
Treatment by Mycophenolate Mofetil of Advanced Graft Vascular Disease in Non-Human Primate...
13
Treatment by Mycophenolate Mofetil of Advanced Graft Vascular Disease in Non-Human Primate Recipients of Orthotopic Aortic Allografts Jochen Klupp a,d, *, Camille Dambrin a , Kiyoshi Hibi b , Jorge Luna b , Takeshi Suzuki b , Bernard Hausen a , Tudor Birsan a , Teun van Gelder a , Peter J. Fitzgerald b , Gerald Berry c and Randall E. Morris a a Transplantation Immunology, Department of Cardiothoracic Surgery, b Division of Cardiovascular Medicine, c Depart- ment of Pathology, Stanford University School of Medi- cine, 300 Pasteur Drive, Stanford, CA 94305–5407, USA d Department of Surgery, Charite ´ -Virchow, Humboldt- University Berlin, Augustenburger Platz 1, D-13353 Berlin, Germany *Corresponding author: Jochen Klupp, jochen.klupp@ charite.de Failure to control chronic graft dysfunction [e.g. graft vascular disease (GVD)] is the primary cause of immunologic graft failure. This is the first study of mycophenolate mofetil (MMF) for the treatment of GVD in non-human primate recipients of aortic allografts. Abdominal aortic allografts were exchanged between mixed leukocyte reaction (MLR) -mismatched, blood-group-compatible cynomolgus monkeys. Six control recipients were untreated. Individualized treatment with frequent dose adjust- ments of MMF insured that treatment was close to the maximum tolerated dose (mean 99.2 mg/kg/day). Immune-mediated injury proceeded unhindered until day 45, after which MMF treatment began. Changes in intimal volume (IV) were quantified by intravascular ultrasound (IVUS) and compared to histology on day 105. Serial IVUS measurements of IV (mm 3 ) in controls showed progressive GVD. In four out of six animals, MMF was well tolerated, thus enabling optimum treatment; in all these animals, IV was significantly less than in the control animals (p = 0.02). In the two remaining animals, high doses were not tolerated; at day 105, there was no significant difference in IV between them and the controls. We found a signifi- cant correlation between the mean MMF tolerated dose and the inhibition of progression of IV (r = 0.88, p = 0.015). When high MMF doses were tolerated, MMF slowed progression of GVD. Key words: Chronic rejection, mycophenolate mofetil, non-human primates, pharmacodynamics, pharmaco- kinetics Received 15 February 2002, revised and accepted for publication 4 March 2003 Introduction Graft vascular disease (GVD) and neointimal thickening are pathognomonic for chronic rejection after heart, kidney and other solid organ transplantations. The pathophysiological mechanisms of GVD development are becoming increas- ingly well understood, and smooth muscle cell prolifer- ation plays a central role in the development of intimal thickening. The mechanism of action of mycophenolic acid (MPA), the active metabolite of mycophenolate mofe- til (MMF), makes MMF attractive to investigate for the treatment and prevention of GVD. As previously well described (1), MPA inhibits inosine-monophosphate- dehydrogenase isoenzymes I and II, and thereby de novo purine synthesis. Proliferating lymphocytes and, to a lesser extent, smooth muscle cells, fibroblasts and endothelial cells depend on de novo purine synthesis (2,3). Therefore, these cells may be targets for the treatment of chronic rejection by MMF. In vitro inhibition of growth-factor- stimulated smooth muscle cells by MPA (3,4) led to several animal studies that investigated the effect of MPA and MMF on intimal thickening in rodent models of chronic rejection (5–8) and on re-stenosis after mechanical arterial injury (9,10). After xeno-heart-transplantation MMF reduced vascular rejection and graft coronary disease (11). In addition, early clinical results suggest that MMF reduces chronic graft dysfunction after heart (12,13), kidney (14–16) and liver transplantation (17,18). These previous studies encouraged us to investigate the effect of MMF on GVD after allogenic aortic transplant- ation in non-human primates. This procedure (19,20) is the first – and so far only one – reported for the study of GVD in non-human primates. Using this procedure, the effect of immunosuppressive drugs can be tested for their ability to impede progression of pre-existing graft vascular disease. With serial intravascular ultrasound (IVUS) morphometry, the time-course of development of intimal thickening can be monitored in vivo in individual monkeys. Furthermore, the effects on the immune system and the pharmacokinetics, pharmacodynamics and toxicology of MMF in non-human primates are similar to those in humans. Most important, however, the intimal lesions in aortic grafts are histologically indistinguishable from human allograft vasculopathy (21). Our primary objective was to test whether MMF could halt or impede the progression of advanced intimal thickening in an individualized treatment regimen in this American Journal of Transplantation 2003; 3: 817–829 Copyright # Blackwell Munksgaard 2003 Blackwell Munksgaard ISSN 1600-6135 817
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Treatment by Mycophenolate Mofetil of Advanced Graft Vascular Disease in Non-Human Primate...

Treatment by Mycophenolate Mofetil of AdvancedGraft Vascular Disease in Non-Human PrimateRecipients of Orthotopic Aortic Allografts
Jochen Kluppa,d,*, Camille Dambrina, KiyoshiHibib, Jorge Lunab, Takeshi Suzukib, BernardHausena, Tudor Birsana, Teun van Geldera,Peter J. Fitzgeraldb, Gerald Berryc andRandall E. Morrisa
aTransplantation Immunology, Department of CardiothoracicSurgery, bDivision of Cardiovascular Medicine, cDepart-ment of Pathology, Stanford University School of Medi-cine, 300 Pasteur Drive, Stanford, CA 94305–5407, USAdDepartment of Surgery, Charite-Virchow, Humboldt-University Berlin, Augustenburger Platz 1, D-13353 Berlin,Germany*Corresponding author: Jochen Klupp, [email protected]
Failure to control chronic graft dysfunction [e.g. graftvascular disease (GVD)] is the primary cause ofimmunologic graft failure. This is the first study ofmycophenolate mofetil (MMF) for the treatmentof GVD in non-human primate recipients ofaortic allografts. Abdominal aortic allografts wereexchanged between mixed leukocyte reaction (MLR)-mismatched, blood-group-compatible cynomolgusmonkeys. Six control recipients were untreated.Individualized treatment with frequent dose adjust-ments of MMF insured that treatment was close tothe maximum tolerated dose (mean 99.2 mg/kg/day).Immune-mediated injury proceeded unhindered untilday 45, after which MMF treatment began. Changes inintimal volume (IV) were quantified by intravascularultrasound (IVUS) and compared to histology on day105. Serial IVUS measurements of IV (mm3) in controlsshowed progressive GVD. In four out of six animals,MMF was well tolerated, thus enabling optimumtreatment; in all these animals, IV was significantlyless than in the control animals (p =0.02). In the tworemaining animals, high doses were not tolerated; atday 105, there was no significant difference in IVbetween them and the controls. We found a signifi-cant correlation between the mean MMF tolerateddose and the inhibition of progression of IV(r =�0.88, p= 0.015). When high MMF doses weretolerated, MMF slowed progression of GVD.
Key words: Chronic rejection, mycophenolate mofetil,non-human primates, pharmacodynamics, pharmaco-kinetics
Received 15 February 2002, revised and accepted forpublication 4 March 2003
Introduction
Graft vascular disease (GVD) and neointimal thickening are
pathognomonic for chronic rejection after heart, kidney and
other solid organ transplantations. The pathophysiological
mechanisms of GVD development are becoming increas-
ingly well understood, and smooth muscle cell prolifer-
ation plays a central role in the development of intimal
thickening. The mechanism of action of mycophenolic
acid (MPA), the active metabolite of mycophenolate mofe-
til (MMF), makes MMF attractive to investigate for the
treatment and prevention of GVD. As previously well
described (1), MPA inhibits inosine-monophosphate-
dehydrogenase isoenzymes I and II, and thereby de novo
purine synthesis. Proliferating lymphocytes and, to a lesser
extent, smooth muscle cells, fibroblasts and endothelial
cells depend on de novo purine synthesis (2,3). Therefore,
these cells may be targets for the treatment of chronic
rejection by MMF. In vitro inhibition of growth-factor-
stimulated smooth muscle cells by MPA (3,4) led to
several animal studies that investigated the effect of
MPA and MMF on intimal thickening in rodent models of
chronic rejection (5–8) and on re-stenosis after mechanical
arterial injury (9,10). After xeno-heart-transplantation MMF
reduced vascular rejection and graft coronary disease (11).
In addition, early clinical results suggest that MMF
reduces chronic graft dysfunction after heart (12,13),
kidney (14–16) and liver transplantation (17,18).
These previous studies encouraged us to investigate the
effect of MMF on GVD after allogenic aortic transplant-
ation in non-human primates. This procedure (19,20) is
the first – and so far only one – reported for the study of
GVD in non-human primates. Using this procedure, the
effect of immunosuppressive drugs can be tested for
their ability to impede progression of pre-existing graft
vascular disease. With serial intravascular ultrasound
(IVUS) morphometry, the time-course of development of
intimal thickening can be monitored in vivo in individual
monkeys. Furthermore, the effects on the immune
system and the pharmacokinetics, pharmacodynamics
and toxicology of MMF in non-human primates are similar
to those in humans. Most important, however, the intimal
lesions in aortic grafts are histologically indistinguishable
from human allograft vasculopathy (21).
Our primary objective was to test whether MMF could
halt or impede the progression of advanced intimal
thickening in an individualized treatment regimen in this
American Journal of Transplantation 2003; 3: 817–829 Copyright # Blackwell Munksgaard 2003Blackwell Munksgaard
ISSN 1600-6135
817

demanding non-human primate model of graft vascular
disease.
Materials and Methods
Experimental design
To optimize MMF tolerability and efficacy, we performed phase I dose-
finding pre-studies with extensive pharmacokinetic and pharmacodynamic
assays in four nontransplanted cynomolgus monkeys.
In the phase II transplant study, six cynomolgus monkeys received MLR-
mismatched infrarenal artery aortic interposition allografts. To allow for the
formation of substantial GVD, the recipients received no immunosuppres-
sive treatment through day 44 and animals in the MMF group were treated
with MMF from day 45 until day 103 after transplantation using individual
treatment to ensure MMF exposures were close to the maximal tolerated
dose. The treatment group was compared to an untreated control group of
six transplanted animals. In all animals, serial IVUS was performed on
postoperative days (POD) 21, 42, 63, 84 and 105, when the study was
terminated and the animals were euthanized. Grafts were then removed
for histological examination.
Animals
Sixteen healthy male Macaca fascicularis monkeys (5.9–8.3 kg), screened
to be disease free, were purchased from Charles River BRF Inc. (Houston,
TX, USA), and kept in quarantine at Stanford for 6 weeks before release for
scientific use. Four animals were used for the phase I dose-finding study,
and from the 12 animals in the phase II transplant groups, each animal
served as both a donor and a recipient for aortic transplantation. Pairs were
ABO matched, and the mixed leukocyte reaction was used to ensure histo-
incompatibility [Stimulation Index (SI) 2.7–38.3].
Husbandry
Before each procedure, the animals were acclimated for at least 1 week in
controlled conditions of temperature and humidity in the room where they
were housed during the study. Water and primate chow were provided ad
libitum, and the monkeys were cared for according to the standards of the
US Public Health Policy of the Humane Care and Use of Laboratory Animals
(PHS Manual, Ch. 143) and the guide for the Care and Use of Laboratory
Animals (NIH Publication no. 8523, revised 1985). The study protocol was
approved by the Institutional Laboratory Animal Committee.
Anesthesia and postoperative care
For surgical procedures, the animals were anesthetized with ketamine
hydrochloride (Ketaset1) 10 mg/kg s.c., atropine sulfate 0.04 mg/kg i.v.
and buprenorphine hydrochloride (Buprenex1) 0.01 mg/kg i.m. After endo-
tracheal intubation, anesthesia was maintained with continuous propofol
(2.5 mg/mL; 0.1 mg/kg/min) and midazolam infusion (1 mg/mL; 0.35 mg/kg/
min). Until extubation in stable conditions, ECG, body temperature, oxygen
saturation, respiration rate and end-expiratory CO2 concentrations were
monitored continuously. Blood pressure was measured at 3-min intervals,
and all vital signs were recorded at 15-min intervals. Postoperatively, the
animals were transferred to special ICU units with individually controlled
cage temperatures and oxygen concentrations for 24 h. To control for
postoperative pain, 0.03 mg/kg buprenorphine hydrochloride (Buprenex1)
was administered i.m. Cefazolin (25 mg/kg i.m.) and gentamycin (5 mg/kg
s.c.) were used for perioperative antibiotic prophylaxis.
Aortic transplantation
After deep anesthesia, a midline laparotomy was performed. The abdominal
aorta was exposed. After heparinization (70 IU/kg) and aortic clamping, a
3.0-cm segment of the abdominal aorta distally to the inferior mesenteric
artery was removed, flushed with cold saline and anastomosed (beveled to
avoid anastomotic strictures) to the recipients aorta using 7–0 Prolene1.
After homeostasis, the retro-peritoneum was sutured and the abdominal
wall was closed.
Intravascular ultrasound methodology
Intravascular ultrasound methodology was performed on POD 21, 42, 63,
84, and 105. After deep anesthesia, the femoral artery was exposed, and a 5
French sheath was introduced into the vessel under heparinization (70 IU/kg).
After injecting 20mg nitroglycerin into the catheter, intra-aortic pressures
were recorded with a 5-French Swan-Ganz catheter (Baxter Healthcare
Corp., Deerfield, IL, USA), and the peak-to-peak gradient over each anasto-
mosis was assessed by a pullback technique. Sequential IVUS imaging was
performed using an intravascular ultrasound system (CardioVascular
Imaging Systems/Boston Scientific, Sunnyvale, CA, USA) with a 40-MHz,
2.6 French ultrasound catheter (SciMed/Boston Scientific, Sunnyvale, CA,
USA). The imaging probe was positioned proximal to the graft, and with-
drawn at a constant speed of 0.5 mm/ s. The IVUS images were recorded
for later analyses. After completion of the IVUS measurements, the sheath
was removed, and the femoral arteriotomy was repaired with 7–0 Prolene1
sutures.
Off-line 3-D reconstruction of the IVUS data was performed with Echo-
Plaque1 software (Indec Systems, Inc., Mountain View, CA, USA) using a
digitization frame rate of 15 images/ s, resulting in the corresponding planar
3-D image of each studied segment. Contour drawings of intima and lumen
outer borders were performed manually at 1-mm intervals, and the inter-
polated contours for the remaining frames were automatically generated
by the system (Figure 1). Areas and diameters for all lumen and intima
contours were measured, and volumes were calculated automatically
using the following formula:
Volume ¼ nX
i¼1:n
ðAi � HÞ
where Ai is the measured area of segment, i; H is the thickness of the
segment and n is the number of IVUS images in the 3-D data set. Volu-
metric [intimal-lumen volume (VV), intimal volume (IV), lumen volume (LV)]
and cross-sectional values [cross-sectional intimal-lumen area (VA), cross-
sectional intimal area (IA), cross-sectional lumen area (LA)] were assessed
for segments in the middle 10 mm of the graft segments. The minimal
lumen cross-sectional area within each segment was selected and meas-
ured accordingly.
Mycophenolate mofetil (MMF; CellCept�) treatment
In phase I studies, MMF powder (a gift from Roche Bioscience, Palo Alto,
CA, USA) was dissolved in vehicle and was administered by oral gavage
under ketamine sedation (Ketaset1, 5 mg/kg s.c.). The vehicle was pre-
pared by dissolving sodium carboxymethylcellulose (CMC, City Chemical
Corp., New York, NY, USA; viscosity of 1300–2200 centipoises at 25 �C in a
1% weight/volume in deionized water solution) in 0.9% benzyl alcohol
(volume/volume), 0.4% polysorbate 80 (weight/volume) and 0.9% sodium
chloride (weight/volume) in water to produce a 0.2% CMC solution, which
was stored at room temperature. In the phase II transplant study, MMF
treatment started on day 45 after transplantation. Initially, 50 mg/kg MMF
hydrochloride solution (CellCept1IV, a gift from Roche Laboratories Inc.,
Nutley, NJ, USA) was administered twice daily (b.i.d.) subcutaneously for
7 days and subsequently administered by oral gavage BID. MMF was
dosed individually according to maximal tolerability: total weight loss
exceeding 10% or a 3% weight loss in 3 days, substantial diarrhea or
vomiting prompted dose reduction. In case of toxicity, food was supple-
mented with high calorie gruel gavage once or twice daily to a maximal
gruel volume of 30 mL/kg. Dehydration was treated with subcutaneous
Klupp et al.
818 American Journal of Transplantation 2003; 3: 817–829

fluid administration (10–20 mL/kg lactate-Ringer solution). Diarrhea was
treated with loperamide (25–50 mg p.o. daily).
In addition to the assessment of toxicity, MMF pharmacokinetics and
pharmacodynamics were considered for MMF dosing. We defined MPA
plasma levels below 2.0 mg/L and more than 5 abs% (absolute percentage)
proliferating cells in the peripheral blood (see methods below) as subthera-
peutic immunosuppression.
Pharmacokinetic (PK) and pharmacodynamic (PD) monitoring
In phase I studies, in vitro assays evaluating the effect of MPA on immune
functions in cynomolgus blood and complete in vivo pharmacokinetic (PK)
and pharmacodynamic (PD) profiles were performed. Blood was collected
after ketamine hydrochloride (Ketaset1, 5 mg/kg s.c.) sedation. For in vitro
assays, blood was incubated with different concentrations of mycophen-
olic acid for 30 min before the mitogen stimulation. For in vivo studies
blood was collected before drug treatment in the morning, and 2, 10 and
24 h thereafter. The plasma MPA PK area under the curve (AUC) and blood
MPA PD area under effect (AUE) were calculated using the trapezoidal
rule. In the phase II transplant study, PK and PD assays were done twice
weekly, just before the morning MMF dose (trough levels).
Mycophenolic acid (MPA) concentrations were measured by gradient
HPLC in heparinized plasma (50 mL). A method described previously for
rats (22) was modified and validated for monkey plasma: mean intraday
precision was 2.5%, mean interday precision was 9.2%, and linearity was
better than 0.99.
Lymphocyte proliferation after mitogen stimulation was measured by flow
cytometry to assess the pharmacodynamic effects of the MMF treatment.
The method was modified from our previous publications (23–27). Eighty
microliters of whole, heparinized (100 IU/mL) blood, diluted 1 : 10 in culture
Figure 1: Digitized 3-D intravascular ultrasound image using Echoplaque� Software. Contour drawings of both intima and lumen
outer borders were performed manually at 1-mm intervals, and the interpolated contours for the remaining frames were automatically
generated by the system.
Treatment of Graft Vascular Disease by MMF
American Journal of Transplantation 2003; 3: 817–829 819

medium (RPMI 1640 supplemented with penicillin, streptomycin and
glutamine; all reagents obtained from Life technologies, Inc., Grand Island
NY, USA), was incubated for 72 h at 37 �C with 7.5 mg/mL concanavalin
A (Con A) (Vector Laboratories, Burlingame CA, USA). After lysing the
erythrocytes, leukocytes were washed, fixed with 1% formaldehyde and
resuspended in 2 mL of methanol for 10 min at 4 �C. After washing, cells
were treated for 25 min at 37 �C with permeabilizing buffer (1% heat-
inactivated fetal calf serum (Hyclone, Logan, UT, USA), 0.1% saponin
(Calbiochem, La Jolla, CA, USA), 0.1% sodium azide (Sigma Chemical
Co., St. Louis, MO, USA) in (PBS), RNAse A (100 mg/mL in water; Sigma
Chemical Co., St. Louis, MO, USA), propidium iodine (PI) and anti-
proliferating cell nuclear antigen (PCNA)-FITC mAb (Dako Corp., Carpinteria,
CA, USA). The washed cells were then resuspended in PBS containing PI.
All samples were assessed by two-color analysis (Epics XL-MCL/498 nm
air-cooled argon laser, Beckman-Coulter, Fullerton, CA, USA) within 6 h of
preparation. Emitted fluorescence was collected with bandpass filters
through 525 nm (– 20 nm; FITC) and 675 nm (660–700 nm; PI). Forward-
sideward scatter gates differentiated cells of interest from debris, and
5000 light scatter-gated cells were analyzed per sample. Cell proliferation
was determined as percentage of cells in the S/G2M phase of the cell cycle
expressing PCNA. As controls, mAbs were added to unstimulated blood
identically processed as stimulated samples and inactive immunoglobulin
isotype controls were added to cultures of stimulated cells.
Pharmacokinetic and pharmacodynamic analysis
Absolute percentages (abs%) of proliferating cells were normalized at each
time point to the individual pretreatment values for both phase I and phase II
studies as 100 relative per cent (rel%). Analogous to the calculation of the
AUC0�24h, the area under the pharmacodynamic effect time – curve
(AUE0�24h) was calculated using the linear trapezoidal rule. The inhibitory
effect was expressed as per cent inhibition of lymphocyte proliferation,
analyzed by flow cytometry and calculated as follows:
%inhibition ¼ ½1 � ðTreatment=PretreatmentÞ� � 100
MPA plasma concentrations (C), which produced a 50% inhibition (IC50) of
the maximum inhibitory effect (Emax), were calculated after fitting the
concentration-effect curves in an Emax sigmoidal pharmacodynamic
model (28)
E ¼ Emax � ðEmax � E0Þ½CGamma=ðCGamma þ IC50GammaÞ�
using WinNonlin Software version 1.1 (Scientific Consulting, Inc., Cary, NC,
USA).
CBC and blood chemistry
Hemograms, sodium, potassium and chloride were obtained every
3 weeks in untreated monkeys, and once a week during immunosuppres-
sive treatment. Every 3 weeks, blood chemistry screens were performed
for total serum protein, albumin, BUN, creatinine, triglycerides, cholesterol,
liver enzymes, alkaline phosphatase, lactate dehydrogenase (LDH) and
lipase.
Graft removal, histology and immunohistochemistry
After the final IVUS-examination on POD 105, a thoraco-laparotomy was
performed under deep anesthesia. The aorta was mobilized, all visceral
branches ligated and the animal euthanized. The whole infra-diaphragmatic
aorta, including the graft, was flushed with saline and perfused with a total
volume of 250 cc of 10% formaldehyde solution for 15–20 min in situ, with
a pressure of 100 mmHg. Thereafter, the graft was removed and perfused
ex vivo under the same pressure for 18 h with a 10% formaldehyde solu-
tion. From 4-mm thick transverse sections from the paraffin-embedded
graft and the proximal native aorta, hematoxylin & eosin (HE) and elastin
van Gieson staining was performed. Deparaffinized sections prepared at
4mm thickness were stained with anti-a-smooth muscle actin (1 : 4000
dilution, Sigma Corp, St Louis, MO, USA) on a Ventana-Nexus automated
stainer (Ventana Medical Systems, Inc., Tucson, AZ, USA).
Morphometric analysis
Video images of elastin van Gieson-stained aortic sections were recorded
with a Dage MTI-81 high-resolution color camera mounted on a Leica
DMAB microscope and analyzed with a C-imaging 1280 morphometric
system (Compix Inc., Imaging Systems, Cranberry Township, PA, USA).
Lumen area (LA), intimal area (IA) the area inside the internal elastic lamina
corresponding to the vessel area assessed (VA) by IVUS, and media area,
were assessed.
Statistics
For statistical analysis, SPSS version 10.0 (SPSS Corp., Birmingham, AL,
USA) was used. All data are expressed as mean – standard error of mean
(SEM). The two-tailed Student’s t-test or the Mann–Whitney U-test was
used to estimate the levels of significance for the differences between two
groups, according to its applicability. The general linear model for repetitive
measurements was used to differentiate between the two groups over the
time. For n�n tables chi-square statistics were computed. Correlations
between PD or PK measurements or both and histology scores were
determined using the Pearson correlation factor. A p-value of less than
0.05 was considered significant.
Results
In vitro study to quantitate the effects of mycophenolicacid on monkey whole blood lymphocyte proliferationTo evaluate the in vitro effects of mycophenolic acid
(MPA) on lymphocyte proliferation, blood from four
untreated animals was incubated with different MPA con-
centrations between 0 and 100 mg/L. Fifty per cent inhibi-
tory undiluted blood concentrations (IC50) varied between
0.3 and 1.2 mg/L among the animals. The maximal effects
(Emax) were reached with 7.7 rel% PCNA expression. The
coefficient of correlation between MPA concentration and
inhibition of proliferation was 0.95.
Tolerability phase I PK and PD study evaluating 100mg/kg MMF once daily for 28daysOf four cynomolgus monkeys (P1 – P4; Figure 2), the dose
of 100 mg/kg MMF orally once a day had to be reduced
after 14 days of treatment due to toxicity in two animals
(P2, P3). For animal P3, drug withdrawal for 1 day was
necessary. After 21 days, in all animals the dose was
reduced to 50 mg/kg QD due to side-effects.
Toxicity. Significant weight loss occurred, and reached
an average of 11.6% after 21 days of MMF treatment
(range 7.6–19.4%; p< 0.02 vs. pretreatment weight).
Diarrhea was observed in all animals beginning between
days 10 and 21 of treatment. Additionally, two animals
became anorectic, and two animals started vomiting
during treatment. Signs of toxicity were reversible after
MMF dose reduction to 50 mg/kg orally once a day.
Klupp et al.
820 American Journal of Transplantation 2003; 3: 817–829

Pharmacokinetics and pharmacodynamics. After the first
single dose of 100 mg/kg, a high variability in drug PK and
PD was observed: two animals reached their highest drug
levels (Tmax) 2 h after dosing and two animals reached
Tmax 10 h after dosing. Also, the maximal MPA plasma
concentrations varied from 1.88 to 21.68 mg/L and the
inhibition of proliferation varied, with lowest relative
PCNA expressions being between 17.3 and 34.2%.
On day 7 of treatment with 100 mg/kg MMF PO QD,
another PK/PD profile was performed and later compared
with the results on day 28, when all animals had received
a 50-mg/kg MMF dose for at least 7 days (Figure 3). After
multiple doses of 100 mg/kg of MMF QD, mean MPA
trough levels (Figure 3a) were 6.45 mg/L with a range of
2.04–13.46 mg/L, and MPA peak levels were now reached
in all animals after 2 h (32.02– 12.7 mg/L). In contrast, after
multiple days of 50 mg/kg MMF QD treatment, MPA
plasma levels before dosing and 2 h after dosing were
lower (C0: 2.2– 0.6 mg/L; p¼ 0.06, C2: 10.7– 2.7 mg/L;
p¼ 0.06). Pharmacodynamics (Figure 3b) after multiple
doses of 100 mg/kg MMF PO QD showed complete inhib-
ition of proliferation at all times, whereas after a dose of
50 mg/kg MMF daily incomplete inhibition of proliferation
at all times except 2 h after dosing was shown.
Phase I study evaluating tolerability andpharmacokinetics of 50 mg/kg mycophenolate mofetiltreatment given twice a day (b.i.d.) subcutaneously ororallyTreatment with 50 mg/kg MMF given twice daily as a s.c.
solution prepared with CellCept IV1 produced MPA levels
of 11.3 – 0.6 mg/L within 2 h after the first dose. Ten hours
after the first s.c. dose, mean MPA levels were
2.7– 0.9 mg/L, and 24-h trough levels were 3.7–1.1 mg/L.
After 14 daily doses of b.i.d. treatment s.c., trough MPA
plasma levels were 7.0– 0.9 and 2 h after dosing, MPA
plasma levels were 14.2 –0.25 mg/L. Weight loss (5.2–
10.1%) and other side-effects were less frequent compared
to the 100 mg/kg MMF QD phase I study.
To evaluate oral absorption of the CellCept IV1 formulation,
another single-dose study was performed: 2 h after the
initial 50 mg/kg oral dose, MPA plasma levels of 2.9 mg/L
(range 0.4–5.5 mg/L) were reached; the 24 h MPA trough
levels were 3.9– 2.3 mg/L (range 0.3–7.9 mg/L).
Phase II study evaluating the efficacy of mycophenolatemofetil for treatment of advanced graft vascular diseaseafter aortic transplantation in cynomolgus monkeys
Demographics and morbidity of operative procedures.
Demographics of the transplanted male cynomolgus
monkeys are shown in Table 1. No mortality occurred
during the transplant study, including five IVUS proced-
ures per animal. One animal experienced an
intussusception and needed a small bowel resection on
day 8 after transplantation; GVD progression was not
affected.
Out of 60 IVUS procedures, one animal of each group
(3.3%) experienced an intimal dissection caused by the
IVUS probe without residual injuries, as noted in the sub-
sequent IVUS. Additionally, in one animal an IVUS proced-
ure on day 42 had to be terminated prematurely, due to
uncontrollable arterial spasm. However, no temporary or
continuous limb ischemia was noted in any of the monkeys.
Mycophenolate mofetil treatment and its specific toxicity
and side-effects. All animals in the MMF group began
020406080
100120140
0 14 21 28
P1
020406080
100120140
P2
0
5
10
15
20
25P3
0
5
10
15
20
25P4
0 14 21 28
0 14 21 28
0 14 21 28
Wei
ght L
oss
Afte
r S
tart
of T
reat
men
t (%
)
MMF dose
Time After Starting MMF Treatment (Days)
weight loss diarrhea vomiting loss of appetite
7
7
7
7
Tot
al D
aily
MM
F Q
D D
ose
PO
(m
g/kg
/day
)
Figure 2: Pre-study on treated, but
not transplanted animals. Four
cynomolgus monkeys (P1–P4) were
treated with a maximal tolerated dose
(MTD) of mycophenolate mofetil
(MMF) starting with 100 mg/kg
body-weight given orally once daily
(QD). Figures express the individual
tolerability for each monkey and the
resulting MMF dose, which was
adjusted according to animal safety.
Treatment of Graft Vascular Disease by MMF
American Journal of Transplantation 2003; 3: 817–829 821

treatment on postoperative day 45 with 50 mg CellCept
IV1 twice daily administered s.c. and switched to oral
administration from treatment day 8 on. Absorption and
efficacy of drug treatment were monitored closely (see
below). After 5 days of treatment (POD 50), the MMF
dose was adjusted for each animal based on individual
toxicity, PK and PD values (Figure 4). The mean total
daily dose for the whole treatment period of 58 days
was 99.2 – 4.2 mg/kg/day. In none of the animals MMF
was withdrawn completely, but in two animals (Rx4,
Rx5) temporary dose reduction below 50 mg/kg/day was
necessary.
As shown in phase I studies, the major sign of MMF
toxicity was the decrease in body weight. Through POD
42, there was no difference in body weight changes
between the animals assigned to the control and MMF-
treated groups (Figure 5a). The individual response to the
drug showed a high variation (Figure 5b), and maximal
weight loss differed between 2.5% and 14.2% among
animals treated with MMF. The general behavior of all
animals was unimpaired during the study period. During
the time of treatment (58 days), the appetite of three
animals was reduced for 4–29 days. These animals
stopped eating for a range of 1–8 days. Gruel feeding
was initiated after 4 days of anorexia. Diarrhea occurred
in four animals for a period of 1–15 days.
No other adverse events were noted during the study or
revealed by autopsy on day 105. Changes in hemograms
and in blood chemistries are shown in Table 2.
Pharmacokinetics and pharmacodynamics during myco-
phenolate mofetil treatment in transplanted animals. Before
treatment started, in vitro analysis of immune functions was
performed in all animals. The calculated MPA IC50 of lympho-
cyte proliferation varied between 0.3 mg/L and 0.61mg/L.
The variation for Emax (0–18.75 abs% expression of PCNA)
was higher than in the phase I studies, and the coefficients of
correlation between inhibition of proliferation and MPA
plasma concentration ranged from 0.96 to 0.99.
After the first dose of MMF on POD 45, mean trough
MPA plasma levels were 2.3 mg/L (range 1.8–2.8 mg/L).
A corresponding PCNA expression of 2.1– 0.3 abs% was
noted. Throughout the entire study, trough MPA plasma
levels showed a higher inter- and intra-monkey variation
than did the pharmacodynamics of suppression of lympho-
cyte proliferation (Figure 6).
0 2 10 240
10
20
50
40
30
24100 20
20
60
80
100
40
Time After Oral MMF Dose (h)
Mea
n P
CN
A E
xpre
ssio
n N
orm
aliz
ed to
Pre
trea
tmen
t Val
ues
(%)
SE
±
100 mg/kg PO MMF QD
50 mg/kg PO MMF QD
Time After Oral MMF Dose (h)
100 mg/kg PO MMF QD
50 mg/kg PO MMF QD
Mea
n M
PATr
ough
Pla
sma
Con
cent
ratio
n (m
g/L)
SE
±A
B
Figure 3: Pre-study on treated, but not transplanted animals
(n = 4). Complete pharmacokinetic (a) and pharmacodynamic
profiles (b) were performed on day 7 (MMF dose 100 mg/kg
orally once daily) and compared to day 28 (MMF dose 50 mg/kg
orally once daily) after starting the treatment. Mean mycophenolic
acid levels (a) were similar at all time-points except for higher
levels 2 h after dosing. In contrast, pharmacodynamic assays (b)
showed complete inhibition of lymphocyte proliferation at all time-
points only when 100 mg/kg MMF was administered. Fifty mg/kg
MMF given once daily, was not able to suppress lymphocyte
proliferation completely, suggesting an insufficient immuno-
suppressive effect of that dose.
Table 1: Demographic characteristics (all calculations: mean–SEM) for untreated and mycophenolate mofetil (MMF)-treated
cynomolgus monkeys after aortic transplantation to study
treatment of graft vascular disease
Untreated MMFa p-valuesb
Blood group B (n¼4),
AB (n¼ 2)
A (n¼ 6) – c
Cross-match neg. n¼6 n¼6 – c
MLR index (SI) 9.69– 5.73 7.3– 1.3 n.s.d
Preoperative weight (kg) 8.0– 0.27 6.81–0.03 0.03
Weight mismatch (kg) 1.0– 0.78 0.91–0.4 n.s.d
Transplant time (min) 112.8–3.8 128.6– 8.1 n.s.d
Graft ischemia time (min) 46.5– 3.7 61.6–12.1 n.s.d
Mean IVUS time (min) 41.1– 2.5 39.4–1.6 n.s.d
aMMF treatment from day 45–103.bMann–Whitney U-test.cSignificance not computed.dNot significant.
Klupp et al.
822 American Journal of Transplantation 2003; 3: 817–829

In a retrospective analysis after the end of the study, in vivo
PK/PD relationships were calculated. The coefficient of
correlation between MPA plasma levels and PCNA expres-
sion was much lower than in the in vitro study and than in
the phase I studies (r2¼ 0.58) and showed a high inter-
individual variation (range r2¼ 0.37–0.99). Calculated MPA
IC50s varied between 0.01 and 2.2 mg/L (mean 0.82 mg/L),
and the maximal effect of inhibition of PCNA expression
was 9.9 rel% (range 0.4–29.9 rel%).
Intravascular ultrasound studies and development of
graft vascular disease. In untreated controls, mid-graft
vessel volumes decreased from 192 –15 mm3 on day 21
to 160– 16 mm3 on day 105. After day 42, significant
intimal thickening was noted (p< 0.028; Figure 7), with
the most rapid increase between PODs 42 and 63
(44.6 –4.3 mm3). Lumen volumes decreased significantly
(p< 0.02) between POD 21 (167– 15 mm3) and POD
105 (105– 16 mm3), with a minimal lumen volume of
105
0
50
100
150
100
150
63 84 10563 84 10542 63
50
084
Rx1 Rx2 Rx3
Rx6Rx5Rx4
Time After Transplantation (Days)In
divi
dual
Tot
al M
MF
Dos
e (m
g/kg
/day
)
Figure 4: Individual dosage of myco-
phenolate mofetil in six cynomolgus
monkeys starting treatment on day
45 after aortic transplantation. Dose
was adjusted according to animal
tolerability, PK and PD, with the
intention of reaching an individual
maximal tolerated dose. A mean total
MMF dose of 99.2–4.2 mg/kg was
reached for 9 treatment weeks.
105
+/–0
+15
–15
+/–0
+15
–1563 84 10563 84 10542 63 84
Rx1 Rx2 Rx3
Rx6Rx5Rx4
Time After Transplantation (Days)
Indi
vidu
al W
eigh
t Cha
nge
Afte
r S
tart
of T
reat
men
t (%
)
0–8
–6
–4
–2
21 42 63 84 105
0
2
4
6
8
10
A
B
controlMMFcontrol p = 0.02
Wei
ght C
hang
e A
fter
Tra
nspl
anta
tion
(mea
n %
± S
E)
Time After Transplantation (Days)
MMF treatment
Figure 5: Weight change normal-
ized to the preoperative weight as
an indicator of drug toxicity.
(a) From POD 63 on weight loss
was significantly different between
the two groups (p ¼ 0.02). (b)
Individual weight changes after start
of MMF treatment in combination
with gastrointestinal side-effects
resulted in dose adjustments
(compare to Figure 4).
Treatment of Graft Vascular Disease by MMF
American Journal of Transplantation 2003; 3: 817–829 823

87.8 –12 mm3 on day 105. However, this remodeling did
not have any clinical effects: mean intraluminal blood pres-
sure differences proximal and distal to the graft did not
change significantly between POD 21(1.5 –0.9 mmHg)
and POD 105 (5.3 –1.6 mmHg; p¼ 0.3).
Overall influence on graft vascular disease of delayed
MMF treatment starting 45 days after aortic transplant-
atio assessed by serial IVUS measurements. Before
starting MMF treatment on day 45, IVUS values were
not statistically significantly different between the control
42 63 84 105
Time After Transplantation (Days)
0
5
10
15
20
25
30
0
2
4
6
8
10
Mea
n A
bsol
ute
PC
NA
Exp
ress
ion
(%)
SE
±
Mea
n M
PATr
oug h
Pla
sma
Con
cent
r atio
n (m
g /L)
SE
±
PCNA expression
MPA plasma level
Figure 6: Pharmacokinetic and
pharmacodynamic monitoring of
animals treated with MMF after
aortic transplantation. Trough MPA
levels were measured twice weekly
and MPA levels of higher than 2 mg/L
were aimed for. Pharmacodynam-
ics was assessed by measuring
lymphocyte proliferation using flow
cytometry. After mitogen stimulation,
absolute intracellular PCNA expres-
sion was detected in cells, which
were in the S, G2 or M phase of the
cell cycle. Five per cent of absolute
PCNA expression or less was aimed
for.
Table 2: Means–SEM of hemogram and blood chemistry results from untreated and MMF treated cynomolgus monkeys with aortic
allografts on day 42 before start of treatment and at the end of the treatment on day 105 and the levels of significance for differences
p-value d
Control a p-value b MMF c p-value b (Control vs. MMF)
Hemogram & chemistry day 42 day 105 (42–105) day 42 day 105 (42–105) day 42 day 105
Hemoglobin (mg/dL) 13.2–0.3 12.8– 0.3 0.5 12.6– 0.3 11.1– 0.8 0.1 0.3 0.1
Hematocrit (%) 41 –0.8 40.5– 1.1 0.4 39.9– 0.9 35.5– 0.8 0.3 0.1 0.1
RBC (103/nL) e 6.5 – 0.1 6.3 – 0.2 0.2 6.1– 0.2 5.2 –0.4 0.05 0.07 0.03
WBC (/nL) e 9.2 – 1.3 8.2 – 0.6 0.7 11.2– 0.9 7.5 –1.4 0.1 0.3 0.7
Platelet count (/nL) 356– 33 331– 23 0.5 399– 30 306–33 0.1 0.3 0.6
Total protein (mg/dL) 7.1 – 0.1 6.9 – 0.1 0.2 6.8– 0.2 6.3 –0.2 0.1 0.2 0.01
Albumin (mg/dL) 3.9 – 0.1 3.9 – 0.2 0.9 3.9– 0.1 3.8 –0.2 0.3 0.5 0.3
Amylase (IU/L) 303– 31 278– 33 0.2 340– 50 261–20 0.4 0.8 1.0
Lipase (IU/L) 10.8– 1.6 15– 2.9 0.2 9.4– 1.9 6.7 –1.5 0.05 0.6 0.02
Creatinine (mg/dL) 1.2 – 0.1 1.1 – 0.05 0.3 0.9– 0.05 0.8 –0.1 0.3 0.08 0.09
BUN (mg/dL) e 13.5–1.8 11.5– 0.5 0.7 10.2– 0.8 9 –1.6 0.8 0.2 0.5
Total bilirubin (mg/dL) 0.2– 0.05 0.18– 0.02 0.8 0.2– 0.05 0.13– 0.02 0.02 0.8 0.09
Conj. bilirubin (mg/dL) 0.05–0.02 0.03– 0.01 0.5 0.04– 0.001 0.03– 0.01 0.01 1.0 0.3
AST (IU/L) e 40 –3 35– 2 0.3 34– 3 24– 1 0.04 0.3 0.01
ALT (IU/L) e 19 –5 33– 16 0.6 24– 3 18– 3 0.3 0.3 0.8
AP (IU/L) e 164– 17 141– 14 0.5 229– 19 192–15 0.3 0.04 0.06
Cholesterol (mg/dL) 98 –6 92– 8 0.8 94– 4 75– 8 0.05 0.7 0.2
Triglycerides (mg/dL) 49 –6 74– 12 0.06 55– 5 50– 8 0.5 0.4 0.1
Glucose (mg/dL) 42.1–5.3 55.8– 7.1 0.13 45.3– 4.3 53.3– 4.3 0.4 0.5 0.7
LDH (IU/L) e 508– 96 413–71 0.5 460– 83 273–30 0.1 0.7 0.2
CPK (IU/L) 356– 80 233–71 0.2 488– 205 285–147 0.18 0.6 0.8
aControl animals did not receive any immunosuppressive treatment from day 0 to 105.bWilcoxon signed-rank test for two dependent samples.cMMF treatment from days 45 to 103.dMann–Whitney U-test for independent samples.
RBC – Red blood cell count, WBC – White blood cell count, BUN – urea, AST – aspartate amino transferase, ALT – alanine amino
transferase, AP – alkaline phosphatase, LDH – lactate dehydrogenase, CPK – Creatinine phosphokinase.
Klupp et al.
824 American Journal of Transplantation 2003; 3: 817–829

and the treatment groups: mean vessel volumes for animals
in the treatment group were 166– 15 mm3 vs. 183– 17 mm3
in the control group; intimal volumes 25–3 mm3 vs.
25–2 mm3; and lumen volumes 141– 13 mm3 vs.
158– 17 mm3, respectively. The intraluminal blood pres-
sures differences were not significantly different (control:
3.2– 2 mmHg, MMF 5.5– 1.9 mmHg; p¼ 0.3).
In contrast to the control group (p¼ 0.028), VV in the
treatment group did not change significantly between
the beginning of the study (154 – 18 mm3) and day 105
(138– 13 mm3). However, due to high inter-individual
differences within the animals of the MMF group, no
statistically significant differences in mean VV were
found between treatment and control group on day 105
(p¼ 0.3).
Lumen volumes (LV) did not differ significantly among
animals in the control and MMF treatment groups. On
POD 105, mean LV was 104 –16 mm3 in the control and
90 –6 mm3 in the treatment group. Cross-sections with
minimal lumen areas (LA) were 7.8 –0.5 mm2 and
8.7– 1.2 mm2 and with maximal LA 9.7– 0.7 and
11.5– 1.8 mm2 in MMF and control groups, respectively.
Overall, the progression of intimal volume did increase
significantly between start of treatment on day 45 and
the end of the study on day 105 in both the control
(p< 0.028) and MMF groups (p< 0.043). In a general
linear model, evaluating the overall difference in
development of intimal volumes between days 42 and
105, there were no significant differences among animals
in the control and MMF treatment groups (p¼ 0.3;
Figure 7). The progression of graft vascular disease
decreased in MMF-treated animals, but the differences
between MMF and control groups were not statistically
significant on day 84 (43– 7 vs. 52 – 4 mm3, respectively,
p¼ 0.32) or on day 105 (47 –7 vs. 55 – 2 mm3, respec-
tively, p¼ 0.37).
Overall influence of MMF treatment on graft vascular
disease assessed by histology. Grafts from untreated
animals showed histological signs of graft vascular dis-
ease that were indistinguishable from human allograft
vasculopathy. The GVD consisted of concentric fibrointimal
proliferation of smooth muscle cells and myofibroblasts,
containing scattered macrophages and lymphocytes in a
collagenous matrix of intima. Smooth muscle cell a-actin
staining confirmed that the intima in allografts was com-
prised predominantly of smooth muscle cells. The internal
elastic membrane was partly fractured, and partly pre-
served with reduplication. The medial layer was obscured
by fibrous tissue that extended into the surrounding
adventitial soft tissue. Perivascular inflammation was min-
imal in one graft, focal in one, band-like in one and multifocal
in three. No calcifications or cholesterol plaques were
noticed. Semi-quantitative assessment of GVD was mild in
one animal, moderate in two animals and severe in three.
In contrast, in the MMF-treated animals GVD was mild in
two animals, moderate in three and severe in one graft.
This histology did not differ significantly from results in
the untreated controls (p¼ 0.3). Also, the damage to the
internal elastic membrane and the perivascular inflam-
mation were not statistically different.
The histomorphometric analysis correlated highly with the
IVUS morphometry (r2¼ 0.88, p< 0.001). However,
despite the pressurized preservation with formalin, the
grafts shrank, and intimal areas measured by histomorpho-
metry were by 31.6% smaller than areas measured by
IVUS.
Mean intimal areas measured by histomorphometry failed
to be statistically different between the control
(4.2– 0.4 mm2) and MMF treatment groups (2.9– 0.5 mm2;
p¼ 0.078). Differences in mean intimal thickening, how-
ever, were close to being significant between the groups
(control: 504– 44 mm, MMF 410– 47 mm; p¼ 0.065).
The medial areas were significantly lower in the MMF-
treated animals (1.5 –0.1 mm2) than in the untreated
animals (2.3 – 0.3 mm2 (p¼ 0.016). However, there was
no difference in lumen areas between the groups
(control: 4.2– 0.5 mm2; MMF: 3.9 – 0.4 mm2; p¼ 0.87).
Individual development of graft vascular disease after
delayed MMF treatment starting on day 45 after aortic
transplantation. In contrast to the grafts from control
animals, the extent of development of graft vascular dis-
ease showed a high variation among the MMF-treated
monkeys. Whereas the IVUS measurements in all the
untreated animals showed a homogenous distribution in
intimal volume between 47 and 67 mm3 in the aortic grafts
on day 105, the animals in the treatment group could be
divided into two subpopulations: four out of six animals
showed significantly less intimal thickening, than each of
the control animals (p< 0.02; Figure 8). In the other two
Mea
n IV
US
–In
timal
Vol
ume
SE
(m
m)
±3
Time After Transplantation (Days)
0
10
20
30
40
50
60
70
0 21 42 63 84 105
controlMMF
MMF treatment
p = 0.3
Figure 7: Mean intimal volume in the mid-segment of aortic
allografts from untreated and MMF treated cynomolgus
monkeys assessed by IVUS studies at 3-week intervals.
Treatment of Graft Vascular Disease by MMF
American Journal of Transplantation 2003; 3: 817–829 825
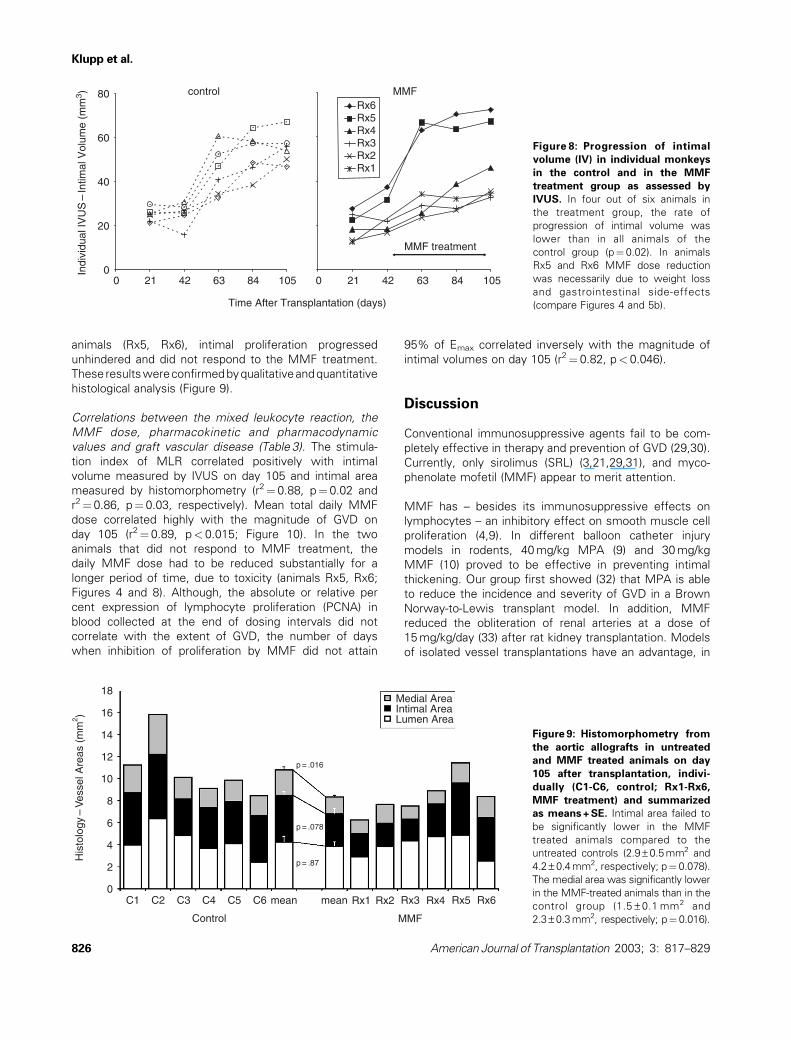
animals (Rx5, Rx6), intimal proliferation progressed
unhindered and did not respond to the MMF treatment.
These resultswereconfirmedbyqualitativeandquantitative
histological analysis (Figure 9).
Correlations between the mixed leukocyte reaction, the
MMF dose, pharmacokinetic and pharmacodynamic
values and graft vascular disease (Table 3). The stimula-
tion index of MLR correlated positively with intimal
volume measured by IVUS on day 105 and intimal area
measured by histomorphometry (r2¼ 0.88, p¼ 0.02 and
r2¼ 0.86, p¼ 0.03, respectively). Mean total daily MMF
dose correlated highly with the magnitude of GVD on
day 105 (r2¼ 0.89, p< 0.015; Figure 10). In the two
animals that did not respond to MMF treatment, the
daily MMF dose had to be reduced substantially for a
longer period of time, due to toxicity (animals Rx5, Rx6;
Figures 4 and 8). Although, the absolute or relative per
cent expression of lymphocyte proliferation (PCNA) in
blood collected at the end of dosing intervals did not
correlate with the extent of GVD, the number of days
when inhibition of proliferation by MMF did not attain
95% of Emax correlated inversely with the magnitude of
intimal volumes on day 105 (r2¼ 0.82, p< 0.046).
Discussion
Conventional immunosuppressive agents fail to be com-
pletely effective in therapy and prevention of GVD (29,30).
Currently, only sirolimus (SRL) (3,21,29,31), and myco-
phenolate mofetil (MMF) appear to merit attention.
MMF has – besides its immunosuppressive effects on
lymphocytes – an inhibitory effect on smooth muscle cell
proliferation (4,9). In different balloon catheter injury
models in rodents, 40 mg/kg MPA (9) and 30 mg/kg
MMF (10) proved to be effective in preventing intimal
thickening. Our group first showed (32) that MPA is able
to reduce the incidence and severity of GVD in a Brown
Norway-to-Lewis transplant model. In addition, MMF
reduced the obliteration of renal arteries at a dose of
15 mg/kg/day (33) after rat kidney transplantation. Models
of isolated vessel transplantations have an advantage, in
Time After Transplantation (days)
1058463422100
20
40
60
80 controlIn
divi
dual
IVU
S –
Intim
al V
olum
e (m
m3 )
105846342210
MMF
MMF treatment
Rx6Rx5Rx4Rx3Rx2Rx1
Figure 8: Progression of intimal
volume (IV) in individual monkeys
in the control and in the MMF
treatment group as assessed by
IVUS. In four out of six animals in
the treatment group, the rate of
progression of intimal volume was
lower than in all animals of the
control group (p¼ 0.02). In animals
Rx5 and Rx6 MMF dose reduction
was necessarily due to weight loss
and gastrointestinal side-effects
(compare Figures 4 and 5b).
C1 C2 C3 C4 C5 C6 mean mean Rx1 Rx2 Rx3 Rx4 Rx5 Rx6
p = .87
p = .078
p = .016
0
2
4
6
8
10
12
14
16
18
Control MMF
His
tolo
gy–
Ves
sel A
reas
(m
m)2
Medial AreaIntimal AreaLumen Area
Figure 9: Histomorphometry from
the aortic allografts in untreated
and MMF treated animals on day
105 after transplantation, indivi-
dually (C1-C6, control; Rx1-Rx6,
MMF treatment) and summarized
as means + SE. Intimal area failed to
be significantly lower in the MMF
treated animals compared to the
untreated controls (2.9–0.5 mm2 and
4.2– 0.4 mm2, respectively; p¼ 0.078).
The medial area was significantly lower
in the MMF-treated animals than in the
control group (1.5 – 0.1 mm2 and
2.3–0.3 mm2, respectively; p¼ 0.016).
Klupp et al.
826 American Journal of Transplantation 2003; 3: 817–829

that no initial immunosuppressive therapy is needed to
secure graft function (34,35) and GVD can be investigated
independently. In an ACI-to-Lewis model of orthotopic
aortic transplantation, intimal proliferation was reduced
by 76.1% with the daily treatment of 40–30 mg/kg MMF
(8). MMF was less, but still significantly effective, when
treatment was delayed by 2 weeks or 4 weeks.
These results in rodents encouraged us to investigate the
effect of MMF after allogenic aortic transplantation in
non-human primates. As previously published, this pro-
cedure has many advantages over the rodent studies
(19,21,36,37). Additionally, this present study investigated
the effect of MMF on advanced GVD: in the first 6 weeks
after orthotopic aortic transplantation cynomolgus
monkeys did not receive any immunosuppressive treat-
ment at all. During this time, intimal proliferation developed
unhindered and drug efficacy in treating advanced
lesions could be studied. Our protocol was designed in
such a way that each animal was treated with an indi-
vidualized, maximal tolerated dose of MMF. We intended,
thereby, to evaluate the efficacy of ideal MMF treatment
for GVD.
To determine the maximal tolerated dose for a 2-month
period of treatment in cynomolgus monkeys, various pre-
studies were performed. Previous toxicological studies in
non-human primates (Roche data on file) showed that
MMF at a dose of 150 mg/kg/day leads to gastrointestinal
toxicity, necessitating MMF withdrawal within 4 weeks. In
our phase I pharmacokinetic and pharmacodynamic pre-
studies, we showed that, with 100 mg/kg/day MMF QD
dosing, all animals suffered from severe weight loss and
gastrointestinal toxicity (Figure 2). After 14 and 21 days of
MMF treatment, in all animals the dose had to be reduced
stepwise to 50 mg/kg/day. However, the pharmacokinetics
and pharmacodynamics in this experiment showed that the
lower dosage was not able to provide sufficient MPA
plasma levels for inhibition of lymphocyte proliferation, as
measured by intracellular PCNA expression.
In rodent studies (27,28,38), we showed earlier that PK
and PD parameters correlate highly with the immunosup-
pressive efficacy of MMF. We were even able to prove
that sustained suppression of lymphocyte proliferation
throughout the dosing interval was necessary to prevent
graft rejection and to show the beneficial effect of BID vs.
QD dosing (27).
With our BID therapeutic regimen in cynomolgus monkeys,
we were able to dose the animals starting on day 45 after
transplantation for 2 months with a mean total daily MMF
dose of 99.2– 4.2 mg/kg. The individual susceptibility to
MMF toxicity showed a high variation, resulting in daily
MMF doses between 30 and 120 mg/kg (Figure 4). How-
ever, none of the animals was withdrawn from the study
due to uncontrollable toxicity.
The primary endpoint of our present study was the intimal
thickening on day 105 after transplantation. Three days
before beginning treatment in the MMF group, the intimal
volume was identical in both groups. By day 105, IV in the
mid-graft in the control group increased to 55.2 –2.8 mm3,
and in the MMF group to 47.8 – 7.2 mm3 and there was no
overall difference between the groups (p ¼0.3). The dif-
ferences in histomorphometry between the two groups
just failed to be significant (p¼ 0.07), but the postmortem
shrinkage of the grafts made histomorphometry less
reliable than IVUS measurements.
However, and most important, there was a clear inter-
animal variability for progression of GVD in the MMF
0
20
40
60
80
0 80 90 100 110 120
Mean Total Daily MMF Dose (mg/kg/day)Between Day 45–103 After Aortic Transplantation
IVU
S –
Intim
al V
olum
e D
ay 1
05 (
mm
3 )
r2 = 0.89p < 0.015
Rx6Rx5Rx4Rx3Rx2Rx1
Figure 10: Total daily MMF dose (mg/kg/day) correlates
significantly with the intimal volume on day 105 assessed
using IVUS morphometry (r2 = 0.89; p< 0.015).
Table 3: Correlation between mixed leukocyte reaction (MLR),
ischemia time, pharmacokinetics, pharmacodynamics and graft
vascular disease measured by intravascular ultrasound (IVUS) and
histomorphometry on day 105 after aortic transplantation in the
mycophenolate mofetil (MMF) treatment group
IVUS (IV) Histology (IA)
r2 p r2 p
MLR 0.88 0.02 0.86 0.03
Ischemia time 0.18 0.5 0.34 0.3
Mean daily MMF dose 0.89 0.015 0.85 0.03
Mean MPA trough levels 0.07 0.9 0.02 0.9
Days with MPA trough 0.15 0.7 0.21 0.6
<2.0 mg/L
Mean PCNA expression 0.16 0.7 0.21 0.7
Days with PCNA expression 0.14 0.7 0.10 0.8
>5.0 abs%
Days with PCNA expression 0.82 0.046 0.80 0.058
<95% Emax
IV –intimal volume, IA – intimal area, MPA – mycophenolic acid,
PCNA – proliferating cell nuclear antigen.
Treatment of Graft Vascular Disease by MMF
American Journal of Transplantation 2003; 3: 817–829 827

treatment group: four out of six MMF-treated animals
showed an intimal volume that was lower than in each
of the control animals. In the other two animals, progres-
sion of GVD was unhindered (Figure 8). In the treatment
group, the stimulation index (SI) of the MLR correlated
with GVD, and both ‘non-responding’ animals (Rx5, Rx6)
had SI’s above 10.
Mean total daily MMF dose correlated highly with IV meas-
ured by IVUS on day 105 and with IA as measured by
histomorphometry (Figure 10; Table 3). In both ‘non-
responding’ animals, the dose of MMF had to be reduced
substantially for more than 50% of the treatment days due
to MMF toxicity.
Neither MMF pharmacokinetics nor trough pharmaco-
dynamic markers correlated with IV or IA on day 105
(Table 3). However, taking the drug sensitivity of each
animal into account, the number of days when 95% of
inhibition of maximal lymphocyte proliferation was not
reached correlated significantly with the extension of
GVD. This finding, as well as the results from our rodent
studies (27), supports the hypothesis that an insufficient
immunosuppressive effect, measured by pharmaco-
dynamics in the peripheral blood, predicts acute or chronic
rejection of the graft.
In summary, there was no overall statistically significant
difference in progression of GVD between the untreated
control and the MMF treatment groups. However, there
was a high correlation between the total daily MMF dose
and intimal hyperplasia. Depending on the individual
tolerability of MMF in cynomolgus monkeys, MMF was
effective for treatment of advanced GVD after aortic trans-
plantation. This efficacy was achieved when intimal prolif-
eration had already proceeded unhindered for more
than 6 weeks after transplantation due to lack of any
immunosuppression. Since we have shown in rodent
studies that MPA and SRL more effectively inhibit intimal
thickening than either drug alone (9), combination
therapy of MMF and SRL may be even more effective
for controlling GVD in non-human primates or patients.
With this study in non-human primates, the foundation
has been laid for randomized, double-blind clinical,
studies investigating the value of MMF for prevention or
treatment of GVD.
Acknowledgments
We gratefully acknowledge the technical assistance of Randi Shorthouse
and the editorial support of Kate Hinke. We also thank Dr Elsie Eugui for
her excellent advice. This study was funded in part by Roche Laboratories,
Inc. (Nutley, NJ). It has also been supported by the Ralph and Marian Falk
Trust and by the Hedco Foundation. Dr Jochen Klupp received grants (KL
1214/1–1/1–2) from the ‘Deutsche Forschungsgemeinschaft’; Dr Teun van
Gelder, from the Dutch Kidney Foundation, and Dr Camille Dambrin, from
the French Federation of Cardiology.
References
1. Hager PW, Collart FR, Huberman E, Mitchell BS. Recombinant
human inosine monophosphate dehydrogenase type I and type II
proteins. Purification and characterization of inhibitor binding.
Biochem Pharmacol 1995; 49: 1323–1329.
2. Allison AC, Eugui EM. Preferential suppression of lymphocyte
proliferation by mycophenolic acid and predicted long-term
effects of mycophenolate mofetil in transplantation. Transplant
Proc 1994; 26: 3205–3210.
3. Mohacsi P, Tuller D, Hulliger B, Wijngaard P. Different inhibitory
effects of immunosuppressive drugs on human and rat aortic
smooth muscle and endothelial cell proliferation stimulated by
platelet-derived growth factor or endothelial cell growth factor. J
Heart Lung Transplant 1997; 16: 484–492.
4. Gregory CR, Pratt RE, Huie P et al. Effects of treatment with
cyclosporine, FK 506, rapamycin, mycophenolic acid, or deoxy-
spergualin on vascular muscle proliferation in vitro and in vivo.
Transplant Proc 1993; 25: 770–771.
5. Raisanen-Sokolowski A, Myllarniemi M, Hayry P. Effect of myco-
phenolate mofetil on allograft arteriosclerosis (chronic rejection).
Transplant Proc 1994; 26: 3225.
6. Raisanen-Sokolowski A, Vuoristo P, Myllarniemi M, Yilmaz S,
Kallio E, Hayry P. Mycophenolate mofetil (MMF, RS-61443) inhibits
inflammation and smooth muscle cell proliferation in rat
aortic allografts. Transpl Immunol 1995; 3: 342–351.
7. Morris R, Wang J, Blum J et al. Immunosuppressive effects of
the morpholinoethyl ester of mycophenolic acid (RS-61443) in rat
and nonhuman primate recipients of heart allografts. Transplant
Proc 1991; 23 (Suppl. 2): 19–25.
8. Steele D, Hullett D, Bechstein W et al. Effects of immunosup-
pressive therapy on the rat aortic allograft model. Transplant
Proc 1993; 25: 754–755.
9. Gregory C, Huang X, Pratt R et al. Treatment with rapamycin and
mycophenolic acid reduces arterial intimal thickening produced
by mechanical injury and allows endothelial replacement. Trans-
plantation 1995; 59: 655–661.
10. Fraser-Smith E, Rosete J, Schatzman R. Suppression by myco-
phenolate mofetil of the neointimal thickening caused by vascu-
lar injury in a rat arterial stenosis model. J Pharmacol Exp Ther
1995; 275: 1204–1208.
11. O’Hair DP, McManus RP, Komorowski R. Inhibition of chronic
vascular rejection in primate cardiac xenografts using myco-
phenolate mofetil. Ann Thorac Surg 1994; 58: 1311–1315.
12. Kobashigawa J. Mycophenolate mofetil in cardiac transplantation.
Curr Opin Cardiol 1998; 13: p117–121.
13. Orbaek AH. Heart allograft vascular disease: an obliterative
vascular disease in transplanted hearts. Atherosclerosis 1999;
142: 243–263.
14. Jirasiritham S, Sumethkul V, Mavichak V, Chiewsilp P,
Leenanupunth C, Kochakarn W. Treatment of chronic rejection
in renal transplantation by mycophenolate mofetil (MMF): a
preliminary report of six-month experience. Transplant Proc
1998; 30: 3576–3577.
15. Campistol J, Mazuecos A, Segura J et al. Mycophenolate mofetil
slows the decline of renal function in patients with biopsy-
proven chronic rejection: a collaborative pilot study. Transplant
Proc 1999; 31: 2267–2269.
16. Ferraris J, Tambutti M, Redal M, Bustos D, Ramirez J,
Prigoshin N. Conversion from azathioprine [correction of azathio-
prina] to mycophenolate mofetil in pediatric renal transplant
recipients with chronic rejection. Transplantation 2000; 70:
297–301.
Klupp et al.
828 American Journal of Transplantation 2003; 3: 817–829

17. Klupp J, Bechstein W, Platz K et al. Mycophenolate mofetil
added to immunosuppression after liver transplantation – first
results. Transpl Int 1997; 10: 223–228.
18. Kato T, De Ruiz PFW, Weppler D et al. Mycophenolate mofetil
rescue therapy in patients with chronic hepatic allograft rejec-
tion. Transplant Proc 1999; 31: 396.
19. Ikonen T, Briffa N, Gummert J et al. Multidimensional assess-
ment of graft vascular disease (GVD) in aortic grafts by serial
intravascular ultrasound in rhesus monkeys. Transplantation
2000; 70: 420–429.
20. Gummert J, Ikonen T, Briffa N et al. A new large-animal model for
research of graft vascular disease. Transplant Proc 1998; 30: 4023.
21. Ikonen T, Gummert J, Serkova N et al. Efficacies of sirolimus
(rapamycin) and cyclosporine in allograft vascular disease in non-
human primates: trough levels of sirolimus correlate with inhib-
ition of progression of arterial intimal thickening. Transpl Int
2000; 13 (Suppl. 1): S314–S320.
22. Gummert JF, Christians U, Barten M, Silva H, Morris RE. High-
performance liquid chromatographic assay with a simple extrac-
tion procedure for sensitive quantification of mycophenolic acid
in rat and human plasma. J Chromat B 1999; 721: 321–326.
23. Barten MJ, Gummert JF, van Gelder T, Shorthouse R, Morris RE.
Flow cytometric quantitation of calcium-dependent and
-independent mitogen-stimulation of T cell functions in whole
blood: inhibition by immunosuppressive drugs in vitro. J Immunol
Meth 2001; 253: 95–112.
24. Gummert JF, Barten MJ, van Gelder T, Billingham M, Morris RE.
Pharmacodynamics of mycophenolic acid in heart allograft recipi-
ents: correlation of lymphocyte proliferation and activation with
pharmacokinetics and graft histology. Transplantation 2000; 70:
1038–1049.
25. Silva HT, Slauson S, Sherwood S et al. Monitoring of pharmaco-
dynamic (PD), but not pharmacokinetics (PK), differentiate the
relative immunosuppressive potencies of leflunomide and its
malononitrilamide (MNA) analogs [abstract]. Transplantation
1998; 65: S42.
26. Slauson SD, Silva HT, Sherwood SW, Morris RE. Flow cyto-
metric analysis of the molecular mechanisms of immunosup-
pressive action of the active metabolite of leflunomide and its
malononitrilamide analogues in a novel whole blood assay.
Immunol Lett 1999; 67: 179–183.
27. Klupp J, van Gelder T, Dambrin C et al. Sustained suppression of
peripheral blood immune functions by treatment with myco-
phenolate mofetil throughout the dosing interval correlates
with reduced histologic severity of heart allograft rejection.
J Heart Lung Transplant 2003; in press.
28. Gummert JF, Barten MJ, Sherwood SW, van Gelder T, Morris RE.
Pharmacodynamics of immunosuppression by mycophenolic
acid: inhibition of both lymphocyte proliferation and activation
correlates with pharmacokinetics. J Pharmacol Exp Ther 1999;
291: 1100–1112.
29. Ikonen T, Gummert J, Hayase M et al. Sirolimus (rapamycin)
halts and reverses progression of allograft vascular disease in
non-human primates. Transplantation 2000; 70: 969–975.
30. Weis M, von Scheidt W. Cardiac allograft vasculopathy: a
review. Circulation 1997; 96: 2069–2077.
31. Gregory CR, Huie P, Billingham ME, Morris RE. Rapamycin
inhibits arterial intimal thickening caused by both alloimmune
and mechanical injury. Its effect on cellular, growth factor, and
cytokine response in injured vessels. Transplantation 1993; 55:
1409–1418.
32. Morris RE, Wang J. Comparison of the immunosuppressive
effects of mycophenolic acid and the morpholinoethyl ester of
mycophenolic acid (RS-61443) in recipients of heart allografts.
Transplant Proc 1991; 23: 493–496.
33. Azuma H, Binder J, Heemann U, Schmid C, Tullius SG, Tilney NL.
Effects of RS61443 on functional and morphological changes in
chronically rejecting rat kidney allografts. Transplantation 1995;
59: 460–466.
34. Hayry P, Mennander A, Tiisala S, Halttunen J, Yilmaz S,
Paavonen T. Rat aortic allografts: an experimental model for
chronic transplant arteriosclerosis. Transplant Proc 1991; 23:
611–612.
35. Mennander A, Tiisala S, Halttunen J, Yilmaz S, Paavonen T,
Hayry P. Chronic rejection in rat aortic allografts. An experimen-
tal model for transplant arteriosclerosis. Arterioscler Thromb
1991; 11: 671–680.
36. Ikonen T, Gummert J, Honda Y et al. Development of models of
graft vascular disease in nonhuman primates: evaluation of GVD
by intravascular ultrasound in a new cynomolgus model with
arterial allograft exchange. Transplant Proc 1999; 31: 687.
37. Mehra MR, Ventura HO, Stapleton DD et al. Allograft aorto-
pathy: an in vivo study of donor aorta involvement in cardiac
allograft vasculopathy. Am Heart J 1997; 133: 698–702.
38. Barten MJ, van Gelder T, Gummert JF et al. Pharmacodynamics
of mycophenolate mofetil (CellCept) after heart transplantation:
New mechanism of action and correlation with histologic sever-
ity of graft rejection. Am J Transplant 2002; 2: 719–732.
Treatment of Graft Vascular Disease by MMF
American Journal of Transplantation 2003; 3: 817–829 829














