Recent Perspective on Coronary Bifurcation Intervention: Statement of the “Bifurcation Club in...
10
C 2010, Wiley Periodicals, Inc. DOI: 10.1111/j.1540-8183.2010.00570.x Recent Perspective on Coronary Bifurcation Intervention: Statement of the “Bifurcation Club in KOKURA” YOSHINOBU MURASATO, M.D., 1 YUTAKA HIKICHI, M.D., 2 SUNAO NAKAMURA, M.D., 3 FUMIHIKO KAJIYA, M.D., 4 KIYOTAKA IWASAKI, M.D., 5 YOSHIHISA KINOSHITA, M.D., 6 MASAHIRO YAMAWAKI, M.D., 7 TOSHIRO SHINKE, M.D., 8 SHNICHIRO YAMADA, M.D., 9 TAKEHIRO YAMASHITA, M.D., 10 GIM-HOOI CHOO, M.D., 11 CHANG-WOOK NAM, M.D., 12 YOUNG-HAK KIM, M.D., 13 NIGEL JEPSON, M.D., 14 and MIROSLAW FERENC, M.D. 15 From the 1 New Yukuhashi Hospital, Japan; 2 Saga University, Japan; 3 New Tokyo Hospital, Japan; 4 Kawasaki University of Medical Welfare, Japan; 5 Waseda University, Japan; 6 Toyohashi Heart Center, Japan; 7 Saiseikai Yokohama-Eastern Hospital, Japan; 8 Kobe University, Japan; 9 Himeji Cardiovascular Center, Japan; 10 Cardiovascular Center Hokkaido Ohno Hospital, Japan; 11 KPJ Selangor Specialist Hospital, Malaysia; 12 Keimyung University, Korea; 13 Asan Medical Center, Korea; 14 Eastern Heart Clinic, Australia; and 15 Herz-Zentrum Bad Krozingen, Germany The treatment of coronary bifurcation lesion remains a challenging issue even in the drug-eluting stent era. Frequent restenosis and stent thrombosis have been recently shown to be related not only to geometrical gap or stent structural deformation but also to rheological disturbance. Low wall shear stress at the lateral side of the bifurcation is likely to cause atherosclerotic changes due to easy access of the macrophages that induce chemical mediators. The turbulent flow over stent metal may facilitate accumulation of platelets, which results in thrombosis. The jailed strut and excess metal overlap may increase these risks. Since dramatic changes of the coronary flow pattern at the bifurcation are closely related to the genesis of atherosclerosis, future bifurcation intervention technique should be considered to restore the original physiological state as well as the anatomical structure. This article summarizes the global consensus of the members of the Asian Bifurcation Club and European Bifurcation Club at the KOKURA meeting. It also provides a perspective of basic sciences relating to bifurcation anatomy, physiology, and pathology, in the search for a best strategy for bifurcation intervention. (J Interven Cardiol 2010;23:295–304) Introduction Coronary bifurcation lesions are frequently encoun- tered by the interventional cardiologist, as evidenced by the high prevalence of bifurcation lesions (>60%) in the SYNTAX (synergy between percutaneous coro- nary intervention with TAXUS and cardiac surgery) trial. 1 However, coronary bifurcation intervention is still a challenging issue even in the era of drug-eluting Address for reprints: Yoshinobu Murasato, M.D., Department of Cardiovascular Medicine, Heart Center, New Yukuhashi Hospital, 1411, Dojoji, Yukuhashi 824-0026, Japan. Fax: +81-930-22-5551; e-mail: [email protected] stent (DES). Difficulties and controversies persist, es- pecially in relation to stenting technique, strategy (one- stent vs. two-stent), or complications (frequent resteno- sis, side branch (SB) occlusion, and stent thrombosis (ST). This is why it is necessary to understand the com- plex nature of the bifurcation in anatomical, physiolog- ical, and pathological aspects in order to allow better understanding of the mechanism of frequent resteno- sis and helping the engineering development of new dedicated devices. The “Bifurcation Club in KOKURA” was held in a special session focusing on coronary bifurcation inter- vention at the 26th Live Demonstration in KOKURA on May 30, 2009. This session was attended by Vol. 23, No. 4, 2010 Journal of Interventional Cardiology 295
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Recent Perspective on Coronary Bifurcation Intervention: Statement of the “Bifurcation Club in...

C©2010, Wiley Periodicals, Inc.DOI: 10.1111/j.1540-8183.2010.00570.x
Recent Perspective on Coronary Bifurcation Intervention: Statement of the
“Bifurcation Club in KOKURA”
YOSHINOBU MURASATO, M.D.,1 YUTAKA HIKICHI, M.D.,2 SUNAO NAKAMURA, M.D.,3
FUMIHIKO KAJIYA, M.D.,4 KIYOTAKA IWASAKI, M.D.,5 YOSHIHISA KINOSHITA, M.D.,6
MASAHIRO YAMAWAKI, M.D.,7 TOSHIRO SHINKE, M.D.,8 SHNICHIRO YAMADA, M.D.,9
TAKEHIRO YAMASHITA, M.D.,10 GIM-HOOI CHOO, M.D.,11 CHANG-WOOK NAM, M.D.,12
YOUNG-HAK KIM, M.D.,13 NIGEL JEPSON, M.D.,14 and MIROSLAW FERENC, M.D.15
From the 1New Yukuhashi Hospital, Japan; 2Saga University, Japan; 3New Tokyo Hospital, Japan; 4Kawasaki University of Medical Welfare,Japan; 5Waseda University, Japan; 6Toyohashi Heart Center, Japan; 7Saiseikai Yokohama-Eastern Hospital, Japan; 8Kobe University, Japan;9Himeji Cardiovascular Center, Japan; 10Cardiovascular Center Hokkaido Ohno Hospital, Japan; 11KPJ Selangor Specialist Hospital,Malaysia; 12Keimyung University, Korea; 13Asan Medical Center, Korea; 14Eastern Heart Clinic, Australia; and 15Herz-Zentrum BadKrozingen, Germany
The treatment of coronary bifurcation lesion remains a challenging issue even in the drug-eluting stent era.Frequent restenosis and stent thrombosis have been recently shown to be related not only to geometrical gap orstent structural deformation but also to rheological disturbance. Low wall shear stress at the lateral side of thebifurcation is likely to cause atherosclerotic changes due to easy access of the macrophages that induce chemicalmediators. The turbulent flow over stent metal may facilitate accumulation of platelets, which results in thrombosis.The jailed strut and excess metal overlap may increase these risks. Since dramatic changes of the coronary flowpattern at the bifurcation are closely related to the genesis of atherosclerosis, future bifurcation interventiontechnique should be considered to restore the original physiological state as well as the anatomical structure.This article summarizes the global consensus of the members of the Asian Bifurcation Club and EuropeanBifurcation Club at the KOKURA meeting. It also provides a perspective of basic sciences relating to bifurcationanatomy, physiology, and pathology, in the search for a best strategy for bifurcation intervention. (J IntervenCardiol 2010;23:295–304)
Introduction
Coronary bifurcation lesions are frequently encoun-tered by the interventional cardiologist, as evidencedby the high prevalence of bifurcation lesions (>60%)in the SYNTAX (synergy between percutaneous coro-nary intervention with TAXUS and cardiac surgery)trial.1 However, coronary bifurcation intervention isstill a challenging issue even in the era of drug-eluting
Address for reprints: Yoshinobu Murasato, M.D., Department ofCardiovascular Medicine, Heart Center, New Yukuhashi Hospital,1411, Dojoji, Yukuhashi 824-0026, Japan. Fax: +81-930-22-5551;e-mail: [email protected]
stent (DES). Difficulties and controversies persist, es-pecially in relation to stenting technique, strategy (one-stent vs. two-stent), or complications (frequent resteno-sis, side branch (SB) occlusion, and stent thrombosis(ST). This is why it is necessary to understand the com-plex nature of the bifurcation in anatomical, physiolog-ical, and pathological aspects in order to allow betterunderstanding of the mechanism of frequent resteno-sis and helping the engineering development of newdedicated devices.
The “Bifurcation Club in KOKURA” was held in aspecial session focusing on coronary bifurcation inter-vention at the 26th Live Demonstration in KOKURAon May 30, 2009. This session was attended by
Vol. 23, No. 4, 2010 Journal of Interventional Cardiology 295

MURASATO, ET AL.
members of the European Bifurcation Club and AsianBifurcation Club. This article summarizes the presenta-tions of original investigations and randomized clinicaltrials by their authors-investigators.
Anatomy and Physiology
Kajiya summarized the advances in the understand-ing of anatomy and physiology for coronary bifurca-tion. The endothelium in the cardiovascular system ishighly sensitive to hemodynamic shear stresses thatact on the vessel luminal surface in the direction ofblood flow.2 Asakura and Karino demonstrated in theirobservations of isolated, transparent human coronaryarteries that the atherosclerotic plaque formation wasclosely related to the low and oscillatory flow at thelateral area of the bifurcated and tortuous lesion.3 Soany interventions that change the local arterial geome-try, e.g., by stenting, could influence the flow-mediatedendothelial responses.
Vascular branching according to Murray’s law pro-poses the consideration of minimizing energy costfunction (Fig. 1).4 The mechanical energy is obtainedas the product of the vascular flow and the pressure gra-dient from the proximal to the distal part of the vessel.The metabolic energy is assumed to be in proportion tothe vessel volume. Since the cost function is expressed
Figure 1. Murray’s law of vascular branching. See detail in the text. Q, �P, K, a, and L are vessel flow, pressure gradient,constant, radius, and length of vessel, respectively. Q0, Q1, and Q2 are the vessel flows in the mother branch and eachdaughter branch, respectively, and a0, a1, and a2 are defined in the same manner.
as the sum of these energies, the numerical formula ofthe cost function could be calculated as
Cost function = Q�P + Kπa2L= (8 μL/πa4)Q2 + Kπa2L
where Q, �P, K, a, L, and μ are vessel flow according toPoiseuille’s formula (top in Fig. 1), pressure gradient,constant, vascular radius and length, and coefficient ofviscosity, respectively. To minimize the cost function,d (Cost Function)/da must vanish. This yields the so-lution on the second line from the bottom. Hence, theoptional radius of a blood vessel is proportional to Q tothe 1/3 power. The equation of continuity is Q0 = Q1+Q2, and then a3
0 = a31 + a3
2, which is often referred toas Murray’s law. Fung also described the optimal bi-furcation pattern, i.e., θ and � of Figure 1, for givenmother and daughter radii in his text.4
Pathology
Pathological studies have demonstrated thatatherosclerotic changes usually occurred in the lat-eral area of the bifurcation with low shear stress andrarely involved the carinal area where high flow wasobserved.5 DES deployment is an excellent option forthe bifurcation lesion as many true bifurcation lesionsrequired a two-stent technique. However, the healing
296 Journal of Interventional Cardiology Vol. 23, No. 4, 2010

STATEMENT OF “BIFURCATION CLUB IN KOKURA”
process after implantation of two DES in the bifurca-tion lesion has not yet been elucidated. High volumeof metal overlap and high amount of antiproliferativedrug could delay the endothelialization of the DES.6
The risk of ST after discontinuation of antiplatelettherapy also increased.7 The J-Cypher registry studydemonstrated a higher frequency of ST after two-stentdeployment when compared with a one-stent strategy.7
An autopsy study demonstrated that ST occurred at thesite of nonendothelialization of struts at the bifurcationcarina area and the protruded stent struts at the prox-imal main vessel (MV).8 Delayed healing at the areaof stent overlap was also suggested to be a critical riskfactor for ST.
Flow Study
In vitro flow studies under physiological conditionsare ideal for the analysis of the impact of the coro-nary flow on atherosclerotic plaque formation. Thefollowing aspects of the flow model are related to anideal physiological condition: (1) elasticity of the sili-con tube similar to that in human coronary artery, (2)three-dimensional structure of the bifurcation model,(3) stenotic model that has similar geometry and com-pliance to the real atherosclerotic lesion, and (4) visu-alization using pulsatile coronary flow.
Iwasaki developed a left main coronary artery(LMCA) bifurcation model that enclosed the first threestructural characteristics noted above. This model alsodemonstrated a high-speed visualization of the pul-satile flow using double pulse Nd: YLF laser. There re-sults showed flow delay at the lateral area and high flow
Figure 2. High-speed flow visualizationin the three-dimensional left main coro-nary artery (LMCA) bifurcation model. A:Stenotic model which has 60% stenosisfrom the LMCA to the LAD and 50% steno-sis in the LCX. The flow retardation wasprominent in the distal lateral area neigh-boring to the stenosis (arrows). B: Aftermini-crush stenting. The flow retardationat the lateral area was relieved by the stent-ing; however, flow disturbance was newlydeveloped in the carina where the stent strutdid not cover (triangle) and in the overdi-lated area close to the MV ostium (dottedarrows).
at the flow-divider in the normal bifurcation model.The flow delay was more prominent in the distal lat-eral area neighboring the stenosis in the stenotic model(Fig. 2A, arrows). The flow delay was relieved aftera mini-crush stenting procedure. However, new flowdisturbance developed at the carina in the area lackingstrut coverage (Fig. 2B, triangle) and in the overdilatedarea close to the MV ostium (Fig. 2B, dotted arrows).
Bench Study
Bench study is essential for understanding the mech-anism of bifurcation stenting. Microfocus computedtomography (MFCT) provided clearer images withhigher resolution compared to the clinically availableimaging tools, such as fluoroscopy and intravascularsound (IVUS), and better analyzed the detailed stentdeformation and strut apposition to the vessel wall.9,10
Three-dimensional reconstruction of the images is es-pecially useful for the analysis of the strut configura-tion, deformation and reapposition (Fig. 3A–C). Stud-ies using MFCT have demonstrated the limitation oftwo-stent deployment in any technique. There remainsan unstented area at the opposite site of the crushedstent after crush stenting; incomplete crush at the prox-imal MV has also been observed in some cases. Hikichidemonstrated in the cross-sectional MFCT analysis ofcrush stenting that the success rate in recrossing theguidewire through the appropriate route in the SB os-tium to permit final kissing balloon inflation was notas high as was expected. Although the procedure wasperformed under fluoroscopy, only 6 of 16 attempts
Vol. 23, No. 4, 2010 Journal of Interventional Cardiology 297

MURASATO, ET AL.
Figure 3. Stent configuration after deployment in the MV followed by kissing balloon inflation in Cypher stent (A), TaxusExpress stent (B), and Endeavor stent (C). Although the Cypher stent had the limitation of the cell dilation for the SB to3 mm, the closed cell based structure was likely to maintain its original configuration in the MV. The Taxus Express stenthad ability for the adequate cell expansion for the SB; however, more prominent deformation was observed in the proximalMV after kissing balloon inflation (B, arrows). Although the Endeavor stent also had ability for the adequate expansion forthe SB, excessive dilation caused the gap around the carina in the MV (C, dotted circle). (D): Guidewire recrossing throughthe central area of the SB. Although the procedure was performed under the fluoroscopy, only 6 of 16 attempts (37.5%) weresuccessful in recrossing through the appropriate point.
(37.5%) were successful at recrossing through the cen-tral area of the SB (Fig. 3D).
Review of Clinical Trials: Provisional Stentingversus Two-Stent Strategy
Murasato reviewed several recent randomized tri-als from Europe and revealed the lack of benefitsof planned SB stenting. In the NORDIC bifurcationstudy,11 413 patients were randomized to routine SBstenting or one-stent strategy using sirolimus-elutingstent (SES). The excellent point of this study was oftoo low frequency (4.3%) of switch from a one-stentstrategy to additional SB stenting. In general, rou-tine SB stenting was more time-consuming and wasassociated with higher levels of irradiation and con-trast usage. Procedure-related biomarker release wasalso higher in the routine two-stent group and therewas no difference in MACE between the two groupsduring follow-up. In the British Bifurcation CoronaryStudy: Old, New, and Evolving Strategies (BBC-ONE)study,12 500 patients were randomized to provisional T-stenting and complex stenting using paclitaxel-elutingstent (PES). Although there was no difference in thefrequency of death or target vessel failure, myocar-dial infarction (MI) occurred more frequently in the
complex stenting group (11.2% vs. 3.6%), resulting ina higher frequency of MACE (15.2% vs. 8.0%, P <
0.01). In the Coronary Bifurcations: Application of theCrushing Technique Using Sirolimus-Eluting Stents(CACTUS) study,13 350 true bifurcation lesions wererandomized to either crush or provisional stenting afterpredilatation of both branches. SB stenting was neces-sary in one-third of the cases of the provisional stentinggroup. The percentages of binary restenosis in the MV(4.6% in the crush stenting group vs. 6.7% in the pro-visional stenting group) and the SB (13.2% vs. 14.7%)at 6 months were not significantly different. The dou-ble stent strategy was also not associated with a higherincidence of MACE. This study suggests the appropri-ateness of a two-stent strategy for the true bifurcationlesion with severe SB stenosis.
Ferenc et al. compared routine and provisional T-stenting using SES in the bifurcations bad Krozingen(BBK) randomized study.14 There were 101 patientsenrolled in each group and 19% of cases in the pro-visional group required double stenting. There was nosignificant difference in binary restenosis of the MVor the SB in the 9-month follow-up angiography. Tar-get lesion revascularization (TLR), MI, and death inthe routine and provisional stenting groups after 1-yearfollow-up were 8.9% versus 10.9%, 2.0% versus 1.0%,and 1.0% versus 2.0%, respectively, and no significant
298 Journal of Interventional Cardiology Vol. 23, No. 4, 2010
STATEMENT OF “BIFURCATION CLUB IN KOKURA”
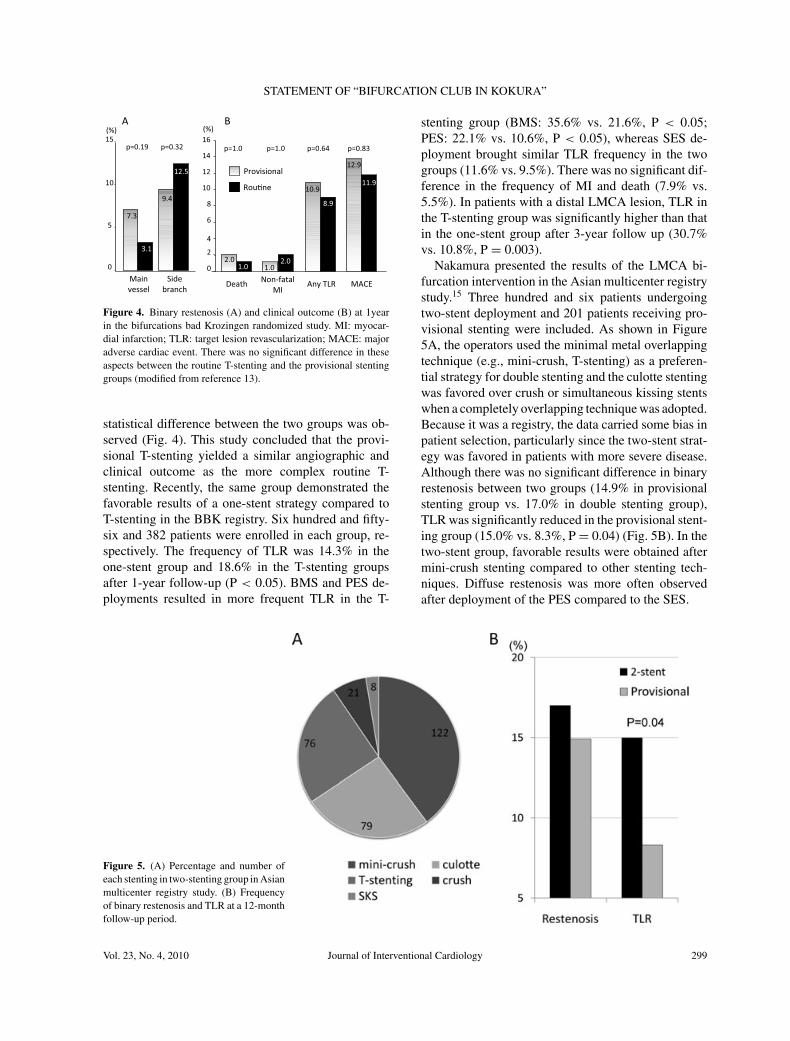
Figure 4. Binary restenosis (A) and clinical outcome (B) at 1yearin the bifurcations bad Krozingen randomized study. MI: myocar-dial infarction; TLR: target lesion revascularization; MACE: majoradverse cardiac event. There was no significant difference in theseaspects between the routine T-stenting and the provisional stentinggroups (modified from reference 13).
statistical difference between the two groups was ob-served (Fig. 4). This study concluded that the provi-sional T-stenting yielded a similar angiographic andclinical outcome as the more complex routine T-stenting. Recently, the same group demonstrated thefavorable results of a one-stent strategy compared toT-stenting in the BBK registry. Six hundred and fifty-six and 382 patients were enrolled in each group, re-spectively. The frequency of TLR was 14.3% in theone-stent group and 18.6% in the T-stenting groupsafter 1-year follow-up (P < 0.05). BMS and PES de-ployments resulted in more frequent TLR in the T-
Figure 5. (A) Percentage and number ofeach stenting in two-stenting group in Asianmulticenter registry study. (B) Frequencyof binary restenosis and TLR at a 12-monthfollow-up period.
stenting group (BMS: 35.6% vs. 21.6%, P < 0.05;PES: 22.1% vs. 10.6%, P < 0.05), whereas SES de-ployment brought similar TLR frequency in the twogroups (11.6% vs. 9.5%). There was no significant dif-ference in the frequency of MI and death (7.9% vs.5.5%). In patients with a distal LMCA lesion, TLR inthe T-stenting group was significantly higher than thatin the one-stent group after 3-year follow up (30.7%vs. 10.8%, P = 0.003).
Nakamura presented the results of the LMCA bi-furcation intervention in the Asian multicenter registrystudy.15 Three hundred and six patients undergoingtwo-stent deployment and 201 patients receiving pro-visional stenting were included. As shown in Figure5A, the operators used the minimal metal overlappingtechnique (e.g., mini-crush, T-stenting) as a preferen-tial strategy for double stenting and the culotte stentingwas favored over crush or simultaneous kissing stentswhen a completely overlapping technique was adopted.Because it was a registry, the data carried some bias inpatient selection, particularly since the two-stent strat-egy was favored in patients with more severe disease.Although there was no significant difference in binaryrestenosis between two groups (14.9% in provisionalstenting group vs. 17.0% in double stenting group),TLR was significantly reduced in the provisional stent-ing group (15.0% vs. 8.3%, P = 0.04) (Fig. 5B). In thetwo-stent group, favorable results were obtained aftermini-crush stenting compared to other stenting tech-niques. Diffuse restenosis was more often observedafter deployment of the PES compared to the SES.
Vol. 23, No. 4, 2010 Journal of Interventional Cardiology 299

MURASATO, ET AL.
Provisional Stenting
Choo suggested that the provisional T-stenting is anattractive technique for bifurcation intervention. It wassuitable in up to 90% of bifurcation lesions and theevidence suggested high success rates and low ratesof restenosis that were comparable if not better thanprimary two-stent strategy.11–14 Additional advantagesinclude enhanced safety (less biomarker rise11 andST6), technical ease, less time-consuming,11,12 andlower cost. The ability to cross-over to a two-stentstrategy was not compromised in the event of subop-timal result or threatened closure in the SB. Neverthe-less, there were situations when provisional T-stentingstrategy was not optimal such as in cases of a nar-row bifurcation angle and large SB with long proximaldisease.
Two-Stent Strategy and SB StentingTechnique
Culotte Stenting. Although culotte stenting re-quired a complex procedure entailing double guide-wire exchange and KBI, culotte stenting has been con-sidered an optimal technique for the true bifurcationlesion because of the excellent apposition of the strutsto the vessel wall. The Nordic II study, which wasthe randomized comparison of culotte and crush stent-ing using SES in 424 patients, demonstrated less SBrestenosis in culotte stenting compared to crush stent-ing (9.8% vs. 3.8%, P = 0.04). There was no differencein MV restenosis at the 6-month follow-up.16 A previ-ous report documented the 12-month clinical outcomesof culotte stenting in 134 lesions in 132 patients.17 Theincidence of binary restenosis was 22% for the wholebifurcation lesion, 0% in the proximal MV, 9.1% in thedistal MV, and 16% in the SB. The frequency of TLRand ST was 21% and 1.5%, respectively, and compa-rable to other two-stent techniques. In another reportthat compared culotte and T-stenting in 75 patients,culotte stenting resulted in a lower frequency of TLR(8.9% vs. 27.3%, P = 0.014) and a tendency to a lowerincidence of MACE (13.3% vs. 27.3%, P = 0.051).18
Although the open-cell-based stent is ideal for the com-plete apposition to the vessel, a numerical trend towarda higher incidence of restenosis with Endeavor (28.6%)and Taxus (34.6%) was reported compared to Cypher(18.0%) despite the limitation of strut dilation for the
SB.17 Further examination is required to clarify whichis the optimal stent for this technique.
Shunt Technique. Jepson et al. demonstrated theeffectiveness of their unique SB stenting method,the shunt technique. The SB stent is positioned withthe proximal end protruding minimally from the ostiumwhile the MV balloon is positioned at the bifurcation.The SB stent is first inflated with low pressure and thenthe MV balloon is inflated. This results in the move-ment of the SB stent downstream to the appropriateposition with minimal protrusion or overlap in the MV.Finally, the SB stent is inflated to high pressure fol-lowed by MV stenting. The SB is rewired and KBI isperformed to complete the procedure. This techniqueprotects the MV, SB patency, and is applicable to DESpermitting complete coverage.
The authors reported the favorable results of the ran-domized trial of the shunt technique in the Re-Wiretrial.19 The frequency of MACE, clinically driven TLR,and late/very late ST at 1-year follow-up were 9.2%,4.4%, and 0.8%, respectively.
Flower/Stenting with Protruding Strut intoSide Branch Technique
Kinoshita found that the structural limitations ofconventional stent platform for bifurcation interventioninclude: restricted diameter of maximal cell expansionfor the SB ostium, conformability of stent fitting tothe bifurcation angle, durability of stent against hingemotion, and damage of polymer. They proposed thenew stenting technique (Flower/SPRINT technique)that can provide the complete coverage of the carinaand adequate expansion of the stented branch ostium(Fig. 6).20,21
In this technique, the following preparation out ofthe body before stenting is necessary: stent dilationmounting the distal cap except for the proximal 1 to 3struts, guidewire crossing through the dilated strut, andreinstallation of the dilated strut to the balloon. The fas-tened guidewire is inserted to the nontargeted branchand the prepared strut still remains in the nontargetedbranch after stent deployment at the targeted branch.These struts are reflected to the distal direction by theballoon inflation in the nontargeted branch with strutdilation (flower technique) or without it (SPRINT tech-nique). In cases with rich plaque burden or hard cal-cification, plaque modification is necessary to ensureadequate expansion and coverage of the SB ostium.
300 Journal of Interventional Cardiology Vol. 23, No. 4, 2010

STATEMENT OF “BIFURCATION CLUB IN KOKURA”
Figure 6. Stenting with protruding strut into side branch (SPRINT)technique. The proximal strut of the SB stent was minimally pro-truded at the carina due to detainment of the strut by the guide-wire that crossed through the proximal one strut toward the oppositebranch (asterisk). In the case of planned two-stent deployment, prox-imal part of the SB ostium was covered by the protruded MV stent(cross). This technique brought minimal metal overlapping at thebifurcation.
Left Main Coronary Bifurcation
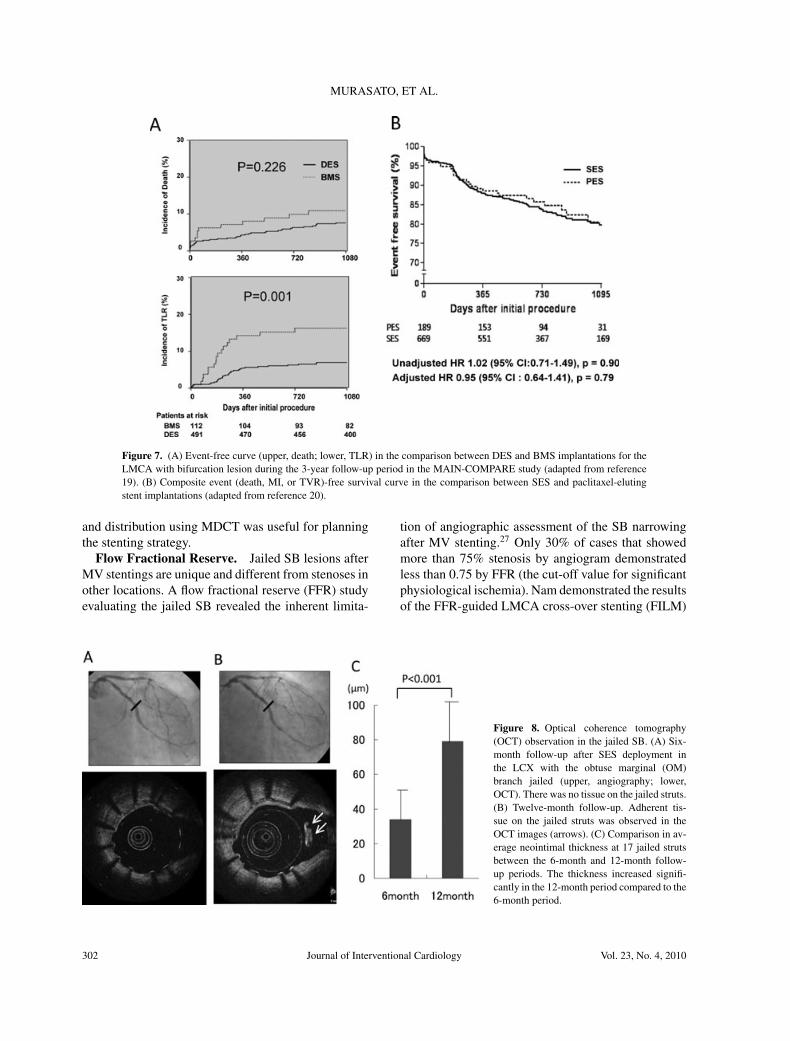
Kim summarized the Revascularization for Unpro-tected LMCA Stenosis: Comparison of PercutaneousCoronary Angioplasty versus Surgical Revasculariza-tion (MAIN-COMPARE) study22 and its substudyanalysis.23,24 His group compared the MACE between1,102 patients with unprotected LMCA disease whounderwent stent implantation and 1,138 patients whounderwent CABG. The study showed that there was nosignificant difference in death, MI, or stroke betweenthe stenting and the CABG groups. However, the rateof TVR was significantly higher in the stenting groupthan in the CABG group (hazard ratio, 4.76; 95% CI,2.80 to 8.11).22 In the subanalysis of the stenting group,they demonstrated superiority of the DES to the BMSin causing fewer TLR at 3-year follow-up period (5.4%vs. 12.1%; hazard ratio, 0.40; 95% CI, 0.22 to 0.73; P= 0.009) despite worse patient background. The use ofDES did not yield any significant benefit in terms of thefrequency of death or MI for the entire group.23 How-ever, it brought significant reduction in MI and TLRin the LMCA with a bifurcation lesion (Fig. 7A).23
In the comparison between SES (n = 669) and PES(n = 189), both stent groups showed a similar 3-yearclinical outcome: death (9.1% vs. 11.0%, HR: 0.92,95% CI: 0.47 to 1.80, P = 0.82), MI (8.1% vs. 8.0%,HR: 0.80, 95% CI: 0.43 to 1.48, P = 0.47), and TVR
(12.1% vs. 10.6%, HR: 1.10, 95% CI: 0.53 to 2.29,P = 0.81) (Fig. 7B).24 The 3-year rates of ST were0.6% in the SES group and 1.6% in the PES group;however, the difference was not statistically significant(P = 0.18).24
Imaging and Physiological Assessment
Intravascular Ultrasound. Yamawaki investi-gated the mechanism of SB narrowing after MV stent-ing in nontrue bifurcation lesions using IVUS. Theplaque volume in the proximal MV was higher inthe SB narrowing group than that in the nonnarrow-ing group (45.7 ± 19.7 mm3 vs. 34.2 ± 13.5 mm3, P< 0.01). Both plaque volume and vessel volume werehigher in the SB narrowing group (12.7 ± 6.1 mm3
vs. 7.3 ± 3.2 mm3 and 24.8 ± 9.3 mm3 vs. 18.8 ± 5.9mm3, P < 0.05, respectively). Such results suggest thatthe accumulated plaque in the SB ostium or plaque bur-den ranging from the proximal MV to the SB were riskfactors for the SB narrowing after the MV stenting.
Optical Coherence Tomography. Shinke inves-tigated the condition of the jailed strut at the SB ostiumafter MV stenting using serial optical coherence to-mography (OCT). They found neointimal tissue grow-ing on the jailed struts in OCT follow-up (Fig. 8A, B).The average neointimal thickness was higher at 12-month follow-up period compared to 6-month (79.0 ±26.0 μm vs. 34.0 ± 17.0 μm, P < 0.001) (Fig. 8C). Theclinical and pathological significance of delayed tissuecoverage of the jailed strut has not yet been clarified inlong-term follow-up results.
Multislice-Detected Raw Computed Tomogra-phy. Yamada revealed the advantage of multislice-detected raw computed tomography (MDCT) assess-ment in bifurcation intervention. Optimal evaluationof bifurcation angle is possible in the appropriate viewwhen the angle is most widely opened in the MDCT.The previous MDCT study showed that the frequencyof high-angle bifurcation (>80◦) in the LMCA bifur-cation was more than twice that in other bifurcations.25
In addition, the authors demonstrated that the angle be-tween the LMCA and the LAD was wider than betweenthe LMCA and the LCX (142◦ vs. 131◦, P < 0.0001).The authors also confirmed good correlation in thepercentage plaque area between the assessments byMDCT and by IVUS.26 They suggested that preinter-ventional assessment of plaque morphology, volume,
Vol. 23, No. 4, 2010 Journal of Interventional Cardiology 301
MURASATO, ET AL.
Figure 7. (A) Event-free curve (upper, death; lower, TLR) in the comparison between DES and BMS implantations for theLMCA with bifurcation lesion during the 3-year follow-up period in the MAIN-COMPARE study (adapted from reference19). (B) Composite event (death, MI, or TVR)-free survival curve in the comparison between SES and paclitaxel-elutingstent implantations (adapted from reference 20).
and distribution using MDCT was useful for planningthe stenting strategy.
Flow Fractional Reserve. Jailed SB lesions afterMV stentings are unique and different from stenoses inother locations. A flow fractional reserve (FFR) studyevaluating the jailed SB revealed the inherent limita-
Figure 8. Optical coherence tomography(OCT) observation in the jailed SB. (A) Six-month follow-up after SES deployment inthe LCX with the obtuse marginal (OM)branch jailed (upper, angiography; lower,OCT). There was no tissue on the jailed struts.(B) Twelve-month follow-up. Adherent tis-sue on the jailed struts was observed in theOCT images (arrows). (C) Comparison in av-erage neointimal thickness at 17 jailed strutsbetween the 6-month and 12-month follow-up periods. The thickness increased signifi-cantly in the 12-month period compared to the6-month period.
tion of angiographic assessment of the SB narrowingafter MV stenting.27 Only 30% of cases that showedmore than 75% stenosis by angiogram demonstratedless than 0.75 by FFR (the cut-off value for significantphysiological ischemia). Nam demonstrated the resultsof the FFR-guided LMCA cross-over stenting (FILM)
302 Journal of Interventional Cardiology Vol. 23, No. 4, 2010

STATEMENT OF “BIFURCATION CLUB IN KOKURA”
pilot study. Although there was a negative correla-tion between percent stenosis and FFR (r = −0.469,P = 0.01), no lesion with ≤50% diameter stenosishad FFR <0.80. QCA demonstrated significant steno-sis (>50%) in the ostial LCX in 58.6% (17/29) byplaque and carina shifting from LM and LAD. How-ever, functionally significant obstruction by pressurewire criteria was seen in just 17.2% (5/29) of cases.Therefore, physiological assessments are also impor-tant in the jailed LCX and routine LCX treatment maybe unnecessary. FFR may avoid overtreatment and un-necessary two-stent deployment.
Stent Thrombosis
ST results in MI and carries a poor prognosis. It hasbeen demonstrated that the frequency of recurrence andthe rate of death were approximately 20% and 10%,respectively, at a 3-year follow-up period.28 Yamashitapointed out the low frequency of ST in the J-Cypherregistry6 compared to Bern/Rotterdam registry (cumu-lative frequency at 2 year; 0.8% vs. 2.3%).29 However,ST increased at a stable rate in both registries (0.25%and 0.6% per year, respectively).
Bifurcation lesions have been recognized to be ahigh-risk subset for ST and one report showed a hazardratio of up to 6.42.30 Flow disturbance and stent overlapare probably responsible for delayed reendothelializa-tion and subsequent ST in bifurcation lesions. It wasreported that IVUS had a potential to decrease acuteand subacute thrombosis but no impact on late throm-bosis.31 A large-scale randomized trial is needed toconfirm its efficacy on bifurcation stenting.
Conclusion
Coronary bifurcation lesion treatment remains achallenging issue even in the DES era. Frequentrestenosis and ST have been recently shown to be re-lated not only to geometrical gap or stent structuraldeformation but also to rheological disturbance. Lowwall shear stress at the lateral side of the bifurcationis likely to cause atherosclerotic changes due to easyaccess of the macrophages that induce chemical medi-ators. The turbulent flow over stent metal may facilitateaccumulation of platelets, which results in thrombosis.The jailed strut and excess metal overlap may increasethese risks. Since dramatic changes of the coronary
flow pattern at the bifurcation are closely related tothe genesis of atherosclerosis, future bifurcation inter-vention technique should be considered to restore theoriginal physiological state as well as the anatomicalstructure.
Acknowledgment: The authors extend thanks particularly to Drs.Masakiyo Nobuyoshi and Hiroyoshi Yokoi (President and Vice Pres-ident of the Live Demonstration in KOKURA, Kokura MemorialHospital, Japan) for their contribution on holding the session.
References
1. Serruys PW, Morice MC, Kappetein AP, et al. Percuta-neous coronary intervention versus coronary-artery bypassgrafting for severe coronary artery disease. N Engl J Med2009;360:961–972.
2. Caro CG. Discovery of the role of wall shear in atherosclerosis.Arterioscler Thromb Vasc Biol 2009;29:158–161.
3. Asakura T, Karino T. Flow patterns and spatial distribution ofatherosclerotic lesions in human coronary arteries. Circ Res1990;66:1045–1066.
4. Fung FC. Biomechanics: Circulation. 2nd ed. Chap.3, NewYork: Springer-Verlag, 1996.
5. Nakazawa G, Yazdani SK, Finn AV, et al. Pathological find-ings at bifurcation lesions: The impact of flow distribution onatherosclerosis and arterial healing after stent implantation. JAm Coll Cardiol 2010;55:1679–1687.
6. Nakazawa G, Finn AV, Joner M, et al. Delayed arterial healingand increased late stent thrombosis at culprit sites after drug-eluting stent placement for acute myocardial infarction patients:An autopsy study. Circulation 2008;118:1138–1145.
7. Kimura T, Morimoto T, Nakagawa Y, et al. Antiplatelet therapyand stent thrombosis after sirolimus-eluting stent implantation.Circulation 2009;119:987–995.
8. Joner M, Finn AV, Farb A, et al. Pathology of drug-elutingstents in humans: Delayed healing and late thrombotic risk. JAm Coll Cardiol 2006;48:193–202.
9. Hikichi Y, Inoue T, Node K. Benefits and limitations of cypherstent-based bifurcation approaches: In vitro evaluation usingmicro-focus CT scan. J Interv Cardiol 2009;22:128–134.
10. Murasato Y, Hikichi Y, Horiuchi M. Examination of stent de-formation and gap formation after complex stenting of leftmain coronary artery bifurcations using microfocus computedtomography. J Interv Cardiol 2009;22:135–144.
11. Steigen TK, Maeng M, Wiseth R, et al. Nordic PCI StudyGroup. Randomized study on simple versus complex stentingof coronary artery bifurcation lesions: The Nordic bifurcationstudy. Circulation 2006;114:1955–1961.
12. Hildick-Smith D, de Belder AJ, Cooter N, et al. Random-ized trial of simple versus complex drug-eluting stenting forbifurcation lesions: The British Bifurcation Coronary Study:old, new, and evolving strategies. Circulation 2010;121:1235–1243.
13. Colombo A, Bramucci E, Sacca S, et al. Randomized study ofthe crush technique versus provisional side-branch stenting intrue coronary bifurcations: The CACTUS (Coronary Bifurca-tions: Application of the Crushing Technique Using Sirolimus-Eluting Stents) Study. Circulation 2009;119:71–78.
Vol. 23, No. 4, 2010 Journal of Interventional Cardiology 303

MURASATO, ET AL.
14. Ferenc M, Gick M, Kienzle RP, et al. Randomized trial onroutine vs. provisional T-stenting in the treatment of de novocoronary bifurcation lesions. Eur Heart J 2008;29:2859–2867.
15. Nakamura S, Ogawa H, Bae JH, et al. Systematic double stent-ing versus simple provisional T-stenting for true bifurcationlesions of left main coronary artery disease using drug elutingstents: Multicenter registry in Asia. Am Coll Cardiol i2 Summit2009.
16. Erglis A, Kumsars I, Matti Niemela M, et al. Randomized com-parison of coronary bifurcation stenting with the crush versusthe culotte technique using sirolimus eluting stents. The Nordicstent technique study. Circ Cardiovasc Intervent 2009;2:27–34.
17. Adriaenssens T, Byrne RA, Dibra A, et al. Culotte stenting tech-nique in coronary bifurcation disease: Angiographic follow-upusing dedicated quantitative coronary angiographic analysisand 12-month clinical outcomes. Eur Heart J 2008;29:2868–2876.
18. Kaplan S, Barlis P, Dimopoulos K, et al. Culotte versus T-stenting in bifurcation lesions: Immediate clinical and angio-graphic results and midterm clinical follow-up. Am Heart J2007;154:336–343.
19. Prasan AM, Pitney MR, Ramsay D, et al. New bifurcationstenting technique: Shunt stenting. Catheter Cardiovasc Interv2004;63:474–481.
20. Habara M, Kinoshita Y. Stenting with PRotruding strutINTo side branch (SPRINT) technique: A novel techniquefor coronary bifurcation stenting. Catheter Cardiovasc Interv2009;73:336–343.
21. Kinoshita Y. First clinical experience of “flower petal stenting”:A novel technique for the treatment of coronary bifurcationlesions. J Am Coll Cardiol Interv, 2010;3:58–65.
22. Seung KB, Park DW, Kim YH, et al. Stents versus coronary-artery bypass grafting for left main coronary artery disease. NEngl J Med 2008;358:1781–1792.
23. Kim YH, Park DW, Lee SW, et al. Long-term safety and ef-fectiveness of unprotected left main coronary stenting withdrug-eluting stents compared with bare-metal stents. Circula-tion 2009;120:400–407.
24. Lee JY, Park DW, Yun SC, et al. Long-term clinical outcomesof sirolimus- versus paclitaxel-eluting stents for patients withunprotected left main coronary artery disease: Analysis of theMAIN-COMPARE (revascularization for unprotected left maincoronary artery stenosis: Comparison of percutaneous coronaryangioplasty versus surgical revascularization) registry. J AmColl Cardiol 2009;54:853–859.
25. Kawasaki T, Koga H, Serikawa T, et al. The bifurcation studyusing 64 multislice computed tomography. Catheter CardiovascInterv 2009;73:653–658.
26. Hara T, Yamada S, Hayashi T, et al. Accuracy of nonstenoticcoronary atherosclerosis assessment by multi-detector com-puted tomography. Circ J 2007;71:911–914.
27. Koo BK, Kang HJ, Youn TJ, et al. Physiologic assessment ofjailed side branch lesions using fractional flow reserve. J AmColl Cardiol 2005;46:633–637.
28. van Werkum JW, Heestermans AA, de Korte FI, et al. Long-term clinical outcome after a first angiographically confirmedcoronary stent thrombosis: An analysis of 431 cases. Circula-tion 2009;119:828–834.
29. Wenaweser P, Daemen J, Zwahlen M, et al. Incidence andcorrelates of drug-eluting stent thrombosis in routine clinicalpractice. 4-year results from a large 2-institutional cohort study.J Am Coll Cardiol 2008;52:1134–1140.
30. Iakovou I, Schmidt T, Bonizzoni E, et al. Incidence, predictors,and outcome of thrombosis after successful implantation ofdrug-eluting stents. JAMA 2005;293:2126–2130.
31. Roy P, Torguson R, Okabe T, et al. Angiographic and pro-cedural correlates of stent thrombosis after intracoronary im-plantation of drug-eluting stents. J Interv Cardiol 2007;20:307–313.
304 Journal of Interventional Cardiology Vol. 23, No. 4, 2010