Salvage Allogeneic Hematopoietic Cell Transplantation with Fludarabine and Low-Dose Total Body...
18
Salvage allogeneic hematopoietic cell transplantation with fludarabine and low-dose total body irradiation after rejection of first allografts Boglarka Gyurkocza 1 , Thai M. Cao 2 , Rainer F. Storb 1 , Thoralf Lange 3 , Wendy Leisenring 1 , Georg N. Franke 3 , Mohamed Sorror 1 , Richard Hoppe 2 , David G. Maloney 1 , Robert S. Negrin 2 , Judith A. Shizuru 2,* , and Brenda M. Sandmaier 1,* 1 Fred Hutchinson Cancer Research Center and the University of Washington School of Medicine, Seattle, Washington 2 Stanford University Medical Center, Palo Alto, California 3 University of Leipzig, Leipzig, Germany Abstract We summarized results in 38 consecutive patients (median age = 56 years) with hematologic malignancies (n=33), aplastic anemia (n=2) or renal cell carcinoma (n=1), who underwent salvage hematopoietic cell transplantation (HCT) for allograft rejection. In 14 patients the original donors were used for salvage HCT, and in 24 cases different donors were used. Conditioning for salvage HCT consisted of fludarabine and either 3 or 4 Gy total body irradiation (TBI). Sustained engraftment was achieved in 33 patients (87%). Grafts were rejected in 5 patients (13%), 4 of whom had myelofibrosis. With a median follow-up of 2 (range, 0.3 to 7.8) years, the 2 and 4 year estimated survivals were 49% and 42%, respectively. The 2-year relapse rate and non-relapse mortality were 36% and 24%, respectively. The 2-year cumulative incidences of grades 2–4 acute and moderate- severe chronic graft-versus-host disease were 42% and 41%, respectively. In this cohort, TBI dose, grafts from original vs. different donors, related vs. unrelated donors, and HCT comorbidity scores did not impact outcomes. We concluded that graft rejection after allogeneic HCT could be overcome by salvage transplantation using conditioning with fludarabine and low dose TBI. © 2009 The American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved. Correspondence and reprints to, Brenda M Sandmaier, M.D., Fred Hutchinson Cancer Research Center, 1100 Fairview Avenue N., Mail Stop D1-100, P.O. Box 19024, Seattle, WA 98109-1024, United States, phone: (206) 667-4961, fax: (206) 667-6124, e-mail: [email protected]. * JAS and BMS contributed equally to this article Authorship B.G. contributed to data collection, analyzed and interpreted data, wrote the manuscript, participated in patient care; T.M.C. contributed to data collection, analyzed and interpreted data, participated in patient care; R.F.S. designed study, analyzed and interpreted data, wrote the manuscript, participated in patient care; T.L. contributed to data collection, analyzed and interpreted data, participated in patient care; W.L. performed statistical analysis, wrote the manuscript; G.N.F. contributed to data collection, participated in patient care; M.S. analyzed and interpreted data; R.H. analyzed and interpreted data, acted as radiation consultant, participated in patient care; D.M. analyzed and interpreted data, participated in patient care; R.S.N. analyzed and interpreted data, participated in patient care; J.A.S. designed study, analyzed and interpreted data, wrote the manuscript, participated in patient care; B.M.S. designed study, analyzed and interpreted data, wrote the manuscript, participated in patient care Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain. Presented as poster presentation at the 50th annual meeting of the American Society of Hematology, San Francisco, CA, December 8, 2008 (Abstract #3272). The authors have no relevant financial relationship(s) to disclose. NIH Public Access Author Manuscript Biol Blood Marrow Transplant. Author manuscript; available in PMC 2010 October 1. Published in final edited form as: Biol Blood Marrow Transplant. 2009 October ; 15(10): 1314–1322. doi:10.1016/j.bbmt.2009.06.011. NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Salvage Allogeneic Hematopoietic Cell Transplantation with Fludarabine and Low-Dose Total Body...
Salvage allogeneic hematopoietic cell transplantation withfludarabine and low-dose total body irradiation after rejection offirst allografts
Boglarka Gyurkocza1, Thai M. Cao2, Rainer F. Storb1, Thoralf Lange3, Wendy Leisenring1,Georg N. Franke3, Mohamed Sorror1, Richard Hoppe2, David G. Maloney1, Robert S.Negrin2, Judith A. Shizuru2,*, and Brenda M. Sandmaier1,*1Fred Hutchinson Cancer Research Center and the University of Washington School of Medicine,Seattle, Washington2Stanford University Medical Center, Palo Alto, California3University of Leipzig, Leipzig, Germany
AbstractWe summarized results in 38 consecutive patients (median age = 56 years) with hematologicmalignancies (n=33), aplastic anemia (n=2) or renal cell carcinoma (n=1), who underwent salvagehematopoietic cell transplantation (HCT) for allograft rejection. In 14 patients the original donorswere used for salvage HCT, and in 24 cases different donors were used. Conditioning for salvageHCT consisted of fludarabine and either 3 or 4 Gy total body irradiation (TBI). Sustained engraftmentwas achieved in 33 patients (87%). Grafts were rejected in 5 patients (13%), 4 of whom hadmyelofibrosis. With a median follow-up of 2 (range, 0.3 to 7.8) years, the 2 and 4 year estimatedsurvivals were 49% and 42%, respectively. The 2-year relapse rate and non-relapse mortality were36% and 24%, respectively. The 2-year cumulative incidences of grades 2–4 acute and moderate-severe chronic graft-versus-host disease were 42% and 41%, respectively. In this cohort, TBI dose,grafts from original vs. different donors, related vs. unrelated donors, and HCT comorbidity scoresdid not impact outcomes. We concluded that graft rejection after allogeneic HCT could be overcomeby salvage transplantation using conditioning with fludarabine and low dose TBI.
© 2009 The American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.Correspondence and reprints to, Brenda M Sandmaier, M.D., Fred Hutchinson Cancer Research Center, 1100 Fairview Avenue N.,Mail Stop D1-100, P.O. Box 19024, Seattle, WA 98109-1024, United States, phone: (206) 667-4961, fax: (206) 667-6124, e-mail:[email protected].*JAS and BMS contributed equally to this articleAuthorshipB.G. contributed to data collection, analyzed and interpreted data, wrote the manuscript, participated in patient care; T.M.C. contributedto data collection, analyzed and interpreted data, participated in patient care; R.F.S. designed study, analyzed and interpreted data, wrotethe manuscript, participated in patient care; T.L. contributed to data collection, analyzed and interpreted data, participated in patient care;W.L. performed statistical analysis, wrote the manuscript; G.N.F. contributed to data collection, participated in patient care; M.S. analyzedand interpreted data; R.H. analyzed and interpreted data, acted as radiation consultant, participated in patient care; D.M. analyzed andinterpreted data, participated in patient care; R.S.N. analyzed and interpreted data, participated in patient care; J.A.S. designed study,analyzed and interpreted data, wrote the manuscript, participated in patient care; B.M.S. designed study, analyzed and interpreted data,wrote the manuscript, participated in patient carePublisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customerswe are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resultingproof before it is published in its final citable form. Please note that during the production process errors may be discovered which couldaffect the content, and all legal disclaimers that apply to the journal pertain.Presented as poster presentation at the 50th annual meeting of the American Society of Hematology, San Francisco, CA, December 8,2008 (Abstract #3272).The authors have no relevant financial relationship(s) to disclose.
NIH Public AccessAuthor ManuscriptBiol Blood Marrow Transplant. Author manuscript; available in PMC 2010 October 1.
Published in final edited form as:Biol Blood Marrow Transplant. 2009 October ; 15(10): 1314–1322. doi:10.1016/j.bbmt.2009.06.011.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
INTRODUCTIONGraft rejection is an infrequent but life-threatening complication of allogeneic hematopoieticcell transplantation (HCT), occurring historically at a frequency of 6% or less after bonemarrow transplantation with myeloablative conditioning [1,2]. However, with expandingindications for HCT and widespread use of alternative donors and non-myeloablativeconditioning regimens, graft rejection rates of 12–15% have been reported [3–5]. Factorsinfluencing graft rejection include underlying diseases, previous chemotherapy, graft sourcesand composition, degrees of HLA disparity, intensity of conditioning regimens and graft-versus-host disease (GVHD) prophylaxis. In general, graft rejection has been associated withpoor outcome [6].
Management of graft rejection is challenging, due to cytopenias, infections and organ toxicityresulting from the preparative regimens. Salvage allogeneic HCT represented a possibletherapeutic strategy, although the available literature has been limited to small, singleinstitution series [7–12]. The early experience with second allogeneic HCTs usingmyeloablative conditioning at the Fred Hutchinson Cancer Research Center was summarizedby Radich et al [13]. Seventy seven patients with hematologic malignancies underwent secondallogeneic HCTs for relapse after allogeneic marrow transplantation following high-dosechemotherapy and total body irradiation (TBI). In this series, patients older than 10 years hada 60% risk of non-relapse mortality (NRM) at 1 year. Second allogeneic HCTs were moresuccessful in patients with severe aplastic anemia, who received cyclophosphamide-basedconditioning regimens for both their first and second transplants (10-year survival was 83%for patients undergoing 2nd HCT between 1982 and 1996) [14].
In general, second myeloablative HCT, particularly in adults, has been associated with serioustoxicities. For this reason, reduced intensity regimens were designed to escalate hostimmunosuppression necessary for successful engraftment. Baron et al. [15] describedallogeneic HCTs after nonmyeloablative conditioning (2 Gy of TBI with or withoutfludarabine) in patients who had experienced relapse after autologous (n=137) or allogeneic(n=10) myeloablative HCT. The overall 3-year NRM rate was approximately 30%.
Here we summarize the multicenter experience with salvage allogeneic HCT in 38 patientswith primary or secondary allograft rejection, using fludarabine and TBI of 3 or 4 Gy aspreparative regimen.
PATIENTS AND METHODSPatients
This retrospective analysis included 38 consecutive patients with primary (n=18) or secondary(n=20) allograft rejection who underwent salvage allogeneic HCT after conditioning withfludarabine and low dose TBI (3 or 4 Gy) between March 2000 and November 2007 at 3participating centers: the Fred Hutchinson Cancer Research Center (FHCRC; n=16), StanfordUniversity (SU; n=11) and the University of Leipzig (UL; n=11). Primary graft rejection wasdefined as failure to detect more than 5% donor CD3+ T cells in the peripheral blood at anytime point after HCT. Engraftment with mixed chimerism was defined as attainment of between5% to 95% donor peripheral blood CD3+ T-cells at day 28. Following initial engraftment, adecline in donor peripheral blood CD3+ T-cells to ≤ 5% was considered secondary graftrejection. Patients with evidence of relapse/progression of their underlying disease followingtheir first allograft were not included in this study.
Gyurkocza et al. Page 2
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
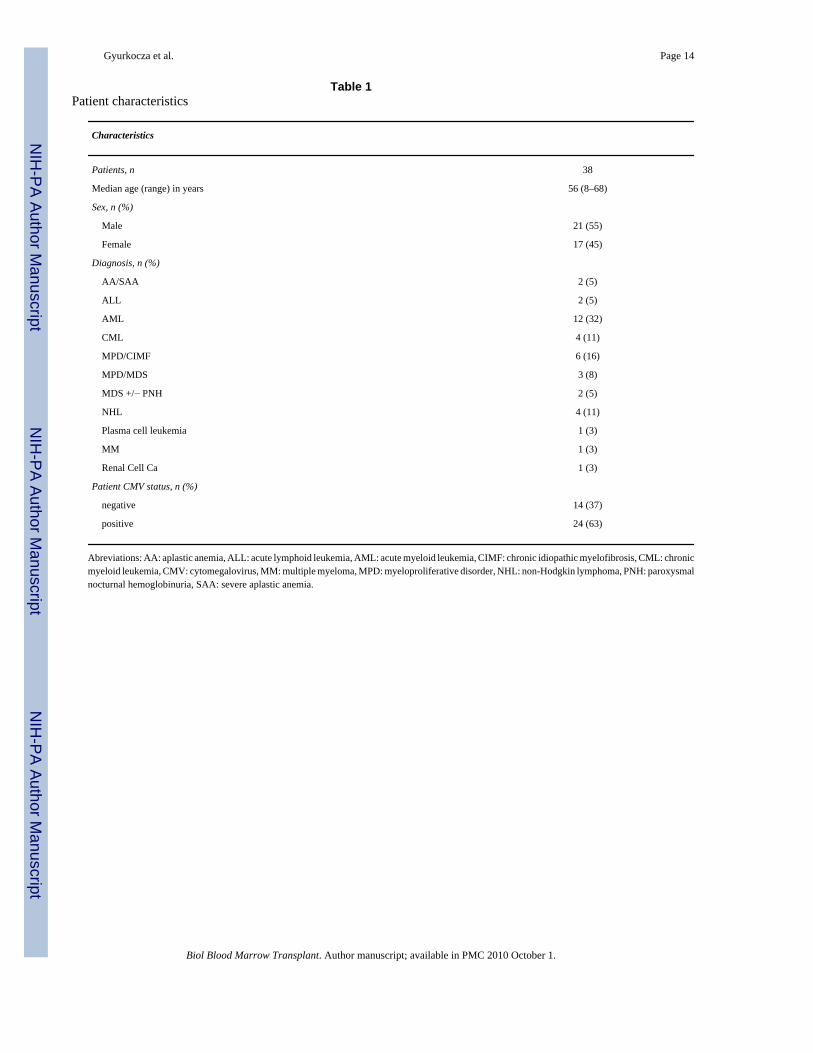
Results were analyzed as of July 28, 2008. Patient characteristics are summarized in Table 1.Thirty-six patients had failed one, one patient had failed two and one patient failed threepreceding allogeneic transplants. Three patients had autologous HCTs before their firstallogeneic HCTs. There were 21 males and 17 females. Median age of patients was 56 (range:8 – 68) years; with one exception patients were older than 21 years. Diagnoses includedhematologic malignancies (acute myeloid leukemia, n=12; myeloproliferative disorder/chronic idiopathic myelofibrosis, n=6; chronic myeloid leukemia, n=4; non-Hodgkinlymphoma, n=4; myelodysplastic syndrome(MDS)/myeloproliferative disorder (MPD)overlap syndrome, n=3; acute lymphoid leukemia n=2; MDS with or without paroxysmalnocturnal hemoglobinuria, n=2; multiple myeloma, n=1; plasma cell leukemia, n=1); aplasticanemia, (n=2); and renal cell cancer, (n=1).
A retrospective chart review and waiver of informed consent for chart review were approvedby the institutional review boards of all 3 participating Centers.
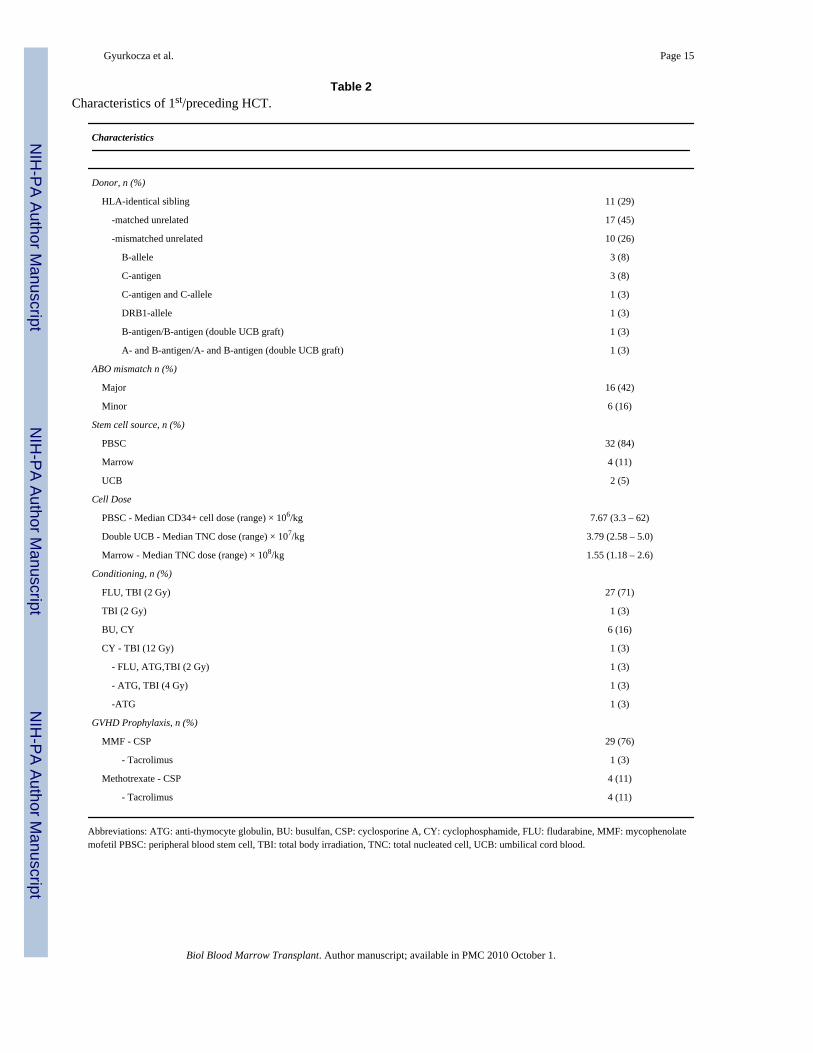
First/Preceding HCTsCharacteristics of the first/preceding allogeneic HCT are summarized in Table 2. With theexception of the unrelated umbilical cord blood units (UCB), patients and donors were testedfor HLA-A, -B, -C and -DQB1 by at least intermediate-resolution DNA typing and for HLA-DRB1 by high-resolution techniques. Cord blood units were tested for HLA-A and B antigensand DRB1 alleles. Grafts were from HLA-identical siblings (n=11), HLA-matched unrelateddonors (n=17) and HLA-mismatched unrelated donors (n=10, including 2 patients whoreceived double unrelated UCB grafts). Additional details of HLA-disparity, including thenumber of mismatched HLA loci are summarized in Table 2. The stem cell sources weregranulocyte colony-stimulating factor-mobilized peripheral blood stem cell (PBSC; n=32),bone marrow (n=4) or UCB (n=2). The median CD34+ cell dose for PBSC grafts was 7.67 ×106 CD 34+ cells/kg recipient weight. The median total nucleated cell count of bone marrowand double UCB grafts were 1.55 × 108/ kg and 3.79 × 107/kg recipient weight, respectively.A total of 28 patients received non-myeloablative conditioning with 2 Gy TBI on day 0 with(n=27) or without (n=1) fludarabine 30 mg/m2/day on days −4 through −2. Seven patientsreceived myeloablative conditioning with busulfan (n=6) or 12 Gy fractionated TBI (n=1)combined with cyclophosphamide. Three patients received anti-thymocyte globulin (ATG)combined with either cyclophosphamide (n=1), cyclophosphamide/4 Gy TBI (n=1), orcyclophosphamide/fludarabine/2 Gy TBI (n=1). Postgrafting immunosuppression for the 29patients receiving non-myeloablative or ATG/low dose TBI-based conditioning consisted ofmycophenolate mofetil (MMF) and cyclosporine (CSP), as described [16].
One patient given non-myeloablative conditioning received tacrolimus and MMF. Patientsundergoing myeloablative conditioning received methotrexate and either CSP (n=4) ortacrolimus (n=4), as described [17,18]. Following HCT, patients were monitored with dailyblood counts for evidence of engraftment. Donor chimerism was evaluated in peripheral bloodCD3+ T-cells and granulocytes (CD33+ cells at FHCRC and CD15+ cells at SU and UL)separated by flow cytometry. Donor-host chimerism levels were evaluated on day 28, and, onmost patients on days 84, 180 and 360 after HCT using polymerase chain reaction-basedamplification of variable-number tandem repeat or short-tandem repeat sequences unique todonors and hosts, or by fluorescent in situ hybridization for X and Y chromosomes in somecases when patients and donors were sex mismatched.
Primary graft rejection was defined as inability to detect more than 5% donor CD3+ T cells inthe peripheral blood at any time point after HCT. Following initial engraftment, a reduction indonor peripheral blood CD3+ T-cells to ≤ 5% was considered secondary graft rejection, asdetailed above. Based on these definitions 18 of 38 patients experienced primary graft rejection;the remaining 20 had secondary graft rejection.
Gyurkocza et al. Page 3
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

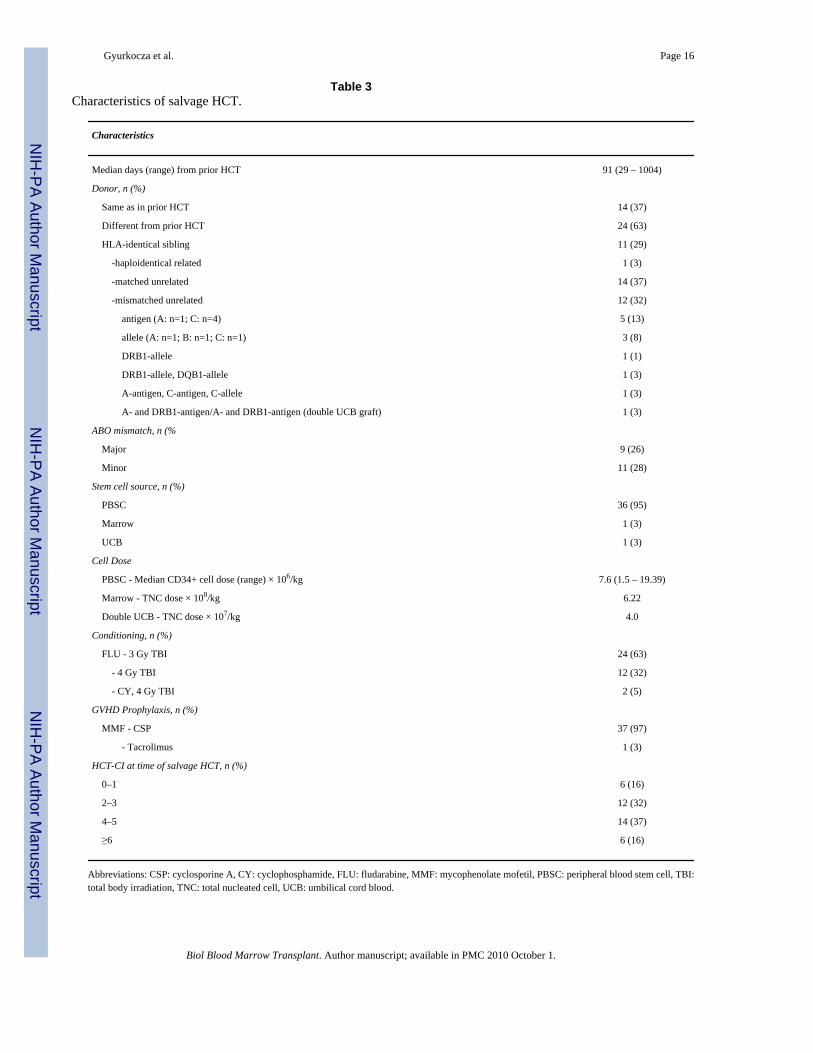
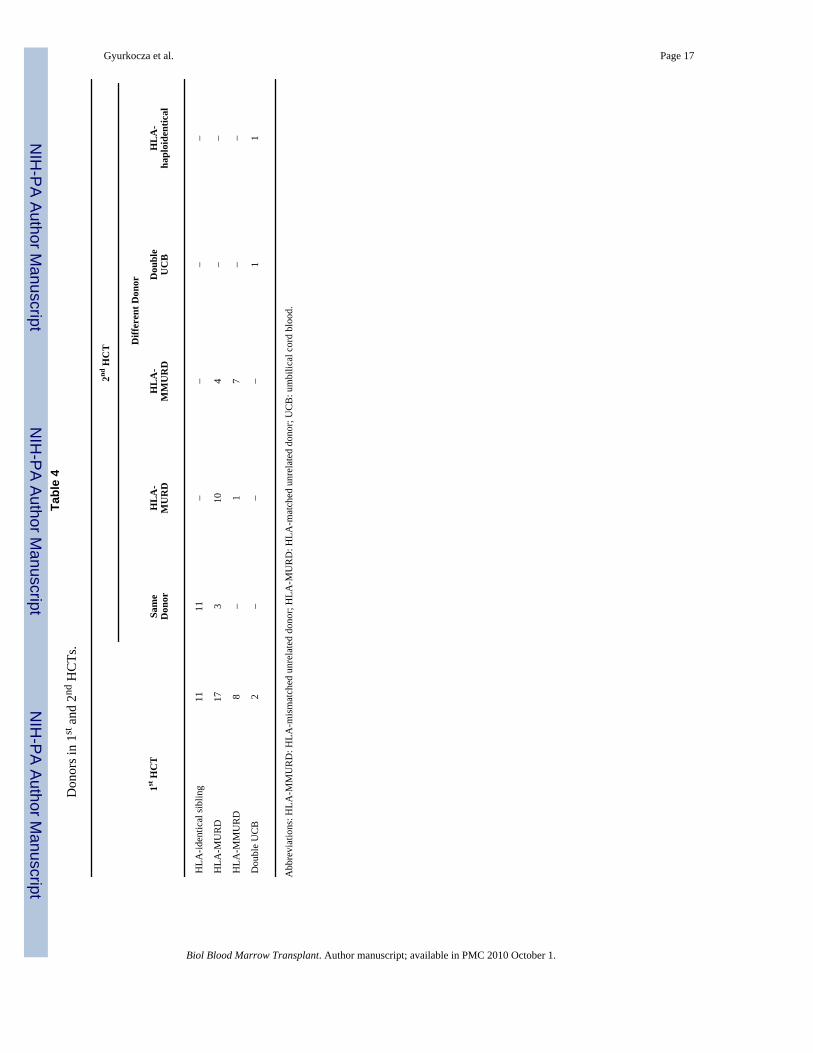
Second/Salvage HCTsCharacteristics of the 2nd/salvage allogeneic HCT are summarized in Table 3. HLA typing,patient monitoring and chimerism testing were carried out as described above. None of thepatients included in this analysis had evidence of relapse/progression of their underlyingdisease at the time of salvage allogeneic HCT. Pretransplantation comorbidities weredetermined retrospectively using an HCT-specific comorbidity index (HCT-CI) [19]. SalvageHCTs were performed at a median of 91 (range: 29 – 1004) days after the preceding HCT. Ifpatients had HLA-identical sibling donors for their preceding HCT, the same donors were usedfor salvage HCT, depending on their availability. When patients had HLA-matched unrelateddonors for their previous HCT, different donor were utilized for salvage HCT, except in 3patients. In summary, donors for the second HCT were the same as for the first in 14 cases; 11were HLA-identical siblings and 3 HLA-matched unrelated donors. In the remaining 24 casesdifferent donors were used; 11 were HLA-matched unrelated, 11 HLA-mismatched unrelated,one HLA-haploidentical related and one double UCB graft (Table 4). Additional details ofHLA-disparity, including the number of mismatched HLA loci are shown in Table 3. The stemcell sources were PBSC (n=36), bone marrow (HLA-haploidentical donor, n=1) or UCB (n=1).The median CD34+ cell count for PBSC grafts was 7.6 × 106 CD 34+ cells/kg recipient weight,the TNC counts were 6.22 × 108/kg recipient weight and 4.0 × 107/kg recipient weight for themarrow and double UCB grafts, respectively. The conditioning regimens consisted offludarabine 30mg/m2/day on days −4 to −2, followed by 3 Gy TBI (n=24) or 4 Gy TBI (n=12)on day 0. The determination of the TBI dose (3 vs. 4 Gy) was center-dependent. Except for 2patients with HLA-identical sibling donors, all patients treated at FHCRC received 4 Gy TBI.All patients treated at SU and at the UL received 3 Gy TBI. One HLA-haploidentical recipientreceived fludarabine, 30 mg/m2/day on days −6 to −2, cyclophosphamide, 25 mg/kg on days−6 and −5, and 4 Gy TBI on day −1. Another patient given a double UCB graft was conditionedwith fludarabine, 40 mg/m2/day on days −6 to −2, cyclophosphamide, 50 mg/kg on day −6,and 4 Gy TBI on day −1. Postgrafting immunosuppression for 37 patients consisted of CSPand MMF, as described [16] and tacrolimus and MMF for one patient. Acute and chronicGVHD were graded as described [20,21]. Toxicities occurring within the first 100 days werescored using the Common Terminology Criteria for Adverse Events v3.0.
Causes of deathIn patients who relapsed or progressed, relapse/progression was listed as primary cause of deathregardless of other associated events. In patients with GVHD requiring immunosuppressivetherapy who subsequently died from infections, GVHD/infection were listed as cause of death.Infection was listed as cause of death when it occurred in the absence of relapse/progressionor GVHD. All deaths occurring in the absence of relapse/progression were considered non-relapse mortality (NRM).
Statistical AnalysisSummary statistics were reported using standard measures as appropriate for categorical andcontinuous data. The primary end point of this retrospective analysis was engraftment.Secondary end points included: overall survival, NRM, relapse/progression, acute and chronicGVHD.
Overall survival was estimated using the Kaplan-Meier method. Cumulative incidenceestimates were used for engraftment, relapse/progression, acute and chronic GVHD and NRM,treating death prior to the event of interest as a competing risk for engraftment, relapse andacute GVHD, and relapse as competing risk event for NRM [22]. Associated 95% confidenceintervals were calculated using Greenwood’s formula for Kaplan-Meier estimates and themethod described by Marubini and Valsecchi for cumulative incidence [23]. Comparisons
Gyurkocza et al. Page 4
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
between hazards of time to event outcomes were compared using the logrank test. All reportedp-values were two-sided and p-values less than 0.05 were considered significant.
RESULTSEngraftment
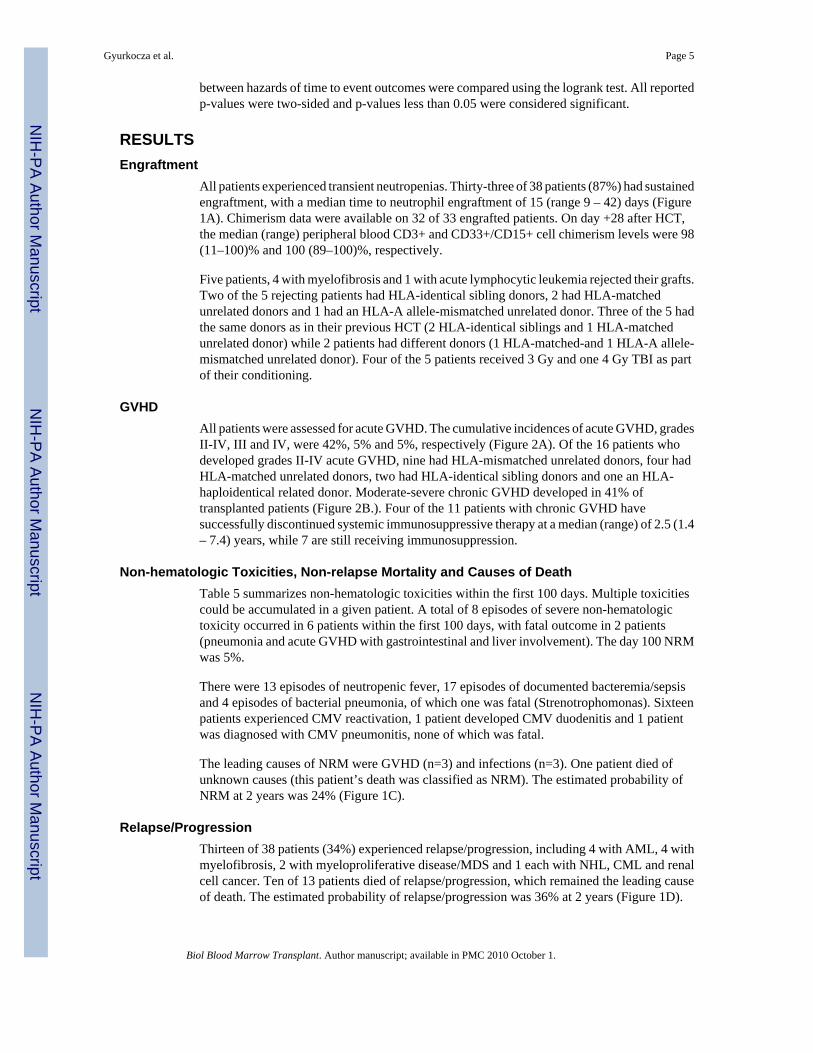
All patients experienced transient neutropenias. Thirty-three of 38 patients (87%) had sustainedengraftment, with a median time to neutrophil engraftment of 15 (range 9 – 42) days (Figure1A). Chimerism data were available on 32 of 33 engrafted patients. On day +28 after HCT,the median (range) peripheral blood CD3+ and CD33+/CD15+ cell chimerism levels were 98(11–100)% and 100 (89–100)%, respectively.
Five patients, 4 with myelofibrosis and 1 with acute lymphocytic leukemia rejected their grafts.Two of the 5 rejecting patients had HLA-identical sibling donors, 2 had HLA-matchedunrelated donors and 1 had an HLA-A allele-mismatched unrelated donor. Three of the 5 hadthe same donors as in their previous HCT (2 HLA-identical siblings and 1 HLA-matchedunrelated donor) while 2 patients had different donors (1 HLA-matched-and 1 HLA-A allele-mismatched unrelated donor). Four of the 5 patients received 3 Gy and one 4 Gy TBI as partof their conditioning.
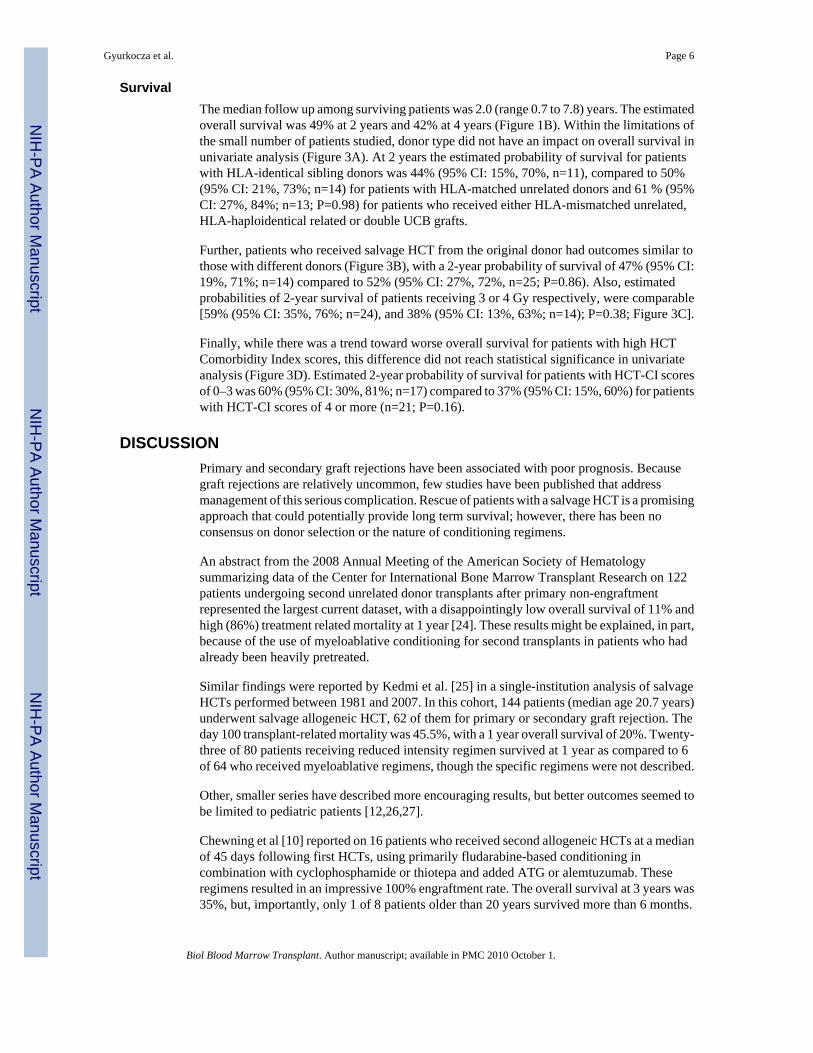
GVHDAll patients were assessed for acute GVHD. The cumulative incidences of acute GVHD, gradesII-IV, III and IV, were 42%, 5% and 5%, respectively (Figure 2A). Of the 16 patients whodeveloped grades II-IV acute GVHD, nine had HLA-mismatched unrelated donors, four hadHLA-matched unrelated donors, two had HLA-identical sibling donors and one an HLA-haploidentical related donor. Moderate-severe chronic GVHD developed in 41% oftransplanted patients (Figure 2B.). Four of the 11 patients with chronic GVHD havesuccessfully discontinued systemic immunosuppressive therapy at a median (range) of 2.5 (1.4– 7.4) years, while 7 are still receiving immunosuppression.
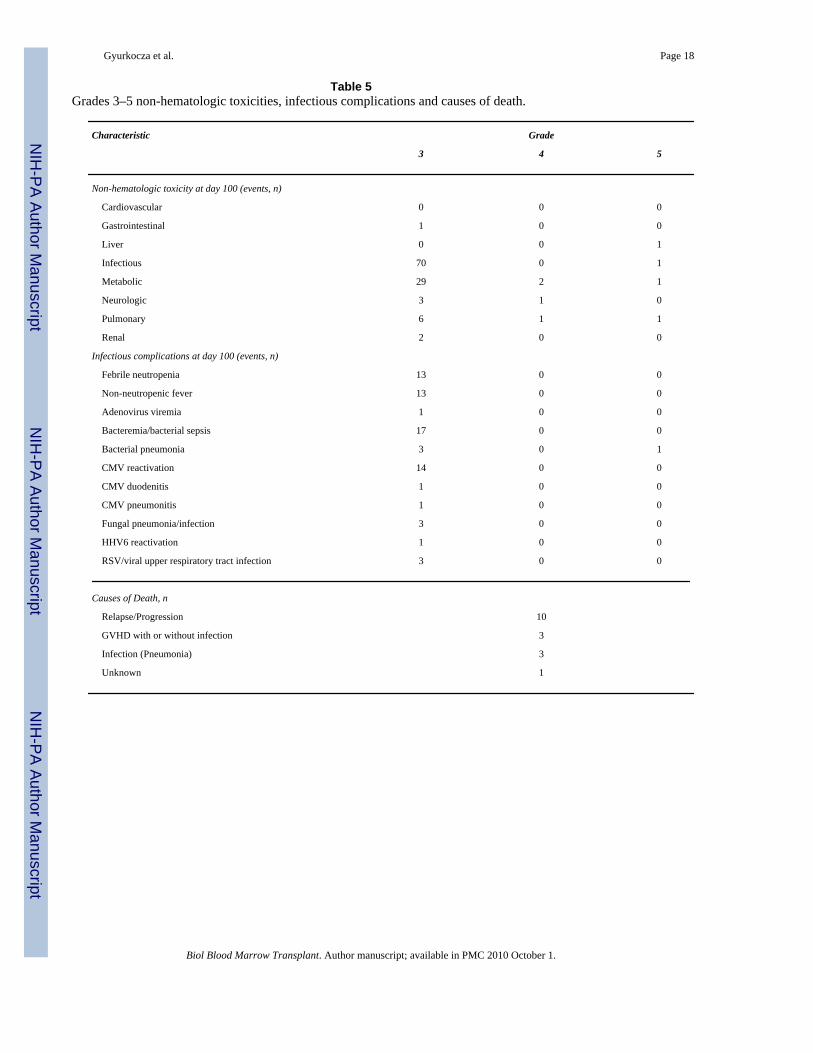
Non-hematologic Toxicities, Non-relapse Mortality and Causes of DeathTable 5 summarizes non-hematologic toxicities within the first 100 days. Multiple toxicitiescould be accumulated in a given patient. A total of 8 episodes of severe non-hematologictoxicity occurred in 6 patients within the first 100 days, with fatal outcome in 2 patients(pneumonia and acute GVHD with gastrointestinal and liver involvement). The day 100 NRMwas 5%.
There were 13 episodes of neutropenic fever, 17 episodes of documented bacteremia/sepsisand 4 episodes of bacterial pneumonia, of which one was fatal (Strenotrophomonas). Sixteenpatients experienced CMV reactivation, 1 patient developed CMV duodenitis and 1 patientwas diagnosed with CMV pneumonitis, none of which was fatal.
The leading causes of NRM were GVHD (n=3) and infections (n=3). One patient died ofunknown causes (this patient’s death was classified as NRM). The estimated probability ofNRM at 2 years was 24% (Figure 1C).
Relapse/ProgressionThirteen of 38 patients (34%) experienced relapse/progression, including 4 with AML, 4 withmyelofibrosis, 2 with myeloproliferative disease/MDS and 1 each with NHL, CML and renalcell cancer. Ten of 13 patients died of relapse/progression, which remained the leading causeof death. The estimated probability of relapse/progression was 36% at 2 years (Figure 1D).
Gyurkocza et al. Page 5
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
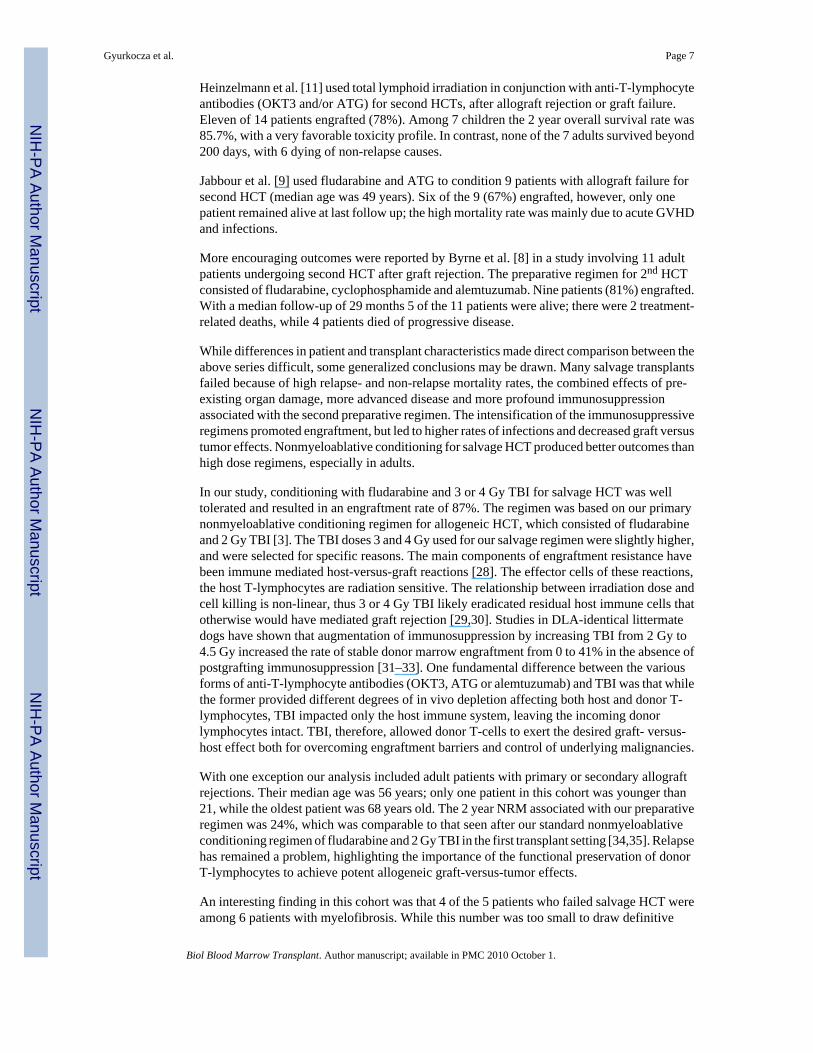
SurvivalThe median follow up among surviving patients was 2.0 (range 0.7 to 7.8) years. The estimatedoverall survival was 49% at 2 years and 42% at 4 years (Figure 1B). Within the limitations ofthe small number of patients studied, donor type did not have an impact on overall survival inunivariate analysis (Figure 3A). At 2 years the estimated probability of survival for patientswith HLA-identical sibling donors was 44% (95% CI: 15%, 70%, n=11), compared to 50%(95% CI: 21%, 73%; n=14) for patients with HLA-matched unrelated donors and 61 % (95%CI: 27%, 84%; n=13; P=0.98) for patients who received either HLA-mismatched unrelated,HLA-haploidentical related or double UCB grafts.
Further, patients who received salvage HCT from the original donor had outcomes similar tothose with different donors (Figure 3B), with a 2-year probability of survival of 47% (95% CI:19%, 71%; n=14) compared to 52% (95% CI: 27%, 72%, n=25; P=0.86). Also, estimatedprobabilities of 2-year survival of patients receiving 3 or 4 Gy respectively, were comparable[59% (95% CI: 35%, 76%; n=24), and 38% (95% CI: 13%, 63%; n=14); P=0.38; Figure 3C].
Finally, while there was a trend toward worse overall survival for patients with high HCTComorbidity Index scores, this difference did not reach statistical significance in univariateanalysis (Figure 3D). Estimated 2-year probability of survival for patients with HCT-CI scoresof 0–3 was 60% (95% CI: 30%, 81%; n=17) compared to 37% (95% CI: 15%, 60%) for patientswith HCT-CI scores of 4 or more (n=21; P=0.16).
DISCUSSIONPrimary and secondary graft rejections have been associated with poor prognosis. Becausegraft rejections are relatively uncommon, few studies have been published that addressmanagement of this serious complication. Rescue of patients with a salvage HCT is a promisingapproach that could potentially provide long term survival; however, there has been noconsensus on donor selection or the nature of conditioning regimens.
An abstract from the 2008 Annual Meeting of the American Society of Hematologysummarizing data of the Center for International Bone Marrow Transplant Research on 122patients undergoing second unrelated donor transplants after primary non-engraftmentrepresented the largest current dataset, with a disappointingly low overall survival of 11% andhigh (86%) treatment related mortality at 1 year [24]. These results might be explained, in part,because of the use of myeloablative conditioning for second transplants in patients who hadalready been heavily pretreated.
Similar findings were reported by Kedmi et al. [25] in a single-institution analysis of salvageHCTs performed between 1981 and 2007. In this cohort, 144 patients (median age 20.7 years)underwent salvage allogeneic HCT, 62 of them for primary or secondary graft rejection. Theday 100 transplant-related mortality was 45.5%, with a 1 year overall survival of 20%. Twenty-three of 80 patients receiving reduced intensity regimen survived at 1 year as compared to 6of 64 who received myeloablative regimens, though the specific regimens were not described.
Other, smaller series have described more encouraging results, but better outcomes seemed tobe limited to pediatric patients [12,26,27].
Chewning et al [10] reported on 16 patients who received second allogeneic HCTs at a medianof 45 days following first HCTs, using primarily fludarabine-based conditioning incombination with cyclophosphamide or thiotepa and added ATG or alemtuzumab. Theseregimens resulted in an impressive 100% engraftment rate. The overall survival at 3 years was35%, but, importantly, only 1 of 8 patients older than 20 years survived more than 6 months.
Gyurkocza et al. Page 6
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Heinzelmann et al. [11] used total lymphoid irradiation in conjunction with anti-T-lymphocyteantibodies (OKT3 and/or ATG) for second HCTs, after allograft rejection or graft failure.Eleven of 14 patients engrafted (78%). Among 7 children the 2 year overall survival rate was85.7%, with a very favorable toxicity profile. In contrast, none of the 7 adults survived beyond200 days, with 6 dying of non-relapse causes.
Jabbour et al. [9] used fludarabine and ATG to condition 9 patients with allograft failure forsecond HCT (median age was 49 years). Six of the 9 (67%) engrafted, however, only onepatient remained alive at last follow up; the high mortality rate was mainly due to acute GVHDand infections.
More encouraging outcomes were reported by Byrne et al. [8] in a study involving 11 adultpatients undergoing second HCT after graft rejection. The preparative regimen for 2nd HCTconsisted of fludarabine, cyclophosphamide and alemtuzumab. Nine patients (81%) engrafted.With a median follow-up of 29 months 5 of the 11 patients were alive; there were 2 treatment-related deaths, while 4 patients died of progressive disease.
While differences in patient and transplant characteristics made direct comparison between theabove series difficult, some generalized conclusions may be drawn. Many salvage transplantsfailed because of high relapse- and non-relapse mortality rates, the combined effects of pre-existing organ damage, more advanced disease and more profound immunosuppressionassociated with the second preparative regimen. The intensification of the immunosuppressiveregimens promoted engraftment, but led to higher rates of infections and decreased graft versustumor effects. Nonmyeloablative conditioning for salvage HCT produced better outcomes thanhigh dose regimens, especially in adults.
In our study, conditioning with fludarabine and 3 or 4 Gy TBI for salvage HCT was welltolerated and resulted in an engraftment rate of 87%. The regimen was based on our primarynonmyeloablative conditioning regimen for allogeneic HCT, which consisted of fludarabineand 2 Gy TBI [3]. The TBI doses 3 and 4 Gy used for our salvage regimen were slightly higher,and were selected for specific reasons. The main components of engraftment resistance havebeen immune mediated host-versus-graft reactions [28]. The effector cells of these reactions,the host T-lymphocytes are radiation sensitive. The relationship between irradiation dose andcell killing is non-linear, thus 3 or 4 Gy TBI likely eradicated residual host immune cells thatotherwise would have mediated graft rejection [29,30]. Studies in DLA-identical littermatedogs have shown that augmentation of immunosuppression by increasing TBI from 2 Gy to4.5 Gy increased the rate of stable donor marrow engraftment from 0 to 41% in the absence ofpostgrafting immunosuppression [31–33]. One fundamental difference between the variousforms of anti-T-lymphocyte antibodies (OKT3, ATG or alemtuzumab) and TBI was that whilethe former provided different degrees of in vivo depletion affecting both host and donor T-lymphocytes, TBI impacted only the host immune system, leaving the incoming donorlymphocytes intact. TBI, therefore, allowed donor T-cells to exert the desired graft- versus-host effect both for overcoming engraftment barriers and control of underlying malignancies.
With one exception our analysis included adult patients with primary or secondary allograftrejections. Their median age was 56 years; only one patient in this cohort was younger than21, while the oldest patient was 68 years old. The 2 year NRM associated with our preparativeregimen was 24%, which was comparable to that seen after our standard nonmyeloablativeconditioning regimen of fludarabine and 2 Gy TBI in the first transplant setting [34,35]. Relapsehas remained a problem, highlighting the importance of the functional preservation of donorT-lymphocytes to achieve potent allogeneic graft-versus-tumor effects.
An interesting finding in this cohort was that 4 of the 5 patients who failed salvage HCT wereamong 6 patients with myelofibrosis. While this number was too small to draw definitive
Gyurkocza et al. Page 7
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
conclusions, results suggested that alternative conditioning regimens should be developed forpatients with myelofibrosis, who have failed their first HCT. Graft rejection has been aconsiderable problem in these patients after other conditioning regimens as well [36].
Based on the current analysis, we concluded that graft rejection following allogeneic HCTcould be effectively corrected by salvage transplantation using conditioning with fludarabineand 3 or 4 Gy TBI, with resultant long-term survival in 40–50% of patients. This treatmentmodality could be offered to older patients, to those lacking HLA-identical sibling donors andto patients with comorbid conditions.
ACKNOWLEDGMENTSThe authors wish to thank the research nurses Michelle Bouvier and Hsien-Tzu Chen and data manager GresfordThomas for their invaluable help in making the study possible. The authors also wish to thank Helen Crawford, BonnieLarson and Sue Carbonneau for manuscript preparation, and the transplant teams, physicians, nurses, and supportpersonnel for their care of patients on this study.
Grant support
This study was supported by grants CA78902, CA18029, CA15704 and CA49605 from the National Cancer Institute,HL088021 and HL36444 from the National Heart, Lung, and Blood Institute.
REFERENCES1. Thomas ED, Storb R, Clift RA, et al. Bone-marrow transplantation. N Engl J Med 1975;292:832–843.
[PubMed: 234595]895–9022. Kernan NA, Bartsch G, Ash RC, et al. Analysis of 462 transplantations from unrelated donors facilitated
by The National Marrow Donor Program. N Engl J Med 1993;328:593–602. [PubMed: 8429851]3. Niederwieser D, Maris M, Shizuru JA, et al. Low-dose total body irradiation (TBI) and fludarabine
followed by hematopoietic cell transplantation (HCT) from HLA-matched or mismatched unrelateddonors and postgrafting immunosuppression with cyclosporine and mycophenolate mofetil (MMF)can induce durable complete chimerism and sustained remissions in patients with hematologicaldiseases. Blood 2003;101:1620–1629. [PubMed: 12393457]
4. Maris MB, Niederwieser D, Sandmaier BM, et al. HLA-matched unrelated donor hematopoietic celltransplantation after nonmyeloablative conditioning for patients with hematologic malignancies.Blood 2003;102:2021–2030. [PubMed: 12791654]
5. Laport GG, Sandmaier BM, Storer BE, et al. Reduced-intensity conditioning followed by allogeneichematopoietic cell transplantation for adult patients with myelodysplastic syndrome andmyeloproliferative disorders. Biol Blood Marrow Transplant 2008;14:246–255. [PubMed: 18215785]
6. Rondon G, Saliba RM, Khouri I, et al. Long-term follow-up of patients who experienced graft failurepostallogeneic progenitor cell transplantation. Results of a single institution analysis. Biol BloodMarrow Transplant 2008;14:859–866. [PubMed: 18640568]
7. Ruiz-Arguelles GJ, Gomez-Almaguer D, Tarin-Arzaga LD, Morales-Toquero A, Cantu-RodriguezOG, Manzano C. Second allogeneic peripheral blood stem cell transplants with reduced-intensityconditioning. Revista de Investigacion Clinica 2006;58:34–38. [PubMed: 16789597]
8. Byrne BJ, Horwitz M, Long GD, et al. Outcomes of a second non-myeloablative allogeneic stem celltransplantation following graft rejection. Bone Marrow Transplant 2008;41:39–43. [PubMed:17982503]
9. Jabbour E, Rondon G, Anderlini P, et al. Treatment of donor graft failure with nonmyeloablativeconditioning of fludarabine, antithymocyte globulin and a second allogeneic hematopoietictransplantation. Bone Marrow Transplant 2007;40:431–435. [PubMed: 17603511]
10. Chewning JH, Castro-Malaspina H, Jakubowski A, et al. Fludarabine-based conditioning securesengraftment of second hematopoietic stem cell allografts (HSCT) in the treatment of initial graftfailure. Biol Blood Marrow Transplant 2007;13:1313–1323. [PubMed: 17950918]
11. Heinzelmann F, Lang PJ, Ottinger H, et al. Immunosuppressive total lymphoid irradiation-basedreconditioning regimens enable engraftment after graft rejection or graft failure in patients treated
Gyurkocza et al. Page 8
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

with allogeneic hematopoietic stem cell transplantation. Int J Radiat Oncol Biol Phys 2008;70:523–528. [PubMed: 17869449]
12. Ahmed N, Leung KS, Rosenblatt H, et al. Successful treatment of stem cell graft failure in pediatricpatients using a submyeloablative regimen of campath-1H and fludarabine. Biol Blood MarrowTransplant 2008;14:1298–1304. [PubMed: 18940685]
13. Radich JP, Sanders JE, Buckner CD, et al. Second allogeneic marrow transplantation for patients withrecurrent leukemia after initial transplant with total-body irradiation-containing regimens. J ClinOncol 1993;11:304–313. [PubMed: 8426208]
14. Stucki A, Leisenring W, Sandmaier BM, Sanders J, Anasetti C, Storb R. Decreased rejection andimproved survival of first and second marrow transplants for severe aplastic anemia (a 26-year oldretrospective analysis). Blood 1998;92:2742–2749. [PubMed: 9763558]
15. Baron F, Storb R, Storer BE, et al. Factors associated with outcomes in allogeneic hematopoietic celltransplantation with nonmyeloablative conditioning after failed myeloablative hematopietic celltransplantation. J Clin Oncol 2006;24:4150–4157. [PubMed: 16896000]
16. Baron F, Baker JE, Storb R, et al. Kinetics of engraftment in patients with hematologic malignanciesgiven allogeneic hematopoietic cell transplantation after nonmyeloablative conditioning. Blood2004;104:2254–2262. [PubMed: 15226174]
17. Storb R, Deeg HJ, Whitehead J, et al. Methotrexate and cyclosporine compared with cyclosporinealone for prophylaxis of acute graft versus host disease after marrow transplantation for leukemia.N Engl J Med 1986;314:729–735. [PubMed: 3513012]
18. Ratanatharathorn V, Nash RA, Devine SM, et al. Phase III study comparing tacrolimus (PrografFK506) with cyclosporine for graft-versus-host disease (GVHD) prophylaxis after HLA-identicalsibling bone marrow transplantation (BMT). Blood 1996;88(Part 1)459a, #1826[abstr.]
19. Sorror ML, Maris MB, Storb R, et al. Hematopoietic cell transplantation (HCT)-specific comorbidityindex: a new tool for risk assessment before allogeneic HCT. Blood 2005;106:2912–2919. [PubMed:15994282]
20. Przepiorka, D.; Weisdorf, D.; Martin, P., et al. Bone Marrow Transplant; 1994 Consensus conferenceon acute GVHD grading; 1995. p. 825-828.
21. Filipovich AH, Weisdorf D, Pavletic S, et al. National Institutes of Health consensus developmentproject on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and StagingWorking Group report. Biol Blood Marrow Transplant 2005;11:945–956. [PubMed: 16338616]
22. Gooley TA, Leisenring W, Crowley J, Storer BE. Estimation of failure probabilities in the presenceof competing risks: new representations of old estimators. Stat Med 1999;18:695–706. [PubMed:10204198]
23. Marubini, E.; Valsecchi, MG. Analyzing Survival Data from Clinical Trials and ObservationalStudies. Chichester, NY: John Wiley and Sons; 1995.
24. Schriber JR, Agovi MA, Ballen KK, et al. Second unrelated donor (URD) transplant as a rescuestrategy for 122 patients with primary non engraftment: results from CIBMTR. Blood 2008;112:295.[PubMed: 18332228]#794[abstr.]
25. Kedmi M, Resnick IB, Dray L, et al. A retrospective review of the outcome after second or subsequentallogeneic transplantation. Biol Blood Marrow Transplant 2009;15:483–489. [PubMed: 19285636]
26. Grandage VL, Cornish JM, Pamphilon DH, et al. Second allogeneic bone marrow transplants fromunrelated donors for graft failure following initial unrelated donor bone marrow transplantation. BoneMarrow Transplant 1998;21:687–690. [PubMed: 9578308]
27. Lang P, Mueller I, Greil J, et al. Retransplantation with stem cells from mismatched related donorsafter graft rejection in pediatric patients. Blood Cells Molecules and Diseases 2008;40:33–39.
28. Storb R, Yu C, Barnett T, et al. Stable mixed hematopoietic chimerism in dog leukocyte antigen-identical littermate dogs given lymph node irradiation before and pharmacologic immunosuppressionafter marrow transplantation. Blood 1999;94:1131–1136. [PubMed: 10419907]
29. Vriesendorp HM. Radiobiological speculations on therapeutic total body irradiation. Oncology/Hematology 1990;10:211–224.
30. Tarbell, NJ.; Chin, LM.; Mauch, PM. Total body irradiation for bone marrow transplantation. In:Mauch, PM.; Loeffler, JS., editors. Radiation Oncology: Technology and Biology. Philadelphia, PA:W.B. Saunders; 1994.
Gyurkocza et al. Page 9
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

31. Yu C, Storb R, Mathey B, et al. DLA-identical bone marrow grafts after low-dose total bodyirradiation: Effects of high-dose corticosteroids and cyclosporine on engraftment. Blood1995;86:4376–4381. [PubMed: 7492799]
32. Storb R, Raff RF, Appelbaum FR, et al. Fractionated versus single-dose total body irradiation at lowand high dose rates to condition canine littermates for DLA-identical marrow grafts. Blood1994;83:3384–3389. [PubMed: 8193376]
33. Storb R, Yu C, Wagner JL, et al. Stable mixed hematopoietic chimerism in DLA-identical littermatedogs given sublethal total body irradiation before and pharmacological immunosuppression aftermarrow transplantation. Blood 1997;89:3048–3054. [PubMed: 9108426]
34. Hegenbart U, Niederwieser D, Sandmaier BM, et al. Treatment for acute myelogenous leukemia bylow-dose, total-body, irradiation-based conditioning and hematopoietic cell transplantation fromrelated and unrelated donors. J Clin Oncol 2006;24:444–453. [PubMed: 16344316]
35. Rezvani AR, Norasetthada L, Gooley T, et al. Non-myeloablative allogeneic haematopoietic celltransplantation of relapsed diffuse large B-cell lymphoma: a multicentre experience. Br J Haematol2008;143:395–403. [PubMed: 18759762]
36. Kerbauy DMB, Gooley TA, Sale GE, et al. Hematopoietic cell transplantation as curative therapy foridiopathic myelofibrosis, advanced polycythemia vera, and essential thrombocythemia. Biol BloodMarrow Transplant 2007;13:355–365. [PubMed: 17317589]
Gyurkocza et al. Page 10
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
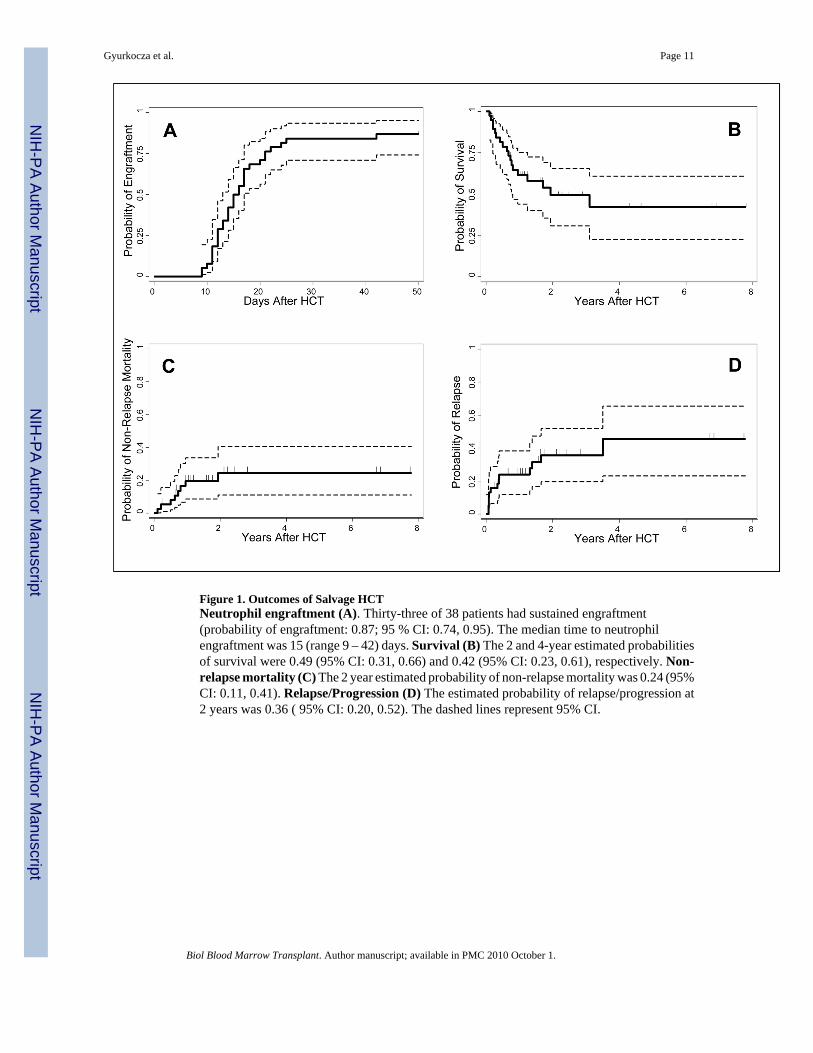
Figure 1. Outcomes of Salvage HCTNeutrophil engraftment (A). Thirty-three of 38 patients had sustained engraftment(probability of engraftment: 0.87; 95 % CI: 0.74, 0.95). The median time to neutrophilengraftment was 15 (range 9 – 42) days. Survival (B) The 2 and 4-year estimated probabilitiesof survival were 0.49 (95% CI: 0.31, 0.66) and 0.42 (95% CI: 0.23, 0.61), respectively. Non-relapse mortality (C) The 2 year estimated probability of non-relapse mortality was 0.24 (95%CI: 0.11, 0.41). Relapse/Progression (D) The estimated probability of relapse/progression at2 years was 0.36 ( 95% CI: 0.20, 0.52). The dashed lines represent 95% CI.
Gyurkocza et al. Page 11
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
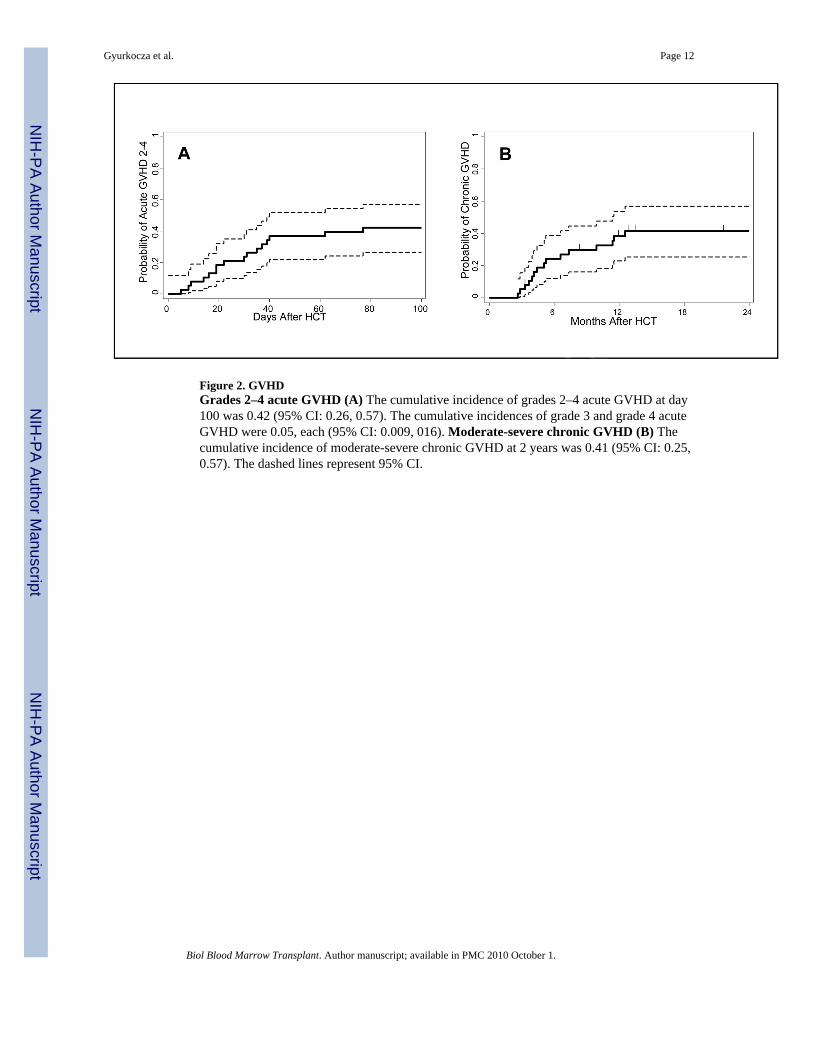
Figure 2. GVHDGrades 2–4 acute GVHD (A) The cumulative incidence of grades 2–4 acute GVHD at day100 was 0.42 (95% CI: 0.26, 0.57). The cumulative incidences of grade 3 and grade 4 acuteGVHD were 0.05, each (95% CI: 0.009, 016). Moderate-severe chronic GVHD (B) Thecumulative incidence of moderate-severe chronic GVHD at 2 years was 0.41 (95% CI: 0.25,0.57). The dashed lines represent 95% CI.
Gyurkocza et al. Page 12
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
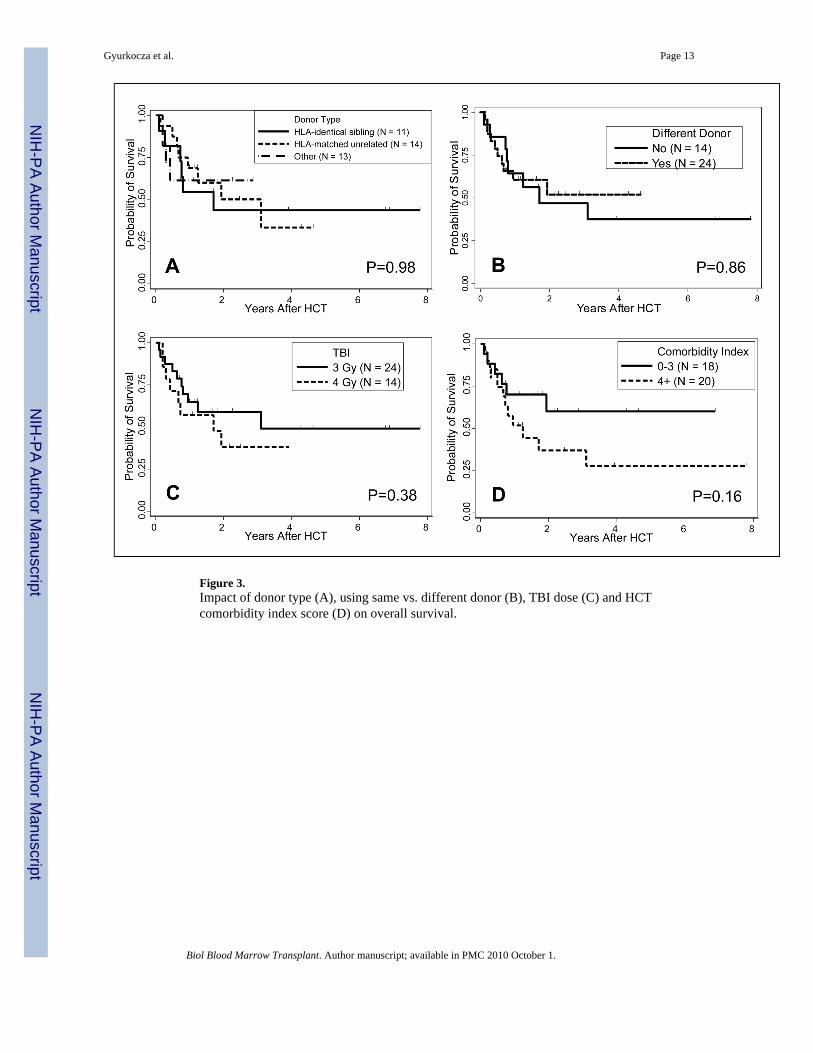
Figure 3.Impact of donor type (A), using same vs. different donor (B), TBI dose (C) and HCTcomorbidity index score (D) on overall survival.
Gyurkocza et al. Page 13
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Gyurkocza et al. Page 14
Table 1Patient characteristics
Characteristics
Patients, n 38
Median age (range) in years 56 (8–68)
Sex, n (%)
Male 21 (55)
Female 17 (45)
Diagnosis, n (%)
AA/SAA 2 (5)
ALL 2 (5)
AML 12 (32)
CML 4 (11)
MPD/CIMF 6 (16)
MPD/MDS 3 (8)
MDS +/− PNH 2 (5)
NHL 4 (11)
Plasma cell leukemia 1 (3)
MM 1 (3)
Renal Cell Ca 1 (3)
Patient CMV status, n (%)
negative 14 (37)
positive 24 (63)
Abreviations: AA: aplastic anemia, ALL: acute lymphoid leukemia, AML: acute myeloid leukemia, CIMF: chronic idiopathic myelofibrosis, CML: chronicmyeloid leukemia, CMV: cytomegalovirus, MM: multiple myeloma, MPD: myeloproliferative disorder, NHL: non-Hodgkin lymphoma, PNH: paroxysmalnocturnal hemoglobinuria, SAA: severe aplastic anemia.
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Gyurkocza et al. Page 15
Table 2Characteristics of 1st/preceding HCT.
Characteristics
Donor, n (%)
HLA-identical sibling 11 (29)
-matched unrelated 17 (45)
-mismatched unrelated 10 (26)
B-allele 3 (8)
C-antigen 3 (8)
C-antigen and C-allele 1 (3)
DRB1-allele 1 (3)
B-antigen/B-antigen (double UCB graft) 1 (3)
A- and B-antigen/A- and B-antigen (double UCB graft) 1 (3)
ABO mismatch n (%)
Major 16 (42)
Minor 6 (16)
Stem cell source, n (%)
PBSC 32 (84)
Marrow 4 (11)
UCB 2 (5)
Cell Dose
PBSC - Median CD34+ cell dose (range) × 106/kg 7.67 (3.3 – 62)
Double UCB - Median TNC dose (range) × 107/kg 3.79 (2.58 – 5.0)
Marrow - Median TNC dose (range) × 108/kg 1.55 (1.18 – 2.6)
Conditioning, n (%)
FLU, TBI (2 Gy) 27 (71)
TBI (2 Gy) 1 (3)
BU, CY 6 (16)
CY - TBI (12 Gy) 1 (3)
- FLU, ATG,TBI (2 Gy) 1 (3)
- ATG, TBI (4 Gy) 1 (3)
-ATG 1 (3)
GVHD Prophylaxis, n (%)
MMF - CSP 29 (76)
- Tacrolimus 1 (3)
Methotrexate - CSP 4 (11)
- Tacrolimus 4 (11)
Abbreviations: ATG: anti-thymocyte globulin, BU: busulfan, CSP: cyclosporine A, CY: cyclophosphamide, FLU: fludarabine, MMF: mycophenolatemofetil PBSC: peripheral blood stem cell, TBI: total body irradiation, TNC: total nucleated cell, UCB: umbilical cord blood.
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Gyurkocza et al. Page 16
Table 3Characteristics of salvage HCT.
Characteristics
Median days (range) from prior HCT 91 (29 – 1004)
Donor, n (%)
Same as in prior HCT 14 (37)
Different from prior HCT 24 (63)
HLA-identical sibling 11 (29)
-haploidentical related 1 (3)
-matched unrelated 14 (37)
-mismatched unrelated 12 (32)
antigen (A: n=1; C: n=4) 5 (13)
allele (A: n=1; B: n=1; C: n=1) 3 (8)
DRB1-allele 1 (1)
DRB1-allele, DQB1-allele 1 (3)
A-antigen, C-antigen, C-allele 1 (3)
A- and DRB1-antigen/A- and DRB1-antigen (double UCB graft) 1 (3)
ABO mismatch, n (%
Major 9 (26)
Minor 11 (28)
Stem cell source, n (%)
PBSC 36 (95)
Marrow 1 (3)
UCB 1 (3)
Cell Dose
PBSC - Median CD34+ cell dose (range) × 106/kg 7.6 (1.5 – 19.39)
Marrow - TNC dose × 108/kg 6.22
Double UCB - TNC dose × 107/kg 4.0
Conditioning, n (%)
FLU - 3 Gy TBI 24 (63)
- 4 Gy TBI 12 (32)
- CY, 4 Gy TBI 2 (5)
GVHD Prophylaxis, n (%)
MMF - CSP 37 (97)
- Tacrolimus 1 (3)
HCT-CI at time of salvage HCT, n (%)
0–1 6 (16)
2–3 12 (32)
4–5 14 (37)
≥6 6 (16)
Abbreviations: CSP: cyclosporine A, CY: cyclophosphamide, FLU: fludarabine, MMF: mycophenolate mofetil, PBSC: peripheral blood stem cell, TBI:total body irradiation, TNC: total nucleated cell, UCB: umbilical cord blood.
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Gyurkocza et al. Page 17Ta
ble
4D
onor
s in
1st a
nd 2
nd H
CTs
.
2nd H
CT D
iffer
ent D
onor
1st H
CT
Sam
eD
onor
HL
A-
MU
RD
HL
A-
MM
UR
DD
oubl
eU
CB
HL
A-
hapl
oide
ntic
al
HLA
-iden
tical
sibl
ing
1111
––
––
HLA
-MU
RD
173
104
––
HLA
-MM
UR
D8
–1
7–
–
Dou
ble
UC
B2
––
–1
1
Abb
revi
atio
ns: H
LA-M
MU
RD
: HLA
-mis
mat
ched
unr
elat
ed d
onor
; HLA
-MU
RD
: HLA
-mat
ched
unr
elat
ed d
onor
; UC
B: u
mbi
lical
cor
d bl
ood.
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2010 October 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Gyurkocza et al. Page 18
Table 5Grades 3–5 non-hematologic toxicities, infectious complications and causes of death.
Characteristic Grade
3 4 5
Non-hematologic toxicity at day 100 (events, n)
Cardiovascular 0 0 0
Gastrointestinal 1 0 0
Liver 0 0 1
Infectious 70 0 1
Metabolic 29 2 1
Neurologic 3 1 0
Pulmonary 6 1 1
Renal 2 0 0
Infectious complications at day 100 (events, n)
Febrile neutropenia 13 0 0
Non-neutropenic fever 13 0 0
Adenovirus viremia 1 0 0
Bacteremia/bacterial sepsis 17 0 0
Bacterial pneumonia 3 0 1
CMV reactivation 14 0 0
CMV duodenitis 1 0 0
CMV pneumonitis 1 0 0
Fungal pneumonia/infection 3 0 0
HHV6 reactivation 1 0 0
RSV/viral upper respiratory tract infection 3 0 0
Causes of Death, n
Relapse/Progression 10
GVHD with or without infection 3
Infection (Pneumonia) 3
Unknown 1
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2010 October 1.