizes, other measures were available at the time of the study
Up to 6.00 mm*
Up to 3.75 mm*
Up to 6.50 mm*
Up to 4.25 mm*
Ø 3.0 mm Ø 3.5 mm

E Goal is to span both vessels with coverage of the proximal lesion segment E Cover the ostium of SB and distal MV without compromising access to SB:
E 2 distal stent markers in one branch and one in the other E Convenient markers for placing overlapped distal or proximal stents
The AXXESSTM stent

How the Axxess stent works
• The Axxess stent, when delivered op(mally (black dots), pushes atheroma away from the flow divider leaving no drug elu(ng struts near the carina.
• Atheroma and in(mal hyperplasia are not thought to occur at the carina.
• With many alterna(ve sten(ng techniques it is non-‐endothelialized carina struts that are associated with thrombus.
Ormiston modified from Virmani

Ormiston, 2012

Distal sheath
Ormiston, 2012

The Axxess™ stent: a specific delivery system
• The different markers are located as follows
Source: Axxess™ Instruction For Use
Marker 1 – Tip marker • The most distal marker is located on the
inner delivery catheter (p • This marker will not move with respect
to stent during the deployment procedure
Marker 2 – Distal sheath marker • The second marker is located at the end
of the cover sheath, distal to the 3 gold markers on the stent
• This marker will move as the cover sheath is retracted during deployment, at first to cover the three distal stent markers, then proximal toward Marker 3 as the sheath is retracted

The Axxess™ stent: a specific delivery system
• The different markers are located as follows
Source: Axxess™ Instruction For Use
Marker 3 • The third marker – also called the
deployment marker – is located on the inner catheter shab approximately mid-‐stent
• This marker serves as visual reference to aid the user during withdrawal
• This marker will not move with respect to stent during the deployment procedure
Marker 4 • The fourth marker – also called the pull
wire marker – is located on the cover sheath proximal to the stent an will also move when the sheath is retracted
• This marker is part of the sheath body and serves no purpose in stent placement

Coronary Artery Bifurcation Narrowing treated By AXxess Stent Implantation (CARINAX) registry
Inclusion criteria 1) Significant (≥70% diameter stenosis) bifurcation lesion;
a) both protected and unprotected left main bifurcation lesions were allowed to be included, provided that all other angiographic criteria were satisfied.
2) MV reference diameter between 2.75 and 4.75 mm by visually estimated,
3) SB reference diameter ≥2.25 mm by visual estimate; 4) Bifurcation angle (between the distal MV and the SB) <70° by visual
estimate.
Exclusion criteria 1) Patients with contraindications to prolonged DAPT, 2) Known sensitivity to “limus” compounds, stainless steel, titanium, or
nickel; 3) Inclusion in others studies; and 4) All bifurcation lesions not satisfying the angiographic inclusion criteria
reported above. This study was registered with http://www.clinicaltrial.gov (trial ID NCT02486315).

Coronary Artery Bifurcation Narrowing treated By AXxess Stent Implantation (CARINAX) registry
Sample size
The sample size was selected to demonstrate a 9-month MACE rate similar to the provisional SB stenting group (simple approach) of the major trials1-5. v Expecting a 10% MACE rate at 9-month similar to the provisional SB
stenting, a total of at least 150 patients provides the study 80% power (using a one-sided Chi square test with a significance level of 0.05) and 95% confidence interval to proof the above hypothesis.
v Expecting a 8% attrition, the sample size increases to 162 patients.
1. Behan MW et al. Circ Cardiovasc Interv 2011;4:57-64 2. Colombo A. et al. Circulation 2009;119:71-8 3. Chen SL et al. Eur J Clin Invest 2008;38:361-71 4. Chen SL. Et al. J Am Coll Cardiol;57:914-20 5. Ferenc M. et al. Eur Heart J 2008;29:2859-67
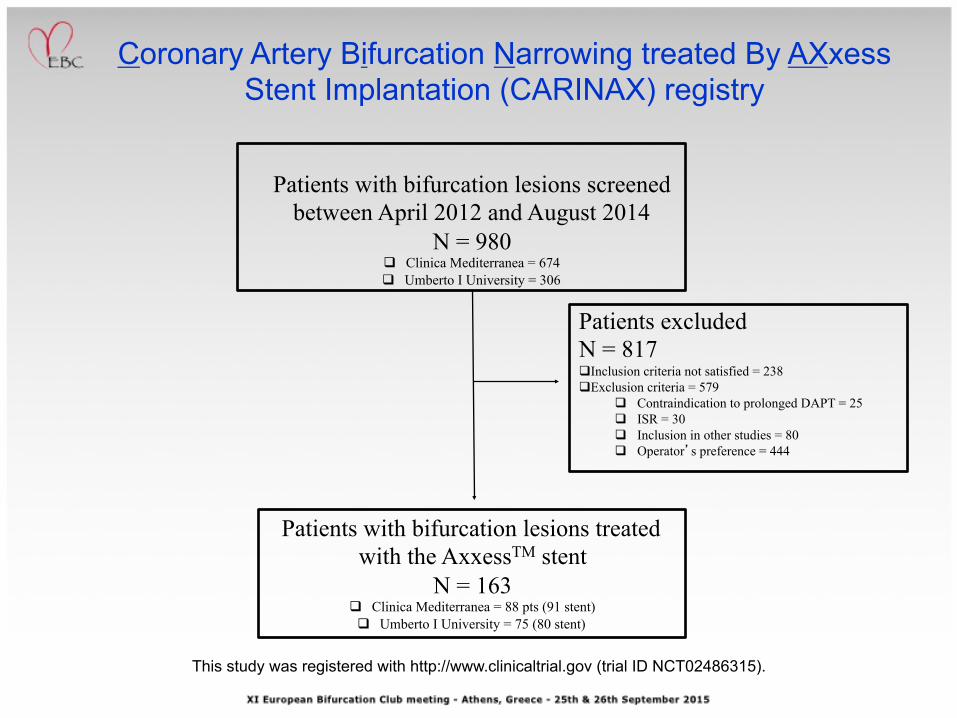
Patients with bifurcation lesions screened between April 2012 and August 2014
N = 980 q Clinica Mediterranea = 674 q Umberto I University = 306
Patients with bifurcation lesions treated with the AxxessTM stent
N = 163 q Clinica Mediterranea = 88 pts (91 stent) q Umberto I University = 75 (80 stent)
Patients excluded N = 817 q Inclusion criteria not satisfied = 238 q Exclusion criteria = 579
q Contraindication to prolonged DAPT = 25 q ISR = 30 q Inclusion in other studies = 80 q Operator’s preference = 444
Coronary Artery Bifurcation Narrowing treated By AXxess Stent Implantation (CARINAX) registry
This study was registered with http://www.clinicaltrial.gov (trial ID NCT02486315).

Clinical Characteris(cs Axxess DES (n = 163)
Age, years 65 ± 11
Male 131 (80.5%)
Diabetes mellitus 124 (76%)
Systemic Hypertension 124 (76%)
Silent ischemia or Stable angina 123 (75.5%)
UA/NSTEMI 25 (15.5%)
STEMI 15 (9%)
Previous MI 27 (16.5%)
Previous CABG 9 (5.5%)
Previous PCI 42 (26%)
Active smoking 49 (30 %)
CKD 36 (22%)
hyperlipidemia 95 (58%)
Family history of CAD 61 (37.5%)
Left Ventricular Ejection Fraction, % 51 ± 9
Multivessel PCI 58 (35.6%)

Angiographic Characteris(cs Axxess DES (n=163)
Target Vessel Left main coronary artery Left anterior descending/diagonal Circumflex/obtuse marginal Rigth coronary artery/posterior descending
171 15 (9%)
104 (61%) 41 (24%) 11 (6%)
Medina classification 1:1:1 1:1:0 1:0:0 1:0:1 0:1:1 0:1:0 0:0:1
171 67 (39%) 13 (7.5%)
23 (13.5%) 45 (26%) 15 (9%) 4 (2.5%) 4 (2.5)
Bifurcation angle (°) 61 ± 17
Chronic total occlusion 17 (9.9%)
Calcification (moderate-severe) 47 (27.5%)
Lesion Type A B1 B2 C
171 0
55 (32%) 74 (43%) 42 (25%)

Procedural Characteris(cs Axxess DES (n=163)
Axxess stent diameter (mm) 3.0 3.5 4.0
105 (61.5%)
63 (37%) 3 (1.5%)
Axxess stent length (mm) 9 11 14
3 (1.5%) 92 (54%)
76 (44.5%)
Maximal inflation pressure (atmospheres) MV SB
18 ± 4 12 ± 4
Final balloon diameter (mm) MV SB
3.3 ± 0.3 2.5 ± 0.3
Use of rotational atherectomy 16 (9.5%)
Contrast media volume (ml)
144 ± 59

Quan(ta(ve coronary artery analysis
Pre-procedure Post-procedure Pre-procedure Post-procedure
Reference diameter,mm 3.2 ± 0.45 3.5 ± 0.52
2.4 ± 0.55
2.55 ± 0.60
MLD, mm 0.57 ± 0.57 3.33 ± 0.59 0.78 ± 0.94 2.34 ± 0.64
Diameter Stenosis (%) 81 ± 16 0.82 ± 2.1 63 ± 34 2.49 ± 6.5
Lesion Length, mm 17 ± 10 10 ± 12
Main Vessel Side branch

Pattern I (n = 57)
1,0,0 18 1,0,1 29 1,1,1 6 1,1,0 2 0,1,1 2
1,0,0 5 1,0,1 4 1,1,1 26 1,1,0 9 0,1,1 4 0,0,1 1 0,1,0 4
Pattern II (n = 53)
Pattern III (n = 22)
1,0,1 8
1,1,1 10
0,1,1 3
0,0,1 1
Pattern IV (n = 39)
1,0,1 4
1,1,1 25
0,1,1 6
0,0,1 2
1,1,0 2

Coronary Artery Bifurcation Narrowing treated By AXxess Stent Implantation (CARINAX) registry
v Device success was obtained in 162/163 (99.5%) of patients and in
170/171 (99.5%) lesions. v We reported one Axxess stent deployment failure due to malfunction of
the delivery system consisting of the unsuccessful retraction of the cover sheath
v Inaccurate AxxessTM stent implantation occurred in 15.8% of cases,
which is almost the double than the 7% reported in the DIVERGE trial1
1. Verheye S et al. J Am Coll Cardiol 2009;53:1031-9.

Procedural and angiographic characteris(cs according to the accuracy of Axxess stent implanta(on
Accurate position group (n=144)
Inaccurate position group (n=27)
p
Lesion site proximal middle distal
48 (33%) 72(50%) 24 (17%)
8 (29.5%) 14 (52%) 5 (18.5%)
0.25
Angle between branches (°) 62 ± 13 59 ± 18 0.31
Contrast media volume (ml) 140 ± 55 170 ± 71 0.014
Number of guidewires used 1.9 ± 0.27 1.82 ± 0.4 0.21
Calcification (moderate-severe) 32 (22%) 15 (52%) 0.012
Medina classification 1:1:1 1:1:0 1:0:0 1:0:1 0:1:1 0:1:0 0:0:1
53 (37%) 11 (7.5%) 19 (13%)
41 (28.5%) 14 (10%)
3 (2%) 3 (2%)
14 (51.5%)
2 (7.5%) 4 (15%) 4 (15%) 1 (3.5%) 1 (3.5%) 1 (3.5%)
0.62
Lesion Type A B1 B2 C
0
48 (33%) 60 (42%) 36 (25%)
0
9 (33%) 11 (41%) 7 (26%)
0.93
Predilatation MV SB Both
21 (14.5%)
9 (6%) 119 (82.5%)
1 (4%) 1 (4%)
25 (92%) 0.66
Fluoroscopic times (minutes) 20 ± 9 27 ± 14 0.040

0
2
4
6
8
10
12
14
16
18
20
I Quartile ( n = 40)
II Quartile (n = 42)
III Quartile (n = 40)
IV Quartile (n = 49)
17.5% 16.7%
17.5%
14.5%
%
p = 0.97
Inaccurate Axxess DES deployment overt (me

In-‐hospital and 30-‐day major adverse cardica events
Axxess DES (n=163)
Cumulative events 14 (8.5%)
Cardiac death 0
Myocardial infarction Q-wave Non-Q wave periprocedural
13 (12.9%) 2 (1.2%)
11 (11.6%) 10 (11.6%)
TLR 3 (1.8%)
Stent thrombosis acute subacute
2 (1.2%) 2 (1.2%)
0

9-‐month major adverse cardiac events
Axxess DES (n=163)
Cumulative events 16 (9.8%)
Cardiac death 0
Myocardial infarction Q-wave Non-Q wave
14 (8.5%) 2 (1.2%)
12 (7.3%)
TLR 4 (2.4%)
Stent thrombosis acute subacute late
2 (1.2%) 2 (1.2%)
0 0

Log rank p = 0.43
1.0
0.8
0.6
0.4
0.2
0.0
0 50 100 150 200 250 300
Even
t-fre
e su
rviv
al
Time (days)
Pattern I Pattern II Pattern III Pattern IV
9-‐month major adverse cardiac events

Case 1

PCI has been performed using a 7 F EBU 3.75 guide catheter. With a Pilot 200 guidewire and the support of a 1.25 mm OTW balloon the occlusion at the os(um of the diagonal branch has been crossed.
PTCA

Predila(on has been performed with a 2.5 x 15 mm semi-‐compliant balloon. A TIMI 3 flow was obtained.
PTCA
0:1:1 bifurcation lesion

Axxess stent 3.5 x 11 mm was succefully deployed at the level of the carina with the three distal markers protruding into the distal branches.
PTCA

PTCA
Easy crossing of the diagonal branch os(um covered by AXXESSTM by a 2.5 mm SC balloon Kissing balloon (2,5 mm SC balloons)

A Resolute Integrity 2.5 x 30 mm was implanted in the proximal diagonal branch, overlapped to the AxxessTM
A Resolute Integrity 3.0 x 30 mm was implanted in the mid LAD, overlapped to the AxxessTM
PTCA
Final kissing balloon (3.0 mm NC balloon in both branches)
PTCA

• Op(mal stent apposi(on • Op(mal carine reconstruc(on • Op(mal stent expansion
IVUS MLA: 7,60 mm2 MLA: 6,21 mm2 MLA: 14,38 mm2
MLA: 7,54 mm2 MLA: 7,02 mm2

LCX bifurca(on

LCX bifurca(on

LCX bifurca(on

LCX bifurca(on

LCX bifurca(on

LCX bifurca(on

LCX bifurca(on

Case 3

Case 3

Case 3

Case 3

Case 3

Case 3

Case 3

Case 2

Case 2

Case 3

Case 3

Case 4 Inaccurate Implanta(on

Case 4 Inaccurate Implanta(on

Case 4 Inaccurate Implanta(on

Case 4 Inaccurate Implanta(on

Case 4 Inaccurate Implanta(on

Case 5 Acute thrombosis

Case 5 Acute thrombosis

Case 5 Acute thrombosis

Case 5 Acute thrombosis

Case 5 Acute thrombosis

Case 5 Acute thrombosis

Case 5 Acute thrombosis

Conclusions The use of the AXXESS™ stent for treatment of bifurca(on lesions: • May solve the problem of
– Size selec(on & – Side-‐branches access – Technical strategy of carina reconstruc(on
• Issues – overlapping stents in case addi(onal stents are implanted in the distal MV and/or in the SB
– bifurca(on lesions with specific anatomic features (i.e., MV reference diameter between 2.75 and 4.75 mm; SB reference diameter ≥2.25 mm; and bifurca(on angle <70°).

Study Limitations
ü Lack of a control group ü A propensity-‐matched control group has been selected from our database.
ü The rela(vely small sample size and the short term follow-‐up
ü Inaccurate AxxessTM stent implanta(on was higher in case of moderate-‐to-‐severe calcifica(ons. These bifurca(on lesions should have been excluded as in the DIVERGE trial.




















