Thesis - Jamil Alyan s2701483 Chpt 1-6 +SH signature (digital)
197
Maxillary Sinus Augmentation - a histological, clinical, radiographic and patient centred assessment Author Alayan, Jamil Published 2018 Thesis Type Thesis (PhD Doctorate) School School of Dentistry&Oral Hlth DOI https://doi.org/10.25904/1912/3162 Copyright Statement The author owns the copyright in this thesis, unless stated otherwise. Downloaded from http://hdl.handle.net/10072/381656 Griffith Research Online https://research-repository.griffith.edu.au
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Thesis - Jamil Alyan s2701483 Chpt 1-6 +SH signature (digital)

Maxillary Sinus Augmentation - a histological, clinical,radiographic and patient centred assessment
Author
Alayan, Jamil
Published
2018
Thesis Type
Thesis (PhD Doctorate)
School
School of Dentistry&Oral Hlth
DOI
https://doi.org/10.25904/1912/3162
Copyright Statement
The author owns the copyright in this thesis, unless stated otherwise.
Downloaded from
http://hdl.handle.net/10072/381656
Griffith Research Online
https://research-repository.griffith.edu.au

Maxillary Sinus Augmentation – a
histological, clinical, radiographic
and patient centred assessment
Jamil Alayan
BSc, BDSc, MDSc (perio), FRACDS (perio), FICD
School of Dentistry & Oral Health
Faculty of Health
Griffith University
Submitted in fulfilment of the requirements of the degree of
Doctor of Philosophy
11-May-2018

i
ABSTRACT
Maxillary sinus pneumatization is a frequently encountered problem in the dental
implant rehabilitation of the posterior maxilla. Maxillary sinus augmentation
(MSA) using a lateral wall approach is a well-established and commonly utilized
surgical technique for overcoming this bone deficiency and allowing implant
placement. MSA is still in the refinement process with a large degree of variation
in all aspects of the technique including; the surgical protocol, the anatomical site,
the choice of material, the site of autogenous bone harvesting, the timing of implant
surgery and the use of barrier membranes. Generally, however, prospective
controlled clinical trials critically assessing these domains remain rare, especially
studies applying well defined success criteria for implant supported restorations
placed in sites of MSA.
The maxillary sinus grafting procedure is invasive and surgically demanding, but
appears to have limited interference with maxillary sinus physiology when
performed well. In addition, reported surgical complications are generally well
tolerated and followed by normal recovery in the vast majority of cases. Most of
this data however is derived from medium to low level evidence (clinical case
series, retrospective analyses). Patients undergoing this procedure also expect to be
counselled about their expectations regarding pain and the impact of this procedure
on their daily life in the post-operative period. Such information is not available.
There is also limited long term outcome data on implants placed in MSA.
Historically, autogenous bone grafts have been considered the gold standard due to
their inherent osteoinductivity. Their significant limitations in MSA however has
driven intense research into various bone substitutes. Anorganic bovine bone
mineral (ABBM) is a very well documented xenograft in MSA when used alone or
as a composite graft with autogenous bone (AB) (ABBM + AB). More recently,
collagen stabilized ABBM using 10% porcine type-1 collagen matrix has also
become available for use (ABBM-C) (Bio-Oss Collagen®). This formulation may
have clinical utility in its use as a sole biomaterial in MSA especially in situations

ii
of Schneiderian membrane perforation. There are however, no published studies on
this grafting material in MSA.
Whilst material selection influences the histological appearance and characteristics
of the regenerated bone, other factors can also play a role including defect anatomy
and implant surface. Chemical modification of implant surfaces has resulted in a
surface with increased surface energy and hydrophilicity (SLActive®). These
surfaces have demonstrated enhanced bone apposition during the early stages of
osseointegration and improved bone regeneration in bone defects when compared
to traditional microrough implant surfaces (SLA®). To date however, very few
studies have compared these two implant surfaces in MSA and none at the early
stages of osseointegration.
As such, this thesis aims to assess the histological, clinical (surgical), volumetric
and patient centered outcomes of ABBM-C in MSA when compared to ABBM +
AB. In addition, the influence of implant surface microtopography on early
osseointegration in MSA regenerated sites was assessed. This is continued further
to assess the outcomes of implant supported restorations placed into MSA sites
using these two biomaterials and well defined success criteria including survival,
biological and technical outcomes.
In the first part of the thesis, qualitative and quantitative histological assessment
was used to compare ABBM-C with ABBM + AB in both pre-clinical and clinical
MSA models. In the first experimental chapter (Chapter 2), a randomized
controlled trial utilized histomorphometric assessment in a pre-clinical model
(ovine) to show that both healing time and proximity to the resident sinus walls had
a positive impact on histomorphometric outcomes. Both biomaterials exhibited
very similar histomorphometric parameters in the proximal zones but the presence
of AB seemed advantageous in regions distant from resident sinus wall. In chapter
3, the histomorphometric assessment was performed in a prospective controlled
clinical trial. Both biomaterials exhibited very similar histomorphometric
parameters but the ABBM+AB group exhibited a more mature graft with a greater
proportion of lamellar bone. Based on these histological assessments, ABBM-C
appeared to be a suitable bone substitute for the purposes of MSA. In chapter 4,

iii
the influence of implant surface microtopography on early osseointegration in MSA
was assessed in a pre-clinical (ovine) model by placing implants with a hydrophilic
and hydrophobic surface in sites previously receiving the MSA procedure. Both
time and the use of a hydrophilic implant surface had a positive impact on %BIC
around implants placed into augmented maxillary sinuses. Hydrophilic implant
surfaces also had a positive impact on the surrounding tissue composition.
The second part of this thesis explores the clinical, radiographic and patient centred
outcomes of MSA using these two biomaterials, as well as the survival and success
of the implant supported restorations placed into these sites. In chapter 5, a
prospective clinical trial compared both groups of biomaterials in MSA with
material allocation based on specific clinical presentations (sinus membrane
perforation / local AB bone availability). It indicated that MSA using the lateral
wall technique is safe and associated with mild to moderate pain and restrictions to
daily activities for 48-72hrs. Patient reporting of morbidity was greater with AB
harvesting. Volumetric analysis using 3-D imaging showed that C-ABBM provides
comparable bone volume to AB + ABBM that is sufficient for placement of
implants of adequate size with no need for further vertical augmentation. Engaging
the surrounding sinus walls had a significant positive impact on graft volume. In
chapter 6, the same patient population was followed to assess implant supported
restorations after 12 months of function using well defined success criteria. Both
groups revealed high implant survival rates. Marginal bone levels & peri-implant
parameters were consistent with health in both groups. The majority of the
restorations were screw retained single crowns or small fixed partial dentures. The
incidence of mucositis was dependent on the definition threshold. Absence of peri-
implantitis and low rates of technical complications were reported in both groups.
Within the limitation of this trial, it can be concluded that collagen stabilized
ABBM can be successfully used alone for maxillary sinus augmentation and
subsequent implant rehabilitation. Its clinical utility is most relevant in cases of
sinus membrane perforation and insufficient autogenous bone in the local area.

iv
STATEMENT OF ORIGINALITY
I, Jamil Alayan declare that this work has not previously been submitted for a
degree or diploma in any university. To the best of my knowledge and belief, the
thesis contains no material previously published or written by another person
except where due reference is made in the thesis itself.
Jamil Alayan
04th May 2018

v
Table of Contents
ABSTRACT .............................................................................................................i
STATEMENT OF ORIGINALITY ............................................................................. iv
LIST OF APPENDICES .......................................................................................... vii
ACKNOWLEDGEMENTS ..................................................................................... viii
RESEARCH OUTPUTS ARISING FROM THESIS ...................................................... ix
STATEMENT OF ETHICS APPROVAL ...................................................................... x
STATEMENT OF INCLUSION OF ONLY CO-AUTHORED PAPERS ............................ xi
CHAPTER 1 – INTRODUCTION ..............................................................................1
BACKGROUND & SURGICAL TECHNIQUE ................................................................... 2
PRE-OPERATIVE ASSESSMENT ................................................................................... 4
Relevant Anatomical Features ............................................................................................ 5 Relevant Sinus Physiology ................................................................................................... 7 Common Pathological Conditions ..................................................................................... 10 Maxillary Sinus Pathology & Patient Assessment ............................................................... 11
POST-OPERATIVE CONSIDERATIONS ........................................................................11
Impact of MSA on Sinus Physiology ................................................................................... 11 Surgical & Post-operative Complications ........................................................................... 13
BONE GRAFTS & MSA ...............................................................................................16 Biomaterials – types and characteristics ........................................................................... 17 Bone Graft Healing & MSA ................................................................................................ 20 Characteristics of MSA Sites .............................................................................................. 25
DENTAL IMPLANTS & SUPPORTED RESTORATIONS IN MSA .....................................30
Dental implant surface microtopography .......................................................................... 30 Outcomes of implant supported restorations in MSA ........................................................ 33
RESEARCH HYPOTHESIS ............................................................................................38
AIMS.........................................................................................................................39
REFERENCES .............................................................................................................41
PART 1 – HISTOLOGICAL & HISTOMORPHOMETIRC ASSESSMENT OF USING
COLLAGEN STABILIZED ABBM IN MSA ...............................................................66

vi
Chapter 2 - A histomorphometric assessment of collagen stabilized anorganic
bovine bone mineral in maxillary sinus augmentation – a randomized controlled
trial in sheep. ...........................................................................................................67
Chapter 3 - A histomorphometric assessment of collagen stabilized anorganic
bovine bone mineral in maxillary sinus augmentation – a prospective clinical trial. 79
Chapter 4: Comparison of early osseointegration of SLA® and SLActive® implants in
maxillary sinus augmentation: a pilot study. ............................................................90
PART 2 – CLINICAL & RADIOGRAPHIC ASSESSMENT OF COLLAGEN STABILIZED
ABBM IN MSA .................................................................................................. 101
Chapter 5: A prospective controlled trial comparing xenograft/autogenous bone
and collagen-stabilized xenograft for maxillary sinus augmentation – Complications,
patient reported outcomes and volumetric analysis. .............................................102
Chapter 6: A prospective controlled trial comparing xenograft/autogenous bone
and collagen-stabilized xenograft for maxillary sinus augmentation – biological and
technical implant outcomes. ..................................................................................119
CHAPTER 7 – DISCUSSION & FUTURE DIRECTIONS........................................... 156
APPENDIX A ..................................................................................................... 177

vii
LIST OF APPENDICES
Appendix A: Ethics approval certificates
1. Human Ethics Approval - Dental Sciences Ethics Committee, School of
Dentistry, University of Queensland, Australia.
2. Animal Ethics approval certificate – University Animal Research
Committee, Queensland University of Technology, Australia.
3. Animal Ethics Committee – Griffith University, Australia.

viii
ACKNOWLEDGEMENTS
This doctoral thesis was carried out under the primary supervision of Prof. Saso
Ivanovski. I would like to sincerely thank Saso for the opportunity to work under
his guidance, his supervision and within his research team. It has been a wonderful
learning experience.
I would also like to acknowledge the following members of the research team for
their invaluable contribution and assistance throughout the research project:
• Dr Cedryck Vaquette for his assistance with the histological components of
this project.
• Dr Siamak Saifzadeh for his assistance with the animal model and surgery.
• Dr Dimitrios Vagenas for his assistance with the statistical analysis of this
project.
• Dr Raahib Dudhia for his assistance with the radiological component of this
study.
Furthermore, I would also like to acknowledge the love, support and sacrifice of
my family throughout this long journey.

ix
RESEARCH OUTPUTS ARISING FROM THESIS
Published Refereed Journal Articles
1. Alayan J, Vaquette C, Saifzadeh S, Hutmacher D, Ivanovski S. (2016) A
histomorphometric assessment of collagen stabilized anorganic bovine bone
mineral in maxillary sinus augmentation – a randomized controlled trial in
sheep. Clinical Oral Implants Research 27: 734 – 743. doi: 10.1111/clr.12652.
2. Alayan J, Vaquette C, Farah C, Ivanovski S. (2016) A histomorphometric
assessment of collagen stabilized anorganic bovine bone mineral in maxillary
sinus augmentation – a prospective clinical trial. Clinical Oral Implants
Research 27: 850 – 858. doi: 10.1111/clr.12694.
3. Alayan J, Vaquette C, Saifzadeh S, Hutmacher D, Ivanovski S. (2017)
Comparison of early osseointegration of SLA® and SLActive® implants in
maxillary sinus augmentation: a pilot study. Clinical Oral Implants Research
28: 1325 – 1333. doi: 10.1111/clr.12988.
4. Alayan J, Ivanovski S. (2018) A prospective controlled trial comparing
xenograft/autogenous bone and collagen-stabilized xenograft for maxillary
sinus augmentation – Complications, patient reported outcomes and volumetric
analysis. Clinical Oral Implants Research 29: 248 – 262. doi:
10.1111/clr.13107.
Articles In Final Preparations
1. Alayan J, Ivanovski S. (2018) A prospective controlled trial comparing
xenograft/autogenous bone and collagen-stabilized xenograft for maxillary
sinus augmentation – biological and technical implant outcomes. Clinical Oral
Implants Research (submitted).

x
STATEMENT OF ETHICS APPROVAL
I confirm that ethical clearance for this research was granted by the following
organisations (Appendix A):
1. Human Ethics Approval - Dental Sciences Ethics Committee, School of
Dentistry, University of Queensland, Australia (Project number: 1010).
2. Animal Ethics approval certificate – University Animal Research Committee,
Queensland University of Technology, Australia (QDPI Scientific Use
Registration Number 0052. Approval number: 1100001051).
3. Animal Ethics Committee – Griffith University, Australia (GU Ref No:
DOH/02/13/AEC).
I can confirm that research was conducted in accordance with the approved
protocols.
Jamil Alayan
04th May 2018

xi
STATEMENT OF INCLUSION OF ONLY CO-AUTHORED PAPERS
Included in this thesis are papers in Chapters 2, 3, 4, 5 and 6 which are co-authored
with other researchers. My contribution to each co-authored paper is outlined at the
front of the relevant chapter. The bibliographic details for these papers including
all authors, are:
Chapter 2: Alayan J, Vaquette C, Saifzadeh S, Hutmacher D, Ivanovski S. (2016)
A histomorphometric assessment of collagen stabilized anorganic bovine bone
mineral in maxillary sinus augmentation – a randomized controlled trial in sheep.
Clinical Oral Implants Research 27: 734 – 743. doi: 10.1111/clr.12652. Copyright
status: permission to reproduce granted. License number: 4342510031510.
Chapter 3: Alayan J, Vaquette C, Farah C, Ivanovski S. (2016) A
histomorphometric assessment of collagen stabilized anorganic bovine bone
mineral in maxillary sinus augmentation – a prospective clinical trial. Clinical Oral
Implants Research 27: 850 – 858. doi: 10.1111/clr.12694. Copyright status:
permission to reproduce granted. License number: 4342510448961.
Chapter 4: Alayan J, Vaquette C, Saifzadeh S, Hutmacher D, Ivanovski S. (2017)
Comparison of early osseointegration of SLA® and SLActive® implants in
maxillary sinus augmentation: a pilot study. Clinical Oral Implants Research 28:
1325 – 1333. doi: 10.1111/clr.12988. Copyright status: permission to reproduce
granted. License number: 4342510697065.
Chapter 5: Alayan J, Ivanovski S. (2018) A prospective controlled trial comparing
xenograft/autogenous bone and collagen-stabilized xenograft for maxillary sinus
augmentation – Complications, patient reported outcomes and volumetric analysis.
Clinical Oral Implants Research 29: 248 – 262. doi: 10.1111/clr.13107. Copyright
status: permission to reproduce granted. License number: 4342510860031.
Chapter 6: Alayan J, Ivanovski S. (2018) A prospective controlled trial comparing
xenograft/autogenous bone and collagen-stabilized xenograft for maxillary sinus

xii
augmentation – biological and technical implant outcomes. Clinical Oral Implants
Research (submitted).
Appropriate acknowledgements of those who contributed to the research but did
not qualify as authors are included in each paper.
Jamil Alayan
04th May 2018
(Countersigned) ___________________________ (Date) 16th May 2018
Supervisor: Stephen Hamlet

CHAPTER 1 – INTRODUCTION

2
BACKGROUND & SURGICAL TECHNIQUE
The rehabilitation of partial and fully edentulous patient with dental implants is
considered to be a predictable therapeutic modality with favourable long term
functional results (Buser, et al. 2012, Jung, et al. 2012, Pjetursson, et al. 2012).
Reduced alveolar bone height and bone density however, are common limitations
when considering implant rehabilitation of the posterior maxilla (Jemt & Lekholm
1995). Bone deficiency in this anatomical region is caused by post-extraction ridge
resorption and maxillary sinus pneumatization (Farina, et al. 2011). Maxillary sinus
floor elevation (MSA) using a trans-alveolar or a lateral window approach (Boyne
& James 1980, Summers 1994) are the most commonly utilized procedures to
overcome maxillary sinus pneumatization. MSA using the lateral window approach
has been shown to support predictable survival of implants placed into the
augmented bone (Bornstein, et al. 2008, Del Fabbro, et al. 2008, Pjetursson, et al.
2008, Nkenke & Stelzle 2009).
The lateral window or modified Caldwell-Luc approach has its roots in the 19th
century. George Caldwell in 1893; Scanes Spicer in 1894 and Henri Luc in 1897,
independently advocated the creation of an anterior maxillary antrostomy through
the canine fossa with nasal drainage to cure maxillary sinusitis. This became known
as the Caldwell-Luc procedure (Macbeth 1971). This procedure involved a buccal
vestibular incision form the region of the canine eminence to the first molar
(DeFreitas & Lucente 1988). The elevated mucoperiosteal flap exposed the lateral
maxillary wall and the inferior orbital nerve, which can be identified and protected.
The anterior antrostomy is placed above the roots of the maxillary teeth or it may
be created more posteriorly depending on the pathological condition. Sinus mucosa
was then removed and the amount of this removal was dictated by the extent of
disease, with healthy mucosa preserved. After the antrum is adequately cleared, an
inferior meatal antrostomy is created and the buccal flap is closed.
Philip Byone used the Caldwell-Luc technique to augment the maxillary sinus floor
with corticocancellous bone graft harvested from the iliac crest (Boyne & James
1980) After 3 months, Boyne carried out an alveolar osteoplasty of the posterior
maxilla without risk of penetrating the maxillary sinus and created the necessary

3
interarch distance in patients needing full removable dentures with advanced sinus
pneumatisation.
Subsequently, the same surgical procedure was utilised in patients with advanced
sinus pneumatisation for the purposes of placing a dental implant. Both Boyne
(Boyne & James 1980) and Tatum (Tatum 1986) used a modified Caldwell-Luc
approach to the antrum where a buccal antrostomy was created in the lateral wall
of the maxilla and the Schneiderian membrane was carefully elevated. Autogenous
particulate bone graft was subsequently placed in the sub-antral space after it was
harvested from the iliac crest. The dental implants were placed some months later
and the prosthetic reconstructions comprised of fixed and removable prostheses.
In the same period, Tatum also further developed and improved the surgical
technique. Tatum’s modification of the technique involved the creation of a trap
door from the buccal antrostomy, which was pushed into the antrum to create a new
roof. Implants were also placed simultaneously at the time of grafting. (Tatum
1977, Tatum 1986)
Since these early reports, treatment options have developed further for the
management of the deficient posterior maxilla with the advent of MSA via the
transcrestal approach and short implants (<8mm). Both options are associated with
good outcomes (Del Fabbro, et al. 2004, Esposito, et al. 2014, Schincaglia, et al.
2015). However, both of these options require a residual ridge height typically
ranging from a minimum of 4 or 5mm up to 7mm (Markovic, et al. 2016, Pohl, et
al. 2017). In contrast, MSA using the lateral window approach can achieve adequate
grafted ridge height even in cases with complete loss of an intact maxillary sinus
floor, (Cortes, et al. 2015). Furthermore, the MSA using the lateral approach is
necessary if the required gain in bone height is greater than 3-4mm in order to
accommodate the desired implant dimension (Zitzmann & Scharer 1998). A recent
systematic review comparing these options for the rehabilitation of the deficient
posterior maxilla reiterated that the three options are all viable but not strictly
equivalent, and treatment decision needs to be based on the particular features of
each individual (Corbella, et al. 2015).
4
Whilst the original Caldwell-Luc technique is based on solid principles, this
surgical technique is still being refined, with a large degree of variation in many
aspects. Some of these include the location (Tatum 1986) and method of creating
buccal antrostomy (Galindo-Moreno, et al. 2007), the use of various bone grafting
materials (Schmitt, et al. 2013), and the timing of both implant placement (Peleg,
et al. 1999).
If the initial bone height allows primary implant stability, simultaneous implant
placement can be performed (Jensen & Terheyden 2009). Several case series have
presented favourable results for simultaneous implant placement (Cordioli, et al.
2001, Mangano, et al. 2007). If primary stability cannot be achieved, then the sinus
floor should be elevated in a separate procedure followed by delayed implant
placement. A mean ridge height of 4.4mm was reported in studies using
simultaneous implant placement and 2.9mm for staged placement (Jensen &
Terheyden 2009).
The position of the antrostomy and the technique for its creation are determined by
the size and location of the maxillary sinus and anatomical features such as
vasculature, septa, lateral sinus wall thickness and internal sinus dimensions. While
rotary instruments are commonly used for window preparation the recent
development of piezoelectric surgery has specifically been adapted for sinus
surgery (Vercellotti, et al. 2001). This technology may contribute to reducing intra-
operative complications such as membrane perforation and haemorrhage (Wallace,
et al. 2007). However, a small scale clinical study with a randomised controlled
design failed to confirm this difference (Barone, et al. 2008) and further trials are
warranted on the merits of using piezoelectric surgery compared with rotary
instruments.
PRE-OPERATIVE ASSESSMENT
Post-surgical complications tend to be associated with pre-existing sinus disease or
documented susceptibility to sinus disease (Raghoebar, et al. 1999, Timmenga, et
al. 2003). Therefore, proper pre-operative evaluation of the sinus health is expected
to minimise postoperative adverse events. Sinus health assessment in the dental
setting is performed through a detailed history and a radiographic examination and

5
relies on a sound understanding of the relevant anatomy, physiology and pathology
of the region.
Relevant Anatomical Features
Osteomeatal Complex and Related Structures
The anterior osteomeatal complex (OMC) (Figure 1) is the key region to the
drainage of the anterior sinuses (frontal, anterior ethmoid and maxillary) and the
sphenoethmoidal recess drains the posterior sinuses (posterior ethmoid and
sphenoid) and is also called the posterior OMC (Naumann 1965). The anterior
OMC comprises the maxillary sinus ostia and ethmoid infundibulum, hiatus
semilunaris, middle meatus, anterior ethmoidal air cells and frontal recess (Beale,
et al. 2009).
The maxillary ostium is located in the superior-medial aspect of the maxillary sinus
(Schatz & Becker 1984). The ostium leads into the second passage, the ethmoid
infundibulum, which is a funnel shaped passage that conducts mucous from the
maxillary sinus into the middle meatus via the third passage, the hiatus semilunaris
(Roithmann, et al. 1992). A fourth passage, the frontal recess is a part of the anterior
ethmoid complex and drains the frontal sinus (Rao & El-Noueam 1994) also into
the middle meatus (Oliverio, et al. 1995). The middle meatus drains into the back
of the nasal cavity and into the nasopharynx where mucous is ultimately swallowed.
From a functional standpoint the infundibular space represents the confluence of
drainage from the frontal, anterior ethmoid and maxillary sinuses. Anatomic
abnormalities or disease states affecting any of these neighbouring structures could
obstruct this space and cause sinusitis in any or all of the adjacent structures
(Kennedy, et al. 1985).

6
Figure 1 OMC - radiographic (CT) features (from Sarna A et al. 2002)

7
Relevant Sinus Physiology
Sinus health in any patient depends on three interrelated factors (Senior & Kennedy
1996):
1. Secretion of mucous with normal viscosity, volume and composition;
2. Normal mucociliary flow to prevent mucous stasis and subsequent infection
3. Open sinus ostia to allow adequate drainage and ventilation.
In the rhino-sinus-pharyngeal district, there are three important sites from anterior
to posterior: the osteomeatal complex (OMC), the sphenoethmoidal recess and the
rhinopahrynx. The correct ventilation and effective mucociliary clearance (MCC)
of these three patho-physiologic regions maintains the healthy physiology of the
whole respiratory system (Varricchio, et al. 2010).
Schneiderian Membrane
The maxillary sinus is internally lined with a thin mucosa of ciliated respiratory
epithelium, also known as the Schneiderian membrane, that is continuous with that
of the nose (McGowan, et al. 1993) and other paranasal sinuses through their ostia.
The mucosa of the paranasal sinuses is a mucoperiosteum (Figure 2) consisting of
a layer of pseudostratified columnar ciliated epithelium with mucous secreting
goblet cells. This overlies a thin lamina propria of loose connective tissue and
elastic fibres that is continuous with the periosteum. All cells are attached on the
basal membrane. Basal cells lie on the membrane and show no contact with the
epithelial surface and utilise desmosomes for cell adhesion (Gudis & Cohen 2010).
Mucociliary Clearance (MCC)
MCC is an essential homeostatic mechanism of the respiratory system and is
designed to remove both healthy and pathological secretions from the airway. MCC
in the sinuses was demonstrated in a pre-clinical model after the removal of mucosa
from the frontal sinuses resulted in significant interference with mucociliary
transport (Hilding 1932). It was also demonstrated that each of the large sinus
cavities has distinct mucosal flow patterns (Messerklinger 1966). These
observations remain valid today. It has since been demonstrated that mucosal flow
is accomplished through the coordinated beating of cilia in a specific direction

8
resulting in organised ciliary waves propelling particulate matter out of the cavity.
The mucociliary flow from the anterior sinuses converges at the OMC before
travelling posteriorly to the nasopharynx. Once the mucous layer is in the
nasopharynx, further mucociliary action and swallowing assists its ingestion.
Microscopic cilia dysfunction at any step of this intricate transport system can result
in significant and clinically evident sinonasal pathology. It is important to
emphasize that the upper airway paranasal sinuses are almost completely dependent
on the activity of cilia for removal of mucous, whereas in the lower airway deficient
MCC may be compensated for by coughing (Wagenmann & Naclerio 1992).
Figure 2. (A) Schematic representation of the components of the Schneiderian
membrane (B) Light microscope micrograph of histological section of the
Schneiderian membrane (From Sourji et al 2009)

9
Inter-sinus Connections
Paranasal sinuses are interconnected via accessory ostia and many sinuses do not
drain directly into the nasal cavity but rather indirectly through adjacent sinuses. A
research group indicated that 37% of maxillary sinuses drained exclusively into the
middle meatus via the nasal ostium, 19% drained via the nasal ostium and ethmoid
nasal route and 52% exclusively via the ethmoid nasal route (Prott 1971, Prott 1973)
(Vogt & Schrade 1979). Similarly, nasal ostia for ethmoidal cells were seen
draining directly into the middle meatus in 15% of patients, with 33% of patients,
drainage occurred via the maxillary sinus or a shared common drainage canal with
the maxillary sinus in 19% of individuals (Prott 1971, Prott 1973, Vogt & Schrade
1979).
Ostial Patency & Ventilation
It is generally accepted fact that free air communication between the nasal cavity
and its paranasal sinus via patent ostia is a pre-requisite for physiological conditions
within the sinuses (Mann, et al. 1977). Oxygen pressure within the maxillary sinus
is dependent on the functional ostial diameter. When the ostial diameter is less than
2mm, oxygen pressure falls (Aust & Drettner 1974). This reduction of the ostial
patency leads to alterations in pO2 and pCO2 resulting in early inflammation (Aust,
et al. 1994). Pressure recordings in humans indicate identical pressure exists within
the maxillary sinus cavity and ipsilateral nasal cavity during inspiration and
expiration (Proetz 1932, Jannert, et al. 1984). Also, sinuses with patent ostia
showed pressure curves synchronous with the respiratory cycle (Scharf, et al. 1995).
Microbiological Features
Knowledge of the bacterial flora of normal sinuses is mandatory to understand the
pathogenicity of species isolated in disease sinuses (Busaba, et al. 2004). Healthy
maxillary sinuses have been considered to be sterile (Su, et al. 1983). Nonetheless,
other papers have discovered bacteria in healthy sinuses (Brook 1981, Cook &
Haber 1987, Jiang, et al. 1999). Brook et al. reported for the first time the presence
of aerobic and anaerobic bacteria in normal maxillary sinuses (Brook 1981). Also,
Jiang et al detected culturable bacteria in 46.7% from swab specimens and 41.2%

10
from mucosal specimens in healthy individuals using a puncture and aspiration
method (Jiang, et al. 1999).
Studies on this topic vary significantly in many ways, including the techniques used
for sampling and culturing, and most importantly the definition of maxillary sinus
health. While some authors based their definition of normality on the absence of
clinical symptoms (Brook 1981), others used clinical presentation, history and
radiographic appearance (Cook & Haber 1987) or normal endoscopic appearance
(Jiang, et al. 1999).
A study in 2009 (Abou-Hamad, et al. 2009) used strict criteria for defining the
normal maxillary sinus: asymptomatic patients with normal CT scan and normal
endoscopic findings. Comprehensive exclusion criteria and parameters were used
to reduce confounding factors, and included controlled sampling methods, storage
media and transportation time. The majority of sinuses were found to be sterile
(82.1%). It should be noted that all of the species recovered from healthy sinuses
(17.8%) were aerobes and no anaerobes were isolated despite the use of appropriate
methods for anaerobic detection.
Further studies with the same strict inclusion criteria and well-controlled
parameters as the study above, reported similar results for the frontal sinus, with
85.72% found to be sterile (Albu & Florian 2013). On the other hand, bacterial
growth was reported in 94.3% of normal and un-diseased anterior ethmoid sinuses
(Kirtsreesakul, et al. 2008). Anaerobes however, were not found.
Common Pathological Conditions
The maxillary sinus may become involved with several types of diseases including
inflammatory, benign and malignant neoplasms (Diecidue, et al. 1999, Sciubba
1999). Most pathologic processes in the maxillary sinus are asymptomatic and often
found incidentally. Studies report very few cases of sinus pathology that are
absolute contra-indicate MSA (Pignataro, et al. 2008, Torretta, et al. 2013). In
contrast, more than a third of patients exhibit relative contra-indications that require
further management (medical or surgical) (Beaumont, et al. 2005, Torretta, et al.
11
2013). Most frequent conditions diagnosed include chronic sinusitis, cysts,
odontogenic sinusitis and foreign bodies.
Maxillary Sinus Pathology & Patient Assessment
A key issue is interpretation of anatomical variants or radiological signs of
pathology and relating this to clinical presentation or history provided. This
important step dictates whether the MSA procedure proceeds as planned or is
contraindicated and necessitates a referral to an ENT specialist.
A prospective study assessing patients for chronic rhino-sinusitis reported that
sensitivity of symptoms alone was high for the diagnosis of CRS at 88.75. But since
CRS symptoms are non-specific and associated with many other conditions, the
positive predictive value (PPV) was only 39.9% (Bhattacharyya & Lee 2010). The
addition of endoscopy significantly increased the PPV to 66%. Relying on the
presence of symptoms alone is likely to lead to diagnostic errors. Primarily
rhinosinusitis is a clinical diagnosis that is supported by endoscopic findings.
Reliance on endoscopy however for screening of all potential patients planning to
undergo MSA is likely to lead to unnecessary referrals to ENT specialists.
Radiography however is an accessible and familiar assessment tool in the dental
setting and will assist in carrying a risk assessment of prospective patients. A
prospective study assessed the accuracy of CT in the diagnosis of CRS has shown
them to exhibit good sensitivity and above average specificity especially when
extensive or widespread opacification is seen (Bhattacharyya & Fried 2003).
POST-OPERATIVE CONSIDERATIONS
Impact of MSA on Sinus Physiology
Whilst it has been suggested that Schneiderian membrane elevation may cause
interim inhibition of ciliary activity, clinical evidence suggests that maxillary sinus
augmentation has limited effects on sinus physiology (Timmenga, et al. 1997,
Timmenga, et al. 2003). A retrospective study (Timmenga, et al. 1997) examined
the impact of MSA on sinus function. The occurrence of postoperative chronic
sinusitis was limited to patients with a predisposition for this condition. This
highlights the concept of ‘sinus compliance’ which depends on the baseline

12
anatomical and physiological condition of the sinus (Torretta, et al. 2013). The
better the health of the sinus the lower the risk of complications due to its improved
ability to regain homeostasis after MSA.
In a prospective study (Timmenga, et al. 2003), 17 patients underwent endoscopic,
microbiological and morphological examination of their maxillary sinuses after
MSA. These evaluations were performed immediately preceding MSA, and then at
3 months (at implant insertion) and 9 months (at uncovering of implants) post-
operatively. Pre-operative screening was carried out to exclude those with
maxillary sinusitis. The 3 month microbiological evaluation showed a significant
increase in bacterial growth, while the 9-months results were comparable to the pre-
operative status. Morphologically, neither fibrosis nor thickening of the epithelium
and lamina propria was observed postoperatively. The number of goblet cells in the
epithelial layer was increased. This mild inflammatory reaction observed using
endoscopic evaluation should be interpreted as a normal physiological response of
the mucosal airway. MSA does not appear to have clinical consequences in patients
without signs of pre-existing sinusitis.
A similar conclusion was reached by Sul et al. (Sul, et al. 2008), after examining
the sinus mucosa under both light and electron microscopy post-sinus membrane
elevation. The implant was placed 5mm into the sinus cavity after sinus membrane
elevation and without a bone graft. The contralateral side was left untreated and
used as a control. There were no morphologic or ultrastructural changes in the sinus
membrane between groups. Furthermore, the cilia were all synchronously arrayed,
uniformly leaning in the same direction in both sinuses. This implies that the
insertion of dental implants into the maxillary sinus cavity after elevating the
membrane without adding any graft seems to be well tolerated. An important factor
to be considered in these studies is that the membrane was not perforated in any of
these samples.
Complete regeneration of the mucous membrane including cilia occurs within five
months after total surgical removal (Selden 1974). There is also agreement that the
sinus membrane will recover form sinusitis once proper ventilation is restored
(Stammberger 1986). This was also shown by Huang et al. (Huang, et al. 2006)

13
whereby endoscopic surgery in patients with chronic maxillary sinusitis resulted in
recovery of antral mucosa and MCC with improved ventilation and drainage. In
addition, cilia were significantly regenerated compared to the pre-operative state.
Alterations in voice quality secondary to nasal cavity and paranasal sinus surgery
have been reported (Chen & Metson 1997, Hosemann, et al. 1998). A study in 2003
(Tepper, et al. 2003) examined the effects of reduction in sinus volume on voice
quality in a specific group of patients who depend on the quality of their voice for
their livelihood (e.g. speakers, singers, actors). An exhaustive list of sound / voice
parameters were analysed with no changes detected in any of the evaluated
parameters. It was concluded that sinus grafting does not appear to jeopardise the
individuals voice pattern even when the sinus volume was reduced by as much as
22%.
Surgical & Post-operative Complications
Maxillary sinus grafting is a procedure with well documented clinical success and
founded on sound biological principles. The procedure however is not free of
complications (Chanavaz 1990, Regev, et al. 1995). It is technique sensitive and
dependent on careful patient selection.
A review carried out in 2009 reported that perforation of the Schneiderian
membrane was the most common intra-operative complication (Schwartz-Arad, et
al. 2004, Chiapasco, et al. 2009). Other intra-operative complications including
excessive bleeding, displacement of implant or grafting material into the sinus
cavity, and damage to the infra-orbital nerve were reported in only a few cases
(Chiapasco, et al. 2009). The most frequent post-operative complications was
infection and /or postoperative maxillary sinusitis. Partial or total bone graft loss
occurred in less than 1% of the patients (Chiapasco, et al. 2009).
Schneiderian Membrane Perforation
Perforation of the Schneiderian membrane is the most common intra-operative
complication of sinus elevation surgery (Chiapasco, et al. 2009). The reported

14
incidence in the literature varies from 7.5% (Cortes, et al. 2015) to 35% (Jensen, et
al. 1994) and 44% (Schwartz-Arad, et al. 2004).
Few studies have reported a negative impact of perforations on implant survival,
especially in cases of larger perforations (Proussaefs, et al. 2004, Hernandez-
Alfaro, et al. 2008). In most studies however, no significant impact were seen on
implant survival rates (Barone, et al. 2006, Zijderveld, et al. 2008) even for larger
perforations (Testori, et al. 2008). Furthermore, perforations have not been shown
to negatively affect the height of regenerated bone post-augmentation (Shlomi, et
al. 2004).
Reported causes of membrane perforations include the presence of a thin
membrane, presence of septa and adhesions or previous sinus surgery (Becker, et
al. 2008, Zijderveld, et al. 2008). The angulation between the medial and lateral
walls of the maxillary sinus seems to exert an influence on the incidence of
membrane perforation during membrane elevation. A study by Cho et al. (Cho, et
al. 2001) showed a correlation between the percentage of perforation and the
anatomy of the sinus. The patient population was divided into groups based on the
internal angle of the medial and lateral sinus walls. The perforation rates were
significantly higher in the group with narrow angles. These are typically found in
the second bicuspid region (Velloso, et al. 2006).
Since the presence of septa are also associated with an increased risk of membrane
perforation, a modification of the conventional surgical technique is required (Betts
& Miloro 1994). Boyne and James recommended their cutting and removal (Boyne
& James 1980), others subdivided the trapdoor into an anterior and posterior part
(Tidwell, et al. 1992), or followed the contour of the sinus floor by making a W-
shaped preparation at smaller septa (Zijderveld, et al. 2008).
Post-grafting sinusitis & infection
When using generally accepted ENT criteria for diagnosing sinusitis, the
development of post-sinus grafting chronic maxillary sinusitis has been reported to
occur in 4.4% (2/45) of MSA cases (Timmenga, et al. 1997). Previously, maxillary
sinusitis post-sinus membrane elevation was considered to be a major drawback,

15
but many of these studies were based on poorly defined criteria for sinus
examination (Doud Galli, et al. 2001).
The occurrence of post-grafting sinusitis appears to be associated with pre-existing
structural or mucosal features that compromise the sinus ability for adequate MCC
and ventilation after the surgical challenge or due to physical obstruction caused by
endo-antral displacement of particulate bone graft into the maxillary sinus proper
(van den Bergh, et al. 2000).
Barone et al. experienced post-grafting sinusitis in 10% of their study population
(7/70 patients) (Barone, et al. 2006). These cases were treated by drainage through
the bony window and systemic antibiotics. In a small fraction of these cases
endoscopic surgery was required where infection persisted despite conservative
treatment. Endoscopy in these patients confirmed a stenotic OMC. Other case
reports of post-grafting sinusitis have confirmed overfilling of the subantral space
in-conjunction with pre-existing structural risk factors, such as pneumatization of
the middle turbinate leading to narrowing of the middle meatus (Felisati, et al.
2008).
Other reports of post-grafting sinusitis report the cause to be endo-antral
displacement of bone graft particles leading to obstruction of OMC (Regev, et al.
1995, Wiltfang, et al. 2000, Doud Galli, et al. 2001). Many of these cases required
endoscopic surgery (middle meatal antrostomy) to resolve the symptoms after
systemic antibiotics and local measures failed to manage this condition. These case
reports have been supported by Timmenga et al. (Timmenga, et al. 2001), who
reported chronic purulent maxillary sinusitis post-grafting that was non-responsive
to conservative therapy including systemic antibiotics, nasal decongestant and
corticosteroids. Functional endoscopic surgery was required. The authors
recommended surgical intervention if post-grafting sinusitis is non-responsive to
conservative measures, in order to re-establish adequate drainage and remove the
obstructing particles that may be responsible for persistent symptoms.

16
Prompt and appropriate post-operative management is required in these cases. It
also highlights the importance of adequate screening of patients to identify those
with diminished sinus compliance and the prevention of endo-antral displacement.
BONE GRAFTS & MSA
The ideal grafting material should provide an osteoconductive matrix,
osteoinductive factors and be osteogenic with viable cells contained inside the bone
graft, capable of laying new bone matrix.
Osteoinduction is a healing process in which local growth factors cause
mesenchymal cells to disaggregate, migrate, re-aggregate, proliferate and later
differentiate into chondroblasts or osteoblasts (Urist 1965, Reddi, et al. 1987).
Osteoconduction is a process where the implanted material serves as a scaffold for
ingrowth of capillaries, peri-vascular tissue and osteoprogenitor cells from the
recipient bed (Burchardt 1983). The host tissue has a specific effect on these
materials that may vary depending on the site in which they are placed (Donath, et
al. 1992) such that bone formation is seen when a biomaterial is placed into host
bone, whereas its insertion into subcutaneous tissue results only in connective tissue
encapsulation.
Consequently, the gold standard for bone grafting procedures is traditionally
considered to be autogenous bone because of its combination of osteoconduction
and osteoinduction. Despite these benefits, considerable drawbacks, such as
additional surgical procedures, donor site morbidity (Clavero & Lundgren 2003,
Cricchio & Lundgren 2003), limited availability and unpredictable resorption
(Davis, et al. 1984, Clavero & Lundgren 2003, Wiltfang, et al. 2005, Sbordone, et
al. 2013), have necessitated the pursuit of alternatives. These include bone
allografts from human donors, xenografts and various alloplastic materials (Kao &
Scott 2007). Other strategies incorporate growth factors and cell based alternatives,
used either alone or in combination with other materials (Jabbarzadeh, et al. 2008).

17
Biomaterials – types and characteristics
The ideal bone substitute must be biocompatible and allow for proliferation of new
blood vessels and ultimately the growth of new bone into the augmented area. The
ideal bone substitute maintains this biological support during healing and is
gradually replaced by newly formed bone (Jensen, et al. 2006).
From a tissue engineering perspective, (Woodruff & Hutmacher 2010) the
following characteristics are desirable for scaffolds: a three-dimensional and highly
porous structures with an interconnected pore network for cell growth and transport
of nutrients and metabolic waste, a biocompatible and bioresorbable material with
controllable degradation and resorption rate to match cell/tissue growth, suitable
surface chemistry for cell attachment, proliferation and differentiation and
mechanical properties to match those of the tissues at the site of implantation.
Although much effort has been put into the search for the ideal bone substitute
material, such a material probably does not exist. The ideal grafting material for
MSA procedures is not necessarily ideal for onlay bone grafting. For many years,
autogenous bone from the iliac crest has been considered the gold standard in
reconstructive osseous surgery. However, its pronounced resorption, resulting in
loss of almost 50% of its original volume after 6 months of healing (Johansson, et
al. 2001), implies that it cannot be considered an ideal material for MSA.
Various substitutes have been used to fill the sub-antral space after sinus membrane
elevation, including allografts, xenografts, alloplasts and composites of various
materials (Wheeler, et al. 1996, Artzi, et al. 2001, Schlegel, et al. 2003, Wiltfang,
et al. 2003, Thorwarth, et al. 2005, Schlegel, et al. 2007, Artzi, et al. 2008). To date,
a variety of bone substitute materials have been clinically demonstrated to promote
acceptable outcomes (Jensen & Terheyden 2009, Nkenke & Stelzle 2009, Klijn, et
al. 2010, Jensen, et al. 2012). The search continues for the optimal bone substitute
for sinus floor augmentation.
Anorganic Bovine Bone Mineral (ABBM)
Bio-Oss® (Geistlich AG, Wollhusen, Switzerland) is a widely used preparation of
ABBM and is a bone substitute with osteoconductive properties and high

18
biocompatibility (Jensen, et al. 1996). It is one of the best documented biomaterials,
especially in MSA.
Bio-Oss® is a xenograft consisting of deproteinised, sterilized bovine bone with
75-80% porosity and a crystal size of approximately 10 microns in the form of
cortical granules. It has a natural, non-antigenic porous matrix that is chemically
and physically identical to the mineral phase of human bone, and it has been
reported to be highly osteoconductive (Jensen, et al. 1996, Berglundh & Lindhe
1997, Haas, et al. 2002, Orsini, et al. 2005). It is available in two particle sizes, 0.25
– 1.0 mm or 1.0 – 2.0 mm.
Bio-Oss® contains macroscopic and microscopic structures with an
interconnecting pore system that serves as a physical scaffold for osteogenesis
(Tapety, et al. 2004). The pores in Bio-Oss® are of optimal size and configuration
for vascular ingrowth, which is necessary for new bone formation (Daculsi &
Passuti 1990).
Jensen et al. (Jensen, et al. 1996) examined the osteoconductive and biocompatible
features of ABBM and three other bone substitutes in a pre-clinical model. Defects
filled with Bio-Oss® exhibited normal bone healing with initial woven bone
undergoing remodeling to form haversian systems. Bio-Oss® was completely
osseointegrated with intimate contact between the surfaces of the porous system of
ABBM and the newly formed bone.
Understanding the mechanism and the rate of resorption of the different
biomaterials is clinically relevant (Artzi, et al. 2001). It has been debated whether
ABBM is truly resorbable since remnants of Bio-Oss® particles have been reported
to be present many years after their insertion, including in MSA (Piattelli, et al.
1999, Schlegel, et al. 2003).
Some studies have reported signs of resorption of the Bio-Oss® particles
(Berglundh & Lindhe 1997, Hurzeler, et al. 1997, Hammerle, et al. 1998, Yildirim,
et al. 2000) whereas others have reported a lack of resorption (Valentini & Abensur
1997, Hallman, et al. 2002, Schlegel, et al. 2003). Osteoclasts have been described

19
to be present around Bio-Oss® particles (Hurzeler, et al. 1997, Stavropoulos, et al.
2004), while others could not identify this cell type (Artzi, et al. 2001). Some
authors believe that despite the absence of osteoclasts, the ingrowth of bone and the
progressive increase in relative bone volume over a period of time could indicate a
slow resorption of the xenograft material (Sartori, et al. 2003).
A study by Orsini et al. (Orsini, et al. 2007) analyzed Bio-Oss® particles at both a
histological and ultrastructural level from samples taken at 20 months and 7 years
post-sinus grafting in a single patient. In the 7-year specimen, the Bio-Oss®
particles seemed smaller compared with the 20-month specimen at the ultra-
structural level. In contrast, human mandibular ridge defects of varying size and
parameters were assessed histologically after grafting with ABBM (Schlegel &
Donath 1998). Biopsies were taken 6 years post-grafting. The particles exhibited
no change in size or shape over the 6 years. The surface of Bio-Oss® was smooth
with no signs of resorption, not even on surfaces that contained mononuclear
macrophages and multinuclear giant cells.
Jensen et al. (Jensen, et al. 2005) demonstrated osteoclast-like multinucleated giant
cells in close approximation to where osteoblasts formed new bone on the ABBM
surface. However, the characteristic osteoclast associated resorption lacunae were
absent and no quantitative reduction of graft volume could be demonstrated. It was
suggested that the observed multinucleated giant cells had a macrophage-like role
of cleaning the surface of the graft particles, rather than resorption. Mordenfeld et
al. (Mordenfeld, et al. 2010) also evaluated histologically the long-term tissue
response to ABBM and compared particles size after 6 months and 11 years in the
same 11 patients, to determine possible resorption. After 11 years, the ABBM
particles were well integrated and surrounded by lamellar bone with no obvious
sign of resorption. There were no statistically significant differences between the
size of the particles after 11 years compared with those measured after 6 months or
when compared with sterile particles. The area fraction of the Bio-Oss® particles
(17.3%) and the individual particle area (0.063 mm2) after 11 years were similar
with results from specimens retrieved in the same patients at 6 months (14.5% and
0.066 mm2).

20
Overall the evidence seems to indicate that ABBM behaves as a semi-permanent
grafting material with no evidence of significant resorption.
Bio-Oss Collagen® is comprised of ABBM granules with the addition of 10%
highly purified porcine type-1collagen. The collagen acts, according to the
manufacturer, as a cohesive for the granules (Araujo, et al. 2010). Histological
assessment of Bio-Oss Collagen® was carried out in extraction sockets of beagle
dogs at 1 and 3 days, as well as 1, 2 and 4 weeks (Araujo, et al. 2010). The amount
of bovine bone mineral remained unchanged in the socket during the entire 4-week
healing period, whereas the collagen portion was rapidly removed. It was
hypothesized by the authors that hydrolytic enzymes (collagenase) released from
activated PMN cells were involved in the rapid degradation of the porcine collagen
portion of the graft.
Bone Graft Healing & MSA
Irrespective of the model or defect, bone formation and healing require the
recruitment, migration, and differentiation of osteogenic cells into osteoblasts,
resulting in deposition of a collagenous extracellular matrix for mineralization. The
osteoblasts are derived from progenitor cells of the mesenchymal lineage (Bruder,
et al. 1994, Bianco & Robey 2001). Mesenchymal progenitor cells can originate
from various sources such as the bone marrow, the cambrium layer of the
periosteum, and from pericytes surrounding capillaries (Bruder, et al. 1994, Bianco
& Robey 2001). Differentiation of mesenchymal progenitor cells into osteoblasts is
a multistep process, which is stimulated by local growth factors (Reddi 1998,
Gerstenfeld, et al. 2003). Members of the bone morphogenetic protein family are
likely candidates to be involved in this process as they are expressed during bone
repair and have the potential to induce bone formation at ectopic sites.
Schenk described the parameters needed for successful osteogenesis (Schenk
1987):
• Sufficient blood supply: osteoblasts require a high partial oxygen tension to
produce bone matrix. When oxygen tension is low, cells produce cartilage
or fibrous tissue

21
• Mechanical stability: this contributes to formation of stable coagulation and
granulation tissue that is rich in blood vessels.
• Solid surface: osteoblasts can only deposit lamellar bone starting from a
solid stable surface.
• Size of the defect: when a defect is overly large it will not heal through
formation of complete rapid bone bridge between defect walls. It will
instead need several months to completely fill the defect.
• Competition between cells: soft tissue cells proliferate more rapidly than
osteoprogenitor cells and can fill the defect before formation of new bone.
Fibrous tissue formed faster than bone tissue.
Neo-osteogenesis and graft consolidation
After grafts are inserted into maxillary sinus, osteogenesis is activated by surgical
trauma which ultimately causes the release of a large quantity of growth factors
(TGF-β1, aFGF, bFGF, BMP-2, BMP-7) with osteogenic effects (Joyce, et al. 1990,
Bolander 1992, Bostrom, et al. 1995, Sakou 1998, Trippel 1998). It stands to reason
that the osteogenic stimuli released by the surgical trauma and exposure of resident
sinus bone walls allows for the induction and attachment of osteoblasts leading to
deposition of osteoid on the exposed solid walls, similar to early pre-clinical models
of guided bone regeneration (Schenk, et al. 1994, Hammerle, et al. 1995).
Boyne and James (1980) showed that elevation of the Schneiderian membrane
could induce bone formation directly from the sinus floor. There is evidence that
osteogenesis extends progressively towards the centre and apical areas of the graft
and may continue for months after surgery, starting from the sinus floor and lateral
walls and creating a gradient of graft consolidation, as demonstrated in pre-clinical
models (Margolin, et al. 1998, Haas, et al. 2002, Haas, et al. 2002, Scala, et al.
2010). GBR models have suggested that gradients of graft consolidation are
specific for each biomaterial, as reflected by the osteogenic response of the host
bone and the degradation profile of the bone substitutes (Busenlechner, et al. 2008).
In 2009, a pre-clinical study (Busenlechner, et al. 2009) was carried out to assess
graft consolidation in augmented sinuses. A sequential histomorphometric analysis

22
of samples from augmented sinuses using two materials with contrasting
degradation profiles – slow (Bio-Oss®) and rapid (Ostim®) – carried out at various
distances from the resident maxillary bone wall. New bone formation increased
with time and with proximity to the resident bony wall. Residual volume of Ostim®
but not of Bio-Oss® was strongly influenced by the distance from the host bone.
The process of graft consolidation is complex and involves the interaction of the
bone substitute with cells, extracellular matrix and signalling molecules provided
by the host (Khan, et al. 2005). The microenvironment of the maxilla can influence
the behaviour of bone substitutes and the microenvironment of bone substitutes can
influence the osteogenic response of the resident maxilla.
Role of Schneiderian membrane & coagulum in MSA
In-vitro studies have demonstrated that Schneiderian membrane cells can develop
an osteogenic phenotype when cultured in the presence of osteoinductive factors
(Gruber, et al. 2004) and could be induced to express the osteogenic markers
alkaline phosphatase, BMP-2, Oteopontin, Osteonectin and Osteoclacin, in addition
to exhibiting ectopic bone formation in-conjunction with an osteoconductive
scaffold (Srouji, et al. 2009). A pre-clinical (monkey) study placed protruded
implants into the sinus cavity by 5mm, after sinus membrane elevation via a lateral
window (Boyne 1993). One side received a bone graft and the contralateral side
was allowed to fill with a coagulum. Histomorphometric evaluation indicated that
implants placed without bone grafting resulted in bone formation around the first
1-3mm of the protruding implant only. Implants that received the bone graft,
exhibited greater bone coverage around the apical portion. This suggests that the
Schneiderian membrane alone was insufficient to fully support implant integration
in the sinus and the addition of a space maintaining grafting material results in
enhanced bone volume at the implant interface.
There have however been reports of clinically successful implant integration in the
sinus floor by simply elevating the maxillary sinus membrane and simultaneously
inserting dental implants without the use of adjunctive grafting material (Lundgren,
et al. 2004, Palma, et al. 2006). Ten patients were recruited for investigating the
clinical and radiologic results of elevating the Schneiderian membrane without

23
adding any grafting materials and simultaneous implants placement (Lundgren, et
al. 2004). Implants were placed such that a minimum of 5 mm protruded into the
sub-antral space. Comparison of pre- and post-operative CT scans (6 months later)
clearly demonstrated new bone formation within the sub-antral space created by
membrane elevation only. The new bone formed however did not cover the apex of
the implant rather it was only visible around the portion of the protruding implant
proximal to the native bone wall of the maxillary sinus floor. The above technique
was subsequently repeated in monkeys (Palma, et al. 2006) with one side receiving
no grafting material, whilst the contralateral side was augmented using autogenous
bone. Histologically, the apex was in direct contact with a normal Schneiderian
membrane unless there was a thin layer of intervening bone. Below that, membrane
collapse was seen into the underlying space, irrespective of the treatment group to
form a tent shaped figure. In the mid portion of the implants, sites treated with
membrane elevation only tended to exhibit more bone at the periphery in contact
with the Schneiderian membrane. This series of studies suggests that the surgical
stimuli of sinus membrane elevation and coagulum filling the sub-antral alone leads
to bone formation. This is limited to the sinus floor due to the lack of space
maintenance and instability of the coagulum leaving the apex of the implant
supporting the membrane. This tenting effect also maintains space in the immediate
vicinity of the implant that widens gradually in the coronal direction allowing
maturation of the regenerated bone in this region. The absence of grafting material
ensures this healing process is not impeded.
In 2010, a pre-clinical study (Scala, et al. 2010) reported on the early healing after
sinus membrane elevation and simultaneous implant placement. No bone
substitutes were used and a coagulum was allowed to fill the sub-antral space. After
10 days of healing, a higher amount of woven bone was noted in continuity with
the walls of the sinus that was often preceded by a dense connective tissue layer.
The newly formed bone became more mature and organised with primary osteons
and primitive bone marrow noted. Shrinkage of the elevated area was observed
during the healing period and the formation of new bone sprouting from the resident
bony walls of the sinus, growing towards the middle of the elevated area was noted.
No bone formation from the Schneiderian membrane was identified. These findings
are in agreement with previous pre-clinical studies (Xu, et al. 2003, Xu, et al. 2004)

24
with new bone formation initiated from the walls of the sinus after maxillary sinus
elevation and not beneath the Schneiderian membrane, regardless of whether a bone
graft or a blood clot alone was used. As healing progressed, the augmented space
significantly reduced in size when using a coagulum only, corroborating other
studies showing that bone formation as a result of a coagulum is unstable (Xu, et
al. 2005).
Haas et al. (Haas, et al. 2002) also showed a tenting effect of implants placed into
the maxillary sinuses cavity after sinus membrane elevation with no additional bone
grafting in sheep. The apex of the implant was mostly in direct contact with the
Schneiderian membrane, with new bone formation noted around the part of the
implant proximal to the resident bone walls. The new bone appeared to originate
from these cortical walls. Sporadic bone islands were noted along the Schneiderian
membrane but their origin is unclear.
These studies demonstrate the importance of space maintenance in neo-
osteogenesis and that a coagulum has the potential for neo-osteogenesis if the space
can be maintained. New bone is unstable in areas where the membrane collapses
due to the instability of the blood clot and a lack of mechanical support (absence of
biomaterials and / or implant). Whilst in-vitro and some in-vivo experiments have
shown that the Schneiderian membrane may have osteogenic potential, pre-clinical
studies are not in agreement as to the role of the membrane in bone formation,
especially in the early stages of bone healing. There is overwhelming evidence that
early bone formation begins at the periphery of the defect using surrounding
resident bony walls as a stable base for neo-osteogenesis, but the osteogenic
potential of the Schneiderian membrane is questionable.
Impact of sinus pneumatization on maxillary sinus grafting
Ventilation of the maxillary sinus is accomplished by air exchange with the nasal
cavity through the sinus ostium (Scharf, et al. 1995). The presence of prolonged air
pressure has shown sinus enlargement and bony wall displacement (Zizmor, et al.
1975). As such, sinus pressure may have an impact on sinus floor location post-
grafting.

25
A study by Asai et al. (Asai, et al. 2002) investigated the impact of occluding the
maxillary sinus ostium on bone formation in a pre-clinical model. The sub-antral
space was allowed to fill with a coagulum only and initially resulted in formation
of granulation tissue with bone formation at the periphery. Occluding the ostium
resulted in regenerated bone matrix after 3 weeks which matured by week 6. Not
occluding the ostium resulted in almost complete replacement by a normal sinus
airspace after 3 weeks of healing. In a similar pre-clinical model (Xu, et al. 2004),
the same research group compared the addition of a deproteinised bone graft into
the sub-antral space with a coagulum only after sinus membrane elevation. The new
bone that had formed subsequently resorbed in the coagulum only group, but
remained in the grafted group and showed further consolidation. The authors
concluded that the coagulum did not withstand the sinus pressure during the first
several weeks, and re-pneumatization of the sinus or ‘slumping’ was noted. The
grafted sinus however maintained the space and the deproteinised bone grafts
particles resisted pressure induced bone resorption.
Characteristics of MSA Sites
Histological & histomorphometric
Large variations in the area fraction of biomaterials such as ABBM have been
reported (Valentini, et al. 2000, Yildirim, et al. 2000, Hallman, et al. 2001) and may
depend on the pressure at application of the grafting material, the initial percentage
of the material, the particle size, the biopsy technique, or the histological
preparation technique.
Biopsy harvesting techniques have been reported to have a significant impact on
histomorphometric outcomes, at least in the early phase of graft healing (Margolin,
et al. 1998, Artzi, et al. 2005). Artzi et al. histomorphometrically assessed the
variation in area fraction of residual bone substitutes and new bone in samples
harvested via a trephine from grafted maxillary sinuses (Artzi, et al. 2005). The
depth of the samples influenced both parameters. This has been corroborated by
another study reporting biopsy harvesting depth and location as important aspects
to consider, since they influence the mineralization and degree of bone formation

26
(Avila, et al. 2010). Furthermore, there is overwhelming evidence that
histomorphometric parameters vary depending on proximity to resident bony walls
(Busenlechner, et al. 2009). As such, another determining factor may be the
horizontal dimension of the lateral window and proximity of the lateral walls of the
sinus to the harvesting site (Suarez-Lopez Del Amo, et al. 2015). Further
confounding variables include the histological slice thickness (Klijn, et al. 2010)
and residual ridge height (Corbella, et al. 2015).
Haas et al. (Haas, et al. 1998) published a histological assessment of MSA sites in
an ovine model, which had simultaneous implants placement. The sinuses received
either ABBM (Bio-Oss®), AB (iliac crest) or they were left as empty controls filled
with only a coagulum. New bone formation around the ABBM particles was
observed in areas in which the material was in direct contact with local bone. None
of the specimens showed new bone formation around the particles further away
from this contact area. Great variation was noted in the degree of osseointegration
of the ABBM particles irrespective of the healing time. Grafting had no additional
osteoconductive effect in the region of the implant proximal to the resident bony
wall.
These histological changes leading to improved integration between new bone and
ABBM particles correlated well with mechanical testing carried out by the same
group (Haas, et al. 1998). The pull-out strengths of implants in the group augmented
with ABBM showed the highest values. Time also had a significantly positive
impact on pull-out strengths.
If de novo bone formation is the reference parameter however, then AB remains the
gold standard. An RCT by Schmitt et al. (Schmitt, et al. 2013) reported on the
histological and histomorphometric characteristics of samples harvested 5 months
after two stage MSA with various materials in 30 patients. The amount of newly
formed bone was significantly higher in the AB (42.74 ± 2.10 %) group when
compared to ABBM (24.90 ± 5.67 %). The measured mineralized components were
comparable between these two materials (ABBM - 46.26 ± 8.11 %) (AB - 42.74 ±
2.12 %) which is consistent with the increased fraction of residual bone substitute

27
in ABBM samples. This has been further confirmed in systematic reviews
(Corbella, et al. 2016) using comparative studies.
The composite graft of ABBM and AB has been utilized in multiple studies of
maxillary sinus floor augmentation (Maiorana, et al. 2000, Hallman, et al. 2001,
Hallman, et al. 2001, Hallman, et al. 2002, Hatano, et al. 2004, Hallman, et al. 2005,
Cannizzaro, et al. 2009, Hallman, et al. 2009, Kim, et al. 2009, Avila, et al. 2010,
de Vicente, et al. 2010, Galindo-Moreno, et al. 2010), but few comparative studies
exist with ABBM or to AB alone. The proportion of vital bone within the sinuses
after using two different ratios of ABBM and AB was evaluated in humans
(Galindo-Moreno, et al. 2011). No statistically significant differences in newly
formed bone and non-mineralized tissue were noted for 50% ABBM and 50% AB
group when compared to the 80% ABMM and 20% AB group. Additional
comparative studies also failed to show an advantage of adding AB to ABBM in
terms of %NB when analysed in a recent systematic review (Corbella, et al. 2016).
The impact of using a non-resorbing material such as ABBM is of interest when
considering the degree of bone-to-implant contact (BIC) of a dental implant. Early
reports indicated no direct contact between ABBM particles and the implant surface
(Valentini & Abensur 1997). In a pre-clinical study, Jensen et al. (Jensen, et al.
2013) examined the impact of varying the proportion of ABBM (Bio-Oss®) and
AB on BIC in mini-pigs after 12 weeks after MSA and implantation. This was
performed using (a) 100% AB, (b) 75% AB and 25% Bio-Oss®, (c) 50% AB and
50% Bio-Oss®, (d) 25% AB and 75% Bio-Oss®, and (e) 100% Bio-Oss®. Samples
were harvested 12 weeks post-grafting and BIC was calculated. The median BIC
was (a) 42.9%, (b) 37.8%, (c) 43.9%, (d) 30.2%, (e) 13.9%, respectively. BIC was
significantly higher when autogenous bone or Bio-Oss® mixed with AB was used
in varying ratios as compared to Bio-Oss® alone.
Hallman et al. (Hallman, et al. 2002) examined BIC of micro-implants placed into
augmented maxillary sinuses in humans after 6 months of healing. The sinuses were
augmented with 100% ABBM, a mixture of 80% ABMM and 20% AB and 100%
AB. No statistically significant differences in mean BIC were reported for ABBM
(mean 31.6% ± 19.1) when compared to ABBM mixed with AB (mean 54.3% ±

28
33.1) or 100% AB (mean 34.6% ± 9.5). Variations in species, model design and
healing time may explain the different results obtained in this study when compared
to the study carried out by Jensen et al.
Whilst histomorphometirc outcomes using a biopsy technique are influenced by
many factors it remains the most commonly reported method of assessing the
biological success of the graft after MSA. Whilst many pre-clinical and clinical
studies have shown the effectiveness of ABBM in MSA, a systematic review has
shown that the use of AB alone provides the greatest amount of new bone (Corbella,
et al. 2016). Furthermore, the addition of AB to ABBM yields little advantage when
compared to ABBM alone (Corbella, et al. 2016).
Impact of barrier membranes on MSA
Studies on the benefits of using barrier membranes over the buccal antrostomy once
graft placement has been completed are conflicting, with very few trials actually
carrying out controlled trials comparing the use of a membrane against no
membrane. Excluding studies using smooth surface implants, the reported survival
rates of implants placed into MSA sites with a barrier membrane appear similar
(mean 98.5% & range 92-100%) when compared to rates without the use of a
membrane (mean 98.5% & range 93-100%) (Chiapasco, et al. 2009).
Whilst earlier studies by Tarnow et al. (Tarnow, et al. 2000) and Wallace et al.
(Wallace, et al. 2005) did show improved new bone formation with the use of the
membrane, subsequent small RCTs have not replicated these results (Choi, et al.
2009, Barone, et al. 2013) with equivalent %NB reported in for both groups.
Interestingly however both of these RCTs reported significantly greater %ST when
not using a barrier membrane. Furthermore, systematic reviews using
histomorphometric data from clinical samples after MSA using AB only (Klijn, et
al. 2010) or a variety of materials (Suarez-Lopez Del Amo, et al. 2015) indicated
that the use of barrier membranes did not influence the amount of new bone
formation.

29
As discussed previously, the location and depth of the biopsy and proximity to the
lateral wall will influence histomorphometric outcomes. Since the barrier
membrane is placed on the buccal surface of the lateral wall of the maxilla and most
biopsy samples are taken from the crest, this may not be representative of its true
barrier function. Interestingly, the histological samples used in the RCT by Tarnow
et al. were taken through the lateral window. They demonstrated that the mean
percentage of new bone formation was 25.5% with and 11.9% without a covering
barrier. Overall, the evidence suggests that the presence or absence of a membrane
has no significant effect on implant survival or on %NB formation, with some
evidence of increased %ST in the absence of a barrier membrane.
Linear & volumetric changes
Re-pneumatization after MSA using a variety of grafting materials has been
reported by a variety of authors and may represent time dependent graft remodelling
leading to re-pneumatization of the maxillary sinus. One can only hypothesize as to
whether barometric pressure within sinuses exerts an effect on the remodelling
process, as was discussed earlier in the section ‘role of Schneiderian membrane &
coagulum in MSA’. Studies measuring linear changes of graft height using a variety
of bone substitutes, including AB (Wiltfang, et al. 2005, Zijderveld, et al. 2009,
Schmitt, et al. 2012), beta-tricalcium phosphate (Zijderveld, et al. 2009) and a
composite of AB and ABBM (Hatano, et al. 2004), suggest that the greatest extent
of graft height occurred early after grafting, with subsequent resorption slowing
down and eventually stabilizing. Sbordone et al. (Sbordone, et al. 2011)
hypothesized that the amount of linear graft remodelling depends on the nature of
the graft (AB or ABBM). Reduced linear changes were seen in the ABBM group
when compared to AB, especially when sourced from the iliac crest.
Considering the obvious limitations of two-dimensional radiographs, three
dimensional methods were subsequently applied to assess this remodelling
phenomenon. The earliest prospective clinical study using CT assessment of graft
volume reported a mean volume reduction using 100% AB from iliac crest of 49.5%
(31-78%) 6 months after grafting (Johansson, et al. 2001). Arasawa et al. (Arasawa,
et al. 2012) assessed the volumetric changes in 9 patients grafted with only AB

30
harvested from either the iliac crest or the mandibular ramus at 3 months and at
least 1 year after sinus augmentation. A mean volume reduction of 24.8% (SD
6.1%) was reported over this period.
A pre-clinical model examined the impact of varying the proportion of ABBM
(Bio-Oss®) and AB on bone graft volume after sinus floor elevation (Jensen, et al.
2012). CT scans of the maxillary sinus were taken immediately post-grafting and
then 12 weeks later. The volumetric reduction was significantly influenced by the
ratio of ABBM and AB, but not by the origin of the AB. The greater the proportion
of AB, the greater the reduction in volume.
A more recent systematic review of three dimensional graft volumetric change was
performed on controlled studies published up to 2013 (Shanbhag, et al. 2014).
Using a variety of bone grafting materials, weighted mean volume reductions of
63.24% (±14.29) were reported for particulate AB, 30.37% (±11.98) for allografts,
18.30% (±2.35) for bone substitutes (included: ABBM, biphasic calcium
phosphate) and 21.88% (±7.38) for composite grafts (any combination of two or
more materials). ABBM (Bio-Oss®) was the most frequently utilized material in
the reported studies. Most of these studies had short term follow up and therefore it
remains to be seen if volumetric data is similar to previous 2D linear measurements,
which indicated stabilization of the graft loss in the long term.
Overall, there is sufficient evidence to suggest that MSA using AB as the sole
material is not recommended, based on a lack of volumetric stability. In addition,
ABBM appears to exhibit superior volumetric stability.
DENTAL IMPLANTS & SUPPORTED RESTORATIONS IN MSA
Dental implant surface microtopography
Implant surface topography and chemistry affects the osseointegration process
(Gittens, et al. 2014). It has been shown to play a critical role in the predictability
of the bone response to implant placement (Junker, et al. 2009) and is a major
determinant of the rate and extent of dental implant osseointegration (Wennerberg
& Albrektsson 2009). Animal studies have shown that microrough titanium

31
implants result in superior BIC compared to minimally rough implants (Cochran,
et al. 1998), as well as superior torque removal values (Buser, et al. 1998).
Histological analysis of the sequential healing events associated with the placement
of microrough surface titanium implants showed that initial bone formation around
these implants occurs not only at the exposed bone wall of the osteotomy site, as is
the case with minimally rough surface implants, but also along an osteophylic
implant surface (Berglundh, et al. 2003). Furthermore, Abrahamsson et al.
(Abrahamsson, et al. 2004) compared the temporal healing events associated with
osseointegration to microrough and minimally rough surfaces. They demonstrated
histological evidence of superior early healing associated with the microrough
surfaces, with a higher level of wound organization as early as 4 days following
implantation, ultimately leading to greater BIC one week post-insertion.
The clinically utilized microrough SLA® surface is achieved by sand blasting
minimally rough (Ra 0.5 - 1µm) titanium with large grit followed by etching with
acid to give a microrough (Ra 1 - 2µm) surface topography. The use of such
microscale modified implant surfaces has been credited with being one of the key
factors in increasing the clinical success rate of implants, especially in areas of
compromised bone quality (Ivanovski 2010).
Chemical modification of the SLA surface to remove surface contamination
resulting in a surface with increased surface energy and hydrophilicity
(SLActive®), has further demonstrated enhanced bone apposition during the early
stages of osseointegration compared to the SLA surface (Bornstein, et al. 2008). In
vitro studies have demonstrated that the early cell response to the modified
hydrophilic surface (SLActive®) were significantly enhanced (Rausch-fan, et al.
2008). Further, Mamalis et al. (Mamalis, et al. 2011) showed that the SLActive®
surface promotes an ‘osteoprotective microenvironment’ which up-regulates
osteoblastic differentiation, whilst suppressing osteoclastogenesis. In-vivo human
studies also showed that compared with the SLA surface, SLActive® exerts a pro-
osteogenic and pro-angiogenic influence on gene expression as early as 7 days post
implantation (Donos, et al. 2011).

32
When compared with SLA, pre-clinical studies demonstrated that SLActive®
achieved significantly greater BIC at 2 weeks after placement, although
equivalence was reached at 8 weeks (Buser, et al. 2004). Similarly, Bornstein et al.
(Bornstein, et al. 2008) also showed an initially greater BIC at 2 weeks that reached
equivalence by week 4 when compared to SLA implants. SLActive® implant
surfaces have also shown significantly greater removal torque values compared to
SLA (Ferguson, et al. 2006). A histological analysis of human samples by Lang et
al. (Lang, et al. 2011) showed a superior degree of osseointegration for SLActive®
implants after 2 and 4 weeks of healing when compared to a conventional SLA
surface, but this difference was not evident by 42 days after placement.
In a review of the evidence for the chemically modified hydrophilic implant surface
(SLActive®) it was concluded that a stronger bone response was present during the
early healing. The later stages however, exhibited similar biological response to the
non-chemically modified surface (Wennerberg, et al. 2011). Nonetheless, the early
histological advantage has translated to successful earlier loading protocols, as
demonstrated by Morton et al. (Morton, et al. 2010). Loading of these implants was
achievable in 95.6% of cases at 21 days without incident. At 2 years after
placement, they reported a success rate of 97.7%. Using an identical loading
protocol, clinical parameters for SLActive implants exhibited signs consistent with
peri-implant health after 3 years of function (Bornstein, et al. 2010).
Various authors have also advocated the use of SLActive surfaces in compromised
sites, such as those experienced in diabetes and osteoporosis. Pre-clinical studies in
rabbits (Mardas, et al. 2011) and pigs (Schlegel, et al. 2013) have indicated
significantly improved BIC around the modified implant surface (SLActive®)
when compared to the conventional surface (SLA).
Studies comparing these modified implant surfaces in bone defects or grafted sites
are rare. Schwarz et al. (Schwarz, et al. 2008) evaluated such implant surfaces in
dehiscence-type defects in a canine model. At 8 weeks, the modified implants
(SLActive®) exhibited significantly greater defect bone fill and %BIC when
compared to both a standard surface (SLA) and a calcium phosphate modified dual
acid etched surface (Nanotite®) (Schwarz, et al. 2010).

33
These improvements were not however observed in a pre-clinical study assessing
the influence of this implant surface modification in grafted maxillary sinuses
(Philipp, et al. 2013). Half of the sheep received a bone graft (hydroxyapatite and
beta-tricalcium phosphate) and the other half underwent sinus floor elevation only.
Using a paired design, a conventional implant was simultaneously placed on one
side of the animal and the modified surface on the other side. The animals were
sacrificed at 12 and 26 weeks. There was no significant difference in BIC when the
two surfaces were compared in either grafted or ungrafted sites at both time points.
In light of previous studies, the sacrifice at even the earlier time-point of 12 weeks
may have been too late in the healing process to detect a significant difference.
It has been suggested that many factors influence osseointegration of implants, and
the ability to withstand functional load, in augmented maxillary sinuses (Jensen, et
al. 1998). This multitude of variables may explain the seemingly arbitrary loading
intervals reported in different studies. A recent study using a composite bone graft
(ABBM+AB 1:1) utilized a loading time of 6 months (Galindo-Moreno, et al.
2015). Another study using SLA implants placed into biphasic beta-tricalcium
phosphate or ABBM reported a mean loading time of 10 weeks (Bornstein, et al.
2008), yet a clinical trial using SLActive implants placed into ABBM or biphasic
calcium phosphate loaded at a mean of 16.8 weeks after placement (Mordenfeld, et
al. 2016). Systematic reviews report a mean loading time between 5 to 6.5 months
(Chiapasco, et al. 2009, Jensen & Terheyden 2009), irrespective of the biomaterial
used or implant surface. A review of only rough implant surfaces reported a range
of loading periods from 0.3 to 10 months with no impact on survival rates (Nkenke
& Stelzle 2009).
Outcomes of implant supported restorations in MSA
Implant Survival
Implant survival rates in MSA are enhanced when using microrough implant
surfaces, as has been reported in a number of systematic reviews (Pjetursson, et al.
2008, Chiapasco, et al. 2009, Jensen & Terheyden 2009, Nkenke & Stelzle 2009,
Rickert, et al. 2012). A median survival rate of 100% (88-100%) is reported for
microrough implant surfaces when compared to 89% (61.2 – 100%) using

34
machined implant surfaces (Jensen & Terheyden 2009). Indeed, a 100% survival
rate has been reported in a clinical study using one-piece SLA implants in MSA at
12 and 60 months after implant placement (Bornstein, et al. 2008). The enhanced
outcomes for micro-rough compared with machined implant surfaces is consistent
with superior histologically documented outcomes (Abrahamsson, et al. 2004) and
improved bone-to-implant contact (BIC) and stability (Buser, et al. 1998, Cochran,
et al. 1998). Interestingly, a survival rate of 86% was reported in a study with 10
year follow up, using commercially pure implants with a turned surface, with the
majority of their failures occurring prior to loading (Mordenfeld, et al. 2014).
The 5-year implant survival rate in MSA sites grafted using composite graft
AB+ABBM (1:1) was reported to be 92.86% (Schmitt, et al. 2015) in a small
number of patients.
Overall the survival rates for microrough implant surfaces placed into MSA sites
using ABBM or composite grafts of ABBM + AB is high even at 5 years, and is
comparable to implants placed into pristine bone.
Implant Success
Implant success is measured using a wide variety of composite or single outcomes,
with little or no consistency between studies (Tonetti, et al. 2012). The four most
frequently used parameters for assessing success are related to the implant level,
peri-implant soft tissue, prosthesis and patient’s subjective assessment
(Papaspyridakos, et al. 2012). Similarly, based on consensus reports published at
the 8th European Workshop on Periodontology, outcome measures should capture
patient reported outcomes (McGrath, et al. 2012), peri-implant health (Derks &
Tomasi 2015) and restoration outcomes (Pjetursson, et al. 2012). As such, for
implant health it was recommended to report on marginal bone levels, tissue
inflammation (BOP) and probing depth. For implant restorations, it was advised to
report on longevity of the restorations, functional / occlusal related outcomes and
technical complications. One group of researchers has recommended success
criteria report the long term outcomes of the implant-prosthetic complex as a whole

35
(Papaspyridakos, et al. 2012) rather than report each outcome separately
(Pjetursson, et al. 2012, Sanz, et al. 2012, Tonetti, et al. 2012).
Since the case definitions for peri-implant health and disease vary significantly in
terms of defined threshold (Derks & Tomasi 2015), significant variations in
reported success rates would be expected (Karoussis, et al. 2003).
The success criteria utilized in this study are based on the consensus reports
published at the 8th European Workshop on Periodontology (Pjetursson, et al. 2012,
Sanz, et al. 2012).
• Biological complications: included implants that exhibited signs of mucositis
or peri-implantitis. Mucositis was defined as any bleeding on gentle probing
without loss of supporting bone (Lang, et al. 2011). Peri-implantitis was
defined as bleeding on probing and / or suppuration with or without
concomitant deepening of peri-implant pockets, accompanied by marginal
bone level changes of greater than 1.0mm after baseline (Sanz, et al. 2012)
(Lang, et al. 2011). Furthermore, any treatment performed on the implant that
was not part of routine maintenance was by default classified as a
complication.
• Technical complications: included any implant-supported restorations that
presented with features as defined above (Pjetursson, et al. 2012). These were
divided into (1) major: such as implant fracture, loss of super-structure, (2)
medium: such as abutment fracture, veneer or framework fracture and (3)
minor: abutment and screw loosening, loss of screw hole sealing, veneer
chipping (requiring polishing) and occlusal adjustments. In addition, any
treatment performed on the restoration that was not part of routine maintenance
was by default classified as a complication. If the implant was incorporated into
an FPD, then any technical complication affecting any part of the FPD was
included in the analysis.

36
Biological Outcomes
For one-piece rough surface implants, the marginal bone remodelling process
begins immediately following implant placement and is influenced by the location
of the rough-smooth junction (Hammerle, et al. 1996, Hermann, et al. 2000,
Hermann, et al. 2001, Hermann, et al. 2001). Continued change in marginal bone
levels after this initial remodelling period has been observed in many studies. This
change may represent bone loss due to exposure to bacterial load (Lang, et al. 2011)
and masticatory forces (Marcelis, et al. 2012), rather than an adaptation to implant
placement and biologic width formation. Most studies exhibit reduced changes in
marginal bone levels after the first year of function.
A case series with a 10 year follow up (Mordenfeld, et al. 2014), reported on
marginal bone levels and pocket depths (PPD) around two-piece implants with a
turned surface and placed into MSA sites using 80% AB and 20% ABBM. Baseline
was measured at the time of abutment connection. Stable marginal bone levels were
seen after the first, third and tenth year of function with mean marginal bone loss
(ABL) of 0.4mm during the first interval (year 1-to-3) followed by a further 0.4mm
in the longer second interval (year 3-to-10). A mean pocket depth of 3.3 ±1.4mm
was reported at the 10 year follow up. No significant differences were found
between peri-implant parameters for implants placed into augmented bone or
pristine bone. Whilst the long follow up period makes this study an important one,
it does not include well defined parameters for success for marginal bone levels or
PPD. This is important as values reported in some patients for marginal bone levels
reached 5.9mm and PPD of 9mm.
Generally, there is a paucity of studies reporting on implant outcomes using well
defined success criteria when placed into the widely used composite graft of 50%
AB and 50% ABBM (Bornstein, et al. 2008, Galindo-Moreno, et al. 2015), and no
studies using collagen stabilized ABBM. Marginal bone levels ranging from 0 to
5.89mm at 18 months after loading have been reported after performing MSA using
the composite graft and subsequently placing implants with an internal or external
connection (Galindo-Moreno, et al. 2015). These as measurements however, were
taken using panoramic radiographs.

37
A 5 year prospective study reported on a range of outcomes using tissue level
(transmucosal, SLA and TPS) implants placed into MSA augmented with ABBM
or beta-tri-calcium phosphate. Stable marginal bone levels were seen with a mean
marginal bone loss of 0.25mm in the first year of function after baseline and only
0.08mm at the five year review. All patient exhibited good plaque control, a low
mean bleeding index and mean PPD of 4.14mm (± 0.11). The five year success rate
of 98% is attributed to the strict patient selection and defined conditions. A trial by
Schincaglia et al. (Schincaglia, et al. 2015) comparing two-piece (bone level),
rough surface implants placed into MSA sites using ABBM reported a mean
marginal bone loss of 0.22mm (±0.46) in the interval between implant placement
and insertion of prosthesis (baseline) and 0.39mm (±0.69) between baseline and at
the 12 months review in the MSA group. A mean PPD of 2.3mm (±1.4) was
reported in the MSA group.
Recent evidence indicates that rough implants placed into MSA sites can exhibit
high success rates with stable marginal bone levels and peri-implant parameters.
Technical Outcomes
Fixed single (SC) and fixed partial denture (FPD) implant restorations are well
documented in the literature (Pjetursson, et al. 2007, Jung, et al. 2008, Jung, et al.
2012, Pjetursson, et al. 2012). To the best of our knowledge there are no prospective
studies reporting on well-defined technical outcomes for implant supported
restorations in MSA in the partially dentate patient.
Systematic reviews have reported a 5 year survival of 96.3% for SCs and 95.4% for
FPDs (Jung, et al. 2012, Pjetursson, et al. 2012). Whilst screw and cement forms
of retention have their advantages and disadvantages (Michalakis, et al. 2003, Chee
& Jivraj 2006), more recent publications indicate a preference for screw retained
restorations based on retrievability and a lower rate of biological complications
(Gotfredsen, et al. 2012, Wismeijer, et al. 2014). Overall, the 5 year survival rates
for fixed implant supported reconstructions is 96.03% (CI: 93.85 – 97.43%) and
95.55% (CI: 92.96 – 97.19%) for screw retained and cement retained

38
reconstructions respectively (Wittneben, et al. 2014). When assessed according to
prosthesis type, the estimated 5-year survival rate of screw retained SC and FPD
reconstructions is similar to that of cemented reconstructions (Sailer, et al. 2012,
Wittneben, et al. 2014, Millen, et al. 2015).
The overall rate of technical complications of fixed implant reconstructions has
been reported to be significantly greater for cement retained when compared to
screw retained fixed restorations (Wittneben, et al. 2014, Millen, et al. 2015). When
the data is analysed according to the type of prosthesis however, screw retained SC
restorations exhibit greater rates of technical complications due to their
significantly greater rates of abutment screw loosening (Sailer, et al. 2012, Millen,
et al. 2015). Whilst an earlier review reported no significant difference in rate of
technical complications for FPDs (Sailer, et al. 2012) a more recent review reported
a significantly greater rate of technical complications for screw retained FPDs
(Millen, et al. 2015). The incidence of technical complications seems to be
dependant more upon prosthesis and retention type than prosthesis or abutment
material (Millen, et al. 2015).
The overall incidence of biological complications is significantly greater for cement
retained when compared to screw retained restorations (Wittneben, et al. 2014,
Millen, et al. 2015). No statistically significant differences were identified for
biological complications relative to retention type for SC restorations in a recent
review (Millen, et al. 2015). This review reported increased aesthetic complications
in screw retained restorations (Millen, et al. 2015). This parameter was not reported
by an earlier systematic review (Sailer, et al. 2012) and it offset the greater
incidence of bone loss (>2mm) and presence of fistula / suppuration noted in
cement retained restorations. Data for FPD’s remains scarce especially for cement
retained FPD’s hence preventing a statistical comparison.
RESEARCH HYPOTHESIS
A priori hypothesis in this project includes the demonstration of equivalence across
a range of outcomes (histomorphometric, volumetric and clinical) for the test graft
of collagen stabilized anorganic bovine bone mineral (ABBM) when compared to

39
the control graft of ABBM + autogenous bone (AB) in both a pre-clinical and
clinical model of maxillary sinus augmentation (MSA).
Furhtermore, with regard to assessing the impact of implant surfaces, we
hypothesized that modified hydrophilic implants (SLActive®) will exhibit a similar
degree of BIC and tissue compoistion when compared to a hydrophobic surface
with the same geometry and surface microroughness (SLA®).
AIMS
Broad objectives of this research:
This research aims to evaluate the performance of the collagen stabilized ABBM
grafting material in MSA under the specific clinical scenarios of Schneiderian
membrane perforation and insufficient local autogenous bone. The impact of dental
implant surface modification on early osseointegration was also assessed.
More broadly, the research also aims to report on patient reported outcome
measures (PROMs) for MSA and on the outcomes for implant supported
restorations placed in MSA sites using well defined criteria in a private practice
setting.
The thesis has been divided into two parts to address the following items:
• Part 1 – Histological & histomorphometric assessment of using collagen
stabilized ABBM in MSA (Chapters 2, 3 and 4).
• Part 2 – Clinical & radiographic assessment of using collagen stabilized
ABBM in MSA (Chapters 5 and 6).
The specific objectives of this thesis include:
• Histomorphometrically compare the use of collagen stabilized ABBM to
ABBM + autogenous bone in a pre-clinical model (ovine) of MSA. The
secondary objectives were to assess the impact of resident wall proximity
and healing time on histomorphometric outcomes (Chapter 2).
• Histomorphometrically compare the use of collagen stabilized ABBM to
ABBM + autogenous bone in MSA in a clinical model. Our secondary
40
objective was to assess the impact of the resident sinus floor proximity on
histomorphometric outcomes (Chapter 3).
• Compare the early osseointegration of implants with a hydrophilic surface
(SLActive®) to those with a hydrophobic surface with the same geometry
and surface microroughness (SLA®), in a pre-clinical model of MSA. Our
secondary objective was to characterize the tissue composition in the
immediate vicinity of the implant surface in these augmented sites (Chapter
4).
• Determine whether the use of collagen stabilized ABBM in defined clinical
scenarios (i.e. reduced local autogenous bone availability and/or sinus
membrane perforation), performs equivalently to the ABBM + autogenous
bone in a clinical model of MSA, in terms of the prevalence of surgical
complications, patient reported and volumetric outcomes (Chapter 5).
• Test whether or not implant supported restorations have similar biological
and technical outcomes when placed into previously augmented maxillary
sinuses using stabilized ABBM, as used in defined clinical scenarios (i.e.
reduced local autogenous bone availability and/or sinus membrane
perforation), when compared to those placed into a composite graft of
ABBM and autogenous bone (Chapter 6).

41
REFERENCES
Abou-Hamad, W., Matar, N., Elias, M., Nasr, M., Sarkis-Karam, D., Hokayem,
N. & Haddad, A. (2009) Bacterial flora in normal adult maxillary sinuses. Am J
Rhinol Allergy 23: 261-263.
Abrahamsson, I., Berglundh, T., Linder, E., Lang, N. P. & Lindhe, J. (2004) Early
bone formation adjacent to rough and turned endosseous implant surfaces. An
experimental study in the dog. Clin Oral Implants Res 15: 381-392.
Albu, S. & Florian, I. S. (2013) Bacteriology of normal frontal sinuses. Am J
Otolaryngol 34: 327-330.
Arasawa, M., Oda, Y., Kobayashi, T., Uoshima, K., Nishiyama, H., Hoshina, H.
& Saito, C. (2012) Evaluation of bone volume changes after sinus floor
augmentation with autogenous bone grafts. Int J Oral Maxillofac Surg 41: 853-
857.
Araujo, M. G., Liljenberg, B. & Lindhe, J. (2010) Dynamics of bio-oss collagen
incorporation in fresh extraction wounds: An experimental study in the dog. Clin
Oral Implants Res 21: 55-64.
Artzi, Z., Kozlovsky, A., Nemcovsky, C. E. & Weinreb, M. (2005) The amount of
newly formed bone in sinus grafting procedures depends on tissue depth as well
as the type and residual amount of the grafted material. J Clin Periodontol 32:
193-199.
Artzi, Z., Nemcovsky, C. E. & Tal, H. (2001) Efficacy of porous bovine bone
mineral in various types of osseous deficiencies: Clinical observations and
literature review. Int J Periodontics Restorative Dent 21: 395-405.
Artzi, Z., Nemcovsky, C. E., Tal, H. & Dayan, D. (2001) Histopathological
morphometric evaluation of 2 different hydroxyapatite-bone derivatives in sinus
augmentation procedures: A comparative study in humans. J Periodontol 72: 911-
920.
Artzi, Z., Tal, H. & Dayan, D. (2001) Porous bovine bone mineral in healing of
human extraction sockets: 2. Histochemical observations at 9 months. J
Periodontol 72: 152-159.
Artzi, Z., Weinreb, M., Carmeli, G., Lev-Dor, R., Dard, M. & Nemcovsky, C. E.
(2008) Histomorphometric assessment of bone formation in sinus augmentation
utilizing a combination of autogenous and hydroxyapatite/biphasic tricalcium

42
phosphate graft materials: At 6 and 9 months in humans. Clin Oral Implants Res
19: 686-692.
Asai, S., Shimizu, Y. & Ooya, K. (2002) Maxillary sinus augmentation model in
rabbits: Effect of occluded nasal ostium on new bone formation. Clin Oral
Implants Res 13: 405-409.
Aust, R. & Drettner, B. (1974) Experimental studies of the gas exchange through
the ostium of the maxillary sinus. Ups J Med Sci 79: 177-186.
Aust, R., Stierna, P. & Drettner, B. (1994) Basic experimental studies of ostial
patency and local metabolic environment of the maxillary sinus. Acta Otolaryngol
Suppl 515: 7-10; discussion 11.
Avila, G., Wang, H. L., Galindo-Moreno, P., Misch, C. E., Bagramian, R. A.,
Rudek, I., Benavides, E., Moreno-Riestra, I., Braun, T. & Neiva, R. (2010) The
influence of the bucco-palatal distance on sinus augmentation outcomes. J
Periodontol 81: 1041-1050.
Barone, A., Ricci, M., Grassi, R. F., Nannmark, U., Quaranta, A. & Covani, U.
(2013) A 6-month histological analysis on maxillary sinus augmentation with and
without use of collagen membranes over the osteotomy window: Randomized
clinical trial. Clin Oral Implants Res 24: 1-6.
Barone, A., Santini, S., Marconcini, S., Giacomelli, L., Gherlone, E. & Covani, U.
(2008) Osteotomy and membrane elevation during the maxillary sinus
augmentation procedure. A comparative study: Piezoelectric device vs.
Conventional rotative instruments. Clin Oral Implants Res 19: 511-515.
Barone, A., Santini, S., Sbordone, L., Crespi, R. & Covani, U. (2006) A clinical
study of the outcomes and complications associated with maxillary sinus
augmentation. Int J Oral Maxillofac Implants 21: 81-85.
Beale, T. J., Madani, G. & Morley, S. J. (2009) Imaging of the paranasal sinuses
and nasal cavity: Normal anatomy and clinically relevant anatomical variants.
Semin Ultrasound CT MR 30: 2-16.
Beaumont, C., Zafiropoulos, G. G., Rohmann, K. & Tatakis, D. N. (2005)
Prevalence of maxillary sinus disease and abnormalities in patients scheduled for
sinus lift procedures. J Periodontol 76: 461-467.
Becker, S. T., Terheyden, H., Steinriede, A., Behrens, E., Springer, I. & Wiltfang,
J. (2008) Prospective observation of 41 perforations of the schneiderian
membrane during sinus floor elevation. Clin Oral Implants Res 19: 1285-1289.

43
Berglundh, T. & Lindhe, J. (1997) Healing around implants placed in bone
defects treated with bio-oss. An experimental study in the dog. Clin Oral Implants
Res 8: 117-124.
Betts, N. J. & Miloro, M. (1994) Modification of the sinus lift procedure for septa
in the maxillary antrum. J Oral Maxillofac Surg 52: 332-333.
Bhattacharyya, N. & Fried, M. P. (2003) The accuracy of computed tomography
in the diagnosis of chronic rhinosinusitis. Laryngoscope 113: 125-129.
Bhattacharyya, N. & Lee, L. N. (2010) Evaluating the diagnosis of chronic
rhinosinusitis based on clinical guidelines and endoscopy. Otolaryngol Head Neck
Surg 143: 147-151.
Bianco, P. & Robey, P. G. (2001) Stem cells in tissue engineering. Nature 414:
118-121.
Bolander, M. E. (1992) Regulation of fracture repair by growth factors. Proc Soc
Exp Biol Med 200: 165-170.
Bornstein, M. M., Chappuis, V., von Arx, T. & Buser, D. (2008) Performance of
dental implants after staged sinus floor elevation procedures: 5-year results of a
prospective study in partially edentulous patients. Clin Oral Implants Res 19:
1034-1043.
Bornstein, M. M., Valderrama, P., Jones, A. A., Wilson, T. G., Seibl, R. &
Cochran, D. L. (2008) Bone apposition around two different sandblasted and acid-
etched titanium implant surfaces: A histomorphometric study in canine
mandibles. Clin Oral Implants Res 19: 233-241.
Bornstein, M. M., Wittneben, J. G., Bragger, U. & Buser, D. (2010) Early loading
at 21 days of non-submerged titanium implants with a chemically modified
sandblasted and acid-etched surface: 3-year results of a prospective study in the
posterior mandible. J Periodontol 81: 809-818.
Bostrom, M. P., Lyden, J. P., Ernberg, J. J., Missri, A. A. & Berberian, W. S.
(1995) A biomechanical evaluation of the long stem intramedullary hip screw. J
Orthop Trauma 9: 45-52.
Boyne, P. J. (1993) Analysis of performance of root-form endosseous implants
placed in the maxillary sinus. J Long Term Eff Med Implants 3: 143-159.
Boyne, P. J. & James, R. A. (1980) Grafting of the maxillary sinus floor with
autogenous marrow and bone. J Oral Surg 38: 613-616.

44
Brook, I. (1981) Aerobic and anaerobic bacteriology of adenoids in children: A
comparison between patients with chronic adenotonsillitis and adenoid
hypertrophy. Laryngoscope 91: 377-382.
Brook, I. (1981) Aerobic and anaerobic bacteriology of cholesteatoma.
Laryngoscope 91: 250-253.
Bruder, S. P., Fink, D. J. & Caplan, A. I. (1994) Mesenchymal stem cells in bone
development, bone repair, and skeletal regeneration therapy. J Cell Biochem 56:
283-294.
Burchardt, H. (1983) The biology of bone graft repair. Clin Orthop Relat Res: 28-
42.
Busaba, N. Y., Siegel, N. S. & Salman, S. D. (2004) Microbiology of chronic
ethmoid sinusitis: Is this a bacterial disease? Am J Otolaryngol 25: 379-384.
Busenlechner, D., Huber, C. D., Vasak, C., Dobsak, A., Gruber, R. & Watzek, G.
(2009) Sinus augmentation analysis revised: The gradient of graft consolidation.
Clin Oral Implants Res 20: 1078-1083.
Busenlechner, D., Tangl, S., Mair, B., Fugger, G., Gruber, R., Redl, H. & Watzek,
G. (2008) Simultaneous in vivo comparison of bone substitutes in a guided bone
regeneration model. Biomaterials 29: 3195-3200.
Buser, D., Broggini, N., Wieland, M., Schenk, R. K., Denzer, A. J., Cochran, D.
L., Hoffmann, B., Lussi, A. & Steinemann, S. G. (2004) Enhanced bone
apposition to a chemically modified sla titanium surface. J Dent Res 83: 529-533.
Buser, D., Janner, S. F., Wittneben, J. G., Bragger, U., Ramseier, C. A. & Salvi,
G. E. (2012) 10-year survival and success rates of 511 titanium implants with a
sandblasted and acid-etched surface: A retrospective study in 303 partially
edentulous patients. Clin Implant Dent Relat Res 14: 839-851.
Buser, D., Nydegger, T., Hirt, H. P., Cochran, D. L. & Nolte, L. P. (1998)
Removal torque values of titanium implants in the maxilla of miniature pigs. Int J
Oral Maxillofac Implants 13: 611-619.
Cannizzaro, G., Felice, P., Leone, M., Viola, P. & Esposito, M. (2009) Early
loading of implants in the atrophic posterior maxilla: Lateral sinus lift with
autogenous bone and bio-oss versus crestal mini sinus lift and 8-mm
hydroxyapatite-coated implants. A randomised controlled clinical trial. Eur J Oral
Implantol 2: 25-38.

45
Chanavaz, M. (1990) Maxillary sinus: Anatomy, physiology, surgery, and bone
grafting related to implantology--eleven years of surgical experience (1979-1990).
J Oral Implantol 16: 199-209.
Chee, W. & Jivraj, S. (2006) Screw versus cemented implant supported
restorations. Br Dent J 201: 501-507.
Chen, M. Y. & Metson, R. (1997) Effects of sinus surgery on speech. Arch
Otolaryngol Head Neck Surg 123: 845-852.
Chiapasco, M., Casentini, P. & Zaniboni, M. (2009) Bone augmentation
procedures in implant dentistry. Int J Oral Maxillofac Implants 24 Suppl: 237-
259.
Cho, S. C., Wallace, S. S., Froum, S. J. & Tarnow, D. P. (2001) Influence of
anatomy on schneiderian membrane perforations during sinus elevation surgery:
Three-dimensional analysis. Pract Proced Aesthet Dent 13: 160-163.
Choi, K. S., Kan, J. Y., Boyne, P. J., Goodacre, C. J., Lozada, J. L. &
Rungcharassaeng, K. (2009) The effects of resorbable membrane on human
maxillary sinus graft: A pilot study. Int J Oral Maxillofac Implants 24: 73-80.
Clavero, J. & Lundgren, S. (2003) Ramus or chin grafts for maxillary sinus inlay
and local onlay augmentation: Comparison of donor site morbidity and
complications. Clin Implant Dent Relat Res 5: 154-160.
Cochran, D. L., Schenk, R. K., Lussi, A., Higginbottom, F. L. & Buser, D. (1998)
Bone response to unloaded and loaded titanium implants with a sandblasted and
acid-etched surface: A histometric study in the canine mandible. J Biomed Mater
Res 40: 1-11.
Cook, H. E. & Haber, J. (1987) Bacteriology of the maxillary sinus. J Oral
Maxillofac Surg 45: 1011-1014.
Corbella, S., Taschieri, S. & Del Fabbro, M. (2015) Long-term outcomes for the
treatment of atrophic posterior maxilla: A systematic review of literature. Clin
Implant Dent Relat Res 17: 120-132.
Corbella, S., Taschieri, S., Weinstein, R. & Del Fabbro, M. (2016)
Histomorphometric outcomes after lateral sinus floor elevation procedure: A
systematic review of the literature and meta-analysis. Clin Oral Implants Res 27:
1106-1122.

46
Cortes, A. R., Pinheiro, L. R., Cavalcanti, M. G., Arita, E. S. & Tamimi, F. (2015)
Sinus floor bone failures in maxillary sinus floor augmentation: A case-control
study. Clin Implant Dent Relat Res 17: 335-342.
Cricchio, G. & Lundgren, S. (2003) Donor site morbidity in two different
approaches to anterior iliac crest bone harvesting. Clin Implant Dent Relat Res 5:
161-169.
Daculsi, G. & Passuti, N. (1990) Effect of the macroporosity for osseous
substitution of calcium phosphate ceramics. Biomaterials 11: 86-87.
Davis, W. H., Martinoff, J. T. & Kaminishi, R. M. (1984) Long-term follow up of
transoral rib grafts for mandibular atrophy. J Oral Maxillofac Surg 42: 606-609.
de Vicente, J. C., Hernandez-Vallejo, G., Brana-Abascal, P. & Pena, I. (2010)
Maxillary sinus augmentation with autologous bone harvested from the lateral
maxillary wall combined with bovine-derived hydroxyapatite: Clinical and
histologic observations. Clin Oral Implants Res 21: 430-438.
Del Fabbro, M., Rosano, G. & Taschieri, S. (2008) Implant survival rates after
maxillary sinus augmentation. Eur J Oral Sci 116: 497-506.
Del Fabbro, M., Testori, T., Francetti, L. & Weinstein, R. (2004) Systematic
review of survival rates for implants placed in the grafted maxillary sinus. Int J
Periodontics Restorative Dent 24: 565-577.
Derks, J. & Tomasi, C. (2015) Peri-implant health and disease. A systematic
review of current epidemiology. J Clin Periodontol 42 Suppl 16: S158-171.
Diecidue, R. J., Streck, P. D. & Spera, J. F. (1999) Diagnosis of benign lesions of
the maxillary sinus. Oral and Maxillofacial Clinics of North America 11: 83-100.
Donath, K., Laass, M. & Gunzl, H. J. (1992) The histopathology of different
foreign-body reactions in oral soft tissue and bone tissue. Virchows Arch A Pathol
Anat Histopathol 420: 131-137.
Donos, N., Hamlet, S., Lang, N. P., Salvi, G. E., Huynh-Ba, G., Bosshardt, D. D.
& Ivanovski, S. (2011) Gene expression profile of osseointegration of a
hydrophilic compared with a hydrophobic microrough implant surface. Clin Oral
Implants Res 22: 365-372.
Doud Galli, S. K., Lebowitz, R. A., Giacchi, R. J., Glickman, R. & Jacobs, J. B.
(2001) Chronic sinusitis complicating sinus lift surgery. Am J Rhinol 15: 181-186.

47
Esposito, M., Felice, P. & Worthington, H. V. (2014) Interventions for replacing
missing teeth: Augmentation procedures of the maxillary sinus. Cochrane
Database Syst Rev: CD008397.
Farina, R., Pramstraller, M., Franceschetti, G., Pramstraller, C. & Trombelli, L.
(2011) Alveolar ridge dimensions in maxillary posterior sextants: A retrospective
comparative study of dentate and edentulous sites using computerized
tomography data. Clin Oral Implants Res 22: 1138-1144.
Felisati, G., Borloni, R., Maccari, A., Mele, V. & Chiapasco, M. (2008)
Endoscopic removal of alloplastic sinus graft material via a wide middle
antrotomy. Int J Oral Maxillofac Surg 37: 858-861.
Ferguson, S. J., Broggini, N., Wieland, M., de Wild, M., Rupp, F., Geis-
Gerstorfer, J., Cochran, D. L. & Buser, D. (2006) Biomechanical evaluation of the
interfacial strength of a chemically modified sandblasted and acid-etched titanium
surface. J Biomed Mater Res A 78: 291-297.
Galindo-Moreno, P., Avila, G., Fernandez-Barbero, J. E., Aguilar, M., Sanchez-
Fernandez, E., Cutando, A. & Wang, H. L. (2007) Evaluation of sinus floor
elevation using a composite bone graft mixture. Clin Oral Implants Res 18: 376-
382.
Galindo-Moreno, P., Fernandez-Jimenez, A., O'Valle, F., Silvestre, F. J., Sanchez-
Fernandez, E., Monje, A. & Catena, A. (2015) Marginal bone loss in implants
placed in grafted maxillary sinus. Clin Implant Dent Relat Res 17: 373-383.
Galindo-Moreno, P., Moreno-Riestra, I., Avila, G., Fernandez-Barbero, J. E.,
Mesa, F., Aguilar, M., Wang, H. L. & O'Valle, F. (2010) Histomorphometric
comparison of maxillary pristine bone and composite bone graft biopsies obtained
after sinus augmentation. Clin Oral Implants Res 21: 122-128.
Galindo-Moreno, P., Moreno-Riestra, I., Avila, G., Padial-Molina, M., Paya, J.
A., Wang, H. L. & O'Valle, F. (2011) Effect of anorganic bovine bone to
autogenous cortical bone ratio upon bone remodeling patterns following maxillary
sinus augmentation. Clin Oral Implants Res 22: 857-864.
Gerstenfeld, L. C., Cullinane, D. M., Barnes, G. L., Graves, D. T. & Einhorn, T.
A. (2003) Fracture healing as a post-natal developmental process: Molecular,
spatial, and temporal aspects of its regulation. J Cell Biochem 88: 873-884.
48
Gittens, R. A., Scheideler, L., Rupp, F., Hyzy, S. L., Geis-Gerstorfer, J.,
Schwartz, Z. & Boyan, B. D. (2014) A review on the wettability of dental implant
surfaces ii: Biological and clinical aspects. Acta Biomater 10: 2907-2918.
Gotfredsen, K., Wiskott, A. & Working, G. (2012) Consensus report -
reconstructions on implants. The third eao consensus conference 2012. Clin Oral
Implants Res 23 Suppl 6: 238-241.
Gruber, R., Kandler, B., Fuerst, G., Fischer, M. B. & Watzek, G. (2004) Porcine
sinus mucosa holds cells that respond to bone morphogenetic protein (bmp)-6 and
bmp-7 with increased osteogenic differentiation in vitro. Clin Oral Implants Res
15: 575-580.
Gudis, D. A. & Cohen, N. A. (2010) Cilia dysfunction. Otolaryngol Clin North
Am 43: 461-472, vii.
Haas, R., Baron, M., Donath, K., Zechner, W. & Watzek, G. (2002) Porous
hydroxyapatite for grafting the maxillary sinus: A comparative histomorphometric
study in sheep. Int J Oral Maxillofac Implants 17: 337-346.
Haas, R., Donath, K., Fodinger, M. & Watzek, G. (1998) Bovine hydroxyapatite
for maxillary sinus grafting: Comparative histomorphometric findings in sheep.
Clin Oral Implants Res 9: 107-116.
Haas, R., Haidvogl, D., Dortbudak, O. & Mailath, G. (2002) Freeze-dried bone
for maxillary sinus augmentation in sheep. Part ii: Biomechanical findings. Clin
Oral Implants Res 13: 581-586.
Haas, R., Mailath, G., Dortbudak, O. & Watzek, G. (1998) Bovine hydroxyapatite
for maxillary sinus augmentation: Analysis of interfacial bond strength of dental
implants using pull-out tests. Clin Oral Implants Res 9: 117-122.
Hallman, M., Cederlund, A., Lindskog, S., Lundgren, S. & Sennerby, L. (2001) A
clinical histologic study of bovine hydroxyapatite in combination with autogenous
bone and fibrin glue for maxillary sinus floor augmentation. Results after 6 to 8
months of healing. Clin Oral Implants Res 12: 135-143.
Hallman, M., Lundgren, S. & Sennerby, L. (2001) Histologic analysis of clinical
biopsies taken 6 months and 3 years after maxillary sinus floor augmentation with
80% bovine hydroxyapatite and 20% autogenous bone mixed with fibrin glue.
Clin Implant Dent Relat Res 3: 87-96.
Hallman, M., Mordenfeld, A. & Strandkvist, T. (2005) A retrospective 5-year
follow-up study of two different titanium implant surfaces used after

49
interpositional bone grafting for reconstruction of the atrophic edentulous maxilla.
Clin Implant Dent Relat Res 7: 121-126.
Hallman, M., Mordenfeld, A. & Strandkvist, T. (2009) Bone replacement
following dental trauma prior to implant surgery--status. Dent Traumatol 25: 2-
11.
Hallman, M., Sennerby, L. & Lundgren, S. (2002) A clinical and histologic
evaluation of implant integration in the posterior maxilla after sinus floor
augmentation with autogenous bone, bovine hydroxyapatite, or a 20:80 mixture.
Int J Oral Maxillofac Implants 17: 635-643.
Hammerle, C. H., Bragger, U., Burgin, W. & Lang, N. P. (1996) The effect of
subcrestal placement of the polished surface of iti implants on marginal soft and
hard tissues. Clin Oral Implants Res 7: 111-119.
Hammerle, C. H., Chiantella, G. C., Karring, T. & Lang, N. P. (1998) The effect
of a deproteinized bovine bone mineral on bone regeneration around titanium
dental implants. Clin Oral Implants Res 9: 151-162.
Hammerle, C. H., Schmid, J., Lang, N. P. & Olah, A. J. (1995) Temporal
dynamics of healing in rabbit cranial defects using guided bone regeneration. J
Oral Maxillofac Surg 53: 167-174.
Hatano, N., Shimizu, Y. & Ooya, K. (2004) A clinical long-term radiographic
evaluation of graft height changes after maxillary sinus floor augmentation with a
2:1 autogenous bone/xenograft mixture and simultaneous placement of dental
implants. Clin Oral Implants Res 15: 339-345.
Hermann, J. S., Buser, D., Schenk, R. K. & Cochran, D. L. (2000) Crestal bone
changes around titanium implants. A histometric evaluation of unloaded non-
submerged and submerged implants in the canine mandible. J Periodontol 71:
1412-1424.
Hermann, J. S., Buser, D., Schenk, R. K., Schoolfield, J. D. & Cochran, D. L.
(2001) Biologic width around one- and two-piece titanium implants. Clin Oral
Implants Res 12: 559-571.
Hermann, J. S., Schoolfield, J. D., Nummikoski, P. V., Buser, D., Schenk, R. K.
& Cochran, D. L. (2001) Crestal bone changes around titanium implants: A
methodologic study comparing linear radiographic with histometric
measurements. Int J Oral Maxillofac Implants 16: 475-485.

50
Hernandez-Alfaro, F., Torradeflot, M. M. & Marti, C. (2008) Prevalence and
management of schneiderian membrane perforations during sinus-lift procedures.
Clin Oral Implants Res 19: 91-98.
Hilding, A. (1932) The physiology of drainage of nasal mucous: 3. Experimental
work on the accesory sinuses. Am J Physiol 100: 664-670.
Hosemann, W., Gode, U., Dunker, J. E. & Eysholdt, U. (1998) Influence of
endoscopic sinus surgery on voice quality. Eur Arch Otorhinolaryngol 255: 499-
503.
Huang, H. M., Cheng, J. J., Liu, C. M. & Lin, K. N. (2006) Mucosal healing and
mucociliary transport change after endoscopic sinus surgery in children with
chronic maxillary sinusitis. Int J Pediatr Otorhinolaryngol 70: 1361-1367.
Hurzeler, M. B., Quinones, C. R., Kirsch, A., Gloker, C., Schupbach, P., Strub, J.
R. & Caffesse, R. G. (1997) Maxillary sinus augmentation using different grafting
materials and dental implants in monkeys. Part i. Evaluation of anorganic bovine-
derived bone matrix. Clin Oral Implants Res 8: 476-486.
Hurzeler, M. B., Quinones, C. R., Kirsch, A., Schupbach, P., Krausse, A., Strub,
J. R. & Caffesse, R. G. (1997) Maxillary sinus augmentation using different
grafting materials and dental implants in monkeys. Part iii. Evaluation of
autogenous bone combined with porous hydroxyapatite. Clin Oral Implants Res 8:
401-411.
Ivanovski, S. (2010) Osseointegration--the influence of implant surface. Ann R
Australas Coll Dent Surg 20: 82-85.
Jabbarzadeh, E., Starnes, T., Khan, Y. M., Jiang, T., Wirtel, A. J., Deng, M., Lv,
Q., Nair, L. S., Doty, S. B. & Laurencin, C. T. (2008) Induction of angiogenesis in
tissue-engineered scaffolds designed for bone repair: A combined gene therapy-
cell transplantation approach. Proc Natl Acad Sci U S A 105: 11099-11104.
Jannert, M., Andreasson, L., Ivarsson, A. & Nielsen, A. (1984) Patency of the
maxillary sinus ostium in healthy individuals. Acta Otolaryngol 97: 137-149.
Jemt, T. & Lekholm, U. (1995) Implant treatment in edentulous maxillae: A 5-
year follow-up report on patients with different degrees of jaw resorption. Int J
Oral Maxillofac Implants 10: 303-311.
Jensen, J., Sindet-Pedersen, S. & Oliver, A. J. (1994) Varying treatment strategies
for reconstruction of maxillary atrophy with implants: Results in 98 patients. J
Oral Maxillofac Surg 52: 210-216; discussion 216-218.

51
Jensen, O. T., Shulman, L. B., Block, M. S. & Iacono, V. J. (1998) Report of the
sinus consensus conference of 1996. Int J Oral Maxillofac Implants 13 Suppl: 11-
45.
Jensen, S. S., Aaboe, M., Pinholt, E. M., Hjorting-Hansen, E., Melsen, F. &
Ruyter, I. E. (1996) Tissue reaction and material characteristics of four bone
substitutes. Int J Oral Maxillofac Implants 11: 55-66.
Jensen, S. S., Broggini, N., Hjorting-Hansen, E., Schenk, R. & Buser, D. (2006)
Bone healing and graft resorption of autograft, anorganic bovine bone and beta-
tricalcium phosphate. A histologic and histomorphometric study in the mandibles
of minipigs. Clin Oral Implants Res 17: 237-243.
Jensen, S. S., Broggini, N., Weibrich, G., Hjorting-Hansen, E., Schenk, R. &
Buser, D. (2005) Bone regeneration in standardized bone defects with autografts
or bone substitutes in combination with platelet concentrate: A histologic and
histomorphometric study in the mandibles of minipigs. Int J Oral Maxillofac
Implants 20: 703-712.
Jensen, S. S. & Terheyden, H. (2009) Bone augmentation procedures in localized
defects in the alveolar ridge: Clinical results with different bone grafts and bone-
substitute materials. Int J Oral Maxillofac Implants 24 Suppl: 218-236.
Jensen, T., Schou, S., Gundersen, H. J., Forman, J. L., Terheyden, H. &
Holmstrup, P. (2013) Bone-to-implant contact after maxillary sinus floor
augmentation with bio-oss and autogenous bone in different ratios in mini pigs.
Clin Oral Implants Res 24: 635-644.
Jensen, T., Schou, S., Stavropoulos, A., Terheyden, H. & Holmstrup, P. (2012)
Maxillary sinus floor augmentation with bio-oss or bio-oss mixed with
autogenous bone as graft: A systematic review. Clin Oral Implants Res 23: 263-
273.
Jensen, T., Schou, S., Svendsen, P. A., Forman, J. L., Gundersen, H. J.,
Terheyden, H. & Holmstrup, P. (2012) Volumetric changes of the graft after
maxillary sinus floor augmentation with bio-oss and autogenous bone in different
ratios: A radiographic study in minipigs. Clin Oral Implants Res 23: 902-910.
Jiang, R. S., Liang, K. L., Jang, J. W. & Hsu, C. Y. (1999) Bacteriology of
endoscopically normal maxillary sinuses. J Laryngol Otol 113: 825-828.

52
Johansson, B., Grepe, A., Wannfors, K., Aberg, P. & Hirsch, J. M. (2001)
Volumetry of simulated bone grafts in the edentulous maxilla by computed
tomography: An experimental study. Dentomaxillofac Radiol 30: 153-156.
Johansson, B., Grepe, A., Wannfors, K. & Hirsch, J. M. (2001) A clinical study of
changes in the volume of bone grafts in the atrophic maxilla. Dentomaxillofac
Radiol 30: 157-161.
Joyce, M. E., Roberts, A. B., Sporn, M. B. & Bolander, M. E. (1990)
Transforming growth factor-beta and the initiation of chondrogenesis and
osteogenesis in the rat femur. J Cell Biol 110: 2195-2207.
Jung, R. E., Pjetursson, B. E., Glauser, R., Zembic, A., Zwahlen, M. & Lang, N.
P. (2008) A systematic review of the 5-year survival and complication rates of
implant-supported single crowns. Clin Oral Implants Res 19: 119-130.
Jung, R. E., Zembic, A., Pjetursson, B. E., Zwahlen, M. & Thoma, D. S. (2012)
Systematic review of the survival rate and the incidence of biological, technical,
and aesthetic complications of single crowns on implants reported in longitudinal
studies with a mean follow-up of 5 years. Clin Oral Implants Res 23 Suppl 6: 2-
21.
Junker, R., Dimakis, A., Thoneick, M. & Jansen, J. A. (2009) Effects of implant
surface coatings and composition on bone integration: A systematic review. Clin
Oral Implants Res 20 Suppl 4: 185-206.
Kao, S. T. & Scott, D. D. (2007) A review of bone substitutes. Oral Maxillofac
Surg Clin North Am 19: 513-521, vi.
Karoussis, I. K., Salvi, G. E., Heitz-Mayfield, L. J., Bragger, U., Hammerle, C. H.
& Lang, N. P. (2003) Long-term implant prognosis in patients with and without a
history of chronic periodontitis: A 10-year prospective cohort study of the iti
dental implant system. Clin Oral Implants Res 14: 329-339.
Kennedy, D. W., Zinreich, S. J., Rosenbaum, A. E. & Johns, M. E. (1985)
Functional endoscopic sinus surgery. Theory and diagnostic evaluation. Arch
Otolaryngol 111: 576-582.
Khan, S. N., Cammisa, F. P., Jr., Sandhu, H. S., Diwan, A. D., Girardi, F. P. &
Lane, J. M. (2005) The biology of bone grafting. J Am Acad Orthop Surg 13: 77-
86.

53
Kim, Y. K., Yun, P. Y., Kim, S. G. & Lim, S. C. (2009) Analysis of the healing
process in sinus bone grafting using various grafting materials. Oral Surg Oral
Med Oral Pathol Oral Radiol Endod 107: 204-211.
Kirtsreesakul, V., Tuntaraworasin, J. & Thamjarungwong, B. (2008)
Microbiology and antimicrobial susceptibility patterns of commensal flora in the
middle nasal meatus. Ann Otol Rhinol Laryngol 117: 914-918.
Klijn, R. J., Meijer, G. J., Bronkhorst, E. M. & Jansen, J. A. (2010) A meta-
analysis of histomorphometric results and graft healing time of various
biomaterials compared to autologous bone used as sinus floor augmentation
material in humans. Tissue Eng Part B Rev 16: 493-507.
Klijn, R. J., Meijer, G. J., Bronkhorst, E. M. & Jansen, J. A. (2010) Sinus floor
augmentation surgery using autologous bone grafts from various donor sites: A
meta-analysis of the total bone volume. Tissue Eng Part B Rev 16: 295-303.
Lang, N. P., Berglundh, T. & Working Group 4 of Seventh European Workshop
on, P. (2011) Periimplant diseases: Where are we now?--consensus of the seventh
european workshop on periodontology. J Clin Periodontol 38 Suppl 11: 178-181.
Lang, N. P., Salvi, G. E., Huynh-Ba, G., Ivanovski, S., Donos, N. & Bosshardt, D.
D. (2011) Early osseointegration to hydrophilic and hydrophobic implant surfaces
in humans. Clin Oral Implants Res 22: 349-356.
Lundgren, S., Andersson, S., Gualini, F. & Sennerby, L. (2004) Bone reformation
with sinus membrane elevation: A new surgical technique for maxillary sinus
floor augmentation. Clin Implant Dent Relat Res 6: 165-173.
Macbeth, R. (1971) Caldwell, luc, and their operation. Laryngoscope 81: 1652-
1657.
Maiorana, C., Redemagni, M., Rabagliati, M. & Salina, S. (2000) Treatment of
maxillary ridge resorption by sinus augmentation with iliac cancellous bone,
anorganic bovine bone, and endosseous implants: A clinical and histologic report.
Int J Oral Maxillofac Implants 15: 873-878.
Mamalis, A. A., Markopoulou, C., Vrotsos, I. & Koutsilirieris, M. (2011)
Chemical modification of an implant surface increases osteogenesis and
simultaneously reduces osteoclastogenesis: An in vitro study. Clin Oral Implants
Res 22: 619-626.
Mann, W., Beck, C. & Apostolidis, T. (1977) Liability of ultrasound in maxillary
sinus disease. Arch Otorhinolaryngol 215: 67-74.

54
Marcelis, K., Vercruyssen, M., Nicu, E., Naert, I. & Quirynen, M. (2012)
Sleeping vs. Loaded implants, long-term observations via a retrospective analysis.
Clin Oral Implants Res 23: 1118-1122.
Mardas, N., Schwarz, F., Petrie, A., Hakimi, A. R. & Donos, N. (2011) The effect
of slactive surface in guided bone formation in osteoporotic-like conditions. Clin
Oral Implants Res 22: 406-415.
Margolin, M. D., Cogan, A. G., Taylor, M., Buck, D., McAllister, T. N., Toth, C.
& McAllister, B. S. (1998) Maxillary sinus augmentation in the non-human
primate: A comparative radiographic and histologic study between recombinant
human osteogenic protein-1 and natural bone mineral. J Periodontol 69: 911-919.
Markovic, A., Misic, T., Calvo-Guirado, J. L., Delgado-Ruiz, R. A., Janjic, B. &
Abboud, M. (2016) Two-center prospective, randomized, clinical, and
radiographic study comparing osteotome sinus floor elevation with or without
bone graft and simultaneous implant placement. Clin Implant Dent Relat Res 18:
873-882.
McGowan, D. A., Baxter, P. W. & James, J. (1993) The maxillary sinus and its
dental implications: Oxford: Wright, Butter-worth-Heinemann Ltd.
McGrath, C., Lam, O. & Lang, N. (2012) An evidence-based review of patient-
reported outcome measures in dental implant research among dentate subjects. J
Clin Periodontol 39 Suppl 12: 193-201.
Messerklinger, W. (1966) [on the drainage of the human paranasal sinuses under
normal and pathological conditions. 1]. Monatsschr Ohrenheilkd Laryngorhinol
100: 56-68.
Michalakis, K. X., Hirayama, H. & Garefis, P. D. (2003) Cement-retained versus
screw-retained implant restorations: A critical review. Int J Oral Maxillofac
Implants 18: 719-728.
Millen, C., Bragger, U. & Wittneben, J. G. (2015) Influence of prosthesis type and
retention mechanism on complications with fixed implant-supported prostheses:
A systematic review applying multivariate analyses. Int J Oral Maxillofac
Implants 30: 110-124.
Mordenfeld, A., Albrektsson, T. & Hallman, M. (2014) A 10-year clinical and
radiographic study of implants placed after maxillary sinus floor augmentation
with an 80:20 mixture of deproteinized bovine bone and autogenous bone. Clin
Implant Dent Relat Res 16: 435-446.
55
Mordenfeld, A., Hallman, M., Johansson, C. B. & Albrektsson, T. (2010)
Histological and histomorphometrical analyses of biopsies harvested 11 years
after maxillary sinus floor augmentation with deproteinized bovine and
autogenous bone. Clin Oral Implants Res 21: 961-970.
Morton, D., Bornstein, M. M., Wittneben, J. G., Martin, W. C., Ruskin, J. D.,
Hart, C. N. & Buser, D. (2010) Early loading after 21 days of healing of
nonsubmerged titanium implants with a chemically modified sandblasted and
acid-etched surface: Two-year results of a prospective two-center study. Clin
Implant Dent Relat Res 12: 9-17.
Naumann, H. (1965) Patholische anatomic der chronischen rhinitis and sinusitis
8th International Congress of Oto-rhinolaryngology, 12. Amsterdam: Excerpta
Medica.
Nkenke, E. & Stelzle, F. (2009) Clinical outcomes of sinus floor augmentation for
implant placement using autogenous bone or bone substitutes: A systematic
review. Clin Oral Implants Res 20 Suppl 4: 124-133.
Oliverio, P. J., Benson, M. L. & Zinreich, S. J. (1995) Update on imaging for
functional endoscopic sinus surgery. Otolaryngol Clin North Am 28: 585-608.
Orsini, G., Scarano, A., Degidi, M., Caputi, S., Iezzi, G. & Piattelli, A. (2007)
Histological and ultrastructural evaluation of bone around bio-oss particles in
sinus augmentation. Oral Dis 13: 586-593.
Orsini, G., Traini, T., Scarano, A., Degidi, M., Perrotti, V., Piccirilli, M. &
Piattelli, A. (2005) Maxillary sinus augmentation with bio-oss particles: A light,
scanning, and transmission electron microscopy study in man. J Biomed Mater
Res B Appl Biomater 74: 448-457.
Palma, V. C., Magro-Filho, O., de Oliveria, J. A., Lundgren, S., Salata, L. A. &
Sennerby, L. (2006) Bone reformation and implant integration following
maxillary sinus membrane elevation: An experimental study in primates. Clin
Implant Dent Relat Res 8: 11-24.
Papaspyridakos, P., Chen, C. J., Singh, M., Weber, H. P. & Gallucci, G. O. (2012)
Success criteria in implant dentistry: A systematic review. J Dent Res 91: 242-
248.
Peleg, M., Mazor, Z. & Garg, A. K. (1999) Augmentation grafting of the
maxillary sinus and simultaneous implant placement in patients with 3 to 5 mm of
residual alveolar bone height. Int J Oral Maxillofac Implants 14: 549-556.

56
Philipp, A., Duncan, W., Roos, M., Hammerle, C., Attin, T. & Schmidlin, P. R.
(2013) Comparison of sla or slactive implants in the maxillary sinus with or
without synthetic bone graft materials - an animal study in sheep. Clinical Oral
Implants Research 0: 1-7.
Piattelli, M., Favero, G. A., Scarano, A., Orsini, G. & Piattelli, A. (1999) Bone
reactions to anorganic bovine bone (bio-oss) used in sinus augmentation
procedures: A histologic long-term report of 20 cases in humans. Int J Oral
Maxillofac Implants 14: 835-840.
Pignataro, L., Mantovani, M., Torretta, S., Felisati, G. & Sambataro, G. (2008)
Ent assessment in the integrated management of candidate for (maxillary) sinus
lift. Acta Otorhinolaryngol Ital 28: 110-119.
Pjetursson, B. E., Bragger, U., Lang, N. P. & Zwahlen, M. (2007) Comparison of
survival and complication rates of tooth-supported fixed dental prostheses (fdps)
and implant-supported fdps and single crowns (scs). Clin Oral Implants Res 18
Suppl 3: 97-113.
Pjetursson, B. E., Tan, W. C., Zwahlen, M. & Lang, N. P. (2008) A systematic
review of the success of sinus floor elevation and survival of implants inserted in
combination with sinus floor elevation. J Clin Periodontol 35: 216-240.
Pjetursson, B. E., Thoma, D., Jung, R., Zwahlen, M. & Zembic, A. (2012) A
systematic review of the survival and complication rates of implant-supported
fixed dental prostheses (fdps) after a mean observation period of at least 5 years.
Clin Oral Implants Res 23 Suppl 6: 22-38.
Pjetursson, B. E., Zwahlen, M. & Lang, N. P. (2012) Quality of reporting of
clinical studies to assess and compare performance of implant-supported
restorations. J Clin Periodontol 39 Suppl 12: 139-159.
Pohl, V., Thoma, D. S., Sporniak-Tutak, K., Garcia-Garcia, A., Taylor, T. D.,
Haas, R. & Hammerle, C. H. (2017) Short dental implants (6 mm) versus long
dental implants (11-15 mm) in combination with sinus floor elevation procedures:
3-year results from a multicentre, randomized, controlled clinical trial. J Clin
Periodontol 44: 438-445.
Proetz, A. W. (1932) Some intimate studies of nasal function. Ann Otol Rhinol
Laryngol 41: 125.
Prott, W. (1971) [two efferent ducts of frontal sinuses--an antomical variant]. Z
Laryngol Rhinol Otol 50: 821-822.

57
Prott, W. (1973) [normal and atypical nasal sinus drainage duct examined by
endoscopy and x-rays]. Z Laryngol Rhinol Otol 52: 96-109.
Proussaefs, P., Lozada, J., Kim, J. & Rohrer, M. D. (2004) Repair of the
perforated sinus membrane with a resorbable collagen membrane: A human study.
Int J Oral Maxillofac Implants 19: 413-420.
Raghoebar, G. M., Batenburg, R. H., Timmenga, N. M., Vissink, A. & Reintsema,
H. (1999) Morbidity and complications of bone grafting of the floor of the
maxillary sinus for the placement of endosseous implants. Mund Kiefer
Gesichtschir 3 Suppl 1: S65-69.
Rao, V. M. & El-Noueam, K. I. (1994) Sinonasal imaging. Radiol Clin North Am
36: 921-939.
Rausch-fan, X., Qu, Z., Wieland, M., Matejka, M. & Schedle, A. (2008)
Differentiation and cytokine synthesis of human alveolar osteoblasts compared to
osteoblast-like cells (mg63) in response to titanium surfaces. Dent Mater 24: 102-
110.
Reddi, A. H. (1998) Initiation of fracture repair by bone morphogenetic proteins.
Clin Orthop Relat Res: S66-72.
Reddi, A. H., Wientroub, S. & Muthukumaran, N. (1987) Biologic principles of
bone induction. Orthop Clin North Am 18: 207-212.
Regev, E., Smith, R. A., Perrott, D. H. & Pogrel, M. A. (1995) Maxillary sinus
complications related to endosseous implants. Int J Oral Maxillofac Implants 10:
451-461.
Rickert, D., Slater, J. J., Meijer, H. J., Vissink, A. & Raghoebar, G. M. (2012)
Maxillary sinus lift with solely autogenous bone compared to a combination of
autogenous bone and growth factors or (solely) bone substitutes. A systematic
review. Int J Oral Maxillofac Surg 41: 160-167.
Roithmann, R., Shankar, L. & Hawke, M. (1992) Ct imaging in the diagnosis and
treatment of sinus disease. Journal of Otolaryngology 22: 253-260.
Sailer, I., Muhlemann, S., Zwahlen, M., Hammerle, C. H. & Schneider, D. (2012)
Cemented and screw-retained implant reconstructions: A systematic review of the
survival and complication rates. Clin Oral Implants Res 23 Suppl 6: 163-201.
Sakou, T. (1998) Bone morphogenetic proteins: From basic studies to clinical
approaches. Bone 22: 591-603.

58
Sanz, M., Chapple, I. L. & Working Group 4 of the, V. E. W. o. P. (2012) Clinical
research on peri-implant diseases: Consensus report of working group 4. J Clin
Periodontol 39 Suppl 12: 202-206.
Sartori, S., Silvestri, M., Forni, F., Icaro Cornaglia, A., Tesei, P. & Cattaneo, V.
(2003) Ten-year follow-up in a maxillary sinus augmentation using anorganic
bovine bone (bio-oss). A case report with histomorphometric evaluation. Clin
Oral Implants Res 14: 369-372.
Sbordone, C., Sbordone, L., Toti, P., Martuscelli, R., Califano, L. & Guidetti, F.
(2011) Volume changes of grafted autogenous bone in sinus augmentation
procedure. J Oral Maxillofac Surg 69: 1633-1641.
Sbordone, C., Toti, P., Guidetti, F., Califano, L., Bufo, P. & Sbordone, L. (2013)
Volume changes of autogenous bone after sinus lifting and grafting procedures: A
6-year computerized tomographic follow-up. J Craniomaxillofac Surg 41: 235-
241.
Scala, A., Botticelli, D., Rangel, I. G., Jr., de Oliveira, J. A., Okamoto, R. & Lang,
N. P. (2010) Early healing after elevation of the maxillary sinus floor applying a
lateral access: A histological study in monkeys. Clin Oral Implants Res 21: 1320-
1326.
Scharf, K. E., Lawson, W., Shapiro, J. M. & Gannon, P. J. (1995) Pressure
measurements in the normal and occluded rabbit maxillary sinus. Laryngoscope
105: 570-574.
Schatz, C. J. & Becker, T. S. (1984) Normal ct anatomy of the paranasal sinuses.
Radiol Clin North Am 22: 107-118.
Schenk, R. K. (1987) Cytodynamics and histodynamics of primary bone repair In:
Lane, J. M., ed. Fracture healing, 23-32. Edinburgh: Churchill Livingstone.
Schenk, R. K., Buser, D., Hardwick, W. R. & Dahlin, C. (1994) Healing pattern
of bone regeneration in membrane-protected defects: A histologic study in the
canine mandible. Int J Oral Maxillofac Implants 9: 13-29.
Schincaglia, G. P., Thoma, D. S., Haas, R., Tutak, M., Garcia, A., Taylor, T. D. &
Hammerle, C. H. (2015) Randomized controlled multicenter study comparing
short dental implants (6 mm) versus longer dental implants (11-15 mm) in
combination with sinus floor elevation procedures. Part 2: Clinical and
radiographic outcomes at 1 year of loading. J Clin Periodontol 42: 1042-1051.

59
Schlegel, A. K. & Donath, K. (1998) Bio-oss--a resorbable bone substitute? J
Long Term Eff Med Implants 8: 201-209.
Schlegel, K. A., Fichtner, G., Schultze-Mosgau, S. & Wiltfang, J. (2003)
Histologic findings in sinus augmentation with autogenous bone chips versus a
bovine bone substitute. Int J Oral Maxillofac Implants 18: 53-58.
Schlegel, K. A., Kloss, F. R., Schultze-Mosgau, S., Neukam, F. W. & Wiltfang, J.
(2003) [osseous defect regeneration using autogenous bone alone or combined
with biogran or algipore with and without added thrombocytes. A microradiologic
evaluation]. Mund Kiefer Gesichtschir 7: 112-118.
Schlegel, K. A., Prechtl, C., Most, T., Seidl, C., Lutz, R. & von Wilmowsky, C.
(2013) Osseointegration of slactive implants in diabetic pigs. Clin Oral Implants
Res 24: 128-134.
Schlegel, K. A., Zimmermann, R., Thorwarth, M., Neukam, F. W., Klongnoi, B.,
Nkenke, E. & Felszeghy, E. (2007) Sinus floor elevation using autogenous bone
or bone substitute combined with platelet-rich plasma. Oral Surg Oral Med Oral
Pathol Oral Radiol Endod 104: e15-25.
Schmitt, C., Karasholi, T., Lutz, R., Wiltfang, J., Neukam, F. W. & Schlegel, K.
A. (2012) Long-term changes in graft height after maxillary sinus augmentation,
onlay bone grafting, and combination of both techniques: A long-term
retrospective cohort study. Clin Oral Implants Res.
Schmitt, C. M., Doering, H., Schmidt, T., Lutz, R., Neukam, F. W. & Schlegel, K.
A. (2013) Histological results after maxillary sinus augmentation with
straumann(r) boneceramic, bio-oss(r), puros(r), and autologous bone. A
randomized controlled clinical trial. Clin Oral Implants Res 24: 576-585.
Schmitt, C. M., Moest, T., Lutz, R., Neukam, F. W. & Schlegel, K. A. (2015)
Anorganic bovine bone (abb) vs. Autologous bone (ab) plus abb in maxillary
sinus grafting. A prospective non-randomized clinical and histomorphometrical
trial. Clin Oral Implants Res 26: 1043-1050.
Schwartz-Arad, D., Herzberg, R. & Dolev, E. (2004) The prevalence of surgical
complications of the sinus graft procedure and their impact on implant survival. J
Periodontol 75: 511-516.
Schwarz, F., Sager, M., Ferrari, D., Herten, M., Wieland, M. & Becker, J. (2008)
Bone regeneration in dehiscence-type defects at non-submerged and submerged

60
chemically modified (slactive) and conventional sla titanium implants: An
immunohistochemical study in dogs. J Clin Periodontol 35: 64-75.
Schwarz, F., Sager, M., Kadelka, I., Ferrari, D. & Becker, J. (2010) Influence of
titanium implant surface characteristics on bone regeneration in dehiscence-type
defects: An experimental study in dogs. J Clin Periodontol 37: 466-473.
Sciubba, J. J. (1999) Diagnosis of malignant tumours of the maxillary sinus. Oral
and Maxillofacial Clinics of North America 11: 117-123.
Selden, H. S. (1974) The interrelationship between the maxillary sinus and
endodontics. Oral Surg Oral Med Oral Pathol 38: 623-629.
Senior, B. A. & Kennedy, D. W. (1996) Management of sinusitis in the asthmatic
patient. Ann Allergy Asthma Immunol 77: 6-15; quiz 15-19.
Shanbhag, S., Shanbhag, V. & Stavropoulos, A. (2014) Volume changes of
maxillary sinus augmentations over time: A systematic review. Int J Oral
Maxillofac Implants 29: 881-892.
Shlomi, B., Horowitz, I., Kahn, A., Dobriyan, A. & Chaushu, G. (2004) The
effect of sinus membrane perforation and repair with lambone on the outcome of
maxillary sinus floor augmentation: A radiographic assessment. Int J Oral
Maxillofac Implants 19: 559-562.
Srouji, S., Kizhner, T., Ben David, D., Riminucci, M., Bianco, P. & Livne, E.
(2009) The schneiderian membrane contains osteoprogenitor cells: In vivo and in
vitro study. Calcif Tissue Int 84: 138-145.
Stammberger, H. (1986) Nasal and paranasal sinus endoscopy. A diagnostic and
surgical approach to recurrent sinusitis. Endoscopy 18: 213-218.
Stavropoulos, A., Kostopoulos, L., Nyengaard, J. R. & Karring, T. (2004) Fate of
bone formed by guided tissue regeneration with or without grafting of bio-oss or
biogran. An experimental study in the rat. J Clin Periodontol 31: 30-39.
Su, W. Y., Liu, C., Hung, S. Y. & Tsai, W. F. (1983) Bacteriological study in
chronic maxillary sinusitis. Laryngoscope 93: 931-934.
Suarez-Lopez Del Amo, F., Ortega-Oller, I., Catena, A., Monje, A., Khoshkam,
V., Torrecillas-Martinez, L., Wang, H. L. & Galindo-Moreno, P. (2015) Effect of
barrier membranes on the outcomes of maxillary sinus floor augmentation: A
meta-analysis of histomorphometric outcomes. Int J Oral Maxillofac Implants 30:
607-618.

61
Sul, S. H., Choi, B. H., Li, J., Jeong, S. M. & Xuan, F. (2008) Histologic changes
in the maxillary sinus membrane after sinus membrane elevation and the
simultaneous insertion of dental implants without the use of grafting materials.
Oral Surg Oral Med Oral Pathol Oral Radiol Endod 105: e1-5.
Summers, R. B. (1994) A new concept in maxillary implant surgery: The
osteotome technique. Compendium 15: 152, 154-156, 158 passim; quiz 162.
Tapety, F. I., Amizuka, N., Uoshima, K., Nomura, S. & Maeda, T. (2004) A
histological evaluation of the involvement of bio-oss in osteoblastic
differentiation and matrix synthesis. Clin Oral Implants Res 15: 315-324.
Tarnow, D. P., Wallace, S. S., Froum, S. J., Rohrer, M. D. & Cho, S. C. (2000)
Histologic and clinical comparison of bilateral sinus floor elevations with and
without barrier membrane placement in 12 patients: Part 3 of an ongoing
prospective study. Int J Periodontics Restorative Dent 20: 117-125.
Tatum, H., Jr. (1986) Maxillary and sinus implant reconstructions. Dent Clin
North Am 30: 207-229.
Tatum, O. H. (1977) Maxillary sinus grafting for endosseous implants Lecture,
Alabama Implant Study Group, Annual Meeting. Birmingham, AL, USA.
Tatum, O. H. (1986) Maxillary and sinus implant reconstruction. Dent Clin North
Am 30: 207-229.
Tepper, G., Haas, R., Schneider, B., Watzak, G., Mailath, G., Jovanovic, S. A.,
Busenlechner, D., Zechner, W. & Watzek, G. (2003) Effects of sinus lifting on
voice quality. A prospective study and risk assessment. Clin Oral Implants Res
14: 767-774.
Testori, T., Wallace, S. S., Del Fabbro, M., Taschieri, S., Trisi, P., Capelli, M. &
Weinstein, R. L. (2008) Repair of large sinus membrane perforations using
stabilized collagen barrier membranes: Surgical techniques with histologic and
radiographic evidence of success. Int J Periodontics Restorative Dent 28: 9-17.
Thorwarth, M., Srour, S., Felszeghy, E., Kessler, P., Schultze-Mosgau, S. &
Schlegel, K. A. (2005) Stability of autogenous bone grafts after sinus lift
procedures: A comparative study between anterior and posterior aspects of the
iliac crest and an intraoral donor site. Oral Surg Oral Med Oral Pathol Oral
Radiol Endod 100: 278-284.
Tidwell, J. K., Blijdorp, P. A., Stoelinga, P. J., Brouns, J. B. & Hinderks, F.
(1992) Composite grafting of the maxillary sinus for placement of endosteal

62
implants. A preliminary report of 48 patients. Int J Oral Maxillofac Surg 21: 204-
209.
Timmenga, N. M., Raghoebar, G. M., Boering, G. & van Weissenbruch, R.
(1997) Maxillary sinus function after sinus lifts for the insertion of dental
implants. J Oral Maxillofac Surg 55: 936-939;discussion 940.
Timmenga, N. M., Raghoebar, G. M., Liem, R. S., van Weissenbruch, R.,
Manson, W. L. & Vissink, A. (2003) Effects of maxillary sinus floor elevation
surgery on maxillary sinus physiology. Eur J Oral Sci 111: 189-197.
Timmenga, N. M., Raghoebar, G. M., van Weissenbruch, R. & Vissink, A. (2001)
Maxillary sinusitis after augmentation of the maxillary sinus floor: A report of 2
cases. J Oral Maxillofac Surg 59: 200-204.
Tonetti, M., Palmer, R. & Working Group 2 of the, V. E. W. o. P. (2012) Clinical
research in implant dentistry: Study design, reporting and outcome measurements:
Consensus report of working group 2 of the viii european workshop on
periodontology. J Clin Periodontol 39 Suppl 12: 73-80.
Torretta, S., Mantovani, M., Testori, T., Cappadona, M. & Pignataro, L. (2013)
Importance of ent assessment in stratifying candidates for sinus floor elevation: A
prospective clinical study. Clin Oral Implants Res 24 Suppl A100: 57-62.
Trippel, S. B. (1998) Potential role of insulinlike growth factors in fracture
healing. Clin Orthop Relat Res: S301-313.
Urist, M. R. (1965) Bone: Formation by autoinduction. Science 150: 893-899.
Valentini, P. & Abensur, D. (1997) Maxillary sinus floor elevation for implant
placement with demineralized freeze-dried bone and bovine bone (bio-oss): A
clinical study of 20 patients. Int J Periodontics Restorative Dent 17: 232-241.
Valentini, P., Abensur, D., Wenz, B., Peetz, M. & Schenk, R. (2000) Sinus
grafting with porous bone mineral (bio-oss) for implant placement: A 5-year study
on 15 patients. Int J Periodontics Restorative Dent 20: 245-253.
van den Bergh, J. P., ten Bruggenkate, C. M., Disch, F. J. & Tuinzing, D. B.
(2000) Anatomical aspects of sinus floor elevations. Clin Oral Implants Res 11:
256-265.
Varricchio, A., Avvisati, F., Varricchio, A. M., Tortoriello, G. & Ciprandi, G.
(2010) The nose and paranasal sinuses. Int J Immunopathol Pharmacol 23: 1-3.

63
Velloso, G. R., Vidigal, G. M., Jr., de Freitas, M. M., Garcia de Brito, O. F.,
Manso, M. C. & Groisman, M. (2006) Tridimensional analysis of maxillary sinus
anatomy related to sinus lift procedure. Implant Dent 15: 192-196.
Vercellotti, T., De Paoli, S. & Nevins, M. (2001) The piezoelectric bony window
osteotomy and sinus membrane elevation: Introduction of a new technique for
simplification of the sinus augmentation procedure. Int J Periodontics Restorative
Dent 21: 561-567.
Vogt, K. & Schrade, F. (1979) [anatomical variations of frontal sinus duct system.
Results of radioresistometric examinations (author's transl)]. Laryngol Rhinol Otol
(Stuttg) 58: 783-794.
Wagenmann, M. & Naclerio, R. M. (1992) Anatomic and physiologic
considerations in sinusitis. J Allergy Clin Immunol 90: 419-423.
Wallace, S. S., Froum, S. J., Cho, S. C., Elian, N., Monteiro, D., Kim, B. S. &
Tarnow, D. P. (2005) Sinus augmentation utilizing anorganic bovine bone (bio-
oss) with absorbable and nonabsorbable membranes placed over the lateral
window: Histomorphometric and clinical analyses. Int J Periodontics Restorative
Dent 25: 551-559.
Wallace, S. S., Mazor, Z., Froum, S. J., Cho, S. C. & Tarnow, D. P. (2007)
Schneiderian membrane perforation rate during sinus elevation using
piezosurgery: Clinical results of 100 consecutive cases. Int J Periodontics
Restorative Dent 27: 413-419.
Wennerberg, A. & Albrektsson, T. (2009) Effects of titanium surface topography
on bone integration: A systematic review. Clin Oral Implants Res 20 Suppl 4:
172-184.
Wennerberg, A., Galli, S. & Albrektsson, T. (2011) Current knowledge about the
hydrophilic and nanostructured slactive surface. Clin Cosmet Investig Dent 3: 59-
67.
Wheeler, S. L., Holmes, R. E. & Calhoun, C. J. (1996) Six-year clinical and
histologic study of sinus-lift grafts. Int J Oral Maxillofac Implants 11: 26-34.
Wiltfang, J., Schlegel, K. A., Schultze-Mosgau, S., Nkenke, E., Zimmermann, R.
& Kessler, P. (2003) Sinus floor augmentation with beta-tricalciumphosphate
(beta-tcp): Does platelet-rich plasma promote its osseous integration and
degradation? Clin Oral Implants Res 14: 213-218.

64
Wiltfang, J., Schultze-Mosgau, S., Merten, H. A., Kessler, P., Ludwig, A. &
Engelke, W. (2000) Endoscopic and ultrasonographic evaluation of the maxillary
sinus after combined sinus floor augmentation and implant insertion. Oral Surg
Oral Med Oral Pathol Oral Radiol Endod 89: 288-291.
Wiltfang, J., Schultze-Mosgau, S., Nkenke, E., Thorwarth, M., Neukam, F. W. &
Schlegel, K. A. (2005) Onlay augmentation versus sinuslift procedure in the
treatment of the severely resorbed maxilla: A 5-year comparative longitudinal
study. Int J Oral Maxillofac Surg 34: 885-889.
Wismeijer, D., Bragger, U., Evans, C., Kapos, T., Kelly, J. R., Millen, C.,
Wittneben, J. G., Zembic, A. & Taylor, T. D. (2014) Consensus statements and
recommended clinical procedures regarding restorative materials and techniques
for implant dentistry. Int J Oral Maxillofac Implants 29 Suppl: 137-140.
Wittneben, J. G., Buser, D., Salvi, G. E., Burgin, W., Hicklin, S. & Bragger, U.
(2014) Complication and failure rates with implant-supported fixed dental
prostheses and single crowns: A 10-year retrospective study. Clin Implant Dent
Relat Res 16: 356-364.
Wittneben, J. G., Millen, C. & Bragger, U. (2014) Clinical performance of screw-
versus cement-retained fixed implant-supported reconstructions--a systematic
review. Int J Oral Maxillofac Implants 29 Suppl: 84-98.
Woodruff, M. A. & Hutmacher, D. W. (2010) The return of a forgotten polymer -
polycaprolactone in the 21st century. Progress in Polymer Science 35: 1217-1256.
Xu, H., Shimizu, Y., Asai, S. & Ooya, K. (2003) Experimental sinus grafting with
the use of deproteinized bone particles of different sizes. Clin Oral Implants Res
14: 548-555.
Xu, H., Shimizu, Y., Asai, S. & Ooya, K. (2004) Grafting of deproteinized bone
particles inhibits bone resorption after maxillary sinus floor elevation. Clin Oral
Implants Res 15: 126-133.
Xu, H., Shimizu, Y. & Ooya, K. (2005) Histomorphometric study of the stability
of newly formed bone after elevation of the floor of the maxillary sinus. Br J Oral
Maxillofac Surg 43: 493-499.
Yildirim, M., Spiekermann, H., Biesterfeld, S. & Edelhoff, D. (2000) Maxillary
sinus augmentation using xenogenic bone substitute material bio-oss in
combination with venous blood. A histologic and histomorphometric study in
humans. Clin Oral Implants Res 11: 217-229.

65
Zijderveld, S. A., Schulten, E. A., Aartman, I. H. & ten Bruggenkate, C. M.
(2009) Long-term changes in graft height after maxillary sinus floor elevation
with different grafting materials: Radiographic evaluation with a minimum
follow-up of 4.5 years. Clin Oral Implants Res 20: 691-700.
Zijderveld, S. A., van den Bergh, J. P., Schulten, E. A. & ten Bruggenkate, C. M.
(2008) Anatomical and surgical findings and complications in 100 consecutive
maxillary sinus floor elevation procedures. J Oral Maxillofac Surg 66: 1426-
1438.
Zitzmann, N. U. & Scharer, P. (1998) Sinus elevation procedures in the resorbed
posterior maxilla. Comparison of the crestal and lateral approaches. Oral Surg
Oral Med Oral Pathol Oral Radiol Endod 85: 8-17.
Zizmor, J., Bryce, M., Schaffer, S. L. & Noyek, A. M. (1975) Pneumocele of the
maxillary sinus. A second case report. Arch Otolaryngol 101: 387-388.
66
PART 1 – HISTOLOGICAL & HISTOMORPHOMETIRC ASSESSMENT
OF USING COLLAGEN STABILIZED ABBM IN MSA
This section of the thesis includes the following chapter:
Chapter 2: A histomorphometric assessment of collagen stabilized anorganic
bovine bone mineral in maxillary sinus augmentation – a randomized controlled
trial in sheep.
Chapter 3: A histomorphometric assessment of collagen stabilized anorganic
bovine bone mineral in maxillary sinus augmentation – a prospective clinical trial.
Chapter 4: Comparison of early osseointegration of SLA® and SLActive® implants
in maxillary sinus augmentation: a pilot study.

67
Chapter 2 - A histomorphometric assessment of collagen stabilized anorganic
bovine bone mineral in maxillary sinus augmentation – a randomized
controlled trial in sheep.

68
STATEMENT OF CONTRIBUTION TO CO-AUTHORED PUBLISHED
PAPER
This chapter includes a co-authored paper. The bibliographic details of the
co-authored paper, including all authors, are:
Alayan J, Vaquette C, Saifzadeh S, Hutmacher D, Ivanovski S. (2016) A
histomorphometric assessment of collagen stabilized anorganic bovine bone
mineral in maxillary sinus augmentation – a randomized controlled trial in sheep.
Clinical Oral Implants Research 27: 734 – 743. doi: 10.1111/clr.12652.
My contribution to the paper involved:
Design of the project, the provision of the data, the preliminary analysis and
categorization of the data into a usable format, the provision of direction on the
scope and structure of the analysis, the interpretation of results and drafting of the
article.
04th May 2018
Jamil Alayan
(Countersigned) 16th May 2018
Corresponding author of paper: Saso Ivanovski
(Countersigned) ___________________________ 16th May 2018
Supervisor: Stephen Hamlet

Jamil AlayanCedryck VaquetteSiamak SaifzadehDietmar HutmacherSaso Ivanovski
A histomorphometric assessment ofcollagen-stabilized anorganic bovinebone mineral in maxillary sinusaugmentation – a randomizedcontrolled trial in sheep
Authors’ affiliations:Jamil Alayan, Saso Ivanovski, School of Dentistryand Oral Health, Centre for Medicine and OralHealth, Griffith University, Southport, Qld,AustraliaCedryck Vaquette, Siamak Saifzadeh, DietmarHutmacher, Institute for Health and BiomedicalInnovation, Queensland University of Technology,Kelvin Grove, Qld, Australia
Corresponding author:Saso IvanovskiSchool of Dentistry and Oral Health, Centre forMedicine and Oral HealthGold Coast Campus Griffith UniversitySouthport, Qld 4215AustraliaTel.: +61 75 678 0741Fax: +61 75 678 0708e-mail: [email protected]
Key words: animal model, bone grafting, bone regeneration, bone substitute, histomorphom-
etry, maxillary sinus augmentation
Abstract
Objective: To histomorphometrically compare the use of collagen-stabilized anorganic bovine
bone (ABBM-C) (test) to anorganic bovine bone + autogenous bone (ABBM + AB) (control) in
maxillary sinus augmentation.
Materials and methods: Nine sheep underwent bilateral sinus augmentation. Each sinus was
randomized to receive either control or test bone graft. Three animals were sacrificed at 8 weeks,
and six animals were sacrificed at 16 weeks post-grafting. The 18 sinuses were processed for
histomorphometry, which assessed the area fraction of new bone (%NB), residual graft (%RG) and
soft tissue components (% STM), as well as graft particle osseointegration (% OI), within three
zones equally distributed from the augmented sinus floor.
Results: At week 16, a significant increase in %NB was evident across all three zones in the control
group when compared to week 8. A significantly greater %NB was evident in the control group
when compared to the test group in zones 2 (P < 0.001) and 3 (P < 0.001). There was a significant
increase in %OI in week 16 when compared to week 8 across all three zones in the control group
(P < 0.001). %OI in the control group was significantly greater across all three zones when
compared to the test group at week 16 (P < 0.001). Zone was found to be a significant main effect
(P < 0.001) that was independent of time and treatment with decreasing %OI in distant zones. %
RG did not significantly change with time for both groups. There was a significant reduction in %
ST in week 16 when compared to week 8 across all three zones in the control group (P < 0.001). %
ST in the test group was significantly greater across all zones when compared to the control group
at week 16 (P < 0.001).
Conclusion: Both groups exhibited very similar histomorphometric measurements in the zones
proximal to the resident sinus wall. The % NB and % OI were greatest in the zones proximal to
resident bony walls and gradually decreased as the distance from the proximal walls increased.
There was greater % NB and % OI in the control group when compared to the test group in the
distant zone.
Implant placement in the posterior maxilla is
often prevented by insufficient bone volume
as a result of bone resorption and sinus pneu-
matization. Maxillary sinus floor elevation is
the technique most frequently used to over-
come this limitation and is considered a safe
and effective procedure with high implant
survival rates (Del Fabbro et al. 2004). Clini-
cally this surgical technique is still being
refined, with a large degree of variation in all
aspects of the procedure.
Autogenous bone, allografts, xenografts and
alloplastic materials, as well as various
mixtures of these, are currently used in sinus
grafting (Del Fabbro et al. 2004). Autogenous
bone grafts exhibit osteogenic properties, as
well as osteoconductivity and osteoinductivi-
ty, (Burchardt 1983) and have long been con-
sidered to be the gold standard grafting
material. Autogenous bone harvesting how-
ever can be associated with post-operative
patient morbidity (Clavero & Lundgren 2003;
Cricchio & Lundgren 2003) and is only pres-
ent in limited quantities intra-orally. Autoge-
nous bone grafts can also exhibit
unpredictable resorption (Davis et al. 1984;
Date:Accepted 25 May 2015
To cite this article:Alayan J, Vaquette C, Saifzadeh S, Hutmacher D, Ivanovski S.A histomorphometric assessment of collagen-stabilizedanorganic bovine bone mineral in maxillary sinusaugmentation – a randomized controlled trial in sheep.Clin. Oral Impl. Res. 27, 2016, 734–743doi: 10.1111/clr.12652
734 © 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd

Clavero & Lundgren 2003; Wiltfang et al.
2005; Sbordone et al. 2013) which may not
be a desirable characteristic in sinus grafting
where a slower resorbing osteoconductive
material can provide superior space mainte-
nance for de novo bone formation. These
limitations of autogenous bone have resulted
in considerable research into various alterna-
tive bone substitutes.
Bio-Oss! (Geistlich AG, Wollhusen, Swit-
zerland) is a widely utilized commercial prod-
uct consisting of anorganic bovine bone
mineral (ABBM) in the form of cortical gran-
ules. It has a natural, non-antigenic porous
matrix and is chemically and physically iden-
tical to the mineral phase of human bone. It
has been reported to be highly osteoconduc-
tive and to have a very low resorption rate
(Jensen et al. 1996; Berglundh & Lindhe
1997; Haas et al. 2002a; Orsini et al. 2005)
The pores in Bio-Oss! are of optimal size and
configuration to facilitate vascular ingrowth,
which is essential for new bone formation
(Klawitter et al. 1976; Daculsi & Passuti
1990). Bio-Oss! is one of the best docu-
mented biomaterials used in maxillary sinus
augmentation (Artzi et al. 2001; Hallman
et al. 2002b; Valentini & Abensur 2003).
The combined utilization of ABBM and
particulate autogenous bone has been
reported in multiple studies of maxillary
sinus floor augmentation (Hallman et al.
2001a,b, 2002a,b; Galindo-Moreno et al.
2010; Schmitt et al. 2014). Recent animal
studies have shown that, compared with
autogenous bone and ABBM alone, the com-
bination of autogenous bone and ABBM has
the advantages of reduced graft resorption
and increased bone-to-implant contact (Jen-
sen et al. 2012, 2013).
Bio-Oss Collagen! (ABBM-C; Geistlich
AG) is also composed of ABBM particles but
stabilized in 10% porcine type-1 collagen
matrix. ABBM-C is made available for clini-
cal use in block form, rather than as a partic-
ulate graft. The contained nature of the block
may be advantageous in maxillary sinus aug-
mentation. The impact of this altered formu-
lation of ABBM has not been investigated in
terms of bone regeneration and graft stability
in maxillary sinus augmentation. This is an
important consideration as it has been shown
that surface characteristics and the geometry
of a material has a significant impact on neo-
osteogenesis (Hing et al. 2005).
Therefore, the primary aim of this study
was to histomorphometrically compare the
use of collagen-stabilized anorganic bovine
bone (ABBM-C) to anorganic bovine
bone + autogenous bone (ABBM + AB) in an
animal (ovine) model of maxillary sinus floor
augmentation. Our secondary objectives were
to assess the impact of resident wall proxim-
ity and healing time on histomorphometric
outcomes in augmented sinuses.
Material and methods
Animal care and handling
All animal handling and surgical procedures
were conducted according to the Australian
code of practice for the care and use of ani-
mals for scientific purposes at the Medical
Engineering Research Facility (MERF),
Queensland University of Technology (QUT),
Queensland, Australia. Ethical approval was
provided by the QUT Animal Research Eth-
ics Committee (QDPI Scientific Use Registra-
tion Number: 0052). All sheep underwent a
health assessment, especially to check for
the presence of upper respiratory tract infec-
tions, and were continually monitored by a
veterinary surgeon for the duration of the
study.
The surgical procedures were performed
under general anaesthesia (2.5% pentothal
sodium I.V and halothane 2% I.V) with
multi-modal pain management including
local analgesia (bupivacaine 0.5% w/v
1 : 200,000 adrenalin), an NSAID (ketorolac,
0.5 mg/kg, SC) and an opioid analgesic (bupr-
enorphine, 0.01 mg/kg IM). During surgery,
animals received cephalothin and gentami-
cin, which were continued for 5 days after
surgery.
Bone grafting materials
Animals were randomly assigned to one of
the following groups:
• Control group – small diameter particles
(0.25–1.0 mm) of deproteinized bovine
bone mineral (Bio-Oss!, Geistlich
AG) + autogenous bone (ABBM + AB) in a
1 : 1.
• Test group – 250 mg blocks of deprotei-
nized bovine bone mineral + collagen
(ABBM-C) (Bio-Oss Collagen!, Geistlich
AG).
Animal allocation and study design
The study used nine (x9) skeletally mature
wether sheep (Ovis aries), 3–4 years old.
Each animal underwent bilateral sinus aug-
mentation procedures randomly receiving on
one side the control and the other the test
grafting material. A total of x9 sinuses
received the control graft (ABBM + AB), and
a total of x9 sinuses received the test graft
(ABBM-C).
Three animals were then sacrificed at
8 weeks, and another six animals were sacri-
ficed at 16 weeks after grafting. The 18
sinuses were then processed for histology and
histomorphometry.
Surgical procedure
All animals were treated using the same sur-
gical technique utilizing an extra-oral
approach. The anterior wall of the maxillary
sinus was exposed inferior to the lower orbi-
tal rim using an oblique sagittal skin incision
of approximately 6–8 cm followed by dissec-
tion of the masseter muscle (Fig. 1a). A full
circular antrostomy was created in the lateral
wall of the maxilla using a bone scraper
(Safescraper Twist, META, C.G.M Sp.A, Reg-
gio Emilia, Italy) and a Piezo-electric surgical
unit (Implant Center, Satelec, Acteon,
France) to gain access to the maxillary sinus
(Fig. 1b). The size of the antrostomy was
standardized using a circular sterile template
with a diameter of 2.0 cm. The sinus mem-
brane was then dissected and elevated in a
dorsocranial direction using a combination of
piezoelectric surgical tips and hand sinus
membrane elevators to create an intrasinus
space (Fig. 1c). The prepared sinus was then
randomly allocated to receive the grafting
material, which is then carefully packed into
the sub-antral space ensuring contact with as
many of the residual bony walls as possible
whilst avoiding over-packing (Fig. 1d).
The autogenous bone chips collected using
the bone scraper were used as the autogenous
bone component in the control group. To
ensure a 1 : 1 ratio was maintained, a stan-
dardized chamber was utilized to ensure that
the same volume of Bio-Oss! and autogenous
particles was used. The reconstructed sites
were covered with a resorbable porcine colla-
gen membrane (Bio-Gide!, Geistlich AG)
(Fig. 1e). The masseter muscle and skin flap
were then sutured separately using a resorb-
able polyglactin suture (Vicryl 4/0, Ethicon,
Johnson & Johnson, CA, USA) followed by a
non-resorbable polypropylene suture (Prolene
4/0, Ethicon, Johnson & Johnson) for the skin
flap to achieve primary closure (Fig. 1f).
Post-operative treatment and sacrifice
A combination analgesic was given (bupr-
enorphine, 0.01 mg/kg IM, and Ketorolac,
0.5 mg/kg, SC) for 2–3 days post-operatively
to alleviate pain.
The oral surgical wounds were checked on
a daily basis for any evidence of post-opera-
tive complications, such as failure in suture
integrity (wound dehiscence), bleeding,
inflammation and infection.
© 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 735 | Clin. Oral Impl. Res. 27, 2016 / 734–743
Alayan et al !Bio-Oss Collagen in Sinus Augmentation

Post-operatively, each sheep was trans-
ferred to a covered pen and was cradled in a
sheep sling. To protect the operated sinus
from masticatory load immediately after the
surgery, the animals were fed on peripheral
parenteral nutrition for 24 h. Throughout the
fluid administration, the sheep remained cra-
dled in the sling and were monitored con-
stantly. From the second day after surgery,
the sheep were fed a soft diet for 1 week
post-operatively, and eating and drinking
were closely monitored following parenteral
nutrition.At the completion of the 8- and 16-week
healing periods, the animals were sacrificed
by a lethal injection of Lethabarb (320 mg/ml
Pentobarbital Sodium, 0.5 ml/kg).
Histological preparation andHistomorphometry
Blinding during histological preparation of
tissue samples was achieved by coding each
animal and by using a different operator for
the surgery (JA) and histomorphometry
(CV). Undecalcified resin embedded tissue
sections were prepared as previously
described (Donath & Breuner 1982; Boss-
hardt et al. 2011; Lang et al. 2011). The ini-
tial trimming of the fixed tissue samples
was performed to exclusively contain the
maxillary sinus. Two coronal samples (each
sample = 3 mm thick) were subsequently
obtained from the centre of each augmented
sinus by cutting perpendicular to the dorso-
ventral axis of the augmented sinus (Fig. 2a,
b). One sample was kept and not processed
further, whilst the other was dehydrated in
a graded series of ethanol and resin infil-
trated (methyl methacrylate/glycol methac-
rylate, Technovit 7200, Heraeus Kulzer,
Germany). Once cured, resin blocks were
ground using an EXAKT 400 CS microgrind-
ing system to expose the samples, glued
onto a glass slide and subsequently sec-
tioned to a thickness of 150 lm using an
EXAKT 300 cutting system (Exact Apparate-
bau, GmbH Norderstedt Germany). A single
slide per sinus was polished down to a
thickness of 20 lm using the EXAKT 400
CS microgrinding system. The thin speci-
mens were then stained with 0.1% tolui-
dine blue (Sigma Aldrich, St Louis, MO,
USA) for light microscopy.
Histomorphometric measurements were
performed blinded and carried out using a
specialized histomorphometric software pro-
gram (Aperio ImageScope version 12.1, Ape-
rio Technologies Inc©, Nussloch, Germany).
A single specimen was examined from each
augmented sinus. The sinus sample was
divided into three zones. The delineation of
the three zones was made after examining
the microscopic appearance of the whole
sample and dividing it into three regions of
equal surface area size (Fig. 3). Zone 1 repre-
(a) (b)
(c) (d)
(e) (f)
Fig. 1. A clinical photograph outlining the surgical steps of maxillary sinus augmentation in the sheep model. (a)
Extra-oral incision, (b) Full flap elevation & antrostomy preparation, (c) Schneiderian membrane elevation, (d) Bone
substitute selection and delivery, (e) Resorbable membrane placement, (f) Primary wound closure.
(a)
(b)
Fig. 2. (a) The maxilla was orientated such that coronal
cuts can be made within each sinus perpendicular to
the dorsoventral axis of the maxilla. (b) The cuts
yielded 3 mm sections that were then prepared histo-
logically. SW, superior wall (or roof) of the maxillary
sinus; MW, medial wall of the maxillary sinus; IW,
inferior wall (or floor) of the maxillary sinus; LW, lat-
eral wall of the maxillary sinus; AS, augmented sinus.
736 | Clin. Oral Impl. Res. 27, 2016 / 734–743 © 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Alayan et al !Bio-Oss Collagen in Sinus Augmentation

sented the region immediately adjacent to
the resident wall of bone. Zone 2 represented
the middle zone and zone 3 the zone furthest
from the resident wall and adjacent to the
sinus membrane. Histomorphometric analy-
sis assessed the percentages (i.e. area fraction)
of mineralized bone, residual graft and soft
tissue components (i.e. connective tissue
and/or bone marrow) within each zone. In
addition, the degree of graft particle osseoin-
tegration in each of the three zones was also
assessed and expressed as a percentage of the
total graft particle surface area.
The definitions of each parameter are as
follows (Fig. 4):
• % NB = area of newly formed bone/total
zonal area
• % RG = area residual graft particles/total
zonal area
• % STM = area of soft tissue and marrow
spaces/total zonal area
• % OI = area ABBM particles in direct
contact with bone/total ABBM particle
area
Statistics
Quantitative data were analysed using IBM
SPSS Statistics for Windows version 21.0
(IBM Corporation 2012©, Armonk, NY,
USA). Generalized estimating equations were
used using individual animals as the cluster-
ing variable. Zone, time and treatment were
used as explanatory variables along with all
two-way interactions. A backward elimina-
tion procedure was used for arriving to the
most parsimonious model. A P ≤ 0.05 was
considered to represent statistically signifi-
cant differences.
Results
The surgical wounds in all animals healed
completely within 10–14 days with no signs
of complications.
Gross histological features
The augmented region within the intact
sinus cavity was identified by the obvious
retained volume and change in the Schneide-
rian membrane topography. The graft parti-
cles from both groups were also easily
identified (Fig. 5). Bone of varying degrees of
maturity was observed over both time points
in both treatment groups. This ranged from
woven bone to mature bone with longitudi-
nal and concentric lamellae (Fig. 5). The
presence of BMUs is also apparent in both
groups (Figs 5 and 6). Bridging between graft
particles was evident with new bone forma-
tion seen to be continuous around and
between graft particles (Fig. 6). Most samples
exhibited residual graft particles and minimal
new bone directly in contact with the Schne-
iderian membrane in both groups at both
time points (Fig. 7). Figs 8 and 9 represent
sections of the test and control groups at
weeks 8 and 16, respectively.
% New Bone (%NB)
We tested all two-way interactions and main
effects (Fig. 10a,b). Given that all two-way
interactions were significant, we subse-
quently tested the three-way interaction.
This was found to be statistically significant
and the most parsimonious model. Thus, the
final model included the three-way interac-
tion, all two-way interactions and the main
effects.
At week 8, both the control group
(ABBM + AB) and the test group (ABBM-C)
exhibited significantly decreased %NB the
further the zone is located from the resident
wall. In the control group (ABBM + AB) at
week 8, the order of presentation of %NB is
as follows: zone 1 > 2 > 3 (P < 0.001). Simi-
larly, in the test group at week 8, %NB in
zone 1 is >2 (P < 0.001), zone 1 is >3
(P < 0.001) and zone 2 is >3 (P < 0.01). A sta-
tistically significant greater %NB was noted
in the test group when compared to the con-
trol group at week 8 in zone 1 (P < 0.01).
At week 16, a significant increase in %NB
was evident across all three zones in the con-
trol group (ABBM + AB) when compared to
week 8 in zone 1 (P < 0.01), zone 2
(P < 0.001) and zone 3 (P < 0.001). This was
especially apparent in zone 3. As such, the
impact of zone is not readily apparent in this
group with only zone 2 having a greater %
NB than zone 3 (P < 0.001). In the test group
however, there was a little change in % NB
over time with only zone 2 exhibiting a sig-
nificant increase (P < 0.01). The zonal pattern
as such in the test group (ABMM-C)
remained the same, zone 1 > 2 (P < 0.05),
zone 1 > 3 (P < 0.001) and zone 2 > 3
(P < 0.001). As such, a significantly greater %
NB was evident in the control group when
compared to the test group in zones 2
(P < 0.001) and 3 (P < 0.001).
% Osseointegration (%OI)
Time*Treatment was the only significant 2-
way interaction (P < 0.001) (Fig. 10c,d). There
was a significant increase in %OI in week 16
when compared to week 8 across all three
Fig. 3. Augmented maxillary sinus divided into three
equal zones for histomorphometric assessment. Zone 1
represents the region immediately adjacent to the resi-
dent wall of bone. Zone 2 represents the middle zone,
and zone 3 is the zone furthest from the resident wall
and adjacent to the sinus membrane.
Fig. 4. A part histological image illustrating the histomorphometric method employed. This method involves out-
lining the area of new bone (%NB), residual graft particles (%RG), soft tissue/marrow spaces (%STM) and particle
osseointegration (%OI) within the entire augmented sinus, thus allowing the calculation of the relative fractions of
each parameter.
© 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 737 | Clin. Oral Impl. Res. 27, 2016 / 734–743
Alayan et al !Bio-Oss Collagen in Sinus Augmentation

zones in the control group (ABBM + AB)
(P < 0.001). There were no significant
changes in %OI over time in the test group
(ABBM-C) (P > 0.05). %OI in the control
group was significantly greater across all
three zones when compared with the test
group at week 16 (P < 0.001) but not at week
8 (P > 0.05).
Zone was found to be a significant main
effect (P < 0.001) that was independent of
time and treatment with decreasing %OI
noted in distant zones. Zone 2 had 12.58%
("6.36) less OI than zone 1 (P < 0.05). Zone 3
had 41.25% ("6.37) less OI than zone 1
(P < 0.001). Zone 3 had 28.68% less OI than
zone 2 (P < 0.001).
% Residual Graft (%RG)
Zone*Treatment was the only significant 2-
way interaction (P < 0.01) (Fig. 11a,b). %RG
significantly increased in the test group
(ABBM-C) in the more distant zones from the
resident bone wall. At both weeks 8 and 16
in the test group, %RG in zone 3 > 2 > 1
(P < 0.01). In addition, the test group (ABBM-
C) had significantly greater % RG when com-
pared to control group in both zones 2
(P < 0.001) and 3 (P < 0.05). %RG did not sig-
nificantly change with time (P > 0.05) for
both groups.
% Soft Tissue (%ST)
Time*Treatment was the only significant 2-
way interaction (P < 0.001) (Fig. 11c,d). There
was a significant reduction in %ST in week
16 when compared to week 8 across all three
zones in the control group (ABBM + AB)
(P < 0.001). There were no significant
changes in %ST over time in the test group
(ABBM-C) (P > 0.05). %ST in the test group
was significantly greater across all three
zones when compared to the control group at
week 16 (P < 0.001) but not at week 8
(P > 0.05).
Zone was found to be a significant main
effect (P < 0.001) that was independent of
time and treatment with increasing %ST
noted in distant zones. Zone 2 had 10.01%
("4.44) more ST than zone 1 (P < 0.05). Zone
3 had 21.1% ("3.63) more ST than zone 1
(P < 0.001). Zone 3 had 11.08% more ST than
zone 2 (P < 0.001).
Discussion
The aim of this study was primarily to com-
pare the histological and histomorphometric
features of collagen-stabilized anorganic
bovine bone (test, ABBM-C) to anorganic
bovine bone + autogenous bone (control,
ABBM + AB) grafting materials in augmented
sheep maxillary sinuses. Sheep is a well-
established animal model for maxillary sinus
augmentation using an extra-oral approach
(Haas et al. 1998a, 2002a; Philipp et al. 2013).
The characteristics of the Schneiderian mem-
brane in sheep are anatomically comparable
with humans (Estaca et al. 2008), and it does
not have the disadvantage of an excessively
thick cortical bone layer such as that found
in pigs (Estaca et al. 2008).
The composite graft of anorganic bovine
bone and autogenous bone was chosen as the
control group as this combination has been
utilized in multiple studies of maxillary
sinus floor augmentation (Maiorana et al.
2000; Hallman et al. 2001a,b, 2002b; Hatano
et al. 2004; Hallman, et al. 2005; Galindo-
Moreno et al. 2010). Recent studies indicate
that this combination of autogenous bone
and Bio-Oss (ABBM) has the advantages of
Fig. 5. A histological image illustrating the varying degrees of maturity in the regenerated bone (test group week
16). Note the presence of woven bone, lamellar bone and BMUs (asterisks). ABBM, anorganic bovine bone mineral
particles; LB, lamellar bone; WB, woven bone. Toluidine blue staining.
Fig. 6. A histological image illustrating the bridging of ABBM particles by regenerated new bone (control group
week 16). ABBM, anorganic bovine bone mineral particles; NB, new bone. Toluidine blue staining.
Fig. 7. A histological image illustrating the lack of bone in the Schneiderian membrane region and the lack of
osseointegration of graft particles (test group week 16). ABBM, anorganic bovine bone mineral particles; ST, soft tis-
sue; SM, Schneiderian membrane. Toluidine blue staining.
738 | Clin. Oral Impl. Res. 27, 2016 / 734–743 © 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Alayan et al !Bio-Oss Collagen in Sinus Augmentation

reduced graft resorption and increased bone-
to-implant contact formation (Jensen et al.
2012, 2013).
The test group received Bio-Oss Collagen!
(ABBM-C) which is comprised of ABBM gran-
ules with the addition of 10% highly purified
porcine type 1 collagen. The role of the colla-
gen is to act as a cohesive for the granules,
and the material is delivered in a block for-
mat. As such, this format may have some
advantages in sinus augmentation, especially
where a particulate material is to be avoided
such as during minor sinus membrane perfo-
ration. A histological assessment of ABBM-C
in extraction sockets of beagle dogs found
that the amount of residual bovine bone min-
eral remained unchanged in the socket dur-
ing the entire healing period, whereas the
collagen portion was rapidly removed (Araujo
et al. 2010). It was hypothesized that hydro-
lytic enzymes (collagenase) released from
activated PMN cells were involved in the
rapid degradation of the porcine collagen por-
tion of the graft. However, there are no
studies reporting on the outcome of this
material after maxillary sinus floor elevation.
The histomorphometric analysis of the
augmented sinuses was performed at various
distances from the resident maxillary bone
wall to assess the impact of resident wall
proximity on the outcomes. Further, two
time points were included to gain some
insight into the temporal healing patterns in
augmented sinuses.
A decline in new bone formation was
observed within the most distant zone away
from the resident bone walls, as evidenced by
the reduced % NB in zones 2 and 3 when
compared to zone 1 in both the test (ABBM-
C) and control groups (ABBM + AB) at week
8. New bone formation in any bone defect
including the augmented sub-antral space of
maxillary sinuses occurs via a widely con-
served process of neo-osteogenesis. This pro-
cess requires the recruitment, migration and
differentiation of osteogenic cells into osteo-
blasts, leading to synthesis and deposition
of a collagenous extracellular matrix for
mineralization (Lundgren et al. 2004). It also
requires an environment with adequate blood
supply (Ham & Harris 1971), mechanical sta-
bility and sufficient space availability
(Schenk 1987).
The process of osteogenesis is modified
with the introduction of grafting materials as
there is interaction of the inserted bone sub-
stitutes with host cells, extracellular matrix
and signalling molecules (Khan et al. 2005).
Thus, there is bidirectional interaction
between the microenvironment of the maxil-
lary sinus and the properties of a given bone
substitute which can significantly influence
the osteogenic response (Donath 1991; Busen-
lechner et al. 2009). As osteogenesis extends
progressively towards the central and distal
areas of the graft (Haas et al. 2002a,b), it is
important for the biomaterial to be highly os-
teoconductive and therefore promote the
ingrowth of capillaries, peri-vascular tissue
and osteoprogenitor cells from the recipient
bed (Burchardt 1983).
A gradient of new bone formation was
observed in this study, with more new bone
formation in regions proximal to the resident
walls and reduced new bone formation at
more distant regions proximal to the elevated
membrane. This gradient of new bone forma-
tion was also observed by a number of other
studies (Fuerst et al. 2004; Busenlechner
et al. 2009; Scala et al. 2010).
Early studies of sinus augmentation sug-
gested that the source of the osteogenic cells
and molecules could be the floor (Boyne &
James 1980) or lateral wall (Misch & Dietsh
1991) of the maxillary sinus. Our results sup-
port the premise that the process of osteogen-
esis begins and is enhanced in regions
proximal to the maxillary sinus bony walls.
This observation has been further supported
by more recent studies in mini-pigs (Fuerst
et al. 2004; Busenlechner et al. 2009), rabbits
(Xu et al. 2003, 2004), primates (Margolin
et al. 1998; Scala et al. 2010, 2012) and
humans (Boyne et al. 1997; Lundgren et al.
2004).
In this study, minimal new bone formation
was seen in direct contact with the Schneide-
rian membrane (Fig. 7). Sporadic bone islands
have been noted along the Schneiderian
membrane by previous authors, but their ori-
gin remained unclear (Haas et al. 2002a). In a
study of early healing (1 month) after sinus
membrane elevation in monkeys (Scala et al.
2010), new bone formation was seen to origi-
nate from the resident bony walls of the
sinus, but not from the Schneiderian mem-
brane even though the membrane was found
to be in direct contact with bone. These
(a)
(b)
Fig. 8. Histological images representing week 8 samples from (a) control (anorganic bovine bone mineral
(ABBM) + AB) and (b) test (ABBM-C) groups. Toluidine blue staining.
© 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 739 | Clin. Oral Impl. Res. 27, 2016 / 734–743
Alayan et al !Bio-Oss Collagen in Sinus Augmentation

results are in contrast to in vitro and in vivo
studies, which suggest that the sinus mucosa
has osteogenic potential (Gruber et al. 2004;
Srouji et al. 2009). In a pre-clinical study in
which sinus membrane elevation and simul-
taneous implant placement were performed
in monkeys (Palma et al. 2006), the Schne-
iderian membrane was seen to be in contact
with newly formed bone after 1 month of
healing, but there was no evidence that it
participated in the early phase of hard tissue
formation.
Increased healing time improved the per-
centage of new bone formed in ABBM + AB
group in the distant zones (zones 2 and 3)
where a greater amount of new bone was
noted at week 16 when compared to week 8
in the control group. This may indicate a
rapid bone healing response in the zone prox-
imal to the resident wall (zone 1), which did
not subsequently benefit from additional
healing time. The distant zones, however,
may have experienced delayed neo-osteogene-
sis and therefore benefited from the extended
healing time and the addition of autogenous
bone. This may also explain why the
improved %NB was only seen in the
ABBM + AB in zone 3 at week 16 but not at
week 8. Notably, this improvement in new
bone formation was not seen in ABBM-C
group in the distant zone. These findings
would suggest that the nature of the grafting
material had a greater influence over the
degree of new bone formation in regions dis-
tant from the resident walls especially when
given sufficient time and had minimal influ-
ence in regions proximal to the resident wall,
where there is enhanced inherent osteogenic
potential. These findings were supported by
another study that histologically assessed
maxillary sinus elevation in sheep using
ABBM, autogenous bone or no filler (Haas
et al. 1998b) and reported that grafting had
no additional osteoconductive effect in
regions proximal to the resident bony wall.
Indeed, elevation of the Schneiderian mem-
brane alone resulted in new bone formation
in the region proximal to the resident bony
wall.
These findings for %NB are in contrast to
what was observed for % ST. Greater soft tis-
sue fractions were observed in the distant
zones in both treatment groups.
The increase in bone formation seen in the
control group (ABBM + AB) over time inver-
sely correlated with a reduction in soft tissue
seen over time in this group. This was espe-
cially so in the most distant zone.
A reduced degree of particle osseointegra-
tion was seen in the distant zones (zones 2
(a)
(b)
Fig. 9. Histological images representing week 16 samples from (a) control (anorganic bovine bone mineral
(ABBM) + AB) and (b) test (ABBM-C) groups. Toluidine blue staining.
Fig. 10. Area fraction of new bone (%NB) and degree of anorganic bovine bone mineral Particle osseointegration (%
OI) at week 8 and week 16. C, control group; T, test group; 1, zone 1; 2, zone 2; 3, zone 3; #, mean.
740 | Clin. Oral Impl. Res. 27, 2016 / 734–743 © 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Alayan et al !Bio-Oss Collagen in Sinus Augmentation

and 3). This correlates with the decrease in
new bone formation in these zones. The
observed increase in bone formation over
time in the distant zone in the control
ABBM + AB group may have promoted fur-
ther osseointegration of particles in this
group. As this increase in bone formation
over time was not observed in the test
ABBM-C group, the degree of particle osseo-
integration similarly did not improve and
was lower than the control group. Similar
findings were reported in a study of aug-
mented sheep sinuses (Haas et al. 1998a)
where no new bone formation was found in
contact with the ABBM particles distant to
the resident bone. It is unclear whether the
reduced new bone formation and particle
osseointegration in the ABBM-C group in the
distant zones is due to an absence of autoge-
nous bone or due to the characteristics of the
material.
Large variation in the degree of particle
osseointegration was evident in the current
study, as reflected in the wide standard devia-
tions recorded for this parameter in both
groups at both time points. This may have
been exacerbated by the small number of ani-
mals used in the week 8 group.
In summary, ABBM-C exhibited very simi-
lar histomorphometric parameters to the
composite graft of ABBM + AB in regions
proximal to the resident sinus wall. The per-
centage of new bone and residual graft parti-
cle osseointegration were greatest in the
zones proximal to the resident bony walls
and gradually decreased as the distance from
the proximal walls increased. In the distant
zone however, there was significantly greater
percentage of new bone and residual graft
particles osseointegration in the ABBM + AB
group when compared to the ABBM-C group.
The clinical implications of these results
is that the choice of graft material
(ABBM + AB vs. ABBM-C) is only relevant if
the intention is to utilize the regenerated
bone in the distant third of the augmented
sinus, in which case ABBM + AB is the
superior material.
Acknowledgements: Jamil Alayan is
the recipient of a scholarship from the
National Health & Medical Research
Council of Australia (ID: APP1056633). Bio-
Oss!, Bio-Oss Collagen! and Bio-Gide! were
kindly provided by Geistlich AG, Wollhusen,
Switzerland. We would like to thank Dr
Dimitrios Vagenas (Biostatistician, Institute
for Health and Biomedical Innovation,
Queensland University of Technology,
Kelvin Grove, Australia) for his assistance
and contribution to the statistical analysis in
this project.
References
Araujo, M.G., Liljenberg, B. & Lindhe, J. (2010)
Dynamics of bio-oss collagen incorporation in fresh
extraction wounds: an experimental study in the
dog. Clinical Oral Implants Research 21: 55–64.
Artzi, Z., Nemcovsky, C.E., Tal, H. & Dayan, D.
(2001) Histopathological morphometric evalua-
tion of 2 different hydroxyapatite-bone derivatives
in sinus augmentation procedures: a comparative
study in humans. Journal of Periodontology 72:
911–920.
Berglundh, T. & Lindhe, J. (1997) Healing around
implants placed in bone defects treated with bio-
oss. An experimental study in the dog. Clinical
Oral Implants Research 8: 117–124.
Bosshardt, D.D., Salvi, G.E., Huynh-Ba, G., Ivanov-
ski, S., Donos, N. & Lang, N.P. (2011) The role of
bone debris in early healing adjacent to hydro-
philic and hydrophobic implant surfaces in man.
Clinical Oral Implants Research 22: 357–364.
Boyne, P.J. & James, R.A. (1980) Grafting of the
maxillary sinus floor with autogenous marrow
and bone. Journal of Oral Surgery 38: 613–616.
Boyne, P.J., Marx, R.E., Nevins, M., Triplett, G.,
Lazaro, E., Lilly, L.C., Alder, M. & Nummiko-
ski, P. (1997) A feasibility study evaluating
rhbmp-2/absorbable collagen sponge for maxil-
lary sinus floor augmentation. The International
Journal of Periodontics & Restorative Dentistry
17: 11–25.
Burchardt, H. (1983) The biology of bone graft
repair. Clinical Orthopaedics & Related
Research 174: 28–42.
Busenlechner, D., Huber, C.D., Vasak, C., Dobsak,
A., Gruber, R. & Watzek, G. (2009) Sinus aug-
mentation analysis revised: the gradient of graft
consolidation. Clinical Oral Implants Research
20 : 1078–1083.
Clavero, J. & Lundgren, S. (2003) Ramus or chin
grafts for maxillary sinus inlay and local onlay
augmentation: comparison of donor site morbid-
ity and complications. Clinical Implant Dentistry
and Related Research 5 : 154–160.
Cricchio, G. & Lundgren, S. (2003) Donor site mor-
bidity in two different approaches to anterior iliac
crest bone harvesting. Clinical Implant Dentistry
and Related Research 5 : 161–169.
Daculsi, G. & Passuti, N. (1990) Effect of the
macroporosity for osseous substitution of calcium
phosphate ceramics. Biomaterials 11: 86–87.
Davis, W.H., Martinoff, J.T. & Kaminishi, R.M.
(1984) Long-term follow up of transoral rib grafts
for mandibular atrophy. Journal of Oral and Max-
illofacial Surgery 42: 606–609.
Del Fabbro, M., Testori, T., Francetti, L. & Wein-
stein, R. (2004) Systematic review of survival
rates for implants placed in the grafted maxillary
sinus. The International Journal of Periodontics
& Restorative Dentistry 24: 565–577.
Donath, K. (1991) Fundamentals of pathologic anat-
omy and pathophysiology for implantation suc-
cess. Niedersachs Zahnarztebl 26: 203–205.
Donath, K. & Breuner, G. (1982) A method for the
study of undecalcified bones and teeth with
attached soft tissues. The sage-schliff (sawing and
grinding) technique. Journal of Oral Pathology &
Medicine 11: 318–326.
Fig. 11. Area fraction of residual graft (%RG) and area fraction of soft tissue (%ST) at week 8 and week 16. C,
control group; T, test group; 1, zone 1; 2, zone 2; 3, zone 3; #, mean.
© 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 741 | Clin. Oral Impl. Res. 27, 2016 / 734–743
Alayan et al !Bio-Oss Collagen in Sinus Augmentation

Estaca, E., Cabezas, J., Uson, J., Sanchez-Margallo,
F., Morell, E. & Latorre, R. (2008) Maxillary
sinus-floor elevation: an animal model. Clinical
Oral Implants Research 19 : 1044–1048.
Fuerst, G., Tangl, S., Gruber, R., Gahleitner, A.,
Sanroman, F. & Watzek, G. (2004) Bone forma-
tion following sinus grafting with autogenous
bone-derived cells and bovine bone mineral in
minipigs: preliminary findings. Clinical Oral
Implants Research 15 : 733–740.
Galindo-Moreno, P., Moreno-Riestra, I., Avila, G.,
Fernandez-Barbero, J.E., Mesa, F., Aguilar, M.,
Wang, H.L. & O’Valle, F. (2010) Histomorpho-
metric comparison of maxillary pristine bone and
composite bone graft biopsies obtained after sinus
augmentation. Clinical Oral Implants Research
21: 122–128.
Gruber, R., Kandler, B., Fuerst, G., Fischer, M.B. &
Watzek, G. (2004) Porcine sinus mucosa holds
cells that respond to bone morphogenetic protein
(bmp)-6 and bmp-7 with increased osteogenic dif-
ferentiation in vitro. Clinical Oral Implants
Research 15 : 575–580.
Haas, R., Baron, M., Donath, K., Zechner, W. &
Watzek, G. (2002a) Porous hydroxyapatite for
grafting the maxillary sinus: a comparative histo-
morphometric study in sheep. The International
Journal of Oral & Maxillofacial Implants 17:
337–346.
Haas, R., Donath, K., Fodinger, M. & Watzek, G.
(1998a) Bovine hydroxyapatite for maxillary sinus
grafting: comparative histomorphometric findings
in sheep. Clinical Oral Implants Research 9 :
107–116.
Haas, R., Haidvogl, D., Dortbudak, O. & Mailath,
G. (2002b) Freeze-dried bone for maxillary sinus
augmentation in sheep. Part ii: biomechanical
findings. Clinical Oral Implants Research 13:
581–586.
Haas, R., Mendorff-Pouilly, N., Mailath, G. &
Bernhart, T. (1998b) Five-year results of maxil-
lary intramobile zylinder implants. British Jour-
nal of Oral and Maxillofacial Surgery 36: 123–
128.
Hallman, M., Cederlund, A., Lindskog, S., Lund-
gren, S. & Sennerby, L. (2001a) A clinical histo-
logic study of bovine hydroxyapatite in
combination with autogenous bone and fibrin
glue for maxillary sinus floor augmentation.
Results after 6 to 8 months of healing. Clinical
Oral Implants Research 12: 135–143.
Hallman, M., Hedin, M., Sennerby, L. & Lundgren,
S. (2002a) A prospective 1-year clinical and radio-
graphic study of implants placed after maxillary
sinus floor augmentation with bovine hydroxyap-
atite and autogenous bone. Journal of Oral and
Maxillofacial Surgery 60 : 277–284; discussion
285–276.
Hallman, M., Lundgren, S. & Sennerby, L. (2001b)
Histologic analysis of clinical biopsies taken
6 months and 3 years after maxillary sinus floor
augmentation with 80% bovine hydroxyapatite
and 20% autogenous bone mixed with fibrin glue.
Clinical Implant Dentistry and Related Research
3: 87–96.
Hallman, M., Sennerby, L. & Lundgren, S. (2002b)
A clinical and histologic evaluation of implant
integration in the posterior maxilla after sinus
floor augmentation with autogenous bone, bovine
hydroxyapatite, or a 20:80 mixture. The Interna-
tional Journal of Oral & Maxillofacial Implants
17: 635–643.
Hallman, M., Sennerby, L., Zetterqvist, L. & Lundg-
ren, S. (2005) A 3-year prospective follow-up
study of implant-supported fixed prostheses in
patients subjected to maxillary sinus floor aug-
mentation with a 80:20 mixture of deproteinized
bovine bone and autogenous bone Clinical, radio-
graphic and resonance frequency analysis. Inter-
national Journal of Oral and Maxillofacial
Surgery 34: 273–280.
Ham, A.W. & Harris, W.R. (1971) Repair and trans-
plantation of bone. In: Bourne, G.H., ed. The Bio-
chemistry and Physiology of Bone, 337–399. New
York, NY: Academic Press.
Hatano, N., Shimizu, Y. & Ooya, K. (2004) A clini-
cal long-term radiographic evaluation of graft
height changes after maxillary sinus floor aug-
mentation with a 2:1 autogenous bone/xenograft
mixture and simultaneous placement of dental
implants. Clinical Oral Implants Research 15 :
339–345.
Hing, K.A., Annaz, B., Saeed, S., Revell, P.A. &
Buckland, T. (2005) Microporosity enhances bio-
activity of synthetic bone graft substitutes. Jour-
nal of Materials Science: Materials in Medicine
16: 467–475.
Jensen, S.S., Aaboe, M., Pinholt, E.M., Hjorting-
Hansen, E., Melsen, F. & Ruyter, I.E. (1996)
Tissue reaction and material characteristics of
four bone substitutes. The International Jour-
nal of Oral & Maxillofacial Implants 11: 55–
66.
Jensen, T., Schou, S., Gundersen, H.J., Forman,
J.L., Terheyden, H. & Holmstrup, P. (2013)
Bone-to-implant contact after maxillary
sinus floor augmentation with bio-oss and
autogenous bone in different ratios in mini
pigs. Clinical Oral Implants Research 24: 635–
644.
Jensen, T., Schou, S., Svendsen, P.A., Forman, J.L.,
Gundersen, H.J., Terheyden, H. & Holmstrup, P.
(2012) Volumetric changes of the graft after max-
illary sinus floor augmentation with bio-oss and
autogenous bone in different ratios: a radiographic
study in minipigs. Clinical Oral Implants
Research 23: 902–910.
Khan, S.N., Cammisa, F.P., Jr, Sandhu, H.S., Diwan,
A.D., Girardi, F.P. & Lane, J.M. (2005) The
biology of bone grafting. The Journal of the Amer-
ican Academy of Orthopaedic Surgeons 13: 77–
86.
Klawitter, J.J., Bagwell, J.G., Weinstein, A.M. &
Sauer, B.W. (1976) An evaluation of bone
growth into porous high density polyethylene.
Journal of Biomedical Materials Research 10 :
311–323.
Lang, N.P., Salvi, G.E., Huynh-Ba, G., Ivanovski, S.,
Donos, N. & Bosshardt, D.D. (2011) Early osseo-
integration to hydrophilic and hydrophobic
implant surfaces in humans. Clinical Oral
Implants Research 22: 349–356.
Lundgren, S., Andersson, S., Gualini, F. & Senner-
by, L. (2004) Bone reformation with sinus mem-
brane elevation: a new surgical technique for
maxillary sinus floor augmentation. Clinical
Implant Dentistry and Related Research 6: 165–
173.
Maiorana, C., Redemagni, M., Rabagliati, M. & Sal-
ina, S. (2000) Treatment of maxillary ridge resorp-
tion by sinus augmentation with iliac cancellous
bone, anorganic bovine bone, and endosseous
implants: a clinical and histologic report. The
International Journal of Oral & Maxillofacial
Implants 15 : 873–878.
Margolin, M.D., Cogan, A.G., Taylor, M., Buck, D.,
McAllister, T.N., Toth, C. & McAllister, B.S.
(1998) Maxillary sinus augmentation in the non-
human primate: a comparative radiographic and
histologic study between recombinant human
osteogenic protein-1 and natural bone mineral.
Journal of Periodontology 69 : 911–919.
Misch, C.E. & Dietsh, F. (1991) Autogenous bone
grafts for endosteal implants–indications and fail-
ures. The International Journal of Oral Implan-
tology 8: 13–20.
Orsini, G., Traini, T., Scarano, A., Degidi, M., Per-
rotti, V., Piccirilli, M. & Piattelli, A. (2005) Max-
illary sinus augmentation with bio-oss particles:
a light, scanning, and transmission electron
microscopy study in man. Journal of Biomedical
Materials Research Part B: Applied Biomaterials
74: 448–457.
Palma, V.C., Magro-Filho, O., de Oliveria, J.A.,
Lundgren, S., Salata, L.A. & Sennerby, L. (2006)
Bone reformation and implant integration follow-
ing maxillary sinus membrane elevation: an
experimental study in primates. Clinical Implant
Dentistry and Related Research 8: 11–24.
Philipp, A., Duncan, W., Roos, M., Hammerle,
C.H., Attin, T. & Schmidlin, P.R. (2013)
Comparison of sla or slactive implants placed
in the maxillary sinus with or without syn-
thetic bone graft materials – an animal study in
sheep. Clinical Oral Implants Research 25 :
1142–1148.
Sbordone, C., Toti, P., Guidetti, F., Califano, L.,
Bufo, P. & Sbordone, L. (2013) Volume changes of
autogenous bone after sinus lifting and grafting
procedures: a 6-year computerized tomographic
follow-up. Journal of Cranio-maxillo-facial Sur-
gery 41: 235–241.
Scala, A., Botticelli, D., Faeda, R.S., Garcia Rangel,
I., Jr, Americo de Oliveira, J. & Lang, N.P. (2012)
Lack of influence of the schneiderian membrane
in forming new bone apical to implants simulta-
neously installed with sinus floor elevation: an
experimental study in monkeys. Clinical Oral
Implants Research 23: 175–181.
Scala, A., Botticelli, D., Rangel, I.G., Jr, de Oliveira,
J.A., Okamoto, R. & Lang, N.P. (2010) Early heal-
ing after elevation of the maxillary sinus floor
applying a lateral access: a histological study in
monkeys. Clinical Oral Implants Research 21:
1320–1326.
Schenk, R. (1987) Cytodynamics and histodynamics
of primary bone repair. In: Lane, J.M., ed. Fracture
Healing, 23–32. New York, Edinburgh, London,
Melbourne: Churchill Livingstone.
Schmitt, C.M., Moest, T., Lutz, R., Neukam, F.W.
& Schlegel, K.A. (2014) Anorganic bovine
742 | Clin. Oral Impl. Res. 27, 2016 / 734–743 © 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Alayan et al !Bio-Oss Collagen in Sinus Augmentation

bone (abb) vs. Autologous bone (ab) plus abb in
maxillary sinus grafting. A prospective non-ran-
domized clinical and histomorphometrical
trial. Clinical Oral Implants Research 26: 1043–
1050.
Srouji, S., Kizhner, T., Ben David, D., Riminucci,
M., Bianco, P. & Livne, E. (2009) The schneideri-
an membrane contains osteoprogenitor cells:
in vivo and in vitro study. Calcified Tissue Inter-
national 84: 138–145.
Valentini, P. & Abensur, D.J. (2003) Maxillary sinus
grafting with anorganic bovine bone: a clinical
report of long-term results. The International Jour-
nal of Oral & Maxillofacial Implants 18: 556–560.
Wiltfang, J., Schultze-Mosgau, S., Nkenke, E., Thor-
warth, M., Neukam, F.W. & Schlegel, K.A. (2005)
Onlay augmentation versus sinuslift procedure in
the treatment of the severely resorbed maxilla: a
5-year comparative longitudinal study. Interna-
tional Journal of Oral and Maxillofacial Surgery
34: 885–889.
Xu, H., Shimizu, Y., Asai, S. & Ooya, K. (2003)
Experimental sinus grafting with the use of de-
proteinized bone particles of different sizes. Clini-
cal Oral Implants Research 14: 548–555.
Xu, H., Shimizu, Y., Asai, S. & Ooya, K. (2004)
Grafting of deproteinized bone particles inhibits
bone resorption after maxillary sinus floor eleva-
tion. Clinical Oral Implants Research 15 : 126–
133.
Supporting Information
Additional Supporting Information may be
found in the online version of this article:
Appendix S1. CONSORT Statement 2001
Checklist.
© 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 743 | Clin. Oral Impl. Res. 27, 2016 / 734–743
Alayan et al !Bio-Oss Collagen in Sinus Augmentation

79
Chapter 3 - A histomorphometric assessment of collagen stabilized anorganic
bovine bone mineral in maxillary sinus augmentation – a prospective clinical
trial.

80
STATEMENT OF CONTRIBUTION TO CO-AUTHORED PUBLISHED
PAPER
This chapter includes a co-authored paper. The bibliographic details of the
co-authored paper, including all authors, are:
Alayan J, Vaquette C, Farah C, Ivanovski S. (2016) A histomorphometric
assessment of collagen stabilized anorganic bovine bone mineral in maxillary sinus
augmentation – a prospective clinical trial. Clinical Oral Implants Research 27: 850
– 858. doi: 10.1111/clr.12694.
My contribution to the paper involved:
Design of the project, the provision of the data, the preliminary analysis and
categorization of the data into a usable format, the provision of direction on the
scope and structure of the analysis, the interpretation of results and drafting of the
article.
04th May 2018
Jamil Alayan
(Countersigned) 16th May 2018
Corresponding author of paper: Saso Ivanovski
(Countersigned) ___________________________ 16th May 2018
Supervisor: Stephen Hamlet

Jamil AlayanCedryck VaquetteCamile FarahSaso Ivanovski
A histomorphometric assessment ofcollagen-stabilized anorganic bovinebone mineral in maxillary sinus aug-mentation – a prospective clinical trial
Authors’ affiliations:Jamil Alayan, Saso Ivanovski, School of Dentistryand Oral Health, Centre for Medicine and OralHealth, Griffith University, Southport, AustraliaCedryck Vaquette, Institute of Health andBiomedical Innovation, Queensland University ofTechnology, Kelvin Grove, AustraliaCamile Farah, UQ Centre for Clinical Research,University of Queensland, Brisbane, Australia
Corresponding author:Saso IvanovskiSchool of Dentistry and Oral HealthCentre for Medicine and Oral HealthGold Coast Campus Griffith UniversitySouthport QLD 4215AustraliaTel.: +61 75 678 0741Fax: +61 75 678 0708e-mail: [email protected]
Key words: anorganic bovine bone, Bio-Oss, Bio-Oss Collagen, bone grafting, bone regenera-
tion, bone substitute, clinical trial, histomorphometry, maxillary sinus augmentation, sinus
floor elevation
Abstract
Objective: To histomorphometrically compare the use of collagen-stabilized anorganic bovine
bone (ABBM-C) (test) to anorganic bovine bone + autogenous bone (ABBM + AB) (control) in
maxillary sinus augmentation.
Materials and Methods: Forty (n = 40 sinuses) patients underwent sinus augmentation and
received either control (20 sinuses) or test bone graft (20 sinuses). Bone samples were harvested
from the augmented sinuses 5 months postgrafting. The samples were processed for
histomorphometry, which assessed within the primary region of interest (ROI-1), the area fraction
of new bone (%NB), graft particle osseointegration (% OI), residual graft (%RG), and soft tissue
components (% STM). The same analysis was also carried out in a second region of interest (ROI-2)
located in a zone 1 mm proximal to the previous maxillary sinus floor.
Results: In both ROI-1 and ROI-2, the mean % NB, %RG, and %STM in the control group were
similar to mean values in the test group. The % OI was significantly greater in the control group
(42.0 +/! 26.8) when compared to the test group (19.6 +/! 27.3) in ROI-2 (P < 0.05). No statistically
significant differences were seen when ROI-1 and ROI-2 were compared except for improved %OI
in ROI-2 in the control group. The mean proportion of lamellar bone to woven bone in the control
group (1.22 " 1.48) was significantly greater than the test group (0.38 " 0.29) (P < 0.05).
Conclusion: ABBM-C exhibited very similar histomorphometric parameters to the composite graft
of ABBM + AB. The ABBM + AB group was more mature as indicated by the significantly greater
proportion of lamellar bone when compared to the ABBM-C. Improved % OI was seen in the zone
proximal to the resident bony floor in the ABBM + AB group. Based on histological assessment,
ABBM-C is a suitable bone substitute for the purposes of maxillary sinus augmentation. Its clinical
utility may be indicated in cases of sinus membrane perforation and insufficient autogenous bone
in the local area.
Implant placement in the posterior maxilla is
often prevented by insufficient bone volume
as a result of bone resorption and sinus
pneumatization. Maxillary sinus floor eleva-
tion is the technique most frequently used to
overcome this limitation and is considered a
safe and effective procedure with high
implant survival rates (Del Fabbro et al.
2004; Chiapasco et al. 2009). Nevertheless,
clinically this surgical technique is still being
refined, with a large degree of variation in
many aspects of the procedure.
To date, a variety of bone substitute mate-
rials have demonstrated clinically acceptable
outcomes (Froum et al. 2006; Cordaro et al.
2008; Nkenke & Stelzle 2009; Klijn et al.
2010). However, despite the established clini-
cal efficacy of the technique, the search con-
tinues for a bone substitute with optimal
properties including rapid osteogenesis as
well as long-term stability and space mainte-
nance.
If de novo bone formation is the reference
parameter, then autogenous bone remains
the gold standard (Klijn et al. 2010; Schmitt
et al. 2013). Autogenous bone harvesting,
however, can be associated with postopera-
tive patient morbidity (Clavero & Lundgren
2003; Cricchio & Lundgren 2003) and pro-
longed surgical time and is only present in
Date:Accepted 16 August 2015
To cite this article:Alayan J, Vaquette C, Farah C, Ivanovski S. Ahistomorphometric assessment of collagen-stabilizedanorganic bovine bone mineral in maxillary sinusaugmentation – a prospective clinical trial.Clin. Oral Impl. Res. 27, 2016, 850–858doi: 10.1111/clr.12694
850 © 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd

limited quantities. Autogenous bone grafts
can also exhibit unpredictable resorption
(Davis et al. 1984; Clavero & Lundgren 2003;
Wiltfang et al. 2005; Sbordone et al. 2013),
which may not be a desirable characteristic
in sinus grafting. Indeed, sinuses augmented
using autogenous bone as the sole grafting
material have been shown to undergo signifi-
cant re-pneumatization and loss of aug-
mented volume (Johansson et al. 2001;
Arasawa et al. 2012). These limitations of
autogenous bone have resulted in consider-
able research into alternative bone substi-
tutes. It has been proposed that a slower
resorbing osteoconductive material may pro-
vide superior space maintenance for de novo
bone formation.
Anorganic deproteinized bovine bone min-
eral (ABBM) (Bio-Oss!; Geistlich AG, Woll-
husen, Switzerland) is a widely utilized
commercial product in the form of cortical
granules. It has a natural, non-antigenic por-
ous matrix and is chemically and physically
identical to the mineral phase of human
bone. It has been reported to be highly
osteoconductive and to have a very low
resorption rate (Jensen et al. 1996; Berglundh
& Lindhe 1997; Haas et al. 2002; Orsini
et al. 2005). The pores in Bio-Oss! are of
optimal size and configuration to facilitate
vascular ingrowth, which is essential for
new bone (NB) formation (Klawitter et al.
1976; Daculsi & Passuti 1990). Bio-Oss! is
one of the best-documented biomaterials
used in maxillary sinus augmentation (Artzi
et al. 2001; Hallman et al. 2002; Valentini
& Abensur 2003).
ABBM is also available in a block form that
is stabilized in 10% porcine type-1 collagen
matrix (ABBM-C) (Bio-Oss Collagen!; Geis-
tlich AG). The contained nature of the block
may be advantageous in maxillary sinus aug-
mentation when the common surgical com-
plication of Schneiderian membrane
perforation occurs (Chiapasco et al. 2009).
The impact of this altered formulation of
ABBM has not been investigated in terms of
bone regeneration in maxillary sinus aug-
mentation. This is an important considera-
tion because it has been shown that surface
characteristics and the geometry of a material
have a significant impact on neo-osteogenesis
(Hing et al. 2005).
Therefore, the primary aim of this con-
trolled clinical trial was to histomorphomet-
rically compare the use of collagen-stabilized
anorganic bovine bone (ABBM-C) vs. anor-
ganic bovine bone + autogenous bone
(ABBM + AB) in maxillary sinus floor aug-
mentation. Our secondary objective was to
assess the impact of the resident sinus floor
proximity on histomorphometric outcomes.
Material and methods
Ethics and consent
The University of Queensland School of Den-
tistry Dental Sciences Research Ethics Com-
mittee provided ethical approval for this
project (Project Number: 1010). The project
complies with the provisions contained in
the National Statement on Ethical Conduct
in Research Involving Humans and complies
with the regulations governing experimenta-
tion on humans.
All patients provided informed consent
prior to enrolling in the study.
Inclusion criteria
To be considered eligible for the study, the
following inclusion criteria were applied:
• Males and females, over 21 years of age at
the time of surgery
• Must present with a bone deficiency in
the maxillary sinus region, which necessi-
tates sinus floor augmentation to facili-
tate the placement of one or more dental
implants.
• If bilateral sinus augmentation was
required, only one sinus was used for the
purposes of this study.
• Residual alveolar bone height of the eden-
tulous maxilla below the floor of the
maxillary sinus ≤5 mm and ≥ 1 mm, as
measured on a CT scan in the deepest
floor of the sinus
• Residual alveolar bone width of ≥6 mm as
measured on a CT scan
• Absence of sinus infection
• Generally fit and healthy and able to
undergo oral surgical procedures under
local anesthesia
• Patients with a history of chronic peri-
odontitis were required to be treated first
and subsequently enrolled in a supportive
maintenance program
• Teeth at the surgical site which required
removal were extracted a minimum of
8 weeks prior to sinus floor elevation
Exclusion criteria
Patients were considered ineligible if any of
the following criteria were met:
• Any systemic medical condition that
could interfere with the surgical proce-
dure
• Current pregnancy at the time of recruit-
ment
• Physical handicaps that would interfere
with the ability to perform adequate oral
hygiene
• Alcoholism or chronic drug abuse
• Patients who smoke more than 10 cigar-
ettes per day
• Medications which interferes with bone
formation
• Mucosal diseases such as erosive Lichen
Planus
• History of local radiation therapy
• Severe bruxism or clenching habits
• Signs and symptoms consistent with
acute sinus infections
• Previous guided bone regeneration (bone
graft) or dental implant treatment in the
posterior segments of the maxilla
• Benign or malignant tumors of the maxil-
lary sinus
• Pathological conditions that severely
impact mucociliary clearance including;
chronic sinusitis, primary ciliary dyskine-
sia, or cystic fibrosis.
Bone graft materials and dental implants
Patients were randomly assigned to one of
the following groups:
• Control group – small diameter particles
(0.25–1.0 mm) of deproteinized bovine
bone mineral (Bio-Oss!; Geistlich
AG) + autogenous bone (ABBM + AB) in a
1 : 1 ratio, as determined using a stan-
dardized 2 cc bone collecting chamber.
• Test group – 250 mg blocks of depro-
teinized bovine bone mineral + collagen
(ABBM-C) (Bio-Oss Collagen!, Geistlich
AG).
All patients’ received a single Straumann
(Institut Straumann AG, Basel, Switzerland)
tissue level dental implant 5 months post-
grafting. The implant had a standard micro-
roughened sandblasted and acid-etched (SLA)
surface. The dimensions of the implants were
chosen according to the specific site charac-
teristics.
Participant allocation and study design
The study included 42 (n = 42) patients that
underwent the informed consent process
after meeting the outlined criteria. It was cal-
culated that a sample size of 16 patients per
group was required to detect a 10% difference
in the means of the primary parameter (%
NB), based on 95% confidence level, 80%
power and a predicted variance of 100 (10%
deviation from mean). Twenty-one patients
were recruited per group to allow for possible
dropouts. All patients were recruited prospec-
© 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 851 | Clin. Oral Impl. Res. 27, 2016 / 850–858
Alayan et al #Bio-Oss collagen in human sinus grafting

tively from the School of Dentistry at the
University of Queensland and from a special-
ist private practice from July 2010 to March
2014. All patients were referred specifically
for replacement of teeth with implant-sup-
ported restorations.
Allocation of each patient to either the test
(ABBM-C) or the control group (ABBM + AB)
was based on two clinical parameters; the
presence of Schneiderian membrane perfora-
tion and/or availability of adequate autoge-
nous bone in the vicinity of the surgical site.
ABBM-C was selected if mild (≤3 mm) sinus
membrane perforations occurred (four cases)
or if there was insufficient autogenous bone
available for harvesting from the buccal
aspect of the posterior maxilla within the
same surgical region. ABBM + AB was alter-
natively used if the Schneiderian membrane
remained intact and if there was sufficient
autogenous bone that could be harvested
from the buccal wall of the maxilla.
Five months later, all participants under-
went surgical implant placement whereby
they received a single implant in the aug-
mented site. At this time, a single bone
biopsy was harvested during the osteotomy
preparation and collected from a total of 40
patients (920 from test group and 920 from
the control group). These samples were used
for the histological assessment.
The same clinician (JA) performed all of
the surgical procedures. While clinician
blinding was not possible at the time of the
augmentation surgery, it was possible during
the data collection and analysis stages of this
project.
Presurgical procedures
Prior to surgery 3-dimensional CT scanning
was carried on all patients to determine the
site anatomy and to identify patients with
significant sino-nasal pathology. All partici-
pants started systemic antibiotic therapy
(1000 mg amoxycillin or 300 mg clin-
damycin) 24 h prior to surgery. A 0.2%
chlorhexidine mouth rinse was utilized for
60 s immediately prior to grafting surgery.
Surgical procedure – sinus floor elevation
All patients were treated with the same sur-
gical technique consisting of sinus floor ele-
vation via a lateral wall (modified Caldwell-
Luc) approach. After elevation of a full buccal
mucoperiosteal flap, a full antrostomy was
created in the lateral wall of the maxilla
using a bone scraper (Safescraper Twist,
META, C.G.M Sp.A, Reggio Emiia, Italy) and
a Piezo-electric surgical unit (Implant Center,
Satelec, Acteon, France) to gain access to the
maxillary sinus. The size, shape, and location
of the antrostomy were variable and tailored
to the site and patient’s characteristics. The
only consistent feature of the antrostomy
was the superior osteotomy, which was
located 10 mm superior/apical to the alveolar
bony crest. The sinus membrane was then
dissected and elevated in all directions to cre-
ate an intra-sinus space that received one of
the two grafting materials (Fig. 1). The mem-
brane was elevated superiorly to allow for
grafting material packing up to 10 mm apical
to the alveolar bone crest. This was achieved
using standard sinus membrane elevator
spoons. Sufficient material was placed until
the desired 10 mm of vertical height was
achieved. The material was carefully packed
to ensure maximum contact with resident
bony walls, with care taken to avoid over-
packing.
Autogenous bone chips collected using a
bone scraper were used for the autogenous
bone component needed for the control
group. If additional autogenous bone was
required, it was harvested from the zygo-
matic buttress within the same surgical field.
The reconstructed sites were covered with a
porcine collagen membrane (Bio-Gide; Geis-
tlich AG). The mucoperiosteal flaps were
then sutured using a non-resorbable thermo-
plastic polyether-ester monofilament suture
(Dyloc 5/0; Dynek, Adelaide, Australia) to
achieve primary closure.
A postoperative regimen of amoxycillin
500 mg t.d.s for 7 days (or if allergic 150 mg
clindamycin q.i.d for 6 days) was prescribed,
as was paracetamol 500 mg, ibuprofen
200 mg and 0.2% chlorhexidine mouth rinse
b.d for 7 days. Patients were reviewed at 1
and 2 weeks postoperatively.
Surgical procedure – dental implant placementand biopsy
A preimplant placement CT scan was taken
5 months later when dental implant place-
ment was performed. All participants began
systemic antibiotic therapy (1000 mg amoxy-
cillin or 300 mg of clindamycin) 60 min prior
to surgery. A 0.2% chlorhexidine mouth
rinse was utilized for 60 s immediately prior
to surgery. A single bone biopsy was har-
vested from each participant during the
osteotomy preparation using a standard tre-
phine bur with an internal/external diameter
of 2.0/3.0 mm, respectively. Drilling with the
trephine was taken as far apically as possible
without perforating the Schneiderian mem-
brane, as predetermined on the preimplant
CT scan. The trephine was directed in the
exact three dimensional position/axis as the
dental implant osteotomy. The osteotomy
preparation was then completed, and the
implant was delivered. The mucoperiosteal
flap was then sutured using a non-resorbable
thermoplastic polyether-ester monofilament
suture (Dyloc 5/0; Dynek) to achieve primary
closure.
A postoperative regimen of amoxycillin
500 mg three times daily for 7 days was pre-
scribed, together with paracetamol 500 mg,
ibuprofen 200 mg, and 0.2% chlorhexidine
mouth rinse twice daily for 7 days. Patients
were reviewed 1-week postoperatively.
The bone samples were immediately stored
in paraformaldehyde until further histological
processing.
Histological preparation and histomorphometry
Blinding during histological preparation of
tissue samples was achieved by coding each
sample and using a different operator for the
surgery (JA) and histomorphometry (CV).
Undecalcified resin embedded tissue sections
were prepared as previously described
(Donath & Breuner 1982; Schlegel & Donath
1998; Schmitt et al. 2015). Each sample was
fixed in 4% paraformaldehyde phosphate-buf-
fered formalin. The samples were cut along
the long axis of the biopsy and divided into
two. One sample was kept and not processed
further, while the other was dehydrated in a
graded series of ethanol and resin infiltrated
(Methyl Methacrylate/Glycol Methacrylate,
Fig. 1. Clinical photographs showing the surgical place-
ment of the test group grafting material (ABBM-C). (a)
An ABBM-C block. (b) The ABBM-C blocks after they
were delivered into the maxillary intra-sinus space.
852 | Clin. Oral Impl. Res. 27, 2016 / 850–858 © 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Alayan et al #Bio-Oss collagen in human sinus grafting

Tecknovit 7200, Heraeus Kulzer, Hanau, Ger-
many). Once cured, resin blocks were ground
using an EXAKT 400 CS microgrinding sys-
tem to expose the samples, glued onto a glass
slide and subsequently sectioned to a thick-
ness of 150 lm using an EXAKT 300 cutting
system (Exact Apparatebau GmbH, Norderst-
edt, Germany). A single slide per sample was
polished down to a thickness of 20 lm using
the EXAKT 400 CS microgrinding system.
The specimens were then stained with 0.1%
toluidine blue (Sigma-Aldrich, St Louis, MO,
USA) for light microscopy.
Histomorphometric measurements were
performed blinded and carried out using a
specialized histomorphometric analysis soft-
ware program (Aperio ImageScope version
12.1; Aperio Technologies Inc©, Nussloch,
Germany) (Fig. 2) by the same operator (JA).
Two regions of interest (ROI) were delineated
after carefully studying the microscopic
appearance of the whole biopsy. The first
region of interest (ROI-1) represented the area
from the junction of the preexisting or native
bone (i.e., the former floor of the sinus cav-
ity) to where the biopsy broke during the har-
vesting procedure (Fig. 2). The second region
of interest (ROI-2) represented the area from
the junction of the preexisting or native bone
(i.e., the former floor of the sinus cavity) and
ended 1 mm apically into the sample (Fig. 2).
Histomorphometric analysis assessed the
percentages (i.e., area fraction) of mineralized
bone (% NB), residual graft (%RG), and soft
tissue components (i.e., connective tissue
and/or bone marrow) (%STM) within each
ROI. In addition, the degree of graft particle
osseointegration (%OI) in each ROI was also
assessed and expressed as a percentage of the
total graft particle surface area (Fig. 3).
The definitions of each parameter are as
follows (Fig. 3):
• % NB = area of newly formed bone/area
ROI.
• % RG = area residual graft particles/area
ROI.
• % STM = area of soft tissue and marrow
spaces/area ROI.
• % OI = area particles in direct contact
with bone/total particles area ROI.
In addition, the ratio of lamellar bone to
woven bone was compared between control
and test groups.
Statistics
Area fractions and the ratio of lamellar bone
to woven bone were analyzed using IBM
SPSS Statistics for Windows version 21.0
(IBM Corporation 2012©, Armonk, NY,
USA). A two-sample, two-tailed t-test was
performed after assessing normality of the
data set using histogram, skewness, and kur-
tosis. Homogeneity of variance was assessed
using the Levene’s test. Mean difference, con-
fidence intervals, and P-values were adjusted
if equal variance could not be assumed. Simi-
larly, baseline parameters, including residual
radiological bone height and the area of ROI,
were compared between test and control
groups using a t-test. If data were not found
to be normally distributed, then a Mann–
Whitney U-test was used. The null hypothe-
sis was that of no difference between control
and test groups for all histomorphometric
parameters. A P ≤ 0.05 was considered to rep-
resent statistically significant differences
between test and control groups. All nor-
mally distributed data were expressed as
mean " standard deviation. The median was
reported for values calculated using a Mann–
Whitney U-test. In addition, mean difference
and the 95% confidence interval of the differ-
ence are provided where applicable for com-
parative analysis (Tables 1 and 2).
The primary outcome measure includes
the area fractions in control and test samples
in ROI-1. The secondary outcome measure
includes the area fractions in control and test
samples in ROI-2.
Results
Study population
Forty-two (n = 42) patients were enrolled in
this study and underwent sinus augmenta-
tion. Prior to sinus grafting, the mean resi-
dent bone ridge height in the deepest portion
of the maxillary sinuses floor was
2.4 " 0.75 mm in the control group and
2.2 " 0.87 mm in the test group. The mean
difference was 0.19 mm (95% CI !0.34–0.71)
and was not significant (P ≤ 0.49). A total of
40 patients (n = 40) underwent sample har-
vesting and histomorphometric analysis (con-
trol group n = 20) (test group n = 20) with
one sample harvested per sinus and a single
dental implant placed in each site (n = 20
control group) (n = 20 test group). Two
patients could not undergo sample harvesting
in the implant site due to limited access.
The mean patient age in the control group
was 57.70 years with a female/male ratio of
2.3. The mean patient age in the test group
was 54.60 years with a female/male ratio of
3.0. Wound healing proceeded as expected
with no signs of impaired wound healing or
wound dehiscence. A total of four membrane
perforations occurred in the test group of
patients. These perforations were small
(≤3 mm in diameter) and repaired by creating
a pouch using the placement of a resorbable
Fig. 2. Histological images outlining the histomorpho-
metric analysis after each parameter of interest was
delineated such as the residual graft (RG) particles, new
bone, and RG particle osseointegration. (a) First region
of interest (ROI-1) represents the area from the junction
of the preexisting or native bone (i.e., the former floor
of the sinus cavity) to where the biopsy broke during
the harvesting procedure. (b) Second region of interest
(ROI-2) represents the area from the junction of the pre-
existing or native bone (i.e., the former floor of the
sinus cavity) and ends 1 mm apically into the sample.
Fig. 3. A high magnification part histological image highlighting the area of new bone (%NB), residual graft parti-
cles (%RG), soft tissue/marrow spaces (%STM), and particle osseointegration (%OI) within a region of interest
(ROI) allowing then the calculation of the relative fractions of each parameter.
© 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 853 | Clin. Oral Impl. Res. 27, 2016 / 850–858
Alayan et al #Bio-Oss collagen in human sinus grafting

porcine collagen membrane (Bio-Gide; Geis-
tlich AG) as per Proussaefs & Lozada (Prous-
saefs & Lozada 2003). Symptoms consistent
with postoperative sinusitis were observed in
one patient in the control group, which
resolved spontaneously within 48 h after
sinus grafting.
Gross histological features
Common histological features observed in
both groups included readily identifiable RG
particles, presence of NB around and
between graft particles, and a significant
non-mineralized (soft tissue/marrow) tissue
fraction (Fig. 4). Bone of varying degrees of
maturity was observed in both treatment
groups (Fig. 5). This ranged from woven
bone to mature bone with longitudinal and
concentric lamellae (Fig. 5). The presence of
bone multicellular units (BMUs) was also
apparent in both groups. The mean propor-
tion of lamellar bone to woven bone in the
control group (1.22 " 1.48) was significantly
greater than the test group (0.38 " 0.29).
The mean difference was 0.84 (95% CI
0.14–1.54) and represented a significant dif-
ference (P ≤ 0.021).
Comparison between ROI-1 and ROI-2
The mean area for ROI-1 in the control group
(6.92 " 4.18 mm2) was similar to the ROI-1
in the test group (7.73 " 3.53 mm2) (Fig. 6
and Table 1). The mean difference was
!0.81 mm2 (95% CI !3.29–1.67) and was not
significant (P ≤ 0.51). The mean area for ROI-
2 in the control group (2.09 " 0.82 mm2) was
similar to the ROI-2 in the test group
(1.95 " 0.41 mm2). The mean difference was
0.14 mm2 (95% CI !0.28–0.56) and was not
significant (P ≤ 0.49).
In the control group, ROI-2 had greater %
NB (ROI-1: 29.06 " 13.51 vs. ROI-2:
34.03 " 13.05), greater %OI (ROI-1:
26.34 " 14.30 vs. ROI-2: 42.03 " 26.83),
lower %RG (ROI-1: 19.11 " 8.87 vs. ROI-2:
15.59 " 9.93), and lower %STM (ROI-1:
51.82 " 10.98 vs. ROI-2: 50.38 " 10.96)
when compared to ROI-1 (Fig. 6). The mean
differences were not statistically significant,
except for the %OI (P ≤ 0.03) (Table 1).
In the test group, ROI-2 had greater %NB
(ROI-1: 30.71 " 12.24 vs. ROI-2:
39.68 " 17.36) and lower %OI (ROI-1: 25.93
vs. ROI-2: 4.49), lower %RG (ROI-1: 14.11 vs.
ROI-2: 3.86) and lower %STM (ROI-1:
54.18 " 10.53 vs. ROI-2: 49.82 " 20.47)
when compared to ROI-1 (Fig. 6). These dif-
ferences were not statistically significant
except for the %OI (P ≤ 0.05) and %RG
(P ≤ 0.05) (Table 1).
Comparison between test and control groups
In ROI-1, the control and test groups had
very similar mean values for all parameters:
%NB (control: 29.06 " 13.51 vs. test:
30.71 " 12.24), %OI (control: 26.34 " 14.30
vs. test: 26.57 " 18.14), %RG (control:
19.11 " 8.87 vs. test: 15.11 " 9.65), and %
STM (control: 51.82 " 10.98 vs. test:
54.18 " 10.53) (Fig. 6 and Table 2). These
mean differences were not statistically signif-
icant (Table 2).
Similarly, in ROI-2, the control and test
groups had very similar mean values for the
following parameters: %NB (control:
34.03 " 13.05 vs. test: 39.68 " 17.36) and %
STM (control: 50.38 " 10.96 vs. test:
49.82 " 20.47) (Fig. 6). These mean differ-
ences were not statistically significant
(Table 2). The %OI and %RG, however, were
greater in the control group when compared
to the test group (%OI control: 48.62 vs. test:
4.49) and (%RG control: 13.21 vs. test: 3.86)
(Fig. 6). These differences were statistically
significant (P ≤ 0.05) (Table 2).
Discussion
The aim of this prospective clinical trial
was primarily to compare the histological
and histomorphometric features of colla-
gen-stabilized anorganic bovine bone (test,
ABBM-C) and anorganic bovine bone + au-
togenous bone (control, ABBM + AB) graft-
ing materials in augmented maxillary
sinuses. There are no reported studies
assessing collagen-stabilized anorganic
bovine bone (test, ABBM-C) in maxillary
sinus augmentation.
Table 1. Outcomes of histomorphometric evaluation comparing ROI-1 (total sample area) vs. ROI-2(area proximal to resident wall) within samples taken from grafted maxillary sinuses
Parameter P-value Mean difference
95% Confidenceinterval of themean difference
ROI-1 vs. ROI-2 Group: control (ABBM + AB) (n = 20)
% NB 0.24 !4.97 !13.48–3.53% OI 0.03 !15.69 !29.59–(!1.78)% RG 0.24 3.52 !2.5–9.55% STM 0.68 1.44 !5.57–8.47
ROI-1 vs. ROI-2 Group: test (ABBM-C) (n = 20)
% NB 0.07 8.96 !18.58–0.65% OI* 0.014 NA NA% RG* 0.02 NA NA% STM 0.40 4.36 !6.18–14.89
ABBM, anorganic bovine bone mineral; AB, autogenous bone; ABBM-C, collagen-stabilized anor-ganic bovine bone mineral; ROI-1, border of previous sinus floor-to-most apical portion of the regionof the sample; ROI-2, border previous sinus floor-to-1 mm apical into the sample; NB, new bone; RG,residual graft particles; STM, soft tissue/marrow spaces; OI, particle osseointegration; SD, standarddeviation; P, P-value for inter-group comparison after applying a t-test.*Mann–Whitney U-test was carried out on these parameters.
Table 2. Outcome of histomorphometric evaluation comparing control (ABBM + AB) vs. test(ABBM-C) samples taken from grafted maxillary sinuses
Parameter P-value Mean difference
95% Confidenceinterval of themean difference
Control vs. Test groups ROI-1 (n = 20) total sample area
% NB 0.69 !1.65 !9.90–6.60% OI 0.96 !0.23 !10.69–10.22% RG 0.18 4.01 !1.93–9.94% STM 0.49 !2.35 !9.24–4.53
Control vs. test groups ROI-2 (n = 20) area proximal to resident wall
% NB 0.25 !5.65 !15.48–4.18% OI* 0.01 NA NA% RG* 0.03 NA NA% STM 0.92 0.55 !10.06–11.17
ABBM, anorganic bovine bone mineral; AB, autogenous bone; ABBM-C, collagen-stabilized anor-ganic bovine bone mineral; ROI-1, border of previous sinus floor-to-most apical portion of the regionof the sample; ROI-2, border previous sinus floor-to-1 mm apical into the sample; NB, new bone; RG,residual graft particles; STM, soft tissue/marrow spaces; OI, particle osseointegration; SD, standarddeviation; P, P-value for inter-group comparison after applying a t-test.*Mann–Whitney U-test performed on these parameters.
854 | Clin. Oral Impl. Res. 27, 2016 / 850–858 © 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Alayan et al #Bio-Oss collagen in human sinus grafting
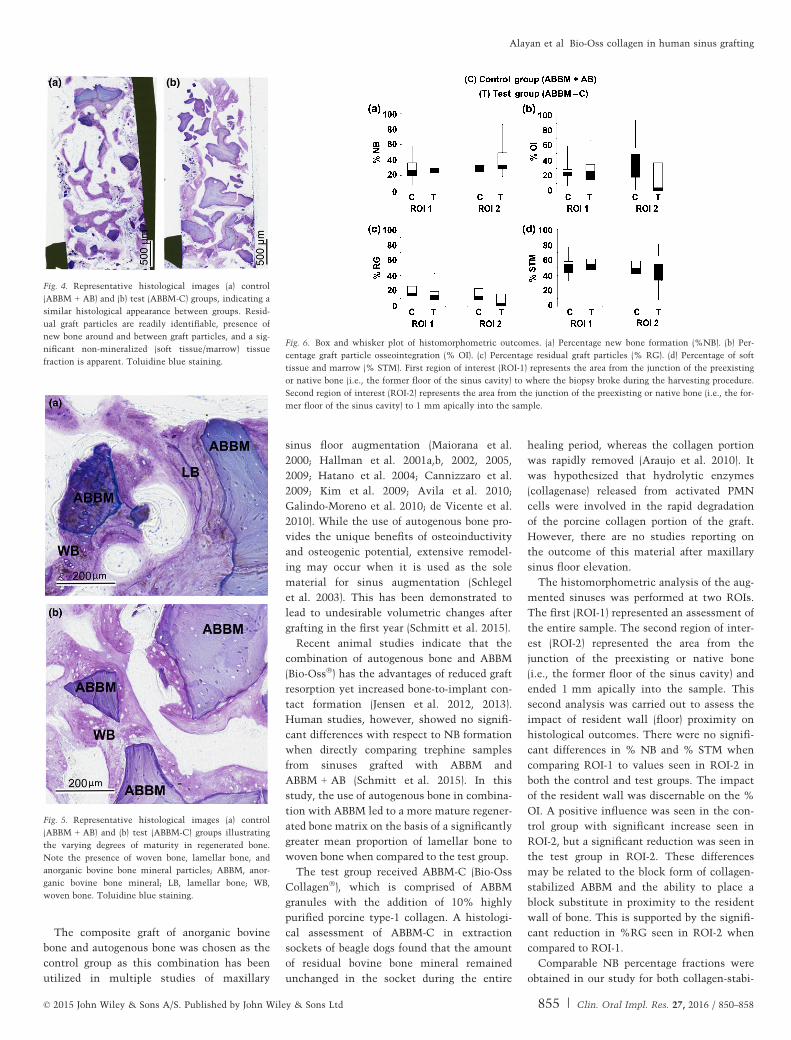
The composite graft of anorganic bovine
bone and autogenous bone was chosen as the
control group as this combination has been
utilized in multiple studies of maxillary
sinus floor augmentation (Maiorana et al.
2000; Hallman et al. 2001a,b, 2002, 2005,
2009; Hatano et al. 2004; Cannizzaro et al.
2009; Kim et al. 2009; Avila et al. 2010;
Galindo-Moreno et al. 2010; de Vicente et al.
2010). While the use of autogenous bone pro-
vides the unique benefits of osteoinductivity
and osteogenic potential, extensive remodel-
ing may occur when it is used as the sole
material for sinus augmentation (Schlegel
et al. 2003). This has been demonstrated to
lead to undesirable volumetric changes after
grafting in the first year (Schmitt et al. 2015).
Recent animal studies indicate that the
combination of autogenous bone and ABBM
(Bio-Oss!) has the advantages of reduced graft
resorption yet increased bone-to-implant con-
tact formation (Jensen et al. 2012, 2013).
Human studies, however, showed no signifi-
cant differences with respect to NB formation
when directly comparing trephine samples
from sinuses grafted with ABBM and
ABBM + AB (Schmitt et al. 2015). In this
study, the use of autogenous bone in combina-
tion with ABBM led to a more mature regener-
ated bone matrix on the basis of a significantly
greater mean proportion of lamellar bone to
woven bone when compared to the test group.
The test group received ABBM-C (Bio-Oss
Collagen!), which is comprised of ABBM
granules with the addition of 10% highly
purified porcine type-1 collagen. A histologi-
cal assessment of ABBM-C in extraction
sockets of beagle dogs found that the amount
of residual bovine bone mineral remained
unchanged in the socket during the entire
healing period, whereas the collagen portion
was rapidly removed (Araujo et al. 2010). It
was hypothesized that hydrolytic enzymes
(collagenase) released from activated PMN
cells were involved in the rapid degradation
of the porcine collagen portion of the graft.
However, there are no studies reporting on
the outcome of this material after maxillary
sinus floor elevation.
The histomorphometric analysis of the aug-
mented sinuses was performed at two ROIs.
The first (ROI-1) represented an assessment of
the entire sample. The second region of inter-
est (ROI-2) represented the area from the
junction of the preexisting or native bone
(i.e., the former floor of the sinus cavity) and
ended 1 mm apically into the sample. This
second analysis was carried out to assess the
impact of resident wall (floor) proximity on
histological outcomes. There were no signifi-
cant differences in % NB and % STM when
comparing ROI-1 to values seen in ROI-2 in
both the control and test groups. The impact
of the resident wall was discernable on the %
OI. A positive influence was seen in the con-
trol group with significant increase seen in
ROI-2, but a significant reduction was seen in
the test group in ROI-2. These differences
may be related to the block form of collagen-
stabilized ABBM and the ability to place a
block substitute in proximity to the resident
wall of bone. This is supported by the signifi-
cant reduction in %RG seen in ROI-2 when
compared to ROI-1.
Comparable NB percentage fractions were
obtained in our study for both collagen-stabi-
Fig. 4. Representative histological images (a) control
(ABBM + AB) and (b) test (ABBM-C) groups, indicating a
similar histological appearance between groups. Resid-
ual graft particles are readily identifiable, presence of
new bone around and between graft particles, and a sig-
nificant non-mineralized (soft tissue/marrow) tissue
fraction is apparent. Toluidine blue staining.
Fig. 5. Representative histological images (a) control
(ABBM + AB) and (b) test (ABBM-C) groups illustrating
the varying degrees of maturity in regenerated bone.
Note the presence of woven bone, lamellar bone, and
anorganic bovine bone mineral particles; ABBM, anor-
ganic bovine bone mineral; LB, lamellar bone; WB,
woven bone. Toluidine blue staining.
Fig. 6. Box and whisker plot of histomorphometric outcomes. (a) Percentage new bone formation (%NB). (b) Per-
centage graft particle osseointegration (% OI). (c) Percentage residual graft particles (% RG). (d) Percentage of soft
tissue and marrow (% STM). First region of interest (ROI-1) represents the area from the junction of the preexisting
or native bone (i.e., the former floor of the sinus cavity) to where the biopsy broke during the harvesting procedure.
Second region of interest (ROI-2) represents the area from the junction of the preexisting or native bone (i.e., the for-
mer floor of the sinus cavity) to 1 mm apically into the sample.
© 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 855 | Clin. Oral Impl. Res. 27, 2016 / 850–858
Alayan et al #Bio-Oss collagen in human sinus grafting

lized ABBM (30.71 " 12.24%) and
ABBM + AB (29.06 " 13.51%) to a recent
study of maxillary sinus grafting in humans
which used ABBM + AB bone also in a 1 : 1
ratio (27.50 " 6.31%) and utilized a similar
biopsy harvesting technique (Schmitt et al.
2015).
Harvesting of autogenous bone can be asso-
ciated with increased postoperative patient
morbidity (Clavero & Lundgren 2003; Cric-
chio & Lundgren 2003) and prolonged surgical
time. These disadvantages are exaggerated if a
second intra-oral surgical site has to be
accessed to gain sufficient autogenous bone
volume. As such, the use of bone substitutes
solely has a distinct clinical advantage. Based
on the histomorphometric outcomes of this
study, the use of collagen-stabilized anorganic
bovine bone mineral (ABBM-C) alone is suit-
able in such clinical situations.
The impact of proximity to the sinus floor
on NB formation was not discernable in this
study as the %NB in ROI-1 and ROI-2 were
not significantly different in both groups. A
recent animal study (Alayan et al. 2015) by
our group noted a positive histomorphometric
impact of proximity to the resident bony
walls on parameters such as %NB and %OI.
This gradient of bone formation has also been
reported in other studies (Haas et al. 1998;
Busenlechner et al. 2009). The differences in
outcomes compared to the current study may
have been due to different sampling tech-
niques. The animal study by Alayan et al.
(Alayan et al. 2015) assessed entire sinus sam-
ples, whereas this study assessed trephine/
biopsy samples. The biopsy harvesting tech-
nique has been reported to have a significant
impact on histomorphometric outcomes at
least in the early phases of graft healing (Mar-
golin et al. 1998; Artzi et al. 2005). Artzi
et al. (2005) histomorphometrically assessed
the variation in area fraction of residual bone
substitutes and NB in samples harvested via a
trephine from grafted maxillary sinuses. The
depth of the samples influenced both the area
fraction of NB and RG particles. As such, the
limitations of the biopsy technique may pre-
vent observation of a gradient of graft consoli-
dation by not being fully representative of the
entire maxillary sinus environment.
Additional sources of variations in the area
fraction of biomaterials such as ABBM have
been reported (Valentini et al. 2000; Yildirim
et al. 2000; Hallman et al. 2001b) and may
depend on the density of the grafting material
at application, the initial percentage of the
material, the particle size, and the histologi-
cal preparation technique. In this study, cer-
tain factors were controlled, as the same
clinician carried out all surgical procedures,
the particle size was identical in all cases
and the proportion of ABMM to autogenous
bone was maintained at 1 : 1 using a stan-
dardized bone collection chamber.
A significant difference was seen in the
degree of particle OI with the control group
showing improved %OI in ROI-2 when com-
pared to the test group. While this mean dif-
ference was statistically significant, a large
variation in the degree of particle OI between
samples was noted. This was reflected in the
wide confidence intervals. This wide varia-
tion in %OI was also seen in a recent animal
study by our group (Alayan et al. 2015), has
also been reported in previous animal studies
(Haas et al. 1998), and may have been influ-
enced by the sample size. These histological
variations may influence the available bone
volume for implantation and bone-to-implant
contact. It would also imply that clinicians
should aim to maximize the regenerative
potential of the procedure by maximizing the
bony walls involved in the healing process
and ensuring intimate contact between the
graft particles and resident walls.
The role of the collagen in the test grafting
material (ABBM-C) is to cohesively bind the
ABBM granules, and hence, the material is
delivered in a block format. As such, it may
have some advantages in sinus augmentation,
especially where a particulate material is to be
avoided such as during sinus membrane perfo-
ration. This is the most frequently reported
surgical complication during maxillary sinus
augmentation and according to a recent review
has a mean occurrence rate of 10% (4.8–58%)
(Chiapasco et al. 2009). This complication
occurred in 9.5% of cases in this study (4 of
42), with all of these allocated to the test
group. All of these perforations were small in
diameter (≤ 3 mm) and were repaired with a
resorbable porcine collagen membrane using a
previously described technique (Proussaefs &
Lozada 2003). ABBM-C is advantageous in
these cases because of its block format incor-
porating stabilized ABBM particles. As such, it
would be less likely to migrate into the maxil-
lary sinus cavity proper and obstruct the osteo-
meatal complex, thereby minimizing the
occurrence of postgrafting sinusitis. Previous
studies have cited particulate migration as a
source of postoperative sinusitis (Quiney et al.
1990; Wiltfang et al. 2000; Doud Galli et al.
2001) which may require endoscopic removal
and re-establishment of drainage (Doud Galli
et al. 2001; Timmenga et al. 2001). The use of
ABBM-C in this manner had no impact on his-
tomorphometric outcomes. The significance
of sinus membrane perforations on implant
survival or graft success remains contentious
with some studies reporting a negative impact
especially in large perforations (Proussaefs
et al. 2004; Hernandez-Alfaro et al. 2008),
while others showed no differences (Becker
et al. 2008).
In summary, ABBM-C exhibited very simi-
lar histomorphometric parameters to the com-
posite graft of ABBM + AB. Improved % OI
was seen in the zone proximal to the resident
bony floor in the anorganic bovine bone + au-
togenous bone group (ABBM + AB). In addi-
tion, the ABBM + AB group was more mature
as indicated by the significantly greater pro-
portion of lamellar bone when compared to
the ABBM-C. It can be concluded that from a
histological standpoint ABBM-C is a suitable
bone substitute for the purposes of maxillary
sinus augmentation. Its clinical utility may be
in cases of sinus membrane perforation and
insufficient autogenous bone in the local area.
This material could potentially be a useful
addition to the armamentarium of clinicians
carrying out maxillary sinus augmentation.
Acknowledgements: This project was
funded by a grant from the Australian Dental
Research Foundation (RM#: 2010001012).
Bio-Oss!, Bio-Oss Collagen! & Bio-Gide!
were kindly provided by Geistlich AG,
Wollhusen, Switzerland. We would like to
thank Dr Dimitrios Vagenas and Lee Jones
(Biostatisticians, Institute for Health and
Biomedical Innovation, Queensland
University of Technology, Kelvin Grove,
Australia) for their assistance and
contribution to the statistical analysis in this
project.
References
Alayan, J., Vaquette, C., Saifzadeh, S., Hutmacher,
D.W. & Ivanovski, S. (2015) A histomorphometric
assessment of collagen stabilized anorganic bovine
bone mineral in maxillary sinus augmentation – a
randomized controlled trial in sheep. Clinical Oral
Implants Research 27: 734–743.
Arasawa, M., Oda, Y., Kobayashi, T., Uoshima, K.,
Nishiyama, H., Hoshina, H. & Saito, C. (2012)
Evaluation of bone volume changes after sinus
floor augmentation with autogenous bone grafts.
International Journal of Oral and Maxillofacial
Surgery 41: 853–857.
856 | Clin. Oral Impl. Res. 27, 2016 / 850–858 © 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Alayan et al #Bio-Oss collagen in human sinus grafting

Araujo, M.G., Liljenberg, B. & Lindhe, J. (2010) Dy-
namics of bio-oss collagen incorporation in fresh
extraction wounds: an experimental study in the
dog. Clinical Oral Implants Research 21: 55–64.
Artzi, Z., Kozlovsky, A., Nemcovsky, C.E. & Wein-
reb, M. (2005) The amount of newly formed bone
in sinus grafting procedures depends on tissue
depth as well as the type and residual amount of
the grafted material. Journal of Clinical Periodon-
tology 32: 193–199.
Artzi, Z., Nemcovsky, C.E., Tal, H. & Dayan, D. (2001)
Histopathological morphometric evaluation of 2 dif-
ferent hydroxyapatite-bone derivatives in sinus aug-
mentation procedures: a comparative study in
humans. Journal of Periodontology 72: 911–920.
Avila, G., Wang, H.L., Galindo-Moreno, P., Misch,
C.E., Bagramian, R.A., Rudek, I., Benavides, E.,
Moreno-Riestra, I., Braun, T. & Neiva, R. (2010)
The influence of the bucco-palatal distance on
sinus augmentation outcomes. Journal of Peri-
odontology 81: 1041–1050.
Becker, S.T., Terheyden, H., Steinriede, A., Behrens,
E., Springer, I. & Wiltfang, J. (2008) Prospective
observation of 41 perforations of the schneiderian
membrane during sinus floor elevation. Clinical
Oral Implants Research 19 : 1285–1289.
Berglundh, T. & Lindhe, J. (1997) Healing around
implants placed in bone defects treated with bio-
oss. An experimental study in the dog. Clinical
Oral Implants Research 8: 117–124.
Busenlechner, D., Huber, C.D., Vasak, C., Dobsak,
A., Gruber, R. & Watzek, G. (2009) Sinus aug-
mentation analysis revised: the gradient of graft
consolidation. Clinical Oral Implants Research
20: 1078–1083.
Cannizzaro, G., Felice, P., Leone, M., Viola, P. &
Esposito, M. (2009) Early loading of implants in
the atrophic posterior maxilla: lateral sinus lift
with autogenous bone and bio-oss versus crestal
mini sinus lift and 8-mm hydroxyapatite-coated
implants. A randomised controlled clinical trial.
European Journal of Oral Implantology 2: 25–38.
Chiapasco, M., Casentini, P. & Zaniboni, M. (2009)
Bone augmentation procedures in implant den-
tistry. International Journal of Oral & Maxillofa-
cial Implants 24(Suppl): 237–259.
Clavero, J. & Lundgren, S. (2003) Ramus or chin
grafts for maxillary sinus inlay and local onlay
augmentation: comparison of donor site morbid-
ity and complications. Clinical Implant Dentistry
and Related Research 5: 154–160.
Cordaro, L., Bosshardt, D.D., Palattella, P., Rao, W.,
Serino, G. & Chiapasco, M. (2008) Maxillary
sinus grafting with bio-oss or straumann bone
ceramic: histomorphometric results from a ran-
domized controlled multicenter clinical trial.
Clinical Oral Implants Research 19 : 796–803.
Cricchio, G. & Lundgren, S. (2003) Donor site mor-
bidity in two different approaches to anterior iliac
crest bone harvesting. Clinical Implant Dentistry
and Related Research 5: 161–169.
Daculsi, G. & Passuti, N. (1990) Effect of the
macroporosity for osseous substitution of calcium
phosphate ceramics. Biomaterials 11: 86–87.
Davis, W.H., Martinoff, J.T. & Kaminishi, R.M.
(1984) Long-term follow up of transoral rib grafts
for mandibular atrophy. Journal of Oral and Max-
illofacial Surgery 42: 606–609.
Del Fabbro, M., Testori, T., Francetti, L. & Wein-
stein, R. (2004) Systematic review of survival
rates for implants placed in the grafted maxillary
sinus. The International Journal of Periodontics
& Restorative Dentistry 24: 565–577.
Donath, K. & Breuner, G. (1982) A method for the
study of undecalcified bones and teeth with
attached soft tissues. The sage-schliff (sawing and
grinding) technique. Journal of Oral Pathology
11: 318–326.
Doud Galli, S.K., Lebowitz, R.A., Giacchi, R.J.,
Glickman, R. & Jacobs, J.B. (2001) Chronic
sinusitis complicating sinus lift surgery. Ameri-
can Journal of Rhinology 15: 181–186.
Froum, S.J., Wallace, S.S., Elian, N., Cho, S.C. &
Tarnow, D.P. (2006) Comparison of mineralized
cancellous bone allograft (puros) and anorganic
bovine bone matrix (bio-oss) for sinus augmenta-
tion: histomorphometry at 26 to 32 weeks after
grafting. The International Journal of Periodon-
tics & Restorative Dentistry 26: 543–551.
Galindo-Moreno, P., Moreno-Riestra, I., Avila, G.,
Fernandez-Barbero, J.E., Mesa, F., Aguilar, M.,
Wang, H.L. & O’Valle, F. (2010) Histomorphome-
tric comparison of maxillary pristine bone and
composite bone graft biopsies obtained after sinus
augmentation. Clinical Oral Implants Research
21: 122–128.
Haas, R., Baron, M., Donath, K., Zechner, W. &
Watzek, G. (2002) Porous hydroxyapatite for graft-
ing the maxillary sinus: a comparative histomor-
phometric study in sheep. The International
Journal of Oral & Maxillofacial Implants 17:
337–346.
Haas, R., Donath, K., Fodinger, M. & Watzek, G.
(1998) Bovine hydroxyapatite for maxillary sinus
grafting: comparative histomorphometric findings
in sheep. Clinical Oral Implants Research 9 :
107–116.
Hallman, M., Cederlund, A., Lindskog, S., Lund-
gren, S. & Sennerby, L. (2001a) A clinical histo-
logic study of bovine hydroxyapatite in
combination with autogenous bone and fibrin
glue for maxillary sinus floor augmentation.
Results after 6 to 8 months of healing. Clinical
Oral Implants Research 12: 135–143.
Hallman, M., Lundgren, S. & Sennerby, L. (2001b)
Histologic analysis of clinical biopsies taken
6 months and 3 years after maxillary sinus floor
augmentation with 80% bovine hydroxyapatite
and 20% autogenous bone mixed with fibrin glue.
Clinical Implant Dentistry and Related Research
3: 87–96.
Hallman, M., Mordenfeld, A. & Strandkvist, T.
(2005) A retrospective 5-year follow-up study of
two different titanium implant surfaces used after
interpositional bone grafting for reconstruction of
the atrophic edentulous maxilla. Clinical Implant
Dentistry and Related Research 7: 121–126.
Hallman, M., Mordenfeld, A. & Strandkvist, T.
(2009) Bone replacement following dental trauma
prior to implant surgery–status. Dental trauma-
tology 25: 2–11.
Hallman, M., Sennerby, L. & Lundgren, S. (2002) A
clinical and histologic evaluation of implant inte-
gration in the posterior maxilla after sinus floor
augmentation with autogenous bone, bovine
hydroxyapatite, or a 20:80 mixture. The Interna-
tional Journal of Oral & Maxillofacial Implants
17: 635–643.
Hatano, N., Shimizu, Y. & Ooya, K. (2004) A clini-
cal long-term radiographic evaluation of graft
height changes after maxillary sinus floor aug-
mentation with a 2:1 autogenous bone/xenograft
mixture and simultaneous placement of dental
implants. Clinical Oral Implants Research 15:
339–345.
Hernandez-Alfaro, F., Torradeflot, M.M. & Marti,
C. (2008) Prevalence and management of schnei-
derian membrane perforations during sinus-lift
procedures. Clinical Oral Implants Research 19 :
91–98.
Hing, K.A., Annaz, B., Saeed, S., Revell, P.A. &
Buckland, T. (2005) Microporosity enhances
bioactivity of synthetic bone graft substitutes.
Journal of Materials Science. Materials in Medi-
cine 16: 467–475.
Jensen, S.S., Aaboe, M., Pinholt, E.M., Hjorting-
Hansen, E., Melsen, F. & Ruyter, I.E. (1996) Tis-
sue reaction and material characteristics of four
bone substitutes. The International Journal of
Oral & Maxillofacial Implants 11: 55–66.
Jensen, T., Schou, S., Gundersen, H.J., Forman, J.L.,
Terheyden, H. & Holmstrup, P. (2013) Bone-to-
implant contact after maxillary sinus floor aug-
mentation with bio-oss and autogenous bone in
different ratios in mini pigs. Clinical Oral
Implants Research 24: 635–644.
Jensen, T., Schou, S., Svendsen, P.A., Forman, J.L.,
Gundersen, H.J., Terheyden, H. & Holmstrup, P.
(2012) Volumetric changes of the graft after max-
illary sinus floor augmentation with bio-oss and
autogenous bone in different ratios: a radiographic
study in minipigs. Clinical Oral Implants
Research 23: 902–910.
Johansson, B., Grepe, A., Wannfors, K. & Hirsch,
J.M. (2001) A clinical study of changes in the vol-
ume of bone grafts in the atrophic maxilla. Den-
tomaxillofacial Radiology 30: 157–161.
Kim, Y.K., Yun, P.Y., Kim, S.G. & Lim, S.C. (2009)
Analysis of the healing process in sinus bone
grafting using various grafting materials. Oral
Surgery Oral Medicine Oral Pathology Oral
Radiology & Endodontics 107: 204–211.
Klawitter, J.J., Bagwell, J.G., Weinstein, A.M. &
Sauer, B.W. (1976) An evaluation of bone growth
into porous high density polyethylene. Journal of
Biomedical Materials Research 10: 311–323.
Klijn, R.J., Meijer, G.J., Bronkhorst, E.M. & Jansen,
J.A. (2010) A meta-analysis of histomorphometric
results and graft healing time of various biomate-
rials compared to autologous bone used as sinus
floor augmentation material in humans. Tissue
Engineering. Part B, Reviews 16: 493–507.
Maiorana, C., Redemagni, M., Rabagliati, M. & Sal-
ina, S. (2000) Treatment of maxillary ridge resorp-
tion by sinus augmentation with iliac cancellous
bone, anorganic bovine bone, and endosseous
implants: a clinical and histologic report. The
International Journal of Oral & Maxillofacial
Implants 15: 873–878.
Margolin, M.D., Cogan, A.G., Taylor, M., Buck, D.,
McAllister, T.N., Toth, C. & McAllister, B.S.
(1998) Maxillary sinus augmentation in the non-
human primate: a comparative radiographic and
histologic study between recombinant human
© 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 857 | Clin. Oral Impl. Res. 27, 2016 / 850–858
Alayan et al #Bio-Oss collagen in human sinus grafting

osteogenic protein-1 and natural bone mineral.
Journal of Periodontology 69 : 911–919.
Nkenke, E. & Stelzle, F. (2009) Clinical outcomes
of sinus floor augmentation for implant place-
ment using autogenous bone or bone substitutes:
a systematic review. Clinical Oral Implants
Research 20(Suppl 4): 124–133.
Orsini, G., Traini, T., Scarano, A., Degidi, M., Per-
rotti, V., Piccirilli, M. & Piattelli, A. (2005) Max-
illary sinus augmentation with bio-oss particles:
a light, scanning, and transmission electron
microscopy study in man. Journal of Biomedical
Materials Research Part B: Applied Biomaterials
74: 448–457.
Proussaefs, P. & Lozada, J. (2003) The “loma linda
pouch”: a technique for repairing the perforated
sinus membrane. The International Journal of
Periodontics & Restorative Dentistry 23: 593–597.
Proussaefs, P., Lozada, J., Kim, J. & Rohrer, M.D.
(2004) Repair of the perforated sinus membrane
with a resorbable collagen membrane: a human
study. The International Journal of Oral & Max-
illofacial Implants 19 : 413–420.
Quiney, R.E., Brimble, E. & Hodge, M. (1990) Max-
illary sinusitis from dental osseointegrated
implants. The Journal of Laryngology and Otol-
ogy 104: 333–334.
Sbordone, C., Toti, P., Guidetti, F., Califano, L.,
Bufo, P. & Sbordone, L. (2013) Volume changes of
autogenous bone after sinus lifting and grafting
procedures: a 6-year computerized tomographic
follow-up. Journal of Cranio-Maxillo-Facial Sur-
gery 41: 235–241.
Schlegel, A.K. & Donath, K. (1998) Bio-oss–a resorb-
able bone substitute? Journal of Long-Term
Effects of Medical Implants 8: 201–209.
Schlegel, A.K., Fichtner, G., Schultze-Mosgau, S. &
Wiltfang, J. (2003) Histologic findings in sinus
augmentation with autogenous bone chips versus
a bovine bone substitute. The International Jour-
nal of Oral & Maxillofacial Implants 18: 53–58.
Schmitt, C.M., Doering, H., Schmidt, T., Lutz, R.,
Neukam, F.W. & Schlegel, K.A. (2013) Histologi-
cal results after maxillary sinus augmentation
with straumann(r) boneceramic, bio-oss(r), puros
(r), and autologous bone. A randomized controlled
clinical trial. Clinical Oral Implants Research
24: 576–585.
Schmitt, C.M., Moest, T., Lutz, R., Neukam, F.W.
& Schlegel, K.A. (2015) Anorganic bovine bone
(ABB) vs. Autologous bone (AB) plus ABB in max-
illary sinus grafting. A prospective non-random-
ized clinical and histomorphometrical trial.
Clinical Oral Implants Research 26: 1043–1053.
Timmenga, N.M., Raghoebar, G.M., van Weis-
senbruch, R. & Vissink, A. (2001) Maxillary
sinusitis after augmentation of the maxillary
sinus floor: a report of 2 cases. Journal of Oral
and Maxillofacial Surgery 59 : 200–204.
Valentini, P. & Abensur, D.J. (2003) Maxillary sinus
grafting with anorganic bovine bone: a clinical
report of long-term results. The International Jour-
nal of Oral & Maxillofacial Implants 18: 556–560.
Valentini, P., Abensur, D., Wenz, B., Peetz, M. &
Schenk, R. (2000) Sinus grafting with porous bone
mineral (bio-oss) for implant placement: a 5-year
study on 15 patients. The International Journal of
Periodontics & Restorative Dentistry 20: 245–
253.
de Vicente, J.C., Hernandez-Vallejo, G., Brana-Abas-
cal, P. & Pena, I. (2010) Maxillary sinus augmen-
tation with autologous bone harvested from the
lateral maxillary wall combined with bovine-
derived hydroxyapatite: clinical and histologic
observations. Clinical Oral Implants Research
21: 430–438.
Wiltfang, J., Schultze-Mosgau, S., Merten, H.A.,
Kessler, P., Ludwig, A. & Engelke, W. (2000) En-
doscopic and ultrasonographic evaluation of the
maxillary sinus after combined sinus floor aug-
mentation and implant insertion. Oral Surgery
Oral Medicine Oral Pathology Oral Radiology &
Endodontics 89 : 288–291.
Wiltfang, J., Schultze-Mosgau, S., Nkenke, E., Thor-
warth, M., Neukam, F.W. & Schlegel, K.A. (2005)
Onlay augmentation versus sinuslift procedure in
the treatment of the severely resorbed maxilla: a
5-year comparative longitudinal study. Interna-
tional Journal of Oral and Maxillofacial Surgery
34: 885–889.
Yildirim, M., Spiekermann, H., Biesterfeld, S. &
Edelhoff, D. (2000) Maxillary sinus augmenta-
tion using xenogenic bone substitute material
bio-oss in combination with venous blood. A
histologic and histomorphometric study in
humans. Clinical Oral Implants Research 11:
217–229.
Supporting Information
Additional Supporting Information may be
found in the online version of this article:
Appendix S1. CONSORT 2010 checklist of
information to include when reporting a ran-
domised trial.
858 | Clin. Oral Impl. Res. 27, 2016 / 850–858 © 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Alayan et al #Bio-Oss collagen in human sinus grafting

90
Chapter 4: Comparison of early osseointegration of SLA® and SLActive®
implants in maxillary sinus augmentation: a pilot study.

91
STATEMENT OF CONTRIBUTION TO CO-AUTHORED PUBLISHED
PAPER
This chapter includes a co-authored paper. The bibliographic details of the
co-authored paper, including all authors, are:
Alayan J, Vaquette C, Saifzadeh S, Hutmacher D, Ivanovski S. (2017) Comparison
of early osseointegration of SLA® and SLActive® implants in maxillary sinus
augmentation: a pilot study. Clinical Oral Implants Research 28: 1325 – 1333. doi:
10.1111/clr.12988.
My contribution to the paper involved:
Design of the project, the provision of the data, the preliminary analysis and
categorization of the data into a usable format, the provision of direction on the
scope and structure of the analysis, the interpretation of results and drafting of the
article.
04th May 2018
Jamil Alayan
(Countersigned)16th May 2018
Corresponding author of paper: Saso Ivanovski
(Countersigned) ___________________________ 16th May 2018
Supervisor: Stephen Hamlet

Jamil AlayanCedryck VaquetteSiamak SaifzadehDietmar HutmacherSaso Ivanovski
Comparison of early osseointegrationof SLA! and SLActive! implants inmaxillary sinus augmentation: a pilotstudy
Authors’ affiliations:Jamil Alayan, Saso Ivanovski, Authors’Affiliations:School of Dentistry and Oral Health,Centre for Medicine and Oral Health, MenziesHealth Institute Queensland, Griffith University,Southport, AustraliaCedryck Vaquette, Siamak Saifzadeh, DietmarHutmacher, Institute for Health and BiomedicalInnovation, Queensland University of Technology,Kelvin Grove, Australia
*Corresponding author:Saso IvanovskiSchool of Dentistry and Oral Health, Centre forMedicine and Oral HealthGold Coast Campus Griffith UniversitySouthport, QLD 4215, AustraliaTel.: +61 75 678 0741Fax: +61 75 678 0708e-mail: [email protected]
Key words: animal model, bone grafting, bone regeneration, bone substitute, dental implant,
histomorphometry, maxillary sinus augmentation
Abstract
Objective: To assess the impact of a hydrophilic implant surface (SLActive!) placed into
augmented maxillary sinuses on bone-to-implant contact (BIC) and surrounding tissue composition
when compared to a hydrophobic surface (SLA!).
Material and methods: Four sheep underwent bilateral sinus augmentation. Each sinus received
anorganic bovine bone mineral + autogenous bone (ABBM + AB). Sixteen implants were
subsequently placed 12 weeks postgrafting with each sinus receiving a control (SLA!) and test
implant (SLActive!). Two animals were sacrificed at 2 weeks and another two animals were
sacrificed at 4 weeks postimplantation. The eight sinuses and 16 implants were processed for
histomorphometry, which assessed bone-to-implant contact (%BIC) and tissue elements (woven
bone – WB, lamellar bone – LB, soft tissue – ST) in the interthread region of implants within the
augmented sinus.
Results: There was a statistically significant increase in %BIC at week 4 compared to the week 2
animals in both test (P < 0.005) and control (P < 0.005) groups. There was a statistically significant
greater %BIC around test implants when compared to control implants in both week 2 (P < 0.05)
and week 4 animals (P < 0.05). Greater %WB (11.17% !6.82) and %LB (11.06% !3.67) were seen
in the test implants when compared to the control implants independent of time. This was only
statistically significant for %LB (P < 0.05). A statistically significant reduction of 16.78% (!6.19) in
%ST was noted in test implants when compared to control implants (P < 0.05) independent of
time.
Conclusion: Both time and the use of hydrophilic implant surface had a positive impact on %BIC
around implants placed into augmented maxillary sinuses. Hydrophilic implant surfaces also had a
positive impact on surrounding tissue composition. Larger trials are needed to better assess and
detect differences between these two surfaces in augmented maxillary sinuses.
Implant surface topography and chemistry
affect the osseointegration process (Gittens
et al. 2014). It has been shown to play a criti-
cal role in the predictability of the bone
response to implant placement (Junker et al.
2009) and is a major determinant of the rate
and extent of dental implant osseointegration
(Wennerberg & Albrektsson 2009).
The SLA! surface is a moderately rough
surface which is commonly utilized clini-
cally and widely documented in the litera-
ture. It is formed by coarse grit blasting with
0.25–0.5 mm corundum followed by acid
etching with sulphuric and hydrochloric acid
(Zhao et al. 2005). Animal studies have
shown that these surface results in superior
bone-to-implant contact compared to
minimally rough implants (Cochran et al.
1998), as well as superior torque removal val-
ues (Buser et al. 1998). Histological analysis
of the sequential healing events associated
with the placement of SLA titanium
implants showed that initial bone formation
around these implants occurs not only at the
exposed bone wall of the surgically created
recipient site (distance osteogenesis), as is
the case with turned minimally rough sur-
face implants, but also along the implant sur-
face (contact osteogenesis; Abrahamsson
et al. 2004).
The SLActive! surface is produced with the
same sandblasting and acid etching technique
as SLA!, but differs in that the SLActive!
implants are rinsed under nitrogen protection
Date:Accepted 7 September 2016
To cite this article:Alayan J, Vaquette C, Saifzadeh S, Hutmacher D, Ivanovski S.Comparison of early osseointegration of SLA! and SLActive!
implants in maxillary sinus augmentation: a pilot study.Clin. Oral Impl. Res. 00, 2016, 1–9doi: 10.1111/clr.12988
© 2016 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 1

to prevent exposure to air and are then stored
in a sealed glass tube containing isotonic
NaCl solution as opposed to dry storage (Zhao
et al. 2005). This method allows the
SLActive! implant to have a higher surface
energy and be more hydrophilic in nature than
the SLA! implant (Rupp et al. 2006).
Preclinical studies showed that SLActive!
implants achieved up to 60% more bone-to-
implant contact at 2 weeks after placement
(Buser et al. 2004), had greater removal tor-
que values (Ferguson et al. 2008), and
demonstrated faster and more mature bone
formation in comparison with SLA! surfaces
(Schwarz et al. 2008, 2009). Similarly, a
human study indicated a superior degree of
osseointegration for SLActive! implants
after 2 and 4 weeks of healing when com-
pared to SLA! implants, but this difference
was not evident by 6 weeks postplacement
(Lang et al. 2011). This supports the hypoth-
esis of accelerated bone healing on
SLActive! at least in the early stages. This
histologically demonstrated advantage has
translated to successful earlier loading proto-
cols (Morton et al. 2010).
Studies on modified hydrophilic implants
in bone defects or grafted sites are rare. Modi-
fied implants have been shown to have sig-
nificantly greater bone regeneration in
dehiscence defects (Schwarz et al. 2008) and
circumferential defects in canines (Lai et al.
2009). To date, however, there is only one
study comparing SLA! and SLActive! in
grafted maxillary sinuses. This animal study
failed to show any significant difference in
BIC between the two types of implants at 12
and 26 weeks postplacement in augmented
maxillary sinuses (Philipp et al. 2014). This
may be because SLActive! has been shown
to have a beneficial effect during early
osseointegration (2–4 weeks), with this effect
not evident at later time points (Buser et al.
2004; Lang et al. 2011).
The primary objective of this in vivo study
was to compare the early osseointegration of
implants with a hydrophilic surface
(SLActive!) to those with a hydrophobic sur-
face with the same geometry and surface
microroughness (SLA!), in augmented maxil-
lary sinuses. Our secondary objective was to
characterize the tissue composition in the
immediate vicinity of the implant surface in
these augmented sites.
Material and methods
Animal care and handling
The ARRIVE guidelines on reporting of
in vivo experiments in animal research were
adhered to in this study (Kilkenny et al.
2010). All animal handling and surgical pro-
cedures were conducted according to the
Australian code of practice for the care and
use of animals for scientific purposes at the
Medical Engineering Research Facility
(MERF), Queensland University of Technol-
ogy (QUT), Queensland, Australia. This facil-
ity is a GLP (good laboratory practice)-
accredited large animal research facility. Eth-
ical approval was provided by the QUT Ani-
mal Research Ethics Committee (QDPI
scientific use registration number: 0052). The
animal experiments were carried out between
January and September 2012. The experimen-
tal animals were sourced from the ex-Univer-
sity of Queensland agricultural research farm
at Mount Cotton, Queensland, Australia.
The sheep were housed either in the QUT
MERF building (animal house) at Chermside,
Queensland, Australia, immediately prior to
and after surgery or the QUT MERF agist-
ment farm in Pinjarra Hills, Queensland,
Australia for the remainder of the study.
All sheep underwent a health assessment,
especially to check for the presence of upper
respiratory tract infections, and were contin-
ually monitored by a veterinary surgeon for
the duration of the study.
The surgical procedures were performed
under general anaesthesia (5 mg/kg propofol
I.V and 2–2.5% isoflurane) with multimodal
pain management including local analgesia
(bupivacaine 0.5% w/v 1:200,000
adrenaline), an NSAID (ketorolac, 0.5 mg/
kg, SC) and an opioid analgesic (buprenor-
phine, 0.01 mg/kg IM). During surgery ani-
mals received cephalothin and gentamicin,
which were continued for 3 days after sur-
gery.
Animal allocation and study design
The study used four skeletally mature wether
sheep (Ovis aries), 3–4 years old. Every ani-
mal underwent bilateral sinus augmentation
procedures, and hence, a total of eight
sinuses received the graft (ABBM + AB).
Twelve weeks following the sinus augmenta-
tion procedure, a control (SLA!) and a test
implants (SLActive!) were placed in each of
the grafted sinuses. A total of two implants
were placed in each sinus with the caudal/
cranial position determined by a coin toss. A
total of 94 implants were therefore placed in
each animal, and hence, a total of 16
implants were placed.
Two animals were then sacrificed at
2 weeks, and another two animals were sacri-
ficed at 4 weeks after implant placement. The
eight sinuses and 16 implants were then pro-
cessed for histology and histomorphometry.
Bone grafting materials
All animals received small diameter particles
(0.25–1 mm) of deproteinized bovine
bone mineral (Bio-Oss!, Geistlich AG,
Wollhusen, Switzerland) + autogenous bone
(ABBM + AB) in a 1 : 1 ratio.
(a) (b)
(c) (d)
Fig. 1. A clinical photograph outlining the surgical steps of maxillary sinus augmentation in the sheep model. (a)
Line demarcating the extra-oral incision, (b) after antrostomy preparation and Schneiderian membrane elevation,
the bone substitute selection and delivery, (c) implant placement 12 weeks later, and (d) harvested sample of
implant containing augmented sinus.
2 | Clin. Oral Impl. Res. 0, 2016 / 1–9 © 2016 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Alayan et al "SLA! and SLActive! implants in maxillary sinus augmentation

Maxillary sinus augmentation
All animals were treated using the same sur-
gical technique utilizing an extra-oral
approach (Fig. 1a), as previously described
(Alayan et al. 2016). The anterior wall of the
maxillary sinus was exposed inferior to the
lower orbital rim using an oblique sagittal
skin incision of approximately 6–8 cm fol-
lowed by dissection of the masseter muscle.
A full circular antrostomy was created in the
lateral wall of the maxilla using a bone scra-
per (Safescraper Twist, META, C.G.M Sp.A,
Reggio Emiia, Italy) and a piezoelectric
surgical unit (Implant Center, Satelec,
Acteon, France) to gain access to the maxil-
lary sinus (Fig. 1b). The size of the antros-
tomy was standardized using a circular
sterile template with a diameter of 2 cm.
The sinus membrane was then dissected and
elevated in a dorso-cranial direction using a
combination of piezoelectric surgical tips and
hand sinus membrane elevators to create an
intra-sinus space. The prepared sinus then
received the grafting material, which was
carefully packed into the subantral space
ensuring contact with as many of the
residual bony walls as possible whilst avoid-
ing over-packing (Fig. 1b).
The autogenous bone chips collected using
the bone scraper were used as the autogenous
bone component in the control group. To
ensure a 1 : 1 ratio was maintained, a stan-
dardized 2 cc chamber was utilized to ensure
that the same volume of Bio-Oss! and auto-
genous particles was used. The reconstructed
sites were covered with a resorbable porcine
collagen membrane (Bio-Gide!, Geistlich
AG, Wolhusen, Switzerland). The masseter
muscle and skin flap were then sutured sepa-
rately using a resorbable polyglactin suture
(Vicryl 4/0, Ethicon, Johnson & Johnson) fol-
lowed by a nonresorbable polypropylene
suture (Prolene 4/0, Ethicon, Johnson & John-
son) for the skin flap to achieve primary clo-
sure.
Dental implant placement
Twelve weeks following the sinus augmenta-
tion procedure, two endosseous dental
implants were placed in each of the grafted
sinuses (Fig. 1c). One control implant had a
standard SLA! surface (SLA-sandblasted and
acid-etched; Institut Straumann AG, Basel,
Switzerland), and the second test implant
had a modified hydrophilic SLA surface
(SLActive!; Institut Straumann AG, Basel,
Switzerland). All implants were bone level in
design with a diameter of 3.3 and 8 mm in
height. A total of 16 implants were placed.
Implant osteotomy preparation was per-
formed using the universally accepted proto-
col of stepwise bone excavation using
progressively increasing diameter drills and
copious sterile physiologic saline cooling.
This protocol was carried out with sharp
drills, light pressure, and intermittent drilling
thereby ensuring minimal bone trauma. The
implants were then submerged under the
mucocutaneous flap and were therefore not
exposed to the external environment.
Postoperative treatment and sacrifice
Practices and procedures used for the care
and management of animals in this study
were based on current best practice, as per
Australian code for the care and use of ani-
mals for scientific purposes (https://www.
nhmrc.gov.au/_files_nhmrc/publications/at
tachments/ea28_code_care_use_animals_1312
09.pdf). This takes into consideration the rel-
evant aspects of species-specific biology,
physiology, and behaviour. It also includes
the potential adverse impact of conditions
and procedures on the well-being of the ani-
mals, and strategies to minimize adverse
impacts on the animals after surgery.
(a)
(b)
(c)
Fig. 2. A histological image illustrating the histomorphometirc method employed. (a) The method excluded the
region of the implant in contact with resident bone. (b) This highlighted region in green represents the implant sur-
face within the augmented sinus. The regions highlighted in red represent those regions of implant surface in con-
tact with bone and within the augmented sinus. (c) Magnified histological image corresponding to the demarcated
region illustrating this methodology.
© 2016 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 3 | Clin. Oral Impl. Res. 0, 2016 / 1–9
Alayan et al "SLA! and SLActive! implants in maxillary sinus augmentation
https://www.nhmrc.gov.au/_files_nhmrc/publications/attachments/ea28_code_care_use_animals_131209.pdf
https://www.nhmrc.gov.au/_files_nhmrc/publications/attachments/ea28_code_care_use_animals_131209.pdf

Postoperatively, each sheep was transferred
to a covered pen and was cradled in a sheep
sling. A combination analgesic was given
(buprenorphine, 0.01 mg/kg IM, and ketoro-
lac, 0.5 mg/kg, SC) for 2–3 days postopera-
tively to alleviate pain. The animals were
housed indoor and monitored three times per
day over the first week and two times daily
thereafter until the end of the experimental
period. Monitoring observations were re-
corded. Interventions were implemented
when signs of discomfort were detected.
Suitable dressing was used postoperatively
to protect the surgical wound, and acute
postoperative monitoring (3 times/day) for
the first seven took place. The extra-oral sur-
gical wounds were checked for any evidence
of postoperative complications, such as fail-
ure in suture integrity (wound dehiscence),
bleeding, inflammation, and infection.
To protect the operated sinus from masti-
catory load immediately after the surgery,
the animals were maintained NPO (nil per
os) with parenteral support for 24 h.
Throughout the fluid administration, the
sheep remained cradled in the sling and were
monitored constantly. From the second day
after surgery, the sheep were fed a soft diet
for 1 week postoperatively, and eating and
drinking were closely monitored following
parenteral nutrition.
At the completion of the 2 and 4 week
healing periods, the animals were sacrificed
by a lethal injection of Lethabarb (320 mg/ml
pentobarbital sodium, 0.5 ml/kg).
Histological preparation and histomorphometry
Blinding during histological preparation of tis-
sue samples was achieved by coding each ani-
mal and by using a different operator for the
surgery (JA) and histological processing (CV).
Undecalcified resin-embedded tissue sections
were prepared as previously described (Donath
& Breuner 1982; Schlegel et al. 1998, 2006;
Bosshardt et al. 2011; Lang et al. 2011). The
initial trimming of the fixed tissue samples
was performed to exclusively contain the
implants within the maxillary sinus (Fig. 1d).
The samples were further sectioned longitudi-
nally to the implant long axis leaving a 1-mm-
thick tissue border around the implant and
subsequently dehydrated in a graded series of
ethanol and resin infiltrated (methyl
methacrylate/glycol methacrylate, Technovit
7200, Heraeus Kulzer, Germany). Once cured,
resin blocks were ground using an EXAKT 400
CS microgrinding system until the threads of
the implant was exposed, glued onto a glass
slide, and subsequently sectioned to a thick-
ness of 150 lm using an EXAKT 300 cutting
system (Exact Apparatebau, GmbH Norderst-
edt Germany). A single slide per implant was
polished down to a thickness of 20 lm using
the EXAKT 400 CS microgrinding system. A
single sample from the central aspect of each
implant was then stained with 0.1% toluidine
blue (Sigma Aldrich, St Louis, MO, USA) for
light microscopy and analysis.
Histomorphometric measurements were
performed blinded and carried out by a single
experienced operator (JA) using a specialized
histomorphometric software program (Aperio
ImageScope version 12.1, Aperio Technolo-
gies Inc.©). Histomorphometric analysis was
carried out as previously described (Bosshardt
et al. 2011; Lang et al. 2011) and the follow-
ing parameters were assessed (Fig. 2): (a) the
proportion of mineralized bone in contact
with the surface of the implants contained
within the augmented sinus and (b) the tis-
sue elements occupying the interthread
region including the proportions of woven
bone, lamellar bone, nonmineralized struc-
tures (residual tissue), and residual graft par-
ticles.
The definitions of each parameter are as
follows and were measured only within the
augmented sinus (Fig. 2):
• % WB = area of woven bone interthread
regions/total interthread area
• % LB = area of lamellar bone interthread
regions/total interthread area
• % RG = area residual graft particles inter-
thread regions/total interthread area
• % STM = area of soft tissue interthread
regions/total interthread area
• % BIC = length implant in contact with
bone/total implant length within aug-
mented sinus
(a)
(b)
Fig. 3. Magnified histological images illustrating peri-implant tissue of (a) control (SLA!) implant after 4 weeks of
healing. New bone, mostly woven bone is seen on both the existing regenerated bone and on residual ABBM. (b)
Further magnification of highlighted area (star) showing woven bone trabeculae extending from the ERB towards
the implant surface. Secondary osteons as part of a BMU (asterisks) are seen indicative of ongoing remodeling.
ABBM, anorganic bovine bone mineral particles; ERB, existing regenerated bone; LB, lamellar bone; NB, new bone;
WB, woven bone. Toluidine blue staining.
4 | Clin. Oral Impl. Res. 0, 2016 / 1–9 © 2016 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Alayan et al "SLA! and SLActive! implants in maxillary sinus augmentation

Statistics
Quantitative data were analysed using IBM
SPSS Statistics for Windows version 21.0
(IBM Corporation 2012©, Armonk, NY, US).
A generalized linear model was used using
individual animals as the clustering variable.
Time and implant surface were used as
explanatory variables. A backward elimina-
tion procedure was used for arriving to the
most parsimonious model. A P ≤ 0.05 was
considered to represent statistically signifi-
cant differences. Our primary outcome mea-
sure was %BIC and our secondary outcomes
measures included tissue composition in the
interthread regions.
The null hypothesis is no difference in degree
of BIC or tissue composition around an
SLActive! surface implant when compared to
an SLA! surface in augmented maxillary
sinuses.
Results
The surgical wounds in all animals healed
completely within 10–14 days with no signs
of complications.
Gross histological features
The augmented region within the intact sinus
cavity was identified by the obvious retained
residual graft particles and change in the Sch-
neiderian membrane topography. Bone of vary-
ing degrees of maturity was observed over both
time points in both treatment groups (Figs 3,
4, 5). This ranged from woven bone to mature
bone with longitudinal and concentric lamel-
lae in addition to the presence of BMUs,
indicative of ongoing bone maturation and
remodeling. Bridging between graft particles
was evident with new bone formation seen to
be continuous around and between graft parti-
cles (Figs 3, 4). A predominance of woven
bone, however, was noted in areas proximal to
the implant surface in both groups (Fig. 4).
Graft particles were located at varying dis-
tances from the implant surface but not seen
in direct contact with the implant surface
except in some areas where the pitch of the
implant thread was in direct contact with
residual ABBM particles. Some of the gaps
between the host bone and the implant surface
were partly filled with debris resulting from
the surgical osteotomy preparation. New bone
was seen in the form of a thin coating on the
implant surfaces, the existing regenerated bone
(ERB), and the residual ABBM particles (ABBM;
Figs 3, 4). In addition, projections of woven
bone trabeculae were seen extending from the
ERB towards the implant surface (Fig. 4).
The impact of time (Figs 6 and 7)
There was a statistically significant increase
in %BIC at week 4 compared to the week 2
animals for both test (SLActive!; P < 0.005;
from 16.48 ! 6.13 at week 2 to 37.78 ! 12 at
week 4; mean ! SD) and control (SLA!)
implants (P < 0.005; from 14.63 ! 8.52 at
week 2 to 26.4 ! 12.67 at week 4;
mean ! SD). The impact of time was indepen-
dent of implant surface with implants in the
week 4 group having 13.23% (!3.92) greater %
BIC than those in the week 2 group.
Greater %WB (9.02% !6.82) and %LB
(6.35% !3.67) was seen in week 4 samples
compared to week 2. Further an 8.59%
(!5.48) reduction in %ST was seen in week 4
samples. Very little difference was noted in
%RG (<1%). None of these differences were
statistically significant.
The impact of treatment (Figs 6 and 7)
There was a statistically significant greater
%BIC in the test implants when compared to
the control implants in both week 2 (test
16.48 ! 6.13 vs. control 14.63 ! 8.52;
mean ! SD; P < 0.05) and week 4 animals
(test 37.78 ! 12 vs. control 26.4 ! 12.67;
mean ! SD; P < 0.05). The impact of implant
surface was independent of time with test
implants showing 9.89% (!3.90) greater %
BIC than control implants.
Greater %WB (11.17% !6.82) and %LB
(11.06% !3.67) were seen in the test implants
when compared to the control implants inde-
pendent of time. This was only statistically
significant for %LB (P < 0.05). A statistically
significant reduction of 16.78% (!6.19) in %
ST was noted in test implants when compared
to control implants (P < 0.05). Very little
(a)
(b)
Fig. 4. Magnified histological images illustrating peri-implant tissue of (a) test (SLActive!) implant after 2 weeks of
healing. (b) Further magnification of highlighted area (star) showing, new bone mostly as woven bone, directly
formed onto the implant surface in addition to residual ABBM particles. ABBM, anorganic bovine bone mineral par-
ticles; ERB, existing regenerated bone; LB, lamellar bone; NB, new bone; WB, woven bone. Toluidine blue staining.
© 2016 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 5 | Clin. Oral Impl. Res. 0, 2016 / 1–9
Alayan et al "SLA! and SLActive! implants in maxillary sinus augmentation

difference was noted in %RG (<1%) between
test and control implants.
Discussion
This histological study was designed to gain
information on the impact of a hydrophilic
microrough surface (SLActive!) on early heal-
ing around implants placed into grafted max-
illary sinuses. Sheep is a well-established
animal model for maxillary sinus augmenta-
tion using an extra-oral approach (Haas et al.
1998, 2002; Aral et al. 2008; Saffarzadeh et al.
2009; Gutwald et al. 2010; Alayan et al.
2016). The characteristics of the Schneiderian
membrane in sheep are anatomically compa-
rable with humans (Estaca et al. 2008), and it
does not have the disadvantage of an
excessively thick cortical bone layer such as
that found in pigs (Estaca et al. 2008).
The design of the study attempted to
closely mimic routine clinical protocols,
whereby a staged implant placement was
undertaken following a 12 week period of
graft consolidation, which has been shown to
result in mature tissue in this model (Alayan
et al. 2016). The composite graft of anorganic
bovine bone and autogenous bone was cho-
sen as the graft of choice as this combination
has been utilized in multiple studies of max-
illary sinus floor augmentation (Maiorana
et al. 2000; Hallman et al. 2001a, 2001b,
2002, 2005, 2009; Hatano et al. 2004; Canniz-
zaro et al. 2009; Kim et al. 2009; Avila et al.
2010; Galindo-Moreno et al. 2010; de Vicente
et al. 2010; Alayan et al. 2016). Recent stud-
ies indicate that the combination of
autogenous bone and Bio-Oss (ABBM) has the
advantages of reduced graft resorption and
increased bone-to-implant contact formation
(Jensen et al. 2012b, 2013). A recent study
utilizing an identical sinus augmentation
procedure (Alayan et al. 2016) showed ade-
quate new bone formation using this
composite grafting material. In addition,
improved histological parameters were re-
ported in the AB-ABBM sites compared to
collagen-stabilized ABBM alone, especially
when assessing regions furthest away from
the resident bone.
In this animal model, healing time (4 vs.
2 weeks) led to significant improvements in
%BIC, %WB, and %LB in both test and con-
trol implants. %BIC around SLA! implants
increased from 14.63 ! 8.52 at week 2 to
26.4 ! 12.67 at week 4 (mean ! SD) and
SLActive! implants significantly increased
from 16.48 ! 6.13 at week 2 to 37.78 ! 12 at
week 4 (mean ! SD). This finding is consis-
tent with a systematic review which con-
cluded that BIC of implants placed in
augmented sinuses improved over time (Jen-
sen et al. 2012a). Studies included in this
review assessed BIC in both simultaneous
and staged implant placement after maxillary
sinus grafting using ABBM (Bio-Oss) via the
lateral window approach. The only other
study comparing SLA! and SLActive!
implants in augmented maxillary sinuses
(Philipp et al. 2014) reported similar %BIC
that also improved with time. %BIC for
SLA! implants increased from 21.5 ! 16.2 at
week 12 to 28.7 ! 13.3 at 26 weeks
(mean ! SD) and for SLActive! implants
from 20.1 ! 9.2 at week 12 to 34.1 ! 13.7 at
26 weeks (mean ! SD), but this was only sig-
nificant around SLActive! implants.
The use of a modified hydrophilic implant
surface (SLActive!) also led to increased %
BIC compared to the SLA! surface at both 2
and 4 weeks. This is consistent with other
studies which have shown improved out-
comes with SLActive! compared with SLA!
in terms of BIC in pristine bone (Buser et al.
2004; Lang et al. 2011) and bone healing in
augmented defects (Schwarz et al. 2008; Lai
et al. 2009). However, Philipp et al. (2014)
did not observe a statistically significant dif-
ference in %BIC between the two surfaces in
grafted sinuses at either 12 or 26 weeks.
They did, however, observe that SLActive!
implants placed into a grafted maxillary sinus
provided the best BIC values after 26 weeks
of healing. The differences between our
results and those from the above-mentioned
study may be due to the different implant
placement protocols (simultaneous vs. staged
(a)
(b)
Fig. 5. Magnified histological images representing samples from a (a) test (SLActive!) implant after 4 weeks of heal-
ing. (b) New bone is seen mostly as lamellar bone directly formed onto the implant surface. ABBM, anorganic
bovine bone mineral particles; ERB, existing regenerated bone; LB, lamellar bone; NB, new bone; WB, woven bone.
Toluidine blue staining.
6 | Clin. Oral Impl. Res. 0, 2016 / 1–9 © 2016 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Alayan et al "SLA! and SLActive! implants in maxillary sinus augmentation

implant placement), the different observation
times (12 and 26 weeks vs. 2 and 4 weeks) or
due to differences in bone graft composition
(hydroxyapatite and beta-tricalcium phos-
phate vs. ABBM + AB). Indeed, a number of
studies have also shown equivalence when
comparing SLActive! vs. SLA! surface at
later time points, after early observations
indicated an initial advantage to SLActive!
surfaces (Buser et al. 2004; Bosshardt et al.
2011; Lang et al. 2011). In review of the
available literature, it was concluded that a
stronger bone response was indeed present
during early healing around SLActive!
implants, which was not evident at later
stages (Wennerberg et al. 2011).
SLActive! implants also positively influ-
enced the bone healing in the vicinity of the
implants, as measured by the amounts of
woven and lamellar bone in the interthread
regions. Greater %WB and %LB were seen in
the test implants when compared to the con-
trol implants independent of time. This was
only statistically significant for %LB and
reflects the greater maturity of the new bone
around the SLActive! implants due to the
accelerated bone formation. Indeed,
transcriptome analysis from human peri-
implant human samples showed that com-
pared with the SLA! surface, SLActive!
exerts a pro-osteogenic and pro-angiogenic
influence on gene expression as early as
7 days postimplantation (Donos et al. 2011).
The outcomes of this pilot study, however,
must be interpreted with caution due to its
low power and higher probability of type-1
errors. These results should be validated in
larger studies with an increased number of
animals. Indeed, there appears to be a lack of
published studies that assess the influence of
surface modification in augmented sites gen-
erally. The small sample size was partly com-
pensated by the placement of a test and
control implant in every augmented sinus,
thus reducing the confounding influence of
variability in the healing potential at the
sinus level.
In conclusion, both time and the use of
hydrophilic implant surface had a positive
impact on %BIC around implants placed into
augmented maxillary sinuses. Hydrophilic
implant surfaces were also associated with a
more mature bone–implant interface. These
findings suggest that implant surface charac-
teristics influence the early wound healing
process at the implant–tissue interface lead-
ing to improved histomorphometric out-
comes.
Acknowledgements: Jamil Alayan is
the recipient of a scholarship from the
National Health & Medical Research
Council of Australia (ID: APP1056633). Bio-
Oss!, Bio-Oss Collagen! & Bio-Gide! were
kindly provided by Geistlich AG, Wollhusen,
Switzerland. We would like to thank Dr
Dimitrios Vagenas (Biostatistician, Institute
for Health and Biomedical Innovation,
Queensland University of Technology,
Kelvin Grove, Australia) for his assistance
and contribution to the statistical analysis in
this project.
References
Abrahamsson, I., Berglundh, T., Linder, E., Lang,
N.P. & Lindhe, J. (2004) Early bone formation
adjacent to rough and turned endosseous implant
surfaces. An experimental study in the dog. Clini-
cal Oral Implants Research 15 : 381–392.
Alayan, J., Vaquette, C., Saifzadeh, S., Hutmacher,
D. & Ivanovski, S. (2016) A histomorphometric
assessment of collagen-stabilized anorganic
bovine bone mineral in maxillary sinus
augmentation – a randomized controlled trial in
sheep. Clinical Oral Implants Research 27: 734–
743.
Aral, A., Yalcin, S., Karabuda, Z.C., Anil, A., Jan-
sen, J.A. & Mutlu, Z. (2008) Injectable calcium
phosphate cement as a graft material for maxil-
lary sinus augmentation: an experimental pilot
study. Clinical Oral Implants Research 19 : 612–
617.
Avila, G., Wang, H.L., Galindo-Moreno, P., Misch,
C.E., Bagramian, R.A., Rudek, I., Benavides, E.,
Moreno-Riestra, I., Braun, T. & Neiva, R. (2010)
The influence of the bucco-palatal distance on
sinus augmentation outcomes. Journal of Peri-
odontology 81: 1041–1050.
Bosshardt, D.D., Salvi, G.E., Huynh-Ba, G., Iva-
novski, S., Donos, N. & Lang, N.P. (2011) The
role of bone debris in early healing adjacent to
hydrophilic and hydrophobic implant surfaces in
man. Clinical Oral Implants Research 22: 357–
364.
Fig. 6. Scatter plot illustrating histomorphometric outcomes in the interthread regions. (a) Area fraction of lamellar
bone (%LB), (b) area fraction of woven bone (%WB), (c) area fraction of residual graft particles (%RG), and (d) area
fraction of soft tissue (%ST) at week 2 and week 4 postimplantation. C, control group (SLA!); T, test group
(SLActive!); 2, week 2 postimplantation; 4, week 4 postimplantation; # mean.
Fig. 7. Scatter plot illustrating the percentage of bone-
to-implant contact (%BIC) for all groups. C, control
group (SLA!); T, test group (SLActive!); 2, week 2
postimplantation; 4, week 4 postimplantation; # mean.
© 2016 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 7 | Clin. Oral Impl. Res. 0, 2016 / 1–9
Alayan et al "SLA! and SLActive! implants in maxillary sinus augmentation

Buser, D., Broggini, N., Wieland, M., Schenk, R.K.,
Denzer, A.J., Cochran, D.L., Hoffmann, B., Lussi,
A. & Steinemann, S.G. (2004) Enhanced bone
apposition to a chemically modified sla titanium
surface. Journal of Dental Research 83: 529–533.
Buser, D., Nydegger, T., Hirt, H.P., Cochran, D.L.
& Nolte, L.P. (1998) Removal torque values of
titanium implants in the maxilla of miniature
pigs. International Journal of Oral and Maxillofa-
cial Implants 13: 611–619.
Cannizzaro, G., Felice, P., Leone, M., Viola, P. &
Esposito, M. (2009) Early loading of implants in
the atrophic posterior maxilla: lateral sinus lift
with autogenous bone and bio-oss versus crestal
mini sinus lift and 8-mm hydroxyapatite-coated
implants. A randomised controlled clinical trial.
European Journal of Oral Implantology 2: 25–38.
Cochran, D.L., Schenk, R.K., Lussi, A., Higginbot-
tom, F.L. & Buser, D. (1998) Bone response to
unloaded and loaded titanium implants with a
sandblasted and acid-etched surface: a histometric
study in the canine mandible. Journal of Biomed-
ical Materials Research 40: 1–11.
Donath, K. & Breuner, G. (1982) A method for the
study of undecalcified bones and teeth with
attached soft tissues. The sage-schliff (sawing and
grinding) technique. Journal of Oral Pathology
11: 318–326.
Donos, N., Hamlet, S., Lang, N.P., Salvi, G.E.,
Huynh-Ba, G., Bosshardt, D.D. & Ivanovski, S.
(2011) Gene expression profile of osseointegration
of a hydrophilic compared with a hydrophobic
microrough implant surface. Clinical Oral
Implants Research 22: 365–372.
Estaca, E., Cabezas, J., Uson, J., Sanchez-Margallo,
F., Morell, E. & Latorre, R. (2008) Maxillary
sinus-floor elevation: an animal model. Clinical
Oral Implants Research 19 : 1044–1048.
Ferguson, S.J., Langhoff, J.D., Voelter, K., von
Rechenberg, B., Scharnweber, D., Bierbaum, S.,
Schnabelrauch, M., Kautz, A.R., Frauchiger, V.M.,
Mueller, T.L., van Lenthe, G.H. & Schlottig, F.
(2008) Biomechanical comparison of different sur-
face modifications for dental implants. Interna-
tional Journal of Oral and Maxillofacial Implants
23: 1037–1046.
Galindo-Moreno, P., Moreno-Riestra, I., Avila, G.,
Fernandez-Barbero, J.E., Mesa, F., Aguilar, M.,
Wang, H.L. & O’Valle, F. (2010) Histomorphome-
tric comparison of maxillary pristine bone and
composite bone graft biopsies obtained after sinus
augmentation. Clinical Oral Implants Research
21: 122–128.
Gittens, R.A., Scheideler, L., Rupp, F., Hyzy, S.L.,
Geis-Gerstorfer, J., Schwartz, Z. & Boyan, B.D.
(2014) A review on the wettability of dental
implant surfaces II: biological and clinical
aspects. Acta Biomaterialia 10: 2907–2918.
Gutwald, R., Haberstroh, J., Stricker, A., Ruther, E.,
Otto, F., Xavier, S.P., Oshima, T., Marukawa, E.,
Seto, I., Enomoto, S., Hoogendijk, C.F., Sch-
melzeisen, R. & Sauerbier, S. (2010) Influence of
rhbmp-2 on bone formation and osseointegration
in different implant systems after sinus-floor ele-
vation. An in vivo study on sheep. Journal of Cra-
nio-Maxillo-Facial Surgery 38: 571–579.
Haas, R., Baron, M., Donath, K., Zechner, W. &
Watzek, G. (2002) Porous hydroxyapatite for
grafting the maxillary sinus: a comparative histo-
morphometric study in sheep. International Jour-
nal of Oral and Maxillofacial Implants 17: 337–
346.
Haas, R., Donath, K., Fodinger, M. & Watzek, G.
(1998) Bovine hydroxyapatite for maxillary sinus
grafting: comparative histomorphometric findings
in sheep. Clinical Oral Implants Research 9 :
107–116.
Hallman, M., Cederlund, A., Lindskog, S., Lund-
gren, S. & Sennerby, L. (2001a) A clinical
histologic study of bovine hydroxyapatite in com-
bination with autogenous bone and fibrin glue for
maxillary sinus floor augmentation. Results after
6 to 8 months of healing. Clinical Oral Implants
Research 12: 135–143.
Hallman, M., Lundgren, S. & Sennerby, L. (2001b)
Histologic analysis of clinical biopsies taken
6 months and 3 years after maxillary sinus floor
augmentation with 80% bovine hydroxyapatite
and 20% autogenous bone mixed with fibrin glue.
Clinical Implant Dentistry and Related Research
3: 87–96.
Hallman, M., Mordenfeld, A. & Strandkvist, T.
(2005) A retrospective 5-year follow-up study of
two different titanium implant surfaces used after
interpositional bone grafting for reconstruction of
the atrophic edentulous maxilla. Clinical Implant
Dentistry and Related Research 7: 121–126.
Hallman, M., Mordenfeld, A. & Strandkvist, T.
(2009) Bone replacement following dental trauma
prior to implant surgery–status. Dental Trauma-
tology 25 : 2–11.
Hallman, M., Sennerby, L. & Lundgren, S. (2002) A
clinical and histologic evaluation of implant inte-
gration in the posterior maxilla after sinus floor
augmentation with autogenous bone, bovine
hydroxyapatite, or a 20:80 mixture. International
Journal of Oral and Maxillofacial Implants 17:
635–643.
Hatano, N., Shimizu, Y. & Ooya, K. (2004) A clini-
cal long-term radiographic evaluation of graft
height changes after maxillary sinus floor aug-
mentation with a 2:1 autogenous bone/xenograft
mixture and simultaneous placement of dental
implants. Clinical Oral Implants Research 15 :
339–345.
Jensen, T., Schou, S., Gundersen, H.J., Forman, J.L.,
Terheyden, H. & Holmstrup, P. (2013) Bone-to-
implant contact after maxillary sinus floor aug-
mentation with bio-oss and autogenous bone in
different ratios in mini pigs. Clinical Oral
Implants Research 24: 635–644.
Jensen, T., Schou, S., Stavropoulos, A., Terheyden,
H. & Holmstrup, P. (2012a) Maxillary sinus
floor augmentation with bio-oss or bio-oss mixed
with autogenous bone as graft: a systematic
review. Clinical Oral Implants Research 23: 263–
273.
Jensen, T., Schou, S., Svendsen, P.A., Forman, J.L.,
Gundersen, H.J., Terheyden, H. & Holmstrup, P.
(2012b) Volumetric changes of the graft after
maxillary sinus floor augmentation with bio-oss
and autogenous bone in different ratios: a radio-
graphic study in minipigs. Clinical Oral Implants
Research 23: 902–910.
Junker, R., Dimakis, A., Thoneick, M. & Jansen,
J.A. (2009) Effects of implant surface coatings and
composition on bone integration: a systematic
review. Clinical Oral Implants Research 20
(Suppl. 4): 185–206.
Kilkenny, C., Browne, W.J., Cuthill, I.C., Emerson,
M. & Altman, D.G. (2010) Improving bioscience
research reporting: the arrive guidelines for
reporting animal research. PLoS Biology 8:
e1000412. doi: 10.1371/journal.pbio.1000412.
Kim, Y.K., Yun, P.Y., Kim, S.G. & Lim, S.C. (2009)
Analysis of the healing process in sinus bone
grafting using various grafting materials. Oral
Surgery, Oral Medicine, Oral Pathology, Oral
Radiology and Endodontics 107: 204–211.
Lai, H.C., Zhuang, L.F., Zhang, Z.Y., Wieland, M.
& Liu, X. (2009) Bone apposition around two dif-
ferent sandblasted, large-grit and acid-etched
implant surfaces at sites with coronal circumfer-
ential defects: an experimental study in dogs.
Clinical Oral Implants Research 20: 247–253.
Lang, N.P., Salvi, G.E., Huynh-Ba, G., Ivanovski, S.,
Donos, N. & Bosshardt, D.D. (2011) Early
osseointegration to hydrophilic and hydrophobic
implant surfaces in humans. Clinical Oral
Implants Research 22: 349–356.
Maiorana, C., Redemagni, M., Rabagliati, M. & Sal-
ina, S. (2000) Treatment of maxillary ridge resorp-
tion by sinus augmentation with iliac cancellous
bone, anorganic bovine bone, and endosseous
implants: a clinical and histologic report. Interna-
tional Journal of Oral and Maxillofacial Implants
15 : 873–878.
Morton, D., Bornstein, M.M., Wittneben, J.G., Mar-
tin, W.C., Ruskin, J.D., Hart, C.N. & Buser, D.
(2010) Early loading after 21 days of healing of
nonsubmerged titanium implants with a chemi-
cally modified sandblasted and acid-etched sur-
face: two-year results of a prospective two-center
study. Clinical Implant Dentistry and Related
Research 12: 9–17.
Philipp, A., Duncan, W., Roos, M., Hammerle,
C.H., Attin, T. & Schmidlin, P.R. (2014) Com-
parison of sla(r) or slactive(r) implants placed in
the maxillary sinus with or without syn-
thetic bone graft materials – an animal study in
sheep. Clinical Oral Implants Research 25 :
1142–1148.
Rupp, F., Scheideler, L., Olshanska, N., de Wild,
M., Wieland, M. & Geis-Gerstorfer, J. (2006)
Enhancing surface free energy and hydrophilicity
through chemical modification of microstruc-
tured titanium implant surfaces. Journal of
Biomedical Materials Research Part A 76 : 323–
334.
Saffarzadeh, A., Gauthier, O., Bilban, M., Bagot
D’Arc, M. & Daculsi, G. (2009) Comparison of
two bone substitute biomaterials consisting of a
mixture of fibrin sealant (tisseel) and mbcp (tri-
cos) with an autograft in sinus lift surgery in
sheep. Clinical Oral Implants Research 20: 1133–
1139.
Schlegel, A.K., Donath, K. & Weida, S. (1998) Histo-
logical findings in guided bone regeneration (gbr)
around titanium dental implants with autogenous
bone chips using a new resorbable membrane.
Journal of Long-Term Effects of Medical Implants
8: 211–224.
Schlegel, K.A., Lang, F.J., Donath, K., Kulow, J.T. &
Wiltfang, J. (2006) The monocortical critical size
8 | Clin. Oral Impl. Res. 0, 2016 / 1–9 © 2016 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Alayan et al "SLA! and SLActive! implants in maxillary sinus augmentation

bone defect as an alternative experimental model
in testing bone substitute materials. Oral Sur-
gery, Oral Medicine, Oral Pathology, Oral Radi-
ology and Endodontics 102: 7–13.
Schwarz, F., Sager, M., Ferrari, D., Herten, M., Wie-
land, M. & Becker, J. (2008) Bone regeneration in
dehiscence-type defects at non-submerged and
submerged chemically modified (slactive) and
conventional sla titanium implants: an immuno-
histochemical study in dogs. Journal of Clinical
Periodontology 35 : 64–75.
Schwarz, F., Wieland, M., Schwartz, Z., Zhao, G.,
Rupp, F., Geis-Gerstorfer, J., Schedle, A., Broggini,
N., Bornstein, M.M., Buser, D., Ferguson, S.J.,
Becker, J., Boyan, B.D. & Cochran, D.L. (2009)
Potential of chemically modified hydrophilic sur-
face characteristics to support tissue integration
of titanium dental implants. Journal of Biomedi-
cal Materials Research. Part B, Applied Biomate-
rials 88: 544–557.
de Vicente, J.C., Hernandez-Vallejo, G., Brana-
Abascal, P. & Pena, I. (2010) Maxillary sinus
augmentation with autologous bone harvested
from the lateral maxillary wall combined with
bovine-derived hydroxyapatite: clinical and histo-
logic observations. Clinical Oral Implants
Research 21: 430–438.
Wennerberg, A. & Albrektsson, T. (2009) Effects of
titanium surface topography on bone integration:
a systematic review. Clinical Oral Implants
Research 20(Suppl. 4): 172–184.
Wennerberg, A., Galli, S. & Albrektsson, T. (2011)
Current knowledge about the hydrophilic and
nanostructured slactive surface. Clinical, Cos-
metic and Investigational Dentistry 3: 59–67.
Zhao, G., Schwartz, Z., Wieland, M., Rupp, F.,
Geis-Gerstorfer, J., Cochran, D.L. & Boyan, B.D.
(2005) High surface energy enhances cell response
to titanium substrate microstructure. Journal of
Biomedical Materials Research Part A 74: 49–58.
© 2016 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 9 | Clin. Oral Impl. Res. 0, 2016 / 1–9
Alayan et al "SLA! and SLActive! implants in maxillary sinus augmentation

101
PART 2 – CLINICAL & RADIOGRAPHIC ASSESSMENT OF
COLLAGEN STABILIZED ABBM IN MSA
This section of the thesis includes the following chapter:
Chapter 5: A prospective controlled trial comparing xenograft/autogenous bone
and collagen-stabilized xenograft for maxillary sinus augmentation –
Complications, patient reported outcomes and volumetric analysis.
Chapter 6: A prospective controlled trial comparing xenograft/autogenous bone
and collagen-stabilized xenograft for maxillary sinus augmentation – Implant
supported restorations outcomes.

102
Chapter 5: A prospective controlled trial comparing xenograft/autogenous
bone and collagen-stabilized xenograft for maxillary sinus augmentation –
Complications, patient reported outcomes and volumetric analysis.

103
STATEMENT OF CONTRIBUTION TO CO-AUTHORED PUBLISHED
PAPER
This chapter includes a co-authored paper. The bibliographic details of the
co-authored paper, including all authors, are:
Alayan J, Ivanovski S. (2018) A prospective controlled trial comparing
xenograft/autogenous bone and collagen-stabilized xenograft for maxillary sinus
augmentation – Complications, patient reported outcomes and volumetric analysis.
Clinical Oral Implants Research 29: 248 – 262. doi: 10.1111/clr.13107.
My contribution to the paper involved:
Design of the project, the provision of the data, the preliminary analysis and
categorization of the data into a usable format, the provision of direction on the
scope and structure of the analysis, the interpretation of results and drafting of the
article.
04th May 2018
Jamil Alayan
(Countersigned) 16th May 2018
Corresponding author of paper: Jamil Alayan
(Countersigned) ___________________________ 16th May 2018
Supervisor: Stephen Hamlet

Clin Oral Impl Res. 2017;1–15. wileyonlinelibrary.com/journal/clr | 1© 2017 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Accepted: 29 October 2017
DOI: 10.1111/clr.13107
O R I G I N A L A R T I C L E
A prospective controlled trial comparing xenograft/autogenous bone and collagen- stabilized xenograft for maxillary sinus augmentation—Complications, patient- reported outcomes and volumetric analysis
Jamil Alayan | Saso Ivanovski
School of Dentistry and Oral Health, Centre for Medicine and Oral Health, Griffith University, Southport, QLD, Australia
CorrespondenceJamil Alayan, School of Dentistry and Oral Health, Centre for Medicine and Oral Health, Gold Coast Campus Griffith University, Southport, QLD, Australia.Email: [email protected]
AbstractObjective: Compare maxillary sinus augmentation (MSA) using two different materi-
als—anorganic bovine bone mineral (ABBM) + autogenous bone (AB) (control group)
vs. collagen- stabilized ABBM (test group) in terms of complications, patient- reported
outcome measures (PROMs) and volumetric analysis.
Materials and Methods: Sixty patients underwent sinus augmentation (30 control + 30
test group). Intra- and postoperative complications were recorded. PROMs measured
the impact of grafting on daily activities, pain and morbidity. CT scans were used to
measure graft volume, ridge height, material selection and degree of contact of graft-
to- surrounding sinus walls. Dental implant placement parameters were also
recorded.
Results: All complications were minor and did not prevent completion of the augmen-
tation or subsequent implant placement. Schneiderian membrane perforation was the
most frequently encountered complication. Both treatment groups reported moderate
limitation in the 1st 48 hr post- surgery but little or none by day 3 or 4. Jaw opening,
chewing and bruising were significantly higher in the control group. The impact on
work and social life was moderate initially but reduced to little or none by the 2nd day.
Mild to moderate pain and interference to daily activities were reported for the first
3 days requiring the use of NSAIDs only. A mean graft volume of 1.46 cm3 (±0.77) was
calculated in the control group and 1.27 cm3 (±0.65) in the test group. Extent of con-
tact between graft and surrounding sinus walls had a significant impact on bone vol-
ume. Shorter (8 mm) implants were utilized more frequently in the test group, which
was also more likely to require additional vertical augmentation, but this was not sta-
tistically significant.
Conclusion: MSA using a lateral wall approach is safe and associated with mild to mod-
erate pain and restrictions to daily activities for 48–72 hr. Patients’ reports of morbid-
ity were greater with autogenous bone harvesting. Collagen- stabilized ABBM provides
comparable bone volume to AB + ABBM that is sufficient for placement of implants of
adequate size with no need for further vertical augmentation. Engaging the surround-
ing sinus walls had a significant positive impact on graft volume.

2 | ALAYAN ANd IVANOVSKI
1 | INTRODUCTION
Implant placement in the posterior maxilla is often prevented by
insufficient bone volume as a result of bone resorption and sinus
pneumatization. Maxillary sinus floor elevation is the technique most
frequently used to overcome this limitation and is considered a safe
and effective procedure with high implant survival rates (Chiapasco,
Casentini & Zaniboni, 2009; Del Fabbro, Testori, Francetti &
Weinstein, 2004). Nevertheless, clinically this surgical technique is
still being refined, with a large degree of variation in many aspects
of the procedure.
To date, a variety of bone substitute materials have demonstrated
clinically acceptable outcomes (Cordaro et al., 2008; Froum, Wallace,
Elian, Cho & Tarnow, 2006; Klijn, Meijer, Bronkhorst & Jansen, 2010;
Nkenke & Stelzle, 2009). Despite the established clinical efficacy of
the technique, the search continues for a bone substitute with optimal
properties including rapid osteogenesis as well as long- term volumet-
ric stability and space maintenance.
The composite graft of anorganic bovine bone mineral (ABBM)
and autogenous bone (AB) is well documented in multiple studies
of maxillary sinus floor augmentation (Avila et al., 2010; Cannizzaro,
Felice, Leone, Viola & Esposito, 2009; Galindo- Moreno et al., 2010;
Hallman, Cederlund, Lindskog, Lundgren & Sennerby, 2001; Hallman,
Mordenfeld & Strandkvist, 2005; Hallman, Sennerby & Lundgren,
2002; Hatano, Shimizu & Ooya, 2004; Kim, Yun, Kim & Lim, 2009;
Maiorana, Redemagni, Rabagliati & Salina, 2000; de Vicente,
Hernandez- Vallejo, Brana- Abascal & Pena, 2010). The ABBM/AB
combination is the most clinically and histologically studied mate-
rial for sinus augmentation (Jensen, Schou, Stavropoulos, Terheyden
& Holmstrup, 2012a,b; Jensen, Schou, Svendsen, et al., 2012) and
provides the advantages of AB whilst limiting its undesirable effects.
AB results in superior de novo bone formation (Schmitt et al., 2013),
but its harvesting is associated with postoperative patient morbidity
(Clavero & Lundgren, 2003; Cricchio & Lundgren, 2003), prolonged
surgical time and is only present in limited quantities. AB grafts can
also exhibit unpredictable resorption (Clavero & Lundgren, 2003;
Davis, Martinoff & Kaminishi, 1984; Sbordone et al., 2013; Wiltfang
et al., 2005), which is not a desirable characteristic in sinus graft-
ing. Indeed, sinuses augmented using AB as the sole grafting mate-
rial have been shown to undergo significant re- pneumatization and
loss of augmented volume (Arasawa et al., 2012; Johansson, Grepe,
Wannfors, Aberg & Hirsch, 2001; Johansson, Grepe, Wannfors &
Hirsch, 2001). The addition of a slower resorbing highly osteocon-
ductive material such as ABBM (Bio- Oss®, Gesitlich, AG, Wollhusen
Switzerland) provides superior space maintenance for de novo
bone formation (Berglundh & Lindhe, 1997; Haas, Baron, Donath,
Zechner & Watzek, 2002; Jensen et al., 1996; Orsini et al., 2005)
and volumetric stability (Galindo- Moreno et al., 2010; Jensen et al.,
2012a,b; Jensen, Schou, Svendsen, et al., 2012).
The supplementation of ABBM to AB grafts has also led to a re-
duction in the amount of autogenous bone needed, which in turn
eliminated the need for extra- oral harvesting thereby reducing pa-
tient morbidity, surgical time and expense (Scheerlinck et al., 2013).
Whilst the symphysis and retromolar regions of the mandible are rel-
atively safe sites to harvest particulate autograft, the need to create
a second surgical site remains. As such, collecting the bone removed
from the buccal wall of the maxilla during preparation of the buc-
cal antrostomy allows for the use of autogenous cortical particles
as part of a composite graft without the need for a second surgi-
cal site. Whilst further reductions in patient morbidity and operating
time would be expected using this technique, previous studies have
only emphasized histological/histomorphometric outcomes (Galindo-
Moreno et al., 2007, 2010, 2011). In general, there is an absence
of patient- reported outcome measures (PROMs) for maxillary sinus
augmentation, yet factors such as pain, bruising, oedema and their
impact on daily activities are an important consideration for patients
considering this treatment option.
ABBM is also available in a block form that is stabilized in 10% por-
cine type 1 collagen matrix (ABBM- C) (Bio- Oss Collagen®, Gesitlich,
AG, Wollhusen Switzerland). The contained nature of the block may
be advantageous in maxillary sinus augmentation when the common
surgical complication of Schneiderian membrane perforation occurs
(Chiapasco et al., 2009). The impact of this altered formulation of
ABBM has been investigated in terms of bone regeneration in max-
illary sinus augmentation (Alayan, Vaquette, Farah & Ivanovski, 2016;
Alayan, Vaquette, Saifzadeh, Hutmacher & Ivanovski, 2016), but there
are no studies reporting on the clinical outcomes of maxillary sinus
grafts using this material.
The primary aim of this controlled clinical trial was to determine
whether the test group (ABBM- C), used in defined clinical scenarios
(i.e., reduced local autogenous bone availability and/or sinus membrane
perforation), performs equivalently to the control group (ABBM+AB)
in terms of the prevalence of surgical complications, patient- reported
and volumetric outcomes.
2 | MATERIAL AND METHODS
2.1 | Ethics and consent
The University of Queensland School of Dentistry Dental Sciences
Research Ethics Committee provided ethical approval for this equiva-
lence non- randomized controlled clinical trial (Project Number: 1010).
The project complies with the provisions contained in the National
Statement on Ethical Conduct in Research Involving Humans and
K E Y W O R D S
anorganic bovine bone, Bio-Oss, Bio-Oss Collagen, bone substitute, clinical trial, guided bone
regeneration, patient-centred outcomes, Sinus floor elevation, volumetric outcomes

| 3ALAYAN ANd IVANOVSKI
complies with the regulations governing experimentation on humans.
The STROBE (Strengthening the Reporting of Observational Studies
in Epidemiology) guidelines were adhered to in the preparation of this
manuscript.
2.2 | Inclusion criteria
To be considered eligible for the study, the following inclusion criteria
were applied:
1. Males and females, over 21 years of age at the time of
surgery
2. Must present with a bone deficiency in the maxillary sinus region,
which necessitates sinus floor augmentation to facilitate the place-
ment of one or more dental implants.
3. If bilateral sinus augmentation was required, only one sinus was
randomly selected and used for the purposes of this study.
4. Residual alveolar bone height of the edentulous maxilla below the
floorofthemaxillarysinus≤4.5mmand≥1mm(measuredatthemid-point of the edentulous space where both the coronal and sag-
ittal planes intersect).
5. Residualalveolarbonewidthof≥6mmasmeasuredonaCTscan.6. Generally fit and healthy and able to undergo oral surgical proce-
dures under local and general anaesthesia.
7. Patients with a history of chronic periodontitis were treated first
and subsequently enrolled in a supportive maintenance programme
prior to recruitment into the study.
8. Teeth at the surgical site which required removal were extracted a
minimum of 12 weeks prior to sinus floor elevation.
2.3 | Exclusion criteria
Patients were considered ineligible if any of the following criteria
were met:
1. Any systemic medical condition that could interfere with the
surgical procedure
2. Current pregnancy at the time of recruitment
3. Physical handicaps that would interfere with the ability to perform
adequate oral hygiene
4. Alcoholism or chronic drug abuse
5. Patients who smoke more than 10 cigarettes per day
6. Medications which interferes with bone formation
7. Mucosal diseases such as lichen planus
8. History of local radiation therapy
9. Severe bruxism or clenching habits
10. Signs and symptoms consistent with acute maxillary sinusitis
11. Significant soft tissue thickening or sinus opacification in the sinus
of interest.
12. Previous GBR (bone graft) or dental implant treatment in the poste-
rior segments of the maxilla
13. Benign or malignant tumours of the maxillary sinus
14. Pathological conditions that severely impact mucociliary clearance
including; chronic sinusitis, primary ciliary dyskinesia or cystic
fibrosis.
2.4 | Participant allocation and study design
To perform a comparison of bone volume between groups in this equiv-
alence study, a power analysis (PASS v. 11.0) indicated that we would
need 30 individuals in each group (total study population = 60 patients) to
achieve a power of 0.83 with a probability of 0.05 for type 1(alpha) errors,
assuming a standard deviation of 0.70 (Gultekin et al., 2016), a true dif-
ference of zero and a zone of clinical equivalence of ±0.55 cm3 (Figure 1).
Patients were prospectively recruited from the School of Dentistry
at the University of Queensland and from a specialist private prac-
tice from July 2010 to December 2015. Those that met the inclusion
F IGURE 1 Flow chart of treatment sequence and data collection, including the number of patients involved in each step. MSFE, maxillary sinus floor elevation; control (ABBM + AB), anorganic bovine bone mineral + autogenous bone; test (ABBM- C), collagen- stabilized anorganic bovine bone mineral; PCO, patient- centred outcomes

4 | ALAYAN ANd IVANOVSKI
criteria then underwent the informed consent process. All patients
were referred specifically for replacement of teeth with implant-
supported restorations. Recruitment continued until 30 patients were
allocated to the control and test groups.
Allocation of each patient to either the test (ABBM- C) or the control
group (ABBM + AB) was based on two intra- operative parameters, the
presence of Schneiderian membrane perforation and availability of ade-
quate autogenous bone in the vicinity of the surgical site. ABBM- C was
selected if sinus membrane perforations occurred or if there was insuf-
ficient autogenous bone available for harvesting from in the site of the
buccal antrostomy. ABBM + AB was alternatively used if the Schneiderian
membrane remained intact and if there was sufficient autogenous bone
that could be harvested from the buccal wall of the maxilla.
Five–six months later, all participants underwent surgical implant
placement whereby they received a single implant in the augmented
site. The same clinician (JA) performed all of the surgical procedures.
Whilst clinician blinding was not possible at the time of the augmen-
tation surgery or implant placement, it was possible during the data
collection and analysis stages of this project.
2.5 | Primary and secondary outcomes
The overall objective of this study was to assess the success of the
maxillary sinus augmentation procedure.
Primary endpoint:
1. Augmented bone volume measured 5–6 months after maxillary
sinus augmentation and prior to implant placement.
Secondary endpoints include the following:
1. Intra-operative complications
2. Postoperative surgical complications and morbidity
3. PROMs such as pain and interference with daily life, in addition to
quality of life measures during the first week after maxillary sinus
augmentation
4. Need for further vertical augmentation at implant placement
5. Placement of implants with adequate dimensions
6. Complications during implant insertion, such as lack of primary
stability
2.6 | Bone graft materials and dental implants
Patients were assigned to one of the following groups:
1. Control group—small diameter particles (0.25 – 1.0 mm) of depro-
teinized bovine bone mineral (Bio-Oss®, Geistlich AG, Wollhusen,
Switzerland) + autogenous bone (ABBM+AB) in a 1:1 ratio, as
determined using a standardized 2 cc bone collecting chamber.
2. Test group—250 mg blocks of deproteinized bovine bone mineral +
collagen (ABBM-C) (Bio-Oss Collagen®, Geistlich AG, Wollhusen,
Switzerland).
All patients received a single Straumann (Institut Straumann AG,
Basel, Switzerland) tissue level dental implant 5 months post- grafting.
The implant had a standard microroughened sandblasted and acid-
etched (SLA) surface. The dimensions of the implants were chosen
according to the specific site characteristics.
2.7 | Pre- surgical procedures
All participants started systemic antibiotic therapy (500 mg amoxycil-
lin or 300 mg clindamycin) and 0.2% chlorhexidine mouth rinse 24 hr
prior to grafting surgery. A single dose of 8 mg dexamethasone was
also given preoperatively. All patients were assessed for periodontal
disease at the initial assessment appointment by specialist periodon-
tists (JA & SI) and according to the criteria of Armitage (Armitage,
1999). Those diagnosed were treated and deemed to be stable prior
to sinus augmentation surgery. Stability was defined as having a full
mouth bleeding score of ≤20% and ≤4sites of residual periodontalprobingdepth≥5mm(Lang&Tonetti,2003).
2.8 | Maxillary sinus floor elevation and grafting
All patients were treated by the same operator (JA) with the same
surgical technique consisting of sinus floor elevation via a lateral
wall (modified Caldwell- Luc) approach. After elevation of a full buc-
cal mucoperiosteal flap, a full antrostomy was created in the lat-
eral wall of the maxilla using a bone scraper (Safescraper Twist,
META, C.G.M Sp.A, Reggio Emilia, Italy). A piezoelectric surgical unit
(Implant Center, Satelec, Acteon, France) was subsequently used to
finalize the osteotomy and gain access to the maxillary sinus. The
size, shape and location of the antrostomy were variable and tai-
lored to the site and patient’s characteristics. The only consistent
feature of the antrostomy was the superior osteotomy, which was
located 10 mm apical to the alveolar bony crest (Figure 2). The full
buccal mucoperiosteal flap was limited in its vertical extension but
provided sufficient access to create this superior osteotomy. The
sinus membrane was then dissected and elevated in all directions
to create an intrasinus space that received one of the two grafting
materials. The membrane was elevated superiorly to allow for graft-
ing material packing to at least 10 mm apical to the alveolar bone
crest. This was achieved using standard sinus membrane elevator
spoons. Sufficient material was placed until the desired 10 mm of
vertical height was achieved. The material was carefully packed to
ensure maximum contact with resident bony walls, with care taken
to avoid over- packing.
The autogenous bone chips harvested during preparation of the
buccal antrostomy were collected using a bone scraper with a stan-
dardized bone collecting chamber (2 cc) and used for the autogenous
bone component needed for the control group. No other autogenous
bone harvesting was performed nor was the mucoperiosteal flap ex-
tended any further to widen the antrostomy zone for the purposes
of further autogenous bone harvesting. Any patient with insufficient
autogenous bone in the local area to achieve a 1:1 ratio with ABBM
was allocated to the test group. The reconstructed sites were covered
with a porcine collagen membrane (Bio- Gide, Geistlich AG, Wolhusen,
Switzerland). The mucoperiosteal flaps were then sutured using a

| 5ALAYAN ANd IVANOVSKI
non- resorbable thermoplastic polyether- ester monofilament suture
(Dyloc 5/0 and 6/0 Dynek, Adelaide, Australia) to achieve primary
closure.
A postoperative regimen of amoxycillin 500 mg t.d.s for 7 days
(or if allergic 150 mg clindamycin q.i.d for 6 days) was prescribed, as
was paracetamol 500 mg, ibuprofen 200 mg and 0.2% chlorhexidine
mouth rinse b.d for 7 days. Narcotic analgesics were not prescribed
unless requested by the patient in cases of recalcitrant pain.
2.9 | Clinical follow- up and evaluation
Intra- operative complications and adverse events relating to the
maxillary sinus augmentation procedure were recorded and included
Schneiderian membrane perforation and intra- operative bleeding re-
quiring intervention. All patients were reviewed at 7 and 14 days post-
operatively. At the 7- day review, the following signs were recorded as
either present or absent: wound dehiscence, wound infection (sup-
puration and oedema), extra- oral bruising, oedema and other signs of
morbidity including altered sensation and nasal bleeding. Maxillary
sinusitis was also recorded and defined according to the clinical prac-
tice guidelines of the American Academy of Otolaryngology—Head
and Neck Surgery Foundation 2007 which defines acute maxillary
sinusitis as up to 4 weeks of purulent discharge accompanied by nasal
obstruction, facial pain/pressure or both as reported by the patient or
clinically observed (Rosenfeld et al., 2007).
Postoperative symptoms and the degree of interference with daily
activities were assessed in all patients that underwent maxillary sinus
augmentation under local anaesthesia. A condition- specific health-
related quality of life (HRQL) instrument was used which contained a
questionnaire and a VAS (Shugars, Benson, White, Simpson & Bader,
1996). The instrument collected data for 6 days postoperatively. The
self- administered questionnaire assessed limitations on daily activities
(jaw opening, chewing, talking, sleeping, work and social life) and post-
operative signs (swelling, bruising, bleeding) that cover oral and gen-
eral function, pain and other symptoms (Hashem, Claffey & O’Connell,
2006). A five- point Likert- type scale was used as the response for-
mat (lots, quite a bit, some, little or none). The VAS evaluated average
pain, and interference with daily activities. It consisted of a 10- cm line
with clearly defined endpoints. One end of the line was labelled “no
pain” and the other end of the line was labelled “most intense pain
imaginable.” A similar VAS was used to record interference with daily
activities. Patients were provided with six copies of the data- collecting
instrument and instructed to complete one instrument each evening
for the first 6 days postoperatively. The instrument was coded and
returned to a staff member but was anonymous to the operator (JA).
2.10 | Radiological/volumetric assessment
Volumetric imaging was performed using either multislice CT or cone
beam CT depending on the imaging centre the patient attended. All
scans were obtained at a small number of specialist imaging centres
under the supervision of an oral and maxillofacial radiologist. Pre-
maxillary sinus augmentation scanning was carried out on all patients
to assess site anatomy and to identify patients with significant sino-
nasal pathology. Subsequent scanning was performed no earlier than
5 months after maxillary sinus augmentation and prior to implant
placement. Patients attended the same centre for both scans to en-
sure scans were obtained on the same machines using the same scan
protocol thereby ensuring compatibility (Table 1). All CT scans were
taken with no gantry tilt. Scans were performed with the occlusal
plane approximately parallel with the primary X- ray beam during
acquisition. The occlusal plane was used as the reference plane for
subsequent image reconstruction.
F IGURE 2 A clinical photograph highlighting the placement of the superior osteotomy 10 mm form the bone crest accompanied by similar extent of membrane elevation
TABLE 1 Summary of CT scan protocols
Company Location Modality Scanner make/model kV Exposure (mAs)
Slice thickness (mm)
Image resolution (mm)
1 1 CT GE Lightspeed VCT 120 43.8 0.625 0.336
1 2, 3 CBCT iCAT/Imaging Science International
120 20 0.25 0.25
1 3 CT Toshiba Aquilion 16 120 40 0.5 0.3
2 1 CBCT Kodak Trophy K9500 90 108 0.2–0.3 0.2–0.3
2 2, 3 CT GE Brightspeed 120 168 0.625 0.336
3 1 CBCT Carestream Health/CS9300 85 60.25 0.25 0.25

6 | ALAYAN ANd IVANOVSKI
All data sets were uploaded into the software and allocated an
identification number. The same operator, an experienced specialist
periodontist, performed all data set reconstruction and measurements
(JA). The protocol was discussed and confirmed with an experienced
oral and maxillofacial radiologist (RD).
DICOM data were then imported into a 3D dental implant plan-
ning software (Simplant Pro 17.0 Dentsply Implants NV, Research
Campus 10 3500 Hasslet Belgium). Only those data sets that in-
cluded the full volume of the maxillary sinus were included in the
study (i.e., from occlusal plane to the superior orbital rim). In addi-
tion, data sets were eliminated from the study if significant soft tis-
sue thickening or sinus opacification was noted that prevented the
accurate volumetric measurement of the maxillary sinus. A mask was
initially created to highlight the air- filled cavities, with subsequent
use of a segmentation tool to manually highlight the volume of the
maxillary sinus cavity proper. This allowed the software to calculate
the sinus volume in cubic centimetres. These measurements were
performed on both the pre- graft (Figure 3a) and post- graft CT data
sets (Figure 3b), and the difference between these measurements
was taken as the graft volume.
Two further radiographic parameters were measured using the
same software and included residual ridge height and contact of graft-
to- surrounding sinus walls (Simplant Pro 17.0 Dentsply Implants NV,
Research Campus 10 3500 Hasslet Belgium). Residual ridge height
was measured using a linear measurement tool at the mid- point of the
edentulous space where both the coronal and sagittal planes intersect.
To determine the degree of graft- to- surrounding sinus wall contact,
linear measurements were performed in regions where the graft con-
tacted resident walls at three predetermined coronal and three sag-
ittal sections through the grafted region. These three sections were
located by dividing the graft into three equal segments in both coronal
and sagittal planes (Figure 4a). Specifically, axial slices were assessed
to identify the slice which displays the maximum volume of graft in
the mesio- distal and transverse dimension. The mid- sagittal and the
mid- coronal bisecting lines were then identified on this axial slice. The
division of the graft into equal thirds was made at this axial slice level.
The division of the graft into equal thirds coronally was carried out
using this mid- sagittal slice, and similarly, the division into equal thirds
sagittally was performed using this mid- coronal slice. An average of
these contact measurements was obtained and used in the analysis
(Figure 4b).
2.11 | Dental implant placement
Dental implant placement was performed 5.5–6 months later. All
participants began systemic antibiotic therapy (1,000 mg amoxycillin
or 300 mg of clindamycin) 60 min prior to surgery. A 0.2% chlorhex-
idine mouth rinse was utilized for 60 s immediately prior to surgery.
Osteotomy preparation was completed using a standard surgical tech-
nique. The implant was placed with the border of the rough surface
approximating the alveolar crest leaving the machined neck portion
in the trans- mucosal area. A healing abutment was secured, and mu-
coperiosteal flaps were sutured using a non- resorbable thermoplastic
polyether- ester monofilament suture (Dyloc 5/0, Dynek, Adelaide,
Australia) to allow for a trans- mucosal healing modality. A small
amount of crestal gingiva was excised to allow for tight flap adapta-
tion, if necessary.
A postoperative regimen of amoxycillin 500 mg three times daily
for 7 days was prescribed, together with paracetamol 500 mg, ibupro-
fen 200 mg and 0.2% chlorhexidine mouth rinse twice daily for 7 days.
F IGURE 3 Volumetric assessment using digital reconstruction. (a) Pre- sinus augmentation CT – maxillary sinus volume (cubic centimetres) calculated by reconstructing the axial, sagittal and coronal segmentation. (b) Measurements repeated on the post- augmentation CT and the difference between these measurements taken as the graft volume
(a) (b)

| 7ALAYAN ANd IVANOVSKI
Patients allergic to penicillin- based antibiotics were prescribed clinda-
mycin 150 mg four times daily for 7 days. Patients were reviewed 7
and 14 days later.
At implant placement, the following parameters were recorded;
implant dimension, the need for further vertical augmentation at
implant placement using osteotomes, and lack of primary stabil-
ity. Implant survival and success will be reported in a subsequent
study.
2.12 | Statistics
All data were analysed using IBM SPSS Statistics for Windows version
21.0 (IBM Corporation 2012©, Armonk, NY, U.S). Surgical outcomes
and complications were analysed using a comparison of proportion
calculator (MedCalc Software®). Generalized estimating equations
were used to analyse PROMs (VAS and survey) due to clustering of
data (VAS and survey were assessed on the same patients six times)
with the individual (subject) used as the clustering variable, and using
an ordinal logistic regression model for categorical and a linear model
for continuous outcomes. Treatment and time were used as explana-
tory variables along with treatment*time interaction. A backward
elimination procedure was used for arriving at the most parsimoni-
ous model. An independent t test was used to compare bone graft
volumetric data and a linear regression model to assess impact of
treatment (test vs. control), residual ridge height and extent of graft
contact with surrounding sinus walls on this parameter. Baseline pa-
rameters such as age and initial ridge height were compared using an
independent t test, and categorical parameters such as gender, smok-
ing and periodontal status were compared using a chi- squared test.
The null hypothesis was taken as non- equivalence in surgical
complications, in patient- centred outcomes and graft volume in aug-
mented maxillary sinuses using ABBM (Bio- Oss®) + AB or blocks of
ABBM- C (Bio- Oss Collagen®) alone. A p ≤ .05 was considered to rep-
resent statistically significant differences.
3 | RESULTS
3.1 | Study population
Sixty (n = 60) patients were enrolled in this study and underwent sinus
augmentation (Table 2). A total of thirty patients (n = 30) were allo-
cated to each group. There were no significant differences between
groups in terms of age, gender ratio or number of patients smoking.
Allsmokersreportedsmoking≤10cigarettesperday.Moderate-to-severe chronic periodontitis was diagnosed in four patients in the
control group and seven in the test group. All of these patients were
treated and were deemed stable (Lang & Tonetti, 2003) prior to place-
ment into a supportive maintenance programme and enrolment into
the study. All patients received maxillary sinus augmentation to allow
for the placement of a single implant in either a site bounded by natu-
ral teeth or in a distal extension situation. There were no significant
differences in the distribution of this arrangement between groups.
3.2 | Intra- operative complications
No major intra- operative complications were encountered during
the procedure or during the postoperative period (Table 3). All minor
complications were successfully managed and did not prevent com-
pletion of the augmentation procedure or subsequent implant place-
ment. Schneiderian membrane perforation was the most frequently
encountered complication with eight patients in total experiencing
sinus perforation and therefore allocated to the test group. These
perforations were small (≤3mm in diameter) to moderate (>3mm≤5mm) and repaired by creating a pouch using the placement ofa resorbable porcine collagen membrane (Bio- Gide, Geistlich AG,
Wolhusen, Switzerland) that was fixed using titanium tacs to the ex-
ternal surface of the lateral wall of the maxilla if needed (Proussaefs
& Lozada, 2003).
F IGURE 4 Representative CT scan showing method of determining degree of graft- to- sinus walls contact. (a) measurements were performed at three coronal (C1, C2, C3) and three sagittal (S1, S2, S3) sections through the grafted regions, located by dividing graft into three equal segments; (b) an average was taken of these linear measurements in regions where the graft contacted the surrounding sinus walls
(a)
(b)

8 | ALAYAN ANd IVANOVSKI
3.3 | Postoperative surgical complications and morbidity
All 60 patients attended for post- surgical review (Table 3). Overall, no
major complications were encountered during the first 2 weeks post-
augmentation surgery. Minor complications were almost all seen at
the one- week review and were resolved by the second review without
specific intervention. Wound dehiscence (10% control and 3.3% test),
bruising (13.3% control and 6.7% test) and oedema (10% control and
3.3% test) were the most frequently recorded signs of morbidity albeit
at low frequencies. Fewer cases of dehiscence, bruising and oedema
were noted in the test group, but this was not statistically significant.
These bruising and oedema were also noted to be of lesser severity
in test patients compared to patients in the control group. This obser-
vation however was not objectively measured. Symptoms consistent
with postoperative sinusitis (nasal congestion and post- nasal drip and
facial pressure) were reported by a single patient in the control group
and resolved spontaneously within 48 hr after sinus grafting. A single
patient in the control group reported an isolated minor incident of
bleeding from the nose after the first 24 hr.
3.4 | Patient- reported outcome measures (PROMs)
A total of 30 patients (15 control + 15 test) completed the question-
naire and VAS for this part of the analysis. All these patients under-
went maxillary sinus augmentation using local anaesthesia only.
3.4.1 | Questionnaire—limitation to daily activities (oral function)
Overall, a trend of gradual and daily decrease in the degree of limita-
tion was seen across all activities. The majority of patients in both
ParametersControl (ABBM+AB) (n = 30)
Test (ABBM- C) (n = 30)
Group comparison (p)
Age (Mean years ± SD) 59.57 (±10.57) 58.87 (±9.43) .93
Gender ratio (f/m) 2.0 (f = 20/m = 10) 3.29 (f = 23/m = 7) .57
Smoking (no. patients) 1 2 1.0
Periodontal disease (no. patients)
4 7 .51
Initial ridge height (mm) (Mean ± SD)
3.13 ± 0.73 3.04 ± 0.72 .62
Implant arrangement—bounded by natural teeth (no. patients)
12 11 .98
Implant arrangement—distal extension (no. patients)
18 19 .99
ABBM, anorganic bovine bone mineral; AB, autogenous bone; ABBM- C, collagen- stabilized anorganic bovine bone mineral; p, p- value for intergroup comparison after proportion or means testing. Mean ± SD for continuous variables and counts for categorical variables.
TABLE 2 Baseline parameters
ParametersControl (ABBM+AB) (n = 30) Number (%)
Test (ABBM- C) (n = 30) Number (%) 95% CI
Group comparison (p)
Perforations - 8 - -
Haemorrhage 0 (0) 0 (0) - -
Wound dehiscence
3 (10.0) 1 (3.33) −9.3,23.5 .30
Wound infection
0 (0) 0 (0) - -
Extra- oral bruising
4 (13.3) 2 (6.67) −11.5,24.9 .40
Extra- oral oedema
3 (10) 1 (3.33) −9.3,23.5 .30
Acute maxillary sinusitis
1 (3.3) 0 (0) −8.7,17.2 .32
Other 1 (3.3) 0 (0) −8.7,17.2 .32
ABBM, anorganic bovine bone mineral; AB, autogenous bone; ABBM- C, collagen- stabilized anorganic bovine bone mineral; 95% CI, 95% confidence interval; p, p- value for intergroup comparison after pro-portion testing.
TABLE 3 Surgical outcomes from augmented maxillary sinuses

| 9ALAYAN ANd IVANOVSKI
treatment groups reported to experience some or quite a bit of limi-
tation to all activities during the first 48 hr post- surgery that reduced
to some or little by day 3. Jaw opening and chewing were affected
by the augmentation procedure to a similar degree and were the oral
functions affected most during the postoperative period. Time was a
significant predictor of all three activities (opening p < .01, chewing
p < .01, talking p < .001) with reductions seen daily. Treatment was a
significant predictor for both opening (p < .005) and chewing (p < .01)
with test group experiencing significantly less interference in both of
these activities. The majority of the control group patients reported
some or lots of interference to both activities on the 1st 24 hr post-
augmentation as opposed to little or some in the test group. The
median interference to opening and chewing was reduced to little
or no interference by the 3rd day in the test group but remained
at some interference in the control group. This delay in reduction
was especially obvious for chewing in the control group. Talking was
mostly restricted in the control group of patients in the first 24 hr and
quickly improved by the 2nd and 3rd days.
3.4.2 | Questionnaire—limitation to daily activities (general function)
The greatest limitation on the first day after surgery was reported to
be on work and social life, but limitation to all three activities (sleeping,
work, social life) was reduced to little or none after the 2nd day. Time
was a significant predictor with reductions seen in all three activi-
ties (sleeping p < .001, work p < .005, social life p < .001) on a daily
basis across all these activities. Treatment group was not a significant
predictor in any of these three activities.
3.4.3 | Questionnaire—postoperative morbidity
Oedema was reported to occur from little to quite a bit by the majority
of patients for the first 3 days post- surgery reducing to some by day 4
and then little or none by days 5 and 6. Time was a significant predictor
for swelling (p < .001) with the median reducing from some to little or
none by the third day in the test group and 4th day in the control group.
Treatment was not a significant predictor. Time was not a significant
predictor of bruising, but treatment group was a significant predictor
(p < .05). The median impact of bruising was none on the first day after
surgery but increased to little on the second day and then to some for
the remainder of the 6 days in the control group, whereas it remained
unchanged and reported to affect patients little or none for the test
group; hence, the time*group interaction was also significant (p < .05).
Whilst time (p < .001) and group (p < .05) were significant predictors for
bleeding, it was reported at a level of little or none in both groups at all
times.
3.4.4 | VAS—average pain and interference to daily activities
Treatment did not significantly affect perception of pain but time
(p < .001) was a predictor of average pain with similar significant re-
ductions reported in both treatment groups. The majority of patients
reported that the average daily pain was mild to moderate for the first
3 days, which was halved by day 4 to become mild pain. Similarly,
treatment did not significantly affect perception of interference with
daily activities but time (p < .001) was a predictor with significant re-
ductions reported in both treatment groups. The majority of patients
reported that the interference with daily activities was mild to mod-
erate for the first 3 days, and this was halved by day 3 to become
mild interference. None of the patients requested narcotic analgesics
(Figure 5).
3.5 | Radiographic/volumetric analysis
The mean graft volume in the control group was 1.46 ± 0.77 cm3 and
1.27 ± 0.65 cm3 in the test group, which was not statistically different
(Tables 4 and 5). The mean initial ridge heights were very similar be-
tween the groups (control = 3.13 ± 0.73 mm; test = 3.04 ± 0.72 mm),
as was the average graft contact to resident walls (con-
trol = 18.67 ± 3.94 mm; test = 17.24 ± 3.08 mm). Multivariable linear
regression analysis performed indicated that treatment group and
initial ridge height were not significant explanatory variables for bone
graft volume but that average contact between graft and surround-
ing sinus walls was a significant explanatory variable with increased
volumes are seen in cases of greater contact (p < .01).
F IGURE 5 Box and whisker plot of VAS for (a) average pain and (b) interference to daily activities for the 1st 6 days post- maxillary sinus augmentation. (c), control group (ABBM + AB); T, test group (ABBM- C). Outliers (o) were identified as responses that lie below Q1 - (1.5IQR) or above Q3 + (1.5IQR)

10 | ALAYAN ANd IVANOVSKI
3.6 | Implant placement outcomes
Two 8- mm implants were placed in the control group and six 8- mm
implants in the test group with the remainder of patients having suf-
ficient bone height for the desired 10- mm implant (Table 6). This
difference did not reach statistical significance. Additional vertical
augmentation using an osteotome mediated sinus floor elevation was
needed in order to place an 8- mm implant in three patients in the test
group with no such cases occurring in the control group. This differ-
ence did not reach statistical significance.
A single implant from both control and test groups did not achieve
primary stability, and these were classed as “spinners.” Adequate pri-
mary stability was achieved for all remaining implants.
4 | DISCUSSION
The aim of this equivalence trial was to prospectively examine a con-
servative approach to maxillary sinus augmentation that utilizes a lim-
ited flap design and locally harvested autogenous bone in combination
with Bio- Oss® (ABBM) versus Bio- Oss Collagen® (ABBM- C) alone and
compare the rates of surgical complications, postoperative morbid-
ity, PROMs and bone graft volume. Both groups were comparable in
terms of age, gender ratio, and rates of periodontal disease and extent
of edentulism.
This patient population did not experience major intra- or post-
operative complications, consistent with previous reviews (Chiapasco
et al., 2009). In addition, the minor complications were manageable
and did not prevent completion of the augmentation procedure. The
most frequent complication was membrane perforation and occurred
in 13% of our patient population (eight of 60). Multiple reviews have
also reported this to be the most frequently reported surgical com-
plication (Chiapasco et al., 2009; Nkenke & Stelzle, 2009; Pjetursson,
Tan, Zwahlen & Lang, 2008). The mean occurrence rates ranged from
10.0% to 19.5%, but some of the included studies reported perfora-
tions in up to 58% of cases. Most of these perforations were small in
diameter(≤3mm)andwererepairedwitharesorbableporcinecolla-gen membrane using a previously described technique (Proussaefs &
Lozada, 2003) with the addition of titanium tacs for additional stability
of the membrane where needed. The role of the collagen in the test
grafting material (ABBM- C) is to cohesively bind the ABBM granules
to form a block. Its advantage in sinus augmentation procedures over
particulate material is evident when perforations of the sinus mem-
brane occur and there is a risk of particulate biomaterial migrating
into the maxillary sinus cavity proper and obstructing the osteome-
atal complex. Previous studies have cited particulate migration into
the sinus cavity proper as a source of postoperative sinusitis (Doud
Galli, Lebowitz, Giacchi, Glickman & Jacobs, 2001; Quiney, Brimble
& Hodge, 1990; Wiltfang et al., 2000) which may require endoscopic
removal and re- establishment of drainage (Doud Galli et al., 2001;
Timmenga, Raghoebar, van Weissenbruch & Vissink, 2001). Our group
has previously shown that the use of ABBM- C for sinus augmentation
had no significant impact on histomorphometric outcomes except for
its delayed maturity as indicated by the lower proportion of lamellar
bone when compared to the control group (Alayan, Vaquette, Farah
& Ivanovski 2016). The significance of sinus membrane perforations
on implant survival or graft success remains contentious with some
studies reporting a negative impact especially in large perforations
(Hernandez- Alfaro, Torradeflot & Marti, 2008; Proussaefs, Lozada,
Kim & Rohrer, 2004), whilst others showed no differences (Becker
et al., 2008).
In terms of PROMs, the majority of patients reported that average
daily pain was mild to moderate for the first 3 days and subsequently
reduced to mild levels using NSAIDs only. The level of average pain
was similar across treatment groups. The majority of patients in both
treatment groups reported a moderate amount of limitation to both
oral and general activities during the first 48 hr post- surgery that re-
duced to little or none by day 3 or 4. The extent of interference to daily
activities was largely similar across the treatment groups, as assessed
using a VAS. A VAS is a valid, easily administered and reproducible tool
to assess dental pain perception (Seymour, Charlton & Phillips, 1983;
Tan, Krishnaswamy, Ong & Lang, 2014). Regardless of the treatment
group, all parameters improved after 48–72 hr. To the best of our
knowledge, this is the first study to report on PROMs for maxillary
TABLE 4 Outcomes of bone graft volume comparing control and test group materials
ParametersControl (ABBM+AB) (Mean ± SD)
Test (ABBM- C) (Mean ± SD) Mean difference 95% CI p value
Bone graft volume (cm3)
1.46 (±077) 1.27 (±0.65) 0.185 −0.18,0.55 .23
ABBM, anorganic bovine bone mineral; AB, autogenous bone; ABBM- C, collagen- stabilized anorganic bovine bone mineral; SD, standard deviation; 95% CI, 95% confidence interval of the mean difference; p, p- value for intergroup comparison after applying a t test.
TABLE 5 Results of linear regression for graft volume—patient used as the unit of analysis
b (SE) 95% CI p value
Treatment group
control 0.064 (0.16) −0.26,0.39 .70
test reference – –
Initial ridge height
−0.09(0.11) −0.31,0.13 .43
Contact sinus walls
0.09 (0.23) 0.045, 0.14 <.001
b, regression estimate coefficient; SE, standard error; 95% CI, 95% confi-dence interval.

| 11ALAYAN ANd IVANOVSKI
sinus augmentation and indicates that 48–72 hr of recovery from this
procedure is needed for patients to resume oral function and daily
activities without limitations or the need for analgesics.
Jaw opening and chewing were the oral functions affected most in
both groups and to a significantly greater extent in the control group,
as was bruising after the first day. Whilst greater prevalence of bruis-
ing and swelling was noted clinically in the control group at the post-
operative review, this did not reach statistical significance. Bruising
and oedema were also noted to be of lesser severity in test patients
compared to patients in the control group, but this observation was
not objectively measured. This perception of increased limitation in
oral functions may reflect the increased morbidity associated with
greater autogenous bone harvesting (Cricchio & Lundgren, 2003).
Patients in the control group typically possessed a thick buccal wall of
bone that provided sufficient volume of autogenous bone needed to
support the elevated Schneiderian membrane at the requisite height.
The test patients on the other hand exhibited a thin buccal wall of
bone and therefore experienced far less bone removal. The inclusion
of the eight patients in the test group due to sinus membrane perfora-
tion may have reduced the extent of this difference in perception and
clinical signs of morbidity. Work and social life were the most affected
general activities with moderate levels of restrictions reported for the
first 48 hr in both treatment groups. It is likely those symptoms of pain
and perception of bruising and oedema translated to this limitation in
social life and work, and is generally consistent with anecdotal reports
from patients of abstaining from work for 48 hr post- surgery.
A slightly increased mean graft volume was measured in the
control group (1.46 ± 0.77 cm3) when compared to the test group
(1.27 ± 0.65 cm3). Whilst the volume of bone graft delivered into
the subantral space was tailored to the individual situation, the area
grafted was controlled in similar ways in both groups and therefore
should have resulted in the delivery of similar initial volume of graft
material. All patients were grafted for the purposes of placing a sin-
gle dental implant, and both groups had a very similar number of
sites bounded by natural teeth and distal extension situations. This
would have limited the mesio- distal dimension to a similar degree
across groups. The superior osteotomy was located 10 mm apical
to the bony crest in all patients and therefore would have similarly
limited the apico- coronal dimension. Interestingly, a cadaveric study
showed that 10 mm of membrane elevation translated to a volume
of 1.81 ± 0.79 cm3 (Uchida, Goto, Katsuki & Akiyoshi, 1998; Uchida,
Goto, Katsuki & Soejima, 1998) which is very similar to what was mea-
sured in our study in both groups. The only dimension not controlled
was the width of the sinus in a bucco- palatal dimension. A previous
study has reported this dimension to be largely consistent and not
influenced greatly by age or gender but influenced by whether the
patient is dentate or edentulous (Uchida, Goto, Katsuki & Akiyoshi,
1998; Uchida, Goto, Katsuki & Soejima, 1998), which was not a dif-
ferentiating factor between the groups in our study. To the authors’
best knowledge, this is the first study to utilize this technique to mea-
sure maxillary sinus graft volume in the context of dental implants. It
is however a utilized technique reported in the orthodontic literature
to measure airway volume and maxillary sinus volume (Darsey, English,
Kau, Ellis & Akyalcin, 2012; Oz, Oz, El & Palomo, 2017; Pangrazio-
Kulbersh, Wine, Haughey, Pajtas & Kaczynski, 2012). By measuring
the volumetric change in the air- filled maxillary sinus cavity, it over-
comes a major disadvantage of traditional techniques such as manual
perimeter tracing of a region of interest (Johansson, Grepe, Wannfors,
Aberg, et al., 2001; Johansson, Grepe, Wannfors, & Hirsch, 2001;
Uchida, Goto, Katsuki & Akiyoshi, 1998; Uchida, Goto, Katsuki &
Soejima, 1998; Wanschitz, Figl, Wagner & Rolf, 2006) or regions grow-
ing segmentation thresholding (Park, Kim, Kim, Kim & Chang, 2010)
by eliminating the need to delineate sinus graft from resident bone
especially after graft consolidation has taken place.
Whilst the use of autogenous bone provides the unique benefits
of osteoinductivity and osteogenic potential, extensive remodelling
may occur when it is used as the sole material for sinus augmenta-
tion (Schlegel, Fichtner, Schultze- Mosgau & Wiltfang, 2003). This has
been demonstrated to lead to undesirable volumetric changes after
grafting in the first year (Schmitt, Moest, Lutz, Neukam & Schlegel,
2014; Schmitt, Karasholi, et al., 2014). Recent animal studies indi-
cate that the combination of autogenous bone and ABBM (Bio- Oss®)
has the advantages of reduced graft resorption yet increased bone-
to- implant contact formation (Jensen, Schou, Svendsen, et al., 2012;
Jensen et al., 2013). Human studies however showed no signifi-
cant differences with respect to new bone formation when directly
Evaluated parameters
Control (ABBM+AB) (n = 30) Number (%)
Test (ABBM- C) (n = 30) Number (%) 95% CI
Group comparison (p value)
Primary stability
29 (96.7) 29 (96.7) −14.2,14.2 1.0
Implant length ≥10mm
28 (93.3) 24 (80.0) −6.4,32.8 .13
Additional vertical augmenta-tion
0 (0) 3 (10.0) −4.0,26.53 .078
ABBM, anorganic bovine bone mineral; AB, autogenous bone; ABBM- C, collagen- stabilized anorganic bovine bone mineral; 95% CI, 95% confidence interval; p, p- value for intergroup comparison after pro-portion testing.
TABLE 6 Implant placement outcomes into augmented maxillary sinuses

12 | ALAYAN ANd IVANOVSKI
comparing trephine samples from sinuses grafted with ABBM and
ABBM + AB (Schmitt, Karasholi, et al., 2014; Schmitt, Moest, et al.,
2014). A recent clinical study showed that percentage fraction of
new bone in samples obtained from maxillary sinuses grafted with
ABBM- C (Bio- Oss Collagen®) are comparable to ABBM + AB (Alayan,
Vaquette, Farah & Ivanovski 2016). To date however, there are no
volumetric studies of the test material (ABBM- C) performance in
sinus augmentation. Even though this study did not assess volumet-
ric changes over time, some volumetric reduction can be assumed to
have taken place during the 6 months of graft consolidation. A re-
view by (Shanbhag, Shanbhag & Stavropoulos, 2014) indicated that
weighted average for volumetric reduction from controlled studies
for composite grafts was 21.88% (±7.38) at 6 months post- grafting.
This volumetric reduction is influenced by a variety of factors includ-
ing the choice of material. Multivariable linear regression analysis in
our study indicated that the choice of material did not correlate with
graft volume 6 months after augmentation and suggests that these
two grating materials exhibit similar volumetric changes over the
short term. Volumetric comparison between the two groups must
be made cautiously as no direct intra- operative measurement of the
graft volume was performed and no immediate postoperative CT
scan was carried out.
Multivariable linear regression analysis indicated that there is a sig-
nificant and positive relationship between the extent of graft contact
with surrounding sinus walls and graft volume. No significant relation-
ship was seen for residual ridge height. This is consistent with other
studies using a range of graft materials, reporting that native bone
height does not have a significant effect on the mean graft height
(Block, Kent, Kallukaran, Thunthy & Weinberg, 1998; Zijderveld,
Schulten, Aartman & ten Bruggenkate, 2009). It has also been shown
that adequate grafted ridge height can be achieved in cases with com-
plete loss of an intact maxillary sinus floor (Cortes, Pinheiro, Cavalcanti,
Arita & Tamimi, 2015). Histological studies have shown a positive im-
pact of increasing number or area of bony walls during healing on graft
outcomes (Alayan, Vaquette, Saifzadeh, Hutmacher & Ivanovski 2016,
Busenlechner et al., 2009; Haas, Donath, Fodinger & Watzek, 1998)
and support the principle ascertained form other models of guided
bone regeneration that surrounding bony walls are an important de-
terminant for de novo bone formation and graft particle incorporation
(Berglundh & Lindhe, 1997; Carmagnola, Adriaens & Berglundh, 2003;
Klinge, Alberius, Isaksson & Jonsson, 1992; Schenk, Buser, Hardwick
& Dahlin, 1994).
This conservative approach to sinus grafting is a safe procedure
that is associated with mild to moderate levels of pain and restric-
tions on oral function and daily activities for 48–72 hr. The use of
both locally harvested autogenous bone combined with ABBM or
collagen- stabilized ABBM solely provided adequate bone volume
for placement of implants of adequate size (8–10 mm) in the major-
ity of cases with no need for further vertical augmentation. The im-
portance of engaging surrounding sinus walls seems to have a more
significant impact on bone graft volume than material selection or
residual ridge height.
ACKNOWLEDGEMENTS
A portion of the Bio- Oss®, Bio- Oss Collagen® and Bio- Gide® uti-
lized in this study were kindly provided by Geistlich AG, Wollhusen,
Switzerland. The authors are grateful to Dr. Dimitrios Vagenas
(Biostatisticians, Institute for Health and Biomedical Innovation,
Queensland University of Technology, Kelvin Grove, Australia) for
his assistance and contribution to the statistical analysis in this pro-
ject. The authors are also grateful to Dr. Raahib Dudhia (RD) (Oral
and Maxillofacial Radiologist, private practice) for his assistance and
contribution to the radiological component of this study.
ORCID
Jamil Alayan http://orcid.org/0000-0003-4191-4776
Saso Ivanovski http://orcid.org/0000-0001-5339-0936
REFERENCES
Alayan, J., Vaquette, C., Farah, C., & Ivanovski, S. (2016). A histomor-phometric assessment of collagen- stabilized anorganic bovine bone mineral in maxillary sinus augmentation - a prospective clin-ical trial. Clinical Oral Implants Research, 27, 850–858. https://doi.org/10.1111/clr.12694
Alayan, J., Vaquette, C., Saifzadeh, S., Hutmacher, D., & Ivanovski, S. (2016). A histomorphometric assessment of collagen- stabilized anorganic bovine bone mineral in maxillary sinus augmentation - a randomized controlled trial in sheep. Clinical Oral Implants Research, 27, 734–743. https://doi.org/10.1111/clr.12652
Arasawa, M., Oda, Y., Kobayashi, T., Uoshima, K., Nishiyama, H., Hoshina, H., & Saito, C. (2012). Evaluation of bone volume changes after sinus floor augmentation with autogenous bone grafts. International Journal of Oral and Maxillofacial Surgery, 41, 853–857. https://doi.org/10.1016/ j.ijom.2012.01.020
Armitage, G. C. (1999). Development of a classification system for peri-odontal diseases and conditions. Annals of Periodontology, 4, 1–6. https://doi.org/10.1902/annals.1999.4.1.1
Avila, G., Wang, H. L., Galindo-Moreno, P., Misch, C. E., Bagramian, R. A., Rudek, I., … Neiva, R. (2010). The influence of the bucco- palatal dis-tance on sinus augmentation outcomes. Journal of Periodontology, 81, 1041–1050. https://doi.org/10.1902/jop.2010.090686
Becker, S. T., Terheyden, H., Steinriede, A., Behrens, E., Springer, I., & Wiltfang, J. (2008). Prospective observation of 41 perforations of the schneiderian membrane during sinus floor elevation. Clinical Oral Implants Research, 19, 1285–1289. https://doi.org/10.1111/j.1600-0501.2008.01612.x
Berglundh, T., & Lindhe, J. (1997). Healing around implants placed in bone defects treated with bio- oss. An experimental study in the dog. Clinical Oral Implants Research, 8, 117–124. https://doi.org/10.1034/j.1600-0501.1997.080206.x
Block, M. S., Kent, J. N., Kallukaran, F. U., Thunthy, K., & Weinberg, R. (1998). Bone maintenance 5 to 10 years after sinus grafting. Journal of Oral and Maxillofacial Surgery, 56, 706–714; discussion 714–705. https://doi.org/10.1016/S0278-2391(98)90801-1
Busenlechner, D., Huber, C. D., Vasak, C., Dobsak, A., Gruber, R., & Watzek, G. (2009). Sinus augmentation analysis revised: The gradient of graft consolidation. Clinical Oral Implants Research, 20, 1078–1083. https://doi.org/10.1111/j.1600-0501.2009.01733.x
Cannizzaro, G., Felice, P., Leone, M., Viola, P., & Esposito, M. (2009). Early loading of implants in the atrophic posterior maxilla: Lateral sinus lift with autogenous bone and bio- oss versus crestal mini sinus lift and

| 13ALAYAN ANd IVANOVSKI
8- mm hydroxyapatite- coated implants. A randomised controlled clini-cal trial. European Journal of Oral Implantology, 2, 25–38.
Carmagnola, D., Adriaens, P., & Berglundh, T. (2003). Healing of human ex-traction sockets filled with bio- oss. Clinical Oral Implants Research, 14, 137–143. https://doi.org/10.1034/j.1600-0501.2003.140201.x
Chiapasco, M., Casentini, P., & Zaniboni, M. (2009). Bone augmenta-tion procedures in implant dentistry. International Journal of Oral and Maxillofacial Implants, 24(Suppl), 237–259.
Clavero, J., & Lundgren, S. (2003). Ramus or chin grafts for maxillary sinus inlay and local onlay augmentation: Comparison of donor site morbid-ity and complications. Clinical Implant Dentistry and Related Research, 5, 154–160. https://doi.org/10.1111/j.1708-8208.2003.tb00197.x
Cordaro, L., Bosshardt, D. D., Palattella, P., Rao, W., Serino, G., & Chiapasco, M. (2008). Maxillary sinus grafting with bio- oss or straumann bone ce-ramic: Histomorphometric results from a randomized controlled multi-center clinical trial. Clinical Oral Implants Research, 19, 796–803. https://doi.org/10.1111/j.1600-0501.2008.01565.x
Cortes, A. R., Pinheiro, L. R., Cavalcanti, M. G., Arita, E. S., & Tamimi, F. (2015). Sinus floor bone failures in maxillary sinus floor augmentation: A case- control study. Clinical Implant Dentistry and Related Research, 17, 335–342. https://doi.org/10.1111/cid.12113
Cricchio, G., & Lundgren, S. (2003). Donor site morbidity in two dif-ferent approaches to anterior iliac crest bone harvesting. Clinical Implant Dentistry and Related Research, 5, 161–169. https://doi.org/10.1111/j.1708-8208.2003.tb00198.x
Darsey, D. M., English, J. D., Kau, C. H., Ellis, R. K., & Akyalcin, S. (2012). Does hyrax expansion therapy affect maxillary sinus volume? A cone- beam computed tomography report. Imaging science in Dentistry, 42, 83–88. https://doi.org/10.5624/isd.2012.42.2.83
Davis, W. H., Martinoff, J. T., & Kaminishi, R. M. (1984). Long- term follow up of transoral rib grafts for mandibular atrophy. Journal of Oral and Maxillofacial Surgery, 42, 606–609. https://doi.org/10.1016/0278-2391(84)90092-2
Del Fabbro, M., Testori, T., Francetti, L., & Weinstein, R. (2004). Systematic review of survival rates for implants placed in the grafted maxillary sinus. International Journal of Periodontics & Restorative Dentistry, 24, 565–577.
Doud Galli, S. K., Lebowitz, R. A., Giacchi, R. J., Glickman, R., & Jacobs, J. B. (2001). Chronic sinusitis complicating sinus lift sur-gery. American Journal of Rhinology, 15, 181–186. https://doi.org/10.2500/105065801779954120
Froum, S. J., Wallace, S. S., Elian, N., Cho, S. C., & Tarnow, D. P. (2006). Comparison of mineralized cancellous bone allograft (puros) and anorganic bovine bone matrix (bio- oss) for sinus augmentation: Histomorphometry at 26 to 32 weeks after grafting. International Journal of Periodontics & Restorative Dentistry, 26, 543–551.
Galindo-Moreno, P., Avila, G., Fernandez-Barbero, J. E., Aguilar, M., Sanchez-Fernandez, E., Cutando, A., & Wang, H. L. (2007). Evaluation of sinus floor elevation using a composite bone graft mixture. Clinical Oral Implants Research, 18, 376–382. https://doi.org/10.1111/j.1600-0501.2007.01337.x
Galindo-Moreno, P., Moreno-Riestra, I., Avila, G., Fernandez-Barbero, J. E., Mesa, F., Aguilar, M., … O’Valle, F. (2010). Histomorphometric com-parison of maxillary pristine bone and composite bone graft biopsies obtained after sinus augmentation. Clinical Oral Implants Research, 21, 122–128. https://doi.org/10.1111/j.1600-0501.2009.01814.x
Galindo-Moreno, P., Moreno-Riestra, I., Avila, G., Padial-Molina, M., Paya, J. A., Wang, H. L., & O’Valle, F. (2011). Effect of anorganic bovine bone to autogenous cortical bone ratio upon bone remodeling patterns fol-lowing maxillary sinus augmentation. Clinical Oral Implants Research, 22, 857–864. https://doi.org/10.1111/j.1600-0501.2010.02073.x
Gultekin, B. A., Cansiz, E., Borahan, O., Mangano, C., Kolerman, R., Mijiritsky, E., & Yalcin, S. (2016). Evaluation of volumetric changes of augmented maxillary sinus with different bone grafting biomaterials. Journal of Craniofacial Surgery, 27, e144–e148. https://doi.org/10.1097/SCS.0000000000002393
Haas, R., Baron, M., Donath, K., Zechner, W., & Watzek, G. (2002). Porous hydroxyapatite for grafting the maxillary sinus: A comparative histomor-phometric study in sheep. International Journal of Oral and Maxillofacial Implants, 17, 337–346.
Haas, R., Donath, K., Fodinger, M., & Watzek, G. (1998). Bovine hydroxy-apatite for maxillary sinus grafting: Comparative histomorphometric findings in sheep. Clinical Oral Implants Research, 9, 107–116. https://doi.org/10.1034/j.1600-0501.1998.090206.x
Hallman, M., Cederlund, A., Lindskog, S., Lundgren, S., & Sennerby, L. (2001). A clinical histologic study of bovine hydroxyapatite in combination with autogenous bone and fibrin glue for maxillary sinus floor augmentation. Results after 6 to 8 months of healing. Clinical Oral Implants Research, 12, 135–143. https://doi.org/10.1034/j.1600-0501.2001.012002135.x
Hallman, M., Mordenfeld, A., & Strandkvist, T. (2005). A retrospective 5- year follow- up study of two different titanium implant surfaces used after interpositional bone grafting for reconstruction of the atrophic edentulous maxilla. Clinical Implant Dentistry and Related Research, 7, 121–126. https://doi.org/10.1111/j.1708-8208.2005.tb00055.x
Hallman, M., Sennerby, L., & Lundgren, S. (2002). A clinical and histologic evaluation of implant integration in the posterior maxilla after sinus floor augmentation with autogenous bone, bovine hydroxyapatite, or a 20:80 mixture. International Journal of Oral and Maxillofacial Implants, 17, 635–643.
Hashem, A. A., Claffey, N. M., & O’Connell, B. (2006). Pain and anxiety fol-lowing the placement of dental implants. International Journal of Oral and Maxillofacial Implants, 21, 943–950.
Hatano, N., Shimizu, Y., & Ooya, K. (2004). A clinical long- term radiographic evaluation of graft height changes after maxillary sinus floor augmen-tation with a 2:1 autogenous bone/xenograft mixture and simulta-neous placement of dental implants. Clinical Oral Implants Research, 15, 339–345. https://doi.org/10.1111/j.1600-0501.2004.00996.x
Hernandez-Alfaro, F., Torradeflot, M. M., & Marti, C. (2008). Prevalence and management of schneiderian membrane perforations during sinus- lift procedures. Clinical Oral Implants Research, 19, 91–98.
Jensen, S. S., Aaboe, M., Pinholt, E. M., Hjorting-Hansen, E., Melsen, F., & Ruyter, I. E. (1996). Tissue reaction and material characteristics of four bone substitutes. International Journal of Oral and Maxillofacial Implants, 11, 55–66.
Jensen, T., Schou, S., Gundersen, H. J., Forman, J. L., Terheyden, H., & Holmstrup, P. (2013). Bone- to- implant contact after maxillary sinus floor augmentation with bio- oss and autogenous bone in different ra-tios in mini pigs. Clinical Oral Implants Research, 24, 635–644. https://doi.org/10.1111/j.1600-0501.2012.02438.x
Jensen, T., Schou, S., Stavropoulos, A., Terheyden, H., & Holmstrup, P. (2012a). Maxillary sinus floor augmentation with bio- oss or bio- oss mixed with autogenous bone as graft in animals: A systematic review. International Journal of Oral and Maxillofacial Surgery, 41, 114–120. https://doi.org/10.1016/j.ijom.2011.08.010
Jensen, T., Schou, S., Stavropoulos, A., Terheyden, H., & Holmstrup, P. (2012b). Maxillary sinus floor augmentation with bio- oss or bio- oss mixed with autogenous bone as graft: A systematic re-view. Clinical Oral Implants Research, 23, 263–273. https://doi.org/10.1111/j.1600-0501.2011.02168.x
Jensen, T., Schou, S., Svendsen, P. A., Forman, J. L., Gundersen, H. J., Terheyden, H., & Holmstrup, P. (2012). Volumetric changes of the graft after maxillary sinus floor augmentation with bio- oss and au-togenous bone in different ratios: A radiographic study in mini-pigs. Clinical Oral Implants Research, 23, 902–910. https://doi.org/10.1111/j.1600-0501.2011.02245.x
Johansson, B., Grepe, A., Wannfors, K., Aberg, P., & Hirsch, J. M. (2001). Volumetry of simulated bone grafts in the edentulous maxilla by computed tomography: An experimental study. Dentomaxillofacial Radiology, 30, 153–156. https://doi.org/10.1038/sj.dmfr.4600600
Johansson, B., Grepe, A., Wannfors, K., & Hirsch, J. M. (2001). A clinical study of changes in the volume of bone grafts in the atrophic maxilla.

14 | ALAYAN ANd IVANOVSKI
Dentomaxillofacial Radiology, 30, 157–161. https://doi.org/10.1038/sj.dmfr.4600601
Kim, Y. K., Yun, P. Y., Kim, S. G., & Lim, S. C. (2009). Analysis of the healing process in sinus bone grafting using various grafting ma-terials. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontics, 107, 204–211. https://doi.org/10.1016/j.tripleo.2008.07.021
Klijn, R. J., Meijer, G. J., Bronkhorst, E. M., & Jansen, J. A. (2010). A meta- analysis of histomorphometric results and graft healing time of various biomaterials compared to autologous bone used as sinus floor aug-mentation material in humans. Tissue Engineering Part B Reviews, 16, 493–507. https://doi.org/10.1089/ten.teb.2010.0035
Klinge, B., Alberius, P., Isaksson, S., & Jonsson, J. (1992). Osseous re-sponse to implanted natural bone mineral and synthetic hydrox-ylapatite ceramic in the repair of experimental skull bone defects. Journal of Oral and Maxillofacial Surgery, 50, 241–249. https://doi.org/10.1016/0278-2391(92)90320-Y
Lang, N. P., & Tonetti, M. S. (2003). Periodontal risk assessment (pra) for pa-tients in supportive periodontal therapy (spt). Oral Health & Preventive Dentistry, 1, 7–16.
Maiorana, C., Redemagni, M., Rabagliati, M., & Salina, S. (2000). Treatment of maxillary ridge resorption by sinus augmentation with iliac cancel-lous bone, anorganic bovine bone, and endosseous implants: A clini-cal and histologic report. International Journal of Oral and Maxillofacial Implants, 15, 873–878.
Nkenke, E., & Stelzle, F. (2009). Clinical outcomes of sinus floor aug-mentation for implant placement using autogenous bone or bone substitutes: A systematic review. Clinical Oral Implants Research, 20(Suppl 4), 124–133. https://doi.org/10.1111/j.1600-0501.2009. 01776.x
Orsini, G., Traini, T., Scarano, A., Degidi, M., Perrotti, V., Piccirilli, M., & Piattelli, A. (2005). Maxillary sinus augmentation with bio- oss particles: A light, scanning, and transmission electron microscopy study in man. Journal of Biomedical Materials Research. Part B, Applied Biomaterials, 74, 448–457. https://doi.org/10.1002/(ISSN)1552-4981
Oz, A. Z., Oz, A. A., El, H., & Palomo, J. M. (2017). Maxillary sinus volume in patients with impacted canines. Angle Orthodontist, 87, 25–32. https://doi.org/10.2319/122915-895.1
Pangrazio-Kulbersh, V., Wine, P., Haughey, M., Pajtas, B., & Kaczynski, R. (2012). Cone beam computed tomography evaluation of changes in the naso- maxillary complex associated with two types of max-illary expanders. Angle Orthodontist, 82, 448–457. https://doi.org/10.2319/072211-464.1
Park, J. W., Kim, N. K., Kim, J. W., Kim, M. J., & Chang, Y. I. (2010). Volumetric, planar, and linear analyses of pharyngeal airway change on computed tomography and cephalometry after mandibular setback surgery. American Journal of Orthodontics and Dentofacial Orthopedics, 138, 292–299. https://doi.org/10.1016/j.ajodo.2009.10.036
Pjetursson, B. E., Tan, W. C., Zwahlen, M., & Lang, N. P. (2008). A sys-tematic review of the success of sinus floor elevation and sur-vival of implants inserted in combination with sinus floor eleva-tion. Journal of Clinical Periodontology, 35, 216–240. https://doi.org/10.1111/j.1600-051X.2008.01272.x
Proussaefs, P., & Lozada, J. (2003). The “loma linda pouch”: A technique for repairing the perforated sinus membrane. International Journal of Periodontics & Restorative Dentistry, 23, 593–597.
Proussaefs, P., Lozada, J., Kim, J., & Rohrer, M. D. (2004). Repair of the perforated sinus membrane with a resorbable collagen membrane: A human study. International Journal of Oral and Maxillofacial Implants, 19, 413–420.
Quiney, R. E., Brimble, E., & Hodge, M. (1990). Maxillary sinusitis from den-tal osseointegrated implants. Journal of Laryngology and Otology, 104, 333–334. https://doi.org/10.1017/S0022215100112630
Rosenfeld, R. M., Andes, D., Bhattacharyya, N., Cheung, D., Eisenberg, S., Ganiats, T. G., … Witsell, D. L. (2007). Clinical practice guideline: Adult
sinusitis. Otolaryngology - Head and Neck Surgery, 137, S1–S31. https://doi.org/10.1016/j.otohns.2007.06.726
Sbordone, C., Toti, P., Guidetti, F., Califano, L., Bufo, P., & Sbordone, L. (2013). Volume changes of autogenous bone after sinus lifting and grafting procedures: A 6- year computerized tomographic follow- up. Journal of Cranio- Maxillo- Facial Surgery, 41, 235–241. https://doi.org/10.1016/j.jcms.2012.09.007
Scheerlinck, L. M., Muradin, M. S., van der Bilt, A., Meijer, G. J., Koole, R., & Van Cann, E. M. (2013). Donor site complications in bone graft-ing: Comparison of iliac crest, calvarial, and mandibular ramus bone. International Journal of Oral and Maxillofacial Implants, 28, 222–227. https://doi.org/10.11607/jomi.2603
Schenk, R. K., Buser, D., Hardwick, W. R., & Dahlin, C. (1994). Healing pattern of bone regeneration in membrane- protected defects: A his-tologic study in the canine mandible. International Journal of Oral and Maxillofacial Implants, 9, 13–29.
Schlegel, K. A., Fichtner, G., Schultze-Mosgau, S., & Wiltfang, J. (2003). Histologic findings in sinus augmentation with autogenous bone chips versus a bovine bone substitute. International Journal of Oral and Maxillofacial Implants, 18, 53–58.
Schmitt, C. M., Doering, H., Schmidt, T., Lutz, R., Neukam, F. W., & Schlegel, K. A. (2013). Histological results after maxillary sinus augmentation with straumann(r) boneceramic, bio- oss(r), puros(r), and autologous bone. A randomized controlled clini-cal trial. Clinical Oral Implants Research, 24, 576–585. https://doi.org/10.1111/j.1600-0501.2012.02431.x
Schmitt, C., Karasholi, T., Lutz, R., Wiltfang, J., Neukam, F. W., & Schlegel, K. A. (2014). Long- term changes in graft height after maxillary sinus aug-mentation, onlay bone grafting, and combination of both techniques: A long- term retrospective cohort study. Clinical Oral Implants Research, 25, e38–e46. https://doi.org/10.1111/clr.12045
Schmitt, C. M., Moest, T., Lutz, R., Neukam, F. W., & Schlegel, K. A. (2014). Anorganic bovine bone (abb) vs Autologous bone (ab) plus abb in maxillary sinus grafting. A prospective non- randomized clini-cal and histomorphometrical trial. Clinical Oral Implants Research, 26, 1043–1050.
Seymour, R. A., Charlton, J. E., & Phillips, M. E. (1983). An evaluation of dental pain using visual analogue scales and the mcgill pain question-naire. Journal of Oral and Maxillofacial Surgery, 41, 643–648. https://doi.org/10.1016/0278-2391(83)90017-4
Shanbhag, S., Shanbhag, V., & Stavropoulos, A. (2014). Volume changes of maxillary sinus augmentations over time: A systematic review. International Journal of Oral and Maxillofacial Implants, 29, 881–892. https://doi.org/10.11607/jomi.3472
Shugars, D. A., Benson, K., White, R. P. Jr, Simpson, K. N., & Bader, J. D. (1996). Developing a measure of patient perceptions of short- term outcomes of third molar surgery. Journal of Oral and Maxillofacial Surgery, 54, 1402–1408. https://doi.org/10.1016/S0278-2391(96)90253-0
Tan, W. C., Krishnaswamy, G., Ong, M. M., & Lang, N. P. (2014). Patient- reported outcome measures after routine periodontal and implant surgical procedures. Journal of Clinical Periodontology, 41, 618–624. https://doi.org/10.1111/jcpe.12248
Timmenga, N. M., Raghoebar, G. M., van Weissenbruch, R., & Vissink, A. (2001). Maxillary sinusitis after augmentation of the maxillary sinus floor: A report of 2 cases. Journal of Oral and Maxillofacial Surgery, 59, 200–204. https://doi.org/10.1053/joms.2001.20494
Uchida, Y., Goto, M., Katsuki, T., & Akiyoshi, T. (1998). A cadaveric study of maxillary sinus size as an aid in bone grafting of the maxillary sinus floor. Journal of Oral and Maxillofacial Surgery, 56, 1158–1163. https://doi.org/10.1016/S0278-2391(98)90761-3
Uchida, Y., Goto, M., Katsuki, T., & Soejima, Y. (1998). Measurement of maxillary sinus volume using computerized tomographic im-ages. International Journal of Oral and Maxillofacial Implants, 13, 811–818.

| 15ALAYAN ANd IVANOVSKI
de Vicente, J. C., Hernandez-Vallejo, G., Brana-Abascal, P., & Pena, I. (2010). Maxillary sinus augmentation with autologous bone harvested from the lateral maxillary wall combined with bovine- derived hydroxyapatite: Clinical and histologic observa-tions. Clinical Oral Implants Research, 21, 430–438. https://doi.org/10.1111/j.1600-0501.2009.01877.x
Wanschitz, F., Figl, M., Wagner, A., & Rolf, E. (2006). Measurement of vol-ume changes after sinus floor augmentation with a phycogenic hy-droxyapatite. International Journal of Oral and Maxillofacial Implants, 21, 433–438.
Wiltfang, J., Schultze-Mosgau, S., Merten, H. A., Kessler, P., Ludwig, A., & Engelke, W. (2000). Endoscopic and ultrasonographic evaluation of the maxillary sinus after combined sinus floor augmentation and implant insertion. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontics, 89, 288–291. https://doi.org/10.1016/S1079-2104(00)70090-4
Wiltfang, J., Schultze-Mosgau, S., Nkenke, E., Thorwarth, M., Neukam, F. W., & Schlegel, K. A. (2005). Onlay augmentation versus sinuslift procedure in the treatment of the severely resorbed maxilla: A 5- year comparative longitudinal study. International Journal of Oral and Maxillofacial Surgery, 34, 885–889. https://doi.org/10.1016/j.ijom.2005.04.026
Zijderveld, S. A., Schulten, E. A., Aartman, I. H., & ten Bruggenkate, C. M. (2009). Long- term changes in graft height after maxillary sinus floor el-evation with different grafting materials: Radiographic evaluation with a minimum follow- up of 4.5 years. Clinical Oral Implants Research, 20, 691–700. https://doi.org/10.1111/j.1600-0501.2009.01697.x
SUPPORTING INFORMATION
Additional Supporting Information may be found online in the sup-
porting information tab for this article.
How to cite this article: Alayan J, Ivanovski S. A prospective
controlled trial comparing xenograft/autogenous bone and
collagen- stabilized xenograft for maxillary sinus
augmentation—Complications, patient- reported outcomes and
volumetric analysis. Clin Oral Impl Res. 2017;00:1–15.
https://doi.org/10.1111/clr.13107

119
Chapter 6: A prospective controlled trial comparing xenograft/autogenous
bone and collagen-stabilized xenograft for maxillary sinus augmentation –
biological and technical implant outcomes.

120
STATEMENT OF CONTRIBUTION TO CO-AUTHORED PUBLISHED
PAPER
This chapter includes a co-authored paper. The bibliographic details of the
co-authored paper, including all authors, are:
Alayan J, Ivanovski S. (2018) A prospective controlled trial comparing
xenograft/autogenous bone and collagen-stabilized xenograft for maxillary sinus
augmentation – biological and technical implant outcomes. Clinical Oral Implants
Research (submitted).
My contribution to the paper involved:
Design of the project, the provision of the data, the preliminary analysis and
categorization of the data into a usable format, the provision of direction on the
scope and structure of the analysis, the interpretation of results and drafting of the
article.
04th May 2018
Jamil Alayan
(Countersigned) 16th May 2018
Corresponding author of paper: Jamil Alayan
(Countersigned) ___________________________ 16th May 2018
Supervisor: Stephen Hamlet

119
A Prospective Controlled Trial comparing Xenograft /
Autogenous Bone and Collagen-stabilized Xenograft for
Maxillary Sinus Augmentation – Biological and Technical
Implant Outcomes
Jamil Alayan, Saso Ivanovski
Authors’ affiliations:
Jamil Alayan & Saso Ivanovski, School of Dentistry and Oral Health, Centre for
Medicine and Oral Health, Griffith University, Southport, Australia.
Corresponding author:
Jamil Alayan
School of Dentistry and Oral Health, Centre for Medicine and Oral Health
Gold Coast Campus Griffith University
Southport, QLD 4215
Australia
Tel: +61 75 678 0741
Fax: +61 75 678 0708
Email: [email protected]
Keywords: Sinus floor elevation, guided bone regeneration, anorganic bovine bone,
Bio-Oss Collagen, Bio-Oss, bone substitute, clinical trial, dental implants.
Running title: Collagen-Stabilized Xenograft in MSA - Implant Outcomes

120
Abstract
Objective: Report on biological and technical outcomes of implant supported
restorations placed into previously augmented maxillary sinuses (MSA) using
anorganic bovine bone (ABBM) + autogenous bone (AB) (control group) or collagen
stabilized ABBM (test group) after 1 year of function.
Materials & Methods: A single implant was placed 6 months (T0) after MSA in 27
control and 26 test patients. Fixed restorations were delivered 12 weeks later (T1 -
baseline) and reviewed 12 months after function (T2). Outcomes measured included
implant survival, marginal bone levels (DIB) and their changes, periodontal
parameters and incidence of biological and technical complications.
Results: A survival rate of 100% was reported. No significant inter-group differences
were noted for all parameters. Radiographic assessment 12 months after loading
revealed a mean (± SD) marginal bone level (DIB) of 0.60mm (0.33) and 0.58mm
(0.40) from the implant shoulder in the control and test group respectively. After 12
months of loading mean DIB loss of 0.32mm (± 0.24) and 0.35mm (±0.23) were
noted in the control and test group respectively. Mucositis (≥1 site BOP) was
diagnosed in 62.9% of control & 69.23% of test patients. Peri-implantitis was not
diagnosed in any patient. Screw retention and single crowns predominated. Technical
complications mostly comprised of ceramic veneer chipping and was noted in 7.4% of
control and 11.54% of test patients.
Conclusion: Based on a short observation period, implant reconstruction of the
partially edentulous posterior maxilla after MSA using ABBM + autogenous bone or
collagen stabilized ABBM led stable marginal bone levels, high implant survival and
low rates of technical complications.

121
Introduction Maxillary sinus floor augmentation using the lateral wall approach (MSA) is well
established as a surgical technique for treating severe reduction of bone height due to
sinus pneumatization, in order to allow successful implant rehabilitation of the
posterior maxilla with high implant survival rates (Del Fabbro, et al. 2004, Chiapasco,
et al. 2009). When using a conservative approach and locally harvested AB, this
technique is also a safe procedure that is associated with mild to moderate pain and
restriction of daily activities for 2-3 days (Alayan & Ivanovski 2018).
The composite graft of anorganic bovine bone mineral (ABBM) and autogenous bone
(AB) is well documented in multiple studies of MSA (Maiorana, et al. 2000, Hallman,
et al. 2001, Hatano, et al. 2004, Galindo-Moreno, et al. 2007, Cannizzaro, et al. 2009,
Kim, et al. 2009, Avila, et al. 2010, de Vicente, et al. 2010, Galindo-Moreno, et al.
2010, Galindo-Moreno, et al. 2011). ABBM is also available in a block form that is
stabilized in 10% porcine type-1 collagen matrix (ABBM-C). The contained nature of
this material has been shown to have clinical utility when perforations of the sinus
membrane occur during MSA, as it eliminates the risk of particulate biomaterial
migrating into the maxillary sinus cavity proper and obstructing the osteomeatal
complex (Alayan & Ivanovski 2018). This altered formulation of ABBM has been
shown to have comparable histomorphometric and volumetric parameters when
compared to the composite graft (ABBM+AB) in MSA (Alayan, et al. 2016, Alayan,
et al. 2016, Alayan & Ivanovski 2018).
Improved implant survival rates have been shown when using rough implant surfaces
with a median survival rate of 100% (88-100%) when compared to 89% (61.2 –
100%) using machined implant surfaces (Jensen & Terheyden 2009). This is likely to
be due to histologically documented effects (Abrahamsson, et al. 2004) of improved
bone-to-implant contact (Buser, et al. 1998, Cochran, et al. 1998). Implant surface has
also been shown to affect the local tissue composition around implants placed into
augmented maxillary sinuses such as the area fraction of woven and lamellar bone in
a pre-clinical model (Alayan, et al. 2017). The SLA surface is a moderately rough
surface which is widely utilized clinically and documented in the literature in various
clinical scenarios (Bornstein, et al. 2005, Roccuzzo, et al. 2008, Buser, et al. 2012,

122
Thoma, et al. 2014). A 100% survival rate has been reported in a clinical study using
one piece SLA implants in MSA at 12 and 60 months after implant placement
(Bornstein, et al. 2008).
Whilst survival data is available, there is a paucity of studies with well defined
success criteria reporting on implants placed into sinuses grafted with the composite
material (ABBM+AB 1:1) (Galindo-Moreno, et al. 2015) especially in terms of
clinical outcomes of the implant supported restorations and their technical
complications. Furthermore, there are no studies reporting on outcomes of implants
placed into augmented maxillary sinuses using ABBM-C.
As such, the aim of this controlled clinical trial was to test whether implant supported
restorations have similar biological and technical outcomes when placed into
previously augmented maxillary sinuses using stabilized ABBM (ABBM-C), as used
in defined clinical scenarios (i.e. reduced local autogenous bone availability and/or
sinus membrane perforation), when compared to those placed into a composite graft
of ABBM and autogenous bone (ABBM+AB).
Materials & Methods Ethics and Consent
The University of Queensland School of Dentistry Dental Sciences Research Ethics
Committee provided ethical approval for this equivalence non-randomized controlled
clinical trial (Project Number: 1010). The project complies with the provisions
contained in the National Statement on Ethical Conduct in Research Involving
Humans and complies with the regulations governing experimentation on humans.
The CONSORT (Consolidated Standards of Reporting Trials) checklist was used in
the preparation of this manuscript.
Study Settings & Participants Patients were prospectively recruited from the School of Dentistry at the University of
Queensland and from a specialist private practice (Brisbane, Australia) between July
2010 to December 2015. Those that met the inclusion criteria then underwent the
informed consent process. All patients were referred specifically for replacement of

123
teeth with implant-supported restorations. Recruitment continued until 30 patients
were allocated into the control and test groups.
Patients were considered eligible for the study if they fulfilled the following criteria:
• Individuals were at least 18 years of age, medically healthy or with mild
controlled systemic disease, able to undergo oral surgical procedures under local
or general anaesthesia (ASA I and II; American Society of Anesthesiologists,
Schaumburg, Illinois, USA).
• Must present with a bone deficiency in the maxillary sinus region, which
necessitates sinus floor augmentation
• If bilateral sinus augmentation was required, only one sinus was randomly
selected and used for the purposes of this study.
• Residual alveolar bone height of the edentulous maxilla below the floor of the
maxillary sinus ≤4.5 mm and ≥ 1 mm (measured at the mid-point of the
edentulous space where both the coronal and sagittal planes intersect) and residual
alveolar bone width of ≥6mm.
• Teeth at the surgical site which required removal were extracted a minimum of 12
weeks prior to sinus floor elevation
• Patients with a history of periodontal disease as assessed by specialist
Periodontists (JA & SI) and according to the criteria of Armitage (Armitage 1999)
were treated and deemed to be stable prior to sinus augmentation surgery.
Stability was defined as having a full mouth bleeding score of ≤20% and no sites
of residual periodontal probing depth ≥5mm (Lang & Tonetti 2003).
Patients were considered ineligible if any of the following factors were evident:
• Pregnancy at the time of recruitment
• Physical handicaps that would interfere with the ability to perform adequate oral
hygiene
• Alcoholism or chronic drug abuse
• Patients who smoke more than 10 cigarettes per day
• Medications which interferes with bone formation
• Mucosal diseases such as Lichen Planus
• History of local radiation therapy
• Severe bruxism or clenching habits

124
• Signs and symptoms consistent with acute maxillary sinusitis
• Significant soft tissue thickening or sinus opacification in the sinus of interest.
• Previous GBR (bone graft) or dental implant treatment in the posterior segments
of the maxilla
• Benign or malignant tumours of the maxillary sinus
• Pathological conditions that severely impact mucociliary clearance including;
Chronic sinusitis, Primary Ciliary Dyskinesia or Cystic Fibrosis.
Sample size
The patients in this study were part of a larger study designed to have sufficient
statistical power to detect differences in maxillary sinus graft volume between the two
groups (Alayan & Ivanovski 2018). Nonetheless, an analysis was performed for this
equivalence study to ensure adequate power to perform a comparison on marginal
bone level changes (G*Power 3.1.9, Faul, F., Erdfelder, E., Lang, A.-G., & Bychnner,
A, Germany). This analysis indicated that 25 individuals in each group (total study
population = 50) would be needed to achieve a power of 0.8 with a probability of 0.05
for type 1 (alpha) errors, assuming a standard deviation of 0.89mm, a true difference
of zero and a zone of clinical equivalence of ± 0.74mm (Galindo-Moreno, et al.
2014).
Participant allocation and study design
Allocation of each patient to either the control or test group was based on two intra-
operative parameters; the presence of Schneiderian membrane perforation and
availability of adequate autogenous bone in the vicinity of the surgical site. ABBM-C
(test) was selected if sinus membrane perforations occurred or if there was
insufficient autogenous bone available for harvesting in the vicinity of the buccal
antrostomy. ABBM + AB (control) was alternatively used if the Schneiderian
membrane remained intact and if there was sufficient autogenous bone that could be
harvested from the buccal wall of the maxilla.
The same clinician (JA) performed all of the surgical procedures. While clinician
blinding was not possible at the time of the augmentation surgery or implant
placement, it was possible during the measurement and analysis stages of this project.

125
Bone graft materials and dental implants
• Control group – MSA with small diameter particles (0.25 – 1.0 mm) of
deproteinised bovine bone mineral (Bio-Oss®, Geistlich AG, Wollhusen,
Switzerland) + autogenous bone (ABBM+AB) in a 1:1 ratio, as determined by
using a standardized 2cc bone collecting chamber.
• Test group – MSA with 250mg blocks of deproteinised bovine bone mineral +
collagen (ABBM-C) (Bio-Oss Collagen®, Geistlich AG, Wollhusen, Switzerland).
All patients received a single (Straumann, Institut Straumann AG, Basel, Switzerland)
one piece dental implant. The implant had a standard micro-roughened sandblasted
and acid-etched (SLA) surface. The dimensions of the implants were chosen
according to the specific site characteristics.
Primary and Secondary Outcomes
Primary end point:
• Interproximal marginal bone levels (DIB) up to a period of 1 year after delivery
of prosthesis
Secondary end points:
• Peri-implant tissue health assessment (Periodontal probing depth, gingival
recession, bleeding on probing, suppuration, plaque index) • Implant supported restoration assessment (technical outcomes) • Implant and restoration survival
Clinical Interventions / Surgical Procedures
Maxillary sinus floor elevation and grafting
All patients received the same surgical technique consisting of sinus floor elevation
via a lateral wall (modified Caldwell-Luc) approach as previously described (Alayan
& Ivanovski 2018).
Dental implant placement
A single dental implant was placed 6 months later as previously described (Alayan &
Ivanovski 2018).

126
Implant supported restorations
Abutment connection was carried out as per the manufacturer’s recommendations at
35Ncm, 3 months after implant placement by a small group of independent restorative
clinicians. No restrictions were made regarding the prosthesis design (single or multi-
unit) material type or type of retention. The baseline assessment was carried out after
insertion of restoration.
Follow Up Evaluations & Outcomes Measurements
Radiographic follow up & evaluation
Marginal bone levels were measured on intra-oral radiographs taken using a long cone
paralleling technique and a paralleling device. An exposure of 0.12s (70kV, 7mA,
Carestream CS2200) was used with a digital sensor (SOPIX2 SOPRO sensor, Acteon,
La Ciotat, France) with a pixel size of 20 x 20µm to acquire the radiographic images.
The digital images were imported into a free and open source code software program
(Horos v2.2.0 sponsored by Purview, Annapolis, MD USA www.horosproject.org).
The distance from the implant shoulder at the implant-abutment connection to the most
coronal bone-to-implant contact (DIB) was measured at the mesial and distal aspects
of each implant and expressed in millimeters (Roccuzzo, et al. 2001, Bornstein, et al.
2005). These linear measurements were calibrated to account for any distortion and
magnification by using the known inter-thread distance of the utilized implant
(1.25mm). The known distance of the smooth surface collar of the implant of 1.8mm
was subtracted to give the distance from the rough-smooth junction to DIB. All
radiographic measurements were recorded at placement (DIB0), at delivery of the
implant supported restoration (baseline) (DIB1) and then at 12 months post-placement
of the restoration (DIB2). The mean change per implant was then calculated between
T0 and T1 and then from T1 to T2 . All measurements were made by a single blinded
experienced periodontist (JA) after the radiographs were allocated an identification
number.
Clinical follow up & evaluation
The following parameters were assessed within 1 month after the placement of the
restoration (T1) (baseline) and then repeated 12 months post-placement of the
restoration (T2):

127
• Assessment of peri-implant tissue – Periodontal probing depth (PPD) and measures
of inflammation were recorded. PPDs were measured at x6 sites per implant using
a manual periodontal probe (UNC 15, Hu Friedy, Chicago, U.S), with gentle force
and rounded off to the nearest millimeter. In addition, the same probe was used to
locate the mucosal margin (DIM) using the occlusal surface of the implant-
supported restoration as a fixed landmark. Recession was calculated as the change
in DIM between T1 and T2. A mean value was then calculated for each implant-
supported restoration. The presence or absence of sites with bleeding on probing
(BOP) and suppuration were assessed dichotomously (0, no bleeding / suppuration;
1, bleeding / suppuration) at six sites per implant supported restoration (Mombelli
& Lang 1994). Similarly, the presence or absence of plaque at the peri-implant
mucosal margin was recorded at six sites per implant supported restoration
dichotomously.
• Implant-supported restorations were assessed to determine if any of the following
features were evident or had taken place: implant fracture, loss of superstructure,
abutment fracture, framework or veneer fracture, abutment screw fracture,
abutment or abutment screw loosening, restoration screw loosening, loss of
retention (luting cement), veneer chipping and loss of access hole restoration
(Pjetursson, et al. 2012).
Definitions & Success Criteria
• % Survival – percentage of implants and restorations in-vivo and in function at the
time of assessment.
• Biological complications: included implants that exhibited signs of peri-implant
mucositis or peri-implantitis. Peri-implant mucositis was defined as any bleeding
on gentle probing without loss of supporting bone (Lang, et al. 2011). Peri-
implantitis was defined as bleeding on probing and / or suppuration with or
without concomitant deepening of peri-implant pockets, accompanied by marginal
bone level changes of greater than 1.0mm after baseline (Sanz, et al. 2012) (Lang,
et al. 2011). Furthermore, any treatment performed on the implant that was not
part of routine maintenance was by default classified as a complication.
• Technical complications (Pjetursson, et al. 2012): These were divided into (1)
major: such as implant fracture, loss of super-structure, (2) medium: such as

128
abutment fracture, veneer or framework fracture and (3) minor: abutment and
screw loosening, loss of screw hole sealing, veneer chipping (requiring polishing)
and occlusal adjustments. In addition, any treatment performed on the restoration
that was not part of routine maintenance was by default classified as a
complication. If the implant was incorporated into an FPD, then any technical
complication affecting any part of the FPD was included in the analysis.
Statistics All data was analyzed using IBM SPSS Statistics for Windows version 25.0 (IBM
Corporation 2017©, Armonk, NY, U.S). Descriptive statistics such as mean (±
standard deviation) in addition to median (inter-quartile range) and range (minimum,
maximum) as well as absolute and relative frequencies were provided for baseline and
outcome parameters. Inter-group comparisons for continuous variables (DIB, PPD,
DIM) were performed using an independent t-test after being assessed for normality.
Homogeneity of variance was assessed using the Levene’s test. Mean difference,
confidence intervals and P values were adjusted if equal variance could not be
assumed. A paired t-test was used for intra-group time comparisons. Comparisons
using count data (BOP and PI) were assessed using a GEE with a Poisson regression
model. Proportions were analyzed using a Chi square or Fisher’s Exact test. A multi-
variable linear regression model was used to assess the impact of treatment group,
initial implant position (depth), residual ridge height, periodontal status, age and
gender on ABL1 and ABL2. The null hypothesis was taken as non-equivalence in
marginal alveolar bone loss, proportions of complications, and peri-implant
parameters around dental implants placed into augmented maxillary sinuses using
ABBM (Bio-Oss®) + AB or blocks of ABBM-C (Bio-Oss Collagen®) alone. A P ≤
0.05 was considered to represent statistically significant differences.
Results Study population & Survival (table 1)
Outcomes related to the maxillary sinus augmentation and implant placement stages
of treatment have been previously published (Alayan & Ivanovski 2018). Originally
sixty (n = 60) patients were enrolled into this study and underwent unilateral sinus
augmentation followed by single implant placement (n = 30 were allocated into each

129
group) 6 months later. A total of 7 patients (3 control, 4 test group) were lost to follow
up as they did not return for their 1 year follow up assessment and were not
contactable. Analysis was performed on 53 patients (control = 27, test = 26). There
were no significant differences between groups in terms of age, gender, ratio or
number of smokers. Patients with chronic periodontitis (control = 3, test = 7 patients)
remained stable and continued to attend for supportive maintenance program (Lang &
Tonetti 2003) at the same private practice (Brisbane, Australia). There were no
significant inter-group differences in the number of weeks between insertion of
restoration and when baseline assessment actually took place (control = 9.29 ± 3.8
weeks) (test = 10.81 ± 2.7). Similarly, there were no significant inter-group
differences in the number of weeks between baseline assessment and the 12 month
assessment (control = 58.07 ± 19.61 weeks) (test = 59.73 ± 13.25). All 53 patients
presented with functional implant supported restorations resulting in a 100% survival
rate for both groups. Ten millimeter long implants were used in 92% of control
patients and 88% of test patients. The dimensions of all implants are shown in table 2.
Radiographic Outcomes
Marginal bone level values are shown table 3. No significant inter-group differences
(control vs. test) for DIB0 (marginal bone level at implant placement), at DIB1
(marginal bone level at delivery of the implant supported restoration) (baseline) or
DIB2 (marginal bone level after 12 months of function) were reported (P>0.05) (table
4). Intra-group comparisons indicated that these dimensions significantly increased at
baseline when compared to implant placement (DIB1 > DIB0) and at the 1 year
follow up when compared to implant placement (DIB2 > DIB1) in both the control
and test groups (P < 0.0001) (table 4).
When considering the change of marginal bone levels over time, there were no
significant inter-group differences (control vs. test) (P>0.05) (table 4). Intra-group
comparisons indicated a significantly greater ABL1 in both the control (P = 0.001)
and test groups (P = 0.001) when compared to ABL2. Multi-variable linear
regression analysis (table 5a) indicated that initial implant position (depth) was a
significant explanatory variable (P<0.0001) for ABL1 but that treatment group,
periodontal status, gender, age and residual ridge height were not significant

130
explanatory variables (P>0.05). None of these variables were significant explanatory
variables for ABL2 (P>0.05) (table 5b). Table 6 displays the frequency (no. of
implants / patients) distribution of marginal bone level changes (ABL) between T0-to-
T1 and between T1-to-T2 for both groups.
Biological Outcomes
All peri-implant parameters (PI, BOP, PPD, DIM) were similar for both groups and at
both time points (table 7). No suppuration was recorded in any site at either time point
for both groups. PI and BOP were low in both groups and at both T1 and T2.
Treatment group (control vs. test) was not a significant predictor for PI (P = 0.56) or
BOP (P = 0.63). Whilst both parameters increased at T2 (vs. T1) in both groups, this
did not reach a level of statistical significance PI (P = 0.07) or BOP (P = 0.09). There
were no significant inter-group differences in PPD at T1 (P = 0.45) (mean difference
0.13, 95%CI -0.49, 0.22) or at T2 (P = 0.81) (mean difference -0.05 & 95%CI -0.35,
0.45). Intra-group comparisons of PPD indicated no significant changes between T1
and T2 in both control (P = 0.39) (mean difference 0.1, 95%CI -0.13, 0.33) and test
groups (P = 0.49) (mean difference -0.85, 95%CI -0.33, 0.16). There were no
significant inter-group differences of DIM at T1 (P = 0.17) (mean difference -0.7,
95%CI -1.69, 0.30) or at T2 (P = 0.13) (mean difference -0.84, 95%CI -1.94, 0.26).
Intra-group comparisons of DIM indicated no significant changes between T1 and T2
in both the control (P = 0.51) (mean difference 0.38, 95%CI -1.51, 0.76) and test
groups (P = 0.28) (mean difference 0.52, 95%CI -1.47, 0.43). Using DIM
measurements to calculate gingival recession, there was minimal gingival recession at
T2 in both control (mean 0.40 ± 0.36) and test groups (mean 0.51± 0.61) with no
significant difference between treatment groups (P = 0.45) (mean difference 0.11,
95%CI -0.39, 0.17). Similar proportion of peri-implant mucositis was noted in both
groups with 62.9% (17/27 patients) of control implants and in 69.23% (18/26
patients) of test implants. There was no statistically significant association between
treatment group and proportion of peri-implant mucositis (P = 0.63). Peri-implantitis
was not diagnosed in any of the patients in this study.
Technical Outcomes

131
All patients were successfully restored without delay 3 months after implant
placement using metal-ceramic restorations. Table 8 summarizes type of restoration
utilized and the method of retention. The majority of patients were restored with a
single crown restoration (SC) in both treatment groups (67% control group and 77%
test group). Fewer number of implants were incorporated as part of a fixed partial
denture (FPD) (33% control group and 23% test group). The majority of FPDs were 3
units without cantilever extension with the distal implant placed into the augmented
maxillary sinus. A small of number of FPDs had a short mesial cantilevered
extension. Screw retention was the predominant type of retention utilized in both
treatment groups (78% control group and 77% test group). There was no statistically
significant association between type of restoration (P = 0.41) or type of retention
utilized (P = 0.94) and treatment group. Technical complications were noted in 7.4%
of patients in the control group (2/27 patients) and 11.54% in the test group (3/26
patients). A full description of these complications is shown in table 9. There was no
statistically significant association between proportion of complications and treatment
group (P = 0.67). All of these minor complications were successfully repaired by the
restoring clinicians.
Discussion
The aim of this equivalence trial was to report on the biological and technical
outcomes of implant supported restorations placed into augmented maxillary sinuses
using a conservative approach and locally harvested autogenous bone in combination
with Bio-Oss® (ABBM) versus Bio-Oss Collagen® (ABBM-C) alone. Both groups
were comparable in terms of age, gender ratio, rates of periodontal disease and
implant dimensions. This study revealed a 100% implant survival during the first year
of function for both groups, which is consistent with those reported in a number of
systematic reviews (Pjetursson, et al. 2008, Chiapasco, et al. 2009, Jensen &
Terheyden 2009, Nkenke & Stelzle 2009, Rickert, et al. 2012).
All patients in the present study were successfully restored without delay 3 months
after implant placement, suggesting that this is a sufficient time interval for
osseointegration to occur when using a moderately rough (SLA) implant surface using
both grafting materials. Systematic reviews report a mean loading time between 5 to

132
6.5 months (Chiapasco, et al. 2009, Jensen & Terheyden 2009) irrespective of the
biomaterial used or implant surface. The absence of autogenous bone from the
ABBM-C group did not lead to delays in restoration or decrease in survival rates even
though it has been shown to exhibit delayed maturity as indicated by a lower
proportion of lamellar bone (Alayan, et al. 2016). .
The one-piece implant system utilized in this study is designed to be placed with the
rough-smooth junction at the bone crest, leaving the implant collar in the trans-
mucosal region. Furthermore, the marginal bone remodeling process begins
immediately following placement of these implants and is influenced by the location
of the rough-smooth junction (Hammerle, et al. 1996, Hermann, et al. 2000, Hermann,
et al. 2001, Hermann, et al. 2001). These characteristics were also observed in this
study with greater initial marginal alveolar bone loss taking place with increasing sub-
crestal location of the rough-smooth junction. Initial implant position (depth)
however did not correlate with marginal bone level changes after 12 months of
functional load. This is in contrast to a previous clinical study (Hammerle, et al. 1996)
which reported greater marginal bone loss beyond initial remodeling in one piece
implants placed with a rough-smooth junction 1mm sub-crestal. Variations in in the
clinical model and the contrasting implant surfaces (TPS vs. SLA) may explain this
discrepancy. The vast majority of implants in the present study were placed with a
rough-smooth junction ranging from at the crest to 1.5mm below the bone crest.
Withstanding the short observation period, this suggests that the risk of excessive
marginal bone loss after initial remodeling due to mild sub-crestal placement of the
rough-smooth junction, is no different from crestal positioning in a group of healthy
compliant patients.
Both treatment groups exhibited stable and similar marginal bone level changes at the
1 year follow up. Significantly less change was seen in marginal bone levels during
functional load in both groups when compared to initial remodeling. This change may
represent bone loss due to exposure to bacterial load (Lang, et al. 2011) and
masticatory forces (Marcelis, et al. 2012) rather than physiological adaptation to
implant placement and biologic width formation. The marginal bone level changes
during the functional loading period in our study compare closely with a recent study

133
(Thoma, et al. 2014) that reported a mean marginal loss after 1 year of function of
0.25mm (±0.35) using the identical dental implant and radiographic protocol. This
study however placed implants in a variety of clinical scenarios with only a small
fraction of implants placed into MSA. Greater changes in marginal bone levels after
12 months of functional load were seen in the present study however than those
reported by Schincaglia et al. (Schincaglia, et al. 2015), who compared long implants
and MSA with short implants without MSA. They reported a mean loss of 0.16mm
(±0.62) in the grafted group. This variation between studies may have been caused by
differences in placement protocol and implant surface / design. Interestingly, whilst
the mean change in marginal bone level is smaller than the present study, the
variations (SD) are greater with 4 patients exhibiting marginal bone loss ranging from
1.0-2.5mm when compared to none in the present study.
Both treatment groups predominantly exhibited signs consistent with peri-implant
health and represent a compliant patient population who attend for maintenance and
performed adequate plaque control. Similar findings were reported in a recent study
on clinical parameters for implants placed into augmented maxillary sinuses after 12
months of functional load (Schincaglia, et al. 2015). They reported a mean PPD of 2.3
(±1.4)mm with 38% of the implants in the augmented sinus group exhibiting BOP.
The present study however diagnosed peri-implant mucositis in the majority of
patients in both treatment groups, when defined as any site of BOP without loss of
supporting bone. This was mostly due to the presence of one or two sites of BOP out
of 6 sites probed. The success criteria utilized in this study are based on the consensus
reports published after the 8th European Workshop on Periodontology (Pjetursson, et
al. 2012, Sanz, et al. 2012). It has been noted that variations in case definitions for
peri-implant disease (Derks & Tomasi 2015) leads to significant variations in reported
success rates (Karoussis, et al. 2003). Whilst the absence of BOP has a high negative
predictive value for disease progression (Jepsen, et al. 1996), the positive predictive
value of BOP becomes a useful parameter only once it reaches a frequency of ≥50%
at a site level (Luterbacher, et al. 2000). The case definition for mucositis also relies
on gentle probing (Lang, et al. 2011) and therefore probing force cannot be
discounted as a source of error in this study especially in the presence of low plaque
scores. Peri-implantitis was not diagnosed in any of the patients in this study.

134
However, recent meta-regression analysis demonstrated a positive association
between implant time in function and the prevalence of peri-implantitis (Derks &
Tomasi 2015). As such, our short observation period may be the main reason for the
absence of peri-implantitis and longer follow up will be required to more accurately
assess this outcome measure.
Fixed single crowns (SC) and multi-unit (FPD) implant restorations are well
documented in the literature (Pjetursson, et al. 2007, Jung, et al. 2008, Jung, et al.
2012, Pjetursson, et al. 2012). To the best of our knowledge this is the first
prospective study reporting on well defined technical outcomes for implant supported
restorations in MSA in the partially dentate patient. After one year of service, 100%
of the implant supported restorations were functional. The majority of patients were
restored with a SC restoration in both treatment groups. Screw retention was the
predominant type of retention utilized in both treatment groups and for both types of
restorations. There was no statistically significant association between type of
restoration or type of retention utilized and treatment group.
In the present study, the great majority of patients (90.56%) presented with
complication free implant supported restorations. Minor technical complications
comprising mostly of ceramic veneer fractures were seen in few patients. This is
consistent with a systematic review indicating that the most common technical
complication of implant supported restorations was veneer fracture (Pjetursson, et al.
2012). In the present study there was no statistically significant association between
proportion of complications and treatment group. From the total of 5 incidents of
reported complications, 4 affected screw retained restorations. This may be due to an
over representation of screw retained restorations in the present study but is also
consistent with a systematic review reporting higher technical complications for
screw retained restorations (Sailer, et al. 2012). Whilst the great majority of FPDs
were without cantilever extension a few 2-unit FPDs with cantilevered extension were
successfully utilized in this study. Whilst there are no comparative studies for this
treatment modality in maxillary sinus augmentation it appears to be consistent with
previous studies and systematic reviews (Aglietta, et al. 2009, Romeo & Storelli
2012, Kim, et al. 2014) on cantilevered restorations.

135
In conclusion, considering the short observation period, implant reconstruction of the
partially edentulous posterior maxilla after MSA using ABBM + autogenous bone or
collagen stabilized ABBM led to similar and stable marginal bone levels, high
implant survival, low rates of technical complications and no peri-implantitis. Whilst
high rates of peri-implant mucositis were similarly seen in both groups, its
significance remains unknown and is mostly related to definition threshold.

136
Acknowledgements The authors are grateful to Dr Dimitrios Vagenas (Biostatisticians, Institute for Health
and Biomedical Innovation, Queensland University of Technology, Kelvin Grove,
Australia) for his assistance and contribution to the statistical analysis in this project.
No external funding was received for this project.

137
References
Abrahamsson, I., Berglundh, T., Linder, E., Lang, N. P. & Lindhe, J. (2004) Early
bone formation adjacent to rough and turned endosseous implant surfaces. An
experimental study in the dog. Clin Oral Implants Res 15: 381-392.
Aglietta, M., Siciliano, V. I., Zwahlen, M., Bragger, U., Pjetursson, B. E., Lang, N. P.
& Salvi, G. E. (2009) A systematic review of the survival and complication rates of
implant supported fixed dental prostheses with cantilever extensions after an
observation period of at least 5 years. Clin Oral Implants Res 20: 441-451.
Alayan, J. & Ivanovski, S. (2018) A prospective controlled trial comparing
xenograft/autogenous bone and collagen-stabilized xenograft for maxillary sinus
augmentation-complications, patient-reported outcomes and volumetric analysis. Clin
Oral Implants Res 29: 248-262.
Alayan, J., Vaquette, C., Farah, C. & Ivanovski, S. (2016) A histomorphometric
assessment of collagen-stabilized anorganic bovine bone mineral in maxillary sinus
augmentation - a prospective clinical trial. Clin Oral Implants Res 27: 850-858.
Alayan, J., Vaquette, C., Saifzadeh, S., Hutmacher, D. & Ivanovski, S. (2016) A
histomorphometric assessment of collagen-stabilized anorganic bovine bone mineral
in maxillary sinus augmentation - a randomized controlled trial in sheep. Clin Oral
Implants Res 27: 734-743.
Alayan, J., Vaquette, C., Saifzadeh, S., Hutmacher, D. & Ivanovski, S. (2017)
Comparison of early osseointegration of sla((r)) and slactive((r)) implants in
maxillary sinus augmentation: A pilot study. Clin Oral Implants Res 28: 1325-1333.
Armitage, G. C. (1999) Development of a classification system for periodontal
diseases and conditions. Ann Periodontol 4: 1-6.
Avila, G., Wang, H. L., Galindo-Moreno, P., Misch, C. E., Bagramian, R. A., Rudek,
I., Benavides, E., Moreno-Riestra, I., Braun, T. & Neiva, R. (2010) The influence of
the bucco-palatal distance on sinus augmentation outcomes. J Periodontol 81: 1041-
1050.
Bornstein, M. M., Chappuis, V., von Arx, T. & Buser, D. (2008) Performance of
dental implants after staged sinus floor elevation procedures: 5-year results of a
prospective study in partially edentulous patients. Clin Oral Implants Res 19: 1034-
1043.

138
Bornstein, M. M., Schmid, B., Belser, U. C., Lussi, A. & Buser, D. (2005) Early
loading of non-submerged titanium implants with a sandblasted and acid-etched
surface. 5-year results of a prospective study in partially edentulous patients. Clin
Oral Implants Res 16: 631-638.
Buser, D., Janner, S. F., Wittneben, J. G., Bragger, U., Ramseier, C. A. & Salvi, G. E.
(2012) 10-year survival and success rates of 511 titanium implants with a sandblasted
and acid-etched surface: A retrospective study in 303 partially edentulous patients.
Clin Implant Dent Relat Res 14: 839-851.
Buser, D., Nydegger, T., Hirt, H. P., Cochran, D. L. & Nolte, L. P. (1998) Removal
torque values of titanium implants in the maxilla of miniature pigs. Int J Oral
Maxillofac Implants 13: 611-619.
Cannizzaro, G., Felice, P., Leone, M., Viola, P. & Esposito, M. (2009) Early loading
of implants in the atrophic posterior maxilla: Lateral sinus lift with autogenous bone
and bio-oss versus crestal mini sinus lift and 8-mm hydroxyapatite-coated implants. A
randomised controlled clinical trial. Eur J Oral Implantol 2: 25-38.
Chiapasco, M., Casentini, P. & Zaniboni, M. (2009) Bone augmentation procedures in
implant dentistry. Int J Oral Maxillofac Implants 24 Suppl: 237-259.
Cochran, D. L., Schenk, R. K., Lussi, A., Higginbottom, F. L. & Buser, D. (1998)
Bone response to unloaded and loaded titanium implants with a sandblasted and acid-
etched surface: A histometric study in the canine mandible. J Biomed Mater Res 40:
1-11.
de Vicente, J. C., Hernandez-Vallejo, G., Brana-Abascal, P. & Pena, I. (2010)
Maxillary sinus augmentation with autologous bone harvested from the lateral
maxillary wall combined with bovine-derived hydroxyapatite: Clinical and histologic
observations. Clin Oral Implants Res 21: 430-438.
Del Fabbro, M., Testori, T., Francetti, L. & Weinstein, R. (2004) Systematic review
of survival rates for implants placed in the grafted maxillary sinus. Int J Periodontics
Restorative Dent 24: 565-577.
Derks, J. & Tomasi, C. (2015) Peri-implant health and disease. A systematic review
of current epidemiology. J Clin Periodontol 42 Suppl 16: S158-171.
Galindo-Moreno, P., Avila, G., Fernandez-Barbero, J. E., Aguilar, M., Sanchez-
Fernandez, E., Cutando, A. & Wang, H. L. (2007) Evaluation of sinus floor elevation
using a composite bone graft mixture. Clin Oral Implants Res 18: 376-382.

139
Galindo-Moreno, P., Fernandez-Jimenez, A., Avila-Ortiz, G., Silvestre, F. J.,
Hernandez-Cortes, P. & Wang, H. L. (2014) Marginal bone loss around implants
placed in maxillary native bone or grafted sinuses: A retrospective cohort study. Clin
Oral Implants Res 25: 378-384.
Galindo-Moreno, P., Fernandez-Jimenez, A., O'Valle, F., Silvestre, F. J., Sanchez-
Fernandez, E., Monje, A. & Catena, A. (2015) Marginal bone loss in implants placed
in grafted maxillary sinus. Clin Implant Dent Relat Res 17: 373-383.
Galindo-Moreno, P., Moreno-Riestra, I., Avila, G., Fernandez-Barbero, J. E., Mesa,
F., Aguilar, M., Wang, H. L. & O'Valle, F. (2010) Histomorphometric comparison of
maxillary pristine bone and composite bone graft biopsies obtained after sinus
augmentation. Clin Oral Implants Res 21: 122-128.
Galindo-Moreno, P., Moreno-Riestra, I., Avila, G., Padial-Molina, M., Paya, J. A.,
Wang, H. L. & O'Valle, F. (2011) Effect of anorganic bovine bone to autogenous
cortical bone ratio upon bone remodeling patterns following maxillary sinus
augmentation. Clin Oral Implants Res 22: 857-864.
Hallman, M., Cederlund, A., Lindskog, S., Lundgren, S. & Sennerby, L. (2001) A
clinical histologic study of bovine hydroxyapatite in combination with autogenous
bone and fibrin glue for maxillary sinus floor augmentation. Results after 6 to 8
months of healing. Clin Oral Implants Res 12: 135-143.
Hammerle, C. H., Bragger, U., Burgin, W. & Lang, N. P. (1996) The effect of
subcrestal placement of the polished surface of iti implants on marginal soft and hard
tissues. Clin Oral Implants Res 7: 111-119.
Hatano, N., Shimizu, Y. & Ooya, K. (2004) A clinical long-term radiographic
evaluation of graft height changes after maxillary sinus floor augmentation with a 2:1
autogenous bone/xenograft mixture and simultaneous placement of dental implants.
Clin Oral Implants Res 15: 339-345.
Hermann, J. S., Buser, D., Schenk, R. K. & Cochran, D. L. (2000) Crestal bone
changes around titanium implants. A histometric evaluation of unloaded non-
submerged and submerged implants in the canine mandible. J Periodontol 71: 1412-
1424.
Hermann, J. S., Buser, D., Schenk, R. K., Schoolfield, J. D. & Cochran, D. L. (2001)
Biologic width around one- and two-piece titanium implants. Clin Oral Implants Res
12: 559-571.

140
Hermann, J. S., Schoolfield, J. D., Nummikoski, P. V., Buser, D., Schenk, R. K. &
Cochran, D. L. (2001) Crestal bone changes around titanium implants: A
methodologic study comparing linear radiographic with histometric measurements.
Int J Oral Maxillofac Implants 16: 475-485.
Jensen, S. S. & Terheyden, H. (2009) Bone augmentation procedures in localized
defects in the alveolar ridge: Clinical results with different bone grafts and bone-
substitute materials. Int J Oral Maxillofac Implants 24 Suppl: 218-236.
Jepsen, S., Ruhling, A., Jepsen, K., Ohlenbusch, B. & Albers, H. K. (1996)
Progressive peri-implantitis. Incidence and prediction of peri-implant attachment loss.
Clin Oral Implants Res 7: 133-142.
Jung, R. E., Pjetursson, B. E., Glauser, R., Zembic, A., Zwahlen, M. & Lang, N. P.
(2008) A systematic review of the 5-year survival and complication rates of implant-
supported single crowns. Clin Oral Implants Res 19: 119-130.
Jung, R. E., Zembic, A., Pjetursson, B. E., Zwahlen, M. & Thoma, D. S. (2012)
Systematic review of the survival rate and the incidence of biological, technical, and
aesthetic complications of single crowns on implants reported in longitudinal studies
with a mean follow-up of 5 years. Clin Oral Implants Res 23 Suppl 6: 2-21.
Karoussis, I. K., Salvi, G. E., Heitz-Mayfield, L. J., Bragger, U., Hammerle, C. H. &
Lang, N. P. (2003) Long-term implant prognosis in patients with and without a
history of chronic periodontitis: A 10-year prospective cohort study of the iti dental
implant system. Clin Oral Implants Res 14: 329-339.
Kim, P., Ivanovski, S., Latcham, N. & Mattheos, N. (2014) The impact of cantilevers
on biological and technical success outcomes of implant-supported fixed partial
dentures. A retrospective cohort study. Clin Oral Implants Res 25: 175-184.
Kim, Y. K., Yun, P. Y., Kim, S. G. & Lim, S. C. (2009) Analysis of the healing
process in sinus bone grafting using various grafting materials. Oral Surg Oral Med
Oral Pathol Oral Radiol Endod 107: 204-211.
Lang, N. P., Berglundh, T. & Working Group 4 of Seventh European Workshop on,
P. (2011) Periimplant diseases: Where are we now?--consensus of the seventh
european workshop on periodontology. J Clin Periodontol 38 Suppl 11: 178-181.
Lang, N. P. & Tonetti, M. S. (2003) Periodontal risk assessment (pra) for patients in
supportive periodontal therapy (spt). Oral Health Prev Dent 1: 7-16.
Luterbacher, S., Mayfield, L., Bragger, U. & Lang, N. P. (2000) Diagnostic
characteristics of clinical and microbiological tests for monitoring periodontal and

141
peri-implant mucosal tissue conditions during supportive periodontal therapy (spt).
Clin Oral Implants Res 11: 521-529.
Maiorana, C., Redemagni, M., Rabagliati, M. & Salina, S. (2000) Treatment of
maxillary ridge resorption by sinus augmentation with iliac cancellous bone,
anorganic bovine bone, and endosseous implants: A clinical and histologic report. Int
J Oral Maxillofac Implants 15: 873-878.
Marcelis, K., Vercruyssen, M., Nicu, E., Naert, I. & Quirynen, M. (2012) Sleeping vs.
Loaded implants, long-term observations via a retrospective analysis. Clin Oral
Implants Res 23: 1118-1122.
Mombelli, A. & Lang, N. P. (1994) Clinical parameters for the evaluation of dental
implants. Periodontol 2000 4: 81-86.
Nkenke, E. & Stelzle, F. (2009) Clinical outcomes of sinus floor augmentation for
implant placement using autogenous bone or bone substitutes: A systematic review.
Clin Oral Implants Res 20 Suppl 4: 124-133.
Pjetursson, B. E., Bragger, U., Lang, N. P. & Zwahlen, M. (2007) Comparison of
survival and complication rates of tooth-supported fixed dental prostheses (fdps) and
implant-supported fdps and single crowns (scs). Clin Oral Implants Res 18 Suppl 3:
97-113.
Pjetursson, B. E., Tan, W. C., Zwahlen, M. & Lang, N. P. (2008) A systematic review
of the success of sinus floor elevation and survival of implants inserted in
combination with sinus floor elevation. J Clin Periodontol 35: 216-240.
Pjetursson, B. E., Thoma, D., Jung, R., Zwahlen, M. & Zembic, A. (2012) A
systematic review of the survival and complication rates of implant-supported fixed
dental prostheses (fdps) after a mean observation period of at least 5 years. Clin Oral
Implants Res 23 Suppl 6: 22-38.
Pjetursson, B. E., Zwahlen, M. & Lang, N. P. (2012) Quality of reporting of clinical
studies to assess and compare performance of implant-supported restorations. J Clin
Periodontol 39 Suppl 12: 139-159.
Rickert, D., Slater, J. J., Meijer, H. J., Vissink, A. & Raghoebar, G. M. (2012)
Maxillary sinus lift with solely autogenous bone compared to a combination of
autogenous bone and growth factors or (solely) bone substitutes. A systematic review.
Int J Oral Maxillofac Surg 41: 160-167.

142
Roccuzzo, M., Aglietta, M., Bunino, M. & Bonino, L. (2008) Early loading of
sandblasted and acid-etched implants: A randomized-controlled double-blind split-
mouth study. Five-year results. Clin Oral Implants Res 19: 148-152.
Roccuzzo, M., Bunino, M., Prioglio, F. & Bianchi, S. D. (2001) Early loading of
sandblasted and acid-etched (sla) implants: A prospective split-mouth comparative
study. Clin Oral Implants Res 12: 572-578.
Romeo, E. & Storelli, S. (2012) Systematic review of the survival rate and the
biological, technical, and aesthetic complications of fixed dental prostheses with
cantilevers on implants reported in longitudinal studies with a mean of 5 years follow-
up. Clin Oral Implants Res 23 Suppl 6: 39-49.
Sailer, I., Muhlemann, S., Zwahlen, M., Hammerle, C. H. & Schneider, D. (2012)
Cemented and screw-retained implant reconstructions: A systematic review of the
survival and complication rates. Clin Oral Implants Res 23 Suppl 6: 163-201.
Sanz, M., Chapple, I. L. & Working Group 4 of the, V. E. W. o. P. (2012) Clinical
research on peri-implant diseases: Consensus report of working group 4. J Clin
Periodontol 39 Suppl 12: 202-206.
Schincaglia, G. P., Thoma, D. S., Haas, R., Tutak, M., Garcia, A., Taylor, T. D. &
Hammerle, C. H. (2015) Randomized controlled multicenter study comparing short
dental implants (6 mm) versus longer dental implants (11-15 mm) in combination
with sinus floor elevation procedures. Part 2: Clinical and radiographic outcomes at 1
year of loading. J Clin Periodontol 42: 1042-1051.
Thoma, D. S., Sanz Martin, I., Benic, G. I., Roos, M. & Hammerle, C. H. (2014)
Prospective randomized controlled clinical study comparing two dental implant
systems: Demographic and radiographic results at one year of loading. Clin Oral
Implants Res 25: 142-149.

Table 1. Baseline Parameters
Parameters
Control
(ABBM+AB)
(n = 27)
Test
(ABBM-C)
(n = 26)
Group
comparison
(P)
Age (Mean years ±SD) 60.26 (±11.0) 61.58 (± 6.89) 0.61
Gender ratio (f/m) 2.0 (f=18/m=9) 2.71 (f= 19/m=7) 0.97
Smoking
(no. patients) 1 2 0.95
Periodontal disease
(no. patients) 3 7 0.89
Initial ridge height
(mm) (Mean ± SD) 3.11 ± 0.76 3.06 ± 0.70 0.81
Time (weeks)
restoration insertion to
baseline assessment
9.29 (3.8) 10.81 (2.7) 0.10
Time (weeks) baseline
assessment to 1 year
assessment
58.07 (19.61) 59.73 (13.25) 0.72
ABBM, anorganic bovine bone mineral; AB, autogenous bone; ABBM-C, collagen
stabilized anorganic bovine bone mineral; 95% CI, 95% confidence interval; P, P-value for
inter-group comparison after proportion testing or independent t-test.

Table 2. Implant dimensions – frequency table (no. of implants). Implants used were one piece with an SLA surface.
Implant
Dimensions
Control
(ABBM+AB)
(n = 27)
Test
(ABBM-C)
(n = 26)
RN 4.1 x 10mm 2 5
RN 4.8 x 10mm 1 0
WN 4.8 x 8mm 2 3
WN 4.8 x 10mm 22 18
ABBM, anorganic bovine bone mineral; AB, autogenous bone; ABBM-C, collagen
stabilized anorganic bovine bone mineral. RN, regular neck; WN, wide neck

Table 3. Marginal bone level (DIB) and changes at various time points (ABL).
Control (ABBM+AB) (n = 27) Test (ABBM-C) (n = 26)
Time Mean (± SD)
Median (± IQR)
Range (min, max)
Mean (± SD)
Median (± IQR)
Range (min, max)
DIB0 -0.38 (0.43)
-0.32 (0.68) -1.62, 0.20 -0.54
(0.45) -0.55 (0.75) -1.63, 0.14
DIB1 0.28 (0.31)
0.29 (0.42) -0.30, 1.12 0.24
(0.37) 0.24
(0.43) -0.70, 0.91
DIB2 0.60 (0.33)
0.58 (0.56) 0.08, 1.37 0.58
(0.40) 0.54
(0.55) -0.24, 1.57
ABL1 -0.66 (0.40)
-0.59 (0.5) -1.74, -0.02 -0.77
(0.48) -0.80 (0.62) -1.94, 0.21
ABL2 -0.32 (0.24)
-0.26 (0.38) -0.88, -0.02 -0.35
(0.23) -0.32 (0.29) -0.97, -0.01
DIB, distance from the implant shoulder at the implant-abutment connection to the
most coronal bone-to-implant contact; DIB0, mean DIB at implant placement (T0);
DIB1, mean DIB at loading of prosthesis (T1 baseline); DIB 2, mean DIB at 12
months after function (T2); ABBM, anorganic bovine bone mineral; AB, autogenous
bone; ABBM-C, collagen stabilized anorganic bovine bone mineral; ABL1, change in
DIB from T0 to T1; ABL2, change in DIB from T1 to T12; SD, standard deviation;
IQR, inter-quartile range. Negative ABL values denote alveolar bone loss.

Table 4. Group comparisons - marginal bone levels (DIB) and changes at various time points.
Inter-group comparison: Control (ABBM+AB) vs. Test (ABBM-C)
Parameter Mean Difference 95% CI P Value
DIB0 0.16 -0.08, 0.40 0.19
DIB1 0.05 -0.14, 0.23 0.61
DIB2 0.02 -0.18, 0.22 0.84
DIB0 - DIB1 -0.11 -0.35, 0.13 0.38
DIB1- DIB2 -0.03 -0.16, 0.10 0.68
Intra-group comparison
Parameter Mean Difference 95% CI P Value
Control
(DIB0 vs. DIB1) -0.66 -0.82, -0.50 <0.0001
Control
(DIB1 vs. DIB2) -0.32 -0.42, -0.22 <0.0001
Test
(DIB0 vs. DIB1) -0.77 -0.97, -0.57 <0.0001
Test
(DIB1 vs. DIB2) -0.35 -0.44, -0.25 <0.0001
Control
(ABL1 vs. ABL2) 0.34 0.15, 0.54 0.001
Test
(ABL1 vs. ABL2) 0.42 0.20, 0.64 0.001
DIB, distance from the implant shoulder at the implant-abutment connection to the
most coronal bone-to-implant contact; DIB0, mean DIB at implant placement (T0);
DIB1, mean DIB at loading of prosthesis (T1 baseline); DIB 2, mean DIB at 12
months after function (T2); ABL1, DIB change from (T0) to (T1); ABL2, DIB change
from (T1) to (T2); ABBM, anorganic bovine bone mineral; AB, autogenous bone;
ABBM-C, collagen stabilized anorganic bovine bone mineral; 95% CI, 95%
confidence interval of the mean difference; P, P-value for group comparison after
applying a t-test.

Table 5a. Results of multi-variable linear regression model for ABL1.
ABL1, marginal bone level changes from implant (T0) placement to baseline (T1); b,
regression estimate coefficient; SE, standard error; 95% CI, 95% confidence interval.
b (SE) 95% CI P value
Treatment group
control -0.02 (0.09) -0.19, 0.14 0.76
test reference - -
Periodontal status
healthy 0.07 (0.12) -0.16, 0.30 0.54
chronic disease reference - -
Gender
male 0.03 (0.09) -0.14, 0.21 0.71
female reference - -
Initial position -0.66 (0.10) -0.86, -0.47 <0.0001
Residual ridge height 0.10 (0.06) -0.02, 0.22 0.09
Age 0.0 (0.0) -0.01, 0.01 0.96

Table 5b. Results of multi-variable linear regression model for ABL2.
ABL2, marginal bone level changes from baseline (T1) to 12 months after function
(T2); b, regression estimate coefficient; SE, standard error; 95% CI, 95% confidence
interval.
b (SE) 95% CI P value
Treatment group
control -0.02 (0.07) -0.15, 0.11 0.72
test reference - -
Periodontal status
healthy 0.07 (0.09) -0.11, 0.24 0.46
chronic disease reference - -
Gender
male -0.11 (0.07) -0.24, 0.03 0.12
female reference - -
Initial position -0.03 (0.08) -0.19, 0.12 0.66
Residual ridge height -0.01 (0.05) -0.09, 0.09 0.95
Age 0.0 (0.0) -0.01, 0.01 0.85

Table 6. Frequency distribution (no. of implants / patients) of marginal bone level changes (ABL) across time.
ABL1, marginal bone level change from T0 to T1; ABL2, marginal bone level change from T1 to T12. T0,
implant placement; T1, insertion restoration (baseline); T2, 12 months after function; ABBM, anorganic bovine
bone mineral; AB, autogenous bone; ABBM-C, collagen stabilized anorganic bovine bone mineral.
ABL1 (T0-T1) ABL2 (T1-T2) ABL Interval
(mm) Control
(ABBM+AB) Test (ABBM-C) Control (ABBM+AB) Test (ABBM-C)
-2.5 < ABL ≤ -2.0 0 0 0 0
-2.0 < ABL ≤ -1.5 1 2 0 0
-1.5 < ABL ≤ -1.0 4 6 0 0
-1.0 < ABL ≤ -0.5 11 11 6 4
-0.5 < ABL ≤ 0 11 6 21 22
0 < ABL ≤ 0.5 0 1 0 0
0.5 < ABL ≤ 1.0 0 0 0 0
Total 27 26 27 26

Table 7. Clinical parameters of implants placed into augmented sinuses at baseline (T1) and after 12 months of function (T2).
Control (ABBM+AB) (n = 27) Test (ABBM-C) (n = 26)
Parameter Time Mean (± SD)
Median (± IQR)
Range (min - max) Parameter Time Mean
(± SD) Median (± IQR)
Range (min - max)
PI (no. sites)
T1 0.22 (0.51)
0.0 (0) 0.0 – 2.0
PI (no. sites)
T1 0.19 (0.49)
0.0 (0) 0.0 – 2.0
T2 0.41 (0.57)
0.0 (1.0) 0.0 – 2.0 T2 0.31
(0.55) 0.0
(1.0) 0.0 – 2.0
BOP (no. sites)
T1 0.96 (1.0)
1.0 (1.0) 0.0 - 3.0
BOP (no. sites)
T1 0.88 (1.03)
1.0 (1.25) 0.0 – 3.0
T2 1.03 (0.94)
1.0 (2.0) 0.0 - 3.0 T2 1.31
(1.16) 1.0
(2.0) 0.0 – 4.0
PPD (mm)
T1 2.34 (0.50)
2.33 (0.67) 1.33 - 3.33
PPD (mm)
T1 2.46 (0.76)
2.33 (1.22) 0.83 – 3.83
T2 2.50 (0.66)
2.33 (0.83) 1.50 – 4.17 T2 2.43
(0.83) 2.33
(1.13) 1.17 – 4.50
DIM (mm)
T1 8.10 (2.0)
7.67 (3.84) 5.17, 12.17
DIM (mm)
T1 8.78 (1.54)
8.84 (2.13) 6.17 – 12.0
T2 8.35 (2.09)
8.0 (3.43) 4.83, 12.33 T2 9.31
(1.94) 8.84
(1.71) 6.33 – 14.33
T1, baseline; T2, 12 months after function; ABBM, anorganic bovine bone mineral; AB,
autogenous bone; ABBM-C, collagen stabilized anorganic bovine bone mineral; PI, plaque index;
BOP, bleeding on probing; PPD, probing pocket depth; DIM, gingival marginal position; SD,
standard deviation; IQR, inter-quartile range.

Table 8. Technical Outcomes – type of prosthesis and retention
Control group (ABBM+AB)
(n = 27)
Type of prosthesis Test group (ABBM-C)
(n = 26)
Type of prosthesis
SC FPD Totals SC FPD Totals
Ret
entio
n Screw 15 6 21/27 (0.78)
Ret
entio
n Screw 16 4 20/26 (0.77)
Cement 3 3 6/27 (0.22) Cement 4 2 6/26
(0.23)
Totals 18/27 (0.67)
9/27 (0.33) Totals 20/26
(0.77) 6/26
(0.23)
ABBM, anorganic bovine bone mineral; AB, autogenous bone; ABBM-C, collagen
stabilized anorganic bovine bone mineral; SC, single crown, FPD, fixed partial denture.

Table 9. Technical Complications.
Patient Complication Category Treatment group Prosthesis Retention
1 Veneer fracture Minor Control SC Screw
2 Veneer fracture Minor Control FPD Screw
3 Restoration screw loosening Minor Test SC Screw
4 Veneer fracture Minor Test SC Screw
5 Veneer fracture Minor Test FPD (cantilever) Cement
Control group (ABBM + AB); Test group (ABBM-C); (ABBM, anorganic bovine bone mineral; AB,
autogenous bone; ABBM-C, collagen stabilized anorganic bovine bone mineral; SC, single crown,
FPD, fixed partial denture.

CONSORT 2010 Flow Diagram
Assessed for eligibility (n=67)
Excluded (n= 7) ¨ Not meeting inclusion criteria (n=3) ¨ Declined to participate (n=4) ¨ Other reasons (n=0)
Analysed (n=27) ¨ Excluded from analysis (n=0)
Lost to follow-up (not contactable = 2, relocated = 1) (n= 3)
Discontinued intervention (n=0)
Allocated to CONTROL (ABBM+AB) (n= 30) ¨ Received allocated intervention (n= 30) ¨ Did not receive allocated intervention (n=0)
Lost to follow-up (not contactable = 3, relocated =1) (n=4)
Discontinued intervention (n=0)
Allocated to TEST (ABBM-C) (n= 30) ¨ Received allocated intervention (n= 30) ¨ Did not receive allocated intervention (n=0)
Analysed (n=26) ¨ Excluded from analysis (n=0)
Allocation
Analysis
Follow-Up
Allocation (n= 60)
Enrollment

156
CHAPTER 7 – DISCUSSION & FUTURE DIRECTIONS

157
DISCUSSION
The rehabilitation of partial and fully edentulous patients with dental implants is
considered to be a predictable therapeutic modality with favourable long term
functional outcomes (Buser, et al. 2012, Jung, et al. 2012, Pjetursson, et al. 2012).
Reduced alveolar bone height and bone density however are common limitations
when considering implant rehabilitation of the posterior maxilla (Jemt & Lekholm
1995). Maxillary sinus floor elevation (MSA) using the lateral window approach
(Boyne & James 1980) is the most commonly utilized procedure to overcome
maxillary sinus pneumatisation, resulting in predictable survival of implant
supported restorations (Bornstein, et al. 2008, Del Fabbro, et al. 2008, Pjetursson,
et al. 2008, Nkenke & Stelzle 2009, Corbella, et al. 2015, Antonoglou, et al. 2018).
Histomrphometric assessment of collagen stabilized ABBM in MSA
The significant limitations of autogenous bone (AB) in MSA has driven intense
research into various bone substitutes. Anorganic bovine bone mineral (ABBM)
(Bio-Oss®) is a very well documented xenograft in MSA when used alone or as a
composite graft with AB (ABBM + AB) (Galindo-Moreno, et al. 2011, Schmitt, et
al. 2015). More recently, collagen stabilized ABBM using 10% porcine type-1
collagen matrix has also become available for use (ABBM-C) (Bio-Oss
Collagen®). This formulation may have clinical utility in its use as a sole
biomaterial in MSA, especially in situations of Schneiderian membrane perforation.
There are however, no published studies on this material in MSA.
As such, the first part of this thesis was to test the suitability of this biomaterial in
a pre-clinical model. Collagen stabilized ABBM exhibited very similar
histomorphometric parameters to the composite graft of ABBM + AB in the
proximal zones to resident bone. The presence of AB however, seemed
advantageous in regions distant from resident sinus walls. This is consistent with
previous pre-clinical models reporting a gradient of graft consolidation
(Busenlechner, et al. 2009) which is dependent on the osteogenic response of the
host bone and the osteogenic profile of the bone substitute (Busenlechner, et al.
2008). This is also in line with early clinical observations of bone formation directly
from the sinus walls (Boyne & James 1980) with little evidence of new bone in
contact with the Schneiderian membrane (Boyne 1993, Scala, et al. 2010). New

158
bone was rarely observed in contact with the Schneiderian membrane in this study.
Whilst there are reports of successful MSA and simultaneous dental implants
placement without the use of adjunctive grafting material (Lundgren, et al. 2004),
bone formation does not appear to be extensive and is only present in areas proximal
to native bone walls of the maxillary sinus (Lundgren, et al. 2004, Palma, et al.
2006). Furthermore, the Schneiderian membrane has been shown to have
osteogenic potential (Gruber, et al. 2004, Srouji, et al. 2009), but this does not seem
to translate into actual bone formation in pre-clinical models (Haas, et al. 2002,
Scala, et al. 2010). It has also been shown that whilst new bone is formed after
membrane elevation only, this is unstable leading to resorption in areas where the
membrane collapses due to instability of the blood clot and a lack of mechanical
support (Xu, et al. 2005).
Whilst previous clinical comparative studies have failed to show an advantage of
adding AB to ABBM (Galindo-Moreno, et al. 2011, Corbella, et al. 2016), its use
in this pre-clinical experiment was associated with significant improvements in new
bone formation and degree of particle osseointegration, but only in the zone distant
to the resident sinus bone walls. When the above experiment was repeated in a
clinical model however, comparable histomorphometric outcomes were observed
for the two materials, with no signs of different gradients of consolidation. This
may be due to variety of reasons, such as differences between animal and human
models or the varying ability to detect a gradient in whole sinus samples compared
with biopsy harvested samples. Whilst there are no studies comparing these two
different sampling techniques, one could postulate that results would vary
depending on the location and depth of the biopsy (Margolin, et al. 1998, Artzi, et
al. 2005, Avila, et al. 2010). Another influencing factor may be the proximity of the
lateral walls of the sinus to the harvesting site (Suarez-Lopez Del Amo, et al. 2015).
Further pre-clinical comparisons between the standard particulate formulation of
ABBM alone and the ABBM+AB composite graft is required to definitively assess
the impact of adding AB to this model. There are currently no pre-clinical
histomorphometric comparative studies using ABBM+AB and ABBM alone.

159
The impact of hydrophilic dental implant surface on early osseointegration in MSA
Whilst grafting material influences the histological make-up of the regenerated
bone, other factors can also play a role including the dental implant surface. This
project assessed the impact of using a chemically modified hydrophilic implant
surface in MSA (SLActive®). Implant surface topography and chemistry have been
shown to affect osseointegration (Gittens, et al. 2012). They play a critical role in
the predictability of the bone response to implant placement (Junker, et al. 2009)
and are a major determinant of the rate and extent of dental implant osseointegration
(Wennerberg, et al. 2011). To date however, very few studies have compared
different implant surfaces in MSA and none at the early stages of osseointegration.
Results from this experiment showed that both time and the use of a hydrophilic
implant surface had a positive impact on BIC. Hydrophilic implant surfaces also
had a positive impact on the surrounding tissue composition. This finding is in
agreement with a number of studies using this same hydrophilic implant surface
(SLActive®, Struamann, Basel, Switzerland), indicating enhanced bone apposition
during the early stages of osseointegration compared to the standard SLA surface
(Lang, et al. 2011). The early advantage however, was not evident when assessing
BIC in a pre-clinical MSA model at later time points (Philipp, et al. 2013). Early
loading of modified hydrophilic implants may remain as an advantage, similar to
what has already been observed in non-grafted clinical models (Morton, et al.
2010).
Volumetric / radiographic assessment of collagen stabilized ABBM in MSA
Studies have shown higher resorption rates resulting in loss of graft volume when
using AB alone in MSA (Johansson, et al. 2001, Arasawa, et al. 2012), and an
increase in volumetric stability following the incorporation of ABBM, which was
positively correlated with increased proportions of ABBM in the ABBM + AB
composite grafts (Jensen, et al. 2012). The volumetric stability of collagen
stabilized ABBM (ABBM-C) was assessed in this study, to further determine its
suitability for use in MSA. A prospective clinical trial compared ABBM-C and
ABBM + AB with allocation based on defined clinical presentations (sinus
membrane perforation and/or insufficient local AB bone). ABBM-C exhibited
comparable bone volume to AB + ABBM that was sufficient for placement of
implants of adequate length, with little or no need for further vertical augmentation.

160
Longer follow up will be needed to determine if further changes in graft volume
takes place in both treatment groups over the long term.
Interestingly, further analysis indicated that engaging the surrounding sinus walls
had a significant positive impact on graft volume but not the residual ridge height.
Whilst previous studies have indicated that adequate graft height can be achieved
even in the presence of a sinus floor fenestration (Cortes, et al. 2015), this is the
first study to report on the association between engaging adjacent walls and graft
volume. Conceptually this finding is consistent with the overall impression that the
resident sinus walls are key defect parameters that influence not only histological
outcomes but also volumetric stability. Histological studies have shown a positive
impact of increasing both the number and total area of engaged bony on graft
healing outcomes (Haas, et al. 1998, Busenlechner, et al. 2009, Alayan, et al. 2017).
This is consistent with the principle, ascertained form other models of guided bone
regeneration, that surrounding bony walls are an important determinant for de novo
bone formation and graft particle incorporation (Klinge, et al. 1992, Schenk, et al.
1994, Carmagnola, et al. 2003).
Surgical complications & PROMs associated with MSA
Most of the clinical outcomes data for MSA is derived from medium to low level
evidence (clinical case series, retrospective analyses). Patients undergoing this
procedure also expect to be counselled about their expectations regarding pain and
the impact on their daily life in the post-operative period. Such information is not
currently available. There are few prospective controlled clinical trials applying
well defined success criteria to implant supported restorations placed in sites of
MSA and there are none on the use of collagen stabilized ABBM grafting material
in MSA. As such, the second part of this thesis explores the clinical, and patient
centred outcomes of MSA using these two biomaterials, followed by assessment of
the survival and success of the implant supported restorations placed into these
sites.
This patient population did not experience major intra- or post-operative
complications, consistent with previous reviews (Chiapasco, et al. 2009). In
addition, the minor complications were manageable and did not prevent completion

161
of the augmentation procedure. The most frequent complication was membrane
perforation, which occurred in 13% of the patient population. Multiple reviews
have also reported this to be the most frequently reported surgical complication
(Pjetursson, et al. 2008, Chiapasco, et al. 2009, Nkenke & Stelzle 2009). Whilst the
reported incidence varies greatly between studies, our rate of perforation is on the
lower end of the range and similar to more recent publications (Becker, et al. 2008,
Cortes, et al. 2015, Holtzclaw 2015). Most of these perforations were small in
diameter (≤ 3mm) and were repaired with a resorbable porcine collagen membrane
using a previously described technique (Proussaefs & Lozada 2003). The role of
the collagen in the test grafting material is to cohesively bind the ABBM granules
to form an intact 3-dimensional block. Its advantage in sinus augmentation
procedures over particulate material is evident when perforations of the sinus
membrane occur and there is a risk of endo-antral displacement of loose particles
and obstruction of the OMC (Quiney, et al. 1990, Wiltfang, et al. 2000, Doud Galli,
et al. 2001). The significance of sinus membrane perforations on implant survival
or graft success remains contentious with some studies reporting a negative impact,
especially in large perforations (Proussaefs, et al. 2004, Hernandez-Alfaro, et al.
2008), while others showed no differences (Becker, et al. 2008). Further follow-up
of our patient population did not reveal any consequences in outcomes on implant
loading, survival or biological / technical outcomes.
In terms of patient reported outcome measures (PROMs), the majority of patients
reported that average daily pain was mild to moderate for the first 3 days and
subsequently reduced to mild levels using non-steroidal anti-inflammatory drugs
(NSAIDs) only. The reported level of pain was similar across treatment groups. The
majority of patients in both treatment groups reported a moderate amount of
limitation to both oral and general activities during the first 48hrs post-surgery that
significantly further reduced by day 3 or 4. To the best of my knowledge, this is the
first study to report on PROMs for maxillary sinus augmentation and indicates that
48-72 hours of recovery from this procedure is needed for patients to resume oral
function and daily activities without limitations or the need for analgesics.
Whilst greater prevalence of bruising and swelling were noted clinically in the
control group at the post-operative review, this did not reach statistical significance.

162
Bruising and oedema was also noted to be of reduced severity in test patients
compared to patients in the control group, but this observation was not objectively
measured. This perception of increased limitation in oral functions may reflect the
increased morbidity associated with greater autogenous bone harvesting (Cricchio
& Lundgren 2003). Patients in the control group typically possessed a thick buccal
wall of bone that provided sufficient volume of autogenous bone needed to support
the elevated Schneiderian membrane at the requisite height. The test patients on the
other hand exhibited a thin buccal wall of bone and therefore experienced far less
bone removal. It is likely those symptoms of pain and perception of bruising and
oedema translated to limitation in social life and work and is generally consistent
with anecdotal reports from patients of abstaining from work for 48 hours post-
surgery.
It’s important to note however, the sample size calculation for this part of the project
was performed for graft volumetric analysis and not for PROMs. Further studies
specifically designed at investigating PROMs after MSA would be needed before
firm conclusions can be made.
Biological & technical outcomes of dental implants placed into MSA sites
The same patient population was followed to assess implant supported restorations
after 12 months of function using well defined success criteria. Both groups
revealed 100% implant survival rates, which is consistent with high survival rates
reported in other MSA studies using micro-rough implant surfaces (Pjetursson, et
al. 2008, Chiapasco, et al. 2009, Jensen & Terheyden 2009, Nkenke & Stelzle 2009,
Rickert, et al. 2012). Whilst many factors may contribute to implant survival,
implant surface and graft composition are two important considerations. A median
survival rate of 100% (88-100%) is reported for rough implant surfaces when
compared to 89% (61.2 – 100%) using machined implant surfaces (Jensen &
Terheyden 2009). A100% survival rate was reported in a clinical study using one-
piece SLA implants in MSA at 60 months after implant placement (Bornstein, et al.
2008). This may be due to the documented favourable histological outcomes
(contact osteogenesis) with moderately rough implant surfaces (Abrahamsson, et
al. 2004), resulting in improved bone-to-implant contact (BIC) and stability
compared to minimally rough surfaces (Buser, et al. 1998, Cochran, et al. 1998).

163
Furthermore, from a graft material perspective, the 5-year implant survival rate of
implants placed in MSA sites grafted using composite graft AB+ABBM (1:1) was
reported to be 92.86% (Schmitt, et al. 2015) in a small number of patients.
It has been suggested that many factors influence osseointegration and the ability
of implants in augmented maxillary sinuses to withstand functional load (Jensen, et
al. 1998). This multitude of variables may explain the seemingly arbitrary loading
interval reported in studies. All patients in the present project were successfully
restored without delay 3 months after implant placement, suggesting that this is a
sufficient time interval for osseointegration to occur when using a moderately rough
(SLA) implant surface in either of the grafting materials. Studies using the same
composite graft (Galindo-Moreno, et al. 2015) or implants surface (Bornstein, et al.
2008) have utilized a loading time of 6 months and 10 weeks respectively.
Systematic reviews report a mean loading time between 5 to 6.5 months
(Chiapasco, et al. 2009, Jensen & Terheyden 2009).
We could speculate, based on our pre-clinical histological findings for the modified
hydrophilic implant surfaces, that these implants may be successfully loaded earlier
than the 12 week protocol we used for the SLA implants. This obviously needs to
be further investigated in an appropriately designed clinical trial.
The four most frequently used parameters for assessing success are related to the
implant level, peri-implant soft tissue, prosthesis and patient’s subjective
assessment (Papaspyridakos, et al. 2012). Similarly, based on consensus reports
published at the 8th European Workshop on Periodontology, outcome measures
should capture patient reported outcomes (McGrath, et al. 2012), peri-implant
health (Derks & Tomasi 2015) and restoration outcomes (Pjetursson, et al. 2012).
As such, for implant health we reported on marginal bone levels, tissue
inflammation (BOP / suppuration) and periodontal probing depth. For implant
restorations, we reported on longevity of the restorations and technical
complications. One limitation of this project was that PROMs were reported for the
MSA procedure only but not for the subsequent implant supported restorations.

164
Furthermore, we reported each success criteria outcome separately instead of
reporting the implant-prosthetic complex as a whole (Papaspyridakos, et al. 2012).
Generally, there is a paucity of studies reporting on implant outcomes using well
defined success criteria when placed into a composite graft (ABBM+AB 1:1)
(Galindo-Moreno, et al. 2015), and no studies on implants inserted in collagen
stabilized ABBM grafts. It has been shown however, that micro-rough implants
placed into MSA sites can exhibit high success rates with stable marginal bone
levels and healthy peri-implant parameters (Bornstein, et al. 2008). In this thesis,
both groups had very similar outcome measures across all categories. A mean
alveolar bone loss of 0.66mm in the control group and 0.77mm in the test group
was noted initially after implant placement (biologic width formation), that was
significantly associated with depth of placement and location of the rough-smooth
junction. This is consistent with studies indicating that marginal bone level changes
for one-piece rough surface implants are associated with remodelling immediately
following implant placement and are influenced by the location of the rough-
smooth junction (Hammerle, et al. 1996, Hermann, et al. 2000, Hermann, et al.
2001, Hermann, et al. 2001).
Significantly lower marginal bone loss was seen during the interval between
baseline and 12 months of function. Continued change in marginal bone levels after
this initial remodelling period has been observed in many studies. In this thesis, a
mean loss of 0.32mm and 0.35mm were noted in the control and test groups
respectively. This change may represent bone loss due to exposure to bacterial load
(Lang, et al. 2011) and masticatory forces (Marcelis, et al. 2012), rather than a
physiological adaptation to implant placement. The bone loss at 12 months in our
patient population approximates that seen in a comparable study with a mean
marginal bone loss of 0.25mm (Bornstein, et al. 2008), but was double that of
another study reporting a mean loss of 0.16mm (±0.62) (Schincaglia, et al. 2015)
during the same interval. These variations between studies may have been caused
by differences in the placement protocol and implant surface / design. The authors
have attributed the small amount of marginal bone loss to the platform switching
feature of the implants utilized in their study.

165
Both treatment groups predominantly exhibited signs consistent with peri-implant
health. At the 12 months follow up, they were characterized by a median of 1 site
of BOP, a mean PPD <3mm and negligible gingival recession. Both treatment
groups represent a compliant patient population who attend for maintenance and
performed adequate plaque control. This is similar to a recent study that reported
on clinical parameters for implants placed into augmented maxillary sinuses after
12 months of functional load (Schincaglia, et al. 2015). They reported a mean PPD
of 2.3mm (±1.4). They also reported that 38% of the implants in the augmented
sinus group exhibited BOP. This is lower than the present study, with mucositis
diagnosed in approximately 2/3 of patients in both treatment groups (62.9% control
patients and 69.23% of test patients), when defined as any site of bleeding on gentle
probing without loss of supporting bone (Pjetursson, et al. 2012, Sanz, et al. 2012).
This was mostly due to the presence of one or two sites of BOP out of 6 sites probed.
Indeed, 96% of control and 85% of test patients had BOP at fewer than 3/6 (i.e. 0,
1 or 2) sites at the 12 months follow up. Whilst the absence of BOP has a high
negative predictive value for disease progression (Luterbacher, et al. 2000, Coli, et
al. 2017), the significance of a single recording of positive BOP in determining
disease progression is not determined and its dichotomous nature limits its
correlation to disease status and severity (Sanz-Sanchez, et al. 2018). Furthermore,
excessive probing force may induce false positive readings (Gerber, et al. 2009).
A high prevalence of peri-implant mucositis was reported by a recent systematic
review estimated the weighted mean prevalence to be 43% (95% CI: 32, 54%)
(Derks & Tomasi 2015). The case definitions for peri-implant disease vary
significantly in terms of threshold (Derks & Tomasi 2015) leading to significant
variations in reported success rates (Karoussis, et al. 2003). The success criteria
utilized in this study are based on the consensus reports published at the 8th
European Workshop on Periodontology (Pjetursson, et al. 2012, Sanz, et al. 2012).
When an alternative, previously proposed definition of mucositis was used (≥1 site
with PPD ≥ 5mm and BOP without loss of supporting bone) (Mombelli & Lang
1994), mucositis was diagnosed in 11.1% in the control group and 15.4% in the test
group. There was no statistically significant association between treatment groups
and proportion of peri-implant mucositis. It is possible that our sample size was
insufficiently powered to detect this difference. Peri-implantitis was not diagnosed

166
in any of the patients in this study. However, it is noteworthy that a recent meta-
regression analysis demonstrated a positive association between implant time in
function and the prevalence of peri-implantitis (Derks & Tomasi 2015). As such,
our short observation period may be the main reason for the absence of peri-
implantitis and longer follow up will be required to more accurately assess this
outcome measure.
To the best of our knowledge there are no prospective studies reporting on well
defined technical outcomes for implant supported restorations placed in MSA sites
in the partially dentate patient. Fixed single (SC) and multi-unit (FPD) implant
restorations are well documented in the literature (Pjetursson, et al. 2007, Jung, et
al. 2008, Jung, et al. 2012, Pjetursson, et al. 2012) with a reported 5 year survival
of 96.3% and 95.4% respectively (Jung, et al. 2012, Pjetursson, et al. 2012). The
majority of the restorations in this study were screw retained SCs or short span
FPDs with a small number of cement retained restorations. Both forms of retention
have their advantages and disadvantages (Michalakis, et al. 2003, Chee & Jivraj
2006). Overall, the 5 year survival rates for fixed implant supported reconstructions
is 96.03% (CI: 93.85 – 97.43%) and 95.55% (CI: 92.96 – 97.19%) for screw
retained and cement retained reconstructions respectively (Wittneben, et al. 2014).
When assessed according to prosthesis type, the estimated 5-year survival rate of
screw retained SC and FPD reconstructions is similar to that of cemented
reconstructions (Sailer, et al. 2012, Wittneben, et al. 2014, Millen, et al. 2015). The
short observation period of this project and the 100% survival rates prevent any
comments or conclusions on restoration survival.
The most common technical complication of implant supported restorations was
reported to be veneer fracture (Pjetursson, et al. 2012), which was consistent with
the findings of this thesis. The overall rate of technical complications of fixed
implant reconstructions has been reported to be significantly greater for cement
retained when compared to screw retained fixed restorations (Wittneben, et al.
2014, Millen, et al. 2015). When the data is analysed according to the type of
prosthesis however, screw retained SC restorations exhibit greater rates of technical
complications due to their significantly greater rates of abutment screw loosening
(Millen, et al. 2015). Whilst our results seem to be consistent with these reports,

167
they are however influenced by the significantly greater number of SCs and screw
form of retention, in addition to the very short observation period of this project.
This prevents any meaningful analysis or conclusion.
FUTURE DIRECTIONS
• There are few studies reporting on long term outcomes for implant supported
restorations placed into MSA using well defined success criteria as well as
volumetric graft stability. A long term follow-up of the present population
would therefore be a useful contribution to the field.
• It would be interesting and novel to assess the histomorphometric and
volumetric outcomes in a controlled clinical MSA model that is analyzed and
stratified according to extent of engagement of maxillary sinus walls.
• The impact of implant surface characteristics on the loading protocols of
implants placed in MSA sites has been underexplored. This thesis showed that
chemical modification can result in accelerated osseointegration as measured
by improved early bone-implant contact. However, the clinical implications of
these findings are not clear and it would be interesting to explore whether using
the chemically modified SLActive implants would facilitate the use of shorter
loading protocols.
• Tissue engineering is a rapidly developing multi-disciplinary field. Continued
development in this area may lead to the production of a bone substitute that is
not only biocompatible and highly osteoconductive but also osteoinductive and
is gradually resorbed and replaced by host tissue. This is likely to involve the
use of 3-dimensional bioresorbable alloplastic scaffolds with or without the
addition of growth factors and cells. This may lead to further reductions in
treatment time and possibly morbidity.

168
REFERENCES
Abrahamsson, I., Berglundh, T., Linder, E., Lang, N. P. & Lindhe, J. (2004) Early
bone formation adjacent to rough and turned endosseous implant surfaces. An
experimental study in the dog. Clin Oral Implants Res 15: 381-392.
Alayan, J., Vaquette, C., Saifzadeh, S., Hutmacher, D. & Ivanovski, S. (2017)
Comparison of early osseointegration of sla((r)) and slactive((r)) implants in
maxillary sinus augmentation: A pilot study. Clin Oral Implants Res 28: 1325-
1333.
Antonoglou, G. N., Stavropoulos, A., Samara, M. D., Ioannidis, A., Benic, G. I.,
Papageorgiou, S. N. & Sandor, G. K. (2018) Clinical performance of dental
implants following sinus floor augmentation: A systematic review and meta-
analysis of clinical trials with at least 3 years of follow-up. Int J Oral Maxillofac
Implants 33: e45-e65.
Arasawa, M., Oda, Y., Kobayashi, T., Uoshima, K., Nishiyama, H., Hoshina, H.
& Saito, C. (2012) Evaluation of bone volume changes after sinus floor
augmentation with autogenous bone grafts. Int J Oral Maxillofac Surg 41: 853-
857.
Artzi, Z., Kozlovsky, A., Nemcovsky, C. E. & Weinreb, M. (2005) The amount of
newly formed bone in sinus grafting procedures depends on tissue depth as well
as the type and residual amount of the grafted material. J Clin Periodontol 32:
193-199.
Avila, G., Wang, H. L., Galindo-Moreno, P., Misch, C. E., Bagramian, R. A.,
Rudek, I., Benavides, E., Moreno-Riestra, I., Braun, T. & Neiva, R. (2010) The
influence of the bucco-palatal distance on sinus augmentation outcomes. J
Periodontol 81: 1041-1050.
Becker, S. T., Terheyden, H., Steinriede, A., Behrens, E., Springer, I. & Wiltfang,
J. (2008) Prospective observation of 41 perforations of the schneiderian
membrane during sinus floor elevation. Clin Oral Implants Res 19: 1285-1289.
Bornstein, M. M., Chappuis, V., von Arx, T. & Buser, D. (2008) Performance of
dental implants after staged sinus floor elevation procedures: 5-year results of a
prospective study in partially edentulous patients. Clin Oral Implants Res 19:
1034-1043.
Boyne, P. J. (1993) Analysis of performance of root-form endosseous implants
placed in the maxillary sinus. J Long Term Eff Med Implants 3: 143-159.

169
Boyne, P. J. & James, R. A. (1980) Grafting of the maxillary sinus floor with
autogenous marrow and bone. J Oral Surg 38: 613-616.
Busenlechner, D., Huber, C. D., Vasak, C., Dobsak, A., Gruber, R. & Watzek, G.
(2009) Sinus augmentation analysis revised: The gradient of graft consolidation.
Clin Oral Implants Res 20: 1078-1083.
Busenlechner, D., Tangl, S., Mair, B., Fugger, G., Gruber, R., Redl, H. & Watzek,
G. (2008) Simultaneous in vivo comparison of bone substitutes in a guided bone
regeneration model. Biomaterials 29: 3195-3200.
Buser, D., Janner, S. F., Wittneben, J. G., Bragger, U., Ramseier, C. A. & Salvi,
G. E. (2012) 10-year survival and success rates of 511 titanium implants with a
sandblasted and acid-etched surface: A retrospective study in 303 partially
edentulous patients. Clin Implant Dent Relat Res 14: 839-851.
Buser, D., Nydegger, T., Hirt, H. P., Cochran, D. L. & Nolte, L. P. (1998)
Removal torque values of titanium implants in the maxilla of miniature pigs. Int J
Oral Maxillofac Implants 13: 611-619.
Carmagnola, D., Adriaens, P. & Berglundh, T. (2003) Healing of human
extraction sockets filled with bio-oss. Clin Oral Implants Res 14: 137-143.
Chee, W. & Jivraj, S. (2006) Screw versus cemented implant supported
restorations. Br Dent J 201: 501-507.
Chiapasco, M., Casentini, P. & Zaniboni, M. (2009) Bone augmentation
procedures in implant dentistry. Int J Oral Maxillofac Implants 24 Suppl: 237-
259.
Cochran, D. L., Schenk, R. K., Lussi, A., Higginbottom, F. L. & Buser, D. (1998)
Bone response to unloaded and loaded titanium implants with a sandblasted and
acid-etched surface: A histometric study in the canine mandible. J Biomed Mater
Res 40: 1-11.
Coli, P., Christiaens, V., Sennerby, L. & Bruyn, H. (2017) Reliability of
periodontal diagnostic tools for monitoring peri-implant health and disease.
Periodontol 2000 73: 203-217.
Corbella, S., Taschieri, S. & Del Fabbro, M. (2015) Long-term outcomes for the
treatment of atrophic posterior maxilla: A systematic review of literature. Clin
Implant Dent Relat Res 17: 120-132.
Corbella, S., Taschieri, S., Weinstein, R. & Del Fabbro, M. (2016)
Histomorphometric outcomes after lateral sinus floor elevation procedure: A

170
systematic review of the literature and meta-analysis. Clin Oral Implants Res 27:
1106-1122.
Cortes, A. R., Pinheiro, L. R., Cavalcanti, M. G., Arita, E. S. & Tamimi, F. (2015)
Sinus floor bone failures in maxillary sinus floor augmentation: A case-control
study. Clin Implant Dent Relat Res 17: 335-342.
Cricchio, G. & Lundgren, S. (2003) Donor site morbidity in two different
approaches to anterior iliac crest bone harvesting. Clin Implant Dent Relat Res 5:
161-169.
Del Fabbro, M., Rosano, G. & Taschieri, S. (2008) Implant survival rates after
maxillary sinus augmentation. Eur J Oral Sci 116: 497-506.
Derks, J. & Tomasi, C. (2015) Peri-implant health and disease. A systematic
review of current epidemiology. J Clin Periodontol 42 Suppl 16: S158-171.
Doud Galli, S. K., Lebowitz, R. A., Giacchi, R. J., Glickman, R. & Jacobs, J. B.
(2001) Chronic sinusitis complicating sinus lift surgery. Am J Rhinol 15: 181-186.
Galindo-Moreno, P., Fernandez-Jimenez, A., O'Valle, F., Silvestre, F. J., Sanchez-
Fernandez, E., Monje, A. & Catena, A. (2015) Marginal bone loss in implants
placed in grafted maxillary sinus. Clin Implant Dent Relat Res 17: 373-383.
Galindo-Moreno, P., Moreno-Riestra, I., Avila, G., Padial-Molina, M., Paya, J.
A., Wang, H. L. & O'Valle, F. (2011) Effect of anorganic bovine bone to
autogenous cortical bone ratio upon bone remodeling patterns following maxillary
sinus augmentation. Clin Oral Implants Res 22: 857-864.
Gerber, J. A., Tan, W. C., Balmer, T. E., Salvi, G. E. & Lang, N. P. (2009)
Bleeding on probing and pocket probing depth in relation to probing pressure and
mucosal health around oral implants. Clin Oral Implants Res 20: 75-78.
Gittens, R. A., Olivares-Navarrete, R., McLachlan, T., Cai, Y., Hyzy, S. L.,
Schneider, J. M., Schwartz, Z., Sandhage, K. H. & Boyan, B. D. (2012)
Differential responses of osteoblast lineage cells to nanotopographically-
modified, microroughened titanium-aluminum-vanadium alloy surfaces.
Biomaterials 33: 8986-8994.
Gruber, R., Kandler, B., Fuerst, G., Fischer, M. B. & Watzek, G. (2004) Porcine
sinus mucosa holds cells that respond to bone morphogenetic protein (bmp)-6 and
bmp-7 with increased osteogenic differentiation in vitro. Clin Oral Implants Res
15: 575-580.

171
Haas, R., Baron, M., Donath, K., Zechner, W. & Watzek, G. (2002) Porous
hydroxyapatite for grafting the maxillary sinus: A comparative histomorphometric
study in sheep. Int J Oral Maxillofac Implants 17: 337-346.
Haas, R., Donath, K., Fodinger, M. & Watzek, G. (1998) Bovine hydroxyapatite
for maxillary sinus grafting: Comparative histomorphometric findings in sheep.
Clin Oral Implants Res 9: 107-116.
Hammerle, C. H., Bragger, U., Burgin, W. & Lang, N. P. (1996) The effect of
subcrestal placement of the polished surface of iti implants on marginal soft and
hard tissues. Clin Oral Implants Res 7: 111-119.
Hermann, J. S., Buser, D., Schenk, R. K. & Cochran, D. L. (2000) Crestal bone
changes around titanium implants. A histometric evaluation of unloaded non-
submerged and submerged implants in the canine mandible. J Periodontol 71:
1412-1424.
Hermann, J. S., Buser, D., Schenk, R. K., Schoolfield, J. D. & Cochran, D. L.
(2001) Biologic width around one- and two-piece titanium implants. Clin Oral
Implants Res 12: 559-571.
Hermann, J. S., Schoolfield, J. D., Nummikoski, P. V., Buser, D., Schenk, R. K.
& Cochran, D. L. (2001) Crestal bone changes around titanium implants: A
methodologic study comparing linear radiographic with histometric
measurements. Int J Oral Maxillofac Implants 16: 475-485.
Hernandez-Alfaro, F., Torradeflot, M. M. & Marti, C. (2008) Prevalence and
management of schneiderian membrane perforations during sinus-lift procedures.
Clin Oral Implants Res 19: 91-98.
Holtzclaw, D. (2015) Maxillary sinus membrane repair with amnion-chorion
barriers: A retrospective case series. J Periodontol 86: 936-940.
Jemt, T. & Lekholm, U. (1995) Implant treatment in edentulous maxillae: A 5-
year follow-up report on patients with different degrees of jaw resorption. Int J
Oral Maxillofac Implants 10: 303-311.
Jensen, O. T., Shulman, L. B., Block, M. S. & Iacono, V. J. (1998) Report of the
sinus consensus conference of 1996. Int J Oral Maxillofac Implants 13 Suppl: 11-
45.
Jensen, S. S. & Terheyden, H. (2009) Bone augmentation procedures in localized
defects in the alveolar ridge: Clinical results with different bone grafts and bone-
substitute materials. Int J Oral Maxillofac Implants 24 Suppl: 218-236.

172
Jensen, T., Schou, S., Svendsen, P. A., Forman, J. L., Gundersen, H. J.,
Terheyden, H. & Holmstrup, P. (2012) Volumetric changes of the graft after
maxillary sinus floor augmentation with bio-oss and autogenous bone in different
ratios: A radiographic study in minipigs. Clin Oral Implants Res 23: 902-910.
Johansson, B., Grepe, A., Wannfors, K. & Hirsch, J. M. (2001) A clinical study of
changes in the volume of bone grafts in the atrophic maxilla. Dentomaxillofac
Radiol 30: 157-161.
Jung, R. E., Pjetursson, B. E., Glauser, R., Zembic, A., Zwahlen, M. & Lang, N.
P. (2008) A systematic review of the 5-year survival and complication rates of
implant-supported single crowns. Clin Oral Implants Res 19: 119-130.
Jung, R. E., Zembic, A., Pjetursson, B. E., Zwahlen, M. & Thoma, D. S. (2012)
Systematic review of the survival rate and the incidence of biological, technical,
and aesthetic complications of single crowns on implants reported in longitudinal
studies with a mean follow-up of 5 years. Clin Oral Implants Res 23 Suppl 6: 2-
21.
Junker, R., Dimakis, A., Thoneick, M. & Jansen, J. A. (2009) Effects of implant
surface coatings and composition on bone integration: A systematic review. Clin
Oral Implants Res 20 Suppl 4: 185-206.
Karoussis, I. K., Salvi, G. E., Heitz-Mayfield, L. J., Bragger, U., Hammerle, C. H.
& Lang, N. P. (2003) Long-term implant prognosis in patients with and without a
history of chronic periodontitis: A 10-year prospective cohort study of the iti
dental implant system. Clin Oral Implants Res 14: 329-339.
Klinge, B., Alberius, P., Isaksson, S. & Jonsson, J. (1992) Osseous response to
implanted natural bone mineral and synthetic hydroxylapatite ceramic in the
repair of experimental skull bone defects. J Oral Maxillofac Surg 50: 241-249.
Lang, N. P., Berglundh, T. & Working Group 4 of Seventh European Workshop
on, P. (2011) Periimplant diseases: Where are we now?--consensus of the seventh
european workshop on periodontology. J Clin Periodontol 38 Suppl 11: 178-181.
Lang, N. P., Salvi, G. E., Huynh-Ba, G., Ivanovski, S., Donos, N. & Bosshardt, D.
D. (2011) Early osseointegration to hydrophilic and hydrophobic implant surfaces
in humans. Clin Oral Implants Res 22: 349-356.
Lundgren, S., Andersson, S., Gualini, F. & Sennerby, L. (2004) Bone reformation
with sinus membrane elevation: A new surgical technique for maxillary sinus
floor augmentation. Clin Implant Dent Relat Res 6: 165-173.

173
Luterbacher, S., Mayfield, L., Bragger, U. & Lang, N. P. (2000) Diagnostic
characteristics of clinical and microbiological tests for monitoring periodontal and
peri-implant mucosal tissue conditions during supportive periodontal therapy
(spt). Clin Oral Implants Res 11: 521-529.
Marcelis, K., Vercruyssen, M., Nicu, E., Naert, I. & Quirynen, M. (2012)
Sleeping vs. Loaded implants, long-term observations via a retrospective analysis.
Clin Oral Implants Res 23: 1118-1122.
Margolin, M. D., Cogan, A. G., Taylor, M., Buck, D., McAllister, T. N., Toth, C.
& McAllister, B. S. (1998) Maxillary sinus augmentation in the non-human
primate: A comparative radiographic and histologic study between recombinant
human osteogenic protein-1 and natural bone mineral. J Periodontol 69: 911-919.
McGrath, C., Lam, O. & Lang, N. (2012) An evidence-based review of patient-
reported outcome measures in dental implant research among dentate subjects. J
Clin Periodontol 39 Suppl 12: 193-201.
Michalakis, K. X., Hirayama, H. & Garefis, P. D. (2003) Cement-retained versus
screw-retained implant restorations: A critical review. Int J Oral Maxillofac
Implants 18: 719-728.
Millen, C., Bragger, U. & Wittneben, J. G. (2015) Influence of prosthesis type and
retention mechanism on complications with fixed implant-supported prostheses:
A systematic review applying multivariate analyses. Int J Oral Maxillofac
Implants 30: 110-124.
Mombelli, A. & Lang, N. P. (1994) Clinical parameters for the evaluation of
dental implants. Periodontol 2000 4: 81-86.
Morton, D., Bornstein, M. M., Wittneben, J. G., Martin, W. C., Ruskin, J. D.,
Hart, C. N. & Buser, D. (2010) Early loading after 21 days of healing of
nonsubmerged titanium implants with a chemically modified sandblasted and
acid-etched surface: Two-year results of a prospective two-center study. Clin
Implant Dent Relat Res 12: 9-17.
Nkenke, E. & Stelzle, F. (2009) Clinical outcomes of sinus floor augmentation for
implant placement using autogenous bone or bone substitutes: A systematic
review. Clin Oral Implants Res 20 Suppl 4: 124-133.
Palma, V. C., Magro-Filho, O., de Oliveria, J. A., Lundgren, S., Salata, L. A. &
Sennerby, L. (2006) Bone reformation and implant integration following

174
maxillary sinus membrane elevation: An experimental study in primates. Clin
Implant Dent Relat Res 8: 11-24.
Papaspyridakos, P., Chen, C. J., Singh, M., Weber, H. P. & Gallucci, G. O. (2012)
Success criteria in implant dentistry: A systematic review. J Dent Res 91: 242-
248.
Philipp, A., Duncan, W., Roos, M., Hammerle, C., Attin, T. & Schmidlin, P. R.
(2013) Comparison of sla or slactive implants in the maxillary sinus with or
without synthetic bone graft materials - an animal study in sheep. Clinical Oral
Implants Research 0: 1-7.
Pjetursson, B. E., Bragger, U., Lang, N. P. & Zwahlen, M. (2007) Comparison of
survival and complication rates of tooth-supported fixed dental prostheses (fdps)
and implant-supported fdps and single crowns (scs). Clin Oral Implants Res 18
Suppl 3: 97-113.
Pjetursson, B. E., Tan, W. C., Zwahlen, M. & Lang, N. P. (2008) A systematic
review of the success of sinus floor elevation and survival of implants inserted in
combination with sinus floor elevation. J Clin Periodontol 35: 216-240.
Pjetursson, B. E., Thoma, D., Jung, R., Zwahlen, M. & Zembic, A. (2012) A
systematic review of the survival and complication rates of implant-supported
fixed dental prostheses (fdps) after a mean observation period of at least 5 years.
Clin Oral Implants Res 23 Suppl 6: 22-38.
Pjetursson, B. E., Zwahlen, M. & Lang, N. P. (2012) Quality of reporting of
clinical studies to assess and compare performance of implant-supported
restorations. J Clin Periodontol 39 Suppl 12: 139-159.
Proussaefs, P. & Lozada, J. (2003) The "loma linda pouch": A technique for
repairing the perforated sinus membrane. Int J Periodontics Restorative Dent 23:
593-597.
Proussaefs, P., Lozada, J., Kim, J. & Rohrer, M. D. (2004) Repair of the
perforated sinus membrane with a resorbable collagen membrane: A human study.
Int J Oral Maxillofac Implants 19: 413-420.
Quiney, R. E., Brimble, E. & Hodge, M. (1990) Maxillary sinusitis from dental
osseointegrated implants. J Laryngol Otol 104: 333-334.
Rickert, D., Slater, J. J., Meijer, H. J., Vissink, A. & Raghoebar, G. M. (2012)
Maxillary sinus lift with solely autogenous bone compared to a combination of

175
autogenous bone and growth factors or (solely) bone substitutes. A systematic
review. Int J Oral Maxillofac Surg 41: 160-167.
Sailer, I., Muhlemann, S., Zwahlen, M., Hammerle, C. H. & Schneider, D. (2012)
Cemented and screw-retained implant reconstructions: A systematic review of the
survival and complication rates. Clin Oral Implants Res 23 Suppl 6: 163-201.
Sanz, M., Chapple, I. L. & Working Group 4 of the, V. E. W. o. P. (2012) Clinical
research on peri-implant diseases: Consensus report of working group 4. J Clin
Periodontol 39 Suppl 12: 202-206.
Sanz-Sanchez, I., Carrillo de Albornoz, A., Figuero, E., Schwarz, F., Jung, R.,
Sanz, M. & Thoma, D. (2018) Effects of lateral bone augmentation procedures on
peri-implant health or disease: A systematic review and meta-analysis. Clin Oral
Implants Res 29 Suppl 15: 18-31.
Scala, A., Botticelli, D., Rangel, I. G., Jr., de Oliveira, J. A., Okamoto, R. & Lang,
N. P. (2010) Early healing after elevation of the maxillary sinus floor applying a
lateral access: A histological study in monkeys. Clin Oral Implants Res 21: 1320-
1326.
Schenk, R. K., Buser, D., Hardwick, W. R. & Dahlin, C. (1994) Healing pattern
of bone regeneration in membrane-protected defects: A histologic study in the
canine mandible. Int J Oral Maxillofac Implants 9: 13-29.
Schincaglia, G. P., Thoma, D. S., Haas, R., Tutak, M., Garcia, A., Taylor, T. D. &
Hammerle, C. H. (2015) Randomized controlled multicenter study comparing
short dental implants (6 mm) versus longer dental implants (11-15 mm) in
combination with sinus floor elevation procedures. Part 2: Clinical and
radiographic outcomes at 1 year of loading. J Clin Periodontol 42: 1042-1051.
Schmitt, C. M., Moest, T., Lutz, R., Neukam, F. W. & Schlegel, K. A. (2015)
Anorganic bovine bone (abb) vs. Autologous bone (ab) plus abb in maxillary
sinus grafting. A prospective non-randomized clinical and histomorphometrical
trial. Clin Oral Implants Res 26: 1043-1050.
Srouji, S., Kizhner, T., Ben David, D., Riminucci, M., Bianco, P. & Livne, E.
(2009) The schneiderian membrane contains osteoprogenitor cells: In vivo and in
vitro study. Calcif Tissue Int 84: 138-145.
Suarez-Lopez Del Amo, F., Ortega-Oller, I., Catena, A., Monje, A., Khoshkam,
V., Torrecillas-Martinez, L., Wang, H. L. & Galindo-Moreno, P. (2015) Effect of
barrier membranes on the outcomes of maxillary sinus floor augmentation: A

176
meta-analysis of histomorphometric outcomes. Int J Oral Maxillofac Implants 30:
607-618.
Wennerberg, A., Frojd, V., Olsson, M., Nannmark, U., Emanuelsson, L.,
Johansson, P., Josefsson, Y., Kangasniemi, I., Peltola, T., Tirri, T., Pankalainen,
T. & Thomsen, P. (2011) Nanoporous tio(2) thin film on titanium oral implants
for enhanced human soft tissue adhesion: A light and electron microscopy study.
Clin Implant Dent Relat Res 13: 184-196.
Wiltfang, J., Schultze-Mosgau, S., Merten, H. A., Kessler, P., Ludwig, A. &
Engelke, W. (2000) Endoscopic and ultrasonographic evaluation of the maxillary
sinus after combined sinus floor augmentation and implant insertion. Oral Surg
Oral Med Oral Pathol Oral Radiol Endod 89: 288-291.
Wittneben, J. G., Buser, D., Salvi, G. E., Burgin, W., Hicklin, S. & Bragger, U.
(2014) Complication and failure rates with implant-supported fixed dental
prostheses and single crowns: A 10-year retrospective study. Clin Implant Dent
Relat Res 16: 356-364.
Wittneben, J. G., Millen, C. & Bragger, U. (2014) Clinical performance of screw-
versus cement-retained fixed implant-supported reconstructions--a systematic
review. Int J Oral Maxillofac Implants 29 Suppl: 84-98.
Xu, H., Shimizu, Y. & Ooya, K. (2005) Histomorphometric study of the stability
of newly formed bone after elevation of the floor of the maxillary sinus. Br J Oral
Maxillofac Surg 43: 493-499.

177
APPENDIX A

SCHOOL OF DENTISTRY
DENTAL SCIENCES RESEARCH ETHICS COMMITTEE
APPROVAL FORM
Chief Investigator: Jamil Alayan Project Title: Randomised clinical trial comparing DBBM vs. BCP with and without autogenous bone deficient maxillary Sinuses for the purpose of dental implant placement. Supervisor: A/Prof CS Farah Co-Investigator(s): N/A Department(s): Dentistry Project Number: 1010 Duration of Approval: 3 years
Comments/Conditions/Restrictions: This project complies with the provisions contained in the National Statement on Ethical Conduct in Research Involving Humans and complies with the regulations governing experimentation on humans. A/Prof Camile Farah Chairperson, Research Committee Date:___________________ Signature: _______________________________________

University Animal Research Ethics CommitteeANIMAL ETHICS APPROVAL CERTIFICATE
QDPI Scientific Use Registration Number 0052
Date of Issue:4/10/11 (supersedes all previously issued certificates)
UAECs must advise investigators and teachers of their decisions in writing as promptly as possible and activities must not commence until written approval has been obtained from the UAEC. This Approval Certificate serves as your written notice.
Within this Approval Certificate are: * Activity Details * Animal Details * Conditions of Approval (Specific and Standard)
The following standard conditions are particularly important: (a) prompt notification to the UAEC of any adverse or unexpected effects that impact on animal wellbeing; (b) submission to the UAEC for consideration, any changes to the project as detailed in the proposal application.
Further information regarding your ongoing obligations regarding animal based research can be found via the Research Ethics website (http://www.research.qut.edu.au/ethics/) or by contacting the Research Ethics Coordinator on 07 3138 2091 or [email protected].
If any details within this Approval Certificate are incorrect please advise Research Ethics within 10 days of receipt of this certificate.
Activity Details
Dear Prof Dietmar Hutmacher
1100001051Approval Number:
Bone regeneration in a sinus model: a comparison between several bone grafting materials
Activity Title:
The aims of this project are to compare the histological appearance, histomorphometric parameters, immunohistochemical features and expressed gene profiles of biopsies harvested from the maxillary sinus cavity in a sheep model (ovis aries)after sinus ?oor augmentation with either deproteinised bovine bone mineral (DBBM; Bio-Oss, Geistlich AG, Wolhusen, Switzerland) or Bio-Oss Collagen (DBBM-C; Bio-Oss Collagen, Geistlich AG, Wolhusen, Switzerland) and to assess the impact of adding autogenous bone on these parameters by means of a prospective randomized clinical trial.
Activity Summary:
Approved Until: 04-Oct-2014 (subject to annual reports to the UAEC)Date Approved: 04-Oct-2011
Location(s): MERF
Chief Investigator: Prof Dietmar Hutmacher
Other Staff/Students:Investigator Name Type RoleAdj/Prof Saso Ivanovski Internal Ethics - Alternative
InvestigatorMr Cedryck Vaquette Internal Associate InvestigatorA/Prof Yin Xiao Internal Associate InvestigatorMr Stephen Hamlet External Associate InvestigatorMr Jamil Alayal External Associate InvestigatorDr Siamak Saifzadeh Internal Ethics - VeterinarianDr Eugene Huang External Associate Investigator
Investigator Details
Animal Details
RM Report No. E802 Version 3.1 Page 1 of 3
University Animal Research Ethics CommitteeANIMAL ETHICS APPROVAL CERTIFICATE
QDPI Scientific Use Registration Number 0052
Date of Issue:4/10/11 (supersedes all previously issued certificates)
Sheep: Domestic Mammals Ovis aries --- 3-4yrs maleFurther Details:Animal Type:No. Used to Date:Total No. Approved: 045
Monitoring of Animals: During procedures, the depth of general anaesthesia will be monitored throughout the operation using the following parameters: physiological parameters (HR, RR), reflexes (palpebral, corneal and web pinch reflexes) and muscle tone (jaw tension), the oxygen saturation of the sheep using pulse oximetry, end tidal CO2 level. After procedures - The oral surgical wounds will be checked on a daily basis for any evidence of post-operative complications, such as failure in suture integrity (wound dehiscence), bleeding, inflammation, and infection.
Housing of Animals: The sheep will be housed in a group of 10/yard. Group of 3/pen for overnight fasting. Environmental enrichment: grass, pellet, trees, and rocks.
Disposal of Animals: As per MERF protocols
Conditions of Approval
Specific Conditions of ApprovalNo special conditions placed on approval by the UAEC. Standard conditions apply.
Standard Conditions of ApprovalUnder its Terms of Reference the UAEC monitors the conduct of approved activities until their completion so as toensure continued compliance with relevant requirements, and may withdraw approval;
Investigators and teachers have personal responsibility for all matters related to the welfare of the animals they use and must act in accordance with all requirements of the Code. This responsibility begins when an animal is allocated to a project and ends with its fate at the completion of a project;
Work must be conducted in accordance with university policy, NHMRC / AVCC guidelines and regulations, and in accordance with the provisions of any legislation which is relevant to your project;
Immediately advise the UAEC, via the Research Ethics Coordinator, of any unforseen events that might affect the continued ethical acceptability of the project;
Immediately advise the UAEC, via the Research Ethics Coordinator, if any complaints are made, or expressions of concern raised in relation to the project;
Report on the progress of the approved project at least annually, or at intervals determined by the Committee. The Committee may also choose to conduct a random audit of your research;
Ensure that adequate records are kept of the acquisition, breeding, health, care, use, transportation, housing, handling and disposal of the animals. The Committee may wish to see these records at the end of the experimentation;
It is the responsibility of all investigators to ensure that all personnel involved, or connected with the project, including research assistant and students, are adequately trained in all handling and safety procedures;
Investigators and teachers must make arrangements so that they, or other responsible persons, can be contacted in the event of emergencies.
Modifying your Ethical ClearanceRequests for variations must be made via submission of a Variation Request Form (available online at http://www.research.qut.edu.au/ethics/forms/ani/var/var.jsp) to the Research Ethics Coordinator. Minor changes will be assessed on a case by case basis.
It generally takes 7-14 days to process and notify the Chief Investigator of the outcome of a request for a variation.
Major changes, depending upon the nature of your request, may require submission of a new application.
Audits
RM Report No. E802 Version 3.1 Page 2 of 3

University Animal Research Ethics CommitteeANIMAL ETHICS APPROVAL CERTIFICATE
QDPI Scientific Use Registration Number 0052
Date of Issue:4/10/11 (supersedes all previously issued certificates)
All active ethical clearances are subject to random audit by the UAEC. You will be contacted by the Research Ethics Unit if this is to occur.
End of Document
RM Report No. E802 Version 3.1 Page 3 of 3

ANIMAL ETHICS COMMITTEE
23 April 2013 Dear Professor Saso Ivanovski, I write further to the additional information provided in relation to the conditional approval granted to your application for ethical clearance for your project "Bone regeneration in a sinus model: a comparison between several bone grafting materials." (GU Ref No: DOH/02/13/AEC) detailed below. Is this submission only for the approval of Dr Alayan to work on the project? Yes Where will the animal work take place? All procedures involving the animals will take place at QUT’s Medical Engineering Research Facility, Chermside, Brisbane. A Griffith University staff member is listed on the original AEC application to QUT. Why was an application not submitted to the Griffith University AEC in 2011? Since all of the animal work was done at QUT, I was not aware that we need Griffith University ethical approval. I have close collaborators at QUT and hold an adjunct appointment there. This application has now been put through the Griffith Ethics Committe, because Dr Alayan, a PhD student who will be doing the sheep surgery, has obtained an NHMRC scholarship, and the Office of Research requires ethics approval through Griffith in order to formally accept the scholarship. The additional information provided in relation to the conditional approval granted to your application for ethical clearance has satisfied all the conditions and you are authorised to immediately commence this research on this basis. Regards Dr Amanda Fernie Animal Ethics Committee Secretary Office for Research Bray Centre, Nathan Campus Griffith University ph: 3735 6618 fax: 3735 7994 email: [email protected] Researchers are reminded that the Griffith University Code for the Responsible Conduct of Research provides guidance to researchers in areas such as conflict of interest, authorship, storage of data, & the training of research students.

2
You can find further information, resources and a link to the University's Code by visiting http://policies.griffith.edu.au/pdf/Code%20for%20the%20Responsible%20Conduct%20of%20Research.pdf PRIVILEGED, PRIVATE AND CONFIDENTIAL This email and any files transmitted with it are intended solely for the use of the addressee(s) and may contain information which is confidential or privileged. If you receive this email and you are not the addressee(s) [or responsible for delivery of the email to the addressee(s)], please disregard the contents of the email, delete the email and notify the author immediately.
Gold Coast Logan Mt Gravatt Nathan South Bank