axxess - European Bifurcation Club
52
AXXESS TM – The Self- Expanding Bifurcation DES – Device Overview and Clinical Data Clinical Data Ricardo A. Costa Instituto Dante Pazzanese de Cardiologia São Paulo, Brazil Ricardo A. Costa Instituto Dante Pazzanese de Cardiologia São Paulo, Brazil 7 7 7 th th th th European Bifurcation Club European Bifurcation Club European Bifurcation Club European Bifurcation Club – – – Lisbon, Portugal, October 14 2011 Lisbon, Portugal, October 14 2011 Lisbon, Portugal, October 14 2011 Lisbon, Portugal, October 14 2011
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of axxess - European Bifurcation Club

AXXESSTM – The Self-
Expanding Bifurcation DES
– Device Overview and Clinical DataClinical Data
Ricardo A. Costa
Instituto Dante Pazzanese de Cardiologia
São Paulo, Brazil
Ricardo A. Costa
Instituto Dante Pazzanese de Cardiologia
São Paulo, Brazil
7777thththth European Bifurcation Club European Bifurcation Club European Bifurcation Club European Bifurcation Club –––– Lisbon, Portugal, October 14 2011Lisbon, Portugal, October 14 2011Lisbon, Portugal, October 14 2011Lisbon, Portugal, October 14 2011

AXXESS Biolimus A9-Coated Stent � Self-expanding nickel-
titanium (Nitinol) alloy
� Conical shape
� Proximal and distal gold
markers to facilitate
implantation
� Coated with Biolimus A9™
DEVICE DESCRIPTION
2
� First self-expanding coronary stent to incorporate a drug
� First drug-eluting stent dedicated for the treatment of
diseased coronary bifurcation lesions
� Coated with Biolimus A9
using a bioabsor-bable
polymer matrix (PLA) in a
dose of 22 µg/mm of
stent length

New Molecular Entity
• Sirolimus analog
• Same macrocyclic “limus” family
• C55H87NO14
• More lipophilic than Sirolimus/Everolimus
• Potent immunosuppressant
BIOLIMUS A9
3
4040--OO--(2(2--ethoxyethyl) Modification, ethoxyethyl) Modification, Most preferred position for stentMost preferred position for stent--based applications,based applications,
as it doesn’t affect FKBP binding propertiesas it doesn’t affect FKBP binding properties
Mechanism of Action
• Anti-proliferative agent
• Binds to FKBP-12
• Inhibits mTOR activity
• Inhibits G1 phase of the cell cycle

� Nitinol self-expanding stent
platform
� 0.006 in. (0.15mm) strut
thickness
� Sizes
� 3.0 and 3.5mm in diameter
� 10 and 14 mm in length
1 Proximal Marker
AXXESS STENT
4
� Drug carrier: bioabsorbable
polymer matrix (PLA)
� Drug release rate: ~ 70% in 30
days, remaining ~ 30% released in
< 6 months
� Polymer absorption: ~ 6-9 months;
then, only the metal strut remains3 Distal Markers

• 4.8-Fr.• 7-Fr. or higher
catheter size compatible system
DELIVERY SYSTEM
Sheath actuator
Safety lock
Covered sheath Rapid Exchange (RX) delivery catheter
5
system
Handle
Flushing port
Catheter tip
Tip marker
Stent sheath markers
AXXESSStent markers

Existing techniques have several
drawbacks:
• T-stenting can leave a gap in coverage at
the SB ostium (1)
• If “crushed” to cover the ostium, 2 or 3
stent layers of stent are left to block side
branch flow (2)
Side BranchParent Vessel 1
2
RATIONALE
6
branch flow (2)
• The crushing action may pull the stent
away from the carina (3)
• The AXXESS approach leaves an
unobstructed side branch and completely
covers the SB ostium with DES (4)
3
4
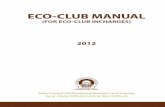
GOAL: SPAN BOTH VESSELS
7
� Cover the proximal lesion segment
� Cover the ostium of the side branch and distal parent vessel without
compromising access to the side branch
� This is accomplished if 2 markers are in 1 branch and 1 is in the other
� Provide a convenient placement marker for additional distal stents

THERAPEUTIC CONCEPT
8
The AXEESS approach:
� Implant a stent with the appropriate shape to treat the
troublesome anatomy of the bifurcation, then
� Provisionally add subsequent stents to cover the lesion as
needed: stent “end to end”, rather than “through the side”

CASE EXAMPLE
� Location: LAD/diagonal
� Both branches
involved
� Calcification
9
AP CRANIAL VIEW LAO CAUDAL VIEW
� Calcification
� Distal angle <60o
� Lesions in distal
branches
DiagonalLAD
LAD
Diagonal

PROCEDURE I
Pre-dilatation
PVPV PV
SB
SB
PV predilatation 1 PV predilatation 2 PV predilatation 3
10
� Both parent vessel (PV) – LAD, and side
branch (SB) – diagonal, pre-dilated with high
pressure balloon inflations
� Pre-dilatation in the PV found “resistan-ce”
(yellow arrow) to fully dilate the lesion
PV
SB
SB SB
PV
SB single predilatation
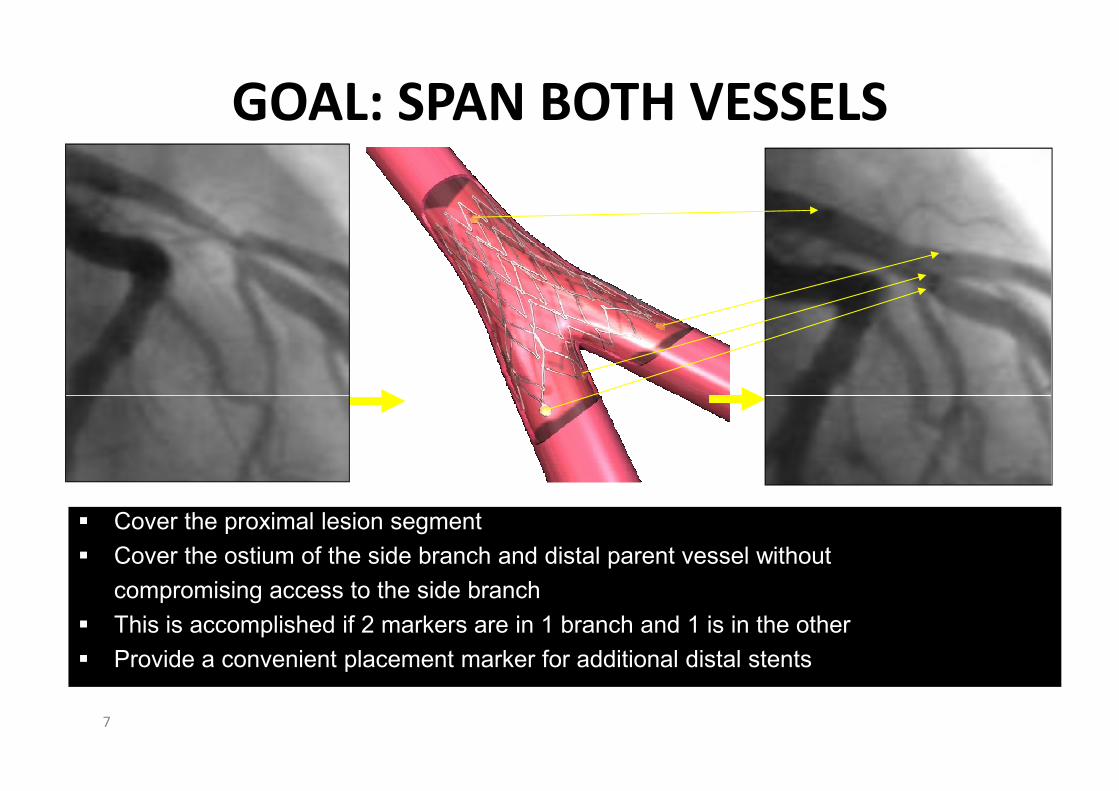
PROCEDURE II
AXXESS ImplantationProximal and distal markers of the AXXESS
stent
Delivery system almost
completely withdrawn, self-
expanding mechanism to
Distal “flared” end
of the AXXESS
stent, covering the
SB angulation
PV angulationDistal markers
alignment not
11
RAO CRANIAL LAO CRANIAL
AXXESS inserted towards
the PV*
expanding mechanism to
“open” and deploy the stent origin of the SB
Alignment of distal markers is visualized in the most
orthogonal view of the SB origin, BEST for AXXESS
stent positioning
* Most angulated branch to the proximal vessel, recommended
alignment not
visualized:
foreshortening
view, SB origin
not well
visualized
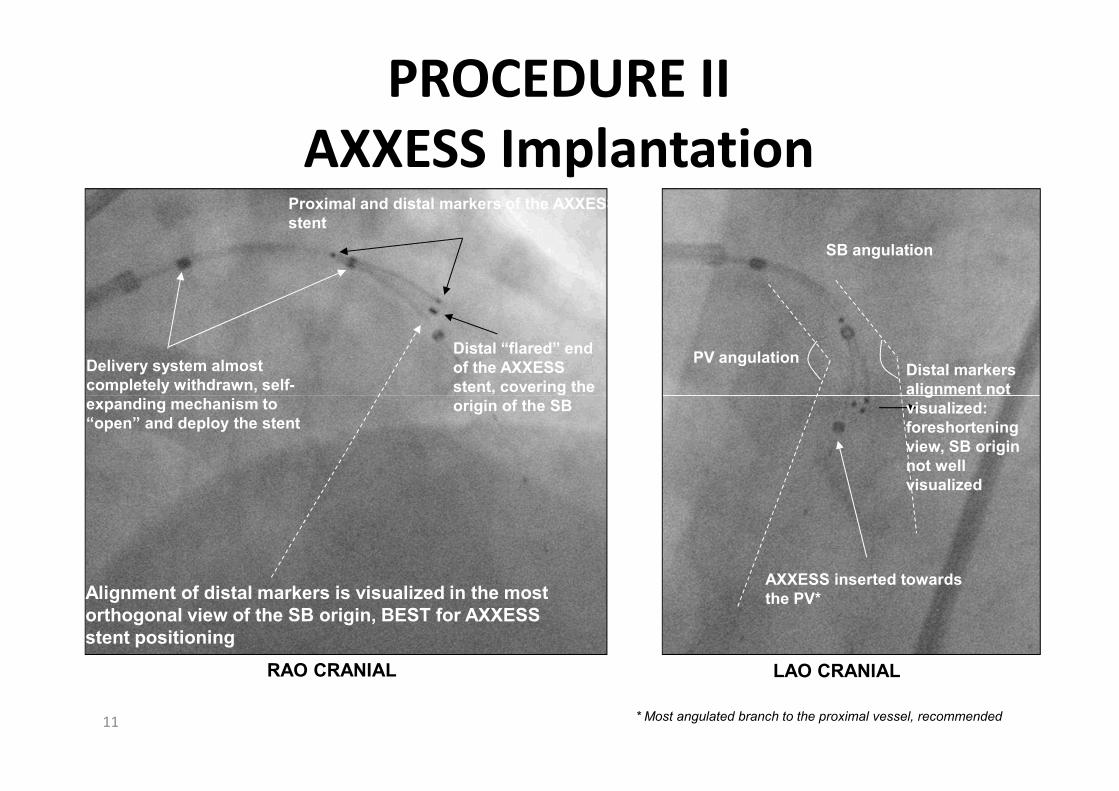
PROCEDURE III
Additional Stents Distal markers of
the
AXXESS stentSES
proximal
marker
Overlap
Overlapping
segment
12
PV post-
dilatation
SESSimultaneous deployment of
PV and SB SES
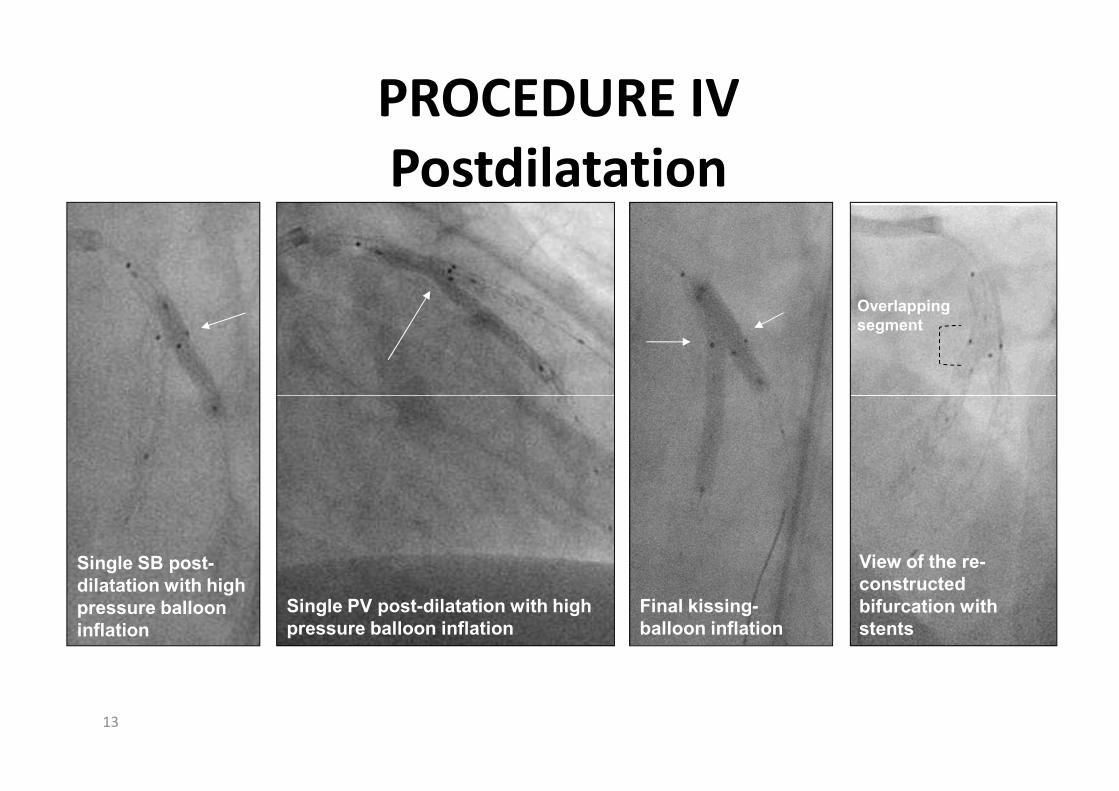
PROCEDURE IV
Postdilatation
Overlapping
segment
13
Single SB post-
dilatation with high
pressure balloon
inflation
Final kissing-
balloon inflation
Single PV post-dilatation with high
pressure balloon inflation
View of the re-
constructed
bifurcation with
stents
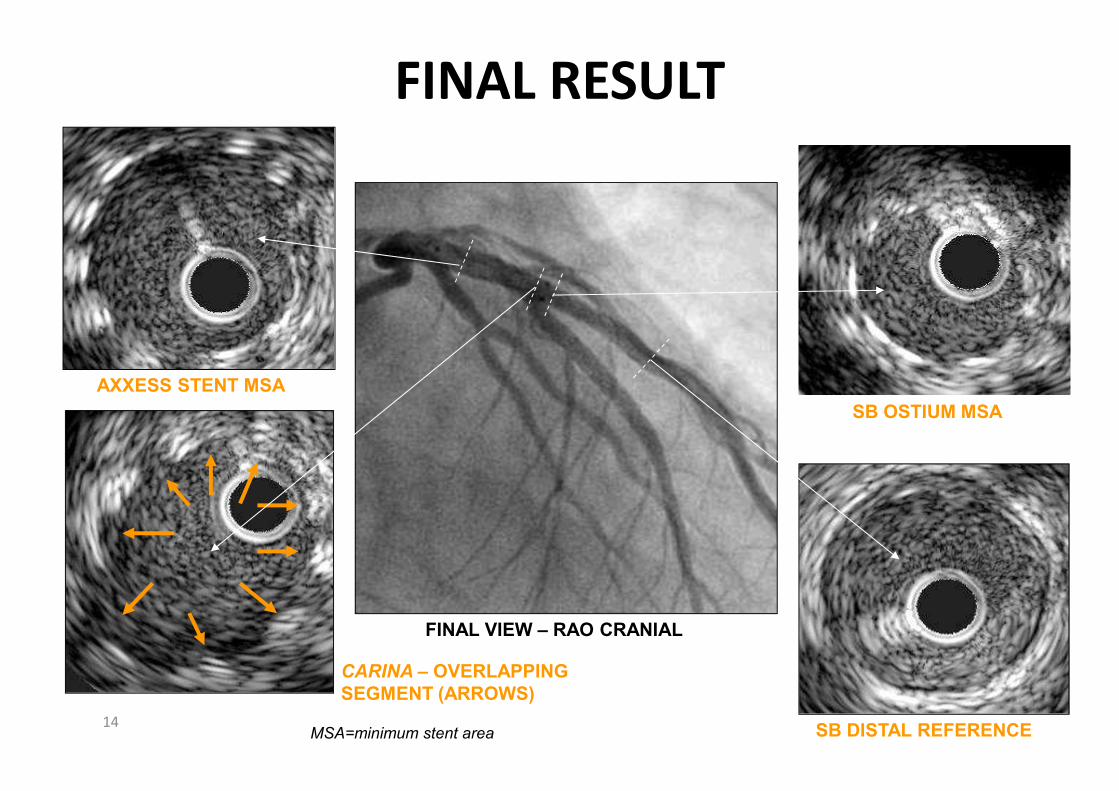
FINAL RESULT
AXXESS STENT MSA
14
FINAL VIEW – RAO CRANIAL
SB OSTIUM MSA
SB DISTAL REFERENCE
CARINA – OVERLAPPING
SEGMENT (ARROWS)
AXXESS STENT MSA
MSA=minimum stent area

AXXESS Clinical Studies
AXXESS
N=43
AXXESS
PLUS
• Bare metal version of AXXESS Stent
• Safety and effectiveness study
• 6 month follow-up completed
• Evaluated drug-eluting AXXESS stent to BMS
• Safety and effectiveness studyPLUS
N=139
DIVERGE
N=302
• Safety and effectiveness study
• Follow-up through 3 years completed
• International safety and effectiveness study
• Evaluated best practices from AXXESS Plus
• 3 year follow-up will be presented at EuroPCR 2011

AXXESS PLUS TRIAL DESIGNAXXESS PLUS TRIAL DESIGNAXXESS PLUS TRIAL DESIGNAXXESS PLUS TRIAL DESIGN
� DESIGN Prospective, non-randomized, single-arm, multi-center
clinical evaluation of the AXXESSTM Plus Bifurcated
Coronary Stent System
� OBJECTIVE To evaluate the acute and long-term safety, tolerabi-
lity and performance of the AXXESS Plus stent
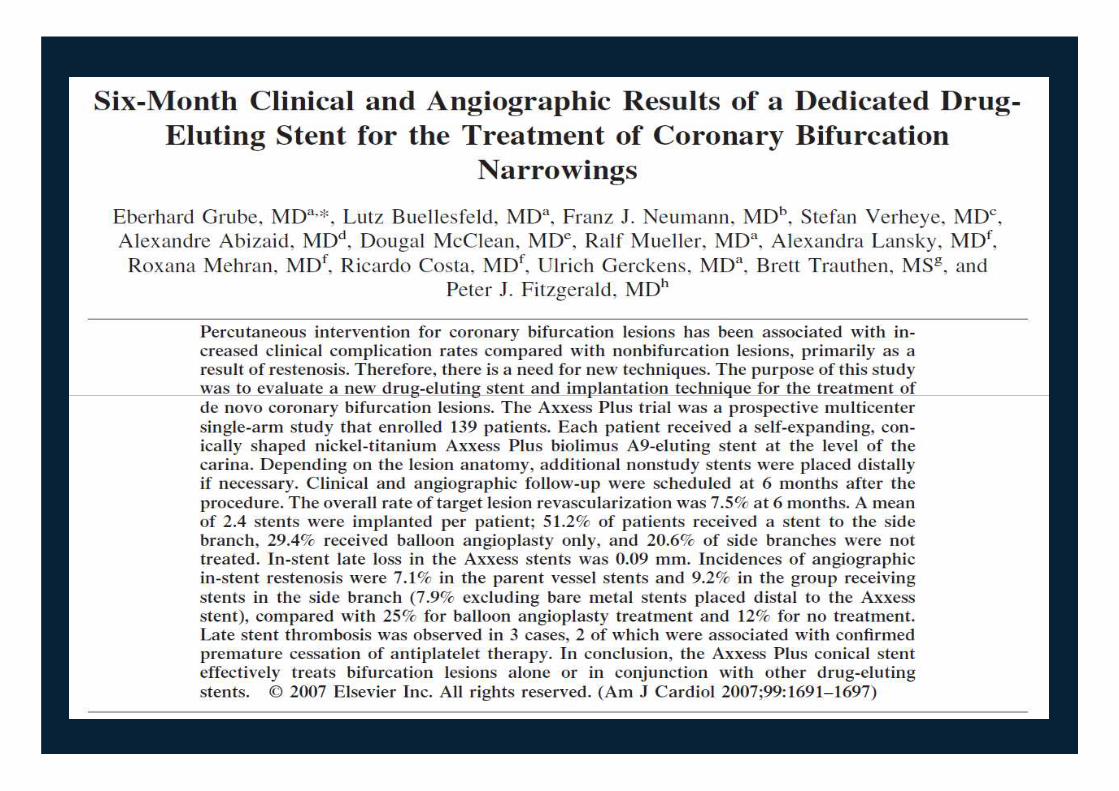
� PRINCIPAL INVESTIGATOR Eberhard Grube, MD
� DESIGN Prospective, non-randomized, single-arm, multi-center
clinical evaluation of the AXXESSTM Plus Bifurcated
Coronary Stent System
� OBJECTIVE To evaluate the acute and long-term safety, tolerabi-
lity and performance of the AXXESS Plus stent
� PRINCIPAL INVESTIGATOR Eberhard Grube, MD� PRINCIPAL INVESTIGATOR Eberhard Grube, MD
Helios Heart Center, Siegburg, Germany
� ANGIOGRAPHIC CORE LAB Alexandra J. Lansky, MD
Cardiovascular Research Foundation, New York, NY
� DATA MANAGEMENT CENTER Roxana Mehran, MD
Cardiovascular Research Foundation, New York, NY
� SPONSOR DEVAX, Inc., Irvine, CA
� PRINCIPAL INVESTIGATOR Eberhard Grube, MD
Helios Heart Center, Siegburg, Germany
� ANGIOGRAPHIC CORE LAB Alexandra J. Lansky, MD
Cardiovascular Research Foundation, New York, NY
� DATA MANAGEMENT CENTER Roxana Mehran, MD
Cardiovascular Research Foundation, New York, NY
� SPONSOR DEVAX, Inc., Irvine, CA

139 patients enrolled between July and December
2004 in 13 clinical sites in Europe, South America and
New Zealand
136 patients with AXXESS conical stent implanted
3 patients not stented
PATIENT FLOWCHARTPATIENT FLOWCHARTPATIENT FLOWCHARTPATIENT FLOWCHART
Clinical follow-up at 12 months
in 96.3% (N=131)
Angiographic follow-up at 6
months in 92.6% (N=126)
Clinical follow-up at 6 months
in 99.3% (N=135)

BASELINE DEMOGRAPHICSBASELINE DEMOGRAPHICSBASELINE DEMOGRAPHICSBASELINE DEMOGRAPHICS
Age, yearsAge, years 64.564.5
FemaleFemale 26.4%26.4%
DiabetesDiabetes 16.4%16.4%
HypertensionHypertension 72.9%72.9%
HyperlipidemiaHyperlipidemia 78.6%78.6%
Variable Variable N=139N=139
HyperlipidemiaHyperlipidemia 78.6%78.6%
SmokingSmoking 51.5%51.5%
Previous MIPrevious MI 31.4%31.4%
Previous PCIPrevious PCI 30%30%
Previous CABGPrevious CABG 4.3%4.3%
Congestive heart failureCongestive heart failure 1.4%1.4%
Left ventricule EF, %Left ventricule EF, % 65.565.5±±13.213.2

LESION LOCATIONLESION LOCATIONLESION LOCATIONLESION LOCATION
5.7%5.7%73.6%73.6%
16.4%16.4%
N=139N=139
4.3%4.3%

LESION SEVERITYLESION SEVERITYLESION SEVERITYLESION SEVERITY
Bifurcation lesion Duke classification
Bifurcation lesion Duke classification
13.2%3.7%
2.9%
Bifurcation lesion Duke classification
60.3% 0.7%18.4%
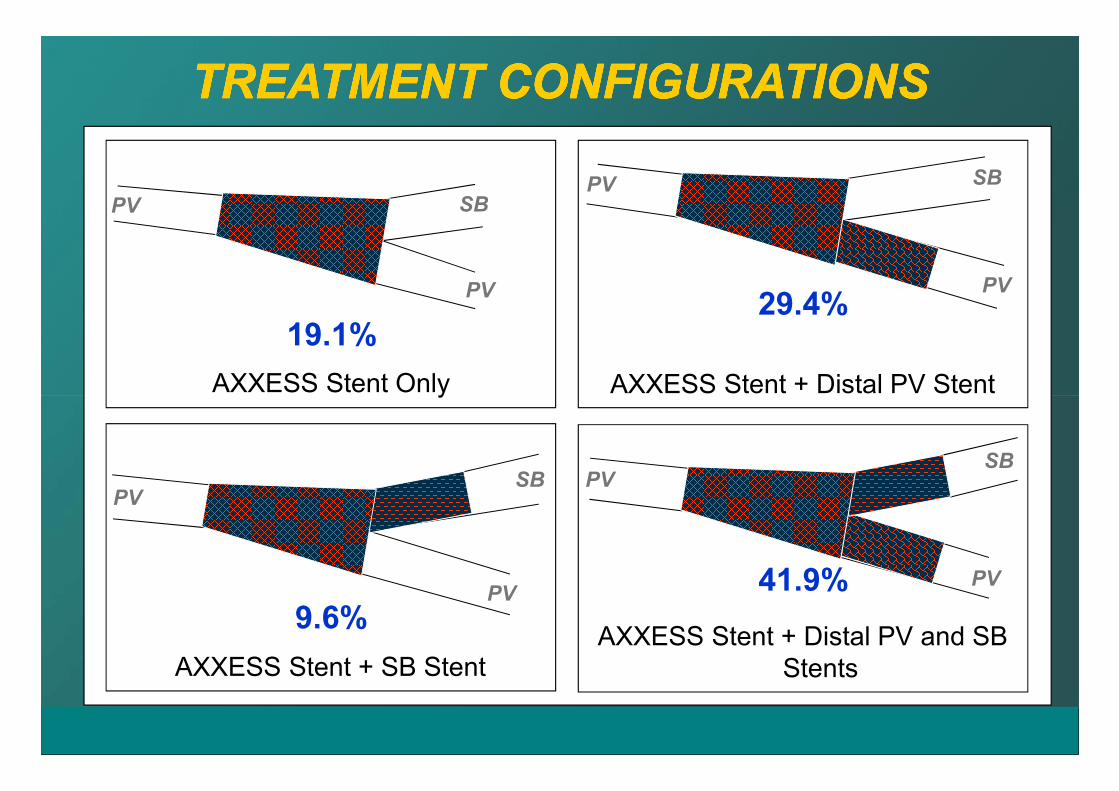
AXXESS Stent Only AXXESS Stent + Distal PV Stent
19.1%29.4%
TREATMENT CONFIGURATIONSTREATMENT CONFIGURATIONSTREATMENT CONFIGURATIONSTREATMENT CONFIGURATIONS
PV
PV
SB
SBPV
PV
AXXESS Stent Only AXXESS Stent + Distal PV Stent
AXXESS Stent + Distal PV and SB
StentsAXXESS Stent + SB Stent
9.6%
41.9%
PV
PV
SBSB
PV
PV

PREPRE-- AND FINAL QCAAND FINAL QCAPREPRE-- AND FINAL QCAAND FINAL QCA
BASELINEBASELINE
Lesion length, mmLesion length, mm 16.2816.28 7.437.43
RD, mmRD, mm 2.862.86 2.342.34
MLD, mmMLD, mm 0.780.78 0.880.88
VariableVariable PVPV SBSB
MLD, mmMLD, mm 0.780.78 0.880.88
% DS% DS 72.972.9 62.262.2
FINALFINAL††
MLD, mmMLD, mm 2.272.27 1.891.89
% DS% DS 23.823.8 22.322.3
Acute gain, mmAcute gain, mm 1.491.49 1.011.01*p<0.05 versus PV; †in-segment analysis

PARENT VESSEL QCA AT FOLLOWPARENT VESSEL QCA AT FOLLOW--UPUPPARENT VESSEL QCA AT FOLLOWPARENT VESSEL QCA AT FOLLOW--UPUP
LATE LUMEN LOSSLATE LUMEN LOSS
AXXESS conical stent, mmAXXESS conical stent, mm 0.090.09
InIn--stent, mmstent, mm 0.210.21
InIn--segment, mmsegment, mm 0.260.26
VariableVariable N=126N=126
InIn--segment, mmsegment, mm 0.260.26
RESTENOSISRESTENOSIS
AXXESS stent, mmAXXESS stent, mm 4%4%
InIn--stent, mmstent, mm 5.6%5.6%
InIn--segment, mmsegment, mm 10.5%10.5%
PRIMARY ENDPOINTPRIMARY ENDPOINT BA9 BMSBA9 BMS
AXXESS late loss, mmAXXESS late loss, mm 0.09 vs. 0.46 (0.09 vs. 0.46 (pp<0.001)<0.001)
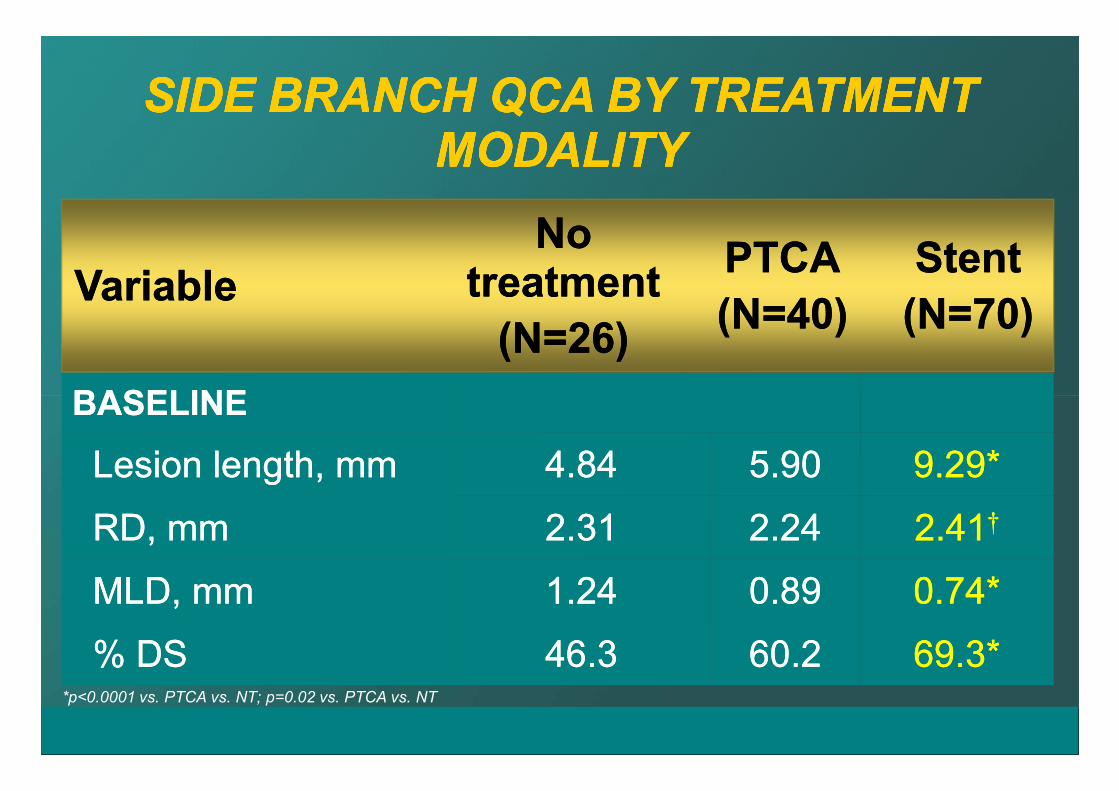
SIDE BRANCH QCA BY TREATMENT SIDE BRANCH QCA BY TREATMENT MODALITYMODALITY
SIDE BRANCH QCA BY TREATMENT SIDE BRANCH QCA BY TREATMENT MODALITYMODALITY
BASELINEBASELINE
VariableVariable
No No treatmenttreatment
(N=26)(N=26)
PTCAPTCA
(N=40)(N=40)
StentStent
(N=70)(N=70)
BASELINEBASELINE
Lesion length, mmLesion length, mm 4.844.84 5.905.90 9.29*9.29*
RD, mmRD, mm 2.312.31 2.242.24 2.412.41††
MLD, mmMLD, mm 1.241.24 0.890.89 0.74*0.74*
% DS% DS 46.346.3 60.260.2 69.3*69.3**p<0.0001 vs. PTCA vs. NT; p=0.02 vs. PTCA vs. NT

InIn--segmentsegment
MLD, mmMLD, mm 1.831.83 1.641.64 2.05*2.05*
%DS %DS 22.422.4 28.128.1 19.019.0††
Acute gain, mmAcute gain, mm 0.590.59 0.750.75 1.311.31‡‡
FINALFINALNo treatmentNo treatment
(N=26)(N=26)
PTCAPTCA
(N=40)(N=40)
StentStent
(N=70)(N=70)
SB SUBSB SUB--SEGMENTAL QCA SEGMENTAL QCA -- IISB SUBSB SUB--SEGMENTAL QCA SEGMENTAL QCA -- II
*p=0.02 vs. NT, and p<0.0001 vs. PTCA; † p=0.002 vs. PTCA; ‡p<0.0001 vs. NT and vs. PTCA; §p=0.003 vs. Stent. Lesion success:
defined as attainment of <50% residual stenosis of the target lesion using any combination of percutaneous devices
Acute gain, mmAcute gain, mm 0.590.59 0.750.75 1.311.31
5mm ostium5mm ostium
MLD, mmMLD, mm 1.851.85 1.691.69 2.422.42‡‡
%DS %DS 21.621.6 26.026.0 3.93.9‡‡
Acute gain, mmAcute gain, mm 0.610.61 0.800.80 1.681.68‡‡
Lesion success, %Lesion success, % 96.296.2 77.577.5§§ 97.197.1
InIn--segmentsegment
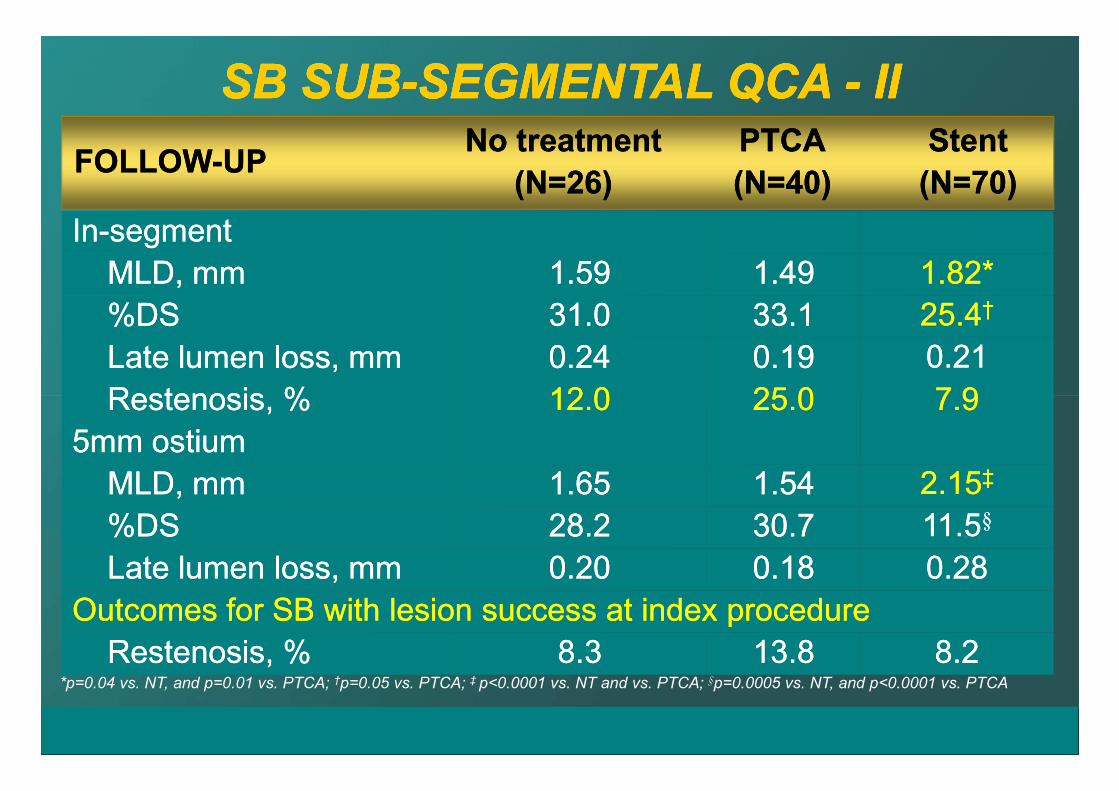
MLD, mmMLD, mm 1.591.59 1.491.49 1.82*1.82*
%DS %DS 31.031.0 33.133.1 25.425.4††
Late lumen loss, mmLate lumen loss, mm 0.240.24 0.190.19 0.210.21
Restenosis, %Restenosis, % 12.012.0 25.025.0 7.97.9
FOLLOWFOLLOW--UPUPNo treatmentNo treatment
(N=26)(N=26)
PTCAPTCA
(N=40)(N=40)
StentStent
(N=70)(N=70)
SB SUBSB SUB--SEGMENTAL QCA SEGMENTAL QCA -- IIIISB SUBSB SUB--SEGMENTAL QCA SEGMENTAL QCA -- IIII
Restenosis, %Restenosis, % 12.012.0 25.025.0 7.97.9
5mm ostium5mm ostium
MLD, mmMLD, mm 1.651.65 1.541.54 2.152.15‡‡
%DS %DS 28.228.2 30.730.7 11.511.5§§
Late lumen loss, mmLate lumen loss, mm 0.200.20 0.180.18 0.280.28
Outcomes for SB with lesion success at index procedureOutcomes for SB with lesion success at index procedure
Restenosis, %Restenosis, % 8.38.3 13.813.8 8.28.2*p=0.04 vs. NT, and p=0.01 vs. PTCA; †p=0.05 vs. PTCA; ‡ p<0.0001 vs. NT and vs. PTCA; §p=0.0005 vs. NT, and p<0.0001 vs. PTCA

PREPRE--, FINAL AND FU ANGIOGRAPHY, FINAL AND FU ANGIOGRAPHYPREPRE--, FINAL AND FU ANGIOGRAPHY, FINAL AND FU ANGIOGRAPHY
Final Result Final Result 6 Months FU6 Months FU

ININ--HOSPITAL MAJOR EVENTSHOSPITAL MAJOR EVENTSININ--HOSPITAL MAJOR EVENTSHOSPITAL MAJOR EVENTS
MACE*MACE* 5% (7)5% (7)
Death Death 0% (0)0% (0)
MIMI 5% (7)5% (7)
Q waveQ wave 0.7% (1)0.7% (1)
Outcome Outcome
Q waveQ wave 0.7% (1)0.7% (1)
NonNon--Q waveQ wave 4.3% (6)4.3% (6)
TLRTLR 0% (0)0% (0)
Acute/subacute thrombosisAcute/subacute thrombosis 0% (0)0% (0)*Defined as death, MI and TLR
MI=myocardial infarction
TLR=target lesion revascularization

OUTOUT--OFOF--HOSPITAL OUTCOMESHOSPITAL OUTCOMESOUTOUT--OFOF--HOSPITAL OUTCOMESHOSPITAL OUTCOMES% of patients
% of patients

AXXESS PLUS TrialAXXESS PLUS TrialMACE CountMACE Count

AXXESS PLUS TRIALAXXESS PLUS TRIAL3 Year KM Curve3 Year KM Curve
MACE Free (%)
50
60
70
80
90
100MACE Free (%)
0
10
20
30
40
50
Time in Years
0 1 2 3


DIVERGE Trial DesignProspective, single-arm,
multi-center trial
1 mo 6 mo 9 mo 12 mo 2 yrs 3 yrs 4 yrs 5 yrs
Clinical FU
302 patients in 16 clinical sites in Europe, Australia and New Zealand
Lesion type:
Any bifurcation with:
• Significant SB’s > 2.25mm
• PV-SB angulation < 70°
Angio/IVUS FU
1° Endpoint: MACE* at 9 months
Key 2° Endpoints: MACE* at 30 days, 6, 9 and 12 months and 2, 3, 4 and 5 yrs
death, cardiac death, MI (Q-wave and non Q-Wave), id-TLR,
id-TVR and stent thrombosis at 30 days, 6, 9 and 12 months
and 2, 3, 4 and 5 yrs
Angiographic: In-stent restenosis and late loss at 9 months
*MACE = Composite of Death, MI and ischemia driven TLR
DAPT recommended: 12 months
Angio/IVUS FU

Lesion Inclusion Criteria
Parent Vessel
Side Branch
Any Type Bifurcation
SB > 2.25 mm
Up to 15 mm
Stents:
Proximal = 10 or 14 mm Axxess
Distal PV or SB = add Cypher to fit
Up to 10 mm
Up to 25 mmDistal
Parent Vessel
70°
Axxess Stent Procedure
Optimal Treatment Strategy
Pre Final

Axxess Stent Procedure
Optimal Treatment Strategy
Pre Final
Complex lesions were emphasized in this study.
Treatment was tailored to the disease with Axxess at the carina
followed by Cypher in the distal vessels.

DIVERGE Follow UpLead in Cases
< 3 per site
Enrollment
N=302
6 Months
Check up (N=302)
9 Months
N=301 (99.7% clin. FU)
Angiography
N=140 (94% FU)
IVUS Evaluation
N=68 (91% FU)
5 Year Annual
Follow Up
12 Months
N=300 (99.4% FU)
2 years
N=300 (99.4% FU)
3 years
N=294 (97.4% FU)
Agostoni P., oral presentation, EuroPCR 2011

DemographicsMean Age (years) 62.8 ± 10.6
Diabetic 18.2%
Insulin Dependent 5.6%
Current + History of Smoking 67.9%
Hypercholesterolemia 78.1%
Hypertension 56.6%
Verheye S. et al., J Am Coll Cardiol, 2009.
53(12): p. 1031-9
Prior MI 29.1%
Prior PCI/CABG 34.1%
Mean LVEF (%) 68.4 ± 11.1
Angina 92.1%
Stable 68.5%
Unstable 23.5%

Medina Class All Patients
1,1,1*1,1,1*1,1,1*1,1,1*
64.5%
6.6%6.3%
77.4%
True Bifurcation ****
1,1,01,1,01,1,01,1,0
12.0%
1,0,1*1,0,1*1,0,1*1,0,1*0,1,1*0,1,1*0,1,1*0,1,1*
1,0,01,0,01,0,01,0,0
6.6%
0,1,00,1,00,1,00,1,0
3.3%
0,0,10,0,10,0,10,0,1
0.7%
Verheye S. et al., J Am Coll Cardiol, 2009.
53(12): p. 1031-9

Procedure OutcomesAll Patients
(N=302)
AXXESS stent placed1 99.0%
Optimal placement1
(by core lab assessment) 93.0%
Branch vessel Cypher stents placed2500
1 Verheye S. et al., J Am Coll Cardiol, 2009.
53(12): p. 1031-92 Verheye S., oral presentation, TCT 2008
Branch vessel Cypher stents placed2
(210 in SB)
Angiographic success1
(Final DS < 50% by QCA)99.3%
Final mean diameter stenosis122.6% (PV)
18.8% (SB)
Procedure success1
(Angio success without in-hospital MACE)96.7%

Stent Distribution Patterns
AXXESS only:
12.3% AXXESS + PV:
17.7%
AXXESS + PV + SB: 64.7%
SB Stent: 68.7%
AXXESS + SB: 4.0%
Verheye S. et al., J Am Coll Cardiol, 2009.
53(12): p. 1031-9

9-month QCA Results
At Follow UpParent Vessel
(N=140)
Side Branch
(N=140)
Late Loss
(mm)
In-stent LL (AXXESS only) 0.18 ± 0.49 -
In-stent LL (all stents) 0.29 ± 0.50 0.29 ± 0.45
In-lesion LL 0.20 ± 0.41 0.17 ± 0.34
In-stent - AXXESS Only 0.7% -
Verheye S. et al., J Am Coll Cardiol, 2009.
53(12): p. 1031-9
Restenosis
Per Vessel
In-stent - AXXESS Only 0.7% -
In-stent - Cypher 2.3% 4.8%
In-lesion restenosis
(all stents + edges)3.6% 4.3%
Overall
Bifurcation
Restenosis
In-stent - PV + SB 5.0% (7/140)
In-stent or edges, within PV + SB 6.4% (9/140)

9 Month RestenosisAny In-segment bifurcation restenosis:
6.4% (9/140 at 9 months)
Side Branch RSSide Branch RSSide Branch RSSide Branch RS
3 pts2 pts
4 pts
Parent Vessel RSParent Vessel RSParent Vessel RSParent Vessel RS
BothBothBothBoth
Proximal edge:
2.8% SB stent:
4.8%(105 SB stents)
Location Analysis:
Verheye S. et al, J Am Coll Cardiol, 2009
3 pts 4 ptsBothBothBothBoth
Distal PV Cypher:
2.1%
AXXESS:
0.7%“Lowest restenosis rates ever reported in a
bifurcation study of any kind”

9-month Clinical Outcomes
*MACE: a composite of Death, MI and id-TLR
Verheye S. et al., J Am Coll Cardiol, 2009. 53(12): p. 1031-9

3-year Clinical OutcomesCumulative Rates
*MACE: a composite of Death, MI and id-TLR
Agostoni P., oral presentation, EuroPCR 2011

MACE (Death, MI, id-TLR)
3-year Outcomes
9.3%
14.0%
16.0%
8
10
12
14
16
18
20%
Number at Risk 302 286 272 262 258 248 201
0
2
4
6
8
0 6 12 18 24 30 36
Month
Agostoni P., oral presentation, EuroPCR 2011

MACE Components3-year Outcomes
8
12
16
20
%
6.0%7.4%
8
12
16
20
%6.0%
8.7%10.1%
8
12
16
20
%
Death MI id-TLR
0.7%2.3%
3.0%
0
4
8
0 12 24 36
Months
4.3%6.0%
0
4
8
0 12 24 36
Months
6.0%
0
4
8
0 12 24 36
Months
Agostoni P., oral presentation, EuroPCR 2011

Antiplatelet Agent UtilizationCumulative incidence
(All patients N=302)
Aspirin
- At 6 months 95.3% (282/296)
- At 1 year 94.3% (280/297)
- At 2 years 93.2% (272/292)
- At 3 years 91.5% (260/284)
Clopidrogel/Thienopyridine
- At 6 months 85.1% (252/296)
- At 1 year 73.1% (217/297)
- At 2 years 43.2% (126/292)
- At 3 years 40.5% (115/284)

Definite Stent Thrombosis*
3-year outcomes
1.3%1.7%
2.4%
2
3
4
5
%
* Definite stent thrombosis defined by ARC
(Cutlip et al,. Circulation, 2007)
Agostoni P., oral presentation, EuroPCR 2011
Number at Risk 302 299 292 288 288 280 224
0
1
0 6 12 18 24 30 36
Months

Stent Thrombosis up to 3 Years
Protocol ARC
Definite* Probable Definite* Probable Possible
Acute
(In-hospital)0 0 0 0 0
Subacute
(30 days)0.7% 0 0.7% 0 0
Late
(>30 days - 1 year)0.7% 0 0.3%§ 0 0
Very Late
(1 year - 3 years)1.0% 0.7% 1.0% 0.7% 2.4%
*All definite stent thrombosis in DIVERGE were confirmed
with angiography.
§One case of asymptomatic chronic total occlusion is
omitted in ARC classification but included in protocol
definition
Agostoni P., oral presentation, EuroPCR 2011

Conclusions
� The safety and efficacy of the Axxess Biolimus A9-eluting stent was
confirmed up to 3 years
� The use of Axxess stent for the treatment of complex bifurcation lesions
resulted in low 3-year event rates:
– all-cause cumulative MACE rate 16.3%
– Ischemia-driven TLR rate 12.2%
– very late definite stent thrombosis 1.0%
– Very low definite VLST not resulting in any death
–Only one definite VLST attributed to the Axxess stent whereas
all events were present in the Cypher stent