
Three-Year Outcomes of Cultured Limbal Epithelial Allografts in Aniridia and Stevens-Johnson...
13
Vernon, Genevieve A. Secker, Stephen J. Tuft and Julie T. Daniels Alex J. Shortt, Catey Bunce, Hannah J. Levis, Peter Blows, Caroline J. Doré, Amanda Surgical Trials Assessment Tool in Stevens-Johnson Syndrome Evaluated Using the Clinical Outcome Assessment Three-Year Outcomes of Cultured Limbal Epithelial Allografts in Aniridia and published online January 17, 2014 Stem Cells Trans Med http://stemcellstm.alphamedpress.org/content/early/2014/01/17/sctm.2013-0025 located on the World Wide Web at: The online version of this article, along with updated information and services, is by Alex Shortt on January 31, 2014 http://stemcellstm.alphamedpress.org/ Downloaded from by Alex Shortt on January 31, 2014 http://stemcellstm.alphamedpress.org/ Downloaded from
Transcript of Three-Year Outcomes of Cultured Limbal Epithelial Allografts in Aniridia and Stevens-Johnson...

Vernon, Genevieve A. Secker, Stephen J. Tuft and Julie T. DanielsAlex J. Shortt, Catey Bunce, Hannah J. Levis, Peter Blows, Caroline J. Doré, Amanda
Surgical Trials Assessment ToolinStevens-Johnson Syndrome Evaluated Using the Clinical Outcome Assessment
Three-Year Outcomes of Cultured Limbal Epithelial Allografts in Aniridia and
published online January 17, 2014Stem Cells Trans Med
http://stemcellstm.alphamedpress.org/content/early/2014/01/17/sctm.2013-0025located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by Alex Shortt on January 31, 2014
http://stemcellstm
.alphamedpress.org/
Dow
nloaded from
by Alex Shortt on January 31, 2014
http://stemcellstm
.alphamedpress.org/
Dow
nloaded from
Tissue Engineering and Regenerative Medicine
Three-Year Outcomes of Cultured Limbal EpithelialAllografts in Aniridia and Stevens-Johnson SyndromeEvaluated Using the Clinical Outcome Assessment inSurgical Trials Assessment Tool
ALEX J. SHORTT,a,b,c CATEY BUNCE,c HANNAH J. LEVIS,b PETER BLOWS,c CAROLINE J. DORE,d
AMANDA VERNON,a,b GENEVIEVE A. SECKER,a STEPHEN J. TUFT,a,c JULIE T. DANIELSa,b
KeyWords. Stemcell x Cornea x Stemcell deficiency x Stemcell transplantation x Outcomemeasures
ABSTRACT
Limbal stemcell deficiency (LSCD) is aneyedisorder inwhich the stemcells responsible for forming thesurface skin of the cornea are destroyed by disease. This results in pain, loss of vision, and a cosmet-ically unpleasant appearance. Many new treatments, including stem cell therapies, are emerging forthe treatment of this condition, but assessment of these new technologies is severely hampered bythe lack of biomarkers for this disease or validated tools for assessing its severity. The aims of thisstudywere to design and test the reliability of a tool for grading LSCD, to define a set of core outcomemeasures for use inevaluating treatments for this condition, and todemonstrate their utility. Thiswasachieved by using our defined outcome set (which included the Clinical Outcome Assessment in Sur-gical Trials of Limbal stemcell deficiency [COASTL] tool) toevaluate the3-yearoutcomes for allogeneicex vivo cultivated limbal epithelial transplantation (allo-CLET) in patientswhohad bilateral total LSCDsecondary to aniridia or Stevens-Johnson syndrome. The results demonstrate that our new gradingtool for LSCD, the COASTL tool, is reliable and repeatable, and that improvements in the biomarkersused in this tool correlate positivelywith improvements in visual acuity. The COASTL tool showed thatfollowing allo-CLET there was a decrease in LSCD severity and an increase in visual acuity up to 12months post-treatment, but thereafter LSCD severity and visual acuity progressively deteriorated.STEM CELLS TRANSLATIONAL MEDICINE 2014;3:1–11
INTRODUCTION
The cornea is the clear window at the front of theeye. Its transparency depends on a complex rela-tionship between collagen fibrils, extracellularma-trix, and several specialized cell types. One of thecell populations, the limbal epithelial stem cells(LESCs), are responsible for generating and main-taining the transparent multilayered epitheliumthat covers theouter surfaceof the cornea forminga protective barrier against the external environ-ment [1–7]. LESCs are located in a specializednichecalled the limbus [8]. The limbus is the semitrans-lucent ring of tissue that forms the junction be-tween the transparent cornea and opaque sclera.
A wide range of diseases can result in damageto the LESCs and/or their niche. If severe, this dam-age can lead to a deficiency in LESC function result-ing in an inability tomaintain an intact transparentepitheliumon the surfaceof the eye. Clinically, thiscondition is known as limbal stem cell deficiency(LSCD). Instead of a healthy transparent cornealepithelium generated by functioning LESCs, pa-tients with LSCD suffer from migration of periph-eral conjunctival epithelial cells and blood vessels
onto the corneal surface, which is associated withlossof visionand intermittentulceration [1–7]. Theleading causes of LSCD in the developed worldare chemical/thermal injury, Stevens-Johnson syn-drome (SJS), aniridia, andocular cicatricial pemphi-goid [1–7]. Following chemical injury, LESCs aredestroyed by direct physical-chemical damage. InSJS, the mechanism of LESC damage is poorly un-derstood, but it may occur as a result of the acuteinflammatory episode simultaneous with orocuta-neous ulceration or develop several years later asa resultofchronicocularsurfacedisease.Thecauseof LSCD in aniridia is related to an abnormality ofthe PAX6 gene. This geneplays a key role in the de-velopment of the anterior segment of the eye andmutations in a single allele result in awide rangeofabnormalities. Interestingly, patients with aniridiahave normal corneal epithelium at birth but beginto develop signs of LSCD in their 20s to 30s; thesesigns slowly progress to LSCD. The mechanism bywhich PAX6mutations result in LSCD is not known.
The severity of LSCD can vary. It may be clas-sified as partial or total and as unilateral or bilat-eral. The treatment of severe LSCD has beenrevolutionized by the introduction of surgical
aCells for SightTransplantation andResearchProgramme and bOcularBiology and TherapeuticsDivision, University CollegeLondon Institute ofOphthalmology, London,United Kingdom; cMoorfieldsEye Hospital National HealthService Foundation Trust,London, United Kingdom;dUniversity College LondonClinical Trials Unit, London,United Kingdom
Correspondence: Alex J. Shortt,M.R.C.Ophth., Ph.D., NationalInstitute for Health ResearchBiomedical Research Centre forOphthalmology, MoorfieldsEye Hospital National HealthService Foundation Trust andUniversity College LondonInstitute of Ophthalmology,162 City Road, London EC1V2PD, United Kingdom.Telephone: 44(0)207-253-3411,ext. 4654; E-Mail: [email protected]
Received February 11, 2013;accepted for publicationSeptember 23, 2013.
©AlphaMed Press
http://dx.doi.org/10.5966/sctm.2013-0025
STEM CELLS TRANSLATIONAL MEDICINE 2014;3:1–11 www.StemCellsTM.com ©AlphaMed Press 2014
TISSUE ENGINEERING AND REGENERATIVE MEDICINE
http://stemcellstm.alphamedpress.org/cgi/doi/10.5966/sctm.2013-0025The latest version is at Published Ahead of Print on January 17, 2014 as 10.5966/sctm.2013-0025
by Alex Shortt on January 31, 2014
http://stemcellstm
.alphamedpress.org/
Dow
nloaded from

techniques for LESC transplantation. There are several differentsurgical options, all of which have been summarized recentlyby the Corneal Society (http://www.corneasociety.org) [9].Broadly, there are two approaches: (a) direct transplantation ofwhole segments of healthy limbal tissue—these can be either autol-ogous (from the fellow eye) or allogeneic (from a cadaveric donor)[10–16]—and (b) transplantation of a bioengineered cell sheet thatis constructed from LESCs in a specialist culture facility. These cellsheets can be constructed fromautologous (the fellow eye) or fromallogeneic (a cadaveric donor) LESCs [17–20]. Direct limbal tissuetransplantation was first reported in 1989 [12] and bioengineeredLESC cell sheets in 1997 [17]. Since then, there have been ever in-creasing numbers of publications reporting the clinical outcomesfor both approaches [6, 21]. A significant problemwhen interpretingdata from these studies is the way in which outcomes have beenmeasured and reported. Outcomes have generally been based onsubjective grading, which is open to bias, or on attempts to stratifyoutcomes based on poorly defined criteria, the reliability of whichhad not been tested [19, 22–26]. This lack of objective outcomemeasures makes it difficult to compare results between studiesand to determine which of the many surgical options has the bestoutcome in a given patient cohort. The increasing use of stem celltechnology to treat thesepatientshas resulted inadditionalpressurefrom regulatory authorities and health care funders to demonstratetheir safety, efficacy, and cost-effectiveness using defined, objective,and reliable outcome criteria. At present, no such outcomes exist.
Theaimsof this studywere to (a) design and test the reliabilityof a grading tool for quantifying the severity of LSCD, (b) definea set of core outcomemeasures for use in treatments for this con-dition, and (c) demonstrate the utility of these core outcomes byreporting the3-year results for allogeneic ex vivo cultivated limbalepithelial transplantation (allo-CLET) in patientswhohadbilateraltotal LSCD secondary to aniridia or SJS.
MATERIALS AND METHODS
Design and Validation of a Grading System
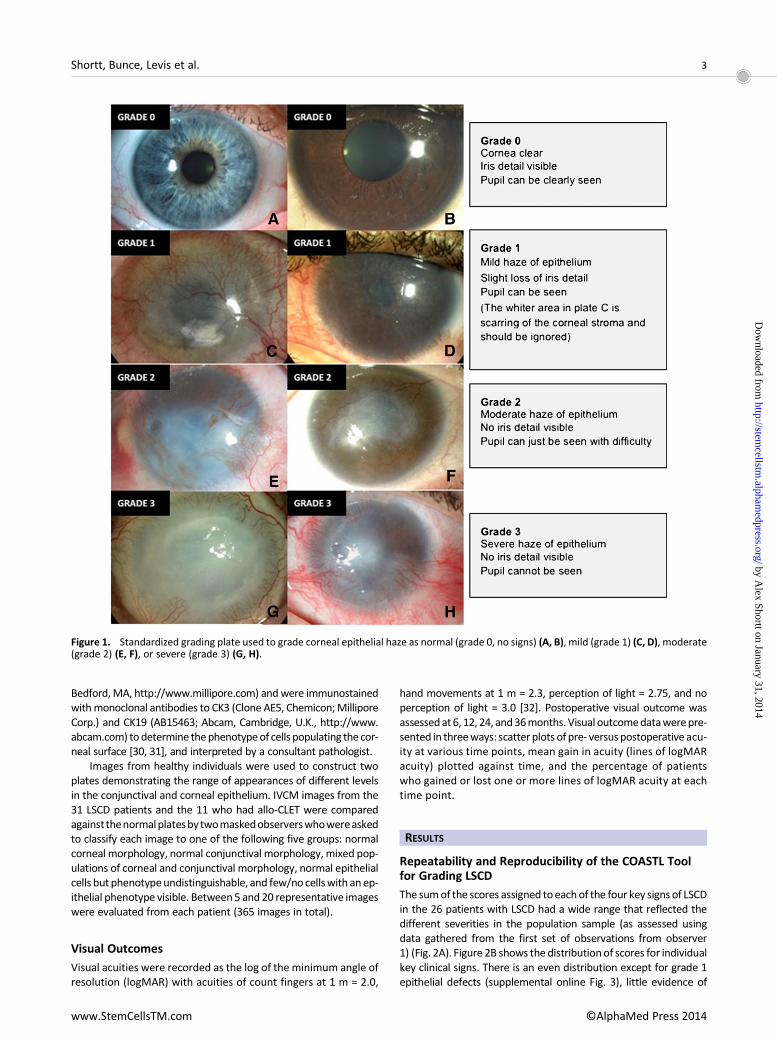
This study adhered to the tenets of theDeclaration ofHelsinki. Eth-ical approval was obtained from the institutionalMedical ResearchEthics Committee, and informed consent was obtained from allpatients prior to treatment. A list of clinical signs useful in the di-agnosis and assessment of LSCD severity was created from out-come measures used in previously published studies in this field.Nine clinicians and scientists with experience in diagnosing andtreating limbal stem cell deficiency anonymously selected fourkey clinical signs of LSCD from this list for use in a new grading tool:corneal epithelial haze, superficial corneal neovascularization,corneal epithelial irregularity, and corneal epithelial defect. Astandardized gradingplatewas produced for each of these para-meters with severity graded from 0 (normal) to grade 3 (severe)(Fig. 1; supplemental online Figs. 1–3). The use of separateplates allowed independent grading of each parameter in cor-neas manifesting multiple abnormalities.
Clinical photographs were formatted using a standardizedtechnique. The protocol required a minimum of two images ofthe whole cornea, with one high (316) magnification image ofthe central cornea and one image under cobalt blue illuminationfollowing instillation of onedrop of fluorescein 2%. The four photo-graphswerearranged intoa single large imageusingAdobe Illustra-torCS4 (AdobeSystems Inc., San Jose, CA, http://www.adobe.com)
(supplemental online Fig. 4). Two observers masked to the clinicalhistory then graded each image against the standardized gradingplates. The scores for each of the four clinical signs of LSCD weresummated to give a score of overall severity (global score, range0 to 12). This system was designated the Clinical Outcome Assess-ment in Surgical Trials of Limbal stem cell deficiency (COASTL) tool.It is a composite ordinal grading scale.
The reliability of the COASTL tool was tested using images from26 patients with varying degrees of LSCD from a range of etiologies.Two observers graded the same set of images in random order ontwo occasions 28 days apart. Repeatability (intraobserver agree-ment) was assessed using weighted k to assess between the re-spective observers’ scores at different time points [27, 28].Reproducibility (interobserver agreement) was assessed using theindividual observers’ initial scores,whichwere again assessed usingweightedk because the scalewasordinal. In all casesofweightedk,we used the following quadratic weighting: 1 2 {(i 2 j)/(k2 1)}2,where i and j index the rows and columns of the ratings by thetwo raters, and k is the maximum number of possible ratings. Be-cause therewas onepatientwho contributedboth eyes to the anal-ysis, we treated eyes as independent (but checked thatmain resultswere robust by sensitivity analyses without this one observation).
Grading of Allo-CLET Outcomes
Fourteeneyes of13patientswith total bilateral LSCDwith aniridia(10 eyes of 9 patients) or SJS (4 eyes of 4 patients)were treated byallo-CLET. The culture and transplantation techniques have beendescribed previously [29]. Patients received postoperative oralprednisolone for 4 weeks and oral cyclosporin or mycophenolatefor 6 months. Corneal photographs were taken before surgeryand at intervals up to 3 years following allo-CLET. These weregraded using the COASTL tool. The effect of treatment on the in-dividual parameters of LSCD and on the global grading score wasevaluated by plotting the mean change in score from baselineover time. We arbitrarily defined success as a 25% reduction inthe global score and using this definition of success createda Kaplan-Meier survival curve for each patient group.
Assessment of Biomarker Impact and Relevance
To confirm the impact and relevance of the four biomarkers (cor-neal epithelial haze, superficial corneal neovascularisation, cor-neal epithelial irregularity, and corneal epithelial defect) eachwas correlated with visual acuity. Data were collected from theaforementioned 14 eyes of the 13 patients that underwentallo-CLET. Changes ineachof thebiomarkers and theglobal (total)score were correlated with changes in visual acuity using Spear-man rank correlation.
In Vivo Confocal Microscopy and Impression Cytology
In vivo confocal microscopy (IVCM)with the Rostock CornealMod-ule and Heidelberg Retina Tomograph II (Heidelberg EngineeringGmbh, Heidelberg, Germany, http://www.heidelbergengineering.com)wasperformedonfivenormalvolunteersand31patientswithLSCD. Eleven of these 31 patients subsequently underwent allo-CLET and IVCMwas then repeated at intervals following surgeryde-termined by patient tolerance and clinical status. Optical sectionswere collected fromat least two locations in the central cornea. Im-pression cytology was also performed before and after surgery inthe 11 allo-CLET patients. Samples were collected using Bioporemembranes (Millicell-CM 0.4 mm PICM 012550; Millipore Corp.,
2 Cultured Limbal Epithelial Allograft Outcomes
©AlphaMed Press 2014 STEM CELLS TRANSLATIONAL MEDICINE
by Alex Shortt on January 31, 2014
http://stemcellstm
.alphamedpress.org/
Dow
nloaded from
Bedford,MA, http://www.millipore.com) andwere immunostainedwithmonoclonal antibodies to CK3 (Clone AE5, Chemicon;MilliporeCorp.) and CK19 (AB15463; Abcam, Cambridge, U.K., http://www.abcam.com) todetermine thephenotypeof cells populating the cor-neal surface [30, 31], and interpreted by a consultant pathologist.
Images from healthy individuals were used to construct twoplates demonstrating the range of appearances of different levelsin the conjunctival and corneal epithelium. IVCM images from the31 LSCD patients and the 11 who had allo-CLET were comparedagainstthenormalplatesby twomaskedobserverswhowereaskedto classify each image to one of the following five groups: normalcorneal morphology, normal conjunctival morphology, mixed pop-ulations of corneal and conjunctival morphology, normal epithelialcells but phenotypeundistinguishable, and few/no cellswith an ep-ithelial phenotype visible. Between5 and 20 representative imageswere evaluated from each patient (365 images in total).
Visual Outcomes
Visual acuities were recorded as the log of the minimum angle ofresolution (logMAR) with acuities of count fingers at 1 m = 2.0,
hand movements at 1 m = 2.3, perception of light = 2.75, and noperception of light = 3.0 [32]. Postoperative visual outcome wasassessedat6, 12, 24, and36months. Visual outcomedatawerepre-sented in threeways: scatter plots of pre- versuspostoperative acu-ity at various time points, mean gain in acuity (lines of logMARacuity) plotted against time, and the percentage of patientswho gained or lost one or more lines of logMAR acuity at eachtime point.
RESULTS
Repeatability and Reproducibility of the COASTL Toolfor Grading LSCD
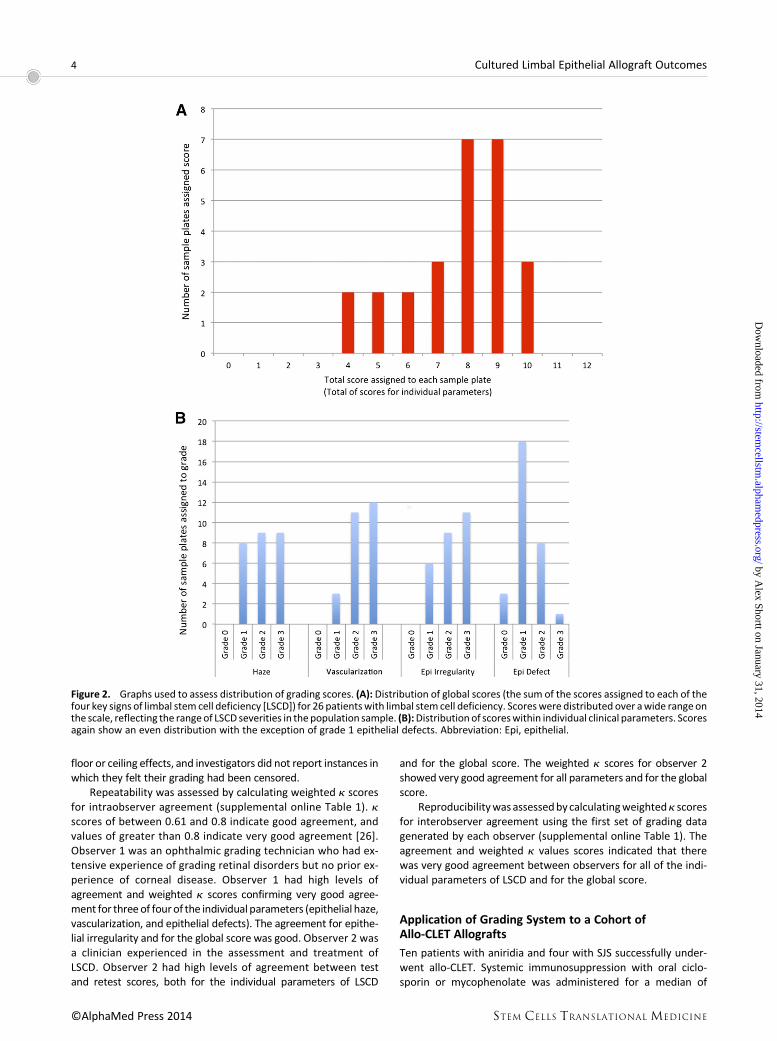
The sumof the scores assigned toeachof the four key signs of LSCDin the 26 patients with LSCD had a wide range that reflected thedifferent severities in the population sample (as assessed usingdata gathered from the first set of observations from observer1) (Fig. 2A). Figure 2B shows the distributionof scores for individualkey clinical signs. There is an even distribution except for grade 1epithelial defects (supplemental online Fig. 3), little evidence of
Figure 1. Standardized grading plate used to grade corneal epithelial haze as normal (grade 0, no signs) (A, B), mild (grade 1) (C, D), moderate(grade 2) (E, F), or severe (grade 3) (G, H).
Shortt, Bunce, Levis et al. 3
www.StemCellsTM.com ©AlphaMed Press 2014
by Alex Shortt on January 31, 2014
http://stemcellstm
.alphamedpress.org/
Dow
nloaded from
floor or ceiling effects, and investigators did not report instances inwhich they felt their grading had been censored.
Repeatability was assessed by calculating weighted k scoresfor intraobserver agreement (supplemental online Table 1). kscores of between 0.61 and 0.8 indicate good agreement, andvalues of greater than 0.8 indicate very good agreement [26].Observer 1 was an ophthalmic grading technician who had ex-tensive experience of grading retinal disorders but no prior ex-perience of corneal disease. Observer 1 had high levels ofagreement and weighted k scores confirming very good agree-ment for three of fourof the individual parameters (epithelial haze,vascularization, and epithelial defects). The agreement for epithe-lial irregularity and for the global score was good. Observer 2 wasa clinician experienced in the assessment and treatment ofLSCD. Observer 2 had high levels of agreement between testand retest scores, both for the individual parameters of LSCD
and for the global score. The weighted k scores for observer 2showed very good agreement for all parameters and for the globalscore.
Reproducibilitywasassessedbycalculatingweightedk scoresfor interobserver agreement using the first set of grading datagenerated by each observer (supplemental online Table 1). Theagreement and weighted k values scores indicated that therewas very good agreement between observers for all of the indi-vidual parameters of LSCD and for the global score.
Application of Grading System to a Cohort ofAllo-CLET Allografts
Ten patients with aniridia and four with SJS successfully under-went allo-CLET. Systemic immunosuppression with oral ciclo-sporin or mycophenolate was administered for a median of
Figure 2. Graphs used to assess distribution of grading scores. (A): Distribution of global scores (the sum of the scores assigned to each of thefour key signs of limbal stem cell deficiency [LSCD]) for 26 patientswith limbal stem cell deficiency. Scoreswere distributed over awide range onthe scale, reflecting the rangeof LSCD severities in the population sample. (B):Distribution of scoreswithin individual clinical parameters. Scoresagain show an even distribution with the exception of grade 1 epithelial defects. Abbreviation: Epi, epithelial.
4 Cultured Limbal Epithelial Allograft Outcomes
©AlphaMed Press 2014 STEM CELLS TRANSLATIONAL MEDICINE
by Alex Shortt on January 31, 2014
http://stemcellstm
.alphamedpress.org/
Dow
nloaded from
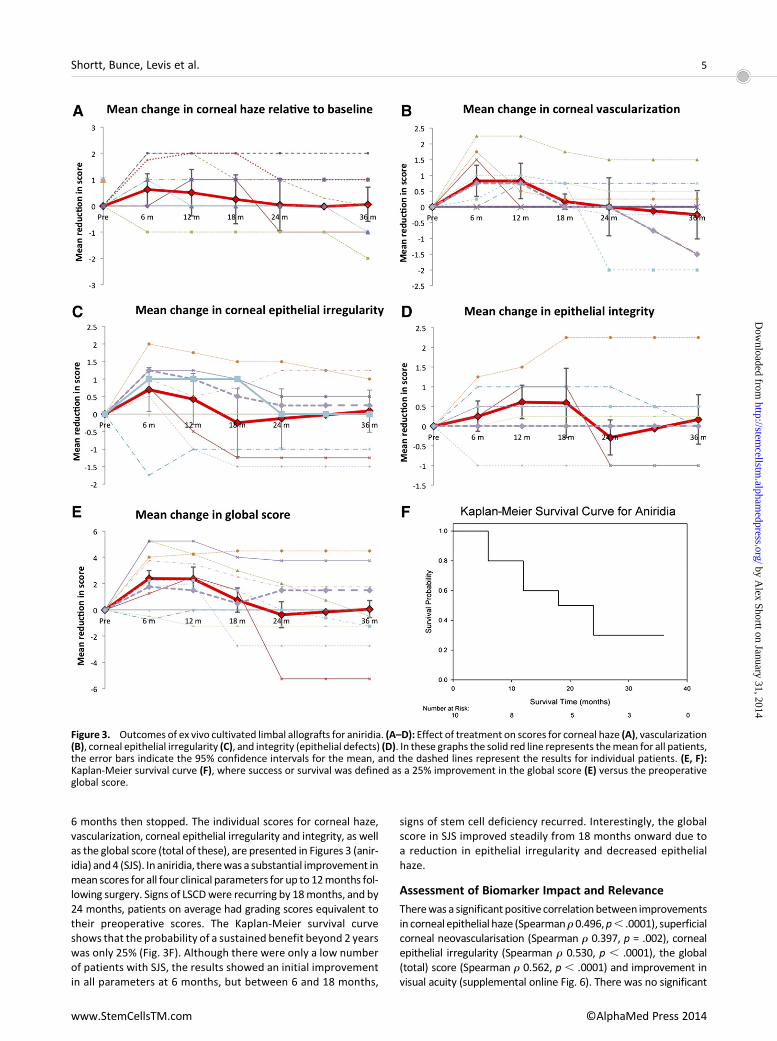
6 months then stopped. The individual scores for corneal haze,vascularization, corneal epithelial irregularity and integrity, as wellas the global score (total of these), are presented in Figures 3 (anir-idia) and4 (SJS). In aniridia, therewas a substantial improvement inmean scores for all four clinical parameters for up to 12months fol-lowing surgery. Signs of LSCDwere recurring by 18months, and by24 months, patients on average had grading scores equivalent totheir preoperative scores. The Kaplan-Meier survival curveshows that the probability of a sustained benefit beyond 2 yearswas only 25% (Fig. 3F). Although there were only a low numberof patients with SJS, the results showed an initial improvementin all parameters at 6 months, but between 6 and 18 months,
signs of stem cell deficiency recurred. Interestingly, the globalscore in SJS improved steadily from 18 months onward due toa reduction in epithelial irregularity and decreased epithelialhaze.
Assessment of Biomarker Impact and Relevance
Therewas a significant positive correlationbetween improvementsin corneal epithelial haze (Spearmanr 0.496,p, .0001), superficialcorneal neovascularisation (Spearman r 0.397, p = .002), cornealepithelial irregularity (Spearman r 0.530, p , .0001), the global(total) score (Spearman r 0.562, p , .0001) and improvement invisual acuity (supplemental online Fig. 6). There was no significant
Figure 3. Outcomes of ex vivo cultivated limbal allografts for aniridia. (A–D): Effect of treatment on scores for corneal haze (A), vascularization(B), corneal epithelial irregularity (C), and integrity (epithelial defects) (D). In these graphs the solid red line represents themean for all patients,the error bars indicate the 95% confidence intervals for the mean, and the dashed lines represent the results for individual patients. (E, F):Kaplan-Meier survival curve (F), where success or survival was defined as a 25% improvement in the global score (E) versus the preoperativeglobal score.
Shortt, Bunce, Levis et al. 5
www.StemCellsTM.com ©AlphaMed Press 2014
by Alex Shortt on January 31, 2014
http://stemcellstm
.alphamedpress.org/
Dow
nloaded from
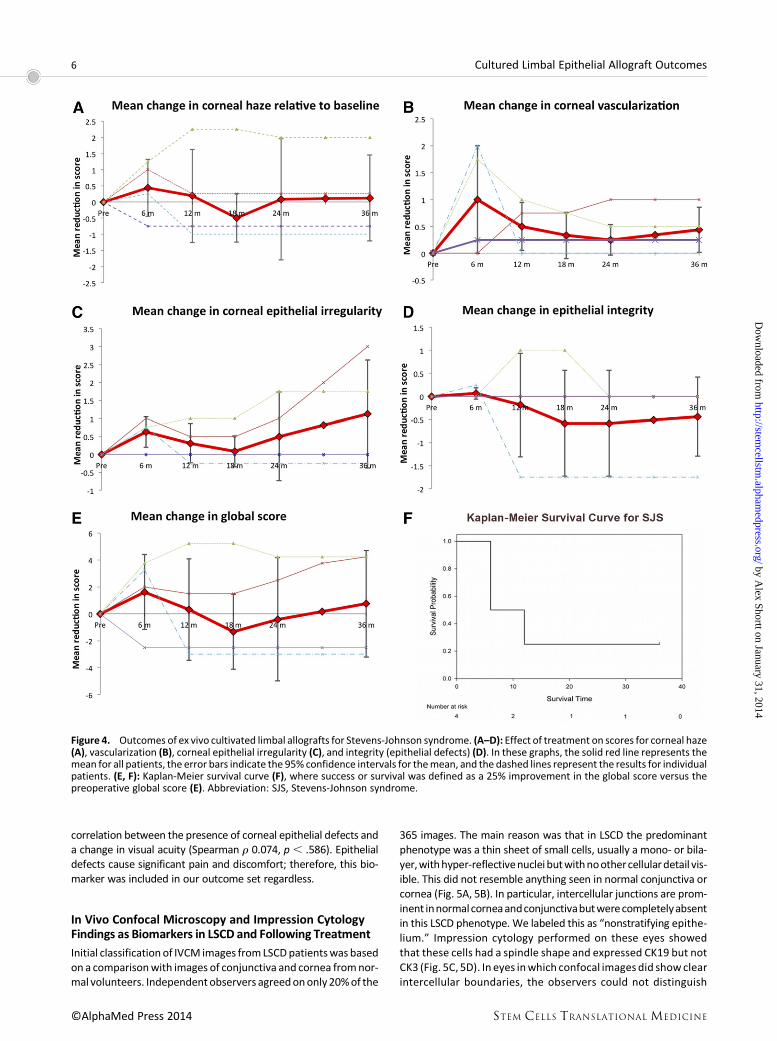
correlation between the presence of corneal epithelial defects anda change in visual acuity (Spearman r 0.074, p , .586). Epithelialdefects cause significant pain and discomfort; therefore, this bio-marker was included in our outcome set regardless.
In Vivo Confocal Microscopy and Impression CytologyFindings as Biomarkers in LSCD and Following Treatment
Initial classification of IVCM images fromLSCDpatientswas basedon a comparisonwith images of conjunctiva and cornea fromnor-mal volunteers. Independentobservers agreedononly 20%of the
365 images. The main reason was that in LSCD the predominantphenotype was a thin sheet of small cells, usually a mono- or bila-yer,withhyper-reflectivenucleibutwithnoothercellulardetail vis-ible. This did not resemble anything seen in normal conjunctiva orcornea (Fig. 5A, 5B). In particular, intercellular junctions are prom-inent innormalcorneaandconjunctivabutwerecompletelyabsentin this LSCD phenotype. We labeled this as “nonstratifying epithe-lium.” Impression cytology performed on these eyes showedthat these cells had a spindle shape and expressed CK19 but notCK3 (Fig. 5C, 5D). In eyes inwhich confocal images did showclearintercellular boundaries, the observers could not distinguish
Figure 4. Outcomes of ex vivo cultivated limbal allografts for Stevens-Johnson syndrome. (A–D): Effect of treatment on scores for corneal haze(A), vascularization (B), corneal epithelial irregularity (C), and integrity (epithelial defects) (D). In these graphs, the solid red line represents themean for all patients, the error bars indicate the 95% confidence intervals for themean, and the dashed lines represent the results for individualpatients. (E, F): Kaplan-Meier survival curve (F), where success or survival was defined as a 25% improvement in the global score versus thepreoperative global score (E). Abbreviation: SJS, Stevens-Johnson syndrome.
6 Cultured Limbal Epithelial Allograft Outcomes
©AlphaMed Press 2014 STEM CELLS TRANSLATIONAL MEDICINE
by Alex Shortt on January 31, 2014
http://stemcellstm
.alphamedpress.org/
Dow
nloaded from

between corneal or conjunctival cells. We concluded that con-focal microscopy could not be used to distinguish conjunctivaland corneal epithelial enotypes.We therefore devised a revisedclassification based on LSCD alone (supplemental online Fig. 5).Images were classified as follows: (a) no epithelial cells visible,interpreted as an epithelial defect, ulcer, or an acellular scar onthe ocular surface; (b) nonstratifying epithelium one or two cellsthick, with hyper-reflective nuclei but absent intercellular junc-tions; or (c) stratified epithelium with clear intercellular bound-aries indicative of normal epithelial differentiation. These couldbe conjunctival or corneal cells.
With this system, the observers agreed on 98% of the 365images from 31 patients. Each of the 31 patients was assignedan overall score (based on the score most commonly recordedby the observer for that patient’s images). We then assessedagreement between overall scores using k and found almost per-fect agreement with a k of 0.91 (SE 0.11).
This modified system of classifying confocal phenotypes wasthen applied to patients undergoing allo-CLET. IVCM images of suf-ficient quality for analysiswere available for 8 eyes before allo-CLETand 10 eyes following surgery. In addition, impression cytology ofsufficientquality for analysiswas available from14eyesbefore allo-CLET and 11 eyes following surgery (supplemental online Table 1).Before surgery, 6 of the 8 eyes that underwent IVCMshowed a thinlayer of hyper-reflective cells without identifiable cell boundaries.One patient had stratified differentiated epithelium and one hada mixed phenotype. Patients with a nonstratifying epithelial phe-notype on IVCM had a correlating conjunctival morphology andCK19-positive (+ve) phenotype on impression cytology consistent
with this as shown in Figure5. Threepatientswereexamined1yearafter surgery, and they showed a multilayered differentiated epi-thelium that was mainly CK3+ve but also some areas of CK19+vecells. Twoof 4eyes examinedat3 years following surgery showedthenonstratifying epithelial phenotype,while the other twodis-played a differentiated epithelium with both CK3 and CK19expression.
Visual Acuity
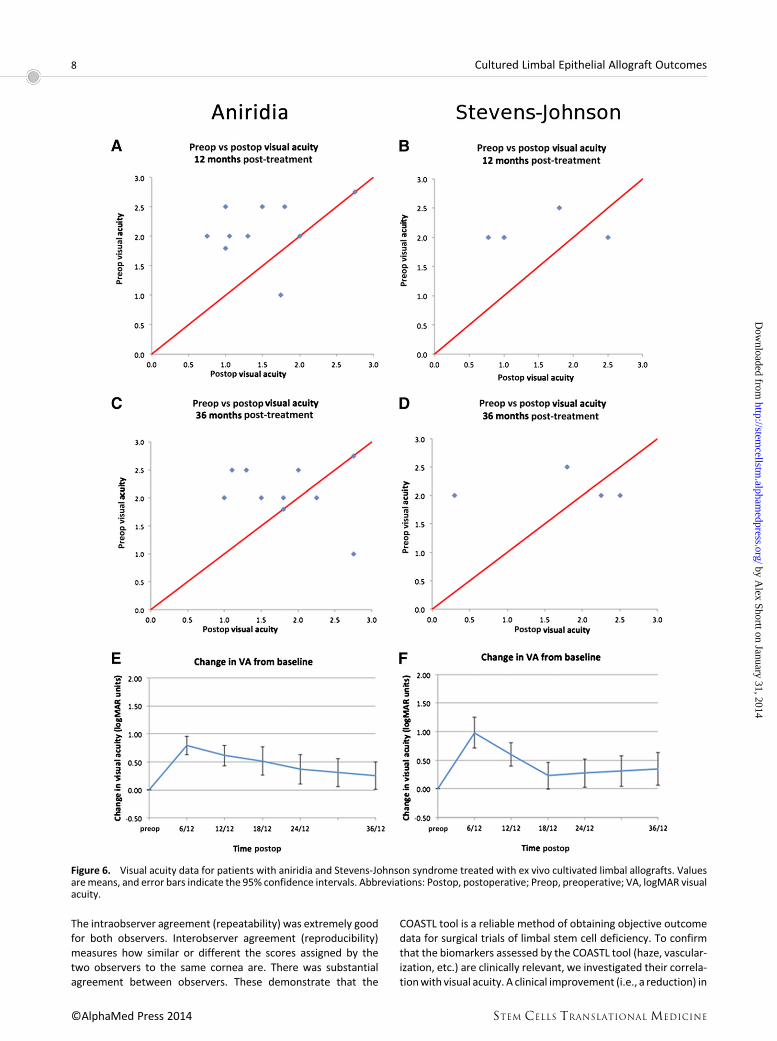
Thepreoperative visual acuitywas6/60 (Snellen acuity 20/200) orworse in all eyes undergoing allo-CLET. Scatter plots of pre- versuspost-treatment acuity showed an improvement in visual acuity in79% of eyes at 6 months, 71% at 12 months, 64% at 18 months,and 57%at both 24 and 36months (Fig. 6A–6C). Visual acuity datawere inspected for normality by plotting distribution at each timepoint. No significant skew was identified; therefore, mean visualacuity is reported. There was an initial improvement in the meanvisual acuity of 0.86 logMAR units at 6 months (aniridia 0.78 log-MAR, SJS 0.98 logMAR). The visual gain gradually reduced overthe subsequent 30 months, but at 36 months, there was a stablemean gain of 0.28 logMAR units (0.26 in aniridic and 0.35 in SJSeyes) (Fig. 6D–6F). The percentage of eyes gaining one line of log-MAR acuity was 57% overall at 6 months (aniridia, 50%; SJS, 75%)and 29% at 36 months (aniridia, 30%; SJS, 25%).
DISCUSSION
The variability of biological systems means that clinical signs canrarely be simplified to exact numerical values, and inmedicine, thisis reflected in the use of therapeutic ranges andgrading scales [33].The laboratory and surgical techniques developed to treat LSCDcontinue to evolve, but an inability to objectively compare treat-ment outcomes has limited progress. There is currently nomethodto track the long-term fate of transplanted corneal epithelial cells,and surrogate measures are the only alternative at present. Regu-latory bodies increasingly require proof of efficacy for new techni-ques, and a subjective assessment of success is insufficient. In thisstudy, we have validated a set of objectivemeasures to describetreatment outcomes for LSCD and demonstrated the use ofthese in reporting the 3-year outcomes of allo-CLET for aniridiaand SJS.
In virtually all studies of limbal stem cell transplantation todate, the clinical outcomehas been assessed subjectively by the in-vestigatingclinician.This is clearlyopentosignificantmeasurementand reporting bias. Some studies have attempted to reduce bias byusinganagreedsetofoutcomemeasuresorassigningascorebasedon the overall interpretation of the observer [19, 22, 23, 25, 26].However, the weakness of these studies is that the parametersassessed were poorly defined and the classification systems werenot validated. An exception is the study by Sotozono et al., whichused a reference plate of clinical signs to grade the ocular surfacechanges inSJS [24]. In thepresent study,wehave reducedpotentialbiasbyusing two independentmaskedobservers tograde four spe-cific indicators of stem cell deficiency. The use of different photo-graphic magnifications and fluorescein staining to highlight areasof epithelial breakdown was specifically designed to enablegrading of four defined and key signs of LSCD.
The utility of the COASTL tool developed for this study wasevaluated by measuring its reliability. Grading systems thatlack reliability are susceptible to random measurement error.
Figure 5. Nonstratifying epithelial phenotype observed in in vivoconfocal microscopy and impression cytology observed in severalpatients with limbal stem cell deficiency. Shown are confocal micros-copy (A, B) and corresponding impression cytology (C, D) images fromthe central cornea of two patients with limbal stem cell deficiencyprior to treatment. (A, B): Confocal microscopy shows a thin sheetof small cells, usually a mono- or bilayer, with hyperfluorescent nu-clei, but no other cellular detail is visible. (C, D): Correlation with im-pression cytology performed on the same patients directly afterconfocal scans showed that these cells had a spindle-like shapeand expressed CK19 (red) but not CK3 (brown) (C, D). This phenotypemay represent conjunctival cell migration onto the corneal stromabut failure of the cell layer to form cell junctions anddifferentiate intoa mature multilayered epithelium. Scale bars = 25 mm.
Shortt, Bunce, Levis et al. 7
www.StemCellsTM.com ©AlphaMed Press 2014
by Alex Shortt on January 31, 2014
http://stemcellstm
.alphamedpress.org/
Dow
nloaded from
The intraobserver agreement (repeatability) was extremely goodfor both observers. Interobserver agreement (reproducibility)measures how similar or different the scores assigned by thetwo observers to the same cornea are. There was substantialagreement between observers. These demonstrate that the
COASTL tool is a reliable method of obtaining objective outcomedata for surgical trials of limbal stem cell deficiency. To confirmthat the biomarkers assessed by the COASTL tool (haze, vascular-ization, etc.) are clinically relevant, we investigated their correla-tionwith visual acuity. A clinical improvement (i.e., a reduction) in
Figure 6. Visual acuity data for patients with aniridia and Stevens-Johnson syndrome treated with ex vivo cultivated limbal allografts. Valuesaremeans, and error bars indicate the 95% confidence intervals. Abbreviations: Postop, postoperative; Preop, preoperative; VA, logMAR visualacuity.
8 Cultured Limbal Epithelial Allograft Outcomes
©AlphaMed Press 2014 STEM CELLS TRANSLATIONAL MEDICINE
by Alex Shortt on January 31, 2014
http://stemcellstm
.alphamedpress.org/
Dow
nloaded from

corneal haze, vascularization, and epithelial irregularity corre-lated significantly with an improvement in visual acuity, confirm-ing the appropriateness of these biomarkers for measuringoutcomes in trials of LSCD treatments. The exception to thiswas corneal epithelial integrity. Changes in this biomarker didnot correlate significantly with changes in visual acuity. Nonethe-less, it was included in the COASTL tool because the inability tomaintain an intact corneal epithelium is a critical sign of LSCD,and furthermore, there is little doubt that epithelial defects resultin significant pain and discomfort.
We used impression cytology with immunostaining forCK3/CK19 and IVCM as indices of biological success of these treat-ments. We hypothesized that IVCM could replace impression cy-tology in the assessment LSCD; however, this was not the case.Insteadweconclude that the two techniques provide complemen-tary data. Confocal microscopy alone could not accurately distin-guish between corneal and conjunctival cell phenotypes, whereasimpression cytology could, basedonCK3orCK19expression.How-ever, IVCM gave more information about the degree of epithelialstratification and the presence of cell-cell junction formation, in-dicating normal epithelial differentiation. A notable finding insomepatients with LSCDwas a central corneal epithelial thicknessof only one to two cell layers formed of elongated spindle-shapedCK19+vecells that appeared tobemigrating conjunctival epithelialcells. To the best of our knowledge, this phenotype has not previ-ously been described.
For studiesof refractiveeyesurgeryprocedures, therearea setof standardized outcomemeasures that should be adhered to andreported [34]. No such standardized set of visual acuity outcomemeasures exists for LSCD treatments, probably because it is a chal-lenge to interpret the wide range of visual acuities seen as well asthe potential gain in vision following treatment. Also, pre-existingcomorbidity, such asmacular hypoplasia andnystagmus in aniridicpatients and stromal corneal scarring in patients with SJS, limit po-tential visual improvement. We showed that pre- versus postop-erative scatter plots are an effective method of evaluating thisoutcome. To the best of our knowledge, this is the first time thatlongitudinal long-term follow-up data on visual acuity has beenpresented. Another measure, the percentage of patients gainingfive letters or more (one line of logMAR acuity) was also usefulin determining the percentage of patients who had a functionallysignificant gain in acuity.
Having developed the COASTL tool and defined a set of out-come measures including standardized visual acuity plots, weapplied this outcome tool to a series of allo-CLET procedures per-formed for aniridiaor SJS. Theoutcomesclearly showan initial suc-cessful reduction in the signs of LSCD. However, in both aniridiaand SJS, the signs of disease gradually returned and, by 24months,reached pretreatment levels. The IVCM and confocal microscopyfindings suggest that this is due to the recurrence of partial LSCDinitially, as indicated by the CK3/19 mosaic and, in some cases, bythe recurrence of total LSCD, as indicated by the nonstratifying ep-ithelial phenotype. The initial improvement in clinical signs andcell phenotypewas associatedwith an improvement in visual acu-ity,which slowly regressedover36months inboth conditions, butit is notable thatdespite recurrenceof clinical signs the visual ben-efit persists in 30% of aniridic and 25% of SJS patients at 36months. This suggests that the treatment can have beneficialeffects on visual function and, potentially, on quality of life, evenin the presence of a recurrence of the signs of LSCD. This raisesthe issue of how a treatment “success” should be defined orwhat
the primary outcome measure for future trials of this therapyshould be.
There are awide variety of surgical treatments for transplant-ing LESCs [9]. Published data suggest that the procedure of choicefor patients with long-standing unilateral alkali injuries is an exvivo cultivated limbal autograft (auto-CLET) [19]. Evidence toguide decisions on the treatment of other disease groups is poor[35]. There is still controversy as to whether transfer of ex vivoexpanded cells offers an advantage over direct tissue transfertechniques for patients with bilateral disease. Until recently,long-term outcome data for keratolimbal allografts (KLAL) showeduniversally poor results [36], but a more potent immunosuppres-sive regimen combining tacrolimus and mycophenolate witha short course of oral steroids can significantly prolong KLALgraft survival [37, 38]. Another novel way of improving outcomesof these allogeneic direct tissue transfer techniques is to com-bine living related conjunctival limbal autograft and KLAL (theCincinnatti Procedure) thus giving superior outcomes toKLALout-comes alone [38]. The closest comparable data to our data onpatients with aniridia was reported by Biber et al. [38], whoreported that at a mean follow-up of 43.4 months, 33% had animproved ocular surface and 75% of eyes had an improvementin vision of at least one line at the last follow-up. This presentstudy found that 22% of aniridia eyes had a persistent improve-ment in clinical signs and 30% had a persistent gain of one lineof logMAR acuity at 36 months. Apart from these data, it is diffi-cult to compare the two sets of outcomes, highlighting the poten-tial benefits of a standardized outcome reporting system.
The discrepancy between the outcomes reported by Biberet al. [38] and the less favorable outcomes in the present studymay be accounted for by differences in immunosuppressiveregimes. In the former study, two immunosuppressive agents(tacrolimus and mycophenolate) were administered indefinitely,whereas in the present study, one agent (cyclosporin or mycophe-nolate)wasadministered for6monthsonly.Thedecisiontousethisregimenwasbasedonevidence thatdonorepithelial cells couldnotbedetectedonthe surfaceof thecorneabeyond8months [39].Wehypothesized that for the 6 months following treatment, trans-planted cells provide a suitable environment for innate cells to re-store corneal epithelial homeostasis. We felt that beyond thisperiod there was unlikely to be a significant benefit from immuno-suppression thatwould justify the riskofpotentially life-threateningcomplications. The alternative hypothesis for themechanism of ac-tion of this treatment is that transplanted cells do indeed survive inthe long term. There are data from animal models of the disease tosuggest thismaybe the case [40]. Theheterogeneous outcomesbe-tween studies using a variety of differing immunosuppressive re-gimes suggests that effective long-term immunosuppression couldpotentially improve outcomes. It is possible, however, that the dif-ference could also be accounted for by inherent differences in thesurgical procedures used.
Fromthepatients’perspective,quality-of-lifeassessments thatquantify the physical, emotional, and socioeconomic aspects oftreatment for LSCD are an important outcome measure [41]. Thequality of life for patients who have had conventional limbal trans-plants has been reported by Miri et al. [42], and that for patientswho have received cultured LESCs has been reported by DiGirolamo et al. [43] and Kolli et al. [25]. A limitation of the presentstudy is that these datawere not collected. Thiswas in part due tothe fact that there is no quality-of-life assessment tool specificallydesigned for or validated for use in this condition. We are
Shortt, Bunce, Levis et al. 9
www.StemCellsTM.com ©AlphaMed Press 2014
by Alex Shortt on January 31, 2014
http://stemcellstm
.alphamedpress.org/
Dow
nloaded from

currently developing such a tool in collaboration with patientsand will use this tool in future studies.
CONCLUSION
The work of the Corneal Society in standardizing the nomencla-ture for ocular surface reconstructive techniques is to be wel-comed [9]. The data presented in this manuscript highlight howasetof standardizedoutcomemeasures canbeused todocumentoutcomes. The Corneal Society is currently facilitating a consulta-tion among the LSCD research community on adopting sucha standardized system for reporting outcomes so that compari-sons between studies and techniques can be made.
ACKNOWLEDGMENTS
This research received a portion of its funding from the Depart-ment ofHealth’sNational Institute ofHealth ResearchBiomedicalResearch Centre for Ophthalmology at Moorfields Eye Hospitaland the University College London Institute of Ophthalmology.Other sources of funding include the Special Trustees ofMoorfields
Eye Hospital (A.J.S. and J.T.D.), the Medical Research Council(A.J.S.), and the Eranda Foundation (J.T.D.). The views expressedin this publication are those of the authors and not necessarilythose of the Department of Health.
AUTHOR CONTRIBUTIONS
A.J.S., S.J.T., and J.T.D.: conception/design, provision of studyma-terial or patients, collection and/or assembly of data, data anal-ysis and interpretation, manuscript writing, final approval ofmanuscript; C.B.: collection and/or assembly of data, data analy-sis and interpretation, manuscript writing, final approval of man-uscript; H.J.L. and P.B.: data analysis and interpretation, finalapproval of manuscript; C.J.D.: data analysis and interpretation,manuscript writing, final approval of manuscript; A.V. and G.A.S.:provision of studymaterial or patients, collection and/or assemblyof data, final approval of manuscript.
DISCLOSURE OF POTENTIAL CONFLICTS OF INTEREST
The authors indicate no potential conflicts of interest.
REFERENCES1 Daniels JT, Dart JK, Tuft SJ et al. Corneal
stem cells in review. Wound Repair Regen2001;9:483–494.2 Grueterich M, Espana EM, Tseng SC. Ex
vivo expansion of limbal epithelial stem cells:amniotic membrane serving as a stem cellniche. Surv Ophthalmol 2003;48:631–646.3 HollandEJ.Epithelial transplantation for the
management of severe ocular surface disease.Trans Am Ophthalmol Soc 1996;94:677–743.4 Kim JY, Djalilian AR, Schwartz GS et al. Oc-
ular surface reconstruction: Limbal stem celltransplantation. Ophthalmol Clin North Am2003;16:67–77.5 Kinoshita S, Adachi W, Sotozono C et al.
Characteristics of the human ocular surface ep-ithelium. Prog Retin Eye Res 2001;20:639–673.6 Shortt AJ, Secker GA, Notara MD et al.
Transplantation of ex vivo cultured limbal ep-ithelial stem cells: A review of techniques andclinical results. Surv Ophthalmol 2007;52:483–502.7 Tseng SC. Concept and application of lim-
bal stem cells. Eye (Lond) 1989;3:141–157.8 Shortt AJ, Secker GA, Munro PM et al.
Characterization of the limbal epithelial stemcell niche: Novel imaging techniques permitin vivo observation and targeted biopsy of lim-bal epithelial stem cells. STEM CELLS 2007;25:1402–1409.9 Daya SM, Chan CC, Holland EJ et al. Cornea
Society nomenclature for ocular surface rehabil-itative procedures. Cornea 2011;30:1115–1119.10 Meallet MA, Espana EM, Grueterich M
et al. Amniotic membrane transplantation withconjunctival limbal autograft for total limbalstem cell deficiency. Ophthalmology 2003;110:1585–1592.11 Santos MS, Gomes JA, Hofling-Lima AL
et al. Survival analysis of conjunctival limbalgrafts and amniotic membrane transplantationineyeswith total limbal stemcell deficiency.AmJ Ophthalmol 2005;140:223–230.
12 Kenyon KR, Tseng SC. Limbal autografttransplantation for ocular surface disorders.Ophthalmology 1989;96:709–722; discussion722–723.13 Daya SM, Ilari FA. Living related conjunc-
tival limbal allograft for the treatment of stemcell deficiency. Ophthalmology 2001;108:126–133; discussion 133–134.14 Tsubota K, Satake Y, KaidoM et al. Treat-
ment of severe ocular-surface disorders withcorneal epithelial stem-cell transplantation. NEngl J Med 1999;340:1697–1703.15 Ilari L, Daya SM. Long-term outcomes of
keratolimbal allograft for the treatment of se-vere ocular surface disorders. Ophthalmology2002;109:1278–1284.16 Solomon A, Ellies P, Anderson DF et al.
Long-term outcome of keratolimbal allograftwith orwithout penetrating keratoplasty for to-tal limbal stem cell deficiency. Ophthalmology2002;109:1159–1166.17 Pellegrini G, Traverso CE, Franzi AT et al.
Long-term restoration of damaged corneal sur-faces with autologous cultivated corneal epi-thelium. Lancet 1997;349:990–993.18 Di Iorio E, Ferrari S, Fasolo A et al. Tech-
niques for culture and assessment of limbalstem cell grafts. Ocul Surf 2010;8:146–153.19 RamaP,Matuska S, PaganoniGet al. Lim-
bal stem-cell therapy and long-term corneal re-generation. N Engl J Med 2010;363:147–155.20 Shortt AJ, Tuft SJ, Daniels JT. Ex vivo cul-
tured limbal epithelial transplantation. A clini-cal perspective. Ocul Surf 2010;8:80–90.21 Baylis O, Figueiredo F, Henein C et al. 13
yearsof cultured limbal epithelial cell therapy:Areview of the outcomes. J Cell Biochem 2011;112:993–1002.22 Nakamura T, Takeda K, Inatomi T et al.
Long-term results of autologous cultivated oralmucosal epithelial transplantation in the scarphase of severe ocular surface disorders. Br JOphthalmol 2011;95:942–946.23 Nakamura T, SotozonoC, BentleyAJ et al.
Long-term phenotypic study after allogeneic
cultivated corneal limbal epithelial transplanta-tion for severeocular surfacediseases.Ophthal-mology 2010;117:2247–2254.e2241.24 Sotozono C, Ang LP, Koizumi N et al. New
grading system for the evaluation of chronic oc-ular manifestations in patients with Stevens-Johnson syndrome. Ophthalmology 2007;114:1294–1302.25 Kolli S, Ahmad S, LakoM et al. Successful
clinical implementation of corneal epithelialstem cell therapy for treatment of unilaterallimbal stem cell deficiency. STEM CELLS 2010;28:597–610.26 Baradaran-Rafii A, Ebrahimi M, Kanavi
MR et al. Midterm outcomes of autologous cul-tivated limbal stem cell transplantation with orwithoutpenetratingkeratoplasty. Cornea2010;29:502–509.27 Altman DG. Practical Statistics for Medi-
cal Research. London, U.K.: Chapman and Hall,1991.28 Streiner DL, Norman GR. Health Mea-
surement Scales: A Practical Guide to Their De-velopment and Use. Oxford, United Kingdom:Oxford University Press, 2008.29 Shortt AJ, Secker GA, Rajan MS et al. Ex
vivo expansion and transplantation of limbalepithelial stem cells. Ophthalmology 2008;115:1989–1997.30 Tole DM, McKelvie PA, Daniell M. Reli-
ability of impression cytology for the diagnosisof ocular surface squamous neoplasia employ-ing the Biopore membrane. Br J Ophthalmol2001;85:154–158.31 Donisi PM, Rama P, Fasolo A et al. Anal-
ysis of limbal stem cell deficiency by corneal im-pression cytology. Cornea 2003;22:533–538.32 Lange C, Feltgen N, Junker B et al. Resolv-
ing the clinical acuity categories “hand motion”and “counting fingers” using the Freiburg VisualAcuity Test (FrACT). Albrecht Von Graefes ArchKlin Exp Ophthalmol 2009;247:137–142.33 Cantrill HL. The diabetic retinopathy
study and the early treatment diabetic retinop-athy study. Int Ophthalmol Clin 1984;24:13–29.
10 Cultured Limbal Epithelial Allograft Outcomes
©AlphaMed Press 2014 STEM CELLS TRANSLATIONAL MEDICINE
by Alex Shortt on January 31, 2014
http://stemcellstm
.alphamedpress.org/
Dow
nloaded from

34 Stulting RD, Dupps WJ Jr, Kohnen T et al.Standardized graphs and terms for refractivesurgery results. Cornea 2011;30:945–947.35 Shortt AJ, Tuft SJ. Ocular surface recon-
struction. Br J Ophthalmol 2011;95:901–902.36 Cauchi PA, AngGS, Azuara-Blanco A et al.
A systematic literature review of surgical inter-ventions for limbal stem cell deficiency inhumans. Am J Ophthalmol 2008;146:251–259.37 Liang L, Sheha H, Tseng SC. Long-term
outcomes of keratolimbal allograft for totallimbal stem cell deficiency using combinedimmunosuppressive agents and correction
of ocular surface deficits. Arch Ophthalmol2009;127:1428–1434.38 Biber JM,SkeensHM,NeffKDetal.TheCin-
cinnati procedure: Technique and outcomes ofcombined living-related conjunctival limbal allog-rafts and keratolimbal allografts in severe ocularsurface failure. Cornea 2011;30:765–771.39 Daya SM,Watson A, Sharpe JR et al. Out-
comes and DNA analysis of ex vivo expandedstemcell allograft for ocular surface reconstruc-tion. Ophthalmology 2005;112:470–477.40 Djalilian AR, Mahesh SP, Koch CA et al.
Survival of donor epithelial cells after limbal
stem cell transplantation. Invest OphthalmolVis Sci 2005;46:803–807.41 Fitzpatrick R, Fletcher A, Gore S et al. Quality
of life measures in health care. I: Applications andissues in assessment. BMJ 1992;305:1074–1077.42 Miri A,MathewM, DuaHS. Quality of life
after limbal transplants. Ophthalmology 2010117:638, 638.e1–638.e3.43 Di GirolamoN, BoschM, Zamora K et al.
A contact lens-based technique for expan-sionand transplantationofautologousepithelialprogenitors for ocular surface reconstruction.Transplantation 2009;87:1571–1578.
See www.StemCellsTM.com for supporting information available online.
Shortt, Bunce, Levis et al. 11
www.StemCellsTM.com ©AlphaMed Press 2014
by Alex Shortt on January 31, 2014
http://stemcellstm
.alphamedpress.org/
Dow
nloaded from

Supplementary Material http://stemcellstm.alphamedpress.org/content/suppl/2014/01/17/sctm.2013-0025.DC1.html
Supplementary material can be found at: by A
lex Shortt on January 31, 2014http://stem
cellstm.alpham
edpress.org/D
ownloaded from




















